What refugees need to know to live healthily - Community ...
84
What refugees need to know to live healthily Living Well in Glasgow Research Report Living Well connecting people, improving lives Prepared by Community InfoSource May 2014
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of What refugees need to know to live healthily - Community ...

1
What refugees need to know to live healthily
Living Well in Glasgow Research Report
Living Well connecting people, improving lives
Prepared by Community InfoSource
May 2014

2
This research report has been supported and written by a number of
people who have each worked on different aspects of it:
Chapter One: Introduction Sheila Arthur
Chapter Two: Literature Review Duncan Sim
Chapter Three: Methodology Sheila Arthur
Chapter Four: Findings - Individuals Jamila Hassan
Chapter Five: Findings - Organisations Jane Balmforth
Chapter Six and Recommendations were written by both Duncan
Sim and Jamila Hassan
The final report was compiled by Community InfoSource
Photograph on front cover:
Final day of the very successful Mental Wellbeing Workshops
December 2013

3
Contents Page
List of figures and tables 4
Acknowledgements 5
Chapter One: Introduction 6
1.1 Introduction and overview
1.2 Project development
Chapter Two: Reviews of previous literature 12
2.1 Barriers and misunderstandings
2.2 Health, happiness and “wellness”
2.3 Conclusion
Chapter Three: Methodology 24
3.1 Introduction
3.2 Methodology
Chapter Four: Research findings - individuals 30
4.1 Overview of respondents
4.2 Food habits
4.3 Access to health services
4.4 Activities
Chapter Five: Research findings - organisations 49
5.1 Aims
5.2 Findings
Chapter Six: Conclusions 60
Recommendations 62
Bibliography 63
Appendices 66
1. Living Well in Glasgow Timeline
2. Letter of introduction and individual survey
3. Letter of introduction and organisational survey
4. Details of organisations surveyed
5. Support provided by individual organisations
4
List of figures and tables
Figures
Figure 1: Respondents by Region
Figure 2: Respondents by Age
Figure 3: Respondents by Residential status
Figure 4: Respondents by Length been in UK
Figure 5: Gender by Age
Figure 6: Gender by Region
Figure 7: Do you mainly cook, or buy fast food?
Figure 8: cooking skill by Gender
Figure 9: cooking skill by Region
Figure 10: do you eat the same kind of food
Figure 11: Kind of food by age
Figure 12: do you eat the same amount of food
Figure 13: Amount of food by gender
Figure 14: Amount of food by Region
Figure 15: Do you eat the same amount of fruit and vegetables
Figure 16: Do you eat different mixture of food?
Figure 17: Mixture of Different food by Gender
Figure 18: Mixture of Different food by Region
Figure 19: Are you registered with doctor
Figure 20: Are you registered with dentist
Figure 21: How has your health been compared in your home country
Figure 22: Do you think people are interested in attending workshops on
Tables
Table 1: Gender of the respondents * Cooking * Region of the
respondents
Table 3: Region * Do you eat the same kind of food?
Table 2: Gender * Do you eat the same kind of food?
Table 4: Gender * Do you eat the same amount of fruit and vegetables?
Table 5: Respondents’ Regions * Do you eat the same amount of fruit
and vegetables? Cross tabulation

5
Acknowledgements
The Living Well in Glasgow Planning Group, which is now up to
meeting number 31.
The Living Well in Glasgow Steering Group, which provided support
and advice in the earlier stages of development, as have individual
members throughout.
All the Living Well in Glasgow volunteers, those who have
supported us in the past and those who still volunteer in the
administration of the project.
All the Living Well in Glasgow volunteers who took part in
developing the research, carrying out the interviews and inputting
much of the data.
Stefan Robert who, in addition, also carried out significant analysis of the
early data.
All those who took part in surveys
102 individuals and 20 representatives of organisations
All of the volunteers who helped fundraise, develop and deliver the
three types of workshops which followed from the research
Finally, the volunteer who made all of this happen, Lori Sullivan, the
Volunteer Coordinator
Our continuing thanks to them all

6
Chapter One: Introduction
1.1 Introduction and overview
The dispersal of large numbers of asylum seekers to Glasgow started in
2000 and is still ongoing. These are people who have asked the UK
government, in the form of the Home Office, to give them refugee status
under the 1951 Refugee Convention and who are currently waiting to
have their applications assessed. There are currently around 3,000
asylum seekers, supported and housed by the Home Office, in the City.
In addition, over these 14 years, many have received status of some kind
which entitles them to stay in the UK, many of whom have decided to
make Glasgow their home rather than moving elsewhere in the UK.
Netto (2011) found that just over two-thirds of her interviewees reported
that they were 'very likely' to stay in Glasgow and she points to the
'connectedness to place' which many refugees felt after living in the city.
Mulvey (2013) similarly found the majority of his research participants
planning to stay in Glasgow.
Terms
Our project Living Well in Glasgow (LWiG) generally uses the term
‘refugee’ to cover all those who have come to the UK seeking refugee
status. In this report we use the word “refugee” to refer to people at
various stages of the process, namely:
British citizens from a refugee background
Those with full refugee status
Those who have indefinite leave to remain
Those who have leave to remain in the UK for a limited time
Those who are still in the formal asylum process and who are on
Home Office section 95, 98 or section 4 support
Those who have been refused asylum, are destitute and are
trying to get back into the system, while living in Glasgow
7
We only differentiate between these categories where it is necessary for
a better understanding of the analysis.
Community InfoSource (CIS) has been involved with refugees and
asylum seekers (referred to as refugees from here, unless there is a
need to differentiate), through its individual directors, since 2000 (and
before). We are a group of six people, four of which come from a
refugee background and two which have worked with refugees.
Living Well in Glasgow came about through conversations between CIS
directors and different refugees about problems to do with health and
well being. Some of the issues for newcomers which are commonly
related to knowledge and information are listed below:
How do people deal with the transition of working with their
community in hard work on the land to being forbidden to work
and so having a sedentary lifestyle, probably living in a high rise
block, and being socially isolated
How do people from a hot climate learn methods of dealing with
our relatively cold weather
How do people learn what food here is nutritious and reasonably
priced and how to cook it
How do people cope with mental health issues from: the
traumas of their previous lives; their lives in the asylum system
here, and then, after receiving status, adjustment to a
completely different life in UK
Cultural differences – how do newcomers learn what behaviour
is acceptable (or not) here, especially if they are isolated
Initially a partnership was set up between CIS and Ypeople Glasgow
Residents’ Association (YGRA), an organisation with an elected
committee of people who lived in housing provided by Ypeople, the main
Home Office accommodation provider in Glasgow at that time (2011).
YGRA was particularly concerned about how to identify mental health
issues and about how to provide some kind of supportive sign- posting
for the many affected people which they could identify from their own
general experiences.

8
YGRA were based in 33 Petershill Drive, in Springburn. This is where
Ypeople rented the whole building, where they had a reception desk on
the ground floor, offices on the 1st and 2nd floors, and temporary housing
where they accommodated people under the Initial Asylum Service for
their first few weeks until they were re-housed. They also provided
accommodation for some large families and some single people in
shared flats. Ypeople also provided a community space (called
Ycommunity) on the 28th floor, using the four flats. They had also
donated a room to YGRA as an office.
The research idea
Originally, the idea being developed was to set up a project which
focussed on the health and well being of newcomers to Glasgow, and in
the spirit of partnership, work alongside Ypeople (who had agreed to
support the project) and National Health Service Greater Glasgow and
Clyde’s asylum seeker base “Health Matters”, on the 1st floor of the
building at 33 Petershill Drive. Ypeople no longer has the asylum
support contract (now held by Serco) and Health Matters has now
become a different project with a change of staff, so this partnership
arrangement became inappropriate. LWiG therefore took the idea
forward independently.
After long discussion, a decision was made to develop the project for
refugees.
The aim of LWiG is to develop a pilot project for health and wellbeing
activities to address what refugees need to know to live healthily. Ideally
these could be incorporated into mainstream services in Glasgow.
The project is to be developed as a pilot one which could be rolled out to
other community groups or neighbourhoods. It was acknowledged that
every community could benefit from awareness raising on the issues we
wish to address, although we focus on ones particularly relevant for
refugees who have come to the UK to escape persecution and violence.
While developing ideas for workshops and starting to fundraise, we
realised that all of the evidence of what refugees needed to know for
9
healthy living and wellbeing was anecdotal up to the present time.
Therefore we decided that the first part of the package has to be the
accumulation of evidence of what is actually needed. So we agreed to
carry out research by and for refugees, with the aim of providing the
information needed to develop activities for LWiG. What better way of
finding out than carrying out an action research project whereby refugees
developed the research methods, carry out the surveys and then analyse
the data.
Fundraising
A successful funding application was made to The Scottish Community
Foundation (now Foundation Scotland) for a grant to facilitate the
research project.
We also accessed a small grant from the European Year of the
Volunteer (through the Voluntary Action Fund) which helped us finance
the setting up of the Volunteer Project and the volunteer costs of
administering the project.
1.2 Project development
From September 2011 onwards Living Well in Glasgow recruited some
volunteers to be trained in office administration and research methods.
A Steering Group was set up, consisting of people who understand the
situation of our target group (the refugees), and had its first meeting in
October 2011. The Steering Group discussed how they could assist
Living Well in Glasgow and suggestions were made for others to join the
support structure. There were small discussion groups to gather
participants’ views on what refugees needed to know to live healthily
here, and how information should be presented to make it accessible for
them. Details from these discussions are in Methodology in Chapter
Four. The second meeting took place at the end of February 2012 and
looked at the findings of the pilot research (the first 50 surveys of
individuals) and involved helpful discussion of some of the issues

10
identified (such as the use of the term GP (General Practitioner) by
professionals and the word Doctor by newcomers).
The research data was collected until April 2012 with the analysis
following. The data from both individual surveys and surveys of staff at
relevant organisations was input to Survey Monkey research package
and the results were generated in excel and pdf formats.
During Refugee Week 2012 we held a successful and professional event
which highlighted some of the results from the individual surveys. Using
some of the data based on what refugees felt they needed to know to
live healthily here, we also delivered two pilot workshops to help teach
stress management techniques, which were very highly acclaimed.
The nature of working with volunteers is that often they find themselves
having access to formal employment, no longer having the time to give to
projects, or gaining the confidence to go on to education courses, which
is as it should be.
By advertising for support, we were very pleased to find a volunteer who
helped us with the detailed analysis of the organisation interviews. The
analysis of the individual interviews took longer to find a successful
volunteer placement, with at least two false starts, but finally in 2013 we
found not only a refugee volunteer but someone who had academic
experience of analysis.
Meanwhile, in spring 2013 we advertised and interviewed for a second
group of volunteers to help develop three types of workshops. We used
the results of primary data analysis to address the highest demand
issues that refugees think they need to know to live healthily in Glasgow.
There was a lot of work involved in the development of workshops:
finding accessible locations where refugees would be comfortable to
come and could get to without too much trouble; finding accessible
premises where everyone could get in; developing the content of the
workshops; finding suitable practitioners with skills and experience of
working with refugees; taking decisions about support for childcare and
even finding a suitable source for the provision of lunch.

11
Three types of workshops took place between October 2013 and
January 2014 and involved: a) Zumba classes on a Saturday, both mixed
gender and women only ones; b) a Healthy Eating & Cooking workshop
on Mondays, both mixed gender in the afternoons and women only in the
morning and c) Mental Wellbeing workshops fortnightly on Tuesday
mornings, for men and women separately.
These workshops were all very well received and there has been great
demand from participants and other professionals, that they should be
repeated for other groups.
Finally, the LWiG Planning Group is still meeting regularly (we are up to
meeting number 31) and has a committed group of six volunteers (four of
whom are from a refugee background) who are eager to move forward
with new ideas which are being developed based both on the research
findings and personal knowledge. Funding applications should be
submitted shortly.
A Timeline of the development of the project to date is attached as
Appendix One
First Steering Group meeting, 2011 Stefan and Mavis preparing for
our Refugee Week event
12
Chapter Two: Review of previous literature
2.1 Barriers and Misunderstandings
There are a considerable number of reports, advice documents and
papers written about the importance of good health and lifestyle in
relation to refugees and asylum seekers.
A significant number of these are concerned with the initial arrival of
refugees and the importance of helping them to register with health
services, most importantly a General Practitioner (GP) but also with a
dentist or other health professional. The Scottish Executive (as it then
was) for example, provided advice to local authorities and other agencies
in 2004, emphasising the importance of alerting refugees to their
entitlements under the NHS, how to register with a GP, and how to
access out-of-hours services through the NHS24 helpline. Similarly, the
Scottish Refugee Council issued guidance in April 2011 on ‘How to
Access Health Care in Scotland’ and, in February 2013, a Health
Information Briefing on the health rights and entitlements of refugees and
asylum seekers in Scotland. As well as providing basic information on
registering with a GP and on, for example, out-of-hours services, the
briefings also provided information on how to obtain help with additional
healthcare costs (such as dental care, glasses, contact lenses and wigs),
and on how to make a complaint in the event of poor service by the NHS.
There have, subsequently, been a number of studies which have
explored the barriers to accessing healthcare which have been
experienced by refugees. In an important study of the health
experiences of refugees in north Glasgow, Roshan (2005) found that
there was a high level of GP registration but that refugees experienced a
number of difficulties in making use of the NHS. Principal among these
was language and communication, with many refugees requiring the use
of an interpreter. Other problems included the length of time some
refugees had to wait for appointments, uncertainties as to their rights and
entitlements, difficulties in travelling to surgeries and health centres, and
interactions with NHS staff – sometimes because staff themselves were
unsure how to deal with refugee patients.

13
In another Glasgow study, O’Donnell et al (2007) noted in relation to
language barriers that there is sometimes a tension between interpreters
translating verbatim and acting as patient advocates. Additionally,
access to interpreters in other settings, for example in-patient hospital
stays could be problematic. They also found that refugee families with
limited resources sometimes found it hard to afford over-the-counter
medication such as children’s paracetamol.
Barriers to health care are particularly significant in the case of older
refugees whose knowledge of English may be poorer and who may be
less able to articulate their needs. Yet they may be experiencing ageing
faster, possibly due to traumatic experiences and many refugee women
require health support during the menopause. Older refugees may be
particularly affected by isolation because of the stereotype that BME
communities ‘look after their own’ and therefore that care support is not
needed (Connelly et al 2006).
Indeed, there has often been a marked variation in the ability of different
parts of the NHS in responding to cultural diversity. In areas with long-
established black and minority ethnic communities, health services have
experience of meeting the needs of people with different religious,
language or cultural backgrounds (Johnson 2006). But perhaps in
Scotland, with a much smaller BME population prior to the late 1990s,
this was not necessarily the case. Nevertheless, the Race Relations
(Amendment) Act 2000 has laid a statutory duty on the NHS and other
public bodies to develop race equality strategies and to ensure equal
treatment of all users.
Szczepura (2005) therefore argues that providing appropriate access to
health care for a diverse population is about more than simply providing
the service. She draws attention to the need for services not just to
demonstrate linguistic competence (in terms of interpreting and
translation services) but also cultural competence. Cultural dimensions
of health might include:
Patients’ health, healing and wellness belief systems
How illness, disease and their causes are perceived

14
The behaviour of patients seeking health care and their attitudes
towards healthcare providers
The views and values of those delivering health care
At the end of the day, as Szczepura points out, the aim is for BME
service users to have equal access to and appropriate information about
the NHS, to have appropriate and sensitive services, and to be able to
use the NHS with ease.
The extent to which users actually feel at ease depends not just on
removing barriers to access but also in improving knowledge of how the
NHS actually functions on a day-to-day basis. Those refugees who have
come from countries without a well-developed system of primary
healthcare, for example, may expect a hospital referral for conditions that
in the UK would be treated by a GP or Practice Nurse (Burnett and Peel
2001). There have therefore been various misunderstandings, where
refugees have used Accident and Emergency services inappropriately,
either for routine health problems (Ager and Strang 2008) or during the
night because of a lack of knowledge of out-of-hours services (Mulvey
2013).
Research by Wasp et al (2004) suggests that heads of households have
a generally better understanding of the workings of the NHS, as do
young refugees, who tend in any case to be healthier and to make less
use of health services. Wasp et al also draw attention to the fact that
many refugees do not understand the treatments administered due to a
lack of explanation compounded by language differences. By way of
example, Papadopoulos et al’s (2004) study of Ethiopian refugees notes
how traditional remedies are more likely to be used in Ethiopia and so
there was a lack of understanding of the treatments prescribed by the
NHS.
Health Promotion
As part of the process of removing barriers to health care, it is widely
recognised that health authorities can do much actively to promote good

15
health and to ensure refugees are made aware of the availability of
services.
A number of cities, for example, have outreach teams who target recent
refugee arrivals. In London, for example, Kensington, Chelsea and
Westminster’s Equal Access to Health Care Project use community
health workers to work with new arrivals, while Lambeth, Southwark and
Lewisham have a special outreach team with a specific focus on single
homeless BME people, many of them refugees (Refugee Health
Consortium 1998). Health visitors do similar work in the West Midlands,
while in Nottingham, there is a community-based asylum seeker and
refugee health outreach team to provide health promotion and to build
knowledge and capacity in mainstream services (Bunting 2009).
There are similar approaches in other countries. In the Australian state of
Victoria, a Refugee Health and Wellbeing Action Plan seeks to work with
refugees to promote improvements in refugee health, sometimes through
promoting access to services and sometimes through improved diet
(Victorian Refugee Health Network 2008). New Zealand has established
a Refugee Health and Wellbeing Project to promote healthy living and
has had considerable success. After a 10-month health education
programme, they reported significant increases in awareness of the
importance of cancer screening, of the symptoms of meningitis and the
availability of immunisation for communicable diseases. There was also
a significant drop in the number of people who said they smoked (New
Zealand Red Cross 2013).
The process of promoting good health amongst refugees has been
portrayed as a ‘journey to wellness’ by Palinkas et al (2003). In an
important study, they draw attention to the ‘health burden’ with which
refugees arrive, including trauma and stress-related disorders,
depression, substance abuse, infectious and parasitic diseases and an
increased susceptibility to chronic diseases. The journey to wellness
therefore focuses on treatment of psychiatric disorders and of infectious
diseases, and prevention of chronic diseases. Working in San Diego,
California, the consortium working with refugees has implemented a
number of health promotion programmes and developed a range of
educational materials aimed at improving knowledge of treatments for
16
cancer, diabetes and cardiovascular diseases. They portray this as a
‘two-way process affecting both the migrant and the organisations
dedicated to helping the migrant on the journey to wellness’.
2.2 Health, happiness and ‘wellness’
This concept of ‘wellness’ or wellbeing as a journey leads us to consider
the importance of wellbeing as a key part of living in the wider society.
Johnson (2006), for example, argues that good health enables better
participation in society and the supply of appropriate health care shows
the responsiveness of society to the needs of new members. Indeed,
although health is not always cited as a core factor in integration,
fieldwork by Ager and Strang (2008) suggests that good health was
widely seen as an important resource for active engagement in a new
society. So good health and wellbeing are key to long-term integration
by the new refugee communities.
In clarifying what is meant by integration, Johnson (2006: 57) suggests
that the key factors must be:
Equity of access to relevant health services;
The ability of health and social care services to respond to the
specific needs of the relevant minority groups; and in the long-term
A parity of health outcomes and life expectancy or disease
experience.
Parity of outcomes can be achieved not necessarily through refugees
adopting the lifestyle choices of the host population – which may not
always be healthy ones! Rather, the long-term aim should be to ensure
that there are no statistical differences between the health of the host
and refugee communities.
Health and wellbeing are closely linked in many of the studies of refugee
health. Wasp et al (2004) interviewed a number of refugees who found
that the simple act of talking to others helped to relieve stress and had a
positive effect on health. Papadopoulos et al’s (2004) study of Ethiopian
refugees identified six ‘meanings’ of health, namely:
17
Happiness
The ability to fulfil material needs and ambitions
Harmonious relationships
Positive personal qualities and attributes
Physical, mental and spiritual wellbeing
A healthy environment.
For the Ethiopians, ‘desta’ or happiness was the most important
prerequisite and indication of health.
Finally, Lewis (2009) identifies the centrality of food to the long-term
happiness and wellbeing of refugees. She identifies the importance of
food to refugees’ sense of community and the lengths to which some
refugees will go to obtain traditional produce. The emotional value of
food lies in a link to specific places and times that people have left
behind. Western diets may be unappealing to many refugees and are
not always healthy; therefore a focus on traditional eating and cooking
practices may assist with long-term health and wellbeing,
We move on now therefore to consider the wider aspects of diet, nutrition
and the links to health.
Nutrition and diet
Deficiencies in diet and nutrition are common amongst refugees and
asylum seekers. Pre-arrival factors which will affect nutrition include
prolonged deprivation, malnutrition, drinking contaminated water,
untreated or undiagnosed illnesses such as parasitic infections and
chronic diarrhoea, and dental problems which cause difficulties when
eating (Victorian State Government 2012).
However, once settled in a safe country, refugees continue to face
nutritional challenges and research suggests that they often become
accustomed to poor eating habits. Two American studies (Barnes and
Almasy 2005, Rondinelli et al 2011) show how refugees became
accustomed to an American lifestyle, including consumption of high-

18
calorie, nutrient-poor foods and this was a particular problem amongst
children who were targeted by the fast food industry. In Barnes and
Almasy’s study, only 13% of refugees thought they ate healthily,
acknowledging that they ate too many calories, too many sweets and too
much fat. Closer to home, an Irish study (Manandhar et al 2006)
identified a similar problem, with refugees eating too much protein and
saturated fats and fewer carbohydrates. Although the intake of fruit and
vegetables was adequate, it was perceived to be low by the refugees
compared to their previous diets.
Although refugees recognised the fact that their eating habits were often
poor, there were considerable barriers to eating better. These included
the high cost of some fresh fruits and vegetables, the general cost of
food in many western countries, the limited amount of time available to
prepare food when adults had to work outside the home and the
cheapness and easy availability of fast food (Barnes and Almasy 2005).
Manandhar et al (2006) suggest that many parts of Ireland are ‘food
deserts’ for refugees, especially when they are accommodated in
peripheral housing with limited access to shops stocking preferred
‘ethnic’ foods and affordable healthy food options. This scenario would
also apply to many parts of the UK.
Southcombe (2008), writing about refugees in Australia, defines the
problem as ‘food insecurity’ which exists ‘whenever the availability of
nutritionally adequate and safe foods or the ability to acquire acceptable
foods in socially acceptable ways is limited or uncertain’. She notes the
high prevalence of food insecurity among refugees resettled in
developed countries, associated with poor dietary practices, overweight
and morbidity and she refers to various local Australian studies
identifying a prevalence of food insecurity among refugees of over 70%.
The impacts of food insecurity and poor nutrition are significant. In
Barnes and Almasy’s (2005) study, 52% of refugees believed that they
were overweight and 74% believed that they were less active than they
should be to be healthy. 61% thought that they were less active since
arriving in the United States, a key factor being an increased use of cars.
There was a negative impact on oral health and vitamin deficiency and,
in terms of disease, Rondinelli et al (2011) found that rates of diseases
19
that are commonly nutritionally influenced (such as diabetes, heart
disease and high blood pressure) were increasing linearly with the length
of time that refugees were living in the US. Poor diet was also impacting
negatively on breastfeeding by reducing women’s ability to eat and feed
on demand, and refugees were increasingly using processed feeding
products. Indeed, Sellen and Tedstone (2000) refer specifically to the
nutritional risks posed to children because of refugee poverty and the
difficulties of adapting eating and child feeding practices to new social,
cultural and economic conditions. They suggest, however, that we have
insufficient knowledge of these risks and call for more research.
There is therefore a growing recognition of the need to work with
refugees to help them identify appropriate and healthy diets. In America,
for example, the US Committee for Refugees and Immigrants has
developed a Nutrition Outreach Toolkit and a range of educational
materials for those working with the refugee communities1, while in
Australia, the government developed the Fairfield Refugee Nutrition
Project2 and, in Perth, the ‘Good Food for New Arrivals’ training
resource3. These resources comprise a variety of materials, including
advice to community workers and presentations and activities for using
with refugees themselves.
The challenge in seeking to tackle the problem of poor nutrition in
refugees is to change behaviour (Barnes and Amasy 2005). The easy
availability and relative cheapness of fast food is clearly attractive.
Research shows that refugees from many countries have a knowledge of
healthy food choices, physical activity needs and the risks associated, for
example with smoking. But knowledge does not always translate directly
into healthy behaviours.
1 http://www.refugees.org/resources/for-refugees--immigrants/health/healthy-living-toolkit/ 2 http://www.aifs.gov.au/cafca/ppp/profiles/cfc_fairfield_nutrition.html 3 http://nutrition.asetts.org.au/

20
Specific health needs
So far, we have discussed the health and nutritional needs of refugees
as a whole, but it is clear that, within the overall refugee population,
specific health needs have emerged and have often been the subject of
specific studies.
Mental health
Mental health is a significant issue for refugees and asylum seekers, with
the trauma of migration leading to depression, stress, sleeplessness and
anxiety. Social isolation and poverty in their new country can have a
compounding effect on mental health. In a Cardiff study (Cardiff Health
Alliance 2011), for example, a third of refugees were receiving medical
treatment, most notably treatment for depression in the form of anti-
depressants and / or counselling. We need to recognise, however, that
refugees more often need social care than psychiatric treatment and so a
standard medical model of care may not necessarily be appropriate
(Simich et al 2010).
What is particularly significant in relation to mental health problems is
their persistence. Mulvey’s (2013) study in Glasgow uses a ‘Warwick
Edinburgh Mental Well Being Scale (WEMWBS) to measure problems.
He found that, despite refugees accessing employment, being in more
secure housing, securing status and often bringing family to Scotland,
nevertheless WEMWBS scores actually rose over time. This appeared
to be a hangover effect resulting partly from the trauma of migration and
partly from the asylum process, so mental health problems were
ongoing. Mulvey also noted significant under-reporting by refugees.
Women
Research suggests that women may have an insufficient voice in
articulating their health problems and needs. Partly this may be a result
of their being isolated at home in a childcare role, partly it may reflect
(perhaps as a result) a poorer knowledge of English, and partly it may

21
reflect the fact that they may be from a patriarchal society, where
women’s voices are not well heard.
Some women may be reluctant to consult with a GP (particularly a male)
if rape or sexual abuse has occurred. And there appears to be a low
uptake of health promotion programmes, for example prevention
measures amongst refugee women, in relation to cancer screening
(Refugee Health Consortium 1998).
We have already referred to reduced breastfeeding rates, often caused
by poor nutrition. McCarthy and Haith-Cooper (2013) also refer to the
insufficient use made of maternity services by refugee women and their
complex care needs, which midwives have to meet. They find that
befriending schemes have had an impact in helping to remedy the
position.
Older people
We have referred earlier to the particular difficulties facing older people
in accessing health services, including poorer language skills, isolation
and a belief that minority ethnic families ‘look after their own’ elders. But
older people often need additional health support, linked to the process
of ageing, possible disabilities and frailty. Carers too may need support,
something that is increasingly recognised.
Older people may be financially disadvantaged and may struggle to
understand pension provision and this may affect their ability to access
support (Connelly et al 2006).
Children and young people
Children and young people may be particularly affected by the trauma of
migration, if they are unsure what is happening to them and such trauma
may lead to drug or alcohol abuse. Adolescence is in any case, a time of
transition from childhood to adulthood and a period often associated with

22
mental disorders and behavioural difficulties. For young refugees, it can
clearly be a particularly complex process (Milosevic 2002).
Where young people attend school, their language skills will improve
markedly and they may find themselves as the main interpreter or
advocate for their family’s health needs. They therefore take on a
responsibility unmatched to their age and this can be somewhat
traumatic in itself.
Schools need to be alert to health issues affecting refugee children and
adolescents and have an important role to play, for example, in
promoting immunisation in young people (Refugee Health Consortium
1998)
2.3 Conclusion
The literature clearly demonstrates a situation where refugees need
substantial support and advice in relation to health and wellbeing,
including a healthy lifestyle. The initial arrival of refugees prompts a
focus on GP registration and access to health services but longer-term
settlement means that the focus of support needs to shift towards the
promotion of good health, good diet and good nutrition, while recognising
that certain groups within the refugee population need particularly
intensive support.
Some researchers have stressed the value of befriending schemes,
particularly for women who may experience isolation and who may
require advice and support in relation to issues such as childcare and
breastfeeding (McCarthy and Haith-Cooper 2013). Counselling services
are also valuable in relation to mental health and other sensitive issues.
The concept may be unfamiliar to many refugees but it can be helpful if it
is culturally sensitive to the needs of ethnic minorities; indeed there is a
strong case for refugee communities to develop their own counselling
skills (Burnett and Peel 2001).
Finally, there are various ways in which the wellbeing of refugees can be
supported. We have already referred to nutritional advice but other

23
approaches can be highly successful. In Manchester, the Refugee
Wellbeing Project4 delivered a wide range of activities including gym
sessions, cycling, self-defence, laughter workshops, trips around the city,
multi-sports sessions and cookery contests. As well as the group
sessions, practical help and health advocacy was provided and the
project appears to have been highly successful.
Ready to leave after another invigorating Zumba class,
November 2013, Vivace Theatre School in Sauchiehall Street
4 http://www.groundwork.org.uk/Sites/targetwellbeing/pages/refugee-well-being-project-tw
24
Chapter Three: Methodology
3.1 Introduction
The information for this study was gathered in a variety of different ways,
including background information on refugees, obtained from ‘desk top’
research, a survey of 100 refugees, using a questionnaire and interviews
with key professionals involved in the refugee process in Glasgow,
including staff in the Scottish Refugee Council, British Red Cross and
Freedom from Torture.
The main driver for the type of methodology using “action research” was
the principle of using researchers from the group of people being
interviewed to develop and carry out the research. Therefore we aimed
to recruit around 80% of the research planners, interviewers and
analysts from refugee backgrounds. The inclusion of 20% from a local
background was expected to aid integration and could provide additional
local knowledge for the group.
Accordingly therefore, the interviews with individual refugees and
organisations were also conducted by refugees. This approach has
been shown to have a number of advantages (Mestheneos 2006).
Participation in the research can be a valuable professional experience,
enhancing skills and boosting self-esteem. In addition, there is
satisfaction in working on a project which has the ability to influence
policy and practice and to benefit others. We also found that refugee
researchers have a clearer understanding of the issues facing other
refugees.
This ‘peer research’ approach, in which individuals are interviewed by
their ‘peers’, has been used successfully in other studies. Within
Glasgow, Roshan (2005) assessed the health needs of refugees and
asylum seekers in north Glasgow using peer researchers, suggesting
that they gained both professionally and personally from their
involvement in the work. In London, Dumper’s (2002) skills audit of
refugee women for the Mayor of London’s office used other refugee
women to carry out the interviews. Dumper suggests that barriers
arising out of a mistrust of strangers and people in authority were

25
overcome, and the exercise helped to empower those refugee women
who became involved.
Identifying potential research and administration volunteers
Potential researchers were identified through advertising widely and by
the provision of information about the benefits of volunteering in such a
project. Organisations which had contact with refugee communities were
provided with the advertising (emails, flyers and posters) and it was also
sent to individual refugees who were contacts of our organisations. As
the project was developed and managed by people who were either
refugees or who worked with refugees, there was significant word of
mouth advertising as well.
At the same time, Living Well in Glasgow was also advertising for
administrative volunteers. The development of the whole project was
being taken forward by volunteers, from the Volunteer Coordinator to the
Planning Group. The administration of the project was also supported by
volunteers who had learnt office skills or practised them in college but
had not had the opportunity to use them in a professional setting.
Potential researchers were asked to complete an application form and
were then to come for a discussion with the Team. These meetings took
place in the Ycommunity space on the 28th floor of 33 Petershill Drive,
which is a building which still houses induction stage asylum seekers
during their first weeks in Glasgow, and some asylum seekers. The
Residents’ Association had been provided with office space on there,
which was used for the interviews.
The applicants had already been asked to decide whether they wanted
to volunteer on the research or the administration parts of the project.
The work involved and the commitment being made by both the
volunteer and the project team was discussed by a person from a
refugee background from the Planning Group plus the Volunteer
Coordinator. By October 2011 we had recruited a starting group of 4
administration and 6 research volunteers.

26
The whole Living Well in Glasgow volunteer project started with an
induction into the organisations involved in the project and with
information about what Living Well in Glasgow was hoping to be able to
do as a result of the research. There was also a discussion opportunity
for the new volunteers to contribute their thoughts.
3.2 Methodology
Aim of the study
This study is a baseline study with the aim of providing information
needed to develop activities for the Living Well in Glasgow (LWiG)
project. The aim of LWiG is to develop pilot health and wellbeing
activities to address what refugees need to know to live healthily here
and which could ideally be incorporated into mainstream services in
Glasgow.
Training research volunteers
In total, ten research volunteers were recruited during the research
period. Seven were female and three male. The research volunteers
came from Algeria, Cameroon, England, Kurdistan (Iraq, Kurdish Sorani
speaker), Scotland/France, Sierra Leone, Sudan and Zimbabwe. The
range of countries of origin meant that we were able to use a wide range
of languages during the interviewing process.
Each researcher was asked to commit to volunteering until the interviews
were completed and the data uploaded for analysis, as a minimum
(unless they had a change of circumstance).
Following recruitment, training was provided by Community InfoSource.
The training focused on types of survey development, interviewing skills,
cultural and ethical issues, methods of recording interviews and analysis,
dissemination and, where necessary, IT skills.

27
The training also sought to provide support in terms of confidence
building for the interviewers, in order to enable them to carry out the
survey. In addition, support was put in place in case the interviews
raised difficult issues for the interviewers and/or interviewees.
Developing the research methods and analysis
Following the training, the research group started development of the
research plan. They met twice a week to do this. It was agreed that the
main research would focus on the views of individual refugees and
additional information would be requested from organisations or
individuals who worked closely with refugees.
The research method used for both individual and organisational surveys
was individual interviews where a questionnaire with mostly closed-
ended questions was used (Appendix Two and Three).
Both the individual and organisational surveys were developed by the
volunteer researchers who were mainly refugees, plus one or two people
living in Glasgow who had close contact with the refugee communities.
Each interview was expected to last about 30 minutes, but could take
longer if an interpreter had to be used. The interviews mainly took place
in local community facilities where the interviewee and interviewer felt
comfortable, although some took place at other locations to suit the
interviewee.
The volunteers who carried out the primary analysis used Survey
Monkey software for this initially.
After consideration, it was decided to use Survey Monkey to produce a
basic analysis of the information collected in the individual survey
interviews. Two of the volunteers taught themselves how to use this
format and set up the survey based on questions the group decided were
appropriate. After piloting this, a hard copy was then used in the actual
interviews. The resulting data from the interviews was then input to
Survey Monkey and the completed survey forms returned to the office.

28
Unfortunately the volunteer who started the analysis had to leave before
the report was done. As a result the work stopped for a while until a new
volunteer resumed it.
The new volunteer decided to use SPSS statistics software, and she
trained a volunteer to help her with data entry, after which the analysis
was developed.
The interview process and sample
Individuals
Prior to the interviews, a request letter with basic information about the
project, its aims and objectives, contact details for the team, and how the
results would be used was given to the expected respondents. This letter
emphasised the confidential nature of the process. (see Appendix Two).
This letter was translated into several languages including Arabic and
French.
To overcome the language barrier we used an interviewee’s mother
tongue whenever it was possible, otherwise we used interpreters.
The sampling method was opportunistic whereby we accessed
interviewees wherever we came across them, although we tried to cover,
as far as possible, a range of different countries, different lengths of time
living in the UK, different age groups, as well as achieving a gender
balance. The sample size was 50 for the pilot study. A further 52 took
part in the final study. As little change was made to the questionnaire
after the pilot research, it was decided to amalgamate the two samples.
However, two questionnaires were excluded from the analysis due to
incomplete data leaving a total of 100 respondents.
Organisations
A list of suitable organisations and individuals who were known to work
with refugees and be sympathetic to their needs was drawn up by the
research volunteers. It was agreed that this list should be limited to 20

29
organisations in order to be manageable. The survey form which was
developed was much shorter than the one for individuals and was
intended to gather organisational information, details of any services
which were provided and the views of the individual taking part on what
was needed to help refugees live healthily here.
The Steering Group were asked the basic questions below in a workshop
at their first meeting (before the formal interviews took place). Their
answers are amalgamated.
A- From your experience, what do you think asylum seekers and refugees need to know to live healthily in Glasgow? A number of responses were received, with the main ones being:
How to access cheap/healthy food (fruit and vegetables etc)
Correct signposting: language needs, where to get own country food
What GP offers & other health services they are entitled to
Mentoring, befriending, preventing isolation
Accessible information on health, housing, education, lawyers, sport,
budgeting and travel
B- How can information be presented to people whose first language is not English? Responses included:
Forming Languages groups
Have multi-lingual audio/video resources & provide information in all
useful formats
Use social media/Facebook etc
Combination of different choices: DVDs, leaflets in all languages,
translators.
Using images rather than words but make sure to get the basic signs
translated with the help of volunteer translators/interpreters
30
Chapter Four: Individual survey results
This section covers the core part of the report: data analysis and
findings. It is divided into four main parts: the first one describes the
statistics of the target group, the second is an exploration of their food
habits, the third part is on access to health services, and the last is on a
subjective estimation of the gaps of knowledge among the target group.
4.1 Overview of respondents
The sample used in this study was composed of 100 refugees and
asylum seekers, 40 of them females. They were of different cultural
backgrounds, ages and residential status as well as length of time living
in the UK. These factors will be considered in turn.
4.1.1 Cultural background
Knowing the cultural background is important to explain barriers that face
integration of newcomers in their host society and access to public
resources, as well as indicating needs for each group that might help
policy makers to target specific group(s). Cultural background, here, is
indicated by the country of origin of the respondent. Respondents were
originally from 30 different countries. However, for simplicity and
research ethic they are divided into three groups based on geography
and cultural similarity: Middle East and North Africa (MENA)5, Africa6, and
East and South Asia (Asians).
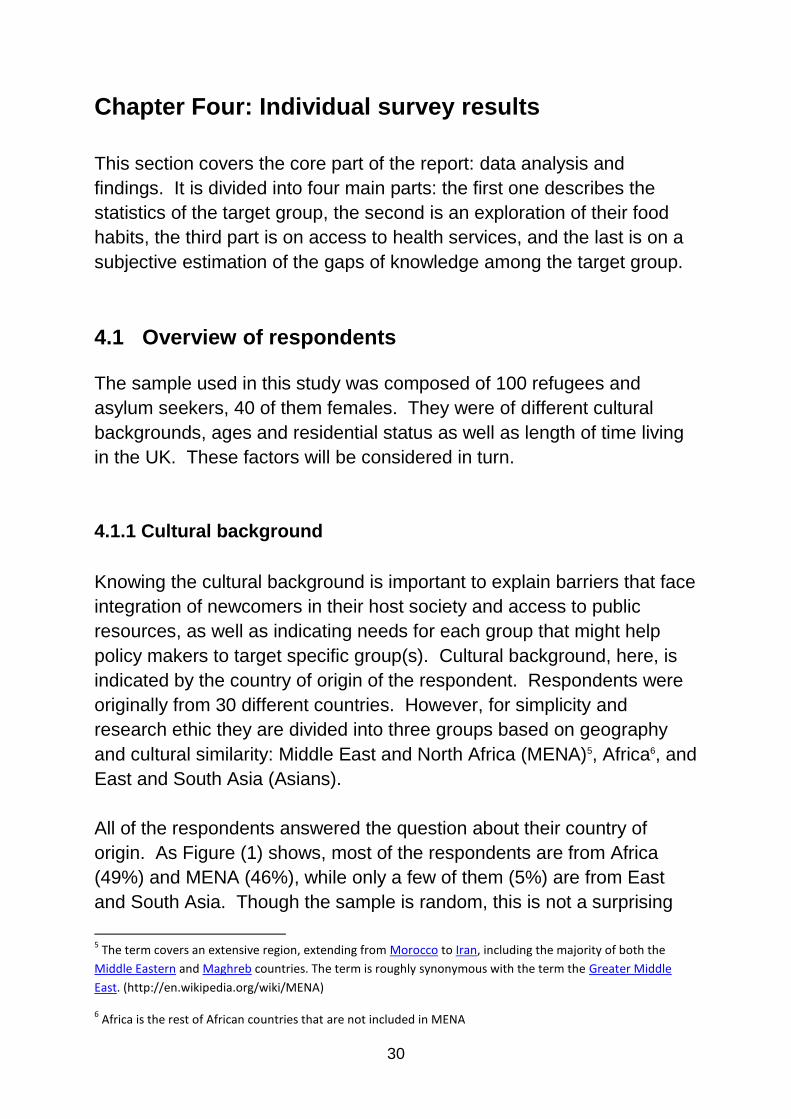
All of the respondents answered the question about their country of
origin. As Figure (1) shows, most of the respondents are from Africa
(49%) and MENA (46%), while only a few of them (5%) are from East
and South Asia. Though the sample is random, this is not a surprising
5 The term covers an extensive region, extending from Morocco to Iran, including the majority of both the
Middle Eastern and Maghreb countries. The term is roughly synonymous with the term the Greater Middle
East. (http://en.wikipedia.org/wiki/MENA)
6 Africa is the rest of African countries that are not included in MENA
31
Africa 49%
MENA 46%
South & East Asia
5%
result, since Africa and the Middle East have been suffering from
protracted political instability and economic crisis for decades.
Figure (1): Respondents by Region
4.1.2 Age
The ages of the respondents might reveal barriers that face specific age groups, and help in accurately addressing such barriers. As mentioned above, for example, old people have different barriers in accessing health services, and young ones have different health needs. 98 per cent of the respondents stated their ages. The age of the respondents is grouped into five categories. Though the sample was random, as mentioned above, we tried to cover different age groups as shown in Figure (2). The sample is dominated by those between 25 and 34 years old (51%), followed by those between 35 and 59 years old (23%), and the group between 18 and 24 (19%), while four percent are under 18 and two percent are seniors. Under-representation of those under 18 and senior people in the sample could be explained by restricted mobility of these categories.

32
Refugee 27%
Asylum seeker 62%
Asylum seeker in section 4 support
4%
Asylum seeker on no
support 8%
Figure (2): Respondents by Age
4.1.3 Residential Status
The residential status of the respondents varies between refugees, asylum seekers, asylum seekers in section 4 support and asylum seekers without support. The question about the residential status was added to the questionnaire after the pilot study, and as a result 48 respondents were not included. As Figure (3) shows 62% of the sample consists of asylum seekers, 27% are refugees, 8% are refused asylum seekers and destitute, and 4% are asylum seekers on section 4 support.
Figure (3): Respondents by Residential Status
Under 18 4%
18-24 19%
25-34 52%
35-59 23%
60+ 2%

33
4.1 4 Length of time living in the UK
The period immigrants live in host countries is positively correlated with
immigrants’ integration. Therefore, we asked about the length of time
each respondent has stayed in the UK. Two of the respondents did not
answer this question.
The period of time respondents lived in the UK, in this study, was divided
into three categories: ‘less than one year’, ‘less than three years’, and
‘three years and more’. Most of the respondents (54%) are newcomers;
having lived less than a year in the UK, while fourteen percent have lived
for less than three years, and the rest have been living in the UK for
three years or more (Figure 4).
Figure (4): Respondents by length of time in UK
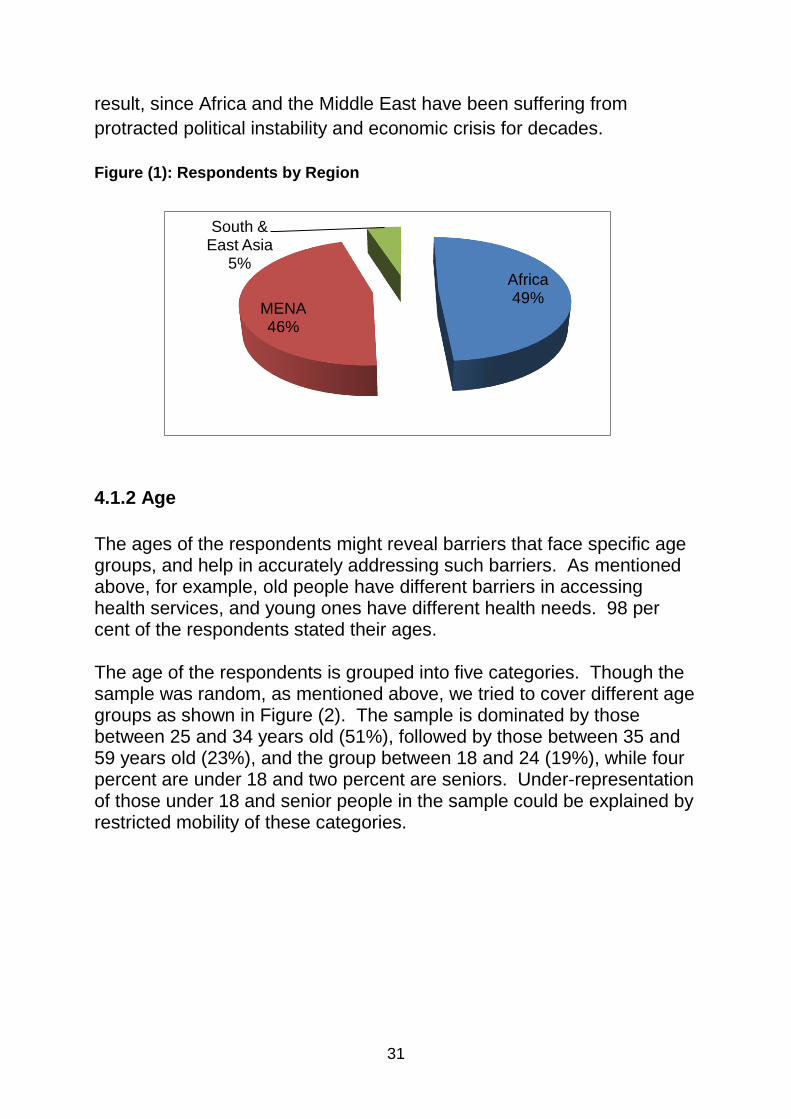
4.1.5 Gender
As mentioned above 40 percent of the sample are female. Gender,
however, is an essential factor in the analysis; therefore we will break it
down by age and cultural background. The dominant age category of
both genders is between 25 and 34, followed by the older category
among the females, and the younger among the males (see Figure 6).
Considering the cultural background, while most of the women are from
Africa, most of the male are from MENA (see Figure 5).
Less than one year
54%
Less than 3 years
14%
3 years or more 32%
34
4.2 Food habits
Five questions were addressed to the respondents in order to assess
their cooking skills, changes in their food habits and in their food intake
both in quantity and quality. Additional questions were posed in order to
find the reasons behind the changes (if any). In this section we analyse
these questions broken down by some of the respondents’
characteristics introduced in the previous section.
4.2.1 Cooking skills and access to nutritious food
Cooking is an essential daily activity for both genders in Northern
countries, yet the situation might not be the same in the Southern
countries. This skill is essential for accessing nutritious food, rather than
buying fast food. Therefore, assessing newcomers’ cooking skills
reveals whether it is necessary to help them with developing such skills.
To assess their cooking skill respondents were asked whether they
mainly cook by themselves, bought fast food or used a mixture of both
methods. Twelve percent of the respondents were found to depend
totally on fast food, while sixteen percent used a mixture of both (Figure
7). This indicates that around 28% of the respondents need to develop
their cooking skills, or to be helped to raise awareness of the importance
of healthy food. Though no direct question was posed about the need
0
20
40
60
80
100
Female Male
Figure (5): Gender by Region
Africa MENA Asia
0
10
20
30
40
50
60
70
80
90
Under 18
18-24 25-34 35-59 60+
Figure (6): Gender by Age
Female Male

35
for developing cooking skills, this result does not imply that the rest have
no need to develop these skills,
Figure (7): Do you mainly cook, or buy fast food
The sample reflects the gender division of labour in the South, where
mostly cooking is females’ responsibility. As Figure (8) shows, 84% of
females cook their own food, while only 60% of males do so.
Considering cultural background, Figure (9) shows that all south-Asians
mainly cook their food, while Africans cook more than the MENA people.
This could be explained by gender division of labour, where in the culture
of most MENA countries cooking is a females’ role. Our sample
supports this argument, as table (1) shows none of the MENA women
depends on fast food, while a fifth of the men do.
72%
12% 16%
Mainly cook Mainly buy fast food Both

36
Figure (8): Cooking Skill by Gender Figure (9): Cooking Skill by Region
------------------------------------------------------------------------------------------------ Table 1: Gender and Region in relation to Cooking Skills
Region of the respondents
Do you mainly cook or buy fast
foods?
Total Mainly cook
Buy fast
food Both
Africa Female 88% (28) 3% (1) 9% (3) 100% (32)
Male 69% (11) 19% (3) 12% (2) 100% (16)
Total 81% (39) 8% (4) 11% (5) 100% (48)
MENA Female 80% (4) 0% (0) 20% (1) 100% (5)
Male 56% (23) 20% (8)
24%
(10) 100% (41)
Total 59% (27) 17% (8)
24%
(11) 100% (46)
South & East
Asia
Female 100% (3) 0% (0) 0% (0) 100% (3)
Male 100% (3) 0% (0) 0% (0) 100% (3)
Total 100% (6) 0% (0) 0% (0) 100% (6)
0
20
40
60
80
100
Female Male
Mainly cook Maily buy fast food Both
0
20
40
60
80
100
120
Africa MENA Asians
Mainly cook
Mainly buy fast food/ take-away
Both

37
To sum up, at least 29% of the respondents need to develop their
cooking skills and have their awareness of the importance of healthy
food raised. The group that need this most are the men from MENA.
4.2.2 Kind of food
In the previous section around one third of the sample were shown to
have poor cooking skills, which raises the question “Has this effect been
due to the kind and amount of food they were used to in their home
countries?” The second question addressed to the respondents was
about whether they eat the same type of food they used to eat in their
home country. 99 percent answered this question, and 45 percent of
them gave an affirmative response. This result indicates that the
majority of the respondents have experienced changes in the kind of
food they were accustomed to. Considering the gender factor, we found
slight difference where males (56%) were more likely to have changed
their food kinds than females (53%). (See Table 2).
Considering the region, more Asians (67%) have not changed their kind
of food, where the opposite is true in the case of the other groups
(around 44% for each). This result indicates cultural similarity between
Scottish and Asian people in term of food habits, while indicating a wider
cultural distance between the host and the other two groups.
Figure (10): Do you eat the same kind of food?
-----------------------------------------------------------------------------------------------
Yes 45%
No 55%

38
Table 2: By Gender * Do you eat the same kind of food?
---------------------------------------------------------------------------------------------------------------- Table 3: By Region * Do you eat the same kind of food?
The majority of the respondents have experienced changes from the kind of food they were accustomed to; males being more adaptive to the new food than females.
Do you eat the same kind of food
Yes No Total
Female 47.5% (19)
52.5% (21)
100.0% (40)
Male 44.1% (26)
55.9% (33)
100.0% (59)
Total 45.5% (45) 54.5% (54) 100.0% (99)
Do you eat the same kind of
food?
Total Yes No
Africa 43.8% (21)
56.2% (27)
100.0% (48)
MENA 44.4%(20)
55.6% (25
100.0% (45)
South & East Asia
66.7% (4) 33.3% (2) 100.0% (6)
Total 45.5% (45)
54.5% (54)
100.0% (99)

39
Figure (11): Kind of Food by Age Figure (12): Amount of food eaten
Considering the age of the respondents, the group that experienced most change in the kind of food they ate were those between 18 and 24 years old. This might be explained by poor cooking skills, or easy adaptation to the new culture. 4.2.3 Do you eat the same amount of food?
Regarding the amount of food, a considerable number of the participants (41%), took almost the same amount of food, while 35 percent took less amount and 24 percent took more. Figure (13): Amount of Food by Gender Figure (14): Amount of Food by Region
More 38%
About the
same 38%
Less 24%
0
5
10
15
20
25
30
35
40
45
50
Female Male
More About the same Less
0
10
20
30
40
50
60
Africa MENA South & East Asia
More About the same Less
0
20
40
60
80
100
120
Under 18
18 - 24 25 - 34 35- 59 60 +
Yes No
40
While most of the women eat more food than they used to before coming
to the UK, most of the men eat less food. This difference might be
related to the cooking skills mentioned above.
Most of the Africans and Asians said they eat about the same amount,
while most participants from MENA countries eat less food.
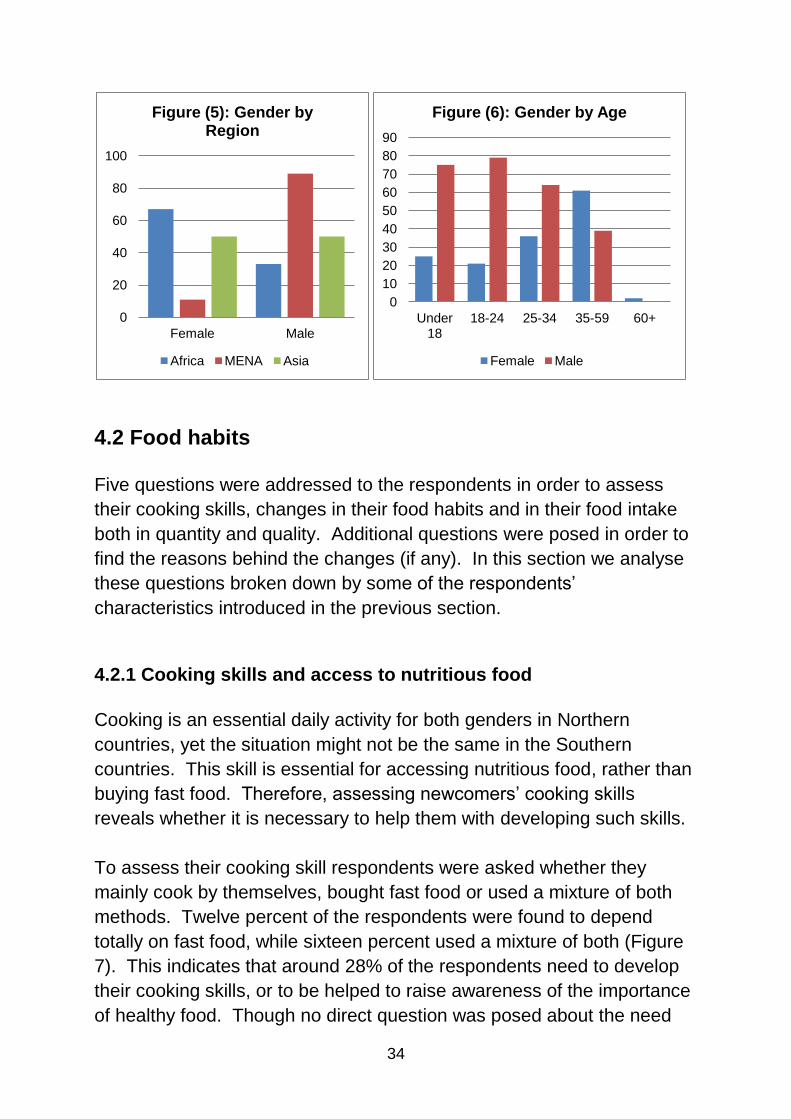
4.2.4 Do you eat the same amount of fruit and vegetables?
67 respondents answered the question about fruit and vegetable
consumption. 45 percent of them consume the same amount as they
used to in their country of origin, 30 percent consume more, while 25
percent consume less.
Figure (15): Do you eat the same amount of fruit and vegetables?
Most of the females either consume the same amount of fruit and vegetables that they used to (50%), or more (37%); while 41 percent of the males consume the same amount, 24 percent more, and 35 percent less.
Table 4: By Gender * Do you eat the same amount of fruit and vegetables?
More 30%
About the
same 45%
Less 25%
Do you eat the same amount of fruit and
vegetables?
Total
More About the same Less
Female 37% (11) 50% (15) 13% (4) 100% (30)
Male 24% (9) 41% (15) 35% (13) 100% (37)
Total 30% (20) 45% (30) 25% (17) 100% (67)

41
Table 5: Respondents’ Regions * Do you eat the same amount of fruit and vegetables? Cross tabulation
Considering the regions of the participants, 75 percent of Asians, and 50
percent of MENA said they consume the same amount of fruit and
vegetables as before, while only 39 percent of the Africans did. None of
the Asians consumed more, while 41 percent of the Africans and 19
percent of the MENA did. Respondents from MENA are dominant
among those who consume less (31%), followed by the Asians (25%),
and then the Africans (22%).
Numerous contradictory reasons are cited for changing habit of fruit and
vegetables consumption. The most frequent cited reasons for those who
consume more are: Affordable, available, cheaper, back home eat only
rice or not eating it, I like it, I think it is good for health.
Those who consumed less fruit and vegetables than before explained it
as a financial problem (affordability). Other reasons given are: Don’t like
it, back home I eat fresh fruit, no appetite, expensive, financial reasons,
not affordable, I don’t value it, not used to it.
4.2.5 Do you eat the same mixture of different foods?
Earlier we explored whether respondents ate the same kind and amount
of food, and fruit and vegetables they used to consume before moving to
the UK. In this section we are going to study whether they change the
mixture of fruit and vegetables they used to eat in their home countries.
Do you eat the same amount of fruit and
vegetables?
Total
More About the same Less
Africa 40.5% (15) 37.8% (14) 21.6% (8) 100.0% (37)
MENA 19.2% (5) 50.0% (13) 30.8% (8) 100.0% (26)
South & East Asia 0% (0) 75.0% (3) 25.0% (1) 100.0%(4)
Total 29.9%(20) 44.8% (30) 25.4% (17) 100.0%(67)

42
The answer to this question highlights whether people’s diets had
changed significantly since their arrival and whether they were accessing
a diverse range of different foodstuffs. The overall result (Figure 16),
shows that 24 percent of the respondents said they consume ‘less
mixture’ of different kinds of food, while the rest of the sample divided
equally between ‘same’ and ‘more’ mixture.
Figure (16): Do you eat a different mixture of foods?
As shown in Figure (17), more females (56%) said they consume ‘more’
mixture of different kinds of food than they were used to in their home
countries, compared to males (27%). In contrast, more males (31%)
said they consume ‘less’ mixture of food than what they were used to in
their home countries compare to women (12%). This indicates that men
and women have slightly different approaches to eating and health, and
that female respondents demonstrated that they had more control over
their eating habits than males.
More 38%
About the same 38%
Less 24%

43
Considering cultural backgrounds, as shown in Figure (18), we found
that only Africans ate ‘more’ mixtures of different kinds of food (56%)
than they used to in their home countries. While a high proportion (45%)
of people from MENA ate the ‘same’ mixture of different kinds of food
they used to in their home countries, people from Asia divided equally
between the three options.
4.3 Access to health services
To assess the respondents’ ability to access health services, two main
questions were posed, followed by three follow up questions to find more
detailed information. The main questions asked whether respondents
were registered with a family doctor (General Practitioner or GP) and a
dentist. Below we will explore the findings.
4.3.1 Are you registered with a doctor?
The first question was answered by all the respondents, and 21 percent
of them had not registered with a GP.
0
10
20
30
40
50
60
Female Male
Figure (17): Mixture of Different Food by Gender
More
About the same
Less
0
10
20
30
40
50
60
Aferica MENA Asia
Figure (18): Mixture of Different Food by Region
More About the same Less

44
Figure (19): Are you registered with a doctor?
Of those who had registered at a GP, 49 percent had managed to do it in
less than a month, 42 percent within three months and the rest after
more than six months. The last group cited ‘lack of information’ as their
reason for taking so long time.
Those who had not registered at a GP at the time of the interview cited
different reasons, such as: ‘my health is good’, ‘ I am fit’, ‘I am not
educated so I could not understand’, ‘I am still in the asylum process’, ‘I
didn’t receive any paper about it’, ‘I don’t know where GP could be
found’. These reasons could be summed up in one reason: ‘lack of
knowledge’.
4.3.2 Are you registered with a dentist?
98 of the respondents answered the second question: Are you registered
with a dentist? As shown in Figure (20) 37 percent were not registered
with a dentist at the time of the interview.
Figure (20): Are registered with a dentist?
Yes 79%
No 21%
Yes 63%
No 37%

45
Of those who had registered with a dentist, 39 percent took less than a
month to register, 45 percent between one and three months, five
percent three to six months, and three percent more than six months.
Those who took more than three months to get a dentist gave reasons
such as: not needed, didn’t know how, a long waiting process, shortage
of time, don’t like dentistry, still in the asylum process, have no problem
with my teeth, I don’t know how and where to go a dentist, I don’t like
doctors, I lost an appointment, I need very much to go to dentist, but I
don’t know how, waiting for GP, paper.
This study shows that lack of knowledge of the way the health system
operates is the main reason for delaying registration with a GP or a
dentist. Many people have come from countries where access to health
services is different from the system in the UK. Despite the fact that
some organisations provide written information on how to access the
health services, a considerable number could not access the services at
suitable times due to their lack of information / knowledge. Therefore,
we argue that it would be useful either to review or to change the method
by which the information is provided.
4.3.3 How has your health been since you have come to UK?
The third question addressed to the respondents concerned their
subjective feelings about their health since their arrival in the UK
compared to what they experienced in their home countries. 41 percent
of the respondents said their health had improved since their arrival in
the UK, while 22 percent felt the opposite.

46
Figure (21): How has your health been compared to in your country?
Two types of examples of the statements made by respondents follow:-
From respondents who felt better:
Back home I used to suffer from depression and had no money to
pay for my treatment,
Because I am very happy, and I don`t have problem of killing,
punishment and capital punishment.
So I feel freedom, because in the U.K I have more freedom, but in
Iran I have not any freedom, and I don`t have any problem like my
country in social life and political,
Because l do some exercises,
Because I feel safe, eating is better.
The air is better and the life is more comfortable,
Warm people in Glasgow, and
Fewer problems, good freedom and the human equality in this
country.
From respondents who felt worse:
stressed about my on-going immigration case, which had taken too
long, Bad weather and housing,
because for being foreign and stressed,
Because I miss my family and I have problem with different culture
and language.
Also I have problem with my case,
Better 41%
Same 37%
Worse 22%
47
Because still I did not get a paper so it is affecting me and affects
my mental health,
During my journey I was faced the more health problem then in
there I have many problem with my case. So that my mental
situation was changed to bad,
I am very worried and I have mental problem,
I have not work, and I miss my family,
I find it very difficult to cope with the weather and also, No sunshine
and too dark,
So much stress, spending most of the time at home without doing
anything that effected lot on my health, and
Suffering depression because still not got papers.
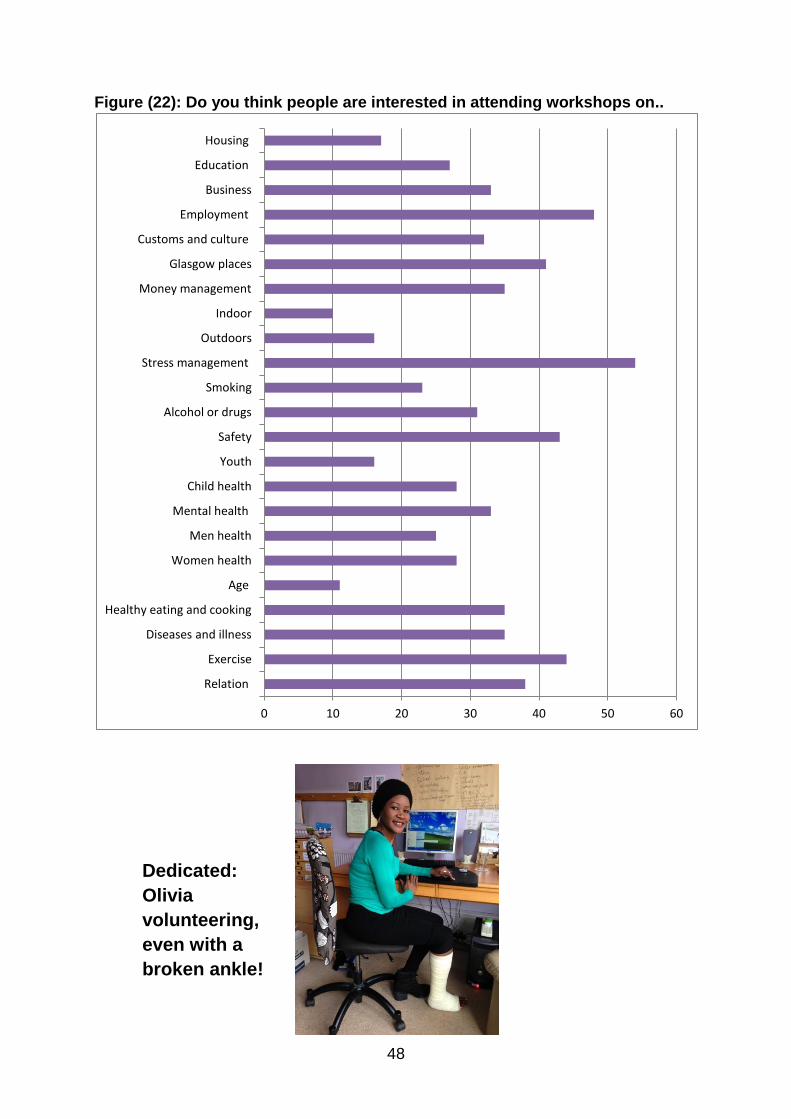
4.4 Activities
In order to assess the respondents’ needs, that would improve their
wellbeing in Glasgow, various training activities were listed and the
respondents were asked to choose which one(s) people might be
expected to attend. Each respondent could select more than one
activity. Figure (22) summarises the answers.
For example, 88 percent said that people could be expected to attend
workshops related to mental wellbeing (54% stress management
activities and 34% mental health); this is a good indicator of the stress
and mental health of the newcomers.
In addition to what the refugees and asylum seekers experienced in their
home country, and the process of fleeing the situation there, they also
suffer a lot during the process of establishing their lives in UK. 81 per
cent would like to improve their access to the labour market (48 percent
employment, and 33 percent for business establishment), 78 percent
want to improve their health by doing exercises (44 per cent), and/ or by
healthy eating and cooking (34 per cent) .
48
Figure (22): Do you think people are interested in attending workshops on..
Dedicated:
Olivia
volunteering,
even with a
broken ankle!
0 10 20 30 40 50 60
Relation
Exercise
Diseases and illness
Healthy eating and cooking
Age
Women health
Men health
Mental health
Child health
Youth
Safety
Alcohol or drugs
Smoking
Stress management
Outdoors
Indoor
Money management
Glasgow places
Customs and culture
Employment
Business
Education
Housing

49
Chapter Five: Organisation survey results
5.1 Aims and Objectives
The main aims and objectives of this part of the research project were to:
Ask organisations what type of support they currently provide for
refugees and asylum seekers.
Find out what organisations think new refugees and asylum
seekers need in order to live healthily in Glasgow
Find out what organisations think are the best ways of presenting
information to people who do not have English as their first
language.
Sample
Twenty organisations which work closely with refugees and are based in
Glasgow were approached and asked to participate in the survey. It was
thought they could provide additional information and insights.
5.2 Findings
Question 1.
Background Information
Please see spread sheet of organisations and the contact person there
(Appendix Four).
Question 2.
What support does your organisation provide to refugees and
asylum seekers?
Please see spread sheet for responses (Appendix Five).

50
Question 3.
Please tell me about your role in the organisation.
The roles were all individual – they are briefly summarised on the spread
sheet for Question 1 (Appendix Four) and listed here for information.
I am the Project Coordinator and am responsible for the day-to-day
running of the organisation and service delivery (Unity Centre).
I am a religious sister, l am also a local superior; I live a simple life
as any poor person would live (Missionaries of Charity).
I am manager of the Scotland Centre. I work strategically across 5
locations of the organisation. I am also a therapist and work with
individuals (Freedom from Torture).
I signpost and pass on information. I run and organise the group. I
listen to people's stories, help them with any problems I can, help
them build relationships and share their experiences as single
mothers. I help them build their confidence and independence
(Umoja).
I am the Female Outreach Worker. I work with awareness raising
over HIV testing, condom use and condom distribution. To provide
information about access to information to these issues. I am
involved in running workshops. I also signpost to other
organisations who can help with their needs should issues like
housing arise (Waverley Care).
Provision of emotional support, advice and information on services
available to asylum and refugee women (Ethnic Minorities Law
Centre).
I am one of the founding members of the organisation and ex-chair
person and acting chair for around three years. Due to this I assist
the current management when I am required to and contribute
towards the improvement of the organisation’s functions. I do also
address some queries from other organisations and funders who
use to contact me every now and then and signpost them
accordingly (Ypeople Residents’ Association).
The Health Service: 1. knows and understands the inequalities &
discrimination faced by its patients and population; 2. engages
with those experiencing inequality & discrimination; 3. knows that
people’s experience of inequality affects the health choices they
make; 4. removes obstacles to services and health information

51
caused by inequality; 5. uses an understanding of inequality and
discrimination when devising treatment and care; 6. uses its core
budget and staff resources differently to tackle inequality (NHS).
My role is development of people and projects in Glasgow
Edinburgh, Stirling, Fife, Newcastle and Inverness (Destiny
Angels).
A member of the Management Committee: at one time I was chair
of the organisation (Karibu Scotland).
I help run the drop-in and support volunteers and work with the
community flat (G&CIN).
I help run all the above activities as a volunteer support worker
(Ycommunity).
I manage housing advice and the destitution project. There are 2
teams. One provides housing advice, the other money skills
advice and runs the drop-in (Positive Action in Housing).
Office Manager (Bridges Programmes).
I am the campaign coordinator (NCADC).
Development worker, general manager (Unity in Community).
Life Skill Programme Manager (British Red Cross Refugee
Service).
Women`s policy development officer (Scottish Refugee Council).
Question 4.
What field does your organisation provide support in?
See spread sheet for a tabular summary of the different fields of support
(Appendix Five)
The support was mostly in providing general information (15
organisations) and training (11).
Many organisations offer general advice (9), clothing (9), employability
help (8) and food (8).
Less common are organisations that offer immigration information (4),
legal support (3), money (3), stress management (3) and
accommodation (3).

52
Support was provided for cultural issues by 7 organisations and issues of
violence (5), minority ethnic issues (6) and mental health support (6).
Question 5.
How do you provide that support?
Some organisations provide a drop-in service: Ycommunity, Unity
Women’s Project, GCIN, Karibu and Destiny Angels.
Destiny Angels also run a helpline and mobile food banks.
Freedom from Torture provides therapy, which is open-ended. Clients
have to be referred.
Emotional support is also provided by Umoja and Waverley Care.
Waverley Care also direct people to relevant organisations for their
needs.
Ypeople runs a weekly surgery to have first-hand knowledge of the
problems and needs of the residents and liaise with the appropriate
department.
Positive Action in Housing and Unity also sign post people to other
organisations.
Karibu, Destiny Angels and EMLC run one to one support sessions.
Bridges Programme and NCADC provide training.
Question 6.
What do you think people need to live a healthy life?
Fifteen respondents answered this question.
Most respondents (12) stated that people need healthy food/a healthy
diet in order to live a healthy life.
53
Five respondents replied that (a) information about healthy living was
important and (b) information about exercise and sport was important.
Three respondents named housing/shelter, medical services/healthcare,
community support and social activities and good mental health as
important factors.
Two respondents named hope or having a meaning in life as important.
Safety and security, money, and advice about entitlements were
considered necessary by one respondent.
Question 7.
What do you think refugees and asylum seekers need to know to
live healthily in Glasgow?
The responses of organisations to this question can be divided into
seven sections.
Section 1: Food
Where to get cheap, healthy food
Awareness of what is healthy and unhealthy food
Cookery lessons/demonstrations
Section 2: Exercise
Where to go for free/cheap exercise e.g. parks, exercise groups,
football groups
Section 3: Healthcare
How the NHS and the GP system work
Reproductive health
Children’s health
Section 4: Mental health
Assistance in dealing with past trauma
Assistance in dealing with present and future uncertainty

54
Orientation to work through and accept cultural and life style
differences
Section 5: Financial
Help with travel costs
How to survive on very little money
Budgeting advice
Section 6: Networking
Access to community activities
Informal support structures
Help to integrate
More English classes
Information about drop-ins
Information about women’s groups
Section 7: Rights
Knowledge of rights and entitlements regarding asylum
Knowledge of benefits/rights to work
How organisations are structured
Question 8.
From your experience do you have any suggestions about how
health information can be shared with people whose first language
is not English?
There were a variety of responses to this question, with some
disagreement about the most effective approaches. All respondents
except one answered this question (19 out of 20).
The most popular solutions to sharing health information with people
whose first language is not English were (a) using multi-media
methods (9 respondents) and (b) using people-oriented events (9
respondents).
(a) Visual and audio methods were recommended as effective ways of
presenting health issues; for example, picture cards, photographs,
videos, posters, documentaries.

55
(b) The importance of people-centred events for passing on
information was also highlighted e.g. having a mixture of one-to-
one sessions and group discussions, demonstrations or
workshops; involving key people from the community; having a
system of befriending/mentoring in the community.
Examples given were of one-to-one help with using the internet and groups for cookery classes and First Aid.
Two respondents recommended offering women-only groups: one to explore issues such as sexual and domestic violence and the other to provide an opportunity to speak to an expert e.g. a midwife about women’s specific health issues.
Several respondents recommended using interpreters (8 respondents) although one respondent disagreed and warned that using an interpreter can ‘skew the relationships and the transfer of knowledge.’ However another respondent stated that ‘the only way is to have translators’.
Another suggestion was translating leaflets into different languages (5 respondents). One respondent suggested providing information leaflets at drop-in centres used by asylum seekers and another suggestion was to provide information in packs when people first arrive from their induction. However, two respondents did not consider this effective due to literacy issues, expense and the difficulty of keeping information up to date. It was suggested that having material available on-line would be cheaper. Other suggestions were to make recipe books combining recipes from different countries, and to use sporting activities as a way of getting people together and sharing information. Question 9. Do you know any organisations or groups who could provide
Healthy Living workshops for us?
There were many suggestions of suitable organisations and groups:
Wise Women: http://www.wisewomen.org.uk/
Sure Start:
http://www.direct.gov.uk/en/Parents/Preschooldevelopmentandlearnin
g/NurseriesPlaygroupsReceptionClasses/DG_173054

56
North West Women's Centre:
http://www.maryhillwomenscentreglasgow.org.uk/
Karibu Scotland:
http://www.karibuscotland.org.uk
Lifelink: http://www.lifelink.org.uk/
Nutritionists from the NHS
We (Freedom from Torture) can do psycho-educational programs.
We look specifically at post-traumatic symptoms. In groups people
can get help and advice and it doesn't have to be personal.
Unity Centre
Scottish Refugee Council
Refugee Women’s Strategy Group (RWSG)
We (Waverley) provide sexual health workshops but we focus on HIV.
Asda Community Events: http://your.asda.com/community
Health and Well-being centre in Kingsway; there is also a centre in a
Royston.
Govan and Craigton Integration Network developed a book which
included healthy recipes from all different countries.
NHS also had a project last year where they gave information.
EMLC Leisure classes for women
Ethnic Enable- befriending and Workshops: www.ethnicenable.org.uk
Glasgow women's library-courses and workshops:
http://womenslibrary.org.uk/
Bridging the Gap:
http://www.educationscotland.gov.uk/Images/Bridging_The_Gap_tcm
4-552837.pdf
Ankur -0141 248 8889 - workshops
Food for Thought - healthy eating and cooking- not free
Simple Pleasures - access to green space – free:
http://www.snh.gov.uk/enjoying-the-outdoors/simple-pleasures/
BTCV: Conservation volunteering
http://www2.tcv.org.uk/display/btcv_scotland
Glasgow Life -taster session for all of their services:
http://www.glasgowlife.org.uk/Pages/default.aspx
Compass- mental health awareness sessions ( capacity issues):
http://www.nhsggc.org.uk/content/default.asp?page=home_compass
Health Team (Dr Anne Douglas).

57
integration networks and YMCA
Hidden Gardens , Red Cross,
Freedom from Torture
Work Glasgow Community Food Interactive:
http://www.communityfoodandhealth.org.uk/
Work Glasgow Healthy Living Community:
http://www.healthynorthglasgow.co.uk/nghlc/work-areas
Question 10.
Do you know any asylum seekers or refugees who may have skills
or information about healthy living?
Most respondents did not know anyone with appropriate skills or
information about healthy living.
Other respondents suggested that the following agencies could help:
Barnardos has a group that works with refugees over HIV
Waverley Care
Scottish Refugee Council (SRC)
British Red Cross
Refugee Women’s Strategy Group (RWSG)
Question 11.
Do you have any other comments you would like to make about
healthy living in Glasgow?
Comments from the organisations centred around the difficulties of
accessing information:
Life Skill Programme only works with the most vulnerable young
people (30 each year) with information about healthy living: [it is]
also valuable for the vast majority of young asylum seekers that we
do not have capacity to support e.g. information on access to
sexual /mental health services and support to access education.
I do think there is a gap in information and services provided.
58
I think that it is worthwhile explaining this. It would be effective if
the balance between what people knew and needed to have the
confidence to do things themselves could be bridged. Walking,
being taken to different clinics and services to show people would
help. Being encouraged to role play and dialogue with other
mental professionals would help. People are often too
embarrassed to say if they don't understand (Umoja).
You can't force people to change but you can give them the
information to help themselves. There can be great benefits to
awareness raising. I would like to be invited to any workshops and
events (Waverley Care).
Need to encourage/ educate asylum seekers and refuges about
the benefit of physical activity to health e.g. walks, running,
swimming etc.
Other comments dealt with the political aspects of support:
Many of the women we support have major difficulties accessing
basic and specialist services because of their vulnerabilities and
the discrimination they experience. This coupled with the stress of
an ongoing asylum case creates huge barriers to women asylum
seekers having healthy lifestyles (Unity).
Are you going to use any information featured from your sessions
to explain to politicians how hard it is to live a healthy life when you
are under the stress, both financial and emotional of going through
the asylum process?
I think it is a good idea, if there is some focussed work in this area,
it will have an impact on the mental health of asylum seekers.
Especially for destitute people as they need advice on how they
can buy and prepare food healthily on limited budget and not eat
things like fish and chips all the time
Living in real poverty, sometimes with no money at all, is a big
issue. As is living under threat of detention/deportation/removal.

59
Stress. Losing your GP when refused asylum and having to move
and became homeless.
The biggest health effect for asylum seekers in Glasgow would be
to give them their papers.
Sharing food after one of the Healthy Eating & Cooking Workshops
(This one delivered by Soghra from Woodlands Community Garden)

60
Chapter 6: Conclusions
This study is pioneering action research carried out by Living Well in
Glasgow with the support of Community InfoSource. The research was
a baseline study which aimed to provide information needed to develop
activities for the refugees in order to improve their living standard, health
and wellbeing in Glasgow. The research was designed and
implemented by refugees. They used mainly quantitative and some
qualitative research methods to collect the data, the bulk of which was
analysed by SPSS statistical software.
Respondents were 100 refugees from Africa, Middle East and North
Africa (MENA) and South and East Asia. In addition supplementary data
was collected from 20 key informants from organisations that provide
services to the target group. Questions addressed to the refugees were
clustered into three groups: access to healthy food and change in their
food intake; access to health services and change in their health status;
and their subjective gap of knowledge that prevented them from having
good health and wellbeing in Glasgow.
The first part of the individual surveys explored cooking skills and access
to nutritious food. It became clear that almost one third of interviewees
needed to improve their cooking skills and to have their awareness
raised of healthy eating. The group in most need of these were males
from MENA.
We also explored the extent to which people had changed the food that
they ate, and if they continued to eat healthily with an appropriate intake
of fruit and vegetables. Results appeared rather complex and
contradictory and there were no clear trends. Where changes had taken
place, sometimes this seemed to lead to improvements in diet and
sometimes the opposite. Improvements were attributed to security,
better standards of living and better access to health services, while
those whose diet had not improved spoke of the stress they had felt
during the asylum and settlement process, together with feelings of
longing and loneliness. They stated that they used to eat better in their
home country.

61
Regarding access to services, the majority of interviewees were
registered with a GP and a dentist, but a significant minority were not
registered and, in some cases, there had been a considerable delay in
registering. The most cited reason for this was a lack of information.
There was a relatively even split between those interviewees who felt
that their health had improved since coming to the UK and those whose
health remained the same. In 22% of cases, their health was felt to be
worse. Those who felt better attributed this to freedom from persecution
and threat, to safety and a more comfortable existence. Those who felt
worse highlighted the stress of getting used to a different culture and
language, as well as being separated from family.
Finally, in relation to activities, it was clear that interviewees were keen to
improve their employability and access to the labour market, and were
also concerned to improve their health. This could be achieved by
exercise and leisure activity as well as by healthy eating and cooking.
The organisations interviewed offered a wide range of support – both
emotional and practical. Some offered advice sessions and had drop-in
services; others had ‘helplines’. Practical support included advice on
housing and employment, training mobile food banks.
All organisations stressed the importance of healthy eating, of exercise
and sport, and of safety and security in helping refugees to ‘live well’.
This echoes many of the findings of other studies elsewhere and which
are described in Chapter Two. There was general agreement that
refugees needed to know about food, exercise and sport, healthcare
provision and the availability of community activities. In addition, for
long-term safety and security, refugees need information on their rights
and entitlements, and financial advice.
In terms of advising refugees on these matters, organisations suggested
a wide range of methods, including the use of visual and audio material,
for those needing support with English language, and group sessions,
possibly with interpreters. These suggestions echo some of the refugee
toolkits developed by outreach workers in America and Australia, and
described in Chapter Two.

62
Recommendations
In accordance with the Scottish Government’s strategy paper of 2013:
“New Scots: Integrating Refugees in Scotland’s Communities 2014 to
2017”, we make the following 10 recommendations:
Partnership working should be arranged to support the
development of workshops on all key topics requested by refugees
Refugees must be involved as key partners in any new workshops
being developed
Putting funding in place to provide more mental wellbeing
workshops as developed by Living Well in Glasgow, these being
the highest priority identified in the research. Current provision in
Glasgow is extremely stretched and tends to only reach those who
are in an emergency situation
Putting funding in place to provide additional employability support
Dissemination of good practice and audio-visual learning methods
of delivering information for refugees
Investment in development of multi media types of information
provision and person centred events for refugees
Provision of a ‘Training for Trainers’ specialised package to support
good practice in delivering information to refugees
Provision of information in improved and accessible formats for
newly arrived asylum seekers
Provision of orientation support for new asylum seekers to learn
about Glasgow and the types and locations of services in it
Provision of culturally sensitive and inexpensive physical activities
in the city

63
Bibliography
Chapter One Introduction
Netto, G. (2011), 'Identity negotiation, pathways to housing and "place :
the experience of refugees in Glasgow', Housing Theory and
Society 28.2, pp.123-143
Mulvey, G. (2013), In search of normality: refugee integration in
Scotland, Glasgow: Scottish Refugee Council
Chapter Two Background and literature review
Ager, A. and Strang, A. (2008), ‘Understanding integration: a conceptual
framework’, Journal of Refugee Studies 21.2, pp.166-191
Barnes, D. and Almasy, N. (2005), ‘Refugees’ perceptions of healthy
behaviors’, Journal of Immigrant Health 7.3, pp.185-193
Bunting, R. (2009), Asylum seeker and refugee health needs
assessment, Nottingham: NHS
Burnett, A. and Peel, M. (2001), ‘Health needs of asylum seekers and
refugees’, British Medical Journal 322, pp.544-547
Cardiff Health Alliance (2011), Cardiff health, social care and well being
operational plan 2011-2014, Cardiff: CHA
Connelly, N., Forsythe, L., Njike, G. and Rudiger, A. (2006), Older
refugees in the UK: a literature review, London: Age Concern
England and Refugee Council.
Johnson, M. (2006), ‘Integration of new migrants: health’ in Spencer, S.
(ed.), Refugees and other new migrants: a review of the evidence on
successful approaches to integration, Oxford: COMPAS, pp.57-72
Lewis, H. (2009), Food, gender and ‘refugee community’ moments,
Unpublished paper, SOAS Food and Migration Workshop,
https://www.soas.ac.uk/migrationdiaspora/seminarsevents/food_mig
ration_abstracts/file49328.pdf
Manandhar, M., Share, M., Friel, S., Walsh, O. and hardy, F. (2006),
Food, nutrition and poverty among asylum-seekers in north-west
Ireland, Galway: Health Service Executive
64
McCarthy, R. and Haith-Cooper, M. (2013), ‘Evaluating the impact of
befriending for pregnant asylum-seeking and refugee women’,
British Journal of Midwifery 21.6, pp.404-409
Milosevic, D. (2002), Refugee young people and mental health, Sydney:
NSW Youth Action and Policy Association
Mulvey, G. (2013), In search of normality: refugee integration in
Scotland, Glasgow: Scottish Refugee Council
New Zealand Red Cross (2013), The Refugee Health and Wellbeing
Project: changes in knowledge, attitude and practice of participants
in the health and wellbeing programme, Wellington: NZRC
O’Donnell, C., Higgins, M., Chauhan, R. and Mullen, K. (2007), ‘”They
think we’re OK and we know we’re not”. A qualitative study of
asylum seekers’ access, knowledge and views to health care in the
UK’, BMC Health Services Research 7.75
Palinkas, L., Pickwell, S., Brandstein, K., Clark, T., Hill, L., Moser, R. and
Osman, A. (2003), ‘The journey to wellness: stages of refugee
health promotion and disease prevention’, Journal of Immigrant
Health 5.1, pp.19-28
Papadopoulos, I., Lees, S., Lay, M. and Gebrehiwot, A. (2004),
‘Ethiopian refugees in the UK: migration, adaptation and settlement
experiences and their relevance to health’, Ethncity and Health 9.1,
pp.55-73
Refugee Health Consortium (1998), Promoting the health of refugees,
London: RHC
Rondinelli, A., Morris, M., Rodwell, T., Moser, K., Paida, P., Popper, S.
and Brouwer, K. (2011), ‘Under- and over-nutrition among refugees
in San Diego County, California’, Journal of Immigrant Minority
Health 13, pp.161-168
Roshan, N. (2005), Supporting new communities: a qualitative study of
health needs among asylum seekers and refugee communities in
north Glasgow, Glasgow: NHS
Scottish Executive (2004), Providing information to refugees: a good
practice checklist, Edinburgh: Scottish Executive
Scottish Refugee Council (2011), How to access health care in Scotland,
Glasgow: SRC
Scottish Refugee Council (2013), Health rights and entitlements of
refugees and asylum seekers in Scotland, Glasgow: SRC Health
Information Briefing

65
Sellen, D. and Tedstone, A. (2000), ‘Nutritional needs of refugee children
in the UK’, Journal of the Royal Society of Medicine 93, pp.360-364
Simich, L., Este, D. and Hamilton, H. (2010), ‘Meanings of home and
mental well-being among Sudanese refugees in Canada’, Ethncity
and Health 15.2, pp.199-212
Southcombe, F. (2008), Feeding the family in an unfamiliar environment:
food insecurity among recently resettled refugees, Sydney: NSW
Refugee Health Service
Szczepura, A. (2005), ‘Access to health care for ethnic minority
populations’, Postgraduate Medical Journal 81, pp.141-147
Victorian Refugee Health Network (2008), Healthy eating resource kit for
community workers, Melbourne: VRHN
Victoria State Government Department of Health (2012), Victorian
refugee health and wellbeing action plan, Melbourne
Wasp, D. with Noel, A., Farah, I. and Habib, D. (2004), Mapping health
access for Afghan, Iranian and Somali refugees and asylum seekers
in Harrow, London: Mind in Harrow
Chapter Three: Methodology
Dumper, H. (2002), Missed opportunities: a skills audit of refugee women
in London from the teaching, nursing and medical professions,
London: Mayor of London
Mestheneos, E. (2006), ‘Refugees as researchers: experiences from the
project “Bridges and fences: paths to refugee integration in the EU”’
in Temple, B. and Moran, R. (eds.), Doing research with refugees:
issues and guidelines, Bristol: Policy Press, pp. 21-36
Roshan, N. (2005) ), Supporting new communities: a qualitative study of
health needs among asylum seekers and refugee communities in
north Glasgow, Glasgow: NHS

66
Appendices
Appendix One Timeline
January 2011
Ypeople Glasgow Residents’ Association (now Scottish Asylum Seekers
Residents’ Association [SASRA]) and Community InfoSource CIC (CIS)
agree to develop the Living Well in Glasgow project
April 2011
Formal agreement in place between YGRA and CIS
1st Planning Group Meeting of Living Well in Glasgow (LWiG) takes
place, agree to meet monthly
Application made to Voluntary Action Fund’s European Year of the
Volunteer grant for the Administration side of the project in the
office
May 2011
Grant application made to Scottish Community Foundation for the
Research Project
June 2011
A Volunteer Co-ordinator takes up the voluntary position and we start
working towards Volunteer Friendly Accreditation
August 2011
Grants awarded for the two projects:
o £995 from European Year of the Volunteer grant (Voluntary
Action Fund)
o £1,966 from the Hilden Charitable Trust and RND Community
Cash Fund (through Scottish Community Foundation, now
Foundation Scotland)
Volunteer Policy agreed by the Planning Group
September 2011
Planning Group agrees recruitment information and dates for
volunteers for both projects

67
Advertising takes place for the volunteer positions
Shortlisting and interviewing takes place for both projects and
volunteers are recruited
October 2011
Introductory meeting for all volunteers takes place
Administration volunteers start working in YGRA and CIS’s office
Research volunteers start training in Ycommunity in Springburn
Steering Group Meeting 1 takes place with advisers to the project
November 2011
A survey is developed by the researchers and piloting starts
Financial accounting spreadsheets are set up by the Administration
volunteers
December 2011
A corporate image starts to be developed
The pilot survey takes in 50 respondents and the analysis starts
using Survey Monkey
A Christmas night out takes place at the CCA with food and a
poetry night
January 2012
The Survey Monkey analysis method is completed and the 50
surveys are input
The main survey is developed and individuals start to be
interviewed
A separate survey is developed for organisations
February 2012
The main Survey Monkey method of analysis is finalised and
surveys start to be input
Interviews start with organisations and individual surveys continue
Volunteers have a general meeting & support & supervision
meetings are arranged
LWiG emails are functioning

68
The analysis of the pilot survey is completed and a report is
compiled
Method of analysing the organisations surveys is completed
Steering Group Meeting 2 takes place to hear about the pilot
survey and progress
March and April 2012
Interviews continue with organisations and analysis is ongoing
Individual surveys continue and analysis is ongoing
Logo and website developed and live
June 2012
Refugee Week event to launch the research and carry out two pilot
workshops for stress management
September 2012 to January 2013
Volunteers developed and submitted funding applications for
workshops based on survey & interview information.
Grants awarded for the two projects:
o £1,995 from Communities 2014 grant (Big Lottery Fund) for
Zumba classes
o £9,282 from Awards for All (Big Lottery Fund) for two sets of
workshops plus the launch of the research and analysis once
complete.
A new volunteer supports the project by analysing the information
gathered from organisations
March to September 2013
Planning Group agrees recruitment information and dates for
volunteers for the workshop development
Advertising takes place for the volunteer positions
Shortlisting and interviewing takes place and volunteers are
recruited
An additional volunteer is recruited to help with the analysis of the
research data from individuals
Volunteers start to develop the format and programme for
workshops, based on the research findings

69
Advice is sought from professionals with experience in our fields of
interest
Agreements are reached with support organisations for delivery of
parts of workshops
Advertising takes place to access participants
October 2013 to January 2014
Pilot workshops take place to help us decide what works best in practice:
1. Mental Wellbeing – separate sessions for men and women
2. Healthy Eating & Cooking – mixed sessions in the afternoons and
women only in the mornings
3. Zumba – exercise classes, women only and mixed
These workshops were all very well received and there has been great
demand from participants and other professionals, that they run again.
Celebration of current volunteers takes place followed by Christmas
meal. See the results: www.lwig.org.uk
February to April 2014
Research analysis completed and report written up
Report on Zumba workshops completed
Launch of research prepared for May 2014
Projects for future decided on and starting to be developed
Fundraising applications being prepared
Volunteer fundraisers urgently required!
April 2014
70
Appendix Two
Letter of Introduction and Individual Survey
Research project: Healthy Living Needs of Newcomers Who We Are Living Well in Glasgow is a partnership between Community InfoSource and Ypeople Glasgow Residents’ Association which is developing this project. The research Living Well in Glasgow is a Healthy Living Pilot project being developed to provide health and well being information for people who have come to live in Britain from a different culture. The research is being carried out by asylum seekers and refugees who have been trained for this project and who are volunteering. You will be asked about how you live now compared to before you came here and about what would have been helpful for you to know when you arrived. Your Role Without you, this research would not be possible – we need you to talk to us about the information you felt you needed to live in a healthy way when you came to stay in Glasgow. The interviews will be completely anonymous and you do not have to answer any question if you do not wish to do so. Each interview should last about half an hour. Thank you very much for your support and help
LWiG, C/o YGRA Mailbox, 33 Petershill Drive, Glasgow G21 4QQ;
YGRA phone: 0141 557 6112; CIS phone: 0141 946 6193; Email: [email protected]
Tear off here and return to researcher I have read the information sheet and understand the reasons for the research. I understand that any comments that I make will be kept anonymous. Name: Signed: Date:
71
Living Well in Glasgow
Living Well connecting people, improving lives
Introduction
Thank you for meeting me today. Check: are you still happy to be involved with the
research?
(Give participant LWiG sheet). Suggest they put it in a safe and/or prominent place e.g.
notice board, so they can see it easily if they need to contact LWiG at anytime).
Points to discuss with participant before they give Consent:
What we are going to discuss today is health and food. I am going to ask you some questions about healthy living and whether you feel your health or lifestyle has changed since you came to Glasgow. Also whether you would like to receive more information about health. The reason we are asking is that we want to set up some workshops where we can provide talks and information to new arrivals about health topics.
There are some personal questions such as about age or nationality but these are only for our records and won’t be shared. You do not have to answer anything you do not wish to share.
If there is anything you don’t want to talk about just say so. This interview is about me having the opportunity to understand what life is like for you and your family at this time - you are the expert, and I hope to be following your lead in what we talk about today. If however we do stray onto a subject that you don’t want to discuss now or at any other time during the research, then please don’t be afraid to tell me and we can talk about something else.
We can stop whenever you like. If you want to take a break, feel upset or unwell; please just let me know and we can finish the session.
You will not be named in anything I write about this research, it will be anonymous.
So that I can protect your identity I will ask for your name and contact details at the end but will only if you are interested in future events that we are planning.
Signing Consent Form
You have a sheet to give the participant, with a tear-off sheet on the end of it.
Make sure the participant is giving his / her consent to take part in the research.
Does this all sound okay? Would you like to ask me to explain anything, or do you have any
questions?
72
Begin interview
Living Well in Glasgow Research First stage No. ___
Circle or tick the correct answer
1. Food you are eating now, compared to before in your own country:
a. Are you eating the same foods? Yes / No
b. Do you mainly cook for yourself or do you buy more fast foods or take-away?
Mainly cook; Mainly buy fast food/take-away; Both
c. Are you eating the same mixture of different foods?
More of a mixture; About the same Less of a mixture
Less - why is that?
Too expensive; Not available; Takes too long to cook; No time; No
cooking skills; No appetite; Life style changes;
Other / what:
_____________________________________________________________________________________________
More - why is that?
Less expensive; More available; Easily available; More time; More
appetite; More money to buy; Life style changes;
Other / what:
_____________________________________________________________________________________________
d. Are you eating the same amount of fruit and vegetables?
More; About the same Less
Why is that (if different)?
______________________________________________________________
______________________________________________________________
e. Are you eating the same amount of food?
More; About the same Less
Why is that (if different)?
______________________________________________________________
______________________________________________________________
2. What country are you from?
________________________________________________________________

73
3. How long since you came to UK?
Under 1 month; Less than 6 months; Less than 1 year;
Less than 3 years; 3+ years
4. How long since you came to Glasgow?
Under 1 month; Less than 6 months; Less than 1 year;
Less than 3 years; 3+ years
5. What is your status?
Refugee; asylum seeker; asylum seeker on section 4 support;
asylum seeker on no support (destitute); other ________________
6. Are you registered with a doctor? Yes / No
a. Yes: how long did it take you?
Under 1 month; 1 - 3 months; 4 – 6 months; Over 6 months
If over 3 months: why did it take so long?
________________________________________________________
b. No: why is that?
______________________________________________________________
7. Are you registered with a dentist? Yes / No
a. Yes: how long did it take you?
Under 1 month; 1 - 3 months; 4 – 6 months; Over 6 months
If over 3 months: why did it take so long?
______________________________________________________________
b. No: why is that
8. Since you arrived in Glasgow, how has your health been?
a. How has your health been, compared to in your country?
Better Same Worse
b. Why do you think that is (only if better or worse)?
______________________________________________________________
______________________________________________________________

74
9. Do you think people would be interested to attend special events or
workshops on the following issue
Other: _________________________________________________________
______________________________________________________________
10. Is there anything you would like to know about health?
__________________________________________________________
__________________________________________________________
11. What would you need to be able to attend a workshop?
a. Would you need childcare?
Childcare: how many would need it? _____________________________
What ages of children? ______________________________________
b. What gender are you?
Female Male Other
c. Would you like separate times for men and women?
Yes / No
d. What would be the best time of day for you?
10am – 2pm; 12 noon – 4pm; 2pm to 6pm; 4pm – 8pm
e. What would be the best day of the week?
Monday; Tuesday; Wednesday; Thursday; Friday; Saturday; Sunday; Any
If Saturday or Sunday, which times?
10am – 2pm; 12 noon – 4pm; 2pm to 6pm;
f. Interpreter?
Yes / No If yes, what languages?
_________________________________________________
a. Relationships b. Women’s health
c. Smoking d. Employment
e. Activities & exercise f. Men’s health g. Stress management
h. Business
i. Diseases & illnesses j. Mental health k. Outdoors l. Education m. Healthy eating /
cooking n. Children’s
health o. Indoors p. Housing
q. Parenting r. Youth s. Money management
t. Special needs u. Safety v. Glasgow places w. 50 + x. Alcohol or
drugs y. Customs &
culture

75
g. In which area of Glasgow would you like workshops to be held?
______________________________________________________
h. Would you have any personal difficulties or support needs to be able to attend
a workshop?
Yes / No If yes, what?
___________________________________________________________
i. Transport expenses?
Yes / No
j. What age are you?
Under 18; 18-24; 25-34; 35-59; 60+
12. How can health information be presented to people whose first language is
not English?
__________________________________________________________
13. Do you, or anyone you know, who is an asylum seeker or refugee have
skills or information about healthy living, to share?
Could you ask them to contact us? Or tell us their name?
_________________________________________________________
14. How did you find this discussion?
Interesting; useful; hard to understand the questions; good
Other? ____________________________________________________
15. Any other comment you would like to make?
___________________________________________________________
16. When the Living Well project is starting, would you like us to invite you to
it? If yes:
Name: ________________________________________________________
Address: ______________________________________________________
Phone: ________________________________________________________
Email: _________________________________________________________
17. Could we talk to you again when we have developed the plans more?
Yes / Maybe / No / Don’t know
Name of researcher:
Date of interview:
Researcher comments:

76
Appendix Three
Letter of introduction and organisational survey
Research project: Healthy Living Needs of Newcomers
Who We Are Living Well in Glasgow is a partnership between Community InfoSource and Ypeople Glasgow Residents’ Association which is developing this project. The research Living Well in Glasgow is a Healthy Living Pilot project being developed to provide health and well being information for people who have come to live in Glasgow from a different background. The research is being carried out by asylum seekers and refugees who have been trained for this project and who are volunteering. Your Role We would like you to talk to us about the information you feel refugees and asylum seekers who are new to Glasgow need to know to live in a healthy way, especially when they have come from a different climatic or cultural background. Also how you think that information should be presented. Thank you very much for your support and help
LWiG, C/o YGRA Mailbox, 33 Petershill Drive, Glasgow G21 4QQ;
YGRA phone: 0141 557 6112; CIS phone: 0141 946 6193; Email: [email protected]
Tear off here and return to researcher
I have read the information sheet and understand the reasons for the research.
Name:
Signed: Date:

77
Living Well in Glasgow
Living Well connecting people, improving lives
Introduction First Stage Research for Organisations
Thank you for meeting me today. Check: are you still happy to be involved with this
research? (Give participant LWiG details).
Points to discuss with participant from an organisation:
What we are going to discuss today is what you think new refugees and asylum
seekers need to know to live healthily in Glasgow
We will also ask about methods of presenting information to people who do not
have English as their first language
You do not have to answer anything you do not wish to.
We would like to quote you in our research report. If there are certain things you
say that you would rather NOT be quoted then please just tell me.
Let me reassure you, if you wish we can offer you pseudo-anonymity. This is
when your name is changed in any reports or publications so no one can
recognise you. You can even pick the name you wish to be called in our report!
Signing Consent Form
You have a sheet to give the participant, with a tear-off sheet on the end of it.
Ask the participant to give his / her consent to take part in the research.
Does this all sound okay? Would you like to ask me to explain anything, or do you
have any questions?
Begin interview
Living Well in Glasgow Research Organisation No. ___
Organisation’s full name:
__________________________________________________
Your name and position:
___________________________________________________
Organisation’s Email address:
_____________________________________________
Organisation’s Phone number:
_____________________________________________

78
1. What support does your organisation provide to refugees and asylum
seekers?
_____________________________________________________________
______________________________________________________________
1a) Please tell me about your role in the organisation:
_____________________________________________________________
______________________________________________________________
Circle or tick the correct answer
2. What field does your organisation provide support in?
a. Medical treatment
b. Information general
c. Advice general
d. Legal
e. Money
f. Food
g. Clothing
h. Training
i. Mental heath
j. Stress
k. Education
l. Employability skills
m. Accommodation
n. Immigration
o. Minority ethnic issues
p. Violence
q. Cultural
Other / what: _______________________
2a) How do you provide that support?
_____________________________________________________________
______________________________________________________________
2b) What do you think people need to live a healthy life?
______________________________________________________________
______________________________________________________________

79
3. What do you think refugees and asylum seekers need to know to live
healthily in Glasgow?
______________________________________________________________
______________________________________________________________
4. From your experience, do you have any suggestions about how health
information can be shared with people whose first language is not English?
______________________________________________________________
______________________________________________________________
5. Do you know any organisations or groups who could provide Healthy
Living workshops for us?
______________________________________________________________
______________________________________________________________
6. Do you know any asylum seekers or refugees who may have skills or
information about healthy living, to share?
Could you tell us their name? Or ask them to contact us?
______________________________________________________________
______________________________________________________________
7. Do you have any other comments you would like to make about
healthy living in Glasgow?
______________________________________________________________
8. Do you wish a copy of our research findings?
Yes No
Name of researcher:
Date of interview:
Researcher comments:
Time interview took to conduct?
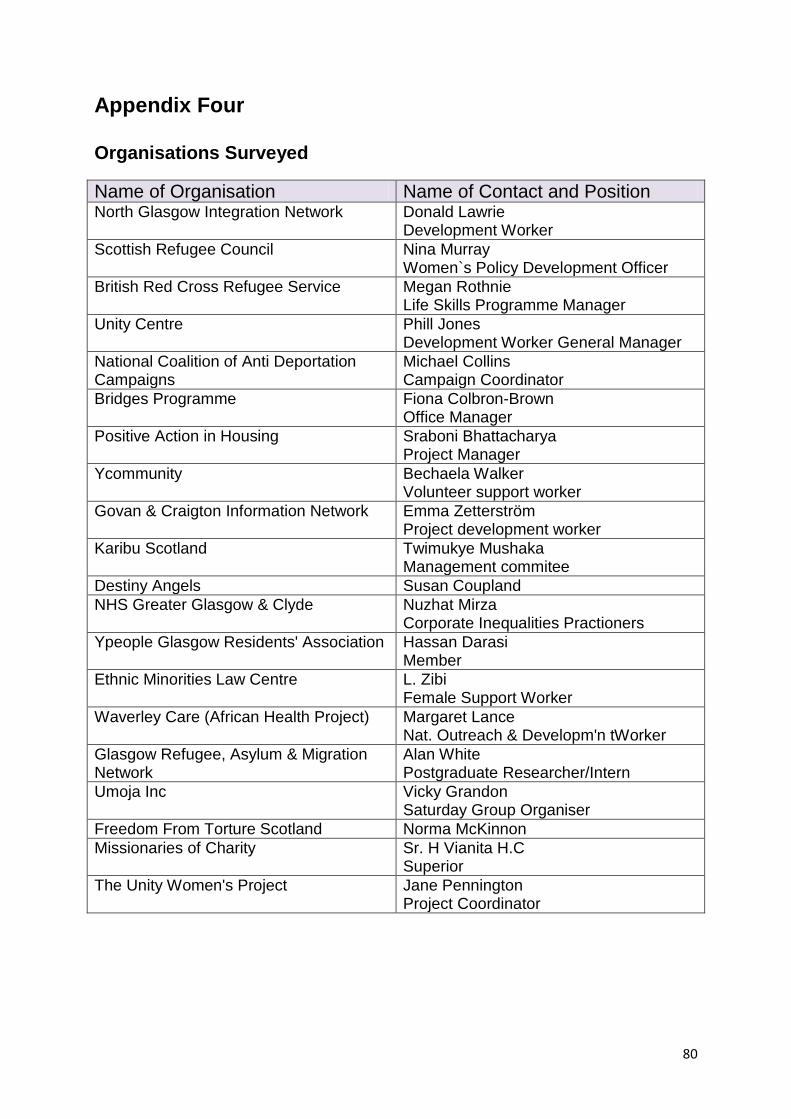
80
Appendix Four
Organisations Surveyed
Name of Organisation Name of Contact and Position North Glasgow Integration Network Donald Lawrie
Development Worker
Scottish Refugee Council Nina Murray Women`s Policy Development Officer
British Red Cross Refugee Service Megan Rothnie Life Skills Programme Manager
Unity Centre Phill Jones Development Worker General Manager
National Coalition of Anti Deportation Campaigns
Michael Collins Campaign Coordinator
Bridges Programme Fiona Colbron-Brown Office Manager
Positive Action in Housing Sraboni Bhattacharya Project Manager
Ycommunity Bechaela Walker Volunteer support worker
Govan & Craigton Information Network Emma Zetterström Project development worker
Karibu Scotland Twimukye Mushaka Management commitee
Destiny Angels Susan Coupland
NHS Greater Glasgow & Clyde Nuzhat Mirza Corporate Inequalities Practioners
Ypeople Glasgow Residents' Association Hassan Darasi Member
Ethnic Minorities Law Centre L. Zibi Female Support Worker
Waverley Care (African Health Project) Margaret Lance Nat. Outreach & Developm'n tWorker
Glasgow Refugee, Asylum & Migration Network
Alan White Postgraduate Researcher/Intern
Umoja Inc Vicky Grandon Saturday Group Organiser
Freedom From Torture Scotland Norma McKinnon
Missionaries of Charity Sr. H Vianita H.C Superior
The Unity Women's Project Jane Pennington Project Coordinator

81
Appendix Five
Support Provided by Organisations Surveyed
Name General Information
General Advice
Legal Money Food Clothing Training
Mental Health
North Glasgow Integration Network Yes Yes - - Yes Yes Yes Yes
Scottish Refugee Council Yes Yes Yes Yes - - Yes Yes
British Red Cross Refugee Service Yes Yes Yes - Yes - -
Unity Centre Yes Yes - - Yes Yes - -
National Coalition of Anti Deportation Campaigns Yes Yes - - - - Yes -
Bridges Programmes Yes - - - - Yes -
Positive action in Housing Yes Yes - Yes Yes Yes Yes Yes
Ycommunity Yes - - Yes Yes (planned) -
Govan & Craigton Information network Yes Yes - - Yes Yes Yes -
Karibu Scotland Yes Yes - - Yes Yes Yes -
Destiny Angels Yes - - - Yes Yes Yes -
NHS Greater Glasgow & Clyde Yes - - - - - Yes Yes
Ypeople Glasgow Residents' Association - - -
- - - - -
Ethnic Minorities Law Centre - - Yes - - - - -
Waverley Care (African Health Project) Yes Yes - - - - - -
Glasgow Refugee, Asylum and Migration Network Yes - -
- - - Yes -
Umoja Inc - - - - - - -
Freedom From Torture Scotland - - - - - - - Yes
Missionaries of Charity - - - - Yes Yes - -
The Unity Women's Project Yes Yes - - - - - Yes
Totals 15 9 3 3 8 9 11 6
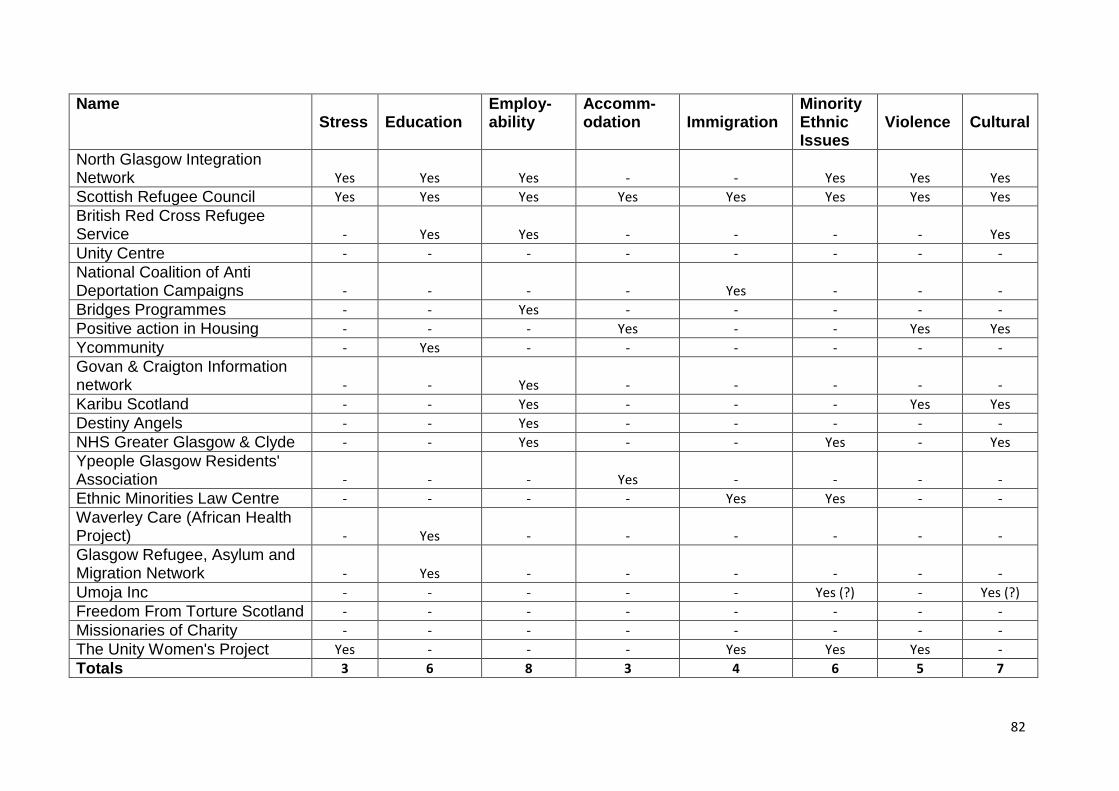
82
Name Stress
Education
Employ-ability
Accomm-odation
Immigration
Minority Ethnic Issues
Violence
Cultural
North Glasgow Integration Network Yes Yes Yes - - Yes Yes Yes
Scottish Refugee Council Yes Yes Yes Yes Yes Yes Yes Yes
British Red Cross Refugee Service - Yes Yes - - - - Yes
Unity Centre - - - - - - - -
National Coalition of Anti Deportation Campaigns - - - - Yes - - -
Bridges Programmes - - Yes - - - - -
Positive action in Housing - - - Yes - - Yes Yes
Ycommunity - Yes - - - - - -
Govan & Craigton Information network - - Yes - - - - -
Karibu Scotland - - Yes - - - Yes Yes
Destiny Angels - - Yes - - - - -
NHS Greater Glasgow & Clyde - - Yes - - Yes - Yes
Ypeople Glasgow Residents' Association - - - Yes - - - -
Ethnic Minorities Law Centre - - - - Yes Yes - -
Waverley Care (African Health Project) - Yes - - - - - -
Glasgow Refugee, Asylum and Migration Network - Yes - - - - - -
Umoja Inc - - - - - Yes (?) - Yes (?)
Freedom From Torture Scotland - - - - - - - -
Missionaries of Charity - - - - - - - -
The Unity Women's Project Yes - - - Yes Yes Yes -
Totals 3 6 8 3 4 6 5 7

83
Name Other Comments
North Glasgow Integration Network
Scottish Refugee Council
British Red Cross Refugee Service
Unity Centre Volunteering opportunities
National Coalition of Anti Deportation Campaigns Anti-deportation support
Bridges Programmes
Positive action in Housing
Ycommunity
Govan & Craigton Information network
Karibu Scotland
Destiny Angels Furniture
NHS Greater Glasgow & Clyde Marginalised people
Ypeople Glasgow Residents' Association
Ethnic Minorities Law Centre
Waverley Care (African Health Project)
Glasgow Refugee, Asylum and Migration Network
Umoja Inc None of these are really applicable
Freedom From Torture Scotland Have a relief fund for people with problems. People are referred to us when they are in psychological treatment
Missionaries of Charity
The Unity Women's Project Violence against women including sexual and domestic violence, trafficking and torture

84
Voluntary Action Fund Administration Volunteers Mental Wellbeing Workshops
Healthy Eating & Cooking Workshops
Research Launch
Research funding
Communities 2014 Zumba workshops
www.lwig.org.uk
Community InfoSource • Company No SC291462 272 Bath Street • Glasgow • G2 4JR • Tel: 0141 946 6111
Email: [email protected]
Printed on FSC accredited mix paper