The Influence of Rural and Urban Substance Abuse Treatment Counselor Characteristics on Client...
14
PLEASE SCROLL DOWN FOR ARTICLE This article was downloaded by: [University of Kentucky] On: 8 June 2011 Access details: Access Details: [subscription number 931144696] Publisher Routledge Informa Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House, 37- 41 Mortimer Street, London W1T 3JH, UK Journal of Social Service Research Publication details, including instructions for authors and subscription information: http://www.informaworld.com/smpp/title~content=t792306968 The Influence of Rural and Urban Substance Abuse Treatment Counselor Characteristics on Client Outcomes Carrie B. Oser a ; Elizabeth P. Biebel b ; Erin L. Pullen a ; Kathi L. H. Harp a a Department of Sociology, Center on Drug & Alcohol Research, University of Kentucky, Lexington, KY b Department of Sociology, Social Work, & Criminology, Morehead State University, Morehead, KY First published on: 08 June 2011 To cite this Article Oser, Carrie B. , Biebel, Elizabeth P. , Pullen, Erin L. and Harp, Kathi L. H.(2011) 'The Influence of Rural and Urban Substance Abuse Treatment Counselor Characteristics on Client Outcomes', Journal of Social Service Research,, First published on: 08 June 2011 (iFirst) To link to this Article: DOI: 10.1080/01488376.2011.582020 URL: http://dx.doi.org/10.1080/01488376.2011.582020 Full terms and conditions of use: http://www.informaworld.com/terms-and-conditions-of-access.pdf This article may be used for research, teaching and private study purposes. Any substantial or systematic reproduction, re-distribution, re-selling, loan or sub-licensing, systematic supply or distribution in any form to anyone is expressly forbidden. The publisher does not give any warranty express or implied or make any representation that the contents will be complete or accurate or up to date. The accuracy of any instructions, formulae and drug doses should be independently verified with primary sources. The publisher shall not be liable for any loss, actions, claims, proceedings, demand or costs or damages whatsoever or howsoever caused arising directly or indirectly in connection with or arising out of the use of this material.
Transcript of The Influence of Rural and Urban Substance Abuse Treatment Counselor Characteristics on Client...

PLEASE SCROLL DOWN FOR ARTICLE
This article was downloaded by: [University of Kentucky]On: 8 June 2011Access details: Access Details: [subscription number 931144696]Publisher RoutledgeInforma Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK
Journal of Social Service ResearchPublication details, including instructions for authors and subscription information:http://www.informaworld.com/smpp/title~content=t792306968
The Influence of Rural and Urban Substance Abuse Treatment CounselorCharacteristics on Client OutcomesCarrie B. Osera; Elizabeth P. Biebelb; Erin L. Pullena; Kathi L. H. Harpa
a Department of Sociology, Center on Drug & Alcohol Research, University of Kentucky, Lexington,KY b Department of Sociology, Social Work, & Criminology, Morehead State University, Morehead, KY
First published on: 08 June 2011
To cite this Article Oser, Carrie B. , Biebel, Elizabeth P. , Pullen, Erin L. and Harp, Kathi L. H.(2011) 'The Influence of Ruraland Urban Substance Abuse Treatment Counselor Characteristics on Client Outcomes', Journal of Social ServiceResearch,, First published on: 08 June 2011 (iFirst)To link to this Article: DOI: 10.1080/01488376.2011.582020URL: http://dx.doi.org/10.1080/01488376.2011.582020
Full terms and conditions of use: http://www.informaworld.com/terms-and-conditions-of-access.pdf
This article may be used for research, teaching and private study purposes. Any substantial orsystematic reproduction, re-distribution, re-selling, loan or sub-licensing, systematic supply ordistribution in any form to anyone is expressly forbidden.
The publisher does not give any warranty express or implied or make any representation that the contentswill be complete or accurate or up to date. The accuracy of any instructions, formulae and drug dosesshould be independently verified with primary sources. The publisher shall not be liable for any loss,actions, claims, proceedings, demand or costs or damages whatsoever or howsoever caused arising directlyor indirectly in connection with or arising out of the use of this material.

Journal of Social Service Research, 1–13, 2011Copyright c© Taylor & Francis Group, LLCISSN: 0148-8376 print / 1540-7314 onlineDOI: 10.1080/01488376.2011.582020
The Influence of Rural and Urban Substance AbuseTreatment Counselor Characteristics on Client Outcomes
Carrie B. OserElizabeth P. Biebel
Erin L. PullenKathi L. H. Harp
ABSTRACT. Focus group data were collected from 28 substance abuse treatment counselors employedin rural and urban areas to examine their perceptions of factors influencing treatment outcomes. Theinfluence of the counselor characteristics (i.e., education, experience, and recovery status) on clientoutcomes and geographic differences is explored. Focus group data were analyzed by three ratersusing line-by-line coding, focused coding, and memoing. This analytic approach revealed geographicdifferences in the counselors’ perceptions of the effect of counselor education, experience, and recoverystatus on client outcomes. Recommendations for treatment planning and future research are provided.
KEYWORDS. Substance abuse treatment counselors, treatment outcomes, rural
Much of the existing knowledge surround-ing substance abuse treatment outcomes is de-rived from three national, multisite longitudinaltreatment evaluation studies sponsored by theNational Institute on Drug Abuse since the late1960s (Fletcher, Tims, & Brown, 1997). How-ever, limitations of these studies include the lackof information gathered at the counselor contex-tual level, exclusion of nonmetropolitan areas,and the sole focus on quantitative survey datacollection. In fact, the counselor context maybe one of the most important factors in effec-tive substance abuse treatment. Therefore, the
Carrie B. Oser, PhD, is an Associate Professor at University of Kentucky, Department of Sociology, Centeron Drug & Alcohol Research, Lexington, KY.
Elizabeth P. Biebel, PhD, is an Assistant Professor at Morehead State University, Department of Sociology,Social Work, & Criminology, Morehead, KY.
Erin L. Pullen, MA, and Kathi L. H. Harp, MA, are Doctoral Students at University of Kentucky,Department of Sociology, Center on Drug & Alcohol Research, Lexington, KY.
Address correspondence to: Carrie B. Oser, PhD, University of Kentucky, Department of Sociol-ogy, Center on Drug & Alcohol Research, 1531 Patterson Office Tower, Lexington, KY 40506 (E-mail:[email protected]).
purpose of this qualitative study is to examineboth rural and urban substance abuse treatmentcounselors’ perceptions of factors influencingtreatment outcomes. Specifically, the influencesof the counselor characteristics (i.e., education,experience in the field, and recovery status) onclient outcomes are explored and geographic dif-ferences are examined.
Counselor Characteristics
Some research has suggested that the therapistand the therapeutic relationship are two of the
1
Downloaded By: [University of Kentucky] At: 19:21 8 June 2011

2 C. B. Oser et al.
most significant factors related to positive sub-stance abuse treatment outcomes (Luborsky etal., 1986; Luborsky, McLellan, Diguer, Woody,& Seligman, 1997). In fact, when determin-ing predictors for early dropout from treat-ment, Kleinman and colleagues (1990) discov-ered therapist assignment was found to be thestrongest predictor of early dropout from treat-ment, while no patient characteristics were deter-mined to be significant. One study revealed thatclients with positive perceptions of their coun-selors had more favorable treatment outcomes(e.g., improved psychological functioning and alonger length of stay in outpatient treatment) ascompared with clients with negative perceptionsof their counselors (see Kasarabada, Hser, Boles,& Huang, 2002). In addition, Rohrer, Thomas,and Yasenchak (1992) examined client percep-tions of the ideal characteristics of a substanceabuse counselor. The top five positive coun-selor traits included being understanding of theclient, concerned, caring, experienced, and hon-est, while negative traits included being an “ass-hole,” dishonest, treating clients like children,and uneducated (Rohrer et al., 1992).
One counselor characteristic that has beenshown to be an important factor related to pos-itive client treatment outcomes is a counselor’slevel of educational attainment. The educationalrequirements to be a substance abuse counselorvary by state, which differentiates substanceabuse counseling from other types of mentalhealth counseling (e.g., 45% of states do notrequire a college degree to be a substance abusecounselor while 98% of states require a master’sdegree for mental health counseling; Kerwin,Walker-Smith, & Kirby, 2006). In return, sub-stance abuse counselors are typically required tocomplete more supervised hours than other men-tal health counselors, which enforces the ideathat substance abuse counselors participate in anapprentice-style training model, where much ofthe skills are developed on the job under the di-rection of a mentor, while other types of mentalhealth counselors participate in a professional-style training where classroom instruction is em-phasized (Kerwin et al., 2006). And althoughthere has been a movement to professionalizethe field, there are still a number of “parapro-fessionals” practicing substance abuse counsel-
ing (Mulvey, Hubbard, & Hayashi, 2003). Previ-ous research in substance abuse counseling hasfound that education level and cognitive func-tioning among counselors are positively corre-lated (Sias, Lambie, & Foster, 2006). Counselorswith higher levels of education have also beenfound to purposively have a more limited rangeof treatment goals as based on the Addiction Re-search Foundation’s Goal Inventory—an inven-tory that includes dealing with family problems,obtaining residential care for the client, help-ing clients obtain employment, assisting clientsin social adjustment, helping clients to stop us-ing illegal drugs and/or alcohol, and enhanc-ing the client’s ability to cope with problemsof living (Stoffelmayr, Mavis, Sherry, & Chiu,1999). Furthermore, Stoffelmayr and colleagues(1999) found that residential program counselorswith less education utilized a broader repertoireof treatment techniques. In addition, Sias andcolleagues (2006) also found that counselorswith higher education levels had higher levelsof moral reasoning.
Many of the “paraprofessionals” practicingin the field are counselors that are in recov-ery from alcohol and drug dependence. Thesecounselors are thought to have an “edge” overcounselors not in recovery when it comes to rap-port building with clients due to their shared ex-periences (Martino, Ball, Nich, Frankforter, &Carroll, 2009). When a counselor is able to con-vey to their clients a genuine understanding ofthe difficulties in obtaining sobriety and avoid-ing relapse because they too have “walked intheir shoes,” a bond is created that is difficult tomatch for those counselors who are not in recov-ery. In fact, “shared experiences” are the basis ofthe recovery process in self-help programs suchas Alcoholics Anonymous (AA) and NarcoticsAnonymous (Martino et al., 2009). However, nosignificant differences have been found in clientoutcomes based on the counselors’ recovery sta-tus (Culbreth, 2000). Although some differenceshave been found between counselors who arein recovery and those who are not, the differ-ences are in the counseling methods utilized andin the way substance addiction is viewed (Cul-breth, 2000) but not in actual client treatmentoutcomes. For example, counselors in recov-ery have been found to be less flexible in their
Downloaded By: [University of Kentucky] At: 19:21 8 June 2011

Influence of Counselor Characteristics on Outcomes 3
treatment approach and less likely to allow forclient input into their treatment goals (Moyers &Miller, 1993). However, Stoffelmayr, Mavis, andKasim (1998) determined that recovering coun-selors actually utilize a greater range of treat-ment practices.
Rural Versus Urban Substance AbuseTreatment and Counselors
Several recent studies—the National Epi-demiological Survey on Alcohol and RelatedConditions (Dawson, Grant, Stinson, Chou,Huang, & Ruan, 2005), the National Survey onDrug Use and Health (Wright, Sathe, & Spag-nola, 2007), and the National Survey of Sub-stance Abuse Treatment Services (Lenardson &Gale, 2008)—have reported that rural residentsseeking substance abuse treatment must still dealwith limited availability and utilization. In fact,although more than a quarter of the U.S. popula-tion resides in a rural area, less than 10% of avail-able treatment facilities are located in rural ar-eas (Lenardson & Gale, 2008). This forces ruraldwellers seeking substance abuse treatment totravel greater distances, which has been shown tohave a negative impact on both length of stay andtreatment completion (Beardsley, Wish, Fitzelle,O’Grady, & Arria, 2003; Fortney, Booth, Blow,Bunn, & Cook, 1995). When this is combinedwith the lack of public transportation in ruralareas, the result is an additional barrier that ru-ral substance abuse counselors must assist theirclients in overcoming while attempting to en-gage them in treatment.
There are also cultural differences that sub-stance abuse counselors in rural areas face thatcounselors in urban areas do not, such as thehigh value placed on self-reliance in rural areasand a distrust of mental health services, whichmakes treatment utilization more difficult for ru-ral clients (Sullivan, Hasler, & Otis, 1993). Fur-thermore, rural clients entering treatment mustdo so without the benefit of anonymity that mosturban clients have, because they may be recog-nized while attending a 12-step meeting or groupcounseling session. These are all obstacles coun-selors must overcome when trying to treat ruralsubstance abusers.
The literature is limited in examining sub-stance abuse treatment counselor differences ineducation, experience, and recovery status bygeographic region. The few existing studies thatare available suggest that there minimal demo-graphic differences between rural and urban sub-stance abuse counselors. In fact, a study by Elia-son and Hughes (2004) determined that whilethe urban substance abuse counselor workforceis more culturally diverse, rural counselors hadslightly higher levels of educational attainment.However, urban substance abuse counselors aremore likely to be specifically trained in sub-stance abuse treatment (17.8% compared with6.6%; Condelli, Bonito, Ennett, & Fairbank,1996). Although this may be a disadvantagein some respects, it may also benefit the ruralcounselor because they typically take on therole of a generalist due to the lack of men-tal health treatment options available to theirclients. Another study of rural versus urban sub-stance abuse treatment found no demographicvariations among urban and rural counselorsother than urban counselors had slightly moreexperience than their rural counterparts (Bouf-fard & Smith, 2005). There are no known studiesexamining the role of recovering counselors inrural versus urban areas.
This study makes a contribution to the lit-erature by collecting qualitative data on coun-selor perceptions of the counselor characteris-tics that affect client substance abuse treatmentoutcomes. Specifically, the research questionsexamined are threefold. First, does a counselor’seducation affect the counselor’s perceptions ofa client’s substance abuse treatment outcomesdifferently in rural versus urban areas? Second,how do geographic differences in a counselor’sexperience (e.g., the number of years workingin the field) affect the counselor’s perceptions ofclient’s treatment outcomes? Third, does a coun-selor’s recovery status affect the counselor’s per-ceptions of a client’s substance abuse treatmentoutcomes, and does this vary by rural versus ur-ban locales? There are no known studies thathave examined the counselor characteristics ofeducation, experience in the field, and recoverystatus among both rural and urban counselors. Itis expected that the counselor characteristics ofeducation, experience in the field, and recovery
Downloaded By: [University of Kentucky] At: 19:21 8 June 2011

4 C. B. Oser et al.
status will affect client substance abuse treat-ment outcomes differently in rural versus urbanareas; however, the directionality of these rela-tionships is not expressed a priori because thisqualitative study is exploratory in nature.
METHOD
Participants
Data were collected from 28 substance abusetreatment counselors who participated in fourfocus groups. Focus group counselor partici-pants were recruited from an annual regionalconference that provides continuing educationfor drug prevention and treatment profession-als. Institutional review board (IRB)- and publicrelations-approved recruitment flyers requestingparticipation in a 1- to 2-hour focus group weredistributed in continuing education sessions anddisplayed at an information booth.
Counselors employed in a Kentucky state-funded substance abuse treatment program wereeligible to participate in one of two focusgroups for rural counselors or one of two fo-cus groups for urban counselors. During thescreening process, counselors were also askedto provide the county in which they were em-ployed. Rural–urban continuum codes were usedfor classification purposes in the present studybecause they distinguish metropolitan countiesby the population size of their metropolitanarea and nonmetropolitan counties by degreeof urbanization and adjacency to a metropolitanarea(s). Specifically, there are nine rural–urbancontinuum codes, which have been subdividedinto three metropolitan and six nonmetropolitangroupings. Counselors employed in metropoli-tan counties (i.e., counties coded as a 1, 2, and3) were categorized as urban, and counselors inthe remainder of the counties were classified asbeing employed in a rural county.
Procedures
For the focus group participants, informedconsent was obtained by the focus group facilita-tor, who is the lead author. IRB-approved studypersonnel, the first and second authors, met withpotential focus group participants, described thestudy and the informed consent procedures, as-
sured the prospective participants that decidingnot to participate would have no adverse ef-fects, and answered any questions. All coun-selors agreed to participate in the focus groupand signed the informed consent document.
In the four focus groups, 10 participants wereemployed in rural counties and 18 were em-ployed in urban counties. Three focus groupparticipants were African American (11%), andthe remaining 25 participants were White (89%),which is similar to Kentucky’s racial distribution(U.S. Census Bureau, 2008). Ten participantswere male (36%). Each focus group lasted ap-proximately 60 to 90 minutes and was conductedon site at the Kentucky School of Alcohol andOther Drug Studies in a private room. After ob-taining permission from all the focus group par-ticipants, each focus group was audio recorded.In addition, the first author moderated the focusgroup using a scripted protocol that introducedthe study purpose, outlined the agenda, reempha-sized confidentiality, outlined the procedures forincentives, and provided the ground rules. Thesecond author took detailed notes. Because par-ticipants may feel uncomfortable disclosing theirpersonal experiences, participants were also en-couraged to provide more general responses thatwere common to the “typical counselor.” Focusgroups were conducted in July 2008. Each coun-selor received $50 for participating in a focusgroup, and food was provided.
Focus Group Questions
The focus group protocol included the focusgroup questions, which were developed to gatherin-depth, qualitative data on the factors impact-ing client behavioral treatment outcomes froma provider perspective on a variety of topics.Specifically, the purpose of this article was toexamine how substance abuse treatment coun-selors’ education, experience in the field, and re-covery status could affect client outcomes. In ad-dition, differences in themes between counselorsemployed in rural versus urban areas were iden-tified. Feedback on the focus group questionswas obtained from two experts in the substanceabuse treatment field, and revisions were madeto the focus group protocol. The focus groupquestions for this article included:
Downloaded By: [University of Kentucky] At: 19:21 8 June 2011

Influence of Counselor Characteristics on Outcomes 5
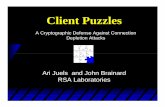
TABLE 1. Education, Experience in the Counseling Occupation, and Recovery Status FocusGroup Themes
Topic Area Theme
Education Education is beneficial.Experience matters more than education.Counseling is an innate ability.
∗
Experience in the Counseling Occupation Depends on the individual counselor.Provides a large clinical skill set.Outcomes depend primarily on client.
∗
Recovery Status Recovery status is a rapport-building tool.Recovery status can serve as an excuse for a lack of client engagement.Knowledge of a counselor’s recovery status is more central to clients earlier
in the recovery process.All people are in some form of recovery.
∗
∗Denotes themes specific to urban counselors only.
• How do you think a counselor’s educationaffects a client’s substance abuse treatmentoutcomes?
• How do you think a counselor’s experi-ence (e.g., the number of years working inthe field) affects a client’s substance abusetreatment outcomes?
• Do you think a counselor’s recovery status(e.g., whether or not the counselor has apersonal history of substance abuse prob-lems) affects a client’s substance abusetreatment outcomes?
Content Analysis
Immediately following the focus groups, sec-ond author transcribed the audio recordings ofthe four focus groups. Individual research par-ticipants were not identified on the transcripts.A content analysis approach was used to de-velop themes from the qualitative focus groupdata (e.g., Hall, Baldwin, & Prendergast, 2001).Three raters independently used a line-by-linecoding scheme of each focus group transcript.Specifically, initial coding, also known as opencoding, was first used to condense and catego-rize the data (Strauss & Corbin, 1990). Next, fo-cused coding took place to build upon the initialcoding (Lofland, Snow, Anderson, & Lofland,2006). Throughout the process of both initialand focused coding, memoing occurred. Memo-ing has been defined as the step between codingand the first draft of the data analysis (Char-
maz, 2001). This strategy allowed for theoreti-cal extension and refinement of the existing lit-erature on substance abuse treatment outcomesfrom a counselor’s perspective. From this an-alytic approach, three education themes, threeexperience themes, and four recovery statusthemes emerged (see Table 1 for overview of the-matic findings). Geographic differences betweenthemes were also discovered during the contentanalysis approach. Illustrative quotes were se-lected from the focus group transcripts to sup-port each theme.
RESULTS
Education
Three themes regarding education emergedfrom the focus group data, including thateducation is beneficial, experience mattersmore than education, and counseling is aninnate ability. First, substance abuse treatmentcounselors felt that formal education (e.g., abachelor’s or advanced graduate degree) wasbeneficial and could improve clients’ behavioraloutcomes. Both urban and rural counselorsbelieve that education results in enhancing andlearning new clinical skills (e.g., new treatmentmethods). However, rural counselors alsocited other benefits. Rural counselors thoughteducation made them more marketable andallowed them to claim more billable hours. In
Downloaded By: [University of Kentucky] At: 19:21 8 June 2011

6 C. B. Oser et al.
addition, one rural counselor said “ . . . I thinkhigher education helps us to do our paperworkbetter, which we have plenty of.” Managedcare and accountability standards have ledto ever-growing amounts of paperwork, andcounselors felt as though paperwork distractedfrom the clinical aspect of their jobs.
Second, both urban and rural counselors be-lieved that although education was important,experience mattered more. Examples of on-the-job training, such as learning from and listen-ing to clients as well as other counselors, werethought to be critical in producing positive clientoutcomes. An urban focus group participantsaid, “Categorically no. It [education] doesn’tautomatically translate. I have seen people verywell credentialed that I would not let counsel mydog. And I don’t own one, but if I had one, theywouldn’t touch him.” The notion of some coun-selors not being qualified enough to treat a non-human being, such as a dog, was also related toanother theme. Specifically, the third theme thatemerged from only the urban counselors was theperception that counseling was an innate ability,regardless of education level. One urban focusgroup participant said: “I am a true believer thatcounselors are born, not made. I’ve known somevery, very good counselors who were just recov-ering people, and I’ve known some who havePhDs that I wouldn’t send my dog to.” The no-tion that being an effective counselor is an in-herent ability was discussed in both urban focusgroups.
Experience in the Counseling Occupation
In addition to education, focus group partic-ipants were also asked how they think tenurein the counseling field affects clients’ sub-stance abuse treatment outcomes. Three themesemerged from the focus group; however, onlyone theme was specific to being employed inan urban treatment program. In regards to thefirst theme, both rural and urban focus groupparticipants thought that experience could pro-duce better client outcomes, but it could also bedetrimental to clients’ outcomes—depending onthe individual counselor. For example, one urbancounselor said:
If you have somebody who is in recoveryand has a lot of experience, has no educa-tion . . . I heard a good comment the otherday, they can “crack the egg.” They crackthat egg just right out front, and everythingjust falls forward from that point. Whereassomeone with high degrees of, you know,PhDs . . ., they can talk to them for monthson end and nothing ever happens. On theother side, it could just be reversed.
A rural counselor also discussed that the affectof a counselor’s experience on client outcomesdepends on the individual counselor. Specif-ically, this participant used the double-edgedsword analogy by stating:
I think it can go either way . . . . It [expe-rience] can be a two-edged sword in that itcan be real easy to start putting someonein a box. And all of a sudden, “you remindme of so-and-so” so I am going to do theexact same treatment with you that I didwith them, and maybe that is not proper.So, I don’t . . . if it does anything, it proba-bly on the whole helps out, but again it canbe a two-edged sword.
Both rural and urban counselors cited thebenefits of experience, including a large clini-cal skill set. Counselors who have honed anddeveloped an extensive set of clinical skillsare able to tailor their therapeutic approachto meet the client’s needs. A rural counselorstated “Ahhh, they still get over on you afteryears of experience . . . I think experience helpsin that again, it gives you more exposure todifferent ways, different activities you can dowith clients.” Interestingly, being sensitive todifferent cultures was an example of a clini-cal skill that was only mentioned in the urbanfocus groups. Counselors who have been em-ployed in the substance abuse treatment fieldfor numerous years may be more adept at iden-tifying and addressing the culturally specificneeds of their clients. As one urban counselorsaid:
I think if the older counselors, as long asthey keep their education, their knowledge
Downloaded By: [University of Kentucky] At: 19:21 8 June 2011

Influence of Counselor Characteristics on Outcomes 7
base, you know, maintain, in my opinion,I would think that they would make a bet-ter counselor just based on their experienceand exposure to different kinds of personal-ities, cultural factors, you know, the wholegambit, than the new person who is eagerand has all the book knowledge, ready totake off running.
The notion that client outcomes depend pri-marily on the client was a theme that emergedfrom only the urban focus groups. Regardlessof the number of years that the counselor hasbeen employed in the field, urban counselors ex-pressed that individualized client treatment plan-ning is needed. One urban counselor stated:
The stuff that I have read and the stuffthat I have experienced is based on, it’smore of an individual response from theclient, irrespective of education and expe-rience, either one. And under the umbrellaof client-focused treatment plan or client-focused program, where you take the clientfrom where they are, I think it all comesinto play. And the education by itself, orexperience by itself, will not yield a betteroutcome, unless it is applied to the clientin the client’s interest, based on what theclient needs.
Another urban counselor reaffirmed this sen-timent in stating, “And that’s how . . . you know,if it’s experience or the education, it dependson where that client is as to what piece theymight need . . . But then someone who is fromthe street and needs ‘in the face’ or direct isnot going to get it when you are trying to dotheory. [It’s a] very important piece, the individ-uality.” It is interesting to note that despite thepurpose of the focus groups (which was to illicitresponses on counselor characteristics that affectclients’ treatment outcomes), the urban partici-pants repeatedly brought the discussion back tothe individual client.
Recovery Status
Counselors were asked how recovery statusplays into their clients’ treatment success. Four
recovery status themes emerged from the focusgroup data, including that it helps as a rapport-building tool, it can serve as an excuse for a lackof client engagement, it is more central to clientsearlier in the recovery process, and all peopleare in some form of recovery. Overall, both ruraland urban counselors stated that having a coun-selor who is in recovery could be helpful in theirclient’s recovery process, but it still depends onthe individual client. Focus group participantsfelt that it would be easier for counselors in re-covery to establish rapport with clients and not“look down” on them. One urban counselor dis-cussed the need for recovering counselors to alsohave education, by stating:
And when I talk about clinical compe-tence, there is clinical competence and thenthere’s experiential competence—I havegone through recovery, I’m in recovery, soI have that piece, and I think that we justneed to learn how to blend that. So it’snot one’s better than the other. I think it’sjust one’s different than the other, and to-gether, we make a pretty good team andgood package.
An additional theme that emerged, regardlessof the geographic region of the counselor, wasthat a counselor’s recovery status could be anexcuse for the client’s lack of engagement inthe recovery process. Clients who may not befully committed to the recovery process—forexample, those mandated to treatment—couldbe looking for any reason to justify their lackof treatment success. One reason clients coulduse to neutralize their lack of treatment successcould be that their counselor is not in recoveryand has not “walked a mile in their shoes.” Arural counselor stated, “I think clients who wantto make that [a counselor’s recovery status] atreatment issue are looking for an issue. A lotof times I protect my anonymity being in re-covery, and I’ll hear that and then they’ll laterfind out that I am in recovery and so then it willswitch to—‘You’re Caucasian,’ or ‘You’re notfrom Kentucky’ . . . it will be something. So Idon’t give that a lot of credence.” In a relatedfashion, one urban focus group participant dis-cussed how recovery status became so central in
Downloaded By: [University of Kentucky] At: 19:21 8 June 2011

8 C. B. Oser et al.
their organization that the management directedstaff not to discuss their status. Specifically, thisurban counselor said:
I worked at an inpatient treatment centerin the past, and when I started workingthere, we had staff who were in recoveryand staff that were not in recovery and thatwas talked about a lot. Well, it got to thepoint where the management decided thatwe were no longer allowed to disclose ourrecovery status because they felt it wasalmost becoming a distraction and that itwas hurting the client’s recovery becausethey didn’t maybe respect the knowledgeof the people who weren’t in recovery, andthe people who were in recovery couldn’twork with everybody. And it is a good mixto have people who are in recovery andhave that perspective, but also people whoknow how to live without substances andhave that knowledge base from education,from experience, not of using but of theireducation and working with folks. So theyended up just not even allowing staff toshare anymore whether or not they were inrecovery.
Disclosing one’s recovery status to a clientseemed to be an individual decision among thefocus group participants, with the exception ofthe aforementioned participant who said man-agement mandated that staff not discuss theirrecovery status. Some experienced counselorshad developed strategies to negate the questionabout their recovery status, while some focusgroup participants knew counselors who werenew to the field who made up addictions to es-tablish rapport with clients.
Another theme that emerged from both therural and urban focus group participants wasthat recovery status was more central to clientsin the earlier stages of change. The Stages ofChange Model, also known as the transtheo-retical perspective, is a public health model ofbehavior that examines an individual’s progres-sion through four distinct stages of readiness tochange their perceptions and behaviors regard-ing substance use (Prochaska & DiClemente,1983). These four stages include precontempla-
tion, contemplation, action, and maintenance.An urban counselor stated:
I just want to say that I get asked that ques-tion [if I’m in recovery] almost all of thetime. And I have talked to other colleaguesabout what their responses have been, andjust based on what I can see, it seems tobe more important to the clients that areearlier in the stages of change. Those thatare progressed a little bit further into thechange process, it doesn’t seem to make asmuch of a difference to them.
This may be related to the excuse theme dis-cussed above, because clients earlier in the re-covery process may not have made a consciousdecision (e.g., they are either in the precontem-plation or contemplation stage) to change theirsubstance use behaviors.
The final theme that emerged from the focusgroup transcripts was the notion that we are all inrecovery. This theme was specific to the urbanfocus groups. The urban counselors expressedthat to some degree, it did not matter whethera counselor was in recovery, because he or shewas trying to improve his or her behavior in someway. Counselors could be struggling with otherhealth behaviors such as smoking or overeating.One urban counselor stated:
I’m not in recovery, but when I first gotinto the business, I told a friend of minethat I never learned anything about alco-hol in school, we really didn’t have anyclasses about that. And I wanted to learnabout alcoholism, and he said, “Fine, comewith me,” and he took me to an AA Meet-ing. And I went to AA for 6 years. We allhave something to recover from, and oncewe understand the process in recovery, andwe understand 12 steps, and we understandthat community, we become part of thatcommunity. It’s easier to be with clients,and clients have more respect even thoughI’m not an alcoholic. Because, and most ofthe professionals that I’ve known through-out the years all assume I’m in recoverybecause . . . so when I was in an AA meet-ing, I would always say, “Hi, my name is
Downloaded By: [University of Kentucky] At: 19:21 8 June 2011

Influence of Counselor Characteristics on Outcomes 9
. . ., and I am a recovering human being,”and that was accepted. And so, I think ifyou’re not recovering and you want to workwith this clientele, you better learn aboutrecovery and learning about it personallyby going to AA once a week for 6 years;[it] really does a lot for understanding theprocess.
This counselor used AA as a self-help forumto address his specific behavior issues, whichwere not alcohol related, as well as to learn aboutthe specific struggles related to alcohol and drugdependence.
DISCUSSION
The results of this study indicate that sub-stance abuse counselors in both rural and urbanvenues share many of the same opinions regard-ing the activities involved in the occupation ofcounseling, the benefits of counselor educationand experience, and the meaning of counselorrecovery status. Both urban and rural counselorsagree that counselor experience can have ben-efits, including a more diverse treatment reper-toire. Though this may seem an obvious con-clusion, it is important to note that past findingsindicate that the quality of such experience is im-portant (Sias et al., 2006). That is, having workedin a variety of treatment settings, both urban andrural, experimenting with a variety of treatmenttechniques, and being exposed to different typesof clients creates a greater wealth of experiencethan working in a less-varied environment.
Though the substance abuse counselors par-ticipating in this research indicate that expe-rience was useful, rural and urban counselorsagree that it may or may not produce better out-comes. Although counselors from both settingshighlight that prolonged work in the substanceabuse treatment field can result in burnout andnegative attitudes about the likelihood of sus-tained recovery among clients, only the urbancounselors espouse the belief that client out-comes often depend more on the particular clientthan the counselor. There is extant literature thatreflects on the occupational burnout that is preva-lent among those working in the substance abuse
treatment field and that discusses both the causesand effects of this burnout (Burke & Greenglass,2001; Elman & Dowd, 1997; Garner, Knight, &Simpson, 2007; Knudsen, Ducharme, & Roman,2006; Lacoursiere, 2001; Shoptaw, Stein, &Rawson, 2000). Though substance abuse coun-selor burnout and pessimistic attitudes aboutclient outcomes contribute to negative client ex-perience and lower recovery rates, it is clear fromthis research that it is a substantial concern forsubstance abuse counselors. The sentiment ex-pressed by participants in the urban focus groupsthat the client’s recovery status was more depen-dent on the client than the counselor may reflectan attempt to manage negative client outcomesin a way that relieves urban counselors from ex-periencing some of the difficult emotions thatcan become involved when the substance abusecounseling process does not result in client ab-stinence.
Although experience in the field for sub-stance abuse counselors can have both posi-tive and negative aspects, rural and urban coun-selors agreed that additional education and train-ing can only improve counselor functioning inthe treatment setting. Despite the belief amongfocus group participants that experience is amore significant factor, this study found thatsubstance abuse counselors in urban and ruralcommunities have overwhelmingly positive at-titudes about the value of education. Even urbancounselors—who also suggested that counselingwas an innate ability—agreed that formal educa-tion and staying current on new treatment strate-gies can improve counselor efficacy. Past re-search supports these conclusions, with findingsthat indicate counselor education and counselorcognitive functioning are positively correlated(Rest & Narvaez, 1994; Sias et al., 2006; Thoma,1986). Specifically, more educated counselorshave been found to possess characteristics likethe ability to “read” clients and assess their in-dividual needs, which may improve client out-comes (Sias et al., 2006).
In this research, rural counselors cited addi-tional benefits of education that urban substanceabuse counselors did not, such as having a com-petitive edge when on the job market and be-ing able to claim more billable hours. These arelikely greater concerns for those working in the
Downloaded By: [University of Kentucky] At: 19:21 8 June 2011

10 C. B. Oser et al.
rural setting because their counseling job op-portunities are more limited than those in urbanvenues and they may have fewer opportunitiesto use their counseling skill set to supplementtheir income (e.g., working part time at anothertreatment facility or hospital).
With regard to recovery status among sub-stance abuse counselors, both the urban and ruralfocus groups asserted the belief that substanceabuse counselors in recovery often have an eas-ier time establishing rapport with clients. Al-though both groups perceived recovery status asa potential rapport-building tool, past researchindicates that it may have few enduring positiveeffects on the client–counselor relationship andon client recovery (Culbreth, 2000). Recoveringcounselors are typically less educated than theirnonrecovering colleagues and may feel less mo-tivated to pursue additional training than coun-selors who are not in recovery (Culbreth, 2000;Sias et al., 2006; Stoffelmayr et al., 1998). Addi-tionally, substance abuse counselors who are inrecovery may have a more rigid treatment styleand lower levels of autonomy, perhaps due totheir lower levels of education (Culbreth, 2000);however, recovering counselors’ more firm treat-ment styles may be acceptable by clients if theyknow their counselor is successful in their ownrecovery process. Other research has yielded dif-ferent results, suggesting that substance abusecounselors in recovery tend to use a more eclec-tic approach to treatment (Humphreys, Noke,& Moos, 1996; Stoffelmayr et al., 1998). Re-gardless of whether or not recovering counselorshave better client outcomes, results of both thecurrent and past research indicate that being acounselor in recovery seems to ease the initialtension between these substance abuse treatmentprofessionals and their clients, though it is un-clear if this initial rapport established throughshared experience has a continuing impact onthe counselor–client relationship or client out-comes.
Though counselors from urban and ruraltreatment facilities shared many of the samethoughts regarding topics discussed, some dif-ferent themes did emerge during the focus groupsessions. It appears that substance abuse coun-selors from urban areas expressed more var-ied attitudes regarding the effects of counselors’
level of experience and recovery status than didtheir rural counterparts. Urban counselors, forexample, identified such skills as being able torecognize the culturally specific needs of theirclients as useful and potentially predictive ofclient success. Given past literature that hasfound a significant positive correlation betweencounselor–client gender and ethnicity matchingand treatment success, it is clear that identify-ing a client’s culturally specific needs and in-corporating them into the treatment process canbe an important part of the therapeutic process(Kasarabada et al., 2002). Further, it is not sur-prising that substance abuse counselors in ru-ral Kentucky did not identify this as an impor-tant skill because the racial and ethnic make-up of these rural communities is relatively ho-mogenous, with counselors and clients matchedracially and culturally more often than in urbancommunities.
Though the findings of this research are cer-tainly important, there are some limitations thatmust also be considered. First, generalizabilitymay be limited as these findings are based onfour focus groups. Second, these analyses didnot consider how different themes were pat-terned by counselor gender—rather, the focuswas mainly on rural–urban counselor differ-ences. Past research has found that counselorgender can be a significant factor when consider-ing such diverse themes as treatment strategies,rate of burnout, and in certain circumstances,even client outcomes (Green, Polen, Dickinson,Lynch, & Bennett, 2002; Jones & Zoppel, 1982;Price & Spence, 1994; Sterling, Gottheil, Win-stein, & Serota 1998; Vredenburgh, Carlozzi, &Stein, 1999). Another factor not considered bythese analyses—counselor caseload—has alsobeen found to be significantly correlated withcounselor burnout and with negative client out-comes in some instances (Garner et al., 2007;Luborsky et al., 1997). Specifically, as substanceabuse counselors become overworked, they areless able to effectively serve their clients on anindividual basis. In addition to these limitations,it is important to note that states differ in theirrequirements for substance abuse counselors, sothe attitudes expressed by participants in the ur-ban and rural focus groups, especially their per-ceptions of the value of education, may not be
Downloaded By: [University of Kentucky] At: 19:21 8 June 2011

Influence of Counselor Characteristics on Outcomes 11
generalizable to counselors in all states (Kerwinet al., 2006).
CONCLUSIONS
Regardless of the limitations of this study,these findings can provide an important contri-bution to the literature on substance abuse treat-ment and can guide future research. Althoughthere is a great wealth of past research that quan-titatively investigates counselor characteristicsand their correlation to client recovery, burnout,and other themes, this research provides insightinto the perceptions of the substance abuse coun-selors themselves. Understanding their observa-tions about the value of counselor experience,education, and recovery status can provide ad-ministrators and others working with these pro-fessionals a better sense of the use value of thesevarious counselor characteristics in the field.This can assist those preparing to work in thesubstance abuse treatment field or those over-seeing substance abuse counselors with prepar-ing themselves or others for the kinds of chal-lenges they will experience in this occupation.Specifically, results of this research suggest thatcounselors would benefit from increased train-ing opportunities that would help them remaincurrent regarding treatment options and alterna-tive therapies. Further, the results of this researchsuggest that being a counselor in recovery doesnot exempt one from the gains of these educa-tional opportunities, as additional counselor edu-cation can provide practitioners with knowledgethat will have sustained benefits for clients andcounselors alike. Given the proliferation of para-professionals working as substance abuse coun-selors, increased access to educational opportu-nities is also advisable (Mulvey et al., 2003).
In addition to creating more opportunities forsubstance abuse counselors to further their ed-ucation, the findings of this study indicate thatproviding clients with supplementary services(e.g., medical services, transportation assistance,and family/social services) would also createbenefits for their counselors (Ducharme, Mello,Roman, Knudsen, & Johnson, 2007). While ed-ucation, experience, and recovery status are in-dividual counselor characteristics that can im-
pact the success of the treatment process, pro-viding more comprehensive services to clientswould improve client retention and outcomes(Ducharme et al., 2007). Though the responsibil-ity for providing these core and support serviceshas to come from sources other than the coun-selors, many of whom are often already overbur-dened, their availability in the treatment settingwould create an environment that is better forboth clients and their counselors.
ACKNOWLEDGMENTS
This research was supported by the NationalInstitute on Drug Abuse (K01-DA21309).
REFERENCES
Beardsley, K., Wish, E. D., Fitzelle, D. B., O’Grady, K.,& Arria, A. M. (2003). Distance traveled to outpatientdrug treatment and client retention. Journal of Sub-stance Abuse Treatment, 25(4), 279–285.
Bouffard, J. A., & Smith, S. (2005). Programmatic, coun-selor, and client-level comparison of rural versus urbandrug court treatment. Substance Use & Misuse, 40(3),321–342.
Burke, R. J., & Greenglass, E. R. (2001). Hospital re-structuring, work–family conflict, and psychologicalburnout among nursing staff. Psychology and Health,16, 583–594.
Charmaz, K. (2001). Qualitative interviewing and groundedtheory analysis. In N. Denzin & Y. Lincoln (Eds.),Handbook of qualitative research: Context and method(pp. 675–694). Thousand Oaks, CA: Sage Publications.
Condelli, W. S., Bonito, A. J., Ennett, S. T., & Fairbank,J. A. (1996). Drug abuse among non-metropolitan andrural adolescents: The need and availability of services.Research Triangle Park, NC: Research Triangle Insti-tute.
Culbreth, J. R. (2000). Substance abuse counselors withand without a personal history of chemical dependency.Alcoholism Treatment Quarterly, 18(2), 67–82.
Dawson, D. A., Grant, B. F., Stinson, F. S., Chou, P. S.,Huang, B., & Ruan, W. J. (2005). Recovery from DSM-IV alcohol dependence: United States, 2001–2002. Ad-diction, 100, 281–292.
Ducharme, L. J., Mello, H. L., Roman, P. M., Knudsen,H. K., & Johnson, A. J. (2007). Service delivery insubstance abuse treatment: Reexamining “comprehen-sive” care. Journal of Behavioral Health Services andResearch, 34(2), 121–136.
Eliason, M. J., & Hughes, T. L. (2004). Substance user treat-ment counselors’ attitudes about lesbian, gay, bisexual,
Downloaded By: [University of Kentucky] At: 19:21 8 June 2011

12 C. B. Oser et al.
and transgender clients: Urban versus rural settings.Journal of Substance Use and Misuse, 39(4), 625–644.
Elman, B. D., & Dowd, E. T. (1997). Correlates of burnoutin inpatient substance user treatment therapists. Journalof Addictions & Offender Counseling, 17, 56–65.
Fletcher, B. W., Tims, F. M., & Brown, B. S. (1997). Na-tional treatment evaluations and the Drug Abuse Treat-ment Outcome Study (DATOS). Psychology of Addic-tive Behaviors, 11, 216–229.
Fortney, J. C., Booth, B. M., Blow, F. C., Bunn, J. Y., &Cook, C. A. L. (1995). The effects of travel barriersand age on the utilization of alcoholism treatment after-care. The American Journal of Drug and Alcohol Abuse,21(3), 391–406.
Garner, B. R., Knight, K., & Simpson, D. D. (2007).Burnout among corrections-based drug treatment staff:Impact of individual and organizational factors. Inter-national Journal of Offender Therapy and ComparativeCriminology, 51(5), 510–522.
Green, C. A., Polen, M. R., Dickinson, D. M., Lynch,F. L., & Bennett, M. D. (2002). Gender differencesin predictors of initiation, retention, and completionin an HMO-based substance abuse treatment pro-gram. Journal of Substance Abuse Treatment, 23(4),285–295.
Hall, E. A., Baldwin, D. M., & Prendergast, M. L. (2001).Women on parole: Barriers to success after substanceabuse treatment. Human Organization, 60(3), 225–233.
Humphreys, K., Noke, J. M., & Moos, R. H. (1996). Re-covering substance abuse staff members’ beliefs aboutaddiction. Journal of Substance Abuse Treatment, 13(1),75–78.
Jones, E. E., & Zoppel, C. L. (1982). Impact of clientand therapist gender on psychotherapy process and out-come. Journal of Consulting and Clinical Psychology,50(2), 259–272.
Kasarabada, N. D., Hser, Y., Boles, S. M., & Huang,Y. C. (2002). Do patients’ perceptions of their coun-selors influence outcomes of drug treatment? Journal ofSubstance Abuse Treatment, 23, 327–334.
Kerwin, M. E., Walker-Smith, K., & Kirby, K. C. (2006).Comparative analysis of state requirements for the train-ing of substance abuse and mental health counselors.Journal of Substance Abuse Treatment, 30, 173–181.
Kleinman, P. H., Woody, G. E., Todd, T. C., Millman, R.B., Kang, S., Kemp, J., & Lipton, D. S. (1990). Crackand cocaine abusers in outpatient psychotherapy. Na-tional Institute on Drug Abuse Research Monograph,104, 24–38.
Knudsen, H. K., Ducharme, L. J., & Roman, P. M. (2006).Counselor emotional exhaustion and turnover intentionin therapeutic communities. Journal of Substance AbuseTreatment, 31(2), 173–180.
Lacoursiere, R. B. (2001). “Burnout” and sub-stance user treatment: The phenomenon and theadministrator–clinician’s experience. Substance Use &Misuse, 36(13), 1839–1874.
Lenardson, J., & Gale, J. A. (2008). Distribution of sub-stance abuse treatment facilities across the rural–urbancontinuum. Retrieved from http://muskie.usm.maine.edu/Publications/rural/pb35bSubstAbuseTreatmentFacilities.pdf
Lofland, J., Snow, D. A., Anderson, L., & Lofland, L. H.(2006). Analyzing social settings: A guide to qualita-tive observation and analysis (4th ed.). Belmont, CA:Wadsworth Publishing.
Luborsky, L., Crits-Cristoph, P., McLellan, A. T., Woody,G., Piper, W., Liberman, B., Imber, . . . Pilkonis, P.(1986). Do therapists vary much in their success? Find-ings from four outcome studies. American Journal ofOrthopsychiatry, 56, 501–512.
Luborsky, L., McLellan, A. T., Diguer, L., Woody, G., &Seligman, D. A. (1997). The psychotherapist matters:Comparison of outcomes across twenty-two therapistsand seven patient samples. Clinical Psychology: SciencePractice, 4, 53–65.
Martino, S., Ball, S. A., Nich, C., Frankforter, T. L., &Carroll, K. M. (2009). Informal discussions in substanceabuse treatment sessions. Journal of Substance AbuseTreatment, 36, 366–375.
Moyers, T. B., & Miller, W. R. (1993). Therapists’ concep-tualizations of alcoholism: Measurement and implica-tions for treatment decisions. Psychology of AddictiveBehaviors, 7, 238–245.
Mulvey, K. P., Hubbard, S., & Hayashi, S. (2003). A na-tional study of the substance abuse treatment work-force. Journal of Substance Abuse Treatment, 24, 51–57.
Price, L., & Spence, S. H. (1994). Burnout symptomsamongst drug and alcohol service employees: Genderdifferences in the interaction between work and homestressors. Anxiety, Stress, & Coping, 7(1), 67–84.
Prochaska, J. O., & DiClemente, C. C. (1983). Stages andprocesses of self-change of smoking: Toward an inte-grative model of change. Journal of Consulting andClinical Psychology, 51(3), 390–395.
Rest, J. R., & Narvaez, D. (1994). Moral development in theprofessions: Psychology and applied ethics. Hillsdale,NJ: Erlbaum.
Rohrer, G. E., Thomas, M., & Yasenchak, A. B. (1992).Client perceptions of the ideal addictions counselor. TheInternational Journal of the Addictions, 27(6), 727–733.
Shoptaw, S., Stein, J. A., & Rawson, R. A. (2000). Burnoutin substance abuse counselors: Impact of environment,attitudes, and clients with HIV. Journal of SubstanceAbuse Treatment, 19, 117–126.
Sias, S. M., Lambie, G. W., & Foster, V. A. (2006). Concep-tual and moral development of substance abuse coun-selors: Implications for training. Journal of Addictionsand Offender Counseling, 26, 99–110.
Sterling, R. C., Gottheil, E., Winstein, S. P., & Serota, R.(1998). Therapist/patient race and sex matching: Treat-ment retention and 9-month follow-up outcome. Addic-tion, 93(7), 1043–1050.
Downloaded By: [University of Kentucky] At: 19:21 8 June 2011

Influence of Counselor Characteristics on Outcomes 13
Stoffelmayr, B. E., Mavis, B. E., & Kasim, R. M. (1998).Substance abuse treatment staff: Recovery status andapproaches to treatment. Journal of Drug Education,28(2), 135–145.
Stoffelmayr, B. E., Mavis, B. E., Sherry, L. A., &Chiu, C. W. (1999). The influence of recovery sta-tus and education on addiction counselors’ approachto treatment. Journal of Psychoactive Drugs, 31(2),121–127.
Strauss, A., & Corbin, J. (1990). Basics of qualitative re-search: Grounded theory, procedures, and techniques.Newbury Park, CA: Sage Publications.
Sullivan, W. P., Hasler, M. D., & Otis, A. G. (1993). Ruralmental health practice: Voices from the field, families insociety. Journal of Contemporary Human Service, 74,493–502.
Thoma, S. J. (1986). Estimating gender differences in com-prehension and preference of moral issues. Develop-mental Review, 6, 165–180.
U.S. Census Bureau. (2008). State & county quick facts:Kentucky. Retrieved from http://quickfacts.census.gov/qfd/states/21000.html
Vredenburgh, L. D., Carlozzi, A. F., & Stein, L. B. (1999).Burnout in counseling psychologists: Type of practicesetting and pertinent demographics. Counseling Psy-chology Quarterly, 12(3), 293–302.
Wright, D., Sathe, N., & Spagnola, K. (2007). State esti-mates of substance use from the 2004–2005 NationalSurveys on Drug Use and Health (DHHS PublicationNo. SMA 07–4235, NSDUH Series H-31). Rockville,MD: Substance Abuse and Mental Health Services Ad-ministration, Office of Applied Studies.
Downloaded By: [University of Kentucky] At: 19:21 8 June 2011