







Bahasa
Halaman
Hukum


65
CHAPTER THREE OSTEOARTHRITIS: RECONSTRUCTING MOBILITY
AND ACTIVITY PATTERNS
3.1 Introduction
Osteoarthritis, or degenerative joint disease, is perhaps the most commonly
documented pathological condition of the human skeleton. The disorder involves
degenerative changes in diarthrodial joints characterized by a loss of cartilage and the
resulting bony lesions caused by direct interosseous contact (Aufderheide and
Rodríguez-Martín 1998:93). Skeletal modifications resulting from osteoarthritis
include hypertrophy of joint margins through osteophytic development (lipping) and
erosion and eburnation (polishing) of subchondral bone. While degenerative changes
involving amphiarthrodial intervertebral joints are not osteoarthritis by strict
definition, the pathological response is virtually identical. Following the lead of
numerous other scholars (Bridges 1991, Griffin and Larsen 1989, Hemphill 1999,
Jurmain 1990, Jurmain and Kilgore 1995, Kilgore 1984, Larsen 1982, 1987, Larsen et
al. 1995, Larsen and Hutchinson 1999, Merbs 1983, Pickering 1984, Walker and
Hollimon 1989), they will be subsumed under the term osteoarthritis for this study.
Osteoarthritis is a multifactorial condition, with patterns of response
representing a number of underlying causes (Hoffman 1993, Sokoloff 1969, Rogers
and Waldron 1995). Sex, body build, nutrition, endocrine status, and heredity may all
play a role in its etiology, but physical activity and mechanical stress are the primary
contributing factors (Engel 1968, Jurmain 1977, Kellgren and Moore 1952, Kellgren
and Lawrence 1958, Larsen 1997, Moskowitz 1972, McCarty and Koopman 1993,
Radin 1982, 1983). Thus, while osteoarthritis is generally associated with advancing
age, it is not age per se, but rather the cumulative effects of physiological wear and
tear, which are reflected on joint surfaces and margins. This relationship between

66
osteoarthritis and activity has been well documented, in large part due to the former’s
frequent nonsystemic manifestation. Not only are osteoarthritic prevalence and
severity increased in human populations exhibiting high levels of activity or engaged
in physically stressful occupations, but joint distribution patterns also reflect the
specific activities undertaken (Kennedy 1989, Larsen 1997). Thus, osteoarthritis
provides a valuable record of activity and mechanical stress levels experienced by
individuals throughout their adult lives (Bridges 1991, Jurmain and Kilgore 1995,
Larsen et al. 1995)
A conspicuous feature of the Cis-Baikal’s richly-documented mid-Holocene
past is the substantial interruption of cultural continuity during the fifth millennium
BC. The late Mesolithic/early Neolithic Kitoi culture (6800-4900 BC) appears to have
been replaced, after a 700-year hiatus, by the culturally and biologically distinct
Serovo-Glaskovo cultural complex (4200-1700 BC), which spanned the middle
Neolithic through early Bronze Age (Weber 1995, Weber et al. 2002). In this study,
skeletal remains from five mid-Holocene Cis-Baikal cemetery sites – two pre-dating
the hiatus and three post-dating it – are examined for evidence of osteoarthritis. The
objective is to investigate osteoarthritic prevalence and distribution (patterning) within
and among these populations in order to reconstruct mobility and activity patterns
among Cis-Baikal foragers, and to test for possible disparities which may reflect
differing adaptive strategies. Because the five populations lie on either side of the
alleged hiatus, they provide an excellent opportunity not only to characterize mid-
Holocene hunter-gatherer adaptation as a whole, but also to investigate cultural change
in the Cis-Baikal.

67
3.2 Materials and Methods
This study investigates human skeletal remains from five distinct Cis-Baikal
cemetery populations. They represent the pre-hiatus Kitoi sites of Lokomotiv and
Shamanka II, the early post-hiatus Serovo site of Ust’-Ida I Serovo, and the late post-
hiatus Glaskovo sites of Ust’-Ida I Glaskovo and Khuzhir-Nuge XIV. Two of these
sites – Shamanka II and Khuzhir-Nuge XIV – are newly excavated (since the late
1990’s) and their human remains previously unanalyzed. In both cases, the skeletal
material was examined for osteoarthritis and other osteobiographical features
immediately or shortly after excavation, and curatorial methods maintained both
individual and element integrity. However, despite careful excavation and curation,
variable but generally poor skeletal condition at Khuzhir-Nuge XIV and numerous
commingled and incompletely-represented individuals at Shamanka II have presented
some challenges to the investigation of skeletal and dental material from these two
sites. Remains from the other three sites (Lokomotiv, Ust’-Ida I Serovo, and Ust’-Ida
I Glaskovo) were excavated in the 1980’s and early 1990’s and examined for a
previous study in 1995, in some cases more than ten years after their initial excavation
(Link 1996, 1999, Weber et al. 2002). Unfortunately, poor curation of the skeletal
material during that period resulted in extensive commingling, misplaced, fragmented,
or otherwise unobservable elements, and sometimes completely missing individuals.
Many of these problems have recently been rectified, resulting in the substantial
modification to and enhancement of the previously-collected data, and warranting the
inclusion of these three sites in the current study. However, the negative effects of
poor curation could not be completely obliterated: numerous individuals remain
incompletely represented by their skeletal elements, particularly small bones such as
those of the hands and feet. Because of the challenges presented by all five skeletal
assemblages, care has been taken in the current investigation to control for the effects

68
of poor preservation (i.e., Khuzhir-Nuge XIV) and inadequate element representation
(i.e., Shamanka II, Lokomotiv, Ust’-Ida I Serovo, and Ust’-Ida I Glaskovo). This has
been accomplished through the establishment of specific criteria by which to consider
individuals observable for osteoarthritic examination and the exclusion from analyses
of those not deemed so.
Of the total 308 individuals represented by the five sites investigated, only 175
were deemed observable for osteoarthritis and considered in this examination (Table
3.1). Observability was based on two main criteria: age at death and skeletal
condition. Because osteoarthritis is largely associated with advancing age, and
because no subadult individuals (those under 20 years of age) were afflicted by the
condition at any of the five sites, only adults (those 20 years of age and older) were
included in the analyses. Furthermore, osteoarthritis was considered observable only
for those adult individuals exhibiting good skeletal preservation, specifically with
regards to joint surfaces and margins. Since the disorder appears to be especially
common among vertebrae in the Cis-Baikal (see below), and since these elements are
particularly susceptible to postmortem taphonomic degradation due to their largely
trabecular composition (Henderson 1987, Janaway 1996, Micozzi 1991:54-57,
Nawrocki 1995), any adult individual with vertebrae exhibiting well preserved
articular facets was considered observable for osteoarthritis. In almost every instance,
these individuals also presented a number of other major joint surfaces in a good state
of preservation. Finally, any adult individual visibly affected by osteoarthritis,
regardless of overall skeletal condition, was also deemed observable for this study.
The examination of osteoarthritis was limited to macroscopic, noninvasive, and
nondestructive techniques. Joint surfaces and margins were cleaned of debris with
plastic implements and soft brushes, and documentation included the description of
arthritic extent and location (element and joint surface), as well as photography of

69
Table 3.1 Individuals Observable for Osteoarthritis (n=175) Site Individ. Age Sex OA Site Individ. Age Sex OA Lok L 2-1-1 20-25 U 1 Lok L 25-1-1 35-40 F 2 Lok L 2-2 35-39 U 2 Lok L 25-2 20-22 F 2 Lok L 2-3-1 25-35 F 1 Lok L 25-3 25-35 F 1 Lok L 2-4-1 25-35 U 2 Lok L 25-4-1 35-45 M 2 Lok L 4-1-1 35-50 F 1 Lok L 25-5-1 35-50 M 2 Lok L 6-1-1 20+ M 2 Lok L 26-1-1 20+ M 2 Lok L 7-1-1 40-45 F 1 Lok L 28-1-1 35-40 F 2 Lok L 8-1-1 40-45 M 1 Lok L 29-1-1 30-40 F 1 Lok L 9-1-1 20+ F 1 Lok L 30-1-1 35-40 M 2 Lok L 10-1-1 20-25 M 2 Lok L 30-2-1 35-40 M 2 Lok L 10-2-1 20-25 M 2 Lok L 31-1-1 35-50 U 2 Lok L 10-3-1 25-30 M 2 Lok L 31-2-1 25-30 M 2 Lok L 10-4 30-35 M 2 Lok L 33-1-1 35-45 M 1 Lok L 11-1-1 50+ M 1 Lok L 34-1-1 35-45 F 1 Lok L 12-1-1 18-22 F 1 Lok L 35-1-1 20+ U 1 Lok L 13-1-1 25-30 M 1 Lok L 36-1-1 20-25 F 1 Lok L 14-1-4 25-30 F 1 Lok L 37-1-1 25-29 F 1 Lok L 14-4-4 19-22 M 2 Lok L 38-1-1 50+ F 1 Lok L 15-1-1 20-35 M 1 Lok L 38-2-1 35-45 F 1 Lok L 16-1-1 45-55 M 1 Lok L 39-1-1 20-25 F 2 Lok L 17-1-1 45-55 F 1 Lok L 40-1-1 20+ M 2 Lok L 18-1-1 50+ F 1 Lok L 41-3-1 20+ U 2 Lok L 20-1-1 20-29 F 1 Lok L 42-1-1 40-50 M 1 Lok L 20-2-1 35-50 M 1 Lok L 43-2-1 40-44 F 2 Lok L 21-1-1 50+ F 1 Lok L 44-1-1 35-39 M 1 Lok L 22-1 20+ M 2 Lok L 44-2-1 30-39 M 1 Lok L 22-2 20-25 M 2 Lok R 1-1-1 30-34 M 1 Lok L 22-3 20-25 M 2 Lok R 3-1-1 30-45 M 2 Lok L 22-5 20+ U 2 Lok R 6-1-1 35-39 M 1 Lok L 22-6 25-30 F 2 Lok R 6-2-1 35-39 M 1 Lok L 22-7 20+ F 2 Lok R 7-1-1 50+ M 1 Lok L 22-8 20+ M 2 Lok R 13-3 25-35 F 2 Lok L 23-1-1 20-25 M 2 Lok R 13-4 20-25 F 2 Lok L 24-2-1 40-45 M 1 Lok R 14-1 30-39 M 1 Lok L 24-5-2 45-50 M 1 Lok R 15-1 20-35 F 2 Lok L 24-6-2 25-35 F 2 Lok R 15-2 35-40 F 2 Sham 7-1 20-25 F 2 Sham 13-2 35-50 M 1 Sham 8-1 35-40 M 1 Sham 14-1 25-30 M 2 Sham 10-1 25-30 M 1 Sham 14-2 20-25 F 2 Sham 11-2 30-40 M 1 Sham 15-1 25-35 M 1 Sham 12-1 20-35 U 1 Sham 16-1 20-25 U 1 Sham 13-1 25-35 F 1 Sham 17-1 30-40 M 1

70
Table 3.1 (Continued) Site Individ. Age Sex OA Site Individ. Age Sex OA Sham 17-2 20-22 M 2 Sham 25-1 20-22 F 2 Sham 18-1 20-25 M 2 Sham 25-3 20+ F 1 Sham 19-1 25-35 M 2 Sham 26-1 20+ F 1 Sham 21-1 25-35 M 2 Sham 26-2 20+ M 2 Sham 21-2 25-30 M 1 Sham 27-1 35-50 M 1 Sham 22-1 19-22 M 2 Sham 27-2 25-30 M 2 Sham 23-1 35-45 M 1 Sham 29-1 20-30 M 1 Sham 23-2 20+ F 2 Sham 30-1 35-50 M 1 Sham 23-3 20+ U 1 Sham 32-1 35-45 M 1 Sham 23-4 20+ U 1 Sham 33-1 35-45 M 1 Sham 23-5 20+ U 2 Sham 34-1 35-45 M 1 Sham 24-1 25-35 M 2 U-I S 6-1-1 35-50 M 1 U-I S 36-1-2 30-40 F 2 U-I S 11-1-1 35-50 F 1 U-I S 38-1-1 45-60 M 1 U-I S 16-1-1 25-35 M 2 U-I S 41-1-1 35-50 M 1 U-I S 16-2-1 25-35 M 1 U-I S 43-1-1 20+ M 2 U-I S 20-1-1 18-24 M 2 U-I S 52-1-1 60+ F 1 U-I S 20-2-1 30-40 F 2 U-I S 54-1-1 50+ M 1 U-I S 30-1-1 50+ F 1 U-I S 56-1 35-50 M 1 U-I G 1-1 20+ F 2 U-I G 40-1-1 25-35 F 2 U-I G 7-1-1 20+ M 2 U-I G 42-1-1 50+ F 1 U-I G 12-1-1 35-50 M 1 U-I G 45-1-1 22-30 M 1 U-I G 19-1-1 30-35 M 1 U-I G 47-1-1 30-40 M 2 U-I G 29-1-1 50+ M 1 U-I G 48-1-1 50+ M 1 U-I G 39-1-1 25-35 F 2 U-I G 51-1-1 20+ M 1 Kh-N 9-1 50+ M 1 Kh-N 49-1 50+ U 1 Kh-N 11-1 35-50 M 1 Kh-N 52-1 25-35 U 2 Kh-N 14-1 35-50 M 2 Kh-N 53-1 35-50 M 1 Kh-N 15-1 25-35 M 2 Kh-N 54-1 20+ U 1 Kh-N 19-1 35-50 F 1 Kh-N 55-1 35-50 M 1 Kh-N 21-1 20+ U 2 Kh-N 57-2 35-50 M 2 Kh-N 22-1 20+ U 1 Kh-N 58-1 25-35 U 1 Kh-N 25-1 35-50 M 2 Kh-N 58-2 35-50 M 1 Kh-N 27-1 35-50 M 1 Kh-N 60-1 50+ F 1 Kh-N 29-1 50+ M 1 Kh-N 61-1 20+ U 2 Kh-N 32-1 50+ F 1 Kh-N 62-1 20+ M 2 Kh-N 34-1 25-35 M 1 Kh-N 64-1 25-35 M 1 Kh-N 36-1 35-50 U 2 Kh-N 66-1 35-50 M 2 Kh-N 38-1 35-50 M 2 Kh-N 68-1 25-35 M 1 Kh-N 43-1 25-35 M 1 Kh-N 72-1 20+ U 2 Kh-N 44-1 35-50 M 1 Kh-N 73-1 20+ U 2 Kh-N 46-1 25-35 M 1 Kh-N 74-1 25-35 M 1

71
Table 3.1 (Continued) Site Individ. Age Sex OA Site Individ. Age Sex OA Kh-N 76-1 20+ U 1 Kh-N 81-1 35-50 M 2 Kh-N 78-1 20+ U 1 Kh-N 82-1 20-25 U 2 Kh-N 79-1 20+ U 2 Kh-N 86-1 20-25 U 2 Kh-N 80-2 50+ M 1 Kh-N 87-1 35-50 M 1 Age: Years of age at death Sex: M = Male/probable male; F = Female/probable female; U = Undetermined OA (Osteoarthritis): 1 = Present; 2 = Absent on skeletal elements observed
extreme or unusual cases. However, for the purpose of the current examination, the
disorder has been designated as simply present or absent, whether referring to an
entire individual or a specific joint region. Afflicted individuals are those exhibiting
osteoarthritic degeneration of at least one joint region, while affected joint regions
(following the procedures employed by Larsen and colleagues [1995]) are those in
which the condition is present on at least one articular surface within that region.
Osteoarthritis was scored as present if any one or a combination of the following
modifications were observed on an articular surface: periarticular bone formation
(except in cases where it was deemed as “very slight” or “barely discernible”),
subchondral bone resorption, and eburnation. Seven major joint regions were
considered in this study: vertebral, shoulder, elbow, wrist and hand, hip, knee, and
ankle and foot (Table 3.2). While these regions do not represent every human joint
possibly affected by osteoarthritis, they do reflect all major weight and non-weight
bearing articulations (Hemphill 1999, Larsen 1992, Larsen et al. 1995). Before
analyses were conducted, bilateral joint regions (those of the upper and lower limbs)
were examined for patterns of side and limb distribution.
To provide a general understanding of osteoarthritis in the mid-Holocene Cis-
Baikal, prevalence and distribution were compared between and within each of the
five skeletal populations. Overall prevalence, or the proportion of all observable

72
Table 3.2 Seven Major Joint Regions and their Articular Surfaces Observed for Osteoarthritis (adapted from Larsen 1982 and Larsen et al. 1995)
Joint Region Articular Surfaces Vertebral cervical, thoracic, and lumbar intervertebral bodies and superior and inferior articular facets; occipital condyles; thoracic costal facets; superior intervertebral body of sacrum Shoulder humeral caput; glenoid fossa and acromial-clavicular facet of scapula; acromial facet of clavicle Elbow trochlea and capitulum of humerus; caput and tuberosity of radius; trochlear notch, radial notch, and coronoid process of ulna Wrist & Hand lunate and scaphoid articular surfaces and ulnar notch of radius; caput and styloid process of ulna; all carpal, metacarpal, and manual phalangeal facets Hip femoral caput; acetabulum Knee lateral and medial condyles of femur; condylar surfaces of patella; lateral and medial condyles of tibia Ankle & Foot medial malleolus and inferior facets of tibia; lateral malleolus facet of fibula; all tarsal, metatarsal, and pedal phalangeal facets
individuals afflicted, was examined between sites, as was prevalence by sex, age of
onset, and both sex and age together. Age of onset was represented categorically, with
observable individuals being grouped into one of three broad age categories following
Buikstra and Ubelaker (1994:9): young adult (20-35 years), middle adult (35-50
years), and old adult (50+ years). Individuals unable to be aged more specifically than
‘adult’ (20+ years) were excluded from age of onset (but not sex) analyses.
Distribution, or the proportion of affected individuals exhibiting osteoarthritis for each
joint region, was also investigated between populations, both for all afflicted
individuals together, as well as for males and females separately. In addition,
prevalence by age of onset was examined within each site. In all cases, binomial
statistics were utilized to compare proportions of affectation between or within each of
the five sites (H0: πx = πy; HA: πx ≠ πy, α = 0.01), and Fisher’s Exact tests were
employed when sample sizes were small (less than five).

73
Numerous researchers have observed substantial sexual differences in
osteoarthritic prevalence and distribution, reflecting disparities in male and female
activity patterns (Anderson 1976, Fahlström 1981, Goodman et al. 1984, Griffin and
Larsen 1989, Hemphill 1999, Jurmain 1977, Lallo 1973, Larsen 1982, 1987, Larsen et
al. 1995, Larsen and Hutchinson 1999, McCafferty et al. 1992, Merbs 1983, Pickering
1979, Pierce 1987, Pfeiffer 1977, Waldron 1992, Walker and Hollimon 1989, Webb
1989, 1995). In order to examine the possible effects of sex on osteoarthritis in the
Cis-Baikal, analyses focused on comparing male and female proportions within each
site. Prevalence was evaluated by sex alone and by both sex and age of onset together,
while distribution was compared between the sexes for each of the seven joint regions.
Again, binomial statistics and Fisher’s Exact tests were employed (H0: πx = πy; HA: πx
≠ πy, α = 0.01).
3.3 Presentation of Results
Of the total 287 joint regions exhibiting osteoarthritis for the five skeletal
populations considered (Table 3.3), 206 were bilateral, or those of the upper and lower
limbs. One hundred and sixty-six bilateral joint regions were affected on both the left
and right sides, while only 40 exhibited unilateral affectation. Bilateral joint regions
exhibiting degenerative changes on both sides were most common among the lower
limbs for Khuzhir-Nuge XIV and Shamanka II (80.0% and 77.8% respectively), but
least common among them for Ust’-Ida I Glaskovo, Ust’-Ida I Serovo, and Lokomotiv
(22.2%, 33.3%, and 45.9%, respectively). A probable explanation for this difference
is the substantially poorer representation of pedal elements at the latter three sites,
particularly when taking into consideration the high prevalence of ankle and foot
osteoarthritis at Khuzhir-Nuge XIV and Shamanka II (Table 3.3, Figure 3.1). It is
reasonable to expect a higher prevalence of bilaterally-afflicted joint regions among

74
Ank
le/F
oot
2 2 2 2 2 2 1B
2 1B
2 2 2 2 2 2 2 2 2 1L
Kne
e 2 1B
2 1B
1B
2 1B
2 1B
2 2 1B
2 2 2 2 1B
2 1R
Hip
2 2 2 2 2 2 1B
2 2 2 2 2 2 1B
2 2 2 2 2
Wris
t/Han
d 2 2 2 2 2 2 2 2 2 2 2 2 2 2 2 2 2 2 2
Elbo
w
2 2 2 1B
1B
2 2 2 1B
1B
2 2 2 2 2 2 1B
2 1B
Shou
lder
2 2 2 1B
2 2 1B
2 2 2 2 1B
2 2 2 1B
1B
1B
1B
Ver
tebr
al
1 2 1 1 1 1 1 1 1 2 1 1 1 2 1 1 2 1 1
Jo
int R
egio
n
Indi
vidu
al
L
2-1-
1
L 2-
3-1
L
4-1-
1
L 7-
1-1
L
8-1-
1
L 9-
1-1
L
11-1
-1
L
12-1
-1
L
13-1
-1
L
14-1
-4
L
15-1
-1
L
16-1
-1
L
17-1
-1
L
18-1
-1
L
20-1
-1
L
20-2
-1
L
20-2
-1
L
24-2
-1
L
24-5
-2
Tabl
e 3.
3 Jo
int R
egio
ns A
ffec
ted
by O
steo
arth
ritis
(n=2
87)
Site
Loko
mot
iv
Loko
mot
iv
Loko
mot
iv
Loko
mot
iv
Loko
mot
iv
Loko
mot
iv
Loko
mot
iv
Loko
mot
iv
Loko
mot
iv
Loko
mot
iv
Loko
mot
iv
Loko
mot
iv
Loko
mot
iv
Loko
mot
iv
Loko
mot
iv
Loko
mot
iv
Loko
mot
iv
Loko
mot
iv
Loko
mot
iv

75
Ank
le/F
oot
1B
2 2 2 2 1R
2 2 2 1B
2 2 2 2 2 1B
2 1B
1R
Kne
e 2 2 2 2 2 2 2 2 2 1B
1B
2 2 2 2 1B
2 1B
1R
Hip
2 2 2 2 2 2 2 2 2 2 2 2 2 2 2 1B
2 2 2
Wris
t/Han
d 2 2 2 2 2 2 2 2 2 2 2 2 2 2 2 2 2 2 2
Elbo
w
2 2 2 1R
2 2 1B
1B
2 1B
1B
2 2 1B
2 1B
2 2 1R
Shou
lder
2 2 2 2 2 2 2 2 2 2 1B
2 2 2 2 1B
2 2 2
Ver
tebr
al
1 1 1 2 1 1 1 1 1 2 1 1 1 1 1 1 1 1 1
Jo
int R
egio
n
Indi
vidu
al
L
25-3
L 29
-1-1
L 33
-1-1
L 34
-1-1
L 35
-1-1
L 36
-1-1
L 37
-1-1
L 38
-1-1
L 38
-2-1
L 42
-1-1
L 44
-1-1
L 44
-2-1
R 1
-1-1
R 6
-1-1
R 6
-2-1
R 7
-1-1
R 1
4-1
8-
1 10
-1
Tabl
e 3.
3 (C
ontin
ued)
Si
te
Lo
kom
otiv
Lo
kom
otiv
Lo
kom
otiv
Lo
kom
otiv
Lo
kom
otiv
Lo
kom
otiv
Lo
kom
otiv
Lo
kom
otiv
Lo
kom
otiv
Lo
kom
otiv
Lo
kom
otiv
Lo
kom
otiv
Lo
kom
otiv
Lo
kom
otiv
Lo
kom
otiv
Lo
kom
otiv
Lo
kom
otiv
S
ham
anka
II
Sha
man
ka II

76
Ank
le/F
oot
2 2 2 1B
1B
1L
1B
2 1U
2 1B
1B
1B
1B
2 1B
1B
2 2
Kne
e 2 2 2 1L
2 2 1B
2 2 1R
2 2 2 1B
2 1R
1L
2 1B
Hip
2 2 2 2 2 2 2 2 2 2 2 2 2 2 2 2 2 2 2
Wris
t/Han
d 2 2 2 2 1L
2 1L
2 2 2 2 2 2 2 2 2 2 2 2
Elbo
w
2 2 2 2 2 2 1B
2 1L
2 2 2 2 1B
2 2 1R
2 2
Shou
lder
2 2 2 2 1B
2 1R
2 2 2 2 2 2 1B
2 2 2 2 2
Ver
tebr
al
1 1 1 1 1 2 1 1 1 2 2 2 2 1 1 1 1 1 1
Jo
int R
egio
n
Indi
vidu
al
11
-2
12
-1
13
-1
13
-2
15
-1
16
-1
17
-1
21
-2
23
-1
23
-3
23
-4
25
-3
26
-1
27
-1
29
-1
30
-1
32
-1
33
-1
34
-1
Tabl
e 3.
3 (C
ontin
ued)
Si
te
S
ham
anka
II
Sha
man
ka II
Sha
man
ka II
Sha
man
ka II
Sha
man
ka II
Sha
man
ka II
Sha
man
ka II
Sha
man
ka II
Sha
man
ka II
Sha
man
ka II
Sha
man
ka II
Sha
man
ka II
Sha
man
ka II
Sha
man
ka II
Sha
man
ka II
Sha
man
ka II
Sha
man
ka II
Sha
man
ka II
Sha
man
ka II

77
Ank
le/F
oot
2 2 2 2 1B
2 1R
2 2 2 2 2 2 2 2 2 1L
2 2
Kne
e 2 2 2 2 1B
2 1R
2 2 1B
2 1B
2 2 2 2 2 2 2
Hip
2 2 2 2 2 2 2 1B
2 2 2 2 2 2 2 2 2 2 2
Wris
t/Han
d 2 2 2 2 1B
2 1B
2 2 1B
2 1B
2 2 2 2 1R
2 2
Elbo
w
2 2 2 2 1B
2 1B
2 2 1B
1B
1B
2 1B
1L
2 2 2 2
Shou
lder
2 2 2 2 2 2 1B
1B
2 1B
2 2 2 2 2 2 2 1R
2
Ver
tebr
al
1 1 1 1 1 1 1 1 1 1 1 1 1 1 2 1 1 1 1
Jo
int R
egio
n
Indi
vidu
al
6-
1-1
11-1
-1
16
-2-1
30-1
-1
38
-1-1
41-1
-1
52
-1-1
54-1
-1
56
-1
12
-1-1
19-1
-1
29
-1-1
42-1
-1
45
-1-1
48-1
-1
51
-1-1
9-1
11-1
19-1
Tabl
e 3.
3 (C
ontin
ued)
Si
te
U
st’-
Ida
I S
Ust
’-Id
a I S
U
st’-
Ida
I S
Ust
’-Id
a I S
U
st’-
Ida
I S
Ust
’-Id
a I S
U
st’-
Ida
I S
Ust
’-Id
a I S
U
st’-
Ida
I S
Ust
’-Id
a I G
U
st’-
Ida
I G
Ust
’-Id
a I G
U
st’-
Ida
I G
Ust
’-Id
a I G
U
st’-
Ida
I G
Ust
’-Id
a I G
K
h-N
XIV
K
h-N
XIV
K
h-N
XIV

78
Ank
le/F
oot
2 1L
1B
1L
2 2 1R
1L
1L
2 2 2 2 2 1B
1B
1B
1R
1B
Kne
e 1R
2 2 2 2 2 2 2 2 2 2 1R
2 2 2 2 2 2 2
Hip
2 2 2 2 2 2 2 2 2 2 2 2 2 2 1L
2 2 2 2
Wris
t/Han
d 2 2 2 2 2 2 2 1R
2 2 1R
2 2 2 2 2 2 2 2
Elbo
w
2 2 1B
2 2 2 2 1B
2 2 2 2 2 2 2 2 2 2 2
Shou
lder
2 2 1R
2 2 2 2 2 2 2 2 2 2 2 1L
2 2 2 2
Ver
tebr
al
2 1 1 1 1 1 1 1 1 1 2 1 1 1 1 2 1 2 1
Jo
int R
egio
n
Indi
vidu
al
22
-1
27
-1
29
-1
32
-1
34
-1
43
-1
44
-1
46
-1
49
-1
53
-1
54
-1
55
-1
58
-1
58
-2
60
-1
64
-1
68
-1
74
-1
76
-1
Tabl
e 3.
3 (C
ontin
ued)
Si
te
K
h-N
XIV
K
h-N
XIV
K
h-N
XIV
K
h-N
XIV
K
h-N
XIV
K
h-N
XIV
K
h-N
XIV
K
h-N
XIV
K
h-N
XIV
K
h-N
XIV
K
h-N
XIV
K
h-N
XIV
K
h-N
XIV
K
h-N
XIV
K
h-N
XIV
K
h-N
XIV
K
h-N
XIV
K
h-N
XIV
K
h-N
XIV

79
Ank
le/F
oot
1B
1B
2
Kne
e 1B
2 2
Hip
2 2 2
Wris
t/Han
d 2 2 2
Elbo
w
2 2 1R
Shou
lder
2 2 2
Ver
tebr
al
2 1 1
Jo
int R
egio
n
Indi
vidu
al
78
-1
80
-2
87
-1
Tabl
e 3.
3 (C
ontin
ued)
Si
te
K
h-N
XIV
K
h-N
XIV
K
h-N
XIV
1 =
Ost
eoar
thrit
is p
rese
nt (R
- rig
ht si
de; L
- le
ft si
de; B
- bo
th si
des;
U -
side
unk
now
n)
2 =
Ost
eoar
thrit
is a
bsen
t or u
nobs
erva
ble

80
Figure 3.1 Proportion of All Affected Individuals Exhibiting Osteoarthritis for Each Joint Region
the lower rather than the upper limbs because individual handedness can result in
considerable side disparity in hand and arm usage (Wilczak and Kennedy 1998). Of
the 40 bilateral joint regions affected by osteoarthritis on only one side, no marked
discrepancies in left-right distribution were observed. Because of this, sides were
combined for analyses: that is, osteoarthritis was not scored twice for a particular joint
region if degenerative changes were present on both the right and left sides.
Overall osteoarthritic prevalence – the proportion of all observable individuals
affected by the condition – was not significantly different among the five Cis-Baikal
cemetery sites examined (Figure 3.2). This similarity in prevalence held true when
observable males and females were considered separately, with the possible exception
of Khuzhir-Nuge XIV, whose females appeared to be more commonly affected by the
condition than those from the other sites (Figure 3.2). However, this difference was
most likely a reflection of the small sample size and relatively advanced age of onset
characterizing observable Khuzhir-Nuge XIV females (Table 3.4). Therefore, in order
to increase the power of the tests, sample size was enlarged by pooling observable
females from the two Glaskovo sites (Khuzhir-Nuge XIV and Ust’-Ida I Glaskovo),

81
Figure 3.2 Proportion of Observable Individuals Affected by Osteoarthritis
with results indicating statistically similar osteoarthritic prevalence among all females.
A comparison of prevalence by age of onset suggested further similarities among the
five populations. While middle adults at Lokomotiv and Khuzhir-Nuge XIV exhibited
significantly less skeletal degeneration than did fellow members of their age cohort
from Shamanka II, no differences in osteoarthritic prevalence were noted between any
of the skeletal populations for observable young and old adult individuals (Table 3.4,
Figure 3.3). Finally, to control for the effects of both sex and age of onset, observable
individuals for each site were separated into males and females representing the
young, middle, and old adult age categories (Table 3.4). In those cases where sample
sizes were adequate for statistical comparisons, no significant differences in
osteoarthritic prevalence were observed. Thus, while instances of disparity cannot be
disregarded, no patterns were discerned which suggested substantial differences in the
general prevalence of osteoarthritis across the five skeletal populations.
Comparisons of overall osteoarthritic distribution – the proportion of affected
individuals exhibiting the condition for each joint region – revealed additional
similarities among the five sites (Figure 3.1). In all cases, osteoarthritic degeneration

82
%
100 * 100
100
100
Fem
ale
N 3 0 2 1 2
%
100 * 100
100
100
Mal
e N
2 0 2 2 3
%
100 * 100
100
100
O
ld A
dult
(50+
yea
rs)
All
N 5 0 4 3 6
%
55.6
* 100 * 100
Fem
ale
N 9 0 1 0 1
%
66.7
10
0 10
0 10
0 53
.9
Mal
e N
15
8 3 1 13
%
60.0
10
0 10
0 10
0 53
.3
M
iddl
e A
dult
(35-
50 y
ears
) A
ll N
25
8 4 1 15
%
53.3
25
.0
0.0
0.0 *
Fem
ale
N
15
4 2 2 0
%
35.7
42
.9
33.3
66
.7
85.7
Mal
e N
14
14
3 3 7
%
43.8
45
.0
20.0
40
.0
63.6
Y
oung
Adu
lt (2
0-35
yea
rs)
All
N
32
20
5 5 11
Tabl
e 3.
4 A
ge o
f Ost
eoar
thrit
ic O
nset
Acr
oss S
ites
Site
Lo
k Sh
am
U-I
S
U-I
G
Kh-
N
N
: Num
ber o
f ind
ivid
uals
obs
erva
ble
for o
steo
arth
ritis
%:
Perc
enta
ge o
f obs
erva
ble
indi
vidu
als
affe
cted
by
oste
oarth
ritis
* M
issi
ng d
ata

83
Figure 3.3 Age of Osteoarthritic Onset Across Sites
was most common among the vertebrae and least common for hip joints. Its
frequency among the other five joint regions (i.e., shoulder, elbow, wrist and hand,
knee, and ankle and foot) varied somewhat between the sites, but was only
significantly different in a few cases. The prevalence of osteoarthritis among elbow
joints was higher at Ust’-Ida I Glaskovo than at either Khuzhir-Nuge XIV or
Shamanka II, as well as at Lokomotiv compared to Khuzhir-Nuge XIV. Although
osteoarthritic degeneration of the knees appears to have been more common at
Shamanka II than at the other sites (Figure 3.1), statistically significant differences in
occurrence were only observed between Khuzhir-Nuge XIV and Shamanka II.
Finally, osteoarthritis of the ankles and feet was observed substantially more
frequently at Khuzhir-Nuge XIV and Shamanka II than at the other three sites, as well
as at Lokomotiv compared to Ust’-Ida I Glaskovo (Figure 3.1). However, these
apparent differences in ankle and foot osteoarthritis were undoubtedly a reflection of
the differential representation of pedal elements at the five sites. It cannot be
coincidental that the three sites consisting of numerous incompletely-represented
individuals (see above) were also affected considerably less often by osteoarthritis of
84
the ankles and feet. Thus, while some significant differences were noted in the
distribution of osteoarthritis, the general trend remained that of similarity rather than
disparity among the skeletal populations.
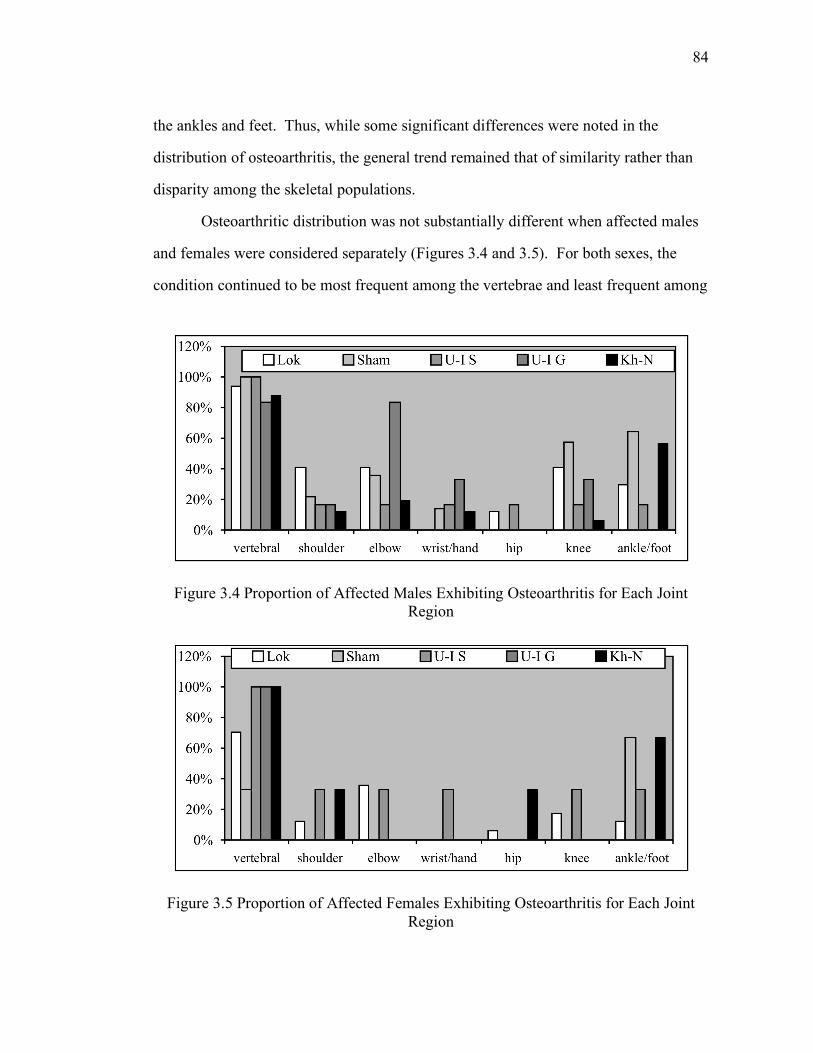
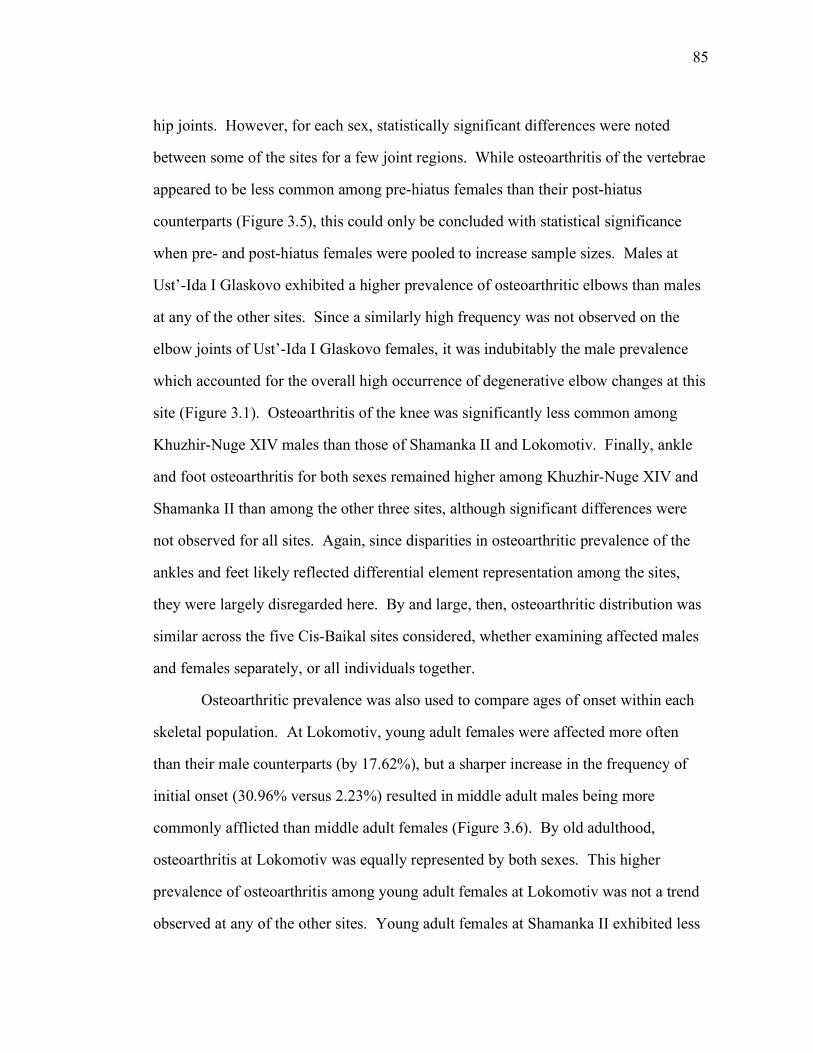
Osteoarthritic distribution was not substantially different when affected males
and females were considered separately (Figures 3.4 and 3.5). For both sexes, the
condition continued to be most frequent among the vertebrae and least frequent among
Figure 3.4 Proportion of Affected Males Exhibiting Osteoarthritis for Each Joint Region
Figure 3.5 Proportion of Affected Females Exhibiting Osteoarthritis for Each Joint Region
85
hip joints. However, for each sex, statistically significant differences were noted
between some of the sites for a few joint regions. While osteoarthritis of the vertebrae
appeared to be less common among pre-hiatus females than their post-hiatus
counterparts (Figure 3.5), this could only be concluded with statistical significance
when pre- and post-hiatus females were pooled to increase sample sizes. Males at
Ust’-Ida I Glaskovo exhibited a higher prevalence of osteoarthritic elbows than males
at any of the other sites. Since a similarly high frequency was not observed on the
elbow joints of Ust’-Ida I Glaskovo females, it was indubitably the male prevalence
which accounted for the overall high occurrence of degenerative elbow changes at this
site (Figure 3.1). Osteoarthritis of the knee was significantly less common among
Khuzhir-Nuge XIV males than those of Shamanka II and Lokomotiv. Finally, ankle
and foot osteoarthritis for both sexes remained higher among Khuzhir-Nuge XIV and
Shamanka II than among the other three sites, although significant differences were
not observed for all sites. Again, since disparities in osteoarthritic prevalence of the
ankles and feet likely reflected differential element representation among the sites,
they were largely disregarded here. By and large, then, osteoarthritic distribution was
similar across the five Cis-Baikal sites considered, whether examining affected males
and females separately, or all individuals together.
Osteoarthritic prevalence was also used to compare ages of onset within each
skeletal population. At Lokomotiv, young adult females were affected more often
than their male counterparts (by 17.62%), but a sharper increase in the frequency of
initial onset (30.96% versus 2.23%) resulted in middle adult males being more
commonly afflicted than middle adult females (Figure 3.6). By old adulthood,
osteoarthritis at Lokomotiv was equally represented by both sexes. This higher
prevalence of osteoarthritis among young adult females at Lokomotiv was not a trend
observed at any of the other sites. Young adult females at Shamanka II exhibited less

86
Figure 3.6 Age of Osteoarthritic Onset among Lokomotiv Males and Females
osteoarthritis than their male counterparts (by 17.86%), and the latter exhibited a
dramatic increase in occurrence with age (57.14%). Unfortunately, females older than
young adult were not observable for comparison (Figure 3.7). At Ust’-Ida I Serovo,
young adult females were less commonly affected by osteoarthritis than young adult
males (by 33.33%), but they exhibited a sharper increase in the prevalence of initial
onset with age than did their male colleagues (100.00% versus 66.67%). By middle
and old adulthood, osteoarthritic occurrence was identical for both sexes (Figure 3.8).
Figure 3.7 Age of Osteoarthritic Onset among Shamanka II Males and Females

87
Figure 3.8 Age of Osteoarthritic Onset among Ust'-Ida I Serovo Males and Females
Similarly, at Ust’-Ida I Glaskovo, osteoarthritis among young adult females was less
frequent than among males (by 66.67%), and an increase in prevalence with advancing
age was more dramatic among the former (100.00% versus 33.33%). As a result,
osteoarthritis was equally common among middle-old adult males and females alike
(Figure 3.9). Finally, no young adult females from Khuzhir-Nuge XIV were
observable for osteoarthritis, so comparisons could not be made with young adult
males. Interestingly, the latter exhibited a decrease in the frequency of initial onset to
Figure 3.9 Age of Osteoarthritic Onset among Ust'-Ida I Glaskovo Males and Females
88
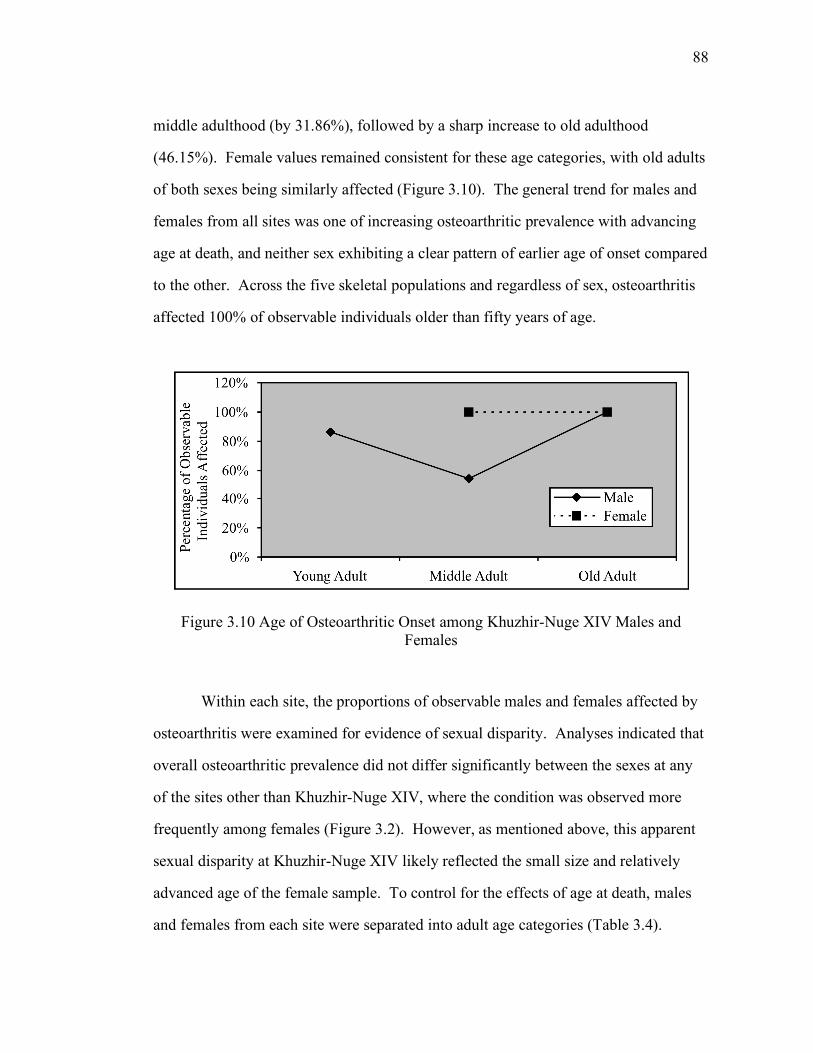
middle adulthood (by 31.86%), followed by a sharp increase to old adulthood
(46.15%). Female values remained consistent for these age categories, with old adults
of both sexes being similarly affected (Figure 3.10). The general trend for males and
females from all sites was one of increasing osteoarthritic prevalence with advancing
age at death, and neither sex exhibiting a clear pattern of earlier age of onset compared
to the other. Across the five skeletal populations and regardless of sex, osteoarthritis
affected 100% of observable individuals older than fifty years of age.
Figure 3.10 Age of Osteoarthritic Onset among Khuzhir-Nuge XIV Males and Females
Within each site, the proportions of observable males and females affected by
osteoarthritis were examined for evidence of sexual disparity. Analyses indicated that
overall osteoarthritic prevalence did not differ significantly between the sexes at any
of the sites other than Khuzhir-Nuge XIV, where the condition was observed more
frequently among females (Figure 3.2). However, as mentioned above, this apparent
sexual disparity at Khuzhir-Nuge XIV likely reflected the small size and relatively
advanced age of the female sample. To control for the effects of age at death, males
and females from each site were separated into adult age categories (Table 3.4).

89
Significant differences were observed only between young adult males and females at
Ust’-Ida I Glaskovo, with males exhibiting a higher occurrence of osteoarthritis, and
middle adult males and females at Khuzhir-Nuge XIV, with the condition being more
common among females. None of the results indicated a propensity among any of the
five populations for one sex to be consistently affected by osteoarthritis more than the
other.
Osteoarthritic distribution for each site was compared between affected males
and females, as graphically depicted in Figures 3.11 through 3.15. Males from both
pre-hiatus sites (Lokomotiv and Shamanka II) appeared to exceed females in
osteoarthritic occurrence throughout the body (Figures 3.11 and 3.12). However,
statistically significant differences were noted only when males and females from both
sites were pooled to increase sample size, with osteoarthritis of the vertebrae and knee
being more common among pre-hiatus males than females. For the three post-hiatus
sites, males and females varied in terms of highest affectation among joint regions
(Figures 3.13, 3.14, and 3.15), but no significant differences were observed between
the sexes. This conclusion held even when the post-hiatus male and female samples
Figure 3.11 Proportion of Affected Lokomotiv Males and Females Exhibiting Osteoarthritis for Each Joint Region

90
Figure 3.12 Proportion of Affected Shamanka II Males and Females Exhibiting Osteoarthritis for Each Joint Region
Figure 3.13 Proportion of Affected Ust'-Ida I Serovo Males and Females Exhibiting Osteoarthritis for Each Joint Region
were pooled together. Across sites and for both sexes, skeletal degeneration was most
common among vertebrae and least common among hip joints. These results
reiterated assertions made above that osteoarthritic distribution in the Cis-Baikal was
more or less consistent across skeletal populations, whether males and females were
considered separately or together. With only two pre-hiatus exceptions, the

91
prevalence of osteoarthritis appears to have been similar between the sexes for all
seven joint regions.
Figure 3.14 Proportion of Affected Ust'-Ida I Glaskovo Males and Females Exhibiting Osteoarthritis for Each Joint Region
Figure 3.15 Proportion of Affected Khuzhir-Nuge XIV Males and Females Exhibiting Osteoarthritis for Each Joint Region
3.4 Discussion
In the archaeological literature, the presence of formal cemeteries among
prehistoric hunter-gatherers is often associated with increased sedentism, subsistence

92
intensification, and increasing territoriality (e.g., Charles and Buikstra 1983, Goldstein
1981, Price and Brown 1985). The Cis-Baikal mid-Holocene is somewhat unique in
this regard, as large formal cemeteries were utilized by highly mobile foragers
exploiting a wide range of potential resources. However, the mobility patterns and
subsistence strategies employed in the region appear to have varied over time, even
though environmental conditions remained relatively consistent (Weber et al. 2002).
Recent examinations of archaeological and stable isotope data from the Cis-Baikal
suggest that pre-hiatus Kitoi and post-hiatus Serovo-Glaskovo peoples may have
differed in their respective adaptive regimes (Katzenberg and Weber 1999, Weber
1995, Weber and Katzenberg 1998, Weber et al. 2002). If this assertion is accurate,
then this disparity should be reflected in the prevalence and distribution of
osteoarthritis among the pre- and post-hiatus skeletal material.
The current understanding of pre-hiatus Kitoi and post-hiatus Serovo-Glaskovo
adaptive strategies proposes decreased mobility due to a narrower subsistence base
among the former. It is thought that Kitoi annual ranges were quite small, focusing on
aquatic (specifically fish) resources whether or not these were the most abundant or
accessible. Residential mobility was low, particularly during the fishing season, with
home bases being occupied for extended periods of time. In addition, mobility was
restricted within annual ranges, as increased reliance on aquatic resources would have
tethered groups to specific waterways. By contrast, the Serovo-Glaskovo people
appear to have exhibited broader subsistence patterns focusing on both aquatic (fish
and seal) and terrestrial resources. As a result, residential mobility was high, home
bases were small and infrequently-occupied, and annual ranges were large,
encompassing much, or all, of the Cis-Baikal region (Katzenberg and Weber 1999,
Weber 1995, Weber and Katzenberg 1998, Weber et al. 2002).

93
These apparent differences in Kitoi and Serovo-Glaskovo subsistence regimes
are supported by archaeological and stable isotope (particularly δ15N) data. Although
both cultural complexes encompass the entire Cis-Baikal region, most Kitoi sites are
limited to river mouths, shallow coves, and river confluences, with site density
corresponding to (modern) fish availability. Furthermore, stable isotope analyses have
documented noticeable differences in both δ13C and δ15N values among skeletal
material from different Kitoi sites, two of which are located only 100 km apart. In
contrast, isotopic variation among the Serovo-Glaskovo samples appears to be
minimal across the entire Cis-Baikal, suggesting higher interregional travel. Fishing
paraphernalia such as composite hooks and carved fish lures are frequent and
abundant among Kitoi grave goods and within their habitation horizons. Serovo-
Glaskovo grave goods and tool kits, on the other hand, are largely represented by
hunting paraphernalia such as bows, arrowheads, harpoons, and spears. Finally, stable
isotope values suggest a greater reliance on fish by the Kitoi people and an increased
reliance on terrestrial foods by the Serovo-Glaskovo. However, some of these isotopic
differences appear to reflect proximity to Lake Baikal itself, with adjacent populations
of both temporal periods utilizing more aquatic resources than distant ones
(Katzenberg and Weber 1999, Khlobystin 1969, Lam 1994, Okladnikov 1950, 1955,
1959, Weber et al. 1998, 2002, Weber 1995).
If these interpretations of distinct Kitoi and Serovo-Glaskovo adaptive regimes
are correct, then skeletal material from pre- and post-hiatus sites should reflect the
variable physical stress associated with each strategy. For example, post-hiatus
individuals engaged in greater residential mobility would have suffered from increased
levels of osteoarthritis throughout the body due to heavy and repetitive physical
activity placing higher levels of stress on all the major joint regions. Traversing over
the Cis-Baikal’s rough and topographically severe terrain, particularly while
94
transporting goods and resources, would have resulted in a higher prevalence of
arthritic degeneration and an earlier age of onset for both males and females alike.
Pre-hiatus peoples, on the other hand, appear to have been less residentially mobile
and to have largely limited their movements within small annual ranges tethered to
topographically milder waterways. If this is accurate, then the decreased physical
stress associated with this lifestyle would have resulted in a lower prevalence of
osteoarthritis throughout the body and a later age of onset compared to that
experienced by post-hiatus peoples.
The results presented above do not appear to support this interpretation of the
effects of mobility and physical activity on osteoarthritis in the Cis-Baikal. Overall
osteoarthritic prevalence, and indeed that of males and females within each of the
adult age categories, did not differ substantially between the pre-hiatus Kitoi sites (i.e.,
Lokomotiv and Shamanka II) and the post-hiatus Serovo-Glaskovo ones (i.e., Ust’-Ida
I Serovo, Ust’-Ida I Glaskovo, and Khuzhir-Nuge XIV). In fact, the osteoarthritic data
suggest that activity levels remained relatively constant throughout the mid-Holocene,
specifically on either side of the fifth millennium hiatus. The most logical explanation
for this inconsistency is the fact that residential mobility does not necessarily reflect
individual mobility. Among the Kitoi, acquisition of terrestrial resources, both floral
and faunal, likely resulted in increasingly extensive logistical forays by individuals the
greater the amount of time spent in residentially stable units (Weber et al. 2002). As
such, individual mobility may have been equally high among both pre- and post-hiatus
peoples, despite their apparent differences in residential mobility. This interpretation
may be supported by the osteoarthritic data.
If the pre- and post-hiatus occupants of the Cis-Baikal did indeed engage in
substantially different levels of logistical mobility, then one would expect to find
evidence of this in the osteoarthritic data. Kitoi peoples, tethered to specific water

95
courses and subsequently employing high levels of logistical foraging to exploit
terrestrial resources, should exhibit increased sexual disparity in osteoarthritic
prevalence compared to Serovo-Glaskovo peoples. Because the bulk of the terrestrial
resource acquisition appears to have been represented by male-dominated hunting of
large mammals, particularly ruminants such as red deer (Cervus elaphus), roe deer
(Capreolus capreolus), moose (Alces alces), and reindeer (Rangifer tarandus)
(Katzenberg and Weber 1999, Weber et al. 2002), Kitoi males would have
experienced considerably more logistical mobility than females. Furthermore, since
residential movement would have been undertaken more or less equally by both sexes,
overall mobility of Kitoi males – and thus the amount of degenerative changes
exhibited by their joints – would have been substantially higher than that of females.
By contrast, more equitable overall mobility resulting from decreased logistical
foraging among Serovo-Glaskovo individuals should have resulted in decreased sexual
discrepancy in osteoarthritic prevalence.
Analyses indicate that no or only minimal differences in osteoarthritic
prevalence existed between males and females at all five Cis-Baikal sites. While this
lack of sexual disparity supports the findings of previous archaeological and isotopic
research suggesting high residential mobility among the Serovo-Glaskovo people
(Katzenberg and Weber 1999, Weber 1995, Weber and Katzenberg 1998, Weber et al.
2002), it may call into question interpretations of low residential and high logistical
mobility among the Kitoi. However, there are two explanations which may account
for this apparent inconsistency between the pre-hiatus osteoarthritic data and those
obtained from other sources. First, mobility – both residential and logistical – may
have varied considerably throughout the mid-Holocene Cis-Baikal as a result of
seasonal and annual fluctuations in environmental conditions. The Kitoi focus on
aquatic resources, for example, was likely limited to seasonal fishing periods when

96
waterways were most accessible (Weber et al. 2002). During the rest of the year,
when fish harvesting was more difficult and resource acquisition focused on terrestrial
resources, residential mobility may have been substantially higher, lowering the level
of sexually-disparate logistical mobility.
Second, it is possible that the pre-hiatus occupants of the Cis-Baikal engaged
in physically stressful occupational activities despite their low levels of residential
mobility, thus resulting in more sexually-equitable osteoarthritic prevalence. If this
hypothesis is true, then the Kitoi should exhibit distinctive osteoarthritic distribution
patterns compared to the Serovo-Glaskovo. Also, as side differences in osteoarthritic
degeneration typically represent the effects of specific physical activities over normal
age-related changes (Wilczak and Kennedy 1998), pre-hiatus individuals should
exhibit fewer instances of bilateral affectation across joint regions, particularly those
of the upper limb, than post-hiatus people. Unfortunately, the osteoarthritic data do
not readily support these assertions. With only one exception, that of less frequent
vertebral affection among pre-hiatus females than post-hiatus ones, osteoarthritic
distribution for all joint regions was similar across populations, whether considering
all individuals together or males and females separately. In addition, with only two
exceptions (vertebral and knee degeneration), the distribution of osteoarthritis among
Kitoi males was not significantly different than that among their female counterparts.
Thus, joint distribution data indicate that activity patterns were quite similar for both
pre- and post-hiatus individuals, males and females alike. Bilateral joint affectation
was also equally common among the Kitoi and Serovo-Glaskovo, further evidence to
suggest that pre- and post-hiatus peoples did not engage in markedly different patterns
of occupational activity or mobility.
Reconstructing specific activity patterns from the distribution of osteoarthritis
among joints has met with some success by other scholars (e.g., Bridges 1990, 1992,

97
Merbs 1983). Of the major joint regions of the body, osteoarthritic degeneration of
the enarthroses of the shoulder and hip is generally least correlated with activity levels
and most correlated with age, while the opposite is true for the ginglymus and trochoid
joints of the elbow and knee (Bridges 1992, Jurmain 1991a). As such, degenerative
changes of the elbows and knees may best represent the activity patterns undertaken in
the mid-Holocene Cis-Baikal, especially those reflecting high physical exertion and/or
repetitive stress. Osteoarthritis of the elbow was significantly more common for Ust’-
Ida I Glaskovo males than for those of the other four sites, whereas arthritic
degeneration of the knee occurred more frequently among pre-hiatus (Lokomotiv and
Shamanka II) males than those of Khuzhir-Nuge XIV. Furthermore, significant
differences in the sexual distribution of osteoarthritis were observed for the two pre-
hiatus sites, with males exhibiting considerably more degeneration of the knee than
females. While these differences are not absolute across the five skeletal populations,
they do suggest some variation in specific activity patterns. For all sites, osteoarthritis
of the elbow was most commonly represented by degenerative changes to the trochlea,
capitulum, radial head, and olecranon and coronoid processes, reflecting overuse and
stress during pronation, supination, flexion, and extension. Thus, activities involving
these movements, such as spear-throwing, paddling, and skin-scraping (Angel 1966,
Haney 1974, Merbs 1983, Nagy and Hawkey 1993, Ortner 1968, Tainter 1980), may
have been engaged in more frequently and/or more intensively by post-hiatus males
compared to pre-hiatus ones. Osteoarthritis of the knee was typically represented by
degeneration of the medial and lateral articular surfaces of the femoral condyle, tibial
condyle, and patella, reflecting joint stress during flexion and hyperextension. Data
suggest that activities affecting these joint surfaces, such as squatting and walking
over rough, steep, and/or snow-covered terrain (Dahl et al. 1981, Jurmain 1977) may
have been undertaken more frequently by pre-hiatus males than their post-hiatus

98
counterparts, as well as pre-hiatus males compared to pre-hiatus females. The latter
lends support to previous assertions of possible sexual disparity in pre-hiatus logistical
foraging. Increased male mobility resulting from extensive hunting forays is
compatible with higher levels of knee osteoarthritis compared to that exhibited by
females.
Vertebral osteoarthritis can be a poor indicator of specific activity patterns
because it often reflects the stresses associated with bipedality and thus experienced
by all individuals (Wilczak and Kennedy 1998). This is particularly true when the
condition is located at points of maximum curvature – and thus weight-bearing stress –
within each (cervical, thoracic, and lumbar) vertebral segment (Nathan 1962).
Furthermore, degenerative changes occurring on joint surfaces (erosion and
eburnation) are more likely to reflect physical activity, while those occurring on joint
margins (lipping and osteophytes) are more commonly associated with the normal
aging process (Jurmain 1991a). The vast majority of vertebral arthritis observed at all
five Cis-Baikal cemetery sites was represented by osteophytic development on
vertebral bodies and periarticular lipping on superior and inferior facets. However,
despite its common association with advancing age, vertebral degeneration can
provide a number of insights into the specific activities undertaken in the Cis-Baikal,
as variation in activity patterns is the most plausible explanation for differences which
cannot be accounted for by sex and age at death. Osteoarthritis of the cervical spine
often results from extension and compression of the neck, while that of the thoracic
and lumbar spine most typically reflects load-bearing stress on the back (Bridges
1994, Merbs 1983, Stirland 1985). Data suggest that activities such as these were
engaged in more frequently by post-hiatus (Khuzhir-Nuge XIV, Ust’-Ida I Glaskovo,
and Ust’-Ida I Serovo) females than their pre-hiatus (Lokomotiv and Shamanka II)
counterparts and by pre-hiatus males compared to pre-hiatus females. This also

99
supports earlier interpretations of decreased residential mobility and increased sexual
disparity in logistical foraging among pre-hiatus people. High levels of vertebral
stress would result from the increased residential mobility experienced by post-hiatus
females as well as the frequent hunting forays undertaken by pre-hiatus males, as both
activities would have included the regular transportation of goods and resources
without the assistance of animal or mechanical power.
Finally, osteoarthritis of the ankle and foot joints warrants discussion here
because of its high prevalence among two of the skeletal populations considered –
Shamanka II and Khuzhir-Nuge XIV. As mentioned previously, its relatively low
occurrence at the other three cemetery sites is most likely a reflection of the under-
representation of pedal elements resulting from poor curation techniques, and not an
accurate indicator of the condition at these sites. As such, it is probable that
osteoarthritis of the ankles and feet was common for both the pre- and post-hiatus
occupants of the Cis-Baikal, males and females alike. At Shamanka II and Khuzhir-
Nuge XIV, where pedal elements were adequately represented among the skeletal
remains, osteoarthritis of the ankles and feet affected the distal tibia, tarsals
(particularly talus and calcaneus), metatarsals, and phalanges more or less equally.
Degenerative changes reflected stress and overuse during ankle and digit flexion and
extension, resulting from a myriad of possible activities such as extensive walking,
particularly over steep or uneven terrain, squatting (squatting facets were observed on
a number of occasions), and kneeling with dorsiflexion (Merbs 1983, Molleson 1989).
As locomotion involves major biomechanical stress throughout the ankle and foot, it is
likely responsible for much of the osteoarthritis affecting this joint region for all Cis-
Baikal individuals.
100
3.5 Summary and Conclusions
The overall similarities in osteoarthritic prevalence and distribution among the
five skeletal populations investigated are most easily explained by parallels in mobility
and activity patterns undertaken by both the pre- and post-hiatus occupants of the Cis-
Baikal. Prevalence data provide little direct support for interpretations of different
adaptive strategies involving distinct mobility patterns between the Kitoi and Serovo-
Glaskovo people. However, it is probable that mobility varied considerably
throughout the mid-Holocene as an adaptive response to environmental fluctuations,
both seasonal and annual. As such, low residential mobility among the Kitoi during
certain seasons may have been offset by higher mobility at other times of the year.
Furthermore, annual fluctuations in resource availability likely resulted in equally
variable modifications to mobility patterns by both the Kitoi and Serovo-Glaskovo
alike. This variation, over the course of whole lifetimes, could have equalized overall
individual mobility among the pre- and post-hiatus peoples, resulting in similar
osteoarthritic prevalence for both groups.
Minimal sexual disparity in osteoarthritic prevalence was also noted for each
of the five Cis-Baikal cemetery sites, suggesting similar mobility and activity levels
for Kitoi and Serovo-Glaskovo males and females. Again, this seems to contradict
earlier interpretations of Kitoi adaptation, in which low residential mobility would
have resulted in sexually-disparate individual mobility due to increased levels of
largely male-dominated logistical foraging. However, a more compatible explanation
for the apparent sexual equity in overall levels of osteoarthritis throughout the mid-
Holocene Cis-Baikal is the probable seasonal and annual variation in mobility
experienced by both pre- and post-hiatus individuals over the course of their lives.
This variability may have largely balanced out the effects of sexual differences in

101
mobility, resulting in the more or less equitable osteoarthritic prevalence observed
here.
While osteoarthritic distribution was also remarkably similar among the five
populations and between the sexes, several significant differences were noted which
suggest distinctions in the specific activities undertaken by them, if not in kind, then in
frequency and intensity. Activities resulting in elbow degeneration, such as spear-
throwing and paddling, may have been more commonly engaged in by post-hiatus
males than pre-hiatus males. Those involving stress to the knee, such as squatting and
traveling over steep and uneven terrain, appear to have been more frequently
undertaken by pre-hiatus males than their post-hiatus counterparts, as well as pre-
hiatus males compared to pre-hiatus females. Finally, activities such as carrying
heavy items on the back and head may have been engaged in more frequently by post-
hiatus females than their pre-hiatus counterparts and by pre-hiatus males compared to
pre-hiatus females. These lend credible support to previous assertions of increased
(and sexually disparate) logistical foraging among the Kitoi due to decreased
residential mobility. Thus, rather than overturning earlier interpretations of distinct
subsistence strategies employed by the Kitoi and Serovo-Glaskovo, it is more likely
that the parallels observed in osteoarthritic prevalence and distribution across the five
populations examined reflect variation in mobility and activity patterns over time. As
such, the osteoarthritic data presented here shed additional light on mid-Holocene
adaptive regimes in the Cis-Baikal by drawing attention to the likelihood of high
variability employed by both the pre- and post-hiatus occupants of the region.
Copyright © 2022 FDOKUMEN

