
Privacy in instant messaging: an impression management model
Upload
independentCategory
view
5download
0
Text4baby: Development and Implementation of a NationalText Messaging Health Information Service
Text4baby is the first free
national health text mes-
saging service in the United
States that aims to provide
timely information to preg-
nant women and new
mothers to help them im-
prove their health and the
health of their babies.
Here we describe the de-
velopment of the text mes-
sages and the large public–
private partnership that led
to the national launch of the
service in 2010. Promotion
at the local, state, and na-
tional levels produced rapid
uptake across the United
States. More than 320 000
people enrolled with text4-
babybetweenFebruary2010
andMarch 2012.
Further evaluations of the
effectiveness of the service
areongoing;however,impor-
tant lessons can be learned
from its development and
uptake. (Am J Public Health.
2012;102:2207–2213. doi:
10.2105/AJPH.2012.300736)
Robyn Whittaker, MBChB, PhD, MPH, Sabrina Matoff-Stepp, PhD, Judy Meehan, BS, Juliette Kendrick, MD,Elizabeth Jordan, DNSc, Paul Stange, MPH, Amanda Cash, DrPH, Paul Meyer, JD, Julie Baitty, Pamela Johnson, PhD,Scott Ratzan, MD, MPA, MA, and Kyu Rhee, MD, MPP
THE US INFANT MORTALITY
rate (6.59/1000 live births) ishigher than in most developedcountries.1 In the United States,the infant mortality rate for non-Hispanic African Americanwomen is 2.4 times the rate fornon-Hispanic White women.1
Rates are also elevated for NativeAmerican Indian and Alaska Na-tive women. In 2008, 12.3% ofthe 4 251095 babies born in theUnited States were born prema-turely and 8.2% had a low birthweight.2 Health-related behaviorsin the prenatal and postnatal pe-riods, such as nutrition, tobaccosmoking, breastfeeding, safe sleeppractices, and vaccination areknown to affect maternal and in-fant outcomes.3 Women withoutaccess to affordable and appropri-ate care may not be receivinginformation needed to supportprenatal and postnatal pediatriccare. Recent studies have alsoshown limited health literacy inthe United States to be related toa lack of prenatal planning, suchas taking folic acid, and difficultieswith informed parental decision-making.4,5
Mobile phones may be an ap-propriate means for addressingthe challenges of health literacy6
and for reaching women fromunderserved communities. Mobilephone ownership in the UnitedStates is similar across racial/eth-nic groups (80% of Whites and87% of African Americans andHispanics). African Americans(79%) and Hispanic Americans(83%) are more likely than are
White Americans (68%) to sendtext messages.7 Americans livingin or near poverty are more likelyto live in cell phone---only house-holds (no fixed phone line), andthose living in cell phone---onlyhouseholds are more likely tohave experienced numerous bar-riers to health care.8
Mobile phone text messaginghas been used to support healthybehavior change and health caredelivery processes.9---12 Successfulbehavior change interventionshave used text messaging tosupport smoking cessation,13---15
weight management through dietor physical activity,16---19 and man-agement of anxiety symptoms.20
Health care process interventionshave included appointment re-minders21---24 and reminders totake medications.25---30
Here we describe the develop-ment of text4baby, a free nationaltext messaging service that pro-vides timely information to preg-nant women and new mothers tohelp them improve their healthand the health of their babies.More than 320 000 people en-rolled with text4baby between itslaunch in February 2010 andMarch 2012. Little has been pub-lished in peer-reviewed journalson mobile health initiatives of thisscale in the United States. Pub-lished international examples ofnational-scale services includea text messaging smoking cessa-tion service in New Zealand,which was established after a ran-domized trial and registered 3905clients in the first year,13,31 and
a public health campaign in SouthAfrica, which sent 968 millionHIV/AIDS awareness messagesembedded in free “Please call me”text messages over two years.32,33
Lessons from the development oftext4baby could guide similarmobile health developments.
PARTNERSHIPDEVELOPMENT
Interest in developing a modelof how mobile health could betaken to scale in the United Statesled to discussions between stafffrom the US Centers for DiseaseControl and Prevention (CDC) andVoxiva Inc, a private mobilehealth company, in January 2009.These discussions focused on cre-ating a public---private partnershipto support a program that woulddeliver health messages via textmessaging to pregnant women andmothers of infants. The NationalHealthy Mothers, Healthy BabiesCoalition, a nonprofit group of100 local, state, and national or-ganizations focusing on improvingthe quality and reach of public andprofessional maternal and chil-dren’s health education, joined thepartnership to lead the program.
An exploratory meeting heldin the second quarter of 2009brought together representativesfrom private partners (Voxiva,Johnson and Johnson), nonprofitpartners (HealthyMothers, HealthyBabies, CTIA---The Wireless Foun-dation), and interested public or-ganizations (White House Officeof Science Technology and Policy;
COMMENTARY
December 2012, Vol 102, No. 12 | American Journal of Public Health Whittaker et al. | Peer Reviewed | Commentary | 2207

within the US Department of Healthand Human Services [HHS], theOffice on Women’s Health, CDC,and the Health Resources and Ser-vices Administration [HRSA]; USDepartment of Defense; US De-partment of Agriculture; VirginiaState Health Commissioner; andGeorge Washington University).
In January 2010, HHS (repre-sented by Howard Koh, MD, MPH,Assistant Secretary for Health)and Healthy Mothers, HealthyBabies signed a memorandum ofunderstanding that designatedHealthy Mothers, Healthy Babiesas the lead partner, with overallresponsibility for the delivery ofthe service. The memorandumstated that HHS would oversee adepartment-wide effort to promotethe initiative and that HHS com-ponents (the Office on Women’sHealth, CDC, HRSA, and Centersfor Medicare and Medicaid Ser-vices) would provide guidance andinput on the content of text mes-sages, have final approval of thetext message content, and be in-volved in the design, development,and evaluation of the service. (Laterin 2010, HHS announced fundingfor an evaluation of the program.)The memorandum stated thegoals of the program as demon-strating the potential of mobilehealth technology to address acritical national health priority forunderserved populations, devel-oping an evidence base on theeffectiveness of mobile health in-terventions, and catalyzing newmodels for public---private part-nerships in mobile health.
Healthy Mothers, HealthyBabies and Voxiva directly ap-proached potential importantsponsors and partners throughtheir existing networks. In Febru-ary 2010, Voxiva and HealthyMothers, Healthy Babies reachedout to Johnson and Johnson, amultinational consumer health
care, pharmaceuticals, and diag-nostics company that had previousrelationships with some partnersand an interest in digital health.The company signaled interest inserving as the founding sponsor.Through its relationships withthe wireless networks, Voxivaapproached CTIA, a nonprofitfoundation representing the wire-less communications industry. Thefoundation saw it as an opportu-nity to help quantify the value ofmobile health and worked with thewireless carriers to garner theirsupport. This resulted in 18 wire-less carriers absorbing messagingcosts so that text4baby could beprovided free to the end users.CTIA and Healthy Mothers,Healthy Babies agreed to supportthe service for its first two years(2010---2011). This was a first fora health service of this kind in theUnited States and has since beenextended to the end of 2013. GrayHealthcare Group, a marketingand design firm with an existingrelationship with Voxiva, provideda marketing strategy, includinga logo and promotional materials.
Also in February 2010, formerUS Chief Technology Officer,Aneesh Chopra, announced thelaunch of the service.34 HealthyMothers, Healthy Babiesapproached organizations in itsnetworks about actively promot-ing the program directly to preg-nant women and new mothers.Among the organizations thatsigned up to be outreach andpromotional partners were stategovernment organizations; na-tional, state, and local nonprofitorganizations; county and cityhealth departments; healthplans; and state-based teams (afull list of current partners isavailable at http://www.text4-baby.org/index.php/get-involved-pg/partners). Outreach partners havebeen supported via a Web portal
with customizable resources,weekly Webinars, ande-newsletters with aggregatedenrollment information.
MESSAGE DEVELOPMENT
CDC staff (medical epidemiolo-gists and experts in obstetrics, pe-diatrics, family practice, and healthcommunication) identified topicsaccording to evidence-informedguidelines, particularly the Ameri-can Congress of Obstetriciansand Gynecologists guidelines forcare35 and the Bright FuturesGuidelines for Health Supervisionof Infants, Children, and Adoles-cents.36 Identified topics rangedfrom tobacco effects on motherand infant to the importance ofprenatal and well-baby care tothe positive effects of breastfeed-ing. HHS staff prioritized topicsby public health importance.Topics would be timed to themother’s stage of gestation or theinfant’s age.
Healthy Mothers, HealthyBabies held informal discussiongroups with women from com-munity health centers in six citiesacross the United States. Theyasked attending women about thetypes of topics they would like tosee covered and the frequency ofmessages they would find accept-able. This input informed finaltopic selection and the regimen ofthree messages per week.
CDC and Healthy Mothers,Healthy Babies staff drafted the150-character messages. The Mo-bile Marketing Association’s best-practice guidelines recommendedthat each message begin with thephrase “Free msg” to reassure re-cipients that the service was in-deed free.37 The writers designedthe messages to be understand-able to low-literacy populations(approximately sixth-grade read-ing level). The draft messages
underwent several levels of reviewand testing; among the reviewerswere staff from across HHS, toensure consistency with agencymission and policy, and expert con-sultants representing the AmericanCongress of Obstetricians and Gy-necologists, the American Academyof Pediatrics, and others. BabyCen-ter en Español translated the mes-sages into Spanish, and the NationalAlliance for Hispanic Healthreviewed the translations.
The final 117 prenatal mes-sages covered usual symptomsduring pregnancy; when and howto access health care; emotionalsupport for the pregnant woman;safety; nutrition; smoking, alcohol,and drugs; infectious diseases; la-bor and delivery; postnatal infor-mation; and exercise. The 147postnatal messages focused oncare for the baby according tonormal developmental stages;safety, feeding, and nutrition;when and how to access healthcare; emotional support for themother; immunizations; andsmoking. Toll-free numbers insome messages (e.g., 1---800-311-BABY) connected callers to theirrespective state or local maternaland children’s health services. Thebox at the top of the followingpage provides examples.
The messages continue to bereviewed and refined. In 2010,Healthy Mothers, Healthy Babiescontracted with a team at EmoryUniversity to recruit pregnantwomen in a Women, Infants, andChildren Program waiting room ata large city hospital in Atlanta,Georgia. These women (n = 100)were predominantly AfricanAmerican (96%), single (66%),and low income (100% had< $35 000/year). The team askedparticipants to review the mes-sages for their level of under-standing. The team suggestedrevisions derived from its
COMMENTARY
2208 | Commentary | Peer Reviewed | Whittaker et al. American Journal of Public Health | December 2012, Vol 102, No. 12

members’ expertise in health lit-eracy and the women’s feedback,which were incorporated.
In addition, messages onemerging urgent issues were de-veloped by CDC and HealthyMothers, Healthy Babies; for ex-ample, a message about whoopingcough immunization went to Cal-ifornia enrollees in response to anoutbreak, and a message went toall enrollees in response to a Foodand Drug Administration recallalert.
Voxiva conducted extensive in-ternal testing of the interactivemobile health platform, which en-abled matching of each woman’sstage of pregnancy and baby’sdevelopment (from their self-reported dates) to the appropriatemessages. The Virginia healthcommissioner and the state’s
Infant Mortality Task Forceformed a multistakeholder text4-baby implementation team; thisteam provided input into enroll-ment processes and resources andacted as a beta testing site of themessaging platform in November2009 (prior to launch). In additionto the stakeholder team, the taskforce enrolled a small group ofmothers (n = 10) to test the mes-saging processes.
TEXT4BABY IN ACTION
The service launched in Febru-ary 2010, and outreach partnersimmediately began promoting it topregnant women, new mothers,and families in their communitiesand clinics. Healthy Mothers,Healthy Babies supplied promo-tional posters, flyers, tear pads,
referral cards, and other items. Allpromotions advised women toenroll online or by texting “baby,”or “bebe” for the Spanish version,to 511411. After providing theirzip code and estimated due date,women received three free textmessages per week relevant totheir stage of pregnancy or stage oftheir babies’ development (up toage one year). The program col-lected no health information, in-cluded no advertisements in themessages, and adhered to a strictprivacy policy for registrationdata. Enrollees received regularnotifications by text message thatthey could opt out at any time.Over the last few weeks of preg-nancy, they received 11 text mes-sages advising them to update thesystem by texting their deliverydate to receive postnatal messages.
Local partners promoted theservice through, for example, bill-boards, mall displays, birth certif-icate mailings, mass e-mails,newsletters, health fairs, babyshower events, home-visiting pro-grams, Medicaid member mail-ings, media events, and parentingclasses. Virginia’s implementationteam developed its own outreachplan (see the box at the bottom ofthe page). In October 2010,Healthy Mothers, Healthy Babiesdetermined that Virginia was thestate with the third highest enroll-ment rate (3.5% of the estimatedannual number of pregnancies).The maternal and children’shealth epidemiologist for the VirginiaDepartment of Health examined thezip codes of the 3987 Virginiaenrollees from February throughAugust 2010 and concluded that
The Six Initial Messages to All Enrollees in text4baby, a Text Messaging Health Service for Pregnant Women and New Mothers,
February 2010, Version 1
Free msg: Congratulations, you’re going to be a mom! Text4baby wishes you a happy and healthy pregnancy. Thanks for including us in this special time.
Free msg: You can choose who you see for pregnancy care. Midwives, family docs, OBs & nurse practitioners can all provide care. Call 800-311-2229 for free/low-cost care & to find
a provider who’s right for you.
Free msg: The flu can be dangerous for pregnant women & their babies. Talk to your doctor about seasonal flu & H1N1 flu shots. More from CDC: 1-800-232-4636.
Free msg: Get your baby off to a great start! You can help your baby’s development by taking a prenatal vitamin each day. It should have 600 mcg of folic acid.
Free msg: For a healthy baby, visit a doctor or midwife early & keep all of your appointments. Hear your baby’s heartbeat. See how fast she grows!
Free msg: Give your baby a good start by not drinking alcohol, smoking or using drugs. For help, call 800-784-8669 (smoking); 800-662-4357 (drugs & alcohol).
Note. CDC = Centers for Disease Control and Prevention; OB = obstetrician.
Virginia Outreach Plan for text4baby, a Text Messaging Health Service for Pregnant Women and New Mothers, 2010
Point of contact designations for 35 health districts
Press conference and press release
Stakeholders meetings and webinars
Promotion to women in WIC clinics
Information e-mails to members of local sections of AAP, ACOG, and AWHONN
Distribution of materials to clients and presentation at meetings by Richmond City Healthy Start Initiative and Virginia Healthy Start Initiative/Loving Steps
Information dissemination by Medicaid via Web site, letters to women, training conducted at eligibility entry points, and managed care outreach program
Information e-mails from a local health system to obstetric providers, recruitment of women in prenatal clinics
Promotion to women at a local hospital via obstetric and outreach staff
Note. AAP = American Academy of Pediatrics; ACOG = American Congress of Obstetricians and Gynecologists; AWHONN = Association of Women’s Health, Obstetric, and Neonatal Nurses; WIC =Women, Infants and Children Program.
COMMENTARY
December 2012, Vol 102, No. 12 | American Journal of Public Health Whittaker et al. | Peer Reviewed | Commentary | 2209

higher enrollment rates occurredin zip codes with higher propor-tions of families living in povertyand of low-birth-weight babies(Derek Chapman, maternal andchildren’s health epidemiologist,Virginia Department of Health,oral communication, October 26,2010). To augment these efforts,the partners promoted the text4-baby service via a Web site(http://www.text4baby.org) andsocial networking sites. In Feb-ruary 2010, an episode of TeenMom on MTV highlighted theservice, with an ensuing jump inenrollment rates of several thou-sand new enrollees (similar in-creases occurred after the NewYork Times ran two articles inFebruary 2011).
In the first 10 months of ser-vice, 109 201 women enrolled(including those who subsequentlystopped the service and thosetesting or investigating the ser-vice). Most enrolled in the prenatalmessage module (75.6%; n = 82548), likely because the majorityof initial promotional activitiestargeted pregnant women (as op-posed to new mothers). Of these,approximately one third (33.1%;n = 27 313) enrolled in the firsttrimester or earlier, according tothe estimated due date they pro-vided. Of total enrollments, 5.4%(n = 5869) chose the Spanish-language version. This proportionis much lower than the 12% of thepopulation who speak Spanishat home, although 53% of thesesay they also speak English“very well.”38 It may be thatSpanish speakers opted for theEnglish version, or it may be thatthe service has not penetratedinto Spanish-speaking popula-tions on a large scale. HealthyMothers, Healthy Babies hassince partnered with the Na-tional Latino Research Center toexamine this more closely and
has employed a multiculturaloutreach coordinator to identifystrategies for reaching this pop-ulation effectively.
At one month prior to their duedate, enrollees were sent two textmessage questions asking them torate the service (1---10, with 10highest) and whether they wouldrecommend text4baby to a friend.At the time of our analysis,15% (4533/30 064 enrollees)responded by text to both ques-tions. The average rating was 7.7(SD=2) and 95% (4308/4533 re-spondents) said they would recom-mend it. After 10 months, 27749(25.4%) enrollees had opted out bytexting in the word STOP.
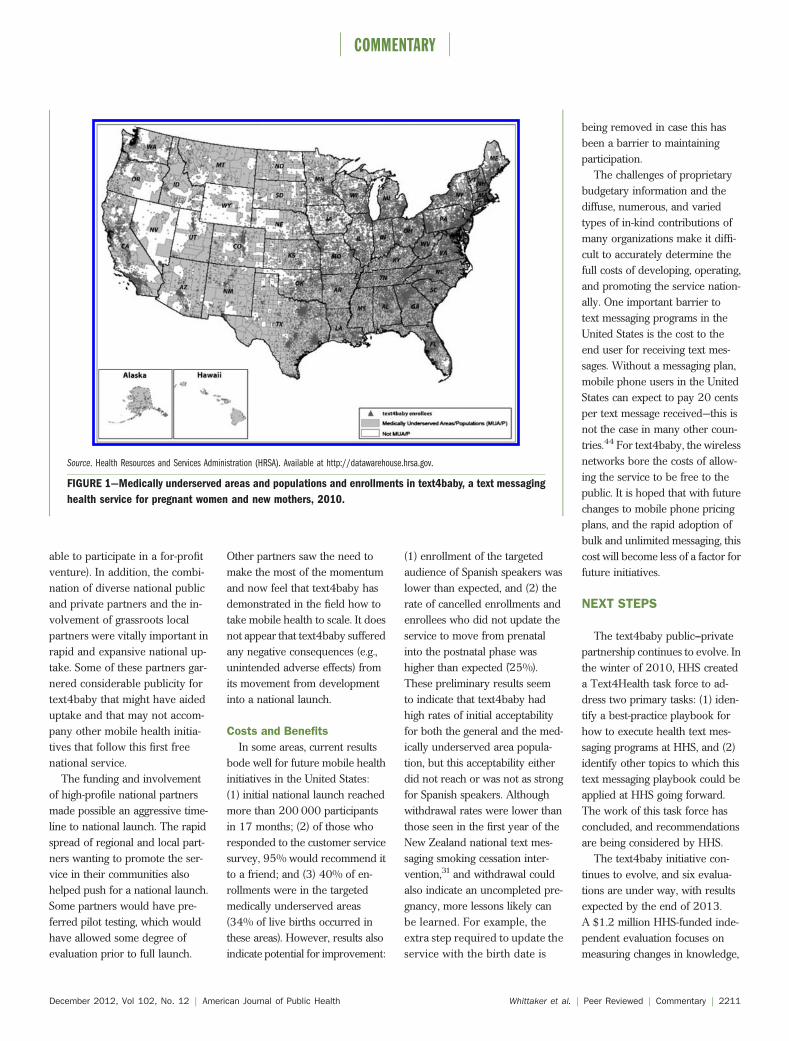
Two authors (J. B, R.W.) map-ped zip code data in relation tothe geographic distribution ofhigh-need populations, such asmedically underserved areas(counties, groups of counties,civil divisions, or urban censustracts designated as having toofew primary care providers, highinfant mortality, high povertyrate, or a large elderly popula-tion).39 Approximately 40% ofall text4baby enrollments and34% of total live births (from2002---2006, the most recentdata available) came from medi-cally underserved areas.40
Nearly one third of all medicallyunderserved areas (n = 1318)had no enrollments in the first10 months (Figure 1). This en-rollment information should beinterpreted with caution. Forexample, although enrollmentsoccurred within medically under-served areas, it is not knownwhether the actual enrollees werethose in need of the service.
LESSONS LEARNED
The launch of text4baby pro-vided valuable lessons about part-nership and message development,
promotion, and dissemination. Thiswas the first national-scale public---private partnership mobile healthinitiative in the United States (asrecognized by an HHSinnovatesaward for HHS innovative activi-ties and programs that can helpHHS better accomplish its mis-sion41), and these lessons may beuseful for future text messaginghealth programs.
Public---private partnerships canbring distinct benefits and chal-lenges to collaborative projects.42
In Austin’s 7 pillars of strategiccollaboration, of particular impor-tance is the challenge of creatingvalue.43 In the development ofthis project, all partners broughtsomething of unique and signifi-cant value:
1. Federal partners had the con-tent expertise for message de-velopment and brought credi-bility with clinical,governmental, and communitypartners;
2. Healthy Mothers, HealthyBabies had a national andgrassroots local network andcould negotiate a memoran-dum of understanding withHHS;
3. Voxiva brought mobile healthexpertise and a proven scalableplatform, championed the ini-tial vision, and obtained thesupport of CTIA and the wire-less industry;
4. Johnson and Johnson provideda broad range of in-kind sup-port and a multimillion dollar,multiyear pledge; and
5. CTIA and the wireless industrysupported the initiative by pro-viding free messages.
Austin also states that strategiccollaborations need internalchampions and that not all suc-cessful alliances start from thetop.43 Champions were important
within all partner organizations,perhaps particularly in HHS,where the momentum began atnonmanagerial levels within CDCand moved incrementally to thosewho were able to navigate supportat higher levels.
Partnership challenges includedinformation sharing and efforts toestimate the actual and in-kindcosts of the initiative, some confu-sion in defined roles and responsi-bilities, and differing perspectivesand priorities in evolving to thenext stage of the partnership.
Elements of Success
The text4baby initiative’sstrengths were that it was a simpleidea that used a popular and fa-miliar technology that was wellintegrated into daily life, con-cerned a topic with a strong evi-dence base, was universallyappealing (healthy pregnantwomen and healthy babies), andwas noncontroversial. The in-volvement of federal scientificagencies (CDC and the HRSA) inmessage development and the as-surance that messages accordedwith existing national guidelineswere critical to the initiative’scredibility. Testing messages withthe target audience and revisingthem according to participants’feedback was important; for ex-ample, each text message deliv-ered just one action point, andparticipants received no morethan three messages per week.Message development benefittedfrom federal agency scientists’ andprofessional organizations’ inputas well as engagement from pro-spective end users.
Providing the service free tothe end user appears to be animportant element for rapid up-take, as well as for ensuring theinvolvement of public and non-profit partners (governmentalagencies might not have been
COMMENTARY
2210 | Commentary | Peer Reviewed | Whittaker et al. American Journal of Public Health | December 2012, Vol 102, No. 12
able to participate in a for-profitventure). In addition, the combi-nation of diverse national publicand private partners and the in-volvement of grassroots localpartners were vitally important inrapid and expansive national up-take. Some of these partners gar-nered considerable publicity fortext4baby that might have aideduptake and that may not accom-pany other mobile health initia-tives that follow this first freenational service.
The funding and involvementof high-profile national partnersmade possible an aggressive time-line to national launch. The rapidspread of regional and local part-ners wanting to promote the ser-vice in their communities alsohelped push for a national launch.Some partners would have pre-ferred pilot testing, which wouldhave allowed some degree ofevaluation prior to full launch.
Other partners saw the need tomake the most of the momentumand now feel that text4baby hasdemonstrated in the field how totake mobile health to scale. It doesnot appear that text4baby sufferedany negative consequences (e.g.,unintended adverse effects) fromits movement from developmentinto a national launch.
Costs and Benefits
In some areas, current resultsbode well for future mobile healthinitiatives in the United States:(1) initial national launch reachedmore than 200 000 participantsin 17 months; (2) of those whoresponded to the customer servicesurvey, 95% would recommend itto a friend; and (3) 40% of en-rollments were in the targetedmedically underserved areas(34% of live births occurred inthese areas). However, results alsoindicate potential for improvement:
(1) enrollment of the targetedaudience of Spanish speakers waslower than expected, and (2) therate of cancelled enrollments andenrollees who did not update theservice to move from prenatalinto the postnatal phase washigher than expected (e25%).These preliminary results seemto indicate that text4baby hadhigh rates of initial acceptabilityfor both the general and the med-ically underserved area popula-tion, but this acceptability eitherdid not reach or was not as strongfor Spanish speakers. Althoughwithdrawal rates were lower thanthose seen in the first year of theNew Zealand national text mes-saging smoking cessation inter-vention,31 and withdrawal couldalso indicate an uncompleted pre-gnancy, more lessons likely canbe learned. For example, theextra step required to update theservice with the birth date is
being removed in case this hasbeen a barrier to maintainingparticipation.
The challenges of proprietarybudgetary information and thediffuse, numerous, and variedtypes of in-kind contributions ofmany organizations make it diffi-cult to accurately determine thefull costs of developing, operating,and promoting the service nation-ally. One important barrier totext messaging programs in theUnited States is the cost to theend user for receiving text mes-sages. Without a messaging plan,mobile phone users in the UnitedStates can expect to pay 20 centsper text message received—this isnot the case in many other coun-tries.44 For text4baby, the wirelessnetworks bore the costs of allow-ing the service to be free to thepublic. It is hoped that with futurechanges to mobile phone pricingplans, and the rapid adoption ofbulk and unlimited messaging, thiscost will become less of a factor forfuture initiatives.
NEXT STEPS
The text4baby public---privatepartnership continues to evolve. Inthe winter of 2010, HHS createda Text4Health task force to ad-dress two primary tasks: (1) iden-tify a best-practice playbook forhow to execute health text mes-saging programs at HHS, and (2)identify other topics to which thistext messaging playbook could beapplied at HHS going forward.The work of this task force hasconcluded, and recommendationsare being considered by HHS.
The text4baby initiative con-tinues to evolve, and six evalua-tions are under way, with resultsexpected by the end of 2013.A $1.2 million HHS-funded inde-pendent evaluation focuses onmeasuring changes in knowledge,
Source. Health Resources and Services Administration (HRSA). Available at http://datawarehouse.hrsa.gov.
FIGURE 1—Medically underserved areas and populations and enrollments in text4baby, a text messaging
health service for pregnant women and new mothers, 2010.
COMMENTARY
December 2012, Vol 102, No. 12 | American Journal of Public Health Whittaker et al. | Peer Reviewed | Commentary | 2211

behavior, processes, and outcomesamong program participants andnonparticipating comparisongroups. It also includes key stake-holder interviews to gain greaterinsight into lessons learned. Otherevaluations being undertaken bya variety of partners include pro-spective trials with pregnantwomen and research on accept-ability for Spanish-speakingwomen.
The text4baby public---privatepartnership has set an ambitiousgoal of reaching one million en-rollments by the end of 2012. Thecurrent evaluations should pro-vide much-needed informationabout its reach into high-riskgroups and about its effectivenessin behavior change. j
About the AuthorsAt the time of the study, Robyn Whittakerwas with The Commonwealth Fund, NewYork, NY. Sabrina Matoff-Stepp was withthe Office of Women’s Health, Julie Baittywas with the Office of Information Tech-nology, and Kyu Rhee was with the Imme-diate Office of the Administrator, HealthResources and Services Administration,Rockville, MD. Judy Meehan was with theNational Healthy Mothers, Healthy BabiesCoalition, Alexandria, VA. Juliette Ken-drick and Paul Stange were with the Cen-ters for Disease Control and Prevention,Atlanta, GA. Elizabeth Jordan was with theCommunity and Public Health School ofNursing, Johns Hopkins University,Baltimore, MD. Amanda Cash was withthe Office of the Assistant Secretary forPlanning and Evaluation, US Departmentof Health and Human Services, Washing-ton, DC. Paul Meyer and Pamela Johnsonwere with Voxiva Inc, Washington, DC.Scott Ratzan was with Johnson and John-son, New Brunswick, NJ.Correspondence should be sent to Dr. S.
Matoff-Stepp, Director HRSA Office ofWomen’s Health, 5600 Fishers Ln,Rockville, MD 20857 (email: [email protected]) or Dr. J. Kendrick,Division of Reproductive Health, NationalCenter for Chronic Disease Prevention andHealth Promotion, Centers for DiseaseControl and Prevention, Atlanta GA(email: [email protected]). Reprints can beordered at http://www.ajph.org by clickingthe “Reprints” link.This commentary was accepted February
8, 2012.
Note. The findings and conclusions inthis article are those of the authors anddo not necessarily represent the officialposition of the US Department of Healthand Human Services or Johnson andJohnson.
ContributorsAll authors except R. Whittaker andJ. Baitty were involved in developingtext4baby. R. Whittaker and J. Baittyanalyzed the data. All authors helpedwrite and edit the article.
AcknowledgmentsRobyn Whittaker was a CommonwealthFund Harkness Fellow at the time of thestudy. Paul Meyer and Pamela Johnsonare stockholders and board members ofVoxiva Inc. No funding was provided forthis article.
Human Participant ProtectionNo protocol approval was required be-cause the study used only de-identifieddata.
References1. MacDorman S, Mathews T. RecentTrends in Infant Mortality in the UnitedStates. Atlanta, GA: Centers for DiseaseControl and Prevention; 2008. Availableat: http://www.cdc.gov/nchs/data/databriefs/db09.htm. Accessed July 23,2011.
2. Heron M, Sutton PD, Xu J, VenturaSJ, Strobino DM, Guyer B. Annual sum-mary of vital statistics: 2007. Pediatrics.2010;125(1):4---15.
3. Health, United States, 2009: WithSpecial Feature on Medical Technology.Hyattsville, MD: National Center forHealth Statistics; 2010.
4. Yin HS, Johnson M, Mendelsohn AL,Abrams MA, Sanders LM, Dreyer BP. Thehealth literacy of parents in the UnitedStates: a nationally representative study.Pediatrics. 2009;124(suppl 3):S289---S296.
5. Endres LK, Sharp LK, Haney E,Dooley SL. Health literacy and preg-nancy preparedness in pregestationaldiabetes. Diabetes Care. 2004;27(2):331---334.
6. Nielsen-Bohlman L, Panzer A, KindigD, eds. Health Literacy: A Prescription toEnd Confusion. Washington, DC: NationalAcademies Press; 2004.
7. Smith A. Pew Internet and AmericanLife Project. Mobile Access 2010. Wash-ington, DC: Pew Research Center; 2010.
8. Blumberg S, Luke J. Wireless Sub-stitution: Early Release of Estimates Fromthe National Health Interview Survey,
January---June 2009. Atlanta, GA: Na-tional Center for Health Statistics; 2009.
9. Cole-Lewis H, Kershaw T. Textmessaging as a tool for behaviourchange in disease prevention and man-agement. Epidemiol Rev. 2010;32(1):56---69.
10. Fjeldsoe BS, Marshall AL, MillerYD. Behavior change interventions de-livered by mobile telephone short-message service. Am J Prev Med.2009;36(2):165---173.
11. Whittaker R, Borland R, Bullen C,Lin RB, McRobbie H, Rodgers A. Mobilephone-based interventions for smokingcessation. Cochrane Database Syst Rev.2009;7(4):CD006611.
12. Krishna S, Boren SA, Balas EA.Healthcare via cell phones: a systematicreview. Telemed J E Health. 2008;15(3):231---240.
13. Rodgers A, Corbett T, Bramley C,et al. Do u smoke after txt? Results ofa randomised trial of smoking cessationusing mobile phone text messaging. TobControl. 2005;14(4):255---261.
14. Brendryen H, Kraft P. Happyending: a randomized controlled trialof a digital multi-media smoking cessa-tion intervention. Addiction. 2008;103(3):478---484; discussion 485---486.
15. Brendryen H, Drozd F, Kraft P.A digital smoking cessation programdelivered through internet and cellphone without nicotine replacement(happy ending): randomized controlledtrial. J Med Internet Res. 2008;10(5):e51.
16. Joo N-S, Kim B- T. Mobile phoneshort messaging service messaging forbehaviour modification in a community-based weight control programme inKorea. J Telemed Telecare. 2007;13(8):416---420.
17. Hurling R, Catt M, De Boni M, et al.Using internet and mobile phone tech-nology to deliver an automated physicalactivity program: randomized con-trolled trial. J Med Internet Res. 2007;9(2):e7.
18. Haapala I, Barengo NC, Biggs S,Surakka L, Manninen P. Weight loss bymobile phone: a 1-year effectivenessstudy. Public Health Nutr. 2009;12(12):2382---2391.
19. Patrick K, Raab F, Adams M, et al.A text message-based intervention forweight loss: randomized controlled trial.J Med Internet Res. 2009;11(1):e1.
20. Riva G, Preziosa A, Grassi A,Villani D. Stress management usingUMTS cellular phones: a controlledtrial. Stud Health Technol Inform.2006;119:461---463.
21. Downer SR, Meara JG, Da Costa AC,Sethuraman K. SMS text messaging im-proves outpatient attendance. Aust HealthRev. 2006;30(3):389---396.
22. da Costa TM, Salomão PL, MarthaAS, Pisa IT, Sigulem D. The impact ofshort message service text messagessent as appointment reminders to pa-tients’ cell phones at outpatient clinicsin São Paulo, Brazil. Int J Med Inform.2010;79(1):65---70.
23. Koshy E, Car J, Majeed A. Effective-ness of mobile-phone short messageservice (SMS) reminders for ophthal-mology outpatient appointments: ob-servational study. BMC Ophthalmol.2008;8:9.
24. Liew SM, Tong SF, Lee VK, Ng CJ,Leong KC, Teng CL. Text messagingreminders to reduce non-attendance inchronic disease follow-up: a clinicaltrial. Br J Gen Pract. 2009;59(569):916---920.
25. Mao Y, Zhang Y, Zhai S. Mobilephone text messaging for pharmaceuticalcare in a hospital in China. J TelemedTelecare. 2008;14(8):410---414.
26. Strandbygaard U, Thomsen SF,Backer V. A daily SMS reminder increasesadherence to asthma treatment: a three-month follow-up study. Respir Med.2010;104(2):166---171.
27. Miloh T, Annunziato R, Arnon R,et al. Improved adherence and outcomesfor pediatric liver transplant recipients byusing text messaging. Pediatrics. 2009;124(5):e844---e850.
28. Franklin VL, Waller A, Pagliari C,Greene SA. A randomized controlledtrial of Sweet Talk, a text-messagingsystem to support young people withdiabetes. Diabet Med. 2006;23(12):1332---1338.
29. Vilella A, Bayas JM, Diaz MT, et al.The role of mobile phones in improvingvaccination rates in travelers. Prev Med.2004;38(4):503---509.
30. Cocosila M, Archer N, Haynes RB,Yuan Y. Can wireless text messagingimprove adherence to preventive ac-tivities? Results of a randomised con-trolled trial. Int J Med Inform. 2009;78(4):230---238.
31. Milne K, Bowler S, Li J, Salmon P.Evaluation of the first year of theTxt2Quit service: 17 June 2008---16 June2009. The Quit Group. 2009. Availableat: http://www.quit.org.nz/file/research/FINAL%202008-09%20Txt2Quit%20evaluation%20report%2020090731.pdf. Accessed July 23, 2011.
32. Yale School of Management. Designand social enterprise case series; projectM: texting and testing to fight HIV/AIDSin South Africa. Available at: http://
COMMENTARY
2212 | Commentary | Peer Reviewed | Whittaker et al. American Journal of Public Health | December 2012, Vol 102, No. 12

nexus.som.yale.edu/design-project-m/?q=node/99. Accessed July 23, 2011.
33. PopTech. Project Masiluleke: abreakthrough initiative to combatHIV/AIDS utilizing mobile technologyand HIV self-testing in South Africa.Available at: http://poptech.org/system/uploaded_files/27/original/Project_Masiluleke_Brief.pdf. Accessed July 23,2011.
34. Chopra A. New mothers get digitalhelper right on their phones. The WhiteHouse Blog. Available at: http://www.whitehouse.gov/blog/2010/02/04/new-mothers-get-digital-helper-right-their-phones. Accessed July 23, 2011.
35. American Congress of Obstetriciansand Gynecologists. You and your baby:
prenatal care, labor and delivery, andpostpartum care. Available at: http://www.acog.org/publications/patient_education/ab005.cfm. Accessed Decem-ber 12, 2010.
36. American Academy of Pediatrics.Bright Futures 3rd edition guidelines,pocket guide, tool and resource kit. Avail-able at: http://brightfutures.aap.org/3rd_Edition_Guidelines_and_Pocket_Guide.html. Accessed March 1, 2011.
37. Mobile Marketing Association. U.S.consumer best practices version 6.1.2011. Available at: http://mmaglobal.com/Consumer_Best%20Practices_6.1%20Update-02May2011FINAL_MMA.pdf. Accessed July 23, 2011.
38. US Census Bureau. 2005---2009American Community Survey. Availableat: http://www.census.gov/acs/www.Accessed January 14, 2011.
39. Health Resources and ServicesAdministration. Data sources. Datawarehouse. Available at: http://datawarehouse.hrsa.gov/sources.aspx.Accessed July 23, 2011.
40. Centers for Disease Control andPrevention, National Center for HealthStatistics. Births and infant deaths2002---2006. Available at: http://www.cdc.gov/nchs/linked.htm. Accessed July23, 2011.
41. Text4Baby wins outstanding inno-vation award. Available at: http://www.whitehouse.gov/blog/2010/08/04/
text4baby-wins-outstanding-innovation-award. Accessed July 23, 2011.
42. Reich M, ed. Public-Private Partner-ships for Public Health. Cambridge, MA:Harvard Center for Population and De-velopment Studies; 2002.
43. Austin J. The Collaboration Challenge:How Nonprofits and Businesses SucceedThrough Strategic Alliances. San Fran-cisco, CA: Jossey-Bass Publishers; 2000.Available at: http://hbswk.hbs.edu/item/1263.html. Accessed July 23, 2011.
44. Costhelper. Text messaging cost.Available at: http://www.costhelper.com/cost/electronics/text-messaging.html.Accessed July 23, 2011.
COMMENTARY
December 2012, Vol 102, No. 12 | American Journal of Public Health Whittaker et al. | Peer Reviewed | Commentary | 2213
Copyright © 2022 FDOKUMEN




















