
The relationship between body dysmorphic concerns and the effects of image suppression: Implications...
7
The relationship between body dysmorphic concerns and the effects of image suppression: Implications for models of body dysmorphic disorder Melissa Onden-Lim n , Jessica R. Grisham School of Psychology, University of New South Wales, Sydney, NSW 2052, Australia article info Article history: Received 12 December 2011 Received in revised form 2 May 2012 Accepted 18 May 2012 Available online 26 May 2012 Keywords: Body dysmorphic disorder Body image Thought suppression Imagery abstract A key clinical feature of body dysmorphic disorder (BDD) is the use of avoidance behaviours to minimise discomfort associated with perceived defects in appearance. While overt avoidance, such as avoidance of social situations, has been well-documented (e.g., Phillips, 2005), covert avoidance, such as image suppression, has not been explored. This study investigated the role of suppression of negative self-imagery in the maintenance of dysmorphic concern. Undergraduate participants completed a thought suppression paradigm with an experimentally-constructed negative self-image as the target. Dysmorphic concern was associated with how distressing and vivid an appearance-related intrusion was, although it did not affect whether participants engaged in suppression of the intrusion. Instructions to suppress the image led to reduced intrusion frequency and discomfort but it did not affect the quality (e.g., vividness) of intrusions. In addition, participants high in dysmorphic concern were more likely to internalise distorted appearance-related information and be disgusted by that information. Implications for models of body dysmorphic disorder are discussed. & 2012 Elsevier Ltd. All rights reserved. 1. Introduction Body dysmorphic disorder (BDD) is a disorder characterised by a distressing or impairing preoccupation with a perceived defect in appearance that is often accompanied by repetitive or compul- sive behaviour directed toward the defect. BDD shares many similarities with OCD in clinical features, demographic features, psychiatric comorbidity and similar treatment response to ser- otonin reuptake inhibitor medication (e.g., Phillips et al., 2007). For this reason BDD has widely been considered to be an OCD spectrum disorder. BDD patients have been found to engage in a number of behavioural avoidance strategies intended to reduce anxiety and other negative emotional states associated with negative judge- ments of their own appearance (e.g., Didie, Kelly, & Phillips, 2010). While these overt avoidance patterns, such as mirror avoidance and social withdrawal, have been well-documented, more covert meth- ods of avoidance have not yet been investigated. Thought suppres- sion is one such method by which individuals with BDD may attempt to avoid internal reminders of their appearance flaws. BDD patients have been shown to report more vivid and negative intrusive appearance-related images that are viewed from an observer (third-person) perspective compared to controls (Osman, Cooper, Hackmann, & Veale, 2004). In addition, preli- minary data from our laboratory suggests that body dysmorphic disorder patients and undergraduates high in dysmorphic concern engage in more suppression of appearance-related imagery than anxious control participants and undergraduates lower in dys- morphic concern (Onden-Lim & Grisham, Unpublished). We posit that suppression of these appearance-related images may con- tribute to the maintenance of the disorder. A large body of research on thought suppression suggests that efforts to suppress unwanted cognitions are likely to be ineffec- tive and ultimately maladaptive, since unwanted thoughts can paradoxically increase after a period of suppression (Abramowitz, Tolin, & Street, 2001; Wenzlaff & Wegner, 2000). Furthermore, increases in target thought frequency are often accompanied by negative emotions such as frustration and distress, which in turn fuel further suppression efforts and other avoidance behaviours (Purdon, 1999; Salkovskis & Campbell, 1994). These mechanisms have been shown to play a major role in the maintenance of other disorders (e.g., Purdon, 1999; Purdon, Rowa & Antony, 2005). Much of this previous thought suppression research, however, has failed to distinguish between cognitions that are primarily verbal in nature and those that are imagery-based. Semantic and imagery-based cognitions differ qualitatively (Paivio, 1971) and in their relation with memories and emotions (Holmes & Mathews, 2010; Holmes, Mathews, Mackintosh, & Dalgeish, 2008). The verbal thought-imagery distinction may be particularly important Contents lists available at SciVerse ScienceDirect journal homepage: www.elsevier.com/locate/jocrd Journal of Obsessive-Compulsive and Related Disorders 2211-3649/$ - see front matter & 2012 Elsevier Ltd. All rights reserved. http://dx.doi.org/10.1016/j.jocrd.2012.05.001 n Corresponding author. Tel.: þ612 938 53196; fax: þ612 938 5364. E-mail addresses: [email protected] (M. Onden-Lim), [email protected] (J.R. Grisham). Journal of Obsessive-Compulsive and Related Disorders 1 (2012) 189–195
-
Upload
independent -
Category
Documents
-
view
4 -
download
0
Transcript of The relationship between body dysmorphic concerns and the effects of image suppression: Implications...
Journal of Obsessive-Compulsive and Related Disorders 1 (2012) 189–195
Contents lists available at SciVerse ScienceDirect
Journal of Obsessive-Compulsive and Related Disorders
2211-36
http://d
n Corr
E-m
jessicag
journal homepage: www.elsevier.com/locate/jocrd
The relationship between body dysmorphic concerns and the effects of imagesuppression: Implications for models of body dysmorphic disorder
Melissa Onden-Lim n, Jessica R. Grisham
School of Psychology, University of New South Wales, Sydney, NSW 2052, Australia
a r t i c l e i n f o
Article history:
Received 12 December 2011
Received in revised form
2 May 2012
Accepted 18 May 2012Available online 26 May 2012
Keywords:
Body dysmorphic disorder
Body image
Thought suppression
Imagery
49/$ - see front matter & 2012 Elsevier Ltd. A
x.doi.org/10.1016/j.jocrd.2012.05.001
esponding author. Tel.: þ612 938 53196; fax
ail addresses: [email protected] (
@unsw.edu.au (J.R. Grisham).
a b s t r a c t
A key clinical feature of body dysmorphic disorder (BDD) is the use of avoidance behaviours to
minimise discomfort associated with perceived defects in appearance. While overt avoidance, such as
avoidance of social situations, has been well-documented (e.g., Phillips, 2005), covert avoidance, such
as image suppression, has not been explored. This study investigated the role of suppression of negative
self-imagery in the maintenance of dysmorphic concern. Undergraduate participants completed a
thought suppression paradigm with an experimentally-constructed negative self-image as the target.
Dysmorphic concern was associated with how distressing and vivid an appearance-related intrusion
was, although it did not affect whether participants engaged in suppression of the intrusion.
Instructions to suppress the image led to reduced intrusion frequency and discomfort but it did not
affect the quality (e.g., vividness) of intrusions. In addition, participants high in dysmorphic concern
were more likely to internalise distorted appearance-related information and be disgusted by that
information. Implications for models of body dysmorphic disorder are discussed.
& 2012 Elsevier Ltd. All rights reserved.
1. Introduction
Body dysmorphic disorder (BDD) is a disorder characterised bya distressing or impairing preoccupation with a perceived defectin appearance that is often accompanied by repetitive or compul-sive behaviour directed toward the defect. BDD shares manysimilarities with OCD in clinical features, demographic features,psychiatric comorbidity and similar treatment response to ser-otonin reuptake inhibitor medication (e.g., Phillips et al., 2007).For this reason BDD has widely been considered to be an OCDspectrum disorder.
BDD patients have been found to engage in a number ofbehavioural avoidance strategies intended to reduce anxiety andother negative emotional states associated with negative judge-ments of their own appearance (e.g., Didie, Kelly, & Phillips, 2010).While these overt avoidance patterns, such as mirror avoidance andsocial withdrawal, have been well-documented, more covert meth-ods of avoidance have not yet been investigated. Thought suppres-sion is one such method by which individuals with BDD mayattempt to avoid internal reminders of their appearance flaws.
BDD patients have been shown to report more vivid andnegative intrusive appearance-related images that are viewed
ll rights reserved.
: þ612 938 5364.
M. Onden-Lim),
from an observer (third-person) perspective compared to controls(Osman, Cooper, Hackmann, & Veale, 2004). In addition, preli-minary data from our laboratory suggests that body dysmorphicdisorder patients and undergraduates high in dysmorphic concernengage in more suppression of appearance-related imagery thananxious control participants and undergraduates lower in dys-morphic concern (Onden-Lim & Grisham, Unpublished). We positthat suppression of these appearance-related images may con-tribute to the maintenance of the disorder.
A large body of research on thought suppression suggests thatefforts to suppress unwanted cognitions are likely to be ineffec-tive and ultimately maladaptive, since unwanted thoughts canparadoxically increase after a period of suppression (Abramowitz,Tolin, & Street, 2001; Wenzlaff & Wegner, 2000). Furthermore,increases in target thought frequency are often accompanied bynegative emotions such as frustration and distress, which in turnfuel further suppression efforts and other avoidance behaviours(Purdon, 1999; Salkovskis & Campbell, 1994). These mechanismshave been shown to play a major role in the maintenance of otherdisorders (e.g., Purdon, 1999; Purdon, Rowa & Antony, 2005).
Much of this previous thought suppression research, however,has failed to distinguish between cognitions that are primarilyverbal in nature and those that are imagery-based. Semantic andimagery-based cognitions differ qualitatively (Paivio, 1971) and intheir relation with memories and emotions (Holmes & Mathews,2010; Holmes, Mathews, Mackintosh, & Dalgeish, 2008). Theverbal thought-imagery distinction may be particularly important

M. Onden-Lim, J.R. Grisham / Journal of Obsessive-Compulsive and Related Disorders 1 (2012) 189–195190
in BDD since appraisals about the self are often based on internalperceptual representations of actual and ideal selves (Veale &Neziroglu, 2010). Furthermore, imagery appears to be moreclosely tied to the affective system than verbal thoughts(Holmes & Mathews, 2010). Thus, the overarching aim of thecurrent study was to conduct a preliminary investigation of therole of suppression of negative self-images in the maintenanceof BDD.
In order to accomplish this aim, we induced negative self-images in an undergraduate population using a distorted photo-graph of each participant. First, we examined the associationbetween level of dysmorphic concern and reaction to the negativeself-image prior to any explicit instructions. Second, we investi-gated the effect of experimental instructions to suppress theinduced negative self-imagery.
We hypothesised that dysmorphic concern would predictmore frequent intrusions of negative self-imagery, more effortsto suppress that imagery, and more discomfort experiencedduring intrusions. We also predicted that higher dysmorphicconcern would be associated with more vivid, longer intrusionsand more use of the observer perspective in line with Osmanet al.’s (2004) study, as well as more disgust toward and reportedbelievability of the negative self-imagery. Disgust and believabil-ity of an induced negative self-image were introduced as addi-tional variables based on BDD case reports of high levels ofreported disgust toward appearance and the tendency for patientsto use distorted non-mirror reflecting surfaces for feedback aboutthe appearance (Phillips, 2005; Veale & Riley, 2001). We predictedthat the above associations would remain significant controllingfor general psychopathology and baseline mood.
Consistent with previous thought suppression research (e.g.,Abramowitz et al., 2001), we hypothesised that suppression ofnegative self-imagery would result in more frequent intrusions inthe post-suppression period, and more discomfort experiencedduring intrusions both during and after the suppression period.We also predicted that suppression would decrease the durationof intrusions, since they would be terminated earlier, but notaffect their quality (vividness and perspective).
2. Method
2.1. Participants
Ninety-two first year undergraduate students (67 female) were recruited from
the University of New South Wales and participated in exchange for course credit.
Mean age of the students was 19.92 (SD¼2.61) years and mean years in education
was 14.19 (SD¼1.41). The majority of the sample was Asian (n¼39) or Anglo-
saxon (n¼32), with the remaining participants describing themselves as mixed or
other race (n¼22). Two participants who met diagnostic criteria for BDD were
excluded for ethical reasons.
2.2. Materials
2.2.1. Distorted photograph
A portrait photograph of the participant displaying a neutral expression was
digitally altered to include a prominent dry white wart in the nasal region of the
face (lateral side or tip of nose, depending on facial structure). The modified
photograph [17�23 cm] was presented to the participant against a black back-
ground on-screen.
2.2.2. Body Dysmorphic Disorder Diagnostic Module for Adults (BDD Diagnostic
Module; Phillips, 2005)
This is a brief semi-structured clinician-administered diagnostic measure that
maps onto the DSM-IV diagnostic criteria for BDD. The BDD Diagnostic Module has
excellent interrator reliability (kappa¼ .96; Phillips, 2005).
2.2.3. Body Image Concern Inventory (BICI; Littleton, Axsom & Pury, 2005)
The BICI is a 19-item self-report measure of dysmorphic concern. That is,
concern about, and preoccupation with, a perceived defect in appearance,
excessive checking or camouflaging of the defect, social avoidance and reassur-
ance seeking. It has good internal consistency in college and multiethnic commu-
nity samples (Cronbach’s alpha¼ .93–.94), good concurrent validity (r¼ .83, BDDE-
SR; r¼ .60, BDD Y-BOCS), reasonable convergent validity with eating disorder
measures (r¼ .62), and has excellent sensitivity (96%) (Littleton et al., 2005;
Littleton & Breitkopf, 2008). The BICI was also selected because it was developed
using an undergraduate population (Littleton et al., 2005). In the current study
Cronbach’s alpha was .91.
2.2.4. 21-Item Depression Anxiety Stress Scales (DASS21;
Lovibond & Lovibond, 1995)
The DASS21 consists of three 7-item self report scales taken from the full
version of the Depression Anxiety Stress Scales. The subscales show good
concurrent validity, excellent construct validity and excellent reliability (Cron-
bach’s alphas¼ .94 for depression, .87 for anxiety, and .91 for stress; Antony,
Bieling, Cox, Enns, & Swinson, 1998; Clara, Cox, & Enns, 2001). Furthermore, each
of these subscales haven been shown to tap a more general dimension of
psychological distress (Henry & Crawford, 2005). In this study Cronbach’s alphas
for the depression, anxiety and stress subscales were. 83, .78, and .83, respectively.
2.2.5. Monitor forms
There were four self-report forms in total. These contained questions asking
participants to rate their current mood (10-point scale), discomfort experienced
when the intrusions occurred (11-point scale), and effort to suppress intrusions
during the Monitor/Suppression periods (10-point scale). Participants also were
asked to report how many times intrusions about the target story or image
occurred; how many times intrusions related to the target story or image
occurred; and to report the vividness (10-point scale), perspective (as if from
one’s own eyes vs. as if from a third person point of view; 7-point scale), average
duration of intrusions (s), believability of the modified photo (10-point scale), and
how disgusting they found the modified photo (10-point scale).
2.3. Procedure
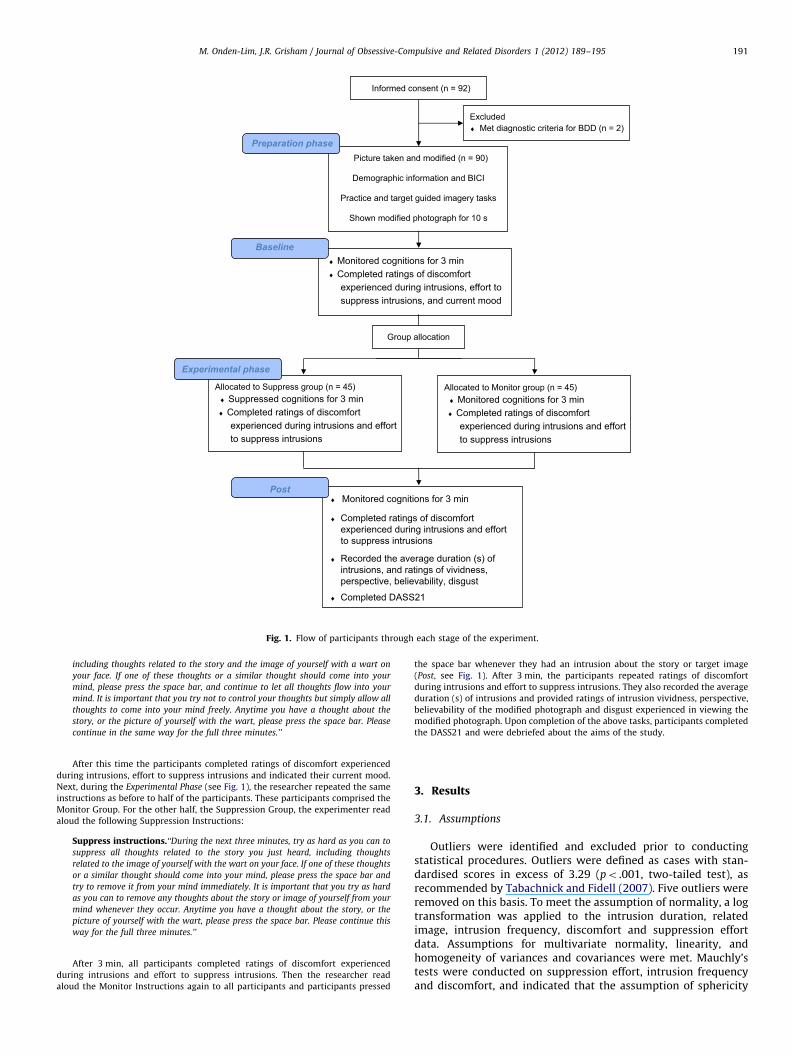
Fig. 1 shows the flow of participants through each stage of the experiment.
Participants signed statements of informed consent and were tested individually
by one female graduate level researcher. The experimenter first administered the
BDD Diagnostic Module. If participants met criteria for BDD they were debriefed
and the experiment was terminated. The remaining participants stood next to a
white backdrop and the experimenter took a picture of the participant’s face and
neck (neutral expression). Participants then completed the BICI and reported their
demographic information. BICI scores were collected at the start of the experiment
for matching purposes. Meanwhile, the researcher uploaded and digitally altered
the image to include a prominent crusty wart on nasal region of the face using the
programme Paint.net. Next, the researcher guided participants through a brief
practice visualisation task of cutting a lemon to engage participants in the use of
imagery. This procedure has been adopted in previous studies (e.g. Holmes,
Mathews, Dalgeish, & Mackintosh, 2006).
Afterward, the researcher asked participants take part in another visualisation
task and that they should ‘‘try to imagine the scenario as vividly as possible’’. The
researcher read aloud the following passage:
‘‘Imagine you are entering the university food court. You are on your way to a
group meeting over lunch with 4 other students. You feel quite hot and flustered
because you’ve been hurrying in order to get there on time. As you enter you
notice that it is very crowded and noisy with the sound of people chatting away.
The wonderful smells of food in the air make your stomach rumble and your
mouth water. After a short look around you spot your group members sitting at a
table at the back. You head over to greet them. As you say hi, you notice two of
them looking at you strangely. One of them asks you, ‘‘What’s that on your nose?’’
You run your hand across your face and feel a large pea-sized lump. It feels dry,
rough and bumpy. Hurriedly, you head to the bathroom. You look into the mirror
and this is what you seey’’
The researcher immediately presented the participants’ own modified images
(target image) back to the participants on a computer screen for 10 s, a period
intended to be sufficient for participants to engage with the image without
becoming bored. If a participant looked away from the screen during this time, the
researcher gently directed his or her gaze back to the image. At the end of the
viewing time, all participants were instructed to monitor their thoughts for 3 min
and press the space bar if they experienced a thought about the story or target
image during this time (Baseline, see Fig. 1). The key press procedure was utilised
in this study because it is less intrusive than other means (e.g., verbalising one’s
stream of consciousness) and may therefore be less likely to affect response rates
and incur problems of participants wanting to appear compliant with the
instructions (Purdon, 2004).
Monitor instructions. ‘‘During the next three minutes, you will be asked to
monitor your thoughts. During this time you may think about anything you like,
Allocated to Monitor group (n = 45) ♦ Monitored cognitions for 3 min
♦ Completed ratings of discomfort experienced during intrusions and effort to suppress intrusions
Allocated to Suppress group (n = 45) ♦ Suppressed cognitions for 3 min
♦ Completed ratings of discomfort experienced during intrusions and effort to suppress intrusions
♦ Monitored cognitions for 3 min ♦ Completed ratings of discomfort
experienced during intrusions, effort to suppress intrusions, and current mood
Baseline
Experimental phase
Picture taken and modified (n = 90)
Demographic information and BICI
Practice and target guided imagery tasks
Shown modified photograph for 10 s
Informed consent (n = 92)
♦ Monitored cognitions for 3 min
♦ Completed ratings of discomfort experienced during intrusions and effort to suppress intrusions
♦ Recorded the average duration (s) ofintrusions, and ratings of vividness, perspective, believability, disgust
♦ Completed DASS21
Post
Group allocation
Preparation phase
Excluded ♦ Met diagnostic criteria for BDD (n = 2)
Fig. 1. Flow of participants through each stage of the experiment.
M. Onden-Lim, J.R. Grisham / Journal of Obsessive-Compulsive and Related Disorders 1 (2012) 189–195 191
including thoughts related to the story and the image of yourself with a wart on
your face. If one of these thoughts or a similar thought should come into your
mind, please press the space bar, and continue to let all thoughts flow into your
mind. It is important that you try not to control your thoughts but simply allow all
thoughts to come into your mind freely. Anytime you have a thought about the
story, or the picture of yourself with the wart, please press the space bar. Please
continue in the same way for the full three minutes.’’
After this time the participants completed ratings of discomfort experienced
during intrusions, effort to suppress intrusions and indicated their current mood.
Next, during the Experimental Phase (see Fig. 1), the researcher repeated the same
instructions as before to half of the participants. These participants comprised the
Monitor Group. For the other half, the Suppression Group, the experimenter read
aloud the following Suppression Instructions:
Suppress instructions.‘‘During the next three minutes, try as hard as you can to
suppress all thoughts related to the story you just heard, including thoughts
related to the image of yourself with the wart on your face. If one of these thoughts
or a similar thought should come into your mind, please press the space bar and
try to remove it from your mind immediately. It is important that you try as hard
as you can to remove any thoughts about the story or image of yourself from your
mind whenever they occur. Anytime you have a thought about the story, or the
picture of yourself with the wart, please press the space bar. Please continue this
way for the full three minutes.’’
After 3 min, all participants completed ratings of discomfort experienced
during intrusions and effort to suppress intrusions. Then the researcher read
aloud the Monitor Instructions again to all participants and participants pressed
the space bar whenever they had an intrusion about the story or target image
(Post, see Fig. 1). After 3 min, the participants repeated ratings of discomfort
during intrusions and effort to suppress intrusions. They also recorded the average
duration (s) of intrusions and provided ratings of intrusion vividness, perspective,
believability of the modified photograph and disgust experienced in viewing the
modified photograph. Upon completion of the above tasks, participants completed
the DASS21 and were debriefed about the aims of the study.
3. Results
3.1. Assumptions
Outliers were identified and excluded prior to conductingstatistical procedures. Outliers were defined as cases with stan-dardised scores in excess of 3.29 (po .001, two-tailed test), asrecommended by Tabachnick and Fidell (2007). Five outliers wereremoved on this basis. To meet the assumption of normality, a logtransformation was applied to the intrusion duration, relatedimage, intrusion frequency, discomfort and suppression effortdata. Assumptions for multivariate normality, linearity, andhomogeneity of variances and covariances were met. Mauchly’stests were conducted on suppression effort, intrusion frequencyand discomfort, and indicated that the assumption of sphericity
M. Onden-Lim, J.R. Grisham / Journal of Obsessive-Compulsive and Related Disorders 1 (2012) 189–195192
had not been violated (respectively, w2¼5.48, p¼ .07; w2
¼2.22,p¼ .33; w2
¼4.01, p¼ .13).
3.2. Group assignment and manipulation checks
Participants were matched across groups for BICI scores andtime of day. Each group contained 45 participants, and the meanBICI scores for the Suppress and Monitor groups were 43.3(SD¼11.9) and 43.2 (SD¼12.01), respectively. DASS21 scores forthe Suppress and Monitor groups were 12.6 (SD¼9.0) and 13.0(SD¼8.8), respectively.
Independent samples t-tests and w2 were used to examinewhether any group differences existed in sex, age, years ofeducation, time of testing, baseline mood, and scores on the BICIand DASS21. There were no significant group differences on anyof these variables. Further, there was no significant differencebetween the groups in how realistic participants perceived theactual distorted computerised photo to be, t(88)¼�1.01, p¼ .32.Mean believability scores for the Suppress and Monitor groupswere 6.48 (SD¼2.29) and 5.96 (SD¼2.61) out of 10, respectively.
Participant efforts to suppress were also analysed to ensurethe condition instructions were followed. A one way 3 (time)�2(group) repeated measures multivariate analysis of variance (RM-MANOVA) was conducted to investigate the impact of suppres-sion and monitoring (control) on suppression effort, intrusionfrequency and discomfort experienced during intrusions. Resultsfor intrusion frequency and discomfort are presented later inSection 3.7. There was a main effect of time, Wilks’ L¼ .27, F(6,74)¼32.70, po .001, and a significant time by group interaction,Wilks’ L¼ .32, F(6, 74)¼25.95, po .001. Follow-up pairwisecomparisons confirmed that the Suppression group (M¼7.77,
Table 2Hierarchical multiple regression analyses predicting frequency, suppression effort an
(Baseline).
Frequency Su
Predictor DR2 b DR
Step 1 .10n .14
Baseline mood .22n
DASS21 .27n
Step 2 o .01 � .03 .02
BICI
Total R2 .10n .16
n po .05.nn po .01.
Table 1Zero order correlations.
Variable 1 2 3 4 5 6
1. BICI – .40nn� .03 .09 .28nn .3
2. DASS21 – � .17 .23n .29nn .2
3. Baseline mood – .05 � .06 �
4. Intrusion frequency – .28nn .2
5. Suppression effort – .3
6. Discomfort –
7. Vividness
8. Perspective
9. Duration
10. Believability
11. Disgust
12. Related intrusion
n po .05.nn po .01.
SD¼2.56) attempted to suppress their intrusions more than theMonitor group (M¼3.02, SD¼2.09) during the Experimental Phase,
F(1, 84)¼67.83, po .01. As expected, there were no groupdifferences in suppression effort at Pre, F(1, 84)¼2.28, p¼ .14, orPost, F(1, 84)¼3.32, p¼ .07.
3.3. The relationship between dysmorphic concern and intrusion
frequency, suppression efforts and discomfort prior to manipulation
(baseline)
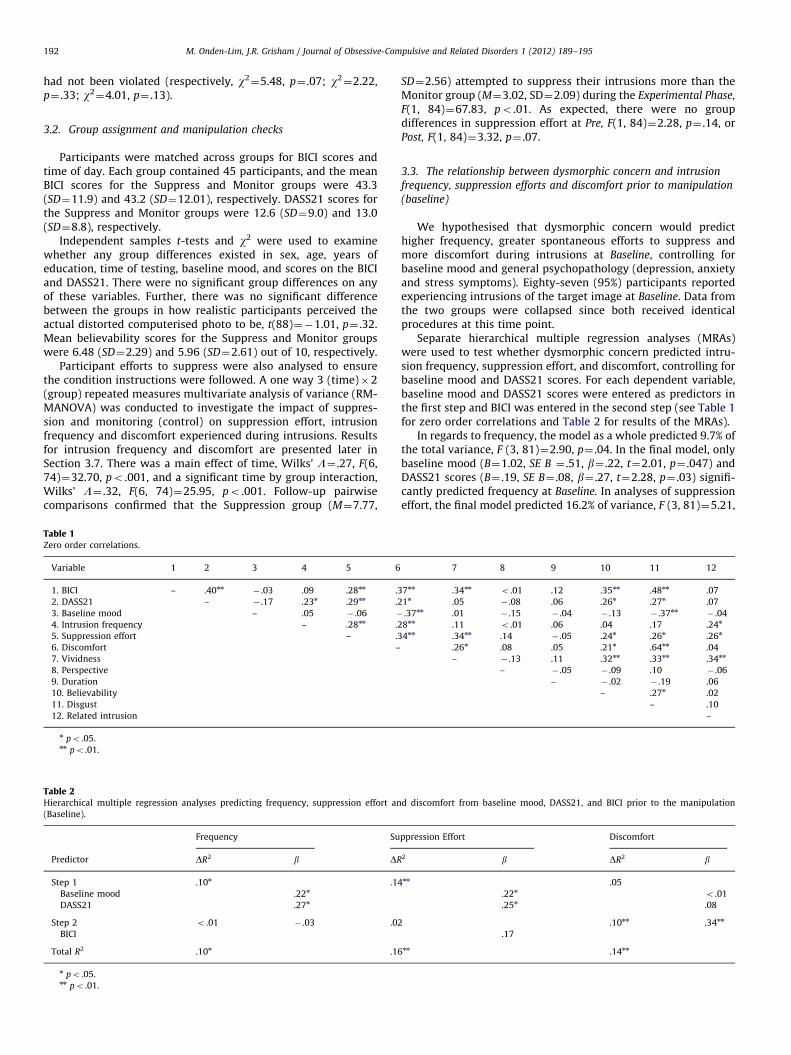
We hypothesised that dysmorphic concern would predicthigher frequency, greater spontaneous efforts to suppress andmore discomfort during intrusions at Baseline, controlling forbaseline mood and general psychopathology (depression, anxietyand stress symptoms). Eighty-seven (95%) participants reportedexperiencing intrusions of the target image at Baseline. Data fromthe two groups were collapsed since both received identicalprocedures at this time point.
Separate hierarchical multiple regression analyses (MRAs)were used to test whether dysmorphic concern predicted intru-sion frequency, suppression effort, and discomfort, controlling forbaseline mood and DASS21 scores. For each dependent variable,baseline mood and DASS21 scores were entered as predictors inthe first step and BICI was entered in the second step (see Table 1for zero order correlations and Table 2 for results of the MRAs).
In regards to frequency, the model as a whole predicted 9.7% ofthe total variance, F (3, 81)¼2.90, p¼ .04. In the final model, onlybaseline mood (B¼1.02, SE B ¼ .51, b¼ .22, t¼2.01, p¼ .047) andDASS21 scores (B¼ .19, SE B¼ .08, b¼ .27, t¼2.28, p¼ .03) signifi-cantly predicted frequency at Baseline. In analyses of suppressioneffort, the final model predicted 16.2% of variance, F (3, 81)¼5.21,
d discomfort from baseline mood, DASS21, and BICI prior to the manipulation
ppression Effort Discomfort
2 b DR2 b
nn .05
.22n o .01
.25n .08
.10nn .34nn
.17
nn .14nn
7 8 9 10 11 12
7nn .34nn o .01 .12 .35nn .48nn .07
1n .05 � .08 .06 .26n .27n .07
.37nn .01 � .15 � .04 � .13 � .37nn� .04
8nn .11 o .01 .06 .04 .17 .24n
4nn .34nn .14 � .05 .24n .26n .26n
.26n .08 .05 .21n .64nn .04
– � .13 .11 .32nn .33nn .34nn
– � .05 � .09 .10 � .06
– � .02 � .19 .06
– .27n .02
– .10
–
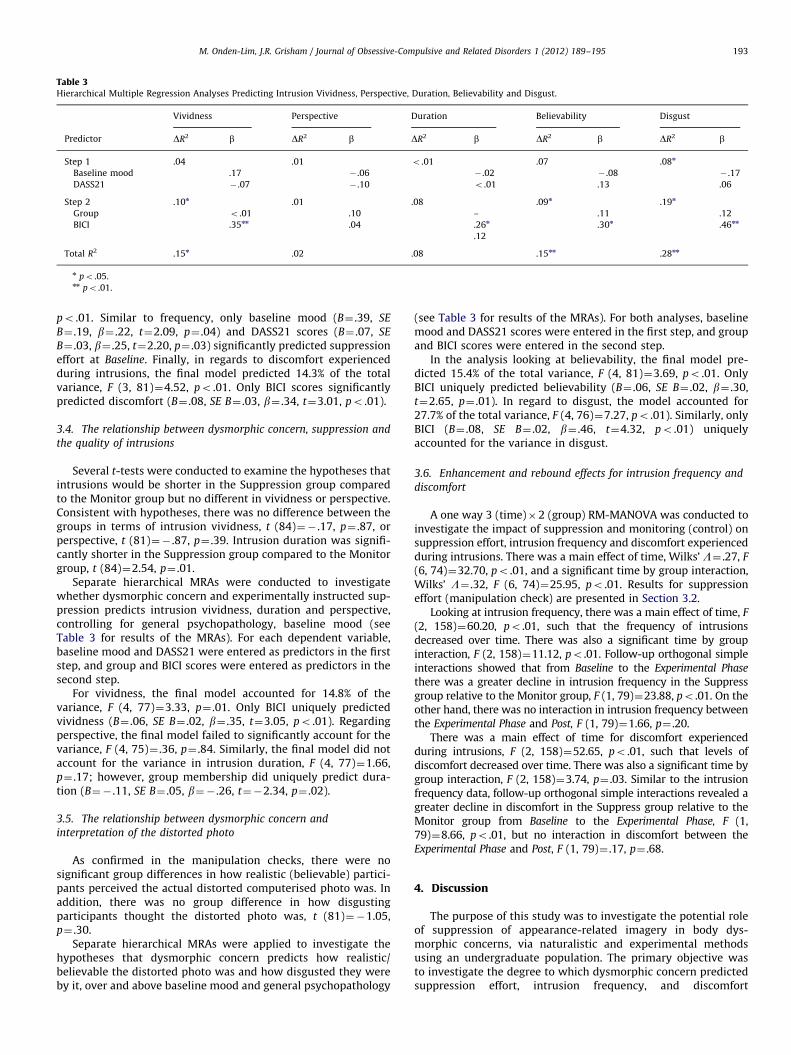
Table 3Hierarchical Multiple Regression Analyses Predicting Intrusion Vividness, Perspective, Duration, Believability and Disgust.
Vividness Perspective Duration Believability Disgust
Predictor DR2 b DR2 b DR2 b DR2 b DR2 b
Step 1 .04 .01 o .01 .07 .08n
Baseline mood .17 � .06 � .02 � .08 � .17
DASS21 � .07 � .10 o .01 .13 .06
Step 2 .10n .01 .08 .09n .19n
Group o .01 .10 – .11 .12
BICI .35nn .04 .26n .30n .46nn
.12
Total R2 .15n .02 .08 .15nn .28nn
n po .05.nn po .01.
M. Onden-Lim, J.R. Grisham / Journal of Obsessive-Compulsive and Related Disorders 1 (2012) 189–195 193
po .01. Similar to frequency, only baseline mood (B¼ .39, SE
B¼ .19, b¼ .22, t¼2.09, p¼ .04) and DASS21 scores (B¼ .07, SE
B¼ .03, b¼ .25, t¼2.20, p¼ .03) significantly predicted suppressioneffort at Baseline. Finally, in regards to discomfort experiencedduring intrusions, the final model predicted 14.3% of the totalvariance, F (3, 81)¼4.52, po .01. Only BICI scores significantlypredicted discomfort (B¼ .08, SE B¼ .03, b¼ .34, t¼3.01, po .01).
3.4. The relationship between dysmorphic concern, suppression and
the quality of intrusions
Several t-tests were conducted to examine the hypotheses thatintrusions would be shorter in the Suppression group comparedto the Monitor group but no different in vividness or perspective.Consistent with hypotheses, there was no difference between thegroups in terms of intrusion vividness, t (84)¼� .17, p¼ .87, orperspective, t (81)¼� .87, p¼ .39. Intrusion duration was signifi-cantly shorter in the Suppression group compared to the Monitorgroup, t (84)¼2.54, p¼ .01.
Separate hierarchical MRAs were conducted to investigatewhether dysmorphic concern and experimentally instructed sup-pression predicts intrusion vividness, duration and perspective,controlling for general psychopathology, baseline mood (seeTable 3 for results of the MRAs). For each dependent variable,baseline mood and DASS21 were entered as predictors in the firststep, and group and BICI scores were entered as predictors in thesecond step.
For vividness, the final model accounted for 14.8% of thevariance, F (4, 77)¼3.33, p¼ .01. Only BICI uniquely predictedvividness (B¼ .06, SE B¼ .02, b¼ .35, t¼3.05, po .01). Regardingperspective, the final model failed to significantly account for thevariance, F (4, 75)¼ .36, p¼ .84. Similarly, the final model did notaccount for the variance in intrusion duration, F (4, 77)¼1.66,p¼ .17; however, group membership did uniquely predict dura-tion (B¼� .11, SE B¼ .05, b¼� .26, t¼�2.34, p¼ .02).
3.5. The relationship between dysmorphic concern and
interpretation of the distorted photo
As confirmed in the manipulation checks, there were nosignificant group differences in how realistic (believable) partici-pants perceived the actual distorted computerised photo was. Inaddition, there was no group difference in how disgustingparticipants thought the distorted photo was, t (81)¼�1.05,p¼ .30.
Separate hierarchical MRAs were applied to investigate thehypotheses that dysmorphic concern predicts how realistic/believable the distorted photo was and how disgusted they wereby it, over and above baseline mood and general psychopathology
(see Table 3 for results of the MRAs). For both analyses, baselinemood and DASS21 scores were entered in the first step, and groupand BICI scores were entered in the second step.
In the analysis looking at believability, the final model pre-dicted 15.4% of the total variance, F (4, 81)¼3.69, po .01. OnlyBICI uniquely predicted believability (B¼ .06, SE B¼ .02, b¼ .30,t¼2.65, p¼ .01). In regard to disgust, the model accounted for27.7% of the total variance, F (4, 76)¼7.27, po .01). Similarly, onlyBICI (B¼ .08, SE B¼ .02, b¼ .46, t¼4.32, po .01) uniquelyaccounted for the variance in disgust.
3.6. Enhancement and rebound effects for intrusion frequency and
discomfort
A one way 3 (time)�2 (group) RM-MANOVA was conducted toinvestigate the impact of suppression and monitoring (control) onsuppression effort, intrusion frequency and discomfort experiencedduring intrusions. There was a main effect of time, Wilks’ L¼ .27, F
(6, 74)¼32.70, po .01, and a significant time by group interaction,Wilks’ L¼ .32, F (6, 74)¼25.95, po .01. Results for suppressioneffort (manipulation check) are presented in Section 3.2.
Looking at intrusion frequency, there was a main effect of time, F
(2, 158)¼60.20, po .01, such that the frequency of intrusionsdecreased over time. There was also a significant time by groupinteraction, F (2, 158)¼11.12, po .01. Follow-up orthogonal simpleinteractions showed that from Baseline to the Experimental Phase
there was a greater decline in intrusion frequency in the Suppressgroup relative to the Monitor group, F (1, 79)¼23.88, po .01. On theother hand, there was no interaction in intrusion frequency betweenthe Experimental Phase and Post, F (1, 79)¼1.66, p¼ .20.
There was a main effect of time for discomfort experiencedduring intrusions, F (2, 158)¼52.65, po .01, such that levels ofdiscomfort decreased over time. There was also a significant time bygroup interaction, F (2, 158)¼3.74, p¼ .03. Similar to the intrusionfrequency data, follow-up orthogonal simple interactions revealed agreater decline in discomfort in the Suppress group relative to theMonitor group from Baseline to the Experimental Phase, F (1,79)¼8.66, po .01, but no interaction in discomfort between theExperimental Phase and Post, F (1, 79)¼ .17, p¼ .68.
4. Discussion
The purpose of this study was to investigate the potential roleof suppression of appearance-related imagery in body dys-morphic concerns, via naturalistic and experimental methodsusing an undergraduate population. The primary objective wasto investigate the degree to which dysmorphic concern predictedsuppression effort, intrusion frequency, and discomfort

M. Onden-Lim, J.R. Grisham / Journal of Obsessive-Compulsive and Related Disorders 1 (2012) 189–195194
experienced during intrusions, as well as the vividness, durationand perspective of those intrusions. The second aim was toinvestigate the degree to which dysmorphic concern predictedhow believable and disgusting the distorted photograph wasperceived to be. The final objective was to experimentallyexamine the effect of suppression on discomfort and intrusionfrequency, as well as intrusion vividness, perspective andduration.
We found that dysmorphic concern predicted vividness anddiscomfort experienced during intrusions but not suppression effort,frequency, perspective or duration. Dysmorphic concern also pre-dicted the degree to which participants viewed the distortedphotograph as believable and how disgusted they were by it. Thefindings are consistent with Osman et al. (2004), who found thatBDD patients experience more vivid and distressing imagery thancommunity controls. Our results also suggest that this vivid anddistressing imagery may in part a result of the greater likelihood ofindividuals with high levels of dysmorphic concern to internalisedistorted appearance-related information (because they view it asrealistic) and experience disgust toward it. Interestingly, dysmorphicconcern was not associated with the perspective taken duringintrusions and duration, thereby failing to support the hypothesisthat higher dysmorphic concern is associated with use of theobserver perspective, and longer intrusion duration.
Experimentally-instructed suppression reduced intrusion fre-quency, discomfort and duration but did not affect intrusionvividness or perspective. Together with the above results, thesefindings suggest that while dysmorphic concern affects howdistressing and vivid an appearance-related intrusion will be, itdoes not affect intrusion frequency or whether one engages insuppression to reduce distress associated with that intrusion.However, suppression of a negative self-image may reduce intru-sion frequency and discomfort in the short term, although it willnot affect the quality (vividness and perspective) of intrusions.The finding that intrusions were significantly shorter in theSuppression group suggests that this group terminated intrusionsearlier than the Monitor group, and is consistent with lesserintrusion discomfort in this group.
These findings have interesting implications for the role ofcovert avoidance in BDD. They show that suppression of appear-ance-related imagery reduces intrusion frequency and discomfort,at least in the short term. If image suppression is negativelyreinforced by this decrease in discomfort, it may function as asafety behaviour for those high in dysmorphic concern. Thefindings are also consistent with models of body image andBDD (e.g., Cash, 2011; Veale & Neziroglu, 2010) that predict thatgreater body image investment and negative evaluation leads tonegative appraisals of appearance-related information, which inturn leads to more distress experienced during intrusions. How-ever, it does not support the models’ prediction that negativeappraisals lead to more use of thought suppression (or, covertavoidance). Our study found that only baseline mood and generalpsychopathology uniquely predicted intrusion frequency andsuppression effort. In view of the models, this suggests intrusionfrequency and suppression effort may not be due to investment inand negative evaluations of body image but rather stem frommore general factors. One reason why mood may be important isthat cognitions consistent with current mood states (e.g., negativeself-images and negative mood) may be more difficult to managethan thoughts inconsistent with current mood state (e.g.,Reynolds & Salkovskis, 1992; Wenzlaff, Wegner, and Klein, 1991).
The failure to find increases in intrusion frequency during andafter experimental instructions to suppress is inconsistent withmuch of the literature on thought suppression of personallyrelevant cognitions (e.g., Abramowitz et al., 2001; Purdon,1999). One possible reason for this divergence may be due to
methodological differences. In the present study, the target storyand modified photograph were presented once only before thefirst monitoring period (Baseline), whereas in other thoughtsuppression studies the target thought is presented duringinstructions at the beginning of each monitor/suppress period(e.g., ‘‘you may think about a white bear, but you don’t have to’’;Tolin, Abramowitz, Przeworski, & Foa, 2002, pp. 1261). Thus, astime progressed, the target story and image may have faded suchthat any immediate and post-suppression rebound effects couldnot be observed. Evidence in support of this assertion is thefinding that intrusion frequency decreased over time for bothgroups.
To counter fading of the target story and image, future studiesmay wish to incorporate a target story and image reminder (e.g.,re-presentation of the modified photo) prior to the commence-ment of each monitor/suppress period. Furthermore, investiga-tions into level of suppression success, level of personal andemotional relevance (in this case, dysmorphic concern and mood),and multiple periods of suppression may be important in experi-mental investigations, as these have been shown to modulate theemergence of immediate and post-suppression rebound effects(e.g., Corcoran & Woody, 2009; Reynolds & Salkovskis, 1992;Williams & Moulds, 2007). Should rebound effects fail to beobserved following such manipulations, this may indicate thatthe effects of image suppression in body image preoccupation donot follow standard rebound patterns as observed in other statescharacterised by obsessive or recurrent cognitions (e.g., OCD andother obsessive-compulsive spectrum disorders). However, giventhat this study was conducted on a non-clinical sample, it isnecessary to replicate findings within a clinical BDD sample. Asalluded to above, rebound effects may be evident in this popula-tion since target images (e.g., images of one’s deformed appear-ance) are likely to be of greater personal and emotional relevancein BDD populations than in non-clinical ones.
One limitation of the present study is that the target story hasovert implications for negative social evaluation (e.g., being in abusy food court). As a result it is difficult to separate whetherintrusions represented incidence of negative self-imagery orincidence of fears of negative social evaluation that are indepen-dent of dysmorphic concern. Given that we were interested inimplications for models of BDD we attempted to address theconcerns that are typical to this disorder. One key feature in thephenomenology of BDD is the high degree of social evaluativeconcern and shame surrounding the perceived defect (e.g., Veale& Neziroglu, 2010). Social concerns are also a key component ofdysmorphic concern (Castle, Molton, Hoffman, Preston, & Phillips2004). As this was the first study to address negative imagerywith application to BDD models, we elected to include a socialcomponent. However, this was at the cost of being unable toseparate out social evaluative concerns that were independent ofdysmorphic concern. Future studies may wish to modify andcompare target visualisations with and without social compo-nents in order to isolate their relative effect. In addition, futurestudies may also wish to investigate the actual content ofthoughts and images being suppressed in order to allow identi-fication of cognitions focused on body dysmorphic tendencies andthose better characterised by social anxiety.
5. Conclusion and future directions
In sum, the present study demonstrated a possible role forsuppression of appearance-related imagery in BDD, and providedsome initial evidence as to the nature of internal distortedappearance-related imagery. A noteworthy contribution of thisstudy is the use of a novel, standardised facial disfigurement

M. Onden-Lim, J.R. Grisham / Journal of Obsessive-Compulsive and Related Disorders 1 (2012) 189–195 195
added to participants’ photographs to serve as a component of thesuppressed imagery. This approach permitted greater experimen-tal control over the target concern because participants did nothave direct (only related) prior experiences with that concern.However, in order to increase applicability of the concern toparticipants, it would be useful for future studies to complementsuch studies by using idiosyncratic concerns as part of thesuppressed imagery.
The current study also extended the suppression literaturethrough the investigation of more qualitative factors, includingintrusion vividness, perspective and duration. Future researchshould investigate the effect of longer-term suppression anddelineate what individual characteristics distinguish whether ornot one engages in suppression as a strategy to respond tonegative thoughts and images.
Acknowledgements
This research was supported by an Australian PostgraduateAward of the Australian Federal Government awarded to the firstauthor.
References
Abramowitz, J. S., Tolin, D. F., & Street, G. P. (2001). Paradoxical effects of thoughtsuppression: A meta-analysis of controlled studies. Clinical Psychology Review,21, 683–703.
Antony, M. M., Bieling, P. J., Cox, B. J., Enns, M. W., & Swinson, R. P. (1998).Psychometric properties of the 42-item and 21-item versions of the Depres-sion Anxiety Stress Scales in clinical groups and a community sample.Psychological Assessment, 10, 176–181.
Cash, T. F. (2011). Cognitive-behavioral perspectives on body image. In T. F. Cash, &L. Smolak (Eds.), Body Image: A Handbook of Science, Practice and Prevention (pp.39–47). New York, NY: Guilford Press.
Castle, D. J., Molton, M., Hoffman, K., Preston, N. J., & Phillips, K. A. (2004).Correlates of dysmorphic concern in people seeking cosmetic enhancement.Australian and New Zealand Journal of Psychiatry, 38, 439–444.
Clara, I. P., Cox, B. J., & Enns, M. W. (2001). Confirmatory factor analysis of theDepression-Anxiety-Stress Scales in depressed and anxious patients. Journal ofPsychopathology and Behavioral Assessment, 23, 61–67.
Corcoran, K. M., & Woody, S. R. (2009). Effects of suppression and appraisals onthought frequency and distress. Behaviour Research and Therapy, 47,1024–1031.
Didie, E. R., Kelly, M. M., & Phillips, K. A. (2010). Clinical features of bodydysmorphic disorder. Psychiatric Annals, 40, 310–316.
Henry, J. D., & Crawford, J. R. (2005). The short-form version of the DepressionAnxiety Stress Scales (DASS-21): Construct validity and normative data in alarge non-clinical sample. British Journal of Clinical Psychology, 44, 227–239.
Holmes, E. A., & Mathews, A. (2010). Mental imagery in emotion and emotionaldisorders. Clinical Psychology Review, 30, 349–362.
Holmes, E. A., Mathews, A., Dalgeish, T., & Mackintosh, B. (2006). Positiveinterpretation training: Effects of mental imagery versus verbal training onpositive mood. Behavior Therapy, 37, 237–247.
Holmes, E. A., Mathews, A., Mackintosh, B., & Dalgeish, T. (2008). The causal effectof mental imagery on emotion assessed using picture-word cues. Emotion, 8,
395–409.Littleton, H. L., Axsom, D., & Pury, C. L. S. (2005). Development of the body image
concern inventory. Behaviour Research and Therapy, 43, 229–241.Littleton, H., & Breitkopf, C. R. (2008). The body image concern inventory:
Validation in a multiethnic sample and initial development of a Spanish
language version. Body Image, 5, 381–388.Lovibond, S. H., & Lovibond, P. F. (1995). Manual for the depression anxiety stress
scales (2nd Ed). Sydney, Australia: Psychology Foundation.Onden-Lim, M., & Grisham, J.R. (2011). [Intrusive imagery experiences in a high
dysmorphic concern population].Unpublished raw data.Osman, S., Cooper, M., Hackmann, A., & Veale, D. (2004). Spontaneously occurring
images and early memories in people with body dysmorphic disorder.Memory, 12, 428–436.
Paivio, A. (1971). Imagery and verbal processes. New York: Holt, Rinehart, andWinston.
Phillips, K. A. (2005). The broken mirror: Understanding and treating body dys-
morphic disorder. New York: Oxford University Press.Phillips, K. A., Pinto, A., Menard, W., Eisen, J. L., Mancebo, M., & Rasmussen, S. A.
(2007). Obsessive-compulsive disorder versus body dysmorphic disorder: Acomparison study of two possibly related disorders. Depression and Anxiety, 24,
399–409.Purdon, C. (1999). Thought suppression and psychopathology. Behaviour Research
and Therapy, 37, 1029–1054.Purdon, C. (2004). Empirical investigations of thought suppression in OCD. Journal
of Behavior Therapy and Experimental Psychiatry, 35, 121–136.Purdon, C., Rowa, K., & Antony, M. M. (2005). Thought suppression and its effects
on thought frequency, appraisal and mood state in individuals with obsessive-compulsive disorder. Behaviour Research and Therapy, 43, 93–108.
Reynolds, M., & Salkovskis, P. M. (1992). Comparison of positive and negativeintrusive thoughts and experimental investigation of the differential effects ofmood. Behaviour Research and Therapy, 30, 273–281.
Salkovskis, P. M., & Campbell, P. (1994). Thought suppression induces intrusionin naturally occurring negative intrusive thoughts. Behaviour Research and
Therapy, 32, 1–8.Tabachnick, B. G., & Fidell, L. S. (2007). Using Multivariate Statistics (5th ed.).
Boston: Pearson Education.Tolin, D. F., Abramowitz, J. S., Przeworski, A., & Foa, E. B. (2002). Thought suppression in
obsessive-compulsive disorder. Behaviour Research and Therapy, 40, 1255–1274.Veale, D., & Neziroglu, F. (2010). Body dysmorphic disorder: A treatment manual.
Chichester: Wiley-Blackwell.Veale, D., & Riley, S. (2001). Mirror, mirror on the wall, who is the ugliest of them
all? The psychopathology of mirror gazing in body dysmorphic disorder.
Behaviour Research and Therapy, 39, 1381–1393.Wenzlaff, R. M., & Wegner, D. M. (2000). Thought suppression. Annual Review of
Psychology, 51, 59–91.Wenzlaff, R. M., Wegner, D. M., & Klein, S. B. (1991). The role of thought
suppression in the bonding of thought and mood. Journal of Personality and
Social Psychology, 60, 500–508.Williams, A. D., & Moulds, M. L. (2007). Investigation of the indulgence cycles
hypothesis of suppression on experimentally induced visual intrusions indysphoria. Behaviour Research and Therapy, 45, 2780–2788.




















