The role of the clinical trial nurse in Italy
7
The role of the clinical trial nurse in Italy Gianluca Catania a, * , Ilaria Poirè b , Matteo Bernardi c , Laura Bono a , Francesco Cardinale d , Beatrice Dozin d a Regional Palliative Care Network, Istituto Nazionale per la Ricerca sul Cancro, Largo Rosanna Benzi, 10 Genoa, Italy b Secondary Prevention and Screening, Istituto Nazionale per la Ricerca sul Cancro, Largo Rosanna Benzi, 10 Genoa, Italy c Pediatric Oncohematology Unit, II Clinica di Pediatria, Azienda Ospedaliera, Via Giustiniani, 2 Padova, Italy d Clinical Epidemiology, Istituto Nazionale per la Ricerca sul Cancro, Largo Rosanna Benzi, 10 Genoa, Italy Keywords: Nurse's Role Clinical trials Cancer care abstract Purpose: To assess the role of the Clinical Trials Nurse (CTN) and to evaluate the quality of the job per- formed by Clinical Trials Nurses (CTNs) in Italy. Methods: The study design was descriptive. The sample included 30 CTNs in Italy who were involved in conducting clinical trials in the last years. Respondents completed the Italian Clinical Trials Nursing Questionnaire (CTNQ) developed to measure frequency and importance of clinical trials nursing activi- ties. Data analyses included descriptive statistics, Student’s t-test and ChieSquare test. Results: Thirty out of 34 CTNs consented to participate. Respondents were more involved in the exper- imental drug management, in the protocol implementation and, partially, in the informed consent process. CTNs have a marginal position with respect to the protocol assessment and planning, subject recruitment, data management. CTNs reported high rates for the importance evaluation. Number of years in the nursing role was significantly associated with data management related activities (p ¼ 0.016). Items with minor response rate differences between frequency and importance were not statistically significant (p values ranging from 0.087 to 0.911). The CTNs reported to be autonomous and competent; however, they lack and/or do not perform some nursing-related responsibilities and/or activities. Conclusions: Although CTNs are not involved in all of the activities listed on the CTNQ, most of them are fully aware to be a key member of research teams. Overall, the Italian CTN role is mostly practical task- oriented and focuses little on data management and organizational activities. Ó 2011 Elsevier Ltd. All rights reserved. Introduction Clinical trial is one of the final steps of a long and careful research process. According to the National Cancer Institute (NCI), clinical studies are carried out on cancer patients to investigate whether new promising approaches to prevent, diagnose or treat cancer are both safe and effective (NCI, 2008). As cancer has become a major concern worldwide, oncology is now one of the most investigated medical fields. In Italy the number of clinical trials has increased considerably over the last six years; and data from the National Monitoring Centre on Clinical Trials of Drugs (Osservatorio Nazionale sulla Sperimentazione Clinica dei Medicinali [OsSC]) report that 4465 clinical trials were registered between 2004 and 2009 (OsSC, 2010). It is worth mentioning that whereas, phase III trials have progres- sively decreased since 2005, falling below 40% in 2009, phase I and II studies rose to 43.5% of the total number of registered studies in the same year. Most of such studies were multi-centered (80%), international (74.3%) and/or sponsored by pharmaceutical compa- nies (63.5%). In Italy, as in the rest of the world, oncology is nowadays the most investigated therapeutic branch (29.4%) (OsSC, 2010); indeed, it was estimated that in 2008 approximately 250,000 Italians were diagnosed with cancer and that in 2006, 122,000 people died of cancer (AIRTUM Working Group, 2009). Clinical research is a long and complex process involving large numbers of patients in a wide variety of clinical settings, and anecdotal evidence suggests that Clinical Trials Nurses (CTNs) are paramount both in giving optimal care to patients and their fami- lies, and in successfully designing, implementing, and evaluating clinical trials (Jenkins and Hubbard, 1991). Although the role of CTNs has not as yet been greatly looked into in Italy, literature from the UK and the USA offers considerable insight into their position and many authors (Hubbard, 1982; White-Hersheyand Nevidjon, 1990; Eaton and Pratt, 1990; Cassidy and MacFarlane, 1991; McEvoy et al., 1991; Wheeler, 1991; Arrigo et al., 1994; Berry et al., 1996; Di Giulio et al., 1996; Rosse and Krebs, * Corresponding author. Tel.: þ39 010 5600 948; fax: þ39 010 5600 794. E-mail address: [email protected] (G. Catania). Contents lists available at ScienceDirect European Journal of Oncology Nursing journal homepage: www.elsevier.com/locate/ejon 1462-3889/$ e see front matter Ó 2011 Elsevier Ltd. All rights reserved. doi:10.1016/j.ejon.2011.04.001 European Journal of Oncology Nursing 16 (2012) 87e93
Transcript of The role of the clinical trial nurse in Italy

lable at ScienceDirect
European Journal of Oncology Nursing 16 (2012) 87e93
Contents lists avai
European Journal of Oncology Nursing
journal homepage: www.elsevier .com/locate/ejon
The role of the clinical trial nurse in Italy
Gianluca Catania a,*, Ilaria Poirè b, Matteo Bernardi c, Laura Bono a, Francesco Cardinale d, Beatrice Dozin d
aRegional Palliative Care Network, Istituto Nazionale per la Ricerca sul Cancro, Largo Rosanna Benzi, 10 Genoa, Italyb Secondary Prevention and Screening, Istituto Nazionale per la Ricerca sul Cancro, Largo Rosanna Benzi, 10 Genoa, Italyc Pediatric Oncohematology Unit, II Clinica di Pediatria, Azienda Ospedaliera, Via Giustiniani, 2 Padova, ItalydClinical Epidemiology, Istituto Nazionale per la Ricerca sul Cancro, Largo Rosanna Benzi, 10 Genoa, Italy
Keywords:Nurse's RoleClinical trialsCancer care
* Corresponding author. Tel.: þ39 010 5600 948; faE-mail address: [email protected] (G. Catan
1462-3889/$ e see front matter � 2011 Elsevier Ltd.doi:10.1016/j.ejon.2011.04.001
a b s t r a c t
Purpose: To assess the role of the Clinical Trials Nurse (CTN) and to evaluate the quality of the job per-formed by Clinical Trials Nurses (CTNs) in Italy.Methods: The study design was descriptive. The sample included 30 CTNs in Italy who were involved inconducting clinical trials in the last years. Respondents completed the Italian Clinical Trials NursingQuestionnaire (CTNQ) developed to measure frequency and importance of clinical trials nursing activi-ties. Data analyses included descriptive statistics, Student’s t-test and ChieSquare test.Results: Thirty out of 34 CTNs consented to participate. Respondents were more involved in the exper-imental drug management, in the protocol implementation and, partially, in the informed consentprocess. CTNs have a marginal position with respect to the protocol assessment and planning, subjectrecruitment, data management. CTNs reported high rates for the importance evaluation. Number of yearsin the nursing role was significantly associated with data management related activities (p ¼ 0.016).Items with minor response rate differences between frequency and importance were not statisticallysignificant (p values ranging from 0.087 to 0.911). The CTNs reported to be autonomous and competent;however, they lack and/or do not perform some nursing-related responsibilities and/or activities.Conclusions: Although CTNs are not involved in all of the activities listed on the CTNQ, most of them arefully aware to be a key member of research teams. Overall, the Italian CTN role is mostly practical task-oriented and focuses little on data management and organizational activities.
� 2011 Elsevier Ltd. All rights reserved.
Introduction
Clinical trial is one of the final steps of a long and carefulresearch process. According to the National Cancer Institute (NCI),clinical studies are carried out on cancer patients to investigatewhether new promising approaches to prevent, diagnose or treatcancer are both safe and effective (NCI, 2008). As cancer hasbecome a major concern worldwide, oncology is now one of themost investigated medical fields.
In Italy the number of clinical trials has increased considerablyover the last six years; and data from the National MonitoringCentre on Clinical Trials of Drugs (Osservatorio Nazionale sullaSperimentazione Clinica dei Medicinali [OsSC]) report that 4465clinical trials were registered between 2004 and 2009 (OsSC, 2010).It is worth mentioning that whereas, phase III trials have progres-sively decreased since 2005, falling below 40% in 2009, phase I and
x: þ39 010 5600 794.ia).
All rights reserved.
II studies rose to 43.5% of the total number of registered studies inthe same year. Most of such studies were multi-centered (80%),international (74.3%) and/or sponsored by pharmaceutical compa-nies (63.5%). In Italy, as in the rest of the world, oncology isnowadays the most investigated therapeutic branch (29.4%) (OsSC,2010); indeed, it was estimated that in 2008 approximately250,000 Italians were diagnosed with cancer and that in 2006,122,000 people died of cancer (AIRTUM Working Group, 2009).
Clinical research is a long and complex process involving largenumbers of patients in a wide variety of clinical settings, andanecdotal evidence suggests that Clinical Trials Nurses (CTNs) areparamount both in giving optimal care to patients and their fami-lies, and in successfully designing, implementing, and evaluatingclinical trials (Jenkins and Hubbard, 1991).
Although the role of CTNs has not as yet been greatly lookedinto in Italy, literature from the UK and the USA offers considerableinsight into their position and many authors (Hubbard, 1982;White-Hersheyand Nevidjon, 1990; Eaton and Pratt, 1990; Cassidyand MacFarlane, 1991; McEvoy et al., 1991; Wheeler, 1991; Arrigoet al., 1994; Berry et al., 1996; Di Giulio et al., 1996; Rosse and Krebs,

G. Catania et al. / European Journal of Oncology Nursing 16 (2012) 87e9388
1999; Coulson and Phelan, 2000; Ocker and Plank, 2000; Barrett,2002; Carlson et al., 2005) and organizations of oncology profes-sionals such as the Oncology Nursing Society (ONS) (Klimaszewskiet al., 2008) have reported on how the role of CTNs has developedto include and integrate organizational, clinical and ethicalresponsibilities.
Regarding ethical responsibilities, Davis et al. (2002) identifiedthree different CTN advocacy roles and described the commitmentrequired by each: in order to address and balance the rights of thepatients, to ensure the protection of research subjects, and toguarantee the quality of clinical studies. As a direct result of botheducational and certification programmes in the research area,Deininger (2008) describes how CTNs have both the knowledgeand the skills required in supporting and monitoring both theintegrity of studies and the safety of patients.
Unlike other European and American countries, where the roleof the CTN is well acknowledged, in Italy this specific nursing role isrelatively new and has only just begun to develop and to spreadinto the area of clinical research in oncology (Bryce, 2008). Theoverall purpose of this survey was to delineate the role of the CTNin Italy, with a two-fold focus on (1) role assessment and (2) qualityof job performance.
Methods
A nationwide survey for Italy was carried out among oncologyCTNs with the aim of validating the national version of the ClinicalTrials Nursing Questionnaire (CTNQ). Italian CTNQ validationresults, including tests of validity and reliability, are reportedelsewhere (Catania et al., 2008) and described briefly in theInstrument section below. For the current study, gathered infor-mation was further analyzed in a specific attempt to delineate therole of the CTN in Italy.
Sample
The study sample comprised oncology CTNs working at cancerhospitals located in northern, central and southern Italy.
All 34 CTNs listed in the Libro Bianco dell’Oncologia Italiana(Associazione Italiana Oncologia Medica (AIOM, 2004) - an ongoing
Table 1Structure of the Italian CTNQ.
Area Topic Section(n� of item)
Co
1 Clinical researchactivities/responsibilities
1 (15) Pro2 (14) Pro3 (13) Su4 (14) Inf5 (10) Inv6 (23) Im7 (18) Da8 (10) Nu
2 Professional Perception 9 (10) Nu
3 Nursing Role Characteristics 10 (11) Hiex
4 Organizational Characteristics 11 (8) Pritit
5 Demographic Information 12 (3) Ge
census compiled by the National Association of Medical Oncology(Associazione Italiana di Oncologia Medica [AIOM]) regardingItalian cancer centres - were duly contacted.
Instrument
The instrument used in this study was the validated Italianversion of the CTNQ (Catania et al., 2008) originally developedby Ehrenberger and Lillington in 2004 (Ehrenberger andLillington, 2004) to measure frequency and importance of clin-ical trials nursing activities. For the Italian validation of theCTNQ, a total of 30 CTNs were recruited from different areas inItaly. Linguistic and content validation were accomplishedthrough a forward translation, a backward translation, anda review by experts in clinical trial nursing. An analysis of theinternal consistency showed a Cronbach a coefficient of 0.98 onthe frequency scale and 0.96 on the importance scale. Acomparison of the test-retest reliability was conducted withina 2-week interval on a sample of 10 CTNs out of the 30 recruitedparticipants, and an overall k coefficient of 0.98 was obtained onthe frequency scale while 0.99 was obtained on the importancescale (Catania et al., 2008). The Italian CTNQ is structured intofive areas divided into a total of 12 sections featuring 149 itemsin total (Table 1). In order to define (1) the frequency with whichCTNs perform each activity and (2) the importance of eachactivity for the safety and effectiveness of nursing practice, theitems listed in sections 1e8 are scored by respondents throughreference to two separate five-point Likert-style rating scales.Section 9 assesses the level of perception of the professionalnursing role, as respondents choose one out of six agreement/disagreement options. Sections 10, 11, and 12 investigate nursingrole, organizational characteristics and demographics, respec-tively (Table 1).
Procedure
A description of the study, and instructions for completing thestudy questionnaire were emailed to potential participants.
Out-going e-mails clearly stated that, by returning a completedquestionnaire, respondents were consenting to the survey.
ntent Score
tocol Assessment Frequency Scale:tocol Planning �0 (never, not part of my role)bject Recruitment �1 (once or twice)ormed Consent Process �2 (occasionally, as needed)estigational Product �3 (repeatedly)plementation/Evaluation �4 (extremely frequently)ta Management Importance Scale:rsing Role Performance �0 (not important)
�1 (somewhat important)�2 (important)�3 (moderately important)�4 (very important)
rsing Role Perception - Strongly Agree- Agree- Strongly Disagree- Disagree- Undecided- Not Applicable
ghest degree completed; Years ofperience; Certification.
Not Applicable
mary work setting; Assigned positionle; Opportunity for advancement.
Not Applicable
nder, Age, Geographic Region Not Applicable

Table 2Demographic, educational and professional characteristics.
Characteristic Mean SD Median Range
Age (years) 38 5.2 38 27e49Years in nursing 13.8 6.2 12 2e29Years in oncology 8 6.3 7 0e23Years in clinical research 2.8 2.6 2 0e12
Characteristic N %
GenderMale 23 76Female 7 24
Geographic AreaNorth of Italy 19 64Centre of Italy 7 23South of Italy 4 13
Highest Nursing EducationRegional Diploma (þMaster) 18 (3) 60 (10)University Diploma (þMaster) 1 (0) 3 (0)Bachelor’s (þMaster) 3 (0) 10 (0)
Education in Clinical ResearchFormal (e.g. academic coursework) 8 26Informal (e.g. self taught) 21 70
Table 3Descriptive statistics for the main sections of Italian CTNQ.
Frequency Scale Importance Scale
Section Mean Range Mean Range
1.Protocol Assessment 1.46 0.00e3.27 3.01 1.8e42.Protocol Planning 1.58 0.00e3.79 3.15 1.29e43.Subject Recruitment 1.77 0.00e3.46 2.89 0.92e44.Informed Consent Process 2.29 0.00e4 3.42 1.5e45.Investigational Product 2.66 0.40e4 3.37 1.5e46.Implementation/Evaluation 2.51 0.33e3.91 3.4 1.91e47.Data Management 1.53 0.00e3.39 2.58 0.00e48.Nursing Role Performance 2.15 0.00e4 3.39 0.5e4
G. Catania et al. / European Journal of Oncology Nursing 16 (2012) 87e93 89
Completed questionnaires were then returned by mail or handdelivered. Non-respondents were sent a reminder two weeks afterthe first email. The name and phone number of the principalinvestigator were included in all e-mails as a contact for theparticipants, if they required additional information on the study.
Eligibility criteria
To be eligible for inclusion in the study, nurses had to beworking either directly (e.g., research nurse, clinical researchcoordinator) or indirectly (e.g., clinical research associate, nursemanager) in the support of clinical trials.
Data analysis
SPSS� (version 17.0 for Windows) was used to carry out statis-tical analyses. Descriptive statistics were first computed for allitems in sections 1e8. For each item, the response rates wereaccrued in order to obtain preliminary results. On the basis of suchresults, low scores (0, 1 and 2) in the Likert scales were thenexcluded from the analysis since they indicated marginal contri-bution by the CTNs. Subsequently, to facilitate the interpretation ofresults, response rates of scores 3 and 4 in the Likert scales,measuring either frequency or importance of activities, werepooled. Unpaired Student’s t-tests were performed on those itemswith minor response rate differences between frequency andimportance scales in order to evaluate any significant differencesbetween the scales.
Within each section, the median score of each item was calcu-lated both for frequency and importance. The median of all thesemedian scores was in turn calculated and allocated into one of thetwo following groups defined by a threshold value of 2: a medianvalue �2 corresponded to low frequency or importance whereasa median value >2 corresponded to high frequency or importance.These frequency or importance median values were correlated byusing the Pearson ChieSquare test with the following parameterspossibly influencing CTN expertise: number of years in oncology,education and training level in clinical research (formal or informal),number of years in nursing, and number of Continuing Education(CE) programmes attended specifically related to clinical trial topics.
Results
Participant characteristics
Thirty (88%) out of 34 CTNs who were contacted and invited totake part in this study consented, emailed or hand-returned thefilled out Italian CTNQ to the investigator and were thus included inthe final data analyses. Demographic, educational and professionalcharacteristics of these 30 CTNs are summarized in Table 2.
Evaluation of the CTN activities and responsibilities (sections 1e8)
Descriptive analysis of frequency and importance for section 1e8Table 3 presents the frequency and importance of the CTN role
for the main sections of the questionnaire. The informed consentprocess (mean ¼ 2.29), implementation and evaluation of all studycomponents (mean ¼ 2.51), and investigational product manage-ment (mean ¼ 2.66) scored highest for frequency. All sectionsreceived mean importance scores> 3, except for data management(mean ¼ 2.58) and subject recruitment (mean ¼ 2.89).
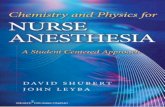
Fig. 1 compares pooled scores (3 and 4) for section 1e8 byimportance and frequency, thereby yielding the discrepancyexisting between perceived importance of activities and actualfrequency of performance. Since no reference value for CTN role is
available in the literature, an arbitrary cut-off value of 50% wasadopted to identify specific activities defining nursing contribu-tions to clinical trials in Italy. Accordingly, as regards importance,safety- and effectiveness-related activities in nursing practicescored highly in all sections. As regards frequency, most activitiesrelated to informed consent process (Section 4), investigationalproduct management (Section 5), implementation and evaluationof research protocol (Section 6), and professional nursing role(Section 8) scored highly, thus indicating major CTN contributions.Only a few activities in protocol assessment and planning (Sections1 and 2), subject recruitment (Section 3) and data management(Section 7) scored highly, thus indicating a lower level of involve-ment by CTNs.
Table 4 reports response rates that scored above 50% for the 3and 4 pooled scores which correspond to activities frequentlyperformed and highly important for the safety and effectiveness ofnursing practice. In most cases, the response rate for importancewas higher than the response rate for frequency. Where responserates were similar, a Student’s t-test was performed to verify thelack of significance of such differences. As reported in Table 5, nodifferences were statistically significant (all p values ranging from0.087 to 0.911).
Clinical trials activity and CTN professional characteristicsFor each section, a ChieSquare test was performed to examine
the relationship between CTN professional characteristics and the

Fig. 1. Comparison between pooled scores (3 and 4) for sections 1e8 by importance and frequency.
G. Catania et al. / European Journal of Oncology Nursing 16 (2012) 87e9390
two groups of median scores created for frequency or importancescales. No statistical significance was found for any of these cate-gories, except for the frequency scale, where fewer years in nursingpractice was significantly correlated with lower likelihood of per-forming datamanagement-related activities (p¼ 0.016, not shown).
Evaluation of perception of the professional nursing role (section 9)
CTNs reported being competent in their activities (77%) andsatisfied (80%) with their role (items 1 and 4). Most respondents(74%) believed they communicated effectively with prospective andcurrent subjects and their families (item 5), as well as with comembers of the healthcare and research team (item 6). Moreover,CTNs perceived their role as being accepted and supported byphysicians (63%), non-research nurses (40%), and administrativestaff (30%) (items 7, 9 and 10, respectively). Finally, seventy percentof CTNs reported being autonomous and independent when per-forming their professional role (item 8).
Discussion
Whereas in a small number of other countries the role of CTNsand the quality of their performance have been extensively delin-eated (Mori et al., 2007; Nagel et al., 2010), in Italy this is the firststudy specifically designed to define such aspects of nursing care.
Although the number of participants in this study was relativelysmall (N ¼ 30), the high response rate (88%) exemplifies the strongresearch interests by the nurses involved. In addition, CTNs mayhave considered completion of the CTNQ as a meaningful way ofenhancing recognition of nursing contribution to clinical trials,thereby acquiring greater role-related visibility.
This study reports scores both for frequency and importancescales, related to CTN activities. With reference to scores 3 and 4,results show that CTNs scored highly on the importance scale,whereas rates were lower on the frequency scale. Such findingsindicate that Italian CTNs are fully aware of being key members ofresearch teams, potentially able to share the common goals of

Table 4Activities mainly performed and retained important by CTNs.
Fa Ia
Section 1. Protocol AssessmentAssess a protocol for possible risks and inconveniences to the subject 60 90Consider the ability to maintain the rights, safety, and well-being of subject 51 83Determine facility and equipment availability 51 86Identify concerns about the study 50 76
Section 2. Protocol PlanningDevelop appropriate patient education materials 52 88Participate in study initiation meetings 55 91
Section 3. Subject RecruitmentEnsure compliance with the regulations for the recruitment of subjects 53 76Ensure all screening eligibility and enrolment procedures are completed 63 72Maintain subjects enrolment logs 53 82Verify that only eligible subjects are enrolled 63 79
Section 4. Informed Consent (IC) ProcessEnsured that the appropriate language was used in the IC document and discussion 50 73Assess the ability and willingness of subjects to follow and complete study procedures and visits 53 83Assess the potential subject’s understanding of the consent form information 57 90Verify that the IC document is signed and dated by the subject and by the person
who conducted the IC discussion60 83
Verify that the subject received a copy of the signed and dated written IC document 63 77Verify that written IC document was obtained before each subject’s participation in the study 60 80Serves as a patient advocate for subjects in all matters related to study participation 70 90Verify the subject’s continued consent throughout the course of the study 60 80
Section 5. Investigational Product (IP)Order/obtain the IP 50 67Verify record are maintained of the IP 53 67Verify the proper storage and handling of the IP 70 90Educate members of the research team about the use of the IP 64 80Verify the dose of IP to be administered 75 83Verify adequate documentation of the administered IP in the subject’s medical record 63 80Ensure that the IP is used only in accordance with the approved protocol. 86 90
Section 6. Implementation and EvaluationEnsure conduct of the study is in compliance with the approved protocol 52 77Schedule procedures and tests per protocol RQMTs 83 87Perform clinical procedures and tests per protocol RQMTs 79 90Ensure the proper collection, processing, and shipment of specimens 93 90Administer research treatments or interventions to subjects 83 93Establish mechanism for subjects to report all signs and symptoms to research team 72 87Coordinate clinical care to provide continuity and assist in subject compliance with study RQMTs 69 94Review diaries and/or questionnaires completed by subject 67 77Communicate with members of the research team for determination of seriousness,
causality, and intervention for toxicities/adverse events67 90
Assess and document identified toxicities/adverse events per protocol-specific criteria 63 87Assess and document the subject’s concurrent use of either complementary or alternative therapies 55 87Evaluate subject participation and identify barriers to protocol compliance 50 67Identify the subject’s need for additional resources and facilitate referrals 59 80Ensure the long-term follow-up of subjects 57 83Communicate with the Principal Investigator about the progress of the study 69 77
Section 7. Data ManagementMaintain source documentation for all case report form entries 50 63Participate in sponsor audits/review of records and documents 50 67Prepare for regulatory inspections of records and documents 57 60Ensure subject records are protected in accordance with applicable regulatory RQMT 62 67
Section 8. Professional nursing role performanceReceive updated information about the administration, side effects and patient monitoring RQMTs of IPs 62 90Seek additional experiences to maintain and expand knowledge of clinical research and nursing expertise 62 87Contribute to the professional development of peers, colleagues, and others 61 87
Abbreviations: F, Frequency; I, Importance; IC, Informed Consent; IP, Investigational Product; RQMT, Requirement. Values are presented as %.a Values correspond to pooled scores 3 and 4 of the Likert scales.
G. Catania et al. / European Journal of Oncology Nursing 16 (2012) 87e93 91
clinical studies, as well as supporting protocol integrity and patientsafety. However, results also indicate that most CTNs are notactively involved in protocol assessment, protocol planning, subjectrecruitment, or data management.
Overall, the present study clearly indicates that in Italy the roleof CTNs is mostly practical and focuses little on data managementand organizational activities. Indeed, the position of researchcoordinator is often held by a non-nursing professional - usually

Table 5Results of Student’s t-tests for minor differences between frequency and importance response rates.
Frequency Scalea Importance Scalea
Section 5. Investigational product N Mean SD N Mean SD p value
Verify the dose of investigational product to be administered 28 3.21 1.315 29 3.48 1.122 0.407Ensure that the investigational product is used only in accordance
with the approved protocol29 3.28 1.131 30 3.57 0.774 0.254
Section 6. Implementation and EvaluationSchedule procedures and tests per protocol requirements 29 3.31 1.198 30 3.60 0.724 0.263Ensure the proper collection, processing, and shipment of specimens 29 3.69 0.712 30 3.67 0.661 0.911Administer research treatments or interventions to subjects 29 3.38 1.208 30 3.70 0.596 0.200Review diaries and/or questionnaires completed by subject 30 2.73 1.461 29 3.28 0.882 0.087
Section 7. Data ManagementPrepare for regulatory inspections of records and documents 30 2.10 1.689 29 2.72 1.486 0.140
a Values correspond to pooled scores 3 and 4 of the Likert scales.
G. Catania et al. / European Journal of Oncology Nursing 16 (2012) 87e9392
a Data Manager (DM). Consequently, specific CTN managementskills may possibly be under-used and/or entirely unacknowledged.According to section one, CTNs occasionally assess adherence topolicies of local/institutional conflict of interest, an activity thusconsidered of low importance by respondents. Neglecting thisethical part of professional practice may well be a limitation ofpatient advocacy rights.
Most activities listed under protocol planning (Section 2) anddata management (section 7) are not performed by CTNs but ratherby other research team members, most likely the DM. As describedby Bryce et al. (2008) DMs in Italy usually deal with protocolplanning, are involved in transcribing and reporting source data,carry out query resolution, and attend to administrative,supportive, and coordinative functions related to clinical trials.
Nursing support during protocol planning is regarded as animportant activity, although the results of the frequency scale revealsome difficulty in implementing such practice. CTNs rarely educateclinical staff on research protocols. However, specifically educatednursing staffe through using nursing summary, for instance - couldpositively influence and guide the care process, possibly allowingfor a full accomplishment of research protocol objectives.
At present, patient recruitment in Italy is not a specificresponsibility of CTNs. Indeed, the principal investigator is mostlya physician. However, more specific information about the study isoften provided to the patient by CTNs. During the recruitmentphase, CTNs also ensure that all clinical investigations prior toenrolment are performed and that results meet inclusion criteria.Patient recruitment primarily depends on the informed consentprocess as CTNs ensure that patients are fully informed on the aimsand procedures of the trial and have been allowed enough time todecide whether or not to consent. Finally, CTNs are responsible forobtaining legal consent. In agreement with the findings of Moriet al. (2007), our results also suggest that Italian CTNs havea secondary role in the assessment of patient expectations throughtheir participation in a trial.
Moreover, in keeping with Deininger (2008), our study clearlyindicates that in order to handle the complexities and sensitivitiesof patient education, including inherent clinical and administrativeresponsibilities, CTNs should hold post-basic and advancedcurricular qualifications. Indeed, most CTNs in our sample lackedcertification in Clinical Trial Nursing and had mostly informalprimary education and training in clinical research, which mayhave led to practice which was only partially advanced andautonomous.
Investigational product (Section 5) and implementation andevaluation (Section 6) were the most highlighted domains. Withreference to section 5, CTNs frequently perform drug-related
activities since they have always had greater experience in drugmanagement compared with other healthcare professionals. Withreference to section 6, CTNs are fully responsible for such tasks asadministering experimental treatment; ensuring the appropriatecollection, processing and shipment of biological specimens;scheduling procedures and tests according to protocol require-ments; and assessing and documenting toxicities/adverse events.Respondents may have thought highly of the latter activitiesbecause they clearly delineate the nursing role in clinical trials andhave a major impact on a study’s outcome.
In conclusion, the role of CTNs in Italy has gained importanceover the last decade. For example, as a result of the following majorchanges: nowadays, nursing education ranges from a basic degreeto a Ph.D. degree in nursing, most nursing education programmesare taught by nurse educators and not only by medical doctors; inthe healthcare system, organization and planning of all nursingactivities are the responsibility of nurse managers rather thanmedical managers, and the increasing complexity of clinical trialsrequires a wider array of both quality and safety procedures to befulfilled by nurses. By delineating the role of the Italian CTN, thisstudy found that the Italian CTN is primarily task-oriented and fullyaware of trial demands. As such, the CTN has the potential to servea prominent role as a key member of research teams.
As shown by the present study, CTNs play a key role in themanagement of experimental drugs as well as in the imple-mentation and evaluation of protocols. Nevertheless, they are onlypartially involved in the informed consent process. Italian CTNs alsohave a marginal position in protocol assessment and planning,subject recruitment, data management and participation in thedissemination of clinical research findings.
A recent CTNQ web-based survey (Nagel et al., 2010) conductedin the United States and Canada aiming at describing the CTN rolein a Pediatric Cooperative Clinical Trials Group, found thatrespondents rated all role components as very important. Suchfindings are in keeping with results from this study andwith resultsreported by Mori et al. (2007). However, only in Nagel’s study, didthe consent process and data management sections have thehighest frequency scores. This observation, as reported by Bacon(2008) may be accounted for by the fact that Canadian CTNsfrequently perform a dual role as nurse and data manager. Thus, inItaly the strengthening of CTN organizational activities may beimplemented through greater training and more specific educa-tional programmes. In addition, our results may help nursemanagers to better promote the integration of the CTN’s role withinthe healthcare system.
A limitation of the present study might be the sample size,which may be deemed somewhat small; nevertheless, this number

G. Catania et al. / European Journal of Oncology Nursing 16 (2012) 87e93 93
of participants in itself shows that the role of the CTN is not as yetwidespread in Italy, although some universities cater for coursesaimed at developing specific advanced skills in clinical trialsnursing.
Role perception appeared to reveal awareness of Italian CTNs asto their professional autonomy and competence; however, the datareport that certain nursing-related responsibilities and activitiesare actually not performed by this category of professionals. Thereasons of such a discrepancy between role perception and nursingperformance might become the subject of further investigation inorder to allow for a more empowered, effective and efficientdeployment of available human resources within the oncologysetting of clinical trials.
Conflict of interestNone declared.
Acknowledgements
We would like to thank all study participants who agreed to fillthe questionnaire and to Dr. Alexia Piaggio for her English languageediting of the manuscript.
References
Associazione Italiana Registro Tumori (AIRTUM), 2009. AIRTUM working group.Epidemiologia & Prevenzione 33 (1e2 Suppl. 2), e6ee9.
Arrigo, C., Gall, H., Delogne, A., Molin, C., 1994. The involvement of nurses in clinicaltrials. Results of the EORTC oncology nurses study group survey. Cancer Nursing17 (5), 429e433.
Associazione Italiana Oncologia Medica (AIOM), 2004. Il Libro Bianco Dell’OncologiaItaliana, Terza Edizione. http://www.aiom.it/default.asp (accessed December2009).
Bacon, M., 2008. Canada. In: Klimaszewski, A.D., Bacon, M., Deininger, H.E.,Ford, B.A., Westendorp, J.G. (Eds.), Manual for Clinical Trials Nursing. OncologyNursing Society, Pittsburgh, PA, pp. 383e390.
Barrett, R., 2002. A nurse’s primer on recruiting participants for clinical trials.Oncology Nursing Forum 29 (7), 1091e1098.
Berry, D., Dodd, M., Hinds, P., Ferrel, B., 1996. Informed consent: process and clinicalissues. Oncology Nursing Forum 23 (3), 507e512.
Bryce, J., Connola, M., Falanga, M., 2008. Italy. In: Klimaszewski, A.D., Bacon, M.,Deininger, H.E., Ford, B.A., Westendorp, J.G. (Eds.), Manual for Clinical TrialsNursing. Oncology Nursing Society, Pittsburgh, PA, pp. 429e437.
Carlson, C., Reilly, M., Hitchens, A., 2005. An innovative approach to the care ofpatients on phase I and phase II clinical trials: the role of the experimentaltherapeutics nurse. Journal of Pediatric Oncology Nursing 22 (6), 353e364.
Cassidy, J., Macfarlane, D.K., 1991. The role of the nurse in clinical cancer research.Cancer Nursing 14 (3), 124e131.
Catania, G., Poirè, I., Dozin, B., Bernardi, M., Boni, L., 2008. Validating a measure todelineate the clinical trials nursing role in Italy. Cancer Nursing 31 (5), E11eE15.
Coulson, S., Phelan, L., 2000. Clinical research in paediatric oncology and the role ofthe research nurse in the UK. European Journal of Oncology Nursing 4 (3),154e161.
Davis, A.M., Hull, S.C., Grady, C., Wilfond, B.S., Henderson, G.E., 2002. The invisiblehand in clinical research: the study coordinator’s critical role in human subjectsprotection. The Journal of Law, Medicine & Ethics 30 (3), 411e419.
Deininger, H.E., 2008. Specialization in clinical trials nursing. In: Klimaszewski, A.D.,Bacon, M., Deininger, H.E., Ford, B.A., Westendorp, J.G. (Eds.), Manual for ClinicalTrials Nursing. Oncology Nursing Society, Pittsburgh, PA, pp. 353e356.
Di Giulio, P., Arrigo, C., Gall, H., Molin, C., Nieweg, R., Strohbucker, B., 1996.Expanding the role of the nurse in clinical trials: the nursing summaries. CancerNursing 19 (5), 343e347.
Eaton, T., Pratt, C.M., 1990. A clinic’s perspective on screening, recruitment and datacollection. Statistics in Medicine 9 (1e2), 137e144.
Ehrenberger, H.E., Lillington, L., 2004. Development of a measure to delineate theclinical trials nursing role. Oncology Nursing Forum 31 (3), E64eE68.
Hubbard, S., 1982. Cancer treatment research: the role of the Nurse in clinical trialsof cancer therapy. The Nursing Clinics of North America 17 (4), 763e783.
Jenkins, J., Hubbard, S., 1991. History of clinical trials. Seminars in Oncology Nursing7 (4), 228e234.
Klimaszewski, A.D., Bacon, M., Deininger, H.E., Ford, B.A., Westendorp, J.G., 2008.Manual for Clinical Trials Nursing, second ed. Oncology Nursing Society, Pitts-burgh, PA.
McEvoy, M.D., Cannon, L., MacDermott, M.L., 1991. The professional role for nursesin clinical trials. Seminars in Oncology Nursing 7 (4), 268e274.
Mori, C., Mullen, N., Hill, E.E., 2007. Describing the role of the clinical research nurse.Research Practitioner 8 (6), 220e228.
Nagel, K., Gender, J., Bonner, A., 2010. Delineating the role of a cohort of clinicalresearch nurses in a pediatric cooperative clinical trials group. OncologyNursing Forum 37 (3), E180eE185.
National Cancer Institute, 2008. Clinical Trials. http://www.cancer.gov/clinicaltrials/learning/what-is-a-clinical-trial (accessed February 2011).
Ocker, B., Plank, D., 2000. The research nurse role in a clinic-based oncologyresearch setting. Cancer Nursing 23 (4), 286e292.
Osservatorio Nazionale sulla Sperimentazione Clinica dei MedicinaliOsSC, 2010.Bulletin Clinical Trials of Drugs in Italy. 9� Rapporto Nazionale. http://ricerca-clinica.agenziafarmaco.it/sites/default/files/files_wysiwyg/files/Pubblicazioni_OsSC/boll_ing_2010.pdf (accessed February 2011).
Rosse, P., Krebs, L., 1999. The nurse’s role in the informed consent process. Seminarsin Oncology Nursing 15 (2), 116e123.
Wheeler, V.S., 1991. Preparing nurses for clinical trials: the cancer center approach.Seminars in Oncology Nursing 7 (4), 275e279.
White-Hershey, D., Nevidjon, B., 1990. Fundamentals for oncology nurse/datamanagers. Preparing for a new role. Oncology Nursing Forum 17 (3), 371e377.




















