Usefulness of 2 Questions About Age and Year of Birth in the Case-Finding of Dementia
6
Original Study Usefulness of 2 Questions About Age and Year of Birth in the Case-Finding of Dementia Tirso Ventura MD, PhD a, b, c, d , Concepción De-la-Cámara MD, PhD b, c, d, e , Raúl Lopez-Anton PhD c, f , Javier Santabárbara MStat c, g , Guillermo Marcos MD, PhD c, d, g, h , Miguel Angel Quintanilla MD, PhD b, e , Antonio Campayo MD, PhD b, c, d, e , Elena Lobo PhD c, g , Juan Francisco Roy PhD c, f , Pedro Saz MD, PhD b, c , Beatriz Olaya PhD c, i , Josep María Haro MD, PhD c, i , Leocadio Rodríguez-Mañas MD, PhD j , Norman Sartorius MD k , Antonio Lobo MD, PhD b, c, d, e, * a Psychiatry Service, Hospital Universitario Miguel Servet, Zaragoza, Spain b Department of Medicine and Psychiatry, Universidad de Zaragoza, Zaragoza, Spain c Centro de Investigación Biomédica en Red de Salud Mental (CIBERSAM), Ministry of Science and Innovation, Madrid, Spain d Instituto de Investigación Sanitaria de Aragón (IIS Aragón), Zaragoza, Spain e Psychiatry Service, Hospital Clínico Universitario, Zaragoza, Spain f Department of Psychology and Sociology, Universidad de Zaragoza, Zaragoza, Spain g Department of Preventive Medicine and Public Health, Universidad de Zaragoza, Zaragoza, Spain h Medical Records Service, Hospital Clínico Universitario, Zaragoza, Spain i Parc Sanitari Sant Joan de Déu, Universitat de Barcelona, Sant Boi de Llobregat, Barcelona, Spain j Hospital Universitario de Getafe, Getafe, Madrid, Spain k Association for the Improvement of Mental Health Programmes (AMH), Geneva, Switzerland Keywords: Longitudinal community study dementia ultra-short test aging diagnostic tests geriatric psychiatry screening case-finding abstract Objective: To test the hypothesis that the efficacy of 2 simple questions commonly used in clinical practice, asking the age and year of birth of individuals, will be satisfactory to rule out cases of dementia. Design: Population-based, longitudinal, prospective study focused on the incidence of dementia. In the baseline, a 2-phase procedure for identifying cases and noncases of dementia was implemented. Setting: Zaragoza, Spain. Participants: Individuals 65 years or older without previous diagnoses of dementia (n ¼ 3613) drawn from the population-based random sample of the ZARADEMP project. Measurements: Standardized instruments were used, including the Geriatric Mental State (GMS) and the History and Aetiological Schedule (HAS); cases were diagnosed according to DSM-IV criteria (“reference standard”). The simple cognitive test used in this study consists of the following 2 compulsory questions: “How old are you?” and “What year were you born?” Results: The test was well accepted by the participants and took less than 30 seconds to complete. Compared with the “reference standard,” validity coefficients for incorrect answers in both questions were as follows: sensitivity 61.2%, specificity 97.8%, positive predictive value 44.4%, negative predictive value 98.9%. Conclusions: This ultra-short test has very good specificity and negative predictive power. Its use to rule out cases of dementia might be generalized, as it has the best efficiency reported to date. Copyright Ó 2013 - American Medical Directors Association, Inc. Alzheimer disease and other dementias rank among the leading causes of global burden of mental and neurological disorders world- wide. 1,2 In view of the incidence and lifetime risk 3 and the expected rise in the prevalence, 4 dementia is considered to be a public health priority, and a research priority calling for urgent action and investment. 5,6 Most authors conclude that systematic screening of dementia should be postponed until there is convincing evidence that it helps more than harms. 7,8 However, enhanced detection and good case- finding has been recommended both in primary care (PC) 9 and in geriatrics, although it should be tailored to the needs of the individual patient. 10 The integration of case-finding and care packages of services into routine primary health care has been suggested, 1 but national surveys of physicians have documented that the proportion of PC physicians (PCPs) doing systematic screening for dementia is The authors designed and undertook the study, had full access to the raw data, did the analyses, wrote the report, and had final responsibility for the decision to submit for publication. The funder had no role in design, data collection, analysis, interpretation or writing of the report. The authors declare no conflicts of interest. * Address correspondence to Antonio Lobo, MD, PhD, Servicio de Psiquiatría, Hospital Clínico Universitario, planta 3, Avd. San Juan Bosco, 15, 50009 Zaragoza, Spain. E-mail address: [email protected] (A. Lobo). JAMDA journal homepage: www.jamda.com 1525-8610/$ - see front matter Copyright Ó 2013 - American Medical Directors Association, Inc. http://dx.doi.org/10.1016/j.jamda.2013.05.006 JAMDA 14 (2013) 627.e7e627.e12
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Usefulness of 2 Questions About Age and Year of Birth in the Case-Finding of Dementia

JAMDA 14 (2013) 627.e7e627.e12
JAMDA
journal homepage: www.jamda.com
Original Study
Usefulness of 2 Questions About Age and Year of Birth in the Case-Findingof Dementia
Tirso Ventura MD, PhD a,b,c,d, Concepción De-la-Cámara MD, PhD b,c,d,e, Raúl Lopez-Anton PhD c,f,Javier Santabárbara MStat c,g, Guillermo Marcos MD, PhD c,d,g,h, Miguel Angel Quintanilla MD, PhD b,e,Antonio Campayo MD, PhD b,c,d,e, Elena Lobo PhD c,g, Juan Francisco Roy PhD c,f, Pedro Saz MD, PhD b,c,Beatriz Olaya PhD c,i, Josep María Haro MD, PhD c,i, Leocadio Rodríguez-Mañas MD, PhD j,Norman Sartorius MD k, Antonio Lobo MD, PhD b,c,d,e,*a Psychiatry Service, Hospital Universitario Miguel Servet, Zaragoza, SpainbDepartment of Medicine and Psychiatry, Universidad de Zaragoza, Zaragoza, SpaincCentro de Investigación Biomédica en Red de Salud Mental (CIBERSAM), Ministry of Science and Innovation, Madrid, Spaind Instituto de Investigación Sanitaria de Aragón (IIS Aragón), Zaragoza, Spaine Psychiatry Service, Hospital Clínico Universitario, Zaragoza, SpainfDepartment of Psychology and Sociology, Universidad de Zaragoza, Zaragoza, SpaingDepartment of Preventive Medicine and Public Health, Universidad de Zaragoza, Zaragoza, SpainhMedical Records Service, Hospital Clínico Universitario, Zaragoza, Spaini Parc Sanitari Sant Joan de Déu, Universitat de Barcelona, Sant Boi de Llobregat, Barcelona, SpainjHospital Universitario de Getafe, Getafe, Madrid, SpainkAssociation for the Improvement of Mental Health Programmes (AMH), Geneva, Switzerland
Keywords:Longitudinal community studydementiaultra-short testagingdiagnostic testsgeriatric psychiatryscreeningcase-finding
The authors designed and undertook the study, hadid the analyses, wrote the report, and had final respsubmit for publication. The funder had no role in desinterpretation or writing of the report.
The authors declare no conflicts of interest.* Address correspondence to Antonio Lobo, MD,
Hospital Clínico Universitario, planta 3, Avd. San JuaSpain.
E-mail address: [email protected] (A. Lobo).
1525-8610/$ - see front matter Copyright � 2013 - Ahttp://dx.doi.org/10.1016/j.jamda.2013.05.006
a b s t r a c t
Objective: To test the hypothesis that the efficacy of 2 simple questions commonly used in clinicalpractice, asking the age and year of birth of individuals, will be satisfactory to rule out cases of dementia.Design: Population-based, longitudinal, prospective study focused on the incidence of dementia. In thebaseline, a 2-phase procedure for identifying cases and noncases of dementia was implemented.Setting: Zaragoza, Spain.Participants: Individuals 65 years or older without previous diagnoses of dementia (n ¼ 3613) drawnfrom the population-based random sample of the ZARADEMP project.Measurements: Standardized instruments were used, including the Geriatric Mental State (GMS) and theHistory and Aetiological Schedule (HAS); cases were diagnosed according to DSM-IV criteria (“referencestandard”). The simple cognitive test used in this study consists of the following 2 compulsory questions:“How old are you?” and “What year were you born?”Results: The testwaswell accepted by the participants and took less than30 seconds to complete. Comparedwith the “reference standard,” validity coefficients for incorrect answers in both questions were asfollows: sensitivity 61.2%, specificity 97.8%, positive predictive value 44.4%, negative predictive value 98.9%.Conclusions: This ultra-short test has very good specificity and negative predictive power. Its use to ruleout cases of dementia might be generalized, as it has the best efficiency reported to date.
Copyright � 2013 - American Medical Directors Association, Inc.
Alzheimer disease and other dementias rank among the leading in theprevalence,4 dementia is considered tobeapublichealthpriority,
causes of global burden of mental and neurological disorders world-wide.1,2 In viewof the incidence and lifetime risk3 and the expected rised full access to the raw data,onsibility for the decision toign, data collection, analysis,
PhD, Servicio de Psiquiatría,n Bosco, 15, 50009 Zaragoza,
merican Medical Directors Associa
and a research priority calling for urgent action and investment.5,6
Most authors conclude that systematic screening of dementiashould be postponed until there is convincing evidence that it helpsmore than harms.7,8 However, enhanced detection and good case-finding has been recommended both in primary care (PC)9 and ingeriatrics, although it should be tailored to the needs of the individualpatient.10 The integration of case-finding and care packages ofservices into routine primary health care has been suggested,1 butnational surveys of physicians have documented that the proportionof PC physicians (PCPs) doing systematic screening for dementia is
tion, Inc.

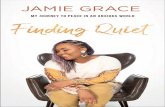
Fig. 1. Flow of participants through the study.
T. Ventura et al. / JAMDA 14 (2013) 627.e7e627.e12627.e8
low.11 Although the unwillingness of clinicians such as PCPs to do thissystematic screen may be because of limited resources, or negativeattitudes toward the value of detecting and managing these condi-tions,12 there is also important evidence suggesting that they havedifficulty identifying dementia.12,13 In the geriatric field, there isconsensus that appropriate diagnosis of dementia benefits patients,but a large proportion of patients under geriatric care in both acuteand rehabilitation settings remains undiagnosed.14
In relation to this, a stepped approach, sometimes called algorithmscreening, has been proposed by both geriatricians10 and PCPs.15 Asimple test might be used in the first step to exclude those individualswithout significant cognitive impairment and then a more extensivecase-finding method would be implemented by either the PCP ora specialist, such as a geriatrician, neurologist, or psychiatrist, in thosewho screenpositive in thefirst step.11 Thorough reviewof the literaturehas found a considerable number of robust studies that examineddiagnostic validity of brief, single, or multidomain screening methodsin comparisonwith a validated diagnostic standard of dementia. In thisreview, theMini-Mental Status Examination (MMSE)16 is the testmostfrequently used for screening, and a recent meta-analysis supports itsvalidity in community studies.17 However, one of the main problemswith the MMSE relates to its use in busy clinical practices, as theadministration time has been estimated to be 7 to 10 minutes13,18 and
15 minutes in patients with some cognitive problems.17 Studies in thegeneral population and primary care settings18,19 have raised the needto develop screening tools shorter and easier to apply. We previouslyreported good validity coefficients of individual items in the MMSE20
and Mitchell and Malladi,21 in a careful meta-analysis of simpledomain tests, concluded that validity coefficients were surprisinglysimilar to the fullMMSE, and that tests suchas theMemory ImpairmentTest (MIS) may be an efficient first step in identifying cognitiveimpairment. Nevertheless, there is no evidence that the use of thesetests is systematic, and no consensus onwhat test should be preferred.
The objective of this study was to test the following hypothesisemerging from our clinical and research experience: the efficacy ofa simple cognitive test based on 2 routine questions commonly usedin clinical practice and well accepted by both patients and clinicians(asking the age and year of birth of individuals) will be satisfactory torule out cases of dementia.
Methods
Background, Design, and Sampling Technique
The data in this report come from the baseline of the ZARADEMPproject, a longitudinal, prospective study focused on the incidence of

T. Ventura et al. / JAMDA 14 (2013) 627.e7e627.e12 627.e9
dementia. The project, designed on the basis of results of previousinvestigations in the same population, started in 1994, and thegeneral objectives, as well as the setting and eligibility criteria ofparticipants, have been described elsewhere.3,22 A population-basedrepresentative random sample of individuals aged 55 and older(n ¼ 157,787), stratified with proportional allocation by age (5-yeargroups) and sex, was drawn from census lists. Although specialstrategies were implemented to minimize losses, a considerablerefusal rate was anticipated by design, so that oversampling wasapplied. Refusal rate (20.5%) was considered to be acceptable andultimately 4803 people were interviewed. The specific characteristicsof nonrespondents have also been previously described.22 For thisparticular study, only the individuals 65 years or older were consid-ered (Figure 1). The principles of the Declaration of Helsinki werefollowed throughout; the Ethics Committee of the University of Zar-agoza and the Fondo de Investigación Sanitaria (FIS) approved thisstudy protocol, according to Spanish Law, and all individuals providedwritten informed consent.
Instruments
The following validated instruments incorporated in the ZAR-ADEMP interview were administered:
� Geriatric Mental State (GMS), a semistructured standardizedclinical interview for assessing the mental state of elderlypersons.23 The GMS provides a syndrome case-finding rating,the GMS-B “threshold global score” discriminating between“noncases” and “cases” of dementia.
� The History and Aetiology Schedule (HAS), a standardizedmethod of collecting history data from a caregiver, or directlyfrom the respondent when he or she is judged to be reliable.19
It includes items to explore history of dementia.� The MMSE16,20 was also used to detect cognitive difficulty; theLawton and Brody scale and Katz index to assess instrumentaland basic activities of daily living, respectively; and theEURODEM risk factors questionnaire, which includes data onmedical conditions.
The simple cognitive test used in this study consists of thefollowing 2 compulsory questions: “How old are you?” and “Whatyear were you born?”
Procedure
In the baseline study, a 2-phase epidemiological screening designwas used to identify cases of dementia that should be excluded forthe follow-up cohort of individuals without dementia. In Phase I,well-trained, reliable, and regularly supervised lay interviewers and
Table 1Demographic Characteristics of the Interviewed Sample
Individuals WithoutDementia n ¼ 3495
n %
Sex Men 1458 41.7Women 2037 58.3
Age 65e79 2281 65.3>80 1214 34.7
Educational level* Illiterate 411 11.9Primary 2560 73.9Medium/high 495 14.3
*The number of individuals listed for educational level in both categories of individubecause the few individuals in whom information was uncertain were excluded.
senior medical students conducted the 25- to 90-minute ZARADEMPinterview at each participant’s residence. The compulsory 2 questionsof the brief cognitive test were asked in this phase. The answers wererecorded and afterward were contrasted with official data forcorrectness. The lay interviewers were blind to the study hypothesis.Participants were considered to be “probable cases” of dementia onthe basis of GMS threshold “global” score (1/2) and/or MMSE (23/24)standard cutoff points.20,23 In phase II, triggered by predeterminedcriteria, using the same interview, a trained research psychiatristreassessed participants suspected of dementia to confirm the diag-nosis. These interviews were also conducted in participants’ resi-dences. For the diagnosis of dementia, assessments werecomplemented by medical reports and laboratory data, frequentlyavailable at most people’s homes in Spain. Outside caregivers wereinterviewed when the participant was considered to be unreliable.Identified cases of dementia were presented to a panel of 4 researchpsychiatrists who made the final diagnosis according to DSM-IVcriteria. Previously, variables in the ZARADEMP interview were op-erationalized to conform to this diagnostic system. The validity of thisprocess has been previously established.24
For thepurposeof this report, individuals completing theassessmentprocesswere classified as cases of dementia previously diagnosed, casesof dementia diagnosed for the first time, and noncases of dementia. Toavoid selection bias for this particular study, individuals with history ofdementia were excluded from the analysis, so that only the cases ofdementia sequentially detected and not previously diagnosed wereincluded. The research psychiatrists in phase II and those in the diag-nostic panel remained blind to the results of the brief cognitive test.
Statistical Analysis
Standard statistical techniques were used, and 2-sided tests wereapplied throughout. For the analysis, the test with the compulsoryquestions was considered an ordinal scale with 3 categories: “0” wasused for “correct” answers in both questions; and “1” or “2” for“incorrect” answers in one or both questions, respectively. To calculatevalidity coefficients, sensitivity, specificity, and positive and negativepredictive values (PPV and NPV, respectively) were calculatedfollowing standard procedures. DSM-IV diagnosis of dementia wasused as the “reference standard” for this purpose. Predictive values and95% confidence intervals for different base rates of dementiawere alsocalculated following previously reported procedures.25
Results
All individuals aged 65 years or older and previously undiagnosedfor dementia (n ¼ 3613) were interviewed in the baseline of theZARADEMP project. This cohort had a mean age of 76.7 years (SD ¼8.2). Most individuals had primary education (n ¼ 2634, 72.9%), 440
Individuals With Dementian ¼ 118
c2 P
n %
37 31.4 5.05 .02481 68.619 16.1 119.2 <.00199 83.929 27.4 29.9 <.00174 69.83 2.8
als, with or without dementia, does not add-up to the total number in the sample,

Table 2Sensitivity, Specificity, and Predictive Values of the Simple Cognitive Test
Sensitivity, % Specificity, % PositivePredictiveValue, %
NegativePredictiveValue, %
Fails one or both(vs fails none)
80.1 90.1 20.0 99.4
Fails both(vs fails oneor none)
61.2 97.8 44.4 98.9
T. Ventura et al. / JAMDA 14 (2013) 627.e7e627.e12627.e10
were illiterate (12.1%), and 498 (13.8%) had higher educational level,including university education. Forty-three individuals (1.2%) withincomplete information in the 2 compulsory questions were excludedfrom the analysis (Figure 1). The excluded individuals were signifi-cantly older than individuals in whom information was complete(mean age 84 years, SD ¼ 6.27, P < .001), but did not differ in otherdemographic characteristics. Twenty of them were cases of dementiaand 23 were noncases. Table 1 shows the demographic characteristicsof individuals included in the analysis, with and without dementia.Statistically significant differences were observed between bothsubgroups, the persons with dementia being more frequently womenand older, and having lower educational level.
The test was well accepted by the participants and took less than30 seconds to complete. Most individuals (3176; 88.9%) answeredcorrectly both questions related to age and year of birth, 259 (7.3%)failed 1 of the questions, and 135 (3.8%) failed both. Sixty (61.2%)individuals with dementia and 75 (2.2%) without dementia failedboth questions (Figure 1).
Table 2 shows validity data related to the 2 questions studied. Thesensitivity coefficientwas 61.2%whenonly individualswith “incorrect”answers in both questions in the test are considered to be probablecases of dementia, and PPV was low (44.4%). On the contrary, bothspecificity (97.8%) and NPV (98.9%) were quite high. Specificity wasconsiderably lower if individuals with “incorrect” answers in one orboth questions were considered to be probable cases of dementia.
To assess potential bias, we performed a sensitivity analysis byincorporating in the calculations of validity coefficients the individ-uals excluded because of incomplete information in the test. In theworst possible hypothesis that all cases of dementia excluded werefalse negatives, and all noncases of dementia excluded were falsepositives, the following coefficients were obtained when individualswith “incorrect” answers in both questions are considered: sensitivitywas 50.8%, specificity was 97.8%, PPV was 44.4%, and NPV was 98.3%.
Predictive values for different base rates of prevalence of dementiaare shown in Table 3. If only individuals with “incorrect” answers inboth questions were considered to be probable cases of dementia, thePPV was 59.6% for a prevalence of 5.0%, but increased to 87.1% fora prevalence of 20.0%. On the contrary, NPV was 98.0% for a 5.0%prevalence, but decreased to 91.0% for a prevalence of 20.0%. Similarchanges in PPV and NPV were observed when individuals with“incorrect” answers in one or both questions were considered to beprobable cases of dementia.
Table 3Predictive Values and 95% CIs of the Simple Cognitive Test for Different Base Rates of De
Base Rates Positive PredictiveValue, % (95% CI)
5% 10% 15% 20%
Fails one or both(vs fails none)
29.9 (21.7e38.0) 47.6 (39.9e55.5) 59.0 (52.1e66.0) 67.1 (60.9e
Fails both(vs fails oneor none)
59.6 (45.3e73.9) 75.3 (65.3e85.3) 82.9 (75.4e90.3) 87.1 (81.2e
CI, confidence interval.
Discussion
This article supports the hypothesis that the efficacy of a simplecognitive test, with 2 questions asking the age and year of birth ofindividuals, is acceptable to rule out cases of dementia in the firstphase of case-finding procedures in older adults. First, these ques-tions are commonly used in clinical practice and were well acceptedby individuals. Second, in terms of efficiency, the test takes less than30 seconds to complete, and therefore may be considered to be ultra-short. Clinical, screening tools with 1 to 4 items, taking less than2 minutes to complete, have been considered to be ultra-short.26
Third, both specificity and NPV in this test are very good. Specificityand NPV are considered to be the most important coefficients ina first phase of case-finding, as it is possible to rule out the noncasesof dementia and unnecessary concern is avoided.13 In this particularcase, the specificity was 97.8%, meaning that the great majority ofnoncases may be correctly identified by the test; and the NPV was98.9%, meaning that fewer than 2 of 100 individuals classified by thetest as probable noncases would be false-negative cases.
Although specificity in this test is very good, it might be arguedthat the sensitivity (61.2%) is not good for screening processes. Thereis no consensus about what level of sensitivity and specificity wouldbe acceptable for the screening and case-finding in the field ofdementia, but coefficients of 80% or higher have been considered tobe acceptable in the field of biological testing.17 However, shouldresearchers or clinicians aim at better sensitivity, they could selectfailures in 1 of the 2 questions in the test (sensitivity ¼ 80.6%) as thethreshold to identify probable cases of dementia.
It is remarkable that the efficacy coefficients of this simple test areso good. In fact, some authors have commented on the potential ofbrief tests,27 and Mitchell et al21 concluded in their meta-analysesthat single domain tests, commonly exploring memory items,episodic memory, or fluency, also have validity coefficients surpris-ingly similar to those offered by cognitive batteries such as the MMSE.Particularly good efficacy coefficients were reported for some of thecommonly used single-domain, brief tests reviewed, such asthe Clock Drawing Test, Verbal Fluency Test, or 3-Word Recall, but theMIS was considered in this meta-analysis to be “the optimal indi-vidual method.”21 Two relevant studies support the validity of theMIS,28,29 but none of them used a random community sample, andthe second study was limited to patients with Alzheimer disease andcontrols without dementia. Therefore, these studies may be difficultto compare with our study aimed at overall dementia and conductedin a large, random community sample. The MIS requires 4 minutes tocomplete, and the efficacy coefficients reported for this test were asfollows: sensitivity ¼ 80% and specificity ¼ 96% in the study onoverall dementia. Consequently, for the purpose of a first phase ofcase-finding, our method improves the results of the “optimal” one,because the efficiency is better (30 seconds) and the specificity is alsoslightly better. A particular advantage in this study is the design, asthe consecutive cases of dementia sequentially identified in a randomsample from the population were included in the analysis and theyhad not been diagnosed previously. This design minimizes the risk of
mentia (5%, 10%, 15%, and 20%)
Negative PredictiveValue, % (95% CI)
5% 10% 15% 20%
73.2) 98.9 (98.1e99.6) 97.7 (96.6e98.8) 96.4 (95.0e97.7) 94.9 (93.2e96.5)
93.0) 98.0 (97.1e98.9) 95.8 (94.4e97.1) 93.5 (91.8e95.2) 91.0 (89.1e93.0)

Box 1. Key points of the simple cognitive test for the case-
finding of dementia
� Ultra-short cognitive test (<30 seconds)
� Two clinical routine questions
B How old are you?B What year were you born?B These questions need no idiomatic standardization
� Well accepted by both patients and clinicians
� Very good specificity and negative predictive value in
first phase of case-finding
� More efficient than previous, similar tests
T. Ventura et al. / JAMDA 14 (2013) 627.e7e627.e12 627.e11
selection bias by excluding from the analysis the potentially hetero-geneous patients previously diagnosed in different disease stages.30
The importance of studies related to screening instruments andusing random sampling conducted in the community has beenemphasized.13 Other strengths in the study include the objectivity ofthe test, as the answers were contrasted with official data forcorrectness, or the fact that lay interviewers were blind to the studyhypothesis and the diagnosticians were blind to the results of the test.
Previous studies have shown that a large proportion of individualswith dementia remain undiagnosed, even among patients undergeriatric care.14 Broad-based dementia screening programs in olderadults have not been widely advocated, given the lack of evidencethat earlier detection helps more than harms.7 However, expertgroups and international committees have emphasized the impor-tance of improving the accuracy of case-finding techniques andstrategies in target situations, to allow the PCP to detect probablecases of dementia that might then be confirmed by the specialist.31
The development of parsimonious and cost-effective consensusmodels of case-finding in such settings should take into account timeconstraints and costs, as well as the documented difficulty of prac-titioners to identify cases of dementia.4,8 The models should includethe availability of a simple, safe, and validated test, which is accept-able to both practitioners and the population.32 We believe that ourmethod fulfills such criteria. The test might be used in the first step ofa diagnostic algorithm to rule out those individuals without signifi-cant cognitive impairment. Then, a more extensive case-findingmethod by either the PCP or a specialist, such as a geriatrician,could be implemented in those who screen positive in the first step.11
It might be argued that the method we propose needs specificstudies in different settings. In particular, the NPV reported here forthe general population might be exceedingly optimistic, and wouldbe lower in medical settings where the prevalence of dementia isexpected to be higher. However, we show here, in calculations forhigher base rate of dementia, that the NPV decreases as the preva-lence increases is modest (98.0% at 5.0% prevalence, and 93.5% at15.0% prevalence, if failures in the 2 questions is selected as thethreshold for probable cases of dementia). Furthermore, the expectedincrease in the PPV is considerable (59.6% at 5.0% prevalence, and82.9% at 15.0% prevalence, if failures in both questions are selected asthe threshold). The possibility that the effectiveness of this screeningwas affected by the illiterate status of a significant proportion ofindividuals has also been considered, and the PPV and NPV for literateand illiterate groups have been calculated separately. For the preva-lence of dementia observed in this sample for each subgroup, PPVwas 65.6% (95% confidence interval [CI] 52.8%e78.3%) among theilliterate, and 41.7% (95% CI 24.2%e59.2%) among the literate, thecorresponding values of NPV being 97.2% (95% CI 96.1%e98.3%) and98.9% (95% CI 98.2%e99.6%). Therefore, the effectiveness of this test isnot altered significantly by illiterate status.
The applicability of this simple test might be extended to otherdomains, including the epidemiological type of studies and theassessment of mental capacity, an area of increasing relevance, bothethical and legal. Failure to recall the date of birth has been used tojudge medical inpatients not to have mental capacity, but no datawere reported to support the judgment.33 An additional advantage isthat the questions in this test do not need idiomatic standardization.However, studies in other cultural settings may be required beforeaccepting a widespread use of the test.
Other limitations in this study must be noted, including thesubstantial attrition from sampling to enrollment. However, theattrition rate was expected by design and we previously argued that itis comparable to rates reported in other 2-stage epidemiologicalstudies.22 Another limitation is that we do not have hospital-baseddiagnosis in this baseline of the ZARADEMP project. Nonetheless,
we have shown in the same population a good agreement betweenhome-based diagnosis and hospital-based diagnosis.3 We believe theindividuals excluded from the analysis because of incomplete infor-mation in the brief cognitive test did not influence the main results.In the worst possible hypothesis that all cases of dementia excludedwere misclassified as noncases by the test, and all noncases ofdementia excluded were misclassified as cases by the test, bothsensitivity and PPV would be reduced, but specificity and NPV wouldnot. Specificity and NPV are considered to be the most importantcoefficients for this particular test, which is intended for a first phaseof case-finding processes.
Conclusion
In conclusion (see key points in Box 1), the test based on thecombined use of 2 routine questions about the age and year of birthof individuals, that need no idiomatic adaptation, are commonlyformulated in clinical practice and well accepted by both patients andclinicians, has very good specificity and negative predictive value torule out cases of dementia. These coefficients are better than those inother single-domain ultra-short cognitive tests and the time tocomplete the test is shorter (30 seconds). We therefore believe thatthis test for a first-phase, case-finding of dementia will be useful andused in many settings because it is ultra-short, easy to apply, inex-pensive, and does not involve any physical or psychological burdenfor the patient or the physician.
Acknowledgments
The authors acknowledge the contribution of the lay interviewers,senior medical students, and members of the ZARADEMP Workgroupwho participated in the study.
References
1. Collins PY, Patel V, Joestl SS, et al. Grand challenges in global mental health.Nature 2011;475:27e30.
2. Mitchell SL, Black BS, Ersek M, et al. Advanced dementia: State of the art andpriorities for the next decade. Ann Intern Med 2012;156:45e51.
3. Lobo A, Lopez-Anton R, Santabárbara J, et al. Incidence and lifetime risk ofdementia and Alzheimer’s disease in a Southern European population. ActaPsychiatr Scand 2011;124:372e383.
4. Stephan BC, Kurth T, Matthews FE, et al. Dementia risk prediction in thepopulation: Are screening models accurate? Nat Rev Neurol 2010;6:318e326.
5. Public health planning for dementia must start now. Lancet Neurol 2012;11:477.6. Waldemar G, Phung KT, Burns A, et al. Access to diagnostic evaluation and
treatment for dementia in Europe. Int J Geriatr Psychiatry 2007;22:47e54.7. Brunet MD, McCartney M, Heath I, et al. There is no evidence base for proposed
dementia screening. BMJ 2012;345:e8588.8. Screening for Dementia, Topic Page. June 2003. US Preventive Services Task Force.
Available at: http://www.uspreventiveservicestaskforce.org/uspstf/uspsdeme.htm.AccessedMarch 19, 2013.
9. Brayne C, Fox C, Boustani M. Dementia screening in primary care: Is it time?JAMA 2007;298:2409e2411.

T. Ventura et al. / JAMDA 14 (2013) 627.e7e627.e12627.e12
10. Christensen MD, White HK. Dementia assessment and management. J Am MedDirAssoc 2007;8:e89ee98.
11. Boustani M, Peterson B, Hanson L, et al. Screening for dementia in primarycare: A summary of the evidence for the U.S. Preventive Services Task Force.Ann Intern Med 2003;138:927e937.
12. Iliffe S, Robinson L, Brayne C, et al. Primary care and dementia: 1. diagnosis,screening and disclosure. Int J Geriatr Psychiatry 2009;24:895e901.
13. Holsinger T, Deveau J, Boustani M, Williams JW Jr. Does this patient havedementia? JAMA 2007;297:2391e2394.
14. Russ TC, Shenkin SD, Reynish E, et al. Dementia in acute hospital inpatients:The role of the geriatrician. Age Ageing 2012;41:282e284.
15. Buntinx F, De Lepeleire J, Paquay L, et al. Diagnosing dementia: No easy job.BMC Fam Pract 2011;12:60.
16. Folstein MF, Folstein SE, Mchugh PR. Mini-Mental State. A practical method forgrading the cognitive state of patients for the clinician. J Psychiatr Res 1975;12:189e198.
17. Mitchell AJ, Malladi S. Screening and case finding tools for the detection ofdementia. Part I: Evidence-based meta-analysis of multidomain tests. Am JGeriatr Psychiatry 2010;18:759e782.
18. BrodatyH, LowL,GibsonL,BurnsK.What is thebestdementia screeninginstrumentfor general practitioners to use? Am J Geriatr Psychiatry 2006;14:391e400.
19. Ismail Z, Rajji TK, Shulman KI. Brief cognitive screening instruments: Anupdate. Int J Geriatr Psychiatry 2010;25:111e120.
20. Lobo A, Saz P, Marcos G, et al. [Revalidation and standardization of the cognitionmini-exam (first Spanish version of the Mini-Mental Status Examination) in thegeneral geriatric population]. Med Clin (Barc) 1999;112:767e774. Spanish.
21. Mitchell AJ, Malladi S. Screening and case-finding tools for the detection ofdementia. Part II: Evidence-based meta-analysis of single-domain tests. Am JGeriatr Psychiatry 2010;18:783e800.
22. Lobo A, Saz P, Marcos G, et al. The ZARADEMP Project on the incidence,prevalence and risk factors of dementia (and depression) in the elderlycommunity: II. Methods and first results. Eur J Psychiatry 2005;19:40e54.
23. Copeland JR, Dewey ME, Wood N, et al. Range of mental illness amongst theelderly in the community: Prevalence in Liverpool using the GMS-AGECATpackage. Br J Psychiatry 1987;150:815e823.
24. Lobo A, Saz P, Marcos G, et al. The prevalence of dementia and depression inthe elderly community in a southern European population. The Zaragoza study.Arch Gen Psychiatry 1995;52:497e506.
25. Fletcher RH, Fletcher SW, Wagner EH. Clinical Epidemiology: The Essentials.Philadelphia, PA: Lippincott Williams & Wilkins; 2005.
26. Mitchell AJ, Coyne JC. Do ultra-short screening instruments accurately detectdepression in primary care? A pooled analysis and meta-analysis of 22 studies.Br J Gen Pract 2007;57:144e151.
27. Hirsch C. ACP Journal Club. The Mini-Cog had sensitivity similar to the longer3MS for detecting cognitive impairment or dementia. Ann Intern Med 2012;157:JC4eJC8.
28. Buschke H, Kuslansky G, Katz M, et al. Screening for dementia with thememory impairment screen. Neurology 1999;52:231e238.
29. Kuslansky G, Buschke H, Katz M, et al. Screening for Alzheimer’s disease: Thememory impairment screen versus the conventional three-word memory test.J Am Geriatr Soc 2002;50:1086e10891.
30. Straus SE, Richardson WS, Glasziou P, Haynes RB. Evidence-based Medicine:How to Practice and Teach EBM. 3rd ed. Edinburgh, Scotland: ChurchillLivingstone; 2005.
31. Kansagara D, Freeman M. A Systematic Evidence Review of the Signs andSymptoms of Dementia and Brief Cognitive Tests Available in VA.Washington, DC: Department of Veterans Affairs (US). Available at:http://www.ncbi.nlm.nih.gov/books/NBK49021/; 2010. Accessed March19, 2013.
32. Wilson JM, Jungner YG. Principles and practice of mass screening for disease.Geneva: WHO; 1968.
33. Raymont V, Bingley W, Buchanan A, et al. Prevalence of mental incapacity inmedical inpatients and associated risk factors: cross-sectional study. Lancet2004;364:1421e1427.