Target and Achievement of MDGs: A Study on Factors Affecting Reduction of Child Mortality
9
SUST Jornd of Public Adminsration Vol l, No I, December 2008 ISSN:2073 8293 TARGET AND ACHIEVEMENT OF MDG: A STUDY ON FACTORS AFFECTING REDUCTION OF CHILD MORTALITY Mohammad Nashir Uddin' Chowdhury Abdullah AI - Hossienie" Chowdhury Abddlah At - Baki"' In this ariicle atlempts has been made to show rhe achicvemenr ofMDc goal 4 in Bangladesh rnd rhal is reducrion ol child mortat;ty rare. Child motality refers to the death ol irrfants and child.en under the age of five. About 25.000 young.hild.en die cvery dry. mrinly lrom prevenlable causes. In developing countrics, one child in cveryt0 dies beforc its fiftb birthday, compared to.l in every 143 in high income counrr;es. According to an estimare by Lr].UCEF, one miltion child deaths coutd be prevented annudly at a cost ol $US I billion per year. Reduction ofchild mo.tality is the fou h of the United Narions' Millennium Devetopnenl Goals. The objective of the study is to know how far Bangladesh could achi€ve "MDG Goal 4" of reducing under-five morraliry by exa'nining different variables affecting child mortality. The study has done on the basis of secondary data which were collected from differenr data sources. reporls, joumals and published lirerarure. So far Bangladesh could ach;eve fte rate more tban the expecred target. For rhis reason. Bangladesh has 10 conrinue this pace towards reducing rhe chitd mortali!y. Key Words: Child Morrality, Achievemenr of MDG, Inmurization, 'Asntutu Prcfesor, Depa 'rcnt oJPubllc Adninistt4tiah, Shahjatal Unirelsitt ot Sr.nr, an t l "chhotoe \, : lt t pt t l 1 r'. Bonelad.,h. E ngil: [email protected] "MSS, DepLltnrent of Publi. A.lninniaiaa, shahjdlal unire1it! oJ science andT.chnolosy, sllhet 3114, Ban8latl^h. E hail: [email protected] "'Gratuate Studeht, Depa.tnenl of Ecohonics, Shohjalal Unbe$it-r of Scietue aDd Technoloet, Stlhzt3 1 11, BoapladeslL E-Mil: aobia [email protected] SUST Joumal of Publi. Adminisldtion S LIST JoLmrl ol Public Adminishr i.n
Transcript of Target and Achievement of MDGs: A Study on Factors Affecting Reduction of Child Mortality
SUST Jornd of Public AdminsrationVol l, No I, December 2008
ISSN:2073 8293
TARGET AND ACHIEVEMENT OF MDG: A STUDY ONFACTORS AFFECTING REDUCTION OF CHILD MORTALITY
Mohammad Nashir Uddin'Chowdhury Abdullah AI - Hossienie"
Chowdhury Abddlah At - Baki"'
In this ariicle atlempts has been made to show rhe achicvemenr ofMDcgoal 4 in Bangladesh rnd rhal is reducrion ol child mortat;ty rare. Childmotality refers to the death ol irrfants and child.en under the age of five.About 25.000 young.hild.en die cvery dry. mrinly lrom prevenlablecauses. In developing countrics, one child in cveryt0 dies beforc its fiftbbirthday, compared to.l in every 143 in high income counrr;es.According to an estimare by Lr].UCEF, one miltion child deaths coutd beprevented annudly at a cost ol $US I billion per year. Reduction ofchildmo.tality is the fou h of the United Narions' Millennium DevetopnenlGoals. The objective of the study is to know how far Bangladesh couldachi€ve "MDG Goal 4" of reducing under-five morraliry by exa'niningdifferent variables affecting child mortality. The study has done on thebasis of secondary data which were collected from differenr data sources.reporls, joumals and published lirerarure. So far Bangladesh couldach;eve fte rate more tban the expecred target. For rhis reason.Bangladesh has 10 conrinue this pace towards reducing rhe chitdmortali!y.
Key Words: Child Morrality, Achievemenr of MDG, Inmurization,
'Asntutu Prcfesor, Depa 'rcnt
oJPubllc Adninistt4tiah, Shahjatal Unirelsittot Sr.nr, an t l "chhotoe \, : lt t pt t l 1 r'. Bonelad.,h.E ngil: [email protected]
"MSS, DepLltnrent of Publi. A.lninniaiaa, shahjdlal unire1it! oJ scienceandT.chnolosy, sllhet 3114, Ban8latl^h. E hail: [email protected]
"'Gratuate Studeht, Depa.tnenl of Ecohonics, Shohjalal Unbe$it-r of ScietueaDd Technoloet, Stlhzt3 1 11, BoapladeslL E-Mil: aobia [email protected]
SUST Joumal of Publi. AdminisldtionS LIST JoLmrl ol Public Adminishr i.n
Ta.gel and Achievement ofMDG
lntroduction
In order to lchieve some targeted progress in poverty. education, health,gender equality, sustainAble e.vironment and strcngthening inlcrcountry co'o.dinaiion for developm€nl, lhe Millennium Developrnentcoals (MDGS) havc been adopred by thc United Nalions (uN). whichcontain a scl of developtnent lctiviries agrecd upon during a se.ies ofglobal conle.ences over thc preceding decade. Alter review ud editingby rhe United Narions Sccrclariat. IMII, OECD and World Ba.k, lheobjecrivcs were publishcd in Septcmbcr 2(X)l as n ser of 8 major goals
accompanicd by 18 rargcts and 48 iMicrtors for nLasuring p.ogrcss
As a mernber counlry of the Unitcd Nnlions. Bogl desh has trken a
comprehensive appro{ch lo achieve rhe millcnni rn development 8oals.Governmcnl of Bangladesh h$ prepared a policy document enritlcd''Unl(xking ihe potential: Nltional SlruteSy for Accclcrated PovenyReduction which is rermed as PRSP. This document has outlined a
number ol policy measures lor achieving the tnillennium developmentgoais.
Declaration ofgoals may mcan nothing if efforts are nol made to achieve
the 8oals. ln order to ensurc the mvcment of the cconomy along the
raght track to achieve lhc goals, it ;s imponant lhal the progr€ss towards
atta;nment of goals is rcgularly monitored. This paper trics to show thcp.ogress ol Lhe MDC goll 4 ol rcducing Lrnder five motulity rate froml5l dcrths pcr rhousand lile Siths in 1990 {o 50 by 2015. Childmonaliry rate is a rctlection of the carc. henkh and nutrilion status olchildren bclow rhc lgo of fivc yerrs and also indicales thc social,
cultural. and ccononric progrrss in thc country. As children are (he
futures oi our count.y. il is trrli:rlly r rcscu.ch on how much wc are
concerrred about fuLurt gcncrrlion as wcll us soc economic and culLural
progress of the country.
A good nu'nber ofstudics assessed lhc cxlent of achievemenl of the 8oal.Child health in general has improved, though thc neonatal monalily ratc
remains high and contibutes disproponionn(ely to overall inlantmorlality The immunization prograrnme hls been recognized for itssustain€d high coveragei however. only Tlak of infanrs are f llyimmunized. Measles presents an additional challenge !o theimmunizarion programne wirh an eslimated 20.000 children dying fromthe disease €ach year. Effons musl be inlensified to ensure access to safe
immunizathn as well as strengthening surveillance of all vaccine"
p.eventable diseases. Ma lnutrition conlin ues to be a serious problem wilh
Nashir Uddin, C. A. A. Hossienie& C. A. A. Baki
nearly half of the children b€ing modemrely underweight, one-thirdsuffering from stunti.g aod a Iarge number of adolescenrs, girls inparticular, being mlnourished. Adolescent healrh requires closerattenlion. particularly in the contexr ofreproductive health (WHO 2007).Under'fives. neonatal and prrcnralcauses contribure to48 percenr of thedcaths. Othel factors include very low mtes of instirutional deliveries(8.6%), low attendancc ofdelivcries by skilled personnet (12%), and lowutilizalion of antenatal care (48%). More rhm 71 percent of theseneonatrl deaths were due to non-commuricable diseases, mainly birrh-rclated ailments as well as neonaral teranus. Odrcr majorcauscs of under-five duths are pneurnooia (18%), diarhea (6%), injuries and drownins(8%), and rneasles wirh malnutriiion underlying mosr othcr causes(13%). Poor care-seeking behavior and practices are also importanrcontributing faclors. Only 8 percent ofparenrs ofsick children under rheage offive seek care liom qualified fiealth care provideG (MDc 2005).
Bangladsh has made rrctrLndoos progrcss in erpatditrg chirdimmunization coverage over lhe last lwo decades. The WHO VaccinePrevenaable Diselses Monitoring System indicalcs rhrr Bangladesh wenrfrom virtLrally no measles vaccination coleragc in 1980 Lo 72% coverageby 1998. The empiricrl resulls sllggesr thal disrricl-level immunizationcovcmge of mcaslcs has a strong (inverse) associarion with under fivemonaliry, with each percenrlge poinr increas€ in trEasles vacine.coferage beinS associaied with a reduction of0.4 child deaths p€r 1,000live births. These estirutes imply that universal measles vaccinecoverage would be associaied with a reducrion in undef-five
'nortatity of
about 16 deaths pcr 1,000 live births (WHO 2005). While asked,villagers also identificd a ser ofcontribuling facrors to rhis positive trendin r€ducing inf.rnr and child monalily panicularly from th€ 1990s. Thefactors werei increased coverage of immunizarion program, improvedmon;toring syslcm by UP, Numb€r of doclors ;ncr€ased. Devetopedcomnrun;carion systen (easy to reach hospitalt, Improved medjcalscience, Avaihbility of cquipment inc.eased. Doctors behaviorsimproved, GOs (Gove.n"rent OrSanizarions) and NGOS are cottaboraringon health issues (PFM 2005). Effecr;ve m€chanisns for financing theintcrventions (tbr achieving heshh MDC in Africa) in the shorr-run,recxplored. wjlh I focus on the role of social healrh insurancc. It isconcluded that national or social insurance hrs a rimited rote in achievinghealrh MDGS in Af.ica over the nexr seven years. However, it can playan important supplemnrary function. Revenue from general hxarion isrccommended as the main financing option. This revenue is proposed rolinance f.ee basic health care in public clinics in rural aDd slum areas,with health crre services at higher levels of lhe public sysrcm being
Sl iST Joumrl of Public Administarion 52SUST toumal oa Public Adminiskdion
Target and AchieverreDt ofMDG
funded mainly by social insufrnce. Additiotrll supportivcrecommeDdations in areas ol private insurance and instilutional reformsare offered (Mwab'r 2008).
Rationale of the SfudJ
Across the world, childr€n are tlt higher risk of dying if they arc poor'Child morlalily is a greal problcm in th€ world especially for the
dcvelopine cooDlries likc Bangladesh. To reduce lhe child monality,govearmenl ofdiffereDl counnics took vuious policies d srategics. Inspite of thcse initialives, ratc of child moflalny, in many developingcounlries is not dcc.easing. So to reduce drc rnle of child monality UNenclosed Coal 4 in MDCS. ln Ban8ladesh child monality;s relativelyhigh in rural areas than those of towns. On lhe olher hand, msl of the
people otour counlry live in villages. Child morlalily depcnds on sevcral
facrors. Wc have ro know rhc factors affecting the child motulily toreduce i1. Finally it can be said lhat the rationlle of tlE study iscnormous, which helps us ro know aboul the factors ot child monality.the way to reduce it and its future trends in the stipulaled time
Obj€ctivcs of the Siudy
The objeclive of the study is to analyzc lhe achievemcnt ofMDC Goal 4
For lhis end in thc view. sorne specific objeclivcs were fixed 1o perform:
a. To observe diffcrent variables atfecting child monalily.
b. To show in what cxtenl (he affecb of the variables havc been
c. To predict \that cotrld hc lhe positio of Bangladcsh if the
Nashir Uddin. C. A. A. Hossicnie& C. A- A. Baki
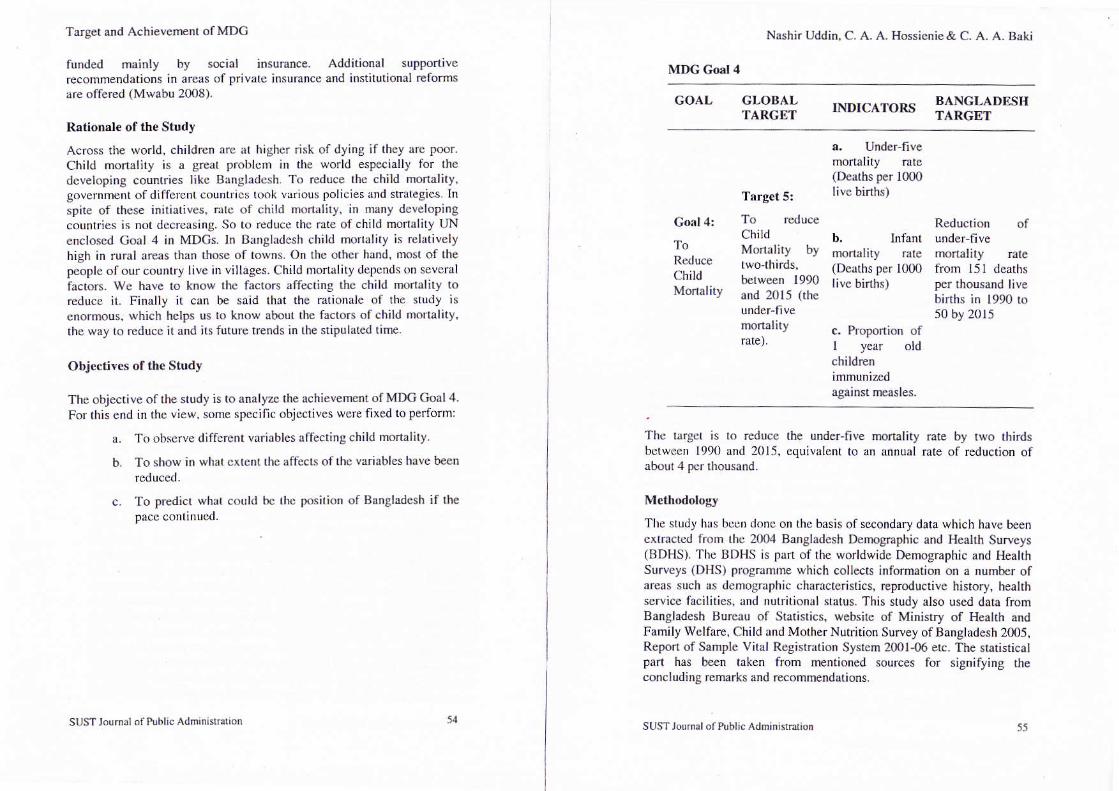
MDG God 4
GOAL GLOBALTARCET INDICATORS BANGLADESII
Go.l 4:
To
ChiIdMonaliry
Target 5:
chitdMonaliry bytwo-thirds,between 1990and 2015 (rhe
nlortalityrate).
a, UndeFfive
(Deaths per l0O0livc binhs)
b. Infant
(Dcaths per 1000livc bhths)
I yedr oldchildren
againstm€isles.
undsr.five
from i5l deaths
births in 1990 to50 by 2015
Tho la.gcr is 10 reduce the under-fi\€ monaliry mre by r1{o thirdsbetween 1990 and 2015, equivalcnt to an annual rate oi reduct;on ofaboul 4 pcr thousand.
MethodoloKt'
The study has bcon donc on ihc basis ofsecondary data which have beenexlractcd liom thc 2004 Bangladesh Denographic and Health Srrvcys(BDHS). The BDHS is part of the worldwide Demographic and HeahhSurvcys (DHS) programne which collccts inforrnation on a number ofareas such as demographic characteristics, reproductive history, healthservice faciliries, and nutritional sLatus- This study also used data fromBangladesh Burcau of Statisti€s, websirc of Ministry of Heahh andFamily Welfare. Child and MotherNutrition Survey ofBangladesh 2005.Repon of Sarnple Vital Registr.rtion Sy$em 200l{6 erc. The sraristicalpad has been taken from mentioned sources for signifying rheconcluding rcrnarks and recoftmendations.
sUST Joumll ol P!blic AdEinislhlion SUST Joun!l of Public AdDinishrion 55
Target and Achievemenl ofMDC
The depcndent variable of the study was conside.ed as Child MonalhyRate of under fivc cbildren and a ser of independent variables such as
measles immunization, malnulrition. fcmale literacy, Thana Health
Centre and Regislered Doctors.
ln this study some tabular analyss through shtistical packages have
been applied for proccssing and analyzing the dara. A tabular analvsis
rechnique has b€en used tofind out lhe asso.iation or difference b€tween
varilbles. ln this sludy, tabular lecbnique has been followed to illuslraterhe overall situalion. Tabulated datl werc analyzed and.ondensed byusing average, sum, p€rcentage etc. wilh the holP ol Software packuges
namely MS word, MS Exceland SPSS
In this study, quanlitative method has bccn uscd Lo explrin the rffect ofvarious factors on child monality,rnd to find out lhe level ofachieverEnr of MDCS Coal 4 in Bdgladesh.
Specification of Vsriabl€s witb Operations Defi nition
CMR (<5y".,) =,f (MlM' MalNu! FeLi' THC' ResDoc)
Nashir Uddin, C. A. A. Hossienie & (1. A A. Baki
Resulls
Tlre resuhs ofthe stud), alc prescrtcd in two ways. Firstly.lhc nAturc andextent ol lhe reduction of child mortaliry has been analyzed and
'discussed in tabular format. Secondly. thc audy focused on statisticalanalysis ofthc rcduclion ofchild
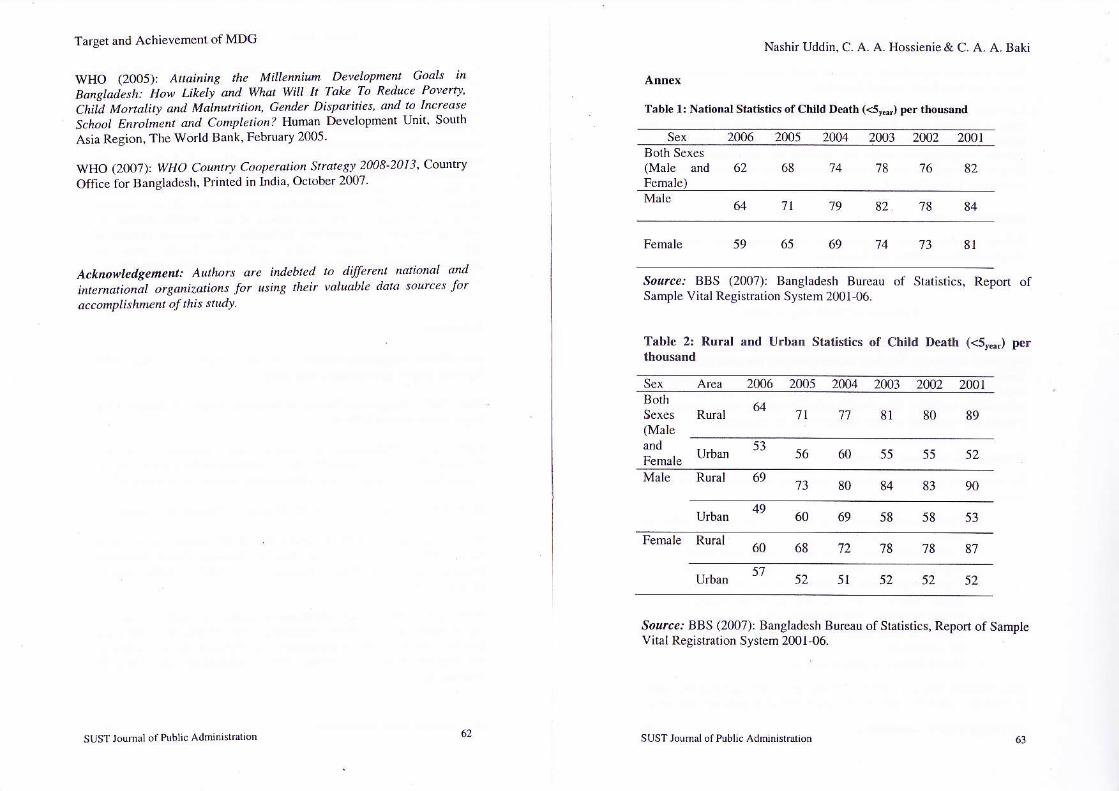
'nodality.ln Table-l it is secn lhat child nronal;ty is rcducing dry by day;n ourcounlry. ll is also seetr that lifc cxpcclancy ofmale childrcn arc lcss rllanfemale children. Although i1 is see ihat the nutrition ol children aregeider bias, icnale children has long ilc expectancy
Table-2 shows that rural areas ofour couftry are facing lack ol mcdicalcarc iDd hcilities. So the child monaliry rate is higher ill lhesc areas thannalional and urban nreas. But il also has shown the good lrend ofredrcing child
'nortalilJ--'. On lh€ other hand. urban areas are facililared
wilh modem mcdicallechnology aod highcrcdncat;vc knowledge. So thechild monality rale is k)wcr hcrc lha lhc nilidral a d nrrrl nrcas.
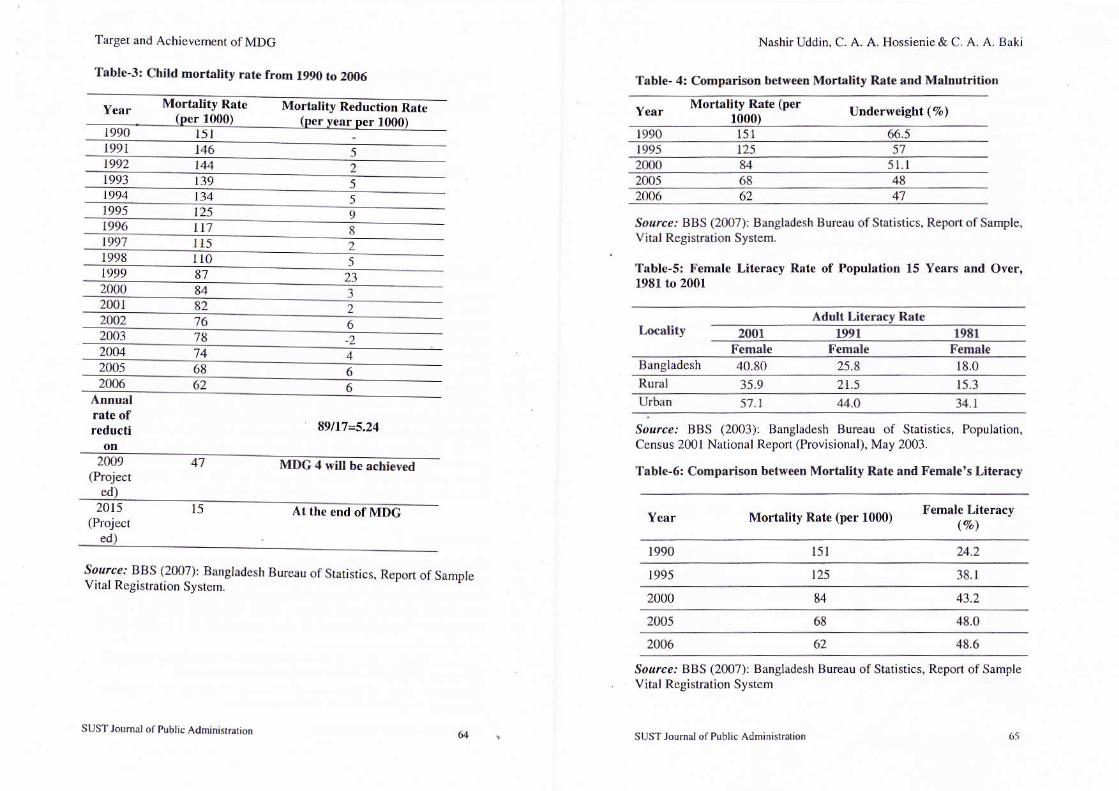
From lablc-3 il can bc said thrit chikl m)n.lit) rrrc I'cr thouirnd was 84in 2000 llo r l5l in l9tl0 and ir 200(r il wNs 61. Ahrxxi snne data has
been found lionr world llanl and LJNICL;l:rcports. World Bank's MDC.BaDgladclh Progress Reporl (2005) also srpp.rts these dala except three
]€ars 1002. 20{)l and 2004 and child mortalil} .ates oflho$c ycars were16. 78 ai<I '74 rcspeclively. World Bank nnd UNICEF also poblisheddata of2007. in !'hich child mortalily rates were rcduced lo ?2 and 6l
An annual rate ofreduction olaboLt 4 is neccssary lo achicvc th€ MDOgoal 4 but accordlng to the Tablc-3. Bangladesh has achieved 5.24. Ifwccan kecp this pace. we car achicve the Boal within 2009 and withirr 2015child morlalily rate sill be l5 per thousand (as per calcLrlation). In 1999child morlalit] rarc was reduced siSnificaDtly. So it can bc said thatBn'rgladcsh car nclr,eve the Soalso casily.
Mahulrili()n conlributes lo ovcr onc halfofchild dcalhs. wilh low binhweighr csrin)alcd lo affect l0 ro 50 perc€nr of infanrs (MDG 2005: 28).over thc ycars. approprialc intcr\rentions have helped to reduce theproponion oJ underwei8ht children fronr 66.5 pcrceni irr 1990 ro 51.1
percerl in 2000. and child stunting liorr 65.5 to 48.8 percent. In spite ofthis. thc prevalencc ol child stuntirB and underweight is still very lrighaccording to Wllo criteria. Ib addrcss child malnutrition, it is csscntialto improv€ lhe utritional slalus ofadolesccnl girls and molhcrs. becauseifmorhers are malnourished, theh childr€'r a.e much more likely to have
low birrh wcighr. aDd to rcDaiD malnourished rhrouglronl the; liv€s.
Here,
Depend€trr Vrriablc
Indepcndent V6riables
: CMR (<5r-.) = Child Mor.ality Rateof under fivc children
: MIM = % of Measles ;mmun izalion
MalNut = MalnutriLnrn (Numbcr ofChildren in per 1000 is suffering lromM.rlnulrition)
FeLi = Fc,nllc LiteruY (Numbcr ofLiterdtc fcmales Per 100)
THC = Thana Health Centre (Total
Number ofThana Health Cenke)
RegDo = Rcgistered Doctor (TolalNumber of Rcgistered Doctors)
This study assumes tha( measles immunization' fernale litcracy. Thana
Heahh Cenre and regislered doctors are negatively and malnulrition is
posirively relaled with child monalily rale
56 sUSl Jo! ilolhh ic Adtrrin(rlLLonsl Js l ldunal oi Public Admihhrrdion
Target and Achiev€ment ofMDG
Although chronjc ene.gy deficiency in non-pregnant women has declinedfrom 52 percenl in 1997 to 45 percenl in 2000. it still rcmrins atunaccept,bly high levels.
Fron Table-4 wc can see that there is a positive relation b€twccn childmortality nte and malnutriaion. Both of lhem are reducing significantly.It is observed lhal malnutrition rale was 66.570 in 1990 and it decreasedb 41qa in 2006. So to achieve MDO goal 4 malnutrition is reducins
Female lirerlcy rate is rn import nt indicrlu of past perforrnance ofcducalional alLainmcnl by the popululbr of lhc counlry. Female literacyrare obtaincd from different ceDsuscs ol lhe country has bcen presenled
in Tablc 5. It is obscrved that femalc li(eracy rate was 18% in l98l and itincrcased ro 40.80% in 2001. Indicaring 22.8 pcrcentage poants increase
ovcr rhe lasl two decades. The increasc for the females olcr th€ lastdecades more th n doubled. It is notable that iocrcase in the lemale
literacy rate is more pronounccd in the rural areas compared to urban
From Tablc-6 we can see thal therc is a negative relation belwccn childmortality rrte and female literacy. Fenule liteacy is doubled from l99rt)
lo 2006- It is observed lhat female literacy rate was 24.2% in 1990 and iIincreased 1o 48.6% in 2fi)6 Femalc lilcracy ;s very significant to reduce
child monality because educated molher can take belter cffe of lheirchild.
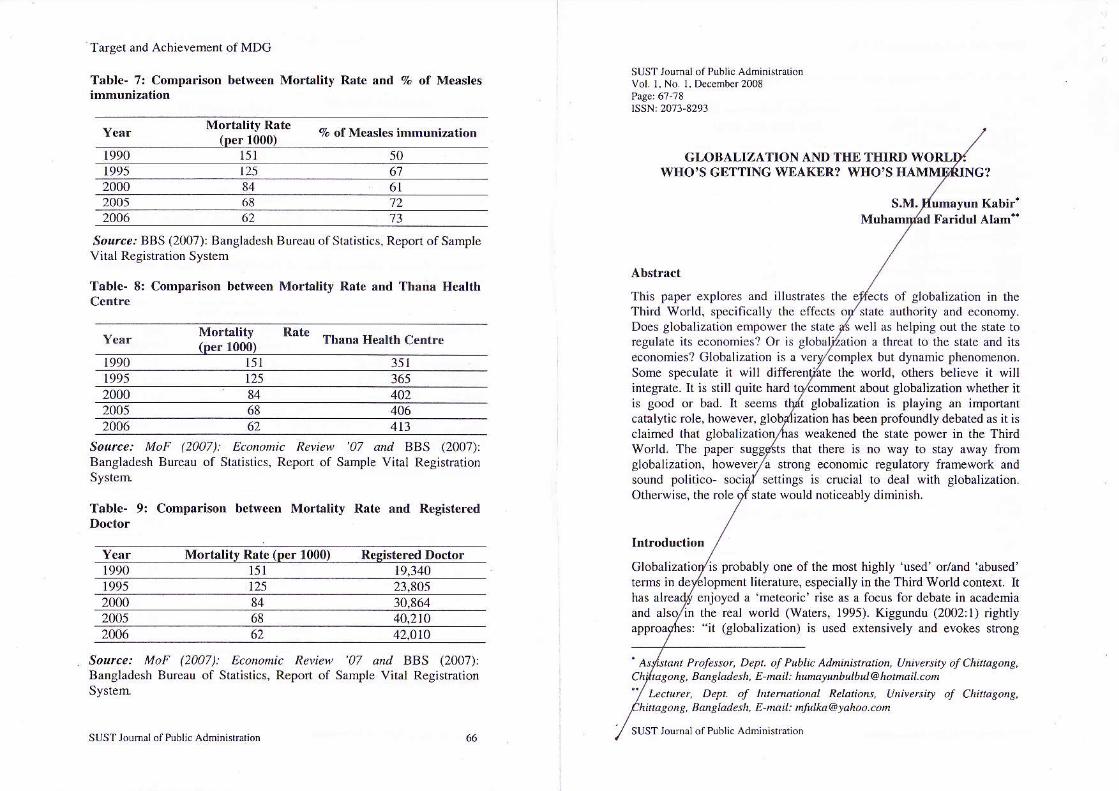
Thc proportion of children aged by 12 months who received
immunization rgainst mcrlcs hrs been shown in Table 7. lt is seen that
covc.rge of immunizllrion doscs lgrinst lnc sles incteascd ovcr the years
at national levcl. Alld fro'n Tablc-? it is .rlso scen thrt immuniT-ttion is a
viral factor of reducins child trn'lality. The'c is ncgative relationshipbetween child monalily and me0slcs immunization.
Access to vaccination has b€en rmong the foremost interventions thal
have helped rcduce mort. ily rales in Bangladesh. Nationallmmunization Drys (NlD) has been obscrvcd for many ycals and has
proved very successful. Since 2001 not a single case of wild tolio vnustransmission has been confirrned in the country. The percentage of fullyimmunized children increas€d from 53 percent in the l9ms lo69 percent
in 2000 but thc covera8e renains below erpcctalions- According to the
world Heahh Orsanization (wHo) repon 2004, in 2m3 BCG coveragervas 96 percenl while measles coverage was only 69 percenl.
Nashir Uddin. C. A. A. Hossienie& C. A. A. Baki
From Table-8 illuslrates that there is r ncgatile relaiion betweeD childmortalily rate and Thana Health Centre. It is obscrved thar Thana HealthCcntrc was 351 in 1990 and it incrclsed to 413 in 2006. Thlna HealtbCentrc is vcry significant to reducc child monality. Thana Health Centreis the vein of rural health system. But it is a matter of sonow that ThanaHealth Cent.e has not incrased enough to meet the demand of vast ruralpeoplc. According to the World Health Repon 2m6, betw€en l99l and2001 rhere was a 250% increase in the number of private hospitals from280 to 712 iacilities whereas govemment laciliries increased by onlyl0'/.. lrom 610 to 670.
From Table-9 we can see that rhere is a negative relalion between childmortality ratc and regislered doctor. It is observed thrt reginercd doctorwas 19.340 in 1990 and it increascd ro 42.010in 2006. lt is doubledwithin lhis time. Registered doclor has very sign;ficanl role to reducechild monaliry because thcre nre no other options of M.B.B.S doctors inmost of thc villages in Bangladcsh. In the rural areas of Bansladeshmxny quack doctoF are avail blc. Thcy hNve no institutional knowledgeof moden mcdical science and thcy rrc drngcrous for ruml healthsystem. According to the World Ilcrlth Rcpon 2006, in 2l[4lhcre wcrc38485 medical doctors, 20134 rcgistered nurses. 5658 mcdicaltechnologists, 5743 public and environrnenral health wor&ers. and 46202conmunily heakh wor'{ers (CtMt in Bangladesh. Addilionally, abour72fi)O village health voluntcen (VHV) have b€en trained ro serve (he
codnunity.
Discussion
ln Bangladcsh child moriality is reducing day by day. Il is also seel lhatlife expectancy ot male children are less rhan female children. On theother hand rural arcas ofour country are facing lack ofrncdicalcare andfa.ilities. So lhc child rnodality rate is higher in these areas than nationa,and urban are:ls. An annual rale of red$lion of abour 4 is necessary toachieve thc MDG goal 4. In Bangladesh child nortality rate per thousandreached 62 in 2006 kom 151 in 1990. Bangladesh has achieved 5.24. Sothere is a grcat ch,rnce for Bangladesh 1o achieve the goal so easily.
It is obscrvcd that nalnut.ition rote is decreasing bry by day inBanglrdesh and it has a positivc rclalion wilh the reduction of childmonalily. So to achieve 'MDC gorl 4 malnutrition is rcducingmoderatcly. Female lileracy has a great impact on the child mortality.There is a negalive relalion betwecn ch;ld nonality nle lnd femalelileracy. Female literacy is doubled in last o.e and halfdecades. Female
sl rST lormri ol P!b|. Adninslralion 53SIJST JrJu'.d ol Prhli. Adm'nirrrirhn
Target and Achievement ofMDG
literacy is very significant to reduce child mortality because educatedmother can take better care oftheir child.
Coverage of immunization doses against measles irrcreased over theyears al national lc\,el. Immunization is a vital factor of reducing childmonality. There is negative .elationship beiween child nortaljry andmeasles immunization. Wilh thc inc.ease of immunization coveragethere is reduction of rate in child mortality. This was also same for theincrease ofThana Health Ccntrc and rcgistered Doctors.
Statistical Analysis
Pulting all lhe values of depcDdent and indep€ndent variables nrstatistical software SPSS, we found dr t,
Rl= 0.971
F statistic : 73.019 (Sig. =.000)
The R1 under the sludy is 0.9?1, which indicares thal rhe function 00 iscapable ofexplaining 97.Iol. of the variabilily of the child mortalily rate.The adjusted R2 indicate that 95 percent of the variation in ihe dependenlvanable in ihe study used here is explained by variations in theindependent variables- The F ratio indicates that the study significanrlyexplains the variations in child motality rate in Bangladesh.
Recomm€ndations ard Conclusion
For improv;ng the present situation following recommendations can be
. Proper coordination among rll concerned agencies (atnational and local levels).
. Create opponunities for fenale in higher education.
. Implementation ofrhe laws regarding child rnariage.
. Create ernploymenl opportonities for the women.r Ensure supply of safe water and improved sanitation.. Proper implemenhtion ofhealth poli€y.. t-esson on nutritional issues for mother and child healtb in
the cudculum.. Health literacy at grass root level.
Child mortality rate is a reflection ofthe care, health and nutrition statusof children below tfie a8e of five years and ako indicates the socio-
Nashir Uddin, C. A. A. Hossienie& C. A. A. Baki
economic and cultural prog.ess in the country. This study found thai ifwe can keep pace with reduction of child morraliry rale, we can easilyachieve MDG goal4". Child health in general has improved, rhough rheneonatal mortality .ate remains high and conrributes disproporrionarelyto overall infant mortaliry. The immunizalion proeramme has beenrecognized for its sustained high coverage; however, only 7l% of infantsare fully immunized. Measles presents an additional challenge to theimmunizalion programme with an eslirnated 20,000 children dyins fronrthe disease each year. Effons musr be intensified to ensure access 10 safeimmunizaijon and of strengthening survcillance oi all vaccine-preventablc diseases. Nowadays numbers of under weighi children arereducirg because of govemment facilitation of increasing number ofregistered doctors, norses, hospitals and Thana Health Cenlre. Sogovemment, NGOS and our developmenl painer should be more concemabout our health sector.
BBS (2001): Bangladesh Bureau of Sratisrics, Popularion Census 2001National Report (Provisional), May 2003.
BBS (2007): Bangladesh Bureau oI Statisrjcs. Reporr of Sample ViralRegislration Systern 2001 06.
MDG (2005): Millenniun Developntent Goals: Bangla.lesh ProSrcssRepon 2045. Joially ptepared by the covemmenr ofBansladesh and theUnited Nations Country Team in Bangladesh, Dhaka. l0 February 2005.
MoF (2007): Economic Review '07, Ministry ofFinance. Bangladesh.
Mwabu, Germrno (20O8): Achietiry HeaLth Millennium DevelopmentGoals (MDC|) h Afii.a: The Role oJ Natio al Health ln'uranceS.reDsr. Analytical Report Prepared for LTNECA, Addis Ababa,Ethiopia, April 7, 2008.
PFM (2005): Mlllennitrm Dewlopnent Coals: a people s prosressrepo Bdngladeth Or"nie,, September 2005. Prblished by People'sForum on MDG (PFM) in associalion with Manusher Jonno, Campaisnfor Popular Education, Social Watch Bangladesh and UnnayanShamannay.
SUST Jounal otPublic Adninistdrion SUST Jounal olPnblic Adninktnii.n
Target and Achievemenl of MDG
WHO (2005): Attainins the Millennium Developnent Goals in
Baflsladesh: How Likelr and What WiII k TakE To Reduce Powltv'
ChiLi Moftality anl Molnutition, Gendet Dispatities and to Incredse
School Enrolme t and Comptetion? ll],:rman Developrnent UDit. South
Asia Region, The World Bank, Februarv 2m5.
WHO (2007): WHO Country C.'operution StrakgJ 2008'2013, Corntrv
Office for Bangladesh, Printed in India, October 2007
Nashi Uddin. C. A. A- Hossienie& C. A. A. Baki
Annex
Table l: National Stlthtis of Child Derth (<5,.-) pe. thoGand
Acknov'ledgement: Autho^ arc ihdebted
inrernational organizarions Jor using theitaccomplishment ol this studY
to tl.iffercnt national abnvluable datu sources for
73
Srr.e. BBS (200?)i Bangladesh Bureau of Statistics, Report ofSrmple Vital Reg;stration System 200146.
Sex 2006 2005 2(n4 2OO3 2OO2 2(nlBoth Sexes(Mare and 62Female)
't8 76
'71 '78
2006 2005 2004 2003 200) 2001BothSexes(Male
'n 8l
Tablc 2; Rural and Urban Slatistics of Child Death (<5y*.) per
821468
848219
81't46959
89801l
5255556056
90838480
5358586960
7878726860
52525252
64Rural
53Urban
Male Rural 6911
49Urban
87
57Urban JI
Sorc€. BBS (2007): Bangladesb Bureau ofstatistics, Reporr of SampleVital Registration System 200146.
slJsT Joumal olPublic AdninnMlion 67 SUSTJounal of Public Adninishtiob
Tarset and Achievemenr of MDC
Table-3: Child mortality rrtc from l9m to 20(|6
NashirUddin, C. A. A. Hossienie& C. A. A. Baki
Tablc- 4: ComprrisoD bclween Morlslity Rlte and Mtlnutrition
Mortallty Rat€ (per1000)
litJ Rste Mo.tality R€ducrion Rate Undcrweisht (%)
l9go l5t 66.5t99l 57lL5t46
48681i9
84
19951992 144 2{no 5l. tt993 2005t994 l.l4 622006 471995 1251996 I t'l So!.ce-' BBS (2007): Bnngladesh Burcau of Statistics, Report of Sample,
Vihl Regisrdtion Sysrem-
Table-s: Female Literacy Rar€ of Population 15 Years ond Over,1981 ro 2001
1991 51998 ll01999 8'l 712000 8420012(n2 76 Aduli Litemcy Rate
78 lacality l99l t98l2
2004 74 Femalc Fcmalc Femal€
20{)5 68 Bangladesh 40.80 25.4 18.0
2006 62 Rural 2t5 t5.3
reducti
57.1
Sot rce. BBS (2003): Bangladesh Bureau of Statistics, Population.Census 2001 National Report (Provisional), May 2003.
Tabl€-6: Comparison betu,e€n Mortality Rate and F€lnalc's Literacy
F€male Lit€racy(%)
34.tM.O
89/17=5.24
MDC 4 will be schiev€d
At thc cnd of MDC Ycar Mortality Rate (per 1000)
t 990 r5t 24.2
Sorrc?r BBS (2007): Bangladesh Bureau ofSrarisrics, Report ofSampleVkal Registration System.
1995 125 38.r
2000 43.2
2005 68 48.0
2U)6 62 48.6
So .c?. BBS (2007 ): Bangladesh Burcau of Starisdcs, Report of SampleVital Regislration System
20n9(Projecr
ed)
SUSTJoum,l ol Pubt. Adni.ist6tionSUS_r Joumal oi Public Adminnldioi
Target and Achievemeni of MDG
Table- 7: Comparison between Morlality Rate snd 7, of MeaslesSUST Jouoal of Public AdmioistralionVol. I, No l. De.enber2008
This paper explores and illustrates the
Mortality Rate(D€r l0O0)
9, of Measles immunization
1990 151 50 GI,OBAI,IZATION AND THE THIRD WOWHO'S GETTING WEAKER? WI{O'S HA NC?
Fa.idul Alam"
1995 125
6l2005 't2682006 t362
Sor."i BBS (2007): Bangladesh Bureau ofStaiistics, Report ofSampleVital Registration Syslcm
Table- 8: Comparison b€tween Mortaliiy Rate and Thana Hcalth
Mortality(per 1000)
Rat€ Thana Herlrh cent'.e
Third World. specifically thc cficcts oy'state audrority and economy.Doe. globali/drion empo$er rlr qah l. s,ll as hrlping our rhe sr.re roregulate its economies? Or is
economies? Globalization is aSome speculare iI will di the world- others belicve it willintegrare. Ir is srill quite hard t about globalization whether it
of globalization in the
a threar to the state and its
rq90 l5l i5l but dynamic phenomenon.
1995 165125
402842000406682005
622(n6 413
globalization is playing an importantcatalytic role, however. has been profoundly debated as it isciaimed thar globali weakened the state power in the Third
is good or bad. It seerN
world. The paper that there is no way to stay away fromglobalization, however^ strong ecoromic regulatory framework and,ound polirico. sociy' selrings i" crucial ro deJl wrrh globalizarion.
Source: MoF (2007): Eco onic Reriew 07 d d BBS (200?)lBangladesh Bureau of Statislics, Rcport of Sarnple Vital RegistrationSystem.
Table- 9: Comparison betw€en Mortality Rate and R€gisa€red
Morlslitv Rate (pcr 1000) Resist€red Doctor1990 151 19,340
Orherwise. the role 9{,rdre qould noliceabl) dininish
Globalizalio probably one of the most highly 'used' or/and 'abused'opmcnt literature, especially in the Third World context. It
enioyed a 'meteori€' dse as a focus for debate in academiain the real world (Waters, 1995)- Kisgundu (200211) ishtlys: "it (globalizatio.) is used extensively and evokes strong
1995 125 23,805842000 30 R64
2005 40,2102006 42.01o
Sowce: MoF (2007): Econonic Re|kt', 07 .,,./ BBS (2007):Bangladesh Bureau of Statistics, Report of Sample Vital RegistrationSyslelrl
P.ofesso/, Dept. of Public A.lhi isttdtion, Universitr oJChitasone,
62
Banstadesh, E-nait: hunatunb tbut@hot ait.con
tact rct, Depl. of tnternatiandl R.lalions, Univ.^iry of ChitaBons,nhranp, Bahpladesh, E ,tuil: nfulka@yohoo-coh
SITST I. mrl.lP,'hli. Adninistsrinn 66SIIST Jormrl olPubli. AdminMation