Service User Involvement: How do we know it's a reality?
74
Service User Involvement: How do we know it’s a reality? Clive Willis MBA in Health Services Management Greenwich School of Management Dissertation 14 th Fedruary 2011
-
Upload
independent -
Category
Documents
-
view
2 -
download
0
Transcript of Service User Involvement: How do we know it's a reality?
Service User Involvement: How do
we know it’s a reality?
Clive Willis
MBA in Health Services Management
Greenwich School of Management
Dissertation
14th Fedruary 2011
Greenwich School of Management
Dissertation: Master of Business Administration in Health Services
Management
Title: Service User Involvement: How do we know it’s a reality?
Student: Clive Willis
Student Ref: H52017PE
Submission date: 14th February 2011
Dissertation Supervisor: David Schofield

Content: Page
Abstract 1
Chapter 1 Introduction 1
Chapter 2 Literature Review
2.1 Service User Involvement (SUI) in Substance Misuse Delivery 8
2.2 Service User Involvement (SUI) in Health & Social Care 10
2.3 Evaluating User Involvement 12
2.4 Summary 17
Chapter 3 Methodology 18
Chapter 4 Data Collection 24
Chapter 5 Findings & Analysis 27
5.1 Drug Action Team (DAT) 1, Semi-structured Interviews 28
5.1.1 Efficacy of the Tool to Support, Plan and Monitor User Involvement 35
5.1.2 Amendments to Process and/or Assessment Tool 39
5.2 Drug Action Team (DAT) 2, Semi-structured Interviews 41
5.2.1 Efficacy of the Tool to Support, Plan and Monitor User Involvement 48
5.2.2 Workshop 51
Chapter 6 Conclusions 57
Chapter 7 Recommendations 60
References 62

1
Service User Involvement: How do we know it’s a reality?
Abstract
Service User Involvement (SUI) is a requirement in the planning, commissioning and
delivery of health and social care services and leads to improved choices and control for
people who use them. However, the ability to both measure and monitor this activity at a
national level has continued to elude us.
This study seeks to support the future planning, delivery and monitoring of SUI through the
development and piloting of an assessment tool for local drug partnerships (or equivalent
structure i.e. Drug Action Teams (DAT)). It highlights how the identification of baseline
activity of SUI in planning and development processes provides a platform from which these
partnerships can better understand and embed user participation into decision making. It is
only by understanding the why, where and when of user involvement, that we can appreciate
and comprehend the HOW.
Chapter 1. Introduction
Total estimates for problematic drug use (PDU1, opiate and/or crack cocaine use) in England
are around 350,000 across the whole population; this number does not account for other drug
use such as cannabis, ecstasy, benzodiazepines, etc. The complexity of need of these
1 Problem drug use (PDU) is defined as ‘injecting drug use or long-duration/regular use of opioids, cocaine and/or amphetamines’.
2
individuals presents a significant challenge nationally, regionally and locally in terms of
engagement and treatment. Current policy and legislation (Department of Health: The
National Health Services Act, 2006a; Our health, our care our say, 2006b; NHS Constitution,
2010) places a requirement on organisations providing or commissioning NHS or local
authority care to ensure that the local community and service users are involved in the
planning, development and decision-making of their services. Guidance from the National
Treatment Agency (NTA2) reflects these requirements in the commissioning and provision of
substance misuse services (NTA, 2006, 2009, 2010). However, there is little evidence to
support the view that SUI is sufficiently integrated into policy and planning across health and
social care, or specifically within substance misuse provision (Carr, 2004; Patterson et al,
2007; DH, 2008a).
Whilst community participation has been a key principle of NHS delivery since its inception
in 1948, the ability to performance assure organisations and services against this activity has
continued to prove difficult. Some of the difficulties associated with evaluating performance
have been how participation is defined; the absence of validated and jointly owned
frameworks or models for measurement and the consistency of outputs being measured.
Within the substance misuse field this is exacerbated by the fact that the cohort of individuals
affected by substance misuse is variable in terms of the substance used, the level of usage
(from recreational use to PDU) and demographics. This variability requires a multitude of
approaches in ensuring effective engagement when assessing the need of a community and
future planning.
2 A Special Health Authority whose role is to performance assure delivery of local drug partnerships (or equivalent i.e. Drug Action Teams)
3
Although guidance on how and when to involve users is abundant (GLADA, 2005; DH,
2008b; Welsh Assembly, 2008; Jürgens 2008), there is little evidence to support the
effectiveness of involvement methods (Nicholson, 2005). In addition, the evaluation models
currently being used lack the ability, either due to the limitations of the model or through
their implementation, to be replicated across different programs (Rowe & Frewer, 2004).
Existing evaluations have also been limited to specific intervention programs or
organisations. Consequently, it is not currently possible to develop a consistent understanding
of SUI at a national level. In order to inform national guidance to support the ongoing
development and integration of user participation, we first need to establish a baseline of
activity in relation to process (Rifkin et al, 1988; Tritter & McCallum, 2006), from which
organisations can begin to explore what works best in terms of engagement in a given
locality.
This is not suggesting that there is not some excellent and innovative service user
engagement going on, but the inability to use comparative analysis across organisations
impedes benchmarking and future development through research and national guidance.
This study will seek to support future planning, delivery and monitoring of SUI through the
development and piloting of an assessment tool for local drug partnerships. This will be
limited to establishing the extent to which user involvement is embedded into these activities,
rather than the success of user involvement. The way in which users are engaged to
participate in the activity being evaluated is a separate issue and has purposely not been
included on the basis that what works in any given locality is dependent on the demographics
of the community (or subgroup) seeking to be served and the outcomes being sought. It is
envisaged that the identification of baseline activity in policy and planning will provide a
4
platform from which organisations can better understand and embed user participation into
decision making, which in turn will support and drive future evaluation of engagement
methods or tools at a local level.
The objectives of the study are to:
1. Evaluate how accurately the assessment is able to identify baseline activity.
Responses to the assessment questions will be analysed and then reviewed in a focus
group to measure individual perception of activity against actual delivery (Delphi
technique, Fiander & Burns, 2000).
2. Evaluate how the assessment process informs future delivery.
The assessment tools ability to identify deficits in user involvement and subsequent
action planning (Robinson, 2004) will be used as a measurement of how processes
inform future delivery.
3. Evaluate the efficacy of the tool to support, plan and monitor user involvement.
This will be undertaken through participant questionnaires which will capture how
they perceived the tool’s ease-of-use and ability to support planning and monitoring
of user involvement.
5
An adaptation of the model proposed by Rifkin et al (1988) was developed to map the current
level of user participation within local drug partnerships. The model focuses on key factors of
delivery within an organisation and where SUI is encompassed within them. This enables an
understanding of where within the organisation, user participation is predominant.
Adaptations of the model centred on the factors originally stated by Rifkin et al (1988) and
their relevance to local drug partnerships.
The five factors being measured in this study were modified to the following:
• Needs Assessment – how the engagement and participation of service users inform
and support the identification and prioritisation of ‘need’ locally.
• Leadership – the influence of Leadership on engagement and implementation of user
participation.
• Programme/Policy Development – the ability of service users to inform both the
context and content of a new initiative or programme.
• Programme/Policy Implementation – the ability of service users to inform and
support programme implementation.
• Resource Mobilisation – the organisations ability to effectively utilise user
participation.
For each factor stated above a continuum was developed with wide SUI (users plan;
implement and evaluate activity, with professionals used as a resource) at one end and narrow
SUI (professionals plan; implement and evaluate activity, with no SUI) at the other. The
continuum was then divided into a series of points. By placing a mark at the point that most
describes activity in the local drug partnership, process indicators were defined for SUI in the
local drug partnership as the width of SUI on the continuum of each factor. Placing a mark on
6
the continuum, and connecting those marks in a spoke arrangement, provided the base for
where SUI is most narrow.
In order to plot the marks on the continuum, it is necessary to establish a consensus as to
where the organisation sees its activities for each factor in relation to SUI. The Delphi
technique (Fiander & Burns, 2000) was used to collect this information as it allowed for
individual views and/or perceptions to be captured through questionnaires, alongside a group
process via a workshop to establish consensus on where SUI should be placed on the
continuum for each factor. An assessment tool questionnaire was developed to capture
individual team member perceptions on where SUI should be placed on the continuum for
each factor.
Questionnaires were completed as part of a semi structured interview. The use of semi-
structured interviews allowed for the interviewer to note any difficulties experienced by the
respondent in completing the questionnaire and ask additional questions to ascertain the
tool’s ease-of-use and ability to support planning and monitoring of user involvement.
Data from the completed assessment tool questionnaires were collated and analysed to
produce an initial outline of perceived activity and feedback to the team in a workshop. The
initial outline was used as the basis for discussion of current activity to inform a final
decision by the group on where marks should be placed on the continuum for each factor.
This enabled staff to evaluate activity based on a collective understanding rather than
individual perceptions. In addition, this process allowed for a wider discussion on gaps in
delivery to inform action planning.
7
The study has shown that by focusing on organisational processes and where users’ are
involved in its planning, development and decision-making processes, we are able to:
a) recognise gaps in delivery and identify actions to improve and/or sustain user
involvement
b) support individuals and teams to understand and consider activity to support effective
SUI
c) effectively plan and monitor SUI
However, further testing of the assessment tool should be undertaken in organisations with a
range of user involvement experience and organisational support for user involvement. In
addition, wider testing of the assessment tool should also consider the independence of the
facilitator (interviewer) and co-facilitation by a representative of the local user group.
Key to any further evaluation of the assessment tools efficacy is the support and/or
involvement of those with responsibility for the oversight and governance of the
organisations (local drug partnerships, or equivalent i.e. DAT) being assessed.
Chapter 2
Literature Review
8
Chapter 2. Literature Review
2.1 Service User Involvement (SUI) in Substance Misuse Delivery
SUI in health and social care is today commonplace and perceived as much as a part of
normal business as the delivery of the services themselves. However, SUI within the
substance misuse field has been slower to develop, largely as a result of the myriad of
government departments and organisations tasked with responding to this multi dimensional
agenda. The NTA was created in 2001 as part of the Government’s overall Drug Strategy
(Home Office, 1998) and presented the first opportunity to develop user involvement in a
consistent and meaningful manner. As a consequence, few studies to-date have attempted to
provide insight into SUI in substance misuse provision at a national level, given the infancy
of its development as a national platform.
The two most referenced studies were considered, each focusing on distinct areas of user
involvement. The Department of Psychological Medicine, Imperial College London study
(Patterson et al, 2007) explores user involvement in planning, commissioning and delivery of
drug treatment services, whereas, the Joseph Rowntree Foundation study (Fischer et al, 2007)
explores SUI in treatment decisions. It is important to note the difference in focus of these
studies as this highlights an important question in relation to which studies are pertinent to
this literature review. Whilst user involvement in making treatment decisions is integral to the
wider SUI agenda i.e. personalisation and individual budgets (Department of Health, 2008a),
those decisions are limited within the context of what services are available locally. This
literature review will predominantly focus on SUI at a policy and planning level, therefore
9
impacting the availability of choice, and draw from wider studies (e.g. Fischer et al 2007)
where a reference to policy-making and planning is made.
Patterson et al (2007) surveyed service commissioners, providers and users in a
representative 50 of the 149 local Drug Action Teams (DAT) and conducted in-depth case
studies in six DAT areas. Their findings concluded that there was significant variability in the
level, type and quality of SUI nationally. Key findings included:
• “wide variation in the degree to which UI systems and structures had been
established.
• disparity between and within DATs in terms of models and mechanisms used and the
degree to which user involvement was integrated in planning, commissioning and
development of services.
• fewer than half (47%) had formal user representation at commissioning level.
• findings indicated a lack of strategic UI planning in many DATs.
• processes to enable user input to contribute systematically to commissioning and
service level development are often not well defined.
• a significant minority of DATs (n=16; 36%) evidenced no user involvement at
strategic levels with fragmented and inconsistent UI within services.” (Patterson et
al, 2007, p2)
In addition, Patterson et al (2007, p1) found only 22% of DATs surveyed had “user
involvement workers”. This might be seen as a missed opportunity by DATs given Fischer et
al (2007, p1) noted “user involvement co-ordinators” in DATs as a positive development.
10
The Patterson et al study (2007), although surveying a broad spectrum of participants, was
limited in the breadth of partnerships it included and raises questions on whether national
comparisons can be made. However, a recent report on how well local drug partnerships
planned and commissioned services for diverse populations made the following statements as
priorities for action.
• “Commissioners should ensure that all contracts include requirements for
compliance with all relevant equality and diversity legislation.
• Local drug partnerships should focus on ensuring that services are accessible and
relevant to crack users, to increase the proportion accessing services.
• Service providers and local drug partnerships should consult more broadly with the
communities they service, including with diverse groups and communities
(particularly those not currently accessing drug treatment) and involve them in
service planning.” (Commission for Healthcare Audit and Inspection, 2009, p8)
These indicate wider consultation and involvement is required and goes to support some of
the findings of Patterson et al (2007).
2.2 Service User Involvement (SUI) in Health & Social Care
Studies on SUI tend to fall into the following categories: those that evaluate methods or tools
in engaging service users; those that evaluate the usefulness of SUI, and those that evaluate
the evaluations. Few however attempt to clarify a national position of existing levels of
participation or involvement. The Department of Health (DH) acknowledges the lack of
evidence to support a view that SUI is embedded in NHS day-to-day delivery and goes as far
as to state:
11
“There is scant evidence to show that involvement activity is stitched into all the strands of
NHS organisations’ work, including their decision-making processes......” (DH, 2008a, p10)
There are numerous guidance documents available on service user involvement such as: Real
Involvement (DH, 2008b), User Involvement Framework (Welsh Assembly, 2008) and
Lessons Learnt (GLADA 2005). The guidance addresses both the principles and legislation
upon which SUI is built, alongside methods and tools of engagement and/or involvement.
However, there does not appear to be research on the extent to which these methods or tools
are used across the NHS. Nevertheless, Young (2006) does explore SUI and its influence
across both NHS and Social Care. The study considers government strategy, in terms of SUI,
and its impact on those whose treatment and support crosses the boundaries of the two
distinct organisational cultures (NHS & Social Care).
Previous studies being considered by Young (2006) include those that comment on the
implementation and flexibility of section 31 agreements, partnership working, and the NHS
changing workforce programme. Two key lessons learnt from this study were firstly that
consultation was more likely to take place “ex-post” i.e. service users being asked to confirm
or critique decisions already made, as opposed to “ex-ante” and influencing thinking before
the decision is made (p265). The second lesson was that "real involvement takes a long time
to achieve" (p266). In addition, Speak Up (2007) identified that the most used forms of user
participation methods by Local Authorities were focus groups (84%), postal questionnaires
(79%), whereas the use of service user advocates were used less (35%) followed by peer
reviews (25%).
A review of the literature available found no empirical evidence to suggest that SUI in the
12
planning or delivery of substance misuse services is, to a greater or lesser extent, a mirror of
SUI across the broader spectrum of NHS and Social Care delivery.
2.3 Evaluating User Involvement
The most commonly occurring method of measuring the meaningfulness of user involvement
methods or tools (Robinson, 2004; GLADA, 2005; Welsh Assembly, 2008; DH, 2008b;
Participation Works, 2008; McLaughlin, 2009), as opposed to successful outcomes,
incorporate adaptations to the Ladder of Participation (Arnstein, 1969). A visual
interpretation of citizen participation is provided by Arnstein within eight rungs on the ladder
of citizen participation, ranging from manipulation (rung 1) to citizen power (rung eight). The
rungs in between identify varying layers of participation that move through tokenism to
empowerment. This method of measurement would see the most used participation methods
referred to previously (Speak Up, 2007) on the lower rung of the ladder and regarded as
tokenistic. In general, studies utilising Arnstein’s model note the limitations of its approach
i.e. its view that participation is hierarchical. Nonetheless despite this view the approach is
not often modified to remove this hierarchical structure.
Arnstein’s study was undertaken against the backdrop of political imperatives and debates in
relation to tokenism of participation and the power or influence participation brings to the
governed. Arnstein emphasises the way in which consultation can be frustrating for those
being consulted unless it includes the real ability for the powerless to exert power. Whilst
Arnstein recognises the simplistic interpretation of a complex interaction between those that
govern and those that are governed, the baseline of this approach appears to accept an
underlying principle that those that seek to consult are unwilling or unable to inform
13
decisions based on this interaction i.e. tokenistic engagement. In addition the rungs are
hierarchical and place a distinct value on each rung and therefore are unable to appreciate the
limitations sometimes incumbent in user participation - the focus being the distribution of
power in decision making rather than the process of engagement. Tritter & McCallum, (2006,
p163) make the comment that: "it is the process rather than the outcome that has the greatest
potential for changing organisational culture”. Arnstein’s approach needs to be viewed
within the context of the situation or issues being discussed and there are still similarities
today in terms of the perception of those that see themselves as the powerless. We therefore
need to consider the meaningfulness of participation to the participant (citizen, user or
consumer) and the level to which participation empowers the individual or group, as opposed
to organisational judgements and/or perception of what is meaningful.
In reviewing Arnstein's study in today’s context, consideration should be given to the
evolution of clinical governance in the delivery of health and social care, which has seen
greater accountability for decision making. It could be argued that what may have been
previously seen as tokenism is now an integral part of decision-making and provides a clear
platform for challenge by those that seek to be heard. Available studies on SUI range in their
findings on the emphasis that power in decision-making should be given to service users.
Some of these studies see Arnstein's model still relevant today (Welsh Assembly, 2008),
some seeking to move beyond Arnstein (Tritter & McCallum, 2006) and those that seek to
embrace both sides of the debate (Participation Works, 2008).
What is clear is the need to recognise the availability of choice regarding how the individual
or group wishes to participate. Additionally, there needs to be recognition of who is being
sought to be involved, alongside their desire to be involved. Given the diverse populations (or

14
groups of individuals) being sought for participation by equally diverse agendas, it is
unrealistic to envisage equal levels of involvement or participation across all agendas. In
relation to substance misuse, it is reasonable to argue that due to the nature of drug use and a
desire by the user to remain unnoticed by the larger community, involvement in decision-
making will continue to be problematic and require innovative ways to support and engage
the user's voice in decision-making. As Lessons Learned (GLADA, 2005, pvii) notes:
"Drug users are a diverse group with different needs, expectations and skills. Therefore it’s
unlikely that there is a single approach that would support them to be involved and
enthusiastic about participating more fully in public life."
Studies concerning the usefulness of SUI or participation will continue to provide a positive
(and essential) forum to question and evolve the who, how and why we seek to ensure SUI in
decision-making. However, the reality today is that organisations are required by legislation
(DH, 2006a) to ensure user involvement in decision-making and will continue to be measured
on how effectively this activity is undertaken. SUI and participation in the delivery of
services to vulnerable, excluded or marginalised groups, is often considered to provide
additional benefits beyond that of organisational delivery for example: developing non-
cognitive skills such as perseverance, motivation, self-esteem, verbal and interpersonal skills.
Fischer et al (2007, p36) concluded that:
“...user involvement and retention in treatment can go hand in hand and, by facilitating the
former, agencies have the potential to increase the latter.”
15
Additionally, Listen and Change (Participation Works, 2008, p20), in referring to the added
benefits of user involvement in children’s services, noted that, “if this participation were
tokenistic....... there would be fewer benefits and possibly even some negative
consequences”.
It is important to consider the broad spectrum of studies evaluating user involvement or
participation to understand or gauge the validity of the findings being made. Rowe & Frewer
(2004) consider some of the complexities of defining success, highlighting that participation
is never a clear measurement between A and B (speed or distance). Instead it requires the
understanding of the nature of the participation (e.g. open public consultation, questionnaires,
formal meeting of representatives) and the variables contained within each type of
participation and the outcome produced. An additional point to consider is whether success is
measured purely by the fact that a decision was made, or whether it is measured through
positive outcomes that emerge from the actual decision itself. Also, in considering the variety
of models or techniques that might be utilised in any one area when engaging the public in
consultation or decision-making processes, can the criteria for defining success be applied to
all?
Individual areas, i.e. local drug partnerships, may be seeking different outcomes via the same
or different levels of engagement or consultation. One would also need to consider the
attributes of those they seek to engage and their ability to participate, for example substance
misusers who are positively engaged in treatment versus a transient cohort of substance
misusers not engaged in treatment. The levels of, and category for, successful engagement
within these cohorts would therefore need to be measured differently. Rowe & Frewer (2004)
were unable to establish consistency among previously conducted evaluations on
16
participation. The study went as far as to state that previous research had been disorganised
and sporadic in nature and as such does not provide a platform from which ongoing
evaluation of participation could take place. In addition the lack of detailed evidence of
methodology used meant that few, if any, of these evaluations could be duplicated.
Additionally, Nicholson (2005, p52) noted that: “a greater understanding of what
participation activity works best in what context is curtailed by the lack of a body of robust,
empirical evidence on which to draw conclusions.”
Rifkin et al (1988), in considering measurements of equity and participation in community
development projects, considered whether an analytical framework could be developed to
assess participation. In reviewing existing studies that sought to evaluate either outcomes
derived from participation and/or levels of participation reached, they concluded that: “the
development of process indicators is critical to the understanding of health improvements
and community participation” (Rifkin et al, 1988, p933). Their conclusion being based on
similar arguments already noted previously in this paper such as: limitations of existing
methods in terms of replicating, and/or, the ability to account for nuances in social, cultural or
participant determinants. Rifkin et al propose a methodology to define indicators for
participation in health care programs as to how wide participation is on a continuum
developed for five factors: Needs Assessment, Leadership, Organisation, Resource
Mobilisation, and Management.
The methodology used enabled the evaluator to measure levels of participation within a
program or organisation rather than the effectiveness of participation. The premise here is
that community participation works, rather than establishing whether it works. In addition
there are no judgements as to which of the five factors is more important, but instead
17
recognises that participation may vary at any given time across these factors. The assertion
being made is that this methodology enables a programme or organisation to better
understand where levels of community participation are concentrated and where necessary,
undertake an evaluation at distinct points of engagement.
2.4 Summary
Whilst user involvement in health and social care is often considered as commonplace and
guidance on how and when to involve users is abundant, there is little evidence to support the
effectiveness of involvement methods, or, that user involvement is sufficiently integrated into
policy and planning. In addition the evaluation models currently being used lack the ability,
either due to the limitations of the model or through their implementation, to be replicated
across different programs. Existing evaluations have also been limited to specific intervention
programs or organisations. Consequently, it is not currently possible to develop a consistent
understanding of SUI at a national level. In order to inform national guidance to support the
ongoing development and integration of user participation, we first need to establish a
baseline of activity in relation to process, from which organisations can begin to explore what
works best in terms of engagement in a given locality.
Chapter 3
Methodology
18
Chapter 3. Methodology
An adaptation of the model proposed by Rifkin et al (1988) was developed to map the current
level of user participation within local drug partnerships. This model allows us to understand
where within the organisation, user participation is predominant. This is not to say that any
one function within the organisation is best served by user participation, as this may be
variable at any given time, but to better understand where it occurs.
Rifkin et al (1988, p933) defined factors impacting on participation in Primary Health Care
(PHC) as:
• “Needs Assessment
• Leadership
• Organisation
• Management
• Resource Mobilisation, and
• Focus on the Poor.”
However, Focus on the Poor was not included in the final matrix as it was not able to be
plotted on a continuum. Additionally, its inclusion might have been seen as limiting the
framework’s wider use i.e. programmes targeting specific community groups.
Rifkin (1990, p10) states:
“...participation can best be defined by asking questions about its concrete components.”
19
Therefore, adaptations of the model centred on the factors above and their relevance to local
drug partnerships. In addition, consideration was given to the context within which the
factors were developed i.e. PHC implementation within a community (in its widest sense). In
considering Rifkin’s descriptions of organisation and management, that can be summarised
as:
• Organisation created by the community (either in existence or subsequently created)
designed to improve health services.
• Management refers to programme management and the inclusion of community
leaders within its framework.
We begin to question their relevance to local drug partnerships.
In the delivery of substance misuse provision there has been a significant increase in recent
years of services being either created by, or, delivered in partnership with users. However,
these tend to have been developed to address specific treatment requirements or expression of
views (user groups) within a multidiscipline approach delivered as part of the National Drug
Strategy (Home Office, 2008). Therefore it would be difficult to argue that they represent or
address the needs of the whole user community. In addition, it might be considered that the
ability to create community organisations within the substance misuse field is impacted upon
by the inherent difficulties experienced by such a diverse group with varying needs,
expectations and skills (GLADA, 2005).
20
The ability to categorise community in the context of substance misuse has not featured in
existing research and would be a key addition to the further understanding of SUI in local
drug partnerships. Additionally, those that represent the user view, tend to be individuals
(service users) who have either stabilised, for example through substitute prescribing, and/or
abstinent. This raises additional questions as to when those representatives can still be
considered to represent a community that they themselves are no longer a part of, i.e. a
community that encompasses those that are actively using and/or those actively engaged in
treatment. Whilst some may consider abstinence (recovery) as part of the treatment journey,
the needs, expectations and skills of those individuals shift significantly over time. This shift,
alongside changes in the populations’ drug use and patterns over relatively short periods of
time, would indicate a gap between the community and those that seek to represent it. The
latter becoming a professional advocate over time, as opposed to a member of the community
they seek to serve.
To address the points raised above, the two factors (Organisation and Management) were
replaced by the following:
• Programme/Policy Development: participation of service users in the development
of a programme or policy ensures that the programme or policy has relevance to, and
ownership from, those that it seeks to support – therefore having a greater chance of
success.
• Programme/Policy Implementation: this can often falter because those that it is
intended for or delivered by are not provided with contextual information in a way
that is understandable to them and/or is seen to favour someone else’s agenda –
21
leading to resistance. User participation across all aspects of implementation can
significantly affect the way in which a programme is received by others.
The inclusion of these two factors provides an increased focus on process relevant to local
drug partnership activity (DH, 2006a). And in turn, encompasses components of
‘Organisation’ and ‘Management’, in that SUI in these factors ensures their inclusion within
the organisational decision-making structure and presents a visible presence to the
community.
In further considering the wider impact of removing management as a factor, consideration
was also given to the role of Leadership. Rifkin (1990) viewed Leadership in relation to those
within the community that either through political or natural selection, influenced or
determined the implementation of an initiative. The leader(s) was seen by Rifkin to have a
direct impact on participation residing within the elite of a community or broadening out to
the participation of the wider community. Given the structure of local drug partnerships and
their relatively small staff group (4 – 12), and the points raised above relating to the
substance misuse community, Leadership in this instance was seen to have more significance
by measuring the influence of those who lead within the organisation (local drug partnership),
rather than leaders within the community. This view is in part supported by Patterson et al
(2003), whose findings included leaders (Chief Executive Officers) having significant
influence on the decision-making process of the teams they lead.
22
The factors being measured in this study were subsequently modified to the following:
• Needs Assessment – how the engagement and participation of service users inform
and support the identification and prioritisation of ‘need’ locally.
• Leadership – the influence of Leadership on engagement and implementation of user
participation.
• Programme/Policy Development – the ability of service users to inform both the
context and content of a new initiative or programme.
• Programme/Policy Implementation – the ability of service users to inform and support
programme implementation.
• Resource Mobilisation – the organisations ability to effectively utilise user
participation.
For each factor stated above we can develop a continuum with wide SUI (users plan;
implement and evaluate activity, with professionals used as a resource) at one end and narrow
SUI (professionals plan; implement and evaluate activity, with no SUI) at the other. The
continuum is then divided into a series of points. By placing a mark at the point that most
describes activity in the local drug partnership, we can define process indicators for SUI in
local drug partnerships as the width of SUI on the continuum of each factor. When a mark is
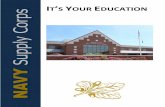
placed on the continuum, those marks can be connected in a spoke arrangement (Figure 1,
below), which provides the base for where SUI is most narrow (outlined in blue). The first
point on the continuum is however not where the spokes connect as it is recognised that
wherever an organisation interacts with a community, there will always be some degree to
which service users will influence delivery. In the example provided (Figure 1, below) we
can see that by placing a mark on the continuum for each factor, which denotes the activity of
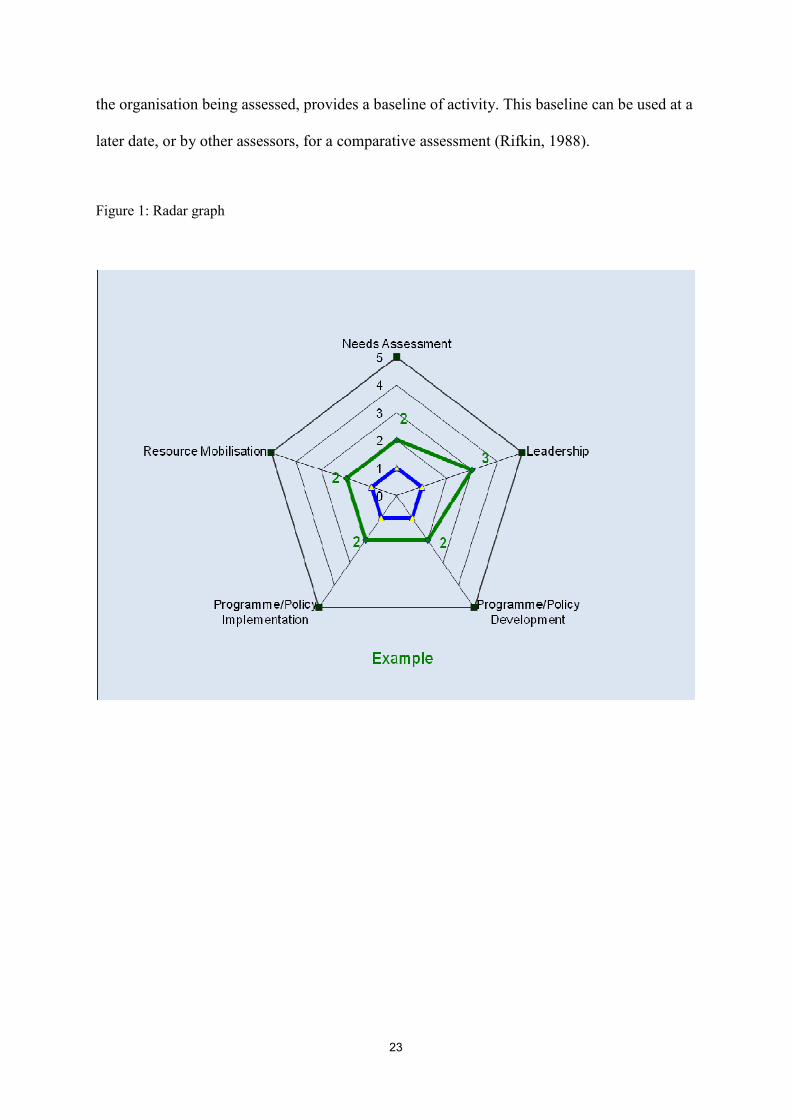
23
the organisation being assessed, provides a baseline of activity. This baseline can be used at a
later date, or by other assessors, for a comparative assessment (Rifkin, 1988).
Figure 1: Radar graph
Chapter 4
Data Collection

24
Chapter 4. Data collection
In order to plot the marks on the continuum, it is necessary to establish a consensus as to
where the organisation sees its activities for each factor in relation to SUI. The Delphi
technique (Fiander & Burns, 2000) was used to collect this information as it allowed for
individual views and/or perceptions to be captured through questionnaires, alongside a group
process via a workshop to establish consensus on where SUI should be placed on the
continuum for each factor. An assessment tool questionnaire was developed (Appendix 1 -
Draft Assessment Tool Questionnaire) to capture individual team member perceptions on
where SUI should be placed on the continuum for each factor. The questionnaire provided a
series of questions for each factor, which capture activities mirrored in national guidance and
best practice. These questions were designed to provide an overview to the respondent on
what SUI activity might look like in practice and therefore help them visualise and compare
the activity of the organisation. In addition, this is followed by a brief statement against each
mark (level) on the continuum allowing the respondent to be clear about the statement being
made when selecting where to place the organisational activity.
DAT teams and/or commissioning teams, acting on behalf of the wider partnership, are
relatively small (4-12 staff members) and therefore enabled the questionnaires to be
completed as part of a semi structured interview. The use of semi-structured interviews
allowed for the interviewer to note any difficulties experienced by the respondent in
completing the questionnaire and ask additional questions (Appendix 2 - Assessment Tool
Evaluation Questionnaire) to ascertain the tool’s ease-of-use and ability to support planning
and monitoring of user involvement.
25
The selection of interviewees was made by the participating organisation and the criteria for
selection were that interviewees represented a range of grades with varying responsibility and
experience within the factors being assessed. In addition to staff interviews, a member of the
local user group was also included in the interview process. It is important to note here that
the measurement being undertaken is of where SUI is predominant across the factors
identified and not how well the organisation engages service users. As such, the inclusion of
a member of the service user group was not to illicit their experience of being engaged but to
ascertain when (and if) they are involved in planning, development and decision-making, and
at what stage within the factors being assessed.
Data from the completed assessment tool questionnaires were collated and analysed to
produce an initial outline of perceived activity and feedback to the team in a workshop. The
initial outline, detailed in an interim report, was used as the basis for discussion of current
activity to inform a final decision by the group on where marks should be placed on the
continuum for each factor. The further questioning of scores in the workshop recognised that
at times activity or policies exist but may not have been effectively communicated throughout
the organisation. This enabled staff to evaluate activity based on a collective understanding
rather than individual perceptions. In addition, this process allowed for a wider discussion on
gaps in delivery to inform action planning.
The process described above was undertaken in two organisations, DAT 1 and DAT 2.
However, the process undertaken with DAT 1 did not include the workshop event. DAT 1
was used to further refine the tool, prior to the tool being piloted in DAT 2. The refining of
the tool and questionnaire in DAT 1 was undertaken to allow for the assessment of the
proposed data analysis techniques and the tool’s ease of use to uncover potential problems,
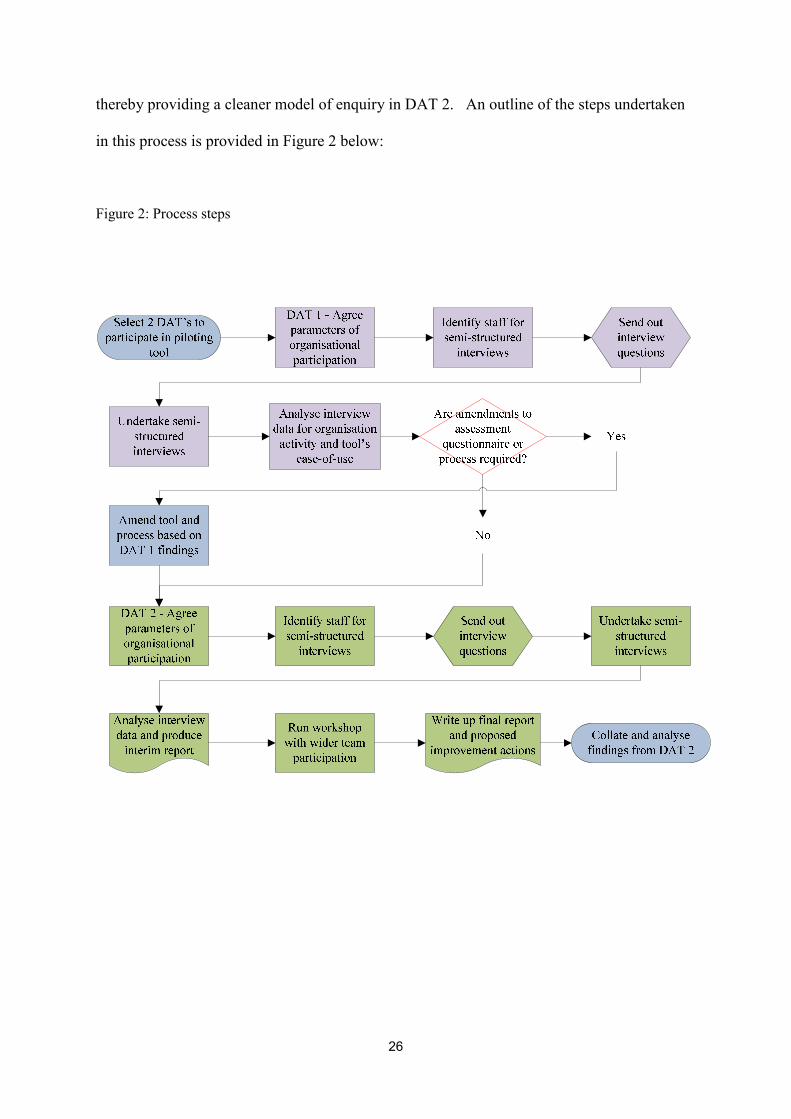
26
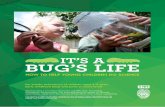
thereby providing a cleaner model of enquiry in DAT 2. An outline of the steps undertaken
in this process is provided in Figure 2 below:
Figure 2: Process steps
Chapter 5
Findings & Analysis
27
Chapter 5. Findings & Analysis
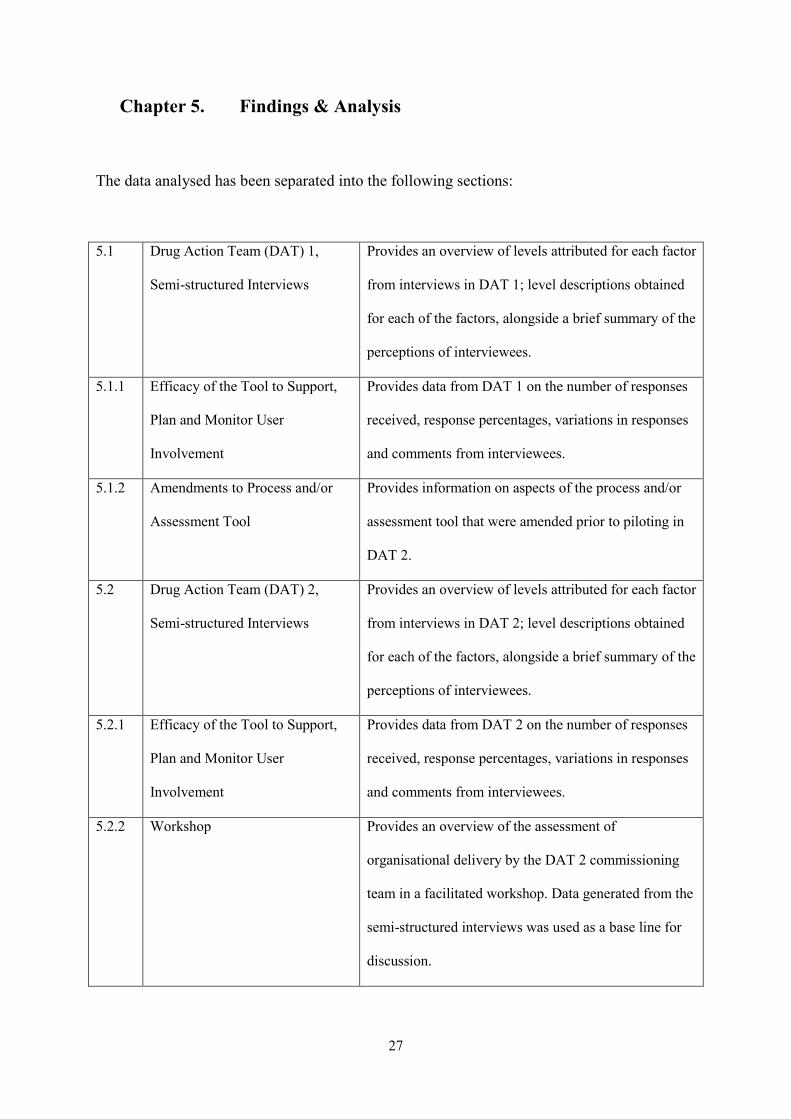
The data analysed has been separated into the following sections:
5.1 Drug Action Team (DAT) 1,
Semi-structured Interviews
Provides an overview of levels attributed for each factor
from interviews in DAT 1; level descriptions obtained
for each of the factors, alongside a brief summary of the
perceptions of interviewees.
5.1.1 Efficacy of the Tool to Support,
Plan and Monitor User
Involvement
Provides data from DAT 1 on the number of responses
received, response percentages, variations in responses
and comments from interviewees.
5.1.2 Amendments to Process and/or
Assessment Tool
Provides information on aspects of the process and/or
assessment tool that were amended prior to piloting in
DAT 2.
5.2 Drug Action Team (DAT) 2,
Semi-structured Interviews
Provides an overview of levels attributed for each factor
from interviews in DAT 2; level descriptions obtained
for each of the factors, alongside a brief summary of the
perceptions of interviewees.
5.2.1 Efficacy of the Tool to Support,
Plan and Monitor User
Involvement
Provides data from DAT 2 on the number of responses
received, response percentages, variations in responses
and comments from interviewees.
5.2.2 Workshop Provides an overview of the assessment of
organisational delivery by the DAT 2 commissioning
team in a facilitated workshop. Data generated from the
semi-structured interviews was used as a base line for
discussion.
28
5.1 Drug Action Team (DAT) 1, Semi-structured Interviews
The total number of staff (officers) in DAT 1 is seven and four officers were interviewed. In
addition to the four officers, a member of the local user group was also interviewed and the
total number of interviewees was five. The initial questionnaire presented to DAT 1 officers
contained only the five factors previously identified (Needs Assessment, Leadership,
Programme/Policy Development, Programme/Policy Implementation, Resource
Mobilisation).
However, feedback from the interview process resulted in questions, which combined
‘programme and policy’, being separately asked for each. That amendment increased the
factors being assessed from five to seven. The rationale for this decision was that
interviewees felt that programme development and implementation was a more organic
process than policy development and implementation and offered greater opportunity for
SUI. Whereas, a percentage of policies were nationally driven and presented less opportunity
for SUI, therefore adversely affecting the assessment of programme development and
implementation. Therefore the data presented below reflects interviewees separate
assessments of programme and policy, as distinct factors, and presents data for the following
seven factors:
• Needs Assessment
• Leadership
• Programme development
• Policy development
• Programme implementation

29
• Policy implementation
• Resource Mobilisation
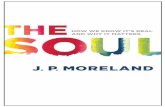
Data from the completed questionnaires was collated and analysed and has been presented
below for each of the seven factors assessed. This section provides: an overview of levels
attributed for each factor (Figure 3, below), level descriptions obtained for each of the
factors, alongside a brief summary of the perceptions of interviewees.
Figure 3: Factor levels attained
30
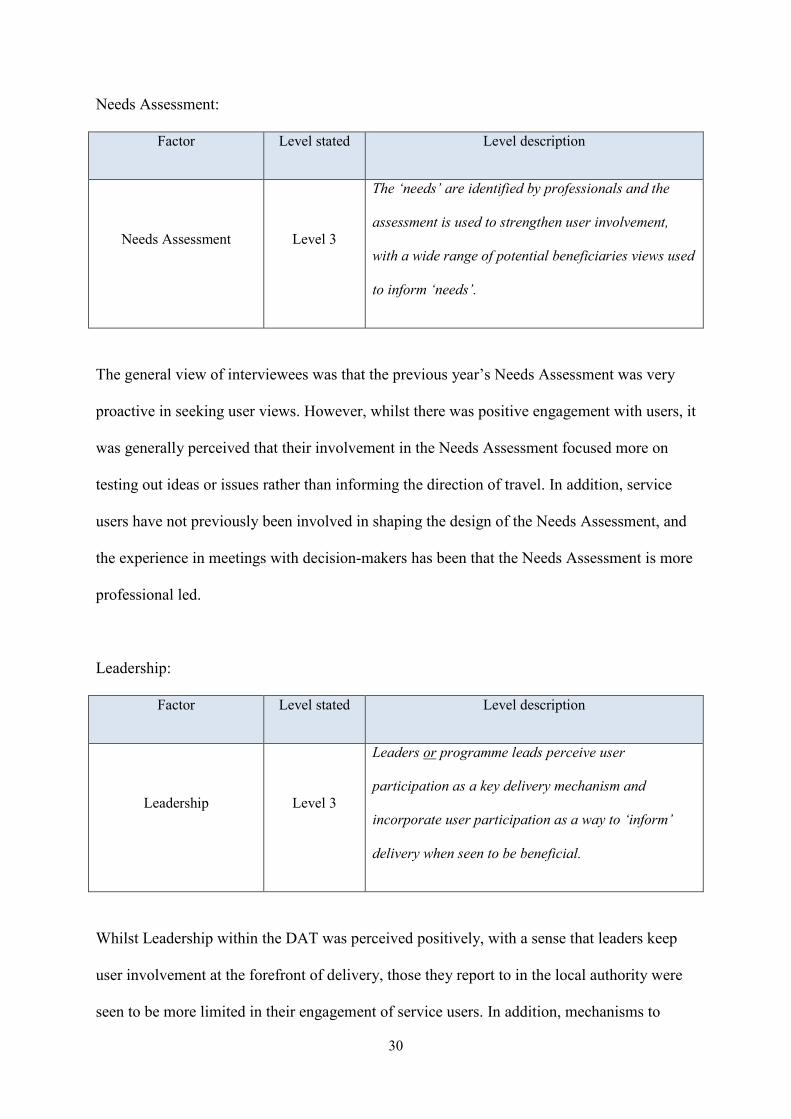
Needs Assessment:
Factor Level stated Level description
Needs Assessment Level 3
The ‘needs’ are identified by professionals and the
assessment is used to strengthen user involvement,
with a wide range of potential beneficiaries views used
to inform ‘needs’.
The general view of interviewees was that the previous year’s Needs Assessment was very
proactive in seeking user views. However, whilst there was positive engagement with users, it
was generally perceived that their involvement in the Needs Assessment focused more on
testing out ideas or issues rather than informing the direction of travel. In addition, service
users have not previously been involved in shaping the design of the Needs Assessment, and
the experience in meetings with decision-makers has been that the Needs Assessment is more
professional led.
Leadership:
Factor Level stated Level description
Leadership Level 3
Leaders or programme leads perceive user
participation as a key delivery mechanism and
incorporate user participation as a way to ‘inform’
delivery when seen to be beneficial.
Whilst Leadership within the DAT was perceived positively, with a sense that leaders keep
user involvement at the forefront of delivery, those they report to in the local authority were
seen to be more limited in their engagement of service users. In addition, mechanisms to
31
support service users in decision-making were not felt to be fully implemented and although
service user views were valued and heard, there was a question as to the level of influence
they bring to decision-making at a strategic level i.e. “they have a voice but not a vote”.
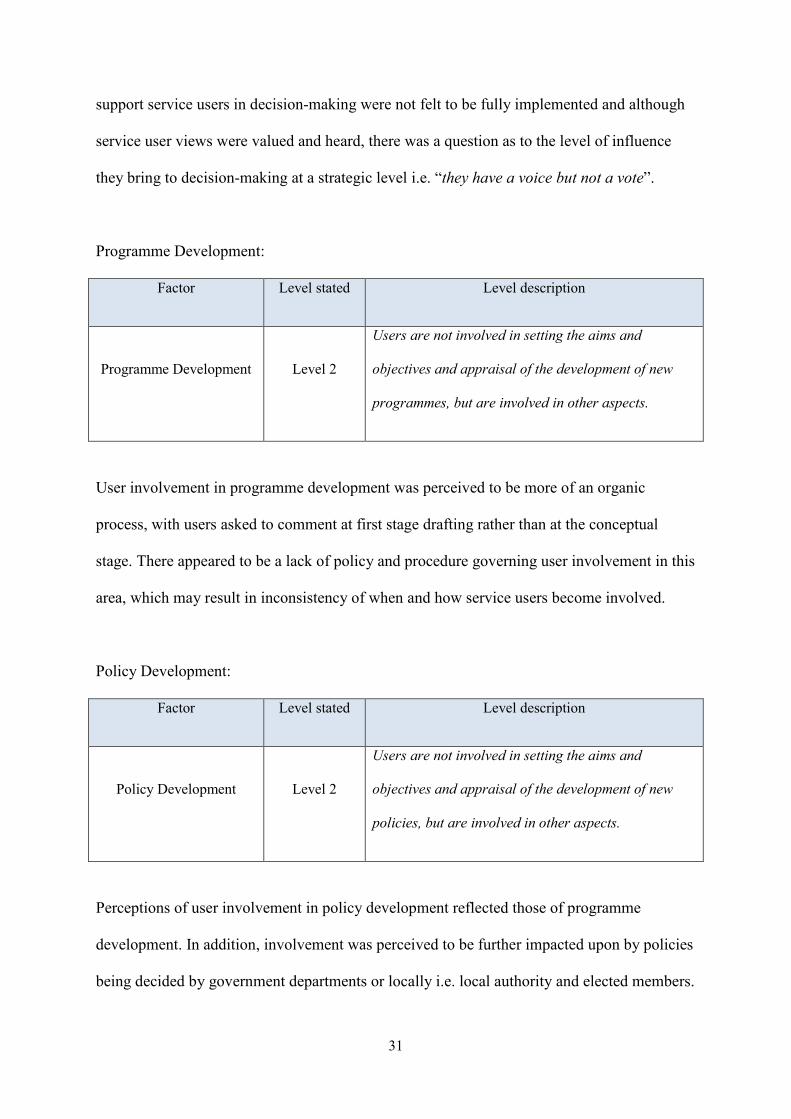
Programme Development:
Factor Level stated Level description
Programme Development Level 2
Users are not involved in setting the aims and
objectives and appraisal of the development of new
programmes, but are involved in other aspects.
User involvement in programme development was perceived to be more of an organic
process, with users asked to comment at first stage drafting rather than at the conceptual
stage. There appeared to be a lack of policy and procedure governing user involvement in this
area, which may result in inconsistency of when and how service users become involved.
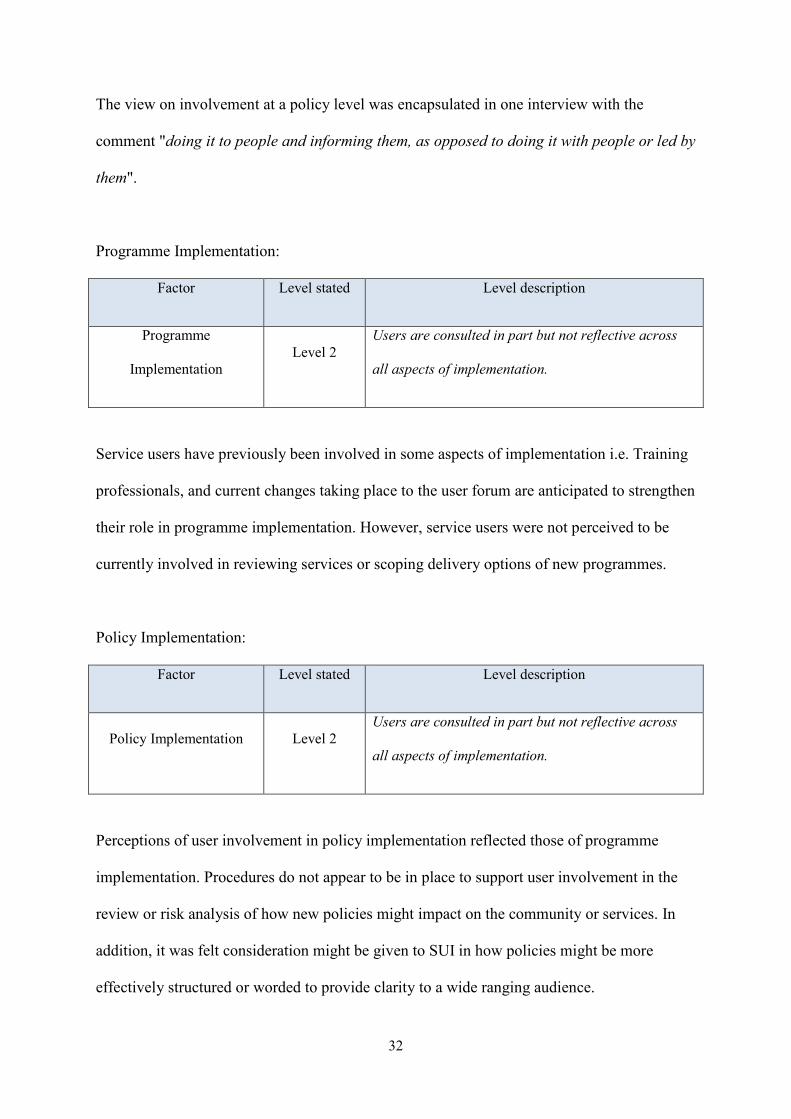
Policy Development:
Factor Level stated Level description
Policy Development Level 2
Users are not involved in setting the aims and
objectives and appraisal of the development of new
policies, but are involved in other aspects.
Perceptions of user involvement in policy development reflected those of programme
development. In addition, involvement was perceived to be further impacted upon by policies
being decided by government departments or locally i.e. local authority and elected members.
32
The view on involvement at a policy level was encapsulated in one interview with the
comment "doing it to people and informing them, as opposed to doing it with people or led by
them".
Programme Implementation:
Factor Level stated Level description
Programme
Implementation Level 2
Users are consulted in part but not reflective across
all aspects of implementation.
Service users have previously been involved in some aspects of implementation i.e. Training
professionals, and current changes taking place to the user forum are anticipated to strengthen
their role in programme implementation. However, service users were not perceived to be
currently involved in reviewing services or scoping delivery options of new programmes.
Policy Implementation:
Factor Level stated Level description
Policy Implementation Level 2 Users are consulted in part but not reflective across
all aspects of implementation.
Perceptions of user involvement in policy implementation reflected those of programme
implementation. Procedures do not appear to be in place to support user involvement in the
review or risk analysis of how new policies might impact on the community or services. In
addition, it was felt consideration might be given to SUI in how policies might be more
effectively structured or worded to provide clarity to a wide ranging audience.
33
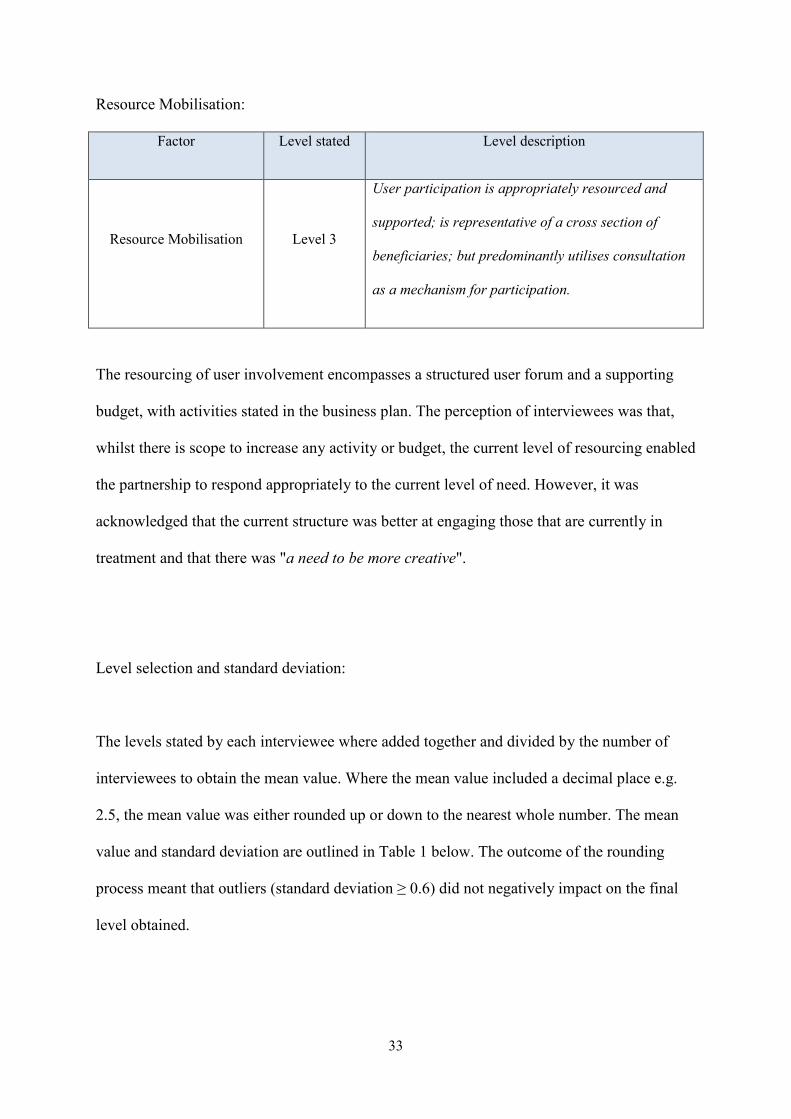
Resource Mobilisation:
Factor Level stated Level description
Resource Mobilisation Level 3
User participation is appropriately resourced and
supported; is representative of a cross section of
beneficiaries; but predominantly utilises consultation
as a mechanism for participation.
The resourcing of user involvement encompasses a structured user forum and a supporting
budget, with activities stated in the business plan. The perception of interviewees was that,
whilst there is scope to increase any activity or budget, the current level of resourcing enabled
the partnership to respond appropriately to the current level of need. However, it was
acknowledged that the current structure was better at engaging those that are currently in
treatment and that there was "a need to be more creative".
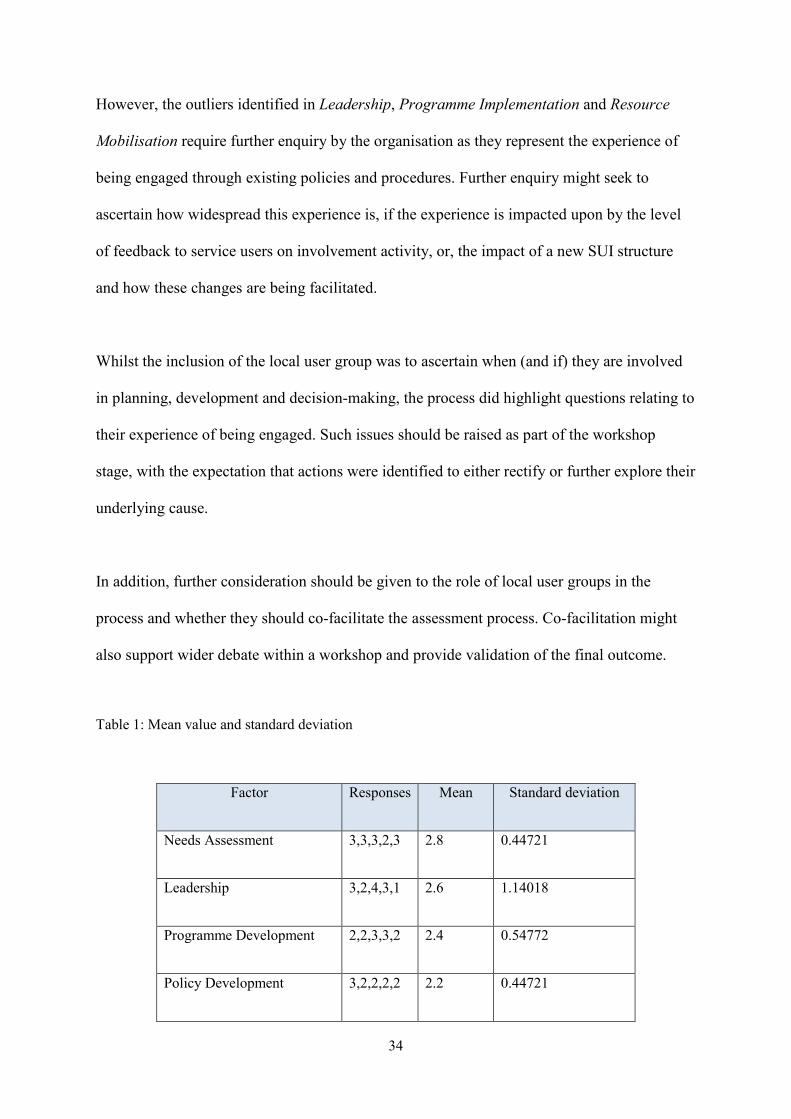
Level selection and standard deviation:
The levels stated by each interviewee where added together and divided by the number of
interviewees to obtain the mean value. Where the mean value included a decimal place e.g.
2.5, the mean value was either rounded up or down to the nearest whole number. The mean
value and standard deviation are outlined in Table 1 below. The outcome of the rounding
process meant that outliers (standard deviation ≥ 0.6) did not negatively impact on the final
level obtained.
34
However, the outliers identified in Leadership, Programme Implementation and Resource
Mobilisation require further enquiry by the organisation as they represent the experience of
being engaged through existing policies and procedures. Further enquiry might seek to
ascertain how widespread this experience is, if the experience is impacted upon by the level
of feedback to service users on involvement activity, or, the impact of a new SUI structure
and how these changes are being facilitated.
Whilst the inclusion of the local user group was to ascertain when (and if) they are involved
in planning, development and decision-making, the process did highlight questions relating to
their experience of being engaged. Such issues should be raised as part of the workshop
stage, with the expectation that actions were identified to either rectify or further explore their
underlying cause.
In addition, further consideration should be given to the role of local user groups in the
process and whether they should co-facilitate the assessment process. Co-facilitation might
also support wider debate within a workshop and provide validation of the final outcome.
Table 1: Mean value and standard deviation
Factor Responses Mean Standard deviation
Needs Assessment 3,3,3,2,3 2.8 0.44721
Leadership 3,2,4,3,1 2.6 1.14018
Programme Development 2,2,3,3,2 2.4 0.54772
Policy Development 3,2,2,2,2 2.2 0.44721
35
Programme Implementation 3,2,2,2,1 2 0.70711
Policy Implementation 2,2,2,2,1 1.8 0.44721
Resource Mobilisation 4,2,4,3,2 3 1
5.1.1 Efficacy of the Tool to support, Plan and Monitor User Involvement
Each interviewee was presented with nine statements (Assessment Tool Evaluation
Questionnaire, Appendix 2) relating to the assessment tools overall ease-of-use, the factors
being measured and the tool’s ability to support future planning and monitoring of SUI.
However, it should be noted that statements 3, 4, 5, 6, and 7 were replicated for each of the
factors being assessed and therefore the number of statements being responded to in total was
thirty nine. Interviewees were asked to rate their level of agreement with each statement by
stating whether they either: strongly agree; disagree; neither agree or disagree; agree;
strongly agree; not known. This was undertaken as part of the semi structured interviews
conducted to facilitate the completion of the assessment tool.
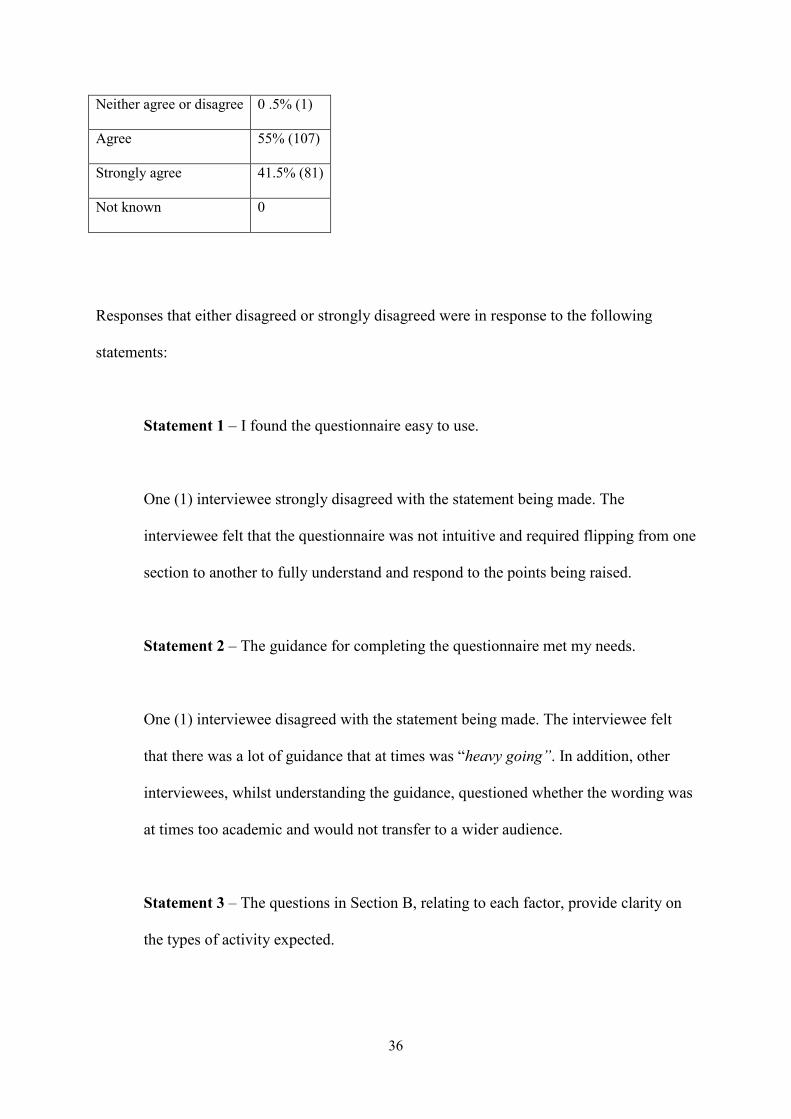
A total of 195 responses from the five interviewees where recorded. Table 2 (below) shows
that a significant percentage (96.5%) of responses were positive (agree/strongly agree).
Table 2: Response percentages
Strongly disagree 0 .5% (1)
Disagree 2.5% (5)
36
Neither agree or disagree 0 .5% (1)
Agree 55% (107)
Strongly agree 41.5% (81)
Not known 0
Responses that either disagreed or strongly disagreed were in response to the following
statements:
Statement 1 – I found the questionnaire easy to use.
One (1) interviewee strongly disagreed with the statement being made. The
interviewee felt that the questionnaire was not intuitive and required flipping from one
section to another to fully understand and respond to the points being raised.
Statement 2 – The guidance for completing the questionnaire met my needs.
One (1) interviewee disagreed with the statement being made. The interviewee felt
that there was a lot of guidance that at times was “heavy going”. In addition, other
interviewees, whilst understanding the guidance, questioned whether the wording was
at times too academic and would not transfer to a wider audience.
Statement 3 – The questions in Section B, relating to each factor, provide clarity on
the types of activity expected.
37
One (1) interviewee disagreed with the statement being made when applied to
Programme/Policy Development and Programme/Policy Implementation. The
interviewee’s response was based on the view that programme and policy could not
be assessed together due to new policies being, at times, nationally driven. It is worth
noting that other interviewees had provided positive responses to this statement for
each of the factors stated but with the caveat that the two items (programme and
policy) were separated as factors.
All interviewees responded positively (agree/strongly agree) to all other statements as
outlined below:
Statement 4 – The questions in Section B, relating to each factor, helped me decide
where to place my organisation on the continuum. (Agree 57.2%, strongly agree
42.8%)
Statement 5 – The levels stated for each factor were fair. (Agree 77.1%, strongly
agree 22.9%)
Statement 6 – The factors used represent key factors for SUI in organisational
planning, development and decision-making processes. (Agree 40%, strongly agree
60%)
Statement 7 – The assessment tool supported me in understanding the types of
activity I should consider for effective SUI. (Agree 40%, strongly agree 60%)
38
Statement 8 – The assessment tool would help me plan SUI more effectively. (Agree
40%, strongly agree 60%)
Statement 9 – The assessment tool would help me monitor how SUI is being
delivered. (Agree 20%, strongly agree 80%)
Comments made by interviewees during the completion of the questionnaire included:
• "A lot of guidance! Methodology was interesting....... personally I could have lived
without it."
• "Could too easily be used as a tick box exercise if not conducted as part of an
interview."
• "You got the answers out because you've asked me, if you are just reading from this
you wouldn't understand where I'm coming from."
• "The questions (Section B) were more helpful than the levels."
• "Thought-provoking (Section B)"
• "It does make you question the kinds of support you give to people to actually take
part."
• "It raised a couple of issues for me (previous planning)."
Data from semi structured interviews and the questionnaire on the tool’s ease-of-use show
that interviewees perceived that: a) the content and structure of the assessment tool supported
them in its completion, and, b) that the assessment tool itself was effective in supporting
planning and monitoring of SUI. However, the volume of guidance needed to be reduced; the
wording should be more reader friendly and that programme and policy should be separated

39
into individual factors. In addition, all interviewees reported that the iterative process of a
semi-structured interview enabled them to better understand their rationale for the levels
chosen and where improvements in the system could be considered. The interviewer found
that the interview process provided context for the levels attributed, which might contribute
to providing a richer picture to present in the workshop stage and form the basis for a wider
debate in planning future actions.
5.1.2 Amendments to Process and/or Assessment Tool
In response to data collected from the Draft Assessment Tool Questionnaire (Appendix 1),
the Assessment Tool Evaluation Questionnaire (Appendix 2) and general comments from
DAT 1, elements of the process and the questionnaires were amended. Amendments to the
process and questionnaires were as follows:
1. Semi-structured interviews were incorporated as part of the data collection process.
The use of semi-structured interviews was initially undertaken to a) enable the
interviewer to note any difficulties experienced by the respondent in completing the
assessment tool questionnaire, and, b) ask additional questions to ascertain the tool’s
ease-of-use and ability to support planning and monitoring of user involvement.
However, interviewees reported that the iterative process of a semi-structured
interview supported their decision-making and the interviewer identified that the
process supported the collection of additional data to support the next stage
40
(workshop). In addition, using interviews as the vehicle for data collection allowed for
a reduction in the level of guidance required for completing the questionnaire.
2. Factors that combined ‘programme and policy’ were separated and the factors being
assessed were increased from five to seven.
Interviewees felt that programme development and implementation was a more
organic process than policy development and implementation and offered greater
opportunity for SUI. Whereas, a percentage of policies were nationally driven and
presented less opportunity for SUI, therefore adversely affecting the assessment of
programme development and implementation.
3. The Assessment tool questionnaire was re-configured and the methodology section
was removed. (NB The questionnaire was subsequently renamed as ‘User
Involvement Questionnaire’)
Interviewees felt that there was a significant amount of guidance in the questionnaire.
It was noted by the interviewer, alongside one comment, that interviewees needed to
constantly refer to different sections of the questionnaire to fully consider their
responses. Changes to the questionnaire were undertaken to reduce the necessity to
refer to Section B to enable completion. In addition, incorporating semi-structured
interviews as the vehicle for data collection also removed the necessity for the
methodology section as this could be conveyed by the interviewer during the
interview.
41
The amendment to the number of factors being assessed (item 2, above) also required these
changes to be incorporated into the Assessment Tool Evaluation Questionnaire.
It should be noted that data from DAT 1 was utilised to refine the assessment process and
questionnaires. Therefore, conclusions drawn from findings and analysis will refer only to
DAT 2 as the pilot site. The revised questionnaires (User Involvement Questionnaire,
Appendix 3 and Assessment Tool Evaluation Questionnaire v2, Appendix 4) were
subsequently used to run the pilot in DAT 2.
5.2 Drug Action Team (DAT) 2, Semi-structured Interviews
The total number of staff (officers) in DAT 2 is ten and seven officers were interviewed. In
addition to the seven officers, a member of the local user group was also interviewed and the
total number of interviewees was eight.
Data from the completed questionnaires was collated and analysed and has been presented
below for each of the seven factors assessed. This section provides: an overview of levels
attributed for each factor (Figure 4, below), level descriptions obtained for each of the
factors, alongside a brief summary of the perceptions of interviewees.
42
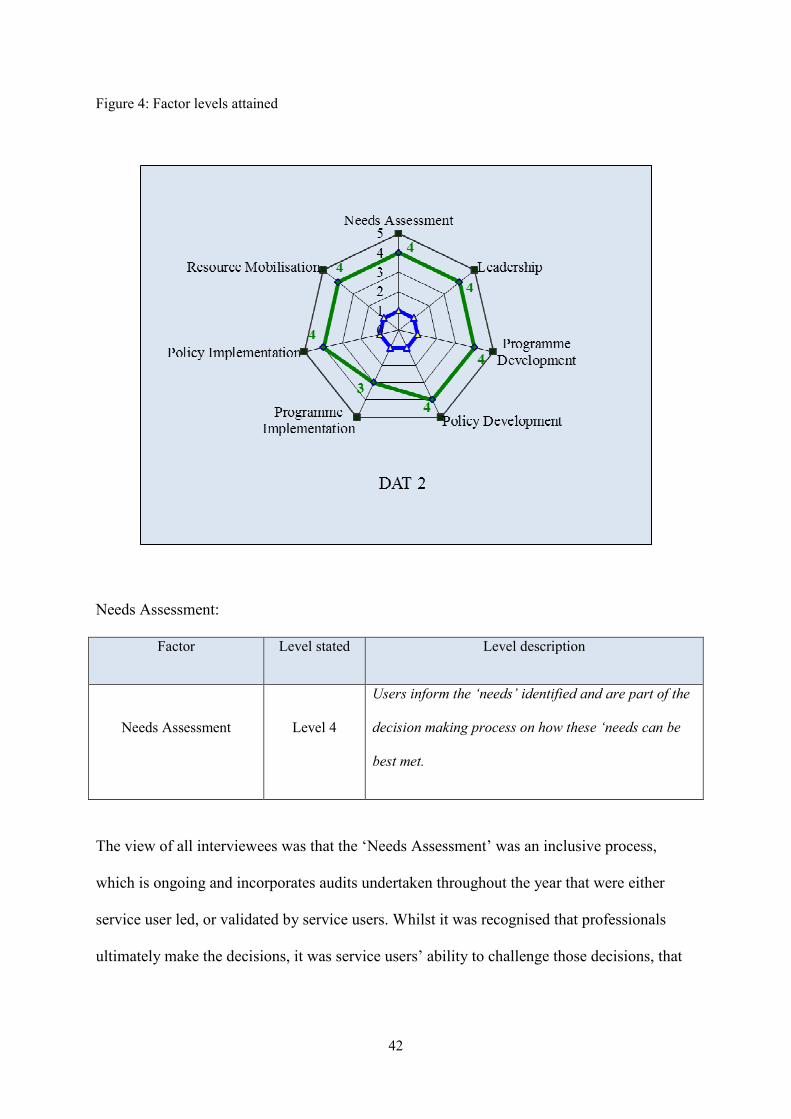
Figure 4: Factor levels attained
Needs Assessment:
Factor Level stated Level description
Needs Assessment Level 4
Users inform the ‘needs’ identified and are part of the
decision making process on how these ‘needs can be
best met.
The view of all interviewees was that the ‘Needs Assessment’ was an inclusive process,
which is ongoing and incorporates audits undertaken throughout the year that were either
service user led, or validated by service users. Whilst it was recognised that professionals
ultimately make the decisions, it was service users’ ability to challenge those decisions, that

43
holds those responsible accountable. However, the DAAT appeared reliant on the service
user council to provide users’ views from a breadth of possible beneficiaries.
Leadership:
Factor Level stated Level description
Leadership Level 4
Leaders and programme leads perceive user
participation as a key delivery mechanism and actively
seek it to inform delivery wherever possible.
Leadership within the DAAT was perceived positively, with a sense that service user
involvement is so “embedded” in individual culture and practice that “they wouldn’t think of
doing anything without user involvement”. However, there was recognition from some
interviewees that whilst this is the case, this position is reliant on current culture and working
practice. As such, further exploration of this might consider how existing governance
structures would sustain user involvement should the culture and practice of individuals
change i.e. changes in senior management.
Programme Development:
Factor Level stated Level description
Programme Development Level 4
User participation is incorporated in all aspects of
programme development and is encompassed in
organisational policy and procedures to guide
professionals.
44
User involvement in programme development was perceived to be embedded at a policy
level, which was evident throughout the recent service redesign with service users
participating in planning, tendering and interviewing. This view was encapsulated in one
interview with the comment “we make sure service users have their fingers in all the pies”.
However, some interviewees questioned if involvement consistently began at the first stage
of development and whether there was sufficient understanding of the objectives for
involvement and clarity of roles and responsibilities.
Policy Development:
Factor Level stated Level description
Policy Development Level 3
User participation is incorporated in aspects of policy
development, including either setting aims and
objectives or appraisal but is not encompassed in
organisational policy or procedures to guide
professionals.
User involvement in policy development was perceived as positive with anecdotal evidence
of the service user council being pro-active in identifying changes and recommendations for
policy reviews. However, where policies are developed locally there was a perception by
some that whilst there were checks and balances in place to ensure user involvement, with
national policies a gap was perceived in guidance to ensure policies were referred back into
local processes.
45
Programme Implementation:
Factor Level stated Level description
Programme
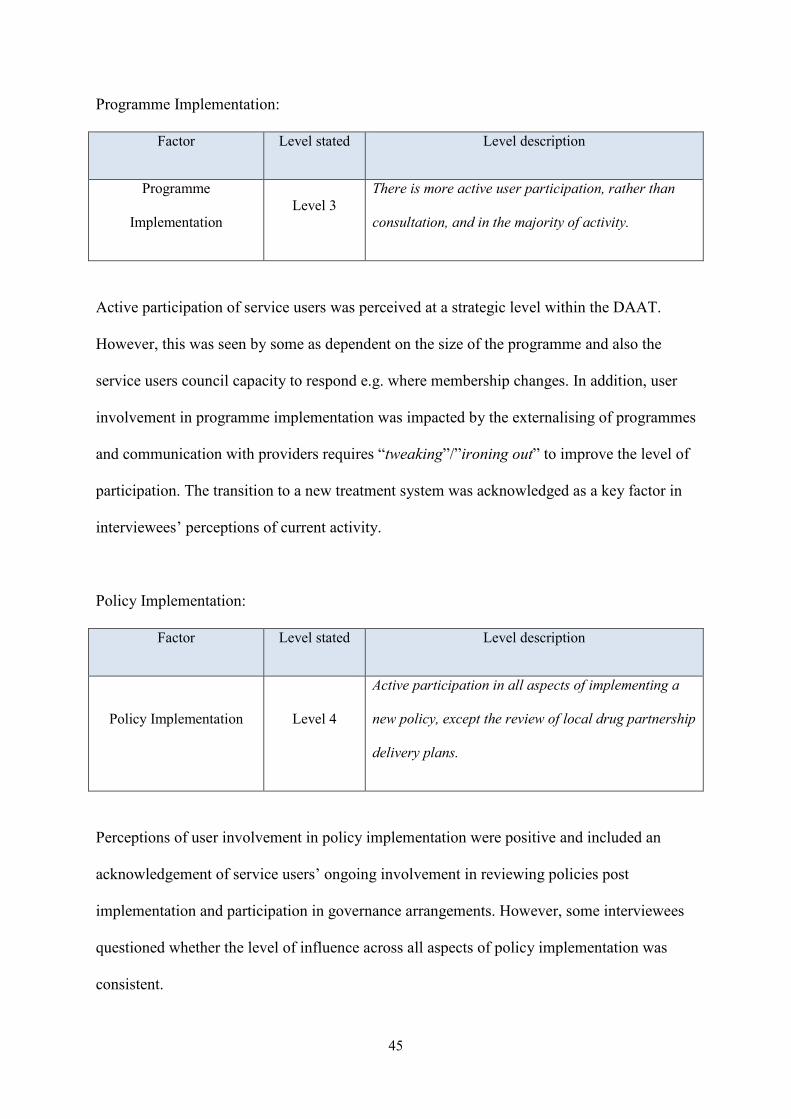
Implementation Level 3
There is more active user participation, rather than
consultation, and in the majority of activity.
Active participation of service users was perceived at a strategic level within the DAAT.
However, this was seen by some as dependent on the size of the programme and also the
service users council capacity to respond e.g. where membership changes. In addition, user
involvement in programme implementation was impacted by the externalising of programmes
and communication with providers requires “tweaking”/”ironing out” to improve the level of
participation. The transition to a new treatment system was acknowledged as a key factor in
interviewees’ perceptions of current activity.
Policy Implementation:
Factor Level stated Level description
Policy Implementation Level 4
Active participation in all aspects of implementing a
new policy, except the review of local drug partnership
delivery plans.
Perceptions of user involvement in policy implementation were positive and included an
acknowledgement of service users’ ongoing involvement in reviewing policies post
implementation and participation in governance arrangements. However, some interviewees
questioned whether the level of influence across all aspects of policy implementation was
consistent.
46
Resource Mobilisation:
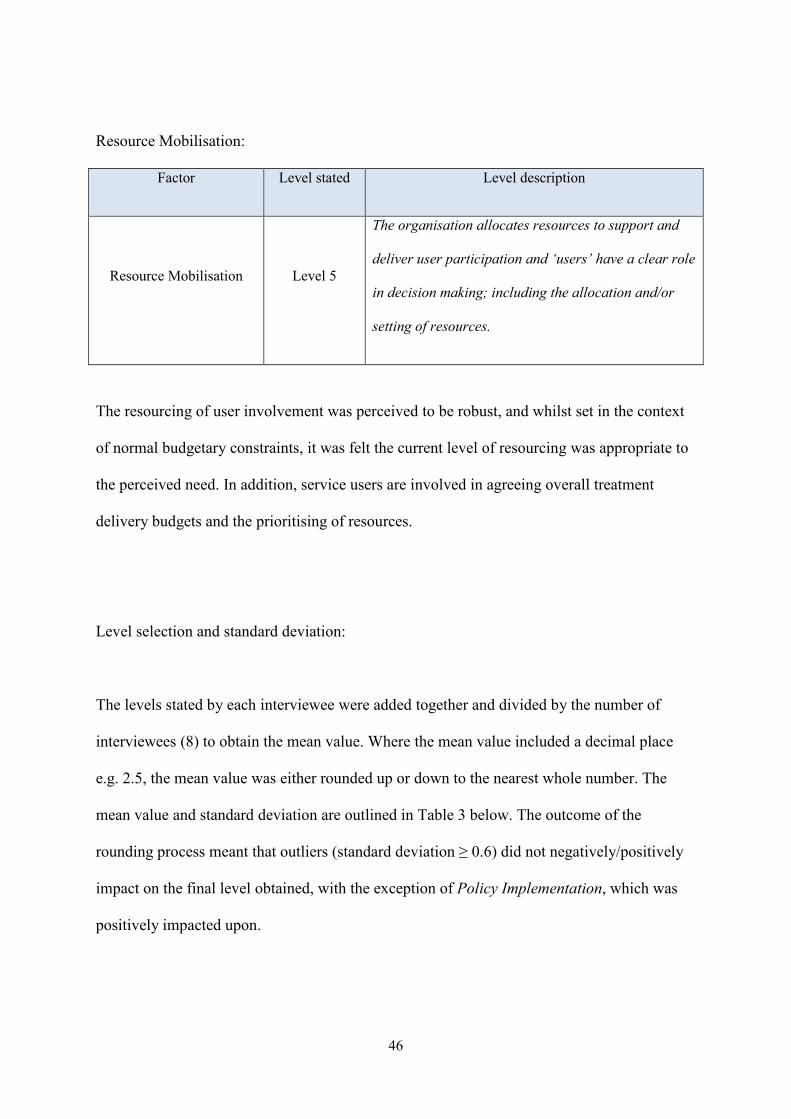
Factor Level stated Level description
Resource Mobilisation Level 5
The organisation allocates resources to support and
deliver user participation and ‘users’ have a clear role
in decision making; including the allocation and/or
setting of resources.
The resourcing of user involvement was perceived to be robust, and whilst set in the context
of normal budgetary constraints, it was felt the current level of resourcing was appropriate to
the perceived need. In addition, service users are involved in agreeing overall treatment
delivery budgets and the prioritising of resources.
Level selection and standard deviation:
The levels stated by each interviewee were added together and divided by the number of
interviewees (8) to obtain the mean value. Where the mean value included a decimal place
e.g. 2.5, the mean value was either rounded up or down to the nearest whole number. The
mean value and standard deviation are outlined in Table 3 below. The outcome of the
rounding process meant that outliers (standard deviation ≥ 0.6) did not negatively/positively
impact on the final level obtained, with the exception of Policy Implementation, which was
positively impacted upon.
47
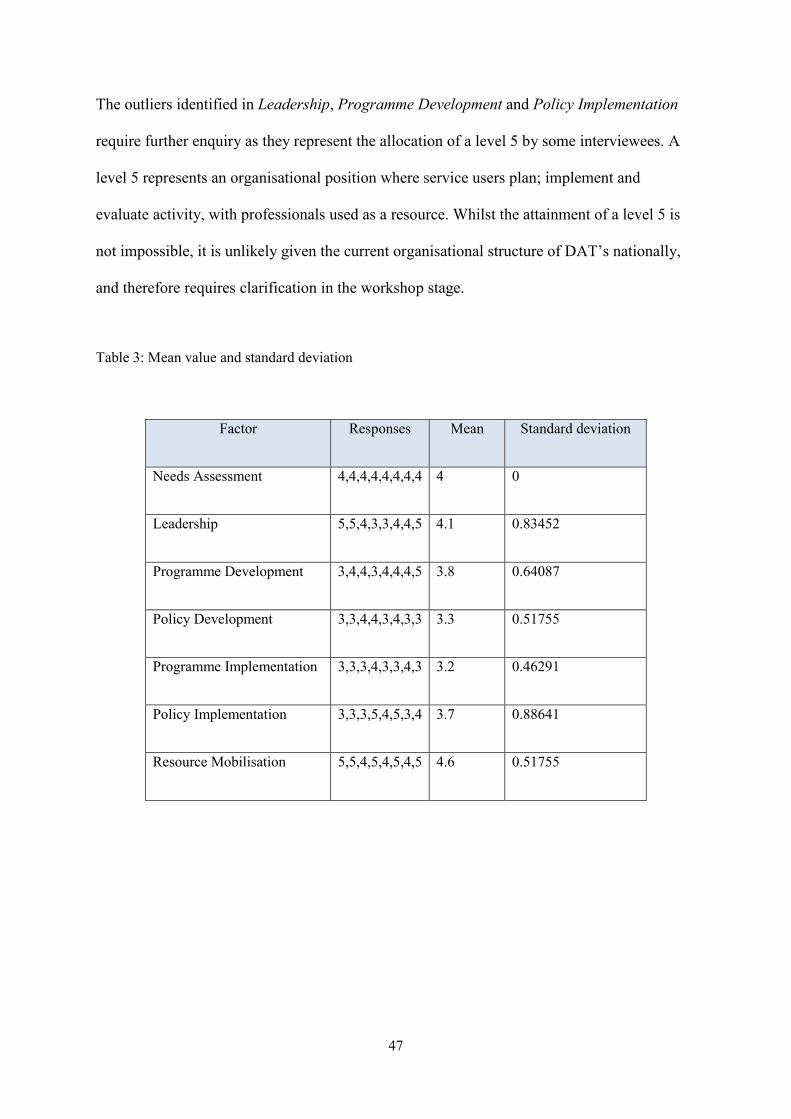
The outliers identified in Leadership, Programme Development and Policy Implementation
require further enquiry as they represent the allocation of a level 5 by some interviewees. A
level 5 represents an organisational position where service users plan; implement and
evaluate activity, with professionals used as a resource. Whilst the attainment of a level 5 is
not impossible, it is unlikely given the current organisational structure of DAT’s nationally,
and therefore requires clarification in the workshop stage.
Table 3: Mean value and standard deviation
Factor Responses Mean Standard deviation
Needs Assessment 4,4,4,4,4,4,4,4 4 0
Leadership 5,5,4,3,3,4,4,5 4.1 0.83452
Programme Development 3,4,4,3,4,4,4,5 3.8 0.64087
Policy Development 3,3,4,4,3,4,3,3 3.3 0.51755
Programme Implementation 3,3,3,4,3,3,4,3 3.2 0.46291
Policy Implementation 3,3,3,5,4,5,3,4 3.7 0.88641
Resource Mobilisation 5,5,4,5,4,5,4,5 4.6 0.51755
48
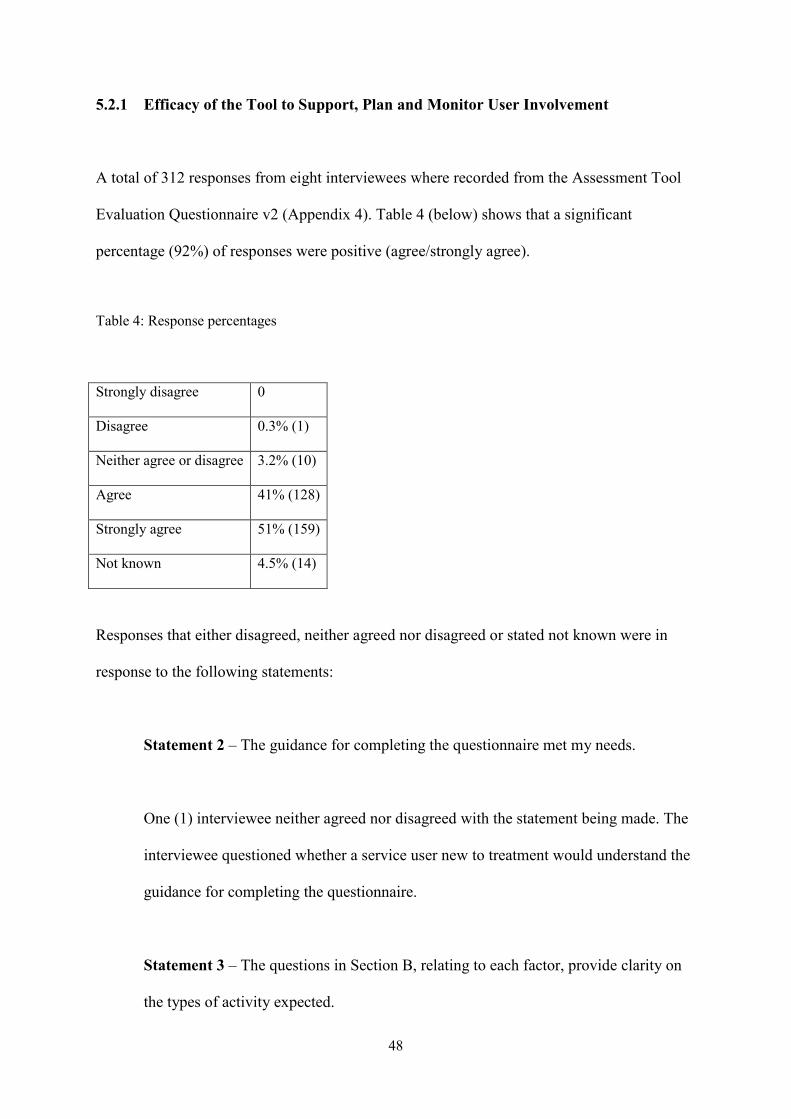
5.2.1 Efficacy of the Tool to Support, Plan and Monitor User Involvement
A total of 312 responses from eight interviewees where recorded from the Assessment Tool
Evaluation Questionnaire v2 (Appendix 4). Table 4 (below) shows that a significant
percentage (92%) of responses were positive (agree/strongly agree).
Table 4: Response percentages
Strongly disagree 0
Disagree 0.3% (1)
Neither agree or disagree 3.2% (10)
Agree 41% (128)
Strongly agree 51% (159)
Not known 4.5% (14)
Responses that either disagreed, neither agreed nor disagreed or stated not known were in
response to the following statements:
Statement 2 – The guidance for completing the questionnaire met my needs.
One (1) interviewee neither agreed nor disagreed with the statement being made. The
interviewee questioned whether a service user new to treatment would understand the
guidance for completing the questionnaire.
Statement 3 – The questions in Section B, relating to each factor, provide clarity on
the types of activity expected.
49
One (1) interviewee felt they could not answer the question (Not known) as they had
not used the questions in Section B and therefore could not comment.
Statement 4 – The questions in Section B, relating to each factor, helped me decide
where to place my organisation on the continuum.
One (1) interviewee felt they could not answer the question (Not known) as they had
not used the questions in Section B and therefore could not comment.
One (1) interviewee disagreed with the statement being made for ‘Leadership’ only as
they felt the questions were not as expansive as those for other factors.
Statement 5 – The levels stated for each factor were fair.
One (1) interviewee neither agreed nor disagreed with the statement being made. The
interviewee felt that the statements against each level were at times too prescriptive
and did not lend themselves to the complexity of the situation “not enough wriggle
room”.
One (1) interviewee neither agreed nor disagreed with the statement being made for
Programme and Policy Development respectively. The interviewee felt that the level
statements for these two factors did not fully reflect their view.
50
All interviewees responded positively (agree/strongly agree) to all other statements as
outlined below:
Statement 1 – I found the questionnaire easy to use. (Agree 62.5%, strongly agree
37.5%)
Statement 6 – The factors used represent key factors for SUI in organisational
planning, development and decision-making processes. (Agree 62.5%, strongly agree
37.5%)
Statement 7 – The assessment tool supported me in understanding the types of
activity I should consider for effective SUI. (Strongly agree 100%)
Statement 8 – The assessment tool would help me plan SUI more effectively. (Agree
37.5%, strongly agree 62.5%)
Statement 9 – The assessment tool would help me monitor how SUI is being
delivered. (Agree 62.5%, strongly agree 37.5%)
Comments made by interviewees during the completion of the questionnaire included:
• “Reading this made me very aware that I don’t always reflect on where I could ask
more of SUI to support various work streams.”
• "Required dialogue to fully understand all the statements."

51
• "Near enough, language appropriate for professionals but would question
understanding for individuals with less experience.”
• "I felt at times it was too prescriptive.”
• "Would look at different process for engaging young people.”
Data from semi structured interviews and the questionnaire on the tool’s ease-of-use show
that interviewees perceived that: a) the content and structure of the assessment tool supported
them in its completion, and, b) that the assessment tool itself was effective in supporting
planning and monitoring of SUI. However, the statements for each of the levels were at times
too prescriptive and/or required dialogue with the interviewer to understand their relation to
organisational activity.
5.2.2 Workshop
A workshop (2 hours) with the DAT 2 commissioning team, and a member of the local user
group, was held to facilitate a final decision on where marks should be placed on the
continuum for each factor. Data from the semi-structured interviews (4.2, above) was used as
the basis for discussion. The process used to reach agreement was as follows:
1. An overview of the data from semi-structured interviews was presented to the group,
followed by the outcome for each factor and general perceptions of current activity.
2. For each factor, the group were asked to:

52
• Consider whether the level attained from the interview process was a fair
representation of organisational delivery
• Discuss why, or why it is not a fair representation
• Vote on which level they believe is a fair representation of organisational
delivery
• Identify actions that would either improve, or, sustain current levels of
delivery
At the beginning of the process (above) the group where asked to agree how levels would be
attributed where there was not unanimous agreement in the group. The group decided a
majority vote would identify each level. Where there was no majority, the mean would be
established, as per the interview process (see Table 3, above). However, where the mean
contained a fraction, the number would be rounded down at 0.5, as opposed to ‘up’ which
was undertaken in the interview process. The rationale for this decision was that they felt
there needed to be proportionally more positive than negative actions to warrant rounding up.
The levels attributed at the workshop (final outcome) and comparisons to those attributed
from interviews are contained below in Table 5.
53
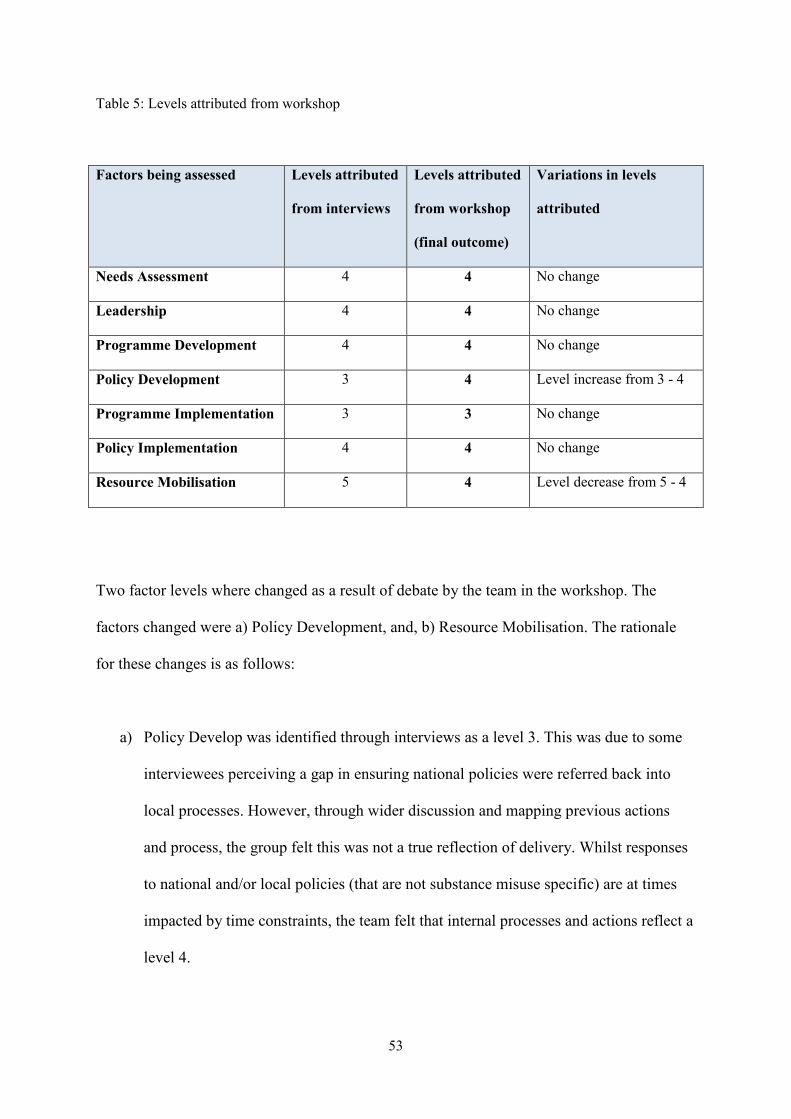
Table 5: Levels attributed from workshop
Factors being assessed Levels attributed
from interviews
Levels attributed
from workshop
(final outcome)
Variations in levels
attributed
Needs Assessment 4 4 No change
Leadership 4 4 No change
Programme Development 4 4 No change
Policy Development 3 4 Level increase from 3 - 4
Programme Implementation 3 3 No change
Policy Implementation 4 4 No change
Resource Mobilisation 5 4 Level decrease from 5 - 4
Two factor levels where changed as a result of debate by the team in the workshop. The
factors changed were a) Policy Development, and, b) Resource Mobilisation. The rationale
for these changes is as follows:
a) Policy Develop was identified through interviews as a level 3. This was due to some
interviewees perceiving a gap in ensuring national policies were referred back into
local processes. However, through wider discussion and mapping previous actions
and process, the group felt this was not a true reflection of delivery. Whilst responses
to national and/or local policies (that are not substance misuse specific) are at times
impacted by time constraints, the team felt that internal processes and actions reflect a
level 4.
54
b) Resource Mobilisation was identified through interviews as a level 5. This represents
an organisational position where service users plan, implement and evaluate activity,
with professionals used as a resource. However, during discussions it was
acknowledged that ‘professional’s’ ultimately have responsibility for decision-
making. The selection of level 5 by some interviewees’ had been governed by the
level description used in the assessment tool itself. The wording of a level 4
description was subsequently replaced by the original level 5 description and the team
allocated a level 4 for this factor. This was undertaken to reflect organisational
activity but acknowledged that professional’s ultimately have responsibility for
decision-making.
Recommendations to support and maintain future user involvement of the DAT included:
• Support the local user group to link with other user groups within the borough. This
action is reliant on the ongoing development of the user group and its resourcing,
alongside a borough wide identification of need and structure to support such an
initiative.
• Recommend the consideration of borough wide service user involvement in
forthcoming Partnership Board reviews.
• Monitor the impact of NHS and public sector reform on service user involvement
within the DAT.
• Ensure the completion of appropriate levels of documentation to support and monitor
service user involvement e.g. project initiation documents. This action is reliant on
both team and departmental/partnership compliance. Departmental/partnership
55
compliance is often more difficult to influence and could be supported through a
structured feedback process.
• Continue to monitor and support the levels of, and requirements for, skills within the
local user group. Membership of user groups naturally changes over time as new
service users are engaged, and as such, skills and knowledge will vary. Organisations
must therefore maintain a balance between supporting individuals to participate in
user groups, in a way that does not negatively impact on their treatment journey,
whilst ensuring the group has an appropriate skill set to effectively represent the
views of the community it seeks to serve.
• Maintain the inclusion of service users in the risk analysis of programme and policy
implementation. This action can be impacted upon jointly by timescales and the
capacity within the local user group. Timescale and capacity relates to a) where
implementation is for services that are not substance misuse specific and are
implemented by other departments or partners, and, b) implementation by
organisation’s commissioned by the DAT. Consideration should be given to the level
of user involvement required on a case-by-case basis. In situation ‘a’, where full user
involvement is not undertaken, the reasons for the level of involvement undertaken
and any subsequent risks should be noted. In situation ‘b’, levels of user involvement
should be supported, monitored and/or challenged through contracting processes.
The data from the semi-structured interviews provided a rich picture from which to generate
debate and challenge perceptions of organisational delivery during the workshop. In addition,
whilst there were minimal changes to the levels attained, those that did change have a clear
rationale for doing so.
56
However, the ability of the team to openly debate organisational delivery was seen as a
reflection on the level of ease that was apparent between the team and senior management
present. In addition, the teams’ willingness and ability to question individual practice and
organisational deliver supported the piloting of the assessment tool. As such, future
assessment of the tools’ use might consider the impact on the final outcome where senior
management (Leadership) appears less supportive of user involvement.
Whilst there is no expectation that outcomes from semi-structured interviews should mirror
those of the workshop, any significant and/or multiple shifts in levels should be fully
explored by the facilitator. In addition, the independence of the facilitator (interviewer)
should be explored as a factor in establishing a fair representation of organisational delivery.
In the piloting of the assessment tool, a member of the Alliance monitored both the semi-
structured interviews and the workshop. Their prior knowledge and perception of DAT 2’s
organisational delivery was comparable to the outcome of the assessment.
Chapter 6
Conclusions
57
Chapter 6. Conclusions
Whilst current policy and guidance seeks to support and guide user involvement, far less
attention has been given to where and how involvement takes place in organisations. As such,
we find ourselves in the position whereby we are unable to:
• routinely measure levels of activity,
• benchmark activity to support future development and research, or
• provide accountability.
The focus of this study was to establish whether an assessment tool could a) measure user
involvement in the planning, development and decision-making activity of a DAT, and, b) be
used to support future planning and monitoring of user involvement.
The piloting of the assessment tool has shown that by focusing on organisational processes
and where users’ are involved in its planning, development and decision-making processes,
we are able to:
d) recognise gaps in delivery and identify actions to improve and/or sustain user
involvement
e) support individuals and teams to understand and consider activity to support effective
SUI
f) effectively plan and monitor SUI
58
The use of individual interviews provided an effective vehicle for staff members to reflect on
their own practice and wider organisational delivery. This reflection provided the interviewer
with a rich picture to inform wider debate in the team workshop and challenge perceptions of
practice and process. The open debate and challenge of the workshop enabled the team to not
only identify areas for improvement but also recognise good practice that takes place and
what the strengths and weaknesses of the team were.
In addition, individual and team reflection of practice during the assessment may yield future
outcomes through greater understanding and focus. Those that participated in the pilot
strongly agreed with the statement that:
• The assessment tool supported me in understanding the types of activity I should
consider for effective SUI (strongly agree 100%).
“Understanding user involvement as a small part of a larger system helps bridge the divide
between micro level changes and system-wide reforms.”
(Tritter & McCallum, 2006, p166)
Whilst some comments on the assessment tools ease-of-use require further consideration i.e.
the wording for ‘level descriptions’, all participants agreed that:
• The assessment tool would help plan SUI more effectively.
• The assessment tool would help monitor how SUI is being delivered.
59
Levels of service user engagement will always be variable from organisation to organisation,
and impacted upon by a multitude of factors such as: rural versus urban; those in treatment
versus treatment naive; methods of engagement; resources; skills and experience. However,
effective user engagement is underpinned by an organisation with:
• a clear understanding of why, where and when users’ should be involved
• the ability to continually and consistently review policy and practice, and
• accountability to those they seek to serve.
Whilst we must continue to evolve the methods and tools of engagement, we first need to
assure ourselves that we, and the organisations we work in, fully understand the why, where
and when of user involvement. Only then can we appreciate and comprehend the HOW.
Chapter 7
Recommendations
60
Chapter 7. Recommendations
The piloting of the assessment tool was undertaken in a DAT that has been recognised within
their region as having progressive user involvement activity. This was reflected in their
willingness and ability to question individual practice and organisational delivery and was
perceived as a contributing factor to the outcome of the pilot. However, to fully understand
the limitations and/or challenges of undertaking such an assessment, further testing of the
assessment tool should take place in organisations with a range of user involvement
experience and organisational support for user involvement.
Wider testing of the assessment tool would also need to consider the need for the
independence of the facilitator (interviewer). Whilst the independence of the facilitator might
be seen to bring a level of validation to the outcome of the process, facilitation by a member
of the organisation may provide oversight of proposed actions and integration of
organisational learning.
Co-facilitation by a representative of the local user group would be seen as a key addition to
any future testing or implementation of the assessment tool. The inclusion of a representative
of the local user group not only supports wider debate throughout the process but would also
support the consideration of next steps and how future engagement takes place. In addition,
where involvement is less evolved, co-facilitation may also support the longer-term
relationship between staff and users.
Key to any further evaluation of the assessment tool’s efficacy is the support and/or
involvement of those with responsibility for the oversight and governance of the

61
organisations (local drug partnerships, or equivalent i.e. DAT) being assessed. Whilst there
are organisations that recognise and value user involvement, the inclusion of those with less
organisational support for it, presents a greater challenge.
62
References:
• Arnstein, S. R; 1969, A Ladder Of Citizen Participation, Journal of the American
Planning Association,35:4,216 – 224
• Carr, Sarah; 2004, Has service user participation made a difference to social care
services?, Social Care Institute for Excellence, British Library Cataloguing in
Publication Data, ISBN 1 904812 10 4
• Commission for Healthcare Audit and Inspection, January 2009, Improving services
for substance misuse, Diversity, and inpatient and residential rehabilitation services.
ISBN 978-1-84562-212-1
• Department of Health, 2006a, The National Health Services Act (modified 13 April
2007), viewed online 02/06/2010
http://www.dh.gov.uk/en/Publicationsandstatistics/Legislation/Actsandbills/DH_0641
03
• Department of Health, 2006b, Our health, our care our say – a new direction for
community services, The Stationary Office, ISBN 0-10-167372-8
• Department of Health, 30th June 2008a, High quality care for all: NHS Next Stage
Review final report, ISBN 978-0-10-174322-8
• Department of Health, 2008b, Real Involvement, Gateway reference 10546,
www.dh.gov.uk/publications
• Department of Health, 2010, NHS Constitution, viewed online 02/06/2010
http://www.dh.gov.uk/prod_consum_dh/groups/dh_digitalassets/@dh/@en/@ps/docu
ments/digitalasset/dh_113645.pdf
• Fiander, M; Burns, T; 2000, Psychiatric Services Vol. 51 No. 5 A Delphi Approach to
Describing Service Models of Community Mental Health Practice, Psychiatric
63
Services Vol. 51 No. 5 viewed on line 04/10/09
http://psychservices.psychiatryonline.org/cgi/reprint/51/5/656
• Fischer, J; Jenkins, N; Bloor, M; Neale, J; Berney, L; 17 March 2007, Drug user
involvement in treatment decisions, Joseph Rowntree Foundation, ISBN 978 1 85935
565 7 (pdf: available at www.jrf.org.uk)
• GLADA (Greater London alcohol and drugs alliance), 2005, Lessons Learned,
Greater London Authority, ISBN 1 85261 707 1
• Home Office, 1 January 1998, Tackling Drugs To Build a Better Britain, Product
number: 0101394527
• Home Office, February 2008, Drugs: protecting families and communities – the 2008
drug strategy, ISBN 978-1-84726-615-6
• Jürgens, R; 2008, “Nothing about us without us” — Greater, meaningful involvement
of people who use illegal drugs, Canadian HIV/AIDS Legal Network, International
HIV/AIDS Alliance, Open Society Institute ISBN 978-1-896735-92-4
• McLaughlin, H; 2009, ‘Keeping Service User Involvement in Research Honest’,
Oxford University Press.
• National Treatment Agency, June 2006, NTA Guidance for local partnerships on user
and carer involvement. viewed online 12/06/2010
http://www.nta.nhs.uk/areas/users_and_carers/publications/nta_guide_to_u&c_involv
ement6.6.pdf
• National Treatment Agency, July 2009, Undertaking needs assessment, viewed online
12/06/2010
http://www.nta.nhs.uk/areas/treatment_planning/treatment_plans_2010_11/needs_ass
essment_2010_11.pdf
64
• National Treatment Agency for Substance Misuse, 2010, Commissioning for recovery
Drug treatment, reintegration and recovery in the community and prisons: a guide for
drug partnerships. London: NTA Gateway number: 12944. Available as download:
http://www.nta.nhs.uk/uploads/summary_c4r_2010.pdf
• Nicholson, L; 2005, Civic Participation in Public Policy-Making: a Literature Review,
The Research Shop, ISBN 0 7559 2700 1 (Web only publication)
http://www.scotland.gov.uk/Publications/2005/09/16120247/02537
• Participation Works, 2008, Listen and Change, Children’s Rights Alliance for
England, ISBN: 978-1-898961-19-2
• Patterson, S; Crawford, M.J; Weaver T; Rutter, D; Agath, K; Albert, E; Hunt, A;
Jones, V; 2007, User involvement in efforts to improve the quality of drug misuse
services: factors that promote and hinder successful working, London: Department of
Health; 2007.
• Patterson, R, S., Smith, D, B., Martorana, P, V., Owens, P, D., 2003. The Impact of
Chief Executive Officer Personality on Top Management Team Dynamics: One
Mechanism by Which Leadership Affects Organizational Performance, Journal of
Applied Psychology 2003, Vol. 88, No. 5, 795–808
• Rifkin, S, B; Muller, F; Bichmann, B; 1988, Primary health care: on measuring
participation, Social Science and Medicine, vol 26 (9) pp.931-940.
• Rifkin, S, B., 1990. Community Participation in maternal and child health/family
planning programmes: An analysis based on case study material, WHO/UNICEF,
Geneva, In press.
• Robinson, S.K; 2004, Consumer and Community Participation Self-Assessment Tool,
Version 2.0, National Resource Centre for Consumer Participation in Health, ISBN 0-
9750924-8-0
65
• Rowe, G; Frewer, L.J.; 2004, Evaluating Public-Participation Exercises, Science,
Technology, & Human Values, Vol. 29, No. 4 (Autumn, 2004), pp. 512-557
Published by: Sage Publications
• Speak Up, 2007, Bolton Council, national service user involvement survey, viewed
online, 26/03/2010 http://www.serviceuserinvolvement.co.uk/
• Tritter, J.Q.; McCallum, A; 2006, The snakes and ladders of user involvement:
Moving beyond Arnstein, Science Direct Health Policy 76 (2006) 156–168
• Welsh Assembly, 2008, User Involvement Framework,
http://www.adjudicationpanelwales.org.uk/dsjlg/publications/commmunitysafety/sub
misusetreatframework/usere.pdf;jsessionid=4rwyKPhK9DnC8T2SG0d1szL0Hp2zzR
wC4Df2NvjMpfFBVRtv7sYV!-692465818?cr=4&lang=en&ts=1
• Young, S; 2006, ‘Introducing Role and Service Changes in Health and Social Care:
The Impact and Influence of User Involvement in England and Wales’ Social Policy
& Society 5:2, 249–268