Spoligotyping of isolates from patients with pulmonary tuberculosis in Mumbai, India
9
Research in Microbiology 156 (2005) 588–596 www.elsevier.com/locate/resmic Spoligotyping of Mycobacterium tuberculosis isolates from patients with pulmonary tuberculosis in Mumbai, India Savita Kulkarni a , Christophe Sola b , Ingrid Filliol b , Nalin Rastogi b , Gururaj Kadival a,∗ a Laboratory Nuclear Medicine Section, Isotope Group, Bhabha Atomic Research Centre C/o T.M.H. Annexe, Parel, Mumbai 400012, India b Unité de la Tuberculose et des Mycobactéries, Institut Pasteur de Guadeloupe, Pointe-à-Pitre, Guadeloupe Received 3 May 2004; accepted 6 January 2005 Available online 11 March 2005 Abstract Tuberculosis remains a major health problem in India, with 2 million new cases and 421000 deaths each year. In this paper, we describe the spoligotyping results of 216 Mycobacterium tuberculosis culture isolates from patients with pulmonary tuberculosis in Mumbai, India. As spoligotyping data from India have rarely been described until now, and as there is limited information on the major circulating clades of M. tuberculosis, the data obtained were also compared to an international spoligotype database (SpolDB4) that contained patterns from 22 546 isolates from more than 100 countries. Eighty-four (39%) of the isolates were definitively marked as orphan strains, indicating the paucity of such data from India. The remaining 132 isolates clustered among 59 shared types; among these, 42 shared types were already present in the database, 17 were newly created, and 5 of them were specifically reported from Mumbai. A total of 9 major types in this study clustered 32% of the isolates. At the phylogenetic level, 30% of the isolates belonged to the Central Asian families CAS1 and CAS2, of the major genetic group (MGG) 1, 29% to MGG 2 and 3 families (spacers 33–36 missing) and 17% to the ancestral East African Indian (EAI) family. Finally, nearly 10% of the isolates belonged to the W-Beijing family in a broad sense, also in the MGG 1 group. In conclusion, historic clones of the MGG 1 group of M. tuberculosis are responsible for roughly 60% of all tuberculosis cases in Mumbai. Together with the fact that organisms presumably of European descent (such as the Haarlem family) were only rarely found, our observations suggest that tuberculosis in Mumbai, India is essentially caused by historical clones of tubercle bacilli undergoing active circulation due to uncontrolled demography, high prevalence of the disease, and a paucity of resources. 2005 Elsevier SAS. All rights reserved. Keywords: Mycobacterium tuberculosis; Spoligotyping; Mumbai, India; SpolDB4 database; Dendrogram 1. Introduction Tuberculosis has re-emerged as one of the leading causes of death worldwide. Currently, more than one-third of the world’s population is infected by Mycobacterium tubercu- losis, and 8 million new cases and approximately 2 million deaths are reported each year [9]. Tuberculosis remains a major health problem, especially in India, with 2 million new cases and 500 000 deaths per year [1]. Mumbai (for- merly Bombay) is a densely populated metropolis with a population of 12 million, 4.8 million (40%) of whom live in * Corresponding author. E-mail address: [email protected] (G. Kadival). crowded slums. A resurgence of tuberculosis has occurred since 1990 and is characterized by a 70–140% increase in deaths due to tuberculosis among adults. Multidrug-resistant (MDR) tuberculosis has also increased, with two different studies reporting 11% MDR cases in 1991–1995 and 58% in 1994–1995 [7,33]. As tuberculosis is a highly contagious disease that is mainly transmitted from person to person, tracing individuals who might have been in contact with infected persons is a major strategy in limiting the dissem- ination of M. tuberculosis. The typing of strains from in- fected individuals could play an important role in tracking the source of infection and helping in epidemiological stud- ies. Most molecular strain typing methods for tuberculosis are based on genetic elements that contribute to DNA poly- 0923-2508/$ – see front matter 2005 Elsevier SAS. All rights reserved. doi:10.1016/j.resmic.2005.01.005
-
Upload
campus-paris-saclay -
Category
Documents
-
view
5 -
download
0
Transcript of Spoligotyping of isolates from patients with pulmonary tuberculosis in Mumbai, India

c
e describedia.g cladeserns fromating theere alreadythis studyCAS2, ofan Indianclusion,with
uggest thatontrolled
Research in Microbiology 156 (2005) 588–596
www.elsevier.com/locate/resmi
Spoligotyping ofMycobacterium tuberculosis isolates from patientswith pulmonary tuberculosis in Mumbai, India
Savita Kulkarnia, Christophe Solab, Ingrid Filliol b, Nalin Rastogib, Gururaj Kadivala,∗
a Laboratory Nuclear Medicine Section, Isotope Group, Bhabha Atomic Research Centre C/o T.M.H. Annexe, Parel, Mumbai 400012, Indiab Unité de la Tuberculose et des Mycobactéries, Institut Pasteur de Guadeloupe, Pointe-à-Pitre, Guadeloupe
Received 3 May 2004; accepted 6 January 2005
Available online 11 March 2005
Abstract
Tuberculosis remains a major health problem in India, with 2 million new cases and 421 000 deaths each year. In this paper, wthe spoligotyping results of 216Mycobacterium tuberculosis culture isolates from patients with pulmonary tuberculosis in Mumbai, InAs spoligotyping data from India have rarely been described until now, and as there is limited information on the major circulatinof M. tuberculosis, the data obtained were also compared to an international spoligotype database (SpolDB4) that contained patt22 546 isolates from more than 100 countries. Eighty-four (39%) of the isolates were definitively marked as orphan strains, indicpaucity of such data from India. The remaining 132 isolates clustered among 59 shared types; among these, 42 shared types wpresent in the database, 17 were newly created, and 5 of them were specifically reported from Mumbai. A total of 9 major types inclustered 32% of the isolates. At the phylogenetic level, 30% of the isolates belonged to the Central Asian families CAS1 andthe major genetic group (MGG) 1, 29% to MGG 2 and 3 families (spacers 33–36 missing) and 17% to the ancestral East Afric(EAI) family. Finally, nearly 10% of the isolates belonged to the W-Beijing family in a broad sense, also in the MGG 1 group. In conhistoric clones of the MGG 1 group ofM. tuberculosis are responsible for roughly 60% of all tuberculosis cases in Mumbai. Togetherthe fact that organisms presumably of European descent (such as the Haarlem family) were only rarely found, our observations stuberculosis in Mumbai, India is essentially caused by historical clones of tubercle bacilli undergoing active circulation due to uncdemography, high prevalence of the disease, and a paucity of resources. 2005 Elsevier SAS. All rights reserved.
Keywords: Mycobacterium tuberculosis; Spoligotyping; Mumbai, India; SpolDB4 database; Dendrogram
usehe
onins an
(for-a
rredse intant
ent8%us
son,ithm-
-ngud-sis
1. Introduction
Tuberculosis has re-emerged as one of the leading caof death worldwide. Currently, more than one-third of tworld’s population is infected byMycobacterium tubercu-losis, and 8 million new cases and approximately 2 millideaths are reported each year [9]. Tuberculosis remamajor health problem, especially in India, with 2 millionew cases and 500 000 deaths per year [1]. Mumbaimerly Bombay) is a densely populated metropolis withpopulation of 12 million, 4.8 million (40%) of whom live in
* Corresponding author.
E-mail address: [email protected] (G. Kadival).0923-2508/$ – see front matter 2005 Elsevier SAS. All rights reserved.doi:10.1016/j.resmic.2005.01.005
s
crowded slums. A resurgence of tuberculosis has occusince 1990 and is characterized by a 70–140% increadeaths due to tuberculosis among adults. Multidrug-resis(MDR) tuberculosis has also increased, with two differstudies reporting 11% MDR cases in 1991–1995 and 5in 1994–1995 [7,33]. As tuberculosis is a highly contagiodisease that is mainly transmitted from person to pertracing individuals who might have been in contact winfected persons is a major strategy in limiting the disseination of M. tuberculosis. The typing of strains from infected individuals could play an important role in trackithe source of infection and helping in epidemiological sties. Most molecular strain typing methods for tuberculo
are based on genetic elements that contribute to DNA poly-
S. Kulkarni et al. / Research in Microbiology 156 (2005) 588–596 589
ers.ain
ileemse-with
g-useites
smis
encent
em-
s
iche.
r,
ogi-
r-mostyp-ingnce
itive
om-samandesa
iquee asinsn.typathortre-18,imi-
et-
ffin-
iso-.as
un-. Attternsibe a
onaltotalun-
ntslesear.co-andean-onerialfiedhewth12
for
theereand
an-d.etri-r43tlyuth,n-
. To
morphism and may be exploited as strain-specific markVarious repetitive DNA elements that contribute to strvariation have been discovered inM. tuberculosis. Two ofthese, IS6110 and IS1081, are insertion sequences, whothers, like direct repeats (DRs), major polymorphic tandrepeats (MPTRs), and polymorphic GC-rich repetitivequences (PGRs), are short repetitive DNA sequencesno known function or phenotype.
IS6110 was evaluated as a probe for restriction frament length polymorphism (RFLP) analysis [6,35] becaof the highly variable number of copies and the variable sof integration into the chromosome. Strains ofM. tuber-culosis display an extremely high degree of polymorphiof IS6110 containing restriction fragments [6,20,21]. Thpolymorphism is presumably due to the ability of IS6110 totranspose within the genome without much target sequspecificity [21]. IS6110 has been proven to be an excellegenetic marker for tracing individualM. tuberculosis strainsduring outbreaks, nosocomial infections and clonal dissination of MDR strains [4,15,24,35]. Though IS6110 RFLPhas been used widely forM. tuberculosis strain typing, itsmajor limitation is its low discriminating power for isolateharboring fewer than six copies of IS6110 [39], along withthe requirement for large amounts of pure intact DNA whcan be obtained only by culture which takes a long timIn some strains ofM. tuberculosis, especially from Indiaand other Asian countries, IS6110 may be absent. Moreovesystematic fingerprinting of all bacterial isolates by IS6110RFLP analysis remains cumbersome in large epidemiolcal studies, particularly in developing countries.
With the aim of overcoming the limitations of RFLP, vaious PCR-based methodologies were developed. Thepopular typing method among these is DR-based spoligoing. The DR locus, which is the basis for the spoligotyptechnique, consists of a series of directly repeated sequeof 36 bp, with each DR being separated by a non-repetunique spacer DNA of 35–41 bp in length. MostM. tuber-culosis strains contain a copy of IS6110 at a site within theDR region. When the DR regions of several strains are cpared, the order of spacers appears to be about theamong all strains, but insertions or deletions of spacersDR do occur [13,25,34]. The spoligotyping method involvPCR amplification of the DR locus and hybridization toseries of oligonucleotides representing each of the unspacer sequences in the DR locus. The most attractivpect of the method is the ability to rapidly fingerprint strawithout the need to subculture isolates for DNA isolatioThus, the technique can be used for detection as well asing of M. tuberculosis strains, and is a rapid method thallows a large number of isolates to be handled in a stime [18]. Spoligotyping has been extensively used incent years for epidemiological studies of tuberculosis [28,38], and has been shown to be useful in strain discrnation when used in association with IS6110-RFLP, variablenumber of tandem DNA repeats (VNTR), and double rep
itive element (DRE)-PCR [12,32]. Spoligotyping can alsot
s
e
-
-
be performed directly fromM. tuberculosis organisms, eventhose that are non-viable or are found in tissues in paraembedded blocks or in archeological samples.
In the present study, spoligopatterns of 216 culturelates ofM. tuberculosis from Mumbai, India were analyzedSince Mumbai is a densely populated metropolis, it winteresting to study the spoligo pattern in an effort toderstand the extent of polymorphism of the organismsthe same time, a possible association between these paand MDR tuberculosis was also analyzed. We also descrdendrogram of theM. tuberculosis population structure fromMumbai and compare the data obtained with an internatispoligotyping database that contained patterns from aof 22 546 isolates from more than 100 countries, so as toderstand the origin of the organism.
2. Materials and methods
2.1. Patient population and bacterial isolates
Our analysis was based on 216M. tuberculosis cultureisolates which originated from sputum samples of patiefrom two government hospitals in Mumbai. Sputum sampwere collected from 681 patients over a period of one yPatients from all parts of the city belonged to the lowest enomic strata and used the two hospitals for diagnosistreatment. The male to female ratio was 8:1 and the mage of the group was 35 years. Six-hundred and eightycultures were set up, 347 of which showed mycobactegrowth. Three-hundred and twelve of these were identiasM. tuberculosis by conventional biochemical tests and tremaining samples showed atypical mycobacterial groand were exluded from further analysis. Among the 3M. tuberculosis cultures, 216 were randomly selectedspoligotyping analysis.
2.2. MDR status
The isolates were also tested for drug sensitivity bystandard proportion method. Fifty-three of the isolates wclassified as MDR on the basis of resistance to isoniazidrifampicin.
2.3. DNA extraction and spoligotyping
DNA was extracted from all culture isolates by the stdard cetyl-trimethyl ammonium bromide (CTAB) methoThe DNA concentration was estimated spectrophotomcally and stored in TE1x (10 mM Tris, 1 mM EDTA) buffeat 4◦C until use. For spoligotyping, a membrane witholigonucleotides in parallel lines, immobilized covalenon a Biodyne C membrane (Pall Biosystems, PortsmoUK), was provided as part of an International Atomic Eergy Agency coordinated research project (No. 10039)
avoid typing errors, the results obtained were systematically
590 S. Kulkarni et al. / Research in Microbiology 156 (2005) 588–596
nest desing
ingor-edde-tter-
gateilu-m,
vel-
ataentdataer-B4)Pasthiseur-in-
redhannedaredl of
ailedionrld:raler-),e
al-typerldersin-
aseters)p-theredeivetheon-ibed
itherm-
l thethegesicsol-
5].
Theem-
yre
pat-clus-andere
with, 84nd
ain-tudytheyun-tal
omevi-rentre-
ypese re-basehedl of 5frompesle 1istri-
e-32%heseent-from4),
reconfirmed on another batch of spoligotyping membraprepared and supplied by the Unité de la Tuberculose eMycobactéries, Institut Pasteur, Guadeloupe. Spoligotypwas performed as previously described [18], by amplifythe spacer regions of the DR locus with primers Dra (fward) and Drb (reverse). The amplified DNA was hybridizto a membrane containing 43 oligonucleotide probes totect spacer regions in test strains with a 45-lane blo(Miniblotter 45, Immunetics, Cambridge, MA). The membrane was incubated with streptavidin-peroxidase conjuand hybridized DNA was detected by an enhanced chemminescence detection liquid (ECL detection kit, AmershaBuckinghamshire, UK). The autoradiograms were deoped using standard photochemicals after 10 min to 2 h ofexposition on X-ray films.
2.4. Data analysis
Spoligopatterns were analyzed using MS-Excel dsheets and grouped together for similarity. The differclusters were labeled with arbitrary numbers and thewere further analyzed by comparison with the fourth vsion of an international spoligotyping database (SpolDwhich has been created and maintained at the Institutteur of Guadeloupe (IPG). The latest public release ofdatabase (SpolDB3) may be downloaded at www.pastguadeloupe.fr/tb/spoldb3 (see also Ref. [11]). Beforetroduction of the Mumbai results(n = 216), the databasecontained a total of 22 546 isolates split into 1310 shatypes totaling 20 408 clustered isolates and 2138 orppatterns. After matching analysis, the spolDB4 contai22 762 isolates corresponding to a new total of 1327 shtypes totaling 20 552 clustered isolates and a new tota2210 orphan types. The database also provided detcountry origin information about the geographic distributof the shared types within 8 predefined regions of the woAfrica (AFR), Far East/Asia (FEA), Middle East and CentAsia (MECA), Europe (EUR), Oceania (OCE), South Amica (SAM), Central America and the Caribbean (CAMand North America (NAM). The strains with spoligotypsimilar to any pattern of anM. tuberculosis strain alreadyfound in the database were automatically labeled with anready defined ‘shared type’ number, whereas a spoligoexhibiting a profile not yet found anywhere in the wowas termed an ‘orphan strain’. New shared type numbwere automatically created when orphan profiles of theput dataset matched with orphan profiles of the databNew clusters present in the input dataset (specific cluswere treated similarly. Although quality control in genotying, and in particular in spoligotyping, has not yet beenfocus of numerous studies [10], the principle of the shatype nomenclature (only patterns seen at least twice reca label) is a simple and efficient means of controllingincreasing entropy within the spoligotyping database. Csequently, we assume that the genetic variability descr
in this study is due to true polymorphism of the DR re--
.
gion, and that shared type definitions indeed represent econvergence or true synapomorphy (similarity due to comon ancestors). A spoligotype-based dendrogram of alMumbai isolates was built using the Jaccard index andunweighted pair group method using arithmetic avera(UPGMA). This task was performed using Bionumersoftware (Applied Maths, St. Marten-Latems, Belgium), flowing the manufacturer’s recommendations.
2.5. RFLP analysis
RFLP was performed by the conventional method [3Briefly, M. tuberculosis DNA was digested withPvuII for 4 hat 37◦C and subjected to agarose gel electrophoresis.separated fragments were then transferred to a nylon mbrane (Biodyne, USA) and hybridized with a32P-labeledinternal probe specific to IS6110.
3. Results
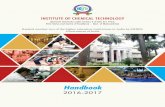
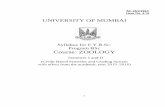
A total of 216M. tuberculosis isolates were analyzed bspoligotyping. Ninety-four strains (43.5%) out of 216 wepresent in 21 different clusters. Fig. 1 shows the spoligoterns of these strains (named as SP-1 to SP-21). Twelveters of 2 isolates, two clusters of 3, 4 and 5 isolates eachthree big clusters (2 of 16 isolates and 1 of 14 isolates) wobserved. The spoligopatterns were further comparedthe SpolDB4 database. Out of the remaining 122 isolateswere definitively marked as orphan strains from India athe spoligotypes of these are shown in Fig. 2. The reming 38 isolates were present as unique patterns in our spopulation, and were declared to be shared types, asexhibited patterns similar to orphan strains from other cotries after matching with SpolDB4. This increased the tonumber of clustered strains to 132/216 (61.1%), since sof the orphan strains of the input file matched with preously described shared types. Thus, a total of 143 diffespoligotypes were observed with 84 orphan types, themaining 59 being shared types. Among the 59 shared tfound, our strains created 17 new shared types, while thmaining 42 shared types were already found in the datawithin various geographic regions, and our strains enricthese already defined shared types. There were a totanew shared types created uniquely among our isolatesMumbai, India, whereas the remaining 12 new shared tywere created with orphan types from other countries. Tabshows these shared types with their broad geographic dbution.
A total of 9 major types from Mumbai, India were dfined that contain 3 or more isolates each and containof all isolates in the present study. Table 2 represents tmajor types, their geographic distribution, and their percage in the present study and the database. It is clearTable 2 that predominant cluster SP-1 (type 1 in spolDB
called the Beijing strain, is present in 7.4% of our study
S. Kulkarni et al. / Research in Microbiology 156 (2005) 588–596 591
Fig. 1. Spoligopatterns of theM. tuberculosis culture isolates in clusters.
:
ralrth
-14o-B4)nlyins
senthanour
igo-
psntedS1) 1ec-
iso-p ofers
lem,ll-s.
har-udyo-thisns.ngtes.9%rlya
, thisata-
f the
ble4
ma-inug-
tive
Table 1Geographic distribution of new shared types
1A. Five new shared types created uniquely among Indian strains
Type numberin database
Number(% of isolates in present study)
Geographicdistribution
1314 3 (1.4%) India1319 2 (0.9%) India1320 2 (0.9%) India1323 2 (0.9%) India1325 2 (0.9%) India
1B. Twelve new shared types created with orphan types from othercountries
Type number in database(number in our study)
Geographic distributioncommon to a single isolate each, from
1313, 1315, 1316, 1317 (1) EUR1326, 1327 (1) MECA1321, 1322, 1324 (1) NAM1321 (1) SAM1311 (2) OCE1318 (4) AFR
Geographic distribution: AFR, Africa; MECA, Middle East and CentAsia; EUR, Europe; OCE, Oceania; SAM, South America; NAM, NoAmerica.
which is comparable to 8.85% of the database. Also SP(type 53 in spolDB4) is present in 6.5% of our culture islates and 6.44% in the database. SP-3 (type 26 in spolDwhich is a major type in our study (7.4%) is present oas a minor type in the database, with only 0.87% strawith that spoligotype. 50 other shared types were preas minor types from Mumbai, India and contained less t3 isolates each; they represented 29% of all isolates instudy.
We then built a dendrogram based on the 216 spol
typing results (Fig. 3) using the Jaccard index and the UP-,
GMA method. At the phylogenetic level, at least 5 grouof strains were observed. The most frequently represefamily was made up of the Central Asian families CAand CAS2, belonging to the major genetic group (MGGwith prototypic spoligotypes type 26 and type 288, resptively. This family represented as much as 30% of thelates studied. A second large cluster contained a grouMGG 2 and 3 families that had in common missing spac33–36. This cluster comprised well-defined clades HaarX, Latin-American and Mediterranean (LAM), and an idefined “T” clade [11], accounting for 29% of the isolateWithin the same large group, we also noted a yet poorly cacterized group of strains baptized “Manu” in a recent stfrom Delhi [27], that represented an additional 5% of islates from Bombay. It is possible that in some cases,specific spoligotype could represent polyclonal infectioThe ancestral East African Indian (EAI) family, belongito the MGG 1, represented one sixth (17%) of total isolaIt was followed by a “miscellaneous” group representingof poorly defined clinical isolates. Last but not least, nea10% of the isolates belonged to the W-Beijing family inbroad sense, and also the MGG 1 group (sensu strictofamily is represented by a single shared type 1 in the dbase, i.e., characterized by hybridization only to 3′ terminalspacers of 35–43; such strains represented only 7.4% oisolates in the present study).
When this dendrogram was compared to all availaspoligotypes from different parts of India in the SpolDB(n = 500; results not shown), the same structure of 5jor families was maintained with only slight variationsthe percentages shown in Fig. 3. This observation sgests that the structure of theM. tuberculosis complex inthe present study from Mumbai is probably representa
of the major circulating clades ofM. tuberculosis in In-
592 S. Kulkarni et al. / Research in Microbiology 156 (2005) 588–596
Fig. 2. Spoligopatterns of orphan strains ofM. tuberculosis in Mumbai.
to
i-tureedis-
pat-urnoden
be-P-3pat-waswasis
so-
dia. Although more data will undoubtedly be neededprecisely define the specific population structure ofM. tu-berculosis for a country as huge as India, these prelimnary results underline a deeply rooted population strucof tubercle bacilli in India. Further diversity data acquirfrom various regions of India should shed light on thissue.
Further analysis was done to determine whether anytern was preferentially present in MDR strains. Fifty-foMDR isolates were well distributed in all groups, andparticular pattern preference was observed. In patterns itified as the W-Beijing family ofM. tuberculosis, only 2
isolates were MDR (data not shown).-
RFLP analysis was carried out on 46 isolates thatlonged to the three major clusters, SP-1 (16 isolates), S(16 isolates) and SP-14 (14 isolates). Fig. 4 depicts theterns obtained by spoligotyping and RFLP. The analysisdepicted on an MS Excel sheet. As seen in Fig. 4, thereextensive polymorphism by RFLP, indicating that RFLPmore discriminative than spoligotyping.
4. Discussion
This study describes the spoligotyping of 216 culture i
lates ofM. tuberculosis from Mumbai, India which has a
S. Kulkarni et al. / Research in Microbiology 156 (2005) 588–596 593
Fig. 3. Spoligotype-based dendrogram of Mumbai isolates (n = 216) using the Jaccard index and the UPGMA method.
la-ase,
ibedthe
.5%theo-rged towithhavebut
-14,Thegedthe
ionwnsia,t forlencinpa-o-its
ing-
k ofer,re
ifi-oftesDRthyDRotins
tudyab-
tizedlytricny
andtherins
s inas awn
is26 ised toob-
tuberculosis incidence of 1%. In spite of the high popution density and conditions for the spread of the dise38.8% of the patients were infected with anM. tuberculo-sis isolate having a spoligotype that had not been descrin the global database of more than 22 500 isolates. Atsame time, the study showed that a fair percentage (43of strains were present as clusters. Although Mumbai isindustrial capital of India, with a great deal of travel by peple from various countries, tuberculosis still affects a lapopulation in the lower middle class, which is not exposeinternational travel and does not have frequent contactpeople who travel a great deal. Thus, these strains mayspread within Mumbai and some areas of the country,have remained as clusters within the country.
Three major clusters, SP-1 (W-Beijing), SP-3 and SPcomprised 48.9% of the total clustered strains present.analysis clearly shows that around 7.4% of isolates belonto spoligotype SP-1 (type-1 in database), referred to asW-Beijing genotype that is characterized by hybridizatonly to 3′ terminal spacers of 35–43. This strain is knoto be prevalent in China and neighboring countries in Abut it is uncommon in Europe and the Caribbean excepCuba [3,8,29,36]. Recent studies have reported a prevaof about 3–5% of strains belonging to the Beijing familyIndia [22,36]. Soini et al. reported that a large number oftients from Houston, TX were infected by this family of islates [28]. The importance of the W-Beijing genotype isreported association with drug resistance [3]. A W-Beijsubclone ofM. tuberculosis isolates, a group of closely re
lated MDR strains, belongs to the W-Beijing lineage and)
e
has also been shown to be responsible for an outbreaMDR tuberculosis in New York and Paris [2,5]. Howevonly 2 out of the 16 (12.5%) W-Beijing type isolates wemultidrug-resistant in our study. This figure is not signcantly different from that of other circulating genotypesM. tuberculosis in our setting, suggesting that these isolamay have been present in India prior to the outbreak of MBeijing clones in the US and Europe. It is also noteworthat no particular pattern was associated with the 53 Mstrains from Mumbai, indicating that spoligotyping cannbe used to differentiate MDR strains from sensitive strain our setting.
The other most prevalent spoligotype in the present swas type 26 observed in 16 strains, characterized by thesence of spacers 4–7 and 23–34. This pattern was bapthe “Delhi” type in a former study [37]; it was concomitantand independently defined as the CAS1 in a multicenstudy, since its geographic distribution is linked to macountries in Central Asia [11], such as Pakistan [14],it was also reported to be present in Sudan [26] and oAfrican countries (our unpublished observations). As strapresenting a high similarity with this pattern are numerouthe present study (Fig. 3), this type may be consideredmajor type in Mumbai. Three out of nine major types shoin Table 2 belonged to this group. This group of strainsunderrepresented in the spolDB4 database, e.g., typepresent in 7.4% strains in the present study as comparonly 0.87% of isolates in the database. Although this
servation probably represents an affinity of this type for the
594 S. Kulkarni et al. / Research in Microbiology 156 (2005) 588–596
Fig. 4. Comparison of spoligotype and RFLP using 3 major clusters.
uit-
0]oste oopaeded
har-1].
andes,ingncemaseenul-
va-i-nce
lent
a-nant
bai
theul-
8].ro-o
inDRor-ed
ever,typ-e its by
erede ofen
Indian subcontinent, it may also be partly due to a recrment bias in the SpolDB4.
A previous spoligotyping study performed in Sicily [3showed that type 42, an ubiquitous pattern, was the mfrequent (26%) spoligotype characterized by the absencspacers 21–24 and spacers 33–36, whereas in our spoligterns, only 2.3% of strains accounted for similar derivspoligotypes. This family of strains covers a yet undefinnumber of subclades belonging to MGG 2 organisms,boring 2 alleles of an exact tandem repeat (ETR)-A [3Thus it appears that this group, mainly found in Europethe Americas, is not prevalent in Asia. Along the same linin spite of the presence of a predominant group showthe absence of spacers 33–36, and presumed to be atral to the Haarlem family, only one strain of the Haarlefamily (type 50, with missing spacers 31, and 33–36) wseen in the present study in Mumbai. As this type has blinked to be a major clade of European descent in a mticentric study [19], this suggests a relatively lower prelence of circulatingM. tuberculosis clades of European orgin presently in India. However, the presence or abseof spacer 31 discriminates between two highly preva
spoligotypes worldwide (types 50 and 53), with its absenceft-
s-
being linked to IS6110 insertional events [13]. This observtion suggests that a phylogenetical study of the predomigroup showing the absence of spacers 33–36 from Mummay shed light onM. tuberculosis evolution.
Since spoligotyping is a PCR-based method, it hasadvantage of rapidity, robustness and the ability to simtaneously detect and typeM. tuberculosis isolates, not onlyfrom cultures but also directly from clinical specimens [2The sensitivity of the technique is shown to be 10 fg of chmosomalM. tuberculosis DNA, an amount corresponding tabout 2–3 mycobacterial genomes.
Overall, our analysis shows a high degree of diversityclinical isolates in the Mumbai area, suggesting that thespacers in the strains from Mumbai are sufficiently polymphic to be typed by spoligotyping. The study also showthat 43.5% of the strains were present as clusters. Howit should be emphasized that, in many settings, spoligoing alone does not permit investigating outbreaks, sincoverestimates the number of recent transmission caseat least 30%. Instead, spoligotyping should be considas first screening information on the population structurbacterial diversity in a given setting, and clonality betwe
isolates should be investigated by at least one other fin-
S. Kulkarni et al. / Research in Microbiology 156 (2005) 588–596 595
M
a; CAM,
Table 2The geographic distribution of major spoligotypes present in Mumbai
Type numberin database
Number: Geographic distribution
of isolates in present study (%) in database (%)
1a 16 (7.4%) 2014 (8.85%) FEA, NAM, MECA, EUR, AFR, OCE, SAM, CAM26b 16 (7.4%) 197 (0.87%) MECA, EUR, OCE, CAM, NAM53 14 (6.5%) 1465 (6.44%) AFR, FEA, MECA, EUR, OCE, SAM, CAM, NA11d 5 (2.3%) 146 (0.64) MECA, EUR, OCE, SAM, CAM, NAM
288e 5 (2.3%) 18 (0.08%) MECA, EUR, OCE, NAM48c 4 (1.9%) 155 (0.68%) AFR, MECA, FEA, EUR, OCE, NAM
1318 4 (1.9%) 5 (0.02%) AFR, MECA141f 3 (1.4%) 9 (0.04%) MECA, EUR, NAM
1314f 3 (0.01%) 3 (0.01%) MECA
Geographic distribution: AFR, Africa; FEA, Far East/Asia; MECA, Middle East and Central Asia; EUR, Europe; OCE, Oceania; SAM, South AmericCentral America and Caribbean; NAM, North America.
a W. Beijing type.b Prototype of the Delhi CAS1 family (Filliol et al., Emerg. Infect. Dis. 8 (2002) 1347–1349).c Prototype of the EAI1 family (Filliol et al., Emerg. Infect. Dis. 8 (2002) 1347–1349).d Prototype of the EAI3 family (Filliol et al., Emerg. Infect. Dis. 8 (2002) 1347–1349).e Prototype of CAS2 family (Filliol et al., Emerg. Infect. Dis. 8 (2002) 1347–1349).
f Variants of the CAS1 family.ajorrns.or-al et
ofr-an-rlemestbyu-of
i-archcon-weree auAs-aiselted
past
s,
5–
,
.J.T.os-
nts,
L..T.ead
ord,
5
esis-
J.A.na,
96
en-nce,
and
.igh-
-K.el-yne-sa-P.si,
idell,
gerpriting method such as IS6110-RFLP, LM-PCR,VNTR,MIRU or even DRE-PCR [23]. Indeed, when IS6110-RFLPwas carried out on 46 isolates that were present in 3 mspoligo clusters, the strains showed polymorphic patteSimilar results showing spoligo clusters and RFLP polymphism have been reported by Horgen et al. [17] and Goyal. [16].
In conclusion, historic clones of the MGG 1 groupM. tuberculosis are responsible for roughly 60% of all tubeculosis cases in Mumbai. Together with the fact that orgisms presumably of European descent (such as the Haafamily) were only rarely found, our observations suggthat tuberculosis in Mumbai, India is essentially causedhistorical clones of tubercle bacilli undergoing active circlation due to uncontrolled demography, high prevalencethe disease and a paucity of resources.
Acknowledgements
We thank the International Atomic Energy Agency, Venna for financial support as part of Collaborative ReseProject 10039. The international spoligotype databasestruction projects at the Institut Pasteur de Guadeloupesupported through grants from the Délégation GénéralRéseau International des Instituts Pasteur et Institutssociés, Institut Pasteur, Paris, and the Fondation françRaoul Follereau, Paris, France. SpolDB3 may be consuonline at http://www.pasteur-guadeloupe.fr/tb/spoldb3.
References
[1] S.P. Agarwal, TB across the globe: 2. Tuberculosis in India—theand prospects for the future, Scott. Med. J. 45 (2000) 11–13.
[2] T.B. Agerton, S.E. Valway, R.J. Blinkhorn, K.L. Shilkret, R. Reve
W.W. Schluter, B. Gore, C.J. Pozsik, B.B. Plikaytis, C. Woodley, I.M.Onorato, Spread of strain W, a highly drug-resistant ofMycobacteriumtuberculosis, across the United States, Clin. Infect. Dis. 29 (1999) 895.
[3] D.D. Anh, M.W. Borgdorff, L.N. Van, N.L.T. Lan, T. van GorkomK. Kremer, D. van Soolingen,Mycobacterium tuberculosis “Beijing”genotype emerging in Vietnam, Emerg. Inf. Dis. 6 (2000) 302–305
[4] C. Beck-Sague, S.W. Dooley, M.D. Hutton, J. Otten, A. Breeden,Crawford, A.E. Pitchenik, C. Woodley, G. Cauthen, W.R. Jarvis, Hpital outbreak of multidrug-resistantMycobacterium tuberculosis in-fections: Factors in transmission to staff and HIV-infected patieJAMA 268 (1992) 1280–1286.
[5] P.J. Bifani, B.B. Plykaitis, V. Kapur, K. Stockbauer, X. Pan, M.Lutfey, S.L. Moghazh, W. Eisner, T.M. Daniel, M.H. Kaplan, JCrawford, J.M. Musser, B.N. Kreiswirth, Origin and interstate sprof a New York City multidrug-resistantMycobacterium clone family,JAMA 275 (1996) 452–457.
[6] M.D. Cave, K.D. Eisenach, P.F. McDermott, J.H. Bates, J.T. CrawfIS6110 conservation of sequence in theMycobacterium tuberculosiscomplex and its utilization in DNA fingerprinting, Mol. Cell. Probes(1991) 73–80.
[7] R.V. Chowgule, L. Deodhar, Pattern of secondary acquired drug rtance to antituberculosis drugs in Mumbai, India, 1991–1995.
[8] R. Diaz, R. Gomez, E. Restrepo, R. Rumbaut, J. Sevy-Court,Valdivia, D. van Soolingen, Transmission of tuberculosis in HavaCuba: A molecular epidemiological study by IS6110 restriction frag-ment length polymorphism typing, Mem. Inst. Oswaldo Cruz(2001) 437–443.
[9] C. Dye, S. Scheele, P. Dolin, V. Pathania, M.C. Raviglione, Conssus statement. Global burden of tuberculosis: Estimated incideprevalence, and mortality by country, WHO Global SurveillanceMonitoring Project, JAMA 282 (1999) 677–686.
[10] K.R. Ewen, M. Bahlo, S.A. Treloar, D.F. Levinson, B. Mowry, J.WBarlow, S.J. Foote, Identification and analysis of error types in hthroughput genotyping, Am. J. Hum. Genet. 67 (2000) 727–736.
[11] I. Filliol, J.R. Driscoll, D. van Soolingen, B.N. Kreiswirth, K. Kremer, G. Valétudie, D.D. Anh, R. Barlow, D. Banerjee, P.J. Bifani,Brudey, A. Cataldi, R.C. Cooksey, D.V. Cousins, J.W. Dale, O.A. Dlagostin, F. Drobniewski, G. Engelmann, S. Ferdinand, D. GascoBinzi, M. Gordon, M.C. Gutierrez, W.H. Haas, H. Heersma, E. KasKelembho, H.M. Ly, A. Makristathis, C. Mammina, G. Martin,Moström, I. Mokrousov, V. Narbonne, O. Narvskaya, A. NastaS.N.N. Eyangoh, J.W. Pape, V. Rasolofo-Razanamparany, M. R
M.L. Rossetti, F. Stauffer, P.N. Suffys, H. Takiff, J. Texier-Maugein, V.
596 S. Kulkarni et al. / Research in Microbiology 156 (2005) 588–596
and
lin.
larf
with
ed
A.ant
Evi-05
aw,
n.
ofesS
lin-al,
ntia-,
.M.ey,th-ing-9)
tes,ith
cu-
ns
,
In-
sedn-
l,
1)
M.
of
vanly-
J. In-
.C.dom-10
r,
0)
d,nu-erg.
etic-isonClin.
i,
etic
gi,pidl
ta,96)
.M.ori-
D.A.es inr-emi-
ore,mb-
38..M.
82
for
iony
18.
Vincent, J.H. de Waard, C. Sola, N. Rastogi, Snapshot of movingexpanding clones ofMycobacterium tuberculosis and their global dis-tribution assessed by spoligotyping in an International study, J. CMicrobiol. 41 (2003) 1963–1970.
[12] I. Filliol, S. Ferdinand, L. Negroni, C. Sola, N. Rastogi, Molecutyping of Mycobacterium tuberculosis based on variable number otandem DNA repeats (VNTR) used alone, and in associationspoligotyping, J. Clin. Microbiol. 38 (2000) 2520–2524.
[13] I. Filliol, C. Sola, N. Rastogi, Detection of a previously unamplifispacer within the DR locus ofMycobacterium tuberculosis: Epidemi-ological implications, J. Clin. Microbiol. 38 (2000) 1231–1234.
[14] D.M. Gascoyne-Binzi, R.E. Barlow, A. Essex, R. Gelletlie, M.Khan, S. Hafiz, T.A. Collyns, R. Frizzell, P.M. Hawkey, PredominVNTR family of strains ofMycobacterium tuberculosis isolated fromSouth Asian patients, Int. J. Tuberc. Lung Dis. 6 (2002) 492–496.
[15] P. Godfrey-Faussett, P.R. Mortimer, P.A. Jenkins, N.G. Stocker,dence of transmission of tuberculosis by DNA fingerprinting, BMJ 3(1992) 221–223.
[16] M. Goyal, N.A. Saunders, J.D.A. van Embden, D.B. Young, R.J. ShDifferentiation ofMycobacterium tuberculosis isolates by spoligotyp-ing and IS6110 restriction fragment length polymorphism, J. CliMicrobiol. 35 (1997) 647–651.
[17] L. Horgen, C. Sola, A. Devallois, K.S. Goh, N. Rastogi, Follow-upMycobacterium tuberculosis transmission in the French West Indiby IS6110-DNA fingerprinting and DR-based spoligotyping, FEMImmunol. Med. Microbiol. 21 (1998) 203–212.
[18] J. Kamerbeek, L. Schouls, A. Kolk, M. van Agterveld, D. van Soogen, S. Kuijper, A. Bunschoten, H. Molhuizen, R. Shaw, M. GoyJ.D.A. van Embden, Simultaneous detection and strain differetion of Mycobacterium tuberculosis for diagnosis and epidemiologyJ. Clin. Microbiol. 35 (1997) 907–914.
[19] K. Kremer, D. van Soolingen, R. Frothingham, W.H. Haas, P.WHermans, C. Martin, P. Palittapongarnpim, B.B. Plikaytis, L.W. RilM.A. Yakrus, J.M. Musser, J.D.A. van Embden, Comparison of meods based on different molecular epidemiologial markers for typof Mycobacterium tuberculosis strains: Interlaboratory study of discriminatory power and reproducibility, J. Clin. Microbiol. 37 (1992607–2618.
[20] G.H. Mazurek, M.D. Cave, K.D. Eisenach, R.J. Wallace Jr., J.H. BaJ.T. Crawford, Chromosomal DNA fingerprint patterns produced wIS6110 as strain-specific markers for epidemiologic study of tuberlosis, J. Clin. Microbiol. 29 (1991) 2030–2033.
[21] M.V. Mendiola, C. Martin, I. Otal, B. Gicquel, Analysis of the regioresponsible for IS6110-RFLP in a singleMycobacterium tuberculosisstrain, Res. Microbiol. 143 (1992) 767–772.
[22] N.F. Mistry, A.M. Iyer, D.T. D’Souza, G.M. Taylor, D.B. YoungN.H. Antia, Spoligotyping ofMycobacterium tuberculosis isolatesfrom multiple drug resistant tuberculosis patients from Bombay,dia, J. Clin. Microbiol. 40 (2002) 2677–2680.
[23] P. Moström, M. Gordon, M. Ridell, C. Sola, N. Rastogi, Methods uin the molecular epidemiology of tuberculosis, Clin. Microbiol. Ifect. 8 (2002) 694–704.
[24] I. Otal, C. Martin, V. Vincent-Levy-Frébault, D. Thierry, B. GicqueRestriction fragment length polymorphism analysis using IS6110 as anepidemiological marker in tuberculosis, J. Clin. Microbiol. 29 (1991252–1254.
[25] S.L. Sampson, R.M. Warren, M. Richardson, T.C. Victor, A.Jordaan, G.D. van der Spuy, P.D. van Helden, IS6110-mediated dele-
tion polymorphism in the direct repeat region of clinical isolatesMycobacterium tuberculosis, J. Bacteriol. 185 (2003) 2856–2866.
[26] G.S. Sharaf-Eldin, N.S. Saeed, M.E. Hamid, A.M. Jordaan, G.D.der Spuy, R.M. Warren, P.D. van Helden, T.C. Victor, Molecular anasis of clinical isolates ofMycobacterium tuberculosis collected frompatients with persistent disease in the Khartoum region of Sudan,fect. 44 (2002) 244–251.
[27] U.B. Singh, N. Suresh, N.V. Bhanu, J. Arora, H. Pant, S. Sinha, RAggarwal, S. Singh, J.N. Pande, C. Sola, N. Rastogi, P. Seth, Preinant tuberculosis spoligotypes, Delhi, India, Emerg. Infect. Dis.(2004) 1138–1142.
[28] H. Soini, X. Pan, A. Amin, E.A. Graviss, A. Siddiqui, J.M. MusseCharacterization ofMycobacterium tuberculosis isolates from patientsin Houston, Texas, by spoligotyping, J. Clin. Microbiol. 38 (200669–676.
[29] C. Sola, A. Devallois, L. Horgen, J. Maïsetti, I. Filliol, E. LegranN. Rastogi, Tuberculosis in the Caribbean: Using spacer oligocleotide typing to understand strain origin and transmission, EmInfect. Dis. 5 (1999) 404–414.
[30] C. Sola, S. Ferdinand, C. Mammina, A. Nastasi, N. Rastogi, Gendiversity of Mycobacterium tuberculosis in Sicily based on spoligotyping and variable number of tandem DNA repeats and comparwith a spoligotyping database for population-based analysis, J.Microbiol. 39 (2001) 1559–1565.
[31] C. Sola, I. Filliol, C. Guttierez, I. Mokrousov, V. Vincent, N. RastogSpoligotype database ofMycobacterium tuberculosis: Biogeographi-cal distribution of shared types and epidemiological and phylogenperspectives, Emerg. Infect. Dis. 7 (2001) 390–396.
[32] C. Sola, L. Horgen, J. Maïsetti, A. Devallois, K.S. Goh, N. RastoSpoligotyping followed by double-repetitive element PCR is a raalternative methodology to IS6110-fingerprinting for epidemiologicastudies of tuberculosis, J. Clin. Microbiol. 36 (1998) 1122–1124.
[33] Z.F. Udwadia, A. Hakimiyan, C. Rodrigues, T. Jillisgar, A. MehA profile of drug resistant tuberculosis in Bombay, Chest 110 (19228.
[34] J.D.A. van Embden, T. van Gorkom, K. Kremer, R. Jansen, B.Avan der Zeijst, L.M. Schouls, Genetic variation and evolutionarygin of the direct repeat locus ofMycobacterium tuberculosis complexbacteria, J. Bacteriol. 182 (2000) 2393–2401.
[35] D. van Soolingen, P.W.M. Hermans, P.E.W. de Haas, D.R. Sool, J.van Embden, The occurrence and stability of insertion sequencMycobacterium tuberculosis complex strains: Evaluation of an insetion sequence-dependent DNA polymorphism as a tool in the epidology of tuberculosis, J. Clin. Microbiol. 29 (1991) 2576–2586.
[36] D. van Soolingen, L. Qian, P.E.W. de Haas, J.T. Douglas, H. TraF. Portaels, H.Z. Qing, D. Enkhsaikan, P. Nymadawa, J.D.A. van Eden, Predominance of a single genotype ofMycobacterium tuberculo-sis in countries of East Asia, J. Clin. Microbiol. 33 (1995) 3234–32
[37] N. Vijaya-Bhanu, D. van Soolingen, J.D.A. van Embden, L. Dar, RPandey, P. Seth, Predominance of a novelMycobacterium tuberculo-sis genotype in the Delhi region of India, Tuberculosis (Edinburg)(2002) 105–112.
[38] S.M. Wilson, S. Gross, F. Drobniewski, Evaluation of strategiesmolecular fingerprinting for use in the routine work of aMycobac-terium reference unit, J. Clin. Microbiol. 36 (1998) 3385–3388.
[39] L.K.W. Yuen, B.C. Ross, K.M. Jackson, B. Dwyer, Characterizatof Mycobacterium tuberculosis strains from Vietnamese patients bSouthern blot hybridization, J. Clin. Microbiol. 31 (1993) 1615–16