Should California's Film Script Cases Be Merged into Trade ...

State Policies and Language Access in California’s HMOs:Public Reporting and Regulation of HMOs’ Language Services
Christopher J. MorelandDominique RitleyJulie A. RainwaterPatrick S. Romano
Journal of Health Care for the Poor and Underserved, Volume 23, Number1, February 2012, pp. 474-498 (Article)
Published by The Johns Hopkins University PressDOI: 10.1353/hpu.2012.0020
For additional information about this article
Access Provided by your local institution at 02/20/13 10:17PM GMT
http://muse.jhu.edu/journals/hpu/summary/v023/23.1.moreland.html

Part 2: Original PaPer
© Meharry Medical College Journal of Health Care for the Poor and Underserved 23 (2012): 474–498.
State Policies and language access in California’s HMOs: Public reporting and regulation of HMOs’ language Services
Christopher J. Moreland, MD, MPH Dominique Ritley, MPHJulie A. Rainwater, PhD
Patrick S. Romano, MD, MPH
Abstract: Objective. Describe the status of language access services for California’s lim-ited English proficient (LEP) health maintenance organization (HMO) members within the context of voluntary public reporting and anticipated state regulation. Study design. Descriptive analysis of longitudinal data provided by health plans. Methods. Retrospec-tive, descriptive analysis of responses to voluntary annual/biennial surveys of commercial, Medicare, Medicaid, and Healthy Families HMOs, 2003–2008. results. From 2003 to 2008, during California’s public reporting of HMO language services, the percentage of HMOs providing in-person interpretation free of charge to consumers increased to over 80% across all product lines. By 2008, the percentage of commercial HMO plans matching new LEP members to providers by language increased to 70%, while 79% provided telephone interpretation services in at least seven languages. Conclusions. Increasingly HMOs provide language access services for LEP Californians, perhaps resulting from public reporting and anticipated state regulation, although similar trends in other states cannot be ruled out.
Key words: Limited English proficiency, health communication, health maintenance orga-nizations, interpreter, access to care.
Language barriers contribute to disparities in health care in the United States. In 2000, about 12.5 million (39.5%) Californians spoke a language other than Eng-
lish at home.1 Of these, 20% spoke English less than “very well” and were classified as limited English proficient (LEP). In 2007, more than one million Californian health
Christopher Moreland (corresponding author—[email protected]), Assistant Professor of Medicine at the University of Texas Health Science Center at San Antonio, works on the identification and reduction of disparities, particularly those affecting the health of the limited–English proficient. doMinique ritley is a senior research analyst at the University of California–Davis, Center for Health Care Policy and Research; her current work includes public health policy implications of mandated health insurance benefits and measuring quality of health care. Julie rainwater is Director of the Evaluation Program at the Clinical and Translational Science Center at the University of California–Davis. patriCk roMano is Professor of General Internal Medicine and General Pediatrics at the University of California–Davis School of Medicine, works on developing, testing, and validating health care quality measures, and evaluating the impact of reporting programs.

475Moreland, Ritley, Rainwater, and Romano
maintenance organization (HMO) members were LEP.2 These individuals have signifi-cant difficulty accessing health care3 because they are often unable to find providers who speak their preferred language.4–6 Trained, professional interpreters can improve access to care, with fewer errors than ad hoc interpreters and with improved quality of care, patient satisfaction, clinical outcomes, and health services utilization.7–11 One previous qualitative study explored health plans’ language services, but no quantitative study has described such services.9
The federal government and many states require provision of translation services for some LEP patients, usually at point of service, but implementation appears to be inconsistently instituted throughout the health care system. California, considered a leader in improving access to language services, initiated several actions during the last decade.12 For example, the California Office of the Patient Advocate (OPA) developed and began conducting an annual Survey of Cultural and Language Access Services Pro-vided by California Health Plans (SCLAS) in 2002, with public reporting of key survey results. After the first year of the survey, the California legislature passed Senate Bill 853, which mandated that commercial health plans provide language assistance services. Regulations were published by the Department of Managed Health Care (DMHC) in 2006 and implemented in January 2009. These new regulations require all health plans to assess the linguistic needs of their members and to provide interpretation services for members who meet the DMHC’s “threshold language” requirements (calculated as a formulaic percentage of a plan’s member population with non-English language preferences). As a brief example, health plans are required to survey their enrollees to determine the most prevalent spoken languages. Health plans with one million or more enrollees must translate key documents into the two most common threshold languages (other than English), while health plans with 300,000 to less than one million enrollees must translate into the single most common threshold non-English language.13 To our knowledge, California’s only preceding legislation regarding language services in health care (from 1990) requires acute care hospitals to create policies for language assistance.14 In our article, we focus on HMOs, a subgroup of health care service plans that typically direct enrollees to health care providers within specified networks and geographic service areas; although SB 853 does not apply exclusively to HMOs, HMOs cover the majority of the insured California population.
The DMHC HMO Help Center uses several tools to track health plan compliance with SB 853 provisions, including the language assistance program provision. SB 853 directs the HMO Help Center to evaluate health plans every three years and permits periodic use of secret-shopper calls and appointments to monitor compliance between survey years. To encourage compliance efforts, the Help Center also provides on-line, program-specific Technical Assistance Guides that health plans may use as checklists to optimize compliance. Additionally, The Help Center investigates enrollee- and provider-initiated complaints and grievances, including those related to language bar-riers. Potential violations are referred for review to the DMHC Office of Enforcement, which is authorized to enforce SB 853 through corrective action notification and civil penalties and fines, ranging up to $2,500 daily for each violation or enrollee harmed.
The present study was designed to explore the impact of this changing policy envi-ronment on LEP HMO members’ access to language services, using SCLAS survey

476 State policies and language access in California’s HMOs
data. In undertaking this analysis, we recognize that it is difficult to disentangle the independent contributions of public reporting, legislation, and regulatory actions. Nonetheless, our findings highlight the role that health plans can play in improving LEP patient-provider communications.
Methods
The SCLAS has been administered annually from 2002–2008 (except 2007) to California’s nine largest full-service HMOs and to those HMOs that serve by contract the state’s Medicaid (Medi-Cal) population. These HMOs represent over 90% of California HMO members.13 The 2002 survey questions differed from those in subsequent surveys, so we were unable to include that year’s responses in our analyses. Because this survey was actually a census of all eligible HMOs, and because the response rate was 100% in all years (except four commercial HMOs in 2004 and one Medi-Cal HMO in 2006), statistical hypothesis testing was not appropriate. Instead, readers should focus on whether reported differences are meaningful from the clinical and policy perspectives. Survey respondents (who were typically HMO representatives for cultural and language services) were asked about their specific HMO product lines including commercial, Medi-Cal (California’s Medicaid program), Healthy Families (California’s Children’s Health Insurance Program), Medicare, and Healthy Kids (Appendix A). We exclude Healthy Kids from analyses because few HMOs reported this product line. When the SCLAS asked about Medi-Cal language services at the county level, we report only responses that applied to all counties. Due to state contract requirements predating SB 853, Medi-Cal and Healthy Families HMOs provided nearly complete language services across the survey years, while Medicare HMOs are not subject to state law. We thus focus on commercial product lines in some analyses, as these commercial HMOs had no language access requirements prior to SB 853’s implementation.
We summarize 36 of the 59 items in the 2008 SCLAS (Appendix B, available at http://www.ucdmc.ucdavis.edu/chpr/downloads/moreland1.pdf). We categorized the questions and their responses by their relevance to non-English language identification, provi-sion of language services during medical encounters, provision of language services at HMO points of contact, and HMO operations in managing language-related issues. The languages assessed by the SCLAS in all survey years were Armenian, Chinese, Korean, Russian, Spanish, Tagalog, and Vietnamese; the OPA added Arabic, Farsi, Hmong, and Khmer in 2006. For questions about specific languages, the denominator consisted of the number of HMOs offering the relevant product line, while the numerator consisted of the number of those HMOs that reported offering services in that language.
We do not report results from 23 questions. The seven items addressing signed language services for the deaf and hard of hearing are discussed elsewhere.14 Three questions identify contact information or other technical data. We omit responses to one question about which respondents expressed confusion. Four questions (about “member-informing” documents in certain languages, written policies on language services beyond the grievance process, tracking requests for interpretation services, and 24-hour advice nurse access) were not analyzed because respondents commented that the response choices were inadequate. Nor did we include 11 questions about delega-

477Moreland, Ritley, Rainwater, and Romano
tion of services to independent contractors, member satisfaction surveys, or whether HMOs used data from the Health care Effectiveness Data and Information Set (HEDIS), because many respondents stated they were not applicable. We are unable to report data from early survey years for some questions, either because the question was added in later versions of the SCLAS, or because the data were unavailable from the OPA.
results
Table 1 outlines the number of HMOs per year with each product line.language identification. To provide language-appropriate services, HMOs must
first identify members’ primary languages. Spanish and Chinese were the most com-mon “threshold languages” across all product lines. No more than 20% of responding HMOs identified any other language as meeting the regulatory threshold (Table 2).
At least 95% of Medi-Cal and Healthy Families HMOs stated they documented cur-rent members’ primary languages from 2004–2008. Only 44% and 64% of Medicare and commercial HMOs, respectively, did so in 2004, but 95% of both did so in 2008. From 2004 through 2008, Medi-Cal and Healthy Families generally (84% to 100%) reported capturing this information from the government agencies that administer these programs. In contrast, Medicare and commercial HMOs more often (55% to 100%) captured pri-mary language data themselves and/or through a contractor, except that 56% of Medicare HMOs reported obtaining primary language data from Medicare itself in 2008.
When asked whether member language information was shared with contracted health care providers in 2006, most Medi-Cal and Healthy Families HMOs responded affirmatively (95% and 89%, respectively), while about half of Medicare and commer-cial HMOs did so (45% and 53%, respectively). In 2008, language information sharing increased to 100% for Medi-Cal and Healthy Families HMOs, 61% for Medicare HMOs, and 74% for commercial HMOs.
Provider point of contact services. Providing medical interpretation in specified languages. In 2006, 64% of commercial HMOs provided medical interpretation in
table 1.nUMBer OF HMOS WitH eaCH PrODUCt line aMOng reSPOnDentS tO tHe SClaS, 2003–2008
line of business
Year of SClaS administration
2003 2004 2005 2006 2008
Commercial 14 14 14 17 19Medi-Cal 20 20 20 20 21Healthy Families 19 19 19 19 20Medicare 9 9 9 11 18
SCLAS 5 Survey of Cultural and Language Access Services

478 State policies and language access in California’s HMOs
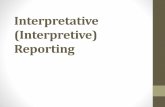
“threshold languages,” as required by DMHC regulations that took effect in 2009, compared with 94% in 2008. The percentage of commercial HMOs providing face-to-face interpretation during medical encounters increased for nearly all languages, including non-threshold languages (Figure 1). In 2005, 64% and 71% of commercial HMOs provided interpretation services in Chinese and Spanish, respectively. These percentages increased to 79% and 84%, respectively, by 2008.
To a lesser degree, provision of services in languages other than Spanish and Chinese also increased. For Russian, Spanish, Tagalog, and Vietnamese, interpretation services seemed to drop between 2005 and 2006, but ultimately rose to higher levels in 2008. However, these dips may have been artifactual, because four of the 15 commercial HMOs that responded in both 2006 and 2008 reportedly switched from providing interpretation in no languages in 2006 to providing interpretation in all languages in 2008. Reported reasons for this switch included new contracts with interpretation vendors, incorrect survey responses, and categorization of bilingual staff as interpreters, suggesting that respondent variation may explain the unexpected changes between 2005 and 2008.
Focusing on free services, the percentage of Medi-Cal and Healthy Families HMOs providing free interpretation for LEP consumers at medical encounters remained high throughout the survey period, while the corresponding percentages for Medicare and commercial HMOs increased from 2004 to 2008 (Figure 2). The percentage of com-
table 2.tHreSHOlD langUageS OF CaliFOrnia’S HMOS, aS iDentiFieD BY PerCentage OF SUrVeY reSPOnDentS, 2006 anD 2008
languagea
Medi-Calb Healthy Families Medicare Commercial
2006 2008 2006 2008 2006 2008 2006 2008
ArabicArmenianChinese 15% 21% 35% 9% 11% 47% 58%FarsiHmongKhmer 5%Korean 5% 5% 6% 11%Russian 6% 5%Spanish 10% 100% 95% 73% 67% 76% 84%Tagalog 12% 5%Vietnamese 10% 15% 11% 12% 20%
aBlank cells indicate that the language was not claimed by the HMO as a threshold language. bBlank cells indicate that the language was not claimed Medi-Cal as a threshold languages at the county level. We report threshold languages only for those Medi-Cal plans which identified a threshold language across all counties.

479Moreland, Ritley, Rainwater, and Romano
mercial HMOs providing interpretation services in any language without charge to members transiently dropped from 79% in 2003 to 58% in 2004, but rebounded to 84% in 2008. For Medicare HMOs, the percentage rose to 83% in 2008, but remained lower than the 95% mark achieved by Healthy Families and Medi-Cal HMOs.
Regarding who actually conducts interpretation at medical points of contact from 2003–2008, at least 90% of Medi-Cal HMOs and 89% of Healthy Families HMOs discour-aged use of either adult family and friends or children as ad hoc interpreters in 2003, with 100% of both ultimately doing so in 2008. However, only 33% of Medicare HMOs and 43% of commercial HMOs consistently discouraged such ad hoc interpretation in 2003, increasing to 78% of Medicare HMOs and 89% of commercial HMOs in 2008.
Obtaining 24-hour telephone interpretation. In 2006, 71% of commercial HMOs provided telephone interpretation in their “threshold languages,” compared with 82% in 2008. The percentage of commercial HMOs providing telephone interpretation in all seven languages (including non-threshold languages) increased from 64% in 2005 to 76% in 2006 and 79% in 2008; the percentage for Medicare HMOs likewise rose from 56% in 2005 to 73% in 2006 and 83% in 2008. Four commercial HMOs switched from providing telephone interpretation in no languages in 2006 to all languages in 2008, reportedly due to new contracts with telephone interpretation vendors. Between 90% and 100% of Medi-Cal and Healthy Families HMOs provided telephone interpretation in all seven languages across all three surveys.
Figure 1. The percentage of commercial plans that provided medical interpretation in specified languages at medical encounters, 2005–2008.

480 State policies and language access in California’s HMOs
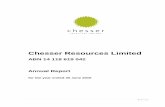
Matching LEP members with PCPs by language. If LEP members do not choose a primary care provider (PCP), HMOs have the option of language matching. Although commercial HMOs’ overall use of language matching increased from 50% to 71% between 2004 and 2008 (Figure 3), two commercial HMOs ceased the practice between 2006 and 2008. At least 90% of Medi-Cal HMOs continued the practice throughout the study period, while language matching by Healthy Families HMOs rose from 21% in 2004 to 95% in 2008. However, HMOs’ tracking of whether current LEP members had a PCP who used the same primary language changed minimally from 2006 to 2008 for Medi-Cal (75% to 71%), Healthy Families (79% to 75%), Medicare (55% to 67%), and commercial HMOs (59% to 58%).
Training providers and office staff. One question addressed whether HMOs provided at least four hours of training that focused on culturally appropriate care to office staff and providers within HMO networks in the year preceding the survey. The percentage of HMOs responding affirmatively fluctuated from 71% in 2005 to 56% in 2006 and 62% in 2008; the question did not stratify by product line. This training reportedly included skills and practices regarding cultural health care, concepts of cultural com-petency, and how to access and use medical interpretation for 60% of HMOs; 48% also included information about how to locate translated materials. In 2008, the percentages of HMOs incorporating these categories into their training programs rose to 62% for cultural skills and practices and cultural competency, 70% for utilizing interpretation services, and 54% for locating translated materials.
HMO point of contact services. Qualified, bilingual staff members. From 2005 through 2008, the overall percentage of commercial HMOs with qualified bilingual
Figure 2. Percentage of plans by product line that provided free interpretation to consumers at medical encounters, 2003–2006 and 2008. The survey was not conducted in 2007.

481Moreland, Ritley, Rainwater, and Romano
staff members available to assist LEP consumers during HMO business contacts was generally stable at 16–29% for Armenian and Korean, 21–36% for Russian and Tagalog, 47–57% for Chinese and Vietnamese, and 94–100% for Spanish (Figure 4). Korean and Russian were the only two languages with increasing numbers of qualified bilingual staff.
In 2006, 79% of HMOs trained bilingual member services staff in providing culturally appropriate services; this percentage rose to 88% in 2006 and 92% in 2008. For bilingual staff who functioned as interpreters, 44–48% of all (except 28% of commercial) HMOs incorporated interpreting protocols, basic medical terminology, culture’s impact on communication, and interpreting ethics into the training. In 2008, the percentages of HMOs addressing each category were 61%, 63%, 63%, and 44%, respectively (without stratification by product line).
Informing HMO members about in-person interpretation services. In 2006 and 2008, all HMOs stated that their LEP members could obtain information in their primary languages about enrollment, disenrollment, and health education and wellness pro-grams, either by telephone or in writing, with the exception of one commercial HMO (in 2006 and 2008) and one Medicare HMO (in 2008).
Communication with LEP members about medical interpretation availability via handbooks and newsletters, respectively, in non-English languages has remained relatively unchanged between 2003 and 2008 (Tables 3 and 4). However, Medicare and commercial HMOs markedly enhanced the use of handbooks and newsletters in Spanish. In 2006, all respondents reported providing oral interpretations of written materials on request, versus 92% in 2008.
HMOs almost invariably reported using the same methods as above to inform LEP members about telephone services, so those data are not shown here.
Informing HMO members about filing written grievances or complaints. In addition to communicating with HMO members about accessing interpretation services, HMOs
Figure 3. The percentage of plans by product line that reported matching patients and providers by language, 2004–2008.

482 State policies and language access in California’s HMOs
can provide member handbooks, newsletters, or websites to inform members in their primary languages about how to file grievances or complaints. In 2006 and 2008, all Medi-Cal and Healthy Families HMOs used handbooks in this manner, but the per-centage using newsletters or websites rose from 79–85% in 2006 to 85–95% in 2008. Medicare HMOs similarly increased the use of handbooks and newsletters (from 55% to 67%) and websites (from 64% to 72%). Commercial HMOs, however, decreased their use of handbooks (from 82% to 74%) and newsletters (from 76% to 63%) in favor of websites (from 76% to 84%).
Translating provider directories. HMOs frequently offer health provider directories in English and non-English languages, either online or in print or both (Table 5). For both media, HMOs most often translated directories to Spanish and Chinese. Provider directories were available on HMO websites less frequently than in print. Seventy-nine to 82% of all HMOs across product lines reported a provider directory in English on their websites in 2006, while 92–95% did so in 2008. However, only 45–58% reported providing a version in at least one non-English language in 2006, while 67–85% reported doing so in 2008.
Website-based information about language access. From 2004–2008, HMOs across all product lines steadily increased website-based communication in English about language access services. Only 60% of Medi-Cal and 58% of Healthy Families HMOs provided such information in 2004, but 90% of both did so in 2008. In contrast, only
Figure 4. The percentage of commercial plans with qualified staff members fluent in specified languages, 2005–2008.

tabl
e 3.
t
He
lan
gU
ag
eS i
n W
HiC
H P
lan
S in
FOr
M l
eP M
eMB
erS
OF
MeD
iCa
l
int
erPr
eta
tiO
n S
erV
iCeS
Via
MeM
Ber
Ha
nD
BO
OK
, 200
3–20
08
lang
uage
a
Med
i-Cal
Hea
lthy
Fam
ilies
Med
icar
eC
omm
erci
al
2003
2006
2008
2003
2006
2008
2003
2006
2008
2003
2006
2008
Ara
bic
20%
24%
5%5%
9%6%
6%5%
Arm
enia
n30
%29
%5%
10%
9%6%
6%5%
Chi
nese
60%
55%
52%
32%
32%
38%
22%
27%
33%
36%
35%
42%
Fars
i30
%29
%11
%10
%9%
6%6%
5%H
mon
g30
%24
%5%
5%9%
6%6%
5%K
hmer
35%
33%
11%
10%
9%6%
6%5%
Kor
ean
30%
30%
29%
11%
11%
14%
11%
9%6%
14%
18%
16%
Russ
ian
55%
52%
11%
14%
18%
11%
18%
16%
Span
ish10
0%10
0%10
0%84
%10
0%95
%33
%73
%61
%43
%88
%74
%Ta
galo
g30
%30
%29
%16
%5%
10%
11%
9%6%
14%
6%5%
Vie
tnam
ese
60%
60%
62%
21%
16%
29%
11%
18%
17%
21%
24%
26%
a Blan
k ce
lls in
dica
te th
at d
ata
wer
e no
t ava
ilabl
e fo
r th
is la
ngua
ge in
yea
rs p
rece
ding
200
6.

tabl
e 4.
tH
e la
ng
Ua
geS
in
WH
iCH
Pla
nS
inFO
rM
leP
MeM
Ber
S O
F M
eDiC
al
int
erPr
eta
tiO
n
SerV
iCeS
Via
MeM
Ber
neW
Slet
ter
S O
r a
nn
Ua
l n
Ot
iCeS
, 200
3–20
08
lang
uage
a
Med
i-Cal
Hea
lthy
Fam
ilies
Med
icar
eC
omm
erci
al
2003
2006
2008
2003
2006
2008
2003
2006
2008
2003
2006
2008
Ara
bic
15%
14%
11%
10%
9%6%
6%5%
Arm
enia
n30
%19
%21
%10
%9%
6%12
%5%
Chi
nese
35%
55%
43%
32%
42%
43%
33%
9%28
%43
%47
%47
%Fa
rsi
25%
19%
21%
10%
9%6%
12%
5%H
mon
g35
%19
%16
%10
%9%
6%6%
5%K
hmer
35%
24%
26%
14%
9%6%
12%
11%
Kor
ean
10%
30%
24%
11%
26%
14%
11%
9%6%
14%
29%
16%
Russ
ian
50%
43%
26%
19%
18%
17%
18%
16%
Span
ish80
%10
0%10
0%74
%95
%95
%33
%73
%83
%50
%88
%84
%Ta
galo
g10
%30
%19
%5%
16%
10%
11%
9%11
%14
%18
%5%
Vie
tnam
ese
30%
60%
52%
26%
42%
43%
0%18
%22
%21
%41
%37
%
a Blan
k ce
lls in
dica
te th
at d
ata
wer
e no
t ava
ilabl
e fo
r th
is la
ngua
ge in
yea
rs p
rece
ding
200
6.

485Moreland, Ritley, Rainwater, and Romano
table 5.PerCentage OF PlanS tHat tranSlateD PrOViDer DireCtOrieS intO VariOUS langUageS On tHeir WeBSiteS Or in Print, 2006–2008
language Medium
Medi-CalaHealthy Families Medicare Commercial
2006 2008 2006 2008 2006 2008 2006 2008
Arabic Website 5% 5% 0% 0% 0% 0% 0% 0%Print directory 5% 0% 53% 65% 55% 67% 41% 58%
Armenian Website 15% 19% 5% 5% 0% 0% 0% 0%Print directory 5% 0% 58% 65% 55% 67% 41% 52%
Chinese Website 20% 29% 16% 20% 9% 17% 12% 16%Print directory 0% 0% 79% 80% 55% 78% 53% 58%
Farsi Website 15% 19% 5% 5% 0% 0% 0% 0%Print directory 5% 0% 58% 65% 55% 67% 41% 52%
Hmong Website 10% 5% 5% 0% 0% 0% 0% 0%Print directory 5% 0% 53% 65% 55% 67% 41% 52%
Khmer Website 15% 19% 5% 5% 0% 0% 0% 0%Print directory 5% 0% 63% 65% 55% 67% 41% 52%
Korean Website 15% 19% 11% 10% 0% 0% 6% 5%Print directory 5% 0% 63% 65% 55% 67% 41% 52%
Russian Website 15% 24% 5% 5% 9% 6% 0% 0%Print directory 5% 0% 58% 65% 55% 67% 46% 52%
Spanish Website 55% 86% 58% 85% 45% 50% 53% 58%Print directory 0% 0% 100% 100% 91% 94% 94% 100%
Tagalog Website 15% 19% 5% 5% 9% 6% 0% 0%Print directory 5% 0% 58% 70% 55% 72% 41% 52%
Vietnamese Website 20% 38% 11% 25% 0% 11% 12% 11%Print directory 0% 0% 63% 75% 55% 72% 46% 52%
aMedi-Cal data shown are those applying to all counties only; responses applying only to specific counties are not shown.
11% of Medicare and 29% of commercial HMOs posted language services information in English on their websites in 2004, but these percentages jumped to 94% and 84%, respectively, in 2008.
The number of HMOs reporting that their websites contained information about language access services in a non-English language generally increased from 2006 to 2008 across product lines, although percentages varied due to changes in the denomi-nator of responding HMOs (Table 6). Spanish was the only language for which HMO use increased consistently across product lines.

tabl
e 6.
Pe
rC
enta
ge
OF
Pla
nS
tH
at
Pr
OV
iDeD
WeB
Sit
e-Ba
SeD
in
FOr
Ma
tiO
n O
n
lan
gU
ag
e a
CC
eSS
FOr
MeM
Ber
S, i
n V
ar
iOU
S la
ng
Ua
geS
, 200
5–20
08
lang
uage
Med
i-Cal
bH
ealth
y Fa
mili
esM
edic
are
Com
mer
cial
2005
2006
2008
2005
2006
2008
2005
2006
2008
2005
2006
2008
Ara
bica
10%
5%11
%5%
9%0%
6%0%
Arm
enia
n15
%20
%14
%16
%16
%15
%0%
9%0%
7%12
%5%
Chi
nese
20%
35%
29%
21%
32%
30%
0%27
%22
%29
%41
%32
%Fa
rsia
20%
14%
16%
15%
9%0%
12%
5%H
mon
ga15
%10
%16
%10
%9%
6%6%
0%K
hmer
a25
%14
%21
%15
%9%
0%12
%5%
Kor
ean
10%
20%
14%
11%
16%
15%
0%18
%11
%14
%24
%16
%Ru
ssia
n20
%30
%24
%16
%21
%20
%0%
9%6%
7%12
%5%
Span
ish80
%85
%86
%74
%79
%90
%56
%64
%72
%71
%76
%74
%Ta
galo
g10
%20
%14
%11
%16
%15
%0%
9%0%
7%12
%5%
Vie
tnam
ese
25%
35%
33%
26%
32%
35%
0%18
%22
%14
%24
%21
%
a This
lang
uage
was
add
ed to
the
SCLA
S in
200
6; n
o da
ta a
vaila
ble
for
2005
.b M
edi-C
al re
sults
are
acr
oss
all c
ount
ies
only
; res
pons
es a
pply
ing
only
to sp
ecifi
c co
untie
s ar
e no
t sho
wn.

487Moreland, Ritley, Rainwater, and Romano
HMO operations. HMO policies and staff training. HMOs have opportunities to encourage language services through administrative policy. Respondent HMOs con-sistently increased the incorporation of cross-cultural competencies into corporate strategies across product lines from 2004 through 2008, with a greater change for Medicare (44% to 83%) and commercial (57% to 90%) HMOs than for Medi-Cal (80% to 91%) and Healthy Families (84% to 90%) HMOs. Medi-Cal and Healthy Families HMOs almost universally reported incorporating language services into their quality improvement programs (95% and 89% of responding HMOs in 2004 to 100% in 2008, respectively) while Medicare and commercial HMOs increased this practice from 44% and 64% in 2004 to 89% and 95%, respectively, in 2008. In 2004, 95% of Medi-Cal and Healthy Families, 56% of Medicare, and 57% of commercial HMOs instructed member services staff regarding written policies on language services. In 2008, all HMOs across product lines did so, except for one Medicare HMO.
Monitoring and assessing language services. In addition to documenting and training bilingual staff and health providers, HMOs have evaluated their non-English language proficiency levels in several ways (Table 7). HMOs (especially commercial and Medi-care HMOs) have trended away from relying on self-reporting and academic credits for bilingual staff, opting for evaluation by either the HMO itself or an independent appraiser. Assessment of providers’ linguistic fluency, however, has relied predominantly on self-reporting across the survey years.
Management of grievances and complaints. At least 90% of HMOs in each product line tracked language-related grievances independently from other complaints in 2003, but this percentage fluctuated in subsequent years between 90% and 100% for Medi-Cal and Healthy Families HMOs, and between 67% and 89% for Medicare and commercial HMOs. The SCLAS also asked whether HMOs monitor the percentage of self-disenrolling members who report reasons that might be language-related. The percentage of HMOs doing so remained relatively stable between 2005 and 2008 for Medi-Cal (35%–45%), Healthy Families (40%–53%), and commercial product lines (21%–24%), but rose among Medicare HMOs from 33% in 2005 and 18% in 2006 to 50% in 2008.
To file a complaint, Medi-Cal and Healthy Families HMO members were more likely to have non-English forms available than Medicare and commercial HMO members (Table 8). For each language, only one or two additional HMOs offered complaint forms in non-English languages by written or telephone request only (and not by website).
Discussion
To our knowledge, previous studies have not quantitatively described HMOs’ practices with regard to language services, although the link between interpretation services and improved health outcomes has been documented at the patient level.7,8,10,11 We report the results of a series of comprehensive annual surveys completed by representatives of nearly all eligible HMOs in California. According to these surveys, California HMOs are increasingly providing services to improve LEP members’ linguistic access to health care through face-to-face and telephone interpretation, as well as by offering translated documents and bilingual staff for HMO service contacts. The improvement in services provided by commercial and Medicare HMOs is notable because Medi-Cal and Healthy

tabl
e 7.
M
etH
OD
S BY
WH
iCH
Pla
nS
aSS
eSSe
D t
He
lan
gU
ag
e Pr
OFi
Cie
nC
Y O
F Bi
lin
gU
al
Sta
FF
(in
MeM
Ber
Ser
ViC
eS) a
nD
Hea
ltH
PrO
ViD
erS
(WH
O O
FFer
eD C
ar
e
Wit
Hin
tH
e Pl
an
net
WO
rK
), 20
04–2
008
Prod
uct l
ine
ass
esse
d by
Staff
Hea
lth p
rovi
ders
2004
2005
2006
2008
2004
2005
2006
2008
Med
i-Cal
No
form
al a
sses
smen
t10
%0%
0%0%
10%
5%0%
0%Se
lf-re
port
ing
30%
35%
20%
24%
90%
100%
100%
100%
Aca
dem
ic/s
tudy
cre
dits
15%
10%
10%
5%10
%5%
5%0%
Form
al b
y Pl
an45
%55
%30
%43
%5%
10%
15%
10%
Plan
con
trac
ts45
%50
%65
%62
%5%
5%0%
14%
Hea
lthy
Fam
ilies
No
form
al a
sses
smen
t11
%0%
0%0%
16%
0%0%
0%Se
lf-re
port
ing
26%
37%
21%
25%
95%
100%
100%
100%
Aca
dem
ic/s
tudy
cre
dits
16%
11%
11%
5%11
%5%
5%0%
Form
al b
y Pl
an42
%47
%26
%35
%5%
11%
16%
10%
Plan
con
trac
ts47
%53
%68
%70
%5%
11%
0%15
%M
edic
are
No
form
al a
sses
smen
t44
%22
%18
%17
%56
%22
%18
%11
%Se
lf-re
port
ing
22%
56%
55%
39%
67%
100%
91%
94%
Aca
dem
ic/s
tudy
cre
dits
11%
0%0%
0%11
%0%
0%0%
Form
al b
y Pl
an33
%11
%9%
28%
0%0%
0%6%
Plan
con
trac
ts11
%33
%27
%44
%0%
0%0%
11%
Com
mer
cial
No
form
al a
sses
smen
t36
%21
%0%
5%43
%14
%12
%5%
Self-
repo
rtin
g43
%64
%41
%21
%71
%93
%88
%75
%A
cade
mic
/stu
dy c
redi
ts14
%7%
6%0%
7%0%
0%0%
Form
al b
y Pl
an50
%43
%35
%26
%0%
7%12
%5%
Plan
con
trac
ts0%
36%
41%
68%
0%0%
0%16
%

489Moreland, Ritley, Rainwater, and Romano
table 8.PerCentage OF PlanS in WHiCH MeMBerS COUlD aCCeSS COMPlaint FOrMS in langUageS OtHer tHan engliSH, 2006–2008
language
Medi-Cala Healthy Families Medicare Commercial
2006 2008 2006 2008 2006 2008 2006 2008
Arabic 20% 29% 21% 30% 9% 11% 6% 16%Armenian 25% 33% 21% 35% 9% 6% 12% 21%Chinese 50% 52% 53% 55% 36% 28% 41% 53%Farsi 25% 33% 21% 35% 9% 6% 12% 21%Hmong 20% 29% 21% 25% 9% 11% 6% 16%Khmer 30% 38% 32% 40% 9% 6% 12% 26%Korean 25% 33% 26% 35% 9% 6% 12% 21%Russian 40% 53% 37% 45% 9% 11% 18% 26%Spanish 95% 100% 95% 95% 64% 72% 71% 90%Tagalog 25% 33% 21% 35% 9% 6% 12% 21%Vietnamese 45% 62% 47% 65% 9% 22% 24% 37%
aMedi-Cal results are across all counties only; responses applying only to specific counties are not shown.
Families HMOs have served as a benchmark with high levels of language services, due to state contracts that require language access services. Spanish and Chinese were the two languages in which commercial HMOs most frequently provided services, consistent with the distribution of non-English languages in California.
HMOs have increased efforts to identify current and new LEP members and match them with providers by language, which should decrease the need for interpretation services and presumably lower interpretation costs; however, patient-provider language concordance does not ensure access at points of contact beyond the provider (such as with front office staff). While language concordance has been shown to improve patient satisfaction,5 a number of other factors used in assigning patients to providers might be of higher priority to HMOs, such as distance to or capacity of a clinic. Medicare and commercial HMOs appear to have room for improvement with regard to sharing LEP members’ language data with their providers.
To access in-person and telephone interpretation services, as well as information about how to submit complaints, Spanish-speaking members seem to have increasing options available via multiple media. Chinese and Vietnamese speakers have less access to written materials in their own languages; other languages are rarely used in print materials. However, HMOs do provide oral interpretation and translations of docu-ments if asked, thus requiring members who prefer less frequently spoken languages to submit a special request. Yet, HMOs also infrequently communicate information in those languages about the opportunity to obtain such services.

490 State policies and language access in California’s HMOs
HMOs increasingly rely on professional interpreters and over-the-phone interpreta-tion vendors. These vendors appear to provide a significant portion of language access services; HMOs view them as easily accessible and potentially cost-effective.9 However, hospital-trained, face-to-face interpreters have been viewed by patients as more effec-tive than telephone interpreters;15 telephonic services should thus not be emphasized as an adequate surrogate for professional on-site interpretation. Nor should ad hoc interpreters take precedence over professional interpreters, a principle reflected in policies adopted by the majority of HMOs to discourage family and friends from act-ing as medical interpreters.
HMOs’ training programs generally incorporate cultural awareness into corporate policy. The SCLAS defines such training as four or more hours of instruction, which provides little insight into the actual time or effort devoted to this activity. While most HMOs train bilingual staff who interpret, less than three-quarters of respondents incorporated all of the four relevant categories of content (protocols, terminology, cultural communication, and ethics). Fewer HMOs trained health providers and their in-office staff, with relatively little change in stated content across survey years. The difference may reflect the relatively complex logistics of training providers in multiple locations. Along the same lines, we note HMOs’ persistent reliance on self-reporting of providers’ language proficiency, as compared to their focus on more formal methods of evaluating their own staff.
This study has three main strengths. First, since the respondent HMOs’ members constitute over 90% of California’s HMO members, the results are representative of California HMOs. HMO respondents range in member size from less than 13,000 to over three million. Nearly 100% response was obtained. Finally, the results span at least four years and are unlikely to be influenced by transient events, such as economic fluctuations.
Several limitations exist. First, the results cannot be generalized to other states, given that California is the only state to conduct such a survey, to report key responses publicly, and to mandate the provision of language services by commercial health plans; however, our data suggest how other states’ health plans might respond to legislative and regula-tory actions like the one taken in California. To our knowledge, no similar legislation to SB 853 has been enacted elsewhere in the United States.12 Second, it is difficult to validate these results without great expense; the SCLAS relies on self-reporting with validation only by asking HMO managers to review their own organizations’ responses and then posting key responses for public education and comment. We attempted to validate a subset of responses about HMO member documentation and websites in non-English languages, but were unable to do so due to changes between the most recent survey (May 2008) and our analyses of the data (June 2009). Third, the survey questions do not address patients’ actual language needs beyond simple identification of their primary languages. Fourth, these results represent the HMO perspective and provide little insight into actual consumer experiences, either with HMOs or at health care provider organizations at the point of care. It would build upon our results to explore consumers’ perspectives via member interviews and H-CAHPS survey responses.
Despite these limitations, California’s public reporting program appears to have moderately improved language access for the LEP among the largest HMOs, particularly

491Moreland, Ritley, Rainwater, and Romano
among commercial HMOs that are not bound by state contract or federal law to provide interpretation services. This trend has affected both “threshold languages” designated under SB 853 and non-threshold languages. Evidence from public reporting programs at the hospital level suggest that such reporting programs can stimulate substantial internal quality improvement activity18 and may improve patient care performance measures19 despite little or no migration of patients from lower-performing facilities to higher-performing facilities. In other words, patients consider many factors other than quality in making health care decisions, but having more quality-related information in the market appears to affect provider behavior. Our findings are consistent with this prior research, although it is difficult to attribute the changes that we observed to a single cause. We cannot yet measure the effects of the SB 853 regulations, which were implemented in 2009, and we cannot distinguish the impact of public reporting, which has been ongoing since 2004, from the impact of these long-anticipated regulations. It would be instructive to conduct another SCLAS in future years to compare provision of language services before and after regulation.
Contemporaneous comparative data from another diverse state would also be infor-mative. Future research should explore whether similar trends are occurring among preferred provider organizations, and how such language services are affecting plan members’ experiences and clinical outcomes. In the meantime, California’s experience suggests that public reporting, combined with the threat of state regulation, may improve the availability of language access services to LEP health plan members.
acknowledgments
Funding: Grant D55HP10337-02-00 from the Health Resources and Services Admin-istration; Interagency Agreement 05MC-1A016 from the California Department of Managed Health Care.
appendix a—California HMOS and Product lines in 2008
Health Plans—2008
lines of business in 2008
Commercial MedicareHealthy Families
Healthy Kids Medi-Cal
Aetna Health of California, Inc. X X Anthem Blue Cross X X X XBlue Shield of California X X X CIGNA HMO X Health Net X X X X XKaiser Permanente—Northern CA X X X XKaiser Permanente—Southern CA X X X XPacifiCare of California X X Western Health Advantage X X XAlameda Alliance for Health X X X X X

492 State policies and language access in California’s HMOs
CalOptima X X X XCare1st Health Plan X X X XCenCal Health X X X XCentral Coast Alliance for Health X X X XChinese Community Health Plan X X Community Health Plan X X XContra Costa Health Plan X X X XHealth Plan of San Joaquin X X X XHealth Plan of San Mateo X X X X XInland Empire Health Plan X X X XKern Family Health Care X XL.A. Care Health Plan X X XMolina Healthcare X X XPartnership Health Plan X X XSan Francisco Health Plan X X X XSanta Clara Family Health Plan X X X X
X 5 Product Lines
appendix B—Questions in the 2008 Office of the Patient advocate Survey of Cultural and language Services Provided by California Health Plans
1. Check the Plan’s lines of business below and provide the name(s) of Plans as marketed as well as the approximate enrollment as of March 1, 0008.
• Medi-Cal• HealthyFamilies• HealthyKids• Medicare• Commercial
2. Please provide the name(s), title/department(s) and telephone number(s) and email of the person(s) completing this survey.
3. For Medi-Cal, please indicate the Type of Coverage for the county and whether the county coverage is partial or full.
4. For the following lines of business, please indicate which are your Plan’s non-English threshold languages?
5. For the following lines of business, please indicate who captures the Plan
Health Plans—2008
lines of business in 2008
Commercial MedicareHealthy Families
Healthy Kids Medi-Cal

493Moreland, Ritley, Rainwater, and Romano
member’s primary language upon enrollment or at eligibility determination? (Mark all that apply)
• PlanOnly• Contractor• BothPlan/Contractor• GovernmentAgency
6. Does the Plan document a member by language in the IS system or member database?
7. Does the Plan share member language information with your contracted providers?
8. When LEP members fail to choose a primary care provider, does the Plan match member and provider language capacity in assigning a primary care provider?
9A. Are LEP members informed on the availability of access to telephone interpreter services in non-English languages using Evidence of Coverage / Member Handbook?
9B. Are LEP members informed on the availability of access to telephone interpreter services in non-English languages using Member Newsletters/Annual Notice (including web based communication)?
10A. Are LEP members informed in non-English languages on the availability of interpreters at medical visits by using Evidence of Coverage / Member Handbook?
10B. Are LEP members informed in non-English languages on the availability of interpreters at medical visits by using Member Newsletters/Annual Notice (includes web based communication)?
11. Are oral translations of the Plan’s written materials for LEP members available upon request?
12. Does the Plan provide or arrange for access to face-to-face interpreter during business hours at medical points of contact in the following non-English languages?
13. Are face-to-face interpretation services in medical settings provided free of charge for LEP members?
14. Does the Plan provide or arrange for twenty-four hour telephone interpretation at medical points of contact in the following non-English languages?
15. Does the Plan provide or arrange for twenty-four hour Advice Nurse in the following non-English languages?
16. Does the Plan’s Call Center(s) and/or Member Services department(s) have qualified bilingual staff that can speak to a LEP member in their preferred language?
17. Can a Plan member obtain the following services in their primary language upon request either by telephone or in writing?
• Explanationand/orassistancewithenrollmentanddisenrollment• Informationabouthealtheducationandwellnessprograms
18. Except when explicitly requested by the patient, does the Plan discourage adult family members and friends from serving as interpreters at medical visits?

494 State policies and language access in California’s HMOs
19. Except when explicitly requested by the patient, does the Plan expressly discourage the use of children (under 18) from serving as interpreters at medical visits?
20. Are TTY/TDD capacities (including the California Relay Services) available to hearing-impaired Plan members?
21. How are hearing impaired members informed on how to access sign language interpreter services?
• Memberhandbook• Membernewsletters• Website
22. Except when explicitly requested by the patient, does the Plan discourage adult family members and friends from serving as sign-language interpreters at medical visits?
23. Except when explicitly requested by the patient, does the Plan expressly discourage the use of children (under 18) from serving as sign-language interpreters at medical visits?
24. What is the Plan’s website address? 25. Does the Plan’s website have information on language access services in
English? 26. Does the Plan’s website have information on language access in a non-English
language? 27. Is the Provider Directory on the Plan’s web site? 28. Is there a non-English version of the Provider Directory on the Plan’s web site? 29. In what non-English languages is the Provider Directory available on the Plan’s
website? 30. Are member informing documents available to Limited English Proficient
(LEP) members in the following non-English languages?
A. Evidence of Coverage / Member HandbookB. Grievance/Complaint and Appeals Materials (e.g., Grievance submission
forms, Notices of Rights to Appeal, etc. C. Notices for LEP members pertaining to modification, reduction, denial or
termination of services and benefits D. Consent Forms (informed consent used by Providers)E. Member Newsletters/Annual Notice (may include web based
communications)
31. If the Plan offers a written translated Provider Directory, in what non-English languages is it available?
32. Over the past year, have the Plan’s bilingual/multilingual staff in member services been trained in providing culturally appropriate services?
33. Did the Plan provide training(s) that focused on culturally appropriate care to office staff/providers in its network within the last year?
34. Which of the following describes the type of training office staff/providers in its network received in the past year (January thru December 2005)? (Training may be in-service or vendor class of 4 or more hours.)
• Skillsandpracticesregardingculture-relatedhealthcareissues?

495Moreland, Ritley, Rainwater, and Romano
• Conceptsofculturalcompetencyanditseffectsonqualitycareandaccesstocare?
• Howtolocatetranslatedmaterial?• Howtoaccessandutilizeinterpreterservicesinamedicalhealthencounter?
35. Which of the following describes the type of training bilingual staff who function as interpreters received in the past year (January thru December 2007)? (Training may be an in-service or vendor class of 4 or more hours.)
• Interpretingprotocols?• BasicmedicalterminologyinEnglishandothernon-Englishlanguages?• Cultureanditsimpactoncommunication?• Ethicalprinciplesofhealthcareinterpreting?
36. Does the Plan keep track of how often Plan members request interpretation services . . .? (Mark all that apply)
• Yes,viaMemberServices• Yes,whenmakingmedicalappointments• Yes,other• Notmonitored
37. How are the non-English language proficiency and language skills of the Plan’s bilingual or multilingual staff in member services assessed? (Mark all that apply)
• Noformalassessment• Proficiencythroughself-reporting• Academicorstudycredits• FormallanguageproficiencyassessmentbyPlan• Plancontractsforformallanguageassessment
38. Does the Plan monitor the delegated contractor’s language proficiency assessment methods or policies for provider/office staff?
39. How are the non-English language proficiency and language skills of bilingual providers who offer care assessed? (Mark all that apply)
• Noformalassessment• Proficiencythroughself-reporting• Academicorstudycredits• FormallanguageproficiencyassessmentbyPlan• Plancontractsforformallanguageassessment
40. How are the non-English language proficiency and sign language skills of sign language interpreters assessed? (Mark all that apply)
• Noformalassessment• Proficiencythroughself-reporting• Academicorstudycredits• FormallanguageproficiencyassessmentbyPlan• Plancontractsforformallanguageassessment

496 State policies and language access in California’s HMOs
41. If the Plan contracts for sign language interpreters, does the Plan monitor the contractor’s proficiency assessment methods or policies?
42. Does the Plan track whether the Plan’s LEP members have a primary care provider who speaks their primary language?
43. Does the Plan monitor the availability of face-to-face interpreter services at the delegated contractor site through . . .? (Mark all that apply)
• ContractorReportsasrequiredbycontract• SiteVisits• Auditsortestsofservices• Other• Notapplicable(notdelegated)
44. Does the Plan monitor the availability of sign language interpreter services at the delegated contractor site through . . .? • ContractorReportsasrequiredbycontract• SiteVisits• Auditsortestsofservices• Other• Notapplicable(notdelegated)
45. Does the Plan track language barrier grievances/complaints independent from general complaints?
46. Does the Plan monitor delegated contractor’s services for language problems or complaints?
47. Does the Plan maintain records of self-disenrollments from the Plan that may be attributable to language service issues?
48. How does the Plan inform its members in their primary preferred languages about how to file a written Grievance or Complaint?
a. Member Handbook or Evidence of Coverageb. Member Newsletters/Annual Notice (may include web based
communications)c. Plan Website
49. Are non-English language forms available for an LEP member to file a written complaint?
50. Are non-English Grievance and Complaint forms available on the Plan’s website?
51. In what non-English languages does the Plan administer CAHPS Member Satisfaction Surveys?
52. In what non-English languages does the Plan survey LEP members using a tool other than CAHPS to track satisfaction with the health Plan?
53. Does the Plan have written policies on the provision of language access services beyond the grievance process?
54. Are health Plan Member Services staff given and made aware of the written policies regarding language access services?
55. Does the Plan provide a stand alone notice to LEP Plan members in a language they understand of the right to language assistance free of cost?
56. Does the health Plan incorporate language access services in its quality improvement program?

497Moreland, Ritley, Rainwater, and Romano
57. Does the Plan incorporate cross-cultural competencies in its Strategic Plan? 58. Does the Plan review its HEDIS data to examine scores by race and ethnicity? 59. Does the Plan review its HEDIS data to examine scores by language groups?
LEP 5 Limited English ProficientHEDIS 5 Health Care Effectiveness Data and Information Set
notes 1. Shin HB, Bruno R. Language use and English speaking ability: 2000. Washington,
DC: U.S. Census Bureau, 2003. Available at: http://www.census.gov/prod/2003pubs /c2kbr-29.pdf.
2. Kominski GF, Reifman C, Cameron ME, et al. Language barriers pose a risk for Cali-fornia HMO enrollees. Los Angeles, CA: UCLA Center for Health Policy Research, 2006. Available at: http://www.healthpolicy.ucla.edu/pubs/files/lang_barrier_hmo_pb .050806.pdf.
3. Masland M, Snowden L. California’s limited English proficient population (LEP) and strategies to promote health care access. Berkeley, CA: UC Berkeley/California Program on Access to Care, 2009. Available at: http://cpac.berkeley.edu/documents /snowden_proof.pdf.
4. Baker DW, Hayes R, Fortier JP. Interpreter use and satisfaction with interpersonal aspects of care for Spanish-speaking patients. Med Care. 1998 Oct;36(10):1461–70.
5. Quan K. Assessing the impact of physician-patient communication barriers on health-care costs and quality. Presented to the OMH Expert Panel, Rockville, MD. 2003 Oct 16.
6. Diamond LC, Schenker Y, Curry L, et al. Getting by: underuse of interpreters by resident physicians. J Gen Intern Med. 2009 Feb;24(2):256–62.
7. Flores G, Laws MB, Mayo SJ, et al. Errors in medical interpretation and their potential clinical consequences in pediatric encounters. Pediatrics. 2003 Jan;111(1):6–14.
8. Jacobs EA, Lauderdale DS, Meltzer D, et al. Impact of interpreter services on deliv-ery of health care to limited-English-proficient patients. J Gen Intern Med. 2001 Jul; 16(7):468–74.
9. Brach C, Fraser I, Paez K. Crossing the language chasm: an in-depth analysis of what language-assistance programs look like in practice. Health Affairs. 2005;24(2):424–34.
10. Flores G. The impact of medical interpreter services on the quality of health care: a systematic review. Med Care Res Rev. 2005 Jun 2005;62(3):255–99.
11. Karliner LS, Jacobs EA, Chen AH, et al. Do professional interpreters improve clinical care for patients with limited English proficiency? A systematic review of the literature. Health Serv Res. 2007 Apr;42(2):727–54.
12. Au M, Taylor EF, Gold M. Improving access to language services in health care: a look at national and state efforts. Washington, DC: Mathematica Policy Research Inc., 2009 Apr. Available at: http://www.ahrq.gov/populations/languageservicesbr.pdf.
13. State of California/Department of Managed Health Care. Title 28: California Code of Regulations. Sacramento, CA: State of California/Department of Managed Health Care, 2006. Available at: http://www.dmhc.ca.gov/library/reports/news/lart.pdf.
14. State of California/Legislative Counsel. California Health & Safety Code Section 1259. Sacramento, CA: State of California/Legislative Counsel. Available at: http://www .leginfo.ca.gov/cgi-bin/calawquery?codesection5hsc.
15. State of California/Office of the Patient Advocate. Why isn’t my health plan listed?

498 State policies and language access in California’s HMOs
Sacramento, CA: State of California/Office Patient Advocate, 2011. Available at: http://opa.ca.gov/report_card/hmonotlisted.aspx.
16. Moreland CJ, Ritley D, Romano PS. Interpreting for California’s insured deaf and hard of hearing: HMOs’ language access services. J Disability Policy Studies. 2011 Dec; 22(3):172–80.
17. Garcia EA, Roy LC, Okada PJ, et al. A comparison of the influence of hospital-trained, ad hoc, and telephone interpreters on perceived satisfaction of limited English-proficient parents presenting to a pediatric emergency department. Pediatr Emerg Care. 2004 Jun;20(6):373–8.
18. Fung CH, Lim YW, Mattke S, et al. Systematic review: the evidence that publish-ing patient care performance data improves quality of care. Ann Intern Med. 2008 Jan;148(2):111–23.
19. Werner RM, Konetzka RT, Stuart EA, et al. Impact of public reporting on quality of postacute care. Health Serv Res. 2009 Aug;44(4):1169–87.
Copyright © 2022 FDOKUMEN