Summary of the Recommendations on Sexual Dysfunctions in Women
17
REPORT Summary of the Recommendations on Sexual Dysfunctions in MenFrancesco Montorsi, MD,* Ganesan Adaikan, MD, † Edgardo Becher, MD, ‡ Francois Giuliano, MD, PhD, § Saad Khoury, MD, ¶ Tom F. Lue, MD,** Ira Sharlip, MD,** Stanley E. Althof, PhD, †† Karl-Eric Andersson, PhD, ‡‡ Gerald Brock, MD, §§ Gregory Broderick, MD, ¶¶ Arthur Burnett, MD,*** Jacques Buvat, MD, ††† John Dean, MD, ‡‡‡ Craig Donatucci, MD, §§§ Ian Eardley, MD, ¶¶¶ Kerstin S. Fugl-Meyer, PhD,**** Irwin Goldstein, MD, †††† Geoff Hackett, MD, ‡‡‡‡ Dimitris Hatzichristou, MD, §§§§ Wayne Hellstrom, MD, ¶¶¶¶ Luca Incrocci, MD,***** Graham Jackson, MD, ††††† Ates Kadioglu, MD, ‡‡‡‡‡ Laurence Levine, MD, §§§§§ Ronald W. Lewis, MD, ¶¶¶¶¶ Mario Maggi, MD,****** Marita McCabe, PhD, †††††† Chris G. McMahon, MD, ‡‡‡‡‡‡ Drogo Montague, MD, §§§§§§ Piero Montorsi, MD, ¶¶¶¶¶¶ John Mulhall, MD,******* Jim Pfaus, PhD, ††††††† Hartmut Porst, MD, ‡‡‡‡‡‡‡ David Ralph, MD, §§§§§§§ Raymond Rosen, PhD, ¶¶¶¶¶¶¶ David Rowland, MD,******** Hossein Sadeghi-Nejad, MD, †††††††† Ridwan Shabsigh, MD, ‡‡‡‡‡‡‡‡ Christian Stief, MD, §§§§§§§§ Yoram Vardi, MD, ¶¶¶¶¶¶¶¶ Kim Wallen, PhD,********* and Marlene Wasserman, MD ††††††††† *Department of Urology, San Raffaele Hospital, Milan, Italy; † National University of Singapore Department of Obstetrics and Gynaecology, Singapore; ‡ Division of Urology, University of Buenos Aires. Buenos Aires, Argentina; § Raymond Poincare Hospital, Department of Neurouroandrology Garches, Garches, France; ¶ Department of Urology, Hopital de la Pitié, Paris, France; **University of California, San Francisco, Department of Urology San Francisco, CA, USA; †† University of Miami School of Medicine Psychiatry, West Palm Beach, FL, USA; ‡‡ Wake Forest Institute for Regenerative Medicine, Winston-Salem, NC, USA; §§ Department of Surgery, University of Western Ontario, London, Ontario, Canada; ¶¶ Department of Urology, Mayo Clinic of Jacksonville, Jacksonville, Florida, USA; ***Department of Urology, Johns Hopkins University, Baltimore, MD, USA; ††† CETPARP, LeGrand Hunier, Lille, France; ‡‡‡ Court Gate House, Harbourneford—South Brent, UK; §§§ Department of Urology, Duke University, Durham, NC, USA; ¶¶¶ Spire Leeds Hospital, Leeds, UK; ****Centre for Andrology & Sexual Medicine Department of Medicine Karolinska University Hospital, Huddinge, Stockholm, Sweden; †††† Department of Sexual Medicine, Alvarado Hospital, San Diego, CA, USA; ‡‡‡‡ Holly Cottage Clinic, Lichfield, UK; §§§§ 2nd Department of Urology, Papageorgiou General Hospital and Center for the Study of Prostate Diseases (CSPD), Aristotle University of Thessaloniki, Thessaloniki, Greece; ¶¶¶¶ Tulane University, Urology Department, New Orleans, LA, USA; *****Erasmus MC Department of Radiation Oncology, Rotterdam, the Netherlands; ††††† Department of Cardiology, London Bridge Hospital Cardiology, London, United Kingdom; ‡‡‡‡‡ Department of Urology, University of Istanbul Urology, Istanbul, Turkey; §§§§§ Department of Urology, Rush University Medical Center, Chicago, IL, USA; ¶¶¶¶¶ Department of Surgery/Urology, Medical College of Georgia, Augusta, GA, USA; ******Andrology Unit University of Florence, Florence, Italy; †††††† Department of Psychology, Deakin University, Burwood, Australia; ‡‡‡‡‡‡ Australian Centre for Sexual Health, Sydney, Australia; §§§§§§ Glickman Urological and Kidney Institute, Cleveland Clinic, Cleveland, OH, USA; ¶¶¶¶¶¶ University of Milan, Department of Cardiovascular Sciences, Centro Cardiologio Monzino, IRCCS, Milan, Italy; *******Department of Urology/Sexual Medicine, Memorial Sloan-Kettering Cancer Center, New York, NY, USA; ††††††† Concordia University, Department of CSBN/Psychology, Montreal, Quebec, Canada; ‡‡‡‡‡‡‡ Private Practice for Urology and Andrology, Hamburg, Germany; §§§§§§§ Department of Urology, St Peter Andrology Centre, London, UK; ¶¶¶¶¶¶¶ New England Research Institutes, Watertown, MA, USA; ********Valparaiso University Graduate School, Valparaiso, IN, USA; †††††††† Department of Urology, UMDNJ—Hackensack, Hackensack, NJ, USA; ‡‡‡‡‡‡‡‡ Department of Urology, Maimonides Medical Center, Brooklyn, NY, USA; §§§§§§§§ Department of Urology, Klinikum Universitat Munchen, Munich, Germany; ¶¶¶¶¶¶¶¶ Department of Neuro Urology, Rambam Health Care Campus, Haifa, Israel; *********Department of Psychology, Emory University, Atlanta, GA, USA; ††††††††† Sexual Health Centre, Sea Point Cape Town, South Africa DOI: 10.1111/j.1743-6109.2010.02062.x ABSTRACT Introduction. Sexual health is an integral part of overall health. Sexual dysfunction can have a major impact on quality of life and psychosocial and emotional well-being. Aim. To provide evidence-based, expert-opinion consensus guidelines for clinical management of sexual dysfunc- tion in men. 3572 J Sex Med 2010;7:3572–3588 © 2010 International Society for Sexual Medicine
-
Upload
independent -
Category
Documents
-
view
4 -
download
0
Transcript of Summary of the Recommendations on Sexual Dysfunctions in Women
REPORT
Summary of the Recommendations on Sexual Dysfunctionsin Menjsm_2062 3572..3588
Francesco Montorsi, MD,* Ganesan Adaikan, MD,† Edgardo Becher, MD,‡
Francois Giuliano, MD, PhD,§ Saad Khoury, MD,¶ Tom F. Lue, MD,** Ira Sharlip, MD,**Stanley E. Althof, PhD,†† Karl-Eric Andersson, PhD,‡‡ Gerald Brock, MD,§§ Gregory Broderick, MD,¶¶
Arthur Burnett, MD,*** Jacques Buvat, MD,††† John Dean, MD,‡‡‡ Craig Donatucci, MD,§§§
Ian Eardley, MD,¶¶¶ Kerstin S. Fugl-Meyer, PhD,**** Irwin Goldstein, MD,†††† Geoff Hackett, MD,‡‡‡‡
Dimitris Hatzichristou, MD,§§§§ Wayne Hellstrom, MD,¶¶¶¶ Luca Incrocci, MD,*****Graham Jackson, MD,††††† Ates Kadioglu, MD,‡‡‡‡‡ Laurence Levine, MD,§§§§§ Ronald W. Lewis, MD,¶¶¶¶¶
Mario Maggi, MD,****** Marita McCabe, PhD,†††††† Chris G. McMahon, MD,‡‡‡‡‡‡
Drogo Montague, MD,§§§§§§ Piero Montorsi, MD,¶¶¶¶¶¶ John Mulhall, MD,******* Jim Pfaus, PhD,†††††††
Hartmut Porst, MD,‡‡‡‡‡‡‡ David Ralph, MD,§§§§§§§ Raymond Rosen, PhD,¶¶¶¶¶¶¶
David Rowland, MD,******** Hossein Sadeghi-Nejad, MD,†††††††† Ridwan Shabsigh, MD,‡‡‡‡‡‡‡‡
Christian Stief, MD,§§§§§§§§ Yoram Vardi, MD,¶¶¶¶¶¶¶¶ Kim Wallen, PhD,********* andMarlene Wasserman, MD†††††††††
*Department of Urology, San Raffaele Hospital, Milan, Italy; †National University of Singapore Department of Obstetricsand Gynaecology, Singapore; ‡Division of Urology, University of Buenos Aires. Buenos Aires, Argentina; §RaymondPoincare Hospital, Department of Neurouroandrology Garches, Garches, France; ¶Department of Urology, Hopital de laPitié, Paris, France; **University of California, San Francisco, Department of Urology San Francisco, CA, USA;††University of Miami School of Medicine Psychiatry, West Palm Beach, FL, USA; ‡‡Wake Forest Institute for RegenerativeMedicine, Winston-Salem, NC, USA; §§Department of Surgery, University of Western Ontario, London, Ontario, Canada;¶¶Department of Urology, Mayo Clinic of Jacksonville, Jacksonville, Florida, USA; ***Department of Urology, JohnsHopkins University, Baltimore, MD, USA; †††CETPARP, Le Grand Hunier, Lille, France; ‡‡‡Court Gate House,Harbourneford—South Brent, UK; §§§Department of Urology, Duke University, Durham, NC, USA; ¶¶¶Spire Leeds Hospital,Leeds, UK; ****Centre for Andrology & Sexual Medicine Department of Medicine Karolinska University Hospital,Huddinge, Stockholm, Sweden; ††††Department of Sexual Medicine, Alvarado Hospital, San Diego, CA, USA; ‡‡‡‡HollyCottage Clinic, Lichfield, UK; §§§§2nd Department of Urology, Papageorgiou General Hospital and Center for the Study ofProstate Diseases (CSPD), Aristotle University of Thessaloniki, Thessaloniki, Greece; ¶¶¶¶Tulane University, UrologyDepartment, New Orleans, LA, USA; *****Erasmus MC Department of Radiation Oncology, Rotterdam, the Netherlands;†††††Department of Cardiology, London Bridge Hospital Cardiology, London, United Kingdom; ‡‡‡‡‡Department of Urology,University of Istanbul Urology, Istanbul, Turkey; §§§§§Department of Urology, Rush University Medical Center, Chicago, IL,USA; ¶¶¶¶¶Department of Surgery/Urology, Medical College of Georgia, Augusta, GA, USA; ******Andrology UnitUniversity of Florence, Florence, Italy; ††††††Department of Psychology, Deakin University, Burwood, Australia;‡‡‡‡‡‡Australian Centre for Sexual Health, Sydney, Australia; §§§§§§Glickman Urological and Kidney Institute, ClevelandClinic, Cleveland, OH, USA; ¶¶¶¶¶¶University of Milan, Department of Cardiovascular Sciences, Centro CardiologioMonzino, IRCCS, Milan, Italy; *******Department of Urology/Sexual Medicine, Memorial Sloan-Kettering Cancer Center,New York, NY, USA; †††††††Concordia University, Department of CSBN/Psychology, Montreal, Quebec, Canada;‡‡‡‡‡‡‡Private Practice for Urology and Andrology, Hamburg, Germany; §§§§§§§Department of Urology, St Peter AndrologyCentre, London, UK; ¶¶¶¶¶¶¶New England Research Institutes, Watertown, MA, USA; ********Valparaiso UniversityGraduate School, Valparaiso, IN, USA; ††††††††Department of Urology, UMDNJ—Hackensack, Hackensack, NJ, USA;‡‡‡‡‡‡‡‡Department of Urology, Maimonides Medical Center, Brooklyn, NY, USA; §§§§§§§§Department of Urology, KlinikumUniversitat Munchen, Munich, Germany; ¶¶¶¶¶¶¶¶Department of Neuro Urology, Rambam Health Care Campus, Haifa,Israel; *********Department of Psychology, Emory University, Atlanta, GA, USA; †††††††††Sexual Health Centre, Sea PointCape Town, South Africa
DOI: 10.1111/j.1743-6109.2010.02062.x
A B S T R A C T
Introduction. Sexual health is an integral part of overall health. Sexual dysfunction can have a major impact onquality of life and psychosocial and emotional well-being.Aim. To provide evidence-based, expert-opinion consensus guidelines for clinical management of sexual dysfunc-tion in men.
3572
J Sex Med 2010;7:3572–3588 © 2010 International Society for Sexual Medicine

Methods. An international consultation collaborating with major urologic and sexual medicine societies convened inParis, July 2009. More than 190 multidisciplinary experts from 33 countries were assembled into 25 consultationcommittees. Committee members established scope and objectives for each chapter. Following an exhaustive reviewof available data and publications, committees developed evidence-based guidelines in each area.Main Outcome Measures. New algorithms and guidelines for assessment and treatment of sexual dysfunctions weredeveloped based on work of previous consultations and evidence from scientific literature published from 2003 to2009. The Oxford system of evidence-based review was systematically applied. Expert opinion was based onsystematic grading of medical literature, and cultural and ethical considerations.Results. Algorithms, recommendations, and guidelines for sexual dysfunction in men are presented. These guide-lines were developed in an evidence-based, patient-centered, multidisciplinary manner. It was felt that all sexualdysfunctions should be evaluated and managed following a uniform strategy, thus the International Consultation ofSexual Medicine (ICSM-5) developed a stepwise diagnostic and treatment algorithm for sexual dysfunction. Themain goal of ICSM-5 is to unmask the underlying etiology and/or indicate appropriate treatment options accordingto men’s and women’s individual needs (patient-centered medicine) using the best available data from population-based research (evidence-based medicine). Specific evaluation, treatment guidelines, and algorithms were developedfor every sexual dysfunction in men, including erectile dysfunction; disorders of libido, orgasm, and ejaculation;Peyronie’s disease; and priapism.Conclusions. Sexual dysfunction in men represents a group of common medical conditions that need to be managedfrom a multidisciplinary perspective. Montorsi F, Adaikan G, Becher E, Giuliano F, Khoury S, Lue TF, SharlipI, Althof SE, Andersson K-E, Brock G, Broderick G, Burnett A, Buvat J, Dean J, Donatucci C, Eardley I,Fugl-Meyer KS, Goldstein I, Hackett G, Hatzichristou D, Hellstrom W, Incrocci L, Jackson G, Kadioglu A,Levine L, Lewis RW, Maggi M, McCabe M, McMahon CG, Montague D, Montorsi P, Mulhall J, Pfaus J, PorstH, Ralph D, Rosen R, Rowland D, Sadeghi-Nejad H, Shabsigh R, Stief C, Vardi Y, Wallen K, and WassermanM. Summary of the recommendations on sexual dysfunctions in men. J Sex Med 2010;7:3572–3588.
Key Words. Erectile Dysfunction; Testosterone; Premature Ejaculation; Delayed Ejaculation; Peyronie’s Disease;Priapism; Prostate Cancer; Radical Prostatectomy; Guidelines
Introduction
T he 2009 International Consultation onSexual Dysfunctions was convened in Paris
in 2009. It identified the following fundamentalconcepts as the basis for the management of sexualdysfunctions in men and women:
• Sexual health is an integral part of overallhealth.
• Healthcare providers should seek, receive, andimpart information related to sexuality. Indi-viduals have the right to receive the highestattainable standard of sexual health, includingaccess to sexual and reproductive healthcare ser-vices, as a fundamental sexual right.
• Sexual dysfunctions can have a major impact onquality of life (QoL) as well as psychosocial andemotional well-being.
• The three principles for clinical evaluation andmanagement of sexual dysfunctions are (i) adop-tion of a patient-centered framework, with anemphasis on cultural competence in medicalpractice; (ii) application of evidence-basedmedicine in diagnostic and treatment planning;
and (iii) use of a unified management approachin evaluating and treating sexual problems inboth men and women.
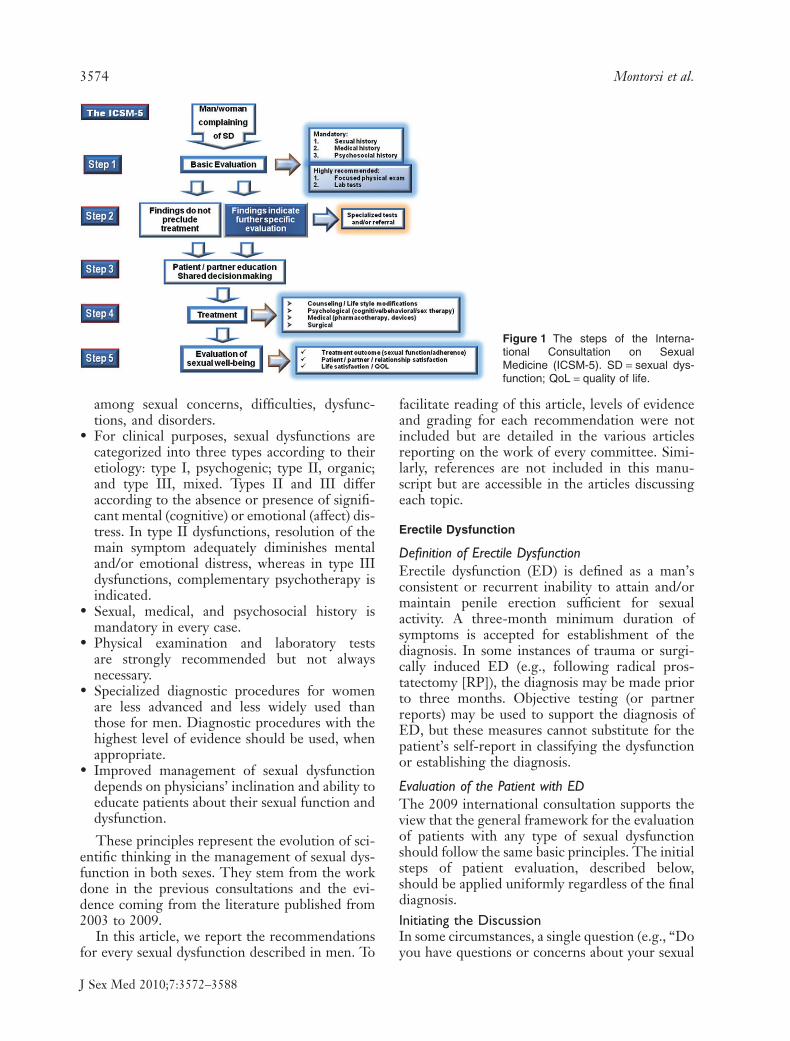
• Sexual dysfunctions are essentially self-reportedconditions. Therefore, diagnostic tests or pro-cedures should not be recommended withoutcontrolled clinical data or research-based evi-dence supporting their use. The InternationalConsultation of Sexual Medicine (ICSM-5(Figure 1) is a stepwise diagnostic and treatmentalgorithm for sexual dysfunction in men andwomen. The main goal of the ICSM-5 is tounmask the underlying etiology and/or to indi-cate appropriate treatment options according tomen’s and women’s individual needs (patient-centered medicine) using the best available datafrom population-based research (evidence-based medicine).
• Ignorance and knowledge gaps about sexualfunction and dysfunction are commonplace.Misinformation or myths may lead touninformed sexual decisions with seriousconsequences. During the initial phase ofassessment, physicians must discriminate
Summary of the Recommendations on Sexual Dysfunctions in Men 3573
J Sex Med 2010;7:3572–3588
among sexual concerns, difficulties, dysfunc-tions, and disorders.
• For clinical purposes, sexual dysfunctions arecategorized into three types according to theiretiology: type I, psychogenic; type II, organic;and type III, mixed. Types II and III differaccording to the absence or presence of signifi-cant mental (cognitive) or emotional (affect) dis-tress. In type II dysfunctions, resolution of themain symptom adequately diminishes mentaland/or emotional distress, whereas in type IIIdysfunctions, complementary psychotherapy isindicated.
• Sexual, medical, and psychosocial history ismandatory in every case.
• Physical examination and laboratory testsare strongly recommended but not alwaysnecessary.
• Specialized diagnostic procedures for womenare less advanced and less widely used thanthose for men. Diagnostic procedures with thehighest level of evidence should be used, whenappropriate.
• Improved management of sexual dysfunctiondepends on physicians’ inclination and ability toeducate patients about their sexual function anddysfunction.
These principles represent the evolution of sci-entific thinking in the management of sexual dys-function in both sexes. They stem from the workdone in the previous consultations and the evi-dence coming from the literature published from2003 to 2009.
In this article, we report the recommendationsfor every sexual dysfunction described in men. To
facilitate reading of this article, levels of evidenceand grading for each recommendation were notincluded but are detailed in the various articlesreporting on the work of every committee. Simi-larly, references are not included in this manu-script but are accessible in the articles discussingeach topic.
Erectile Dysfunction
Definition of Erectile DysfunctionErectile dysfunction (ED) is defined as a man’sconsistent or recurrent inability to attain and/ormaintain penile erection sufficient for sexualactivity. A three-month minimum duration ofsymptoms is accepted for establishment of thediagnosis. In some instances of trauma or surgi-cally induced ED (e.g., following radical pros-tatectomy [RP]), the diagnosis may be made priorto three months. Objective testing (or partnerreports) may be used to support the diagnosis ofED, but these measures cannot substitute for thepatient’s self-report in classifying the dysfunctionor establishing the diagnosis.
Evaluation of the Patient with EDThe 2009 international consultation supports theview that the general framework for the evaluationof patients with any type of sexual dysfunctionshould follow the same basic principles. The initialsteps of patient evaluation, described below,should be applied uniformly regardless of the finaldiagnosis.Initiating the DiscussionIn some circumstances, a single question (e.g., “Doyou have questions or concerns about your sexual
Figure 1 The steps of the Interna-tional Consultation on SexualMedicine (ICSM-5). SD = sexual dys-function; QoL = quality of life.
3574 Montorsi et al.
J Sex Med 2010;7:3572–3588

functioning?”) may be sufficient to clarify thepatient’s primary issue; in other situations, a seriesof questions is indicated. Sexual inquiry is mostoften conducted in a face-to-face interview withthe patient, although paper-and-pencil question-naires or Internet-based methods may be of value.The style or manner in which sexual inquiry isconducted is important: It should reflect a highlevel of sensitivity and regard for each individual’sunique ethnic, cultural, and personal background.
The aim of taking a sexual history should beascertaining the severity, onset, and duration of theproblem as well as the presence of concomitantmedical or psychosocial factors. It is necessary todetermine whether the presenting complaint (e.g.,ED, anorgasmia) is the primary or major sexualproblem or if some other aspect of the sexualresponse cycle (desire, ejaculation, orgasm) isinvolved. Other sexual problems may exist as con-comitant disorders (e.g., hypoactive sexual desire)or as secondary disorders to the primary sexualcomplaint.
The medical and sexual history is essential andfrequently the most revealing aspect of the assess-ment process. A comprehensive sexual history isessential in confirming the patient’s diagnosis aswell as in the evaluation of the patient’s overallsexual function. Questions apply specifically to theevaluation of male arousal, desire, and orgasm/ejaculation difficulties. In principle, these ques-tions can be addressed to all patients presentingwith sexual difficulties.
Medical HistoryAlthough not always definitive, a detailed medicalhistory may provide suggestive evidence for oragainst the role of specific organic or psychogenicfactors and should be obtained in all cases of sexualdysfunction. Documenting a medical history hasseveral goals. First, the physician must evaluate thepotential role of underlying or comorbid medicalconditions. Sexual dysfunction may be symptom-atic of an underlying medical disorder, such asatherosclerosis or diabetes. Second, the physicianmust actively investigate the possible associationwith cardiovascular conditions to differentiateamong potential organic and psychogenic causesin the etiology of a patient’s sexual problem.Third, the history helps the physician assess theuse of concomitant medications. Some of thesemedications can either cause or contribute to thepatient’s sexual difficulties, and a change in medi-cation may result in an improvement in sexualfunction. Additionally, the use of certain medica-
tions may be important contraindications for spe-cific treatments. Medical history may include allmedical conditions that could interfere with sexualfunction.
Psychosocial HistoryPotential etiologies for sexual dysfunction includea wide range of organic and medical factors, butmultiple psychological or interpersonal factors(e.g., anxiety, depression, relationship distress) canalso be causes. A detailed psychosocial assessmentis essential in every case of sexual dysfunction.Given the interpersonal context of sexual prob-lems in men and women, the physician shouldcarefully assess past and present partner relation-ships. Sexual dysfunction may affect the patient’sself-esteem and coping ability as well as his or hersocial relationships and occupational performance.These aspects should be assessed in each case.
The physician should not assume that everypatient is involved in a monogamous, heterosexualrelationship. For this reason, it is advisable to beginthe history with broad questions: “Are you sexuallyactive at the moment?,” “Do you have a regular sexpartner?” Then ask a follow-up question, such as,“Is this a same-sex or opposite-sex relationship?”The early stages in the development of a problemare often of crucial significance to assessment andtreatment. Were there particular times of change inthe sexual relationship? If so, what events occurredin the patient’s life at those times? In addition, thephysician should ask questions about other relevantaspects of the patient’s life, including interpersonalrelationships, occupational status, financial secu-rity, family life, and social support.
Physical ExaminationThe etiology or causal factors for sexual dysfunc-tion may or may not be apparent from the patient’shistory alone. In specific sexual dysfunctions (e.g.,anatomic problems, ED), further investigation bymeans of a physical examination and selected labo-ratory testing may be of value in confirming orruling out specific etiologies or comorbidities. Inmost cases, the physical examination will not iden-tify the specific etiology or cause of sexual dysfunc-tion; however, a focused physical examination isstrongly recommended. This examination shouldinclude a general screening for medical risk factorsor comorbidities that are associated with sexualdysfunction, such as body habitus (secondarysexual characteristics) and assessment of the car-diovascular, neurologic, and genital systems, withparticular focus on the genitalia and secondary sexcharacteristics.
Summary of the Recommendations on Sexual Dysfunctions in Men 3575
J Sex Med 2010;7:3572–3588

The physical examination may corroborateaspects of the medical history and can sometimesreveal unsuspected physical findings (e.g.,decreased peripheral pulses, hypertension, atrophictestes, penile plaque). In addition to identifyingspecific etiologies or comorbidities, the physicalexamination may provide an opportunity to informthe patient about aspects of his sexual anatomy orphysiology as well as to provide reassurance aboutbody appearance and function. It should be recog-nized that the physical examination can also be asource of shame, embarrassment, or discomfortfor many patients. Every effort should be made toensure the patient’s privacy, confidentiality, andpersonal comfort during the examination.
The physician should always review the majorfindings of the examination and should address anyquestions or concerns of the patient regarding hisphysical appearance or normality. In some set-tings, it may be advisable for the physician toperform the physical examination in the presenceof a nurse or chaperone.
Laboratory TestingRecommended laboratory tests for men withsexual problems typically include fasting glucose,cholesterol, lipids, and a hormone profile. As withthe physical examination, these tests are per-formed primarily to identify or confirm specificetiologies (e.g., hypogonadism) or to assess therole of potential medical comorbidities or con-comitant illnesses (e.g., diabetes, hyperlipidemia).Additional laboratory tests (e.g., thyroid function)may be performed at the physician’s discretionbased on the patient’s medical history and the phy-sician’s judgment.
Specialized Testing for EDThe classical specialized tests—with the exceptionof pharmaco-penile duplex ultrasound and mea-surements of nocturnal penile tumescence orsleep-related erections—are not equipped to spe-cifically and accurately assess cavernosal neuro-endothelial function. On the contrary, these testsfrequently do not add to data already availablefrom the medical history and assessments based onpatient self-report (e.g., self-administered ques-tionnaires, event logs, patient diaries), physicalexamination, and laboratory testing. At best, theytypically confirm an expected diagnosis. Moreover,these tests are expensive, time-consuming, inva-sive, prone to complications (prolonged erections),and rarely conclusive except in experienced hands.A thorough description of the available specialized
test can be found in the chapter devoted to theevaluation of patients with ED.
Treatment of EDPsychological Treatment for EDPsycho-sexologic literature has made an importantcontribution to the description, etiology, and diag-nosis of ED, but large, randomized, and controlledstudies demonstrating the efficacy of the psycho-therapeutic treatment are lacking. Psychologicaltreatment of ED consists of a variety of interven-tions, including psychodynamic interpretationsregarding transference or anxiety, systematicdesensitization, sensate focus, couples therapy,behavioral assignments, sex education, communi-cation and sexual skills training, and masturbationexercises. It is not clear which of these interventionsin combination or alone has the greatest efficacy.
Clinical experience highlights that these inter-ventions help the patient and/or couple to improvetheir relationship and sexual life. Men withacquired ED demonstrated more gains than menwith lifelong ED. Four goals of psychotherapy forED have been described:
• Reduce or eliminate performance anxiety.• Understand the context in which men or a
couple make love.• Implement psycho-education and modification
of sexual scripts.• Identify and reduce resistance to premature dis-
continuation of pharmacotherapy.
Medical Treatment for EDOral Agents. Medical treatment for ED has beenrevolutionized by the advent of phosphodiesterasetype 5 (PDE5) inhibitors (PDE5-Is), which virtu-ally represent the unique form of oral treatmentfor ED. A chapter is completely devoted to dis-cussing all medical therapies for ED, and wereport only the final recommendations issued bythe responsible committee.
The reason for the clinical efficacy of PDE5-Isis easily understood by considering their effect onthe physiology of smooth muscle relaxation. Insummary, the normal pathway for penile erectionis initiated by sexual arousal, which stimulatesrelease of nitric oxide (NO) at nerve endings in thepenis (Figure 2). Another source of NO is vascularendothelial cells. NO diffuses into vascular smoothmuscle cells in the penile corpus cavernosum tocause stimulation of guanylyl cyclase and elevationof cyclic guanosine monophosphate (cGMP) inthese cells. This process leads to activation of
3576 Montorsi et al.
J Sex Med 2010;7:3572–3588

cGMP-dependent protein kinase G (PKG), phos-phorylation of several proteins, and either lower-ing of cell calcium or reducing sensitivity tocalcium, finally resulting in smooth muscle relax-ation. The increased accumulation of blood in thecorpus cavernosum caused by this relaxation isthe underlying basis for penile erection.
Lack of proper cGMP elevation could be theresult (at least in part) of insufficient release of NOfrom nerve endings or endothelium. PDE5-Isenhance erectile function during sexual stimula-tion by penetrating into smooth muscle cells andinhibiting PDE5, which is an enzyme thatdegrades cGMP. This results in decreased degra-dation of cGMP, which maintains higher cellularlevels of cGMP in both corpus cavernosum andthe vessels supplying it. This decreased degrada-tion increases relaxation of the smooth muscle,which dilates the corporeal sinusoids, resulting inincreased blood flow and allowing an erectionto occur. The pathway shown in Figure 2 maynot work properly if the cGMP level in corpus
cavernosum smooth muscle cells is not elevatedsufficiently or if relaxation of smooth muscle in thetissue is deficient or incomplete.
In most countries, the PDE5-Is are the initialform of pharmacotherapy for men with ED. Threesuch drugs—sildenafil, tadalafil, and vardenafil—are licensed for use around the world. A number ofother PDE-Is are available in a few countries(udenafil, mirodenafil), and still others (avanafil,lodenafil, SLx-2101) are currently under develop-ment (Table 1).
There is robust evidence that PDE5-Is areeffective, safe, and well-tolerated therapies for thetreatment of men with ED. Most currently avail-able evidence relates to sildenafil, tadalafil, andvardenafil. PDE5-Is are the first-line therapy formost men with ED who do not have a specificcontraindication to their use. There is no evidenceof significant differences in efficacy, safety, or tol-erability among the PDE5-Is, but it is importantto recognize that patients who are using nitratescannot use PDE5-Is at the same time.
Figure 2 Regulation of penile corpuscavernosum smooth muscle relaxationand effect of phosphodiesterase type 5inhibitors. GTP = guanosine triphos-phate; cGMP = cyclic guanosinemonophosphate; PKG = proteinkinase G; ATP = adenosine triphos-phate; ADP = adenosine diphosphate;PDE5 = phosphodiesterase type 5.
Neurons or Endothelium
ATP
ADP
Nitric Oxide
GuanylylCyclase
PKGcGMPSLOW
5’-GMP
Protein
Protein P
Lower Ca2+
Relaxation of Smooth MuscleOther Effects
PDE5
PDE5 Inhibitor
inhibition
ATP
ADP
GTP
FAST
Table 1 Pharmacokinetics of the phosphodiesterase type 5 inhibitors
ParameterTadalafil,20 mg
Sildenafil,100 mg
Vardenafil,20 mg
Udenafil,100 mg SLx-2101
Avanafil,100 mg
Mirodenafil,100 mg
Lodenafil,160 mg
Cmax, ng/mL 378 450 20.9 416.2 No data No data No data 157Tmax, h 2 0.8 0.7–0.9 1.1.5 1 0.5–1.5 1.25 1.2T1/2, h 17.5 3–5 4–5 11–13 9–14 <1.5 2.5 2.4Bioavailability — 40% 14.5% — — — — —
Cmax = maximum plasma concentration; Tmax = time to maximum plasma concentration.
Summary of the Recommendations on Sexual Dysfunctions in Men 3577
J Sex Med 2010;7:3572–3588

Local Therapies. The dawn of the age of pharma-cologic treatment began 25 years ago with therecognition that vasoactive drugs, when injectedinto the penile erectile tissue, were capable ofinitiating and maintaining erection. Currently,alprostadil, papaverine, and the combinationphentolamine plus vasoactive intestinal polypep-tide are the main licensed agents for intracavern-osal injection (ICI) therapy. Alprostadil is alsoavailable as an intraurethral suppository.
Both ICI and intraurethral therapy with alpros-tadil are effective and well-tolerated treatments formen with ED. It is recognized that the intraure-thral route of administration is less effective thanthe intracavernosal route. Local therapies are con-sidered second-line therapy and should be consid-ered in patients in whom PDE5-Is are not effectiveand in men who have contraindications to theiruse. ICIs should not be used in men withconditions that predispose them to priapism—most notably, men with sickle cell disease, multi-ple myeloma, and leukemia. Anticoagulation,however, is not a contraindication to ICI.
Vacuum Constriction DevicesVacuum constriction devices (VCD) are ED treat-ment devices that use negative pressure to engorgethe penis with blood while constriction rings arti-ficially trap blood in the penis. VCDs are a safeand effective form of therapy for men with ED.The British Society for Sexual Medicine Guide-lines, an evidence-based guideline for the diagno-sis and treatment of ED, concluded that oralpharmacotherapy with PDE5-Is and VCDs are thefirst-line therapy for ED. However, one has torecognize that a number of studies have reportedthat erections obtained with a VCD are unnaturaland therefore are distinctly different from physi-ological erections. The most common VCD sideeffects are painful ejaculation, inability to ejacu-late, generalized pain, petechiae, bruising, andnumbness.
Serious complications from VCD use are rarebut include penile skin necrosis, urethral varicosi-ties, capture of scrotal tissues within the penileshaft, development of Peyronie’s disease, andFournier’s gangrene The importance of properpatient selection improves outcome results, asconfirmed by the experience of a number ofauthors. VCDs may be offered preferentially toelderly patients who partake in limited intercourseattempts versus younger patients, who documentlower preference for VCDs because of unnaturalerections and cumbersome application.
Surgical Treatment for EDArterial Revascularization. Many retrospectivestudies report outcome data for penile revascular-ization surgery for arteriogenic ED. These studiesare limited by variable inclusion and exclusion cri-teria, short length of follow-up, and lack ofobjective follow-up data. Young men who havesustained traumatic arterial lesions appear to havebetter outcomes compared to elderly patients.
No comparative prospective, randomizedstudies have assessed the outcome of penile revas-cularization surgery for arteriogenic ED. Based onthe evidence within the literature, this surgery maybe offered to men younger than 55 years of agewho are nonsmokers and nondiabetic, who haveno evidence of venous leakage, and who demon-strate an isolated stenosis of the internal pudendalartery.
Surgery for Cavernous Veno-Occlusive Dysfunction.At the time of this writing, cavernous veno-occlusive dysfunction (CVOD) surgery in themanagement of ED remains controversial, and theweight of available evidence is contrary to routineuse as a treatment option for ED. CVOD surgery,as it is practiced today, does not conform to thedesiderata of good clinical practice or evidence-based medicine. The normal diagnostic values foravailable tests, universal diagnostic criteria for caseselection for surgery, and consensus on choice ofoperation in a given patient have not beenunequivocally established. This said, althoughCVOD surgery is still considered investigational,it may be offered in special situations, such as foryoung patients with site-specific congenital, post-traumatic, or postinflammatory venous leaks. IfCVOD surgery is undertaken, the physicianshould be required to follow an operated patientlong term (48 months).
Penile Prosthetic Surgery For ED. A patient wouldcurrently be considered a good candidate for apenile prosthesis if he had failed medical therapyor if medical therapy were contraindicated and theother therapies (e.g., penile injections, intraure-thral therapy, VCDs) have also failed or do notsatisfy the patient. Patients who eventually opt foran implant are usually highly motivated to con-tinue with sexual activity.
In many instances, the physician helps thepatient decide which prosthesis type to choose.This decision is usually based on the physician’scomfort with the surgical approach, assessment ofbody habitus, manual dexterity of the patient, andoverall cost. Patients with a larger penis will be
3578 Montorsi et al.
J Sex Med 2010;7:3572–3588

best served by a three-piece inflatable device, asthese devices deliver the best rigidity. Similarly,patients with shorter penises often choose thethree-piece device because semirigid rods andtwo-piece implants are more difficult to conceal.Patients with limited manual dexterity or thosewho have difficulty manipulating hydraulic devicesare directed toward a semirigid rod. An exceptionto this rule is when a motivated partner manipu-lates the hydraulic device for the patient.
It is important for the patient receiving a three-piece inflatable implant to understand that thepostimplant size of his penis will invariably beslightly shorter than his natural erection when hewas fully potent. Also, unlike a normal erection,the prosthetic erection does not result in anincrease in the size of the glans. Preoperative con-sultation with the implant candidate shouldexplain this loss of length but emphasize that thegirth of the penis may be greater than a naturalerection and that girth, not length, is responsiblefor penile rigidity.
Sensitivity of the penis, ejaculatory abilities, andsexual drive are for the most part unchanged fol-lowing placement of a prosthesis. The patientneeds to clearly understand that penile implantsonly restore the ability to penetrate. They do notrestore any special sensitivity or sexual drive thatmay have been present in earlier years. If the cyl-inders are removed at a later date, the capsuleremains, and the empty space will partially fill withproliferating scar tissue. This may make it difficultfor the patient to respond adequately to othertreatments, such as medication or a VCD.
It is important that the patient have realisticexpectations for his penile prosthesis. Along thisline of reasoning, the patient should be informedof the following possible complications related tothe prosthesis prior to implantation: infection andits consequences, pain, mechanical failure, penileshortening, and autoinflation. Numerous studieshave shown high satisfaction rates for bothpatients and partners.
Clinical Correlates between ED and CoronaryArtery DiseaseWhen dealing with the ED patient, the followingconsiderations should be always discussed indetail: (i) ED and coronary artery disease (CAD)share the same risk factors; (ii) sexual activity forcouples in a stable relationship does not increasecardiac events; (iii) sex is not an undue stress to theheart; (iv) men with ED should have their CADrisks assessed and treated; (v) sexual activity safety
can be assessed using noninvasive stress testing;and (vi) exercise stress testing and computed coro-nary angiography can be used to detect occultCAD.
The correlation between ED and the metabolicsyndrome should also be considered with attentionand discussed with the ED patient taking the fol-lowing points into account: ED is closely linkedto the metabolic syndrome, and the metabolicsyndrome is associated with hypogonadism andreduces the effectiveness of PDE5-Is. Testosteroneshould be measured when the metabolic syndromeis present.
Clinical Correlates between Testosterone Deficiencyand EDTestosterone deficiency (TD) is a clinical and bio-chemical syndrome frequently associated with ageand comorbidities and is characterized by a defi-ciency in testosterone and relevant symptoms. Itmay affect the function of multiple organ systemsand result in significant detriment to QoL, includ-ing alterations in sexual function. The clinicalmanifestations of TD are variable. Sexual dysfunc-tion, particularly hypoactive sexual desire, ED, anddelayed ejaculation (DE) are prominent and oftenthe presenting symptoms. Visceral obesity is oftenassociated, and muscle mass and very likely bonemineral density are diminished. Diminishedstrength and alterations in spatial cognition andmood may be associated.
Physical examination is frequently unhelpful,but small testicular size, alterations in testicularconsistency and hair distribution, gynecomastia,and small prostate size can be detected. It is impor-tant to recognize that cardiovascular disease isoften associated with low testosterone. All menwith TD as well as all men over 40 years of age orthose younger with a strong family history shouldhave their cardiovascular risk factors assessed andaddressed.
Although a number of questionnaires have beenproposed to support screening for or diagnosingTD, they typically show good sensitivity but lowspecificity. The diagnosis of TD must be based onboth symptoms and serum testosterone values.Although there are no generally accepted lowerlimits of normal total testosterone (TT), thereis general agreement that TT > 12 nmol/L(3.5 ng/mL or 350 ng/dL) does not usually requiresubstitution, whereas men with TT < 8 nmol/l(2.3 ng/mL or 230 ng/dL) usually benefit fromtestosterone treatment. Between these levels, mea-suring free testosterone by equilibrium dialysis or
Summary of the Recommendations on Sexual Dysfunctions in Men 3579
J Sex Med 2010;7:3572–3588

calculating it from TT and sexual hormone-binding globulin levels may be helpful. A lowerlimit of 225 pmol/L (65 pg/mL) is accepted bymany experts.
The indication to start testosterone therapymust be based on a clear clinical picture togetherwith evidence of hypoandrogenism. Absence of anappropriate response after adequate testosteronetreatment for 3–6 months calls for further investi-gation to rule out associated comorbidities.
Current commercially available preparations oftestosterone (with the exception of the 17a-alkylated options) are safe and effective. Thetreating physician should have sufficient knowl-edge and adequate understanding of the advan-tages and drawbacks of each preparation. Finally,the patient should be given the opportunity toactively participate in the choice of testosteroneformulation. The contraindications and cautionsfor the use of testosterone remain controversial.Testosterone therapy is contraindicated in menwith clinical evidence of prostate cancer (PCa)until more evidence on safety is available; thatsaid, there is no compelling evidence that test-osterone treatment causes PCa or PCa progres-sion in noncastrated men. Men with significanterythrosis (hematocrit > 52%) or severe symp-toms of bladder outlet obstruction should not starttestosterone therapy without prior improvementin the comorbid condition.
Clinical Correlates between ED and RPIt is becoming increasingly recognized that anumber of sexual dysfunctions may occur after RP,the most commonly used treatment for clinicallylocalized PCa. These dysfunctions include ED,libido reduction, changes in orgasm, anejaculation,penile size changes, and possibly Peyronie’sdisease. These sexual dysfunctions should beextensively discussed with the patient prior tosurgery.
It is recommended that physicians use a vali-dated instrument with recognized cutoffs for nor-mality and severity in their preoperative andpostoperative evaluation of erectile function intheir patients. Physicians should discuss the recog-nized predictors of erectile function recovery:patient age, baseline erectile function, and nerve-sparing status. It should also be pointed out topatients that other factors such as comorbiditystatus and surgeon experience have been shown tobe significant contributors to recovery. Physiciansmust provide patients with a realistic time framefor recovery of erectile function.
Penile rehabilitation is defined as the use of amedication, a combination of medications, ordevices (alone or in combination with medication)in the early stages after RP. The goal of rehabili-tation is to maximize preservation of all compo-nents of the local erectile mechanism and optimizerecovery of erectile function. It is recommendedthat based on the strong animal and basic scienceevidence, understanding the strengths and weak-nesses of the existing human studies and the nega-tive consequences of long-term ED after RP,physicians should discuss with patients that penilerehabilitation has significant potential benefits forthe patient or partner and should be consideredafter RP.
No specific recommendations regarding thestructure of the optimal rehabilitation regimen canbe given. Unfortunately, numerous variablesremain undefined with regard to the ideal rehabili-tative approach. These variables include definingthe best time to start rehabilitation after RP; thefrequency of medication use, specifically dailyversus on-demand exposure, the best dosingschedule (low dose vs. maximum dose), the dura-tion of rehabilitation after its commencement, andthe strategies used (PDE5-Is, ICI, transurethralprostaglandin suppository, vacuum therapy).Unfortunately, no definitive evidence exists favor-ing one rehabilitation strategy over another.
Orgasm and Ejaculation Disorders in Men
Premature EjaculationDefinition of Premature EjaculationIn August 2007, the International Society forSexual Medicine convened a panel of experts toreview criteria for premature ejaculation (PE;Table 2). This panel proposed the followingevidence-based definition of lifelong PE: “ejacula-tion which always or nearly always occurs prior toor within about one minute of vaginal penetration,and the inability to delay ejaculation on all ornearly all vaginal penetrations, and negative per-sonal consequences such as distress, bother, frus-tration and/or the avoidance of sexual intimacy.”The panel concluded that there was insufficientevidence to propose definitions for acquired PE,although it is recognized that men with acquiredPE have acquired this disorder at some point afterexperiencing normal ejaculatory latencies and thatonset may be either sudden or gradual. Theappearance of PE may be the result of urologicdysfunctions, thyroid dysfunction, or psychologi-cal or relationship problems.
3580 Montorsi et al.
J Sex Med 2010;7:3572–3588
The possibility that other sexual problemscoexist with PE should be investigated routinely.Although most men with lifelong PE do not sufferfrom concomitant ED, PE coexists in about one-third of patients complaining of ED. In someinstances, PE and ED may form a vicious cycle inwhich a man trying to control his ejaculationinstinctively reduces his level of excitation (whichcan lead to ED) or a man trying to achieve anerection basically attempts to do so by increasinghis excitation and arousal (which can lead to PE).Although reduced time to ejaculation is only rarelyan early manifestation of ED, it may occur when
the man has an unstable erection because of afluctuation in penile blood flow. In this case, theman may reach ejaculation quickly to compensatefor the weak erection.
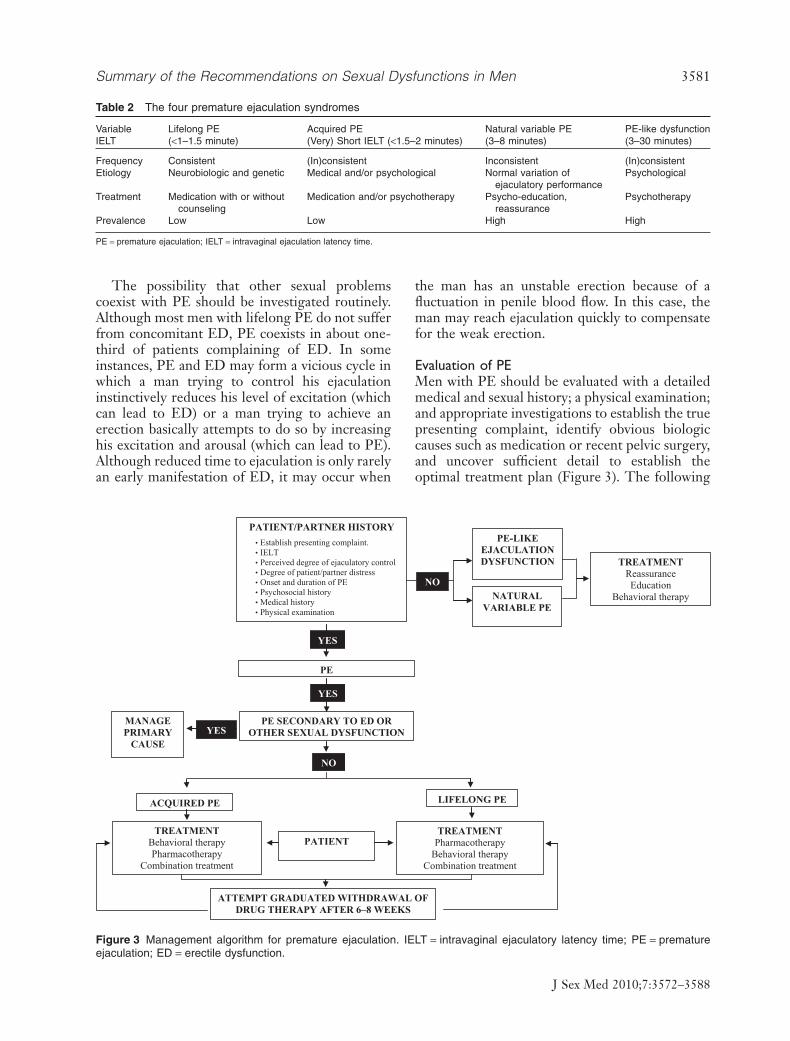
Evaluation of PEMen with PE should be evaluated with a detailedmedical and sexual history; a physical examination;and appropriate investigations to establish the truepresenting complaint, identify obvious biologiccauses such as medication or recent pelvic surgery,and uncover sufficient detail to establish theoptimal treatment plan (Figure 3). The following
Table 2 The four premature ejaculation syndromes
Variable Lifelong PE Acquired PE Natural variable PE PE-like dysfunctionIELT (<1–1.5 minute) (Very) Short IELT (<1.5–2 minutes) (3–8 minutes) (3–30 minutes)
Frequency Consistent (In)consistent Inconsistent (In)consistentEtiology Neurobiologic and genetic Medical and/or psychological Normal variation of
ejaculatory performancePsychological
Treatment Medication with or withoutcounseling
Medication and/or psychotherapy Psycho-education,reassurance
Psychotherapy
Prevalence Low Low High High
PE = premature ejaculation; IELT = intravaginal ejaculation latency time.
MANAGE PRIMARY
CAUSEYES
PATIENT/PARTNER HISTORY
PE
YES
PE SECONDARY TO ED OR OTHER SEXUAL DYSFUNCTION
ATTEMPT GRADUATED WITHDRAWAL OF DRUG THERAPY AFTER 6–8 WEEKS
ACQUIRED PE
TREATMENTBehavioral therapyPharmacotherapy
Combination treatment
LIFELONG PE
TREATMENTPharmacotherapy
Behavioral therapyCombination treatment
PATIENT
YES
NO
NATURALVARIABLE PE
PE-LIKEEJACULATIONDYSFUNCTION
NO
• Establish presenting complaint.• IELT• Perceived degree of ejaculatory control• Degree of patient/partner distress• Onset and duration of PE• Psychosocial history • Medical history• Physical examination
TREATMENTReassuranceEducation
Behavioral therapy
Figure 3 Management algorithm for premature ejaculation. IELT = intravaginal ejaculatory latency time; PE = prematureejaculation; ED = erectile dysfunction.
Summary of the Recommendations on Sexual Dysfunctions in Men 3581
J Sex Med 2010;7:3572–3588

relevant information should be obtained from thepatient:
• A basic medical history, including the use ofprescribed and recreational medications
• The cultural context and developmental historyof the disorder, including whether the PE isglobal or situational, lifelong or recent in itsdevelopment
• Quality measures of each of the three phases ofthe sexual response cycle (desire, arousal, andejaculation); the desire and arousal phases mayaffect the ejaculatory response
• Details about the ejaculatory response, includ-ing the patient’s subjective assessment of hisintravaginal ejaculatory latency time and senseof ejaculatory control, the level of sexual dissat-isfaction and distress, and the frequency ofsexual activity
• The partner’s assessment of the situation,including whether the partner suffers fromfemale sexual dysfunction
• Assessment of the sexual and overallrelationship
Treatment of PEPsychological Therapy. Present-day psychotherapyfor PE is an integration of psychodynamic,systems, behavioral, and cognitive approacheswithin a short-term psychotherapy model. Theguiding principles of treatment are to learn tocontrol ejaculation while understanding themeaning of the symptom and the context in whichit occurs. Besides teaching self-control techniquesto delay ejaculation, modern psychosexual thera-pies try to achieve the following aims:
• Help the patient recover his self-confidence andconfidence in his sexual performance.
• Reduce performance anxiety.• Solve relational problems.• Increase communication between the partners.• Resolve interpersonal issues that precipitate and
maintain the dysfunction.
In addition, psychotherapists seek to modifyrigid sexual repertoires and help the coupleremove barriers to intimacy. The majority of psy-chotherapy treatment outcome studies can becharacterized as uncontrolled, unblinded trials;none meets the requirements for high-level,evidenced-based studies. The literature comprisesreports on small to moderately sized cohorts ofsubjects who received different forms of psycho-logical interventions with limited or no follow-up.
In most studies, active treatment was not com-pared to placebo, control, or wait-list groups.
Medical Treatment for PE. The efficacy and safetyof off-label daily dosing of selective serotoninreuptake inhibitors (SSRI; paroxetine, sertraline,citalopram, fluoxetine) and the serotonergic tricy-clic, clomipramine, and off-label on-demanddosing of clomipramine for the treatment of PE iswell established. Within this group of drugs, ameta-analysis of published data suggests that par-oxetine (an SSRI) exerts the strongest ejaculationdelay. The use of SSRIs is limited by the lack ofapproval by the U.S. Food and Drug Administra-tion, the European Medicines Agency, or otherregulatory agency and therefore must be pre-scribed off label. Recently, dapoxetine has beenofficially approved in Europe and other extra-European countries for the on-demand treatmentof PE. The efficacy and safety of dapoxetine is wellestablished. The decision to treat PE with eithercurrent off-label SSRI daily dosing or on-demanddosing of dapoxetine must be based on the treatingphysician’s assessment of individual patientrequirements.
The efficacy and safety of off-label on-demandtopical anesthetic agents in the treatment of PEhas also been shown. The efficacy and safety ofoff-label on-demand or daily dosing of PDE5-Ishas been shown in the treatment of lifelong PE inmen with normal erectile function, although thelevel of evidence is lower. There is no evidence tosuggest that selective dorsal nerve neurotomy orhyaluronic acid gel glans penis augmentation areeffective treatments for PE. Surgery may be asso-ciated with permanent loss of sexual function andis contraindicated in the management of PE.
Orgasmic DysfunctionDefinition of Orgasmic DysfunctionOrgasmic dysfunction is the inability to achieve anorgasm or markedly diminished intensity of orgas-mic sensations; it can also be the marked delay oforgasm during any kind of sexual stimulation.There can be self-report of high sexual arousal orexcitement in this disorder, and orgasmic dysfunc-tion can occur together with ejaculatory function.
DE, retarded ejaculation, and inhibited ejacula-tion (IE) are probably the least common, leaststudied, and least understood male sexual dysfunc-tions. Yet, the impact of these conditions is signifi-cant in that they typically result in a lack of sexualfulfillment for both the man and his partner, aneffect further compounded when procreation is
3582 Montorsi et al.
J Sex Med 2010;7:3572–3588
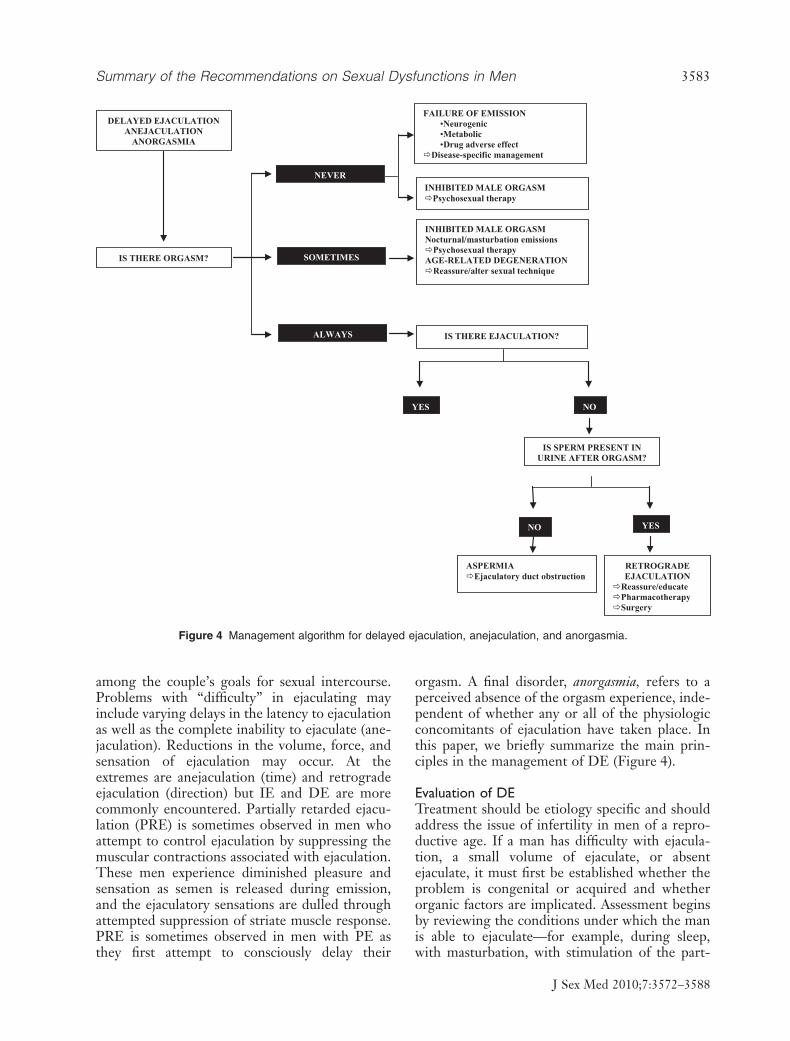
among the couple’s goals for sexual intercourse.Problems with “difficulty” in ejaculating mayinclude varying delays in the latency to ejaculationas well as the complete inability to ejaculate (ane-jaculation). Reductions in the volume, force, andsensation of ejaculation may occur. At theextremes are anejaculation (time) and retrogradeejaculation (direction) but IE and DE are morecommonly encountered. Partially retarded ejacu-lation (PRE) is sometimes observed in men whoattempt to control ejaculation by suppressing themuscular contractions associated with ejaculation.These men experience diminished pleasure andsensation as semen is released during emission,and the ejaculatory sensations are dulled throughattempted suppression of striate muscle response.PRE is sometimes observed in men with PE asthey first attempt to consciously delay their
orgasm. A final disorder, anorgasmia, refers to aperceived absence of the orgasm experience, inde-pendent of whether any or all of the physiologicconcomitants of ejaculation have taken place. Inthis paper, we briefly summarize the main prin-ciples in the management of DE (Figure 4).
Evaluation of DETreatment should be etiology specific and shouldaddress the issue of infertility in men of a repro-ductive age. If a man has difficulty with ejacula-tion, a small volume of ejaculate, or absentejaculate, it must first be established whether theproblem is congenital or acquired and whetherorganic factors are implicated. Assessment beginsby reviewing the conditions under which the manis able to ejaculate—for example, during sleep,with masturbation, with stimulation of the part-
DELAYED EJACULATIONANEJACULATION
ANORGASMIA
NEVER
IS THERE ORGASM?
IS SPERM PRESENT IN URINE AFTER ORGASM?
RETROGRADE EJACULATION
Reassure/educatePharmacotherapySurgery
ASPERMIAEjaculatory duct obstruction
SOMETIMES
ALWAYS IS THERE EJACULATION?
INHIBITED MALE ORGASMPsychosexual therapy
FAILURE OF EMISSION•Neurogenic•Metabolic•Drug adverse effect
Disease-specific management
INHIBITED MALE ORGASMNocturnal/masturbation emissions
Psychosexual therapyAGE-RELATED DEGENERATION
Reassure/alter sexual technique
YES NO
YESNO
Figure 4 Management algorithm for delayed ejaculation, anejaculation, and anorgasmia.
Summary of the Recommendations on Sexual Dysfunctions in Men 3583
J Sex Med 2010;7:3572–3588

ner’s hand or mouth, or infrequently with varyingcoital positions. The course of the problem isdocumented, and variables that improve or worsenperformance are noted. Questions concerning theman’s ability to relax, sustain, and heighten arousaland the degree to which he can concentrate onsensations are posed.
If orgasmic attainment had been possible previ-ously, the life events and circumstances tempo-rarily related to orgasmic cessation are reviewed.The events in question may be pharmaceutical orrelated to congenital problems, illness, trauma, ora variety of life stressors and other psychologicalfactors (e.g., following his wife’s mastectomy, theman is afraid of hurting her and therefore is onlypartially aroused). Societal and religious attitudesthat may interfere with excitement are noted, suchas the spilling of seed as a sin. Finally, questionsconcerning the quality of the nonsexual relation-ship are posed and problems explored. This assess-ment, in conjunction with appropriate physicalexamination and laboratory results, will provideunderstanding and help determine an appropriatetreatment path.
Treatment of DEAs indicated previously, before considering a psy-chological or behavioral approach toward thetreatment of DE, physicians need to exclude prob-able iatrogenic and pathophysiologic causes. Theyshould be alert for various medical conditions aswell as medications that might delay ejaculationand, in the case of antidepressants, consider areduction in dose or use of an antidote (Table 3).Vascular or neuropathic damage that causes DE isusually irreversible; therefore, the patient might becounseled to seek alternative methods to achieve
mutual sexual satisfaction with his partner. Andro-gen deficiency—another potential cause forDE—requires appropriate testosterone replace-ment therapy.
Regardless of whether a clear pathophysiologiccause is present or absent, patients might be coun-seled to consider lifestyle changes, includingenjoying more time together to achieve greaterintimacy; minimizing alcohol consumption;making love when not tired; and practicing tech-niques that maximize penile stimulation, such aspelvic floor training. Patient education regardingexisting factors that can exacerbate DE is animportant first step and may represent a segue intoeither short-term or long-term counseling. Treat-ment of DE or IE with pharmaceuticals has metwith limited success. No drugs have been approvedby regulatory agencies for this purpose, and mostdrugs that have been identified for potential usehave limited efficacy, impart significant sideeffects, or are considered experimental in nature.
Priapism
Definition of PriapismPriapism is an uncommon medical condition inmen that is defined as an unwanted erection notassociated with sexual desire or sexual stimulationand lasting for more than four hours. Three dif-ferent types of priapism are recognized, althoughthere may be some overlap among these catego-ries. Ischemic or veno-occlusive priapism is themost common form of priapism and is associatedwith a failure of detumescence, increasing anoxia,and ultimately necrosis of the cavernous muscle ifuntreated. It is an example of the compartmentsyndrome and requires urgent treatment. Nonis-
Table 3 Adjunctive drug therapy for selective serotonin reuptake inhibitor-induced sexual dysfunction
Drug Symptom
Dosage
As needed Daily
Amantadine Anorgasmia 100–400 mg (for 2 d prior to coitus) 75–100 mg bid or tidDecreased libidoED
Bupropion Anorgasmia 75–150 mg 75 mg bid or tidBuspirone Anorgasmia 15–60 mg 5–15 mg bid
Decreased libidoED
Cyproheptadine Anorgasmia 4–12 mg On demandDecreased libidoED
Yohimbine Anorgasmia 5.4–10.8 mg 5.4 mg tidDecreased libidoED
ED = erectile dysfunction; bid = twice daily; tid = three times daily.
3584 Montorsi et al.
J Sex Med 2010;7:3572–3588

chemic or high-flow priapism is less common thanthe first type and often occurs following bluntstraddle injury of the penis. It may also be con-genital or idiopathic in origin. The third type,recurrent or stuttering priapism, commonly occursin men with sickle cell disease but is not confinedto them. Such priapism usually starts with a high-flow state but may become typical ischemicpriapism.
Diagnosis of PriapismCareful history and physical examination are suf-ficient in most cases to make the diagnosis andclassification of priapism. The physical examina-tion should focus on the rigidity of the penis, theseverity of pain, and the presence of potential caus-ative or comorbid factors, such as secondarytumors in the penis.
An initial corporal blood aspirate is essential todifferentiating ischemic from nonischemic pri-apism. A corporal blood gas test (if this technologyis available) on the initial aspirate is recommendedin the emergency evaluation of priapism. ColorDoppler ultrasonography (if this technology isavailable) of the penis and perineum is recom-mended in the evaluation of priapism when thehistory or examination suggests penile trauma.
Ischemic Priapism (Veno-Occlusive)Treatment of Ischemic PriapismThe recommended initial treatment for ischemicpriapism is the decompression of the corpora cav-ernosa by aspiration. Aspiration immediatelysoftens the erection and relieves pain, and it shouldbe repeated until no more dark blood can be seencoming out of the corpora and fresh, red blood isobtained. This process of repeated aspiration leadsto a marked decrease in the intracavernous pres-sure and resuscitates the corporal environment,removing anoxic, acidotic, and hypercarbic blood.
Aspiration should be followed by the intracav-ernous injection of a sympathomimetic drug.Worldwide availability of adrenergic agentsvaries, and effective reversal of priapism has beendocumented with dilute injections of ephedrine,epinephrine, etilefrine, metaraminol, or phenyle-phrine. Regardless of the intracavernous sym-pathomimetic agent chosen for the managementof ischemic priapism, physicians should consulttheir pharmacies and develop clear mixingand dosing protocols for safe administration.Some sympathomimetic drugs are activators ofboth a- and b-adrenergic receptors. Significant
a-mediated effects on peripheral vasculature andb-mediated ionotropic and chronotropic effectson the heart may occur.
During ICI of sympathomimetic drugs, thephysician should monitor the patient for subjectivecomplaints and objective findings consistent withknown undesirable effects of sympathomimeticagents: headache, chest discomfort, acute hyper-tension, reflex bradycardia, tachycardia, palpita-tions, and cardiac arrhythmia. Patients (andparents of child patients) should be informedabout these potential complications. Blood pres-sure monitoring is recommended if repeated sym-pathomimetic dosing is given in an attempt toreverse ischemic priapism. In patients with signifi-cant cardiovascular risks, a medication historyshould be taken, and electrocardiogram monitor-ing is recommended.
Ischemic priapism associated with sickle celldisease requires intracavernous treatment. Ahematologist may provide concurrent systemictherapies, but the best resolution rates areachieved with therapies directed at the penis. Oraltherapy is not recommended for the treatment ofacute ischemic priapism.
Shunt surgery should be considered for all casesof veno-occlusive priapism failing aspiration andICI of sympathomimetics. Patients should becounseled that erectile function outcomes declinesignificantly when priapism has lasted longer than24–36 hours and that complete ED is anticipated ifpriapism persists for longer than 36 hours. In menpresenting with ischemic priapism longer than 48hours in duration or failing interventions for up to48 hours, severe ED is inevitable. Considerationmay be given to implantation of a penile prosthesisafter 48–72 hours of unresolved ischemic priapism.Treatment of Stuttering Ischemic PriapismThe goals of managing a patient with stutteringischemic priapism are prevention of future epi-sodes, preservation of erectile function, and bal-ancing of risks vs. benefits of various treatmentoptions. A trial of either daily oral sympathomi-metic therapy (a-adrenergic) or PDE5-I therapymay be used in the management of patients (adultsand children) with stuttering ischemic priapismassociated with hemoglobinopathies. Androgenablation therapy is also an effective therapy.Dosing efficacy should be monitored and mayneed adjustment.
Nonischemic Priapism (High-Flow, Arterial)In the management of nonischemic priapism, cor-poral aspiration has only a diagnostic role. Aspira-
Summary of the Recommendations on Sexual Dysfunctions in Men 3585
J Sex Med 2010;7:3572–3588

tion with or without injection of sympathomimeticagents is not recommended as treatment. ColorDoppler ultrasonography (if this technology isavailable) of the penis and perineum is recom-mended in the evaluation and management ofhigh-flow priapism. The initial management ofnonischemic priapism may be observation. Imme-diate invasive interventions (embolization orsurgery) can be performed at the request of thepatient but should be preceded by a thorough dis-cussion of the chances for spontaneous resolution,the risks of treatment-related ED, and the lack ofsignificant consequences expected from delaying(immediate) interventions. Penile arteriographyshould be reserved for the management of high-flow priapism when embolization is elected.
Selective arterial embolization is recommendedfor the management of nonischemic priapism inpatients who request treatment. Autologous clotand absorbable gels, which are not permanent, arepreferable to coils and ablative chemicals, whichare permanent.
Peyronie’s Disease (La Peyronie)
Definition of Peyronie’s DiseasePeyronie’s disease is considered a wound-healingdisorder that presents with a fibrous inelastic scarof the tunica albuginea; it is currently believed tooccur in genetically susceptible individuals follow-ing some form of trauma to the penis. A palpablescar develops in the flaccid state and causes avariety of deformities in the erect state, includingcurvature, shortening, narrowing, and hingeeffect. In the early phase, an inflammatory compo-nent often causes pain. This inflammatory paintends to resolve with time, but because of thedeformity, intercourse may be compromised orimpossible. Peyronie’s disease is also frequentlyassociated with ED and a variety of other comor-bid disorders, including diabetes, hypertension,dyslipidemia, and low testosterone.
Evaluation of Peyronie’s DiseaseThe diagnosis of Peyronie’s disease is usuallyapparent from the patient history and penileexamination. A detailed history should beobtained focusing on onset, duration, pain, defor-mity, and presence of ED. This data collectioncan be facilitated by using a disease-specific ques-tionnaire. Plaque measurement is inaccurate byany modality and is operator dependent; there-fore, it is not a reliable assessment for treatment
response. An assessment of the curvature on erec-tion is best made by an ICI of a vasoactive agent.This test is more accurate than a home photo-graph or a vacuum-assisted erection test.Dynamic duplex ultrasound—a useful but unnec-essary test—provides assessment of plaque calci-fication, vascular flow parameters, and objectivemeasures of deformity. It is imperative that thestretched penile length be measured preopera-tively so that the patient realizes that the lengthloss postoperatively is mainly the result of thedisease itself, not the surgery.
Treatment of Peyronie’s DiseaseNonsurgical TreatmentMen with early-phase disease (i.e., longer than 12months in duration) manifest by unstable or pro-gressive deformity and painful erections as well asthose men not psychologically ready or interestedin surgery may be considered candidates for non-surgical therapy. In general, nonsurgical treatmenthas limited evidence of benefit, but multiplereports of deformity stabilization or reductionmake it reasonable to offer electromotive drugadministration and/or intralesional injection ofverapamil or interferon and/or traction therapy.
Surgical TreatmentSurgery remains the gold standard for correctingerect penile deformity in the man with stabledisease. Surgical reconstruction is indicated for theman who has had stable disease for more than 6months, painless deformity, compromised abilityor inability to engage in coitus secondary to defor-mity, and/or inadequate rigidity when there isextensive plaque calcification as well as for the manwho desires the most rapid and reliable result.Preoperative consent is critical to setting properoutcome expectations for the patient. It is impera-tive to have a discussion about the risks of persis-tent or recurrent curvature, loss of erect length,diminished rigidity, and decreased sexual sensa-tion. Several surgical algorithms have been pub-lished, with general agreement that for men withadequate preoperative rigidity, some form oftunica plication procedure is best for those withcurvature of less than 60° and with no hourglassdeformity resulting in a hinge effect. For thosewith more severe deformity (more than 60° and/orhourglass) and good preoperative rigidity, incisionor partial excision and grafting is recommended.Penile prosthesis implantation with additionalmaneuvers to correct the deformity is recom-
3586 Montorsi et al.
J Sex Med 2010;7:3572–3588

mended when there is preoperative ED that is notresponsive to oral medication (PDE5-Is).
Penile Trauma
Definition of Penile FracturePenile fracture is defined as the traumatic rupture ofthe tunica albuginea. It usually occurs duringsexual intercourse when the erect penis is thrustagainst the partner’s symphysis pubis or perineum.
Evaluation of Penile FractureA careful history and physical examination areessential. The classical presentation includes acracking sound at the moment of injury, a sharppain, detumescence, swelling, and ecchymosis.The typical appearance has been described aseggplant deformity or aubergine sign by someauthors. A palpable defect in the tunica albugineacan occasionally be felt, but usually the swellingconceals this sign. It is important to rememberthat a concomitant urethral injury—partial orcomplete—may occur in 2–20% of patients.Imaging (cavernosography, ultrasound, or mag-netic resonance imaging) can be used forlocalization of the injury, whereas retrograde ure-throgram (preoperative or perioperative) can beperformed if a urethral injury is suspected. Theultimate decision for surgery is based on clinicalfindings; once diagnosed, there is no indicationfor conservative management.
Treatment of Penile FractureConservative management of a penile fracture withcatheterization, compression dressings, analgesia,antibiotics, and erection-inhibiting agents shouldbe avoided. Once penile fracture is diagnosed, sur-gical exploration is widely accepted as the goldstandard therapeutic option, even in the event of adelayed presentation (48 hours after injury).
Penile Augmentation and Lengthening Surgery
This area of research and practice is controversialbecause an increasing number of patients now pre-sents with an anatomically normal penis that thepatient perceives to be inadequate in size. The riskof performing unjustified surgery in these cases isobvious.
Both penile lengthening and augmentationtechniques have been described with variablesuccess rates. A critical analysis of the pertinentliterature, however, does not reveal proven efficacy
outcome data. On the contrary, findings clearlydemonstrate that the complications related tothese procedures may be significant. Stretchingdevices may be viable alternative treatmentoptions, whereas liquid silicone injection shouldbe discouraged. It is mandatory to recommendthat the patient undergo a thorough psychologicalassessment prior to considering any surgicalapproach.
A penis with stretched length of <7 cm shouldbe considered a micropenis. These patients shouldundergo a thorough multidisciplinary assessment.Many surgical techniques are recommended forthese rare cases.
Sexually Transmitted Infections
There is a paucity of state-of-the-art informationabout sexually transmitted infections (STIs) affect-ing sexual function. The problem is underscoredby high prevalence rates: It is estimated that 35%of adult men suffer from sexual dysfunctions andthat 340 million people live with STIs.
Patients with HIV frequently suffer from sexualdysfunctions due to both pathology (i.e., HIV lipo-dystrophy and HIV neuropathy/encephalopathy)and HIV therapies (i.e., highly active antiretroviraltherapy). HIV-associated sexual dysfunction isideally addressed by a multidisciplinary team, andthe importance of education as a protective factoragainst HIV must be emphasized.
PDE5-Is prescribed for ED, as well as recre-ational drugs and unprotected sexual behavior,may play a role in HIV transmission among HIV-infected and HIV-negative men having sex withmen. Disclosure of HIV status among partnersshould be encouraged (especially with newlyregained erectile function following PDE5-I orsexual-aid use), and stigmatizing attitudes shouldbe discouraged to promote voluntary counselingand testing. Male circumcision will reduce the riskof acquisition of HIV in heterosexual men andis not associated with high-risk sexual behavior(disinhibition).
Patients with frequent recurrences of genitalherpes should be evaluated on a regular basis forcoexisting psychological and psychosexual illnessand given appropriate treatment including pos-sible continuous antiviral medications. Chlamydiatrachomatis, gonorrhea, and human papillomavirusmay also be associated with sexual dysfunction, butmore information is needed before causality can beestablished.
Summary of the Recommendations on Sexual Dysfunctions in Men 3587
J Sex Med 2010;7:3572–3588

Prostatitis and chronic pelvic pain syndrome(CPPS) are associated with sexual dysfunction.The severity of the pain and illness in acutebacterial prostatitis interferes with sexual func-tion. Chronic bacterial prostatitis (CBP) andCPPS are frequently associated with ejaculatorypain or PE (77%) as well as with ED in 15–72%of cases. The efficacy of PDE5-Is for ameliora-tion of the symptoms of prostatitis in patientswith CBP or CPPS and disturbed sexualityremains unclear.
Conclusion
The 2009 International Consultation on SexualDysfunctions in men convened all the recognizedexperts in the field and produced evidence-based
guidelines and an evaluation-treatment algorithm.It is recognized that most patients with any of theknown sexual dysfunctions should be approachedin a multidisciplinary fashion. The contemporarysexual medicine expert must be knowledgeable inmany scientific areas, including urology, androl-ogy, endocrinology, and internal medicine. Thepatient’s psychological perspective remains a keyparameter to be considered for successful manage-ment of these conditions.
Corresponding Author: Francesco Montorsi, MD,Department of Urology, San Raffale ScientificInstitute, Via Olgettina 60, 20132 Milan, Italy.Tel: +390226436438; Fax: +390226436450; E-mail:[email protected]
Conflict of Interest: None.
3588 Montorsi et al.
J Sex Med 2010;7:3572–3588