RMO®'s Guide to - Rocky Mountain Orthodontics
27
AAO Give Away Inside this issue Practice Management RMO ® ’s Guide to put the pieces together for growth Orthodontic CLINICALREVIEW Clinician’s Study of Direct vs. Indirect Bonding Become a ‘Big Deal’ Uncover Your True Identity New Product Developments from RMO ®
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of RMO®'s Guide to - Rocky Mountain Orthodontics

AAOGive Away
Inside this issue
Practice ManagementRMO®’s Guide to
put the pieces together for growth
OrthodonticCLINICALREVIEW
Clinician’s Study of Direct vs. Indirect Bonding
Become a ‘Big Deal’ Uncover Your True Identity
New Product Developments
from RMO®

3Clinical Review
Dear Doctor, I am excited to share some thoughts with you concerning this edition of the Clinical Review. As you know from reading past issues, the focus has normally been on new products, services and techniques that help to improve clinical treatment results and efficiencies. In this year’s edition we have selected some of these product related articles. However, we have also decided to include some other themes related to Practice Management.
The reason for this change in content is quite simple – staying abreast of new products and technological improvements does not in itself guarantee that you will automatically have a successful business. You must also learn how to manage your office as an efficient and profitable company. It is this union of clinical expertise and Practice Management that will lead to true, long term success.
RMO® has been involved with Practice Management for over 40 years. In the early 1970’s we opened a branch of our company called The Millenium Society. This was one of the first endeavors directed solely at the Management/Marketing side of exclusive orthodontic practices. The Millenium Society was focused on high volume offices that wanted to become more profitable and efficient, while improving care and service for the patients.
Some of the concepts that were shared include many that have become required components in todays’ best offices. Some examples of scheduling include: Doctor scheduling, staff scheduling, specific chairs for specific uses, time allocation by procedure, etc. Other areas include: An effective treatment coordinator, patient motivation, reward programs, marketing plans - internal and external, referrals - by patients and dental colleagues.
RMO® continues to support advances in Practice Management. We are proud of our long involvement in this important aspect of your business. We have more experience in this field than any of our competitors in the world. We are working hard to help make this expertise available to you. We want to help you to succeed!
Tony Zakhem
Chairman and CEO
In this issue I’m also excited to showcase RMO®’s new image and focus. Please see more about this by visiting the RMO® Web Page, Facebook and YouTube sites.
Lingualjet Pascal Baron DDS, MSc, PhD and Christophe Gualana, DDS
Clinician’s Study of Direct vs. Indirect Bonding
Glenn Burkland, DMD and Catehrine Berg, RDH
6
Zenman and the Art of Web DevelopmentWhat your website should do for you
Keith Roberts, Zenman Productions 20
44
14 Maximizing Office Efficiency Three steps to operating an elite orthodontic office Neal D Kravitz, DMD, MS
18 Liberty Bielle: Removable/Fixed Eric Marie-Catherine, DDS
New Patient Enrollment ProcessKen Alexander, Millenium Management Group
4280/20 Rule- Could a wise use of the “80/20 rule” increase your practice clinical efficiency and profitability?
Ray McLendon, DDS
Become a ‘Big Deal’ Uncover Your True Identity Bridgette Owens, 7 Group
32
TABLE of CONTENTS
On-Time Doctor
Time Scheduling
Ken Alexander,
Millenium Management Group
34
24
OFFICE MANAGEMENT MARKETING AND BRANDING
CLINICAL The JOE Cephalometric
System Bruce Haskell, DMD, PhD
10

5Clinical Review
Contributors
For the past 25 years Ken Alexander has been one of the top consultants in orthodontic management, serving over five hundred clients in North America and Europe. He lectures regularly at the AAO Meetings and across the country on every area of orthodontic practice management and practice transitions. If you have not had the opportunity to meet Ken you will find him and the Millenium Management Group at the RMO booth at the AAO. Ken has a wealth of knowledge on every area of orthodontic management and many of his clients have some of the most successful practices in the world. You may contact Ken at [email protected] or visit his website at www.KenAlexander.com.
Ken Alexander
Dr. McLendon is a 1983 graduate of the University of Texas Orthodontic program at Houston. He is the founding partner of Clear Choice Orthodontic Associates, a group practice with 7 locations serving the greater Houston area. Dr. McLendon is a past president of both the Houston Regional Society of Orthodontics as well as the Texas Association or Orthodontics. He served as a Board Member on the Southwestern Society of Orthodontics. He has been a popular speaker on the business issues that relate to the field of orthodontics at a number of the countries orthodontic society meetings.
Raymond McClendon, DDS
Dr. Bruce Haskell is Professor of Orthodontics, (Part Time), at the University of Kentucky, Department of Orthodontics, where he joined the faculty in 2010. His prior experience includes orthodontic practice in the U.S. Air Force Dental Corps, at the Churchill Hospital in Oxford, England, and Clinical Professor at the University of Louisville, School of Dentistry, where he has taught since 1977. Currently, Dr. Haskell also works in his private practice in Louisville with his daughter, Jennifer. He is a dental and Arts and Sciences graduate of the University of Pittsburgh, with a doctorate in Physical Anthropology, majoring in Cranio-facial Biology. Dr. Haskell obtained his orthodontic specialty training at the University of Rochester, Eastman Dental Center (The Eastman Institute for Oral Health). His publications include works on habit modification, bio-mechanics, cranio-facial computer modeling and forensic anthropology.
Bruce Haskell, DMD, PhD
Glenn Burkland, DMDDr. Burkland is a board-certified orthodontist with a private practice in West Chester, PA. He graduated first in his class from the University of Pennsylvania Dental School before receiving his certificate in orthodontics from Harvard University. He subsequently taught at both institutions, as well as Temple University School of Orthodontics. He has lectured both nationally and internationally and has published many research articles.
Catherine Berg, RDHCatherine obtained her dental hygiene license after completing her education at Harcum College. There she earned numerous academic and clinical awards and gained national recognition for her skills. In her professional career, she is a vital member of the orthodontic team at a private practice in West Chester, PA and has published several research articles.
become a FAN of RMO®’s facebook page!www.facebook.com/rmortho
www.rmortho.com
rocky mountain orthodonticsTM
Synergistic Solutions for Progressive OrthodonticsTM
800.525.6375 | www.rmortho.com650 West Colfax Avenue, Denver, Colorado 80204P 303.592.8200 F 303.592.8209 E [email protected]
Pascal Baron studied at the University of Toulouse, where he gained a DDS, an MSc in orthodontics, and a PhD in biomathematics. He is a specialist in orthodontics and titular professor at Toulouse University, head of the Orthodontics and Dentofacial Orthopedics Department of Toulouse University, and head of the Clinical Orthodontics Unit at Toulouse Rangueil Hospital. He is a member of the European College of Orthodontics (CEO), a member of the French Society of Dentofacial Orthopedics (SFODF), a member of the European Society of Lingual Orthodontics (ESLO), Member of the European Francophone Association of Research in Odontology (AFEERO), CNRS Laboratory of Anatomy Imaging UMR5288, and is on the editorial board of International Orthodontics. He maintains a private practice in Toulouse (France) and is a co-inventor of Lingualjet.
Pascal Baron, DDS, MSc, PhD
Christophe Gualano, DDSChristophe Gualano has earned a DDS and a postgraduate qualification in orthodontics, and is a specialist in orthodontics. He is ex-assistant professor of the Orthodontics Department of Toulouse University, a member of the European College of Orthodontics (CEO), and a member of the European Society of Lingual Orthodontics (ESLO). He runs a private practice in Toulouse (France) and is a co-inventor of LingualJet.
Neal D Kravitz, DMD, MSNeal D. Kravitz, D.M.D., M.S. is a Diplomate of the American Board of Orthodontics. He is also clinical faculty & research adviser at the University of Maryland & Washington Hospital Center. Dr. Kravitz received his undergraduate degree from Columbia University, received a D.M.D. at the University of Pennsylvania School of Dental Medicine (where he graduated as Valedictorian) & completed his orthodontic
A combination of skills in the creative, business development and marketing arenas has resulted in Bridgette earning a reputation as a creative and astute marketer with the ability to not only recognize opportunities, but to convert
Bridgette Owens
Dr. Eric Marie-Catherine is a specialist in orthodontics, graduated from the University of Clermont-Ferrand where he became an instructor in orthodontics. He is a member of the SPPD and the SFODF and teaches many courses and conferences in Europe. He is the co-inventor of Liberty Bielle system.
Eric Marie-Catherine, DDS
training at the prestigious University of Illinois-Chicago with an M.S. in Oral Sciences. A prolific writer, Dr. Kravitz continues to publish his cases in numerous journals, including the AJO-DO, JCO, JADA, Angle Orthodontist, Orthodontist & Orthodontic Products, among others. Dr. Kravitz lectures throughout the country & internationally on modern advancements in orthodontics, including early-interceptive (Phase I treatment) & invisible lingual braces. He has presented numerous times at the AAO, dental & orthodontic society meetings, & orthodontic residencies throughout the country.
Keith founded Zenman in 1998, which has grown to one of the top web development firms. His inventive concepts unfailingly result in visually pleasing, informative and provoking designs that penetrate to the target audience, ultimately resulting in sales. Keith has been working as a marketing expert and web designer for 15 years. www.zenmanproductions.com
Keith Roberts
them into effective marketable solutions. Bridgette received a Bachelor of Fine Arts from the University of Auckland, Elam Art School, New Zealand. With over 10 years experience in Marketing and advertising she is the founder for 7 Group USA which launched in June 2010. Contact Bridgette at [email protected].
Check out NEWlook!
RMO’s®

6 Clinical Review
By Glenn Burkland, DMD and Catherine Berg, RDH
The study to be shared was undertaken in one dental office by one doctor. It involved 200 consecutively treated patients who were randomly and alternatively assigned to two methods of treatment. The first involved indirect bonding and the second was direct bonding. Treatment times and deviations from the averages were recorded. Bond failure was rigorously recorded and, to the best ability of the clinician, the reason for failure was determined. The average time to place initial bonds was recorded using both techniques.
There is a paucity of literature on indirect versus direct bonding. In this study, the single treating clinician has over 30 years experience in orthodontics with a distinguished clinical career. He wanted to re-examine the two bonding modes because previous literature is outdated, did not have standard treatment approaches, bonding techniques, or have the same operator performing the procedures. These variations make it difficult, if not impossible, to make conclusions about indirect and direct bonding.
To eliminate a significant variable, a single doctor was responsible for placement of all bonds, whether placed indirectly or directly. Care was taken to ensure accuracy of placement and maintenance of ideal bonding conditions in either modality.
He concluded that it was far easier and much more accurate to place brackets indirectly on a model, which can be manipulated for easy viewing, than directly while dealing with access, viewing and isolation challenges.
Materials and Methods
The 200 treated patients were randomly and alternately assigned to one of the treatment modes, resulting in 100 cases bonded directly and 100 cases bonded indirectly. The direct method was performed on the posterior teeth (the molars and premolars), quadrant by quadrant, with isolation of the teeth using cotton rolls and dri-angles. The anterior teeth (canines, laterals, and centrals) were isolated with the use of a cheek retractor.
Teeth to be bonded were prepared by etching with 37% phosphoric acid for 30 seconds according to manufacturer’s instructions, then rinsed and air-dried, followed by a seal of Unitek MIP* (moisture insensitive primer). Brackets were adhered to the tooth with a thin coat of Unitek Transbond XT* (10). Once the brackets were positioned and checked for accuracy, pressure was applied to ensure complete incorporation of the cement into the mesh pad of the bracket and light cured.
The indirect method was done as follows: An alginate impression was taken and poured in green stone for its hardness. The models, dried for 24 hours, were then painted with two coats of separator (liquid foil). The brackets were then carefully placed on the teeth using Unitek Transbond XT* cement (see figure 1). The cement, which normally adheres the bracket to the bonding surface, in this case creates a custom base for the bracket ensuring proper fit on any tooth, despite the presence of a possible structural
anomaly that exists in many dentitions (12). If the bracket in its proper position on the tooth impinged on the gum tissue, the bracket base was trimmed to ensure comfort and to allow for proper hygiene.
Articulating the models checks for interferences and ensures brackets are not being occluded. If the bite was extremely deep and interferences were observed, bite turbos were placed on the lingual surface on the upper centrals to prevent breakages. Then the models were lined on the edges with rope wax and the soft tray, RMO® Inner Tray material**, was applied to a thickness of about 3 mm over the brackets. The tray was smoothed using RMO® Tray Finish** and trimmed of any excess with a surgical blade. The tray and the brackets were removed as one piece.
Finally, the custom pads made earlier are micro-etched with a 50-micron aluminum oxide powder to restore
surface area for better adhesion to the tooth surface. Chairside, NOLA cheek retractors are placed in the patient’s mouth, which provide adequate suction to eliminate moisture from all areas, eliminating the need for antisialogogues as suggested in previous studies (17,18). The teeth are etched and sealed with RMO® Bonding Resin**. A small amount of RMO® Flowable Adhesive** is applied to the back of each bracket and the trays inserted (see figure 2). Upper and lower trays are seated one right after another then the cement cured, through the clear tray. Once completely cured, trays are peeled away, leaving the brackets in their proper position.
Data Analysis Even though there are more preparation steps for IDB, its advantages far outweigh any additional prep time spent. First of all, the majority of time that goes into preparing for IDB can be done whenever there is down time or done by the lab tech; each step is not time intensive. IDB preparation can be stopped and started at any point, allowing for flexibility if something more pressing comes up during the day.
Secondly, the amount of time spent chairside at the initial bonding appointment is almost cut in half. An average of 127 minutes were spent at the initial visit for direct bonding versus an average of 66 minutes for IDB. Plus, that hour is much more comfortable for both the patient and clinician. The clinician is not straining his/her neck and back
Clinician’s Study of Direct vs. Indirect Bonding
A solo dental practice evaluated 200 consecutively treated patients and compared the resulting treatment of direct and indirect bonding.
to gain access to difficult to view teeth and all of the teeth are prepped at one time instead of by quadrants. The patient doesn’t have to strain to stay open, or stay open nearly as long, since the NOLA retractors have a built in bite block for resting the jaw. NOLAs are only in the mouth for an average of 15 minutes then all the braces are bonded.
The chief advantage of indirect placement of brackets is increased accuracy of positioning. It is far easier for the operator to place brackets at their correct height and angulations on a model than it is in the mouth, especially for molars and premolars.
Another advantage of indirect bonding is less bond failure, averaging 6% failure with direct bonding, reduced to 3% failure using indirect bonding (see table 1). This is the result of:
The chief advantage of indirect
placement of brackets is increased accuracy of
positioning.
a. Better tooth isolation
b. Decreased time need to place brackets and maintain isolation
c. Excellent adaptation of bracket base to the tooth
d. Increased control of bonding materials
Figure 1
Figure 2
7Clinical Review

rocky mountain orthodonticsTM
Synergistic Solutions for Progressive OrthodonticsTM
800.525.6375 | www.rmortho.com650 West Colfax Avenue, Denver, Colorado 80204P 303.592.8200 F 303.592.8209 E [email protected]
8 Clinical Review
Energy ChainTM
Since the braces are initially placed on a model, much more time can be spent ensuring proper positioning (6, 7, 8, 13). This allows for shorter overall treatment time. We have seen a 25% reduction in treatment time from about 24 months to around 18. This is due to less bracket repositioning and fewer bends having to be put in the wire, which eliminates the human error factor (2). Treatment time is also reduced due to less bond failure. When the brackets are positioned ideally, there is less stress on the bracket (1, 5, 9, 14, 18).
Failures Total Brackets Places
Intact Bonds
Failed Bonds Percentage of Failures
Direct Bonding 20,246 18,954 1292 6.4%
Indirect Bonding 20,872 20,235 637 3.1%
Treatment Time Average Months in Treatment Deviation in Months
Direct Bonding 24.2 2.1 +/-
Indirect Bonding 18.4 2.6 +/-
Table 2
Table 1
A disadvantage to the IDB system, although minor, exists in transitional dentition. No more than two weeks can lapse from the impressions to the bonding appointment. Otherwise there can be too many changes in the oral cavity to accommodate the custom fitted trays.
Conclusion
The results of this study suggest indirect bonding as superior due to shorter treatment time, less bond failure and increased ease for the patient and
operator. This study was controlled in that one clinician administered the two treatment modes. Further study needs to be completed to see if the results can be extrapolated to more treating clinicians with the results remaining consistent.
*3M Unitek, 3M Corporate Headquarters, 3M Center, St.Paul, MN 55144 www.solutions.3m.com
**Rocky Mountain Orthodontics, 650 West Colfax Avenue, Denver, CO 80204 www.rmortho.com
Bibliography:
As good as it getsRMO®’s Energy ChainTM is the proven leader in elastomeric chain material, outperforming other elastic chains in numerous independent clinical tests. Stain resistant, latex free, 4 sizes and a variety of colors.
RMO®’s patented formula provides light, continuous force for weeks resulting in brilliant closure and very..very..happy patients.
1. Aguirre MJ, King GJ, Waldron JM. Assessment of Bracket Placement and Bond Strength When Comparing Direct Bonding to Indirect Bonding Techniques. AM J Orthod 1982; 82:269-76.
2. Andrews LF. The Straight-Wire Appliance. BR J Orthod. 1979; 6:125-43.
3. Collins J. A Precise and Predictable Laboratory Procedure for Indirect Bonding. AM J Orthod. 2000; 34:702-705.
4. Deahl ST, Salome N, Hatch J, Rugh JD. Practice-based Comparison of Direct and Indirect Bonding. AM J Orthod Dentofacial Orthop. 2007; 132:738-742.
5. Gia K, Dunn W, Taloumis LJ. Shear Bond Strength Comparison Between Direct and Indirect Bonded Orthodontic Brackets. AM J Ortho Dentofacial Orthop. 2003; 124:577-581.
6. Hickman. Predictable Indirect Bonding. 1993;27:215-217.
7. Hodge TM, et al. The Burton Approach to Indirect Bonding. AM J Orthod 2001;28:267-270.
8. Hodge TM, et al. A Randomized Clinical Trial Comparing the Accuracy of Direct
Versus Indirect Bracket Placement. AM J Orthod 2004;31:132-137.
9. Hocevar RA, Vincent HF. Indirect versus Direct Boding: Bond Strength and Failure Location. AM J Orthod Dentofacial Orthop 1988;94:367-71.
10. Jost-Brinkmann PG, Schiffer A, Miethke RR. The Effect of Adhesive Layer Thickness on Bond Strength. AM J Orthod. 1992; 26:718-720.
11. Kasrovi PM, Timmins S, Shen A. A New Approach to Indirect Bonding Using Light-Cure Composites. AM J Orthod Dentofacial Orthop. 1997;111:652-656.
12. Klocke A, Shi J, et al. Bond Strength with Custom Base Indirect Bonding Techniques. Angle Orthod 2003;73;176-80.
13. Koo BC, Chung CH, Vanardsall RL. Comparison of the Accuracy of Bracket Placement Between Direct and Indirect Bonding Techniques. Am J Orthod Dentofacial Orthop 1999;116:346-51.
14. Milne JW, Andreasen GF, Jakobsen JR. Bond Strength Comparison: A Simplified
Indirect Technique Versus Direct Placement of Brackets. AM J Orthod Dentofacial Orthop 1989;96:8-15.
15. Moskowitz EM, Knight LD, Shreidan JJ, et al. A New Look at Indirect Bonding. AM J Orthod. 1996;30:277-281.
16. Read MJ, Pearson AI. A Method for Light-Cured Indirect Bonding. AM J Orthod. 1998;32:502-503.
17. Sondhi A. Efficient and Effective Indirect Bonding. AM J Orthod Dentofacial Orthop. 1999;115:352-359.
18. Thiyagarajah S, Spary DJ, Rock WP. A Clinical Comparison of Bracket Bond Failures in Association with Direct and Indirect Bonding. AM J Orthod 2006;33:198-204.
19. Thomas RG. Indirect Bonding: Simplicity in Action. AM J Orthod. 1979; 13:93-106.
20. Wendl B, Droschl H, Muchitsch P. Indirect Bonding-A New Transfer Method. EU J of Orthod 2008;30:100-107.

11Clinical Review 10 Clinical Review
I have been fortunate to use the JOE Cephalometric System in my practice for the last 20 (20? not sure!) years. It has allowed clarity and simplicity in Cephalometric Interpretation, a field unusually complex and often confusing.
Now that tracing can be done directly on the computer screen with digital radiography, the process has been additionally simplified. It is possible to view the computerized tracing superimposed directly upon a digital cephalometric image.
This includes showing asymmetric discrepancies to your patient (or their parents), to the referring doctor as well as to insurance companies if they so require. It is the application of the unique RMO® “visual norm”, a compensated and individually adjusted image available for each patient which makes this a singular product for the orthodontist. The “red” computer tracing shows an ideal or “norm”, compensated for age, race, sex and volumetric size of the patient, and compares it through superimposition to an “actual” anatomical tracing image.
This combined image easily highlights any dental and skeletal discrepancies. The orthodontist has the choice of more than a score of superimpositions in which
to highlight exactly where the differences between the ideal and anatomical error may lie.
This is a really fantastic communication tool. In a Class II situation, for example, the need of either a functional appliance, or instead the use of maxillary distalizing mechanics for classification may be easily illustrated depending upon which jaw is the problem structure; upper or lower. In surgical situations, it also demonstrates the degree and amount of movement necessary in which to plan for improving facial and skeletal balance. I have never had an insurance company analyst balk at the need for an orthognathic surgical correction when the Joe tracing presents a maxillary or mandibular discrepancy of two or more clinical deviations from an
The JOE Cephalometric SystemBy Bruce Haskell, DMD, PhD
The use of JOE is one of the best communication devices I know of to demonstrate the nature of dental and skeletal imbalance.
established norm. A clear and concise print-out highlighting the degree of every abnormal measurement is a convenient tool for me to send to the oral surgeon. This assists decision making as to whether a one or two jaw procedure is necessary in an individual patient, or how much actual surgical correction may be required for an ideal skeletal or facial balance. I make certain my oral surgeon has this report to include in his treatment request to the insurance company.
I often have my Treatment Coordinator do a preliminary discussion of the treatment at our consultation visit. Our staff was once horrified when I tried to use a new conventional digital analysis which came (included), with our office software. My Coordinator felt that the free analysis simply showed a “bunch of numbers” without a proper explanation and illustration of what was specifically wrong with the patient. I switched back to JOE!
The actual use of JOE may be illustrated here in a few examples. This first patient illustrates a need for anterior retraction. The “red” is the computer generated “ideal” norm while the “gray” shows the actual anatomy. Anterior retraction of the dentition together with lip position reduction is illustrated as is extra lower facial height. This report may make the difference between choosing an extraction vs. a non-extraction treatment plan. It easily shows a concerned parent
The retraction of the anteriors seen in gray, compared to the position of the ideal norm, in red, illustrates an ideal orthodontic treatment plan. The cephalometric analysis is Ricketts.
There are many reasons why I would feel lost without JOE.
the need for one plan above another. The opposite situation of a patient with retroclined anteriors and extreme lower crowding requiring the advancement of incisors for non-extraction therapy might also be simply and effectively communicated with this program.
The Colorado Orthodontic Foundation is a community focused organization that is dedicated to promoting superior orthodontic treatment
and care by orthodontic specialists within Colorado.
MissionTo provide affordable orthodontic treatment and education to as many
financially challenged children and families as possible.
w w w . t h e c o f . o r g
Dedicated to promoting orthodontic health in local communities….
VisionTo foster a greater awareness and understanding among the general
public about the benefits of orthodontic treatment by doctors that specialize in orthodontic prevention and care. We hope to provide care to an underserved community in order to help foster better health, beautiful smiles, and confident children that can become leaders in the community.

Synergistic Solutions for Progressive OrthodonticsTM
800.525.6375 | www.rmortho.com650 West Colfax Avenue, Denver, Colorado 80204P 303.592.8200 F 303.592.8209 E [email protected]
12 Clinical Review
rocky mountain orthodonticsTM
JOE Ceph®
This is one of the very few programs that contain norms for Asians, African Americans, Hispanics, Mixed Ethnicity, Caucasians, etc. This means that calculated norms exist for these groups of peoples based upon the samples of scores and often many thousands of peoples derived from sample populations at a number of universities. This knowledge is critical is being able to communicate with patients and referring doctors concerning what is “visually” normal for patients of distinct or mixed ethnicities. This method helps eliminate misunderstandings about what is actually desired for an individual of a specific ethnic background. I have been amazed as to how much this has helped me communicate in my practice, showing concerned parents that I am ethnically “aware”.
This analysis shows an African American male. The maxillary base is normal for a person of this ethnicity, together with a full and mildly protrusive denture. This is normal, and demonstrates that the lower anteriors should be advanced in order to gain proper inter-incisal angulations for this particular individual.
There are many reasons why I would feel lost without JOE. Some reasons include the automated print-out summary indicating the type of major discrepancy and malocclusion with each cephalometric point highlighted. A 2-year facial growth forecast, a built in golden proportions divider, a ruler, superimpositions of progress films, etc. are also reasons I like JOE. The actual list of features is very extensive. I suggest you contact your RMO® representative for a full display of the capability of this unique product, an incalculable asset to my orthodontic practice and to communication with patient and the referring doctor.
Another unique feature of JOE is in the area of specifying ethnicity in your particular cephalometric analysis.
A full profile is normal for this ethnic type. Advancement of the lower anteriors for incisal guidance correction is appropriate for this patient.
There are many reasons why I would feel lost without JOE.
In-office Software Package
On Screen Digitizing
Cephalometric Analyses
Custom Analysis
Upper and Lower Arch Analysis
Visual Norms
Airway Analysis
Excessive Mandibular Growth Alert
24 Month Growth Forecast without Treatment
Superimpositions of Different Time Points
Management of Patient Images

15Clinical Review 14 Clinical Review
goal is to always improve and to always evolve. Mastering product advancements such as the RMbond® Indirect Bonding System, Dual-Top® temporary anchorage devices with torsion-controlled drivers, myofunctional retainers, and non-ligating Synergy-R® brackets with Thermaloy Plus wires have enabled my office to create beautifully finished cases in a comfortable, timely manner.
When developing any new system, the first step is to truly make the decision. All members of my office team are informed that a new product or technique will be implemented. My decision is not up for democratic vote. If given the option, most people will
Simply stated, efficiency means finding a better way to work. As the sole orthodontist of two thriving offices that together start nearly nine-hundred cases per year, maximizing office efficiency is crucial not only to managing my busy schedule, but also most importantly, providing a higher standard of orthodontic care to my patients. Operating with efficiency requires working each day with organization, time-management, and resolute commitment toward continual self-improvement. The premise of this article is to share three steps used in my offices that maximize clinical efficiencies so your team may provide exceptional orthodontic care.
As an orthodontist, I strive to produce work that is clean and organized. Organization of my cases first begins with organization of my inventory. Amazingly, I find that many offices have inventory expenses (excluding laboratory expenses) from more than ten vendors: two or three companies may provide brackets, another two may provide the bands or molar tubes, another two may provide wires, another two discount product companies may provide a variety of auxiliaries, and still others may provide adhesives, laboratory materials, and dental sundries.
In my office I order from four companies, with the vast majority of products from Rocky Mountain Orthodontics. I think many clinicians would be surprised to learn the wide variety of products offered
by Rocky Mountain Orthodontics, including fixed appliances, sundries, adhesives and instruments. (Page 17)
Condensing my inventory to a minimal number of vendors reduces office overhead, ensures items are delivered in a timely manner, and enables my clinical staff to gain expertise with the orthodontic products. Simplification is fundamental to organization and operating at maximum efficiency. What gets organized gets measured; and what gets measured gets monitored.
Success in my professional life is directly related to my time management. Properly managing my schedule is integral to operating an office that is efficient and focused on premium patient services. Lack of time
creates a lack of control, which is the very essence of stress. As the saying goes, “time is a wonderful servant but a terrible master.” Step 2: Cherish your time
I have three simple rules in regards to clinical time management:
(1) Abide by the Terry Sellke principle of scheduling like-with - like. Long appointments are scheduled together in the morning with other long appointments. Short appointments are scheduled in the afternoon together with other short appointments. Finishing the appointment on time so the patient can continue with his/her day is equally important as starting the appointment on time. My time is not more important than my patient’s time.
Maximizing Office Efficiency
Three steps to operating an elite orthodontic office
Neal D Kravitz, DMD, MS
Step 1: Simplify your inventory
(2) Schedule challenging malocclusions or demanding patients in the morning. Not all malocclusions are created equal. Those patients that require more attention are seen during quieter times in the day when I can focus on their needs. Sometimes, the most productive appointment with a challenging patient is to schedule them to return in two weeks for a longer appointment in the morning for extensive evaluation.
(3) Maximize each treatment appointment. If the patient presents with a broken bracket, I perform all necessary bracket repositionings at this time; if the patient presents for an emergency wire-poke, I proceed to their next visit when possible; if there is a lull in the schedule, I perform as much work as possible for those patients sitting in the treatment chairs. Carpe diem!
The challenge with patient scheduling is that any rules are written in sand. At the last moment, appointments may be added, canceled, or lengthened; employees may need meetings for instruction or disciplining; impromptu phone calls may need answering; and administrative decisions may require immediate attention. Therefore, to maximize treatment efficiency, I cherish my clinical time and always try to create more of it. “Work when at work,” as I like to say.
Step 3: Invest in quality and advancements
The speed of the workplace demands that systems or proper routines are established to maximize office efficiency.
Steps to Maximize Office Efficiencies1. Simplify your inventory by
reducing the number of product vendors.
2. Continually organize and reorganize your schedule, so as to take full advantage of each appointment.
3. Constantly improve yourself by staying current with advancements in products and techniques. Commit yourself to change. The seven costliest words ever uttered in business may just be, “that’s the way I’ve always done it.”
As orthodontists, we have systems in place for preparing the treatment units, bonding and banding, organizing laboratory cases, sterilization and packaging, and so forth. However, our demanding schedule often gives little flexibility to incorporate new technology, particularly those that may require experimenting with a new system. Such a folie à deux! We often find ourselves too busy to learn to use advancements that would otherwise enable us to work more efficiently.
In my office, I am firmly committed to incorporating advancements immediately no matter how steep the learning curve with the understanding that my staff will soon be able provide an even higher standard of care in the future. The
When developing any new system, the first step is to truly make the decision. All members of my office team are informed that a new product or technique will be implemented. My decision is not up for democratic vote. If given the option, most people will choose to take the familiar route; but changing old habits is never comfortable. Everything will be hard until it’s easy.
17Clinical Review 16 Clinical Review
1 3 6
7
24
5 8
RMO®’s Energy Chain™ is a proven elastic chain material leader. Numerous universities and clinical researchers have shown that
RMO®’s Energy Chain™ outperforms virtually all other elastic chains available. Energy Chain™ is a tough elastic chain material that is stain resistant, tasteless, and delivers a uniform continuous force over significantly longer periods of time in comparison to most other elastic chains.
RMO®’s Dual-Top Temporary Anchorage Device (TAD) system provides eff icient and f lexible biomechanics.
Dual-Top TADs signif icantly enhance treatment capabil it ies and can be extremely effective in reducing treatment t ime, surgeries, and extractions. Appliances can be inserted chairside by the doctor and forces can be applied immediately. Experience the next generation of appliances: RMO®’s Dual-Top TADs.
Synergy R ®
IDB Wires
Dual-Top ®
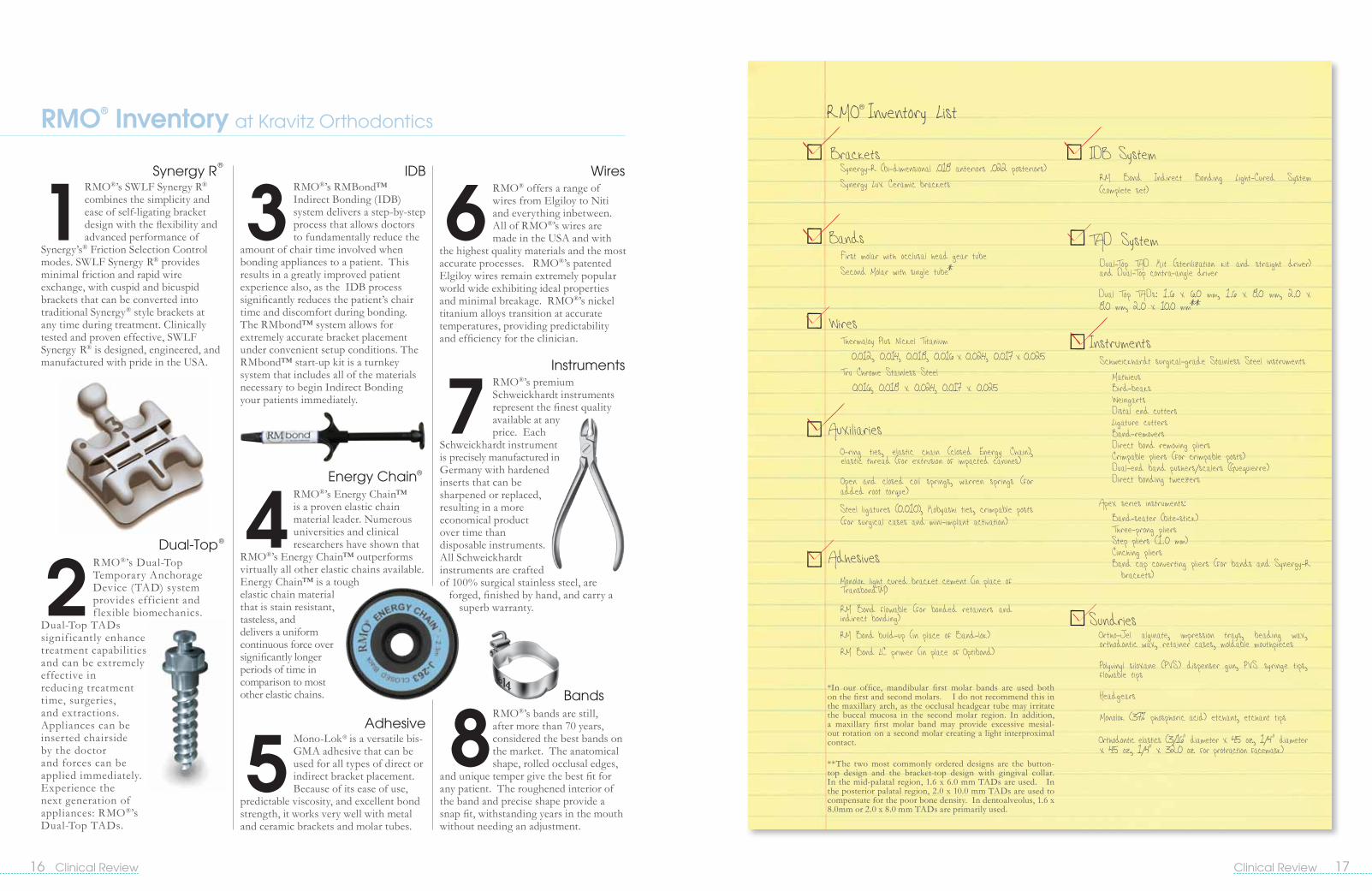
RMO®’s SWLF Synergy R® combines the simplicity and ease of self-ligating bracket design with the flexibility and advanced performance of
Synergy’s® Friction Selection Control modes. SWLF Synergy R® provides minimal friction and rapid wire exchange, with cuspid and bicuspid brackets that can be converted into traditional Synergy® style brackets at any time during treatment. Clinically tested and proven effective, SWLF Synergy R® is designed, engineered, and manufactured with pride in the USA.
RMO®’s RMBond™ Indirect Bonding (IDB) system delivers a step-by-step process that allows doctors to fundamentally reduce the
amount of chair time involved when bonding appliances to a patient. This results in a greatly improved patient experience also, as the IDB process significantly reduces the patient’s chair time and discomfort during bonding. The RMbond™ system allows for extremely accurate bracket placement under convenient setup conditions. The RMbond™ start-up kit is a turnkey system that includes all of the materials necessary to begin Indirect Bonding your patients immediately.
RMO® Inventory at Kravitz Orthodontics
RMO® offers a range of wires from Elgiloy to Niti and everything inbetween. All of RMO®’s wires are made in the USA and with
the highest quality materials and the most accurate processes. RMO®’s patented Elgiloy wires remain extremely popular world wide exhibiting ideal properties and minimal breakage. RMO®’s nickel titanium alloys transition at accurate temperatures, providing predictability and efficiency for the clinician.
RMO®’s premium Schweickhardt instruments represent the finest quality available at any price. Each
Schweickhardt instrument is precisely manufactured in Germany with hardened inserts that can be sharpened or replaced, resulting in a more economical product over time than disposable instruments. All Schweickhardt instruments are crafted of 100% surgical stainless steel, are
forged, finished by hand, and carry a superb warranty.
Instruments
RMO®’s bands are still, after more than 70 years, considered the best bands on the market. The anatomical shape, rolled occlusal edges,
and unique temper give the best fit for any patient. The roughened interior of the band and precise shape provide a snap fit, withstanding years in the mouth without needing an adjustment.
Energy Chain®
Adhesive
Bands
Mono-Lok® is a versatile bis-GMA adhesive that can be used for all types of direct or indirect bracket placement. Because of its ease of use,
predictable viscosity, and excellent bond strength, it works very well with metal and ceramic brackets and molar tubes.
*In our office, mandibular first molar bands are used both on the first and second molars. I do not recommend this in the maxillary arch, as the occlusal headgear tube may irritate the buccal mucosa in the second molar region. In addition, a maxillary first molar band may provide excessive mesial-out rotation on a second molar creating a light interproximal contact.
**The two most commonly ordered designs are the button-top design and the bracket-top design with gingival collar. In the mid-palatal region, 1.6 x 6.0 mm TADs are used. In the posterior palatal region, 2.0 x 10.0 mm TADs are used to compensate for the poor bone density. In dentoalveolus, 1.6 x 8.0mm or 2.0 x 8.0 mm TADs are primarily used.
RMO® Inventory List
Brackets Synergy-R (bi-dimensional .018 anteriors .022 posteriors) Synergy Lux Ceramic brackets
Bands First molar with occlusal head gear tube Second Molar with single tube*
Wires Thermaloy Plus Nickel Titanium 0.012, 0.014, 0.018, 0.016 x 0.024, 0.017 x 0.025 Tru Chrome Stainless Steel 0.016, 0.018 x 0.024, 0.017 x 0.025
Auxiliaries O-ring ties, elastic chain (closed Energy Chain), elastic thread (for extrusion of impacted canines)
Open and closed coil springs, warren springs (for added root torque)
Steel ligatures (0.010), Kobyashi ties, crimpable posts (for surgical cases and mini-implant activation)
Adhesives Monolok light cured bracket cement (in place of TransbondTM)
RM Bond flowable (for bonded retainers and indirect bonding)
RM Bond build-up (in place of Band-lok)
RM Bond LC primer (in place of Optibond)
IDB System RM Bond Indirect Bonding Light-Cured System (complete set)
TAD System Dual-Top TAD Kit (sterilization kit and straight driver) and Dual-Top contra-angle driver
Dual Top TADs: 1.6 x 6.0 mm, 1.6 x 8.0 mm, 2.0 x 8.0 mm, 2.0 x 10.0 mm**
SundriesOrtho-Jel alginate, impression trays, beading wax, orthodontic wax, retainer cases, moldable mouthpieces
Polyvinyl siloxane (PVS) dispenser gun, PVS syringe tips, flowable tips
Headgears
Monolok (37% phosphoric acid) etchant, etchant tips
Orthodontic elastics (3/16" diameter x 4.5 oz., 1/4" diameter x 4.5 oz., 1/4" x 32.0 oz. for protraction facemask)
InstrumentsSchweickhardt surgical-grade Stainless Steel instruments
Mathieus Bird-beaks Weingarts Distal end cutters Ligature cutters Band-removers Direct bond removing pliers Crimpable pliers (for crimpable posts) Dual-end band pushers/scalers (Guequierre) Direct bonding tweezers
Apex series instruments: Band-seater (bite-stick) Three-prong pliers Step pliers (1.0 mm) Cinching pliers Band cap converting pliers (for bands and Synergy-R brackets)

19Clinical Review 18 Clinical Review
The Liberty Bielle Fixed / Removable has unique configurations that allows it to rotate 360 degrees, maximizing lateral movement and providing comfort, flexibility for the patient and treatment efficiency to the doctor. The unique components increase the durability of the appliance by minimizing destructive lateral forces and allowing the maximum movement of the mandible in many directions.
Libery Bielle: Removable / Fixed
VS.
Was Removable Now Fixed
No Cheek irritation
Yes Patient cooperation
No Pain
No Cheek irritation
No Patient cooperation
No Pain
Initi
al
6 M
ont
hsOrthopedic
Changes and Orthodontic Changes
Orthopedic Changes and Orthodontic Changes
Patient Comfort | 360 Degree Movement | Lateral Flexibility | Efficient Design
In progress
3 M
ont
hs
Initi
al
Eric Marie-Catherine, DDSThe freedom of movement...

21Clinical Review 20 Clinical Review
Zenman and theArt of Web DevelopmentBy Keith Roberts, Zenman Productions
The answer is obvious. Your website is the first impression that a potential client has of your practice. Before a phone call is made to set up the consultation you are being researched online. Some users will just look at your website while more tech-savvy users will read online reviews and browse social networking sites. The website is an online face of your practice and must accomplish two things. First, it needs to have a design that conveys the same experience a patient would get walking into your practice. The look and feel of your website should match your brand and office culture. All of your marketing should have a cohesiveness based on solid brand guidelines and a website is no different. Next, the site must be intuitive and easy to navigate. The user should be able to get to any page on the site with one click making information available with little to no effort.
Why are these two things critical?
The web is the first place a decision maker goes when looking for a new service, even if a referring doctor makes a recommendation the potential patient (or mom/dad). The potential customer is going to Google your practice name, and the website must show up. Having a good website doesn’t just mean that it looks cool. Your website needs to be developed to the current industry standards in order to minimize extraneous code that can impact the density of keywords used for organic search engine placement. It is also important to have a CMS (Content Management System). The site should
quickly engage the user and drive them to CTAs (calls to action) or key areas of the site (example: services or contact information).
SEO (Search Engine Optimization)
What exactly is SEO? Search engine optimization (SEO) is the process of improving the visibility of a website or a web page in search engines via the “natural” or un-paid (“organic” or “algorithmic”) search results. As a marketing strategy, SEO considers how search engines work, what people search for, the actual search terms typed into search engines and which search engines are preferred by their targeted audience. Statistics show that when a user searches for something on Google they will visit the first result 48% of the time, the second result 18% and the third result 7%. If you’re not in the top three organic search results you are losing potential patients.
Pay-per-click vs. Organic search results
Ideally your practice should appear in both the organic search results and in the sponsored or paid advertiser section. Research has shown that if a business appears in both places the user is far more likely to click on your link…and the best part is 70% of the time the user will click on the organic results so you’re only paying for 30% of the traffic. Pay-per-click campaigns like Google AdWords work on a bidding system. You can set a maximum bid for individual keywords
(example: “clear braces “might sell for $5.69 in Phoenix, AZ), set geographic specifications so your only appearing in your target area and manage your daily/weekly/monthly budgets. This means that you can pay a few extra dollars to appear when someone searches “orthodontic care” in Houston, TX for example. This is a much more targeted approach to marketing. If you place a traditional print advertisement or do a direct mail campaign the audience might not be looking for your services and your best hope is a little brand awareness. With the paid search results you know the user is searching specifically for your specialty and in your town.
“Once you have them at your site keep them...”
The average bounce rate* is 50%, that means half the users that find your website never get past the home page. If half the customers that walked into your practice turned around and walked out wouldn’t you make a change? The photography of your practice should be inviting and showcase images of the staff, patient interaction/lifestyle, and the practice interior. The user should be able to quickly and intuitively find information about your experience, services and contact information
* Bounce rate – Google defines this as the percentage of single-page visits (i.e. visits in which the person left your site from the entrance page).
“The site we have had forever is fine. Why should I update the site that we have had for years?”
“Why do I need a website?” { {Keep it current
Your website can’t become stale. The content must be updated frequently to keep users returning to your site. From tracking rewards program to updating the smile gallery or news and events, the website must be current. This doesn’t have to be a daunting task. We recommend planning a few posts throughout the month and have the practice manager update the site once a week. With an easy to use CMS, the website updates will only take a few minutes and the impact is dramatic.
Analytics – track your results
Google Analytics is a free service that generates detailed statistics about the
visitors to a website. Google Analytics is currently in use in 57% of the top 1,000,000 websites. This allows you to track visitors from referrers, search engines, pay-per-click campaigns and email marketing. By tracking the user experience you can easily see which marketing mediums are getting the best ROI (Return on Investment).
CMS
A Content Management System is a software system which provides website authoring, collaboration and administrative tools designed to allow users with little knowledge of web programming to create and manage the site’s content with ease. The CMS will allow you to edit/add/remove content and images along with creating
Keys to effective web design
1.Easy to use
2.Focus the users attention (CTAs, animation, etc)
3.SEO
4.Current content
5.Strong design
new pages. With current systems like WordPress the average computer user can administer the content of your site via the GUI (Graphical User Interface).
* SEO within CMS – The SEO can be managed at the individual page level within certain systems.
What should it cost?
I always make the comparison to food. You can eat fast food for little cost but it’s not the best quality. The industry standard would be around $7,000-$12,000 depending on functionality, size, and other variables like SEO, copy writing, etc. The important thing is to get a firm that understands your needs and can develop a website that will be appealing to your target audience.

22 Clinical Review
Social Media
If you are not leveraging any means of social media, it’s time your practice embraced the phenomenon. Social media is the use of web-based and mobile technologies to turn communication into interactive dialogue. One of the key components in achieving highly visible brands are the social networks (Facebook, Twitter, Blogs, YouTube, etc). By creating networks via these tools you can dramatically increase your market penetration at little to no cost to set up or maintain. The only critical rule you must follow is that you have to be active in your social media. If you create a blog, which is a great way to drive traffic to your site, I would recommend at least one post per week. For Facebook and Twitter accounts
www.zenmanproductions.com
you should have 1-3 posts per day. Start slow and build your social networking up as you feel comfortable with the maintenance. Facebook is easy to set up and would be the best place to establish your network.
Marketing
Effective marketing campaigns increase the awareness of your practice/brand. By tracking the ROI on different techniques (direct mail, pay-per-click, etc) you can maximize your marketing budget. Your campaign should start with a strategy for the next year. The plan should evolve based on results from each medium. Remember, you can be the best but if potential patients don’t know you exist, the practice will not continue to grow.
rocky mountain orthodonticsTM
Synergistic Solutions for Progressive OrthodonticsTM
800.525.6375 | www.rmortho.com650 West Colfax Avenue, Denver, Colorado 80204P 303.592.8200 F 303.592.8209 E [email protected]
bondTM
Happy Patients and Happy OrthodontistsThe sum of all RMbondTM products equal
Tray Finish
LC Model Adhesive
Model Storage Box
Inner Tray Material
Dispensing Gun
LC Bonding Resin
LC Flowable Adhesive
Separating Medium
Round Rope Wax
LC Turbo Material
Mention this Clinical Review article or Rocky Mountain OrthodonticsTM to receive a free consultation with Keith at Zenman Productions.

25Clinical Review 24 Clinical Review
One of my best friends has sold everything from real estate, custom computer chips, and wealth building accounts. His secret to fabulous success has always been to capture the moments where the little things mean a lot in a relationship. Each time he would visit a prospective buyer or client he would listen carefully, not for the sale, but for the little personal things that the person would say to him about life, love, and the things that were important to him. This listening was about all he did the first meeting and then he would jump into his BMW at the end of the visit, and instead of scurrying off to the next sale, he would write down everything he could remember about the new potential buyer, especially those things that were personal.
“Yes, my wife just had a baby and there were some complications so she cannot come home for three to four days.”
Immediately after writing such things down he flew into action by calling his secretary, and the next day flowers arrived at the hospital with a note remarkably written with wonderful praise and appreciation telling the new mother how much her husband glowed when he spoke of her and their new baby daughter.
The sales tools of listening and responding in a caring manner with praise and appreciation are a lost art, especially in the busy orthodontic practice.
“Five exams and two consults are on the books today,” Sandy blurts out as she shakes her head. “When will it ever slow down?” she thinks to herself as she walks towards the Exam Room to get ready for battle. Sure she loves her job as Treatment Coordinator. She especially loves the thrill of getting the Start and making the numbers each month. But really? “When would I ever have time to listen, to care, and to respond in a personal way that builds a relationship? I am just too busy!”
I have seen it over and over again in practices large and small. TCs who see three exams a day and others who see ten and few feel they have the time or energy to build a relationship that will be not only the foundation for the Start, but also for future referrals.
There is one TC who used to see 8-10 New Patient Exams a day. We will call her Pat, just because that is her name. Pat is a master of relationship selling from the very first smile that she gives as she greets the patient and parent in the reception area to the time that she gets the signature on the contract. Pat can have the patient and parent smiling and laughing with her in less than five minutes, and when she goes to get the doctor she just has to whisper to him with a smirk, “They’re sold, so don’t screw it up!”
Patient The New Enrollment Process
The Art Of Relationship Selling
By Ken Alexander, Millenium Management Group
Find a Rockstar TC who loves the job
The Pats in the TC world exist, but they are few and far between. To be a Pat, you have to be in love, by actually loving people, loving your patients, loving your doctor, loving your practice and in love with your job. That love and affection comes through in hundreds of verbal and non-verbal ways, and the results are that the patients Start, and they refer their friends. Often not because of anything more than the fact that they have fallen in love with Pat and the joy she exudes!
One time I videotaped Pat to use the tape as a training tool and when I left the room, I left the camera on the table filming the patient and parent paging through the Before and After Album. All of a sudden the patient blurted out, “I like this doctor!”
The Mom retorts, “She is not the doctor. She is just the nurse.” “I know,” replied the patient, ‘but I really like her!”
Needless to say, the patient signed up to start that day. It was their third opinion and Pat’s practice was charging $500 more than the others for the treatment. Having the right TC who loves others and knows her stuff, and most of ALL knows how to win over new patients with a smile, a laugh, praise and appreciation; this TC is worth her weight in gold. For great sales is all about relationships and there is so much more to selling orthodontics than just giving information or getting a patient to Start.
Great practices have super stars who fill all of the key positions in the practice. Find a Super Star TC who loves her job because she loves people, and great success is bound to follow.
Will You Dance The One Step Or Two-StepA lot has been made over a relatively new concept of going to a One-Step New Patient Exam process. All this means is that the practice tries to cut out the Consultation, or Treatment Conference and the doctor does his diagnosis at the first visit and gives a clear and relatively accurate treatment approach. Records can be taken the same visit, and if the doctor’s suggested approach at the Exam Visit matches his diagnosis, all proceeds as planned. In the 10% of cases that the doctor is unsure as to a treatment, especially if extractions or surgery may be required, the doctor punts back to a two-step approach and asks that the TC set up the patient for a separate Consultation Visit to discuss the treatment options. In the very rare case after the review of records the doctor discovers something in the records that makes him second guess his original treatment plan given at the Exam Visit, he asks the TC to set up a phone consult or a separate consultation so that he, or the TC, may review the new findings with the patient or parent.
One-Step Exams work great for many of my clients, but they are not for everyone. As a matter of fact, no matter how hard some consultants push for a One-Step to be done in the practice…,
“There is actually no real statistical difference in exam-to-start percentages between a One-Step or Two-Step Exam when both approaches are done correctly…and, in some communities, a One-Step will kill a practice’s exam-to-start ratio as the Moms perceive it as
too aggressive and many must go home and talk to Dad before making a final decision.”
There is one more thing that really messes things up with a One-Step and that is that too often “everything but the kitchen sink” is thrown into the discussion; tooth brushing, wearing retainers, taking your fair share of appointments during school hours, paperwork galore. The patient’s head is spinning by the time the visit is done. After putting the patient’s mind into overload we then wonder why she doesn’t remember anything about what we just told her.
All the patient cooperation information and risks and limitations and other facts of the case are vital and must be communicated, but it is best to give only the bare minimum of facts on the first date and focus on the benefits of orthodontics and all the reasons why they should desire …,
One-Step, Two-Step or Three-Step, whatever dance you want to do for your New Patient Enrollment Process is A-OK with this consultant as long as each step is well-choreographed and it works to take the patient from a point of an inquiring mind to a happy, satisfied patient who sings your praises and cannot wait to get started. To achieve this goal, it will require Relationship Selling from a terrific TC with every step and every line of the process must be properly choreographed and scripted for maximum effectiveness.
A Beautiful Smile that Lasts a Lifetime! and w h y , Dr. Alexander is the Best Orthodontist in world for their little Suz y!
[ [There is actually no real statistical difference in exam-to-start percentages between a One-Step or Two-Step Exam when both approaches are done correctly…

27Clinical Review 26 Clinical Review
Welcome To Our Home
No you did not misread the line… it does say, “Home,” not “Practice.” The TC and all staff should think of a New Patient as if they are a welcomed guest in their home. Think about it for a second, but do you ever recall a time when you met a person coming into your home and you did not pause for a moment and welcome them with a smile? Yes, even your son Joey’s friends who you do not really like all that much, you pause, you give them a smile and hello, then head back to the kitchen or to wherever you are going.
Should we not expect at least the same from every one of our team members? When the office tour begins it is not just for the front staff and the TC to be welcoming, but every assistant should lift her head and smile, or say “hello” or “welcome”; especially an assistant who is running by the new patient on a mission to seat her next patient or stir the doctor from his office. Our practice must be welcoming, and if Dad sits in his big Lazy Boy with only a frown as he watches the tube when guests come over, few friends want to come to visit, or they just tip-toe up away to a bedroom.
Being a welcoming practice takes lots of time and energy, but it is the foundation on which all great customer service and marketing rests. Don’t stop with just New Patients but welcome every patient at every visit with big smiles and warm hellos. What the heck, we only see them once every six to eight weeks, can’t we at
least be warm and inviting when they do come to visit?
L’Image De Mark
I love the way this sounds, “L’Image de Mark !” It’s the French way of kind of saying “trademark” but it encompasses so much more in that your “L’Image de Mark” sets you apart from others in an exciting way. I just visited a practice in Lincoln, Nebraska where the doctor has captured this concept of L’Image de Mark” so beautifully in her Harrewood practice. The theme is Hollywood and the movies, with a built in theater and lots of movie stars posted all around. When the patients walk through the front door they know they are in for something special in this place, and it truly is special, but especially because of the fabulous glassed in New Patient Room and a relationship selling TC, named Suzy. Really… her name is Suzy.
Suzy has a huge advantage over other TC’s because the office facility is a WOW, and then with Suzy’s warmth and experience, getting patients to Start is normally a breeze.
The Right Room And The Right Tools
Not every office facility can be a WOW, but every New Patient Room can be. Whatever you do when designing your facility never skimp on the TC Room, or on getting all the right tools to sell your cases. I am constantly amazed at how poorly designed many TC rooms can be and that they do not have the fabulous ICAT or Dolphin Aquarium programs that make selling orthodontics so easy. Your TC Room should have a long, narrow table that allows at least the patient and parent, and perhaps two parents, to sit comfortably across from the TC. There should be an Exam Chair in the room so you do not have to switch rooms or go to the operatory to do the clinical exam. Having the right TC, TC Room, and the right tools can easily increase the exam to Starts by a good 7-12%.
Years ago I watched an exam being done with the right TC and no exam room. It was one humorous interruption after another. The coup de grâce was just after the patient signed the contract using a Good Housekeeping magazine to write on in the computer room that was
being used for consultations. We had to carefully extricate ourselves from the room one-by-one as the doorway was blocked with one assistant at the top of the attic stairs throwing toilet tissue down to another assistant impeding the passageway. Within months we had built a beautiful TC Room by bumping out into the parking lot and the exam-to-Start percentages rose 15% the next year. OK, it wasn’t just the room as we changed many things about the New Patient process, but if you are going to sell a million or two in braces, you really should have the right place to do it properly, and the right tools. And if you are less than a million, you need the room more than the next practice does.
Show And Tell
I mentioned that you need the right tools, but no tool is more effective than a Before and After Album when used properly. Would you ever buy a car without first test driving it and kicking the tires? What makes you think patients want to buy a beautiful smile without first seeing what it has done for your other patients? I particularly like it when I walk into a TC Room and all around are beautiful pictures of your best finished cases. Sometimes I see monstrous pictures up and down halls and in the operatory, all professionally taken and showing off the practice’s terrific work. There’s so much more to selling orthodontics than just saying the right things and smiling. Knowing when and how to use your Before and After Album can be just the thing to get your patients begging for what you have to offer, instead of you begging them to Start!
Dr. Who?
Well, Dr. Who is a great TV series in the UK, but that is not what I mean. One of the most effective sales tools in orthodontics and in all of dentistry is when your terrific TC says nice things about the doctor and the practice and actually means it! This is one of those areas that is so weak in most New Patient Exam presentations and yet can be so powerful in getting the Start if it is just scripted well, and done in the right timing. “Dr. Alexander is a warm and friendly doctor who treats his patients and his staff with kindness and excellence. It is not by accident that the
average staff member has been here for 7 years.”
OK, you don’t have to say that your office manager and lab person have been with the doctor for 25 years, skewing the stats, but find all the great things about the doctor and the practice that you can artfully communicate in a genuine
way, and spill the beans with each and every New Patient. Are these glowing comments not the things you want said about you in the community? If so, start the rumor and you will soon find Moms coming to the practice repeating what they have heard,
“I heard that Dr. Alexander has a super reputation for quality.”
“And Mrs. Jones, whom may we thank for saying such nice things about us?”
“My sister Gloria had her daughter Taryn start in your practice two months ago and she told me all about you guys.”
Look at that… positive rumors about the doctor can be a powerful marketing tool to create confidence in the practice. Who better to start the rumor with than the New Patient?
Dr. Who Has Arrived
We almost got through an entire article on New Patient Enrollment without having the doctor even come in the room. Yes, the doctor plays an important role, but in most of my clients’ practices, and most are seeing over 75 patients a day, the doctor needs to play just a small role. This
should be the TC’s show and the doctor comes in with just enough time to look in the mouth, dictate his or her findings and make recommendations. Ten to twelve minutes is usually enough time to show off a warm, caring and knowledgeable doctor without having the doctor screw up the sale. Anything longer than fifteen minutes and an assistant should come to
the door and stand quietly and smile, until the doctor acknowledges her and quickly wraps things up.
If the TC has done her job properly of showing off the doctor’s work and telling the patient and parent wonderful things about him, the doctor does not need to try too hard. Just spend a few minutes talking about things you may have found out you have in common with the patient; sports, hobbies, etc. Then have the patient hop up into the exam chair. Yes, I much prefer not to have the patient in the exam chair until the doctor invites them to jump in. Then a few more seconds of banter about the flavored gloves and off the doctor goes dictating the clinical findings while the TC types furiously. Anything the doctor forgets in his dictation the TC can ask the questions. “But really doctor?” Within just an hour you can memorize the dictation sequence and so not to keep forgetting things. It is quite impressive if you can get the teamwork with the dictation to match up perfectly.
Then all that is left is to show the patient and parent what is going on in the patient’s mouth and what will be necessary to lasso the teeth to bring them into their proper place in the mouth. This is where taking photos prior to the doctor’s
“Dr. Alexander is a warm and friendly doctor who treats his patients and his staff with kindness and excellence. It is not by accident that the average staff member has been here for 7 years.”[ [

28 Clinical Review
arrival is indispensable for excellent communications. Seat the patient back around the consult table and show them on a big 24”-28” screen exactly what is happening with their teeth and what you would like to correct. Answer any questions then get out of there to keep the assistants on time, leaving the TC to do her job selling the case.
When “No” Means Maybe
In sales we are taught to be a little hard of hearing. When someone says “No, I am not interested” or “I need to talk to my husband,” the best TCs take this on as a personal challenge to find out if “No” really means “Maybe.” Often a parent is not prepared to make the decision that day, or really does need to go home and discuss it with their spouse, yet the TC’s head starts hanging and her throat starts tightening up as she thinks that the doctor wants the Start and I am a failure if I do not get it today!
No, not everyone will Start in your practice, especially not at the first visit. Besides, we believe in relationships and so we maintain our smile and enthusiasm all they way through the exam. Hey, many patients do come back, so give it your best shot and don’t take “No” for an answer. Instead look at how you might overcome any objections. You will never know the objections if you do not ask, and then you must have the right scripts to be able to overcome the objections without fumbling around for the right words. The TC position is a sales job, and great sales people know how to turn a “no” into a “yes” in an intelligent and caring manner.
Track’em & Follow’er Up!
Anyone who gets out of the New Patient Exam without making an appointment needs to get onto a tracking system and then followed up within 7-14 days.
“Mrs. Jones, I came across Suzy’s chart on my desk today and I was just wondering if there is anything I can do to help her get started with her beautiful smile?”
Now you are back to listening and to finding those things that will regain the relationship and bridge the gap between the buyer’s needs and what the practice has to offer them. Listen well and be
creative in overcoming objections and you will find cases you never thought would Start coming back into the office for braces. Unfortunately, many TCs are on to the next Exam and have no time for this relationship business that requires persistence in getting follow-up patients into treatment.
And yet we will spend a lot of time, money and energy trying to get another New Patient into the practice before using some of that energy to love a busy parent enough to check in on them to see how we can help move them into a Start. Follow-up work is not the glamorous part of the job, but it can pay the entire salary of a good TC each year with the extra Starts she gets going in the practice, all because she cared.
It’s All About Relationships
If you have been one of Ken Alexander’s terrific clients over the years you know that:
Hands down nothing else comes close. That is why being a TC is the most fun job ever in orthodontics. Thank you Frank Edwards, Dean Bellevia and Ellen Grady for designing the original TC role and allowing doctors to save oodles of doctor time while giving TCs the opportunity to help others. If it is only about the sale, you will often lose the sale. But if it is about the relationships, you will be creating a foundation where your happy, satisfied patients and their parents go back to your community and to their family dentists shouting your praises. Now, isn’t that a lot more fun than advertising in the newspaper or taking on a discounted insurance plan? Get your New Patient Enrollment Process in tip-top shape and watch your practice grow by adding to your family of happy patients who you have given something to smile about. Always remember what my a ten year old told me one day and you will never take your eyes off of what counts in life:
“If you are not helping others, you are not helping yourself.” Cassi Alexander
...And that is why being a TC is the most fun job ever in orthodontics.
Relationships are the Most Important Things in Life!
Functional EducationTM
The Multi FamilyTM System, Functional Education Appliances, is an integrated system of appliances that allow the doctor to choose the ideal appliance according to the age and the malocclusion of the patient.
rocky mountain orthodonticsTM
Synergistic Solutions for Progressive OrthodonticsTM
800.525.6375 | www.rmortho.com650 West Colfax Avenue, Denver, Colorado 80204P 303.592.8200 F 303.592.8209 E [email protected]
2 16+ 2 16+ 2 16+ 2 16+
Multi-STM
Multi-P®
Multi -T®
Multi-TBTM
Why wait for the perfect smile?

30 Clinical Review Synergistic Solutions for Progressive OrthodonticsTM
800.525.6375 | www.rmortho.com
FLI® TwinFacial, mesial and distal flared lead ins for easy wire insertion and minimal binding
Low profile design
Color quadrant for easy identification
FLI® ClearIdeal clarity to match tooth color
Small design for patient comfort
Ideal base construction for great bond strength and easy debonding
FLI® TubesSimplifies wire insertion
Smooth comfortable contours
Notches for easy positioning
FLI® WireAesthetic wire that will last until your next wire change
Maintains all of the thermal properties of the Niti wire
Available in round rectangular and square sizes
FLI® Ceramic AdhesiveSpecifically formulated for use with RMO®’s wide range of clear and ceramic brackets
Light cure adhesive provides extended working time and quick cure application
Optimum balance of high strength and easy removal offers enhanced bonding efficiency
Get your winning team together...
rocky mountain orthodonticsTM

33Clinical Review 32 Clinical Review
By Bridgette Owens, 7 Group Advertising
“So what is a brand? I already have a logo - isn’t that enough?”
A brand is the sum of the subconscious, sensory and emotional elements that make up the total experience of your medical practice. It encompasses every touch-point you have with the world, patients and prospective patients, making it so much more than a ‘logo’ or an advertising campaign.
Everything you do reflects upon your brand. The moment a patient intersects with any part of your practice they are forming an opinion of their experience and the services to follow.
Therefore, the positioning of a brand in the minds of the target market happens whether you’re pro-active, reactive or passive, making it important to take charge and actively manage at every step. The world is a stage, so let’s start performing!
It’s an attitude thing
No matter how different you make the logo it will not reflect your brand unless you change the attitude and put life back into the brand at all levels. Brands are experiences that live in the hearts and minds of people and this starts with your team and core beliefs. It is difficult for a potential customer to buy into your brand if your team does not reinforce it’s core values. A strong, well loved brand breeds pride.
Defining your brand
By not clearly defining a brand personality or a relationship with all stakeholders the major potential of the brand is ignored.
Become A ‘Big Deal’ - Uncover Your True Identity
R&DIn order to strengthen your brand and improve campaign validity you must ‘do your research’. Who is your target market? What are their values? Spend some time understanding what drives this demographic to make decisions and/or instigate change.
Make sure to keep an open mind as the answers may differ from your personal values. By correctly targeting your demographic the probability to ignite buzz and create the desired response from your campaigns increase significantly.
It’s not too late
Yes, sometimes brands do lose their way and can be seen as being unloved! However, the good news is that with a little care and attention you can initiate the road to recovery. Begin small by updating your business card; this will ‘start the ball rolling’ reminding you of your commitment to change every time you present it.
Be consistent
It’s easy to become absorbed in the design of each marketing piece, but ask yourself, how does this relate to my other campaigns? Am I maximizing my marketing dollars spent by cross advertising? Investing a little thought in your marketing initiatives will create a whirlpool effect, leading your efforts full circle.
Consistency is the key to great exposure. Assign a brand guardian in order to sustain campaign coherence. Seek someone who has the experience, the knowledge and most importantly the passion to provide you with this service.
For example, your business card, magazine advertisement, direct mail, Facebook fan page, online banner advertisements etc. should all correlate to one another.
The consistency of your product along with the frequency and visibility of your campaigns greatly increase your chance of a prospective patient choosing YOU when the time is right.
Make your marketing dollars work
Creativity drives innovation, inspires actions and provokes reactions. It is the art of selling, not telling. Be creative!!! It doesn’t always have to be costly in order to grab attention; with modern social media products such as Facebook, Twitter and YouTube you can obtain maximum exposure with minimal costs.
In our experience the best results are always achieved through a stimulating combination of pleasure, pain and open, honest communication.
There’s nothing more enjoyable than taking a bunch of communication goals, giving them a good shake-up and coming
The ‘7 Group’ Guide To Brand Development And Strategic Planning
It is a promise of value to different audiences and the manifestation of your mission and strategic priorities.
Think about the things that make you and your practice unique. Is your marketing material clearly portraying the attention to detail you posses in your work? Is your material current and up to date? Out of date material suggests that you are out of touch, opening the door for doubt regarding future services.
Defining your brand ultimately unites your team in a common goal and vision. It informs your audience how to react, presenting them with the tools needed to participate and the vision to identify.
out the other end with a solution that exceeds everyone’s expectations. That’s the element of surprise!
Plan ahead
Developing strong campaigns take time and effort, so give yourself the opportunity to participate by setting your projects and deadlines ahead of time i.e. start planning your Valentines day promotions at the beginning of January. By clearly defining your goals you allow time to strategically plan and cross promote your marketing initiatives, giving you the best value for your dollar.
“I don’t know how to put this but... I’m kind of a BIG deal”*
In today’s competitive market it’s more important than ever to deliver a fresh, inspiring brand identity. By defining your unique proposition and market position
you can begin to develop a strategic road map – improving your touch points and cultivating your message through any given media. It is essential to find the right resources to make your ‘BIG Deal’ dreams a reality. Source an agency that will engage you in an open and honest relationship, willing to take on the hard tasks, and with the experience and vision to say ‘how it is’. An independent and objective view on all marketing decisions will help you to be that one step above the rest.
So understand it, believe in it and get out there and promote it in everything you do!
*Anchorman: The Legend of Ron Burgundy, Dir. Adam McKay, Will Ferrell, 2004
www.7groupus.com
Uncover Your True Identity
Mention this Clinical Review article or Rocky Mountain OrthodonticsTM to receive a free consultation with Bridgette at 7 Group Advertising.

35Clinical Review 34 Clinical Review
By Ken Alexander, Millenium Management Group
I find no greater challenge or enjoyment as a consultant than in helping my clients develop a scheduling system that gets them on time, keeps them on time and allows the practice to grow. Creating such a system takes time, usually a day’s worth of consulting, but as Abe Lincoln once said,
Most practices have heard of a Doctor Time Scheduling and most computer systems can easily pre-code each day to allow for the Templates to juggle doctor time for maximum efficiency. But the
difference between what a practice can do in designing a Template and what any of the top scheduling consultants can do for you, is the difference between a sharp axe and a dull one. Many doctors cave in to a short-term solution of throwing another new hire at the scheduling problem instead of taking the time to
work through a complete system with an experienced consultant; a system that will often last them their entire career, with just a few sharpening sessions.
Over the past 28 years I have been a large part of popularizing the concept of Doctor Time Scheduling that is used in a majority of orthodontic offices. The concept is simple... plan out an entire day for all necessary procedures
with the doctor time built into them and make sure that the doctor is not needed at more than one place at one time. This is easier said than done and often requires the experienced consultant to coach the orthodontic team towards healthy standards and habits. For the growing practice the challenge may hit big obstacles as the fish may have outgrown the aquarium and the practice needs 8 hours of doctor time in a 7 hour work day, or the office does not have enough treatment chairs, or maybe the size of the office is too small. Proper planning requires good decisions as to where the doctor can delegate more, speed up or improve efficiency, but nothing can hold a schedule back more than a lack of the basic resources so that the fish can fit and survive in the aquarium.
On-Time Doctor Time Scheduling
“If I had eight hours to chop down a tree, I’d spend six hours sharpening my axe.”
It is important that assistant time is managed appropriately. Nothing eats away at assistant time more than a doctor who cannot, or will not, get to his/her chair in a timely manner. While consulting, I often ask the question, “If you could have the doctor at your chair the instant you needed him/her, how much time could you save each day?” Would it astonish you to know that the typical answer is 2 hours and sometimes 3-4 hours of lost or less productive time... per assistant!?!
For some scheduled days, commitment can overcome a poorly designed Template, but when the Template is poorly planned and executed every day, then frustration turns to apathy and both doctor and staff may give up on trying staying on
time. Obviously if you have given up on your schedule you have reached your maximum and your potential for growth is being squandered. The only way to reach your peak performance and greatest potential is to plan for it with On-Time – Doctor Time Scheduling.
Being on Time is Vital to Practice Growth
Maintaining an efficient scheduling system is the single most important factor in growing and sustaining an orthodontic practice. The goal of every doctor should be to not only reach their peak potential, but also to practice each day at their highest level of efficiency and competence. Practices tend to grow to their level of maximum capacity, or should I say slight incompetence, and then stop growing. The understanding of the key components of On-Time - Doctor Time Scheduling is the first step towards building your foundation for peak performance and sustained success.
A Doctor Time Schedule will keep the doctor and team on time, but just as importantly it gives the signal to patients that you can handle more growth. Why would a patient send their friends to a practice that cannot meet their needs
and is perceived of being too busy? Those who fail in the timeliness of each appointment make an implicit declaration to their clients that they are at their maximum capacity. Worse yet, many scheduling templates do not allow the practice to capture all of the new patients and Starts who would want to join the practice because the delay in the peak months pushes some Starts off to other more efficient practices.
There is no number of patients per day that will dictate if a practice can stay on time. I have worked with practices who were not able to stay on time at 30 patients a day, and yet some of my shining stars see 120-150 patients and stay relatively on-time. Many factors play into developing the right Doctor Time Templates and the
ideal scheduling system that is customized for each practice to stay on time. Here is a quick look at the main components for designing an On-Time - Doctor Time Scheduling system.
It’s a Chess Match
One of my greatest assets as a consultant is that I was a big chess player all the way through college. I once was challenged by a dorm mate that he could beat me if I did not look at the board. Three days later I said: “checkmate” and won the match. OK, I got really lucky. Consulting is much like a chess game with many pieces that must be discovered and understood,
then organized in the most effective manner to win the game, and winning means achieving the doctor’s goals. Yes, it requires experience, an analytical mind and proper planning, but if the consultant has done his job correctly at the end of the process he often hears from a staff member,
“This is so easy, why didn’t we think of that?”
Working with the right consultant who has been properly trained and has visited hundreds of other practices is vital to getting the most out of your practice scheduling system. Some practices can get good at it, but I have yet to find a practice where the scheduling system could not be greatly enhanced. Remember, the goal is not to complicate things but to make things as simple as possible. As Albert Einstein rightfully stated,
“Everything should be made as simple as possible, but not one bit simpler.” Albert Einstein
Make it too simple and it’s not very effective, make it too complex and no one can follow it or make it work. To make it effective means getting every team member on board with understanding their individual role in staying on time.
Most of the time the scheduling problem is not that the lack of assistants, but that the doctor and assistant time is poorly planned.

37Clinical Review 36 Clinical Review
The Puzzle Pieces
The first step is to determine the puzzle pieces. The vast majority of practices that stay on time are those that have identified each of their routine procedures in treatment and established an appropriate amount of doctor and assistant time, at the right times, to complete the work, on time.
The top companies such as airlines and factories schedule for success to stay on time. Imagine Continental Airlines not having gate agents arrive on time to check passengers onto the plane, the food truck being late, the gas man forgets to come, pilots showing up at the last minute, and the list goes on. Hundreds of little things must all be scheduled properly for the flight to take off on time, and this must happen over and over again for the thousands of flights each day. If airlines can stay relatively on time, except for the occasional bad weather, so too must the orthodontic practice juggle its many pieces to develop a daily game plan that, if followed each day, will lead to daily success. With a little hard work and proper planning, the orthodontic practice can determine its many puzzle pieces and get them all to fit properly into a daily on-time schedule.
Steps to Scheduling Success
Step #1: Look at all your procedures and develop an assistant/doctor/assistant time for each procedure you see routinely. Determining accurately exactly where the doctor time falls in each and every procedure and for how long in exact minutes is vital to developing any workable Scheduling Template.
Step #2: Try to combine as many treatment procedures into
as few scheduling codes as possible while insuring the doctor time and assistant time matches up relatively well. Remember, we are not looking for perfection, but something that is workable. So keep it simple by having fewer than 25 total scheduling codes that will serve your hundreds of procedures by appropriately taking into account the doctor and assistant time.
Step #3: Determine how many of each scheduling code you will need to see each year, each month and finally each day. Many of the computer systems today will tell you how many of each procedure you have seen for a month or year, and you simply must divide the procedure numbers by the number of days worked in the period surveyed to determine how many of each procedure, or scheduling code, you will need on your daily template. Barring that, count up two months worth of scheduled patients and divide by the number of days worked those two months. For the consultants, you can tell us your treatment technique and we can get pretty close to planning the right numbers if we know how many patients the practice wants to Start. Getting it
right with the number of scheduling codes needed per day is a set of math equations that only an experienced consultant best understands.
Step #4: Now go ahead and design the Templates. If you know all of your puzzle pieces or scheduling codes, and you know how many you need each day in your Template, armed with a pencil and large eraser you can begin to create your game plan by putting together your puzzle in such a way that the doctor time is juggled properly. Ideally, the doctor time never conflicts and the doctor is never needed at more than one place at a time. This job can be greatly enhanced by the Millenium Template Designer software program that I have used for the last eight years to greatly simply Template design, it may hit the market soon.
Oh! by the Way!
Did I forget to tell you that you really should calculate if you have enough of the practice resources of assistant time, doctor time and total number of chairs before you start designing your Templates? Designing a Template that is missing a key resource, like not enough chairs, or not enough doctor time in the day, can lead to the futile exercise of rearranging the chairs on the Titanic. It might be a little better when you are done than had you made no attempt to improve the scheduling system, but it will sink each day because your problem is the lack of necessary resources. You will just keep bailing water until you discover the missing resources and make the right decisions that will resolve the deficits.
You will just keep bailing water until you discover the missing resources...
rocky mountain orthodonticsTM
Treat the parents like you treat their kids...

39Clinical Review 38 Clinical Review
Consistency is the Road to Success
When I go into a practice I am often asked to try and “fix” the scheduling without significantly changing the basic system. I usually ask, “Which schedule do you want fixed, Tuesday’s or Thursday’s; a week ago Tuesday’s or Wednesday’s?” Any practice that does not fill in a defined Template essentially is asking the receptionist to bake a different cake or pie each day and then in the morning huddle she says, “Surprise, look what I have baked for you! It’s upside-down cake or mincemeat pie!”
So what if your practice could see the same number and the same types of procedures at the same time every day. Don’t you think you might get good at it? Seeing the same Template’s worth of patients each day allows a practice to not only get good at knowing when the doctor is needed,
and when the doctor or an assistant can take a break, but it also allows the practice to know where modifications are necessary. If the schedule is always falling behind at 9:00 a.m. and it is slow at 11:00 a.m., sometimes just taking an observation patient out at 9:00 a.m. and moving it to 11:00 a.m. makes the Template flow beautifully again. It takes a few hours to design a great Template, but most often, it takes only minutes to properly modify well designed Templates to keep them humming at maximum capacity and efficiency.
Another attractiveness of a well designed Template is that it is somewhat “self-regulating” in that it will tell you if you have planned too many or too few of any particular scheduling code. If the receptionists are constantly searching for a specific code that is not available within the normal rotation then the weekly set
of Templates may not contain enough of these missing codes. It is also possible that the assistants may be requesting an incorrect code, and with a little retraining to get all the assistants to select the ten minute “A” Activation code for reties instead of the 20 minute “AW” Archwire Code, this could solve the problem as it gets everyone back to using the Template as designed. But if more AW’s are needed, all one has to do is look for where there are consistently unused codes in the Template and place some extra AW’s in these excess code spots making sure to properly juggle doctor and assistant time. Viola! Another 3-6 months of an effective Template.
It Takes a Village to Run a Practice On-Time
Everyone must participate to effectively run an On-Time – Doctor Time Scheduling system, even the patients. Proper
It’s Not Evolution... It’s by Design
It is in the actual design of the Templates that most practices fail. What often happens is that the Template starts looking really good with 50 codes and then the designers realize that there still are 10 more codes that have to get in but they are out of resources! So the extra codes get shoved into a column with no chair or assistant, or placed in columns where the doctor time is overbooked. Worse yet, the new Template may not plan any breaks for the assistants as each appointment is stacked one upon the other with no time for a late patient or breakage patient. The consultant is a realist and he will guide a practice into how to overcome the lack of resources so that the practice can stay on time and continue to grow. Planning an extra 8-10% more codes each day than the practice needs will insure not only continued growth, but also room for rebooking cancellations, repairing breakages and seeing patients in 3-4 weeks to finish them up.
training in your scheduling principles will allow patients to participate in keeping you on time with calling in advance with breakage, arriving five minutes ahead of their scheduled time to be brushed and ready to go, and being courteous to call early if they must cancel an appointment.
Critical to staying on time is to have scheduling coordinators who will fill in the Templates as designed and use the proper substitutions if they cannot find the appropriate code that meets the patient’s needs. Obviously long procedures during school hours and short procedures after school is the only way to meet the majority of patient needs without working until 8:00 p.m. Too much deviation from the Template and its legal substitutions will put a practice right back to where they are eating mincemeat pie.
The doctor must be on his/her best behavior throughout the day to focus on being on time, and talking to patients and parents is quite acceptable and a part of the job, but most of the talking must be done when the doctor is not needed at a chair. Assistants must work to the time allotted them for the procedure and be aware of when the doctor is to arrive in their chair. They must always be at the chair when the doctor gets to their chair so as not to cause any loss of doctor time
throughout the day. Everyone must be disciplined enough to do their jobs or their part of the teamwork to make the scheduling system run on time. About 60% of a great scheduling system is properly designed Templates, but the final 40% is the teamwork needed from all parts of your village to make things go smoothly and to stay on time.
Discipline is Another Way of Saying “I Love You!”It makes the consultant a bit crazy when he arrives at a practice that has a big scheduling problem and he watches the clock strike 8:00 a.m. and the morning huddle discussion continues on. Finally at 8:03 a.m. the assistants scurry to their positions to grab the 8:00 a.m. patients, yet one or two still have some coffee to finish, restrooms to use and to chat in a corner while their patient is waiting. Discipline is all about love, because without discipline you cannot show your patients that you truly esteem them and value their time. I find it ideal when instead of being late to the operatory in the morning, the morning huddle finishes five minutes in advance and at least two assistants who are ready to go, run into the waiting room and grab the early arrivals to take them back to the chairs to get started. That is honoring your
patients, or as Betty Sanders rightfully points out in her book Fabled Service,
“After all, service is nothing more than the reflection of esteem in which you hold others.” Betty Sanders
Do you love your patients and parents, and most importantly do you esteem them and their time? Then you have no choice but to get on-time and stay on-time. Running consistently more than ten minutes behind tells your patients that you are either too busy for them or you do not highly esteem them as you should, or could. Sure mistakes or unplanned occurrences will happen that may set you behind by 20 or 30 minutes in a day, but it is no worry, if you can consistently stay on time with the vast majority of your appointments.
I Heart You
Run your day on time...

41Clinical Review 40 Clinical Review
The Principle of Patient Cooperation
Every good team needs to know the rules, but some rules are not rules at all, but simply principles and good guidelines. Ask this consultant what to do about a patient that arrives late or has something broken and he will always say, “It depends.” There is no hard fast rule that governs these moments of truth, but rather a principle that says,
Too often assistants want to establish a rule that says arrive more than ten minutes late, or break a brace and get reappointed. When it comes to great service it is not so easy or obvious as to how to handle poor cooperation and each circumstance takes thinking through the best approach to both stay on time with regularly scheduled patients while still meeting the needs of the poor cooperator. Also, if it is the first offense it will be treated differently than if it is the fourth broken bracket in three months. Each situation needs a Clinical Coordinator who will explore the options while insuring that the final decision maintains the principle of patient cooperation stated above. Keep the poor cooperator waiting and move on with regularly scheduled patients, squeezing the offender back into the schedule as best you can while staying on time.
It’s a Natural Disaster
Breakage is a natural disaster in any busy orthodontic practice but its effects are often compounded by the rescue team’s panic. I have watched one assistant run to another, who then runs to the doctor, and then all three waste five minutes looking at the schedule, while during this time the repair could have already been done. In today’s world of one-step etch and seal with light cure, a bond can be replaced in minutes and often the regularly planned procedure can still be performed. Having everyone alerted to the breakage and having disaster repair trays ready to go in case of breakage, can keep this natural
“No regularly scheduled patient should be kept waiting because of a poor cooperator!”
Ken Alexander
occurrence under control and avoid the nuclear meltdowns that often occur because we panic and are not properly prepared to make quick repairs. If there is not extra time to do the planned procedure, make the patient comfortable, change their ties and then reappoint for the procedure a few weeks down the road.
Late patients are another natural disaster in the practice that again must be handled with the best customer service while not
trampling on the needs of your good cooperators. Whatever you decide to do, make sure the parent is completely informed, especially if they must wait as they may have other errands, or a child who needs to get to ballet, or soccer practice.
“Mrs. Jones, it looks like Joey is running ten minutes late today and has a bracket that needs repaired. No worries, we can take care of him, but it will be about 20 minutes before we can work him back into the schedule and another 20-25 to have him repaired. If he had told you about the breakage you could have called us and we could have given you a more convenient appointment time. Are you OK with being here for 45-50 minutes as we work Joey back into the schedule and stay on time with our regularly scheduled patients? Or would you rather reappoint to a more convenient time?”
Isn’t it Always About Relationships?
No system in the practice will affect the relationships more than poor scheduling. The stress from being late often filters into the relationships between doctor and staff and staff members with each other. Needless to say, patients and parents do not look fondly on the practice that cannot meet their needs by staying on time, and some may stop referring their friends. Referral sources hate to look bad by sending one of their valued patients to a practice that is regularly tardy. I have often quipped to my clients,
“In orthodontics, staying on time is close to godliness.” Ken Alexander
On-Time – Doctor Time Scheduling is the secret to the super success of most of my busiest clients because no matter how many patients want into the practice we figure out a way to keep them on time. Sure it takes hard work and discipline, but the system itself has been turned into a science by this consultant and with a set of mathematical equations then coupled with great principles and the right mix of discipline and goodwill. Soon each client finds a stress free day that allows for rescheduled appointments, breakage, and practice growth, but most of all they are able to meet the patient’s definition of being on-time, which is:
“Meeting or beating the expectations of the busy patient and parent in the
timeliness of each appointment and total treatment time.” Ken Alexander
So now you know how to build an effective scheduling system. Give it a try and spend some time sharpening you axe so that you can easily cut through your work load each and every day. If you need help, call on an experienced consultant who understands On-Time – Doctor Time Scheduling, and do not give up until you are once again running your practice, instead of your practice running you!
Mention this Clinical Review article or Rocky Mountain OrthodonticsTM to receive a free consultation with Ken at Millenium Management Group.

43Clinical Review 42 Clinical Review
By Ray McLendon, DDS
Efficient treatment planning of routine orthodontic cases as well as a wise choice of orthodontic appliances can help keep a practice more competitive by keeping the cost to start the case lower as well as keeping the effort to finish the case lower.
Although there are many different clinical treatment philosophies, a common interest is treatment efficiency. Rather than debate various philosophies, I would like to propose that once you have chosen the one that you like the best; it would
be helpful to the efficiency of your practice to identify and treat routine cases in the same way. This same or “routine” treatment plan idea will help you and your team deliver the care in a more predictable and efficient way. When your team knows in advance the routine way that you approach “normal” cases, the less stress and effort that all of you can expend. This idea in return can help you and your entire team expend the needed extra time, effort and expertise needed to treat the “non routine” cases.
Many specialists have told me over the last 25 years “I wonder who is treating all of the Class I cases, because I am not seeing them anymore?” as well as “I wonder why the simple cases do not
come in often?” What I mean by this is that although every patient and every treatment is “special” it could be that the “80 / 20” may apply to orthodontics as it seems to apply to so many other parts of life. A strategy that defines up to 80% of cases as routine cases, and as we define
in advance how we will treat them every time, may create a specific strategy to help make sure that our practices will attract all cases that are available to be treated, and
at the same time maximize our clinical efficiency. Increased clinical efficiency helps us be more profitable, more efficient, and more affordable.
Some practices (and not necessarily specialist practices) offer “low” or at least the appearance of lower fees, as well as low or no down payments. A practice can put itself into a competitive disadvantage by having a high cost of starting a patient. If a practice has a significantly higher cost of starting a case due to much higher cost of the appliances or other lab or technology fees associated with treating the case, the less options that they can offer the patient. As a fair analogy, even the “highest quality” car companies offer many different models. All of the models are considered high and good quality, and yet the highest trim model might literally be priced at twice as much as the basic model. High quality companies do not attempt a “one offering fits all”
8020
Could a wise use of the “80/20 rule” increase your practice clinical efficiency and profitability?
RULE
Get your ducks in a row so... when your team knows in advance the routine way that you approach ”normal” cases, the less stress and effort that all of you can expend. approach. As an alternative, they commit
to a level of quality, but still have several offerings to stay competitive. It may even be possible that a good volume in the lower priced “good sellers” allow the company to sell a much smaller number of the “high end” models that they have every reason to be proud of.
In our practice we value a detailed written treatment plan for each patient. With modern software we have the ability to save these treatment plans and apply them to other similar cases. The more often that we can use a “saved” treatment plan, the more efficient I believe that we can be. If 80% of our cases can be treated with our “routine” written treatment plans on file, we can use our expertise to treat those “20%” of cases that need absolute custom treatment plans. These are by definition, more difficult, higher fee cases. If these cases do not have a higher fee, they are not profitable cases. We believe that this concept is fair to the patients and fair to the practice.
My final thought is to discuss the costs associated with starting a case, including
High quality companies do not attempt a “one offering fits all” approach.
the cost of the actual appliances. We like high quality appliances and we like indirect bonding as well. If, however, we forced every patient to accept indirect bonding, we would have a higher fixed cost than if we did not. If we forced every patient to accept clear brackets (rather than metal ones) we would have a higher cost of doing business and our fees would need to be higher.
Back in the 1990’s RMO® introduced the first low or no friction Synergy® bracket system. This idea was very attractive to me and I have used this system for almost 20 years now. There have been a number of imitators and of course, other “systems” that claim great results due to low friction qualities. Although there is debate over how scientifically significant the lower friction may be, there is little debate that orthodontist can pay well over $50,000 per year for more expensive “low friction” appliance systems compared to the Synergy® system.
I personally believe that much of our clinical efficiency with less appointments and less wire changes is necessary in
these competitive times. Some cases can be treated with as few as three wires and with much longer intervals than were ever thought before. I fear that some orthodontists were not introduced to this wire technology until they were introduced to much more expensive self ligation systems.
Even if a doctor felt that there were some advantages to SL brackets (which I personally do not) I must wonder if they make sense for the 80% of cases that are routine. I also wonder if offering only this option could cause a practice to loose competitiveness due to much higher cost to just start the case.
Since there has been an old business concept to compare the difference between “buy” versus “build” when it comes to a business. I would suggest that it is much more cost effective to decide how to “build” your own clinical system to treat cases rather than “buy” someone else’s system of clinical orthodontic treatment.
Routine
Custom Treatment
[ [

45Clinical Review 44 Clinical Review
Lingualjet Technology has recently developed a new appliance concept including customized lingual brackets, a straight wire technique and 3D numerical processes. These technical improvements are combined into a unified bracket system by Lingualjet™ providing a highly advanced tailor-made appliance.
The principle of Lingualjet™ is built on four advanced components:
1. A numerical set-up: A set-up of the final positioning of the teeth is generated after obtaining 3D information of the dental arches.
2. A custom made bracket: The brackets are manufactured utilizing CAD/CAF technology. 3D software is used to design each individual bracket. Features include low profiles, smooth contours and special pad surface design.
3. A flat archwire: the archwire has a standard shape and is adjusted to fit exactly in the center of the arch slots. The archwire is fixed to one plane and results in a very precise and accurate straight wire system.
4. 3D Imaging: As an option, the patient’s facial details can be captured via CT Scan or Cone Beam technology. A 3D image report utilizing individualized parameters can then be generated.
Similar ideas have been described by other inventors regarding specific components of this system including: straight-wire 1, 2, 3, numerical set-up 4, customized brackets 5, 6 or imaging applications 7,8,9. But Lingualjet™ is the only method which combines all of these hi-tech advances into one system 10, 11.
The combination of these four technologies results in a unique appliance which creates many advantages. Some of these include:
• Ahighdegreeofindividualization for each patient
• Theorthodontisthasthefreedom to adjust the clinical outcome
• Theorthodontistmaintainshis/her preferred methods of treatment
• Abilitytousestandardarchwires and ligatures
• Helpstolowerclinicalcosts
• Featurescombinetoallowforenhanced sliding mechanics and reduced friction
• Highbondstrength
• AbilitytocombineStraightwireconcepts with custom made brackets and 3D numerical technology
• Optionof3Dimagingtoimprove diagnostic and treatment protocols
The Lingualjet Appliance: a one-piece customized lingual bracket incorporating the straight-wire technique.
Lingualjet
Figure 1A: Brackets designed by CDA
Figure 1B: After bonding at levelling step
Figure 2: Comparison between Conventional and LJ Bracket
Figure 3: The LJ Pores (patent pending) avoid the composite fusing towards the gingival margin
Figure 4: The LJ bracket slot (left) is closer to the center of resistance than a conventional bracket (right)
Figure 1A Figure 1B
Figure 2
The main objective of the system is to give the practitioner all of the clinical advantages of a reliable lingual attachment.
1. Optimized bond strength: retention is substantially increased by the larger than normal surface area of the pad and a specific treatment of the pad, along with special design features.
The pad of the bracket is manufactured to fit the lingual surface of the tooth exactly. The large surface area of the pad is designed to cover a major part of the lingual surface area of the crown. This facilitates correct positioning as well as enhances bond strength. (Fig. 1A)
Direct Bonding procedures can also be utilized according to the doctor’s preferences. (Fig. 1B)
Another feature which results in better bond strength relates to the amount of adhesive that is required. The LJ bracket is connected to the tooth as two isotropic bodies of comparable resistance. Conventional lingual brackets require a thicker zone of resin, which can be deformed and weakens the bond. (Fig. 2)
In addition, the pad design minimizes interference with the opposing teeth during mastication.
A new manufacturing process creates pierced pores of a specific geometric shape within the pads. This improves bond strength and decreases the quantity of adhesive needed near the gingiva (Fig. 3). The practitioner can begin treatment mechanics including rapid correction of rotation and dystopic positioning of the teeth without fear of the bracket loosening or debonding.
2. Control features are built into the bracket instead of the archwire: the computer generated numerical process creates a precise arch slot which incorporates the 3 orders of control. The arch slot, with a cross section of .018 x .025, is positioned so that the center is positioned more gingivally. Thus, the application point of the orthodontic force is closer to the center of resistance of the tooth, compared to techniques using standard brackets (Fig 4). These features help to enhance treatment mechanics while taking anchorage considerations into account.
3. The bracket is adapted to each individual tooth: it takes into account the anatomy of each tooth. It works on all types of surfaces, including enamel, metal, resin, etc. By creating customized brackets with CDA technology, different geometric factors are incorporated and designed for optimal results. This includes things like the actual position of the arch slot compared to the position of the bracket relative to the pad and tooth surface.
The Lingualjet bracket (LJ bracket)
Figure 3
Figure 4
Pascal Baron, DDS, MSc, PhD and Christophe Gualano, DDS

47Clinical Review 46 Clinical Review
The advantages of using a straight-wire technique with lingual brackets are obvious:
• Nobendingneededinthearchwires
• Useofpreformedarchwiresateach phase of treatment
• Differentwirematerialscanbeutilized
• Differentwiresizescanbeused
• Reductionofcostsandchairtime
• Bettercontroloftransverseandvertical movements
• Controloflevelingandalignment without interference of the canine offsets
• Enhancedslidingmechanics
• Savesanchoragebecauseofthereduced friction between the wire and the slots
Using transversal scanner slices, it’s easy to demonstrate the justification of a lingual straightwire. Figure 5A shows that at half height of the crowns, the guide line of the arch describes a mushroom shape. Repositioning upward of the level of the arch-wire plane, an appropriate location can be found to be compatible with a standard straight wire form (Figure 5B).
Bringing the arch closer to the crown root junction eliminates the requirement for a canine off-set. This is because the difference between the palatine side of the canine and pre-molar disappears. There is thus no need for offset bends in the arch. Preformed arches can be made for this technique. A new arch shape has been developed, and the 3 sizes – narrow, medium and large, will cover all clinical situations.
A guide line chart is generated and will be helpful during treatment to check and control the exact position of each tooth. The crossing point between the bucco-lingual axis and the guide line of the wire is the same as the center of the bracket slot.
After the patients’ malocclusion has been recorded, the numerical setup of the final occlusion can be prepared. The PVS impressions must be broad enough to include all of the crowns and sufficient gingival surface. The details that are obtained are used in the optical scanning phase and provide a numerical capture of the malocclusion. On the resulting virtual model each tooth will be separated from adjacent teeth by using specialized software to manipulate three dimensional objects. Once the segmentation is made, the composition of the set-up can begin. A separate software program allows the construction of the final set-up which incorporates the practitioner’s preferred prescription (Fig 7).
The practitioner can check the final occlusion on his/her own computer. The images can be reviewed from different perspectives and magnification levels (Fig 8).
Straighwire technique A numerical setup
Figure 5A
Figure 5B
Figure 6A Figure 6B
Figure 6A: LJ Chart Figure 6B: Corresponding location of the brackets
Figure 7: Set-Up phase
The numerical set-up is a very user friendly and precise tool for defining the final positions and relationships of the dental arches. With a few simple clicks of the mouse, the therapeutic prescription can be personalized for the ideal set-up. The dental axes can be modified and adjusted without difficulty until the desired occlusion is obtained.
Before manufacturing the brackets, it is possible to add or modify the position of one or more teeth to adjust the end of treatment occlusion.
Mechanical effects can be anticipated as well. Effects of V-bends or anti-rotating bends can be simulated and thus can be integrated into the bracket slot prior to the manufacture of the bracket.
The ability to individually position each tooth also includes the possibility of
Figure 9
Figure 7
Figure 8: Numerical set-up can be displayed by shareware program i.e. Meshlab
TM
enabling the practitioner to verify the intra-arch and inter-arch relationships.
Figure 8
preparing anchorage by inputting the desired tip-back on molars and second premolars at the mandibular arch (Fig 9).
The same modifications can be done on upper incisors for instance, by increasing aesthetic tipping in the case of dento-dental discrepancy. All of these possibilities provide complete management of anchorage thereby facilitating the achievement of the treatment goals.
Figure 9: Anchor preparation on L6 and L7 by modifying the numerical set-up
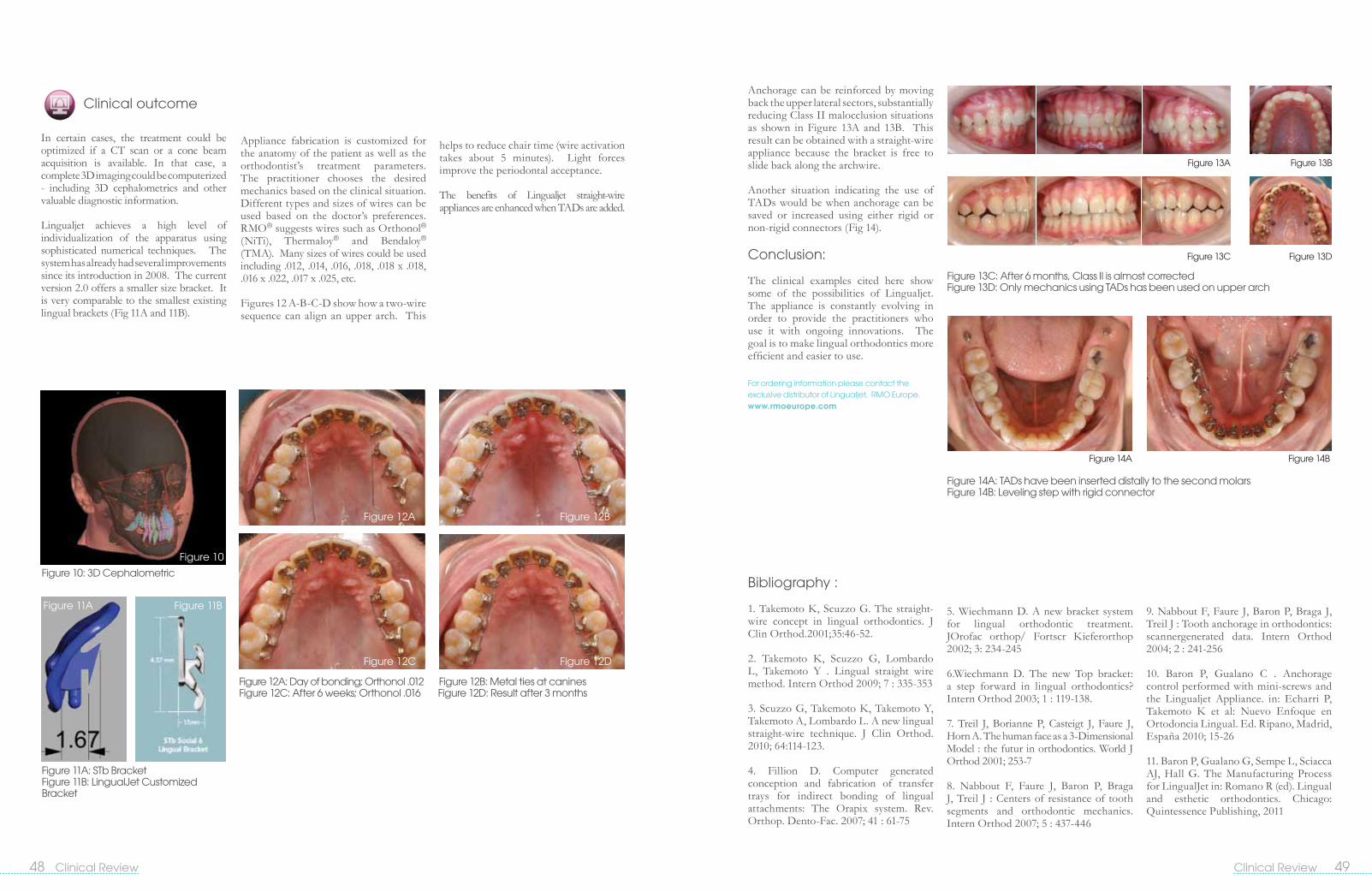
49Clinical Review 48 Clinical Review
Clinical outcome
In certain cases, the treatment could be optimized if a CT scan or a cone beam acquisition is available. In that case, a complete 3D imaging could be computerized - including 3D cephalometrics and other valuable diagnostic information.
Lingualjet achieves a high level of individualization of the apparatus using sophisticated numerical techniques. The system has already had several improvements since its introduction in 2008. The current version 2.0 offers a smaller size bracket. It is very comparable to the smallest existing lingual brackets (Fig 11A and 11B).
Bibliography :
1. Takemoto K, Scuzzo G. The straight-wire concept in lingual orthodontics. J Clin Orthod.2001;35:46-52.
2. Takemoto K, Scuzzo G, Lombardo L, Takemoto Y . Lingual straight wire method. Intern Orthod 2009; 7 : 335-353
3. Scuzzo G, Takemoto K, Takemoto Y, Takemoto A, Lombardo L. A new lingual straight-wire technique. J Clin Orthod. 2010; 64:114-123.
4. Fillion D. Computer generated conception and fabrication of transfer trays for indirect bonding of lingual attachments: The Orapix system. Rev. Orthop. Dento-Fac. 2007; 41 : 61-75
Appliance fabrication is customized for the anatomy of the patient as well as the orthodontist’s treatment parameters. The practitioner chooses the desired mechanics based on the clinical situation. Different types and sizes of wires can be used based on the doctor’s preferences. RMO® suggests wires such as Orthonol® (NiTi), Thermaloy® and Bendaloy® (TMA). Many sizes of wires could be used including .012, .014, .016, .018, .018 x .018, .016 x .022, .017 x .025, etc.
Figures 12 A-B-C-D show how a two-wire sequence can align an upper arch. This
helps to reduce chair time (wire activation takes about 5 minutes). Light forces improve the periodontal acceptance.
The benefits of Lingualjet straight-wire appliances are enhanced when TADs are added.
Anchorage can be reinforced by moving back the upper lateral sectors, substantially reducing Class II malocclusion situations as shown in Figure 13A and 13B. This result can be obtained with a straight-wire appliance because the bracket is free to slide back along the archwire.
Another situation indicating the use of TADs would be when anchorage can be saved or increased using either rigid or non-rigid connectors (Fig 14).
Conclusion:
The clinical examples cited here show some of the possibilities of Lingualjet. The appliance is constantly evolving in order to provide the practitioners who use it with ongoing innovations. The goal is to make lingual orthodontics more efficient and easier to use.
Figure 10: 3D Cephalometric
Figure 10
Figure 11BFigure 11A
Figure 12A
Figure 12C
Figure 12B
Figure 12D
Figure 11A: STb Bracket Figure 11B: LingualJet Customized Bracket
Figure 12A: Day of bonding; Orthonol .012 Figure 12B: Metal ties at canines Figure 12C: After 6 weeks; Orthonol .016 Figure 12D: Result after 3 months
Figure 13C: After 6 months, Class II is almost corrected Figure 13D: Only mechanics using TADs has been used on upper arch
5. Wiechmann D. A new bracket system for lingual orthodontic treatment. JOrofac orthop/ Fortscr Kieferorthop 2002; 3: 234-245
6.Wiechmann D. The new Top bracket: a step forward in lingual orthodontics? Intern Orthod 2003; 1 : 119-138.
7. Treil J, Borianne P, Casteigt J, Faure J, Horn A. The human face as a 3-Dimensional Model : the futur in orthodontics. World J Orthod 2001; 253-7
8. Nabbout F, Faure J, Baron P, Braga J, Treil J : Centers of resistance of tooth segments and orthodontic mechanics. Intern Orthod 2007; 5 : 437-446
9. Nabbout F, Faure J, Baron P, Braga J, Treil J : Tooth anchorage in orthodontics: scannergenerated data. Intern Orthod 2004; 2 : 241-256
10. Baron P, Gualano C . Anchorage control performed with mini-screws and the Lingualjet Appliance. in: Echarri P, Takemoto K et al: Nuevo Enfoque en Ortodoncia Lingual. Ed. Ripano, Madrid, España 2010; 15-26
11. Baron P, Gualano G, Sempe L, Sciacca AJ, Hall G. The Manufacturing Process for LingualJet in: Romano R (ed). Lingual and esthetic orthodontics. Chicago: Quintessence Publishing, 2011
Figure 14A
Figure 13A Figure 13B
Figure 13C Figure 13D
Figure 14B
Figure 14A: TADs have been inserted distally to the second molars Figure 14B: Leveling step with rigid connector
For ordering information please contact the exclusive distributor of Lingualjet, RMO Europe. www.rmoeurope.com

RMO® would like to invite you to join us in the excitement and buzz generated about the new RMO®! Our Executive Group and our entire company staff, with an average tenure of 15 years, share our enthusiasm for this new corporate re-launch. RMO® continues to be privately owned, and this will enable us to maintain flexibility to make decisions based on current orthodontic needs and visions for the future.
RMO®
You will see a new slogan, a new logo, and new colors to reflect our current and future directions. This will be incorporated in our Web Page, E-mail Communications, Social Networking Sites, Brochures, Company Letterhead, Booth Exhibit, and so on, moving forward. This will help to identity and unify our products, services and projects.
The majestic mountains are a key feature of our new logo. They tie in to the name that we are still known by in many parts of the world “Rocky Mountain® Orthodontics”. We see the mountains from our home office everyday, and they help to remind us of our history and development here
“Synergistic Solutions for Progressive OrthodonticsTM”
New Look: in Colorado. We know that these mountains will continue to endure – and this is a characteristic that RMO® wants to emulate.
RMO® believes strongly in orthodontic systems, and how their component parts when used together create a result that is greater than the sum of their individual effects.
Progressive Orthodontics refers to looking ahead, and keeping the big picture in mind. Orthodontics is about treating the patient as a whole – not just straightening their teeth. Treatment options and protocols continue to evolve and improve – and this is what makes the profession as challenging and stimulating as it is.
Putting our BEST
foot forward
650 West Colfax Avenue, Denver, Colorado 80204P 303.592.8200 F 303.592.8209 E [email protected]
Tony Zakhem & Jody Hardy
New Manufacturing AdvancementsRMO® has always been at the forefront of manufacturing technologies. This will continue. Some of the technological areas that will receive special attention are:Microsoft Dynamics AX – ERP System
Laser Welding
Advancements in Metal Injection Molding
CNC – Updated Technology
Laser Product Etching
Automated Product Identification/Marking
Continued Legacy of Innovative Products and ServicesThis will include ongoing efforts related to:SWLF Synergy®
FLI ® Family Systems – Twin Brackets, Ceramic Brackets, Bucal Tubes
Diagnostics – Moving to the Global Internet delivery model
Functional EducationTM – Multi Family TM, Liberty BielleTM, Wilson® System
IDB – Indirect Bonding SystemDual Top Temporary Anchorage Device System
Focus on the Total Customer Service ExperienceThis starts with the first contact with our Sales Reps and Inside Office Support. It continues with order entry, delivery of products and clinical use. Feedback mechanisms regarding product design and quality, as well as customer service, feed into an ongoing loop to enhance our continuous improvement philosophy. We are expanding our channels of communication to include the new RMO® Website, E-mail, and Social Networks. Our attendance at
conventions, seminars and study clubs will also be focused on providing useful information and interfacing with the orthodontic community.In summary, we would like to reiterate that we are proud to be the new owners of RMO®. We are proud of our past and what it has taught us. We are equally excited to be moving in new directions. We value our
long time customers, and also look forward to forming new relationships. We are committed to keeping RMO® as a privately held company and to maintain our manufacturing facilities in the USA. We are excited about our continuing involvement in the stimulating and ever changing world of orthodontics!
Tony Zakhem, Chairman and CEO
Jody Hardy, President and COO
rocky mountain orthodonticsTM
Synergistic Solutions for Progressive OrthodonticsTM
800.525.6375 | www.rmortho.com

52 Clinical Review
See enclosed flyer for your chance to win a variety of prizesincluding trips to Hawaii
AAOPRIZES
650 West Colfax AvenueDenver, Colorado 80204