





Bahasa
Halaman
Hukum

Technical Assistance Consultant’s Report
Project Number: 53266-001 December 2020
Accelerating Sanitation for Allin Asia and the Pacific
Water, Sanitation, Hygiene, and Health (WASH+H) Integration in ADB Projects
Prepared by
Bronwyn Powell
For Asian Development Bank
This consultant’s report does not necessarily reflect the views of ADB or the Government concerned, and ADB and the Government cannot be held liable for its contents.
WASH + Health Consultancy Final Report
December 2020
Contents 1 Executive Summary ............................................................................................................................... 1
2 Background and Introduction ............................................................................................................... 1
2.1 Background ................................................................................................................................... 1
2.2 WASH situation in the Asian region .............................................................................................. 2
2.3 COVID-19 pandemic impacts on WASH services .......................................................................... 4
2.4 Assignment objectives .................................................................................................................. 6
2.5 Methodology ................................................................................................................................. 6
2.6 Definitions ..................................................................................................................................... 8
3 ADB institutional context ...................................................................................................................... 8
3.1 WASH+H in ADB policies and strategies ....................................................................................... 8
3.2 Measuring performance ............................................................................................................. 10
4 Findings ............................................................................................................................................... 12
4.1 Urban Development and Water .................................................................................................. 12
4.2 Education .................................................................................................................................... 17
4.3 Health .......................................................................................................................................... 19
4.4 Environment, Agriculture and Natural Resources ...................................................................... 21
4.5 Social protection, gender and inclusion ...................................................................................... 22
4.6 Operations .................................................................................................................................. 23
4.6.1 Enablers and entry points ................................................................................................... 23
4.6.2 Barriers ................................................................................................................................ 24
4.6.3 Financing ............................................................................................................................. 24
4.7 Capacities and knowledge .......................................................................................................... 26
4.8 WASH+H reflected Country Partnership Strategies .................................................................... 27
4.9 Partnering ................................................................................................................................... 28
4.9.1 UNICEF ................................................................................................................................ 28
4.10 Sustainability ............................................................................................................................... 29
4.11 Support requests and knowledge gaps ....................................................................................... 30
5 Sector evidence for WASH+H .............................................................................................................. 31
5.1 Health from WASH ...................................................................................................................... 31
5.1.1 Anti-microbial resistance .................................................................................................... 32
5.1.2 Nutrition and Stunting ........................................................................................................ 33
5.1.3 Neglected Tropical Diseases ............................................................................................... 33
5.1.4 COVID-19 ............................................................................................................................. 34
5.2 Multi-sectoral and economic benefits of WASH ......................................................................... 34
5.3 Hygiene: emphasizing the ‘H’ in WASH....................................................................................... 36
5.4 Addressing hygiene at scale ........................................................................................................ 43
6 Analysis ............................................................................................................................................... 44
6.1 Exploring integration ................................................................................................................... 44
6.1.1 WASH+H project types ........................................................................................................ 44
6.1.2 Multi-sectoral approaches .................................................................................................. 45
6.1.3 Holistic approach ................................................................................................................ 51
6.2 Capture the moment for WASH, especially in schools and HCFs ............................................... 51
6.3 Strengthening the WASH+H narrative ........................................................................................ 51
6.4 Evidence and knowledge gaps .................................................................................................... 52
6.4.1 Hygiene ............................................................................................................................... 52
6.4.2 Measuring health impacts .................................................................................................. 53
6.5 Partnerships ................................................................................................................................ 54
7 Conclusions and recommendations .................................................................................................... 55
7.1 Recommendations ...................................................................................................................... 57
8 Guidance and tools ............................................................................................................................. 61
8.1 Types of projects ADB provides DMCs in WASH+H .................................................................... 61
8.2 Roadmap to increase country-level interest in WASH for health investments .......................... 63
8.3 Strengthen systems to capture and share good practice ........................................................... 64
8.4 Monitoring WASH and HyBC ....................................................................................................... 64
Annexes
Annex 1. References ................................................................................................................................... 69
Annex 2. Key Informant Interviewees ......................................................................................................... 73
Annex 3. Consultancy methodology diagram ............................................................................................. 76
Annex 4. Projects with WASH+H elements mentioned during ADB KIIs .................................................... 77
Annex 5. Novel SARS-CoV-2 virus in WASH systems................................................................................... 79
Annex 6. Tools to assess the WASH enabling environment ....................................................................... 81
Annex 7 Guidance for designing good practice HyBC programs ................................................................ 82
Annex 8. Examples of Improving HyBC in ADB COVID-19 Response projects ............................................ 83
Annex 9. WASH in Healthcare Facilities: Practical guidelines and tools ..................................................... 85
Annex 10. WASH in Schools: Practical guidelines and tools ....................................................................... 87
Figure 1. Infographic showing gaps in access to handwashing facilities with soap in households, schools
and HCFs in South Asia, East Asia and Pacific and Southeast Asia ............................................................... 3
Figure 2. Breakdown of water-related loans and grants by area of investment (2011 – 2021) ................. 12
Figure 3. WASH attributable disease where disease burden estimates quantifiable ................................ 32
Figure 4. Summary of WASH-attributable disease burden (Prüss-Ustün, 2019) ........................................ 32
Figure 5. One Health conceptual model ..................................................................................................... 34
Figure 6. Behavior Centered Design components and process .................................................................. 38
Figure 7. FOAM framework for handwashing with soap ............................................................................ 41
Figure 8. SaniFOAM Framework ................................................................................................................. 42
Figure 9. Financial support for hygiene promotion plans (WHO, 2020) ..................................................... 43
Figure 10. Proportion of projects by main sector ....................................................................................... 44
Figure 11. Diagram of core and overlapping responsibilities of WASH and health sectors ....................... 48
Figure 12. WB multi-sectoral convergence programming for improved nutrition and stunting reduction in
Laos (World Bank , 2019) ............................................................................................................................ 48
Figure 13. Spectrum of WASH+H integration project implementation with examples indicated .............. 50
Figure 14. Diagram showing water and sanitation infrastructure as foundational to desired hygiene
behavior change and health impacts. ......................................................................................................... 52
Tables
Table 1. Water and sanitation in SDG regions (JMP 2017) ........................................................................... 2
Table 2. ADB policies and operational plans pertinent to WASH and health ............................................... 9
Table 3. WUS projects mentioned during interviews as having aspects of WASH+H ................................ 15
Table 4. Education projects mentioned during interviews as having aspects of WASH+H ........................ 18
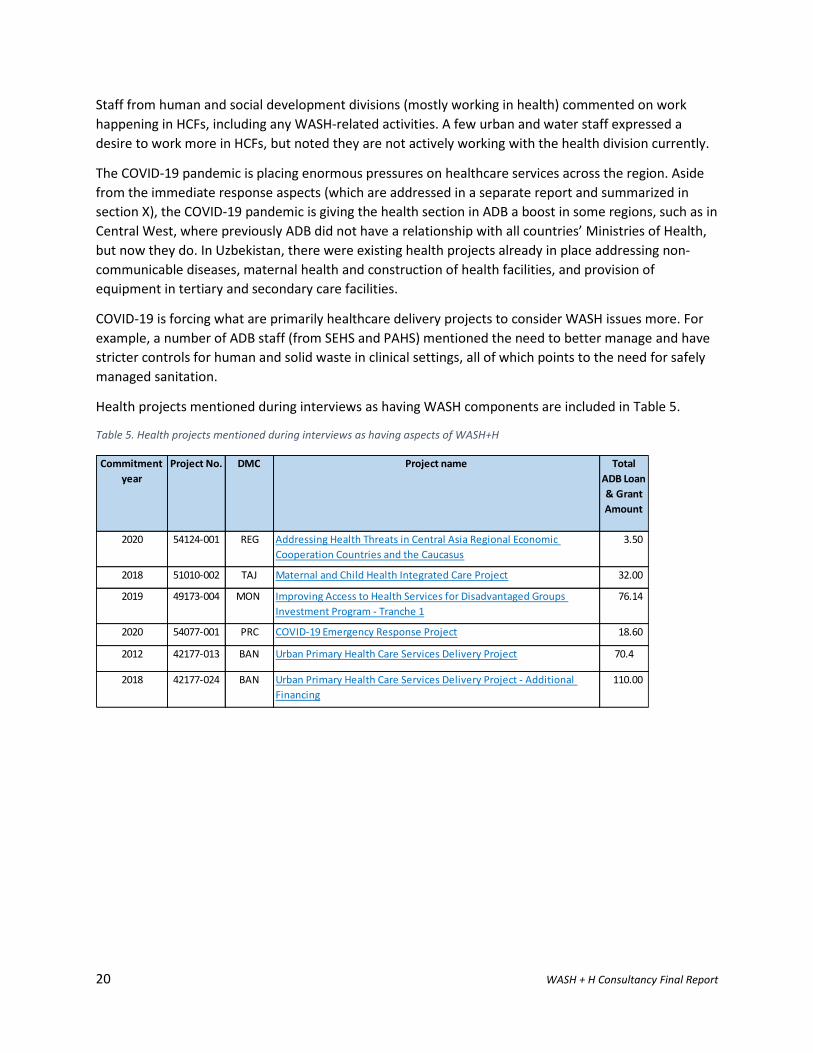
Table 5. Health projects mentioned during interviews as having aspects of WASH+H ............................. 20
Table 6. ANR projects mentioned during interviews as having aspects of WASH+H ................................. 22
Table 7. Donor, knowledge and civil society organizations mentioned as by ADB interviewees ............... 28
Table 8. Number of projects mentioned during interviews by country and region ................................... 44
Table 9. Twelve types of WASH+H projects ADB implements .................................................................... 45
Table 10. Recommendations for short, medium and long-term actions to increase ADB focus on WASH
and health integration ................................................................................................................................ 57
Table 11. Suggested steps for increasing interest in WASH for Health investments in DMCs ................... 63
Table 12. Current and potential WASH indicators for inclusion in Design and Monitoring Frameworks .. 64
Figures
ACRONYMS
ADB Asian Development Bank AIIB Asian Infrastructure Investment Bank ANR Agriculture and Natural Resources AUD Australian dollars AWA Australian Water Association AWDO Asian Water Development Outlook BMGF Bill and Melinda Gates Foundation CoP Community of Practice COVID-19 Coronavirus disease CWIS City Wide Inclusive Sanitation CWSS Central West Social Sector Division CWUW Central West Urban Development and Water Division DFAT Australian Department of Foreign Affairs and Trade DFID United Kingdom Department for International Development DMC Developing Member Country DP Development Partner EASS East Asia Urban and Social Sectors Division EBRD European Bank for Reconstruction and Development EGF Pan-European Guarantee Fund EIB European Investment Bank EURO Euro currency FCDO Foreign, Commonwealth and Development Office (previously DFID) FFD Financing for Development FSM Fecal Sludge Management ICU Intensive Care Unit IPC Infection Prevention and Control IWC International WaterCentre HCF Healthcare Facility HyBC Hygiene Behavior Change JFPR Japan Fund for Poverty Reduction KII Key Informant Interview MHM Menstrual Hygiene Management MOU Memorandum of Understanding O&M Operations and Maintenance PAUW Pacific Urban Development, Water Supply and Sanitation Division PPE Personal Protective Equipment PPSF PSA SAER South Asia Environment, Natural Resources and Agriculture Division SAHS South Asia Human and Social Development Division SARS-CoV-2 Severe acute respiratory syndrome coronavirus 2 SAUW South Asia Urban Development and Water Division SDCC Sustainable Development and Climate Change SEER Southeast Asia Environment, Natural Resources and Agriculture
Division
SEHS Southeast Asia Human and Social Development Division SEUW Southeast Asia Urban Development and Water Division
Special Fund Window Small and medium-sized enterprises Netherlands Development Organisation
SWA Sanitation and Water for All TOR Terms of Reference UNESCAP United Nations Economic and Social Commission for Asia and the
Pacific UNICEF United Nations Children's Fund UNOPS United Nations Office for Project Services USD US dollars WASH Water, Sanitation and Hygiene WHAT Water and Health Advisory Team WHO World Health Organization WUS Water and Other Urban Infrastructure Services
1 WASH + H Consultancy Final Report
1 Executive Summary The COVID-19 disease pandemic has swept across the globe with enormous health, economic and
societal impacts. Safe water supply, sanitation and hygiene (WASH) are more critical than ever for
infection prevention and control (IPC). The COVID-19 pandemic is increasing and entrenching
vulnerabilities and inequalities, including access to WASH services. Handwashing with soap (HWWS) and
water is a particularly critical IPC measure but 1 in 4 healthcare facilities globally have no clean water on
site. In the South East Asian region, 40% of households do not have access to handwashing facilities with
soap and water, and 50% of schools do not have this access.
The COVID-19 pandemic presents a chance to reorient ADB initiatives to more comprehensively and
effectively address hygiene in interventions, policies, strategies and knowledge activities. There is
evidence of this already occurring through project pivots and specific hygiene focused grants. This
consultancy considered how WASH and health aspects has been integrated elements of ADB urban,
health and water strategies, knowledge and lending programs over the last 10 years and provide
recommendations for how these elements could be further integrated in the future. The consultancy
followed a mixed methods approach consisting of: review of ADB policies, projects and strategy
documents and project pipeline; interviews with 49 ADB staff and 9 external organizations; and,
verification of preliminary findings and further data collection via presentations.
Considering WASH and health and WASH for health integration in ADB’s past decade of programming as
well as existing and future programming, the review identified 44 projects that contain WASH and
health components and/or integration across water, urban, health, agriculture and natural resources,
social protection and education sectors. These represent a diverse set of projects across 17 Developing
Member Countries (DMCs).
Peoples’ Republic of China (PRC) had the most projects (6) with WASH and health integration identified,
and it is reported that multi-sectoral health city approaches are the norm. The South Asian region had
the most WASH and health integration projects identified (15). Health projects in India (e.g. National
Urban Health Mission) and Bangladesh (e.g. Urban Primary Health Care Services Delivery Project) in
particular provide examples of interesting innovative and multi-sectoral approaches. Pacific region
water sector projects consistently include WASH components, often explicitly aiming to reduce WASH-
related disease and with community-outreach hygiene components (e.g. South Tarawa Water Supply
Project and Ebeye Water Supply and Sanitation Project).
Some of the key findings and subsequent recommendations from the analysis of WASH and health in the
ADB portfolio include that:
- Urban and water infrastructure projects are strongly weighted to increasing access, with less
emphasis on how beneficiaries use services, hygiene behavior change (HyBC) and related health
impacts. A more holistic approach to WASH will be important to ensuring the health impact of
water and urban infrastructure investments.
- There is evidence of greater emphasis on sustainability and ‘software’ across the board but
more is needed to fully address poor rates of sustainability to ensure the continuity of services
which provide the foundation for improved WASH behaviors.
2 WASH + H Consultancy Final Report
- Where HyBC components are included in projects these are small and effectiveness is almost
never assessed. There is a strong case and rationale to improve the effectiveness of HyBC
components and suggestions on how this can be done are included in the guidance section.
- DMC willingness to borrow for ‘software’ and preventative health remains low and more work is
needed to make the case for the development benefits of these. On this, there remain gaps in
the knowledge base, particularly return on investment from WASH infrastructure and hygiene
specifically.
- There is a committed cohort of ADB officers with a wide range of backgrounds for managing
infrastructure and social development projects. ADB could either increase in-house skills or
partner to increase HyBC and WASH skills which will be needed to increase program
effectiveness.
- There are internal and external factors which both inhibit and assist multi-sectoral and holistic
programming approaches within ADB.
Over 50 recommendations are made for short and medium/long term actions ADB could take to shift to
greater WASH and health integration across the following categories:
i) Capacity development and learning;
ii) Information, evaluation, innovation and knowledge;
iii) Implementation and Operations;
iv) Resources and financing;
v) Policy, strategy and institutional arrangements; and
vi) Partnerships.
Promoting HyBC should be advocated for now as part of COVID-19 pandemic responses and also to
address a longer-term goal to broadly embed and upscale hygiene in ADB’s activities. This will need to
be multi-pronged and long-term effort. Multi-sectoral, holistic approaches can have wide reaching
health benefits and should be promoted. In time the understanding that health-based messaging and
awareness raising alone is insufficient to shift behaviors like HWWS should be mainstream within ADB.
Practical guidance for increasing emphasis on WASH and health is provided from project
conceptualization, design through to monitoring and evaluation. There are already numerous tools and
resources available on effective WASH and HyBC programming across multiple settings for ADB to
access outlined in this report, as well as possibilities to deepen or expand partnerships with recognized
knowledge and implementation partners. Steps to shift strategic priorities from access to infrastructure
to use and health benefits of that access will require a long-term change program. There are suggested
steps to shift the agenda with DMCs and within ADB so that WASH services are further prioritized not
only as a foundation of public health, but also as essential services underpinning economic growth and
development.

1 WASH + H Consultancy Final Report
2 Background and Introduction
2.1 Background Water supply, sanitation and hygiene (WASH) are accepted foundations of public health, as well as
essential services that underpin economic growth and development. There are serious gaps in service
provision globally, with the most acute challenges in vulnerable and poor populations of lower income
and lower middle-income countries. Globally over 2 billion people still do not have basic sanitation
facilities and 785 million people lack even a basic drinking-water service (WHO, 2020). Handwashing
with soap and water are critical IPC measures, and the low levels of access for adequate hygiene
practices are particularly alarming in light of the unfolding COVID-19 pandemic. Globally 1 in 3 people do
not have basic handwashing facilities at home (WSSCC, 2020). The situation in healthcare facilities
globally is also of concern with 1 in 4 having no clean water on site and 1 in 5 not having basic sanitation
(WaterAid). In South East Asia 40% of households do not have access to handwashing facilities with soap
and water, and 50% of schools do not have this access (WHO/UNICEF, JMP WASH data , 2020). Overlaid
on these gaps in basic WASH services are two unfolding crises: the COVID-19 pandemic and climate
change.
The COVID-19 disease pandemic has swept across the globe with enormous health, economic and societal impacts. The disease is caused by the SARS-CoV-2 virus, which is passed human-to-human primarily through respiratory droplets and direct contact. In efforts to contain the virus governments have rapidly implemented numerous containment measures restricting movement and economic activity and worked to strengthen health system preparedness, containment and tracing. Frequent and correct hand hygiene1 is one of the most important measures to prevent infection with SARS-CoV-2 (WHO/UNICEF, Water, sanitation, hygiene, and waste management for SARS-CoV-2, the virus that causes COVID-19: Interim guidance, 2020). Thus, assuring that people have access to soap and continuous water supply and/or other hand hygiene supplies (e.g. sanitizers) at this time of COVID-19 pandemic is more critical than ever. Additionally, governments should guarantee that everyone has access to a minimum level of water and sanitation during the pandemic, for example ensuring people are not be cut of when they are temporary unable to pay bills.
Water security is being affected by the climate change impacts of increasing incidence of extreme and unpredictable climatic events and increasing global temperatures (UNEP, 2020). The increasingly regular disturbances caused by floods, droughts, fires, typhoons and cyclones, storm surge, etc, make the provision of continuous and reliable water and sanitation services all the more challenging. Acknowledging mitigation measures are essential to reducing a worsening future outlook, countries must also focus on developing and implementing adaptation policies, building resilience and increasing preparedness measures.
1 Correct hand hygiene practices include either handwashing with soap for 40-60 seconds following 11 steps or use of alcohol-based sanitizers for 20-30 seconds following 8 steps. These steps are outlined by WHO in a visual guide: https://www.who.int/gpsc/5may/Hand_Hygiene_Why_How_and_When_Brochure.pdf.
2 WASH + H Consultancy Final Report
2.2 WASH situation in the Asian region People’s ability to perform hygiene behaviors recommended during the COVDI-19 pandemic in
household, public, healthcare, education or other settings is contingent on the availability of water. An
overview of the WASH situation in sub-regions provided here shows the extent of gaps in water and
sanitation services and handwashing station availability for millions across the region. The cost to
achieve SDG 6 targets was calculated by the World Bank at US$114 billion of investment per year.
Water and sanitation
Table 1 presents the number of people without access to at least basic drinking water supplies and
sanitation. Basic drinking water access is defined by the WHO/UNICEF Joint Monitoring Program2 as
drinking water sources as those that have the potential to deliver safe water by nature of their design
and construction, and include: piped water, boreholes or tube wells, protected dug wells, protected
springs, rainwater, and packaged or delivered water. Basic sanitation as the use of improved facilities
which are not shared with other households. Improved sanitation facilities are those designed to
hygienically separate excreta from human contact, and include: flush/pour flush to piped sewer system,
septic tanks or pit latrines; ventilated improved pit latrines, composting toilets or pit latrines with slabs.
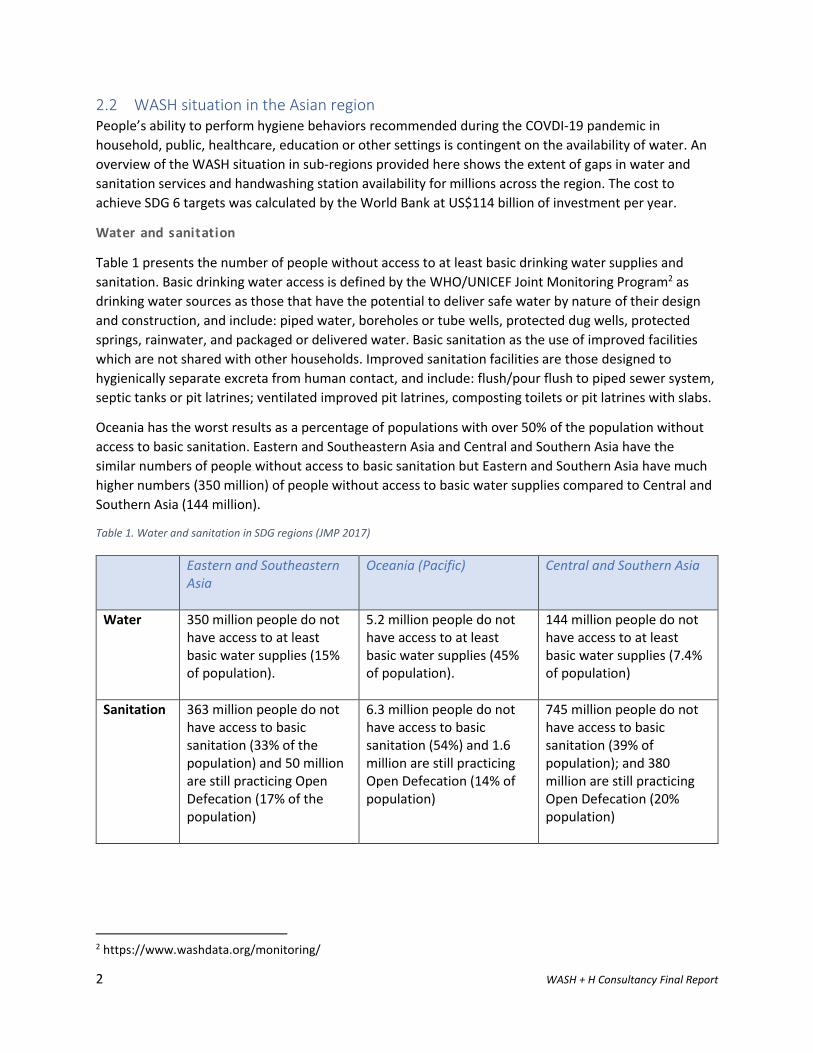
Oceania has the worst results as a percentage of populations with over 50% of the population without
access to basic sanitation. Eastern and Southeastern Asia and Central and Southern Asia have the
similar numbers of people without access to basic sanitation but Eastern and Southern Asia have much
higher numbers (350 million) of people without access to basic water supplies compared to Central and
Southern Asia (144 million).
Table 1. Water and sanitation in SDG regions (JMP 2017)
Eastern and Southeastern Asia
Oceania (Pacific) Central and Southern Asia
Water 350 million people do not have access to at least basic water supplies (15% of population).
5.2 million people do not have access to at least basic water supplies (45% of population).
144 million people do not have access to at least basic water supplies (7.4% of population)
Sanitation 363 million people do not have access to basic sanitation (33% of the population) and 50 million are still practicing Open Defecation (17% of the population)
6.3 million people do not have access to basic sanitation (54%) and 1.6 million are still practicing Open Defecation (14% of population)
745 million people do not have access to basic sanitation (39% of population); and 380 million are still practicing Open Defecation (20% population)
2 https://www.washdata.org/monitoring/
3 WASH + H Consultancy Final Report
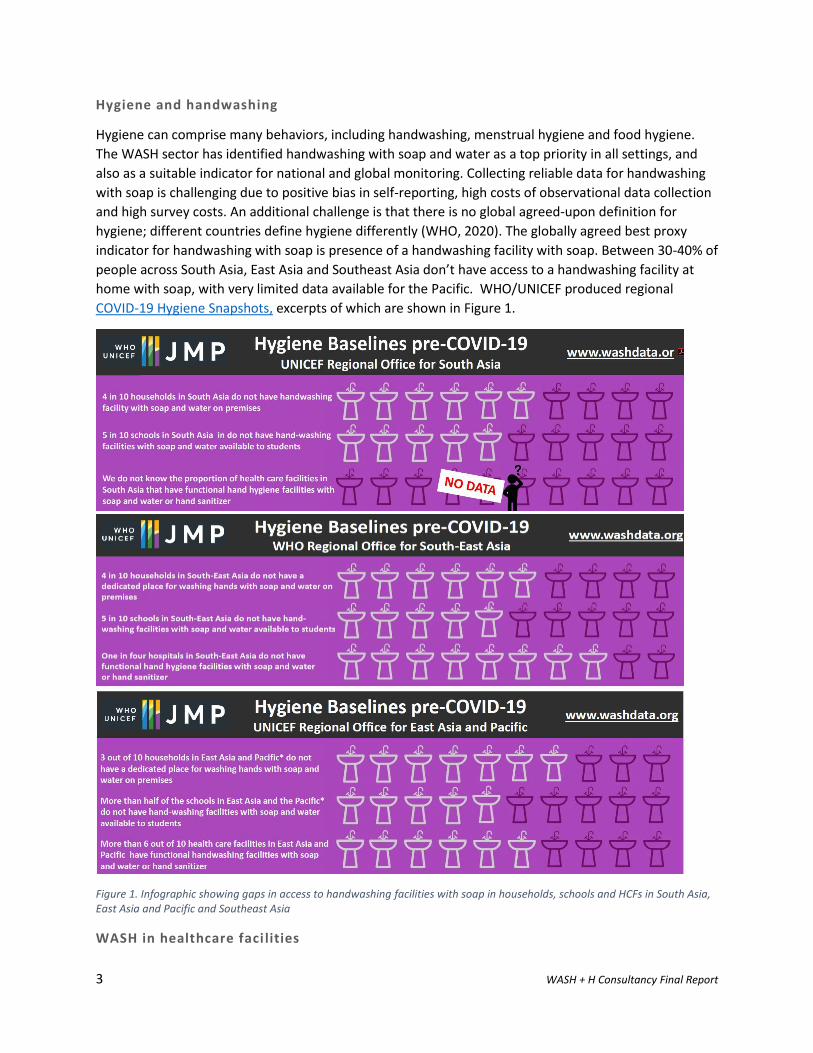
Hygiene and handwashing
Hygiene can comprise many behaviors, including handwashing, menstrual hygiene and food hygiene.
The WASH sector has identified handwashing with soap and water as a top priority in all settings, and
also as a suitable indicator for national and global monitoring. Collecting reliable data for handwashing
with soap is challenging due to positive bias in self-reporting, high costs of observational data collection
and high survey costs. An additional challenge is that there is no global agreed-upon definition for
hygiene; different countries define hygiene differently (WHO, 2020). The globally agreed best proxy
indicator for handwashing with soap is presence of a handwashing facility with soap. Between 30-40% of
people across South Asia, East Asia and Southeast Asia don’t have access to a handwashing facility at
home with soap, with very limited data available for the Pacific. WHO/UNICEF produced regional
COVID-19 Hygiene Snapshots, excerpts of which are shown in Figure 1.
Figure 1. Infographic showing gaps in access to handwashing facilities with soap in households, schools and HCFs in South Asia, East Asia and Pacific and Southeast Asia
WASH in healthcare faci lities
4 WASH + H Consultancy Final Report
The lack of WASH in HCFs is particularly concerning and a barrier to the delivery of universal and high- quality healthcare, for example:
- 74% of health care facilities globally have basic water services, meaning water is available froman improved source on the premises.
- 21% of health care facilities globally have no sanitation service, meaning they have unimprovedtoilets or no toilets at all.
- The proportion of health care facilities without sanitation services ranges from 5% in Easternand South-Eastern Asia to 40% in Central and Southern Asia.
- One out of three health care facilities (36%) in Eastern and South-Eastern Asia has basic hygieneservices (WHO/UNICEF, 2019 ).
The Global Baseline Report (WHO/UNICEF, 2019 ) identifies that HCFs in rural areas have poorer access than those in urban areas. Additionally, non-government facilities are more than twice as likely to have no sanitation service (36%) than government facilities (16%) globally. Due to the heterogeneity of the sector, such as having government and non-government HCFs, the reasons for poor WASH services in HCFs vary from country to country. Some common issues identified for improvement by include: need for comprehensive national policies and standards; setting targets; improving and managing WASH services; and monitoring and operational research (WHO/UNICEF, 2015).
WASH in schools
Gaps in WASH in schools mean that children do not have the benefit of a safe and hygienic learning environment, which can in turn affect not only their health but also their longer-term educational achievements. Some figures that illustrate the scale of the problem include:
- Of 92 countries with data, 69% of schools have a basic drinking water service, defined as animproved source with water available at the time of the survey.
- Less than half of schools in Oceania and only two thirds of schools in Central and Southern Asiahave a basic drinking water service.
- Out of 101 countries with data, 23% of schools have no sanitation service, defined as anunimproved facility or no facility at all. One third of schools in Central and Southern Asia havelimited or no service, and in Oceania 50% have limited or no service (WHO/UNICEF, 2018).
2.3 COVID-19 pandemic impacts on WASH services Urban water and sanitation
The impacts of the COVID-19 pandemic and flow-on economic impacts on urban water utilities are still
unfolding, and this section is a combination of what is known and predicted to affect utilities.
Sustaining services and protecting staff
Ensuring continuity of essential water services has been of utmost concern as border and local
lockdowns have meant that more people are forced to stay at home and also increase their hygiene
measures that require water. Risks to service continuity and quality may be hampered by local
unavailability of and disrupted supply chains for consumables and spare parts needed for treatment
plants, pumping stations, distribution networks and storage tanks. There have been changes to water
demand, with a 10–15% increase in demand for water at household level due to people working from
home and increased handwashing and hygiene measures (WaterAid, 2020).
5 WASH + H Consultancy Final Report
Utilities face the risk of increased staff shortages because of illness and staff concerns about catching
the virus. Any increased risk to staff is also an increased risk to their families and communities,
increasing a company’s or utilities’ responsibilities ‘beyond the company fence line’ (Schulte, 2020)
Utilities have widely recognized their responsibilities to protect staff and various international
collaborative platforms have been formed to share lessons. Useful guidance materials are now available
such as the Practical Guidance notes (in English, Khmer, Indonesian and Vietnamese) on keeping water
utility workers safe as part of the Australian Telenetwork Partnership3 in additional to more general
guidelines like UNICEF’s Guidance on COVID-19 Back-To-Work Preparedness4.
Extending services and reducing contagion risks
Lockdowns have increased hardship for people without existing access to water and sanitation and reaching the poorest and most marginalized people has become more challenging. Utilities and governments may lack capacity to service informal settlements, peri-urban areas and slums with either emergency or new connections (WaterAid, 2020). Large cities face the highest risks stemming from population density and informal settlements, and those areas without adequate WASH are at highest risk of becoming contagion centers (IFC, June 2020).
Financial risks
In the short-term water utilities are facing significant revenue shortfalls due to a reduction in demand from large industrial and commercial users and tariff waivers for households facing economic hardship. This is predicted to be between 15-40% or more in many cases (WaterAid , 2020; IFC, June 2020). In the longer-term reducing government budgets from economic down-turns will likely mean similar declines in capital expenditures in capital and operational expenditures (Capex and Opex). A downward adjustment of 7% in the global water sector Capex projections for 2020 is expected (IFC, June 2020). Unless shortfalls are addressed, many utilities will be unable to maintain current service levels nor will they be able to scale-up and expand existing networks to service vulnerable and unserved populations.
Rural WASH
There is very little documented as yet on the impacts of COVID-19 on rural WASH. Despite important improvements over the last decade or more, service levels and access to water and sanitation in rural areas are worse than urban areas across the board. A review in 2019 showed that 21 countries had rural-urban coverage gaps of fewer than ten percentage points in access to basic drinking water services but 45 countries had gaps of over 20 points, while 15 countries had gaps of over 40 points. The same review showed that for basic sanitation coverage (UNICEF/WHO, 2019).
3 https://watersource.awa.asn.au/business/partnerships/australian-telewater-network-for-international-development/ http://ozwater.org/Watersource/wp-content/uploads/2020/03/COVID-19-Fact-Sheet-for-Water-Utilities-English.pdf http://ozwater.org/Watersource/wp-content/uploads/2020/05/Riverina-Water-Pandemic-Planned-Response.pdf http://ozwater.org/Watersource/wp-content/uploads/2020/05/Aqwest-Water-OHS-Handbook.pdf https://watersource.awa.asn.au/wp-content/uploads/2020/05/FAQs-on-COVID-19-in-English.pdf https://watersource.awa.asn.au/wp-content/uploads/2020/05/COVID_Surveillance_Activity_Overview_MK_Countries_English.pdf 4 https://www.unicef.org/nepal/media/7551/file
6 WASH + H Consultancy Final Report
2.4 Assignment objectives The consultancy considered how WASH plus health (WASH+H) aspects should be integrated elements of
ADB’s urban, health and water strategies, knowledge and lending programs. The assignment aimed to
analyze ADB’s past decade of programming as well as existing and future programming to capture
lessons learnt to inform short, medium and long-term urban and water ADB investments. The initial
scope was to assess how to better incorporate health aspects into the ADB water and urban pipeline
and ADB health and social sector investments to better incorporate water, sanitation and hygiene
aspects. Over the course of the consultancy the scope has widened to also consider education, social
development, gender, agriculture (food security), natural resource and private sector interventions
where these include WASH components.
The analysis has resulted in recommendations on how to improve ‘integration’ of ADB’s WASH and
health investments at a strategic through to operational levels. The consultancy also reviewed the
extent of WASH in COVID-19 responses and makes recommendations to enhance priority areas such as
hygiene promotion and handwashing with soap to increase effectiveness of interventions for IPC.
2.5 Methodology The consultancy took a mixed-methods approach with a number of elements running consecutively (see Annex 3). The first step included a desktop review of key ADB policy documents and project pipelines to propose a sampling methodology to review projects where WASH+H could be assessed. Through discussion with ADB staff it was agreed that rather than undertake a stratified sample of projects to review, projects for further analysis would be identified via key informants with ADB staff via voluntary interviews. Another first step was to discuss the scope of analysis and definition of WASH+H for the purposes of the review (see definitions section).
The first stage of internal data collection was ADB via key informant interviews with 49 directors and
staff of regional departments and sector and thematic groups in Sustainable Development and Climate
Change (SDCC). 22 interviews were held between early August 2020 and mid-November 2020. The
scope of internal ADB interviews was to gather:
i. Trends in WASH and health sectors over the last 10 years in policies, strategies knowledge,
evidence-base gathering/impact evaluation and DMC support requests or borrowing;
ii. Reflections on internal and external operational and strategy factors that inhibit investment in
WASH, health or hygiene in the pipeline, effective models of intervention, lessons learned and
ideas on upscaling and mainstreaming WASH;
iii. Project examples that ADB staff consider to have WASH+H integration elements;
iv. Evidence-base and knowledge base that already exists or is still required to further mainstream
WASH+H;
v. Observations on financing for WASH+H including amounts committed to hygiene behavior
change (HyBC) or WASH broadly;
vi. Collaboration and/or integration across sectors within ADB or DMC engagement, especially
WUS, health, education and social protection; and
vii. Key Development Partners (DPs) working in WASH+H and existing partnerships with ADB.
Internal interviews were transcribed, coded using NVivo software and analyzed according to key themes
(trends, operations, strategies, financing, capacity, partnerships, knowledge and evidence, COVID-19
responses) as well as emergent and cross-cutting themes (e.g. gender, climate change).
7 WASH + H Consultancy Final Report
Nine external key informant interviews with 22 interviewees were undertaken with an agreed list of DPs
and Civil Society Organizations (CSOs). These included: ADB, World Bank, UNICEF, WHO, DFAT, BMGF,
SNV, WaterAid. Interviews were transcribed and analyzed for trends and lessons relevant to ADB’s
internal review. The scope of external interviews was to gather:
i. Views and experience on mainstreaming and integrating WASH and Health in DP policies and
programming;
ii. Views on strengths, gaps and opportunities in financing, evidence and modalities for increasing
health aspects in water and sanitation and urban initiatives, and WASH aspects in health
initiatives in the short, medium and long-term; and
iii. Information on DP COVID-19 responses including partnerships.
A list of projects was collated from those mentioned during internal key informant interviews (KIIs).
Available reports were reviewed for these projects for level of intervention (e.g. sector strengthening,
private sector, community, utility), settings (e.g. households, schools, healthcare facilities, public
spaces), location (urban, peri-urban or rural), main sector/s of intervention (e.g. urban development,
water supply, sanitation, skills development, etc) and hygiene promotion activities, where they exist
(e.g. handwashing promotion, HyBC, menstrual hygiene management (MHM)). Reports reviewed for
each project were those publicly available including reports such as: Report and Recommendation of the
President to the Board of Directors; Project Readiness Financing Project Administration Manual; Social
Safeguard Monitoring Reports; Project Readiness Financing Reports; Initial Poverty and Social Analysis
(PSA) Reports; Gender Action Plans; Consultant Reports; Technical Assistance (TA) Reports and Concept
Notes for projects in early design phases shared by Project Officers. Over fifty reports were reviewed
paying particular attention to:
- Presence/absence of water, sanitation and/or hygiene in health, water, urban, education or
agriculture and natural resource (ANR) projects, and type of intervention where they exist;
- Presence/absence of HyBC components, and type, delivery modality and monitoring of
intervention where they exist, across all sector interventions;
- Notable examples of pro-poor targeting, gender components, innovative approaches and
measurement of health impacts;
- Use of previous lessons learned for effective cross- or multi-sectoral interventions.
A rapid assessment of COVID-19 WASH responses was undertaken in parallel with this work. The
methodology and results of that are presented in a separate stand-alone report, the first draft of which
was submitted to ADB on 16 October 2020. The scope of the consultancy was to consider short, medium
and long-term WASH+H integration issues. COVID-19 pandemic initial responses are considered short-
term and immediate, thus justifying a separate report with a quicker turnaround. Certain sections of the
COVID-19 Rapid Assessment Report are included above (Section 2.2, 2.3 and Annex 5).
The project analysis was used to develop and gather insights from a typology of ADB projects that
include WASH+H integration elements. The KII and project analyses were used to develop and inform
recommendations. Preliminary findings were presented to the Water and Health Advisory Team
(WHAT) to validate early findings and seek further inputs. This step led to inclusion of additional projects
and interviews with social protection and private sector divisions.
8 WASH + H Consultancy Final Report
2.6 Definitions For the purposes of this review and report the following definitions are assumed:
Sanitation: is used to refer to all components of the sanitation services chain in rural and urban settings,
and so includes toilet facilities, fecal sludge management, septage, sewerage networks and wastewater
treatment and disposal. Where is it necessary to separate the different components of sanitation this is
included.
WASH: is the collective term for Water, Sanitation and Hygiene. While each a separate field of work,
each is dependent on the presence of the other (UNICEF, 2016). The significance of hygiene being
included in conjunction with water and sanitation is that hygiene behaviors (e.g. use of a latrine,
handwashing with soap) are essential to create pathogen infection barriers for the individual and thus to
enjoy the full potential health benefits of services.
WASH+H: An initial conceptualization of WASH plus health discussed with ADB included three
interpretations of the term:
i. integrated programming of WASH and health sectors to address priority issues;
ii. WASH for health, i.e. WASH as fundamental building block to public health and development;
iii. WASH in health services, i.e. addressing need for WASH to provide adequate health services.
Through the consultancy process it became clear that a wider range of WASH+H aspects are considered
important, reaching into the education, rural development, social protection and other sectors. There is
a section in the analysis outlining the challenges, advantages and disadvantages of the WASH+H
terminology as well as recommendations for consistent terminology usage.
3 ADB institutional context
3.1 WASH+H in ADB policies and strategies ADB’s overall Strategy 2030 (ADB, July 2018) outlines seven Operational Priorities (OPs) and ADB’s
Water Sector contributes to all seven of these in various ways. Water especially contributes to OP1,
Addressing Remaining Poverty and Reducing Inequalities and OP2, Accelerating Progress in Gender
Equality. OP1 encompasses health, education, social protection and inequality in access to
opportunities. A lack of access to quality WASH and/or health services entrenches and exacerbates
existing inequalities and reduces possibilities to move out of poverty. Health is present in multiple OPs,
especially OP1 subcomponent “achieving better health for all”. This sub-component identifies ADB’s
health priority areas as: universal health coverage by improving the quality and coverage of government
and private health-care services; supporting health financing reforms (e.g. health insurance, quality
health-care and reducing out-of-pocket expenses for the poor). Through strengthening water
management, the governance and institutional capacity (OP6) of public and private institutions are
improved. Healthy urban areas (cities), water services as well as transport and energy improvements
optimize indirect health benefits. The Water Sector contributes to OP3, Tackling Climate Change and
OP4, Livable cities, through flood risk management, water-based solutions and water supply and
sanitation provision. In rural areas improvements to irrigation systems contribute to development and
food security (OP5), and related watershed management and water security contribute to fostering
regional cooperation (OP7).
9 WASH + H Consultancy Final Report
Multi-sectoral approaches are supported as a common operational approach in Strategy 2030. For
example, the livable cities approach should include almost all sectors and themes through multisector
projects or programmatic approaches that support physical capital investments (e.g., transport, water,
and energy infrastructure) and human capital investments (e.g., social protection, health care, and
education) (ADB, Sept 2019 ).
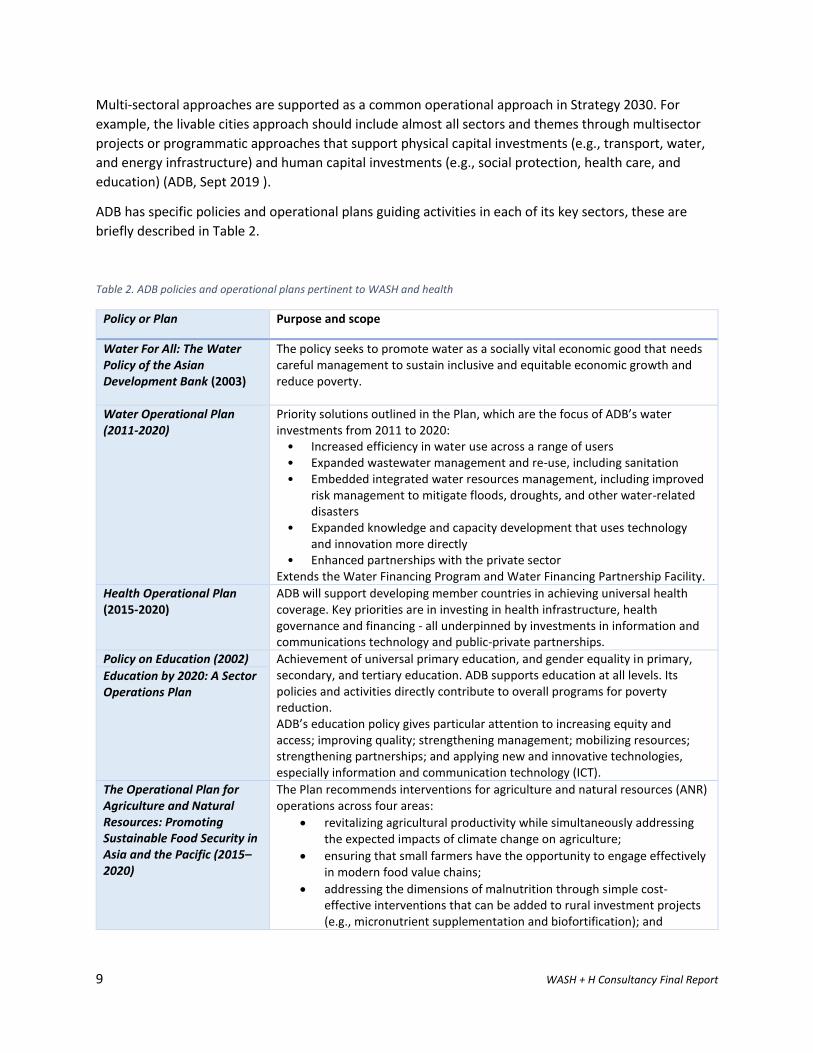
ADB has specific policies and operational plans guiding activities in each of its key sectors, these are
briefly described in Table 2.
Table 2. ADB policies and operational plans pertinent to WASH and health
Policy or Plan Purpose and scope
Water For All: The Water Policy of the Asian Development Bank (2003)
The policy seeks to promote water as a socially vital economic good that needs careful management to sustain inclusive and equitable economic growth and reduce poverty.
Water Operational Plan (2011-2020)
Priority solutions outlined in the Plan, which are the focus of ADB’s water investments from 2011 to 2020:
• Increased efficiency in water use across a range of users• Expanded wastewater management and re-use, including sanitation• Embedded integrated water resources management, including improved
risk management to mitigate floods, droughts, and other water-relateddisasters
• Expanded knowledge and capacity development that uses technologyand innovation more directly
• Enhanced partnerships with the private sectorExtends the Water Financing Program and Water Financing Partnership Facility.
Health Operational Plan (2015-2020)
ADB will support developing member countries in achieving universal health coverage. Key priorities are in investing in health infrastructure, health governance and financing - all underpinned by investments in information and communications technology and public-private partnerships.
Policy on Education (2002) Achievement of universal primary education, and gender equality in primary, secondary, and tertiary education. ADB supports education at all levels. Its policies and activities directly contribute to overall programs for poverty reduction. ADB’s education policy gives particular attention to increasing equity and access; improving quality; strengthening management; mobilizing resources; strengthening partnerships; and applying new and innovative technologies, especially information and communication technology (ICT).
Education by 2020: A Sector Operations Plan
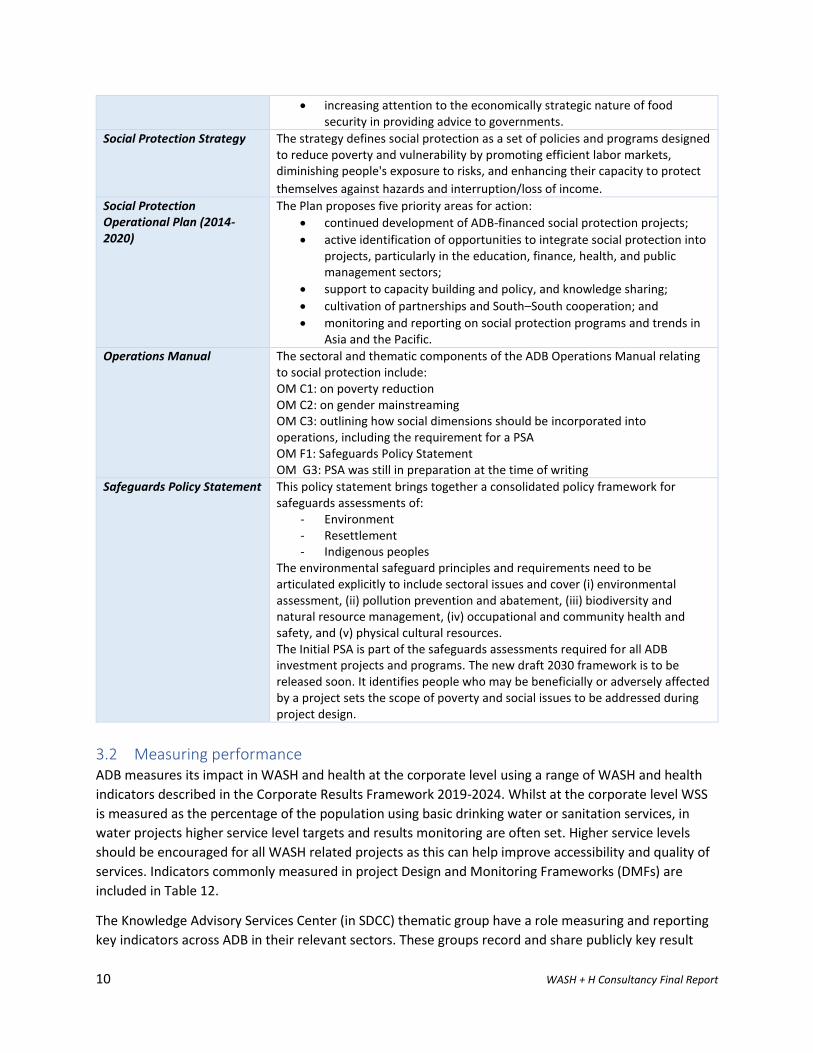
The Operational Plan for Agriculture and Natural Resources: Promoting Sustainable Food Security in Asia and the Pacific (2015–2020)
The Plan recommends interventions for agriculture and natural resources (ANR) operations across four areas:
• revitalizing agricultural productivity while simultaneously addressingthe expected impacts of climate change on agriculture;
• ensuring that small farmers have the opportunity to engage effectivelyin modern food value chains;
• addressing the dimensions of malnutrition through simple cost-effective interventions that can be added to rural investment projects(e.g., micronutrient supplementation and biofortification); and
10 WASH + H Consultancy Final Report
• increasing attention to the economically strategic nature of foodsecurity in providing advice to governments.
Social Protection Strategy The strategy defines social protection as a set of policies and programs designed to reduce poverty and vulnerability by promoting efficient labor markets, diminishing people's exposure to risks, and enhancing their capacity to protect
themselves against hazards and interruption/loss of income.
Social Protection Operational Plan (2014-2020)
The Plan proposes five priority areas for action:
• continued development of ADB-financed social protection projects;
• active identification of opportunities to integrate social protection intoprojects, particularly in the education, finance, health, and publicmanagement sectors;
• support to capacity building and policy, and knowledge sharing;
• cultivation of partnerships and South–South cooperation; and
• monitoring and reporting on social protection programs and trends inAsia and the Pacific.
Operations Manual The sectoral and thematic components of the ADB Operations Manual relating to social protection include: OM C1: on poverty reduction OM C2: on gender mainstreaming OM C3: outlining how social dimensions should be incorporated into operations, including the requirement for a PSA OM F1: Safeguards Policy Statement OM G3: PSA was still in preparation at the time of writing
Safeguards Policy Statement This policy statement brings together a consolidated policy framework for safeguards assessments of:
- Environment- Resettlement- Indigenous peoples
The environmental safeguard principles and requirements need to be articulated explicitly to include sectoral issues and cover (i) environmental assessment, (ii) pollution prevention and abatement, (iii) biodiversity and natural resource management, (iv) occupational and community health and safety, and (v) physical cultural resources. The Initial PSA is part of the safeguards assessments required for all ADB investment projects and programs. The new draft 2030 framework is to be released soon. It identifies people who may be beneficially or adversely affected by a project sets the scope of poverty and social issues to be addressed during project design.
3.2 Measuring performance ADB measures its impact in WASH and health at the corporate level using a range of WASH and health
indicators described in the Corporate Results Framework 2019-2024. Whilst at the corporate level WSS
is measured as the percentage of the population using basic drinking water or sanitation services, in
water projects higher service level targets and results monitoring are often set. Higher service levels
should be encouraged for all WASH related projects as this can help improve accessibility and quality of
services. Indicators commonly measured in project Design and Monitoring Frameworks (DMFs) are
included in Table 12.
The Knowledge Advisory Services Center (in SDCC) thematic group have a role measuring and reporting
key indicators across ADB in their relevant sectors. These groups record and share publicly key result

11 WASH + H Consultancy Final Report
indicators with cumulative figures over last 15-20 years. Education and water indicators are readily
available on the website, and health indicators are included in publications. Some multi-sectoral
indicators which cross water, gender and education are included.
12 WASH + H Consultancy Final Report
4 Findings This section presents the results of KIIs and project reviews with the main consideration being the
extent of WASH+H efforts in ADB’s WUS, rural WASH, education, health, ANR and social protection
departments and sector and thematic groups across the topics of trends, operations, strategies,
financing, capacity, partnerships and knowledge and evidence. KII findings on emergent and cross-
cutting themes such as hygiene, gender and climate change are presented.
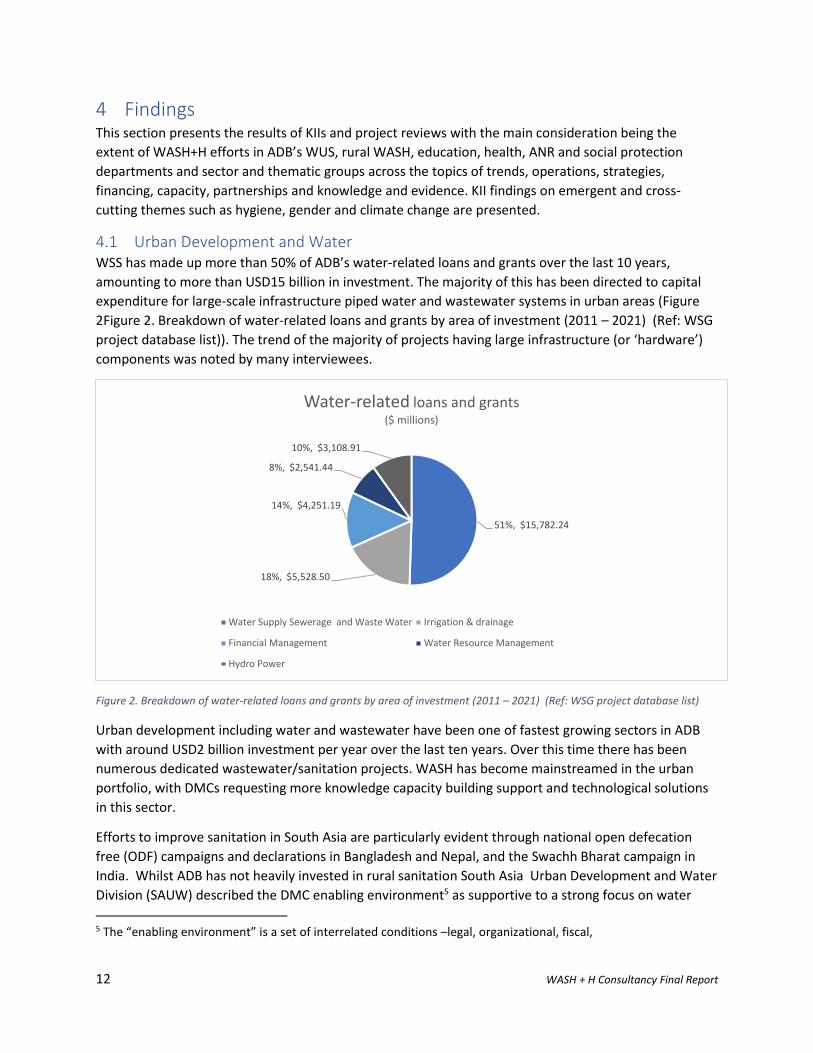
4.1 Urban Development and Water WSS has made up more than 50% of ADB’s water-related loans and grants over the last 10 years,
amounting to more than USD15 billion in investment. The majority of this has been directed to capital
expenditure for large-scale infrastructure piped water and wastewater systems in urban areas (Figure
2Figure 2. Breakdown of water-related loans and grants by area of investment (2011 – 2021) (Ref: WSG
project database list)). The trend of the majority of projects having large infrastructure (or ‘hardware’)
components was noted by many interviewees.
Figure 2. Breakdown of water-related loans and grants by area of investment (2011 – 2021) (Ref: WSG project database list)
Urban development including water and wastewater have been one of fastest growing sectors in ADB
with around USD2 billion investment per year over the last ten years. Over this time there has been
numerous dedicated wastewater/sanitation projects. WASH has become mainstreamed in the urban
portfolio, with DMCs requesting more knowledge capacity building support and technological solutions
in this sector.
Efforts to improve sanitation in South Asia are particularly evident through national open defecation
free (ODF) campaigns and declarations in Bangladesh and Nepal, and the Swachh Bharat campaign in
India. Whilst ADB has not heavily invested in rural sanitation South Asia Urban Development and Water
Division (SAUW) described the DMC enabling environment5 as supportive to a strong focus on water
5 The “enabling environment” is a set of interrelated conditions –legal, organizational, fiscal,
51%, $15,782.24
18%, $5,528.50
14%, $4,251.19
8%, $2,541.44
10%, $3,108.91
Water-related loans and grants ($ millions)
Water Supply Sewerage and Waste Water Irrigation & drainage
Financial Management Water Resource Management
Hydro Power
13 WASH + H Consultancy Final Report
supply systems, and greater focus on sanitation and hygiene. This has in turn moved to fit-for-purpose
approaches like fecal sludge management and city-wide basic sanitation. This trend is reflected in East
Asia and Southeast Asia regional departments as well, with urban sanitation investments over recent
years including mixed-investment portfolios of decentralized and non-networked sanitation via city-
wide inclusive sanitation (CWIS)6 approaches.
When asked the extent to which non-structural elements formed part of WSS investments, most
divisions noted that only a very small percentage of WSS projects go to ‘software’ or non-structural
components. Central, South and Southeast Asia (SEUWD) argued that engagement in urban areas is
driven by links to institutions, not links with communities, and that because of this hygiene and WASH
(considered to be community-level work) is often not within scope.
Projects or programs with non-infrastructure components to complement water and sanitation
infrastructure and service provision range across a number of areas and include, for example:
- Policy level: Policy and strategy development; analytical research;
- Institutional level: Business operations and management support; capacity building;
institutional strengthening;
- Community level: Awareness raising; information education communication (IEC) programs;
HyBC promotion.
During interviews different people expressed different understandings of what constitutes non-
infrastructure components. HyBC, especially handwashing with soap (HWWS), was especially explored
and through that it was evident that whilst ‘soft’ (i.e. institutional support) components are standard,
HyBC components are not and appear only in some WUS projects. SEUW reported that hygiene and
WASH components are not standard, either being not included or included late in the project design
process. SAUW on the other hand reported increasing demand from DMCs to include hygiene in WUS
projects. The Pacific and Central West indicated that hygiene and awareness campaigns are standard for
WUS projects, with the Pacific consistently naming these ‘WASH’ components and often involving
utilities. Peoples Republic of China (PRC) is a unique case compared since ADB has been involved in
water and sanitation sector many years and there is consistent demand for integrated approaches.
There are some utility-led hygiene and community outreach programs reported, mostly in the Pacific. These include:
- Solomon Islands: Urban Water Supply and Sanitation Sector Project (51271-001) has acomponent led by Solomon Islands Water Authority to ensure sustainability from the customeror user perspective through a comprehensive awareness and behavior campaign to promotegood hygiene practices, water conservation and importance to pay the tariffs in thecommunities.
- Fiji: Urban Water Supply and Wastewater Management Investment Program (49001-003 ) has aWASH campaign mostly targeting water demand management to be led by the Water Authorityof Fiji with the Ministry of Health in project areas and informal settlements.
regulatory, informational, political and cultural – that impact on the capacity of development partners to engage in developmental processes in a sustained and effective manner. 6 City Wide Inclusive Sanitation is a public service approach to planning and implementing urban sanitation systems aiming to ensure everyone has access to safely managed sanitation by promoting a range of solutions.
14 WASH + H Consultancy Final Report
Interviewees mentioned that the success of these is mixed depending on the utilities’ understanding of its mandate.
Interviewees noted a need to focus on systems strengthening, institutional capacity building and
sustainability so as to improve overall sector performance and sustainability of services provision. For
example, in Uzbekistan, the vicious cycle in water supply sector was noted, with low salaries not
attracting best talent and with resulting performance reductions also reducing financial viability and
resources to maintain infrastructure. In South Asia as water and sanitation coverage has increased,
there is a trend for DMCs to consider increasing the sustainability of interventions and service level
quality.
The rural WASH component of ADB’s portfolio is small, with only three projects mentioned during
interviews. Emphasis on and financing for rural WASH was observed to have declined over the last
decade (SEUW, EAER). PRC presents a unique case where urban WSS infrastructure has already received
a great deal of attention with widespread improvements in access. PRC has a national HWWS campaign
and attention has now turned to rural sanitation which is now it’s priority concern with 80% of
wastewater directly discharging to rivers without treatment in rural areas and many people lacking
appropriate and simple sanitation facilities.
The lack of ADB or other multilateral development bank (MDB) investments in rural WASH has left a gap
in infrastructure financing according to some. One interviewee argued that unlike in urban water, that
the pendulum has swung too far to ‘soft’ interventions such as Community Led Total Sanitation (CLTS)
led by NGOs, and that infrastructure has been neglected. Rural WASH projects mentioned appeared in
either the WUS or the ANR pipeline.
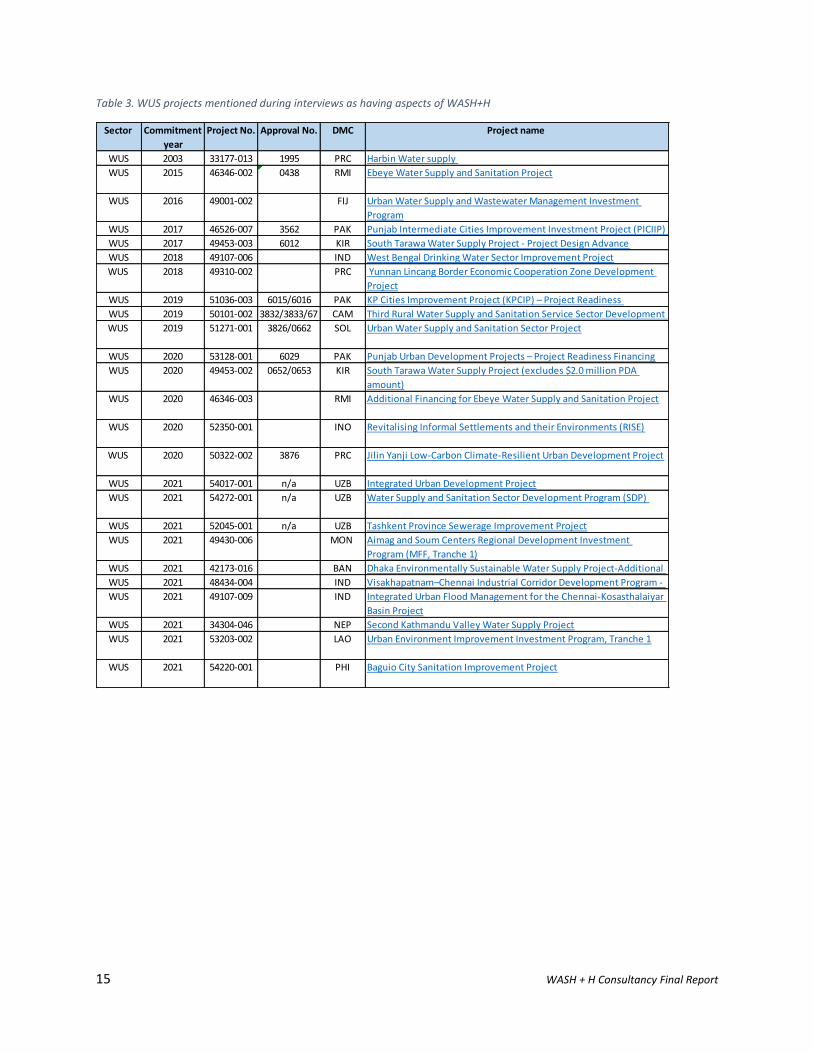
All of the WUS projects mentioned during interviews as having WASH+H components are included in
Table 3. There are a number of projects in design stages which are pivoting to respond to the COVID-19
pandemic, such as the Laos Urban Environment Improvement Investment Program and Philippines
Baguio City Sanitation Improvement Project.
15 WASH + H Consultancy Final Report
Table 3. WUS projects mentioned during interviews as having aspects of WASH+H
Sector Commitment
year
Project No. Approval No. DMC Project name
WUS 2003 33177-013 1995 PRC Harbin Water supply
WUS 2015 46346-002 0438 RMI Ebeye Water Supply and Sanitation Project
WUS 2016 49001-002 FIJ Urban Water Supply and Wastewater Management Investment
Program
WUS 2017 46526-007 3562 PAK Punjab Intermediate Cities Improvement Investment Project (PICIIP)
WUS 2017 49453-003 6012 KIR South Tarawa Water Supply Project - Project Design Advance
WUS 2018 49107-006 IND West Bengal Drinking Water Sector Improvement Project
WUS 2018 49310-002 PRC Yunnan Lincang Border Economic Cooperation Zone Development
Project
WUS 2019 51036-003 6015/6016 PAK KP Cities Improvement Project (KPCIP) – Project Readiness
WUS 2019 50101-002 3832/3833/67 CAM Third Rural Water Supply and Sanitation Service Sector Development
WUS 2019 51271-001 3826/0662 SOL Urban Water Supply and Sanitation Sector Project
WUS 2020 53128-001 6029 PAK Punjab Urban Development Projects – Project Readiness Financing
WUS 2020 49453-002 0652/0653 KIR South Tarawa Water Supply Project (excludes $2.0 million PDA
amount)
WUS 2020 46346-003 RMI Additional Financing for Ebeye Water Supply and Sanitation Project
WUS 2020 52350-001 INO Revitalising Informal Settlements and their Environments (RISE)
WUS 2020 50322-002 3876 PRC Jilin Yanji Low-Carbon Climate-Resilient Urban Development Project
WUS 2021 54017-001 n/a UZB Integrated Urban Development Project
WUS 2021 54272-001 n/a UZB Water Supply and Sanitation Sector Development Program (SDP)
WUS 2021 52045-001 n/a UZB Tashkent Province Sewerage Improvement Project
WUS 2021 49430-006 MON Aimag and Soum Centers Regional Development Investment
Program (MFF, Tranche 1)
WUS 2021 42173-016 BAN Dhaka Environmentally Sustainable Water Supply Project-Additional
WUS 2021 48434-004 IND Visakhapatnam–Chennai Industrial Corridor Development Program -
WUS 2021 49107-009 IND Integrated Urban Flood Management for the Chennai-Kosasthalaiyar
Basin Project
WUS 2021 34304-046 NEP Second Kathmandu Valley Water Supply Project
WUS 2021 53203-002 LAO Urban Environment Improvement Investment Program, Tranche 1
WUS 2021 54220-001 PHI Baguio City Sanitation Improvement Project
16 WASH + H Consultancy Final Report
Box 3. UZB: Tashkent Province Sewerage Improvement Project (52045-001: 2021)
The project is upgrading the centralized wastewater systems of six cities and the Chinaz urban center,
improving sanitation practices in two districts’ rural areas, and building wastewater planning and
operational capacity of the water and sanitation service provider. Interestingly, the project includes the
design and implementation of a sanitation and hygiene awareness program to improve community
awareness and understanding of sanitation best practices. It sets indicator targets for households in rural
areas of Chinaz and Yangiyul and public schools including youth to have increased awareness on sanitation
and hygiene. It is not clear, however, if baseline was taken to measure progress against. Sanitation and
hygiene awareness program to be undertaken in areas where decentralized sanitation systems to be
installed.
Box 1. KIR: South Tarawa Water Supply Project (49453-002: 2020)
The project aims to combat factors that result in the high incidence of waterborne disease in South Tarawa, the capital of Kiribati, through the delivery and effective management of new and rehabilitated climate-resilient water supply assets and of improved hygiene practices. It is of particular interest because:
- Overcrowding as well as inadequate WASH coverage are linked to waterborne diseases (diarrhea and dysentery) in Kiribati;
- The hygiene component goes beyond general awareness raising and outlines specific target behaviors it aims to address: handwashing with soap, household water treatment and safe storage, and menstrual hygiene management;
- The project will collect gender impacts from improved WASH by undertaking studies and collecting evidence over the project life of to measure positive impacts on women’s daily lives resulting from 24/7 access to safe water. A variety of qualitative survey techniques will be used at project base-, mid- and end-line.
This project is co-financed between ADB, DFAT, World Bank, Global Climate Fund. Total project USD 34.72m
with ADB USD13m loan component. There is a USD2.5m component for WASH and CC awareness raising.
Box 2. NEP: Second Kathmandu Valley Water Supply Project (34304-046: 2021)
This project is an example of how water supply projects can address individual behaviors to facilitate more
sustainable functioning of the water supply system. It consists of two loans which with components that: (i)
raw water transfer and treatment; (ii) transmission mains and distribution network; (iii) small water supply
projects; (iv) institutional strengthening; and (v) planning for future WSS service delivery.
Project stages two and three both have community awareness raising and behavior change components.
The target behaviors relate to improving use of water services and include: reducing illegal connections,
regularly paying tariffs, contributing to maintenance, preventing leakages, and taking measures to protect
and conserve water. Approaches used to shift behaviors include: public education activities (including in
schools); community mobilization (through two hired Community Awareness consultants); and a
Stakeholder Communication Strategy with social marketing, jingles, social media and messages tailored to
different groups. Hygiene practices were incorporated into messaging and the project’s social monitoring
report states that hand hygiene improved, but no quantitative measures to support this were not included.
17 WASH + H Consultancy Final Report
4.2 Education It was observed by a number of interviewees that social sector divisions (education, health and social
protection) are increasingly dealing with WASH components. The projects listed by interviews support
this and it is particularly true for education.
The Education Sector Group (ESG) reported two key ways that WASH+H are addressed by the education
sector. These include:
i. Access to facilities for water and sanitation services, hygiene promotion and health in schools.
ii. Education curriculum support and skills development to support relevant topics and sectors.
Education sector has had a clear and focused effort on universalizing elementary education and ensuring
WASH access for girls to primary and secondary education has been a key part of this (e.g. provision of
gender separated facilities and drinking water). Long-term sector support programs in Nepal and
Bangladesh provide good examples of this. Despite these efforts more than 20% schools or maybe more
don’t meet basic requirements. ESG reported that there is increasing realization that WASH is a lot more
than providing facilities and infrastructure, and also requires HyBC, advocacy and awareness raising and
operations and maintenance (O&M) of facilities.
Education projects that had supported infrastructure found that in some places where there were
toilets, they were not being used, or had no water. ESG commented that in developing and poor
contexts WASH requires far more than facilities, it also requires behavior change.
The Education sector and future is changing rapidly with impacts of COVID-19 lockdowns and remote
learning; there are major concerns about long-term educational gaps affecting life-long learning and
employment opportunities for the ‘lock down generation’. SEHS education is already partnering to
develop guidelines for schools re-opening to manage health risks and transmission of the SARS COVID-2
virus. SEHS commented that most counterparts have integrated water and sanitation guidelines when
re-opening schools, indicating they use UNICEF guidelines for better hygiene in schools.
Through interviews a few divisions agreed that schools are a good entry point for increasing hygiene
efforts, especially in the context of COVID-19 pandemic, with providing systematic approaches to return-
to-school a big challenge. ESG also point out that schools also often used for health sessions and
vaccinations and thus the necessity for them to be well equipped, have necessary safety protocols and
hygiene practices is even greater.
Education projects mentioned during interviews as having WASH components are included in Table 4.
18 WASH + H Consultancy Final Report
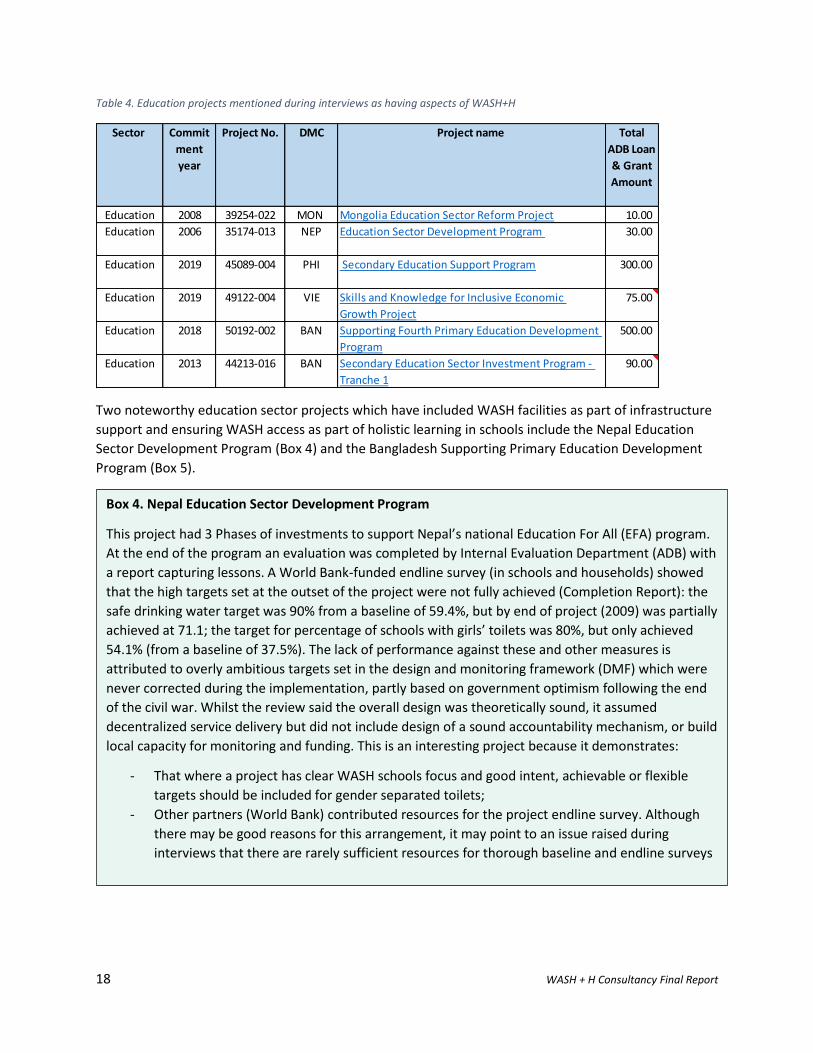
Table 4. Education projects mentioned during interviews as having aspects of WASH+H
Two noteworthy education sector projects which have included WASH facilities as part of infrastructure
support and ensuring WASH access as part of holistic learning in schools include the Nepal Education
Sector Development Program (Box 4) and the Bangladesh Supporting Primary Education Development
Program (Box 5).
Sector Commit
ment
year
Project No. DMC Project name Total
ADB Loan
& Grant
Amount
Education 2008 39254-022 MON Mongolia Education Sector Reform Project 10.00
Education 2006 35174-013 NEP Education Sector Development Program 30.00
Education 2019 45089-004 PHI Secondary Education Support Program 300.00
Education 2019 49122-004 VIE Skills and Knowledge for Inclusive Economic
Growth Project
75.00
Education 2018 50192-002 BAN Supporting Fourth Primary Education Development
Program
500.00
Education 2013 44213-016 BAN Secondary Education Sector Investment Program -
Tranche 1
90.00
Box 4. Nepal Education Sector Development Program
This project had 3 Phases of investments to support Nepal’s national Education For All (EFA) program.
At the end of the program an evaluation was completed by Internal Evaluation Department (ADB) with
a report capturing lessons. A World Bank-funded endline survey (in schools and households) showed
that the high targets set at the outset of the project were not fully achieved (Completion Report): the
safe drinking water target was 90% from a baseline of 59.4%, but by end of project (2009) was partially
achieved at 71.1; the target for percentage of schools with girls’ toilets was 80%, but only achieved
54.1% (from a baseline of 37.5%). The lack of performance against these and other measures is
attributed to overly ambitious targets set in the design and monitoring framework (DMF) which were
never corrected during the implementation, partly based on government optimism following the end
of the civil war. Whilst the review said the overall design was theoretically sound, it assumed
decentralized service delivery but did not include design of a sound accountability mechanism, or build
local capacity for monitoring and funding. This is an interesting project because it demonstrates:
- That where a project has clear WASH schools focus and good intent, achievable or flexible
targets should be included for gender separated toilets;
- Other partners (World Bank) contributed resources for the project endline survey. Although
there may be good reasons for this arrangement, it may point to an issue raised during
interviews that there are rarely sufficient resources for thorough baseline and endline surveys
19 WASH + H Consultancy Final Report
4.3 Health Aligning with ADB’s Health Operational Plan, types of health sector operations mentioned in interviews
include: health infrastructure (building HCFs and hospitals); health governance (supporting health
systems); and health financing (via policy loans and results-based loans). Trends in the health sector
noted during interviews included a shift away from just thinking about infrastructure to considering
universal healthcare and the quality of primary health care. The Health Sector Group (HSG) noted that in
the past there has been a focus on infrastructure delivery with the result being limited responsibility
taken for outcomes and impacts beyond building hospitals. They noted that this view is changing and
that more consideration is given to the broader universal healthcare system.
In conjunction with a trend towards universal healthcare is a move towards financial protection and
ensuring accessibility and affordability of health services to all, especially the poor and vulnerable.
ADB has a number of long-term health partnerships with DMCs. Those noted during interviews were
with China, Mongolia (>25 years engagement, 6 health sector projects) and Bangladesh (> 25 years
engagement) and cover support areas ranging from policy assistance through to operations and
management of infectious diseases and health hazards. The SDCC health section which provides
knowledge and sector support to operations has not had the same longevity: after being disbanded for
some years it was reformed in 2016. This means the SDCC section has not had continuity of interaction
with projects such as the long-term sector support projects which may benefit sector learning and
knowledge sharing across the Bank.
The health sector expressed that WASH, as an explicit area of work, is relatively limited in the health
pipeline. The Southeast Asia Human Social Development Division (SEHS) said that hospitals usually have
good guidelines and integrated policies between WASH and health for hospital settings. The Health
Sector Group noted that projects follow government standards, and it is assumed that these are
comprehensive enough to include WASH. The extent to which this assumption is ever tested was not
clear.
Box 5. Bangladesh Supporting Fourth Primary Education Development Program
Significant WASH facility improvements make up part of this large education sector strengthening
program as part of "equitable access and participation" outputs and activities. The project has a target
of building an additional 43,500 gender-segregated WASH blocks, 11,250 safe drinking water sources,
and 30,000 classrooms completed according to the government’s Infrastructure Planning Guideline
and meeting the standards of the Bangladesh National Building Code. Aside from the Government of
Bangladesh, project partners include EU, UNICEF, World Bank as well as ADB in a pooled fund ($15bn)
through Sovereign Results Based Lending (Concessional Loan). This is an interesting project because it
demonstrates large scale WASH infrastructure developed through education sector investments.
20 WASH + H Consultancy Final Report
Staff from human and social development divisions (mostly working in health) commented on work
happening in HCFs, including any WASH-related activities. A few urban and water staff expressed a
desire to work more in HCFs, but noted they are not actively working with the health division currently.
The COVID-19 pandemic is placing enormous pressures on healthcare services across the region. Aside
from the immediate response aspects (which are addressed in a separate report and summarized in
section X), the COVID-19 pandemic is giving the health section in ADB a boost in some regions, such as in
Central West, where previously ADB did not have a relationship with all countries’ Ministries of Health,
but now they do. In Uzbekistan, there were existing health projects already in place addressing non-
communicable diseases, maternal health and construction of health facilities, and provision of
equipment in tertiary and secondary care facilities.
COVID-19 is forcing what are primarily healthcare delivery projects to consider WASH issues more. For
example, a number of ADB staff (from SEHS and PAHS) mentioned the need to better manage and have
stricter controls for human and solid waste in clinical settings, all of which points to the need for safely
managed sanitation.
Health projects mentioned during interviews as having WASH components are included in Table 5.
Table 5. Health projects mentioned during interviews as having aspects of WASH+H
Commitment
year
Project No. DMC Project name Total
ADB Loan
& Grant
Amount
2020 54124-001 REG Addressing Health Threats in Central Asia Regional Economic
Cooperation Countries and the Caucasus
3.50
2018 51010-002 TAJ Maternal and Child Health Integrated Care Project 32.00
2019 49173-004 MON Improving Access to Health Services for Disadvantaged Groups
Investment Program - Tranche 1
76.14
2020 54077-001 PRC COVID-19 Emergency Response Project 18.60
2012 42177-013 BAN Urban Primary Health Care Services Delivery Project 70.4
2018 42177-024 BAN Urban Primary Health Care Services Delivery Project - Additional
Financing
110.00

21 WASH + H Consultancy Final Report
The Bangladesh projects are particularly noteworthy for their focus on HyBC as well as having climate
change resilience components.
4.4 Environment, Agriculture and Natural Resources Interviews with three Agriculture and Natural Resources (ANR) regional divisions opened the discussion of possible intersection of WASH+H with agriculture, irrigation, agribusiness, river management and other ANR sub-sectors. One interviewee’s observation was that, whereas in the past rural projects would have typically had rural WASH components, this has not been so evident over the last ten years. The Southeast Asia Environment, Natural Resources and Agriculture (SAER) division indicated that they aim to fund at least one multi-sectoral ANR and WASH project each year. An example of this was developing irrigation systems that also provide drinking water to surrounding communities.
Box 6. Bangladesh Urban Primary Health Care Services Delivery Project: The project scope
encompasses not only primary health care services but also community HyBC programs. The core
output areas are: 1) Strengthening institutional governance and local government capacity to deliver
urban primary health care services sustainably; 2) Accessibility, quality, and utilization of urban primary
health care services (with a focus on the poor, women, and children) improved through public–private
partnership; and 3) Effective support for decentralized project management provided. The project has
multiple loans and grants working in parallel, with financing from Urban Climate Change Resilience
Trust Fund (with BMGF support), Government of Sweden and ADB in partnership with Government of
Bangladesh.
At the institutional level the project is supporting city and municipal health departments to develop
organograms and reorganization plans and integrate with other determinants of health and related
climate-sensitive subsectors (e.g., water, sanitation, and waste management) in a holistic manner to
improve public health. HyBC campaigns will include multimodal BCC campaigns in communities, and
the RRP indicated that HyBC communication and marketing programs will be aligned with an updated
BCC strategy with “an innovative, interactive, multi-platform campaign". This will include television,
radio, newspaper, mobile, social media, website, and interpersonal communication through door-to-
door, clinic, community theater, and community events.
The project is building “green clinics” which expand on previous efforts to include climate change
mitigation and adaptation measures such as (i) conducting climate risk and vulnerability assessments;
(ii) adopting climate-resilient infrastructure (solar panels, rain -water harvesting systems, and flood
protection drain systems); (iii) training on medical waste management; and (iv) building capacity on
climate change resilience (water and electricity conservation, disaster and emergency response, disease
surveillance, and outbreak response). This is project is of interest because it demonstrates:
- The ability of targeted grants and Trust Funds to foster and pilot more complex, evidence-
based and innovative project designs; and
- Climate change resilient ‘green clinics’ which integrate WASH, energy and risk considerations
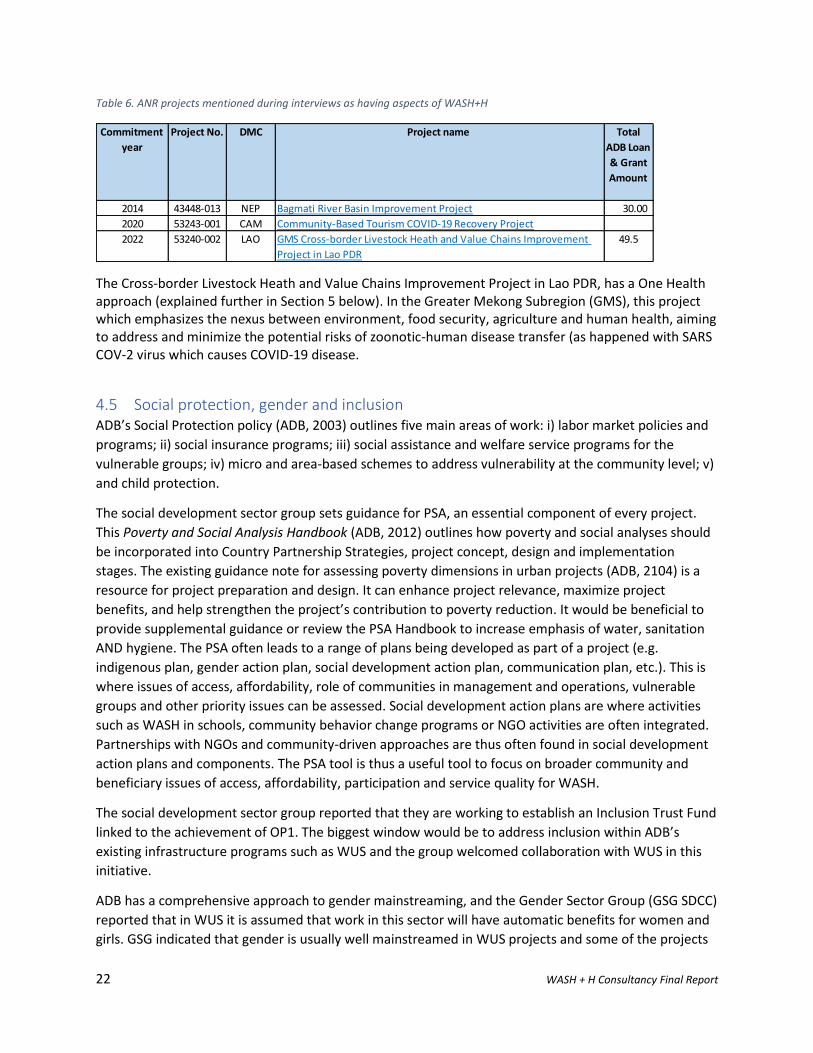
22 WASH + H Consultancy Final Report
Table 6. ANR projects mentioned during interviews as having aspects of WASH+H
The Cross-border Livestock Heath and Value Chains Improvement Project in Lao PDR, has a One Health approach (explained further in Section 5 below). In the Greater Mekong Subregion (GMS), this project which emphasizes the nexus between environment, food security, agriculture and human health, aiming to address and minimize the potential risks of zoonotic-human disease transfer (as happened with SARS COV-2 virus which causes COVID-19 disease.
4.5 Social protection, gender and inclusion ADB’s Social Protection policy (ADB, 2003) outlines five main areas of work: i) labor market policies and
programs; ii) social insurance programs; iii) social assistance and welfare service programs for the
vulnerable groups; iv) micro and area-based schemes to address vulnerability at the community level; v)
and child protection.
The social development sector group sets guidance for PSA, an essential component of every project.
This Poverty and Social Analysis Handbook (ADB, 2012) outlines how poverty and social analyses should
be incorporated into Country Partnership Strategies, project concept, design and implementation
stages. The existing guidance note for assessing poverty dimensions in urban projects (ADB, 2104) is a
resource for project preparation and design. It can enhance project relevance, maximize project
benefits, and help strengthen the project’s contribution to poverty reduction. It would be beneficial to
provide supplemental guidance or review the PSA Handbook to increase emphasis of water, sanitation
AND hygiene. The PSA often leads to a range of plans being developed as part of a project (e.g.
indigenous plan, gender action plan, social development action plan, communication plan, etc.). This is
where issues of access, affordability, role of communities in management and operations, vulnerable
groups and other priority issues can be assessed. Social development action plans are where activities
such as WASH in schools, community behavior change programs or NGO activities are often integrated.
Partnerships with NGOs and community-driven approaches are thus often found in social development
action plans and components. The PSA tool is thus a useful tool to focus on broader community and
beneficiary issues of access, affordability, participation and service quality for WASH.
The social development sector group reported that they are working to establish an Inclusion Trust Fund
linked to the achievement of OP1. The biggest window would be to address inclusion within ADB’s
existing infrastructure programs such as WUS and the group welcomed collaboration with WUS in this
initiative.
ADB has a comprehensive approach to gender mainstreaming, and the Gender Sector Group (GSG SDCC)
reported that in WUS it is assumed that work in this sector will have automatic benefits for women and
girls. GSG indicated that gender is usually well mainstreamed in WUS projects and some of the projects
Commitment
year
Project No. DMC Project name Total
ADB Loan
& Grant
Amount
2014 43448-013 NEP Bagmati River Basin Improvement Project 30.00
2020 53243-001 CAM Community-Based Tourism COVID-19 Recovery Project
2022 53240-002 LAO GMS Cross-border Livestock Heath and Value Chains Improvement
Project in Lao PDR
49.5

23 WASH + H Consultancy Final Report
reviewed (Pakistan KPCIP and Nepal Urban Water Supply and Sanitation (Sector) Project) have the
highest possible gender rating. Despite these positive reviews, some areas for improvement, knowledge
gathering and innovation were noted. This included the need to:
- Ensure that increasing women’s responsibilities in WASH-related activities does not add to their
unpaid burden of work. For example, it is assumed in some projects that women will voluntarily
assume roles educating children, raising awareness or being part of decision-making bodies in
the community as these have been their traditional roles. Whilst this may be well intentioned it
may in fact have unintended negative consequences.
- Assess the extent to which WASH interventions are assisting gender disparity, and better
understanding if and how improved services are supporting women to allocate time to more
productive activities. There is an opportunity for GSG and WSG to work together to gather more
evidence on this issue and produce a joint study. Such a study would have benefits for
quantifying and qualifying the value of WASH for OP2.
- Strengthen the use of gender inclusive language in WASH messaging. There is the potential for
HyBC messaging to reinforce existing gender norms, and GSG sees potential to ensure messages
are more consistent with respect to gender as well as being appropriately tailored to the cultural
context.
The COVID-19 pandemic has made pre-existing gender equality issues more pronounced, and projects
are working to understand and address rapidly changing situations and ensure women and girls are
supported by strong health support programs. In addition, GSG is focused on: the redistributive care
economy; women’s unpaid care burden, particularly during COVID-19; and women’s leadership and
employment opportunities in non-traditional sectors.
4.6 Operations
4.6.1 Enablers and entry points Integration between WSS and hygiene is not strongly emphasized by ADB policy and strategy
documents. Where this link has been made strongly in operations, interviewees said that some
individual ADB Project Officers have a key role in pushing certain agendas, including hygiene behavior
change or other ‘soft’ components. DMC enabling environments also play a role: for example, South
Asian countries like India, Pakistan and Nepal have strong national WASH campaigns as well as high
profile champions.
Country Partnership Strategies, safeguards policy and PSA processes are key entry points to influence
WASH+H in the pipeline. One interviewee indicated that the safeguards policy is too weighted to ‘green’
environment issues (such as biodiversity protection) and would be more balanced with more emphasis
on ‘brown’ or pollution issues arguing that increased focus on health and safety would identify issues
relating to poorly managed sanitation. Whilst the safeguards policy focuses primarily on issues of
resettlement and issues faced by the immediately affected population and indigenous people, the PSA
has a wider mandate to consider broader community and beneficiary concerns and issues. The PSA is
the most useful tool to consider all possible beneficiaries of a project in terms of WASH access, quality
and affordability and all of the potential equity issues attached those.
There is a desire to think about WASH+H more deeply amongst ADB staff. Staff don’t want to treat the ‘software’ or HyBC components of projects as a ‘check box’ activity, but want to more deeply
24 WASH + H Consultancy Final Report
understand these issues, efficacious approaches and the potential and challenges to enhancing investments.
4.6.2 Barriers Interviewees mentioned a range of barriers to successful WASH+H integration in operations, including:
- Delivery of projects through Project Management Offices (PMOs) has limitations in terms of
range of skills available, including leadership skills and expanding beyond normal ministerial
boundaries. For example, a WASH project may be led by Executing Agency’s (EA) Water Division
and not properly resource sanitation and hygiene components.
- Insufficient use of data and evidence in operations as well as ability to access technical
expertise across divisions within ADB results in less effective projects.
- Financing arrangements and procurement constraints make engaging NGOs more difficult,
which is problematic where NGOs might be the best partners for HyBC components.
- Operational units face numerous challenges in implementation such as governance, human
resources, lack of skills, and WASH is seen as only one of many challenging aspects.
- While the ADB Strategy 2030 encourages multi-sectoral approaches, institutional arrangements
for personal incentives and recognition processes within ADB do not encourage multi-sectoral
efforts. Staff reported that incentives rather encourage quick processing and large loans with
uncomplicated designs.
- Working across sectors where it is necessary to facilitate cross-ministerial engagement slows
down processing and can be very time-consuming if they are siloed ministries. Cross-ministerial
coordination is difficult and requires a higher level of government to set priorities for
integration, especially if aiming to have cross-ministerial collaboration and integrated projects
(e.g. between Ministries of Public Works, Health, Local Government, etc) (SEUW).
- Whilst both health and water sectors are supportive of integration in theory, implementation
is complex as ministries are siloed.
- A lack of tools and resources was mentioned, particularly in relation to addressing COVID-19
related WASH and HyBC program design. (SAUW)
4.6.3 Financing Interviewees mentioned a range number of issues to do with financing WASH+H integration in
operations.
Where water and sanitation infrastructure projects include hygiene and institutional strengthening,
they are only a small component of projects. Cost elements of these ‘software’ components usually
include people’s time (consultant fees, NGOs, etc) and do not include more costly construction or
equipment costs. Estimates of percentages of ‘software’ components in WSS projects included:
- Less than 1% of USD100 million loans in PRC going to non-structural aspects (e.g. awareness
campaigns, capacity building) (EASS).
- Solomon Islands Urban Water Supply and Sanitation Sector Project is a USD90 million project and USD2 million of that is for WASH. PAUW commented this is a small but still significant component.
- Approximately 3% of the water supply project in Kiribati (South Tarawa Water Supply Project, worth USD62 million) is going to non-structural aspects (e.g. hygiene and community outreach) (PAUW).

25 WASH + H Consultancy Final Report
SAER is consciously increasing multi-sectoral projects that include WASH in their pipeline as a way to
find maximum benefit to communities from water resource management projects. SAER plans to
increase the amount for cross-sectoral projects and are at least one integrated project per year. For
example, the Bagmati River protection project (Nepal) includes construction of wastewater treatment
plant and sewerage system. Similarly, where hydropower dams are being planned SEER will look for
opportunities provide for community water supply needs.
Climate change focused trust funds have opened up opportunities for innovative WASH+H
interventions across a few regions. In the Pacific, GEF, Internal Trust Funds, the Green Global Fund and
others are available for climate change projects. PAUW commented that it’s possible to include
additionalities such as water in climate-related projects. The Urban Climate Change Resilience Trust
Fund (multi-donor trust fund) project in Bangladesh is an example of a Trust Fund project that builds on
a larger health sector program with innovative models that build climate change resilience through
innovative clinic design with WASH provision.
It is difficult to quantify the proportion of health and education sector projects going to WASH-related
infrastructure. WASH facilities are folded into broader infrastructure investments such as HCFs, schools,
training centers, etc. However, education projects usually set targets and monitor numbers of latrines
built for girls and boys as part of their project results monitoring framework. WASH facilities are
significant components of some education projects, especially where they are long-term and sector-
wide programs. ESG commented that WASH components in education sector developments might be
able to be estimated from national programs with UNICEF support.
It is common for grants to be used for pilot and demonstration projects, as well as for the ‘software’
components which DMCs are less willing to borrow against. This model is widespread across all sectors.
Grants are also used to demonstrate new and innovative approaches. Successful pilots in grant
projects have been demonstrated as convincing governments to include these components in loans.
Grants can leverage more government finance for scaling up when they demonstrate and prove a
particular approach. South Asian colleagues reported that this model has been successful in
demonstrating the effectiveness of fecal sludge treatment plants in Rajastan, India. After grant projects
supporting FS treatment plans the government agreed to include additional inclusive sanitation
investments as a loan.
The Pacific has unique financing issues, constraints and opportunities. Most PICs only receive grant
funding which limits the type and scale of interventions. In addition, Pacific governments are aware that
many donors are keen to finance WASH programs, so DMCs are not keen to put their own money into
WASH. Even in PNG which has some of the worst WASH statistics in the world, it is still struggling to get
government investment. Additionally, there is very limited investment in the health sector in the Pacific
(PASP).
The consistent and persistent underfunding from national budgets for WASH in the Pacific means that
more work is needed to increase importance of WASH in national budgets as Ministries of Finance do
not yet understand broader economic benefits.
There was one view from the Pacific (PARD) that the finance available to run and scale ‘soft’/ hygiene
behaviour change projects is insufficient. The view was that resources are insufficient to do the scale of
hygiene awareness operations they would like to see.
26 WASH + H Consultancy Final Report
The competition for Bank grant funds is too high and some regions do not have sufficient access to
grant funds. The Pacific in particular mentioned a lack of opportunities to access grant funds or find
support for WASH initiatives. The Central West region also has limited access to grant funds due to their
development status.
Water utilities are a key client for ADB investments in urban water supply and sanitation. Interviewees
consistently reported that utilities only want to borrow where they can see a direct return on
investment. In the Pacific, where the most utility-led WASH components were reported, PAWD and
PASP both reported that utilities will only borrow for loans that are 100% commercially interesting.
Some perceptions are that utilities do not take a holistic view and do not, for example, take into
consideration the possible financial impact of poor customer health on their ability to pay. Only grants
have been used on utility-led WASH components.
Very few interviewees mentioned results-based financing. These kinds of financing mechanisms
(program clusters, multi-tranche financing facility, and results-based lending) and performance-based
disbursements were identified as important to enhancing sustainability of projects by IED’s WSS
evaluation (ADB, 2015).
When discussing COVID-19 Rapid Response financing, the likely increased interest in financing services
from utilities was mentioned (PARD). Budgetary support for COVID-19 provided by ADB broadly
supports a broad-spectrum of DMC health, economic, social protection and other responses. The
structure of these COVID-19 related loans does not have an obvious mechanism for ADB to track
whether funding is used on WASH and hygiene. Such monitoring might be useful if ADB wants to track
their impact in WASH related COVID-19 responses. Nonetheless some sections (SAHS) said they expect
that all country recovery packages included some WASH components.
4.7 Capacities and knowledge Internal ADB and external DMC, client and partner capacities affect how and how well WASH+H
integration is understood and included in operations.
ADB staff includes a large range of professionals from financiers, economics, engineers, project
managers through to thematic specialists (health, education, water, water resources, urban
development, social development, safeguards, gender, irrigation, agriculture, etc). A number of ADB
staff reflected during interviews that they are known as the infrastructure bank. This acknowledges the
internal skills in managing the complex processes of negotiating grants and loans and procurement for
large-scale infrastructure investments.
Whilst there are many strong skillsets within the Bank, HyBC skills appear lacking and there appear to be
no HyBC specialists, social marketing specialists or psychologists on staff. CWUW commented that DMCs
don’t think of ADB when seeking support for hygiene initiatives. ADB internal capacity in hygiene
behavior change is limited compared to water and sanitation services. To date ADB has partnered (see
partnering section) to include HyBC skills on projects or included HyBC components in TORs of
consultants. In projects reviewed HyBC was often included in the gender component of the project and
within the TORs of gender specialists.
HSG interviewees argued that there is a need for capacity building for ADB’s staff to shift from pure
infrastructure provision outlook (e.g. health care facilities) to understanding universal health care.
27 WASH + H Consultancy Final Report
Although COVID-19 pandemic has increased focus on hygiene, the full benefits of WSS infrastructure
may not always be maximized as how beneficiaries use services is not explicitly or implicitly internalized
by all project staff.
It would be valuable for ADB to undertake a survey of skills required across institution and prepare skills
development plan. If ADB choses to build in-house capacity in HyBC then an on-going program to build
knowledge and skills would be useful, as is further described in the Recommendations section.
4.8 WASH+H reflected Country Partnership Strategies The level of engagement in integration is dependent on maturity, size of ADB engagement as well as
policy, strategy and cross-ministerial engagement. Country Partnership Strategies (CPSs) were
mentioned as enablers of WASH+H integration efforts as they set the framework for country level
investment pipelines and Country Operations Business Plans.
A brief analysis of the 26 CPSs (one for each DMC except for 11 Pacific DMCs which are included in one CPS) showed that all mentioned water supply and education. Sanitation was mentioned as an area of ADB investment by all DMCs except three in Central West region (Afghanistan, Azerbaijan, Turkmenistan) and health by all except three countries (Azerbaijan, Cambodia, Georgia). Hygiene was not explicitly mentioned in CPSs except for Papua New Guinea’s, which was published this post COVID-19 pandemic outbreak. In PNG’s case hygiene is mentioned in the context of the National Water, Sanitation and Hygiene policy (2015 – 2030), with the CPS stating that ADB will align support implementation of this policy. CPSs often mention ADB’s support to national policy implementation, but rarely explicitly mention water sector policies in the way PNG has. PNG’s CPS also states that ADB will provide capacity building support to agencies involved in WASH as part of responses to disease outbreaks such as the COVID-19 pandemic. Indonesia’s CPS was also published since the pandemic started, but does not mention hygiene. This coarse analysis shows that sanitation has been successfully prioritized in the majority ADB CPSs, which has likely happened over the last 10-15 years in conjunction with the increasing profile of sanitation in DMCs and global initiatives and commitments. As part of CPS country context analysis economic, poverty and environment indicators and progress over recent years are included. For poverty these usually include:
- Life expectancy at birth (years) - Adult literacy (%) - Primary school gross enrollment (%) - Child malnutrition (% below 5 years old) - Population below poverty line (%) - Population with access to safe water (%) - Population with access to basic sanitation (%)
In future it would be beneficial to add the indicator, population with access to handwashing facility with soap (%). The benefits of handwashing with soap to education, health, broader economic development and poverty reduction are expanded on in Section 0. A deeper analysis of a handful of CPSs shows that the extent to which WASH+H is integrated varies, and is dependent on both the maturity of the sectors and extent of ADB engagement. In Bangladesh for example, ADB co-chairs the Local Consultative Group energy and education working groups so has a central role in inter-ministerial engagement. The Indonesia CPS shows that water investments cut across
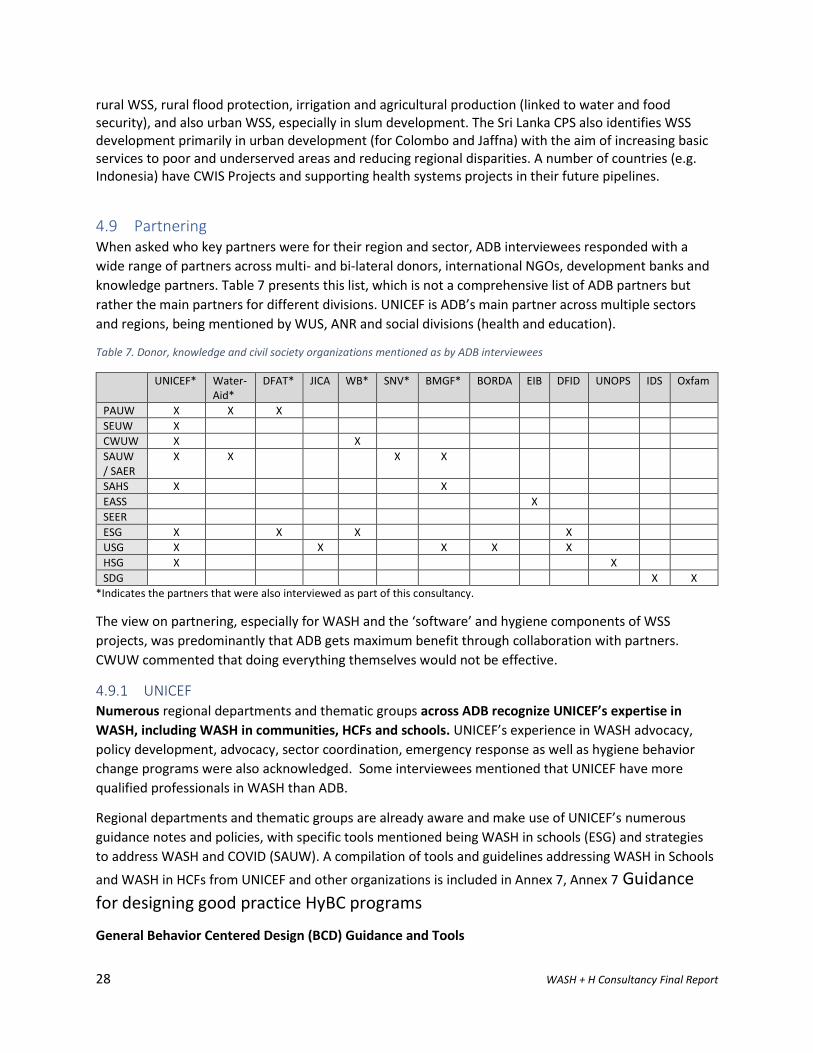
28 WASH + H Consultancy Final Report
rural WSS, rural flood protection, irrigation and agricultural production (linked to water and food security), and also urban WSS, especially in slum development. The Sri Lanka CPS also identifies WSS development primarily in urban development (for Colombo and Jaffna) with the aim of increasing basic services to poor and underserved areas and reducing regional disparities. A number of countries (e.g. Indonesia) have CWIS Projects and supporting health systems projects in their future pipelines.
4.9 Partnering When asked who key partners were for their region and sector, ADB interviewees responded with a
wide range of partners across multi- and bi-lateral donors, international NGOs, development banks and
knowledge partners. Table 7 presents this list, which is not a comprehensive list of ADB partners but
rather the main partners for different divisions. UNICEF is ADB’s main partner across multiple sectors
and regions, being mentioned by WUS, ANR and social divisions (health and education).
Table 7. Donor, knowledge and civil society organizations mentioned as by ADB interviewees
UNICEF* Water-Aid*
DFAT* JICA WB* SNV* BMGF* BORDA EIB DFID UNOPS IDS Oxfam
PAUW X X X
SEUW X
CWUW X X
SAUW / SAER
X X X X
SAHS X X
EASS X
SEER
ESG X X X X
USG X X X X X
HSG X X
SDG X X
*Indicates the partners that were also interviewed as part of this consultancy.
The view on partnering, especially for WASH and the ‘software’ and hygiene components of WSS
projects, was predominantly that ADB gets maximum benefit through collaboration with partners.
CWUW commented that doing everything themselves would not be effective.
4.9.1 UNICEF Numerous regional departments and thematic groups across ADB recognize UNICEF’s expertise in
WASH, including WASH in communities, HCFs and schools. UNICEF’s experience in WASH advocacy,
policy development, advocacy, sector coordination, emergency response as well as hygiene behavior
change programs were also acknowledged. Some interviewees mentioned that UNICEF have more
qualified professionals in WASH than ADB.
Regional departments and thematic groups are already aware and make use of UNICEF’s numerous
guidance notes and policies, with specific tools mentioned being WASH in schools (ESG) and strategies
to address WASH and COVID (SAUW). A compilation of tools and guidelines addressing WASH in Schools
and WASH in HCFs from UNICEF and other organizations is included in Annex 7, Annex 7 Guidance
for designing good practice HyBC programs
General Behavior Centered Design (BCD) Guidance and Tools
29 WASH + H Consultancy Final Report
https://www.lshtm.ac.uk/research/centres-projects-groups/bcd#resources
LSHTM has produced a range of resources on BCD and its practical application. These include papers,
manuals for practitioners and for researchers, formative research protocols and checklists. There is also
a series of online webinars available for free. The webinars cover BCD theory and process for designing
behavior change programs, with a focus on hygiene, and some general background on behavior change.
Behavior Centered Design (BCD) Guidance and Tools during COVID-19
https://gh.bmj.com/content/bmjgh/5/8/e002780.full.pdf
Designing effective hand hygiene campaigns during COVID-19 pandemic is possible and requires a
number of stages in addition to standard BCD. LSHTM academics led by the late Prof Val Curtis published
a guidance paper outlining ten necessary steps to developing a national communications strategy for
COVID-19 prevention :
i. Set up a task force and appoint a national focal person.
ii. Mobilize resources and involve the private sector.
iii. Define exactly which behaviors need to change and by whom.
iv. Review what is already being done internationally and locally.
v. Review what is known about the drivers of these behaviors and rapidly fill in gaps in knowledge.
vi. Produce a creative brief and theory of change.
vii. Develop a unifying national brand.
viii. Develop executions employing the most relevant channels for the target audiences.
ix. Rapidly pretest and continually revise content.
x. Deliver, monitor, evaluate and share lessons.
Promotional Approaches to WASH Behavior Change
https://www.3ieimpact.org/sites/default/files/2019-04/srs-handwash.pdf
International Initiative for Impact Evaluation (3iE) produced a systematic review of the effectiveness of
WASH program design for behavior change. It shows that community-based activities and social
marketing are far more effective than messaging in resulting adherence to desired behaviors.
Handwashing Promotion: Monitoring and Evaluation Module
https://www.unicef.org/wash/files/M_and_E_Toolkit_.pdf
UNICEF has published this monitor and evaluation (M&E) guide which identifies the steps and processes
required to monitor and evaluate handwashing promotion programs irrelevant of implementation
design. It outlines appropriate indicators and sample questions for handwashing advocacy, education
and HyBC. Usefully it outlines the caveats and limitations that should be placed on measuring health
impact assessment.
Training programs available on WASH Behavior Change
International WaterCentre WASH and Behavior Change online training course:
http://www.watercentre.org/courses/wash-and-behaviour-change/
30 WASH + H Consultancy Final Report
Annex 8. Examples of Improving HyBC in ADB COVID-19 Response projects
A number of ADB projects in design phases are pivoting to respond to the COVID-19 pandemic. The
following provide examples of hygiene components and related consultant terms of reference (TOR) if
available. Only components relevant to HyBC are included (see project documents for other
information).
1) Lao PDR: Urban Environment Improvement Investment Program. Proposed Multi-tranche
Financing Facility and Administration of Loan and Grant (53203-001)
Output 1: Policy and regulatory environment improved
Output 2: Urban infrastructure improved
Output 3: Institutional effectiveness improved
Output 4: Women’s leadership and employment enhanced. The program will improve women’s
participation in MPWT employment and leadership roles through the following activities in the water
supply and sanitation sector: (i) a Technical and Vocational Education and Training certification program
for women at the community level, (ii) a higher education scholarship and internship program, (iii) a
leadership training program for female civil servants to achieve decision-making roles, (iv) a
communication and outreach campaign on employment opportunities for women, (v) investment in
handwashing and toilet facilities including menstrual equipment in schools and health centers,
accompanied by an awareness raising program for WASH, effective menstrual and personal hygiene
practices, including hygiene behaviors for post COVID-19, and (vi) a monitoring and evaluation system to
enhance women’s participation.
2) TA 8899-IND: Strengthening Capacity of the National Urban Health Mission
Actions: Intervention pilot will undertake a gap analysis of the prevailing COVID-19 situation; assess
access to general health (preventive and curative), laboratory and WASH services; study existing referral
linkages with higher level of care for COVID-19 as well as for non-COVID-19 emergency and chronic care
needs; efficacy of community level mechanisms, municipal initiatives on managing the outbreak (and its
effectiveness) and access to other essential non-health services (e.g. food security). These would feed
into development and implementation of a tailored, humane and a comprehensive containment
strategy for COVID-19 for the slum, including community and household level quarantine and isolation
strategies, and community led provision and monitoring of services. Further, the pilot will look beyond
the current COVID-19 crisis and from a systems outlook it will attempt to demonstrate solutions for
maintenance or resumption of general health services, propose community level structures for
improved response in preventing and managing future outbreaks, and propose models of leveraging
local health systems (public as well as private) for meeting holistic health needs and demonstrate
assured referral linkages to higher levels of care. Similarly, coordination mechanisms envisaged at slum,
ward and municipal levels to ensure access to essential services will be engaged and models on assured
access to critical WASH and other public services during mass health emergencies will be demonstrated.
The consultant team members hired to undertake this work will include with example TOR include:
31 WASH + H Consultancy Final Report
i. Team Leader The team leader will, be responsible for guiding the collective work of the
consulting team and for timely preparation and quality control of all reports submitted to ADB.
The consultant will work closely with the Ministry of Health and Family Welfare (MOHFW) and
selected states, agencies, resource centers, and other consultants fielded by ADB.
ii. Social Scientist/Program Manager The program manager will, be responsible for overseeing the
implementation of intervention pilot and day-to-day management of the field team, guiding the
collective work of the consulting team for timely preparation and quality control of all reports
submitted to ADB. The consultant will work closely with the Ministry of Health and Family
Welfare (MOHFW) and selected states, agencies, resource centers, and other consultants
fielded by ADB.
iii. Public Health Expert The Public Health Expert will be responsible for on-ground
implementation of intervention pilot, ensuring execution of baseline and endline assessment as
per design, lead capacity building of pilot staff and partners, engage community leaders and
platforms, lead interaction with various local stakeholders to ensure support for intervention
pilot, ensure timely completion of pilot reports and escalate relevant issues and concerns to
Program Manager for quick redressal. The consultant will work closely with selected
municipalities, agencies, resource centers, and other consultants fielded by ADB.
32 WASH + H Consultancy Final Report
Annex 9 and Annex 10. SAUW also noted that UNICEF has many decades working with local NGOs on
ground to implement projects in some countries.
ADB’s role and comparative advantage vis-à-vis other DPs is primarily in infrastructure, and the links
between infrastructure and community development and has access to high level policy makers and
Ministries of Finance. UNICEF does not have access to resources for large-scale infrastructure as ADB
does. Interviewees argued that ADB has its own strengths.
UNICEF work is seen as complementing ADB initiatives in the education sector. SEHS noted UNICEF as
one of the best partners when operating with schools. UNICEF has health promotion and pilot activities,
awareness raising with parents and communities.
UNICEF’s role successfully coordinating emergency responses, especially for COVID-19 was noted. For
example, in Nepal. SAHS reported that UNICEF did a very good job coordinating the WASH sector
through a Sector Wide Approach which was especially important for managing Sars COVID-2 IPC in
quarantine camps for returning expatriate workers.
ADB either works with or alongside UNICEF, and the method of engagement varies from country to
country. In some countries ADB provides the loan and the government decides who to work with and
contracts UNICEF or an NGO. UNICEF has a Memorandum of Understanding (MOU) ADB, and DMCs,
which allow DMCs to accept grants and engage UNICEF directly (for emergency and other responses). An
example of this is vaccine procurement in Pacific. This same agreement also allowed for rapid
procurement of good and equipment as part of COVID-19 pandemic responses.
In the Southeast Asia region, ADB is in negotiations with UNICEF to develop a partnership to advocate
for HyBC and WASH+H in strategy, policy and budgets. The aim of this is to ensure focus on HyBC in new
projects which will be developed in the coming years, as well as longer-term mainstreaming of ‘WASH
Plus’ into projects and government policy.
4.10 Sustainability ADB staff raised sustainability concerns across different sectors, but this was mostly raised by WUS
and education divisions. Many divisions acknowledged the importance of systems strengthening, sector
reforms and building institutional capacity to improve overall sector performance as essential to
sustainability of investments. Only two staff (USG, CWUW) acknowledged the problems the Bank and
DMCs have ensuring sustainability of WSS and education infrastructure once it had been built, a
problem which is clearly evident in reviews of WUS projects undertaken by the Independent Evaluation
Department (IED).
IED reviews of urban WSS investments (2003-2016) found poor levels of financial and service provision
sustainability of infrastructure investments, including for WASH in schools. Just over 50% (13/20) of
projects reviewed were found to be “less than likely sustainable or lower” (ADB, 2015). Reasons given
for this low rating by Project Officers ranged from financial issues (e.g. tariffs, nonrevenue water), loan
conditions (e.g. ambitious covenants and assurances) to capacity constraints of responsible institutions
as a necessary condition for sustainable WSS operations.
For sanitation, a further review (ADB, 2018) of success and failure factors in sanitation investments over
the same timeframe found that in the case of failures, ADB did not adequately adopt global best
33 WASH + H Consultancy Final Report
practices or was not able to fully implement some of its initiatives. Some of the same factors identified
in that review were noted again during interviews:
Success factors: Long-term relationships for policy dialogue; national campaigns for investment in
sanitation; and encouraging demonstration effects of pilot fecal sludge management at
municipality level for a wider effect.
Failure factors: No targets for the poor in inclusive planning; and not monitoring environment and
health impacts indicators.
The lack of pro-poor targeting further reduces the potential health benefits of infrastructure projects
because poverty is a correlated to poor health outcomes. In other words, the greatest gains in health
improvements can be gained by investing to improve WASH services of the poor and vulnerable and to
not do so reduces the potential health impacts.
A USG interviewee argued that institutional capacity is the most important project component, noting
that the competence of water and sanitation user committees, government agencies and management
committees as well as the systems, guidelines and operations they develop and manage are critical.
“[Our efforts] currently not sufficient to sustain quality and operations of our investments. O&M to
sustain services to citizens’ are a more critical part and there is not enough focus on this in project
loans.” Sustainability is not sufficiently considered at design phase of the project and only is considered
at the last minute when the project is completed. CWUW noted that systems strengthening can be
pursued through policy-based loans.
ADB has recognized the sustainability issue and set up a special internal group. The concept of
sustainability has been broadened and deepened so that it considers more than financial sustainability.
USG wants to set up projects on knowledge and sustainability improvements as there are limited ways
for ADB to engage infrastructure post-completion. One way the challenge has been addressed is
through have long-term O&M contracts for complex assets (like wastewater treatment plants) with 15-
year terms plus construction period, ensuring the EA earmarks expenditure for O&M.
The worsening economic impacts of the COVID-19 pandemic are having negative and worsening impacts
on utilities and the sustainability of the services they provide. A recent study showed that very few
countries in Asia are taking proactive steps to correct the operation of services of extend financial or
technical support to utilities. This lack of assistance will impact utilities’ short-term financial viability
(UNICEF, 2020). PARD reported that water utilities in the Pacific are being affected by increase in non-
revenue water, increases in illegal connections and income losses linked to customers’ reduced ability to
pay bills.
4.11 Support requests and knowledge gaps Support requests and knowledge gaps raised by ADB staff during KIIs are included here.
COVID-19 pandemic related
- How to improve COVID-19 pandemic responses, adapt and design effective programs. Topics
mentioned: hygiene and social behaviors within the family; continuity of education; distance
learning; TV and mass media campaigns; monitoring current and future status; preparedness for
reopening schools. (CWUW)
34 WASH + H Consultancy Final Report
- COVID-19 knowledge gaps, for example transmission risks from fecal matter and how to safely
handle feces, especially in clinical settings (PASD).
- Capture lessons on how to build health systems that address any future pandemics, but also
keep quality of health services and any diseases that address public health with HyBC and access
to better sanitation. (SESH)
- Many divisions are concerned about lack of WASH in schools being a problem for return to
school and IPC risk (EAER, ESG). Aside from WASH elements attention needs to be given to the
nuances of gender, disability and social inclusion in schools to ensure equitable education access
throughout return-to-school and pandemic economic impacts.
- Lack of sanitation in HCFs posing a high IPC risk is also a concern. (EAER, PEHS)
- Good guidance is needed for developing country contexts on what are adequate precautions to
prevent disease transmission where they do not have HW facilities. COVID has exacerbated and
hastened the need to address this existing issue to take that dialogue forward. (ESG)
- Social protection is challenging as people’s vulnerabilities and poverty profiles are changing
rapidly with COVID-19 impacts. There is a need for social assistance programs that are agile and
can adapt to needs of people affected by ongoing crises. (SESH)
Specific topics raised for additional knowledge support included:
- Tools, guidance documents and/or trainings on:
o WASH and Health with urban focus (HSG)
o Return on investment assessments of HyBC and WASH
- Impact stories or pilot project examples of WASH/health integration
- Examples of innovative project arrangements and modalities which include private sector
The WSG run Water and Health Advisory Team (WHAT) webinars were mentioned as valuable and
useful. Including presentations on the topics mentioned above would be useful to include in a WHAT
Learning Plan (see Section 8.3). The COVID-19 and WASH Rapid Assessment Report addresses some of
topics raised here, and a COVID-19 and WASH series would be a useful addition to a WHAT Learning
Plan.
5 Sector evidence for WASH+H The case for the public health benefits of WASH are well-documented and evidenced, with examples
reaching back to late 1800s. Rather than repeat this evidence base in this report, the latest evidence of
remaining global gaps and emerging health concerns which link to WASH are highlighted.
5.1 Health from WASH The global burden of disease from inadequate WASH was updated in 2019 (Prüss-Ustün, 2019) and can
be calculated for 16 health outcomes. Figure 3 lists those 16 health outcomes and the WASH exposure
pathway leading to the condition.
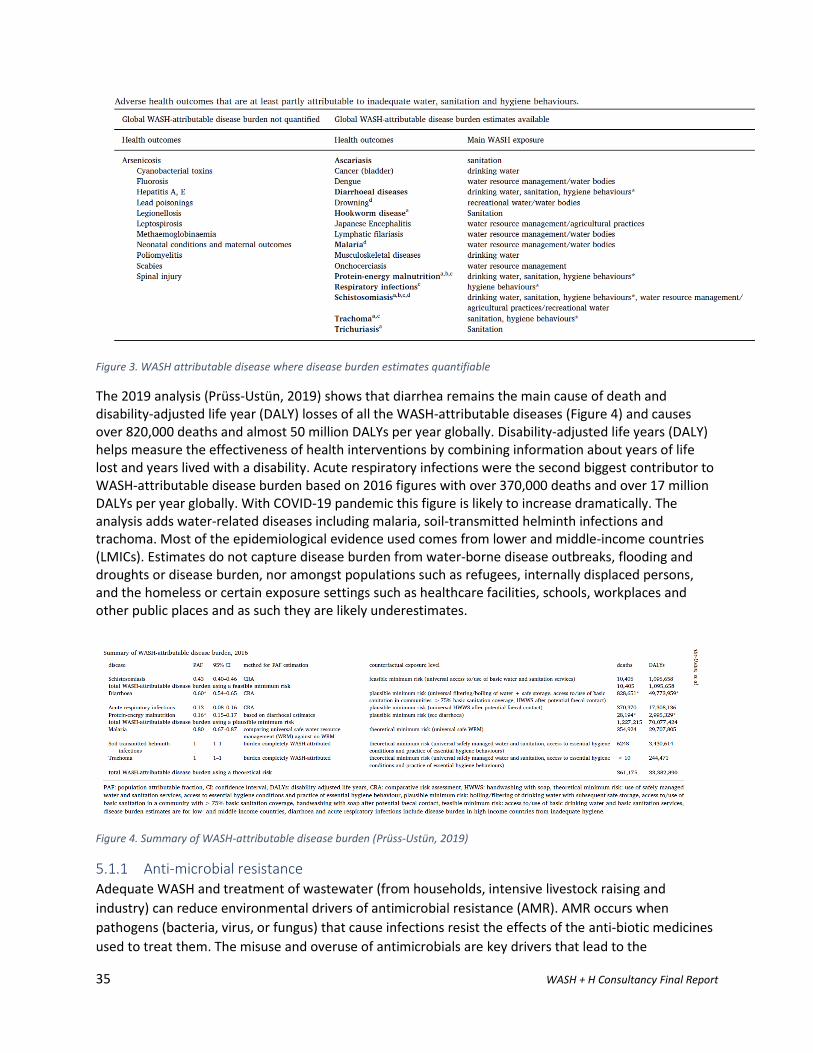
35 WASH + H Consultancy Final Report
Figure 3. WASH attributable disease where disease burden estimates quantifiable
The 2019 analysis (Prüss-Ustün, 2019) shows that diarrhea remains the main cause of death and disability-adjusted life year (DALY) losses of all the WASH-attributable diseases (Figure 4) and causes over 820,000 deaths and almost 50 million DALYs per year globally. Disability-adjusted life years (DALY) helps measure the effectiveness of health interventions by combining information about years of life lost and years lived with a disability. Acute respiratory infections were the second biggest contributor to WASH-attributable disease burden based on 2016 figures with over 370,000 deaths and over 17 million DALYs per year globally. With COVID-19 pandemic this figure is likely to increase dramatically. The analysis adds water-related diseases including malaria, soil-transmitted helminth infections and trachoma. Most of the epidemiological evidence used comes from lower and middle-income countries (LMICs). Estimates do not capture disease burden from water-borne disease outbreaks, flooding and droughts or disease burden, nor amongst populations such as refugees, internally displaced persons, and the homeless or certain exposure settings such as healthcare facilities, schools, workplaces and other public places and as such they are likely underestimates.
Figure 4. Summary of WASH-attributable disease burden (Prüss-Ustün, 2019)
5.1.1 Anti-microbial resistance Adequate WASH and treatment of wastewater (from households, intensive livestock raising and
industry) can reduce environmental drivers of antimicrobial resistance (AMR). AMR occurs when
pathogens (bacteria, virus, or fungus) that cause infections resist the effects of the anti-biotic medicines
used to treat them. The misuse and overuse of antimicrobials are key drivers that lead to the

36 WASH + H Consultancy Final Report
development of drug-resistant pathogens. A lack of clean water and sanitation and inadequate IPC
promotes the spread of microbes, including those resistant to antibiotics. WHO has declared that AMR is
one of the top 10 global public health threats facing humanity (WHO, 2020).
5.1.2 Nutrition and Stunting The link between undernutrition, failure to thrive and stunting with enteric diseases has been a major area of focus for WASH researchers and funders over the last decade. Off the back of evidence from India (Spears, 2013) three large-scale randomized control trials (RCTs) were undertaken in Kenya (WASH-Benefits), Bangladesh (WASH-Benefits) and Zimbabwe (SHINE). These tested the effect of targeted effect of basic WASH interventions on childhood stunting and childhood diarrhea. The results found no clear evidence that the specific interventions had any effect on childhood linear growth, and mixed effects on childhood diarrhea. However, a review of the results by leading academics and funders released a Consensus Paper stating that more comprehensive or ambitious WASH interventions may be needed to achieve a major impact on child health (Cumming, 2019 ). Current evidence recognizes poor sanitation is the second leading risk factor for stunting worldwide (WaterAid, 2020). The World Bank WASH Poverty Diagnostic Initiative7 demonstrates that WASH investments targeted at areas or groups whose risk of diarrhea and stunting is high are likely to accomplish more in improving overall human development outcomes than efforts to achieve universal coverage by reducing the WASH gaps between poor and rich, rural and urban. An effort to improve WASH, coordinated with other health interventions, can have effects greater than the sum of its parts. The Diagnostic approach uses a UNICEF conceptual framework as a guide, the analysis highlights the need to look across the determinants of poor health indicators, such as stunting, to understand the multidimensional deprivations of a child. UNICEF identifies four determinants of stunting: a lack of (i) food security, (ii) adequate personal care and feeding, (iii) a healthy environment (that is, WASH), and (iv) adequate health-care services. Stunting can be reduced to a greater degree when children are given simultaneous access to both adequate WASH and specific health services than when they gain access to only WASH or only health services.
5.1.3 Neglected Tropical Diseases WHO has established a list of 20 “official” neglected tropical diseases (NTDs): Buruli ulcer, Chagas
disease, cysticercosis, dengue, dracunculiasis, echinococcosis, endemic treponematoses, foodborne
trematode infections, human African trypanosomiasis, leishmaniasis, leprosy, lymphatic filariasis,
onchocerciasis, rabies, schistosomiasis, soil-transmitted helminthiases, trachoma, romoblastomycosis
and other deep mycoses, scabies and other ectoparasites and snakebite envenoming8. WASH has been
included as critical to disease eradication in the global NTD Roadmap (2021-2030, currently in
preparation) as NTDs are worst in communities that also lack WASH.
Other DPs have expanded the scope of the WASH+H concerns beyond water-borne diseases (i.e. those
that are transmitted by ingestion of contaminated water) to also account for other disease pathways
and human-environment interactions. From interviews with external organizations the following
priorities were noted for WASH+H integration:
- UNICEF’s priority is the elimination of open defecation (OD) and they have a 4 year target of 148
million less people practicing OD. This focus is due to the direct link between OD and health and
7 https://www.worldbank.org/en/topic/water/publication/wash-poverty-diagnostic 8 https://www.who.int/neglected_diseases/diseases/en/
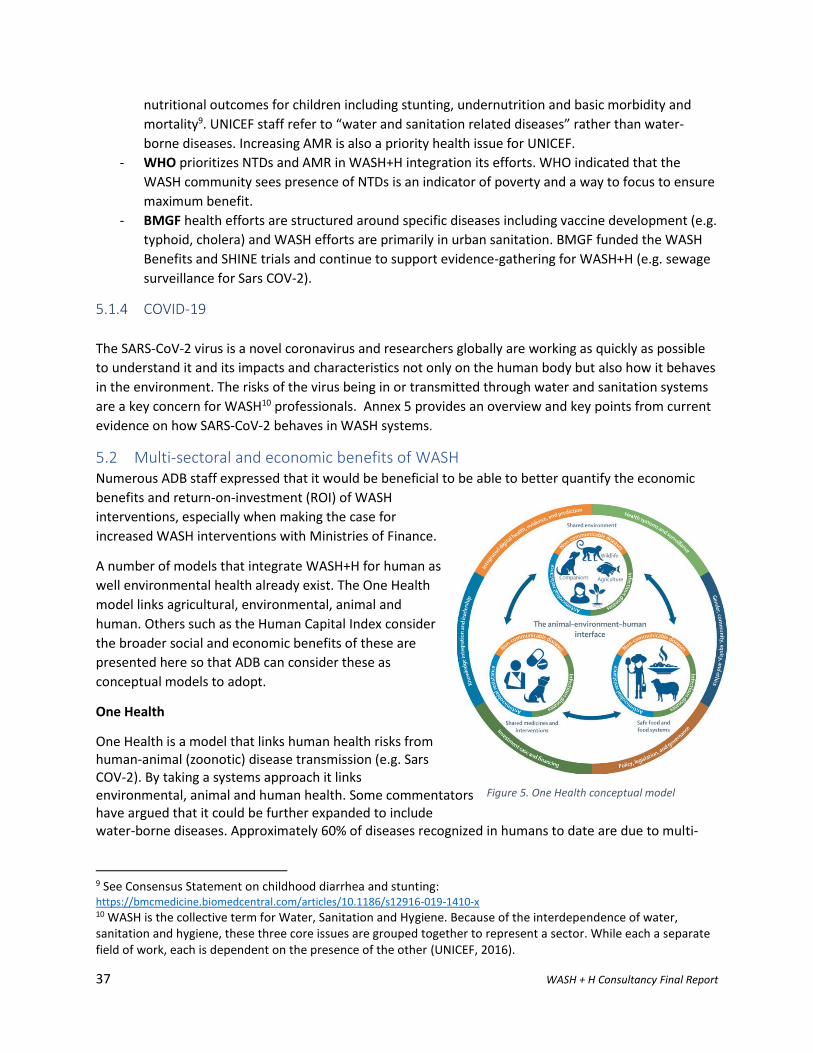
37 WASH + H Consultancy Final Report
nutritional outcomes for children including stunting, undernutrition and basic morbidity and
mortality9. UNICEF staff refer to “water and sanitation related diseases” rather than water-
borne diseases. Increasing AMR is also a priority health issue for UNICEF.
- WHO prioritizes NTDs and AMR in WASH+H integration its efforts. WHO indicated that the
WASH community sees presence of NTDs is an indicator of poverty and a way to focus to ensure
maximum benefit.
- BMGF health efforts are structured around specific diseases including vaccine development (e.g.
typhoid, cholera) and WASH efforts are primarily in urban sanitation. BMGF funded the WASH
Benefits and SHINE trials and continue to support evidence-gathering for WASH+H (e.g. sewage
surveillance for Sars COV-2).
5.1.4 COVID-19
The SARS-CoV-2 virus is a novel coronavirus and researchers globally are working as quickly as possible
to understand it and its impacts and characteristics not only on the human body but also how it behaves
in the environment. The risks of the virus being in or transmitted through water and sanitation systems
are a key concern for WASH10 professionals. Annex 5 provides an overview and key points from current
evidence on how SARS-CoV-2 behaves in WASH systems.
5.2 Multi-sectoral and economic benefits of WASH Numerous ADB staff expressed that it would be beneficial to be able to better quantify the economic
benefits and return-on-investment (ROI) of WASH
interventions, especially when making the case for
increased WASH interventions with Ministries of Finance.
A number of models that integrate WASH+H for human as
well environmental health already exist. The One Health
model links agricultural, environmental, animal and
human. Others such as the Human Capital Index consider
the broader social and economic benefits of these are
presented here so that ADB can consider these as
conceptual models to adopt.
One Health
One Health is a model that links human health risks from human-animal (zoonotic) disease transmission (e.g. Sars COV-2). By taking a systems approach it links environmental, animal and human health. Some commentators have argued that it could be further expanded to include water-borne diseases. Approximately 60% of diseases recognized in humans to date are due to multi-
9 See Consensus Statement on childhood diarrhea and stunting: https://bmcmedicine.biomedcentral.com/articles/10.1186/s12916-019-1410-x 10 WASH is the collective term for Water, Sanitation and Hygiene. Because of the interdependence of water, sanitation and hygiene, these three core issues are grouped together to represent a sector. While each a separate field of work, each is dependent on the presence of the other (UNICEF, 2016).
Figure 5. One Health conceptual model

38 WASH + H Consultancy Final Report
host pathogens. Around 75% of newly emerging human infectious diseases, including the recent coronavirus disease (COVID-19), are zoonotic.11 Human Capital
The Human Capital Index (HCI) measures which countries are best in mobilizing the economic and
professional potential of its citizens and is promoted as a holistic development approach that
preferences the human potential over quick economic returns. It measures the human capital that a
child born today can expect to attain by her 18th birthday, given the risks of poor health and poor
education prevailing in her country (World Bank , 2020). HCI = Survival x Health x Education. It can be
argued that WASH is important to all aspects of HCI, with WASH intersecting all three elements through,
for example:
1. Survival – Prevention of water-borne diseases in first 5 years of life is critically important to
survival (as diarrhea still main killer of under 5s and makes up highest DALYs of all WASH-
attributable disease burden);
2. Health – stunting prevalence is the main measure, and lack of adequate WASH is a contributor
to stunting;
3. Education – availability of adequate WASH facilities has a direct bearing on years and quality of
school attendance, especially by girls.
The HCI approach includes a call to action for a “whole-of-government” approach which (World Bank ,
2018): sustain effort across political cycles; link sectoral programs; and expand the evidence base for
policy design to identify which interventions deliver the highest returns to investment. Country-level HCI
profiles are available12.
Economic benefits of WASH
There are numerous and well-recognized economic benefits that result from improved WASH. Reduced
burden of disease (outlined above) is the main benefit, and it in turn provides for other benefits such as
increased economic participation (reduced time lost to disease or caring for others) as well as reduced
time lost to carrying water and reduced premature mortality. Hutton’s analysis of benefits and costs of
WASH targets in the Post-2015 agenda (Hutton., 2015) assessed return on investment at a global level
through achievement of key SDG WASH goals (e.g. end to Open Defecation). The cost estimation
approach and assumed benefits are clearly described in the methodology. For instance, time of adults
too sick to work is valued at 30% of average GDP per capita on an hourly basis and for school-age
children and adults caring for under-fives, time is valued at 15% of GDP per capita. Mortality is valued
using the human capital approach. Non-health benefits accounted for included time saved from not
having to walk to collect water and not having to walk to open defecation sites.
This study estimated the cost of achieving SDG targets globally, and found return on investment from
specific targets (dependent on assumptions) was as follows:
- The global benefit-cost ratio of ending open defecation is 5.8 - 7.3
11 There is an ADB project in Laos designed with One Health Approach: https://www.adb.org/projects/53240-002/main#project-pds 12 https://www.worldbank.org/en/publication/human-capital
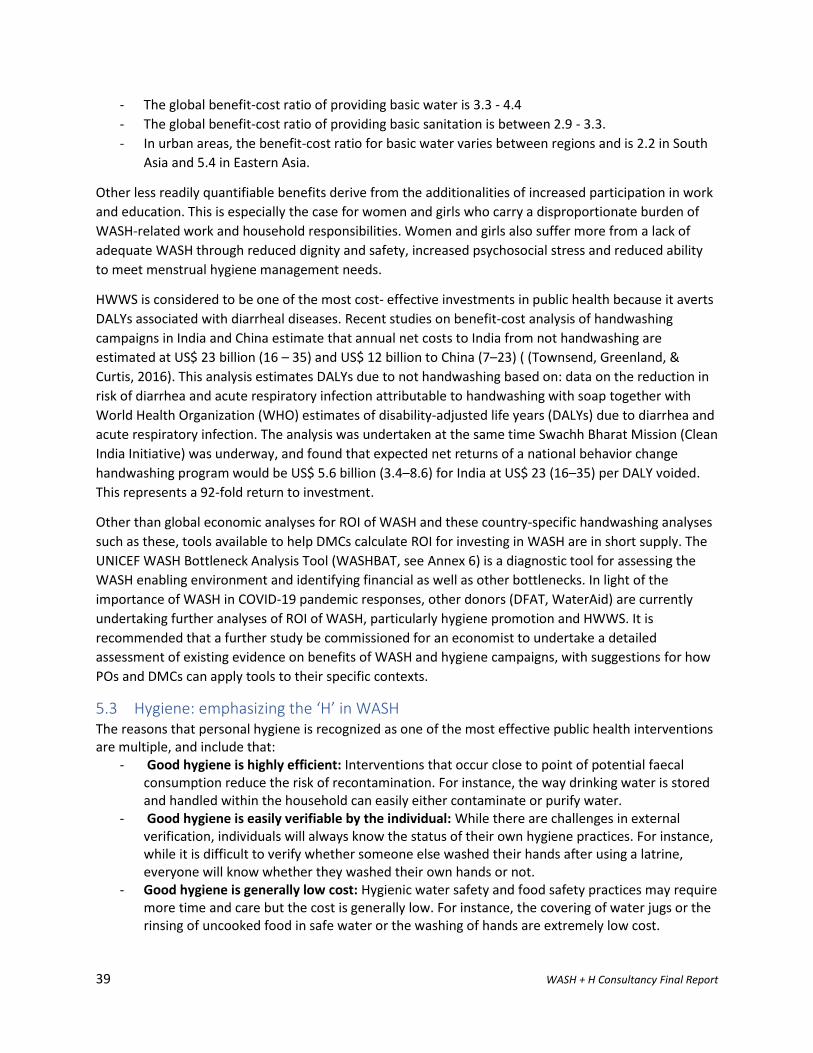
39 WASH + H Consultancy Final Report
- The global benefit-cost ratio of providing basic water is 3.3 - 4.4
- The global benefit-cost ratio of providing basic sanitation is between 2.9 - 3.3.
- In urban areas, the benefit-cost ratio for basic water varies between regions and is 2.2 in South
Asia and 5.4 in Eastern Asia.
Other less readily quantifiable benefits derive from the additionalities of increased participation in work
and education. This is especially the case for women and girls who carry a disproportionate burden of
WASH-related work and household responsibilities. Women and girls also suffer more from a lack of
adequate WASH through reduced dignity and safety, increased psychosocial stress and reduced ability
to meet menstrual hygiene management needs.
HWWS is considered to be one of the most cost- effective investments in public health because it averts
DALYs associated with diarrheal diseases. Recent studies on benefit-cost analysis of handwashing
campaigns in India and China estimate that annual net costs to India from not handwashing are
estimated at US$ 23 billion (16 – 35) and US$ 12 billion to China (7–23) ( (Townsend, Greenland, &
Curtis, 2016). This analysis estimates DALYs due to not handwashing based on: data on the reduction in
risk of diarrhea and acute respiratory infection attributable to handwashing with soap together with
World Health Organization (WHO) estimates of disability-adjusted life years (DALYs) due to diarrhea and
acute respiratory infection. The analysis was undertaken at the same time Swachh Bharat Mission (Clean
India Initiative) was underway, and found that expected net returns of a national behavior change
handwashing program would be US$ 5.6 billion (3.4–8.6) for India at US$ 23 (16–35) per DALY voided.
This represents a 92-fold return to investment.
Other than global economic analyses for ROI of WASH and these country-specific handwashing analyses
such as these, tools available to help DMCs calculate ROI for investing in WASH are in short supply. The
UNICEF WASH Bottleneck Analysis Tool (WASHBAT, see Annex 6) is a diagnostic tool for assessing the
WASH enabling environment and identifying financial as well as other bottlenecks. In light of the
importance of WASH in COVID-19 pandemic responses, other donors (DFAT, WaterAid) are currently
undertaking further analyses of ROI of WASH, particularly hygiene promotion and HWWS. It is
recommended that a further study be commissioned for an economist to undertake a detailed
assessment of existing evidence on benefits of WASH and hygiene campaigns, with suggestions for how
POs and DMCs can apply tools to their specific contexts.
5.3 Hygiene: emphasizing the ‘H’ in WASH The reasons that personal hygiene is recognized as one of the most effective public health interventions are multiple, and include that:
- Good hygiene is highly efficient: Interventions that occur close to point of potential faecal consumption reduce the risk of recontamination. For instance, the way drinking water is stored and handled within the household can easily either contaminate or purify water.
- Good hygiene is easily verifiable by the individual: While there are challenges in external verification, individuals will always know the status of their own hygiene practices. For instance, while it is difficult to verify whether someone else washed their hands after using a latrine, everyone will know whether they washed their own hands or not.
- Good hygiene is generally low cost: Hygienic water safety and food safety practices may require more time and care but the cost is generally low. For instance, the covering of water jugs or the rinsing of uncooked food in safe water or the washing of hands are extremely low cost.

40 WASH + H Consultancy Final Report
Individual hygiene can cover many behaviors, and those relating to water and sanitation include, inter
alia:
1) Sanitation hygiene: use of a latrine, safe disposal of human feces
2) Water hygiene: use and protection of safe water sources, household water treatment
3) Personal hygiene: hand hygiene (handwashing with soap and use of alcohol-based sanitizers),
menstrual hygiene
4) Food hygiene: proper food preparation and handling
Other aspects of WASH, such as use of proper drainage and water source protection are usually
collective (community or institutional) responsibilities and differ from individual behaviors. Hygiene
behavior change promotion is best focused on a single or a few key behaviors at a time, so selection of
the target hygiene behavior(s) and target audience(s) is critical to having the biggest impact on health
outcomes. Of WASH behaviors listed above, handwashing with soap (HWWS) is one of the most
effective but most difficult to shift and measure.
Why focus on handwashing with soap?
Handwashing with soap (HWWS) is a highly effective intervention
and has been found to:
- Reduce diarrheal disease between 23-40% (Freeman, 2014)
- Reduce children’s school absenteeism by 29-57% (Wang,
2017 )
- Reduce respiratory illnesses, like colds, in the general
population by 16-21% (Rabie, 2006).
Whilst studies show how beneficial handwashing is, they have also
shown that HWWS is very poorly practiced, estimating that between
19-25% of the world population washes hands after contact with
excreta (i.e. own or children’s feces) (Freeman, 2014; Wolf, 2019). Studies have also shown that
knowledge about the health benefits of handwashing and/or the critical times to wash hands have been
insufficient to change people’s handwashing behaviors.
One contributing factor to poor handwashing behaviors is a lack of infrastructure. Between 30-40% of
people across South Asia, East Asia and Southeast Asia don’t have access to a handwashing facility at
home with soap, with very limited data available for the Pacific. There are worrying gaps in handwashing
facilities in schools and HCFs which are highlighted in regional snapshots13 produced by JMP
(WHO/UNICEF) in 2020 after the COVID-19 pandemic started. To provide environments conducive to
HWWS facilities should be available and HWWS behavior encouraged in all settings.
The hygiene indicator chosen for national and global monitoring by the JMP (WHO/UNICF) is a proxy
indicator because collecting reliable data for handwashing with soap is unreliable due to positive bias in
self-reporting, high costs of observational data collection and high survey costs. An additional challenge
is that there is no global agreed-upon definition for hygiene; different countries define hygiene
differently (WHO, 2020). The globally agreed best proxy indicator for handwashing with soap is presence
13 https://washdata.org/reports
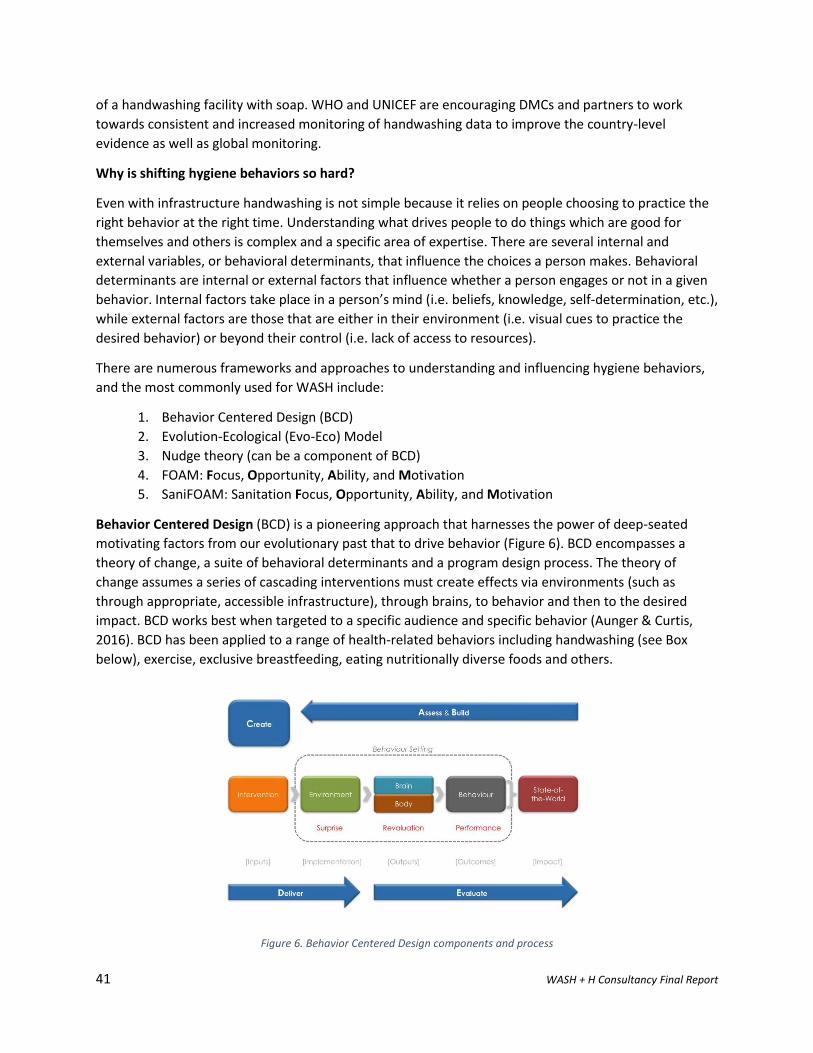
41 WASH + H Consultancy Final Report
of a handwashing facility with soap. WHO and UNICEF are encouraging DMCs and partners to work
towards consistent and increased monitoring of handwashing data to improve the country-level
evidence as well as global monitoring.
Why is shifting hygiene behaviors so hard?
Even with infrastructure handwashing is not simple because it relies on people choosing to practice the
right behavior at the right time. Understanding what drives people to do things which are good for
themselves and others is complex and a specific area of expertise. There are several internal and
external variables, or behavioral determinants, that influence the choices a person makes. Behavioral
determinants are internal or external factors that influence whether a person engages or not in a given
behavior. Internal factors take place in a person’s mind (i.e. beliefs, knowledge, self-determination, etc.),
while external factors are those that are either in their environment (i.e. visual cues to practice the
desired behavior) or beyond their control (i.e. lack of access to resources).
There are numerous frameworks and approaches to understanding and influencing hygiene behaviors,
and the most commonly used for WASH include:
1. Behavior Centered Design (BCD)
2. Evolution-Ecological (Evo-Eco) Model
3. Nudge theory (can be a component of BCD)
4. FOAM: Focus, Opportunity, Ability, and Motivation
5. SaniFOAM: Sanitation Focus, Opportunity, Ability, and Motivation
Behavior Centered Design (BCD) is a pioneering approach that harnesses the power of deep-seated
motivating factors from our evolutionary past that to drive behavior (Figure 6). BCD encompasses a
theory of change, a suite of behavioral determinants and a program design process. The theory of
change assumes a series of cascading interventions must create effects via environments (such as
through appropriate, accessible infrastructure), through brains, to behavior and then to the desired
impact. BCD works best when targeted to a specific audience and specific behavior (Aunger & Curtis,
2016). BCD has been applied to a range of health-related behaviors including handwashing (see Box
below), exercise, exclusive breastfeeding, eating nutritionally diverse foods and others.
Figure 6. Behavior Centered Design components and process
42 WASH + H Consultancy Final Report
Evolution-Ecological (Evo-Eco) Model – This model was also developed by LSHTM (Aunger & Curtis,
2014) and is a as a precursor to BCD and is called ‘Evo-Eco’ because it derives from evolutionary biology
and ecological psychology theory. It is based on the insight that brains evolved to provide adaptive
behavioral responses to rapidly changing or complex environmental conditions. From this foundation,
we have developed a model with three basic components (as seen in the diagram below).
These components are:
1. The environment, which presents a challenge or opportunity to the individual;
2. The brain, which produces potential responses to that challenge;
3. The body, which engages in interactions with the environment (i.e., produces behaviour) that
changes that environment.

43 WASH + H Consultancy Final Report
Nudge theory - Nudges are environmental cues engaging unconscious decision-making processes to
prompt behavior change. Nudges change the way choices are presented, and can make people more
Box 7. Behavior Centered Design for improving handwashing with soap in Bhutan
Bhutan’s Public Health Engineering Division (PHED) of the Ministry of Health (MoH) found that despite high
levels of basic sanitation coverage, expected health benefits did not materialize and Bhutan still experienced
some of the highest stunting in the region. In response to this, the Royal Government of Bhutan (RGoB) set
national targets for improved sanitation >85% in its Five-Year Plan and scaled up its national Rural Sanitation
and Hygiene Program (RSAHP). RSAHP integrates sanitation demand creation, supply chain development,
behavior change communication and governance.
To strengthen handwashing with soap activities in its national approach, PHED trialed an innovative Behavior
Centered Design (BCD) approach to improve handwashing practices in partnership with SNV Bhutan and
LSHTM, supported by DFAT’s Civil Society WASH Fund (CS WASH Fund, 2017). The BCD approach used level by
evolved from the fields of evolutionary biology and ecological psychology and comprises three basic
components:
1. The environment, which presents a challenge or opportunity to the individual 2. The brain, which produces potential responses to that challenge 3. The body, which engages in interactions with the environment (i.e. produces behavior) or changes that environment. Through a creative research process, the pilot identified nurture and disgust as the most powerful motivators of hygiene behavior. Further research means of associating nurture with hygiene identified the strongest association as a farming metaphor of three different where the growth of seeds into healthy plants mirrors the growth of children into healthy adults. Conveying this metaphor through stories was a powerful means of encouraging good hygiene practices. This was then translated into a joint commitment or pledge, “Like how a sapling needs water to grow, my child needs good behavior like hand washing with soap”.
Where previously the HWWS messaging was strongly health-message-based, relying on health assistants and
information, education and communication (IEC) materials, the BCD approach relied on emotional messages of
nurture and disgust delivered through a Community Development for Health approach. A combination of tools
were used to deliver these messages including workshops, household visits, reminder stickers, story books and
habit record sheets. The pilot study design measured the following indicators at baseline and endline:
- Self-reported handwashing with soap at key times (structured recall with pictures) - Presence of soap & water at latrine and kitchen (spot-check observations) - Handwashing awareness and normative beliefs (questionnaire) The results showed increases in HWWS across all indicators, and PHED has gone on to undertake a Cost Benefit
Analysis (Dem, June 2018)and scale-up the program nationally.

44 WASH + H Consultancy Final Report
likely to do something desirable (Dreibelbis, 2016). Nudges for HWWS have been trialed with good
results (see Box 8 on nudges in schools in the Philippines) and are now widespread as part of COVID-19
responses to encourage social distancing (e.g. through marking out 1.5m spaces in queues, spacing out
seating in public areas etc.).
FOAM - The FOAM framework was developed by the World Bank’s (WB) Water Sanitation Program
(WSP) can be used to design, monitor, and evaluate handwashing behavior change interventions
(Coombes, Y & Devine, J, 2010). The four FOAM components represent behavioral determinants: Focus,
Opportunity, Ability, and Motivation. Three of these categories are derived from systems used in social
marketing and organizational management, such as:
- Opportunity: Is it possible to practice the behavior (in the specific physical and social environment)?
- Ability: Are people capable of practicing the behavior (do they have the knowledge, money, time)?
- Motivation: Do people want to practice the behavior (beliefs, attitudes; are they willing to change)?
Figure 7. FOAM framework for handwashing with soap
SaniFOAM – The SaniFOAM framework also developed by WB WSP, uses the same FOAM categories,
but adds additional behavioral determinants that are influencing factors for individuals’ behaviors
towards using improved sanitation (Devine, 2009). Additional determinants included in SaniFOAM
include: sanctions/enforcements; skills and self-efficacy; roles and decisions that influence household
members in sanitation-related decision-making; affordability; values, attitudes and beliefs; emotional,
physical, social drivers; and competing priorities; and willingness to pay.14
14 FOAM and SaniFOAM information adapted from International WaterCentre’s Behavior Change in WASH training modules.
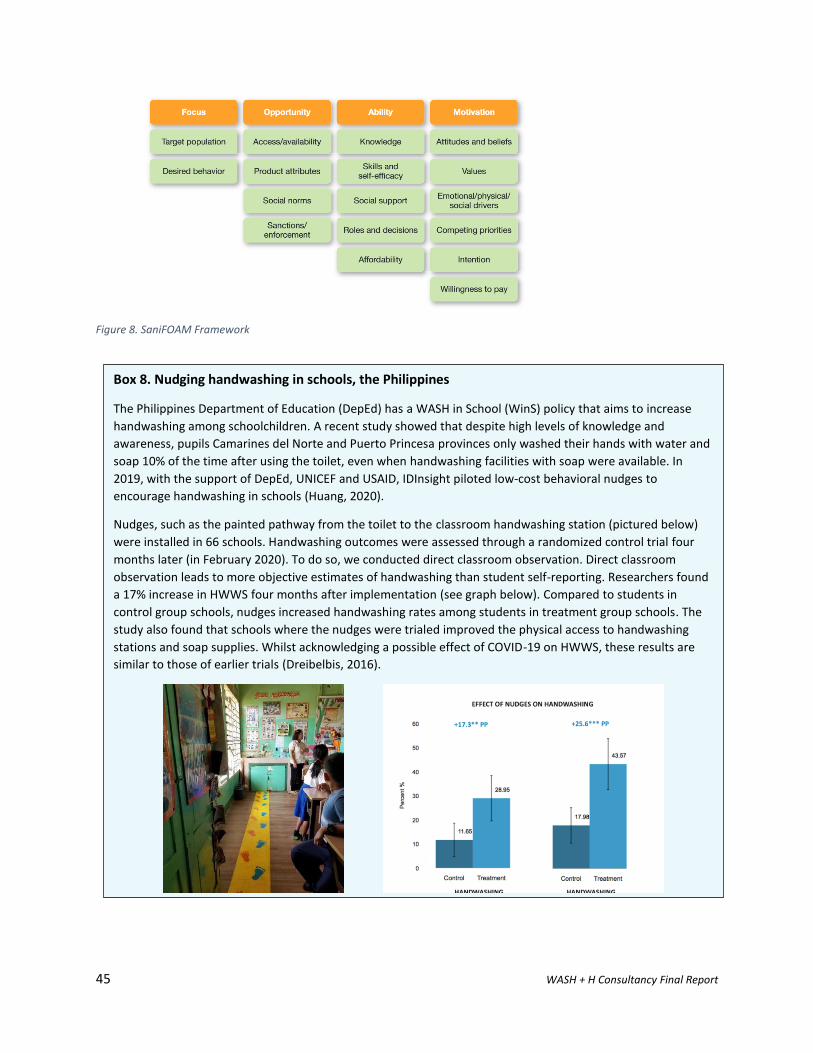
45 WASH + H Consultancy Final Report
Figure 8. SaniFOAM Framework
Box 8. Nudging handwashing in schools, the Philippines
The Philippines Department of Education (DepEd) has a WASH in School (WinS) policy that aims to increase
handwashing among schoolchildren. A recent study showed that despite high levels of knowledge and
awareness, pupils Camarines del Norte and Puerto Princesa provinces only washed their hands with water and
soap 10% of the time after using the toilet, even when handwashing facilities with soap were available. In
2019, with the support of DepEd, UNICEF and USAID, IDInsight piloted low-cost behavioral nudges to
encourage handwashing in schools (Huang, 2020).
Nudges, such as the painted pathway from the toilet to the classroom handwashing station (pictured below)
were installed in 66 schools. Handwashing outcomes were assessed through a randomized control trial four
months later (in February 2020). To do so, we conducted direct classroom observation. Direct classroom
observation leads to more objective estimates of handwashing than student self-reporting. Researchers found
a 17% increase in HWWS four months after implementation (see graph below). Compared to students in
control group schools, nudges increased handwashing rates among students in treatment group schools. The
study also found that schools where the nudges were trialed improved the physical access to handwashing
stations and soap supplies. Whilst acknowledging a possible effect of COVID-19 on HWWS, these results are
similar to those of earlier trials (Dreibelbis, 2016).
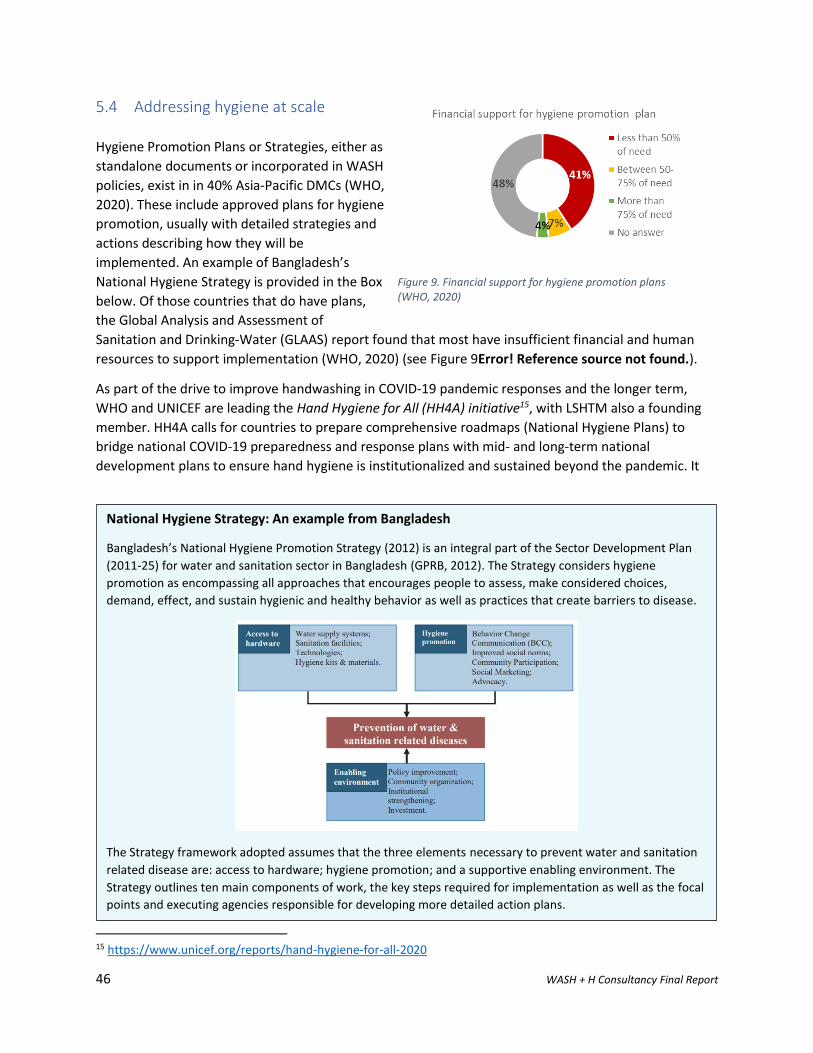
46 WASH + H Consultancy Final Report
5.4 Addressing hygiene at scale
Hygiene Promotion Plans or Strategies, either as
standalone documents or incorporated in WASH
policies, exist in in 40% Asia-Pacific DMCs (WHO,
2020). These include approved plans for hygiene
promotion, usually with detailed strategies and
actions describing how they will be
implemented. An example of Bangladesh’s
National Hygiene Strategy is provided in the Box
below. Of those countries that do have plans,
the Global Analysis and Assessment of
Sanitation and Drinking-Water (GLAAS) report found that most have insufficient financial and human
resources to support implementation (WHO, 2020) (see Figure 9Error! Reference source not found.).
As part of the drive to improve handwashing in COVID-19 pandemic responses and the longer term,
WHO and UNICEF are leading the Hand Hygiene for All (HH4A) initiative15, with LSHTM also a founding
member. HH4A calls for countries to prepare comprehensive roadmaps (National Hygiene Plans) to
bridge national COVID-19 preparedness and response plans with mid- and long-term national
development plans to ensure hand hygiene is institutionalized and sustained beyond the pandemic. It
15 https://www.unicef.org/reports/hand-hygiene-for-all-2020
National Hygiene Strategy: An example from Bangladesh
Bangladesh’s National Hygiene Promotion Strategy (2012) is an integral part of the Sector Development Plan
(2011-25) for water and sanitation sector in Bangladesh (GPRB, 2012). The Strategy considers hygiene
promotion as encompassing all approaches that encourages people to assess, make considered choices,
demand, effect, and sustain hygienic and healthy behavior as well as practices that create barriers to disease.
The Strategy framework adopted assumes that the three elements necessary to prevent water and sanitation
related disease are: access to hardware; hygiene promotion; and a supportive enabling environment. The
Strategy outlines ten main components of work, the key steps required for implementation as well as the focal
points and executing agencies responsible for developing more detailed action plans.
Figure 9. Financial support for hygiene promotion plans (WHO, 2020)
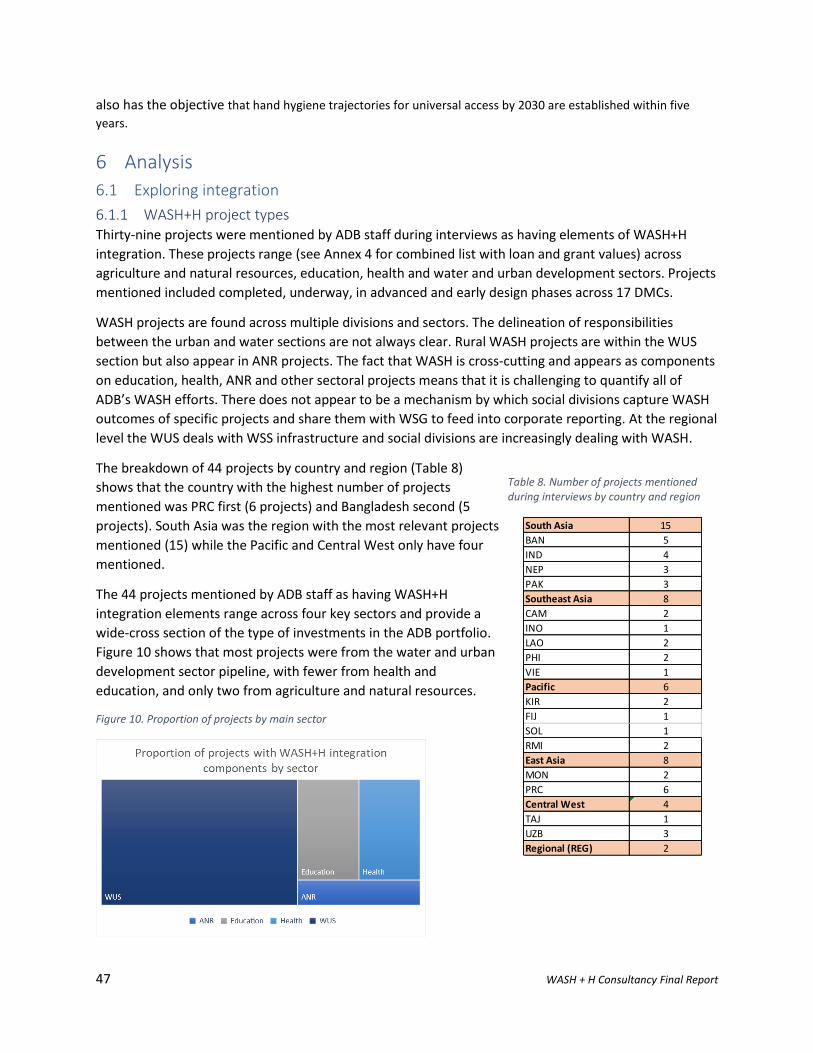
47 WASH + H Consultancy Final Report
also has the objective that hand hygiene trajectories for universal access by 2030 are established within five
years.
6 Analysis
6.1 Exploring integration
6.1.1 WASH+H project types Thirty-nine projects were mentioned by ADB staff during interviews as having elements of WASH+H
integration. These projects range (see Annex 4 for combined list with loan and grant values) across
agriculture and natural resources, education, health and water and urban development sectors. Projects
mentioned included completed, underway, in advanced and early design phases across 17 DMCs.
WASH projects are found across multiple divisions and sectors. The delineation of responsibilities
between the urban and water sections are not always clear. Rural WASH projects are within the WUS
section but also appear in ANR projects. The fact that WASH is cross-cutting and appears as components
on education, health, ANR and other sectoral projects means that it is challenging to quantify all of
ADB’s WASH efforts. There does not appear to be a mechanism by which social divisions capture WASH
outcomes of specific projects and share them with WSG to feed into corporate reporting. At the regional
level the WUS deals with WSS infrastructure and social divisions are increasingly dealing with WASH.
The breakdown of 44 projects by country and region (Table 8)
shows that the country with the highest number of projects
mentioned was PRC first (6 projects) and Bangladesh second (5
projects). South Asia was the region with the most relevant projects
mentioned (15) while the Pacific and Central West only have four
mentioned.
The 44 projects mentioned by ADB staff as having WASH+H
integration elements range across four key sectors and provide a
wide-cross section of the type of investments in the ADB portfolio.
Figure 10 shows that most projects were from the water and urban
development sector pipeline, with fewer from health and
education, and only two from agriculture and natural resources.
Figure 10. Proportion of projects by main sector
Table 8. Number of projects mentioned during interviews by country and region
South Asia 15
BAN 5
IND 4
NEP 3
PAK 3
Southeast Asia 8
CAM 2
INO 1
LAO 2
PHI 2
VIE 1
Pacific 6
KIR 2
FIJ 1
SOL 1
RMI 2
East Asia 8
MON 2
PRC 6
Central West 4
TAJ 1
UZB 3
Regional (REG) 2
48 WASH + H Consultancy Final Report
Given the scope and range of ADB’s pipeline it was useful to typify projects that have WASH+H elements
to describe the breadth and scope work underway and planned. Table 9 shows a categorization of
WASH+H projects identified through KIIs the across ANR, education, health and WUS portfolios. Five
projects mentioned are in preparatory stages and do not have sufficient information available yet to
categorize. A further more in-depth description of the types of WASH+H projects underway is included
in Guidance Section 8.1.
Table 9. Twelve types of WASH+H projects ADB implements
1 ANR project with human health link ANR
2 ANR project with WSS infrastructure 3 Education project with WASH infrastructure EDU 4 Education project with skills building for WASH 5 Health project (no WASH component evident)
Health
6 Health project with community HyBC component 7 Holistic rural water supply and sanitation project WUS 8 Integrated urban development with WSS and/or HyBC components 9 Water supply project
10 WASH and health knowledge building and innovation 11 WSS project with community and/or schools and/or HFCs HyBC components 12 Convergence WSS and Health projects
The breadth and depth of projects that fit within a WASH+H scope shows that ADB already has well-
established examples of integrated approaches to draw upon and learn more from. Many of the projects
mentioned could be write as project impact studies and given more profile.
6.1.2 Multi-sectoral approaches WASH is by its nature multi-sectoral and this complexity means that related responsibilities are usually
shared across multiple levels of government and ministries. PASP noted that this sometimes results in
no single government agency taking a leadership role. Some of the factors identified through KIIs as
influencing the extent of WASH+H in designs are:
- Appetite for project design complexity from PO, DMC and country offices;
- WASH enabling environment and extent to which WASH and HyBC is a DMC priority;
- Knowledge, attitude and resources available to POs and EAs for non-infrastructure components
as well as willingness to pursue and design these into projects; and
- Priority health and WASH challenges of the country.
Some countries are already implementing integrated multi-sector approaches as standard practice. This
is the case for urban development and health cities projects in PRC. These kinds of projects include
advanced elements on health (protect against water borne diseases, clean water, sanitation, life style)
green spaces with green infrastructure approach. With PRC recently announcing that 100% rural water
supply has been achieved, it is now adopting an integrated approach to rural projects, with WASH, solid
waste management and wastewater treatment also considered. EAER reported that PRC is innovating
with respect to: rural and urban water linkages; public-private partnership models for wastewater
49 WASH + H Consultancy Final Report
treatment; cost-effective technologies and solutions in village situations. PRC’s WASH enabling
environment allows for multi-sectoral approaches that are more challenging in other countries.
A few ADB projects are primarily implemented by one sector, but with measurable impacts across
multiple sectors. The Ebeye Water Supply and Sanitation Project is an example where water sector
benefits to public health have been measured (Box 9).
In South Asian countries there are more examples of health and WSS projects running in parallel in
urban settings. Lessons learned include that multi-sectoral efforts, such as development of health and
urban development road maps, are most effectively mobilized at lower levels of government. This is
demonstrated well by the Indian National Urban Health Mission project (see Box 10).
Box 9. ADB’s work in Marshall Islands: Convergence of Water and Health investments
The Ebeye Water Supply and Sanitation Project (EWSSP) has upgraded the Marshall Island’s capital
drainage system to mitigate flooding, constructed saltwater wells adding volume to the island’s
desalination plant, and undertaken community hygiene awareness raising. The desalination plant's
design-build-operate (DBO) contract finishes in September 2020. Additional financing (Grant 0749-
RMI) is support to build the utilities (KAJUR) technical capacity to operate and maintain the new
desalination plant. In parallel with this, the Health Expenditure and Livelihoods Support Program
Grant is being supported.
ADB’s parallel health and water programming can be considered an example of convergence
programming, with additional benefits across multiple areas. Already through ADB’s involvement
across both sectors ADB has been found measurable progress towards project's target impact and
outcome, reducing diarrheal incidence. The average monthly number of cases of diarrhea reported
by the Ebeye Hospital has declined by almost 20% since following the implementation of the
project's hygiene awareness and education program and the commissioning of the new desalination
plant. All 1,465 household on Ebeye now have access to freshwater, saltwater, and sewerage
networks service.
EWSSP Funding is: ABD Special Fund resources: USD5 million; Government of Australia grant USD4
million; Government of Marshall Islands: USD10.02 million equivalent in counterpart funds
exemption of taxes and duties.
50 WASH + H Consultancy Final Report
Box 10. Supporting National Urban Health Mission, India
National Urban Health Mission (NUHM) is a US$300 million and US$3.8 million TA program with a
core strategy to enhance the public health system to improve the health of people living in cities,
especially the poor. Infrastructure support includes establishing a network of urban primary health
centers (UPHCs) covering all cities with a population above 50,000. Linked with community outreach
and referral services, UPHCs will expand health service access and strengthen primary health care.
The rollout of the NUHM at the same time as the introduction of the Swachh Bharat Mission (Clean
India Initiative) to provide universal access to sanitation facilities in urban areas, led to the project
pursuing a convergence approach to ensure support and momentum at all levels of government.
Activities to build dialogue between the two agendas (NUHM and Swachh Bharat) included
multisectoral interventions, joint development of plans and road maps and module development and
training across sectors (health, urban local bodies and nutrition). The efforts included training
different functionaries from different bodies together so they could engage in single classroom and
build dialogue and relationship between two agendas.
Some ADB reflections on the successes and challenges of these convergence approaches include:
- Lending to a single line Ministry (Health) is a challenge, especially as health is a State
responsibility with decentralized delivery.
- Whilst ideally convergence would be seen at every level of government through
implementation, governance and policy, that is challenging in India where there are >700
districts and it is difficult to have a unified approach across all.
- Initiating policy at the central level does not always percolate to States, resulting in very
weak implementation. Convergence and joint planning are more achievable at district rather
than national Ministry level.
- Whilst joint training programs have been emphasized, the effects have not been as hoped as
people are regularly transferred to new jobs. Re-training of new functionaries is regularly
required, showing the need for ongoing training programs.
“[Convergence is] one of the most challenging components of lending portfolio. We continue to see
this component of loan as something we need to continually push and adapt, as needs and policies
change. We need to keep adapting our convergence model to needs on the ground.”
The COVID-19 pandemic has put more strain on Indian urban health services, and NUHM is
responding by developing an intervention pilot to demonstrate contextual implementation of various
COVID-19 guidelines, aid in control of the COVID-19 outbreak in high density urban areas and
empower the local health system and community to sustain interventions (including improved access
to WASH).
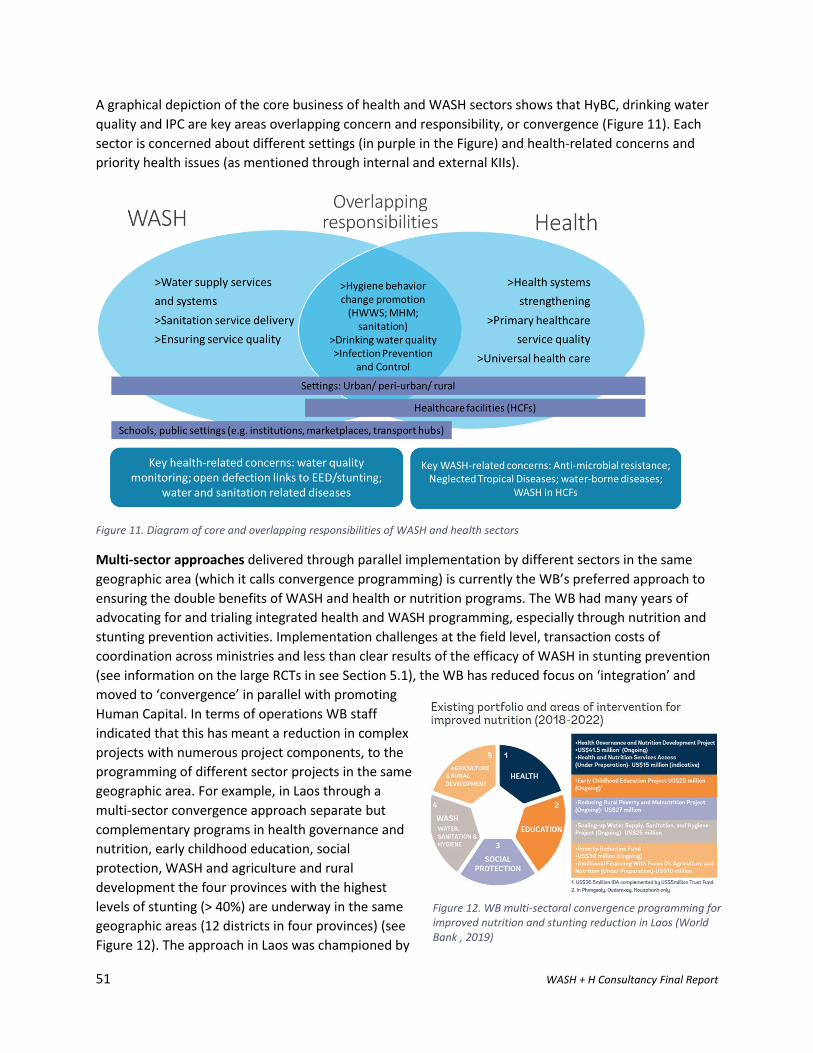
51 WASH + H Consultancy Final Report
A graphical depiction of the core business of health and WASH sectors shows that HyBC, drinking water
quality and IPC are key areas overlapping concern and responsibility, or convergence (Figure 11). Each
sector is concerned about different settings (in purple in the Figure) and health-related concerns and
priority health issues (as mentioned through internal and external KIIs).
Figure 11. Diagram of core and overlapping responsibilities of WASH and health sectors
Multi-sector approaches delivered through parallel implementation by different sectors in the same
geographic area (which it calls convergence programming) is currently the WB’s preferred approach to
ensuring the double benefits of WASH and health or nutrition programs. The WB had many years of
advocating for and trialing integrated health and WASH programming, especially through nutrition and
stunting prevention activities. Implementation challenges at the field level, transaction costs of
coordination across ministries and less than clear results of the efficacy of WASH in stunting prevention
(see information on the large RCTs in see Section 5.1), the WB has reduced focus on ‘integration’ and
moved to ‘convergence’ in parallel with promoting
Human Capital. In terms of operations WB staff
indicated that this has meant a reduction in complex
projects with numerous project components, to the
programming of different sector projects in the same
geographic area. For example, in Laos through a
multi-sector convergence approach separate but
complementary programs in health governance and
nutrition, early childhood education, social
protection, WASH and agriculture and rural
development the four provinces with the highest
levels of stunting (> 40%) are underway in the same
geographic areas (12 districts in four provinces) (see
Figure 12). The approach in Laos was championed by
Figure 12. WB multi-sectoral convergence programming for improved nutrition and stunting reduction in Laos (World Bank , 2019)
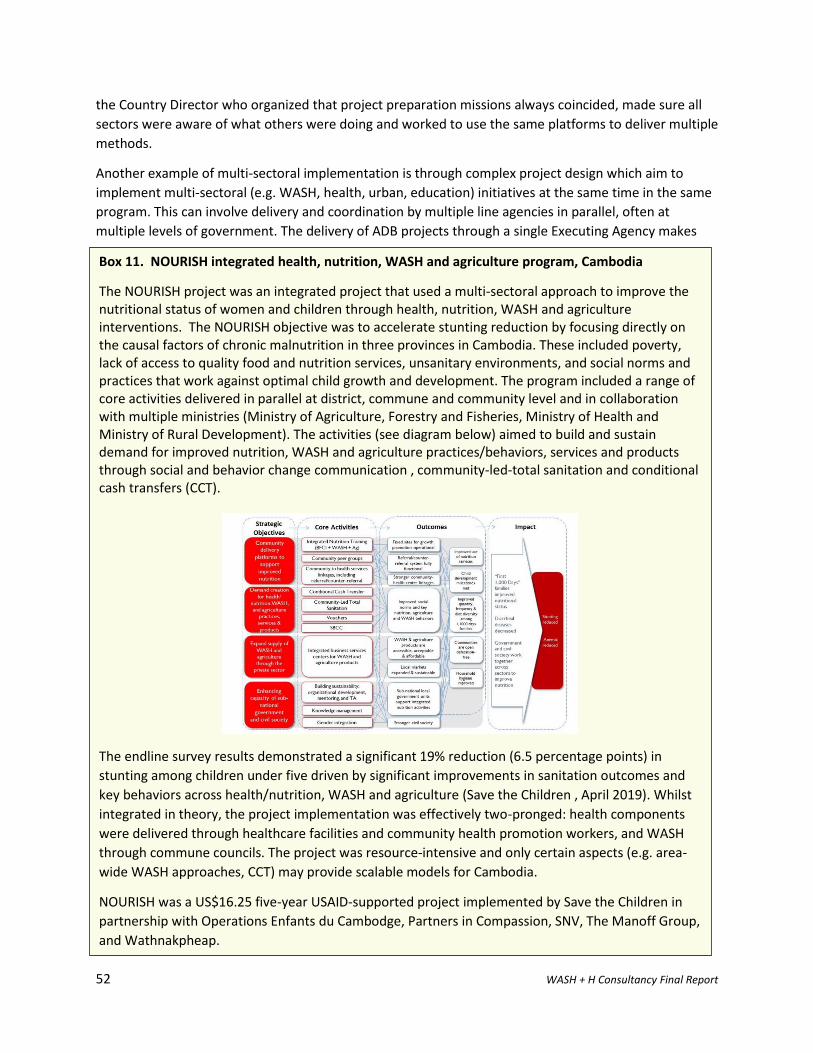
52 WASH + H Consultancy Final Report
the Country Director who organized that project preparation missions always coincided, made sure all
sectors were aware of what others were doing and worked to use the same platforms to deliver multiple
methods.
Another example of multi-sectoral implementation is through complex project design which aim to
implement multi-sectoral (e.g. WASH, health, urban, education) initiatives at the same time in the same
program. This can involve delivery and coordination by multiple line agencies in parallel, often at
multiple levels of government. The delivery of ADB projects through a single Executing Agency makes
Box 11. NOURISH integrated health, nutrition, WASH and agriculture program, Cambodia
The NOURISH project was an integrated project that used a multi-sectoral approach to improve the nutritional status of women and children through health, nutrition, WASH and agriculture interventions. The NOURISH objective was to accelerate stunting reduction by focusing directly on the causal factors of chronic malnutrition in three provinces in Cambodia. These included poverty, lack of access to quality food and nutrition services, unsanitary environments, and social norms and practices that work against optimal child growth and development. The program included a range of core activities delivered in parallel at district, commune and community level and in collaboration with multiple ministries (Ministry of Agriculture, Forestry and Fisheries, Ministry of Health and Ministry of Rural Development). The activities (see diagram below) aimed to build and sustain demand for improved nutrition, WASH and agriculture practices/behaviors, services and products through social and behavior change communication , community-led-total sanitation and conditional cash transfers (CCT).
The endline survey results demonstrated a significant 19% reduction (6.5 percentage points) in
stunting among children under five driven by significant improvements in sanitation outcomes and
key behaviors across health/nutrition, WASH and agriculture (Save the Children , April 2019). Whilst
integrated in theory, the project implementation was effectively two-pronged: health components
were delivered through healthcare facilities and community health promotion workers, and WASH
through commune councils. The project was resource-intensive and only certain aspects (e.g. area-
wide WASH approaches, CCT) may provide scalable models for Cambodia.
NOURISH was a US$16.25 five-year USAID-supported project implemented by Save the Children in
partnership with Operations Enfants du Cambodge, Partners in Compassion, SNV, The Manoff Group,
and Wathnakpheap.
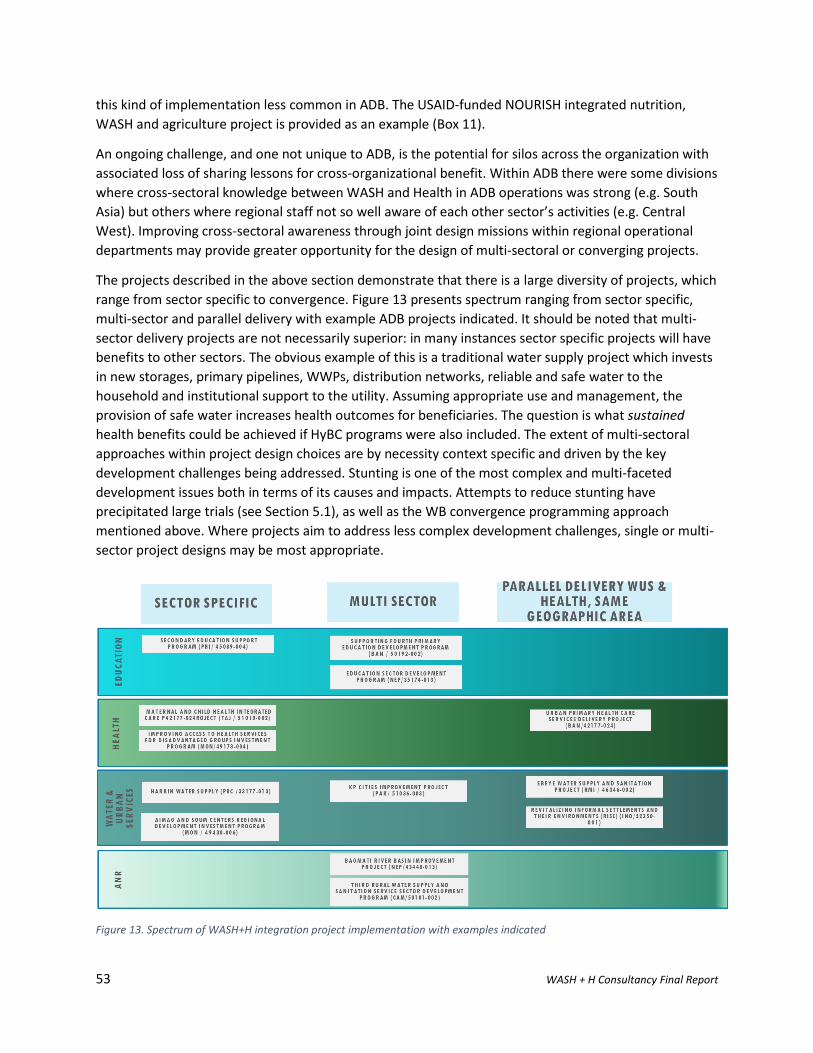
53 WASH + H Consultancy Final Report
this kind of implementation less common in ADB. The USAID-funded NOURISH integrated nutrition,
WASH and agriculture project is provided as an example (Box 11).
An ongoing challenge, and one not unique to ADB, is the potential for silos across the organization with
associated loss of sharing lessons for cross-organizational benefit. Within ADB there were some divisions
where cross-sectoral knowledge between WASH and Health in ADB operations was strong (e.g. South
Asia) but others where regional staff not so well aware of each other sector’s activities (e.g. Central
West). Improving cross-sectoral awareness through joint design missions within regional operational
departments may provide greater opportunity for the design of multi-sectoral or converging projects.
The projects described in the above section demonstrate that there is a large diversity of projects, which
range from sector specific to convergence. Figure 13 presents spectrum ranging from sector specific,
multi-sector and parallel delivery with example ADB projects indicated. It should be noted that multi-
sector delivery projects are not necessarily superior: in many instances sector specific projects will have
benefits to other sectors. The obvious example of this is a traditional water supply project which invests
in new storages, primary pipelines, WWPs, distribution networks, reliable and safe water to the
household and institutional support to the utility. Assuming appropriate use and management, the
provision of safe water increases health outcomes for beneficiaries. The question is what sustained
health benefits could be achieved if HyBC programs were also included. The extent of multi-sectoral
approaches within project design choices are by necessity context specific and driven by the key
development challenges being addressed. Stunting is one of the most complex and multi-faceted
development issues both in terms of its causes and impacts. Attempts to reduce stunting have
precipitated large trials (see Section 5.1), as well as the WB convergence programming approach
mentioned above. Where projects aim to address less complex development challenges, single or multi-
sector project designs may be most appropriate.
Figure 13. Spectrum of WASH+H integration project implementation with examples indicated
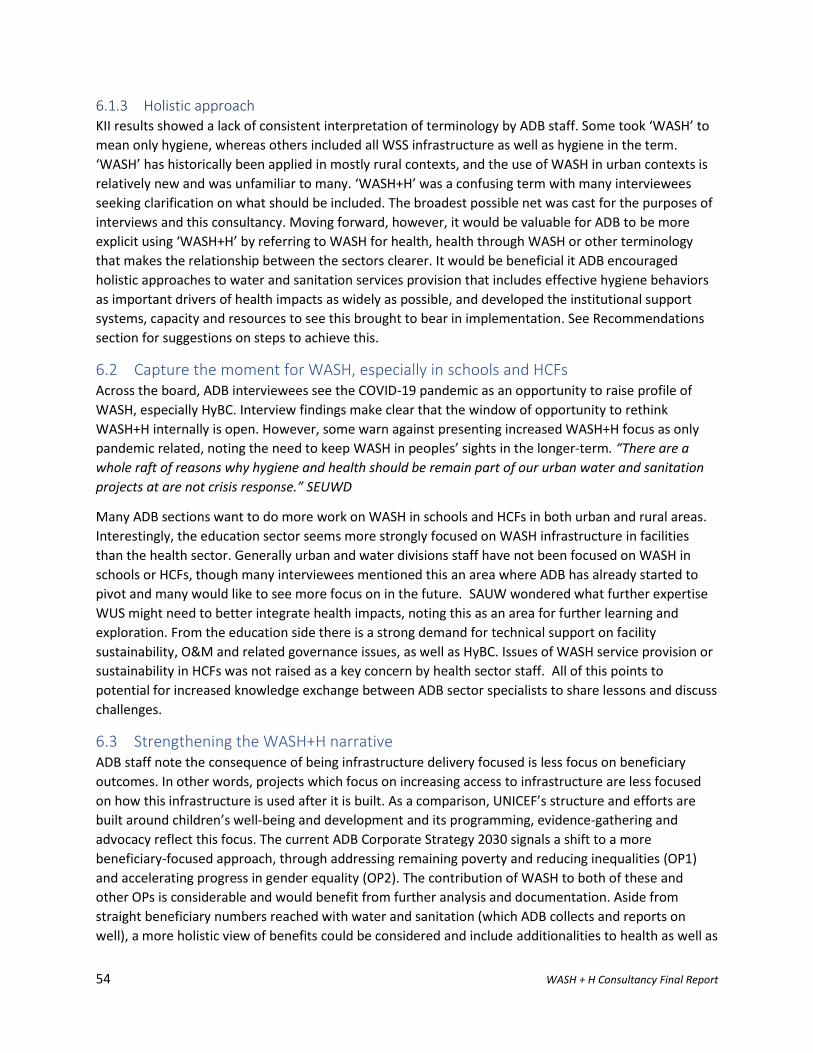
54 WASH + H Consultancy Final Report
6.1.3 Holistic approach KII results showed a lack of consistent interpretation of terminology by ADB staff. Some took ‘WASH’ to
mean only hygiene, whereas others included all WSS infrastructure as well as hygiene in the term.
‘WASH’ has historically been applied in mostly rural contexts, and the use of WASH in urban contexts is
relatively new and was unfamiliar to many. ‘WASH+H’ was a confusing term with many interviewees
seeking clarification on what should be included. The broadest possible net was cast for the purposes of
interviews and this consultancy. Moving forward, however, it would be valuable for ADB to be more
explicit using ‘WASH+H’ by referring to WASH for health, health through WASH or other terminology
that makes the relationship between the sectors clearer. It would be beneficial it ADB encouraged
holistic approaches to water and sanitation services provision that includes effective hygiene behaviors
as important drivers of health impacts as widely as possible, and developed the institutional support
systems, capacity and resources to see this brought to bear in implementation. See Recommendations
section for suggestions on steps to achieve this.
6.2 Capture the moment for WASH, especially in schools and HCFs Across the board, ADB interviewees see the COVID-19 pandemic as an opportunity to raise profile of
WASH, especially HyBC. Interview findings make clear that the window of opportunity to rethink
WASH+H internally is open. However, some warn against presenting increased WASH+H focus as only
pandemic related, noting the need to keep WASH in peoples’ sights in the longer-term. “There are a
whole raft of reasons why hygiene and health should be remain part of our urban water and sanitation
projects at are not crisis response.” SEUWD
Many ADB sections want to do more work on WASH in schools and HCFs in both urban and rural areas.
Interestingly, the education sector seems more strongly focused on WASH infrastructure in facilities
than the health sector. Generally urban and water divisions staff have not been focused on WASH in
schools or HCFs, though many interviewees mentioned this an area where ADB has already started to
pivot and many would like to see more focus on in the future. SAUW wondered what further expertise
WUS might need to better integrate health impacts, noting this as an area for further learning and
exploration. From the education side there is a strong demand for technical support on facility
sustainability, O&M and related governance issues, as well as HyBC. Issues of WASH service provision or
sustainability in HCFs was not raised as a key concern by health sector staff. All of this points to
potential for increased knowledge exchange between ADB sector specialists to share lessons and discuss
challenges.
6.3 Strengthening the WASH+H narrative ADB staff note the consequence of being infrastructure delivery focused is less focus on beneficiary
outcomes. In other words, projects which focus on increasing access to infrastructure are less focused
on how this infrastructure is used after it is built. As a comparison, UNICEF’s structure and efforts are
built around children’s well-being and development and its programming, evidence-gathering and
advocacy reflect this focus. The current ADB Corporate Strategy 2030 signals a shift to a more
beneficiary-focused approach, through addressing remaining poverty and reducing inequalities (OP1)
and accelerating progress in gender equality (OP2). The contribution of WASH to both of these and
other OPs is considerable and would benefit from further analysis and documentation. Aside from
straight beneficiary numbers reached with water and sanitation (which ADB collects and reports on
well), a more holistic view of benefits could be considered and include additionalities to health as well as
55 WASH + H Consultancy Final Report
to education, well-being, economic participation, women’s economic participation and girls’ education
(as the Human Capital Index aims to do). The benefits of increasing focus beyond access to use and
health impacts are described graphically (Figure 14), with good quality and sustainable water and
sanitation infrastructure being the foundation for both of these.
Figure 14. Diagram showing water and sanitation infrastructure as foundational to desired hygiene behavior change and health impacts.
6.4 Evidence and knowledge gaps
6.4.1 Hygiene As described in Section 5.4, hygiene behaviors are important for IPC and breaking pathogen pathways.
However, the centrality of hygiene as a key WASH pillar to ensure health outcomes was only expressed
by one interviewee. “Without the [hygiene] element there is no point investing in [water and sanitation]
because we won’t get health outcomes. The whole objective is health-based.” PARD. The case needs to
be made more strongly within ADB for the health and economic benefits of hygiene investments,
especially so that it is pushed further up the national priority list with Ministries of Finance. Convincing
arguments and data to make this case will vary depending on context and the specific interests and
priorities in that DMC. Providing a range of tools and guidance documents could be provided to POs to
make this case at DMC level including data on economic, social and human development benefits from
investment in WASH (see Section 8).
There were no examples of measuring the effectiveness of HyBC components mentioned during KIIs and
none were found through review of publicly available project documentation. Interviewees also
reported that education and health projects with HyBC components have rarely been evaluated to
56 WASH + H Consultancy Final Report
gather lessons learned. SEHS commented that there is a lack of evidence-based lessons from the
integration of WASH into health and education interventions. There is a need to capture more lessons
from HyBC components and investigate effective delivery modalities, as well as government and CSO
roles and responsibilities. Social protection projects where interventions that target the household and
combine social protection, nutrition and livelihoods enhancement would be valuable to understand
more.
6.4.2 Measuring health impacts There is a need for internal dialogue on the question of whether to measure health impacts from WASH
(or other sector) interventions. The HSG proposes that WASH projects should give more serious
attention to health outcomes, and keep track of health outcomes of WASH projects. However, WASH is
itself a determinant of public health leading to improved health outcomes and the broader existing
evidence base and literature already makes a clear case for this.
WHO’s advice on whether projects should measure WASH outcomes and impacts is that they should
not. WHO points out that health impact assessments are tricky and expensive, they require
sophisticated statistical design, large sample sizes, independent teams, usually needing a control area.
Meeting these criteria can be difficult and also ethically problematic. Ideally assessment teams would be
blinded to the intervention, which is also challenging. Population level health impacts may also only be
apparent many years after a given intervention.
WHO argues that WASH projects should focus attention on monitoring more proximal determinants of
health impacts, such as outputs rather than impacts. For example, monitoring the following: whether
behaviors change; people use different water and sanitation infrastructure; wash hands more often;
manage child feces differently; etc. It’s also important to monitoring outputs that would lead to the
Revitalizing Informal Settlements and their Environments (RISE) in Indonesia and Fiji (52350-001)
The goal of the project is to demonstrate nature-based water and sanitation solutions for reducing
vulnerabilities of the urban poor in Fiji and Indonesia. This will be through diversifying water resources
through rainwater and stormwater harvesting and introducing nature-based flood mitigation
infrastructure to improve local environment and health conditions. The pilot aims to demonstrate
approaches for further deployments in the region and globally.
Parallel research is measuring the impact on health from improved water supply and sanitation
through a randomized control trial (RCT) gathering empirical evidence. The health assessment focuses
predominantly on children under 5 years of age, assessing the impact of interventions on pathogen
burden, markers of intestinal inflammation and function, and drug-resistance markers detected in
feces. Reported symptoms such as fever and diarrhea, child anthropometric markers, and frequency of
healthcare visits are also monitored. Since COVID-19 RISE has analyzed the correlation between
COVID-19 and poverty, population density and access to urban services in its case study sites. The
research is led by Monash University and Wellcome Trust UK.
RISE should produce robust research results on health impacts from RISE interventions, contributing to
the broader evidence of health benefits from improved WASH. This level of resourcing to analyse
health impacts is unusual in the ADB portfolio and unlikely to be a scalable model for other projects.

57 WASH + H Consultancy Final Report
impacts. For example, how well was the intervention implemented? How good were the trainings, or
the construction of infrastructure? How many people were reached by the mass media and BCC?
Without outputs and outcomes impacts will not be achieved.
6.5 Partnerships Current and future partners expressed a desire to collaborate with ADB in the push towards more
WASH+H integration work, especially HyBC and hand hygiene including WHO, LSHTM, WaterAid, and
UNICEF. ADB’s existing regional and sectoral partnerships described in section 4.11 show a diversity of
financing and delivery partners. ADB can take advantage of the window of opportunity currently open,
increase the focus on WASH in COVID-19 response, recovery and future pandemic preparedness and
join other international partners advocating coalescing for HWWS and HyBC in responses. Ensuring the
gains in HWWS during COVID-19 pandemic are institutionalized and sustained is a key area of focus for
many countries and multi-lateral agencies is an active discussion now.
58 WASH + H Consultancy Final Report
7 Conclusions and recommendations The analysis of WASH+H integration in ADB’s portfolio over the last ten years provides examples of
interventions which can be grouped into 12 main types across water, urban, health, ANR and education
sectors. The scope of ADB’s WASH+H projects fall across a spectrum of interventions from sector-
specific to integration to convergence.
There is evidence of a shift to greater emphasis on sustainability in ADB projects and ‘software’:
elements to strengthen institutions and capacities are standard components of infrastructure projects.
This goes some of the way to address the very poor rates of sustainability (financial and service
provision) identified by IED evaluations of urban water and sanitation infrastructure, though a number
of KIIs indicated more needs to be done. Linked to this is the need to front-end project effort to ensure
sufficient data and evidence is gathered and used in preparatory stages, and that infrastructure is well
targeted to reach poor and vulnerable populations, and deliver planned infrastructure with
sustainability and O&M in mind at the outset of design stages. These will not be new recommendations
to ADB, but are emphasized because they are essential for delivering the infrastructure which in turn
provides the environments and opportunities for individuals to practice good hygiene and realize
potential health impacts.
Albeit in tragic circumstances, the COVID-19 pandemic presents a chance to reorient ADB initiatives to
more comprehensively and effectively address hygiene in interventions, policies, strategies and
knowledge activities. There is evidence of this already occurring through, for example, project pivots,
hygiene focused TAs and inclusion of WASH in CPSs released in 2020. Through interviews it was clear
that there are numerous engaged and committed officers already working to adjust programs to the
current crisis and increase WASH+H efforts moving forward. At the risk of oversimplifying ADB’s complex
past investment portfolio, until this juncture there has been limited evidence that ADB’s efforts in
hygiene promotion have been informed by the growing literature on best practice HyBC. Where projects
have hygiene components they are mostly described as awareness raising and community promotion,
and rarely identify target behaviors or hygiene behavior change programs. Through this consultancy no
evidence of attempts to assess the effectiveness of hygiene components was found through either KIIs
or in publicly available project documentation.
Promoting HyBC, especially HWWS, should be advocated for now, not only in COVID-19 Rapid Response
initiatives but also to address a longer-term goal to embed and upscale hygiene in ADB’s activities
broadly. This will need to be multi-pronged and long-term effort. ADB should consider to what extent it
wants to build in-house HyBC expertise or engage external expertise through implementation and
knowledge partners and/or consultants. If building-in house expertise is preferred ADB should consider
building capacities in hygiene promotion and the nuances of effective and evidenced practice. ADB can
make use of available tools, resources and training programs as well as seek inputs from knowledge
partners. In time the understanding that health-based messaging and awareness raising alone is
insufficient to shift behaviors like HWWS should be mainstream within ADB.
There are factors which both inhibit and assist multi-sectoral and holistic programming approaches
within ADB. Multi-sectoral, holistic approaches can have wide reaching health benefits and should be
promoted. The framing of this could be driven by programming approaches (multi-sectoral vs
integration vs convergence), economic models (such as Human Capital), the Corporate Strategy, or other
frameworks which resonate with ADB’s modus operandi. Suggestions for how all this might be achieved
59 WASH + H Consultancy Final Report
are included in Recommendations (Table 10) and some practical steps and guidance to get there
included in Section 8. Recommendations are grouped as short and medium to long-term against six
categories:
vii) Capacity development and learning;
viii) Information, evaluation, innovation and knowledge;
ix) Implementation and Operations;
x) Resources and financing;
xi) Policy, strategy and institutional arrangements; and
xii) Partnerships.
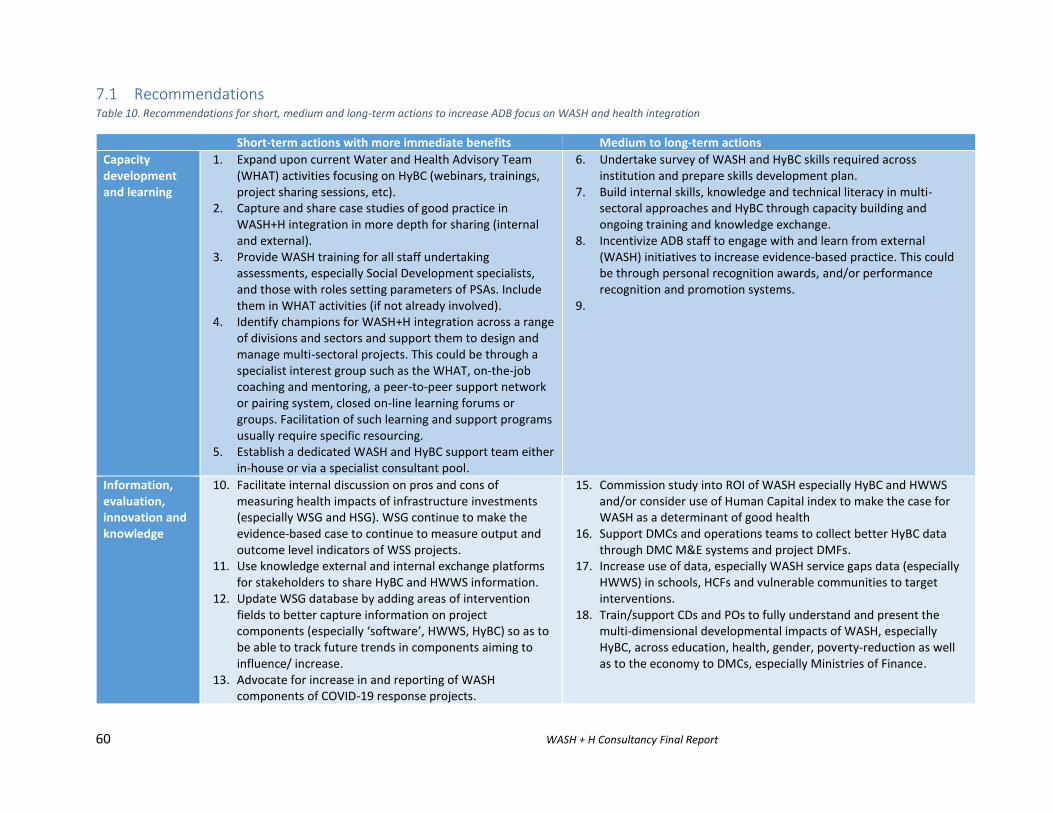
60 WASH + H Consultancy Final Report
7.1 Recommendations Table 10. Recommendations for short, medium and long-term actions to increase ADB focus on WASH and health integration
Short-term actions with more immediate benefits Medium to long-term actions
Capacity development and learning
1. Expand upon current Water and Health Advisory Team (WHAT) activities focusing on HyBC (webinars, trainings, project sharing sessions, etc).
2. Capture and share case studies of good practice in WASH+H integration in more depth for sharing (internal and external).
3. Provide WASH training for all staff undertaking assessments, especially Social Development specialists, and those with roles setting parameters of PSAs. Include them in WHAT activities (if not already involved).
4. Identify champions for WASH+H integration across a range of divisions and sectors and support them to design and manage multi-sectoral projects. This could be through a specialist interest group such as the WHAT, on-the-job coaching and mentoring, a peer-to-peer support network or pairing system, closed on-line learning forums or groups. Facilitation of such learning and support programs usually require specific resourcing.
5. Establish a dedicated WASH and HyBC support team either in-house or via a specialist consultant pool.
6. Undertake survey of WASH and HyBC skills required across institution and prepare skills development plan.
7. Build internal skills, knowledge and technical literacy in multi-sectoral approaches and HyBC through capacity building and ongoing training and knowledge exchange.
8. Incentivize ADB staff to engage with and learn from external (WASH) initiatives to increase evidence-based practice. This could be through personal recognition awards, and/or performance recognition and promotion systems.
9.
Information, evaluation, innovation and knowledge
10. Facilitate internal discussion on pros and cons of measuring health impacts of infrastructure investments (especially WSG and HSG). WSG continue to make the evidence-based case to continue to measure output and outcome level indicators of WSS projects.
11. Use knowledge external and internal exchange platforms for stakeholders to share HyBC and HWWS information.
12. Update WSG database by adding areas of intervention fields to better capture information on project components (especially ‘software’, HWWS, HyBC) so as to be able to track future trends in components aiming to influence/ increase.
13. Advocate for increase in and reporting of WASH components of COVID-19 response projects.
15. Commission study into ROI of WASH especially HyBC and HWWS and/or consider use of Human Capital index to make the case for WASH as a determinant of good health
16. Support DMCs and operations teams to collect better HyBC data through DMC M&E systems and project DMFs.
17. Increase use of data, especially WASH service gaps data (especially HWWS) in schools, HCFs and vulnerable communities to target interventions.
18. Train/support CDs and POs to fully understand and present the multi-dimensional developmental impacts of WASH, especially HyBC, across education, health, gender, poverty-reduction as well as to the economy to DMCs, especially Ministries of Finance.
61 WASH + H Consultancy Final Report
14. Undertake a joint analysis and knowledge piece to quantify gendered health impacts of WUS projects in collaboration with gender thematic group. This will help demonstrate WASH’s contribution to OP2, accelerating progress in gender equality. The possible gendered nature of HyBC work such as community hygiene promotion should be explored in this study. From the analysis seek Trust Fund support to test innovative approaches to reduce unintended consequences of ADB WASH-related projects on women’s burden of work.
19. Develop guidance document on mainstreaming HyBC into infrastructure projects (preferably in conjunction with a knowledge partner) and include HyBC consultant positions in project designs.
20. Review extent to which IED WUS evaluation recommendations have been responded to at institutional level, and document what remains unactioned to improve sustainability of ADB and DMC interventions.
21. Include comprehensive HyBC programs and undertake effectiveness evaluations of HyBC project components in conjunction with knowledge partners/specialists.
22. Include HWWS indicator (% population using at least basic
handwashing facility on premises with soap and water) into DMFs,
CPSs, PSA and Corporate Strategy Results Framework to elevate its importance to be at level with access to basic water and sanitation.
Implementation and Operations
23. Enhance guidance for WASH (especially HyBC) in PSA Guidelines, to improve multi-dimensional poverty targeting and advocate for WASH as a precondition to good health and full economic, educational and societal participation, especially for women and girls.
24. Advocate for and provide technical support as needed to DMCs linked to COVID-19 Rapid Response loans to increase WASH, especially HWWS, for IPC.
25. Urban, Water Divisions provide cross-divisional technical support to education and schools WASH programs for O&M and HyBC as part of COVID-19 recovery.
26. ADB rapidly pivot existing projects and increase support to WASH and hygiene promotion in education projects as part of COVID-19 recovery.
27. Develop a guidance document of best practice project design elements and components (see Section 8).
28. Undertake cross-sectoral project design missions across regional and operational departments, sector and thematic groups for WASH+H integration and multi-sectoral projects and programming.
29. Increase incentives and avail necessary resources to POs/DMCs to incorporate HyBC and BCD into projects, e.g. including HyBC specialist consultants to be involved in project preparatory and implementation stages.
30. Embed effective HyBC programs, BCD, WASH O&M and sustainability guidance in education and health infrastructure project designs and modalities.
31. Encourage more widespread use of Health Impact Assessment in PPTA.
32. For WASH in HCFs, schools and public places, embed WASH O&M and sustainability guidance and requirements in infrastructure project designs and modalities. Data on WASH in HCFs, schools and public places be monitored.
33. Develop systems to capture and share lessons learned from project reviews and effectiveness evaluations of HyBC to influence future design and implementation.
34. Assess ease of partnering with partners like WHO, local NGOs, UNICEF in ADB’s procurement processes.
Resources and financing
35. Make support available in the form of WASH, HyBC and
health specialist inputs to increase HyBC focus in pipeline
36. Develop joint Inclusion Trust Fund with Social Development Section with focus on innovation and mainstreaming WASH+H.
62 WASH + H Consultancy Final Report
projects, including for COVID-19 response projects. This
could be through specialist inputs from a pre-selected
consultants and/or knowledge partners consultant pools
or internally from WSG and additional resources could be
sought from Trust Funds or partnerships with other
donors. For example, ADB operational departments can
seek inputs from the pre-selected panel of WASH+H
Specialists.
37. Increase availability of resources (e.g. Trust Funds resources) to pilot comprehensive and evidence-based HyBC programs at scale, especially in conjunction with infrastructure loans – Also loan resources?
38. Increase resources available (e.g. Trust Fund resources) to pilot and demonstrate innovative programs in: HyBC at scale, BCD, sustainability and O&M initiatives, WASH+H integration, etc.
39. Increase proportion of loans and TA spent on strengthening the WASH enabling environment (capacity building, institutional strengthening, policies, planning and regulation, financial support, etc.) with view to improving sustainability and O&M.
40. Encourage DMCs to borrow more for rural WASH to address urban/rural inequalities as well as urban WASH to address existing gaps
41. Increase emphasis and mention of HyBC and water-related health in CPSs.
Policy, strategy and institutional arrangements
42. Support DMCs to implement and/or develop and resource National Hygiene Plans or Strategies as part of COVID-19 responses .
43. Promote and advocate for WASH, especially HyBC, in conjunction with other divisions (e.g. gender, social protection, health) as contributor to multiple Corporate OPs (see Section 8)
44. Promote holistic approaches to water and sanitation services provision AND hygiene as an important determinants of health through strategies, operations and knowledge platforms.
45. Recognize hygiene as separate to sanitation in ADB policy and strategy documents, and advocate for consistent use of HWWS indicator in DMFs and other results frameworks.
46. Consistently adopt and encourage DMCs to adopt targets and indicators for safely managed drinking water services and sanitation services to align with SDGs and drive towards higher quality service levels.
47. Increase beneficiary-focused decision-making (project targeting, design, implementation, monitoring and impact evaluation).
48. Recognize broader human health benefits of WASH through systems approaches considering not only water-borne diseases, but also AMR, stunting, NTDs as well as climate change health and water impacts.
Partnerships 49. Explore private sector partnerships for HWWS solutions in COVID-19 responses, especially for upscaling use of simple affordable handwashing technologies in low-income areas with poor water service provision.
52. As part of ADB’s MOU with UNICEF, consider implementation-level partnering for delivery of specific ‘software’ project components as well as endorsing and advocating for use of specific UNICEF tools (e.g. WASH in Schools, enabling environment analysis) as
63 WASH + H Consultancy Final Report
50. Establish knowledge and technical support partnerships to progressively develop ADB’s in-house WASH and HyBC expertise in SDCC and Regional Departments. This could be with e.g. LSHTM, IWC or other specialist groups able to provide ongoing training and mentoring as well as project design and review support in HyBC.
51. Seek additional co-financing partnerships with other donors for Trust Funds that can support innovative designs across WASH, health, gender and inclusion, education and social protection
appropriate to DMC context. This would be preferrable to developing ADB guidance tools with similar content.
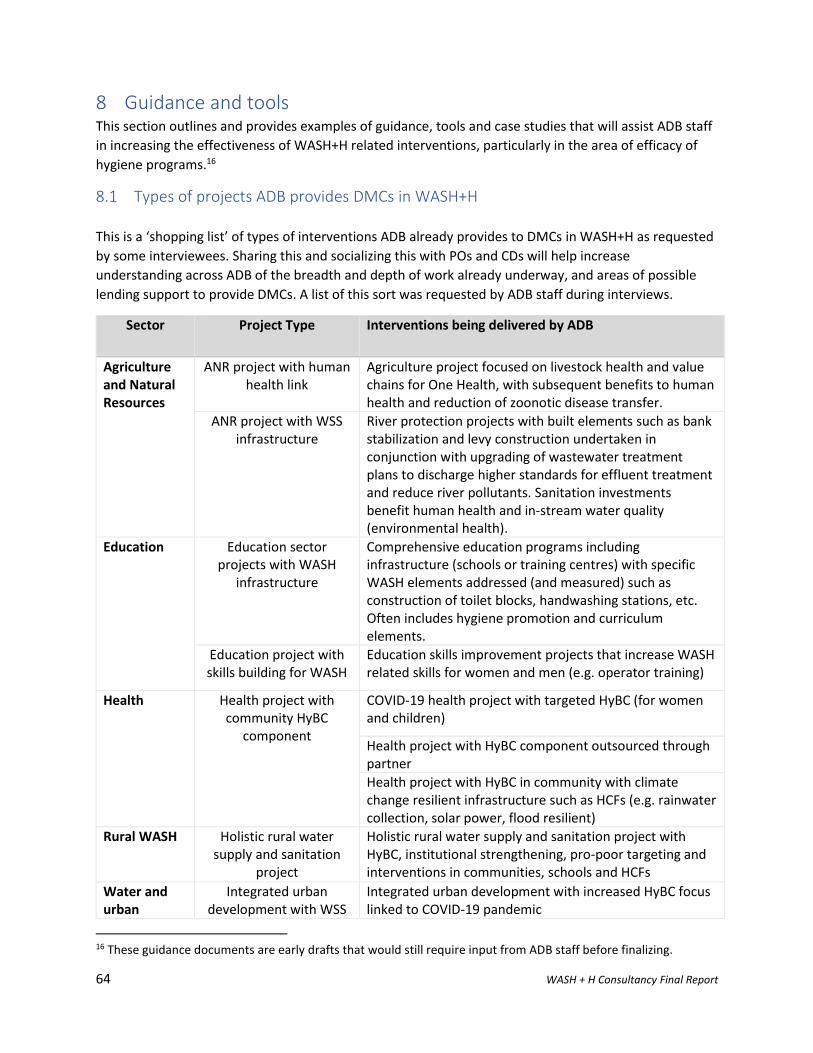
64 WASH + H Consultancy Final Report
8 Guidance and tools This section outlines and provides examples of guidance, tools and case studies that will assist ADB staff
in increasing the effectiveness of WASH+H related interventions, particularly in the area of efficacy of
hygiene programs.16
8.1 Types of projects ADB provides DMCs in WASH+H
This is a ‘shopping list’ of types of interventions ADB already provides to DMCs in WASH+H as requested
by some interviewees. Sharing this and socializing this with POs and CDs will help increase
understanding across ADB of the breadth and depth of work already underway, and areas of possible
lending support to provide DMCs. A list of this sort was requested by ADB staff during interviews.
Sector Project Type Interventions being delivered by ADB
Agriculture and Natural Resources
ANR project with human health link
Agriculture project focused on livestock health and value chains for One Health, with subsequent benefits to human health and reduction of zoonotic disease transfer.
ANR project with WSS infrastructure
River protection projects with built elements such as bank stabilization and levy construction undertaken in conjunction with upgrading of wastewater treatment plans to discharge higher standards for effluent treatment and reduce river pollutants. Sanitation investments benefit human health and in-stream water quality (environmental health).
Education
Education sector projects with WASH
infrastructure
Comprehensive education programs including infrastructure (schools or training centres) with specific WASH elements addressed (and measured) such as construction of toilet blocks, handwashing stations, etc. Often includes hygiene promotion and curriculum elements.
Education project with skills building for WASH
Education skills improvement projects that increase WASH related skills for women and men (e.g. operator training)
Health Health project with community HyBC
component
COVID-19 health project with targeted HyBC (for women and children)
Health project with HyBC component outsourced through partner
Health project with HyBC in community with climate change resilient infrastructure such as HCFs (e.g. rainwater collection, solar power, flood resilient)
Rural WASH Holistic rural water supply and sanitation
project
Holistic rural water supply and sanitation project with HyBC, institutional strengthening, pro-poor targeting and interventions in communities, schools and HCFs
Water and urban
Integrated urban development with WSS
Integrated urban development with increased HyBC focus linked to COVID-19 pandemic
16 These guidance documents are early drafts that would still require input from ADB staff before finalizing.
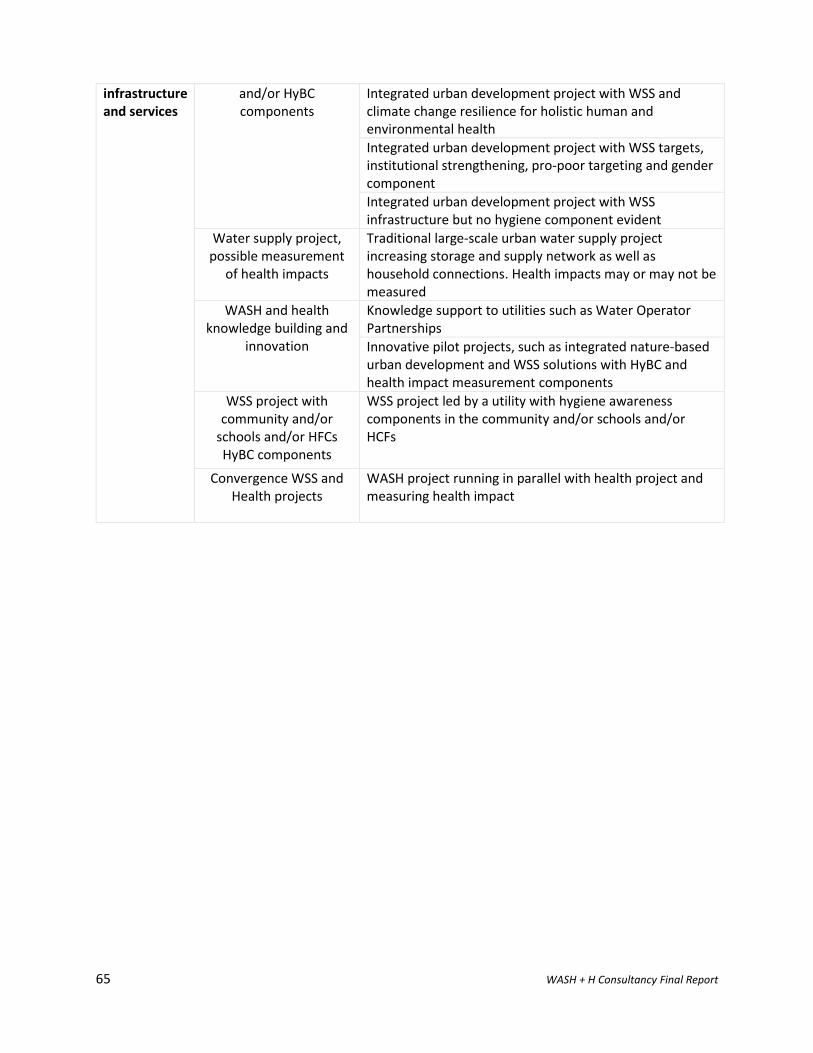
65 WASH + H Consultancy Final Report
infrastructure and services
and/or HyBC components
Integrated urban development project with WSS and climate change resilience for holistic human and environmental health
Integrated urban development project with WSS targets, institutional strengthening, pro-poor targeting and gender component
Integrated urban development project with WSS infrastructure but no hygiene component evident
Water supply project, possible measurement
of health impacts
Traditional large-scale urban water supply project increasing storage and supply network as well as household connections. Health impacts may or may not be measured
WASH and health knowledge building and
innovation
Knowledge support to utilities such as Water Operator Partnerships
Innovative pilot projects, such as integrated nature-based urban development and WSS solutions with HyBC and health impact measurement components
WSS project with community and/or
schools and/or HFCs HyBC components
WSS project led by a utility with hygiene awareness components in the community and/or schools and/or HCFs
Convergence WSS and Health projects
WASH project running in parallel with health project and measuring health impact
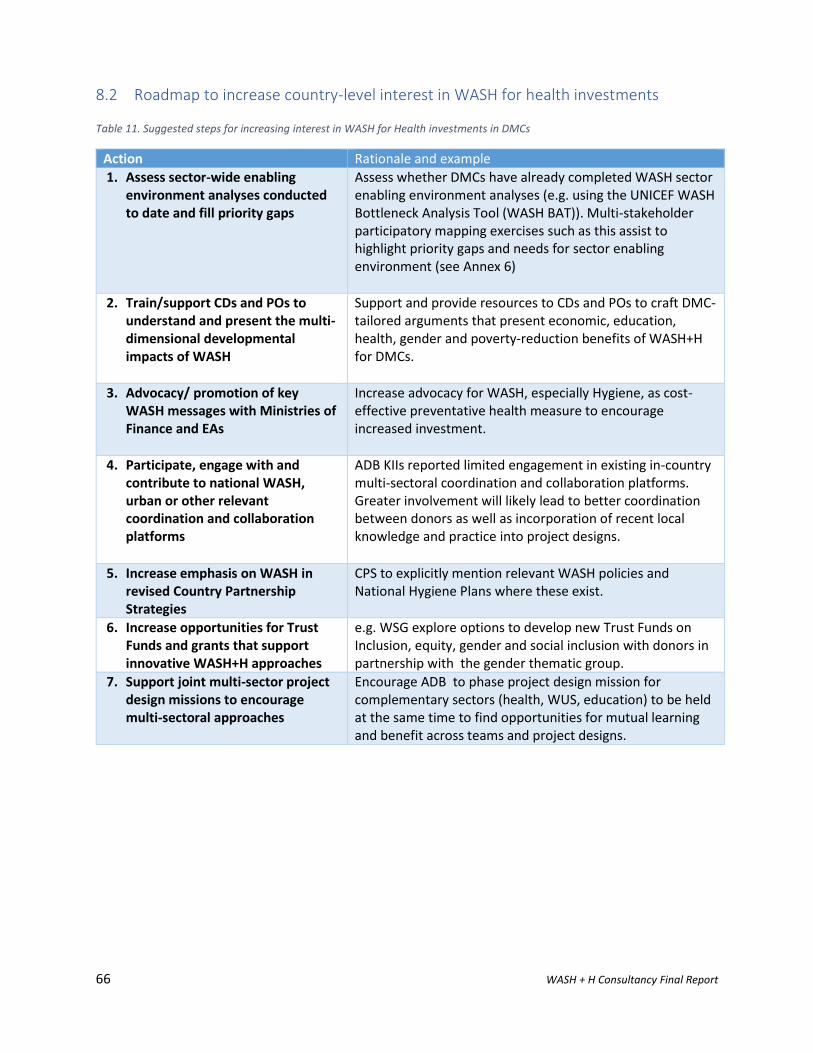
66 WASH + H Consultancy Final Report
8.2 Roadmap to increase country-level interest in WASH for health investments Table 11. Suggested steps for increasing interest in WASH for Health investments in DMCs
Action Rationale and example
1. Assess sector-wide enabling environment analyses conducted to date and fill priority gaps
Assess whether DMCs have already completed WASH sector enabling environment analyses (e.g. using the UNICEF WASH Bottleneck Analysis Tool (WASH BAT)). Multi-stakeholder participatory mapping exercises such as this assist to highlight priority gaps and needs for sector enabling environment (see Annex 6)
2. Train/support CDs and POs to understand and present the multi-dimensional developmental impacts of WASH
Support and provide resources to CDs and POs to craft DMC-tailored arguments that present economic, education, health, gender and poverty-reduction benefits of WASH+H for DMCs.
3. Advocacy/ promotion of key WASH messages with Ministries of Finance and EAs
Increase advocacy for WASH, especially Hygiene, as cost-effective preventative health measure to encourage increased investment.
4. Participate, engage with and contribute to national WASH, urban or other relevant coordination and collaboration platforms
ADB KIIs reported limited engagement in existing in-country multi-sectoral coordination and collaboration platforms. Greater involvement will likely lead to better coordination between donors as well as incorporation of recent local knowledge and practice into project designs.
5. Increase emphasis on WASH in revised Country Partnership Strategies
CPS to explicitly mention relevant WASH policies and National Hygiene Plans where these exist.
6. Increase opportunities for Trust Funds and grants that support innovative WASH+H approaches
e.g. WSG explore options to develop new Trust Funds on Inclusion, equity, gender and social inclusion with donors in partnership with the gender thematic group.
7. Support joint multi-sector project design missions to encourage multi-sectoral approaches
Encourage ADB to phase project design mission for complementary sectors (health, WUS, education) to be held at the same time to find opportunities for mutual learning and benefit across teams and project designs.
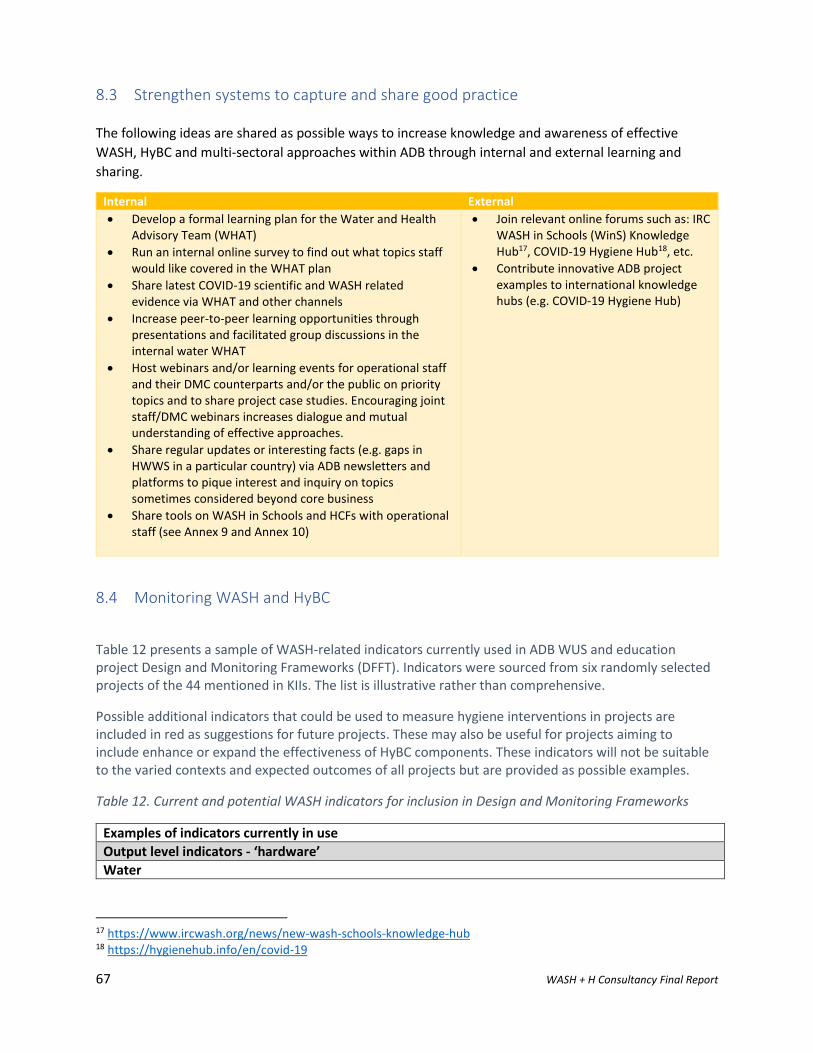
67 WASH + H Consultancy Final Report
8.3 Strengthen systems to capture and share good practice
The following ideas are shared as possible ways to increase knowledge and awareness of effective
WASH, HyBC and multi-sectoral approaches within ADB through internal and external learning and
sharing.
Internal External
• Develop a formal learning plan for the Water and Health Advisory Team (WHAT)
• Run an internal online survey to find out what topics staff would like covered in the WHAT plan
• Share latest COVID-19 scientific and WASH related evidence via WHAT and other channels
• Increase peer-to-peer learning opportunities through presentations and facilitated group discussions in the internal water WHAT
• Host webinars and/or learning events for operational staff and their DMC counterparts and/or the public on priority topics and to share project case studies. Encouraging joint staff/DMC webinars increases dialogue and mutual understanding of effective approaches.
• Share regular updates or interesting facts (e.g. gaps in HWWS in a particular country) via ADB newsletters and platforms to pique interest and inquiry on topics sometimes considered beyond core business
• Share tools on WASH in Schools and HCFs with operational staff (see Annex 9 and Annex 10)
• Join relevant online forums such as: IRC WASH in Schools (WinS) Knowledge Hub17, COVID-19 Hygiene Hub18, etc.
• Contribute innovative ADB project examples to international knowledge hubs (e.g. COVID-19 Hygiene Hub)
8.4 Monitoring WASH and HyBC
Table 12 presents a sample of WASH-related indicators currently used in ADB WUS and education project Design and Monitoring Frameworks (DFFT). Indicators were sourced from six randomly selected projects of the 44 mentioned in KIIs. The list is illustrative rather than comprehensive.
Possible additional indicators that could be used to measure hygiene interventions in projects are included in red as suggestions for future projects. These may also be useful for projects aiming to include enhance or expand the effectiveness of HyBC components. These indicators will not be suitable to the varied contexts and expected outcomes of all projects but are provided as possible examples.
Table 12. Current and potential WASH indicators for inclusion in Design and Monitoring Frameworks
Examples of indicators currently in use
Output level indicators - ‘hardware’
Water
17 https://www.ircwash.org/news/new-wash-schools-knowledge-hub 18 https://hygienehub.info/en/covid-19
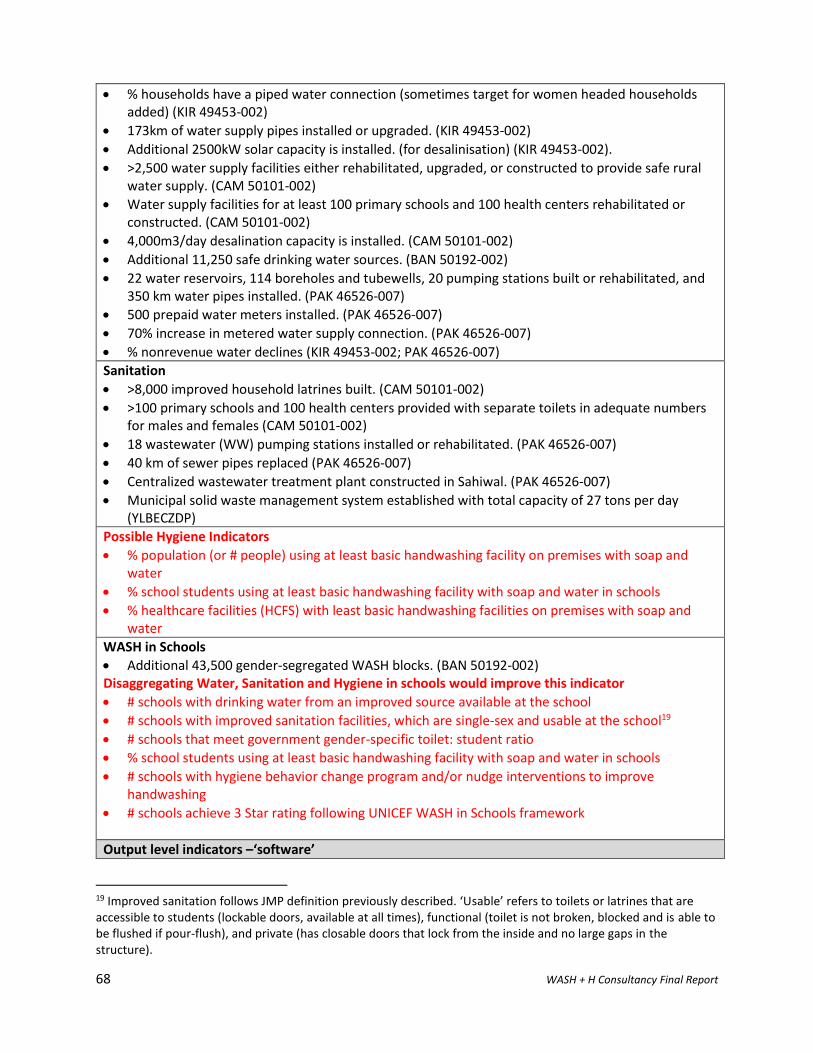
68 WASH + H Consultancy Final Report
• % households have a piped water connection (sometimes target for women headed households added) (KIR 49453-002)
• 173km of water supply pipes installed or upgraded. (KIR 49453-002)
• Additional 2500kW solar capacity is installed. (for desalinisation) (KIR 49453-002).
• >2,500 water supply facilities either rehabilitated, upgraded, or constructed to provide safe rural water supply. (CAM 50101-002)
• Water supply facilities for at least 100 primary schools and 100 health centers rehabilitated or constructed. (CAM 50101-002)
• 4,000m3/day desalination capacity is installed. (CAM 50101-002)
• Additional 11,250 safe drinking water sources. (BAN 50192-002)
• 22 water reservoirs, 114 boreholes and tubewells, 20 pumping stations built or rehabilitated, and 350 km water pipes installed. (PAK 46526-007)
• 500 prepaid water meters installed. (PAK 46526-007)
• 70% increase in metered water supply connection. (PAK 46526-007)
• % nonrevenue water declines (KIR 49453-002; PAK 46526-007)
Sanitation
• >8,000 improved household latrines built. (CAM 50101-002)
• >100 primary schools and 100 health centers provided with separate toilets in adequate numbers for males and females (CAM 50101-002)
• 18 wastewater (WW) pumping stations installed or rehabilitated. (PAK 46526-007)
• 40 km of sewer pipes replaced (PAK 46526-007)
• Centralized wastewater treatment plant constructed in Sahiwal. (PAK 46526-007)
• Municipal solid waste management system established with total capacity of 27 tons per day (YLBECZDP)
Possible Hygiene Indicators
• % population (or # people) using at least basic handwashing facility on premises with soap and water
• % school students using at least basic handwashing facility with soap and water in schools
• % healthcare facilities (HCFS) with least basic handwashing facilities on premises with soap and water
WASH in Schools
• Additional 43,500 gender-segregated WASH blocks. (BAN 50192-002) Disaggregating Water, Sanitation and Hygiene in schools would improve this indicator
• # schools with drinking water from an improved source available at the school
• # schools with improved sanitation facilities, which are single-sex and usable at the school19
• # schools that meet government gender-specific toilet: student ratio
• % school students using at least basic handwashing facility with soap and water in schools
• # schools with hygiene behavior change program and/or nudge interventions to improve handwashing
• # schools achieve 3 Star rating following UNICEF WASH in Schools framework
Output level indicators –‘software’
19 Improved sanitation follows JMP definition previously described. ‘Usable’ refers to toilets or latrines that are accessible to students (lockable doors, available at all times), functional (toilet is not broken, blocked and is able to be flushed if pour-flush), and private (has closable doors that lock from the inside and no large gaps in the structure).
69 WASH + H Consultancy Final Report
Water
• >80% of district administrations implement water quality testing procedures. (CAM 50101-002)
• # behavior change activities delivered following BCD approach to target household water management behaviors affecting utility performance (NRW, illegal connections, paying tariffs etc)
Sanitation and Hygiene
• >40,000 households residing in at least 11 districts have reported improved awareness and/or knowledge of sanitation and hygiene. (CAM 50101-002)
• >95% of the population is reached directly or indirectly by WASH and climate change awareness programs, which use gender-sensitive materials (CAM 50101-002)
Possible Hygiene Indicators
• Formative research and behavior centered design (BCD) hygiene behavior change program developed to target X (specific behavior such as HWWS, household water treatment etc)
• # behavior change initiatives/ nudges/ activities delivered as part of BCD program
• # people reached and # ‘touchpoints’ (i.e. amount of exposure) through BCD program
WASH
• % of the population is reached directly or indirectly by WASH and climate change awareness programs, which use gender-sensitive materials (KIR 49453-002)
• 1,000 people have visited the WASH and climate change visitor education center. (CAM 50101-002)
Training and capacity
• 250 national and subnational staff (at least 40% women) participated in technical, financial, management, and leadership training. (RWSSDP)
• PUB customers (75% of them women) in 250 communities report improved financial literacy. (CAM 50101-002)
• Utility and EA staff report positive outcomes from exposure to training and/or monitoring programs (KIR 49453-002)
Possible indicators
• # (non-volunteer) hygiene behavior change specialists trained in HyBC messaging
Business management and operational improvements
• Private operator supporting utility operations is in place and operational (KIR 49453-002)
• Utility meets dispursement and reporting requirements (KIR 49453-002)
• Standard procedure for septage management in rural areas is issued. (Cambodia WSS)
• Utility (PUB) achieves 95% collection ratio. (CAM 50101-002)
• New supervisory control and data administration system established. (PAK 46526-007)
• Utility meets disbursement and reporting requirements (CAM 50101-002)
• Utility and EA staff report positive outcomes from exposure to training and/or monitoring programs (CAM 50101-002)
• Private operator supporting utility operations is in place and operational (CAM 50101-002)
Gender
• % of new technical recruits to Utility and EA are women (KIR 49453-002)
• 50% of community mobilizers contracted through the WASH and climate change program are women (KIR 49453-002)
• >40% women members in 2,500 WSUG boards. (CAM 50101-002)
• >20% of new technical recruits to Utility and EA are women. (CAM 50101-002)
• PUB customers (75% of them women) in 250 communities report improved financial literacy. (CAM 50101-002)
70 WASH + H Consultancy Final Report
• >50% of community mobilizers contracted through the WASH and climate change program are women. (CAM 50101-002)
• Additional 43,500 gender-segregated WASH blocks. (BAN 50192-002)
• 250 national and subnational staff (at least 40% women) participated in technical, financial, management, and leadership training. (RWSSDP)
• >20% women among all (75) technical and financial management staff of the project management unit and city implementation units, and Water Sanitation Company trained. (PAK 46526-007)
• > 50% of MCH health workers trained on gender sensitive referral protocols. (TMHC)
• Utility delivers project progress and semi-annual gender action plan reports, including sex-disaggregated data. (CAM 50101-002)
Evidence
• Using a variety of social science techniques, qualitative data is collected over the life of the project in 4–6 project areas to measure positive impacts on women’s daily lives resulting from 24/7 access to safe water. These would include baseline, mid and end of project surveys.(KIR 49453-002)
• All 10 target provinces produce an annual water quality monitoring report based on the rural drinking water quality standard (2019 baseline: not applicable) (CAM 50101-002)
• Integrated web-based information with sex-disaggregated data (including for social groups) made operational in DPE. (BAN 50192-002)
• At least one study or development plan completed on each of the following: […] v) health care services and hospital management improvement, […] and (viii) policy dialogue on water tariff system to meet the PRC regulations. (PRC 49310-002)
Possible Indicators
• Baseline, mid and end line project surveys (quantitative and qualitative) assess impact on behaviors targeted through BCD program
Outcome level indicators (note only WASH contributing outcomes are listed)
• The cost of acquiring safe drinking water in at least 11 districts reduced by 50%. (CAM 50101-002)
• At least 90% of water quality tests conducted in at least 11 districts show that the quality of rural drinking water meets the standard. (CAM 50101-002)
• Access of South Tarawa’s population to safe, climate-resilient water supplies increased.
• By 2027, at least 95% of South Tarawa’s population (51.5% of them women) has access to safe, climate-resilient water supplies. (CAM 50101-002)
• Access to quality urban services by the residents of Sialkot and Sahiwal cities improved. (PAK 46526-007)
• Total population in Sialkot and Sahiwal city consuming improved water supplies increased from existing 50% to 70%
• Volume of wastewater treatment increased to at least 80,000 cubic meters per day in Sialkot and Sahiwal respectively.
• Competitiveness of urban centers, logistics and industrial parks, and land ports in project counties and LBECZ enhanced. (PRC 49310-002)
• Urban residents’ rate of satisfaction with use of road, water supply, wastewater, and municipal solid waste increased to 60%.
Possible Indicators
• % population (or # people) using at least basic handwashing facility on premises with soap and water increases from X to Y.
• Water provider develops comprehensive and evidence-based HyBC plan and allocates sufficient resources for implementation
71 WASH + H Consultancy Final Report
Projects included are: Bangladesh Supporting Fourth Primary Education Development Program (BAN 50192-002);
Cambodia Third Rural Water Supply and Sanitation Services Sector Development Program (CAM 50101-002) ;
Yinnan Lincang Border Economic Cooperation Zone Development Project (PRC 49310-002); Punjab Intermediate
Cities Improvement Investment Project (PAK 46526-007); South Tarawa Water Supply Project (KIR 49453-002);
Vietnam Skills and Knowledge for Inclusive Economic Growth Project (VIE 49122-004).
72 WASH + H Consultancy Final Report
Annex 1. References
ADB. (2003). Social Protection Policy . Manilla: Asian Development Bank.
ADB. (2012). Handbook on Poverty and Social Analysis: A Working Document. Mandaluyong City: Asian
Development Bank .
ADB. (2015). Topical Paper: Sustainability of Urban Water Supply and Sanitation Operations Findings and
Lessons. Independent Evaluation Asian Development Bank .
ADB. (2017). Meeting Asia's Infrastructure Needs . Mandaluyong City: Asian Development Bank .
ADB. (2018). Leading Factors of Success and Failure in Asian Development Bank Urban Sanitation
Projects. Manilla: Independent Evaluation Asian Development Bank.
ADB. (2104). Guidance note: Poverty and social dimensions in urban projects. . Mandaluyong City,
Philippines : Asian Development Bank .
ADB. (July 2018). STRATEGY 2030: Achieving a Prosperous, Inclusive, Resilient, and Sustainable Asia and
the Pacific. Manilla: Asian Development Bank .
ADB. (Sept 2019 ). Strategy 2030 Operational Plans Overview . Manilla : Asian Development Bank .
Aunger, R., & Curtis, V. (2014). The Evo-Eco approach to behaviour change’. In D. L. Gibson, Applied
Evolutionary Anthropology. Springer.
Aunger, R., & Curtis, V. (2016). Behaviour Centred Design: towards an applied science of behaviour
change. Health Psychology Review, 10:4, 425-446.
Coombes, Y & Devine, J. (2010). Introducing FOAM: A Framework to Analyze Handwashing Behaviors to
Design Effective Handwashing Programs. Washington D.C. : Water and Sanitation Program,
World Bank.
CS WASH Fund. (2017). Hygiene Behaviour Change in the Civil Society WASH Fund. Brisbane: Civil Society
WASH Fund, Palladium & DFAT.
Cumming, O. E. (2019 ). The implications of three major new trials for the effect of water, sanitation and
hygiene on childhood diarrhea and stunting: a consensus statement. BMC Medicine , 17:173.
Curtis, V. (2020). How to set up government-led national hygiene communication campaigns to combat
COVID-19: a strategic blueprint. BMJ Global Health, 1-11.
Dem, T. a. (June 2018). Hygiene Cost Effectiveness Study in Bhutan. SNV and IRC.
Devine, J. (2009). Introducing SaniFOAM: A Framework to Analyse Sanitation Behaviours to Design
Effective Sanitation Programs. Washington D.C. : Water Sanitation Program, World Bank .
Dreibelbis, R. A. (2016). Behavior Change without Behavior Change Communication: Nudging
Handwashing among Primary School Students in Bangladesh. Int J Environ Res Public Health,
13(1): 129.
73 WASH + H Consultancy Final Report
Freeman, M. S. (2014). al. Hygiene and health: Systematic review of handwashing practices worldwide
and update of health effects. Tropical Medicine & International Health, 19: 906–916.
GPRB. (2012). National Hygiene Promotion Strategy for Water Supply and Sanitation Sector in
Bangladesh 2012. Government of the People's Republic of Bangladesh Ministry of Local
Government, Rural Development and Cooperatives Local Government Division.
Howard, G. J. (2020). COVID-19: urgent actions, critical reflections and future. Journal of Water,
Sanitation and Hygiene for Development, in press.
Huang, C. N. (2020, May). A nudge toward hand hygiene: simple design features improved handwashing
among Filipino students. Retrieved from IDInsight Blog: https://medium.com/idinsight-blog/a-
nudge-toward-hand-hygiene-simple-design-features-improved-handwashing-among-filipino-
students-ae4fab1c94db
Hutton., G. (2015). Benefits and Costs of the Water Sanitation and Hygiene Targets for the Post-2015
Development Agenda Post-2015 Consensus. Copenhagen Consensus Centre Working Paper. .
World Bank.
IFC. (June 2020). The Impact of COVID-19 on the Water and Sanitation Sector. International Finance
Corporation (IFC): World Bank Group.
Prüss-Ustün, A. W. (2019). Burden of disease from inadequate water, sanitation and hygiene for
selected adverse health outcomes: An updated analysis with a focus on low and middle-income
countries. International Journal of Hygiene and Environmental Health, 765-777.
Rabie, T. a. (2006). Handwashing and risk of respiratory infections: a quantitative systematic review .
Tropical Medicine & International Health, 11(3): 258-67.
Save the Children . (April 2019). NOURISH Project Endline Survey . Phnom Penh : Save the Children .
Schulte, P. R. (2020, July). Water and the COVID-19 Pandemic: A Business Framework for Water and
COVID-19. Retrieved from Pacific Institute: https://pacinst.org/wp-
content/uploads/2020/07/Pacific-Institute_Business-Framework-for-Water-COVID-19.pdf
Spears, D. G. (2013). Open Defecation and Childhood Stunting in India: An Ecological Analysis of New
Data from 112 Districts. PLOS ONE, 8(9).
Townsend, J., Greenland, K., & Curtis, V. (2016). Costs of diarrhoea and acute respiratory infection
attributable to not handwashing: the cases of India and China. Tropical Medicine & International
Health.
UNEP. (2020, August 6). United Nations Environment Program . Retrieved from
https://www.unenvironment.org/explore-topics/climate-change/facts-about-climate-
emergency
UNICEF. (2016). UNICEF . Retrieved from Water, Sanitation and Hygiene :
https://www.unicef.org/wash/3942_3952.html
UNICEF. (2020). Overview of Water, Sanitation and Hygiene (WASH) COVID-19 Responses from
Governments, Regulators, Utilities and other Stakeholders in 84 Countries. UNICEF.
74 WASH + H Consultancy Final Report
UNICEF/WHO. (2019). Progress on household drinking water, sanitation and hygiene 2000-2017: Special
focus on inequalities. New York : United Nations Children’s Fund (UNICEF) and World Health
Organization (WHO).
Wang, Z. L. (2017 ). The effect of hand-hygiene interventions on infectious disease-associated
absenteeism in elementary schools: A systematic literature review. American Journal of Infection
Control , 45: 682–689.
WaterAid . (2020, September 14). Retrieved from WaterAid :
https://washmatters.wateraid.org/blog/water-and-sanitation-service-providers-and-the-
challenges-of-covid-19
WaterAid. (2020, September 1). Water and sanitation service providers and the challenges of COVID-19.
Retrieved from WaterAid: https://washmatters.wateraid.org/blog/water-and-sanitation-service-
providers-and-the-challenges-of-covid-19
WaterAid. (2020, September 10). WaterAid . Retrieved from
https://washmatters.wateraid.org/publications/practical-pathways-nutrition-wash
WHO. (2020). Hygiene: UN-Water GLAAS findings on national policies, plans, targets and finance.
Geneva: World Health Organization.
WHO. (2020). Hygiene: UN-Water GLAAS Findings on National Policies, Plans, Targets and Finance.
Geneva: World Health Organization .
WHO. (2020, August 5). World Health Organisation. Retrieved from 785 million people lack even a basic
drinking-water service,
WHO. (2020). World Health Organization. Retrieved from Anti-Microbial Resistance:
https://www.who.int/news-room/fact-sheets/detail/antimicrobial-resistance
WHO/UNICEF. (2015). Water, sanitation and hygiene in health care facilities: Status in low- and middle-
income countries and way forward. Geneva: World Health Organization.
WHO/UNICEF. (2018). Drinking Water, Sanitation and Hygiene in Schools: Global baseline report 2018.
Geneva: World Health Organisation (WHO) and United Nations Children's Fund (UNICEF).
WHO/UNICEF. (2019 ). WASH in Healthcare Facilities: Global Baseline Report . Geneva: World Health
Organisation (WHO) and United Nations Children's Fund (UNICEF) .
WHO/UNICEF. (2020, July). Retrieved from JMP WASH data : https://washdata.org/
WHO/UNICEF. (2020). Water, sanitation, hygiene, and waste management for SARS-CoV-2, the virus that
causes COVID-19: Interim guidance. 29 July 2020.
Wolf, J. ,.-U. (2019). Handwashing with soap after potential faecal contact: global, regional and country
estimates. International Journal of Epidemiology, 1204–1218.
World Bank . (2018). The Human Capital Project. Washington DC: International Bank for Reconstruction
and Development / The World Bank.
75 WASH + H Consultancy Final Report
World Bank . (2019, June). The World Bank . Retrieved from
https://www.worldbank.org/en/country/lao/brief/multi-sector-convergence-approach-to-
reducing-malnutrition-in-lao-pdr
World Bank . (2020). The Human Capital Index 2020 Update: Human Capital in the time of COVID-19 .
Washington DC: International Bank for Reconstruction and Development / The World Bank.
WSSCC. (2020, July). Water Supply and Sanitation Collaborative Council . Retrieved from
https://www.wsscc.org/media/resources/frequently-asked-questions-wsscc-evolving-
sanitation-and-hygiene-fund-2021
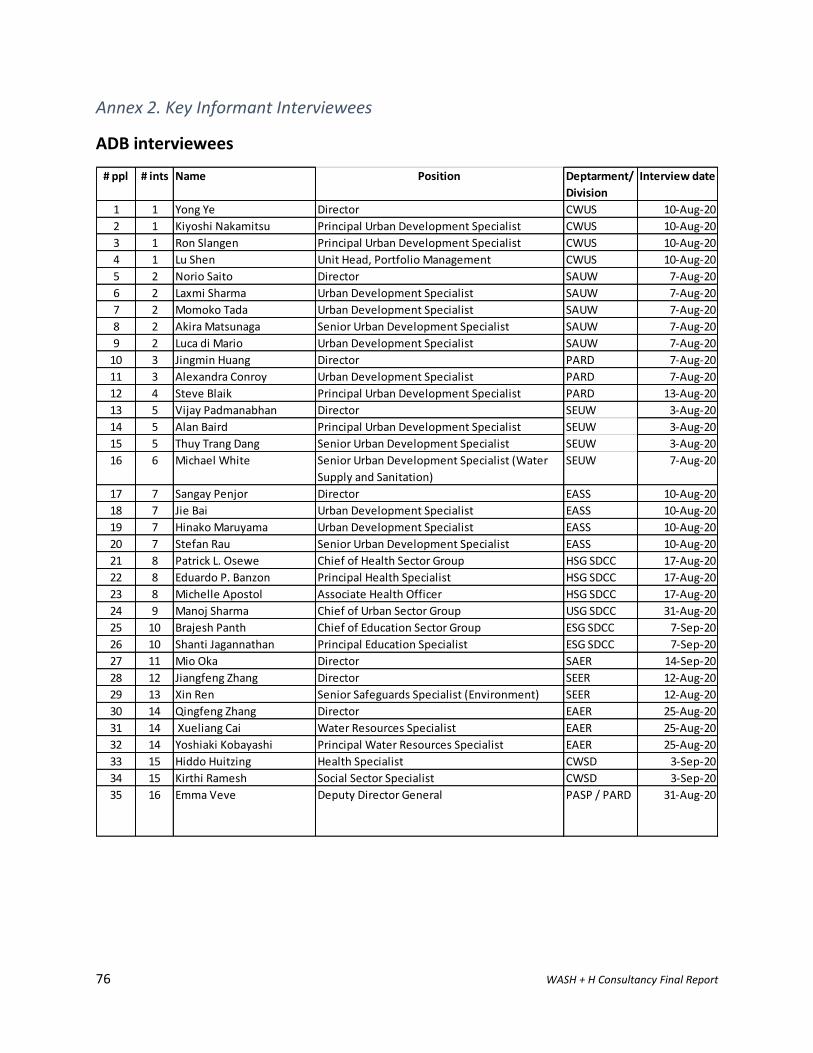
76 WASH + H Consultancy Final Report
Annex 2. Key Informant Interviewees
ADB interviewees
# ppl # ints Name Position Deptarment/
Division
Interview date
1 1 Yong Ye Director CWUS 10-Aug-20
2 1 Kiyoshi Nakamitsu Principal Urban Development Specialist CWUS 10-Aug-20
3 1 Ron Slangen Principal Urban Development Specialist CWUS 10-Aug-20
4 1 Lu Shen Unit Head, Portfolio Management CWUS 10-Aug-20
5 2 Norio Saito Director SAUW 7-Aug-20
6 2 Laxmi Sharma Urban Development Specialist SAUW 7-Aug-20
7 2 Momoko Tada Urban Development Specialist SAUW 7-Aug-20
8 2 Akira Matsunaga Senior Urban Development Specialist SAUW 7-Aug-20
9 2 Luca di Mario Urban Development Specialist SAUW 7-Aug-20
10 3 Jingmin Huang Director PARD 7-Aug-20
11 3 Alexandra Conroy Urban Development Specialist PARD 7-Aug-20
12 4 Steve Blaik Principal Urban Development Specialist PARD 13-Aug-20
13 5 Vijay Padmanabhan Director SEUW 3-Aug-20
14 5 Alan Baird Principal Urban Development Specialist SEUW 3-Aug-20
15 5 Thuy Trang Dang Senior Urban Development Specialist SEUW 3-Aug-20
16 6 Michael White Senior Urban Development Specialist (Water
Supply and Sanitation)
SEUW 7-Aug-20
17 7 Sangay Penjor Director EASS 10-Aug-20
18 7 Jie Bai Urban Development Specialist EASS 10-Aug-20
19 7 Hinako Maruyama Urban Development Specialist EASS 10-Aug-20
20 7 Stefan Rau Senior Urban Development Specialist EASS 10-Aug-20
21 8 Patrick L. Osewe Chief of Health Sector Group HSG SDCC 17-Aug-20
22 8 Eduardo P. Banzon Principal Health Specialist HSG SDCC 17-Aug-20
23 8 Michelle Apostol Associate Health Officer HSG SDCC 17-Aug-20
24 9 Manoj Sharma Chief of Urban Sector Group USG SDCC 31-Aug-20
25 10 Brajesh Panth Chief of Education Sector Group ESG SDCC 7-Sep-20
26 10 Shanti Jagannathan Principal Education Specialist ESG SDCC 7-Sep-20
27 11 Mio Oka Director SAER 14-Sep-20
28 12 Jiangfeng Zhang Director SEER 12-Aug-20
29 13 Xin Ren Senior Safeguards Specialist (Environment) SEER 12-Aug-20
30 14 Qingfeng Zhang Director EAER 25-Aug-20
31 14 Xueliang Cai Water Resources Specialist EAER 25-Aug-20
32 14 Yoshiaki Kobayashi Principal Water Resources Specialist EAER 25-Aug-20
33 15 Hiddo Huitzing Health Specialist CWSD 3-Sep-20
34 15 Kirthi Ramesh Social Sector Specialist CWSD 3-Sep-20
35 16 Emma Veve Deputy Director General PASP / PARD 31-Aug-20
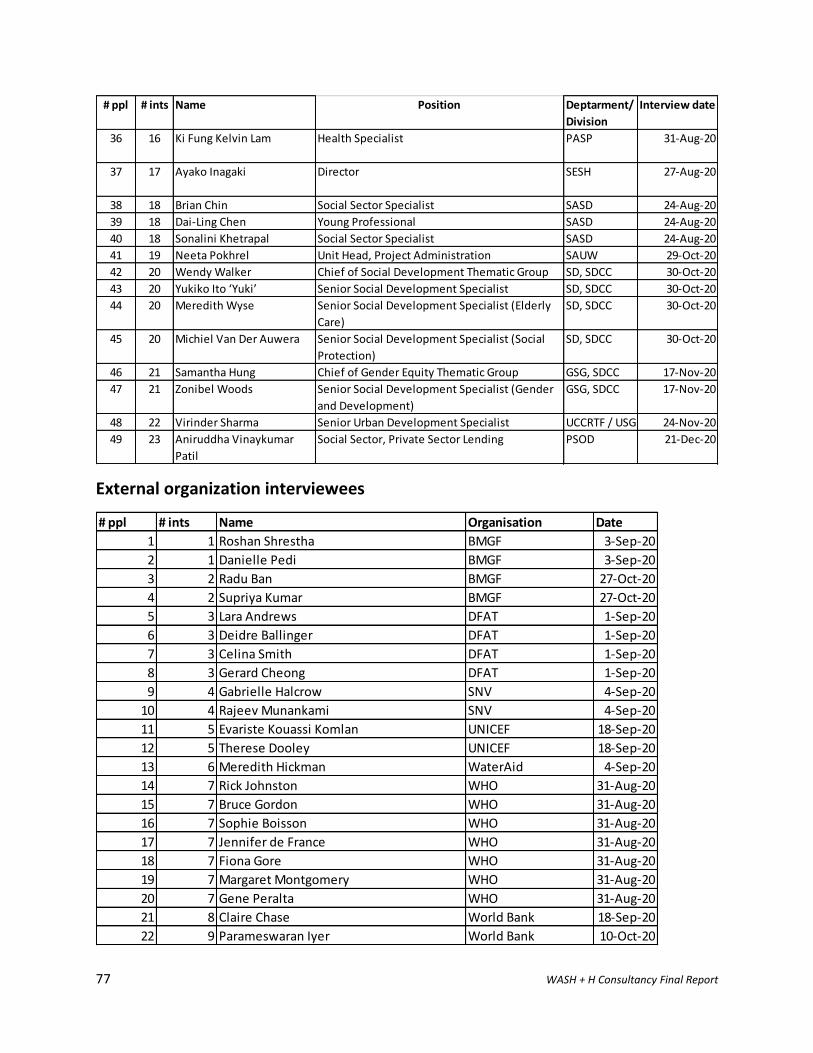
77 WASH + H Consultancy Final Report
External organization interviewees
# ppl # ints Name Position Deptarment/
Division
Interview date
36 16 Ki Fung Kelvin Lam Health Specialist PASP 31-Aug-20
37 17 Ayako Inagaki Director SESH 27-Aug-20
38 18 Brian Chin Social Sector Specialist SASD 24-Aug-20
39 18 Dai-Ling Chen Young Professional SASD 24-Aug-20
40 18 Sonalini Khetrapal Social Sector Specialist SASD 24-Aug-20
41 19 Neeta Pokhrel Unit Head, Project Administration SAUW 29-Oct-20
42 20 Wendy Walker Chief of Social Development Thematic Group SD, SDCC 30-Oct-20
43 20 Yukiko Ito ‘Yuki’ Senior Social Development Specialist SD, SDCC 30-Oct-20
44 20 Meredith Wyse Senior Social Development Specialist (Elderly
Care)
SD, SDCC 30-Oct-20
45 20 Michiel Van Der Auwera Senior Social Development Specialist (Social
Protection)
SD, SDCC 30-Oct-20
46 21 Samantha Hung Chief of Gender Equity Thematic Group GSG, SDCC 17-Nov-20
47 21 Zonibel Woods Senior Social Development Specialist (Gender
and Development)
GSG, SDCC 17-Nov-20
48 22 Virinder Sharma Senior Urban Development Specialist UCCRTF / USG 24-Nov-20
49 23 Aniruddha Vinaykumar
Patil
Social Sector, Private Sector Lending PSOD 21-Dec-20
# ppl # ints Name Organisation Date
1 1 Roshan Shrestha BMGF 3-Sep-20
2 1 Danielle Pedi BMGF 3-Sep-20
3 2 Radu Ban BMGF 27-Oct-20
4 2 Supriya Kumar BMGF 27-Oct-20
5 3 Lara Andrews DFAT 1-Sep-20
6 3 Deidre Ballinger DFAT 1-Sep-20
7 3 Celina Smith DFAT 1-Sep-20
8 3 Gerard Cheong DFAT 1-Sep-20
9 4 Gabrielle Halcrow SNV 4-Sep-20
10 4 Rajeev Munankami SNV 4-Sep-20
11 5 Evariste Kouassi Komlan UNICEF 18-Sep-20
12 5 Therese Dooley UNICEF 18-Sep-20
13 6 Meredith Hickman WaterAid 4-Sep-20
14 7 Rick Johnston WHO 31-Aug-20
15 7 Bruce Gordon WHO 31-Aug-20
16 7 Sophie Boisson WHO 31-Aug-20
17 7 Jennifer de France WHO 31-Aug-20
18 7 Fiona Gore WHO 31-Aug-20
19 7 Margaret Montgomery WHO 31-Aug-20
20 7 Gene Peralta WHO 31-Aug-20
21 8 Claire Chase World Bank 18-Sep-20
22 9 Parameswaran Iyer World Bank 10-Oct-20

78 WASH + H Consultancy Final Report
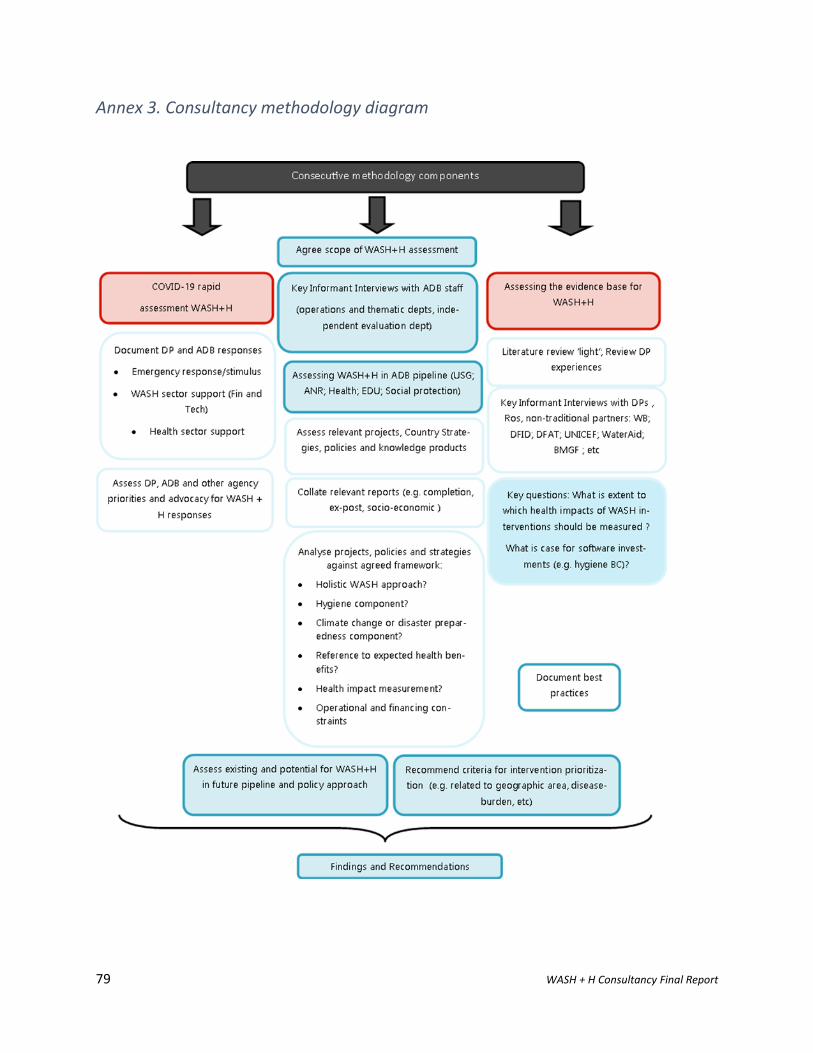
79 WASH + H Consultancy Final Report
Annex 3. Consultancy methodology diagram
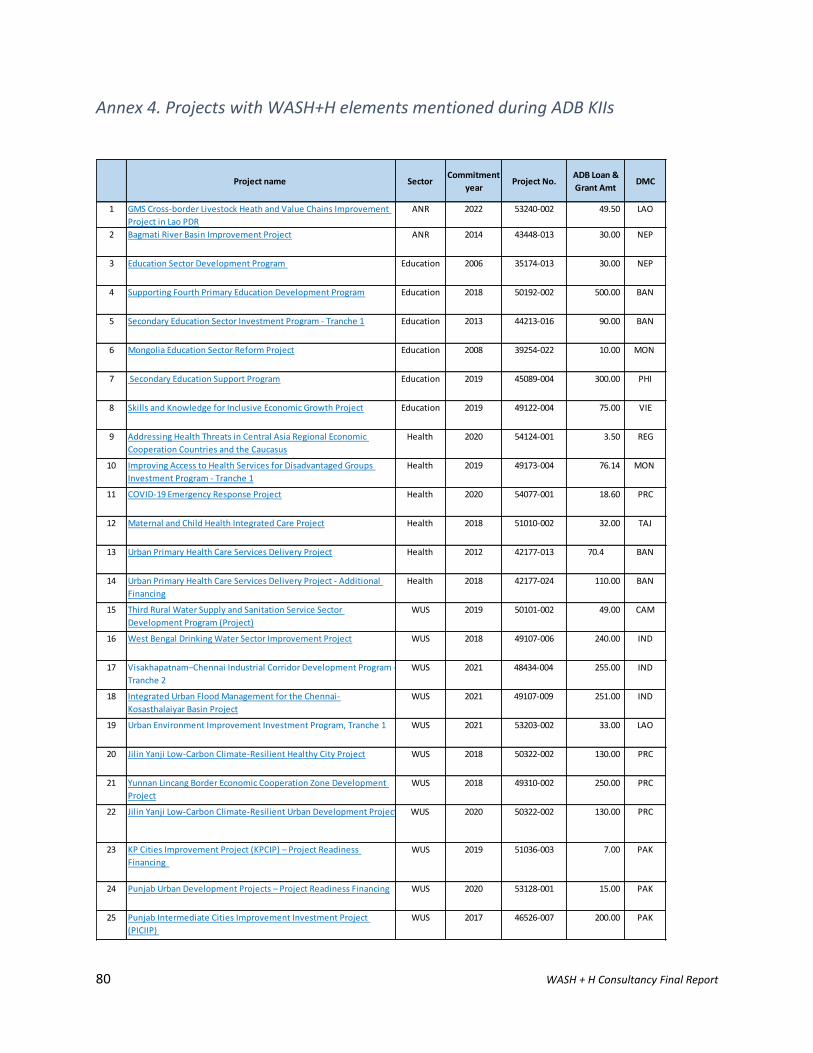
80 WASH + H Consultancy Final Report
Annex 4. Projects with WASH+H elements mentioned during ADB KIIs
Project name Sector Commitment
year Project No.
ADB Loan &
Grant AmtDMC
1 GMS Cross-border Livestock Heath and Value Chains Improvement
Project in Lao PDR
ANR 2022 53240-002 49.50 LAO
2 Bagmati River Basin Improvement Project ANR 2014 43448-013 30.00 NEP
3 Education Sector Development Program Education 2006 35174-013 30.00 NEP
4 Supporting Fourth Primary Education Development Program Education 2018 50192-002 500.00 BAN
5 Secondary Education Sector Investment Program - Tranche 1 Education 2013 44213-016 90.00 BAN
6 Mongolia Education Sector Reform Project Education 2008 39254-022 10.00 MON
7 Secondary Education Support Program Education 2019 45089-004 300.00 PHI
8 Skills and Knowledge for Inclusive Economic Growth Project Education 2019 49122-004 75.00 VIE
9 Addressing Health Threats in Central Asia Regional Economic
Cooperation Countries and the Caucasus
Health 2020 54124-001 3.50 REG
10 Improving Access to Health Services for Disadvantaged Groups
Investment Program - Tranche 1
Health 2019 49173-004 76.14 MON
11 COVID-19 Emergency Response Project Health 2020 54077-001 18.60 PRC
12 Maternal and Child Health Integrated Care Project Health 2018 51010-002 32.00 TAJ
13 Urban Primary Health Care Services Delivery Project Health 2012 42177-013 70.4 BAN
14 Urban Primary Health Care Services Delivery Project - Additional
Financing
Health 2018 42177-024 110.00 BAN
15 Third Rural Water Supply and Sanitation Service Sector
Development Program (Project)
WUS 2019 50101-002 49.00 CAM
16 West Bengal Drinking Water Sector Improvement Project WUS 2018 49107-006 240.00 IND
17 Visakhapatnam–Chennai Industrial Corridor Development Program -
Tranche 2
WUS 2021 48434-004 255.00 IND
18 Integrated Urban Flood Management for the Chennai-
Kosasthalaiyar Basin Project
WUS 2021 49107-009 251.00 IND
19 Urban Environment Improvement Investment Program, Tranche 1 WUS 2021 53203-002 33.00 LAO
20 Jilin Yanji Low-Carbon Climate-Resilient Healthy City Project WUS 2018 50322-002 130.00 PRC
21 Yunnan Lincang Border Economic Cooperation Zone Development
Project
WUS 2018 49310-002 250.00 PRC
22 Jilin Yanji Low-Carbon Climate-Resilient Urban Development Project WUS 2020 50322-002 130.00 PRC
23 KP Cities Improvement Project (KPCIP) – Project Readiness
Financing
WUS 2019 51036-003 7.00 PAK
24 Punjab Urban Development Projects – Project Readiness Financing WUS 2020 53128-001 15.00 PAK
25 Punjab Intermediate Cities Improvement Investment Project
(PICIIP)
WUS 2017 46526-007 200.00 PAK
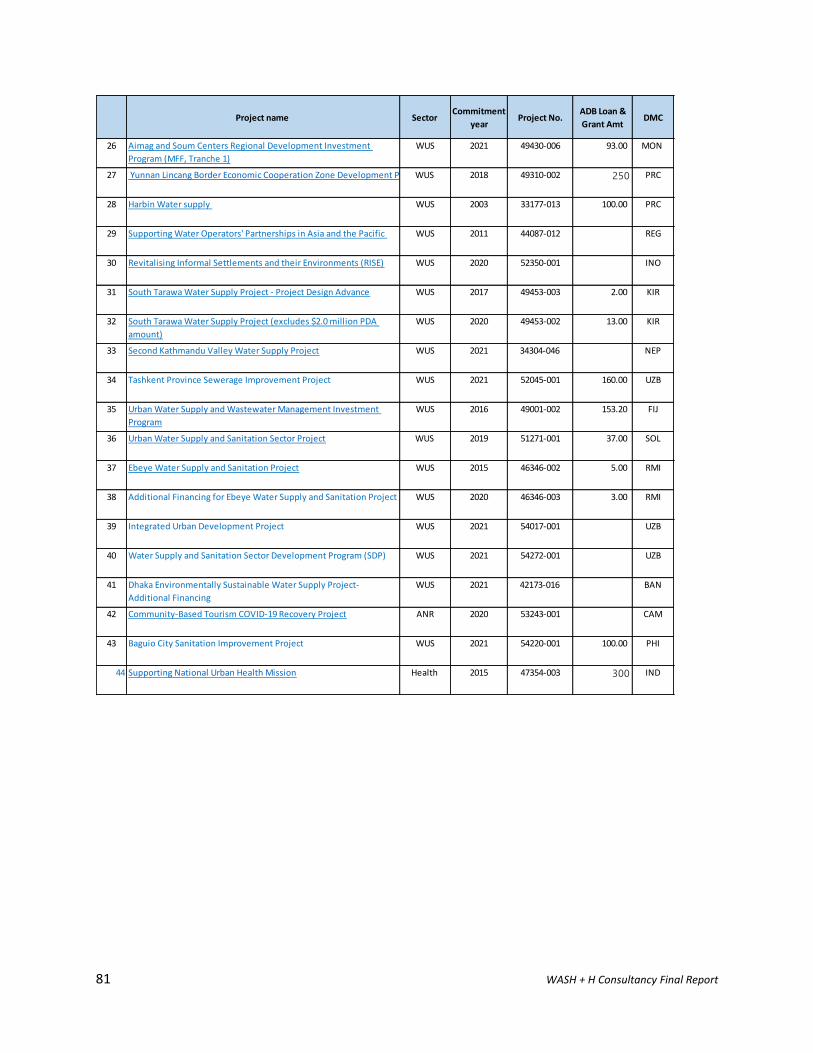
81 WASH + H Consultancy Final Report
Project name Sector Commitment
year Project No.
ADB Loan &
Grant AmtDMC
26 Aimag and Soum Centers Regional Development Investment
Program (MFF, Tranche 1)
WUS 2021 49430-006 93.00 MON
27 Yunnan Lincang Border Economic Cooperation Zone Development ProjectWUS 2018 49310-002 250 PRC
28 Harbin Water supply WUS 2003 33177-013 100.00 PRC
29 Supporting Water Operators' Partnerships in Asia and the Pacific WUS 2011 44087-012 REG
30 Revitalising Informal Settlements and their Environments (RISE) WUS 2020 52350-001 INO
31 South Tarawa Water Supply Project - Project Design Advance WUS 2017 49453-003 2.00 KIR
32 South Tarawa Water Supply Project (excludes $2.0 million PDA
amount)
WUS 2020 49453-002 13.00 KIR
33 Second Kathmandu Valley Water Supply Project WUS 2021 34304-046 NEP
34 Tashkent Province Sewerage Improvement Project WUS 2021 52045-001 160.00 UZB
35 Urban Water Supply and Wastewater Management Investment
Program
WUS 2016 49001-002 153.20 FIJ
36 Urban Water Supply and Sanitation Sector Project WUS 2019 51271-001 37.00 SOL
37 Ebeye Water Supply and Sanitation Project WUS 2015 46346-002 5.00 RMI
38 Additional Financing for Ebeye Water Supply and Sanitation Project WUS 2020 46346-003 3.00 RMI
39 Integrated Urban Development Project WUS 2021 54017-001 UZB
40 Water Supply and Sanitation Sector Development Program (SDP) WUS 2021 54272-001 UZB
41 Dhaka Environmentally Sustainable Water Supply Project-
Additional Financing
WUS 2021 42173-016 BAN
42 Community-Based Tourism COVID-19 Recovery Project ANR 2020 53243-001 CAM
43 Baguio City Sanitation Improvement Project WUS 2021 54220-001 100.00 PHI
44 Supporting National Urban Health Mission Health 2015 47354-003 300 IND
82 WASH + H Consultancy Final Report
Annex 5. Novel SARS-CoV-2 virus in WASH systems
SARS-CoV-2 in water supplies
1) While the presence of SARS-CoV-2 in untreated drinking-water is possible, normal water
treatment processes that meet World Health Organization (WHO) Drinking Water Quality
Standards should significantly reduce the concentration of SARS-CoV-2.
2) Conventional, centralized water treatment methods that utilize filtration and disinfection should
significantly reduce the concentration of SARS-CoV-2. For effective centralized disinfection,
there should be a free chlorine residual concentration of ≥0.5 mg/L after at least 30 minutes of
contact time at pH < 8.0. A chlorine residual should be maintained throughout the distribution
system.
3) Protecting drinking water should include treating water at the point of distribution, collection or consumption and ensuring that treated water is safely stored at home. These steps can be planned, implemented and monitored using WSPs.
4) For effective water treatment in centralized treatment systems, water utility managers can adopt several other preventive measures in a WSP approach. These include: securing adequate stocks of chemical additives and consumable reagents for water-quality testing, ensuring that critical spare parts, fuel and contractors can still be accessed and that there are contingency plans for staff and training to maintain the required supply of safe drinking-water.
5) Water utilities personnel should be briefed on COVID-19 preventive measures. They may wear masks (dependent on local government policy), they may respect physical distancing between workers and with the public, and practice hand hygiene frequently.
6) In places where decentralized water sources are used, household water treatment technologies that are effective in removing or destroying viruses include: boiling or using high-performing ultrafiltration or nanomembrane filters, solar irradiation and, in non-turbid waters, ultraviolet (UV) irradiation and appropriately dosed chlorine products such as sodium hypochlorite and NaDCC (WHO/UNICEF, 2020).
SARS-CoV-2 in fecal sludge and sewage
1) Within wastewater, infectious SARS-CoV-2 has not been detected in untreated or treated
sewage. RNA fragments of SARS-CoV-2 have been detected in untreated sewage and sludge.
2) SARS-CoV-2 is enveloped and thus less stable in the environment compared to non-enveloped
human enteric viruses with known waterborne transmission (such as adenoviruses, norovirus,
rotavirus and hepatitis A virus) (WHO/UNICEF, 2020).
Sewage surveillance
1) Research is underway in many countries to detect non-infective viral fragments (RNA) of SARS-
CoV-2 in wastewater and sludge. Further research and capacity building are needed on the
analytical methods (particularly for settings with low sewerage coverage), modelling, and data
interpretation to inform decision making and public health actions (WHO/UNICEF, 2020).
2) Sewage surveillance should not be used as a substitute for robust surveillance of COVID-19 cases. In addition, the primary aim of governments, utilities and investments should focus on
83 WASH + H Consultancy Final Report
continuity and expanding safely managed sanitation services to protect against COVID-19 and a number of other infectious diseases (WHO/UNICEF, 2020).
3) Preliminary evidence suggests that such monitoring can identify the presence of SARS-CoV-2 before the detection of clinical cases, in part because asymptomatic cases shed SARS-CoV-2. These approaches could be part of pandemic preparedness and early warning systems (Howard, 2020).
General hygiene
1) Overall hygiene approaches to IPC being widely promoted are: avoiding touching the eyes, nose or mouth with unwashed hands, sneezing into one’s sleeve or a disposal tissue, practicing physical distancing while working and travelling to and from work, and staying home if one develops symptoms associated with COVID-19 (e.g. fever, dry cough, fatigue) (WHO/UNICEF, 2020).
Hand hygiene practices
1) Frequent and correct hand hygiene is one of the most important measures to prevent infection with SARS-CoV-2.
2) WASH practitioners should work to enable, inform and motivate more frequent and regular hand hygiene by building a supportive environment to improve and sustain access to hand hygiene facilities and using a multimodal strategy.
3) It is critical that people not only have access to soap and continuous water supply and/or other hand hygiene supplies (e.g. alcohol-based sanitizers) but also know how to wash hands properly and thoroughly in line with advice provided by WHO (WHO/UNICEF, 2020).
Hygiene in healthcare facilities
4) Hand hygiene is extremely important to prevent the spread of SARS-CoV-2. All health care facilities (HCFs) should have regular programs aimed at promoting best hand hygiene practices and ensuring the availability of the necessary infrastructure (equipment and supplies) as well as operation and maintenance protocols.
5) Frequent hygiene practices are needed in healthcare settings including: a. hand hygiene using appropriate techniques; b. implementing regular environmental cleaning and disinfection practices; c. managing excreta (feces and urine) safely; d. safely managing health-care waste produced by COVID-19 cases; and e. safely managing dead bodies (WHO/UNICEF, 2020).
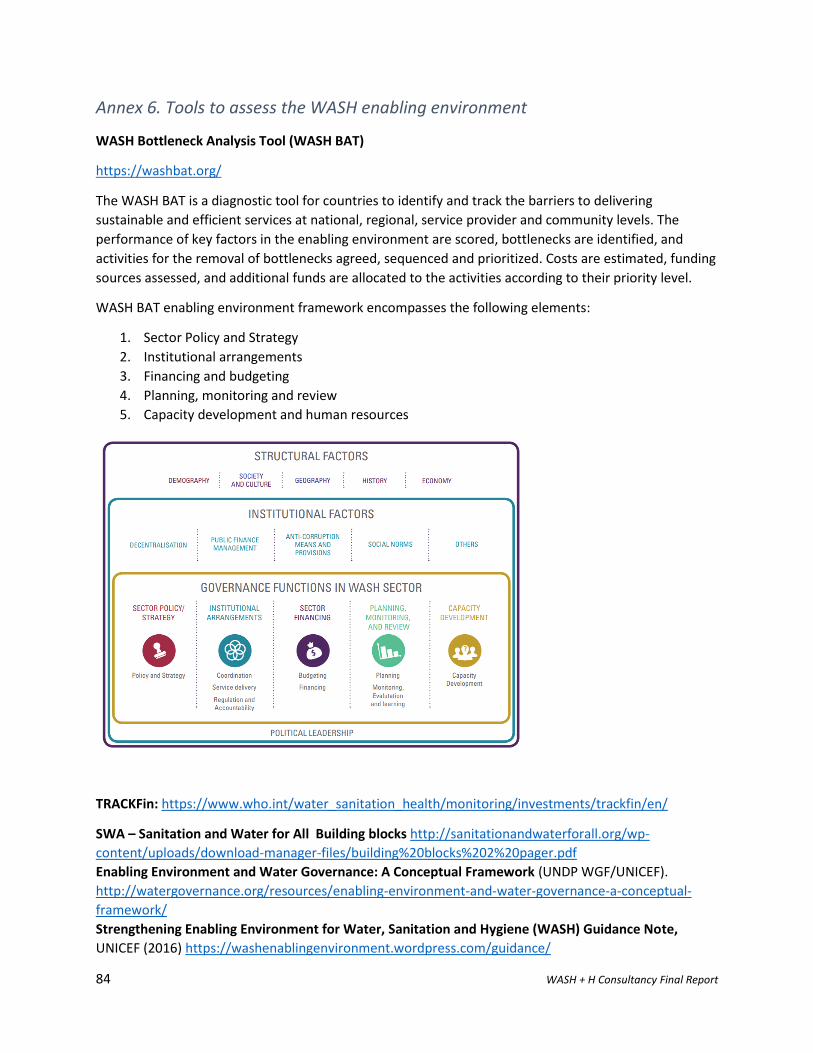
84 WASH + H Consultancy Final Report
Annex 6. Tools to assess the WASH enabling environment
WASH Bottleneck Analysis Tool (WASH BAT)
https://washbat.org/
The WASH BAT is a diagnostic tool for countries to identify and track the barriers to delivering
sustainable and efficient services at national, regional, service provider and community levels. The
performance of key factors in the enabling environment are scored, bottlenecks are identified, and
activities for the removal of bottlenecks agreed, sequenced and prioritized. Costs are estimated, funding
sources assessed, and additional funds are allocated to the activities according to their priority level.
WASH BAT enabling environment framework encompasses the following elements:
1. Sector Policy and Strategy
2. Institutional arrangements
3. Financing and budgeting
4. Planning, monitoring and review
5. Capacity development and human resources
TRACKFin: https://www.who.int/water_sanitation_health/monitoring/investments/trackfin/en/
SWA – Sanitation and Water for All Building blocks http://sanitationandwaterforall.org/wp-
content/uploads/download-manager-files/building%20blocks%202%20pager.pdf
Enabling Environment and Water Governance: A Conceptual Framework (UNDP WGF/UNICEF).
http://watergovernance.org/resources/enabling-environment-and-water-governance-a-conceptual-
framework/
Strengthening Enabling Environment for Water, Sanitation and Hygiene (WASH) Guidance Note,
UNICEF (2016) https://washenablingenvironment.wordpress.com/guidance/
85 WASH + H Consultancy Final Report
Annex 7 Guidance for designing good practice HyBC programs
General Behavior Centered Design (BCD) Guidance and Tools
https://www.lshtm.ac.uk/research/centres-projects-groups/bcd#resources
LSHTM has produced a range of resources on BCD and its practical application. These include papers,
manuals for practitioners and for researchers, formative research protocols and checklists. There is also
a series of online webinars available for free. The webinars cover BCD theory and process for designing
behavior change programs, with a focus on hygiene, and some general background on behavior change.
Behavior Centered Design (BCD) Guidance and Tools during COVID-19
https://gh.bmj.com/content/bmjgh/5/8/e002780.full.pdf
Designing effective hand hygiene campaigns during COVID-19 pandemic is possible and requires a
number of stages in addition to standard BCD. LSHTM academics led by the late Prof Val Curtis published
a guidance paper outlining ten necessary steps to developing a national communications strategy for
COVID-19 prevention (Curtis, 2020):
xi. Set up a task force and appoint a national focal person.
xii. Mobilize resources and involve the private sector.
xiii. Define exactly which behaviors need to change and by whom.
xiv. Review what is already being done internationally and locally.
xv. Review what is known about the drivers of these behaviors and rapidly fill in gaps in knowledge.
xvi. Produce a creative brief and theory of change.
xvii. Develop a unifying national brand.
xviii. Develop executions employing the most relevant channels for the target audiences.
xix. Rapidly pretest and continually revise content.
xx. Deliver, monitor, evaluate and share lessons.
Promotional Approaches to WASH Behavior Change
https://www.3ieimpact.org/sites/default/files/2019-04/srs-handwash.pdf
International Initiative for Impact Evaluation (3iE) produced a systematic review of the effectiveness of
WASH program design for behavior change. It shows that community-based activities and social
marketing are far more effective than messaging in resulting adherence to desired behaviors.
Handwashing Promotion: Monitoring and Evaluation Module
https://www.unicef.org/wash/files/M_and_E_Toolkit_.pdf
UNICEF has published this monitor and evaluation (M&E) guide which identifies the steps and processes
required to monitor and evaluate handwashing promotion programs irrelevant of implementation
design. It outlines appropriate indicators and sample questions for handwashing advocacy, education
and HyBC. Usefully it outlines the caveats and limitations that should be placed on measuring health
impact assessment.
Training programs available on WASH Behavior Change
International WaterCentre WASH and Behavior Change online training course:
http://www.watercentre.org/courses/wash-and-behaviour-change/
86 WASH + H Consultancy Final Report
Annex 8. Examples of Improving HyBC in ADB COVID-19 Response projects
A number of ADB projects in design phases are pivoting to respond to the COVID-19 pandemic. The
following provide examples of hygiene components and related consultant terms of reference (TOR) if
available. Only components relevant to HyBC are included (see project documents for other
information).
3) Lao PDR: Urban Environment Improvement Investment Program. Proposed Multi-tranche
Financing Facility and Administration of Loan and Grant (53203-001)
Output 1: Policy and regulatory environment improved
Output 2: Urban infrastructure improved
Output 3: Institutional effectiveness improved
Output 4: Women’s leadership and employment enhanced. The program will improve women’s
participation in MPWT employment and leadership roles through the following activities in the water
supply and sanitation sector: (i) a Technical and Vocational Education and Training certification program
for women at the community level, (ii) a higher education scholarship and internship program, (iii) a
leadership training program for female civil servants to achieve decision-making roles, (iv) a
communication and outreach campaign on employment opportunities for women, (v) investment in
handwashing and toilet facilities including menstrual equipment in schools and health centers,
accompanied by an awareness raising program for WASH, effective menstrual and personal hygiene
practices, including hygiene behaviors for post COVID-19, and (vi) a monitoring and evaluation system to
enhance women’s participation.
4) TA 8899-IND: Strengthening Capacity of the National Urban Health Mission
Actions: Intervention pilot will undertake a gap analysis of the prevailing COVID-19 situation; assess
access to general health (preventive and curative), laboratory and WASH services; study existing referral
linkages with higher level of care for COVID-19 as well as for non-COVID-19 emergency and chronic care
needs; efficacy of community level mechanisms, municipal initiatives on managing the outbreak (and its
effectiveness) and access to other essential non-health services (e.g. food security). These would feed
into development and implementation of a tailored, humane and a comprehensive containment
strategy for COVID-19 for the slum, including community and household level quarantine and isolation
strategies, and community led provision and monitoring of services. Further, the pilot will look beyond
the current COVID-19 crisis and from a systems outlook it will attempt to demonstrate solutions for
maintenance or resumption of general health services, propose community level structures for
improved response in preventing and managing future outbreaks, and propose models of leveraging
local health systems (public as well as private) for meeting holistic health needs and demonstrate
assured referral linkages to higher levels of care. Similarly, coordination mechanisms envisaged at slum,
ward and municipal levels to ensure access to essential services will be engaged and models on assured
access to critical WASH and other public services during mass health emergencies will be demonstrated.
The consultant team members hired to undertake this work will include with example TOR include:
87 WASH + H Consultancy Final Report
iv. Team Leader The team leader will, be responsible for guiding the collective work of the
consulting team and for timely preparation and quality control of all reports submitted to ADB.
The consultant will work closely with the Ministry of Health and Family Welfare (MOHFW) and
selected states, agencies, resource centers, and other consultants fielded by ADB.
v. Social Scientist/Program Manager The program manager will, be responsible for overseeing the
implementation of intervention pilot and day-to-day management of the field team, guiding the
collective work of the consulting team for timely preparation and quality control of all reports
submitted to ADB. The consultant will work closely with the Ministry of Health and Family
Welfare (MOHFW) and selected states, agencies, resource centers, and other consultants
fielded by ADB.
vi. Public Health Expert The Public Health Expert will be responsible for on-ground
implementation of intervention pilot, ensuring execution of baseline and endline assessment as
per design, lead capacity building of pilot staff and partners, engage community leaders and
platforms, lead interaction with various local stakeholders to ensure support for intervention
pilot, ensure timely completion of pilot reports and escalate relevant issues and concerns to
Program Manager for quick redressal. The consultant will work closely with selected
municipalities, agencies, resource centers, and other consultants fielded by ADB.
88 WASH + H Consultancy Final Report
Annex 9. WASH in Healthcare Facilities: Practical guidelines and tools
WHO (2019) Water, sanitation and hygiene in health care facilities: practical steps to achieve universal
access. Geneva: World Health Organization
https://www.unicef.org/media/51591/file/WASH-in-health-care-facilities-practical-steps-2019%20.pdf
The document presents eight practical steps that countries can take at the national and sub-national
level to improve WASH in health care facilities. It also summarizes the global response to the UN
Secretary-General’s Call to Action on WASH in Health Care Facilities.
WHO & UNICEF (2019) WASH in health care facilities: Global Baseline Report 2019, World Health
Organization and the United Nations Children’s Fund, Geneva
https://washdata.org/sites/default/files/documents/reports/2019-04/JMP-2019-wash-in-hcf.pdf
This report defines JMP service ladders for monitoring basic WASH services in health care facilities. It
presents a compilation and analysis of existing monitoring data that countries have already collected
and reviewed. The report sets out eight steps countries can take to improve WASH in health care
facilities. These are:
1. Conduct situation analysis and assessment
2. Set targets and define roadmap
3. Establish national standards and regulation
4. Improve infrastructure and maintenance
5. Monitor and review data
6. Develop health workforce
7. Engage communities
8. Conduct operational research and share learning
Situational Analysis and Assessment of WASH in Primary Healthcare Facilities Toolkit. Centres for
Disease Control and Prevention
https://www.cdc.gov/healthywater/global/healthcare-facilities/tools.html
This toolkit is designed to evaluate access to WASH infrastructure and services in primary healthcare facilities. It provides a template of indicators to assess that align with the JMP service ladders for monitoring basic WASH services in HCFs and consists of an interview with the healthcare facility director and a walk-through of the facility. The tool is a downloadable form that can be completed to help health officials understand the current WASH situation and gaps in a primary healthcare facility.
WASH Conditions Assessment Tool (WASHCon) Center for Global Safe Water, Sanitation, and Hygiene at
Emory University
http://washconhcf.org/research-tools/washcon/
The WASHCon is a data collection tool using surveys, observational checklists and water quality testing to assess WASH conditions across the domains (water, sanitation, hygiene, waste disposal, cleanliness)defined by the JMP. A rapid assessment can be conducted on mobile devices and uploaded

89 WASH + H Consultancy Final Report
into pre-programmed dashboards which present findings graphically using a simple traffic light system. The WASH Con can:
1. Develop a comprehensive overview of the status of WASH conditions, infrastructure and resources in a given HCF.
2. Provide data to inform and prioritize programmatic activities to improve WASH in HCF. 3. Contribute to the evidence base for advocacy and action in the area of WASH in HCF.
Water and Sanitation for Health Facility Improvement Tool (WASH FIT). World Health Organization
(2017)
https://apps.who.int/iris/bitstream/handle/10665/254910/9789241511698-
eng.pdf;jsessionid=D3ABFF09211E7618FBBC4F10FD463957?sequence=1
WASH FIT guide contains practical step-by-step directions and tools for assessing and improving services
in HCFs. It outlines a step-by-step approach and is adapted from the WHO water safety plan approach
but goes beyond water safety to include sanitation and hygiene, health care waste, management and
staff empowerment. WASH FIT is a multistep, iterative process to facilitate improvements in WASH
services, quality and experience of care. The tool includes forms and templates to complete a HCF
assessment and develop and continuous improvement plan.
90 WASH + H Consultancy Final Report
Annex 10. WASH in Schools: Practical guidelines and tools
Field Guide: Three Star Approach to WASH in Schools. UNICEF and GIZ, 2013
https://www.unicef.org/wash/schools/files/UNICEF_Field_Guide-3_Star-Guide.pdf
The Three Star Approach for WASH in Schools is designed to improve the effectiveness of hygiene
behavior change programs. The approach ensures that healthy habits are taught, practised and
integrated into daily school routines. Schools are encouraged to take simple, inexpensive steps outlined
in this Field Guide. These steps are designed to ensure that all students wash their hands with soap,
have access to drinking water, and are provided with clean, gender-segregated toilets at school every
day.
Improving Water, Sanitation and Hygiene in Schools: A Guide for Practitioners and Policy Makers in
Mongolia, ADB, April 2013
https://www.adb.org/publications/improving-water-sanitation-hygiene-schools-mongolia
This Guide is intended for use in schools, particularly by school management, teachers, social workers,
and school doctors as well as others involved in designing and constructing school WASH facilities. The
main sections of the Guide provide information for planning, implementing, and managing improved
WASH in schools, covering legislation, standards, and norms on school WASH in Mongolia. It also
outlines steps in planning improved WASH in schools, roles and responsibilities, and tasks involved in
implementing and managing improved WASH in schools and health impacts of WASH and hygiene
education. Whilst written for Mongolia, many of the approaches and processes described would apply
to WASH in schools in any country.
Water, Sanitation and Hygiene (WASH) In Schools: Guidelines for Timor-Leste. Ministry of Education
and the Government of Timor-Leste, 2016
https://www.unicef.org/timorleste/media/506/file/WinS_Guidelines_Final_English_version.pdf.pdf
These guidelines provide an example of the adaptation of global guidelines to a specific country context,
in this case Timor-Leste. The guidelines clear levels of acceptable standards for water supply, provision
of sanitation facilities and hygiene promotion in schools and provide a common framework and policy
direction for all sub-sector actors. All implementers (implementing agencies, planners, architects, water
and sanitation technicians, teaching staff, school directors, school boards, district WASH committees,
local authorities and NGOs) should follow these guidelines.
WASH in Schools Implementation Guideline. Live and Learn Environmental Education, 2020.
https://www.waterforwomenfund.org/en/learning-and-resources/resources/KL/200528-
WinS_Guide_Final_LR.pdf
This guide provides an overview of the NGO, Live & Learn’s approach to WASH in Schools, which
operates in the Pacific countries of Papua New Guinea, Solomon Islands and Vanuatu. Live & Learn
works with schools to improve WASH through a bottom-up capacity-building approach and risk-based
tools based in an ‘Assess-Plan-Act-Monitor’ cycle. The Guideline provides information on the steps
required.
91 WASH + H Consultancy Final Report
UNICEF hosts a WASH in Schools Website with numerous resources across advocacy, MHM, Design,
Standards and Guidelines, M&E, WASH in schools in emergencies, and education and research.
https://www.unicef.org/wash/schools/washinschools_53115.html.
There is also a WASH in Schools (WinS) Knowledge Hub supported by IRC which hosts key WinS
publications.
https://www.ircwash.org/news/new-wash-schools-knowledge-hub
Top Related
Copyright © 2022 FDOKUMEN

