Scientific Studies on Narcotics Anonymous
9
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Scientific Studies on Narcotics Anonymous
"WE DO RECOVER"
W I L L I AM WH I T E , M . A . , MARC GA L AN T E R , M . D . ,
K E I T H HUMPHRE Y S , PH . D . , AND J OHN K E L L Y , PH . D .
S C I E N T I F I C S T UD I E S ON
NARCO T I C S ANONYMOUS
Narcotics Anonymous is a widely-knownand well-attended addiction recoverymutual aid fellowship, but what doesscience really know about who attendsand the effects of such participation? Thisbrief pamphlet summarizes a report on227 scientific studies of the effects ofparticipation in Narcotics Anonymous.The review includes NA-specific studiesand studies of 12-Step participation thatincluded NA members. The full reportwith citation of all studies is available forfree download at williamwhitepapers.com When did formal scientific studies
of NA begin? Brief announcements of NA’s existence asa potential addiction recovery supportresource first appeared in medical andlegal journals in the 1950s and early1960s. Rigorous studies of NA began inthe 1980s with a progressive increase inthe quality of the research in the decadesthat followed. What is the international scope of
NA research studies? The majority of NA studies emanate fromthe Islamic Republic of Iran, the UnitedStates, the United Kingdom, andAustralia, with a smaller number ofstudies conducted in Greece, India, Israel,and Norway. We anticipate the continuedgrowth of NA studies as NA groupscontinue to expand internationally.
What is the relative growth andavailability of NA in the U.S. and
Internationally? NA has experienced substantialworldwide growth and adaptation acrossdiverse cultural, political, and religiouscontexts. In 2020, there are 71,000weekly NA meetings worldwide; it hasmore than doubled in the past 15 years.
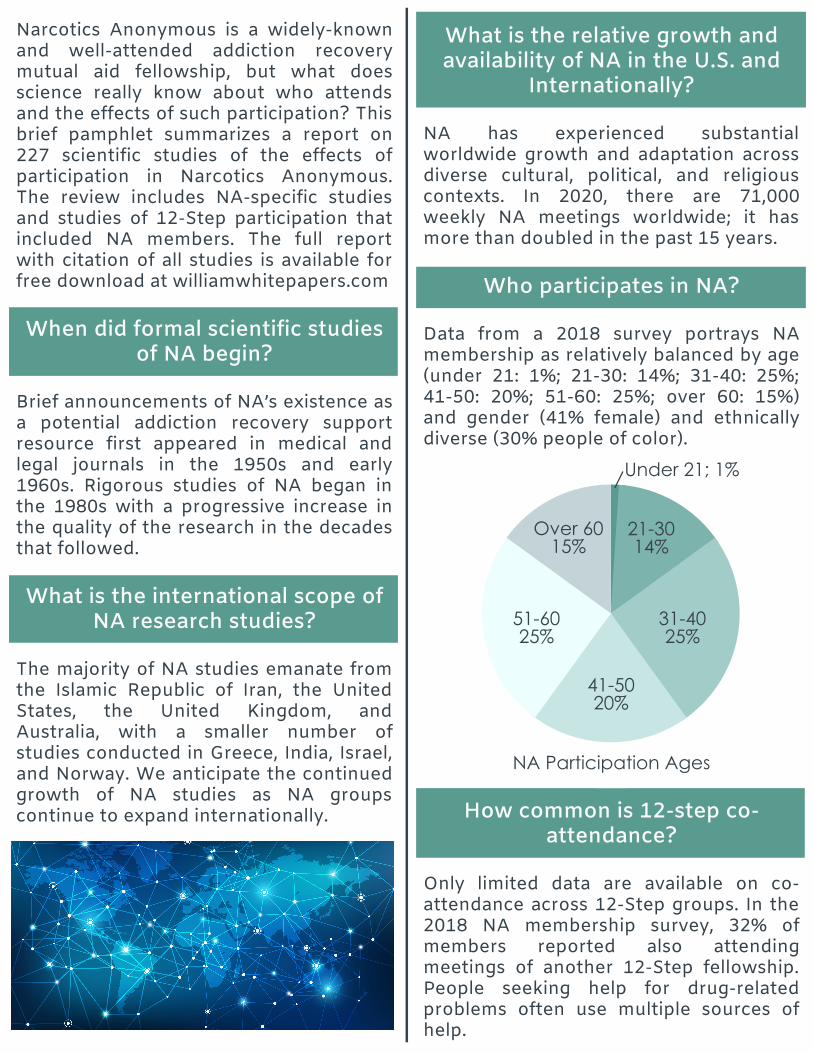
Who participates in NA? Data from a 2018 survey portrays NAmembership as relatively balanced by age(under 21: 1%; 21-30: 14%; 31-40: 25%;41-50: 20%; 51-60: 25%; over 60: 15%)and gender (41% female) and ethnicallydiverse (30% people of color).
How common is 12-step co-attendance?
Only limited data are available on co-attendance across 12-Step groups. In the2018 NA membership survey, 32% ofmembers reported also attendingmeetings of another 12-Step fellowship.People seeking help for drug-relatedproblems often use multiple sources ofhelp.
25%
25%
20%
15%
14%
1%Under 21; 1%
21-30
14%
31-40
25%
41-50
20%
51-60
25%
Over 60
15%
NA Participation Ages

How do people get to NA? Active drug users express generallypositive attitudes toward NA and makeinitial contact with NA through a varietyof influences, including contact with anNA member, referral by a treatmentagency, or encouragement from familymembers. Factors such as personality,problem severity, religious orientation,and social network norms also influencethe degree of attraction to NA.
What are the major obstacles to
NA participation?
Reported obstacles to NA participationinclude NA’s expectation of alcoholabstinence; the perceived religiousorientation of NA; aversion to theconcepts of powerlessness, surrender,and higher power; social anxiety; and NA’sposition on the use of medications as asupport for recovery from opioid usedisorders.
What is the retention/dropout rate
of NA?
The dropout rate from NA is comparableto that in AA (approximately 40% at one-year follow-up) and is lower than thedropout rates of other interventions intoalcohol and other drug problems (e.g.,addiction treatment). NA retention rate isalso superior to rates of adherence toprescribed management of other chronichealth conditions. NA dropout rates callfor professional encouragement ofsustained mutual aid involvement, closemonitoring of responses to mutual aidparticipation, and, when needed, re-linkage or exploration of recovery mutualaid group alternatives. Disengagementfrom mutual aid participation increases
the risk of addiction recurrence in theabsence of alternative recovery support.This suggests the need for closemonitoring and heightened levels ofcontact by addiction professionals andother helpers following disengagementfrom NA participation.
What are the effects of NA
participation on drug use andremission/recovery from substance
use disorders?
NA studies, NA-inclusive 12-Step studies,and published reviews of 12-Stepresearch (including Twelve-StepFacilitation treatment approaches) allreport a strong association between NAparticipation and reduced drug use andincreased rates of abstinence. Theavailable evidence suggests the potentialvalue of NA participation in recoveryinitiation and long-term recoverymaintenance.
What is the average duration ofcontinuous recovery among NA
members?
In a 2018 survey of 28,495 NA membersconducted by NA World Services,members with a wide variety of pastprimary drug choices reported an averageof 11.4 years of continuous abstinence,with 85% of members reporting five ormore years of stable recovery. Withineach community in which NA starts, theprogressive increase in memberssustaining stable recovery provides thefoundation for a strong local NA recoveryculture. That degree of organizational andpersonal stability now exists within manycommunities and provides role models inlong-term recovery who can providesupport to new members.
What are the major risk factors forrecurrence of drug use and
addiction among NA members?
Studies to date identify four risk factorsrelated to addiction recurrence among NAmembers: 1) unemployment, 2) changesin income, 3) decreased levels of NAparticipation, and 4) disengagement fromNA. Research studies are needed thatilluminate the patterns of drug use ordrug abstinence across the long-termcourse of NA involvement and changes insuch patterns preceding and followingdisengagement from NA.
What are the broader effects of NAparticipation on health and quality
of life outcomes?
NA participation is associated withimprovements in global health and socialfunctioning. Studies are limited andneeded on the effects of NA participationon intimate relationships, familyfunctioning, and changes in the person-community relationship.
What factors related to NA
participation predict substance useand quality of life outcomes?
Positive outcomes related to NAparticipation increase in tandem withintensity of participation and duration ofparticipation. Broader involvement in NAactivities and great frequency of theseactivities predict better outcomes thansimply attending occasional NA meetings.Activities beyond meeting attendanceinclude having a home group, active Stepwork, having a sponsor, sponsoringothers, participating in the NA servicestructure, reading NA literature, andbroader acts of helping others. Positive
addiction outcomes decline on thecontinuum from continuous NAparticipation (best outcomes), sporadicNA attendance, and no attendance (worstoutcomes). Time is also a criticalingredient. While reduced drug use andinitiation/stabilization of abstinence canoccur early within NA participation,recovery of psychological health may takeup to five years following cessation ofdrug use.
Do such positive effects differ
across demographic, cultural, andclinical characteristics?
Studies to date suggest that the positiveeffects of NA extend to diversedemographic and clinical populations andacross diverse geographical and culturalcontexts.
Is NA participation associated withbetter recovery outcomes among
adolescents?
Studies to date of 12-Step participationamong adolescents enrolled in SUDtreatment reveal variable, but generallypositive, effects on substance useoutcomes. Effects of 12-Step participationon reductions of drug use and increasedrates of abstinence warrant referral ofadolescents to these recoverymanagement resources, particularly tomeetings with higher youthrepresentation. Youth should bepresented with both 12-Step andalternative recovery mutual aid options,particularly if they are uncomfortable withthe spiritual orientation of NA.

Is NA safe for adolescents andother vulnerable populations?
Published studies on attraction to NA,obstacles to NA participation, or retentionin NA have not identified safety concernsamong those surveyed. We suggest thatprofessionals referring to NA and otherrecovery mutual aid groups closelymonitor the potential for harmful effectsamong youth referred. Mutual aidmeetings vary in the presence of activeingredients known to promote recoveryand vary in their degree of adherence totheir own espoused principles andpractices. Knowledge of the character oflocal meetings should inform referral ofyouth to mutual aid groups.
Is NA safe for people with less
religious or spiritual orientation?What is the role of spirituality in
NA's program of recovery?
While NA’s perceived religious orientationmay be an obstacle to NA participationfor some individuals, research to datesuggests that recovery outcomes in NAare not contingent upon degree ofreligious orientation. At a practice level,professional helpers can explore thisissue prior to potential referral, clarify theNA distinction between religion andspirituality, and provide orientation to NASteps as well as secular interpretations ofthe Steps. It is also advisable toencourage those with less religiousorientation to sample various NAmeetings and as well as available secularalternatives.
Is NA appropriate for people withco-occurring psychiatric illness?
Research findings differ on theequivalence of NA effectiveness amongpeople with and without co-occurringSUD and other psychiatric disorders. Thelargest number of studies suggest thatpeople with co-occurring disorders attendand benefit from NA at similar levels asthose with only an SUD, but those withmore severe forms of mental illness mayrequire additional professional supportsto maximize the positive effects of NAparticipation. When individuals in thelatter group appear to experience amismatch with NA, it is advisable toconsider referral to a dual focus supportgroup, e.g., Dual Diagnosis Anonymous,Double Trouble in Recovery.
How does concurrent participationin addiction treatment and NA
affect long-term recoveryoutcomes?
Research to date suggests that individualswho participate concurrently in bothaddiction treatment and 12-Stepprograms during and following treatmenthave higher rates of abstinence thanthose who participated only in treatmentor only in 12-Step programs.
Research suggests that:
Adolescents and othervulnerable populations
Those with less religiousorientation, and
Those with co-occurringpsychiatric illness
CAN benefit from participation
in Narcotics Anonymous

Is NA appropriate for people inmedication-assisted treatment?
NA involvement may be of potentialbenefit to people in medication-assistedtreatment (MAT) as a complementaryrecovery support during MAT and as asource of post-MAT recovery support.Referral of such patients to NA shouldinclude: 1) preparatory orientation aboutNA policies on medication, 2) assertivelinkage to medication-friendly NAmeetings, 3) monitoring of MAT patientresponses to NA meetings, and, 4) if andwhen needed, linkage to alternativerecovery support resources such asMethadone Anonymous, Moms onMethadone, Medication-AssistedRecovery Support, or All RecoveriesAnonymous.
What mechanisms might helpexplain the positive changes
people experience through NAparticipation?
Mechanisms of change within NAidentified within existing studies includeincreased hope and confidence in one’srecovery potential, increased motivationfor abstinence, personal mentoring(sponsorship), social support, socialnetwork reconstruction, and restructuringof leisure time. Other noted mechanismsinclude transformations in personalidentity and worldview, enhanced self-esteem, improved coping strategies,prestige acquisition from helping others,spiritual renewal, and decreases in stress,anxiety, depression, hostility, and shame. The sheer number of mechanisms ofchange operating within NA identifiedwithin the above noted studies mayaccount for its wide adaptability acrosscultural contexts and its viability across
diverse demographic and clinicalpopulations. The NA program of recoverylikely involves multiple mediatorsoperating simultaneously with factorssuch as sex/gender, age, addictionseverity, and cultural context influencingthese mediators.
Does NA lead to isolation frommainstream community life or
greater civic involvement?
Studies that address this question havedrawn three conclusions. First, 12-Stepmembers are actively involved incommunity life. Second, 12-Stepparticipation can elicit a sense ofempowerment, a reconnection tocommunity life, and increased concern forothers. Finally, NA can serve as aconnecting bridge between the drugculture and the mainstream community.
What is the cost-effectiveness ofNA participation?
The limited data available suggest thatencouraging NA involvement leads tosignificant cost reductions in health careutilization. Additional social cost savingscould accrue from decreased involvementin the criminal justice and child welfaresystems as well as cost offsets related toincreased employment.

What are the attitudes toward NAamong helping professionals and
addiction treatment personnel andrelated referral practices?
Addiction treatment professionals andallied health professionals in the U.S. holdgenerally positive views toward NA, butNA attitudes and referral rates vary bycountry, by professional discipline, andthe nature and degree of training inaddiction treatment and related services.Attitudes toward NA evolve over time asNA groups become more accessible andpredict greater levels of recovery stabilityamong their members. Forty-five percentof NA members’ first contact with NA isdue to referral by a treatment facility orcounseling agency.
What can treatment centers do toincrease patient participation in
NA?
Hosting onsite 12-Step meetings duringtreatment increases 12-Step participation.Assertive linkage versus passive referralprocedures and involving patients in widevariety of 12-Step activities (e.g., reading12-Step literature, service work, etc.) isassociated with increased participationand better long-term abstinenceoutcomes. Linking youth to meetings withhigher youth representation enhancesparticipation rates and recoveryoutcomes.
What are the major limitations ofpublished research on NA?
Limitations of NA research span thelimited number of international studies onNA, the limited range of issues studied,and the historically weak but improvingmethodological rigor of NA and related
12-Step studies. Preliminary answers tokey questions exist but requirereplication, with many questionsremaining uninvestigated. The voluntary,anonymous, and highly decentralizedorganizational structure of NA posesinnumerable research obstacles as NApractices may differ markedly acrossgroups/meetings and across culturalcontexts. Conclusions related to the effects of NAparticipation are often based on “12-Step”studies that use mixed samples of NA andother 12-Step members withoutdisaggregating and analyzing data byrecovery fellowship. This practice castsNA as a clone of AA and defies the realitythat NA constitutes a distinct program ofrecovery with its own unique history,culture, core ideas, language, andrecovery support rituals. Most NA-relatedstudies also utilize treatment samples,findings from which may not apply NAmembers without involvement inaddiction treatment. A final complication is the failure toadequately distinguish studies of NA asan addiction recovery mutual aidfellowship and studies of professionally-directed treatment approaches that relyon NA principles and linkage to NA ascentral ingredients of the clinicalintervention (e.g., Twelve-StepFacilitation studies and studies oftreatment programs that embrace some12-Step principles). In spite of these limitations, the morethan 125 NA-related studies reviewed doilluminate the degree of effectiveness ofNA in real world conditions.

Will NA work for everyone?
No. Effects of participation in NA or otherrecovery mutual aid groups vary acrossindividuals. The menu of secular, spiritual,and religious recovery mutual aidsocieties is growing in the U.S. andinternationally. We encourage individualsand families seeking recovery support tofreely sample these resources and findthe best possible personal fit. A directoryof recovery mutual aid resources isposted at facesandvoicesofrecovery.org/resources/mutual-aid-resources/
Conclusion
Future research will continue toilluminate questions related to the effectsof NA participation on recoveryoutcomes. The scientific evidence wereviewed possesses both consistency andcoherence. NA members and NAliterature boldly assert “We do Recover.”The studies we reviewed providescientific confirmation and context to thatassertion. It is our hope that this analysiswill offer evidential grounding for futurediscussions of the potential role of NA inrecovery initiation, recovery maintenance,and enhanced quality of life in long-termaddiction recovery.
Implications For Individuals Seeking RecoverySupport: Sustained participation in multiple NA-related activities is associated withincreased abstinence and improvementsin global health and quality of life. NA isan accessible, affordable, and potentiallyeffective recovery support resource.
For Treatment Addiction Treatment andAllied Health Professionals and RecoveryCoaches: The positive effects of addictiontreatment can be improved and extendedwhen combined with assertive referral toNA or other recovery mutual aid groups. For Research Scientists: Addiction-related research interests aremoving beyond studies of addiction-related pathologies and the effects ofshort-term interventions to the study ofpathways and styles of long-termaddiction recovery and related supportresources. Additional studies are neededto evaluate the effects of NA participationand particular mechanisms of changewithin NA. Participatory researchinvolving NA membership stakeholderswill expand knowledge of the effects ofNA participation across diversepopulations and cultural contexts. For Policy Makers: Encouraging the expansion of NA andother recovery mutual aid alternatives isassociated with enhanced effectiveness ofaddiction treatment and cost-savingsrelated to reduced health care utilization.

About the Authors
William White, M.A., is Emeritus SeniorResearch Consultant at Chestnut HealthSystems. Marc Galanter, M.D., is Professor ofPsychiatry at New York University Schoolof Medicine and former president of theAmerican Society of Addiction Medicine. Keith Humphreys, Ph.D., is the Esther TingMemorial Professor in the Department ofPsychiatry and Behavioral Sciences atStanford University, a Senior ResearchCareer Scientist at the VA Health ServicesResearch Center, Honorary Professor ofPsychiatry at the Institute of Psychiatry,King’s College, London, and a formerSenior Policy Advisor at the White HouseOffice of National Drug Control Policy. John Kelly, Ph.D., is the Elizabeth R.Spallin Professor of Psychiatry inAddiction Medicine at Harvard MedicalSchool, the Founder and Director of theRecovery Research Institute / Center forAddiction Medicine at the MassachusettsGeneral Hospital (MGH), and formerPresident of the American PsychologicalAssociation (APA) Society of AddictionPsychology.