Teacher Training for Implementation of Teaching Strategies ...
14
Teacher Education and Special Education 34(2) 119–132 © 2011 Teacher Education Division of the Council for Exceptional Children Reprints and permission: sagepub.com/journalsPermissions.nav DOI: 10.1177/0888406410376660 http://tese.sagepub.com Teacher Training for Implementation of Teaching Strategies for Students With Autism Spectrum Disorders Michael J. Morrier 1,2 , Kristen L. Hess 2 , and L. Juane Heflin 2 Abstract Training received by teachers of students with autism spectrum disorders (ASD) in one southern state was investigated. Teachers (n = 90) reported training received via an online version of the Autism Treatment Survey. The most common type of training reported was attendance at a full- or half-day workshop; fewer than 15% reported receiving training from teacher preparation programs at colleges or universities. The types of training received did not predict the use of evidence-based practices. Individual factors related to training were not significant for education level, years of teaching students with ASD, and type of class (i.e., general or special education). The need for an increased role for personnel preparation programs for teachers of students with ASD is discussed. Keywords autism, early childhood, elementary education, instructional practices, professional development, secondary education Recent federal legislation related to the edu- cation of general and special education stu- dents has emphasized the scientific basis of teaching strategies used with students as well as the training teachers receive to implement these strategies (Individuals With Disabilities Education Improvement Act [IDEIA], 2004; No Child Left Behind Act [NCLB], 2002). These mandates for “high-quality teachers” are especially important for teachers who have children with autism spectrum disorders (ASD) in their classrooms (McGee & Morrier, 2005). As the prevalence of ASD continues to rise (Centers for Disease Control and Pre- vention [CDC], 2007a, 2007b; Kogan et al., 2009; Rogers, 1999; Wing & Potter, 2002; Yeargin-Allsopp et al., 2003), it is inevitable that both general and special education teach- ers will have children with this disability in their classrooms. In an era of a national spe- cial education teacher shortage (Billingsley, 2003), training and support for individuals teaching students with ASD has become an important topic in the field of education (National Research Council [NRC], 2001; Odom et al., 2003; Scheuermann, Webber, 1 Emory University School of Medicine, Atlanta, GA, USA 2 Georgia State University, Atlanta, GA, USA Corresponding Author: Michael J. Morrier, Emory University School of Medicine, Emory Autism Center, 1551 Shoup Court, Atlanta, GA 30322, USA Email: [email protected] at PENNSYLVANIA STATE UNIV on May 17, 2016 tes.sagepub.com Downloaded from
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Teacher Training for Implementation of Teaching Strategies ...
Teacher Education and Special Education34(2) 119 –132© 2011 Teacher Education Division of the Council for Exceptional Children Reprints and permission: sagepub.com/journalsPermissions.navDOI: 10.1177/0888406410376660http://tese.sagepub.com
Teacher Training for Implementation of Teaching Strategies for Students With Autism Spectrum Disorders
Michael J. Morrier1,2, Kristen L. Hess2, and L. Juane Heflin2
Abstract
Training received by teachers of students with autism spectrum disorders (ASD) in one southern state was investigated. Teachers (n = 90) reported training received via an online version of the Autism Treatment Survey. The most common type of training reported was attendance at a full- or half-day workshop; fewer than 15% reported receiving training from teacher preparation programs at colleges or universities. The types of training received did not predict the use of evidence-based practices. Individual factors related to training were not significant for education level, years of teaching students with ASD, and type of class (i.e., general or special education). The need for an increased role for personnel preparation programs for teachers of students with ASD is discussed.
Keywords
autism, early childhood, elementary education, instructional practices, professional development, secondary education
Recent federal legislation related to the edu-cation of general and special education stu-dents has emphasized the scientific basis of teaching strategies used with students as well as the training teachers receive to implement these strategies (Individuals With Disabilities Education Improvement Act [IDEIA], 2004; No Child Left Behind Act [NCLB], 2002). These mandates for “high-quality teachers” are especially important for teachers who have children with autism spectrum disorders (ASD) in their classrooms (McGee & Morrier, 2005). As the prevalence of ASD continues to rise (Centers for Disease Control and Pre-vention [CDC], 2007a, 2007b; Kogan et al., 2009; Rogers, 1999; Wing & Potter, 2002; Yeargin-Allsopp et al., 2003), it is inevitable
that both general and special education teach-ers will have children with this disability in their classrooms. In an era of a national spe-cial education teacher shortage (Billingsley, 2003), training and support for individuals teaching students with ASD has become an important topic in the field of education (National Research Council [NRC], 2001; Odom et al., 2003; Scheuermann, Webber,
1Emory University School of Medicine, Atlanta, GA, USA2Georgia State University, Atlanta, GA, USA
Corresponding Author:Michael J. Morrier, Emory University School of Medicine, Emory Autism Center, 1551 Shoup Court, Atlanta, GA 30322, USAEmail: [email protected]
at PENNSYLVANIA STATE UNIV on May 17, 2016tes.sagepub.comDownloaded from

120 Teacher Education and Special Education 34(2)
Boutot, & Goodwin, 2003; Simpson, 2004). The NRC (2001) proposed 12 quality indica-tors for programs serving students with ASD. Three of these apply to teachers and staff: (a) highly trained staff, (b) comprehensive professional resources, and (c) staff supervi-sion and program evaluation mechanisms.
The rise in prevalence combined with the current educational legislation (IDEIA, 2004; NCLB, 2002) has resulted in an increased focus and commitment to teacher training for students on the autism spectrum. Each student with ASD possesses a unique set of educa-tional needs, making teacher training for this population of students fundamentally chal-lenging and complex (McGee & Morrier, 2005; Simpson & Myles, 1998). Children with ASD are a heterogeneous population; educational approaches that prove successful for some students are not successful for others (Handleman & Harris, 2001, 2006, 2008; Harris & Handleman, 1994; NCR, 2001). In an attempt to guide teachers in best practice, some national intervention models for indi-viduals with ASD prescribe a single teaching methodology (Handleman & Harris, 2008; Izeman, 1995). Specific teaching techniques frequently advocated for children with ASD, including one-to-one discrete trial training, pivotal response training, incidental teaching, positive behavioral support, and Picture Exchange Communication System, have demonstrated efficacy with specific sub-groups of children with ASD (Stahmer, Collings, & Palinkas, 2005). Demonstrated efficacy is critical for establishing empirical validation for branding a strategy or interven-tion as evidence based. NCLB (2002) man-dates that teachers implement strategies that are scientifically based. Unfortunately, Hess, Morrier, Heflin, and Ivey (2008) found that educators rarely use evidence-based strategies with students with ASD.
In addition to meeting the challenges of understanding a heterogeneous population, teachers working with students with ASD must function in an educational environment in which families and school systems have become increasingly litigious, even about the
best educational practices. Moreover, leaders in the field acknowledge there are many dif-ferent methods currently employed to work with this student population (Meyers, Goin-Kochel, & Mackintosh, 2005; Simpson et al., 2005), and there is little, if any, consensus with regard to the most effective practices for working with students with ASD in educa-tional settings (Heflin & Simpson, 1998). Given this lack of consensus, it is difficult for colleges and universities to target pedagogy and content priorities, so many teachers may not be adequately prepared to effectively edu-cate their students (Simpson, 2004).
Teacher Training in ASDPre-service training for general education teachers on issues related to special education has generally involved a single introductory course (Turner, 2003), which typically focuses on legal requirements and eligibility classifi-cation (Winn & Blanton, 2005). These courses do not focus on either the specific social, lan-guage, and academic needs of students with ASD or evidence-based strategies that are suc-cessful for students with disabilities in general (Holdheide & Reschly, 2008). Although pre-service training for special educators focuses on instructional strategies and accommoda-tions for students with disabilities, it provides little content on general education curriculum (Winn & Blanton, 2005). Therefore, neither training sequence prepares teachers to suc-cessfully include students with ASD in gen-eral education classrooms or to assist with meeting students’ individualized educational needs. To ensure success for all students, effective teacher training and support needs to incorporate multiple approaches (Scheuermann et al., 2003; Simpson, 2004) and emphasize practices that have a strong evidence base of effectiveness for students with ASD.
PurposeThis study was part of a larger study investigat-ing evidence-based practices, teacher charac-teristics, and diversity issues related to services
at PENNSYLVANIA STATE UNIV on May 17, 2016tes.sagepub.comDownloaded from

Morrier et al. 121
children with autism receive in one state’s public school system (Hess et al., 2008; Morrier, Hess, & Heflin, 2008). The specific purpose of this study was to investigate the characteristics of teachers instructing stu-dents with ASD in one southern state. In this study, the characteristics of teachers (e.g., level of teachers’ education, length of their teach-ing experience) using evidence-based prac-tices were compared to the characteristics of those who were not using evidence-based practices. The researchers also explored the ways teachers had been trained to implement the strategies they reported using in their classrooms. The relationship between indi-vidual teacher characteristics and the type of training received was investigated.
MethodProcedure
Special education directors and autism spe-cialists or autism consultants (N = 249) in all 159 of Georgia’s counties were contacted by the first two authors in an email letter. The let-ter described the Autism Treatment Survey (ATS) and provided information on accessing the survey online. Those contracted were asked to forward the URL link for accessing the ATS to teachers with children with ASD in their district classrooms. Approximately one week later, an invitation to disseminate the URL to district teachers was sent. A third email reminding special education directors and consultants to forward the URL survey link and password was sent. A thank-you email was sent approximately three weeks later, which served as the final reminder that the survey was still available for teachers to complete.
The Autism Treatment SurveyThe ATS was developed to survey public school teachers regarding the most common treatment strategies used with children with ASD across the preschool to high school lev-els (Hess et al., 2008). ATS survey items were based on a review of research on strategies
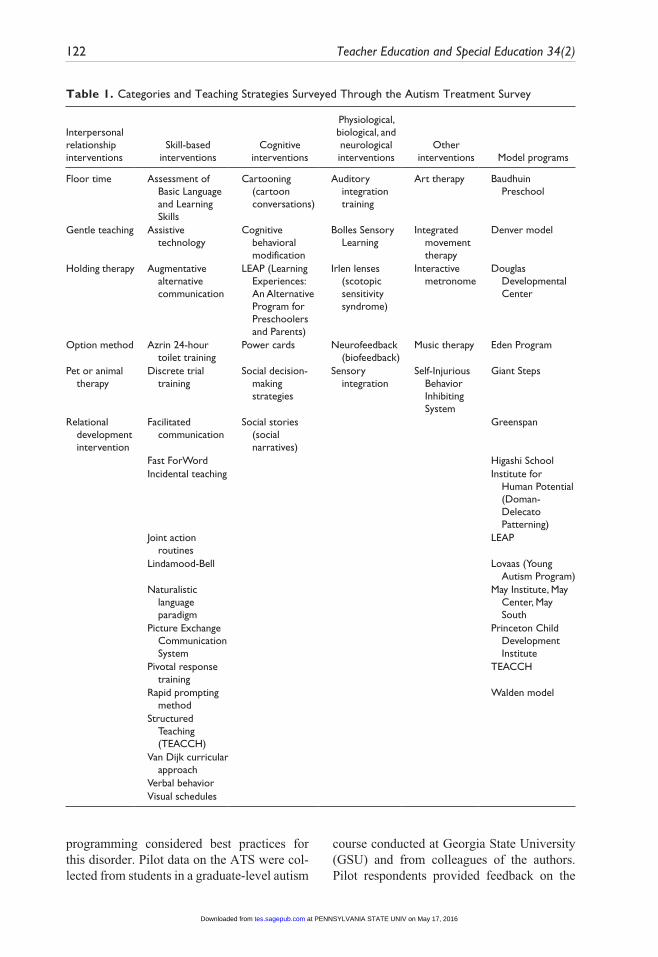
used for educating children with autism and categorized into intervention categories devel-oped by Simpson et al. (2005). Categories included (a) interpersonal relationships strate-gies (6 strategies); (b) skill-based strategies (18 strategies); (c) cognitive strategies (6 strat-egies); (d) physiological, biological, and neu-rological strategies (5 strategies); and (e) other strategies (5 strategies). Table 1 provides all of the teaching strategies queried under each intervention category. Each teaching strategy was provided with an exemplar to assist teach-ers completing the ATS to select the correct method. For example, cognitive behavioral therapy was defined as “includes cognitive learning strategies, cognitive scripts.” At the end of the survey, there was a place for the respondent to list additional treatments not specified previously. The survey item was repeated three times for participants to respond for up to three treatments used within a given category. The appendix provides an example of the text of one survey item. Teachers also were asked to select which of 10 methods of training (e.g., workshop, university course) they had received to implement the strategy chosen. Teachers were specifically asked,
You have indicated that you currently use, or have used <strategy name> in your classroom with children with ASD. We are interested in the method of training you received for implement-ing <strategy name>. Please choose the training methods that you have received.
Teachers could choose only one training method for each strategy. Each of the methods was defined in drop-down menus (see Table 2).
Prior to final administration of the ATS, four experts in autism treatment and research were provided a draft of the survey to deter-mine the validity of the survey constructs and format. Expert feedback was incorporated into a second draft, and feedback was again solic-ited from the experts. Experts reviewing the ATS were knowledgeable on autism diagno-sis, treatment interventions, and educational
at PENNSYLVANIA STATE UNIV on May 17, 2016tes.sagepub.comDownloaded from
122 Teacher Education and Special Education 34(2)
Table 1. Categories and Teaching Strategies Surveyed Through the Autism Treatment Survey
Interpersonal relationship interventions
Skill-based interventions
Cognitive interventions
Physiological, biological, and neurological interventions
Other interventions Model programs
Floor time Assessment of Basic Language and Learning Skills
Cartooning (cartoon conversations)
Auditory integration training
Art therapy Baudhuin Preschool
Gentle teaching Assistive technology
Cognitive behavioral modification
Bolles Sensory Learning
Integrated movement therapy
Denver model
Holding therapy Augmentative alternative communication
LEAP (Learning Experiences: An Alternative Program for Preschoolers and Parents)
Irlen lenses (scotopic sensitivity syndrome)
Interactive metronome
Douglas Developmental Center
Option method Azrin 24-hour toilet training
Power cards Neurofeedback (biofeedback)
Music therapy Eden Program
Pet or animal therapy
Discrete trial training
Social decision-making strategies
Sensory integration
Self-Injurious Behavior Inhibiting System
Giant Steps
Relational development intervention
Facilitated communication
Social stories (social narratives)
Greenspan
Fast ForWord Higashi SchoolIncidental teaching Institute for
Human Potential (Doman-Delecato Patterning)
Joint action routines
LEAP
Lindamood-Bell Lovaas (Young Autism Program)
Naturalistic language paradigm
May Institute, May Center, May South
Picture Exchange Communication System
Princeton Child Development Institute
Pivotal response training
TEACCH
Rapid prompting method
Walden model
Structured Teaching (TEACCH)
Van Dijk curricular approach
Verbal behaviorVisual schedules
programming considered best practices for this disorder. Pilot data on the ATS were col-lected from students in a graduate-level autism
course conducted at Georgia State University (GSU) and from colleagues of the authors. Pilot respondents provided feedback on the
at PENNSYLVANIA STATE UNIV on May 17, 2016tes.sagepub.comDownloaded from

Morrier et al. 123
format and ease of access of the survey. Respondent feedback was incorporated into the final version of the ATS. The Institutional Review Board at GSU provided oversight and approval of the research study.
ResultsA total of 234 teachers completed the ATS during the 3-month data collection period. A total of 185 (79%) surveys were considered useable. To be considered useable, teachers had to provide data on at least one child with ASD and report self-demographic and/or training data.
Total SampleStudents with ASD. Teachers provided data
on 219 students with ASD from preschool through high school. Students’ mean age was 9.45 years (range = 3–19 years). Approximately 88% of students were male (n = 190). Ethnicity was 35.62% African American, 1.37% Asian, 58.90% Caucasian, 0.46% Hispanic or Latino, 2.28% other ethnicity, and 1.37% multiracial. Approximately 19% of students were reported to qualify for the federal reduced-price lunch
program (19.30%; range = 0%–100%), yielding an average of 2.55 students per teacher report. Approximately 40% of students quali-fied for the federal free lunch program (40.14%; range = 0%–100%), yielding an average of 4.64 students per teacher report.
Teachers working with students with ASD (respondents). Almost 99% of the respondents were female, ranging in age from 22 to 59 (M = 40.72, SD = 9.59). This sample of teach-ers provided data for 57% of the school dis-tricts in Georgia, representing all regions of the state. Approximately 8.0% of the respon-dents taught preschool-aged children (i.e., 3- to 5-year-olds), 49.4% taught elementary-aged children (i.e., 6- to 10-year-olds), 29.2% taught middle-school-aged children (i.e., 11- to 13-year-olds), and 13.5% taught high-school-aged students (i.e., 12- to 21-year-olds). Total years of teaching experience ranged from 1 to 35 years (M = 12.28, SD = 8.45), and experi-ence with students with ASD ranged from 2 months to 30 years (M = 5.13, SD = 5.05). Approximately 7.0% of the participants were African American, 84.0% were Caucasian, 1.1% were Hispanic, 5.7% were another eth-nicity, and 2.3% were multiracial. The majority of teachers (58.9%) taught in special education
Table 2. Response Definitions Provided to Respondents via the Autism Treatment Survey
Training method Response definition
Teacher preparation program Undergraduate, graduate, or certification courses provided by a college or university
Half-day workshop Workshop lasting less than 4 hoursFull-day workshop Workshop lasting 4 hours or moreWorkshop provided by
program developer or representative
Workshop provided by the individual who is responsible for developing the program or a person who works with that individual
Local school system in-service Training provided by your school lead teacher, special education coordinator, etc.; must occur at your local school
Peer teacher/therapist A professional colleague told you about or showed you how to use the strategy
Hands-on training Training received by working directly with the children as you learned the method
Self-taught Could include journal articles or book chapters read by you, or information from the Internet
Parent The parent of one of your current or former students told you about or showed you how to use the strategy
County school system in-service
Training provided by the district or county
at PENNSYLVANIA STATE UNIV on May 17, 2016tes.sagepub.comDownloaded from

124 Teacher Education and Special Education 34(2)
classrooms (e.g., autism self-contained, other self-contained), and 26.7% taught in general education classes. The remaining teachers taught in mixed or other types of classrooms (14.4% each). The mean total class size was 12.64 students, with a range from 3 to 39 stu-dents. The mean number of children with ASD taught was 2.51, with a range of 1 to 18 students with ASD. In terms of education, 59.3% of the respondents held master’s degrees, 29.1% held bachelor’s degrees, 10.5% held educational specialist degrees, and 1.2% held doctoral-level degrees. Based on the Georgia Professional Standards Com-mission (2007), reports of certification cate-gories indicated that 87.1% of respondents held clear renewable certifications, 5.9% held performance-based renewable certifications, 4.7% held nonrenewable professional certifi-cations, and 2.4% held nonrenewable waivers.
Teachers Using Evidence-Based PracticesSlightly fewer than 5% of teachers (4.89%) reported using best practices for students with ASD in their classrooms. Table 3 displays the characteristics of teachers who reported the use of best practices versus those who did not report the use of best practices. Best practices were those identified by Simpson et al. (2005) as being scientifically based. As reported by Hess et al. (2008), scientifically based best practices reported by teachers included (a) dis-crete trial training (5.95%), (b) Learning Experiences: An Alternative Program for Pre-schoolers and Parents (3.24%), and (c) pivotal response training (1.62%). An independent-samples t test was conducted to determine if there were differences between the teachers who reported best practice use and those who did not. Results indicated no significant dif-ferences between the groups of teachers.
Training Methods ReceivedFewer than half of the 185 teachers who responded to the ATS reported on the type of training they received. Percentages for the source of training as reported by respondents
Table 3. Characteristics Teachers Who Reported Use of and Nonuse of Best Practices for Autism Spectrum Disorders (ASD)
Reported use of best practices
Did not report use
of best practices
Age M 41.63 40.56 SD 9.516 10.266Education level (%) Bachelor’s 22.22 26.79 Master’s 66.67 66.07 Educational
specialist11.11 5.36
Doctorate 0.00 1.78Grade level taught (%) Preschool 0.00 8.62 Elementary 66.67 39.66 Middle 22.22 34.48 High 11.11 17.24Type of classroom (%) General education 12.5 18.33 Special education 37.5 53.33 Mixed 25.0 15.0 Other 25.00 13.33Overall class size M 8.88 12.98 SD 4.324 8.178ASD in class M 3.00 2.40 SD 2.204 2.039Years of teaching experience M 10.125 12.760 SD 5.842 9.099Years of teaching ASD M 7.125 5.167 SD 6.446 5.479Certification level (%) Clear renewable 88.89 87.72 Performance-based
professional11.11 5.26
Nonrenewable professional
0.0 3.51
Nonrenewable waiver
0.0 3.51
for all interventions implemented with stu-dents with ASD in Georgia public school sys-tems are presented in Figure 1. The most commonly reported methods for training
at PENNSYLVANIA STATE UNIV on May 17, 2016tes.sagepub.comDownloaded from

Morrier et al. 125
were attendance at workshops (i.e., full- and half-day workshops; 20.54%), hands-on train-ing with students with ASD (18.92%), and self-taught methods (18.38%). Teachers were least likely to be trained by the parent of a student with ASD (2.16%) or the program developer (1.08%). Fewer than 15.0% of the teachers reported being trained by university-based teacher preparation programs.
Table 4 presents specific training methods for each of the categories of intervention developed by Simpson et al. (2005). Teachers were more likely to be self-taught and taught through hands-on training for interpersonal relationship strategies. Skill-based strategies were primarily learned through full-day workshops or by self-teaching. For teachers who reported the use of cognitive strategies, full-day workshops and teacher preparation programs were the sources of training. Physi-ological, biological, and neurological strate-gies were learned through hands-on training and full-day workshops. The use of other strategies was learned through peer teachers or therapists or was self-taught.
Factors Related to Teachers’ Use of Evidence-Based Practices
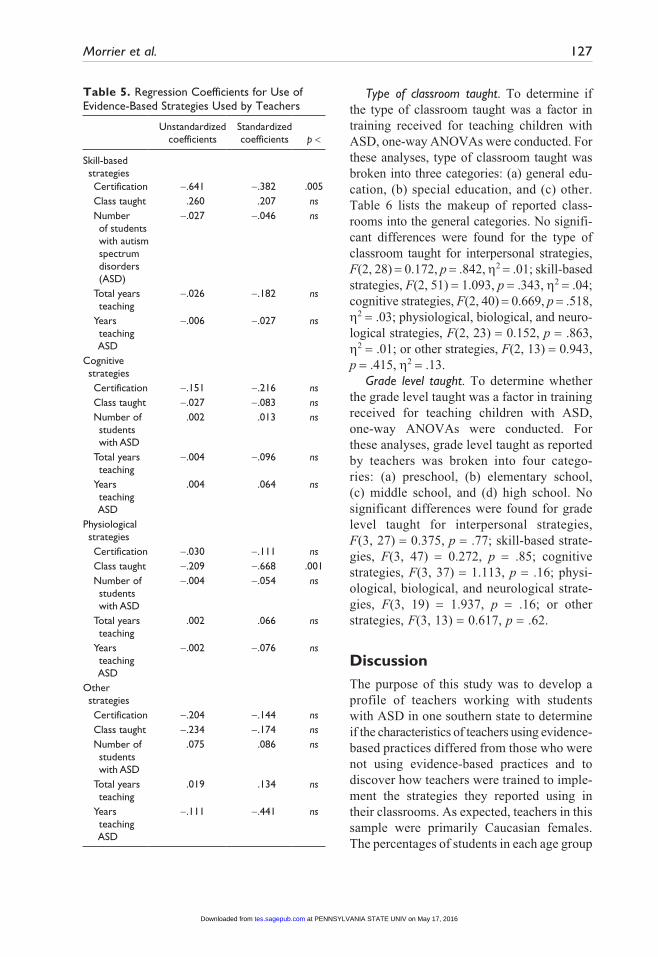
A multiple regression analysis was con-ducted to evaluate factors related to the use of evidence-based practices for each category of teaching strategies used. The predictors were (a) certification level obtained, (b) type of class taught, (c) the number of children with ASD in a class, (d) total years of teaching experience, and (e) total years of experience teaching children with ASD. Coefficients could not be calculated for interpersonal strat-egies because few teachers reported using these strategies. The standardized coefficients for the predictor variables for the remaining four strategies can be found in Table 5. The linear combination of these predictors was sta-tistically significant for the use of physiologi-cal, biological, and neurological strategies, F(5, 19) = 3.450, p = .02, because of signifi-cant differences in the type of classroom taught (t = –3.793, p = .001). Predictors were not significantly related to the use of evidence-based strategies in the skill-based strategies,
Figure 1. Reported training received across all categories and methods of strategies by teachers for strategies used with students with autism spectrum disorders
at PENNSYLVANIA STATE UNIV on May 17, 2016tes.sagepub.comDownloaded from

126 Teacher Education and Special Education 34(2)
F(5, 46) = 2.312, p = .06, although there were significant differences based on the certifica-tion category of the teacher (t = –2.806, p = .007), cognitive strategies, F(5, 36) = 0.469, p = .80, and other, F(5, 16) = 0.793, p = .57.
Individual Factors That May Influence Training Reported by Teachers
Education level. To analyze the effects of edu-cation level on reported methods of training received to use the strategies, teachers were dichotomized as either (a) undergraduate degree recipients (i.e., bachelor’s) or (b) graduate degree recipients (i.e., master’s, educational specialist, doctorate). An independent-samples t test was conducted to evaluate the hypothesis that education level would influence the type of training reported. The test results indicated that education level was not significant for training received in all categories of strategies: interpersonal t(31) = –0.395, p = .70; skill-based strategies, t(51) = 1.174, p = .25; cognitive strategies, t(40) = 0.384, p = .70; physiological, biological, and neurological strategies, t(23) = 0.988, p = .33; and other strategies, t(15) = –0.456, p = .66.
Teaching experience. Researchers indicate that almost 40% of teachers leave the profes-sion within the first 3 years of entry (Singer, 1992). To analyze the hypothesis that the num-ber of years taught would influence the use
of evidence-based strategies, teachers were grouped according to number of years taught and dichotomized as either (a) initial (i.e., 0–3 years of teaching) or experienced (i.e., 4 or more years teaching). An independent-samples t test was conducted to evaluate this hypothesis that years of experience were related to the use of evidence-based practices for students with ASD. Interpersonal strategies were not signifi-cant because teachers reported limited use of these strategies. The test was not significant for skill-based strategies used, t(50) = –1.765, p = .08; cognitive strategies, t(41) = –1.569, p = .12; physiological, biological, and neuro-logical strategies, t(23) = –0.678, p = .50; or other strategies, t(20) = 0.839, p = .41.
Years of teaching experience with students with ASD. To analyze the effects of years of teaching experience on the reported training received, an independent-samples t test was conducted to evaluate initial teachers (i.e., 0–3 years) versus experienced teachers (i.e., 4 or more years). Test results indicated that years of teaching experience did not significantly affect the type of train-ing received in interpersonal relationship strategies, t(30) = 0.636, p = .53; skill-based strategies, t(50) = 0.415, p = .68; cognitive strat-egies, t(39) = 0.076, p = .94; physiological, biological, and neurological strategies, t(23) = 0.509, p = .62; or other strategies, t(16) = –0.366, p = .72.
Table 4. Reported Training for Use of Teaching Strategies
Interpersonal relationship (%) Skill based (%) Cognitive (%)
Physiological, biological,
neurological (%) Other (%)
Teacher prep program
9.7 13.0 23.3 11.5 6.3
Workshop 12.9 22.2 37.2 19.2 6.3Program
developer0.0 3.7 0.0 0.0 0.0
School in-service
6.5 14.9 7.0 11.5 12.6
Peer teacher 0.0 11.1 2.3 15.4 31.3Hands-on 32.3 16.7 16.3 19.2 18.8Self-taught 35.5 18.5 11.6 15.4 25.0Parent 3.2 0.0 2.3 7.7 0.0
at PENNSYLVANIA STATE UNIV on May 17, 2016tes.sagepub.comDownloaded from
Morrier et al. 127
Type of classroom taught. To determine if the type of classroom taught was a factor in training received for teaching children with ASD, one-way ANOVAs were conducted. For these analyses, type of classroom taught was broken into three categories: (a) general edu-cation, (b) special education, and (c) other. Table 6 lists the makeup of reported class-rooms into the general categories. No signifi-cant differences were found for the type of classroom taught for interpersonal strategies, F(2, 28) = 0.172, p = .842, h2 = .01; skill-based strategies, F(2, 51) = 1.093, p = .343, h2 = .04; cognitive strategies, F(2, 40) = 0.669, p = .518, h2 = .03; physiological, biological, and neuro-logical strategies, F(2, 23) = 0.152, p = .863, h2 = .01; or other strategies, F(2, 13) = 0.943, p = .415, h2 = .13.
Grade level taught. To determine whether the grade level taught was a factor in training received for teaching children with ASD, one-way ANOVAs were conducted. For these analyses, grade level taught as reported by teachers was broken into four catego-ries: (a) preschool, (b) elementary school, (c) middle school, and (d) high school. No significant differences were found for grade level taught for interpersonal strategies, F(3, 27) = 0.375, p = .77; skill-based strate-gies, F(3, 47) = 0.272, p = .85; cognitive strategies, F(3, 37) = 1.113, p = .16; physi-ological, biological, and neurological strate-gies, F(3, 19) = 1.937, p = .16; or other strategies, F(3, 13) = 0.617, p = .62.
DiscussionThe purpose of this study was to develop a profile of teachers working with students with ASD in one southern state to determine if the characteristics of teachers using evidence-based practices differed from those who were not using evidence-based practices and to discover how teachers were trained to imple-ment the strategies they reported using in their classrooms. As expected, teachers in this sample were primarily Caucasian females. The percentages of students in each age group
Table 5. Regression Coefficients for Use of Evidence-Based Strategies Used by Teachers
Unstandardized coefficients
Standardized coefficients p <
Skill-based strategies Certification -.641 -.382 .005 Class taught .260 .207 ns Number
of students with autism spectrum disorders (ASD)
-.027 -.046 ns
Total years teaching
-.026 -.182 ns
Years teaching ASD
-.006 -.027 ns
Cognitive strategies Certification -.151 -.216 ns Class taught -.027 -.083 ns Number of
students with ASD
.002 .013 ns
Total years teaching
-.004 -.096 ns
Years teaching ASD
.004 .064 ns
Physiological strategies Certification -.030 -.111 ns Class taught -.209 -.668 .001 Number of
students with ASD
-.004 -.054 ns
Total years teaching
.002 .066 ns
Years teaching ASD
-.002 -.076 ns
Other strategies Certification -.204 -.144 ns Class taught -.234 -.174 ns Number of
students with ASD
.075 .086 ns
Total years teaching
.019 .134 ns
Years teaching ASD
-.111 -.441 ns
at PENNSYLVANIA STATE UNIV on May 17, 2016tes.sagepub.comDownloaded from

128 Teacher Education and Special Education 34(2)
with which teacher respondents were work-ing were similar to those in the state of Geor-gia (Office of Student Achievement, State of Georgia, 2005). It is also not surprising that half of the teachers (49%) taught in self-contained classrooms. Despite current legis-lation to educate students with ASD in the least restrictive environment possible (IDEIA, 2004), many students with special needs are not served in environments with peers who are typically developing. It is interesting to note that teachers using evidence-based prac-tices do not differ statistically from those who are not using evidence-based practices. Individual characteristics that might influ-ence awareness of and willingness to employ best practice strategies (e.g., teacher educa-tion level, age, etc.) do not seem to affect cur-ricular choices teachers are making in this sample. Future research would be helpful in establishing ways to encourage teachers to select evidence-based practices in their classroom.
The increase of students with ASD in both general and special education classrooms (CDC, 2007a) necessitates the need for com-prehensive training in the unique social, lan-guage, and academic needs characterized
by this population of students (McGee & Morrier, 2005). Previous research has demon-strated that teachers of this population tend to use a variety of strategies (Hess et al., 2008), most of which do not have an evidence base to support their use. Results from this study demonstrate that teachers receive training to implement these strategies from a variety of sources. Fewer than 20% of respondents reported learning how to implement the strat-egies used in the classrooms through their university-based teacher preparation program. These data support the previous literature on the lack of interface between pre-service edu-cation and teaching for both general and spe-cial education teachers (Turner, 2003; Winn & Blanton, 2005).
Most of the teachers reported that they were trained in the implementation of strate-gies used with students with ASD through attendance at full- or half-day didactic work-shops. Didactic presentations enable a large number of attendees to hear information pro-vided and learn rationales behind strategies used, but they offer little in the hands-on prac-tice that is often needed to learn the subtle ways strategies must be changed to meet the needs of the heterogeneous population of stu-dents with ASD. McGee and Morrier (2005) proposed a training continuum to assist edu-cators with children with ASD in their class-rooms. This training continuum begins with substantive content concerning the heteroge-neous and unique needs of students with ASD and stresses the importance of hands-on train-ing rather than relying on didactic training. Through direct experience working with stu-dents with ASD, teachers are able to compre-hend the range of characteristics each student with ASD may bring into the classroom.
The results are encouraging in indicating that teachers receive training from a variety of sources, including collaboration with the parents of students with ASD. However, it is striking that time, effort, and expense are being expended on training in strategies that are not always evidence based. Pre-service and in-service teachers need to be trained in the use of evidence-based practices specific to students with ASD. Given traditional access
Table 6. Types of Classrooms Comprising Classroom Categories
Category
Type of classroom and
descriptionUse
reported (%)
General education
General education, full inclusion (more than three fourths of the day), collaborative
26.7
Special education
Resource, self-contained autism, other self-contained, combination
58.9
Other classroom type
Other 14.4
at PENNSYLVANIA STATE UNIV on May 17, 2016tes.sagepub.comDownloaded from

Morrier et al. 129
to research, university-based preparation pro-grams should be well positioned to provide training to facilitate the development of skills in evidence-based practices.
None of the individual factors that were hypothesized to influence training demon-strated any statistical significance. Education level, years of experience, type of classroom environment, and grade level did not contrib-ute to the type of training a teacher received. Given that 72% of the respondents had gradu-ate degrees, it was hoped that education level would be significantly correlated with the use of evidence-based practices. This absence of influence should raise concerns related to what college and university programs are pri-oritizing in their personnel preparation pro-grams for teachers who want to work with students with ASD. Unfortunately, most state certification boards are responding to the mandates of NCLB (2002) and IDEIA (2004) by creating generalized certification (e.g., “gen-eral curriculum” vs. “adapted curriculum” in Georgia), and teacher training programs in higher education are modifying certification programs accordingly, resulting in less spe-cialized training on evidence-based practices for students with ASD. Interestingly, teacher preparation programs were reported to empha-size cognitive interventions more than any other type of intervention, based on the responses from teachers in this sample.
Limitations and Future ResearchThere are several limitations to these results that should be noted. First, only a small number of respondents reported on the training received for implementing strategies with the students with ASD. Also, these data are from one south-ern state, limiting the generalizability of the results to the nation as a whole. Future investi-gations into how teachers are trained to work with students with ASD in educational settings should include larger samples from diverse geo-graphical locations to truly make policy recom-mendations regarding teacher training.
Second, teachers were provided access to the ATS from their county special education
directors and/or autism specialists. This may have reduced the actual types of training that teachers received because they may have felt that the results could influence adminis-trational attitudes. Future research efforts should go directly to the teachers themselves to eliminate any reporting bias. Perhaps a similar survey could be distributed through national teachers organizations (e.g., Coun-cil for Exceptional Children, National Teach-ers Association) to get a wider variety of responses and a more accurate picture of the country as a whole.
Third, teachers who responded were not able to choose more than one option for each strategy reported. This forced choice may have elimi-nated some training methods that have been received and limited the results. Future research should allow teachers to report on all training received as well as combinations of training received for implementing educational strate-gies. Even with these limitations, the data pre-sented demonstrate that there is room for improvement in the training of teachers working with students with ASD.
The results of this study can be interpreted to indicate that teachers are resourceful in seeking a variety of providers for their train-ing needs and many are self-taught or learn simply by trial and error with their students. Didactic training provided through workshops is an efficient method of dissemination but may not result in applied use. Although it is discouraging that a greater percentage of teachers who received graduate training did not report more use of evidence-based prac-tices, it is encouraging that other teacher char-acteristics were not correlated with more or less use of evidence-based practice. The message to be derived from this finding is that teachers will be open to using evidence-based practices if those are the ones they are trained to use. The format and content of training delivered to teachers of students with ASD need to be evaluated more carefully, with data collected to document applied use. Personnel training programs can lead the way in estab-lishing the standards for training to emphasize the use of evidence-based practices as well as the unique needs of students with ASD.
at PENNSYLVANIA STATE UNIV on May 17, 2016tes.sagepub.comDownloaded from
130 Teacher Education and Special Education 34(2)
AppendixExample of Autism Treatment Survey Item
2. Skill-Based Interventions and Treatments1. Which strategy do you use the most frequently in your classroom?a,b
• None • Assessments of Basic Language and Learning Skills (ABLLS) • Assistive Technology (AT; for example adapted utensils, talking calculators, pencil
grips, audible word scanning devices, software, talking word processors with text, or van adaptations)
• Augmentative Alternative Communication (AAC; aided and unaided communica-tion devices and symbol systems, excluding Picture Exchange Communication System—PECS)
• Azrin 24-hour Toilet Training • Discrete Trial Training • Facilitated Communication • Fast ForWord • Incidental Teaching • Joint Action Routines (JAR) • Lindamood-Bell • Naturalistic Language Paradigm • Picture Exchange Communication System (PECS) • Pivotal Response Training • Rapid Prompting Method • Structured Teaching (TEACCH) • Van Dijk Curricular Approach • Verbal Behavior • Visual Schedules
2. With how many students do you use this strategy? The value must be between 1 and 20, inclusive.
3. How were you trained in this strategy. Choose the answer that has contributed the most substantially to your use of this technique. • Teacher Preparation Program • Half-day Workshop • Full-day Workshop • Program Developer • Local School in-service • Peer Teacher/Therapist • Hands-On/Practical Experience • Self-Taught • Parent Instruction • County School System in-service • None
a. This question is repeated two more times so that the participant may list secondary treatments and other treatments.b. Results of best practices are provided in Hess, Morrier, Heflin, and Ivey (2008).
at PENNSYLVANIA STATE UNIV on May 17, 2016tes.sagepub.comDownloaded from

Morrier et al. 131
Declaration of Conflicting Interests
The author(s) declared that they had no conflicts of interests with respect to their authorship or the pub-lication of this article.
Funding
The author(s) declared that they received no finan-cial support for their research and/or authorship of this article.
References
Billingsley, B. S. (2003, April). Special education teacher retention and attrition: A critical analy-sis of the literature. Gainesville: University of Florida, Center on Personnel Studies in Special Education. Retrieved from http://www.copsse .org
Centers for Disease Control and Prevention. (2007a, February 9). Prevalence of autism spectrum disorders—Autism and Developmen-tal Disabilities Monitoring Network, 14 sites, United States, 2002. Surveillance summa-ries. Morbidity and Mortality Weekly Report, 56(SS-1), 12-28.
Centers for Disease Control and Prevention. (2007b, February 9). Prevalence of autism spectrum disorders—Autism and Developmental Dis-abilities Monitoring Network, six sites, United States, 2000. Surveillance summaries. Mor-bidity and Mortality Weekly Report, 56(SS-1), 1-11.
Georgia Professional Standards Commission. (2007). Certificate categories. Retrieved from http://www.gapsc.com/Certification/Classifica-tionofCertificates.asp
Handleman, J. S., & Harris, S. L. (Eds.). (2001). Preschool education programs for children with autism (2nd ed.). Austin, TX: Pro-Ed.
Handleman, J. S., & Harris, S. L. (Eds.). (2006). School-age education programs for children with autism. Austin, TX: Pro-Ed.
Handleman, J. S., & Harris, S. L. (Eds.). (2008). Preschool education programs for children with autism (3rd ed.). Austin, TX: Pro-Ed.
Harris, S. L., & Handleman, J. S. (Eds.). (1994). Preschool education programs for children with autism. Austin, TX: Pro-Ed.
Heflin, L. J., & Simpson, R. S. (1998). Interven-tions for children and youth with autism: Pru-dent choices in a world of exaggerated claims and empty promises. Part I: Intervention and treatment option review. Focus on Autism and Other Developmental Disabilities, 13, 194-211.
Hess, K. L., Morrier, M. J., Heflin, L. J., & Ivey, M. L. (2008). Autism Treatment Survey: Services received by children with autism spec-trum disorders in public school classrooms. Journal of Autism and Developmental Dis-orders, 38, 961-971. doi:10.1007/s10803-007-0470-5
Holdheide, L. R., & Reschly, D. J. (2008). Teacher preparation to deliver inclusive services to students with disabilities. Washington, DC: National Comprehensive Center for Teacher Quality.
Individuals With Disabilities Education Improve-ment Act, Pub. L. No. 108-446, 118 Stat. 2647 (2004).
Izeman, S. (1995). Embedding teaching techniques for young children with autism into daily activi-ties. Early Intervention, 6(2), 1-3.
Kogan, M. D., Blumberg, S. J., Schieve, L. A., Boyle, C. A., Perrin, J. M., Ghandour, R. M., . . . van Dyck, P. C. (2009). Prevalence of parent-reported diagnosis of autism spectrum disorder among children in the US, 2007. Pediatrics, 124, 1395-1403. doi:10.1542/peds.2009-1522
McGee, G. G., & Morrier, M. J. (2005). Prepara-tion of autism specialists. In F. R. Volkmar, R. Paul, A. Klin, & D. Cohen (Eds.), Handbook of autism and pervasive developmental dis-orders: Vol. II. Assessment, interventions, and policy (pp. 1123-1160). New York, NY: Wiley.
Meyers, B. J., Goin-Kochel, R. P., & Mackintosh, V. H. (2005, April). Therapies for children with autism spectrum disorders: How many are children using? Poster presented at the biennial meeting of the Society for Research in Child Development, Atlanta, GA.
Morrier, M. J., Hess, K. L., & Heflin, L. J. (2008). Ethnic disproportionality in students with autism spectrum disorders. Multicultural Education, 16, 31-38.
National Research Council. (2001). Educating chil-dren with autism. Committee on Educational
at PENNSYLVANIA STATE UNIV on May 17, 2016tes.sagepub.comDownloaded from

132 Teacher Education and Special Education 34(2)
Interventions for Children with Autism, Division of Behavioral and Social Sciences and Education. Washington, DC: National Academy Press.
No Child Left Behind Act, Pub. L. No. 107-110, 115 Stat. 1425 (2002).
Odom, S. L., Brown, W. H., Frey, T., Karasu, N., Smith-Canter, L. L., & Strain, P. S. (2003). Evidence-based practices for young children with autism: Contributions for single-subject design research. Focus on Autism and Other Developmental Disabilities, 18, 166-175.
Office of Student Achievement, State of Geor-gia. (2005). 2003-2004 state of Georgia K-12: Report card for state of Georgia. Atlanta, GA: Author.
Rogers, S. J. (1999). Intervention for young children with autism: From research to practice. Infants and Young Children, 12(2), 1-16.
Scheuermann, B., Webber, J., Boutot, A., & Goodwin, M. (2003). Problems with personnel preparation in autism spectrum disorders. Focus on Autism and Other Developmental Disabilities, 18, 197-206.
Simpson, R. L. (2004). Finding effective interven-tion and personnel preparation practices for students with autism spectrum disorders. Excep-tional Children, 70, 135-144.
Simpson, R. L., de Boer-Ott, S. R., Griswold, D. E., Myles, B. S., Byrd, S. E., Ganz, J. B., . . . Adams, L. G. (2005). Autism spectrum disor-ders: Interventions and treatments for chil-dren and youth. Thousand Oaks, CA: Corwin.
Simpson, R. L., & Myles, B. S. (1998). Educat-ing children and youth with autism: Strat-egies for effective practice. Austin, TX: Pro-Ed.
Singer, J. D. (1992). Are special educators’ career paths special? Results from a 13-year longitudinal study. Exceptional Children, 59, 262-279.
Stahmer, A. C., Collings, N. M., & Palinkas, L. A., (2005). Early intervention practices for children with autism: Descriptions from community providers. Focus on Autism and Other Devel-opmental Disabilities, 20, 66-79.
Turner, N. D. (2003). Preparing preservice teach-ers for inclusion in secondary classrooms. Education, 123, 491-495.
Wing, L., & Potter, D. (2002). The epidemiology of autistic spectrum disorders: Is the prevalence rising? Mental Retardation and Developmental Disabilities, 8, 151-161.
Winn, J., & Blanton, L. (2005). The call for collab-oration in teacher education. Focus on Excep-tional Children, 38(2), 1-10.
Yeargin-Allsopp, M., Rice, C., Karapurkar, T., Doernberg, N., Boyle, C., & Murphy, C. (2003). Prevalence of autism in a U.S. metro-politan area. Journal of the American Medical Association, 289, 49-55.
Bios
Michael J. Morrier, PhD, BCBA-D, is an assis-tant director for research and program evaluation at the Emory Autism Center in the Department of Psychiatry and Behavioral Sciences at Emory University School of Medicine. His primary research interests focus on early diagnosis of ASD, peer-related social behaviors, use of evi-dence-based practices for treating and educating students with ASD, and disproportionate repre-sentation of ethnically diverse preschoolers, chil-dren, and youth with disabilities.
Kristen L. Hess, PhD, teaches third- and fourth-grade students at The Atlanta School in Atlanta, Georgia. She also works as an ASD consultant sup-porting students, parents, and teachers. Her pri-mary research interests focus on stress and ASD, as well as use of evidence-based practices for educat-ing students with ASD, and how teachers come to use these practices.
L. Juane Heflin, PhD, is an associate professor in the Department of Educational Psychology and Special Education at Georgia State University, where she coordinates the personnel preparation program for teaching students with ASD. Her research emphasizes the support of students with ASD in educational settings.
at PENNSYLVANIA STATE UNIV on May 17, 2016tes.sagepub.comDownloaded from