TRISTAR SKYLINE MEDICAL CENTER CN2101-003 April 28 ...
489
TRISTAR SKYLINE MEDICAL CENTER CN2101-003 April 28, 2021 PAGE 1 HEALTH SERVICES AND DEVELOPMENT AGENCY MEETING APRIL 28, 2021 APPLICATION SUMMARY NAME OF PROJECT: TriStar Skyline Medical Center PROJECT NUMBER: CN2101-003 ADDRESS: 3441 Dickerson Pike Nashville (Davidson County), TN 37207 LEGAL OWNER: HTI Memorial Hospital Corporation 3441 Dickerson Pike Nashville (Davidson County), TN 37207 OPERATING ENTITY: Not Applicable CONTACT PERSON: Cody Adams, Assistant Administrator TriStar Skyline Medical Center 615-769-7107 DATE FILED: January 15, 2021 PROJECT COST: $5,411,637 FINANCING: Cash Reserves PURPOSE FOR FILING: Initiation of a burn unit DESCRIPTION: TriStar Skyline Medical Center (Skyline) is seeking approval for initiation of a 12- bed burn unit that will be located at the TriStar Skyline Medical Center main campus at 3441 Dickerson Pike, Nashville, Tennessee 37207. 1
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of TRISTAR SKYLINE MEDICAL CENTER CN2101-003 April 28 ...

TRISTAR SKYLINE MEDICAL CENTER CN2101-003
April 28, 2021 PAGE 1
HEALTH SERVICES AND DEVELOPMENT AGENCY MEETING APRIL 28, 2021
APPLICATION SUMMARY NAME OF PROJECT: TriStar Skyline Medical Center
PROJECT NUMBER: CN2101-003 ADDRESS: 3441 Dickerson Pike Nashville (Davidson County), TN 37207 LEGAL OWNER: HTI Memorial Hospital Corporation 3441 Dickerson Pike Nashville (Davidson County), TN 37207 OPERATING ENTITY: Not Applicable CONTACT PERSON: Cody Adams, Assistant Administrator TriStar Skyline Medical Center 615-769-7107 DATE FILED: January 15, 2021 PROJECT COST: $5,411,637 FINANCING: Cash Reserves PURPOSE FOR FILING: Initiation of a burn unit DESCRIPTION: TriStar Skyline Medical Center (Skyline) is seeking approval for initiation of a 12-bed burn unit that will be located at the TriStar Skyline Medical Center main campus at 3441 Dickerson Pike, Nashville, Tennessee 37207.
1

TRISTAR SKYLINE MEDICAL CENTER CN2101-003
April 28, 2021 PAGE 2
SPECIFIC CRITERIA AND STANDARDS REVIEW: BURN UNITS
1. There should be no more than one burn unit bed per 225,000 persons.
This standard may be adjusted to reflect actual incidence in geographical medical service area as documented by the applicant.
Vanderbilt University Medical Center (VUMC) operates the only existing burn unit in this service area which has 25 beds. The applicant’s proposed service area includes 51 counties in Tennessee, and 46 additional counties in Alabama and Kentucky. The Service Area Map (Exhibit 17) for the project is provided below
Source: Original Application Page 55
When the need formula of one bed per 225,000 population is applied to Tennessee (ONLY) counties in the service area there is a need for 24.2 beds based on the 2021 projected population (5,459,036 / 225,000 per bed = 24.26 beds). The 2025 population projection increases to 5,660,589 which supports the need for 25.16 beds in the service area. When this criterion is applied to a Tennessee ONLY service area, it is nearly met in 2021 and is projected to be partially met in 2025 with a need
2

TRISTAR SKYLINE MEDICAL CENTER CN2101-003
April 28, 2021 PAGE 3
for only an additional 0.16 new beds (25.16 bed need in 2025 – 25.0 existing beds), which is less than the 12 additional beds being requested.
Service Area Population and Bed Need Projections Tennessee ONLY Primary and Secondary Service Areas
Service Area 2021 Population
2021 Bed Need per 225,000
2025 Population
2025 Bed Need per 225,000
Beds Available
2025 Bed Need Surplus / Deficit
Primary Service Area (PSA) PSA – Tennessee (51 Counties) 3,508,937 15.6 3,668,534 16.3 25 (8.7) Secondary Service Area (SSA) SSA – Tennessee (27 Counties) 1,950,105 8.7 1,992,055 8.9 0 8.9 TOTAL PSA and SSA (Tennessee Only – 78 Counties)
5,459,042 24.2 5,660,589 25.2 25 0.2
Source: Tennessee Department of Health Population Projections 2018-2030
When the need formula of one bed per 225,000 population is applied to the full Tennessee, Kentucky and Alabama service area there is a need for 33.8 beds based on the 2021 projected population (7,615,770 / 225,000 per bed = 33.8 beds). The 2025 population projection increases to 7,846,715 which supports the need for 34.9 beds in the service area. When this criterion is applied to a the full Tennessee, Kentucky, and Alabama service area, it is met in 2021 and is projected to be met in 2025 with a need for only an additional 9.9 new beds (34.9 bed need in 2025 – 25.0 existing beds), which is less than the 12 additional beds being requested.
Service Area Population and Bed Need Projections
Full Tennessee, Kentucky and Alabama Service Primary and Secondary Service Areas Service Area 2021
Population 2021 Bed Need per 225,000
2025 Population
2025 Bed Need per 225,000
Beds Available
2025 Bed Need Surplus / Deficit
Primary Service Area (PSA) PSA – Tennessee (51 Counties) 3,508,937 15.6 3,668,534 16.3 25 PSA – Alabama (7 Counties) 833,898 3.7 843,915 3.7 0 PSA – Kentucky (39 Counties) 1,070,234 4.7 1,087,560 4.8 0 TOTAL PSA (97 Counties) 5,413,069 24.0 5,600,009 24.9 25 (0.1) Secondary Service Area (SSA) SSA – Tennessee (27 Counties) 1,950,105 8.7 1,992,055 8.9 0 SSA – Kentucky (7 Counties) 252,596 1.1 254,651 1.1 0 TOTAL SSA (34 Counties) 2,202,701 9.8 2,246,706 10.0 0 TOTAL PSA and SSA (Tennessee Only – 78 Counties)
5,459,042 24.3 5,660,589 25.2 25 0.2
TOTAL PSA and SSA (Tennessee, Kentucky and
7,615,770 33.8 7,846,715 34.9 25 9.9
3

TRISTAR SKYLINE MEDICAL CENTER CN2101-003
April 28, 2021 PAGE 4
Alabama – 131 Counties) Source: Tennessee Department of Health Population Projections 2018-2030
The applicant’s projected service area includes 46 counties in Kentucky, but does not include Jefferson County Kentucky, which is the location of the regional burn center at the University of Louisville. The UL facility potentially overlaps with the applicant’s proposed Kentucky service area. The burn center at the University of Louisville increased its bed capacity from 5 to 16 between 2017 and 2018 and was operating at 22.9% occupancy as of 2019. A table with burn unit data for the University of Louisville is provided below and is based on data from the 2014-2019 Kentucky Annual Hospital Utilization and Services Report produced by the Kentucky Cabinet for Health and Family Services, Office of Health Data and Analytics, Division of Analytics. The applicant’s proposed service area also potentially overlaps with the University of Alabama Birmingham (UAB) which operates a (19) bed burn unit located outside of the proposed service area in Birmingham (Shelby County AL). There are additional pediatric burn center beds at the UAB Children’s Hospital (6) and (19) beds at the University of South Alabama in Mobile (Mobile County, AL). Occupany rates could not be determined for the UAB facilities or the University of South Alabama facility by agency staff for this analysis.
University of Louisville Burn Center Beds and Occupancy 2014-2019
County Facilty Type of Service
Licensed Beds
Discharge / Inpatient Days
Licensed Bed Days Open
Licensed Beds % Occupancy
2019 University of Louisville Burn 16 1335 5840 22.9% 2018 University of Louisville Burn 16 1789 5840 30.6% 2017 University of Louisville Burn 5 1455 1825 79.7% 2016 University of Louisville Burn 5 6542 1825 358.5% 2015 University of Louisville Burn 5 3281 1825 179.8% 2014 University of Louisville Burn 5 1705 1825 93.4%
Source: Kentucky Annual Hospital Utilization and Services Report 2014-2019 It appears that this criterion has been partially met.
Note to Agency Members: The applicant provides an extensive criticism and proposed reformulation of the current bed to population standard for burn units from pages 21-31. There is additional
4

TRISTAR SKYLINE MEDICAL CENTER CN2101-003
April 28, 2021 PAGE 5
narrative provided from pages 33-49 to support the applicant’s assertions that:
• There is a large enough population to support more than one burn center in the region.
• There are many patients who meet ICD-10 burn criteria for referral to a burn center who are being service in local hospitals instead.
• There is significant outmigtration of burn patients to other states that can be served in Tennessee.
• The quality of care will be improved over existing services as the applicant is proposing to meet all requirements to become an ABA verified burn center which VUMC is not.
• The applicant has sufficient resources in the areas of local post-discharge comntinuum of care, emergency transportation, local provider outreach and education, to support a regional program of this type.
2. The need shall be based upon the current year's population projected four
years forward. Based upon population projections for 2025 in the project’s Tennessee ONLY
service area there will be a need for 25.16 beds. This support a need for additional beds of 0.16 which is less than the 12 additional beds proposed by the applicant.
Based upon population projections for 2025 in the project’s Tennessee, Kentucky, and Alabama service area there will be a need for 34.9 beds. This support a need for additional beds of 9.9 which is less than the 12 additional beds proposed by the applicant.
It appears that this criterion has been partially met.
3. Each new burn unit proposed shall have a minimum of 12 beds with 6-9 beds designated for adults and 3-6 beds for pediatric patients.
The applicant is proposing to develop a burn unit with 12 beds with 9 beds designated for adults and 3 beds designated for pediatric patients. It appears that this criterion has been met.
4. All existing specialized burn care beds in a service area must have an
annual occupancy rate of 70% before any additional beds are approved.
5

TRISTAR SKYLINE MEDICAL CENTER CN2101-003
April 28, 2021 PAGE 6
Joint Annual Reports (JAR) for the period of 2014-2019 contain two different schedules which reflect burn center utilization. The applicant presents data based upon (Schedule D – Services) in its response to this criterion. For member’s consideration, data from (Schedule G – Utilization) is also included in the analysis below, as the occupancy rates for existing specialized burn care beds in the service area may reflect patients who are not diagnosed with a burn injury. In the case of existing VUMC burn unit beds, the annual occupancy rates using (Schedule D – Services) are much higher - 71.3% in 2019, than when using data from (Schedule G – Utilization), 35.2% in 2019. Data from both Schedule D – Services, and Schedule G – Utilization is presented below for consideration. Schedule D – Services, Item K for each report reflects the Utilization of Services for the 25-bed burn unit at VUMC. Section G – Utilization, Item 2, reflects Utilization by Major Diagnostic Categories. Line #22 of Schedule G reflects the following for individuals admitted or discharged with a burn as their reported diagnosis category:
1. the Number of Admissions or Discharges 2. the Number of Inpatient Days or Discharge Patient Days
Burn Unit Utilization – Vanderbilt University Medical Center
Utilization Data Based on Schedule D – Services of the Joint Annual Report
Vanderbilt Joint Annual Reports of Hospitals (2014-2019) 2014 2015 2016 2017 2018 2019 5-year
% change
5-year CAGR
Burn Unit Admissions 933 860 1,020 1,032 905 901 -3.4% -0.7% Burn Unit Patient Days 6,235 6,125 6,376 6,390 6,694 6,510 4.4% 0.9% Number of Burn Unit Beds 25 25 25 25 25 25 0.0% 0.0% Average Length of Stay (ALOS) 6.7 7.1 6.3 6.2 7.4 7.2 8.1% 1.6% Average Daily Census (ADC) 17.1 16.8 17.5 17.5 18.3 17.8 4.4% 0.9% Burn Unit Occupancy 68.3% 67.1% 69.9% 70.0% 73.4% 71.3% 4.4% 0.9% Source: 2014-2019 Joint Annual Reports of Hospitals
Source: Joint Annual Reports of Hospitals 2014-2019 Section D – Services. Application page 24.
Based upon Schedule D – Services, the Vanderbilt University Medical Center Burn Unit served 901 burn patients for a total of 6,510 patient days in 2019 according to their Joint Annual Report. The average daily census for the 25
6

TRISTAR SKYLINE MEDICAL CENTER CN2101-003
April 28, 2021 PAGE 7
bed VUMC burn unit was 17.8 patients and its annual licensed occupancy rate was 71.3% which is above the 70% threshold for this standard.
Burn Unit Utilization – Vanderbilt University Medical Center
Utilization Data Based on Schedule G – Utilization of the Joint Annual Report
Vanderbilt Joint Annual Reports of Hospitals (2014-2019) 2014 2015 2016 2017 2018 2019 5-year
% change
5-year CAGR
Burn Unit Admissions 355 368 407 398 385 386 8.7% 1.7% Burn Unit Patient Days 3,320 3,417 3,491 3,302 3,250 3,208 -3.3% -0.7% Number of Burn Unit Beds 25 25 25 25 25 25 0.0% 0.0% Average Length of Stay (ALOS) 9.4 9.3 8.6 8.3 8.4 8.3 -11.7% -2.3% Average Daily Census (ADC) 9.1 9.4 9.6 9.2 9.0 8.9 -2.2% -0.7% Burn Unit Occupancy 36.4% 37.4% 38.3% 36.2% 35.6% 35.2% -3.3% -0.7% Source: 2014-2019 Joint Annual Reports of Hospitals
Source: Joint Annual Reports of Hospitals 2014-2019 Section G - Utilization.
Based upon Schedule G – Utilization, the Vanderbilt University Medical Center Burn Unit served 386 burn patients for a total of 3,208 patient days in 2019 according to their Joint Annual Report. The average daily census for the 25 bed VUMC burn unit was 8.8 patients and its annual licensed occupancy rate was 35.2% which is below the 70% threshold for this standard.
It appears that this criterion may be met depending upon the interpretation of VUMC’s annual occupancy rate for its burn unit. i.e. whether to utilize Schedule D or Schedule G of the Joint Annual Reports.
5. Each proposed burn unit should document that a minimum of 50 patients
with a major burn injury to moderate uncomplicated burn injury will be treated each year.
The applicant is projecting that it will serve 212 patients in Year One (2022) increasing by approximately 55.2% to 329 patients in Year Two (2023). It appears that this criterion will be met.
6. Each burn unit shall have availalable, either through direct control or
through a network of clearly identified relationships, a system of transportation sufficient to bring patients to the unit.
The applicant maintains a network relationships with emergency transportation providers including both ground and air transport services in the Tennessee, Kentucky and Alabama service areas.
7

TRISTAR SKYLINE MEDICAL CENTER CN2101-003
April 28, 2021 PAGE 8
It appears that this criterion will be met.
7. A network of relationships should be available to tranport patients to
other units when there are no beds available at a particular site.
The applicant states that its transportation network will be available to transport patients to other units. It appears that this criterion will be met.
CONSTRUCTION, RENOVATION, EXPANSION, AND REPLACEMENT OF HEALTH CARE INSTITUTIONS
1. Any project that includes the addition of beds, services, or medical equipment will be reviewed under the standards for those specific activities.
The application addresses the burn unit standards. It appears that this criterion will be met.
2. For relocation or replacement of an existing licensed health care
institution: a. The applicant should provide plans which include costs for both
renovation and relocation, demonstrating the strengths and weaknesses of each alternative. It appears that this criterion is not applicable.
b. The applicant should demonstrate that there is an acceptable existing
or projected future demand for the proposed project.
It appears that this criterion is not applicable.
3. For renovation or expansions of an existing licensed health care institution: a. The applicant should demonstrate that there is an acceptable existing
demand for the proposed project.
8

TRISTAR SKYLINE MEDICAL CENTER CN2101-003
April 28, 2021 PAGE 9
The applicant discusses the unmet demand in the service area in pages 21-31 and 33-49 of the original application and in the responses to questions 9-27 of Supplemental #1. The applicant’s primary patient base is projected to come from patients who are currently served in local hospitals for burn injuries who meet ICD criteria for referral to a burn center. There is a table on page 27 of Supplemental #1 which details the number of “Service Area Burn Patients Excluding Patients Treated by Vanderbilt or Children Treated at a Pediatric Hospital” which shows 244 patients served in Tennessee in 2019 who met criteria for referral to a burn center but were instead served in a local hospital.
b. The applicant should demonstrate that the existing physical plant's condition warrants major renovation or expansion.
The applicant is proposing to renovate space within an existing ICU to convert it into a burn unit that meets ABA verified burn center standards.
Staff Summary
Note to Agency members: This staff summary is a synopsis of the original application and supplemental responses submitted by the applicant. Any HSDA Staff comments will be presented as a "Note to Agency members" in bold italic.
Application Synopsis TriStar Skyline Medical Center (Skyline) is seeking approval for initiation of a burn unit that will be located at the TriStar Skyline Medical Center main campus at 3441 Dickerson Pike, Nashville, Tennessee 37207. If approved, the applicant plans to initiate the burn unit services in January 2022. Facility Information
• TriStar Skyline Medical Center is a 407 bed acute care, tertiary hospital, an American College of Surgeons (“ACS”) verified Level II trauma center, and a comprehensive stroke center. Currently, Skyline treats burn patients who do not require treatment in a dedicated burn unit or patients with less than moderate to major burn injuries.
• According to the applicant “Skyline recently completed a $69 million expansion that added two floors and 54 additional beds. The project also
9

TRISTAR SKYLINE MEDICAL CENTER CN2101-003
April 28, 2021 PAGE 10
included an expanded ED, additional trauma capacity, and a third helipad which is currently underway. Skyline’s focused tertiary mission and infrastructure provides a foundation for developing a fully integrated, comprehensive burn program.”
• The proposed burn unit will involve the renovation of an existing intensive care unit (ICU) for conversion into a 12-bed burn unit. The 12-bed burn unit will be located on the 2nd Floor of the Hospital and will be 8,994 square feet. It will include 9 beds designated for adults and 3 beds designated for pediatric patients. Renovations are also planned to a 427 square foot debridement/intake room.
• A plot plan and floor plan drawing for the burn unit is included as Attachments A-6B (1) and (2).
According to the 2019 Joint Annual Report, TriStar Skyline Medical Center’s main campus is licensed for 286 beds and staffed for 278 beds. The 2019 licensed bed occupancy was 70.9%, while the staffed bed occupancy was 73.0%. Licensed Beds- The maximum number of beds authorized by the appropriate state licensing (certifying) agency or regulated by a federal agency. This figure is broken down into adult and pediatric beds and licensed isolettes (neonatal intensive or intermediate care isolettes). Staffed Beds-The total number of adult and pediatric beds set up, staffed and in use at the end of the reporting period. This number should be less than or equal to the number of licensed beds. Ownership
• TriStar is wholly owned by HTI Memorial Hospital Corporation. Through subsidiaries, HCA Healthcare, Inc. indirectly owns the applicant’s owner.
• An organizational chart can be found in Attachment A-Project Details-A-4AB, page 114 of the application.
Need Project Need The applicant provides the following justification in the application:
• Existing burn unit beds in the service area are not sufficient to address the needs of the growing population.
• There are limited options for burn patients in East Tennessee, which does not have a burn center.
• The lack of burn center beds leads to the outmigration of patients to other states, or in patients who meet ICD-10 burn referral criteria being treated in non-burn center hospital facilities resulting in a sub-optimal level of
10

TRISTAR SKYLINE MEDICAL CENTER CN2101-003
April 28, 2021 PAGE 11
care.* Data provided by the applicant shows 121 Tennessee service area patients traveling to a burn center in Georgia from 2017-2019. The same table shows no Tennesse patients traveling to a burn center in Kentucky. For more detail regarding the please reference page 35 of the original application as well as pages 13-17 of Supplemental #1.
• There are no ABA verified burn centers in the service area and the applicant will seek ABA verification.
• Burn injury services for residents of the Tennessee service area increased 5.0% from 490 patients in 2017 to 540 in 2019.** *Source: Tennessee, Georgia, and Kentucky State Hospital Associations data set 2017-2019. Supplemental #1 page 17 **Source: Tennessee, Georgia, and Kentucky State Hospital Associations. Supplemental #1 page 14
Service Area Demographics Primary Service Area Skyline’s declared primary service area in Tennessee includes the following 52 counties: Bedford Dickson Jackson Morgan Sumner Benton Fentress Lawrence Overton Trousdale Bledsoe Franklin Lewis Perry Van Buren Cannon Giles Lincoln Pickett Warren Cheatham Grundy Macon Putnam Wayne Clay Hamilton Marion Rhea White Coffee Hardin Marshall Robertson Williamson Cumberland Henry Maury Rutherford Wilson Davidson Hickman Montgomery Sequatchie Decatur Houston Moore Smith DeKalb Humphreys Morgan Stewart Skyline’s declared secondary service area in Tennessee includes the following 27 counties: Anderson Cocke Jefferson Monroe Unicoi Blount Grainger Johnson Polk Union Bradley Greene Knox Roane Washington Campbell Hamblen Loudon Scott Carter Hancock McMinn Sevier Claiborne Hawkins Meigs Sullivan The applicant bases this service area on the the following according to page 53 of its application:
11
TRISTAR SKYLINE MEDICAL CENTER CN2101-003
April 28, 2021 PAGE 12
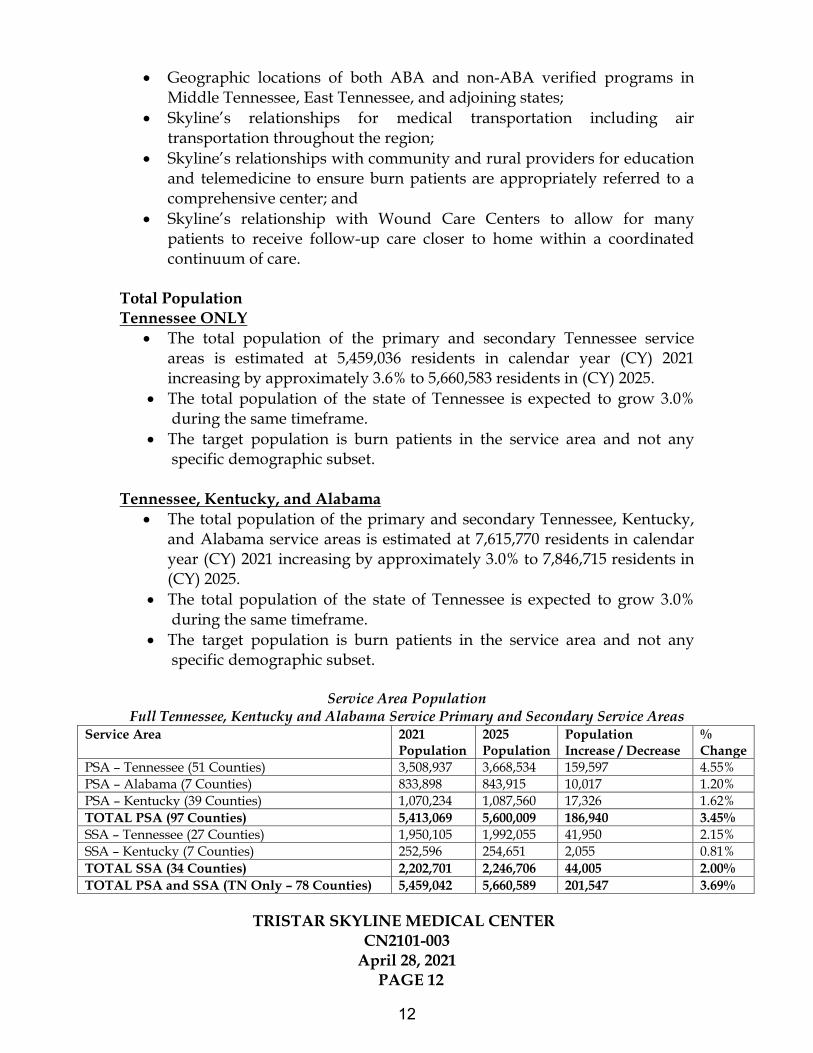
• Geographic locations of both ABA and non-ABA verified programs in Middle Tennessee, East Tennessee, and adjoining states;
• Skyline’s relationships for medical transportation including air transportation throughout the region;
• Skyline’s relationships with community and rural providers for education and telemedicine to ensure burn patients are appropriately referred to a comprehensive center; and
• Skyline’s relationship with Wound Care Centers to allow for many patients to receive follow-up care closer to home within a coordinated continuum of care.
Total Population Tennessee ONLY
• The total population of the primary and secondary Tennessee service areas is estimated at 5,459,036 residents in calendar year (CY) 2021 increasing by approximately 3.6% to 5,660,583 residents in (CY) 2025.
• The total population of the state of Tennessee is expected to grow 3.0% during the same timeframe.
• The target population is burn patients in the service area and not any specific demographic subset.
Tennessee, Kentucky, and Alabama
• The total population of the primary and secondary Tennessee, Kentucky, and Alabama service areas is estimated at 7,615,770 residents in calendar year (CY) 2021 increasing by approximately 3.0% to 7,846,715 residents in (CY) 2025.
• The total population of the state of Tennessee is expected to grow 3.0% during the same timeframe.
• The target population is burn patients in the service area and not any specific demographic subset.
Service Area Population Full Tennessee, Kentucky and Alabama Service Primary and Secondary Service Areas
Service Area 2021 Population
2025 Population
Population Increase / Decrease
% Change
PSA – Tennessee (51 Counties) 3,508,937 3,668,534 159,597 4.55% PSA – Alabama (7 Counties) 833,898 843,915 10,017 1.20% PSA – Kentucky (39 Counties) 1,070,234 1,087,560 17,326 1.62% TOTAL PSA (97 Counties) 5,413,069 5,600,009 186,940 3.45% SSA – Tennessee (27 Counties) 1,950,105 1,992,055 41,950 2.15% SSA – Kentucky (7 Counties) 252,596 254,651 2,055 0.81% TOTAL SSA (34 Counties) 2,202,701 2,246,706 44,005 2.00% TOTAL PSA and SSA (TN Only – 78 Counties) 5,459,042 5,660,589 201,547 3.69%
12

TRISTAR SKYLINE MEDICAL CENTER CN2101-003
April 28, 2021 PAGE 13
TOTAL PSA and SSA (TN, KY and AL – 131 Counties)
7,615,770 7,846,715 230,945 3.03%
Source: Tennessee Department of Health Population Projections 2018-2030 TennCare Population
• The latest 2021 percentage of the Tennessee service area population enrolled in the TennCare program is approximately 20.0%, as compared to the statewide enrollment proportion of 21.8%.
Source: The University of Tennessee Center for Business and Economic Research Population Projection Data Files, Reassembled by the Tennessee Department of Health, Division of Policy, Planning and Assessment, Office of Health Statistics.
Service Area Historical Utilization There are 2 burn centers in Tennessee and only one – Vanderbilt University Medical Center (VUMC) located within the service area of this project. The following tables reflect the burn unit service utilization for VUMC and Regional One Health. The application includes burn-unit utilization data for both VUMC and Regional One Health based on (Section D – Services) of the Joint Annual Reports for each facility from 2014-2019. This data is provided below for reference, but it may represent inflated utilization data based upon the utilization of licensed burn unit beds by non-burn unit patients.
Burn Unit Utilization – Vanderbilt University Medical Center Vanderbilt Joint Annual Respots of Hospitals (2014-2019)
2014 2015 2016 2017 2018 2019 5-year %
change
5-year CAGR
Burn Unit Admissions 933 860 1,020 1,032 905 901 -3.4% -0.7% Burn Unit Patient Days 6,235 6,125 6,376 6,390 6,694 6,510 4.4% 0.9% Number of Burn Unit Beds
25 25 25 25 25 25 0.0% 0.0%
Average Length of Stay (ALOS)
6.7 7.1 6.3 6.2 7.4 7.2 8.1% 1.6%
Average Daily Census (ADC)
17.1 16.8 17.5 17.5 18.3 17.8 4.4% 0.9%
Burn Unit Occupancy 68.3% 67.1% 69.9% 70.0% 73.4% 71.3% 4.4% 0.9% Source: 2014-2019 Joint Annual Reports of Hospitals Source: Joint Annual Reports of Hospitals 2014-2019 Section D – Services. Application page 24.
Burn Unit Utilization – Regional One Health
Regional One Health Joint Annual Respots of Hospitals (2014-2019) 2014 2015 2016 2017 2018 2019 5-year
% change
5-year CAGR
Burn Unit Admissions 279 453 423 566 603 677 142.7% 19.4% Burn Unit Patient Days 3,867 4,364 4,336 4,219 4,318 4,608 19.2% 3.6%
13

TRISTAR SKYLINE MEDICAL CENTER CN2101-003
April 28, 2021 PAGE 14
Number of Burn Unit Beds
14 16 16 14 14 14 0.0% 0.0%
Average Length of Stay (ALOS)
13.9 9.6 10.3 7.5 7.2 6.8 -50.9% -13.3%
Average Daily Census (ADC)
10.6 12.0 11.9 11.6 11.8 12.6 19.2% 3.6%
Burn Unit Occupancy 75.7% 74.7% 74.2% 82.6% 84.5% 90.2% 19.2% 3.6% Source: 2014-2019 Joint Annual Reports of Hospitals Source: Joint Annual Reports of Hospitals 2014-2019 Section D – Services. Application page 24.
The charts above displays the following when using JAR Schedule D – Services for analysis:
• VUMC has exceeded 70% burn unit occupancy from 2017-2019. VUMCs highest level of occupany for burn patients was 2018 at 73.4% occupancy
• Average Length of Stay (+8.1%) and Average Daily Census (+4.4%) both increased from 2014-2019 for the VUMC burn unit. Burn Unit Admissions have decreased (-3.4%) over the same period.
• Average Length of Stay (-50.9%) decreased from 2014-2019 at the Regional One Health burn unit while number of Burn Unit Admissions (+142.7%) and the Average Daily Census (+19.2%) increased over the same period.
Burn Unit Utilization – Vanderbilt University Medical Center
Vanderbilt Joint Annual Reports of Hospitals (2014-2019) 2014 2015 2016 2017 2018 2019 5-year %
change 5-year CAGR
Burn Unit Admissions 355 368 407 398 385 386 8.7% 1.7% Burn Unit Patient Days 3,320 3,417 3,491 3,302 3,250 3,208 -3.3% -0.7% Number of Burn Unit Beds
25 25 25 25 25 25 0.0% 0.0%
Average Length of Stay (ALOS)
9.4 9.3 8.6 8.3 8.4 8.3 -11.7% -2.3%
Average Daily Census (ADC)
9.1 9.4 9.6 9.2 9.0 8.9 -2.2% -0.7%
Burn Unit Occupancy 36.4% 37.4% 38.3% 36.2% 35.6% 35.2% -3.3% -0.7% Source: 2014-2019 Joint Annual Reports of Hospitals Source: Joint Annual Reports of Hospitals 2014-2019 Section G - Utilization
Burn Unit Utilization – Regional One Health
Regional One Health Joint Annual Reports of Hospitals (2014-2019) 2014 2015 2016 2017 2018 2019 5-year %
change 5-year CAGR
Burn Unit Admissions 225 260 220 214 261 283 25.7% 4.7% Burn Unit Patient Days 2,741 3,035 3,152 2,379 2,698 2,791 1.8% 3.6% Number of Burn Unit Beds
14 16 16 14 14 14 0.0% 0.0%
Average Length of Stay (ALOS)
12.2 11.7 14.3 11.1 10.3 9.9 -18.8% -4.1%
14

TRISTAR SKYLINE MEDICAL CENTER CN2101-003
April 28, 2021 PAGE 15
Average Daily Census (ADC)
7.5 8.3 8.6 6.5 7.4 7.6 1.3% 0.3%
Burn Unit Occupancy 53.6% 52.0% 54.0% 46.6% 52.8% 54.6% 1.8% 0.4% Source: 2014-2019 Joint Annual Reports of Hospitals Source: Joint Annual Reports of Hospitals 2014-2019 Section G - Utilization
The charts above displays the following when using JAR Schedule G – Utilization for analysis::
• VUMC has not exceeded 70% burn unit occupancy from 2017-2019. VUMCs highest level of occupany for burn patients was 2016 at 38.3% occupancy
• Average Length of Stay (-11.7%) and Average Daily Census (-2.2%) both decreased from 2014-2019 for the VUMC burn unit. Burn Unit Admissions have increased (+8.7%) over the same period.
• Average Length of Stay (-18.8%) decreased from 2014-2019 at the Regional One Health burn unit while number of Burn Unit Admissions (+25.7%) and the Average Daily Census (+1.3%) increased over the same period.
The applicant provides an analysis of service area trends in admissions for burn diagnoses based upon hospital admission data from Tennessee, Kentucky and Alabama’ State Hospital Assosications.
Service Area Trend in Admissions for Burn Diagnoses Meeting ABA ICD-10 Diagnosis Referral Criteria
Area 2017 2018 2019 2-Year CAGR Primary Service Area 422 489 530 12.1% Secondary Service Area 235 222 228 -1.5% Grand Total 657 711 758 7.4% Source: Tennessee Georgia, and Kentucky State Hospital Associations. Burn Diagnoses Meeting ICD-10 Diagnosis Referral Criteria on page 34 (Exhibit 10) of the original application. Primary Service Area Burn Patients Meeting ICD-10 Burn Criteria by Facility
Type Primary Service Area: 2017 2018 2019 Non-Burn Center Hospital 29.4% 38.0% 29.6% Non-ABA Verified Burn Center 68.7% 60.3% 69.6% Verfied Burn Center 1.9% 1.6% 0.8% Grand Total 100% 100% 100% Source: Tennessee, Georgia, and Kentucky State Hospital Associations. Does not include Alabama data. page 35 (Exhibit 11) of the original application. According to the applicant, 29.9% of burn patients meeting ICD-10 criteria in the primary service area received care at a non-burn center hospital facility in 2019.
Secondary Service Area Burn Patients Meeting ICD-10 Burn Criteria by Facility Type
15

TRISTAR SKYLINE MEDICAL CENTER CN2101-003
April 28, 2021 PAGE 16
Secondary Service Area: 2017 2018 2019 Non-Burn Center Hospital 59.6% 55.4% 57.0% Non-ABA Verified Burn Center 37.9% 42.3% 40.8% Verfied Burn Center 2.6% 2.3% 2.2% Grand Total 100% 100% 100% Source: Tennessee, Georgia, and Kentucky State Hospital Associations. Does not include Alabama data. page 35 (Exhibit 11) of the original application. According to the applicant, 57.0% of burn patients meeting ICD-10 criteria in the secondary service area received care at a non-burn center hospital facility in 2019.
Vanderbilt Estimated Burn Patient Origin (2017-2018)
Middle Tennessee 63.7% Eastern Tennessee 15.9% Central Tennessee 11.2% Midwest US 1.9% Western Tennessee 1.7% Other Southeast Region 1.7% Northern Alabama 1.2% Southeastern Kentucky 1.0% Other Kentucky 0.6% Other Alabama 0.3% Southwest US 0.3% Northeast US 0.1% Western US 0.0% Unknown 0.6% TOTAL 100%
Source: THA data, burn diagnoses *Skyline PSA **Skyline SSA. Supplemental #1 page 5. The applicant provides data on VUMC burn patient origin for the period of 2017-2018 which shows that (90.8%) of patient came from Middle TN (63.7%), Eastern TN (15.9%), and Central Kentucky (11.2%) which are all included in the project’service area. A review of historical utilization of TriStar Skyline Medical Center’s patient origin data demonstrates that the majority of all patients (97% or greater) receiving services at the facility for the period of 2014-2019 were residents of Tennessee, Kentucky or Alabama.
16

TRISTAR SKYLINE MEDICAL CENTER CN2101-003
April 28, 2021 PAGE 17
State 2014 Admissions/ Discharges
Number of Inpatient Days or Discharge Patient Days
% of Admissions/ Discharges by State
% of Patient Days by County
Tennessee 9,953 54,368 91.0% 98.9% Kentucky 708 338 6.5% 0.6% Alabama 14 292 0.1% 0.5% Subtotal 10,675 54,998 97.6% 100.0% Grand Total All Areas Served
10,938 60,163 100.0% 100.0%
CY 2014: Source JAR Facility Report TriStar Skyline Medical Center - Schedule G State 2015 Admissions/
Discharges Number of Inpatient Days or Discharge Patient Days
% of Admissions/ Discharges by State
% of Patient Days by County
Tennessee 10,733 56,912 89.4% 88.3% Kentucky 882 5,514 7.3% 8.6% Alabama 22 113 0.2% 0.2% Subtotal 11,637 62,539 97% 97% Grand Total All Areas Served
12,002 64,461 100% 100%
CY 2015: Source JAR Facility Report TriStar Skyline Medical Center - Schedule G State 2016 Admissions/
Discharges Number of Inpatient Days or Discharge Patient Days
% of Admissions/ Discharges by State
% of Patient Days by County
Tennessee 11,035 60,506 90.3% 90.3% Kentucky 827 4,872 6.8% 7.3% Alabama 21 104 0.2% 0.2% Subtotal 11,883 65,482 97% 98% Grand Total All Areas Served
12,227 67,020 100% 100%
CY 2016: Source JAR Facility Report TriStar Skyline Medical Center - Schedule G State 2017 Admissions/
Discharges Number of Inpatient Days or Discharge Patient Days
% of Admissions/ Discharges by State
% of Patient Days by County
Tennessee 12,034 63,443 92.0% 90.8% Kentucky 819 5,378 6.3% 7.7% Alabama - - 0.0% 0.0% Subtotal 12,853 68,821 98% 98% Grand Total All Areas Served
13,074 69,901 100% 100%
CY 2017: Source JAR Facility Report TriStar Skyline Medical Center - Schedule G
17

TRISTAR SKYLINE MEDICAL CENTER CN2101-003
April 28, 2021 PAGE 18
State 2018 Admissions/
Discharges Number of Inpatient Days or Discharge Patient Days
% of Admissions/ Discharges by State
% of Patient Days by County
Tennessee 11,883 63,861 88.5% 87.4% Kentucky 1,058 6,741 7.9% 9.2% Alabama 30 108 0.2% 0.1% Subtotal 12,971 70,710 97% 97% Grand Total 13,420 73,104 100% 100% CY 2018: Source JAR Facility Report TriStar Skyline Medical Center - Schedule G State 2019 Admissions/
Discharges Number of Inpatient Days or Discharge Patient Days
% of Admissions/ Discharges by State
% of Patient Days by County
Tennessee 12,193 65,984 89.4% 88.7% Kentucky 1,015 6,161 7.4% 8.3% Alabama 32 193 0.2% 0.3% Subtotal 13,240 72,338 97% 97% Grand Total 13,642 74,375 100% 100% CY 2019: Source JAR Facility Report TriStar Skyline Medical Center - Schedule G
Applicant’s Projected Utilization The following chart reflects the projected burn unit admissions in Year 1 and Year 2.
Source: CN2101-003, Supplemental #1 Page 25
Skyline Projected Admissions by Service Area & State Service Area/State Year 1 -
2022 Year 2 - 2023
Year 3 – 2024
Total Admissions Years 1-3
% Change Year 1 – Year 3
% of Total
Primary Service Area Tennessee 71 111 138 320 +94.3% 33.7% Kentucky 46 71 89 206 +93.4% 21.7% Alabama 21 32 38 91 +80.9% 9.5% Secondary Service Area Tennessee 60 94 117 271 +95.0% 28.5% Kentucky 14 21 26 61 +85.7% 6.4%
TriStar Skyline Medical Center-Projected Burn Unit Admissions Year One (2022) % of Total Patients Primary Service Area Tennessee 71 33.4% Kentucky 46 21.7% Alabama 21 10.0% Secondary Service Area Tennessee 60 28.4% Kentucky 14 6.5% Total 212 100.0%
18

TRISTAR SKYLINE MEDICAL CENTER CN2101-003
April 28, 2021 PAGE 19
Total 212 329 408 949 +92.4% 100% Source: CN2101-003, Supplemental #1 Page 27
• The applicant projects 138 patients will be admitted from its primary service area and 74 patients from its secondary service area for a total of 212 patients in Year 1 of the project. 131 (61.7%) of those patients are projected to reside in Tennessee in Year 1 of the project.
• The applicant is projecting a 92.4% increase in admissions from Year 1 of the Project (2022) to Year 3 (2024).
ECONOMIC FEASIBILITY Project Cost The total project cost is $5,411,637. Major costs are:
• Construction Costs - $2,589,367, or 47.8% of project costs. • Mobile Equipment (Fair Market Value) - $1,921,558 or 35.5%% of total
cost. • Contingency Fund - $271,691, or 5.0% of project costs. • Architectural and Engineering Fees - $225,000, or 4.1% of project costs. • For other details on Project Cost, see the Project Cost Chart on page 68 of
the original application. Financing
• A January 6, 2021 letter signed by the CFO of HCA’s TriStar Division – Wes Fountain, confirms that the hospital will fund the proposed project Cash Reserves.
• Review of HCA Healthcare, Inc. Consolidated Balance Sheet for the period ending December 31, 2019 revealed $621,000,000 in cash and cash equivalents, $11,196,000,000 total current assets, total current liabilities of $7,757,000,000 and a current ratio of 1.44 to 1.0.
Note to Agency Members: current ratio is a measure of liquidity and is the ratio of current assets to current liabilities, which measures the ability of an entity to cover its current liabilities with its existing current assets. A ratio of 1:1 would be required to have the minimum amount of assets needed to cover current liabilities. Net Operating Margin Ratio
• The applicant projects a net operating margin ratio for the total facility of 29.6% in Year 1 and 30.1% Year 2.
• The applicant projects a net operating margin ratio for the project only of 30.3% in Year 1 and 37.2% in Year 2.
19

TRISTAR SKYLINE MEDICAL CENTER CN2101-003
April 28, 2021 PAGE 20
Note to Agency Members: The net operating margin demonstrates how much revenue is left over after all the variable or operating costs have been paid. Capitalization Ratio
• The applicant indicated the capitalization ratio for HCA Healthcare, Inc. is -103.25%. The applicant explains this percentage does not accurately reflect its ability to fund the project. For a more detailed explanation, see page 80 in the original application.
The capitalization ratio measures the proportion of debt financing in a business’s permanent financing mix.
Historical Data Chart
• There is no existing burn unit to reference for the Historical Data Chart, but data is provided for the total TriStar Skyline Medical Center facility.
• According to the Historical Data Chart, Skyline experienced a net balance (net operating income – annual capital expenditure) of $63,073,823 for 2017; $54,669,325 for 2018 and $55,505,119 for 2019.
Projected Data Chart Total Facility The Projected Data Chart for Skyline in total reflects $2,793,436,984 in total gross operating revenue in Year 1 increasing by approximately 10.4% to $3,084,384,293 in Year 2. The Projected Data Chart reflects the following:
• Net operating revenue after bad debt, charity care, and contractual adjustments is expected to average approximately 11.4% of gross revenue in Year 1 and 10.9% in Year 2 of the project.
• The net balance is projected to equal $92,124,483 in Year 1 increasing to $98,121,541 in Year 2.
Proposed Burn Unit Project The Projected Data Chart for the applicant’s proposed burn unit reflects $36,734,047 in total gross operating revenue on 212 patient admissions in Year 1 ($173,274/patient) increasing to $61,635,035 on 329 patient admissions in Year 2. The Projected Data Chart reflects the following:
• Net operating revenue after bad debt, charity care, and contractual adjustments is expected to average approximately 17.1% in Year 1 and 16.1% in Year 2 of the proposed project.
• The net balance is projected to equal $1,612,615 in Year 1 increasing to $3,632,842 in Year 2.
20

TRISTAR SKYLINE MEDICAL CENTER CN2101-003
April 28, 2021 PAGE 21
Charges A summary of the applicant’s charges for Year 1 of the project are as follows:
• The proposed average gross charge is $173,274 per burn unit patient in Year 1 and $187,341 in Year 2.
• The average net charge per patient for Year 1 is projected to be $29,717 and $30,198 in Year 2.
Medicare/TennCare Payor Mix • The expected payor mix in Year 1 includes 31.5% for Medicare and 22.7%
for TennCare. • The applicant intends to contract with all TennCare MCOs in the service
area: AmeriGroup, BlueCare, United Healthcare Community Plan, and TennCare Select.
• The projected payor mix in Year 1 is noted in the following table. Projected Burn Unit Service Payor Mix, Year 1
Payor Source Gross Revenue Amount
as a % of Total Gross Revenue
Medicare $11,577,806 31.5% TennCare $8,332,144 22.7% Commercial/Other Managed Care $8,671,243 23.6% Self-pay $3,100,333 8.4% Other: Workers Comp, Champus, HIX, Other Fed
$3,245,661 8.8%
Total Excluding Charity Care $34,927,187 95.1% Charity Care $1,792,380 4.9% Total $36,719,567 100%
Source: CN2101-003, page 81R2 Note to Agency Members: The difference between the total gross revenue in the Projected Data Chart ($36,734,047) and the Projected Burn Unit Service Payor Mix ($36,719,567) is $14,480 from the “Other Operating Revenue – Non-patient income” listed in the Projected Data Chart Totals. PROVIDE HEALTHCARE THAT MEETS APPROPRIATE QUALITY STANDARDS
Licensure
• The Tennessee Department of Health licenses TriStar Skyline Medical Center.
Certification • The applicant is Medicare and TennCare certified.
Accreditation
21

TRISTAR SKYLINE MEDICAL CENTER CN2101-003
April 28, 2021 PAGE 22
• Skyline is accredited by the Joint Commission.
Other Quality Standards • The applicant commits to obtaining and/or maintaining the following:
o Maintaining staffing comparable to the staffing chart presented in the CON application.
o Licenses in good standing o TennCare/Medicare certifications o Three years compliance with federal and state regulations o Has not been decertified in last three years o The hospital will be accredited by The Joint Commission. o The applicant will pursue verification through the American Burn
Association (ABA).
CONTRIBUTION TO THE ORDERLY DEVELOPMENT OF HEALTHCARE Agreements
• The applicant is a full service hospital so that a transfer agreement is not needed. • The hospital has discharge relationships with 37 providers which are listed in
Attachment Section B – Orderly Development – 1 Discharge Relationships with Local Facilities..
Impact on Existing Providers • The applicant does not believe there will be any significant competitive
impacts to other burn unit providers if this project is approved. • One page 49 of the original application, the applicant states that its project
will not impact VUMCs program and that its projected utilization data submitted in the application assume that it will not capture service area patients who have historically sought care at VUMC or who have gone through pediatric hospitals. The applicant states that its patients will be drawn from individuals who received burn care in local non-burn center hospitals who will be better served at a comprehensive burn program.
• The applicant provides analyis of two other burn centers in the region – Regional One Health in Shelby County and the University of Louisville to demonstrate that service area residents for this project only comprised 1.3% of Regional One’s burn patients and 15.4% of the University of Lousville’s patients.* *Source: Supplemental #1 page 20. Tennessee Hospital Association and Kentucky Hospital Association burn diagnoses data.
Staffing
22

TRISTAR SKYLINE MEDICAL CENTER CN2101-003
April 28, 2021 PAGE 23
The applicant provided the facility staffing complement in the table on page 82R2 of the original application. As noted in the table, total direct patient care in Year 1 is expected to be as follows:
• 11.2 FTE RNs • 0.6 FTE Pharmacy • 0.6 FTE Lab Technician • 0.6 FTE Imaging • 1.2 FTE Therapists • 0.6 FTE Respiratory Therapy • 2.2 FTE Surgical Techs • 0.2 Child Life Specialist
• 17.2 Total Direct Care FTEs
• 1.0 FTE VP of Burn Operations • 1.0 FTE Burn Resitry/PI • 2.0 Total Non-Patient Care Staff Positions • 19.2 FTE Total Staff
Note to Agency Members: One FTE means an employee who works 2,080 regular hours per year.
The applicant has submitted the required information on corporate documentation, title and deeds, leases, and professional service agreement. Staff will have a copy of these documents available for member reference at the meeting. Copies are also available for review at the Health Services and Development Agency's office. Should the Agency vote to approve this project, the CON would expire in three years. CERTIFICATE OF NEED INFORMATION FOR THE APPLICANT: There are no other Letters of Intent, denied applications, pending applications, or Outstanding Certificates of Need for this applicant. HCA has financial interests in this project and the following: Outstanding Certificates of Need TriStar Southern Hills Emergency Department at Antioch, CN1803-017A, has an outstanding Certificate of Need that will expire on August 1, 2021. The project was approved at the June 27, 2018 Agency meeting for the establishment
23

TRISTAR SKYLINE MEDICAL CENTER CN2101-003
April 28, 2021 PAGE 24
of a freestanding satellite emergency department (FSED). It will be operated as an off-campus department of the hospital. The satellite ED with 11 treatment rooms will be located in a newly constructed 12,794 square foot (SF) single story building on a 1.83 acre site west of I-24 Exit 60, on the east side of Cane Ridge Parkway at its intersection with Century Farms Parkway in Antioch (Davidson County). The site will be 7.3 miles southeast of the host hospital, TriStar Southern Hills Medical Center. The estimated project cost was $13,883,982. Project Status Update: Construction is in process and the anticipated date of project completion is April of 2021 with opening expected in June of 2021. Stonecrest Surgery Center, CN1707-023A, has an outstanding Certificate of Need that will expire on June 1, 2022. The project was approved at the October 25, 2017 Agency meeting to establish a multi-specialty ambulatory surgical treatment center (ASTC) with two operating rooms and one procedure room located at an unaddressed site within the campus of StoneCrest Medical Center at 200 StoneCrest Boulevard, Smyrna, (Rutherford County), TN 37167. The estimated project cost was $10,556,553. Project Status Update: After CON was granted and before construction began, Medical Care America, an HCA affiliate, was able to acquire an existing surgery center in Rutherford County. Since that acquisition, StoneCrest has been evaluating whether and to what extent that facility will satisfy StoneCrest’s need for ambulatory surgical facilities at least for the foreseeable future. StoneCrest requested and was granted an extension in March of 2021 to allow additional time to fully evaluate the situation, especially in light of recent pandemic events. Southern Hills Surgery Center, CN1411-047A, has an outstanding Certificate of Need that will expire July 1, 2022. The project was approved at the May 27, 2015 Agency meeting for the relocation of Southern Hills Surgery Center from 360 Wallace Road, Nashville (Davidson County), TN 37211, to leased space in a building to be constructed at an unaddressed site in the northeast corner of the intersection of Old Hickory Boulevard and American Way, Brentwood (Davidson County), TN 37250. The estimated project cost was $17,357,832.00. Project Status Update: Construction is in process. Building shell is completed and buildout is underway with expected completion date in early 2021. TriStar Skyline Medical Center - CN1909-035A for the initiation of mobile positron emission tomography (PET) services up to 2 days a week at the campus of TriStar Skyline Medical Center located at 3441 Dickerson Pike, Nashville (Davidson County), TN 37207. The primary service area includes Cheatham, Davidson, Robertson, Sumner, and Wilson Counties. The applicant is owned by HCA Healthcare, Inc. The estimated project cost is $610,000. Project Status Update: Project was approved January 2020. Services have been implemented as of 10/15/2020. Final project report will be filed.
24

TRISTAR SKYLINE MEDICAL CENTER CN2101-003
April 28, 2021 PAGE 25
CERTIFICATE OF NEED INFORMATION FOR OTHER SERVICE AREA FACILITIES: There are no other Letters of Intent or denied applications for other health care organizations proposing this type of service.
PLEASE REFER TO THE REPORT BY THE DEPARTMENT OF HEALTH, DIVISION OF HEALTH STATISTICS, FOR A DETAILED ANALYSIS OF THE STATUTORY CRITERIA OF NEED, ECONOMIC FEASIBILITY, HEALTH CARE THAT MEETS APPROPRIATE QUALITY STANDARDS, AND CONTRIBUTION TO THE ORDERLY DEVELOPMENT OF HEALTH CARE IN THE AREA FOR THIS PROJECT. THAT REPORT IS ATTACHED TO THIS SUMMARY IMMEDIATELY FOLLOWING THE COLOR DIVIDER PAGE. TPP (4/22/2021)
25

HF-0004 Revised 7/1/2019 1
State of Tennessee Health Services and Development Agency Andrew Jackson Building, 9th Floor, 502 Deaderick Street, Nashville, TN 37243 www.tn.gov/hsda Phone: 615-741-2364 Fax: 615-741-9884
CERTIFICATE OF NEED APPLICATION
SECTION A: APPLICANT PROFILE IDENTIFYING INFORMATION
1. Name of Facility, Agency, or Institution TriStar Skyline Medical Center______________________________________________________________ Name 3441 Dickerson Pike Davidson______________ Street or Route County
Nashville_______________________ TN____ 37207______________ City State Zip Code
Website address: https://tristarhealth.com/locations/tristar-skyline _____________________________ Note: The facility’s name and address must be the name and address of the project and must be consistent with the Publication of Intent.
2. Contact Person Available for Responses to Questions
Cody Adams__________________________________ ______Assistant Administrator_____ Name Title
TriStar Skyline Medical Center____________________ [email protected]__ Company Name Email address 3441 Dickerson Pike_________________ ___Nashville_____ __TN__ ____37207_____ Street or Route City State Zip Code
_Assistant Administrator______________ __615-769-7107______ Association with Owner Phone Number
Please answer all questions on 8½” X 11” white paper, clearly typed and spaced, single sided, in order and sequentially numbered. In answering, please type the question and the response. All questions must be answered. If an item does not apply, please indicate “N/A” (not applicable). Attach appropriate documentation as an Appendix at the end of the application and reference the applicable Item Number on the attachment, i.e., Attachment A.1, A.2, etc. The last page of the application should be a completed signed and notarized affidavit.
26

HF-0004 Revised 7/1/2019 2
3. EXECUTIVE SUMMARY
A. Overview Please provide an overview not to exceed three pages in total explaining each numbered point.
1) Description – Address the establishment of a health care institution, initiation of health services, bed complement changes, and/or how this project relates to any other outstanding but unimplemented certificates of need held by the applicant;
TriStar Skyline Medical Center (“Skyline”) proposes to develop a comprehensive burn program on its campus, and therefore seeks approval for the initiation of a burn unit. The proposed burn unit will involve the conversion of existing ICU beds to dedicated burn unit beds and does not involve a change in the hospital’s total bed complement. The Skyline comprehensive burn program, which will serve primarily the residents of Middle and East Tennessee as well as parts of southern Kentucky and northern Alabama, will address the need in this service area for high-quality, comprehensive burn services offered by a program that is verified by the American Burn Association (“ABA”).
2) Ownership structure;
Skyline is indirectly wholly owned by HCA Healthcare, Inc. (“HCA”). Skyline operates in HCA’s TriStar Division (“TriStar Division”), specifically as part of the TriStar Health network. HCA is one of the nation’s leading providers of healthcare services and is composed of 186 hospitals and more than 2,000 sites of care including surgery centers, freestanding ERs, urgent care centers, diagnostic and imaging centers, walk-in clinics and physician clinics in 21 states and the United Kingdom. With its founding in 1968, Nashville-based HCA created a new model for hospital care in the United States. The facilities within this system collectively benefit from the data and expertise of not only corporate-level resources, but also each of the affiliated facilities.
TriStar Division is composed of a network of 20 hospitals and multiple access points including 11 surgery centers, 22 urgent care centers and 88 physician practices throughout Tennessee, Southern Kentucky, and Northwest Georgia. TriStar Division’s culture is firmly planted in a commitment to provide superior healthcare with warmth and compassion for its patients, colleagues, and communities.
TriStar Division provides the latest in clinical technology and innovative procedures, while delivering the highest quality care. TriStar Division facilities continue to lead the industry with patient safety initiatives and practices grounded in evidence-based medicine while using the most advanced diagnostic tools and innovative treatment modalities to improve outcomes and reduce recovery times. As a research and learning health system, it collects and analyzes data from millions of patient encounters to develop technologies and best practices that improve patient care in the facilities.
The TriStar Health network is the portion of TriStar Division that serves Middle Tennessee and Southern Kentucky and is the largest and most comprehensive healthcare provider in the region. This healthcare network consists of 10 hospitals, 21 imaging centers, 80 physician practices, 4 freestanding ERs, 6 outpatient surgery centers, 15 CareNow® Urgent Care centers and 9 medical parks. The TriStar Health network had over 2.2 million encounters in 2019, including 459,988 ER visits, 60,927 inpatient admissions and 7,087 babies delivered.
27

HF-0004 Revised 7/1/2019 3
Additionally, TriStar Health provides approximately $132 million annually in uncompensated care to the communities it serves.
TriStar Health has a number of nationally recognized programs and accredited services throughout its network, including:
Cardiac Care Center Behavioral Health Stroke Care Trauma Services Pediatrics Obstetrics Oncology Research and Services
All seven Middle Tennessee TriStar Health hospitals were awarded an ‘A’ in the spring 2020 Leapfrog Hospital Safety Grade, a national distinction recognizing TriStar Health’s achievements providing safer health care. TriStar Health is committed to raising the bar by investing in new construction, campus expansion projects and the addition of new technology and services. A recent example of this commitment is its collaboration with Belmont University to establish a new College of Medicine in Nashville contributing HCA’s experience as a leading provider of graduate medical education nationally as well as TriStar Health’s local clinical expertise to address the growing shortage of physicians in the United States.
3) Service area;
As a regional service, Skyline anticipates that its comprehensive burn program will treat patients from a broad area. The primary service area consists of 51 counties in Middle Tennessee, 39 counties in southern Kentucky, 7 counties in northern Alabama; and the secondary service area consists of 27 counties in East Tennessee and 7 counties in southeast Kentucky. The service area will be discussed at length below.
4) Existing similar service providers;
The only existing provider of comprehensive burn services in the geographically broad service area is Vanderbilt University Medical Center (“VUMC”), which is not an ABA-verified burn center. For its burn unit, VUMC has not had direct local competition in Middle Tennessee for 35 years or in East Tennessee for the past several years. As will be discussed, VUMC is well utilized and has reported stable burn volume in recent years. The service area size, the lack of an accessible burn provider in East Tennessee, and the continued population growth warrant an alternative provider of comprehensive burn services. As will be demonstrated, Skyline’s proposed burn center will not negatively impact VUMC’s existing burn program.
5) Project cost; The proposed project involves the development of a comprehensive burn program that will be fully integrated into Skyline’s immediate and long-term facility development plans. The proposed project is estimated to cost $5,411,637.
28

HF-0004 Revised 7/1/2019 4
6) Funding; This project will be funded by HCA, the ultimate parent of Skyline. HCA will finance the proposed project with accumulated reserves. See Attachment Section B – Economic Feasibility-2 for supporting documentation.
7) Financial Feasibility including when the proposal will realize a positive financial margin; and Using reasonable and conservative assumptions, the proposed project is financially feasible as shown in Projected Data Chart in the Economic Feasibility Section, Question 4 of this project. The proposed project will realize a positive financial margin in Year 1.
8) Staffing. As the proposed project is a new service line, Skyline projects an additional 19.2 FTEs will be required for the implementation of the comprehensive burn program. As a reputable provider of healthcare services in the community for over 20 years with a robust human resources department and an existing network of nine other hospitals in the service area, Skyline does not anticipate any issues recruiting the necessary staff to support this project.
B. Rationale for Approval
A certificate of need can only be granted when a project is necessary to provide needed health care in the area to be served, can be economically accomplished and maintained, will provide health care that meets appropriate quality standards, and will contribute to the orderly development of adequate and effective health care in the service area.
Provide a brief description of how the project meets the criteria necessary for granting a CON using the data and information points provided in Section B of the application.
1) Need;
Skyline proposes to renovate existing space in the main hospital to house the comprehensive burn program, including a burn unit with 12 dedicated burn unit beds and dedicated support services such as physical and occupational therapy, wound care, and surgical services, to better serve both Middle and East Tennessee as well as other surrounding communities in Kentucky and Alabama. Skyline has recently completed extensive new construction on its campus and will have the requisite facilities, personnel, and resources to provide high quality burn services. Skyline has determined that access to only one existing provider of complex burn services in Middle Tennessee, VUMC, is not sufficient to address the need for burn care in the service area. The large and growing population of the proposed service area coupled with the high utilization of the existing program merits an alternative provider to meet the needs of burn victims. No burn units exist in Tennessee east of Nashville, leaving patients in many parts of the state, including Chattanooga and Knoxville, with limited options. Residents of Kentucky and northern Alabama will also benefit from the introduction of a second burn center in Nashville.
The Skyline project will satisfy this need in several respects. First, the only existing program in the region is operated by VUMC, and its burn unit beds are well utilized, exceeding 70% occupancy in 2019. An additional program at Skyline will complement
29

HF-0004 Revised 7/1/2019 5
VUMC’s burn program, providing not only needed additional capacity but also critical redundancy for a region that is experiencing tremendous growth in population, an influx of new business and industry, and booming tourism. As Nashville has evolved into a “destination tourism” capital and hosts events like the NFL draft that ballooned the population by 600,000, it also experiences the parallel risk of a catastrophic event. The recent Christmas Day bombing in downtown Nashville could have been one such event if it had occurred during a busy workday or popular tourist time. With only one program serving such a broad geographic area, a single catastrophic event would easily exceed the capacity constraints at VUMC, leaving patients without ready access to comprehensive and complex burn care and compromising patient safety and quality of care. Redundancy for critical tertiary services like trauma and burn prepare the health system in the region for a catastrophic event. Vanderbilt and Skyline both provide complex trauma care, and the addition of a second burn center will further prepare the region.
The utilization projections for the Skyline burn unit, detailed below, demonstrate that Skyline’s proposed beds can reach efficient utilization without materially impacting the existing burn programs and pediatric hospitals serving this patient population. Moreover, through Skyline’s planned education and outreach services relating to burn care, it is expected that patients with moderate to major burns now being served less appropriately in community hospitals will instead be transferred to Skyline for comprehensive treatment. Clinical research documents that more severely burned patients have better outcomes when treated in a comprehensive burn program. Additionally, with a second burn program in-state, more patients can stay within the service area for care instead of out-migrating to Georgia and other more distant states for care.
The purpose of this project is to augment the available resources in the region with a burn program that will operate at the highest standards. American Burn Association (“ABA”) verification is important because it verifies that a burn center is meeting the highest current standards of care for burn-injured patients. Skyline will seek ABA verification for its proposed burn program upon approval. The only ABA-verified burn program in Tennessee is Regional One Health’s Firefighters Burn Center in Memphis, over 200 miles southwest of Nashville, and the occupancy of its burn beds exceeded 90% in 2019. Although VUMC is located in Nashville where Skyline proposes its burn program, the large, growing, and aging population of the service area can support more than one program.
Further, burn patients are unique, representing the most severe model of trauma. This uniqueness necessitates a provider that can offer a full, comprehensive, and integrated continuum of care from the initial trauma response through subsequent inpatient admissions and follow-up outpatient services. As an ABA-certified program, Skyline will be able to offer this full range of services and ensure the highest quality care is provided to all burn patients.
Skyline is a 407-bed acute care, tertiary hospital, an American College of Surgeons (“ACS”) verified Level II trauma center, and a comprehensive stroke center. Currently, Skyline treats burn patients who do not require treatment in a dedicated burn unit or patients with less than moderate to major burn injuries. Skyline has the leadership and clinical staff with burn experience to offer a foundation for the development of a more comprehensive burn program. The only service necessary for providing burn treatment that Skyline does not yet offer is a dedicated burn unit, which necessitates the submission of this application.
Skyline’s location just north of downtown Nashville and along the I-65 and I-24 corridors will allow patients and their family unique access, avoiding downtown congestion and
30

HF-0004 Revised 7/1/2019 6
ensuring convenience as they endure what can often be months and even years of follow-up care. TriStar Health’s hub and spoke health system seeks to ensure patients receive appropriate care close to home. The Skyline burn program will utilize the TriStar network of hospitals throughout Middle Tennessee, Chattanooga, Southern Kentucky, and Northwest Georgia to provide appropriate follow-up care at outpatient wound centers, coordinating with Skyline-based burn and wound experts through the existing telemedicine infrastructure.
Affiliated facilities within HCA operate 15 burn centers across the United States with multiple verified burn centers, including one of the world’s leading burn treatment facilities, Joseph M. Still Burn Center in Augusta, Georgia. Through its affiliation with HCA, Skyline has broad access to the resources and expertise necessary to operate a state-of-the-art, high quality burn program and to meet the needs of Middle and East Tennessee and surrounding communities.
2) Economic Feasibility;
Skyline has access to the resources and knowledge of HCA to develop a comprehensive burn program that will operate in an economically feasible manner. Skyline has the financial resources to undertake the necessary construction, and the expected utilization of Skyline’s burn program, coupled with experience of HCA affiliates in operating other burn programs, will allow the program to operate with a positive operating margin. Moreover, Skyline has and will invest the resources to ensure that its burn program successfully completes the ABA verification process.
3) Quality Standards;
Skyline is committed to the overall quality of care of the patients it serves and is consistently ranked in the top of quality ranking within HCA, particularly for Oncology, Stroke, and Trauma services. Skyline is licensed by the Tennessee Board for Licensing Health Care Facilities, and its license is in good standing.
Skyline is renowned as the first comprehensive stroke center in the state as well as a national leader in neuroscience. Skyline’s operations include an ACS Verified Level II Trauma Center and an Accredited Chest Pain Center with Percutaneous Coronary Intervention or “PCI”, deeming it a leader in providing emergency care. Skyline has developed the first new Level II trauma program in more than 15 years in the state and is one of only four hospitals in Tennessee to have received national recognition. The hospital’s inpatient rehabilitation unit, which will support the proposed burn unit, is accredited by the Commission on Accreditation of Rehabilitation Facilities (“CARF”).
Skyline’s notable awards and recognition include an Outstanding Achievement Award from the Commission on Cancer, Top Performer recognition in Key Quality Measures by the Joint Commission, and notoriety as the only CARF accredited program in Middle Tennessee. Skyline’s 407-bed facility is staffed with over 1,400 employees and 820 credentialed physicians and offers medical and surgical programs including heart and vascular, oncology, orthopedics/spine, and CARF accredited rehabilitation.
All seven Middle Tennessee TriStar Health hospitals, including Skyline, were awarded an ‘A’ in the Spring 2020 Leapfrog Hospital Safety Grade, a national distinction recognizing TriStar Health’s achievements in providing safer health care.
31

HF-0004 Revised 7/1/2019 7
As a system, TriStar Health has a number of nationally recognized programs and accredited services including:
Cardiac Care – TriStar Health is nationally recognized for quality outcomes in
cardiovascular surgery. TriStar Health cardiac surgeons perform the most complex surgeries with success rates above the national average. The cardiac surgery program at TriStar Centennial Medical Center is recognized by the Society of Thoracic Surgeons as being the only program in Tennessee to receive three stars (out of a possible three) in four out of five categories, an achievement very few hospitals across the country have obtained. TriStar Health has a network of over 100 cardiologists in 50 locations who are equipped to offer care ranging from treatment of cardiovascular disease to thoracic surgery. The system has seven accredited chest pain centers within the market.
Stroke Care –TriStar Health has seven primary Stroke Centers, a Comprehensive Stroke Center at Skyline, Neuroscience Centers of Excellence and one of the first and largest tele-neurology networks across three states and over 35 locations.
Oncology - Sarah Cannon Cancer Institute is a cancer research center that also offers integrated cancer treatments with convenient access to cutting-edge therapies in nine locations throughout Middle Tennessee. The network of accredited oncology programs provides a full range of services from diagnosis through survivorship. TriStar Health is a leader in cancer research and provides access to a robust trial menu that investigates more than 200+ unique agents through trials each year, with over 3,000 patients enrolled.
Pediatrics - The Children’s Hospital at TriStar Centennial Medical Center is a comprehensive, multi-disciplinary healthcare facility committed to delivering high-quality care and an exceptional patient experience across more than 20 pediatric specialties and a 24/7 pediatric ER.
Obstetrics - TriStar Health has five locations that offer labor and delivery services
with two Level III NICUs and three Level II NICUs, where pediatricians and neonatologists specialize in Advanced Fetal Medicine.
Trauma - With over 6,000 trauma activations each year, TriStar Health hospitals
offer advanced trauma care for those with life-threatening injuries. TriStar Summit Medical Center, TriStar StoneCrest Medical Center, TriStar Horizon Medical Center and TriStar Hendersonville Medical Center are designated as Level III Trauma, and Skyline is designated as a Level II American College of Surgeons (ACS) verified trauma center.
Behavioral Health - TriStar Health operates five behavioral health hospitals
providing critical access and comprehensive care through a variety of behavioral health specialties, three of which are located in the Nashville market: TriStar Skyline Madison Campus, TriStar Centennial Parthenon Pavilion, and Pinewood Springs. TriStar Skyline Madison Campus is the region's most comprehensive provider of inpatient and outpatient behavioral health. TriStar Centennial Parthenon Pavilion is the first Behavioral Health hospital in Tennessee to have received the Joint Commission advanced certification for dementia and violence prevention.
32

HF-0004 Revised 7/1/2019 8
Pinewood Springs, located in Columbia, TN, is a new free-standing psychiatric facility and was recently opened as a joint venture with Maury Regional Health.
TriStar Health and Skyline’s many accolades are evidence of their commitment to maintaining high quality standards. Skyline commits to maintaining adequate staffing and resources and is committed to treating all patients, regardless of ability to pay. This includes maintaining its TennCare and Medicare certifications. Skyline has maintained and will continue to maintain its compliance with all applicable federal and state regulations. As it relates to the proposed project, Skyline commits to pursuing and anticipates achieving ABA verification to ensure quality of care and will participate in the National Burn Repository.
4) Orderly Development of adequate and effective health care.
This comprehensive burn program will contribute to the orderly development of health services in the region in several ways.
Skyline’s burn program will provide additional needed capacity to serve victims of
burns throughout the region as well as needed redundancy in the event of a catastrophic event. VUMC’s program is currently well utilized.
The development of Skyline’s burn program will positively impact the health system
by becoming the first program to pursue ABA verification in Middle Tennessee. This commitment is consistent with Skyline’s history of clinical leadership in the region, including becoming the state’s first primary stroke center, the state’s first comprehensive stroke center, and most recently the first ACS-verified trauma center in Middle Tennessee. These clinical advancements and consistent commitment to “gold standard” verification have raised the bar and influenced other health systems and hospitals to similarly advance their programs, collectively elevating the overall quality of healthcare in the region and state.
Additionally, Skyline will address access by utilizing its network of hospitals and
wound centers for follow-up care close to home, when appropriate, leveraging its existing telemedicine system to link patients receiving outpatient care in their communities with clinical experts at Skyline. This network of geographically diverse access points is particularly important for burn-injured patients, who require an average of five follow-up visits per year after an inpatient stay at a burn center.
TriStar Division launched an air ambulance service, “SKYLIFE”, in December 2020.
This air ambulance service is provided through a partnership with Global Medical Response, which maintains 37 air ambulances serving the southern region of the United States, including five in East Tennessee, where a significant void in burn services exists.
33

HF-0004 Revised 7/1/2019 9
Skyline is a tertiary hospital providing care to some of the most acutely ill and severely injured in an expanding region. Nearly 50% of Skyline’s patients receive their initial care at outlying hospitals before being transferred to Skyline for a higher level of care. To support this medical complexity and acuity, Skyline has continued to develop needed infrastructure, including a recently completed $69M expansion that added two floors and 54 additional ICU beds. The project also included an expanded emergency department, additional trauma capacity, and a third helipad that is currently under construction. Skyline’s focused tertiary mission and infrastructure provides a natural framework for developing a comprehensive burn program.
TriStar Health recently announced a partnership with Belmont University to start a
new College of Medicine, which will help address the significant physician shortage nationally estimated at between 54,100 and 139,000 physicians by 2033. TriStar Health and Skyline will provide clinical rotations for Belmont University’s medical students and further augment training with critical residencies and fellowships through Graduate Medical Education. Skyline will play an integral role in the training of these new physicians and the burn program will further expand and augment their vital clinical experiences. TriStar Health’s commitment to medical education in part drives its motivation to expand its service offerings such as the proposed comprehensive burn program.
C. Consent Calendar Justification
If Consent Calendar is requested, please provide the rationale for an expedited review. A request for Consent Calendar must be in the form of a written communication to the Agency’s Executive Director at the time the application is filed.
The Applicant is not requesting Consent Calendar scheduling.
34

HF-0004 Revised 7/1/2019 10
4. PROJECT DETAILS
A. Owner of the Facility, Agency or Institution
HTI Memorial Hospital Corporation 615-769-2000______ Name Phone Number 3441 Dickerson Pike______________ Davidson Street or Route County Nashville________________________ ___TN_____ ______37207__________ City State Zip Code
B. Type of Ownership of Control (Check One)
1) 2) 3) 4) 5)
Sole Proprietorship Partnership Limited Partnership Corporation (For Profit) Corporation (Not-for- Profit)
________ ________ ________ ___X____ ________
6)
7) 8) 9)
Government (State of TN or Political Subdivision) Joint Venture Limited Liability Company Other (Specify)_________
_______
_______ _______
_______
Attach a copy of the partnership agreement, or corporate charter and certificate of corporate existence. Please provide documentation of the active status of the entity from the Tennessee Secretary of State’s web-site at https://tnbear.tn.gov/ECommerce/FilingSearch.aspx. Attachment Section A-4AB.
See Attachment Section A-4AB for copies of the Applicant’s corporate documentation.
Describe the existing or proposed ownership structure of the applicant, including an ownership structure organizational chart. Explain the corporate structure and the manner in which all entities of the ownership structure relate to the applicant. As applicable, identify the members of the ownership entity and each member’s percentage of ownership, for those members with 5% ownership (direct or indirect) interest.
TriStar Skyline Medical Center is owned by HTI Memorial Hospital Corporation. The applicant is ultimately owned by HCA Healthcare, Inc. the parent company of HCA. See Attachment Section A-4AB for a copy of Skyline’s organizational chart.
5. Name of Management/Operating Entity (If Applicable)
Not Applicable.______________________________________________________________ Name _________________________________________________ ________________ Street or Route County __________________________________ __________ ________________ City State Zip Code Website address: ___________________________________
For new facilities or existing facilities without a current management agreement, attach a copy of a draft management agreement that at least includes the anticipated scope of management services to be provided, the anticipated term of the agreement, and the anticipated management fee payment methodology and schedule. For facilities with existing management agreements, attach a copy of the fully executed final contract. Attachment Section A-5.
35

11R
6A. Legal Interest in the Site (Check the appropriate line and submit the following documentation) The legal interest described below must be valid on the date of the Agency consideration of the certificate
of need application. ☒
Ownership (Applicant or applicant’s parent company/owner)Submit a copy of the title/deed.
Lease (Applicant or applicant’s parent company/owner) Attach a fully executed lease that includes the terms of the lease and the actual lease expense.
Option to Purchase Attach a fully executed Option that includes the anticipated purchase price
Option to Lease Attach a fully executed Option that includes the anticipated terms of the Option and anticipated lease expense
Other (Specify)
Check appropriate line above: For applicants or applicant’s parent company/owner that currently own the building/land for the project location, attach a copy of the title/deed. For applicants or applicant’s parent company/owner that currently lease the building/land for the project location, attach a copy of the fully executed lease agreement. For projects where the location of the project has not been secured, attach a fully executed document including Option to Purchase Agreement, Option to Lease Agreement, or other appropriate documentation. Option to Purchase Agreements must include anticipated purchase price. Lease/Option to Lease Agreements must include the actual/anticipated term of the agreement and actual/anticipated lease expense. The legal interests described herein must be valid on the date of the Agency’s consideration of the certificate of need application. Response: Please see Attachment Section A-6A for a copy of the deed.
6B. Briefly describe the following and attach the requested documentation on an 8 ½” x 11” sheet of white paper, legibly labeling all requested information.
1) Plot Plan must include:
a) Size of site (in acres)The burn unit will be located on Skyline’s existing campus (approximately 40 acres).
b) Location of structure on the siteSee Attachment Section A-6B-1 for the plot plan.
c) Location of the proposed construction/renovationSee Attachment Section A-6B-1 for the plot plan.
d) Names of streets, roads, or highway that cross or border the siteRoads that cross or border the site:
• 31W/41 (Dickerson Pike)• Old Due West Ave.• Due West Ave. North
Highways that cross or border the site: • Highway 155 (Briley Parkway)• Interstate 65
Supplemental 1 January 28, 2021
36

HF-0004 Revised 7/1/2019 12
2) Floor Plan – If the facility has multiple floors, submit one page per floor. If more than
one page is needed, label each page.
a) Patient care rooms (private or semi-private) b) Ancillary areas c) Equipment areas d) Other (specify)
See Attachment Section A-6B2.
3) Public Transportation Route - Describe the relationship of the site to public transportation routes, if any, and to any highway or major road developments in the area. Describe the accessibility of the proposed site to patients/clients. Response: Skyline is located at the intersection of several major highways: I-24, I-65, 155, 31E, and 31W. There are also several major bus routes that have stops both on and within proximity to the campus. In particular, Bus Route 43 stops at Skyline. See Attachment Section A-6B-3. All combined, the campus and its location offer convenient and uncongested access for those who would typically have to travel into the city or outside of the area for medical care, treatments, and follow-up visits.
Attachment Section A-6B-1 a-d, 6B-2, 6B-3.
7. Type of Institution (Check as appropriate--more than one response may apply) A.
B. C. D. E. F. G.
Hospital (Specify)General Acute Care Ambulatory Surgical Treatment Center (ASTC), Multi-Specialty ASTC, Single Specialty Home Health Agency Hospice Mental Health Hospital Intellectual Disability Institutional Habilitation Facility ICF/IID
__X__ _____ _____ _____ _____ _____ _____
H I. J. K. L.
M.
Nursing Home Outpatient Diagnostic Center Rehabilitation Facility Residential Hospice Nonresidential Substitution-Based Treatment Center for Opiate Addiction Other (Specify)___________
_____ _____ _____ _____ _____ _____
8. Purpose of Review (Check appropriate lines(s) – more than one response may apply)
A. B. C. D. E. F.
Establish New Health Care Institution Change in Bed Complement Initiation of Health Care Service as Defined in TCA 68-11-1607(4) (Specify) Burn Unit_____ Relocation and/or Replacement Initiation of MRI Initiation of Pediatric MRI
_____ _____ __X__ _____ _____ _____
G. H. I. J. K.
MRI Unit Increase Satellite Emergency Department Addition of ASTC Specialty Addition of Therapeutic Catheterization Other (Specify)____________
_____ _____ _____ _____ _____
37

HF-0004 Revised 7/1/2019 13
9. Medicaid/Encore, Medicare Participation
MCO Contracts [Check all that apply] _X_AmeriGroup _X_United Healthcare Community Plan __X_BlueCare _X_TennCare Select
Medicare Provider Number 44-0006_____________________________________
Medicaid Provider Number 044006_______________________________________
Certification Type General Acute Care Hospital__________ If a new facility, will certification be sought for Medicare and/or Medicaid/TennCare? Medicare __Yes __No _X_N/A Medicaid/TennCare __Yes __No _X_N/A
38

HF-0004 Revised 7/1/2019 14
10. A.
Bed Complement Data Please indicate current and proposed distribution and certification of facility beds.
Current
Licensed Beds
Staffed Beds
Proposed *Beds
Approved **Beds
Exempted
TOTAL Beds at
Completion 1) Medical _170___ _170___ _______ _______ _______ _170___ 2) Surgical _______ _______ _______ _______ _______ _______ 3) ICU/CCU 75___ 75___ _______ _______ _______ __75____ 4) Obstetrical _______ _______ _______ _______ _______ _______ 5) NICU _______ _______ _______ _______ _______ _______ 6) Pediatric ___ _______ _______ _______ _______ _______ 7) Adult Psychiatric 84___ 70___ _______ _______ _______ 84___ 8) Geriatric Psychiatric 16___ 16___ _______ _______ _______ 16___ 9) Child/Adolescent Psychiatric 21___ 21___ _______ _______ _______ 21___
10) Rehabilitation 41___ 41___ _______ _______ _______ 41___ 11) Adult Chemical Dependency _______ _______ _______ _______ _______ _______ 12) Child/Adolescent Chemical
Dependency _______ _______ _______ _______ _______ _______ 13) Long-Term Care Hospital _______ _______ _______ _______ _______ _______ 14) Swing Beds _______ _______ _______ _______ _______ _______ 15) Nursing Home – SNF
(Medicare only) _______ _______ _______ _______ _______ _______ 16) Nursing Home – NF
(Medicaid only) _______ _______ _______ _______ _______ _______ 17) Nursing Home – SNF/NF (dually
certified Medicare/Medicaid) _______ _______ _______ _______ _______ _______ 18) Nursing Home – Licensed
(non-certified) _______ _______ _______ _______ _______ _______ 19) ICF/IID _______ _______ _______ _______ _______ _______ 20) Residential Hospice _______ _______ _______ _______ _______ _______
TOTAL _407___ _393___ _______ _______ _______ _407___ *Beds approved but not yet in service **Beds exempted under 10% per 3-year provision
B. Describe the reasons for change in bed allocations and describe the impact the bed change
will have on the applicant facility’s existing services. Not applicable.
C. Please identify all the applicant’s outstanding Certificate of Need projects that have a licensed
bed change component. If applicable, complete chart below.
CON Number(s) CON Expiration
Date Total Licensed Beds
Approved _______N/A_________ _____N/A______ _______N/A________ ___________________ ______________ __________________ ___________________ ____________ __________________ ___________________ ______________ __________________ ___________________ ______________ __________________
39

HF-0004 Revised 7/1/2019 15
11. Home Care Organizations – Home Health Agency, Hospice Agency (excluding Residential Hospice), identify the following by checking all that apply:
Not applicable.
Existing Licensed County
Parent Office
County
Proposed Licensed County
Existing Licensed County
Parent Office
County
Proposed Licensed County
Anderson Lauderdale Bedford Lawrence Benton Lewis Bledsoe Lincoln Blount Loudon Bradley McMinn Campbell McNairy Cannon Macon Carroll Madison Carter Marion Cheatham Marshall Chester Maury Claiborne Meigs Clay Monroe Cocke Montgomery Coffee Moore Crockett Morgan Cumberland Obion Davidson Overton Decatur Perry DeKalb Pickett Dickson Polk Dyer Putnam Fayette Rhea Fentress Roane Franklin Robertson Gibson Rutherford Giles Scott Grainger Sequatchie Greene Sevier Grundy Shelby Hamblen Smith Hamilton Stewart Hancock Sullivan Hardeman Sumner Hardin Tipton Hawkins Trousdale Haywood Unicoi Henderson Union Henry Van Buren Hickman Warren Houston Washington Humphreys Wayne Jackson Weakley Jefferson White Johnson Williamson Knox Wilson Lake
40

HF-0004 Revised 7/1/2019 16
12. Square Footage and Cost Per Square Footage Chart
Unit/Department Existing Location
Existing SF
Temporary Location
Proposed Final
Location
Proposed Final Square Footage
Renovated New Total Burn Unit 2nd floor 8,994 N/A N/A 8,994 N/A 8,994
Debridement/Intake 1st floor 427 N/A N/A 427 N/A 427
Unit/Department GSF Sub-Total
Other GSF Total
Total GSF 9,421 9,421 9,421
*Total Cost $2,589,367 $2,589,367
**Cost Per Square Foot
$274.85 $ 274.85
Cost per Square Foot Is Within Which Range (For quartile ranges, please refer to the Applicant’s Toolbox on
www.tn.gov/hsda)
Below 1st Quartile
Between
1st and 2nd Quartile
Between
2nd and 3rd Quartile
Above 3rd Quartile
Below 1st Quartile
Between
1st and 2nd Quartile
Between
2nd and 3rd Quartile
Above
3rd Quartile
Below 1st Quartile
Between 1st
and 2nd Quartile
Between 2nd
and 3rd Quartile
Above 3rd Quartile
* The Total Construction Cost should equal the Construction Cost reported on line A5 of the Project Cost Chart.
** Cost per Square Foot is the construction cost divided by the square feet. Please do not include contingency costs.
41

HF-0004 Revised 7/1/2019 17
A. Describe the construction and renovation associated with the proposed project. If applicable, provide a description of the existing building, including age of the building, and the use of space vacated due to the proposed project. Skyline opened a $69M expansion in late 2019 that included the addition of 54 new inpatient beds, providing needed capacity that also allows for the development of a comprehensive burn program. An existing 12-bed intensive care unit located directly above the Emergency Department will be retrofitted to accommodate burn patients. The unit will include adjustable acuity bed capabilities, and as required, maintain 3 beds dedicated to pediatric burn patients. The west wing of the unit will be renovated to appropriately serve the pediatric burn population. The adjustable acuity beds will allow the rooms to flex between ICU and med/surg without the patient physically requiring relocation. The unit is a closed unit that will be developed according to ABA standards, including appropriate air flow requirements, whirlpool room and large walk-in shower access. The 12-bed burn unit was previously a Trauma ICU that has relocated to a space adjacent to the ED, allowing for needed additional trauma capacity. The close proximity of the trauma and burn programs allow for natural synergies and continuity of care with common overlap of care of the burn and trauma patients. Ultimately, the burn platform located all within the main hospital provides seamless continuity and comfort for patients who require significant follow-up and familial support. Many burn patients may originate in the emergency department with other clinical needs such as trauma, and there will be a dedicated ambulance bay for burn patients. Emergent burn patients and transfers arriving by ambulance will have their own dedicated entrance that flows directly into Intake/Debridement in a low traffic corner of the current ED. The intake/debridement bay will take over a currently vacant space, and will include a debridement table, med gasses, surgical lighting, and trauma capabilities. An existing operating room (OR #12) will be dedicated to burn cases, ensuring burn and wound patients have timely access to operative services and are cared for in a dedicated environment. OR #12 is the closest operating room to the PACU, allowing for direct access and appropriate separation for infection control purposes. Supporting services will also be developed including outpatient burn services, an outpatient wound clinic, and hyperbaric oxygen treatment. These services will be co-located in a clinic on the first floor, directly across from Outpatient Registration. The first-floor location will provide easy access via the main entrance. This area will be staffed with valet services and include the telemedicine infrastructure for burn/wound specialists to connect with patients and providers in outlying areas so patients can receive follow-up care close to home, when clinically appropriate. The comprehensive burn program has also been incorporated into Skyline’s long-term development and facilities plans.
42

HF-0004 Revised 7/1/2019 18
13. MRI, PET, and/or Linear Accelerator Not applicable. This proposal is for a burn unit and does not involve MRI, PET, or Linear Accelerator services. 1. Describe the acquisition of any Magnetic Resonance Imaging (MRI) scanner that is adding
an MRI scanner in counties with population less than 250,000 or initiation of pediatric MRI in counties with population greater than 250,000 and/or
2. Describe the acquisition of any Positron Emission Tomographer (PET) or Linear Accelerator if initiating the service by responding to the following:
A. Complete the chart below for acquired equipment. – Not applicable.
Linear
Accelerator Mev Types: □ SRS □ IMRT □ IGRT □ Other
□ By Purchase Total Cost*: □ By Lease Expected Useful Life
(yrs)
□ New □ Refurbished □ If not new, how old? (yrs)
MRI Tesla: Magnet: □ Breast □ Extremity □ Open □ Short Bore □ Other
□ By Purchase Total Cost*: □ By Lease Expected Useful Life
(yrs)
□ New □ Refurbished □ If not new, how old? (yrs)
PET □ PET only □ PET/CT □ PET/MRI □ By Purchase Total Cost*: □ By Lease Expected Useful Life
(yrs)
□ New □ Refurbished □ If not new, how old? (yrs)
* As defined by Agency Rule 0720-9-.01(4)(b)
B. In the case of equipment purchase, include a quote and/or proposal from an equipment vendor. In the case of equipment lease, provide a draft lease or contract that at least includes the term of the lease and the anticipated lease payments along with the fair market value of the equipment.
Not applicable.
C. Compare lease cost of the equipment to its fair market value. Note: Per Agency Rule, the
higher cost must be identified in the project cost chart. Not applicable.
43

HF-0004 Revised 7/1/2019 19
D. Schedule of Operations: Not applicable.
Location Days of Operation (Sunday through Saturday)
Hours of Operation (example: 8 am – 3 pm)
Fixed Site (Applicant) Mobile Locations
(Applicant) (Name of Other Location) (Name of Other Location)
E. Identify the clinical applications to be provided that apply to the project.
Not applicable.
F. If the equipment has been approved by the FDA within the last five years provide documentation of the same.
Not applicable.
44

HF-0004 Revised 7/1/2019 20
SECTION B: GENERAL CRITERIA FOR CERTIFICATE OF NEED In accordance with T.C.A. § 68-11-1609(b), “no Certificate of Need shall be granted unless the action proposed in the application for such Certificate is necessary to provide needed health care in the area to be served, can be economically accomplished and maintained, will provide health care that meets appropriate quality standards, and will contribute to the orderly development of health care.” In making determinations, the Agency uses as guidelines the goals, objectives, criteria, and standards provided in the State Health Plan. Additional criteria for review are prescribed in Chapter 11 of the Agency’s Rules, Tennessee Rules and Regulations 01730-11. The following questions are listed according to the four criteria: (1) Need, (2) Economic Feasibility, (3) Quality Standards, and (4) Contribution to the Orderly Development of Health Care. Please respond to each question and provide underlying assumptions, data sources, and methodologies when appropriate.
QUESTIONS NEED
The responses to this section of the application will help determine whether the project will provide needed health care facilities or services in the area to be served. 1. Provide a response to the applicable criteria and standards for the type of institution or
service requested. https://www.tn.gov/hsda/hsda-criteria-and-standards.html
Please see the applicant’s responses below to the applicable criteria and standards as set forth by the by the State Health Planning Division:
Criteria and Standards for Burn Units
1. There should be no more than one burn unit bed for every 225,000 persons. This standard
may be adjusted to reflect actual incidence in a geographical medical service area as documented by the applicant.
The Criteria and Standards for Burn Units indicates that there should be no more than one burn unit bed for every 225,000 persons; however, this criterion also allows for an adjustment to reflect actual incidence in a geographical service area as documented by the applicant. As will be shown, the actual need for burn services warrants adjustment to this standard to reflect actual incidence. The adjustment is supported by actual incidence as shown by the current providers operating in excess of the 70% occupancy criterion stated in the State Health Plan and the national burn data which shows that 27 additional burn beds are needed in the service area. In addition, the need for Skyline’s proposed burn beds is supported by patients in the service area being treated in non-burn unit facilities most likely due to the limited availability of specialized burn beds and the out-migration of burn patients due to the limited access to burn treatment facilities. The baseline criterion of 1 burn bed per 225,000 persons is not supported by empirical data and was created approximately 20 years ago by VUMC, the first burn provider in Tennessee. While the basis for this standard is unknown, national burn data shows that there is a disparity in accessibility to burn services for residents of the South, including Tennessee, Kentucky, and Alabama – the three states where the proposed service area counties are located, thereby further supporting the need for additional burn beds in the service area. When appropriately adjusted to the actual national average bed-to-population ratio, the standard demonstrates that there is a need for 27 additional burn beds in the service area. This adjusted ratio reflects the growing trends in burn utilization and disparities in access to burn services in the services.
45

HF-0004 Revised 7/1/2019 21
To further support this bed need, Skyline will demonstrate that actual service area utilization data reflect a large and growing base of patients in the service area that should be but are not being treated in comprehensive burn programs. Skyline has used current clinical treatment protocols to identify the patients that should be served in a comprehensive burn program who are instead receiving care in community hospitals with limited resources. Additionally, service area patients are out-migrating to Georgia and other distant states for care when they should be able to receive care closer to home. Skyline has quantified the patient base in these situations that it expects to redirect to its comprehensive burn program, and this projected demand coupled with population growth justifies the beds requested in this application. Background and History of the Bed-to-Population Standard The landscape of burn services in Tennessee has changed drastically since the inception of burn services over 20 years ago. The CON Criteria and Standards for Burn Units were developed in the late 1990s from available research at that time. In 2000, there were 5.6 million residents in Tennessee according to the Census Bureau. Led by the growth of Middle Tennessee, the population of Tennessee is estimated to be 6.8 million in 2020. Despite this 20 percent increase in population, the number of dedicated burn beds in Tennessee have decreased with the closure of the burn unit at Erlanger Baroness Medical Center (“Erlanger”) in Chattanooga in 2008 according to an article in The Chattanoogan. Thus, there are currently only two burn units in Tennessee, VUMC in Nashville and Regional One Medical Center (“Regional One”) in Memphis. This limited inventory of burn providers has been the state of burn services in Tennessee for more than 10 years. More specifically, according to the 2019 Joint Annual Reports, Regional One operates 14 burn unit beds and VUMC operates 25 burn unit beds for a total of 39 beds in Tennessee for over a decade. Meanwhile, Nashville and Middle Tennessee have experienced significant growth during this time. The Nashville-Davidson-Murfreesboro Metropolitan Statistical Area (“MSA”) population has increased from 1,593,050 residents in 2010 to 1,871,903 in July 2019, an increase of 17.5%. The 2020 Census is expected to show that Metro Nashville exceeds 2 million residents. State Health Plan Criterion #1 set a target ratio of 1 burn unit bed per 225,000 population (the “burn bed-to-population ratio”), which the criterion also states, “may be adjusted to reflect actual incidence.” This ratio was established some 20 years ago without any documentation of its reasonableness based on empirical data. While the details of the rationale of this criterion are unclear at best, it is important to note that the burn criteria and standards were developed by representatives of VUMC, the only providers of burn services at that time. When determining a bed-to-population ratio, it is good healthcare planning to consider many contributing factors, including incidence rates for burn, admission rates of burn patients, admissions trends to burn centers versus non-burn centers, and average length of stay (“ALOS”). There is no information available regarding which, if any, of these underlying factors were considered at the time the State Health Plan standards were adopted. Evidence Indicates that this Standard is not Justifiable Based on Actual Utilization Present day evidence indicates that the burn bed-to-population ratio is not justifiable in determining the need for burn unit beds in Tennessee. Existing burn unit beds in Tennessee are all well-utilized, and the burn bed-to-population ratio is inconsistent with this empirical data:
46

HF-0004 Revised 7/1/2019 22
The 39 existing burn unit beds in Tennessee would require a population of 8,775,000 under the burn bed-to-population ratio; however, the entire population of Tennessee was estimated at 6,853,435 in 2020.
In 2019, the 39 existing burn unit beds at VUMC and Regional One, which are 30% more than called for under the burn bed-to-population ratio, were all highly utilized.
If the number of existing burn unit beds in 2019 was consistent with the burn bed-to-population ratio, the statewide burn unit beds would need to have been reduced from 39 to 30. As a result:
o The statewide aggregate burn unit bed utilization would have been 101%. o Alternatively, if the beds would have been removed from Regional One until its
utilization exceeded full capacity and the remainder from VUMC, the resulting utilization would have been 100% for Regional One and 93% for VUMC.
The utilization levels resulting from an unadjusted compliance with the State Health Plan ratio as discussed above would have severely stressed the existing burn programs and potentially jeopardized the care available to Tennessee residents. In addition, the utilization of burn services nationally, in Tennessee, and in the service area, continue to increase. Further, ALOS for burn patients has been increasing over time. The burn bed-to-population ratio set forth in the State Health Plan does not reflect the data, current trends, utilization patterns, or ALOS.
Most importantly, the State Health Plan burn criteria are internally inconsistent, further proving that the burn bed-to-population is not reasonable. Specifically, Criterion #4 sets 70% occupancy as a threshold minimum utilization to support the need for an additional burn provider. This criterion is met by VUMC within the service area and by both VUMC and Regional One statewide. However, the total beds operated by these providers exceed the burn bed-to-population ratio as set forth in Criterion #1. In other words, the occupancy rate criterion is met (Criterion #4), but the burn bed-to-population ratio does not even support the existing burn beds that are clearly well utilized. This disconnect further demonstrates that the burn bed-to-population ratio is inaccurate and therefore should be adjusted as allowed for within the criterion. Because the burn bed-to-population ratio is not justified based on publicly available data, standard health planning concepts, and published research, and because Criterion #1 expressly allows for an adjustment to the burn bed-to-population ratio, Skyline has made an appropriate adjustment based on actual incidence and the national incidence rate which accurately reflects the identified need for the proposed project in the service area. The discussion below details the national, regional, and statewide trends in burn services that not only justifies the adjustment to the burn bed-to-population ratio but also supports the overall need for the proposed project.
Trend in Burn Injury Admission
Nearly 500,000 patients in the United States require medical treatment for burn injuries annually. The American Burn Association (ABA) estimates that 30,000 to 40,000 of those patients require acute inpatient hospitalization each year.1 Fortunately, significant advances in the burn care industry have led to improved survival rates among all age groups. In the mid-twentieth century, half of patients with burn wounds in excess of 43% total body surface area (TBSA) would die; now, most patients are expected to survive with burn areas up to 60% or 70% TBSA.2 According to the Center for Disease Control (CDC), national burn-injury admissions have increased over time. See Exhibit 1. The CDC reports approximately 33,500 inpatient admissions
1 https://ameriburn.org/who-we-are/media/burn-incidence-fact-sheet/ 2 AMA J Ethics. 2018;20(6):560-566. doi: 10.1001/journalofethics.2018.20.6.medu1-1806.
47

HF-0004 Revised 7/1/2019 23
in 2018. From 2008 to 2018, there has been a 5.6 percent annual increase in admissions due to burn-related injuries in the United States.
Source: Center for Disease Control
Similarly, the CDC reports an increase in the crude incidence rates for burn-related injury admissions as shown in Exhibit 2.
Source: Center for Disease Control
19,51620,613
25,82327,724 27,413
32,44029,953
32,62733,914
35,51333,514
0
5,000
10,000
15,000
20,000
25,000
30,000
35,000
40,000
2008 2009 2010 2011 2012 2013 2014 2015 2016 2017 2018
Exhibit 1Burn Injury Admissions
6.42 6.72
8.36 8.90 8.73
10.26
9.41 10.17
10.50 10.92
10.24
-
2.00
4.00
6.00
8.00
10.00
12.00
2008 2009 2010 2011 2012 2013 2014 2015 2016 2017 2018
Exhibit 2Burn-Related Injury Admissions: Crude Rate
48

HF-0004 Revised 7/1/2019 24
The national trends for burn injury admissions support the need for additional burn programs to meet the growing, regionalized need for burn care.
Utilization of Tennessee Burn Programs As previously established, there are two current comprehensive burn programs in Tennessee: VUMC and Regional One, and according to their 2019 JARs, VUMC operates 25 burn beds and Regional One operates 14 burn beds, for a total of 39 burn beds in the Tennessee. Erlanger had a burn program; however, this unit closed in 2008. The closure of Erlanger created a reduced capacity to accommodate burn patients during a time of rapid growth in population in Tennessee, generally, and Middle and East Tennessee, specifically. The utilization of Regional One and VUMC is presented below. Over the past five years, the VUMC program has grown at a moderate rate with the driving factor being increasing ALOS. Regional One, by contrast, has experienced significant growth in demand and is now operating at over 90% occupancy. Both programs are well utilized and the average occupancy across both programs is over 80%. The high occupancy rates of the existing burn unit beds at VUMC and Regional One evidence the need for additional burn unit capacity in Tennessee.
Disparities in Access to Dedicated, Verified Burn Care The Southeast U.S. faces disparities in access to burn services geographically and from a travel time perspective. Skyline’s project will address these disparities by increasing access within its proposed service area. The optimal distribution of burn centers has long been debated.3 Several aspects of early post-injury burn care including airway assessment, estimation of burn extent and depth, and initiation of fluid administration are important to initial survival. Errors in estimating burn size and depth made by physicians who are inexperienced with burn care occur commonly at
3 Klein MB, Kramer CB, Nelson J, Rivara FP, Gibran NS, Concannon T. Geographic Access to Burn Center Hospitals. JAMA. 2009;302(16):1774–1781. doi:10.1001/jama.2009.1548
2014 2015 2016 2017 2018 20195-year % Change
5-year CAGR
Burn Unit Admissions 933 860 1,020 1,032 905 901 -3.4% -0.7%Burn Unit Patient Days 6,235 6,125 6,376 6,390 6,694 6,510 4.4% 0.9%Number of Burn Unit Beds 25 25 25 25 25 25 0.0% 0.0%Average Length of Stay (ALOS) 6.7 7.1 6.3 6.2 7.4 7.2 8.1% 1.6%Average Daily Census (ADC) 17.1 16.8 17.5 17.5 18.3 17.8 4.4% 0.9%Burn Unit Percent Occupancy 68.3% 67.1% 69.9% 70.0% 73.4% 71.3% 4.4% 0.9%
Vanderbilt Joint Annual Reports of Hospitals (2014-2019)
Source: 2014-2019 Joint Annual Reports of Hospital
2014 2015 2016 2017 2018 20195-year % Change
5-year CAGR
Burn Unit Admissions 279 453 423 566 603 677 142.7% 19.4%Burn Unit Patient Days 3,867 4,364 4,336 4,219 4,318 4,608 19.2% 3.6%Number of Burn Unit Beds 14 16 16 14 14 14 0.0% 0.0%Average Length of Stay (ALOS) 13.9 9.6 10.3 7.5 7.2 6.8 -50.9% -13.3%Average Daily Census (ADC) 10.6 12.0 11.9 11.6 11.8 12.6 19.2% 3.6%Burn Unit Percent Occupancy 75.7% 74.7% 74.2% 82.6% 84.5% 90.2% 19.2% 3.6%
Regional One Trend in Burn Unit Utilization (2014-2019)
Source: 2014-2019 Joint Annual Reports of Hospital
49

HF-0004 Revised 7/1/2019 25
hospitals, especially those without dedicated burn centers, and may lead to complications associated with either over resuscitation or under resuscitation.4,5 Therefore, timely access to a burn center is vital to burn patients, especially those who are severely burned. In addition, with the increasing complexity of medical and surgical aspects of burn care, there is a need to ensure equitable access to quality definitive care. Published findings from a population-level analysis have highlighted regional disparities in access to burn center care across the United States with the southern region of the country identified as one of the most underserved regions of the country. The lack of access is compounded by the fact that approximately half of these centers are not verified by the ABA. Skyline is committed to completing the ABA-verification process for the proposed burn center in order to ensure that all comprehensive services and quality metrics are in place to treat the vulnerable burn-injured population in the service area. A study was conducted recently by Heather E. Carmichael, MD, a general surgery resident at the University of Colorado School of Medicine, in Aurora.6 The report showed that although only 2.9% of the population was found to live in an area with no verified center within 300 miles, nearly one-fourth of Americans (24.7%) live in areas with low access. Moreover, access was shown to vary dramatically by region, with the southern and western regions having the lowest access to burn center care. According to Dr. Carmichael, however, there were notable differences with respect to these regions. With only 59 adult burn centers verified by the ABA, nearly 25% of Americans currently live in areas with low access, according to research presented at the 2019 Annual Scientific Meeting of the Eastern Association for the Surgery of Trauma.7 Furthermore, when analyzed by region, significant differences were observed. More than 37% of the population in the southern region, for example, was identified as having low access compared with just over 10% in the northeastern region. Tennessee is no exception to this statistic. With the closure of the Erlanger burn program, East Tennessee is especially underserved geographically. As will be discussed, a large percentage of burn centers are self-designated and not verified by the ABA, thus, the quality of care and ability to meet the need for comprehensive, multidisciplinary burn care at non-verified burn centers are not evaluated or independently monitored. In Tennessee, only Regional One has received ABA verification. Within the states containing a portion of the service area, the ABA recognizes the following verified and self-reporting burn centers in Exhibit 3:
4 Berkebile BL, Goldfarb IW, Slater H. Comparison of burn size estimates between prehospital reports and burn center evaluations. J Burn Care Rehabil. 1986;7(5):411-4123639879 5 Hammond JS, Ward CG. Transfer from the emergency room to burn center: errors in burn size estimate. J Trauma. 1987;27(10):1161-11653669110 6 https://www.generalsurgerynews.com/In-the-News/Article/03-19/Where-There-s-Smoke-There-May-Not-Be-a-Burn-Center/54309?sub=AE71C110BFBDFD1E89C24A693D937BA1FDD79031D7BA9664E7D6C12AA1EDB 7 It is acknowledged that since this article was published, the number verified burn centers nationwide has increased due to active efforts undertaken by the Verification Review Committee (VRC) of the ABA. There is still a lack of ABA verified burn centers in the service area.
50

HF-0004 Revised 7/1/2019 26
Exhibit 3 Service Area States Inventory of Burn Centers - 2020
State Verification Reported
Beds State Total
Tennessee Regional One Yes 14
39 Vanderbilt No 25 Kentucky University of Louisville No 16 16 Alabama University of Alabama Birmingham No 19
44 UAB Children’s Hospital No 6 University of South Alabama No 19 Source: ABA website
Exhibit 4 below provides a table presented in a study published in 2009 by The Journal of the American Medical Association (JAMA). The Exhibit shows that the South, specifically including Tennessee, Kentucky, and Alabama, have far less access than other regions both in terms of Ground Transport and Air or Ground Transport. This 2009 study does not consider that Erlanger closed its program, which would significantly reduce even air transport times for East Tennessee.
Exhibit 4
Source: Klein MB, Kramer CB, Nelson J, Rivara FP, Gibran NS, Concannon T. Geographic Access to Burn Center Hospitals. JAMA. 2009;302(16):1774–1781. doi:10.1001/jama.2009.1548. Table 2.
This 2009 JAMA study also analyzed access to ABA-verified and non-verified centers in not only transport times but in terms of beds and programs per 100,000 population. It is important to note that since this article was published, the number of burn centers in the United States, both verified and non-verified, have increased, while the number of burn centers in the service area and Tennessee has decreased. When this study was published, Kentucky had 3 self-reported burn centers; currently, Kentucky only has one non-verified burn center at University of Louisville Hospital in Louisville, located in the northern region of the state. The current inventory of burn centers in the states that are, in part, covered by the service area was presented in Exhibit 3 above.
Only one non-verified center, VUMC, is located in the service area. Regional One is over 200 miles to the west. University of Louisville is over 170 miles to the north and University of Alabama-Birmingham is 192 miles to the south. Only one of these providers is ABA-verified, Regional One.
<= 1 <= 2 <= 1 <= 2United States 41.1 68.5 75.3 96.4Northeast 52.7 83.1 89.9 99.9Midwest 41.8 71.5 77.8 97.1South 27.4 54.8 63.5 96.2
Tennessee 31.9 53.3 62.1 100.0Kentucky 34.2 58.8 73.0 100.0Alabama 22.6 44.4 49.1 97.2
West 52.4 74.6 78.8 92.9
RegionAll Centers (n = 128)
Ground Transport Air or Ground Transport% of Population by Hours in Transit
All Centers (n = 128)
51

HF-0004 Revised 7/1/2019 27
Skyline has replicated the analysis from the 2009 JAMA study with updated population and the current inventory of verified and non-verified centers by region and state based on data from the ABA website. This analysis shows that the South continues to have less access to burn beds than all other regions. Both Tennessee and Kentucky have bed to population ratios less than even the Southern region, which is below the national ratio. While Alabama has a higher rate of beds to population, all of these beds are located in central and southern Alabama with 43% of its beds located on the Gulf coast.
Exhibit 5 Summary of Burn Beds per 100,000 Population - 2020
Region Burn Unit
Beds Population Beds per 100,000
Population United States 2,210 330,342,293 0.67 Northeast 440 63,954,231 0.69 Midwest 274 40,051,405 0.68 Eastern Great Lakes 231 28,471,536 0.81 South 687 118,795,019 0.58 Tennessee 39 6,853,435 0.57 Kentucky 16 4,488,567 0.36 Alabama 53 4,904,805 1.08 West 538 79,070,102 0.68 Source: ABA website, Claritas Spotlight population
This analysis demonstrates the comparative lack of access to dedicated burn unit beds in Tennessee and the service area. Enhancing geographic access through Skyline’s extensive medical transport relationships is a critical component of this project particularly for areas of eastern Tennessee and southeastern Kentucky, which are distant from all existing providers. As will be shown, the lack of geographic access results in greater numbers of patients who should be referred to comprehensive burn programs currently staying in their local community hospitals for care. Please see the “Further Need Discussion Responding to the Criteria and Standards” section below for additional discussion supporting the volume of burn injured patients who should be served in burn center but instead are served in hospitals without such capability. Regardless, This Criterion is Met When the Standard is Appropriately Adjusted
Strict application of the burn bed-to-population ratio results in a 10-bed need in the service area; however, for the reasons above, the burn bed-to-population ratio is unreasonable and masks the true need for burn services in the service area. Nonetheless, the State Health Plan criteria expressly states that this ratio “may be adjusted to reflect actual incidence in a geographic medical service area as documented by the applicant.” As will be shown, when the bed need is adjusted using the national incidence rate as allowed for in Criterion #1, the service area defined by Skyline has a need for 27 burn beds.
Service Area Definition In order to quantify the need for the proposed burn beds in the defined service area, the service area must first be defined. Please see Section B.3 for detailed demographic data related to the proposed service area. Skyline considered a variety of factors in defining its service area, including road travel/transport times, air-transport times and Skyline’s extensive air-transport relationships, locations of existing burn centers, Skyline’s telemedicine and outreach/education footprint, and the types of patients currently accessing comprehensive burn services in the area. Skyline has also considered its relationships with wound care centers in the service area, which
52

HF-0004 Revised 7/1/2019 28
will allow for burn patients to be served locally in their communities for follow up care within the comprehensive continuum of Skyline’s proposed program. Each of these components considered in determining the service area will be discussed in detail. The proposed service area includes a primary service area consisting of 51 counties in Middle Tennessee, 39 counties in southern Kentucky, and 7 counties in northern Alabama; and the secondary service area consists of 27 counties in East Tennessee and 7 counties in southeast Kentucky. The primary service area generally aligns with a 150-mile travel radius around Skyline, recognizing the existing ABA-verified program at Regional One (Firefighters Regional Burn Center) in Memphis to the west, the non-verified program at University of Louisville to the north, and the non-verified program at UAB to the south. Given the complete lack of a burn unit in East Tennessee and southeast Kentucky, the secondary service area extends to the east to increase access to these communities through Skyline’s extensive air medical transport relationships throughout the secondary service area as shown.
53

HF-0004 Revised 7/1/2019 29
Exhibit 6 Driving Distance Radius for ABA-Verified Burn Care
54

30 44819987 v1
Unadjusted Bed-to-Population Standard The following table presents the current and projected need for burn unit beds utilizing the unadjusted burn bed-to-population ratio of 1 bed per 225,000 persons. This analysis demonstrates a need for 10 additional beds in 2025, which Skyline believes to be conservative based on national, regional, and service area trends as demonstrated above.
Source: Tennessee Department of Health Population Projections 2018-2030, Claritas Spotlight Kentucky, and Alabama populations.
Adjustment Warranted as Shown by National Standard As permitted under this criterion, the burn bed-to-population ratio has been adjusted to reflect current national bed-population-ratio. In 2020, there were 2,210 burn unit beds reported to the ABA with an estimated population of 330 million residents. This equates to roughly 1 bed per 150,000 population. Skyline believes this is a reasonable adjustment to the burn bed-to-population ratio. Using the national burn bed-to-population ratio, there is a need in the service area for 27 beds in 2025. This more than supports the need for the proposed 12-bed burn unit.
Other Factors that Influence the Bed Need for the Proposed Project As will be shown, the need for the proposed project is demonstrated by a myriad of factors that cannot be reflected in a simple bed-to-population ratio. The proposed project will increase access to a full range of comprehensive burn care services to a large regional area with insufficient access. Moreover, as will be discussed, bed-to-population ratio does not consider the need for redundancy for burn services, as this critical service must be available to meet high levels of demand, particularly related to catastrophic, burn-related events or burn mass casualty incidents. Available capacity of burn beds is even more important considering that both existing burn programs in the State are well utilized. The 2020 Christmas bombing is an example of an event that could have been catastrophic, potentially resulting in multiple burn-injured patients had the explosion taken place on any other typical day. Based on reported occupancy rate, there are few burn beds in the service area that would have been available to meet the potential sudden increase in demand for burn services.
2021 2025Primary Service Area 5,413,066 5,600,006 Secondary Service Area 2,202,698 2,246,703 Total Service Area 7,615,764 7,846,709 Bed Need at 1 Bed per 225,000 34 35 Less Vanderbilt Beds 25 25Bed Need Surplus (+)/Deficit (-) (9) (10)
Service Area Bed Need at 1 Bed per 225,000 Population
2021 2025Primary Service Area 5,413,066 5,600,006 Secondary Service Area 2,202,698 2,246,703 Total Service Area 7,615,764 7,846,709 Bed Need at 1 Bed per 150,000 51 52 Less Vanderbilt Beds 25 25Bed Need Surplus (+)/Deficit (-) (26) (27)
Service Area Bed Need at 1 Bed per 150,000 Population
55

31 44819987 v1
For more information related to the need for the proposed project, please see the “Further Need Discussion Responding to the Criteria and Standards” section below.
2. The need shall be based upon the current year’s population projected four years forward. As of 2021, there are estimated to be 7,615,764 residents living within the proposed service area, which is projected to increase to 7,846,709 residents in 2025. The 2025 population is four years forward from the submission of this application. See the discussion in response to the first criterion above.
3. Each new burn unit proposed shall have a minimum of 12 beds with 6-9 beds designated for adults and 3-6 beds designated for pediatric patients. Skyline proposes a new burn unit with a minimum of 12 beds, with 9 beds designated for adults and 3 beds designated for pediatric patients. Skyline has extensively analyzed the utilization of burn patients in the service area by age group and has determined that pediatric burn patients, while an important component of comprehensive burn care, comprise a small percentage of the overall burn admissions in the service area. Moreover, pediatric burn patients are appropriately being referred to burn centers at a greater rate than adult patients. For this reason, Skyline will more heavily focus on increasing access to adult service area burn patients, who are either leaving the area for care or being served in their local community hospital when such care does not meet clinically accepted burn referral criteria. The result can be long-term suffering and poor outcomes that could be avoided if patients are appropriately referred to comprehensive burn programs. Throughout this application, Skyline has relied on ICD-10 diagnosis definitions and clinically accepted burn referral criteria and has accessed data from the Tennessee Hospital Association (“THA”), the Kentucky Hospital Association (“KHA”), and the Georgia Hospital Association (“GHA”) to analyze the service area in detail. Similar data is not available for Alabama service area counties. These data demonstrate a significant disparity in access to care for service area residents, especially adults and older adults. Far too many patients are leaving the service area and/or receiving care at hospitals that are not equipped to meet the need of patients requiring comprehensive burn care. These data identified all service area burn admissions in 2019 as shown in Exhibit 7. Referral criteria indicate that all pediatric patients should be referred to a comprehensive burn program. In 2019, 72.2% of pediatric patients were referred to a non-verified burn center and 3.2% were referred to an ABA verified burn center, leaving just 24.6% served in local community hospitals without burn center resources. This small percentage can be better served through education and coordination with community and rural hospitals as well as training and education of appropriate air transport for such patients. Skyline will seek to serve these patients.
Exhibit 7 2019 All Service Area Pediatric Burn Admissions
by Hospital Burn Program Type
Age Non-Burn
Center Hospital Non-Verified Burn Center
Verified Burn Center
Grand Total
0 - 17 24.6% 72.2% 3.2% 100.0% Source: Tennessee, Georgia, and Kentucky State Hospital Associations. Does not include Alabama data.
56

32 44819987 v1
By contrast, adult patients are referred less frequently to a comprehensive burn program. Moreover, adults age 60 and over, who may have other complications and co-morbidities, are referred to a comprehensive burn program at an even lower rate, as shown in Exhibit 8 below. These data demonstrate that 34% of burn patients age 18-59 who meet burn referral criteria are served in local community and rural hospitals instead of being appropriately referred to a comprehensive burn program. Moreover, almost 50% of adults age 60 and over are staying in their local communities at hospitals that are neither ABA verified burn centers or non-verified burn centers. These hospitals do not have the resources including specialized medical staff and a comprehensive continuum of both acute and post-acute services to meet the emergent and ongoing needs of these patients.
Exhibit 8
2019 Service Area Adult Burn Admissions by Hospital Burn Program Type
(Patient Meeting ICD-10 Burn Referral Criteria)
Age Non-Burn Center
Hospital Non-Verified Burn Center
Verified Burn Center
Grand Total
18-59 34.0% 64.8% 1.2% 100.0% 60+ 49.4% 50.0% 0.6% 100.0% Source: Tennessee, Georgia, and Kentucky State Hospital Associations. Does not include Alabama data.
These adult burn patients currently being treated in hospitals without a burn center, along with pediatric patients who are not served at a burn center or pediatric hospital, serve as the base of patients that Skyline proposes to serve through its proposed comprehensive burn program and its extensive linkages to emergency air transport, telemedicine, education and outreach programs, and wound care network.
4. All existing specialized burn care beds in a service area must have an annual occupancy rate of 70 percent before any additional beds are approved. As of 2019, the existing specialized burn care beds in the service area have an annual occupancy of 71.3% according to the existing provider’s 2019 Joint Annual Report (JAR).
Vanderbilt University Medical Center Burn Unit Bed Occupancy
Number of Patients 901 Patient Days 6,510 ALOS 7.2 Average Daily Census 17.8 % Occupancy (25 Burn unit beds) 71.3%
Source: Vanderbilt 2019 JAR
5. Each proposed burn unit should document that a minimum of 50 patients with major burn injury to moderate uncomplicated burn injury will be treated each year.
As shown in the projected utilization analysis below, the proposed burn unit has documented that it projects to treat 212 inpatients in Year 1, 329 inpatients in Year 2, and 408 inpatients in Year 3, with major burn injury to moderate burn injury. These projections exceed the minimum of 50 patients with major burn injury to moderate uncomplicated burn injury each year. In addition, Skyline will serve ongoing patients recovering from burn on an outpatient basis as
57

33 44819987 v1
well as minor burns not requiring admission on an outpatient basis. Finally, Skyline will work with its telemedicine partners to ensure that patients with lower acuity burns served by these community hospitals receive the specialized expertise of Skyline’s comprehensive burn program.
6. Each burn unit shall have available, either through direct control or through a network
of clearly identified relationships, a system of transportation sufficient to bring patients to the unit.
As detailed throughout this application, the Applicant has documented that its proposed burn unit will have available, either through direct control or through a network of clearly identified relationships, a system of transportation sufficient to bring patients to the unit. Namely, the Applicant has a number of medical transport agreements in place, including both ground and air transportation providers. As will be discussed in detail below, Skyline and the TriStar Division have an extensive relationship with emergency air transport organizations throughout the service area, including not only middle Tennessee but also, Kentucky, northern Alabama, and eastern Tennessee. For instance, last year TriStar partnered with Global Medical Response (GMR) to launch its “SKYLIFE” program, providing emergency air transport for all patients in need of such services. TriStar’s existing medical transport relationships will allow for increased access to comprehensive burn care for service area residents ensuring that patients will be referred appropriately as needed for comprehensive burn care.
7. A network of relationships should be available to transport patients to other units when
there are no beds available at a particular site.
A network of relationships is available to transport patients to other units when there are no beds available at the proposed burn unit. Skyline’s relationship with medical transport will ensure that patients in the service area will have access to other burn providers when a bed is not available in the proposed unit.
Further Need Discussion Responding to the Criteria and Standards Although the need for the proposed project is generally supported utilizing the criteria and standards above and Skyline meets all of the Criteria and Standards for Burn Units as set forth in the State Health Plan, it is important to note several other factors that further support the need for the proposed project. These factors are discussed at length below. Need Based on Demand and Burn Patient Care Trends in the Service Area Skyline’s market analysis has identified a large base of burn patients who are not being served appropriately and most proximally. Skyline will develop a program that will serve patients who are traveling outside of the service area for burn treatment or receiving burn care in community hospitals that do not offer a full range of burn services. This market analysis relied on detailed data from THA, KHA, and GHA available at an ICD-10 diagnosis code level to identify patients admitted for burn care following the ABA definitional standards. Patients with follow up or sequel admissions were excluded as well as patients served by other than general acute care hospitals such as rehabilitation, behavioral health, or LTAC hospitals.8 This detailed analysis revealed important trends and service
8 Patients’ needs for subsequent admissions and follow up care for rehabilitation and behavioral health services both inpatient and outpatient is a critical component of comprehensive burn care that Skyline recognizes and will provide; however, for this analysis, Skyline has focused on the utilization of and demand for initial access to burn care services.
58

34 44819987 v1
characteristics that document a need and demand for additional access to comprehensive burn services. Demand for Burn Care is Increasing Exhibit 9 documents an overall increase in admissions for burn injured patients in the service area. In fact, the primary service area demand has increased by 3.8% annually over the last two years. While the secondary service area demand has declined, Skyline has explored access factors that may have contributed to this decline as will be discussed.
Exhibit 9 Service Area Trend in Total Admissions for Burn Diagnoses
Area 2017 2018 2019 2-Year CAGR
Primary Service Area 658 677 709 3.8% Secondary Service Area 333 315 304 -4.5% Grand Total 991 992 1,013 1.1% Source: Tennessee, Georgia, and Kentucky State Hospital Associations. Does not include Alabama data.
When this analysis is focused on patients meeting ABA criteria that would indicate the need for comprehensive burn care services, the trend shows an even more striking increase in demand as shown below in Exhibit 10. See Attachment Section B - Need-1A for a list of the ICD-10 codes and referral criteria identified by the ABA.
Exhibit 10 Service Area Trend in Admissions for Burn Diagnoses
Meeting ABA ICD-10 Diagnosis Referral Criteria Area 2017 2018 2019 2-Year CAGR Primary Service Area 422 489 530 12.1% Secondary Service Area 235 222 228 -1.5% Grand Total 657 711 758 7.4% Source: Tennessee, Georgia, and Kentucky State Hospital Associations. Does not include Alabama data.
This trend contradicts the relatively flat utilization trend experienced by VUMC, the only existing burn program in the service area. This further raises the question of where patients are receiving inpatient care for burn injuries. Service Area Burn Patients Leaving the Area for Burn Care Skyline has identified a sizable number of service area burn patients that are leaving the area for care out of state at distant burn center and non-burn center hospitals. Data from the Georgia Hospital Association allows for analysis of Tennessee and Kentucky patients who are migrating to Georgia hospitals for burn services. Most of these patients are traveling to Doctor’s Hospital of Augusta (BRCA affiliate and ABA-verified center), Grady Hospital in Atlanta (ABA-verified center), and Wellstar Cobb Hospital in Metro Atlanta (non-ABA verified center). In particular, patients from East Tennessee are traveling greater distances into Georgia for care when they could be served closer to home and remain in Tennessee. Outmigration to Georgia is significant, and it is likely that additional patients also were transported to North Carolina, Ohio, Virginia, and other more distant locations for care.
59

35 44819987 v1
Not only are these patients transported and admitted to distant hospitals for their initial burn injury, but also many are traveling this significant distance for follow up services. This travel is time consuming, expensive, and may be nearly an impossible demand on the family and caregivers of a severely burn injured patient. Skyline’s goal is to ensure that these burn victims can receive care at an ABA verified burn center closer to home and receive their follow up care as part of a coordinated comprehensive approach to burn care to the greatest extent possible in their local community. Service Area Burn Patients Are Receiving Care at Hospitals without Burn Programs As the service area includes larger rural areas of Middle and East Tennessee, southern Kentucky and northern Alabama, there are numerous rural and small community hospitals throughout these areas that play an important role in local healthcare but do not provide the comprehensive range of burn services needed to address severe burns or pediatric patients. Failure to refer patients appropriately to burn centers can result in poor outcomes. Exhibit 11 shows that in the primary service area, less than two percent of patients are being served in an ABA-verified center, which is likely because the only provider within the primary service area, VUMC, is not ABA verified. Moreover, approximately 30 percent of patients that should have been served in a comprehensive burn program are being served in non-burn center hospitals including small community and rural hospitals.
Exhibit 11 Primary Service Area Burn Patients
Meeting ICD-10 Burn Criteria by Facility Type Primary Service Area: 2017 2018 2019 Non-Burn Center Hospital 29.4% 38.0% 29.6% Non-Verified Burn Center 68.7% 60.3% 69.6% Verified Burn Center 1.9% 1.6% 0.8% Grand Total 100.0% 100.0% 100.0% Source: Tennessee, Georgia, and Kentucky State Hospital Associations. Does not include Alabama data.
The secondary service area trend is also concerning with respect to access to care as shown in Exhibit 12. While just over 2% of secondary service area patients are admitted to ABA-verified centers, 57% of burn injured patients in this area were cared for in their local and community hospital without burn programs in 2019.
Exhibit 12 Secondary Service Area Burn Patients
Meeting ICD-10 Burn Criteria by Facility Type Facility Type 2017 2018 2019 Non-Burn Center Hospital 59.6% 55.4% 57.0% Non-Verified Burn Center 37.9% 42.3% 40.8% Verified Burn Center 2.6% 2.3% 2.2% Grand Total 100% 100% 100% Source: Tennessee, Georgia, and Kentucky State Hospital Associations. Does not include Alabama data.
60

36 44819987 v1
This analysis confirms the lack of access to care shown by the transport distance maps indicating that secondary service area residents are not within a 150-mile travel radius of any verified or non-verified burn program and completely without reasonable access to care as shown previously on the map provided as Exhibit 6. This includes most of East Tennessee since the closure of Erlanger’s burn program in 2008. As discussed previously under the burn unit criteria, a higher percentage of pediatric patients are being appropriately referred to burn centers and specialized pediatric hospitals; however, the percentage of adult patients served in non-burn center hospitals including local community hospitals is especially large. This is the population that Skyline targets to serve. Research Verifies Better Outcomes for Burn Injured Patients Served at Burn Centers Despite joint referral criteria from the ABA and American College of Surgeons, many severely burn-injured patients are not treated at verified centers with specialized care. This is further supported by multiple research studies. For example, one study analyzed adult patients who sustained burn injuries requiring hospital admission. Of these patients, 70% met ABA referral criteria. 48% of the burns treated entirely at non-burn center hospital met referral criteria but were not transferred. Importantly, all deaths occurring at non-burn center hospitals met the ABA referral criteria.9 Further, a significantly higher percentage of patients with Medicare at non-burn center hospitals were not transferred to a burn center, and a significantly higher percentage of patients were discharged to nursing homes as opposed to home from non-burn center hospitals. It is clear that failure to transfer burn patient to a dedicated burn center can potentially have a negative impact on the patient’s outcome. This is further emphasized in a letter of support written by Sharon Hannan, a service area resident and a burn-injured patient. In her letter, Sharon writes in excruciating detail about her treatment experience with severe burns to her arms, hand, face, neck, and head. After the initial burn, Sharon was brought to the local hospital by EMS. She states that:
“Once they were able to manage my pain, they gave me the option to transfer to a burn center, which was over an hour away, or remain at their facility. At the time I had no idea how severe my injuries were or how much pain and suffering the decision I was making would cause. I opted to receive my care locally so that I would not burden my family and friends who I knew would want to be there to support me.”
While Sharon expresses gratitude for the hospital and its staff which did the best that they could with the knowledge they had to help her, Sharon’s health continued to deteriorate. In her letter, Sharon revisits her painful treatment process while in the hospital and following her discharge home:
“After approximately a month in the hospital and multiple surgeries I was discharged home. Once home my situation became significantly worse. … I became increasingly ill and had difficulty communicating with my surgeon through his office staff. … I was left alone to try and figure out how to salvage my grafts. Dressing changes at home were unbearably painful due to the amount of drainage and dressing adherence to my healthy tissue, yet they were ordered 2x a day. I felt hopeless.”
9 Carter JE, Neff LP, Holmes JH 4th. Adherence to burn center referral criteria: are patients appropriately being referred? J Burn Care Res. 2010 Jan-Feb;31(1):26-30. doi: 10.1097/BCR.0b013e3181cb8efb. PMID: 20061833.
61

37 44819987 v1
Sharon’s burns ultimately healed, and many years later, she became an advocate for other burn survivors. It was then that Sharon realized what could have and should have been done differently in relation to her burn care:
“I also learned about the benefits of working with a trained wound team and why remaining at a hospital without the resources to treat patients with extensive burns was a mistake that I paid for through much pain and suffering. Having an inpatient burn team available to me who coordinated a plan for my outpatient recovery and pain management throughout my care would have reduced my pain and suffering without question.”
Sharon goes on to highlight the benefit the Skyline’s proposed burn program on access to high quality, comprehensive burn care for the community:
“Allowing more hospitals to develop burn programs would positively impact the lives of so many patients and families who have suffered accidents resulting in burns. The fact that this treatment is limited in growing cities like Nashville and patients could suffer just like I did is heartbreaking to me. … As a member of this community, I am grateful that hospitals like TriStar Skyline are willing to make this investment in equipment, training, and personnel to better serve us as our populations and industry’s [sic] grow. Not to mention the benefit to patients in rural areas that TriStar also serves.”
See Attachment Section B - Need-1B for Sharon’s full letter of support along with additional letters. Sharon’s experience is heartbreaking but unfortunately not unique as studies have shown. Many smaller community hospitals serving more rural communities lack education on the implications of failing to transfer burn injured patients to facilities that are better equipped with the expertise to meet their unique needs. Accordingly, these hospitals cannot educate the patient on the importance of treatment in a verified burn center and the potential long-term ramifications of choosing to not be transferred. Skyline is committed to changing this paradigm in the service area. Skyline’s proposed project will help remedy the existing disparities in high-quality burn care in the southern region of the country by offering a verified burn program and engaging in community and patient education that is currently lacking in the service area. Research Also Supports the Need for More Verified Burn Centers Many studies document that treatment of severely burned patients at verified burn centers can improve quality of care. For example, one study documented that while mortality rates related to burn injuries have decreased over time, significant improvements have occurred at verified burn centers while mortality rates at non-designated centers vary widely.10 Although this study was conducted in Canada, the findings are relevant. Regardless, several U.S. studies have demonstrated that patients who receive optimal burn care at verified centers may have a better functional outcome after discharge.11,12
10 Mason, Stephanie A et al. “Trends in the epidemiology of major burn injury among hospitalized patients: A population-based analysis.” The journal of trauma and acute care surgery vol. 83,5 (2017): 867-874. doi:10.1097/TA.0000000000001586 11 American College of Surgeons. Committee on T Resources for optimal care of the injured patient 2006. Chicago, IL.: American College of Surgeons; 2006. 12 Brigham PA, Dimick AR. The evolution of burn care facilities in the United States. J Burn Care Res. 2008;29:248–256.
62

38 44819987 v1
Despite the rise in the number of verified burn centers nationally over the past several years, a high proportion of patients continue to receive care outside of burn centers. This data suggests there are further opportunities to regionalize burn care in comprehensive programs and in so doing, potentially lower burn-related mortality. Skyline will work with its partner Burn and Reconstructive Centers of America (“BRCA”) to meet all criteria to become an ABA burn center. Moreover, Skyline will undertake education and outreach efforts throughout its service area to increase awareness of the benefits of serving burn patients in specialized centers such as Skyline’s proposed unit. There is Enough Demand for More Than One Burn Program in Nashville Economic Growth in Nashville Beyond its booming tourism industry, Nashville’s rapidly growing economy is a strong driving force of corresponding business growth in Tennessee and the southeast region as a whole. Contributing factors to this growth result from a balance of diverse industries such as health care, technology, corporate operations, manufacturing, and supply chain management. Additionally, low unemployment paired with a steady influx of new residents mark Nashville as a favorable target for companies to relocate operations or expand their existing operations— companies such as Amazon, for example, which recently announced a new fulfilment warehouse coming to Nashville. As such, this explosion of economic growth has helped Nashville secure a ranking as one of the top 10 large metro areas for job growth and population growth throughout the previous eight years. In fact, Nashville’s population growth over the last decade directly corresponds to job growth in Nashville, outpacing national numbers, as shown in the table below.13
The booming economy and population growth in Nashville can be seen as a double-edged sword. On one hand, it can lead to a strengthened economy and further metropolitan expansion; on the other hand, a populous environment may result in existing medical services being stretched thin and placing particular pressure on highly specialized medical services. Furthermore, large metropolitan populations coupled with catastrophic events and natural disasters are difficult to navigate and pre-emptively prepare for.
13 https://www.tylercauble.com/blog/new-construction-renovation-and-the-future-for-commercial-real-estate-in-nashville
63

39 44819987 v1
Currently, VUMC is the only burn program supporting a vastly expanding population in Nashville. In the event of a catastrophic incident such as the 2016 Great Smoky Mountains wildfires in Gatlinburg or other burn-related incidents in the service area, some of which have been described herein, those 25 beds can easily reach maximum capacity utilization. A second burn program is justified to minimize burn-related casualties and provide service area residents with adequate specialized burn care. Preparedness for Burn Mass Casualty Incident A burn mass casualty incident (burn MCI) is a disaster that includes patients with burn injuries. A burn MCI can further be defined as any catastrophic event in which the number of burn victims exceeds the capability (resources) of local or regional burn centers to provide optimal burn care. Extensive burns require vast amounts of resources (personnel, equipment, and time). Capability includes availability of burn unit beds, burn surgeons, burn nurses, other support staff, operating rooms, equipment, supplies, and related resources. Despite the infrequent nature of burn disasters, their initial management and the subsequent surge in burn treatment capacity that necessarily follows quickly becomes the greatest challenge for, and potential threat to, a given hospital, health care system, or region. Whether it is a major, isolated fire with multiple burn injuries or a catastrophic widespread burn MCI, it is important that communities are prepared to meet the immediate needs of burn injured patients. This is particularly true for Nashville, as its record-setting tourism, congested and growing metropolitan area, and large and growing population put the city even more at risk for a burn MCI that overwhelms the existing burn program. Below are several examples of major fires that occurred in Nashville and other cities across the nations over the past several years: Community Fires:
NHC Healthcare Center in Nashville – in September 2003, a fire broke out in a second-floor room that caused the death of 8 nursing home residents in Nashville. 82 residents and one nursing home employee were treated for burns and smoke inhalation, and 16 were critically injured. While Vanderbilt accommodated most of these patients, some patients were still served in non-burn center hospitals.
Plane Crash in Nashville – an F-14 Navy fighter jet on a training flight crashed, and a massive fireball erupted on the morning of January 29, 1996. Two crew members were killed, and three people were found dead in the house that was hit by the falling plane. Two other homes also burned. The event could have been significantly worse if the plane had landed in a more populated area like one of the regions dense neighborhoods or crowded business centers.
Seton Hall University Campus in New Jersey – In January 2000, a fatal fire in the freshman dormitory, Boland Hall, resulted in one of the deadliest college fires in recent U.S. history. Three students died, and 58 were severely injured with severe burns.
Industrial Fires:
West Fertilizer Company facility in Texas – 15 people were killed, more than 160 injured during an ammonium nitrate explosion in April 2013.
Imperial Sugar in Port Wentworth, Georgia – 14 people were killed and 40 injured, including 14 with serious and life-threatening burns, when a dust explosion occurred at a sugar refinery.
The examples above are just a few of the many scenarios that could cause a burn MCI. Nashville’s recent Christmas morning explosion could have easily been one such event had this occurred during business hours, popular tourist times, or a large tourism event. On such an occasion, the same types
64

40 44819987 v1
of redundancy and capacity that Nashville has for trauma should be available for burns and inhalation injuries. Burn Disasters Often Exceed Local and Regional Capability An estimated 20% to 30% of injuries related to mass casualty events are burn related, and a major event could quickly overwhelm this resource-limited system.14 Events that result in multiple burn injuries can occur in any community. They occur anywhere people congregate—schools, churches, housing units, dormitories, workplaces, factories, airports, and entertainment establishments. They can also occur as a result of natural disasters such as wild land fires, earthquakes, etc. Each community has its own high-risk locations. Nashville, in particular, is a growing urban community with large universities, major highways, massive sporting events and concerts that cause the area’s population to swell well beyond its approximately 1.93 million reported residents.15 Tourism is Nashville’s second-largest industry, second only to healthcare.16 In fact, a record 16.1 million tourists visited Nashville in 2019, an increase of over 6 percent in comparison to the previous record of 15.2 million set in 2018, according to data released January 27, 2020 by the Nashville Convention & Visitors Corp.17 See Exhibit 13.
Exhibit 13 2010 – 2019 Trend in Tourism in Nashville
Definitive Care of Burn Injuries Requires Highly Specialized and Extensive Care
14 Conlon KM, Martin S. “Just send them all to a burn centre”: managing burn resources in a mass casualty incident. J Bus Contin Emer Plan. 2011;5(2):150-160. 15 Nashville Metropolitan area including Nashville, Davidson, Murfreesboro, and Franklin had a population of approximately 1.93 million residents as of July 1, 2019. 16 https://www.visitmusiccity.com/media/press-release/2019/nashville-leads-tennessee-tourism-with-7-billion-in-visitor-spending#:~:text=Hospitality%20is%20Nashville's%20second%2Dlargest%20industry%2C%20behind%20healthcare 17 https://www.visitmusiccity.com/research
65

41 44819987 v1
As previously established, definitive care of burn patients with a major burn injury should take place at a burn center. In the United States, under usual conditions, severe burns should be immediately referred to the nearest burn center for care.18 Since a relatively small number of patients would quickly overwhelm any burn center, this referral paradigm may be detrimental for disaster response. Thus, it is imperative that local/regional disaster planning consider the resources of the burn center(s). Nashville has one, non-verified burn program with 25 beds serving all of Middle and East Tennessee and surrounding southern Kentucky and northern Alabama. The existing program would most certainly be quickly overwhelmed by the surge of burn patient admissions as a result of a burn MCI, especially given their baseline high occupancy. A second, verified burn provider would not only increase quality in general but also would ensure ready access to qualified burn specialists and resources to properly treat burn injured patients, which is particularly important in the event of an unpredictable, catastrophic burn MCI. Redundancy for critical services like burn is of paramount importance for our region. Skyline will leverage its relationships with existing, affiliated burn programs—including the HCA-affiliated Doctors Hospital of Augusta, the largest burn center in America—to develop a comprehensive Health Emergency Preparedness and Disaster Response plan. Skyline will work with all hospitals and hospital systems in the greater Nashville area and surrounding communities for the common goal of ensuring the safety and preparedness of the healthcare delivery system to adequately treat all burn patients from the service area. There is Enough Population to Support More Than One Burn Program in the Service Area As previously established, there is currently one non-verified burn program located in Nashville where Skyline proposes to locate its ABA-verified burn program. It is not uncommon, however, for there to be more than one burn program in a large metropolitan area. See Exhibit 14 below. Note that there are 11 metropolitan areas that are similarly sized or smaller than the Nashville metropolitan area with more than one burn center. It is acknowledged that, for some of these metropolitan areas, one of two programs is a dedicated pediatric unit. Even when these metropolitan areas are excluded, there are at least four other metropolitan areas that are similarly sized or smaller than the Nashville metropolitan area supporting more than one comprehensive burn program.
18 American Burn Association. (2018). Advanced Burn Life Support Course Provider Manual 2018 Update. Chicago: American Burn Association.
66

42 44819987 v1
Exhibit 14 Comparison of Metropolitan Areas with More Than One Burn Program
Geographic Area State
Number of Centers in Proximity Facility Names
Population per 2019 US Census
Centers per 1 Million Population
Nashville-Davidson--Murfreesboro--Franklin, TN Metro Area TN 1 Vanderbilt University Medical Center 1,934,317 0.517
Sacramento-Roseville-Folsom, CA Metro Area CA 2
Shriners Hospitals for Children - Northern California*UC Davis Regional Burn Center 2,363,730 0.846
Pittsburgh, PA Metro Area PA 2UPMC Mercy Burn CenterThe Western Pennsylvania Hospital Burn Center 2,317,600 0.863
Las Vegas-Henderson-Paradise, NV Metro Area NV 2
Sunrise Hospital & Medical Center*Lions Burn Center 2,266,715 0.882
Cincinnati, OH-KY-IN Metro Area OH 2
Shriners Hospitals for Children - Cincinnati*University of Cincinnati Medical Center UC Healthcare 2,221,208 0.900
Kansas City, MO-KS Metro Area MO 2
The Burnett Burn Center at the University of Kansas HospitalChildren's Mercy Hospital Burn Unit* 2,157,990 0.927
Philadelphia, PA Metro Division PA 3
Stuart J. Hulnick Burn Center*Temple University Burn CenterThomas Jefferson University Hospital Burn Center 2,150,811 1.395
Columbus, OH Metro Area OH 2Nationwide Children's Hospital*The Ohio State University Wexner Medical Center 2,122,271 0.942
Indianapolis-Carmel-Anderson, IN Metro Area IN 2
Eskenazi Health Services Richard M. Fairbanks Burn CenterIndiana University Riley Burn Unit Pediatric Burn Care Facility* 2,074,537 0.964
San Francisco-San Mateo-Redwood City, CA Metro Division CA 2
San Francisco General Hospital Burn UnitBothin Burn Center at Saint Francis Memorial Hospital 1,648,122 1.214
Milwaukee-Waukesha, WI Metro Area WI 2
Children's Hospital of Wisconsin*Columbia St. Mary's Hospital Regional Burn Center 1,575,179 1.270
Richmond, VA Metro Area VA 2VCU Health Evans-Haynes Burn CenterDeCamp Wound Healing Center Burn Program 1,291,900 1.548
Source: American Burn Association Website; U.S. Census Bureau*Pediatric Burn Programs
Proposed Burn Unit Location
Similarly-Sized or Smaller Metropolitan Areas with More Than One Existing Burn Program
67

43 44819987 v1
Skyline Has the Infrastructure and Programs in Place to Increase Access to Care Not only has Skyline identified a need for increased access to comprehensive burn services, but Skyline also has the infrastructure in place to implement educational programs that increase awareness of the benefits of comprehensive burn care throughout the service area and ensure appropriate transport of such patients. Skyline’s proposed burn program implementation will parallel the efforts to develop the Skyline trauma/stroke network through existing relationships within TriStar Division and other hospitals throughout the region for education and outreach. TriStar Division has proven its extended outreach with its trauma program, and the proposed comprehensive burn program is a logical overlay to these existing affiliations, linkages, and educational efforts. Burn and Reconstructive Centers of America Through its TriStar Division affiliation, Skyline has established a relationship with Burn and Reconstructive Centers of America (BRCA) to assist with the development of its burn program. For more than 40 years, BRCA has continued to grow and partner with hospitals across the country to provide patients a continuum of care from initial injury through long-term rehabilitation, while ensuring no patient is turned away. As discussed, this relationship will support Skyline in its initial implementation through successfully achieving ABA verification including policies and procedures, recruiting, clinical protocols, and access to the latest advances in burn care nationally. BRCA will work closely with Skyline through the implementation of all aspects of the proposed comprehensive burn program from physical plant and operational considerations to recruiting to ongoing quality of care and best practices working towards ABA verification. BRCA’s collaboration will ensure a stable cadre of the top trained physicians and surgeons available to support Skyline’s program. In fact, BRCA already has multiple physicians interested and willing to move to Nashville to support Skyline’s program. Another aspect of BRCA’s support involves a dedicated staff member to assist Skyline with education and outreach to its referral sources, community hospitals, and medical transport providers. Skyline’s coordination with BRCA for outreach and education will overlay Skyline and TriStar Division’s extensive community outreach program. Based in both Nashville and Chattanooga, TriStar Division has dedicated individuals focused on EMS relationships and community hospital outreach and education. Critical clinical referral protocols can be quickly and readily shared throughout this platform to increase the understanding of decision makers (both medical and transport) regarding appropriate referral criteria for burn injured patients to comprehensive burn programs. This should help address the high percentage of patients with burn injuries that should be served in a burn center that today are continuing to be served in local and community hospitals. Ground and Air Medical Transport Coordination Skyline partners with several ambulance and heli-transport vendors, including Ambulnz, American Medical Response (AMR), First Call Ambulance, Medic One, and Air Evac. Importantly, this year TriStar Division began to connect local Global Medical Response assets to provide integrated air and ground transportation for HCA-affiliated hospitals. TriStar Division’s recently launched “SKYLIFE” program, a twin-engine EC-145 helicopter based at TriStar Centennial Medical Center, is provided through a partnership with Global Medical Response (GMR), which operates 37 air ambulance bases in Tennessee, Kentucky, Georgia, and Alabama. Skyline’s medical transport network was considered in defining the service area, particularly with the ability to increase access to areas of East Tennessee and southeast Kentucky that are more than 150 miles from any verified or non-verified burn centers. Coordination with Skyline and SKYLIFE will ensure patients in need of comprehensive burn care will
68

44 44819987 v1
be appropriately transported. Please see map of air transport base locations with respect to the proposed service area previously presented. TriStar Trauma/Stroke Network, Telemedicine, and Education Skyline has been designated a Level II Trauma Center by the State of Tennessee Department of Health since 2016 and has now become one of only four hospitals in the state to achieve additional, national recognition via verification as an American College of Surgeons (ACS) verified Level II Trauma Center. In 2018, Skyline treated over 3,200 trauma patients injured in Middle Tennessee and southern Kentucky. Comprehensive burn services are a logical and appropriate expansion of this trauma designation. Trauma and burn often go hand in hand. Catastrophic events and accidents can result in both burn and inhalation injuries along with other musculoskeletal injuries soft tissue injuries, and other internal injuries. Skyline will have a full range of specialists to support all traumatic needs of such patients. Additionally, Skyline is proud to be recognized as Tennessee's first Comprehensive Stroke Center by The Joint Commission, American Heart Association, and American Stroke Association. Beyond local access to the highest-level stroke care and comprehensive trauma care services, Skyline serves as the hub for TriStar Division’s telemedicine network. This technology gives patients access to an instantaneous evaluation by remote specialists upon their arrival at many rural emergency departments. Telemedicine gives patients access to a higher level of care where it otherwise may not be available and has the capacity to revolutionize the delivery of healthcare. Additionally, telemedicine technology can be used to evaluate patients to determine whether they should receive appropriate care in their home community or require a higher level of care and coordinated transfer. TriStar Division has conducted 26,655 telehealth consults year-to-date as of November 2020 across 38 strategic telehealth hospital partners – 23 of which are part of the TriStar Division, and 15 of which are community partners that are not affiliated with TriStar Division. This network will allow local physicians direct access to Skyline’s burn experts to help assess burn injuries and make appropriate decisions if these patients should be transported for care. This is important, as there is a shortage of burn specialists nationwide and many service area patients who fit the burn referral criteria are often not appropriately referred to dedicated burn centers. TriStar Division’s existing telemedicine program is only one component of a long-term commitment to partnering with rural hospitals in order to foster enhanced education and community outreach. In addition to telemedicine, TriStar representatives go out to hospitals in rural communities to build authentic relationships through grassroot efforts. TriStar Division’s goal is to bring value to partner hospitals by assisting them to enhance the level of care provided in the local community and keep more patients in the local hospital when appropriate. TriStar Division educational offerings enhance collaborative relationships with rural and community hospital partners, bringing awareness of the TriStar Division’s services and programs to physicians, nurses, EMS personnel and other providers in these rural communities. Examples of these educational offerings include but are not limited to:
Treatment protocols for sepsis, stroke, trauma, and cardiogenic shock Heart anatomy and interpretation of EKGs Cardiogenic shock for emergency providers Pediatric airway management and respiratory emergencies
69

45 44819987 v1
TriStar Division provided education to over 38 rural hospital partners in 2019 and continues this trend across Middle Tennessee and Southern Kentucky in 2020. This significant coverage equates to the education of over 2,644 EMS personnel YTD in 2020 and 4,603 personnel in 2019. TriStar Division’s robust community and rural hospital outreach initiatives provide the perfect model for outreach and education for community hospitals with burn-injured patients. Skyline will work with existing and new community partners to expand education, outreach, and telemedicine relationships specific to burn care. TriStar Division’s telemedicine and outreach programs coupled with its multiple wound care centers throughout the service area provide a unique convenience for patients who may have to travel further from home for their initial burn care. Through TriStar Division’s network, patients can return home after their initial treatment and continue with their long-term care closer to home, reducing the need for the patient to travel far distances for follow-up care. The map in Exhibit 15 depicts Skyline’s outreach footprint including telemedicine within the proposed burn program service area.
70

46 44819987 v1
Exhibit 15 Service Area with Wound Care, Telemedicine, and Educational Outreach Sites
71

47 44819987 v1
Local Post Discharge Care Continuum Beyond the initial inpatient admission, patients treated in burn unit beds often require long-term outpatient follow-up, including rehabilitation, mental health treatment, and wound care. Skyline has all of the resources in place to provide high quality, comprehensive burn care to service area residents both locally and when appropriate, outpatient care through a network of affiliated hospitals and outpatient centers across a multi-state region. Wound Care Linkages Wound care is an important component of burn care that Skyline will be developing on its campus. TriStar Division has a network of wound care centers that will offer outpatient services closer to the patients’ residences and reduce the travel back to Skyline. In addition to Skyline’s wound care capabilities, TriStar Division offers Advanced Wound Care and Vascular Services at the following facilities throughout Tennessee.
TriStar Centennial Medical Center – Nashville, TN TriStar Hendersonville Medical Center – Hendersonville, TN TriStar Southern Hills Medical Center – Nashville, TN TriStar Summit Medical Center – Hermitage, TN Parkridge Medical Center – Chattanooga, TN TriStar Horizon Medical Center – Dickson, TN
TriStar Division’s Wound Care program is composed of a multi-disciplinary team of dedicated physicians supplemented with advanced treatment options, and Hyperbaric Oxygen treatment (when appropriate), can heal wounds that have resisted traditional treatments over the span of months or even years. The programs features:
Comprehensive evaluations by a physician to develop individualized care plans based on protocols and patient-specific needs.
All clinics, with the exception of TriStar Horizon Medical Center, are equipped with Monoplace Hyperbaric Oxygen chambers to help treat serious infections and wounds that may not heal as a result of diabetes or radiation burn injury.
Team of specialists to work with the patient and patient’s existing healthcare providers. A nurse navigator to help patients and families with communication and coordination of healthcare
among various providers. Education: including nutrition and diabetes management skills for home use. Prevention: including off-loading, pressure relief and routine foot care. Long-term follow-ups. Wound care centers are designed for various types of wounds, including but not limited to:
o Diabetic wounds o Pressure ulcers o Venous stasis ulcers o Traumatic wounds o Vasculitic ulcers o Surgical wounds
With wound care centers covering a broad geographic region throughout the service area, Skyline is well positioned to provide access to follow-up care closer to home for much of the service area, easing the travel burden that is often associated with a regionalized service such as burn care.
72

48 44819987 v1
Behavioral Health Services at Skyline Many burn-injured patients have compounding behavioral health conditions resulting from the initial traumatic injury and/or the lasting effects and potential limitations of their injury. Skyline has the resources to provide this support for its burn-injured patients. Skyline maintains a 110-bed behavioral health facility, TriStar Skyline at Madison. This facility maintains robust clinical infrastructure and expertise with psychiatrists, therapists, therapeutic programs, and counselors. The behavioral health hospital includes geriatric, adult, as well as adolescent programs, providing a comprehensive span of expertise. Skyline’s mental health expertise will be expanded and integrated with the comprehensive burn program. In addition, TriStar Division has a network of behavioral health programs to assist burn care patients locally within their communities including areas of east Tennessee:
TriStar Centennial Parthenon Pavilion – Nashville, TN Parkridge Valley Adult and Senior Campus – Chattanooga, TN Parkridge Valley Child and Adolescent Campus – Chattanooga, TN Parkridge Valley Cleveland Outpatient Program – Cleveland, TN Parkridge Valley West Hospital – Jasper, TN Pinewood Springs – Columbia, TN
Rehabilitation Services at Skyline Burn patients often require extensive physical and occupational therapy to regain maximum mobility, function, and independence following a catastrophic burn event. Skyline maintains a 41-bed CARF accredited inpatient rehabilitation program, providing critical continuity and restorative expertise for a variety of patients, including stroke, traumatic brain injury, and spinal cord injury. Inpatient rehabilitation is also frequently needed for burn patients, which Skyline can and will provide to ensure continuity of care and aggressive therapies for the burn patient population. Additionally, Skyline maintains outpatient rehabilitation services, including physical, occupational, and speech therapy. TriStar will extend the availability of these services for burn follow-up care within the service area through:
TriStar Centennial Medical Center (Nashville, TN) – Outpatient Rehabilitation TriStar Southern Hills Medical Center (Nashville, TN) – Inpatient and Outpatient Rehabilitation TriStar StoneCrest Medical Center (Smyrna, TN) – Outpatient Rehabilitation TriStar Hendersonville Medical Center (Hendersonville, TN) – Outpatient Rehabilitation TriStar Summit Medical Center (Hermitage, TN) – Inpatient and Outpatient Rehabilitation TriStar Horizon Medical Center (Dickson, TN) – Inpatient Rehabilitation Parkridge Medical Center (Chattanooga, TN) – Inpatient and Outpatient Rehabilitation TriStar Greenview Medical Center (Bowling Green, KY) Outpatient Rehabilitation Frankfort Regional Medical Center (Frankfort, KY) – Outpatient Rehabilitation
Skyline Will Work to Become ABA Verified Skyline has and will design every aspect of its comprehensive burn program with the goal of being ABA verified. Each aspect of the ABA criteria has been considered from physical plant, equipment, and operational aspects to staffing, policies and procedures, as well as clinical protocols and best practices. Skyline with work with BRCA to meet these requirements. Attachment Section B – Need-1C provides a review of each ABA criteria and how Skyline will meet each item.
73

49 44819987 v1
Skyline Projected Utilization Will Not Impact VUMC’s Program Skyline’s burn unit can achieve efficient utilization without diminishing VUMC’s program. In projecting its utilization, Skyline has focused on the previously identified large base of patients that are being served in community hospitals without a burn program who would be better served in a hospital with a comprehensive burn program as proposed by Skyline. Utilization projections for Skyline’s burn program assume that it will not capture service area burn patients who have historically sought care at VUMC or who have gone to pediatric hospitals. As discussed above, Skyline’s burn program will focus on adult patients, who have a greater need. Demand for pediatric patients is smaller and these patients are more often referred for comprehensive burn care today. Skyline will be equipped and staffed to accommodate pediatric burn patients and will have at least 3 beds available for pediatric patients. Please see question 6 below for detailed utilization projections and supporting assumptions and methodology. Criteria and Standards for Construction, Renovation, Expansion, & Replacement of Health Care Institutions
1. Any project that includes the addition of beds, services, or medical equipment will be reviewed under the standards for those specific activities.
The foregoing discussion addresses the criteria and standards for burn units.
2. For relocation or replacement of existing licensed health care institutions: a. The applicant should provide plans which include costs for both renovation and
relocation, demonstrating the strengths and weaknesses of each alternative. b. The application should demonstrate that there is an acceptable existing or projected
future demand for the project.
Not applicable. This project does not involve relocation or replacement of an existing licensed health care institutions. The responses to the State Health Plan Criteria and Standards for Burn Units demonstrate that there is sufficient future demand for the proposed burn unit.
3. For renovation or expansion of an existing licensed health care institution:
a. The applicant should demonstrate that there is an acceptable existing demand for the proposed project.
Skyline will demonstrate below that there is an acceptable existing demand for the proposed project in its projected utilization using conservative and reasonable assumptions and without material impact on existing providers.
b. The applicant should demonstrate that the existing physician plant’s condition
warrants major renovation or expansion.
In order to accommodate a dedicated comprehensive burn program, Skyline must either renovate existing space or expand the physical footprint of the existing facility. Skyline proposes to locate the burn center in the existing patient tower by converting an existing ICU to a dedicated burn unit. This unit will require only minor renovations and engineering to comply with ABA requirements.
74

50 44819987 v1
2. Describe how this project relates to existing facilities or services operated by the applicant including previously approved Certificate of Need projects and future long-range development plans.
Background on the Applicant
Skyline is the applicant for the initiation of a burn unit that will be integral to its proposed comprehensive burn program. Skyline is renowned as the first comprehensive stroke center in the state as well as a national leader in neuroscience. Skyline’s operations include an ACS Verified Level II Trauma Center and an Accredited Chest Pain Center with PCI, deeming it a leader in providing emergency care. The hospital offers trauma surgeons on-site 24/7. Skyline proposes to be the first ABA-verified burn program serving central and eastern Tennessee as well as surrounding communities. Support Services for Burn Patients Burn injuries are complicated to treat and are associated with substantial morbidity and mortality. The injury affects not only the physical health, but also the mental health and quality of life of the patient. Accordingly, burn injury leads to long-term profound alterations that must be addressed to optimize quality of life. Burn care providers are often faced with a plethora of challenges including acute and critical care management, long-term care, and rehabilitation. Throughout its network, Skyline has access to all of the services necessary to provide adequate access to both burn care and associated support services such as rehabilitation and behavioral health. Behavioral Health Services at Skyline Skyline maintains a 110-bed behavioral health facility, TriStar Skyline at Madison. This facility maintains robust clinical infrastructure and expertise with psychiatrists, therapists, therapeutic programs, and counselors. The behavioral health hospital includes geriatric, adult, as well as adolescent programs, providing a comprehensive span of expertise. Skyline’s mental health expertise will be expanded and integrated with the comprehensive burn program. Rehabilitation Services at Skyline Skyline maintains a 41-bed CARF accredited inpatient rehabilitation program, providing critical continuity and restorative expertise for a variety of patients, including stroke, traumatic brain injury, and spinal cord injury. Inpatient rehabilitation is also frequently needed for burn patients, which Skyline can and will provide to ensure continuity of care and aggressive therapies for the burn patient population. Additionally, Skyline maintains outpatient rehabilitation services, including physical, occupational, and speech therapy. TriStar Health Pediatric Care Children are one of the populations most susceptible to severe burn injury. Ensuring ready access to comprehensive burn care for all patients, including pediatric patients, is of the utmost importance. Skyline’s affiliate, The Children’s Hospital at TriStar Centennial, is a comprehensive healthcare facility delivering excellence in children’s services. The Children’s Hospital boasts an elite team of board-certified pediatricians, pediatric intensivists, and pediatric subspecialists specially trained to meet the unique needs of children. The Children’s Hospital offers a wide array of services including pediatric surgery, pediatric intensive care unit, neonatal intensive care unit (NICU), as well as emergency and outpatient care. Hospital staff includes Child Life Specialists to help children understand why they are in the hospital in an age-appropriate way. The Children’s
75

51 44819987 v1
Hospital at TriStar Centennial will integrate with Skyline’s burn program, including its pediatric intensivists service providing medical coverage at Skyline for pediatric burn patients. Perhaps even more so than an adult burn patient, pediatric burn patients require comprehensive burn care and support services catered specifically to their unique needs. While Skyline will recruit necessary staff to support its pediatric burn patients, its relationship with the nearby Children’s Hospital at TriStar Centennial ensures that pediatric patients and their families have access to a full continuum of care beyond their initial burn treatment. TriStar Wound Care Centers As discussed previously and in addition to Skyline’s wound care capabilities, TriStar Division offers Advanced Wound Care and Vascular Services at a network of facilities throughout Tennessee and Georgia. Skyline’s relationships with these programs will allow patients to stay in their community to received lower acuity follow up services without the costly and time-consuming travel to Nashville for their follow up care. Skyline will use telemedicine to make its burn expertise available to patients at these wound care centers including lower acuity burns and more extensive burns needing follow up from their initial care at Skyline. Skyline Expansion Projects Skyline is committed to providing care to some of the most acutely ill and severely injured in an expanding region. Approximately 50% of Skyline’s patients receive their initial care at outlying hospitals before being transferred to Skyline for a higher level of care. Accordingly, Skyline has developed needed infrastructure and expanded services to better meet the growing and diverse needs of its patients. Namely, Skyline recently completed a $69 million expansion that added two floors and 54 additional beds. The project also included an expanded ED, additional trauma capacity, and a third helipad which is currently underway. Skyline’s focused tertiary mission and infrastructure provides a foundation for developing a fully integrated, comprehensive burn program. HCA, TriStar Division, Skyline Medical Center Partnerships As a member of the largest hospital system in the world and a tertiary hospital provider in Nashville for over 20 years, Skyline is committed to leveraging its existing resources and expansive network to further reinforce the quality of the proposed burn program and the ancillary services that will support the program. These partnerships extend to trauma region coordination, telemedicine services, and wound care coordination, all of which benefit burn patients from their initial injury through their long-term recovery. Burn and Reconstructive Centers of America Through its TriStar Division affiliation, Skyline has established a relationship with BRCA to assist with the development of its burn program. For more than 40 years, BRCA has continued to grow and partner with hospitals across the country to provide patients a continuum of care from initial injury through long-term rehabilitation, while ensuring no patient is turned away. As discussed, this relationship will support Skyline in its initial implementation through successfully achieving ABA verification including policies and procedures, recruiting, clinical protocols, and access to the latest advances in burn care nationally.
76

52 44819987 v1
Medical Transport Because burn care is a regionalized service, a broad network of medical transport services is invaluable to ensuring timely access to care for critical burn patients. Skyline partners with several ambulance and heli-transport vendors, including Ambulnz, American Medical Response (AMR), First Call Ambulance, Medic One, and Air Evac. Importantly, this year TriStar Division began to connect local Global Medical Response assets to provide integrated air and ground transportation for HCA-affiliated hospitals. TriStar Division’s “SKYLIFE” program is provided through a partnership with Global Medical Response (GMR), who operates 37 air ambulance bases in Tennessee, Kentucky, Georgia, and Alabama. The varied forms of medical transport offered by TriStar Division facilities through its relationship with GMR will ensure that burn patients in the service are have expedited access to burn care services at Skyline. Beyond the initial inpatient admission, patients treated in the burn unit beds often require long-term outpatient follow-up, including rehabilitation, mental health treatment, and wound care. Skyline has all of the resources in place to provide high quality, comprehensive burn care to service area residents both locally and when appropriate, outpatient care through a network of affiliated hospitals and outpatient centers across a multi-state region. Clinical Training and Residencies Skyline offers many training opportunities through its partnerships with local medical training programs, colleges, and universities. Significantly, TriStar Health recently partnered with Belmont University to develop a new College of Medicine. The new college will help address the significant national physician shortage estimated between 54,100 and 139,000 physicians by 2033.19 TriStar also partners with existing education programs to offer clinical training opportunities for other students in other areas, including nursing, pharmacy, physical therapy, occupational therapy, speech therapy, and respiratory therapy, amongst others. The unique exposure to a comprehensive burn program at Skyline will offer a broader range of clinical education and experience to its future medical professionals. A letter of support written by Dr. Robert Fisher, President of Belmont University, emphasizes the positive impact the proposed project will have on healthcare for the Nashville community and far beyond, citing the explosive growth in population and tourism in Nashville as support for the need for redundancy in critical healthcare services, including burn services. Dr. Fisher goes on to write:
Especially given Nashville’s status as a premier center for healthcare provision, it is vital that the city be equipped and prepared to manage any large scale health care emergency, whether experience by residents or visitors. In addition to enhancing healthcare offerings, the opening of a burn unit at Skyline would create opportunities for clinical rotations and residencies for Belmont’s Pharmacy, Nursing, Physical Therapy, and soon-to-be medical students. With HCA’s demonstrated commit[ment] to healthcare education, these providers would enter their respective fields in Nashville and beyond even better equipped to meet the needs of their communities.
TriStar Health and Skyline will provide clinical rotations for Belmont University’s medical students and enhance physician training with critical residencies and fellowships through Graduate Medical
19 https://www.aamc.org/news-insights/us-physician-shortage-growing
77

53 44819987 v1
Education. Not only is there an overall shortage of physicians nationwide, but also there is an ongoing, documented shortage of burn specialists.20 Skyline will play an integral role in the training of new physicians in order to assist in addressing the shortage of physicians across many services lines including burn care. TriStar Health’s commitment to medical education in part drives its enthusiasm to expand its service offerings such as the proposed burn program.
3. Identify the proposed service area and provide justification for its reasonableness. Submit a county level map for the Tennessee portion of the service area using the map on the following page, clearly marked and shaded to reflect the service area as it relates to meeting the requirements for CON criteria and standards that may apply to the project. Please include a discussion of the inclusion of counties in the border states, if applicable. Attachment Section B - Need-3.
The service area for the proposed burn program at Skyline consists of 131 counties in Middle Tennessee, East Tennessee, southern Kentucky, and northern Alabama. See Exhibits 16 and 17 below. As has been described, Skyline’s burn service area is based on the following factors:
Geographic locations of both ABA-verified and non-verified programs in Middle Tennessee, East Tennessee, and adjoining states;
Skyline’s relationships for medical transportation including air transport throughout this region;
Skyline’s relationships with community and rural providers for education and telemedicine to ensure burn patients are appropriately referred to a comprehensive center; and
Skyline’s relationships with Wound Care Centers to allow for many patients to receive follow up care closer to home within a coordinated continuum of care.
Because burn care is a regionalized service, Skyline’s proposed service area is intentionally broad and recognizes geographic areas of Tennessee, Kentucky, and Alabama that are rural and have less access to specialized services such as burn care. The East Tennessee portion of the service area will be primarily focused on tertiary/heli-transport services for burn patients provided by a relationship between TriStar Division and Global Medical Response (“GMR”) called SKYLIFE. Through HCA’s collaboration with GMR, TriStar hospitals will have immediate access to air transport via GMR’s five Med-Trans bases which are sufficiently staffed by skilled critical care nurses and paramedical personnel to ensure continuity of quality care in dire situations.
It is likely that when patients experience a burn injury, they will travel to their local hospital for care initially. Whenever a burn patient reaches a local hospital, physicians on site may have limited familiarity with burn treatment. This is particularly true for rural, underserved communities, like some in East Tennessee and southern parts of Kentucky. Under such circumstances, post-treatment care in consultation with a remote burn specialist using telemedicine technology becomes highly valuable. Telemedicine can be appropriately used for a substantial portion of the long-term management of patients after a burn, alleviating some of the travel burdens faced by patients and their families. Additionally, telemedicine can be a helpful tool during an acute transfer process if the ED physician is questioning whether or not referral to a burn center is clinically appropriate.
Skyline also has a robust telemedicine program, currently touting agreements with 35 hospitals in rural communities throughout Tennessee and Kentucky. Skyline intends to continue to develop its telemedicine program by developing additional agreements with hospitals throughout the
20 Vrouwe SQ, Pham CH, Minasian RA, et al. The State of Burn Care Training During Plastic Surgery Residency. Annals of Plastic Surgery. 2020 Aug;85(2):122-126. DOI: 10.1097/sap.0000000000002267.
78

54 44819987 v1
region and plans to include outpatient burn care in its telemedicine program in order to better reach rural and underserved communities throughout its broad geographic service area.
Exhibit 16
List of Service Area Counties
TN Bedford KY Adair TN AndersonTN Benton KY Allen TN BlountTN Bledsoe KY Barren TN BradleyTN Cannon KY Breckinridge TN CampbellTN Cheatham KY Butler TN CarterTN Clay KY Caldwell TN ClaiborneTN Coffee KY Calloway TN CockeTN Cumberland KY Christian TN GraingerTN Davidson KY Clinton TN GreeneTN Decatur KY Crittenden TN HamblenTN DeKalb KY Cumberland TN HancockTN Dickson KY Daviess TN HawkinsTN Fentress KY Edmonson TN JeffersonTN Franklin KY Graves TN JohnsonTN Giles KY Grayson TN KnoxTN Grundy KY Green TN LoudonTN Hamilton KY Hancock TN McMinnTN Hardin KY Hart TN MeigsTN Henry KY Henderson TN MonroeTN Hickman KY Hopkins TN PolkTN Houston KY Livingston TN RoaneTN Humphreys KY Logan TN ScottTN Jackson KY Lyon TN SevierTN Lawrence KY Marshall TN SullivanTN Lewis KY McCracken TN UnicoiTN Lincoln KY McLean TN UnionTN Macon KY Metcalfe TN WashingtonTN Marion KY Monroe KY McCrearyTN Marshall KY Muhlenberg KY WhitleyTN Maury KY Ohio KY CaseyTN Montgomery KY Russell KY PulaskiTN Moore KY Simpson KY BellTN Morgan KY Taylor KY KnoxTN Overton KY Todd KY LaurelTN Perry KY Trigg TN Pickett KY Union TN Putnam KY Warren TN Rhea KY Wayne TN Robertson KY Webster TN Rutherford AL ColbertTN Sequatchie AL JacksonTN Smith AL LauderdaleTN Stewart AL LawrenceTN Sumner AL LimestoneTN Trousdale AL MadisonTN Van Buren AL MorganTN WarrenTN WayneTN WhiteTN WilliamsonTN Wilson
Primary Service Area Secondary Service Area
79

55 44819987 v1
Exhibit 17 Service Area Map
80

56 44819987 v1
Complete the following utilization tables for each county in the service area, if applicable:
Service Area Counties
Historical Utilization-County Residents – Most Recent Year (YEAR = _______)
% of total procedures cases patients Other ___________.
County #1 Not Applicable. Skyline does not currently operate a burn program.
Not Applicable. Skyline does not currently operate a burn program. County #2
County #3 County #4 Etc. Total 100%
Service Area Counties* Projected Utilization-County Residents-Year 1
(YEAR = 1/1/2022-12/31/2022)
% of total procedures cases patients Other ___________.
Primary Service Area Tennessee 71 33.4% Kentucky 46 21.7% Alabama 21 10.0% Secondary Service Area Tennessee 60 28.4% Kentucky 14 6.5% Total 212 100.0% Note: With a total of 131 counties in this regional service area, it is not possible to predict from year to year the individual county patient origin. For many rural counties, there may not be a single burn admission in every year. Patient origin has been projected by service area designation and state.
See Exhibit 16 for a list of all counties in each respective service area.
81

57 44819987 v1
Cou
nty
Leve
l Map
82

58 44819987 v1
4. A. 1) Describe the demographics of the population to be served by the proposal.
As of 2021, there are approximately 7,615,764 residents living within the proposed service area. Within the next five years, the population is projected to increase by 2.9% to approximately 7,846,709 residents. Exhibit 18 is a summary of service area population by age group. The service area is aging with the growth rate of residents age 65 and over increasing at more than twice the rate of the population as a whole. The senior age group is an important burn referral group targeted by this project. As noted previously, a high percentage of patients age 60 and older are not appropriately referred to comprehensive burn programs and instead remain in local community hospitals for care, which may result in poor outcomes.
Exhibit 18 Summary of Service Area Population by Age Group
Further, data from Healthcare Cost and Utilization Project (HCUP), shows that:
The rate of burn-related inpatient stays was highest among infants and the oldest
adults and lowest among children and younger adults. The rate of inpatient stays for burn-related injuries was highest among individuals
living in low-income ZIP Codes, rural areas, and the southern United States.
It should be noted that the south has the highest rate of inpatient stays for burn injuries yet has a lower number of burn unit beds per population as shown in Exhibit 19. Skyline’s service area reflects a large and growing base of older adults and a large geographic area of rural counties in the southern United State.
0-19* 20-44 45-64 65+ Total2021Primary Service Area 1,075,048 2,049,793 1,367,043 921,182 5,413,066 Secondary Service Area 375,970 790,899 586,318 449,510 2,202,698
Total 1,451,018 2,840,693 1,953,361 1,370,692 7,615,764
2025Primary Service Area 1,083,516 2,166,543 1,318,486 1,031,461 5,600,006 Secondary Service Area 376,332 800,591 577,280 492,500 2,246,703
Total 1,459,848 2,967,133 1,895,766 1,523,961 7,846,709
CAGR 2021-2025Primary Service Area 0.2% 1.4% -0.9% 2.9% 0.9%Secondary Service Area 0.0% 0.3% -0.4% 2.3% 0.5%
Total 0.2% 1.1% -0.7% 2.7% 0.7%Source: Tennessee population from Tennessee State data. All other state's data from Claritas Spotlight.*Tennessee data provides residents age 0-19, while other data sources provide 0-18.
83

59 44819987 v1
Exhibit 19
Note: Inpatient stays are based on all-listed diagnoses. Source: Agency for Healthcare Research and Quality (AHRQ), Center for Delivery, Organization, and Markets, Healthcare Cost and Utilization Project (HCUP), National Inpatient Sample (NIS), 2013
At 15.4% in 2018 and 16.5% in 2019, Nashville’s poverty levels remain higher than pre-Great Recession, equating to the highest number of residents in three years, according to the U.S. Census, even amid high levels of overall economic growth. Further, according to a 2019 Community Need Assessment for Nashville and Davidson County published by the Metro Government of Nashville, half of Nashville’s workforce is earning $35,460 or less, far from sufficient for meeting basic household expenses; thus, half of Davidson County workers do not earn enough to afford a Fair Market Rent.21 It has been established that young children and the elderly as well as those living in impoverished and/or rural areas in the South have the highest rate of burn injury requiring hospitalization. The proposed service area population is significantly made up of these populations which contributes to the additional need for expanded access to burn care. As previously described, although VUMC is located in Nashville where TriStar Skyline proposes its burn program, the large growing and aging population of the service area can clearly support more than one program.
21 https://www.nashville.gov/Portals/0/SiteContent/SocialServices/docs/cne/CNE-2019.pdf
84

60 44819987 v1
2) Provide the following data for each county in the service area using current and projected population data from the Department of Health (https://www.tn.gov/content/tn/health/health-program-areas/statistics/health-data/con.html ), the most recent enrollee data from the Division of TennCare (https://www.tn.gov/tenncare/information-statistics/enrollment-data.html ), and US Census Bureau demographic information (http://factfinder.census.gov/faces/nav/jsf/pages/index.xhtml ),.
TennCare Enrollment Data: https://www.tn.gov/tenncare/information-statistics/enrollment-data.html
Census Bureau Fact Finder: http://factfinder.census.gov/faces/nav/jsf/pages/index.xhtml
85

61 44819987 v1
Primary Service Area
BEDFORD 50,850 53,139 4.3% 50,850 53,139 4.3% 100.0% 37.9 $50,415 7,420 14.3% 13,061 25.7%BENTON 16,243 16,273 0.2% 16,243 16,273 0.2% 100.0% 47.9 $37,512 3,122 19.5% 4,275 26.3%BLEDSOE 15,143 15,592 2.9% 15,143 15,592 2.9% 100.0% 44.5 $42,889 2,721 20.3% 3,164 20.9%CANNON 14,717 14,985 1.8% 14,717 14,985 1.8% 100.0% 42.0 $49,523 2,194 15.9% 3,320 22.6%CHEATHAM 41,035 41,665 1.5% 41,035 41,665 1.5% 100.0% 40.4 $58,641 4,516 11.5% 6,882 16.8%CLAY 7,761 7,773 0.2% 7,761 7,773 0.2% 100.0% 48.8 $31,487 2,026 26.7% 2,096 27.0%COFFEE 56,797 58,146 2.3% 56,797 58,146 2.3% 100.0% 40.1 $47,998 7,624 14.1% 14,401 25.4%CUMBERLAND 61,705 63,995 3.6% 61,705 63,995 3.6% 100.0% 50.7 $43,893 8,782 15.2% 13,035 21.1%DAVIDSON 711,359 732,649 2.9% 711,359 732,649 2.9% 100.0% 34.3 $56,507 83,113 12.4% 143,342 20.2%DECATUR 11,715 11,683 -0.3% 11,715 11,683 -0.3% 100.0% 46.4 $42,031 2,016 17.6% 3,050 26.0%DEKALB 20,593 21,109 2.4% 20,593 21,109 2.4% 100.0% 41.2 $44,134 3,364 17.5% 5,341 25.9%DICKSON 55,163 57,239 3.6% 55,163 57,239 3.6% 100.0% 39.4 $50,549 7,333 14.3% 11,477 20.8%FENTRESS 18,402 18,550 0.8% 18,402 18,550 0.8% 100.0% 45.0 $35,084 3,855 21.8% 5,890 32.0%FRANKLIN 42,201 42,538 0.8% 42,201 42,538 0.8% 100.0% 41.9 $49,038 5,841 14.8% 8,297 19.7%GILES 29,438 29,259 -0.6% 29,438 29,259 -0.6% 100.0% 43.4 $47,528 4,162 14.7% 6,600 22.4%GRUNDY 13,142 12,840 -2.4% 13,142 12,840 -2.4% 100.0% 43.2 $36,987 3,184 24.3% 4,487 34.1%HAMILTON 372,453 382,321 2.6% 372,453 382,321 2.6% 100.0% 39.6 $53,035 47,360 13.7% 69,013 18.5%HARDIN 25,803 25,731 -0.3% 25,803 25,731 -0.3% 100.0% 45.3 $40,682 5,075 20.1% 7,129 27.6%HENRY 32,586 32,767 0.6% 32,586 32,767 0.6% 100.0% 45.8 $40,502 6,382 20.1% 7,856 24.1%HICKMAN 25,486 25,951 1.8% 25,486 25,951 1.8% 100.0% 40.8 $41,998 4,160 18.1% 5,891 23.1%HOUSTON 8,355 8,458 1.2% 8,355 8,458 1.2% 100.0% 43.7 $43,964 1,266 15.9% 2,113 25.3%HUMPHREYS 18,589 18,675 0.5% 18,589 18,675 0.5% 100.0% 41.6 $41,510 3,230 18.0% 4,699 25.3%JACKSON 11,928 12,085 1.3% 11,928 12,085 1.3% 100.0% 46.6 $36,703 2,241 19.7% 2,878 24.1%LAWRENCE 44,196 44,637 1.0% 44,196 44,637 1.0% 100.0% 39.4 $41,553 8,029 19.0% 11,188 25.3%LEWIS 12,125 12,135 0.1% 12,125 12,135 0.1% 100.0% 43.9 $37,139 2,385 20.3% 3,152 26.0%LINCOLN 34,547 35,032 1.4% 34,547 35,032 1.4% 100.0% 43.1 $45,736 5,280 15.9% 7,813 22.6%MACON 25,104 26,154 4.0% 25,104 26,154 4.0% 100.0% 39.4 $36,246 4,119 17.9% 6,874 27.4%MARION 28,552 28,424 -0.4% 28,552 28,424 -0.4% 100.0% 43.1 $48,024 5,084 18.2% 7,056 24.7%MARSHALL 34,706 35,965 3.5% 34,706 35,965 3.5% 100.0% 39.0 $49,370 4,661 14.7% 7,124 20.5%MAURY 98,912 104,649 5.5% 98,912 104,649 5.5% 100.0% 38.8 $54,249 10,986 12.4% 19,836 20.1%MONTGOMERY 218,941 236,050 7.2% 218,941 236,050 7.2% 100.0% 30.6 $55,972 26,016 13.5% 41,795 19.1%MOORE 6,475 6,546 1.1% 6,475 6,546 1.1% 100.0% 45.3 $52,294 492 7.9% 918 14.2%MORGAN 21,836 22,100 1.2% 21,836 22,100 1.2% 100.0% 41.1 $40,166 4,093 22.0% 4,602 21.1%OVERTON 22,486 22,961 2.1% 22,486 22,961 2.1% 100.0% 42.9 $36,558 3,687 17.0% 5,359 23.8%PERRY 8,161 8,278 1.4% 8,161 8,278 1.4% 100.0% 43.2 $41,034 2,099 26.9% 2,013 24.7%PICKETT 5,037 4,967 -1.4% 5,037 4,967 -1.4% 100.0% 49.7 $41,004 862 17.2% 1,150 22.8%PUTNAM 81,448 84,710 3.9% 81,448 84,710 3.9% 100.0% 36.3 $40,888 14,310 19.5% 19,245 23.6%RHEA 33,689 34,459 2.2% 33,689 34,459 2.2% 100.0% 40.2 $39,451 6,901 21.9% 9,319 27.7%ROBERTSON 73,499 76,586 4.0% 73,499 76,586 4.0% 100.0% 39.1 $61,774 7,923 11.6% 13,793 18.8%RUTHERFORD 349,087 381,646 8.5% 349,087 381,646 8.5% 100.0% 33.3 $63,846 35,604 11.8% 58,891 16.9%SEQUATCHIE 15,362 15,951 3.7% 15,362 15,951 3.7% 100.0% 43.3 $51,750 2,410 16.6% 4,116 26.8%SMITH 20,317 20,746 2.1% 20,317 20,746 2.1% 100.0% 40.7 $46,404 2,858 14.9% 4,458 21.9%STEWART 13,718 13,880 1.2% 13,718 13,880 1.2% 100.0% 44.5 $42,269 2,159 16.5% 3,173 23.1%SUMNER 196,582 208,748 5.8% 196,582 208,748 5.8% 100.0% 39.6 $64,631 16,833 9.5% 31,277 15.9%TROUSDALE 11,302 11,621 2.7% 11,302 11,621 2.7% 100.0% 36.0 $52,864 1,458 15.9% 2,091 18.5%VAN BUREN 5,755 5,718 -0.6% 5,755 5,718 -0.6% 100.0% 47.1 $37,127 1,060 19.0% 1,414 24.6%WARREN 41,107 41,320 0.5% 41,107 41,320 0.5% 100.0% 40.2 $37,715 9,103 22.9% 11,598 28.2%WAYNE 16,433 16,234 -1.2% 16,433 16,234 -1.2% 100.0% 43.0 $41,427 2,635 18.0% 3,333 20.3%WHITE 27,740 28,492 2.6% 27,740 28,492 2.6% 100.0% 43.1 $40,745 4,542 17.4% 7,452 26.9%WILLIAMSON 250,192 274,604 8.9% 250,192 274,604 8.9% 100.0% 39.2 $109,026 9,474 4.3% 13,954 5.6%WILSON 150,164 162,498 7.6% 150,164 162,498 7.6% 100.0% 40.2 $71,513 10,674 8.2% 20,531 13.7%
*Tar
get P
opul
atio
n- T
otal
SA
Pr
ojec
t Yea
r 202
5
Targ
et P
opul
atio
n-
% C
hang
eDemographic Variable/Geographic Area
Department of Health/Health Statistics Census Bureau TennCare
Tota
l Pop
ulat
ion-
Cur
rent
Ye
ar 2
021
Tota
l Pop
ulat
ion-
Proj
ecte
d Ye
ar 2
025
Tota
l Pop
ulat
ion-
% C
hang
e
Targ
et P
opul
atio
n Pr
ojec
ted
Year
as
% o
f Tot
al
Med
ian
Age
Med
ian
Hou
seho
ld In
com
e
Pers
on B
elow
Pov
erty
Lev
el
Pers
on B
elow
Pov
erty
Lev
el
as %
of T
otal
Tenn
Car
e En
rolle
es
Tenn
Car
e En
rolle
es a
s %
of
Tota
l
*Tar
get P
opul
atio
n- T
otal
SA
C
urre
nt Y
ear 2
021
86

62 44819987 v1
Question 4 A. 2) Continued
Secondary Service Area
NOTE: The tables above includes only Tennessee service area counties. Additional Kentucky and Alabama Counties are provided in Attachment Section B – Need-3.
* Target Population is population that project will primarily serve. For example, nursing home, home health agency, hospice agency projects typically primarily serve the Age 65+ population; projects for child and adolescent psychiatric services will serve the Population Ages 0-17. Projected Year is defined in select service-specific criteria and standards. If Projected Year is not defined, default should be four years from current year, e.g., if Current Year is 2019, then default Projected Year is 2023.
Be sure to identify the target population, e.g., Age 65+, the current year and projected year being used.
ANDERSON 77,459 78,500 1.3% 77,459 78,500 1.3% 100.0% 43.3 $50,392 12,481 16.7% 17,340 22.4%BLOUNT 134,982 139,287 3.1% 134,982 139,287 3.1% 100.0% 43.7 $56,667 14,179 11.1% 22,661 16.8%BRADLEY 109,446 112,852 3.0% 109,446 112,852 3.0% 100.0% 39.5 $51,331 16,333 16.00% 23,645 21.6%CAMPBELL 39,423 39,055 -0.9% 39,423 39,055 -0.9% 100.0% 44.1 $39,803 8,158 21.00% 12,565 31.9%CARTER 55,935 55,145 -1.4% 55,935 55,145 -1.4% 100.0% 45.4 $38,092 12,079 22.10% 13,266 23.7%CLAIBORNE 32,113 32,461 1.1% 32,113 32,461 1.1% 100.0% 43.1 $36,835 6,825 22.40% 9,222 28.7%COCKE 36,130 36,417 0.8% 36,130 36,417 0.8% 100.0% 45.2 $36,716 8,242 23.50% 11,968 33.1%GRAINGER 23,496 23,832 1.4% 23,496 23,832 1.4% 100.0% 45 $44,064 4,146 18.10% 6,077 25.9%GREENE 69,695 70,205 0.7% 69,695 70,205 0.7% 100.0% 44.7 $42,595 11,119 16.70% 16,549 23.7%HAMBLEN 65,553 66,747 1.8% 65,553 66,747 1.8% 100.0% 40.7 $43,619 10,828 17.30% 17,143 26.2%HANCOCK 6,462 6,328 -2.1% 6,462 6,328 -2.1% 100.0% 44.5 $30,136 1,814 28.60% 2,333 36.1%HAWKINS 56,627 56,482 -0.3% 56,627 56,482 -0.3% 100.0% 44.9 $41,924 10,621 19.10% 13,870 24.5%JEFFERSON 55,314 56,788 2.6% 55,314 56,788 2.6% 100.0% 43.9 $49,139 6,822 13.20% 13,156 23.8%JOHNSON 17,731 17,624 -0.6% 17,731 17,624 -0.6% 100.0% 46 $36,004 3,892 11.60% 4,646 26.2%KNOX 478,242 494,503 3.3% 478,242 494,503 3.3% 100.0% 37.4 $57,470 65,448 14.50% 81,837 17.1%LOUDON 55,127 57,606 4.3% 55,127 57,606 4.3% 100.0% 47.6 $58,065 5,845 11.30% 9,333 16.9%MCMINN 54,007 54,782 1.4% 54,007 54,782 1.4% 100.0% 42.6 $43,285 9,937 19.30% 13,199 24.4%MEIGS 12,540 12,814 2.1% 12,540 12,814 2.1% 100.0% 46 $49,167 2,006 16.90% 3,279 26.1%MONROE 47,278 48,244 2.0% 47,278 48,244 2.0% 100.0% 43.9 $42,429 8,326 18.40% 11,893 25.2%POLK 17,150 17,425 1.6% 17,150 17,425 1.6% 100.0% 45.6 $43,306 2,473 15.00% 4,122 24.0%ROANE 53,340 53,386 0.1% 53,340 53,386 0.1% 100.0% 46.4 $53,367 7,237 13.80% 11,688 21.9%SCOTT 22,147 22,212 0.3% 22,147 22,212 0.3% 100.0% 39.4 $38,864 4,687 21.90% 7,813 35.3%SEVIER 102,002 107,095 4.8% 102,002 107,095 4.8% 100.0% 42.9 $49,610 13,078 13.70% 21,544 21.1%SULLIVAN 158,406 158,824 0.3% 158,406 158,824 0.3% 100.0% 45.1 $46,684 24,615 15.90% 34,365 21.7%UNICOI 17,885 17,982 0.5% 17,885 17,982 0.5% 100.0% 46.5 $41,890 3,142 18.10% 4,165 23.3%UNION 19,858 19,984 0.6% 19,858 19,984 0.6% 100.0% 43 $44,671 4,216 22.00% 5,371 27.0%WASHINGTON 131,757 135,475 2.7% 131,757 135,475 2.7% 100.0% 40.2 $48,334 18,955 15.40% 25,460 19.3%Service AreaTotal 5,459,036 5,660,583 3.6% 5,459,036 5,660,583 3.6% 100.00% - - - - 1,090,332 20.0%State of TNTotal 6,886,369 7,102,950 3.0% 6,886,369 7,102,950 3.0% 100.00% 39.0 56,071 922176 13.90% 1,504,151.00 21.8%
Tenn
Car
e En
rolle
es a
s %
of
Tota
l
Targ
et P
opul
atio
n Pr
ojec
ted
Year
as
% o
f Tot
al
Med
ian
Age
Med
ian
Hou
seho
ld In
com
e
Pers
on B
elow
Pov
erty
Lev
el
Pers
on B
elow
Pov
erty
Lev
el
as %
of T
otal
Tenn
Car
e En
rolle
es
Demographic Variable/Geographic Area
Department of Health/Health Statistics Census Bureau TennCareTo
tal P
opul
atio
n-C
urre
nt
Year
202
1
Tota
l Pop
ulat
ion-
Proj
ecte
d Ye
ar 2
025
Tota
l Pop
ulat
ion-
% C
hang
e
*Tar
get P
opul
atio
n- T
otal
SA
C
urre
nt Y
ear 2
021
*Tar
get P
opul
atio
n- T
otal
SA
Pr
ojec
t Yea
r 202
5
Targ
et P
opul
atio
n-
% C
hang
e
87

63 44819987 v1
B. Describe the special needs of the service area population, including health disparities, the accessibility to consumers, particularly the elderly, women, racial and ethnic minorities, TennCare or Medicaid recipients, and low-income groups. Document how the business plans of the facility will take into consideration the special needs of the service area population.
The service area population consist of all residents of the service area counties in need of burn care. As previously established, children and elderly populations experience burns that require inpatient hospitalization at rates that are higher than other populations. Further, a recent analysis conducted by the ABA revealed that approximately 25.1 percent and 13.0 percent of burn patients nationwide are Medicaid and self-pay, respectively.22 In other words, 38 percent of burn patients are medically underserved populations. This statistic aligned with the fact that those living in low-income ZIP Code and/or rural areas have the highest rate of admissions for burn-related injuries.
TriStar Division and Skyline are committed to providing care for all patients, regardless of ability to pay. Its partnership with BRCA, and BRCA’s mission to ensure equitable access to burn services, reinforces TriStar’s commitment to serving the underserved. Further, as previously discussed, Skyline is affiliated with the Children’s Hospital at TriStar Centennial. Not only will Skyline hire pediatric specialists to support its program, but Skyline will also collaborate with the Children’s Hospital to combine expert resources on pediatric care and offer a full continuum of specialized and comprehensive care for pediatric burn patients.
Skyline has a specific plan to implement resources and support services necessary to address the special needs of burn patients in the service area. See Attachment Section B – Need-1C for a summary of Skyline’s plan to meet the ABA criteria for verification which will ensure adequate access to necessary resources and support services for burn care.
5. Describe the existing and approved but unimplemented services of similar healthcare providers in the service area. Include utilization and/or occupancy trends for each of the most recent three years of data available for this type of project. List each provider and its utilization and/or occupancy individually. Inpatient bed projects must include the following data: Admissions or discharges, patient days, average length of stay, and occupancy. Other projects should use the most appropriate measures, e.g., cases, procedures, visits, admissions, etc. This doesn’t apply to projects that are solely relocating a service.
Please see Exhibit 20 below. Skyline’s broad burn service area consists of one primary provider of burn services, VUMC, which reports 25 burn unit beds. The table below was prepared based on the data presented by VUMC on its 2017-2019 JARs. Despite the decline in the number of patients at VUMC, the burn unit has maintained relatively high occupancy rates due to increasing ALOS. As referenced in Question 4A under service area population analysis, Nashville’s large and growing population is sufficient in supporting an alternative provider that is ABA/ACS certified.
22 American Burn Association. (2019). National Burn Repository 2019 Update. Chicago: American Burn Association. Page 21.
88

64 44819987 v1
Exhibit 20
6. Provide applicable utilization and/or occupancy statistics for your institution services for each of the past three years and the projected annual utilization for each of the two years following completion of the project. Additionally, provide the details regarding the methodology used to project utilization. The methodology must include detailed calculations or documentation from referral sources, and identification of all assumptions.
Because the proposed program is a new service, there is no historical utilization. The projected utilization for Skyline’s proposed burn program is based on conservative and reasonable assumptions and will be described below.
First, Skyline obtained detailed burn services data for the service area from Tennessee (THA), Kentucky (KHA), and Georgia Hospital Associations (GHA). Then, Skyline used the ABA referral criteria (see Attachment Section B – Need-1A) to identify patients who qualify for referral to a burn center based on ICD-10 codes and DRGs. See the discussion of ABA referral criteria in the Need Discussion in Section B, Question 2.
Skyline analyzed the trend in these patients in the service area from 2017-2019.
From this set of patients, Skyline excluded the following service area patients treated in 2019: (1) service area burn patients treated at VUMC and (2) additional pediatric burn patients not captured in the referral criteria by DRG or ICD-10 but who were treated at pediatric hospitals. This allowed Skyline to identify the burn patients in the service area who have been previously served at hospitals without burn programs that would likely be better treated at the only other dedicated burn center in the service area (the proposed burn center).
2017 2018 20195-year % Change
5-year CAGR
Burn Unit Admissions 1,032 905 901 -3.4% -0.7%Burn Unit Patient Days 6,390 6,694 6,510 4.4% 0.9%Number of Burn Unit Beds 25 25 25 0.0% 0.0%Average Length of Stay (ALOS) 6.2 7.4 7.2 8.1% 1.6%Average Daily Census (ADC) 17.5 18.3 17.8 4.4% 0.9%Burn Unit Percent Occupancy 70.0% 73.4% 71.3% 4.4% 0.9%
Vanderbilt Joint Annual Reports of Hospitals (2014-2019)
Source: 2014-2019 Joint Annual Reports of Hospital
2017 2018 20192-Year CAGR
Primary Service Area 452 530 561 5.7%Secondary Service Area 253 235 236 -1.7%Total Service Area 705 765 797 3.2%
Trend in Total Service Area Burn Patients That Meet Burn Referral Criteria Including DRGs for Inhalation Injuries
Source: THA/KHA/GHA Data. Does not Include AL data.
89

65 44819987 v1
Skyline projected growth of burn patients who meet the referral criteria through Year 3 based on the historical compound annual growth rate (CAGR) of historical burn patients for the primary service area and population growth rates for the secondary service area.
Skyline then applied the percentage of patients better served at a comprehensive burn center identified above to project the number of service area patients that could be redirected to be served in the proposed dedicated burn beds from Tennessee and Kentucky counties.
Next, Skyline estimated the same type of demand for northern Alabama counties by applying the admission rate of burn patients from the Tennessee and Kentucky service area counties and applied this to the Alabama population. The average service area rate of appropriate referral was applied to identify the pool of patients that Skyline would serve.
From there, Skyline also assumed a conservative ramp-up period over the first three fiscal years of operation, as Skyline makes concerted efforts to better educate and raise awareness among burn patients and service area hospitals of the benefits of referring patients to a dedicated burn center based on ABA burn referral criteria.
2019 Total SA Patients Who
Meet ABA Referral Criteria
2019 SA Patients Better
Served at Skyline*
% of TotalAppropriate
Referral RateProjected
Growth RatePrimary Service Area 561 198 35.3% 5.7%Secondary Service Area 236 146 61.9% -1.7%Total Service Area 797 344 43.2% 3.2%Source: THA/KHA/GHA Data. Does not Include AL data.*Excludes patients who met the referral criteria but were treated at VUMC and pediatric patients not captured by DRG or ICD-10 who were treated at pediatric hospitals
FY 1 FY 2 FY 31/1/2022-
12/31/20221/1/2023-
12/31/20231/1/2024-
12/31/2024Primary Service Area 663 700 740Secondary Service Area 240 241 242Total Service Area 902 941 982
Projected Service Area Patients who Meet Referral Criteria
FY 1 FY 2 FY 31/1/2022-
12/31/20221/1/2023-
12/31/20231/1/2024-
12/31/2024Primary Service Area 234 247 261Secondary Service Area 148 149 150Total Service Area 382 396 411*Excludes patients who met the referral criteria but were treated at VUMC and pediatric patients not captured by DRG or ICD-10 who were treated at pediatric hospitals
Appropriate Referral Rates Applied to Patient Base
90

66 44819987 v1
Based on historical service area ALOS, Skyline projects the following utilization of its proposed 12-bed burn unit:
FY 1 FY 2 FY 31/1/2022-
12/31/20221/1/2023-
12/31/20231/1/2024-
12/31/2024Primary Service Area(excluding Alabama) 117 185 235Secondary Service Area 74 112 135Alabama Estimate 21 32 38Total Service Area 212 329 408Ramp Up 50% 75% 90%
Projected Utilization of Proposed 12 Burn Beds
FY 1 FY 2 FY 31/1/2022-
12/31/20221/1/2023-
12/31/20231/1/2024-
12/31/2024Patients, Inpatient 212 329 408Average Length of Stay (ALOS) 7.0 7.0 7.0Patient Days 1,486 2,303 2,858 Number of Beds 12 12 12Average Daily Census (ADC) 4.1 6.3 7.8Percent Occupancy 33.9% 52.6% 65.2%
Projected Utilization Summary
91

67 44819987 v1
ECONOMIC FEASIBILITY The responses to this section of the application will help determine whether the project can be economically accomplished and maintained.
1. Project Cost Chart Instructions A. All projects should have a project cost of at least $15,000 (the minimum CON Filing
Fee) (See Application Instructions for Filing Fee)
B. The cost of any lease (building, land, and/or equipment) should be based on fair market value or the total amount of the lease payments over the initial term of the lease, whichever is greater. Note: This applies to all equipment leases including by procedure or “per click” arrangements. The methodology used to determine the total lease cost for a "per click" arrangement must include, at a minimum, the projected procedures, the "per click" rate and the term of the lease.
C. The cost for fixed and moveable equipment includes, but is not necessarily limited to,
maintenance agreements covering the expected useful life of the equipment; federal, state, and local taxes and other government assessments; and installation charges, excluding capital expenditures for physical plant renovation or in-wall shielding, which should be included under construction costs or incorporated in a facility lease.
D. The Total Construction Cost reported on line 5 should equal the Total Cost reported
on the Square Footage Chart.
E. For projects that include new construction, modification, and/or renovation—documentation must be provided from a licensed architect or construction professional that support the estimated construction costs. Provide a letter that includes the following:
1) A general description of the project; 2) An estimate of the cost to construct the project; 3) A description of the status of the site’s suitability for the proposed project; and 4) Attesting the physical environment will conform to applicable federal standards,
manufacturer’s specifications and licensing agencies’ requirements including the AIA Guidelines for Design and Construction of Hospital and Health Care Facilities or comparable document in current use by the licensing authority.
Please see Attachment Section B – Economic Feasibility-1A for documentation of cost estimate in the Architect Attestation Letter.
92

68 44819987 v1
PROJECT COST CHART
A. Construction and equipment acquired by purchase: 1. Architectural and Engineering Fees $225,000
2. Legal, Administrative (Excluding CON Filing Fee), Consultant Fees $195,000
3. Acquisition of Site $0
4. Preparation of Site $100,217
5. Total Construction Costs $2,589,367
6. Contingency Fund $271,691
7. Fixed Equipment (Not included in Construction Contract) $71,040
8. Moveable Equipment (List all equipment over $50,000 as separate attachments) $ 1,921,558
9. Other (Specify) _Building Permit____________________ $6,825 B. Acquisition by gift, donation, or lease:
1. Facility (inclusive of building and land)
2. Building only
3. Land only
4. Equipment (Specify)______________________
5. Other (Specify) __________________________ C. Financing Costs and Fees:
1. Interim Financing
2. Underwriting Costs
3. Reserve for One Year’s Debt Service
4. Other (Specify) ___________________________ D. Estimated Project Cost
(A+B+C)
$5,380,698
E. CON Filing Fee $30,939 F. Total Estimated Project Cost
(D+E) TOTAL $5,411,637
Please see Attachment Section B – Economic Feasibility-1B for a detailed list of equipment over moveable equipment threshold ($50,000).
93

69 44819987 v1
2. Identify the funding source(s) for this project.
Check the applicable item(s) below and briefly summarize how the project will be financed. (Documentation for the type of funding MUST be inserted at the end of the application, in the correct alpha/numeric order and identified as Attachment Section B-Economic Feasibility-2.)
__ A. Commercial loan – Letter from lending institution or guarantor stating favorable initial contact, proposed loan amount, expected interest rates, anticipated term of the loan, and any restrictions or conditions;
__ B. Tax-exempt bonds – Copy of preliminary resolution or a letter from the issuing authority stating favorable initial contact and a conditional agreement from an underwriter or investment banker to proceed with the issuance;
__ C. General obligation bonds – Copy of resolution from issuing authority or minutes from the appropriate meeting;
__ D. Grants – Notification of intent form for grant application or notice of grant award;
X E. Cash Reserves – Appropriate documentation from Chief Financial Officer of the organization providing the funding for the project and audited financial statements of the organization; and/or
Please see Attachment Section B - Economic Feasibility-2 for a funding letter showing the availability of funds.
__ F. Other – Identify and document funding from all other sources.
3. Complete Historical Data Charts on the following two pages—Do not modify the Charts provided or submit Chart substitutions!
Historical Data Chart(s) provide revenue and expense information for the last three (3) years for which complete data is available. The “Project Only Chart” provides information for the services being presented in the proposed project while the “Total Facility Chart” provides information for the entire facility. Complete both, if applicable.
Note that “Management Fees to Affiliates” should include management fees paid by agreement to the parent company, another subsidiary of the parent company, or a third party with common ownership as the applicant entity. “Management Fees to Non-Affiliates” should include any management fees paid by agreement to third party entities not having common ownership with the applicant.
94

70 44819987 v1
Total Facility
Year 2017 Year 2018 Year 2019A.
13,309 13,433 13,643 B.
1 $ 1,171,562,153 $1,308,151,159 $ 1,422,350,112
2 $ 283,126,068 $ 296,181,642 $ 319,617,461
3 $ 412,515,376 $ 424,151,236 $ 471,875,324
4 $ 1,479,342 $ 1,675,175 $ 1,450,864 $ 1,868,682,939 $2,030,159,212 $ 2,215,293,761
C.1 $ 1,557,774,235.00 $1,670,934,305 $ 1,801,631,879
2 $ 25,994,176.00 $ 54,821,663 $ 108,792,453
3 $ 28,112,588.00 $ 50,566,068 $ 43,506,304 $ 1,611,880,999 $1,776,322,036 $ 1,953,930,636 $ 256,801,940 $ 253,837,176 $ 261,363,125
D.1
a. Direct Patient Care $ 55,236,084 $ 54,718,991 $ 56,437,302 b. Non-Patient Care $ 35,314,873 $ 34,984,273 $ 36,082,865
2 $ - $ - $ - 3 $ 40,222,747 $ 41,757,463 $ 44,486,227 4 $ 2,013,139 $ 2,572,307 $ 2,618,553
a. Paid to Affiliates
b. Paid to Non-Affiliates
5a. Paid to Affiliates $ 16,613,468 $ 17,421,934 $ 16,949,998 b. Paid to Non-Affiliates
6 $ 45,807,603 $ 50,473,208 $ 52,373,634 $ 195,207,914 $ 201,928,176 $ 208,948,579
E. $ 61,594,026 $ 51,909,000 $ 52,414,546 F.
1 $ - $ - $ - 2 $ 8,489,018 $ 8,946,326 $ 9,948,668 3 $ (9,968,815) $ (11,706,651) $ (12,746,241)
4 $ - $ - $ (293,000)
$ (1,479,797) $ (2,760,325) $ (3,090,573) $ 63,073,823 $ 54,669,325 $ 55,505,119
Depreciation
Interest
Other Non-Operating Expenses
Total Non-Operating Expenses
NET INCOME (LOSS)Chart Continues Onto Next Page
Rent
Total Operating Expenses
Earnings Before Interest, Taxes and Depreciation
Non-Operating ExpensesTaxes
Revenue from Services to PatientsInpatient ServicesOutpatient ServicesEmergency ServicesOther Operating Revenue: Non pt income, Cafeteria
HISTORICAL DATA CHART□ Project Only
Give information for the last three (3) years for which data are available for the facility or agency. The fiscal year begins in January (Month).
Utilization Data Specify Unit of Measure: Admissions
Other Operating Expenses (D6)
Gross Operating Revenue
Management Fees:
Deductions from Gross Operating RevenueContractual AdjustmentsProvision for Charity CareProvisions for Bad Debt
Total DeductionsNET OPERATING REVENUE
Operating ExpensesSalaries and Wages
Physician’s Salaries and Wages
Supplies
95

71 44819987 v1
NOTE: Income taxes are not paid at a facility level and are, instead, paid at the corporate level.
$ 63,073,823 $ 54,669,325 $ 55,505,119
G.1 $ - $ - $ -
2 $ - $ - $ -
$ - $ - $ - $ 63,073,823 $ 54,669,325 $ 55,505,119 $ 8,489,018 $ 8,946,326 $ 9,948,668
$ 71,562,841 $ 63,615,651 $ 65,453,787
Other DeductionsEstimated Annual Principal Debt Repayment
NET INCOME (LOSS)
Annual Capital Expenditure
Total Other DeductionsNET BALANCE
DEPRECIATION
FREE CASH FLOW (Net Balance + Depreciation)
Total Facility
Year 2017 Year 2018 Year 2019(D6)1 $ 9,020,044 $ 9,319,563 $ 9,669,828
2 $ 24,259,880 $ 26,934,306 $ 28,118,664
3 $ 5,092,597 $ 5,595,395 $ 5,775,056
4 $ 2,276,212 $ 2,176,218 $ 2,263,137
5 $ 1,198,889 $ 1,888,039 $ 2,077,544
6 $ 1,121,216 $ 1,172,111 $ 1,166,673
7 $ 2,838,765 $ 3,387,576 $ 3,302,732 $ 45,807,603 $ 50,473,208 $ 52,373,634
HISTORICAL DATA CHART-OTHER EXPENSES
OTHER OPERATING EXPENSES CATEGORIES
*Total Other Expenses
Professional Fees
*Total other expenses should equal Line D.6. In the Historical Data Chart
Contracted ServicesMaintenance and RepairsUtilitiesInsuranceTaxes-Non IncomeOther
□ Project Only
96

72 44819987 v1
4. Complete Projected Data Charts on the following two pages – Do not modify the Charts provided or submit Chart substitutions!
Projected Data Chart(s) provide information for the two years following the completion of the project. The “Project Only Chart” should reflect revenue and expense projections for the project (i.e., if the application is for additional beds, include anticipated revenue from the proposed beds only, not from all beds in the facility). The “Total Facility Chart” should reflect information for the total facility. Complete both, if applicable.
Note that “Management Fees to Affiliates” should include management fees paid by agreement to the parent company, another subsidiary of the parent company, or a third party with common ownership as the applicant entity. “Management Fees to Non-Affiliates” should include any management fees paid by agreement to third party entities not having common ownership with the applicant.
97

73R2
Chart Continues Onto Next Page
Year 2022 Year 2023
A.
212 329
B.
1 $ 35,429,917 $ 59,451,061
2
3 $ 1,289,650 $ 2,161,503
4 $ 14,480 $ 22,471
$ 36,734,047 $ 61,635,035
C.
1 $ 28,046,399 $ 47,693,465
2 $ 1,836,702 $ 3,081,752
3 $ 551,011 $ 924,526
$ 30,434,112 $ 51,699,743
$ 6,299,935 $ 9,935,292
D.
1Salaries and
Wages
a. Direct Patient Care $ 1,496,346 $ 2,380,150
b. Non-Patient Care $ 223,300 $ 227,766
2 $ - $ -
3 $ 1,218,637 $ 1,932,190
4
a. Paid to Affiliates $ - $ -
b. Paid to Non-Affiliates $ 5,936 $ 9,212
5
a. Paid to Affiliates $ 37,800 $ 59,612
b. Paid to Non-Affiliates $ - $ -
6 $ 1,406,791 $ 1,627,425
$ 4,388,810 $ 6,236,355
E. $ 1,911,125 $ 3,698,937
F.
1 $ - $ -
2 $ 546,957 $ 546,957
3 $ (248,446) $ (480,862)
4 $ - $ -
$ 298,511 $ 66,095
$ 1,612,614 $ 3,632,842
Total Operating Expenses
Earnings Before Interest, Taxes and Depreciation
Non-Operating Expenses
Taxes
Depreciation
Interest
Other Non-Operating Expenses
Total Non-Operating Expenses
NET INCOME (LOSS)
Other Operating Expenses (D6)
Deductions from Gross Operating Revenue
Contractual Adjustments
Provision for Charity Care
Provisions for Bad Debt
Total Deductions
NET OPERATING REVENUE
Operating Expenses
Physician’s Salaries and Wages
Supplies
Rent
Management Fees:
Gross Operating Revenue
PROJECTED DATA CHART
□ Project Only
□ Total Facility
Give information for the two (2) years following the completion of this proposal. The fiscal year begins in
January (Month).
Utilization Data
Specify Unit of Measure: Admissions
Revenue from Services to Patients
Inpatient Services
Outpatient Services
Emergency Services
Other Operating Revenue: Non pt income, Cafeteria
Supplemental 2 January 29, 2021
98

74 44819987 v1
NOTE: Professional fees include call coverage. Contracted Services include management service agreements.
G.1 $ - $ - $ - 2 $ - $ - $ -
$ - $ - $ - $ 1,612,615 $ 3,632,842 $ 5,018,934 $ 546,957 $ 546,957 $ 546,957 $ 2,159,572 $ 4,179,799 $ 5,565,891
Estimated Annual Principal Debt Repayment
Annual Capital Expenditure
Total Other DeductionsNET BALANCE
DEPRECIATIONFREE CASH FLOW (Net Balance + Depreciation)
Other DeductionsNET INCOME (LOSS)
Project Only
Year 2022 Year 2023(D6)1 $ 543,936 $ 545,024
2 $ 647,012 $ 766,743
3 $ 80,772 $ 127,856
4 $ 41,393 $ 41,641
5 $ 21,626 $ 33,897
6 $ 27,301 $ 42,121
7 $ 44,751 $ 70,143 $ 1,406,791 $ 1,627,425
*Total other expenses should equal Line D.6. In the Projected Data Chart
Maintenance and RepairsUtilitiesInsuranceTaxes-Non IncomeOther*Total Other Expenses
□ Total FacilityPROJECTED DATA CHART-OTHER EXPENSES
OTHER OPERATING EXPENSES CATEGORIES
Professional FeesContracted Services
99

75R
Chart Continues Onto Next Page
□
Total Facility incl
project
Year 2022 Year 2023
A.
14,777 15,142
B.
1 $ 1,946,186,649 $ 2,159,503,454
2 $ 337,975,490 $ 368,663,665
3 $ 508,252,886 $ 555,157,000
4 $ 1,021,959 $ 1,060,174
$ 2,793,436,984 $ 3,084,384,293
C.
1 $ 2,289,201,403 $ 2,544,110,720
2 $ 142,682,965 $ 158,582,388
3 $ 40,647,532 $ 45,192,896
$ 2,472,531,900 $ 2,747,886,004
$ 320,905,084 $ 336,498,289
D.
1Salaries and
Wages
a. Direct Patient Care $ 61,837,779 $ 66,353,210
b. Non-Patient Care $ 38,802,249 $ 39,437,061
2 $ - $ -
3 $ 50,436,145 $ 53,020,410
4
a. Paid to Affiliates $ - $ -
b. Paid to Non-Affiliates $ 2,389,748 $ 2,416,862
5
a. Paid to Affiliates $ 1,897,473 $ 1,937,881
b. Paid to Non-Affiliates $ - $ -
6 $ 70,516,684 $ 72,062,128
$ 225,880,078 $ 235,227,552
E. $ 95,025,006 $ 101,270,737
F.
1 $ - $ -
2 $ 14,848,541 $ 15,563,620
3 $ (11,948,017) $ (12,414,424)
4 $ - $ -
$ 2,900,524 $ 3,149,196
$ 92,124,482 $ 98,121,541
Other Non-Operating Expenses
Total Non-Operating Expenses
NET INCOME (LOSS)
Interest
Operating Expenses
Physician’s Salaries and Wages
Supplies
Rent
Management Fees:
Other Operating Expenses (D6)
Total Operating Expenses
Earnings Before Interest, Taxes and Depreciation
Non-Operating Expenses
Taxes
Depreciation
NET OPERATING REVENUE
Revenue from Services to Patients
Inpatient Services
Outpatient Services
Emergency Services
Other Operating Revenue: Non pt income, Cafeteria
Gross Operating Revenue
Deductions from Gross Operating Revenue
Contractual Adjustments
Provision for Charity Care
Provisions for Bad Debt
Total Deductions
PROJECTED DATA CHART
□ Project Only
Give information for the two (2) years following the completion of this proposal. The fiscal year begins in January
(Month).
Utilization Data
Specify Unit of Measure: Admissions
Supplemental 2 January 29, 2021
100

76 44819987 v1
NOTE: (1) Professional fees include call coverage. Contracted Services include management service agreements. (2) Income taxes are not paid at a facility level and are, instead, paid at the corporate level.
G.1 $ - $ -
2 $ - $ -
$ - $ - $ 92,124,483 $ 98,121,541 $ 14,848,541 $ 15,563,620 $ 106,973,024 $ 113,685,161
Estimated Annual Principal Debt Repayment
Annual Capital Expenditure
Total Other DeductionsNET BALANCE
DEPRECIATIONFREE CASH FLOW (Net Balance + Depreciation)
NET INCOME (LOSS)Other Deductions
Total Facility incl project
Year 2022 Year 2023(D6)1 $ 13,301,101 $ 13,327,703
2 $ 27,901,835 $ 28,641,456
3 $ 5,712,422 $ 5,815,822
4 $ 2,387,021 $ 2,410,726
5 $ 3,259,062 $ 3,364,733
6 $ 2,115,057 $ 2,196,483
7 $ 15,840,186 $ 16,305,204 $ 70,516,683 $ 72,062,128
*Total other expenses should equal Line D.6. In the Projected Data Chart
Maintenance and RepairsUtilitiesInsuranceTaxes-Non IncomeOther*Total Other Expenses
□ Project Only
PROJECTED DATA CHART-OTHER EXPENSES
OTHER OPERATING EXPENSES CATEGORIES
Professional FeesContracted Services
101

77R
5. A. Please identify the project’s average gross charge, average deduction fromoperating revenue, and average net charge using information from the Projected Data Charts for Year 1 and Year 2 of the proposed project. Complete Project Only Chart and Total Facility Chart, if applicable.
Project Only Chart Previous Year to Most Recent Year Year 2018
Most Recent Year Year 2019
Year One Year 2022
Year Two Year 2023
% Change (Current Year
to Year 2)
Gross Charge (Gross Operating Revenue/Utilization Data)
N/A N/A $173,274 $187,341 N/A
Deduction from Revenue (Total Deductions/Utilization Data)
N/A N/A $143,557 $157,142 N/A
Average Net Charge (Net Operating Revenue/Utilization Data)
N/A N/A $29,717 $30,198 N/A
Total Facility Chart (including Project) Previous Year to Most Recent Year Year 2018
Most Recent Year Year 2019
Year One Year 2022
Year Two Year 2023
% Change (Current Year to Year 2)
Gross Charge (Gross Operating Revenue/Utilization Data)
$151,132 $162,376 $189,033 $203,696 $219,448
Deduction from Revenue (Total Deductions/Utilization Data)
$132,236 $143,219 $167,318 $181,473 $196,747
Average Net Charge (Net Operating Revenue/Utilization Data)
$18,897 $19,157 $21,716 $22,223 $22,701
B. Provide the proposed charges for the project and discuss any adjustment tocurrent charges that will result from the implementation of the proposal.Additionally, describe the anticipated revenue from the project and theimpact on existing patient charges.
The proposed charges for patients admitted to the burn unit represent a complexarray of components from room and board to ancillary and support services. Thecharges were developed based on BRCA affiliated facilities actual experience inserving burn injured patients by DRG. The proposed project will not result in anyadjustments to the current charges at Skyline. The anticipated revenue from theproject also will not impact existing patient charges.
Supplemental 1 January 28, 2021
102

78 44819987 v1
C. Compare the proposed charges to those of similar facilities/services in the service area/adjoining service areas, or to proposed charges of recently approved Certificates of Need. If applicable, compare the proposed charges of the project to the current Medicare allowable fee schedule by common procedure terminology (CPT) code(s).
There is only one similar facility/service in the services area operated by VUMC. There is no publicly available source of data that would allow for comparison of charges for inpatient burn admissions to this program. There are also no recently approved Certificate of Need applications with which to compare. Skyline relied on comparable charges from other burn programs affiliated with BRCA to project the charges for this project. CPT codes are not relevant for this service because it is so complex and involves so many ancillary and support services for the treatment of each patient. Skyline considered the Medicare reimbursement rates for projected burn patients at the DRG level in projecting its charges.
6. A. Discuss how projected utilization rates will be sufficient to support financial performance.
1) Noting when the project’s financial breakeven is expected, and The proposed project is projected to experience positive net income in Year 1, as shown in the projected data chart above.
2) Demonstrating the availability of sufficient cash flow until financial viability is achieved. Provide copies of the balance sheet and income statement from the most recent reporting period of the institution and the most recent audited financial statements with accompanying notes, if applicable. For all projects, provide financial information for the corporation, partnership, or principal parties that will be a source of funding for the project. Copies must be inserted at the end of the application, in the correct alpha-numeric order and labeled as Attachment Section B-Economic Feasibility-6A See Attachment Section B-Economic Feasibility-6A.
103

79 44819987 v1
B. Net Operating Margin Ratio: The Net Operating Margin Radio demonstrates how much revenue is left over after all the variable or operating costs have been paid. The formula for this ratio is: (Earnings before interest, Taxes, and Depreciation/Net Operating Revenue).
Utilizing information from the Historical and Projected Data Charts please report the net operating margin ratio trends in the following tables. Complete Project Only Chart and Total Facility Chart, if applicable.
Project Only Chart
Year
2nd Previous Year to Most Recent Year Year 2017
1st Previous Year to Most Recent Year Year 2018
Most Recent Year
Year 2019
Projected Year 1
Year 2022
Projected Year 2
Year 2023
Net Operating Margin Ratio
N/A N/A N/A 30.3% 37.2%
Total Facility Chart
Year
2nd Previous Year to Most Recent Year Year 2017
1st Previous Year to Most Recent Year Year 2018
Most Recent Year
Year 2019
Projected Year 1
Year 2022
Projected Year 2
Year 2023
Net Operating Margin Ratio
24.0% 20.4% 20.1% 29.6% 30.1%
104

80 44819987 v1
C. Capitalization Ratio: The Long-term debt to capitalization ratio measures the
proportion of debt financing in a business’s permanent (long-term) financing mix. This ratio best measures a business’s true capital structure because it is not affected by short-term financing decisions. The formula for this ratio is: ((Long-Term Debt)/Long-Term Debt + Total Equity {Net Assets}) X 100.
For self or parent company funded projects, provide the capitalization ratio using the most recent year available from the funding entity’s audited balance sheet, if applicable. Capitalization Ratios are not expected from outside the company lenders that provide funding. This question is applicable to all applications regardless of whether or not the project is being partially or totally funded by debt financing. The capitalization ratio is reflected below. Although the traditional capitalization ratio is negative, this does not accurately reflect the financial standing of HCA. This is because the 2006 merger and related transactions were accounted for as "recapitalization" of HCA, Inc. rather than a "sale"; therefore, the Company's liabilities currently exceed its assets on its books. A more accurate depiction of the Company’s financial standing is the Value of Equity calculation also reflected below.
105

81R2
7. Discuss the project’s participation in state and federal revenue programs, including adescription of the extent to which Medicare, TennCare/Medicaid and medically indigentpatients will be served by the project. Report the estimated gross operating revenue dollaramount and percentage of projected gross operating revenue anticipated by payorclassification for the first year of the project by completing the table below. CompleteProject Only Chart and Total Facility Chart, if applicable.
Applicant’s Projected Payor Mix, Year 1
Project Only Chart
Payor Source Projected Gross
Operating Revenue As a % of total
Medicare/Medicare Managed Care $ 11,577,806 31.5%
TennCare/Medicaid $ 8,332,144 22.7%
Commercial/Other Managed Care $ 8,671,243 23.6%
Self-Pay $ 3,100,333 8.4%
Other: Work Comp, Champus, HIX, Other Fed $ 3,245,661 8.8%
Total Excluding Charity $ 34,927,187 95.1%
Charity $ 1,792,380 4.9%
Total* $ 36,719,567 100.0%
*Needs to match Gross Operating Revenue Year One on Projected Data Chart
Applicant’s Projected Payor Mix, Year 1
Total Facility Chart
Payor Source Projected Gross
Operating Revenue As a % of total
Medicare/Medicare Managed Care $ 1,369,611,911 49.0%
TennCare/Medicaid $ 407,261,530 14.6%
Commercial/Other Managed Care $ 521,712,774 18.7%
Self-Pay/Charity $ 216,462,437 7.8%
Other: Work Comp, Champus, HIX, Other Fed $ 153,369,400 5.5%
Total Excluding Charity $ 2,668,418,052 95.6%
Charity $ 123,996,973 4.4%
Total* $ 2,792,415,025 100.0%
*Needs to match Gross Operating Revenue Year One on Projected Data Chart
Supplemental 2 January 29, 2021
106

82R2
8. Provide the projected staffing for the project in Year 1 and compare to the current staffing forthe most recent 12-month period, as appropriate. This can be reported using full-timeequivalent (FTEs) positions for these positions. Identify projected salary amounts by positionclassifications and compare the clinical staff salaries to prevailing wage patterns in theproposed service area as published by the Department of Labor & Workforce Developmentand/or other documented sources, such as the US Department of Labor. Wage data pertainingto healthcare professions can be found at the following link:https://www.bls.gov/oes/current/oes_tn.htm.
Position Classification Existing FTEs ƚ
2019
Projected FTEs Year 1
Average Wage (Contractual
Rate)
Area Wide/Statewide Average Wage
A. Direct Patient CarePositions
RN's 500 11.2 $34.56 $30.08
LPN's 6 $22.42 $19.84
Pharmacy 44 0.6 $48.18 $59.40
Lab 36 0.6 $28.02 $25.47
Dieticians 6 - $29.61 $26.53
Imaging 36 0.6 $36.27 $28.92
Therapists 51 1.2 $37.76 $40.73
Respiratory Therapy 31 0.6 $31.61 $25.08
Surgical Techs 30 2.2 $39.16 $21.41
Child Life Specialist* 0 0.2 $25.27 $22.59
Total Direct Patient Care Positions
740 17.2 - -
B. Non-Patient CarePositions
RN Administrative 25 - $52.64 $46.40
VP of Burn Operations* - 1 $60.09 $66.66
Burn Registry/PI** - 1 $37.50 N/A
Total Non-Patient Care Positions
202 2 $34.79 -
Total Employees (A+B)
227 19.2 - -
C. Contractual Staff 104 - $34.39 -
Total Staff (A+B+C)
1,071 19.2 - -
ƚ Based on Skyline Medical Center FTEs
*Based on research of open positions and/or national averages. Statewide averages were not available for
these position in the U.S. Bureau of Labor Statistics Database.
** National nor statewide averages can be found using publicly available data.
Supplemental 2 January 29, 2021
107

83 44819987 v1
9. What alternatives to this project were considered? Discuss the advantages and disadvantages of each, including but not limited to:
A. The availability of less costly, more effective and/or more efficient methods of providing the benefits intended by the project. If development of such alternatives is not practicable, justify why not, including reasons as to why they were rejected.
Skyline considered the status quo which would be to do nothing. This alternative was quickly dismissed, as the proposed project is necessary in order to offer service area residents with an alternative, ABA-verified comprehensive burn provider. Maintaining the status quo would not be an effective method of providing the benefits intended by the proposed project.
B. Document that consideration has been given to alternatives to new construction, e.g., modernization or sharing arrangements. Not applicable. The proposed project does not involve new construction.
108

84 44819987 v1
QUALITY STANDARDS
1. Per PC 1043, Acts of 2016, any receiving a CON after July 1, 2016 must report annually using forms prescribed by the Agency concerning continued need and appropriate quality measures Please verify that annual reporting will occur. The Applicant will report annually using forms prescribed by the Agency concerning continued need and appropriate quality measures.
2. Quality-The the proposal shall provide health care that meets appropriate quality standards. Please address each of the following questions:
A. Does the applicant commit to the following? (See Attachment Section B – Quality 2A)
1) Maintaining the staffing comparable to the staffing chart presented in its CON application; The Applicant is committed to maintaining the staffing comparable to the staffing chart presented in its CON application.
2) Obtaining and maintaining all applicable state licenses in good standing;
The Applicant is committed to obtaining and maintaining all applicable state licenses in good standing.
3) Obtain and maintaining TennCare and Medicare certification(s), if participation in such programs was indicated in the application;
The Applicant is committed to obtaining and maintaining TennCare and Medicare certification(s).
4) For an existing healthcare institution applying for a CON - Has it maintained substantial compliance with applicable federal and state regulation for the three years prior to the CON application. In the event of non-compliance, the nature of non-compliance and corrective action should be discussed to include any of the following: suspension of admissions, civil monetary penalties, notice of 23-day or 90-day termination proceedings from Medicare/Medicaid/TennCare, revocation/denial of accreditation, or other similar actions and what measures the applicant has or will put into place to avoid similar findings in the future. The Applicant has maintained compliance with applicable federal and state regulation for three years prior to the CON application. The Applicant is not aware of any non-compliance measures and actions.
5) For an existing healthcare institution applying for a CON - Has the entity been
decertified within the prior three years? If yes, please explain in detail. (This provision shall not apply if a new, unrelated owner applies for a CON related to a previously decertified facility)
The Applicant has not been decertified within the prior three years.
109

85 44819987 v1
B. Respond to all of the following and for such occurrences, identify, explain and provide documentation:
1) Has any of the following:
a. Any person(s) or entity with more than 5% ownership (direct or indirect) in the
applicant (to include any entity in the chain of ownership for applicant);
b. Any entity in which any person(s) or entity with more than 5% ownership (direct or indirect) in the applicant (to include any entity in the chain of ownership for applicant) has an ownership interest of more than 5%; and/or
c. Any physician or other provider of health care, or administrator employed by any
entity in which any person(s) or entity with more than 5% ownership in the applicant (to include any entity in the chain of ownership for applicant) has an ownership interest of more than 5%.
The Applicant has made a good faith effort to respond to this question regarding the entities identified in the organizational chart for direct upstream ownership of Skyline, to the best of its knowledge, information, and belief. Due to the breadth of the question and lack of definition of key terms, the Applicant cannot represent these responses are totally comprehensive, but no responsive information is being intentionally withheld. Because there is no central repository for the information sought, and because the length of time some of the entities have been in existence, the Applicant’s responses are limited to the past 5 years as a reasonable look-back period, unless the applicable question specifically calls for a different time period.
2) Been subjected to any of the following:
a. Final Order or Judgment in a state licensure action;
The Applicant assumes for the purpose of this question that “state licensure action” refers to facility licensure. Skyline has not been subjected to a Final Order or Judgment in a state licensure action. The other entities in the chain of ownership do not hold a hospital license.
b. Criminal fines in cases involving a Federal or State health care offense;
None.
c. Civil monetary penalties in cases involving a Federal or State health care offense;
None. The Applicant is not aware that any of its entities upstream have been involved in civil litigation whereby a judgment or settlement was entered into resulting in payment of Civil Monetary Penalty.
d. Administrative monetary penalties in cases involving a Federal or State health care offense; None. The Applicant is not aware that any of its entities upstream have been involved in civil litigation whereby a judgment or settlement was entered into resulting in payment of Administrative Monetary Penalty.
110

86 44819987 v1
e. Agreement to pay civil or administrative monetary penalties to the federal
government or any state in cases involving claims related to the provision of health care items and services; and/or Please see the responses to (c) and (d) above.
f. Suspension or termination of participation in Medicare or Medicaid/TennCare
programs. None.
g. Is presently subject of/to an investigation, regulatory action, or party in any civil or criminal action of which you are aware.
In light of the breadth and scope of services provided and the business conducted by the entities upstream from the Applicant, it is likely that at any given time one or more are involved, in some capacity, in some type of investigation, regulatory action or civil action. However, neither Skyline nor any of its upstream entities are the subject of a criminal action.
h. Is presently subject to a corporate integrity agreement. None.
C. Does the applicant plan, within 2 years of implementation of the project, to participate in self-assessment and external assessment against nationally available benchmark data to accurately assess its level of performance in relation to established standards and to implement ways to continuously improve? Note: Existing licensed, accredited and/or certified providers are encouraged to describe their process for same.
Please complete the chart below on accreditation, certification, and licensure plans.
1) If the applicant does not plan to participate in these types of assessments, explain why since quality healthcare must be demonstrated.
2) Based upon what was checked/completed in above table, will the applicant accept a condition placed on the certificate of need relating to obtaining/maintaining license, certification, and/or accreditation?
Credential Agency Status (Active or Will Apply)
Licensure ☒ ☐ ☐
Health Intellectual and Developmental Disabilities Mental Health and Substance Abuse Services
Active
Certification ☒ Medicare ☒ Medicaid/TennCare ☐ Other_________________
Active
Accreditation The Joint Commission Active
111

87 44819987 v1
Not applicable. The Applicant is active and up to date on all licensures, certifications, and accreditations.
D. The following list of quality measures are service specific. Please indicate which standards you will be addressing in the annual Continuing Need and Quality Measure report if the project is approved. Not applicable. None of these requirements apply to burn units.
For Ambulatory Surgical Treatment Center projects: Estimating the number of physicians by specialty expected to utilize the facility, developing criteria to be used by the facility in extending surgical and anesthesia privileges to medical personnel, and documenting the availability of appropriate and qualified staff that will provide ancillary support services, whether on- or off-site?
For Cardiac Catheterization projects: a. Documenting a plan to monitor the quality of its cardiac catheterization program, including
but not limited to, program outcomes and efficiencies; and
b. Describing how the applicant will agree to cooperate with quality enhancement efforts sponsored or endorsed by the State of Tennessee; and
c. Describing how cardiology staff will be maintaining: d. Adult Program: 75 cases annually averaged over the previous 5 years; e. Pediatric Program: 50 cases annually averaged over the previous 5 years.
For Open Heart projects:
f. Describing how the applicant will staff and maintain the number of who will perform the volume of cases consistent with the State Health Plan (annual average of the previous 2 years), and maintain this volume in the future;
g. Describing how at least a surgeon will be recruited and retained (at least one shall have 5
years’ experience); h. Describing how the applicant will participate in a data reporting, quality improvement,
outcome monitoring, and external assessment system that benchmarks outcomes based on national norms (demonstrated active participation in the STS National Database is expected and shall be considered evidence of meeting this standard).
For Comprehensive Inpatient Rehabilitation Services projects: Retaining or recruiting a physiatrist?
For Home Health projects: Documenting the existing or proposed plan for quality data reporting, quality improvement, and an outcome and process monitoring system.
For Hospice projects: Documenting the existing or proposed plan for quality data reporting, quality improvement, and an outcome and process monitoring system.
For Megavoltage Radiation Therapy projects: Describing or demonstrating how the staffing and quality assurance requirements will be met of the American Society of Therapeutic Radiation and Oncology (ASTRO), the American College of Radiology (ACR), the American College of Radiation Oncology (ACRO), National Cancer Institute (NCI), or a similar accrediting authority.
112

88 44819987 v1
For Neonatal Intensive Care Unit projects: Documenting the existing or proposed plan for data reporting, quality improvement, and outcome and process monitoring systems; document the intention and ability to comply with the staffing guidelines and qualifications set forth by the Tennessee Perinatal Care System Guidelines for Regionalization, Hospital Care Levels, Staffing and Facilities; and participating in the Tennessee Initiative for Perinatal Quality Care (TIPQC).
For Nursing Home projects: Documenting the existing or proposed plan for data reporting, quality improvement, and outcome and process monitoring systems, including in particular details on its Quality Assurance and Performance Improvement program.
For Inpatient Psychiatric projects:
Describing or demonstrating appropriate accommodations for:
Seclusion/restraint of patients who present management problems and children who need quiet space, proper sleeping and bathing arrangements for all patients);
Proper sleeping and bathing arrangements;
Adequate staffing (i.e., that each unit will be staffed with at least two direct patient care
staff, one of which shall be a nurse, at all times);
A staffing plan that will lead to quality care of the patient population served by the project.
An existing or proposed plan for data reporting, quality improvement, and outcome and process monitoring systems; and
If other psychiatric facilities are owned or administered, providing information on
satisfactory surveys and quality improvement programs at those facilities.
Involuntary admissions if identified in CON criteria and standard review
For Freestanding Emergency Department projects: Demonstrating that it will be accredited with the Joint Commission or other applicable accrediting agency, subject to the same accrediting standards as the licensed hospital with which it is associated.
For Organ Transplant projects: Describing how the applicant will achieve and maintain institutional membership in the national Organ Procurement and Transportation Network (OPTN), currently operating as the United Network for Organ Sharing (UNOS), within one year of program initiation. Describing how the applicant shall comply with CMS regulations set forth by 42 CFR Parts 405, 482, and 498, Medicare Program; Hospital Conditions of Participation: Requirements for Approval and Re-Approval of Transplant Centers to Perform Organ Transplants.
For Relocation and/or Replacement of Health Care Institution projects: Describing how facility and/or services specific measures will be met.
113

89 44819987 v1
CONTRIBUTION TO THE ORDERLY DEVELOPMENT OF HEALTH CARE The responses to this section of the application helps determine whether the project will contribute to the orderly development of healthcare within the service area.
1. List all existing health care providers (i.e., hospitals, nursing homes, home care organizations, etc.), managed care organizations, alliances, and/or networks with which the applicant currently has or plans to have contractual and/or working relationships, that may directly or indirectly apply to the project, such as, transfer agreements, contractual agreements for health services.
Please see Attachment Section B – Orderly Development-1.
2. Describe the effects of competition and/or duplication of the proposal on the health care system, including the impact to consumers and existing providers in the service area. Discuss any instances of competition and/or duplication arising from your proposal including a description of the effect the proposal will have on the utilization rates of existing providers in the service area of the project.
As previously discussed, there is only one existing provider of burn services in the service area, serving all of central and east Tennessee: VUMC. VUMC is located in Nashville where Skyline proposes to locate its ABA-verified burn program. Nashville is a growing, large metropolitan area that is easily accessible to the broad service area. The service area can support, and in fact needs, more than one burn provider.
A. Positive Effects
Competition in health care markets, including burn services, benefits consumers because it helps contain costs, improve quality, and encourage innovation. Skyline proposes to offer a needed alternative to the only existing burn provider in the service area. In the event of a burn MCI, Skyline will be able to assist in meeting the needs of the surge of patients that will need immediate access to burn care. Further, Skyline will be the only ABA-verified program in the area which will improve innovation and quality of care.
B. Negative Effects
Unnecessary duplication can have a negative impact on existing providers; however, as evidenced in this application, there is a need for a second burn unit in Skyline’s service area. Skyline has shown in its projections that its project will not have any material effect on VUMC’s burn program which is already highly utilized. Skyline proposes to serve patients in the service area not currently served by VUMC. Further, the service area population is large enough to support two burn services providers.
114

90 44819987 v1
3. A. Discuss the availability of and accessibility to human resources required by the proposal, including clinical leadership and adequate professional staff, as per the State of Tennessee licensing requirements, CMS, and/or accrediting agencies requirements, such as the Joint Commission and Commission on Accreditation of Rehabilitation Facilities.
TriStar Health has significant resources that it employs in recruiting needed clinical and administrative staff for its existing facilities and new facilities. The Applicant is confident that any staff required for the facility can be readily recruited both from that source and from Middle Tennessee.
The Applicant’s owner operates 7 hospitals in metro Nashville and surrounding areas as well as over 10 burn programs across 10 states. Skyline will also be partnering with BRCA, in the creation and operation of the burn center. BRCA has over 40 years of experience as a preeminent burn care provider. With these partnerships, and Skyline’s demonstrated experience as a Level II Trauma Center, this program will have all of the necessary components as well as access to the experience and training necessary to provide exceptional care to this patient population. HCA currently has 3 ABA verified burn programs with additional programs in various stages of that process. Skyline will also seek ABA verification and is committed to meeting all of the staffing requirements set forth by the American Burn Association. Skyline will also partner with the Children’s Hospital at Centennial Medical Center to assist with resources and training for the needed pediatric specialties necessary to treat pediatric burns. These will include Pediatric: Critical Care, Anesthesiology, Pharmacy, Nursing and Therapy. The Applicant fully understands the staffing requirements for this type of unit and is committed to meeting and exceeding those needs. The Applicant is also aware of and familiar with all human resource requirements of the Tennessee Board for Licensing Healthcare Facilities and the Joint Commission.
B. Document the category of license/certification that is applicable to the project and why. These include, without limitation, regulations concerning clinical leadership, physician supervision, quality assurance policies and programs, utilization review policies and programs, record keeping, clinical staffing requirements, and staff education.
Skyline is licensed by the Tennessee Board for Licensing Health Care Facilities and the license is in good standing. As it relates specifically to the proposed burn program, there is no license required; however, Skyline is committed to providing high quality burn care and will seek ABA verification. All of the hospital’s existing and applicable policies and procedures related to quality assurance, utilization review, record keeping, clinical staffing, and staff education will be incorporated into the burn program upon implementation.
C. Discuss the applicant’s participation in the training of students in the areas of medicine, nursing, social work, etc. (e.g., internships, residencies, etc.).
Skyline is committed to providing education opportunities for medical and other clinical staff in training. See Attachment Section B – Orderly Development-3C for a list of the training programs with which Skyline has agreements and serves as a training site.
Additionally, TriStar Health is partnering with Belmont University to start a new College of Medicine. TriStar Health and Skyline will provide clinical rotations for Belmont University’s medical students and further augment training with critical residencies and fellowships through Graduate Medical Education. Skyline will play an integral role in the training of these new physicians, and the burn program will further expand and augment their vital clinical experiences.
115

91 44819987 v1
4. Outstanding Projects:
A. Complete the following chart by entering information for each applicable outstanding CON by applicant or share common ownership; and
Outstanding Projects
CON Number Project Name Date Approved
*Annual Progress Report(s) Expiration Date Due Date Date Filed
CN1411-047 Southern Hills Surgery Center
3/25/2015 7/1/20 7/7/20 7/1/21
CN1803-017 TriStar Southern Hills Emergency Department at Antioch
6/27/2018 8/1/20 8/4/20 8/1/21
CN1707-023 StoneCrest Surgery Center
10/25/17 6/1/20 5/27/2020 (1-year extension
approved)
6/1/21
CN1909-035 TriStar Skyline Medical Center
1/23/20 2/1/21 N/A 2/1/22
* Annual Progress Reports – HSDA Rules require that an Annual Progress Report (APR) be submitted each year. The APR is due annually until the Final Project Report (FPR) is submitted (FPR is due within 90 ninety days of the completion and/or implementation of the project). Brief progress status updates are requested as needed. The project remains outstanding until the FPR is received.
116

92 44819987 v1
B. Describe the current progress, and status of each applicable outstanding CON.
Project Name CON # Project Type Update Expiration
Date
Southern Hills Surgery
Center CN1411-
047 Relocation of ASTC
Construction is in process. Building shell is completed and buildout is underway with expected completion date in early 2021.
7/1/2021
TriStar Southern
Hills Emergency Department at Antioch
CN1803-017
FSED in Antioch
Construction is in process and the anticipated date of project completion is April of 2021 with opening expected in June of 2021.
8/1/2021
StoneCrest Surgery Center
CN1707-023
Addition of a surgery
center
After CON was granted and before construction began, Medical Care America, an HCA affiliate, was able to acquire an existing surgery center in Rutherford County. Since that acquisition, StoneCrest has been evaluating whether and to what extent that facility will satisfy StoneCrest’s need for ambulatory surgical facilities at least for the foreseeable future. StoneCrest requested and was granted an extension in May of 2020 to allow additional time to fully evaluate the situation, especially in light of recent pandemic events.
6/1/2021
TriStar Skyline Medical Center
CN1909-035
Initiation of mobile PET service up
to 2 days/week
Project was approved January 2020. Services have been implemented as of 10/15/2020. Final project report will be filed.
2/1/2022
5. Equipment Registry – For the applicant and all entities in common ownership with the
applicant.
A. Do you own, lease, operate, and/or contract with a mobile vendor for a Computed Tomography scanner (CT), Linear Accelerator, Magnetic Resonance Imaging (MRI), and/or Positron Emission Tomographer (PET)? Yes_____
B. If yes, have you submitted their registration to HSDA? If you have, what was the date of submission? February 25, 2020 _____
C. If yes, have you submitted your utilization to Health Services and Development Agency? If
you have, what was the date of submission? Yes, February 25, 2020. The mobile PET and second MRI unit were recently implemented in October 2020 and will show utilization in the 2021 filing with the Health Services and Development Agency. _____
117

93 44819987 v1
SECTION C: STATE HEALTH PLAN QUESTIONS T.C.A. §68-11-1625 requires the Tennessee Department of Health’s Division of Health Planning to develop and annually update the State Health Plan (found at https://www.tn.gov/health/health-program-areas/health-planning/state-health-plan.html) The State Health Plan guides the State in the development of health care programs and policies and in the allocation of health care resources in the State, including the Certificate of Need program. The 5 Principles for Achieving Better Health are from the State Health Plan’s framework and inform the Certificate of Need program and its standards and criteria. Discuss how the proposed project will relate to the 5 Principles for Achieving Better Health found in the State Health Plan. 1. The purpose of the State Health Plan is to improve the health of Tennesseans.
Skyline and TriStar Health are committed to the care and improvement of human life by striving to deliver high quality and cost-effective healthcare in their communities. TriStar Health believes the following value statements as crucial to achieving its goals:
We recognize and affirm the unique and intrinsic worth of each individual. We treat all those we serve with compassion and kindness. We act with absolute honesty, integrity, and fairness in the way we conduct our
business and the way we live our lives. We trust our colleagues as valuable members of our healthcare team and pledge to
treat one another with loyalty, respect, and dignity.
TriStar Health has been committed to the care and improvement of the health of Tennesseans for decades. More specifically, Skyline has been serving Nashville and surrounding communities for more than 20 years. The proposed project will improve the health of Tennesseans by offering a verified, comprehensive burn care provider with the resources, reputation, and commitment to ensuring that residents have adequate access to high quality burn care.
TriStar Health is committed to raising the bar by investing in new construction, campus expansion projects, and the addition of new technology and services. TriStar Health’s large capital investment underscores its commitment to providing care across its network. In accordance with this commitment, the proposed comprehensive burn program is essential to ensuring adequate access to high quality burn care for Tennessee residents.
2. Every citizen should have reasonable access to health care. The TriStar Health network had over 2.2 million encounters last year, including 459,988 ER visits, 60,927 inpatient admissions and 7,087 babies delivered. Besides paying taxes and employing many people in the communities TriStar Health serves, it provides approximately $1.2 billion annually in uncompensated care to the communities served.
3. The state’s health care resources should be developed to address the needs of Tennesseans while encouraging competitive markets, economic efficiencies and the continued development of the state’s health care system. Skyline proposes to develop a new comprehensive burn program to address the needs of Tennesseans. The proposed project will also encourage competitive markets, as currently only one non-verified burn program is serving middle and eastern Tennessee. Enhancing competition will improve cost of care for patients. With only one existing burn program, Tennesseans residing
118

94 44819987 v1
in the service area are subject to risk due to lack of access to burn services in the event of a burn MCI. Skyline proposes to work with the existing healthcare delivery system to ensure adequate access to burn services as well as preparedness in the event of a catastrophic burn MCI.
4. Every citizen should have confidence that the quality of health care is continually monitored
and standards are adhered to by health care providers. Skyline’s burn program will institute quality monitoring and improvement programs that have been developed over many years. The objective of these programs is to ensure that patients receive safe and effective care. Further, Skyline’s commitment to ABA verification will ensure that its program meets national standards.
5. The state should support the development, recruitment, and retention of a sufficient and
quality health care workforce. TriStar Health has a well-developed human resources division that will assist Skyline in recruiting and retaining any needed incremental staff. In addition, Skyline’s partnership with BRCA will facilitate additional resources specifically related to burn services. Skyline has a robust continuing education and training program that will apply to its burn program for staff development.
PROOF OF PUBLICATION
Attach the full page of the newspaper in which the notice of intent appeared with the mast and dateline intact or submit a publication affidavit from the newspaper that includes a copy of the publication as proof of the publication of the letter of intent.
Date LOI was Submitted: January 8, 2021 Date LOI was Published: January 10, 2021
119

95 44819987 v1
NOTIFICATION REQUIREMENTS
1. T.C.A. §68-11-1607(c)(9)(A) states that “…Within ten (10) days of the filing of an application for a nonresidential substitution-based treatment center for opiate addiction with the agency, the applicant shall send a notice to the county mayor of the county in which the facility is proposed to be located, the state representative and senator representing the house district and senate district in which the facility is proposed to be located, and to the mayor of the municipality, if the facility is proposed to be located within the corporate boundaries of a municipality, by certified mail, return receipt requested, informing such officials that an application for a nonresidential substitution-based treatment center for opiate addiction has been filed with the agency by the applicant.”
2. T.C.A §68-11-1607(c)(9)(B) states that “… If an application involves a healthcare facility in which a county or municipality is the lessor of the facility or real property on which it sits, then within ten (10) days of filing the application, the applicant shall notify the chief executive officer of the county or municipality of the filing, by certified mail, return receipt requested.”
Failure to provide the notifications described above within the required statutory timeframe will result in the voiding of the CON application. Please provide documentation of these notifications. Please see Attachments “Letter of Intent” and “Public Notice.”
DEVELOPMENT SCHEDULE
T.C.A. §§68-11-1609(c) provides that a Certificate of Need is valid for a period not to exceed three (3) years (for hospital projects) or two (2) years (for all other projects) from the date of its issuance and after such time shall expire; provided, that the Agency may, in granting the Certificate of Need, allow longer periods of validity for Certificates of Need for good cause shown. Subsequent to granting the Certificate of Need, the Agency may extend a Certificate of Need for a period upon application and good cause shown, accompanied by a non-refundable reasonable filing fee, as prescribed by rule. A Certificate of Need which has been extended shall expire at the end of the extended time period. The decision whether to grant such an extension is within the sole discretion of the Agency, and is not subject to review, reconsideration, or appeal. 1. Complete the Project Completion Forecast Chart on the next page. If the project will be
completed in multiple phases, please identify the anticipated completion date for each phase. 2. If the CON is granted and the project cannot be completed within the standard completion
time period (3 years for hospital projects and 2 years for all others), please document why an extended period should be approved and document the “good cause” for such an extension.
120

96 44819987 v1
PROJECT COMPLETION FORECAST CHART
Assuming the Certificate of Need (CON) approval becomes the final HSDA action on the date listed in Item 1. below, indicate the number of days from the HSDA decision date to each phase of the completion forecast. Phase
Days Required
Anticipated Date [Month/Year]
1. Initial HSDA decision date 4/28/2021
2. Architectural and engineering contract signed 3 5/1/2021
3. Construction documents approved by the Tennessee Department of Health 64 7/1/2021
4. Construction contract signed 94 7/31/2021
5. Building permit secured 95 8/1/2021
6. Site preparation completed 109 8/15/2021
7. Building construction commenced 156 10/1/2021
8. Construction 40% complete 201 11/15/2021
9. Construction 80% complete 247 12/31/2021
10. Construction 100% complete (approved for occupancy) 248 1/1/2022
11. *Issuance of License 248 1/1/2022
12. *Issuance of Service 248 1/1/2022
13. Final Architectural Certification of Payment 248 1/1/2022
14. Final Project Report Form submitted (Form HR0055) 279 2/1/2022 *For projects that DO NOT involve construction or renovation, complete Items 11 & 12 only.
NOTE: If litigation occurs, the completion forecast will be adjusted at the time of the final determination to reflect the actual issue date
121

122

Letter of Intent
123

124

Public Notice
125

126

127

128

TriStar Skyline Medical Center Burn Bed CON Application
Attachments Table of Contents
Section A Attachments
Section A-4AB Certificate of Corporate Existence
Section A-4AB Articles of Incorporation
Section A-4AB List of Skyline Officers and Directors
Section A-4AB Organizational Chart
Section A-4AB Entity Status Documentation
Section A-6A Deed
Section A-6B-1 Campus Map with Proposed Site
Section A-6B-2 Floor Plan
Section A-6B-3 Public Transportation Map
Section B Attachments
Section B-Need-1A ABA ICD-10 Diagnosis Codes
Section B-Need-1B Physician and Other Letters of Support
Section B-Need-1C American Burn Association Verification Criteria and Plan
Section B-Need-3 Population Analysis Table
Section B-Economic Feasiblity-1A Documentation of Cost Estimate - Architect Attestation Letter
Section B-Economic Feasiblity-1B Detailed Equipment List
Section B-Economic Feasiblity-2 Documentation of Availability of Funding
Section B-Economic Feasiblity-6A Financial Statements - 10K
Section B-Quality-2A Facility License
Section B-Quality-2A The Joint Commission Accreditation
Section B-Quality-2A Inpatient Rehab Accreditation
Section B-Quality-2A Financial Assistance Policy and Charity Care Documentation
Section B-Quality-2A Accessibility Documentation
Section B-Orderly Development-1 Managed Care Contracts
Section B-Orderly Development-1 Discharge Relationships with Local Facilities
Section B-Orderly Development-3C Clinical Training Programs
129

Attachment Section A-4AB Certificate of Corporate Existence
130

November 2, 2020
Tre Hargett
Division of Business ServicesDepartment of State
State of Tennessee
Nashville, TN 37243-1102312 Rosa L. Parks AVE, 6th FL
Secretary of State
BRENTWOOD, TN 370271000 HEALTH PARK DRIVE, SUITE 500DUSTIN GREENE
Date Formed:Formation/Qualification Date: 12/06/1993Active Formation Locale:Status:
Control # :For-profit Corporation - Domestic
Perpetual
HTI MEMORIAL HOSPITAL CORPORATIONFiling Type:
Inactive Date:
273093
Duration Term:TENNESSEE
12/06/1993
Regarding:
DAVIDSON COUNTYBusiness County:
Receipt # : 005870669
Document Receipt
$20.00Filing Fee:
$20.00Payment-Credit Card - State Payment Center - CC #: 3792090233
I, Tre Hargett, Secretary of State of the State of Tennessee, do hereby certify that effective as ofthe issuance date noted above
* is a Corporation duly incorporated under the law of this State with a date of incorporation andduration as given above;* has paid all fees, interest, taxes and penalties owed to this State (as reflected in the records ofthe Secretary of State and the Department of Revenue) which affect the existence/authorizationof the business;* has filed the most recent annual report required with this office;* has appointed a registered agent and registered office in this State;* has not filed Articles of Dissolution or Articles of Termination. A decree of judicial dissolution hasnot been filed.
HTI MEMORIAL HOSPITAL CORPORATION
CERTIFICATE OF EXISTENCE
Cert Web UserProcessed By: Verification #: 042627424
Tre HargettSecretary of State
Issuance Date:0388249Certificate of Existence/Authorization 11/02/2020
Request #:Request Type:
Copies Requested: 1
Phone (615) 741-6488 * Fax (615) 741-7310 * Website: http://tnbear.tn.gov/131

Attachment Section A-4AB Articles of Incorporation
132

133

Attachment Section A-4AB List of Skyline Officers and Directors
134

February 13, 2020
OFFICERS AND DIRECTORS
OF HTI MEMORIAL HOSPITAL CORPORATION
* Samuel N. Hazen President One Park Plaza Nashville, TN 37203 Jon M. Foster Senior Vice President One Park Plaza Nashville, TN 37203 A. Bruce Moore, Jr. Senior Vice President One Park Plaza Nashville, TN 37203 J. William B. Morrow Senior Vice President and Treasurer One Park Plaza Nashville, TN 37203 Heather Rohan Senior Vice President 1000 Health Park Drive, Ste 500 Brentwood, TN 37027 Joseph A. Sowell, III Senior Vice President One Park Plaza Nashville, TN 37203 Robert A. Waterman Senior Vice President One Park Plaza Nashville, TN 37203 * Christopher F. Wyatt Senior Vice President One Park Plaza Nashville, TN 37203 Kevin A. Ball Vice President and Assistant Secretary One Park Plaza Nashville, TN 37203 Mike T. Bray Vice President One Park Plaza Nashville, TN 37203 Monica Cintado Vice President One Park Plaza Nashville, TN 37203 Natalie H. Cline Vice President and Secretary One Park Plaza Nashville, TN 37203 John L. Crothers Vice President One Park Plaza Nashville, TN 37203 Wes Fountain Vice President 1000 Health Park Drive, Ste 500 Brentwood, TN 37027 * John M. Franck II Vice President and Assistant Secretary One Park Plaza Nashville, TN 37203 Shirley Fuller Cooper Vice President 1100 Dr. Martin L. King, Jr. Blvd Suite 1500 Nashville, TN 37203 Dennis Green Vice President One Park Plaza Nashville, TN 37203
135

Dustin Greene Vice President 3441 Dickerson Pike Nashville, TN 37207 Ronald Lee Grubbs, Jr. Vice President One Park Plaza Nashville, TN 37203 John M. Hackett Vice President One Park Plaza Nashville, TN 37203 Ashley Johnson Vice President One Park Plaza Nashville, TN 37203 Seth A. Killingbeck Vice President and Assistant Secretary One Park Plaza Nashville, TN 37203 L. Erik Larsen Vice President One Park Plaza Nashville, TN 37203 T. Scott Noonan Vice President One Park Plaza Nashville, TN 37203 Nicholas L. Paul Vice President 1100 Dr. Martin L. King, Jr. Blvd Suite 1500 Nashville, TN 37203 Doug L. Downey Assistant Secretary One Park Plaza Nashville, TN 37203 Deborah H. Mullin Assistant Secretary One Park Plaza Nashville, TN 37203 Shirley E. Scharf Assistant Secretary One Park Plaza Nashville, TN 37203 John I. Starling Assistant Secretary One Park Plaza Nashville, TN 37203 *Directors Persons employed in the capacity of Chief Executive Officer, Chief Financial Officer, Chief Operating Officer, Administrator and Assistant Administrator of facilities owned and/or operated by this Company or by a partnership for which this Company acts as general partner or by a limited liability company for which this Company acts as managing member, are hereby authorized to, subject to the Company’s policies and procedures, (a) manage the facilities and all day-to-day operations of, and the employees and agents of the Company at, such facilities, and take such other acts as are necessary or appropriate for the proper functioning of the facilities, and (b) negotiate and enter into contracts and agreements necessary to conduct the day-to-day business of such facilities, including, but not limited to, physician contracts, personal property leases, purchase agreements, cost reports, and similar documents (but specifically excluding any contracts or leases relating to real estate, except for leases to tenants in buildings owned by or leased to the Company entered into pursuant to the Company’s policies and procedures) which with the advice of legal counsel shall be deemed appropriate and advisable, and to execute and deliver Certificates of Resolution required in connection with such contracts and agreements.
136

Attachment Section A-4AB Organizational Chart
137

Approved By: ____________________________________________Chief Executive OfficerEffective: October 1, 2020
Marketing/PRAnna-Lee Cockrill
Food & Nutrition Services
Therese Flesch
AccountingLorie Carpenter
Supply ChainHeather Topley
PASHumberto Hernandez
Chief Quality & Patient Safety Officer
Heather Leeper
Human Resources Andy Hooper HIM
Irene Arnold
Chief Operating Officer Skyline Madison Campus &
Ethics and Compliance OfficerMark Fisher
Chief Nursing OfficerVacant
Case ManagementDonna Pote
EVSKevin Heflin
Sarah Cannon Cancer Center
Dyra Harris
Chief Executive OfficerDustin Greene
PharmacyAdam Wilcox
Neuroscience ProgramMichelle Bertotti
Trauma ServicesDavid Kerley
Laboratory ServicesJohn Daniels
Perioperative Services
Martha Stratton, Interim
Director of Admissions& Clinical Operations
Emily Hawkins
MICU/NVICU/TICU & 5th Floor / PCU
& Dialysis Christine Lunger
FacilitiesGary Uselton
Director of NursingDebra McGuire, Interim
CardioPulmonary Services
Angela Hodges
SalesKimberly Ward
Chief Operating OfficerNick Howald
4th & 6th FloorDorcas Churchill
3rd & 7th Floor, CDU Jenna Chapman
I T & STroy Sypien
Advanced ClinicalServices
Rhonda Blackwell
VolunteersJulie Davis
Chief Financial Officer Michael Morrison
EmergencyServices
Brittani Downey
Chief Medical OfficerJason Thurman, MD
Resource Management Flex Pool Hospital Supervisors Resource Pool Sitters
Imaging ServicesDawn Warren
Associate CNO Amy Higgins
Administrative DirectorClinical Operations
Michael Owens
Board of Trustees
Medical ExecutiveCommittee
EducationCarolynn Burton
Associate AdministratorCody Adams
EmergencyManagementZachary Oatis
Graduate MedicalEducation
Program DirectorRehab Services
Patrick Nicks
Inpatient RehabNursing Director
Annie Greer
Director of StaffingJantzen Pendley
Division Report
Contract Report
Endo Central Sterile Operating Room Pre-op Testing Same Day Services Sterile Processing
CT CVOD EEG/EKG/Holters Echo General Rad MRI Nuc Med Patient Transport US
Cardiac Rehab Cath Lab Respiratory Sleep Lab Specials
PBX Plant Ops Security
Adjunctive Therapy BH Intake Case Management IOP/PHP Lead Clinicians Lead Patient Flow Wellness
Acute A Acute B Adolescent & ECO Mood & Stress Nursing Supervisors Safety Attendants Senior Life Staffing Treatment Mall
IP / OP Therapy Wound Care
Infection Prevention Medical Staff Services Risk Management
138

Attachment Section A-4AB Entity Status Documentation
139

Tre Hargett
Division of Business ServicesDepartment of State
State of Tennessee
Nashville, TN 37243-1102312 Rosa L. Parks AVE, 6th FL
Secretary of State
Date Filed Filing Description
The following document(s) was/were filed in this office on the date(s) indicated below:
General Information
Image #
12/06/1993 9:16 AMFor-profit Corporation - Domestic000273093
Filing Type:SOS Control #
PerpetualDuration Term:Status: Active
Date Formed:TENNESSEEFormation Locale:12/06/199312Fiscal Year Close
KNOXVILLE, TN 37919-5546300 MONTVUE RD
Registered Agent AddressC T CORPORATION SYSTEM
NASHVILLE, TN 37203-65271 PARK PLZPrincipal Address
2019 Annual Report03/26/2020 B0847-0694
2018 Annual Report03/20/2019 B0673-7126
2017 Annual Report03/07/2018 B0512-0524
Registered Agent Change (by Agent)01/26/2018 *B0478-4994
Registered Agent Physical Address 1 Changed From: 800 S GAY ST To: 300 MONTVUE RDRegistered Agent Physical Address 2 Changed From: STE 2021 To: No ValueRegistered Agent Physical Postal Code Changed From: 37929-9710 To: 37919-5546
Assumed Name Renewal04/19/2017 B0337-9234
Assumed Name Changed From: TriStar Skyline Medical Center To: TriStar Skyline Medical CenterExpiration Date Changed From: 05/18/2017 To: 04/19/2022
Assumed Name Renewal04/19/2017 B0337-9237
Assumed Name Changed From: TriStar Skyline Madison Campus To: TriStar Skyline Madison CampusExpiration Date Changed From: 05/18/2017 To: 04/19/2022
2016 Annual Report02/22/2017 B0349-6845
2015 Annual Report02/28/2016 B0204-8368
2014 Annual Report03/17/2015 B0062-8243
Assumed Name Renewal10/03/2014 B0003-7269
Assumed Name Changed From: SKYLINE MEDICAL CENTER To: SKYLINE MEDICAL CENTER
Filing Information
Name: HTI MEMORIAL HOSPITAL CORPORATION
Page 1 of 39/17/2020 1:04:20 PM140

Filing Information
Name: HTI MEMORIAL HOSPITAL CORPORATION
Expiration Date Changed From: 10/12/2014 To: 10/03/20192013 Annual Report03/27/2014 7312-1669
2012 Annual Report03/28/2013 7178-1119
Assumed Name05/18/2012 7056-2240
New Assumed Name Changed From: No Value To: TriStar Skyline Medical CenterAssumed Name05/18/2012 7056-2241
New Assumed Name Changed From: No Value To: TriStar Skyline Madison Campus2011 Annual Report03/26/2012 7020-1561
Principal Address 1 Changed From: ONE PARK PLAZA To: 1 PARK PLZPrincipal Postal Code Changed From: 37203 To: 37203-6527Principal County Changed From: No value To: DAVIDSON COUNTY
Assumed Name Renewal11/08/2011 6955-2895
Assumed Name Changed From: SKYLINE MADISON CAMPUS To: SKYLINE MADISON CAMPUSExpiration Date Changed From: 12/13/2011 To: 11/08/2016
2010 Annual Report03/30/2011 6867-0738
2009 Annual Report02/26/2010 A0007-3222
Assumed Name Renewal10/12/2009 6610-1565
Assumed Name Changed From: SKYLINE MEDICAL CENTER To: SKYLINE MEDICAL CENTERExpiration Date Changed From: 11/30/2009 To: 10/12/2014
2008 Annual Report04/15/2009 6519-1024
2007 Annual Report03/11/2008 6240-2028
2006 Annual Report03/14/2007 5984-1180
Assumed Name12/13/2006 5899-1306
2005 Annual Report03/17/2006 5723-1309
2004 Annual Report03/09/2005 5383-2206
Assumed Name Renewal11/22/2004 5286-1503
Registered Agent Change (by Agent)09/27/2004 5243-0482
Registered Agent Physical Address Changed2003 Annual Report03/12/2004 5062-1496
2002 Annual Report04/07/2003 4786-3318
2001 Annual Report03/27/2002 4460-2865
Registered Agent Change (by Entity)12/18/2001 4371-0132
Registered Agent Physical Address ChangedRegistered Agent Changed
Assumed Name Cancellation04/12/2001 4177-1528
Assumed Name Cancellation04/12/2001 4177-1529Page 2 of 39/17/2020 1:04:20 PM
141

Filing Information
Name: HTI MEMORIAL HOSPITAL CORPORATION
2000 Annual Report03/20/2001 4152-1149
Mail Address ChangedAssumed Name Change08/08/2000 3971-1011
Registered Agent Change (by Agent)05/08/2000 3904-0007
Registered Agent Physical Address Changed1999 Annual Report03/29/2000 3866-0586
Assumed Name11/30/1999 3773-2095
Assumed Name Renewal07/02/1999 3708-0500
CMS Annual Report Update02/26/1997 3296-1327
Mail Address ChangedAssumed Name05/20/1996 3173-1391
Assumed Name11/30/1995 3080-2120
CMS Annual Report Update11/02/1995 3072-1303
Principal Address ChangedFiscal Year Close Changed
Registered Agent Change (by Entity)09/14/1995 3053-1262
Registered Agent Physical Address ChangedRegistered Agent Changed
CMS Annual Report Update02/07/1995 2953-1880
Fiscal Year Close ChangedAssumed Name08/22/1994 2881-1046
Initial Filing12/06/1993 2762-1907
Active Assumed Names (if any) Date ExpiresTriStar Skyline Madison Campus 04/19/202205/18/2012TriStar Skyline Medical Center 04/19/202205/18/2012
Page 3 of 39/17/2020 1:04:20 PM142

Attachment Section A-6A Deed
143

144

145

146

147

148

149

Attachment Section A-6B-1 Plot Plan with Proposed Site
150

151

152

Attachment Section A-6B-2 Floor Plan
153

FEC
FAA
FHC
FHC
FHC
FHC
FHC
FHC
FHC
FHC
FHC
FHC
FHC
FHC
FHC
FHC
FEC
FEC
FEC
FEC
FEC
FEC
FEC
FEC
FEC
FEC FEC
FEC
FEC
FEC
FEC
FEC
FEC
FEC
FEC
FEC
FEC
FEC
FEC
F
F
F
FF
F
F
F
F
F
F
F
READING
ADATLT.
HOLDING
1 2
3
SCRUB
NURSEWORK
CASSETTESTORAGE
CATH LABNO 1.
CATH LAB NO. 2
CORRIDOR
ST
ER
ILE
CO
RR
IDO
R
CLEAN UTILITY
COMPUTER EQUIP. RM.
ANGIO/ SPECIALPROCEDURESNO. 1
SUPERV.
LOCKER/LOUNGE
ELEC.
TLT.
SCRUB
ANGIOCONTROL
ANGIOSTORAGE
ANGIO/ SPECIALPROCEDURESNO.2
COMP. EQUIP. RM.
CONTROL
COMM.
ELEC.
COMP.EQUIP. RM.
PASS.1-0106
JAN1-0109
W PUBTLT1-0108
EMERGENCYWALK-INCANOPY
AMBULANCEENTRYCANOPY
EMERGENCYPARKING DECK
LWR
DN
DN
UP
DN
UP
DN
UP
UP
E63431
037500
E63418
EXAM 1EXAM 2
EXAM 3
EXAM 4 EXAM 5 EXAM 6
P TS
ELEV #8
PTS
#3
#4#5
#6
NOURNOUR
NOUR
PTS
LAR
LAR
LA
R
LAR
LAR
1 2 3 4 56
7
8
9
10
11121314
1
2
34 5 6 7 8
9
10
11
LW
R
LWR
PT
S
LW
R
LWR
LWR LW
R
LW
RLWR
PT
S
ST
AIR
#3
STAIR #1
ELEV #1
ELEV #2
ELEV #3
ELEV #4
ELEV #5
ELEV #6
ELEV #7
VP 1
VP 2
VP 3
VP 4
DRS
1 2 3
STAIR #5
ST
AIR
#2
STAIR #4
PTS
PT
S
PTS
PTS
REC
PT
EWC
DOWN
DO
WN
DOWN
DO
WN
FINCOUN
CONSULT
BREAKROOM
OFFICE
OFFICE
DRESS1-0361A
DRESS1-0342A
DRESS1-0343A
DRS1-0374A
FINCOUN/CASH1-0122
CNTRL1-0466.1
OPEN TOATRIUMBELOW
OPEN TOATRIUMBELOW
DRESS1-0375A
DRESS1-0360B
ACCEWC
ACC PAYPH ALC1-0129
CORR1-0442
ACC TLT1-0207
RADDIR OFF1-0337
STAFFACC T/S1-0370A
STF ACCTLT1-0120
PATACC TLT1-0246
PATACC TLT1-0318
PATACCTLT1-0344B
PATACCTLT1-0361B
PATACCTLT1-0365B
STFACC TLT1-0380A
ACCPATTLT1-0374B
ACC DRS1-0379B
EQPTALC
ACC PATTLT1-0421
STFACCTLT1-0438A
PAT ACCTLT1-0468
ACCF. PUB.TLT1-0133
ACCM. PUB.TLT1-0132
CHAPEL1-0369
ADMITCONTROL1-0111
SAME DAYREG1-0128A
WAIT1-0313
ACCTLT1-0448A
WCH ALC1-0103
ADMIT 61-0115
ELEC.1-0135
WORK1-0346
C U/ C. STO.1-0426B
STORAGE1-0426A
CONT1-0345
TLT1-0446A
ACC.DRESS1-0342B
ACC.DRESS1-0343B
DRESS1-0361B
SU1-0334
CU1-0335
CONT1-0340
CORR1-0130
PATACC TLT1-0215
PAT TLT1-0235A
S.U.1-0229
BREAK RM1-0231
STAFFACC TLT1-0230
VASC LAB1-0236
PAT ACCTLT1-0227A
PAT ACCTLT1-0236A
PATACC TLT1-0242
PATACC TLT1-0241
BIOPSY1-0238
DAY PROC1-0349
ACCDRESS1-0360A
ACCDRESS1-0365A
JAN1-0134
ALC1-0475
SUPPLY1-0477
JAN1-0476
ALC1-0474
ALC1-0423
ALC1-0412
ETHERNET1-0366
HOLD 21-0354
HOLD 11-0350
RECPT1-0310
ALC1-0325
ADMIT 81-0117
ADMIT 71-0116
ADMIT 51-0114
ADMIT 41-0113
ADMIT 31-0112
ADMIT 21-0110
ADMIT 11-0109
STO1-0228
ERCP1-0466
LOUNGE1-0450
NS1-0427
COMM1-0311
ON CALL1-0370
CORR1-0472
TRANSPORTOFFICE1-0333
VP1-0245
TLT1-0313A
ADMITWAIT1-0127
COURTYARDBELOW
COURTYARDBELOW
VEST1-0131
ELEC1-0439
EYELASER1-0471
CLINCOORD1-0470
CLINCOORD1-0469
DARKROOM1-0467
WORK1-0465
BRONC ENDO1-0464
GI ENDO1-0463
WORK1-0462
GI ENDO1-0461
NURSESTATION1-0460
EXAM1-0459
S.U.1-0458
PASS1-0457
PREP 181-0456
ACCTLT1-0455A
PREP 191-0455
PREP 201-0454
TLT1-0454A
TLT1-0453A
PREP 211-0453
CU1-0452
SU1-0451
PREP 221-0449
PREP 231-0448
CORR1-0447
PREP 241-0446
TLT1-0445A
PREP 251-0445
TLT1-0444A
PREP 81-0444
TLT1-0443A
PREP 91-0443
PREP 101-0441
TLT1-0441A
TLT1-0440A
PREP 111-0440
STAFFLKR/LNGE1-0438
CORR1-0437
PREP 121-0436
TLT1-0436A
TLT1-0435A
PREP 131-0435
CORR1-0434
PREP 171-0433
TLT1-0433A
TLT1-0432A
PREP 161-0432 CORR
1-0431
CLN1-0430
PREP 151-0429
TLT1-0429A
TLT1-0428A
PREP 141-0428
NOUR1-0425
DICT1-0424
NS1-0422
TLT1-0420A
PREP 51-0420
TLT1-0419A
PREP 61-0419
ACCTLT1-0418A
PREP 71-0418
JAN1-0417
CORR1-0409
PREP 41-0416
TLT1-0416A
TLT1-0415A
PREP 31-0415
TLT1-0414A
PREP 21-0414
TLT1-0413A
PREP 11-0413
PAT 21-0411
PAT 11-0410
PAT 41-0408
CORR1-0407
ALCOVE1-0406
CORR1-0405
PAT 31-0404
COMM1-0403
CONSULT1-0402
CONSULT1-0401
CORR1-0400
LNG1-0380
VEST1-0379
RAD 21-0378
CONTROL1-0377
RAD 11-0376
VEST1-0375
VEST1-0374
R&F 11-0373
CONTROL1-0372
PASS1-0368
TECHWORK1-0367
R & T1-0365
CONTROL1-0364
C-ARMALCOVE1-0363
R&F 31-0362
VEST1-0361
VEST1-0360
CHESTROOM1-0359
CO
NT
RO
L1
-03
58
OFFICE1-0357
DAY P1-0356
PASS1-0355
VIEWING/RADWORK 41-0353
VIEWING/RADWORK 31-0352
VIEWING/RADWORK 21-0351
OFFICE1-0348
R&F 21-0344
VEST1-0343
VEST1-0342
RAD 31-0341
CONTRASTMEDIA1-0339 PASS
1-0338
JAN1-0336
CORR1-0332
ACTIVE FILES1-0331
VIEWING 41-0330
VIEWING 31-0329
VIEWING 21-0328
VIEWING 11-0327
FILMSORTING1-0326
STRESS1-0324
HOTLAB1-0323
PASS1-0319
NUC MED 31-0322 NUC MED 2
1-0321
NUC MED 11-0320
TECHWORK1-0317
SUPER1-0316
PASS1-0315
CORR1-0314
COMMRISER
CORR1-0309
CORR1-0301
ELEVLOBBY1-0300
WORK1-0244
WAIT1-0243
WORK/LASER1-0240
ECHO 21-0239
ECHO 11-0237
US 21-0235
PASS1-0234
PASS1-0233
READ1-0232
US 11-0227
FILE1-0226
EKG1-0225
EEG1-0224
PFT1-0223
PASS1-0222STRESS
TEST1-0221
PASS1-0220
STOR1-0219
DRS1-0218
MAMMO 11-0217
DRS1-0216
READ1-0214
DK RM1-0213
WORK1-0212
PASS1-0209
DRS1-0211
MAMMO 21-0210
DRS1-0208
BONE1-0206
DRS1-0205
MAMMO 31-0204
DRS1-0203
PASS1-0202
WAIT1-0201
PASS1-0200
SAME DAYSURGERYWAIT1-0128
ELEVLOBBY1-0125
CORR1-0123
FINCOUN1-0121
CENTRALSCHED1-0119
ADMIT/WORK1-0108
PASS1-0118
PASS1-0105
CORR1-0106
INFO1-0102
VEST1-0100
LOBBY1-0101
M STFACCT/S1-0620A
F STFACCT/S1-0619A
PATACCTLT1-0607
STFACCTLT1-0611
PATACCTLT1-0623
M STFACCT/S1-0632A
F STFACCT/S1-0631A
NS/CHART1-0612
MEDS1-0672B
DICT1-0672A
JAN1-0674
JAN1-0673
SU1-0668
C.U.1-0646
AIRCOMP1-0670
DICT1-0671
SCRUB1-0667
SCRUB1-0641
SCRUB1-0669
CONTROL1-0649A
SCRUB1-0665
SCRUB1-0666
AL
CO
VE
1-0
651
ELEC1-0637
EQUIPSTO1-0643
PRE-OP1-0621
EXITACCESSCORR1-0473
NEURO OR 11-0659
NEUROSTOR.1-0658
NEURO OR 21-0657
ORTHO OR 21-0656
ORTHOSTOR.1-0655
ORTHO OR 11-0654
GEN OR 31-0653
GEN OR 21-0652
GEN OR 11-0650
CYSTO1-0649
EQUIPSTO1-0645
CORR1-0639
STRCHR ALCOVE1-0638
STERILESTORAGE1-0636
PROCESS/PACKING1-0635
DECONTAM1-0634
STAFFF. LKR1-0631
STAFFM. LKR1-0632
STAFFLOUNGE1-0630
CORR1-0640
CORR1-0629NS
1-0647
CORR1-0644
OFF1-0628
OFF1-0627
OFF1-0626
CORR1-0625
CORR1-0624
NS1-0622
M. LKR.1-0620
F. LKR.1-0619
PHYSLKR/LNG1-0618
ANESTHWORK1-0617
CORR1-0616
STOR1-0614
ISOL1-0613
SU1-0615
PACU1-0610CU
1-0608PM 51-0605
PM 41-0604
NS1-0609
PM 31-0603
PM 21-0602
PM 11-0601
PASS1-0606
PASS1-0600
CORR1-0500
CORR1-0303
S.U.1-0850
STF ACCTLT1-0813A
STFACC TLT1-0846
STFACC TLT1-0843W
CH
/ST
RA
LC
EQUIPALC1-0816
EMERGSHOWER1-1059
WCH/STORALCOVE1-1058
ICU FAMWAITING1-0804A
VEND1-0804B
C.U./CLN STOR1-0852A
CLEANLINEN1-0852B
X-RAYALCOVE1-1065
COMM1-0856
JAN1-0849
DICT/READ1-0848
OFFICE1-0853
ICULKR/LNG1-0841
NURSESTATION1-0845
MEDS1-0840
R.T.LKR/LNG1-0813
RT STOR/WORK1-0809
CORR1-0802
CONSULT1-0806
ANTE1-0817
EQUIPSTOR1-0854
BLOODGAS1-0812
DECONT1-0811
CORR1-0844
PASS1-0808
NURSESTATION1-0807
R.T.OFF1-0810
NURSESTATION1-0814
CORR1-0815
ISOLICU #11-0818
ICU #21-0819
ICU #31-0820
ICU #41-0821
ICU #51-0822
ICU #61-0823
ICU #71-0824
ICU #81-0825
ICU #91-0826
ICU #101-0827
ICU #111-0828
ICU #121-0829
ICU #131-0830
ICU #141-0831
ICU #151-0832
ICU #161-0833
OBSERVATION1-1070
TRAUMA 31-1068
CARDIAC 11-1067
CARDIAC 21-1066
CONTROL1-1064
X-RAY1-1063
CORR1-1062
TRAUMA 21-1061
TRAUMA 11-1060
VEST1-1056
CORR1-1053
CORR1-0529
PLUMBING/MED GAS1-0705B
PLUMBING/MED GAS1-0705A
CONTROLROOM1-0710
BOILERS1-0711
CHILLERS1-0704
GEN ROOM1-0709
ELEC1-0708
MECH ROOM1-0707
FIRE PUMP1-0706
MAINTENGR OFF1-0703
SEC/FILES1-0702
LOCKEDSUPPLYSTORAGE1-0701
BIO-MEDEQUIP WORK/REPAIR STAGING1-0700
ACCDRS1-1109
ACC TLT1-1051B
PBX/SECUR1-1057
LKR/WORK1-1058
DISCHARGE1-0129
MRI1-1112
E.M.S. /POLICE/WORK1-1055
CONT1-1116
ACC DRS1-1108
PUB TLT1-1004
ACCPH
ACCEWC
PUBACC TLT1-1005
PAT ACCTLT1-1049
CU/CLN STO1-1046A
CL1-1046B
PUB ACCTLT1-1125
PATACCTLT1-1101
PATACCTLT1-1106
STFACCTLT1-1210
STFACCTLT1-1211
PATACC TLT1-1051A
PATACC T/S1-1048A
PATACC T/S1-1047A
PATACCTLT1-1014
PATACCTLT1-1028
PATACCTLT1-1027
ENTEXAM1-1037
EXAM 61-1017
MRI1-1115
COORDOFF1-1200
FILE ALC1-1219
HISTOLOGY/CYTOLOGY1-1217
SUPERPTS
SCRUB1-1011B
MICRO1-1206
CORR1-1012
ELEC1-1010
EXAM 51-1025
ALC1-1220
OFF1-1208
NOURISHMENT1-1118
SOILEDUTIL1-1127
INTERVIEW1-1121
SECUREHOLD1-1044
JAN1-1026
DICT1-1050
STRCHHOLD #2
STRCHHOLD #1
HOLDING1-1126
GROSSCUT RM1-1218
PATHOFF1-1216
PATHOFF1-1215
PATHOFF1-1214
PASS1-1213
LKR/LNGE1-1212
STOR1-1209
HEMATOLOGY1-1207
DIROFF1-1205
ASSISTDIR OFF1-1204
BLOODBANK1-1202
CENTRALPROCESSING1-1201
CHEMISTRY1-1203
STO1-1128
DRS1-1124
DRS1-1123
DRS1-1122
OP WAIT1-1120
READING1-1117
MRICOMPUTER RM1-1114
CONTROL1-1111
SUPPLIES1-1110
CT SCANNER #21-1105
CTCOMP1-1104
CT CONTROL1-1103
CT SCANNER #11-1102
BREAKROOM1-1113
PASS1-1119
PASS1-1107
PASS1-1100
TRAUMA 41-1054ISOL/
INFECTEXAM1-1051
GYNEXAM 11-1048
GYNEXAM 21-1047
SU/SL1-1045 NS
1-1042
EXAM 11-1041
EXAM 21-1040
EXAM 31-1039
EXAM 41-1038
NOUR1-1036
MEDS1-1035
STATLAB1-1034
NS1-1033
ORTHO/CAST 11-1031
ORTHO/CAST 21-1030
SL1-1019
MED1-1018
NURSESTATION1-1015
FAST TRACK1-1013
PASS1-1006
VEND1-1003
ENTRYVEST1-1000
CORR1-1052
CORR1-1011
CORR1-1032CORR
1-0305
CORR1-0307
CORR1-0306
CORR1-0304
2-200
PASS.
2-204
STAFF
TLT.
2-205
OFFICE
2-201
OFFICE
2-206
OFFICE
2-203
STAFF
LNGE/
LCKRS
2-202
OFFICE
2-303
PAT. TLT
2-302
EXAM
2-301
EXAM
2-300
EXAM
2-0903
2-1070
OBSERV.
#1
OBSERV.
2-1074
STOR.
2-1073
PAT. TLT
#2
OBSERV.
#8
OBSERV.
#7
OBSERV.
2-116
MEDS
2-117
N.S.
2-113
SUB -
NS
2-112
CORR.
2-103
OBSERV 2
2-104
OBSERV 3
2-114
MEDS
2-105
OBSERV 4
2-106
OBSERV 5
2-111
TLT.
2-107
OBSERV 62-108
OBSERV 7
2-110
SOILED
UTILITY
2-109
OBSERV 8
CORR1-0501
CORR1-0803
CORR1-0805
AMBULANCEENTRYCANOPY
AL - 01 A - S T 7
1 1 0 C
AS - 01 A - 1 0 0 A
10 9 B
AS - 01A - 1 0 0 B
1 1 0 A
OH - 01 E - 1 0 0
24
26 2827 29 31.3
ZE
ZB
Z Z
Y Y
X.7
X
W.5
W W
U U
S
R.1
M
L
Q
30
H
F
E
D.4
D
B
20
2019
19
31
L.9
G.7
G.6
E.1
B.1
V
ZC
32 33 34 35
18
17
17
16
16
15
15
14
14
13
13
12
12
2
4
4
5.9
5.9 7.7
8.8
8.8
9.5
W.3
29.8
29.8
M.2
V.5
ZD
11
11 16.55 7
A.5
A.1
A.0
30.6
C1 C2
CC
CA
CB
A.9
A.4
20.2 20.8
21.219.9
36
C0
220220
VEST1-0473AVEST1-0473A
OUT-PATENTRYCANOPY
DARKROOM1-0642037500
220
CCTCCT
1A-101SECURITY
1A-129TLT-PAT
1A-149MEDS
1A-143
LINENALCOVE
1A-125
WC
STORAGE
1A-135TLT-PAT.
1A-130LAB
1A-147EKG
1A-141
SOILHOLD
1A-131SUB-WAIT
1A-ST7STAIR#7
162 SF1A-132
EXAM
ROOM
126 SF1A-133
LOWACUITY
113 SF1A-134
LOWACUITY
168 SF1A-136
LOWACUITY
154 SF1A-137
LOW
ACUITY
151 SF1A-138
LOWACUITY
158 SF1A-139
LOWACUITY
157 SF1A-140
LOWACUITY
1A-100VEST
1A-102
E DWAITING
1A-103VEND
1A-108SECURITY
1A-110
TLT/
SHWR1A-111
O R
ON-CALL
1A-112
CONFERENCE
RM
1A-124ADMIT
1A-126TLT-STAFF
1A-121
PUBELEV.
LOBBY1A-113TDR
1A-114STORAGE
1A-120EVS
1A-118WORK
1A-122OFFICE
1A-116CONSULT
1A-145TRIAGE
1A-144TRIAGE
1A-146TRIAGE
1A-127RECEPTION
1A-151
NURSE
STATION
1A-148
CLEAN
SUPPLY
1A-115
PAT/STAFFELEV-LOBBY
1A-128KIOSK
1C-ST6STAIR#6
1A-117DISCHARGE
1A-104TLT-F
1A-106TLT-M
1B-100
EMSLOUNGE
1B-101
FAMILY
WAITING
1A-150NOUR
1A-142EVS
1A-COR.4CORRIDOR
1A-COR.5CORRIDOR
1A-COR.6CORRIDOR
1A-COR.7CORRIDOR
1A-COR.8CORRIDOR
1A-COR.3CORRIDOR
1A-COR.9CORRIDOR
1A-COR.2CORRIDOR
1A-COR1CORRIDOR
1-0803CORRIDOR
1-0501CORRIDOR
1A-119ELEC
1A
-PA
SS.1
PA
SSA
GE
1A-EL1
PUB
ELEV-1
1A-EL2
PUBELEV-2
1A-EL3
STAFFELEV-3
1A-EL4
STAFFELEV-4
1D-100CHILLERS
1B-103ALCOVE
LW
R
LWR
LWR
LWR
SCRUB1-0662
GEN OR 41-0664
GEN OR 51-0663
EYE OR 11-0661
EYE OR 21-0660
FHC
UP
UP
1A-105OFFICE
1A-109
SURGERY
STORAGE
1A-107OFFICE
1-0633CORRIDOR CORR
1-0633
S
S
S
S
S
S
MINOR RENOVATION
NEW CONSTRUCTION
MAJOR RENOVATION
COSMETIC
VERTICAL CIRCULATION
CANOPY
COMPONENT 1
BURN OR
COMPONENT 1
DEBRIDEMENT ROOM
GS PROJ. NO.
of
FIR
ST
FL
OO
R -
OV
ER
AL
L -
PR
OP
OS
ED
112/30/2020
TRISTARSKYLINEMEDICALCENTER
44859.00
BU
RN
PR
OG
RA
M R
EN
OV
AT
ION
NASHVILLE, TN
4
0' 30' 120'60' 180'1" = 60'-0"1
FIRST FLOOR - OVERALL - PROPOSED154

FHC
FHC
FHC
FHC
FHC
FEC
FEC
FEC
F
F
COMPUTER EQUIP. RM.
ANGIO/ SPECIAL
SUPERV.
LOCKER/LOUNGE
ELEC.
TLT.
LWR
UP
DN
EXAM 1EXAM 2
EXAM 3
EXAM 4 EXAM 5 EXAM 6
PTS
ELEV #8
PTS
#3
#4#5
#6
NOUR
LAR
LAR
LA
R
LAR
LAR
ST
AIR
#3
OFFICE
OFFICE
DRESS1-0342A
DRESS1-0343A
DRESS1-0360B
RADDIR OFF1-0337
STAFFACC T/S1-0370A
PATACCTLT1-0344BACC.
DRESS1-0342B
ACC.DRESS1-0343B
ACCDRESS1-0360A
ON CALL1-0370
C-ARMALCOVE
R&F 31-0362
VEST1-0361
VEST1-0360
CO
NT
RO
L1-0
358
OFFICE1-0357
DAY P1-0356
R&F 21-0344
VEST1-0343
VEST1-0342
RAD 31-0341
JAN1-0336
COMMRISER
WC
H/S
TR
ALC
EMERGSHOWER1-1059
WCH/STORALCOVE1-1058
ICU FAMWAITING1-0804A
VEND1-0804B
X-RAYALCOVE1-1065
COMM1-0856
R.T.LKR/LNG1-0813
RT STOR/WORK1-0809
CORR1-0802
CONSULT1-0806
ANTE1-0817
EQUIPSTOR1-0854
DECONT1-0811
R.T.OFF1-0810
ISOLICU #11-0818
ICU #21-0819
OBSERVATION1-1070
TRAUMA 31-1068
CARDIAC 11-1067
CARDIAC 21-1066
CONTROL1-1064
X-RAY1-1063
CORR1-1062
TRAUMA 21-1061
TRAUMA 11-1060
VEST1-1056
CORR1-1053
CORR1-0529
ACCDRS1-1109
ACC TLT1-1051B
PBX/SECUR1-1057
LKR/WORK1-1058
DISCHARGE1-0129
E.M.S. /POLICE/WORK1-1055
CONT1-1116
ACC DRS1-1108
PUB TLT1-1004
ACCPH
ACCEWC
PUBACC TLT1-1005
PAT ACCTLT1-1049
CU/CLN STO1-1046A
CL1-1046B
PUB ACCTLT1-1125
PATACCTLT1-1101
PATACCTLT1-1106
PATACC TLT1-1051A
PATACC T/S1-1048A
PATACC T/S1-1047A
PATACCTLT1-1014
PATACCTLT1-1028
PATACCTLT1-1027
ENTEXAM1-1037
EXAM 61-1017
MRI1-1115
SCRUB1-1011B
CORR1-1012
ELEC1-1010
EXAM 51-1025
NOURISHMENT1-1118
SOILEDUTIL1-1127
INTERVIEW1-1121
SECUREHOLD1-1044
JAN1-1026
DICT1-1050
STRCHHOLD #2
STRCHHOLD #1
HOLDING1-1126
STO1-1128
DRS1-1124
DRS1-1123
DRS1-1122
OP WAIT1-1120
READING1-1117
MRICOMPUTER RM1-1114
CT SCANNER #2
CT CONTROL
CT SCANNER #1
BREAKROOM1-1113
PASS1-1119
PASS1-1107
PASS1-1100
TRAUMA 41-1054ISOL/
INFECTEXAM1-1051
GYNEXAM 11-1048
GYNEXAM 21-1047
SU/SL1-1045 NS
1-1042
EXAM 11-1041
EXAM 21-1040
EXAM 31-1039
EXAM 41-1038
NOUR1-1036
MEDS1-1035
STATLAB1-1034
NS1-1033
ORTHO/CAST 11-1031
ORTHO/CAST 21-1030
SL1-1019
MED1-1018
NURSESTATION1-1015
FAST TRACK1-1013
PASS1-1006
VEND1-1003
ENTRYVEST1-1000
CORR1-1052
CORR1-1011
CORR1-1032CORR
1-0305
CORR1-0306
CORR1-0304
2-200
PASS.
2-205
OFFICE
2-201
OFFICE
2-206
OFFICE
2-202
OFFICE
2-303
PAT. TLT
2-302
EXAM
2-301
EXAM
2-300
EXAM
2-0903
2-1070
OBSERV.
#1
OBSERV.
2-1074
STOR.
2-1073
PAT. TLT
#2
OBSERV.
#8
OBSERV.
#7
OBSERV.
2-116
MEDS
2-117
N.S.
2-113
SUB -
NS
2-112
CORR.
2-103
OBSERV 2
2-104
OBSERV 3
2-114
MEDS
2-105
OBSERV 4
2-106
OBSERV 5
2-111
TLT.
2-107
OBSERV 62-108
OBSERV 7
2-110
SOILED
UTILITY
2-109
OBSERV 8
CORR1-0803
Y
W
201716151412
7.7
8.8
8.8
9.5
11 16.5
1A-116CONSULT
PAT/STAFF
1B-100
EMS
LOUNGE
1B-101
FAMILY
WAITING
1-0803CORRIDOR
CORRIDOR
1B-103ALCOVE
MINOR RENOVATION
NEW CONSTRUCTION
MAJOR RENOVATION
COSMETIC
VERTICAL CIRCULATION
CANOPY
DEBRIDEMENT
PAT TLT / SHOWER
GS PROJ. NO.
of
FIR
ST
FL
OO
R P
RO
PO
SE
D -
CO
MP
ON
EN
T 1
-
EN
LA
RG
ED
212/30/2020
TRISTARSKYLINEMEDICALCENTER
44859.00
BU
RN
PR
OG
RA
M R
EN
OV
AT
ION
NASHVILLE, TN
4
0' 8' 16'
36' 48'3/64" = 1'-0"1
FIRST FLOOR PROPOSED - ENLARGED155

UP
DN
W PUBTLT
3-0106
JAN3-0107
PASS.3-0104
SECOND FLOOR ROOF BELOW
SECOND FLOOR ROOF
FIRST FLOOR ROOF BELOW
FIRST FLOOR ROOF BELOW
FIRSTFLOORROOF
BELOW
SECOND FLOOR ROOF
ROOF
PB
COURTYARD 2A-149
STAFFLOUNGE2A-104
TLT- PAT.
ICU253
2A-107
ICU250
2A-111
ISOL.ICU249
2A-113
ANTE2A-114
2A-112 CHART
ICU251
2A-110
2A-109 CHART
ICU252
2A-108
2A-COR.2 CORRIDOR
CHART 2A-106
TLT.-STAFF2A-105
ON-CALL1
2B-111
ON-CALL2
2B-110
ICU272
2B-115
ICU271
2B-116
ICU270
2B-117
ISOL. ICU269
2B-118
ANTE2B-128
2B-COR.5 CORRIDOR
WAITINGALCOVE
2B-COR.1A
EQUIPSTORAGE
2A-103
CHART 2A-135
ICU254
2A-136
MEDS2A-137
NURSE WORK 2A-138
ICU248
2A-139
CHART 2A-140
2A-115 ALCOVE
ICU247
2A-116
ICU245
2A-118
CHART 2A-117
ICU246
2A-141
TLT.PAT.
ICU255
2A-134
SOILWORK2A-102
CORRIDOR 2B-COR.1
TDR2B-108
T R2B-104
DECONTAM
RESPIRATORY THERAPY 2B-107
NOUR2B-120
NURSESTATION2B-119
MEDI2B-121
CORRIDOR 2B-COR.4
ICU268
2B-132
ICU267
2B-133
STAFFLOUNGE2B-134
PHYS/ANC WORK 2B-127
SOILWORK2B-126
CLEANSUPPLY2B-122
STORAGE 2B-103TLT-F2B-105
CLEANSUPPLY2A-101
CORRIDOR 2A-COR.1
CHART 2A-132
ICU256
2A-133
NOUR2A-148
OFFICE 2A-147
MEDS2A-145
NURSE WORK 2A-146
TLT.PAT.
ICU244
2A-142
CORRIDOR 2A-COR.3
CHART 2A-143
CHART 2A-119
ICU243
2A-120
EVS2A-144
2A-COR.4 CORRIDOR
LINENALCOVE2A-131
NURSESTATION
2A-100
ELEC2B-102
TLT-M2B-106
CONSULT 2B-1232B-COR.1 CORRIDOR
OFFICE 2B-124
TLT.STAFF2B-125
MULTIPURPOSE
2B-182
CORRIDOR 2B-COR.14
ALCOVE 2B-179
STAFFELEV-122B-EL4
SOILWORK2B-178
STAFFELEV-112B-EL3 PHYS/ANC WORK 2B-177
PUBELEV-102B-EL2
CLEANSUPPLY2B-172
PUBELEV-92B-EL1
TLT.STAFF2B-170
EVS2B-171
WAITING 2B-101
ICU237
2A-129
ICU238
2A-127
2A-128 CHART
ICU239
2A-126
2A-125 CHART
ICU240
2A-124
ICU241
2A-123
ICU242
2A-121
2A-122 CHART
2A-ST6 STAIR#6
ICU266
2B-181
PASSAGE2B-COR.16
ICU257
2B-131
ICU258
2B-166
CORRIDOR 2B-COR.17
NURSESTATION2B-173
MEDS2B-174
NOUR2B-175
NURSESTATION2B-176
ICU265
2B-180
ANTE2B-208
ISOL.ICU 2642B-157
ICU263
2B-158
STAIR#7 2B-ST7
ICU262
2B-159
ICU261
2B-160
2B-COR.15 CORRIDOR
ICU260
2B-161
ICU259
2B-162
EQUIPMENT STORAGE 2B-114
TLT.PAT.
TLT.PAT.
TLT.PAT.
TLT.PAT.
TLT. PAT.
TLT. PAT.
TLT. PAT.
TLT. PAT.
TLT. PAT.TLT. PAT. TLT. PAT.
TLT. PAT.
TLT. PAT.
TLT. PAT.
TLT. PAT.
TLT. PAT.
TLT. PAT.
TLT. PAT.
TLT. PAT.
TLT. PAT.
TLT. PAT.
TLT. PAT.
TLT. PAT.
SS
S
S
S
S
OB
OB
OBO
B
OB
OB
OB
OB
OB
OB
OB
OB
FEC
CRASHCART
CRASHCARTPTS
Me d . S t a .40 0 06 D ra w e r
Me d . S t a .40 0 07 D ra w e r
M e d . S t a .40 0 0 S i n g l eC o l u m n A u x .
ICE
PTSPTSPTS
REF
ICU33
2-0306
TLT.2-0307
TLT.2-0309
ICU34
2-0308
ICU35
2-0310
TLT.2-0311
TLT.2-0313
ICU36
2-0312
WAITING 2-0314
CORR3-0236
ICU 13-0235
CORR3-0258
CHART3-0222B
ICU 23-0222
ELECCLOSET3-0255A
ICU 33-0236
ICU 43-0239
CHART3-0236A
CORR 3-0225
SU3-0234
PASS3-0253
MEDROOM3-0242
ELEV#5
STAFFBREAKROOM 3-0244
STAFFTLT
3-0244A
MEDS3-0111
DICT3-0114/3-0115
MICRO&
COFFEE
LO
CK
ER
S
ELEV#4
2-0202
CHART 2-0203
TLT.2-0206
ICU31
2-0302
TLT.2-0303
TLT.2-0305
ICU32
2-0304
ISOL.ICU30
2-0205
ICU29
2-0207
TLT.2-0208
TLT.2-0210
ICU28
2-0209
CORRIDOR 2-0204
NURSESTATION
2-0201
ELEV#7
ELEVLOBBY3-0120
ELEV#6
JAN3-0238
PASS3-0255
WORK3-0252 STAFF
TLT3-0220B
DICT3-0257NOUR
3-0256
CU3-0250
NURSESTATION 3-0254
NURSESTATION/
CHART3-0223
CHART3-0240A
ICU 53-0240
ICU 63-0241
ICU 73-0243
ICU 83-0245
ISOLATION9 3-0246
CHART3-0246A
ICU 103-0247
CORR3-0220
ICU 113-0248
CHART3-0248A
ICU 123-0249
MED.2-0218
MGR.OFFICE2-0219
SOILHOLD2-0216
C.U./EQUIP.2-0217
CORRIDOR 2-0215
H.C.ICU26
2-0213
STAIR #4
H.C.TLT.
2-0214TLT.
2-0212
ICU27
2-0211
SUPPLIES3-0110
NOUR3-0125
ELEVLOBBY3-0100
ELEC3-0104
WCHALC
3-0129
JAN3-0128
CORR3-0123
CORR3-0102
C.U./CLN
STOR3-0105
ANTE4-0143
CORR3-0142
CORR3-0132
ISOLP.P.#103-0144
T/S3-0144A
P.P.#93-0145
T/S3-0145A
P.P.#83-0146
T/S3-0146A
P.P.#73-0147
T/S3-0147A
P.P.#33-0151
T/S3-0151A
P.P.#23-0152
T/S3-0152A
MECHANICAL3-0303
P.P.#13-0153
T/S3-0153A
NURSESTATION/
CHART3-0117
ACCP.P.#53-0149
T/S3-0149A
T/S3-0150A
ACCP.P.#43-0150
PUB.TLT
3-0101
ACC P.P.3-0148
T/S3-0148A
ALCOVE
STAIR #2
WAIT
STAIR #1
WAIT
NURSESTATION
2-0103
STAIR#3
CORR 3-0118
STAFFLOUNGE
3-0121
STAFFTLT
3-0121A
DIRECTOR OFFICE 3-0122
3-0124 STRCH ALCOVE
S.U.3-0107
COMM 3-0126
MECHANICAL 3-0300
CORR 3-0200
MECHANICAL 3-0302
CORR 3-0218
ELEV #3
ELEV #2
ELEV #1
PTS
LOCKERS
H H
HH
HH
HH
HH
HH
HH
HH
HH
HHH H
H H
UP
DN
UP
DN
UP
DN
PAYTELE
COMPONENT 1
BURN ICU RENOVATION
FAMILY WAITING
MINOR RENOVATION
NEW CONSTRUCTION
MAJOR RENOVATION
COSMETIC
VERTICAL CIRCULATION
CANOPY
GS PROJ. NO.
of
SE
CO
ND
FL
OO
R -
OV
ER
AL
L -
PR
OP
OS
ED
312/30/2020
TRISTARSKYLINEMEDICALCENTER
44859.00
BU
RN
PR
OG
RA
M R
EN
OV
AT
ION
NASHVILLE, TN
4
0' 25' 100'50' 150'1" = 50'-0"1
SECOND FLOOR - OVERALL - PROPOSED156

UP
DN
SECOND FLOOR ROOF BELOW
SECOND FLOOR ROOF
FIRST FLOOR ROOF BELOW
FIRSTFLOORROOF
BELOW
PB
STAFFLOUNGE2A-104
TLT- PAT.
ICU253
2A-107
2A-COR.2 CORRIDOR
CHART 2A-106
TLT.-STAFF2A-105
ON-CALL1
2B-111
ON-CALL2
2B-110
ICU272
2B-115
ICU271
2B-116
ICU270
2B-117
ISOL. ICU269
2B-118
ANTE2B-128
2B-COR.5 CORRIDOR
WAITINGALCOVE
2B-COR.1A
EQUIPSTORAGE
2A-103
CHART 2A-135
ICU254
2A-136
ICU255
2A-134
SOILWORK2A-102
CORRIDOR 2B-COR.1
TDR2B-108
T R2B-104
DECONTAM
RESPIRATORY THERAPY 2B-107
NOUR2B-120
NURSESTATION2B-119
MEDI2B-121
CORRIDOR 2B-COR.4
ICU268
2B-132
ICU267
2B-133
PHYS/ANC WORK 2B-127
STORAGE 2B-103
CLEANSUPPLY2A-101
CORRIDOR 2A-COR.1
2A-133
TLT.PAT.
TLT.PAT.
OB
OB
OBO
B
OB
OB
OB
OB
OB
OB
OB
OB
FEC
CRASHCART
CRASHCARTPTS
Med.Sta.40006 Drawer
Med.Sta.40007 Drawer
Med.Sta.4000 SingleColumn Aux.
ICE
PTSPTSPTS
REF
WAITING 2-0314
CORR3-0236
ICU 13-0235
CORR3-0258
CHART3-0222B
ICU 23-0222
ELECCLOSET3-0255A
ICU 33-0236
ICU 43-0239
CHART3-0236A
CORR 3-0225
SU3-0234
PASS3-0253
MEDROOM3-0242
ELEV#5
STAFFBREAKROOM 3-0244
STAFFTLT
3-0244A
MEDS3-0111
DICT3-0114/3-0115
MICRO&
COFFEE
LO
CK
ER
S
ELEV#4
2-0202
CHART 2-0203
TLT.2-0206
ISOL.ICU30
2-0205
ICU29
2-0207
TLT.2-0208
TLT.2-0210
ICU28
2-0209
CORRIDOR 2-0204
NURSESTATION2-0201
ELEV#7
ELEVLOBBY3-0120
ELEV#6
JAN3-0238
PASS3-0255
WORK3-0252
STAFFTLT
3-0220B
DICT3-0257NOUR
3-0256
CU3-0250
NURSESTATION 3-0254
NURSESTATION/
CHART3-0223
CHART3-0240A
ICU 53-0240
ICU 63-0241
ICU 73-0243
ICU 83-0245
ISOLATION9 3-0246
CHART3-0246A
ICU 103-0247
CORR3-0220
ICU 113-0248
CHART3-0248A
ICU 123-0249
MED.2-0218
MGR.OFFICE2-0219
SOILHOLD2-0216
C.U./EQUIP.2-0217
CORRIDOR 2-0215
H.C.ICU26
2-0213
STAIR #4
H.C.TLT.
2-0214TLT.
2-0212
ICU27
2-0211
SUPPLIES3-0110
NOUR3-0125
ELEVLOBBY3-0100
ELEC3-0104
WCHALC
3-0129
JAN3-0128
CORR3-0123
CORR3-0102
C.U./CLN
STOR3-0105
ANTE4-0143
CORR3-0142
ISOLP.P.#103-0144
T/S3-0144A
P.P.#93-0145
T/S3-0145A
P.P.#83-0146
T/S3-0146A
P.P.#73-0147
T/S3-0147A
P.P.#33-0151
T/S3-0151A
P.P.#23-0152
T/S3-0152A
P.P.#13-0153
T/S3-0153A
NURSESTATION/
CHART3-0117
ACCP.P.#53-0149
T/S3-0149A
T/S3-0150A
ACCP.P.#43-0150
PUB.TLT
3-0101
ACC P.P.3-0148
T/S3-0148A
ALCOVE
STAIR #2
WAIT
WAIT
NURSESTATION2-0103
STAIR#3
CORR 3-0118
STAFFLOUNGE3-0121
STAFFTLT
3-0121A
DIRECTOR OFFICE 3-0122
3-0124 STRCH ALCOVE
S.U.3-0107
COMM 3-0126
CORR 3-0200 CORR 3-0218
ELEV #3
ELEV #2
ELEV #1
PTS
LOCKERS
H H
HH
HH
HH
HH
HH
HH
HH
HH
HHH H
H H
UP
DN
UP
DN
PAYTELE
WHIRLPOOLSUPPLY ROOM
EQUIP. STORAGE
PAT TLT / SHOWER
CLEAN LINEN
EQUIP. STORAGE
OFFICE
MINOR RENOVATION
NEW CONSTRUCTION
MAJOR RENOVATION
COSMETIC
VERTICAL CIRCULATION
CANOPY
GS PROJ. NO.
of
SE
CO
ND
FL
OO
R P
RO
PO
SE
D -
CO
MP
ON
EN
T
1 -
EN
LA
RG
ED
412/30/2020
TRISTARSKYLINEMEDICALCENTER
44859.00
BU
RN
PR
OG
RA
M R
EN
OV
AT
ION
NASHVILLE, TN
4
0' 8' 16'
36' 48'3/64" = 1'-0"1
SECOND FLOOR PROPOSED - ENLARGED157

Attachment Section A-6B-3 Public Transportation Map
158

CUMBERL AND RIVER
4th N
Rosa L. Parks
9th N
3rd NDr. Martin
L. King Jr.
James
Robertson
Main
Union
Dick
erso
n
Ellin
gton
N 1s
t
Spring
Trinity
Dick
erso
n
Wal
ton
Broadmoor
HuntersLaneOld HickoryLi
ckto
nMaplewood
Dicker
son
Ellington
24
155 155
31E
40
Jam
es Robertson
24
65
65
65
4T
14 T
23 T 56
8 7
4
2
1
3
1
Map KeyNon-stop service
Timepoint
Transfer point
Transfer route
T
4
DOWNTOWNNASHVILLE
WHITESCREEK
43Hickory
Hills
159
Anjello Luciano
Rectangle

CUMBE
RLA
ND
RIV
ER
DO
WN
TOW
NN
ASH
VILL
E
WH
ITES
CREE
K
43 Hic
kory
Hill
s
WeG
oTra
nsit.
com
cust
omer
.com
men
ts@
nash
ville
.gov
Cust
omer
Car
e61
5-86
2-59
506:
30 a
.m. t
o 8:
00 p
.m. –
Mon
day-
Frid
ay8:
00 a
.m. t
o 5:
00 p
.m. –
Sat
urda
y10
:30
a.m
. to
2:30
p.m
. – S
unda
y Ce
ntra
l40
0 Dr
. Mar
tin L
. Kin
g Jr.
Blv
d.5:
15 a
.m. t
o 11
:15
p.m
. – M
onda
y-Fr
iday
6:00
a.m
. to
10:15
p.m
. – S
atur
day
6:00
a.m
. to
9:15
p.m
. – S
unda
ys a
nd h
olid
ays
Adm
inis
trat
ive
O�
ces
615-
862-
5969
430
Mya
tt D
rive
8:00
a.m
. to
4:30
p.m
. – M
onda
y-Fr
iday
Clos
ed w
eeke
nds a
nd h
olid
ays
WeG
oTra
nsit
@W
eGoT
rans
it
@W
eGoT
rans
itW
eGoT
rans
it.co
m/a
lert
s
For M
ore
Info
rmat
ion
Stay
Con
nect
ed
Fare
s & P
asse
s
All f
ares
incl
ude
one
free
tran
sfer
with
in tw
o ho
urs o
f boa
rdin
g.
1-Ri
de ..
......
......
......
......
......
......
......
......
...$2
.00
1-Ri
de D
isco
unte
d* ...
......
......
......
......
....$
1.00
All-D
ay P
ass .
......
......
......
......
......
......
.....
$4.0
0
7-Da
y Pa
ss ...
......
......
......
......
......
......
....$
20.0
0
31-D
ay P
ass .
......
......
......
......
......
......
.....$
65.0
0
Child
ren
age
4 an
d yo
unge
r rid
e fr
ee.
*You
th, s
enio
rs, p
erso
ns w
ith d
isab
ilitie
s, a
nd
Med
icar
e ca
rdho
lder
s are
elig
ible
for d
isco
unte
d fa
res a
nd p
asse
s with
pro
per I
.D.
ADAW
eGo Public Transit makes reasonable
accomm
odations in order for individuals with
disabilities to fully use transit services. All requests should be m
ade in advance by filling out and subm
itting a Reasonable Accomm
odation Request form
. For more inform
ation on Reasonable Accom
modations, visit W
eGoTransit.com
.
Title VITitle VI of the Civil Rights Act of 1964 states that “N
o Person in the United States shall, on the ground of race, color, or national origin, be excluded from
participation in, be denied the benefits of, or be subjected to discrim
ination under any program
or activity receiving Federal financial assistance.” For m
ore information on
Title VI, visit WeG
oTransit.com.
Weekdays to DowntownWhites
Creek High School
Hunters Lane High
School
Skyline Medical Center Walmart
Maplewood High School
Dickerson & Trinity
North 1st & Spring Central
8 7 5 6 4 3 2 16:50 – – – – – – 7:207:15 – – – – – – 7:458:59 9:11 9:21 9:26 9:32 9:40 9:46 9:55
11:04 11:16 11:26 11:31 11:37 11:45 11:51 12:001:20 1:35 1:45 1:50 1:56 2:05 2:11 2:202:13 2:25 2:35 2:40 2:46 2:54 3:01 3:103:42 3:54 4:04 4:09 4:15 4:23 4:30 4:404:17 4:29 4:39 4:44 4:50 4:58 5:04 5:145:24 5:36 5:46 5:51 5:57 6:05 6:11 6:206:40 – – – – – – 7:00
No service Saturdays, Sundays, or holidays.
Weekdays from Downtown
Central Bay 24
North 1st & Spring
Dickerson & Trinity
Maplewood High School
Skyline Medical Center Walmart
Hunters Lane High
School
Whites Creek High
School
1 2 3 4 5 6 7 85:50 5:56 6:03 6:09 6:15 6:20 6:30 6:456:15 – – 6:29 6:35 – 6:45 7:057:24 7:30 7:37 7:46 7:52 7:57 8:06 8:21
10:00 10:06 10:13 10:19 10:25 10:30 10:39 10:5412:05 12:11 12:18 12:24 12:30 12:35 12:44 12:59
2:25 2:31 2:38 2:44 2:50 2:55 3:04 3:193:40 – – – – – – 4:104:40 – – – – – – 5:105:30 5:36 5:44 5:53 5:59 6:04 6:13 6:28
Bold times denote p.m. hours.
This bus operates as an express via Ellington Parkway to Maplewood High School and does not serve Walmart.
For additional service to this area, please see schedule for Route 23 - Dickerson Road.
Sept
embe
r 29,
201
9
160
Anjello Luciano
Rectangle
Anjello Luciano
Rectangle

Section B-Need-1A ABA ICD-10 Diagnosis Codes
161

Courtesy of the
AAmmeerriiccaann BBuurrnn AAssssoocciiaatt iioonn Advanced Burn Life Support (ABLS) Learn more about the ABA and ABLS at www.ameriburn.org
Burn Center Referral Criteria
A burn center may treat adults, children, or both.
Burn injuries that should be referred to a burn
center include:
1. Partial thickness burns greater than 10% total body surface area (TBSA).
2. Burns that involve the face, hands, feet, genitalia, perineum, or major joints.
3. Third degree burns in any age group.
4. Electrical burns, including lightning injury.
5. Chemical burns.
6. Inhalation injury.
7. Burn injury in patients with preexisting medical disorders that could complicate management, prolong recovery, or affect mortality.
8. Any patient with burns and concomitant trauma (such as fractures) in which the burn injury poses the greatest risk of morbidity or mortality. In such cases, if the trauma poses the greater immediate risk, the patient may be initially stabilized in a trauma center before being transferred to a burn unit. Physician judgment will be necessary in such situations and should be in concert with the regional medical control plan and triage protocols.
9. Burned children in hospitals without qualified personnel or equipment for the care of children.
10. Burn injury in patients who will require special social, emotional, or rehabilitative intervention.
Excerpted from Guidelines for the Operation of Burn Centers (pp. 79-86),
Resources for Optimal Care of the Injured Patient 2006, Committee on
Trauma, American College of Surgeons
Severity Determination First Degree (Partial Thickness)
Superficial, red, sometimes
painful.
Second Degree (Partial Thickness)
Skin may be red, blistered,
swollen. Very painful.
Third Degree (Full Thickness)
Whitish, charred or translucent, no
pin prick sensation in burned area.
Percentage Total Body
Surface Area (TBSA)
162

ABA Burn Center Referral Criteria Coding Scheme in AnalysisPartial thickness burns greater than 10% total body surface area (TBSA) Initial encounters for partial thickness burn TBSA over 10% based on ICD-10 CM
Third degree burns in any age group Intitial encounters for third degree burns based on ICD-10 CMBurns that involve the face, hands, feet, genitalia, perineum, or major joints. Initial encounters for burns that involves face, hands, feet, genital, perineum,
and major hands, feet, genital, perineum, and major joints (Knee, ankle, waist, elbows, shoulders) based on ICD-10 CM
Chemical burns All Corrosion ICD-10 CM noted as intial encountersElectrical burns, including lightning injury Initial encounters for electrical injuryInhalation injury ICD-10 CM: (1) T27.1XXA - Burn involving larynx and trachea with lung, initial
encounter, (2) T27.5XXA - Corrosion involving larynx and trachea with lung, initial encounter
Inhalation injury patients based on DRGBurn injury patients with preexisting medical disorders that could complicate management, prolong recovery, or affect mortality
NA
Any patient with burns and concomitant trauma (such as fractures) in which the urn injury poses the greatest risk of morbidity or mortality. In such cases, if the trauma poses the greater immediate risk, the patient may be initially stabilized in a trauma center before being transferred to a burn unit. Physician judgment will be necessary in such situations and should be in concert with the regional medical control plan and triage protocols.
NA
Burned children in hospitals without qualified personnel or equipment for the care of children.
Primary diagnosis is burn and age 0-17, but excluding those initially treated in children’s hospitals
Burn injury in patients who will require special social, emotional, or rehabilitative intervention
NA
ABA BURN CENTER REFERRAL CRITERIA AND CODING SCHEME FOR ANALYSIS
163

Skyline Medical Center Burn Unit CONList of ICD-10 Codes that Meet American Burn Association Referral Criteria
Code DescriptionT2000XA Burn of unsp degree of head, face, and neck, unsp site, initT2005XA Burn of unspecified degree of scalp, initial encounterT2006XA Burn of unsp degree of forehead and cheek, init encntrT2009XA Burn of unsp deg mult sites of head, face, and neck, initT2010XA Burn first degree of head, face, and neck, unsp site, initT2015XA Burn of first degree of scalp [any part], initial encounterT2016XA Burn of first degree of forehead and cheek, init encntrT2019XA Burn of first deg mult sites of head, face, and neck, initT2020XA Burn second degree of head, face, and neck, unsp site, initT2025XA Burn of second degree of scalp [any part], initial encounterT2026XA Burn of second degree of forehead and cheek, init encntrT2029XA Burn of 2nd deg mul sites of head, face, and neck, initT2030XA Burn third degree of head, face, and neck, unsp site, initT20311A Burn of third degree of right ear, initial encounterT20312A Burn of third degree of left ear, initial encounterT20319A Burn of third degree of unspecified ear, initial encounterT2032XA Burn of third degree of lip(s), initial encounterT2033XA Burn of third degree of chin, initial encounterT2034XA Burn of third degree of nose (septum), initial encounterT2035XA Burn of third degree of scalp [any part], initial encounterT2036XA Burn of third degree of forehead and cheek, init encntrT2037XA Burn of third degree of neck, initial encounterT2039XA Burn of 3rd deg mu sites of head, face, and neck, initT2040XA Corros unsp degree of head, face, and neck, unsp site, initT20411A Corrosion of unspecified degree of right ear, init encntrT20412A Corrosion of unspecified degree of left ear, init encntrT20419A Corrosion of unsp degree of unspecified ear, init encntrT2042XA Corrosion of unspecified degree of lip(s), initial encounterT2043XA Corrosion of unspecified degree of chin, initial encounterT2044XA Corrosion of unsp degree of nose (septum), init encntrT2045XA Corrosion of unspecified degree of scalp, initial encounterT2046XA Corrosion of unsp degree of forehead and cheek, init encntrT2047XA Corrosion of unspecified degree of neck, initial encounterT2049XA Corros unsp deg mult sites of head, face, and neck, initT2050XA Corros first degree of head, face, and neck, unsp site, initT20511A Corrosion of first degree of right ear, initial encounterT20512A Corrosion of first degree of left ear, initial encounterT20519A Corrosion of first degree of unspecified ear, init encntrT2052XA Corrosion of first degree of lip(s), initial encounterT2053XA Corrosion of first degree of chin, initial encounterT2054XA Corrosion of first degree of nose (septum), init encntrT2055XA Corrosion of first degree of scalp, initial encounterT2056XA Corrosion of first degree of forehead and cheek, init encntrT2057XA Corrosion of first degree of neck, initial encounterT2059XA Corros first deg mult sites of head, face, and neck, initT2060XA Corros second deg of head, face, and neck, unsp site, init
164

Skyline Medical Center Burn Unit CONList of ICD-10 Codes that Meet American Burn Association Referral Criteria
T20611A Corrosion of second degree of right ear, initial encounterT20612A Corrosion of second degree of left ear, initial encounterT20619A Corrosion of second degree of unspecified ear, init encntrT2062XA Corrosion of second degree of lip(s), initial encounterT2063XA Corrosion of second degree of chin, initial encounterT2064XA Corrosion of second degree of nose (septum), init encntrT2065XA Corrosion of second degree of scalp, initial encounterT2066XA Corrosion of second degree of forehead and cheek, initT2067XA Corrosion of second degree of neck, initial encounterT2069XA Corrosion of 2nd deg mul sites of head, face, and neck, initT2070XA Corros third degree of head, face, and neck, unsp site, initT20711A Corrosion of third degree of right ear, initial encounterT20712A Corrosion of third degree of left ear, initial encounterT20719A Corrosion of third degree of unspecified ear, init encntrT2072XA Corrosion of third degree of lip(s), initial encounterT2073XA Corrosion of third degree of chin, initial encounterT2074XA Corrosion of third degree of nose (septum), init encntrT2075XA Corrosion of third degree of scalp, initial encounterT2076XA Corrosion of third degree of forehead and cheek, init encntrT2077XA Corrosion of third degree of neck, initial encounterT2079XA Corrosion of 3rd deg mu sites of head, face, and neck, initT2106XA Burn of unsp degree of male genital region, init encntrT2107XA Burn of unsp degree of female genital region, init encntrT2116XA Burn of first degree of male genital region, init encntrT2117XA Burn of first degree of female genital region, init encntrT2126XA Burn of second degree of male genital region, init encntrT2127XA Burn of second degree of female genital region, init encntrT2130XA Burn of third degree of trunk, unspecified site, init encntrT2131XA Burn of third degree of chest wall, initial encounterT2132XA Burn of third degree of abdominal wall, initial encounterT2133XA Burn of third degree of upper back, initial encounterT2134XA Burn of third degree of lower back, initial encounterT2135XA Burn of third degree of buttock, initial encounterT2136XA Burn of third degree of male genital region, init encntrT2137XA Burn of third degree of female genital region, init encntrT2139XA Burn of third degree of other site of trunk, init encntrT2140XA Corrosion of unsp degree of trunk, unsp site, init encntrT2141XA Corrosion of unspecified degree of chest wall, init encntrT2142XA Corrosion of unsp degree of abdominal wall, init encntrT2143XA Corrosion of unspecified degree of upper back, init encntrT2144XA Corrosion of unspecified degree of lower back, init encntrT2145XA Corrosion of unspecified degree of buttock, init encntrT2146XA Corrosion of unsp degree of male genital region, init encntrT2147XA Corrosion of unsp degree of female genital region, initT2149XA Corrosion of unsp degree of other site of trunk, init encntrT2150XA Corrosion of first degree of trunk, unsp site, init encntrT2151XA Corrosion of first degree of chest wall, initial encounter
165

Skyline Medical Center Burn Unit CONList of ICD-10 Codes that Meet American Burn Association Referral Criteria
T2152XA Corrosion of first degree of abdominal wall, init encntrT2153XA Corrosion of first degree of upper back, initial encounterT2154XA Corrosion of first degree of lower back, initial encounterT2155XA Corrosion of first degree of buttock, initial encounterT2156XA Corrosion of first degree of male genital region, initT2157XA Corrosion of first degree of female genital region, initT2159XA Corrosion of first degree of oth site of trunk, init encntrT2160XA Corrosion of second degree of trunk, unsp site, init encntrT2161XA Corrosion of second degree of chest wall, initial encounterT2162XA Corrosion of second degree of abdominal wall, init encntrT2163XA Corrosion of second degree of upper back, initial encounterT2164XA Corrosion of second degree of lower back, initial encounterT2165XA Corrosion of second degree of buttock, initial encounterT2166XA Corrosion of second degree of male genital region, initT2167XA Corrosion of second degree of female genital region, initT2169XA Corrosion of second degree of oth site of trunk, init encntrT2170XA Corrosion of third degree of trunk, unsp site, init encntrT2171XA Corrosion of third degree of chest wall, initial encounterT2172XA Corrosion of third degree of abdominal wall, init encntrT2173XA Corrosion of third degree of upper back, initial encounterT2174XA Corrosion of third degree of lower back, initial encounterT2175XA Corrosion of third degree of buttock, initial encounterT2176XA Corrosion of third degree of male genital region, initT2177XA Corrosion of third degree of female genital region, initT2179XA Corrosion of third degree of oth site of trunk, init encntrT2200XA Burn unsp deg of shldr/up lmb, ex wrs/hnd, unsp site, initT22021A Burn of unspecified degree of right elbow, initial encounterT22022A Burn of unspecified degree of left elbow, initial encounterT22029A Burn of unspecified degree of unspecified elbow, init encntrT22091A Burn unsp deg mult sites of r shldr/up lmb, ex wrs/hnd, initT22092A Burn unsp deg mult site of l shldr/up lmb, ex wrs/hnd, initT22099A Burn unsp deg mult sites of shldr/up lmb, ex wrs/hnd, initT2210XA Burn first deg of shldr/up lmb, ex wrs/hnd, unsp site, initT22121A Burn of first degree of right elbow, initial encounterT22122A Burn of first degree of left elbow, initial encounterT22129A Burn of first degree of unspecified elbow, initial encounterT22191A Burn 1st deg mult sites of r shldr/up lmb, ex wrs/hnd, initT22192A Burn 1st deg mult site of l shldr/up lmb, ex wrs/hnd, initT22199A Burn first deg mult sites of shldr/up lmb, ex wrs/hnd, initT2220XA Burn second deg of shldr/up lmb, ex wrs/hnd, unsp site, initT22221A Burn of second degree of right elbow, initial encounterT22222A Burn of second degree of left elbow, initial encounterT22229A Burn of second degree of unspecified elbow, init encntrT22291A Burn 2nd deg mul sites of r shldr/up lmb, ex wrs/hnd, initT22292A Burn 2nd deg mul site of left shldr/up lmb, ex wrs/hnd, initT22299A Burn 2nd deg mul sites of shldr/up lmb, except wrs/hnd, initT2230XA Burn third deg of shldr/up lmb, ex wrs/hnd, unsp site, init
166

Skyline Medical Center Burn Unit CONList of ICD-10 Codes that Meet American Burn Association Referral Criteria
T22311A Burn of third degree of right forearm, initial encounterT22312A Burn of third degree of left forearm, initial encounterT22312S Burn of third degree of unspecified forearm, init encntrT22321A Burn of third degree of right elbow, initial encounterT22322A Burn of third degree of left elbow, initial encounterT22329A Burn of third degree of unspecified elbow, initial encounterT22331A Burn of third degree of right upper arm, initial encounterT22332A Burn of third degree of left upper arm, initial encounterT22339A Burn of third degree of unspecified upper arm, init encntrT22341A Burn of third degree of right axilla, initial encounterT22342A Burn of third degree of left axilla, initial encounterT22349A Burn of third degree of unspecified axilla, init encntrT22351A Burn of third degree of right shoulder, initial encounterT22352A Burn of third degree of left shoulder, initial encounterT22359A Burn of third degree of unspecified shoulder, init encntrT22361A Burn of third degree of right scapular region, init encntrT22362A Burn of third degree of left scapular region, init encntrT22369A Burn of third degree of unsp scapular region, init encntrT22391A Burn 3rd deg mu sites of r shldr/up lmb, ex wrs/hnd, initT22392A Burn 3rd deg mu sites of left shldr/up lmb, ex wrs/hnd, initT22399A Burn 3rd deg mu sites of shldr/up lmb, except wrs/hnd, initT2240XA Corros unsp deg of shldr/up lmb, ex wrs/hnd, unsp site, initT22411A Corrosion of unsp degree of right forearm, init encntrT22412A Corrosion of unspecified degree of left forearm, init encntrT22419A Corrosion of unsp degree of unspecified forearm, init encntrT22421A Corrosion of unspecified degree of right elbow, init encntrT22422A Corrosion of unspecified degree of left elbow, init encntrT22429A Corrosion of unsp degree of unspecified elbow, init encntrT22431A Corrosion of unsp degree of right upper arm, init encntrT22432A Corrosion of unsp degree of left upper arm, init encntrT22439A Corrosion of unsp degree of unsp upper arm, init encntrT22441A Corrosion of unspecified degree of right axilla, init encntrT22442A Corrosion of unspecified degree of left axilla, init encntrT22449A Corrosion of unsp degree of unspecified axilla, init encntrT22451A Corrosion of unsp degree of right shoulder, init encntrT22452A Corrosion of unsp degree of left shoulder, init encntrT22459A Corrosion of unsp degree of unsp shoulder, init encntrT22461A Corrosion of unsp degree of right scapular region, initT22462A Corrosion of unsp degree of left scapular region, initT22469A Corrosion of unsp degree of unsp scapular region, initT22491A Corros unsp deg mult site of r shldr/up lmb,ex wrs/hnd, initT22492A Corros unsp deg mult site of l shldr/up lmb,ex wrs/hnd, initT22499A Corros unsp deg mult sites of shldr/up lmb, ex wrs/hnd, initT2250XA Corros first deg of shldr/up lmb, ex wrs/hnd unsp site, initT22511A Corrosion of first degree of right forearm, init encntrT22512A Corrosion of first degree of left forearm, initial encounterT22519A Corrosion of first degree of unsp forearm, init encntr
167

Skyline Medical Center Burn Unit CONList of ICD-10 Codes that Meet American Burn Association Referral Criteria
T22521A Corrosion of first degree of right elbow, initial encounterT22522A Corrosion of first degree of left elbow, initial encounterT22529A Corrosion of first degree of unspecified elbow, init encntrT22531A Corrosion of first degree of right upper arm, init encntrT22532A Corrosion of first degree of left upper arm, init encntrT22539A Corrosion of first degree of unsp upper arm, init encntrT22541A Corrosion of first degree of right axilla, initial encounterT22542A Corrosion of first degree of left axilla, initial encounterT22549A Corrosion of first degree of unspecified axilla, init encntrT22551A Corrosion of first degree of right shoulder, init encntrT22552A Corrosion of first degree of left shoulder, init encntrT22559A Corrosion of first degree of unsp shoulder, init encntrT22561A Corrosion of first degree of right scapular region, initT22562A Corrosion of first degree of left scapular region, initT22562D Corrosion of first degree of left scapular region,T22562S Corrosion of first degree of left scapular region,T22569A Corrosion of first degree of unsp scapular region, initT22591A Corros 1st deg mult site of r shldr/up lmb, ex wrs/hnd, initT22592A Corros 1st deg mult site of l shldr/up lmb, ex wrs/hnd, initT22599A Corros 1st deg mult sites of shldr/up lmb, ex wrs/hnd, initT2260XA Corros 2nd deg of shldr/up lmb, ex wrs/hnd, unsp site, initT22611A Corrosion of second degree of right forearm, init encntrT22612A Corrosion of second degree of left forearm, init encntrT22619A Corrosion of second degree of unsp forearm, init encntrT22621A Corrosion of second degree of right elbow, initial encounterT22622A Corrosion of second degree of left elbow, initial encounterT22629A Corrosion of second degree of unspecified elbow, init encntrT22631A Corrosion of second degree of right upper arm, init encntrT22632A Corrosion of second degree of left upper arm, init encntrT22639A Corrosion of second degree of unsp upper arm, init encntrT22641A Corrosion of second degree of right axilla, init encntrT22642A Corrosion of second degree of left axilla, initial encounterT22649A Corrosion of second degree of unsp axilla, init encntrT22651A Corrosion of second degree of right shoulder, init encntrT22652A Corrosion of second degree of left shoulder, init encntrT22659A Corrosion of second degree of unsp shoulder, init encntrT22661A Corrosion of second degree of right scapular region, initT22662A Corrosion of second degree of left scapular region, initT22669A Corrosion of second degree of unsp scapular region, initT22691A Corros 2nd deg mul sites of r shldr/up lmb, ex wrs/hnd, initT22692A Corros 2nd deg mul site of l shldr/up lmb, ex wrs/hnd, initT22699A Corros 2nd deg mul sites of shldr/up lmb, ex wrs/hnd, initT2270XA Corros 3rd deg of shldr/up lmb, ex wrs/hnd, unsp site, initT22711A Corrosion of third degree of right forearm, init encntrT22712A Corrosion of third degree of left forearm, initial encounterT22719A Corrosion of third degree of unsp forearm, init encntrT22721A Corrosion of third degree of right elbow, initial encounter
168

Skyline Medical Center Burn Unit CONList of ICD-10 Codes that Meet American Burn Association Referral Criteria
T22722A Corrosion of third degree of left elbow, initial encounterT22729A Corrosion of third degree of unspecified elbow, init encntrT22731A Corrosion of third degree of right upper arm, init encntrT22732A Corrosion of third degree of left upper arm, init encntrT22739A Corrosion of third degree of unsp upper arm, init encntrT22741A Corrosion of third degree of right axilla, initial encounterT22742A Corrosion of third degree of left axilla, initial encounterT22749A Corrosion of third degree of unspecified axilla, init encntrT22751A Corrosion of third degree of right shoulder, init encntrT22752A Corrosion of third degree of left shoulder, init encntrT22759A Corrosion of third degree of unsp shoulder, init encntrT22761A Corrosion of third degree of right scapular region, initT22762A Corrosion of third degree of left scapular region, initT22769A Corrosion of third degree of unsp scapular region, initT22791A Corros 3rd deg mu sites of r shldr/up lmb, ex wrs/hnd, initT22792A Corros 3rd deg mu site of l shldr/up lmb, ex wrs/hnd, initT22799A Corros 3rd deg mu sites of shldr/up lmb, ex wrs/hnd, initT23001A Burn of unsp degree of right hand, unsp site, init encntrT23002A Burn of unsp degree of left hand, unsp site, init encntrT23009A Burn of unsp degree of unsp hand, unsp site, init encntrT23011A Burn of unsp degree of right thumb (nail), init encntrT23012A Burn of unspecified degree of left thumb (nail), init encntrT23019A Burn of unsp degree of unspecified thumb (nail), init encntrT23021A Burn unsp degree of single r finger except thumb, initT23022A Burn unsp degree of single l finger except thumb, initT23029A Burn unsp degree of unsp single finger except thumb, initT23031A Burn unsp deg mult right fingers (nail), not inc thumb, initT23032A Burn unsp deg mult left fingers (nail), not inc thumb, initT23039A Burn unsp degree of unsp mult fngr, not inc thumb, initT23041A Burn of unsp deg mult right fingers (nail), inc thumb, initT23042A Burn of unsp deg mult left fingers (nail), inc thumb, initT23049A Burn unsp degree of unsp mult fngr (nail), inc thumb, initT23051A Burn of unspecified degree of right palm, initial encounterT23052A Burn of unspecified degree of left palm, initial encounterT23059A Burn of unspecified degree of unspecified palm, init encntrT23061A Burn of unsp degree of back of right hand, init encntrT23062A Burn of unspecified degree of back of left hand, init encntrT23069A Burn of unsp degree of back of unspecified hand, init encntrT23071A Burn of unspecified degree of right wrist, initial encounterT23072A Burn of unspecified degree of left wrist, initial encounterT23079A Burn of unspecified degree of unspecified wrist, init encntrT23091A Burn of unsp deg mult sites of right wrist and hand, initT23092A Burn of unsp deg mult sites of left wrist and hand, initT23099A Burn of unsp deg mult sites of unsp wrist and hand, initT23101A Burn of first degree of right hand, unsp site, init encntrT23102A Burn of first degree of left hand, unsp site, init encntrT23109A Burn of first degree of unsp hand, unsp site, init encntr
169

Skyline Medical Center Burn Unit CONList of ICD-10 Codes that Meet American Burn Association Referral Criteria
T23111A Burn of first degree of right thumb (nail), init encntrT23112A Burn of first degree of left thumb (nail), initial encounterT23119A Burn of first degree of unsp thumb (nail), init encntrT23121A Burn first degree of single r finger except thumb, initT23122A Burn first degree of single l finger except thumb, initT23129A Burn first degree of unsp single finger except thumb, initT23131A Burn first deg mult right fngr (nail), not inc thumb, initT23132A Burn first deg mult left fingers (nail), not inc thumb, initT23139A Burn first degree of unsp mult fngr, not inc thumb, initT23141A Burn of first deg mult right fingers (nail), inc thumb, initT23142A Burn of first deg mult left fingers (nail), inc thumb, initT23149A Burn first degree of unsp mult fngr (nail), inc thumb, initT23151A Burn of first degree of right palm, initial encounterT23152A Burn of first degree of left palm, initial encounterT23159A Burn of first degree of unspecified palm, initial encounterT23161A Burn of first degree of back of right hand, init encntrT23162A Burn of first degree of back of left hand, initial encounterT23169A Burn of first degree of back of unsp hand, init encntrT23171A Burn of first degree of right wrist, initial encounterT23172A Burn of first degree of left wrist, initial encounterT23179A Burn of first degree of unspecified wrist, initial encounterT23191A Burn of first deg mult sites of right wrist and hand, initT23192A Burn of first deg mult sites of left wrist and hand, initT23199A Burn of first deg mult sites of unsp wrist and hand, initT23201A Burn of second degree of right hand, unsp site, init encntrT23202A Burn of second degree of left hand, unsp site, init encntrT23209A Burn of second degree of unsp hand, unsp site, init encntrT23211A Burn of second degree of right thumb (nail), init encntrT23212A Burn of second degree of left thumb (nail), init encntrT23219A Burn of second degree of unsp thumb (nail), init encntrT23221A Burn second degree of single r finger except thumb, initT23222A Burn second degree of single l finger except thumb, initT23229A Burn second degree of unsp single finger except thumb, initT23231A Burn 2nd deg mul right fingers (nail), not inc thumb, initT23232A Burn of 2nd deg mul left fingers (nail), not inc thumb, initT23239A Burn second degree of unsp mult fngr, not inc thumb, initT23241A Burn of 2nd deg mul right fingers (nail), inc thumb, initT23242A Burn of 2nd deg mul left fingers (nail), inc thumb, initT23249A Burn second degree of unsp mult fngr (nail), inc thumb, initT23251A Burn of second degree of right palm, initial encounterT23252A Burn of second degree of left palm, initial encounterT23259A Burn of second degree of unspecified palm, initial encounterT23261A Burn of second degree of back of right hand, init encntrT23262A Burn of second degree of back of left hand, init encntrT23269A Burn of second degree of back of unsp hand, init encntrT23271A Burn of second degree of right wrist, initial encounterT23272A Burn of second degree of left wrist, initial encounter
170

Skyline Medical Center Burn Unit CONList of ICD-10 Codes that Meet American Burn Association Referral Criteria
T23279A Burn of second degree of unspecified wrist, init encntrT23291A Burn of 2nd deg mul sites of right wrist and hand, initT23292A Burn of 2nd deg mul sites of left wrist and hand, initT23299A Burn of 2nd deg mul sites of unsp wrist and hand, initT23301A Burn of third degree of right hand, unsp site, init encntrT23302A Burn of third degree of left hand, unsp site, init encntrT23309A Burn of third degree of unsp hand, unsp site, init encntrT23311A Burn of third degree of right thumb (nail), init encntrT23312A Burn of third degree of left thumb (nail), initial encounterT23319A Burn of third degree of unsp thumb (nail), init encntrT23321A Burn third degree of single r finger except thumb, initT23322A Burn third degree of single l finger except thumb, initT23329A Burn third degree of unsp single finger except thumb, initT23331A Burn of 3rd deg mu right fingers (nail), not inc thumb, initT23332A Burn of 3rd deg mu left fingers (nail), not inc thumb, initT23339A Burn third degree of unsp mult fngr, not inc thumb, initT23341A Burn of 3rd deg mu right fingers (nail), inc thumb, initT23342A Burn of 3rd deg mu left fingers (nail), inc thumb, initT23349A Burn third degree of unsp mult fngr (nail), inc thumb, initT23351A Burn of third degree of right palm, initial encounterT23352A Burn of third degree of left palm, initial encounterT23359A Burn of third degree of unspecified palm, initial encounterT23361A Burn of third degree of back of right hand, init encntrT23362A Burn of third degree of back of left hand, initial encounterT23369A Burn of third degree of back of unsp hand, init encntrT23371A Burn of third degree of right wrist, initial encounterT23372A Burn of third degree of left wrist, initial encounterT23379A Burn of third degree of unspecified wrist, initial encounterT23391A Burn of 3rd deg mu sites of right wrist and hand, initT23392A Burn of 3rd deg mu sites of left wrist and hand, initT23399A Burn of 3rd deg mu sites of unsp wrist and hand, initT23401A Corrosion of unsp degree of right hand, unsp site, initT23402A Corrosion of unsp degree of left hand, unsp site, initT23409A Corrosion of unsp degree of unsp hand, unsp site, initT23411A Corrosion of unsp degree of right thumb (nail), init encntrT23412A Corrosion of unsp degree of left thumb (nail), init encntrT23419A Corrosion of unsp degree of unsp thumb (nail), init encntrT23421A Corros unsp degree of single r finger except thumb, initT23422A Corros unsp degree of single l finger except thumb, initT23429A Corros unsp degree of unsp single finger except thumb, initT23431A Corros unsp deg mult right fngr (nail), not inc thumb, initT23432A Corros unsp deg mult left fngr (nail), not inc thumb, initT23439A Corros unsp degree of unsp mult fngr, not inc thumb, initT23441A Corros unsp deg mult right fingers (nail), inc thumb, initT23442A Corros unsp deg mult left fingers (nail), inc thumb, initT23449A Corros unsp degree of unsp mult fngr (nail), inc thumb, initT23451A Corrosion of unspecified degree of right palm, init encntr
171

Skyline Medical Center Burn Unit CONList of ICD-10 Codes that Meet American Burn Association Referral Criteria
T23452A Corrosion of unspecified degree of left palm, init encntrT23459A Corrosion of unsp degree of unspecified palm, init encntrT23461A Corrosion of unsp degree of back of right hand, init encntrT23462A Corrosion of unsp degree of back of left hand, init encntrT23469A Corrosion of unsp degree of back of unsp hand, init encntrT23471A Corrosion of unspecified degree of right wrist, init encntrT23472A Corrosion of unspecified degree of left wrist, init encntrT23479A Corrosion of unsp degree of unspecified wrist, init encntrT23491A Corrosion of unsp deg mult sites of right wrs/hnd, initT23492A Corrosion of unsp deg mult sites of left wrs/hnd, initT23499A Corrosion of unsp deg mult sites of unsp wrs/hnd, initT23501A Corrosion of first degree of right hand, unsp site, initT23502A Corrosion of first degree of left hand, unsp site, initT23509A Corrosion of first degree of unsp hand, unsp site, initT23511A Corrosion of first degree of right thumb (nail), init encntrT23512A Corrosion of first degree of left thumb (nail), init encntrT23519A Corrosion of first degree of unsp thumb (nail), init encntrT23521A Corros first degree of single r finger except thumb, initT23522A Corros first degree of single l finger except thumb, initT23529A Corros first degree of unsp single finger except thumb, initT23531A Corros first deg mult right fngr (nail), not inc thumb, initT23532A Corros first deg mult left fngr (nail), not inc thumb, initT23539A Corros first degree of unsp mult fngr, not inc thumb, initT23541A Corros first deg mult right fingers (nail), inc thumb, initT23542A Corros first deg mult left fingers (nail), inc thumb, initT23549A Corros first degree of unsp mult fngr, inc thumb, initT23551A Corrosion of first degree of right palm, initial encounterT23552A Corrosion of first degree of left palm, initial encounterT23559A Corrosion of first degree of unspecified palm, init encntrT23561A Corrosion of first degree of back of right hand, init encntrT23562A Corrosion of first degree of back of left hand, init encntrT23569A Corrosion of first degree of back of unsp hand, init encntrT23571A Corrosion of first degree of right wrist, initial encounterT23572A Corrosion of first degree of left wrist, initial encounterT23579A Corrosion of first degree of unspecified wrist, init encntrT23591A Corrosion of first deg mult sites of right wrs/hnd, initT23592A Corrosion of first deg mult sites of left wrs/hnd, initT23599A Corrosion of first deg mult sites of unsp wrs/hnd, initT23601A Corrosion of second degree of right hand, unsp site, initT23602A Corrosion of second degree of left hand, unsp site, initT23609A Corrosion of second degree of unsp hand, unsp site, initT23611A Corrosion of second degree of right thumb (nail), initT23612A Corrosion of second degree of left thumb (nail), init encntrT23619A Corrosion of second degree of unsp thumb (nail), init encntrT23621A Corros second degree of single r finger except thumb, initT23622A Corros second degree of single l finger except thumb, initT23629A Corros second deg of unsp single finger except thumb, init
172

Skyline Medical Center Burn Unit CONList of ICD-10 Codes that Meet American Burn Association Referral Criteria
T23631A Corros 2nd deg mul right fingers (nail), not inc thumb, initT23632A Corros 2nd deg mul left fingers (nail), not inc thumb, initT23639A Corros second degree of unsp mult fngr, not inc thumb, initT23641A Corros 2nd deg mul right fingers (nail), inc thumb, initT23642A Corros 2nd deg mul left fingers (nail), inc thumb, initT23649A Corros second degree of unsp mult fngr, inc thumb, initT23651A Corrosion of second degree of right palm, initial encounterT23652A Corrosion of second degree of left palm, initial encounterT23659A Corrosion of second degree of unspecified palm, init encntrT23661A Corrosion of second degree back of right hand, init encntrT23662A Corrosion of second degree back of left hand, init encntrT23669A Corrosion of second degree back of unsp hand, init encntrT23671A Corrosion of second degree of right wrist, initial encounterT23672A Corrosion of second degree of left wrist, initial encounterT23679A Corrosion of second degree of unspecified wrist, init encntrT23691A Corrosion of 2nd deg mul sites of right wrist and hand, initT23692A Corrosion of 2nd deg mul sites of left wrist and hand, initT23699A Corrosion of 2nd deg mul sites of unsp wrist and hand, initT23701A Corrosion of third degree of right hand, unsp site, initT23702A Corrosion of third degree of left hand, unsp site, initT23709A Corrosion of third degree of unsp hand, unsp site, initT23711A Corrosion of third degree of right thumb (nail), init encntrT23712A Corrosion of third degree of left thumb (nail), init encntrT23719A Corrosion of third degree of unsp thumb (nail), init encntrT23721A Corros third degree of single r finger except thumb, initT23722A Corros third degree of single l finger except thumb, initT23729A Corros third degree of unsp single finger except thumb, initT23731A Corros 3rd deg mu right fingers (nail), not inc thumb, initT23732A Corros 3rd deg mu left fingers (nail), not inc thumb, initT23739A Corros third degree of unsp mult fngr, not inc thumb, initT23741A Corros 3rd deg mu right fingers (nail), inc thumb, initT23742A Corros 3rd deg mu left fingers (nail), including thumb, initT23749A Corros third degree of unsp mult fngr, inc thumb, initT23751A Corrosion of third degree of right palm, initial encounterT23752A Corrosion of third degree of left palm, initial encounterT23759A Corrosion of third degree of unspecified palm, init encntrT23761A Corrosion of third degree of back of right hand, init encntrT23762A Corrosion of third degree of back of left hand, init encntrT23769A Corrosion of third degree back of unsp hand, init encntrT23771A Corrosion of third degree of right wrist, initial encounterT23772A Corrosion of third degree of left wrist, initial encounterT23779A Corrosion of third degree of unspecified wrist, init encntrT23791A Corrosion of 3rd deg mu sites of right wrist and hand, initT23792A Corrosion of 3rd deg mu sites of left wrist and hand, initT23799A Corrosion of 3rd deg mu sites of unsp wrist and hand, initT24001A Burn unsp deg of unsp site right lower limb, ex ank/ft, initT24002A Burn unsp deg of unsp site left lower limb, ex ank/ft, init
173

Skyline Medical Center Burn Unit CONList of ICD-10 Codes that Meet American Burn Association Referral Criteria
T24009A Burn unsp deg of unsp site unsp lower limb, ex ank/ft, initT24021A Burn of unspecified degree of right knee, initial encounterT24022A Burn of unspecified degree of left knee, initial encounterT24029A Burn of unspecified degree of unspecified knee, init encntrT24091A Burn unsp deg mult sites of right low limb, ex ank/ft, initT24092A Burn unsp deg mult sites of left lower limb, ex ank/ft, initT24099A Burn unsp deg mult sites of unsp lower limb, ex ank/ft, initT24101A Burn 1st deg of unsp site right lower limb, ex ank/ft, initT24102A Burn first deg of unsp site left lower limb, ex ank/ft, initT24109A Burn first deg of unsp site unsp lower limb, ex ank/ft, initT24121A Burn of first degree of right knee, initial encounterT24122A Burn of first degree of left knee, initial encounterT24129A Burn of first degree of unspecified knee, initial encounterT24191A Burn 1st deg mult sites of right lower limb, ex ank/ft, initT24192A Burn 1st deg mult sites of left lower limb, ex ank/ft, initT24199A Burn 1st deg mult sites of unsp lower limb, ex ank/ft, initT24201A Burn 2nd deg of unsp site right lower limb, ex ank/ft, initT24202A Burn 2nd deg of unsp site left lower limb, ex ank/ft, initT24209A Burn 2nd deg of unsp site unsp lower limb, ex ank/ft, initT24221A Burn of second degree of right knee, initial encounterT24222A Burn of second degree of left knee, initial encounterT24229A Burn of second degree of unspecified knee, initial encounterT24291A Burn 2nd deg mul sites of right lower limb, ex ank/ft, initT24292A Burn 2nd deg mul sites of left lower limb, ex ank/ft, initT24299A Burn 2nd deg mul sites of unsp lower limb, ex ank/ft, initT24301A Burn third deg of unsp site right low limb, ex ank/ft, initT24302A Burn third deg of unsp site left lower limb, ex ank/ft, initT24309A Burn third deg of unsp site unsp lower limb, ex ank/ft, initT24311A Burn of third degree of right thigh, initial encounterT24312A Burn of third degree of left thigh, initial encounterT24319A Burn of third degree of unspecified thigh, initial encounterT24321A Burn of third degree of right knee, initial encounterT24322A Burn of third degree of left knee, initial encounterT24329A Burn of third degree of unspecified knee, initial encounterT24331A Burn of third degree of right lower leg, initial encounterT24332A Burn of third degree of left lower leg, initial encounterT24339A Burn of third degree of unspecified lower leg, init encntrT24391A Burn 3rd deg mu sites of right lower limb, ex ank/ft, initT24392A Burn 3rd deg mu sites of left lower limb, ex ank/ft, initT24399A Burn 3rd deg mu sites of unsp lower limb, ex ank/ft, initT24401A Corros unsp deg of unsp site right low limb, ex ank/ft, initT24402A Corros unsp deg of unsp site left low limb, ex ank/ft, initT24409A Corros unsp deg of unsp site unsp low limb, ex ank/ft, initT24411A Corrosion of unspecified degree of right thigh, init encntrT24412A Corrosion of unspecified degree of left thigh, init encntrT24419A Corrosion of unsp degree of unspecified thigh, init encntrT24421A Corrosion of unspecified degree of right knee, init encntr
174

Skyline Medical Center Burn Unit CONList of ICD-10 Codes that Meet American Burn Association Referral Criteria
T24422A Corrosion of unspecified degree of left knee, init encntrT24429A Corrosion of unsp degree of unspecified knee, init encntrT24431A Corrosion of unsp degree of right lower leg, init encntrT24432A Corrosion of unsp degree of left lower leg, init encntrT24439A Corrosion of unsp degree of unsp lower leg, init encntrT24491A Corros unsp deg mult sites of r low limb, ex ank/ft, initT24492A Corros unsp deg mult sites of left low limb, ex ank/ft, initT24499A Corros unsp deg mult sites of unsp low limb, ex ank/ft, initT24501A Corros 1st deg of unsp site right low limb, ex ank/ft, initT24502A Corros 1st deg of unsp site left lower limb, ex ank/ft, initT24509A Corros 1st deg of unsp site unsp lower limb, ex ank/ft, initT24511A Corrosion of first degree of right thigh, initial encounterT24512A Corrosion of first degree of left thigh, initial encounterT24519A Corrosion of first degree of unspecified thigh, init encntrT24521A Corrosion of first degree of right knee, initial encounterT24522A Corrosion of first degree of left knee, initial encounterT24529A Corrosion of first degree of unspecified knee, init encntrT24531A Corrosion of first degree of right lower leg, init encntrT24532A Corrosion of first degree of left lower leg, init encntrT24539A Corrosion of first degree of unsp lower leg, init encntrT24591A Corros 1st deg mult sites of right low limb, ex ank/ft, initT24592A Corros 1st deg mult sites of left low limb, ex ank/ft, initT24599A Corros 1st deg mult sites of unsp low limb, ex ank/ft, initT24601A Corros 2nd deg of unsp site right low limb, ex ank/ft, initT24602A Corros 2nd deg of unsp site left lower limb, ex ank/ft, initT24609A Corros 2nd deg of unsp site unsp lower limb, ex ank/ft, initT24611A Corrosion of second degree of right thigh, initial encounterT24612A Corrosion of second degree of left thigh, initial encounterT24619A Corrosion of second degree of unspecified thigh, init encntrT24621A Corrosion of second degree of right knee, initial encounterT24622A Corrosion of second degree of left knee, initial encounterT24629A Corrosion of second degree of unspecified knee, init encntrT24631A Corrosion of second degree of right lower leg, init encntrT24632A Corrosion of second degree of left lower leg, init encntrT24639A Corrosion of second degree of unsp lower leg, init encntrT24691A Corros 2nd deg mul sites of right low limb, ex ank/ft, initT24692A Corros 2nd deg mul sites of left lower limb, ex ank/ft, initT24699A Corros 2nd deg mul sites of unsp lower limb, ex ank/ft, initT24701A Corros third deg of unsp site r low limb, ex ank/ft, initT24702A Corros third deg of unsp site left low limb, ex ank/ft, initT24709A Corros third deg of unsp site unsp low limb, ex ank/ft, initT24711A Corrosion of third degree of right thigh, initial encounterT24712A Corrosion of third degree of left thigh, initial encounterT24719A Corrosion of third degree of unspecified thigh, init encntrT24721A Corrosion of third degree of right knee, initial encounterT24722A Corrosion of third degree of left knee, initial encounterT24729A Corrosion of third degree of unspecified knee, init encntr
175

Skyline Medical Center Burn Unit CONList of ICD-10 Codes that Meet American Burn Association Referral Criteria
T24731A Corrosion of third degree of right lower leg, init encntrT24732A Corrosion of third degree of left lower leg, init encntrT24739A Corrosion of third degree of unsp lower leg, init encntrT24791A Corros 3rd deg mu sites of right lower limb, ex ank/ft, initT24792A Corros 3rd deg mu sites of left lower limb, ex ank/ft, initT24799A Corros 3rd deg mu sites of unsp lower limb, ex ank/ft, initT25011A Burn of unspecified degree of right ankle, initial encounterT25012A Burn of unspecified degree of left ankle, initial encounterT25019A Burn of unspecified degree of unspecified ankle, init encntrT25021A Burn of unspecified degree of right foot, initial encounterT25022A Burn of unspecified degree of left foot, initial encounterT25029A Burn of unspecified degree of unspecified foot, init encntrT25031A Burn of unsp degree of right toe(s) (nail), init encntrT25032A Burn of unsp degree of left toe(s) (nail), init encntrT25039A Burn of unsp degree of unsp toe(s) (nail), init encntrT25091A Burn of unsp deg mult sites of right ankle and foot, initT25092A Burn of unsp deg mult sites of left ankle and foot, initT25099A Burn of unsp deg mult sites of unsp ankle and foot, initT25111A Burn of first degree of right ankle, initial encounterT25112A Burn of first degree of left ankle, initial encounterT25119A Burn of first degree of unspecified ankle, initial encounterT25121A Burn of first degree of right foot, initial encounterT25122A Burn of first degree of left foot, initial encounterT25129A Burn of first degree of unspecified foot, initial encounterT25131A Burn of first degree of right toe(s) (nail), init encntrT25132A Burn of first degree of left toe(s) (nail), init encntrT25139A Burn of first degree of unsp toe(s) (nail), init encntrT25191A Burn of first deg mult sites of right ankle and foot, initT25192A Burn of first deg mult sites of left ankle and foot, initT25199A Burn of first deg mult sites of unsp ankle and foot, initT25211A Burn of second degree of right ankle, initial encounterT25212A Burn of second degree of left ankle, initial encounterT25219A Burn of second degree of unspecified ankle, init encntrT25221A Burn of second degree of right foot, initial encounterT25222A Burn of second degree of left foot, initial encounterT25229A Burn of second degree of unspecified foot, initial encounterT25231A Burn of second degree of right toe(s) (nail), init encntrT25232A Burn of second degree of left toe(s) (nail), init encntrT25239A Burn of second degree of unsp toe(s) (nail), init encntrT25291A Burn of 2nd deg mul sites of right ankle and foot, initT25292A Burn of 2nd deg mul sites of left ankle and foot, initT25299A Burn of 2nd deg mul sites of unsp ankle and foot, initT25311A Burn of third degree of right ankle, initial encounterT25312A Burn of third degree of left ankle, initial encounterT25319A Burn of third degree of unspecified ankle, initial encounterT25321A Burn of third degree of right foot, initial encounterT25322A Burn of third degree of left foot, initial encounter
176

Skyline Medical Center Burn Unit CONList of ICD-10 Codes that Meet American Burn Association Referral Criteria
T25329A Burn of third degree of unspecified foot, initial encounterT25331A Burn of third degree of right toe(s) (nail), init encntrT25332A Burn of third degree of left toe(s) (nail), init encntrT25339A Burn of third degree of unsp toe(s) (nail), init encntrT25391A Burn of 3rd deg mu sites of right ankle and foot, initT25392A Burn of 3rd deg mu sites of left ankle and foot, initT25399A Burn of 3rd deg mu sites of unsp ankle and foot, initT25411A Corrosion of unspecified degree of right ankle, init encntrT25412A Corrosion of unspecified degree of left ankle, init encntrT25419A Corrosion of unsp degree of unspecified ankle, init encntrT25421A Corrosion of unspecified degree of right foot, init encntrT25422A Corrosion of unspecified degree of left foot, init encntrT25429A Corrosion of unsp degree of unspecified foot, init encntrT25431A Corrosion of unsp degree of right toe(s) (nail), init encntrT25432A Corrosion of unsp degree of left toe(s) (nail), init encntrT25439A Corrosion of unsp degree of unsp toe(s) (nail), init encntrT25491A Corrosion of unsp deg mult sites of right ank/ft, initT25492A Corrosion of unsp deg mult sites of left ank/ft, initT25499A Corrosion of unsp deg mult sites of unsp ank/ft, initT25511A Corrosion of first degree of right ankle, initial encounterT25512A Corrosion of first degree of left ankle, initial encounterT25519A Corrosion of first degree of unspecified ankle, init encntrT25521A Corrosion of first degree of right foot, initial encounterT25522A Corrosion of first degree of left foot, initial encounterT25529A Corrosion of first degree of unspecified foot, init encntrT25531A Corrosion of first degree of right toe(s) (nail), initT25532A Corrosion of first degree of left toe(s) (nail), init encntrT25539A Corrosion of first degree of unsp toe(s) (nail), init encntrT25591A Corrosion of first deg mult sites of right ank/ft, initT25592A Corrosion of first deg mult sites of left ank/ft, initT25599A Corrosion of first deg mult sites of unsp ank/ft, initT25611A Corrosion of second degree of right ankle, initial encounterT25612A Corrosion of second degree of left ankle, initial encounterT25619A Corrosion of second degree of unspecified ankle, init encntrT25621A Corrosion of second degree of right foot, initial encounterT25622A Corrosion of second degree of left foot, initial encounterT25629A Corrosion of second degree of unspecified foot, init encntrT25631A Corrosion of second degree of right toe(s) (nail), initT25632A Corrosion of second degree of left toe(s) (nail), initT25639A Corrosion of second degree of unsp toe(s) (nail), initT25691A Corrosion of second degree of right ankle and foot, initT25692A Corrosion of second degree of left ankle and foot, initT25699A Corrosion of second degree of unsp ankle and foot, initT25711A Corrosion of third degree of right ankle, initial encounterT25712A Corrosion of third degree of left ankle, initial encounterT25719A Corrosion of third degree of unspecified ankle, init encntrT25721A Corrosion of third degree of right foot, initial encounter
177

Skyline Medical Center Burn Unit CONList of ICD-10 Codes that Meet American Burn Association Referral Criteria
T25722A Corrosion of third degree of left foot, initial encounterT25729A Corrosion of third degree of unspecified foot, init encntrT25731A Corrosion of third degree of right toe(s) (nail), initT25732A Corrosion of third degree of left toe(s) (nail), init encntrT25739A Corrosion of third degree of unsp toe(s) (nail), init encntrT25791A Corrosion of 3rd deg mu sites of right ankle and foot, initT25792A Corrosion of 3rd deg mu sites of left ankle and foot, initT25799A Corrosion of 3rd deg mu sites of unsp ankle and foot, initT2600XA Burn of unspecified eyelid and periocular area, init encntrT2601XA Burn of right eyelid and periocular area, initial encounterT2602XA Burn of left eyelid and periocular area, initial encounterT2610XA Burn of cornea and conjunctival sac, unsp eye, init encntrT2611XA Burn of cornea and conjunctival sac, right eye, init encntrT2612XA Burn of cornea and conjunctival sac, left eye, init encntrT2620XA Burn w resulting rupture and dest of unsp eyeball, initT2621XA Burn w resulting rupture and dest of right eyeball, initT2622XA Burn w resulting rupture and dest of left eyeball, initT2630XA Burns of oth parts of unsp eye and adnexa, init encntrT2631XA Burns of oth parts of right eye and adnexa, init encntrT2632XA Burns of oth parts of left eye and adnexa, init encntrT2640XA Burn of unsp eye and adnexa, part unspecified, init encntrT2641XA Burn of right eye and adnexa, part unspecified, init encntrT2642XA Burn of left eye and adnexa, part unspecified, init encntrT2650XA Corrosion of unsp eyelid and periocular area, init encntrT2651XA Corrosion of right eyelid and periocular area, init encntrT2652XA Corrosion of left eyelid and periocular area, init encntrT2660XA Corrosion of cornea and conjunctival sac, unsp eye, initT2661XA Corrosion of cornea and conjunctival sac, right eye, initT2662XA Corrosion of cornea and conjunctival sac, left eye, initT2670XA Corrosion w resulting rupture and dest of unsp eyeball, initT2671XA Corros w resulting rupture and dest of right eyeball, initT2672XA Corrosion w resulting rupture and dest of left eyeball, initT2680XA Corrosions of oth parts of unsp eye and adnexa, init encntrT2681XA Corrosions of oth parts of right eye and adnexa, init encntrT2682XA Corrosions of oth parts of left eye and adnexa, init encntrT2690XA Corrosion of unsp eye and adnexa, part unsp, init encntrT2691XA Corrosion of right eye and adnexa, part unsp, init encntrT2692XA Corrosion of left eye and adnexa, part unsp, init encntrT270XXA Burn of larynx and trachea, initial encounterT271XXA Burn involving larynx and trachea with lung, init encntrT272XXA Burn of other parts of respiratory tract, initial encounterT273XXA Burn of respiratory tract, part unspecified, init encntrT274XXA Corrosion of larynx and trachea, initial encounterT275XXA Corrosion involving larynx and trachea w lung, init encntrT276XXA Corrosion of other parts of respiratory tract, init encntrT277XXA Corrosion of respiratory tract, part unsp, init encntrT280XXA Burn of mouth and pharynx, initial encounter
178

Skyline Medical Center Burn Unit CONList of ICD-10 Codes that Meet American Burn Association Referral Criteria
T281XXA Burn of esophagus, initial encounterT282XXA Burn of other parts of alimentary tract, initial encounterT283XXA Burn of internal genitourinary organs, initial encounterT285XXA Corrosion of mouth and pharynx, initial encounterT286XXA Corrosion of esophagus, initial encounterT287XXA Corrosion of other parts of alimentary tract, init encntrT288XXA Corrosion of internal genitourinary organs, init encntrT2890XA Corrosions of unspecified internal organs, initial encounterT28911A Corrosions of right ear drum, initial encounterT28912A Corrosions of left ear drum, initial encounterT28919A Corrosions of unspecified ear drum, initial encounterT2899XA Corrosions of other internal organs, initial encounter
T304 Corrosion of unspecified body region, unspecified degreeT3110 Burns of 10-19% of body surfc w 0% to 9% third degree burnsT3111 Burns of 10-19% of body surface w 10-19% third degree burnsT3120 Burns of 20-29% of body surfc w 0% to 9% third degree burnsT3121 Burns of 20-29% of body surface w 10-19% third degree burnsT3122 Burns of 20-29% of body surface w 20-29% third degree burnsT3130 Burns of 30-39% of body surfc w 0% to 9% third degree burnsT3131 Burns of 30-39% of body surface w 10-19% third degree burnsT3132 Burns of 30-39% of body surface w 20-29% third degree burnsT3133 Burns of 30-39% of body surface w 30-39% third degree burnsT3140 Burns of 40-49% of body surfc w 0% to 9% third degree burnsT3141 Burns of 40-49% of body surface w 10-19% third degree burnsT3142 Burns of 40-49% of body surface w 20-29% third degree burnsT3143 Burns of 40-49% of body surface w 30-39% third degree burnsT3144 Burns of 40-49% of body surface w 40-49% third degree burnsT3150 Burns of 50-59% of body surfc w 0% to 9% third degree burnsT3151 Burns of 50-59% of body surface w 10-19% third degree burnsT3152 Burns of 50-59% of body surface w 20-29% third degree burnsT3153 Burns of 50-59% of body surface w 30-39% third degree burnsT3154 Burns of 50-59% of body surface w 40-49% third degree burnsT3155 Burns of 50-59% of body surface w 50-59% third degree burnsT3160 Burns of 60-69% of body surfc w 0% to 9% third degree burnsT3161 Burns of 60-69% of body surface w 10-19% third degree burnsT3162 Burns of 60-69% of body surface w 20-29% third degree burnsT3163 Burns of 60-69% of body surface w 30-39% third degree burnsT3164 Burns of 60-69% of body surface w 40-49% third degree burnsT3165 Burns of 60-69% of body surface w 50-59% third degree burnsT3166 Burns of 60-69% of body surface w 60-69% third degree burnsT3170 Burns of 70-79% of body surfc w 0% to 9% third degree burnsT3171 Burns of 70-79% of body surface w 10-19% third degree burnsT3172 Burns of 70-79% of body surface w 20-29% third degree burnsT3173 Burns of 70-79% of body surface w 30-39% third degree burnsT3174 Burns of 70-79% of body surface w 40-49% third degree burnsT3175 Burns of 70-79% of body surface w 50-59% third degree burnsT3176 Burns of 70-79% of body surface w 60-69% third degree burns
179

Skyline Medical Center Burn Unit CONList of ICD-10 Codes that Meet American Burn Association Referral Criteria
T3177 Burns of 70-79% of body surface w 70-79% third degree burnsT3180 Burns of 80-89% of body surfc w 0% to 9% third degree burnsT3181 Burns of 80-89% of body surface w 10-19% third degree burnsT3182 Burns of 80-89% of body surface w 20-29% third degree burnsT3183 Burns of 80-89% of body surface w 30-39% third degree burnsT3184 Burns of 80-89% of body surface w 40-49% third degree burnsT3185 Burns of 80-89% of body surface w 50-59% third degree burnsT3186 Burns of 80-89% of body surface w 60-69% third degree burnsT3187 Burns of 80-89% of body surface w 70-79% third degree burnsT3188 Burns of 80-89% of body surface w 80-89% third degree burnsT3190 Burns of 90%/more of body surfc w 0% to 9% third deg burnsT3191 Burns of 90%/more of body surfc w 10-19% third degree burnsT3192 Burns of 90%/more of body surfc w 20-29% third degree burnsT3193 Burns of 90%/more of body surfc w 30-39% third degree burnsT3194 Burns of 90%/more of body surfc w 40-49% third degree burnsT3195 Burns of 90%/more of body surfc w 50-59% third degree burnsT3196 Burns of 90%/more of body surfc w 60-69% third degree burnsT3197 Burns of 90%/more of body surfc w 70-79% third degree burnsT3198 Burns of 90%/more of body surfc w 80-89% third degree burnsT3199 Burns of 90%/more of body surfc w 90%/more third deg burnsT320 Corrosions involving less than 10% of body surface
T3210 Corros 10-19% of body surface w 0% to 9% third degree corrosT3211 Corros 10-19% of body surface w 10-19% third degree corrosT3220 Corros 20-29% of body surface w 0% to 9% third degree corrosT3221 Corros 20-29% of body surface w 10-19% third degree corrosT3222 Corros 20-29% of body surface w 20-29% third degree corrosT3230 Corros 30-39% of body surface w 0% to 9% third degree corrosT3231 Corros 30-39% of body surface w 10-19% third degree corrosT3232 Corros 30-39% of body surface w 20-29% third degree corrosT3233 Corros 30-39% of body surface w 30-39% third degree corrosT3240 Corros 40-49% of body surface w 0% to 9% third degree corrosT3241 Corros 40-49% of body surface w 10-19% third degree corrosT3242 Corros 40-49% of body surface w 20-29% third degree corrosT3243 Corros 40-49% of body surface w 30-39% third degree corrosT3244 Corros 40-49% of body surface w 40-49% third degree corrosT3250 Corros 50-59% of body surface w 0% to 9% third degree corrosT3251 Corros 50-59% of body surface w 10-19% third degree corrosT3252 Corros 50-59% of body surface w 20-29% third degree corrosT3253 Corros 50-59% of body surface w 30-39% third degree corrosT3254 Corros 50-59% of body surface w 40-49% third degree corrosT3255 Corros 50-59% of body surface w 50-59% third degree corrosT3260 Corros 60-69% of body surface w 0% to 9% third degree corrosT3261 Corros 60-69% of body surface w 10-19% third degree corrosT3262 Corros 60-69% of body surface w 20-29% third degree corrosT3263 Corros 60-69% of body surface w 30-39% third degree corrosT3264 Corros 60-69% of body surface w 40-49% third degree corrosT3265 Corros 60-69% of body surface w 50-59% third degree corros
180

Skyline Medical Center Burn Unit CONList of ICD-10 Codes that Meet American Burn Association Referral Criteria
T3266 Corros 60-69% of body surface w 60-69% third degree corrosT3270 Corros 70-79% of body surface w 0% to 9% third degree corrosT3271 Corros 70-79% of body surface w 10-19% third degree corrosT3272 Corros 70-79% of body surface w 20-29% third degree corrosT3273 Corros 70-79% of body surface w 30-39% third degree corrosT3274 Corros 70-79% of body surface w 40-49% third degree corrosT3275 Corros 70-79% of body surface w 50-59% third degree corrosT3276 Corros 70-79% of body surface w 60-69% third degree corrosT3277 Corros 70-79% of body surface w 70-79% third degree corrosT3280 Corros 80-89% of body surface w 0% to 9% third degree corrosT3281 Corros 80-89% of body surface w 10-19% third degree corrosT3282 Corros 80-89% of body surface w 20-29% third degree corrosT3283 Corros 80-89% of body surface w 30-39% third degree corrosT3284 Corros 80-89% of body surface w 40-49% third degree corrosT3285 Corros 80-89% of body surface w 50-59% third degree corrosT3286 Corros 80-89% of body surface w 60-69% third degree corrosT3287 Corros 80-89% of body surface w 70-79% third degree corrosT3288 Corros 80-89% of body surface w 80-89% third degree corrosT3290 Corros 90%/more of body surfc w 0% to 9% third degree corrosT3291 Corros 90%/more of body surface w 10-19% third degree corrosT3292 Corros 90%/more of body surface w 20-29% third degree corrosT3293 Corros 90%/more of body surface w 30-39% third degree corrosT3294 Corros 90%/more of body surface w 40-49% third degree corrosT3295 Corros 90%/more of body surface w 50-59% third degree corrosT3296 Corros 90%/more of body surface w 60-69% third degree corrosT3297 Corros 90%/more of body surface w 70-79% third degree corrosT3298 Corros 90%/more of body surface w 80-89% third degree corrosT3299 Corros 90%/more of body surfc w 90%/more third degree corros
181

Section B-Need-1B Physician and Other Letters of Support
182

183

184

185

186

187

188

189

12/1/2020 Mr. Logan Grant Executive Director Tennessee Health Services and Development Agency Andrew Jackson Building, Ninth Floor 502 Deaderick Street Nashville, Tennessee 37243 Re: TriStar Skyline Medical Center Burn Center CON Application Dear Mr. Logan:
The Madison-Rivergate Area Chamber of Commerce would like to support TriStar Skyline Medical Center’s application for their Burn Center CON. TriStar is an incredibly valuable health care system to our community, and we are proud to see their continued advances and efforts to serve our swiftly growing community. Just within a few miles of this hospital, there are currently many hundreds of new homing units being built. We are thrilled with the growth that Madison and its nearby areas are experiencing. However, with increased density in our population in the immediate area comes the need for expanded care.
In addition, please also consider the following points in support of this application: Fire death rates vary considerably by state, with 2013-2017 average death rates per million
population ranging from a low of 4.6 to a high of 23.5. The U.S. average was 9.9. It is alarming that nine of the ten states with the highest overall fire death rates in 2013-2017 were in the South. This is a disturbing realization when we consider our region and the capabilities to respond to victims of fire appropriately.
Nashville's growth, exacerbated by the incredible tourism industry, underscores the need for redundancy in critical healthcare services like burn.
o The region grew by 30,377 people last year, and it is estimated that the population of the Greater Nashville Area is expected to surpass 2.5 million people. The population growth for residents alone is enormous, but our region's population peaks exponentially as our area hosts visitors. Sources say that visitors to the city have swelled from 2 million a year in 1998 to more than 14 million today.
o Visitors attend large and small events alike – and some simultaneously. Events that draw huge crowds like the NFL Draft, pro sports teams, national concert series, fairs, fashion weeks, music festivals (like Bonnaroo and CMA Music Fest), and others that shut down all of Lower Broad affords an environment for disaster.
At present, Vanderbilt Medical Center is the only burn center in our region (it is not ABA Burn Verified). The time is now for our region to add an additional burn center to meet our growing population's needs adequately.
Our community has found that adding the Trauma Center at TriStar Skyline Medical Center has benefited greatly. Not only has the hospital served the patients in need of their service, but they have also raised the bar on the quality of care provided by becoming an American College of Surgeons Verified Trauma Center - the first Verified Center in Middle Tennessee. Currently,
190

there is only one American Burn Association Verified Center in the state – which is in Memphis; thus, the most severe burn patients in the area have to be transported significant distances to a Verified Burn Center, which is a hardship on the patient and their family given the extended duration of burn care and follow-up services.
Of particular concern, o Universities have a historical risk with fires. It was reported that in 2011-2015 U.S. fire
departments responded to an estimated annual of 4,100 structure fires in dorms, fraternity/sorority houses, and barracks. An example was at Seton Hall when a prank turned deadly, resulting in a major fire and three students died with 58 additional severely injured.
o It’s reported that approximately 86 percent of all battlefield deaths occur within the first 30 minutes after wounding, emphasizing the importance of rapidly diagnosing and rendering appropriate initial burn resuscitation and immediate treatment. Middle Tennessee is home to U.S. Army Garrison - Fort Campbell and the 101st Airborne Division (Air Assault). The Garrison integrates and delivers installation services and base support to enable readiness and global response capabilities of Soldiers and Units assigned to Fort Campbell. Our brave soldiers prepare with battlefield maneuvers and put their lives at risk daily. Preparing in advance for an unforeseen accident while training is of the utmost importance. If such a situation arose, the proximity to a verified burn center could be the difference in life or death. Our rapidly growing region only has one burn center – with only 34 beds. A military disaster would overwhelm this center. o Long term care facilities, assisted living facilities, rest and convalescent homes, all help care for some our most vulnerable citizens – our elderly and disabled population. Tennessee contains 316 certified Medicare and Medicaid nursing homes with over 36 thousand skilled nursing residents. The U.S. Census Bureau projects that the number of persons 60 and over will increase from 13% of the population in 2010 to 20% of the population by 2050, from the current 40.3 million to 88 million. With this increase of life expectancy, additional facilities to help care for this segment of the population has increased exponentially in Middle Tennessee. Vulnerability is high for residents in long term care facilities. A majority of residents are immobile and cannot move without assistance. Some are unfortunately mentally challenged and would not understand what was happening or how to react in an emergency. They need our protection. An example of a blaze that caused the death of 16 nursing home residents in Nashville was in September of 2003 when an NHC home experienced a devastating fire.
We hope this letter helps elucidate the need for this expanded care in our community. Sincerely,
Laura J. Knotts MRACC President 615-589-6644
191

House of Representatives State of Tennessee
NASHVILLE
VINCENT DIXIE STATE REPRESENTATIVE
54th LEGISLATIVE DISTRICT
Minority Caucus Treasurer Black Caucus Treasurer
425 5TH Ave. North
Suite 550 Cordell Hull NASHVILLE, TN 37243-0131
(615) 741-1997
DISTRICT ADDRESS: 4020 Drakes Branch Road
Nashville, TN 37218 615-423-5379
MEMBER OF COMMITTEES
HEALTH
EDUCATION
PUBLIC HEALTH SUB
K-12 SUB
11/30/2020 Mr. Logan Grant Executive Director Tennessee Health Services and Development Agency Andrew Jackson Building, Ninth Floor 502 Deaderick Street Nashville, Tennessee 37243 Re: TriStar Skyline Medical Center Burn Center CON Application Dear Mr. Logan: On behalf of Tennesseans in Davidson County and the surrounding area, I am writing to support TriStar Skyline’s certificate of need application to establish a Burn Center.
Over the course of my career, I have seen the growth of our community skyrocket. When our city surges in population due to sporting, civic, and cultural events, we have a significant number of people at risk in the event of an unthinkable disaster. It is time for our community to be supported by an additional Burn Center.
Our community has found that adding the Trauma Center at TriStar Skyline Medical Center has benefited greatly. Not only has the hospital served the patients in need of their service, but they have also raised the bar on the quality of care provided by becoming an American College of Surgeons Verified Trauma Center - the first Verified Center in Middle Tennessee. Currently, there is only one American Burn Association Verified Center in the State – which is in Memphis. The most severe burn patients in the area have to be transported significant distances to a Verified Burn Center, which is a hardship on the patient and their family given the extended duration of burn care and follow-up services.
Our residents, and the visitors to our city, deserve to have access to a Verified Burn Center that adheres to the highest rigor of quality. I am confident that TriStar Skyline will provide that service if approved to establish a Burn Center.
Patients in Davidson County and the surrounding region need more local comprehensive verified burn care services, and TriStar Skyline has the ability and resources to provide this service.
I urge you to support this certificate of need. Thank you for your consideration.
Sincerely, Rep. Vincent Dixie
192

193

194

195

196

197

198

199

200

11/30/2020
Mr. Logan Grant Executive Director Tennessee Health Services and Development Agency Andrew Jackson Building, Ninth Floor 502 Deaderick Street Nashville, Tennessee 37243 Re: TriStar Skyline Medical Center Burn Center CON Application Dear Mr. Logan:
I am very proud of the fearless work that the men and women at TriStar Skyline Medical Center do everyday, 24 hours a day. At present, Vanderbilt Medical Center is the only burn center in our region (it is not ABA Burn Verified). The time is now for our region to add an additional burn center to meet our growing population's needs adequately.
Our community has found great benefit adding the Trauma Center at TriStar Skyline Medical Center. Not only has the hospital served the patients in need of their service, but they have also raised the bar on the quality of care provided by becoming an American College of Surgeons Verified Trauma Center - the first Verified Center in Middle Tennessee. Currently, there is only one American Burn Association Verified Center in the state – which is in Memphis; thus, the most severe burn patients in the area have to be transported significant distances to a Verified Burn Center, which is a hardship on the patient and their family given the extended duration of burn care and follow-up services.
Nashville's growth, exacerbated by the incredible tourism industry, underscores the need for redundancy in critical healthcare services like burn. The region grew by 30,377 people last year, and it is estimated that the population of the Greater Nashville Area is expected to surpass 2.5 million people. The population growth for residents alone is enormous, but our region's population peaks exponentially as our area hosts visitors. Sources say that visitors to the city have swelled from 2 million a year in 1998 to more than 14 million today.
Visitors attend large and small events alike – and some simultaneously. Events that draw huge crowds like the NFL Draft, pro sports teams, national concert series, fairs, fashion weeks, music festivals (like Bonnaroo and CMA Music Fest), and others that shut down all of Lower Broad affords an environment for disaster. Nashville is also under consideration for the FIFA World Cup in 2026.
Additional burn beds are needed and Skyline Medical Center is the ideal place to place them.
Sincerely,
Hon. Nancy VanReece Nashville and Davidsson County Metro Councilmember | District 8, 2015-2023 [email protected] | 615-432-1308
201

METROPOLITAN COUNCIL
Member of Metro Council
204 Metropolitan Courthouse Nashville, Tennessee 37201 615/862-6780 Fax 615/862-6784
Jennifer Gamble Councilmember, District 3
December 2, 2020
Mr. Logan Grant, Executive Director Tennessee Health Services and Development Agency Andrew Jackson Building, Ninth Floor 502 Deaderick Street Nashville, Tennessee 37243 Re: TriStar Skyline Medical Center Burn Center CON Application Dear Mr. Logan: I, Jennifer Gamble, Davidson County Metropolitan Council Member, express my sincere support and enthusiasm for TriStar Skyline Medical Center’s decision to apply for a planned burn center Certificate of Need. This is a wonderful opportunity for the community and city of Nashville in which I serve. Our community has benefited greatly by the Trauma Center at TriStar Skyline Medical Center. Not only has the hospital served the patients in need of their service, but they have also raised the bar on the quality of care provided by becoming an American College of Surgeons Verified Trauma Center - the first Verified Center in Middle Tennessee. Furthermore, the need for quality trauma care in the community is great. Nashville's growth, exacerbated by the incredible tourism industry, underscores the need for redundancy in critical healthcare services like burn. The region grew by 30,377 people last year, and it is estimated that the population of the Greater Nashville Area is expected to surpass 2.5 million people. Currently, Vanderbilt Medical Center is the only burn center in our region though it is not an American Burn Association Verified Center. There is only one ABA Verified Center in the state located in Memphis, which means that the most severe burn patients in the area have to be transported significant distances to a verified burn center. This presents a hardship on the patient and their family given the extended duration of burn care and follow-up services. The time is now for our region to add an additional burn center to meet our growing population's needs. TriStar Skyline Medical Center is a valued health and certified trauma care facility with a proven track record of providing quality care and support to communities in need. Adding a certified burn center will enhance the quality of care and services needed in our city, and I appreciate your consideration for approval of their burn center certification application. Sincerely,
Jennifer Gamble Davidson County Metropolitan Council Member
202

203

3443 Dickerson Pike | Suite 100 | Nashville, TN 37207
12/12/20 Mr. Logan Grant Executive Director Tennessee Health Services and Development Agency Andrew Jackson Building, Ninth Floor 802 Deaderick Street Nashville, Tennessee 37243
Re: TriStar Skyline Medical Center Burn Center CON Application
Dear Mr. Logan,
As the Vice Chief of Staff at TriStar Skyline Medical Center and a practicing, board certified oral and maxillofacial surgeon, I have treated thousands of patients with complex facial injuries in the middle Tennessee region.
Currently, the only verified burn care provider in the state is located in western Tennessee. Therefore, patients from the eastern and middle regions must travel hundreds of miles for burn care. If that is not possible, they must leave the state and travel to Georgia or northern Kentucky to be treated at an American Burn Association verified facility. Quite frankly, this is an unacceptable situation for our injured fellow citizens and places an undue hardship upon their families to provide support.
Approval of TriStar Skyline’s petition to established a verified burn center will help address the deficiency in accessible local care. TriStar Skyline already serves low severity burn patients with our Level II trauma program. We have the capability to provide skin grafts, growth factors, skin substitutes and advanced reconstructive procedures. Unfortunately we cannot operate a comprehensive burn care program without approval from the Tennessee Health Services and Development Agency.
The growth of trauma centers in middle Tennessee over the past seven years was required due to the explosive growth of the region and has proven highly successful in improving the care of our citizens. The addition of a verified burn center by TriStar Skyline Medical Center is necessary to address the comprehensive needs of middle Tennessee and the surrounding region. I fully support their efforts and will be honored to participate in the care of their patients. Thank you for your consideration, please contact me if you have any further questions at (615) 496-9701.
Sincerely,
Steven G Press, DDS Vice Chief of Staff - TriStar Skyline Medical Center President - Tennessee Society of Oral and Maxillofacial Surgeons [email protected]
204

One Public Square, Suite 204 Nashville, Tennessee 37201 TONYA HANCOCK
Councilor, District 9
(615) 398-1373 (615) 432-1309
Monday, November 30, 2020
Mr. Logan Grant Executive Director Tennessee Health Services and Development Agency Andrew Jackson Building, Ninth Floor 502 Deaderick Street Nashville, Tennessee 37243
Re: TriStar Skyline Medical Center Burn Center CON Application
Dear Mr. Logan:
I am reaching out to support TriStar Skyline’s planned Burn Center program. TriStar Skyline is an exemplary Hospital that serves the Madison and North Nashville community. I myself have used their facilities to see my general practitioner, for breast exams, and most recently for sinus surgery. Every step of the way, the facility was professional, trustworthy, and efficient. Likewise, as COVID-19 started to infiltrate Nashville, TriStar Skyline quickly implemented world class safety practices for both their patients and their employees. Every “i” is dotted and every “t” is crossed. This is the type of excellence that is absolutely imperative in a burn center, as infection is such a high risk. TriStar Skyline consistently provides excellent care and I know they would do the same for this much needed burn center here. I strongly support their Certificate of Need (CON) in this case, and I hope you will consider it as well.
Please let me know if you need any additional information.
Wash Your Hands, Wear a Mask, & Get a Flu Shot
Tonya Hancock Metro Councilor, District 9
205

Section B-Need-1C
American Burn Association Verification Criteria and Plan
206

Criterion Number Criterion Criterion Level Response
1.1. (1) The burn center hospital is currently accredited by the Joint Commission or equivalent. 1 Accredited by Joint Commission. 1.2. (2) The burn center has an identifiable medical and administrative commitment to the care of the patient with burns. 1 Medical and administrative personnel are committed to the development of
the burn program and will continue to add incremental burn capabilities and will seek CON approval if required.
1.3. (3) The burn center hospital maintains a specialized unit dedicated to acute burn care. 1 TriStar Skyline has developed and submitted plans for a unit dedicated to acute burn care as well as OP burn followup. There are also additional long term plans to develop a space to house all portions of the burn unit- intake, inpatient, and outpatient.
1.4. (4) The burn center has designated ICU capable beds. 1 Burn Center will have 6 designated ICU beds with 6 Step Down beds that also have ICU capabilities.
1.5. (5) The burn center maintains an appropriate policy and procedure manual that is easily accessible by the burn team and reviewed regularly with appropriate documentation by the burn center director and the nurse leader.
1 HCA currently has 10+ burn programs and will be in partnership with BRCA. There is already a library of best practices and policies available and experience implementing them. Suggestion for last sentence: Medical Director and nurse leader will develop and regualrly review the Skyline policies and procedures manual and will make it easily accessible to the burn team.
1.6. (6) Multi-disciplinary patient care conferences are held and documented at least weekly. 1 Multidisciplinary rounds are done daily in ICU's and on Trauma patients. TriStar Skyline is experienced with this process and will ensure these patients are also handled in a similar format.
1.7. (7) Renal dialysis, radiological services, including computed tomography scanning, and clinical laboratory services are available 24 hours per day.
2 These services are already available at Skyline as a Level 2 Trauma Center.
1.8. (10) The burn center hospital's policies and procedures regarding the use of allograft tissues are in compliance with all federal, state, and The Joint Commission (or equivalent) requirements, and, when feasible and appropriate, with standards of the American Association of Tissue Banks (or equivalent).
1 HCA has more than 3 ABA verified burn centers with others currently in the pipeline. Skyline will partner with other HCA burn centers and BRCA on policies and procedures that meet federal, state, Joint Commission and American Association of Tissue Banks.
1.9. (11) The burn center has liaisons with a designated trauma center to coordinate care of patients with multi-trauma. 1 TriStar Skyline is a Lvl 2 Trauma Center, a very small percentage of our trauma patients require a level of care that we cannot accommodate. However, we do transfer to the local Lvl 1 trauma centers and have appropriate communications and feedback channels as well as participating in the Trauma Care Advisory Council for state of Tennessee.
2.1 (12.) The burn center must have a sufficient volume of acute burn admissions on an ongoing basis. 1 Currently projecting 212 burn admission YR1 and growing to 408 by YR3.
2.2. (13.) Majority of admissions to the burn center are burn patients. 1 Majority of admissions to the burn center will be burn patients and patients covered in ABA registry.
2.3. (15.) The burn center maintains and average daily census of 3 or more patients with acute burns. 1 TriStar Skyline is projecting average daily census of 3 or more patients with Acute Burns.
2.4. (16.) No more than 5% of all patients with a primary diagnosis of a burn injury are admitted to another service per year (e.g. geriatrics, pediatrics, medicine).
1 Burn patients will be admitted to the burn service, unless there is a major multi trauma patient where primary injuries require admission to the Trauma service. In those scenarios, there will be MDT rounds and the services will collaborate on patient care, with the patient being transferred to the burn service when appropriate.
2.5 (88.) No more than 5% of hospital admissions are transferred to another acute care facility. 1 As a Level 2 Trauma Center with high acuity service lines, TriStar Skyline already has low transfer rates, and could care for a minimum of 95% of the hospital burn admissions.
3.1 (26.) The burn center director is a licensed surgeon (MD or DO) with board certikcation by American Board of Surgery or American Board of Plastic Surgery (or equivalent for international burn centers in which case a surgeon must co-manage the center).
1 Burn and Reconstructive Centers of America is the nation’s largest burn network with more than 340 beds and 15 facilities spread over eight states including Idaho, Colorado, Texas, Nevada, South Carolina, Georgia, Mississippi and Florida. In partnership with BRCA we will identify the Burn Center Director that meets these criteria.
3.2 (27.) The burn center director has completed a one-year fellowship in burn treatment and/or has experience in the care of patients with acute burn injuries for two or more years during the previous five years.
1 In partnership with BRCA we have identified a candidate that meets this criteria.
3.3 (28.) The burn center director has ABLS (or equivalent) training. 1 In partnership with BRCA we have identified a candidate that meets this criteria.
3.4 (29.) The burn center director is responsible for the direction of burn center administrative functions. 1 In partnership with BRCA we have identified a candidate that meets this criteria.
3.5 (30.) The burn center director is responsible for the creation of policies and procedures within the burn center specifying all aspects of care for burned patients.
1 Burn Center Director will work closely with BRCA, trauma team, hospital depts, and other HCA accredited burn centers in development of policies and procedures.
3.6 (31.) The burn center director is responsible for ensuring that all burn center team members conform to the burn center’s locally established policies and procedures.
1 Burn Center Director will work with all members of the hospital team to ensure that all policies and procedures are followed to ensure best care for burn patients.
3.7 (33.) The burn center director is responsible for the approval of privileges for physicians participating in the burn service based on medical staff credentialing process.
1 Burn Center Director will be responsible for the approval of privileges for physicians participating in burn service, in patnership with the Medical Executive Committee.
3.8 (34.) The burn center director is responsible for the development and active participation in internal and external continuing medical education programs in the care and prevention of burn injuries.
1 In partnership with BRCA and HCA's established burn centers, the program director will develop and ensure compliance with CME programs and requirements.
3.9 (36.) The burn center director is responsible for the communications on a regular basis with referring physicians regarding patients who have been transferred.
1 Burn center director will establish formal and informal processes of providing feedback to referring physicians of transferred burn patients. Similar processes are already in place for Lvl 2 Trauma program.
3.10 (37.) In the event that the burn center director is not available, an accessible burn center staff surgeon is designated for administrative or clinical decisions.
1 Burn Center will have multiple burn surgeons, and in the event of the burn center director not being available, one of the other surgeons will take over in the interim, in partnership with Hospital Administration and existing Medical Leadership structures for additional support.
3.11 (38.) The burn center director regularly participates in regional, national or international burn meetings. 1 Burn center director will regularly participate in regional, national, or international burn meetings.
3.12P The burn center director demonstrates CME or evidence of education in pediatric burn care annually (i.e. Pediatric Advanced Life Support, pediatric topic review, local regional meetings, invited speakers, journal clubs etc.)
2 The burn center director will demonstrate CME or evidence of education in pediatric burn care annually (i.e. Pediatric Advanced Life Support, pediatric topic review, local regional meetings, invited speakers, journal clubs etc.)
3.13 (39.) The burn center director has directed the total burn care of 50 or more acutely burned patients annually over a three- year period.
1 In partnership with BRCA we have identified a candidate that meets this criteria.
3.14P The burn center director is involved in at least 25 pediatric cases annually. 2 In partnership with BRCA we have identified a candidate that meets this criteria.
3.15 (40.) The burn center director demonstrates ongoing involvement in burn-related research, community education, continuing medical education, prevention efforts and local regional or national burn advocacy.
1 TriStar Skyline will install outreach programs similar to programs already in place as a Level 2 trauma center, but also in partnership with BRCA and HCA's other burn centers as part of a larger network of burn outreach, education, and advocacy.
4.1 (41.) Burn surgeons are licensed surgeons with board certification by American Board of Surgery, American Board of Plastic Surgery or equivalent based on review by Verification Committee.
1 In partnership with BRCA we will be identifying burn surgeons that meet ABA criteria and ensuring they stay current on their continued training needs.
4.2 (42.) Burn surgeons have demonstrated expertise in burn treatment, by two or more years of mentored experience in the management of patients with acute burn injuries.
1 In partnership with BRCA we will be identifying burn surgeons that meet ABA criteria and ensuring they stay current on their continued training needs.
4.3 (45.) Each burn surgeon has participated, including primary decision-making, in the care of sufficient acutely burned patients annually.
1 In partnership with BRCA we will be identifying burn surgeons that meet ABA criteria and ensuring they stay current on their continued training needs.
4.4 (43.) Each burn surgeon must participate in continuing medical education in burn treatment. 1 In partnership with BRCA we will be identifying burn surgeons that meet ABA criteria and ensuring they stay current on their continued training needs.
Verification Criteria Effective October 1, 2019American Burn Association
207

4.5 (44.) Burn surgeons have had ABLS (or equivalent) training. 2 In partnership with BRCA we will be identifying burn surgeons that meet ABA criteria and ensuring they stay current on their continued training needs.
4.6 (49.) Assigned burn center medical staff are promptly available on a 24-hour basis. 1 TriStar Skyline has reviewed appropriate stafffing and call schedules to ensure the appropriate providers are available 24/7.
4.7 (46.) The burn center maintains an on-call schedule for residents, qualified healthcare professionals and burn surgeons for continuous responsibility of burn patients.
1 TriStar Skyline has reviewed appropriate stafffing and call schedules to ensure the appropriate providers are available 24/7.
4.8 (109) For centers that have residents involved in care of the burn patients an orientation program is provided for new residents.
2 Skyline currently does not have residents, but in partnership with Belmont and the future College of Medicine residents may be involved in burn care and would receive appropriate orientation and training. BRCA is experienced with the training and onboarding of residents. They offer residency and training in many of their programs across the country.
4.9P Burn center has physicians who are board certified or eligible for certification in one of the following: · pediatric critical care medicine, pediatric surgery, or surgical critical care
2 In partnership with BRCA we will be identifying burn surgeons that meet ABA criteria and are certified in pediatric critical care medicine, pediatric surgery, or surgical critical care.
4.10P Burn surgeons have pediatric burn fellowship training or mentored clinical experience in pediatric burn surgery. 2 In partnership with BRCA we will be identifying burn surgeons that meet ABA criteria and ensuring they stay current on their continued training needs.
4.11P All burn surgeons demonstrate CME in pediatric care or equivalent internal burn education in pediatric burn care annually.
2 In partnership with BRCA we will be identifying burn surgeons that meet ABA criteria and ensuring they stay current on their continued training needs.
5.1 (47.) All advanced practice providers who are routinely responsible for the care of burn patients conform to burn center criteria documenting appropriate training, patient care experience, continuing medical education, and commitment to the care of the burned patient.
1 APP's will follow burn center criteria regarding training, patient care, CME, and commitment to the care of the burned patient.
5.2 (48.) All advanced practice providers participating in the burn service are credentialed by the hospital medical staff credentialing process and are approved by the burn center director.
1 APP's will follow normal credntialing process as set forth by Medical Staff guidelines with additional approval from burn center director.
6.1 (52.) The burn nurse leader or equivalent is a licensed Registered Nurse (RN) with a minimum of a baccalaureate degree in nursing.
2 Burn nurse leader will be an RN with appropriate education and background.
6.2 (53.) There is at least one nurse leader or equivalent who is administratively responsible for the nursing care provided within the burn center.
1 Program will have nursing director that will be responsible for the administrative nursing functions of burn center.
6.3 (54.) A burn nurse leader or equivalent must have sufficient experience in burns and nursing leadership to lead the staff and manage the nursing program of the burn center.
1 Nursing leader will have sufficient experience in burns and leadership. Nurse leader will manage staff and nursing of burn center.
6.4 (55.) A metric-based staffing system is in place to determine nurse-staffing needs for patients in the burn center. 2 TriStar Skyline already follows a metric-based staffing system that determines nurse staffing needs throughout the hospital.
6.5 (56.) There is a burn-specific competency-based training and continuing educational program for all nurses assigned to the burn center.
1 In partnership with BRCA and the HCA burn center network, Skyline will develop competency-based training and continuing education programs for all nurses in burn center.
6.6 (57.) The burn nurse leader or equivalent routinely participates in multi- disciplinary patient care rounds and there is dissemination to the nursing staff.
1 Burn nurse leader or desginee will regularly participate in mutli-disciplinary rounds and disseminate information to the nursing staff, similar to process as currently demonstrated in Lvl 2 Trauma rounds.
6.7 (58.) The burn nurse leader or designee attends burn-specifc continuing educational opportunities at least once every two years. These requirements can be addressed by attending regional, national or international burn meetings; being an ABLS Instructor; and being involved in the ABA.
1 Burn nurse leader will attend burn specific continuing educational opportunity bi-annually.
6.8 (59.) There is nurse representation within burn center quality improvement processes. 1 Burn nurse leader will be on QI team. 6.9P Nurses have pediatric certification or participate in pediatric specific continuing education or equivalent internal
burn programming in pediatric burn care annually.2 Burn center will ensure Nurses have pediatric certifications and take part in
continuing education or equivalent programming in pediatric burn care annually.
7.1 (60.) A comprehensive rehabilitation program is designed for burned patients within 24 hours of admission. 1 TriStar Skyline has PT/OT/ST- and will have dedicated therapy staff for burn patients. Patients will be identified at admission and team will begin designing program as patient is stabilized.
7.2 (61.) Physical and occupational therapists in the burn center are appropriately licensed in their respective disciplines and demonstrate ongoing continuing education in burn rehabilitation.
1 Physical and Occupational therapists employed by the hospital will have appropriate licenses in their respective discplines as well as continuing to pursue continuing education in burn rehab.
7.3 (62.) Therapy staffing is based upon burn center inpatient and therapy specific outpatient activity with at least one designated full-time equivalent burn physical therapist and one occupational therapist, but more depending on center volume.
1 There will be at least one designated FTE burn PT/OT and addtional based on volumes.
7.4 (63.) Inpatients with an active rehabilitation plan must have care delivered as prescribed in the evaluation which should determine duration and frequency based on acuity, include goals, outcome and plan for follow up.
1 Designated burn therapy team will work with physicians to establish plan of care, that considers duration and frequency, based on established goals, outcomes, and additional OP followup and ensure those needs a are met during the inpatient stay.
7.5 (64.) Burn therapy services are provided 7 days per week for care of burn inpatients. 1 IP Therapy service will be provided 7 days/week. 7.6 (65.) Burn therapists participate in multi- disciplinary rounds and quality improvement. 1 Burn therapists will participate in multidiscplinary rounds and QI7.7 (66.) Therapists assigned to the burn center must show evidence of ongoing burn specific competency training. 1 Therapists assigned to the burn center will be held responsible for ongoing
burn specific competency training.7.8 (67.) Therapists must participate in burn-related CEU activity on a regular basis. 1 Therapists will be required to participate in burn-related CEU activity on a
regular basis.7.9P Therapy staff participates in pediatric specific continuing education. 2 Therapy staff will be required to participate in continuing education for
pediatrics. 7.10P Therapy department has pediatric age-appropriate therapeutic equipment. 2 Therapy dept. has evaluated and will ensure that age-appropriate therapeutic
equipment is available.8.1 (68.) Social service consultation is available to the burn service, as needed. 1 As a Level 2 Trauma Center, TriStar Skyline deals with many social issues,
and social service programs. Social workers are available and will work with care team to identify needs.
8.2 (69.) A dietitian with adequate critical care and burn experience is available on a daily basis for consultation. 1 We currently have dietitians available on a daily basis for consultation. In partnership with BRCA we will add burn experience through hiring and training.
8.3P A pediatric dietitian with adequate critical care and burn experience is available on a daily basis for consultation. 2 In partnership with Children's Hospital at Centennial Medical Center a pediatric detitian with adequate qualifications/experience will be available daily for consultation.
8.4 (70.) A pharmacist with adequate critical care and burn experience is available on a 24-hour basis. 1 We currently have pharmacist available on a 24 hour basis as a Level 2 Trauma Center. In partnership with BRCA we will add burn experience through hiring and training.
8.5P A pediatric pharmacist with adequate critical care and burn experience is available on a 24-hour basis. 2 In partnership with Children's Hospital at Centennial Medical Center a pediatric pharmacist will be available on a 24-hour basis to manage pediatric patients.
8.6 (71.) Respiratory therapists are available for the assessment and management of patients on the burn service on a continuous basis.
1 Respiratory Therapy is currently available and in house 24/7.
8.7 (73.) A psychologist or psychiatrist is available to the burn service on an as needed basis. 1 TriStar Skyline also operates an 86 bed psych unit at its Skyline Madison campus. Psychiatric physicians are available for follow up and consultation.
8.8P (72.) A child life/recreational therapist is available for children cared for in the program. 2 In partnership with Children's Hospital at Centennial Medical Center a child life/recreational therapist will partner with burn team and medical providers anytime Peds patients are admitted.
8.9 (106) Burn team members are provided with a minimum of one regional, national or international burn-related continuing education opportunity annually OR demonstrate annual participation in internal educational process specific to burn care.
1 TriStar Skyline will work in partnership with BRCA and the broader HCA burn network to develop internal education processes specific to burn care, while also offering regional, national, and international opportunities as well to the burn team members.
8.10 (107) A burn center orientation and ongoing continuing education program documents staff competencies specific to age appropriate care and treatment of burn patients, including critical care, wound care, and rehabilitation.
1 Burn center administration will develop orientation and ongoing education program as well as working with facility education team to document staff competencies specific to age appropriate care and treatment of burn patients, including critical care, wound care, and rehabilitation.
9.1 (102) The burn center develops ongoing quality improvement projects to create a culture of safety and promote value- based programs.
1 Similar to Trauma, with Performance Improvement Coordinator, Performance Improvement Meetings and Peer Commitees, the burn program will evaluate all improvement opportunities as identified and maintain a culture of safety and value based care.
208

9.2P The pediatric burn center develops ongoing quality improvement projects to create a culture of safety and promote value-based programs.
2 Pediatric healthcare representatives, in partnership with Centennial Children's Hospital will participate in all of the same Quality Improvement programs and meetings as the adult team, and pursue any Improvement Opportunities through the same pipeline.
9.3 (94.) Sufficient QI documentation is available to verify problems, identify opportunities for improvement, resolve the problem and provide loop-closure.
1 As a Level 2 Trauma Center, Skyline is familiar with the QI process and the documentation necessary for efficient tracking and loop closure.
9.4 (35.) The burn center director is responsible for direction and active participation in the burn center Quality & Process Improvement Programs.
1 Burn Center Director will lead Quality and Process Improvement Program similar to Trauma Medical Director leading Trauma QI programs.
9.5 (92.) The burn center director is responsible for the risk adjusted quality improvement program. 1 Burn Center Director will lead Quality and Process Improvement Program similar to Trauma Medical Director leading Trauma QI programs.
9.6 (93.) A multidisciplinary burn center committee participates in the quality improvement program, meets at least quarterly and is integrated into the hospital QI structure.
1 Burn center leadership will meet regularly amongst themselves for QI, but also as an integrated portion of Trauma and other hospital wide QI teams and meetings.
9.7 (97.) All life-threatening complications and deaths are discussed in a forum that includes specialist peers outside the core burn team, and are classified in a systemic fashion, so as to identify opportunities for improvement
1 Peer review committee will review filters specifically for life threatening complications and deaths, among others, and will include specialists from inside and outside of the burn program. Opportunities will be identified and addressed in a standard fashion as is currently demonstrated in the Trauma Peer Review Process.
9.8 (95.) The morbidity and mortality conferences are held at least monthly. 1 Morbidity and mortality reviews occur at least biweekly currently, with conferences held monthly.
9.9 (96.) The morbidity and mortality conferences include specialist peer staff members other than those practicing in the burn center.
1 Morbidity and mortality will be deliberate in the inclusion of physician leader and specialist both from inside and outside of the burn program.
9.10 (98.) The morbidity and mortality conferences include documentation of loop closure. 1 Morbidity and mortality conferences already evaluate and document loop closure, and burn center patients would be folded into this previously established process.
9.11 (99.) Clinical team members involved in the direct care of the burn patients participate in at least 50% of the morbidity and mortality conferences.
1 Clinical team members involved in the direct care of burn patients will be added to the morbidity and mortality for their feedback in processes, and for the opportunity to discover best practice and identified process delinquencies.
9.12 (100) Sentinel events are discussed in a timely manner at multi-disciplinary intensive reviews during which time a non- involved peer leads a discussion with all involved parties and areas for improvement and loop closure are identified.
1 Sentinel events will be tracked via Burn Center Administration and through the TriStar Skyline Quality dept utilizing current processes. There are internal guidelines for the timeliness of reviews.
9.13 (101) The burn program conducts audits of their benchmarked outcomes data (using available resources such as NBR, UHC, NHSN, or CMS) at least quarterly.
1 TriStar Skyline is familiar with benchmarking outcomes data at least quarterly amongst national databases as well as more specific comparisons across other HCA facilities.
9.14 (103) The burn center has policies for infection control with regular monitoring for hospital-acquired infections, multi-drug resistant organisms and compliance.
1 Burn team will work with infection prevention and quality dept, BRCA and the broader HCA burn network to implement best practices and policies for infection control.
9.15 (104) The burn center participates in the ABA’s National Burn Repository or other equivalent data collection/analysis tool and submits data every year.
1 TriStar Skyline is familiar with collecting, maintaining, and submitting data for national repositories.
9.16 (105) The burn center database includes all patients who are admitted to the burn center hospital for burn care. 1 Burn center registry will include all patients admitted for burn care.
9.17P Evidence of at least one on-going QI metric in pediatric specific rehabilitation issues (i.e., garment compliance, splint compliance, rates of contracture, success with release, etc.)
2 Pediatric specific rehab issues will be a priority for the burn center leadership and QI coordinator. They will ensure they mainatain at least one on-going intitiative in this area.
10.1 (17.) The burn center has written guidelines for the triage, treatment, and transfer of burned patients from other facilities. 1 Burn center in partnership with BRCA and best practice throughout HCA burn network will develop guidelines for the triage, treatment, and transfer of burned patients from other facilities.
10.2 (32.) The burn center director is responsible for the coordination with regional EMS authorities regarding triage and transport of burn patients.
1 Burn center director will coordinate with regional EMS authorities regarding triage and transport of burn patients in coordination with Trauma Outreach and EMS outreach team that is already established and has great working relationships with local, regional, and even interstate EMS providers.
10.3 (18.) The burn center maintains access to an EMS system for the transport of patients with burns from referral sources within the service area.
1 As Level 2 Trauma Center TriStar Skyline has several contracts with local EMS providers as well as a preferred provider agreement with AirEvac (rural air transport provider)
10.4 (19.) The burn center offers input into the quality improvement of pre-hospital care of burn patients. 1 As a Level 2 Trauma Center, TriStar Skyline already has to review and provide input into the pre-hospital care of trauma patients and will be able to include burn patients into this process.
11.1 (20.) Written protocols developed with input from the burn center guide the care of burn patients in the emergency department.
1 Written protocols will be developed with input of burn center team and will guide care in burn patients in ED, in consultation with BRCA and other ED/burn centers in the HCA burn network.
11.2 Emergency department is available 24/7. 2 Currently established11.3P Emergency physicians are board certified or eligible for certification by an appropriate emergency medicine board
according to current requirements in pediatric emergency medicine.2 Currently established
11.4P Evidence of collaborative clinical practice and educational activities between the burn program and the emergency services.
2 Burn program will work closely with Emergency physicians through efficient well informed patient handoffs and consults, as well as through the QI process to ensure processes are working efficiently.
11.5P Emergency service representative serves as a liaison to the burn quality care program. 2 Emergency Dept Nursing Director and Medical Director will hold positions on QI team and will be available for addressing questions and issues.
12.1 (14.) Burn centers caring for critically ill patients must demonstrate facilities, protocols and personnel specific to the care of critically ill patients.
1 TriStar Skyline currently operates 70 ICU rooms and has the facilities, protocols, and personnel for the care of critically ill patients.
12.2P The burn program works collaboratively with the pediatric critical care providers, although all significant therapeutic decisions involving burn patients are approved by the burn program, and the burn program is made aware of all significant clinical changes.
2 In partnership with Children's Hospital at Centennial Medical Center, pediatric critical care providers will partner with burn surgeons and burn program to manage pediatric patients.
12.3P A PICU representative serves as a liaison to the burn quality improvement program. 2 PICU representative will serve in Performance Improvement/Peer Committees similar to ICU leaders in PIPS/PEER for Trauma.
12.4P There are protocols for burn specific care in collaboration with the PICU. 2 In partnership with Peds resources at Centennial Children's Hospital, the burn team and Peds teams will collaborate in development of procedures for PICU.
12.5P PICU works in concert with the Burn Center Director to develop protocols for intensive care. 2 PICU will work with Burn Center Director, Nurse leader, and Centennial Childrens hospital to develop protocols for Peds ICU.
13.1 (8) The burn center has timely access to operating rooms. 1 Currently, multiple OR's are blocked for Trauma surgeries. An OR has been designated for burn.
13.2 (9) A dedicated OR team with burn experience is available for the burn operating theatre. 2 OR team with burn experience will be on call and available, after normal hours.
13.3 (51.) A dedicated anesthesia team with burn experience is available for the burn operating theatre. 2 Many of Skyline's anesthesiologist have burn center experience, and would be dedicated to the burn OR's.
13.4P For centers admitting patients under 2 years of age and requiring surgery, an anesthesiologist with certification in pediatric anesthesiology is available 24/7.
2 In partnership with Children's Hospital at Centennial Medical Center a pediatric anesthesiologist with adequate qualifications/experience will be available 24/7.
13.5P A pediatric anesthesiology representative serves as a liaison to burn quality improvement program. 2 Pediatric Anesthesiology Representative via partnership with Centennial Children's Hospital will be on Quality Improvement Team.
14.1 (89.) Physiatrist consultation is available. 2 Physiatrist consultation is already available 24/7 due to On-Site IP Rehab.
14.2 (90.) The burn center coordinates with local and/or regional rehabilitation centers for inpatient rehabilitation. 1 TriStar Skyline has an on-site IP Rehab Unit and is a part of a 4 facilty network of IP Rehabs in the Nashville market.
14.3 (91.) The burn center coordinates with local and/or regional outpatient facilities for ongoing outpatient therapy needs of patients needing rehabilitation after discharge.
1 As a Level 2 Trauma and Comprehensive Stroke Center, Skyline receives patients needing OP therapy daily. Due to the nature of Trauma and the transfer network, Skyline is experienced in coordinating patient OP Therapy needs in and out of the main market.
209

15.1 (74.) The burn center has appropriate outpatient facilities, including adequate facilities for wound care. 1 TriStar Skyline has operated a wound center in its recent past has identified space to reopen the wound center. It is also a part of a network of 9 Wound Centers in the TriStar Division, all of which can be consulted and involved in treating Skyline wound patients, offering high quality coordinated services closer to home.
15.2 (75.) The outpatient facility must be able to provide for appropriate pain management during wound care. 2 TriStar Skyline has recently managed wound operations and is part of a larger network of 9 OP wound centers in the TriStar Division. Many of these patients have difficult, painful, chronic wounds. Each facility takes great care in multimodal pain management.
15.3 (80.) The burn center provides appropriate multi-disciplinary follow-up. 1 OP Burn Center will provide mutlidisciplinary followup to the patients as needed, and any IP services will be available for consult or followup in the OP setting.
15.4 (76.) For continuity of care, staffing of the outpatient area should be by multi- disciplinary experienced burn team members, approved by the burn center director and nurse leader.
2 Outpatient will also have designated caregivers for burn care and director and nurse leader will have final approval of all burn designated staff.
15.5 (86.) The burn center provides access to outpatient social service, pharmacist and dietary consultations, as needed. 2 Social service, pharmacy, and dietary will be integrated in the burn patients ongoing OP care and will be available for consultation.
15.6 (77.) A representative of the outpatient staff participates in weekly multi-disciplinary burn conferences and the burn center QI program.
1 Managers/Directors of OP burn depts will participate in mutli-disciplinary conferences and QI program.
16.1 (79.) The burn center provides coordinated transition of care to the outpatient status. 1 TriStar Skyline has experience in OP wound and therapy, and transitioning discharged inpatients into those programs. They will coordinate this process for all burn patients, and the build out of the Wound Center on the first floor of the hospital, will allow those patients additional ease of access.
16.2 (78.) The burn center follows >75% of all patients who transition to the outpatient setting. 1 Burn patients often require long term, specialized followup care in the OP setting. It would be our goal to manage greater than 75% of these patients, but for those who cannot due to distance or social issues, we will coordinate OP care for a location more convenient to them and continure to be available for questions, followup, and treatment.
16.3 (83.) A burn therapist is available in the outpatient clinic to provide services, including follow up, as needed. 1 OP therapy dept is located nearby new Wound Center and therapist will be available as needed.
16.4 (81.) The burn center provides brief psychological screening/intervention. 1 TriStar Skyline also operates an 86 bed psych unit at its' Skyline Madison campus. Psych physicians are available 24 hours/day for follow up and consultation. There are also Psych NP's and additional psych resources that can be easily accessed for screening and intervention.
16.5P (82.) The burn center provides evaluation of patient developmental status (for children). 2 Skyline Madison manages an Adolescent Psych program that is experienced in the evaluating childrens developmental status, as well as TriStar Centennial Childrens Hospital who will also be in partnership, supporting the children admitted to the burn program.
16.6 (84.) The burn center provides timely access to reconstructive surgery. 2 Burn center will have access to plastic surgeons that are part of the burn program as well as plastic surgeons that are already involved in Level 2 Trauma services.
16.7 (85.) The burn center facilitates access to peer-to peer and burn survivor resources for patient and family support. Provides access to peer support (such as but not exclusively a Phoenix Society SOAR program).
1 Facility in partnership with BRCA and HCA burn network will facilitate access to peer-to peer and burn survivor resources for patient and family support.
16.8 (87.) The burn center provides access to vocational counseling. 2 As part of a portfolio of patient resources to assist in regaining and retraining for living with burns, Skyline is committed to offering access to vocational counseling.
16.9 P Burn center has established relationship with one of the many camps and demonstrated active attempts at recruitment for children to attend.
2 TriStar Skyline burn program will partner with childrens camps and engage in active recruitment.
17.1 (111) Burn program is involved in local, regional, national, or international prevention outreach efforts. 1 In partnership with BRCA and the additional 10+ burn programs in the HCA network, TriStar Skyline will be involved in many local, regional, national burn initiatives for prevention and outreach. As a Lvl 2 Trauma Center injury prevention is already an expectation for this hospital.
17.2 (108) The burn program regularly participates in regional education related to burn care. 1 As a Level 2 Trauma Center, TriStar Skyline participates in regional education. TriStar Skyline will rely on its current education/outreach networks, and implement the new Burn specific education with BRCA's specialties and expertise. TriStar Skline is also a member of a broader TriStar trauma network that consists of 6 Lvl 3 Trauma Center's, 4 surrounding the Nashville market and 2 in Georgia. The burn program will tie into this network and provid burn education to these facilities as well as using their networks to further burn education.
17.3 (110) The burn center participates regularly in community burn outreach programs. 2 As a Level 2 Trauma Center, TriStar Skyline participates in regional education. TriStar Skyline will rely on its current education/outreach networks, and implement the new Burn specific education with BRCA's specialties and expertise. TriStar Skline is also a member of a broader TriStar trauma network that consists of 6 Lvl 3 Trauma Center's, 4 surrounding the Nashville market and 2 in Georgia. The burn program will tie into this network and provid burn education to these facilities as well as using their networks to further burn education.
18.1 (112) Burn Center multi-disciplinary staff, under the leadership of the burn center director, work locally, regionally, or nationally to advocate for burn related health care issues.
2 Burn Center staff will coordinate with Director/BRCA/other HCA burn centers on any local, regional, national healthcare issues related to burn.
18.2 (113) The burn center multi-disciplinary staff is involved in research (including basic science, clinical, industry-sponsored, QI, multi-center) and presents posters or oral presentations at hospital based, regional national or international meetings.
2 In partnership with BRCA and the additional 10+ burn programs in the HCA network, TriStar Skyline will be involved in many local, regional, national burn initiatives for prevention and outreach. As a Lvl 2 Trauma Center injury prevention is already an expectation for this hospital.
19.1 (21.) The burn center interfaces with regional trauma centers to coordinate care of patients with multiple injuries and to develop regional educational programs, disaster planning and advocacy efforts.
2 As a Level 2 Trauma Center, TriStar Skyline already interfaces with regional trauma centers to coordinate care of patients with multiple injuries and to develop regional educational programs, disaster planning and advocacy efforts. Burn Center Director will be added to this outreach team, upon hiring.
19.2 (22.) The burn center has a written Mass Casualty Disaster Plan for the triage and treatment of those patients burned in a mass casualty incident occurring within its service area.
1 Christmas Day bombing, while thankfully not a mass casualty event, illustrated the need for constant readiness. As a Level 2 Trauma Center, TriStar Skyline is constantly preparing for a disaster and regularly reviews the MCI Disaster Plan and will appropriately include the burn program into this process.
19.3 (23.) The Mass Casualty Disaster Plan is reviewed and updated as needed and on an annual basis by EMS representatives and the burn center director.
2 As a Level 2 Trauma Center, TriStar Skyline is constantly preparing for a disaster and regularly reviews the MCI Disaster Plan and will appropriately include the burn program into this process.
19.4 (24.) There are current (within the past 3 years) written memoranda of understanding with other burn centers regarding secondary triage.
1 Upon inception of the program and officially taking burn IP's, TriStar Skyline will work with other burn centers for secondary triage and handoff processes.
19.5 (25.) The burn center must maintain accurate and up to date contact information for burn surgeons and managers on the ABA website.
2 RN program director will be responsible for updating ABA, for the maintenance of their website with contact info for burn surgeons and managers. This can be maintained from program inception.
Source: American Burn Association Verification Review Program http://ameriburn.org/quality-care/verification/verification-criteria/verification-criteria-effective-october-1-2019/
210

Section B-Need-3
Population Analysis Table
211

ADAIR 19,205 19,468 1.4% 19,205 19,468 1.4% 100.0% 41.8 $38,021 3,655 20.5% 8,607 44.8%ALLEN 21,559 22,023 2.1% 21,559 22,023 2.1% 100.0% 40.7 $44,036 3,866 18.7% 7,315 33.9%BARREN 44,541 45,734 2.6% 44,541 45,734 2.6% 100.0% 40.5 $43,884 10,368 24.2% 16,458 37.0%BRECKINRIDGE 20,625 20,979 1.7% 20,625 20,979 1.7% 100.0% 43.1 $47,190 3,674 18.6% 7,134 34.6%BUTLER 12,941 12,901 -0.3% 12,941 12,901 -0.3% 100.0% 41.3 $41,763 2,407 19.3% 4,940 38.2%CALDWELL 12,736 12,684 -0.4% 12,736 12,684 -0.4% 100.0% 44.0 $44,775 2,112 16.8% 4,294 33.7%CALLOWAY 39,147 40,423 3.2% 39,147 40,423 3.2% 100.0% 35.6 $42,273 7,541 21.5% 9,954 25.4%CHRISTIAN 69,742 70,764 1.4% 69,742 70,764 1.4% 100.0% 28.3 $43,919 12,635 19.6% 22,076 31.7%CLINTON 10,228 10,240 0.1% 10,228 10,240 0.1% 100.0% 41.9 $32,184 2,423 24.1% 5,628 55.0%CRITTENDEN 8,687 8,648 -0.5% 8,687 8,648 -0.5% 100.0% 43.6 $45,244 1,258 14.5% 2,559 29.5%CUMBERLAND 6,554 6,559 0.1% 6,554 6,559 0.1% 100.0% 46.0 $35,344 1,406 21.4% 3,537 54.0%DAVIESS 102,277 104,555 2.2% 102,277 104,555 2.2% 100.0% 38.9 $51,673 16,174 16.6% 32,927 32.2%EDMONSON 12,136 12,543 3.2% 12,136 12,543 3.2% 100.0% 44.3 $43,401 2,182 18.2% 4,566 37.6%GRAVES 37,223 37,637 1.1% 37,223 37,637 1.1% 100.0% 39.7 $44,043 7,165 19.6% 13,237 35.6%GRAYSON 26,545 26,868 1.2% 26,545 26,868 1.2% 100.0% 40.3 $38,612 6,585 25.4% 10,333 38.9%GREEN 10,889 11,043 1.4% 10,889 11,043 1.4% 100.0% 44.6 $35,899 1,953 18.0% 4,275 39.3%HANCOCK 8,725 8,915 2.1% 8,725 8,915 2.1% 100.0% 39.9 $57,217 1,015 11.8% 2,504 28.7%HART 19,203 19,576 1.9% 19,203 19,576 1.9% 100.0% 40.5 $38,396 3,944 21.5% 7,620 39.7%HENDERSON 44,839 44,977 0.3% 44,839 44,977 0.3% 100.0% 41.2 $48,926 8,273 18.5% 14,604 32.6%HOPKINS 44,224 44,024 -0.5% 44,224 44,024 -0.5% 100.0% 41.8 $47,170 8,534 19.4% 16,326 36.9%LIVINGSTON 9,146 9,178 0.3% 9,146 9,178 0.3% 100.0% 46.0 $50,839 1,331 14.6% 2,839 31.0%LOGAN 27,186 27,343 0.6% 27,186 27,343 0.6% 100.0% 40.7 $48,014 4,507 17.0% 9,124 33.6%LYON 8,169 7,733 -5.6% 8,169 7,733 -5.6% 100.0% 50.6 $52,528 1,100 15.8% 1,865 22.8%MARSHALL 31,030 31,279 0.8% 31,030 31,279 0.8% 100.0% 44.9 $55,113 3,177 10.4% 8,729 28.1%MCCRACKEN 65,426 65,680 0.4% 65,426 65,680 0.4% 100.0% 42.2 $46,080 10,042 15.8% 21,838 33.4%MCLEAN 9,145 9,138 -0.1% 9,145 9,138 -0.1% 100.0% 42.4 $51,861 1,471 16.1% 2,968 32.5%METCALFE 10,082 10,088 0.1% 10,082 10,088 0.1% 100.0% 43.9 $37,386 2,304 23.2% 4,677 46.4%MONROE 10,626 10,810 1.7% 10,626 10,810 1.7% 100.0% 41.4 $34,879 2,493 23.8% 4,798 45.2%MUHLENBERG 30,400 30,360 -0.1% 30,400 30,360 -0.1% 100.0% 42.4 $43,590 4,587 15.2% 11,617 38.2%OHIO 23,955 24,304 1.4% 23,955 24,304 1.4% 100.0% 40.3 $45,564 4,435 18.9% 9,161 38.2%RUSSELL 17,999 18,100 0.6% 17,999 18,100 0.6% 100.0% 43.3 $38,390 4,054 23.2% 8,223 45.7%SIMPSON 18,820 19,615 4.1% 18,820 19,615 4.1% 100.0% 39.0 $48,623 2,770 15.6% 6,160 32.7%TAYLOR 25,930 26,103 0.7% 25,930 26,103 0.7% 100.0% 37.6 $44,522 4,365 17.9% 10,075 38.9%TODD 12,262 12,310 0.4% 12,262 12,310 0.4% 100.0% 37.8 $44,005 2,254 13.2% 3,997 32.6%TRIGG 14,747 15,184 2.9% 14,747 15,184 2.9% 100.0% 46.2 $50,536 1,673 11.8% 4,093 27.8%UNION 14,206 14,073 -0.9% 14,206 14,073 -0.9% 100.0% 38.1 $46,673 2,905 20.4% 4,755 33.5%WARREN 136,050 142,467 4.5% 136,050 142,467 4.5% 100.0% 32.8 $52,270 20,285 16.8% 43,325 31.8%WAYNE 20,196 20,262 0.3% 20,196 20,262 0.3% 100.0% 42.5 $34,914 5,073 25.3% 10,548 52.2%WEBSTER 12,833 12,972 1.1% 12,833 12,972 1.1% 100.0% 41.0 $42,119 2,897 23.0% 4,451 34.7%MCCREARY 17,053 16,992 -0.4% 17,053 16,992 -0.4% 100.0% 39.4 $28,105 5,330 33.4% 9,799 57.5%WHITLEY 36,362 36,861 1.4% 36,362 36,861 1.4% 100.0% 36.6 $39,005 8,037 23.6% 24,129 66.4%CASEY 16,287 16,051 -1.5% 16,287 16,051 -1.5% 100.0% 42.6 $34,819 3,936 25.5% 7,305 44.9%PULASKI 65,341 66,098 1.1% 65,341 66,098 1.1% 100.0% 42.0 $39,998 14,330 22.7% 30,030 46.0%BELL 25,481 25,319 -0.6% 25,481 25,319 -0.6% 100.0% 41.7 $26,272 9,218 35.5% 17,142 67.3%KNOX 30,983 31,089 0.3% 30,983 31,089 0.3% 100.0% 40.0 $30,181 10,113 33.2% 23,016 74.3%LAUREL 61,089 62,241 1.9% 61,089 62,241 1.9% 100.0% 40.0 $41,526 13,790 23.2% 34,544 56.5%Service AreaTotal 1,322,830 1,342,211 1.4% 1,322,830 1,342,211 1.4% 100.00% 518,102 39.2%State of KYTotal 4,481,065 4,567,764 1.9% 4,481,065 4,567,764 1.9% 100.00% 39.2 $52,295 747,010 16.30% 1,571,733 35.1%
Med
ian
Age
Med
ian
Hou
seho
ld
Inco
me
Pers
on B
elow
Po
vert
y Le
vel
Pers
on B
elow
Po
vert
y Le
vel a
s %
of T
otal
Medicaid
Med
icai
d En
rolle
es
Med
icai
d En
rolle
es a
s %
of
Tota
l
Demographic Variable/Geographic Area
Department of Health/Health Statistics Census Bureau
Tota
l Pop
ulat
ion-
Cur
rent
Yea
r 20
21
Tota
l Pop
ulat
ion-
Proj
ecte
d Ye
ar
2025
Tota
l Pop
ulat
ion-
% C
hang
e
*Tar
get
Popu
latio
n- T
otal
SA
Cur
rent
Yea
r 20
21
*Tar
get
Popu
latio
n- T
otal
SA
Pro
ject
Yea
r 20
25
Targ
et
Popu
latio
n-
% C
hang
e
Targ
et
Popu
latio
n Pr
ojec
ted
Year
as
% o
f Tot
al
212

COLBERT 55,470 55,505 0.1% 55,470 55,505 0.1% 100.0% 42.4 $48,065 8,390 15.5% 11,961 1.1%JACKSON 51,379 51,057 -0.6% 51,379 51,057 -0.6% 100.0% 43.1 $41,769 9,536 18.6% 10,493 1.0%LAUDERDALE 92,746 92,576 -0.2% 92,746 92,576 -0.2% 100.0% 41.0 $48,094 13,175 14.6% 17,044 1.6%LAWRENCE 32,762 32,433 -1.0% 32,762 32,433 -1.0% 100.0% 42.4 $44,886 5,906 18.0% 7,314 0.7%LIMESTONE 101,763 104,053 2.2% 101,763 104,053 2.2% 100.0% 39.7 $59,686 12,436 13.6% 14,833 1.4%MADISON 379,966 388,709 2.2% 379,966 388,709 2.2% 100.0% 38.5 $65,449 44,038 12.5% 52,212 5.0%MORGAN 119,812 119,582 -0.2% 119,812 119,582 -0.2% 100.0% 40.6 $52,156 17,126 14.6% 23,521 2.2%Service AreaTotal 833,898 843,915 1.2% 833,898 843,915 1.2% 100.00% 137,378State of ALTotal 9,841,260 9,944,908 1.0% 9,841,260 9,944,908 1.0% 100.00% 39.4 $51,734 795,989 26.3% 1,045,966
Med
icai
d El
igib
les
as %
of
Tota
l 20
19
Targ
et
Popu
latio
n Pr
ojec
ted
Year
as
% o
f Tot
al
Med
ian
Age
Med
ian
Hou
seho
ld
Inco
me
Pers
on B
elow
Po
vert
y Le
vel
Pers
on B
elow
Po
vert
y Le
vel a
s %
of T
otal
Med
icai
d El
igib
les
2019Demographic
Variable/Geographic Area
Department of Health/Health Statistics Census Bureau Medicaid
Tota
l Pop
ulat
ion-
Cur
rent
Yea
r 20
21
Tota
l Pop
ulat
ion-
Proj
ecte
d Ye
ar
2025
Tota
l Pop
ulat
ion-
% C
hang
e
*Tar
get
Popu
latio
n- T
otal
SA
Cur
rent
Yea
r 20
21
*Tar
get
Popu
latio
n- T
otal
SA
Pro
ject
Yea
r 20
25
Targ
et
Popu
latio
n-
% C
hang
e
213

Section B-Economic Feasibility-1A Documentation of Cost Estimate
Architect Attestation Letter
214

Genuine Ingenuity
222 Second Avenue South
Suite 1400
Nashville, TN 37201
615.770.8100
GreshamSmith.com
January 12, 2021
Nickolas Howald
Skyline Medical Center
1850 Town Center Parkway
Nashville, TN 37214
Subject: Burn Program Renovation
Skyline Medical Center
Gresham Smith Project No. 44859.00
Dear Nick:
Our firm has reviewed the cost estimate provided for the renovation of an existing
twelve bed ICU, on the second floor of the tower, to house burn patients and
renovation in the Emergency Department to house Burn Debridement and Intake.
The estimated total construction costs include the following:
Building Permit
$6,825
Preparation of Site
$100,217
Construction
$2,589,367
Contingency
$271,691
Total $2,968,100
To the best of our knowledge, based on historical data and past experience, we
believe the estimate is accurate for the defined scope of work.
Further, we believe the site is suitable for the proposed project. The physical
environment will conform to applicable federal standards, manufacturer’s
specifications, and licensing agencies’ requirements.
Sincerely,
Margaret Sutton
Principal
SM
Copy Steve Ryan-HCA
215

Section B-Economic Feasibility-1B Detailed Equipment List
216

Item Description QTY Unit Cost Subtotal TaxTotal Cost (Inc.
Tax and Shipping)
Force Triad Bovie 4 20,974.00$ $ 83,896.00 7,551$ $ 91,446.64 Mesher 1:1- Molnycke 8 6,695.00$ $ 53,560.00 4,820$ $ 58,380.40 Misonix Debrider 1 174,956.80$ $ 174,956.80 15,746$ $ 190,702.91 Cormed Drill with Attachments 1 53,581.68$ $ 53,581.68 4,822$ $ 58,404.03 ScaarFx and M22- Lumenis 1 458,226.00$ $ 458,226.00 41,240$ $ 499,466.34 Transport Defibrillator Monitors 16 13,977.78$ 207,644 18,688$ $ 226,332.48 Ventilator (Pediatric and Adult) 172,000 15,480$ $ 187,480.00
Skyline Medical Center Proposed Burn Unit CONList of Moveable Equipment over $50,000
217

Section B-Economic Feasibility-2 Documentation of Availability of Funding
218

HCA+Healthcare”
January 6, 2021
Mr. Logan GrantExecutive DirectorTennessee Health Services and Development AgencyAndrew Jackson Bldg., Ninth Floor502 Deaderick StreetNashville, TN 37243
RE: Funding Availability for TriStar Skyline Medical Center’s Proposal Seeking CON Approval toEstablish an ABA-Verified Burn Unit in Davidson County, Tennessee
Dear Mr. Grant,
TriStar Skyline Medical Center (“Skyline”) is filing an application to establish an ABA-verified, 12-bedburn unit in Nashville, Davidson County, Tennessee. Skyline is a part of the TriStar Health system inMiddle Tennessee, and our system’s hospitals are owned by HCA Healthcare, Inc., through wholly ownedsubsidiaries.
As Chief Financial Officer of TriStar Health, the HCA Division Office for Middle Tennessee, I am writingto confirm that HCA Healthcare, Inc. is committed to provide through TriStar Health up to $5.5 millionto fully fund the proposed project from cash reserves. HCA Healthcare, Inc.’s audited financialstatements are provided as an attachment to this application.
Sincerely,
es untainChief Financial OfficerHCA TriStar Division
1000 Health Park DriveBuilding Three. Suite 500Nashville, TN 37027HCAhealthcare.,com
219

Section B-Economic Feasibility-6A
Financial Statements -10K
220

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 1/137
Table of Contents
UNITED STATESSECURITIES AND EXCHANGE COMMISSION
Washington, D.C. 20549
Form 10-K
(Mark One)
☒ ANNUAL REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934 For the fiscal year ended December 31, 2019
Or
☐ TRANSITION REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934 For the transition period from to
Commission File Number 1-11239
HCA Healthcare, Inc.(Exact Name of Registrant as Specified in its Charter)
Delaware 27-3865930
(State or Other Jurisdiction ofIncorporation or Organization)
(I.R.S. EmployerIdentification No.)
One Park PlazaNashville, Tennessee
37203
(Address of Principal Executive Offices) (Zip Code) Registrant’s telephone number, including area code: (615) 344-9551
Securities Registered Pursuant to Section 12(b) of the Act:
Title of Each Class Trading
Symbol(s) Name of Each Exchange
on Which RegisteredCommon Stock, $0.01 Par Value HCA New York Stock Exchange
Securities Registered Pursuant to Section 12(g) of the Act: None
Indicate by check mark if the Registrant is a well-known seasoned issuer, as defined in Rule 405 of the Securities Act. Yes ☒ No ☐Indicate by check mark if the Registrant is not required to file reports pursuant to Section 13 or Section 15(d) of the Act. Yes ☐ No ☒Indicate by check mark whether the Registrant (1) has filed all reports required to be filed by Section 13 or 15(d) of the Securities Exchange Act of 1934 during the
preceding 12 months (or for such shorter period that the Registrant was required to file such reports), and (2) has been subject to such filing requirements for the past90 days. Yes ☒ No ☐
Indicate by check mark whether the Registrant has submitted electronically every Interactive Data File required to be submitted pursuant to Rule 405 ofRegulation S-T (§ 232.405 of this chapter) during the preceding 12 months (or for such shorter period that the Registrant was required to submit suchfiles). Yes ☒ No ☐
Indicate by check mark whether the Registrant is a large accelerated filer, an accelerated filer, a non-accelerated filer, a smaller reporting company, or an emerginggrowth company. See the definitions of “large accelerated filer,” “accelerated filer,” “smaller reporting company” and “emerging growth company” in Rule 12b-2 of theExchange Act.
Large accelerated filer ☒ Accelerated filer ☐
Non-accelerated filer ☐ Smaller reporting company ☐
Emerging growth company ☐ If an emerging growth company, indicate by check mark if the registrant has elected not to use the extended transition period for complying with any new or revisedfinancial accounting standards provided pursuant to Section 13(a) of the Exchange Act. ☐
Indicate by check mark whether the Registrant is a shell company (as defined in Rule 12b-2 of the Act). Yes ☐ No ☒As of January 31, 2020, there were 338,427,300 outstanding shares of the Registrant’s common stock. As of June 30, 2019, the aggregate market value of the
common stock held by nonaffiliates was approximately $36.403 billion. For purposes of the foregoing calculation only, Hercules Holding II and the Registrant’s directorsand executive officers have been deemed to be affiliates.
DOCUMENTS INCORPORATED BY REFERENCEPortions of the Registrant’s definitive proxy materials for its 2020 Annual Meeting of Stockholders are incorporated by reference into Part III hereof.
221

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 2/137
Table of Contents
INDEX
Page
Reference Part I
Item 1. Business 3
Item 1A. Risk Factors 30
Item 1B. Unresolved Staff Comments 47
Item 2. Properties 47
Item 3. Legal Proceedings 48
Item 4. Mine Safety Disclosures 48
Part II
Item 5. Market for Registrant’s Common Equity, Related Stockholder Matters and Issuer Purchases of Equity Securities 49
Item 6. Selected Financial Data 51
Item 7. Management’s Discussion and Analysis of Financial Condition and Results of Operations 53
Item 7A. Quantitative and Qualitative Disclosures about Market Risk 73
Item 8. Financial Statements and Supplementary Data 73
Item 9. Changes in and Disagreements with Accountants on Accounting and Financial Disclosure 73
Item 9A. Controls and Procedures 73
Item 9B. Other Information 75
Part III
Item 10. Directors, Executive Officers and Corporate Governance 75
Item 11. Executive Compensation 75
Item 12. Security Ownership of Certain Beneficial Owners and Management and Related Stockholder Matters 76
Item 13. Certain Relationships and Related Transactions, and Director Independence 76
Item 14. Principal Accountant Fees and Services 76
Part IV
Item 15. Exhibits and Financial Statement Schedules 77
Item 16. Form 10-K Summary 90
Signatures 91
2
222

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 3/137
Table of Contents
PART I
Item 1. Business General
HCA Healthcare, Inc. is one of the leading health care services companies in the United States. At December 31, 2019, we operated 184 hospitals,comprised of 179 general, acute care hospitals; three psychiatric hospitals; and two rehabilitation hospitals. In addition, we operated 123 freestandingsurgery centers. Our facilities are located in 21 states and England.
The terms “Company,” “HCA,” “we,” “our” or “us,” as used herein and unless otherwise stated or indicated by context, refer to HCA Healthcare,Inc. and its affiliates. The term “affiliates” means direct and indirect subsidiaries of HCA Healthcare, Inc. and partnerships and joint ventures in whichsuch subsidiaries are partners. The terms “facilities” or “hospitals” refer to entities owned and operated by affiliates of HCA, and the term “employees”refers to employees of affiliates of HCA.
Our primary objective is to provide a comprehensive array of quality health care services in the most cost-effective manner possible. Our general,acute care hospitals typically provide a full range of services to accommodate such medical specialties as internal medicine, general surgery, cardiology,oncology, neurosurgery, orthopedics and obstetrics, as well as diagnostic and emergency services. Outpatient and ancillary health care services areprovided by our general, acute care hospitals, freestanding surgery centers, freestanding emergency care facilities, urgent care facilities, walk-in clinics,diagnostic centers and rehabilitation facilities. Our psychiatric hospitals provide a full range of mental health care services through inpatient, partialhospitalization and outpatient settings.
Our common stock is traded on the New York Stock Exchange (symbol “HCA”). Through our predecessors, we commenced operations in 1968.The Company was incorporated in Delaware in October 2010. Our principal executive offices are located at One Park Plaza, Nashville, Tennessee37203, and our telephone number is (615) 344-9551.
Available Information
We file certain reports with the Securities and Exchange Commission (the “SEC”), including annual reports on Form 10-K, quarterly reports onForm 10-Q and current reports on Form 8-K. The SEC maintains an Internet site at http://www.sec.gov that contains the reports, proxy and informationstatements and other information we file. Our website address is www.hcahealthcare.com. Please note that our website address is provided as an inactivetextual reference only. We make available free of charge, through our website, our annual report on Form 10-K, quarterly reports on Form 10-Q, currentreports on Form 8-K and all amendments to those reports filed or furnished pursuant to Section 13 or 15(d) of the Exchange Act, as soon as reasonablypracticable after such material is electronically filed with or furnished to the SEC. The information provided on our website is not part of this report, andis therefore not incorporated by reference unless such information is specifically referenced elsewhere in this report.
Our Code of Conduct is available free of charge upon request to our Corporate Secretary, HCA Healthcare, Inc., One Park Plaza, Nashville,Tennessee 37203, and is also available on the Ethics and Compliance and Corporate Governance portion of our website at www.hcahealthcare.com.
3
223

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 4/137
Table of Contents
Business Strategy
We are committed to providing the communities we serve with high quality, cost-effective health care while growing our business and creatinglong-term value for our stockholders. To achieve these objectives, we align our efforts around the following growth agenda:
• grow our presence in existing markets; • achieve industry-leading performance in clinical and satisfaction measures; • recruit and employ physicians to meet the need for high quality health services; • continue to leverage our scale and market positions to grow the Company; and • pursue a disciplined development strategy.
Health Care Facilities
We currently own, manage or operate hospitals, freestanding surgery centers, freestanding emergency care facilities, urgent care facilities, walk-inclinics, diagnostic and imaging centers, radiation and oncology therapy centers, comprehensive rehabilitation and physical therapy centers, physicianpractices and various other facilities.
At December 31, 2019, we owned and operated 179 general, acute care hospitals with 48,443 licensed beds. Most of our general, acute carehospitals provide medical and surgical services, including inpatient care, intensive care, cardiac care, diagnostic services and emergency services. Thegeneral, acute care hospitals also provide outpatient services such as outpatient surgery, laboratory, radiology, respiratory therapy, cardiology andphysical therapy. Each hospital has an organized medical staff and a local board of trustees or governing board, made up of members of the localcommunity.
At December 31, 2019, we operated three psychiatric hospitals with 412 licensed beds. Our psychiatric hospitals provide therapeutic programs,including child, adolescent and adult psychiatric care and adolescent and adult alcohol and drug abuse treatment and counseling.
We also operate outpatient health care facilities, which include freestanding ambulatory surgery centers (“ASCs”), freestanding emergency carefacilities, urgent care facilities, walk-in clinics, diagnostic and imaging centers, comprehensive rehabilitation and physical therapy centers, radiation andoncology therapy centers, physician practices and various other facilities. These outpatient services are an integral component of our strategy to developcomprehensive health care networks in select communities. Most of our ASCs are operated through partnerships or limited liability companies, withmajority ownership of each partnership or limited liability company typically held by a general partner or member that is an affiliate of HCA.
Certain of our affiliates provide a variety of management services to our health care facilities, including patient safety programs, ethics andcompliance programs, national supply contracts, equipment purchasing and leasing contracts, accounting, financial and clinical systems, governmentalreimbursement assistance, construction planning and coordination, information technology systems and solutions, legal counsel, human resourcesservices and internal audit services.
Sources of Revenue
Hospital revenues depend upon inpatient occupancy levels, the medical and ancillary services ordered by physicians and provided to patients, thevolume of outpatient procedures and the charges or payment rates for such services. Reimbursement rates for inpatient and outpatient services varysignificantly depending on the type of third-party payer, the type of service (e.g., medical/surgical, intensive care or psychiatric) and the geographiclocation of the hospital. Inpatient occupancy levels fluctuate for various reasons, many of which are beyond our control.
4
224

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 5/137
Table of Contents
We receive payments for patient services from the federal government under the Medicare program, state governments under their respectiveMedicaid or similar programs, managed care plans (including plans offered through the American Health Benefit Exchanges (“Exchanges”)), privateinsurers and directly from patients. Our revenues by primary third-party payer classification and other (including uninsured patients) for the years endedDecember 31, 2019, 2018 and 2017 are summarized in the following table (dollars in millions):
Years Ended December 31, 2019 Ratio 2018 Ratio 2017 Ratio
Medicare $10,798 21.0% $ 9,831 21.1% $ 9,285 21.3%Managed Medicare 6,452 12.6 5,497 11.8 4,680 10.7 Medicaid 1,572 3.1 1,358 2.9 1,316 3.0 Managed Medicaid 2,450 4.8 2,403 5.1 2,165 5.0 Managed care and other insurers 26,544 51.6 24,467 52.4 23,342 53.5 International (managed care and other insurers) 1,162 2.3 1,156 2.5 1,097 2.5 Other 2,358 4.6 1,965 4.2 1,729 4.0 Revenues $51,336 100.0% $46,677 100.0% $43,614 100.0%
Medicare is a federal program that provides certain hospital and medical insurance benefits to persons age 65 and over, some disabled persons,persons with end-stage renal disease and persons with Lou Gehrig’s Disease. Medicaid is a federal-state program, administered by the states, thatprovides hospital and medical benefits to qualifying individuals who are unable to afford health care. All of our general, acute care hospitals located inthe United States are eligible to participate in Medicare and Medicaid programs. Amounts received under Medicare and Medicaid programs aregenerally significantly less than established hospital gross charges for the services provided.
Our hospitals generally offer discounts from established charges to certain group purchasers of health care services, including private healthinsurers, employers, health maintenance organizations (“HMOs”), preferred provider organizations (“PPOs”) and other managed care plans, includinghealth plans offered through the Exchanges. These discount programs generally limit our ability to increase revenues in response to increasing costs. SeeItem 1, “Business — Competition.” For services under Medicare, Medicaid, HMOs, PPOs and other managed care plans, patients are generallyresponsible for any exclusions, deductibles or coinsurance features of their coverage. The amount of such exclusions, deductibles and coinsurancecontinues to increase. Collection of amounts due from individuals is typically more difficult than from government health care programs or other third-party payers. We provide discounts to uninsured patients who do not qualify for Medicaid or for financial relief under our charity care policy. We mayattempt to provide assistance to uninsured patients to help determine whether they may qualify for Medicaid, other federal or state assistance or charitycare under our charity care policy. If an uninsured patient does not qualify for these programs, the uninsured discount is applied.
Medicare
In addition to the reimbursement reductions and adjustments discussed below, the Budget Control Act of 2011 (the “BCA”) requires automaticspending reductions to reduce the federal deficit, including Medicare spending reductions of up to 2% per fiscal year, with a uniform percentagereduction across all Medicare programs. In 2013, the Centers for Medicare & Medicaid Services (“CMS”) began imposing a 2.0% reduction onMedicare payments, and these reductions have been extended through 2029.
Inpatient Acute Care
Under the Medicare program, we receive reimbursement under a prospective payment system (“PPS”) for general, acute care hospital inpatientservices. Under the hospital inpatient PPS, fixed payment amounts per inpatient discharge are established based on the patient’s assigned Medicareseverity diagnosis-related group
5
225

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 6/137
Table of Contents
(“MS-DRG”). MS-DRGs classify treatments for illnesses according to the estimated intensity of hospital resources necessary to furnish care for eachprincipal diagnosis. MS-DRG weights represent the average resources for a given MS-DRG relative to the average resources for all MS-DRGs.MS-DRG payments are adjusted for area wage differentials. Hospitals, other than those defined as “new,” receive PPS reimbursement for inpatientcapital costs based on MS-DRG weights multiplied by a geographically adjusted federal rate. When the cost to treat certain patients falls well outside thenormal distribution, providers typically receive additional “outlier” payments. These payments are financed by offsetting reductions in the inpatient PPSrates. A high-cost outlier threshold is set annually at a level that will result in estimated outlier payments equaling 5.1% of total inpatient PPS paymentsfor the fiscal year.
MS-DRG rates are updated, and MS-DRG weights are recalibrated, using cost-relative weights each federal fiscal year (which begins October 1).The index used to update the MS-DRG rates (the “market basket”) gives consideration to the inflation experienced by hospitals and entities outside thehealth care industry in purchasing goods and services. Each federal fiscal year, the annual market basket update is reduced by a productivity adjustmentbased on the Bureau of Labor Statistics (“BLS”) 10-year moving average of changes in specified economy-wide productivity, as required by the PatientProtection and Affordable Care Act, as amended by the Health Care and Education Reconciliation Act of 2010 (collectively, the “Affordable Care Act”).A decrease in payment rates or an increase in rates that is below the increase in our costs may adversely affect our results of operations.
For federal fiscal year 2019, CMS increased the MS-DRG rate by approximately 1.85%. This increase reflected a market basket update of 2.9%,adjusted by the following percentage points: a 0.75 reduction required by the Affordable Care Act, a negative 0.8 productivity adjustment, and a positive0.5 adjustment in accordance with the Medicare Access and CHIP Reauthorization Act of 2015 (“MACRA”). For federal fiscal year 2020, CMSincreased the MS-DRG rate by approximately 3.1%. This increase reflects a market basket update of 3.0%, adjusted by the following percentage points:a negative 0.4 productivity adjustment and a positive 0.5 adjustment required by MACRA. Additional adjustments may apply, depending on patient-specific or hospital-specific factors. For example, the two midnight rule limits payments to hospitals when services to Medicare beneficiaries arepayable as inpatient services. In addition, under the post-acute care transfer policy, Medicare reimbursement rates may be reduced when an inpatienthospital discharges a patient in a specified MS-DRG to certain post-acute care settings, including, effective October 1, 2018, hospice care.
CMS has implemented and is implementing a number of programs and requirements intended to transform Medicare from a passive payer to anactive purchaser of quality goods and services. For example, hospitals that do not successfully participate in the Hospital Inpatient Quality ReportingProgram are subject to a 25% reduction of the market basket update. Hospitals that do not demonstrate meaningful use of electronic health records(“EHRs”) are subject to a 75% reduction of the market basket update.
Medicare does not allow an inpatient hospital discharge to be assigned to a higher paying MS-DRG if certain designated hospital acquiredconditions (“HACs”) were not present on admission and the identified HAC is the only condition resulting in the assignment of the higher payingMS-DRG. In this situation, the case is paid as though the secondary diagnosis was not present. There are currently 14 categories of conditions on the listof HACs. In addition, the 25% of hospitals with the worst risk-adjusted HAC scores in the designated performance period receive a 1% reduction intheir inpatient PPS Medicare payments. CMS has also established three National Coverage Determinations that prohibit Medicare reimbursement forerroneous surgical procedures performed on an inpatient or outpatient basis.
Payments to hospitals may also be reduced based on readmission rates. Each federal fiscal year, inpatient payments are reduced if a hospitalexperiences “excess” readmissions within the 30-day time period from the date of discharge for conditions designated by CMS. For federal fiscal year2017 and subsequent years, CMS has designated six conditions or procedures, including heart attack, pneumonia and total hip arthroplasty. Hospitalswith what CMS defines as excess readmissions for these conditions or procedures receive reduced payments for
6
226

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 7/137
Table of Contents
all inpatient discharges, not just discharges relating to the conditions or procedures subject to the excess readmission standard. The amount by whichpayments are reduced is determined by assessing a hospital’s performance relative to hospitals with similar proportions of dual eligible patients, subjectto a cap established by CMS. The reduction in payments to hospitals with excess readmissions can be up to 3% of a hospital’s base payments. Eachhospital’s performance is publicly reported by CMS.
In addition, CMS reduces the inpatient PPS payment amount for all discharges by 2.0%. The total amount collected from these reductions ispooled and used to fund payments to reward hospitals that meet certain quality performance standards established by CMS. CMS scores each hospitalbased on achievement (relative to other hospitals) and improvement ranges (relative to the hospital’s own past performance) for each applicableperformance standard. Because the Affordable Care Act provides that the pool will be fully distributed, hospitals that meet or exceed the qualityperformance standards receive greater reimbursement under the value-based purchasing program than they would have otherwise. Hospitals that do notachieve the necessary quality performance receive reduced Medicare inpatient hospital payments. Hospitals are scored on a number of individualmeasures that are categorized into four domains: clinical outcomes; efficiency and cost reduction; safety; and person and community engagement. CMSestimates that $1.9 billion will be available to hospitals as incentive payments in federal fiscal year 2020 under the Hospital Value-Based PurchasingProgram.
Outpatient
CMS reimburses hospital outpatient services (and certain Medicare Part B services furnished to hospital inpatients who have no Part A coverage)on a PPS basis. CMS uses fee schedules to pay for physical, occupational and speech therapies, durable medical equipment, clinical diagnosticlaboratory services, nonimplantable orthotics and prosthetics, freestanding surgery center services and services provided by independent diagnostictesting facilities. In addition, certain items and services furnished by off-campus provider-based departments, subject to certain exceptions, are notcovered as outpatient department services under the outpatient PPS, but are reimbursed under the Medicare Physician Fee Schedule (“Physician FeeSchedule”), subject to adjustments as specified by CMS. In calendar year 2019, CMS began a two-year phase-in of an expanded site-neutral policyunder which clinic visit services provided at all off-campus provider-based departments are reimbursed at the Physician Fee Schedule rate, which isgenerally lower than the PPS rate. Previously, this rate did not apply to “excepted” provider-based departments. However, in September 2019, a federaljudge invalidated the expansion of the site-neutral payment policy for 2019. CMS is appealing this decision, but it is reprocessing the 2019 claims paidat the lower rates. For calendar year 2020, CMS issued a final rule implementing year two of the policy phase-in. Hospitals have also challenged thepolicy for 2020, but the case has not yet been decided.
Hospital outpatient services paid under PPS are classified into groups called ambulatory payment classifications (“APCs”). Services for each APCare similar clinically and in terms of the resources they require. A payment rate is established for each APC. Depending on the services provided, ahospital may be paid for more than one APC for a patient visit. The APC payment rates are updated for each calendar year. Each calendar year, theannual market basket update is further reduced by a productivity adjustment based on the BLS 10-year moving average of changes in specifiedeconomy-wide productivity as required by the Affordable Care Act. For calendar year 2019, CMS increased APC payment rates by an estimated 1.35%.This increase reflected a market basket increase of 2.9% with a negative 0.8 percentage point productivity adjustment and a negative 0.75 percentagepoint adjustment required by the Affordable Care Act. For calendar year 2020, CMS increased APC payment rates by an estimated 2.6%. This increasereflects a market basket increase of 3.0% with a negative 0.4 percentage point productivity adjustment. Together with other policy changes, CMSestimates that the calendar year 2020 rates will increase Medicare outpatient PPS payments by 1.3%. CMS requires hospitals to submit quality datarelating to outpatient care to avoid receiving a 2.0 percentage point reduction in the annual payment update under the outpatient PPS.
The 340B program allows participating hospitals to purchase certain outpatient drugs from manufacturers at discounted rates. These hospitals arereimbursed for the discounted drugs under the same Medicare payment
7
227

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 8/137
Table of Contents
methodology and rates as are applied to non-340B-discounted drugs. In a final rule effective January 1, 2018, the U.S. Department of Health and HumanServices (“HHS”) reduced the Medicare payments under the outpatient PPS for most drugs obtained at the 340B-discounted rates. HHS continued toapply the reduced rates in 2019. On May 6, 2019, the United States District Court for the District of Columbia reaffirmed its ruling that the adoption ofthe 2018 rule had exceeded HHS’ statutory authority and reached the same conclusion with respect to a final rule for the 2019 rates. The court hasremanded to the agency to craft appropriate remedies to implement the holding. HHS is appealing the decision but has also announced its intent tosurvey hospitals for drug acquisition cost data, which it may use to craft a remedy. Depending upon the remedy and the outcome of any appeal, this casecould result in a decrease to the Company’s outpatient Medicare reimbursement. For calendar year 2020, HHS will continue to pay the reduced rates thattook effect in 2018, although this is also the subject of ongoing litigation.
Rehabilitation
CMS reimburses inpatient rehabilitation facilities (“IRFs”) on a PPS basis. Under the IRF PPS, patients are classified into case mix groups thatreflect the relative resource intensity typically associated with the patient’s clinical condition. The case mix groups are based upon impairment, age,functional motor and cognitive scores, and comorbidities (additional diseases or disorders from which the patient suffers). IRFs are paid a predeterminedamount per discharge that reflects the patient’s case mix group and is adjusted for facility-specific factors, such as area wage levels, proportion oflow-income patients, and location in a rural area. Each federal fiscal year, the IRF rates are updated using a market basket index, which is reduced by aproductivity adjustment based on the BLS 10-year moving average of changes in specified economy-wide productivity. For federal fiscal year 2019,CMS increased IRF payment rates by an estimated 1.3%, reflecting an IRF market basket update of 2.9% with a negative 0.8 percentage pointproductivity adjustment and a 0.75 percentage point reduction required by the Affordable Care Act, among other payment adjustments. For federal fiscalyear 2020, CMS increased IRF payment rates by an estimated 2.5%, reflecting an IRF market basket update of 2.9% with a negative 0.4 percentagepoint productivity adjustment. In addition, CMS requires IRFs to report quality measures to avoid receiving a reduction of 2.0 percentage points to themarket basket update. CMS has indicated that it is working toward a unified payment system for post-acute care services, including those provided byIRFs.
In order to qualify for classification as an IRF, at least 60% of a facility’s inpatients during the most recent 12-month CMS-defined review periodmust have required intensive rehabilitation services for one or more of 13 specified conditions. IRFs must also meet additional coverage criteria,including patient selection and care requirements relating to pre-admission screenings, post-admission evaluations, ongoing coordination of care andinvolvement of rehabilitation physicians. A facility that fails to meet the 60% threshold, or other criteria to be classified as an IRF, will be paid undereither the acute care hospital inpatient or outpatient PPS, which generally provide for lower payment amounts. As of December 31, 2019, we had tworehabilitation hospitals and 63 hospital rehabilitation units.
Psychiatric
Inpatient hospital services furnished in psychiatric hospitals and psychiatric units of general, acute care hospitals and critical access hospitals arereimbursed on a PPS basis. The inpatient psychiatric facility (“IPF”) PPS is based upon a per diem payment, with adjustments to account for certainpatient and facility characteristics. The IPF PPS contains an “outlier” policy for extraordinarily costly cases and an adjustment to a facility’s basepayment if it maintains a full-service emergency department. CMS has established the IPF PPS payment rate in a manner intended to be budget neutral.Each federal fiscal year, IPF payment rates are updated using a market basket index, which is reduced by a productivity adjustment based on the BLS10-year moving average of changes in specified economy-wide productivity. For federal fiscal year 2019, CMS increased IPF payment rates by anestimated 1.1%, which reflects a 2.9% IPF market basket update with a negative 0.8 percentage point productivity adjustment, a negative 0.75percentage point adjustment as required by the Affordable Care Act, and other payment adjustments. For federal fiscal year 2020, CMS increased IPFpayment
8
228

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 9/137
Table of Contents
rates by an estimated 1.75%, which reflects a 2.9% IPF market basket increase with a negative 0.4 percentage point productivity adjustment and a 0.75percentage point reduction required by statute, among other payment adjustments. Inpatient psychiatric facilities are required to report quality measuresto CMS to avoid receiving a 2.0 percentage point reduction to the market basket update. As of December 31, 2019, we had three psychiatric hospitalsand 55 hospital psychiatric units.
Ambulatory Surgery Centers
CMS reimburses ASCs using a predetermined fee schedule. Reimbursements for ASC overhead costs are limited to no more than the overheadcosts paid to hospital outpatient departments under the Medicare hospital outpatient PPS for the same procedure. If CMS determines that a procedure iscommonly performed in a physician’s office, the ASC reimbursement for that procedure is limited to the reimbursement allowable under the PhysicianFee Schedule, with limited exceptions. All surgical procedures, other than those that pose a significant safety risk or generally require an overnight stay,are payable as ASC procedures. From time to time, CMS expands the services that may be performed in ASCs, which may result in more Medicareprocedures that historically have been performed in hospitals being moved to ASCs, reducing surgical volume in our hospitals. Also, more Medicareprocedures that historically have been performed in ASCs may be moved to physicians’ offices. Some commercial third-party payers have adoptedsimilar policies.
Historically, CMS updated reimbursement rates for ASCs based on changes to the consumer price index. However, for calendar years 2019through 2023, CMS updates to ASC reimbursement rates will be based on the hospital market basket index, partly to promote site-neutrality betweenhospitals and ASCs. For each federal fiscal year, the ASC payment system update is reduced by a productivity adjustment based on the BLS 10-yearmoving average of changes in specified economy-wide productivity. For calendar year 2019, CMS increased ASC payment rates by 2.1%, whichreflected a market basket increase of 2.9%, less a 0.8 percentage point productivity adjustment. For calendar year 2020, CMS increased ASC paymentrates by 2.6%, which reflects a market basket increase of 3.0% and a negative 0.4 percentage point productivity adjustment. In addition, CMS hasestablished a quality reporting program for ASCs under which ASCs that fail to report on specified quality measures receive a 2.0 percentage pointreduction to the consumer price index update.
Physician Services
Physician services are reimbursed under the Physician Fee Schedule system, under which CMS has assigned a national relative value unit(“RVU”) to most medical procedures and services that reflects the various resources required by a physician to provide the services, relative to all otherservices. Each RVU is calculated based on a combination of work required in terms of time and intensity of effort for the service, practice expense(overhead) attributable to the service and malpractice insurance expense attributable to the service. These three elements are each modified by ageographic adjustment factor to account for local practice costs and are then aggregated. While RVUs for various services may change in a given year,any alterations are required by statute to be virtually budget neutral, such that total payments made under the Physician Fee Schedule may not differ bymore than $20 million from what payments would have been if adjustments were not made. CMS annually reviews resource inputs for select services aspart of the potentially misvalued code initiative. To determine the payment rate for a particular service, the sum of the geographically adjusted RVUs ismultiplied by a conversion factor. For 2020, CMS updated the conversion factor based on a budget neutrality adjustment of 0.14%.
Medicare payments are adjusted based on participation in the Quality Payment Program (“QPP”), a payment methodology intended to rewardhigh-quality patient care. Physicians and certain other health care clinicians are required to participate in one of two QPP tracks. Under both tracks,performance data collected in each performance year will affect Medicare payments two years later. CMS expects to transition increasing financial riskto providers as the QPP evolves. The Advanced Alternative Payment Model (“APM”) track makes incentive payments available for participation inspecific innovative payment models approved by CMS. Providers may earn a 5% Medicare incentive payment between 2019 and 2024 and will beexempt from the reporting
9
229

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 10/137
Table of Contents
requirements and payment adjustments imposed under the Merit-Based Incentive Payment System (“MIPS”) if the provider has sufficient participation(based on percentage of payments or patients) in an Advanced APM. Alternatively, providers may participate in the MIPS track. Currently, providerselecting this option may receive payment incentives or be subject to payment reductions based on their performance with respect to clinical quality,resource use, clinical improvement activities, and meeting Promoting Interoperability standards related to the meaningful use of EHRs. Performancedata collected in 2020 will result in payment adjustments of up to 9% in 2022. MIPS consolidates components of three previously established physicianincentive programs: the Physician Quality Reporting System, the Physician Value-Based Payment Modifier, and the Medicare EHR Incentive Program.
Other
Under PPS, the payment rates are adjusted for area differences in wage levels by a factor (“wage index”) reflecting the relative wage level in thegeographic area compared to the national average wage level and taking into account occupational mix. The redistributive impact of wage index changesis not anticipated to have a material financial impact for 2020.
Medicare reimburses hospitals for a portion (65%) of deductible and coinsurance amounts that are uncollectable from Medicare beneficiaries.
CMS has implemented contractor reform whereby CMS competitively bids the Medicare fiscal intermediary and Medicare carrier functions toMedicare Administrative Contractors (“MACs”), which are geographically assigned across 12 jurisdictions to service both Part A and Part B providers.While providers with operations across multiple geographies had the option of having all hospitals use one home office MAC, we chose to use theMACs assigned to the geographic areas in which our hospitals are located. CMS periodically re-solicits bids, and the MAC servicing a geographic areacan change as a result of the bid competition. MAC transition periods can impact claims processing functions and the resulting cash flows.
CMS contracts with third parties to promote the integrity of the Medicare program through reviews of quality concerns and detections, andcorrections of improper payments. Quality Improvement Organizations (“QIOs”), for example, are groups of physicians and other health care qualityexperts that work on behalf of CMS to ensure that Medicare pays only for goods and services that are reasonable and necessary, and that are provided inthe most appropriate setting. Under the Recovery Audit Contractor (“RAC”) program, CMS contracts with RACs on a contingency basis to conductpost-payment reviews to detect and correct improper payments in the fee-for-service Medicare program. The compensation for RACs is based on theirreview of claims submitted to Medicare for billing compliance, including correct coding and medical necessity, and the amount of overpayments andunderpayments they identify. CMS limits the number of claims that RACs may audit by limiting the number of records that RACs may request fromhospitals based on each provider’s claim denial rate for the previous year. CMS has implemented the RAC program on a permanent, nationwide basisand expanded the RAC program to the Managed Medicare program and Medicare Part D. CMS is transitioning some of its other integrity programs to aconsolidated model by engaging Unified Program Integrity Contractors (“UPICs”) to perform audits, investigations and other integrity activities.
We have established policies and procedures to respond to requests from and payment denials by RACs and other Medicare contractors. Paymentrecoveries resulting from reviews and denials are appealable through administrative and judicial processes, and we pursue reversal of adversedeterminations at appropriate appeal levels. We incur additional costs related to responding to requests and denials, including costs associated withresponding to requests for records and pursuing the reversal of payment denials and losses associated with overpayments that are not reversed uponappeal. Currently, there are significant delays in the Medicare appeals process. Depending upon changes to and the growth of the RAC program andother Medicare integrity programs and our success in appealing claims in future periods, our cash flows and results of operations could be negativelyimpacted.
10
230

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 11/137
Table of Contents
Medicare reimburses teaching hospitals for portions of the direct and indirect costs of graduate medical education (“GME”) through statutoryformulas that are generally based on the number of medical residents and which take into account patient volume or the number of hospital beds.Accrediting organizations review GME programs for compliance with educational standards. Many of our hospitals operate GME or other residencyprograms to train physicians and other allied health professionals.
Managed Medicare
Under the Managed Medicare program (also known as Medicare Part C, or Medicare Advantage), the federal government contracts with privatehealth insurers to provide members with Medicare Part A, Part B and Part D benefits. Managed Medicare plans can be structured as HMOs, PPOs orprivate fee-for-service plans. In addition to covering Part A and Part B benefits, the health insurers may choose to offer supplemental benefits andimpose higher premiums and plan costs on beneficiaries. CMS makes fee payment adjustments based on service benchmarks and quality ratings andpublishes star ratings to assist beneficiaries with plan selection. According to CMS, over one-third of all Medicare enrollees participate in managedMedicare plans.
Medicaid
Medicaid programs are funded jointly by the federal government and the states and are administered by states under approved plans. Most stateMedicaid program payments are made under a PPS or are based on negotiated payment levels with individual hospitals. Medicaid reimbursement isoften less than a hospital’s cost of services. The Affordable Care Act requires states to expand Medicaid coverage to all individuals under age 65 withincomes effectively at or below 138% of the federal poverty level. However, states may opt out of the expansion without losing existing federalMedicaid funding. A number of states, including Texas and Florida, have opted out of the Medicaid expansion. Some states use, or have applied to use,waivers granted by CMS to implement expansion, impose different eligibility or enrollment restrictions, or otherwise implement programs that varyfrom federal standards. The presidential administration and a number of members of Congress have indicated their intent to increase state flexibility inthe administration of Medicaid programs, including allowing states to condition enrollment on work or other community engagement.
Because most states must operate with balanced budgets and because the Medicaid program is often the state’s largest program, states can beexpected to adopt or consider adopting legislation designed to reduce their Medicaid expenditures. Budgetary pressures have, in recent years, resultedand likely will continue to result in decreased spending, or decreased spending growth, for Medicaid programs in many states. Certain states in whichwe operate have adopted broad-based provider taxes to fund the non-federal share of Medicaid programs. Many states have also adopted, or areconsidering, legislation designed to reduce coverage, enroll Medicaid recipients in managed care programs and/or impose additional taxes on hospitalsto help finance or expand the states’ Medicaid systems.
Federal funds under the Medicaid program may not be used to reimburse providers for medical assistance provided to treat certain provider-preventable conditions. Each state Medicaid program must deny payments to providers for the treatment of health care-acquired conditions designatedby CMS as well as other provider-preventable conditions that may be designated by the state.
Congress has expanded the federal government’s involvement in fighting fraud, waste and abuse in the Medicaid program through the MedicaidIntegrity Program. CMS employs UPICs to perform post-payment audits of Medicaid claims, identify overpayments, and perform other programintegrity activities, many of which were previously performed by Medicaid Integrity Contractors. The UPICs collaborate with states and coordinateprovider investigations across the Medicare and Medicaid programs. In addition, state Medicaid agencies are required to establish Medicaid RACprograms. These programs vary by state in design and operation.
11
231

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 12/137
Table of Contents
Managed Medicaid
Enrollment in managed Medicaid plans has increased in recent years, as state governments seek to control the cost of Medicaid programs.Managed Medicaid programs enable states to contract with one or more entities for patient enrollment, care management and claims adjudication. Thestates usually do not relinquish program responsibilities for financing, eligibility criteria and core benefit plan design. We generally contract directlywith one or more of the designated entities, usually a managed care organization. The provisions of these programs are state-specific. Many states directmanaged care plans to pass through supplemental payments to designated providers, independent of services rendered, to ensure consistent funding ofproviders that serve large numbers of low-income patients. However, in an effort to more closely tie funds to delivery and outcomes, CMS beganlimiting these “pass-through payments” to managed Medicaid plans in 2016 and will ultimately prohibit such payments by 2027.
Accountable Care Organizations and Bundled Payment Initiatives
An Accountable Care Organization (“ACO”) is a network of providers and suppliers that work together to invest in infrastructure and redesigndelivery processes to attempt to achieve high quality and efficient delivery of services. Promoting accountability and coordination of care, ACOs areintended to produce savings as a result of improved quality and operational efficiency. ACOs that achieve quality performance standards established byHHS are eligible to share in a portion of the amounts saved by the Medicare program. There are several types of ACO programs, including the MedicareShared Savings Program, which was established pursuant to the Affordable Care Act, and the Next Generation ACO Model.
The Center for Medicare & Medicaid Innovation (“CMMI”) is responsible for establishing demonstration projects and other initiatives in order toidentify, develop, test and encourage the adoption of new methods of delivering and paying for health care that create savings under the Medicare andMedicaid programs, while improving quality of care. For example, providers participating in bundled payment initiatives agree to receive one paymentfor services provided to Medicare patients for certain medical conditions or episodes of care, accepting accountability for costs and quality of care. Byrewarding providers for increasing quality and reducing costs and penalizing providers if costs exceed a set amount, these models are intended to lead tohigher quality, more coordinated care at a lower cost to the Medicare program. Hospitals may receive supplemental Medicare payments or owerepayments to CMS depending on whether overall CMS spending per episode exceeds or falls below a target specified by CMS and whether qualitystandards are met. The CMMI has implemented bundled payment models, including the Bundled Payment Care Improvement Advanced (“BPCIAdvanced”) program, which is voluntary and expected to run through December 2023. Participation in bundled payment programs is generallyvoluntary, but CMS has required providers in selected geographic areas to participate in a mandatory bundled program for specified orthopedicprocedures, which is scheduled to run through December 2020. HHS has indicated that it plans to implement additional bundled payment programs,some of which will be mandatory.
HHS continues to focus on shifting from traditional fee-for-service reimbursement models to alternative payment models that tie reimbursement toquality and/or value, including bundled payment and pay-for-performance programs. Several private third-party payers are increasingly employing suchreimbursement models, which may increasingly shift financial risk to providers.
Disproportionate Share Hospital and Medicaid Supplemental Payments
In addition to making payments for services provided directly to beneficiaries, Medicare makes additional payments to hospitals that treat adisproportionately large number of low-income patients (Medicaid and Medicare patients eligible to receive Supplemental Security Income).Disproportionate Share Hospital (“DSH”) payment adjustments are determined annually based on certain statistical information required by HHS andare paid as a percentage addition to MS-DRG payments. CMS also distributes a payment to each DSH hospital that is allocated according to thehospital’s proportion of uncompensated care costs relative to the uncompensated care amount of other DSH hospitals.
12
232

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 13/137
Table of Contents
Some states make additional payments to providers through the Medicaid program for certain specific claims. These supplemental payments maybe in the form of Medicaid DSH payments, which help to offset hospital uncompensated care costs, or upper payment limit supplemental payments,which are intended to address the difference between Medicaid fee-for-service payments and Medicare reimbursement rates. CMS is consideringchanges to both types of payments. The federal government distributes federal Medicaid DSH funds to each state based on a statutory formula. Thestates then distribute the DSH funding among qualifying hospitals. States have broad discretion to define which hospitals qualify for Medicaid DSHpayments and the amount of such payments. The Affordable Care Act and subsequent legislation provide for reductions to the Medicaid DSH hospitalprogram. Under the budget bill signed into law in February 2018, Medicaid DSH payments will be reduced by $4 billion in 2020 and by $8 billion peryear from 2021 through 2025. However, Congress has delayed the implementation of these reductions until May 23, 2020.
TRICARE
TRICARE is the Department of Defense’s health care program for members of the armed forces. For inpatient services, TRICARE reimburseshospitals based on a DRG system modeled on the Medicare inpatient PPS. For outpatient services, TRICARE reimburses hospitals based on a PPS thatis similar to that utilized for services furnished to Medicare beneficiaries.
Annual Cost Reports
All hospitals participating in the Medicare, Medicaid and TRICARE programs, whether paid on a reasonable cost basis or under a PPS, arerequired to meet certain financial reporting requirements. Federal and, where applicable, state regulations require the submission of annual cost reportscovering the revenues, costs and expenses associated with the services provided by each hospital to Medicare beneficiaries and Medicaid recipients.
Annual cost reports required under the Medicare and Medicaid programs are subject to routine audits, which may result in adjustments to theamounts ultimately determined to be due to us under these reimbursement programs. These audits often require several years to reach the finaldetermination of amounts due to or from us under these programs. Providers also have rights of appeal, and it is common to contest issues raised inaudits of cost reports.
Managed Care and Other Discounted Plans
Most of our hospitals offer discounts from established charges to certain large group purchasers of health care services, including managed careplans and private health insurers. Admissions reimbursed by commercial managed care and other insurers were 28% of our total admissions for each ofthe years ended December 31, 2019, 2018 and 2017, respectively. Managed care contracts are typically negotiated for terms between one and threeyears. While we generally received contracted annual average increases of approximately 4% from managed care payers during 2019, there can be noassurance that we will continue to receive increases in the future. Price transparency initiatives may impact our ability to obtain or maintain favorablecontract terms. Further, it is not clear what impact, if any, health reform efforts at the federal and state levels, consolidation within the third-party payerindustry and vertical integration among third-party payers and health care providers will have on our ability to negotiate reimbursement rates.
13
233

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 14/137
Table of Contents
Uninsured and Self-Pay Patients
Self-pay revenues are derived from providing health care services to patients without health insurance coverage and from the patient responsibilityportion of payments for our health care services that are not covered by an individual’s health plan. Collection of amounts due from individuals istypically more difficult than collection of amounts due from government health care programs or private third-party payers. Any increases in uninsuredindividuals, changes to the payer mix or greater adoption of health plan structures that result in higher patient responsibility amounts could increaseamounts due from individuals.
A high percentage of our uninsured patients are initially admitted through our emergency rooms. For the year ended December 31, 2019,approximately 84% of our admissions of uninsured patients occurred through our emergency rooms. The Emergency Medical Treatment and Labor Act(“EMTALA”) requires any hospital that participates in the Medicare program to conduct an appropriate medical screening examination of every personwho presents to the hospital’s emergency room for treatment and, if the individual is suffering from an emergency medical condition, to either stabilizethat condition or make an appropriate transfer of the individual to a facility that can handle the condition. The obligation to screen and stabilizeemergency medical conditions exists regardless of an individual’s ability to pay for treatment. In addition, health insurers are required to reimbursehospitals for emergency services provided to enrollees without prior authorization and without regard to whether a participating provider contract is inplace. The financial impact of the obligation to screen for and stabilize emergency medical conditions has been offset, in part, by provisions of theAffordable Care Act that decrease the number of uninsured individuals. However, effective January 1, 2019, Congress eliminated the financial penaltyassociated with the individual mandate. Further, final rules issued in 2018 expand the availability of association health plans and allow the sale of short-term, limited-duration health plans, neither of which are required to cover all of the essential health benefits mandated by the Affordable Care Act. It isdifficult to predict the impact of these changes, but they may result in fewer individuals electing to obtain public or private health insurance or affect thescope of such coverage, if purchased.
Hospital Utilization
We believe the most important factors relating to the overall utilization of a hospital are the quality and market position of the hospital and thenumber and quality of physicians and other health care professionals providing patient care within the facility. Generally, we believe the ability of ahospital to be a market leader is determined by its breadth of services, level of technology, quality and condition of the facilities, emphasis on quality ofcare and convenience for patients and physicians. Other factors that impact utilization include the growth in local population, local economic conditionsand market penetration of managed care programs.
14
234

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 15/137
Table of Contents
The following table sets forth certain operating statistics for our health care facilities. Health care facility operations are subject to certain seasonalfluctuations, including decreases in patient utilization during holiday periods and increases in the cold weather months.
Years Ended December 31, 2019 2018 2017 2016 2015
Number of hospitals at end of period 184 179 179 170 168 Number of freestanding outpatient surgery centers at end of period 123 123 120 118 116 Number of licensed beds at end of period(a) 49,035 47,199 46,738 44,290 43,771 Weighted average licensed beds(b) 48,480 46,857 45,380 44,077 43,620 Admissions(c) 2,108,927 2,003,753 1,936,613 1,891,831 1,868,789 Equivalent admissions(d) 3,646,335 3,420,406 3,286,432 3,191,519 3,122,746 Average length of stay (days)(e) 4.9 4.9 4.9 4.9 4.9 Average daily census(f) 28,134 26,663 26,000 25,340 25,084 Occupancy rate(g) 58% 57% 57% 58% 58%Emergency room visits(h) 9,161,129 8,764,431 8,624,137 8,378,340 8,050,159 Outpatient surgeries(i) 1,009,947 971,537 941,231 932,213 909,386 Inpatient surgeries(j) 566,635 548,220 540,304 537,306 529,900 (a) Licensed beds are those beds for which a facility has been granted approval to operate from the applicable state licensing agency. (b) Represents the average number of licensed beds, weighted based on periods owned. (c) Represents the total number of patients admitted to our hospitals and is used by management and certain investors as a general measure of
inpatient volume. (d) Equivalent admissions are used by management and certain investors as a general measure of combined inpatient and outpatient volume.
Equivalent admissions are computed by multiplying admissions (inpatient volume) by the sum of gross inpatient revenue and gross outpatientrevenue and then dividing the resulting amount by gross inpatient revenue. The equivalent admissions computation “equates” outpatient revenueto the volume measure (admissions) used to measure inpatient volume, resulting in a general measure of combined inpatient and outpatientvolume.
(e) Represents the average number of days admitted patients stay in our hospitals. (f) Represents the average number of patients in our hospital beds each day. (g) Represents the percentage of hospital licensed beds occupied by patients. Both average daily census and occupancy rate provide measures of the
utilization of inpatient rooms. (h) Represents the number of patients treated in our emergency rooms. (i) Represents the number of surgeries performed on patients who were not admitted to our hospitals. Pain management and endoscopy procedures
are not included in outpatient surgeries. (j) Represents the number of surgeries performed on patients who have been admitted to our hospitals. Pain management and endoscopy procedures
are not included in inpatient surgeries.
Competition
Generally, other hospitals in the communities we serve provide services similar to those offered by our hospitals. Additionally, in recent years thenumber of freestanding specialty hospitals, surgery centers, emergency departments, urgent care centers and diagnostic and imaging centers in thegeographic areas in which we operate has increased significantly. As a result, most of our hospitals operate in a highly competitive environment. Insome cases, competing facilities are more established than our hospitals. Some competing facilities are physician-owned or are owned by tax-supportedgovernment agencies and many others are owned by not-for-profit entities that may be supported by endowments, charitable contributions and/or taxrevenues and are exempt from sales, property and income taxes. Such exemptions and support are not available to our hospitals and may provide thetax-supported or not-for-profit entities an advantage in funding capital expenditures. In
15
235

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 16/137
Table of Contents
certain localities there are large teaching hospitals that provide highly specialized facilities, equipment and services that may not be available at most ofour hospitals. We also face competition from specialty hospitals and from both our own and unaffiliated freestanding ASCs for market share in certainhigh margin services. Psychiatric hospitals frequently attract patients from areas outside their immediate locale and, therefore, our psychiatric hospitalsand units compete with both local and regional hospitals, including the psychiatric units of general, acute care hospitals.
Trends toward clinical and pricing transparency may impact our competitive position in ways that are difficult to predict. For example, hospitalsare currently required to publish online a list of their standard charges for items and services. In 2019, CMS issued a final rule that, beginning in 2021,will require hospitals to publish additional types of standard charges for all items and services, including discounted cash prices and payer-specific andde-identified negotiated charges, in a publicly accessible online file. Hospitals will also be required to publish a consumer-friendly list of charges forcertain “shoppable” services (i.e., services that can be scheduled by a patient in advance) and associated ancillary services. The 2019 rule is the subjectof ongoing court challenges.
Our strategies are designed to ensure our hospitals are competitive. We believe our hospitals compete within local communities on the basis ofmany factors, including the quality of care, ability to attract and retain quality physicians, skilled clinical personnel and other health care professionals,location, breadth of services, technology offered, and quality and condition of the facilities. We focus on operating outpatient services with accessibilityand convenient service for patients and predictability and efficiency for physicians.
Two of the most significant factors to the competitive position of a hospital are the number and quality of physicians affiliated with or employedby the hospital. Although physicians may at any time terminate their relationship with a hospital we operate, our hospitals seek to retain physicians withvaried specialties on the hospitals’ medical staffs and to attract other qualified physicians. We believe physicians refer patients to a hospital on the basisof the quality and scope of services it renders to patients and physicians, the quality of physicians on the medical staff, the location of the hospital andthe quality of the hospital’s facilities, equipment and employees. Accordingly, we strive to maintain and provide quality facilities, equipment, employeesand services for physicians and patients. Our hospitals face competition from competitors that are implementing physician alignment strategies, such asemploying physicians, acquiring physician practice groups and participating in ACOs or other clinical integration models.
Another major factor in the competitive position of our hospitals is our ability to negotiate service contracts with group purchasers of health careservices. Managed care plans attempt to direct and control the use of hospital services and obtain discounts from hospitals’ established gross charges.Similarly, employers and traditional health insurers continue to attempt to contain costs through negotiations with hospitals for managed care programsand discounts from established gross charges. Generally, hospitals compete for service contracts with group purchasers of health care services on thebasis of price, market reputation, geographic location, quality and range of services, quality of the medical staff and convenience. Our future successwill depend, in part, on our ability to retain and renew our contracts with third-party payers and enter into new contracts on favorable terms. Other healthcare providers may impact our ability to enter into contracts with third-party payers or negotiate increases in our reimbursement and other favorableterms and conditions. For example, some of our competitors may negotiate exclusivity provisions with managed care plans or otherwise restrict theability of managed care companies to contract with us. Price transparency initiatives and increasing vertical integration efforts involving third-partypayers and health care providers, among other factors, may increase these challenges. Moreover, the trend toward consolidation among private third-party payers tends to increase payer bargaining power over fee structures. In addition, health reform efforts, such as the Affordable Care Act’slimitations on rescissions of coverage and pre-existing condition exclusions, may lead to private third-party payers increasingly demanding reduced feesor being unwilling to negotiate reimbursement increases. Health plans increasingly utilize narrow networks that restrict the number of participatingproviders or tiered networks that impose significantly higher cost sharing obligations on patients that obtain services from providers in a disfavored tier.These trends may continue regardless of potential repeal or replacement of, or changes to, the
16
236

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 17/137
Table of Contents
Affordable Care Act, or other health reform efforts. The importance of obtaining contracts with group purchasers of health care services varies fromcommunity to community, depending on the market strength of such organizations.
State certificate of need (“CON”) laws, which place limitations on a health care facility’s ability to expand services and facilities, make capitalexpenditures and otherwise make changes in operations, may also have the effect of restricting competition. We currently operate health care facilities ina number of states with CON laws or that require other types of approvals for the establishment or expansion of certain facility types or services. Beforeissuing a CON or other approval, these states consider the need for additional, changes in, or expanded health care facilities or services. Removal ofthese requirements could reduce barriers to entry and increase competition in our service areas. In those states that do not require state approval or thatset relatively high levels of expenditures before they become reviewable by state authorities, competition in the form of new services, facilities andcapital spending is more prevalent. See Item 1, “Business — Regulation and Other Factors.”
We and the health care industry as a whole face the challenge of continuing to provide quality patient care while dealing with rising costs andstrong competition for patients. Changes in medical technology, existing and future legislation, regulations and interpretations and contracting forprovider services by third-party payers remain ongoing challenges.
Admissions, average lengths of stay and reimbursement amounts continue to be negatively affected by third-party payer pre-admissionauthorization requirements, utilization review and pressure to maximize outpatient and alternative health care delivery services for less acutely illpatients. Increased competition, admission constraints and third-party payer pressures are expected to continue. To meet these challenges, we intend toexpand and update our facilities or acquire or construct new facilities where appropriate, enhance the provision of a comprehensive array of outpatientservices, offer market competitive pricing to group purchasers of health care services, upgrade facilities and equipment and offer new or expandedprograms and services.
Regulation and Other Factors
Licensure, Certification and Accreditation
Health care facility construction and operation are subject to numerous federal, state and local regulations relating to the adequacy of medicalcare, equipment, personnel, operating policies and procedures, maintenance of adequate records, fire prevention, rate-setting, building codes andenvironmental protection. Facilities are subject to periodic inspection by governmental and other authorities to assure continued compliance with thevarious standards necessary for licensing and accreditation. We believe our health care facilities are properly licensed under applicable state laws. Eachof our acute care hospitals located in the United States is eligible to participate in Medicare and Medicaid programs and is accredited by The JointCommission. If any facility were to lose its Medicare or Medicaid certification, the facility would be unable to receive reimbursement from federalhealth care programs. From time to time, we may acquire a facility that is not accredited but for which we will seek accreditation. If any facility were tolose accreditation, the facility would be subject to state surveys, potentially be subject to increased scrutiny by CMS and likely lose payment fromprivate third-party payers. Management believes our facilities are in substantial compliance with current applicable federal, state, local and independentreview body regulations and standards. The requirements for licensure, certification and accreditation are subject to change, and, in order to remainqualified, it may become necessary for us to make changes in our facilities, equipment, personnel and services. The requirements for licensure,certification and accreditation also include notification or approval in the event of the transfer or change of ownership or certain other changes. Failureto provide required notifications or obtain necessary approvals in these circumstances can result in the inability to complete an acquisition or change ofownership, loss of licensure, lapses in reimbursement or other penalties.
Certificates of Need
In some states where we operate hospitals and other health care providers, the construction or expansion of health care facilities, the acquisition ofexisting facilities, the transfer or change of ownership, capital
17
237

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 18/137
Table of Contents
expenditures and the addition of new beds or services may be subject to review by and prior approval of, or notifications to, state regulatory agenciesunder a CON program. Such laws generally require the reviewing state agency to determine the public need for additional or expanded health carefacilities and services or other change. Failure to provide required notifications or obtain necessary state approvals can result in the inability to expandfacilities, complete an acquisition or expenditure or change ownership or other penalties.
State Rate Review
Some states have adopted legislation mandating rate or budget review for hospitals or have adopted taxes on hospital revenues, assessments orlicensure fees to fund indigent health care within the state. In the aggregate, indigent tax provisions have not materially, adversely affected our results ofoperations. Although we do not currently operate facilities in states that mandate rate or budget reviews, we cannot predict whether we will operate insuch states in the future, or whether the states in which we currently operate may adopt legislation mandating such reviews.
Federal Health Care Program Regulations
Participation in any federal health care program, including the Medicare and Medicaid programs, is heavily regulated by statute and regulation. Ifa hospital or other provider fails to substantially comply with the numerous conditions of participation in the Medicare and Medicaid programs orperforms certain prohibited acts, the provider’s participation in the federal health care programs may be terminated, or civil and/or criminal penaltiesmay be imposed. Civil monetary penalties are adjusted annually based on updates to the consumer price index and were increased under the BipartisanBudget Act of 2018.
Anti-kickback Statute
A section of the Social Security Act known as the “Anti-kickback Statute” prohibits providers and others from directly or indirectly soliciting,receiving, offering or paying any remuneration with the intent of generating referrals or orders for services or items covered by a federal health careprogram. Courts have interpreted this statute broadly and held that there is a violation of the Anti-kickback Statute if just one purpose of theremuneration is to generate referrals, even if there are other lawful purposes. Furthermore, the Affordable Care Act provides that knowledge of the lawor the intent to violate the law is not required. Violations of the Anti-kickback Statute may be punished by criminal fines of up to $100,000 per violation,imprisonment, substantial civil monetary penalties per violation that are subject to annual adjustment based on updates to the consumer price index anddamages of up to three times the total amount of the remuneration and/or exclusion from participation in federal health care programs, includingMedicare and Medicaid. In addition, submission of a claim for services or items generated in violation of the Anti-kickback Statute may be subject toadditional penalties under the federal False Claims Act (“FCA”) as a false or fraudulent claim.
The HHS Office of Inspector General (the “OIG”), among other regulatory agencies, is responsible for identifying and eliminating fraud, abuseand waste. The OIG carries out this mission through a nationwide program of audits, investigations and inspections. The OIG provides guidance to theindustry through various methods, including advisory opinions and “Special Fraud Alerts.” These Special Fraud Alerts do not have the force of law, butidentify features of arrangements or transactions that the government believes may cause the arrangements or transactions to violate the Anti-kickbackStatute or other federal health care laws. The OIG has identified several incentive arrangements that constitute suspect practices, including: (a) paymentof any incentive by a hospital each time a physician refers a patient to the hospital, (b) the use of free or significantly discounted office space orequipment in facilities usually located close to the hospital, (c) provision of free or significantly discounted billing, nursing or other staff services,(d) free training for a physician’s office staff in areas such as management techniques and laboratory techniques, (e) guarantees which provide, if thephysician’s income fails to reach a predetermined level, the hospital will pay any portion of the remainder, (f) low-interest or interest-free loans, or loanswhich may be forgiven if a physician refers patients to the hospital, (g) payment of
18
238

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 19/137
Table of Contents
the costs of a physician’s travel and expenses for conferences, (h) coverage on the hospital’s group health insurance plans at an inappropriately low costto the physician, (i) payment for services (which may include consultations at the hospital) which require few, if any, substantive duties by the physician,(j) purchasing goods or services from physicians at prices in excess of their fair market value, (k) rental of space in physician offices, at other than fairmarket value terms, by persons or entities to which physicians refer, and (l) physician-owned entities (frequently referred to as physician-owneddistributorships or PODs) that derive revenue from selling, or arranging for the sale of, implantable medical devices ordered by their physician-ownersfor use on procedures that physician-owners perform on their own patients at hospitals or ASCs. The OIG has encouraged persons having informationabout hospitals who offer the above types of incentives to physicians to report such information to the OIG.
The OIG also issues “Special Advisory Bulletins” as a means of providing guidance to health care providers. These bulletins, along with theSpecial Fraud Alerts, have focused on certain arrangements that could be subject to heightened scrutiny by government enforcement authorities,including: (a) contractual joint venture arrangements and other joint venture arrangements between those in a position to refer business, such asphysicians, and those providing items or services for which Medicare or Medicaid pays, and (b) certain “gainsharing” arrangements, i.e., the practice ofgiving physicians a share of any reduction in a hospital’s costs for patient care attributable in part to the physician’s efforts.
In addition to issuing Special Fraud Alerts and Special Advisory Bulletins, the OIG issues compliance program guidance for certain types ofhealth care providers. The OIG guidance identifies a number of risk areas under federal fraud and abuse statutes and regulations. These areas of riskinclude compensation arrangements with physicians, recruitment arrangements with physicians and joint venture relationships with physicians.
As authorized by Congress, the OIG has published safe harbor regulations that outline categories of activities deemed protected from prosecutionunder the Anti-kickback Statute. Currently, there are statutory exceptions and safe harbors for various activities, including the following: certaininvestment interests, space rental, equipment rental, practitioner recruitment, personnel services and management contracts, sale of practice, referralservices, warranties, discounts, employees, group purchasing organizations, waiver of beneficiary coinsurance and deductible amounts, managed carearrangements, obstetrical malpractice insurance subsidies, investments in group practices, freestanding surgery centers, ambulance replenishing, andreferral agreements for specialty services.
The fact that conduct or a business arrangement does not fall within a safe harbor or is identified in a Special Fraud Alert, Special AdvisoryBulletin or other guidance does not necessarily render the conduct or business arrangement illegal under the Anti-kickback Statute. However, suchconduct and business arrangements may lead to increased scrutiny by government enforcement authorities.
We have a variety of financial relationships with physicians and others who either refer or influence the referral of patients to our hospitals, otherhealth care facilities and employed physicians, including employment contracts, leases, medical director agreements and professional serviceagreements. We also have similar relationships with physicians and facilities to which patients are referred from our facilities and other providers. Inaddition, we provide financial incentives, including minimum revenue guarantees, to recruit physicians into the communities served by our hospitals.While we endeavor to comply with the applicable safe harbors, certain of our current arrangements, including joint ventures and financial relationshipswith physicians and other referral sources and persons and entities to which we refer patients, do not qualify for safe harbor protection.
Although we believe our arrangements with physicians and other referral sources and referral recipients have been structured to comply withcurrent law and available interpretations, there can be no assurance regulatory authorities enforcing these laws will determine these financialarrangements comply with the Anti-kickback Statute or other applicable laws. An adverse determination could subject us to liabilities under the SocialSecurity Act and other laws, including criminal penalties, civil monetary penalties and exclusion from participation in Medicare, Medicaid or otherfederal health care programs.
19
239

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 20/137
Table of Contents
Stark Law
The Social Security Act also includes a provision commonly known as the “Stark Law.” The Stark Law prohibits physicians from referringMedicare and Medicaid patients to entities with which they or any of their immediate family members have a financial relationship, if these entitiesprovide certain “designated health services” reimbursable by Medicare or Medicaid unless an exception applies. The Stark Law also prohibits entitiesthat provide designated health services reimbursable by Medicare and Medicaid from billing the Medicare and Medicaid programs for any items orservices that result from a prohibited referral and requires the entities to refund amounts received for items or services provided pursuant to theprohibited referral on a timely basis. “Designated health services” include inpatient and outpatient hospital services, clinical laboratory services andradiology services. Sanctions for violating the Stark Law include denial of payment, substantial civil monetary penalties per claim submitted andexclusion from the federal health care programs. Failure to refund amounts received as a result of a prohibited referral on a timely basis may constitute afalse or fraudulent claim and may result in civil penalties and additional penalties under the FCA. The statute also provides for a penalty for acircumvention scheme. These penalties are updated annually based on changes to the consumer price index.
There are exceptions to the self-referral prohibition for many of the customary financial arrangements between physicians and providers,including employment contracts, leases and recruitment agreements. Unlike safe harbors under the Anti-kickback Statute with which compliance isvoluntary, a financial relationship must comply with every requirement of a Stark Law exception or the arrangement is in violation of the Stark Law.Although there is an exception for a physician’s ownership interest in an entire hospital, the Affordable Care Act prohibits physician-owned hospitalsestablished after December 31, 2010 from billing for Medicare or Medicaid patients referred by their physician owners. As a result, the law effectivelyprevents the formation of new physician-owned hospitals that participate in Medicare or Medicaid. While the Affordable Care Act grandfathers existingphysician-owned hospitals, it does not allow these hospitals to increase the percentage of physician ownership and significantly restricts their ability toexpand services.
Through a series of rulemakings, CMS has issued final regulations implementing the Stark Law. While these regulations were intended to clarifythe requirements of the exceptions to the Stark Law, it is unclear how the government will interpret many of these exceptions for enforcement purposes.Further, we do not always have the benefit of significant regulatory or judicial interpretation of the Stark Law and its implementing regulations. Weattempt to structure our relationships to meet an exception to the Stark Law, but the regulations implementing the exceptions are detailed and complex,and are subject to continuing legal and regulatory change. We cannot assure that every relationship complies fully with the Stark Law.
Similar State Laws
Many states in which we operate also have laws similar to the Anti-kickback Statute that prohibit payments to physicians for patient referrals andlaws similar to the Stark Law that prohibit certain self-referrals. These state laws often apply regardless of the source of payment for care, and littleprecedent exists for their interpretation or enforcement. These statutes typically provide for criminal and civil penalties, as well as loss of licensure.
Other Fraud and Abuse Provisions
Certain federal fraud and abuse laws apply to all health benefit programs and provide for criminal penalties. The Social Security Act also imposescriminal and civil penalties for making false claims and statements to Medicare and Medicaid. False claims include, but are not limited to, billing forservices not rendered or for misrepresenting actual services rendered in order to obtain higher reimbursement, billing for unnecessary goods and servicesand cost report fraud. Federal enforcement officials have the ability to exclude from Medicare and Medicaid any business entities and any investors,officers and managing employees associated with business entities that have committed health care fraud, even if the officer or managing employee hadno knowledge of the fraud. Criminal and civil penalties may be imposed for a number of other prohibited activities, including failure
20
240

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 21/137
Table of Contents
to return known overpayments, certain gainsharing arrangements, billing Medicare amounts that are substantially in excess of a provider’s usualcharges, offering remuneration to influence a Medicare or Medicaid beneficiary’s selection of a health care provider, contracting with an individual orentity known to be excluded from a federal health care program, making or accepting a payment to induce a physician to reduce or limit services, andsoliciting or receiving any remuneration in return for referring an individual for an item or service payable by a federal health care program. Like theAnti-kickback Statute, these provisions are very broad. Civil penalties may be imposed for the failure to report and return an overpayment within 60days of identifying the overpayment or by the date a corresponding cost report is due, whichever is later. To avoid liability, providers must, among otherthings, carefully and accurately code claims for reimbursement, promptly return overpayments and accurately prepare cost reports.
Some of these provisions, including the federal Civil Monetary Penalty Law, require a lower burden of proof than other fraud and abuse laws,including the Anti-kickback Statute. Substantial civil monetary penalties may be imposed under the federal Civil Monetary Penalty Law. These penaltieswill be updated annually based on changes to the consumer price index. In some cases, violations of the Civil Monetary Penalty Law may result inpenalties of up to three times the remuneration offered, paid, solicited or received. In addition, a violator may be subject to exclusion from federal andstate health care programs. Federal and state governments increasingly use the federal Civil Monetary Penalty Law, especially where they believe theycannot meet the higher burden of proof requirements under the Anti-kickback Statute. Further, individuals can receive up to $1,000 for providinginformation on Medicare fraud and abuse that leads to the recovery of at least $100 of Medicare funds under the Medicare Integrity Program.
The Federal False Claims Act and Similar State Laws
We are subject to state and federal laws that govern the submission of claims for reimbursement and prohibit the making of false claims orstatements. One of the most prominent of these laws is the FCA, which may be enforced by the federal government directly or by a qui tam plaintiff, orwhistleblower, on the government’s behalf. The government may use the FCA to prosecute Medicare and other government program fraud in areas suchas coding errors, billing for services not provided and submitting false cost reports. In addition, the FCA covers payments made in connection with theExchanges created under the Affordable Care Act, if those payments include any federal funds. When a private party brings a qui tam action under theFCA, the defendant is not made aware of the lawsuit until the government commences its own investigation or makes a determination whether it willintervene. If a defendant is determined by a court of law to be liable under the FCA, the defendant may be required to pay three times the actualdamages sustained by the government, plus substantial mandatory civil penalties for each separate false claim. These penalties are updated annuallybased on changes to the consumer price index.
There are many potential bases for liability under the FCA. Liability often arises when an entity knowingly submits a false claim forreimbursement to the federal government. The FCA defines the term “knowingly” broadly. Though simple negligence will not give rise to liability underthe FCA, submitting a claim with reckless disregard to its truth or falsity constitutes a “knowing” submission under the FCA and, therefore, may createliability. Submission of claims for services or items generated in violation of the Anti-kickback Statute constitutes a false or fraudulent claim under theFCA. Whistleblowers and the federal government have taken the position, and some courts have held, that providers who allegedly have violated otherstatutes, such as the Stark Law, have thereby submitted false claims under the FCA. False claims under the FCA also include the knowing and improperfailure to report and refund amounts owed to the government in a timely manner following identification of an overpayment. An overpayment is deemedto be identified when a person has, or should have through reasonable diligence, determined that an overpayment was received and quantified theoverpayment.
Every entity that receives at least $5 million annually in Medicaid payments must have written policies for all employees, contractors or agents,providing detailed information about false claims, false statements and whistleblower protections under certain federal laws, including the FCA, andsimilar state laws. In addition,
21
241

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 22/137
Table of Contents
federal law provides an incentive to states to enact false claims laws comparable to the FCA. A number of states in which we operate have adopted theirown false claims provisions as well as their own whistleblower provisions under which a private party may file a civil lawsuit in state court. We haveadopted and distributed policies pertaining to the FCA and relevant state laws.
HIPAA Administrative Simplification and Privacy and Security Requirements
The Administrative Simplification Provisions of the Health Insurance Portability and Accountability Act of 1996 (“HIPAA”) and implementingregulations require the use of uniform electronic data transmission standards and code sets for certain health care claims and payment transactionssubmitted or received electronically. In addition, HIPAA requires that each provider use a National Provider Identifier. These provisions are intended toencourage electronic commerce in the health care industry.
The privacy and security regulations promulgated pursuant to HIPAA extensively regulate the use and disclosure of individually identifiablehealth information, known as “protected health information,” and require covered entities, including health plans and most health care providers, toimplement administrative, physical and technical safeguards to protect the security of such information. Certain provisions of the security and privacyregulations apply to business associates (entities that handle protected health information on behalf of covered entities), and business associates aresubject to direct liability for violation of these provisions. In addition, a covered entity may be subject to penalties as a result of a business associateviolating HIPAA, if the business associate is found to be an agent of the covered entity.
Covered entities must report breaches of unsecured protected health information to affected individuals without unreasonable delay but not toexceed 60 days after discovery of the breach by a covered entity or its agents. Notification must also be made to HHS and, in certain situations involvinglarge breaches, to the media. HHS is required to publish on its website a list of all covered entities that report a breach involving more than500 individuals. All non-permitted uses or disclosures of unsecured protected health information are presumed to be breaches unless the covered entityor business associate establishes that there is a low probability the information has been compromised. Various state laws and regulations may alsorequire us to notify affected individuals in the event of a data breach involving individually identifiable information.
Violations of the HIPAA privacy and security regulations may result in criminal penalties and in substantial civil penalties per violation. Thesecivil penalties are updated annually based on updates to the consumer price index. HHS enforces the regulations and performs compliance audits. Inaddition to enforcement by HHS, state attorneys general are authorized to bring civil actions seeking either injunction or damages in response toviolations that threaten the privacy of state residents. HHS may resolve HIPAA violations through informal means, such as allowing a covered entity toimplement a corrective action plan, but HHS has the discretion to move directly to impose monetary penalties and is required to impose penalties forviolations resulting from willful neglect. We enforce compliance in accordance with HIPAA privacy and security regulations. The InformationProtection and Security Department monitors our compliance with the HIPAA privacy and security regulations. The HIPAA privacy regulations andsecurity regulations have and will continue to impose significant costs on our facilities in order to comply with these standards.
There are numerous other laws and legislative and regulatory initiatives at the federal and state levels addressing privacy and security concerns.Our facilities remain subject to any federal or state privacy-related laws that are more restrictive than the privacy regulations issued under HIPAA. Theselaws vary and could impose additional penalties. For example, the Federal Trade Commission uses its consumer protection authority to initiateenforcement actions in response to data breaches. The California Consumer Privacy Act of 2018 (the “CCPA”) affords consumers expanded privacyprotections effective January 1, 2020. The potential effects of this legislation are far-reaching and may require us to modify our data processing practicesand policies and to incur substantial costs and expenses to comply. For example, the CCPA gives California residents expanded rights to access andrequire deletion of their personal information, opt out of certain personal information sharing and
22
242

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 23/137
Table of Contents
receive detailed information about how their personal information is used. The CCPA provides for civil penalties for violations, as well as a private rightof action for data breaches.
Many foreign data privacy regulations (including the European Union’s General Data Protection Regulation (the “GDPR”)) are more stringentthan those in the United States. In the case of non-compliance with a material provision of the GDPR (such as non-adherence to the core principles ofprocessing personal data), regulators have the authority to levy a fine in an amount that is up to the greater of €20 million or 4% of global annualturnover in the prior year. If it is determined that non-compliance is related to a non-material provision (such as failure to comply with technicalmeasures), regulators may impose a fine in an amount that is up to the greater of €10 million or 2% of the global annual turnover from the prior year.These administrative fines are discretionary and based, in each case, on a multi-factored approach.
EMTALA
All of our hospitals in the United States are subject to EMTALA. This federal law requires any hospital participating in the Medicare program toconduct an appropriate medical screening examination of every individual who presents to the hospital’s emergency room for treatment and, if theindividual is suffering from an emergency medical condition, to either stabilize the condition or make an appropriate transfer of the individual to afacility able to handle the condition. The obligation to screen and stabilize emergency medical conditions exists regardless of an individual’s ability topay for treatment. There are severe penalties under EMTALA if a hospital fails to screen or appropriately stabilize or transfer an individual or if thehospital delays appropriate treatment in order to first inquire about the individual’s ability to pay. Penalties for violations of EMTALA include exclusionfrom participation in the Medicare program and civil monetary penalties. These civil monetary penalties are adjusted annually based on updates to theconsumer price index. In addition, an injured individual, the individual’s family or a medical facility that suffers a financial loss as a direct result of ahospital’s violation of the law can bring a civil suit against the hospital.
The government broadly interprets EMTALA to cover situations in which individuals do not actually present to a hospital’s emergency room, butpresent for emergency examination or treatment to the hospital’s campus, generally, or to a hospital-based clinic that treats emergency medicalconditions or are transported in a hospital-owned ambulance, subject to certain exceptions. At least one court has interpreted the law also to apply to ahospital that has been notified of a patient’s pending arrival in a non-hospital owned ambulance. EMTALA does not generally apply to individualsadmitted for inpatient services. The government has expressed its intent to investigate and enforce EMTALA violations actively.
Corporate Practice of Medicine/Fee Splitting
Some of the states in which we operate have laws prohibiting corporations and other entities from employing physicians, practicing medicine for aprofit and making certain direct and indirect payments to, or entering into fee-splitting arrangements with, health care providers designed to induce orencourage the referral of patients to, or the recommendation of, particular providers for medical products and services. Possible sanctions for violationof these restrictions include loss of license and civil and criminal penalties. In addition, agreements between the corporation and the physician may beconsidered void and unenforceable. These statutes vary from state to state, are often vague and have seldom been interpreted by the courts or regulatoryagencies.
Health Care Industry Investigations
Significant media and public attention has focused in recent years on the hospital industry. This media and public attention, changes ingovernment personnel and other factors have led to increased scrutiny of the health care industry. Except as may be disclosed in our SEC filings, we arenot aware of any material investigations of the Company under federal or state health care laws or regulations. It is possible that governmental entitiescould initiate investigations or litigation in the future at facilities we operate and that such matters could result in
23
243

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 24/137
Table of Contents
significant penalties, as well as adverse publicity. It is also possible that our executives and managers could be included in governmental investigationsor litigation or named as defendants in private litigation.
Our substantial Medicare, Medicaid and other governmental billings result in heightened scrutiny of our operations. We continue to monitor allaspects of our business and have developed a comprehensive ethics and compliance program that is designed to meet or exceed applicable federalguidelines and industry standards.
Because the law in this area is complex and constantly evolving, governmental investigations or litigation may result in interpretations that areinconsistent with our practices or industry practices.
In public statements surrounding current investigations, governmental authorities have taken positions on a number of issues, including some forwhich little official interpretation previously has been available, that appear to be inconsistent with practices that have been common within the industryand that previously have not been challenged in this manner. In some instances, government investigations that have in the past been conducted underthe civil provisions of federal law may now be conducted as criminal investigations.
Both federal and state government agencies have increased their focus on and coordination of civil and criminal enforcement efforts in the healthcare area. The OIG and the Department of Justice (“DOJ”) have, from time to time, established national enforcement initiatives, targeting all hospitalproviders that focus on specific billing practices or other suspected areas of abuse. The Affordable Care Act includes additional federal funding of$350 million over 10 years to fight health care fraud, waste and abuse, including $10 million in federal fiscal year 2020. In addition, governmentalagencies and their agents, such as MACs, fiscal intermediaries and carriers, may conduct audits of our health care operations. Private third-party payersmay conduct similar post-payment audits, and we also perform internal audits and monitoring.
In addition to national enforcement initiatives, federal and state investigations have addressed a wide variety of routine health care operations suchas: cost reporting and billing practices, including for Medicare outliers; financial arrangements with referral sources; physician recruitment activities;physician joint ventures; and hospital charges and collection practices for self-pay patients. We engage in many of these routine health care operationsand other activities that could be the subject of governmental investigations or inquiries. For example, we have significant Medicare and Medicaidbillings, numerous financial arrangements with physicians who are referral sources to our hospitals, and joint venture arrangements involving physicianinvestors. Certain of our individual facilities have received, and other facilities may receive, government inquiries from, and may be subject toinvestigation by, federal and state agencies. Any additional investigations of the Company, our executives or managers could result in significantliabilities or penalties to us, as well as adverse publicity.
Health Care Reform
The health care industry is subject to changing political, regulatory, and other influences, along with various scientific and technologicalinitiatives. In recent years, the U.S. Congress and certain state legislatures have passed a large number of laws and regulations intended to effect majorchange within the U.S. health care system, including the Affordable Care Act. The Affordable Care Act affects how health care services are covered,delivered and reimbursed through expanded health insurance coverage, reduced growth in Medicare program spending, reductions in Medicare andMedicaid DSH payments, and the establishment of programs that tie reimbursement to quality and integration. However, there is uncertainty regardingthe future of the Affordable Care Act. The law has been subject to legislative and regulatory changes and court challenges. The presidentialadministration and a number of members of Congress have stated their intent to repeal or make additional significant changes to the Affordable CareAct, its implementation or interpretation. For example, final rules issued in 2018 expand the availability of association health plans and allow the sale ofshort-term, limited-duration health plans, neither of which are required to cover all of the essential health benefits mandated by the Affordable Care Act.Further, the President of the United States signed an executive order that directs agencies to minimize “economic and regulatory burdens” of theAffordable Care Act, which may result in additional changes
24
244

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 25/137
Table of Contents
in how the law is implemented. Effective January 1, 2019, the penalty associated with the individual mandate to maintain health insurance waseliminated. As a result of this change, in December 2018, the United States District Court for the North District of Texas found the individual mandateto be unconstitutional and determined that the rest of the Affordable Care Act was, therefore, invalid. In December 2019, the Fifth Circuit Court ofAppeals upheld this decision with respect to the individual mandate, but remanded for further consideration of how this affects the rest of the law.Pending the appeals process, the law remains in place. The elimination of the individual mandate penalty and other changes may impact the number ofindividuals that elect to obtain public or private health insurance or the scope of such coverage, if purchased.
As currently structured, the Affordable Care Act expands coverage through a combination of private sector health insurance requirements, publicprogram expansion and other reforms. Expansion of coverage through the private sector has been driven by requirements applicable to health insurers,employers, and individuals. For example, health insurers are prohibited from imposing annual coverage limits, dropping coverage, excluding personsbased upon pre-existing conditions or denying coverage for any individual who is willing to pay the premiums for such coverage. Expansion in publicprogram coverage has been driven primarily by expanding the categories of individuals eligible for Medicaid coverage and permitting individuals withrelatively higher incomes to qualify. A number of states, including Texas and Florida, have opted out of the Medicaid expansion provisions, which theymay do without losing federal funding. For states that have not participated in the Medicaid expansion, the maximum income level required forindividuals and families to qualify for Medicaid varies widely from state to state. Some states are using waivers granted by CMS to expand theirMedicaid programs, impose different eligibility or enrollment restrictions, or otherwise implement programs that vary from federal standards. Inaddition, some states are proposing or have implemented various health reform initiatives at the state level. For example, some states have proposedpublic health insurance options, and some states have passed or are considering legislation to address out-of-network billing.
The Affordable Care Act has had a net positive effect on the Company to date, before considering the impact of Medicare reductions that began in2010, and it is expected that the law, as presently implemented, will continue to have a positive contribution to the Company’s results of operations.However, there is uncertainty regarding the ongoing net effect of the Affordable Care Act due to efforts to change, repeal or replace the Affordable CareAct, court challenges, and the development of agency guidance, among other factors. There is also uncertainty regarding the potential impact of otherreform efforts at the federal and state levels. For example, some presidential candidates and members of Congress have proposed measures that wouldexpand government-sponsored coverage, including single-payer proposals (often referred to as “Medicare for All”), and some states are consideringsimilar measures. Other initiatives and proposals, including those aimed at price transparency and out-of-network charges, may impact prices and therelationships between health care providers and insurers. These issues are further discussed in Item 1A, “Risk Factors.”
General Economic and Demographic Factors
The health care industry is impacted by the overall United States economy. Budget deficits at federal, state and local government entities have hada negative impact on spending for many health and human service programs, including Medicare, Medicaid and similar programs, which representsignificant payer sources for our hospitals and other providers. We anticipate that the federal deficit, the growing magnitude of Medicare and Medicaidexpenditures and the aging of the United States population will continue to place pressure on government health care programs. Other risks we faceduring periods of economic weakness and high unemployment include potential declines in the population covered under managed care agreements,increased patient decisions to postpone or cancel elective and nonemergency health care procedures (including delaying surgical procedures), potentialincreases in the uninsured and underinsured populations, increased adoption of health plan structures that shift financial responsibility to patients andincreased difficulties in collecting patient receivables for copayment and deductible amounts.
25
245

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 26/137
Table of Contents
Compliance Program
We maintain a comprehensive ethics and compliance program that is designed to meet or exceed applicable federal guidelines and industrystandards. The program is intended to monitor and raise awareness of various regulatory issues among employees and to emphasize the importance ofcomplying with governmental laws and regulations. As part of the ethics and compliance program, we provide annual ethics and compliance training toour employees and encourage all employees to report any violations to their supervisor, an ethics and compliance officer or to the Company’s ethics lineavailable 24 hours a day by phone and internet portal.
Antitrust Laws
The federal government and most states have enacted antitrust laws that prohibit certain types of conduct deemed to be anti-competitive. Theselaws prohibit price fixing, market allocation, bid-rigging, concerted refusal to deal, market monopolization, price discrimination, tying arrangements,acquisitions of competitors and other practices that have, or may have, an adverse effect on competition. Violations of federal or state antitrust laws canresult in various sanctions, including criminal and civil penalties. Antitrust enforcement in the health care industry is currently a priority of the FederalTrade Commission and the DOJ. We believe we are in compliance with such federal and state laws, but courts or regulatory authorities may reach adetermination in the future that could adversely affect our operations.
Environmental Matters
We are subject to various federal, state and local statutes and ordinances regulating the discharge of materials into the environment. We do notbelieve that we will be required to expend any material amounts in order to comply with these laws and regulations.
Insurance
As is typical in the health care industry, we are subject to claims and legal actions by patients in the ordinary course of business. Subject, in mostcases, to a $15 million per occurrence self-insured retention, our facilities are insured by our 100% owned insurance subsidiary for losses up to$50 million per occurrence. The insurance subsidiary has obtained reinsurance for professional liability risks generally above a retention level of$25 million per occurrence. We also maintain professional liability insurance with unrelated commercial carriers for losses in excess of amounts insuredby our insurance subsidiary.
We purchase, from unrelated insurance companies, coverage for cyber security incidents, directors and officers liability and property loss inamounts we believe are adequate. The cyber security and directors and officers liability coverage each include a $5 million corporate deductible. Inaddition, we will continue to purchase coverage for our directors and officers on an ongoing basis. The property coverage includes varying deductiblesdepending on the cause of the property damage. These deductibles range from 2% to 5% of the affected property values for certain flood and wind andearthquake related incidents.
Employees and Medical Staffs
At December 31, 2019, we had approximately 280,000 employees, including approximately 70,000 part-time employees. References herein to“employees” refer to employees of our affiliates. We are subject to various state and federal laws that regulate wages, hours, benefits and other termsand conditions relating to employment. At December 31, 2019, certain employees at 37 of our domestic hospitals are represented by various laborunions. One election was held in January 2020 that resulted in the addition of a number of employees to an existing bargaining unit at one of ourfacilities in California. While no other elections are scheduled in 2020, it is possible that employees at additional hospitals may unionize in the future.We consider our employee relations to be good and have not experienced work stoppages that have materially, adversely affected our business or results
26
246

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 27/137
Table of Contents
of operations. Our hospitals, like most hospitals, have experienced rising labor costs. In some markets, nurse and medical support personnel availabilityhas become a significant operating issue to health care providers. To address this challenge, we have implemented several initiatives to improveretention, recruiting, compensation programs and productivity.
Our hospitals are staffed by licensed physicians, including both employed physicians and physicians who are not employees of our hospitals.Some physicians provide services in our hospitals under contracts, which generally describe a term of service, provide and establish the duties andobligations of such physicians, require the maintenance of certain performance criteria and fix compensation for such services. Any licensed physicianmay apply to be accepted to the medical staff of any of our hospitals, but the hospital’s medical staff and the appropriate governing board of the hospital,in accordance with established credentialing criteria, must approve acceptance to the staff. Members of the medical staffs of our hospitals often alsoserve on the medical staffs of other hospitals and may terminate their affiliation with one of our hospitals at any time.
We may be required to continue to enhance wages and benefits to recruit and retain nurses and other medical support personnel or to hire moreexpensive temporary or contract personnel. As a result, our labor costs could increase. We also depend on the available labor pool of semi-skilled andunskilled employees in each of the markets in which we operate. If there is additional union organizing activity and to the extent a significant portion ofour employee base unionizes, our costs could increase materially. In addition, the states in which we operate could adopt mandatory nurse-staffing ratiosor could reduce mandatory nurse-staffing ratios already in place. State-mandated nurse-staffing ratios could significantly affect labor costs, and have anadverse impact on revenues if we are required to limit patient admissions in order to meet the required ratios.
Information about our Executive Officers
As of February 1, 2020, our executive officers were as follows:
Name Age Position(s)Samuel N. Hazen 59 Chief Executive Officer and DirectorJennifer L. Berres 49 Senior Vice President and Chief Human Resource OfficerPhillip G. Billington 52 Senior Vice President — Internal Audit ServicesJeff E. Cohen 48 Senior Vice President — Government RelationsMichael S. Cuffe, M.D. 54 President — Physician Services GroupJane D. Englebright 62 Senior Vice President and Chief Nursing OfficerJon M. Foster 58 President — American GroupCharles J. Hall 66 President — National GroupA. Bruce Moore, Jr. 59 President — Service Line and Operations IntegrationSandra L. Morgan 57 Senior Vice President — Provider RelationsJ. William B. Morrow 49 Senior Vice President — Finance and TreasurerP. Martin Paslick 60 Senior Vice President and Chief Information OfficerJonathan B. Perlin, M.D. 58 President — Clinical Services Group and Chief Medical OfficerDeborah M. Reiner 58 Senior Vice President — Marketing and CommunicationsWilliam B. Rutherford 56 Executive Vice President and Chief Financial OfficerJoseph A. Sowell, III 63 Senior Vice President and Chief Development OfficerKathryn A. Torres 56 Senior Vice President — Payer Contracting and AlignmentRobert A. Waterman 66 Senior Vice President and General CounselKathleen M. Whalen 56 Senior Vice President and Chief Ethics and Compliance OfficerChristopher F. Wyatt 42 Senior Vice President and Controller
Samuel N. Hazen was appointed Chief Executive Officer effective January 1, 2019 and was appointed as a director in September 2018. FromNovember 2016 through December 2018, Mr. Hazen served as the Company’s President and Chief Operating Officer. Prior to that, he served as ChiefOperating Officer of the Company from
27
247

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 28/137
Table of Contents
January 2015 to November 2016 and as President — Operations of the Company from 2011 to 2015. He also served as President — Western Groupfrom 2001 to 2011 and as Chief Financial Officer — Western Group of the Company from 1995 to 2001. Prior to that time, Mr. Hazen served in varioushospital, regional and division Chief Financial Officer positions with the Company, Humana Inc. and Galen Health Care, Inc.
Jennifer L. Berres was appointed Senior Vice President and Chief Human Resource Officer effective November 1, 2019. Ms. Berres joined HCAin 1993 and served in various capacities, including as Vice President — Human Resources from April 2013 through October 2019.
Phillip G. Billington was appointed Senior Vice President — Internal Audit Services effective January 1, 2019. Mr. Billington previously servedas Vice President — Corporate Internal Audit from June 2005 to December 2018. Prior to joining HCA, Mr. Billington worked as a managing directorfor FTI Consulting, Inc., a director for KPMG LLP and was a senior manager at Arthur Andersen LLP.
Jeff E. Cohen was appointed Senior Vice President — Government Relations effective October 1, 2019. Prior to joining HCA, Mr. Cohen spent 20years with the Federation of American Hospitals, most recently as Executive Vice President of Public Affairs, where he managed all advocacy, publicaffairs and communications for the association.
Dr. Michael S. Cuffe has served as President — Physician Services Group since October 2011. From October 2011 to January 2015, Dr. Cuffe alsoserved as a Vice President of the Company. Prior to that time, Dr. Cuffe served Duke University Health System as Vice President for AmbulatoryServices and Chief Medical Officer from March 2011 to October 2011 and Vice President Medical Affairs from June 2005 to March 2011. He alsoserved Duke University School of Medicine as Vice Dean for Medical Affairs from June 2008 to March 2011, Deputy Chair of the Department ofMedicine from August 2009 to August 2010 and Associate Professor of Medicine from March 2005 to October 2011. Prior that time, Dr. Cuffe served invarious leadership roles with the Duke Clinical Research Institute, Duke University Medical Center and Duke University School of Medicine.
Dr. Jane D. Englebright was appointed Senior Vice President and Chief Nursing Officer in January 2015. Dr. Englebright previously served asVice President and Chief Nursing Officer from 2007 to January 2015. Dr. Englebright joined HCA in 1992 as a critical care nurse at Lewisville MedicalCenter in Texas and became Chief Nursing Officer of HCA’s San Antonio Community Hospital in 1996. Dr. Englebright currently serves on The JointCommission’s Board of Commissioners.
Jon M. Foster was appointed President — American Group in January 2013. Prior to that, Mr. Foster served as President — Southwest Groupfrom February 2011 to January 2013 and as Division President for the Central and West Texas Division from January 2006 to February 2011. Mr. Fosterjoined HCA in March 2001 as President and CEO of St. David’s HealthCare in Austin, Texas and served in that position until February 2011. Prior tojoining the Company, Mr. Foster served in various executive capacities within the Baptist Health System in Knoxville, Tennessee and The MethodistHospital System in Houston, Texas.
Charles J. Hall was appointed President — National Group in February 2011. Prior to that, Mr. Hall served as President — Eastern Group fromOctober 2006 to February 2011. Mr. Hall had previously served the Company as President — North Florida Division from April 2003 until October2006, as President of the East Florida Division from January 1999 until April 2003, as a Market President in the East Florida Division from January1998 until December 1998, as President of the South Florida Division from February 1996 until December 1997, and as President of the SouthwestFlorida Division from October 1994 until February 1996, and in various other capacities since 1987.
A. Bruce Moore, Jr. was appointed President — Service Line and Operations Integration in February 2011. Prior to that, Mr. Moore had served asPresident — Outpatient Services Group since January 2006. Mr. Moore served as Senior Vice President and as Chief Operating Officer — OutpatientServices Group from July 2004 to
28
248

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 29/137
Table of Contents
January 2006 and as Senior Vice President — Operations Administration from July 1999 until July 2004. Mr. Moore served as Vice President —Operations Administration of the Company from September 1997 to July 1999, as Vice President — Benefits from October 1996 to September 1997,and as Vice President — Compensation from March 1995 until October 1996.
Sandra L. Morgan was appointed Senior Vice President — Provider Relations in January 2015. Prior to that time, she served as Vice President —National Sales from April 2008 to January 2015. From 2000 to 2008, Ms. Morgan served in various capacities with Pfizer Inc., including Vice Presidentof Managed Care for the Customer Business Unit from 2005 to 2008.
J. William B. Morrow was appointed Senior Vice President — Finance and Treasurer in February 2017. Mr. Morrow served as Vice President —Finance and Treasurer from July 2016 through January 2017. From 2011 to 2016, Mr. Morrow served the Company as Vice President —Development/Special Assets. Mr. Morrow served as a partner in the law firm of Waller Lansden Dortch & Davis from 2006 to October 2011. Prior tobecoming a partner, Mr. Morrow was an associate at Waller Lansden Dortch & Davis and at Cleary Gottlieb Steen & Hamilton.
P. Martin Paslick was appointed Senior Vice President and Chief Information Officer in June 2012. Prior to that time, he served as Vice Presidentand Chief Operating Officer of Information Technology & Services from March 2010 to May 2012 and Vice President — Information Technology &Services Field Operations from September 2006 to February 2010. From January 1998 to September 2006, he served in various Vice President roles inthe Company’s Information Technology & Services department. Mr. Paslick joined the Company in 1985.
Dr. Jonathan B. Perlin was appointed President — Clinical Services Group and Chief Medical Officer in November 2007. Dr. Perlin had served asChief Medical Officer and Senior Vice President — Quality of the Company from August 2006 to November 2007. Prior to joining the Company,Dr. Perlin served as Under Secretary for Health in the U.S. Department of Veterans Affairs since April 2004. Dr. Perlin joined the Veterans HealthAdministration in November 1999 where he served in various capacities, including as Deputy Under Secretary for Health from July 2002 to April 2004,and as Chief Quality and Performance Officer from November 1999 to September 2002. He also served as Senior Advisor to the Acting Secretary of theU.S. Department of Veterans Affairs from July 2014 to September 2014 and as Chairman for the American Hospital Association in 2015.
Deborah M. Reiner was appointed Senior Vice President — Marketing and Communications in October 2017. Prior to that time, she served asVice President of Marketing and Customer Relationship Management from August 2017 to October 2017 and Vice President of Customer RelationshipManagement from January 2012 to August 2017. Ms. Reiner joined the Company in 2000 and served in various roles with the Company’s MountainDivision from 2000 to 2012.
William B. Rutherford has served as Executive Vice President and Chief Financial Officer since January 2014. Mr. Rutherford previously servedas Chief Operating Officer of the Company’s Clinical and Physician Services Group from January 2011 to January 2014 and Chief Financial Officer ofthe Company’s Outpatient Services Group from November 2008 to January 2011. Prior to that time, Mr. Rutherford was employed by SummitConsulting Group of Tennessee from July 2007 to November 2008 and was Chief Operating Officer of Psychiatric Solutions, Inc. from March 2006 toJune 2007. Mr. Rutherford also previously served in various positions with the Company from 1986 to 2005, including Chief Financial Officer of whatwas then the Company’s Eastern Group, Director of Internal Audit and Director of Operations Support.
Joseph A. Sowell, III was appointed as Senior Vice President and Chief Development Officer in December 2009. From 1987 to 1996 and againfrom 1999 to 2009, Mr. Sowell was a partner at the law firm of Waller Lansden Dortch & Davis where he specialized in the areas of health care law,mergers and acquisitions, joint
29
249

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 30/137
Table of Contents
ventures, private equity financing, tax law and general corporate law. He also co-managed the firm’s corporate and commercial transactions practice.From 1996 to 1999, Mr. Sowell served as the head of development, and later as the Chief Operating Officer of Arcon Healthcare.
Kathryn A. Torres was appointed Senior Vice President — Payer Contracting and Alignment (formerly Senior Vice President — Employer andPayer Engagement) in July 2016. Ms. Torres joined HCA in 1993 and served in various capacities, including as Vice President of Employer and PayerEngagement and Vice President — Strategy.
Robert A. Waterman has served as Senior Vice President and General Counsel since November 1997. Mr. Waterman served as a partner in the lawfirm of Latham & Watkins from September 1993 to October 1997; he was Chair of the firm’s health care group during 1997.
Kathleen M. Whalen was appointed Senior Vice President and Chief Ethics and Compliance Officer effective January 1, 2019. Prior to that time,Ms. Whalen served as Vice President — Ethics and Compliance from August 2013 through December 2018 and Assistant Vice President — Ethics andCompliance Program Development from March 2000 through July 2013. Prior to joining HCA in January 1998, Ms. Whalen served as AssociateCounsel to President Clinton with responsibility for the White House’s ethics program. She began her government service in the ethics division of theGeneral Counsel’s Office at the U.S. Commerce Department. Prior to that, she practiced labor and employment law in Dayton, Ohio.
Christopher F. Wyatt was appointed Senior Vice President and Controller in April 2016. Prior to that time, Mr. Wyatt served the Company as VicePresident and Chief Financial Officer — IT&S from January 2013 to April 2016 and Chief Financial Officer — Clinical Services Group from October2010 until January 2013. From 2000 to 2010, Mr. Wyatt served in various capacities with Ernst & Young LLP.
Item 1A. Risk Factors
If any of the events discussed in the following risk factors were to occur, our business, financial position, results of operations, cash flows orprospects could be materially, adversely affected. Additional risks and uncertainties not presently known, or currently deemed immaterial, may alsoconstrain our business and operations.
Our substantial leverage could adversely affect our ability to raise additional capital to fund our operations, limit our ability to react to changes inthe economy or our industry, expose us to interest rate risk to the extent of our variable rate debt and prevent us from meeting our obligations.
We are highly leveraged. As of December 31, 2019, our total indebtedness was $33.722 billion. As of December 31, 2019, we had availability of$1.967 billion under our senior secured revolving credit facility and $1.270 million under our asset-based revolving credit facility, after giving effect toletters of credit and borrowing base limitations. Our high degree of leverage could have important consequences, including:
• increasing our vulnerability to downturns or adverse changes in general economic, industry or competitive conditions and adverse changesin government regulations;
• requiring a substantial portion of cash flows from operations to be dedicated to the payment of principal and interest on our indebtedness,therefore reducing our ability to use our cash flows to fund our operations, capital expenditures and future business opportunities;
• exposing us to the risk of increased interest rates to the extent that our existing unhedged borrowings are at variable rates of interest or weseek to refinance our debt in a rising rate environment;
• limiting our ability to make strategic acquisitions or causing us to make nonstrategic divestitures;
30
250

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 31/137
Table of Contents
• limiting our ability to obtain additional financing for working capital, capital expenditures, share repurchases, dividends, product or serviceline development, debt service requirements, acquisitions and general corporate or other purposes; and
• limiting our ability to adjust to changing market conditions and placing us at a competitive disadvantage compared to our competitors whoare less highly leveraged.
We and our subsidiaries have the ability to incur additional indebtedness in the future, subject to the restrictions contained in our senior securedcredit facilities and the indentures governing our outstanding notes. If new indebtedness is added to our current debt levels, interest rates and the relatedrisks that we now face could intensify.
We may not be able to generate sufficient cash to service all of our indebtedness and may not be able to refinance our indebtedness on favorableterms. If we are unable to do so, we may be forced to take other actions to satisfy our obligations under our indebtedness, which may not besuccessful.
Our ability to make scheduled payments on or to refinance our debt obligations depends on our financial condition and operating performance,which are subject to prevailing economic and competitive conditions and to certain financial, business and other factors beyond our control. We cannotassure you we will maintain a level of cash flows from operating activities sufficient to permit us to pay the principal, premium, if any, and interest onour indebtedness.
In addition, we conduct our operations through our subsidiaries. Accordingly, repayment of our indebtedness is dependent on the generation ofcash flows by our subsidiaries and their ability to make such cash available to us by dividend, debt repayment or otherwise. Our subsidiaries may not beable to, or may not be permitted to, make distributions to enable us to make payments in respect of our indebtedness. Each subsidiary is a distinct legalentity, and, under certain circumstances, legal and contractual restrictions may limit our ability to obtain cash from our subsidiaries.
We may find it necessary or prudent to refinance our outstanding indebtedness, the terms of which may not be favorable to us. Our ability torefinance our indebtedness on favorable terms, or at all, is directly affected by the then current global economic and financial conditions which affect theavailability of debt financing and the rates at which such financing is available. In addition, our ability to incur secured indebtedness (which wouldgenerally enable us to achieve better pricing than the incurrence of unsecured indebtedness) depends in part on the value of our assets, which depends, inturn, on the strength of our cash flows and results of operations, and on economic and market conditions and other factors.
If our cash flows and capital resources are insufficient to fund our debt service obligations or we are unable to refinance our indebtedness, we maybe forced to reduce or delay investments and capital expenditures, or to sell assets, seek additional capital or restructure our indebtedness. Thesealternative measures may not be successful and may not permit us to meet our scheduled debt service obligations. If our operating results and availablecash are insufficient to meet our debt service obligations, we could face substantial liquidity problems and might be required to dispose of materialassets or operations to meet our debt service and other obligations. We may not be able to consummate those dispositions, or the proceeds from thedispositions may not be adequate to meet any debt service obligations then due.
Our debt agreements contain restrictions that limit our flexibility in operating our business.
Our senior secured credit facilities and, to a lesser extent, the indentures governing our outstanding notes contain various covenants that limit ourability to engage in specified types of transactions. These covenants limit our and certain of our subsidiaries’ ability to, among other things:
• incur additional indebtedness or issue certain preferred shares;
31
251

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 32/137
Table of Contents
• pay dividends on, repurchase or make distributions in respect of our capital stock or make other restricted payments;
• make certain investments;
• sell or transfer assets;
• create liens;
• consolidate, merge, sell or otherwise dispose of all or substantially all of our assets; and
• enter into certain transactions with our affiliates.
Under our asset-based revolving credit facility, borrowing availability is subject to a borrowing base of 85% of eligible accounts receivable lesscustomary reserves, with any reduction in the borrowing base commensurately reducing our ability to access this facility as a source of liquidity. Inaddition, under the asset-based revolving credit facility, when (and for as long as) the combined availability under our asset-based revolving creditfacility and our senior secured revolving credit facility is less than a specified amount for a certain period of time or, if a payment or bankruptcy event ofdefault has occurred and is continuing, funds deposited into any of our depository accounts will be transferred on a daily basis into a blocked accountwith the administrative agent and applied to prepay loans under the asset-based revolving credit facility and to collateralize letters of credit issuedthereunder.
Under our senior secured credit facilities, we are required to satisfy and maintain specified financial ratios. Our ability to meet those financialratios may be affected by events beyond our control, and there can be no assurance we will continue to meet those ratios. A breach of any of thesecovenants could result in a default under both the cash flow credit facility and the asset-based revolving credit facility. Upon the occurrence of an eventof default under these senior secured credit facilities, the lenders thereunder could elect to declare all amounts outstanding under the senior securedcredit facilities to be immediately due and payable and terminate all commitments to extend further credit, which would also result in an event of defaultunder a significant portion of our other outstanding indebtedness. If we were unable to repay those amounts, the lenders under the senior secured creditfacilities could proceed against the collateral granted to them to secure such indebtedness. We have pledged a significant portion of our assets under oursenior secured credit facilities and that collateral is also pledged as collateral under our first lien notes. If any of the lenders under the senior securedcredit facilities accelerate the repayment of borrowings, there can be no assurance there will be sufficient assets to repay the senior secured creditfacilities, the first lien notes and our other indebtedness.
Our results of operations may be adversely affected by health care reform efforts, including court challenges to, and efforts to repeal, replace orotherwise significantly change the Affordable Care Act. We are unable to predict what, if any, and when such changes will be made in the future.
In recent years, the U.S. Congress and certain state legislatures have passed a large number of laws and regulations intended to effect majorchange within the U.S. health care system, including the Affordable Care Act. The Affordable Care Act affects how health care services are covered,delivered and reimbursed through expanded health insurance coverage, reduced growth in Medicare program spending, reductions in Medicare andMedicaid DSH payments, and the establishment of programs that tie reimbursement to quality and integration. However, there is uncertainty regardingthe future of the Affordable Care Act. The law has been subject to legislative and regulatory changes and court challenges. The presidentialadministration and a number of members of Congress have stated their intent to repeal or make additional significant changes to the Affordable CareAct, its implementation or interpretation. For example, final rules issued in 2018 expand the availability of association health plans and allow the sale ofshort-term, limited-duration health plans, neither of which are required to cover all of the essential health benefits mandated by the Affordable Care Act.Further, the President of the United States signed an executive order that directs agencies to minimize “economic and regulatory burdens” of theAffordable Care Act, which may result in additional changes in how the law is implemented.
32
252

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 33/137
Table of Contents
Effective January 1, 2019, the penalty associated with the individual mandate to maintain health insurance was eliminated. As a result of this change, inDecember 2018, the United States District Court for the North District of Texas found the individual mandate to be unconstitutional and determined thatthe rest of the Affordable Care Act was, therefore, invalid. In December 2019, the Fifth Circuit Court of Appeals upheld this decision with respect to theindividual mandate, but remanded for further consideration of how this affects the rest of the law. Pending the appeals process, the law remains in place.The elimination of the individual mandate penalty and other changes may impact the number of individuals that elect to obtain public or private healthinsurance or the scope of such coverage, if purchased, either of which may have an adverse effect on our business.
There is uncertainty regarding whether, when, and how the Affordable Care Act may be further changed, the ultimate outcome of court challengesand how the law will be interpreted and implemented. Changes by Congress or government agencies could eliminate or alter provisions beneficial to us,while leaving in place provisions reducing our reimbursement or otherwise negatively impacting our business. There is also uncertainty regardingwhether, when, and what other health reform initiatives will be adopted and the impact of such efforts on providers and other health care industryparticipants. Further, the outcome of the 2020 federal election and its potential impact on health reform efforts is unknown. Some presidential candidatesand members of Congress have proposed measures that would expand government-sponsored coverage, including single-payer proposals (often referredto as “Medicare for All”), and some states are considering similar measures. CMS has indicated that it intends to increase flexibility in state Medicaidprograms, including by expanding the scope of waivers under which states may implement Medicaid expansion provisions, impose different eligibilityor enrollment restrictions, or otherwise implement programs that vary from federal standards. CMS administrators have also signaled interest inchanging Medicaid payment models. Other health reform initiatives and proposals, such as those addressing out-of-network charges, may impact prices,our relationships with patients and payers, and our competitive position. Other industry participants, such as private payers and large employer groupsand their affiliates, may also introduce financial or delivery system reforms. We are unable to predict the nature and success of such initiatives. Healthcare reform initiatives, including changes to or repeal or invalidation of the Affordable Care Act, may have an adverse effect on our business, results ofoperations, cash flow, capital resources, and liquidity.
Changes in government health care programs may adversely affect our revenues.
A significant portion of our patient volume is derived from government health care programs, principally Medicare and Medicaid. Specifically, wederived 41.5% of our revenues from the Medicare and Medicaid programs in 2019. Changes in government health care programs, including Medicaidwaiver programs, may reduce the reimbursement we receive and could adversely affect our business and results of operations. The Affordable Care Acthas made significant changes to Medicare and Medicaid, and future health reform efforts or further efforts to repeal or significantly change theAffordable Care Act may impact these programs.
In recent years, legislative and regulatory changes have resulted in limitations on and, in some cases, reductions in levels of payments to healthcare providers for certain services under the Medicare program. Congress has established automatic spending reductions that extend through 2029.However, the percentage reduction for Medicare may not be more than 2% for a fiscal year, with a uniform percentage reduction across all Medicareprograms. We are unable to predict what other deficit reduction initiatives may be proposed by Congress. These reductions are in addition to reductionsmandated by the Affordable Care Act and other laws. Further, from time to time, CMS revises the reimbursement systems used to reimburse health careproviders, including changes to the MS-DRG system and other payment systems, which may result in reduced Medicare payments. For example, undera site neutrality policy, clinic visit services provided by off-campus provider-based departments that were formerly paid under the outpatient PPS arenow paid under the Physician Fee Schedule, subject to certain exceptions that are being phased out through calendar years 2019 and 2020. Although afederal judge invalidated the expansion of the policy for calendar year 2019, in a decision that CMS is appealing, CMS issued a final rule implementingyear two of the policy phase-in for 2020. CMS is also considering proposals to reduce drug costs and has reduced Medicare payment rates under theoutpatient PPS for
33
253

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 34/137
Table of Contents
most drugs obtained at 340B discounted rates, although the final rules implementing the 340B reductions are the subject of ongoing court challenges.CMS may implement changes to how items or services are reimbursed that result in payment reductions for other services.
Because most states must operate with balanced budgets and because the Medicaid program is often a state’s largest program, some states haveenacted or may consider enacting legislation designed to reduce their Medicaid expenditures. Further, many states have also adopted, or are considering,legislation designed to reduce coverage, enroll Medicaid recipients in managed care programs, dis-enroll Medicaid recipients who fail to meet workrequirements and/or impose additional taxes on hospitals to help finance or expand the states’ Medicaid systems. Periods of economic weakness mayincrease the budgetary pressures on many states, and these budgetary pressures may result in decreased spending, or decreased spending growth, forMedicaid programs and the Children’s Health Insurance Program in many states. Some states that provide Medicaid supplemental payments arereviewing these programs or have filed waiver requests with CMS to replace these programs, and CMS has performed and continues to performcompliance reviews of some states’ programs and is considering changes to the requirements for such programs, which could result in Medicaidsupplemental payments being reduced or eliminated. Further, legislation and administrative actions at the federal level may significantly alter thefunding for, or structure of, the Medicaid program. For example, from time to time, Congress considers proposals to restructure the Medicaid program toinvolve block grants that would be administered by the states. CMS has announced its intent to introduce additional flexibilities for Medicaid programoperation, including block grants and increased use of value-based care models.
In some cases, private third-party payers rely on all or portions of Medicare payment systems to determine payment rates. Changes to governmenthealth care programs that reduce payments under these programs may negatively impact payments from private third-party payers.
Current or future health care reform and deficit reduction efforts, changes in laws or regulations regarding government health care programs, otherchanges in the administration of government health care programs and changes by private third-party payers in response to health care reform and otherchanges to government health care programs could have a material, adverse effect on our financial position and results of operations.
Our hospitals face competition for staffing, which may increase labor costs.
Our operations are dependent on the efforts, abilities and experience of our management and medical support personnel, such as nurses,pharmacists and lab technicians, as well as our physicians. We compete with other health care providers in recruiting and retaining qualifiedmanagement and support personnel responsible for the daily operations of each of our hospitals, including nurses and other nonphysician health careprofessionals. In some markets, the availability of nurses and other medical support personnel has been a significant operating issue to health careproviders. We may be required to continue to enhance wages and benefits to recruit and retain nurses and other medical support personnel or to hiremore expensive temporary or contract personnel. As a result, our labor costs could increase. We also depend on the available labor pool of semi-skilledand unskilled employees in each of the markets in which we operate. If there is additional union organizing activity and to the extent a significantportion of our employee base unionizes, it is possible our labor costs could increase materially. When negotiating collective bargaining agreements withunions, whether such agreements are renewals or first contracts, there is the possibility that strikes could occur during the negotiation process, and ourcontinued operation during any strikes could increase our labor costs. In addition, the states in which we operate could adopt mandatory nurse-staffingratios or could reduce mandatory nurse staffing ratios already in place. State-mandated nurse-staffing ratios could significantly affect labor costs andhave an adverse impact on revenues if we are required to limit admissions in order to meet the required ratios. If our labor costs increase, we may not beable to offset these increased costs as a significant percentage of our revenues consists of fixed, prospective payments. Our failure to recruit and retainqualified management, nurses and other medical support personnel, or to control labor costs, could have a material, adverse effect on our results ofoperations.
34
254

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 35/137
Table of Contents
We may be unable to attract, hire, and retain a highly qualified and diverse workforce, including key management.
The talents and efforts of our employees, particularly our key management, are vital to our success. Our management team has significant industryexperience and would be difficult to replace. In addition, institutional knowledge may be lost in any potential managerial transition. We may be unableto retain them or to attract other highly qualified employees, particularly if we do not offer employment terms that are competitive with the rest of thelabor market. Failure to attract, hire, develop, motivate, and retain highly qualified and diverse employee talent, or failure to develop and implement anadequate succession plan for the management team, could disrupt our operations and adversely affect our business and our future success.
Our performance depends on our ability to recruit and retain quality physicians.
The success of our hospitals depends in part on the number and quality of the physicians on the medical staffs of our hospitals, the admitting andutilization practices of those physicians, maintaining good relations with those physicians and controlling costs related to the employment of physicians.Although we employ some physicians, physicians are often not employees of the hospitals at which they practice, and, in many of the markets we serve,most physicians have admitting privileges at other hospitals in addition to our hospitals. We continue to face increasing competition to recruitphysicians. Such physicians may terminate their affiliation with our hospitals at any time. We may face increased challenges in this area as the physicianpopulation reaches retirement age, especially if there is a shortage of physicians willing and able to provide comparable services. If we are unable toprovide adequate support personnel or technologically advanced equipment and hospital facilities that meet the needs of those physicians and theirpatients, they may be discouraged from referring patients to our facilities, admissions may decrease and our operating performance may decline.
Our hospitals face competition for patients from other hospitals and health care providers.
The health care business is highly competitive, and competition among hospitals and other health care providers for patients has intensified inrecent years. Generally, other hospitals in the communities we serve provide services similar to those offered by our hospitals. CMS publicizes on itsHospital Compare website performance data related to quality measures and data on patient satisfaction surveys that hospitals submit in connection withtheir Medicare reimbursement. The Hospital Compare website provides an overall rating that synthesizes various quality measures into a single starrating for each hospital. Federal law provides for the future expansion of the number of quality measures that must be reported. Further, hospitals arecurrently required by law to publish online a list of their standard charges for items and services. A CMS final rule implements expanded transparencyrequirements beginning in 2021, but these additional requirements are the subject of ongoing court challenges. If any of our hospitals achieve poorresults (or results that are lower than our competitors) on quality measures or on patient satisfaction surveys or if our standard charges are higher or areperceived to be higher than our competitors, our competitive position could be negatively affected.
The number of freestanding specialty hospitals, surgery centers, emergency departments, urgent care centers and diagnostic and imaging centers inthe geographic areas in which we operate has increased. Many individuals are seeking a broader range of services at outpatient facilities as a result of thegrowing availability of stand-alone outpatient health care facilities, the increase in payer reimbursement policies that restrict inpatient coverage and theincrease in the services that can be provided on an outpatient basis, including high margin services. Consequently, most of our hospitals operate in ahighly competitive environment, which may put pressure on our pricing, ability to contract with third-party payers and the Company’s strategy forvolume growth. Some of the facilities that compete with our hospitals are physician-owned or are owned by governmental agencies or not-for-profitcorporations supported by endowments, charitable contributions and/or tax revenues and can finance capital expenditures and operations on atax-exempt basis. Recent consolidations of not-for-profit hospital entities may intensify this competitive pressure. There is also increasing consolidationin the third-party payer industry, including vertical integration efforts among third-party payers and health care providers, and
35
255

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 36/137
Table of Contents
increasing efforts by payers to influence or direct the patient’s choice of provider by the use of narrow networks or other strategies. Health care industryparticipants are increasingly implementing physician alignment strategies, such as employing physicians, acquiring physician practice groups andparticipating in ACOs or other clinical integration models. Other industry participants, such as large employer groups and their affiliates, may intensifycompetitive pressure and affect the industry in ways that are difficult to predict.
Our hospitals compete with specialty hospitals and with both our own and unaffiliated freestanding ASCs and other outpatient providers formarket share in certain high margin services and for quality physicians and personnel. If ASCs and other outpatient providers are better able to competein this environment than our hospitals, our hospitals may experience a decline in patient volume, and we may experience a decrease in margin, even ifthose patients use our providers. In states that do not require a CON or other type of approval for the purchase, construction or expansion of health carefacilities or services, competition in the form of new services, facilities and capital spending is more prevalent. Some states that have historicallyimposed CON or similar prior approval requirements have removed or are considering removing these requirements, which may reduce barriers to entryand increase competition in our service areas. If our competitors are better able to attract patients, make capital expenditures and maintain modern andtechnologically upgraded facilities and equipment, recruit physicians, expand services or obtain favorable third-party payer contracts at their facilitiesthan our hospitals and other providers, we may experience an overall decline in patient volume. See Item 1, “Business — Competition.”
A deterioration in the collectability of uninsured and patient due accounts could adversely affect our results of operations.
The primary collection risks for our accounts receivable relate to the uninsured patient accounts and patient accounts for which the primary third-party payer has paid the amounts covered by the applicable agreement, but patient responsibility amounts (exclusions, deductibles and copayments)remain outstanding. Medicare reimburses hospitals for 65% of eligible Medicare bad debts. To be eligible for reimbursement, the amounts claimed mustmeet certain criteria, including that the debt is related to unpaid deductible or coinsurance amounts and that the hospital first attempted to collect the feesfrom the Medicare beneficiary.
The estimates for implicit price concessions are based upon management’s assessment of historical write-offs and expected net collections,business and economic conditions, trends in federal and state governmental and private employer health care coverage, the rate of growth in uninsuredpatient admissions and other collection indicators. At December 31, 2019, estimated implicit price concessions of $6.953 billion had been recorded toadjust our revenues and accounts receivable to the estimated amounts we expect to collect. The estimated cost of total uncompensated care increasedfrom $3.021 billion for 2017 to $3.318 billion for 2018 and to $3.733 billion for 2019.
Any increase in the amount or deterioration in the collectability of uninsured accounts receivable will adversely affect our cash flows and resultsof operations. Our facilities may experience growth in total uncompensated care as a result of a number of factors, including conditions impacting theoverall economy and high unemployment. Effective January 2019, Congress eliminated the financial penalty associated with the Affordable Care Act’sindividual mandate. Further, final rules issued in 2018 expand the availability of association health plans and allow the sale of short-term, limited-duration health plans, neither of which are required to cover all of the essential health benefits mandated by the Affordable Care Act. These changesmay impact the number of individuals that elect to obtain public or private health insurance or the scope of such coverage, if purchased. The presidentialadministration and a number of members of Congress continue to make other efforts to repeal or significantly change the Affordable Care Act, and thelaw remains subject to court challenges. See Item 1A, “Risk Factors — Our results of operations may be adversely affected by health care reformefforts, including court challenges to, and efforts to repeal, replace or otherwise significantly change the Affordable Care Act. We are unable to predictwhat, if any, and when such changes will be made in the future.”
36
256

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 37/137
Table of Contents
We provide uninsured discounts and charity care for individuals, including for those residing in states that choose not to implement the Medicaidexpansion or that modify the terms of the program, for undocumented aliens who are not permitted to enroll in an Exchange or government health careprograms and for certain others who may not have insurance. Some patients may choose to enroll in lower cost Medicaid plans or other health insuranceplans with lower reimbursement levels. We may also be adversely affected by the growth in patient responsibility accounts as a result of increases in theadoption of health plan structures that shift greater responsibility for care to individuals through greater exclusions and copayment and deductibleamounts.
We may not be reimbursed for the cost of expensive, new technology.
As healthcare technology continues to advance, the price of purchasing such new technology has significantly increased for providers. Somepayers have not adapted their payment systems to adequately cover the cost of these technologies for providers and patients. If payers do not adequatelyreimburse us for these new technologies, we may be unable to acquire such technologies or we may nevertheless determine to acquire or utilize thesetechnologies in order to treat our patients. In either case, our results of operations and financial position could be adversely affected.
A cybersecurity incident could result in the compromise of our facilities, confidential data or critical data systems. A cybersecurity incident couldalso give rise to potential harm to patients; remediation and other expenses; and exposing us to liability under HIPAA, consumer protection laws,common law theories or other laws. Such incidents could subject us to litigation and foreign, federal and state governmental inquiries, damage ourreputation, and otherwise be disruptive to our business.
We, directly and through third-party vendors, collect and store on our networks and devices sensitive information, including intellectual property,proprietary business information and personally identifiable information of our patients and employees. We have made significant investments intechnology to adopt and meaningfully use EHR and in the use of medical devices that store sensitive data and are integral to the provision of patientcare. In addition, medical devices manufactured by third parties that are used within our facilities are increasingly connected to the internet, hospitalnetworks and other medical devices. The secure maintenance of this information and technology is critical to our business operations. We haveimplemented multiple layers of security measures to protect the confidentiality, integrity and availability of this data and the systems and devices thatstore and transmit such data. We utilize current security technologies, and our defenses are monitored and routinely tested internally and by externalparties. Despite these efforts, threats from malicious persons and groups, new vulnerabilities and advanced new attacks against information systems anddevices against us or our third-party vendors create risk of cybersecurity incidents, including ransomware, malware and phishing incidents. We areregularly the target of attempted cybersecurity and other threats that could have a security impact. There can be no assurance that we or our third-partyvendors will not be subject to cybersecurity incidents that bypass our security measures, impact the integrity, availability or privacy of personal healthinformation or other data subject to privacy laws or disrupt our information systems, devices or business, including our ability to provide various healthcare services. As a result, cybersecurity, physical security and the continued development and enhancement of our controls, processes and practicesdesigned to protect our facilities, information systems and data from attack, damage or unauthorized access remain a priority for us. As cyber threatscontinue to evolve, we may be required to expend significant additional resources to continue to modify or enhance our protective measures or toinvestigate and remediate any cybersecurity vulnerabilities or incidents. The occurrence of any of these events could result in (i) harm to patients;(ii) business interruptions and delays; (iii) the loss, misappropriation, corruption or unauthorized access of data; (iv) litigation and potential liabilityunder privacy, security, breach notification and consumer protection laws, common law theories or other applicable laws; (v) reputational damage and(vi) foreign, federal and state governmental inquiries, any of which could have a material, adverse effect on our financial position and results ofoperations and harm our business reputation.
37
257

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 38/137
Table of Contents
Our operations could be impaired by a failure of our information systems.
The performance of our information systems is critical to our business operations. In addition to our shared services initiatives, our informationsystems are essential to a number of critical areas of our operations, including:
• accounting and financial reporting;
• billing and collecting accounts;
• coding and compliance;
• clinical systems and medical devices;
• medical records and document storage;
• inventory management;
• negotiating, pricing and administering managed care contracts and supply contracts; and
• monitoring quality of care and collecting data on quality measures necessary for full Medicare payment updates.
Information systems may be vulnerable to damage from a variety of sources, including telecommunications or network failures, human acts andnatural disasters. We have taken precautionary measures to prevent unanticipated problems that could affect our information systems. Nevertheless, weor our third-party vendors that we rely upon may experience system failures. The occurrence of any system failure could result in interruptions, delays,the loss or corruption of data and cessations or interruptions in the availability of systems, all of which could have a material, adverse effect on ourfinancial position and results of operations and harm our business reputation.
If our volume of patients with private health insurance coverage declines or we are unable to retain and negotiate favorable contracts with privatethird-party payers, including managed care plans, our revenues may be reduced.
Private third-party payers, including HMOs, PPOs and other managed care plans, typically reimburse health care providers at a higher rate thanMedicare, Medicaid or other government health care programs. Reimbursement rates are set forth by contract when our facilities are in-network, andpayers utilize plan structures to encourage or require the use of in-network providers. Revenues derived from private third-party payers (domestic only)accounted for 51.6%, 52.4% and 53.5% of our revenues for 2019, 2018 and 2017, respectively. As a result, our ability to maintain or increase patientvolumes covered by private third-party payers and to maintain and obtain favorable contracts with private third-party payers significantly affects therevenues and operating results of our facilities.
Private third-party payers, including managed care plans, continue to demand discounted fee structures, and the ongoing trend towardconsolidation among payers tends to increase their bargaining power over fee structures. Payers may utilize plan structures such as narrow networks andtiered networks that limit beneficiary provider choices or impose significantly higher cost sharing obligations when care is obtained from providers in adisfavored tier. Other health care providers may impact our ability to enter into managed care contracts or negotiate increases in our reimbursement andother favorable terms and conditions. For example, some of our competitors may negotiate exclusivity provisions with managed care plans or otherwiserestrict the ability of managed care plans to contract with us. In addition to increasing negotiating leverage of private third-party payers, alignmentefforts between third-party payers and health care providers may result in other competitive advantages, such as greater access to performance andpricing data. Our future success will depend, in part, on our ability to retain and renew our third-party payer contracts and enter into new contracts onterms favorable to us, which may be impacted by price transparency initiatives. Cost-reduction strategies by large employer groups
38
258

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 39/137
Table of Contents
and their affiliates, such as directly contracting with a limited number of providers, may also limit our ability to negotiate favorable terms in ourcontracts and otherwise intensify competitive pressure. It is not clear what impact, if any, future health reform efforts or the repeal of, or further changesto, the Affordable Care Act will have on our ability to negotiate reimbursement increases and participate in third-party payer networks on favorableterms. If we are unable to retain and negotiate favorable contracts with third-party payers or experience reductions in payment increases or amountsreceived from third-party payers, our revenues may be reduced.
If we fail to comply with extensive laws and government regulations, we could suffer penalties or be required to make significant changes to ouroperations.
The health care industry is required to comply with extensive and complex laws and regulations at the federal, state and local government levelsrelating to, among other things:
• billing and coding for services and properly handling overpayments;
• appropriateness and classification of level of care provided, including proper classification of inpatient admissions, observation services andoutpatient care;
• relationships with physicians and other referral sources and referral recipients;
• necessity and adequacy of medical care;
• quality of medical equipment and services;
• qualifications of medical and support personnel;
• confidentiality, maintenance, data breach, identity theft and security issues associated with health-related and personal information andmedical records;
• screening, stabilization and transfer of individuals who have emergency medical conditions;
• licensure, certification and enrollment with government programs;
• hospital rate or budget review;
• debt collection, limits on balance billing and billing for out of network services;
• communications with patients and consumers;
• preparing and filing of cost reports;
• operating policies and procedures;
• activities regarding competitors;
• addition of facilities and services; and
• environmental protection.
Among these laws are the federal Anti-kickback Statute, the federal Stark Law, the FCA and similar state laws. We have a variety of financialrelationships with physicians and others who either refer or influence the referral of patients to our hospitals, other health care facilities and employedphysicians or who are the recipients of referrals, and these laws govern those relationships. The OIG has enacted safe harbor regulations that outlinepractices deemed protected from prosecution under the Anti-kickback Statute. While we endeavor to comply with the applicable safe harbors, certain ofour current arrangements, including joint ventures and financial relationships with physicians and other referral sources and persons and entities towhich we refer patients, do not qualify for safe harbor protection. Failure to qualify for a safe harbor does not mean the arrangement necessarily violatesthe Anti-kickback Statute but may subject the arrangement to greater scrutiny. However, we cannot offer assurance that practices outside of a safe harborwill not be found to violate the Anti-kickback Statute. Allegations of violations of the Anti-kickback Statute may be brought under the federal CivilMonetary Penalty Law, which requires a lower burden of proof than other fraud and abuse laws, including the Anti-kickback Statute.
39
259

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 40/137
Table of Contents
Our financial relationships with referring physicians and their immediate family members must comply with the Stark Law by meeting anexception. We attempt to structure our relationships to meet an exception to the Stark Law, but the regulations implementing the exceptions are detailedand complex and are subject to continuing legal and regulatory change. Thus, we cannot provide assurance that every relationship complies fully withthe Stark Law. Unlike the Anti-kickback Statute, failure to meet an exception under the Stark Law results in a violation of the Stark Law, even if suchviolation is technical in nature.
Additionally, if we violate the Anti-kickback Statute or Stark Law, or if we improperly bill for our services, we may be found to violate the FCA,either under a suit brought by the government or by a private person under a qui tam, or “whistleblower,” suit. See Item 1, “Business — Regulation andOther Factors.”
We also operate health care facilities in the United Kingdom and have operations and commercial relationships with companies in other foreignjurisdictions and, as a result, are subject to certain U.S. and foreign laws applicable to businesses generally, including anti-corruption laws. The ForeignCorrupt Practices Act regulates U.S. companies in their dealings with foreign officials, prohibiting bribes and similar practices, and requires that theymaintain records that fairly and accurately reflect transactions and appropriate internal accounting controls. In addition, the United Kingdom BriberyAct has wide jurisdiction over certain activities that affect the United Kingdom.
A variety of state, national, foreign and international laws and regulations apply to the collection, use, retention, protection, security, disclosure,transfer and other processing of personal data. For example, the CCPA which affords consumers expanded privacy protections such as the right to knowwhat personal information is collected and how it is used, went into effect on January 1, 2020. California residents also have the right to request abusiness to delete their personal information unless it is necessary for the business to maintain for certain purposes. They have the right to know if theirpersonal information is being sold or shared and the right to opt-out of the sale or disclosure. Failure to comply with the CCPA may result in attorneygeneral enforcement action and damage to our reputation. The CCPA also provides for civil penalties for violations, as well as a private right of actionfor data breaches that may increase data breach litigation. The potential effects of this legislation are far-reaching and may require us to modify our dataprocessing practices and policies and to incur substantial costs and expenses to comply. The European Union’s General Data Protection Regulation (the“GDPR”) contains stricter privacy restrictions than laws and regulations in the United States and provides for significant fines in the event of violations.These administrative fines are based on a multi-factored approach. We expect that there will continue to be new laws, regulations and industry standardsconcerning privacy, data protection and information security proposed and enacted in various jurisdictions, which could impact our operations and causeus to incur substantial costs.
We send short message service, or SMS, text messages to patients. While we obtain consent from these individuals to send text messages, federalor state regulatory authorities or private litigants may claim that the notices and disclosures we provide, form of consents we obtain or our SMS textingpractices are not adequate or violate applicable law. In addition, we must ensure that our SMS texting practices comply with regulations and agencyguidance under the Telephone Consumer Protection Act (the “TCPA”), a federal statute that protects consumers from unwanted telephone calls, faxesand text messages. While we strive to adhere to strict policies and procedures that comply with the TCPA, the Federal Communications Commission, asthe agency that implements and enforces the TCPA, may disagree with our interpretation of the TCPA and subject us to penalties and otherconsequences for noncompliance. Determination by a court or regulatory agency that our SMS texting practices violate the TCPA could subject us tocivil penalties and could require us to change some portions of our business. Even an unsuccessful challenge by patients or regulatory authorities of ouractivities could result in adverse publicity and could require a costly response from and defense by us.
We engage in consumer debt collection and credit reporting for HCA-affiliated hospitals and certain non-affiliated hospitals. The federal Fair DebtCollection Practices Act, the Fair Credit Reporting Act and the TCPA restrict the methods that companies may use to contact and seek payment fromconsumer debtors
40
260

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 41/137
Table of Contents
regarding past due accounts and to report to consumer reporting agencies on the status of those accounts. Many states impose additional requirements ondebt collection and credit reporting practices, and some of those requirements may be more stringent than the federal requirements.
If we fail to comply with these or other applicable laws and regulations, which are subject to change, we could be subject to liabilities, includingcivil penalties, money damages, the loss of our licenses to operate one or more facilities, exclusion of one or more facilities from participation in theMedicare, Medicaid and other federal and state health care programs, civil lawsuits and criminal penalties. The costs of compliance with, and the otherburdens imposed by, these and other laws or regulatory actions may increase our operational costs, result in interruptions or delays in the availability ofsystems and/or result in a patient volume decline. We may also face audits or investigations by one or more domestic or foreign government agenciesrelating to our compliance with these regulations. An adverse outcome under any such investigation or audit could result in liability, result in adversepublicity, and adversely affect our business.
We do not always have the benefit of significant regulatory or judicial interpretation of these laws and regulations. In the future, differentinterpretations or enforcement of, or amendment to, these or other laws and regulations could subject our current or past practices to allegations ofimpropriety or illegality or could require us to make changes in our facilities, equipment, personnel, services, capital expenditure programs andoperating expenses. A determination that we have violated these or other laws, or the public announcement that we are being investigated for possibleviolations of these or other laws, could have a material, adverse effect on our business, financial condition, results of operations or prospects, and ourbusiness reputation could suffer significantly. In addition, other legislation or regulations at the federal or state level may be adopted that adverselyaffect our business.
Changes to physician utilization practices and treatment methodologies, third-party payer controls designed to reduce inpatient services or surgicalprocedures and other factors outside our control that impact demand for medical services may reduce our revenues.
Controls imposed by Medicare, managed Medicare, Medicaid, managed Medicaid and private third-party payers designed to reduce admissions,intensity of services, surgical volumes and lengths of stay, in some instances referred to as “utilization review,” have affected and are expected toincreasingly affect our facilities. Utilization review entails the review of the admission and course of treatment of a patient by third-party payers, andmay involve prior authorization requirements. The Medicare program also issues national or local coverage determinations that restrict thecircumstances under which Medicare pays for certain services. Inpatient utilization, average lengths of stay and occupancy rates continue to benegatively affected by third-party payers’ preadmission authorization requirements, coverage restrictions, utilization review and by pressure tomaximize outpatient and alternative health care delivery services for less acutely ill patients. Efforts to impose more stringent cost controls are expectedto continue. Additionally, trends in physician treatment protocols and health plan design, such as health plans that shift increased costs andaccountability for care to patients, could reduce our surgical volumes and admissions in favor of lower intensity and lower cost treatment methodologies.
Volume, admission and case-mix trends may be impacted by other factors beyond our control, such as changes in volume of certain high acuityservices, variations in the prevalence and severity of outbreaks of influenza and other illnesses and medical conditions, seasonal and severe weatherconditions, changes in treatment regimens and medical technology and other advances. These factors may reduce the demand for services we offer anddecrease the reimbursement that we receive. Significant limits on the scope of services reimbursed, cost controls, changes to physician utilizationpractices, treatment methodologies, reimbursement rates and fees and other factors beyond our control could have a material, adverse effect on ourbusiness, financial position and results of operations.
41
261

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 42/137
Table of Contents
Our overall business results may suffer during periods of general economic weakness.
Budget deficits at federal, state and local government entities have had a negative impact on spending, and may continue to negatively impactspending, for health and human service programs, including Medicare, Medicaid and similar programs, which represent significant third-party payersources for our hospitals. We anticipate that the federal deficit, the growing magnitude of Medicare and Medicaid expenditures and the aging of theUnited States population will continue to place pressure on government health care programs. Other risks we face during periods of economic weaknessand high unemployment include potential declines in the population covered under managed care agreements, increased patient decisions to postpone orcancel elective and nonemergency health care procedures (including delaying surgical procedures), potential increases in the uninsured and underinsuredpopulations, increased adoption of health plan structures that shift financial responsibility to patients and further difficulties in collecting patientreceivables for copayment and deductible receivables.
The industry trend toward value-based purchasing may negatively impact our revenues.
There is a trend in the health care industry toward value-based purchasing of health care services. These value-based purchasing programs includeboth public reporting of quality data and preventable adverse events tied to the quality and efficiency of care provided by facilities. Governmentalprograms including Medicare currently require hospitals to report certain quality data to receive full reimbursement updates. In addition, Medicare doesnot reimburse for care related to certain preventable adverse events (also called “never events”). The Affordable Care Act also prohibits the use offederal funds under the Medicaid program to reimburse providers for medical assistance provided to treat HACs. The 25% of hospitals with the worstrisk-adjusted HAC scores in the designated performance period receive a 1% reduction in their inpatient PPS Medicare payments.
Hospitals with excess readmission rates for conditions designated by HHS receive a reduction in their inpatient PPS operating Medicare paymentsfor all Medicare inpatient discharges, not just discharges relating to the conditions subject to the excess readmission standard. The reduction in paymentsto hospitals with excess readmissions can be up to 3% of a hospital’s base payments.
HHS has implemented a value-based purchasing program for inpatient hospital services that reduces inpatient hospital payments for all dischargesby 2% in each federal fiscal year. HHS pools the amount collected from these reductions to fund payments to reward hospitals that meet or exceedcertain quality performance standards established by HHS. HHS estimates that $1.9 billion in value-based incentive payments will be available tohospitals in federal fiscal year 2020 based on achievement (relative to other hospitals) and improvement (relative to the hospital’s own pastperformance). Hospitals that meet or exceed the quality performance standards will receive greater reimbursement under the value-based purchasingprogram than they would have otherwise.
CMS has developed several alternative payment models that are intended to reduce costs and improve quality of care for Medicare beneficiariesand has signaled its intent to have states apply similar strategies in the Medicaid context. Examples of alternative payment models include bundledpayment models in which, depending on whether overall CMS spending per episode exceeds or falls below a target specified by CMS and whetherquality standards are met, hospitals may receive supplemental Medicare payments or owe repayments to CMS. Generally, participation in bundledpayment programs is voluntary, but CMS requires hospitals in selected markets to participate in a bundled payment initiative for orthopedic services,which is scheduled to run through December 2020. CMS has indicated that it is developing more voluntary and mandatory bundled payment models.Participation in mandatory or voluntary demonstration projects, particularly demonstrations with the potential to affect payment, may negatively impactour results of operations.
Some private third-party payers are also transitioning toward alternative payment models or implementing other value-based care strategies. Forexample, many large private third-party payers currently require hospitals
42
262

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 43/137
Table of Contents
to report quality data, and several private third-party payers do not reimburse hospitals for certain preventable adverse events. Further, we haveimplemented a policy pursuant to which we do not bill patients or third-party payers for fees or expenses incurred due to certain preventable adverseevents.
We expect value-based purchasing programs, including programs that condition reimbursement on patient outcome measures, to become morecommon and to involve a higher percentage of reimbursement amounts. It is unclear whether these and other alternative payment models willsuccessfully coordinate care and reduce costs or whether they will decrease aggregate reimbursement. We are unable at this time to predict our futurepayments or whether we will be subject to payment reductions under these programs or how this trend will affect our results of operations. If we areunable to meet or exceed the quality performance standards under any applicable value-based purchasing program, perform at a level below theoutcomes demonstrated by our competitors, or otherwise fail to effectively provide or coordinate the efficient delivery of quality health care services,our reputation in the industry may be negatively impacted, we may receive reduced reimbursement amounts and we may owe repayments to payers,causing our revenues to decline.
We have been and could become the subject of government investigations, claims and litigation.
Health care companies are subject to numerous investigations by various government agencies. Further, under the FCA, private parties have theright to bring qui tam, or “whistleblower,” suits against companies that submit false claims for payments to, or improperly retain overpayments from, thegovernment. Some states have adopted similar state whistleblower and false claims provisions. Certain of our individual facilities and/or affiliates havereceived, and other facilities and/or affiliates may receive, government inquiries from, and may be subject to investigation by, federal and state agencies.Depending on whether the underlying conduct in these or future inquiries or investigations could be considered systemic, their resolution could have amaterial, adverse effect on our financial position, results of operations and liquidity.
Government agencies and their agents, such as the MACs, fiscal intermediaries and carriers, as well as the OIG, CMS and state Medicaidprograms, conduct audits of our health care operations. CMS and state Medicaid agencies contract with RACs and other contractors on a contingencyfee basis to conduct post-payment reviews to detect and correct improper payments in the Medicare program, including managed Medicare plans, andthe Medicaid programs. RAC denials are appealable; however, there are currently significant delays in the Medicare appeals process, which negativelyimpacts our ability to appeal RAC payment denials. Private third-party payers may conduct similar post-payment audits, and we also perform internalaudits and monitoring. Depending on the nature of the conduct found in such audits and whether the underlying conduct could be considered systemic,the resolution of these audits could have a material, adverse effect on our financial position, results of operations and liquidity.
Should we be found out of compliance with applicable laws, regulations or programs, depending on the nature of the findings, our business, ourfinancial position and our results of operations could be negatively impacted.
Health care technology initiatives, particularly those related to patient data and interoperability, may adversely affect our operations.
The federal government is working to promote the adoption of health information technology and the promotion of nationwide health informationexchange to improve health care. For example, HHS incentivizes the adoption and meaningful use of certified EHR technology through its PromotingInteroperability Programs. Eligible hospitals and eligible professionals, including our hospitals and employed professionals, are subject to reducedpayments from Medicare if they fail to demonstrate meaningful use of certified EHR technology. As these technologies have become widespread, thefocus has shifted to increasing patient access to health care data and interoperability. The 21st Century Cures Act prohibits information blocking byhealth care providers and certain other entities, which is defined as engaging in activities likely to interfere with, prevent, or materially
43
263

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 44/137
Table of Contents
discourage access, exchange or use of electronic health information, except as required by law or specified by HHS as a reasonable and necessaryactivity. Current and future initiatives related to health care technology and interoperability may require changes to our operations, impose new andcomplex compliance obligations and require investments in infrastructure. We may be subject to financial penalties for failure to comply. It is difficult topredict how these initiatives will affect our relationships with providers and vendors, participation in health care information exchanges or networks, theexchange of patient data, and patient engagement.
The emergence and effects related to a pandemic, epidemic or outbreak of an infectious disease could adversely affect our operations.
If a pandemic, epidemic, outbreak of an infectious disease or other public health crisis were to occur in an area in which we operate, ouroperations could be adversely affected. Such a crisis could diminish the public trust in health care facilities, especially hospitals that fail to accurately ortimely diagnose, or are treating (or have treated) patients affected by infectious diseases. If any of our facilities were involved, or perceived as beinginvolved, in treating patients from such an infectious disease, patients might cancel elective procedures or fail to seek needed care at our facilities, andour reputation may be negatively affected. Further, a pandemic, epidemic or outbreak might adversely affect our operations by causing a temporaryshutdown or diversion of patients, by disrupting or delaying production and delivery of materials and products in the supply chain or by causing staffingshortages in our facilities. We have disaster plans in place and operate pursuant to infectious disease protocols, but the potential emergence of apandemic, epidemic or outbreak is difficult to predict and could adversely affect our operations.
State efforts to regulate the construction or expansion of health care facilities could impair our ability to operate and expand our operations.
Some states, particularly in the eastern part of the country, require health care providers to obtain prior approval, often known as a CON, for thepurchase, construction or expansion of health care facilities, to make certain capital expenditures or to make changes in services or bed capacity. Ingiving approval, these states consider the need for additional or expanded health care facilities or services. We currently operate health care facilities in anumber of states with CON laws or that require other types of approvals for the establishment or expansion of certain facility types or services. Thefailure to obtain any required CON or other required approval could impair our ability to operate or expand operations. Any such failure could, in turn,adversely affect our ability to attract patients and physicians to our facilities and grow our revenues, which would have an adverse effect on our resultsof operations.
We may encounter difficulty acquiring hospitals and other health care businesses, encounter challenges integrating the operations of acquiredhospitals and other health care businesses and become liable for unknown or contingent liabilities as a result of acquisitions.
A component of our business strategy is acquiring hospitals and other health care businesses. We may encounter difficulty acquiring new facilitiesor other businesses as a result of competition from other purchasers that may be willing to pay purchase prices that are higher than we believe arereasonable. Some states require CONs in order to acquire a hospital or other facility or to expand facilities or services. In addition, the acquisition ofhealth care facilities often involves licensure approvals or reviews and complex change of ownership processes for Medicare and other payers. Further,many states have laws that restrict the conversion or sale of not-for-profit hospitals to for-profit entities. These laws may require prior approval from thestate attorney general, advance notification of the attorney general or other regulators and community involvement. Attorneys general in states withoutspecific requirements may exercise broad discretionary authority over transactions involving the sale of not-for-profits under their general obligations toprotect the use of charitable assets. These legislative and administrative efforts often focus on the appropriate valuation of the assets divested and the useof the proceeds of the sale by the non-profit seller and may include consideration of commitments for capital improvements and charity care by thepurchaser. Also, the increasingly challenging regulatory and enforcement
44
264

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 45/137
Table of Contents
environment may negatively impact our ability to acquire health care businesses if they are found to have material unresolved compliance issues, suchas repayment obligations. Resolving compliance issues as well as completion of oversight, review or approval processes could seriously delay or evenprevent our ability to acquire hospitals or other businesses and increase our acquisition costs.
We may be unable to timely and effectively integrate hospitals and other businesses that we acquire with our ongoing operations, or we mayexperience delays implementing operating procedures and systems. Hospitals and other health care businesses that we acquire may have unknown orcontingent liabilities, including liabilities for failure to comply with health care and other laws and regulations, medical and general professionalliabilities, workers’ compensation liabilities and tax liabilities. Although we typically exclude significant liabilities from our acquisition transactions andseek indemnification from the sellers for these matters, we could experience difficulty enforcing those obligations, experience liability in excess of anyindemnification obtained or otherwise incur material liabilities for the pre-acquisition conduct of acquired businesses. Such liabilities and related legalor other costs could harm our business and results of operations.
Our facilities are heavily concentrated in Florida and Texas, which makes us sensitive to regulatory, economic, environmental and competitiveconditions and changes in those states.
We operated 184 hospitals at December 31, 2019, and 91 of those hospitals are located in Florida and Texas. Our Florida and Texas facilities’combined revenues represented approximately 48% of our consolidated revenues for the year ended December 31, 2019. This concentration makes usparticularly sensitive to regulatory, economic, environmental and competitive conditions and changes in those states. Any material change in the currentpayment programs or regulatory, economic, environmental or competitive conditions in those states could have a disproportionate effect on our overallbusiness results.
In addition, our hospitals in Florida, Texas and other coastal states are located in hurricane-prone areas. In the past, hurricanes have had adisruptive effect on the operations of our hospitals in Florida, Texas and other coastal states and the patient populations in those states. Our businessactivities could be harmed by a particularly active hurricane season or even a single storm, either of which may be intensified by climate change, and theproperty insurance we obtain may not be adequate to cover losses from future hurricanes or other natural disasters.
We may be subject to liabilities from claims by taxing authorities.
We are subject to examination by federal, state and foreign taxing authorities. Management believes HCA Healthcare, Inc., its predecessors,subsidiaries and affiliates properly reported taxable income and paid taxes in accordance with applicable laws and agreements established with the IRS,state and foreign taxing authorities and final resolution of any disputes will not have a material, adverse effect on our results of operations or financialposition. However, if payments due upon final resolution of any issues exceed our recorded estimates, such resolutions could have a material, adverseeffect on our results of operations or financial position.
We may be subject to liabilities from claims brought against our facilities.
We are subject to litigation relating to our business practices, including claims and legal actions by patients and others in the ordinary course ofbusiness alleging malpractice, product liability or other legal theories. Many of these actions seek large sums of money as damages and involvesignificant defense costs. We insure a portion of our professional liability risks through a 100% owned insurance subsidiary. Management believes ourreserves for self-insured retentions and insurance coverage are sufficient to cover insured claims arising out of the operation of our facilities. Our 100%owned insurance subsidiary has entered into certain reinsurance contracts; however, the subsidiary remains liable to the extent that the reinsurers do notmeet their obligations under the reinsurance contracts. If payments for claims exceed actuarially determined estimates, are not covered by insurance, orreinsurers, if any, fail to meet their obligations, our results of operations and financial position could be adversely affected.
45
265

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 46/137
Table of Contents
We are exposed to market risk related to changes in the market values of securities and interest rate changes.
We are exposed to market risk related to changes in market values of securities. The investments of our 100% owned insurance subsidiaries were$462 million at December 31, 2019. These investments are carried at fair value, with changes in unrealized gains and losses being recorded asadjustments to other comprehensive income. At December 31, 2019, we had a net unrealized gain of $18 million on the insurance subsidiaries’investment securities.
We are exposed to market risk related to market illiquidity. Investment securities of our 100% owned insurance subsidiaries could be impaired bythe inability to access the capital markets. Should the 100% owned insurance subsidiaries require significant amounts of cash in excess of normal cashrequirements to pay claims and other expenses on short notice, we may have difficulty selling these investments in a timely manner or be forced to sellthem at a price less than what we might otherwise have been able to in a normal market environment. We may be required to recognize credit-relatedimpairments on long-term investments in future periods should issuers default on interest payments or should the fair market valuations of the securitiesdeteriorate due to ratings downgrades or other issue specific factors.
We are also exposed to market risk related to changes in interest rates that impact the amount of the interest expense we incur with respect to ourfloating rate obligations as well as the value of certain investments. We periodically enter into interest rate swap agreements to manage our exposure tothese fluctuations. Our interest rate swap agreements involve the exchange of fixed and variable rate interest payments between two parties, based oncommon notional principal amounts and maturity dates. The notional amounts of the swap agreements represent balances used to calculate the exchangeof cash flows and are not our assets or liabilities.
Discontinuation, reform or replacement of LIBOR may adversely affect our business.
As of December 31, 2019, we had $6.205 billion of borrowings under our senior secured credit facilities that bore interest at a floating rate basedon LIBOR and $3.237 billion of unfunded commitments under those facilities. The U.K. Financial Conduct Authority announced in 2017 that it intendsto phase out LIBOR by the end of 2021. If the phase out occurs as planned, the interest rate applicable to our floating rate debt will be calculated basedon an alternative, comparable or successor rate which may have a material adverse impact on the cost of the floating rate portion of our indebtedness.The timing and result of the phase out of LIBOR are unclear, and efforts of industry groups to develop a suitable successor are not guaranteed to resultin a viable or widely adopted replacement for LIBOR. If LIBOR becomes unavailable before a suitable replacement is widely adopted, it could have amaterial adverse impact on the availability of floating rate financing.
As of December 31, 2019, we also had $2.500 billion of interest rate swap agreements based on LIBOR. If LIBOR becomes unavailable, it isunclear how payments under those agreements would be calculated. Relevant industry groups are seeking to create a standard protocol addressing theexpected discontinuation of LIBOR, but there can be no assurance that such a protocol will be developed or implemented with respect to our swapagreements.
There can be no assurance that we will continue to pay dividends.
In January 2018, the Board of Directors initiated a cash dividend program under which the Company commenced and expects to continue to pay aregular quarterly cash dividend. The declaration, amount and timing of such dividends are subject to capital availability and determinations by ourBoard of Directors that cash dividends are in the best interest of our stockholders and are in compliance with all respective laws and our agreementsapplicable to the declaration and payment of cash dividends. Our ability to pay dividends will depend upon, among other factors, our cash flows fromoperations, our available capital and potential future capital requirements for strategic transactions, including acquisitions, debt service requirements,share repurchases and investing in our existing markets as well as our results of operations, financial condition and other factors beyond our control thatour Board of Directors may deem relevant. A reduction in or elimination of our dividend payments could have a negative effect on our stock price.
46
266

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 47/137
Table of Contents
Certain of our investors may continue to have influence over us.
On November 17, 2006, HCA Inc. was acquired by a private investor group, including affiliates of HCA founder, Dr. Thomas F. Frist, Jr. andcertain other investors. Through their investment in Hercules Holding II and other holdings, certain of the Frist-affiliated investors continue to hold asignificant interest in our outstanding common stock (approximately 21% as of January 31, 2020). In addition, pursuant to a shareholders agreement weentered into with Hercules Holding II and the Frist-affiliated investors, certain representatives of these investors have the continued right to nominatecertain of the members of our Board of Directors. As a result, certain of these investors potentially have the ability to influence our decisions to enterinto corporate transactions (and the terms thereof) and prevent changes in the composition of our Board of Directors and any transaction that requiresstockholder approval.
Item 1B. Unresolved Staff Comments
None.
Item 2. Properties
The following table lists, by state, the number of hospitals (general, acute care, psychiatric and rehabilitation) directly or indirectly owned andoperated by us as of December 31, 2019:
State Hospitals Beds Alaska 1 250 California 5 1,858 Colorado 7 2,411 Florida 45 12,410 Georgia 9 2,469 Idaho 2 468 Indiana 1 278 Kansas 4 1,374 Kentucky 2 384 Louisiana 3 914 Mississippi 1 130 Missouri 5 1,058 Nevada 3 1,421 New Hampshire 2 306 North Carolina 7 1,181 South Carolina 3 949 Tennessee 13 2,576 Texas 46 13,395 Utah 8 1,011 Virginia 11 3,300
International England 6 892
184 49,035
In addition to the hospitals listed in the above table, we directly or indirectly operate 123 freestanding surgery centers. We also operate medicaloffice buildings in conjunction with some of our hospitals. These office buildings are primarily occupied by physicians who practice at our hospitals.Fourteen of our general, acute care hospitals and two of our other properties have been mortgaged to support our obligations under our senior securedcash flow credit facility and first lien secured notes.
47
267

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 48/137
Table of Contents
We maintain our headquarters in approximately 2,127,000 square feet of space in the Nashville, Tennessee area. In addition to the headquarters inNashville, we maintain regional service centers related to our shared services initiatives. These service centers are located in markets in which weoperate hospitals.
We believe our headquarters, hospitals and other facilities are suitable for their respective uses and are, in general, adequate for our present needs.Our properties are subject to various federal, state and local statutes and ordinances regulating their operation. Management does not believe thatcompliance with such statutes and ordinances will materially affect our financial position or results of operations.
Item 3. Legal Proceedings We operate in a highly regulated and litigious industry. As a result, various lawsuits, claims and legal and regulatory proceedings have been andcan be expected to be instituted or asserted against us. We are also subject to claims and suits arising in the ordinary course of business, including claimsfor personal injuries or wrongful restriction of, or interference with, physicians’ staff privileges. In certain of these actions the claimants may seekpunitive damages against us which may not be covered by insurance. We are also subject to claims by various taxing authorities for additional taxes andrelated interest and penalties. The resolution of any such lawsuits, claims or legal and regulatory proceedings could have a material, adverse effect onour results of operations, financial position or liquidity.
Government Investigations, Claims and Litigation
Health care companies are subject to numerous investigations by various governmental agencies. Under the federal False Claims Act (“FCA”),private parties have the right to bring qui tam, or “whistleblower,” suits against companies that submit false claims for payments to, or improperly retainoverpayments from, the government. Some states have adopted similar state whistleblower and false claims provisions. Certain of our individualfacilities have received, and from time to time, other facilities may receive, government inquiries from, and may be subject to investigation by, federaland state agencies. Depending on whether the underlying conduct in these or future inquiries or investigations could be considered systemic, theirresolution could have a material, adverse effect on our results of operations, financial position or liquidity.
Texas operates a state Medicaid program pursuant to a waiver from CMS under Section 1115 of the Social Security Act (“Program”). TheProgram includes uncompensated-care pools; payments from these pools are intended to defray the uncompensated costs of services provided by ourand other hospitals to Medicaid eligible or uninsured individuals. Separately, we and other hospitals provide charity care services in several communitiesin the state. In 2018, the Civil Division of the U.S. Department of Justice and the U.S. Attorney’s Office for the Southern District of Texas requestedinformation about whether the Program, as operated in Harris County, complied with the laws and regulations applicable to provider related donations,and the Company cooperated with that request. On May 21, 2019, a qui tam lawsuit asserting violations of the FCA and the Texas Medicaid FraudPrevention Act related to the Program, as operated in Harris County, was unsealed by the U.S. District Court for the Southern District of Texas. Both thefederal and state governments declined to intervene in the qui tam lawsuit. The Company believes that our participation is and has been consistent withthe requirements of the Program and is vigorously defending against the lawsuit being pursued by the relator. We cannot predict what effect, if any, thequi tam lawsuit could have on the Company.
Item 4. Mine Safety Disclosures None.
48
268

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 49/137
Table of Contents
PART II
Item 5. Market for Registrant’s Common Equity, Related Stockholder Matters and Issuer Purchases of Equity Securities During January 2020 and 2019, our Board of Directors authorized share repurchase programs for up to $4 billion ($2 billion for eachauthorization) of our outstanding common stock. Repurchases made during the fourth quarter of 2019, as detailed below, were made pursuant to theJanuary 2019 share repurchase authorization and were made in the open market.
The following table provides certain information with respect to our repurchases of common stock from October 1, 2019 through December 31,2019 (dollars in millions, except per share amounts).
Period
Total Number of Shares
Purchased Average Price
Paid per Share
Total Number of Shares
Purchased as Part of
Publicly Announced
Plans or Programs
Approximate Dollar Value of Shares That
May Yet Be Purchased Under Publicly
Announced Plans or
Programs October 1, 2019 through October 31, 2019 898,323 $ 120.23 898,323 $ 1,405 November 1, 2019 through November 30, 2019 585,739 $ 136.44 585,739 $ 1,325 December 1, 2019 through December 31, 2019 585,429 $ 143.49 585,429 $ 1,241 Total for Fourth Quarter 2019 2,069,491 $ 131.40 2,069,491 $ 1,241
Our common stock is traded on the New York Stock Exchange (“NYSE”) (symbol “HCA”). On January 27, 2020, our Board of Directors declareda quarterly dividend of $0.43 per share on our common stock payable on March 31, 2020 to stockholders of record at the close of business on March 2,2020. Future declarations of quarterly dividends and the establishment of future record and payment dates are subject to the final determination of ourBoard of Directors. Our ability to declare future dividends may also from time to time be limited by the terms of our debt agreements. During 2019, ourBoard of Directors declared four quarterly dividends of $0.40 per share, or $1.60 per share in the aggregate, on our common stock. At the close ofbusiness on February 7, 2020, there were approximately 390 holders of record of our common stock.
49
269

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 50/137
Table of Contents
STOCK PERFORMANCE GRAPHCOMPARISON OF 5 YEAR CUMULATIVE TOTAL RETURN
Among HCA Healthcare, Inc., the S&P 500 Index and the S&P Health Care Index
12/31/2014 12/31/2015 12/31/2016 12/31/2017 12/31/2018 12/31/2019
HCA Healthcare, Inc. $ 100.00 $ 92.15 $ 100.86 $ 119.69 $ 171.61 $ 206.36 S&P 500 100.00 101.38 113.51 138.29 132.23 173.86 S&P Health Care 100.00 106.89 104.01 126.98 135.19 163.34
The graph shows the cumulative total return to our stockholders beginning as of December 31, 2014 through December 31, 2019, in comparisonto the cumulative returns of the S&P 500 Index and the S&P Health Care Index. The graph assumes $100 invested on December 31, 2014 in ourcommon stock and in each index with the subsequent reinvestment of dividends. The stock performance shown on the graph represents historical stockperformance and is not necessarily indicative of future stock price performance.
50
270

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 51/137
Table of Contents
Item 6. Selected Financial Data
HCA HEALTHCARE, INC.SELECTED FINANCIAL DATA
AS OF AND FOR THE YEARS ENDED DECEMBER 31(Dollars in millions, except per share amounts)
2019 2018 2017 2016 2015 Summary of Operations:
Revenues $51,336 $46,677 $43,614 $41,490 $39,678
Salaries and benefits 23,560 21,425 20,059 18,897 18,115 Supplies 8,481 7,724 7,316 6,933 6,638 Other operating expenses 9,481 8,608 8,051 7,496 7,056 Equity in earnings of affiliates (43) (29) (45) (54) (46)Depreciation and amortization 2,596 2,278 2,131 1,966 1,904 Interest expense 1,824 1,755 1,690 1,707 1,665 Losses (gains) on sales of facilities (18) (428) (8) (23) 5 Losses on retirement of debt 211 9 39 4 135 Legal claim (benefits) costs — — — (246) 249
46,092 41,342 39,233 36,680 35,721 Income before income taxes 5,244 5,335 4,381 4,810 3,957 Provision for income taxes 1,099 946 1,638 1,378 1,261 Net income 4,145 4,389 2,743 3,432 2,696 Net income attributable to noncontrolling interests 640 602 527 542 567
Net income attributable to HCA Healthcare, Inc. $ 3,505 $ 3,787 $ 2,216 $ 2,890 $ 2,129 Per common share data:
Basic earnings per share $ 10.27 $ 10.90 $ 6.12 $ 7.53 $ 5.14 Diluted earnings per share $ 10.07 $ 10.66 $ 5.95 $ 7.30 $ 4.99 Cash dividends declared per share $ 1.60 $ 1.40 — — —
Financial Position: Assets $45,058 $39,207 $36,593 $33,758 $32,744 Working capital 3,439 2,644 3,819 3,252 3,716 Long-term debt, net, including amounts due within one year 33,722 32,821 33,058 31,376 30,488 Noncontrolling interests 2,243 2,032 1,811 1,669 1,553 Stockholders’ deficit (565) (2,918) (4,995) (5,633) (6,046)
Cash Flow Data: Cash provided by operating activities $ 7,602 $ 6,761 $ 5,426 $ 5,653 $ 4,734 Cash used in investing activities (5,720) (3,901) (4,279) (3,240) (2,583)Purchase of property and equipment (4,158) (3,573) (3,015) (2,760) (2,375)Cash used in financing activities (1,771) (3,075) (1,061) (2,508) (1,976)
51
271

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 52/137
Table of Contents
2019 2018 2017 2016 2015 Operating Data:
Number of hospitals at end of period 184 179 179 170 168 Number of freestanding outpatient surgical centers at
end of period
123
123
120
118
116 Number of licensed beds at end of period(a) 49,035 47,199 46,738 44,290 43,771 Weighted average licensed beds(b) 48,480 46,857 45,380 44,077 43,620 Admissions(c) 2,108,927 2,003,753 1,936,613 1,891,831 1,868,789 Equivalent admissions(d) 3,646,335 3,420,406 3,286,432 3,191,519 3,122,746 Average length of stay (days)(e) 4.9 4.9 4.9 4.9 4.9 Average daily census(f) 28,134 26,663 26,000 25,340 25,084 Occupancy(g) 58% 57% 57% 58% 58%Emergency room visits(h) 9,161,129 8,764,431 8,624,137 8,378,340 8,050,159 Outpatient surgeries(i) 1,009,947 971,537 941,231 932,213 909,386 Inpatient surgeries(j) 566,635 548,220 540,304 537,306 529,900 Days revenues in accounts receivable(k) 50 51 52 50 53 Outpatient revenues as a % of patient revenues(l) 39% 38% 38% 38% 40%
(a) Licensed beds are those beds for which a facility has been granted approval to operate from the applicable state licensing agency.(b) Represents the average number of licensed beds, weighted based on periods owned.(c) Represents the total number of patients admitted to our hospitals and is used by management and certain investors as a general measure of
inpatient volume.(d) Equivalent admissions are used by management and certain investors as a general measure of combined inpatient and outpatient volume.
Equivalent admissions are computed by multiplying admissions (inpatient volume) by the sum of gross inpatient revenue and gross outpatientrevenue and then dividing the resulting amount by gross inpatient revenue. The equivalent admissions computation “equates” outpatient revenueto the volume measure (admissions) used to measure inpatient volume, resulting in a general measure of combined inpatient and outpatientvolume.
(e) Represents the average number of days admitted patients stay in our hospitals.(f) Represents the average number of patients in our hospital beds each day.(g) Represents the percentage of hospital licensed beds occupied by patients. Both average daily census and occupancy rate provide measures of the
utilization of inpatient rooms.(h) Represents the number of patients treated in our emergency rooms.(i) Represents the number of surgeries performed on patients who were not admitted to our hospitals. Pain management and endoscopy procedures
are not included in outpatient surgeries.(j) Represents the number of surgeries performed on patients who have been admitted to our hospitals. Pain management and endoscopy procedures
are not included in inpatient surgeries.(k) Revenues per day is calculated by dividing the revenues for the fourth quarter of each year by the days in the quarter. Days revenues in accounts
receivable is then calculated as accounts receivable at the end of the period divided by revenues per day.(l) Represents the percentage of patient revenues related to patients who are not admitted to our hospitals.
52
272

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 53/137
Table of Contents
HCA HEALTHCARE, INC.
MANAGEMENT’S DISCUSSION AND ANALYSIS OF FINANCIAL CONDITIONAND RESULTS OF OPERATIONS
Item 7. Management’s Discussion and Analysis of Financial Condition and Results of Operations
The selected financial data and the accompanying consolidated financial statements present certain information with respect to the financialposition, results of operations and cash flows of HCA Healthcare, Inc. which should be read in conjunction with the following discussion and analysis.The terms “HCA,” “Company,” “we,” “our,” or “us,” as used herein, refer to HCA Healthcare, Inc. and its affiliates. The term “affiliates” means directand indirect subsidiaries of HCA Healthcare, Inc. and partnerships and joint ventures in which such subsidiaries are partners.
Forward-Looking Statements
This annual report on Form 10-K includes certain disclosures which contain “forward-looking statements” within the meaning of the federalsecurities laws, which involve risks and uncertainties. Forward-looking statements include statements regarding expected share-based compensationexpense, expected capital expenditures, expected dividends, expected net claim payments and all other statements that do not relate solely to historicalor current facts, and can be identified by the use of words like “may,” “believe,” “will,” “expect,” “project,” “estimate,” “anticipate,” “plan,” “initiative”or “continue.” These forward-looking statements are based on our current plans and expectations and are subject to a number of known and unknownuncertainties and risks, many of which are beyond our control, which could significantly affect current plans and expectations and our future financialposition and results of operations. These factors include, but are not limited to, (1) the impact of our substantial indebtedness and the ability to refinancesuch indebtedness on acceptable terms, (2) the impact of the Patient Protection and Affordable Care Act, as amended by the Health Care and EducationReconciliation Act of 2010 (collectively, the “Affordable Care Act”), including the effects of court challenges to, any repeal of, or changes to, theAffordable Care Act or additional changes to its implementation, the possible enactment of additional federal or state health care reforms and possiblechanges to other federal, state or local laws or regulations affecting the health care industry, including single-payer proposals (often referred to as“Medicare for All”), (3) the effects related to the continued implementation of the sequestration spending reductions required under the Budget ControlAct of 2011, and related legislation extending these reductions, and the potential for future deficit reduction legislation that may alter these spendingreductions, which include cuts to Medicare payments, or create additional spending reductions, (4) increases in the amount and risk of collectability ofuninsured accounts and deductibles and copayment amounts for insured accounts, (5) the ability to achieve operating and financial targets, and attainexpected levels of patient volumes and control the costs of providing services, (6) possible changes in Medicare, Medicaid and other state programs,including Medicaid supplemental payment programs or Medicaid waiver programs, that may impact reimbursements to health care providers andinsurers and the size of the uninsured or underinsured population, (7) the highly competitive nature of the health care business, (8) changes in servicemix, revenue mix and surgical volumes, including potential declines in the population covered under third-party payer agreements, the ability to enterinto and renew third-party payer provider agreements on acceptable terms and the impact of consumer-driven health plans and physician utilizationtrends and practices, (9) the efforts of health insurers, health care providers, large employer groups and others to contain health care costs, (10) theoutcome of our continuing efforts to monitor, maintain and comply with appropriate laws, regulations, policies and procedures, (11) increases in wagesand the ability to attract and retain qualified management and personnel, including affiliated physicians, nurses and medical and technical supportpersonnel, (12) the availability and terms of capital to fund the expansion of our business and improvements to our existing facilities, (13) changes inaccounting practices, (14) changes in general economic conditions nationally and regionally in our markets, (15) the emergence of and effects related topandemics, epidemics and infectious diseases, (16) future divestitures which may result in charges and possible impairments of long-lived assets,(17) changes in business strategy or development plans, (18) delays in receiving payments for services provided, (19) the outcome of pending and anyfuture tax audits, disputes and litigation associated
53
273

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 54/137
Table of Contents
HCA HEALTHCARE, INC.
MANAGEMENT’S DISCUSSION AND ANALYSIS OF FINANCIAL CONDITIONAND RESULTS OF OPERATIONS (Continued)
Forward-Looking Statements (continued)
with our tax positions, (20) potential adverse impact of known and unknown government investigations, litigation and other claims that may be madeagainst us, (21) the impact of potential cybersecurity incidents or security breaches, (22) our ongoing ability to demonstrate meaningful use of certifiedelectronic health record (“EHR”) technology and the impact of interoperability requirements, (23) the impact of natural disasters, such as hurricanes andfloods, or similar events beyond our control, (24) changes in U.S. federal, state, or foreign tax laws including interpretive guidance that may be issuedby taxing authorities or other standard setting bodies, and (25) other risk factors described in this annual report on Form 10-K. As a consequence,current plans, anticipated actions and future financial position and results of operations may differ from those expressed in any forward-lookingstatements made by or on behalf of HCA. You are cautioned not to unduly rely on such forward-looking statements when evaluating the informationpresented in this report.
2019 Operations Summary
Net income attributable to HCA Healthcare, Inc. totaled $3.505 billion, or $10.07 per diluted share, for 2019, compared to $3.787 billion, or$10.66 per diluted share, for 2018. The 2019 results include gains on sales of facilities of $18 million, or $0.04 per diluted share, and losses onretirement of debt of $211 million, or $0.47 per diluted share. The 2018 results include gains on sales of facilities of $428 million, or $0.91 per dilutedshare, and losses on retirement of debt of $9 million, or $0.02 per diluted share. The 2019 results also include revenues of $86 million, or $0.19 perdiluted share, related to the resolution of transaction price differences regarding certain out-of-network services performed in prior periods. The 2018results also include a reduction in our provision for income taxes of $67 million, or $0.19 per share, for the remeasurement of certain of our deferred taxassets and liabilities for which we were unable to record reasonable estimates in 2017. During 2019 and 2018, we recorded reductions to the provisionfor professional liability risks of $50 million, or $0.11 per diluted share, and $70 million, or $0.15 per diluted share, respectively. During 2018, werecorded additional expenses and losses of revenues estimated at approximately $31 million, or $0.07 per diluted share, associated with the impact ofhurricane Michael on our Florida facilities. This amount is prior to any insurance recoveries. During 2018, we recorded a benefit of $49 million, or$0.11 per diluted share, from an insurance recovery related to hurricane Harvey business interruption losses incurred during 2017, and we recorded areduction to the provision for income taxes of $28 million, or $0.08 per diluted share, for tax credits related to certain 2017 hurricane-related expenses.Our provisions for income taxes for 2019 and 2018 included tax benefits of $65 million, or $0.19 per diluted share, and $124 million, or $0.35 perdiluted share, respectively, related to employee equity award settlements. All “per diluted share” disclosures are based upon amounts net of theapplicable income taxes. Shares used for diluted earnings per share were 348.226 million shares and 355.303 million shares for the years endedDecember 31, 2019 and 2018, respectively. During 2019 and 2018, we repurchased 7.949 million and 14.070 million shares, respectively, of ourcommon stock.
Revenues increased to $51.336 billion for 2019 from $46.677 billion for 2018. Revenues increased 10.0% and 5.9%, respectively, on aconsolidated basis and on a same facility basis for 2019, compared to 2018. The consolidated revenues increase can be primarily attributed to thecombined impact of a 3.2% increase in revenue per equivalent admission and a 6.6% increase in equivalent admissions. The same facility revenuesincrease resulted primarily from a 2.3% increase in same facility revenue per equivalent admission and a 3.5% increase in same facility equivalentadmissions.
During 2019, consolidated admissions increased 5.2% and same facility admissions increased 2.8%, compared to 2018. Inpatient surgical volumesincreased 3.4% on a consolidated basis and increased 1.1% on a same facility basis during 2019, compared to 2018. Outpatient surgical volumesincreased 4.0% on a
54
274

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 55/137
Table of Contents
HCA HEALTHCARE, INC.
MANAGEMENT’S DISCUSSION AND ANALYSIS OF FINANCIAL CONDITIONAND RESULTS OF OPERATIONS (Continued)
2019 Operations Summary (continued)
consolidated basis and increased 1.6% on a same facility basis during 2019, compared to 2018. Emergency room visits increased 4.5% on a consolidatedbasis and increased 2.8% on a same facility basis during 2019, compared to 2018.
The estimated cost of total uncompensated care increased $415 million for 2019, compared to 2018. Consolidated and same facility uninsuredadmissions increased 5.8% and 3.7%, respectively, and consolidated and same facility uninsured emergency room visits increased 5.8% and 3.9%,respectively, for 2019, compared to 2018.
Interest expense totaled $1.824 billion for 2019, compared to $1.755 billion for 2018. The $69 million increase in interest expense for 2019 wasdue to the increase in the average debt balance.
Cash flows from operating activities increased $841 million, from $6.761 billion for 2018 to $7.602 billion for 2019. The increase in cash flowsfrom operating activities was primarily related to the increase in net income, excluding gains on sales of facilities and losses on retirement of debt, of$222 million and increases related to income taxes of $322 million and depreciation and amortization of $318 million.
Business Strategy
We are committed to providing the communities we serve with high quality, cost-effective health care while growing our business and creatinglong-term value for our stockholders. To achieve these objectives, we align our efforts around the following growth agenda:
Grow Our Presence in Existing Markets. We believe we are well positioned in a number of large and growing markets that will allow us theopportunity to generate long-term, attractive growth through the expansion of our presence in these markets. We plan to continue recruiting andstrategically collaborating with the physician community and developing comprehensive service lines such as cardiology, neurology, oncology,orthopedics and women’s services. Additional components of our growth strategy include providing access and convenience through developing variousoutpatient facilities, including, but not limited to surgery centers, urgent care clinics, freestanding emergency care facilities and imaging centers.
Achieve Industry-Leading Performance in Clinical and Satisfaction Measures. Achieving high levels of patient safety, patient satisfaction andclinical quality are central goals of our business. To achieve these goals, we have implemented a number of initiatives including infection reductioninitiatives, hospitalist programs, advanced health information technology and evidence-based medicine programs. We routinely analyze operationalpractices from our best-performing hospitals to identify ways to implement organization-wide performance improvements and reduce clinical variation.We believe these initiatives will continue to improve patient care, help us achieve cost efficiencies and favorably position us in an environment whereour constituents are increasingly focused on quality, efficacy and efficiency.
Recruit and Employ Physicians to Meet the Needs for High Quality Health Services. We depend on the quality and dedication of the health careproviders and other team members who serve at our facilities. We believe a critical component of our growth strategy is our ability to successfullyrecruit and strategically collaborate with physicians and other professionals to provide high quality care. We attract and retain physicians by providinghigh quality, convenient facilities with advanced technology, by expanding our specialty services and by building our outpatient operations. We believeour continued investment in the employment, recruitment and retention of physicians will improve the quality of care at our facilities.
55
275

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 56/137
Table of Contents
HCA HEALTHCARE, INC.
MANAGEMENT’S DISCUSSION AND ANALYSIS OF FINANCIAL CONDITIONAND RESULTS OF OPERATIONS (Continued)
Business Strategy (continued)
Continue to Leverage Our Scale and Market Positions to Grow the Company. We believe there is significant opportunity to continue to grow ourcompany by fully leveraging the scale and scope of our organization. We continue to invest in initiatives such as care navigators, clinical data exchangeand centralized patient transfer operations, which will enable us to improve coordination of care and patient retention across our markets. We believe ourcentrally managed business processes and ability to leverage cost-saving practices across our extensive network will enable us to continue to managecosts effectively. We continue to invest in our Parallon subsidiary group to leverage key components of our support infrastructure, including revenuecycle management, health care group purchasing, supply chain management and staffing functions.
Pursue a Disciplined Development Strategy. We continue to believe there are significant growth opportunities in our markets. We will continue toprovide financial and operational resources to analyze and develop our in-market opportunities. To complement our in-market growth agenda, we intendto focus on selectively developing and acquiring new hospitals, outpatient facilities and other health care service providers. We believe the challengesfaced by the hospital industry may continue to spur consolidation and we believe our size, scale, national presence and access to capital will position uswell to participate in any such consolidation.
Critical Accounting Policies and Estimates
The preparation of our consolidated financial statements requires management to make estimates and assumptions that affect the reported amountsof assets and liabilities, the disclosure of contingent liabilities and the reported amounts of revenues and expenses. Our estimates are based on historicalexperience and various other assumptions we believe are reasonable under the circumstances. We evaluate our estimates on an ongoing basis and makechanges to the estimates and related disclosures as experience develops or new information becomes known. Actual results may differ from theseestimates.
We believe the following critical accounting policies affect our more significant judgments and estimates used in the preparation of ourconsolidated financial statements.
Revenues
Revenues are recorded during the period the health care services are provided, based upon the estimated amounts due from payers. Estimates ofcontractual allowances under managed care health plans are based upon the payment terms specified in the related contractual agreements. Laws andregulations governing the Medicare and Medicaid programs are complex and subject to interpretation. The estimated reimbursement amounts are madeon a payer-specific basis and are recorded based on the best information available regarding management’s interpretation of the applicable laws,regulations and contract terms. Management continually reviews the contractual estimation process to consider and incorporate updates to laws andregulations and the frequent changes in managed care contractual terms resulting from contract renegotiations and renewals. We have investedsignificant resources to refine and improve our billing systems and the information system data used to make contractual allowance estimates. We havedeveloped standardized calculation processes and related employee training programs to improve the utility of our patient accounting systems.
The Emergency Medical Treatment and Labor Act (“EMTALA”) requires any hospital participating in the Medicare program to conduct anappropriate medical screening examination of every person who presents to the hospital’s emergency room for treatment and, if the individual issuffering from an emergency medical condition,
56
276

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 57/137
Table of Contents
HCA HEALTHCARE, INC.
MANAGEMENT’S DISCUSSION AND ANALYSIS OF FINANCIAL CONDITIONAND RESULTS OF OPERATIONS (Continued)
Critical Accounting Policies and Estimates (continued)
Revenues (continued)
to either stabilize the condition or make an appropriate transfer of the individual to a facility able to handle the condition. The obligation to screen andstabilize emergency medical conditions exists regardless of an individual’s ability to pay for treatment. Federal and state laws and regulations, includingbut not limited to EMTALA, require, and our commitment to providing quality patient care encourages, the provision of services to patients who arefinancially unable to pay for the health care services they receive.
Prior to November 2017, patients treated at hospitals for non-elective care, who have income at or below 200% of the federal poverty level, wereeligible for charity care. During November 2017, we expanded our charity policy to include patients who have income above 200%, but at or below400%, of the federal poverty level and we limit the patient responsibility amounts for these patients to a percentage of their annual household income,computed on a sliding scale based upon their annual income and the applicable percentage of the federal poverty level. The federal poverty level isestablished by the federal government and is based on income and family size. Because we do not pursue collection of amounts determined to qualify ascharity care, they are not reported in revenues. We provide discounts to uninsured patients who do not qualify for Medicaid or charity care. We mayattempt to provide assistance to uninsured patients to help determine whether they may qualify for Medicaid, other federal or state assistance, or charitycare. If an uninsured patient does not qualify for these programs, the uninsured discount is applied.
Due to the complexities involved in the classification and documentation of health care services authorized and provided, the estimation ofrevenues earned and the related reimbursement are often subject to interpretations that could result in payments that are different from our estimates.Adjustments to estimated Medicare and Medicaid reimbursement amounts and disproportionate-share funds, which resulted in net increases to revenues,related primarily to cost reports filed during the respective year were $51 million, $29 million and $41 million in 2019, 2018 and 2017, respectively. Theadjustments to estimated reimbursement amounts, which resulted in net increases to revenues, related primarily to cost reports filed during previousyears were $13 million, $51 million and $56 million in 2019, 2018 and 2017, respectively. We expect adjustments during the next 12 months related toMedicare and Medicaid cost report filings and settlements will result in increases to revenues generally similar to the amounts recorded during theseyears.
The collection of outstanding receivables for Medicare, Medicaid, managed care payers, other third-party payers and patients is our primarysource of cash and is critical to our operating performance. The primary collection risks relate to uninsured patient accounts, including patient accountsfor which the primary insurance carrier has paid the amounts covered by the applicable agreement, but patient responsibility amounts (deductibles andcopayments) remain outstanding. Implicit price concessions relate primarily to amounts due directly from patients. Estimated implicit price concessionsare recorded for all uninsured accounts, regardless of the age of those accounts. Accounts are written off when all reasonable collection efforts havebeen performed.
The estimates for implicit price concessions are based upon management’s assessment of historical writeoffs and expected net collections,business and economic conditions, trends in federal, state and private employer health care coverage and other collection indicators. Management relieson the results of detailed reviews of historical writeoffs and collections at facilities that represent a majority of our revenues and accounts receivable (the“hindsight analysis”) as a primary source of information in estimating the collectability of our accounts receivable. We perform the hindsight analysisquarterly, utilizing rolling twelve-months accounts receivable collection and writeoff data. We believe our quarterly updates to the estimated implicitprice
57
277

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 58/137
Table of Contents
HCA HEALTHCARE, INC.
MANAGEMENT’S DISCUSSION AND ANALYSIS OF FINANCIAL CONDITIONAND RESULTS OF OPERATIONS (Continued)
Critical Accounting Policies and Estimates (continued)
Revenues (continued)
concession amounts at each of our hospital facilities provide reasonable estimates of our revenues and valuations of our accounts receivable. Theseroutine, quarterly changes in estimates have not resulted in material adjustments to the valuations of our accounts receivable or period-to-periodcomparisons of our results of operations. At December 31, 2019 and December 31, 2018, estimated implicit price concessions of $6.953 billion and$6.280 billion, respectively, had been recorded to adjust our revenues and accounts receivable to the estimated amounts we expect to collect.
To quantify the total impact of and trends related to uninsured patient accounts, we believe it is beneficial to view total uncompensated care,which is comprised of charity care, uninsured discounts and implicit price concessions. A summary of the estimated cost of total uncompensated care forthe years ended December 31, follows (dollars in millions):
2019 2018 2017 Patient care costs (salaries and benefits, supplies, other operating expenses and depreciation and
amortization)
$44,118
$40,035
$37,557 Cost-to-charges ratio (patient care costs as percentage of gross patient charges) 12.0% 12.4% 12.9%Total uncompensated care $31,105 $26,757 $23,420 Multiply by the cost-to-charges ratio 12.0% 12.4% 12.9%Estimated cost of total uncompensated care $ 3,733 $ 3,318 $ 3,021
Days revenues in accounts receivable were 50 days, 51 days and 52 days at December 31, 2019, 2018 and 2017, respectively. Managementexpects a continuation of the challenges related to the collection of the patient due accounts. Adverse changes in the percentage of our patients havingadequate health care coverage, increases in patient responsibility amounts under certain health care coverages, general economic conditions, patientaccounting service center operations, payer mix, or trends in federal, state, and private employer health care coverage could affect the collection ofaccounts receivable, cash flows and results of operations.
Professional Liability Claims
We, along with virtually all health care providers, operate in an environment with professional liability risks. Our facilities are insured by our100% owned insurance subsidiary for losses up to $50 million per occurrence, subject, in most cases, to a $15 million per occurrence self-insuredretention. The insurance subsidiary has obtained reinsurance for professional liability risks generally above a retention level of $25 million peroccurrence. We purchase excess insurance on a claims-made basis for losses in excess of $50 million per occurrence. Provisions for losses related toprofessional liability risks were $497 million, $447 million and $466 million for the years ended December 31, 2019, 2018 and 2017, respectively.During 2019 and 2018, we recorded reductions to the provision for professional liability risks of $50 million and $70 million, respectively, due to thereceipt of updated actuarial information.
Reserves for professional liability risks represent the estimated ultimate cost of all reported and unreported losses incurred through the respectiveconsolidated balance sheet dates. The estimated ultimate cost includes
58
278

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 59/137
Table of Contents
HCA HEALTHCARE, INC.
MANAGEMENT’S DISCUSSION AND ANALYSIS OF FINANCIAL CONDITIONAND RESULTS OF OPERATIONS (Continued)
Critical Accounting Policies and Estimates (continued)
Professional Liability Claims (continued)
estimates of direct expenses and fees paid to outside counsel and experts, but does not include the general overhead costs of our insurance subsidiary orcorporate office. Individual case reserves are established based upon the particular circumstances of each reported claim and represent our estimates ofthe future costs that will be paid on reported claims. Case reserves are reduced as claim payments are made and are adjusted upward or downward as ourestimates regarding the amounts of future losses are revised. Once the case reserves for known claims are determined, information is stratified by losslayers and retentions, accident years, reported years, and geographic location of our hospitals. Several actuarial methods are employed to utilize this datato produce estimates of ultimate losses and reserves for incurred but not reported claims, including: paid and incurred extrapolation methods utilizingpaid and incurred loss development to estimate ultimate losses; frequency and severity methods utilizing paid and incurred claims development toestimate ultimate average frequency (number of claims) and ultimate average severity (cost per claim); and Bornhuetter-Ferguson methods which addexpected development to actual paid or incurred experience to estimate ultimate losses. These methods use our company-specific historical claims dataand other information. Company-specific claim reporting and payment data collected over an approximate 20-year period is used in our reserveestimation process. This company-specific data includes information regarding our business, including historical paid losses and loss adjustmentexpenses, historical and current case loss reserves, actual and projected hospital statistical data, professional liability retentions for each policy year,geographic information and other data.
Reserves and provisions for professional liability risks are based upon actuarially determined estimates. The estimated reserve ranges, net ofamounts receivable under reinsurance contracts, were $1.589 billion to $1.903 billion at December 31, 2019 and $1.514 billion to $1.814 billion atDecember 31, 2018. Our estimated reserves for professional liability claims may change significantly if future claims differ from expected trends. Weperform sensitivity analyses which model the volatility of key actuarial assumptions and monitor our reserves for adequacy relative to all ourassumptions in the aggregate. Based on our analysis, we believe the estimated professional liability reserve ranges represent the reasonably likelyoutcomes for ultimate losses. We consider the number and severity of claims to be the most significant assumptions in estimating reserves forprofessional liabilities. A 2.5% change in the expected frequency trend could be reasonably likely and would increase the reserve estimate by$32 million or reduce the reserve estimate by $31 million. A 2.5% change in the expected claim severity trend could be reasonably likely and wouldincrease the reserve estimate by $117 million or reduce the reserve estimate by $107 million. We believe adequate reserves have been recorded for ourprofessional liability claims; however, due to the complexity of the claims, the extended period of time to resolve the claims and the wide range ofpotential outcomes, our ultimate liability for professional liability claims could change by more than the estimated sensitivity amounts and could changematerially from our current estimates.
The reserves for professional liability risks cover approximately 2,300 and 2,200 individual claims at December 31, 2019 and 2018, respectively,and estimates for unreported potential claims. The time period required to resolve these claims can vary depending upon the jurisdiction and whether theclaim is settled or litigated. The average time period between the occurrence and final resolution for our professional liability claims is approximatelyfour years, although the facts and circumstances of each individual claim can result in an occurrence-to-resolution timeframe that varies from thisaverage. The estimation of the timing of payments beyond a year can vary significantly.
Reserves for professional liability risks were $1.827 billion and $1.741 billion at December 31, 2019 and 2018, respectively. The current portionof these reserves, $457 million and $466 million at December 31, 2019
59
279

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 60/137
Table of Contents
HCA HEALTHCARE, INC.
MANAGEMENT’S DISCUSSION AND ANALYSIS OF FINANCIAL CONDITIONAND RESULTS OF OPERATIONS (Continued)
Critical Accounting Policies and Estimates (continued)
Professional Liability Claims (continued)
and 2018, respectively, is included in “other accrued expenses.” Obligations covered by reinsurance and excess insurance contracts are included in thereserves for professional liability risks, as we remain liable to the extent reinsurers and excess insurance carriers do not meet their obligations. Reservesfor professional liability risks (net of $46 million and $50 million receivable under reinsurance and excess insurance contracts at December 31, 2019 and2018, respectively) were $1.781 billion and $1.692 billion at December 31, 2019 and 2018, respectively. The estimated total net reserves forprofessional liability risks at December 31, 2019 and 2018 are comprised of $695 million and $703 million, respectively, of case reserves for knownclaims and $1.086 billion and $989 million, respectively, of reserves for incurred but not reported claims.
Changes in our professional liability reserves, net of reinsurance recoverable, for the years ended December 31, are summarized in the followingtable (dollars in millions):
2019 2018 2017 Net reserves for professional liability claims, January 1 $1,692 $1,603 $1,494
Provision for current year claims 499 486 467 Favorable development related to prior years’ claims (2) (39) (1)
Total provision 497 447 466 Payments for current year claims 8 3 7 Payments for prior years’ claims 400 355 350
Total claim payments 408 358 357 Net reserves for professional liability claims, December 31 $1,781 $1,692 $1,603
Income Taxes
We calculate our provision for income taxes using the asset and liability method, under which deferred tax assets and liabilities are recognized byidentifying the temporary differences that arise from the recognition of items in different periods for tax and accounting purposes. Deferred tax assetsgenerally represent the tax effects of amounts expensed in our income statement for which tax deductions will be claimed in future periods. Interest andpenalties payable to taxing authorities are included as a component of our provision for income taxes. We have elected to treat taxes incurred on globalintangible low-taxed income as a period expense.
Although we believe we have properly reported taxable income and paid taxes in accordance with applicable laws, federal, state or foreign taxingauthorities may challenge our tax positions upon audit. Significant judgment is required in determining and assessing the impact of uncertain taxpositions. We report a liability for unrecognized tax benefits from uncertain tax positions taken or expected to be taken in our income tax returns. Duringeach reporting period, we assess the facts and circumstances related to uncertain tax positions. If the realization of unrecognized tax benefits is deemedprobable based upon new facts and circumstances, the estimated liability and the provision for income taxes are reduced in the current period. Finalaudit results may vary from our estimates.
60
280

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 61/137
Table of Contents
HCA HEALTHCARE, INC.
MANAGEMENT’S DISCUSSION AND ANALYSIS OF FINANCIAL CONDITIONAND RESULTS OF OPERATIONS (Continued)
Results of Operations
Revenue/Volume Trends
Our revenues depend upon inpatient occupancy levels, the ancillary services and therapy programs ordered by physicians and provided to patients,the volume of outpatient procedures and the charge and negotiated payment rates for such services. Gross charges typically do not reflect what ourfacilities are actually paid. Our facilities have entered into agreements with third-party payers, including government programs and managed care healthplans, under which the facilities are paid based upon the cost of providing services, predetermined rates per diagnosis, fixed per diem rates or discountsfrom gross charges. We do not pursue collection of amounts related to patients who meet our guidelines to qualify for charity care; therefore, they arenot reported in revenues. We provide discounts to uninsured patients who do not qualify for Medicaid or charity care.
Revenues increased 10.0% to $51.336 billion for 2019 from $46.677 billion for 2018 and increased 7.0% for 2018 from $43.614 billion for 2017.The increase in revenues in 2019 can be primarily attributed to the combined impact of a 3.2% increase in revenue per equivalent admission and a 6.6%increase in equivalent admissions compared to the prior year. The increase in revenues in 2018 can be primarily attributed to the combined impact of a2.8% increase in revenue per equivalent admission and a 4.1% increase in equivalent admissions compared to the prior year.
Same facility revenues increased 5.9% for the year ended December 31, 2019 compared to the year ended December 31, 2018 and increased 6.5%for the year ended December 31, 2018 compared to the year ended December 31, 2017. The 5.9% increase for 2019 can be primarily attributed to thecombined impact of a 2.3% increase in same facility revenue per equivalent admission and a 3.5% increase in same facility equivalent admissions. The6.5% increase for 2018 can be primarily attributed to the combined impact of a 3.9% increase in same facility revenue per equivalent admission and a2.5% increase in same facility equivalent admissions.
Consolidated admissions increased 5.2% during 2019 compared to 2018 and increased 3.5% during 2018 compared to 2017. Consolidatedsurgeries increased 3.7% during 2019 compared to 2018 and increased 2.6% during 2018 compared to 2017. Consolidated emergency room visitsincreased 4.5% during 2019 compared to 2018 and increased 1.6% during 2018 compared to 2017.
Same facility admissions increased 2.8% during 2019 compared to 2018 and increased 2.5% during 2018 compared to 2017. Same facilitysurgeries each increased 1.4% during 2019 compared to 2018 and during 2018 compared to 2017. Same facility emergency room visits increased 2.8%during 2019 compared to 2018 and increased 0.1% during 2018 compared to 2017.
Same facility uninsured emergency room visits increased 3.9% and same facility uninsured admissions increased 3.7% during 2019 compared to2018. Same facility uninsured emergency room visits increased 3.8% and same facility uninsured admissions increased 8.5% during 2018 compared to2017.
61
281

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 62/137
Table of Contents
HCA HEALTHCARE, INC.
MANAGEMENT’S DISCUSSION AND ANALYSIS OF FINANCIAL CONDITIONAND RESULTS OF OPERATIONS (Continued)
Results of Operations (continued)
Revenue/Volume Trends (continued)
The approximate percentages of our admissions related to Medicare, managed Medicare, Medicaid, managed Medicaid, managed care andinsurers and the uninsured for the years ended December 31, 2019, 2018 and 2017 are set forth below.
Years Ended December 31, 2019 2018 2017
Medicare 29% 30% 30%Managed Medicare 18 17 16 Medicaid 5 5 6 Managed Medicaid 12 12 12 Managed care and insurers 28 28 28 Uninsured 8 8 8
100% 100% 100%
The approximate percentages of our inpatient revenues related to Medicare, managed Medicare, Medicaid, managed Medicaid, and managed careand insurers for the years ended December 31, 2019, 2018 and 2017 are set forth below.
Years Ended December 31, 2019 2018 2017
Medicare 28% 28% 28%Managed Medicare 15 14 13 Medicaid 5 4 5 Managed Medicaid 5 6 5 Managed care and insurers 47 48 49
100% 100% 100%
At December 31, 2019, we owned and operated 45 hospitals and 33 surgery centers in the state of Florida. Our Florida facilities’ revenues totaled$11.494 billion, $10.892 billion and $10.168 billion for the years ended December 31, 2019, 2018 and 2017, respectively. At December 31, 2019, weowned and operated 46 hospitals and 29 surgery centers in the state of Texas. Our Texas facilities’ revenues totaled $13.101 billion, $12.023 billion and$10.634 billion for the years ended December 31, 2019, 2018 and 2017, respectively. During 2019, 2018 and 2017, 56%, 57% and 56% of ouradmissions and 48%, 49% and 48%, respectively, of our revenues were generated by our Florida and Texas facilities. Uninsured admissions in Floridaand Texas represented 72%, 70% and 70% of our uninsured admissions during 2019, 2018 and 2017, respectively.
We receive a significant portion of our revenues from government health programs, principally Medicare and Medicaid, which are highlyregulated and subject to frequent and substantial changes. In December 2017, the Centers for Medicare & Medicaid Services (“CMS”) announced that itwill phase out federal matching funds for Designated State Health Programs under waivers granted under Section 1115 of the Social Security Act. Texascurrently operates its Healthcare Transformation and Quality Improvement Program pursuant to a Medicaid waiver. In December 2017, CMS approvedan extension of this waiver through September 30, 2022, but
62
282

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 63/137
Table of Contents
HCA HEALTHCARE, INC.
MANAGEMENT’S DISCUSSION AND ANALYSIS OF FINANCIAL CONDITIONAND RESULTS OF OPERATIONS (Continued)
Results of Operations (continued)
Revenue/Volume Trends (continued)
indicated that it will phase out some of the federal funding. Our Texas Medicaid revenues included Medicaid supplemental waiver payments of$416 million, $450 million and $351 million during 2019, 2018 and 2017, respectively.
In addition, we receive supplemental payments in several other states. We are aware these supplemental payment programs are currently beingreviewed by CMS and certain state agencies, and that some states have made waiver requests to CMS to replace their existing supplemental paymentprograms. It is possible these reviews and waiver requests will result in the restructuring of such supplemental payment programs and could result in thepayment programs being reduced or eliminated. Because deliberations about these programs are ongoing, we are unable to estimate the financial impactthe program structure modifications, if any, may have on our results of operations.
63
283

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 64/137
Table of Contents
HCA HEALTHCARE, INC.
MANAGEMENT’S DISCUSSION AND ANALYSIS OF FINANCIAL CONDITIONAND RESULTS OF OPERATIONS (Continued)
Results of Operations (continued)
Operating Results Summary
The following are comparative summaries of operating results for the years ended December 31, 2019, 2018 and 2017 (dollars in millions):
2019 2018 2017 Amount Ratio Amount Ratio Amount Ratio
Revenues $51,336 100.0 $46,677 100.0 $43,614 100.0
Salaries and benefits 23,560 45.9 21,425 45.9 20,059 46.0 Supplies 8,481 16.5 7,724 16.5 7,316 16.8 Other operating expenses 9,481 18.5 8,608 18.5 8,051 18.4 Equity in earnings of affiliates (43) (0.1) (29) (0.1) (45) (0.1)Depreciation and amortization 2,596 5.0 2,278 4.9 2,131 4.9 Interest expense 1,824 3.6 1,755 3.8 1,690 3.9 Gain on sales of facilities (18) — (428) (0.9) (8) — Losses on retirement of debt 211 0.4 9 — 39 0.1
46,092 89.8 41,342 88.6 39,233 90.0 Income before income taxes 5,244 10.2 5,335 11.4 4,381 10.0 Provision for income taxes 1,099 2.1 946 2.0 1,638 3.7 Net income 4,145 8.1 4,389 9.4 2,743 6.3 Net income attributable to noncontrolling interests 640 1.3 602 1.3 527 1.2 Net income attributable to HCA Healthcare, Inc. $ 3,505 6.8 $ 3,787 8.1 $ 2,216 5.1 % changes from prior year:
Revenues 10.0% 7.0% 5.1% Income before income taxes (1.7) 21.8 (8.9) Net income attributable to HCA Healthcare, Inc. (7.4) 70.9 (23.3) Admissions(a) 5.2 3.5 2.4 Equivalent admissions(b) 6.6 4.1 3.0 Revenue per equivalent admission 3.2 2.8 2.1
Same facility % changes from prior year(c): Revenues 5.9 6.5 3.8 Admissions(a) 2.8 2.5 1.1 Equivalent admissions(b) 3.5 2.5 1.5 Revenue per equivalent admission 2.3 3.9 2.2
(a) Represents the total number of patients admitted to our hospitals and is used by management and certain investors as a general measure of
inpatient volume. (b) Equivalent admissions are used by management and certain investors as a general measure of combined inpatient and outpatient volume.
Equivalent admissions are computed by multiplying admissions (inpatient volume) by the sum of gross inpatient revenue and gross outpatientrevenue and then dividing the resulting amount by gross inpatient revenue. The equivalent admissions computation “equates” outpatient revenueto the volume measure (admissions) used to measure inpatient volume, resulting in a general measure of combined inpatient and outpatientvolume.
(c) Same facility information excludes the operations of hospitals and their related facilities that were either acquired, divested or removed fromservice during the current and prior year.
64
284

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 65/137
Table of Contents
HCA HEALTHCARE, INC.
MANAGEMENT’S DISCUSSION AND ANALYSIS OF FINANCIAL CONDITIONAND RESULTS OF OPERATIONS (Continued)
Results of Operations (continued)
Years Ended December 31, 2019 and 2018
Net income attributable to HCA Healthcare, Inc. totaled $3.505 billion, or $10.07 per diluted share, for 2019, compared to $3.787 billion, or$10.66 per diluted share, for 2018. The 2019 results include gains on sales of facilities of $18 million, or $0.04 per diluted share, and losses onretirement of debt of $211 million, or $0.47 per diluted share. The 2018 results include gains on sales of facilities of $428 million, or $0.91 per dilutedshare, and losses on retirement of debt of $9 million, or $0.02 per diluted share. The 2019 results include revenues of $86 million, or $0.19 per dilutedshare, related to the resolution of transaction price differences regarding certain out-of-network services performed in prior periods. The 2018 resultsinclude a reduction in our provision for income taxes of $67 million, or $0.19 per diluted share, for the remeasurement of certain of our deferred taxassets and liabilities for which we were unable to record reasonable estimates in 2017. During 2019 and 2018, we recorded reductions to the provisionfor professional liability risks of $50 million, or $0.11 per diluted share, and $70 million, or $0.15 per diluted share, respectively. During 2018, werecorded additional expenses and losses of revenues estimated at approximately $31 million, or $0.07 per diluted share, associated with the impact ofhurricane Michael on our Florida facilities. This amount is prior to any insurance recoveries. During 2018, we recorded a benefit of $49 million, or$0.11 per diluted share, from an insurance recovery related to hurricane Harvey business interruption losses incurred during 2017, and we recorded areduction to the provision for income taxes of $28 million, or $0.08 per diluted share, for tax credits related to certain 2017 hurricane-related expenses.Our provisions for income taxes for 2019 and 2018 included tax benefits of $65 million, or $0.19 per diluted share, and $124 million, or $0.35 perdiluted share, respectively, related to employee equity award settlements. All “per diluted share” disclosures are based upon amounts net of theapplicable income taxes. Shares used for diluted earnings per share were 348.226 million shares and 355.303 million shares for the years endedDecember 31, 2019 and 2018, respectively. During 2019 and 2018, we repurchased 7.949 million and 14.070 million shares, respectively, of ourcommon stock.
During 2019, consolidated admissions increased 5.2% and same facility admissions increased 2.8% compared to 2018. Consolidated inpatientsurgeries increased 3.4% and same facility inpatient surgeries increased 1.1% during 2019 compared to 2018. Consolidated outpatient surgeriesincreased 4.0%, and same facility outpatient surgeries increased 1.6% during 2019 compared to 2018. Emergency room visits increased 4.5% on aconsolidated basis and increased 2.8% on a same facility basis during 2019 compared to 2018.
Revenues increased 10.0% to $51.336 billion for 2019 from $46.677 billion for 2018. The increase in revenues was primarily due to the combinedimpact of a 3.2% increase in revenue per equivalent admission and a 6.6% increase in equivalent admissions compared to 2018. Same facility revenuesincreased 5.9% due primarily to the combined impact of a 2.3% increase in same facility revenue per equivalent admission and a 3.5% increase in samefacility equivalent admissions compared to 2018.
Salaries and benefits, as a percentage of revenues, were 45.9% each in 2019 and 2018. Salaries and benefits per equivalent admission increased3.1% in 2019 compared to 2018. Same facility labor rate increases averaged 2.7% for 2019 compared to 2018. Share-based compensation expense was$347 million in 2019 and $268 million in 2018.
Supplies, as a percentage of revenues, were 16.5% each in 2019 and 2018. Supply costs per equivalent admission increased 3.0% in 2019compared to 2018. Supply costs per equivalent admission increased 2.8% for medical devices, 8.6% for pharmacy supplies and 1.0% for generalmedical and surgical items in 2019 compared to 2018. Same facility supply costs per equivalent admission increased 1.6% for medical devices and 2.2%for general medical and surgical items and declined 2.1% for pharmacy supplies in 2019 compared to 2018.
65
285

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 66/137
Table of Contents
HCA HEALTHCARE, INC.
MANAGEMENT’S DISCUSSION AND ANALYSIS OF FINANCIAL CONDITIONAND RESULTS OF OPERATIONS (Continued)
Results of Operations (continued)
Years Ended December 31, 2019 and 2018 (continued)
Other operating expenses, as a percentage of revenues, were 18.5% each in 2019 and 2018. Other operating expenses are primarily comprised ofcontract services, professional fees, repairs and maintenance, rents and leases, utilities, insurance (including professional liability insurance) andnonincome taxes. Provisions for losses related to professional liability risks were $497 million and $447 million for 2019 and 2018, respectively.
Equity in earnings of affiliates was $43 million for 2019 and $29 million for 2018.
Depreciation and amortization, as a percentage of revenues, was 5.0% in 2019 and 4.9% in 2018. Depreciation expense was $2.579 billion for2019 and $2.262 billion for 2018, and the $317 million increase was due to both acquisitions and increased capital expenditures in 2019 (same facilitydepreciation amortization increased $154 million).
Interest expense increased to $1.824 billion for 2019 from $1.755 billion for 2018. The increase in interest expense was due to an increase in theaverage debt balance. Our average debt balance was $34.288 billion for 2019 compared to $33.065 billion for 2018. The average interest rate for ourlong-term debt was 5.3% for both 2019 and 2018.
Gains on sales of facilities were $18 million and $428 million, respectively, for 2019 and 2018. The gains on sales of facilities for 2019 relatedprimarily to sales of real estate and other investments. The gains on sales of facilities for 2018 related primarily to the sale of the two hospital facilitiesin our Oklahoma market.
During June 2019, we issued $5.000 billion aggregate principal amount of senior secured notes comprised of $2.000 billion aggregate principalamount of 4 1/8% notes due 2029, $1.000 billion aggregate principal amount of 5 1/8% notes due 2039 and $2.000 billion aggregate principal amount of5 1/4% notes due 2049. During July 2019, we redeemed all $600 million outstanding aggregate principal amount of 4.25% senior secured notes due2019, all $3.000 billion outstanding aggregate principal amount of 6.50% senior secured notes due 2020 and all $1.350 billion outstanding aggregateprincipal amount of 5.875% senior secured notes due 2022. The pretax loss on retirement of debt for these redemptions was $211 million. During 2018,we issued $2.000 billion aggregate principal amount of senior notes comprised of $1.000 billion aggregate principal amount of 5.375% notes due 2026and $1.000 billion aggregate principal amount of 5.625% notes due 2028. We used the net proceeds for general corporate purposes, including fundingthe purchase of a hospital, and the redemption of all $1.500 billion aggregate principal amount of our existing 3.750% senior secured notes maturing inMarch 2019. The pretax loss on retirement of debt was $9 million.
The effective tax rates were 23.9% and 20.0% for 2019 and 2018, respectively. The effective tax rate computations exclude net incomeattributable to noncontrolling interests as it relates to consolidated partnerships. Our provision for income taxes for 2018 included $28 million ofbenefits for tax credits related to certain 2017 hurricane-related expenses and $67 million of benefits related to the remeasurement of our deferred taxassets and liabilities due to the enactment of the Tax Act. Our provisions for income taxes for 2019 and 2018 also included tax benefits of $65 millionand $124 million, respectively, related to employee equity award settlements. Excluding the effect of these adjustments, the effective tax rates for 2019and 2018 would have been 25.3% and 24.6%, respectively.
66
286

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 67/137
Table of Contents
HCA HEALTHCARE, INC.
MANAGEMENT’S DISCUSSION AND ANALYSIS OF FINANCIAL CONDITIONAND RESULTS OF OPERATIONS (Continued)
Results of Operations (continued)
Years Ended December 31, 2019 and 2018 (continued)
Net income attributable to noncontrolling interests increased from $602 million for 2018 to $640 million for 2019. The increase in net incomeattributable to noncontrolling interests related primarily to a joint venture in one of our Texas markets and the operations of our surgery centerpartnerships.
For results of operations comparisons relating to years ending December 31, 2018 and 2017, refer to our annual report on Form 10-K, Item 7.Management’s Discussion and Analysis of Financial Condition and Results of Operations for the year ended December 31, 2018, filed with theSecurities and Exchange Commission on February 21, 2019.
Liquidity and Capital Resources
Our primary cash requirements are paying our operating expenses, servicing our debt, capital expenditures on our existing properties, acquisitionsof hospitals and other health care entities, repurchases of our common stock, distributions to stockholders and distributions to noncontrolling interests.Our primary cash sources are cash flows from operating activities, issuances of debt and equity securities and dispositions of hospitals and other healthcare entities.
Cash provided by operating activities totaled $7.602 billion in 2019 compared to $6.761 billion in 2018 and $5.426 billion in 2017. The$841 million increase in cash provided by operating activities for 2019, compared to 2018, was primarily related to the increase in net income, excludinggains on sales of facilities and losses on retirement of debt, of $222 million and increases related to income taxes of $322 million and depreciation andamortization of $318 million. The $1.335 billion increase in cash provided by operating activities for 2018, compared to 2017, was primarily related tothe increase in net income, excluding gains on sales of facilities, of $1.309 billion. Working capital totaled $3.439 billion at December 31, 2019 and$2.644 billion at December 31, 2018. The increase in working capital of $795 million is primarily related to a decline in long-term debt due within oneyear of $643 million. Cash payments for interest and income taxes increased $147 million for 2019 compared to 2018 and declined $289 million for2018 compared to 2017.
Cash used in investing activities was $5.720 billion, $3.901 billion and $4.279 billion in 2019, 2018 and 2017, respectively. Excludingacquisitions, capital expenditures were $4.158 billion in 2019, $3.573 billion in 2018 and $3.015 billion in 2017. We expended $1.682 billion,$1.253 billion and $1.212 billion for acquisitions of hospitals and health care entities during 2019, 2018 and 2017, respectively. Planned capitalexpenditures are expected to approximate $4.0 billion to $4.2 billion in 2020. At December 31, 2019, there were projects under construction which hadan estimated additional cost to complete and equip over the next five years of approximately $3.0 billion. We expect to finance capital expenditures withinternally generated and borrowed funds. Cash received from sales of hospitals and health care entities declined $747 million for 2019 compared to2018 primarily related to the receipt during 2018 of $758 million from the sale of the two hospitals in our Oklahoma market.
Cash used in financing activities totaled $1.771 billion in 2019, $3.075 billion in 2018 and $1.061 billion in 2017. During 2019, we had a netincrease of $567 million in our indebtedness, paid dividends of $550 million and paid $1.031 billion for repurchases of common stock. During 2018, wehad a net decline of $344 million in our indebtedness, paid dividends of $487 million and paid $1.530 billion for repurchases of common stock. During2017, we had a net increase of $1.509 billion in our indebtedness and paid $2.051 billion for repurchases
67
287

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 68/137
Table of Contents
HCA HEALTHCARE, INC.
MANAGEMENT’S DISCUSSION AND ANALYSIS OF FINANCIAL CONDITIONAND RESULTS OF OPERATIONS (Continued)
Liquidity and Capital Resources (continued)
of common stock. During 2019, 2018 and 2017, we made distributions to noncontrolling interests of $542 million, $441 million and $448 million,respectively.
We, or our affiliates, may in the future repurchase portions of our debt or equity securities, subject to certain limitations, from time to time ineither the open market or through privately negotiated transactions, in accordance with applicable SEC and other legal requirements. The timing, prices,and sizes of purchases depend upon prevailing trading prices, general economic and market conditions, and other factors, including applicable securitieslaws. During January 2020 and 2019, our Board of Directors authorized share repurchase programs for up to $4 billion ($2 billion for eachauthorization) of our outstanding common stock, and at December 31, 2019, there was $1.241 billion of share repurchase authorization that remainedavailable under the January 2019 authorization. Funds for the repurchase of debt or equity securities have, and are expected to, come primarily fromcash generated from operations and borrowed funds. On January 27, 2020, our Board of Directors declared a quarterly dividend of $0.43 per share onour common stock payable on March 31, 2020 to stockholders of record at the close of business on March 2, 2020. During 2019, our Board of Directorsdeclared four quarterly dividends of $0.40 per share, or $1.60 per share in the aggregate, on our common stock. The timing and amount of future cashdividends will vary based on a number of factors, including future capital requirements for strategic transactions, share repurchases and investing in ourexisting markets, the availability of financing on acceptable terms, debt service requirements, changes to applicable tax laws or corporate laws, changesto our business model and periodic determinations by our Board of Directors that cash dividends are in the best interest of stockholders and are incompliance with all applicable laws and agreements of the Company.
In addition to cash flows from operations, available sources of capital include amounts available under our senior secured credit facilities($3.237 billion as of December 31, 2019 and $3.187 billion as of January 31, 2020) and anticipated access to public and private debt and equity markets.
Investments of our insurance subsidiaries, held to maintain statutory equity levels and to provide liquidity to pay claims, totaled $462 million and$409 million at December 31, 2019 and 2018, respectively. The insurance subsidiary maintained net reserves for professional liability risks of$175 million and $183 million at December 31, 2019 and 2018, respectively. Our facilities are insured by our 100% owned insurance subsidiary forlosses up to $50 million per occurrence; however, this coverage is subject, in most cases, to a $15 million per occurrence self-insured retention. Netreserves for the self-insured professional liability risks retained were $1.606 billion and $1.509 billion at December 31, 2019 and 2018, respectively.Claims payments, net of reinsurance recoveries, during the next 12 months are expected to approximate $448 million. We estimate that approximately$394 million of the expected net claim payments during the next 12 months will relate to claims subject to the self-insured retention.
Financing Activities
We are a highly leveraged company with significant debt service requirements. Our debt totaled $33.722 billion and $32.821 billion atDecember 31, 2019 and 2018, respectively. Our interest expense was $1.824 billion for 2019 and $1.755 billion for 2018.
During August 2018, we issued $2.000 billion aggregate principal amount of senior unsecured notes comprised of $1.000 billion aggregateprincipal amount of 5.375% notes due 2026 and $1.000 billion aggregate principal amount of 5.625% notes due 2028. We used the net proceeds forgeneral corporate purposes, including
68
288

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 69/137
Table of Contents
HCA HEALTHCARE, INC.
MANAGEMENT’S DISCUSSION AND ANALYSIS OF FINANCIAL CONDITIONAND RESULTS OF OPERATIONS (Continued)
Liquidity and Capital Resources (continued)
Financing Activities (continued)
funding the purchase of a hospital, and the redemption of all $1.500 billion aggregate principal amount of our existing 3.750% senior secured notesmaturing in March 2019.
During January 2019, we issued $1.500 billion aggregate principal amount of senior unsecured notes comprised of $1.000 billion aggregateprincipal amount of 5.875% notes due 2029 and $500 million aggregate principal amount of 5.625% notes due 2028. We used the net proceeds to fundthe purchase of a seven-hospital health system located in western North Carolina.
During June 2019, we issued $5.000 billion aggregate principal amount of senior secured notes comprised of $2.000 billion aggregate principalamount of 4 1/8% notes due 2029, $1.000 billion aggregate principal amount of 5 1/8% notes due 2039 and $2.000 billion aggregate principal amount of5 1/4% notes due 2049. During July 2019, we redeemed all $600 million outstanding aggregate principal amount of 4.25% senior secured notes due2019, all $3.000 billion outstanding aggregate principal amount of 6.50% senior secured notes due 2020 and all $1.350 billion outstanding aggregateprincipal amount of 5.875% senior secured notes due 2022.
Management believes that cash flows from operations, amounts available under our senior secured credit facilities and our anticipated access topublic and private debt markets will be sufficient to meet expected liquidity needs during the next twelve months.
69
289

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 70/137
Table of Contents
HCA HEALTHCARE, INC.
MANAGEMENT’S DISCUSSION AND ANALYSIS OF FINANCIAL CONDITIONAND RESULTS OF OPERATIONS (Continued)
Contractual Obligations and Off-Balance Sheet Arrangements
As of December 31, 2019, maturities of contractual obligations and other commercial commitments are presented in the table below (dollars inmillions):
Payments Due by Period Contractual Obligations(a) Total Current 2-3 Years 4-5 Years After 5 Years Long-term debt including interest, excluding the senior secured credit
facilities(b)
$42,756
$1,667
$ 6,061
$ 7,227
$ 27,801 Loans outstanding under the senior secured credit facilities, including
interest(b)
7,132
266
3,031
1,284
2,551 Professional liability risks(c) 1,827 457 774 399 197 Right-of-use operating lease obligations 2,530 411 635 410 1,074 Other obligations(d) 25 22 2 1 — Total contractual obligations $54,270 $2,823 $10,503 $ 9,321 $ 31,623
Commitment Expiration by Period Other Commercial Commitments Not Recorded on the
Consolidated Balance Sheet Total Current 2-3 Years 4-5 Years After 5 Years Surety bonds(e) $ 60 $ 59 $ 1 $ — $ — Letters of credit(e) 33 18 15 — — Physician commitments(f) 37 30 7 — — Total commercial commitments $130 $ 107 $ 23 $ — $ —
(a) We have not included obligations related to unrecognized tax benefits of $550 million at December 31, 2019, as we cannot reasonably estimate the
timing or amounts of cash payments, if any, at this time.(b) Estimates of interest payments assume that interest rates and borrowing spreads at December 31, 2019, remain constant during the period
presented.(c) The estimation of the timing of payments for professional liability risks beyond a year can vary significantly. The time period required to resolve
these claims can vary depending upon the jurisdiction and whether the claim is settled or litigated.(d) Amounts include physician commitments that are recorded in our consolidated balance sheet. Amounts also include future other obligations that
are not recorded in our consolidated balance sheet.(e) Amounts relate primarily to instances in which we have agreed to indemnify various commercial insurers and lenders who have provided surety
bonds and letters of credit to cover damages for legal cases which were awarded to plaintiffs by the courts, Medicaid provider bonds, educationaladministrative bonds and utility and construction deposits.
(f) In consideration for physicians relocating to the communities in which our hospitals are located and agreeing to engage in private practice for thebenefit of the respective communities, we make advances to physicians to assist in establishing the physicians’ practices. The actual amount ofthese commitments to be advanced often depends upon the financial results of the physicians’ private practice during the recruitment agreementpayment period. The physician commitments reflected were based on our maximum exposure on effective agreements at December 31, 2019.
70
290

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 71/137
Table of Contents
HCA HEALTHCARE, INC.
MANAGEMENT’S DISCUSSION AND ANALYSIS OF FINANCIAL CONDITIONAND RESULTS OF OPERATIONS (Continued)
Market Risk
We are exposed to market risk related to changes in market values of securities. The investments in our 100% owned insurance subsidiaries were$462 million at December 31, 2019. These investments are carried at fair value, with changes in unrealized gains and losses being recorded asadjustments to other comprehensive income. At December 31, 2019, we had a net unrealized gain of $18 million on the insurance subsidiaries’investment securities.
We are exposed to market risk related to market illiquidity. Investments in debt and equity securities of our 100% owned insurance subsidiariescould be impaired by the inability to access the capital markets. Should the 100% owned insurance subsidiaries require significant amounts of cash inexcess of normal cash requirements to pay claims and other expenses on short notice, we may have difficulty selling these investments in a timelymanner or be forced to sell them at a price less than what we might otherwise have been able to in a normal market environment. We may be required torecognize credit-related impairments on our investment securities in future periods should issuers default on interest payments or should the fair marketvaluations of the securities deteriorate due to ratings downgrades or other issue-specific factors.
We are also exposed to market risk related to changes in interest rates, and we periodically enter into interest rate swap agreements to manage ourexposure to these fluctuations. Our interest rate swap agreements involve the exchange of fixed and variable rate interest payments between two parties,based on common notional principal amounts and maturity dates. The notional amounts of the swap agreements represent balances used to calculate theexchange of cash flows and are not our assets or liabilities. Our credit risk related to these agreements is considered low because the swap agreementsare with creditworthy financial institutions. The interest payments under these agreements are settled on a net basis. These derivatives have beenrecognized in the financial statements at their respective fair values. Changes in the fair value of these derivatives, which are designated as cash flowhedges, are included in other comprehensive income.
With respect to our interest-bearing liabilities, approximately $3.706 billion of long-term debt at December 31, 2019 was subject to variable ratesof interest, while the remaining balance in long-term debt of $30.016 billion at December 31, 2019 was subject to fixed rates of interest. Both thegeneral level of interest rates and, for the senior secured credit facilities, our leverage affect our variable interest rates. Our variable debt is comprisedprimarily of amounts outstanding under the senior secured credit facilities. Borrowings under the senior secured credit facilities bear interest at a rateequal to an applicable margin plus, at our option, either (a) a base rate determined by reference to the higher of (1) the federal funds rate plus 0.50% and(2) the prime rate of Bank of America or (b) a LIBOR rate for the currency of such borrowing for the relevant interest period. The applicable margin forborrowings under the senior secured credit facilities may fluctuate according to a leverage ratio. The average effective interest rate for our long-termdebt was 5.3% for both 2019 and 2018, respectively.
The estimated fair value of our total long-term debt was $37.026 billion at December 31, 2019. The estimates of fair value are based upon thequoted market prices for the same or similar issues of long-term debt with the same maturities. Based on a hypothetical 1% increase in interest rates, thepotential annualized reduction to future pretax earnings would be approximately $37 million. To mitigate the impact of fluctuations in interest rates, wegenerally target a majority of our debt portfolio to be maintained at fixed rates.
We are exposed to currency translation risk related to our foreign operations. We currently do not consider the market risk related to foreigncurrency translation to be material to our consolidated financial statements or our liquidity.
71
291
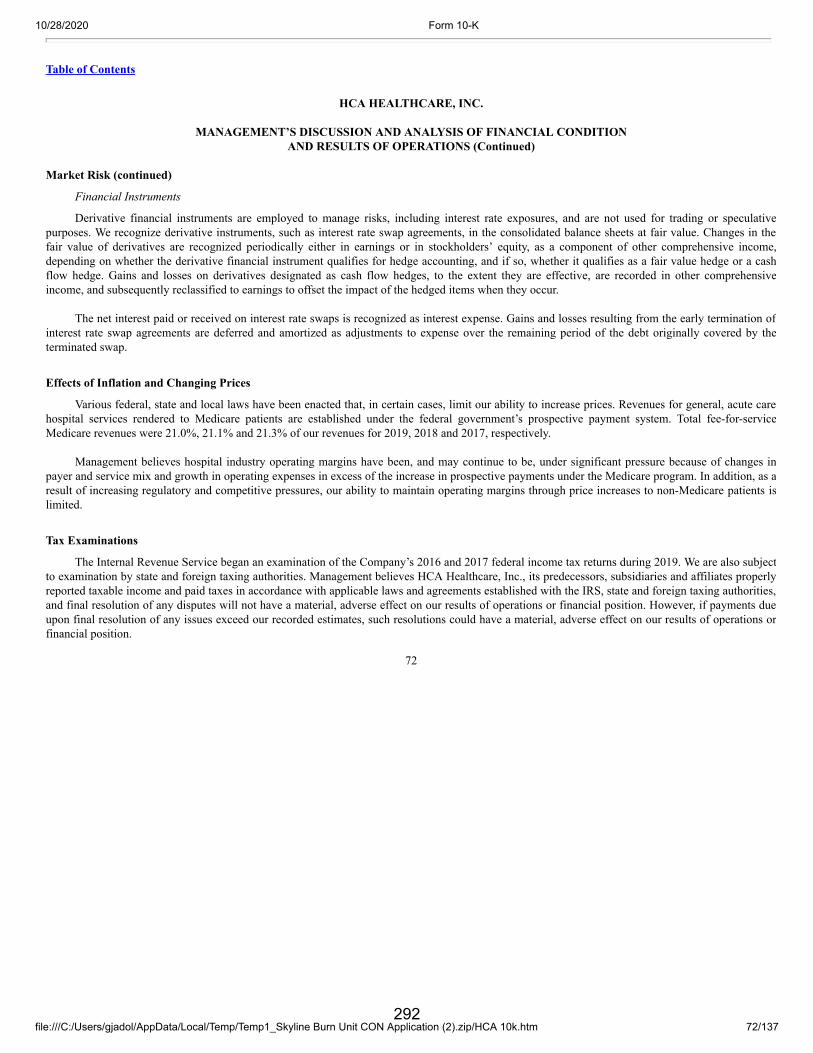
10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 72/137
Table of Contents
HCA HEALTHCARE, INC.
MANAGEMENT’S DISCUSSION AND ANALYSIS OF FINANCIAL CONDITIONAND RESULTS OF OPERATIONS (Continued)
Market Risk (continued)
Financial Instruments
Derivative financial instruments are employed to manage risks, including interest rate exposures, and are not used for trading or speculativepurposes. We recognize derivative instruments, such as interest rate swap agreements, in the consolidated balance sheets at fair value. Changes in thefair value of derivatives are recognized periodically either in earnings or in stockholders’ equity, as a component of other comprehensive income,depending on whether the derivative financial instrument qualifies for hedge accounting, and if so, whether it qualifies as a fair value hedge or a cashflow hedge. Gains and losses on derivatives designated as cash flow hedges, to the extent they are effective, are recorded in other comprehensiveincome, and subsequently reclassified to earnings to offset the impact of the hedged items when they occur.
The net interest paid or received on interest rate swaps is recognized as interest expense. Gains and losses resulting from the early termination ofinterest rate swap agreements are deferred and amortized as adjustments to expense over the remaining period of the debt originally covered by theterminated swap.
Effects of Inflation and Changing Prices
Various federal, state and local laws have been enacted that, in certain cases, limit our ability to increase prices. Revenues for general, acute carehospital services rendered to Medicare patients are established under the federal government’s prospective payment system. Total fee-for-serviceMedicare revenues were 21.0%, 21.1% and 21.3% of our revenues for 2019, 2018 and 2017, respectively.
Management believes hospital industry operating margins have been, and may continue to be, under significant pressure because of changes inpayer and service mix and growth in operating expenses in excess of the increase in prospective payments under the Medicare program. In addition, as aresult of increasing regulatory and competitive pressures, our ability to maintain operating margins through price increases to non-Medicare patients islimited.
Tax Examinations
The Internal Revenue Service began an examination of the Company’s 2016 and 2017 federal income tax returns during 2019. We are also subjectto examination by state and foreign taxing authorities. Management believes HCA Healthcare, Inc., its predecessors, subsidiaries and affiliates properlyreported taxable income and paid taxes in accordance with applicable laws and agreements established with the IRS, state and foreign taxing authorities,and final resolution of any disputes will not have a material, adverse effect on our results of operations or financial position. However, if payments dueupon final resolution of any issues exceed our recorded estimates, such resolutions could have a material, adverse effect on our results of operations orfinancial position.
72
292

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 73/137
Table of Contents
Item 7A. Quantitative and Qualitative Disclosures about Market Risk Information with respect to this Item is provided under the caption “Market Risk” under Item 7, “Management’s Discussion and Analysis ofFinancial Condition and Results of Operations.”
Item 8. Financial Statements and Supplementary Data Information with respect to this Item is contained in our consolidated financial statements indicated in the Index to Consolidated FinancialStatements on Page F-1 of this annual report on Form 10-K.
Item 9. Changes in and Disagreements with Accountants on Accounting and Financial Disclosure None.
Item 9A. Controls and Procedures 1. Conclusion Regarding the Effectiveness of Disclosure Controls and Procedures
Under the supervision and with the participation of our management, including our principal executive officer and principal financial officer, weconducted an evaluation of our disclosure controls and procedures, as such term is defined under Rule 13a-15(e) promulgated under the SecuritiesExchange Act of 1934, as amended (the “Exchange Act”). Based on this evaluation, our principal executive officer and our principal financial officerconcluded that our disclosure controls and procedures were effective as of the end of the period covered by this annual report.
2. Internal Control Over Financial Reporting
(a) Management’s Report on Internal Control Over Financial Reporting
Our management is responsible for establishing and maintaining effective internal control over financial reporting, as such term is defined inExchange Act Rule 13a-15(f). Because of its inherent limitations, internal control over financial reporting may not prevent or detect misstatements.Therefore, even those systems determined to be effective, can provide only reasonable assurance with respect to financial statement preparation andpresentation.
Under the supervision and with the participation of our management, including our principal executive officer and principal financial officer, weconducted an assessment of the effectiveness of our internal control over financial reporting based on the framework in Internal Control — IntegratedFramework issued by the Committee of Sponsoring Organizations of the Treadway Commission (2013 framework). Based on our assessment under theframework in Internal Control — Integrated Framework, our management concluded that our internal control over financial reporting was effective as ofDecember 31, 2019.
Ernst & Young LLP, the independent registered public accounting firm that audited our consolidated financial statements included in this Form10-K, has issued a report on our internal control over financial reporting, which is included herein.
73
293

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 74/137
Table of Contents
(b) Attestation Report of the Independent Registered Public Accounting Firm
Report of Independent Registered Public Accounting Firm
The Board of Directors and StockholdersHCA Healthcare, Inc.
Opinion on Internal Control over Financial Reporting
We have audited HCA Healthcare, Inc.’s internal control over financial reporting as of December 31, 2019, based on criteria established inInternal Control — Integrated Framework issued by the Committee of Sponsoring Organizations of the Treadway Commission (2013 framework) (theCOSO criteria). In our opinion, HCA Healthcare, Inc. (the Company) maintained, in all material respects, effective internal control over financialreporting as of December 31, 2019, based on the COSO criteria.
We also have audited, in accordance with the standards of the Public Company Accounting Oversight Board (United States) (PCAOB), theconsolidated balance sheets of HCA Healthcare, Inc. as of December 31, 2019 and 2018, and the related consolidated statements of income,comprehensive income, stockholders’ deficit, and cash flows for each of the three years in the period ended December 31, 2019, and the related notesand our report dated February 20, 2020 expressed an unqualified opinion thereon.
Basis for Opinion
The Company’s management is responsible for maintaining effective internal control over financial reporting and for its assessment of theeffectiveness of internal control over financial reporting included in the accompanying Management’s Report on Internal Control Over FinancialReporting. Our responsibility is to express an opinion on the Company’s internal control over financial reporting based on our audit. We are a publicaccounting firm registered with the PCAOB and are required to be independent with respect to the Company in accordance with the U.S. federalsecurities laws and the applicable rules and regulations of the Securities and Exchange Commission and the PCAOB.
We conducted our audit in accordance with the standards of the PCAOB. Those standards require that we plan and perform the audit to obtainreasonable assurance about whether effective internal control over financial reporting was maintained in all material respects.
Our audit included obtaining an understanding of internal control over financial reporting, assessing the risk that a material weakness exists,testing and evaluating the design and operating effectiveness of internal control based on the assessed risk, and performing such other procedures as weconsidered necessary in the circumstances. We believe that our audit provides a reasonable basis for our opinion.
Definition and Limitations of Internal Control Over Financial Reporting
A company’s internal control over financial reporting is a process designed to provide reasonable assurance regarding the reliability of financialreporting and the preparation of financial statements for external purposes in accordance with generally accepted accounting principles. A company’sinternal control over financial reporting includes those policies and procedures that (1) pertain to the maintenance of records that, in reasonable detail,accurately and fairly reflect the transactions and dispositions of the assets of the company; (2) provide reasonable assurance that transactions arerecorded as necessary to permit preparation of financial statements in accordance with generally accepted accounting principles, and that receipts andexpenditures of the company are being made only in accordance with authorizations of management and directors of the company; and (3) providereasonable assurance regarding prevention or timely detection of unauthorized acquisition, use, or disposition of the company’s assets that could have amaterial effect on the financial statements.
74
294

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 75/137
Table of Contents
Because of its inherent limitations, internal control over financial reporting may not prevent or detect misstatements. Also, projections of anyevaluation of effectiveness to future periods are subject to the risk that controls may become inadequate because of changes in conditions, or that thedegree of compliance with the policies or procedures may deteriorate.
/s/ Ernst & Young LLP
Nashville, TennesseeFebruary 20, 2020
(c) Changes in Internal Control Over Financial Reporting
During the fourth quarter of 2019, there have been no changes in our internal control over financial reporting that have materially affected or arereasonably likely to materially affect our internal control over financial reporting.
Item 9B. Other Information None.
PART III
Item 10. Directors, Executive Officers and Corporate Governance The information required by this Item regarding the identity and business experience of our directors and executive officers is set forth under theheading “Nominees for Election” and “Election of Directors” in the definitive proxy materials of HCA to be filed in connection with our 2020 AnnualMeeting of Stockholders with respect to our directors and is set forth in Item 1 of Part I of this annual report on Form 10-K with respect to our executiveofficers. The information required by this Item contained in such definitive proxy materials is incorporated herein by reference.
Information on the beneficial ownership reporting for our directors and executive officers required by this Item is contained under the caption“Delinquent Section 16(a) Reports” in the definitive proxy materials to be filed in connection with our 2020 Annual Meeting of Stockholders and isincorporated herein by reference.
Information on our Audit and Compliance Committee and Audit Committee Financial Experts required by this Item is contained under the caption“Corporate Governance” in the definitive proxy materials to be filed in connection with our 2020 Annual Meeting of Stockholders and is incorporatedherein by reference.
We have a Code of Conduct which is applicable to all our directors, officers and employees (the “Code of Conduct”). The Code of Conduct isavailable on the Ethics and Compliance and Corporate Governance pages of our website at www.hcahealthcare.com. To the extent required pursuant toapplicable SEC regulations, we intend to post amendments to or waivers from our Code of Conduct (to the extent applicable to our chief executiveofficer, principal financial officer or principal accounting officer) at this location on our website or report the same on a Current Report on Form 8-K.Our Code of Conduct is available free of charge upon request to our Corporate Secretary, HCA Healthcare, Inc., One Park Plaza, Nashville, TN 37203.
Item 11. Executive Compensation The information required by this Item is set forth under the headings “Executive Compensation” and “Compensation Committee Interlocks andInsider Participation” in the definitive proxy materials to be filed in connection with our 2020 Annual Meeting of Stockholders, which information isincorporated herein by reference.
75
295

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 76/137
Table of Contents
Item 12. Security Ownership of Certain Beneficial Owners and Management and Related Stockholder Matters Information about security ownership of certain beneficial owners required by this Item is set forth under the heading “Security Ownership ofCertain Beneficial Owners and Management and Related Stockholder Matters” in the definitive proxy materials to be filed in connection with our 2020Annual Meeting of Stockholders, which information is incorporated herein by reference.
This table provides certain information as of December 31, 2019 with respect to our equity compensation plans:
EQUITY COMPENSATION PLAN INFORMATION(Share and share unit amounts in millions)
(a) (b) (c)
Number of securities to be issued
upon exercise of outstanding options,
warrants and rights
Weighted-average exercise price of
outstanding options,
warrants and rights
Number of securities remaining available for future issuance
under equity compensation plans (excluding securities reflected in column(a))
Equity compensation plans approved by security holders 16.849(1) $ 71.79(1) 27.211(2)Equity compensation plans not approved by security holders — — — Total 16.849 $ 71.79 27.211 (1) Includes 2.620 million restricted share units which vest solely based upon continued employment over a specific period of time and 3.035 million
performance share units which vest based upon continued employment over a specific period of time and the achievement of predeterminedfinancial targets over time. The performance share units reported reflect the number of performance share units that would vest upon achievementof target performance; the number of performance share units that vest can vary from zero (for actual performance less than 90% of target for2019 grants and 80% of target for 2018 and prior grants) to two times the units granted (for actual performance of 110% or more of target for 2019grants and 120% or more of target for 2018 and prior grants). The weighted average exercise price does not take these restricted share units andperformance share units into account.
(2) Includes 20.328 million shares available for future grants under the 2006 Stock Incentive Plan for Key Employees of HCA Holdings, Inc. and itsAffiliates, as Amended and Restated, and 6.883 million shares of common stock reserved for future issuance under the HCA Holdings, Inc.Employee Stock Purchase Plan.
* For additional information concerning our equity compensation plans, see the discussion in Note 2 — Share-Based Compensation in the notes tothe consolidated financial statements.
Item 13. Certain Relationships and Related Transactions, and Director Independence The information required by this Item is set forth under the headings “Certain Relationships and Related Party Transactions” and “CorporateGovernance” in the definitive proxy materials to be filed in connection with our 2020 Annual Meeting of Stockholders, which information isincorporated herein by reference.
Item 14. Principal Accountant Fees and Services The information required by this Item is set forth under the heading “Ratification of Appointment of Independent Registered Public AccountingFirm” in the definitive proxy materials to be filed in connection with our 2020 Annual Meeting of Stockholders, which information is incorporatedherein by reference.
76
296

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 77/137
Table of Contents
PART IV
Item 15. Exhibits and Financial Statement Schedules (a) Documents filed as part of the report:
1. Financial Statements. The accompanying Index to Consolidated Financial Statements on page F-1 of this annual report on Form 10-K isprovided in response to this item.
2. List of Financial Statement Schedules. All schedules are omitted because the required information is either not present, not present in materialamounts or presented within the consolidated financial statements.
3. List of Exhibits
2.1 — Agreement and Plan of Merger, dated July 24, 2006, by and among HCA Inc., Hercules Holding II, LLC and HerculesAcquisition Corporation (filed as Exhibit 2.1 to the Company’s Current Report on Form 8-K filed July 25, 2006 (File No. 001-11239), and incorporated herein by reference).
2.2 — Merger Agreement, dated November 22, 2010, by and among HCA Inc., HCA Holdings, Inc., and HCA Merger Sub LLC (filed asExhibit 2.1 to the Company’s Current Report on Form 8-K filed November 24, 2010 (File No. 000-18406), and incorporated hereinby reference).
3.1 — Amended and Restated Certificate of Incorporation of the Company (restated for SEC filing purposes only) (filed as Exhibit 3.1 tothe Company’s Quarterly Report on Form 10-Q for the quarter ended June 30, 2019 (File No. 001-11239), and incorporated hereinby reference).
3.2 — Amended and Restated Bylaws of the Company (restated for SEC filing purposes only) (filed as Exhibit 3.2 to the Company’sQuarterly Report on Form 10-Q for the quarter ended June 30, 2019 (File No. 001-11239), and incorporated herein by reference).
4.1 — Description of Registered Securities.
4.2 — Specimen Certificate for shares of Common Stock, par value $0.01 per share, of the Company (filed as Exhibit 4.1 to the Company’sQuarterly Report on Form 10-Q for the quarter ended March 31, 2017 (File No. 001-11239), and incorporated herein by reference).
4.3 — Security Agreement, dated as of November 17, 2006, among HCA Inc., the subsidiary grantors party thereto and The Bank of NewYork, as collateral agent (filed as Exhibit 4.2 to the Company’s Current Report on Form 8-K filed November 24, 2006 (File No. 001-11239), and incorporated herein by reference).
4.4 — Pledge Agreement, dated as of November 17, 2006, among HCA Inc., the subsidiary pledgors party thereto and The Bank of NewYork, as collateral agent (filed as Exhibit 4.3 to the Company’s Current Report on Form 8-K filed November 24, 2006 (File No. 001-11239), and incorporated herein by reference).
4.5(a) — $13,550,000,000 — € 1,000,000,000 Credit Agreement, dated as of November 17, 2006, among HCA Inc., HCA UK CapitalLimited, the lending institutions from time to time parties thereto, Banc of America Securities LLC, J.P. Morgan Securities Inc.,Citigroup Global Markets Inc. and Merrill Lynch, Pierce, Fenner & Smith Incorporated, as joint lead arrangers and jointbookrunners, Bank of America, N.A., as administrative agent, JPMorgan Chase Bank, N.A. and Citicorp North America, Inc., as co-syndication agents and Merrill Lynch Capital Corporation, as documentation agent (filed as Exhibit 4.8 to the Company’s CurrentReport on Form 8-K filed November 24, 2006 (File No. 001-11239), and incorporated herein by reference).
77
297

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 78/137
Table of Contents
4.5(b) — Amendment No. 1 to the Credit Agreement, dated as of February 16, 2007, among HCA Inc., HCA UK Capital Limited, the lendinginstitutions from time to time parties thereto, Bank of America, N.A., as administrative agent, JPMorgan Chase Bank, N.A., andCiticorp North America, Inc., as Co-Syndication Agents, Banc of America Securities, LLC, J.P. Morgan Securities Inc., CitigroupGlobal Markets Inc. and Merrill Lynch, Pierce, Fenner & Smith Incorporated, as joint lead arrangers and bookrunners, DeutscheBank Securities and Wachovia Capital Markets LLC, as joint bookrunners and Merrill Lynch Capital Corporation, as documentationagent (filed as Exhibit 4.7(b) to the Company’s Annual Report on Form 10-K for the fiscal year ended December 31, 2006 (File No.001-11239), and incorporated herein by reference).
4.5(c) — Amendment No. 2 to the Credit Agreement, dated as of March 2, 2009, among HCA Inc., HCA UK Capital Limited, the lendinginstitutions from time to time parties thereto, Bank of America, N.A., as administrative agent, JPMorgan Chase Bank, N.A., andCiticorp North America, Inc., as Co-Syndication Agents, Banc of America Securities, LLC, J.P. Morgan Securities Inc., CitigroupGlobal Markets Inc. and Merrill Lynch, Pierce, Fenner & Smith Incorporated, as joint lead arrangers and bookrunners, DeutscheBank Securities and Wachovia Capital Markets LLC, as joint bookrunners and Merrill Lynch Capital Corporation, as documentationagent (filed as Exhibit 4.8(c) to the Company’s Annual Report on Form 10-K for the fiscal year ended December 31, 2008 (FileNo. 001-11239), and incorporated herein by reference).
4.5(d) — Amendment No. 3 to the Credit Agreement, dated as of June 18, 2009, among HCA Inc., HCA UK Capital Limited, the lendinginstitutions from time to time parties thereto, Bank of America, N.A., as administrative agent, JPMorgan Chase Bank, N.A., andCiticorp North America, Inc., as Co-Syndication Agents, Banc of America Securities, LLC, J.P. Morgan Securities Inc., CitigroupGlobal Markets Inc. and Merrill Lynch, Pierce, Fenner & Smith Incorporated, as joint lead arrangers and bookrunners, DeutscheBank Securities and Wachovia Capital Markets LLC, as joint bookrunners and Merrill Lynch Capital Corporation, as documentationagent (filed as Exhibit 4.1 to the Company’s Current Report on Form 8-K filed June 22, 2009 (File No. 001-11239), andincorporated herein by reference).
4.5(e) — Extension Amendment No. 1 to the Credit Agreement, dated as of April 6, 2010, among HCA Inc., HCA UK Capital Limited, thelending institutions from time to time parties thereto, Bank of America, N.A., as administrative agent and collateral agent (filed asExhibit 10.1 to the Company’s Current Report on Form 8-K filed April 8, 2010 (File No. 001-11239), and incorporated herein byreference).
4.5(f) — Amended and Restated Joinder Agreement No. 1, dated as of November 8, 2010, by and among each of the financial institutionslisted as a “Replacement-1 Revolving Credit Lender” on Schedule A thereto, HCA Inc., Bank of America, N.A., as AdministrativeAgent and as Collateral Agent, and the other parties listed on the signature pages thereto (filed as Exhibit 4.1 to the Company’sQuarterly Report on Form 10-Q for the quarter ended September 30, 2010 (File No. 001-11239), and incorporated herein byreference).
4.5(g) — Restatement Agreement, dated as of May 4, 2011, by and among HCA Inc., HCA UK Capital Limited, the lenders party thereto andBank of America, N.A., as administrative agent and collateral agent to the Credit Agreement, dated as of November 17, 2006, asamended on February 16, 2007, March 2, 2009, June 18, 2009, April 6, 2010 and November 8, 2010 (filed as Exhibit 10.1 to theCompany’s Current Report on Form 8-K filed May 9, 2011 (File No. 001-11239), and incorporated herein by reference).
78
298

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 79/137
Table of Contents
4.5(h) — Extension Amendment No. 1, dated as of April 25, 2012, by and among HCA Inc., HCA UK Capital Limited, each of the U.S.Guarantors, each of the European Guarantors, the lenders party thereto and Bank of America, N.A., as administrative agent,swingline lender and letter of credit issuer (filed as Exhibit 10.1 to the Company’s Current Report on Form 8-K filed April 26, 2012(File No. 001-11239), and incorporated herein by reference).
4.5(i) — Restatement Agreement, dated as of February 26, 2014, to (i) the Credit Agreement, dated as of November 17, 2006 and as amendedand restated as of May 4, 2011, by and among the HCA Inc., HCA UK Capital Limited, the lenders party thereto and Bank ofAmerica, N.A., as administrative agent and collateral agent and (ii) the U.S. Guarantee, dated as of November 17, 2006 by andamong the guarantors party thereto and Bank of America, N.A., as administrative agent (filed as Exhibit 4.1 to the Company’sCurrent Report on Form 8-K filed February 28, 2014 (File No. 001-11239), and incorporated herein by reference).
4.5(j) — Supplement No. 14 dated as of November 9, 2015 to the U.S. Guarantee, dated as of November 17, 2006 and amended and restatedon February 26, 2014, by and among the guarantors party thereto and Bank of America, N.A., as administrative agent (filed asExhibit 4.4(j) to the Company’s Annual Report on Form 10-K filed February 21, 2019 (File No. 001-11239), and incorporatedherein by reference).
4.5(k) — Schedule of Omitted Supplements to the U.S. Guarantee dated as of November 17, 2006 and amended and restated on February 26,2014, filed pursuant to Instruction 2 to Item 601 of Regulation S-K.
4.5(l) — Restatement Agreement, dated as of June 28, 2017, to the Credit Agreement, dated as of November 17, 2006, by and among HCAInc., as borrower, the guarantors party thereto, Bank of America, N.A., as administrative agent and collateral agent, and the lendersparty thereto (filed as Exhibit 4.1 to the Company’s Current Report on Form 8-K filed June 30, 2017 (File No. 001-11239), andincorporated herein by reference).
4.5(m) — Joinder Agreement No. 8, dated as of July 16, 2019, by and among HCA Inc., as borrower, the guarantors party thereto, Bank ofAmerica, N.A., as administrative agent and collateral agent, and the lenders party thereto (filed as Exhibit 4.1 to the Company’sCurrent Report on Form 8-K filed July 22, 2019 (File No. 001-11239), and incorporated herein by reference).
4.5(n) — Joinder Agreement No. 9, dated as of October 8, 2019, by and among HCA Inc., as borrower, the guarantors party thereto, Bank ofAmerica, N.A., as administrative agent and collateral agent, and the lenders party thereto (filed as Exhibit 4.1 to the Company’sCurrent Report on Form 8-K filed October 10, 2019 (File No. 001-11239), and incorporated herein by reference).
4.5(o) — Joinder Agreement No. 10, dated as of November 20, 2019, by and among HCA Inc., as borrower, the guarantors party thereto,Bank of America, N.A., as administrative agent and collateral agent, and the lenders party thereto (filed as Exhibit 4.1 to theCompany’s Current Report on Form 8-K filed November 21, 2019 (File No. 001-11239), and incorporated herein by reference).
4.6(a) — Security Agreement, dated as November 17, 2006, and amended and restated as of March 2, 2009, among the Company, theSubsidiary Grantors named therein and Bank of America, N.A., as Collateral Agent (filed as Exhibit 4.10 to the Company’s AnnualReport on Form 10-K for the fiscal year ended December 31, 2008 (File No. 001-11239), and incorporated herein by reference).
4.6(b) — Supplement No. 2 dated as of October 27, 2011, to the Amended and Restated Security Agreement dated as of March 2, 2009, assupplemented, by and among the subsidiary grantor named therein and Bank of America, N.A., as collateral agent (filed as Exhibit4.5(b) to the Company’s Annual Report on Form 10-K filed February 21, 2019 (File No. 001-11239), and incorporated herein byreference).
79
299

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 80/137
Table of Contents
4.6(c) — Schedule of Omitted Supplements to the Security Agreement dated as of November 17, 2006 and amended and restated as ofMarch 2, 2009, filed pursuant to Instruction 2 to Item 601 of Regulation S-K.
4.7(a) — Pledge Agreement, dated as of November 17, 2006, and amended and restated as of March 2, 2009, among the Company, theSubsidiary Pledgors named therein and Bank of America, N.A., as Collateral Agent (filed as Exhibit 4.11 to the Company’s AnnualReport on Form 10-K for the fiscal year ended December 31, 2008 (File No. 001-11239), and incorporated herein by reference).
4.7(b) — Supplement No. 1 dated as of October 27, 2011 to the Amended and Restated Pledge Agreement dated as of March 2, 2009, by andamong the subsidiary pledgors named therein and Bank of America, N.A., as collateral agent (filed as Exhibit 4.6(b) to theCompany’s Annual Report on Form 10-K filed February 21, 2019 (File No. 001-11239), and incorporated herein by reference).
4.7(c) — Schedule of Omitted Supplements to the Pledge Agreement dated as of November 6, 2006 and amended and restated as of March 2,2009, filed pursuant to Instruction 2 to Item 601 of Regulation S-K.
4.8(a) — $2,500,000,000 Credit Agreement, dated as of September 30, 2011, by and among HCA Inc., the subsidiary borrowers party thereto,the lenders from time to time party thereto and Bank of America, N.A., as administrative agent (filed as Exhibit 4.4 to theCompany’s Current Report on Form 8-K filed October 3, 2011 (File No. 001-11239), and incorporated herein by reference).
4.8(b) — Restatement Agreement, dated as of March 7, 2014, to the Credit Agreement, dated as of September 30, 2011, by and among HCAInc., the subsidiary borrowers party thereto, the lenders party thereto and Bank of America, N.A. as administrative agent andcollateral agent (filed as Exhibit 4.1 to the Company’s Current Report on Form 8-K filed March 11, 2014 (File No. 001-11239), andincorporated herein by reference).
4.8(c) — Joinder Agreement and Amendment No. 1, dated as of October 30, 2014, to the Credit Agreement, dated as of September 30, 2011and amended and restated as of March 7, 2014, by and among HCA Inc., the subsidiary borrowers party thereto, the lenders partythereto and Bank of America, N.A. as administrative agent and collateral agent. (filed as Exhibit 4.1 to the Company’s CurrentReport on Form 8-K filed October 31, 2014 (File No. 001-11239), and incorporated herein by reference).
4.8(d) — Restatement Agreement dated as of June 28, 2017, to the Credit Agreement, dated as of September 30, 2011 by and among HCAInc., as borrower, the subsidiary borrowers party thereto, Bank of America, N.A., as administrative agent and collateral agent, andthe lenders party thereto (filed as Exhibit 4.2 to the Company’s Current Report on Form 8-K filed June 30, 2017 (File No. 001-11239), and incorporated herein by reference).
4.8(e) — Joinder Agreement dated as of January 3, 2018 to the Credit Agreement dated as of September 30, 2011 (as amended and restatedon March 7, 2014, as further amended on October 30, 2014, and as further amended and restated on June 28, 2017), by and amongthe subsidiary borrowers party thereto and Bank of America, N.A., as administrative agent (filed as Exhibit 4.7(e) to the Company’sAnnual Report on Form 10-K filed February 21, 2019 (File No. 001-11239), and incorporated herein by reference).
4.9(a) — Security Agreement, dated as of September 30, 2011, by and among HCA Inc., the subsidiary borrowers party thereto and Bank ofAmerica, N.A., as collateral agent (filed as Exhibit 4.5 to the Company’s Current Report on Form 8-K filed October 3, 2011 (FileNo. 001-11239), and incorporated herein by reference).
80
300

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 81/137
Table of Contents
4.9(b) — Supplement No. 1 dated as of October 27, 2011 to the Security Agreement dated as of September 30, 2011, by and among thesubsidiary borrower party thereto and Bank of America, N.A., as collateral agent (filed as Exhibit 4.8(b) to the Company’s AnnualReport on Form 10-K filed February 21, 2019 (File No. 001-11239), and incorporated herein by reference).
4.9(c) — Schedule of Omitted Supplements to the Security Agreement dated as of September 30, 2011, filed pursuant to Instruction 2 to Item601 of Regulation S-K.
4.10(a) — General Intercreditor Agreement, dated as of November 17, 2006, between Bank of America, N.A., as First Lien Collateral Agent,and The Bank of New York, as Junior Lien Collateral Agent (filed as Exhibit 4.13(a) to the Company’s Registration Statement onForm S-4 (File No. 333-145054), and incorporated herein by reference).
4.10(b) — Receivables Intercreditor Agreement, dated as of November 17, 2006, among Bank of America, N.A., as ABL Collateral Agent, Bankof America, N.A., as CF Collateral Agent and The Bank of New York, as Bonds Collateral Agent (filed as Exhibit 4.13(b) to theCompany’s Registration Statement on Form S-4 (File No. 333-145054), and incorporated herein by reference).
4.10(c) — First Lien Intercreditor Agreement, dated as of April 22, 2009, among Bank of America, N.A. as Collateral Agent, Bank of America,N.A. as Authorized Representative under the Credit Agreement and Law Debenture Trust Company of New York as the InitialAdditional Authorized Representative (filed as Exhibit 4.5 to the Company’s Current Report on Form 8-K filed April 28, 2009, andincorporated herein by reference).
4.10(d) — Additional General Intercreditor Agreement, dated as of August 1, 2011, by and among Bank of America, N.A., in its capacity as FirstLien Collateral Agent, The Bank of New York Mellon, in its capacity as Junior Lien Collateral Agent and in its capacity as trustee forthe Second Lien Notes issued on November 17, 2006, and The Bank of New York Mellon Trust Company, N.A., in its capacity astrustee for the Second Lien Notes issued on February 19, 2009 (filed as Exhibit 4.9 to the Company’s Current Report on Form 8-Kfiled August 1, 2011 (File No. 001-11239), and incorporated herein by reference).
4.10(e) — Additional Receivables Intercreditor Agreement, dated as of August 1, 2011 by and between Bank of America, N.A., as ABLCollateral Agent, and Bank of America, N.A., as New First Lien Collateral Agent (filed as Exhibit 4.10 to the Company’s CurrentReport on Form 8-K filed August 1, 2011 (File No. 001-11239), and incorporated herein by reference).
4.10(f) — Additional General Intercreditor Agreement, dated as of February 16, 2012, by and among Bank of America, N.A., in its capacity asFirst Lien Collateral Agent, The Bank of New York Mellon, in its capacity as Junior Lien Collateral Agent and in its capacity astrustee for the Second Lien Notes issued on November 17, 2006, and The Bank of New York Mellon Trust Company, N.A., in itscapacity as trustee for the Second Lien Notes issued on February 19, 2009 (filed as Exhibit 4.9 to the Company’s Current Report onForm 8-K filed February 16, 2012 (File No. 001-11239), and incorporated herein by reference).
4.10(g) — Additional Receivables Intercreditor Agreement, dated as of February 16, 2012, by and between Bank of America, N.A., as ABLCollateral Agent, and Bank of America, N.A., as New First Lien Collateral Agent (filed as Exhibit 4.10 to the Company’s CurrentReport on Form 8-K filed February 16, 2012 (File No. 001-11239), and incorporated herein by reference).
4.10(h) — Additional General Intercreditor Agreement, dated as of October 23, 2012, by and among Bank of America, N.A., in its capacity asFirst Lien Collateral Agent, The Bank of New York Mellon, in its capacity as Junior Lien Collateral Agent and in its capacity astrustee for the Second Lien Notes issued on November 17, 2006, and The Bank of New York Mellon Trust Company, N.A., in itscapacity as trustee for the Second Lien Notes issued on February 19, 2009 (filed as Exhibit 4.10 to the Company’s Current Report onForm 8-K filed October 23, 2012 (File No. 001-11239), and incorporated herein by reference).
81
301

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 82/137
Table of Contents
4.10(i) — Additional Receivables Intercreditor Agreement, dated as of October 23, 2012, by and between Bank of America, N.A., as ABLCollateral Agent, and Bank of America, N.A., as New First Lien Collateral Agent (filed as Exhibit 4.11 to the Company’s CurrentReport on Form 8-K filed October 23, 2012 (File No. 001-11239), and incorporated herein by reference).
4.11 — Registration Rights Agreement, dated as of November 22, 2010, among HCA Holdings, Inc., Hercules Holding II, LLC and certainother parties thereto (filed as Exhibit 4.4 to the Company’s Current Report on Form 8-K filed November 24, 2010 (File No. 000-18406), and incorporated herein by reference).
4.12 — Registration Rights Agreement, dated as of March 16, 1989, by and among HCA-Hospital Corporation of America and the personslisted on the signature pages thereto (filed as Exhibit 4.14 to the Company’s Registration Statement on Form S-4 (File No. 333-145054), and incorporated herein by reference).
4.13 — Assignment and Assumption Agreement, dated as of February 10, 1994, between HCA-Hospital Corporation of America and theCompany relating to the Registration Rights Agreement, as amended (filed as Exhibit 4.15 to the Company’s Registration Statementon Form S-4 (File No. 333-145054), and incorporated herein by reference).
4.14(a) — Indenture, dated as of December 16, 1993 between the Company and The First National Bank of Chicago, as Trustee (filed asExhibit 4.16(a) to the Company’s Registration Statement on Form S-4 (File No. 333-145054), and incorporated herein by reference).
4.14(b) — First Supplemental Indenture, dated as of May 25, 2000 between the Company and Bank One Trust Company, N.A., as Trustee (filedas Exhibit 4.16(b) to the Company’s Registration Statement on Form S-4 (File No. 333-145054), and incorporated herein byreference).
4.14(c) — Second Supplemental Indenture, dated as of July 1, 2001 between the Company and Bank One Trust Company, N.A., as Trustee (filedas Exhibit 4.16(c) to the Company’s Registration Statement on Form S-4 (File No. 333-145054), and incorporated herein byreference).
4.14(d) — Third Supplemental Indenture, dated as of December 5, 2001 between the Company and The Bank of New York, as Trustee (filed asExhibit 4.16(d) to the Company’s Registration Statement on Form S-4 (File No. 333-145054), and incorporated herein by reference).
4.14(e) — Fourth Supplemental Indenture, dated as of November 14, 2006, between the Company and The Bank of New York, as Trustee (filedas Exhibit 4.1 to the Company’s Current Report on Form 8-K filed November 16, 2006 (File No. 001-11239), and incorporated hereinby reference).
4.15 — Form of 7.5% Debentures due 2023 (filed as Exhibit 4.17 to the Company’s Registration Statement on Form S-4 (File No. 333-145054), and incorporated herein by reference).
4.16 — Form of 8.36% Debenture due 2024 (filed as Exhibit 4.18 to the Company’s Registration Statement on Form S-4 (File No. 333-145054), and incorporated herein by reference).
4.17 — Form of Fixed Rate Global Medium-Term Note (filed as Exhibit 4.19 to the Company’s Registration Statement on Form S-4 (FileNo. 333-145054), and incorporated herein by reference).
4.18 — Form of Floating Rate Global Medium-Term Note (filed as Exhibit 4.20 to the Company’s Registration Statement on Form S-4 (FileNo. 333-145054), and incorporated herein by reference).
4.19 — Form of 7.69% Note due 2025 (filed as Exhibit 4.10 to the Company’s Annual Report on Form 10-K for the fiscal year endedDecember 31, 2004 (File No. 001-11239), and incorporated herein by reference).
4.20 — Form of 7.50% Debenture due 2095 (filed as Exhibit 4.23 to the Company’s Registration Statement on Form S-4 (File No. 333-145054), and incorporated herein by reference).
82
302

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 83/137
Table of Contents
4.21 — Form of 7.05% Debenture due 2027 (filed as Exhibit 4.24 to the Company’s Registration Statement on Form S-4 (File No. 333-145054), and incorporated herein by reference).
4.22 — 7.50% Note due 2033 in the principal amount of $250,000,000 (filed as Exhibit 4.2 to the Company’s Current Report on Form 8-Kfiled November 6, 2003 (File No. 001-11239), and incorporated herein by reference).
4.23 — Form of Indenture of HCA Inc. (filed as Exhibit 4.2 to the Registrant’s Registration Statement on Form S-3 (File No. 333-175791),and incorporated herein by reference).
4.24 — Indenture dated as of August 1, 2011, among HCA Inc., the guarantors named on Schedule I thereto, Delaware Trust Company (assuccessor to Law Debenture Trust Company of New York), as trustee, and Deutsche Bank Trust Company Americas, as paying agent,registrar and transfer agent (filed as Exhibit 4.5 to the Company’s Registration Statement on Form S-3 (File No. 333-226709), andincorporated herein by reference).
4.25 — Supplemental Indenture No. 1, dated as of August 1, 2011, among HCA Inc., HCA Holdings, Inc., Law Debenture Trust Company ofNew York, as trustee, and Deutsche Bank Trust Company Americas, as paying agent, registrar and transfer agent (filed as Exhibit 4.2to the Company’s Current Report on Form 8-K filed August 1, 2011 (File No. 001-11239), and incorporated herein by reference).
4.26 — Form of 7.50% Senior Notes due 2022 (included in Exhibit 4.25).
4.27 — Supplemental Indenture No. 5, dated as of October 23, 2012, among HCA Inc., HCA Holdings, Inc., Law Debenture Trust Companyof New York, as trustee, and Deutsche Bank Trust Company Americas, as paying agent, registrar and transfer agent (UnsecuredNotes) (filed as Exhibit 4.3 to the Company’s Current Report on Form 8-K filed October 23, 2012 (File No. 001-11239), andincorporated herein by reference).
4.28(a) — Supplemental Indenture No. 6, dated as of October 23, 2012, among HCA Inc., HCA Holdings, Inc., the subsidiary guarantors namedtherein, Law Debenture Trust Company of New York, as trustee, and Deutsche Bank Trust Company Americas, as paying agent,registrar and transfer agent (Secured Notes) (filed as Exhibit 4.4 to the Company’s Current Report on Form 8-K filed October 23,2012 (File No. 001-11239), and incorporated herein by reference).
4.28(b) — Supplemental Indenture dated as of January 3, 2018, among the subsidiary guarantors named therein, Delaware Trust Company, astrustee, and Deutsche Bank Trust Company Americas, as paying agent, registrar and transfer agent (filed as Exhibit 4.26(b) to theCompany’s Annual Report on Form 10-K for the fiscal year ended December 31, 2018 (File No. 001-11239), and incorporated hereinby reference).
4.28(c) — Schedule of Omitted Supplemental Indentures to Supplemental Indentures, filed pursuant to Instruction 2 to Item 601 of Regulation S-K.
4.29 — Form of 5.875% Senior Notes due 2023 (included in Exhibit 4.27).
4.30 — Form of 4.75% Senior Secured Notes due 2023 (included in Exhibit 4.28(a)).
4.31 — Indenture, dated as of December 6, 2012, among HCA Holdings, Inc., Law Debenture Trust Company of New York, as trustee, andDeutsche Bank Trust Company Americas, as registrar, paying agent and transfer agent (filed as Exhibit 4.1 to the Company’s CurrentReport on Form 8-K filed December 6, 2012 (File No. 001-11239), and incorporated herein by reference).
4.32 — Supplemental Indenture No. 1, dated as of December 6, 2012, among HCA Holdings, Inc., Law Debenture Trust Company of NewYork, as trustee, and Deutsche Bank Trust Company Americas, as registrar, paying agent and transfer agent (filed as Exhibit 4.2 to theCompany’s Current Report on Form 8-K filed December 6, 2012 (File No. 001-11239), and incorporated herein by reference).
4.33 — Form of 6.25% Senior Notes due 2021 (included in Exhibit 4.32).
83
303

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 84/137
Table of Contents
4.34 — Supplemental Indenture No. 8, dated as of March 17, 2014, among HCA Inc., HCA Holdings, Inc., the subsidiary guarantors namedtherein, Law Debenture Trust Company of New York, as trustee, and Deutsche Bank Trust Company Americas, as paying agent,registrar and transfer agent (filed as Exhibit 4.3 to the Company’s Current Report on Form 8-K filed March 21, 2014 (File No. 001-11239), and incorporated herein by reference).
4.35 — Form of 5.00% Senior Secured Notes due 2024 (included in Exhibit 4.34).
4.36 — Additional Receivables Intercreditor Agreement, dated as of March 17, 2014, by and between Bank of America, N.A., as ABLCollateral Agent, and Bank of America, N.A., as New First Lien Collateral Agent (filed as Exhibit 4.9 to the Company’s CurrentReport on Form 8-K filed March 21, 2014 (File No. 001-11239), and incorporated herein by reference).
4.37 — Supplemental Indenture No. 10, dated as of October 17, 2014, among HCA Inc., HCA Holdings, Inc., the subsidiary guarantorsnamed therein, Law Debenture Trust Company of New York, as trustee, and Deutsche Bank Trust Company Americas, as payingagent, registrar and transfer agent (filed as Exhibit 4.3 to the Company’s Current Report on Form 8-K filed October 17, 2014(File No. 001-11239), and incorporated herein by reference).
4.38 — Form of 5.25% Senior Secured Notes due 2025 (included in Exhibit 4.37).
4.39 — Additional Receivables Intercreditor Agreement, dated as of October 17, 2014, by and between Bank of America, N.A., as ABLCollateral Agent, and Bank of America, N.A., as New First Lien Collateral Agent (filed as Exhibit 4.9 to the Company’s CurrentReport on Form 8-K filed October 17, 2014 (File No. 001-11239), and incorporated herein by reference).
4.40 — Supplemental Indenture No. 11, dated as of January 16, 2015, among HCA Inc., HCA Holdings, Inc., Law Debenture TrustCompany of New York, as trustee, and Deutsche Bank Trust Company Americas, as paying agent, registrar and transfer agent (filedas Exhibit 4.2 to the Company’s Current Report on Form 8-K filed January 16, 2015 (File No. 001-11239), and incorporated hereinby reference).
4.41 — Form of 5.375% Senior Notes due 2025 (included in Exhibit 4.40).
4.42 — Supplemental Indenture No. 12, dated as of May 20, 2015, among HCA Inc., HCA Holdings, Inc., Law Debenture Trust Companyof New York, as trustee, and Deutsche Bank Trust Company Americas, as paying agent, registrar and transfer agent (filed as Exhibit4.4 to the Company’s Current Report on Form 8-K filed May 20, 2015 (File No. 001-11239), and incorporated herein by reference).
4.43 — Supplemental Indenture No. 13, dated as of November 13, 2015, among HCA Inc., HCA Holdings, Inc., Law Debenture TrustCompany of New York, as trustee, and Deutsche Bank Trust Company Americas, as paying agent, registrar and transfer agent (filedas Exhibit 4.2 to the Company’s Current Report on Form 8-K filed November 13, 2015 (File No. 001-11239), and incorporatedherein by reference).
4.44 — Form of 5.875% Senior Notes due 2026 (included in Exhibit 4.43).
4.45 — Supplemental Indenture No. 14, dated as of December 8, 2015, among HCA Inc., HCA Holdings, Inc., Law Debenture TrustCompany of New York, as trustee, and Deutsche Bank Trust Company Americas, as paying agent, registrar and transfer agent (filedas Exhibit 4.4 to the Company’s Current Report on Form 8-K filed December 8, 2015 (File No. 001-11239), and incorporated hereinby reference).
4.46 — Supplemental Indenture No. 15, dated as of March 15, 2016, among HCA Inc., HCA Holdings, Inc., the subsidiary guarantorsnamed therein, Law Debenture Trust Company of New York, as trustee, and Deutsche Bank Trust Company Americas, as payingagent, registrar and transfer agent (filed as Exhibit 4.2 to the Company’s Current Report on Form 8-K filed March 15, 2016 (FileNo. 001-11239), and incorporated herein by reference).
84
304

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 85/137
Table of Contents
4.47 — Form of 5.250% Senior Secured Notes due 2026 (included in Exhibit 4.46).
4.48 — Additional Receivables Intercreditor Agreement, dated as of March 15, 2016, by and between Bank of America, N.A., as ABLCollateral Agent, and Bank of America, N.A., as First Lien Collateral Agent (filed as Exhibit 4.7 to the Company’s Current Reporton Form 8-K filed March 15, 2016 (File No. 001-11239), and incorporated herein by reference).
4.49 — Supplemental Indenture No. 16, dated as of August 15, 2016, among HCA Inc., HCA Holdings, Inc., the subsidiary guarantorsnamed therein, Law Debenture Trust Company of New York, as trustee, and Deutsche Bank Trust Company Americas, as payingagent, registrar and transfer agent (filed as Exhibit 4.3 to the Company’s Current Report on Form 8-K filed August 15, 2016(File No. 001-11239), and incorporated herein by reference).
4.50 — Form of 4.500% Senior Secured Notes due 2027 (included in Exhibit 4.49).
4.51 — Additional Receivables Intercreditor Agreement, dated as of August 15, 2016, by and between Bank of America, N.A., as ABLCollateral Agent, and Bank of America, N.A., as First Lien Collateral Agent (filed as Exhibit 4.8 to the Company’s Current Reporton Form 8-K filed August 15, 2016 (File No. 001-11239), and incorporated herein by reference).
4.52 — Supplemental Indenture No. 17, dated as of December 9, 2016, among HCA Inc., HCA Holdings, Inc., the subsidiary guarantorsnamed therein, Delaware Trust Company, as trustee, and Deutsche Bank Trust Company Americas, as paying agent, registrar andtransfer agent (filed as Exhibit 4.1 to the Company’s Current Report on Form 8-K filed December 9, 2016 (File No. 001-11239), andincorporated herein by reference).
4.53 — Supplemental Indenture No. 18, dated as of June 22, 2017, among HCA Inc., HCA Healthcare, Inc., the subsidiary guarantorsnamed therein, Delaware Trust Company, as trustee, and Deutsche Bank Trust Company Americas, as paying agent, registrar andtransfer agent (filed as Exhibit 4.2 to the Company’s Current Report on Form 8-K filed on June 22, 2017 (File No. 001-11239), andincorporated herein by reference).
4.54 — Form of 5.500% Senior Secured Notes due 2047 (included in Exhibit 4.53).
4.55 — Additional Receivables Intercreditor Agreement, dated as of June 22, 2017, by and between Bank of America, N.A., as ABLCollateral Agent, and Bank of America, N.A., as First Lien Collateral Agent (filed as Exhibit 4.7 to the Company’s Current Reporton Form 8-K filed on June 22, 2017 (File No. 001-11239), and incorporated herein by reference).
4.56 — Supplemental Indenture No. 19, dated as of August 23, 2018, among HCA Inc., HCA Healthcare, Inc., Delaware Trust Company, astrustee, and Deutsche Bank Trust Company Americas, as paying agent, registrar and transfer agent (filed as Exhibit 4.2 to theCompany’s Current Report on Form 8-K filed on August 23, 2018 (File No. 001-11239), and incorporated herein by reference).
4.57 — Form of 5.375% Senior Notes Due 2026 (included in Exhibit 4.56).
4.58 — Supplemental Indenture No. 20, dated as of August 23, 2018, among HCA Inc., HCA Healthcare, Inc., Delaware Trust Company, astrustee, and Deutsche Bank Trust Company Americas, as paying agent, registrar and transfer agent (filed as Exhibit 4.3 to theCompany’s Current Report on Form 8-K filed on August 23, 2018 (File No. 001-11239), and incorporated herein by reference).
4.59 — Form of 5.625% Senior Notes Due 2028 (included in Exhibit 4.58).
4.60 — Supplemental Indenture No. 21, dated as of January 22, 2019, among HCA Inc., HCA Healthcare, Inc., Delaware Trust Company, astrustee, and Deutsche Bank Trust Company Americas, as paying agent, registrar and transfer agent (filed as Exhibit 4.4 to theCompany’s Current Report on Form 8-K filed on January 22, 2019 (File No. 001-11239), and incorporated herein by reference).
85
305

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 86/137
Table of Contents
4.61 — Supplemental Indenture No. 22, dated as of January 30, 2019, among HCA Inc., HCA Healthcare, Inc., Delaware Trust Company, astrustee, and Deutsche Bank Trust Company Americas, as paying agent, registrar and transfer agent (filed as Exhibit 4.2 to theCompany’s Current Report on Form 8-K filed on January 30, 2019 (File No. 001-11239), and incorporated herein by reference).
4.62 — Form of 5.875% Senior Notes Due 2029 (included in Exhibit 4.61).
4.63 — Supplemental Indenture No. 23, dated as of June 12, 2019, among HCA Inc., HCA Healthcare, Inc., the subsidiary guarantors namedtherein, Delaware Trust Company, as trustee, and Deutsche Bank Trust Company Americas, as paying agent, registrar and transferagent (filed as Exhibit 4.2 to the Company’s Current Report on Form 8-K filed on June 12, 2019 (File No. 001-11239), andincorporated herein by reference).
4.64 — Supplemental Indenture No. 24, dated as of June 12, 2019, among HCA Inc., HCA Healthcare, Inc., the subsidiary guarantors namedtherein, Delaware Trust Company, as trustee, and Deutsche Bank Trust Company Americas, as paying agent, registrar and transferagent (filed as Exhibit 4.3 to the Company’s Current Report on Form 8-K filed June 12, 2019 (File No. 001-11239), and incorporatedherein by reference).
4.65 — Supplemental Indenture No. 25, dated as of June 12, 2019, among HCA Inc., HCA Healthcare, Inc., the subsidiary guarantors namedtherein, Delaware Trust Company, as trustee, and Deutsche Bank Trust Company Americas, as paying agent, registrar and transferagent (filed as Exhibit 4.4 to the Company’s Current Report on Form 8-K filed June 12, 2019 (File No. 001-11239), and incorporatedherein by reference).
4.66 — Form of 4 1/8% Senior Secured Notes due 2029 (included in Exhibit 4.63).
4.67 — Form of 5 1/8% Senior Secured Notes due 2039 (included in Exhibit 4.64).
4.68 — Form of 5 1/4% Senior Secured Notes due 2049 (included in Exhibit 4.65).
4.69 — Additional Receivables Intercreditor Agreement, dated as of June 12, 2019, by and between Bank of America, N.A., as ABLCollateral Agent, and Bank of America, N.A., as First Lien Collateral Agent (filed as Exhibit 4.11 to the Company’s Current Reporton Form 8-K filed on June 12, 2019 (File No. 001-11239), and incorporated herein by reference).
10.1 — Form of Indemnity Agreement with certain officers and directors (filed as Exhibit 10.3 to the Company’s Registration Statement onForm S-4 (File No. 333-145054) and incorporated herein by reference).
10.2(a) — 2006 Stock Incentive Plan for Key Employees of HCA Holdings, Inc. and its Affiliates as Amended and Restated (filed asExhibit 10.11(b) to the Company’s Registration Statement on Form S-1 (File No. 333-171369), and incorporated herein byreference).*
10.2(b) — First Amendment to 2006 Stock Incentive Plan for Key Employees of HCA Holdings, Inc. and its Affiliates, as amended and restated(filed as Exhibit 10.1 to the Company’s Quarterly Report on Form 10-Q for the quarter ended June 30, 2011 (File No. 001-11239), andincorporated herein by reference).*
10.2(c) — Second Amendment to the 2006 Stock Incentive Plan for Key Employees of HCA Holdings, Inc. and its Affiliates, as amended andrestated (filed as Exhibit 10.1 to the Company’s Quarterly Report on Form 10-Q for the quarter ended March 31, 2013 (File No. 001-11239), and incorporated herein by reference).*
10.3(a) — Management Stockholder’s Agreement dated November 17, 2006 (filed as Exhibit 10.12 to the Company’s Annual Report onForm 10-K for the fiscal year ended December 31, 2006 (File No. 001-11239), and incorporated herein by reference).
86
306

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 87/137
Table of Contents
10.3(b) — Form of Omnibus Amendment to HCA Holdings, Inc.’s Management Stockholder’s Agreements (filed as Exhibit 10.39 to theCompany’s Registration Statement on Form S-1 (File No. 333-171369), and incorporated herein by reference).
10.4 — Form of Stock Option Agreement (2011) (filed as Exhibit 10.1 to the Company’s Quarterly Report on Form 10-Q for the quarterended September 30, 2011 (File No. 001-11239), and incorporated herein by reference).*
10.5(a) — Form of Stock Appreciation Right Award Agreement Under the 2006 Stock Incentive Plan for Key Employees of HCA Holdings, Inc.and its Affiliates, as Amended and Restated (filed as Exhibit 10.1 to the Company’s Current Report on Form 8-K filedFebruary 14, 2012 (File No. 001-11239), and incorporated herein by reference).*
10.5(b) — Form of 2014 Stock Appreciation Right Award Agreement Under the 2006 Stock Incentive Plan for Key Employees of HCAHoldings, Inc. and its Affiliates, as Amended and Restated (filed as Exhibit 10.17(b) to the Company’s Annual Report on Form 10-Kfor the fiscal year ended December 31, 2013 (File No. 001-11239), and incorporated herein by reference).*
10.6 — Retirement Agreement between the Company and Thomas F. Frist, Jr., M.D. dated as of January 1, 2002 (filed as Exhibit 10.30 to theCompany’s Annual Report on Form 10-K for the fiscal year ended December 31, 2001 (File No. 001-11239), and incorporated hereinby reference).*
10.7 — Amended and Restated HCA Supplemental Executive Retirement Plan, effective December 22, 2010, except as provided therein(filed as Exhibit 10.26 to the Company’s Annual Report on Form 10-K for the fiscal year ended December 31, 2010 (File No. 001-11239), and incorporated herein by reference).*
10.8 — Amended and Restated HCA Restoration Plan, effective December 22, 2010 (filed as Exhibit 10.27 to the Company’s Annual Reporton Form 10-K for the fiscal year ended December 31, 2010 (File No. 001-11239), and incorporated herein by reference).*
10.9(a) — Amended and Restated Employment Agreement dated September 10, 2018 (R. Milton Johnson) (filed as Exhibit 10.1 to theCompany’s Current Report on Form 8-K filed September 12, 2018 (File No. 001-11239), and incorporated herein by reference).*
10.9(b) — Employment Agreement dated November 16, 2006 (Samuel N. Hazen) (filed as Exhibit 10.27(d) to the Company’s Annual Report onForm 10-K for the fiscal year ended December 31, 2006 (File No. 001-11239), and incorporated herein by reference).*
10.9(c) — Employment Agreement dated November 16, 2006 (Charles J. Hall) (filed as Exhibit 10.28(d) to the Company’s Annual Report onForm 10-K for the fiscal year ended December 31, 2012 (File No. 001-11239), and incorporated herein by reference).*
10.9(d) — Amendment to Employment Agreement effective February 9, 2011 (Samuel N. Hazen) (filed as Exhibit 10.29(j) to the Company’sAnnual Report on Form 10-K for the fiscal year ended December 31, 2010 (File No. 001-11239), and incorporated herein byreference).*
10.9(e) — Second Amendment to Employment Agreement effective January 29, 2015 (Samuel N. Hazen) (filed as Exhibit 10.23(i) to theCompany’s Annual Report on Form 10-K for the fiscal year ended December 31, 2014 (File No. 001-11239), and incorporated hereinby reference).*
10.9(f) — Third Amendment to Employment Agreement effective January 27, 2016 (Samuel N. Hazen) (filed as Exhibit 10.23(j) to theCompany’s Annual Report on Form 10-K for the fiscal year ended December 31, 2015 (File No. 001-11239), and incorporated hereinby reference).*
10.9(g) — Amendment to Employment Agreement effective January 27, 2016 (Charles J. Hall) (filed as Exhibit 10.23(k) to the Company’sAnnual Report on Form 10-K for the fiscal year ended December 31, 2015 (File No. 001-11239), and incorporated herein byreference).*
87
307

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 88/137
Table of Contents
10.9(h) — Fourth Amendment to Employment Agreement effective November 14, 2016 (Samuel N. Hazen) (filed as Exhibit 10.16(l) to theCompany’s Annual Report on Form 10-K for the fiscal year ended December 31, 2016 (File No. 001-11239), and incorporated hereinby reference).*
10.9(i) — Fifth Amendment to Employment Agreement effective January 1, 2019 (Samuel N. Hazen) (filed as Exhibit 10.14(i) to theCompany’s Annual Report on Form 10-K for the fiscal year ended December 31, 2018 (File No. 001-11239), and incorporated hereinby reference).*
10.10 — Indemnification Priority and Information Sharing Agreement, dated as of November 1, 2009, between HCA Inc. and certain otherparties thereto (filed as Exhibit 10.35 to the Company’s Annual Report on Form 10-K for the fiscal year endedDecember 31, 2009 (File No. 001-11239), and incorporated herein by reference).
10.11 — Assignment and Assumption Agreement, dated November 22, 2010, by and among HCA Inc., HCA Holdings, Inc. and HCA MergerSub LLC (filed as Exhibit 10.1 to the Company’s Current Report on Form 8-K filed November 24, 2010 (File No. 000-18406), andincorporated herein by reference).
10.12 — Omnibus Amendment to Various Stock and Option Plans and the Management Stockholders’ Agreement, dated November 22, 2010(filed as Exhibit 10.2 to the Company’s Current Report on Form 8-K filed November 24, 2010 (File No. 000-18406), and incorporatedherein by reference).*
10.13 — Omnibus Amendment to Stock Option Agreements Issued Under the 2006 Stock Incentive Plan for Key Employees of HCAHoldings, Inc. and its Affiliates, as amended, effective February 16, 2011 (filed as Exhibit 10.38 to the Company’s Annual Report onForm 10-K for the fiscal year ended December 31, 2010 (File No. 001-11239), and incorporated herein by reference).*
10.14 — Stockholders’ Agreement, dated as of March 9, 2011, by and among the Company, Hercules Holding II, LLC and the other signatoriesthereto (filed as Exhibit 10.1 to the Company’s Current Report on Form 8-K filed March 16, 2011 (File No. 001-11239), andincorporated herein by reference).
10.15 — Amendment, dated as of September 21, 2011, to the Stockholders’ Agreement, dated as of March 9, 2011 (filed as Exhibit 10.2 to theCompany’s Current Report on Form 8-K filed September 21, 2011 (File No. 001-11239), and incorporated herein by reference).
10.16 — Form of Director Restricted Share Unit Agreement Under the 2006 Stock Incentive Plan for Key Employees of HCA Holdings, Inc.and its Affiliates, as Amended and Restated (filed as Exhibit 10.5 to the Company’s Quarterly Report on Form 10-Q for the quarterended March 31, 2011 (File No. 001-11239), and incorporated herein by reference).*
10.17 — Executive Severance Policy (filed as Exhibit 10.46 to the Company’s Annual Report on Form 10-K for the fiscal year endedDecember 31, 2013 (File No. 001-11239), and incorporated herein by reference).*
10.18 — HCA Holdings, Inc. Employee Stock Purchase Plan (filed as Exhibit 10.1 to the Company’s Current Report on Form 8-K filed April25, 2014 (File No. 001-11239), and incorporated herein by reference).*
10.19 — Form of 2015 Stock Appreciation Right Award Agreement Under the 2006 Stock Incentive Plan for Key Employees of HCAHoldings, Inc. and its Affiliates, as Amended and Restated (filed as Exhibit 10.1 to the Company’s Current Report on Form 8-K filedFebruary 4, 2015 (File No. 001-11239), and incorporated herein by reference).*
10.20 — Form of 2016 Stock Appreciation Right Award Agreement Under the 2006 Stock Incentive Plan for Key Employees of HCAHoldings, Inc. and its Affiliates, as Amended and Restated (filed as Exhibit 10.50 to the Company’s Annual Report on Form 10-K forthe fiscal year ended December 31, 2015 (File No. 001-11239), and incorporated herein by reference).*
88
308

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 89/137
Table of Contents
10.21 — Form of Director Restricted Share Unit Agreement (Annual Award) Under the 2006 Stock Incentive Plan for Key Employees of HCAHoldings, Inc. and its Affiliates, as Amended and Restated (filed as Exhibit 10.2 to the Company’s Quarterly Report on Form 10-Qfor the quarter ended March 31, 2016 (File No. 001-11239), and incorporated herein by reference).*
10.22 — Form of 2017 Stock Appreciation Right Award Agreement Under the 2006 Stock Incentive Plan for Key Employees of HCAHoldings, Inc. and its Affiliates, as Amended and Restated (filed as Exhibit 10.42 to the Company’s Annual Report on Form 10-K forthe fiscal year ended December 31, 2016 (File No. 001-11239), and incorporated herein by reference).*
10.23 — Form of 2017 Performance Share Unit Award Agreement Under the 2006 Stock Incentive Plan for Key Employees of HCA Holdings,Inc. and its Affiliates, as Amended and Restated (filed as Exhibit 10.43 to the Company’s Annual Report on Form 10-K for the fiscalyear ended December 31, 2016 (File No. 001-11239), and incorporated herein by reference).*
10.24 — HCA Holdings, Inc. 2017 Senior Officer Performance Excellence Program (filed as Exhibit 10.1 to the Company’s Current Report onForm 8-K filed April 3, 2017 (File No. 001-11239), and incorporated herein by reference).*
10.25 — Form of 2018 Stock Appreciation Right Award Agreement Under the 2006 Stock Incentive Plan for Key Employees of HCAHoldings, Inc. and its Affiliates, as Amended and Restated (filed as Exhibit 10.40 to the Company’s Annual Report on Form 10-K forthe fiscal year ended December 31, 2017 (File No. 001-11239), and incorporated herein by reference).*
10.26 — Form of 2018 Performance Share Unit Award Agreement Under the 2006 Stock Incentive Plan for Key Employees of HCA Holdings,Inc. and its Affiliates, as Amended and Restated (filed as Exhibit 10.41 to the Company’s Annual Report on Form 10-K for the fiscalyear ended December 31, 2017 (File No. 001-11239), and incorporated herein by reference).*
10.27 — HCA Holdings, Inc. 2018 Senior Officer Performance Excellence Program (filed as Exhibit 10.1 to the Company’s Current Report onForm 8-K filed April 5, 2018 (File No. 001-11239), and incorporated herein by reference).*
10.28 — Form of 2019 Stock Appreciation Right Award Agreement Under the 2006 Stock Incentive Plan for Key Employees of HCAHoldings, Inc. and its Affiliates, as Amended and Restated (filed as Exhibit 10.41 to the Company’s Annual Report on Form 10-K forthe fiscal year ended December 31, 2018 (File No. 001-11239), and incorporated herein by reference).*
10.29 — Form of 2019 Performance Share Unit Award Agreement Under the 2006 Stock Incentive Plan for Key Employees of HCA Holdings,Inc. and its Affiliates, as Amended and Restated (filed as Exhibit 10.42 to the Company’s Annual Report on Form 10-K for the fiscalyear ended December 31, 2018 (File No. 001-11239), and incorporated herein by reference).*
10.30 — Form of Restricted Share Unit Agreement (R. Milton Johnson) (filed as Exhibit 10.43 to the Company’s Annual Report on Form 10-Kfor the fiscal year ended December 31, 2018 (File No. 001-11239), and incorporated herein by reference).*
10.31 — HCA Healthcare, Inc. 2019 Senior Officer Performance Excellence Program (filed as Exhibit 10.1 to the Company’s Current Reporton Form 8-K filed April 2, 2019 (File No. 001-11239), and incorporated herein by reference).*
10.32 — Form of 2020 Stock Appreciation Right Award Agreement Under the 2006 Stock Incentive Plan for Key Employees of HCAHoldings, Inc. and its Affiliates, as Amended and Restated.*
10.33 — Form of 2020 Performance Share Unit Award Agreement Under the 2006 Stock Incentive Plan for Key Employees of HCA Holdings,Inc. and its Affiliates, as Amended and Restated.*
21 — List of Subsidiaries.
89
309

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 90/137
Table of Contents
23 — Consent of Ernst & Young LLP.
31.1 — Certification of Chief Executive Officer Pursuant to Section 302 of the Sarbanes-Oxley Act of 2002.
31.2 — Certification of Chief Financial Officer Pursuant to Section 302 of the Sarbanes-Oxley Act of 2002.
32 — Certification Pursuant to 18 U.S.C. Section 1350, as Adopted Pursuant to Section 906 of the Sarbanes-Oxley Act of 2002.
101 — The following financial information from our annual report on Form 10-K for the year ended December 31, 2019, filed with theSEC on February 20, 2020, formatted in Extensible Business Reporting Language (XBRL): (i) the consolidated balance sheets atDecember 31, 2019 and 2018, (ii) the consolidated income statements for the years ended December 31, 2019, 2018 and 2017,(iii) the consolidated comprehensive income statements for the years ended December 31, 2019, 2018 and 2017, (iv) theconsolidated statements of stockholders’ deficit for the years ended December 31, 2019, 2018 and 2017, (v) the consolidatedstatements of cash flows for the years ended December 31, 2019, 2018 and 2017, and (vi) the notes to consolidated financialstatements.
104 — The cover page from the Company’s Annual Report on Form 10-K for the year ended December 31, 2019, formatted in InlineXBRL (included in Exhibit 101).
* Management compensatory plan or arrangement.
Item 16. Form 10-K Summary None.
90
310

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 91/137
HCA HEALTHCARE, INC.
By: /s/ S����� N. H���� Samuel N. Hazen
Chief Executive Officer
Table of Contents
SIGNATURES
Pursuant to the requirements of Section 13 or 15(d) of the Securities Exchange Act of 1934, the Registrant has duly caused this report to be signedon its behalf by the undersigned, thereunto duly authorized.
Dated: February 20, 2020
Pursuant to the requirements of the Securities Exchange Act of 1934, this report has been signed below by the following persons on behalf of theregistrant and in the capacities and on the dates indicated.
Signature Title Date
/s/ S����� N. H����Samuel N. Hazen
Chief Executive Officer and Director(Principal Executive Officer)
February 20, 2020
/s/ W������ B. R���������William B. Rutherford
Executive Vice President andChief Financial Officer
(Principal Financial Officer andPrincipal Accounting Officer)
February 20, 2020
/s/ T����� F. F���� IIIThomas F. Frist III
Chairman and Director February 20, 2020
/s/ M�� G. C������Meg G. Crofton
Director February 20, 2020
/s/ R����� J. D�����Robert J. Dennis
Director February 20, 2020
/s/ N����-A�� D�P����Nancy-Ann DeParle
Director February 20, 2020
/s/ W������ R. F����William R. Frist
Director February 20, 2020
/s/ C������ O. H�������, J�.Charles O. Holliday, Jr.
Director February 20, 2020
/s/ G������� G. M�����Geoffrey G. Meyers
Director February 20, 2020
/s/ M������ W. M��������Michael W. Michelson
Director February 20, 2020
/s/ W���� J. R����Wayne J. Riley
Director February 20, 2020
/s/ J��� W. R���John W. Rowe
Director February 20, 2020
91
311

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 92/137
Table of Contents
HCA HEALTHCARE, INC.
INDEX TO CONSOLIDATED FINANCIAL STATEMENTS
Page Report of Independent Registered Public Accounting Firm F-2
Consolidated Financial Statements:
Consolidated Income Statements for the years ended December 31, 2019, 2018 and 2017 F-5
Consolidated Comprehensive Income Statements for the years ended December 31, 2019, 2018 and 2017 F-6
Consolidated Balance Sheets, December 31, 2019 and 2018 F-7
Consolidated Statements of Stockholders’ Deficit for the years ended December 31, 2019, 2018 and 2017 F-8
Consolidated Statements of Cash Flows for the years ended December 31, 2019, 2018 and 2017 F-9
Notes to Consolidated Financial Statements F-10
Quarterly Consolidated Financial Information (Unaudited) F-46
F-1
312

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 93/137
Table of Contents
Report of Independent Registered Public Accounting Firm
The Board of Directors and StockholdersHCA Healthcare, Inc.
Opinion on the Financial Statements
We have audited the accompanying consolidated balance sheets of HCA Healthcare, Inc. (the Company) as of December 31, 2019 and 2018, the relatedconsolidated statements of income, comprehensive income, stockholders’ deficit and cash flows for each of the three years in the period endedDecember 31, 2019, and the related notes (collectively referred to as the “consolidated financial statements”). In our opinion, the consolidated financialstatements present fairly, in all material respects, the financial position of the Company at December 31, 2019 and 2018, and the results of its operationsand its cash flows for each of the three years in the period ended December 31, 2019, in conformity with U.S. generally accepted accounting principles.
We also have audited, in accordance with the standards of the Public Company Accounting Oversight Board (United States) (PCAOB), the Company’sinternal control over financial reporting as of December 31, 2019, based on criteria established in Internal Control-Integrated Framework issued by theCommittee of Sponsoring Organizations of the Treadway Commission (2013 framework), and our report dated February 20, 2020 expressed anunqualified opinion thereon.
Adoption of New Accounting Standard
As discussed in Note 1 to the consolidated financial statements, effective January 1, 2019, the Company adopted ASU No. 2016-02, Leases (Topic 842),on a modified retrospective basis.
Basis for Opinion
These financial statements are the responsibility of the Company’s management. Our responsibility is to express an opinion on the Company’s financialstatements based on our audits. We are a public accounting firm registered with the PCAOB and are required to be independent with respect to theCompany in accordance with the U.S. federal securities laws and the applicable rules and regulations of the Securities and Exchange Commission andthe PCAOB.
We conducted our audits in accordance with the standards of the PCAOB. Those standards require that we plan and perform the audit to obtainreasonable assurance about whether the financial statements are free of material misstatement, whether due to error or fraud. Our audits includedperforming procedures to assess the risks of material misstatement of the financial statements, whether due to error or fraud, and performing proceduresthat respond to those risks. Such procedures included examining, on a test basis, evidence regarding the amounts and disclosures in the financialstatements. Our audits also included evaluating the accounting principles used and significant estimates made by management, as well as evaluating theoverall presentation of the financial statements. We believe that our audits provide a reasonable basis for our opinion.
Critical Audit Matters
The critical audit matters communicated below are matters arising from the current period audit of the financial statements that were communicated orrequired to be communicated to the audit committee and that: (1) relate to accounts or disclosures that are material to the financial statements and(2) involved our especially challenging, subjective or complex judgments. The communication of critical audit matters does not alter in any way ouropinion on the consolidated financial statements, taken as a whole, and we are not, by communicating the critical audit matters below, providingseparate opinions on the critical audit matters or on the accounts or disclosures to which they relate.
F-2
313

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 94/137
Table of Contents
Revenue Recognition
Description of the Matter For the year ended December 31, 2019, the Company’s revenues were $51.336 billion. As discussed in Note 1 tothe consolidated financial statements, revenues are based upon the estimated amounts the Company expects to beentitled to receive from patients and third-party payers. Estimates of contractual allowances under managed care,commercial, and governmental insurance plans are based upon the payment terms specified in the relatedcontractual agreements or as mandated under government payer programs. Management continually reviews thecontractual allowances estimation process to consider and incorporate updates to laws and regulations and thefrequent changes in managed care contractual terms resulting from contract renegotiations and renewals. Revenuesrelated to uninsured patients and uninsured copayment and deductible amounts for patients who have health careinsurance coverage may have discounts applied (uninsured discounts and contractual discounts). The Company alsorecords estimated implicit price concessions (based primarily on historical collection experience) related touninsured accounts to record these revenues and accounts receivable at the estimated amounts the Company expectsto collect. The primary collection risks relate to uninsured patient accounts, including amounts owed from patientsafter insurance has paid the amounts covered by the applicable agreement. Implicit price concessions relateprimarily to amounts due directly from patients and are based upon management’s assessment of historical write-offs and expected net collections, business and economic conditions, trends in federal, state and private employerhealth care coverage and other collection indicators. Auditing management’s estimates of contractual allowances and implicit price concessions was complex andjudgmental due to the significant data inputs and subjective assumptions utilized in determining related amounts.
How We Addressed the Matterin Our Audit
We tested internal controls that address the risks of material misstatement related to the measurement and valuationof revenues, including estimation of contractual allowances and implicit price concessions. For example, we testedmanagement’s internal controls over the key data inputs to the contractual allowances and implicit priceconcessions models, significant assumptions underlying management’s models, and management’s internal controlsover retrospective hindsight reviews of historical reserve accuracy. To test the estimated contractual allowances and implicit price concessions, we performed audit procedures thatincluded, among others, assessing methodologies and evaluating the significant assumptions discussed above andtesting the completeness and accuracy of the underlying data used by the Company in its estimates. We comparedthe significant assumptions used by management to current industry and economic trends and considered changes,if any, to the Company’s business and other relevant factors. We also assessed the historical accuracy ofmanagement’s estimates as a source of potential corroborative or contrary evidence.
Professional Liability Claims
Description of the Matter At December 31, 2019, the Company’s reserves for professional liability risks were $1.827 billion and theCompany’s related provision for losses for the year ended December 31, 2019 was $497 million. As discussed inNote 1 to the consolidated financial statements, reserves for professional liability risks represent the estimatedultimate cost of all reported and unreported losses incurred and unpaid as of the
F-3
314

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 95/137
Table of Contents
consolidated balance sheet date. Management determines professional liability reserves and provisions for lossesusing individual case-basis valuations and actuarial analyses. Trends in the average frequency (number of claims)and ultimate average severity (cost per claim) of claims are significant assumptions in estimating the reserves. Auditing management’s professional liability claims reserves was complex and judgmental due to the significantestimations required in determining the reserves, particularly the actuarial methodology and assumptions related tothe severity and frequency of claims.
How We Addressed the Matterin Our Audit
We tested management’s internal controls that address the risks of material misstatement over the Company’sprofessional liability claims reserve estimation process. For example, we tested internal controls overmanagement’s review of the actuarial methodology and significant assumptions, and the completeness and accuracyof claims data supporting the recorded reserves. To test the Company’s determination of the estimated professional liability expense and reserves, we performedaudit procedures that included, among others, testing the completeness and accuracy of underlying claims data usedby the Company and its actuaries in its determination of reserves and reviewing the Company’s insurance contractsto assess self-insured limits, deductibles and coverage limits. Additionally, with the involvement of our actuarialspecialists, we performed audit procedures that included, among others, assessing the actuarial valuationmethodologies utilized by management and its actuaries, testing the significant assumptions, includingconsideration of Company-specific claim reporting and payment data, assessing the accuracy of management’shistorical reserve estimates, and developing an independent range of reserves for comparison to the Company’srecorded amounts.
/s/ Ernst & Young LLP
We have served as the Company’s auditor since 1994.
Nashville, TennesseeFebruary 20, 2020
F-4
315

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 96/137
Table of Contents
HCA HEALTHCARE, INC.CONSOLIDATED INCOME STATEMENTS
FOR THE YEARS ENDED DECEMBER 31, 2019, 2018 AND 2017(Dollars in millions, except per share amounts)
2019 2018 2017 Revenues $ 51,336 $ 46,677 $ 43,614
Salaries and benefits 23,560 21,425 20,059 Supplies 8,481 7,724 7,316 Other operating expenses 9,481 8,608 8,051 Equity in earnings of affiliates (43) (29) (45)Depreciation and amortization 2,596 2,278 2,131 Interest expense 1,824 1,755 1,690 Gains on sales of facilities (18) (428) (8)Losses on retirement of debt 211 9 39
46,092 41,342 39,233 Income before income taxes 5,244 5,335 4,381 Provision for income taxes 1,099 946 1,638 Net income 4,145 4,389 2,743 Net income attributable to noncontrolling interests 640 602 527
Net income attributable to HCA Healthcare, Inc. $ 3,505 $ 3,787 $ 2,216 Per share data:
Basic earnings per share $ 10.27 $ 10.90 $ 6.12 Diluted earnings per share $ 10.07 $ 10.66 $ 5.95
Shares used in earnings per share calculations (in millions): Basic 341.210 347.297 362.305 Diluted 348.226 355.303 372.221
The accompanying notes are an integral part of the consolidated financial statements.
F-5
316

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 97/137
Table of Contents
HCA HEALTHCARE, INC.CONSOLIDATED COMPREHENSIVE INCOME STATEMENTSFOR THE YEARS ENDED DECEMBER 31, 2019, 2018 AND 2017
(Dollars in millions)
2019 2018 2017 Net income $4,145 $4,389 $2,743 Other comprehensive income (loss) before taxes:
Foreign currency translation 5 (71) 97
Unrealized gains (losses) on available-for-sale securities 15 (7) 1 Realized gains included in other operating expenses — — (2)
15 (7) (1)
Defined benefit plans (63) 44 (43)Pension costs included in salaries and benefits 13 21 18
(50) 65 (25)
Change in fair value of derivative financial instruments (50) 23 11 Interest (benefits) costs included in interest expense (17) (10) 20
(67) 13 31 Other comprehensive (loss) income before taxes (97) — 102 Income taxes (benefits) related to other comprehensive income items (18) 8 42 Other comprehensive (loss) income (79) (8) 60 Comprehensive income 4,066 4,381 2,803 Comprehensive income attributable to noncontrolling interests 640 602 527 Comprehensive income attributable to HCA Healthcare, Inc. $3,426 $3,779 $2,276
The accompanying notes are an integral part of the consolidated financial statements.
F-6
317

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 98/137
Table of Contents
HCA HEALTHCARE, INC.CONSOLIDATED BALANCE SHEETS
DECEMBER 31, 2019 AND 2018(Dollars in millions)
2019 2018 ASSETS
Current assets: Cash and cash equivalents $ 621 $ 502 Accounts receivable 7,380 6,789 Inventories 1,849 1,732 Other 1,346 1,190
11,196 10,213 Property and equipment, at cost:
Land 2,178 1,944 Buildings 17,669 15,659 Equipment 25,756 23,577 Construction in progress 1,632 1,785
47,235 42,965 Accumulated depreciation (24,520) (23,208)
22,715 19,757
Investments of insurance subsidiaries 315 362 Investments in and advances to affiliates 249 232 Goodwill and other intangible assets 8,269 7,953 Right-of-use operating lease assets 1,834 — Other 480 690
$ 45,058 $ 39,207 LIABILITIES AND STOCKHOLDERS’ DEFICIT
Current liabilities: Accounts payable $ 2,905 $ 2,577 Accrued salaries 1,775 1,580 Other accrued expenses 2,932 2,624 Long-term debt due within one year 145 788
7,757 7,569
Long-term debt, less debt issuance costs and discounts of $239 and $157 33,577 32,033 Professional liability risks 1,370 1,275 Right-of-use operating lease obligations 1,499 — Income taxes and other liabilities 1,420 1,248 Stockholders’ deficit:
Common stock $0.01 par; authorized 1,800,000,000 shares; outstanding 338,445,600 shares — 2019 and 342,895,200shares — 2018
3
3
Accumulated other comprehensive loss (460) (381)Retained deficit (2,351) (4,572)Stockholders’ deficit attributable to HCA Healthcare, Inc. (2,808) (4,950)Noncontrolling interests 2,243 2,032
(565) (2,918) $ 45,058 $ 39,207
The accompanying notes are an integral part of the consolidated financial statements.
F-7
318

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 99/137
Table of Contents
HCA HEALTHCARE, INC.CONSOLIDATED STATEMENTS OF STOCKHOLDERS’ DEFICIT
FOR THE YEARS ENDED DECEMBER 31, 2019, 2018 AND 2017(Dollars in millions)
Equity (Deficit) Attributable to HCA Healthcare, Inc.
Equity
Attributable to Noncontrolling Interests Total
Common Stock
Capital in Excess of Par
Value
Accumulated Other
Comprehensive Loss
Retained Deficit
Shares (in millions)
Par Value
Balances, December 31, 2016 370.536 $ 4 $ — $ (338) $(6,968) $ 1,669 $(5,633)Comprehensive income 60 2,216 527 2,803 Repurchase of common stock (25.092) (271) (1,780) (2,051)Share-based benefit plans 4.648 281 281 Distributions (448) (448)Other (10) 63 53
Balances, December 31, 2017 350.092 4 — (278) (6,532) 1,811 (4,995)Comprehensive income (loss) (8) 3,787 602 4,381 Repurchase of common stock (14.070) (1) (103) (1,426) (1,530)Share-based benefit plans 6.873 115 115 Cash dividends declared ($1.40 share) (496) (496)Distributions (441) (441)Reclassification of stranded tax effects (95) 95 — Other (12) 60 48
Balances, December 31, 2018 342.895 3 — (381) (4,572) 2,032 (2,918)Comprehensive income (loss) (79) 3,505 640 4,066 Repurchase of common stock (7.949) (302) (729) (1,031)Share-based benefit plans 3.500 313 313 Cash dividends declared ($1.60 share) (555) (555)Distributions (542) (542)Other (11) 113 102
Balances, December 31, 2019 338.446 $ 3 $ — $ (460) $(2,351) $ 2,243 $ (565)
The accompanying notes are an integral part of the consolidated financial statements.
F-8
319

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 100/137
Table of Contents
HCA HEALTHCARE, INC.CONSOLIDATED STATEMENTS OF CASH FLOWS
FOR THE YEARS ENDED DECEMBER 31, 2019, 2018 AND 2017(Dollars in millions)
2019 2018 2017 Cash flows from operating activities:
Net income $ 4,145 $ 4,389 $ 2,743 Adjustments to reconcile net income to net cash provided by operating activities:
Increase (decrease) in cash from operating assets and liabilities: Accounts receivable (326) (423) (601)Inventories and other assets (158) (242) (69)Accounts payable and accrued expenses 396 698 374
Depreciation and amortization 2,596 2,278 2,131 Income taxes 250 74 433 Gains on sales of facilities (18) (428) (8)Losses on retirement of debt 211 9 39 Amortization of debt issuance costs 30 31 31 Share-based compensation 347 268 270 Other 129 107 83
Net cash provided by operating activities 7,602 6,761 5,426 Cash flows from investing activities:
Purchase of property and equipment (4,158) (3,573) (3,015)Acquisition of hospitals and health care entities (1,682) (1,253) (1,212)Sales of hospitals and health care entities 61 808 25 Change in investments 25 57 (73)Other 34 60 (4)
Net cash used in investing activities (5,720) (3,901) (4,279)Cash flows from financing activities:
Issuances of long-term debt 6,451 2,000 1,502 Net change in revolving bank credit facilities (560) (640) 760 Repayment of long-term debt (5,324) (1,704) (753)Distributions to noncontrolling interests (542) (441) (448)Payment of debt issuance costs (73) (25) (26)Payment of dividends (550) (487) — Repurchases of common stock (1,031) (1,530) (2,051)Other (142) (248) (45)
Net cash used in financing activities (1,771) (3,075) (1,061)Effect of exchange rate changes on cash and cash equivalents 8 (15) — Change in cash and cash equivalents 119 (230) 86 Cash and cash equivalents at beginning of period 502 732 646 Cash and cash equivalents at end of period $ 621 $ 502 $ 732 Interest payments $ 1,914 $ 1,744 $ 1,700 Income tax payments, net $ 849 $ 872 $ 1,205
The accompanying notes are an integral part of the consolidated financial statements.
F-9
320

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 101/137
Table of Contents
HCA HEALTHCARE, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
NOTE 1 — ACCOUNTING POLICIES
Reporting Entity
HCA Healthcare, Inc. is a holding company whose affiliates own and operate hospitals and related health care entities. The term “affiliates”includes direct and indirect subsidiaries of HCA Healthcare, Inc. and partnerships and joint ventures in which such subsidiaries are partners. AtDecember 31, 2019, these affiliates owned and operated 184 hospitals, 123 freestanding surgery centers and provided extensive outpatient and ancillaryservices. HCA Healthcare, Inc.’s facilities are located in 21 states and England. The terms “Company,” “HCA,” “we,” “our” or “us,” as used herein andunless otherwise stated or indicated by context, refer to HCA Healthcare, Inc. and its affiliates. The terms “facilities” or “hospitals” refer to entitiesowned and operated by affiliates of HCA and the term “employees” refers to employees of affiliates of HCA.
Basis of Presentation
The preparation of financial statements in conformity with generally accepted accounting principles requires management to make estimates andassumptions that affect the amounts reported in the consolidated financial statements and accompanying notes. Actual results could differ from thoseestimates.
The consolidated financial statements include all subsidiaries and entities controlled by HCA. We generally define “control” as ownership of amajority of the voting interest of an entity. The consolidated financial statements include entities in which we absorb a majority of the entity’s expectedlosses, receive a majority of the entity’s expected residual returns, or both, as a result of ownership, contractual or other financial interests in the entity.The accounts of acquired entities are included in our consolidated financial statements for periods subsequent to our acquisition of controlling interests.Significant intercompany transactions have been eliminated. Investments in entities we do not control, but in which we have a substantial ownershipinterest and can exercise significant influence, are accounted for using the equity method.
The majority of our expenses are “cost of revenue” items. Costs that could be classified as general and administrative include our corporate officecosts, which were $370 million, $344 million and $340 million for the years ended December 31, 2019, 2018 and 2017, respectively.
Revenues
Our revenues generally relate to contracts with patients in which our performance obligations are to provide health care services to the patients.Revenues are recorded during the period our obligations to provide health care services are satisfied. Our performance obligations for inpatient servicesare generally satisfied over periods that average approximately five days, and revenues are recognized based on charges incurred in relation to totalexpected charges. Our performance obligations for outpatient services are generally satisfied over a period of less than one day. The contractualrelationships with patients, in most cases, also involve a third-party payer (Medicare, Medicaid, managed care health plans and commercial insurancecompanies, including plans offered through the health insurance exchanges) and the transaction prices for the services provided are dependent upon theterms provided by (Medicare and Medicaid) or negotiated with (managed care health plans and commercial insurance companies) the third-party payers.The payment arrangements with third-party payers for the services we provide to the related patients typically specify payments at amounts less than ourstandard charges. Medicare generally pays for inpatient and outpatient services at prospectively determined rates based on clinical, diagnostic and otherfactors. Services provided to patients having Medicaid coverage are generally paid at prospectively determined rates per discharge, per identified serviceor per covered member. Agreements with commercial insurance carriers, managed care and preferred provider organizations generally provide forpayments based
F-10
321

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 102/137
Table of Contents
HCA HEALTHCARE, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
NOTE 1 — ACCOUNTING POLICIES (continued)
Revenues (continued)
upon predetermined rates per diagnosis, per diem rates or discounted fee-for-service rates. Management continually reviews the contractual estimationprocess to consider and incorporate updates to laws and regulations and the frequent changes in managed care contractual terms resulting from contractrenegotiations and renewals.
Our revenues are based upon the estimated amounts we expect to be entitled to receive from patients and third-party payers. Estimates ofcontractual adjustments under managed care and commercial insurance plans are based upon the payment terms specified in the related contractualagreements. Revenues related to uninsured patients and uninsured copayment and deductible amounts for patients who have health care coverage mayhave discounts applied (uninsured discounts and contractual discounts). We also record estimated implicit price concessions (based primarily onhistorical collection experience) related to uninsured accounts to record these revenues at the estimated amounts we expect to collect. Our revenues byprimary third-party payer classification and other (including uninsured patients) for the years ended December 31, are summarized in the following table(dollars in millions):
Years Ended December 31, 2019 Ratio 2018 Ratio 2017 Ratio
Medicare $10,798 21.0% $ 9,831 21.1% $ 9,285 21.3%Managed Medicare 6,452 12.6 5,497 11.8 4,680 10.7 Medicaid 1,572 3.1 1,358 2.9 1,316 3.0 Managed Medicaid 2,450 4.8 2,403 5.1 2,165 5.0 Managed care and other insurers 26,544 51.6 24,467 52.4 23,342 53.5 International (managed care and other insurers) 1,162 2.3 1,156 2.5 1,097 2.5 Other 2,358 4.6 1,965 4.2 1,729 4.0 Revenues $51,336 100.0% $46,677 100.0% $43,614 100.0%
Laws and regulations governing the Medicare and Medicaid programs are complex and subject to interpretation. Estimated reimbursementamounts are adjusted in subsequent periods as cost reports are prepared and filed and as final settlements are determined (in relation to certaingovernment programs, primarily Medicare, this is generally referred to as the “cost report” filing and settlement process). The adjustments to estimatedMedicare and Medicaid reimbursement amounts and disproportionate-share funds related primarily to cost reports filed during the respective yearresulted in net increases to revenues of $51 million, $29 million and $41 million in 2019, 2018 and 2017, respectively. The adjustments to estimatedreimbursement amounts related primarily to cost reports filed during previous years resulted in net increases to revenues of $13 million, $51 million and$56 million in 2019, 2018 and 2017, respectively.
The Emergency Medical Treatment and Labor Act (“EMTALA”) requires any hospital participating in the Medicare program to conduct anappropriate medical screening examination of every person who presents to the hospital’s emergency room for treatment and, if the individual issuffering from an emergency medical condition, to either stabilize the condition or make an appropriate transfer of the individual to a facility able tohandle the condition. The obligation to screen and stabilize emergency medical conditions exists regardless of an individual’s ability to pay fortreatment. Federal and state laws and regulations require, and our commitment to providing quality patient care encourages, us to provide services topatients who are financially unable to pay for the health care services they receive.
F-11
322

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 103/137
Table of Contents
HCA HEALTHCARE, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
NOTE 1 — ACCOUNTING POLICIES (continued)
Revenues (continued)
Prior to November 2017, patients treated at hospitals for non-elective care, who have income at or below 200% of the federal poverty level, wereeligible for charity care. During November 2017, we expanded our charity policy to include patients who have income above 200%, but at or below400%, of the federal poverty level and we limit the patient responsibility amounts for these patients to a percentage of their annual household income,computed on a sliding scale based upon their annual income and the applicable percentage of the federal poverty level. The federal poverty level isestablished by the federal government and is based on income and family size. Because we do not pursue collection of amounts determined to qualify ascharity care, they are not reported in revenues. We provide discounts to uninsured patients who do not qualify for Medicaid or charity care. We mayattempt to provide assistance to uninsured patients to help determine whether they may qualify for Medicaid, other federal or state assistance, or charitycare. If an uninsured patient does not qualify for these programs, the uninsured discount is applied.
The collection of outstanding receivables for Medicare, Medicaid, managed care payers, other third-party payers and patients is our primarysource of cash and is critical to our operating performance. The primary collection risks relate to uninsured patient accounts, including patient accountsfor which the primary insurance carrier has paid the amounts covered by the applicable agreement, but patient responsibility amounts (deductibles andcopayments) remain outstanding. Implicit price concessions relate primarily to amounts due directly from patients. Estimated implicit price concessionsare recorded for all uninsured accounts, regardless of the age of those accounts. Accounts are written off when all reasonable internal and externalcollection efforts have been performed.
The estimates for implicit price concessions are based upon management’s assessment of historical writeoffs and expected net collections,business and economic conditions, trends in federal, state and private employer health care coverage and other collection indicators. Management relieson the results of detailed reviews of historical writeoffs and collections at facilities that represent a majority of our revenues and accounts receivable (the“hindsight analysis”) as a primary source of information in estimating the collectability of our accounts receivable. We perform the hindsight analysisquarterly, utilizing rolling twelve-months accounts receivable collection and writeoff data. We believe our quarterly updates to the estimated implicitprice concession amounts at each of our hospital facilities provide reasonable estimates of our revenues and valuations of our accounts receivable. Theseroutine, quarterly changes in estimates have not resulted in material adjustments to the valuations of our accounts receivable or period-to-periodcomparisons of our results of operations. At December 31, 2019 and 2018, estimated implicit price concessions of $6.953 billion and $6.280 billion,respectively, had been recorded to adjust our revenues and accounts receivable to the estimated amounts we expect to collect.
F-12
323

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 104/137
Table of Contents
HCA HEALTHCARE, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
NOTE 1 — ACCOUNTING POLICIES (continued)
Revenues (continued)
To quantify the total impact of the trends related to uninsured patient accounts, we believe it is beneficial to view total uncompensated care, whichis comprised of charity care, uninsured discounts and implicit price concessions. A summary of the estimated cost of total uncompensated care for theyears ended December 31, follows (dollars in millions):
2019 2018 2017 Patient care costs (salaries and benefits, supplies, other operating expenses and depreciation and
amortization)
$44,118
$40,035
$37,557 Cost-to-charges ratio (patient care costs as percentage of gross patient charges) 12.0% 12.4% 12.9%Total uncompensated care $31,105 $26,757 $23,420 Multiply by the cost-to-charges ratio 12.0% 12.4% 12.9%Estimated cost of total uncompensated care $ 3,733 $ 3,318 $ 3,021
The total uncompensated care amounts include charity care of $13.260 billion, $8.611 billion and $4.861 billion. The estimated costs of charitycare were $1.591 billion, $1.068 billion and $627 million for the years ended December 31, 2019, 2018 and 2017, respectively.
Cash and Cash Equivalents
Cash and cash equivalents include highly liquid investments with a maturity of three months or less when purchased. Our insurance subsidiaries’cash equivalent investments in excess of the amounts required to pay estimated professional liability claims during the next twelve months are notincluded in cash and cash equivalents as these funds are not available for general corporate purposes. Carrying values of cash and cash equivalentsapproximate fair value due to the short-term nature of these instruments.
Our cash management system provides for daily investment of available balances and the funding of outstanding checks when presented forpayment. Outstanding, but unpresented, checks totaling $486 million and $449 million at December 31, 2019 and 2018, respectively, have been includedin “accounts payable” in the consolidated balance sheets. Upon presentation for payment, these checks are funded through available cash balances or ourcredit facility.
Accounts Receivable
We receive payments for services rendered from federal and state agencies (under the Medicare and Medicaid programs), managed care healthplans, commercial insurance companies, employers and patients. We recognize that revenues and receivables from government agencies are significantto our operations, but do not believe there are significant credit risks associated with these government agencies. We do not believe there are any othersignificant concentrations of revenues from any particular payer that would subject us to any significant credit risks in the collection of our accountsreceivable. Days revenues in accounts receivable were 50 days, 51 days and 52 days at December 31, 2019, 2018 and 2017, respectively. Changes ingeneral economic conditions, patient accounting service center operations, payer mix, or federal or state governmental health care coverage could affectour collection of accounts receivable, cash flows and results of operations.
F-13
324

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 105/137
Table of Contents
HCA HEALTHCARE, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
NOTE 1 — ACCOUNTING POLICIES (continued)
Inventories
Inventories are stated at the lower of cost (first-in, first-out) or market.
Property and Equipment
Depreciation expense, computed using the straight-line method, was $2.579 billion in 2019, $2.262 billion in 2018 and $2.111 billion in 2017.Buildings and improvements are depreciated over estimated useful lives ranging generally from 10 to 40 years. Estimated useful lives of equipment varygenerally from four to 10 years.
When events, circumstances or operating results indicate the carrying values of certain long-lived assets expected to be held and used might beimpaired, we prepare projections of the undiscounted future cash flows expected to result from the use of the assets and their eventual disposition. If theprojections indicate the recorded amounts are not expected to be recoverable, such amounts are reduced to estimated fair value. Fair value may beestimated based upon internal evaluations that include quantitative analyses of revenues and cash flows, reviews of recent sales of similar assets andindependent appraisals.
Long-lived assets to be disposed of are reported at the lower of their carrying amounts or fair value less costs to sell or close. The estimates of fairvalue are usually based upon recent sales of similar assets and market responses based upon discussions with and offers received from potential buyers.
Investments of Insurance Subsidiaries
At December 31, 2019 and 2018, the investments of our 100% owned insurance subsidiaries were classified as “available-for-sale” as defined inAccounting Standards Codification (“ASC”) No. 320, Investments — Debt Securities and are recorded at fair value. The investment securities are heldfor the purpose of providing a funding source to pay liability claims covered by the insurance subsidiaries. We perform quarterly assessments ofindividual investment securities to determine whether declines in fair value are due to credit-related or noncredit-related factors. Our investmentsecurities evaluation process involves subjective judgments, often involves estimating the outcome of future events, and requires a significant level ofprofessional judgment in determining whether a credit-related impairment has occurred. We evaluate, among other things, the financial position and nearterm prospects of the issuer, conditions in the issuer’s industry, liquidity of the investment, changes in the amount or timing of expected future cashflows from the investment, and recent downgrades of the issuer by a rating agency, to determine if, and when, a decline in the fair value of aninvestment below amortized cost is considered to be a credit-related impairment. The extent to which the fair value of the investment is less thanamortized cost and our ability and intent to retain the investment, to allow for any anticipated recovery of the investment’s fair value, are importantcomponents of our investment securities evaluation process.
Goodwill and Intangible Assets
Goodwill is not amortized but is subject to annual impairment tests. In addition to the annual impairment review, impairment reviews areperformed whenever circumstances indicate a possible impairment may exist. Impairment testing for goodwill is done at the reporting unit level.Reporting units are one level below the business segment level, and our impairment testing is performed at the operating division level. We compare thefair value of the reporting unit assets to the carrying amount, on at least an annual basis, to determine if there is potential impairment. If the fair value ofthe reporting unit assets is less than their carrying value, an impairment loss is recognized. Fair value is estimated based upon internal evaluations ofeach reporting unit that include
F-14
325

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 106/137
Table of Contents
HCA HEALTHCARE, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
NOTE 1 — ACCOUNTING POLICIES (continued)
Goodwill and Intangible Assets (continued)
quantitative analyses of market multiples, revenues and cash flows and reviews of recent sales of similar facilities. No goodwill impairments wererecognized during 2019, 2018 or 2017.
During 2019, goodwill increased by $332 million related to acquisitions and declined by $4 million related to foreign currency translation andother adjustments. During 2018, goodwill increased by $636 million related to acquisitions and declined by $60 million related to foreign currencytranslation and other adjustments.
During 2019, identifiable intangible assets declined by $12 million due to amortization, foreign currency translation and other adjustments. During2018, identifiable intangible assets declined by $17 million due to amortization, foreign currency translation and other adjustments. Identifiableintangible assets are amortized over estimated lives ranging generally from three to 10 years. The gross carrying amount of identifiable intangible assetsat both December 31, 2019 and 2018 was $184 million and accumulated amortization was $123 million and $111 million, respectively. The grosscarrying amount of indefinite-lived identifiable intangible assets at both December 31, 2019 and 2018 was $269 million. Indefinite-lived identifiableintangible assets are not amortized but are subject to annual impairment tests, and impairment reviews are performed whenever circumstances indicate apossible impairment may exist.
Debt Issuance Costs and Discounts
Debt issuance costs and discounts are amortized based upon the terms of the respective debt obligations. The gross carrying amount of debtissuance costs and discounts at December 31, 2019 and 2018 was $413 million and $360 million, respectively, and accumulated amortization was$174 million and $203 million, respectively. Amortization of debt issuance costs and discounts is included in interest expense and was $30 million,$31 million and $31 million for 2019, 2018 and 2017, respectively.
Professional Liability Claims
Reserves for professional liability risks were $1.827 billion and $1.741 billion at December 31, 2019 and 2018, respectively. The current portionof the reserves, $457 million and $466 million at December 31, 2019 and 2018, respectively, is included in “other accrued expenses” in the consolidatedbalance sheets. Provisions for losses related to professional liability risks were $497 million, $447 million and $466 million for 2019, 2018 and 2017,respectively, and are included in “other operating expenses” in our consolidated income statements. Provisions for losses related to professional liabilityrisks are based upon actuarially determined estimates. During 2019 and 2018, we recorded reductions to the provision for professional liability risks of$50 million and $70 million, respectively, due to the receipt of updated actuarial information. Loss and loss expense reserves represent the estimatedultimate net cost of all reported and unreported losses incurred through the respective consolidated balance sheet dates. The reserves for unpaid lossesand loss expenses are estimated using individual case-basis valuations and actuarial analyses. Those estimates are subject to the effects of trends in lossseverity and frequency. The estimates are continually reviewed and adjustments are recorded as experience develops or new information becomesknown. Adjustments to the estimated reserve amounts are included in current operating results. The reserves for professional liability risks coverapproximately 2,300 and 2,200 individual claims at December 31, 2019 and 2018, respectively, and estimates for unreported potential claims. The timeperiod required to resolve these claims can vary depending upon the jurisdiction and whether the claim is settled or litigated. During 2019 and 2018,$408 million and $358 million, respectively, of net payments were made for professional and general liability claims. The estimation of the timing ofpayments beyond a year can vary
F-15
326

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 107/137
Table of Contents
HCA HEALTHCARE, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
NOTE 1 — ACCOUNTING POLICIES (continued)
Professional Liability Claims (continued)
significantly. Although considerable variability is inherent in professional liability reserve estimates, we believe the reserves for losses and loss expensesare adequate; however, there can be no assurance the ultimate liability will not exceed our estimates.
A portion of our professional liability risks is insured through a 100% owned insurance subsidiary. Subject, in most cases, to a $15 million peroccurrence self-insured retention, our facilities are insured by our 100% owned insurance subsidiary for losses up to $50 million per occurrence. Theinsurance subsidiary has obtained reinsurance for professional liability risks generally above a retention level of $25 million per occurrence. We alsomaintain professional liability insurance with unrelated commercial carriers for losses in excess of amounts insured by our insurance subsidiary.
The obligations covered by reinsurance and excess insurance contracts are included in the reserves for professional liability risks, as we remainliable to the extent the reinsurers and excess insurance carriers do not meet their obligations under the reinsurance and excess insurance contracts. Theamounts receivable under the reinsurance contracts include $37 million and $40 million at December 31, 2019 and 2018, respectively, recorded in “otherassets,” and $9 million and $10 million at December 31, 2019 and 2018, respectively, recorded in “other current assets.”
Financial Instruments
Derivative financial instruments are employed to manage interest rate risks, and are not used for trading or speculative purposes. We recognize ourinterest rate swap derivative instruments in the consolidated balance sheets at fair value. Changes in the fair value of derivatives are recognizedperiodically in stockholders’ equity, as a component of other comprehensive income (loss), provided the derivative financial instrument qualifies forhedge accounting. Gains and losses on derivatives designated as cash flow hedges, to the extent they are effective, are recorded in other comprehensiveincome (loss), and subsequently reclassified to earnings to offset the impact of the forecasted transactions when they occur. In the event the forecastedtransaction to which a cash flow hedge relates is no longer likely, the amount in other comprehensive income is recognized in earnings and generally thederivative is terminated.
The net interest paid or received on interest rate swaps is recognized as adjustments to interest expense. Gains and losses resulting from the earlytermination of interest rate swap agreements are deferred and amortized as adjustments to interest expense over the remaining term of the debt originallyassociated with the terminated swap.
Noncontrolling Interests in Consolidated Entities
The consolidated financial statements include all assets, liabilities, revenues and expenses of less than 100% owned entities that we control.Accordingly, we have recorded noncontrolling interests in the earnings and equity of such entities.
Reclassifications
Certain prior year amounts have been reclassified to conform to the 2019 presentation.
F-16
327

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 108/137
Table of Contents
HCA HEALTHCARE, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
NOTE 2 — SHARE-BASED COMPENSATION
Stock Incentive Plan
Our stock incentive plan is designed to promote the long term financial interests and growth of the Company by attracting and retainingmanagement and other personnel, motivating them to achieve long range goals and aligning their interests with those of our stockholders throughopportunities for stock-based compensation and stock ownership in the Company. Stock option, stock appreciation right (“SARs”) and restricted shareunit (“RSUs”) grants vest solely based upon continued employment over a specific period of time, and performance share unit (“PSUs”) grants vestbased upon both continued employment over a specific period of time and the achievement of predetermined financial targets over time. AtDecember 31, 2019, there were 20.328 million shares available for future grants under the stock incentive plan.
Employee Stock Purchase Plan
Our employee stock purchase plan (“ESPP”) provides our participating employees an opportunity to obtain shares of our common stock at adiscount (through payroll deductions over three-month periods). At December 31, 2019, 6.883 million shares of common stock were reserved forissuance under the ESPP provisions. During 2019, 2018 and 2017, the Company recognized $12 million, $10 million and $9 million, respectively, ofcompensation expense related to the ESPP.
Stock Option, SAR, RSU and PSU Activity
The fair value of each stock option and SAR award is estimated on the grant date, using valuation models and the weighted average assumptionsindicated in the following table. Awards under our stock incentive plan generally vest based on continued employment (“Time Stock Options and SARs”and “Time RSUs”) and based upon continued employment and the achievement of certain financial targets (“Performance Stock Options and SARs”,“Performance RSUs” and “PSUs”). PSUs have a three-year cumulative earnings per share target, and the number of PSUs earned can vary from zero(for actual performance of less than 90% of target for 2019 grants and 80% of target for 2018 and prior grants) to two times the original PSU grant (foractual performance of 110% or more of target for 2019 grants and 120% or more of target for 2018 and prior grants). Each grant is valued as a singleaward with an expected term equal to the average expected term of the component vesting tranches. The expected term of the share-based award islimited by the contractual term. We use historical exercise behavior data and other factors to estimate the expected term of the options and SARs.
Compensation cost is recognized on the straight-line attribution method. The straight-line attribution method requires that total compensationexpense recognized must at least equal the vested portion of the grant-date fair value. The expected volatility is derived using historical stock priceinformation for our common stock and the volatility implied by the trading of options to purchase our stock on open-market exchanges. The risk-freeinterest rate is the approximate yield on United States Treasury Strips having a life equal to the expected share-based award life on the date of grant. Theexpected life is an estimate of the number of years a share-based award will be held before it is exercised. The expected dividend yield is estimatedbased on the assumption that the dividend yield at date of grant will be maintained over the expected life of the grant.
2019 2018 2017 Risk-free interest rate 2.50% 2.62% 2.13%Expected volatility 27% 29% 31%Expected life, in years 6.18 6.15 6.17 Expected dividend yield 1.16% 1.37% —
F-17
328

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 109/137
Table of Contents
HCA HEALTHCARE, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
NOTE 2 — SHARE-BASED COMPENSATION (continued)
Stock Option, SAR, RSU and PSU Activity (continued)
Information regarding Time Stock Options and SARs and Performance Stock Options and SARs activity during 2019, 2018 and 2017 issummarized below (share amounts in thousands):
Time Stock Options
and SARs
Performance Stock
Options and SARs
Total Stock Options
and SARs
Weighted Average
Exercise Price
Weighted Average
Remaining Contractual Term
Aggregate Intrinsic Value
(dollars in millions) Options and SARs outstanding, December 31,
2016
10,936
6,130
17,066
$ 35.65
Granted 1,879 — 1,879 81.83 Exercised (1,549) (1,366) (2,915) 21.49 Cancelled (110) (178) (288) 52.92
Options and SARs outstanding, December 31,2017
11,156
4,586
15,742
43.47
Granted 2,342 — 2,342 101.96 Exercised (3,917) (1,774) (5,691) 27.86 Cancelled (221) (145) (366) 68.43
Options and SARs outstanding, December 31,2018
9,360
2,667
12,027
61.49
Granted 1,349 — 1,349 138.31 Exercised (1,137) (523) (1,660) 44.45 Cancelled (522) — (522) 93.26
Options and SARs outstanding, December 31,2019
9,050
2,144
11,194
$ 71.79
5.7 years
$ 851
Options and SARs exercisable, December 31,2019
5,273
2,144
7,417
$ 53.09
4.4 years
$ 703
The weighted average fair values of stock options and SARs granted during 2019, 2018 and 2017 were $38.21, $28.90 and $28.47 per share,respectively. The total intrinsic value of stock options and SARs exercised during 2019, 2018 and 2017 was $153 million, $456 million and$177 million, respectively. The total fair value of RSUs and PSUs that vested during 2019, 2018 and 2017 was $346 million, $413 million and$188 million, respectively. As of December 31, 2019, the unrecognized compensation cost related to nonvested stock options and SARs was$73 million.
F-18
329

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 110/137
Table of Contents
HCA HEALTHCARE, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
NOTE 2 — SHARE-BASED COMPENSATION (continued)
Stock Option, SAR, RSU and PSU Activity (continued)
Information regarding Time RSUs, Performance RSUs and PSUs activity during 2019, 2018 and 2017 is summarized below (share amounts inthousands):
Time RSUs Performance
RSUs PSUs Total RSUs
and PSUs
Weighted Average
Grant Date Fair
Value RSUs and PSUs outstanding, December 31, 2016 4,111 790 2,386 7,287 $ 61.21
Granted 1,484 — 1,304 2,788 81.90 Vested (1,824) (430) — (2,254) 51.20 Cancelled (306) (133) (128) (567) 64.06
RSUs and PSUs outstanding, December 31, 2017 3,465 227 3,562 7,254 72.05 Granted 1,464 — 1,261 2,725 101.85 Performance adjustment — — 1,250 1,250 69.27 Vested (1,487) (136) (2,500) (4,123) 67.33 Cancelled (319) (91) (151) (561) 78.82
RSUs and PSUs outstanding, December 31, 2018 3,123 — 3,422 6,545 86.32 Granted 973 — 796 1,769 138.45 Performance adjustment — — 227 227 69.94 Vested (1,216) — (1,251) (2,467) 75.97 Cancelled (260) — (159) (419) 103.27
RSUs and PSUs outstanding, December 31, 2019 2,620 — 3,035 5,655 $105.23
As of December 31, 2019, the unrecognized compensation cost related to RSUs and PSUs was $338 million.
NOTE 3 — ACQUISITIONS AND DISPOSITIONS
During 2019, we paid $1.384 billion to acquire a seven-hospital health system in North Carolina and $298 million to acquire nonhospital healthcare entities. During 2018, we paid $792 million to acquire two hospital facilities and $461 million to acquire nonhospital health care entities. During2017, we paid $1.000 billion to acquire eight hospital facilities and $212 million to acquire nonhospital health care entities. Purchase price amounts havebeen allocated to the related assets acquired and liabilities assumed based upon their respective fair values. The purchase price paid in excess of the fairvalue of identifiable net assets of these acquired entities aggregated $332 million, $636 million and $693 million in 2019, 2018 and 2017, respectively.The consolidated financial statements include the accounts and operations of the acquired entities subsequent to the respective acquisition dates. The proforma effects of these acquired entities on our results of operations for periods prior to the respective acquisition dates were not significant.
During 2019, we received proceeds of $25 million and recognized a pretax loss of $1 million ($1 million after tax) related to the sale of a hospitalfacility from our American Group (a Louisiana market). During 2019, we also received proceeds of $36 million and recognized pretax gains of$19 million ($14 million after tax) related to sales of real estate and other investments. During 2018, we received proceeds of $758 million andrecognized a pretax gain of $353 million ($265 million after tax) related to the sale of two hospital facilities from our American Group (Oklahomamarket). During 2018, we also received proceeds of $50 million and recognized
F-19
330

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 111/137
Table of Contents
HCA HEALTHCARE, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
NOTE 3 — ACQUISITIONS AND DISPOSITIONS (continued)
pretax gains of $75 million ($59 million after tax) related to sales of real estate and other investments. During 2017, we received proceeds of $25 millionand recognized pretax gains of $8 million ($5 million after tax) related to sales of real estate and other investments.
NOTE 4 — INCOME TAXES
The provision for income taxes consists of the following (dollars in millions):
2019 2018 2017 Current:
Federal $ 670 $759 $1,067 State 134 149 120 Foreign 17 23 19
Deferred: Federal 254 9 423 State 29 13 3 Foreign (5) (7) 6
$1,099 $946 $1,638
The 2017 Tax Cuts and Jobs Act (“Tax Act”) significantly revised U.S. corporate income taxes, including lowering the statutory corporate tax ratefrom 35% to 21% beginning in 2018, imposing a mandatory one-time transition tax on undistributed foreign earnings and creating a new U.S. minimumtax on earnings of foreign subsidiaries. Our provision for income taxes for the year ended December 31, 2018 included tax benefits of $613 million(including $67 million related to the remeasurement of certain deferred tax assets and liabilities) related to the reduction in our effective tax rate underthe Tax Act. We completed our analysis of the impact of the Tax Act during the fourth quarter of 2018, reducing our provision for income taxes for theyear ended December 31, 2018 by $67 million related to a remeasurement of certain deferred tax assets and liabilities for which we were unable to makereasonable estimates in 2017. For the year ended, December 31, 2017, a provisional amount of $301 million related to the remeasurement of ourdeferred tax assets and liabilities for which we were then able to make reasonable estimates was recorded as a component of our provision for incometaxes. During 2017 we also reclassified a provisional amount of $127 million from our deferred tax liabilities for the one-time transition tax, based onour estimated undistributed post-1986 foreign earnings and profits. Because we had previously recorded U.S. taxes on these earnings, the transition taxliability, which is payable over an 8-year period, did not affect our 2017 provision for income taxes. Adjustments during 2018 to the provisionalamounts recorded in 2017 were not significant.
During 2018, we recorded a reduction to our provision for income taxes of $28 million for tax credits related to certain 2017 hurricane-relatedexpenses. Our provision for income taxes for the years ended December 31, 2019, 2018 and 2017 included tax benefits of $65 million, $124 million and$82 million, respectively, related to the settlement of employee equity awards. Our foreign pretax income was $50 million, $86 million and $91 millionfor the years ended December 31, 2019, 2018 and 2017, respectively.
F-20
331

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 112/137
Table of Contents
HCA HEALTHCARE, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
NOTE 4 — INCOME TAXES (continued)
A reconciliation of the federal statutory rate to the effective income tax rate follows:
2019 2018 2017 Federal statutory rate 21.0% 21.0% 35.0%State income taxes, net of federal tax benefit 2.7 2.9 2.2 Change in liability for uncertain tax positions 0.4 (0.1) — Tax benefit from settlements of employee equity awards (1.3) (2.4) (2.0)Impact of Tax Act on deferred tax balances — (1.6) 7.8 Other items, net 1.1 0.2 (0.5)Effective income tax rate on income attributable to HCA Healthcare, Inc. 23.9 20.0 42.5 Income attributable to noncontrolling interests from consolidated partnerships (2.9) (2.3) (5.1)Effective income tax rate on income before income taxes 21.0% 17.7% 37.4%
A summary of the items comprising the deferred tax assets and liabilities at December 31 follows (dollars in millions):
2019 2018 Assets Liabilities Assets Liabilities
Depreciation and fixed asset basis differences $ — $ 601 $ — $ 340 Allowances for professional liability and other risks 376 — 355 — Accounts receivable 307 — 274 — Compensation 292 — 256 — Right-of-use lease assets and obligations 369 366 — — Other 461 538 424 491
$1,805 $ 1,505 $1,309 $ 831
At December 31, 2019, federal and state net operating loss carryforwards (expiring in years 2022 through 2038) available to offset future taxableincome approximated $60 million and $128 million, respectively. Utilization of net operating loss carryforwards in any one year may be limited.
The following table summarizes the activity related to our unrecognized tax benefits (dollars in millions):
2019 2018 Balance at January 1 $390 $399 Additions based on tax positions related to the current year 29 22 Additions for tax positions of prior years 119 10 Reductions for tax positions of prior years (3) (14)Settlements — (2)Lapse of applicable statutes of limitations (13) (25)Balance at December 31 $522 $390
Our liability for unrecognized tax benefits was $550 million, including accrued interest of $62 million and excluding $34 million that was
recorded as reductions of the related deferred tax assets, as of December 31, 2019 ($435 million, $48 million and $3 million, respectively, as ofDecember 31, 2018). Unrecognized tax benefits of $160 million ($137 million as of December 31, 2018) would affect the effective rate, if recognized.The increase in our liability for unrecognized tax benefits relates primarily to the effect of certain federal and state legislative and regulatorydevelopments during 2019.
F-21
332

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 113/137
Table of Contents
HCA HEALTHCARE, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
NOTE 4 — INCOME TAXES (continued)
The Internal Revenue Service began an examination of the Company’s 2016 and 2017 federal income tax returns during 2019. We are also subjectto examination by state and foreign taxing authorities. Depending on the resolution of any federal, state and foreign tax disputes, the completion ofexaminations by federal, state or foreign taxing authorities, or the expiration of statutes of limitation for specific taxing jurisdictions, we believe it isreasonably possible that our liability for unrecognized tax benefits may significantly increase or decrease within the next 12 months. However, we arecurrently unable to estimate the range of any possible change.
NOTE 5 — EARNINGS PER SHARE
We compute basic earnings per share using the weighted average number of common shares outstanding. We compute diluted earnings per shareusing the weighted average number of common shares outstanding plus the dilutive effect of outstanding stock options, SARs, RSUs and PSUs,computed using the treasury stock method. During 2019, 2018 and 2017, we repurchased 7.949 million shares, 14.070 million shares and 25.092 millionshares, respectively, of our common stock. The following table sets forth the computations of basic and diluted earnings per share for the years endedDecember 31, 2019, 2018 and 2017 (dollars and shares in millions, except per share amounts):
2019 2018 2017 Net income attributable to HCA Healthcare, Inc. $ 3,505 $ 3,787 $ 2,216
Weighted average common shares outstanding 341.210 347.297 362.305 Effect of dilutive incremental shares 7.016 8.006 9.916 Shares used for diluted earnings per share 348.226 355.303 372.221 Earnings per share:
Basic earnings per share $ 10.27 $ 10.90 $ 6.12 Diluted earnings per share $ 10.07 $ 10.66 $ 5.95
NOTE 6 — INVESTMENTS OF INSURANCE SUBSIDIARIES
A summary of the insurance subsidiaries’ investments at December 31 follows (dollars in millions):
2019
Amortized
Cost
UnrealizedAmounts Fair
Value Gains Losses Debt securities $ 359 $ 18 $ — $ 377 Money market funds and other 85 — — 85
$ 444 $ 18 $ — 462 Amounts classified as current assets (147)Investment carrying value $ 315
F-22
333

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 114/137
Table of Contents
HCA HEALTHCARE, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
NOTE 6 — INVESTMENTS OF INSURANCE SUBSIDIARIES (continued)
2018
Amortized
Cost
Unrealized Amounts Fair
Value Gains Losses Debt securities $ 338 $ 5 $ (2) $341 Money market funds and other 68 — — 68
$ 406 $ 5 $ (2) 409 Amounts classified as current assets (47)Investment carrying value $362
At December 31, 2019 and 2018, the investments in debt securities of our insurance subsidiaries were classified as “available-for-sale.” Changesin unrealized gains and losses are recorded as adjustments to other comprehensive income (loss).
Scheduled maturities of investments in debt securities at December 31, 2019 were as follows (dollars in millions):
Amortized
Cost Fair
Value Due in one year or less $ 9 $ 9 Due after one year through five years 85 88 Due after five years through ten years 190 202 Due after ten years 75 78
$ 359 $377
The average expected maturity of the investments in debt securities at December 31, 2019 was 5.6 years, compared to the average scheduledmaturity of 10.5 years. Expected and scheduled maturities may differ because the issuers of certain securities have the right to call, prepay or otherwiseredeem such obligations prior to their scheduled maturity date.
NOTE 7 — FINANCIAL INSTRUMENTS
Interest Rate Swap Agreements
We have entered into interest rate swap agreements to manage our exposure to fluctuations in interest rates. These swap agreements involve theexchange of fixed and variable rate interest payments between us and our counterparties based on common notional principal amounts and maturitydates. Pay-fixed interest rate swaps effectively convert variable rate obligations to fixed interest rate obligations. The interest payments under theseagreements are settled on a net basis. The net interest payments, based on the notional amounts in these agreements, generally match the timing of therelated liabilities, for the interest rate swap agreements which have been designated as cash flow hedges. The notional amounts of the swap agreementsrepresent amounts used to calculate the exchange of cash flows and are not our assets or liabilities. Our credit risk related to these agreements isconsidered low because the swap agreements are with creditworthy financial institutions.
F-23
334

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 115/137
Table of Contents
HCA HEALTHCARE, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
NOTE 7 — FINANCIAL INSTRUMENTS (continued)
Interest Rate Swap Agreements (continued)
The following table sets forth our interest rate swap agreements, which have been designated as cash flow hedges, at December 31, 2019 (dollarsin millions):
Notional
Amount Maturity Date Fair
Value Pay-fixed interest rate swaps $ 2,000 December 2021 $ 3 Pay-fixed interest rate swaps 500 December 2022 (7)
During the next 12 months, we estimate $1 million will be reclassified from accumulated other comprehensive income (“OCI”) and will beincluded in interest expense.
Derivatives — Results of Operations
The following table presents the effect of our interest rate swaps on our results of operations for the year ended December 31, 2019 (dollars inmillions):
Derivatives in Cash Flow Hedging Relationships
Amount of Loss Recognized in OCI on
Derivatives, Net of Tax
Location of Gain Reclassified from Accumulated OCI into Operations
Amount of Gain Reclassified from Accumulated OCI into Operations
Interest rate swaps $ 37 Interest expense $ 17
Credit-risk-related Contingent Features
We have agreements with each of our derivative counterparties that contain a provision where we could be declared in default on our derivativeobligations if repayment of the underlying indebtedness is accelerated by the lender due to our default on the indebtedness. As of December 31, 2019,we have not been required to post any collateral related to these agreements. If we had breached these provisions at December 31, 2019, we would havebeen required to settle our obligations under the agreements at their aggregate, estimated termination value of $4 million.
NOTE 8 — ASSETS AND LIABILITIES MEASURED AT FAIR VALUE
Accounting Standards Codification 820, Fair Value Measurements and Disclosures (“ASC 820”) emphasizes fair value is a market-basedmeasurement, and fair value measurements should be determined based on the assumptions market participants would use in pricing assets or liabilities.ASC 820 utilizes a fair value hierarchy that distinguishes between market participant assumptions based on market data obtained from sourcesindependent of the reporting entity (observable inputs classified within Levels 1 and 2 of the hierarchy) and the reporting entity’s own assumptionsabout market participant assumptions (unobservable inputs classified within Level 3 of the hierarchy).
Level 1 inputs utilize quoted prices (unadjusted) in active markets for identical assets or liabilities. Level 2 inputs are inputs other than quotedprices included in Level 1 that are observable for the asset or liability, either directly or indirectly. Level 2 inputs may include quoted prices for similarassets and liabilities in active markets, as well as inputs observable for the asset or liability (other than quoted prices), such as interest rates, foreignexchange rates, and yield curves observable at commonly quoted intervals. Level 3 inputs are unobservable inputs for the asset or liability, which aretypically based on an entity’s own assumptions, as there is little, if any,
F-24
335

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 116/137
Table of Contents
HCA HEALTHCARE, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
NOTE 8 — ASSETS AND LIABILITIES MEASURED AT FAIR VALUE (continued)
related market activity. In instances where the determination of the fair value measurement is based on inputs from different levels of the fair valuehierarchy, the level in the fair value hierarchy within which the entire fair value measurement falls is based on the lowest level input significant to thefair value measurement in its entirety. Our assessment of the significance of a particular input to the fair value measurement in its entirety requiresjudgment.
Cash Traded Investments
Our cash traded investments are generally classified within Level 1 or Level 2 of the fair value hierarchy because they are valued using quotedmarket prices, broker or dealer quotations, or alternative pricing sources with reasonable levels of price transparency.
Derivative Financial Instruments
We have entered into interest rate swap agreements to manage our exposure to fluctuations in interest rates. The valuation of these instruments isdetermined using widely accepted valuation techniques, including discounted cash flow analysis on the expected cash flows of each derivative. Thisanalysis reflects the contractual terms of the derivatives, including the period to maturity, and uses observable market-based inputs, including interestrate curves and implied volatilities. We incorporate credit valuation adjustments to reflect both our own nonperformance risk and the respectivecounterparty’s nonperformance risk in the fair value measurements of these instruments.
The following tables summarize our assets and liabilities measured at fair value on a recurring basis as of December 31, 2019 and 2018,aggregated by the level in the fair value hierarchy within which those measurements fall (dollars in millions):
December 31, 2019
Fair Value
Fair Value Measurements Using Quoted Prices in
Active Markets for Identical Assets
and Liabilities (Level 1)
Significant Other
Observable Inputs
(Level 2)
Significant Unobservable
Inputs (Level 3)
Assets: Investments of insurance subsidiaries:
Debt securities $ 377 $ — $ 377 $ — Money market funds and other 85 85 — — Investments of insurance subsidiaries 462 85 377 — Less amounts classified as current assets (147) (83) (64) —
$ 315 2 $ 313 $ — Interest rate swaps (Other) $ 3 $ — $ 3 $ —
Liabilities: Interest rate swaps (Income taxes and other liabilities) $ 7 $ — $ 7 $ —
F-25
336

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 117/137
Table of Contents
HCA HEALTHCARE, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
NOTE 8 — ASSETS AND LIABILITIES MEASURED AT FAIR VALUE (continued)
Derivative Financial Instruments (continued) December 31, 2018
Fair Value
Fair Value Measurements Using Quoted Prices in
Active Markets for Identical Assets
and Liabilities (Level 1)
Significant Other
Observable Inputs
(Level 2)
Significant Unobservable
Inputs (Level 3)
Assets: Investments of insurance subsidiaries:
Debt securities $ 341 $ — $ 341 $ — Money market funds and other 68 68 — — Investments of insurance subsidiaries 409 68 341 — Less amounts classified as current assets (47) (47) — —
$ 362 $ 21 $ 341 $ — Interest rate swaps (Other) $ 63 $ — $ 63 $ —
The estimated fair value of our long-term debt was $37.026 billion and $32.887 billion at December 31, 2019 and 2018, respectively, compared to
carrying amounts, excluding debt issuance costs and discounts, aggregating $33.961 billion and $32.978 billion, respectively. The estimates of fair valueare generally based upon the quoted market prices or quoted market prices for similar issues of long-term debt with the same maturities.
NOTE 9 — LONG-TERM DEBT
A summary of long-term debt at December 31, including related interest rates at December 31, 2019, follows (dollars in millions):
2019 2018 Senior secured asset-based revolving credit facility (effective interest rate of 3.0%) $ 2,480 $ 3,040 Senior secured revolving credit facility — — Senior secured term loan facilities (effective interest rate of 3.3%) 3,725 3,801 Senior secured notes (effective interest rate of 5.1%) 13,850 13,800 Other senior secured debt (effective interest rate of 5.4%) 654 585 Senior secured debt 20,709 21,226 Senior unsecured notes (effective interest rate of 6.3%) 13,252 11,752 Net debt issuance costs (239) (157)Total debt (average life of 8.6 years, rates averaging 5.2%) 33,722 32,821 Less amounts due within one year 145 788
$33,577 $32,033
During January 2019, we issued $1.500 billion aggregate principal amount of senior unsecured notes comprised of $1.000 billion aggregateprincipal amount of 5.875% notes due 2029 and $500 million aggregate principal amount of 5.625% notes due 2028. We used the net proceeds to fundthe purchase of a seven-hospital health system located in western North Carolina.
F-26
337

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 118/137
Table of Contents
HCA HEALTHCARE, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
NOTE 9 — LONG-TERM DEBT (continued)
During June 2019, we issued $5.000 billion aggregate principal amount of senior secured notes comprised of $2.000 billion aggregate principalamount of 4 1/8% notes due 2029, $1.000 billion aggregate principal amount of 5 1/8% notes due 2039 and $2.000 billion aggregate principal amount of5 1/4% notes due 2049. During July 2019, we redeemed all $600 million outstanding aggregate principal amount of 4.25% senior secured notes due2019, all $3.000 billion outstanding aggregate principal amount of 6.50% senior secured notes due 2020 and all $1.350 billion outstanding aggregateprincipal amount of 5.875% senior secured notes due 2022. The pretax loss on retirement of debt for these redemptions was $211 million.
Senior Secured Credit Facilities And Other Senior Secured Debt
We have entered into the following senior secured credit facilities: (i) a $3.750 billion asset-based revolving credit facility maturing on June 28,2022 with a borrowing base of 85% of eligible accounts receivable, subject to customary reserves and eligibility criteria ($2.480 billion outstanding atDecember 31, 2019) (the “ABL credit facility”); (ii) a $2.000 billion senior secured revolving credit facility maturing on June 28, 2022 (noneoutstanding at December 31, 2019 without giving effect to certain outstanding letters of credit); (iii) a $1.106 billion senior secured term loan A-6facility maturing on July 16, 2024; (iv) a $1.474 billion senior secured term loan B-12 facility maturing on March 13, 2025; and (v) a $1.145 billionsenior secured term loan B-13 facility maturing on March 18, 2026. We refer to the facilities described under (ii) through (v) above, collectively, as the“cash flow credit facility” and, together with the ABL credit facility, the “senior secured credit facilities.”
Borrowings under the senior secured credit facilities bear interest at a rate equal to, at our option, either (a) a base rate determined by reference tothe higher of (1) the federal funds rate plus 0.50% or (2) the prime rate of Bank of America or (b) a LIBOR rate for the currency of such borrowing forthe relevant interest period, plus, in each case, an applicable margin. The applicable margin for borrowings under the senior secured credit facilities maybe reduced subject to attaining certain leverage ratios.
The senior secured credit facilities contain a number of covenants that restrict, subject to certain exceptions, our (and some or all of oursubsidiaries’) ability to incur additional indebtedness, repay subordinated indebtedness, create liens on assets, sell assets, make investments, loans oradvances, engage in certain transactions with affiliates, pay dividends and distributions, and enter into sale and leaseback transactions. In addition, weare required to satisfy and maintain a maximum total leverage ratio covenant under the cash flow credit facility and, in certain situations under the ABLcredit facility, a minimum interest coverage ratio covenant.
Senior secured notes consists of (i) $1.250 billion aggregate principal amount of 4.75% first lien notes due 2023; (ii) $2.000 billion aggregateprincipal amount of 5.00% first lien notes due 2024; (iii) $1.400 billion aggregate principal amount of 5.25% first lien notes due 2025;(iv) $1.500 billion aggregate principal amount of 5.25% first lien notes due 2026; (v) $1.200 billion aggregate principal amount of 4.50% first lien notesdue 2027; (vi) $2.000 billion aggregate principal amount of 4 1/8% first lien notes due 2029; (vii) $1.000 billion aggregate principal amount of 5 1/8%first lien notes due 2039; (viii) $1.500 billion aggregate principal amount of 5.50% first lien notes due 2047; and (ix) $2.000 billion aggregate principalamount of 5 1/4% first lien notes due 2049. Finance leases and other secured debt totaled $654 million at December 31, 2019.
We use interest rate swap agreements to manage the variable rate exposure of our debt portfolio. At December 31, 2019, we had entered intoeffective interest rate swap agreements, in a total notional amount of $2.500 billion, in order to hedge a portion of our exposure to variable rate interestpayments associated with the
F-27
338

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 119/137
Table of Contents
HCA HEALTHCARE, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
NOTE 9 — LONG-TERM DEBT (continued)
Senior Secured Credit Facilities And Other Senior Secured Debt (continued)
senior secured credit facilities. The effect of the interest rate swaps is reflected in the effective interest rates for the senior secured credit facilities.
Senior Unsecured Notes
Senior unsecured notes consist of (i) $12.391 billion aggregate principal amount of senior notes with maturities ranging from 2021 to 2033; (ii) anaggregate principal amount of $125 million medium-term notes maturing 2025; and (iii) an aggregate principal amount of $736 million debentures withmaturities ranging from 2023 to 2095.
General Debt Information
The senior secured credit facilities and senior secured notes are fully and unconditionally guaranteed by substantially all existing and future, directand indirect, 100% owned material domestic subsidiaries that are “Unrestricted Subsidiaries” under our Indenture (the “1993 Indenture”) datedDecember 16, 1993 (except for certain special purpose subsidiaries that only guarantee and pledge their assets under our ABL credit facility).
All obligations under the ABL credit facility, and the guarantees of those obligations, are secured, subject to permitted liens and other exceptions,by a first-priority lien on substantially all of the receivables of the borrowers and each guarantor under such ABL credit facility (the “ReceivablesCollateral”).
All obligations under the cash flow credit facility and the guarantees of such obligations are secured, subject to permitted liens and otherexceptions, by:
• a first-priority lien on the capital stock owned by HCA Inc., or by any U.S. guarantor, in each of their respective first-tier subsidiaries;
• a first-priority lien on substantially all present and future assets of HCA Inc. and of each U.S. guarantor other than (i) “Principal Properties”
(as defined in the 1993 Indenture), (ii) certain other real properties and (iii) deposit accounts, other bank or securities accounts, cash,leaseholds, motor-vehicles and certain other exceptions; and
• a second-priority lien on certain of the Receivables Collateral.
Our senior secured notes and the related guarantees are secured by first-priority liens, subject to permitted liens, on our and our subsidiaryguarantors’ assets, subject to certain exceptions, that secure our cash flow credit facility on a first-priority basis and are secured by second-priority liens,subject to permitted liens, on our and our subsidiary guarantors’ assets that secure our ABL credit facility on a first-priority basis and our other cashflow credit facility on a second-priority basis.
Maturities of long-term debt in years 2021 through 2024, excluding amounts under the ABL credit facility, are $1.156 billion, $2.177 billion,$2.770 billion and $3.137 billion, respectively.
NOTE 10 — LEASES
We adopted ASU No. 2016-02, Leases (Topic 842), which requires leases with durations greater than 12 months to be recognized on the balancesheet, effective January 1, 2019, using the modified retrospective approach. Prior period financial statement amounts and disclosures have not beenadjusted to reflect the
F-28
339

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 120/137
Table of Contents
HCA HEALTHCARE, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
NOTE 10 — LEASES (continued)
provisions of the new standard. We elected the package of transition provisions available which allowed us to carry forward our historical assessmentsof whether contracts are or contain leases, the lease classification and the treatment of initial direct costs.
We lease property and equipment under finance and operating leases. For leases with terms greater than 12 months, we record the related assetsand obligations at the present value of lease payments over the term. Many of our leases include rental escalation clauses and renewal options that arefactored into our determination of lease payments, when appropriate. We do not separate lease and nonlease components of contracts. Generally, we useour estimated incremental borrowing rate to discount the lease payments, as most of our leases do not provide a readily determinable implicit interestrate.
The following table presents our lease-related assets and liabilities at December 31, 2019 (dollars in millions):
Balance Sheet Classification December 31,
2019 Assets:
Operating leases Right-of-use operating lease assets $ 1,834 Finance leases Property and equipment 520
Total lease assets $ 2,354 Liabilities:
Current: Operating leases Other accrued expenses $ 350 Finance leases Long-term debt due within one year 87
Noncurrent: Operating leases Right-of-use operating lease obligations 1,499 Finance leases Long-term debt 470
Total lease liabilities $ 2,406 Weighted-average remaining term:
Operating leases 10.8 years Finance leases 12.0 years
Weighted-average discount rate: Operating leases(1) 5.3%Finance leases 6.0%
(1) Upon adoption of the new lease standard, discount rates used for existing leases were established at January 1, 2019.
F-29
340

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 121/137
Table of Contents
HCA HEALTHCARE, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
NOTE 10 — LEASES (continued)
The following table presents certain information related to lease expense for finance and operating leases for the year ended December 31, 2019(dollars in millions):
Year Ended
December 31, 2019 Finance lease expense:
Amortization of leased assets $ 93 Interest on lease liabilities 32
Operating leases(2) 389 Short-term lease expense(2) 316 Variable lease expense(2) 150
$ 980
(2) Expenses are included in “other operating expenses” in our consolidated income statements.
The following table presents supplemental cash flow information for the year ended December 31, 2019 (dollars in millions):
2019 Cash paid for amounts included in the measurement of lease liabilities:
Operating cash flows for operating leases $404 Operating cash flows for finance leases 32 Financing cash flows for finance leases 79
Maturities of Lease Liabilities
The following table reconciles the undiscounted minimum lease payment amounts to the operating and finance lease liabilities recorded on thebalance sheet at December 31, 2019 (dollars in millions):
Operating
Leases FinanceLeases
Year 1 $ 411 $ 110 Year 2 350 105 Year 3 285 99 Year 4 228 58 Year 5 182 60 Thereafter 1,074 368 Total minimum lease payments 2,530 800 Less: amount of lease payments representing interest (681) (243)Present value of future minimum lease payments 1,849 557 Less: current lease obligations (350) (87)Long-term lease obligations $ 1,499 $ 470
F-30
341

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 122/137
Table of Contents
HCA HEALTHCARE, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
NOTE 11 — CONTINGENCIES
We operate in a highly regulated and litigious industry. As a result, various lawsuits, claims and legal and regulatory proceedings have been andcan be expected to be instituted or asserted against us. We are also subject to claims and suits arising in the ordinary course of business, including claimsfor personal injuries or wrongful restriction of, or interference with, physicians’ staff privileges. In certain of these actions the claimants may seekpunitive damages against us which may not be covered by insurance. We are also subject to claims by various taxing authorities for additional taxes andrelated interest and penalties. The resolution of any such lawsuits, claims or legal and regulatory proceedings could have a material, adverse effect onour results of operations, financial position or liquidity.
Government Investigations, Claims and Litigation
Health care companies are subject to numerous investigations by various governmental agencies. Under the federal False Claims Act (“FCA”),private parties have the right to bring qui tam, or “whistleblower,” suits against companies that submit false claims for payments to, or improperly retainoverpayments from, the government. Some states have adopted similar state whistleblower and false claims provisions. Certain of our individualfacilities have received, and from time to time, other facilities may receive, government inquiries from, and may be subject to investigation by, federaland state agencies. Depending on whether the underlying conduct in these or future inquiries or investigations could be considered systemic, theirresolution could have a material, adverse effect on our results of operations, financial position or liquidity.
Texas operates a state Medicaid program pursuant to a waiver from CMS under Section 1115 of the Social Security Act (“Program”). TheProgram includes uncompensated-care pools; payments from these pools are intended to defray the uncompensated costs of services provided by ourand other hospitals to Medicaid eligible or uninsured individuals. Separately, we and other hospitals provide charity care services in several communitiesin the state. In 2018, the Civil Division of the U.S. Department of Justice and the U.S. Attorney’s Office for the Southern District of Texas requestedinformation about whether the Program, as operated in Harris County, complied with the laws and regulations applicable to provider related donations,and the Company cooperated with that request. On May 21, 2019, a qui tam lawsuit asserting violations of the FCA and the Texas Medicaid FraudPrevention Act related to the Program, as operated in Harris County, was unsealed by the U.S. District Court for the Southern District of Texas. Both thefederal and state governments declined to intervene in the qui tam lawsuit. The Company believes that our participation is and has been consistent withthe requirements of the Program and is vigorously defending against the lawsuit being pursued by the relator. We cannot predict what effect, if any, thequi tam lawsuit could have on the Company.
NOTE 12 — CAPITAL STOCK
The amended and restated certificate of incorporation authorizes the Company to issue up to 1,800,000,000 shares of common stock, and ouramended and restated by-laws set the number of directors constituting the board of directors of the Company at not less than three members, the exactnumber to be determined from time to time by resolution adopted by the affirmative vote of a majority of the total number of directors then in office.
Share Repurchase Transactions
During January 2020, January 2019, October 2017 and November 2016, our Board of Directors authorized share repurchase programs for up to$8 billion ($2 billion for each authorization) of our outstanding common stock. During 2019, we repurchased 7.949 million shares of our common stockat an average price of $129.71 per
F-31
342

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 123/137
Table of Contents
HCA HEALTHCARE, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
NOTE 12 — CAPITAL STOCK (continued)
Share Repurchase Transactions (continued)
share through market purchases pursuant to the October 2017 authorization (which was completed during the first quarter of 2019) and the January 2019authorization. At December 31, 2019, we had $1.241 billion of repurchase authorization available under the January 2019 authorization.
During 2018, we repurchased 14.070 million shares of our common stock at an average price of $108.74 per share through market purchasespursuant to the October 2017 authorization. During 2017, we repurchased 25.092 million shares of our common stock at an average price of $81.73 pershare through market purchases pursuant to the November 2016 authorization (which was completed during the fourth quarter of 2017) and the October2017 authorization.
NOTE 13 — EMPLOYEE BENEFIT PLANS
We maintain defined contribution benefit plans that are available to employees who meet certain minimum requirements. Certain of the plansrequire that we match specified percentages of participant contributions up to certain maximum levels (generally, 100% of the first 3% to 9%, dependingupon years of vesting service, of compensation deferred by participants). The cost of these plans totaled $532 million for 2019, $499 million for 2018and $471 million for 2017. Our contributions are funded during the applicable or following year.
We maintain the noncontributory, nonqualified Restoration Plan to provide certain retirement benefits for eligible employees. Eligibility for theRestoration Plan is based upon earning eligible compensation in excess of the Social Security Wage Base and attaining 1,000 or more hours of serviceduring the plan year. Company credits to participants’ account balances (the Restoration Plan is not funded) depend upon participants’ compensation,years of vesting service and certain IRS limitations. Benefits expense under this plan was $44 million for 2019, $22 million for 2018 and $40 million for2017. Accrued benefits liabilities under this plan totaled $227 million at December 31, 2019 and $205 million at December 31, 2018.
We maintain a Supplemental Executive Retirement Plan (“SERP”) for certain executives (the SERP is not funded). The plan is designed to ensurethat upon retirement the participant receives the value of a prescribed life annuity from the combination of the SERP and our other benefit plans.Benefits expense under the plan was $19 million for 2019, $26 million for 2018 and $28 million for 2017. Accrued benefits liabilities under this plantotaled $192 million at December 31, 2019 and $195 million at December 31, 2018.
We maintain defined benefit pension plans which resulted from certain hospital acquisitions in prior years. Benefits expense under these plans was$11 million for 2019, $9 million for 2018, and $14 million for 2017. Accrued benefits liabilities under these plans totaled $63 million at December 31,2019 and $68 million at December 31, 2018.
NOTE 14 — SEGMENT AND GEOGRAPHIC INFORMATION
We operate in one line of business, which is operating hospitals and related health care entities. We operate in two geographically organizedgroups: the National and American Groups. At December 31, 2019, the National Group included 95 hospitals located in Alaska, California, Florida,southern Georgia, Idaho, Indiana, northern Kentucky, Nevada, New Hampshire, North Carolina, South Carolina, Utah and Virginia, and the AmericanGroup included 83 hospitals located in Colorado, northern Georgia, Kansas, southern Kentucky, Louisiana, Mississippi, Missouri, Tennessee and Texas.We also operate six hospitals in England, and these facilities are included in the Corporate and other group.
F-32
343

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 124/137
Table of Contents
HCA HEALTHCARE, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
NOTE 14 — SEGMENT AND GEOGRAPHIC INFORMATION (continued)
Adjusted segment EBITDA is defined as income before depreciation and amortization, interest expense, gains on sales of facilities, losses onretirement of debt, income taxes and net income attributable to noncontrolling interests. We use adjusted segment EBITDA as an analytical indicator forpurposes of allocating resources to geographic areas and assessing their performance. Adjusted segment EBITDA is commonly used as an analyticalindicator within the health care industry, and also serves as a measure of leverage capacity and debt service ability. Adjusted segment EBITDA shouldnot be considered as a measure of financial performance under generally accepted accounting principles, and the items excluded from adjusted segmentEBITDA are significant components in understanding and assessing financial performance. Because adjusted segment EBITDA is not a measurementdetermined in accordance with generally accepted accounting principles and is thus susceptible to varying calculations, adjusted segment EBITDA, aspresented, may not be comparable to other similarly titled measures of other companies. The geographic distributions of our revenues, equity in earningsof affiliates, adjusted segment EBITDA, depreciation and amortization, assets and goodwill and other intangible assets are summarized in the followingtable (dollars in millions):
For the Years Ended December 31, 2019 2018 2017
Revenues: National Group $ 25,913 $ 22,581 $ 20,772 American Group 23,173 21,959 20,912 Corporate and other 2,250 2,137 1,930
$ 51,336 $ 46,677 $ 43,614 Equity in earnings of affiliates:
National Group $ (2) $ (4) $ (21)American Group (44) (40) (37)Corporate and other 3 15 13
$ (43) $ (29) $ (45)Adjusted segment EBITDA:
National Group $ 5,634 $ 4,980 $ 4,600 American Group 4,904 4,593 4,231 Corporate and other (681) (624) (598)
$ 9,857 $ 8,949 $ 8,233 Depreciation and amortization:
National Group $ 1,161 $ 946 $ 867 American Group 1,117 1,027 986 Corporate and other 318 305 278
$ 2,596 $ 2,278 $ 2,131
F-33
344

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 125/137
Table of Contents
HCA HEALTHCARE, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
NOTE 14 — SEGMENT AND GEOGRAPHIC INFORMATION (continued) For the Years Ended December 31, 2019 2018 2017
Adjusted segment EBITDA $ 9,857 $ 8,949 $ 8,233 Depreciation and amortization 2,596 2,278 2,131 Interest expense 1,824 1,755 1,690 Gains on sales of facilities (18) (428) (8)Losses on retirement of debt 211 9 39
Income before income taxes $ 5,244 $ 5,335 $ 4,381
December 31, 2019 2018 2017
Assets: National Group $18,290 $14,839 $13,097 American Group 20,608 19,122 18,136 Corporate and other 6,160 5,246 5,360
$45,058 $39,207 $36,593
National
Group American
Group Corporate
and Other Total Goodwill and other intangible assets: Balance at December 31, 2016 $ 1,458 $ 4,661 $ 585 $6,704
Acquisitions 19 612 62 693 Foreign currency translation, amortization and other (3) (8) 8 (3)
Balance at December 31, 2017 1,474 5,265 655 7,394 Acquisitions 132 504 — 636 Foreign currency translation, amortization and other (9) (40) (28) (77)
Balance at December 31, 2018 1,597 5,729 627 7,953 Acquisitions 155 39 138 332 Foreign currency translation, amortization and other (13) (3) — (16)
Balance at December 31, 2019 $ 1,739 $ 5,765 $ 765 $8,269
F-34
345

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 126/137
Table of Contents
HCA HEALTHCARE, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
NOTE 15 — OTHER COMPREHENSIVE LOSS
The components of accumulated other comprehensive loss are as follows (dollars in millions):
Unrealized Gains on
Available- for-Sale
Securities
Foreign Currency Translation Adjustments
Defined Benefit Plans
Change in Fair Value of Derivative Instruments Total
Balances at December 31, 2016 $ 7 $ (211) $ (146) $ 12 $(338)Unrealized gains on available-for-sale securities 1 — — — 1 Foreign currency translation adjustments, net of $35 of income
taxes
—
62
—
—
62 Defined benefit plans, net of $10 income tax benefit — — (33) — (33)Change in fair value of derivative instruments, net of $4 of income
taxes
—
—
—
7
7 Expense (income) reclassified into operations from other
comprehensive income, net of $1 of income taxes and $7 and $7income tax benefits, respectively
(1)
—
11
13
23 Balances at December 31, 2017 7 (149) (168) 32 (278)
Unrealized losses on available-for-sale securities, net of $2 incometax benefit
(5)
—
—
—
(5)
Foreign currency translation adjustments, net of $8 income taxbenefit
—
(63)
—
—
(63)
Defined benefit plans, net of $10 of income taxes — — 34 — 34 Change in fair value of derivative instruments, net of $5 of income
taxes
—
—
—
18
18 Expense (income) reclassified into operations from other
comprehensive income, net of $5 income tax benefit and $2 ofincome taxes, respectively
—
—
16
(8)
8 Reclassification of stranded tax effects 1 (71) (30) 5 (95)
Balances at December 31, 2018 3 (283) (148) 47 (381)Unrealized gains on available-for-sale securities, net of $4 of
income taxes
11
—
—
—
11 Foreign currency translation adjustments, net of $5 of income taxes — — — — — Defined benefit plans, net of $14 income tax benefit — — (49) — (49)Change in fair value of derivative instruments, net of $13 income
tax benefit
—
—
—
(37)
(37)Expense (income) reclassified into operations from other
comprehensive income, net of $3 income tax benefit and $3 ofincome taxes, respectively
—
—
10
(14)
(4)Balances at December 31, 2019 $ 14 $ (283) $ (187) $ (4) $(460)
F-35
346

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 127/137
Table of Contents
HCA HEALTHCARE, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
NOTE 16 — ACCRUED EXPENSES
A summary of other accrued expenses at December 31 follows (dollars in millions):
2019 2018 Professional liability risks $ 457 $ 466 Defined contribution benefit plan 528 459 Interest 368 429 Right-of-use operating lease 350 — Taxes other than income 325 308 Other 904 962
$2,932 $2,624
NOTE 17 — SUPPLEMENTAL CONDENSED CONSOLIDATING FINANCIAL INFORMATION AND OTHER COLLATERAL-RELATEDINFORMATION
HCA Inc. is a 100% owned direct subsidiary of HCA Healthcare, Inc. HCA Healthcare, Inc. has $1.000 billion aggregate principal amount of6.25% senior unsecured notes due 2021 outstanding. These notes are senior unsecured obligations and are not guaranteed by any of our subsidiaries.
The senior secured credit facilities and senior secured notes described in Note 9 are jointly and severally, and fully and unconditionally guaranteedby substantially all existing and future, direct and indirect, 100% owned material domestic subsidiaries that are “Unrestricted Subsidiaries” under ourIndenture dated December 16, 1993 (except for certain special purpose subsidiaries that only guarantee and pledge their assets under our ABL creditfacility).
Our condensed consolidating balance sheets at December 31, 2019 and 2018 and condensed consolidating statements of comprehensive incomeand cash flows for each of the three years in the period ended December 31, 2019, segregating HCA Healthcare, Inc. issuer, HCA Inc. issuer, thesubsidiary guarantors, the subsidiary non-guarantors and eliminations, follow.
F-36
347

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 128/137
Table of Contents
HCA HEALTHCARE, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
NOTE 17 — SUPPLEMENTAL CONDENSED CONSOLIDATING FINANCIAL INFORMATION AND OTHER COLLATERAL-RELATEDINFORMATION (continued)
HCA HEALTHCARE, INC.CONDENSED CONSOLIDATING COMPREHENSIVE INCOME STATEMENT
FOR THE YEAR ENDED DECEMBER 31, 2019(Dollars in millions)
HCA Healthcare, Inc.
Issuer HCA Inc.
Issuer Subsidiary
Guarantors
Subsidiary Non-
Guarantors Eliminations Condensed
Consolidated Revenues $ — $ — $ 29,220 $ 22,116 $ — $ 51,336
Salaries and benefits — — 12,898 10,662 — 23,560 Supplies — — 4,802 3,679 — 8,481 Other operating expenses 7 — 4,643 4,831 — 9,481 Equity in earnings of affiliates (3,597) — (6) (37) 3,597 (43)Depreciation and amortization — — 1,447 1,149 — 2,596 Interest expense (income) 64 4,025 (2,001) (264) — 1,824 Gains on sales of facilities — — (14) (4) — (18)Losses on retirement of debt — 211 — — — 211 Management fees — — (768) 768 — —
(3,526) 4,236 21,001 20,784 3,597 46,092 Income (loss) before income taxes 3,526 (4,236) 8,219 1,332 (3,597) 5,244 Provision (benefit) for income taxes 21 (976) 1,874 180 — 1,099 Net income (loss) 3,505 (3,260) 6,345 1,152 (3,597) 4,145 Net income attributable to noncontrolling
interests
—
—
91
549
—
640 Net income (loss) attributable to HCA
Healthcare, Inc.
$ 3,505
$ (3,260)
$ 6,254
$ 603
$ (3,597)
$ 3,505 Comprehensive income (loss) attributable to
HCA Healthcare, Inc.
$ 3,426
$ (3,311)
$ 6,215
$ 614
$ (3,518)
$ 3,426
F-37
348

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 129/137
Table of Contents
HCA HEALTHCARE, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
NOTE 17 — SUPPLEMENTAL CONDENSED CONSOLIDATING FINANCIAL INFORMATION AND OTHER COLLATERAL-RELATEDINFORMATION (continued)
HCA HEALTHCARE, INC.CONDENSED CONSOLIDATING COMPREHENSIVE INCOME STATEMENT
FOR THE YEAR ENDED DECEMBER 31, 2018(Dollars in millions)
HCA Healthcare, Inc.
Issuer HCA Inc.
Issuer Subsidiary
Guarantors
Subsidiary Non-
Guarantors Eliminations Condensed
Consolidated Revenues $ — $ — $ 27,482 $ 19,195 $ — $ 46,677
Salaries and benefits — — 12,287 9,138 — 21,425 Supplies — — 4,560 3,164 — 7,724 Other operating expenses 8 — 4,463 4,137 — 8,608 Equity in earnings of affiliates (3,688) — (7) (22) 3,688 (29)Depreciation and amortization — — 1,335 943 — 2,278 Interest expense (income) 64 3,580 (1,635) (254) — 1,755 Gains on sales of facilities — — (357) (71) — (428)Losses on retirement of debt — 9 — — — 9 Management fees — — (639) 639 — —
(3,616) 3,589 20,007 17,674 3,688 41,342 Income (loss) before income taxes 3,616 (3,589) 7,475 1,521 (3,688) 5,335 Provision (benefit) for income taxes (171) (834) 1,714 237 — 946 Net income (loss) 3,787 (2,755) 5,761 1,284 (3,688) 4,389 Net income attributable to noncontrolling
interests
—
—
99
503
—
602 Net income (loss) attributable to HCA
Healthcare, Inc.
$ 3,787
$ (2,755)
$ 5,662
$ 781
$ (3,688)
$ 3,787 Comprehensive income (loss) attributable to
HCA Healthcare, Inc.
$ 3,779
$ (2,745)
$ 5,712
$ 713
$ (3,680)
$ 3,779
F-38
349

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 130/137
Table of Contents
HCA HEALTHCARE, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
NOTE 17 — SUPPLEMENTAL CONDENSED CONSOLIDATING FINANCIAL INFORMATION AND OTHER COLLATERAL-RELATEDINFORMATION (continued)
HCA HEALTHCARE, INC.CONDENSED CONSOLIDATING COMPREHENSIVE INCOME STATEMENT
FOR THE YEAR ENDED DECEMBER 31, 2017(Dollars in millions)
HCA Healthcare, Inc.
Issuer HCA Inc.
Issuer Subsidiary
Guarantors
Subsidiary Non-
Guarantors Eliminations Condensed
Consolidated Revenues $ — $ — $ 25,774 $ 17,840 $ — $ 43,614
Salaries and benefits — — 11,619 8,440 — 20,059 Supplies — — 4,286 3,030 — 7,316 Other operating expenses 6 — 4,249 3,796 — 8,051 Equity in earnings of affiliates (2,476) — (6) (39) 2,476 (45)Depreciation and amortization — — 1,237 894 — 2,131 Interest expense (income) 64 3,088 (1,309) (153) — 1,690 Gains on sales of facilities — — (2) (6) — (8)Losses on retirement of debt — 39 — — — 39 Management fees — — (621) 621 — —
(2,406) 3,127 19,453 16,583 2,476 39,233 Income (loss) before income taxes 2,406 (3,127) 6,321 1,257 (2,476) 4,381 Provision (benefit) for income taxes 190 (1,154) 2,293 309 — 1,638 Net income (loss) 2,216 (1,973) 4,028 948 (2,476) 2,743 Net income attributable to noncontrolling
interests
—
—
108
419
—
527 Net income (loss) attributable to HCA
Healthcare, Inc.
$ 2,216
$ (1,973)
$ 3,920
$ 529
$ (2,476)
$ 2,216 Comprehensive income (loss) attributable to
HCA Healthcare, Inc.
$ 2,276
$ (1,953)
$ 3,898
$ 591
$ (2,536)
$ 2,276
F-39
350

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 131/137
Table of Contents
HCA HEALTHCARE, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
NOTE 17 — SUPPLEMENTAL CONDENSED CONSOLIDATING FINANCIAL INFORMATION AND OTHER COLLATERAL-RELATEDINFORMATION (continued)
HCA HEALTHCARE, INC.CONDENSED CONSOLIDATING BALANCE SHEET
DECEMBER 31, 2019(Dollars in millions)
HCA Healthcare, Inc.
Issuer HCA Inc.
Issuer Subsidiary
Guarantors
Subsidiary Non-
Guarantors Eliminations Condensed
Consolidated ASSETS
Current assets: Cash and cash equivalents $ — $ — $ 118 $ 503 $ — $ 621 Accounts receivable, net — — 4,037 3,343 — 7,380 Inventories — — 1,208 641 — 1,849 Other — — 727 619 — 1,346
— — 6,090 5,106 — 11,196
Property and equipment, net — — 13,418 9,297 — 22,715 Investments of insurance subsidiaries — — — 315 — 315 Investments in and advances to affiliates 36,684 — 29 220 (36,684) 249 Goodwill and other intangible assets — — 5,743 2,526 — 8,269 Right-of-use operating lease assets — — 455 1,379 — 1,834 Other 300 3 29 148 — 480
$ 36,984 $ 3 $ 25,764 $ 18,991 $ (36,684) $ 45,058 LIABILITIES AND STOCKHOLDERS’
(DEFICIT) EQUITY
Current liabilities: Accounts payable $ — $ — $ 1,903 $ 1,002 $ — $ 2,905 Accrued salaries — — 1,070 705 — 1,775 Other accrued expenses 85 341 1,001 1,505 — 2,932 Long-term debt due within one year — 54 50 41 — 145
85 395 4,024 3,253 — 7,757
Long-term debt, net 998 32,016 213 350 — 33,577 Intercompany balances 38,089 (4,314) (33,828) 53 — — Professional liability risks — — — 1,370 — 1,370 Right-of-use operating lease obligations — — 345 1,154 — 1,499 Income taxes and other liabilities 620 7 252 541 — 1,420
39,792 28,104 (28,994) 6,721 — 45,623 Stockholders’ (deficit) equity attributable to HCA Healthcare,
Inc.
(2,808)
(28,101)
54,652
10,133
(36,684)
(2,808)Noncontrolling interests — — 106 2,137 — 2,243
(2,808) (28,101) 54,758 12,270 (36,684) (565) $ 36,984 $ 3 $ 25,764 $ 18,991 $ (36,684) $ 45,058
F-40
351

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 132/137
Table of Contents
HCA HEALTHCARE, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
NOTE 17 — SUPPLEMENTAL CONDENSED CONSOLIDATING FINANCIAL INFORMATION AND OTHER COLLATERAL-RELATED INFORMATION (continued)
HCA HEALTHCARE, INC.CONDENSED CONSOLIDATING BALANCE SHEET
DECEMBER 31, 2018(Dollars in millions)
HCA Healthcare, Inc.
Issuer HCA Inc.
Issuer Subsidiary
Guarantors
Subsidiary Non-
Guarantors Eliminations Condensed
Consolidated ASSETS
Current assets: Cash and cash equivalents $ — $ — $ 174 $ 328 $ — $ 502 Accounts receivable, net — — 3,964 2,825 — 6,789 Inventories — — 1,178 554 — 1,732 Other — — 669 521 — 1,190
— — 5,985 4,228 — 10,213
Property and equipment, net — — 12,450 7,307 — 19,757 Investments of insurance subsidiaries — — — 362 — 362 Investments in and advances to affiliates 33,166 — 29 203 (33,166) 232 Goodwill and other intangible assets — — 5,724 2,229 — 7,953 Other 478 64 35 113 — 690
$ 33,644 $ 64 $ 24,223 $ 14,442 $ (33,166) $ 39,207 LIABILITIES AND STOCKHOLDERS’
(DEFICIT) EQUITY
Current liabilities: Accounts payable $ — $ — $ 1,721 $ 856 $ — $ 2,577 Accrued salaries — — 998 582 — 1,580 Other accrued expenses 142 403 905 1,174 — 2,624 Long-term debt due within one year — 696 55 37 — 788
142 1,099 3,679 2,649 — 7,569
Long-term debt, net 996 30,544 212 281 — 32,033 Intercompany balances 36,951 (6,789) (28,415) (1,747) — — Professional liability risks — — — 1,275 — 1,275 Income taxes and other liabilities 505 — 223 520 — 1,248
38,594 24,854 (24,301) 2,978 — 42,125 Stockholders’ (deficit) equity attributable to HCA Healthcare,
Inc.
(4,950)
(24,790)
48,437
9,519
(33,166)
(4,950)Noncontrolling interests — — 87 1,945 — 2,032
(4,950) (24,790) 48,524 11,464 (33,166) (2,918) $ 33,644 $ 64 $ 24,223 $ 14,442 $ (33,166) $ 39,207
F-41
352

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 133/137
Table of Contents
HCA HEALTHCARE, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
NOTE 17 — SUPPLEMENTAL CONDENSED CONSOLIDATING FINANCIAL INFORMATION AND OTHER COLLATERAL-RELATEDINFORMATION (continued)
HCA HEALTHCARE, INC.CONDENSED CONSOLIDATING STATEMENT OF CASH FLOWS
FOR THE YEAR ENDED DECEMBER 31, 2019(Dollars in millions)
HCA Healthcare, Inc.
Issuer HCA Inc.
Issuer Subsidiary
Guarantors
Subsidiary Non-
Guarantors Eliminations Condensed
Consolidated Cash flows from operating activities:
Net income (loss) $ 3,505 $ (3,260) $ 6,345 $ 1,152 $ (3,597) $ 4,145 Adjustments to reconcile net income (loss) to net cash provided by
(used in) operating activities:
Change in operating assets and liabilities — (62) 17 (43) — (88)Depreciation and amortization — — 1,447 1,149 — 2,596 Income taxes 250 — — — — 250 Gains on sales of facilities — — (14) (4) — (18)Losses on retirement of debt — 211 — — — 211 Amortization of debt issuance costs — 30 — — — 30 Share-based compensation — — 347 — — 347 Equity in earnings of affiliates (3,597) — — — 3,597 — Other 109 — 23 (3) — 129
Net cash provided by (used in) operating activities 267 (3,081) 8,165 2,251 — 7,602 Cash flows from investing activities:
Purchase of property and equipment — — (2,342) (1,816) — (4,158)Acquisition of hospitals and health care entities — — (43) (1,639) — (1,682)Sales of hospitals and health care entities — — 42 19 — 61 Change in investments — — 6 19 — 25 Other — — (7) 41 — 34
Net cash used in investing activities — — (2,344) (3,376) — (5,720)Cash flows from financing activities:
Issuance of long-term debt — 6,451 — — — 6,451 Net change in revolving bank credit facilities — (560) — — — (560)Repayment of long-term debt — (5,227) (59) (38) — (5,324)Distributions to noncontrolling interests — — (104) (438) — (542)Payment of debt issuance costs — (73) — — — (73)Payment of dividends (550) — — — — (550)Repurchases of common stock (1,031) — — — — (1,031)Changes in intercompany balances with affiliates, net 1,457 2,490 (5,714) 1,767 — — Other (143) — — 1 — (142)
Net cash (used in) provided by financing activities (267) 3,081 (5,877) 1,292 — (1,771)Effect of exchange rate changes on cash and cash equivalents — — — 8 — 8 Change in cash and cash equivalents — — (56) 175 — 119 Cash and cash equivalents at beginning of period — — 174 328 — 502 Cash and cash equivalents at end of period $ — $ — $ 118 $ 503 $ — $ 621
F-42
353

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 134/137
Table of Contents
HCA HEALTHCARE, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
NOTE 17 — SUPPLEMENTAL CONDENSED CONSOLIDATING FINANCIAL INFORMATION AND OTHER COLLATERAL-RELATEDINFORMATION (continued)
HCA HEALTHCARE, INC.CONDENSED CONSOLIDATING STATEMENT OF CASH FLOWS
FOR THE YEAR ENDED DECEMBER 31, 2018(Dollars in millions)
HCA Healthcare, Inc.
Issuer HCA Inc.
Issuer Subsidiary
Guarantors
Subsidiary Non-
Guarantors Eliminations Condensed
Consolidated Cash flows from operating activities:
Net income (loss) $ 3,787 $ (2,755) $ 5,761 $ 1,284 $ (3,688) $ 4,389 Adjustments to reconcile net income (loss) to net cash provided by
(used in) operating activities:
Change in operating assets and liabilities — 23 (178) 188 — 33 Depreciation and amortization — — 1,335 943 — 2,278 Income taxes 74 — — — — 74 Gains on sales of facilities — — (357) (71) — (428)Losses on retirement of debt — 9 — — — 9 Amortization of debt issuance costs — 31 — — — 31 Share-based compensation — — 268 — — 268 Equity in earnings of affiliates (3,688) — — — 3,688 — Other 91 — 25 (9) — 107
Net cash provided by (used in) operating activities 264 (2,692) 6,854 2,335 — 6,761 Cash flows from investing activities:
Purchase of property and equipment — — (2,008) (1,565) — (3,573)Acquisition of hospitals and health care entities — — (897) (356) — (1,253)Sales of hospitals and health care entities — — 770 38 — 808 Change in investments — — 12 45 — 57 Other — — (9) 69 — 60
Net cash used in investing activities — — (2,132) (1,769) — (3,901)Cash flows from financing activities:
Issuance of long-term debt — 2,000 — — — 2,000 Net change in revolving bank credit facilities — (640) — — — (640)Repayment of long-term debt — (1,590) (72) (42) — (1,704)Distributions to noncontrolling interests — — (83) (358) — (441)Payment of debt issuance costs — (25) — — — (25)Payment of dividends (487) — — — — (487)Repurchases of common stock (1,530) — — — — (1,530)Changes in intercompany balances with affiliates, net 2,004 2,947 (4,505) (446) — — Other (252) — — 4 — (248)
Net cash (used in) provided by financing activities (265) 2,692 (4,660) (842) — (3,075)Effect of exchange rate changes on cash and cash equivalents — — — (15) — (15)Change in cash and cash equivalents (1) — 62 (291) — (230)Cash and cash equivalents at beginning of period 1 — 112 619 — 732 Cash and cash equivalents at end of period $ — $ — $ 174 $ 328 $ — $ 502
F-43
354

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 135/137
Table of Contents
HCA HEALTHCARE, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
NOTE 17 — SUPPLEMENTAL CONDENSED CONSOLIDATING FINANCIAL INFORMATION AND OTHER COLLATERAL-RELATEDINFORMATION (continued)
HCA HEALTHCARE, INC.CONDENSED CONSOLIDATING STATEMENT OF CASH FLOWS
FOR THE YEAR ENDED DECEMBER 31, 2017(Dollars in millions)
HCA Healthcare, Inc.
Issuer HCA Inc.
Issuer Subsidiary
Guarantors
Subsidiary Non-
Guarantors Eliminations Condensed
Consolidated Cash flows from operating activities:
Net income (loss) $ 2,216 $ (1,973) $ 4,028 $ 948 $ (2,476) $ 2,743 Adjustments to reconcile net income (loss) to net cash provided by
(used in) operating activities:
Change in operating assets and liabilities — (193) (219) 116 — (296)Depreciation and amortization — — 1,237 894 — 2,131 Income taxes 433 — — — — 433 Gains on sales of facilities — — (2) (6) — (8)Losses on retirement of debt — 39 — — — 39 Amortization of debt issuance costs — 31 — — — 31 Share-based compensation — — 270 — — 270 Equity in earnings of affiliates (2,476) — — — 2,476 — Other 78 — — 5 — 83
Net cash provided by (used in) operating activities 251 (2,096) 5,314 1,957 — 5,426 Cash flows from investing activities:
Purchase of property and equipment — — (1,681) (1,334) — (3,015)Acquisition of hospitals and health care entities — — (26) (1,186) — (1,212)Sales of hospitals and health care entities — — 14 11 — 25 Change in investments — — (1) (72) — (73)Other — — — (4) — (4)
Net cash used in investing activities — — (1,694) (2,585) — (4,279)Cash flows from financing activities:
Issuance of long-term debt — 1,500 — 2 — 1,502 Net change in revolving bank credit facilities — 760 — — — 760 Repayment of long-term debt — (628) (77) (48) — (753)Distributions to noncontrolling interests — — (140) (308) — (448)Payment of debt issuance costs — (26) — — — (26)Repurchases of common stock (2,051) — — — — (2,051)Changes in intercompany balances with affiliates, net 1,867 490 (3,404) 1,047 — — Other (66) — — 21 — (45)
Net cash (used in) provided by financing activities (250) 2,096 (3,621) 714 — (1,061)Change in cash and cash equivalents 1 — (1) 86 — 86 Cash and cash equivalents at beginning of period — — 113 533 — 646 Cash and cash equivalents at end of period $ 1 $ — $ 112 $ 619 $ — $ 732
F-44
355

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 136/137
Table of Contents
HCA HEALTHCARE, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
NOTE 17 — SUPPLEMENTAL CONDENSED CONSOLIDATING FINANCIAL INFORMATION AND OTHER COLLATERAL-RELATEDINFORMATION (continued)
Healthtrust, Inc. — The Hospital Company (“Healthtrust”) is the first-tier subsidiary of HCA Inc. The common stock of Healthtrust has beenpledged as collateral for the senior secured credit facilities and senior secured notes described in Note 9. Rule 3-16 of Regulation S-X under theSecurities Act requires the filing of separate financial statements for any affiliate of the registrant whose securities constitute a substantial portion of thecollateral for any class of securities registered or being registered. We believe the separate financial statements requirement applies to Healthtrust due tothe pledge of its common stock as collateral for the senior secured notes. Due to the corporate structure relationship of HCA and Healthtrust, HCA’soperating subsidiaries are also the operating subsidiaries of Healthtrust. The corporate structure relationship, combined with the application of push-down accounting in Healthtrust’s consolidated financial statements related to HCA’s debt and financial instruments, results in the consolidated financialstatements of Healthtrust being substantially identical to the consolidated financial statements of HCA. The consolidated financial statements of HCAand Healthtrust present the identical amounts for revenues, expenses, net income, assets, liabilities, total stockholders’ deficit, net cash provided byoperating activities, net cash used in investing activities and net cash used in financing activities. Certain individual line items in the HCA consolidatedstatements of stockholders’ deficit and cash flows are combined into one line item in the Healthtrust consolidated statements of stockholder’s deficit andcash flows.
Reconciliations of the HCA Healthcare, Inc. Consolidated Statements of Stockholders’ Deficit and Consolidated Statements of Cash Flowspresentations to the Healthtrust, Inc. — The Hospital Company Consolidated Statements of Stockholder’s Deficit and Consolidated Statements of CashFlows presentations for the years ended December 31, are as follows (dollars in millions):
2019 2018 2017 Presentation in HCA Healthcare, Inc. Consolidated Statements of Stockholders’ Deficit:
Repurchases of common stock $(1,031) $(1,530) $(2,051)Share-based benefit plans 313 115 281 Cash dividends declared ($1.60 per share — 2019 and $1.40 per share — 2018) (555) (496) — Other (11) (12) (10)
Presentation in Healthtrust, Inc. — The Hospital Company Consolidated Statements of Stockholder’s Deficit: Distributions to HCA Healthcare, Inc., net of contributions from HCA Healthcare, Inc. $(1,284) $(1,923) $(1,780)
Presentation in HCA Healthcare, Inc. Consolidated Statements of Cash Flows (cash flows from financingactivities):
Repurchases of common stock $(1,031) $(1,530) $(2,051)Payment of dividends (550) (487) —
Presentation in Healthtrust, Inc. — The Hospital Company Consolidated Statements of Cash Flows (cash flowsfrom financing activities):
Cash distributions to HCA Healthcare, Inc. $(1,581) $(2,017) $(2,051)
Due to the consolidated financial statements of Healthtrust being substantially identical to the consolidated financial statements of HCA, exceptfor the items presented in the table above, the separate consolidated financial statements of Healthtrust are not presented.
F-45
356

10/28/2020 Form 10-K
file:///C:/Users/gjadol/AppData/Local/Temp/Temp1_Skyline Burn Unit CON Application (2).zip/HCA 10k.htm 137/137
Table of Contents
HCA HEALTHCARE, INC.QUARTERLY CONSOLIDATED FINANCIAL INFORMATION
(UNAUDITED)(Dollars in millions, except per share amounts)
2019 First Second Third Fourth
Revenues $12,517 $12,602 $12,694 $13,523 Net income $ 1,181(a) $ 927(b) $ 764(c) $ 1,273 Net income attributable to HCA Healthcare, Inc. $ 1,039(a) $ 783(b) $ 612(c) $ 1,071 Basic earnings per share $ 3.03 $ 2.29 $ 1.80 $ 3.16 Diluted earnings per share $ 2.97 $ 2.25 $ 1.76 $ 3.09
2018 First Second Third Fourth
Revenues $11,423 $11,529 $11,451 $12,274 Net income $ 1,282(d) $ 966(e) $ 896(f) $ 1,245(g)Net income attributable to HCA Healthcare, Inc. $ 1,144(d) $ 820(e) $ 759(f) $ 1,064(g)Basic earnings per share $ 3.26 $ 2.35 $ 2.20 $ 3.09 Diluted earnings per share $ 3.18 $ 2.31 $ 2.15 $ 3.01
(a) First quarter results include $1 million of losses on sales of facilities (See Note 3 of the notes to consolidated financial statements).(b) Second quarter results include $14 million of gains on sales of facilities (See Note 3 of the notes to consolidated financial statements).(c) Third quarter results include $162 million of losses on retirement of debt (See Note 9 of the notes to consolidated financial statements).(d) First quarter results include $305 million of gains on sales of facilities (See Note 3 of the notes to consolidated financial statements).(e) Second quarter results include $8 million of gains on sales of facilities (See Note 3 of the notes to consolidated financial statements).(f) Third quarter results include $5 million of gains on sales of facilities (See Note 3 of the notes to consolidated financial statements) and $7 million
of losses on retirement of debt (See Note 9 of the notes to consolidated financial statements).(g) Fourth quarter results include $6 million of gains on sales of facilities (See Note 3 of the notes to consolidated financial statements).
F-46
357

Section B-Quality-2A
Facility License
358

359

Section B-Quality-2A
The Joint Commission Accreditation
360

361

Section B-Quality-2A
Inpatient Rehab Accreditation
362

363

Section B-Quality-2A
Financial Assistance and Charity Care Documentation
364

DEPARTMENT: Vendor Collections Management
POLICY DESCRIPTION: Financial Assistance Policy for Uninsured Patients
PAGE: 1 of 13 REPLACES POLICY DATED: 09/15/2016 APPROVED: 12/22/2014 RETIRED: EFFECTIVE DATE: 11/01/2017 REFERENCE NUMBER: PARA.PP.VCM.015
SCOPE: All Self-Pay patient accounts, excluding elective cosmetic procedures, facility designated self-pay flat rate procedures and scheduled/discounted procedures for International patients will be given an Uninsured Discount. The following also qualify for the Uninsured Discount::
• Accounts where insurance benefits have been exhausted or terminated • Medicare outpatient self-administered drugs
NOTE: If a Parallon Client chooses to participate in the uninsured discount process and the processes are different a client specific policy should be developed using this policy as the guideline and making changes as applicable. Use the reference number identifying the client as defined in the Policy and Procedure Development policy PARA.PP.GEN.001. (Example: PARA.PP.VCM.015L for LifePoint) PURPOSE: To define the process for selecting the appropriate Self-Pay IPLAN, providing patients with information regarding available discounts and processing discounts for patients assigned one of the Uninsured Discount IPLANS. POLICY: All Self-Pay patient accounts will receive an uninsured discount, with the exception of elective cosmetic procedures; facility designated self-pay flat rate procedures, scheduled/discounted procedures for International patients and accounts meeting the charity guidelines. Uninsured discounts will also be applied to accounts where insurance benefits have been exhausted or terminated. Medicare outpatient self-administered drugs will also receive the uninsured discount. Accounts will be assigned one of the following Uninsured Discount IPLANS. IPLAN IPLAN Description LOG ID IP Proc
Code OP Proc
Code 099-40 Uninsured Discount Plan UINS 920970 920980 099-41 Uninsured Discount Plan –
Burn Unit UINB 920971 920981
099-42 Uninsured Discount Plan – Transplant
UINT 920972 920982
099-44 Uninsured State Specific (local) (local) (local) 099-45 Uninsured ESP – Left or Ref (local) (local) (local) 099-46 Uninsured ESP - Treated (local) (local) (local) 099-47 Uninsured Discount Plan –
Patient Non-Compliance UINS 920970 920980
365

DEPARTMENT: Vendor Collections Management
POLICY DESCRIPTION: Financial Assistance Policy for Uninsured Patients
PAGE: 2 of 13 REPLACES POLICY DATED: 09/15/2016 APPROVED: 12/22/2014 RETIRED: EFFECTIVE DATE: 11/01/2017 REFERENCE NUMBER: PARA.PP.VCM.015
099-49 Uninsured – Partially
Exhausted Benefits N/A (local) (local)
N/A Uninsured – Medicare Self-Administered Drugs
N/A N/A 957983
The discount amounts will be provided to each facility in a formal rate schedule document. The patient will receive the Uninsured Discount unless the patient qualifies for a Charity Discount as outlined in the existing Charity Financial Assistance Policy for Uninsured and Underinsured Patients (PARA.PP.VCM.016). Refer to Uninsured Discount FAQ for more information. Patient Notification at the time of Registration: If it is determined the patient is uninsured at the time of registration, the patient/responsible party will be presented with an Uninsured Patient Information document (PARA.FT.VCM.015) that provides information on the Uninsured Discount Policy and other available discounts and payment options. This document will outline the process for uninsured discounts and inform the patient of additional account resolution options (i.e. monthly payments). The patient/responsible party will be asked to sign and date the document. The document will then be scanned into the imaging system and be placed in the imaging Patient Folder document type, as a validation that information regarding discounts has been communicated to all uninsured patients. Patient Access Responsibilities at the Time of Registration: Patient Access will be responsible for determining the appropriate IPLAN assignment from the table above and for presenting the Uninsured Patient Information Document (PARA.FT.VCM.015) to the patient/responsible party. Patient Access will explain the process as documented, answering questions related to the document and obtaining a signature from the patient/responsible party documenting that the information regarding available discounts was provided. All requests for payment will be based on total estimated charges less the uninsured discount. Patient Access will be responsible for requesting from the patient/responsible party the expected patient liability amount by using a facility specific deposit schedule which has been updated to reflect the Uninsured Discount. Patient Access will be responsible for asking the patient/responsible party for payment in full or monthly payment arrangements on the patient liability amount. Inpatient and Outpatient self-pay patients who are able to make payment in full or monthly payment arrangements.
366

DEPARTMENT: Vendor Collections Management
POLICY DESCRIPTION: Financial Assistance Policy for Uninsured Patients
PAGE: 3 of 13 REPLACES POLICY DATED: 09/15/2016 APPROVED: 12/22/2014 RETIRED: EFFECTIVE DATE: 11/01/2017 REFERENCE NUMBER: PARA.PP.VCM.015
• Assign the appropriate Uninsured Discount IPLAN. • The Uninsured Discount IPLAN should reflect proration of 100% of the total charges for
the patient. • A facility/SSC specific prompt pay discount may be applied in addition to the Uninsured
Discount as set forth in the PARA.PP.SS.035 Discount Policy for Patients. Inpatient self-pay patients who are not able to make payment in full or monthly payment arrangements and Outpatient self-pay patients will be considered for Medicaid eligibility.
• Assign the facility designated Pending Medicaid IPLAN as the primary payer. o The Pending Medicaid IPLAN should reflect proration of 100% of the total
charges for the patient. • Assign the Pending Charity IPLAN (099-50) as the secondary payer.
o Present the patient with a Financial Assistance Application for Charity consideration. (Note: Patients who are elective will not qualify for Charity, so the Pending Charity I-plan does not need to be added.)
• Assign the appropriate Uninsured Discount IPLAN as the tertiary payer. Outpatient self-pay patients who are not able to make payment in full or monthly payment arrangements and do not meet the Medicaid eligibility threshold.
• Assign the Pending Charity IPLAN (099-50) as the primary payer. o The Pending Charity IPLAN should reflect proration of 100% of the total charges
for the patient. o Present the patient with a Financial Assistance Application for Charity
consideration. (Note: Patients who are elective will not qualify for Charity, so the Pending Charity I-plan does not need to be added.)
• Assign the appropriate Uninsured Discount IPLAN as the secondary payer. All Inpatient and Outpatient self-pay patients registered for elective cosmetic procedures, facility designated self-pay flat rate procedures and scheduled/discounted procedures for International patients.
• Assign the facility/SSC designated IPLAN for the discounted/flat rate procedure.
Emergency Department self-pay patients who opt out to an ESP process will be assigned an Uninsured ESP IPLAN.
• Assign the Uninsured ESP –Left or Referred IPLAN (099-45) as the primary payer if the patient elects to Leave or be Referred during the ESP process.
• Assign the Uninsured ESP – Treated IPLAN (099-46) as the primary payer if the patient receives treatment via the ESP process.
367

DEPARTMENT: Vendor Collections Management
POLICY DESCRIPTION: Financial Assistance Policy for Uninsured Patients
PAGE: 4 of 13 REPLACES POLICY DATED: 09/15/2016 APPROVED: 12/22/2014 RETIRED: EFFECTIVE DATE: 11/01/2017 REFERENCE NUMBER: PARA.PP.VCM.015
The default of Self-Pay IPLAN 000-00, due to the absence of an IPLAN, should be avoided once this policy is implemented. All accounts that are not assigned an IPLAN and systematically assigned Self-Pay 000-00 should be reviewed and moved to the appropriate IPLAN. All accounts excluding Client/Industrial accounts must be registered with an appropriate IPLAN for the third party payer, Medicaid Pending, Charity Pending, elective cosmetic/facility designated flat rate plan or an Uninsured Discount Plan. A Business Objects script has been developed to assist in identifying accounts without an IPLAN assignment. Financial Counselor/Support Services/Collector/Early Out Agency Responsibilities: If at any time it is determined that the patient is covered for these services by a health plan, the Uninsured Discount IPLAN should be removed and the Uninsured Discount reversed. The Uninsured Discount is limited to patients who have no third party payer source of payment. The IPLAN assignment of the third party payer should be assigned to the account in place of the Uninsured Discount IPLAN. Retroactive consideration for Medicaid eligibility or Charity Discount: Uninsured Discount Plan patients that retroactively are considered for Medicaid eligibility or Charity discounts will have the appropriate Pending Medicaid eligibility and Pending Charity IPLANS assigned as outlined in the Patient Access process above. The Uninsured Discount will be reversed until determination of Medicaid eligibility and Charity can be ruled out. Insurance Denials for Patient Non-Compliance: Accounts where a denial is applied due to the patient’s lack of cooperation are considered “uninsured”. Based on the liability due from the payer, the following collection guidelines will be followed and approval obtained prior to releasing liability to the patient where the patient failed to provide the requested information timely. Once efforts to obtain required information is exhausted, the 09947 Uninsured Discount Iplan is assigned and remaining liability after the uninsured discount will become the patient’s responsibility.
368

DEPARTMENT: Vendor Collections Management
POLICY DESCRIPTION: Financial Assistance Policy for Uninsured Patients
PAGE: 5 of 13 REPLACES POLICY DATED: 09/15/2016 APPROVED: 12/22/2014 RETIRED: EFFECTIVE DATE: 11/01/2017 REFERENCE NUMBER: PARA.PP.VCM.015
Artiva letters 1100 Request for Additional Information Request and 1153 Additional Insurance Information Request are available to send to the patient for 1st and 2nd letter attempts. The letters contain a dropdown to allow the requester to select the information required or enter free form text if not listed in the dropdown. The next follow-up should occur based on the next follow-up cycle after action is taken based on the standard liability stratification (top, high, etc.). Once the appropriate collection activity and approval is completed, ensure both the Uninsured IPLAN 099-47 and discount is applied appropriately. No approval is required for insurance liability less than $1,500 ($2,000 ATL only); however; an audit must be performed monthly on 15 percent of the accounts to ensure liabilities are released appropriately. To retain the original insurance plan information, assign Uninsured IPLAN 099-47 as the primary payer and resequence the original insurance IPLAN as the secondary payer.
• Assign the 099-47 Uninsured Discount IPLAN and resequence to the primary payer retaining the original IPLAN as the secondary payer.
o The Uninsured Discount IPLAN should reflect proration of 100% of the total charges.
Subsequently, if patient complies with the payer request, the uninsured IPLAN can be removed and the original IPLAN information will move to primary intact. Document actions and approvals with user name and ID in a clear and concise manner in the account notes in Artiva. Insurance Denials for Partially Exhausted Benefits: Accounts where a denial is applied due to partially exhausted benefits, the Uninsured – Partially Exhausted Benefits IPLAN (099-49) should be applied to the secondary position, after the payer with partially exhausted benefits. A manual p-line must be performed to adjust the exhausted benefit portion of the account by the facility Uninsured Discount percentage. Guidelines to determine if an uninsured discount qualifies based on Partially Exhausted Benefits (All three guidelines must be met):
• The remit indicates a Final Denial, or verbiage used on the remit such as “Exhausted Benefits” or “Maximum Coverage Exceeded” and
• The patient was considered for Charity for the remaining balance and not approved and • Days being considered for the uninsured discount were not covered by insurer. Also, no
insurance payment or contractual adjustment was received or posted for a portion of the day’s charges.
Medicare Outpatient Accounts containing Self-administered Drugs:
369

DEPARTMENT: Vendor Collections Management
POLICY DESCRIPTION: Financial Assistance Policy for Uninsured Patients
PAGE: 6 of 13 REPLACES POLICY DATED: 09/15/2016 APPROVED: 12/22/2014 RETIRED: EFFECTIVE DATE: 11/01/2017 REFERENCE NUMBER: PARA.PP.VCM.015
Self-administered drugs (SADs) provided to Medicare outpatients are considered a non-covered service by Medicare. SADs will not be tracked using an IPLAN. Charges for SADs will be uniformly discounted 100% for all HCA facilities. Non-HCA will be discounted based on facility Uninsured Discount percentage. A manual p-line using procedure code 957983 must be performed to adjust the SAD portion of the account. Click here for more information. Insurance Denials for no coverage including pre-existing: Accounts where the insurance remits a denial of coverage including pre-existing conditions and there are no other insurance coverage’s on file will be considered self-pay accounts. The IPLAN for the insurance denial should be removed and the Pending Medicaid IPLAN added as primary (if the account meets local screening guidelines), Pending Charity IPLAN assigned as secondary and the Uninsured Discount IPLAN assigned as tertiary. A Financial Assistance Application will need to be forwarded to the patient/responsible party. Patient Statements: Statements should not be sent out until the uninsured discount has been posted. Letters to a Self-Pay patient/responsible party should not include the account balance until the Uninsured Discount has been posted. If you use letters in your Medicaid Pending or Charity Pending process, you will need to remove the account balance reflected on them. Late Charges: Accounts with the Uninsured Discount IPLAN as the primary payer should not have late charges posted. If late credits are posted to the account, the Uninsured Discount should be recalculated to reflect the correct patient liability. The Bill Code master file on Patient Accounting should be modified to reflect no posting of late charges. Late charges after the Late Charge Days have elapsed should be NPST (not posted) from the Late Charge Report. State Specific requirements Each SSC should evaluate whether this policy complies with the applicable State regulations regarding Uninsured Discounts, and if it does not, clearly document exceptions to this policy in either a State specific policy or an addendum to this policy. HCA Trauma Facilities After all efforts to identify funding for Uninsured patients have been exhausted, the trauma activation charge will be discounted at 100% and then the standard uninsured discount will be applied to the remainder of the account. The discount will be applied automatically when the uninsured iplan is applied. PROCEDURE:
Responsible Party Action
370

DEPARTMENT: Vendor Collections Management
POLICY DESCRIPTION: Financial Assistance Policy for Uninsured Patients
PAGE: 7 of 13 REPLACES POLICY DATED: 09/15/2016 APPROVED: 12/22/2014 RETIRED: EFFECTIVE DATE: 11/01/2017 REFERENCE NUMBER: PARA.PP.VCM.015
Self-Pay – Inpatient and Outpatient (able to pay) Patient Access Determines the patient is not seeking services for elective cosmetic, a
flat rate procedure or is a scheduled/discounted International Patient.
Determines the patient can make payment or establish arrangements for payment.
Assigns the Uninsured IPLAN as the primary payer.
Reviews and obtains a signature on the Uninsured Patient Information Document from the patient or responsible party.
Calculates deposit from facility deposit schedule.
Collects deposit and documents account.
Self-Pay – Inpatient (unable to pay) Patient Access Determines the patient is not seeking services for elective cosmetic, a
flat rate procedure or is a scheduled/discounted International Patient.
Determines the patient cannot make payment or establish arrangements for payment.
Assigns the Medicaid Pending IPLAN as the primary payer.
Assigns the Charity Pending IPLAN as the secondary payer.
Assigns the Uninsured Discount IPLAN as the tertiary payer.
Reviews and obtains a signature on the Uninsured Patient Information Document from the patient or responsible party.
Presents the Financial Assistance Application to the patient or responsible party.
Documents account.
371
DEPARTMENT: Vendor Collections Management
POLICY DESCRIPTION: Financial Assistance Policy for Uninsured Patients
PAGE: 8 of 13 REPLACES POLICY DATED: 09/15/2016 APPROVED: 12/22/2014 RETIRED: EFFECTIVE DATE: 11/01/2017 REFERENCE NUMBER: PARA.PP.VCM.015
Self-Pay – Inpatient and Outpatients for an Elective Cosmetic Procedure, Facility Flat Rate or a scheduled/discounted International Patients Patient Access Assigns the facility/SSC designated IPLAN for the elective cosmetic
procedure, facility flat rate procedure or scheduled/discounted International Patient procedure.
Collects payment for elective cosmetic or facility flat rate procedure.
Documents account.
Self-Pay – Non Inpatient (unable to pay and for services that exceed the facility Medicaid Eligibility threshold) Patient Access Determines the patient is not seeking services for elective cosmetic, a
flat rate procedure or is a scheduled/discounted International Patient.
Determines the patient cannot make payment or arrangements for payment.
Determines the charges will be over the Medicaid eligibility threshold.
Assigns the Medicaid Pending IPLAN as the primary payer.
Assigns the Charity Pending IPLAN as the secondary payer.
Assigns the Uninsured Discount IPLAN as the tertiary payer.
Reviews and obtains a signature on the Uninsured Patient Information Document from the patient or responsible party.
Presents the Financial Assistance Application to the patient or responsible party.
Documents account.
Self-Pay – Non Inpatient (unable to pay and charges for services that may not exceed Medicaid eligibility threshold) Patient Access Determines the patient is not seeking services for elective cosmetic, a
flat rate procedure or is a scheduled/discounted International Patient.
Determines the patient cannot make payment or arrangements for payment.
372

DEPARTMENT: Vendor Collections Management
POLICY DESCRIPTION: Financial Assistance Policy for Uninsured Patients
PAGE: 9 of 13 REPLACES POLICY DATED: 09/15/2016 APPROVED: 12/22/2014 RETIRED: EFFECTIVE DATE: 11/01/2017 REFERENCE NUMBER: PARA.PP.VCM.015
Determines the complete charges for services cannot be made at time of registration or
Determines the charges will not be over the Medicaid eligibility threshold.
Assigns the Charity Pending IPLAN as the primary payer.
Assigns the Uninsured Discount IPLAN as the secondary payer.
Reviews and obtains a signature on the Uninsured Patient Information Document from the patient or responsible party.
Presents the Financial Assistance Application to the patient or responsible party.
Documents account.
Self-Pay – Emergency Department Registrations Patient Access EMTALA guidelines must be adhered to for all ED patients.
Assign the Charity Pending IPLAN as the primary payer.
Assign the Uninsured Discount IPLAN as the secondary payer.
Documents account accordingly.
Self-Pay – Emergency Department Departures (able to pay) Patient Access Determines the patient can make payment or arrangements for payment.
Removes the Charity Pending IPLAN (if assigned at time of
registration)
Assigns the Uninsured IPLAN as the primary payer. If the patient opts out for the ESP process, assign the appropriate ESP IPLAN.
Reviews and obtains a signature on the Uninsured Patient Information Document from the patient or responsible party.
Calculates deposit from facility deposit schedule.
373

DEPARTMENT: Vendor Collections Management
POLICY DESCRIPTION: Financial Assistance Policy for Uninsured Patients
PAGE: 10 of 13 REPLACES POLICY DATED: 09/15/2016 APPROVED: 12/22/2014 RETIRED: EFFECTIVE DATE: 11/01/2017 REFERENCE NUMBER: PARA.PP.VCM.015
Collects deposit and documents account. Self-Pay – Emergency Department Departures (unable to pay) Patient Access Determines the patient cannot make payment or arrangements for
payment.
Ensures the Charity Pending IPLAN is the primary payer
Ensures the Uninsured IPLAN is the secondary payer.
Reviews and obtains a signature on the Uninsured Patient Information Document from the patient or responsible party.
Documents account.
Monitoring Inpatient and Outpatient Uninsured Discounts Vendor Collections Management
Reviews Self-Pay accounts with the Uninsured Discount Plan as the primary payer for appropriate posted discount.
Notifies Payment Compliance of accounts with Uninsured Discount Plan as the primary payer that are final billed and do not reflect an Uninsured Discount.
Ensures that all Statements are held until the Uninsured Discount is posted for patients who have the Uninsured Discount Plan as the primary payer.
Ensures that all Letters to a Self-Pay patient/responsible party do not include the account balance until the Uninsured Discount has been posted
Self-Pay - Medicaid Eligibility Denied Vendor Collections Management staff
Determines the patient IS NOT eligible for Medicaid Coverage.
374

DEPARTMENT: Vendor Collections Management
POLICY DESCRIPTION: Financial Assistance Policy for Uninsured Patients
PAGE: 11 of 13 REPLACES POLICY DATED: 09/15/2016 APPROVED: 12/22/2014 RETIRED: EFFECTIVE DATE: 11/01/2017 REFERENCE NUMBER: PARA.PP.VCM.015
Deletes the Medicaid Pending IPLAN and the system will automatically
move the Charity Discount IPLAN to the primary position and the Uninsured Discount IPLAN to the secondary position.
Considers the patient for a Charity Discount based on PARA.PP.VCM.016 Discount Charity Policy for Patients.
Self-Pay – Charity Discount Denied Vendor Collections Management staff
Determines the patient IS NOT eligible for a Charity Discount
Deletes the Charity Pending IPLAN and the system will automatically
move the Uninsured Discount Plan to the primary position
Non-Concuity facilities processes an IZ transaction to ensure that the Uninsured Discount IPLAN Log ID performs discount calculation
Insurance Denials – Patient Non-Compliance Collections and/or Support Services
Third Party payer denies coverage due to patient fails to comply with request for information or payment of premium (QHP 8X addendum). Sends the patient one or two letters and places one or two phone calls depending on the liability due. Obtains appropriate approval to release liability to the patient. Assigns the Uninsured IPLAN – Patient Non-Compliance (099-47) as the primary payer Resequence the original IPLAN to secondary payer. The system will post the uninsured discount. Keeping the original IPLAN on the account retains the insurance information in the event the patient subsequently complies with payer request. Documents Account. For accounts with liability due <$1000, perform an audit on a 15% sample to confirm one letter was sent and time allowed for the patient to respond before releasing liability to the patient.
375

DEPARTMENT: Vendor Collections Management
POLICY DESCRIPTION: Financial Assistance Policy for Uninsured Patients
PAGE: 12 of 13 REPLACES POLICY DATED: 09/15/2016 APPROVED: 12/22/2014 RETIRED: EFFECTIVE DATE: 11/01/2017 REFERENCE NUMBER: PARA.PP.VCM.015
Insurance Denials – No Coverage or Pre-existing Collections and/or Support Services
Third Party payer denies coverage due to no coverage or pre-existing.
Remove Third Party IPLAN from account. Add Pending Medicaid as primary payer and Charity Pending 099-50 as
secondary payer. Send Financial Assistance Application to patient/RP
Insurance Denials – Partially Exhausted Benefits Collections and/or Support Services
Third Party Payer denies for partially exhausted benefits.
Adds the Uninsured – Partially Exhausted Benefits IPLAN (099-49) into the secondary position following the partially exhausted benefits payer IPLAN.
Medicare - Self-administered Drugs MSC Process
Processes a manual p-line for the facility approved Uninsured Discount on the portion of the account partially denied due to exhausted benefits and re-prorates to patient liability. Will identify billed claims from the billing database that require a SADs uninsured discount. Charges for SADs will be uniformly discounted 100% for all HCA facilities. Non-HCA will be discounted based on facility Uninsured Discount percentage. A p-line using procedure code 957983 will be entered in eTran. The p-line follows the standard approval process defined in eTran. Once the uninsured discount is posted to the account; the accounts follow the normal MSC collection process. Click here for more information. NOTE: Encounters reaching a zero balance will be moved to zero balance status and will not require an uninsured discount.
REFERENCE: PARA.FT.VCM.015 Uninsured Patient Information Document Facility Specific Uninsured Discount Plan Deposit Schedule Facility Specific Cosmetic Procedure Plan Policy and Procedure PARA.PP.SS.035 Discount Policy for Patient
376

DEPARTMENT: Vendor Collections Management
POLICY DESCRIPTION: Financial Assistance Policy for Uninsured Patients
PAGE: 13 of 13 REPLACES POLICY DATED: 09/15/2016 APPROVED: 12/22/2014 RETIRED: EFFECTIVE DATE: 11/01/2017 REFERENCE NUMBER: PARA.PP.VCM.015
PARA.PP.VCM.016 Discount Charity Policy for Patients PARA.PP.GEN.001 Policy and Procedure Development Self-Administered Drug Discount effective 04/01/2016
Self-Administered Drugs 04012016.docx QHP- denial code 8X addendum
QHP denial code 8X specific to collection
Uninsured Discount FAQ 04/01/2016
Uninsured Discount Plan FAQ 04012016.d
377

Uninsured Discount Plan FAQ
Uninsured FAQs 04/01/2016
Who is eligible for the Uninsured Discount Plan? All Self Pay patients, excluding patients seeking treatment for elective cosmetic or facility self pay flat rate procedure. International Patients traveling to the US for scheduled/discounted procedures are also eligible for the Uninsured Discount. If the patient becomes eligible for health care coverage retroactively, will they retain the Uninsured Discount? If the patient becomes eligible for health care coverage, the Uninsured Discount will be removed. Are certain charges included in the facility detail charges, such as private room differences and facility based professional fees excluded from the Uninsured Discount? No. All charges reflected on the account are subject to the Uninsured Discount Plan. Are patients who receive an Uninsured Discount eligible for Charity consideration? Yes. If it is determined that the patient should have been processed under the Charity policy, the Uninsured Discount will be removed and the Charity Discount processed. Are patients who receive an Uninsured Discount eligible for Prompt Payment Discounts? Yes. If the facility offers a prompt payment discount, the discount can be applied to the account. The calculation should be based on the account balance net of the uninsured discount. When should the patient be told about the Uninsured Discount? If it is determined at the point of registration that the patient is uninsured, the registrar should explain the Uninsured Discount Plan at the time of registration and the Uninsured Discount Information document should be given to the patient at this time. All EMTALA guidelines should be met prior to discussing the Uninsured Discount Plan in the ED setting. What is the IPLAN for Uninsured Patients? IPLAN IPLAN Description LOG ID IP Proc
Code OP Proc
Code 099-40 Uninsured Discount Plan UINS 920970 920980 099-41 Uninsured Discount Plan –
Burn Unit UINB 920971 920981
099-42 Uninsured Discount Plan – Transplant
UINT 920972 920982
099-44 Uninsured State Specific (local) (local) (local) 099-45 Uninsured ESP – Left or Ref (local) (local) (local) 099-46 Uninsured ESP - Treated (local) (local) (local) 099-47 Uninsured Discount Plan –
Patient Non-Compliance UINS 920970 920980
099-49 Uninsured – Partially Exhausted Benefits
N/A (local) (local)
Can additional Uninsured Discount IPLANS be established at the SSC, Market or Local level? No. It is important for consolidated reporting that only the approved IPLANS be designated for the Uninsured Discount.
378

Uninsured Discount Plan FAQ
Uninsured FAQs 04/01/2016
Can the facility modify the Uninsured Discount in order to remain competitive in the market? No. The Uninsured Discount will be established for the local market and will be updated annually. If a facility wants to request an exception, this request should be sent to the SSC CEO who will work with the Financial Service Division to determine if an exception is warranted. Can a patient file their own private insurance and still receive the Uninsured Discount? No. The Uninsured Discount Plan is only available for patients who have no form of health care coverage. If you become aware of such activity, the discount should be reversed off the account. Are Physicians and Non-US citizens who have no insurance coverage eligible for the Uninsured Discount? Yes, as long as they have no form of health care coverage. International Patients traveling to the US for scheduled/discounted procedures are also eligible. Can an Uninsured Patient obtain a copy of their UB92 and Detail Bill? Yes. The UB04 and the Detail Bill may be given to the patient after it is determined the patient is not eligible for Medicaid or Charity so that the Uninsured Discount will be reflected on the claim. Is the Uninsured Discount Plan available only for facilities associated with a SSC? No. All HCA facilities participate in the Uninsured Discount Plan. Partnership facilities should take this policy to their board for approval as soon as possible. Who is listed as the insured for the Uninsured Discount IPLAN? The responsible party will also be the insured for the Uninsured Discount Plan. Are required fields in the Uninsured Discount IPLAN different from other IPLANS? No. All normally required fields including those for HIPAA, are still required for this IPLAN. If the patient only has a Daily Benefit or Small healthcare policy, are they eligible for the Uninsured Discount Plan? Yes. To determine if an uninsured discount qualifies based on Partially Exhausted Benefits, all three guidelines must be met: • The remit indicates a Final Denial, or verbiage used on the remit such as “Exhausted Benefits” or
“Maximum Coverage Exceeded” and • The patient was considered for Charity for the remaining balance and not approved and • Days being considered for the uninsured discount were not covered by insurer. Also, no insurance
payment or contractual adjustment was received or posted for a portion of the day’s charges. What is the purpose of IPLAN 099-49 Uninsured – Partially Exhausted Benefits? • The purpose of IPLAN 099-49, Uninsured- Partially Exhausted Benefits is to provide an IPLAN that
can reside in the secondary or tertiary position when insurance benefits, regardless of payer, are exhausted AND the patient does not qualify for any other program, such as Medicaid or Charity. In those instances where Medicaid or Charity coverage is available or the patient qualifies, then IPLAN 099-49 should not be applied.
Why must Patient Access list three IPLANS for patient accounts that are under consideration for Medicaid eligibility?
379

Uninsured Discount Plan FAQ
Uninsured FAQs 04/01/2016
For accounts under consideration for Medicaid eligibility the account will reflect Pending Medicaid IPLAN as primary, Pending Charity IPLAN as secondary and Uninsured Discount Plan as tertiary. If Medicaid eligibility is not available, that IPLAN is removed which will set the account up for Charity discount review. If the patient is not eligible for Charity that IPLAN is removed which will set the account up for the Uninsured Discount. Setting these three payers up on the account is a safe guard for review of appropriate discounting and will ensure that the account financial class reflects the current status of the account. It may be possible for the patient to access HPS to make payment prior to the Uninsured Discount being posted. How should this be addressed? The Uninsured Patient Information document includes information regarding the Uninsured Discount process. It will explain that all charges are posted to the patient’s account and after Medicaid and/or Charity eligibility have been ruled out, the patient will receive the Uninsured Discount. It may be possible for the patient to obtain their account balance in IVR prior to the Uninsured Discount being posted. How should this be addressed? Modification to the IVR process is under investigation. Details of the modification will be shared with the SSC when the final determination has been made. If the insurance carrier denies the claim for no coverage or pre-existing, will the patient receive an Uninsured Discount? Yes. If the insurance carrier denied the claim and remits no payment, then the insurance should be removed from the account and the Pending Charity IPLAN should be placed in the primary position with the Uninsured IPLAN assigned as the secondary payer. If the insurance carrier applies the claim towards a deductible, will the patient receive an Uninsured Discount? No. If the patient is covered by insurance then they will not be considered uninsured. Are there any special considerations for self pay patients that are not eligible for the Uninsured Discount? (e.g. PIP – Personal Injury Protection, Elective Cosmetic, Flat Rates, scheduled International Patients, Medicaid Pending and Charity Pending) Yes. All patient accounts must be assigned an IPLAN. Examples of IPLANS established at the local level for self pay patients who will not receive the Uninsured Discount are; PIP – Personal Injury Protection, Elective Cosmetic, Flat Rate (which could include International patient admissions), Medicaid Pending and Charity Pending. If the patient is seeking treatment for an elective cosmetic procedure and the facility does not offer a flat rate or cosmetic procedure discount, do I still assign an IPLAN? Yes. All patients, including all self pay patients, must be assigned an IPLAN. In this case, the facility would assign a locally defined IPLAN with 0% coverage. The Uninsured Discount IPLANS would not be considered for these type patients. If the insurance carrier delays payment, can I still release tracking and bill the patient for total charges or should I apply an Uninsured Discount? No. You must apply the uninsured discount before billing the patient. If the insurance later pays on the account, the uninsured discount should be reversed.
380

Uninsured Discount Plan FAQ
Uninsured FAQs 04/01/2016
Are you required to attempt Medicaid eligibility for all Uninsured Patients? No. You may set thresholds at your facility/SSC regarding the registration types or dollar minimums for accounts that are to be considered for Medicaid eligibility. Are you required to consider Charity Care for all Uninsured Patients? Yes. The Financial Assistance Application was recently modified. The form can now be easily completed by the patient/responsible party prior to leaving the facility. The simplified Financial Application form and Artiva make the process of reviewing, approving or denying Charity discounts easier for the Collections/Support staff. Are special procedures/services such as bariatrics covered under the Uninsured Discount Plan? Yes. If the facility has a flat/discounted rate for special procedures/services such as bariatrics, they can decide to continue to bill the flat/discounted rate or bill the Uninsured Discount rate. How do I determine the patient liability? The facility should update their existing deposit schedules by reducing the deposits based on the Uninsured discount. Is the Uninsured Discount Plan different for Joint Venture facilities? The uninsured discount plan must be approved by each board and the policy amended for any changes. The discount plan schedule is set at a market level, which would include facilities in a Joint Venture. However, approval by the local Joint Venture is required prior to beginning the Uninsured Discount process. What if the patient does not have his insurance information available at the time of admission? The patient would be considered Self Pay until insurance information can be obtained. The Uninsured Discount IPLAN should be assigned. Once the insurance information has been received, the Uninsured Discount IPLAN should be removed. Should Late Charges be posted to Uninsured Discount accounts? No. The Uninsured Discount is based on a discount of total charges at final bill. Posting additional charges would require coordination of holding statements until late charges could be discounting. If the SSC suspects insurance coverage from a third party liability insurance such as auto or third party liability accident or an indemnity policy where the insurance company pays directly to the patient, should the uninsured discount be applied? No. The SSC should pursue the insurance payment from the patient and thoroughly document the patient had received funds directly from the payer and then full charges can be billed to the patient. If patient / guarantor are uncooperative in providing information necessary to process the claim, should the uninsured discount be applied? Yes. Once all efforts are exhausted to obtain the information needed, the uninsured discount should be applied in primary position retaining the original Iplan in the secondary position. If the patient / guarantor subsequently provide the information, resequence the original iplan back to primary which will remove the uninsured discount.
381

104957056\V-2
DEPARTMENT: Vendor Collections Management
POLICY DESCRIPTION: Charity Financial Assistance Policy for Uninsured and Underinsured Patients
PAGE: 1 of 6 REPLACES POLICY DATED: 11/01/2017 APPROVED: RETIRED: EFFECTIVE DATE: 06/14/ 2018 REFERENCE NUMBER: PARA.PP.VCM.016
SCOPE: All SSC and Facility areas responsible for requesting and evaluating Financial Assistance Applications ("FAA") for the purposes of processing a charity write-off for certain patients receiving services at HCA-affiliated, non-partnership, acute-care hospitals ("Hospitals").
PURPOSE: To define the policy for providing partial or full financial relief to patients who (i) have received emergency services, (ii) meet certain income requirements, (iii) do not qualify for state or federal assistance for the date of service, (iv) are uninsured or underinsured, and (v) are unable to make partial or full payment on outstanding balances. In addition, with respect to the FAA and income validation, to establish protocols and supporting documentation requirements.
POLICY: The following types of patients may qualify for a charity write-off based on the patient’s total household income, supporting income verification documentation or processes, as required, and the amount of the patient liability:
1) To be eligible for a charity write-off review, a patient must have incurred emergent, non-elective services.
2) To be eligible for a charity write-off, a patient must be (a) uninsured or underinsured and (b) have an out-of-pocket patient responsibility of $1,500 or more for an individual account. Upon request by a patient and, if there are extenuating circumstances, accounts with out-of-pocket responsibility balances of less than $1,500 may be reviewed and a charity write-off applied if Federal Poverty Guidelines/Level ("FPL") thresholds are met as set forth in Section 9, below.
3) For purposes of this policy, an uninsured patient is one (i) with no third party payer coverage for emergent health care services, (ii) who provides documentation that the patient is unable to pay for some or all of the provided non-elective hospital services and (iii) who satisfies the financial eligibility criteria set forth herein.
4) For purposes of this policy, an underinsured patient is one with some form of third party payer coverage for health care services, but such coverage is insufficient to pay the current bill such that the patient retains a patient liability that they are unable to pay.
382

104957056\V-2
DEPARTMENT: Vendor Collections Management
POLICY DESCRIPTION: Charity Financial Assistance Policy for Uninsured and Underinsured Patients
PAGE: 2 of 6 REPLACES POLICY DATED: 11/01/2017 APPROVED: RETIRED: EFFECTIVE DATE: 06/14/ 2018 REFERENCE NUMBER: PARA.PP.VCM.016
5) A validation will be completed, as required in this Policy, to ensure that if any portion of the patient's medical services can be paid by any federal or state governmental health care program (e.g., Medicare, Medicaid, Tricare, Medicare secondary payer), private insurance company, or other private, non-governmental third-party payer, that the payment has been received and posted to the account. No charity write-off can be applied to any account with any outstanding payer liability.
6) Supporting Income Verification Documentation & Review:
A. Medicare Accounts
i. All Medicare patients (i.e., inpatients and/or outpatients) must submit supporting income verification documentation. Electronic validation of patient income, e.g., Experian, alone is not sufficient. Medicare requires independent income and resource verification for a charity care determination with respect to Medicare beneficiaries (PRM-I § 312). ii. In addition to the FAA, the preferred income documentation will be the most current year’s Federal Tax Return. Any patient/responsible party unable to provide his/her most recent Federal Tax Return may provide two pieces of supporting documentation from the following list to meet this income verification requirement:
• State Income Tax Return for the most current year • Supporting W-2 • Supporting 1099’s • Copies of all bank statements for last 3 months • Most recent bank and broker statements listed in the Federal Tax Return • Current credit report Qualified Medicare Benefits (“QMB”) for inpatients only iii. Dual-Eligible Beneficiaries: A Medicare beneficiary who also qualifies for Medicaid (dual-eligible beneficiary) may be deemed indigent as long as the “Must Bill” requirements are met. That these requirements are met must be supported by a State Medicaid remittance advice. When claiming an amount as Medicare Bad Debt for a dual-eligible beneficiary, Medicaid must be billed. In addition, the remittance advice showing non-payment must be maintained as supporting documentation for the Medicare Bad Debt adjustment. Charity write-offs for Medicaid Exhausted beneficiaries may be less than $1,500.
383

104957056\V-2
DEPARTMENT: Vendor Collections Management
POLICY DESCRIPTION: Charity Financial Assistance Policy for Uninsured and Underinsured Patients
PAGE: 3 of 6 REPLACES POLICY DATED: 11/01/2017 APPROVED: RETIRED: EFFECTIVE DATE: 06/14/ 2018 REFERENCE NUMBER: PARA.PP.VCM.016
B. Non-Medicare Accounts i. Generally, for all non-Medicare Accounts, the following will be acceptable
supporting documentation: (i) the documentation listed in A. above, (ii) or any one of the following:
• Most Recent Employer Pay Stubs • Written documentation from income sources • Proof of Medicaid Eligibility Electronic validation of patient income and family size, such as Experian
ii. Supporting income verification documentation through an electronic validation of patient information/income, such as Experian, shall be obtained where no other income verification is obtained.
iii. To the extent required by state law, a complete FAA shall be obtained for any dollars reported as charity to the state.
iv. Review of assets may take place during the application process where required by state law or regulation.
C. Patients/Responsible Party Deemed Eligible.
The patient/responsible party may be deemed to meet the charity guidelines if:
• the patient/responsible party is determined to be eligible by a local clinic under poverty and income guidelines similar to the ones in this policy; or
• the patient/responsible party presents with Medicaid, and Medicaid does not pay.
D. Charity Processing Based on Extenuating Circumstances, i.e., Potential Charity Write-off Absent Full Documentation. There may be extenuating circumstances where resource testing cannot be completed because the patient/responsible party does not/cannot (i) complete the FAA, or (ii) provide supporting documentation listed in A or B, above. In those circumstances, a
384

104957056\V-2
DEPARTMENT: Vendor Collections Management
POLICY DESCRIPTION: Charity Financial Assistance Policy for Uninsured and Underinsured Patients
PAGE: 4 of 6 REPLACES POLICY DATED: 11/01/2017 APPROVED: RETIRED: EFFECTIVE DATE: 06/14/ 2018 REFERENCE NUMBER: PARA.PP.VCM.016
manager may waive the required documentation and extend a charity care write-off, consistent with this Policy. The following may be considered by the manager to be extenuating circumstances:
i. Patients identified as an undocumented residents or homeless through:
• Medicaid Eligibility screening
• Registration process
• Discharge to a shelter
• Clinical or Case Management documentation
• Absence of a credit report ii. Patients that expire - if it is determined through family contact and/or courthouse records
that an estate does not exist, it may be considered for a charity write-off (even if the patient had a spouse) upon documentation and with the manager’s review and approval of a policy exception.
iii. Medically Indigent – In addition to the above, if a patient/responsible party meets the medically indigent status based upon state guidelines or requirements, a charity write-off may be applied after the manager completes a resource testing process for the patient/responsible party.
7) Pending Medicaid Effect on Charity Write-off: The Pending Medicaid and Pending Charity processes should not be concurrent processes. Determination of Pending Medicaid should be resolved prior to evaluating for potential Pending Charity.
8) Health Insurance Marketplace for Qualified Health Plans: Pending qualification in the Health Insurance Marketplace may take place concurrently with the Pending Charity process. The QHP enrollment is not retroactive. Rather, the coverage becomes effective for future dates of service. Therefore, it is necessary to continue with the Pending Charity process for visits occurring prior to QHP effective dates.
9) Charity Processing based on Federal Poverty Guidelines: A. Patients with individual or household incomes of between 0-200% of Federal Poverty
Guidelines:
385

104957056\V-2
DEPARTMENT: Vendor Collections Management
POLICY DESCRIPTION: Charity Financial Assistance Policy for Uninsured and Underinsured Patients
PAGE: 5 of 6 REPLACES POLICY DATED: 11/01/2017 APPROVED: RETIRED: EFFECTIVE DATE: 06/14/ 2018 REFERENCE NUMBER: PARA.PP.VCM.016
Patients with more than a $1,500 patient liability that fall within 0-200% of the FPL will have the entire patient balance processed as charity write-off. Upon request by a patient and, if there are extenuating circumstances, accounts with out-of-pocket responsibility balances of less than $1,500 may be reviewed and a charity write-off applied.
B. Patients with individual or household incomes of between 201- 400% of Federal Poverty Guidelines: Patients with incomes between 201% and 400% of FPL will have their balances capped at a percentage of their income according to the table below. This percentage will be determined using the patient's FPL.
• 201% - 300% - balances capped at 3% of annual household income
• 301% - 400% - balances capped at 4% of annual household income Upon request by a patient and, if there are extenuating circumstances, accounts with out-of-pocket responsibility balances of less than $1,500 may be reviewed and a charity write-off applied.
C. Patients Who Are Uninsured: Notwithstanding 9)A. and B. above, patients who are uninsured and who provide the supporting income verification documentation and otherwise meet the requirements of this Policy, will have their patient balance capped at the lesser of the amount calculated under 9)A. or 9)B. above, or the amount calculated pursuant to the uninsured discount model. Balances from multiple accounts for the same patient may be considered together to determine out-of-pocket responsibility minimums and for calculating the cap. The write-off will be applied to the entire outstanding patient balance.
10) Refunds on Charity Accounts: The general expectation is that all patients pay for services rendered if they are not fully covered by a third party. Therefore, any amount paid by the patient (even if the patient subsequently meets the charity write-off guidelines for their balance due), will be retained. Only amounts paid by the patient that exceed the amount that patient would have paid had they received the uninsured discount, or that exceed their out of pocket responsibility per their insurance, will be refunded. For those patients that do meet the charity write-off criteria and
386

104957056\V-2
DEPARTMENT: Vendor Collections Management
POLICY DESCRIPTION: Charity Financial Assistance Policy for Uninsured and Underinsured Patients
PAGE: 6 of 6 REPLACES POLICY DATED: 11/01/2017 APPROVED: RETIRED: EFFECTIVE DATE: 06/14/ 2018 REFERENCE NUMBER: PARA.PP.VCM.016
have made a partial payment, the charity write-off will be posted on the remaining patient balance.
11) Patient Dispute Process: In the event a patient wishes to file a dispute and appeal their eligibility for a Charity write-off under this policy, the patient may seek review from the Vendor Collections Management Director, Hospital Chief Financial Officer or an SSC Executive as defined in the Charity Review Appeal Process policy (PARA.PP.VCM.020).
12) Compliance with State regulations: Each SSC should evaluate whether this Policy complies with the applicable state law and regulations regarding charity care, e.g., California, Florida. If this Policy does not comply with state law and regulations, each SSC must clearly document exceptions to this policy in either a State specific policy or an addendum to this Policy.
13) Liens: Under no circumstances will liens be considered on properties less than $300,000 in value.
REFERENCE:
• PARA.FT.VCM.606 Federal Charity Guidelines • PARA.FT.VCM.638 Financial Assistance Application • PARA.MF.VCM.804 Collection Charity Letters • PARA.PARS.PP.009 Medicare Bad Debt and Recovery Logs Policy • PARA.PP.VCM.019 Utilizing the Artiva Charity Process
387

Section B-Quality-2A Accessibility Documentation
388

COPY
Current Status: Active PolicyStat ID: 5939149
Origination: 01/1999 Last Approved: 06/2018 Last Revised: 02/2016 Next Review: 05/2021 Owner: Jodi Thurman: Assistant Director,
Emergency Dept Area: Patient Care References:
EMTALA Tennessee Medical Screening Examination and Stabilization Policy
SCOPE:
Purpose:
Policy:
1. the individual or a representative acting on the individual's behalf requests an examination or treatment for a medical condition; or
2. a prudent layperson observer would conclude from the individual's appearance or behavior that the individual needs an examination or treatment of a medical condition.
TriStar Skyline Medical Center and TriStar Skyline Madison Campus
This policy reflects guidance under the Emergency Medical Treatment and Labor Act ("EMTALA") and associated State laws only. It does not reflect any requirements of The Joint Commission or other regulatory entities. Each facility should ensure it has policies and procedures to address such additional requirements. No facility may edit this policy in a manner that would remove existing language. Additions to this policy should be clearly identifiable (e.g., in another color, different font or italicized text).
The definitions in the Company EMTALA Policy, LL.EM.001, apply to this and all other Company and facility EMTALA policies.
To establish guidelines for providing appropriate medical screening examinations ("MSE") and any necessary stabilizing treatment or an appropriate transfer for the individual as required by EMTALA, 42 U.S.C. § 1395dd, and all Federal regulations and interpretive guidelines promulgated thereunder.
An EMTALA obligation is triggered when an individual comes to a dedicated emergency department ("DED") and:
Such obligation is further extended to those individuals presenting elsewhere on hospital property requesting examination or treatment for an emergency medical condition ("EMC"). Further, if a prudent layperson observer would believe that the individual is experiencing an EMC, then an appropriate MSE, within the capabilities of the hospital's DED (including ancillary services routinely available and the availability of on-call physicians), shall be performed. The MSE must be completed by an individual (i) qualified to perform such an examination to determine whether an EMC exists, or (ii) with respect to a pregnant woman having
EMTALA Tennessee Medical Screening Examination and Stabilization Policy. Retrieved 10/28/2020. Official copy at
http://tristarskyline.policystat.com/policy/5939149/. Copyright © 2020 TriStar Skyline Medical CenterPage 1 of 12
389
www.princexml.com
Prince - Non-commercial License
This document was created with Prince, a great way of getting web content onto paper.

COPY
Procedure:
When an MSE is Required
a. The individual comes to a DED of a hospital and a request is made by the individual or on the individual's behalf for examination or treatment for a medical condition, including where:
a. The individual requests medication to resolve or provide stabilizing treatment for a medical condition.
b. The individual arrives as a transfer from another hospital or health care facility. Upon arrival of a transfer, a physician or qualified medical person ("QMP") must perform an appropriate MSE. The physician or QMP shall provide any additional screening and treatment required to stabilize the EMC. The MSE of the individual must be documented. This type of screening cannot be performed by the triage nurse. If an EMC is determined to exist and the hospital admits the individual as an inpatient for further treatment, the hospital's obligation under EMTALA ceases.
Note: The MSE and other emergency services need not be provided in a location specifically identified as a DED. The hospital may use areas to deliver emergency services that are also used for other inpatient or outpatient services. MSEs or stabilization may require ancillary services available only in areas or facilities of the hospital outside of the DED.
b. The individual arrives on the hospital property other than a DED and makes a request or another makes a request on the individual's behalf for examination or treatment for an EMC.
i. Screening where the individual presented: If an individual is initially screened in a department or location on-campus other than the DED, the individual may be moved to another hospital department or facility on-campus to receive further screening or stabilizing treatment without such movement being a transfer. The hospital shall not move the individual to an off-campus facility or department (such as an urgent care center or satellite clinic) for an MSE.
ii. Transporting to the DED: The hospital may determine that movement of an individual to the hospital's DED may be necessary for screening. However, common sense and individual judgment should prevail. When determining how best to transport the individual to the DED (means of transport, accompanying qualified personnel, equipment, etc.), the following factors should be taken into account but shall not be determinative:
▪ Whether the hospital DED has the personnel and resources necessary to render adequate
contractions, whether the woman is in labor and whether the treatment requested is explicitly for an EMC. If an EMC is determined to exist, the individual will be provided necessary stabilizing treatment, within the capacity and capability of the facility, or an appropriate transfer as defined by and required by EMTALA. Stabilization treatment shall be applied in a non-discriminatory manner (e.g., no different level of care because of age, gender, disability, race, color, ancestry, citizenship, religion, pregnancy, sexual orientation, gender identity or expression, national origin, medical condition, marital status, veteran status, payment source or ability, or any other basis prohibited by federal, state or local law).
A hospital must provide an appropriate MSE within the capability of the hospital's emergency department, including ancillary services routinely available to the DED, to determine whether or not an EMC exists: (i) to any individual, including a pregnant woman having contractions, who requests such an examination; (ii) an individual who has such a request made on his or her behalf; or (iii) an individual whom a prudent layperson observer would conclude from the individual's appearance or behavior needs an MSE. An MSE shall be provided to determine whether or not the individual is experiencing an EMC or a pregnant woman is in labor. An MSE is required when:
EMTALA Tennessee Medical Screening Examination and Stabilization Policy. Retrieved 10/28/2020. Official copy at
http://tristarskyline.policystat.com/policy/5939149/. Copyright © 2020 TriStar Skyline Medical CenterPage 2 of 12
390

COPY
medical treatment to all existing patients in the DED,
▪ Whether responding to the emergency could send hospital personnel into harm's way or unreasonably endanger or jeopardize the lives or health of such personnel, and
▪ Whether non-hospital paramedics, emergency medical technicians, or other qualified personnel are more appropriate to respond.
iii. Transporting to other hospital property: The facility may direct individuals to other hospital-based facilities that are on hospital property and operated under the hospital's provider number. However, the hospital should not move an individual to a hospital-based facility located off-campus, such as a rural health clinic or physician office, for an MSE or other emergency services. Individuals should only be moved to the hospital-based on-campus facility when the following conditions are met:
▪ all persons with the same medical condition are moved to this location regardless of their ability to pay for treatment,
▪ there is a bona fide medical reason to move the individual, and
▪ QMP accompany the individual.
Note: Unless outpatient testing is associated with an individual presenting to the DED with a request for an emergency medical screening, it should not be performed in the emergency department. Individuals presenting for outpatient testing should be registered as outpatients and not as emergency patients.
Note: Anyone may make the request for an MSE or treatment described in both a. and b. above. Specifically,
◦ A minor (child) can request an examination or treatment for an EMC. Hospital personnel should not delay the MSE by waiting for parental consent. If, after screening the minor, it is determined that no EMC is present, the staff may wait for parental consent before proceeding with further examination and treatment. Note: For additional information regarding treatment of minors, please consult your operations counsel.
◦ Emergency Medical Services (EMS) personnel may request an evaluation or treatment on an individual's behalf.
Example: If an individual is on a gurney or stretcher or in an ambulance or on a helipad at the hospital and EMS personnel, the individual, or a legally responsible person acting on the individual's behalf, requests examination or treatment of an EMC from hospital staff, an MSE must be provided.
c. The individual arrives on the hospital property, either in the DED or property other than the DED, and no request is made for evaluation or treatment, but the appearance or behavior of the individual would cause a prudent layperson observer to believe that the individual needed such examination or treatment.
d. An individual is in a ground or air ambulance for purposes of examination and treatment for a medical condition at a hospital's DED, and the ambulance is either:
i. owned and operated by the hospital, even if the ambulance is not on hospital grounds, or
ii. neither owned nor operated by the hospital, but on hospital property.
e. A community-wide plan exists for specific hospitals to treat certain EMCs (e.g., psychiatric, trauma, physical or sexual abuse). Prior to transferring the individual to the community plan hospital, an MSE must be performed and any necessary stabilizing treatment rendered.
EMTALA Tennessee Medical Screening Examination and Stabilization Policy. Retrieved 10/28/2020. Official copy at
http://tristarskyline.policystat.com/policy/5939149/. Copyright © 2020 TriStar Skyline Medical CenterPage 3 of 12
391

COPY
f. A law enforcement official requests hospital emergency personnel to provide medical clearance for incarceration. In such case, the hospital has an EMTALA obligation to provide an MSE to determine whether or not an EMC exists. All facilities must remain in compliance with federal and state HIPAA regulations. Examples:
i. If an individual presents to a facility which does not have the capability to perform a rape kit when one is needed, the hospital's obligation is to provide an appropriate MSE without disturbing the evidence and transfer the individual to a hospital that has the capability to gather the evidence. Transfer must occur only in compliance with hospital policies and procedures that are Medicare Hospital Conditions of Participation (CoP) and licensure compliant.
ii. If a policeman brings a person who is exhibiting behavior that suggests that he or she is intoxicated to the DED for drawing of the blood alcohol and asks for an MSE, or if a prudent lay person observer would believe that the individual needed examination or treatment for an EMC, then an MSE must be performed. Some medical conditions could present behaviors similar to those of an inebriated individual. Alternatively, if a law enforcement official requests that hospital emergency personnel provide clearance for incarceration, then the hospital has an EMTALA obligation to provide an MSE to determine whether or not an EMC exists.
g. Born Alive Infant. When an infant is born alive in the DED, if a request is made on the infant's behalf for screening for a medical condition or if a prudent layperson would conclude based on the infant's appearance or behavior that the infant needed examination or treatment for a medical condition, the hospital and physician must provide an MSE. If the infant is born alive elsewhere on the hospital's campus and a prudent layperson observer would conclude based on the born alive infant's appearance or behavior that the infant was suffering from an EMC, the hospital and medical staff must perform an MSE to determine whether or not an EMC exists. If an EMC exists, the hospital must provide for stabilizing treatment or an appropriate transfer.
h. Off-Campus Provider-Based Emergency Department. An off-campus provider based- emergency
department is a department of the hospital, located no more than 35 miles from the main hospital,
that meets all the provider-based requirements, holds the same Medicare provider number as the
main hospital and either is (i) licensed by the state as an Emergency Department, (ii) is advertised
as providing care for emergency medical conditions on an urgent basis without appointment, or
(iii) provides at least one-third of all its outpatient visits for the treatment of emergency medical
conditions on an urgent basis without requiring previously scheduled appointments. If an individual presents to an off-campus provider-based emergency department (should not be referred to as a "free-standing" emergency department), he or she must be provided an appropriate MSE just as he or she would if the presentation was at the main campus emergency department. Should the individual require additional screening for stabilizing care by a physician specialist, he or she will be moved to the main campus or another non-HCA facility for the additional care required. Such movement would be via an appropriate transport vehicle as designated by the ED Physician with appropriate equipment and personnel as determined by the ED Physician.
When an MSE is NOT Required
a. If an individual presents to a DED in the following circumstances only, no MSE is required by EMTALA:
i. The individual requests services that are NOT examination or treatment for an EMC, such as preventive care services or drugs that are not required to stabilize or resolve an EMC;
Example: An individual presents to the DED and tells the clerk that he needs a flu shot because it is
EMTALA Tennessee Medical Screening Examination and Stabilization Policy. Retrieved 10/28/2020. Official copy at
http://tristarskyline.policystat.com/policy/5939149/. Copyright © 2020 TriStar Skyline Medical CenterPage 4 of 12
392

COPY
now flu season. The hospital is not obligated to provide an MSE under EMTALA because the request for a flu vaccine is a preventive care service.
ii. The individual requests services that are NOT for an EMC such as gathering of evidence for criminal law cases (sexual assault, blood alcohol). When the request made is only to collect evidence, not to analyze the results or otherwise examine or treat the individual, no EMTALA obligation exists;
iii. When an individual appears for non-emergency tests or pursuant to a previously scheduled visit. The hospital must ensure and document that no EMC was present or that no request was made to examine or treat the individual for an EMC.
i. When an individual presents to the DED for medical care that is, by its nature, clearly
unlikely to involve an EMC, the individual's statement that he or she is not seeking
emergency care, together with brief questioning by QMP, is sufficient to establish that
there is no EMC.
ii. A QMP is not required to question or examine the individual if the individual presents to
the DED solely to fill a physician's order for a non-emergency test. The QMP should,
however, question the individual to confirm that no EMC exists if the individual requests
treatment for a non-emergency condition unrelated to the physician's order.
Example: A physician refers an individual to the emergency department for occupational medicine testing.
b. If the individual is in a ground or air ambulance which is:
i. owned and operated by the hospital and operated under community-wide EMS protocols or EMS protocols "mandated by State law" that direct it to transport the individual to a hospital other than the hospital that owns the ambulance (i.e., to the closest appropriate facility). In this case, the individual is considered to have "come to the emergency department of the hospital" to which the individual is transported, at the time the individual is brought onto hospital property; or
ii. not owned by the hospital and not on the hospital's property even if the ambulance personnel contact the hospital by telephone or telemetry communications and inform the hospital that they want to transport the individual to the hospital for examination and treatment; or
iii. owned but not operated by the hospital as where a physician who is not employed or otherwise affiliated with the hospital that owns the ambulance directs its operation and the ambulance is not on hospital property.
Note: A hospital may deny access to individuals when it is in "official diversionary" status because it does not have the capability or capacity to accept any additional emergency individuals at the time. The hospital shall develop and adopt written criteria that describe the conditions under which any or all of the hospital's emergency services are deemed to be at maximum capacity.
Caution: If the ambulance staff disregards the hospital's instructions and brings the individual on to hospital property, the individual has come to the emergency department and the hospital must perform an appropriate MSE. Should a hospital which is not in official diversionary status fail to accept a telephone or radio request for transfer or admission, the refusal could represent a violation of other Federal or State regulations.
EMTALA Tennessee Medical Screening Examination and Stabilization Policy. Retrieved 10/28/2020. Official copy at
http://tristarskyline.policystat.com/policy/5939149/. Copyright © 2020 TriStar Skyline Medical CenterPage 5 of 12
393

COPY
Note: The hospital shall maintain written records documenting the date and time of the start and end of each period of diversionary status.
c. Use of hospital-owned helipad on hospital property for patient transport. No MSE is required for individuals being transported by local ambulance services or other hospitals to tertiary hospitals throughout the state through use of a hospital-owned helipad on the hospital's property by local ambulance services or other hospitals as long as the sending hospital conducted the MSE prior to
transporting the individual to the helipad for medical helicopter transport to a designated recipient hospital. The sending hospital is responsible for conducting the MSE prior to transfer to determine if an EMC exists and implementing stabilizing treatment or conducting an appropriate transfer.
Caution: If the individual's condition deteriorates while being transported to the helipad or while at the helipad, the hospital at which the helipad is located must provide another MSE and stabilizing treatment within its capacity if requested by medical personnel accompanying the individual.
If, as part of the EMS protocol, EMS activates helicopter evacuation of an individual with a potential EMC, the hospital with the helipad does not have an EMTALA obligation if they are not the recipient hospital, unless a request is made by EMS personnel, the individual, or a legally responsible person acting on the individual's behalf for the examination or treatment of an EMC.
d. Off campus, non-DED. If an individual requests emergency care in a hospital department off the hospital's main campus that does not meet the definition of a DED, EMTALA does not apply and the hospital department is not obligated to perform an MSE. However, the off-campus department must have policies and procedures in place as to how to handle patients in need of immediate care.
Extent of the MSE
a. Determine if an EMC exists. The hospital must perform an MSE to determine if an EMC exists. It is not appropriate to merely "log in" or triage an individual with a medical condition and not provide an MSE. Triage is not equivalent to an MSE. Triage entails the clinical assessment of the individual's presenting signs and symptoms at the time of arrival at the hospital in order to prioritize when the individual will be screened by a physician or other QMP.
b. Definition of MSE. An MSE is the process required to reach, with reasonable clinical confidence, the point at which it can be determined whether the individual has an EMC or not. It is not an isolated event. The MSE must be appropriate to the individual's presenting signs and symptoms and the capability and capacity of the hospital.
c. An on-going process. The individual shall be continuously monitored according to the individual's needs until it is determined whether or not the individual has an EMC, and if he or she does, until he or she is stabilized or appropriately admitted or transferred. The medical record shall reflect the amount and extent of monitoring that was provided prior to the completion of the MSE and until discharge or transfer.
d. Judgment of physician or QMP. The extent of the necessary examination to determine whether an EMC exists is generally within the judgment and discretion of the physician or other QMP performing the examination function according to algorithms or protocols established and approved by the medical staff and governing board.
e. Extent of MSE varies by presenting symptoms. The MSE may vary depending on the individual's signs and symptoms:
i. Depending on the individual's presenting symptoms, an appropriate MSE can involve a wide
EMTALA Tennessee Medical Screening Examination and Stabilization Policy. Retrieved 10/28/2020. Official copy at
http://tristarskyline.policystat.com/policy/5939149/. Copyright © 2020 TriStar Skyline Medical CenterPage 6 of 12
394

COPY
spectrum of actions, ranging from a simple process involving only a brief history and physical examination to a complex process that also involves performing ancillary studies and procedures such as (but not limited to) lumbar punctures, clinical laboratory tests, CT scans and other diagnostic tests and procedures.
ii. Pregnant Women: The medical records should show evidence that the screening examination includes, at a minimum, on-going evaluation of fetal heart tones, regularity and duration of uterine contractions, fetal position and station, cervical dilation, and status of membranes (i.e., ruptured, leaking and intact), to document whether or not the woman is in labor. A woman experiencing contractions is in true labor unless a physician, certified nurse-midwife or other QMP acting within his or her scope of practice as defined by the hospital's medical staff bylaws and State medical practice acts, certifies in writing that after a reasonable time of observation, the woman is in false labor. The recommended timeframe for such physician certification of the QMP's determination of false labor should be within 24 hours of the MSE, however, the medical staff bylaws, rules and regulations can provide guidance on the timeframe.
iii. Individuals with psychiatric or behavioral symptoms: The medical records should indicate both medical and psychiatric or behavioral components of the MSE. The MSE for psychiatric purposes is to determine if the psychiatric symptoms have a physiologic etiology. The psychiatric MSE includes an assessment of suicidal or homicidal thoughts or gestures that indicates danger to self or others.
Who May Perform the MSE
a. Only the following individuals may perform an MSE:
i. A qualified physician with appropriate privileges;
ii. Other qualified licensed independent practitioner (LIP) with appropriate competencies and privileges; or
iii. A qualified staff member who:
▪ is qualified to conduct such an examination through appropriate privileging and demonstrated competencies;
▪ is functioning within the scope of his or her license and in compliance with state law and applicable practice acts (e.g., Medical or Nurse Practice Acts);
▪ is performing the screening examination based on medical staff approved guidelines, protocols or algorithms; and
▪ is approved by the facility's governing board as set forth in a document such as the hospital bylaws or medical staff rules and regulations, which document has been approved by the facility's governing body and medical staff. It is not acceptable for the facility to allow informal personnel appointments that could change frequently.
b. Qualified Medical Personnel. QMPs may perform an MSE if licensed and certified, approved by the hospital's governing board through the hospital's bylaws, and only if the scope of the EMC is within the individual's scope of practice.
Non-discrimination. The hospital must provide an MSE and necessary stabilizing treatment to any individual regardless of age, gender, disability, race, color, ancestry, citizenship, religion, pregnancy, sexual orientation, gender identity or expression, national origin, medical condition, marital status, veteran status, payment source or ability, or any other basis prohibited by federal, state or local law.
EMTALA Tennessee Medical Screening Examination and Stabilization Policy. Retrieved 10/28/2020. Official copy at
http://tristarskyline.policystat.com/policy/5939149/. Copyright © 2020 TriStar Skyline Medical CenterPage 7 of 12
395

COPY
i. The designation of QMP is set forth in a document approved by the governing body of the hospital. Each individual QMP approved to provide an MSE under EMTALA must be appropriately credentialed and must meet the requirements for annual evaluations set forth in the protocol agreements with physicians and the State's medical practice act, nurse practice act or other similar practice acts established to govern health care practitioners. Only appropriately credentialed APRNs, PAs and physicians may perform MSEs in the DED.
ii. Psychiatric QMP. The ED physician shall consult the QMP providing the behavioral assessment for psychiatric purposes but shall remain the primary decision-maker with regard to transfer and discharge of the individual presenting to the DED with psychiatric or behavioral emergencies. Should an individual with a psychiatric or behavioral emergency present to a behavioral department of a hospital that meets the requirements of a DED, that department is responsible for ensuring that the individual has the appropriate MSE, including any behavioral examination, and providing necessary stabilizing treatment.
iii. Labor and Delivery QMP. QMPs in the labor and delivery DED may be appropriately-approved RNs and must communicate their findings as to whether or not a woman is in labor to the obstetrician on call, the laborist, or the ED physician.
iv. Limitations. The hospital has established a process to ensure that:
a. a physician examines all individuals whose conditions or symptoms require physician examination;
b. an ED physician on duty is responsible for the general care of all individuals presenting themselves to the emergency department; and
c. the responsibility remains with the ED physician until the individual's private physician or an on-call specialist assumes that responsibility, or the individual is discharged.
No Delay in Medical Screening or Examination
a. Reasonable Registration Process. An MSE, stabilizing treatment, or appropriate transfer will not be delayed to inquire about the individual's method of payment or insurance status, or conditioned on an individual's completion of a financial responsibility form, an advance beneficiary notification form, or payment of a co-payment for any services rendered. The facility may follow reasonable registration processes for individuals for whom examination or treatment is required. Reasonable registration processes may include asking whether the individual is insured, and if so, what that insurance is, as long as these procedures do not delay screening or treatment or unduly discourage individuals from remaining for further evaluation. The hospital may seek non-payment information from the individual's health plan about the individual, such as medical history. In the case of an individual with an EMC, once the hospital has conducted the MSE and has initiated stabilizing treatment, it may seek authorization for all services from the plan as long as doing so does not delay completion of the stabilizing treatment.
b. Managed Care. For individuals who are enrolled in a managed care plan, prior authorization from the plan shall NOT be required or requested before providing an appropriate MSE and initiating any further medical examination and necessary stabilizing treatment.
c. EMS. A hospital has an obligation to see the individual once the individual presents to the DED whether by EMS or otherwise. A hospital that delays the MSE or stabilizing treatment of any individual who arrives via transfer from another facility, by not allowing EMS to leave the individual, could be in violation EMTALA and the Hospital CoP for Emergency Services. Even if the hospital cannot immediately complete an appropriate MSE, the hospital must assess the individual's condition upon arrival of the EMS
EMTALA Tennessee Medical Screening Examination and Stabilization Policy. Retrieved 10/28/2020. Official copy at
http://tristarskyline.policystat.com/policy/5939149/. Copyright © 2020 TriStar Skyline Medical CenterPage 8 of 12
396

COPY
service to ensure that the individual is appropriately prioritized based on his or her presenting signs and symptoms to be seen for completion of the MSE.
d. Contacting the individual's physician. An ED physician or non-physician practitioner may contact the individual's personal physician at any time to seek advice regarding the individual's medical history and needs that may be relevant to medical treatment and screening of the individual, so long as this consultation does not inappropriately delay services.
e. Financial Responsibility Forms. The performance of the MSE and the provision of stabilizing treatment will NOT be conditioned on an individual's completion of a financial responsibility form, an advance beneficiary notification form, or payment of a co-payment for any services rendered.
f. Financial Inquiries. Individuals who inquire about financial responsibility for emergency care should receive a response by a staff member who has been well trained to provide information regarding potential financial liability. The staff member who provides information on potential financial liability should clearly inform the individual that the hospital will provide an MSE and any necessary stabilizing treatment, regardless of his or her ability to pay. Individuals who believe that they have an EMC should be encouraged to remain for the MSE.
Refusal to Consent to Treatment
a. Written Refusal – Partial Refusal of Care or Against Medical Advice. If a physician or QMP has begun the MSE or any stabilizing treatment and an individual refuses to consent to a test, examination or treatment or refuses any further care and is determined to leave against medical advice, after being informed of the risks and benefits and the hospital's obligations under EMTALA, reasonable attempts shall be made to obtain a written refusal to consent to examination or treatment using the form provided for that purpose or document the individuals refusal to sign the Partial Refusal of Care or the Against Medical Advice Form (see Partial Refusal of Care or Against Medical Advice Form). The medical record must contain a description of the screening and the examination, treatment, or both if applicable, that was refused by or on behalf of the individual.
b. Waiver of Right to Medical Screening Examination. If an individual refuses to consent to examination or treatment and indicates his or her intention to leave prior to triage or prior to receiving an MSE or if the individual withdrew the initial request for an MSE, facility personnel must request that the individual sign the Waiver of Right to Medical Screening Examination Form that is part of the Sign-In Sheet or document on the Sign-In Sheet the individual's refusal to sign the Waiver of Right to Medical Screening Examination Form.
c. Documentation of Information. If an individual refuses to sign a consent form, the physician or nurse must document that the individual has been informed of the risks and benefits of the examination and/or treatment but refused to sign the form.
d. Documentation of Unannounced Leave. If an individual leaves the facility without notifying facility personnel, this must be documented upon discovery. The documentation must reflect that the individual had been at the facility and the time the individual was discovered to have left the premises. Triage notes and additional records must be retained. If the individual leaves prior to transfer or leaves prior to an MSE, the information should be documented on the individual's medical record. If an individual has not completed a Sign-In Sheet, an ED staff member should complete a sheet and if the individual's name is
Note: There is no delay in the provision of an MSE or stabilizing treatment if: (i) there is not an open bed in the DED; (ii) there are not sufficient caregivers present to render the MSE and/or stabilizing treatment; and (iii) the individual's condition does not warrant immediate screening and treatment by a physician or QMP.
EMTALA Tennessee Medical Screening Examination and Stabilization Policy. Retrieved 10/28/2020. Official copy at
http://tristarskyline.policystat.com/policy/5939149/. Copyright © 2020 TriStar Skyline Medical CenterPage 9 of 12
397

COPY
not known a description of the individual leaving should be entered on the form. All individuals presenting for evaluation or treatment must be entered into the Central Log.
Stabilizing Treatment Within Hospital Capability
a. Stable. The physician or QMP providing the medical screening and treating the emergency has determined within reasonable clinical confidence, that the EMC that caused the individual to seek care in the DED has been resolved although the underlying medical condition may persist. Once the individual is stable, EMTALA no longer applies. (The individual may still be transferred; however, the "appropriate transfer" requirement under EMTALA does not apply.)
b. Stabilizing Treatment Within Hospital Capability and Transfer. Once the hospital has provided an appropriate MSE and stabilizing treatment within its capability, an appropriate transfer may be effected by following the appropriate transfer provisions. (See Transfer Policy.) If there is a disagreement between the physician providing emergency care and an off-site physician (e.g., a physician at the receiving facility or the individual's primary care physician if not physically present at the first facility) about whether the individual has been provided sufficient stabilized treatment to effect a transfer, the medical judgment of the transferring physician takes precedence over that of the off-site physician.
Refer to the hospital's Transfer Policy for additional directions regarding transfers of those individuals who are not medically stable. If a hospital has exhausted all its capabilities and is unable to stabilize an individual, an appropriate transfer should be implemented by the transferring physician.
c. Stabilizing Treatment and Individuals Whose EMC's Are Resolved. An individual is considered stable and ready for discharge when, within reasonable clinical confidence, it is determined that the individual has reached the point where his or her continued care, including diagnostic work-up and/or treatment, could reasonably be performed as an outpatient or later as an inpatient, provided the individual is given a plan for appropriate follow-up care with the discharge instructions. The EMC that caused the individual to present to the DED must be resolved, but the underlying medical condition may persist. Hospitals are expected within reason to assist/provide discharged individuals the necessary information to secure follow-up care to prevent relapse or worsening of the medical condition upon release from the hospital.
When EMTALA Obligations End
a. That no EMC exists (even though the underlying medical condition may persist);
The determination of whether an individual is stable is not based on the clinical outcome of the individual's medical condition. An individual has been provided sufficient stabilizing treatment when the physician treating the individual in the DED has determined, within reasonable clinical confidence, that no material deterioration of the condition is likely, within reasonable medical probability, to result from or occur during the transfer of the individual from a facility, or with respect to an EMC of a woman in labor, that the woman has delivered the child and placenta; or in the case of an individual with a psychiatric or behavioral condition, that the individual is protected and prevented from injuring himself/ herself or others. For those individuals who are administered chemical or physical restraints for purposes of transfer from one facility to another, stabilization may occur for a period of time and remove the immediate EMC, but the underlying medical condition may persist and, if not treated for longevity, the individual may experience exacerbation of the EMC. Therefore, the treating physician should use great care when determining if the EMC is in fact stable after administering chemical or physical restraints.
The hospital's EMTALA obligation ends when a physician or QMP has made a decision:
EMTALA Tennessee Medical Screening Examination and Stabilization Policy. Retrieved 10/28/2020. Official copy at
http://tristarskyline.policystat.com/policy/5939149/. Copyright © 2020 TriStar Skyline Medical CenterPage 10 of 12
398

COPY
b. That an EMC exists and the individual is appropriately transferred to another facility; or
c. That an EMC exists and the individual is admitted to the hospital for further stabilizing treatment; or
d. That an EMC exists and the individual is stabilized and discharged.
i. EMTALA Waivers and Requirements During Pandemics and Other Declared Emergencies.
i. Alternative Screening Sites on Campus for Screening during a Pandemic (No Waiver Required.) For the screening of influenza like illnesses, the hospital may establish an alternative screening site(s) on campus. Individuals may be redirected to these sites AFTER being logged in. The redirection and logging can take place outside the entrance to the DED. However, the person doing the directing must be qualified (e.g., an RN or QMP) to recognize individuals who are obviously in need of immediate treatment in the DED. The MSEs must be conducted by qualified personnel.
ii. Alternative Screening Site Off-Campus (No Waiver Required.) The hospital may encourage the public to go to an off-campus hospital-controlled site for the screening of influenza like illness. However, the hospital may NOT tell an individual who has already come to the DED to go to the off-site location for the MSE. The off-campus site for influenza like illnesses should not be held out to the public as a place that provides care for EMCs in general on an urgent, unscheduled basis.
iii. EMTALA Waivers.
a. A hospital operating under an EMTALA waiver will not be sanctioned for an inappropriate transfer or for directing or relocating an individual who comes to the DED to an alternative off-campus site, for the MSE if the following conditions are met:
1. The transfer is necessitated by the circumstances of the declared emergency in the emergency area during the emergency period (as those terms are defined in the hospital's EMTALA Transfer Policy);
2. The direction or relocation of an individual to receive medical screening at an alternate location is pursuant to an appropriate State emergency preparedness plan or, in the case of a public health emergency that involves a pandemic infectious disease, pursuant to a State pandemic preparedness plan;
3. The hospital does not discriminate on the basis of an individual's source of payment or ability to pay;
4. The hospital is located in an emergency area during an emergency period; and
5. There has been a determination that a waiver of sanctions is necessary.
b. An EMTALA waiver can be issued for a hospital only if:
1. The President has declared an emergency or disaster under the Stafford Act or the National Emergencies Act; and
Note: A hospital's EMTALA obligation ends when the individual has been admitted in good faith as an inpatient, whether or not the individual has been stabilized.* An individual is considered to be an inpatient when the individual is formally admitted to the hospital by a physician's order. A hospital continues to have a responsibility to meet the patient's emergency needs in accordance with hospital CoPs. A patient in observation status is not considered admitted as an inpatient, therefore, EMTALA obligations continue.
*Case law provides that EMTALA does apply to inpatients who have not been stabilized in Kentucky, Tennessee, Ohio and Michigan. Moses v. Providence Hospital and Medical Centers, Inc. and Paul Lessem, 6th Circuit Court of Appeals, April 6, 2009.
EMTALA Tennessee Medical Screening Examination and Stabilization Policy. Retrieved 10/28/2020. Official copy at
http://tristarskyline.policystat.com/policy/5939149/. Copyright © 2020 TriStar Skyline Medical CenterPage 11 of 12
399

COPY
2. The Secretary of HHS has declared a Public Health Emergency (PHE); and
3. The Secretary invokes his or her waiver authority including notifying Congress at least 48 hours in advance; and
4. The waiver includes waiver of EMTALA requirements and the hospital is covered by the waiver.
c. In the absence of CMS notification of area-wide applications of the waiver, the hospital must contact CMS and request that the waiver provisions be applicable to the hospital.
d. In addition, in order for an EMTALA waiver to apply to the hospital and for sanctions not to apply, (i) the hospital must activate its disaster protocol, and (ii) the State must have activated an emergency preparedness plan or pandemic preparedness plan in the emergency area, and any redirection of individuals for an MSE must be consistent with such plan.
e. Even when a waiver is in effect, there is still the expectation that everyone who comes to the DED will receive an appropriate MSE, if not in the DED, then at the alternate care site to which they are redirected or relocated.
Except in the case of waivers related to pandemic infectious disease, an EMTALA waiver is limited in duration to 72 hours beginning upon activation of the hospital's disaster protocol. In the case of a PHE involving pandemic infectious disease, the general EMTALA waiver authority will continue in effect until the termination of the declaration of the PHE. However, the waiver may be limited to a date prior to the termination of the PHE declaration, as determined by CMS. If a State emergency/pandemic preparedness plan is deactivated in the area where the hospital is located prior to the termination of the PHE, the hospital no longer meets the conditions for an EMTALA waiver and the hospital waiver would cease to be in effect as of the deactivation date. Likewise, if the hospital deactivates its disaster protocol prior to the termination of the PHE, the hospital no longer meets the conditions for an EMTALA waiver and the hospital waiver would cease to be in effect as of the deactivation date.
REFERENCE:
Attachments
No Attachments
Pre-PolicyStat Number: IPC.SUP.020
EMTALA Tennessee Medical Screening Examination and Stabilization Policy. Retrieved 10/28/2020. Official copy at
http://tristarskyline.policystat.com/policy/5939149/. Copyright © 2020 TriStar Skyline Medical CenterPage 12 of 12
400

COPY
Current Status: Active PolicyStat ID: 5941628
Origination: 12/2018 Last Approved: 12/2018 Last Revised: 12/2018 Next Review: 12/2021 Owner: Nicholas Howald: xxx Area: Facilities References:
Accommodating Persons with Service Animals
PURPOSE
RESPONSIBLE PERSONS
DEFINITIONS A. Disability. A person must meet the statutory definition of having a "disability," under federal, state and/or
local laws. These statutes recognize the following broad categories of disabilities:
◦ A sensory, mental, or physical impairment that substantially limits one or more major life activities (such as walking, seeing, hearing, speaking and breathing, working, learning, caring for one's self, performing manual tasks, etc.).
◦ A sensory, mental, or physical condition that is medically cognizable or diagnosable.
B. Handler. A person with a service or therapy animal.
To develop a plan that accommodates individuals pursuant to Section 504 of the Rehabilitation Act of 1973, Section 1557 of the Patient Protection and Affordable Care Act (2010) and the Americans with Disabilities Act of 2008 which prohibits discrimination on the basis of disability in the offering and delivery of healthcare services.
Skyline Medical Center is committed to compliance with federal and state laws prohibiting discrimination on the basis of disability in the offering and delivery of healthcare. Skyline Medical Center recognizes its legal obligation to accommodate service animals and makes every effort to pro-actively assess the accommodation needs as well as providing the most compassionate care.
Service animals are dogs (or miniature horses) that are individually trained to assist people with disabilities. The Americans with Disabilities Act (ADA) definition of service animals is any "dog individually trained to do work or perform tasks for the benefit of an individual with a disability, including a physical, sensory, psychiatric, intellectual, or other mental disability." The work or tasks performed by a service animal must be directly related to an individual's disability.
This policy requires the development of a plan to ensure that persons using service animals have an equal opportunity to participate in and benefit from healthcare services. This policy specifically differentiates "service animals" from "therapy animals," and describes types of service dogs, as well as sets behavioral guidelines.
All Skyline Medical Center staff.
Accommodating Persons with Service Animals. Retrieved 10/28/2020. Official copy at http://tristarskyline.policystat.com/
policy/5941628/. Copyright © 2020 TriStar Skyline Medical CenterPage 1 of 6
401
www.princexml.com
Prince - Non-commercial License
This document was created with Prince, a great way of getting web content onto paper.

COPY
C. Individualized Assessment. An individualized assessment of a service animal must be made by the Equity Compliance Coordinator (ECC) (previously referred to as the 504 Coordinator/ADA Administrator ) or other designee prior to excluding the service animal and is based on reasonable judgment that relies on current medical knowledge or on the best available objective evidence, to ascertain: the nature, duration, and severity of the risk; the probability that the potential injury will actually occur; and whether reasonable modifications of policies, practices, or procedures or the provision of auxiliary aids will mitigate the risk. [28 C.F.R §36.208(b); 28 C.F.R. §35.139(b)]
D. Pet/Comfort Animal. A domestic animal kept for pleasure or companionship. Pets are generally not permitted in the Skyline Medical Center. Permission may be granted by Administration for a pet to be in a campus facility for a specific reason at a specific time.
E. Service Animal. Any dog (or miniature horse) individually trained to do work or perform tasks directly related to the disability that the individual has. A service animal meets the definition of a service animal regardless of the terminology used to describe it. A service animal is sometimes also called an assistance animal. (A non-inclusive list of more common types of service animals is below).
If there is a question about whether an animal is a service animal, contact the ECC.
F. Therapy Animal. An animal with good temperament and disposition, and who has reliable, predictable behavior, selected to visit people with disabilities or people who are experiencing the frailties of aging as a therapy tool. The animal may be incorporated as an integral part of a treatment process. A therapy animal has not been trained to assist an individual with a disability with work or tasks. The therapy animal does not accompany a person with a disability all the time, unlike a service animal that is always with its handler. Thus, a therapy animal is not a service animal.
G. Service Animal in Training. A dog or miniature horse, undergoing training to become a service animal. A trainee will be housebroken and fully socialized. To be fully socialized means the animal will not, except under rare occasions, bark, yip, growl or make disruptive noises; will have a good temperament and disposition; will not show fear; will not be upset or agitated when it sees another animal; and will not be aggressive. A trainee will be under the control of the handler, who may or may not have a disability. If the trainee begins to show improper behavior, the handler will act immediately to correct the animal or will remove the animal from the premises. There is no federal obligation to accommodate service animals that are still in training.
• TYPES OF SERVICE ANIMALS
There are many different types of services animals. A non-inclusive list of some of the most common service animals is below:
◦ A guide service dog is trained to assist in navigation and other tasks for a person who is legally blind or has low vision.
◦ An alert service dog is trained to alert a person with significant hearing loss or who is deaf when a sound occurs, such as a knock on the door.
◦ A mobility service dog is trained to assist a person who has a mobility or health disability. Duties may include carrying, fetching, opening doors, ringing doorbells, activating elevator buttons, steadying a person while walking, helping a person up after a fall, etc. Mobility service dogs sometimes are called assistance animals.
◦ A seizure response service dog is trained to assist a person with a seizure disorder. The animal's service depends on the person's needs. The animal may go for help, or may stand guard over the person during a seizure. Some animals have learned to predict a seizure and warn the person.
Accommodating Persons with Service Animals. Retrieved 10/28/2020. Official copy at http://tristarskyline.policystat.com/
policy/5941628/. Copyright © 2020 TriStar Skyline Medical CenterPage 2 of 6
402

COPY
POLICY STATEMENT
PROCEDURE A. Requirements for Staff
1. Staff cannot ask about the nature of the person's disability, require (or request) any 'proof' of the animal's training (or any other certification) as any inquiry violates various nondiscrimination laws, including the ADA.
If it is NOT readily apparent that the dog is a service animal staff must ONLY ask:
a. IF THE ANIMAL IS REQUIRED BECAUSE OF A DISABILITY? and
b. WHAT WORK OR TASK HAS THE ANIMAL BEEN TRAINED TO PERFORM?
2. Staff CANNOT pet, play with or try to distract the service animal in any way.
3. Staff CANNOT feed or care for the service animal, including toileting.
4. Staff CANNOT charge or require an individual to pay a surcharge in order to accommodate a service animal.
5. Staff should NEVER attempt to separate the service animal from the person with the qualified disability.
6. Staff should ALWAYS remember that the service animal is a working animal and should make every effort to minimize activities that may startle the animal.
B. Requirements of Service Animals and Their Handlers
1. Leash: The service animal must be on a leash, harness or tether at all times, unless either the handler is unable because of a disability to use the harness, leash or other tether; or the use of a
Service animals will be permitted in all areas of the Skyline Medical Center open to the public in accordance with both the Americans with Disabilities Act (ADA) and Section 504 of the Rehabilitation Act (Section 504) and other applicable federal and state laws and regulations prohibiting the discrimination on the basis of a person's disability.
Reasonable modifications must be made to policies, practices and procedures when necessary to accommodate all individuals with a service animal. Generally, this means the waiving of a no animal policy to permit the use of a service animal.
Service animals will be permitted to accompany an individual with a disability to all areas of the Skyline Medical Center where members of the public and/or patients are normally allowed to go, except where the accommodation of the animal would result in a fundamental alteration of the services offered.
Service animals assist with many different tasks, including, but not limited to, assisting individuals who are blind or have low vision with navigation and other tasks, alerting individuals who are deaf or hard-of-hearing to the presence of people or sounds, providing non-violent protection or rescue work, pulling a wheelchair, assisting an individual during a seizure, alerting individuals to the presence of an allergen(s), providing assistance with balance and stability to individuals with mobility disabilities, and helping persons with behavioral health and neurological disabilities by reminding them to take medications or assisting them when they are symptomatic. If an animal meets this definition, it is considered a service animal regardless of whether it has been licensed or certified by a state or local government or a training program.
Accommodating Persons with Service Animals. Retrieved 10/28/2020. Official copy at http://tristarskyline.policystat.com/
policy/5941628/. Copyright © 2020 TriStar Skyline Medical CenterPage 3 of 6
403

COPY
harness, leash or tether would interfere with the service animal's safe, effective performance of the work or task which the service animal was trained to perform. The service animal must still remain under the control of the handler even if the service animal is not on a harness, leash or tether.
2. Under Control of Handler: The handler must be in full control of the animal at all times. The care and supervision of a service animal is solely the responsibility of its handler. If a service animal must be separated from the handler to avoid a fundamental alteration or a threat to safety, it is the responsibility of the handler to arrange for the care and supervision of the animal during the period of separation.
3. Cleanup Rule: The handler must always carry supplies sufficient to clean up the animal's feces. Marked service animal toileting areas should be used when provided.
4. Feeding and Other Care: The handler must provide the service animal with food, water, and other necessary care or make other arrangements for the care of the service animal. Under no
circumstances shall the staff or volunteers care for the service animal.
C. When a Service Animal Can Be Asked to Leave
A person with a disability may only be asked to remove their service animal immediately from the premises if the service animal is out of control and the handler does not take effective action to keep it under control; or the service animal is not house broken.
D. Individualized Assessment
Individuals with disabilities shall be permitted to be accompanied by their service animal in all areas where members of the public and/or patients are permitted to go. However, it may be appropriate to perform an individualized assessment to exclude the service animal from areas such as the operating rooms and burn units where a sterile environment is critical to the services provided.
This assessment shall be based on reasonable judgment that relies on current medical knowledge or on the best available objective evidence to ascertain: the nature, duration and severity of the risk; the probability that a potential injury will actually occur; and whether any reasonable modifications of policies, practices or procedures or the provision of auxiliary aids or services will mitigate the risk.
If it is determined, through an individualized assessment, that the service animal cannot be accommodated; staff shall, upon the request of the patient, arrange for visits between the service animal and the handler in an area of equivalent privacy and amenities.
E. Visitors with Service Animals
Service animals are generally permitted where visitors are permitted unless an individualized assessment is made to exclude a service animal.
Visitors with service animals may not be permitted to access areas that employ greater than general infectious-control measures or when a patient is immunosuppressed. If a determination is made that a service animal cannot be accommodated in a certain area by the use of an individualized assessment; then the visitor will be offered additional accommodations including but not limited to transferring the patient to another comparable room when available to allow unrestricted access. Only if additional accommodations are not available will the visitor be given the option of removing the animal or having friend, family or accompanying persons remove the animal so the visitor may continue with the visit.
F. Emergency Situations
In the event of an emergency, the Emergency Response Team (ERT) that responds should be trained to recognize service animals and to be aware that the animal may be trying to communicate the need for
Accommodating Persons with Service Animals. Retrieved 10/28/2020. Official copy at http://tristarskyline.policystat.com/
policy/5941628/. Copyright © 2020 TriStar Skyline Medical CenterPage 4 of 6
404

COPY
help. The handler and/or animal may be confused from the stressful situation. The ERT should be aware that the animal is trying to be protective and, in its confusion, is not to be considered harmful. The ERT will make every effort to keep the animal with its handler. However, the ERT's first effort is toward the handler; this may necessitate leaving an animal behind in certain emergency evacuation situations. When doing so is possible, the ERT will transport the service animal to a safe location to await being reunited with its handler.
If a patient is unable to care for their service animal and is unable to arrange for someone else to
care for the dog, the Skyline Medical Center may place the dog in a boarding facility until the
patient is released, or make other appropriate arrangements. However, the Skyline Medical Center
must give the patient an opportunity to make arrangements for the dog's care before taking such
steps.
COMPLAINT PROCESS:
RESOURCES: • Rehabilitation Act of 1973, Section 504. • American Disabilities Act of 1990 (42 U.S.C. 12181), including changes made by the ADA Amendments
Act of 2008 (P.L. 110-325). • 28 CFR Part 36, revised as of July 1, 1994 entitled "Non Discrimination on the Basis of Disability by
Public Accommodations and in Commercial Facilities". (http://www.ada.gov/regs2010/titleIII_2010/titleIII_2010_regulations.htm
It is the policy of Skyline Medical Center not to discriminate on the basis of a person's disability in the offering or delivery of healthcare services. An internal grievance procedure has been adopted to provide for the prompt and equitable resolution of complaints alleging any action prohibited by Section 504 of the Rehabilitation Act of 1973 (28 U.S.C. 794), Section 1557 of the Patient Protection and Affordable Care Act (2010) or the Americans with Disabilities Act of 1990 (42 U.S.C. 12181) including changes made by the ADA Amendments Act of 2008 (P.L. 110-325).
Any person who believes he or she has been subjected to discrimination on the basis of his or her disability may file a grievance under this. It is against the law for Skyline Medical Center to retaliate against anyone who files a grievance or participates in the grievance process.
The ECC shall conduct a thorough investigation providing an opportunity for all relevant evidence to be submitted as it relates to the alleged discriminatory act.
The filing of a complaint of discrimination based on a person's disability does not prevent the filing of a complaint with the U.S. Department of Health and Human Services, Office for Civil Rights, electronically through the Office of Civil Rights Complaint Portal, available at:
https://ocrportal.hhs.gov/ocr/portal/lobby.jsf, or by mail or phone at:
U.S. Department of Health and Human Services 200 Independence Avenue, SW Room 509F, HHH Building Washington, DC 20201 1-800-368-1019, 800-537-7697 (TDD)
Complaint forms are available at: http://www.hhs.gov/ocr/office/file/index.html
Accommodating Persons with Service Animals. Retrieved 10/28/2020. Official copy at http://tristarskyline.policystat.com/
policy/5941628/. Copyright © 2020 TriStar Skyline Medical CenterPage 5 of 6
405

COPY
• Access to Services Policy, ADA.001
Attachments
No Attachments
Accommodating Persons with Service Animals. Retrieved 10/28/2020. Official copy at http://tristarskyline.policystat.com/
policy/5941628/. Copyright © 2020 TriStar Skyline Medical CenterPage 6 of 6
406

COPY
Current Status: Active PolicyStat ID: 5909510
Origination: 02/2001 Last Approved: 11/2018 Last Revised: 11/2018 Next Review: 10/2021 Owner: Julie Davis: Volunteer Services
Director Area: Human Resources References:
Accommodations Program for Patients and Families of TriStar Skyline Medical Center
SCOPE:
PURPOSE: 1. To provide an organized structure for meeting the needs of patients/family member (s) on the TriStar
Skyline Medical Center main campus who need overnight accommodations and who do not have the
means to afford the associated costs.
2. To insure a consistent, equitable basis for referral.
3. To fund other patient centered projects as detailed in this policy.
POLICY:
House-wide for TriStar Skyline Medical Center
This program will be administered solely through and at the discretion of Skyline Auxiliary, Inc and approved
by the Skyline Auxiliary President or their designee as funds allow. The policy will provide overnight hotel
accommodations for family member(s) needing these services as determined by the standards set forth in this
document. The person(s) needing this service must be in financial need where all other sources of funding and
family support have been searched and exhausted. The Skyline Auxiliary will maintain a contracted hotel to
provide for adequate services. Transportation to and from the hotel will be arranged for by the patient's family
or by the hospital social worker's department.
Once approved by the Skyline Auxiliary President or designee, funding will be paid directly to the hotel through
a direct billing previous arrangement by the operating funds of the Skyline Auxiliary organization. No cash is
ever given to any patient or their family members. The Skyline Auxiliary will work under a contracted service
agreement and direct billing/ invoice system only. Funding will not exceed $500 per month as combined with
the Friends Fund expenditures. See "Volunteer Accommodations Program Referral Form." Individuals who
use the services provided by this program would be required to sign a document (Travel Liability Release)
releasing Skyline Auxiliary from any liability while the receiving party travels to and from the hotel. Individuals
who do not qualify for this financial assistance will be offered a list of hotels that offer a courtesy of reduced
costs to families of TriStar Skyline Medical Center patients.
Accommodations Program for Patients and Families of TriStar Skyline Medical Center. Retrieved 10/28/2020. Official copy at
http://tristarskyline.policystat.com/policy/5909510/. Copyright © 2020 TriStar Skyline Medical CenterPage 1 of 3
407
www.princexml.com
Prince - Non-commercial License
This document was created with Prince, a great way of getting web content onto paper.

COPY
PROCEDURES: 1. Need may be assessed and referral made by a hospital social worker, case manager, nurse manager,
doctor or supervisor and must be approved by the Auxiliary President or any member of the Auxiliary
Executive Board or their designee. The referring party must have the patient or their family
member(s) fill out a referral form and release of liability form prior to services rendered. Call (615)
769-2200 to request forms. The Director of Volunteers or their designee will talk with the families and will
facilitate the processing of all forms.
2. Referrals must be made during normal business hours, which are Monday through Friday 8 a.m. to 4:00
p.m. A two-hour window of time is needed to process all requests. Accommodations are not arranged
over the weekends.
3. Referred individuals will have a reservation made for them by the Skyline Auxiliary designee only to the
contracted hotel for direct billing purposes. Individuals applying must live outside the seven contiguous
counties surrounding Davidson County (Robertson, Sumner, Wilson, Rutherford, Williamson, Dickson,
and Cheatham). If the need is for the family member, residence will be defined by where the requesting
person in need resides, not necessarily where the patient resides in order for accommodations to be
granted. Any exceptions will be approved or denied by the Skyline Auxiliary President or their designee.
4. Overnight lodging will be restricted to no more than two nights in any given week, but may be re-
evaluated for extenuating circumstances.
5. No more than four members of a family may be accommodated at a time and all will be required to
occupy one room. If this number is violated, accommodations may be cancelled by the Auxiliary President
or their designee.
6. "Family member" is defined as any individual who is the spouse, parent or sibling of the patient or the
caregiver/guardian of the patient.
7. Participants will be required to sign a statement releasing Skyline Auxiliary from any liability for loss of
property, bodily injury or loss of life due to accidents while traveling to/from the hospital or during an
overnight stay in the contracted hotel.
8. Other programs funded by the Accommodations Fund for our TriStar Skyline patients are:
Care Notes for our patients provided in waiting rooms throughout the hospital, Volunteer Visitor patient
necessity products, gifts for patients for Breast Cancer Awareness Month, yarn to produce hand-made
blankets for patients, tray angel materials, and any other programs that are specifically for our hospital
patients as deemed appropriate by the Skyline Auxiliary President, the Skyline Auxiliary Executive Board
of Directors or their designee.
9. Any other additional programs or expenditures in this policy must be approved and voted by the Skyline
Auxiliary Executive Board of Directors before purchase.
10. The Skyline Auxiliary President will oversee the execution of the expenditures for these programs detailed
in this policy whether supported by Grant funding or expensed by the Skyline Auxiliary Organization.
Overall, accumulative funding for this policy will not exceed $500 per month in combination with "The
Friends Fund" for any fiscal year July 1 to June 30th, unless otherwise voted on by the Skyline Auxiliary
Executive Board of Directors.
MISC. REQUESTS FOR FUNDING:
All other request for funding or repeated funding from any other department of TriStar Skyline Medical
Center for misc. items or projects for the fiscal year of July 1st through June 30th must be made in writing
Accommodations Program for Patients and Families of TriStar Skyline Medical Center. Retrieved 10/28/2020. Official copy at
http://tristarskyline.policystat.com/policy/5909510/. Copyright © 2020 TriStar Skyline Medical CenterPage 2 of 3
408

COPY
and submitted to the Skyline Auxiliary before May of any given year to be considered for the new fiscal
year budget beginning July 1st. Submit all requests in writing to the Volunteer Services Office and they
will be transferred to the Skyline Auxiliary Executive Board of Directors for consideration. The Skyline
Auxiliary reviews all requests during their annual planning session, decisions for funding requests will be
addressed, and notification sent in August/September of the fiscal year.
REFERENCES:
Attachments
Volunteer Accommodations Program Referral Form
Attachments:
Volunteer Accommodations Program Referral Form
Pre-PolicyStat Number: IPC.SUP.026
Accommodations Program for Patients and Families of TriStar Skyline Medical Center. Retrieved 10/28/2020. Official copy at
http://tristarskyline.policystat.com/policy/5909510/. Copyright © 2020 TriStar Skyline Medical CenterPage 3 of 3
409

COPY
Current Status: Active PolicyStat ID: 6668041
Origination: 04/2019 Last Approved: 07/2019 Last Revised: 07/2019 Next Review: 07/2022 Owner: Nicholas Howald: xxx Area: Patient Care References:
Accomodating Persons Who are Blind or Have Low Vision
Scope:
Purpose:
RESPONSIBLE PERSONS:
DEFINITIONS: • Auxiliary aid. The term auxiliary aids refers to those auxiliary aids necessary to ensure effective
communication with persons with disabilities and providers so that persons with language needs
are not excluded, denied services, segregated, or otherwise treated differently than other persons
because of the absence of auxiliary aids.
• Effective communication. Communication sufficient to provide individuals that may be blind or have low
Accommodating persons who are blind or have low vision.
To develop a plan that accommodates individuals pursuant to Section 504 of the Rehabilitation Act of 1973,
Section 1557 of the Patient Protection and Affordable Care Act (2010) and the Americans with Disabilities Act
of 2008 which prohibits discrimination on the basis of disability in the delivery of healthcare services. The
regulations implementing the Acts require that people who are blind or have low vision be provided with
auxiliary aids at no cost to allow them an equal opportunity to participate in and benefit from healthcare
services. The decision as to the method to be used for communication requires the input of any individual
requiring auxiliary aids, and their choice must be given primary consideration.
TriStar Skyline Medical Center / TriStar Skyline Madison Campus is committed to compliance with
federal and state laws prohibiting discrimination on the basis of disability in the offering or delivery of
healthcare services. TriStar Skyline Medical Center / TriStar Skyline Madison Campus recognizes
its legal obligation to ensure effective communication with persons with disabilities and makes every
effort to pro-actively assess communication needs as well as providing the most compassionate care.
This policy requires development of a plan that accommodates individuals who are blind or have low vision by
providing auxiliary aids at no cost to allow them an equal opportunity to participate in and benefit from
healthcare services.
All TriStar Skyline Medical Center / TriStar Skyline Madison Campus staff.
Accomodating Persons Who are Blind or Have Low Vision. Retrieved 10/28/2020. Official copy at
http://tristarskyline.policystat.com/policy/6668041/. Copyright © 2020 TriStar Skyline Medical CenterPage 1 of 5
410
www.princexml.com
Prince - Non-commercial License
This document was created with Prince, a great way of getting web content onto paper.

COPY
vision with substantially the same level of services received by individuals who are not blind or have low
vision.
• Language Assistance Services. Oral and written language services needed to assist individuals who
may be blind or have low vision to communicate effectively with staff and to provide such persons
meaningful access to and equal opportunity to, participate fully in the services, activities, or other
programs.
• Low Vision. Even with eyeglasses, contact lenses, medicine or surgery, a person does not see well.
• Meaningful Access. Language assistance that results in accurate, timely, and effective communication
at no cost to the individual who may be blind or have low vision. Meaningful access denotes access that
is not significantly restricted, delayed or inferior as compared to programs or services provided to persons
who are not blind or have low vision.
• Qualified Reader. A qualified reader is a person who is able to read effectively, accurately, and
impartially using any necessary specialized vocabulary.
POLICY:
PROCEDURE: A. Equity Compliance Coordinator
The Equity Compliance Coordinator (ECC) (previously known as the 504 Coordinator/ADA Administrator)
is responsible for the applicable aspects of Section 504 of the Rehabilitation Act of 1973 (28 U.S.C. 794),
Section 1557 of the Patient Protection and Affordable Care Act (2010) and the Americans with Disabilities
Act of 1990 (42 U.S.C. 12181) including changes made by the ADA Amendments Act of 2008 (P.L.
110-325).
The ECC is responsible for the coordination of the required accessibility training, including effective
communication techniques for all staff members annually. They will conduct regular reviews of the
language access needs of the patient population as well as the monitoring and updating of the
implementation of this policy as needed.
B. Identification and Assessment of Need of Persons who may be Blind or have Low Vision
TriStar Skyline Medical Center / TriStar Skyline Madison Campus will identify the language and
communication needs of persons who may be blind or have low vision as needed to ensure effective
communication.
As soon as TriStar Skyline Medical Center / TriStar Skyline Madison Campus becomes aware of such
needs, staff will use the form, “Notice of Auxiliary Aids for Persons who may be Blind or have Low Vision”
TriStar Skyline Medical Center / TriStar Skyline Madison Campus will take appropriate steps to
ensure persons with disabilities, including persons who may be blind or have low vision, have an equal
opportunity to participate in our services, activities and other benefits. The procedures outlined below
are intended to ensure effective communication with patient involving medical conditions, treatment,
services, and benefits. All necessary auxiliary aids and services shall be provided free of charge.
TriStar Skyline Medical Center / TriStar Skyline Madison Campus staff will be provided notice of this policy
and procedure, and staff that may have direct contact with individuals with disabilities will be trained in
effective communication techniques. TriStar Skyline Medical Center / TriStar Skyline Madison Campus
staff will inform all individuals who are blind or have low vision – including individuals seeking access to
services at TriStar Skyline Medical Center / TriStar Skyline Madison Campus and any family member or
friend of such individual who is an appropriate person with whom TriStar Skyline Medical Center / TriStar
Skyline Madison Campus should communicate of the availability, at no cost to them, of auxiliary aids.
Accomodating Persons Who are Blind or Have Low Vision. Retrieved 10/28/2020. Official copy at
http://tristarskyline.policystat.com/policy/6668041/. Copyright © 2020 TriStar Skyline Medical CenterPage 2 of 5
411

COPY
to inform such persons of services and determine what auxiliary aids may be needed to effectively
communicate.
If language services are declined by an individual who may be blind or have low vision, staff will then use
the “Waiver of Auxiliary Aids” to not only document the refusal but also to serve as notice to the individual
that they may still request free auxiliary aids at any time.
The form(s), “Notice of Auxiliary Aids for Persons who may be Blind or have Low Vision” and/or the
“Waiver of Auxiliary Aids” will be included in the patient’s medical record.
C. Providing Notice to Persons who May be Blind or have Low Vision
TriStar Skyline Medical Center / TriStar Skyline Madison Campus shall inform persons that may be blind
or have low vision of the availability of qualified language assistance, free of charge. A nondiscrimination
statement will be posted at intake areas and other points of entry, including but not limited to the
emergency room, outpatient areas, etc.
D. Obtaining Auxiliary Aids
All staff are responsible for obtaining auxiliary aids needed for effective communication. Any and all
agencies under contract (or with other arrangements made) for auxiliary aids are listed in
SECTION VI; the POLICY IMPLEMENTATION section contained within this policy.
E. The Use of Family or Friends for Professional Language Services
Family members or friends will not be used for language assistance unless specifically requested by the
patient and only after an offer of free qualified auxiliary aids is offered and documented by the use of the
form, "Notice of Auxiliary Aids for Persons who are Blind or have Low Vision."
Persons that request (or prefer) the use of a family member or friend for qualified readers or other
language assistance must take into consideration issues of competency, confidentiality, privacy and
conflicts of interest. A "Waiver of Auxiliary Aids" will be used if any language services or auxiliary aids
are provided by persons not procured specifically by the Facility.
Minor children or other patients will not be used to interpret in order to ensure the confidentiality of
information and effective communication.
If a family member or friend is not competent or appropriate for any of the previous reasons then
auxiliary aids must be provided to ensure effective communication.
F. Providing Written Translation
The ECC will coordinate the translation of vital documents into alternative formats as needed which shall
be provided free of charge to persons who may be blind or have low vision.
G. Monitoring Language Needs and ImplementationThe ECC will assess changes in the demographics,
types of services or other needs that may require modifications to the implementation of this policy.
Regular assessment of the effectiveness of these procedures, equipment necessary for the delivery of
qualified language services and the complaint process will be conducted.
POLICY IMPLEMENTATION:
1. Vendor: Stratus
2. Services Available via iPad (available through bed management offices)
3. Available 24/7
4. Procedure: Devices are available on all floors/units. If not availabile/if in use:
a. Sign out Status iPad in Bed Management offices
b. Utilize instruction on iPad stand hangtag
Accomodating Persons Who are Blind or Have Low Vision. Retrieved 10/28/2020. Official copy at
http://tristarskyline.policystat.com/policy/6668041/. Copyright © 2020 TriStar Skyline Medical CenterPage 3 of 5
412

COPY
c. Return equipment and sign-in
COMPLAINT PROCESS:
DOCUMENTATION:
It is the policy of TriStar Skyline Medical Center / TriStar Skyline Madison Campus not to discriminate
on the basis of a person’s disability in the offering or delivery of healthcare services. An internal grievance
procedure has been adopted to provide for the prompt and equitable resolution of complaints alleging any
action prohibited by Section 504 of the Rehabilitation Act of 1973 (28 U.S.C. 794), Section 1557 of the
Patient Protection and Affordable Care Act (2010) and the Americans with Disabilities Act of 1990 (42
U.S.C. 12181) including changes made by the ADA Amendments Act of 2008 (P.L. 110-325).
Any person who believes he or she has been subjected to discrimination on the basis of his or her
disability may file a grievance under this procedure [or under the regular TriStar Skyline Medical Center /
TriStar Skyline Madison Campus grievance policy]. It is against the law for TriStar Skyline Medical
Center / TriStar Skyline Madison Campus to retaliate against anyone who files a grievance or
participates in the grievance process.
The ECC will make appropriate arrangements so that persons who may be Blind or have low vision are
provided other accommodations if needed to participate in the grievance process.
The ECC shall conduct a thorough investigation providing an opportunity for all relevant evidence to be
submitted as it relates to the alleged discriminatory act.
The filing of a complaint of discrimination based on a person's disability does not prevent the filing of a
complaint with the U.S. Department of Health and Human Services, Office for Civil Rights, electronically
through the Office of Civil Rights Complaint Portal, available at:
https://ocrportal.hhs.gov/ocr/portal/lobby.jsf, or by mail or phone at:
U.S. Department of Health and Human Services
200 Independence Avenue, SW
Room 509F, HHH Building
Washington, DC 20201
1-800-368-1019 , 800-537-7697 (TDD)
Complaint forms are available at: http://www.hhs.gov/ocr/office/file/index.html
Any and all contacts with auxiliary aid agencies must be documented in patient records. The staff member will
document in the medical record that assistance has been provided, offered or refused by the use of the form,
"Notice of Auxiliary Aids for Persons who may be Blind or have Low Vision" which is attached to this
policy.
A "Waiver of Auxiliary Aids" will be used if any language services are refused by an individual who may be
blind or have low vision.
Accomodating Persons Who are Blind or Have Low Vision. Retrieved 10/28/2020. Official copy at
http://tristarskyline.policystat.com/policy/6668041/. Copyright © 2020 TriStar Skyline Medical CenterPage 4 of 5
413

COPY
RESOURCES: • Language Services Providers (approved by HealthTrust).
• Comprehensive Accreditation Manual for Hospitals, 2000.
• Rehabilitation Act of 1973, Section 504.
• American Disabilities Act of 1990 (42 U.S.C. 12181), including changes made by the ADA Amendments
Act of 2008 (P.L. 110-325).
• 28 CFR Part 36, revised as of July 1, 1994 entitled "Non Discrimination on the Basis of Disability by
Public Accommodations and in Commercial Facilities". (http://www.ada.gov/regs2010/titleIII_2010/
titleIII_2010_regulations.htm
• Access to Services Policy, ADA.001
Attachments
Notice of Auxillary Aides.pdf
Waiver of Auxillary Aides.pdf
Approval Signatures
Approver Date
Christine Staigl: CNO 07/2019
Shelley Sircy: Chief Quality/Patient Safety Officer 07/2019
John Franck: Associate Administrator 07/2019
Accomodating Persons Who are Blind or Have Low Vision. Retrieved 10/28/2020. Official copy at
http://tristarskyline.policystat.com/policy/6668041/. Copyright © 2020 TriStar Skyline Medical CenterPage 5 of 5
414

COPY
Current Status: Active PolicyStat ID: 6668031
Origination: 04/2019 Last Approved: 07/2019 Last Revised: 07/2019 Next Review: 07/2022 Owner: Nicholas Howald: xxx Area: Patient Care References:
Accomodating Persons Who are Deaf or Hard-of-Hearing
Scope:
Purpose:
A. This policy requires development of a language access plan that accommodates individuals who are deaf
or hard-of-hearing by providing free auxiliary aids in order to ensure equal opportunity to participate in and
benefit from healthcare services.
RESPONSIBLE PERSONS:
DEFINITIONS:
A. Auxiliary aid. Auxiliary aids may include video remote interpreting (VRI) or face-to-face sign-
language interpreters, flash cards, communication boards, telephone amplifiers, amplified hearing
devices, assisted listening devices, or a TDD/TTY.. Lip reading, note writing, and use of finger
spelling or gestures may also aid communication but are not a replacement for interpreters.
Accommodating persons who are deaf or hard-of-hearing.
To develop a plan that accommodates individuals pursuant to Section 504 of the Rehabilitation Act of
1973, Section 1557 of the Patient Protection and Affordable Care Act (ACA 2010) and the Americans
with Disabilities Act of 2008 which prohibits discrimination on the basis of disability in the offering or
delivery of healthcare services. The regulation implementing the Acts requires that persons who are
deaf or hard-of hearing be provided with auxiliary aids at no cost to allow them an equal opportunity to
participate in and benefit from healthcare services. The decision as to the method to be used for
communication requires the input of any individual requiring auxiliary aids, and their choice must be
given primary consideration.
TriStar Skyline Medical Center / TriStar Skyline Madison Campus is committed to compliance with
federal and state laws prohibiting discrimination on the basis of disability in the offering or delivery of
healthcare services. TriStar Skyline Medical Center / TriStar Skyline Madison Campus recognizes
its legal obligation to ensure effective communication with persons with disabilities and makes every
effort to pro-actively assess communication needs as well as providing the most compassionate care.
All TriStar Skyline Medical Center / TriStar Skyline Madison Campus staff.
Accomodating Persons Who are Deaf or Hard-of-Hearing. Retrieved 10/28/2020. Official copy at
http://tristarskyline.policystat.com/policy/6668031/. Copyright © 2020 TriStar Skyline Medical CenterPage 1 of 6
415
www.princexml.com
Prince - Non-commercial License
This document was created with Prince, a great way of getting web content onto paper.

COPY
B. Effective communication. Communication sufficient to provide individuals that may be deaf or hard-of-
hearing with substantially the same level of services received by individuals who are not deaf or hard-of-
hearing.
C. Interpretation. The act of listening to a communication in one language (source language) and orally
converting it to another language (target language) while retaining the same meaning.
D. Language Assistance Services. Oral and written language services needed to assist individuals who
may be deaf or hard-of-hearing to communicate effectively with staff and to provide persons who are deaf
or hard-of-hearing meaningful access to and equal opportunity to, participate fully in the services,
activities, or other programs.
E. Meaningful Access. Language assistance that results in accurate, timely, and effective communication
at no cost to the individual who may be deaf or hard-of-hearing. Meaningful access denotes access that is
not significantly restricted, delayed or inferior as compared to programs or services provided to persons
who are not deaf or hard-of-hearing.
F. Qualified Interpreter. A qualified interpreter (or translator) is an interpreter who has had their specialized
vocabulary (medical or legal terminology) proficiency assessed. A qualified interpreter is able to interpret
effectively, accurately and impartially both receptively and expressively, using any necessary specialized
vocabulary. No certification is needed to be a qualified interpreter and certified interpreters are not
automatically qualified interpreters despite their training and certification. An interpreter's qualification is
based on his/her ability to communicate effectively in a specific situation such as in a healthcare setting
using complex medical terminology and processes.
POLICY STATEMENT:
PROCEDURE: A. Equity Compliance Coordinator
The Equity Compliance Coordinator (ECC) (previously known as the 504 Coordinator/ADA Administrator)
is responsible for the applicable aspects of Section 504 of the Rehabilitation Act of 1973 (28 U.S.C. 794),
Section 1557 of the Patient Protection and Affordable Care Act (2010) and the Americans with Disabilities
Act of 1990 (42 U.S.C. 12181) including changes made by the ADA Amendments Act of 2008 (P.L.
110-325).
TriStar Skyline Medical Center / TriStar Skyline Madison Campus will take appropriate steps to
ensure persons with disabilities, including persons who may be deaf or hard-of-hearing, have an equal
opportunity to participate in our services, activities and other benefits. The procedures outlined below
are intended to ensure the effective communication with all individuals involving medical conditions,
treatment, services and benefits. All necessary language assistance services shall be provided free of
charge.
TriStar Skyline Medical Center / TriStar Skyline Madison Campus staff will be provided notice of this policy
and procedure. Staff that may have direct contact with individuals with disabilities will be trained in effective
communication techniques. TriStar Skyline Medical Center / TriStar Skyline Madison Campus staff will
inform individuals who may be deaf or hard-of-hearing – including individuals seeking access to services at
TriStar Skyline Medical Center / TriStar Skyline Madison Campus and any family member or friend of such
individual who is an appropriate person with whom TriStar Skyline Medical Center / TriStar Skyline
Madison Campus should communicate - of the availability, at no cost to them, of language services in order
to effectively communicate.
Accomodating Persons Who are Deaf or Hard-of-Hearing. Retrieved 10/28/2020. Official copy at
http://tristarskyline.policystat.com/policy/6668031/. Copyright © 2020 TriStar Skyline Medical CenterPage 2 of 6
416

COPY
The ECC is responsible for the coordination of the required accessibility training, including effective
communication techniques for all staff members annually. They will conduct regular reviews of the
language access needs of the patient population as well as the monitoring and updating of the
implementation of this policy as needed.
B. Identification and Assessment of Persons who may be Deaf or Hard-of-Hearing
TriStar Skyline Medical Center / TriStar Skyline Madison Campus will identify the language and
communication needs of persons who may be deaf or hard-of-hearing as needed to ensure effective
communication.
As soon as TriStar Skyline Medical Center / TriStar Skyline Madison Campus becomes aware of such
needs, staff will use the form, “Services for Persons Who are Deaf or Hard-of-Hearing” to inform such
persons of services and determine what language assistance services may be needed.
If language services are declined by an individual who may be deaf or hard-of-hearing, staff will then use
the “Waiver of Language Assistance” to not only document the refusal but also to serve as notice to the
individual that they may still request a free qualified interpreter at any time.
The form(s), “Services for Persons Who are Deaf or Hard-of-Hearing” and/or the form, “Waiver of
Language Assistance” will be included in the patient’s medical record.
C. Providing Notice to Persons who May be Deaf or Hard-of-Hearing
Skyline Medical Center / TriStar Skyline Madison shall inform persons who may be Deaf or Hard of
Hearing of the availability of free qualified language assistance. A nondiscrimination statement will be
posted at intake areas and other points of entry, including but not limited to the emergency room,
admitting and outpatient areas.
D. Obtaining a Qualified Interpreter All staff are responsible for obtaining a qualified interpreter when
needed to effectively communicate. Any and all agencies under contract (or with other arrangements
made) for professional language assistance are listed in SECTION VI; the POLICY
IMPLEMENTATION section contained within this policy.
1. If a person uses sign language, all medical and psychiatric evaluations or discussions regarding a
patient's symptoms, treatment (including individual and group psychotherapy), diagnosis, progress,
and prognosis must be communicated through the use of a qualified sign language interpreter.
2. Examples of situations where an interpreter may be required (this list is not exhaustive):
a. Determining a patient's history or description of ailment or injury;
b. Obtaining informed consent or permission for treatment;
c. Provision of patient's rights;
d. Explanation of living wills or powers of attorney (or their availability);
e. Diagnosis or prognosis of ailments or injures;
f. Explanation of procedures, tests, treatment, treatment options or surgery;
g. Explaining the administration and side effects of medications, including side effects and food or
drug interactions;
h. Discharge instructions or planning;
i. Explaining and discussing advance directives;
j. Explaining blood donations or aphaeresis;
k. Explaining follow-up treatment, test results, or recovery;
Accomodating Persons Who are Deaf or Hard-of-Hearing. Retrieved 10/28/2020. Official copy at
http://tristarskyline.policystat.com/policy/6668031/. Copyright © 2020 TriStar Skyline Medical CenterPage 3 of 6
417

COPY
l. Discussing billing and insurance issues; and
m. During educational presentations, such as classes concerning birthing, nutrition, CPR, and
weight management.
E. The Use of Family or Friends for Professional Language Services
1. Family members or friends will not be used for language assistance except:
a. in an emergency involving an imminent threat to the safety or welfare of an individual or the
public where there is no interpreter available; or
b. where the individual in need of communication services specifically requests that the
accompanying adult interpret or facilitate communication, the accompanying adult agrees to
provide such assistance, and reliance on that adult for such assistance is appropriate under the
circumstances.
2. Except in an emergency, family members or friends may be used for language assistance only after
an offer of free qualified language assistance is offered and documented by the use of the form,
"Services for Persons Who are Deaf or Hard of Hearing."
3. A "Waiver of Language Assistance" will be used if any language services are provided by persons
not procured by the Facility.
4. Minor children or other patients will not be used to interpret in order to ensure the confidentiality of
information and effective communication.
5. If a family member or friend is not competent or appropriate for any of the previous reasons
then a qualified interpreter must be provided to ensure effective communication.
F. Providing Written Translation
The ECC will coordinate the translation of vital documents into alternative formats as needed which shall
be provided free of charge to persons who may be deaf or hard-of-hearing.
G. Monitoring Language Needs and Implementation The ECC will assess changes in the demographics,
types of services or other needs that may require modifications to the implementation of this policy.
Regular assessment of the effectiveness of these procedures, equipment necessary for the delivery of
qualified language services and the complaint process will be conducted.
POLICY IMPLEMENTATION:
1. Vendor: Stratus
2. Services Available via iPad (available through bed management offices)
3. Available 24/7
4. Procedure: Devices are available on all floors/units: If not available/if in use:
a. Sign out Status iPad in Bed Management offices
b. Utilize instruction on iPad stand hangtag
c. Return equipment and sign-in
COMPLAINT PROCESS:
It is the policy of TriStar Skyline Medical Center / TriStar Skyline Madison Campus not to
discriminate on the basis of a person’s disability. An internal grievance procedure has been adopted to
provide for the prompt and equitable resolution of complaints alleging any action prohibited by Section
Accomodating Persons Who are Deaf or Hard-of-Hearing. Retrieved 10/28/2020. Official copy at
http://tristarskyline.policystat.com/policy/6668031/. Copyright © 2020 TriStar Skyline Medical CenterPage 4 of 6
418

COPYDOCUMENTATION:
RESOURCES:
• Language Services Providers (approved by HealthTrust).
• Comprehensive Accreditation Manual for Hospitals, 2000.
• Rehabilitation Act of 1973, Section 504.
• American Disabilities Act of 1990 (42 U.S.C. 12181), including changes made by the ADA Amendments
Act of 2008 (P.L. 110-325).
• 28 CFR Part 36, revised as of July 1, 1994 entitled "Non Discrimination on the Basis of Disability by
Public Accommodations and in Commercial Facilities". (http://www.ada.gov/regs2010/titleIII_2010/
titleIII_2010_regulations.htm
• Access to Services Policy, ADA.001
504 of the Rehabilitation Act of 1973 (28 U.S.C. 794), Section 1557 of the Patient Protection and
Affordable Care Act (2010) and the Americans with Disabilities Act of 1990 (42 U.S.C. 12181) including
changes made by the ADA Amendments Act of 2008 (P.L. 110-325).
Any person who believes he or she has been subjected to discrimination on the basis of his or her
disability may file a grievance under this procedure [or under the regular TriStar Skyline Medical
Center / TriStar Skyline Madison Campus grievance policy]. It is against the law for TriStar Skyline
Medical Center / TriStar Skyline Madison Campus to retaliate against anyone who files a grievance
or participates in the grievance process.
The ECC will make appropriate arrangements so that persons who may be deaf or hard-of-hearing are
provided other accommodations if needed to participate in the grievance process.
The ECC shall conduct a thorough investigation providing an opportunity for all relevant evidence to be
submitted as it relates to the alleged discriminatory act.
The filing of a complaint of discrimination based on a person's disability does not prevent the filing of a
complaint with the U.S. Department of Health and Human Services, Office for Civil Rights, electronically
through the Office of Civil Rights Complaint Portal, available at:
https://ocrportal.hhs.gov/ocr/portal/lobby.jsf, or by mail or phone at:
U.S. Department of Health and Human Services
200 Independence Avenue, SW
Room 509F, HHH Building
Washington, DC 20201
1-800-368-1019 , 800-537-7697 (TDD)
Complaint forms are available at: http://www.hhs.gov/ocr/office/file/index.html
Any and all contacts with interpreting agencies must be documented in patient records. The staff member will
document in the medical record that assistance has been provided, offered or refused by the use of the form
"Services for Persons Who are Deaf or Hard of Hearing" which is attached to this policy.
A "Waiver of Language Assistance" will be used if any language services are refused by an individual who
may be deaf or hard-of-hearing.
Accomodating Persons Who are Deaf or Hard-of-Hearing. Retrieved 10/28/2020. Official copy at
http://tristarskyline.policystat.com/policy/6668031/. Copyright © 2020 TriStar Skyline Medical CenterPage 5 of 6
419

COPY
Attachments
Services for Deaf or Hard of Hearing.pdf
Waiver of Language.pdf
Approval Signatures
Approver Date
Christine Staigl: CNO 07/2019
Shelley Sircy: Chief Quality/Patient Safety Officer 07/2019
John Franck: Associate Administrator 07/2019
Accomodating Persons Who are Deaf or Hard-of-Hearing. Retrieved 10/28/2020. Official copy at
http://tristarskyline.policystat.com/policy/6668031/. Copyright © 2020 TriStar Skyline Medical CenterPage 6 of 6
420

COPY
Current Status: Active PolicyStat ID: 6668019
Origination: 07/2019 Last Approved: 09/2019 Last Revised: 09/2019 Next Review: 09/2022 Owner: Nicholas Howald: xxx Area: Patient Care References:
Accomodating Persons with Limited English Proficiency
Scope:
Purpose:
RESPONSIBLE PERSONS:
DEFINITIONS: A. Effective Communication. Communication sufficient to provide the individual with limited English
proficiency with substantially the same level of services received by individuals who are not limited in
English proficiency.
Accommodating persons with limited English proficiency.
To develop effective guidelines, consistent with Section 504 of the Rehabilitation Act of 1973 (28 U.S.C
794), Section 1557 of the Patient Protection and Affordable Care Act (2010) and Executive Order 13166
which requires persons with limited English proficiency (LEP) have “meaningful access” to healthcare
services. Recipients of federal financial assistance are prohibited from discriminating based on a person’s
primary (or preferred) language, among other things, failing to provide meaningful access to individuals
with limited English proficiency (LEP). Federal fund recipients must also provide the translation of vital
documents as part of their language assistance services when necessary to ensure the patient’s access to
important written information. Failure to properly assess and subsequently provide a reasonable
accommodation is punishable by fine to the provider.
TriStar Skyline Medical Center / TriStar Skyline Madison Campus is committed to compliance with
federal and state laws prohibiting discrimination on the basis of disability. TriStar Skyline Medical Center
/ TriStar Skyline Madison Campus recognizes its legal obligation to ensure effective communication with
persons with disabilities and makes every effort to pro-actively assess communication needs as well as
providing the most compassionate care.
This policy requires the development of a language access plan that accommodates persons with LEP in
order to ensure them meaningful access to participate in and benefit from healthcare services.
All TriStar Skyline Medical Center / TriStar Skyline Madison Campus staff.
Accomodating Persons with Limited English Proficiency. Retrieved 10/28/2020. Official copy at
http://tristarskyline.policystat.com/policy/6668019/. Copyright © 2020 TriStar Skyline Medical CenterPage 1 of 6
421
www.princexml.com
Prince - Non-commercial License
This document was created with Prince, a great way of getting web content onto paper.

COPY
B. Interpretation. The act of listening to a communication in one language (source language) and orally
converting it to another language (target language) while retaining the same meaning.
C. LEP is the acronym for both "Limited English Proficiency" and "Limited English Proficient." The U.S.
Census Bureau's operational definition for LEP is a patient's self-assessed ability to speak English less
than "very well." Individuals who do not speak English as the primary (or preferred) language and who
have limited ability to read, write, speak, or understand English. Individuals with LEP may be competent in
English for certain types of communication (like speaking) but still be with LEP for other purposes (like
reading or writing).
D. Language Assistance Services. Oral and written language services needed to assist individuals with
LEP to communicate effectively with staff and to provide individuals with LEP meaningful access and
equal opportunity to participate fully in the services, activities, or other programs.
E. Meaningful Access. Language assistance that results in accurate, timely, and effective communication
at no cost to the individual with LEP. Meaningful access denotes access that is not significantly restricted,
delayed or inferior as compared to programs or services provided to persons who are proficient in the
English language.
F. Primary Language. An individual's primary language is the language in which the individual most
effectively communicates.
G. Qualified Interpreter or Translator. A qualified interpreter (or translator) is an interpreter who has had
their specialized vocabulary (medical or legal terminology) proficiency assessed.
H. Translation. The replacement of written text from one language (source language) to an equivalent
written text in another language (target language).
I. Vital Documents. A document will be considered vital if it contains information that is critical for obtaining
federal services and/or benefits, or is required by law.
POLICY STATEMENT:
PROCEDURE: A. Equity Compliance Coordinator
The Equity Compliance Coordinator (ECC) (previously known as the 504 Coordinator/ADA Administrator)
is responsible for the applicable aspects of Section 504 of the Rehabilitation Act of 1973 (28 U.S.C. 794),
Section 1557 of the Patient Protection and Affordable Care Act (2010) and Executive Order 13166.
The ECC is also responsible for the coordination of the required accessibility training, including effective
TriStar Skyline Medical Center / TriStar Skyline Madison Campus will take reasonable steps to ensure
that persons with LEP have meaningful access and an equal opportunity to participate in services,
activities, programs and any other benefits offered.
This policy also provides for the communication of information contained in vital documents. All necessary
qualified language assistance shall be provided free of charge. Language assistance will be provided through
the use of qualified interpreters with local organizations or contracted national vendors as well as video remote
interpreting (VRI) and telephonic interpreting.
TriStar Skyline Medical Center / TriStar Skyline Madison Campus staff will be provided notice of this
policy and procedure and will be trained on effective communication techniques. Staff will inform all
individuals with LEP, of the availability, at no cost, of qualified language assistance.
Accomodating Persons with Limited English Proficiency. Retrieved 10/28/2020. Official copy at
http://tristarskyline.policystat.com/policy/6668019/. Copyright © 2020 TriStar Skyline Medical CenterPage 2 of 6
422

COPY
communication techniques for all staff members annually. The Coordinator will oversee the required
translation of vital documents and the postings of notices of nondiscrimination and associated 'taglines' in
various languages spoken in the local area.
The ECC will conduct regular reviews of the language access needs of the patient population as well as
the monitoring and updating of the implementation of this policy as needed.
B. Identification of Persons who may be LEP
TriStar Skyline Medical Center / TriStar Skyline Madison Campus will identify the language and
communication needs of persons with LEP as needed to ensure effective communication. If necessary,
staff may use a language identification card (or “I speak” cards – which are available at www.lep.gov) or
posters to determine the preferred language of the patient (or person involved in healthcare decisions).
As soon as TriStar Skyline Medical Center / TriStar Skyline Madison Campus becomes aware of such
needs, staff will use the form, “Notice of Language Assistance Services” to inform such persons of
services and determine what language services may be needed.
If language services are declined by an individual with LEP, staff will then use the “Waiver of Language
Assistance” to not only document the refusal but also to serve as notice to the individual that they may still
request a free qualified interpreter at any time.
The form(s), “Notice of Language Assistance Services” and/or the form, “Waiver of Language Assistance”
will be included in the patient’s medical record..
C. Providing Notice to Persons with LEP
TriStar Skyline Medical Center / TriStar Skyline Madison Campus shall inform persons with LEP of the
availability of qualified language assistance, free of charge, by providing written notice in the primary (or
preferred) language of the individual with LEP. The Taglines will be posted in fifteen (15) languages
spoken in the community served. At a minimum, notices and signs will be posted at intake areas and
other points of entry, including but not limited to the emergency room, admitting and outpatient areas.
D. Obtaining a Qualified Interpreter
All staff are responsible for obtaining a qualified interpreter when needed to ensure effective
communication. Any and all agencies under contract (or with other arrangements made) for
professional language assistance are listed in SECTION VI; the POLICY IMPLEMENTATION
section contained within this policy.
E. The Use of Family or Friends for Professional Language Services
1. Family members or friends will not be used for language assistance except:
a. in an emergency involving an imminent threat to the safety or welfare of an individual or the
public where there is no interpreter available; or
b. where the individual in need of communication services specifically requests that the
accompanying adult interpret or facilitate communication, the accompanying adult agrees to
provide such assistance, and reliance on that adult for such assistance is appropriate under the
circumstances.
2. Except in an emergency, family members or friends may be used for language assistance only after
an offer of free qualified language assistance is offered and documented by the use of the form,
"Notice of Language Assistance."
3. A "Waiver of Language Assistance" will be used if any language services are provided by persons
not procured by the Facility.
4. Minor children or other patients will not be used to interpret in order to ensure the confidentiality of
information and effective communication.
Accomodating Persons with Limited English Proficiency. Retrieved 10/28/2020. Official copy at
http://tristarskyline.policystat.com/policy/6668019/. Copyright © 2020 TriStar Skyline Medical CenterPage 3 of 6
423

COPY
5. If a family member or friend is not competent or appropriate for any of the previous reasons
then a qualified interpreter may be provided to ensure effective communication.
F. Providing Written Translation
The ECC will coordinate the translation of vital documents into the appropriate frequently encountered
languages as needed. The translation of other written materials, as well as the written notice of availability
of translation services, shall be provided free of charge to persons with LEP.
G. Monitoring Language Needs and
Implementation The ECC
will assess changes in the demographics, types of services or other needs that may require modifications
to the implementation of this policy. Regular assessment of the effectiveness of these procedures,
equipment necessary for the delivery of qualified language services and the complaint process will be
conducted.
POLICY IMPLEMENTATION:
1. Vendor: Stratus
2. Services Available via Stratus iPad
3. Available 24/7
4. Procedure: Devices are available on all floors/units at both Main and Madison.
5. At TriStar Skyline Medical Center only, If device is not available/if in use:
a. Sign out Status iPad in Bed Management offices
b. Utilize instruction on iPad stand hang-tag
c. Return equipment and sign-in
COMPLAINT PROCESS:
It is the policy of TriStar Skyline Medical Center / TriStar Skyline Madison Campus not to discriminate
on the basis of a person’s preferred or primary language. An internal grievance procedure has been
adopted to provide for the prompt and equitable resolution of complaints alleging any action prohibited by
Section 504 of the Rehabilitation Act of 1974 (29 U.S.C. 794), Section 1557 of the Patient Protection and
Affordable Care Act or the U.S. Department of Health and Human Services regulations implementing the
Acts.
Any person who believes he or she has been subjected to discrimination on the basis of his or her primary
or preferred language may file a grievance under this procedure [or under the regular TriStar Skyline
Medical Center / TriStar Skyline Madison Campus grievance policy]. It is against the law for TriStar
Skyline Medical Center / TriStar Skyline Madison Campus to retaliate against anyone who files a
grievance or participates in the grievance process.
The ECC will make appropriate arrangements so that persons with LEP are provided other accommodations if
needed to participate in the grievance process.
The ECC shall conduct a thorough investigation providing an opportunity for all relevant evidence to be
submitted as it relates to the alleged discriminatory act.
The filing of a complaint of discrimination based on a person's LEP does not prevent the filing of a complaint
Accomodating Persons with Limited English Proficiency. Retrieved 10/28/2020. Official copy at
http://tristarskyline.policystat.com/policy/6668019/. Copyright © 2020 TriStar Skyline Medical CenterPage 4 of 6
424

COPY
DOCUMENTATION:
RESOURCES:
1. Language Services Providers (approved by HealthTrust).
2. Rehabilitation Act of 1973, Section 504 (29 U.S.C. 794).
3. 28 CFR Part 36, revised as of July 1, 1994 entitled "Non Discrimination on the Basis of Disability by
Public Accommodations and in Commercial Facilities". (http://www.ada.gov/regs2010/titleIII_2010/
titleIII_2010_regulations.htm
4. Effective Communication Resources for Health Providers: http://www.hhs.gov/civil-rights/for-individuals/
special-topics/hospitals-effective-communication/limited-english-proficiency/index.html
5. Language Access Assessment and Planning Tool for Federally Conducted and Federally Assisted
Programs: Federal Coordination and Compliance Section of the Civil Rights Division of the U. S.
Department of Justice.
6. Access to Services Policy, ADA. 001
Attachments
Notice of Language Assistance.pdf
Waiver of Language.pdf
with the U.S. Department of Health and Human Services, Office for Civil Rights, electronically through the
Office of Civil Rights Complaint Portal, available at:
https://ocrportal.hhs.gov/ocr/portal/lobby.jsf, or by mail or phone at:
U.S. Department of Health and Human Services
200 Independence Avenue, SW
Room 509F, HHH Building
Washington, DC 20201
1-800-368-1019 , 800-537-7697 (TDD)
Complaint forms are available at: http://www.hhs.gov/ocr/office/file/index.html
Any and all contacts with interpreting agencies must be documented in patient records. The staff member will
document in the medical record that assistance has been provided, offered or refused by the use of the form,
"Notice of Language Assistance Services" which is attached to this policy.
A "Waiver of Language Assistance" will be used if any language services are refused by an individual with
LEP.
Accomodating Persons with Limited English Proficiency. Retrieved 10/28/2020. Official copy at
http://tristarskyline.policystat.com/policy/6668019/. Copyright © 2020 TriStar Skyline Medical CenterPage 5 of 6
425

COPY
Approval Signatures
Approver Date
Mark Fisher: Madison COO/ECO 09/2019
Christine Staigl: CNO 09/2019
Shelley Sircy: Chief Quality/Patient Safety Officer 09/2019
Mark Fisher: Madison COO/ECO 09/2019
Susan Sullivan: Madison - Director of Nursing 09/2019
John Franck: Associate Administrator 09/2019
Accomodating Persons with Limited English Proficiency. Retrieved 10/28/2020. Official copy at
http://tristarskyline.policystat.com/policy/6668019/. Copyright © 2020 TriStar Skyline Medical CenterPage 6 of 6
426

COPY
Current Status: Active PolicyStat ID: 6824057
Origination: 04/2019 Last Approved: 08/2019 Last Revised: 08/2019 Next Review: 08/2022 Owner: Nicholas Howald: xxx Area: Patient Care References:
Accomodating Persons with Service Animals
Scope:
Purpose:
I. RESPONSIBLE PERSONS
All Skyline Medical Center staff.
DEFINITIONS A. Disability. A person must meet the statutory definition of having a "disability," under federal, state and/or local laws. These
statutes recognize the following broad categories of disabilities:
B. A sensory, mental, or physical impairment that substantially limits one or more major life activities (such as walking, seeing, hearing, speaking and breathing, working, learning, caring for one's self, performing manual tasks, etc.).
C. A sensory, mental or physical condition that is medically cognizable or diagnosable.
D. Handler. A person with a service or therapy animal.
E. Individualized Assessment. An individualized assessment of a service animal must be made by the Equity Compliance Coordinator (ECC) (previously referred to as the 504 Coordinator/ADA Administrator ) or other designee prior to excluding the service animal and is based on reasonable judgment that relies on current medical knowledge or on the best available objective evidence, to ascertain: the nature, duration, and severity of the risk; the probability that the potential injury will actually occur; and whether reasonable modifications of policies, practices, or procedures or the provision of auxiliary aids will mitigate the risk. [28 C.F.R §36.208(b); 28 C.F.R. §35.139(b)]
F. Pet/Comfort Animal. A domestic animal kept for pleasure or companionship. Pets are generally not permitted in the Skyline Medical Center. Permission may be granted by Administration for a pet to be in a campus facility for a specific reason at a specific time.
G. Service Animal. Any dog (or miniature horse) individually trained to do work or perform tasks directly related to the disability that the individual has. A service animal meets the definition of a service animal regardless of the terminology used to describe it. A
Accommodating persons with service animals.
To develop a plan that accommodates individuals pursuant to Section 504 of the Rehabilitation Act of 1973, Section 1557 of the Patient Protection and Affordable Care Act (2010) and the Americans with Disabilities Act of 2008 which prohibits discrimination on the basis of disability in the offering and delivery of healthcare services.
Skyline Medical Center is committed to compliance with federal and state laws prohibiting discrimination on the basis of disability in the offering and delivery of healthcare. Skyline Medical Center recognizes its legal obligation to accommodate service animals and makes every effort to pro-actively assess the accommodation needs as well as providing the most compassionate care.
Service animals are dogs (or miniature horses) that are individually trained to assist people with disabilities. The Americans with Disabilities Act (ADA) definition of service animals is any "dog/miniature horse individually trained to do work or perform tasks for the benefit of an individual with a disability, including a physical, sensory, psychiatric, intellectual, or other mental disability." The work or tasks performed by a service animal must be directly related to an individual's disability.
This policy requires the development of a plan to ensure that persons using service animals have an equal opportunity to participate in and benefit from healthcare services. This policy specifically differentiates "service animals" from "therapy animals," and describes types of service dogs, as well as sets behavioral guidelines.
Accomodating Persons with Service Animals. Retrieved 10/28/2020. Official copy at http://tristarskyline.policystat.com/policy/
6824057/. Copyright © 2020 TriStar Skyline Medical CenterPage 1 of 5
427
www.princexml.com
Prince - Non-commercial License
This document was created with Prince, a great way of getting web content onto paper.

COPY
service animal is sometimes also called an assistance animal. (Non-inclusive list of more common types of service animals: Section H). If there is a question about whether an animal is a service animal, contact the ECC.
H. Therapy Animal. An animal with good temperament and disposition, and who has reliable, predictable behavior, selected to visit people with disabilities or people who are experiencing the frailties of aging as a therapy tool. The animal may be incorporated as an integral part of a treatment process. A therapy animal has not been trained to assist an individual with a disability with work or tasks. The therapy animal does not accompany a person with a disability all the time, unlike a service animal that is always with its handler. Thus, a therapy animal is not a service animal.
I. Service Animal in Training. A dog or miniature horse, undergoing training to become a service animal. A trainee will be housebroken and fully socialized. To be fully socialized means the animal will not, except under rare occasions, bark, yip, growl or make disruptive noises; will have a good temperament and disposition; will not show fear; will not be upset or agitated when it sees another animal; and will not be aggressive. A trainee will be under the control of the handler, who may or may not have a disability. If the trainee begins to show improper behavior, the handler will act immediately to correct the animal or will remove the animal from the premises. There is no federal obligation to accommodate service animals that are still in training.
J. TYPES OF SERVICE ANIMALS
◦ There are many different types of services animals. A non-inclusive list of some of the most common service animals is below:
• A guide service dog is trained to assist in navigation and other tasks for a person who is legally blind or has low vision.
• An alert service dog is trained to alert a person with significant hearing loss or who is deaf when a sound occurs, such as a knock on the door.
• A mobility service dog is trained to assist a person who has a mobility or health disability. Duties may include carrying, fetching, opening doors, ringing doorbells, activating elevator buttons, steadying a person while walking, helping a person up after a fall, etc. Mobility service dogs sometimes are called assistance animals.
• A seizure response service dog is trained to assist a person with a seizure disorder. The animal's service depends on the person's needs. The animal may go for help, or may stand guard over the person during a seizure. Some animals have learned to predict a seizure and warn the person.
I. POLICY STATEMENT
Service animals will be permitted in all areas of the Skyline Medical Center open to the public in accordance with both the Americans with Disabilities Act (ADA) and Section 504 of the Rehabilitation Act (Section 504) and other applicable federal and state laws and regulations prohibiting the discrimination on the basis of a person's disability. Reasonable modifications must be made to policies, practices and procedures when necessary to accommodate all individuals with a service animal. Generally, this means the waiving of a no animal policy to permit the use of a service animal. Service animals will be permitted to accompany an individual with a disability to all areas of the Skyline Medical Center where members of the public and/or patients are normally allowed to go, except where the accommodation of the animal would result in a fundamental alteration of the services offered (i.e. Sterile Environments). Service animals assist with many different tasks, including, but not limited to, assisting individuals who are blind or have low vision with navigation and other tasks, alerting individuals who are deaf or hard-of-hearing to the presence of people or sounds, providing non-violent protection or rescue work, pulling a wheelchair, assisting an individual during a seizure, alerting individuals to the presence of an allergen(s), providing assistance with balance and stability to individuals with mobility disabilities, and helping persons with behavioral health and neurological disabilities by reminding them to take medications or assisting them when they are symptomatic. If an animal meets this definition, it is considered a service animal regardless of whether it has been licensed or certified by a state or local government or a training program.
PROCEDURE A. Requirements for Staff
1. Staff cannot ask about the nature of the person's disability, require (or request) any 'proof' of the animal's training (or any other certification) as any inquiry violates various nondiscrimination laws, including the ADA.If it is NOT readily apparent that the dog is a service animal staff must ONLY ask:
a. IF THE ANIMAL IS REQUIRED BECAUSE OF A DISABILITY? and
Accomodating Persons with Service Animals. Retrieved 10/28/2020. Official copy at http://tristarskyline.policystat.com/policy/
6824057/. Copyright © 2020 TriStar Skyline Medical CenterPage 2 of 5
428

COPY
b. WHAT WORK OR TASK HAS THE ANIMAL BEEN TRAINED TO PERFORM?
2. Staff CANNOT pet, play with or try to distract the service animal in any way.
3. Staff CANNOT feed or care for the service animal, including toileting.
4. Staff CANNOT charge or require an individual to pay a surcharge in order to accommodate a service animal.
5. Staff should NEVER attempt to separate the service animal from the person with the qualified disability.
6. Staff should ALWAYS remember that the service animal is a working animal and should make every effort to minimize activities that may startle the animal.
B. Requirements of Service Animals and Their Handlers
1. Leash: The service animal must be on a leash, harness or tether at all times, unless either the handler is unable because of a disability to use the harness, leash or other tether; or the use of a harness, leash or tether would interfere with the service animal's safe, effective performance of the work or task which the service animal was trained to perform. The service animal must still remain under the control of the handler even if the service animal is not on a harness, leash or tether.
2. Under Control of Handler: The handler must be in full control of the animal at all times. The care and supervision of a service animal is solely the responsibility of its handler. If a service animal must be separated from the handler to avoid a fundamental alteration or a threat to safety, it is the responsibility of the handler to arrange for the care and supervision of the animal during the period of separation.
3. Cleanup Rule: The handler must always carry supplies sufficient to clean up the animal's feces. Marked service animal toileting areas should be used when provided.
4. Feeding and Other Care: The handler must provide the service animal with food, water, and other necessary care or make other arrangements for the care of the service animal. Under no circumstances shall the staff or volunteers care for the
service animal.
C. When a Service Animal Can Be Asked to Leave
A person with a disability may only be asked to remove their service animal immediately from the premises if the service animal is out of control and the handler does not take effective action to keep it under control; or the service animal is not house broken.
D. Individualized Assessment
Individuals with disabilities shall be permitted to be accompanied by their service animal in all areas where members of the public and/or patients are permitted to go. However, it may be appropriate to perform an individualized assessment to exclude the service animal from areas such as the operating rooms and burn units where a sterile environment is critical to the services provided. This assessment shall be based on reasonable judgment that relies on current medical knowledge or on the best available objective evidence to ascertain: the nature, duration and severity of the risk; the probability that a potential injury will actually occur; and whether any reasonable modifications of policies, practices or procedures or the provision of auxiliary aids or services will mitigate the risk. If it is determined, through an individualized assessment, that the service animal cannot be accommodated; staff shall, upon the request of the patient, arrange for visits between the service animal and the handler in an area of equivalent privacy and amenities.
E. Visitors with Service Animals
Service animals are generally permitted where visitors are permitted unless an individualized assessment is made to exclude a service animal. Visitors with service animals may not be permitted to access areas that employ greater than general infectious-control measures or when a patient is immunosuppressed. If a determination is made that a service animal cannot be accommodated in a certain area by the use of an individualized assessment; then the visitor will be offered additional accommodations including but not limited to transferring the patient to another comparable room when available to allow unrestricted access. Only if additional accommodations are not available will the visitor be given the option of removing the animal or having friend, family or accompanying persons remove the animal so the visitor may continue with the visit.
F. Emergency Situations In the event of an emergency, the Emergency Response Team (ERT) that responds should be trained to recognize service animals and to be aware that the animal may be trying to communicate the need for help. The handler and/or animal may be confused from the stressful situation. The ERT should be aware that the animal is trying to be protective and, in its confusion, is not to be considered harmful. The ERT will make every effort to keep the animal with its handler. However, the ERT's first effort is toward the handler; this may necessitate leaving an animal behind in certain emergency evacuation situations. When doing so is possible, the ERT will transport the service animal to a safe location to await being reunited with its handler.
Accomodating Persons with Service Animals. Retrieved 10/28/2020. Official copy at http://tristarskyline.policystat.com/policy/
6824057/. Copyright © 2020 TriStar Skyline Medical CenterPage 3 of 5
429

COPY
If a patient is unable to care for their service animal and is unable to arrange for someone else to care for the dog, the
Skyline Medical Center may place the dog in a boarding facility until the patient is released, or make other appropriate
arrangements. However, the Skyline Medical Center must give the patient an opportunity to make arrangements for the
dog's care before taking such steps.
1. Unable to Care for Service Animal (Boarding of Service Animal)
In the event that the Handler/Owner and/or caretaker is unable to care for/meet the requirements of Service Animals and Their Handlers, or experiencing an emergency situation, Skyline Medical Center will provide boarding services for the service animal (after the handler/owner has had the opportunity to make arrangements: Skyline Medical Center's Service Animal Boarding Partner: Peace Love and Paws 1221 Brick Church Pike, Nashville, TN 37207 (615-933-7297) Peace Love and Paws can provide transportation of the service animal. Skyline Medical Center will compensate partner for Boarding Services.
COMPLAINT PROCESS:
RESOURCES: • Rehabilitation Act of 1973, Section 504. • American Disabilities Act of 1990 (42 U.S.C. 12181), including changes made by the ADA Amendments Act of 2008 (P.L.
110-325). • 28 CFR Part 36, revised as of July 1, 1994 entitled "Non Discrimination on the Basis of Disability by Public Accommodations and
in Commercial Facilities". (http://www.ada.gov/regs2010/titleIII_2010/titleIII_2010_regulations.htm • Access to Services Policy, ADA.001
Attachments
No Attachments
It is the policy of Skyline Medical Center not to discriminate on the basis of a person's disability in the offering or delivery of healthcare services. An internal grievance procedure has been adopted to provide for the prompt and equitable resolution of complaints alleging any action prohibited by Section 504 of the Rehabilitation Act of 1973 (28 U.S.C. 794), Section 1557 of the Patient Protection and Affordable Care Act (2010) or the Americans with Disabilities Act of 1990 (42 U.S.C. 12181) including changes made by the ADA Amendments Act of 2008 (P.L. 110-325).
Any person who believes he or she has been subjected to discrimination on the basis of his or her disability may file a grievance under this. It is against the law for Skyline Medical Center to retaliate against anyone who files a grievance or participates in the grievance process.
The ECC shall conduct a thorough investigation providing an opportunity for all relevant evidence to be submitted as it relates to the alleged discriminatory act.
The filing of a complaint of discrimination based on a person's disability does not prevent the filing of a complaint with the U.S. Department of Health and Human Services, Office for Civil Rights, electronically through the Office of Civil Rights Complaint Portal, available at:
https://ocrportal.hhs.gov/ocr/portal/lobby.jsf, or by mail or phone at:
U.S. Department of Health and Human Services
200 Independence Avenue, SW
Room 509F, HHH Building
Washington, DC 20201
1-800-368-1019 , 800-537-7697 (TDD)
Complaint forms are available at: http://www.hhs.gov/ocr/office/file/index.html
Accomodating Persons with Service Animals. Retrieved 10/28/2020. Official copy at http://tristarskyline.policystat.com/policy/
6824057/. Copyright © 2020 TriStar Skyline Medical CenterPage 4 of 5
430

COPY
Approval Signatures
Approver Date
Christine Staigl: CNO 08/2019
Shelley Sircy: Chief Quality/Patient Safety Officer 08/2019
John Franck: Associate Administrator 08/2019
Accomodating Persons with Service Animals. Retrieved 10/28/2020. Official copy at http://tristarskyline.policystat.com/policy/
6824057/. Copyright © 2020 TriStar Skyline Medical CenterPage 5 of 5
431

Section B-Orderly Development-1
Managed Care Contracts
432

433

Section B-Orderly Development-1
Discharge Relationships with Local Facilities
434

GroupName DivisionName CoidName Facility Type Provider
AMERICAN GROUP
TRISTAR DIVISION
34293 - SKYLINE MEDICAL CENTER
SNF445460 - AHC Vanco (f/k/a Vanco Manor Nursing Center)
AMERICAN GROUP
TRISTAR DIVISION
34293 - SKYLINE MEDICAL CENTER
SNF445509 - Life Care Center of Old Hickory Village (ID 0179)
AMERICAN GROUP
TRISTAR DIVISION
34293 - SKYLINE MEDICAL CENTER
SNF445516 - Creekside Center for Rehabilitation and Healing
AMERICAN GROUP
TRISTAR DIVISION
34293 - SKYLINE MEDICAL CENTER
SNF445112 - Trevecca Center for Rehabilitation and Healing
AMERICAN GROUP
TRISTAR DIVISION
34293 - SKYLINE MEDICAL CENTER
SNF445075 - Signature HealthCARE of Madison
AMERICAN GROUP
TRISTAR DIVISION
34293 - SKYLINE MEDICAL CENTER
SNF445191 - NHC HealthCare - Hendersonville
AMERICAN GROUP
TRISTAR DIVISION
34293 - SKYLINE MEDICAL CENTER
SNF445513 - WHITE HOUSE HEALTH CARE INC
AMERICAN GROUP
TRISTAR DIVISION
34293 - SKYLINE MEDICAL CENTER
SNF445486 - StoneRidge Healthcare LLC
AMERICAN GROUP
TRISTAR DIVISION
34293 - SKYLINE MEDICAL CENTER
SNF445519 - NHC Place Sumner
AMERICAN GROUP
TRISTAR DIVISION
34293 - SKYLINE MEDICAL CENTER
SNF
445281 - Grace Healthcare of Whites Creek (formerly Briley Nsg)
435

GroupName DivisionName CoidName Facility Type Provider
AMERICAN GROUP
TRISTAR DIVISION
34293 - SKYLINE MEDICAL CENTER
Home Health447558 - Amedisys of Nashville East - 0551
AMERICAN GROUP
TRISTAR DIVISION
34293 - SKYLINE MEDICAL CENTER
Home Health447403 - SunCrest Home Health Services - Madison
AMERICAN GROUP
TRISTAR DIVISION
34293 - SKYLINE MEDICAL CENTER
Home Health447581 - Adoration Home Health /T/ Hospice - Nashville
AMERICAN GROUP
TRISTAR DIVISION
34293 - SKYLINE MEDICAL CENTER
Home Health447276 - NHC HomeCare - Hendersonville
AMERICAN GROUP
TRISTAR DIVISION
34293 - SKYLINE MEDICAL CENTER
Home Health447276 - NHC Homecare - Springfield
AMERICAN GROUP
TRISTAR DIVISION
34293 - SKYLINE MEDICAL CENTER
Home HealthThe Advanced Care Group (TCM)
AMERICAN GROUP
TRISTAR DIVISION
34293 - SKYLINE MEDICAL CENTER
Home Health447163 - Willow Brook Health Systems
AMERICAN GROUP
TRISTAR DIVISION
34293 - SKYLINE MEDICAL CENTER
Home Health447513 - HOME CARE SOLUTIONS NASHVILLE
AMERICAN GROUP
TRISTAR DIVISION
34293 - SKYLINE MEDICAL CENTER
Home Health447517 - All Heart (HHCOMT) - Nashville
AMERICAN GROUP
TRISTAR DIVISION
34293 - SKYLINE MEDICAL CENTER
Home Health447488 - Kindred at Home - Nashville (formerly Gentiva)
436

GroupName DivisionName CoidName Facility Type Provider
AMERICAN GROUP
TRISTAR DIVISION
34293 - SKYLINE MEDICAL CENTER
IRF44T006 - Skyline Medical Center Rehabilitation Center
AMERICAN GROUP
TRISTAR DIVISION
34293 - SKYLINE MEDICAL CENTER
IRF44T003 - Sumner Regional Medical Center - Rehab
AMERICAN GROUP
TRISTAR DIVISION
34293 - SKYLINE MEDICAL CENTER
IRF44T046 - Horizon Rehabilitation Center
AMERICAN GROUP
TRISTAR DIVISION
34293 - SKYLINE MEDICAL CENTER
IRF183029 - Southern Kentucky Rehabilitation Hospital (SKY)
AMERICAN GROUP
TRISTAR DIVISION
34293 - SKYLINE MEDICAL CENTER
IRF44T231 - TrustPoint Hospital - Acute Rehabilitation
AMERICAN GROUP
TRISTAR DIVISION
34293 - SKYLINE MEDICAL CENTER
IRF44T150 - Summit Acute Rehab
AMERICAN GROUP
TRISTAR DIVISION
34293 - SKYLINE MEDICAL CENTER
IRF
Encompass Health Rehabilitation Hospital of Franklin formerly HealthSouth Rehab Hospital of Williamson County
AMERICAN GROUP
TRISTAR DIVISION
34293 - SKYLINE MEDICAL CENTER
IRF
443028 - Vanderbilt Stallworth Rehabilitation Hospital, a partner of Encompass Health formerly Vanderbilt Stallworth Rehabilitation Hospital
AMERICAN GROUP
TRISTAR DIVISION
34293 - SKYLINE MEDICAL CENTER
IRF44T197 - TriStar Southern Hills Medical Center
AMERICAN GROUP
TRISTAR DIVISION
34293 - SKYLINE MEDICAL CENTER
IRF
18T027 - MURRAY CALLOWAY COUNTY HOSPITAL- Inpatient Rehab
437

GroupName DivisionName CoidName Facility Type Provider
AMERICAN GROUP
TRISTAR DIVISION
34293 - SKYLINE MEDICAL CENTER
LTCH442011 - Select Specialty Hospital - Nashville
AMERICAN GROUP
TRISTAR DIVISION
34293 - SKYLINE MEDICAL CENTER
LTCH442006 - CuraHealth Hospital - Nashville
AMERICAN GROUP
TRISTAR DIVISION
34293 - SKYLINE MEDICAL CENTER
LTCH182005 - Commonwealth Regional Specialty Hospital
AMERICAN GROUP
TRISTAR DIVISION
34293 - SKYLINE MEDICAL CENTER
LTCH012014 - North Alabama Specialty Hospital
AMERICAN GROUP
TRISTAR DIVISION
34293 - SKYLINE MEDICAL CENTER
LTCH182008 - ContinueCARE Hospital at Baptist Health Paducah
AMERICAN GROUP
TRISTAR DIVISION
34293 - SKYLINE MEDICAL CENTER
LTCH422009 - Regency Hospital of Greenville (LTAC)
AMERICAN GROUP
TRISTAR DIVISION
34293 - SKYLINE MEDICAL CENTER
LTCHKindred Hospital - Louisville at Jewish Hospital
438

Section B-Orderly Development-3C
Clinical Training Programs
439

School Program School ProgramMed Lab Science (BS) South-Nashville DMS SonographyPhlebotomy South-Nashville OTA PTA/OTA
APSU Nursing Nursing South-Nashville PN NursingAPSU Radiation Radiology South-Nashville PTA PTA/OTABelmont Nursing Nursing South-Nashville Rad RadiologyBelmont OT PT/OT TN Tech NursingBelmont PT PT/OT Trevecca PA Physician AssistantBelmont-Pharm Pharmacy TSU-ASN NursingBethel Nursing Nursing TSU-HIM HIM/HITCumberland U Nursing TSU-OT PT/OT
Clinical Lab Tech (AAS) TSU-PT PT/OTNursing TSU-Resp RespiratoryPharmacy UAB-Nursing NursingPolysomnography Union-H NursingRespiratory Univ of Miss - Speech Speech
ETSU-Nursing Newbern Nursing USA-NP NursingETSU-Nursing Shelby Nursing UTC-PT PT/OTFortis-Nashville-CVT Cardiovascular Tech UTHSC Pharmacy PharmacyFortis-Nashville-Nursing Nursing UTHSC-OT PT/OTGannon PT PT/OT UTHSC-PT PT/OTHarding PT PT/OT UTHSC-Speech SpeechHuntington OT PT/OT Vanderbilt NursingLipscomb Pharm Pharmacy Vol State-Nursing NursingLipscomb-Nursing Nursing EMT/AEMTLipscomb-PA Physician Assistant Paramedic
Nursing Vol-State Lab Clinical Lab Tech (AAS)Nursing Anesthesia PT/OT
MarianU Nursing PTA/OTAMTSA Nursing Anesthesia Vol-State Radiology RadiologyNashville State CST Instrument Sterile Tech Vol-State Respiratory RespiratoryNashville State OTA PT/OT Vol-State Sonography Sonography
PTA/OTA WKYU-ASN NursingNashville State Surg Tech Surg Tech WKYU-BSN NursingNHC Dietetics Dietetics/Nutrition WKYU-PT PT/OTSouth-Nashville BSN Nursing
Marian SRNA
ETSU-Nursing Nash
APSU Lab
Vol-State PTA
Vol-State EMS
440

January 28, 2021
Thomas Pitt HSD Examiner Tennessee Health Services and Development Agency Andrew Jackson State Office Building, 9th Floor 502 Deaderick Street Nashville, TN 37243
RE: TriStar Skyline Medical Center, CN2101-003
Dear Mr. Pitt,
On behalf of TriStar Skyline Medical Center, please accept this supplemental information in response to your January 25, 2021 request regarding the abovereferenced CON application for the initiation of a burn unit that will be located at the TriStar Skyline Medical Center main campus at 3441 Dickerson Pike, Nashville, Tennessee 37207.
Should you have any questions or require additional information, please do not hesitiate to contact me.
Sincerely,
f A'i,r
Supplemental 1 January 28, 2021
441

1
TriStar Skyline Medical Center CN2101-003
Initiation of a Burn Unit Supplemental Response #1
January 28, 2021 ___________________________________________________________________________
TriStar Skyline (“Skyline” or the “Applicant”) provides the following responses to the HSDA staff’s request for supplemental information regarding CN2101-003 for the initiation of a burn unit that will be located at Skyline’s main campus in Nashville, Tennessee.
1. Section A, Executive Summary, Overview, Item A.1., Page 2
Please address the construction component of the project in this section.Provide additional detail about how the designation of the 12 ICU beds asburn unit beds will impact ICU capacity for the hospital facility.
As detailed in Section A, Item A.12, Skyline opened a $69 million expansionin late 2019 that included the addition of 54 new inpatient beds, providingneeded capacity that also allows for the development of a comprehensiveburn program. Since 2019, through expansion and relocation, Skyline hasadded 30 ICU beds on its campus.
To accommodate the proposed project, an existing 12-bed intensive care unitlocated directly above the Emergency Department will be retrofitted toaccommodate burn patients. The 12-bed burn unit was previously a TraumaICU that has relocated to a space adjacent to the ED, allowing for neededadditional trauma capacity. This also created capacity to treat COVID-19patients. It is anticipated that once COVID-19 numbers begin to decrease,additional ICU capacity will be available.
Based on the aforementioned factors, the proposed 12-bed burn unit is notanticipated to impact ICU capacity significantly. See the table below.
Bed Capacity
2019
2019 Occupancy
Bed Capacity
2020
2020 Occupancy
Bed Capacity
Post Project Year 1
Post Project Occupancy
Year 1
Medical ICU 22 86.1% 43 65.8% 31 85.0%Trauma ICU 12 72.7% 16 59.9% 16 55.9%Neuro ICU 11 94.9% 16 82.8% 16 77.2%Burn ICU 0 0.0% 0 0.0% 12 25.4%Total ICU Beds Main 45 84.7% 75 68.2% 75 68.9%
Facility Capacity/Occupancy (Inpatient and Observation Patients)
Note: Bed Expansion project completed Nov 2019 adding 14 ICU beds. In addition, in 2020 Trauma ICU was relocated to 1st floor adding 16 ICU beds and lowered Med/Surg compliment. This enabled the facility to repurpose 12 beds to MICU for COVID cohort unit, with the area will become Burn unit post project. Total COVID ICU patient days of 2,006 or 5.48 ADC incurred in 2020 not anticipated to continue in future years.
Supplemental 1 January 28, 2021
442

2
2. Section A. Executive Summary, Rationale for Approval Item B.1., Page 4&5
What is the applicant's plan to increase patient referrals from EastTennessee? What presence does the applicant have in East TN and otherproposed service areas that will support increased access for these burnpatients?
Skyline has developed several relationships with facilities serving EastTennessee. These relationships serve to promote patient and staff education.These outreach efforts have and will continue to increase Skyline’s patientreferrals from East Tennessee. This is particularly true for regionalizedand/or advanced care services, such as comprehensive burn care. As a LevelII trauma provider and a tertiary hospital, Skyline has the resources necessaryto provide comprehensive care, which is especially important for patientsliving in rural areas of Tennessee, like much of East Tennessee, who lackaccess to such services at their local community hospitals. Skyline iscommitted to expanding its existing outreach and education programs toinclude burn services, providing education to community hospitals on how tostabilize burn patients and when to refer patients to a verified burn center asdetailed in the referral criteria published by ABA.
It should be noted that Skyline has been serving Tennessee residents for over20 years, and through its TriStar affiliation, Skyline has existing relationshipswith several facilities throughout East Tennessee. TriStar Division hospitals inthe Nashville market are already serving hospitals in East Tennessee fortertiary/quaternary services. TriStar Transfer center data shows that TriStarNashville market hospitals have received patients from the followingcounties in East Tennessee and the Eastern Region of Middle Tennessee:
Primary Service Area:o Eastern Region of Middle Tennessee – Putnam, Overton, Smith,
Dekalb, White, Warren, Grundy, Marion (total of 418 patienttransfers to Nashville in 2020)
o East Tennessee – Hamilton, Cumberland, Rhea, Fentress (totalof 92 patient transfers to Nashville in 2020)
Secondary Service Area:o East Tennessee – Bradley, McMinn, Roane, Blount, Knox,
Hamblen, Campbell, Jefferson, and even one transfer fromWashington (total of 47 patient transfers to Nashville in 2020)
Additionally, TriStar hospitals Parkridge Medical Center and Parkridge East Hospital are located in Chattanooga. TriStar Division also has a presence in Knoxville, as its bone marrow transplant physicians have a satellite clinic in Knoxville and provide pre- and post- follow up visits for bone-marrow-transplant oncology services. While these services are not directly related to burn, TriStar Division is confident that the relationships that have been built in Knoxville for other services will serve as an opportunity to develop referral sources for burn services. Lastly, TriStar Division is hiring another patient-physician relationship (PPR) physician and PPR outreach director that will be focused on the eastern region of the state. The PPR directors will visit with physicians and hospital ERs to promote TriStar services and will also promote Skyline’s burn program.
Supplemental 1 January 28, 2021
443

3
Not only does TriStar Division plan to continue to foster relationships through outreach and education in East Tennessee, but TriStar Division also has the resources in place to ensure proper transportation of these patients who are quite a distance away from any existing burn center. TriStar Division has developed a partnership with Global Medical Response (GMR), which operates 37 air ambulance bases in Tennessee, Kentucky, Georgia, and Alabama. Specific to Tennessee, GMR has bases in its Air Evac division serving mostly West and Middle Tennessee as well as bases in its Med-Trans division which primarily services Middle and East Tennessee. At least six of these bases are located in East Tennessee and at least three are located in Southeast Tennessee, thereby increasing access to care for patients in this region. In fact, the Med-Trans Division is partnered with Erlanger’s LifeForce and with UT Medical Center’s LifeStar to enhance access to air ambulance services in East Tennessee. Coordination with Skyline and GMR will ensure patients in need of comprehensive burn care will be appropriately transported.
Skyline’s outreach efforts and extended network are detailed in the Application in Section B, Item 1, beginning on page 43, “Skyline Has the Infrastructure and Programs in Place to Increase Access to Care”.
Are there any national standards for burn unit capacity that speak to the issue of recommended bed capacity necessary to handle a catastrophic event?
Planning for catastrophic events such as burn mass casualty incidents (“burn MCI”) is not based upon burn unit capacity; rather, it is a multi-faceted, area-wide collaborative effort that requires pooling of resources. Those resources, however, must be available to pool. A 2005 article published by International Journal of Disaster Medicine details the appropriate process for managing a burn MCI. The authors wrote: “Mass casualty burn disasters are potentially challenging, in part because the majority of health care providers are inexperienced in the care of thermally injured patients and in part because of the multisystem response elicited by the thermal injury.”1
Because medical professionals trained in burn care are a limited resource nationwide, redundancy in burn care is even more important to ensuring the availability of resources necessary to provide quality care for patients who are impacted by a burn MCI. The study notes that, “failure to … transfer patients to available burn beds elsewhere in a timely fashion, risks degrading the quality of patient care by overwhelming the primary facility.” With a burn MCI it is quite possible that one burn provider serving a large urban area and with no other provider within 150-mile radius would be overwhelmed thereby potentially compromising quality of care.
Importantly, the article makes a distinction between verified and non-verified burn centers: “A mature appreciation on the part of the hospital, region, or nation of its ability to care for burn casualties during a disaster is needed and, when appropriate, should motivate the timely transfer of patients to
1 Cancio, Leopoldo & Pruitt, Basil. (2005). Management of Mass Casualty Burn Disasters. International Journal of Disaster Medicine. 2. 17. 10.1080/15031430510034640.
Supplemental 1 January 28, 2021
444

4
available, qualified facilities. Central to this concept is the understanding that patients with severe thermal injuries should receive their care in nationally recognized burn centers.” [emphasis added]
Skyline contends that its commitment to become the only verified burn center serving Middle and East Tennessee, as well as parts of Kentucky and Alabama, is important to ensuring efficacy of disaster planning for burn MCI. Now more than ever, disaster planning is of the utmost importance. Skyline intends to work collaboratively with providers in the region to ensure that there is a comprehensive plan in place for burn MCI. Part of that plan is to ensure available bed capacity at a verified burn center.
What are the key standards that differentiate an ABA verified center from a non-verified center?
A complete list of the criteria and standards for ABA verification is included in Attachment Section B-Need-1C. The difference between a verified burn center and a non-verified burn center is that non-verified burn centers are not monitored or evaluated by any accrediting body. Burn Center verification provides a true mark of distinction for a burn center. Verification is an indicator to government, third-party payers, patients, families, and accreditation organizations, that the center provides high quality patient care to burn patients based on current industry standards from time of injury through rehabilitation. ABA is the only nationally recognized accrediting body for burn services in the United States. In other words, if a program is not ABA-verified, there is no way to ensure appropriate management, staffing, equipment, and supplies nor is there outside monitoring of patient outcomes to ensure patient safety and quality standards are met. Skyline proposes to be the first ABA-verified burn center in Nashville serving Middle and East Tennessee.
How does the project service area differ from the VUMC burn center service area?
The service area for a burn program cannot be simply defined by patient origin like with other healthcare services. A small community or county may have several burn admissions in one year and no burn admissions the next. Depending on bed availability and transportation availability, patients from communities located a significant distance from exiting centers may be transported to one center in a given year and a different center the following year. Moreover, complete patient origin data for Vanderbilt’s burn program is not available from any one public source. THA data provides the best estimate but relies on burn diagnosis codes and not actual admissions to VUMC’s burn unit.
Using data from THA and transportation time estimates, Skyline believes that Vanderbilt’s burn program serves Middle Tennessee, East Tennessee, and central Kentucky. For 2017-2018, Vanderbilt has admitted patients from 134
Supplemental 1 January 28, 2021
445

5
counties in 16 states, with states and counties varying by year.2 The following table characterizes Vanderbilt’s patient origin at a level that can be used reasonably to define its service area noting overlap with Skyline’s service area.
Vanderbilt Estimated Burn Patient Origin
(2017-2018)2 Middle Tennessee* 63.7% Eastern Tennessee** 15.9% Central Kentucky* 11.2% Midwest US 1.9% Western Tennessee 1.7% Other Southeast Region 1.7% Northern Alabama** 1.2% Southeastern Kentucky** 1.0% Other Kentucky 0.6% Other Alabama 0.3% Southwest US 0.3% Northeast US 0.1% Western US 0.0% Unknown 0.6% Total 100.0% Source: THA data, burn diagnoses *Skyline PSA **Skyline SSA
Please elaborate on the statement "Skyline’s planned education and outreach services relating to burn care, it is expected that patients with moderate to major burns now being served less appropriately in community hospitals will instead be transferred to Skyline for comprehensive treatment." Which hospitals in the primary and secondary service areas will be included in these outreach and education services?"
ABA accredited facilities are required to demonstrate involvement in local, regional, and national prevention, education, and outreach initiatives as well as research and advocating for burn related healthcare issues. The burn program is still in development and is in the process of identifying key leaders who will be integral in developing the outreach program and
2 Please note that THA prohibits presentation of individual hospital data for the most recent year (2019).
Supplemental 1 January 28, 2021
446

6
calendar. Initial goals will include focus on hospitals that have provided burn care to patients that potentially should have been referred to a burn center.
TriStar Division’s BRCA partnership brings a history of dedication to burn education and outreach. BRCA’s Physician and Provider Relations Liaisons will work to build relationships throughout primary and secondary service area. They will identify top 15 facilities from primary and secondary service areas and maintain close personal contact. Their goal will be to visit all hospitals within 50 miles monthly, and all facilities within outlying markets quarterly. They will schedule visits with EMS/Flight services and transfer centers of hospital networks quarterly as they are in their regions.
As it relates to outreach and education, BRCA also provides:
On-site training and shadowing Webinars The only burn dedicated podcast Annual burn education symposium Emergency burn care education for ED’s/urgent cares, EMS/Fire on
site and via WebEx/webinar More ABLS courses than anyone else in the country
BRCA has been providing education and outreach to South and East Tennessee and Northern Alabama for many years now. It already has established relationships and receive referrals from these locations. BRCA will now be able to provide an ABA-verified, BRCA burn center option to these patients much closer to home.
3. Section A. Executive Summary, Rationale for Approval Item B.4., Page 8
Which counties in the proposed service area are being served by SKYLIFE?
As detailed in the CON Application, TriStar Division has partnered withGMR for medical transport services. GMR has bases throughout the servicearea which will expand access to medical transport. Additionally, through itspartnership with GMR, TriStar Division launched its air ambulance servicecalled SKYLIFE. The SKYLIFE helicopter is based at TriStar CentennialMedical Center.
Exhibit 17 in the application provides a map of GMR’s Med-Trans and Air-Evac bases in relation to the proposed service area.
The map below shows the area covered by SKYLIFE in relation to the TriStarhospital market.
Supplemental 1 January 28, 2021
447

SKYLIFE Travel Radius and TriStar Division Hospital
Supplemental 1 January 28, 2021
448

4. Section A, Project Details, Item 5 – Name of Management/Operating Entity,Page 10.
There are Management Fees Paid to Affiliates listed in the Projected DataChart on page 73 Line D.5.a, but there is no management agreement orentity listed here or attached under A-5. Please identify any managementcontracts that will impact this project and attach copies of those contracts asAttachment A-5 if appropriate.
The amounts listed on this line item are intercompany fees paid to HCAaffiliates. The application is a wholly-owned subsidiary of an HCA affiliateand thus there is no management agreement. These are not technically“management fees”; however, this is the line item where Skyline hashistorically reflected these intercompany fees.
5. Section A, Project Details, Item 6B.1.a-d – Plot Plan, Page 11.
Please revise the plot plan to state, Interstate 65 instead of Highway 65.
Please see the attached revised plot plan and the Replacement Page 11R.
6. Section A, Project Details, Item 6B.2.a-d – Floor Plan, Page 12.
Please provide a note on the Floor Plan that the Burn Unit Operating Roomis not included in construction costs for the project.
There is no construction that will take place in the OR. Mechanical upgrades(e.g. HVAC and duct work) that support the dedicated burn OR will takeplace outside of the actual OR. In other words, there is no construction costdirectly associated with the OR to include in the project costs.
7. Section A, Project Details, Item 10.A – Bed Complement Data, Page 14.
In the chart of bed types, do these beds include those at their MadisonCampus?
Yes, the chart of bed types includes Skyline’s Madison campus. Please notepsychiatric beds included on the bed complement data chart.
8. Section A, Project Details, Item 12.A – Square Footage and Cost Per SquareFootage Chart, Page 17.
Please explain why the “burn unit” beds will flex between ICU andMedical/Surgical?
The proposed burn unit will be designed and designated as an ICU.However, the burn beds will be designed as adjustable-acuity beds. In acontinuous effort to improve patient care and satisfaction, an acuity-adjustable room is designed to eliminate the need for patients to betransferred to different care settings as their recovery progresses. Instead, theroom and nursing staff transform to the needs of the patient. It is not
Supplemental 1 January 28, 2021
449

9
uncommon for a patient to move two to three times from admission to discharge. This is particularly cumbersome for vulnerable burn patients who may spend longer in the hospital than the average acute care patient. An acuity-adjustable unit allows the patient to maintain the same care team throughout his or her hospital stay, minimizing concerns about medical errors, falls, and patient anxiety when readjusting to new accommodations.
9. Section B, Need, Item A (Specific Criteria – Burn Units) Item 1, Page 20.
Please explain the methodology used to determine the bed need andprovide a reference to the page number(s) and section(s) of the applicationthat supports the applicant’s statement on page 20 “The adjustment is supported by actual incidence as shown by the current providers operating in excess of the 70% occupancy criterion stated in the State Health Plan and the national burn data which shows that 27 additional burn beds are needed in the service area.”
As noted in detail in the original CON application, there is no known basisfor the bed to population ratio in Criterion 1 – Burn Units. A simplecomparison of the actual bed need in Tennessee based the utilization of theexisting Tennessee burn programs (43.5) and projected bed need based onthis ratio (30.8) shows that this ratio would not demonstrate sufficient beds tomeet current utilization/incidence rates. In fact, the shortfall is 12.76 beds asshown below.
Bed Need Based on Actual Indicence/Utilization:Vanderbilt ADC - 2019 17.8Regional One ADC - 2019 12.6
Total ADC 30.5Bed Need at 70% Occupancy 43.5
Bed Need Based on State Health Plan Criteria 1:Tennessee 2019 Population 6,920,116 Ratio of Beds to Population 1 to 225,000Bed Need 30.8
Variance between Actual Incidence/Utilization and Criteria Bed Ratio: 12.76 Sources: 2019 JAR Data, TN DOH Division of PHA.
Supplemental 1 January 28, 2021
450

10
Please provide a citation for the following statement on page 20 "national burn data shows that there is a disparity in accessibility to burn services for residents of the South, including Tennessee, Kentucky, and Alabama."
Below is the citation for this statement: Klein MB, Kramer CB, Nelson J, Rivara FP, Gibran NS, Concannon T. Geographic Access to Burn Center Hospitals. JAMA. 2009;302(16):1774–1781. doi:10.1001/jama.2009.1548. Table 2.
The table in the published study that supports this statement can be found in Exhibit 4 and was also updated and recreated based on 2020 data in Exhibit 5.
10. Section B, Need, Item A (Specific Criteria – Burn Units) Item 1, Page 22.
What are the actual incidences and national incidences rates?
Burn unit standards are mentioned and are part of the attachment. Thisneeds to be referenced. What is the patient origin of the burn units? Inother words, where are the patients coming from?
1/27/2021 clarification from Mr. Thomas Pitt:
This question should have been combined with Question #15, which asks: “There are other burn units in close proximately of the proposed service area, what are the service areas of the other burn units such as Regional One Health (Memphis), University of Louisville, and UAB (Alabama)? What overlap will there be with these other centers and the new burn center in Nashville? Please disregard Question #10 and respond to Question #15 which references page 29 of the application.
Please see response to Question #15 below.
11. Section B, Need, Item A (Specific Criteria – Burn Units) Item 1, Page 23.
Crude Rate needs to be explained. The term is used in a chart/exhibit.
A crude rate is the number of new cases (or deaths) occurring in a specifiedpopulation per year, usually expressed as the number of cases per 100,000population at risk. A crude rate differs from an age-adjusted rate, whichattempts to normalize differences in the distribution of population by age indifferent geographic areas. A crude rate is appropriate for projecting futureutilization.
12. Section B, Need, Item A (Specific Criteria – Burn Units) Item 1, Page 25.
Provide a definition for Low Access area according to the research citedhere. Which counties in Tennessee fall under the category of no verifiedcenter within 300 miles and which are “low access”. Apply this information
Supplemental 1 January 28, 2021
451

11
to Tennessee specifically. Additional states in the service should be analyzed in separate tables. Will this project be in a low access area?
As it relates to access, Skyline cites two articles: one article that discusses research conducted by Dr. Heather E. Carmichael and presented at the 2019 Annual Scientific Meeting of the Eastern Association for the Surgery of Trauma and one article published in 2005 in published in 2009 by The Journal of the American Medical Association (JAMA). The reference statement referring to “low access” comes from the 2019 research article. The article states that the southern and western regions have the lowest access to burn center care. Separately, the article states that some areas are more than 300 miles away from a verified burn center but does not tie this the definition of “low access”. This article specifically focuses on access to ABA-verified burn centers and conservatively estimates low access to verified burn center care to be less than 0.3 beds per 100,000 population.
Exhibit 5 in the application shows the number of both non-verified and verified burn beds in Tennessee per 100,000 population based on the methodology used in the 2005 JAMA study. If the nonverified burn beds are removed from the analysis to align with the aforementioned 2019 research article, the ratio of verified burn beds in Tennessee per 100,000 population would be 0.2. Tennessee as a whole has low access to verified burn centers as well as all burn centers according to the methodology presented in both studies. Thus, this project will be located in a low access area.
Neither study breaks this analysis down by county, as it would be inappropriate to do so. Burn care services are planned for on a regional basis and cannot be planned for on a county level.
13. Section B, Need, Item A (Specific Criteria – Burn Units) Item 1, Page 26.
Are there any studies that are more current than 2009 study on regionalaccess to transportation referenced for Exhibit 4? Is there any state specificdata available to demonstrate a gap in medical transportation in serviceareas target for this project?
No, Skyline could not find any more current studies on regional access totransportation. However, since the publication of this article, it can bereasonably concluded that access has only declined even more. The 2009study does not consider that Erlanger closed its program. No other burnprogram has opened since then in Tennessee and population has grownsignificantly since 2009.
Please see the Applicant’s response to Question 14 for discussions concerninggaps in medical transport for the service area.
In Exhibit 4, what does “n” mean?
“n” means “number.” So n = 128 means 128 burn centers.
Supplemental 1 January 28, 2021
452

12
14. Section B, Need, Item A (Specific Criteria – Burn Units) Item 1, Pages 30-36.Please address the Need Criteria utilizing a standalone table(s) for the Stateof Tennessee service area the purposes of this application. Additional out-of-state counties can be included in the analysis as separate tables.
On 1/27/2021 via email correspondence, Mr. Thomas Pitt Provided the following clarification:
Please apply this analysis separating the Tennessee specific service area from out-of-state serve areas to all tables, exhibits and narrative analysis contained in Section B from page 30 through the second paragraph of page 36. Please provide county-level data wherever possible to demonstrate the outmigration of patients to other states.
The following bed need tables from page 30 of the application broken out bystate are provided below. It is important to note that using the actual nationalbed to population ratio of 150,000 results in a need for more than 12 beds inSkyline’s Tennessee-only service area.
1:225,000 Population Ratio:
2021 2025Tennessee Service Area 5,459,036 5,660,583 Bed Need at 1 Bed per 225,000 24 25 Less Vanderbilt Beds 25 25Bed Need Surplus (+)/Deficit (-) 0.7 (0.2)
Tennessee Only Service Area Bed Need at 1 Bed per 225,000 Population
2021 2025Kentucky 1,322,830 1,342,211 Alabama 833,898 843,915 Total Non-Tennessee 2,156,728 2,186,126 Bed Need at 1 Bed per 225,000 10 10 Existing Beds 0 0Bed Need Surplus (+)/Deficit (-) (10) (10)
Non-Tennessee Service Area Bed Need at 1 Bed per 225,000 Population
Supplemental 1 January 28, 2021
453

13
National Actual 1:150,000 Ratio:
2021 2025Tennessee Service Area 5,459,036 5,660,583 Bed Need at 1 Bed per 150,000 36 38 Less Vanderbilt Beds 25 25Bed Need Surplus (+)/Deficit (-) (11.4) (12.7)
Tennessee Only Bed Need at 1 Bed per 150,000 Population
2021 2025Kentucky 1,322,830 1,342,211 Alabama 833,898 843,915 Total Non-Tennessee 2,156,728 2,186,126 Bed Need at 1 Bed per 150,000 14 15 Existing Beds 0 0Bed Need Surplus (+)/Deficit (-) (14) (15)
Non-Tennessee Service Area Bed Need at 1 Bed per 225,000 Population
As documented in the original CON application and above, the Criterion 1 bed to population ratio does not align with the actual use of existing beds in Tennessee.
On page 31, the analysis of service area pediatric burn admissions by hospital burn program type is clarified by state below. This detailed data is consistent with the original application showing that the majority of service area pediatric patients are served at a burn center particularly for Tennessee patients. For Kentucky patients, 50 percent are served in a burn center.
Exhibit 7 – Page 31 by State
Service Area/ State
Non-Burn Center
HospitalNon-Verified Burn Center
Verified Burn Center Grand Total
TN 17.8% 78.2% 4.0% 100.0%KY 50.0% 50.0% 0.0% 100.0%
Total 24.6% 72.2% 3.2% 100.0%
2019 All Service Area Burn Pediatric Admissions by Hospital Burn Program Type
Source: Tennessee, Georgia, and Kentucky State Hospital Associations. Does not include Alabama data.
On page 32, the analysis of service area adult burn admissions by hospital burn program type is clarified by state below. This detailed data is consistent
Supplemental 1 January 28, 2021
454

14
with the original application showing that a large percentage of patients meeting ABA referral criteria for a burn center in Tennessee and Kentucky are not being referred appropriately. For each state, it is clear that older patients (60+) are most frequently staying in their local community and not receiving care from a burn center.
Exhibit 8 – Page 32 by State
Age
Non-Burn Center
HospitalNon-Verified Burn Center
Verified Burn Center Grand Total
18-59 34.4% 64.5% 1.2% 100.0%TN 47.8% 52.2% 0.0% 100.0%KY 30.7% 67.8% 1.5% 100.0%
60+ 51.9% 47.6% 0.4% 100.0%TN 61.5% 35.9% 2.6% 100.0%KY 50.0% 50.0% 0.0% 100.0%
2019 Service Area Burn Admissions by Hospital Burn Program -
Source: Tennessee, Georgia, and Kentucky State Hospital Associations. Does not include Alabama data.
On page 34, Skyline provided the trend in burn patient admissions for the service area. These two exhibits are provided below by state of patient residence. The Tennessee portion of the primary service area actually shows the largest increase in burn admissions at 5.0% CAGR for total burn admissions and 12.9% CAGR for burn admissions meeting ABA referral criteria.
Area 2017 2018 20192-Year CAGR
Primary Service Area 658 677 709 3.8%AL 5 11 9 34.2%KY 163 193 160 -0.9%TN 490 473 540 5.0%Secondary Service Area 333 315 304 -4.5%KY 50 40 42 -8.3%TN 283 275 262 -3.8%Grand Total 991 992 1,013 1.1%
Exhibit 9 - By StateService Area Trend in Total Admissions
Source: Tennessee, Georgia, and Kentucky State Hospital Associations. Only includes Alabama patients served in Tennessee.
Supplemental 1 January 28, 2021
455

15
Area 2017 2018 20192-Year CAGR
Primary Service Area 422 489 530 12.1%AL 3 8 9 73.2%KY 101 137 116 7.2%TN 318 344 405 12.9%
Secondary Service Area 235 222 228 -1.5%KY 36 29 28 -11.8%TN 199 193 200 0.3%
Grand Total 657 711 758 7.4%
Exhibit 10 - by StateService Area Trend in Admissions for Burn Diagnoses Meeting
ABA Diagnosis Referral Criteria
Source: Tennessee, Georgia, and Kentucky State Hospital Associations. Does not include Alabama data.
On page 35, Skyline presented the trend in burn patient admissions by type of facility: ABA-verified burn centers, non-verified centers, and non-burn center hospitals. This data has been provided by state below:
Facility Type 2017 2018 2019AL
Non-Burn Center Hospital 0.0% 62.5% 11.1%Non-Verified Burn Center 100.0% 25.0% 88.9%Verified Burn Center 0.0% 12.5% 0.0%
KYNon-Burn Center Hospital 49.5% 54.7% 43.1%Non-Verified Burn Center 49.5% 44.5% 56.0%Verified Burn Center 1.0% 0.7% 0.9%
TNNon-Burn Center Hospital 23.3% 30.8% 26.2%Non-Verified Burn Center 74.5% 67.4% 73.1%Verified Burn Center 2.2% 1.7% 0.7%
Exhibit 11 - by StatePrimary Service Area Burn Patients
Meeting ICD-10 Burn Criteria by Facility Type
Source: Tennessee, Georgia, and Kentucky State Hospital Associations. Alabama data reflect only patients traveling to Tennessee and Kentucky
As the secondary service area is further from existing burn centers, a higher percentage of patients in both Tennessee and Kentucky have been served at non-burn center hospitals.
Supplemental 1 January 28, 2021
456

16
Facility Type 2017 2018 2019Secondary Service Area
KYNon-Burn Center Hospital 80.6% 86.2% 85.7%Non-Verified Burn Center 16.7% 13.8% 14.3%Verified Burn Center 2.8% 0.0% 0.0%
TNNon-Burn Center Hospital 55.8% 50.8% 53.0%Non-Verified Burn Center 41.7% 46.6% 44.5%Verified Burn Center 2.5% 2.6% 2.5%
Exhibit 12 - by StateSecondary Service Area Burn Patients
Meeting ICD-10 Burn Criteria by Facility Type
Source: Tennessee, Georgia, and Kentucky State Hospital Associations. Alabama data reflect only patients traveling to Tennessee and Kentucky
When documenting the out-migration of TN and other service area patients to out-of-state hospitals for burn center services, please detail the movement of patients by county from one state to another with the movement of TN patients being described as a standalone group. Please provide a state and county level breakdown of these patients meeting ICD-10 Burn Referral Criteria to demonstrate where the service need exists. If there is data from THA, KHA, and GHA, show results by state instead of by service area grouping – especially by burn severity.
The follow analysis clarifies the analysis of outmigration on page 34. As discussed above, the significant variation in utilization patterns for this unique and specialized service does not allow for meaningful and predictive analysis at a county level. Skyline only has access to data from THA, KHA, and GHA and thus is limited in identifying service area patients that may be leaving this area entirely. Skyline only has data on Alabama patients that travel to Tennessee, Kentucky, or Georgia from the aforementioned data sets. The follow data at a State/Service Area level reflects all patients in the service area that meet the ABA criteria for referral to a burn center, as defined in the CON application, traveling to a verified or non-verified burn center.
Supplemental 1 January 28, 2021
457

17
Traveling to GA 1210
1396
23100
Source: THA, KHA, GHA data set, 2017-2019
Service Area Patients Traveling to Verfied and Non-Verified Burn Center in TN, KY & GA (2017-2019)
Traveling to KY
Traveling to TNTraveling to GA
Tennessee Service Area Residents
Kentucky Service Area Residents
Alabama Service Area ResidentsTraveling to TNTraveling to GA
Are there any providers in the proposed service area who are currently treating burn patients at their facilities who support this project and/or have expressed support for referring these patients to Skyline?
Skyline has had conversations with several providers throughout the service area who have expressed their support for the proposed project and willingness to refer patients to Skyline when clinically appropriate.
What other air and ground transportation services are available and how will Skyline's transport relationships represent an enhancement to what is currently available to patients in the primary and secondary service areas?
VUMC is the only existing provider in the service area. The map on the following page provides the helicopter medical transport services available through both TriStar Division (TriStar’s SKYLIFE and GMR’s Med-Trans and Air Evac bases) and VUMC (Lifeflight). Note that VUMC’s affiliated helicopter transport bases are concentrated in Middle and West Tennessee, creating a gap in medical transportation for East Tennesseans. Skyline contends that the proposed project will offer additional helicopters transport services for burn care patients residing in East Tennessee.
SKYLIFE is unique in that the twin-engine EC-145 helicopter has the capability to fly in inclement weather. Not all helicopters have the technology to complete an Instrumental Flight Rules (IFR) plan which is necessary to fly in weather where visibility is limited. Often, in severe weather, ground transportation is delayed. SKYLIFE will ensure access to care despite inclement weather conditions. Additionally, the helicopter is larger than the average helicopter, allowing more room for additional staff and equipment necessary to air transport specialty care patients such as severe burn patients and other high acuity patients.
Skyline’s transport relationships will be an enhancement to what is currently available to the service area.
Supplemental 1 January 28, 2021
458

Map of Skyline Burn Unit Service Area with Air Transport Base Location
Supplemental 1 January 28, 2021
459

15. Section B, Need, Item A (Specific Criteria – Burn Units) Item 1, Page 29.
There are other burn units in close proximately of the proposed servicearea, what are the service areas of the other burn units such as RegionalOne Health (Memphis), University of Louisville, and UAB (Alabama)?What overlap will there be with these other centers and the new burncenter in Nashville?
Given that both verified and non-verified burn centers serve broadgeographic areas and even serve patients from other regions of the country,there is expected to be some overlap in service area. It is also important tonote that geography, travel distance, and the location of other existing burncenters influence service areas. On page 29 of the original CON, Skylineprovided the 150-mile drive time contour for each provider in and around theservice area to demonstrate the travel component of the service area.
The only available source for patient origin data for burn patients is THA,KHA, and GHA data, which allow for an estimate of burn patients bydiagnosis code and DRG. However, this data can only provide an estimateand cannot conclusively provide the patient origin of existing providers. Asnoted above, Alabama data is not available in the same detail as THA, KHA,and GHA thus patient origin is not available for UAB.
Although burn center service areas are not limited to a patient origindefinition, the following table summarizes the estimated patient origin bystate and sub-area for Regional One and University of Louisville in the sameformat provided for Vanderbilt above based on THA data for 2017-2018.3
3 Please note that THA prohibits presentation of individual hospital data for the most recent year (2019).
This analysis shows that neither Regional One nor University of Louisvillereceive a substantial portion of their patients from Skyline’s proposed burnservice area. In fact, service area residents comprised just 1.3% of RegionalOne’s admissions based on THA estimates.
Supplemental 1 January 28, 2021
460

20
Region Regional OneUniv of
LouisvilleMiddle Tennessee* 0.9% 0.0%Eastern Tennessee** 0.0% 0.3%Central Kentucky* 0.3% 14.0%Western Tennessee 50.1% 0.0%Midwest US 3.6% 27.5%Other Southeast Region 43.4% 0.3%Northern Alabama** 0.1% 0.0%Southeastern Kentucky** 0.0% 1.1%Other Kentucky 0.0% 55.9%Other Alabama 0.1% 0.0%Northeast US 0.3% 0.0%Western US 0.0% 0.3%Southwest US 0.5% 0.3%Unknown 0.5% 0.3%Total 100.0% 100.0%Source: THA, KHA data, burn diagnoses
*Skyline PSA
**Skyline SSA
Estimated Burn Patient Origin (2017-2018)
16. Section B, Need, Item A (Specific Criteria – Burn Units) Item 1, Page 30.
Define "National Standard" as the term is utilized in the section entitled“Adjustment Warranted as Shown by National Standard”. Which entityhas established this standard?
There is no standard bed to population ratio either nationally applied toTennessee based on any known research. A more accurate term is “NationalRatio”. What is presented is the actual ratio of burn beds per 150,000population for the United States. This ratio is much lower than the ratio setforth in the Burn Unit Criteria and Standards reflecting the fact that there isless availability of beds in Tennessee than in the country as a whole.
17. Section B, Need, Item A (Specific Criteria – Burn Units) Item 1, Page 31.
If focus will be on adult patients, will the three pediatric beds be used foroverflow?
Patient demands will dictate overflow. It is important that the burn bedsremain flexible to adjust to demands which may fluctuate from day to day.While it is possible that the pediatric beds will be used for overflow duringspikes in demand, it is not anticipated that this will happen often; thus, moreoften than not, these beds will be available for pediatric burn patients.
Supplemental 1 January 28, 2021
461

21
18. Section B, Need, Item A (Specific Criteria – Burn Units) Item 1, Page 32.
Reference the specific page and section of the application for the"utilization analysis below". How many are projected to be TN patientsand what data is available on TN burn patients to support the projectedutilization data? Other state data can be analyzed as well, but at aminimum, TN patient data should be presented as a standalone table.
Page 32 references the projected utilization analysis on pages 64 - 66 inresponse Section B, Need, Item B (Special Needs of the Service Area) Item 6.
As described in detail in the original CON application, Skyline used 2017-2019 data from THA, KHA, and GHA to identify service area patientsmeeting ABA criteria for referral to a burn center. This data was analyzed forthe PSA and SSA proposed to be served by Skyline as well as by state. Pleasesee pages 64-66 and response to Questions 26-27 of this supplement.
19. Section B, Need, Item A (Specific Criteria – Burn Units) Item 1, Page 34.
Regarding section titled “Service Area Burn Patients Leaving the Area for Burn Care” on page 34, please provide any data available to demonstratethat patients are traveling significant distance for follow up services. Ifpossible, articulate how TriStar follow-up services will represent a moreaccessible alternate for follow-up care if burn patients are referred to thisnew burn center in Nashville.
Skyline was not able to ascertain specific data for patients traveling forfollow-up care, as this data is not publicly available to the best of Skyline’sknowledge. However, burn care is a regional service, and there is only oneprovider serving all of Middle and East Tennessee. Thus, it logically followsthat patients in the service area not residing in or around Nashville musttravel far distances for their initial burn injury care. While the travel via air orground transport associated with the initial encounter may not becumbersome for the patient, having to travel several hours one way back tothe facility where the initial treatment was administered for subsequentmultiple follow-up visits could pose a significant financial burden on patientsand their families.
TriStar Division has a robust telehealth program and several outpatientwound care clinics throughout the service area. Thus, a patient could come toSkyline for their initial acute care and access follow up care virtually and inan outpatient facility closer to home. This will significantly improveconvenient access to comprehensive care for burn patients in the service area.
Supplemental 1 January 28, 2021
462

22
20. Section B, Need, Item A (Specific Criteria – Burn Units) Item 1, Page 43
What SKYLIFE resources will be available when to support the burn unitwhen this helicopter is out on another call?
TriStar’s air transportation plan is fully integrated into GMR which has 37aircrafts. If one aircraft is out on another call, the next closest aircraft will bedeployed and dispatched.
21. Section B, Need, Item A (Specific Criteria – Burn Units) Item 1, Pages 47.
Regarding Section “Local Post Discharge Care Continuum” please detailany existing hospital relationships in the secondary service area thatsupport a local post discharge care continuum.
As detailed in the Applicant’s response to Question 3 above, TriStar Divisionhas existing hospital relationships throughout the service area, including thesecondary service area, as documented by the patient transfers fromcommunity hospitals in the service area. As noted in the original CON,TriStar Division operates two hospitals in Chattanooga and has a presence inKnoxville as previously discussed above. Additionally, TriStar Division is inthe process of developing a plan to expand its relationships throughout theservice area with additional telehealth and wound care locations independentof this burn unit proposal. Also, Skyline has been in discussion with servicearea hospitals who have expressed support for the proposed project.Accordingly, TriStar Division will work to continue to develop andstrengthen relationships with all hospitals in the secondary service area toidentify appropriate post-discharge care, such as utilizing telehealth, utilizingcommunity hospital wound care programs if they exist, and referring to ruralhospital swing bed programs for continued rehab when clinicallyappropriate.
Regarding Section “Wound Care Linkages,” how will the project representan enhancement to wound care access in the service areas and specificallythe secondary service area of East TN. Are there plans for expansion ofwound care centers into the East TN region?
TriStar Division operates several wound clinics throughout the service areawhich will enhance access to outpatient follow-up care for the service area.TriStar Division plans to expand its telehealth and wound care network,including more locations in East Tennessee. This expansion is in progressregardless of the proposed burn center.
Supplemental 1 January 28, 2021
463

23
22. Section B, Need, Item A (Specific Criteria – Burn Units) Item 1, Pages 49.
Regarding Section “Skyline Projected Utilization Will Not Impact VUMC’s Program”, is any additional detail available about where this project’spatient base will come from that demonstrates it will not overlap with theVUMC patient base?
As noted on page 64-66, all patients from the service area who havehistorically received care at VUMC were removed from the base of patientsused for Skyline’s projected utilization. The remaining patients received burncare either an out-of-state or a non-burn center hospital. This is the base ofpatients that Skyline projects to serve.
Please provide detail about the strategy to generate more transfer referralsfor those patients who are being served at non-burn center hospitals andwhy a greater percentage of those referrals will come to the new burncenter, i.e. (access to transportation resources, local follow-up care,telemedicine, quality of care, etc.).
As discussed herein, TriStar Division will:
Incorporate burn referral and follow-up care education into itsexisting education and outreach program for communityhospitals throughout the region.
Utilize BRCA’s Physician and Provider Relations Liaisons tobuild relationships with specific community hospitals in need ofburn care education.
Continue to develop its relationships with rural communityhospitals throughout the service area.
Continue to expand its existing telehealth and wound centernetwork to include more locations throughout the service area,particularly East Tennessee.
Leverage its existing air and ground transportationrelationships throughout the service area to increase access toburn care.
Seek ABA verification for the proposed burn center.
Each of these initiatives will generate more transfer referrals for patients served in non-burn center hospitals. Patients are more likely to come to the new burn center when they are educated on the implications of their burn injury, the non-burn center in their community refers them, and they trust the quality of care that is provided at the burn center to which they are being referred. While Skyline is committed to high quality care regardless, ABA verification will ensure the public of this commitment.
Supplemental 1 January 28, 2021
464

24
23. Section B, Need, Item A (Specific Criteria – Construction, Renovation,Expansion, and Replacement of Health Care Institutions) Item 3.a, Pages53-54.
What consultation services will be available to the secondary service area? Which areas is the applicant targeting for expansion of these consultation services in order to support this project?
Through its TriStar Division affiliation, Skyline has established a relationship with Burn and Reconstructive Centers of America (BRCA) to assist with the development of its burn program. BRCA maintains a 24/7 Burn Referral Call Center that facilitates physician consultations, referrals, and transfers. Call Center Specialists will take incoming calls and relevant information and then connect the referring provider with a BRCA provider and will remain on the line for documentation. The BRCA provider will guide the referring physician through the process and help them determine the most appropriate plan of care. They also maintain a HIPAA-compliant burn referral mobile app, which can initiate the burn referral and consultation process. Skyline expects to receive referrals through this program. This consultation service will be available to the service area to connect them with area providers including the proposed burn center if approved.
24. Section B, Need, Item 3, Projected Utilization Tables, Page 56.
Please detail Projected Utilization Tables by County and ensure that, at aminimum, TN counties are broken out separately from out-of-state countiesfor the need statement. Please complete the table and resubmit page 56 as(page 56R).
As discussed above, the uniqueness and randomness of burn injury eventsprohibits a reasonable projection of patients by county. This is demonstratedby the fact that VUMC served patients from 134 counties and 16 states overthe period 2017 to 2018.1 From year to year, the projection of burn patients bycounty cannot be reasonably predicted. For this reason, Skyline projecteddata on a service area basis subdivided by state on page 56 and shown below.To project at a more micro-level would not lead to reasonable results or ameaningful projection.
1 Please note that THA prohibits presentation of individual hospital data for the most recent year (2019).
Supplemental 1 January 28, 2021
465

25
25. Section B, Need, Item 4.A.1, Page 59.
The chart is using 2013 data/results. Is there one with more recentdata/results?
No, the data presented is the most recent publicly available data.
26. Section B, Need, Item 6, Page 64.
Regarding Section “Trend in Total Service Area Burn Patients That Meet Burn Referral Criteria Including DRGs for Inhalation Injuries”, pleaseidentify the counties in the service area that are included in this analysis.Where were these patients receiving services? Does this data includepatients who were served at a burn center in Memphis, Kentucky, Alabamaor Georgia?
As discussed in detail, analysis of burn data by county does not provide formeaningful analysis due to the randomness and variability from year to year.The table on page 64 entitled “Trend in Total Service Area Burn Patients thatMeet Burn Referral Criteria Including DRGs for Inhalation Injuries” has beenbroken out by PSA/SSA and state below to identify Tennessee patients alongwith Kentucky (and limited Alabama patients). This data includes patientsthat were served in Memphis, Kentucky, or Georgia. Alabama hospital datais not available.
Supplemental 1 January 28, 2021
466

26
2017 2018 20192-Year CAGR
PSA - TN 341 373 426 5.9%SSA - TN 214 204 207 -0.8%Total Tennessee Service Area 555 577 633 3.4%PSA - KY 108 149 126 4.0%SSA - KY 39 31 29 -6.9%Total Kentucky Service Area 147 180 155 1.3%Alabama (only inmigration)* 3 8 9 36.6%Total Service Area 705 765 797 3.2%
Trend in Total Service Area Burn Patients That Meet Burn Referral CriteriaIncluding DRGs for Inhalation Injuries
Source: THA/KHA/GHA Data. Does not Include AL data except for patients in-migrating to TN
From this data, patients served at Vanderbilt or a specialty children’s hospital were removed to focus on patients who are not served at burn center or were served at a significant distance outside the service area. These data include a few patients treated in Memphis at Regional One (3 in 2017, and 4 in 2018)2.
27. Section B, Need, Item 6, Page 65.
Define what is meant by "2019 SA Patients Better Served at Skyline*". Dothese patients include any individuals who were served at a burn centerother than VUMC or is it entirely patients who were served in a non-burncenter hospital, but met referral criteria for burn-center services?
These patients include patients served at more distant burn centers orpatients who were served at non-burn center hospitals who met referralcriteria for burn-center services. All VUMC patients and those served atspecialized children’s hospitals have been removed. The vast majority ofthese patients were served at non-burn center hospitals.
2 Please note that THA prohibits presentation of individual hospital data for the most recent year (2019).
Supplemental 1 January 28, 2021
467

27
Service Area/StateYear 1 -
2022Year 2 -
2023Year 3 -
2024Primary Service Area
Tennessee 71 111 138 Kentucky 46 71 89 Alabama 21 32 38
Secondary Service AreaTennessee 60 94 117 Kentucky 14 21 26
Total 212 329 408
Skyline Projected Admissions by Service Area & State
2017 2018 2019PSA - TN 95 128 125SSA - TN 138 128 119Total Tennessee Service Area 233 256 244PSA - KY 66 91 72SSA - KY 34 27 27Total Kentucky Service Area 100 118 99Alabama (only inmigration)* - 5 1 Total Service Area 333 379 344
Service Area Burn Patients Excluding Patients Treated by Vanderbilt or Children Treated at a Pediatric Hospital
Source: THA/KHA/GHA Data. Does not Include AL data except for patients in-migrating to TN
Regarding the second table on page 65 - How many of these patients are expected to come from Tennessee Counties? Please breakdown by county.
The follow table presents the information in the second table on page 65 broken out by service area and state. County information would not be consistent across years nor serve as a reliable basis for projection.
The following table presents Skyline’s projected total patient admissions by service area and state updated from page 66 as requested in Question 18 of this supplement.
2017 2018 2019
Burn Center Outside of the Service Area 37 33 39Non-Burn Center Hospital 123 191 159
Burn Center Outside of the Service Area 34 36 20Non-Burn Center Hospital 139 119 126Total 333 379 344
SSA
Service Area Patients Better Served at Skyline
PSA
Supplemental 1 January 28, 2021
468

28
28. Section B, Economic Feasibility, Historical Data Charts, Item 3, Pages 70.
Please explain why a negative amount is listed under F.3. of the HistoricalData Chart – Total Facility. If appropriate, please revise submit areplacement page 70 (labeled as 70R).
HCA is Skyline’s ultimate parent organization. Deposits Skyline make as an HCA affiliate to the parent company pay Skyline interest calculated at prime plus 2%. This positive earnings/cash flow results in negative interest expense, or more accurately interest income that is expected to continue within the project as well. There is no other more appropriate place to show this interest income on the Historical Data Chart.
29. Section B, Economic Feasibility, Projected Data Charts, Item 4, Page 73 &75.
B.1 Project Only - Round up the dollar amount for Inpatient Services in2022 on the Projected Data Chart.
See Replacement Page 73R.
C - Year one Total Deductions is $1 too high. Please revise.
See Replacement Page 73R.
F.3 - Negative interest is listed on both Project Only and Total FacilityProjected Data Charts. Please explain why there are negative amountslisted. Revise and replace both Projected Data Charts as page 73 (labeled as73R) and page 75 (labeled as 75R).
Please see the Applicant’s response to Question 28 above. Interest income is shown on this line item as there is no other appropriate line item on the Projected Data Charts.
30. Section B, Economic Feasibility, Item 5.A, Page 77.
Complete the Percentage Change Fields. Please revise and resubmit theProject Only Gross Revenue Chart on page 77 as (page 77R).
See Replacement Page 77R.
Supplemental 1 January 28, 2021
469

29
31. Section B, Economic Feasibility, Item 7, Page 81.
In the Applicant’s Projected Payor Mix, Year 1 please separate Charity Carefrom Self/Pay. List Charity Care at the bottom of the Chart under the TotalRow. Please revise and resubmit this chart on page 81 as (page 81R).
See Replacement Page 81R.
32. Section B, Economic Feasibility, Item 8, Page 82.
List the Existing FTEs for Direct and Non-Direct Patient Care Positions as 0for the column if there are no positions dedicated to the operation of theburn unit. Please revise and resubmit the table on page 82 as (page 82R)
See Replacement Page 82R.
33. Section B, Quality Standards, Item B.1.c., Page 85.
Question was not answered.
As it relates to this question, Skyline received the following emailcorrespondence from Mr. Thomas Pitt on 1/27/2021:
Please disregard Question #33. Question #34 Section B, Quality Standards, Item C., Page 86. Provide a response to Question C is the only question that required a response.”
Please see the Applicant’s answer to Question 34 below.
34. Section B, Quality Standards, Item C., Page 86.
Provide a response to Question C.
C. Does the applicant plan, within 2 years of implementation of the project,to participate in self-assessment and external assessment against nationallyavailable benchmark data to accurately assess its level of performance inrelation to established standards and to implement ways to continuouslyimprove?
Note: Existing licensed, accredited and/or certified providers are encouraged to describe their process for same.
Supplemental 1 January 28, 2021
470

30
Yes, the applicant plans, within 2 years of implementation of the project, to participate in self-assessment and external assessment against nationally available benchmark data to accurately assess its level of performance in relation to established standards and to implement ways to continuously improve. This process will be incorporated into the Applicant’s ABA verification process which requires a similar assessment.
35. Section B, Contribution to the Orderly Development of Healthcare, Item2.a., Page 89.
Please address any anticipated benefit this project will provide through increased access to air or ground transportation for specific regions of the state, access to follow-up services, insurance plans that are accepted by Tri-Star, but not the existing provider VUMC.
Skyline anticipates that patients will benefit vastly from the proposed project, particularly as it relates to medical transport and access to follow-up care. As detailed throughout this document, TriStar Division has a partnership with GMR which operates 37 air transportation bases in Tennessee, Kentucky, Georgia, and Alabama. TriStar Division SKYLIFE helicopter can fly an IFR plan which allows the helicopter to be flown in inclement weather when visibility is compromised; the helicopter can fly 300 air miles roundtrip, therefore expanding access to care within a 150-mile radius of Nashville.6 TriStar Division’s partner GMR operates several helicopter bases in East Tennessee which further expands the service area’s access to care via air ambulance transport.
TriStar also has a large and growing telehealth and wound care network throughout the service area and is in the process of expanding this network even further into East Tennessee where there is a gap in access to comprehensive burn care.
6 The 150-mile radius is based on the distance the helicopter can travel without the need to re-fuel. The radius is based on air milage, not driving mileage.
Supplemental 1 January 28, 2021
471

AFFIDAVIT
STATE OF TENNESSEE
COUNTY OF (:ijvidson
NAME oF FAc1uTY: Ji:i Shar Skylini /V\i1:Hcal Cmkr
1, Mn l;rwu.r , after first being duly sworn, state under oath that I am the
applicant named in this Certificate of Need application or the lawful agent thereof, that I
have reviewed all of the supplemental information s
accurate, and complete.
Sworn to and subscribed before me, a Notary Public, this the 2B+J> day of s.JaQU4.r\l, 2011.,witness my hand at office in the County of 1)1vtdson I
State of Ten�essee.
My commission expires A�u.&-/- QO
HF-0043
Revised 7/02
. 2021
Supplemental 1 January 28, 2021
472

January 29, 2021
Thomas Pitt HSD Examiner Tennessee Health Services and Development Agency Andrew Jackson State Office Building, 9th Floor 502 Deaderick Street Nashville, TN 37243
RE: TriStar Skyline Medical Center, CN2101-003, Supplemental Response #2
Dear Mr. Pitt,
On behalf of TriStar Skyline Medical Center, please accept this supplemental information in response to your January 28, 2021 request regarding the above-referenced CON application for the initiation of a burn unit that will be located at the TriStar Skyline Medical Center main campus at 3441 Dickerson Pike, Nashville, Tennessee 37207.
Should you have any questions or require additional information, please do not hesitiate to contact me.
Sincerely,
�JU� Cody Adams
Supplemental 2 January 29, 2021
473

TriStar Skyline Medical Center CN2101-003
Initiation of a Burn Unit Supplemental Response #2
January 29, 2021
TriStar Skyline (“Skyline” or the “Applicant”) provides the following responses to the HSDA staff’s second request for supplemental information regarding CN2101-003 for the initiation of a burn unit that will be located at Skyline’s main campus in Nashville, Tennessee.
1. Section B, Economic Feasibility, Projected Data Charts, Item 4, Page 73 & 75 andreplacement page 73R.
The calculation for Net Operating Revenue ($6,299,935) on replacement page73R is $1.00 less than the total of Gross Operating Revenue ($36,734,047) - TotalDeductions ($30,434,111). Please revise the Project Only Projected Data Chartand resubmit as page 73R2.
Please see Replacement Page 73R2.
The calculations on page 75 of the original application - Total Facility ProjectedData Chart for Section C - Deductions form Gross Operating Revenue - TotalDeductions ($2,472,531,899) is $1.00 more than the value of line items 1-3. Thecalculation for Gross Operating Revenue in Year 2023 is $1.00 more than thevalue of line items 1-4. Please revise the Total Facility Projected Data Chart andresubmit as 75R.
Please see Replacement Page 75R.
2. Section B, Economic Feasibility, Item 7, Page 81 and 81R
There are calculation errors of $1.00 on both Projected Gross Operating Revenuecharts on replacement page 81R. Please revised and resubmit as page 81R2.
Please see Replacement Page 81R2.
3. Section B, Economic Feasibility, Item 8, Page 82 and 82R2.
Please include a note on page 82R under the Existing FTEs (enter year) columnstating which facilities operated by TriStar are represented in these FTE figures.Revise and resubmit page 82R as page 82R2.
Please see Replacement Page 82R2.
Supplemental 2 January 29, 2021
474

AFFIDAVIT
STATE OF TEn
SSEE
couNrv oF �!\u i ds W1
NAMEOFFAc1urv: Tr 1sl,w Sk.Jint Metlaj Ctrt-!e.r
I, fi U }b'y\ C-.r CC (ll , after first being duly sworn, state under oath that I am the applicant named in this Certificate of Need application or the lawful agent thereof, that I have reviewed all of the supplemental information accurate, and complete.
Sworn to and subscribed before me, a Notary
witness my hand at office in the County of
My commission expires M LI,) 1� HF-0043
Revised 7/02
blic,,thj,s the {).t,1-t;ay ol°JMHf't
. 20J.:L
I IJS -
, State of Tennessee.
C, d ARY PUBLIC
,:;oof
Supplemental 2 January 29, 2021
475

476







DOH/…CON#2101-003 TriStar Skyline Medical Center Burn Unit
CERTIFICATE OF NEED REVIEWED BY THE DEPARTMENT OF HEALTH
DIVISION OF POLICY, PLANNING AND ASSESSMENT 615-741-1954
DATE: 2-28-2021 APPLICANT:
TriStar Skyline Medical Center
CON#: CN2101-003 CONTACT PERSON: Cody Adams
TriStar Medical Center 3441 Dickerson Pike Nashville, TN 37207
COST: $5,411,637
In accordance with Section 68-11-1608(a) of the Tennessee Health Services and Planning Act of 2002, the Tennessee Department of Health, Division of Policy, Planning, and Assessment, reviewed this certificate of need application for financial impact, TennCare participation, compliance with Tennessee’s State Health Plan, and verified certain data. Additional clarification or comment relative to the application is provided, as applicable, under the heading “Note to Agency Members.”
GENERAL CRITERIA FOR CERTIFICATE OF NEED The applicant responded to all of the general criteria for Certificate of Need as set forth in the document Tennessee’s State Health Plan. SUMMARY: The applicant, TriStar Skyline Medical Center, (TSMC) is seeking Certificate of Need approval to establish a comprehensive Burn Unit at its main campus in Nashville, TN. This project will involve the conversion of existing ICU beds to dedicated burn unit beds and does not change the number of beds in the hospital’s total bed compliment. The applicant is a 407-bed acute care hospital owned by HCA Healthcare, Inc. TriStar Division is composed of 20 hospitals with 11 surgery centers, 22 urgent care centers and 88 physician practices around Tennessee, southern Kentucky, and northwest Georgia. NEED: The applicant’s primary service area includes 51 of the 95 Tennessee counties, plus a large portion of Kentucky counties. The 2020 population estimate for the Tennessee counties is 3,449,536 increasing to 3,604,260 for estimated 2024 population, a 3.9% increase. The applicant also lists 34 additional counties in Tennessee as a secondary service area. Vanderbilt University Medical Center is the only other existing provider for comprehensive burn services in the general service area. The proposed service area will overlap with VUMC’s current service area. This project will offer patients another option and location for burn services.

__________________________________________________________________________________________________ DOH/…CON#2101-003 TriStar Skyline Medical Center
Burn Unit
- 2 -
The applicant maintains that due to limited burn care medical staff, it is important to have redundancy of these services in the event of a mass causality disaster to ensure that primary burn care providers are not overwhelmed and patients can receive the burn care they need. The applicant provides an estimated patient origin chart for Vanderbilt using Tennessee Hospital Association data:
In 2019, TSMC opened an expansion of 54 new inpatient beds providing for needed capacity while allowing for the future development of a comprehensive burn unit. This expansion also added 30 ICU beds to its campus. The proposed project will be located in an existing 12 bed ICU above the Emergency Department. This area will be redesigned and fitted for the burn unit.

__________________________________________________________________________________________________ DOH/…CON#2101-003 TriStar Skyline Medical Center
Burn Unit
- 3 -
TENNCARE/MEDICARE ACCESS: The applicant is accessible to patients with Medicare and TennCare/Medicaid, (#44-0006) The applicant states TriStar Health provides approximately $132 million annually in uncompensated care to the communities it serves. The applicant provides their Financial Assistance and Charity Care documentation in Section B-Quality-2A ECONOMIC FACTORS/FINANCIAL FEASIBILITY: The Department of Health, Division of Policy, Planning, and Assessment have reviewed the Project Costs Chart, the Historical Data Chart, and the Projected Data Chart to determine if they are mathematically accurate and if the projections are based on the applicant’s anticipated level of utilization. The location of these charts may be found in the following specific locations in the Certificate of Need Application or the Supplemental material: Funding for this project will be provided by parent company HCA. HCA will finance the project with accumulated reserves. In Section B-Economic Feasibility the applicant provides a letter from TriStar Division CFO committing to provide the project funding through cash reserves. Project Costs Chart: The project costs chart is located on page 69 of the application with
a total estimated project cost is $5,411,637, including $2,589,367 on construction costs. On page 137 of the application, is a letter from Gresham Smith company detailing the appropriateness of the construction costs and the ability to meet federal and state building regulations. Historical Data Chart: Not applicable, this is a new project. Projected Data Chart: The Projected Data Chart is located on page 74 of the application. The applicant projects to treat 212 inpatients in Year 1, 329 inpatients in Year 2, and 408 inpatients in Year 3, with Net Incomes of $1,612,614 and $3,632,842 respectively.
Proposed Charge Schedule Previous Year Current Year Year One Year Two % Change
Gross Charge n/a n/a $173,274 $187,341 n/a
Average Deduction
n/a n/a $143,557 $157,142 n/a
Average Net Charge
n/a n/a $29,717 $30,198 n/a
The following chart shows the projected payor mix for the first year of the project:
Projected Payor Mix Year One (project only) Payor Source Projected Gross
Operating Revenue
% of Total
Medicare/Medicare Managed Care $11,577,806 31.5% TennCare/Medicaid $8,332,144 22.7%
Commercial/Other Managed Care $8,671,243 23.6% Self-Pay $3,100,333 8.4% Other $3,245,661 8.8% Total $34,927,187 95.1%
Charity Care $1,792,380 4.9%

__________________________________________________________________________________________________ DOH/…CON#2101-003 TriStar Skyline Medical Center
Burn Unit
- 4 -
CONTRIBUTION TO THE ORDERLY DEVELOPMENT OF HEALTHCARE: The proposed burn unit will be designated as an ICU. However, the burn beds will be designed as adjustable acuity beds. This way, the room and staff transform to the needs of the patient which eliminates the need for patients to be transferred to different care areas as their recovery progresses. The applicant will also serve outpatients recovering from burns on an outpatient basis. The applicant has provided historical data showing an increased trend for inpatient burn units in the service areas:
The TriStar Division has partnered with Global Medical Response which operates 37 air ambulance bases in Tennessee, Kentucky, Georgia, and Alabama. This will enable TSMC to coordinate extended transportation for patients requiring comprehensive burn care. The applicant provides a Project Completion Forecast chart with a Final Project Report Form submitted on 2/1/2022. QUALITY MEASURES: The applicant is licensed by the Department of Health, license # 0000000023. The applicant is accredited by The Joint Commission most recently June 20, 2019. TSMC plans to become the only verified burn unit by the American Burn Association in middle and eastern Tennessee. TriStar Health has a number of nationally recognized programs and accredited services throughout its network, including:
• Cardiac Care Center • Behavioral Health • Stroke Care • Trauma Services • Pediatrics • Obstetrics • Oncology Research and Services
All seven Middle Tennessee TriStar Health hospitals were awarded an ‘A’ in the spring 2020 Leapfrog Hospital Safety Grade, a national distinction recognizing TriStar Health’s achievements providing safer health care. The applicant participates in multiple clinical training programs as detailed in Section B-Orderly Development-3C.
BURN UNITS I . There should be no more than one b u r n u nit bed for every 225,000 persons. This
standard may be adjusted to reflect actual incidence in a geographic medical service area as documented by the applicant.
The 2024 population for the 51 Tennessee county service is estimated to be 3,604,260. Using the bed calculation of one burn unit bed for every 225,000 persons, the burn unit
bed needs results in a need for 16 beds in the service area. 2. The need shall be based upon the current year's population projected four years
forward.

__________________________________________________________________________________________________ DOH/…CON#2101-003 TriStar Skyline Medical Center
Burn Unit
- 5 -
Tennessee Population Estimates 2020 and 2024 *
Population
Estimate 2020 Population
Estimate 2024 % Increase
Total Total Total
Tennessee 6,883,34
7 7,097,353 3.1% Primary Service Area Counties Bedford 50,143 52,701 5.1% Benton 15,887 15,719 -1.1% Bledsoe 15,102 15,461 2.4% Cannon 14,193 14,299 0.7% Cheatham 40,536 41,008 1.2% Clay 7,617 7,455 -2.1% Coffee 56,374 57,989 2.9% Cumberland 61,043 63,074 3.3% Davidson 715,491 743,578 3.9% Decatur 11,742 11,662 -0.7% DeKalb 19,716 20,002 1.4% Dickson 54,556 56,694 3.9% Fentress 18,286 18,427 0.8% Franklin 41,998 42,214 0.5% Giles 29,129 28,873 -0.9% Grundy 13,098 12,771 -2.5% Hamilton 369,758 380,765 3.0% Hardin 25,615 25,456 -0.6% Henry 32,538 32,616 0.2% Hickman 24,567 24,754 0.8% Houston 8,146 8,147 0.0% Humphreys 18,372 18,350 -0.1% Jackson 11,779 11,922 1.2% Lawrence 43,607 43,964 0.8% Lewis 11,881 11,813 -0.6% Lincoln 33,960 34,172 0.6% Macon 24,455 25,361 3.7% Marion 28,988 29,407 1.4% Marshall 33,131 34,218 3.3% Maury 94,683 99,145 4.7% Montgomery 212,678 229,426 7.9% Moore 6,408 6,480 1.1% Morgan 21,904 22,163 1.2% Overton 22,425 22,717 1.3% Perry 8,022 8,064 0.5% Pickett 5,116 5,079 -0.7% Putnam 78,839 81,521 3.4% Rhea 33,185 33,842 2.0% Robertson 72,550 75,704 4.3% Rutherford 338,405 368,667 8.9% Sequatchie 15,629 16,287 4.2% Smith 19,964 20,383 2.1% Stewart 13,270 13,317 0.4%

__________________________________________________________________________________________________ DOH/…CON#2101-003 TriStar Skyline Medical Center
Burn Unit
- 6 -
Sumner 191,743 203,030 5.9% Trousdale 8,655 9,012 4.1% VanBuren 5,653 5,587 -1.2% Warren 40,773 40,947 0.4% Wayne 16,617 16,469 -0.9% White 27,267 27,774 1.9% Williamson 241,035 262,948 9.1% Wilson 143,007 152,826 6.9%
3,449,53
6 3,604,260 * TN_CoPopProj_2017 UTCBER Population Projection Series.
3. Each new burn unit proposed shall have a minimum of 12 beds with 6-9 beds designated for adults and 3-6 beds for ped iatric patients.
This project proposes 12 burn unit beds: 9 adult beds and 3 pediatric beds.
4. All existing specialized burn care beds in a service area must have an annual
occupancy rate of 70 percent before any additional beds are approved.
This Occupancy is taken from Schedule D, Intensive Care Bed occupancy data. This data could contain other patient days than burn patients. A more accurate occupancy might be obtained by using the Joint Annual Report data on Schedule G, Utilization By Major Diagnostic Categories. Category Discharges Patient Days Occupancy Burn 386 3208 35%
Source: 2019 JAR VUMC 25 Burn beds x 365 days = 9125 maximum patient days 3208 patient days / 9125 max patient days = .35% Occupancy 5. Each proposed burn unit should document that a minimum of 50 patients with
major burn injury to moderate uncomplicated burn injury will be treated each year.
The applicant projects to treat 212 inpatients in Year 1, 329 inpatients in Year 2, and 408 inpatients in Year 3.

__________________________________________________________________________________________________ DOH/…CON#2101-003 TriStar Skyline Medical Center
Burn Unit
- 7 -
6. Each burn unit shall have available, either through direct control or through a
network of clearly identified relationships, a system of transportation sufficient to bring patients to the un it.
The TriStar Division has partnered with Global Medical Response which operates 37 air ambulance bases in Tennessee, Kentucky, Georgia, and Alabama. This will enable TSMC to coordinate extended transportation for patients requiring comprehensive burn care.
7. A network of relationships should be available to transport patients to other units when there are no beds available at a particular site.
The applicant states they currently have a network of relationships available to transport patients to other bun units when no beds are available at the proposed burn unit.