Wheeler, M (2011) Transitional Space in Clients' Pockets: the cellphone camera
Upload
khangminh22Category
view
1download
0
Written by: Heather Wheeler, Ph.D., C.Psych.
Penny Werthner, Ph.D. Paddy McClusky, MD
Sari Kraft, MD
Adapted with permission from: Swimming Canada Mental Health Strategy (Hoar et al., 2018) &
Cycling Canada Mental Health Strategy (Hoar et al., 2020)
2 | P a g e
Table of Contents Purpose, Rationale, Goals .................................................................................................................................... 4
Purpose ........................................................................................................................................................ 4
Rationale ...................................................................................................................................................... 5
Goals ............................................................................................................................................................ 6
Mental Health Screening ..................................................................................................................................... 7
Early identification and Screening: Pathways and Tools ......................................................................... 7
Mental Health Screening: Content and Logistics ...................................................................................... 8
Mental Health Screen Results and Information Sharing .......................................................................... 9
Intervention & Treatment ................................................................................................................................. 12
Intervention .............................................................................................................................................. 12
General Communication Strategies for Early intervention by any HP Team member ........................ 12
In Mild/Moderate Cases (i.e., Healthy/Green to Reacting/Yellow on the MH Continuum) ................ 12
In Moderate/Severe Cases (i.e., Injured/Orange to Ill/Red on the MH Continuum) ............................ 14
In Crisis Cases (Immediate concerns of imminent harm to self/others) ................................................ 15
Safe Sport Concerns .................................................................................................................................. 15
Treatment .................................................................................................................................................. 15
Funding .............................................................................................................................................................. 16
Exceptional funding for MH treatment ..................................................................................................... 16
Monitoring and Follow-up during Treatment ................................................................................................. 17
Feedback from treating professionals ....................................................................................................... 18
Other relevant aspects to monitoring and follow-up ...................................................................................... 19
MH Pause-play Protocol ............................................................................................................................ 19
MH Return-to-Sport Protocol .................................................................................................................... 19
Promotion of Mental Health ............................................................................................................................. 21
MH Champions .......................................................................................................................................... 23
Other MH Promotion Supports ................................................................................................................. 23
Implementation and Evaluation of the Strategy .............................................................................................. 24
Mental Health Strategy for AC HP Coaches and Staff .................................................................................... 25
References .......................................................................................................................................................... 26
Appendix A ........................................................................................................................................................ 29
Scope of Practice within the Mental Health Continuum Model (from Durand-Bush, 2021)..................... 29

3 | P a g e
Appendix B ......................................................................................................................................................... 30
Sport Mental Health Recognition Tool-1 (SMHRT-1) ................................................................................. 30
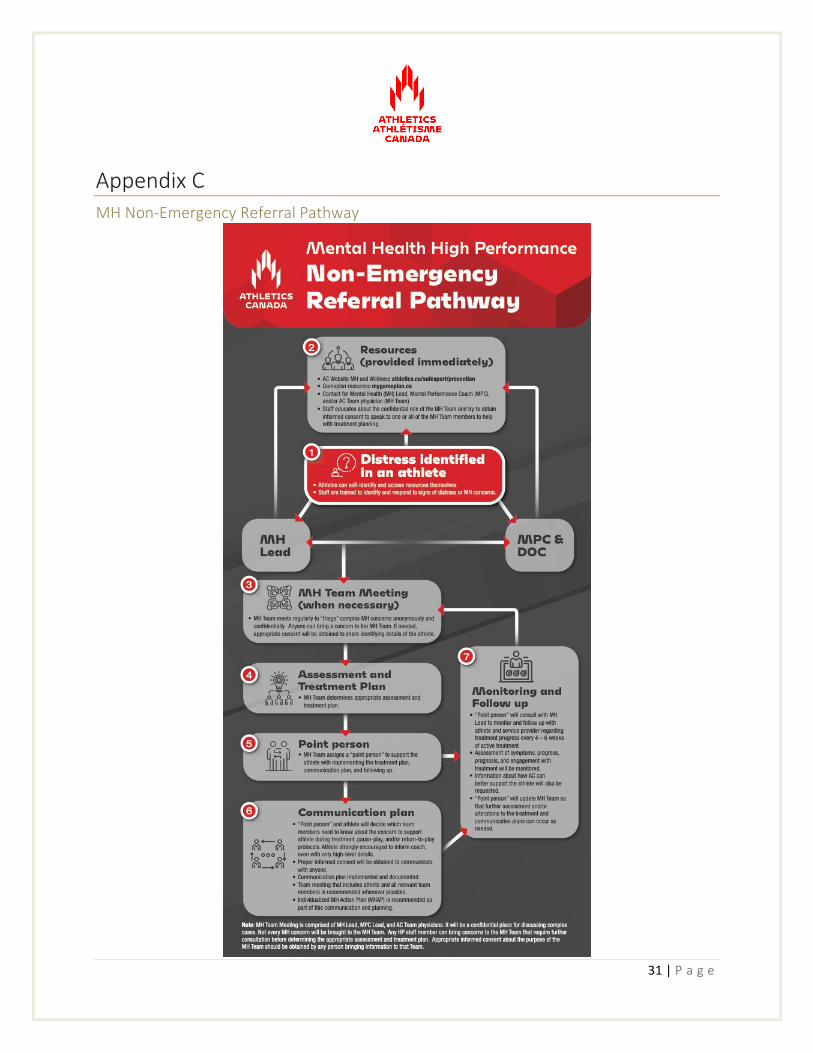
Appendix C ........................................................................................................................................................ 31
MH Non-Emergency Referral Pathway ...................................................................................................... 31
Appendix D ........................................................................................................................................................ 32
MH Assessment Screening procedure (SMHAT-1) .................................................................................... 32
Appendix E ......................................................................................................................................................... 33
Possible List of Life Concerns ..................................................................................................................... 33
Appendix F ......................................................................................................................................................... 34
Athletics Canada Informed Consent for Release of Mental Health Information form .............................. 34
Appendix G ........................................................................................................................................................ 36
Resources for HP Athletes across the MH Continuum .............................................................................. 36
Appendix H ........................................................................................................................................................ 37
Mental Health Action Plan [MHAP] (Example) .......................................................................................... 37
Appendix I .......................................................................................................................................................... 39
MH Emergency Referral Pathway .............................................................................................................. 39

4 | P a g e
Purpose, Rationale, Goals Purpose
This Mental Health (MH) Strategy was developed for Athletics Canada’s (AC) High Performance (HP) program. It outlines the strategy for supporting the psychological health and safety of AC HP members (athletes, coaches, staff, members) and is connected to AC’s Safesport policies and procedures. The MH Strategy for HP members aligns with the overall purpose of the HP program: “To systematically guide and support Canadian athletes along a sustainable pathway to Olympic and Paralympic medals.”
The overall aim of addressing psychological health and safety is to prevent psychological harm through negligence, recklessness, or intent and assist in the resolution of mental health incidents or concerns (CSA, 2013). The goal is also to create a high performance sport environment that is psychologically safe and healthy, as defined by the Mental Health Commission of Canada.
Athletics Canada will strive to promote, protect, and respond to the mental health needs of HP members in a timely manner.
The purpose of this document is to have an established strategy and system in place that supports and improves the speed of care of an individual’s mental health through early identification of mental health issues, the application of timely interventions and return to play/work procedures. Additionally, measures are recommended to promote mental health and literacy among all Athletics Canada High Performance (AC HP) members. Beyond the benefits on the individual level, the hope is for this document to lay the foundation for creating a “culture of excellence” that prioritizes mental skills and psychological health in the same way it does physical health (Own the Podium, 2020).
Adopting A Culture of Excellence (see Hoar et al., 2020)
It is widely understood that fostering and maintaining a “culture of excellence” contributes to podium-performance. High performance sport is a unique environment with many stressors (for example, Olympic/Paralympic competition pressure, risk of injury, selection processes, and large financial costs needed to pursue high performance sport) that must be navigated. Athletics Canada aims to foster a culture of excellence that will empower athletes and coaches with the resilience and mental agility to cope with the inherent stress of high performance sport. This will be best accomplished through training environments that provide for sufficient challenge with the appropriate levels of social support (Sarkar, 2018). Mental health literacy and promotion are key to improving communication among team members, which is part of the foundation for a psychologically safe and healthy organization. Mental health promotion across the organization is likely to reduce burnout rates, increase well-being, and cooperation among team members, including in athlete-coach relationships (OTP, 2020; van Slingerland et al., 2021). Psychological safety describes a shared belief among group members that interpersonal trust and respect within the team exists, and that people are comfortable being themselves (Edmonson, 2014). It is a critical and foundational

5 | P a g e
element for podium performance as well as a protective mechanism for mental well-being of the individuals and the organization.
Rationale
Research has highlighted the negative impact of mental health issues on sport performance (Schinke et al., 2017). It is well-known that stress and pressure is inherent in HP sport. However, as humans have a finite ability to handle stressors and poor performance can be the outcome of too much stress (either in or outside of sport). Podium performances and personal bests require that we attend to the athletes as humans first. We have a duty of care for both physical and mental “injuries” on the road to competition, the podium and beyond. This is the mandate in the NCCP Code of Ethics and Standard of Behaviour: “to preserve and protect the present and future health and well-being” of athletes (Coaching Association of Canada, 2020).
While AC HP members are comfortable seeking help for physical health issues, an internal needs/gap analysis and other conversations with key staff indicate that HP members experience stigma about disclosing mental health issues (Wheeler, October 2020). Stigma around mental health – the sense that one’s entire character will be negatively evaluated because of a mental health concern - is one of the biggest perceived obstacles to getting athletes and staff the help they need.
Reducing stigma involves a multi-pronged approach to understanding, identifying and addressing mental health concerns. One of the key ways to reduce stigma is to increase mental health literacy throughout the organization (e.g., types of mental illnesses and common signs and symptoms) so that all members can help identify problems and connect people to appropriate supports (see Gulliver, Griffiths, Christensen, & Brewer, 2012). Another important step is to reduce fear of what happens with sensitive information that individuals seeking help for mental health concerns share within the organization. Ongoing education about the benefits of sharing information among key team members (i.e., to help individuals get the support they need to reach their potential), in a context of psychological safety and sense of control over what information is shared (with whom and when), is crucial for changing this fear and stigma. Indeed, research shows that we must improve the relationships with key team members and potential providers (Gulliver et al., 2012) to create a sense of safety and allow for growth in this domain.
While it may take years for mental health concerns to be regarded with the same respect as physical health concerns, it is important to start building trust and communication pathways that will support this goal over time. This strategy outlines a plan to ultimately equate mental health concerns with physical injuries and ensure that they are treated with the same respect and attention as part of whole-person wellness on the pathway to podium performances.
From: www.intmath.com
6 | P a g e
This document also aims to serve as a starting point for transparency with regard to mental health concerns so that we can reduce fear and stigma and increase the likelihood that members will seek out and receive the appropriate supports in a timely manner.
Goals
The MH Strategy aims for following outcomes as part of the foundation for podium performances:
1. Promotion of Mental Health and Wellness
a. Mental Health Literacy
b. Improved awareness of Mental Health Resources and mental wellness skills, including suicide prevention
c. Creating a culture of excellence, including psychological safety
2. Prevention of Mental Health concerns and illness
a. Early identification and intervention of mental health issues
b. Improve communication between team members, athletes, and other connected professionals about Mental Health concerns
3. Response
a. Improved speed and responsiveness in Mental Health treatment plan
b. Improved performance as a result of increased health and well-being.

7 | P a g e
Mental Health Screening
Awareness, early detection, building resilience and prevention of mental health issues comes as a result of a supportive environment that monitors for mental health symptoms throughout a calendar year. In some cases, to date, support has been offered only after the athlete asks for help. Asking for help can be difficult, and often people are unable to take this step. Some athletes wait too long to get help and only ask when the pressure before a key competition season arrives and/or their MH (mental health) deteriorates significantly. When this happens, athletes are often surprised and disappointed when they cannot recover (or at least complete a proper course of MH treatment) in time for key performances or Games. By taking a more proactive approach and initiating a conversation with someone when we have concerns about their wellness and mental health, we hope to connect more people with the help they need to be their best.
By screening athletes in a proactive way, we are communicating to our members that we want to support them as a whole person on their way to personal excellence. We want to provide athletes with the best opportunity to build skills and reduce barriers, in both physical and mental domains.
Early identification and screening of mental health concerns is a core part of the recommendations outlined in the National Mental Health Strategy in Sport (van Singerland et al., 2019) and the Gold Medal Performance for Psychology in Sport (OTP, 2020). Evidence shows that proactive screening of athletes has several benefits (Chang et al., 2020; Schinke et al., 2017; Tomalski, 2019).
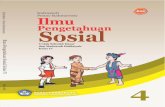
Early identification and Screening: Pathways and Tools At AC, we see mental health concerns lying on a continuum as described by the Mental Health Commission of Canada:
Adapted from Mental Health Commission of Canada/The Working Mind

8 | P a g e
AC’s HP athletes have a variety of supports available to them for MH concerns. AC employs skilled Mental Performance Consultants (MPCs) that are available to athletes for support with mental skill development and the specific skills that promote and maintain mental well-being. AC MPCs are available to most athletes in their Daily Training Environments (DTEs) and are key liaisons with coaches, Athlete Performance Advisors (APAs), and other Integrated Support Team (IST) members to support athlete well-being and healthy communication. MPCs are trained to observe and identify early signs of mental health concerns (Healthy, Reacting, Injured) and refer to appropriate professionals when these concerns extend beyond their scope of practice (see Appendix A).
However, because not all athletes have contact with an MPC employed by AC, it is important that all coaches, appropriate athlete-facing staff, APAs, and IST members be trained in recognizing early warning signs of mental health concerns. As such, all appropriate staff will be trained on the Sport Mental Health Recognition Tool (SMHRT; Gouttebarge et al., see Appendix B). Staff, APAs, IST and coaches will also be provided with continuing education opportunities for recognizing signs of mental health concerns (using the MH Continuum) and how to refer people to appropriate supports within and outside of the organization. This will allow all team members to play a role in early recognition and identification of MH concerns.
When an athlete is identified as someone with potential mental health difficulties, a referral is made to the AC sport physicians or the HP MH Lead for more specific and detailed assessment. It will also be possible for athletes to self-refer to the AC sports physician and/or MH Lead for help as needed.
See Appendix C for an overview of the Non-Emergency Referral Pathway for AC athletes with MH Concerns. More details regarding screening and follow up for individuals with MH concerns is outlined below.
Furthermore, all Athletics Canada HP athletes will be offered formal mental health screening, using the SMHAT-1 (Gouttenbarge et al., 2020) at least once per calendar year. This will be done as part of the yearly intake procedure in the fall and administrated by an AC sport physician and/or appointed designate. 1 The designate will be appropriately trained to administer and interpret the mental health assessment. Yearly screening aims to capture any concerns that may not have been raised through contact with MPCs, APAs, or other IST members, and provides a baseline of functioning for all athletes and will allow for monitoring throughout the quadrennium.
Mental Health Screening: Content and Logistics
Assessment by designated professionals with expertise in MH (AC medical doctors and/or MH Lead) will take the form of an interview and will include the completion of standardized assessment instruments.
1 For those athletes that have a known pre-existing mental illness where diagnosis and treatment plan are clearly documented and available to AC sport physicians, the full SMHAT-1 can be skipped.

9 | P a g e
All athletes will be invited to complete the SMHAT-1 at their yearly physical and/or intake screening, which is consistent with the IOC recommendations (see Gouttebarge et al., 2020). The SMHAT-1 involves a series of steps, using a combination of measurement-based care (i.e., questionnaires) and clinical interviews that determine whether further assessment is needed at each step (see Appendix D).
The SMHAT-1 involves administering Athlete Psychological Strain Questionnaire (APSQ) as a first screen for mental health concerns, followed by the required Athlete Forms as indicated (as per the SMHAT-1; Gouttenbarge et al., 2020). The full SMHAT-1 is available upon request.
The Mental Health Screen will be multi-modal and will also include more general mental health screening including the following:
● Symptoms of possible mental health issues.
● Abnormal patterns of general functioning including (mis)use of drugs and alcohol.
● Current treatment of identified mental health issues.
● Family history of mental illness.
A non-threatening report of potential concerns in the athlete’s life can be very helpful in determining what avenues to explore further in the interview (see Appendix E for an example of such a tool that is optional but helpful as a non-threatening way of naming concerns beyond what is asked in the interview). This tool can be used by MPCs who feel comfortable addressing these issues.
Some of the above will be completed by paper and some will be on the Athletics Canada Sport Database (Smartabase)/delivered electronically. Administrative and program assistants will be employed to help ensure the completion of necessary forms by athletes as required.
Due to reporting biases (mostly due to fear and stigma), some athletes may not be honest in their self-report of symptoms or on the screening questionnaires. As such, it is key that corroborative data be gathered as often as possible. This may include inviting perspectives from coaches, MPCs, Athlete Performance Advisors (APA’s), IST members and/or from family members when indicated (i.e., there are inconsistencies in reporting, nonverbal indicators suggest there may be information that is being withheld, or the professional has a need for more information in order to make an accurate diagnosis/treatment plan).
Mental Health Screen Results and Information Sharing
The mental health screen results will be interpreted by the AC sport physician or MH Lead as part of a larger picture of HP athlete health. The results of the screen are initially shared with the athlete and are to be kept in a private, confidential and secured file.

10 | P a g e
At the start of intake screening/MH assessment, or when MH concerns arise throughout the year, athletes will be informed that their MH screening information may be processed at the MH Team meeting.2 When an athlete screens positive on the SMHRT-1 or SMHAT-1, the MH Team may be notified. The MH Team includes the MH Lead, the AC Sport physicians, and the MPC Lead at a minimum. This MH Team is the forum where athletes’ MH concerns are “triaged” so that the proper level of support and/or treatment can be recommended. The MH Team is mirrored off of the interprofessional teams in our healthcare system that comprise professionals from different training backgrounds or scope of practice and are based on the concept of “two heads are better than one.” The MH Team is essential for helping athletes with MH concerns because we can each bring our expertise and lens to the treatment plan. The MH Team was also developed so that we can work together and provide wrap-around care as the athlete moves up and down the MH Continuum over time.
HP athletes will be educated on the fact that the MH Team members are bound by law to keep their information confidential unless provided with appropriate informed consent. Of note, these professionals have a duty to report where indicated by law. MH Team members will not be sharing beyond their “triage” meeting unless provided with further informed consent by the athlete.
The MH Team is responsible for determining a plan for intervention, monitoring, and treatment. Each plan will be determined on individual basis but there will be at least one “point person” in the AC team that is designated as a safe support to monitor and follow up with the athlete as needed throughout the treatment process. It is recommended that the MPC, AC Sport physician, and/or MH Lead become the “point person” whenever possible, but there may be exceptions (e.g., when an athlete has a closer relationship with a manager or APA and they have the ability to take the lead on information sharing). As appropriate, family members/partners/peers can also be included in these discussions for added support.
After a treatment plan (or at least the first step in care) is determined, a communication plan will be outlined. With the athlete’s consent, the “point person” will take the lead on organizing the communication to key individuals as part of the treatment plan.
Wherever possible, athletes are encouraged to share a high-level summary of MH concerns with their coaches as a way of maintaining a whole-person approach to training and performance goals. To communicate the findings with coaches, APAs, or other IST members, the AC “point person” will work with the athlete to determine what feedback could be helpful for ensuring proper monitoring and supports are in place. It will be important to determine the preferred method and details of what to share and/or schedule a team meeting with coach and athlete together (along with anyone else they trust to support them with this
2 All athletes will be provided with education about the MH Team and it’s role when they complete the yearly MH assessment/intake screening and/or whenever they present with MH concerns. They will be informed that the MH Team is part of AC’s procedure for caring for athletes with “mental injuries” just as much as the Medical team has a procedure for caring for athletes’ physical injuries. Athletes will be encouraged to see the benefits of this process however all athletes will have the ability to revoke consent for their name and identifying information to be shared. in this MH Team meeting. In this case, athletes’ relevant MH concerns and a treatment plan can still be worked through anonymously.

11 | P a g e
MH concern). It is important to consider instances when a particular coach-athlete relationship may not be safe to share information.
HP athlete(s) undergoing mental health screening will be asked to complete the Informed Consent for Release of Mental Health Information form (see Appendix F). Informed consent can vary based on age and understanding. The professionals involved in an HP athlete’s mental health assessment and care need to be sensitive to this issue.
Because of the sensitive nature of mental health assessment, the sharing of the results of HP athletes’ mental health with the AC HP staff is carefully considered on an individual and on-going basis. Open dialogue and collaboration with the athlete is central to the disclosure of information to anyone on the team. It is important that the potential benefits and consequences of sharing the information with key support staff and/or coaches before any sharing is done.3
3 There will be instances where athletes refuse consent to disclose information to anyone. However, as athletes’ willingness to provide informed consent to disclose information can shift over time (with education or increased need to obtain other supports), the point person for each athlete with MH concerns will continue to discuss and encourage safe sharing of information on an ongoing basis.

12 | P a g e
Intervention & Treatment Intervention General Communication Strategies for Early intervention by any HP Team member
In addition to following the protocols for intervention and monitoring noted below, the following is recommended (see Be There - Mental health support for more information):
1. Be approachable – be curious and invite discussion about life, relationships, emotions, and coping beyond sport whenever possible. When an individual indicates a need to talk, make sure you are safe and in a safe place to talk.
2. Give total attention and listen in a non-judgmental manner.
3. Do not express frustration with the individual for having symptoms and do not offer glib advice such as “pull yourself together” or “cheer up”.
4. Encourage and create a sense of hope without dismissing their concerns (e.g., “we’ll figure this out and get you the support you need” vs. “everything is going to be fine.”)
5. Indicate you want to help and ask if there is anything they need from you.
6. Contact the AC sport physician, HP MH Lead and/or registered mental performance consultant – know the limits of your role and inform the athlete of those limits.
7. Tell the athlete that you will follow up with the HP athlete to support them through the process.
In Mild/Moderate Cases (i.e., Healthy/Green to Reacting/Yellow on the MH Continuum)
Athletics Canada has internal mental health referral pathways (see Appendix C) to best support HP athletes who are exhibiting signs of distress or have been referred by IST, APAs or other HP staff. This is also the pathway used to process athletes who have a positive result on a yearly mental health screen.4
In Healthy to Reacting cases, MPCs should be consulted first. AC sport physicians should be notified in cases where there are concerns that decompensation or more serious difficulties could develop. Athletes, APAs, and IST should also be aware that they can reach out directly to the MH Lead if there are concerns regarding their designated MPC or the AC sport physician that is involved. The MH Lead will work to initiate the appropriate support pathways while simultaneously working to increase the trust in the AC staff in order to involve the team at the earliest possible opportunity.
4 There may be slightly different pathways for athletes while at a training camp.
13 | P a g e
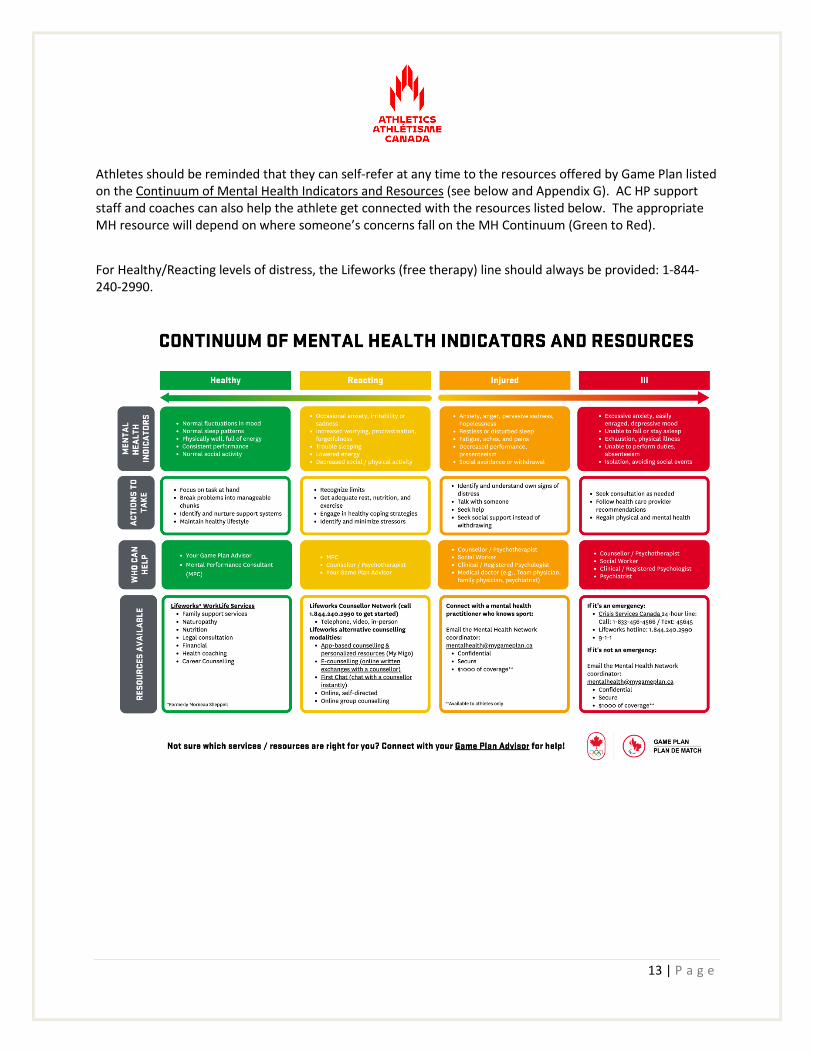
Athletes should be reminded that they can self-refer at any time to the resources offered by Game Plan listed on the Continuum of Mental Health Indicators and Resources (see below and Appendix G). AC HP support staff and coaches can also help the athlete get connected with the resources listed below. The appropriate MH resource will depend on where someone’s concerns fall on the MH Continuum (Green to Red).
For Healthy/Reacting levels of distress, the Lifeworks (free therapy) line should always be provided: 1-844-240-2990.

14 | P a g e
In Moderate/Severe Cases (i.e., Injured/Orange to Ill/Red on the MH Continuum)
When mental health concerns become more persistent, leading to difficulties in functioning (in life and/or in training), and/or are resistant to treatment, all members of the MH Team will be notified as per the referral pathway noted in Appendix C.
A more detailed assessment of symptoms will be conducted by the AC sport physician and/or MH Lead (i.e., qualified professionals). Assessment will take the form of an interview that will include the completion of standardized assessment instruments (e.g., the SMHAT-1) whenever possible. If an assessment cannot be done by an AC sports physician or the AC MH Lead, the results of a MH assessment must come back to the AC physician and/or AC MH Lead to be assured that the proper treatment plan is in place as needed. The AC sports physician and/or MH Lead will follow up with the athlete to obtain consent to receive these assessment results and make recommendations about a treatment plan. Quality Standards for evidence-based treatment (e.g., https://hqontario.ca/; Depression in adults (nice.org.uk)) will be used when determining diagnosis and treatment plan.
The AC sports physician and/or MH Lead (or appropriate program assistants) will follow up with the athlete and/or point person (e.g., MPC, APA) and repeatedly, if necessary, to confirm the athlete was able to be assessed and/or to access treatment.
Follow-up is a crucial but often overlooked step in the process of individuals getting mental health help. The athlete’s designated point person may need to offer practical, emotional, or physical support to make sure they follow through with the treatment plan. This can include things like accompanying the athlete to the treatment appointments or doing more frequent mental health check-ins. It is important to be warm but firm in your recommendation that they get further help and remember that this may need to be repeated many times before the athlete does follow through with further MH assessment/treatment.
In concert with the AC physician, the MPCs and/or MH Lead will also be engaged to help create a Mental Health Action Plan (MHAP), including an Emergency action plan, in case of decompensation (see Appendix H for an example). Athletes will be strongly encouraged to include Coaches in this planning and at the very least, Coaches should be notified about their role in this plan if a crisis or emergency situation develops during the course of training or at a competition. Again, the most common barrier here is consent and athletes not having a feeling of psychological safety when they share their information with coaches and other staff.
All IST, APAs, coaches and staff can help by encouraging HP members to reach out to their medical doctor or a trusted mental health professional when concerns arise that fall outside of their scope of practice.

15 | P a g e
In Crisis Cases (Immediate concerns of imminent harm to self/others)
If there is any chance that the person may hurt him/herself or others, take the immediate steps below. If someone is in imminent danger, 911 should be called.
1. Stay calm.
2. Engage the person in a serious conversation about how they are feeling. Always make sure you are safe before engaging with the person.
3. Ask about suicide (“Are you thinking of killing yourself? Or “Are you having thoughts of suicide?”) and homicidal thoughts (“Do you have thoughts about harming other people?”)
4. Ask them who is their emergency contact person of their choice (don’t assume it is family, may be a friend).
5. Call 911 if the person is imminently at risk of attempting suicide or harm to others, you are concerned that their judgment is not intact and/or you cannot confirm they have a plan to stay safe.
See Appendix I for a summary of the Emergency Referral Pathway for MH concerns.
At risk athletes should be reminded of the Canada-wide Crisis lines and encouraged to use them whenever needed as a first step to reducing distress: 1-833-456-4566/Text 45645.
If the athlete is in the U.S.A., they should be directed to use: 1-800-273-8255 or Lifeline (suicidepreventionlifeline.org)
Safe Sport Concerns
In instances of suspected or confirmed abuse and neglect, it is important that all HP members are aware of and use the Canadian Sport Helpline (see graphic), which is a resource independent of AC. Furthermore, HP members are encouraged to bring Safe Sport concerns to AC’s Commissioner and/or AC’s Safesport officer. Resources for obtaining support for safe sport concerns are outlined in the relevant AC policies (and highlighted on ACs website).
Treatment
For AC’s HP athletes, the first step for treatment should be to determine if they are eligible for support through Game Plan (https://www.mygameplan.ca). HP athletes who are Sport Canada carded are able to receive $1000/ fiscal year (April 1 to March 31st) from Game Plan for MH treatment.

16 | P a g e
Game Plan, in concert with the Canadian Centre for Mental Health in Sport (CCMHS), have developed a network of mental health professionals (the Mental Health Network or MHN), who have an understanding of the demands of high performance sport and the lifestyle it requires. AC’s HP MH Lead has played a role in developing this network but also has other resources beyond the MHN for those who do not find a good therapeutic fit in terms of MH provider.
To access the MHN, athletes can self-refer by contacting the Intake Co-ordinator at [email protected] (also listed in Appendix G in the orange section). Referrals can also be made through the HP mental performance consultant, HP MH Lead and/or AC sport physician. Referrals can be made to either to a member of the MHN, another practitioner, or to specific treatment programs (i.e., addiction treatment centres, eating disorder treatment centres, etc). Any referral for psychiatry must be done through a medical doctor/sport physician. Any difficulties in accessing the MHN or requests for more specific resources (e.g., for a diagnosis for which the MHN does not have expertise) can be aided by consultation with the HP MH Lead.
Funding
Athletics Canada has dedicated resources for mental health counseling services for HP athletes through Game Plan and/or Lifeworks (formerly Morneau-Shepell), depending on severity of the MH concern. Athletes may also access support and resources for local mental health practitioner, including:
● Provincial coverage for psychiatry services
● Private insurance for registered MH practitioners (eg., psychologist, registered psychotherapist or counsellor)
● Athletes registered with the Canadian Olympic and Paralympic Sport Institute Network (COPSIN) may also be eligible for a maximum of $500 per annual carding cycle.
● Upon completion of the appropriate mental health practitioner sessions, the athlete is then responsible for the financial payment of subsequent services and/or can be referred to existing support resources.
● When/if the above resources have been exhausted, athletes may apply to AC for supplementary funding for mental health practitioner support through the MH Lead or HPD. Awards will be determined on an individual case basis (see next section).
Exceptional funding for MH treatment Some exceptional funding may be available for athletes who require more support than what is offered through Game Plan or above resources. Availability will be determined on a case-by-case basis using the following pathway. As a first step, athletes can ask the HP MH Lead to anonymously request an additional block of funding for a discrete number of sessions from either the APA or, if they feel comfortable, the High Performance Director (HPD). However, depending on individual need and availability of funds, the athlete may need to disclose their name as part of the request for funding.

17 | P a g e
To consider need for additional funding, the MH Lead will request a conversation with the athlete and/or treating professional in order to confirm the details outlined in the Feedback section below (i.e., treatment type, engagement, prognosis, collaboration with AC as a support for the athlete). The HP MH Lead will collate feedback from all relevant parties and speak with the athlete about their MH treatment needs. With appropriate consent, the MH Lead will obtain corroborative data as needed (i.e., from coach, APA, or other IST members involved) and consider Quality Standards/Evidence-based care for MH treatment in order to determine the nature of the supports needed in each case. Decisions will incorporate information about chronicity of the illness or MH concern, social supports, financial need, how much treatment has been provided to date, progress, etc. The MH Lead will then bring a specific request for additional funding to the APA or HPD (e.g., this person requires a block of 5 psychological treatment sessions before re-assessment). The APA or HPD will determine what, if any, funds are available to fund this request for addition MH treatment. The MH Lead will then give feedback to the athlete about what additional financial supports, if any, can be provided by AC. In certain cases, a contract for treatment will be written to ensure that there are clear expectations with regard to the use of this funding.
As always, it is the responsibility of each professional and staff member involved to maintain discretion about details to be shared by involving the athlete at every step of information sharing. If there is no explicit consent to share particular information, then it should not be shared (athlete remains in control of their private health information). As informed consent changes over time, it is important that all professionals continue to obtain consent for any information shared.
Monitoring and Follow-up during Treatment
Follow-up and monitoring will depend first of all on the consent provided by the athlete. Athletes who do not feel safe to share their information will likely keep their MH treatment to themselves. As we work on building trust in the system, we hope that athletes will be willing to share key information on their treatment progress with the “AC point person” and MH Team (HP MH Lead, Mental Performance Consultant, or AC sport physician).
When AC is funding treatment (e.g., in non-carded HP athletes and/or when Game Plan funding runs out), it will be an expectation that an update about treatment progress will come back to the AC point person so that ongoing dialogue about best ways to support the athlete can occur. In this vein, the AC point person should make every effort to obtain informed consent to speak to the MH professional chosen by the athlete for treatment (either through the MHN or externally). Reminders that the level of detail shared remains in the athlete’s control is key to building trust and assuring honest dialogue. Further, informed consent requires that both benefits and consequences of sharing the information AND of not sharing the information are discussed with the athlete.

18 | P a g e
Feedback from treating professionals With any treatment (physical or mental), there are likely important pieces of feedback from external professionals that are helpful for AC team members to know in order to prevent undue harm that can occur as part of one’s job as an athlete on the HP team.
With consent, it is recommended that, at a minimum, information between the MH professional and the AC point person would be shared every 4 – 6 weeks regarding the following:
a) Basic information about the type of treatment (e.g., CBT) and expected treatment plan (i.e., frequency and number of sessions to be expected)
b) Engagement in the treatment plan (i.e., interest, attendance, uptake/application of MH skills being taught)
c) Any other relevant information about prognosis (improving, declining, or other concerns), including evidence-based indices from standardized mental health assessment tools
d) Other ways that AC can support the athlete
If the athlete prefers, the feedback to the AC point person can occur with the athlete present.
Athletes are then engaged in a discussion about which members of their team may need to know about their MH treatment in order to support their ongoing ability to train and compete, pause-play, and/or return-to-play. If there is a need to pause-play or return-to-play after a leave due to a MH concern, then the AC medical doctor (in consultation with the MH Lead) must be involved and made aware of this information.
19 | P a g e
Other relevant aspects to monitoring and follow-up
In line with the Canadian Athletics Performance Pathway (CAPP) Selection Policy (https://athletics.ca/wp-content/uploads/2021/07/CAPP-EN-L1.pdf), a number of strategies will be available to an athlete presenting with MH concerns and/or illness, including educating the athlete’s support system and implementing appropriate pause-play and return-to-play5 protocols (to be completed by the AC sport physician in consultation with the HP MH Lead).
An AC sport physician, the treating MH practitioner, or MH Lead will re-administer appropriate standardized mental health assessment tools on a schedule deemed appropriate for the individual athlete. Meetings with key support members will be arranged to ensure that the athlete is involved in the implementation of any relevant protocols.
MH Pause-play Protocol
Any CAPP HP athlete who is unable to train or compete due to MH concerns must communicate and file a report with the APA, as they would for a physical injury. If there is an issue of the athlete not making a national team due to mental health status, a report must be filed with the APA as per selection criteria.
If appropriate, HP coach(es) and staff may be informed of mental health status. The timeline for communication will be handled on a case-by-case basis.
Additionally, athletes may be reassured that their teammate is under professional care, and that other details will not be shared with them because of privacy and confidentiality. Athletes may be offered group or individual counselling if they request it.
At all points, maintaining athletes’ right to confidentiality will be respected and adhered to according to the stipulations outlined on the Informed Consent for Release of Mental Health Information form. Informed Consent is dynamic in nature and therefore should be revisited at when a pause-play protocol is invoked.
MH Return-to-Sport Protocol A return-to-sport protocol will require the athlete to communicate with their coach and AC sport physician, as well as MPC (if they have one). Athletes are encouraged to follow the guidance of an AC sport physician and/or MH Lead when deciding to return to sport. Best practice is for AC’s MH Lead to communicate with the attending practitioner, as per the plan outlined above in terms of Follow-up and Monitoring. The athlete will be encouraged to use the MH Lead’s and/or treating provider’s recommendations, and to complete the relevant forms and assessments as per return-to-sport protocol.
5 Individualized MH Pause-play and Return-to-play protocols will be developed based on the athlete’s unique presentation of symptoms and level of functioning.

20 | P a g e
To avoid relapse once the athlete has returned to training, the athlete will be invited to undergo regular mental health assessment with an AC sport physician and/or licensed practitioner on a schedule determined between practitioner and athlete. A successful return to play is best accomplished with a graduated structured exercise program along with daily monitoring tools. This will be created in collaboration with the athlete’s HP support team.
If the athlete decides to leave Athletics, mental health support resources will be coordinated for continued care in the form of referrals on an individual basis. For example, athletes may be eligible for mental health support through Game Plan for up to 2 years post retirement.

21 | P a g e
Promotion of Mental Health
Mental health promotion in sport includes equipping individuals with the skills and personal resources to help them cope effectively with the demands of life and HP sport. Stigma is the major barrier preventing individuals for seeking help and getting the care that they need (Gulliver et al., 2012; Henriksen et al., 2020). Reducing stigma and educating HP members about how to take care of their mental health as a lifestyle will lay the foundation for physical health, good performances, and therefore longevity in their careers.
Mental health promotion is important for building a “culture of excellence” and improving communication among team members, which is part of the foundation for a psychologically safe and healthy organization. Mental health promotion across the organization is likely to reduce burnout rates, increase well-being, and cooperation among team members, including in athlete-coach relationships (OTP, 2020; van Slingerland et al., 2021).
We can minimize the occurrence of mental health issues in our sport by providing proactive support to help athletes manage the high-performance lifestyle and cope positively with the stresses involved. These needs change throughout each person’s career and are (to some extent) predictable based on our experience with other team members. For example, we know that there are stresses around retirement that can affect athletes in the run-up to the Olympics or Paralympics and post-Games, and that this can affect their performance (Sarkar & Fletcher, 2014; van Slingerland et al., 2021). Extra effort to provide MH support and education for all HP athletes and staff will occur during known times of vulnerability.
MH Promotion Service Delivery Actions
1. MH Lead and AC Lead Mental Performance practitioner (MPC) to develop and deliver MH literacy training for all AC HP members that creates awareness about what mental health is, how it can be impacted through participation in high performance sport, and actions taken to promote mental health (i.e., self-care strategies). The training will also incorporate information about MH referral pathways and resources for members. In addition, discussion about specific mental health literacy components related to addressing negative stereotypes, fears about communicating MH concerns, and the importance of seeking help to reduce stigma will be encouraged. Testimonials from other high performance athletes who have performed with or recovered from mental illness may be included as this has been found to be effective.
2. MH Lead and AC Lead Mental Performance practitioner (MPC) to ensure trainings are available to all HP members, along with other key resources and referral pathways, on the website. Key reminders or updates about resources should be provided through newsletters and other means of communication as much as possible.
3. MH Lead to be a stakeholder in Diversity, Equity, and Inclusion (DEI) and Safesport policies and procedures as they relate to HP members’ mental health. MH Lead will also help ensure that all members within the organization are aware of these policies and procedures, including safe ways of
22 | P a g e
obtaining help when there is a concern or complaint about an HP member who is negatively affecting another member’s mental health.
4. HP coaches will complete, at minimum, the CAC Respect in Sport Mental Health training (via webinar through CAC). HP Coaches will also be offered the opportunity to meet with the MH Lead to discuss the application of this training in the DTE through regular Co-op (peer-to-peer staff) offerings.
5. MH Lead to coordinate crisis intervention and suicide prevention training for all HP coaches and staff.
6. MH Lead and/or MPC to develop and deliver training and resources to assist athletes, coaches, and support staff in integrating mental health action planning into yearly training plans (YTP). Mental Health Action Plans (MHAPs) outline concrete steps to (a) engage in regular self-care, (b) provide support when mental health is compromised, and (c) respond to mental health crises. MHAPs will also be updated routinely with those with identified mental illness or at high risk for difficulty, particularly before major competitions or Games.
7. MPCs (with MH Lead support as needed) to coordinate integration with mental health support programs specific for high performance sport participants (e.g., Game Plan, COPSI network resources).
8. Mental Health Lead and Mental Performance Lead consultant to source and catalogue agencies, resources, and programs for Athletics community to access for mental health and performance support across the country. Establish a referral network of appropriate mental health practitioners (e.g., Registered Clinical Counselors, Registered Psychologists, and Sport Psychiatrists) that can be quickly and easily contacted when needed across Canada and communicated to staff, coaches, and athletes the existence of this resource.
9. MH Lead to support AC sport physician in implementing best practice guidelines for managing mental health during treatment and/or recovery for athletes who continue to train and complete.
10. MH Lead to support AC sport physician in implementing best practice guidelines for re-integrating athletes back into training and competition following an interruption in training due to mental illness.
The MPC role supports the promotion of mental health in many ways, including
1. MPCs identify mental skill competencies and weaknesses in the athletes with whom they work and through a process orientation and relationship, help build mental strengths and skills. The Gold Medal Performance (GMP) for Psychology in Sport and Assessment Guidelines are resource documents for MPCs in this regard (van den Berg et al., 2020; van den Berg & Durand-Bush, 2020).
2. MPCs work with coaches, APAs, and IST staff to identify critical periods of stress (e.g., prior to Olympic Games, World Championships) and develop coping strategies (through education and individualized support) to manage those challenges.
23 | P a g e
3. MPCs educate and facilitate the optimization of coach-athlete relationships among Athletics Canada
high performance coaches and the athletes.
4. MPCs work to identify and reduce/remove modifiable system- and interpersonal risk factors that can trigger or exacerbate mental health challenges or mental illness (for example, safe-sport issues).
In addition to the above roles, Mental Performance practitioners (MPCs) employed by AC will develop and determine best mechanisms to deliver training for all AC athletes in the area of core mental skill competencies (e.g., developing resilience, self-awareness, and self-regulation (cognitively and physiologically); attention; managing stress and determining optimal arousal levels (event specific); facilitating effective athlete-coach relationships; ensuring leadership, teamwork, and communication are effective) and additional mental skill competencies that may be unique to the athlete’s discipline within Athletics (e.g., dealing with weather and wind conditions, equipment failure, etc.). Potential delivery mechanisms include MPC consultation directly with an athlete, MPC consultation indirectly through the coach, and MPC led group education (regional and discipline specific). All programming will ensure a periodized approach to mental skill training across a single year of training and competing, as well as across a quadrennial.
MPCs will facilitate opportunities for athletes and coaches from all athletic disciplines to interact in ways that build interpersonal trust and respect and ensure an environment that is psychologically safe. These activities will be carefully planned for select periods in the yearly training plan.
MH Champions There will be a call to collect MH Champions within the organization so that personal stories of lived experience with MH concerns and/or mental illness can be de-stigmatized. There are already MH Champions in sport leading the way (e.g., Michael Phelps, Clara Hughes) but it is hoped to add the voices of AC athletes to improve resonance. These MH Champions will be encouraged to have a voice in the implementation and evaluation of this MH Strategy.
Other MH Promotion Supports Opportunities for MH promotion also exist for athletes and staff at different stages of their careers through the Canadian Olympic and Paralympic Sport Institute Network (COPSIN), Canadian Olympic Committee (COC)/Canadian Paralympic Committee (CPC), and external providers (see https://mygameplan.ca).
24 | P a g e
Implementation and Evaluation of the Strategy
This High Performance MH Strategy for AC (“the Strategy”) will require time to implement in full. As such, there will be a gradual roll-out of components over time.
To monitor the implementation of the Strategy, a Mental Health (MH) Committee has been established and will aim to meet on a monthly basis. The MH Committee is overseen by the Sport Science Sport Medicine and Innovation (SSSMI) Lead and High Performance Director (HPD) and will provide an update/feedback to these individuals at least twice yearly and upon request.
The MH Committee will provide feedback on the Strategy and its components as they are implemented. Members of the MH Committee will anonymously track MH concerns in athletes to assess the ongoing and changing needs of our members. MH Committee members will report on issues such as:
• the nature/severity/domain of impact with regard to MH concerns, • recommended resources • team members involved • appropriate consent, in particular obstacles to obtaining consent to share information (e.g., stigma,
fear) with an aim to improve help-seeking and team communication in the organization over time.
MH Lead will meet with MPCs and/or AC Sport physicians on a regular basis to consult about specific athlete MH concerns and about the process of implementing the MH assessment and treatment components of this Strategy.
As noted above, MH Champions will be called upon to play a role in the evaluation of this Strategy and its implementation.

25 | P a g e
Mental Health Strategy for AC HP Coaches and Staff
Guidelines for mental health intervention, monitoring, treatment and prevention with coaches and staff exist within AC and Canadian Sport Institute (CSI) employment contracts. Additionally, HP AC employees and HP coaches are eligible for mental health support under Game Plan (contact Game Plan regional advisor at https://mygameplan.ca/ourteam). Support, where required, will be provided to allow for program continuity.
Coaches and staff that are undergoing treatment for mental health issues will continue to follow and fall under the employee support services as outlined through their organization’s human resources policy.
If the coach or staff member decides to discontinue his or her work with AC, mental health support resources may be coordinated for continued care in the form of referrals on an individual basis.

26 | P a g e
References
Chang, C. J., Putukian, M., Aerni, G., Diamond, A. B., Hong, E. S., Ingram, Y. M., Reardon, C. L., & Wolanin, A.
T. (2020). Mental Health Issues and Psychological Factors in Athletes: Detection, Management, Effect
on Performance, and Prevention: American Medical Society for Sports Medicine Position Statement.
Clinical Journal of Sport Medicine, 30(2), e61–e87. https://doi.org/10.1097/JSM.0000000000000817
Coaching Association of Canada (2020, January). NCCP Code of Ethics.
https://coach.ca/sites/default/files/2020-03/NCCP_Code_of_Ethics_2020_EN.pdf
CSA Group (2013). Psychological health and safety in the workplace - Prevention, promotion, and guidance to
staged implementation. (CAN/CSA-Z1003-13/BNQ 9700-803/2013). CSA Group and BNQ.
https://www.csagroup.org/article/cancsa-z1003-13-bnq-9700-803-2013-r2018/
Durand-Bush, N., & Van Slingerland, K. (2021). Mental health strategy for high performance sport in
Canada. The Mental Health Partner Group [Canadian Centre for Mental Health and Sport, Canadian Olympic
and Paralympic Sport Institute Network, Game Plan, and Own The Podium].
Edmonson, A. (2012, May 4). TEDxHGSE. Building a Psychological Safe Workplace.
https://www.youtube.com/watch?v=LhoLuui9gX8&t=82s.
Gouttebarge, V., Bindra, A., Blauwet, C., Campriani, N., Currie, A., Engebretsen, L., Hainline, B., Kroshus, E.,
McDuff, D., Mountjoy, M., Purcell, R., Putukian, M., Reardon, C. L., Rice, S. M., & Budgett, R. (2021).
International Olympic Committee (IOC) Sport Mental Health Assessment Tool 1 (SMHAT-1) and Sport
Mental Health Recognition Tool 1 (SMHRT-1): Towards better support of athletes' mental
health. British Journal of Sports Medicine, 55(1), 30–37. https://doi.org/10.1136/bjsports-2020-102411
Gulliver, A., Griffiths, K.M., & Christensen, H. (2012). Barriers and facilitators to mental health help-
seeking for young elite athletes: a qualitative study. BMC Psychiatry, 12(1), 157– 157.
https://doi.org/10.1186/1471-244X-12-157
Gulliver, A., Griffiths, K.M., Christensen, H., & Brewer, J.L. (2012). A Systematic Review of Help-Seeking
Interventions for Depression, Anxiety, and General Psychological Distress. BMC Psychiatry, 12, 81.
doi:10.1186/1471-244X-12-81.
Health Quality Ontario (2017). Quality Matters: Realizing Excellent Care for All.
https://hqontario.ca/Portals/0/documents/health-quality/realizing-excellent-care-for-all-1704-
en.pdf

27 | P a g e
Hoar, S., Meikle, F., Hadd, V., & Edwards, C. (2020, November). Cycling Canada High
Performance Pathway. Mental Performance & Health Strategy 2021 – 2024. Cycling
Canada.
Hoar, S., Keeler, S., Sedgwick, W., Wrigley, A., Hood, J., Barnes, K., Soulard, A., Holtham, A., & Atkinson, J.
(2018, March). Swimming Canada’s Mental Health Strategy. Swimming Canada Natation.
https://www.swimming.ca/content/uploads/2018/04/Mental-Health-Strategy.pdf
Jack.org. (2021) Be There. https://bethere.org/Home
National Institute for Health and Care Excellence (2011, March). Depression in Adults.
www.nice.org.uk/guidance/qs8
Own the Podium. (2020, August). Position paper: Gold Medal Profile for Psychology in Sport.
Providing Canadian National Sport Organizations with evidence-informed mental performance
competencies for podium success in high-performance sport. Sport Scientist Canada.
Sarkar, M. & Fletcher, D. (2014). Psychological Resilience in Sport Performers: A review of
Stressors and Protective Factors. Journal of Sports Sciences. 32(15):1419-34.
doi: 10.1080/02640414.2014.901551. UK: Loughborough.
Schinke, R. J., Stambulova, N. B., Si, G., & Moore, Z. (2017). International society of sport psychology
position stand: Athletes’ mental health, performance, and development. International Journal of Sport and
Exercise Psychology, 16(6), 622-639.
Tomalski. (2019). Mental health screening for athletes: Program development, implementation, and
evaluation. Journal of Sport Psychology in Action., 10(2), 121–135.
https://doi.org/10.1080/21520704.2019.1604589
van den Berg, F., Baker, J., Bloom, G., Durand-Bush, N., Richard, V., & Tully, B. (2020). Sport
Scientist Canada: Gold Medal Profile (GMP) for Psychology in Sport. Ottawa, ON: Own
The Podium.
van den Berg, F. & Durand-Bush, N. (2020). Sport Scientist Canada: Gold Medal Profile (GMP)
for Psychology in Sport. Assessment Guidelines. Ottawa, ON: Own The Podium.
28 | P a g e
Van Slingerland, K. J., Durand-Bush, N., Bradley, L., Goldfield, G., Archambault, R., Smith, D., … Kenttä, G.
(2019). Canadian Centre for Mental Health and Sport (CCMHS) position statement: Principles of mental
health in competitive and high performance sport. Clinical Journal of Sport Medicine, 29(3), 173-180.
https://doi.org/10.1097/JSM.0000000000000665.
Wheeler, H.A. (2020, October). Needs/Gap Analysis for Mental Health at Athletics Canada. Raw
data and presentation to the MH Committee.

29 | P a g e
Appendix A
Scope of Practice within the Mental Health Continuum Model (from Durand-Bush, 2021)

30 | P a g e
Appendix B Sport Mental Health Recognition Tool-1 (SMHRT-1)
31 | P a g e
Appendix C MH Non-Emergency Referral Pathway

32 | P a g e
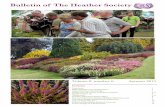
Appendix D MH Assessment Screening procedure (SMHAT-1)
Athlete’s Form 2: Additional questionnaires for more specific MH Symptoms
► General Anxiety Disorder-7 (GAD-7): assesses the presence of symptoms of anxiety
► Patient Health Questionnaire-9 (PHQ-9): assesses the presence of symptoms of depression.
► Athlete Sleep Screening Questionnaire (ASSQ): assesses the presence of sleep disturbance
► Alcohol Use Disorders Identification Test Consumption (AUDIT-C): assesses the presence of alcohol misuse
► Cutting Down, Annoyance by Criticism, Guilty Feeling, and Eye-openers Adapted to Include Drugs (CAGE-AID): assesses the presence of substance misuse, being slightly adapted for the SMHAT (no focus on alcohol use as already explored with the AUDIT-C; additional question to explore which substance was used).
► Brief Eating Disorder in Athletes Questionnaire (BEDA-Q): assesses the presence of disordered eating
Note: The above are only suggested tools for identifying and monitoring mental health concerns. Other assessment tools will be used at the AC physician’s or MH Lead’s discretion.
IOC Sport Mental Health Assessment Tool (SMHAT-1)
Step 1: Triage Tool – Athlete’s Form 1Assessment of sport-related psychological distress with APSQ
Step 2: Screening Tools – Athlete’s Form 2Assessment of 6 mental health symptoms with 6 exis�ng
validated screening instruments
Athleteat pre-, mid- or post-season or in case of any significant event (e.g., injury, illness, surgery, unexplained performance concern,
a�er a major compe��on, end of compe��ve cycle, suspected harassment/abuse, adverse life event, transi�oning out of sport)
No further ac�on needed
Take immediate ac�on to ensure safety of the athlete
Step 3a: Brief Interven�on & Monitoring• Single or combina�on of brief
interven�ons (e.g., psychoeduca�on, mindfulness, stress control, medita�on, resilience training)
• Monitoring with APSQ (Athlete’s Form 1)Step 3b: Clinical Assessment• Assessment of severity, complexity, diagnos�c
uncertainty, previous treatment non-response for each diagnosis.
• Addi�onal informa�on about other mental health symptoms (Athlete’s Form 3)
• Defini�on and applica�on of treatment and support plan• Referral to mental health professional
Score APSQ < 17
6 screening instruments under threshold
Score APSQ ≥ 17
1 or more screening instruments at or above
threshold
Score ≥ 1 PHQ-9 item 9
* IOC = Interna�onal Olympic Commi�ee* APSQ = Athlete Psychological Strain Ques�onnaire
Gou�ebarge V, Bindra A, Blauwet C, et al. Br J Sports Med 2021;55:30–37.

33 | P a g e
Appendix E Possible List of Life Concerns

34 | P a g e
Appendix F Athletics Canada Informed Consent for Release of Mental Health Information form
Members of the High Performance (HP) Integrated Support Team (IST) will be meeting on a regular basis in order to discuss how best to optimize the performance of HP athletes. Members of the IST include (but may not be limited to) coaches, dietitians, massage therapists, physicians, physiotherapists/athletic therapists, mental performance coaches, psychologists, APAs, High Performance Director, physiologists, strength and conditioning coaches, and biomechanists.
During the course of such meetings, IST members may need to share confidential information about a HP athlete amongst the IST. The information that is shared is generally restricted to only that which is required to allow the rest of the IST to understand the status of an athlete within the area of expertise that the member provides to the IST. The athlete may work with the IST member who is sharing sensitive information to determine the preferred wording or narrative for their concerns.
Each IST member will utilize their professional judgement within their scope of practice and will discuss with the athlete in coming to a decision in determining what to share, while still maintaining the integrity of the confidential information. The information shared is expected to be used only to benefit the athlete (i.e., to obtain support from other IST members in order to maintain training and aid performance). If there are reasons to believe that a particular team member or coach does not feel like a safe person to share information with, it is important to discuss other options for you to feel supported while training and in competition. Carefully consider both the potential risks AND benefits when deciding with whom to share this information.
Sharing of information may be verbal, in writing, or within certified electronic medical record systems in Canada. Whenever possible, secure electronic communication will be used to share information. However, in order to facilitate ease of communication, there will at times be the use of SMS messaging and other means (e.g., WhatsApp) in order to coordinate care. All information that is shared is held in the strictest confidence by all HP staff members.
In signing this consent, you state that you have read and understand the purpose for which IST members may share confidential information about you and that you consent to the sharing of information about you. You may withdraw this consent at any time.
Athlete Name (Please Print) Athlete Signature Date

35 | P a g e
Consent for Release of Information
I, ___________________________ herby give permission to _______________________________ to
(Athlete Name) (Consultant Name)
_______________________________
(Consultant Contact Details)
obtain from AND/OR provide to
the following individuals (please list any that apply and provide name of each provider):
COACHING STAFF
________________________
________________________ ADMIN STAFF
High Performance Director (HPD)
Athlete Performance Advisor (APA) ________________________
National Team Unit (NTU) ________________________
MEDICAL TEAM
________________________
________________________
IST Physiotherapy
________________________ Strength & Conditioning Coach
________________________ Biomechanist
________________________ Registered Dietitian
________________________
MH TEAM Dr. Paddy McCluskey, Dr. Sari Kraft, Dr. Penny Werthner, & Dr. Heather Wheeler
the following information: The purpose or need for releasing this information is:
I understand and I am aware of the risks and benefits of consenting, or refusing to consent, to release this information. I also understand that I may withdraw this consent at any time in writing. This Consent for Release of information is valid for one year (until next medical evaluation or intake assessment, unless revoked in writing prior to that time). Any written withdrawal will be effective on the date of receipt of the written notification.
Athlete Signature Date
Witness Signature Date

36 | P a g e
Appendix G
Resources for HP Athletes across the MH Continuum

37 | P a g e
Appendix H Mental Health Action Plan [MHAP] (Example)
My MHAP: __________________ Date: __________________
When I am feeling well, I am:
Describe what you are like when you are feeling good – socially, psychologically, emotionally—in competition and out of competition. Describe your strengths and how you like to be.
What are my triggers for distress?
Describe the events, people, areas, etc., that are likely to trigger unhelpful thoughts, feelings, behaviours.
What are the signs that my mental health is diminishing?
Describe the behaviours/actions, attitudes, emotions that your coach (or supportive other) could observe as an indication that your mental health is diminishing.
As my coach (or supportive other), what can you do when you see the warning signs?
Describe the steps a coach (or supportive other) can take to address the warning signs and help you stay on track.
What is the best way to approach me as a player and person? What sort of motivational tactics do I respond to? What causes me to shut down?
What kind of expectations do I have for myself and others?
The Plan

38 | P a g e
– In competition: Describe the steps, coping techniques, skills, tools, that you will utilize to maintain your mental health in a competitive setting.
– Out of competition: Describe the steps, coping techniques, skills, tools, that you will utilize to maintain your mental health in your daily life away from your sport.
Response to decline in mental health status:
Prior to participation, the coach and athlete should have a discussion and mutually agree on a fair and healthy course of action in the event that the athlete’s mental illness interrupts his or her ability to compete. Use the space provided to get started. Also describe how you feel about disclosing your mental health status to teammates and decide who else be a support during training and competition in this section.
Athlete Signature: ______________________________ Date: __________________________
Coach Signature: _______________________________ Date: __________________________ |
Safety Plan: Who to call in a crisis situation?
Name: __________________________ Contact Number: __________________________
Relationship: __________________________
Name: __________________________
Contact Number: __________________________ Relationship: _________________________
Crisis Lines: _______________________________
Note: If it is an emergency or you feel too unsafe to implement the above plan, call 911 or go to the nearest emergency room.

39 | P a g e
Appendix I
MH Emergency Referral Pathway
Copyright © 2022 FDOKUMEN