Traumatic experience, cannabis use, life satisfaction, and schizotypy
12
This article was downloaded by: [University of Ulster Library] On: 28 January 2015, At: 09:40 Publisher: Routledge Informa Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK Psychosis: Psychological, Social and Integrative Approaches Publication details, including instructions for authors and subscription information: http://www.tandfonline.com/loi/rpsy20 Traumatic experience, cannabis use, life satisfaction, and schizotypy Seamus Fleming a , John Mallett a , Jamie Murphy a & Mark Shevlin a a Psychology Research Institute, University of Ulster , Northern Ireland , UK Published online: 23 Aug 2011. To cite this article: Seamus Fleming , John Mallett , Jamie Murphy & Mark Shevlin (2012) Traumatic experience, cannabis use, life satisfaction, and schizotypy, Psychosis: Psychological, Social and Integrative Approaches, 4:2, 126-136, DOI: 10.1080/17522439.2011.587527 To link to this article: http://dx.doi.org/10.1080/17522439.2011.587527 PLEASE SCROLL DOWN FOR ARTICLE Taylor & Francis makes every effort to ensure the accuracy of all the information (the “Content”) contained in the publications on our platform. However, Taylor & Francis, our agents, and our licensors make no representations or warranties whatsoever as to the accuracy, completeness, or suitability for any purpose of the Content. Any opinions and views expressed in this publication are the opinions and views of the authors, and are not the views of or endorsed by Taylor & Francis. The accuracy of the Content should not be relied upon and should be independently verified with primary sources of information. Taylor and Francis shall not be liable for any losses, actions, claims, proceedings, demands, costs, expenses, damages, and other liabilities whatsoever or howsoever caused arising directly or indirectly in connection with, in relation to or arising out of the use of the Content. This article may be used for research, teaching, and private study purposes. Any substantial or systematic reproduction, redistribution, reselling, loan, sub-licensing, systematic supply, or distribution in any form to anyone is expressly forbidden. Terms & Conditions of access and use can be found at http://www.tandfonline.com/page/terms- and-conditions
Transcript of Traumatic experience, cannabis use, life satisfaction, and schizotypy

This article was downloaded by: [University of Ulster Library]On: 28 January 2015, At: 09:40Publisher: RoutledgeInforma Ltd Registered in England and Wales Registered Number: 1072954 Registeredoffice: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK
Psychosis: Psychological, Social andIntegrative ApproachesPublication details, including instructions for authors andsubscription information:http://www.tandfonline.com/loi/rpsy20
Traumatic experience, cannabis use,life satisfaction, and schizotypySeamus Fleming a , John Mallett a , Jamie Murphy a & Mark Shevlina
a Psychology Research Institute, University of Ulster , NorthernIreland , UKPublished online: 23 Aug 2011.
To cite this article: Seamus Fleming , John Mallett , Jamie Murphy & Mark Shevlin (2012) Traumaticexperience, cannabis use, life satisfaction, and schizotypy, Psychosis: Psychological, Social andIntegrative Approaches, 4:2, 126-136, DOI: 10.1080/17522439.2011.587527
To link to this article: http://dx.doi.org/10.1080/17522439.2011.587527
PLEASE SCROLL DOWN FOR ARTICLE
Taylor & Francis makes every effort to ensure the accuracy of all the information (the“Content”) contained in the publications on our platform. However, Taylor & Francis,our agents, and our licensors make no representations or warranties whatsoever as tothe accuracy, completeness, or suitability for any purpose of the Content. Any opinionsand views expressed in this publication are the opinions and views of the authors,and are not the views of or endorsed by Taylor & Francis. The accuracy of the Contentshould not be relied upon and should be independently verified with primary sourcesof information. Taylor and Francis shall not be liable for any losses, actions, claims,proceedings, demands, costs, expenses, damages, and other liabilities whatsoever orhowsoever caused arising directly or indirectly in connection with, in relation to or arisingout of the use of the Content.
This article may be used for research, teaching, and private study purposes. Anysubstantial or systematic reproduction, redistribution, reselling, loan, sub-licensing,systematic supply, or distribution in any form to anyone is expressly forbidden. Terms &Conditions of access and use can be found at http://www.tandfonline.com/page/terms-and-conditions

Traumatic experience, cannabis use, life satisfaction, andschizotypy
Seamus Fleming*, John Mallett, Jamie Murphy and Mark Shevlin
Psychology Research Institute, University of Ulster, Northern Ireland, UK
(Received 5 November 2010; final version received 9 May 2011)
Research has shown that various environmental factors predict schizotypy. Thisstudy aimed to assess the association of a range of demographic, psycho-socialand experiential factors with schizotypy, based on a sample of 258 universitystudents. Results showed that age, gender, cannabis use, traumatic experienceand life satisfaction significantly predicted overall schizotypy. However, effectsvaried across schizotypy subdimensions. The models that best predicted schizo-typy differed in accordance with the unique combination of facets of each subdi-mension. Differential effects of the predictors in this study continue to validatedimensional representations of the schizotypal construct.
Keywords: schizotypy; psychosis; trauma; cannabis; life satisfaction
Introduction
Schizotypy is a multi-dimensional construct, and to date statistical representationshave identified six discrete, but correlated, dimensions. While early dichotomousrepresentations comprised positive and negative symptom clusters (paralleling thepositive–negative representations of schizophrenia symptomatology), contemporarymodels have recognized three or more dimensions (Fonseca-Pedrero et al., 2008).These include disorganization, social decline or affective disorder and impulsivenon-conformity (Paino-Pinero, Fonseca-Pedrero, Lemos-Giraldez, & Muniz, 2008).A basic assumption of these dimensions is that they parallel the underlying subtypesof schizophrenia (Badcock & Dragovic, 2006). Therefore, given the comparabilitybetween schizotypy and clinical psychosis, the “psychosis proneness” status ofschizotypy affords a valuable opportunity to investigate subclinical dimensionalityand risk, and may further our understanding of psychosis at both clinical and sub-clinical levels.
Previous research has suggested that individuals high on schizotypy are atheightened risk for later development of schizophrenia-spectrum disorders (Kwapil,Miller, Zinser, Chapman, & Chapman, 1997). Moreover, neural correlates of schizo-phrenia-spectrum disorders have also been found to be associated with schizotypy(Skosnik, Krishnan, Aydt, Kuhlenshmidt, & O’Donnell, 2006). These findings sug-gest the existence of a continuum from psychotic disorder (clinical level) to psycho-sis-like experiences (subclinical/schizotypal level), and that psychosis at all levels issusceptible to a common continuum of risk (Paino-Pinero et al., 2008).
*Corresponding author. Email: [email protected]
PsychosisVol. 4, No. 2, June 2012, 126–136
ISSN 1752-2439 print/ISSN 1752-2447 online� 2011 Taylor & Francishttp://dx.doi.org/10.1080/17522439.2011.587527http://www.tandfonline.com
Dow
nloa
ded
by [
Uni
vers
ity o
f U
lste
r L
ibra
ry]
at 0
9:40
28
Janu
ary
2015

Traumatic experiences have been associated with higher levels of schizotypy,with individuals high on schizotypy showing heightened levels of trauma-relatedintrusions (Dumas et al., 2002; Harley et al., 2008; Merckelbach & Giesbrecht,2006). A history of trauma has also been associated with “schizotypal” beliefs andexperiences and is recognized as a risk factor that may precipitate transition to clini-cal disorder (Steel, Marzillier, Fearon, & Ruddel, 2009). Lataster et al. (2006) sug-gested that childhood trauma could lead to negative self/other schemas, which inturn could facilitate external attributions social humiliation and subordination, lead-ing to paranoia, hallucinations and delusions. Campbell and Morrison (2007) foundthat individuals who held negative post-trauma appraisals relating to the self weremore likely to report unusual experiences and adverse beliefs.
Various studies have found that the nature of traumatic experience has a differ-ential effect on the dimensions of schizotypy. For example, individuals who experi-enced bullying were more highly pre-disposed to hallucinations, paranoia and otherpsychotic experiences (Campbell & Morrison, 2007; Lataster et al., 2006). Steel,et al. (2009) found that sexual and physical abuse was associated with higher levelsof paranoia/suspiciousness and unusual perceptual experiences, but not with magicalthinking. Individuals reporting emotional abuse did not show an increase on anyschizotypy dimensions, suggesting that the type of trauma experienced impacteddifferentially on the dimensions of schizotypy. In contrast, Powers, Thomas, Ress-ler, and Bradley (2010) found that emotional childhood abuse predicted symptomssuch as ideas of reference, social anxiety, perceptual illusions and eccentricity; how-ever, childhood sexual and physical abuse displayed no predictive effect.
Cannabis use has also been associated with both a history of traumatic experi-ence and a proneness to psychosis. Inducing a range of transient effects in healthyindividuals, cannabis effects are similar to the attributes of schizotypy and symp-toms of schizophrenia (Sewell, Ranganathani, & D’Souzai, 2009). Longitudinalresearch suggested that cannabis use is causally related to schizophreniform deficitsin later life (Dumas et al., 2002). Its use has been shown to affect the modulationof GABA (inhibitory) and glutamate receptors (excitatory), which have an agonisticeffect on dopamine receptors that are associated with “reward” systems in the brain,resulting in heightened mood and perception (Skosnik et al., 2006). A range ofexperiences similar to aspects of schizotypy can be induced by cannabis use suchas paranoia, ideas of reference, delusions, perceptual illusions and auditory andvisual hallucinations (Sewell et al., 2009).
Moreover, findings have suggested that cannabis use, particularly at an earlyage, can exacerbate a subclinical schizotypy disposition (Degenhardt & Hall, 2001;Ferdinand et al., 2004; Linscott, 2008; Van Dam, Earlywine, & Giacomo, 2008),and it is presumed that consumption may have neuro-developmental implications asadolescence and early adulthood constitute the most vulnerable periods for thoseshowing higher schizotypy levels (Stefanis et al., 2004). Existing research suggeststhat cannabis may also be used to self-medicate (Ferdinand et al., 2004; Raine,2006) and to reduce distress, which may be trauma related (Houston, Murphy,Adamson, Stringer, & Shevlin, 2008; Shevlin, Murphy, Houston & Adamson,2009).
Evidence has also indicated that schizotypy is associated with reduced quality oflife (Henrichs, Hanlon, & Carpenter, 1984). The negative and positive symptoms ofpsychosis-like experiences differ in nature and severity and may adversely affectmood and daily experiences, in turn impacting on the quality of life of those
Psychosis 127
Dow
nloa
ded
by [
Uni
vers
ity o
f U
lste
r L
ibra
ry]
at 0
9:40
28
Janu
ary
2015

affected. Lower levels of life satisfaction induced by a range of experiential factorsmay have an adverse effect on schizotypy levels, potentiating symptoms and result-ing in clinical conditions. Relevant findings have shown that individuals reportingsubclinical psychosis-like experiences were two to three times more likely to engagein “help-seeking behavior”, accessing support from a general practitioner or thera-pist (Murphy, Shevlin, Houston, & Adamson, 2010).
Various studies have found that life satisfaction levels vary in association with awide range of factors such as depression, hope, optimism, perfectionism and inter-personal relationships (Gilman, Ashby, Sverko, Florell, & Varjas, 2005; Wong &Lim, 2009). Research by Cann et al. (2010) found that reduced levels of life satis-faction due to the stress of traumatic life events were negatively associated withindividuals’ assumptive world, impacting on their fundamental beliefs on how oth-ers behave, how events unfold and their ability to influence events. These changesin fundamental beliefs overlap somewhat with the dimensions of schizotypy (Cannet al., 2010). Depression, anxiety and metacognitive beliefs have been shown tocorrelate significantly with the expression of positive schizotypy (Debbane, Van derLinden, Gex-Fabry, & Eliez, 2009). High levels of schizotypy (of clinical relevance)may therefore be associated with lower levels of life satisfaction and may vary inaccordance with the unique nature of the differing schizotypy dimensions.
Consistent with non-clinical sampling methodologies employed by Freemanet al. (2005) and Gracie et al. (2007) the current study utilised a non-clinical univer-sity based sample to examine the distribution of schizotypy while also estimatingassociations with self-reported cannabis use, life satisfaction and traumatic life expe-rience. It was hypothesized that exposure to traumatic experience(s), level of lifesatisfaction and frequency of cannabis use, would differentially be associated withhigher levels of positive aspects of schizotypy while controlling for sociodemo-graphic variables.
Method
Participants
The sample comprised 258 undergraduate students (63% female) who completed abattery of self-report scales in response to an emailed circular advertising the study.The mean age was 24 years (SD = 6.25), with a range of 18 to 51. Participants’cooperation was voluntary and no incentive was offered for participation. The studywas approved by the School of Psychology Ethics Committee.
Measures
The Thinking and Perceptual Style Questionnaire (TPSQ: Linscott & Knight, 2004)was used for the measurement of positive aspects of schizotypy. The full version ofthe TPSQ has a total of 99 items, and a 5-point Likert response format with higherscores indicating increased schizotypal disposition. In this study we did not use theAnhedonia (33 items) section. The remaining sections measured Hallucinations (9items), Social Paranoia and Negative Evaluation (comprising Social Paranoia (4items) and Negative Evaluation (4 items) subscales), Thought Disorder (19 items),Ideation (comprising Magical Ideation (12 items) and Self-referential Ideation (5items) subscales), and Perceptual Illusion (13 items). The TPSQ has been subjected
128 S. Fleming et al.
Dow
nloa
ded
by [
Uni
vers
ity o
f U
lste
r L
ibra
ry]
at 0
9:40
28
Janu
ary
2015

to different taxometric and validity studies, showing high convergent validity withother schizotypy measures (Paino-pinero et al., 2008). Cronbach’s alpha valuesranging from 0.86 (Linscott & Knight, 2004) to 0.91 (Paino-Pinero et al., 2008)have been reported indicating that it has acceptable reliability. Cronbach’s coeffi-cient of the total TPSQ for the current study was 0.93. The internal consistency val-ues of the subscales were acceptable (Hallucinations = 0.86, Social Paranoia andNegative Evaluation = .77, Thought Disorder = .92, Ideation = .89, Perceptual Illu-sion = .87).
The Cannabis Experience Questionnaire (CEQ: Barkus, Stirling, Hopkins, &Lewis, 2006) was used to measure the frequency of cannabis use. An eight-pointLikert scale measured the frequency of cannabis use (1, never used 8, everydayuse). Previous studies reported Cronbach’s alpha values ranging from 0.75 to 0.79(Barkus & Lewis, 2008).
The Traumatic Life Experience (TLE) measure was taken from the British Psy-chiatric Morbidity Survey (Singleton, Bumpstead, O’Brien, Lee & Meltzer, 2001).It comprised a list of traumatic experiences including: (1) Bullying, (2) Violence,(3) Violence in the home, (4) Sexual abuse, (5) Being expelled from school, (6)Running away from home, (7) Being homeless, (8) Serious illness, injury or assaultto yourself, (9) Serious illness, injury or assault to a close relative, (10) Death of aparent, spouse/partner, child, brother or sister of yours, (11) Death of a close familyfriend or other relative, like an aunt, cousin or grandparent, (12) Separation due tomarital difficulties, divorce or steady relationship broken down, (13) Serious prob-lems with a close friend, neighbour or relative. Participants were not required toidentify specific traumas, but rather to report the total number of traumas experi-enced.
The Satisfaction with Life Scale (SWLS: Diener, Emmons, Larsen, & Griffin,1985) was used to measure level of life satisfaction and used five statements suchas “in‘most ways my life is close to my ideal” and “I am satisfied with my life”that were responded to on a seven-point Likert-Scale (strongly disagree to stronglyagree). Cronbach’s alpha estimates of reliability ranging from 0.76 to 0.89 reportedin previous studies indicated good internal consistency and reliability (Wright,Jackson, & Ksiazak, 2006). The Cronbach’s alpha coefficient for the current studywas 0.72.
Socioeconomic Status (SES)
Participants were asked to indicate which category best described the main earnerin their household: (1) professional, (2) intermediate, (3) skilled non-manual, (4)skilled manual, (5) semi-skilled, or (6) unskilled.
Results
Table 1 shows the descriptive statistics for the predictor and criterion variables forthe total sample, and for males and females separately. Results from independent t-tests showed that there was a significant difference in the reported frequency of can-nabis use between males (M = 4.97, SD = 2.93) and females (M = 2.24, SD =2.08); t (256) = 8.74, p < 0.01). There was also a significant sex difference for lev-els of life satisfaction with males (M = 21.55, SD = 6.21) reporting lower levelsthan females (M = 24.13, SD = 6.75); t (254) = –3.05, p < 0.01). No significant
Psychosis 129
Dow
nloa
ded
by [
Uni
vers
ity o
f U
lste
r L
ibra
ry]
at 0
9:40
28
Janu
ary
2015
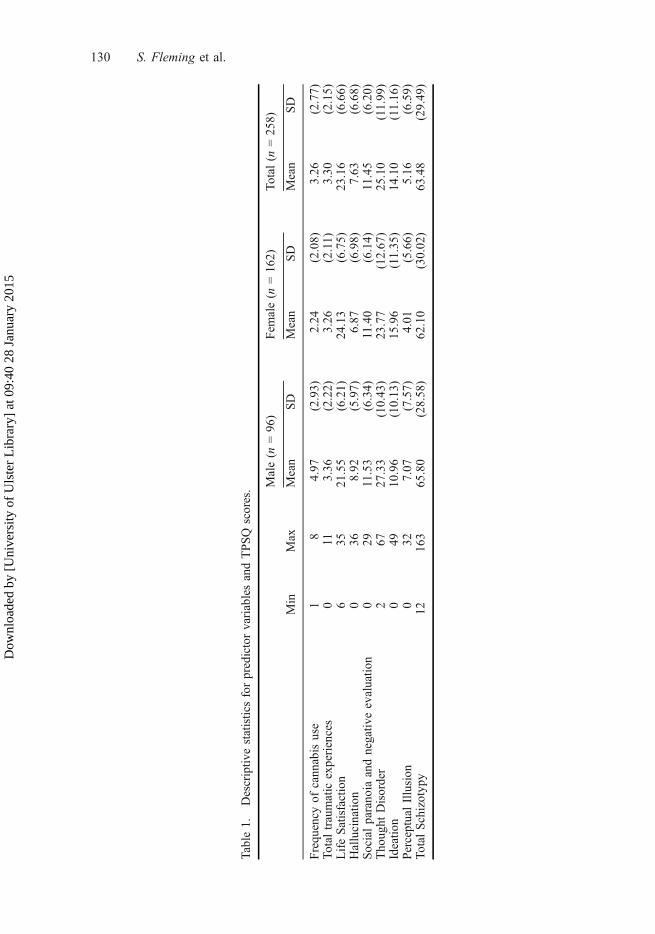
Table1.
Descriptiv
estatisticsforpredictorvariablesandTPSQ
scores. M
ale(n
=96)
Fem
ale(n
=162)
Total
(n=258)
Min
Max
Mean
SD
Mean
SD
Mean
SD
Frequency
ofcannabisuse
18
4.97
(2.93)
2.24
(2.08)
3.26
(2.77)
Totaltraumatic
experiences
011
3.36
(2.22)
3.26
(2.11)
3.30
(2.15)
LifeSatisfaction
635
21.55
(6.21)
24.13
(6.75)
23.16
(6.66)
Hallucinatio
n0
368.92
(5.97)
6.87
(6.98)
7.63
(6.68)
Socialparanoia
andnegativ
eevaluatio
n0
2911.53
(6.34)
11.40
(6.14)
11.45
(6.20)
Thought
Disorder
267
27.33
(10.43)
23.77
(12.67)
25.10
(11.99)
Ideatio
n0
4910.96
(10.13)
15.96
(11.35)
14.10
(11.16)
PerceptualIllusion
032
7.07
(7.57)
4.01
(5.66)
5.16
(6.59)
TotalSchizotypy
12163
65.80
(28.58)
62.10
(30.02)
63.48
(29.49)
130 S. Fleming et al.
Dow
nloa
ded
by [
Uni
vers
ity o
f U
lste
r L
ibra
ry]
at 0
9:40
28
Janu
ary
2015

sex difference was found for total schizotypy scores; however, significant differ-ences were found for the dimensions of schizotypy. Males scored significantlyhigher on Perceptual Illusion (t (255) = 3.70, p < 0.01), Hallucinations (t (256) =2.40, p < 0.05) and Thought Disorder (t (256) = 2.32, p < 0.05), with females scor-ing significantly higher on Ideation (t (256) = –3.55, p < 0.01).
Initially, a hierarchical multivariate regression model (Model 1) was specifiedand estimated using Mplus 5.21 (Muthén & Muthén, 1998–2009). The modelparameters were estimated using robust full information maximum likelihood whichproduces correct standard errors under non-normality. This method also allowedparameters to be estimated using all available information and has been found to besuperior to alternative methods, such as listwise deletion. For this model, Hallucina-tions, Social Paranoia and Negative Evaluation, Thought Disorder, Ideation, andPerceptual Illusions were dependent variables and the predictor variables wereentered in four blocks. In block 1, age, gender and SES were entered; in block 2,life satisfaction was added; in block 3, the cannabis and trauma variables wereadded; and in block 4, the cannabis by trauma interaction was added. This model(Model 2) was estimated again with only the total TPSQ scores used as a dependentvariable.
The standardized regression coefficients (b) and model statistics are reported inTable 2. For the model with the five SPQ subscales as dependent variables, the like-lihood ratio chi-square for block 1 was significant (w2 = 56.11, df = 15, p < .05)and the addition of the second (Dw2 = 25.57.14, D df = 5, p < .05) and third block(Dw2 = 48.81, D df = 10, p < .05) resulted in an improved model. The addition ofthe fourth block (Dw2 = 9.68, D df = 5, p > .05) did not significantly improve themodel. This indicated that the interaction did not significantly improve the model.For the model with the total SPQ scores as the dependent variable, the likelihoodratio chi-square for block 1 was significant (w2 = 12.14, df = 3, p < .05) and theaddition of the second (Dw2 = 5.40, D df = 1, p < .05) and third block (Dw2 =18.52, D df = 2, p < .05) resulted in an improved model. The addition of the fourthblock (Dw2 = 0.02, D df = 1, p > .05) did not significantly improve the model. Thisindicated that the interaction did not significantly improve the model.
Results from the hierarchical multivariate regression for the five TPSQschizotypy dimensions showed that the total variance explained by predictor vari-ables varied in relation to the cumulative R2 of 13% for Total schizotypy. Total var-iance explained ranged from 10% for Hallucinations to 19% for Ideation.Furthermore, the strength and significance of the regression coefficients for the pre-dictor variables in blocks one, two and three differed across the five dimensions ofschizotypy. Model summaries and coefficients in Table 2 show that the predictivestrength of the cannabis use, life satisfaction and traumatic experiences variables onTotal schizotypy scores was differential across the five dimensions of schizotypy.
Age made a significant contribution to the total variance explained for all fivesubdimensions of schizotypy, showing that younger participants tended to havehigher schizotypy levels. Frequency of cannabis was the only significant predictorfor the Perceptual illusion dimension (b = .26, p < .01). Life satisfaction was a sig-nificant predictor for the dimensions of Social paranoia and negative evaluation (b= –.24, p < .01) and Thought Disorder (b = –.22, p < .01). This showed that higherlevels of Social paranoia and negative evaluation and Thought Disorder were asso-ciated with lower levels of life satisfaction. The number of traumatic experienceswas a significant predictor for four dimensions of schizotypy, ranging from (b =
Psychosis 131
Dow
nloa
ded
by [
Uni
vers
ity o
f U
lste
r L
ibra
ry]
at 0
9:40
28
Janu
ary
2015

Table2.
Standardisedregression
coefficients(standarderror)andp-values
formultiv
ariate
hierarchical
regression
models.
Model
1Model
2HN
SP&NE
TD
IDPI
TotalTPSQ
Age
�.16
(.07)
.01
�.15
(.06)
.01
�.25
(.07)
.00
�.12
(.05)
.02
�.17
(.05)
.00
�.26
(.07)
.01
Gender
�.11
(.07)
.11
.02(.07)
.77
�.12
(.07)
.09
.21(.06)
.01
�.12
(.06)
.05
�.01
(.07)
.92
SES
.01(.05)
.89
.04(.06)
.48
.01(.06)
.90
.01(.05)
.79
.05(.06)
.47
�.01
(.06)
.97
LifeSatisfaction
�.01
(.09)
.92
�.242(.070)
.00
�.22
(.06)
.00
.025
(.08)
.75
.07(.08)
.34
�.13
(.08)
.09
Frequency
Cannabisuse
.08(.07)
.23
�.01
(.07)
.92
.04(.06)
.49
.05(.06)
.38
.26(.06)
.00
.09(.10)
.35
Traum
atic
experience
.27(.07)
.00
.15(.07)
.02
.17(.06)
.01
.30(.08)
.00
.04(.07)
.56
.23(.10)
.03
Cannabis�T
raum
a�.
05(.07)
.52
.07(.06)
.22
�.10
(.06)
.086
.16(.08)
.05
�.00
(.06)
.97
.016
(.12)
.90
R2
.10
.12
.15
.19
.12
.13
Note:
p<.05in
bold
(two-tailed).HN,Hallucinatio
ns;SP&NE,SocialParanoiaandNegativeEvaluation;
TD,Tho
ught
Disorder;ID
,Ideatio
n;PI,PerceptualIllusion
;Total
TPSQ,Total
Think
ingandPerceptualStyle
Questionn
aire
scores.
132 S. Fleming et al.
Dow
nloa
ded
by [
Uni
vers
ity o
f U
lste
r L
ibra
ry]
at 0
9:40
28
Janu
ary
2015

.15, p < .05) for Social paranoia and negative evaluation to (b = .30, p < .01) forThought Disorder. The interaction between frequency of cannabis use and traumaticexperiences was not significant and did not add to the variance explained across thedimensions of schizotypy.
Discussion
This study examined the distribution of schizotypy scores in a sample of universitystudents and estimated associations with cannabis use, life satisfaction and traumaticexperiences while controlling for respondent age, gender and SES. The study foundthat age, life satisfaction and traumatic experiences uniquely contributed to theexplained variance in total TPSQ scores. However, these variables did not signifi-cantly predict variance in a consistent way across the TPSQ subscales. Gender andfrequency of cannabis use were also significant predictors of the dimensions ofschizotypy. As schizotypy is multidimensional, with components in each dimensionreflecting differing (dys)functions, the range of associated variables and amount ofvariance explained in schizotypy scores differed in accordance with the symptom-atic nature of each individual schizotypy factor. With the exception of life satisfac-tion, the predictive variables associated with dimensional schizotypy levelsconcurred with previous research (Harley et al., 2008; Paino-Pineiro et al., 2008).
Research has consistently found that schizotypy levels are higher in adolescenceand early adulthood (Paino-Pineiro et al., 2008) and the results of the current studyshowed that a lower age was associated with higher scores on the all of the dimen-sions of schizotypy. This may be explained by neuro-developmental vulnerabilitiesassociated with younger ages and higher schizotypy scores (Stefanis et al., 2004;van Dam et al., 2008). The number of traumatic experiences was significantly asso-ciated with four of the five dimensional factors of schizotypy. Previous research hassuggested that traumatic events can potentiate or exacerbate schizotypy levels (VanDam et al., 2008). The current study showed that the strength of association varieddifferentially across dimensions. Perceptual illusion was not associated with trau-matic experiences which may suggest that its expressive nature and psychosocialfactors that affect its pathology may not be trauma-related; whereas paranoia, hallu-cination or thought disorder can develop due to negative schemas of the self andworld as a result of childhood trauma (Lataster et al., 2006).
Lower levels of life satisfaction were associated with higher schizotypy levelson social paranoia and negative evaluation and thought disorder. In both cases dis-satisfaction with life was significantly associated with traumatic experiences andlower age. The traumagenic neuro-developmental model of Read et al., (2001)asserted that trauma experienced at a young age may lead to abnormal neuro-devel-opmental processes resulting in a high responsivity to stress. It is possible that thestress of traumatic events, experienced at an early age, has impacted on life satisfac-tion levels and may affect fundamental belief systems regarding the behaviour ofothers, how events unfold and abilities to influence events (Cann et al., 2010; VanDam et al., 2008). Life satisfaction did not significantly predict the dimensions ofhallucinations, ideation or perceptual illusion. The differing expressive nature ofSocial paranoia and negative evaluation and Thought Disorder may be producingmore cognitive-perceptual, interpersonal, and disorganized features, resulting inreduced life satisfaction due to deficiencies in interpersonal and social relations(Debbane et al., 2009). Further research would be required to explain why life satis-
Psychosis 133
Dow
nloa
ded
by [
Uni
vers
ity o
f U
lste
r L
ibra
ry]
at 0
9:40
28
Janu
ary
2015

faction has a differential predictive association on the dimensions of schizotypy,particularly with regard to hallucinations, ideation and perceptual illusion.
Frequency of cannabis use showed a significant association with the perceptualillusion factor, however, it was not significant for the other four factors. Numerousstudies have found that cannabis use has been positively associated with higherscores on schizotypy measures and psychosis-like experiences (Van Dam et al.,2008; van Os et al., 2002);therefore, the fact that cannabis use is only significantfor one of the five factors appears inconsistent with previous research. One explana-tion may be that previous research used schitzotypy measures which offer three- orfour-factor solutions and that the perceptual illusion characteristics were loaded onother factors. Second, the sample consisted of higher level education students, 63%of which were females with a mean score well below the overall total mean. How-ever, cannabis use was significant for at least one factor associated with schizotypyscores, which is important as it is related to the subsequent onset of psychotic con-ditions such as schizophrenia (Ferdinand et al., 2004).
A major limitation of the study was that it was cross-sectional. The previous lit-erature is inconclusive with regard to whether cannabis plays a causal role in psy-chosis or is purely associative and more longitudinal studies would address thisquestion better. The study showed the predictive association of traumatic experi-ences on schizotypy, but did not explore the reverse causality argument in relationto how schizotypy may lead to an individual experiencing more traumatic lifeevents (Morrison, Frame, & Larkin, 2003). Furthermore, the relational causalitybetween traumatic life experience, cannabis use, life satisfaction and schizotypy wasnot measured. For example, schizotypy and life events may result in more frequentcannabis use and all three variables may potentially lead to lower life satisfaction.Subsequent studies could look at the effects of therapy for traumatic experiences onschizotypy levels over time to further explore the psychosocial vs. biological argu-ments for schizotypy dispositions. Future studies may benefit from drawing upon amore diverse sample from general and clinical populations. The measure used fortraumatic experience in this study was very basic and could be improved in subse-quent studies by eliciting data on age of traumatic experience, degree of associateddistress and the nature of a particular traumatic experience could be categorized (e.g. life-threatening, emotional, physical or sexual trauma) to ascertain differentialpredictive strengths on schizotypy dimensions.
In conclusion, the current study has demonstrated that variables such as canna-bis, life satisfaction and traumatic experience differentially effect schizotypy levelsand have differing predictive associations across the dimensions of schizotypy. Thissuggests that schizotypy does not appear to be a unitary entity, but rather constitutesa heterogeneous multidimensional construct. Mental health practitioners may wishto focus on the unique nature of, and experiential factors relating to, specific schizo-typy dimensions experienced by individuals (Campbell & Morrison, 2007).
ReferencesBadcock, J., & Dragovic, M. (2006). Schizotypal personality in mature adults. Personality and
Individual Differences, 40, 77–85.Barkus, E., & Lewis, S. (2008). Schizotypy and psychosis-like experiences from recreational can-
nabis in a non-clinical sample. Psychological Medicine, 38, 1267–1276.Barkhouse, E.J., Stirling, J., Hopkins, R.S., & Lewis, S. (2006). Cannabis-induced psychosis-like
experiences are associated with high schizotypy. Psychopathology, 39, 175–178.
134 S. Fleming et al.
Dow
nloa
ded
by [
Uni
vers
ity o
f U
lste
r L
ibra
ry]
at 0
9:40
28
Janu
ary
2015

Campbell, M., & Morrison, A. (2007). The relationship between bullying, psychotic-like experi-ences and appraisals in 14–16 year olds. Behaviour Research and Therapy, 45, 1579–1591.
Cann, A., Calhoun, L., Tedeschi, R., Kilmer, R., Gil-Rivas, V., Vishnevsky, T., et al. (2010). TheCore Beliefs Inventory: A brief measure of disruption in the assumptive world. Anxiety,Stress, and Coping, 23, 19–34.
Debbane, M., Van der Linden, M., Gex-Fabry, M., & Eliez, S. (2009). Cognitive and emotionalassociations to positive schizotypy during adolescence. Journal of Child Psychology and Psy-chiatry, 50, 326–344.
Degenhardt, L., & Hall, W. (2001). The association between psychosis and problematical druguse among Australian adults: Findings from the National Survey of Mental Health and Well-Being. Psychological Medicine, 31, 659–668.
Diener, E., Emmons, R.A., Larsen, R.J., & Griffin, S. (1985). The Satisfaction with Life Scale.Journal of Personality Assessment, 49, 71–75.
Dumas, P., Saoud, M., Bouafia, S., Gutkneckt, C., Ecochard, R., Dale, J., et al. (2002). Cannabisuse correlates with schizotypal personality traits in healthy adults. Psychiatry Research, 109,27–35.
Ferdinand, R., Sondeijker, F., Van der Ende, J., Selten, J., Huizink, A., & Verhulst, F. (2004).Cannabis use predicts future psychotic symptoms and vice versa. Addiction, 100, 612–618.
Fonseca-Pedrero, E., Paíno, M., Lemos-Giráldez, S., García-Cueto, E., Campillo-Álvarez, E.,Villazón-García, U., et al. (2008). Schizotypy assessment: State of the art and future pros-pects. International Journal of Clinical and Health Psychology, 8, 577–593.
Freeman, D., Garety, P.A., Bebbington, P.E., Smith, B., Rollinson, R., Fowler, D., et al. (2005).Psychological investigation of the structure of paranoia in a non-clinical population. BritishJournal of Psychiatry, 186, 427–435.
Gilman, R., Ashby, J.S., Sverko, D., Florell, D., & Varjas, K. (2005). The relationship betweenperfectionism and multidimensional life satisfaction among Croatian and American youth.Personality and Individual Differences, 39, 155–166.
Gracie, A., Freeman, D., Green, S., Garety, P., Kuipers, E., Hardy, A., et al. (2007). The associa-tion between traumatic experience, paranoia and hallucinations: A test of the predictions ofpsychological models. Acta Psychiatrica Scandavica, 116, 280–289.
Harley, M., Kelleher, I., Clarke, M., Lynch, F., Fizpatrick, C., Arsenault, L., et al. (2008). Associ-ations of adolescent cannabis use with mental health disorder: The role of childhood trauma.Schizophrenia Research, 102, 1–279.
Henrichs, D., Hanlon, T., & Carpenter, W. (1984). The Quality of Life Scale: An instrument forrating the schizophrenic deficit syndrome. Schizophrenia Bulletin, 10, 388–398.
Houston, J., Murphy, J., Adamson, G., Stringer, M., & Shevlin, M. (2008). Childhood sexualabuse, early cannabis use, and psychosis: testing an interaction model based on the NationalComorbidity Survey. Schizophrenia Bulletin, 34, 580–585.
Kwapil, T.R., Miller, M.B., Zinser, M.C., Chapman, J.P., & Chapman, L.J. (1997). Magical idea-tion and social anhedonia as predictors of psychosis proneness: A partial replication study.Journal of Abnormal Psychology, 106, 491–495.
Lataster, T., van Os, J., Drukker, M., Henquet, C., Feron, F., Gunther, N., et al. (2006). Childhoodvictimisation and developmental expression of non-clinical delusional ideation and hallucina-tory experiences. Social Psychiatry & Psychiatric Epidemiology, 41, 423–428.
Linscott, R. (2008). Cannabis use versus non-use and the latent structure of schizotypy. Schizo-phrenia Research, 102, 273–279.
Linscott, R.J., & Knight, R.G. (2004). Potentiated automatic memory in schizotypy. Personalityand Individual Differences, 37, 1503–1517.
Merckelbach, H., & Giesbrecht, T. (2006). Subclinical dissociation, schizotypy, and traumatic dis-tress. Personality and Individual Differences, 40, 365–374.
Morrison, A., Frame, L., & Larkin, W. (2003). Relationships between trauma and psychosis: Areview and integration. British Journal of Clinical Psychology, 42, 331–353.
Murphy, J. Shevlin, M., Houston, J., & Adamson, G. (2010). A population based analysis of sub-clinical psychosis and help-seeking behaviour. Schizoprenia Bulletin, Doi:10.1093/schbul/sbq092.
Muthén, L.K., & Muthén, B.O. 1998-2009. Mplus User’s Guide (6th ed.) Los Angeles, CA:Muthén & Muthén.
Psychosis 135
Dow
nloa
ded
by [
Uni
vers
ity o
f U
lste
r L
ibra
ry]
at 0
9:40
28
Janu
ary
2015

Paino-Pinero, M., Fonseca-Pedrero, E., Lemos-Giraldez, S., & Muniz, J. (2008). Dimensionalityof Schizotypy in young people according to sex and age. Personality and Individual Differ-ences, 45, 132–138.
Powers, A., Thomas, K., Ressler, K., & Bradley, B. (2010). The differential effects of child abuseand post-traumatic stress disorder on schizotypal personality disorder. Comprehensive Psychi-atry: doi: 10.1016/j.comppsych.2010.08.001.
Raine, A. (2006). Schizotypal personality: neurodevelopmental and psychosocial trajectories.Annual Review of Clinical Psychology, 2, 291–326.
Read, J., Perry, B., Moskowitz, A., & Connolly, J. (2001). The contribution of early traumaticevents to schizophrenia in some patients: A traumagenic neurodevelopmental model. Psychia-try, 64, 319–345.
Sewell, R., Ranganathani, M., & D’Souzai, D. (2009). Cannabinoids and psychosis. InternationalReview of Psychiatry, 21, 152–162.
Shevlin, M., Murphy, J., Houston, J., & Adamson, G. (2009). Childhood sexual abuse, early can-nabis use, and psychosis. Testing the effects of different temporal orderings based on theNational Comorbidity Survey. Psychosis: Psychological, Social and Integrative Approaches,2, 19–28.
Singleton, N., Bumpstead, R., O’Brien, M., Lee, A., & Meltzer, H. (2001). Psychiatric morbidityamong adults living in private households, 2000: Main Report. London: The StationeryOffice.
Skosnik, P., Krishnan, G., Aydt, E., Kuhlenshmidt, H., & O’Donnell, F. (2006). Psychophysiolog-ical evidence of altered neural synchronization in cannabis use: Relationship to schizotypy.American Journal of Psychiatry, 163, 1798–1805.
Steel, C., Marzillier, S., Fearon, P., & Ruddle, A. (2009). Childhood abuse and schizotypal per-sonality. Social Psychiatry and Psychiatric Epidemiology, 44, 917–923.
Stefanis, N., Smyrnis, N., Avramopoulos, D., Evdokimidis, I., Ntzoufras, I., & Stefanis, C.(2004). Factorial composition of self-rated schizotypal traits among young males undergoingmilitary training. Schizophrenia Bulletin, 30, 335–350.
van Dam, N., Earlywine, M., & Giacomo, G. (2008). Polydrug use, cannabis, and psychosis-likesymptoms. Human Psychopharacology, 23, 475–485.
van Os, J., Bak, M., Hanssen, M., Bijl, R.V., de Graaf, R., & Verdoux, H. (2002). Cannabis useand psychosis: A longitudinal population-based study. American Journal of Epidemiology,156, 319–327.
Wong, S., & Lim, T. (2009). Hope versus optimism in Singaporean adolescents: Contributions todepression and life satisfaction. Personality and Individual Differences, 46, 648–652.
Wright, L., Jackson, Z., & Ksiazak, M. (2006). Relationship of spirituality to work and familyroles and life satisfaction among gifted adults. Journal of Mental Health Counseling, 24,357–364.
136 S. Fleming et al.
Dow
nloa
ded
by [
Uni
vers
ity o
f U
lste
r L
ibra
ry]
at 0
9:40
28
Janu
ary
2015




















