Unit 10 MC Malaria RDT QA
30
The US Agency for International Development (USAID) funded MalariaCare under the terms of Cooperative Agreement No. AID-OAA-A-12-00057. The information provided in this presentation does not necessarily reflect the views or positions of USAID or the US Government. TOT: Refresher Training for Malaria Diagnostics Learning Unit 10: Quality Assurance of Malaria RDTs
-
Upload
independent -
Category
Documents
-
view
5 -
download
0
Transcript of Unit 10 MC Malaria RDT QA

The US Agency for International Development (USAID) funded MalariaCare under the terms of Cooperative Agreement No. AID-OAA-A-12-00057. The information provided in this presentation does not necessarily reflect the views or positions of USAID or the US Government.
TOT: Refresher Training for Malaria Diagnostics
Learning Unit 10: Quality Assurance of Malaria RDTs

Outline
2
• RDT implementation overview • Product testing • Lot testing • Field quality assurance and quality control
• RDT job-aids and training
Learning Objectives
3
On completion of this module, participants will be able to: 1.Demonstrate an understanding of the process used in the Malaria RDT WHO Product Testing programme, including:
- Inclusion criteria for manufacturers- Testing against parasite positive and
negative panels 2.Describe the WHO-FIND Lot Testing programme including:
- Why lot testing is necessary- What tests are performed and how to use
the programme3.Explain how community-level QA/QC contributes to maintaining good quality RDT testing by health workers 4.Know the importance of health worker training and the use of appropriate Job Aids

RDT Implementation: Effort and outcomes
4
Good manufacture
Good procurement
Quality control
Training and
supervision
•Save resources•Reduce pressure to drug resistance
• Reduce mortality• Early referral
• Assess impact• Enable planning• Guide elimination
Accurate malaria diagnosis
Know true malaria rates and results
of interventions
Rational use of anti-malarial
drugs (e.g. ACT)
Early recognition
and management of other diseases
Product testing
Lot testing
Job-aids and training

Quality control of malaria RDT results
5
Product Testing
Lot Testing
Job-aids and Training
Field QA/QCPositive control
wells2011
Available
Now
Available
Manufacturer panels
Round 1 (May 2008-9)Round 2 (April 2009-10)Round 3 (April 2010-11)
Available to manufacturers andtest developers through WHO/TDR

Product testing
6
• Evaluates malaria RDTs to produce comparative performance data to guide procurement and use
• Data relevant to performance in all endemic countries
• Forms basis of WHO RDT procurement recommendations
• Starting point for choosing a product: assurance that product can perform sufficiently well

Product testing results
7
Performance against 200 and 2000 para/µL P. falciparum samples
www.wpro.who.int/sites/rdt
False positive rates
Detection rates (Panel detection Score – PDS)
Invalid rate

Laboratory trials vs. field trials: Why base procurement on laboratory-based results?
8
• Product testing in laboratory:– Can control quality of testing, and parasite density
– Direct comparison of many tests on same samples(e.g. PT Round 1: 40 products, > 30000 tests, >130000 bits of data)

9
• Field trials:– Can only compare a few tests,
– Parasite density can not be controlled (therefore, require very high sample population to achieve statistically-significant differences in test performance at different levels of parasite density
– Require PCR as reference standard, as RDTs may out-perform microscopy, in some settings
– Very expensive to do properly
10
• Why do field trials?– Useful for assessing specific questions such as ease of use, use of results, use in pregnancy etc
– Answering local questions on sensitivity in specific populations (rather than primarily comparison of tests)
– On-going monitoring (later…)

Lot testing
11
Product Testing
Lot Testing
Job-aids and Training
Field QA/QCPositive control
wells2011
Available
Now
Available
Manufacturer panels
Round 1 (May 2008-9)Round 2 (April 2009-10)Round 3 (April 2010-11)
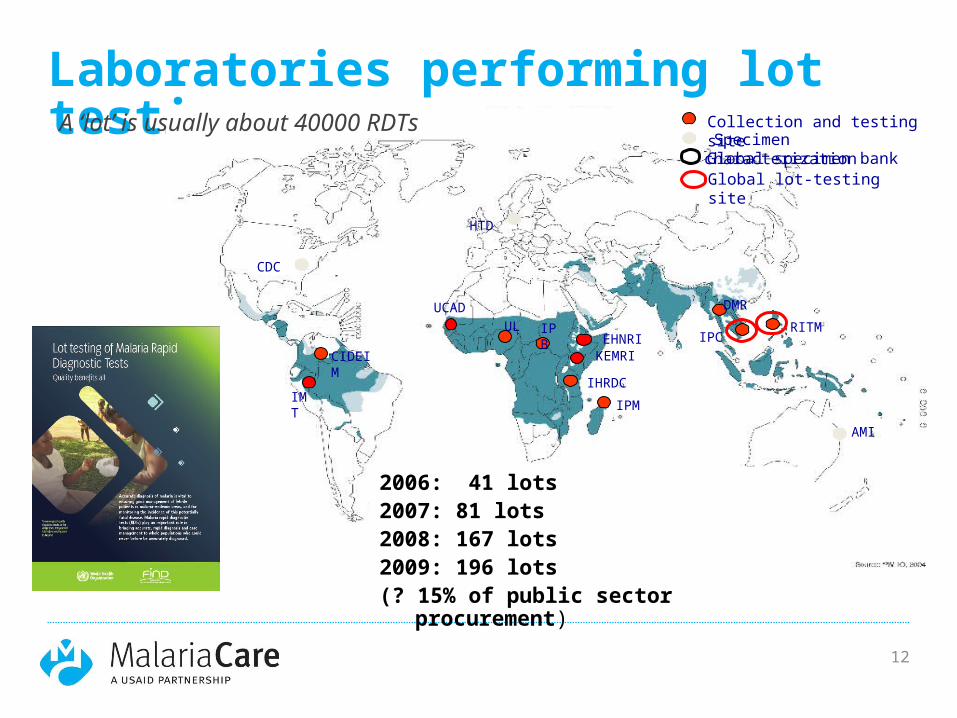
Laboratories performing lot testing
12
Collection and testing site Specimen characterizationGlobal specimen bankGlobal lot-testing site
2006: 41 lots2007: 81 lots2008: 167 lots2009: 196 lots (? 15% of public sector
procurement)
A ‘lot’ is usually about 40000 RDTs
HTD
CDC
UL IPB
RITMIPC
AMI
IHRDCIPM
DMR
CIDEIM
IMT
KEMRIEHNRI
UCAD

Why lot test?
13
• Lot-lot variation noted in most products
• Ensure no damage during transport to country
• Need to convince clinicians / users / regulatory authorities that tests are working

Lot testing requests
14
• WHO-FIND lot testing programme:
• Testing available at no charge through the WHO-FIND network, but sending institution/programme covers cost of RDT shipment to lot-testing lab
• At least 2 weeks prior notice to arrange for testingLot test request form,
obtained fromWHO and FIND: [email protected] nora.champouillon@finddiag
nostics.org

Lot testing procedure
15
Procurement
Release to field
200 para/ul x22000 para/uL x1
x28
Negative x10Report in 5 wk days
200 para/ul x22000 para/uL x1
x6
Negative x2
Report every 6 months
125 Pf RDTs
Country programme
Lot testing lab
Requirements:• 125 Pf RDTs• 175 Pf-pan RDTs
Failures:• Follow re-testing algorithm• Confirm at second lab
End of shelf life
Incubate

Algorithm for lot testing of RDTs
16
QC panels (A & B)PASS
QC panels (A & B) FAIL
discard QC panels
QC panels (A, B, C, D)FAIL
discard QC panels
Test RDTS with more recently prepared QC
panels (If available)(return to top)
If no panel, send RDTS to
confirmatory laboratory
FAIL1) Send out preliminary fail
report2) send RDTS to
confirmatory laboratory
Confirmatory resultsPASS
Confirmatory resultsFAIL
PASS Review Level 1
Laboratory
PASSsend PASS report
report
FAILSend FAIL
PASSsend PASS report
Results suggest two possibilities:1) When prepared QC panels (A&B) had a slightly lower parasite concentration than panels (C&D)2) QC panels (A&B) may have lost some sensitivity since intial
preparation,, but Ag concentration is still adequate enough to be detected by
stock RDTs
QC panels (A,B,C,D)PASS
RDTs tested withPanel A (Pf or Pv): 2 x 200 p/µL, 1 x 5000 p/µL
Panel B (Pf or Pv): 2 x 200 p/µL, 1 x 5000 p/µLPanel C & D For initial testing. 1 x Negative control
Repeat testing with new QC panels (C & D)
QC panels (C & D) FAIL
QC panels (C & D) PASS
PASSsend PASS report
PASS100%
FAILless than 100%
Check QC panels (A & B) areOK with stock RDTS
Check QC panels (A & B) areOK with stock RDTS

Lot test results from (excerpt)
17

% PASS, RITM, IPC, EHNRI lot-testing results (2007-2009)
18
Low failure rate reflects the fact that only 15% of public sector RDTs are being tested, from specific procurers with good procurement policy, and nearly all are products with good performance in product testing
Routine lot-testing
All lot-testing

Future of lot testing
19
• Recombinant antigen lot testing panels
• Stable panels for use at country level
• Available for use in all country programmes
• Accepted common standard for programmes and industry 1 2 3 4 5
6 7 8 9 10Antigen concentration
Antigen types

Field QA/QC
20
Product Testing
Lot Testing
Job-aids and Training
Field QA/QCPositive control
wells2011
Available
Now
Available
Manufacturer panels
Round 1 (May 2008-9)Round 2 (April 2009-10)Round 3 (April 2010-11)

Community-level QA/QC of RDT use and quality
21
• On-site monitoring and supervision1. Check-lists for clinic review
(including waste disposal, storage, record-keeping etc)
2. Observed RDT preparation (following steps of job-aid)
3. Testing against ‘proficiency panels’ of RDT results (photographic quizzes or real RDTs)
4. Review of workplace and safety
• Periodic / focal checking of RDT sensitivity– e.g. Cross-checking against expert
microscopy in sentinel sites (such as those existing for drug efficacy monitoring)

Future of Community level QC: Positive Control Wells
22
• Positive control wells:– Under development by WHO, FIND and partners– Field implementation trials plannedDried
antigen
Water added Contents
placed on RDT
Plastic wells containing stable manufactured parasite antigen, to be diluted with water and placed on an RDT, giving a positive test line if the RDT has good ‘sensitivity’

Quality control of malaria RDTs
23
Product Testing
Lot Testing
Job-aids and Training
Field QA/QCPositive control
wells2011
Available
Now
Available
Manufacturer panels
Round 1 (May 2008-9)Round 2 (April 2009-10)Round 3 (April 2010-11)

Job-aids and training- Zambia
24
Access material: http://www.wpro.who.int/sites/rdt/using_rdts/training/main.htm
http://www.finddiagnostics.org/programs/malaria/find_activities/rdt-job-aids/ QAP, Zambia MoH, WHO, FIND, Malaria
Consortium
- Job-aidSuite of products freely downloaded and assistance for adaptation provided- Proficiency tests - Photographic
result guide - Training manual

2007, Zambia (QAP, URC, Zambia NMCP, WHO, TDR)
25
61%
72%
81%86%
90%96%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Test prep RDT reading
Package directions Job aid only Job aid + training
Harvey SA, et al. Improving community health worker use of malaria rapid diagnostic tests in Zambia: package instructions, job aid and job aid-plus-training. Malar J. 2008 Aug 22;7:160
• Blood safety
• Accuracy• Consisten
cy

Job-aids and training- Zambia12 month follow-up
26
• High retention rates• Good adherence despite low parasite prevalence <5% (currently
being quantified)• Scores for test preparation and interpretation higher after 12
months than at initial training
Zambia NMCP, Malaria Consortium, URC, FIND, WHO, TDR
3 mos (n=62)
6 mos (n=60)
12 mos (n=59)
Mean 87.9% 90.6% 93.4%Median 88.9% 88.9% 94.4%
3 mos (n=62) 6 mos (n=60)
12 mos (n=59)
Mean 88.9% 94.0% 97.0%Median 87.5% 100 % 100%

Use of results in the field…
27
• not always brilliant…• Reyburn et al. 2007 (Tanzania)
– “More than 90% of prescriptions for antimalarial drugs in low-moderate transmission settings were for patients for whom a test requested by a clinician was negative for malaria.”
• Bisoffi et al. 2009 (Burkina Faso)– “In the dry season, 80.8% and 79.8% of patients with a
negative RDT were nevertheless diagnosed and treated for malaria …. an exceedingly and unexpectedly low compliance with the negative test result”.
• …. but successful elsewhere. Why??

Minimum Country Implementation Plan for national programs, funding agencies
28
Timeline for implementation
RDT introduction
Programme planning and managementRegulatory issues
Monitoring and
evaluation
Training and communication
Quality assurance
RDT procurement
and logistics
Couresy: MoH Uganda, WHO
Summary
29
• Buy well:– RDTs vary widely in performance. Products with good sensitivity, specificity, stability are avaialble
• Confirm quality at purchase– Lot-testing of all lots. RDTs are biological tests, and subject to variation in quality at manufacture
• Confirm performance in typical storage conditions– Compare against high-quality microscopy, in selected sites in typical conditions\
• Ensure good preparation and interpretation– Monitor health worker performance

30
• Confirming and demonstrating good performance will:
– Save lives through correct diagnosis and treatment
– Gain and maintain trust of clinicians, health workers and community
– Maintain NMCP morale
Seeing is believing: we need to make the QA programme prominent so that clinicians and patients know that these tests can be relied on. Diagnostic QA is an indispensible part of the malaria programme budget.