





Bahasa
Halaman
Hukum


1
PERUBAHAN LINGKUNGAN INTRA – EKSTRA UTERUS
TERHADAP FISIOLOGI
SISTEM TUBUH
Department of Physiology, Faculty of MedicineDepartment of Physiology, Faculty of MedicineUniversity of Sumatera Utara, MedanUniversity of Sumatera Utara, Medan
IndonesiaIndonesia

PROSES KELAHIRAN
(Perubahan Link. Intrauterine Link. Ekstrauterine)
“at term”“at term”KONTRAKSI uterus
(Frekuensi-Durasi-Intensitas)
KONTRAKSI uterus
(Frekuensi-Durasi-Intensitas)
Sirkulasi (PO2/PCO2) tergangguSirkulasi (PO2/PCO2) terganggu
Asphyxia (PO2 & PCO2 )
Heart Rate :
140x/mnt 160-180x/mnt bila O2 100-120x/mnt
Asphyxia (PO2 & PCO2 )
Heart Rate :
140x/mnt 160-180x/mnt bila O2 100-120x/mnt

3
Perubahan SIRKULASI segera setelah Lahir
Rangs. Dingin pd Kulit + AsphyxiaRangs. Dingin pd Kulit + Asphyxia
Bayi lahir (normal)Bayi lahir (normal)
Bayi MenangisBayi Menangis
PO2 70-80 mmHg
Saturasi Hb-O2 : 80-90%
PO2 70-80 mmHg
Saturasi Hb-O2 : 80-90%

at birth
potong Umbilical cord (tali pusat)
Tahanan peripher
TD. Aorta >> TD. Art.Pulmonal
Sirkulasi Plasenta (-)
Asphyxia (CO2 & O2 )
Menangis Tarik Napas
Paru mengembang
Tahanan paru
TD.Aorta TD. pulmonal
Rangs. Dingin

5

6
Bbrp. Jam postpartumBbrp. Jam postpartum
Aliran Atrium Kiri & Aliran Atrium Kanan
Aliran darah Aorta Arteri Pulmonalis
Konstriksi Duktus Arteriosus (Penutupan Fungsional)
1 - 4 Bulan
Fibrosis Occluded
Sirkulasi Dewasa

7
TD. Aorta >> TD. Art.PulmonalTD. Aorta >> TD. Art.Pulmonal
Aliran darah paru Aliran darah paru
Aliran Atrium Kiri & Aliran Atrium Kanan Aliran Atrium Kiri & Aliran Atrium Kanan
Tek. Atrium Kiri >>Tek. Atrium Kanan Tek. Atrium Kiri >>Tek. Atrium Kanan
Foramen Ovale TertutupForamen Ovale Tertutup

8
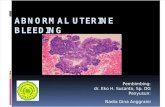
Circulation in Fetus and Newborn

9
PERUBAHAN SIRKULASI
PLASENTA
JARINGAN TUBUH
VENT Ki ATR Ki
PARU
VENT Ka ATR Ka
FETUS PERINATAL (0-1 Bln) BAYI (1-4 Bln) Dewasa
FO : Foramen Ovale
FO
DA
DA : Ductus Arteriosus
JARINGAN TUBUH
VENT Ki ATR Ki
PARU
VENT Ka ATR Ka
DA
PLASENTA
FO
PLASENTA
PARU
JARINGAN TUBUH
FO
VENT Ki ATR Ki
VENT Ka ATR Ka
PARU
JARINGAN TUBUH
DADA

10
MENARIK NAFAS PERTAMA (The First Breath)
Perubahan Respirasi Placenta Respirasi paru
Bayi LahirBayi Lahir
Rangsang sensorik : Kulit & OtotRangsang sensorik : Kulit & Otot Asidosis RinganAsidosis Ringan
Pusat PernapasanPusat Pernapasan
Kontraksi otot-otot PernapasanKontraksi otot-otot Pernapasan
Vol. Intra Thoraks & Tek. Intra Thoraks Vol. Intra Thoraks & Tek. Intra Thoraks
Udara Masuk ke ParuUdara Masuk ke Paru

11
REGULASI SUHU TUBUHREGULASI SUHU TUBUH
BayiBayi Iklim intrauterine (“tropis”) Iklim intrauterine (“tropis”) Iklim Ekstrauterine Iklim Ekstrauterine
STRESSSTRESS
Regulasi Suhu Regulasi Suhu BELUM STABILBELUM STABIL
Suhu Tubuh Suhu Tubuh
TDK STABILTDK STABIL

12
Regulasi Suhu Blm. Stabil
Thermogenesis (Heat Gain) Thermolysis (Heat Loss)
Tak dpt menggigil (respon dingin) Sistem syaraf blm. Sempurna.
Respon dingin :
Metabolisme “brown fat”
Trigliserida
Free fatty acid
Luas permukaan bayi >> Dewasa
Kulit & Jar. Subcutan tipis High Conductance Panas hilang >>
Cairan Tubuh
BB (5-10%) 2-3 Hr pertama

1313
FUNGSI LIVER
Bayi baru lahir Sumber Energi
GLIKOGEN
LIVER, OTOT, JANTUNG, dll
GLIKOGEN
LIVER, OTOT, JANTUNG, dll
Beberapa jam postpartum GLIKOGEN GLIKOGEN

14
REGULASI GLUKOSAREGULASI GLUKOSA
Segera setelah lahir KGD 30-40mg/100mLSegera setelah lahir KGD 30-40mg/100mL
Bbrp. jamBbrp. jam
Glikogen Glikogen
KGD <20mg/100mLKGD <20mg/100mL
GLUKONEOGENESISGLUKONEOGENESIS
Gangguan/gagalGangguan/gagal
Ggn. Syaraf & KomaGgn. Syaraf & Koma
Apnoe + CyanosisApnoe + Cyanosis
Pemberian Glukosa
Pemberian Glukosa

15
METABOLISME PROTEIN & LEMAK
Fetus
Melawati “Barrier Placenta”
- Immunoglobulin
Melawati “Barrier Placenta”
- Immunoglobulin
Tak Melawati “Barrier Placenta”
- Plasma Protein
- Lemak
Tak Melawati “Barrier Placenta”
- Plasma Protein
- Lemak
Sintesa di Hati :
Albumin & Lemak
Sintesa di Hati :
Albumin & Lemak
Aktivasi Met. As.Nukleat & sintesa Protein
Aktivasi Met. As.Nukleat & sintesa Protein
Segera Setelah Lahir

16
BILIRUBIN & FUNGSI DETOXIFIKASI
Fungsi Ekskresi Bilirubin (Hati) & Detoxifikasi Obat-obatan
Fungsi Ekskresi Bilirubin (Hati) & Detoxifikasi Obat-obatan
Physiological Joundice (3-7
Hari)
Physiological Joundice (3-7
Hari)
Blm. SempurnaBlm. Sempurna

1717
TRACT. GASTROINTESTINALIS
“Rute PLACENTA” “Rute INTESTINAL”
Gastric Emptying Time : 3-4 jamGastric Emptying Time : 3-4 jam
Enzym Lambung & HCl, pH : <3
(pencernaan Susu)
Enzym Intestinal, dan Empedu CUKUP
Amilase Pankreas <<<
Enzym Lambung & HCl, pH : <3
(pencernaan Susu)
Enzym Intestinal, dan Empedu CUKUP
Amilase Pankreas <<<
MOTILITAS
MOTILITAS
SEKRESI
SEKRESI
ABSORPSIABSORPSIZat Nutrisi BAIK
Kecuali LEMAK
Zat Nutrisi BAIK
Kecuali LEMAK

18
PENGATURAN ENDOKRIN
PERTUMBUHAN
Foetus Growth Foetus Growth dipengaruhi dipengaruhi ::
““Maternal Nourishment”Maternal Nourishment”
Estrogen & ProgesteronEstrogen & Progesteron
Fetus Growth Fetus Growth Tdk.dipengaruhiTdk.dipengaruhi ::
Growth Hormon FoetusGrowth Hormon Foetus
Thyroxine FoetusThyroxine Foetus

19
Thyroid Gland
IBU
(HYPOTHYROIDISM)
Lahir Bayi
(HYPOTHYROIDISM)
PERKEMBANGANAKTIF segera Stlh Lahir
(respon thd dingin)

2020
Adrenal Korteks
Kortikosteroid (+)
Respon kelenjar (+)
Pada urinePada urine
Keadaan stressKeadaan stress
Adrenal Medula
Saat LahirSaat Lahir
Mempertahankan Sirkulasi Darah Otak
PO2 PO2
ASPHYXIAASPHYXIA
Epinephrin/NEEpinephrin/NE
VASOKONSTRIKSIVASOKONSTRIKSI
Respon Metabolik Thd DINGIN

21
SISTEM SYARAF
Sist. Syaraf Pusat
Pertumbuhan :
- me pd Trimester II & III (maks)
-Berat : ¼ berat Otak Dewasa
Sifat Refleks
Flexion Reflex,menangis wkt. Lapar, memutar Kepala, dll.
Buka mata (respon Cahaya & Suara)
Tidur barbagai posisi

22
PERAN HORMON DALAM PROSES TUMBUH DAN
KEMBANG

23
Multiple hormones, including growth hormone (GH), insulin-like growth factors (IGF-I and -II), insulin, thyroid hormones, glucocorticoids, androgens, and estrogens contribute to the growth process in humans.
Among these, GH and IGF-I have been implicated as the major determinants of growth in normal postuterine life. However, deficiencies (or excesses) of each of the other hormones can seriously affect the normal growth of the musculoskeletal system as well as the growth and maturation of other tissues.

24

25

26

27
Pancreas: Insulin• actions: hypoglycemic (lowers blood
glucose)– increases transport of glucose into muscle and fat
cells (NOTE: does not increase uptake by brain, liver, or kidney)
– inhibits breakdown of glycogen and formation of glucose from amino acids or fatty acids (inhibits glycogenolysis and gluconeogenesis)
– promotes formation of glycogen (liver, skeletal muscles), protein synthesis (muscle), and fat synthesis and storage (adipose)

28
5. Pancreas: Insulin (Control)• stimulated by:
– increased blood glucose
– increased blood amino acid and fatty acid levels
– parasympathetic impulses
– hyperglycemic hormones (GH, glucagon, epinephrine, thyroxine, glucocorticoids) indirectly result in insulin secretion by increasing blood glucose levels
• inhibited by: – low blood glucose and by
somatostatin
– sympathetic impulses

29

30

31
Top Related
Copyright © 2022 FDOKUMEN

