
Report of the Select Committee on GP Out of H ours Services
450
R eport of the S elect C ommittee on GP O ut of H ours S ervices
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of Report of the Select Committee on GP Out of H ours Services
R epo r t o f t h e Selec t C o m m it t ee on G P O u t of H o u rs Ser v ic es
REPORT OF THE SELECT COMMITTEE ON GP OUT OF HOURS SERVICES
At the sitting of Tynwald Court on 18th June 2003 it was resolved that a
Select Committee of five Members be established to -
"investigate the matter o f the General Practitioners 'Out o f Hours Services' being provided throughout the Island, with power to take written and oral evidence pursuant to sections 3 and 4 o f the Tynwald Proceedings Act 1876 and report by October 2003."
The Hon J A Brown SHK (Castletown)(Chairman)
Mr D J Gelling CBE CP MLC
Mr Q B Gill MHK (Rushen)
Mr L I Singer MLC
Mr G H Waft MLC
The powers, privileges and immunities relating to the work of a committee of Tynwald are those conferred by sections 3 and 4 of the Tynwald Proceedings Act 1876, sections 1 to 4 of the Privileges of Tynwald (Publications) Act 1973 and sections 2 to 4 of the Tynwald Proceedings Act 1984.
Copies o f this Report may be obtained from the Tynwald Library, Legislative Buildings, Bucks Road, Douglas IM1 3PW (Tel 01624 685516, Fax 01624 685522) or may be consulted at www.tynwald.org.im
All correspondence with regard to this Report should be addressed to the Clerk o f Tynwald, Legislative Buildings, Bucks Road, Douglas 1M1 3PW.
r
i _
To: The Hon Noel Q Cringle MLC, President of Tynwald, and theHon Council and Keys in Tynwald assembled
REPORT OF THE SELECT COMMITTEE ON GP OUT OF HOURS SERVICES
PART 1: BACKGROUND, HISTORY AND STRATEGY
1.1 Background:
1.1.1 At the sitting of Tynwald Court on 18th June 2003 it was resolved that a Select
Committee of five members be established to -
"investigate the matter o f the General Practitioners 'Out o f Hours Services' being
provided throughout the Island, with -power to take written and oral evidence
pursuant to sections 3 and 4 o f the Tynwald Proceedings Act 1876 and report by
October 2003."
1.1.2 After a ballot Mr Gelling, Mr Gill, Mr Singer, Mr Speaker and Mr Waft were
elected, and at the first meeting Mr Speaker was elected as Chairman.
1.1.3 Your Committee has held fourteen meetings.
1.1.4 The Chairman of your Committee made a Statement to Tynwald Court in
October 2003 to explain that it had proved impossible to meet the deadline of
reporting to the Honourable Court by October 2003 because of the vast
amount of evidence that the Committee had received. Evaluation of this
evidence, together with pursuing various lines of enquiry consequential from
it, have meant that only now is your Committee able to report to Tynwald
Court.
1.2 Strategy:
1.2.1 Your Committee resolved to undertake its inquiry in the following way:
(a) To invite any interested members of the public, or any interested
bodies, to submit views in writing. To facilitate this, your Committee
placed adverts in the local press and on Manx Radio and gave a
deadline of 12th September 2003 for submissions to be received. Due to
the volume of submissions being received the deadline was
subsequently extended by two weeks;
(b) To invite all General Practitioners in the Isle of Man to submit views in
writing. This was facilitated by writing to all General Practitioners and
also to the Chairman of the GP sub-committee of the Isle of Man
Medical Executive;
(c) To invite Members of Tynwald to submit views in writing. To
facilitate this all Members of Tynwald received a letter inviting them to
submit written evidence;
(d) To invite the Minister for Health and Social Security and the Director
of Public Health to submit evidence in writing. To facilitate this the
Minister and Director were written to separately to invite them to
submit written evidence; and
(e) To take oral evidence from selected parties once the written evidence
had been received and analysed. Oral evidence was taken in three
sessions, the first on Thursday 18th December 2003 in Ramsey Town
Hall, the second on Wednesday 28th January 2004 in the Millennium
Conference Room and the third on Friday 7th May 2004 in the
Millennium Conference Room.
2
Those who gave oral evidence on 18th December 2003 were
Dr M Maska on behalf of the GP sub-committee of the IOM Medical
Executive, Mr S Sieling, Deputy Senior Ambulance Officer Isle of Man
Ambulance Service and Mr R Beattie Operations Manager Ambulance
Service, Mr and Mrs Penrose on behalf of the Ramsey Cottage Hospital
League of Friends, Mrs A V Craine MHK, Mr P Gawne MHK,
Hon A R Bell MHK and Hon S C Rodan MHK.
A copy of Hansard recording the oral evidence given to your
Committee on 18th December 2003 is attached to this Report as
Appendix 6.
Those who gave oral evidence on 28th January 2004 were
Mr J D Cannan MHK, Mr R E Quine MHK, the Hon C Christian MLC,
then Minister of the Department of Health and Social Security,
Mr D Killip, Chief Executive of the Department of Health and Social
Security, the late Mr G Newbury, General Manager Primary Health
Care, Mrs S Duke, Family Practitioner Services Manager (who
administers MEDS), and Ramsey Town Commissioners who were
represented by Mr R Radcliffe, Ramsey Town Commissioner and
Mr P Whiteway Ramsey Town Clerk.
Those who gave oral evidence on 7th May 2004 oral evidence were
Mr J Wilson, Head of the Health Services Division and Mr A Jones
Acting General Manager Primary Health Care Service.
Copies of the Hansards recording the oral evidence given to your
Committee on 28th January 2004 and 7th May 2004 are attached to this
Report as Appendix 7.
(f) To carry out visits to Ramsey Cottage Hospital and the Manx
Emergency Doctor Service (MEDS) premises at the new Nobles
Hospital. A pre-arranged visit to Ramsey Cottage Hospital took place
on Thursday 18th December 2003. The MEDS facility was visited,
3
unannounced, on the evening of 10th March 2004. Your Committee
gave prior notice to the Primary Health Care Service that it intended to
visit MEDS during the week of 8th to 14th March but did not indicate
when during that time the visit would occur.
(g) To make specific recommendations, if investigation warranted doing
so, about the out of hours services offered by General Practitioners on
the Isle of Man, and how it may be improved.
1.3 History of Out of Hours General Practitioners Services in the Isle of Man:
1.3.1 Out of hours services are defined as those provided on weekdays between
6.00 pm and 8.00 am and at all times of the day over weekends and bank
holidays. GPs are self employed professionals and until 31st March 2004
worked under terms set down in the National Health Service (Isle of Man)
General Medical and Pharmaceutical Services Regulations 1978. Since
1st April 2004 they work under the terms of the new Contract. The
Regulations in force until 31st March 2004 required that GPs should give
treatment personally or ensure treatment was available by another doctor
acting as a deputy at all times. This meant each GP Practice was responsible
for actually providing, or arranging the provision of, out of hours care for
their patients.
Copies of the National Health Service (Isle of Man) General Medical and
Pharmaceutical Services Regulations 2004 and the new General Practitioners
Contract effective from 1st April 2004 are available for inspection in the
Tynwald Library. These documents were too bulky to be appended to this
report.
1.3.2 Your Committee understands that the out of hours service provided by
General Practitioners consist of the provision of an emergency, but non life
threatening, medical facility for patients who have a condition which requires
treatment before their GP surgery re-opens. It is not designed to provide
treatment for acute life threatening emergencies, for example for heart
4
attacks, strokes etc. Acute life threatening conditions should be dealt with
through the 999 emergency services and the Accident and Emergency
Department at Nobles Hospital.
1.3.3 It was usual for each GP practice to arrange its own out of hours coverage for
patients. In a larger practice this could mean that each doctor was required to
provide cover for one or two sessions a week, but in smaller practices this
could mean that an individual GP had to provide out of hours cover much
more often, or arrange for someone to act on his/her behalf.
1.3.4 The requirement for providing out of hours cover for patients was obviously
demanding, particularly for doctors in smaller practices. Therefore, in July
1998 a number of GP Practices decided to provide out of hours cover through
the establishment of a co-operative. This co-operative was known as
"MannDoc" and eight of the eleven GP practices decided to take part. The
Practices in Laxey, Ramsey and Port Erin were not involved. "MannDoc"
provided for an out of hours co-operative service by which a GP, from one of
the practices involved, provided out of hours cover from a central point
(which was located within the old Nobles Hospital). In evidence your
Committee was advised that the doctors benefited from a significant
reduction in out of hours work and that in turn meant the patients were
treated by less tired doctors.
The service was funded partly through the out of hours element in GPs pay
(which amounted to about £6,000 per annum per doctor, plus £26.30 for each
out of hours home visit undertaken) and partly from the Department of
Health and Social Security. The Department provided premises at the old
Nobles Hospital, the costs of a receptionist and a car and driver for the doctor
to use when visits were required. In the financial year 2001 / 02 this amounted
to £61,560. GPs who participated in "MannDoc" paid into "MannDoc" the
allowance they received from the Department of Health and Social Security
for providing out of hours cover. "MannDoc" used this money to pay fees to
those doctors who undertook "MannDoc" shifts. In the financial year
2001 / 02 participating GPs paid £214,600 into "MannDoc" for this purpose.
5

1.3.5 In the case of the Ramsey Group Practice, prior to April 2003, the GPs
provided out of hours patient care themselves, and did not elect to join
"MannDoc". Under a separate agreement, they also provided staffing for the
Ramsey Cottage Hospital Urgent Treatment Centre on a 24 hours a day, seven
days a week basis, for which an additional payment was provided by the
Department of Health and Social Security.
1.3.6 Following a letter from the General Practitioners to the Chief Minister in
November 2001, the Department of Health and Social Security established a
Joint Negotiating Committee consisting of both GPs and Departmental
officials to work towards the modification of GP contracts on the Isle of Man.
This body began meeting in February 2002. A copy of the letter to the Chief
Minister may be found in Appendix 5.1 of this Report as Appendix 2 of the
evidence supplied by the Department of Health and Social Security dated
10th April 2003.
The negotiating of a new Contract was regarded as necessary because GPs in
England were in the process of negotiating new contracts and it was very
likely that their new contract would remove GP responsibility for out of hours
services. Since England was the chief source of recruitment for Island GPs, a
similar contractual arrangement was thought to be essential. It was put to
your Committee that if the Island's General Practitioners had to work under
terms, they considered, more onerous than those of their colleagues in
England, it could be that doctors would not be willing to work in the Isle of
Man.
1.3.7 One of the major issues this Joint Negotiating Committee dealt with was that
of out of hours services. At a meeting of the Committee on 17th April 2002,
the GPs indicated that they wished out of hours services to be negotiated
separately to the provision of general medical services. In addition, at the
same meeting, their representatives stated that while some younger GPs may
wish to continue to provide out of hours work they would appreciate a choice
in the matter, and that the workload for those involved in "MartnDoc" was
too great. Finally at that meeting the GP representatives stated that GPs had
to pay more to be part of "MannDoc" than they received from the
Department for out of hours cover. The GPs were keen to see the issue of out
of hours services dealt with as a priority.
6
1.3.8 Following the meeting of 17th April 2002 and the evident pressure from GPs to
speedily deal with out of hours services, the Department of Health and Social
Security decided, in negotiation with the GP's representatives, that a new
system for out of hours GP care was required throughout the entire Island,
and that this system would be organised and administered by the
Department. The Department could have insisted that the General
Practitioners continue to provide out of hours care until the new Contract was
agreed and put into effect (1st April 2004) but it was decided to progress the
matter more immediately.
The new scheme established by the Department is known as the Manx
Emergency Doctors Service (MEDS), and it commenced operation on
1st April 2003, replacing "MannDoc". It provides for Island wide out of hours
GP cover, from a central base, which is now at the new Nobles Hospital. This
arrangement was introduced one year before the original GP Contract
expired, under which GP's had the responsibility of providing out of hours
care, and also before the new GP Contract in England came into force which
removed the requirement for GPs to undertake out of hours services.
1.3.9 MEDS is staffed by individual GPs (and a number of other doctors who are
not registered as GPs but who are qualified to undertake this work) who are
willing to participate in it. Of the 46 GPs on the Island the vast majority
perform some work for MEDS, although the number of shifts undertaken by
each individual doctor does vary both between doctors and for individual
doctors over time. A summary of doctors involved in the MEDS rota between
January and March 2004 is included in the Report as part of Appendix 5.2.
However, to preserve the anonymity of the Doctors, random numbers have
been used in place of the names of the individuals concerned.
1.3.10 Between 6.00 pm and 8.00 am each day, one GP is available at the new Nobles
Hospital, with a second on call. The on call doctor would be summoned by
the duty doctor should the workload demand it. Information received from
the Primary Care Service indicates that from the inception of MEDS until
20th February 2004 the standby doctor had only been called out on one
occasion because of excessive workload, and that on four other occasions a
doctor has extended his/her shift because of excessive workload. On a
Saturday, Sunday and public holiday between 8.00 am and 6.00 pm a second
doctor is also on duty at the new Nobles Hospital premises.
1.3.11 On weekdays, doctors work two shifts, one from 6.00 pm to midnight and the
second from midnight to 8.00 am. At the weekend and over bank holidays
there are four shifts, midnight to 8.00 am, 8.00 am to noon, noon to 6.00 pm
and 6.00 pm to midnight.
1.3.12 The duty doctor is contacted by telephone and may choose to give telephone
advice, ask for the patient to visit the MEDS surgery or arrange to visit the
patient at home, although home visits are the least common outcome of
contacting MEDS. During weekday evenings until midnight, and during the
daytime at weekends, the telephone is initially answered by a receptionist.
There are three receptionists who work on a rota basis. The receptionists take
details from the patient in writing and then pass them to the duty doctor. If
the doctor is out on a call, the receptionist will judge whether it is necessary to
contact the doctor by telephone, wait until he/she returns or if necessary
summon an ambulance. After midnight, all calls to MEDS are answered by
the duty doctor.
1.3.13 If the duty doctor believes it is necessary to visit a patient at home, MEDS
provides a car and driver to transport the doctor. In addition, the doctor
carries a mobile phone so that he /she can be contacted by the receptionist.
Both the duty doctor and driver who are on the midnight to 8.00 am shift are
allocated bedrooms in the Hospital complex to enable them to sleep between
calls.
1.3.14 Figures supplied by the Primary Health Care Service for the period
1st April 2003 to 31st December 2003 indicate that of the 10,450 calls received
by MEDS 4,454 (42.6%) resulted in an appointment being made at the MEDS
centre in Douglas, 4,770 (45.6%) resulted in telephone advice being given and
1,226(11.7%) resulted in a doctor visiting the patient at home. During this
period the largest number of contacts made with MEDS was
27th December 2003 when the service received 173 calls during a 24 hour
period, w hilst the fewest num ber of contacts occurred on
20th/21st August 2003 when between 6.00 pm and 8.00 am there was only one.
(Full details of statistics for the period 1st April 2003 to 31st December 2003 are
included in the Report in Appendix 5.2).

1.3.15 Doctors receive an additional payment from the Department of Health and
Social Security for MEDS shifts. The amount depends upon the shift worked;
the payment, per hour, ranging from £42 to £90. The most expensive shift,
paid at £90 per hour, is that between midnight and 8.00 am on a Monday
morning. We were advised that the shifts that offer the highest rates of pay
are those for which it is hardest to attract cover. The standby doctor receives
a flat rate of £10 per hour for being on call but should he/she be called in they
would receive the normal fee for that shift. From oral evidence given on
7th May 2004 by the Head of thé Health Service Division, your Committee
understands that the rates of pay for MEDS shifts are broadly similar to those
paid elsewhere in the British Isles where similar services operate.
GPs have given up the annual payment from the Department of Health and
Social Security of £6,000 plus the fee for each out of hours home visit, which
were part of their original contract for providing out of hours care. However,
an individual GP may well be able to more than compensate for that financial
loss by working a sufficient number of MEDS shifts. Whether a GP is
financially better or worse off under the MEDS system depends on that
individual's level of involvement in MEDS, which is a matter of personal
choice. Your Committee has figures supplied by the Department of Health
and Social Security which indicate some doctors receive as little as £220 a
month for involvement in MEDS while others have earned over £4,000 in a
single month. (A statistical summary of payments made to GPs for MEDS
work is included in this Report in Appendix 5.2).
1.3.16 The DHSS Family Practitioner Services Manager co-ordinates the operation of
MEDS and sends out blank rotas for the participating doctors to fill in. Shifts
are generally filled on a "first come first served basis/. If more than one doctor
should express an interest in a shift where only one is needed, the name of the
first doctor to offer himself/herself for that shift is chosen. Your Committee
understands that on no occasion has it proved impossible to fill a shift
although at certain times, such as school summer holidays, it is more difficult
to find doctors to staff the service.
9
1.3.17 Accommodation for MEDS at the New Nobles Hospital is provided in the
Fracture Clinic. No purpose built accommodation is available for MEDS
largely because the new hospital was planned in the early 1990s before the
introduction of "MannDoc" and subsequently MEDS. Your Committee
understands that the Department of Health and Social Security are aware that
the current premises are not ideal. The issue of accommodation is further
dealt with in paragraphs 2.4.6,2.9.3 and 2.9.4 below.
1.3.18 The new GP Contract came into operation on 1st April 2004. This Contract
formally relieved the GPs from the responsibility of having to provide out of
hours care. A General Practitioner could opt into providing such care if
he / she wished, but the Department correctly believed that no GP would opt
into the provision of out of hours care when the new Contract came into
effect. The new Contract is made under the provisions of Section 31 of the
National Health Service Act 2001, which came into operation on
1st February 2003 (reference NHS (Appointed Day) (No. 2) Order 2002). A
copy of the new GP Contract is available for consultation in the Tynwald
Library.
1.3.19 Removal of the responsibility for providing out of hours care by GPs was
partly the result of pressure from existing GPs and partly because it would be
difficult for the Isle of Man to recruit General Practitioners if there was still a
contractual requirement to provide out of hours services, when such a
requirement did not exist in the United Kingdom. We were advised that the
issue of GP recruitment is a serious one because a large number of Isle of Man
GPs (as many as 50%) might retire within the next ten years particularly if the
old system continued. GP recruitment is already proving to be difficult in
many parts of England. Even in the Isle of Man, where Practices seeking to
recruit do emphasise the benefits of Island life, we were advised that there are
sometimes only a handful of applicants and posts have had to be
re-advertised. We understand that the Department of Health and Social
Security seeks to support GP practices in promoting the Island for
recruitment purposes; for example by offering a Relocation Scheme which
provides for 90% of the costs involved in relocation, up to a maximum set by
the Department.
10
1.3.20 A copy of the Department of Health and Social Security Policy Document
detailing the operation of the Emergency Doctor Service is attached to this
Report as Appendix 5.1.
1.4 Ramsey Cottage Hospital Out of Hours Service:
1.4.1 Your Committee has received a considerable volume of evidence concerning
the present and future role of Ramsey Cottage Hospital, much of which is not
within its remit. However, we are aware that the Department of Health and
Social Security commissioned an independent Review of Ramsey Cottage
Hospital that was laid before Tynwald in March 2004. This Review addresses
many of the issues raised in submissions to this Committee that are beyond
its remit. Debate on the Independent Review was adjourned from the
March 2004 pending the presentation of this Report to Tynwald Court. This
would give an opportunity for Tynwald Court to consider the
recommendations of Review and the Report. A copy of the Independent
Review may be consulted in the Tynwald Library.
1.4.2 Out of hours emergency medical cover at Ramsey Cottage Hospital has
historically been provided by doctors from the Ramsey Group Practice. It has
been organised through a number of contracts between the Department of
Health and Social Security and the Ramsey Group Practice, which were
distinct from the contractual requirement for Ramsey Group Practice to
provide out of hours GP care for its patients. Under the terms of these
contracts, doctors in the Ramsey Group Practice provided medical staffing
24 hours a day seven days a week for the Urgent Treatment Centre at Ramsey
Cottage Hospital, as well as 24 hours a day seven days a week in patient
cover at the Hospital. This Contract could be terminated by either party, with
one month's notice.
On 26th February 2003 the Ramsey Group Practice informed the Department
that it intended to terminate the out of hours staffing of the Urgent Treatment
Centre at the Cottage Hospital with effect from 1st April 2003. Whilst this
contract was terminated, the Group Practice has continued with the contracts
11
that provide for staffing the emergency facility during the day time on week
days and also out of hours in patient cover on a 24 hours a day seven days a
week basis. Because of the removal of medical staffing out of hours in the
Urgent Treatment Unit, the Department of Health and Social Security had to
downgrade this facility to become a Minor Injury Unit. This Unit is covered
by the Ramsey GPs during week days between 8.00 am and 6.00 pm, but its
opening hours in the out of hours periods, have been reduced to 6.00 pm to
10.00 pm on week day evenings only when it is staffed by nurse practitioners.
This Unit is closed after 10.00 pm on week days, at weekends and on bank
holidays. In addition, no patient may be admitted to Ramsey Cottage
Hospital during the out of hours periods, because of the withdrawal of the
medical service provided by the Ramsey Group Practice.
1.4.3 It was clear to your Committee in studying the submissions it received that
many people, particularly in the north of the Island, feel very strongly about
the lack of 24 hours a day seven days a week minor injury provision at
Ramsey Cottage Hospital and also the inability of that Hospital to receive any
admissions during out of hours periods. Many submissions urged that these
facilities needed to be re-introduced. Clearly, this Committee's existence has
been viewed by some as a vehicle for promoting that cause. Your Committee
was also made aware of the strength of feeling expressed at the public
meetings held in Ramsey in May 2003 and May 2004, when large numbers of
people participated in public protests about the alteration to GPs out of hours
arrangements and the reduction in services at the Cottage Hospital.
1.4.4 Your Committee acknowledges the many submissions it has received
regarding the future of Ramsey Cottage Hospital even though this may be
strictly beyond its remit. It has noted the strength of feeling expressed by
many residents in the north of the Island. This issue is discussed further in
Paragraph 3.9 (ii) (a & f) below.
12
PART 2:
EVIDENCE RECEIVED
2.1 Because of the large volume of evidence, your Committee has decided that
the evidence submitted by each group should be considered separately in this
Report:
2.2 Evidence from members of the public:
2.2.1 Your Committee was in receipt of a large number of individual responses
from members of the public. By the closing date for submissions, nearly
130 individual submissions were received from members of the public, some
of which were signed by more than one person. In addition, another
15 individual submissions were received via Ramsey Cottage Hospital
League of Friends and some 125 completed questionnaires, commissioned by
Ramsey Town Commissioners concerning the issue, were also forwarded to
the Committee. Since the closing date for submitting written evidence, your
Committee has continued to receive evidence, particularly from the north of
the Island, regarding problems experienced with out of hours care.
2.2.2 Your Committee noted that a very high percentage of individual submissions
came from the northern part of the Island (defined for this purpose as being
north of a line from Kirk Michael to Laxey). The south of the Island (from
Ballasalla southward) provided the second most numerous geographic source
of individual submissions, with the fewest coming from the Douglas area.
2.2.3 Analysis of these individual responses, particularly those from the north and
south of the Island, indicated a number of common concerns. These may be
summarised principally as:
(a) Concern was expressed at the removal of out of hours GP coverage by
doctors from the patients own Practice. Evidence received indicated
that a MEDS duty doctor would probably not know the medical
history of the patient and many respondents plainly would prefer to be
seen by a General Practitioner from their own practice;
13
(b) Concern was expressed about the time it may take for a patient to
reach the new Nobles Hospital from the north or south of the Island.
Problems of snow, ice and fog were all raised as potential causes for
delay in reaching Nobles Hospital, and road closures for racing or due
to accidents were also considered to be a major problem;
(c) Concern was expressed at the problems which some individuals may
encounter in trying to reach MEDS facility at the new Nobles Hospital
during the out of hours periods if they are unable to drive themselves
or do not have someone who could drive them. Some evidence
received pointed out the difficulty in obtaining a taxi in the middle of
the night as well as the high cost of doing so, and the danger that the
ambulance service would in effect be called upon to deliver patients to
the MEDS unit simply because they had no other way of reaching it.
That would, of course, mean the ambulance may not be available for a
medical emergency. A number of submissions also referred to the
difficulty, in the early hours of the morning, of obtaining transport to
return home once a consultation at MEDS had been completed.
Inquiries made by your Committee suggest that taxis services are
available throughout the night. However, in some parts of the Island
services are not always available throughout every night (particularly
week nights) and it may be that a taxi would have to be called from
Douglas, where there are a number of firms that operate on a 24 hour
basis. The approximate cost of a taxi from either Ramsey or Port Erin
to the MEDS centre in the early hours would be about £30 each way. If
a taxi was unavailable from the area in which a patient lived and one
had to be summoned from Douglas, the time delay in reaching MEDS
would be greater. However, there is no additional cost in having to
call a taxi from Douglas to another part of the Island to pick up a
patient. All taxi fares are charged on a meter at a rate set down by the
Road Transport Licensing Committee.
14
(d) Concern was expressed about the perceived unwillingness of the
MEDS duty doctor to make house calls;
(e) Concern was expressed in evidence received, from the north of the
Island, about the decision of the Ramsey GPs to withdraw staffing
from the Urgent Treatment Centre at Ramsey Cottage Hospital and the
consequent changes at the Hospital which resulted; and
(f) Concern was expressed in a number of submissions regarding the
perceived lack of adequate ambulance cover available in both the north
and south of the Island, and the fact that the ambulance based in the
north would often be away from its locality transporting patients to
Nobles Hospital, This could lead to long delays in an ambulance
arriving in response to a call out. Indeed some evidence received by
your Committee suggested that on occasion ambulances took over
40 minutes to reach a call in the north of the Island.
2.2.4 Your Committee noted that only a relatively small number of individuals
supplied evidence to the effect that the treatment received from MEDS had
been less than adequate or not promptly provided. Of those who did express
concern over the actual treatment received from MEDS, the most common
complaints were that a doctor refused to make a home visit or the doctor had
no knowledge of the patient's medical history. A number of submissions also
believed that there might be a problem in locating a patient's home if a duty
MEDS doctor came from a different part of the Island. However, we
understand that the MEDS driver can telephone the Joint Emergency Services
Control Room for assistance in locating a particular address. It was also clear
from reading quite a number of submissions that many were based on the
"what if" scenario rather than upon actual experience.
2.2.5 Very many of those individuals submitting evidence requested that 24 hour a
day emergency cover be restored forthwith at Ramsey Cottage Hospital. In
total 150 submissions called for this service to be restored. Some argued that
this should be undertaken once again by the doctors from the Ramsey Group
Practice, while others suggested that the Department of Health and Social
Security should employ doctors for the purpose, whilst a few suggested that
24 hour cover by nurse practitioners should be provided.
15
2.2.6 A copy of the press notice inviting members of the public to submit evidence
in writing is included in this Report as Appendix 1. Because of the large
number of individual submissions received, it has not been possible to
include them as an appendix in this Report. However, these submissions
(together with the questionnaires produced by Ramsey Town
Commissioners) are available for consultation in the Tynwald Library.
Appendix 1 does contain a list of the names of those members of the public
who did submit written evidence to your Committee-
2.2.7 Because some of the individual submissions do contain personal medical
information, a number of individuals have asked that their evidence should
not be made public. Therefore, Appendix 1 of this Report also contains a list
of names of those submitting evidence who wish it to remain confidential.
2.3 Evidence received from interested bodies:
2.3.1 Written submissions were received from a variety of interested bodies, these
included Ramsey Cottage Hospital League of Friends, Bride, Lezayre, and
Ramsey Commissioners, Kirk Andreas Women's Institute, and Grest
Residential Home in Ramsey. Oral evidence was also taken from Ramsey
Cottage Hospital League of Friends on 18th December 2003.
2.3.2 Once again your Committee noted that almost all the evidence from
interested bodies came from those working in the north of the Island.
2.3.3 The clear emphasis contained in evidence from these interested bodies was
the perceived inadequacy of out of hours medical care, particularly in the
north of the Island. Issues similar to those voiced by submissions received
from members of the public were raised, such as the difficulty of reaching
Nobles Hospital at night. Some of the evidence cited the unwillingness of
MEDS doctors to make home visits and much of it also expressed strong
reservations about the closure of the Minor Injuries Unit at Ramsey Cottage
Hospital during the out of hours periods. These issues were of particular
concern to residential homes, where the staffing levels necessary to send a
member of staff with a resident to the MEDS centre at Nobles Hospital during
16
the night may not be available. A common thread in the evidence received
from interested bodies was the desire to see the facilities at Ramsey Cottage
Hospital returned to what they had been prior to April 2003.
2.3.4 Whilst all the evidence received from interested bodies was of great value to
your Committee during its investigations; that submitted, both in writing
and orally, by Ramsey Town Commissioners and the Ramsey Cottage
Hospital League of Friends was the most extensive provided by interested
groups. A common thread in the evidence submitted by both these bodies
was the importance of restoring 24 hour a day seven day a week facilities at
the Cottage Hospital and improving access to General Practitioners during
the out of hours periods. Both bodies felt that the distance required to travel
to Douglas to consult a GP during the out of hours periods was excessive
particularly given the problems of possible bad weather and road closures
due to racing or accidents.
2.3.5 A copy of the press notice inviting interested bodies to submit evidence in
writing and the written submissions received by your Committee from
interested bodies are attached to the Report as Appendix 2. A copy of the
Hansard giving the oral evidence from Ramsey Cottage Hospital League of
Friends is included in the Report as Appendix 6.
2.4 Evidence received from General Practitioners:
2.4.1 In total 28 Isle of Man General Practitioners responded to the request from
your Committee for written evidence. Most submissions came from
individual GPs although some were signed by several members of a practice,
for example that received from Kensington Road Group Practice. In addition,
a written submission was received from Dr Maska on behalf of the GP
sub-committee of the Isle of Man Medical Executive, and he also gave oral
evidence to your Committee on 18th December 2003.
2.4.2 Your Committee notes that the majority of submissions received from General
Practitioners indicated that they would not be willing to return to the old
system of each practice having responsibility for its own out of hours patient
care. The growth in the volume of work and demands on the time of family
17
doctors were stressed as being the main reasons why General Practitioners
found it no longer acceptable to undertake practice based out of hours
services. Indeed, some evidence made it abundantly clear that a return to the
old system would, in their opinion, make it very difficult to recruit GPs to the
Isle of Man in future and even to retain existing General Practitioners.
The recruitment of GPs was identified as a major issue given the high age
profile of many present Manx General Practitioners. A high percentage of
Manx GPs would be eligible for retirement (one piece of evidence suggested
this was as high as 50%) within the next 10 years, and if out of hours services
were a requirement for all Island GPs, it was felt that it would be very
difficult to fill these posts. We were advised that this whole issue is set in the
context of extreme difficulties experienced in recruitment of General
Practitioners in the United Kingdom because of the shortage of doctors
entering General Practice. It was also pointed out to your Committee that
many of those who are entering General Practice are female and a significant
proportion of whom do not wish to work full-time because of family
responsibilities.
2.4.3 Some evidence received from GPs indicated that the quality of treatment
given by doctors required to work excessive hours through providing out of
hours cover may well not be to the same standard as that which a GP could
deliver who was not required to provide out of hours care. In addition, some
General Practitioners indicated that such long hours may intrude upon their
social and family lives.
The evidence presented to your Committee by the Doctors suggests that the
traditional ethos of a GP accepting unsociable hours as part of his or her
vocation is no longer acceptable as Gps' expectations have changed in respect
of the right to leisure and family time.
2.4.4 Your Committee also noted that the overwhelming evidence from the GPs
indicated that, in their opinion, the MEDS service was a satisfactory way in
which to provide out of hours cover. Several pieces of evidence argued that
the ratio of doctor to patient provided by MEDS was much higher than in
18
many parts of the United Kingdom and that the geographical area covered by
MEDS was smaller than that covered by many similar organisations within
the United Kingdom. Some evidence also indicated that it was more sensible
for one or two doctors to be on call through MEDS rather than to have one in
each practice who might be disturbed two or three times a night.
Furthermore, several GPs observed that nowhere in the Island is far from the
centrally located MEDS facility and that the vast majority of patients have
access to transport to reach it.
2.4.5 It was also evident from reading some of the evidence supplied by GPs that
some doctors were less inclined to work for MEDS than others. Some GPs
believed the answer to staffing of the out of hours service lay in the
Department of Health and Social Security undertaking to directly employ a
number of doctors to staff MEDS, so that General Practitioners need not be
involved at all.
2.4.6 It is clear to your Committee, from the evidence received from GPs, that one
big problem with the MEDS provision is the lack of adequate facilities for the
service at Nobles Hospital. Twelve GPs made the point that the need to share
accommodation with the Fracture Clinic was less than ideal. (For further
details concerning the problem of accommodation see paragraph 2.9.3 and
2.9.4 below). Furthermore, some General Practitioners submitting evidence
believe that the MEDS premises required fax and computer links, better
signage to assist the public to locate it and more drugs trolleys. A number of
GPs also felt it would be helpful to have access to patient medical records.
However, this was not regarded as critical by the duty doctor to whom your
Committee spoke, during our visit to MEDS. Finally, some GPs suggested it
would be a sensible improvement for MEDS to have a nurse led triage facility
(triage being the assessment of a patient and the decision as to which
treatment route should be taken) by which all incoming calls were taken by a
nurse who could then decide whether the case required the attention of a
doctor or not.
2.4.7 A copy of the letter circulated to all General Practitioners inviting them to
submit evidence in writing together with the written submissions received
from the GPs, except from those that wished their submissions to remain
19
confidential (in such cases a list of names is included at the end of Appendix 3
to indicate that confidential evidence had been received) is attached to the
Report as Appendix 3. A copy of the Hansard detailing the oral evidence
from Dr Maska is included in the Report as Appendix 6.
2.5 Evidence received from Members of Tynwald:
2.5.1 Ten Members of Tynwald provided written submissions to the Committee.
They were Hon A R Bell MHK, Mr J D Q Cannan MHK,
Mrs A V Craine MHK, Mr A J Earnshaw MHK, Mr P A Gawne MHK,
Mrs H Hannan MHK, Mr R E Quine MHK, Hon J Rimington MHK,
Hon S C Rodan MHK and Mr L I Singer MLC
2.5.2 Your Committee noted that the majority of submissions came from Members
in the north of the Island, with Members from the south being the second
most numerous in geographic terms.
2.5.3 Your Committee observed that all the evidence supplied by Members
indicated dissatisfaction with the level of out of hours services currently being
provided. The argument of the Department of Health and Social Security that
the new system provided a better out of hours service was widely discounted.
Members indicated, both in written and oral evidence, that many constituents
had voiced their fears and complaints about MEDS on numerous occasions
and that some complaints were still being received nearly a year after the
introduction of the service. However, in oral evidence some Members did
indicate that the number of comments they were receiving about MEDS had
declined as the system settled down. One Member indicated that he was now
receiving a few positive comments about the service, although another
believed that the reduction in protest may only be temporary, awaiting the
outcome of your Committee's deliberations. We note that letters of concern
are still being circulated to Members of Tynwald and as a Committee we, too,
have also continued to receive such letters. We have taken note of these.
20
2.5.4 It was a general consensus, amongst Members submitting evidence, that
improvements were required. A variety of suggestions were offered. Some
Members suggested that improvements could come via the provision of more
MHDS duty doctors, perhaps one to cover the south and another the north of
the Island; others suggested that resident doctors could be employed at
Ramsey Cottage Hospital; while others suggested a 24 hour a day nurse
practitioner service could be operated at Ramsey Cottage Hospital and in the
south of the Island. One Member proposed that a video conferencing link
should be established between Ramsey Cottage Hospital and Nobles Hospital
to permit doctors at Nobles to give expert advice to the nurse practitioners on
duty at Ramsey.
2.5.5 A copy of the letter inviting Members of Tynwald to submit evidence in
writing together with the written submissions received from Members of
Tynwald is attached to this Report as Appendix 4. A copy of the Hansard
detailing the oral evidence from Hon A R Bell MHK, Mrs A V Craine MHK,
Mr P A Gawne MHK and Hon S C Rodan MHK is included in the Report as
Appendix 6, and a copy of Hansard detailing the oral evidence from
Mr J D Q Cannan MHK and Mr R E Quine MHK is included in the Report as
Appendix 7.
2.6 Evidence received from Government Departments
The Department of Health and Social Security:
2.6.1 The Department of Health and Social Security provided comprehensive
written evidence to the Committee, as did Dr P Emerson, Consultant in Public
Health Medicine on behalf of Dr I Maclean, Director of Public Health. In
addition the then Minister (Hon C M Christian MLC) and Chief Executive of
that Department gave oral evidence. Further written and oral evidence was
supplied by Mr J Wilson, Head of the Health Services Division, the late
Mr G Newbury, Director of Primary Health Care, Mr A Jones, Acting Director
of Primary Health Care, Mrs S Duke, the Family Practitioner Services
21
Manager (who administers MEDS), Mr S Sieling, Deputy Chief Ambulance
Officer of the Isle of Man Ambulance Service and Mr R Beattie, Operations
Manager Isle of Man Ambulance Service.
2.6.2 The Department of Health and Social Security made several written
submissions. The main submission, dated 10th September 2003, came from the
Director of Corporate Affairs, and where reference to it is made within this
section, it will be referred to as "the main Departmental written submission".
The main Departmental written submission outlined the development of out
of hours care provided by GPs, together with responses to various specific
questions asked by your Committee. Your Committee was interested to note,
from the main Departmental written submission, that the evidence indicated
that the DHSS was generally satisfied with the current situation for out of
hours provision. On page 6 of the main Departmental written submission, in
response to the question of whether the Department is satisfied with the
current situation, it was stated that:
"Whilst the extended Service, with its increased medical cover, has only been
in place since 1st April 2003, the early indications are that the out o f hours
cover continues to be effective in meeting the care needs o f patients."
Given the volume of evidence received by the Committee from the public and
other interested bodies, it seems that the Department's view is somewhat at
variance with much of the evidence received. We were also interested to hear
the then Minister (Hon C M Christian MLC) continue to claim, when giving
oral evidence, that MEDS provided an improved out of hours service to that
previously available. Such a view does not coincide with much of the
popular perception concerning the service offered.
2.6.3 Your Committee noted, from the main Departmental written submission, that
complaints received regarding the new system for out of hours care have, in
the main, been related to the principle of the new arrangements with few
formal complaints being received from patients regarding the actual care
provided by MEDS that required investigation. The Departmental evidence
helpfully included a list of comments received regarding MEDS as
22
Appendix 5 of its written evidence. This showed that 33 comments were
received between 1st April 2003 and 18th August 2003, mostly from the north
of the Island, and only two of which contained complaints about specific
issues.
2.6.4 Your Committee was also interested to learn, from the main Departmental
written submission, that the DHSS is seeking to explore ways in which
improvements could be made and noted that these included the possibility of
employing doctors exclusively for MEDS; the possibility of the introduction
of nursing staff to take initial calls from patients and undertake the initial
triage; the provision of some form of transport to MEDS for those who lacked
their own; and the potential for making greater use of paramedics and
improvements to the MEDS premise at Nobles Hospital. The Department
claim that the range of improvements being considered will improve the
service offered by MEDS.
2.6.5 On the question of increasing the number of MEDS centres and duty doctors,
your Committee noted, from the main Departmental written submission, that
the Department had given consideration to this issue but felt it would not be
feasible, partly on the grounds of cost, but primarily, because of the difficulty
of finding sufficient GPs willing to actually undertake the work. In addition,
the Department argue when giving oral evidence, that the number of patients
covered by MEDS was small enough to be dealt with by one central location,
2.6.6 Your Committee received a submission from the Public Health Directorate
which came as part of the Department of Health and Social Security initial
written submission. This evidence identified two basic principles which
should be the core of out of hours service:
(a) patient access to out of hours medical services should be as simple and
straight forward as possible; and
(b) all the health professionals involved in the provision of this care
should work together to ensure the best possible service to patients
and use of resources.
23
In the opinion of the Director of Public Health, MEDS:
"delivers on both these principles"
(page 2 of submission which may be found in Appendix 5.3 of the Report).
2.6.7 The evidence from the Public Health Directorate included seven specific
recommendations to improve the Service. These include:
(a) the recruitment of a small number of salaried General Practitioners,
employed by the Department of Health and Social Security, to staff
MEDS;
(b) providing MEDS with the use of specialist trained nurse practitioners
as the first point of access for the public to the MEDS service; and
(c) a better flow of data between MEDS and the patients own GPs.
(A full list of the seven recommendations will be found on pages 8 and 9 of
the Director's written submission, which is included as Appendix 5.3 in the
Report).
2.6.8 The Health Services Division provided your Committee with details of the
total number of practising GPs in the Island and the ratio of GPs per head of
population both in the Isle of Man and in England, Wales, Scotland and
Northern Ireland. These figures show that there are 46 General Practitioners
on the Isle of Man NHS Medical List, a small number being part-time. There
is an average of one GP per 1,849 residents. The table below compares the
ratio of GPs per patient on the GP Lists in the Isle of Man compared with the
regions of the United Kingdom -
General Practitioners per head of practice population
Isle of Man 1 GP per 1,849
England 1 GP per 1,838
Wales 1 GP per 1,685
Northern Ireland 1 GP per 1,643
Scotland 1 GP per 1,378
24
It is clear from the table that the Isle of Man has the highest ratio of patients to
GPs in these areas. Your Committee was pleased to note that when giving
oral evidence, the Department did indicate that it is seeking to establish a
further GP Practice to help further reduce this ratio. This may help with the
staffing of MEDS because there may be more GPs potentially available.
2.6.9 Oral evidence was also taken from the Primary Health Care Service on two
occasions, the first being on 28th January 2004 and the second, on 7th May 2004.
In addition, during the course of our investigation, a considerable amount of
helpful written evidence was supplied by the Primary Health Care Service.
The Primary Health Care Service is responsible for the organisation of MEDS.
This evidence provided much useful information regarding how MEDS came
into being, how it is administered and how it is monitored. Your Committee
was informed that the service is regularly monitored and that such
monitoring has led to improvements, for example: additional staff being
made available to answer phones at times that have been identified as being
particularly busy. We were also advised that to date it had always been
possible to find sufficient doctors to cover all MEDS shifts. However, your
Committee was concerned to hear that there was no contingency plan in case
it ever proved impossible to staff a MEDS shift. In addition, we were
informed that there was no contingency plan in case of road closures caused
by adverse weather conditions, accidents or other problems preventing
patients from the north, west and south of the Island reaching the MEDS
facility at Nobles Hospital.
2.6.10 Written and oral evidence was also received from the Isle of Man Ambulance
Service. The Service has three responsibilities, providing a 999 emergency
service, responding to requests from GPs for urgent transportation of ill
patients to Hospital and the transportation of patients to out patients and day
care services. The transportation to out patients and day care facilities is
entirely beyond the remit of this Committee.
Since September 2003, to fulfil the 999 emergency service and to respond to
requests from General Practitioners to transport patients to hospital, the
Service provides three ambulances during out of hours periods. One is based
25
in Ramsey, one at Douglas and the third in Port Erin. There are also three fast
responder units available at night to cover the Island, subject to staff
availability. These are home based and can be called out when the ambulance
for an area is unavailable and an emergency call is received. Evidence
obtained from the Ambulance Service suggests such call outs are very rare, as
few as one or two a month. In order to overcome the problem that the fast
responder unit personnel may not be living in the area their vehicle was
designated to cover, the Ambulance Service has been engaged in a six month
trial (ending in August 2004) by which the fast responder units are on
standby for the service as a whole and not for one particular area.
The ambulances are staffed with at least one Paramedic, whilst the fast
response units may be staffed by an Ambulance Technician or a Paramedic.
An Ambulance Technician has completed an eight week approved ambulance
aid course at one of the regional Ambulance Training Centres. This training
involves all aspects of emergency care and Ambulance Technicians can
perform defibrillation and administer drugs for diabetic, asthmatic and
cardiac emergencies. They also undertake a three week advanced driving
course. A Paramedic has the same skills as an Ambulance Technician and in
addition has a further six weeks training at a regional Ambulaince Training
School plus four weeks in Nobles Hospital, This additional training enables
Paramedics to perform additional tasks such as intubation (passing a tube
into a patient's windpipe), infusion (administering fluids through a cannula
into a patient's vein) and the administering of a wider range of drugs.
When an ambulance is dispatched from one of the three stations, the
remaining two ambulances are moved to different locations to enable a
quicker response time to the area from which the ambulance has been called.
For example, if the Douglas ambulance is called out, the Port Erin ambulance
will move to Ballasalla so that it is closer to Douglas; or if the Ramsey
ambulance is called out, the Douglas vehicle will move to Cronk ny Mona.
Should both the Douglas and Ramsey ambulances be called out, then the
Port Erin ambulance is moved to the Douglas Ambulance Station. The
Ambulance Service has a target response time of reaching a 999 call within
8 minutes in 75% of cases and 19 minutes in 95% of cases. For urgent calls
26
from GPs, the response time is 15 minutes for 95% of calls. Your Committee
was informed that these response times are generally met and often the
targets exceeded. (Details of response times will be found in Appendix 5.4).
We were advised that following the introduction of the MEDS service the
number of calls upon the Ambulance Service has not increased significantly.
Figures supplied by the Ambulance Service indicate that in the eight months
April to November 2002 the total number of calls received by the Ambulance
Service for both 999 and GF urgent hospital transportation amounted to 5,049.
For the same period in 2003, which were the first eight months of operation of
the MEDS service, the total was 5,258, which is an increase of about 4%.
When the figures for the north of the Island only are examined, the total
number of calls received by the Ambulance Service (both 999 and GP urgent)
for the eight months April to November 2002 amounted to 1,090. In the same
period for 2003, the number was exactly the same although there were
marginally more calls for the 999 service and marginally fewer from General
Practitioners. This would suggest that the need for patients to travel to
Douglas, both as a 999 emergencies and GP urgent transportation requests,
rather than receive treatment in Ramsey Cottage Hospital, had not increased
the work load of the Ambulance Service to any significant degree.
2.6.11 A copy of the letter inviting the Minister of Health and Social Security and the
Director of Public Health to submit evidence in writing is included in this
Report as Appendix 5.1. All the written submissions received from all
sections within the Department of Health and Social Security are included in
the Report as Appendix 5. Appendix 5.1 contains the main Departmental
written submission dated 10th April 2003 together with subsequent written
submissions from the Health Services Division, Appendix 5.2 contains
evidence received from the Primary Health Care Service, Appendix 5.3
contains evidence received from the Public Health Directorate, and
Appendix 5.4 contains evidence received from the Ambulance Service. A
copy of the Hansard detailing oral evidence provided by the Ambulance
Service is included in the Report as Appendix 6. Copies of the Hansards
detailing oral evidence provided by the Minister and Chief Executive, the
27
Head of the Health Services Division and the Primary Health Care Service are
included in the Report as Appendix 7.
2.7 Department of Home Affairs:
2.7.1 The Department's submission related principally to the problem of
certification of sudden or unexpected death during the out of hours periods.
The evidence indicates that creation of "MannDoc" and now MEDS has
produced an unforeseen problem with regard to certification of sudden or
unexpected death during the out of hours periods.
2.7.2 Prior to April 2003 it was usual for a patient's own General Practitioner, or
one from that practice, to come to certify a sudden or unexpected death that
occurred during the out of hours periods. We were advised that the Police
Surgeon would only be involved where the Police considered the death to be
suspicious or if the patients GP could not be contacted or identified. In
practice these are only a very small proportion of all sudden death cases.
2.7.3 The introduction of "MannDoc" and more recently the MEDS means that the
deceased person's GP is no longer on call to undertake this work and the duty
MEDS doctor is generally unable to undertake the task. Consequently the
volume of work for Police Surgeons has increased.
2.7.4 In the light of this problem the Department of Home Affairs suggest that
some clear definition be given to the role of MEDS in regard to dealing with
sudden and unexpected deaths so that the Police Surgeon would only need to
be called if the circumstances were deemed to be suspicious. Furthermore,
the Department believe that alternative methods of certifying sudden and
unexpected deaths during the out of hours periods might be considered, such
as allowing the task to be initially undertaken by a paramedic so that the
body could then be moved to the Hospital where a duty doctor could confirm
that life is extinct.
28
2.7.5 Since this evidence was received by your Committee, new protocols have
been established which provide that paramedics can pronounce that life is
extinct, and that Police Surgeons need only be called in the cases of where a
body is discovered in a public place, or after the Police have made a forced
entry to a property or in the case of a suspicious death. Your Committee
understands from further correspondence, dated 22nd July 2004, received from
the Department of Home Affairs that these new arrangements seem to be
working satisfactorily.
Furthermore, the Department of Health and Social Security has indicated to
your Committee that there has been some confusion regarding the issues of
notification and certification of sudden or unexpected deaths. Notification of
a death can be undertaken by anyone, notification being made to MEDS, a
General Practitioner, the Police or the Registrar. A doctor is not required to
undertake notification of a death. Certification does need to be undertaken
by a General Practitioner, but does not need to take place at the same time as
notification. Certification can take place some time after notification, and a
body can be removed without certification having occurred. Prior to the
introduction of "MannDoc" and subsequently MEDS, the deceased persons
GP would often undertake both tasks at the same time, but that is not
necessary.
In the case of a sudden or unexpected death in non-suspicious circumstances,
MEDS may be called, and the doctor on duty should respond as quickly as
the urgent needs of living patients permit. However, if the MEDS doctor is
unable to visit to notify death, the death can still be notified since anyone may
do so, the body may be removed, and the deceased person's GP can then
undertake certification of death once the surgery is open. Only in the case of
a suspicious death where a body may be found in a public place, a disused
building, or resulting from a road or other form of accident, does the Police
Surgeon need to be called.
Your Committee understands that there has been some confusion regarding
the two matters of notification and certification and some distress may have
been caused as a result. However, we understand that the Department of
29
Health and Social Security have sought to issue a Policy Statement concerning
Confirmation and Certification of Death, which seeks to clarify these matters
and there is now a greater level of understanding amongst nursing and
residential homes, undertakers and others about the fact that a body can be
removed once death has been notified and that notification does not require
the involvement of a doctor, excepting in suspicious circumstances.
2.7.6 In the light of the new protocols and the clarification from the Department of
Health and Social Security, your Committee feels that no further action is
required with regard to this matter.
2.7.7 The written evidence supplied by the Department, and a copy of the Policy
Statement Issued by the Department of Health and Social Security on
'Confirmation and Certification of Death' are included in the Report as
Appendix 8.
2.8 Evidence obtained from visit by your Committee to Ramsey Cottage
Hospital
2.8.1 Your Committee was given a tour of the facilities available at Ramsey Cottage
Hospital on Thursday 18th December 2003. It was plain that the Hospital was
well equipped, enabling it, if necessary, not only to provide minor injury care
and the stabilisation of patients but also, with appropriate staffing, more
extensive treatments. However, as noted above (see paragraphs 1.4.1 to 1.4.4)
the issue of whether there should be a 24 hour a day seven days a week Minor
Injuries Unit, or other extended usage, at Ramsey Cottage Hospital is largely
beyond the remit of your Committee.
2.8.2 Nevertheless, your Committee feels that it would be remiss of it not to
express concern that some of the medical facilities at Ramsey Cottage
Hospital are not being fully utilised and are idle throughout the out of hours
periods when they could be used for the benefit of patients, the community
and the Health Service.
30
2.9 Evidence obtained from visit by your Committee to the MEDS Facility
2.9.1 An unannounced visit to the MEDS service took place during the evening of
Wednesday 10th March 2004. Your Committee had previously indicated that
it would visit MEDS during the week 8*-l4th March 2004, but had given no
indication as to exactly when the visit would occur or at what time.
2.9.2 On arrival we were immediately concerned to note the lack of any adequate
signage anywhere in the Hospital grounds, directing patients to MEDS. The
absence of such signs made it difficult to find the location particularly in the
dark. When we did locate the facility, we noted that there was only a small,
non-illuminated, sign on the wall immediately outside the access door to
MEDS. When asked about the lack of signs, we were told that all patients
who are given appointments to visit the MEDS surgery are given precise
telephone instructions on its location. However, we still believe that the
MEDS surgery needs proper directional signs at the very least within the
Hospital grounds, as we have received verbal indications that patients are not
always given directions.
2.9.3 In addition, your Committee observed that the premises used by MEDS is
also used by the Fracture Clinic during the day. This means that it is
necessary for all MEDS equipment to be taken out of storage before the
Service begins operating and then stored away at the end of the session. That
is an unsatisfactory use of time, as well as creating the possibility for loss or
damage to equipment and loss of papers.
2.9.4 From our observation, it was clear that there was a lack of sufficient storage
space, a lack of a fax machine or a dedicated computer and no proper kitchen
facilities for staff. We also were advised that the bedroom for the duty doctor
is located some distance from the MEDS facility, and that for the driver is
outside the Hospital itself, at Ballamona House.
2.9.5 During the hour that we were present at MEDS, about ten telephone calls
were received. Three patients were given appointments at the Centre and
others were given telephone advice by the receptionist or the doctor. In
31
addition, the duty doctor was out on a house call when we arrived, although
he arrived back shortly afterwards. He indicated that he would be prepared
to visit a patient even in a more remote part of the Island if that patient's
condition demanded it and the patient was unable to reach MEDS. He
informed us that the decision to visit rather than offer an appointment at
MEDS, or give telephone advice, was primarily a clinical one, made by the
MEDS doctor on duty.
2.9.6 On the night of your Committee's brief visit, one doctor seemed able to deal
with the volume of work. However, we understood that on other occasions,
particularly during the day time at weekends there can be a large workload
and two doctors staff the Service at these times. The duty doctor also told us
that sometimes the two doctors on duty during the morning shift at
weekends remain for a time, when the afternoon shift takes over, to assist
with the clearing of any backlogs that may occur.
PART 3:
CONCLUSIONS
3.1 As a starting point for its conclusions your Committee feels very strongly
that, as a principle, the Island should have a common out of hours doctor
service. It may be argued that the level of demand for night time GP services
can be accommodated by one centrally located facility in Douglas; but your
Committee believes that such an argument fails to take fully into
consideration the geographic, demographic, historical and cultural context of
Manx life. We therefore consider that all areas of the Island should be
provided for by a service that has ease of access for all with an equally high
standard of care.
3.2 From evidence received by your Committee it is apparent that there is serious
concern within the community, which your Committee acknowledges,
regarding the provision of out of hours services provided by GPs. This was
expressed most particularly from the north of the Island. Your Committee
32
noted from the evidence that some of this concern was based upon actual
experiences of the working of the service although some was also based upon
hypothetical "what if" situations.
3.3 Your Committee does feel that the Department of Health and Social Security
could have dealt with the introduction of MEDS more effectively and had
they done so, the level of public concern might have been reduced from the
start. Although it is recognised that the Department did seek to inform the
public concerning the introduction of MEDS, a more extensive publicity and
advertising campaign, commenced earlier, both in the local media and
through Post Offices, the medical, pharmacy, optician and dental services
might have helped reduce public concern and confusion.
3.4 However, your Committee considers that it is largely the General
Practitioners who are chiefly responsible for creating most of the difficulties
relating to the out of hours service (see paragraphs 1.3.4 to 1.3.8 above for
details). From evidence received, it was clear to your Committee that it was
the General Practitioners who -
(a) decided to largely abandon practice based out of hours patient care
and establish "MannDoc";
(b) pressed for the matter of out of hours care to be dealt with speedily
and before the introduction of their new Contract;
(c) required that their new Contract removed the requirement for out of
hours care to be provided by GPs;
(d) did not opt into providing out of hours care under the terms of their
new Contract; and
(e) in the case of the Ramsey Group Practice, decided to stop staffing the
Urgent Treatment Centre at the Cottage Hospital during the out of
hours periods after 1st April 2003, notifying the Department of their
intention in a letter dated 26th February 2003. As a consequence, the
33
Department was forced, within a very short space of time, to alter and
down grade the facilities at that Hospital from an Urgent Treatment
Centre to a Minor Injury Unit.
Evidence that your Committee has received indicates that there may have
been a variety of reasons for the GPs deciding to withdraw from providing
out of hours patient care. Explanations suggested to us include the desire by
doctors to have more free time, to have less pressure of work, to try to ensure
patients are treated by less tired doctors and to ensure the Island remained
competitive in the recruitment of GPs in the future.
We recognise that the demands made on General Practitioners can be
considerable, that many years of providing out of hours care may take their
toll, and we certainly understand that the Island must remain competitive
when it comes to seeking to recruit GPs. We also appreciate the importance
of patients being treated by GPs who are not excessively tired, yet we note
that by choice some General Practitioners are working a considerable number
of MEDS shifts and some are also undertaking hospital based work, which
adds considerably to their work load. (For details of those doctors working
on the MEDS rota between January and March 2004 and those working in the
Hospital see Appendix 5.2).
Therefore, we are not opposed to the concept of GPs sharing out of hours
duties between themselves. However, we feel that the General Practitioners
are well remunerated for their work (including staffing MEDS) and that being
a GP traditionally carries the responsibility of, and dedication to, providing
out of hours care.
Your Committee accepts it is unlikely that some GPs would ever be prepared
to return to the old system of out of hours care being provided by each
Practice. We, therefore, believe that a "MEDS type" system is now probably
the only way to ensure that the provision of an out of hours doctor care
facility continues to be available to the Island's population. However, we feel
that the GPs should be willing to cover more MEDS shifts to enable MEDS
34
centres to operate in other parts of the Island (see paragraph 3.9 (ii) below)
and the General Practitioners should acknowledge that being a well paid
professional in this important area of health care carries with it such a
responsibility to patients and the community.
3.6 It is clear to your Committee that there are problems with the existing MEDS
provision. These have been well documented in the written and oral
evidence received by your Committee. We certainly do not share the general
satisfaction expressed by the Department of Health and Social Security (and
GPs) regarding the operation of MEDS and we believe that there are some
major changes that could improve the service. Furthermore, it seems to your
Committee that there is a certain contradiction on the part of the Department
of Health and Social Security regarding MEDS. Having expressed satisfaction
with the Service, the Department was also keen to point out to us, in both
written and oral evidence, that improvements have already been made and
others are being considered. If MEDS represents such an improvement on the
previous out of hours arrangements (as the Department states) why is it
necessary to be undertaking all these important improvements?
3.7 Any improvement to MEDS should have the dual aims of making the Service
both more accessible to patients and optimising the medical skills and
resources that are available for the benefit of those who need treatment. We
believe that there are a range of improvements that should be undertaken to
enhance the out of hours doctor service. These should be introduced as soon
as possible. Some of them are simply relatively minor practical
improvements to MEDS, while others are more substantive and may have
greater cost implications.
3.8 We believe that there are a number of immediate practical measures that
could improve access to MEDS and the quality of the service that it provides.
These include:
35
(i) The provision of clear signage at Nobles Hospital to indicate the
location of the MEDS facility -
This would assist patients to locate MEDS more easily and not waste
the time of other busy health service professionals at Nobles Hospital
by having to ask for directions. Such signs should be illuminated at
night.
Your Committee's own experiences in visiting MEDS highlighted this
problem (see paragraph 2.9.2 above). Therefore, your Committee
believes that clear signage for MEDS (which clearly explains what
MEDS is) must be provided; commencing at the access road by the
roundabout when entering the hospital grounds and then at
appropriate locations thereafter leading to the MEDS facility. It may
also be that the new signage, which has been provided on the various
approaches to Douglas to direct people to the new Hospital, could also
have a MEDS sign added. That would make it very clear to patients
where MEDS is located, as this could be a time of distress.
(ii) The immediate improvement of the existing facilities for MEDS -
Your Committee believes that whilst the facilities for patients at MEDS
are adequate, we accept the arguments made by a number of GPs, in
evidence, that present facilities for doctors are inadequate. Your
Committee's own visit to MEDS reached similar conclusions (see
paragraph 2.9.3 and 2.9.4 above). We would propose the provision of a
larger secure storage facilities for drugs to enable more than one drugs
trolley to be available if necessary, and the provision of fax and
computer facilities, including intra-net and inter-net links.
During our visit to MEDS we noted that there was a lack of adequate
parking in the immediate vicinity of the MEDS unit, and your
Committee believes that steps should be urgently taken to rectify this.
There does appear to be an area of suitable land adjacent to the MEDS
facility which could be utilised as a MEDS car park during the hours of
36
MEDS operation, and it would then be available to help reduce the
general car parking problem at Nobles Hospital during the day time
when MEDS was not operating.
(iii) The need for a patient education campaign to inform patients when
they should be calling upon MEDS and when they should be
summoning an ambulance -
Your Committee believes, from evidence received, that individuals are
often not the best judges as to whether a medical matter is acute or less
serious, and they should not be expected to make such judgements.
We would strongly urge the Department of Health and Social Security
to provide, on a regular basis, the public with clear advice and
procedures to be followed in the event of a medical emergency,
through the medium of the press and leaflets. Such leaflets should be
available in public places, such as doctor's surgeries, dental surgeries,
pharmacies, post offices, local authority offices, libraries etc. In
addition this information should also be contained prominently in the
telephone directory.
(iv) The provision of free emergency transport to convey patients to and
from the MEDS centre -
Your Committee accepts that there may be a problem with
transportation to MEDS in some cases and it appears from evidence
received that sometimes ambulances have been used for this purpose.
Given the limited resources available to the Ambulance Service it
seems most unwise to utilise an ambulance for a less serious case when
it may be needed for an acute one.
Furthermore, evidence received by your Committee also shows that
the concern at having to drive at night, and possibly in bad weather, is
one that many individuals, especially those who are elderly,
experience. A further concern is driving with someone who is ill or
injured, which could be a potentially dangerous distraction for the
37
driver, especially if there is no-one else accompanying the patient in
the vehicle. Your Committee considers that the Department of Health
and Social Security should investigate ways of providing some form of
free transportation to and from the MEDS centre. This may be through
the use of taxis, a contract scheme similar to that used for patient
transport from Liverpool Airport, a volunteer scheme or some other
method. Criteria for when this service should be called upon would
need to be established so that, as far as possible, it was only used in
genuine cases.
(v) Production of a contingency plan in case of severe weather, accidents
etc -
In evidence, we were concerned to hear from the Primary Health Care
Service, that a contingency plan does not exist to deal with
emergencies, such as severe weather or major accidents, which would
prevent patients from reaching MEDS. Your Committee considers it
reasonable to expect that the Department of Health and Social Security
and the GPs provide specific arrangements for out of hours care in
such extreme situations. A formal contingency plan should be drawn
up by the Primary Health Care Service, in consultation with the
General Practitioners, to ensure that if such circumstances ever arose, a
plan already existed.
Furthermore, the Primary Health Care Service should also devise a
contingency plan in case it ever proved impossible to find a doctor to
staff a MEDS shift. Whilst this may be unlikely, once again it is clearly
better for the Department of Health and Social Security to be prepared
before the event.
3.9 Your Committee believes that there are a whole range of substantive
developments which should be made to improve access to out of hours doctor
care. These developments will have financial implications, but your
38
Committee believes that the issue of the health of the population is a major
responsibility of Government and therefore resources should be made
available. These developments are set out below:
(i) The use of fully trained nurses, with relevant experience, as the first
point of contact with MEDS -
When a patient telephones MEDS, your Committee believes that if the
first point of contact was with a fully trained nurse, with relevant
experience, the patient would have greater confidence in the service
provided. The nurse would make an initial assessment of the patient's
situation. From that assessment, the patient may be given advice over
the telephone by the nurse or the doctor, asked to attend a MEDS unit
to see a doctor, or receive a visit from a MEDS doctor in their home. In
acute cases the nurse would be able to summon an ambulance, as the
Receptionist is currently able to do.
If additional MEDS centres were established (see paragraph 3.9 (ii)
below), your Committee would expect that all calls from patients to
MEDS would be routed to the Douglas MEDS centre, from where the
nurse on duty would contact the duty doctor in the regional MEDS
centre when appropriate.
(ii) The establishment of additional MEDS centres -
(a) Your Committee acknowledges the concern expressed by many
of those who submitted evidence that bad weather conditions,
road closures, the lack of personal transport, the perceived
unwillingness of some MEDS duty doctors to visit more remote
areas etc argue against a sole centrally located MEDS facility.
The geographic nature of the Isle of Man, with its separate
distinct communities, underlines the problem of a centrally
located facility. Your Committee believes that there should be
additional MEDS centres in the north and the south of the
Island. The Department of Health and Social Security owns
39
property in the north (Ramsey Cottage Hospital) and south of
the Island (the former Southlands and the new GP surgeries in
Port Erin, Castletown and Ballasalla), any of which are suitable
to use as locations for these MEDS centres. Your Committee
believes that the Department of Health and Social Security
should establish such additional MEDS centres as soon as
possible.
(b) In determining the most appropriate level of care during out of
hours periods, your Committee believes that the Department of
Health and Social Security should evaluate whether such
centres need to be staffed by a GP or a doctor employed directly
by the Department. The Department could also consider
whether the duty doctor in these additional MEDS units should
be required to be at the MEDS premises all the time, or whether
he/she could be on call from home (providing their residence
was reasonably near the centre) during the night.
(c) None of the above proposals would alter the operation of the
Douglas MEDS centre. Establishing regional MEDS centres
would relieve the Douglas based MEDS doctor of some work
and allow that doctor to concentrate primarily on the provision
of MEDS services for patients in the east, west and central areas
of the Island, where the system appears to be working
reasonably well.
(d) At night the standby doctor, who is on call at home to support
the existing MEDS provision in times of high demand, should
continue to fulfil that role, and be available to all the MEDS
centres. Figures received from the Primary Health Care Service
(see paragraph 6 of their letter dated 20th February 2004 which
can be found in Appendix 5.2 of this Report) indicate that it is
rare for the standby doctor to be called out at night. Therefore,
we believe initially one standby doctor would be sufficient,
although the situation should be reviewed regularly by the
Department of Health and Social Security.
40
(e) The establishment of regional MEDS centres would mean that
many patients would be closer proximity to a MEDS centre than
under the present system. This would have the additional
benefit of helping to overcome problems created by, for
example, adverse weather, accidents, road closures etc and the
lack of personal transport.
While the establishment of additional MEDS centres will require
more resources, your Committee strongly believes that the
provision of such centres will provide a more efficient and
accessible out of hours doctors service for the public, and it is
certainly an option that commands considerable support in the
community.
(f) Based upon evidence which your Committee has received, we
are satisfied that there are a number of alternatives available for
the Department of Health and Social Security to consider
concerning the most appropriate way to staff these MEDS
centres.
These alternatives include:
(i) General Practitioners could staff all the MEDS centres -
A clause could be added into the new GP Contract
requiring all GPs to undertake an agreed number of out
of hours shifts. However, this may prove difficult to
achieve, with some GPS possibly being unwilling to
agree to an amendment to their Contract, which could
mean there were insufficient General Practitioners to staff
the service;
41
(ii) the use of doctors directly employed by the Department
of Health and Social Security -
A small number of doctors could be employed directly by
the Department of Health and Social Security to provide
the bulk of out of hours MEDS cover, with Island GPs
taking only a limited part (or possibly no part) in staffing
the service. There may, of course, be difficulties in
seeking to recruit doctors to posts that involved only
night and weekend work, but we understand that such a
system is employed in some parts of the United Kingdom
to staff out of hours services. We also note that the
Director of Public Health suggested such an option in the
written evidence he supplied to your Committee, (see
Recommendation 1 page 8 of the Director's letter which
may be found in Appendix 5.3 of the Report).
(iii) the use of fully qualified doctors who are not General
Practitioners -
Your Committee understands from the Department of
Health and Social Security that there are currently a
number of fully qualified doctors, who are not GPs, that
undertake some shifts for the existing MEDS facility at
Nobles Hospital. It is possible that greater use of this
source of staffing could be made.
(iv) the northern MEDS centre -
In the case of the proposed northern MEDS centre, the
use of Isle of Man Hospitals Doctors to staff the service.
At present Ramsey Cottage Hospital operates under the
Primary Health Care Service. However, the Hospital
could be transferred back to Isle of Man Hospitals.
Doctors could then be supplied from Nobles Hospital, on
42
a rota basis, 24 hours a day, seven days a week. This
would enable the Minor Injury Unit to function 24 hours
a day, and provide in patients with constant medical
supervision. The doctor on duty at night and at
weekends could also staff the MEDS provision. This
would free the Ramsey Group Practice from any
responsibility at Ramsey Cottage Hospital. Whilst some
hospital doctors may not favour undertaking work for
MEDS, it would seem to be a good use of resources to
employ them in this way.
(g> Your Committee considers that it is the responsibility of the
Department of Health and Social Security to evaluate which of
the above options is the most practical It may be found that the
most practical solution is a combination of several of the
options. However, in the event of failure to reach agreement
with the General Practitioners on the issue of staffing the MEDS
centres, your Committee would prefer the option of the
Department of Health and Social Security directly employing
doctors to staff the MEDS provision, especially as the
Department is fully responsible for funding the Service.
(h) Should a northern MEDS centre be established, your Committee
believes that the Department of Health and Social Security will
need to determine what should happen if a patient arrives at
Ramsey Cottage Hospital during the out of hours period to seek
medical attention, without first having telephoned MEDS. Your
Committee recognises that this is likely to happen and therefore
the Department must be prepared.
(iii) The provision of dedicated accommodation at Nobles Hospital for
M ED S-
Your Committee fully endorses the views of those GPs who argue that
MEDS needs improved facilities. Your Committee has already noted
on several occasions within this report (see paragraphs 2.4.6, 2.9.3 and
43
2.9.4), that the sharing of facilities, at Nobles Hospital, between MEDS
and hospital services is unsatisfactory. There can be no doubt that the
efficient operation of MEDS at Nobles Hospital would benefit from
dedicated accommodation. There would appear to be plenty of space
in the grounds of the new Nobles Hospital site for an additional small
purpose built building, with an adjacent car park, to be constructed for
the sole use of MEDS.
This dedicated accommodation should be easily accessible and ideally
comprise a reception/waiting area, two consulting rooms, a small
kitchen facility, secure storage for drugs and other equipment and two
bedrooms for the night time duty doctor and driver. Such a facility
should be provided whether or not additional regional MEDS centres
were opened, since the Douglas centre obviously serves the main
concentration of population.
(iv) The introduction a common computer system to all GP practices and
M ED S-
Your Committee is firmly of the view that the Department of Health
and Social Security should consider the introduction of a common
computer system across all GP practices and MEDS. This would
enable the MEDS doctors to access patient records where appropriate,
and to input details of treatments given. We understand that such
systems are being introduced in the United Kingdom. Whilst this may
be a long term project, since we understand that not all patient records
are held electronically at present, and where they are held
electronically by practices various systems are employed, we feel such
a system would be beneficial for both doctors and patients, and
therefore progress should be made on this matter as soon as possible.
44
PART 4:
RECOMMENDATIONS
For Immediate Action by the Department of Health and Social
Security
4.1 Your Committee recommends that clear signage, illuminated at night, is
provided on the approaches to, and at Nobles Hospital, to clearly direct
patients to the MEDS facility. (See paragraph 3.8 (i) above).
4.2 Your Committee recommends that the facilities available for MEDS at Nobles
Hospital should be improved by the provision of a larger secure storage
facilities for drugs to enable more than one drugs trolley to be available if
required, and the provision of fax and computer equipment. In addition,
dedicated car parking adjacent to the MEDS unit should be provided. (See
paragraph 3.8 (ii) above).
4.3 Your Committee recommends that the Department of Health and Social
Security should issue clear advice to the public concerning procedures to be
followed in a medical emergency, and that such advice should then be issued
on a regular basis. Such advice should be available in public places as well as
through the media. (See paragraph 3.8 (iii) above).
4.4 Your Committee recommends that the Department of Health and Social
Security should investigate ways of providing free transportation for patients
who cannot reach the MEDS location themselves. (See paragraph 3.8 (iv)
above).
4.5 Your Committee recommends that the Primary Care Service draw up, in
consultation with General Practitioners, contingency plans for the provision
of out of hours GP services in the event of extreme weather or serious
accidents making travel to MEDS in Douglas difficult; and also a contingency
plan in case it proves impossible to staff a MEDS shift. (See paragraph 3.8 (v)
above).
45
Substantive Developments to be undertaken by the Department of Health and Social Security
4.6 Your Committee recommends that the Department of Health and Social
Security seeks to employ and utilise sufficient numbers of fully trained and
experienced nurses based at the Nobles Hospital MEDS centre to receive all
incoming calls to MEDS and decide what course of action is most appropriate.
(See paragraph 3.9 (i) above).
4.7 Your Committee recommends that the Department of Health and Social
Security seeks to establish additional MEDS centres in the north of the Island
(at Ramsey Cottage Hospital) and south of the Island (at either the former
Southlands or one of the new GP surgeries at Port Erin, Castletown or
Ballasalla). The Department of Health and Social Security should investigate
the best way of staffing such centres with doctors. If the General Practitioners
are unwilling to provide the necessary additional staffing, your Committee
favours the concept of the Department directly employing a number of
doctors to deliver the MEDS service. (See paragraphs 3.9 (ii) above).
4.8 Your Committee recommends that the Department of Health and Social
Security should provide the existing Douglas MEDS centre with its own
dedicated accommodation and car parking at Nobles Hospital. (See
paragraph 3.9 (iii) above).
4.9 Your Committee recommends that the Department of Health and Social
Security seek to introduce a generic computer system accessible to all GP
practices and MEDS, so that MEDS could have access to a patients medical
history, if required, and could input details of treatments given directly onto
patient records. (See paragraph 3.9 (iv) above).
4.10 Finally, your Committee wishes to ensure that these recommendations are
implemented by the Department of Health and Social Security. Therefore, we
would recommend that the Department of Health and Social Security be
required to report to Tynwald Court, at least twice within each Parliamentary
session, on progress to implement these Recommendations.
46
Acknowledgements:Your Committee wishes to express its grateful thanks to all those who have
submitted evidence and assisted us with our inquiries. In particular we wish to
express our thanks to -
Mrs C M Christian MLC
Mrs S Duke
Mr A Jones
Mr D Killip
Mr I Maclean
Dr M Maska
The late Mr G Newbury
Mr & Mrs H Penrose
Mr B Pressley
Mr S Sieling
Mr J Wilson
Mr P Whiteway
The doctor, receptionist 10th March 2004.
Minister for Health and Social Security until July 2004;
Family Practitioner Services Manager;
Acting General Manager Primary Health Care Services;
Chief Executive Department of Health and Social Security;
Director of Public Health;
Ramsey Group Practice;
General Manager Primary Health Care Services;
Ramsey Cottage Hospital League of Friends;
Manager Ramsey Cottage Hospital;
Deputy Chief Ambulance Officer Isle of Man Ambulance Service;
Head of Health Services Division;
Clerk to Ramsey Town Commissioners; and
and driver on duty at MEDS on the night of Wednesday
J A Brown (Chairman)
D J Gelling
Q B Gill
L I Singer
G H Waft
November 2003
47
Select Committee of Tynwald on GP Out of Hours Services
Appendix 1:
Appendix 2 :
Appendix 3:
Appendix 4:
Appendix 5:
Summary of Appendices in the Report
A copy of the Press Notice inviting members of the public to submit evidence in writing together with a list of names of those members of the public who have submitted evidence for publication and those who have submitted evidence not for publication. Evidence submitted for publication may be viewed in the Tynwald Library.
A copy of the press notice inviting the submission of written evidence (same notice as for the public) and the written submissions received from interested bodies.
A copy of the letter inviting GPs to submit written evidence together with the written evidence from GPs, together with a list of names of those GPs submitting evidence but who wish it to remain confidential.
A copy of the letter inviting Members to submit written evidence together with the written evidence received from Members.
5.1 A copy of the letter inviting the Minister to submit written evidence and the written evidence from the Minister & Chief Executive dated 10th September 2003 (Appendix 1 of the Department's submission the National Health Service (Isle of Man) General Medical and Pharmaceutical Services Regulations 1978 is not included because of its bulk, and is available for consultation in the Tynwald Library), a copy of the Policy Document on the Emergency Doctor Service, a letter dated 16th December 2003 indicating the ratio of GPs per head of practice population for the Isle of Man, England, Scotland, Wales and Northern Ireland and samples of some publicity material issued by the Department relating to the Emergency Doctor Service and Ramsey Cottage Hospital.
5.2 Written evidence from the Primary Health Care Service
(a) statistical summary of calls received by MEDS 1st April-31st December 2003;
(b) statistical summary of payments made to doctors participating in MEDS 1st April-31st December 2003;
Appendix 6:
Appendix 7:
Appendix 8:
(c) summary of MEDS rota January-March 2004 showing how many shifts each doctor undertook and when these were. To protect the doctors concerned, the names of the doctors on the rota showing which doctor worked which shift have been replaced by random numbers, with each doctor being allocated a number; and
(d) letter dated 20th February 2004 from the late Mr G Newbury General M anager Primary Healthcare Services.
5.3 A copy of the letter inviting the Director of Public Health to submit evidence in writing together with the written evidence from the Director of Public Health.
5.4 Written evidence from the Ambulance Service.
Hansard of oral evidence given on 18ih December 2003 by the Mr S Sieling, Deputy Chief Ambulance Officer and Mr R Beattie, Ambulance Service Operations Manager, Dr M Maska, Ramsey Cottage Hospital League of Friends, Hon A R Bell MHK, Mrs A V Craine MHK, Mr P A Gawne MHK and Hon S C Rodan MHK.
Hansard of oral evidence given on 28th January 2004 by Mr J D Q Cannan MHK, Mr R E Quine MHK, Hon C M Christian MLC, Minister for Health and Social Security and Mr D Killip, Chief Executive Department of Health and Social Security, the late Mr G Newbury, General Manager Primary Health Care Services, and Mrs S Duke, Family Practitioner Services Manager and Mr R Radcliffe, Ramsey Town Commissioner and Mr P White way, Clerk to Ramsey Town Commissioners. Hansard oral evidence given on 7th May 2004 by Mr J Wilson, Head of Health Services Division and Mr A Jones, Acting General Manager Primary Health Care Service.
Written evidence from the Department of Home Affairs, and a copy of the DHSS document on Confirmation & Certification of Death.
Appendix 1
Select Com m ittee of Ty n w a l d o n GP o u t of H o u r s Services
The Select Committee on GP (family doctor) Out of Hours Services invites the submission of written evidence from any interested members of the public regarding their comments on the provision of General Practitioners out of hours services (that is services between 6.00 pm and 8.00 am Mondays to Fridays and over week-ends and bank holidays). The Committee would be interested to hear of how people have been, or feel they may be, affected by the availability of such services. Evidence should be submitted in writing to the under mentioned by Friday 12th September 2003. Oral evidence may be taken at a later date.
For further information please view the Tynwald web site: www.tynwald.org.im
Malachy Comwell-Kelly Clerk of Tynwald
Legislative Buildings, Douglas
IM1 3PW
The following members of the public submitted written evidence to your Committee:
Select Committee of Tynwald on GP Services
Mrs R AdlamM rK AireyMr D AndersonMs G A ArnoldMrs G L ArnoldMrs G AshbyMrs J M AshtonMrs C BallMs M J BarkerMrs E BarryMrs M BarryMr N F BarryMs J M Berrisford-LewisMr & Mrs J R BerrymanMrs S G BeynonMrs D BinderMs B E BonwickMrs A BrophyK BumsBrig N A Butler CBEMr P CaineMr & Mrs J Q CallowMr & Mrs P W Carman
Ms V CannellMr J J CareyMrs A M CarltonMrs J CarterMr R J CaseltonMrs D E CasementMs S CasementMr St Mrs W H CasementMr & Mrs A ChapmanMr D G ChesterMr D P L ChesterMr A J ChineryMrs I ChristianMrs J ChristianM ChrystalMs ] ClagueMiss B ClarkMiss M ClarkMr & Mrs M CleggMr C ClementsMr & Mrs L CliffordMrs M E ComishMrs D ContiMr D M CooperMs H M CorbetMr A RCorkiilMrs IC CorkiHMrs J CorkillMs V Corkill
Mr J Corlett Ms K Coulter Mrs C G Cowell Mr & Mrs S Craggs Mr N Crellin A M B Crookall Mr M Crookall Mr S Crowe P S DaviesMr & Mrs B DenhamMrs A DobrzynskiMr D H DuffMs J DuncalfMr & Mrs D A FairbaimMs V FairbaimMs V FaragherMrs A M FergusonMr & Mrs V R FieldMr L FisherP P FoxR L GarrettMiss C GordonMr & Mrs P Gordon
Miss S GordonMrs K GreenMr & Mrs A GreggMr J GrimsonMr JN HallMr B HallworthMr D R HampshireMs A HannaMs K L HansMs C HardmanMr & Mrs HardyMrs S HardyJ HarrisMrs S Harris-Mayes Mr B Harrison Ms J Harrison E C Harthill L J Har thill Ms A Hayes Mrs J Heginbotham Mrs R W Hinton Ms J Hockings Mr Sc Mrs F Hod son Mr R J Hopkins Ms J Houghton Mrs D Howard Rev B L Humphries Ms S Huyton

The following members of the public submitted written evidence to your Committee:
Select Committee of Tynwald on GP Services
Mrs J Illingworth Mr & Mrs J B QuarkMrs E E Ivory Ms A QuayleMs J James Mr G QuayleMr A Jessopp Mr & Mrs P QuayleMr A Johnson Mrs C A QuirkK J Jones Ms J QuirkMrs J P Jones Mrs J QuirkMr W F Jopson Miss M J QuirkMiss D Kaighen Mrs R QuirkMr J J Kaighen Mr & Mrs R RaddiffeJ J Kaighin Mr S W RandMs J Kaighin Ms C RandallMr & Mrs R Kearsley Mr St Mrs J RatdiffMr R Kellett Mr R F RatdiffeMs S M Kelly Ms L RawlingA Kelsall Mr St Mrs E A RaybonMr & Mrs P J Kelsall Mr & Mrs B A RichardsMr & Mrs J Kennish Mr B J RichardsMr & Mrs E W Kerruish Ms A RobertsMrs P Kind Mrs J RobertsM rsB Kininin Mrs D E RobsonMrs J Kirby Mrs T RushMr W J C Kitto Mrs V SampsonMr J G Knight Ms B SandwellMs K Lace Ms S E M SayerMr J C Lalor-Smith Mrs A ScholesMr D M Legg Mr F SeabyMs D Lovel Mr & Mrs M J SergantMrs A Mansell Mrs H M SewellMs M S Marsden Mr A P ShimminMrs E Marshall Mrs J ShimminM rsT B Maskell R ShimminMr St Mrs H C Maynard Ms L SimmsMr St Mrs McAneney Mr T W SlingsbyMr J McDonough Mrs F StarkeyMr A McGeagh Mrs B StevensonMr R McGregor Mr St Mrs A TeareMrs W McHenry K M TeareJ McLean Ms V TeareMr M Meddings Mr A ThompsonE G Mitchell Mr E C TokeleyP W C Monk Ms A TolandMrs F Moore Mr I R WalkerMs 5 Mylchreest Mr W R WalshMrs P Norman Ms A WellsLady Nugent Mr & Mrs C M WhiteMr & Mrs J Oates Mr P WhitewayMr J Oates Mr T P WhitewayMrs A Oldroyd Mr & Mrs L WillisMrs C Parish Mr A WilsonMr R Peel Prof A Wilson OBEMs K Pendree Mrs M WilsonMr H Penrose R C WilsonMr A S Perdval Mrs S C R WonnacottR Povey Ms F A Woods
Mr H A Priestland Mrs S WrightMrs V A Quane
Select Committee of Tynwald on GP Services
The following members of the public submitted written evidence to your Committee, that they wished to remain confidential:
Mr and Mrs B Beattie Mr W H MagnayMiss J E Beggs Ms M W MogfordMrs I Bennett Miss M MooreMr R Bennett Mr & Mrs T MooreMrs V Bushell Mr P D OwenMiss B V Copeland Mrs A N ParkerMs K Coreen Mr P PerryMrs I and Miss L Cowell Mrs M PickersgillMiss J M Denney Ms C PullingerMrs V Edwards Miss K M PurcellMiss D Gale Mrs E QuayleMrs D Gartside Mrs H RadcliffeMr & Mrs B Graham Mr J C RadcliffeMr D P Hall Mr G F RandMrs M Harper Mr & Mrs E C RatcliffMiss W Higgins Mr & Mrs J RichmondMr & Mrs M Hughes Capt W N SeyboldMr & Mrs R Hudson Mrs P M ShawMrs S M Jelski Mrs R ShawMs M Kelly Mrs M ShearmanMs G Leeming Mr JM WadeMrs C E Lishman Mrs G A WellsMrs M G Lord Mrs J WhiteMrs M Luck Ms K WoodMr } Me Ard
Appendix 2
Select Com m ittee of Ty n w a l d o n GP o u t of H o u r s Services
The Select Committee on GP (family doctor) Out of Hours Services invites the submission of written evidence from any interested members of the public regarding their comments on the provision of General Practitioners out of hours services (that is services between 6.00 pm and 8.00 am Mondays to Fridays and over week-ends and bank holidays). The Committee would be interested to hear of how people have been, or feel they may be, affected by the availability of such services. Evidence should be submitted in writing to the under mentioned by Friday 12th September 2003. Oral evidence may be taken at a later date.
For further information please view the Tynwald web site: www.tynwald.org.im
Malachy Cornwell-Kelly Clerk of Tynwald
Legislative Buildings, Douglas
IM1 3PW
P a r is h
C o m m is s io n e r sBARRANTEE SKYLL VREESHEY
Malachy Comwell-Kelly Clerk of Tynwald Legislative Buildings Douglas IM1 3PW
22ni August, 2003
Dear Sir
Re: GP Out of Hours Services in the North of the Isle of Man
The Bride Parish Commissioners feel veiy strongly about the ongoing problems created in the North of the Island by the removal of an ‘on call, out of hours’ Doctor.
They feel that with little cost, a Doctor could be stationed in the Ramsey Cottage Hospital who would also be available to deal with ‘on call* emergencies, during out of normal working hours and this should be implemented as soon as possible, before a major disaster occurs or someone looses their life.
It is appreciated that an ambulance is available to take patients to Douglas if absolutely necessary but this does'not excuse the lack of a qualified Practitioner in the North.
The time delay in the ambulance arriving at any location in the North would be greatly advanced should there be inclement weather; the roads were closed due to sporting activities or if the team driving the ambulance were to be less experienced in the local vicinity, with regard to finding out of the way locations.
Certainly not all of the local residents possess transport, nor have they friends or neighbours who could easily drive to Douglas in an emergency.
The Commissioners feel that we have good coverage with regard to the Fire Service and it is imperative that a similar standard is achieved with regard to qualified medical assistance.
Yours sincerely,
Lisa SimsClerk to the Commissioners L
Clerk: Lisa Sims Ballacloan, Gardeners Lane, Ramsey, Isle of Man. IM 8 3PN
Tel: 01624 819235 Fax: 01624 819235 e-mail: [email protected]
LEZAYRE PARISH COMMISSIONERSBARRANTTEE SKYLL CHREEST NY H'ARREY
I
b à i f RECEIVEDf P i 1 2 S E P 2003
OFFICE OF THE n.F.RK OF TYNWALD
1 Coollbane C o ttag e B Sulby ■Isle of Man. IM7 2HR
Clerk : Mr R. Peel Tel/Fax : 01624 8970 Please reply to The Clerk.
Mr. P. Lo Bao, 1 1 th. September 2003Joint Clerk to the Committee,Select Committee of Tynwald on G.P. Services.Office of the Clerk of Tynwald,Legislative Buildings,Douglas,1M1 3PW.
Dear Mr. Lo Bao,
Re: Select Committee of Tynwald on G.P. Services.
Points to consider
1. Dedicated doctor for North ofshould provide full cover as in the past2. Sufficient ambulance service and staff. What is the number of ambulances
now compared to the past?
3. Despite the new Nobles Hospital it would be criminal to allow the previous
excellent hospital service to deteriorate.
4. Centralisation is not the answer to everything. Also, of prime consideration
is the remote possibility of something serious happening to Nobles and the
Island has a stand-by in case of National Emergency, just as the North can
provide an alternative airport in Jurby as a back-up for Ronaldsway.
5. The sooner someone is treated the better it is: Early treatment is imperative
if not life-saving.
6. There must be a lack of incentive for doctors to work late or unsocial hours.
7. Can someone sue if the change of hospital practice is shown to be the cause
of death?
Yours sincerely,
Robert PeelClerk to the Commissioners
Ramsey Town Commissioners
Please address all correspondence to the Town Clerk and Chief Executive
Town Clerk and Chief Executive Commissioner for Oaths.
T.P. WHITEWAY
Barrantee Rhumsaa
Your Ref:
Our Ref: TPW/MPC/F 9
Telephone: (01624) 810100
Fax: (01624) 810101 E-mail: enquiries®rtc.gov.im
27th August, 2003.
Malachy Comwell-Kelly,Esq., Clerk of Tynwald,Legislative Buildings, Douglas,Isle of Man. EMI 3PW
CnVM NÄJL dO H K L tIO 3 0 L H 0
COOZ 9 n v 8 I
a a A I H D M
Dear Mr. Comwell-Kelly,
Re: Select Committee of Tynwald on GP out of hours services
At the August, 2003, public meeting of the Ramsey Town Commissioners consideration was given to the Select Committee established to consider GP out of hours services.
The Commission feel that the position regarding the removal of Accident and Emergency Services from the Ramsey Cottage Hospital is intrinsically linked to the GP services. Up to 31st March, 2003, Doctors employed at the Ramsey Group Practice were contracted to provide General Practitioner Services together with in and out patient (A&E) cover at the Ramsey Cottage Hospital and 24 hour on call facilities. Since 1st April, 2003, the contracted services with Ramsey Practice Doctors is for General Practitioner services, Monday to Friday day time surgeries, plus in patient provision at the Ramsey Cottage Hospital. No Doctor cover is provided locally outside surgery hours, and no Doctor cover is provided at any time to the former Accident and Emergency Department which now operates as a Minor Injuries Unit only.
The Health Minister is on record as stating that the difficulties stem from the contracts with the General Practitioners, and that it is not a resource issue. In relation to the Ramsey Cottage Hospital it is clear that its position, which is unique on the Island, is such that it is impractical to expect to be able to reach agreement on staffing through the negotiation of contracted services with the Doctors of the General Practice. Unlike Noble’s Hospital, Ramsey Cottage Hospital falls under the control of Primary Health Care, this part of the DHSS is responsible for services other than Hospital services and predominantly those related to care services within in the community, and it is suggested that it is this position which causes most difficulty.
/1 / 3
Town Hall and Library, Ramsey, Isle of Man. IM8 1RT.Hailey yn Valley as Lioariann, Rhumsaa, Elian Vannin. IM8 1RT
VAT Reg. No. GB 000 0631 62
- 2 -
M. Corwell-Kelly,Esq., Clerk of Tynwald. 27th August, 2003.
2 / 3 ....
The position of the North of the Island is interesting in that historically it has had a Hospital which included 24 hour accident and emergency services, whereas other areas have utilized the services of the Noble’s Hospital. The establishment of the hospital stemmed from the difficulties experienced by people in the North in accessing the hospital and the services of a Doctor in an emergency - which is little different from the present day circumstances. It would appear that access to Doctors is limited by the relationship between Primary Health Care and the General Practitioners, and that the position would be entirely different if the Ramsey Cottage Hospital was able to recruit Doctors itself. The practicality of such is that the Ramsey Cottage Hospital should fall within the general control of IOM Hospitals - in so far as its continued management and operational requirements are concerned - and that the General Practitioner Doctors should no longer be required to provide services to the hospital. This would enable the hospital to recruit its own Doctors to provide in and out patient cover and reinstate A&E. The reduction in the call on Doctors time in providing in-patient cover at the Cottage Hospital could be assessed and possibly enable improved access of patients to doctors surgeries or a review of the number of doctors required to provide the reduced level of services.
The Committee’s remit relates primarily to access to Doctor Services, since 1st April, 2003, access to Doctors is limited to Monday - Friday 8,30 a.m. to 6.00 p.m. Access outside these hours is through a service operated from Noble’s Hospital in Douglas, and staffed by two Doctors. In basic terms the position in the North was such that prior to the 1st April anyone requiring medical assistance had recourse to either 24 hour on-call doctor services, or 24 hour A&E facilities at the Cottage Hospital with doctor cover. Since that date access to Doctors in the North is limited to the Monday - Friday day time surgery provision.
In terms of performance monitoring there is no doubt, with over 75% of the Island population living within a 5 mile radius of the New Hospital, that a high percentage of Doctor or A&E cases can be dealt with within a reasonable timescale, also that a high percentage of ambulance response times will fall within recognized UK national targets (14 minutes urban, 19 minutes rural). What is apparent however is that assessment of these performance ratings by region on the Island would show an entirely different picture, and it is this regional position which is of most concern to the people of the north and south of the Island, where a much lower level of medical service is to be expected due to the apparent policy of seeking to centralise services in the Douglas area.
It is clear that there is a need to establish clear performance criteria suitable for the Island, and recognize that it is legitimate for people living it outlying areas to expect a reasonable level of service. Access to Doctors is a fundamental service, and one which should not be restricted by surgery hours, a clear option therefore is to enable access to be obtained in the north and south through community provision, such as that which was provided at the Ramsey Cottage Hospital prior to 1 st April 2003. Whilst Doctor call out services may not be possible A&E provision would enable emergency cases to be referred to a Doctor in an efficient and timely manner.
.... 2 / 3
- 3 -
M. Corwell-Kelly,Esq., Clerk of Tynwald. 27th August, 2003.
3 / 3 .....
Of fundamental importance to the residents of the North, and South of the Island, is the uncertainty of reasonable access to Douglas during winter months when weather conditions can severely slow or even stop traffic movement. Experience shows that the Mountain Road is no longer considered to be a priority in terms of opening and its availability is left entirely to the influences of the weather conditions - closure is the first option when ice or snow are in evidence. Reliance upon a Douglas based Doctors Service is therefore a matter of great concern especially to the elderly and those less fortunate, including families with members who have known medical conditions where quick access to a Doctor is necessary.
The Commission believes access to Doctors to be of such fundamental importance that emergency access should be provided 24 hours a day 7 days a 2 week. On call provision for GP’s is the ideal however if this is not practicable then having Doctors available in the Community - perhaps at the Cottage Hospital - to deal with emergency admissions is recommended. To achieve this position the Commission feel that the status of the Cottage Hospital should be changed so that it may employ Doctors, either independently or through IOM Hospitals, so that Doctor cover exists for in-patient, A&E, and emergency access.
The Commission wholeheartedly supports the efforts of the Ramsey Cottage Hospital League of Friends in seeking reinstatement of A&E services at the Cottage Hospital. The Commission would also draw attention to the large number of northern and other Island residents who took part in a peaceful march to express their views against the actions of the DHSS in reducing services at the Cottage Hospital, and would respectfully suggest that there is clear evidence that the wishes and aspirations of the residents are not being met and that action must be taken to redress this situation.
Yours sincerely,
Town Clerk & Chief Executive:
The Clerk to Tynwald Isle of Man Government Bucks Road Douglas Isle of Man
10 September 2003
Dear Sir,
There is a great deal of concern felt among the members of Kirk Andreas Women’s Institute with regards to the lack of cover at Ramsey District and Cottage Hospital
It has been noted that people have had to wait for many hours for medical assistance to arrive, sometimes coming from the south of the island.
Our biggest concern is that when the weather deteriorates through the winter and the mountain road may be closed, the residents in the north will be further disadvantaged and lives put at further risk due to delays in transportation of medical relief.
We would be most grateful if you could bring our concerns to the attention of Tynwald.
Yours faithfully,
t to n
Sylvia Beynon Hon. Secretary Kirk Andreas W.I.
RECEIVED1 1 S E P 2003
o f f ic e o f u rnCLERK OF TYNWALD
Elm Cottage, Ballacorey Road, Kirk Andreas, Ramsey, Isle of Man, IM7 4EL

GREST RESIDENTIAL HOMEANDREAS ROAD, LEZAYRE
I.O.M IM7 4EA
Chairman A.S.Percival 1 Chapel Close Ballaugh
Secretary Mrs C.Quayle 18 Rheast Mooar Ave RamseyLO.M. IM8 3LR Tel: 01624 812723
I.O.M. IM7 5EL Tel: 01624 897500
15th August 2003
Mr M Comwell-Kelly Clerk of Tynwald, Lgislative Buildings, Douglas,Isle of Mam. IM1 3PW
1 9 AU G 2003
Dear Sir,
SELECT COMMITTEE OF TYNWALD ON GP OUT OF HOURS SEVICES
I refer to your recent advert in the local press and enclose herewith reports submitted to the Trustees by the Manager of the Grest Home for the consideration of the Select Committee. These illustrate a very worrying, and potentially, life threatening situation caused by the withdrawal of an out of hours GP service in the North of the Island and the closure of A & E services at night in a well equipped Hospital.
The Trustees are fully supportive of the Manager of the Grest Home and of the Ambulance Crews who have an extremely difficult jo b . Apart from the inconvenience and, apparent, lack of interest shown by the duty Mann-Doc, the Minister and Administrators of the Health Service do not seem to realise that elderly people, particularly those in Residential Homes, are frequently very frail, often confused and sometimes suffering from senility. Until recently these residents have known, and been comforted by the fact, that they can call on their Doctor in emergency or can go to the Cottage Hospital where they may be sure of immediate care.
Those residents at the Grest who have been unfortunate enough to suffer the Mann- Doc scheme, either at night or during the weekend, cannot understand why they have to wait for an Ambulance and, probably, be transported to Douglas when ,in their view and that of most people in the North of the Island, there is a well equipped and caring hospital in Ramsey. Many residents at the Home and throughout the north of the Island are concerned that they have contributed large sums to provide improvements at the Cottage Hospital yet their efforts and those of the League of Friends appear to count for nothing in this ,so called, “caring society” . There
Is also disquiet in the knowledge that a Ward in the Cottage Hospital, dedicated to the memory of John Clucas has been converted into a Dental Clinic without reference to his family or those who care for his memory.
The present system puts a heavy load on the Ambulance Crews who have to decide the best course of action to pursue in each case and considerable extra work for the staff at the Grest Home who have to calm and re-settle the residents, as, in the case of Mr Hicks, they are moved from one hospital to another in order to be given a prescription for anti-biotics. Has anyone bothered to work out the cost of these excessive and unnecessary Ambulance journeys and the trauma suffered by our Residents compared with the cost of a duty Doctor in the North of the Island?
The Trustees are of the opinion that the Minister and the Health Service generally have lost sight of their sole function - to provide medical care for the residents of this Island - and have become involved in expensive and grandiose schemes.
The Trustees are grateful for the opportunity to make their views known and they ask that the Select Committee give them, and doubtless many others, due consideration in the fervent hope that there will be an early improvement in the service provided.
A.S.Percival Chairman, Grest Trust.
GREST RESIDENTUL HOME, ANDREAS ROAD, LEZAYRE
Report of incident by MRS SUE WRIGHT - MANAGER
MISS BEATRICE TAYLOR
On Saturday, 31st May 2003 Miss Taylor, aged 89 years and suffering from Senile Dementia, was taken ill. She had a temperature, was vomiting and her urine was very offensive, indicating a severe urinary infection. She became dizzy and unsteady on her feet in the late evening and could not manage the stairs up to her room. Due to her mental condition she could not be persuaded to use the Lift or Stair lift so Mann-Doc was contacted.
An Ambulance was sent at 10.30 pm but Miss Taylor refused to go in the Ambulance and the crew stated that they could not waste time trying to persuade her and, therefore, left. Mann-Doc was contacted again and the Grest Staff were told to contact Miss Taylors own Doctor on Monday morning - a delay of OVER 36 hours! Miss Taylor spent the night in a spare room on the ground floor - she was very agitated and distressed so that the Night staff had great difficulty in calming her.
Miss Taylors symptoms persisted on Sunday morning so Mann-Doc was contacted, again, at 10.30 am. Once again, an Ambulance was dispatched with a different crew who were more persuasive and, with the assistance of her niece Miss Taylor was taken to Nobles Hospital and admitted to Ward 9 where she remained for two days before returning to the Grest Home.
This incident caused a great deal of distress for Miss Taylor who becomes very agitated if her usual routine is changed. Had a Doctor been on duty in Ramsey and the Cottage Hospital permitted to accept patients at night and at weekends this distressing episode could have been avoided.
GREST RESIDENTIAL HOME, ANDREAS ROAD, LEZAYRE
Report of incident by Mrs Sue Wright - Manager
MR LAWRENCE BANNAN
On the morning of June 6th 2003, Mr Lawrence Bannan (a resident at the Grest Home and in his mid 90’s) was sitting eating his breakfast in the dining room of the Grest Home when he collapsed. This was at approximately 08.00 hours. He was grey in colour, sweating, hi s.lips were blue and he was totally unresponsive.I dialled 999 and an Ambulance with Paramedics arrived within about 5 to 10 minutes by which time Mr Bannan had opened his eyes but was not coherent.
The Paramedics gave him Oxygen via a mask which seemed to bring Mr Bannan round quite well and within 10 minutes he was fully conscious again but still very pale and sweating and unable to stand.
At 08.25 hours the Ambulance man decided to take Mr Bannan to hospital. He said they should go to Nobles as no Doctors were on duty in Ramsey until 9.00 am, however, it would be 9.00 am before they got to Nobles anyway.
He (the Paramedic) pondered whether the Nurses on duty at Ramsey Cottage Hospital would accept Mr Bannan at 08.30 but did not think it likely as he was in a “collapsed” state.
Mr Bannan was taken out to the Ambulance at 08.30 hours and was still outside the Grest Home at 08.45 with the Paramedics in attendance. They drove off at 08.50 approximately and I later found out that he had been taken to the Cottage Hospital and admitted via Accident & Emergency.
The Paramedics obviously appreciated it would be far better for Mr Bannan to go to the local Hospital and be seen by his own G.P. or one from the Practice without having to undergo a journey over the mountain to Douglas.

GREST RESIDENTIAL HOME, ANDREAS ROAD, LEZAYRE
Report submitted by Mrs Sue Wright - Manager
MR FREDERICK HICKS
On Saturday 2od August 2003 Mr Frederick Hicks, aged 85 years, became unwell.He had several minor falls and developed a temperature. His condition did not improve so, at 10.00 am on Sunday, 3rd August, the Staff contacted Mann-Doc by telephone. Details were taken by a Nurse and the Doctor ‘phoned back at 10.30 am to say that he was sending an Ambulance. The Ambulance arrived some 20 minutes later when the crew assessed Mr Hicks and decided to take him to Ramsey Cottage Hospital. He was accepted at the A & E Department of the Cottage Hospital but, 30 minutes later, the Hospital ‘phoned the Grest to say that Mr Hicksneeded assessing by a Doctor so they were transferring him to Nobles by Ambulance.
\
Mr Hicks was eventually seen by a Doctor at Nobles Hospital and returned home to the Grest at about 3.00 pm, again by Ambulance, having been prescribed a course of anti-biotics for an infection. Mr Hicks had no lunch and, by the time he returned, was hungry, agitated and quite dis-orientated.
Had a Doctor been available at the Cottage Hospital or on duty in the North of the Island the whole matter could have been dealt with in a veiy short time, the expense of THREE Ambulance journeys avoided and, by far the most important, no trauma or upset for an elderly gentleman and the staff at the Home.
1965 Celebrating 35 years of service ■2000
League o f Fhri ridS-xxtRarasey Hospital
Malachy Cornwell-Kelly Esq.,
Clerk to Tynwald,
Legislative Buildings,
D O U G L A S .
^ e c g f v £ £ >>£P 2003
TYm.â iD
(TREASURER.
H. Penrose
8, Riverbank Road
RAMSEY
IM8 3PP
September 10th2003
Òear Sir,
Select Committee on G .P .'s services.
Enclosed please find a collection of letters submitted
as evidence for the above Committee from:-
Mr H.Penrose, 8 Riverbank Road, Ramsey. IM8 3PP.
Ms Freda Skillicorn, 203 Queens Court Ramsey.
John and Doris Harris, Tan-y-Bryn, Ballavolley, Ballaugh.
Mrs Julia Barker, Nirvana, 50 Claughbane Drive, Ramsey.
Mrs R o s e m a T y Kneale, Thie Grenaugh, Claughbane Road, Ramsey.
Mr & Mrs J.Cushen, 10 Marlborough:* Crescent, Ramsey.
Mrs J.Rawling, 6 Ormly Grove, Ramsey.,
A .P & A.B. Shimmin, 6 Orchard Close, Andreas.
Mr. P.Caine.
Anne Husband, 9 Marlborough Way, Ramsey.
Mrs C.A,Johnson, Àldin Cottage, Glen. Auldyn, Lezayre.
Mrs C.M.RawSfeònj, Manager, Cummal Mooar, Queens P r o m e n a d e ,R a m s e y .
Mrs 6.K.Wynne# Warden, Kerroo Glass Sheltered A c c o m o d a t i o n ,Ramsey
C.J.Martin, -5 Marlborough Way, Ramsey.
Mrs D.S.Crompton, 22 Mountain View, Ballaugh.
Mr & Mrs D. R. Bushe.ll, Swing bridge House, 16 West Quay, Ramsey.
" " M and tEanscript of this letter.
I have also enclosed a copy of the history of Ramsey
Cottage Hospital which I feel may be of interest to the committee
Yours faithfully,
ros e .
Fo Cronk,Riverbank Road,Ramsey. IM 8 3PP.Tel: 812429.
Mai achy Comwell-Kelly Esq. JXB(hons),Cleric of Tynwald, September 9th 2003.Legislative Buildings,DOUGLAS.
Sir,Evidence for the Select Committee on GP Services.
It is very obvious that Government does not comprehend the seriousness of the situation regarding hospital cover and the GFs out of hours service for the people of Ramsey and the north of the Island
A statement was made in Tynwald by the Health Minister, Mrs. Clare Christian, M.L.C., that 'She had to take into consideration the whole Islands needs when making decisions’ and that is understandable.
However, every problem does not fit the rule book and in this instance Ramsey and the north are being denied a basic human right. Due to the removal of the Ramsey GFs cover, the hospital closes at 10pm with only a nurse-led minor injuries unit in operation between 6pm and 10pm ( in other words a sticking plaster clinic). We are, in fact, without medical cover for 14 1/2 hours per day with no doctor cover at night and during weekends and bank holidays. This means we are without doctor cover in emergencies for 120 hours per week and this figure does not include bank holidays.
The Emergency Doctor Service is not working for Ramsey and the north simply because of the mountain terrain. The mountain road is frequently closed for hours by accidents and, of course, fog snow and ice plus the T.T. and M.G.P. races. During the winter it is not unusual for the mountain road to be closed for two months due to snow.
Even on a perfect day with no traffic hold-ups, it takes a minimum of 40 minutes to get to Noble's Hospital.
One must also take into consideration that if an ambulance has had a previous call-out to Noble’s Hospital ( which is often the case) then a return time of 40 minutes must be added before the ambulance collects them with a further 40 minutes before the patient reaches Noble's Hospital making a total of 1 hour 20 minutes before the patient is treated.
The situation with call-out of the Duty Doctor is equally serious. He can be anywhere in the Island If he is in Douglas it will take him 30 minutes with a clear road ( always providing he knows the location of the patient - if he doesn't then there is more delay) and if he is in the south of the Island then it will take him at least an hour to reach parts of the north of the Island We must then add to this time the ambulance response time and the patients survival time has run out!
A very worrying factor is that the Duty Doctor has no access to the patients records which, in a case of a person being allergic to certain drugs which would be noted on the records, could prove fatal.
If Ramsey Hospital was open and working normally the patient could be comfortably in-situ and treated, as it always was before the G.P.’s withdrawal of services.
Previously, people have always been told by their doctors that if they suffer from heart problems, strokes, brain haemorrhage or brain swellings, catatonic seizures, meningitis or burst stomach ulcers to mention but a few conditions, that their survival depends on the response speed of medical attention, TIME BEING OF THE ESSENCE.
Let us not forget there are numerous situations with babies and young children where speedy medical intervention is paramount to survival.
People of the north are so worried that many say they must leave the north because of the lack of medical cover and facilities especially the elderly, the sick and those withe young children. One man said to me, Is this euthanasia under a new name?
One of the problems with the Emergency Doctor Service is that frequently the caller is told by the Duty Doctor that he is not coming out on call and that they are to attend Noble's Hospital to see him/her. There are many in the north who do not drive or find it difficult, being a one parent family, to find a baby-sitter to look after their other chidren whilst the sick child/person goes to Noble's. Also, many find the cost of a taxi to Noble's Hospital exhoibitant and out of their reach. At night, it costs nearly ONE HUNDRED POUNDS RETURN TO JURBY ! To make things worse, the taxi firms in Ramsey close down at lam and it virtually impossible to obtain a taxi in Douglas to return to Ramsey at night.
People are also driving themselves to Noble’s Hospital when in severe pain and in an unfit condition to be driving.
The situation as it stands is totally unacceptable and if this restricted service is allowed to continue there is going to be a tenible tragedy before the Government wakes up to the fact that you cannot put monetary savings before lives,
Therefore, I say to the Health Minister’s remark that 'she has to consider the whole Island when making decisions' that Ramsey and the north have been neglected and the rest of the island has gained at our expense.
I would suggest that we have two doctors, directly employed by the DHSS not under contract, to take over the running of Ramsey Hospital thus enabling the hospital to return to its former status. It is not my intention for these doctors to sit in the hospital waiting for patients. The doctors would live locally and be on call. The morning shift doctor would make his rounds and then be on call, being free to travel locally providing he/she remains within paging distance. The same principle would apply at night with the duty doctor in his own home and able to attend the hospital as and when required.
These doctors would take over the running of the hospital from the Ramsey Group Practice and the savings from this arrangement would go some way towards paying for the new doctors making this a part self-financing viable proposition.
In the event of holidays, sickness and leave days, a locum ccould be employed to cover these situations. Retired doctors could be employed on a part-time locum basis.
If I did not feel that economics were at the bottom of this problem then I would ask for a houseman. However, I feel that two doctors on call (one on, one off) with them being able to stay in their own homes, would be appealing both to the doctors and in economic terms.
The question that needs to be asked is how many people are dying in the ambulance or soon after admission to Noble’s Hospital. These deaths, of course, go down as mere statistics. How many of these would have been saved if Ramsey Hospital had been functioning properly?
Under the present arrangement, the patient has to travel regardless of whether they are fît to do so or not and one asks whether they would have survived if they could have been admitted to Ramsey Hospital until they were in a fit condition to be moved to Noble's Hospital.
Having toured the new Noble's Hospital, there is no doubt that it is a wonderful hospital full of the latest technology. However, as far as the people of the north are concerned, with the distance and the mountain terrain, it is outside our survival times in an emergency.
The two problems of Ramsey Hospital downgrading and doctor coverage are inextricably linked and cannot be dealt with as separate issues
No account should be taken of the after - hours(6pm to 8.30am) attendance figures for Ramsey Hospital. These will not show a true picture due to the fact that after-hours, the ambulance crews by-pass Ramsey Hospital and take the patient direct to Noble's thereby distorting the figures. When you add on the after-hours ambulance journeys to Noble's Hospital you will then get a more realistic figure.
I enclose herewith an enlarged copy of a card, distributed by Ramsey Hospital to the general public in the north of the Island, which shows quite clearly that after- hours the hospital is no more than a clinic or as one person put it yesterday,They are no more than a school nurse1. I have no argument with the nurses, they do a marvellous job but they can only work within the parameters they are given.
Finally, Heaven help us, if we have a severe winter where patients suffer from respiratory problems, flu and cold-induced angina and heart problems or vehicle accidents.
I hope this submission will help the Select Committee to understand some of the problems facing the people of the north of the Island due to the withdrawal of the out-of-hours medical cover.
Yours faithfully,
H - / W o c v .
¡ fL . f i ' b . K . P e n t e Q c
Mr. H. Penrose,Treasurer,League of Friends of Ramsey Hospital,C/o 8, Riverbank Road,Ramsey,IM8 3PP
4th September 2003
Dear Mr. Penrose,
Re. vour article about medical care in the north of IOM
I took part in the protest march through Ramsey and attended the meeting in the church hall. There is no doubt that the voice of the people was heard then but has now been forgotten.
As part of the general picture I can tell only about a personal experience in April 2003 that, after the event, will only come under the category of “if only" or “might have made a difference” or *Sve wiU never know” if or *Ht’s too late now”.
My wife had just got into bed and lifted her head for me to adjust her pillow and then she felt a terrible pain in her head. The time was about 10.45pm on a Tuesday night. She was in agony with arms and legs flailing about, I dialled 999 and while I was spitting out the symptoms my wife slumped into unconsciousness. It was sheer luck that the ambulance was on stand-by at Ramsey and came within a few minutes. The two paramedics had to try and stabilise my wife in the ambulance outside our house and, after about fifteen to twenty minutes, raced her off to Noble’s Hospital, with me following in my car. The journey over the mountain road took about another 20minutes and when she arrived at Noble’s all her functions had shut down apart from a slight pulse. My wife died two days later in ITU because of inoperable bleeding into the brain stem.
I am continually unsettled after the event, as per the second paragraph of this letter, if only my wife had been taken to Ramsey Cottage Hospital. It would have taken only a few minutes but she might have received treatment and in a bed. Instead there was “a delay” of about 40 minutes that included that 20minute bouncy journey. I wonder could it have made some difference? I am like any other ordinary person with little medical knowledge but I feel that my wife might have had a better chance of survival if Ramsey Hospital had been open, i f there had been a doctor on duty and i f there was the equipment there to give her the necessary treatment The doctor tells me that it would have made no difference. “We will never know ” and uit is too late now ” but we must think about other people for the future. What happens if the ambulances are already out, maybe at Nobles? No doubt, someone will die.
Bearing in mind the vast amounts of money the Government has spent on capital projects, I think that the question has to asked, if it would not have made more sense for the Island to have two medium-sized hospitals. One in Ramsey and the other Douglas or towards the South with each hospital properly staffed and equipped with ITU facilities etc. Each hospital capable of offering the same level of treatment and care, thereby the potential to save lives and not knowingly putting lives at risk as with the present system-
Priority should be given to reinstating proper doctor cover, staffing and the upgrading of Ramsey Cottage Hospital
Public Money should be spent on our hospitals rather than on the refurbishment of the Government offices and the like.
If the MHKs for the north and south of the Island who were elected by the people to represent the people had asked the people what to spend the people’s money on then I am sure that the people would have said to spend the people’s money on two hospitals of equal standing. This would have offered a better level of health care to the people overall than with this huge building that caters basically for the people of the Douglas area in an emergency.
The Government supposed to represent all of the people has failed the population of the North, West and South. I believe a calculated risk to the lives of people living in these areas has been made to save on capital costs. I wonder what price tag did the Government put on each life and how the MHK’s can sleep at night.
Yours Sincerely,
Mr. P.Caine
9, Marlborough Way Ramsey
IM83NF 30th August 2003
Dear Mr Penrose
1 understand you are collecting opinions from people in the north of the Island, regarding the medical services provided at weekends and weekday nights.This arrangement seems to me, totally inadequate for single, elderly and disabled people, also young children
I do not know what statistics are being used to assess the use of the on- call doctor and ambulance, but 1 would respectfully suggest that winter figures of illness would be more appropriate than those that have prevailed during the recent good weather
Three years ago a near neighbour, having fallen, had to be transported to the Cottage Hospital, urgently, late one evening. The ambulance was here in a few minutes and the paramedics were excellent. What would happen if this situation arose now, if the ambulance was already in use?
I would be very unhappy to see the facilities at the Cottage Hospital farther diminished. It is a precious asset for Ramsey and a great many people have contributed to providing comforts for patients and staff.
Yours sincerely
Aldin Cottage Glen Auldyn
Lezayre Nr Ramsey Isle o f Man
IM7 2AD
Tel 01624 815504
E-Mail a j @ manx.net
30 August 2003
Ramsey Hospital League o f Friends c/o H Penrose Esq 8 Riverbank Road Ramsey IM8 3PP
Dear Sir
I would like to report to the committee the distress I fe lt over a recent incident regarding my 94 years old Mother.On the 2 9 July last at 7pm my M other who lives with us suffered a serious angina attack, my husband telephoned fo r the ambulance, which arrived without delay. After examination by the ambulance men they decided she needed immediate specialist attention.I asked them i f ¡shou ld follow them in my car, expecting that my M other would be taken to Ramsey Cottage.They then informed me that no one was on duty at Ramsey and that my Mother would be taken to Nobles. I was appalled and shocked that my seriously ill M other was having to fa c e that journey in her condition but the fa ct was there was no choice and I travelled with her in the ambulance.When we arrived at the Bungalow on the mountain road, we had to slop and wait fo r a param edic to attend to my mother as both ambulance men were not qualified to administer the necessary treatment, we then continued to Noble % where she was admitted to the Accident and Emergency department, later that night she was admitted to Ward 6 where on the 4th August she d ied
This trauma would not have happened had the Ramsey Cottage Hospital had a Doctor on duty.
Yours sincerely
Mrs C A Johnson
CMR
26th August 2003
Mr Penrose 8, Riverbank Road,Ramsey Isle of Man
Dear Sir,Thank you for your recent phone call to my colleague re; the concerns since Manndoc put in place.
I have personally found that since Manndoc has been used although the advice has been very helpful ,it has taken rather a long time to get to us . In one instance a Temporary client was having a very violent seizure and because the client was not well known to us I rang Manndoc who said they would pass on the message and the doctor would ring back. After 20 minutes I rang for the ambulance as I had ,had no return call the client was taken to Nobles. After over an hour the Manndoc rang back and was informed that the client had gone to Nobles.The other Concern that we have is if a client dies over the weekend or at night time we have to wait for the client’s own GP to pronounce the client deceased . How can we let the family know that we THINK! The client has passed away as we are untrained and cannot say that someone is dead even if we know they are.I hope this helps .
Yours faithfully
C.M RAWSTRON Deputy Manager Cummal Mooar Queens Promenade Ramsey Isle of Man IM8 1EL
Mrs. Geraldine K. Wynne Resident WardenKerroo Glass Sheltered Accommodation Ramsey IM8 2 NL
12th August 2003.
Mr. H. Penrose 8 Riverbank Road Ramsey IM8 3PP
Dear Mr. Penrose,
Ref. The Tynwald Select Committee on G.P's Services.
I am glad to have the opportunity to comment on the unsatisfactory state of the medical support that we now receive in the north.
I look after 45 elderly residents here at Kerroo Glass and the first thing that I noticed after the ’Manndoc' announcement was the amount of stress and worry caused to my residents. This became apparent when they were talking to each other and also to me.
Recently I had personal experience of this new Manndoc service. My mother, who is elderly and lives in Ramsey telephoned me on a recent Saturday morning. She felt unwell and asked me to take her to Ramsey hospital. The duty nurse did what he could, then contacted the Manndoc doctor at Nobles who decided to examine my mother. So I had to drive to Douglas, leaving my husband to look after my residents at Kerroo Glass.
An ideal solution to the disgraceful service that we receive in Ramsey would be to release our GP's from their hospital contracts ( as they don't wish to provide a full caring service ) and employ Hospital doctors at Ramsey. Please don't say that there is a shortage because adverts could be placed in medical magazines in the Indian sub continent, or in Eastern Europe or for highly trained, western oriented doctors you could advertise in Israel.
Yours sincerely,
Mrs. Geraldine K. Wynne Resident WardenKerroo glass sheltered Accommodation Ramsey IM8 2NL
16th. August 2003.
Mr. H. Penrose 8 Riverbank Road Ramsey IM8 3PP
Dear Mr. Penrose,
Ref. The Tynwald select committee on G.P's Services. ( or lack of services!)
I wrote to you on 12th. August in response to your invitation to comment in the 7th. August Courier.
Once again today I had to avail myself of the poor services at Ramsey Hospital.
Today, one of my residents had a fall on the entrance to Kerroo glass so I took her to the Cottage. After waiting till about 4.30pm. I was asked to take her to Nobles for stitching. I explained that as I had another 40 plus residents to look after, the nurse suggested a taxi or somebody else run her to Nobles. A friend in Ramsey was finally located who gave her a lift with a bleeding nose, forehead and lip.
This further episode - and be assured there will be many more, both more and less serious that will occur in the near future from Kerroo Glass alone - only underlines the need for a full Hospital Doctor service in Ramsey.
Yours sincerely,
G. K. Wynne
5, Marlborough Way Ramsey
Isle of Man IM8 3NF 01624-814751
August 19 2003
M r. Howard Penrose 8 Riverbank Road,Ramsey Isle of Man
Out of hours doctor service: Ramsev
Dear M r. Penrose
I am writing in response to your announcement in The Courier concerning comments and experiences with the new service. Since the Government decided to start the system at the beginning of the summer my wife and myself have not experienced any medical emergency out of hours but when the winter comes things may well be different as we are both aged pensioners. No statistics based on the recent past are of any value. As a statistician who had an international reputation I would advise using the data from the last 2 winters, which should be available as a guide to requirements.
Under the Charter of Human Rights, which the Government has signed, is it not a right to have medical care readily available and close at hand?
I can give an example from past experience which shows how dangerous the present position can be. My wife started vomiting in the middle of the night and I knew that an injection was the only remedy. Without it she would vomit until she would be so exhausted that she would become unconscious. The doctor on duty came and injected her and she slept for 24 hours and was then relatively well. To have had to telephone Noble’s, mahe an appointment and then go to Douglas would have been nigh impossible. May I add that when we lived in Jordan in the Middle East and the same thing happened, a doctor arrived promptly? That country is supposed to be a third world one. W hat does it say of the Isle of Man? Sports stadia and other public buildings including hospitals, do not form the criteria of a developed country. Service, both medical and police need to be available 24 hour each day and both are lacking in the North of the island
22, MOUNTAIN VIEW BALLAUGH
ISLE OF MANIMJ7 5ER 01624-897369
August 19 2003
M r Howard Penrose,8, Riverbank Road,Ramsey Isle of Man
Dear Mr Penrose,
Out of hours doctor service: Ramsev & The North
I am writing as a widow and a pensioner to protest at the withdrawal of the above service from the Cottage Hospital. I live at some distance from Ramsey and it is difficult enough to visit the doctor there. To expect pensioners to visit Douglas in the middle of the night is to refuse us our human rights under the European Charter.
The Government decided to start the system at the beginning of the summer season when illnesses are less and much of the population is on holiday. Accurate information would become available only when the winter months arrive. Does the Government intend to wait until the number of deaths reach a certain figure before taking any real action? The Sunday Times on the occasion of the TT races had an article which demonstrated that a trauma unit was on 24-hour standby at Noble’s at the weekend of Mad Sunday. Surely the resident taxpayers of the island have a right to a similar service close to home.
I, for one, am very fearful of the possibility that the winter months will have a serious effect on my health. Unfortunately any illness will not limit itself to commencing during the period from 9AM to 5PM Monday to Friday.
Yours sincerely,
D. S. Crompton (M rs.)
Transcript of attached letter.
813797 Mr. and Mrs. D.R.Bushell,Mr. H.Penrose, Swingbridge House,Treasurer, Ramsey Hospital League of Friends, 16 West Quay,
Ramsey, IM 8 1DL.Dear Sir,
I am writing in response to your letter in the Aug. 28/2003 Examiner Aug26th.
Last week my husband was attacked with violent pains in the lower abdomen (After hours of course for the Surgery or the Ramsey Hospital) He had an operation for bowel cancer on April 23rd, so naturally we were very worried.
We telephoned the emergency Doctor at Nobles but could not get through, and my husband said he could not face having to make the long and possibly hazardous journey to Douglas, which is now even longer at the Nobles New Hospital.
However, the pain did subside after a warm drink and a couple of pain killers. Fortunately, he had an appointment to see his doctor at 9.30am the following day as he had not been feeling well for several days. The Doctor said that if it happened again he should contact the surgery IMMEDIATELY - as it could be connected with a hernia he had surgery for some years ago. So what if it was after hours AGAIN.
It seems quite incredible that we do not have an emergency doctor based in Ramsey.
Something must be done about it and SOON before we have another death during this long journey.
Yours sincerely,Vivien Bushell.
U- • ^ O S * Mr & Mrs D.R. BushellSwingbridge House
fn < ?u W a ÌCcvttN^ f < ì t 16/WR ^ y
D p O IsleofM anIM81DL
;-rf t J0 V < ? /tJ /J^ Ì Ì y j ^ £ i h < n Ì
]£T}~Q .m rnp^ OoC- Q b / k - ' '
ta^ i- vJ-esA7 f*-j LuoU^c/ì, a UacKZv 1 u.JiL ^<>i /-w
r>d e O J W o ^ ^ f ^ ^ ^ ^ ^
f\^. b a s f l v k f ^ . / l e A a</| a w Q ^ a U ^ - f a i ftimc-m
C"-- O-^otki^ "S'Q cx^fi. o ì3 o&i-p o6n«j viOooRi-é’c /
Vsi-e }-e£-e piescaA /Le em e^e-w :«^ iUt^'e«? al- ^ e t ò - VQt J
ToJV- +?oou.\)£_} m - j h S a /c 4 [_# e s t u a i i J o h Jc< q>
^ ^ i ' o i s i t . C , 1 0 ^ 2 ^ 1 S ^ S jP fc ^ f iu , £■
1 - ^ © v ^ t W , i - ^ t A , vs vS©^> f c c w ^ c a -ìÌj? ù d ~ t e ~ , V é L j
-
ì&tyoGùCÌl. Ca|v>J V i'Cf C-|ifq & \ i/J7 ^ wt? o^J Qy (cèu M
t j^ f a ^ f Q R V u ^ a V f^ k U c i a o ^
A-^l lW ^ S^fr0u3' ' - ± ) t h s j &-> )-f> ¿J ¿¿// f$ <jl~ 4^ q^
^ 0) £ - 0 ^ ^ J ^f Ì)^ c t-O i\ SCHx{ yj ;<f.
P^cÀ * 0 * 1 Cfò^iracT" .-—
(k .^ rW £ow PcÀ ^ fo v ^ C cf-ee /l a fcWio/j c iU
^ < H d . S o i ^ K a l ; j '* <o<n* d f w
^ ^ u V r t^ fo p ^ c U JÌA / ^ v 3^ ^ 0 ^ 0^ J ^ r ? a ^ s ^ a h J .
C w \ ^ < ^ ^ 0 Ì^O tirO ^ 3 > (W ìt1 )-rt
V \ J ^ ^ ^>O0n-p a ^ o o ^ '/(^ JT o q J
t ò c ^ C^1<0 9c^<5^. ^ ^ 7 fLi-r? J
ino
í
Dv <D G > •H O ■H MS U) mDC >,
no¿'no
S c a ni 2 2tu IH 0
S O O ^ 0> mW-M 0 Ë-h1 h oro to oí sCÍ H M M
tr ~
e ri
I
10. Marlborough C rescent Ramsey
5 September 2003. Isle of .Man.IM8 3NE.
RefereiK^ Ramsey_Coflage Hospital Emergency Medical Cover.
Dear Mr Penrose.I understand you are canvassing for support in your quest to have the
recent withdrawal of emergency cover in the evenings and at weekends reinstated
My husband and I fully support your action and have very strong personal reasons in so doing.
About a year ago I had reasons to call for a doctor to attend my husband, and if it had not been for the prompt attendance and diagnosis by our G-P,. which resulted in major surgery for Mr Cushen he would have lost a leg.
The prompt ambulance and paramedics reactions were beyond reproach.
Now Mr Cushen (a war pensioner ) is severly disabled and relies on the services of the Cottage hospital on a regular basis.
We are both senior citizens and feel we are being deprived of having peace of mind iathe event of needing emergency medical treatmentWe cannot emphasis enough our extreme concern at the withdrawal of emergency services and can only hope the powers that be will reconsider their decision and realise what the older residents of Ramsey must have and are entitled to.
We wish you every success and thanks for your efforts.
3\Av^e-Ä^
) K t 9 2 l « L ,
C-J V, S^O^®-U4JBd£t áfi0*2a
I
U a ^ * P e ^ m ^ ^
I C¿SC 'O pr-eÄ proTSf"«
te ^ ¿ x * -*& ^ 4 p 7 kä- p v -Ä ^ ß jJ ' M ^ ì9 c r f t ì^ c f o ^ t j
I p ^ i ^ f f e a o CXI- ^aM^yG-Cj M -o rp tïja Ji ,
« ty- L4* Lvu ö v c c e ^ c r iö Jb t 1& & Jt toß-
r\AA>-e K jo cÂ*zxMov^ cu v^u . (aJfei fo ^
ä a a c ( ÍC a / - p ~ & op te ^^vO kÍ¿4
j ^ p e c i - e ^ i ^ 4 o 4 r ^ i e - L 4 o fO ô ^ k j £ ¿ for*
ij>O tr/-K n eief- -
• Í d>0 (vOpt^ hviVl-
J ^ w ^ y o o r f ^ > fc e ^ \ p iv M iC - <3-uc(
^ftfv^ i~ fo w r l&U-£c> m hfeXie^cf-tiy .
I Çui\ C£>^Xt^ j,
¿ C k ^ C e .
■■sJo-krA X r ib
f i r v n - . __
-----M j- ___ - £ > Ä lk u d ,L
■■I K f t . *T£ flr____ -.. ^ i t e U j t ù ^ - .
I? p g r M /__&L nca% e.2 y\ t^cjptryix- ‘f o j gw' J k t í í r f í\ f h 9 s l^ < r 1
ti-Ks'j 4/Ò&-— *?^ - / d f c I
/£Wi.k« ¿W f a r C.ûv^âJ-rC'— ^ N’ru^J^-
< S e ì j ¡cu— ¿ J r . f â œ r ^ y - / f< d h z $ p _ ttc*/?T F& J.« njiJL^jL
'Yl tr4 X. 1 ^ ÂÀ£L£ i L *S-e ( j i UL* /t ule. j j i K . /-o-iml La^i._____
__ 4 Q íj J Á ~¿n x n - ¿ ^ n ^ e m c ^ ¿ - ¿ m o y W
SPnÄCe b e fiSt\ùicÙ >J ÆT ¿^i
__p c>^ > iûU,..r’ ü x ß i/^ Jb ls j k le^ tx . tU __ÚYW¿Á~aj ¿ótÁ tT j-UrtJtï r fazL&t/it kj) ì fi¿/vtr .______________
Wjfl ft-w— & r ^-to~cr~ cavx ex/-KV_
_______________ y & * jr ì. ____________fa f A P&MÀ-j.
_______— f j - a f / P ï
ouna taarxer Nirvana
50 Claughbane Drive Ramsey
Isle of Man IM8 2BJ Tel. 01624 8143o8'
;;
■
2 ^ è '
â T® *y - i l - *- é -■ ^ <~Ò
a ' l'V
r
4. s
~ r r o
-.*3i - i '2r$ 'Jf
1 ¿ J 4 4«?
-U
4
o - j «4 Q£jö I ^ 1
4»3
<^> c i
<3i - ^ N
?
-O
6 Wt <Q F C L A & J> *7~b ' T f- fe P u & c ^ c . t s t ^ & /* S £ ± £
What can be seen in the Mill?Minor cuts or wounds
Sprain or strain Soft tissue injury/bruising
Bite/sting Minor eye problem Wound infection Pulled elbows
✓
Uncomplicated head injury Small abscesses
Minor burns/scalds
A copy of the history of Ramsey Cottage Hospital - "Ninety
Years Young" an illustrated account of Ramsey and District
Cottage Hospital by Constance Radcliffe provided by the
League of Friends of Ramsey Hospital is available for
viewing in the Tynwald Library.
Appendix 3

OFFICE OF THE CLERK OF TYNWALDLegislative Buildings, Douglas,
Isle of Man, British Isles, IMI 3PW
Our Ref: C /G PS/02/plb
29th July 2003
Isle of Man
Dear Dr
Select Committee of Tynwald on GP Services
I am writing to you at the request of the above Committee, to ask you to supply evidence, in writing, to the Committee concerning any observations you may have on the issue of provision of General Practitioner out of hours services and any changes that you feel may be desirable in the future.
The Committee would be pleased to receive your views by Friday, 12th September 2003. After it has examined the written evidence received, it may wish to call a number of doctors to give oral evidence.
Please find attached a copy of the resolution establishing the Committee.
Yours sincerely
P ¿o Bao
Phil Lo BaoJoint Clerk to the Committee
Enc
At a Tynwald Court held on 17th June 2003
32. General Practitioners Out of Hours Services -
RESOLVED
That Tynwald approves the appointment of a Select Committee of five members to investigate the matter of the General Practitioners 'Out of Hours Services7 being provided throughout the Island, with power to take written and oral evidence pursuant to sections 3 and 4 of the Tynwald Proceedings Act 1876 and report by October 2003.
Mr SpeakerMotion carried.
Mrs Craine, Mr Gelling, Mr Gill, Mr Singer, Mr Speaker and Mr Waft were nominated.
After a ballot Mr Gelling, Mr Gill, Mr Singer, Mr Speaker and Mr Waft were elected.
Telephone 01624 823243 The Surgery,Fax 01624 822947 Mill Road,Dr. C. C. Taggart BALL AS A LLA,Dr. A. M. Blackman Isle of Man.Dr. J. E. Hockings IM9 2EG
3rd September 2003
Mr P Lo BaoJoint Clerk to the CommitteeSelect Committee of Tynwald on GP ServicesOffice of the Clerk to TynwaldLegislative BuildingsDOUGLASIMI 3P
Dear Committee
Re: MEDS / Out of Hours Service
Primary Care Services have developed considerably since the 24-hour cover of the original 1948 Health Service. GPs in the island resisted the development of deputising services many years beyond the UK and only changed the service when we felt we could no longer maintain a satisfactory level of care to meet the daytime workload.
We need more GPs to provide a quality of service and list sizes are already too large to offer a level of service which we consider adequate. As secondary care looks to earlier discharges, shorter hospital stays and less chronic beds the workload continues to increase. More chronic disease management and protected time for specialist services is being taken on by GPs and patients’ expectations of care continue to grow.
I am GP Tutor and the concepts of evidence-based medicine being practiced along with audit requests and clinical governance mean continuing pressures for GPs to undergo regular personal development and education adding to pressures on their evenings and weekends.
The workload pressures have led to increasing problems of recruitment and morale within the GPs, both in the island and the UK. GPs are choosing to retire early and recently a survey of GPs suggested twenty could leave within the next ten years in the Isle of Man along with a shortage of twenty to thirty if list sizes fall from 2000 to 1200 or 1400.
1 0 SEP 2003
OFFICE OF TUE r i F.RK OF TYNWALD
The majority of patient problems can be sorted within the working day of 8.00am to 6.00pm, which is still longer than most professionals’ days. Most feedback from patients and colleagues about Manndoc and now MEDS is positive.
However, there is a need to provide an appropriate working environment for a service which is “open” and “in use” more hours than any secondary care outpatient clinic.There should be a properly designed area including rest facilities for doctor and driver, I feel there is a need for two doctors for most sessions and I elect to only work the sessions with two doctors. I would hope better liaison could be achieved with the A&E department but a drop in service is likely to be abused.
The key to the success of the process is patient education over what is an “emergency” and that telephone advice can be suitable, along with a positive approach from secondary care and administration that this is an appropriate professional development.
Yours faithfully
Dr AM Blackman GP Principal & GP Tutor MBChB DRCOG MRCGP FPCert
Telephone 01624 823243 Fax 01624 822947 Dr. C. C. Taggart
The Surgery, Mill Road, BALLASALLA
Dr. A. M. Blackman Dr. J. E. Hockings
Isle of Man. IM9 2EG
2nd September 2003
Mr P Lo BaoJoint Clerk to the CommitteeSelect Committee of Tynwald on GP ServicesOffice of the Clerk of TynwaldLegislative BuildingsDOUGLASIMI 3PW
Dear Committee
Points to remember to make MEDS an even better service
1. In 1948 health services in Britain were set up with equal access for all patients so GPs were given 24-hour responsibility for their patients. In those days few patients had telephones or cars, now the majority have them.
2. 24-hour cover was covered by mostly single-handed GPs during the 1950s but the advantages of group practices were obvious and by the 1960s GPs were sharing the 24-hour cover with group practices.
3. In the 1970s the burden of their care led to out of hours Deputising Services in the UK - manned by GPs but run by commercial companies.
4. As the cost of Deputising Services rose in the 1980s GP Practices started to band together as cooperatives to cover the out of hours work.
5. On the Isle of Man, before Manndoc was set up, there were seven GPs on call overnight for a population of patients, which on average, phoned three times from0000 until 080D. Given that the day work of GPs is relentless and that some doctors get little rest if on call, this was causing far more disruption to GP lives than was of benefit to the patient.
6. The care of patients since 1948 has increased in complexity, patients’ expectations are high and the elderly population is rapidly expanding. GPs are being stretched in all directions.
7. There is a persistent statement made that when Manndoc started the calls to 999 ambulances fell by 40%. If this is true it shows the great worth of the out of hours service. There appears to be a lot of goodwill between the ambulance service and the out of hours GPs.
8. The island needs more GPs. Many patients cannot register with a practice. To attract more GPs we must have a workable and tolerable out of hours service.
9. GPs are retiring earlier due to increased work whereas, in the 1960s, 70s and 80s GPs would work even to the age of 80 (now not recommended). If the out of hours work was returned to the GPs on the island many more will retire early with loss of many years work from experienced doctors.
10. There have been practical problems with the transfer of the service from old to new Noble’s site but the potential for the service is excellent. That Ramsey patients and Port Erin patients have felt angry at the loss of their previous service is not surprising given the lack of publicity and information. The vast majority of Manndoc patients welcomed the GP co-operative feirly soon after it started because it clearly was a service set up to cope with out of hours problems.
Yours sincerely
Dr JE Hockings MBChB DRCOG DA
RECEIVED1 2 S E P 2003
OfFiCC OF THE CLERK OF TYNWALD
Drs J.E. Brewis & S.M. V. Swainson 46 Arbory Street
Castletown M 91LN
Mr P. Lo BaoJoint Clerk to the Committee Office of the Clerk of Tynwald Legislative Buildings Douglas IMI 3PW
11/9/03
Dear Mr Lo Bao,
Re: Select Committee of Tvnwald on GP Out of Hours Service
When the Emergency out of Hours Doctor Service was set up on the 1st April 2003 to cover the whole of the Island, I had my doubts that one doctor per shift would be able to cover the workload. The single doctor shifts also have the back up of a second on call, should the need arise, and two doctors cover shifts which have been predicted to be busy.I have worked a regular shift (Monday midnight to Sam) since April and I have been pleasantly surprised that the workload, although variable, does not seem to have altered much since I worked for MannDoc, which covered eight of the Island’s practices. We have, however been working a spring and summer period, in which the health of the population tends to better and without additional influenza outbreaks etc. Only time will tell whether this level of cover will be adequate for the winter months. However, I am confident that the Department will address this problem and act appropriately should the need arise.GPs are currently renegotiating their contract and there is great change occurring in General Practice in Britain. Fewer doctors are entering into General Practice, and on the Island, a significant proportion are due to retire in the next 10 years. It is essential therefore, in order to attract and retain GPs, that our working conditions are at least as attractive as those in the U K This is the background to the new Out of Hours arrangements.From the layman’s point of view, the reduced numbers of doctors covering the Island, must have appeared a drastic and sudden change. I can sympathise with his view point, particularly as it happened to coincide with a reduced service in the Minor Injuries Unit at the Ramsey Cottage Hospital and a cessation of admissions to RCH in the out of hours period. However the current conditions are the only ones under which I am prepared to continue to provide out of hours cover. As our representatives have negotiated these conditions, I assume this is the consensus view of my colleagues.Any chafage in the service should only be made in the light of experience and/or statistical evidence and then can only be made if there is available manpower.
Yours sincerely,
Dr. Sm Jy. Swainson
Dr David Chalmers
Dr Frank Vaughan
Dr Juan Garcia
Tel: 01624 629010
F ax: 01624 674515\ , r /
ICushag Roa
Anagh Coai£
Dougla
Isle of Man1
IM2 2SU
30 July 2003
Mr Phil Lo BaoJoint Clerk to the CommitteeOffice of the Clerk of TynwaldLegislative BuildingsDouglasIM1 3PW
Dear Sir,
Re Select Committee of Tynwald on GP Services
My Personal Observations as a GP and former Manndoc Director are as follows:
The Manndoc GP Co-op successfully covered the majority of the islands population for many years
with no problems. In general those that had used the service found that the service was of a high
standard and of quick response, this could be seen by the low level of complaints received against
Manndoc. I have since performed a number of shifts under the new all island system. Obviously
the set up has slightly changed to take into account the extra population covered. Of the evening
shifts and midnight shifts that I have worked I have never needed to call in the back up Doctor and
patients care has not been delayed. Though I do know that this has happened and worked
successfully. Having a back up doctor is something that never occurs when you cover just your own
practice so in the past patient delays always occurred while you were driving around the
countryside trying to find houses.
The out of hours centre at the old Nobles site was well set up with equipment and staff. The new
temporary set up has the same equipment and once a permanent location has been found I am sure
the quality will improve yet further.
The new system mimics that used on the mainland with the exception that our level of cover means
that on average one GP on call on the island covers less patients than the equivalent GP on the
mainland and over the same equivalent topography. So in effect we can respond quicker to patients
on the island.
Emergency/Life Threatening illness cover has remained UNCHANGED since the new GP Out of
hours service. Since the introduction of Paramedics to the ambulance service GPs have ceased to be
involved in these cases which include Heart Attacks, Major Trauma, Epileptic fits, Unconscious
patients etc. The Ambulance service continues as before. Should a patient call MEDS with such a
problem the ambulance is called. I mention this because in the media this was the main concern
raised by the general public. Though not part of this committees remit it should be noted that
Ramsey Cottage Hospital is not a major trauma centre and does not have a Coronary Care Unit so
ambulances going there in my opinion only delayed the care of the patient by the specialists. So
lack of a GP there has no impact, I feel, on true emergencies.
The general public have also stated that transport to the out of hours centre can be problematic. All
terminally ill patients and immobile patients that need a visit are seen. When Manndoc was in force
most if not all of the complaints that we received related to failure to visit. Normally the patient had
requested a visit claiming that they had a lack of transport The Duty Doctor would refuse to visit
on these grounds alone. The complaint letters then usually stated that they had to take the patient to
casualty in a friend’s car etc, i.e. the same building as Manndoc! This is an example of unrealistic
expectations from a medical service. The out of hours emergency service is for medical problems,
transport is provided via ambulance when medically indicated. It is the role of the family, friends,
or social services to provide the transport as would happen during working hours. So far on my
Shifts with MEDS I have had no one who was unable to attend when requested to do so.
In the British Isles there is a shortage of GPs with a further exacerbation of the problem due to
increase this deficit yet further when GPs who came to the UK on the 1960’s retire. The forecast is
not good for recruitment. Newly trained Doctors are used to shift work within the hospital setting
and as such have not been training for General Practice. The On Call 24hr Commitment has
repeatedly been shown to be the main reason for this. As a result the UK GPs have negotiated a new
contract, which is coming into force in the UK, our main recruitment area. This new contract has
removed the 24hr commitment from GPs, because of this the Isle of Man needed to change its
working practices in line with this change, in order to compete in the market place for the few GPs
still training. Hence the timing of the introduction on the island. If this change had not taken place
we would have had NO GPs applying for vacancies on the island. As it is, it is extremely difficult to
persuade people to come, at our practice it took over a year to recruit our new partner. Luckily for
the islands population our Health Minister realises the problem and has acted promptly and her
department is actively negotiating a new GP contract on the island, to allow us to compete with the
UK to retain and recruit new GPs.
In the past when medicine was less complicated Doctors used to work longer hours at a lower
intensity. Now with modem medicine and higher intensity workloads this has been increasingly
detrimental to Patients and Doctors Health. As a society we have decreed that Lorry Drivers, Coach
Drivers and Airline Pilots can only work for limited hours because of the danger of accidents when
tired. Contrary to the publics perception Doctors are human as well and when tired can also make
more mistakes. Hence decreased on call leads to fresher Doctors and potentially less mistakes and a
better quality of life.
In summary the new Out of Hours system and the removal of the 24hr commitment for GPs is
working well, is safe and essential if we are to recruit and retain GPs. Overall the clinical care
offered by this service is an improvement on before. But I accept that the population have to adjust
their view on what to expect out of hours. No one ever likes change.
Yours
Dr A Vaughan
Dr P A Harrison Dr D James Dr N R Hopkinson Dr G Evans Tel (01624)675444 Fax (01624)616290
Hailwood Medical Centre2 Hailwood Court
Governors Hill Douglas
Isle of Man IM2 7EA
31st July 2003
NRH/PP
Mr P Lo-BaoJoint Clark to the CommitteeOffice of the Clark of TynwaldLegislative BuildingsDOUGLASIsle of ManImi 3PW L
R E C E I V E D
- a '¿003
Or'FiCE OF THE r.i >-RK Or TYNWALD
Dear Mr Lo-Bao
Thank you for your letter dated the 29th July (ref: C/GPS/02/PLB) asking for my comments about the general practitioners out of hours services. As you will probably be aware, I have been a GP on the Isle of Man for the last five years, and have worked in the previous MannDoc system and I have also undertaken shifts in the new MEDS out of hours service. It is my firmly held belief that a central singular out of hours service as has been set up is the way forward for the Isle of Man. The Isle of Man has had increasing difficulties in recruiting quality GP’s from the UK, and the move there is definitely towards removing General Practitioners out of hours responsibilities. Now that the department of health has taken over responsibility for out of hours, this puts us in a similar position to the UK and makes the job of attracting GP’s easier. I believe that all GP’s should be given the option to opt out of out of hours provision if they so wish.
The next issue, is with regard to staffing the out of hours service. As you should be aware, despite the fact that levels of remuneration for providing GP services to the out of hours service have increased, it has been difficult for the department to sustain filling these shifts. With this in mind, I thinks the provision of a second out of hours service to cover different parts of the Island would only complicate this issue and cause problems in having sufficient medical cover to provide the necessary out of hours cover. It may be worth pointing out that the out of hours service provides cover to the Island’s GP patients for approximately one hundred and twenty hours per week.
I believe that in terms of man power the current shift system is more than adequate in terms of providing medical cover to the required level. However, there is an issue over visiting patients at home. I firmly believe that the vast majority of problems that we are requested to deal with can be more than adequately dealt with in the out of hours centre where ever this is located. However there is an underlying attitude amongst the general public that they feel that they have some sort of right to have a GP visit them at home. I am totally against this belief and feel that the Government should be strongly be supporting a change in attitude. There is no reason why nearly all patients could not come to a base at Nobles Hospital. After all, if a patient is severely ill enough, they are invariably transported to Hospital for further treatment. However I feel that the Department could help with this in terms of perhaps providing some form of transport option for people who are
Cont
remote and have no access to personal transport. This could be in the form of either a taxi service or perhaps part of the Ambulance services responsibility. I am sure that if this issue was clarified and sorted’ the public’s resistance to centralising the service would be diminished.
Finally I would like to point out that as far as I am aware, amongst the GPs as a whole there is a very strong feeling that centralisation of provision of out of hours is the correct way to go forward. We do not wish to be bullied into providing a service purely to appease the general public or make life easier for politicians.
Yours sincerely
J O — .
Dr N R Hopkinson
Dr P A Harrison Dr D James Dr N R Hopkinson Dr G Evans Tel (01624) 675444 Fax (01624) 616290
Hailwood Medical Centre2 Hailwood Court
Governors Hill Douglas
Isle of Man IM2 7EA
31st July 2003
Our Ref. DJ/SYR
Mr P Lo-BaoJoint Clerk to the CommitteeOffice of the Clerk of TynwaldLegislative BuildingsDOUGLASIsle of ManIM1 3PW
Dear Sir,
Thank you for your letter of the 29th July.
I have been a GP for some 16 years now, of which 12 and a half have been on the Island. I have had experience of all sorts of arrangements for out of hours cover, ranging from one in four on call I did when I first arrived, to a one in ten rota which was shared between four practices, to the Manndoc system and to the use of a commercial deputising service in Liverpool. Of all of these arrangements I found that the most effective for providing rapid easy access to the patients was the Manndoc system where people could attend a central on-call centre to receive attention. People are generally seen a lot more quickly than they were on our previous rotas which involved visiting every patient, when if the work load was heavy there could be long delays between people ringing and being seen. It is very rarely necessary for people to be seen in their own home and most people are perfectly happy to travel to the on-call centre knowing that they will be seen sooner. Under the Manndoc system we regularly saw patients from as far afield as Ballaugh and Kirk Michael and Port St Mary and Port Erin. There is very little criticism of the system or any complaints about the distances that people had to travel to get attention. Since the Emergency Doctor Service has been set up this has just been extended slightly. It still takes people no more than 30 minutes to get to the Centre from any part of the Island and they are still being seen more rapidly than they would have been under their old systems. It is still accepted that some house calls will be necessary and the staffing levels at the Emergency Doctor Service are adequate to provide this without people having to wait too long for their treatment.
I understand the anxieties that some people in the North of the Island felt when the service at Ramsey Cottage was supposedly reduced, but in reality people who attend Ramsey Cottage are now being seen by an enthusiastic team of highly trained nurses who are always there on the premises and who appear to provide an excellent service. 1 feel that there may be scope for a nurse practitioner led service to be set up at Southlands also to reduce the number of people from the South of the Island who have to come to Nobles Hospital.
I am quite sure that there has been no deterioration in the medical care of the Island’s population since the Emergency Doctor Service was set up. In feet the area covered by it is much smaller than many areas in the UK where the system has been in place for a number of years.
As this has now become the accepted system throughout the UK when Doctors are looking for posts that is what they will be expecting, consequently to try and return to the old system you would have extreme difficulty in recruiting Doctors to the Island. I feel you would also have some difficulty in keeping the Doctors on the Island that are already here.
It should also be remembered that the GP out of hours service is not, and never has been, an emergency service. It is never appropriate to do people’s treatment of chest pains and violent abdominal pains by calling the Doctor out. People should attend Hospital as soon as possible. Similarly people should not go to Ramsey Cottage Hospital with potential life threatening conditions as they do not have the facilities to deal with this as it is after all a Cottage Hospital.
I think that if there are any deficiencies in out of hours medical cover it is more in the number of ambulances that are available to transport people from North and South of the Island.Emergency ambulance cover is an integral part of the service and should be looked at alongside the GP cover. Similarly some form of transport could be made available to those few people on the Island who do not have access to a car. This should cut down on a number of the unnecessary house calls that are done at present.
I think that the public should be educated to avoid abuse of the service as it seems to be used as a convenient drop in centre for people in the centre of Douglas who couldn’t be bothered to contact their Doctor or take time off work during the week to seek medical attention. Hopefully this should be less of a problem at the new Hospital.
I feel that it would also be useful to encourage the GP Practice’s to increase the number of appointments they have during the week as it appears that if people have to wait over long for an appointment with their own Doctor they are more likely to use the out of hours service. I know that the UK Government are trying to insist on a 48 hour availability for appointments which may not be totally realistic but I feel that some effort should be made at most Practices to reduce the time that people have to wait for appointments.
Yours sincere]

Dr N G S Gavin Kensington Group Practice,Dr A C Pilling Kensington Road,Dr D M Bull Douglas.Dr C M Blackman Isle of Man, IM1 3PF.Dr Harrop Tel: 01624 676774Dr W J Cowie Fax:01624 614668
Ref C/GPS/02/plb Friday, August 08, 2003
Dear Sir,
Further to your letter of 29th July regarding GP out of hours services Kensington Group Practice would like to express the following observations:
1 Generally we support what is broadly a good, efficient & cost effective system that is essential as the way forward for the issues of retention and recruitment of General Practitioners (GPs) to the Island. To return to a outdated historical model of personal on call duties would, we feel, be a retrograde step and also would be difficult to justify on health & safety grounds for both patients & doctors, not to mention in view of European working time directives regarding maximum working hours.
2 Though it would be ideal to have surgeries in the North and South of the Island, this would seem to be impractical from a staffing and economic point of view.
3 W e also have concerns regarding access both ways across the TT course when roads are closed.
4 W e cannot help but feel we are generally unwelcome within the hospital and within government funding plans.
5 W e have been tacked on within the fracture clinic premises, which may be adequate for a hospital based specialty but would not be used for consultations in primary care.
6 A purpose buitt premises would be more efficient and pleasant for the patients and staff.
7 W e feel there is an ongoing need to communicate to the population that this is an out of hours emergency service and not a second opinion service or because they were too busy working to be sick.
8 Information technology (IT) for the out of hours is non-existent and we are even banned from using the hospital systems. Historically GPs have been at the vanguard of IT and using it to integrate within Primary care to improve records, data flow with practices and safety issues.
9 For a specialty that is present & working for the majority of the week (118 hours per week) we feel it is unacceptable to be wheeling drug trolleys and phones into and out of the room every day. As the fracture clinic has a lower occupancy (40 hours) surely it should be the other way round!
10 The primary care services staff, Ann Marie & Sally, are excellent though we wonder whether a medical director would be beneficial to support them and the doctors, as well as the administration & with clinical governance issues that arise.
11 Uk models of out of hours (OOH) care rely on nurse triage and advice so to be able to get advice direct from a GP shows the high standard of service provided to the Manx people.
12 It would be felt that with the dominance of such large private firms as Nestor (Primecare) in the UK’s OOH care and the higher cost issues such a company would command, the Manx Emergency Doctor service provides excellent value for money.
W e would like to re*iterate our ongoing support for the current system but would afways welcome constructive suggestions for genuine improvement.
Yours sincerely,
Dr N Gavin Dr A Pilling Dr D Bull Dr M Blackman Dr M Harrop Dr W Cowie
Palatine Group Practice
^ j| Tel:(OI624)62393l
IM2 .3TD
Fox:6HTO
11 August 2003
Your ref: C/GPS/02/plb
Mr P Lo BaoJoint Clerk to the CommitteeSelect Committee of Tynwald on GP ServicesOffice of the Clerk of TynwaldLegislative BuildingsDouglasIM1 3PW
Dear Mr Lo Bao
Select Committee of Tynwald on GP Services
Thank you for your letter of 29 July 2003 asking for written evidence for the Select Committee of Tynwald on GP Services. I am a principal in general practice on the Isle of Man for the last 13 years and as such I have participated in out of hours rotas between small groups of practices initially,as part of the MannDoc co-operative and as from 1 April 2003 worked for the Manx Emergency Doctor Service on a sessional basis. I am also one of the negotiators nominated by the GP body on the Isle of Man to negotiate with the DHSS the terms of future GP contracts on the Isle of Man.
The principal need for the change of out of hours cover has come from increasing recruitment and retention problems in general practice in the British Isles over the last 10 years or so. The problems have been particularly acute in the Isle of Man where we have had a number of GP’s retiring at 55 and about a half of practices trying to recruit replacement or additional partners having difficulties.
When GP’s in their fifties were asked what is the single most difficult part of the job that would most influence them to retire early, they said this was having to provide out of hours cover on top of the normal 50 hours a week that surgeries are open. The ability to go without sleep and function safely the following day becomes impaired the older you get. Most other professions or jobs where safety of the general public is involved such as drivers, airline pilots actually have their hours regulated, usually by law in the interests of
2
public safety. It seems very strange that doctors and their patients are offered no such protection.
In the United Kingdom the imposition of the European Working Time directive has resulted in changes in working patterns to hospital and junior doctors and not to treat GP’s in a similar way will further discourage newly qualified doctors from undertaking the higher training to become accredited as specialist General Practitioners.
Another pressure on recruitment and out of hours is that up to 75% of entrants to the medical schools are now women and up to 90% of doctors entering higher training for general practice are also women. In future the Isle of Man will be recruiting from an increasingly female workforce. Not only are female doctors less likely to work full-time in general practice, younger doctors are more likely to have families and as such are already tending to apply for GP principal positions which do not require them to do out of hours.
In the United Kingdom this has been possible for a number of years because of out of hours co-operatives and commercial deputising services who have at least given the doctors the option of paying for somebody else to do their out of hours cover. In the Isle of Man we have never had this option.
One of the fundamental parts of the new UK contract for General Practitioners is that responsibility for providing out of hours services is going to be assumed by primary healthcare trusts for all of the previously mentioned reasons. If we are to have any hope of recruiting to the Isle of Man in future we have to provide at least as good as, if not better, working conditions for our doctors.
As such it was agreed with the Health Services Division of the DHSS that as from 1 April 2003, they would take over responsibility for out of hours cover. As the committee will be aware, there has been an out of hours co-operative running within the Island which included all GP’s except the Ramsey Group Practice, the Southern Group Practice and the Onchan and Laxey Practice.This seems to have worked very well over the last 4 or 5 years with very few problems and was based on UK models of out of hours co-operatives and services where there was a centrally placed out of hours centre appropriately staffed and resourced.
The levels of medical staffing which were basically one doctor with a second one who could be called in if necessary seemed adequate to cope with the level of demand from the areas that the co-operative covered. For the successor to MannDoc which has to cover the whole of the Island, the amount of medical cover at busy times at weekends and Bank Holidays was doubled which seems to have more than covered the increase in workload. I understand that the Manx Emergency Doctor Service has more doctors per head of population than co-operatives in the UK. I also understand that the geographical area that we
2
3
cover from our centrally based out of hours service is much smaller than cooperatives in the UK would cover.
Because the Department has taken responsibility for the service it is now no longer a GP co-operative where only principals in general practice could work within the service, now the service has a much wider pool of doctors to draw upon including a number of fully vocationally trained GP’s who currently work either as non-principals in general practice or locums or doing hospital posts in various other specialties.
I feel the biggest challenge to the out o f hours service is actually finding doctors to work the sessions available. As time goes by the older GP’s in their fifties will be reducing their out of hours commitment and some newer GP’s coming into general practice with family commitments may not wish to work within the service. I think the Department will need to employ increasing numbers of full-time doctors to work within the service and my understanding is that this is the intention of the Department and the process of drawing up job descriptions and recruitment in anticipation of this has already started.
Another direction which the service may develop is in the use of nurses to triage calls at busy times such as during the day and early evenings. This is an approach used in the UK by NHS Direct and many co-operatives where nurses use computerised protocols to assess calls and give advice. With a relatively small population such as the Isle of Man, the fluctuations in demand can be more marked than would be experienced in some of the larger services across and use of nurse triage would enable us to cope better with this.
I think the strength of the current Manx Emergency Doctor Service is that it is staffed by local GP’s who live and work on the Isle of Man and who are familiar with the local set up and services. I feel strongly that this has to be the future of out of hours cover on the Isle of Man. The continuation of the previous service or to try and turn the clock back to the previous service would very rapidly result in retirement of older GP’s and inability to recruit new GP’s to the Island and I suspect a very rapid loss of GP’s on the Island to the UK where better working conditions and remuneration would be available. With average list sizes on the Island per GP greater than England, Scotland, Wales and Northern Ireland currently this would result in a very rapid collapse in NHSGeneral Practitioner services on the Isle of Man which clearly must not be allowed to happen.
Yours sincerely
0bUÄi2ßJÜ)
Dr J K Daniels MB, ChB, MRCGP, DRCOG, DCH, DFFP
3
Palatine Group Practice
5 j ] Tel: (01624)623931Fax:61l7l2
31 July 2003
Your ref: C/GPS/02/plb
Mr P Lo BaoJoint Clerk to the CommitteeSelect Committee of Tynwald on GP ServicesOffice of the Clerk of TynwaldLegislative BuildingsDouglasI Ml 3PW
Dear Mr Lo Bao
Select Committee of Tynwald on GP Services
Thank you for your letter of 29 July 2003.
There are many issues involved here, some national (the GP contract negotiations in the UK are still ongoing) and some are very local (the Ramsey situation).
For an overview from the profession as a whole, it would be better for the committee to approach Dr M Maska, Chairman, GP Sub-Committee of the Isle of Man Medical Society.
From a purely personal point of view, I will be 55 next year and have no intention of doing out of hours work beyond this date and if compelled to do so. then I will resign.
Yours sincerely
R t f
Dr F W Harding
CC Dr M Maska, Ramsey Group Practice
Well established
Virtually universal in UKIsland small compared to UK areas covered.______
Superior manning levels.__________Manndoc covered most of island
Zero obligation April 2004.
PCTs responsibility
OOH.emm -17/08/2003
GP vacanciesRetirement bulge- subcontinent
50%+ female intakeDemography GP male age 50< = 83%
GP male age <30 = 24%
Less attractive hence new contractNon-existent recruitment
25% in 5 years 50% in 10 yearsON-call
Housing/ removal costs
High list size
Worktimedirective
Palatine Group Practice
T el: (01624)633931 Fcx:6117I2
1 September 2003
Your ref: C/GPS/02/plb dated 29 July 2003
Mr P Lo BaoJoint Clerk to the CommitteeSelect Committee of Tynwald on GP ServicesOffice of the Clerk of TynwaldLegislative BuildingsDouglas
Dear Mr Lo Bao
Provision of GP “Out of Hours Services”. “MEDS”
The current provision of GP “out of hours” services came into effect on 1 April 2003 and mirror the recent changes seen in the UK GP contract. The majority of these duties is still provided by the existing GP workforce, but with two fundamental changes;
a) Every GP on the Island “pays in” £6 ,000/year consisting of £3,000 previously paid for out of hours cover and night visits and loss of £3,000 capitation fees.
b) GP’s working “out of hours” have to “opt in” and are paid a variable rate depending on the shift worked.
These changes have benefited GP’s by the fact that they now have to work fewer (but busier) “out of hours” sessions. An unexpected benefit to patients has been an increased availability of “daytime” appointments. This has occurred because a GP has to “volunteer” to do “out of hours” sessions, this effectively makes it a private arrangement between the GP concerned and the Health Service and practices do not now give “time off” following a night duty.
2
Within my practice, Palatine, this has enabled us to offer an extra 60 routine appointments per month. It should not be forgotten that the ambulance service has been unable to meet its “response time” targets largely due to the old MannDoc system.
At the present time, our ability to provide a first rate out of hours service is compromised by the lack of a dedicated “out of hours” centre. When one considers that “out of hours” consists of 118 hours/normal working week. I find it ridiculous that we have to “borrow” the facilities of the Fracture Clinic. Patients have to enter next to the A & E exit where recovering drunks are waiting for taxis. There is no reception area, no fridge, no fax, single drugs trolley (inadequate for Bank Holiday weekend), no rest area for driver/doctor. All of our equipment has to be locked away prior to 0800 on normal working days. On one occasion this month, the duty driver had to sleep 5 minutes drive away as his overnight accommodation had been given to a relative of a patient in the Intensive Care Unit!
Therefore a dedicated “out of hours” area is a priority, this could be a new build on the new hospital site or perhaps use the Union Mills FC clubhouse when this is vacated. This would allow the doctor and driver to sleep on the premises, establish our own fax and computer system and enhance our existing drug stock.
A 4 x 4 vehicle to allow visits to all areas on Island needs to be purchased prior to winter.
Consideration should be given to extending pharmacy opening hours until 2200 weekdays and until 1800 on Sundays/Bank Holidays. This would allow more over the counter (OTC) medication and would reduce the primary care drug bill. Patients discharged from Nobles should be supplied with a 28 day supply of medication as opposed to the current 7 day supply, this would reduce the need for visits and further reduce the primary care drug bill.
I do not feel that there is a medical need to provide satellite “out of hours” centres, no patient is going to be further than 20 miles away. If, however, there is a political need to provide minor casualty facilities, then these should be provided from secondary care as there are clearly insufficient GP’s on the Island to staff these.
There is concern that some patients who do not have their own transport and genuinely cannot get a neighbour/friend to bring then to the “out of hours” centre cannot afford the cost of a taxi eg Bride to Douglas. I am sure that named taxi firms could be used if subsidised by the Health Services.
3
I am confident that with the above proposed changes, we can provide a first rate “out of hours” service and that patients will forget the relative inconvenience of having to travel a few miles in order to achieve 24 hour GP access.
Y
Dr j McDonald Palatine Group Practice
DR V PAUL BRADLEY & DR CLARE HILLAS
For the attention of Phil Lo Bao - Joint Clerk to the Committee
Dear Mr Lo Bao
Re: Select Committee of Tynwald on GP Services
Thank you for your letter requesting observations about the out of hours services.
Personally, I feel that it is going very well. I have not had any complaints from our own patients at this Practice, or those that I have seen whilst working for MEDS. I have also been impressed by the standard of care provided by the nurses at the Ramsey Cottage Hospital minor injuries unit.
My only concerns are that the telephone system is inadequate to cope with the volume of calls on Saturday and Sunday mornings, and that a lot of time is wasted having to go through switchboard to telephone patients if they have only given us a mobile telephone number.
I feel that the MEDS reception Staff and drivers, do a very good job and deserve more remuneration, given the stressful nature of thé work and the anti social hours. Also, if the doctors were better paid, especially for Saturday shifts, it would be easier to fill the rota.
Finally, as the out of hour service is likely to be permanent, and given the number of hours per week for which it is operational, I feel that it merits a permanent site of its own, rather than sharing the Fracture Clinic.
I hope this is of help to you.
Yours sincerely
PROMENADE MEDICAL CENTRE 46 LOCH PROMENADE
DOUGLAS IM1 2RX ISLE OF MAN TELEPHONE: 01624-675490
4 August 2003 RECEIVEDOffice of the Clerk of Tynwald Legislative BuildingsDOUGLAS IMI 3PW
- 7 AUG 2003
OFFICE OF THE CLEFtK OF TYNWALD
DR CLARE HILLAS
RECEIVEDPeel Medical Centre Derby Road PeelIsle of Man
1 2 SEP 2003
Phil Lo BaoJoint Clerk to the CommitteeSelect Committee of Tynwald on GP ServicesOffice of the Clerk of TynwaldLegislative BuildingsDouglasIsle of Man
9/9703
Dear Mir Lo Bao
Select Committee of Tynwald on GP Services
The arrival of OOH Co-ops changed GP’s lives. The removal of responsibility for0 0 H care would be an even bigger improvement, and the present situation where the DHSS threatens collapse of the MEDS system every time there is difficulty in filling a shift is unacceptable. We can’t be opted, out, take a cut in income and still be held responsible.
MEDS needs investment'in terms of equipment (a fax machine to start with - in my previous Co-op all OOH contact details were faxed to the GP surgery the following morning), training and IT. It cannot function well without access to patient records, but SIPS is slow and obstructive. Patients find it hard to believe that we cannot access their GP or hospital records on computer. Give us that access. Consider providing reception staff through the night, and nurse telephone triage at busier times. Put the money saved by not providing OOH dental services into the MEDS fund since it now deals with most dental emergency calls. Give us dedicated premises (the Fracture clinic is open less than 40 hours a week, MEDS is open at least 118, yet we scrabble to clear our equipment into cupboards at 8am weekdays). Consider a new post of Clinical Director for MEDS since it lacks a figurehead, someone to ensure clinical and operational standards are met, and to negotiate changes in OOH practices with interested parties (e.g. the cancer strategy group). Educate the public in what to expect of the OOH service and what is not provided. Ignore the debate on provision of a doctor in the North and South, the workload does not justify it and the public outcry will die away. Above all consider what happened with the dentists when their complaints of rising list sizes and workload went unheeded.
Yours sincerely
Dr.Jones Dr .Hudson Dr.Bloomer Dr.Hanks
PEEL MEDICAL CENTREDerby Road, Peel, Isle of Man, IM5 1HP Tel: 01624 843 636 Fax : 01624 844 543
11.08.03
Mr P.L.BaoJoint Clerk to CommitteeOffice of the Clerk of TynwaldLegislative BuildingsDouglasI.o.MIM1 3PW
Dear
Select Committee of Tynwald on GP Services
It is paramount that the population of the Isle of Man receive high quality out of hours medical cover which is adequately funded and properly staffed. It is essential that the services offered match or preferably better the services offered in the UK. This, as explained later, is crucial to recruitment and retention of medical staff in difficult times so that a service can be offered at all!
You will be aware of the current national GP contract negotiations, a component of this is that by 3 1st December 2004 thé Primary Care Organisations should have taken full responsibility for ‘out of hours’, (from 1830 - 0800 on week days, the whole of weekend, Bank Holidays and public holidays). The current default responsibility of GP’s to provide 24 hour cover is archaic, dangerous and makes general practice unattractive for prospective and current GP’s.
If we do not match or better arrangements in the UK it will be very hard to recruit practitioners to the island. My current commitment to the Peel Practice and MEDS is 50.5 hours a week, in 1992/93 a GP worked an average 43.5 hours and in 1985/86 worked 38 hours a week, UkD.o.H Joint Workload Survey. Our workload potentially is greater than our colleagues in the UK, Isle of Man average list sizes are large —
Isle of Man average list size 2001England 1841Wales 1685Northern Ireland 1649Scotland 1409
The I.o.M average list size is 42% higher than those in Scotland. Our Peel Practice list size has increased by approximately 8% over the last 10 months, average list sizes in the England have remained the same over the last 2 years.
Dr.JonesDr.HudsonDr.BloomerDr.Hanks
PEEL MEDICAL CENTREDerby Road, Peel, Isle of Man, IM5 1HP Tel: 01624 843 636 Fax : 01624 844 543
The proportion of elderly patients on a GP’s list on the I.o.M is considerably higher than in the UK. It is recognized that this cohort of patients utilization of primary care services is high.
People aged 65 years and over per GP by country:
The current unrecognized workload in Primary care is reaching intolerable proportions. The BMA GP Vacancy Survey published January 2003, demonstrated the total number of GP positions vacant at 4.7% of total workforce. There are now 52% of vacancies left unfilled for more than six months.
I personally find the Out of Hours arrangements satisfactory and an improvement on the old commitment. People find it easy to access, figures for Manndoc that preceeded MEDS demonstrated use of the service to be almost the same as for those services in the UK. I believe the number of complaints has not increased. I have had my own patients in Peel praise the service they receive out of hours and value opinions from other doctors.
Out of Hours Co-operatives in the UK cover much larger geographical areas than we do on the I.o.M.
MEDS is not a deputising service but a service covered by knowledgeable, experienced Isle of Man based GPs familiar with local resources.
I feel strongly that the service should be computerized so enabling much improved audit and tracking of frequent inappropriate users. This system should be linked a.s.a.p to a co-ordinated electronic patient record strategy involving primary care. Personally I feel the island has on this occasion been foolish trying to establish it’s own system and should look at developments across with NHSnet.
Isle of man (2001 census)WalesEnglandUK (2000)
306286282272212211
Scotland Northern Ireland
Dr.Jones Dr.Hudson Dr.Bloomer Dr .Hanks
PEEL MEDICAL CENTREDerby Road, Peel, Isle ofMan, ÏM5 1HP Tel: 01624 843 636 Fax : 01624 844 543
The GP’s feel once again second fiddle to hospital care, we need properly designated premises and storage space for our equipment and medicine cabinet
Personally if MEDS was withdrawn and it defaulted to 24 hr GP responsibility I would become a statistic and resign.
Kind regards
A
Dr Andrew Hudson BSc ChB MB MPH(Merit)
Dr. IC J. Jones The Medical Centre
Derby RoadPeel
Isle of Man IMS 1PF
3rd September 2003
Clerk to the Select Committee of Tynwald on GP ServicesLegislative BuildingsDouglasIsle of ManIM1 3PW
Dear Sir,
Thank you for the opportunity for me to pass my personal views to the committee examining evidence on the provision of out of hours community medical services. I do, of course, also expect evidence to be submitted on behalf of the GP body where the mandate of collective opinion is likely to present a very strong feeling that the whole-island GP co-operative should be retained in more or less its present form.
During 22 years experience as a Principal in General Practice I have seen many changes in the style and demands made of the service in particular from a better informed public together with a spiraling beaurocratic mountain. I think this can contribute to increasing standards in the branch of the Medical Profession most commonly accessed by the public and charged with the responsible use of secondary care. The days of frequent out of hours committment in addition to a full time job are now anachronistic and contribute to a lowering of morale, recruitment and undermine the drive to raise the standards of primary care.
I would like to see full time staff recruited to the out of hours force in addition to those doctors who wish to participate occasionally in the rota. It may be necessary for at least part of the OOH period, to operate from two centres.
Yours faithfully
Keith J. Jones
DR.A.ALLINSON RAMSEY GROUP PRACTICE
BOWRING ROAD RAMSEY
ISLE OF MAN, IM8 3EY
3H1 ¿0 HOHaO
£OOZ 9HV S -
TEL: 01624 813881 FAX: 01624 811921
AA/vc
Mr Phil Lo Bao Clerk to the Committee Office of the Clerk of Tynwald Legislative Buildings DOUGLAS.IMI 3 PW.
1 August 2003
Dear Mr Bao,
Thank you very much for your letter dated 29 July, requesting my view on the provision of general practice out of hours services on the Isle of Man.
I came over to Ramsey to work as a GP approximately 18 months ago after working in Central London. During that time 1 worked for numerous practices and took part in the GP out of hours cooperative.
At Ramsey wc used to do our own on calls up until April 1st of this year, and also look after both inpatients and patients arriving in Casualty at the Ramsey District Cottage Hospital.
I view the creation of an all Island GP out of hours service as incredibly encouraging and forward thinking. I have worked numerous shifts since the 1st April and found that it provides a very good service to patients right across the Island
Whilst the service being provided by the GP*s, I think is of a very high standard, I do think operationally there is much that could be done to improve the service given to patients. The Mandoc service was very much set up on an amateur basis, with minimal expenditure. The EDS has taken over from this bat most of the expenditure is currently going into paying the doctors for their sessions rather than infrastructure.
At the moment the entire operation, which is meant to cover the entire population of the Island from 6pm to 8am and weekends and bank holidays, runs out of a small office, temporarily borrowed from the fracture clinic. Given the grounds of the new hospital there is no doubt in my mind that purpose built premises are both desirable and essential. At present calls that come in are written down by hand in an A4 text book then transcribed to small bits of paper with a carbon copy underneath.
All the professional services I have worked for on the mainland now use computerised records, both for accuracy and legibility. With a fairly static population like the Isle of Man there is no obvious problem with having a decent data base of patients with their date of birth, contact details, GP*s and dependants. This would allow decent audit and ensure that much better records are kept.
I feel that a purpose built base for the emergency doctor service is essential, as is the injection of funds to allow the service to develop into a professional» well run and audited organisation. At present the secretaries who take calls work part time and it is up to the Doctors to take calls after midnight.
For medical emergencies GP*s are only one point of access. One also has to consider District Nurses, Community Psychiatric Nurses, Dentists, The Ambulance Service and the A&E Dept at Nobles itself. Ideally I would long to see a centralised point of access for all emergency services. Various organisations have experimented with combining Police, Fire Brigade and Ambulance under one roof. Perhaps one day in the future, one number would also give you access to a range of other medical services that could compliment each other. In this way inappropriate calls to the Ambulance Service could be diverted to a GP or obvious emergency calls could be diverted to the Ambulance Service.This would both utilise shared information and allow greater flexibility for the services involved. It would also promote communication between the different emergency services and save considerable time, money and manpower in the infrastructure of such a call centre.
The above are just a few ideas I have had regarding out of hours provision for the Island. In the case of Ramsey District and Cottage Hospital 1 feel that the current situation of Nurse Practitioners leading patient care is both desirable and successful. Whilst I give all credit to the nurses involved for improving their skills, I do feel that they need more encouragement. With a new Consultant due to be appointed to the A&E dept at Nobles I think integration of the educational opportunities is essential to allow skills to be shared by both centres. I also would encourage the move of having a 24 hour nurse led service over the weekends and bank holidays. I understand that this was not instituted from April due to manpower problems b it feel that with the right planning such a service could be easily brought into being.
Thank you for your invitation to supply evidence to the select committee.
Our ref: JKB/GKS Your ref: C/GPS/02/plb
Dr J K Brownsdon Ramsey Group Practice Bowring Road Ramsey Isle of Man IM8 3EY
Mr.P.LoBao,Joint Clerk to the Committee,Office of the Clerk of Tynwald,Legislative Buildings,Douglas.
1st September 2003
Dear Mr.Lo Bao,
Re; Select Committee of Tynwald on GP Services
Prior to 1st April 2003 out of hours GP provision was provided in different ways in different parts of the island.
Approximately 2/3rds of the population mainly in and around Douglas, through to Peel and down to Castletown had their out of hours services provided by Mann-Doc, an independent co-op of GPs in that area.
The patients of the Port Erin, Laxey and Ramsey practices had their out of hours service provided by their own GPs.
However, it had become apparent for some time that for those GPs providing their own on call out of hours the workload was becoming more and more arduous and that this was having a debilitating effect on their health, their family life and their ability to perform their profession to the high standards that are now expected. This had got to such a state that several of the older GPs, myself included, felt that if the situation did not improve then they would probably opt for early retirement.
Added to this are the problems of recruitment of new GPs. Nowadays there are very few places that require GPs to do their own on call and even fewer newly qualified GPs that are prepared to do it.
It was, therefore, imperative that the DHSS did something about splitting the out of hours responsibility and the day to day care of the GPs1 patients.
The settingup of MED S has been the Department's solution after close consultation with the island’s GPs.
The Ramsey Group Practice thinks that the level of cover provided by MEDS is perfectly acceptable and equates very favourably with most places in the UK for the number of patients and areas covered.
We think that an analysis of the numbers seen will show that the present provision is satisfactory.
If there is perhaps one area of concern it may be that expecting patients to travel to Nobles Hospital by taxi from distant parts of the island is an expensive option. Possibly some form of refund could be provided on receipt of an attendance record to the MEDS base at Nobles Hospital.
We also hope that the ambulance service continues to be fully funded and staffed so that there is an adequate provision of paramedic services when they are required.
i.K.Brownsdon for and on behalf of
'Ramsey Group Practice
DRMS CHAN Ramsey Group Practice
Bowring Road Ramsey
Isle of Man IM8 3EYy r Tel: 01624 813881 Fax: 01624 811921
MSC/LP
11 September 2003
Mr P Lo Bao Clerk of Tynwald Legislative Buildings Douglas.
Dear Mr Lo Bao
Re: Tynwald Select Committee on out of hours GP cover.
You have received letters from Dr J Brownsdon on behalf of the Ramsey Group Practice and Dr M Maska on behalf of the Island GP's.
From a personal point, I find that the out of hours cover extremely difficult to cope with on my return to work in January 2003 after a period of sick leave. It is difficult to work 34 hour shifts once a week and still work 8 - 6.30 Monday to Friday and weekends as well. The out of hours component of our work is being taken out of the GP contract in the UK. There is only a limited pool of GPfs available country wide and unless the terms and conditions of service are as, if not more attractive than the UK, then it will be difficult to recruit and retain GP's in the Isle of Man.
Yours sincerely
¡ M i % t j l
Dr M S Chan.
Tel: Ramsey 813881 Fax 811921
R A M SEY M EDIC AL PR A C TIT IO N ER S
DR M. MASKA GROUP PRACTICE CENTREBOWRING ROAD RAMSEY ISLE OF MAN IM8 3EY1
2 September 2003
Dear Sirs
Further to your letters of thé 29th July and 7th August 2003 please find enclosed a copy of a “mind map” with the relevant factors concerning GP Out of Hours services. Taking each subsection in turn.
Firstly as the Isle of man does not produce GP’s it is almost entirely reliant on the UK for its workforce. Currently there are some 1000 GP vacancies (1). This represents about 1 in 40 of all GP posts. In addition there is a looming retirement bulge of GP’s (1,2) particularly from the Asian subcontinent which will further exacerbate the number of vacancies. More than half the intake of medical schools is now female. This in turn translates into the statistic that 83% of GP’s aged 50 and over are male (2,3). Of those GP’s who are under 30 only 24% are male. The important point of this is that many female doctors do not work full time, nor work out of hours partly for childcare reasons. An increasing number of male GP,s adopt a similar approach. In the year 2001-2002 (9) the number of male GP’s working three-quarter time has increased by 14 %. Therefore despite an increase in the overall number of doctors being trained 2-3+ are needing to be trained to fill one whole time equivalent post.
General Practice in recent years has been seen as a less attractive option by medical graduates (4) hence recruitment has dwindled with many vocational training schemes only partially full or folding altogether and retention an increasing problem. As a way of trying to redress this situation the UK Government in its NHS Plan (5,6,7) has taken steps to make general practice a more popular rewarding choice of career. With the BMA and NHS Confederation a new contract has been proposed (8) and now accepted again as a way of tackling the above issues.
In the NHS Plan it was proposed that GP numbers be increased by 2000 over 3 years: 2001-2004. Workforce figures released in July 2003 (9,10) show that numbers increased by0.1% i.e. 29 in the first year. Hence the overall target is in tatters. The BMA disputes that 2000 GP’s are required and says the figure is nearer 10,000 due to the changes in working practice and increasing retirement as outlined above.
This makes recruitment into General Practice a big problem. In a recent talk that I attended by Chris Town (3) he explained that despite advertising for the past 12 months for GP’s in

Peterborough he had had no expressions of interest yet alone anyone actually apply. At the same meeting Keith Houghton (11) said that Lincolnshire PCT expected to have no GP’s left in east Lincolnshire within the next 2 years. Parts of Derbyshire were running 30% + vacancy rates. It is in this climate that the Isle of Man has to compete to attract and retain GP’s. In many respects conditions offered to GP here have to be better than that of the UK.
On the island 25% of all GP’s could retire within 5 years if they choose and the figure reaches 50% over 10 years. The Isle of Man also has fewer GP’s per capita compared to the UK (UK 63 per 100000, IOM 54.7 per 100000 (2001 figures) population). In addition the age range is skewed heavily to the elderly, 306 over 65 per IOM GP, 272 in the UK. (12). This makes our relative workloads higher. The high cost of housing (13) presents problems as it does to all sectors of the Manx economy. It means GP’s from the cheaper housing areas of the UK are somewhat put off.
Finally on-call. Compared to our UK counterparts we have had a high burden of on-call and despite the new MEDS service compared to large numbers of our UK colleagues continue to do so. For many GP’s this is the biggest issue as to whether they retire (14). Loosing the most experienced members of the workforce is not good for anyone. Taking the BMJ classified ads (15) out of 124 posts advertised that particular week 60 specifically said no on-call, a further 26 specified an out of hours co-op. The vast majority of the remainder of the ads being quite short I feel simply did not specify it; it being taken for granted that that a co-op is in operation. Therefore for a large percentage of GP’s in the UK on call does not exist or is minimal involving a co-op. Recruiting to the island without an all island co-op would severely limit the pool of GP’s likely to apply. Many will look no further if there is any notion of on call. It is simply a must in today’s climate and not some option given the already restricted numbers of GP’s available in the first place.
I already work a 42 hour week before any on-call commitment, various committee meetings, preparatory work plus letters to select committees. If it is all right for Alan Milbum to resign because of lack of family time due to excessive commitments then its all right for me reduce my commitments. The European work time directive will make this mandatory in any case restricting the hours a doctor can work.
Co-op’s for on call are well established having run for many years in the UK. As per the classified ads (as above) they are virtually universal throughout most areas of the UK. Most cover areas much greater geographically than the island yet manning levels on the island are superior in that a GP covers a 76000 population. Some co-ops have one GP for 240000 people. The old Manndoc covered most of the islands population. The change to MEDS is hardly a quantum leap in terms of the UK.
As off April 2004 under the new contract (8) Primary Care Trusts will take over the responsibility for the running of out of hours provision. The default position for GP’s is no on call with zero obligation. This will prove very challenging as large numbers of GP’s intend to do no out of hours. The Department taking over the running of the out of hours on the island has been a satisfactory way of introducing the Department into running an out of hours service.
If the island is to recruit GP’s in the future and retain the existing workforce satisfactory arrangements for out of hours provision have to be in place. The days of individual practices doing their own on-call are dead and buried and relegated to ancient history.
Yours sincerely,
\ A A v^ V » v
DR M MASKA.
References.
1 Press release BMA 21 Feb. 2003 New GP contract heralds new investment for NHS General Practice.
2 Press release BMA 28 Dec. 2001. GP shortage set to worsen.
3 Chris Town. Chief Executive both North and South Peterborough PCT’s, member GMS contract negotiating team.
4 National Survey GP opinion. GPC News 19 Oct. 2001.
5 Press release BMA 17 Oct 2001. Radical action to keep family doctors in the NHS.
6 Valuing General Practice, NHS Plan, The Secretary of State for Health, 2000.
7 Investing in Primary Care, The Department of Health 22 May 2001.
8 New GMS Contract 2003
9 GP News 7 July 2003
10 Pulse Magazine 7 July 2003.
11 Keith Hoghton. Lead Investment Programme, The National Primaiy and Care Trust Development Programme.
12. IOM DoH stats 2001.
13 Money Media. August 2003 p 18.
14 Dr Hardings letter, (copy enclosed)
15 British Medical Journal 5 July 2003
Ramsey Group Practice Bowring Road Ramsey Isle of Man IM8 3EY
Dr G M Wilson
GMW/LPC/GPS/02/pib
11 September 2003
Mr P Lo Bao Clerk of Tynwald Legislative Buildings Douglas.
Dear Mr Lo Bao
Thank you for your letter of 29th July regarding the issue of General Practitioner out of hours services.
I enclose the views expressed by Dr J Brownsdon on behalf of Ramsey Group Practice and Dr M Maska on behalf of the Islands General Practitioners.
I understand the Select Committee is investigating the out of hours services of the Islands General Practitioners and not that provided by Ramsey Group Practice Practitioners under a separate contract to Ramsey & District Cottage Hospital.
Yours sincerely
Dr G M Wilson.
Southern Group PracticeCastletown Road Port Erin Isle of Man IM9 6BD
Tel: (01624) 832226
Dr PH Smith Dr N Mousley Dr CD Blackwell Dr D Wignall Dr V Brewis
M rLoBaoOffice Of The Clerk Of TynwaldLegislative BuildingsDouglasIsle of ManIMI 3PW
4.9.2003
Select Committee of Tvnwald on GP Services
Dear Mr Lo Bao,
The change in the GP out of hours service is an inevitable consequence of the changes in the UK as the new GP contract unfolds. If the Isle of Man does not follow suit then it would be a very short time before there were no GPs on the Island.
So far I have worked Sunday mornings at the manx emergency doctors service at which time there are two doctors on call and I found this to be an entirely practical and satisfactory arrangement. I have had no complaints from my patients at the Southern Group Practice and none from any patients seen whilst on duty.
As far as changes in the future to improve the service are concerned I would envisage the department employing doctors full time in the out of hours service so that the rotamay be filled more easily without any need for filling gaps at the last moment.
/ *I hope you find the above comments helpful.
Yours sincerely t
RECEIVED1 0 SEP 2003
OFHC-. OF l CLERK OF TYNWALD
Dr C D Bläekwell Bsd Ch.B M B
SOUTHERN GROUP PRACTICE CASTLETOWN ROAD, PORT ERIN,
ISLE OF MAN IM9 6BD TELEPHONE (01624) 832226
FAX No. (10624) 836759Dr. P. H. Smith Dr. N. Mousley Dr. D. C. Blackwell Dr. D. Wignall Dr. V. T. Brewis
Mr. P. Lo BaoRECEIVED
Joint Clerk to the Committee 1 0 SEP 2003Office o f the Clerk to TynwaldLegislative Building OrTICE OF THEDouglas CLERK OF TYNWALDIsle o f Man IMK1 3PW
08 September 2003
Dear Mr. Lo Boa, Select Committee of Tvnw ald on GP Services
Thank you for your communication re out o f hours provision; here are my thoughts on the problem.
The system as it was had outgrown its viability; increasing workloads, increasing complexity, increasing expectation made shifts o f 35-56 hours untenable and indeed potentially dangerous.
The system as it is makes better use o f the workforce as shifts are o f a reasonable length and can be arranged by the individual to suit their own working commitments. It makes sense for 1-2 doctors at a time to be doing a steady but finite rate o f work instead o f many being stressed out by being on call for a few for long periods.
From the patient’s point of view it is sensible to be at the hospital as services are immediately available if needed. As most people have their own transport these days (as witnessed by the huge amount o f traffic all times on the roads), very few actually are more than 30-40 minutes away from the hospital and that a tiny number o f our out o f hours calls are for life-threatening emergencies (in which case protocol for some time has been to dial 999), it follows that a centralised service should be practical and viable.
As the system evolves any problems, shortcomings and weaknesses will become apparent and must be addressed as soon as practicable.
I have been doing some weekend morning sessions and so far the system seems to be on course.
Yours sincerely
Dr. V. T. Brewis
SOUTHERN GROUP PRACTICE CASTLETOWN ROAD, PORT ERIN,
ISLE OF MAN IM9 6BD TELEPHONE (01624) 832226
FAX No. (10624) 836759Dr. P. H. Smith Dr. N. Mousley Dr. D. C. Blackwell Dr. D. Wignall Dr. V. T. Brewis
Mr. P. Lo BaoJoint Clerk to the CommitteeOffice of the Clerk to TynwaldLegislative BuildingDouglasIsle of ManIMK1 3PW
Dear Mr. Lo Boa, Select Committee of Tynwald on GP Services
The changeover to the centrally based Manx doctor service has occurred without any apparent problem. Since it began on 1 April 2003 there has been no adverse comment or complaint voiced by our patients.
The centrally based service organised by GPs, namely Mandoc, has already been in operation successfully for most of the Isle of Man for the past five years.
Most of the U.K. population is already served by centralised out of hours services so that it would be very difficult, in future, to recruit new GPs to the Island if this was not available here.
Yours sincerely
SOUTHERN GROUP PRACTICE CASTLETOWN ROAD, PORT ERIN,
ISLE OF MAN IM9 6BD TELEPHONE (01624) 832226
FAX No. (10624) 836759Dr. P, H. Smith Dr. N. Mousley Dr. D. C. Blackwell Dr. D. Wignall Dr. V. T. Brewis
Mr. P. Lo BaoJoint Clerk to the CommitteeOffice o f the Cleric to TynwaldLegislative BuildingDouglasIsle o f ManIMX1 3PW
09 September 2003
Dear Mr. Lo Boa Select Com m ittee o f Tvnw ald on GP Services
My feelings about the current out o f hours service are as follows
1) The system which existed on the Island could not continue. The changes in the U.K. meant that in the future GPs would not come to the Island to work under conditions inferior to those in the U.K. Therefore if no action was taken both daytime and night time primary care service on the Island would deteriorate.
2) The current system is similar to that which is working well throughout the U.K
3) I was disappointed that despite out o f hours responsibility supposedly being relinquished the Island GPs were put under pressure to man the out o f hours service. In the future I would envisage separate out o f hours doctors being employed by the Department o f Health.
Yours sincerely
Dr. D. C. Wignall
Select Committee of Tynwald on GP Services
The following Doctors submitted written evidence to your Committee, that they wished to remain confidential:
Dr A S C Kelsey Ramsey Group Practice
Dr J McAlister Laxey Health Centre
Dr C C Taggart Ballasalla Medical Centre
Appendix 4
OFFICE OF THE CLERK OF TYNWALDLegislative Buildings, Douglas,
Isle of Man, British Isles, IMI 3PW
Our ref: C /G PS/02/plb
16th July 2003
All Members of Tynwald
Dear Member
Select Committee of Tynwald on GP Services
I am writing to you at the request of the above Committee, to ask you to supply evidence, in writing, to the Committee concerning your views on the current provision of GP out of hours services and possible future changes that could be made to the system.
The Committee will in due course also be taking oral evidence and if you are willing to give oral evidence please indicate this in your written submission.
The Committee would be pleased to receive your views by Friday September 12th 2003.
Please find attached a copy of the motion establishing the Committee.
Yours sincerely
Phil Lo BaoJoint Clerk to the Committee
enc
I
LEGISLATIVE BUILDINGSISLE OF MAN
IMI 3PW
Mr Phil La BaoJoint Clerk to the CommitteeSelect Committee of Tynwald on GP ServicesOffice of the Clerk to TynwaldLegislative BuildingsDouglas
29lh August 2003
Dear Sir,
I am writing in response to your invitation to give my views on the current provision of GP out of hours services.
In the main my views will reflect the position in Ramsey but to a degree will of course affect the whole Island.
Until the change in our GP’s contract with the DHSS, Ramsey enjoyed 24 hour GP cover together with the additional facility of night Accident and Emergency cover at the Ramsey Cottage Hospital. This meant that the North of the Island had first class emergency cover which was generally satisfactory to the residents there.
Following the re-negotiation of the GP’s contract, Ramsey lost its locally based out of hours GP emergency cover and at the same time the GPs withdrew from their contract to provide night time cover at the Cottage Hospital. This has led to a limited Accident and Emergency facility, staffed by nurses. However even this service is restricted due to the limited number of properly trained nurses being available.
I appreciate that a large part of the rest of the Island has been served reasonably well by the Mann Doc system which has been based at Noble’s Hospital in Douglas. From a management perspective it might then seem logical to extend that service to the remainder of the Island.
However, under the present circumstances I believe that this is unacceptable. Primarily it undoubtedly dilutes the current quality of service, not only for the North but also the rest of the Island.
I understand that there will only be one doctor on duty and one on call. By extending the area covered to the whole Island, those two doctors will now be responsible for a further 20,000 people.
LEGISLATIVE BUILDINGSISLE OF MAN
IMI 3PW
Additionally, they will have to deal with the problem of travelling to the North, the quickest route being over the Mountain Road. As is well known, in winter the road is often closed due to bad weather and even in summer is frequently affected by fog. This stretch of road is often also restricted because of road traffic accidents which these days nearly always lead to a temporary road closure.
Therefore the speed of access to the North could well be hampered by conditions not usually found elsewhere on the Island.
I fully understand that the current problems have been brought about by changes to the GP’s contract, emanating from the UK. Nevertheless I believe it is most important that there be two doctors on duty to provide out of hours cover, one at Noble’s to cover Douglas and the South, and one based at Ramsey Cottage Hospital to cover the North and possibly the West.
This will help to build greater confidence in the new system and reassure those who presently believe the quality of our GP services is being diminished.
In addition to the Ramsey GP providing emergency cover for the North, he could also be available to support the proposed nurse-led Accident and Emergency service at Ramsey Cottage Hospital
By re-establishing this provision, it will also take the pressure off the Ambulance Service which has previously served the North of the Island very well indeed, but which is now struggling because of its having to take non-urgent cases, (which in the past would have been dealt with routinely at the Ramsey Cottage Hospital), automatically to Noble’s Hospital.
Although there is a promise of a third ambulance to be based at Port Erin, I understand that the personnel are to be moved from Douglas to staff this new service. So far from being a new provision, all that is happening is that the existing Douglas service is being spread more thinly, under the guise of a new service for the South.
This, of course, is going to lead to greater demands on the Ramsey ambulance which is inevitably going to increase its response times to out of hours urgent calls in the North.
As I have said, I fully appreciate the dilemma facing the DHSS. I do think though that an extra GP in Ramsey for out of hours cover could improve the service, not only in Ramsey but throughout the Island. Additionally he could ensure more effective use of the superb facilities at Ramsey Cottage Hospital and restore its 24 hour Accident and Emergency cover.
LEGISLATIVE BUILDINGSISLE OF MAN
IM1 3PW
This in turn will make better use of the Ambulance Service, not just in Ramsey but Island wide, and if the enhanced nurse training schemes are stepped up to ensure more highly trained nurses for the night time Accident and Emergency service, working alongside the extra Mann Doc GP, the service provision in the North will be restored and the level of cover elsewhere will also be improved.
I hope this is of some help.
Yours sincerely,
A R Bell, MHK Minister for the Treasury
LEGISLATIVE BUILDINGSISLE OF MAN
1M1 3PW
Our Ref: DC/ejm
18 August 2003
Mr P Lo BaoJoint Clerk to the Committee Select Committee of Tynwald on GP ServicesOffice of the Clerk of Tynwald Legislative Buildings Douglas
Dear t p ^ ^
Select Committee of Tynwald on GP Services
In response to your letter dated 11 July 2003,1 have the following comments:-
1. Numerous complaints have been received from persons resident in the northernparishes for the failure of the GP out-of-hours service and the resulting non availability of a doctor at Ramsey Cottage Hospital, to provide a satisfactory health care service.
2. Nursing and residential homes can no longer have the comfort of knowing a doctor will visit 'out of hours' to attend an emergency.
3. A GP will not attend "out of hours' at a sudden death at home. Instead, thePolice have to callout a Police doctor to certify death.
There are other examples of the problems relating to healthcare caused by theintroduction of GPs out-of-hours service.
I am willing to attend the Committee to give oral evidence.
I request that the Committee give consideration to the following matter:-
The present downgraded Minor Injuries Unit at the Ramsey Cottage Hospital must be immediately reinstated to an Accident and Emergency Unit with 24 hour doctor cover, 365 days of the year.
-2-
™ S be achieved by the responsibility for the administration of Ramsey Cottage H osptal to be immediately returned to Isle of Man Hospitals and not as at present w ill the Primary Health Care Division of the DHSS.
I look forward to being invited to meet the Committee at some future date.
Yours sincerely
1 d - A A ^ i U , _
David Cannan
LEGISLATIVE BUILDINGSISLE OF MAN
IMI 3PW
10th September 2003
Mr. Malachy Comwell-Kelly,Secretary,Select Committee of Tynwald on GP Services,Office of the Clerk of Tynwald,Legislative Buildings,Bucks Road,Douglas.
Dear Sir,
I attach my submission in respect of GP services for consideration of the Committee in due course.
I would be pleased to attend to give oral evidence to the Committee if they should so desire.
Yours faithfully,
Anne Craine
SELECT COMMITTEE OF TYNWALD ON GP SERVICES SUBMISSION OF ANNE CRAINE MHK FOR RAMSEY
• The position of GP services in Ramsey and the North prior to 1st April 2003 was that GP’s held 3 contracts.
1) General Practitioners services running a surgery and home visits
2) GP services relating to Ramsey Cottage Hospital, tending their own in patients and performing minor surgery
3) Operating an out of hours service, attending emergency call out during the night, to the home or in the majority of cases to the hospital.
• From the 1st April we are left with GP’s in Ramsey continuing with contracts 1 and 2 but declining to continue with contract 3 - delivering the out of hours service.
• This and other outside influences have reduced the service available from Ramsey Cottage Hospital from that of being an Accident and Emergency Unit to that of a Minor Injuries Unit.
• The consequence in Ramsey and the North is to have induced a state of fear for medical well being
• In the DHSS Report to Tynwald of 17th June 2003, it is stated “Regarding specifically the changes to the GP Contract introduced with effect from 1st April 2003, concerning out-of-hours services (which precipitated consequential effects in medical cover for the Ramsey Cottage Hospital Minor Injuries Unit), this was the subject of a Statement to Tynwald on 20th May 2003. That Statement set out the basis of the new arrangements for out-of-hours GP medical cover across the Island, and the reasons why these were necessary. In this respect, the situation remains the same, with the Department continuing to monitor the Service in the interests of patient care. The Department’s stance on this remains unchanged, and is based on a joint view reached with the Medical Profession, that the changes to the GP Contract in relation to out-of-hours care were essential in the interests of sustaining the present and future levels of General Practitioner services for the population. In taking this action, the Department and Profession are satisfied that the enhanced Emergency Doctor Service is satisfactory in maintaining patient care to the level achieved under the previous MannDoc Service. The situation is, however, subject to continual review, for the purpose of identifying and addressing any areas where levels of medical cover pose an unacceptable risk to the care of patients.
I would comment that on the basis of the new arrangements... why these were necessary ... monitor the service in the interests of patient care... The new arrangements were introduced to keep in line with evolving UK practice and as such to attempt to maintain favourable working conditions for presently employed GP’s and to attract new GP’s to the Island. The monitoring of the service in the interests of patients does not appear to have come into the equation. Our GP’s were content to service and receive the remuneration for the two contracts of their choice but were not inclined to continue with the out- of-hours contract in the interests of patient care.
This stance was based on a joint view reached with the Medical Profession... changes to the GP contract in relation to out-of hours care... were essential in interests o f sustaining present and future levels of General Practitioner services for the population.
The one party who was ignored in the changes of these contractual arrangements was the user for whom the service exists. An oversight which was vividly made clear to me- without exception- on every door of every household I canvassed in the run up to the by-election in May. I do not accept that reducing the service can be referred to as sustaining present levels.
The situation is ..subject to continual review... where levels of medical cover pose an unacceptable risk to the care o f the patients. The present situation is putting patients at risk. By the reduction of the GP contract in relation to Ramsey Cottage Hospital the resultant situation is that Ambulance Services are left in untenable quandaries over what to do. I refer to Appendix A attached to this submission We are facing situations where ambulance personnel have to play political games to try and deliver the best service for the patient. Keeping a patient in an ambulance until the doors of the hospital open at 9am is not in the best interests of the patient or the service. I am aware of an occasion where the ambulance service, because of the hospital closure hours, embarked on a journey to Nobles in the knowledge that their journey was not in the best interests of a patient and had they been able to have had that person admitted locally and quickly, their life could have been saved.
The Health Service is being held to ransom by the Medical Profession. GP’s are I understand, employed on the basis of a quota of patient population. The average number of surgery hours per week is 13.5. It is appreciated that in addition they cover house calls. However, despite the reduction of time for out-of-hours service, they have not increased their number of surgery hours. Does the number of hours offered by the Ramsey GP’s equate with those of other surgeries? Or do we have a greater number of GP’s in Ramsey to allow them to offer their services during the day to Ramsey Cottage Hospital?
One of the reasons cited by GP's for the withdrawal of their service to the out of hours provision, was that they were pestered by trivial unnecessary calls at unsociable hours. With the current system the Ramsey GP's operate an on call rota for their patients within Ramsey Cottage Hospital. I believe that we should seek to have Emergency Practice Nurses accepting patients through the doors in Ramsey and that where they deem it necessary, they should have the ability to call upon those doctors who are on call and contract to attend hospital patients anyway. This would eliminate nuisance calls being made directly to the doctor from the patient and would allow Emergency Practice Nurses to make the initial assessment but with GP back up if required. I would be interested to learn how often the GP's are called out to their hospital in-patients these days as compared to how often they were called to the hospital for emergencies pre-April 2003. Does the cost of retaining a GP on call for his hospital patients equate to the separate contract that they used to hold for out of hours calls or the fee applied when they provide doctor for the rota of Emergency Doctor Service?
It has been public perception in the North that the ability to be involved with a Cottage Hospital was an inducement to GP’s when they applied to come here, not a deterrent. If GP’s now find this role burdensome then consideration must be given to removing them entirely from the control of Ramsey Cottage Hospital and allowing the Department of Health to directly control and employ doctors who can deliver the level of service required by the community.
The present Emergency GP service is not satisfactory.- People cannot always get through to the service.- They feel more comfortable with someone who is familiar
with their case.- There are many difficulties over transport in getting to
Nobles from Ramsey and the North, the availability of a car, the discomfort caused in transporting an unwell patient.
- Telephone diagnosis is no substitute for personal contact.- Video assessment of patients at Ramsey Cottage Hospital
should be considered in conjunction with Emergency Practice Nurse provisioa
- All medical records should be able to be accessed by the Emergency GP service and Nobles medical staff so that immediate information about patients can be sought.
- Please see Appendix B
• We are told tired doctors make more errors. The doctors who were, prior to April 1st, on call throughout the night had the option of having locum cover the following day. However in the majority of cases, rather than have to pay that locum themselves opted to work on. Does this indicate that they are not getting adequate remuneration for their services if they do not feel that their salaries can bear the cost of locum cover in such circumstances? Related to this, are those doctors volunteering for the Emergency Doctor Service doing so when they have scheduled time off the following day, or are they so attracted by the rates paid for this new service that they are taking on excessive duties to enhance their contract salaries?
My conclusions are:-
That the current position of GP contracts at the Ramsey Group Practice need examining to see whether they are offering a just service to their patients and in terms of goodwill with the Health Service The possibility of alternate doctor provision to enable the Ramsey Cottage Hospital to operate as an Accident and Emergency Service needs to be given appropriate consideration taking into account the geographically isolated position of Ramsey and the Northern parishes and the recognised difficulties of accessing Nobles Hospital during race weeks and bad weather.Improvement of the Emergency Doctor service at Nobles must be made to appropriately meet the needs of the patient. Greater priority now needs to be given to the Primary Health Care service within DHSS.
Report submitted bv Mr S. WRIGHT. Manager for the GrestResidential Home.
Andreas Road. Lezavre
On the morning of June 6th 2003, Mr Lawrence Bannan (a resident at the Grest Home and in his mid 90’s) was sitting eating his breakfast in the dining room of the Grest Home when he collapsed This was at approximately 08.00 hours. He was grey in colour, sweating, his.lips were blue and he was totally unresponsive.I dialled 999 and an Ambulance with Paramedics arrived within about 5 to 10 minutes by which time Mr Bannan had opened his eyes but was not coherent
The Paramedics gave him Oxygen via a mask which seemed to bring Mr Bannan round quite well and within 10 minutes be was fully conscious again but still very pale and sweating and unable to stand.
At 08.25 hours the Ambulance man decided to take Mr Bannan to hospital. He saidthey should go to Nobles as no Doctors were on duty in Ramsey until 9.00 am, however, it would be 9.00 am before they got to Nobles anyway.
He (the Paramedic) pondered whether the Nurses on duty at Ramsey Cottage Hospital would accept Mr Bannan at 08.30 but did not think it likely as he was in a “collapsed” state.
Mr Bannan was taken out to the Ambulance at 08.30 hours and was still outside the Grest Home at 08.45 with the Paramedics in attodance. They drove off at 08.50 approximately and I later found out that he had been taken to the Cottage Hospital and admitted via Accident & Emergency.
The Paramedics obviously appreciated it would be far better for Mr Bannan to go to the local Hospital and be seen by his own G.P. or one from the Practice without having to undergo a journey over the mountain to Douglas.
APPENDIX B
The following is a situation related verbally to me the mother of the girl involved.
A girl of 18, was taken ill with suspected appendicitis. Her mother is a woman of considerable medical experience.As it was just after lam the mother rang the Emergency Doctor service for advice.She was asked to bring the girl in to be examined by the Emergency Service, This she did arriving just before 2am. She had been told that the entrance was just to the left of the Casualty entrance. Having driven the girl to Douglas wrapped in a blanket and vomiting into a bucket she unloaded her from the car to be told upon entering Casualty that she was in the wrong place and that she would have to take her round to the appropriate entrance. Those in reception could see what condition the girl was in but no assistance was forthcoming. When the mother arrived at the door to the Emergency Doctor Service she rang on the bell for 7 minutes before the doctor responded. Because the door was locked and the girl could not stand any longer the mother had to rest her daughter on the ground, still vomiting whilst she continued to ring the bell. Two policemen with a drunk arrived at Casualty and asked her if she needed any assistance. She responded that she just needed someone to answer the door! The doctor's response when she finally did reach the door was “oh have you been there long”.Whilst the girl was being seen by the doctor three phone calls were also responded to. The girl was subsequently admitted to Casualty where another long series of delays occurred and it appeared to the parent that the feeling was that as this was a patient from the Emergency Doctor service, that Casualty had no responsibility for her. They were left, feeling abandoned for a further 20minutes before the Casualty department came to start procedures with the girl and advise the mother that the doctor had been sent for. It was 5am before she was admitted to Ward 2 where she was cared for.
This whole process was not in the best interests of the patients care. We do not question that it was necessary to make an admission to Nobles in this case but that the surrounding circumstances were not helpful or supportive to the parent. It was a long clumsily drawn out procedure which led to admission. To hear the assertions that the system is working well is callous.
1) Doctors need to be equipped to receive patients when they arrive at the Emergency Doctor service.
2) There appears to be no ‘"joined up” approach between the Emergency Doctor Service and Casualty. Are they paid from different budgets?Even if they are, emphasis must be placed on their duty, between them, to respond to the needs of the patient
LEGISLATIVE BUILDINGSISLE OF MAN
IMI 3PW
Our Ref:-AJE/jw
18th July 2003
Mr Phil Lo Bao Third ClerkOffice of the Clerk of Tynwald Legislative Buildings Douglas
Dear Phil
Select committee of Tynwald on GP Services
Thank you for your letter dated 16th July 2003, regarding the above.
My contribution on this subject is minimal as I have no personal experience in relation to myself or my immediate family, neither have I received any comment negative or positive, from constituents.
The situation as far as I can say appears to be "no news is good news" and I trust this will assist the Committee with its investigations.
Thank you for taking the trouble to seek my views.
Yours sincerely
A J Eamshaw MHK
LEGISLATIVE BUILDINGSISLE OF MAN
IMI 3PW
n t h Septem bér 2003
Dear Sirs,
I am writing to you in response to a letter from Phil Lo Bao which called for evidence to assist your com m ittee in its consideration of the current provision of GP out of hours services and possible future changes that could be made to the system.
You will find attached a sum m ary of my views together with four press releases which I've issued on this m atter (condensed and slightly re-worded to assist your deliberations). I would be happy to give oral evidence should you feel that this would be helpful.
Yours sincerely,
Evidence from Phil Gawne MHK to the Select Committee of Tynwald on GP Services
Summary of my views and thoughts on this matter
I was made very much aware of the widespread anxieties and concerns of Rushen constituents as the new em ergency doctor service was introduced a few days after I began my election campaign in the Rushen by-election. I would estim ate that between 80 - 90 % of constituents I spoke to in the two weeks following the introduction of the service expressed anger an d /or worries about the service.
The level of concern reduced as the initial shock of the ‘out of the blue* change in service wore off but it remained as a significant concern to over half the people I spoke to right up to the election. Since the election I have continued to receive many calls from constituents expressing their concerns over the new service.
The concerns of many of my constituents, which I share, are in two areas: x] concerns over the introduction and promotion of the new service, and2] concerns th at the new service does not m eet their medical needs.
1] The rushed way in which the new service was introduced with little or no warning angered many people and I understand the Departm ent accepts that the introduction of the new service could have been handled better. I believe that if such significant changes to basic health care provision are considered in the future the Departm ent m ust endeavour to undertake open public consultation and flag up changes well in advance of their introduction.
People were also angered that the leaflets delivered at the tim e in which the changes were made, made claim s that this would be an improved service. People are not stupid and in Rushen, Ramsey and the north it was quite clear that what had been introduced was a cut in service.
Cuts in services are hard to justify but had the Departm ent com e clean and explained its difficulties with new GP contracts and the effects of these on out of hours services I feel sure that it would have received a much more sym pathetic response than it received from its cagey, somewhat misleading promotion of the new service. A more open approach from the Department in dealing with difficult issues in the future, might cause a few problems for those politicians and officers concerned, but it also might avoid the PR disaster which developed in this case.
2] There are two areas of concern over whether or not the new emergency doctor service adequately meets people’s medical needs. The first concerns the general operation of the service and the second is in relation to the distance between ‘on call* medical practitioners and people in the south and north during the out of hours period.
1
Concerns are expressed over the unnecessary com plexity of making contact with the new service. People who ring their own GP out of hours get a recorded message asking them to ring a different number to make contact with the service. This could easily and quickly be rectified by arranging for an autom atic transfer of calls directly to the em ergency doctor service.
People were not aware of the location of the Douglas based headquarters of the new services and in some cases described to me considerable time was wasted in tiying to find the place, by people who had been asked to report to the Douglas centre. I understand that the headquarters are now at the new Nobles site though I am unaware of any attem pt made by DHSS to inform the public that the em ergency doctor service has moved. It would certainly help if the DHSS were much m ore proactive in informing people where exactly the MEDS centre is and in rem inding/inform ing people that the centre has moved to the new Nobles site.
One of the m ost difficult aspects of the new service is transport to and from the MEDS centre. People who have been used to doctors coming out to visit them are not happy at having to pay quite high costs for Taxi fares at unsocial hours. These people are of course those who a centrally based doctor believes are not sufficiently ill to deserve a home visit.
This is perhaps the m ost difficult area to resolve as it is popularly believed (whether justifiably or not) that due to pressures on the two doctors manning MEDS, calls which previously received a home visit no longer do so. It is possible at not inconsiderable expense to pay for patients travel costs to the MEDS centre. I understand that patients on low incomes can currently make claims for financial assistance from the DHSS to cover their travel costs, however, this facility is not widely promoted. Perhaps the DHSS could make people aware of this facility and so improve things for at least some patients.
The most significant move which would alleviate people’s concerns would be for MEDS to be manned by three or four doctors. Unfortunately, however, due to the change in doctors working practises recently agreed in contractual negotiations and the shortage of qualified GPs in the UK it is unlikely th at this can be achieved in the short term . If your com m ittee were to recomm end increased staffing levels for MEDS it would have to be quite clear that significant increases in funding and manpower would have to be found to achieve such an increase.
It has been suggested that nurse led services might offer some kind of out of hours medical service. If such a service is provided for Ramsey then a sim ilar service must be offered from one or other of the DHSS buildings at the Four Roads, Rushen.
2
The final issue highlighted hy this change in out of hours GP service, though perhaps not directly related, is the distance which am bulances have to travel to reach patients in the south and the north. W hereas doctors used to be within 10 to 15 m inutes drive of the m ost isolated patients, now the nearest doctor may well be 30 m inutes drive away in Douglas.
Basing a param edic m anned ambulance service at the Four Roads (and a sim ilar service in Ram sey) will be particularly reassuring for many people in the south as it will m ean that in case of em ergency they will receive m edical assistance quickly. It is very im portant that the DHSS’s com m itm ent to these south and north am bulance services is perm anently m aintained.
I had initially intended to be brief and so apologise for extending this submission of evidence. This is, however, a very im portant issue which is seriously affecting the way in which many people access prim ary health care. I wish the com m ittee well in its investigation of this m atter and earnestly hope that an effective, practical solution can be found to this problem.
Press Releases - redrafted and condensed to ease vourconsideration
Petition to the Minister calls for restoration of out of hours GP cover in Rushen.
On Monday 19th May I launched a petition in Rushen which called for the restoration of out of hours GP cover. The petition was undertaken following the expression from constituents of their high level of dissatisfaction over the changes to the out of hours GP service which the Department of Health and Social Security introduced in April 2003.
Over 30 shops and businesses in Port Erin and Port St Mary were keen to take the petition and people in the South who were dissatisfied with the new service were urged to sign the petition. The petition was worded as follows: "we the undersigned call upon the Minister for Health and Social Security to reinstate a level of out of hours GP cover equivalent to that enjoyed prior to the introduction of the all Island Emergency Doctor Service on the 1st April 2003."
Like many people living in Rushen, I am very concerned at the way in which the Department of Health and Social Security has dealt with this cut in prim ary health care in the South. The M inister failed to understand that people are unwilling to accept the reduced out of hours GP service. While we might understand the difficulties her Departm ent faces in GP recruitm ent and retention, people are both worried and angry that in a time of relative prosperity our access to doctors is being cut.
3
2,000 people from Ram sey and the North m arched and 7,000 signed a petition to show their anger at the new arrangem ents in the N orth. As a result the M inister announced in her statem ent to May Tynwald, that some form of nurse led service m ight be introduced in the N orth.
While such a nurse led service would not adequately replace the GP service we’ve lost, Mrs Christian's announcement showed clearly that her Department would bow to the pressure of protest politics and petitions, or perhaps to put it m ore diplomatically, the DHSS was prepared to listen to the genuine concerns expressed by the overwhelming m ajority of people from Ram sey and the north. I therefore strongly urged everyone living in the South who was concerned about the cut in out of hours GP services to sign the petition in the Ports, to write to the M inister and make their voice heard.
Over 2,000 sign Rushen Out of hours GP Petition!
2,117 signed the petition which called on M inister for Health and Social Security, Clare Christian MLC to reinstate in Rushen 'a level of out of hours GP cover equivalent to that enjoyed prior to the introduction of the all Island Em ergency D octor Service on the 1st April 2003.' The petition which I presented to the M inister in Jun e had signatures from around 1,900 separate households in Rushen representing around 45% of properties in the area.
I think that this level of support for the petition confirmed what many of us thought th at concerns over the new out of hours em ergency doctor service are as real in the South as they are in Ram sey and the North. This is a very emotive issue in Rushen and I hope that both the M inister and the Tynwald Select Committee take note of the 2,117 people who have taken the trouble to sign the petition.
I have no wish to add to people's real anxieties on the issue of out of hours GP cover by continually raising the issue but it is clear that people are not happy with the change in service and it is im portant that their concerns are brought to the attention of the DHSS and Tynwald. It is im portant to stress, however, that while the new service is clearly not as good as the previous one it does offer a basic level of out of hours cover.
4
Out of hours GP cover - Minister Offers Some Comfort to People in Rushen!
I was reassured by the M inister for Health and Social Security that a dedicated param edic ambulance service will be based in Port Erin from the beginning of October. I asked the M inister in Tynwald if such a service would be introduced as I was concerned that the cuts in GP out of hours services left people in the south too far away from em ergency medical services.
The M inister's announcement th at a dedicated 24 hours a day, 7 days a week, 52 weeks a year param edic ambulance service will be based at the new am bulance station in Port Erin was very welcome news as it m eans th at the people in the south will have from October a dedicated full tim e emergency service staffed by highly qualified healthcare professionals.
While this does not answer the call from many people in Rushen for a restoration of the previous out of hours service provided by GPs, I hope that it might at least provide some com fort to the many people who have real anxieties and concerns over this m atter.
Out of hours GP cover - New Rushen MHK meets Minister,
On 30th May I m et with the M inister for Health and Social Security, Clare Christian MLC and John Wilson, Head of Health Services, in an attem pt to alleviate the concerns of the people in the South of the Island over the out of hours GP em ergency service.
At the m eeting the M inister made clear that her Departm ent was unable to support the restoration of a level of out of hours GP cover equivalent to that enjoyed by the people of the South prior to 1st April this year. She assured me that the DHSS would be monitoring the new all Island emergency doctor service and she and her Departm ent are keen to hear from anyone who has concerns about the new service.
I was a little disappointed with the M inister’s response. The Minister explained the difficulties which her Department faces in trying to provide an out of hours GP service, but in failing to offer any time scale for improvement of the hurriedly introduced service her Department fails to recognise the views of the people in the South and throughout the Isle of Man.
The Commissioners in Port Erin, Port St M aiy, Rushen, Arbory, Malew and Castletown have all expressed their concern over the new service. It is clear that despite the high level of dissatisfaction already dem onstrated, the DHSS remains unable or unwilling to seriously address our concerns in the South.
5
LEGISLATIVE BUILDINGSISLE OF MAN
IMI 3PW
Our Ref:- H H /jw
11th September 2003
The ChairmanSelect CommitteeG P Services Out of HoursClerk of Tynwald's OfficeLegislative BuildingsBucks RoadDouglas
Dear Sir
Over the last fifty-five years of the National Health Service, the changes in the provision of services have been quite considerable, I fully support a National Health Service which is 'free' at the point of delivery to people in need.
The change in the service provision together with changes in treatment from very basic treatment in the 1940's and 50's to very sophisticated treatment in 2003. With these changes in service provision has come an increase in services, it is not just General Practitioners who are providing a service to the community, but also from Health Centres, District Nurses, Health Visitors and Practice Nurses, in some areas Social Workers and Consultant's visiting to provide much needed community services alongside sophisticated treatments in Hospital.
The provision for members of the public, that is us, has increased out of all expectation from when the National Health Service was set up and I think in some circumstances peoples' expectations have been greater than the service has actually been able to provide. I would urge the Committee not just to look at GP services or out of hours services, but I would hope that the Committee would look at the appointment system, how long people have to wait for an appointment, whether they can be seen in an emergency on the same day, how long they have to wait for a non-urgent appointment, could someone else see the person requiring an appointment other that the Doctor, such as the Health Visitor, District Nurse and Hospital Nurse etc.
I would also urge that the Committee look to see if there is a complaints procedure in place and how complaints are recorded, are they reported to the department.
In relation to out of hours cover, in my own area I was initially opposed to the change to a central unit, but I have received no complaints since the setting up of Mann Doc or Meds.
You might say the people wouldn't complain to me with my husband being a GP, but people quite often ask my advice as to what they should do, this has not happened with the Emergency Doctor Service. People feel genuinely content that they can ring up and speak to someone who is there purely to give an out of hours service, that they can be seen if they go to the centre or the Doctor instead of disturbing the Doctor at home.
I would hope that the Committee will talk to Doctor's especially the younger ones and ask them about the service that they provide now and the service they provided prior to the change to either Mann Doc or Meds. Before the Mann Doc system was set up, Doctor's worked during the day, were on call from 6 p.m. until 8.30 a.m. depending when the surgery opened and depending on how many Doctor's worked in the Practice. In Peel when there were two Doctor's it was every other night and every other weekend on call and when one of the Doctor's were on leave the other Doctor worked every day for two weeks during the day and on call at night and weekends. As the Practice became bigger the cover became less, going from two nights on call a week and a weekend when there were three partners, when they had four Doctor's it was one in four and every forth weekend as well as working during the day. Not only were the Doctor's on call but also their spouses, or their answer machine as things got a little more high tech. Later on it led to mobile phones and that to some extent relieved the pressure on the family member covering the home base. Some patients who knew the spouses of GP's would take exception when asked for information regarding their condition, and it some instances it was very difficult and quite understandably so to gain information to pass on to the GP However, with Mann Doc and Meds that has now changed.
The on-call service is more professional, the Doctor is on call and is expected to give advice on call during the day, the evenings or weekends and during the night from midnight to 8 a.m. While the Doctor can go to sleep when the calls lessen they know they are there to give advice and to go to see patients as and when. It does not matter whether the GP is male or female . When they visit they have a driver who knows the island so the GP. doesn't have to concentrate on driving either during the night or at weekends.
I do hope that the committee will take evidence from young Doctors' because one of the issues of great . concern in future is that it will be very difficult to attract Doctor's as the age profile is quite high now. The number of Doctor's being trained is not that numerous that we can afford to have a service which is different to a service presented in another area, especially when our Doctor's are trained in the United Kingdom and most areas in the United Kingdom have a service such as ours.
To a certain extent I can understand the anger of the people in Ramsey at losing a service which they think is theirs, however, m y area does not have an ambulance service, does not have a hospital type service, we do not have a Nursing Home and therefore for any of these services m y constituents have to travel long distances.
With the development of the Hospital at Braddan now people in Douglas have to travel greater distances for treatment, and I have not noticed any great objections from them, it might only be two miles up the road, but it is a greater distance than before.
W hat I am trying to say is that changes have always taken place within the Health Service since its inception. Everything is much more technical and people expect a more professional treatment and service. The changes which the Doctor's initiated themselves with Mann Doc were received positively by their patients. Three areas were not covered and I believe the Doctor's in those areas did not want to change when Mann Doc was being introduced, however, after seeing the success and how well it was received by GP.'s and their patients was I believe an incentive then for all 'out of hours services' to be delivered from a central area.
I do hope the Committee will take evidence from Doctors and seek from them the information regarding the provisions that they consider need to be in place to provide future services for all our people into the next decade.
Yours sincerely
LEGISLATIVE BUILDINGSISLE OF MAN
IMI 3PW
5th September, 2003.
Mr P. Lo Bao,Joint Clerk to the Committee, Tynwald Office,Legislative Buildings, Douglas.
Dear Mr Lo Bao,
Select Committee of Tynwald on GP Services
I refer to your letter dated the 16th July, 2003. As you are aware, I was not present at the June or July 2003 sitting of Tynwald and have not yet received a copy of the Record of Proceedings for these sittings.
Please find attached a copy of a letter from me to the Minister for Health and Social Services dated 10th June, 2003 which I trust is self explanatory. Attached are copies of a number of letters I have received concerning this matter. Many people residing in the north of the Island have contacted me to voice their objection to the changes in service which have taken place at the Ramsey Cottage Hospital and Ramsey Group Practice.
The 1991 strategy document is based on the redevelopment of an Acute Hospital at the old Nobles Hospital; this materially affects the proposals contained in that document relating to medical services required in the north of the island. An obvious example is the added difficulties for people in the north of the island in gaining access to the new Nobles Hospital on a 24 hour basis.
While the 1991 strategy document lays stress on cost as a factor in determining the extent and nature of acute services to be provided in the regions, it is made clear that this consideration does not stand alone. It is qualified by the words ' and a more accessible service can be provided'. The coupling of these objectives is an important if not critical consideration which has been ignored in implementing the recent changes.
I would invite the Select Committee to note that as recently as July 2001 the DHSS issued a News Release (copy attached) advising, inter alia, that the Ramsey Cottage Hospital would continue to provide a 24 hour service to residents and visitors of the north of the Island, and that medical and nursing staff would be available (for this purpose). The DHSS made this statement 'following reflection on the nature and extent of its (Ramsey Cottage Hospital's) work.'
I can but conclude that the change of policy affecting Ramsey Cottage Hospital has been driven not by sound medical and financial reasons but by pressure exerted by some of the GPs. Part of the answer to the problem therefore may lie in providing dedicated medical cover for Ramsey Cottage Hospital, which could enable some of the services to be recouped if not expanded.
I would be prepared to give oral evidence to the Select Committee.
Yours sincerely,
R. E. Quine. MHK.
Hon. Mrs C,M.Christian, MLC, Minister for Health and Social Security, Markwell House,Douglas,Isle of Man.
Dear Mrs Christian,
Policy on Ramsey and District Cottage Hospital
I refer to the Order Paper for the June 2003 sitting of Tynwald and particular Item 9, and the related Report to Tynwald Court. As I shall not be present in Tynwald for the debate on this item I am taking this opportunity to place my views on record.
The admission in the Report that some of the recent changes in the Island's health services are based on an outdated and questionable strategy is candid but singularly unhelpful. It compounds the mis administration within the Health Services which goes to the root of present difficulties with NHS doctors and dentists contracts and the downgrading of services at the Ramsey Cottage Hospital.
That this deficiency should be seized on by the Department to delay the resolution of the present problems is tantamount to adding insult to injury. I can but conclude that the intention is to produce an 'independent' report by consultants in the hope that the findings can be used to persuade Members of Tynwald to support the existing wholly unacceptable arrangements.
It may be that an urgent review of Health Services strategy is required but a continuation of the present arrangements while it is conducted is emphatically rejected. Additionally, the terms of reference for any such review should be approved by Tynwald as should the membership of the body carrying out the external review.
As a general statement, the evaluation of findings against United Kingdom benchmarks would be unacceptable.
The immediate need is to (a) divide the Emergency Doctor Scheme into two or more operational areas, (b) adjust the placement of ambulances to ensure a fast response in areas outside of Douglas and (c) reintroduce access to Ramsey Cottage Hospital on a 24 hour x 7 day basis. In the absence of such action it is inevitable that the people of Ramsey and the North of the Island will be obliged, amongst other actions, to resort to public protest.
Reverting to the Motion on the Order Papef, I trust that it will not be approved in its present form as this would be to acquiesce to the downgrading of services at the Ramsey Cottage Hospital and elsewhere, and to condone the Department's political manipulation and procrastination. The minimum requirement is for the Motion to be amended to impose the service levels identified m the preceding paragraph.
Yours sincerely,
R. E. Quine, MHK
Plot 32Leodest Road Andreas Isle of Man
22nd May 2003.
I am writing with regard to an extremely painful experience, which I had on the morning of Monday 19th May 2 0 0 3 . Firstly, let m e back track for information, to the night of Wednesday 14th May 2 0 0 3 . At 9 .30p m I becam e overwhelmed by severe chest arid stom ach pains whilst also vomiting blood. My husband becam e worried and telephoned The Emergency Doctor Service. Dr. Allanson, who was on duty, very kindly called to our house in Andreas to deal with m y complaint. He administered much needed Injections of painkillers and advised m e to see my doctor the following morning. With this I have no complaint, as Dr. Allanson was more than helpful.
On Thursday 15th May 2 0 0 3 I tried to make an appointment with my own QP at the Ramsey Group Practice, but he was not available, so alternatively i made an appointment to see Dr. Clarke. I was told that I could possibly have Gallstones. I had blood tests. A request was sent for an Ultra-sound scan and I was advised to start a low-fat diet, which I did. Over the weekend I began to feel much better, but this is where my complaint regarding the new QP led cover com m ences. Please read carefully.
On Monday 1 9 th May 2 0 0 3 1 got up at 6 .45am with the intention of going back to work, as I was feeling so much better. At 7 .30am severe chest and stomach pains again overwhelmed me, and I knew that as on Wednesday night 1 needed to get som e pain relief quickly. My husband who works at the Ramsey Cottage Hospital arranged for som eone to get my children ready for school and take them out of the house, as it was very upsetting for them to see m e in so much distress. He then telephoned his Supervisor at the Hospital at 7 .55am to explain that he would be late for work. According to the recent leaflets received In the post the Emergency Doctor Service Is only available until 8am b u t the Cottage Hospital has OP led cover from 8 .3 0 a m . His Supervisor then said he would ask at the Minor Injury Unit for a Doctor to call out and see me, as I was in far too much pain to sit in the car myself. When he requested a doctor he was informed, quite bluntly, that the Doctors do not start work until 9am ? (I hope you can start to see what I am complaining about.)
Whilst I was still in severe pain and distress my husband then telephoned for an Ambulance which arrived promptly at 8 .20am . The Paramedic did his best to make me m ore comfortable. He then said that the best course of action would be to take m e to Ramsey in order to get my pain under control by a Doctor before taking m e onto Nobles Hospital. He made a telephone call at 8 .28am to ensure
that a Doctor would be waiting at Ramsey for m e, and was told that even if he brought m e in I would have to wait until 9am to see a Doctor. The Paramedic said that that was disgusting and told m e that unfortunately, due to circum stances beyond his control (namely the non-existent doctor cover from 8 .30am at Ramsey)I would have to bear with the pain until we got straight through to nobles.Heedless to say that by this time the pain I was in was unbearable.
We went through to nobles and due to the Paramedic's skill my pain started to subside ju st as we were reaching Douglas. I was then admitted to nobles for pain relief and tests and I have only recently been discharged to await results,
I AM ABSOULTLY DUMMOUHDED, DISGUSTED AND AFPALED BY THE WAY MY CASE WAS HANDLED BY THE ftAMSEY fiOCTOftS.
Why send out leaflets (copy of which is attached) claiming that there Is GP led cover, which 1 would interpret as a Doctor available if required from 8 .3 0 a m In the morning, and yet if som eone like myself requires a Doctor at that time we are told that they do not start work until 9am ?
Why was the Paramedic not allowed to bring me to the Cottage Hospital in order to get the pain relief I required, and so allow me to have a m ore comfortable ride to Nobles?
Do you really think that in this day and age of medicine som eone like myself should have to put up with that amount of severe pain just because a Doctor cannot be bothered to comply with the information which was sent to the public?
The pain I suffered on Monday can only be described as excruciating. I commend the Ambulance Service and the Paramedic for the way they dealt with the situation, but I am damned if I can say the sam e for the Doctors of the Ramsey group Practice. I can only hope and pray that if a Doctor, a m em ber of his/her family or any other m em ber of the public were suffering the pain 1 was, that they would not be fobbed off in the despicable and unsympathetic manner by the Doctors or the Hospital in the sam e way that I was. I would not wish what happened to me on Monday to happen to my worst enemy and I can only hope that I nEVER have to rely on the Emergency cover at the Hospital ever again because in my opinion it is now extremely UNRELIABLE! \
c .c . Mr E Quine, Mr B Pressley, Ramsey Group Practice, Mrs C Christian, Mr G newbry.

ELMVILLE
11ADi ROAD
BALLAUGH
XM7 5KB
Mr R.E. Quine OEE Bareme Ville Clenagh Hoad SulTay
Dear Mr. Quine
RAiSBT COTTAGE HOSPITAL
I feel I must write to you in the hope that you will
support retention of the above Hospital as it is of majdtr
importance to people in the JSorth of the Island. My regret is
that there is no similar facility available in East, West and
South of the island. Progress, if such it can fee termed, has
been too fast in population terms to keep pace with services and
amenities. Projections by the elaborate set-up of the Economic
Affairs Division of Manx Treasury should have formed a safeguard
in this connection - but have they?
I have already written to Mrs. Christian objecting to the
use of the Clucas Wing for dentistry as that is reducing very
necessary medical facilities. The reply that the Wing in
question is under-utilised does not convince me*
In April 1991 a comprehensive Review of Health Services was
carried out by liverpool University. 1 notice you were Junior
Minister for Health at that time and will have made a contrib-
bution to the Heview. Whether a further review has been carried
out I confess to being ignorant as so many other items concerned
with Politics fill me with dismay.
I join with those who consider the retention of what we
already have is vital and would only add that the morale of the
caring band of efficient workers in the medical field will suffer
^Continuedj
with the direction in which matters are heading.
A dismayed member of the Public -
« />
4# Ormfy Road Ramsey Isle of ManIM83LH April 13 2003
Dear Mr Quine,I write to you firstly as a very concerned resident of the
North, with many family and friends living in the North. And secondly, as a concerned Ambulance Technician.
Today, I have received a leaflet in the post\ explaining the procedure to be followed if urgent treatment is needed following the changes in 'out of hours' GP cover. The front of the leaflet claims 'An improved service to patients'! How can this be the case ?
One GP cannot reasonably be expected to cover the entire IOM and likewise, I know the Ambulance Service will be put under immense pressure. When the nurse-led MIU cannot or will not treat a patient, we will have no choice but to transport them to Nobles, regardless of whether they required an Emergency Ambulance and crew in the first instance or not This will reduce the night time Emergency crew to glorified taxi drivers. Then, the North of the island will be covered by one standby first responder.
Myself and my colleagues have no doubt in our abilities to deal with emergencies, but we fear we may not be available to respond when a real emergency call comes in.
I am worried for the residents of the North and, unfortunately, it is a case of when, not if, a life is lost en route to Nobles because we had to bypass Ramsey Cottage Hospital
Isincerely hope it doesn't take a loss of life to show up the inadequacies of this system.
Yours faithfully
Miss A J Chambers
Mr Paul Fisher St. Benedicts Glen Auldyn Lezayre Isle Of Man IM7 2 AD
Date:-24th April,
Dear Mr Edgar Quine,
With regards to the sony state of the health service in the Isle of Man. I would like to convey two experiences that has happened to two of our family members since the service has been changed with regards to the Cottage Hospital.
My partners Daughter two weeks ago had to call for an ambulance at 5.15am due to a very bad admoninal pain. The ambulance took 15 minutes to arrive; she had to be taken to Nobles along with another emergency patient who was already in the ambulance when she was collected. There was no privacy in the ambulance on the 15-mile trip.
A week-ago our G.P had to get an ambulance to take my partners Son who suffers from a heart condition, the ambulance had to come from Castletown!! A waste of Staff time and resources.
Can you imagine a situation when an old lady who has just had a stroke or a pregnant woman having a miscarriage has to share an ambulance on a Saturday night with two drunks who have had a glass fight and endure a 15 mile trip to Douglas. This could happen if the ambulance service turns into a last bus to Douglas on a Saturday night. With the claims culture as it is I hope a personal claims lawyer sues the Manx Government for trauma if someone has to endure a situation such as described.
If this situation is not reversed I see people dying because they can not get access to a hospital on their doorstep during weekends and nights. Does this crazy health minister think people do not require hospital treatment during these hours, cover should be the same 24 hours a day 7 days a week?
Alan Bell recently said on Manx Radio that the problem is nothing to do with funding but the willingness of Doctors to work out of hours. I do not believe him. If you pay the right money you get the cover. It worries me that he represents Ramsey and the nightmare possibility of Anne Craine
the health ministers sister getting elected to also represent Ramsey. You might as well save Archallagan and dump the waste from the power station at the Cottage Hospital site or turn it into a Private Dentist surgery!.
Massive amounts of money has been wasted on the new Hospital. We could have had the best hospital in Europe with private patients bringing in money from all over the world, this would have subsidised the treatment for the island residents and we would all have benefited. Instead this inadequate government has wasted money, allowed the island to get overpopulated without realising that more people means that more services are required. Many people using the health service have never put anything into the Manx economy but are happy to take out and this in turn means we lose out. If the government does not want to listen to the majority of Manx residents who want residence control they better bite the bullet and put up taxes to pay for their policy. Lastly 3 Saturdays ago the wait in A & E at Nobles was 4 Hours this was told to us by a Nurse at the Hospital. I am sad to say we are turning into a mini version of Britain.
Last one to leave turn the light out!! L
44 Ballalough Andreas
Isle of M an IM7 4HX
6th April 2003M r E dgar Quine OBE M HK Barem e Ville Clenagb Road SulbyIsle of M an
D ear M r QuineI am writing with regard to the recent changes to the service provided at the Ramsey &
District Cottage Hospital. Previously you could see a GP at all times daring the day for all emergency, urgent or follow up treatm ents and a t night a GP was available on call for
,— emergencies and urgent cases. ----- ----------------- --------------— " — ’ ‘ --------- — —.j Now yoo can only see aD bctor between 0800b rs and 1800hrs, M onday to Friday. That is a\ total of 50 hours in a week. For the remaining 118 hours in a week you cannot see a GP at J
RDCH if ill. The Nurse Practitioner cannot admit patients to the hospital outside of the above hours.v
-"Quite how M r Pressley (Senior Nurse M anager) can state in the Press that this is not a downgrading and is only an alteration to the service being provided is staggering to say the least.He even goes as far as to call it an exciting development!!
T T th e re was a genuine emergency call made to the Ambulance Service from residents in the North of the Island, who would respond?The Emergency Ambulance crew will be busy transporting everybody with anything from a cut finger which requires a stitch* to a d runk with scraped knuckles received from fighting to Nobles Hospital for treatm ent.All minor ailments / injuries which were previously treated at RDCH will now have to be taken to Douglas for treatm ent, leaving the N orth with what has to be inadequate medical cover.I believe this to be totally unacceptable.People will suffer and undoubtedly lives will be lost, and to someone with family and many friends in the North obviously la m very concerned.
CcM r Richard Corkill Esq Chief M inister Hon. C lare M Christian BSc MLC M r Leonard Singer MRPS MLC M r Allan Bell Esq M HK
Yours Sincerely
M r K S Airey
As an MHK for the North of the Island, I believe you and the general public are aware of the changes due to happen at Ramsey Cottage Hospital as from April 1st 2003.We should be fighting for enhanced health services for the North, not, what seems to be a lack of care and responsibility from our GP’s.
At the very least, the present services should be maintained until a suitable compromise can be attained.
People will suffer and undoubtedly some lose their lives as a result of this move.
Kind RegardsA very concerned member of the public
Select Committee on 'Out of Hours' GP services
Submission by John Rimington MHK
My submission is necessarily brief as I believe there may be little that either the Committee might usefully recommend, or the DHSS deliver, without a major change in priorities and methods of service provision.
The provision of Health services is high on the popular agenda. Any reduction in service, or perceived reduction, invites a public furore and an opportunity for political point scoring against those who have the responsibility for such service provision.
However, there is a popular and legitimate desire for a high proportion of the acquired wealth of society to be spent on Health services whilst the responsible authorities have to balance this desire with the legitimate needs of other services, infrastructure maintenance and development, and the need to generate income to underpin the required expenditure. There is never an end point where the competing demands can be matched to the satisfaction of all.
The Health service budget is under extreme pressure from growing demand, growing expectations and higher and higher standards of service provision which are externally driven. If more resources are to be placed into a particular area, say 'Out of Hours' GP services, then those resources must either be found from another area of the Health budget or from another area of Government. That is the simple reality that cannot be ignored.
Thus it would be easy for the Select Committee to make a recommendation which necessitates significant extra resources. It will be easy for politicians to support that call, as undoubtedly they will, without any responsibility for locating the resources. If the DHSS Minister then reduces another area of provision or the Council of Ministers reduces another service, those same politicians will then have the opportunity to point score again.
The Committee might think that this is simply the nature of politics / democracy. Whilst recognising that the above political traits are evident elsewhere, I would contest that they are particularly acute in the IOM where party politics does not effectively exist. Western parliamentary democracies are generally allied to a party system. This places a responsibility on opposition parties to have a manifesto of some detail which outlines how resources are to be generated and prioritised in allocation. Such manifestos are then open for scrutiny.
Unfortunately, the IOM political system produces no such responsibility on those who criticise and play the populist card.
Primary Health ServicesWhilst recognising that the recent changes of'Out of Hours' provision are a reduction in the level of provision for many - especially those further away from the Douglas area, that reduction is probably not as statistically significant as some would argue. (The rationale of statistics are little comfort if it is a member of your own family that happens to be the exception to the statistical rule.)
We should not forget that, in global terms, our levels of Health care provision are luxurious. This recent change only represents an insignificant reduction in the level of luxury we enjoy.
Unfortunately, health care provision has to be rationed (and this has always been so) to match the available resources. The available resources, in this instance, have Voted with their feet' and are not available to the previous extent.
Is it simply a case of providing more doctors in one configuration or another?
Is this not an opportunity to reappraise 'GP Services' which are a critical element of primary health care?
I would question whether the service currently provided by GPs actually necessitates GPs to the full extent. I would hope that there is some detailed analysis of the service requirements of GPs in terms of reasons for patient contact. Do all the patients (day or night) who wish to see a GP really need to see a GP in the first instance? Is the current structure the right method of providing the services we wish to provide and improving the health of the population?
Philosophically it is logical that more resources should be devoted to primary health care (including health promotion, etc.) at the expense of acute services. Without such a switch in resources, acute provision will soon become unsustainable. Unfortunately a resource switch will be politically unpopular and it will take some years, if not decades, for the benefits to be fully realised. Such a switch of resources may only require the same GPs, or even less, but other health professionals will be required.
I am committed to the concept of'community' service provision. I am not sure that this matches the current methods of providing services in the community. I am not convinced of the efficacy of the rapid expansion in the Public Health Directorate and the desire for more and more 'strategies' for well meaning professionals to interagency themselves.
The Island has an opportunity to be different from the UK. Methodologies which might be appropriate for the UK, or any other large entity, might not apply to a small island community. The Island is also in a straight jacket of national (UK) agreements which we have readily followed. Perhaps we should consider whether there can be a worthwhile life outside of these straight jackets which would give us freedom to innovate and seek new ways of providing primary health care. This is a delicate area which would require willingness from the staff groups to look beyond existing terms and conditions.
My apologies for not focusing on the 'Out of Hours' service in detail. The DHSS and / or the Committee may come up with a remedy but I suspect it will only be a 'patch' job to satisfy political needs. A more fundamental reappraisal is required.
14/09/03
LEGISLATIVE BUILDINGSISLE OF MAN
IMI 3PW
FromHon Stephen C Rodan BSc (Hons), MR Pharm S, MHK
Member of the House of Keys for Garff Minister for Education
Our Ref: SCR/ejm /ecw
9 September 2003
Mr P Lo Baò Clerk to theSelect Committee of Tynwald on GP Services Clerk of Tynwald's Office Legislative Buildings Douglas
Dear Phil
I write in response to your invitation to submit views on the current and future provision of GP out-of-hours services.
As representative for Garff, I would comment on two recent changes which directly affect my constituents:
a) the change by the Laxey GPs from being among the few remaining Island practices to operate a rota system of out-of-hours and night visits directly (rather than Manndoc), to participation in the new Emergency Doctor Service from 1 April; and
b) the change by the Ramsey GPs, who serve many of my Maughold constituents, from operating rota-based out-of-hours and night cover centred on Ramsey Cottage Hospital, to participation in the new Emergency Doctor Service.
In respect of a) many people who had for many years enjoyed high standards of out-of-hours medical care through speedy home visits from their own GP (or another GP from the same practice) were understandably concerned that a centralised service from 1 April would be inferior.
Cont
-2-
"Doctors would not know the medical history of individual patients, not find the house etc". In reality, just as patients in other parts of the Island had found that - on the earlier introduction of the Manndoc Service - these fears were not realised, so has the Emergency Doctor Service, in my experience, not given rise to anticipated’ problems of slower service or inferior standards of care etc for these patients.
The disadvantages of a centralised system are that it is costing twice as much to run as the old system, and that the GPs have to work with patients from first diagnostic principles, due to not being able to access patient records out-of- hours. However, with paperless practices evolving and centralised computer records becoming a future possibility, allowing access to details of allergies, present treatment, past medical history etc, these disadvantages will do doubt disappear.
What will be gained for the NHS will be having doctors on duty out-of-hours because they want to be, not because they have to be.
The momentum for this service is now inexorable and it will secure future recruitment of new GPs to the Isle of Man as the older GPs retire.
From the patients' point of view the Emergency Doctor Service has not, in my opinion, been detrimental to patients who enjoyed the old rota-based system. I cannot speak on behalf of patients of those practices which contracted to Manndoc, other than to say I would be surprised if there were any difference at all.
Certainly the Operational Guidelines are exhaustive, and set high standards of patient care.
However, as far as b) is concerned, I cannot accept that Maughold patients now enjoy similar levels of service from the Emergency Doctor Service that they previously received from their GPs - the reason is, of course, that Ramsey Cottage Hospital facilities, which were made available for what was in effect, out-of-hours consultation, with GPs quasi-emergency provision, and the sort of service that GPs could have delivered through rota-based home visits elsewhere, are no longer available to the public.
Ramsey Cottage Hospital was not an acute general hospital with A & E, but the place where GPs could see patients out-of-hours, and where patients could conveniently receive medical care from a hospital - a much valued facility in the north.
Cont
The loss of such out-of-hours medical facilities to the public was inevitable the moment the Ramsey GPs, like everyone else, switched to a centralised Emergency Doctor Service based in Douglas to look after their patients out-ofhours.
Extending the hours of operation of the nurse-based services can only partially restore the situation. Public confidence will, I feel, never be completely restored in Ramsey Cottage Hospital as a provider of out-of-hours medical care until there is a system where a doctor is actually permanently on duty. The only way to get that will be to set up a salaried medical service, at a consequential cost.
Concerns have been raised about distances from the north to Noble's for emergency treatment, and adverse weather conditions delaying or preventing home visits from Emergency Doctors etc. Such concerns can only be tested and validated from experience, and collating Cottage Hospital and Emergency Doctor data over time. The fear among a number of patients - elderly, housebound, or without cars - is that they are at risk in the meantime. This situation contributes to the loss of confidence.
One way forward might be a temporary trial with salaried medical cover contracted to Ramsey Cottage Hospital, for a period of say 18 months or two years, with' a study then made of the whole range of out-of-hours medical care which had been received by patients - ie at the Cottage Hospital, through the Emergency Doctor Service in Douglas (whether by home visit or otherwise), or emergency admission to Noble's.
An evaluation of the comparative levels of service and patient care could thus be undertaken to establish the cost-effectiveness of such an arrangement being made permanent.
I trust these comments are helpful to the Committee.
Yours sincerely
Steve Rodan
LEGISLATIVE COUNCILLEGISLATIVE BUILDINGS
ISLE OF MAN IMI 3PW
Our Ref: LIS/ecw
3 September 2003
The ChairmanSelect Committee of Tynwald on GP Services Legislative Buildings DOUGLAS Isle of Man
Dear Sir
Whilst I am a member of the above Select Committee, I would like to forward my views on the changes. I am Chairman of the Ramsey Hospital League of Friends, but since my appointment to the sub-committee, I have stood back from their decisions and actions in regard to the changes.
The remit of the Select Committee is to look at GP hours throughout the Island, however, the situation is different depending on where a person lives and how close they are to medical services. I believe it is necessary to therefore make different judgements for particular areas.
I do not wish to repeat matters already contained in correspondence from other sources of which I am aware, and I would, therefore, express my full support for the contents of the letter from Ramsey Town Commissioners as to the way forward.
It is a fact that the Hon Minister for Health and Social Security has stated in public, on more than one occasion, that the difficulty was not lack of finance, but the difficulty in doctor recruitments. The doctors should be recruited through IOM Hospitals, and the Ramsey Hospital returned to the IOM Hospitals for Primary Care. This action would permit the Ramsey Hospital to reinstate an Accident and Emergency service which was its original service, and introduce a flexibility for doctors between there and Noble's Hospital.
Doctors permanently present at Ramsey Cottage Hospital would mean that the Ramsey Grpup Practise would no longer service the Hospital and the outpatients and in-patients would be attended to by the IOM Hospital doctors. Savings would therefore be made, and the Ramsey doctors would offer services similar to those provided by all the other GP practises on the Island (8.00 am to 6.00 pm) which is what they appear to want.
-2-
The consequences of the above changes would take pressure off the Emergency GP "'out of hours" service as those GPs would not have to attend the north of the Island, again generating savings.
I find it interesting that the general view of the Island's GPs is that everything is working well. It may work well within 15 minutes of Noble's Hospital, but it does not work well in the areas more distant such as Ramsey.
As the former MHK for Ramsey, and now as an MLC living in the north of the Island, I am dearly aware that the GPs waiting "on call" in Noble's Hospital are unaware of the difficulties encountered by persons before they eventually contact the doctor.
The nurses at Ramsey are providing an excellent but very limited service "out of hours" in Ramsey, but from 10.00 pm to 8.00 am there is NO SERVICE. I have had recounted to me, since the changes in April, numerous concerns by people living in the north of the difficulties they have encountered and the 'potential for disaster' they believe they are facing. The GPs who think the service is working well have no inkling of these complaints.
People are afraid to complain because they believe that the doctors may well strike them off their lists. Let me give you one personal example to illustrate the problem.
On 30 August (Saturday), I was walking on the Ayres in Bride when my right ankle was damaged when my foot went down a rabbit hole. I went to the Ramsey Hospital at 8.10 pm as I had difficulty walking. I was seen by a nurse who said I needed anti-inflammatory tablets immediately, however, she could not issue them and, of course, there was no doctor. For a person who was not a Pharmacist that would have meant waiting until some time on Monday morning to get a prescription. By that time considerable damage could have been caused to my ankle. A GP would not be aware of these circumstances. Under the suggested changes to IOM Hospitals service this situation would not have arisen and treatment would be available when needed.
Paramedics, quite rightly, on attending a patient, will make the professional decision where they should take the patient. At the moment they have no choice outside the hours of 8.00 am and 6.00 pm, and the patient suffers.
An argument put forward for centralising the "out of hours" GP service in Noble's Hospital is, "why should the north have different treatment"? An answer is that fortunately the north has facilities already available due to the foresight of our ancestors in 1904. Why ignore this facility?
Cont
Similarly, for the majority of the population within a short distance of Noble's Hospital, they already have an excellent Accident and Emergency service. There is no argument to say "take that service away because it is not available to all"!
Each area must be assessed on its needs and the availability of its area services.
Certainly, for the north, an "out of hours" GP service in the north is essential for the future health of the population, and the proposals to move the Ramsey Hospital back to the "umbrella" of IOM Hospitals would ensure that the service would, in fact, be improved from that offered by the Ramsey GPs "on call" as previously.
Yours faithfully
Appendix 5
OFFICE OF THE CLERK OF TYNWALDLegislative Buildings, Douglas,
Isle of Man, British Isles, IM1 3PW
Our ref: C /G PS/02/plb
16th July 2003
Hon C ChristianMinister of Health and Social SecurityMarkwell HouseDouglas
Dear Mrs Christian
Select Committee of Tynwald on GP Services
I am writing to you at the request of the above Committee, to ask you to supply evidence, in writing, to the Committee concerning the following specific issues:
(a) a simple distinction between the services provided by hospitals and those provided through primary care;
(b) why the 'Mann Doc' system was discontinued;
(c) what the precise provision for out of hours GP services is throughout the Island;
(d) whether all GPs are part of the current system;
(e) statistics comparing the number of consultations at hospital and in home visits carried out by 'Man Doc' during the last three months of its operations and the new system in the first three months of its operations and any available statistics indicating how people arrived at 'Mann Doc' and the present out of ours service;
(f) details of the number and nature of any complaints received from the public regarding the provision of the new services; and
(g) whether your Department is satisfied with the current situation or has identified any areas for improvement.
The Committee would be pleased to receive the above information by Friday 12th September 2003. Following its evaluation of evidence received, the Committee may wish to call you and some of your officers and officials, to give oral evidence early in the autumn.
I attach a copy of the Committee's terms of reference for your information.
Yours sincerely
Phil Lo BaoJoint Clerk to the Committee
Ref: 105/3/6
ISLE O F MAN DEPARTMENT O F HEALTH AND SOCIAL SECURITY
To : Select Committee of Tynwald on GP ServicesFrom : Department of Health and Social Security Date 10 September 2003
Subject: General Practitioner Services - Out-Of-Hours Arrangements
1. In responding to the Select Committee, it may be helpful to provide some background to the basis under which General Practitioners (GPs) are contracted to the D.H.S.S. to provide general medical services (G.M.S.) to the Island’s population.
2. The first thing to say is that GPs are part of the National Health Service Primary Care Service, and in common with other Primary Care providers, ie. General Dental Practitioners, Community Pharmacists, and Community Opticians, they are in most cases self-employed individuals who are contracted to the Department to provide N.H.S. services. The statutory basis of the Contract relating to GPs is set down in the National Health Service (Isle of Man) General Medical and Pharmaceutical Services Regulations 1978, as amended. The Regulations, which include the GPs Terms of Service, provide the legal framework within which the business of N.H.S. general practice is conducted. A copy of the consolidated regulations, which include major amendments to GPs contractual responsibilities introduced in 1990 (but exclude a small number of minor amendments made since then) is attached at Appendix 1.
3. Normally, a GP should give treatment personally. However, in the case of G.M.S., other than maternity medical services, child health surveillance, and minor surgery services, a GP is under no obligation to do so if reasonable steps are taken to ensure continuity of treatment by another doctor acting as a deputy, irrespective of whether the other doctor is a partner or an assistant.
4. The principle set out in Paragraph 3 above has been used on a day-to-day basis by GPs in Group Practices, in covering for colleagues and also through the employment of locums to cover periods of Annual and Sick Leave, etc.
5. Whilst the use of deputising services has been commonplace in the United Kingdom for m a n y years, GP Practices on the Island have accepted responsibility for providing cover internally. However, the onerous nature of the 24-hour responsibility on GPs for their patients was increasingly being questioned as no longer sustainable, and this led to the introduction in July 1998 of the “MannDoc” Service, encompassing eight of the eleven GP Practices on the Island. Those not included in these arrangements were Laxey, Ramsey, and Port Erin.
6. Under the MannDoc Service, which was sanctioned by the Department, the eight Practices concerned entered into an agreement under which out*of-hours cover, i.e. evenings, weekends, and Bank Holidays, was provided on a rota basis by a GP from one of the Practices. This effectively meant that GPs within those Practices enjoyed a significant reduction in out-of-hours work, which was seen as an enormous benefit to

individual doctors in achieving an improved work/life balance. In addition, there were perceived benefits for patient care in that GPs, who otherwise were at risk of being tired as a result of regular callouts, etc., were better equipped to handle the rigours of the ensuing day's Practice work, e.g. surgeries, visits to patients, etc.
7. The MannDoc Service was organised entirely by representatives from the Practices involved, with accommodation being provided by the Department at the old Noble’s Hospital.
8. The future of G.M.S. on the Island came to the fore again as a result of a letter dated 23 November 2001, from the GP Sub-Committee, Isle of Man Medical Society, to the Chief Minister (Appendix 2). The letter outlined concerns of local doctors over the arrangements for GP practice on the Island and the steps they considered needed to be taken to secure its future. The approach reflected negotiations taking place in the United Kingdom between the Government and the Profession, who were seeking to re-negotiate their Contract. A key aspect of the request for a re-negotiated Contract concerned recruitment and retention, a situation that was causing equal concern on the Island.
9. Following the approach from the GPs, the Department established a Joint Negotiating Committee, consisting of GP representatives and Department officials, arising out of which agreement was reached in a number of areas aimed at ensuring that the Isle of Man remained competitive in attracting GPs to the Island. Whilst this was partly achieved through additional financial support towards the costs of Practice staff and the development of I.T. services (approximately £600,000 and £40,000 respectively), it was agreed by both sides that a major factor in attracting doctors into GP practice, notwithstanding the MannDoc arrangements, continued to be the on-call commitment, which it was known would be one of the main features of a re-negotiated Contract in the United Kingdom.
10. The subsequent negotiations concentrated on the issue of out-of-hours cover, arising out of which agreement was reached on a variation to the existing Contract under which GPs would be relieved of their out-of-hours responsibilities. The new arrangements, which were based on the principles of the existing MannDoc Service but extended to include all eleven Practices, provided a separate Contract with individual GPs willing to participate in a new Out-Of-Hours Service. The new Service, re-tided “Manx Emergency Doctor Service (M.E.D.S.)”, commenced on 1 April 2003, under the direct control of the Department, and was funded through a limited re-distribution of existing fees, together with a substantial additional amount, in the region of £154,000. Details of the Service which was significantly enhanced to reflect the increased number of patients over a wider geographical spread, are shown at Appendix 3.
11. As indicated above, the approach from local Practitioners was in advance of the outcome of negotiations on a new GP Contract in the United Kingdom. Since then, the new U.K. Contract has been finalised and agreed following a ballot of the Profession. The new Contract contained revised arrangements, under which a General Practitioner or Practice will no longer be required to provide out-of-hours care. Instead, Primary Care Trusts in the United Kingdom will be responsible for providing Emergency Primary Medical Services to their populations out-of-hours (see Briefing Paper at Appendix 4).
2
12. In the event, the Island, in respect of out-of-hours GP cover, has moved ahead of the United Kingdom although the principles governing the new arrangements are in line with the provisions of the new U.K. Contract. The remaining aspects of the Contract are the subject of on-going discussions between the Department and representatives of the Profession.
13. Turning now to the evidence requested by the Select Committee in relation to specific issues, (Select Committee letter dated 16 July 2003, refers), the following information is provided:-
(a) A simple distinction between the services provided bv hospitals and those provided through Primary Care
Primary Care Services are those elements of Health Services directly accessible to the patient. Most of this is provided through Family Health Services, e.g. General Practitioners, Dentists, Pharmacists, and Opticians.
Secondary Care provides specialist diagnosis and treatment facilities, usually in a hospital setting, for both in-patient and out-patient care, following a referral from Primary Care. Secondary Care also includes the main range of diagnostic services such as those provided in X-ray and Pathology Departments.
However, some services directly accessible to patients are located in hospitals; the main example of this is the Accident and Emergency Department.
(b) Whv the MannDoc System was discontinued
Whilst the MannDoc System, in its original format, has been replaced by the Manx Emergency Doctor Service (M.E.D.S.), the principle under which it operated has remained the same. The new arrangements extended the previous Service to take account of the change brought in as a result of the new GP Contract which is being implemented following a vote of support by GPs in the U.K.
In 1998, the MannDoc System was set up as a co-operative by GPs in eight out of the eleven Practices on the Island. At the time, GPs had 24-hour responsibility for the care of their patients, but they were able to delegate that care to other suitably qualified Practitioners, either through internal rotas within Practices or by a number of Practices coming together to share the workload. Under this arrangement, all the GP members of the co-operative were jointly responsible for the funding and running of the Service, although they did receive financial support from the D.H.S.S. for the provision of out-of-hours services.
The new GP Contract recognised that this situation could not continue:-
*The existing default responsibility for all GPs to provide 24-hour care for their patients makes general practice unattractive for many prospective and current general practitioners and works against the achievement o f an appropriate work/life balance. To overcome these problems, if the contract is accepted by the
3
profession, the obligation on practices to ensure the provision of out-ofhours care for their patients will transfer to primary care organisations which will become responsible for commissioning and, where necessary, providing out-of hours services. The out-of- hours period will be defined as 6.30pm to 8.00am on weekdays and also the whole of weekends, bank holidays and public holidays”.
(Reference: New G.M.S. Contract - Investing in General Practice, February 2003).
The above provisions will now be enacted in the U.K. following the acceptance of the GP Contract. It is recognised that if we wish to continue to recruit GPs we must offer Terms and Conditions that are at least as good as those on offer to GPs in the U.K., and this meant that we had to make a similar change in our out- of-hours arrangements.
The result has been the setting-up of an all-island Service as no Practice on the Island has expressed a wish to exercise the option to continue to provide their own Out-Of-Hours Service.
(c) W hat the precise provision for out-of-hours GP services is throughout the Island
The out-of-hours periods are defined as 6.00pm.-8.00pm. every day and all day on Saturdays, Sundays, and Public Holidays.
For the evening and night shifts (6.00pm.-8.00am.) there is one doctor on-duty with a second doctor available on-call should the workload prove too onerous. To date this arrangement has only been activated on one occasion. For daytimes (8.00am.-6.00pm.) on Saturdays, Sundays, and Public Holidays, two doctors are on-duty.
The Out-Of-Hours Service was previously located in shared accommodation in the former Noble’s Hospital and is now located in part of the Fracture Clinic accommodation (adjacent to Accident and Emergency) in the New Hospital.
The initial contact with the Service is by telephone, which allows the doctor to make an assessment of the patient’s condition and decide whether the patient requires a visit, the patient should come to the Centre for further assessment and treatment, or telephoned advice as appropriate (see comments on statistics in Paragraph (e)).
(d) Whether all GPs are part of the current system
All Practices and all patients registered with those Practices are covered by the M.E.D.S. system. Medical cover is undertaken by existing GPs (with the exception of two individuals) as well as by a small number of other doctors who are not GP principals but who are qualified to work on the Service.
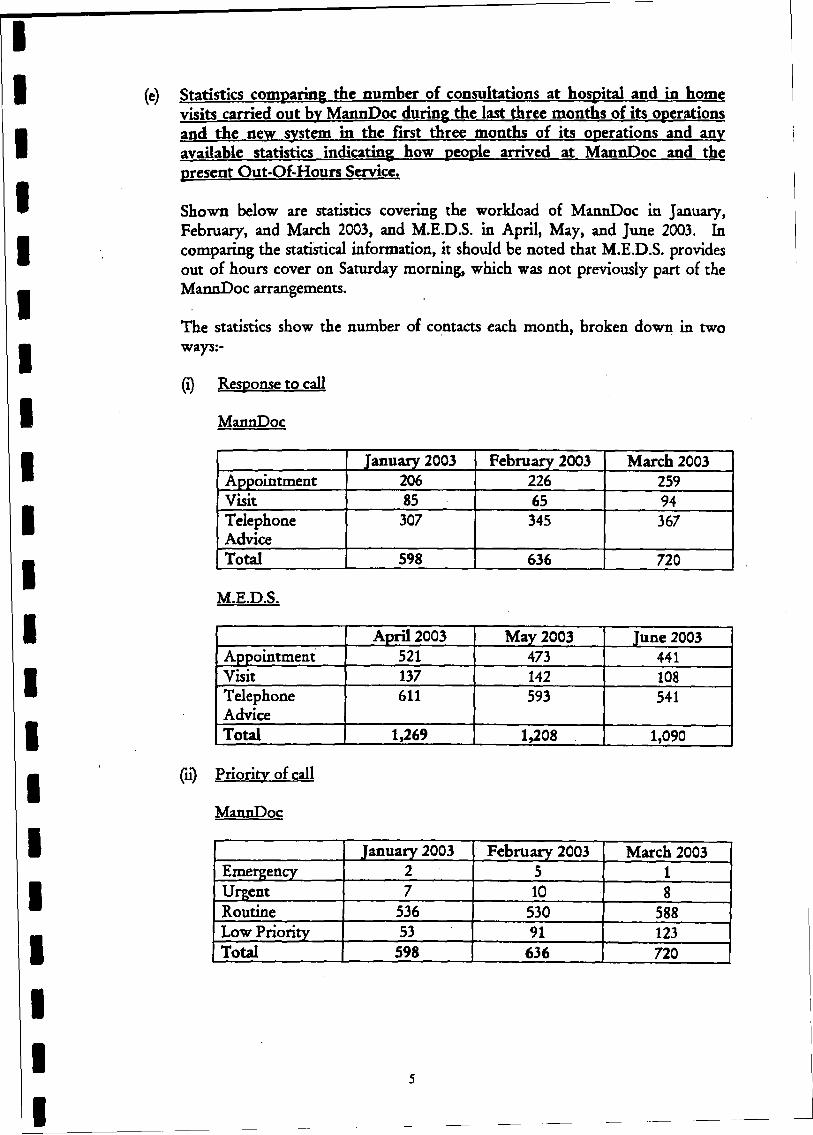
(e) Statistics comparing the number of consultations at hospital and in home visits carried out bv MannDoc during the last three months of its operations and the new system in the first three months of its operations and any available statistics indicating how people arrived at MannDoc and the present Out-Of-Hours Service.
Shown below are statistics covering the workload of MannDoc in January, February, and March 2003, and M.E.D.S. in April, May, and June 2003. In comparing the statistical information, it should be noted that M.E.D.S. provides out of hours cover on Saturday morning, which was not previously part of the MannDoc arrangements.
The statistics show the number of contacts each month, broken down in two ways:-
(¡) Response to call
MannDoc
January 2003 February 2003 March 2003Appointment 206 226 259Visit 85 65 94TelephoneAdvice
307 345 367
Total 598 636 720
M.E.D.S.
April 2003 May 2003 June 2003Appointment 521 473 441Visit 137 142 108TelephoneAdvice
611 593 541
Total 1,269 1,208 1,090
(ii) Priority of call
MannDoc
January 2003 February 2003 March 2003Emergency 2 5 1Urgent 7 10 8Routine 536 530 588Low Priority 53 91 123Total 598 636 720
5
M.E.D.S.
April 2003 May 2003 June 2003Emergency 19 8 12Urgent 104 57 83Routine 1,037 1,036 924Low Priority 109 107 71Total 1,269 1,208 1,090
(f) Details of the number and nature of any complaints received from the public regarding the provision of the new services
A number of concerns have been expressed on behalf of patients regarding the introduction of the extended GP out-of-hours service (see Appendix 5). These concerns have, in the main, been related to the principle of the new arrangements, with no formal complaints from patients regarding the care provided by M.E.D.S. having been received for investigation.
(g) Whether vour Department is satisfied with the current situation or has identified any areas for improvement
In assessing the Out-Of-Hours Service arrangements, the Department is satisfied that over the four-and-a-half years of the MannDoc Service (covering 75% of the Island's population), it proved itself effective in providing general medical services to patients. Whilst the extended Service, with its increased medical cover, has only been in place since 1 April 2003, the early indications are that the out-of-hours cover continues to be effective in meeting the care needs of patients.
Having said that, the Department continues to monitor the Service and to explore ways in which improvements can be made.
One possibility is the employment of doctors who will work for the Service on a full-time basis. This will improve the continuity of service and will also serve to reduce the dependency on existing GPs to provide the Out-Of-Hours Service. This would fit in with the original reasons for introducing these arrangements which were to respond to the unattractiveness to GPs of a commitment to providing an Out-Of-Hours Service.
The other development which is being investigated is the introduction of nursing staff to take the initial calls from patients and to undertake the initial triage. “Triage" is the assessment of the patient’s condition and the decision as to which treatment route should be taken. Nurse triage is well established in other GPs out-of-hours services, and does mean that the most effective use is then made of the medical time available to the Service.
14. It is probably worth clarifying the situation of medical cover at Ramsey and District Cottage Hospital which some have linked to changes in the out-of-hours G.M.S. In so doing, the Select Committee need to be aware that medical services to the Cottage Hospital are provided under Contracts with the Ramsey Group Practice, which are quite separate from their obligations under their G.M.S. Contract.
6
By way of example, the decision of the Group Practice to restrict the level of medical cover provided to the Hospital’s Minor Injuries Unit is not directly related to the new M.E.D.S., in which, since 1 April 2003, the Group has been fully participating. It may of course be that the decision taken by the Group to restrict their commitment to the Minor Injuries Unit reflected the changes in the out-of-hours GP arrangements, but this was a matter solely for the GP Practice and which had financial consequences for them.
That being the case, the issue to be considered in terms of the North, and other areas of the Island, is whether or not the M.E.D.S. arrangements are adequate in providing general medical services to the population as a whole. The views of the Department on this are set out in Paragraph 13(g) above.
As the Committee is aware, Tynwald has called for an independent external review of community services in respect of Ramsey Cottage Hospital, with a report back by January 2004.
15. In concluding this submission, it is clear that the introduction of the three additional Practices into the new arrangements has caused some concern over the extent of the medical cover available out-of-hours. In raising these concerns, emphasis has been directed towards the possibility of providing more than one Emergency Doctor Service, with locations in different parts of the Island.
In considering this possibility, it has to be borne in mind that the decisions in relation to out-of-hours cover, both here and in the United Kingdom, have been taken to address the increasing difficulty in attracting doctors into GP practice. To seek to provide more than one Emergency Doctor Service on the Island would not, in the Department’s view, be feasible. In terms of practicality, the point needs to be made that the M.E.D.S. Service, notwithstanding the additional significant cost, is dependent upon the willingness of GPs to participate. This has, on occasions, presented problems in filling particular slots on the rota which suggests strongly that anything other than a single all-island Out-Of-Hours Service could not be sustained.
Indications from Practices suggest that it is not as easy to recruit and retain GPs as it once was, and that this situation could become more critical in the future given the age profile of existing Practitioners. A survey recently undertaken shows that over 50% of General Practitioners currently in practice on the Island will attain the age of 50 over the next five years, a third of that total reaching 55 years of age in that period, when retirement becomes an option.
Clearly, the Island needs to ensure that the new GP Contract, as it applies locally (including out-of-hours cover), is sufficiently attractive to doctors wishing to work here and this is, and has been, the aim of the on-going negotiations with the Profession.
0 8 /0 8 /2 0 0 3 1 6 :5 4 0 1 624 685710 CHIEF SEC’ S OFFICE ■* 9642682
GP Group IOM Medical Executive
Dear Chief Minister
This paper outlines the actions that the profession feels need to be undertaken to secure the future of General Practice on the Isle of Man. The context of this paper is the need to be able to recruit and retain GP’s to the island in an increasingly competitive market for these skills and the recognition that the UK Government is aware of the need to substantially increase the number of GP's to maintain and improve Primary Care Services.
As you may be aware GP's within the UK are currently renegotiating their contracts. These negotiations are due to conclude by the end of March 2002. We the GP’s on the Isle of Man also intend to renegotiate our contract Following several meeting’s of the GP Group sub-commit tee of the Isle of Man Medical Society it is very apparent there is a deep feeling of discontent amongst GFs. This mirrors the situation within the UK but also highlights pressures peculiar to the Isle of Man.
Foremost in any negotiations the aim would be to provide all on the Isle with the best quality of care available. With greater and greater pressures on workload the only realistic way to provide this is through as is widely acknowledged increased consultation times of 15 minutes duration as recommended by the Royal college of General Practitioners. This in turn would require decreased list sizes and consequently to cover the population greater numbers of GP's.
From the press it is obvious that there is a manpower shortage with the UK government placing advertisements in many countries overseas. By its own initial estimates the UK government thought 2000 extra GP’s were required. With a large number of GP’s particularly those who came from the Indian subcontinent years ago due to retire over the next few years further replacement doctors will be required. Retention is another problem area. I know of no GP's on the Isle of Man who intend to work beyond 60. This again is similar to the UK and most are actively seeking ways to retire even earlier due to low morale stress pooT terms and conditions. This further depletes the pool of GP’s but also robs the public of its most experienced doctors. To compound recruitment problems it is recognized that the increasing number of female medical graduates (80% in Newcastle) means that posts are not being tilled on a one to one basis. Most female graduates wish either to work part-time or take time out to look after children. This also applies to increasing numbers of male graduates also. Hence it takes; more than one trained individual to fill a full time post. The BMA estimates in the region of 10000 extra GP’s being required to fill these gaps.
The Isle of Man therefore needs to provide as good environment as is possible to work in if it is to successfully compete to recruit and retain GP’s in a very competitive market place. For reasons outlined below the isle is£&as an attractive place to practice as it once was. Firstly the £5000 Golden Hello has yet to arrive on these shores. This is being paid to all new GP’s in the UK (£10000 if you work in a deprived area) who take up principal posts. There are no relocation expenses paid to GP’s as there are to consultants more senior departmental employees and civil servants. The cost of housing here means most new applicants unless
NO.345 D01
Apf&cn* 1
0B/Q8/28&3 1 6 :5 4 01624 685710 CHIEF SEC’ S OFFICE * 9642682 NO.345 D02
moving from the most affluent parts of the UK are put off and simply do not apply. Several practices who have recently sought to recruit new partners have struggled. One practice spent two years without success attempting to fill a post.
Investment in Primary Care ifl poor compared to the UK. May I refer you to a document Investing in Primary Care, This may be obtained at www.doh.gov.uk/pricare/investment.htnu This begins with a £100 million investment in Primary Care via Primary Care Groups/Trusts. None of the mechanisms listed in section 25 for funding these initiatives even exist here. The Department has made no moves to equal this in any way whatsoever Investment in Primary Care is poor compared to the UK. May I refer you to a document Investing in Primary Care, This may be obtained at www.doh.gov.uk/pricarc/mvestmenthtm. This begins with a £100 million investment in Primary Care via Primary Care Groups/Trusts. None of the mechanisms listed in section 25 for funding these initiatives even exist here. The Department has made no moves to equal this in any way whatsoever.
■ Going on from this may I refer you to a document called ‘‘Valuing General Practice”. This is a response to the NHS Plan for England and may be obtained from the BMA web site. In addition to the above money there is a £1 billion investment in Primary Care facilities. Sections 1 through 7 outline the plans for Primary Care. Again I have yet to here anything on a comparable basis in the Isle of Man. Whilst numerous housing projects are given the OK scant regard for the infrastructure to support these is taken into consideration. Of late some 200 patients a month were being allocated in the Douglas area simply because practices are at full capacity and simply cannot cope with more patients. There are several practices who have applied for help with both outdated premises and ones which through expansion have been outgrown. Money via the bidding process is currently very unlikely to be made available as these items are destined year after year to a priority level that never sees the light of day. The cumbersome bidding process needs lo be revised to meet the more dynamic changcs in Primary Care rather than “toying “ with them years after they have occurred The age old argument of we will have to see if this appropriate to the Isle of Man will not do as there will be no GP’s left unless there are massive improvements in terms and conditions. Waiting for years to have schemes as enjoyed by our UK counterparts and be financially penalized both in terms of income pension and facilities is not tenable. A simple example of this is the length of time it took to establish a generic prescribing scheme on the isle.
To add to the above there is £30 million for Scottish GP’s, remote and rural incentive schemes also as per Scotland, another £4 million for out of hours development funds, £50 million in ccntrally provided computer software licenses for General Practice, £10000 per practice for triage incentives to name a few. Further more allowances given to GP's reflect UK not Isle of Man costs meaning we are further disadvantaged. These add up to substantive amounts of money which Primary Care here is starved of. The idea of a PCT/PCG locum the “departmental locum” such as are advertised for every week in the BMJ classified ads for various Trusts is again lost in the bidding process. Paying the GP to attend the meetings with mileage and locum cover as happens at PCG/T meetings has not been adopted here. Whereas a consultant can conveniently just cancel a clinic this is a non starter in General Practice.Even a locum docs not mop up the paperwork, phone calls, business administration or outstanding visits. A canceled surgery in GP land is not just a minor blip lost within a waiting list but a farther pressure point on the practice. The Manx Government seems happy to spend vasi amounts on outside advice yet the majority of “inside “ advice is taken for granted and
0 8 /0 8 /2 0 0 3 1 6 :5 4 016 2 4 68 5 7 1 0 CHIEF SEC’ S OFFICE * 9642682 NO.345 003
unrecognized. These locums also have a role in education in that they can provide protected time within the normal working day something which at present is completely impossible. Closing a practice on the island for an afternoon of audit professional development and educational activities as enjoyed across is a pipe dream.
The Health Service in the UK mainly as a consequence of fund holding has become much more Primary Caie led. Hus issue needs to be addressed on the Isle of Man. Secondary care needs are generated and underpinned by Primary Care. The vast majority of health care occurs within Primary and not secondary care.
7116 ahrwf: shows the inequitable situation that exists at present and why the Isle of Mail is not high on the hunting list for many new GP’s. It is also very evident that the NHS is the poor man of Europe. Mr. Blair’s promise to bring the UK upto the European average fails to take account of the fact the UK’s miserly spending on health compared to its continental counterparts. The UK figure decreases the overall total. Taking the UK out of the calculation greatly elevates what is the average.
So what are die goals each vested party wishes. What do we want to achieve.
■ Government. To provide comprehensive and universal access to medical care in a GP setting in a coat effective and accountable way.
* GP. To provide a GP service which has a manageable workload to allow for a high level of service in such a way as to reward hard work but still maintain control of the working environment
* Patient. A high level of service equivalent to other European countries, preferably free at point of contact.
Whilst not wishing to rewrite the entire GP contract there are several areas which need to be urgently seriously and honestly addressed. These include but are not a comprehensive list of all the issues
1. Appropriate and central funding for Out of Hours provision.
2. A fairer system for target remuneration which penalizes neither GP or patient.
3. Lower list sizes.
4. Longer consultation times.
5. Time and fair reimbursement for professional development.
6. Hnchanced pensions/ ability to draw both pension and salary after retirement.
Recent developments within the Isle of Man dental sector should serve to galvanize minds. These issues will not wait for the usual channels that operate but need immediate attention. The above will require the Island to present an attractive package to prospective GP’s and in tum will require a level of investment that at the vejy minimum matches that being directed

0B /08/'2003 1 6 :5 4 01624 685710 CHIEF SEC’ S OFFICE * 9642602 NO.345 004
in the UK to Primary Care plus recognizes the special pressures on the Island. We do not wish simply to be comparable to the UK playing in the third division but intend to be in the European Champions League. Whilst much is being made of the Guernsey option in the UK (please see www.bma.org.uk/gpc.nsf or /pressrcl.nsf for a fuller discussion of the current contract negotiations in the UK) we would prefer that they emulated the Manx Option..
With this in mind may I aak for your initial comments by the I4th December 2001 with a view to starting negotiations in the first two weeks of January 2002.
Yours sincerely
DR M MASKA. Dated. 23rd November 2001.
Chairman GP Subcommittee, Isle of Man Medical Executive
C/oRamsey Group Practice Bowring Road Ramsey IMS 3EV
CcTreasury Minister Minister for DHSS Member for Health
Appenoi X. 3
H E A L T H S E R V I C E S
S h i r v e i s h y n S l a y n t
Emergency Doctor Service
The Island-wide ‘out-of-hours’ emergency CP service will operate from 1st April 2003.This service replaces Mann Doc and will be available when your doctor’s surgery is closed.If you have a medical condition that isn’t life-threatening but cannot wait until the surgery opens, you should telephone your usual doctor’s surgery and a recorded message will inform you of the number to call to speak to the doctor on duty.
The duty doctor will:• offer you medical advice over the telephone or• advise you to attend a consultation at the out-of-hours surgery.• In exceptional circumstances, the doctor may arrange a home visit.
It is not a drop-in service and patients should note that they will not be seen by the duty doctor without an appointment.The service is available from 6pm to 8am Monday to Friday, with 24-hour cover over weekends and bank holidays.If you have chest pain or a life-threatening emergency you should always call 999.
•••••TH E NHS C O N FED ER A T IO N
Appendi K 4-
briefingcsa
Modernisation Agency
www.natpact.nhs.ukNational Primary and Care Trust
Development Programme
Out-of-hours services under the new GMS contractThe NHS Confederation and the National Primary and Care Trust Developm ent Programme (NatPaCT) have developed a series of briefings to help primary care trusts and practices in England prepare for the new General Medical Services (GMS) contract.
This initial briefing focuses on the new roles and responsibilities of Primary Care Trusts (PCTs) and Strategic Health Authorities (SHAs) for ensuring 24-hour patient care. Detailed guidance will follow later.
Paragraphs 2.17 to 2.25 of the new GMS contract - Investing in General Practice - set out a timetable and a process for PCTs to take on out-ofhours responsibility.
JUNE2003 No.2
Briefing 2 • Out-of-hours services
What does this mean in practice?Out-of-hours will, in effect, be a unique form of GMS additional service with a PCT process to allow practices to opt out.The timetable is:
• At the earliest opportunity (by30 September 2003 at the latest), each practice should tell its PCT whether or not they want to opt out. Because the new contract is practice-based, all GPs within a practice will need to agree on this.
• Until April 2004, out-of-hours service will remain the responsibility of the individual GRThe ability to transfer (not just delegate) responsibility to an accredited provider will remain. PCTs will be encouraged to help GPs do this if they wish.
• From April 2004 to Decem ber 2004(subject to legislation), practices may transfer all responsibility for out-of-hours, if the PCT agrees and is ready.
• After 31 Decem ber 2004, it's expected that all practices will be
able to opt out, subject only to a PCT veto in exceptional cases.
Until 31 Decem ber 2004, practices will be able to keep 24-hour responsibility for their patients. Practices that do continue to provide out-of-hours services themselves will need to meet Department of Health quality standard s. They will also be able to delegate this work to an accredited provider, but will still be responsible for the service their delegated agents provide. Practices won't be able to transfer responsibility- opt-out will replace that option.
After 31 Decem ber 2004, opted-out practices and new practices will only be able to do their own out-of-hours work if their PCT agrees.Trusts will take into account the impact on existing services to patients and on other local out-of-hours providers.
Many practices may not want to continue to be responsible for out-ofhours care, but many will want to
ensure their registered patients get a high quality service.
SHAs will manage this process but, in
some exceptional circumstances such as in remote and isolated areas, there may be no alternative to the practice
providing the service. SHAs will, though, manage the process to ensure that exceptions are kept to a minimum.
Implications for PCTs, SHAs and others
PCTsFrom 31 December 2004, PCTs will be responsible for ensuring delivery of emergency primary medical services for an average of 119 hours out of 168 hours each week. GPs and practices may provide as little as 49 hours per week, with PCTs responsible for services for the rest of the time.
PCTs are the key to the success of the new system. Each PCT needs to review its out-of-hours modernisation plan, focusing on how they intend and expect out-of-hours services to be delivered when GPs no longer have to take on 24-hour responsibility.They also-need to consider how they will meet the Carson Report recommendations and Reform of Emergency Care (REC) agenda.
PCTs have to develop robust plans by no later than 31 December 2004. A plan based on commissioning existing local out-of-hours providers is unlikely to be a solution.They need to explore how they will integrate with other services, including accident and emergency, walk-in centres, mental health services, pharmacy, social care and dentistry. A range of service options have already emerged, including:
* GPs working in A&E departments
• out-of-hours providers based in minor injury units (MIUs), A&E departments, NHS Direct and NHS
walk-in centres
Briefing 2 « Out-of-hours services
• nursing and paramedic teams
working in the facilities mentioned above and carrying out home visits out-of-hours
• transport provided by ambulance
services to deliver patients to local primary care centres to reduce
home visiting rates
PCTs should, therefore, be planning to develop or commission new and
integrated services.They should be looking for the most appropriate provider for the range of care required, with more emphasis on triage and a mix of skills.This will provide a much better service for patients, ensuring - for the first time - that they have out-of-hours access to the health professional best suited to their needs.
PCTs will need to make the best possible use of the skills and capacity available in their current arrangements, and to support and encourage the development of providers in their area.
SHAsSHAs have a crucial role in managing the transition.The SHA role is especially vital because:
• PCTs need to organise themselves into networks or consortia to deliver modernised out-of-hours services across more than one area
• providers need to rework some aspects of their current arrangements because integrated working with NHS Direct requires a population of at least 400,000.This
doesn't necessarily mean that small providers have to merge, but it does require co-operation. Providers may have to develop a local network and shared IT.
Out-of-hours service providersGeneral practice co-operatives
(co-ops) and other out-of-hours
providers will need to adapt to a world where fewer practices will want to do out-of-hours work.
GP co-ops may still exist, but these
will have the chance to evolve into organisations capable of designing, implementing and managing new
methods of delivering high quality service.
GP involvement will be at a premium as a smaller, dedicated GP workforce of out-of-hours specialists emerges. They will tend to do this work for relatively short periods within their careers.These GPs will be a scarce and expensive resource and GP co-ops and deputising services will need to develop much wider skills, relying less on GPs and more on a mix of professionals.
It is important that PCTs develop the new arrangements with the support and involvement of their network of practices.This network has great operational and strategic expertise in
providing out-of-hours service. Few other parts of the service are as effective at matching capacity to demand as existing providers.That knowledge and experience will be extremely valuable.
Linking to national initiativesThis represents a major challenge, but the arrangements build on existing developments and modernisation deriving from the Carson Review 2000- Raising Standards for Patients: New
Partnerships in Out-of-Hours Care.
PCTs have been given the job of carrying out the recommendations of the Review.Their plans were last
updated in March 2002.The policy isalso reinforced in the Planning andPriorities Framework (PPF).In particular:
• developing integrated care to
include, for example, nurses, dentists, pharmacists and mental health teams, as well as GPs.This will give
patients access to the most appropriate care for their needs.The
PCT is the key to co-ordinating this approach
■ a number of recent statutory changes have been made’, which introduce PCT accreditation of all • out-of-hours providers (other than GPs doing their own out-of-hours work or working in an informal rota). These require PCTs to manage the performance of the service against quality standards,which currently
focus on responsiveness
• the regulations also allow GPs (and personal medical services providers) to transfer their out-of-hours responsibility to a PCT-accredited provider.The alternative provider takes on full responsibility for delivering the service.This goes further than the previous provisions for out-of-hours delegation, under which the GP or PMS provider remained responsible for the quality of the service
• under the current transfer arrangements, responsibility reverts to the GP only if the contract of the out-of-hours provider is terminated. Primary legislation is needed to allow this responsibility to a provider other than the GP or PMS provider. But PCTs are expected to have contingency plans for a replacement service to help GPs or PMS providers who face this problem
’ The NHS (Out-of-Hours Medical Services) and NHS (General Medical Services) Amendment Regulations 2002 (SI 2003/2548) and NHS (Out-of-Hours Provision of Personal Medical Services and Miscellaneous Amendments) (England) Regulations 2003 (SI 2003/26) and associated amendments to the PMS Implementation Directions
Briefing 2 • Out-of-hours services
• the NHS Plan sets a target for 31 December 2004 for out-of-hours services to be reached through a
single call to NHS Direct. Again,PCTs (especially those working together in local consortia or
networks) have a major part to play in ensuring providers have the IT
and telecoms capability to integrate with NHS Direct
Taken together, these arrangements - which all pre-date the new GMS contract - are a legal and policy framework similar in many respects to that set out in the GMS contract. The key difference is that the new GMS contract sets a clear date of31 December 2004 for PCTs to take on full out-of-hours responsibility.
NHS Direct
The review of NHS Direct-, Developing NHS Direct - a strategy document for the next three years was published on 16 April and details the capacity available for full clinical integration with out-of-hours providers.This reflects:
• com m itm ent in the NHS Plan to single-call access to out-of-hours care, reinforced in the Government's response to the Out-of-Hours Review
• the clear potential benefit that NHS Direct has shown in helping to
reduce GP workload out-of-hours
• the crucial role that this could play in helping introduce the new GP contract, and the impact arrangements for out-of-hours primary care have on A&E and
ambulance services
Reform of emergency care
Out-of-hours planning groups should
be part of the local emergency care network, including representatives
from out-of-hours providers, GPs, the
ambulance service, acute trusts, PCT Professional Executive Committee (PEC) members, mental health services, social services, nursing
services, local out-of-hours coordinators and so on. Such groups can help PCTs investigate and develop
service changes, and the possibilities for integrating GP and other local out- of-hours services.
Accreditation and quality standards
At the moment, all out-of-hours quality standards apply to all accredited providers.The Department of Health has announced a review of accreditation to streamline the system and cut bureaucracy.The review is expected to:
• integrate the separate processes for accreditation and contracting for ' dedicated out-of-hours providers
• review the existing standards to, among other things, take account of the circumstances of practices that continue to do their own out-ofhours work
Practices that continue to do out-ofhours work will be required by their
new GMS (or PMS) contracts to meet the out-of-hours quality standards, or those that apply to practice providers.
Other out-of-hours providers will be required by their PCT contracts to meet the out-of-hours quality standards, or those that apply to nonpractice providers.
Local examples of innovation and good practice
There are already many examples ofinnovative out-of-hours services.These include:
• North Derbyshire Doctors areworking with the A&E department in Chesterfield. Experienced GPs support A&E and look after patients whose needs are'better met by primary care.
• Doctors in Huddersfield and West Yor ks h i re have d eve I o ped dedicated care plans for patients with terminal illnesses.These are available to out-of-hours doctors to enable the most appropriate and timely response to patients'needs.
• In Nottingham, the out-of-hours
co-op employs and trains nurses to support the work of doctors. Referral protocols with the local ambulance service help prevent patients unnecessarily going to A&E departments.
• Exeter has designed an out-ofhours centre that brings together a range of different services including
GPs, district nurses, the social services emergency duty team, and a 24-hour pharmacy.
• Harmoni GP out-of-hours co-ophas 500 GPs and is one of the largest co-ops in the UK.lt incorporates five primary care centres and is linked to NHS Direct West London. All A&E calls are intercepted and routed in the best way. Nurses give triage to patients in the waiting area of the A&E department and there are phone boxes for patients to speak to
NHS Direct.
©
Briefing 2 * Out-of-hours services
■ Northwick Park Urgicare Projecthas been running since April 2002
to provide patients with a consistent service, whether seeking
emergency care in person or by telephone. It's a partnership
between NH5 Direct, the PCT, A&E, the acute trust, Harmoni, community pharmacists, mental health and social services. Patients are categorised into minor illness, minor injury and majors, so that nurse practitioners or GPs can help patients with minor illnesses.
• North Peterborough PCT hasintegrated the local out-of-hours cooperative and the nurse-led walk-in centre onto one site.This is now a base for evening and night community nursing, social services and a paramedic support team.
• East Anglia Ambulance NHS Trustprovides call answering and referral, organisation of GP out-of-hours bases and provision of vehicles, drivers and communications to Norfolk co-ops under pressure from a lack of out-of-hours GPs.
In 2000, the trust based a community paramedic in a very rural surgery.This test project improved ambulance response times.The paramedic now does emergency house calls, takes bloods and performs ECGs, helps practice nurses and responds to 999 calls. In 2001,29 more paramedics took on community roles in GP surgeries.
The trust is also working with the Workforce Development Confederation to incorporate these new skills into higher education
programmes for paramedics.
Quick wins for PCTs
PCTs need to:
• quickly establish whether GPs and practices want to opt out, and
encourage practices and existing out-of-hours providers to work together to ensure those
preferences are met at the same time as maintaining patient care
• consider the Department's guidance on technical links with NHS Direct (see below), and decide which phase best suits their plans and readiness
• complete the technical links registration form (see below)
• start discussions with co-ops and other out-of-hours providers to identify the role they could play in delivering out-of-hours services
• ensure visits to local out-of-hours providers as part of the accreditation process
PCTs and out-of-hours providers should also not overlook the opportunities offered by the new GMS contract, especially as some GMS providers withdraw from providing GMS additional services. Opportunities include:
• in-hours home visiting on behalf of GMS or PMS providers
• patient transport service to take patients to the GP surgery
• support services to staff and the public when caring for and treating violent patients
* dedicated access nursing or GP
services to support the PCT and
practices
SupportIt's a challenging agenda, so extrasupport is available through:
* The Out-of-Hours Provider Development ProjectThe Out-of-Hours Provider Development Project - a
partnership between the NAGPC, the Department of Health and others - has been identifying how existing out-of-hours providers need to develop and adapt to provide integrated and modernised services within the new GMS contract.The first results will be published this summer and GP co-ops and other out-of-hours providers will be able to use them as possible models.
* FundingGPs who opt out will lose an average of £6,000 a year, which will be available to the PCT to fund out- of-hours services. The cost of providing services, though, will be greater than this, so PCTs will be able to use the following:- Existing Out-of-Hours
Developm ent Fund moneyThe rules on using this budget will be relaxed and the statutory ring fence removed to give PCTs greater flexibility in how they use the money.
- Extra moneyAn extra £110m is being made
available to PCTs for out-of-hours modernisation over the next three years: £7m 2003/04, £52m
2004/05, £52m 2005/06.The funding for 2003-04 will be used for development in PCTs outside the existing out-of-hours exemplar
programme, and the funding for 2004/05 and 2005/06 will be
Briefing 2 • Out-of-hours services
made available to all PCTs to
support provision.- Unified budgets
Delivering out-of-hours
modernisation is a key local development plan target and
should be reflected in plans for their unified budgets. Integrating
primary medical out-of-hours services with other out-of-hours services will also lead to savings
that can be reinvested in developing better out-of-hours services.
* Central supportThe Department of Health is strengthening its implementation team so that each SHA will have access to a dedicated person to
help them work with PCTs and the existing out-of-hours co-ordinators. The Department will be issuing more details soon.
• The Out-of-Hours Technical Links ProjectThis Department of Health project will:• help develop a network of
out-of-hours providers capable of linking electronically with NHS Direct. Providers, either individually or in networks, need to be serving a population of around 400,000 people
• manage and fund the programme of electronic links between NHS
Direct and out-of-hours providers• link electronic integration with
wider work on clinical integration and other Carson Review
recommendations
This is a new project, steered by a
board that includes representatives from PCTs, SHAs and the NAGPC. Details of their work have recently been published and include:
* clarification of the NHS Plan and
public/private finance (PPF) target
• how this differs from clinical Integration
• a description of the registration
process and timetable for out-ofhours providers who want to establish a technical link with NHS Direct
• the responsibilities of SHAs and PCTs
• the criteria out-of-hours providers need to meet
* Department of Health out-ofhours websiteThis new website - at w ww .out-of- hours.info - includes details of:• the exemplar programme
* the roles and responsibilities of PCTs,GPs and o.ut-of-hours providers regarding accreditation and reporting
•th e quality standards
• the out-of-hours regulations
* development of the technical links to NHS Direct
* development of out-of-hours providers
* contact details for the national implementation team and regional co-ordinators
* signposts to other useful websites, such as NHS Direct and NatPaCT
• NatPaCTNatPaCT has organised a series of launch events for the REC
Competencies.These give PCTs a
chance to meet local out-of-hours
development team members. NatPaCT will also help PCTs carry out the changes, as part of the wider
Modernisation Agency work and especially in the context of REC.
■ CompetenciesNatPaCT's PCT competency framework is an online self- assessment tool. It is being
extensively revised to take account of the new issues facing PCTs, including the new GMS contract
Under each area, the framework sets out a number of statements of competency and examples of evidence, what should be achieved and how achievement can be recognised. Each domain is linked to discussion forums, relevant new stories, and a growing library of key resources.
Domain 2 of the framework, primary care, is being re-written to take into account material in these briefings, and will be posted shortly at www.natpact.nhs.uk/newcf
Acknowledgements
The NHS Confederation and NatPaCT wish to thank the Department of Health and the NAGPC for an initial draft of this document and to PCT colleagues and others for their contributions.
Briefing 2 » Out-of-hours services
-----------------------------------------------------------------------------------------------------------
Signposting and references
The GMS contract outlines the framework for implementation. You can see
this on the NHS Confederation website.The website also carries supporting documentation and helpful resources such as a series of summary factsheets: wwwinhsconfed.org/gniscontract
The Modernisation Agency and NatPaCT websites have links to local and
national initiatives, programmes and support tools: www.modern.nhs.uk and www.natpact.nhs.uk
The Department of Health Out-of-Hours website carries all the supporting guidance standards and information including the Carson Review: Www.out-of-hours.info
Department of Health: www.doh.gov.uk ;
National Association o f GP. Co-operatives: www .nagpcorg.uk
NHS Direct: www.nhsdirect.nhs.uk- - - - ■ • - r •

Briefing 2 * Out-of-hours services
National Primary and Care Trust Developm ent Programme (NatPaCT) NHS Modernisation Agency 2nd Floor, Blenheim House
West One, Duncombe Street Leeds LSI 4PLTel 0113 254 3800 Fax 011 3 254 3809 E-mail natpact@ doh.gsi.gov.uk w ww .natpact.nhs.uk
The NHS Confederation 1 Warwick Row, London SW1E 5ER
Tel 020 7959 7272 Fax 020 7959 7273 E-mail enquirles@ nhsconfed.org www.nhsconfed.org
Further copies from :
Tel 0870 444 5841 Fax 0870 444 5842
E-mail publications@ nhsconfed.org
Registered C li. in ty no. 1GS0329
Comments Received About the MEDS Service
25/03/03
26/03/03
28/03/03
01/04/03
02/04/03
02/04/03
03/04/03
06/04/03
06/04/03
06/04/03
08/04/03
08/04/03
11/04/03
15/04/03
14/04/03
22/04/03
16/04/03
22/04/03
24/04/03
17/02/03 Mr A Mrs Dicken, 17 Christian Close, Ballastowell Gardens, Ramsey (General concerns regarding change in service)
Mr & Mrs Bushell, 16 West Quay, Ramsey (General concerns regarding change in service)
Mrs P Kinrade, Mountain View, Nassau Road, Bride(General concerns regarding change in service) (Further letter on 04/04/03)
Mr L Singer MLC(Various issues regarding change in services - copied to Members of Tynwald)
Mr J Hall, Ballavane, Fistard Road, Port St Mary(General concerns regarding change in service) (Further letter on 16/06/03)
Mr & Mrs D R Bushell, 16 West Quay, Ramsey (General concerns regarding change in service)
Mr G A Moore CBE, Ballamanaugh, Sulby (General concerns regarding change in service)
Mr Q Gill MHK(General concerns regarding change in service)
Mrs J Wells, 11 Bamile Park, Ramsey (General concerns regarding change in service)
Mr & Mrs Field, 27 Cannan Avenue, Kirk Michael (General concerns regarding change in service)
Mr C Wilson, League of Friends of R&DCH(General concerns regarding change in service - public meeting)
Hon A R Bell MHK(General concerns regarding change in service)
Mrs M Moore, 51 Ballamaddrell, Port Erin (via Mr Gill MHK)(General concerns regarding change in service)
Mr P Gawne, Thie Vaddrell, Cregneash, PSM (General concerns regarding change in service)
Mr R Wilson, Cronk Mooar, Beaumont Road, Ramsey (Medical Practices Committee issues regarding change in service)
The Editor, Isle of Man Newspapers - (Re: copy letter from Mrs Val Exon) (General concerns regarding change in service)
Mrs A Barnett, Ballacamaish Farm, Kirk Andreas (Further letter on 16/05/03) (General concerns regarding change in service)
Kathleen Quine, Ballavayre Cottages, Ballakilpheric (via Mr Gill MHK) (General concerns regarding change in service)
Mrs A Barnett, Ballacamaish Farm, Kirk Andreas (General concerns regarding change in service)
Aibory Parish Commissioners - MrLowey (General concerns regarding change in service)
24/04/03
29/04/03
01/05/03
07/05/03
08/05/03
13/05/03
13/05/03
16/05/03
22/05/03
??/05/03
16/06/03
02/07/03
10/07/03
14/07/03
21/07/03
18/08/03
24/04/03 Mi Q Gill MHK - (Re: letter from constituent Mrs M Moore)(General concerns regarding change in service)
Castletown Commissioners(General concerns regarding change in service)
Mrs G Hayes, 2 Mull View, Kirk Michael (General concerns regarding change in service)
Mrs E Pickard, 2 Scarlett Road, Castletown (Role of the Practices Committee)
Rushen Commissioners - Mrs G Kelly (General concerns regarding change in service)
Mr M J D Pearce, Hyde Mannin Place, Bay View Road, Ramsey (General concerns regarding change in service)
Malew Commissioners - Mr D Barron (General concerns regarding change in service)
Mrs C Beck, Briarcliffe House, Jurby(Complaint regarding a specific incident / General concerns)
Mr M Moyle, Coroner of Inquests - Re: Gail Kyburt deceased (Concerns relating to certification of sudden death - GP out of hours service)
Mrs K Cleator, Plot 32, Leodest Road, Andreas.(Complaint re Ramsey GPs - Positive comments regarding MEDS)
Mrs G Kelly, 2 Larivane Estate, Andreas, (via Mr Quine)(Complaint)
Mr J N Hall, Ballavane, Fistard, PSM (General concerns regarding change in service)
R E Quine MHK(Information re: Operating policies for MEDS)
Mr & Mrs Leece, 8 Douglas Road, Peel (Thanks)
Mrs J Beggs, Cronk Ny Ferrishyn, Ballafesson, Port Erin, (via Mr Gawne MHK) (Complaint re time taken to receive advice from duty doctor)
Ms J Beggs, Cronk Ny Ferrishyn, Ballafesson, Port Erin (General concerns regarding change in service)
Mr A Boult, Colby (Thanks)
Emergency Doctor Service April 2003
DEPARTMENT OF HEALTH AND SOCIAL SECURITY
EMERGENCY DOCTORSERVICE
Policy Document
U:\USER\CHFPAQUA\windows\docs\MEDS - Out of Hours\policy document.doc 1
Emergency Doctor Service April 2003
Aims and Procedures: Operational Guidelines ("Rules")
Quality Statement
"To provide high quality out of hours care for the patients of the Emergency Doctor Service".
Introduction
The Emergency Doctor Service (EDS) aims to provide high quality care, and is responsible to both the patient and the Department of Health and Social Security. In that respect it must have a strategy for achieving predefined and agreed quality targets.
This document is an expression of the standards we want to achieve.
Receiving and Handling Calls
• All calls via Emergency Doctor Service will be tape recorded.• 90% of calls to be answered in 30 seconds all calls to be answered within 90 seconds.• Receptionists to be polite, helpful and efficient• Emergency calls to be handled immediately and not put on hold.• Callers not to be left on hold for more than 2 minutes.• Details to be recorded accurately.• Urgent calls flagged for special handling.• Specific criteria for calling ambulance without prior referral to duty Doctor.• Receptionist not to give medical advice.• Calls passed to the appropriate duty Doctor within 20 minutes.• Receptionists not to commit the duty Doctor to visit.• Call volume constantly monitored.• Standby Doctors activated by doctor where necessary.• Call completion times reported and entered at the first opportunity.• Follow up information transmitted to own GP for next working day.• Clinical outcome recorded and fed back to own GP.• Records of all calls maintained for statutory minimum periods.
Reception Staff Training and Assessment
See Receptionist Handbook.
Doctors1 Conditions
Emergency Doctor Service Doctors will:
• Be a Principal in General Practice, a Locum in General Practice (on the Department’s Locum List) or hold the Certificate issued by JCPTGP.
• Undertake to maintain their registration with the General Medical Council.• Have medical protection insurance.• Endeavor to provide high quality medical care for patients.• Be abreast of current medical practice.
U:\USER\CHFPAQUA\windows\docs\MEDS - Out of Hours\policy document, doc 2
Emergency Doctor Service April 2003
• Ensure familiarity with the drugs and equipment in the Centre and in the vehicle.• Ensure they have sufficient Emergency Doctor Service stationery and emergency drugs for use when on
standby.• Ensure that if they are unable to undertake a shift they have committed to, that they find a
replacement or arrange a locum (see para on Locums).
A n d w h e n o n D uty:
• Be responsible for supplying and ensuring the safety of their own Controlled Drugs.• Be property rested prior to the session.• Undertake to carry a form of identification.• Avoid taking alcohol immediately before or during a duty session.• Refrain from smoking in Emergency Doctor Service vehicles or premises.• Observe the need for punctuality in reporting for Emergency Doctor Service duty.• Remain with the duty driver throughout sessions and stay in communication with Emergency Doctor
Service Base.• Deal with all calls at the first opportunity.• Not allow visits to accumulate before leaving the operating base.• Telephone ahead to offer patients interim advice and reassurance where visits are delayed.• Prioritise workload according to clinical as well as geographical considerations.• Monitor workload and liase with the operating base over activating the standby Doctor.• Where appropriate, remain at the operating base until relieved by the oncoming Doctor• W here appropriate provide a full hand over to the oncoming Doctor including pending visits, earlier
problems etc.• Be responsible for the security of the building during their session and if appropriate locking up and
handing in the key as directed at the end of the session.• Put away Emergency Doctor Service equipment at the end of night time shift.• Ensure that all necessary clinical information is faxed to the patients own GP either by yourself or by the
receptionist by end of your shift.• Complete the duty book and night visit book
Assessing Urgency:
It is recognised that the evaluation of response times is meaningless without reference to the clinical urgency of the patient's condition. For the assessment of response times, duty doctors will therefore be asked to categorise calls handled both before and after the event according to 4 urgency ratings.
Emergency- life threatening conditions*Urgent- urgent intervention necessary.Routine- appropriate but non urgent.Low Priority- spurious or unnecessary visits ( after the event only).
*ln certain life threatening emergencies,(i.e. collapsed & unconscious or stopped breathing), the Emergency Doctor Service reception staff will be under instruction to dial 999 for an ambulance. In such circumstances the call will still be passed to the duty doctor to decide whether or not also to attend.
For the before the event assessment of urgency, doctors should use the above criteria, and the underlisted response time targets, to determine whether to ask for back up support from the stand by doctor.
Response time aims are broadly as follows:
Emergency- All visits within 1 hourUrgent* All visits within 2 hoursRoutine and low priority within 6 hours
U:\USER\CHFPAQUA\windows\docs\MEDS - Out of HouisNpoIicy document.doc 3

Emergency Doctor Service April 2003
* Base staff will be required to pass emergency visits to the appropriate duty driver within 3 minutes of receipt.
Giving Advice:
Emergency Doctor Service receptionists are instructed not to commit the duty doctor to visit unless the seriousness of the reported condition is such that a visit will evidently be the appropriate outcome. It follows that many calls will be passed to the doctor as advice calls as a means of getting the doctor to telephone the patient to make his own assessment of what action is appropriate. Many calls which are initially categorised as "advice" will therefore become home or base visits.
In cases where a base visit is thought appropriate the receptionist can book an appointment without recourse to the doctor.
Duty doctors should make advice calls at the first opportunity, both to ensure that requirements to visit are recognised quickly, and to minimise the number of re-calls from anxious people who are already waiting.
As with home visits, doctors must record fully any telephone consultation on a call slip. Callers must also be advised to call again if the patient's condition continues to cause anxiety. If a patient has called again within a few hours of being advised, doctors should normally undertake to see the patient, either at home or at base.
Remember that your shift is only a short one and that it is better to work with care and minimise mistakes.
Doctors must be careful not to allow considerations of expediency or geography to influence their judgement as to whether to visit or advise. Experience of co-op operations shows that failure to visit is by far the greatest source of sustainable complaint.
Guidelines for telephone advice:
All telephone advice must be documented on a call slip, these forms should be legible, accurate, detailed andcomplete.
1. Even if the patient requests advice the doctor may arrange for a consultation if appropriate.
2. In general, be cautious about giving advice for conditions affecting children below the age of 5 years or for the elderly over the age of 65. It is worth documenting negative symptoms. If there is any doubt, offer a consultation. Endeavor to satisfy yourself that the patient or carer is happy with your advice, and document this fact.
3. Be cautious about giving advice for calls after 11p.m. the call is more likely to be serious and the patient or the carers may be especially anxious. Remember that there is a consultation room available for use at base at any time.
4. At the end of any telephone advice, if you sense that the patient is not entirely happy, offer a consultation at base or at home. In any case make the patient feel happy to contact the service at any stage in the future if the condition appears to be worsening, or their concerns are growing.
5. Avoid giving advice twice for the same condition. It will probably be more appropriate to offer a consultation on the second occasion.
6. Be wary about giving advice to a patient who has already been in touch with their own GP or another health care professional and been instructed to contact the service. It may be useful to contact the relevant professional to discuss the situation before deciding on the most appropriate course of managem ent If the patient's own GP has deemed a consultation necessary, then this should be organized.
U:\USER\CH FPAQUA\windows\docs\MEDS - Out of Hours\policy document.doc 4
Emergency Doctor Service April 2003
7. Regarding acute prescribing, be wary of polypharmacy, and avoid inappropriate prescribing, such as antibiotics for URTIs.
8. Avoid advising the patient to go to hospital without seeing the patient It is generally inappropriate to refer a patient with abdominal pain or headache directly to hospital.
Guidelines for home visits
Criteria for calling ambulance out of hours is the same that applies during the day.
It is for a doctor to decide, based on "reasonable opinion” as to whether a consultation needs to take place before the next time the patient could be seen within normal hours.
Clearly it is for the doctor to decide, based on “the doctors reasonable opinion," whether the patient should attend a doctor’s premises or be visited at home.
Throughout the development of these guidelines, the quality of medical services offered by general practitioners to their patients has been of paramount importance. The emphasis is that clinical effectiveness must, in some circumstances, take precedence over patient convenience.
CLARIFICATION AND EXAMPLES OF VISITING GUIDELINES IN ACTION
The following situations are where GP home visiting makes clinical sense and provides the best way to give a medical opinion:-
1. The terminally ill
2. The truly bedbound patient to whom travel to premises by car would cause a deterioration in medical condition or unacceptable discomfort.
3. The following situations where on occasion visiting may be useful: Where, after initial assessment over the telephone, a seriously ill patient may be helped by a GP's attendance provided that other commitments do not prevent him/her from arriving prior to the ambulance. Examples of such situations are:-
a) Myocardial infarction
b) Severe shortness of breath
c) Severe hemorrhage
d) It must be understood that if a GP has to see a number of patients and a patient is suffering from symptoms suggestive of a myocardial infarct the sensible approach may well be to refer to the emergency paramedical ambulance service rather than attending personally.
situations where visiting is not usually required.
e) Common symptoms of childhood, fevers, cold, cough, earache, headache, diarrhoea/vomiting and most cases of abdominal pain. These patients are almost always well enough to travel by car. The oid wives’ tale that it is unwise to take a child out with a fever is blatantly untrue. It may well be that these children are not indeed fit to travel by bus, or walk, but car transport is sensible and always available from friends, relatives or taxi firms.
f) Adults with common problems of cough, sore throat, “flu-like" symptoms, Chronic back pain, Dental Problems, lost prescriptions/tablets
U:\USERVCHFPAQUA\windows\docs\MEDS - Out of Hours\policy document.doc 5
Emergency Doctor Service April 2003
Calling Standby doctors:
If at any juncture it appears that the response time criteria outlined above cannot be fulfilled, doctors should ask for a standby doctor to be called. This may happen because of simultaneous emergencies, overwhelming workload or, occasionally, time consuming non urgent calls such as sectioning under the Mental Health A ct
Normally, assistance from the standby doctor should be considered once any duty doctor has accumulated 6 outstanding home visits, and where there is a concern that priority or emergency calls are likely to be delayed.
Doctors must continue to accept incoming calls until the end of their duty session so that calls can be prioritised. It matters not that some calls will be passed on to the oncoming duty doctor.
In the event of communication difficulty or exceptionally heavy workload, the base staff will be authorised to call out a standby doctor without prior consultation with the doctor on duty.
Standby doctors obligations:
Standby doctors will be on stand by for the whole of shift. The standby doctor duty rota will notify those affected.
Emergency Doctor Services rule regarding standby availability is as follows:
The standby doctor must ensure that the Emergency Doctor Service receptionists know where he can be contacted either by telephone or pager, and that if called out he is able to be travelling within 10 minutes and in a position to reach the most distant part of his operating area within one hour of being called.
If the standby doctor is required to conduct a visit or visits to relieve overload on the duty doctor he will be paid the appropriate hourly rate in respect of the total commitment during his period of on-call. There will not be a separate mileage allowance. The standby doctor will not normally be expected to report to base, but if called out he must contact base to establish whether any further assistance is required before returning home. The Standby doctor will always use their own car.
If you are on standby for Emergency Doctor Service the receptionist will assume you are contactable on your norma! home phone number. There is no need to report-in when on standby unless you are not at home, in which case you must let the reception staff at the Emergency Doctor Service know how to reach you.
For predictably busy times, such as Bank Holiday or if the Christmas break is extended by a weekend, the standby doctor may be asked to report to the base at the start of their session to collect details of any visits to be done. It will be very important to the flow of work for the doctor undertaking this session to keep the Emergency Doctor Service base aware of progress with calls allocated.
Ensure that Consultation paperwork is returned to the base for forward faxing. Please also ensure that you let the base staff know immediately of any deaths, admissions or re-visits.
Locum s:
Once com m itted to undertaking a shift, it is your responsibility to find a replacem ent - the Manager, Family Practitioner Services will help to find a locum if they can. This can be a swap with another GP or a locum may be used. The Locum must have the approval of Department. Of particular importance is the production of an original GMC certificate, JCPTGP certificate of vocational training and Medical defence cover. A record of approved Locums will be kept by the Department
U:\USER\CHFPAQUA\windows\docs\MEDS * Out of Houis\policy document.doc £
Emergency Doctor Service April 2003
Intra-Partum Care:
Emergency Doctor Service members will not be expected to attend patients requiring intra-partum care except in an emergency and where the alternative arrangements which should have been made by the patient's own practice have broken down. Practices which have undertaken to attend patients electing home confinement should provide Emergency Doctor Service with details of the arrangements made for out of hours care of that patient. Incoming calls will then be appropriately diverted. Practices’ own arrangements will be expected to extend to post-natal care of mother and child for the 48hr period following confinement.
Terminally ill Patients:
Separate practice arrangements can be made should the practice so desire. Emergency Doctor Service will have to be informed of the arrangements for contacting the appropriate doctor.
Documentation of Consultations:
When recording the consultation the doctor should bear in mind that patients have a right to see their medical records. Circumstances will not always be conducive to an open and frank discussion of the duty doctor's findings. However where appropriate, doctors should explain to the patient, parent or carer what is being recorded and include:
Nature of condition Clinical findingsTreatment and /or advice offered Follow up actionHow to contact the doctor again if necessary
Doctors are reminded that the batch number of any drugs issued should be recorded on the appropriate callslip.
Continuity of Information:
All face to face consultations will finish by the doctor giving the carbon copy of the call slip to the patient to give to their own doctor. All important consultations will also be faxed to the surgery.
Practices may wish to provide information to Emergency Doctor Service in order to help with the care of certain patients. This will be especially useful in the area of drug abuse. Members are strongly encouraged to provide any information regarding patients that may help the duty doctor. All drug addicts names must be given.
Assessing Patient Satisfaction:
A suggestion box will be displayed at the base with leaflets asking for name, address and telephone no and asking for comments. The leaflet will also advise the patient that they can make a complaint to the Hospital Complaints Manager advising of the incident which caused their dissatisfaction with the service.
LT:\USER\CHFPAQUA\windows\docs\MEDS - Out of Hours\poUcy documentdoc 7
Emergency Doctor Service April 2003
COMPLAINTS & DISCIPLINE
It should be clearly noted that complaints and disciplinary issues are, and will be dealt with as two completely separate issues.
Complaints Procedure
INTRODUCTIONComplaints will be dealt with under the Department’s Hospital and Community Complaints Procedure and should be sent to :
Mrs K Horn,Complaints and Claims Manager for Health Services,Nobles Hospital,Westmoreland Road,Douglas.
By August 2003 Mrs Horn will have relocated to the New Nobles Hospital, Braddan.
Complaints sent to Mrs Horn will be forwarded to the Manager, Family Practitioner Services (FPS) for a response within 10 days. The Manager, FPS will co-ordinate a response with the doctor. The GP will see the final draft letter back to the patient prior to it being sent.
Disciplinary Procedure
Discipline will be dealt with under the DHSS policy for medical and dental staff.
U:\USER\CHFPAQUA\windows\docs\MEDS - Out of HoursXpolicy document.doc 8
Emergency Doctor Service April 2003
Medical and Performance Audit:
Introduction:
Quality audit and the production of associated statistical information is vital if we are to sustain the perception of the 'Emergency Doctor Service’ as a high quality solution to the problems of providing 24hr primary care. A constructive approach to sensible clinical and operational audit will remain essential to the political credibility of the service, and its acceptability for continued financial support. Such information will also enable the Department to deploy resources effectively at optimum cost. The information may also be useful when dealing with Clinical Auditors, Researchers and the press.
Audit report:
This report with selective content where appropriate will cover the following:
Principals involved and their distribution.Number of patients and geographical area covered.Call incidence, broken down by:i. Call type (visit/advice etc).ii. Urgency grading and response times.iii. Calls from emergency services.iv. Clinical condition.v. Treatments.vi. Time of day and day of week.vii. Seasonal variation.viii. Patient age.
Distribution and incidence of calls handled by standby doctors.Calls handled as Primary Care Centre Visits.Hospital admissions (numbers and percentages) by:ix. Hospitalx. Areaxi. Time of dayxii. Clinical condition Deaths certified.999 calls.Patient Satisfaction.Complaints received/resolved.
It is not envisaged that we will be able to collect all this information until the Emergency Doctor Service is computerised.
U:\USER\CHFPAQUA\windows\docs\MEDS - Out o f HoursVpolicy document.doc 9
Emergency Doctor Service April 2003
Emergency Doctor Service Information Gathering Proforma
Surgery Information:
1. Name by which the surgery is generally known to its patients:2. The surgery's full address and contact details.
Main Surgery Branch Surgery
Address including Postcode
Practice Manager
Telephone 1
Telephone 2
Bypass telephone
Practice Mobile
Fax
1. Practice list size:
2. Drug addicts registered with the practice. Please write on separate sheet, dated. Please up date as appropriate.
3. Other Important patients of note.
U:\USER\CHFPAQUA\windows\docs\MEDS - Out of Hours\policy document.doc l Q
Emergency Doctor Service April 2003
Doctor Information: (please duplicate this form as necessary)
Please let us have the details below for all partners, assistants and regular locum doctors.
Surname First Name ( or name by which known)
Home address
Name of Surgery: Half day:
Status: ( please circle)Principal Assistant Locum Recently retired
Full time or Part time (please indicate 1/2, 2 /3rds etc)
Home telephone: Mobile phone no:
Pager type ( e.g. BT message master) Pager numbers
Email address Fax
GMC Certificate No and Exp date Medical Defence Membership no and Exp date
JCPTGP certificate no:
U:\USER\CHFPAQUA\windows\docs\MEDS - Out of HoursNpolicy document.doc [ 1
Emergency Doctor Service April 2003
Duty Availability:The more choice we have available the more likely we are able to accommodate your wishes.
Practice:
Name of GP:
Holidays:
Days or nights that your are not available:
Name of GP:
Holidays:
Days or nights that your are not available:
Name of GP:
Holidays:
Days or nights that your are not available:
U:\USER\CHFPAQUA\windows\docs\MEDS - Out of HomsVpolicy documcnt.doc 12
DEPARTMENT OF HEALTH AND SOCIAL SECURITY -
HEALTH SERVICES DIVISION
EMERGENCY DOCTOR SERVICE
General Medical Practitioner Out of Hours Contract
The post of NHS Out of Hours General Practitioner is intended to provide high quality out of hours care for patients.
Code of Practice/Statement of Work
Ail work under the auspices of the Emergency Doctor Service will be carried out under the contractual arrangements which are set out in the Department of Health and Social Security’s Emergency Doctor Service Policy Document (Appendix 1). Contractual arrangements are to be strictly adhered to unless varied in writing by The General Manager, Primary Care or nominated deputy.
This Code of Practice is definitive and in force from the date on the code. It is liable to amendment at any time by negotiation between the relevant parties.
Hours of Work
Contracted hours will be on a sessional basis and will be agreed between the General Practitioner and the Department in the form of an Out of Hours Rota.
Sessions will be made up as follows:
Monday to Friday 6.00pm to midnightmidnight to 8.00 am
Weekends and 8.00 am - 12 noonBank Holidays 12 noon - 6.00 pm
6.00 pm - midnight midnight to 8.00 am
V:\windows\docs\MEDS • Out of Hours\doctors contract.doc( i )
Paym ent
Payment will be made on a sessional basis as set out in Appendix 2 of this contract.
Superannuation
You will be entitled to pay into the NHS Superannuation scheme. The relevant deductions will be made in your quarterly payment unless you state otherwise. The Department will pay employer’s contributions towards this scheme.
I. agree to adhere to the Contractual Arrangements as set out in the Emergency Doctor Service Policy Document attached to this Contract as Appendix 1.
Signed:_____________________________________ Date:Practitioner
Signed:_____________________________________ Date:Department
V:\windows\docs\MEDS - Out of Hours\doctors contract.doc(2)
Isle of ManG overnm ent
Rciltvt CÜ0H Vim/n
Department of Health and Social SecurityRheynn Slaynt as Shickyrys Y Theay
ServicesHealth Division Crookall House Demesne Road Douglas, Isle o f Man IMI 3QATelephone (01624)642597Fan (01624)642617 '
Mr P Lo BaoJoint Clerk to the Select Committee o f Tynwald on GP Services
Office of the Clerk o f Tynwald Legislative Buildings Douglas IM I 3PW
Contact :
Our R ef : Your R ef :
Date :
Mr S A Jones
105
16th December 2003
Dear Mr Lo Bao
Sclect Committee of Tvimald on G.P. Services
I am writing in response to your letter of 8th December, 2003, to Mr D Kill ip, Chief Executive, which has been passed for the attention o f the Health Services Division.
In answer to your specific enquiries
(a) The total number o f practising GPs on the Isle o f Man NHS Medical List is currently 46 (43.75 whole time equivalent).
(b) The ratio o f GPs per head o f practice population (i.e. patient capitation figure) is 1 : 1849.
(c) So far as the UK is concerned, the ratio of GPs per head o f practice population is as follows
England 1 : 1838
Scotland 1 : 1378
, - Wales 1 : 1685
NIreland 1 : 1643
Should you require any additional information or clarification, please let me know.
Yours sinccrdy— 's' /
Tony TOnesyC' /7
Deputy Head, He^Hn Services Divisioncopicd to: Mr D Kill ip, C Executive, DHSS
Mr G Newbery, Primary Health Care
Accident and Emergency Department (Casualty)
This service will be unaltered by the new
out-of-hours service. All patients who would normally attend Casualty for their injuries, etc, should continue to do so. Should Casualty tell you that you should, see your CP instead and it is
urgent then contact your own surgery. The out-of-hours doctor’s surgery is not a drop-in
service and patients should note that they will not be seen by the duty doctor without an
appointment.
If you think th a t you have a life-threatening
emergency you should always call 9 9 9 . This service operates 24 hours a day, 7 days
a week.
TH-E ALT'H - S E r V- ICE
Shirveiskyn Slaynt
Emergency Doctor Service
Improved ServicedPatients-
the'H ealtU hf th eN ation i^Ç au r Slaynt yn Àshòórtp ’
The information in this leaflet can be provided in large print or on audio tape, on request.
Issued by:D epartm ent of Health and Social Security
Health Services Division Crookall House,
Demesne Road, Douglas Isle of M an . IM1 3QA
www.gov.im/dhss
Isle of M a nGovernment
DEPARTMENT OF HEALTH AND SOCIAL SECURITY
The Emergency Doctor Service will become an Island-wide scheme from 1 st April 2003. It is an
‘out-of-hours' emergency service that replaces MannDoc and will operate when your doctor’s
surgery is closed.
The service is available from 6pm to 8am Monday to Friday, with 24-hour cover over weekends and bank holidays.
For out-of-hours emergencies you should
telephone your surgery as normal.
You will either get an answerphone service giving
you the number of the out-of-hours service or your calls will be automatically diverted. All calls
are recorded. A trained telephonist will record
your details.
You will be:
1 Given telephone advice by the duty Doctor
2 Invited to attend the Primary Care
out-of-hours Centre, at an appointed time.
3 Visited at home, if considered medically necessary following assessment by the
duty Doctor.
4 Admitted to hospital if considered medically
necessary.
The out-of-hours service is only for emergencies
tha t cannot w ait until the next working day.
Primary Care Out-of-Hours CentreAll patients will be seen by a fully-qualified CP.
The out-of-hours doctors’ surgery is not a drop-in service and patients should note that they will not be seen by the duty doctor without an appointment.
• A Primary Care Centre is a much safer environment in which to treat people.
• A Doctor can see many more patients in the
Centre in the same time that it takes to travel to one house call.
• The Doctor will have direct access to more
medical equipment and drugs within the Centre.
• Tired Doctors make more errors. This service
will allow Doctors more time off duty.
• Home visits will be made when medically
indicated,
• Patients will be responsible for arranging their
own transport to the out-of-hours Centre.
Emergency Dental CareYou should first ring your own Dentist Your dental surgery will inform you how to contact the duty
Dentist. There is a duty Dentist on call for all Emergency Dental Care, They can assess your dental requirements and prescribe appropriate antibiotics, painkillers or provide dental treatment if it is required. Your doctor is not qualified to
treat dental problems.
Chemist RotaChemists open on Sundays and bank holidays. They usually open at lunchtime but for a limited time only. For details of the duty chemist nearest to you and their times of opening see the local press. All chemists display in their window the
name of the duty chemist.
\r\iWO dOO-^MJ '/JoJ 1 Co ■ I
A p r 11 9 u O i .
i
S h i r v e i s b y n S la y n t
Emergency Doctor Service i
i
-■ V - r-;‘ . !. "•?**«( iS’S N M S S ^ ' i S !* • \ V; • . *'. '. r.:'' ,-‘ . M . 'r~ i ->:~T-- ' '
' Ï -1- - ■■ » ■ /
" s S . ' ■: v;*~W
*■ i -1, ¿Ï ÎMB* 1Î. -
■ W <t& ■*îHE-'C" ••* '
©'S^«ae«sï?s -¿«¿flf
W -è' i
*V*riT7‘,m'1 ;*■•*$£»*r,.,. v' r l . i l - " / * -* - * ^ ï - ^ -
I£v_ 'T ---^‘ M * * £Î
The Island-wide ‘out-of-hours’ emergency CP service will operate from 1st April 2003.This service replaces Mann Doc and will be available when your doctor’s surgery is closed.If you have a medical condition that isn’t life-threatening but cannot wait until the surgery opens, you should telephone your usual doctor’s surgery and a recorded message will inform you of the number to call to speak to the doctor on duty.
The duty doctor will:• offer you medical advice over the telephone or• advise you to attend a consultation at the out-of-hours surgery.• In exceptional circumstances, the doctor may arrange a home visit.
It is not a drop-in service and patients should note that they will not be seen by the duty doctor without an appointment.The service is available from 6pm to 8am Monday to Friday, with 24-hour cover over weekends and bank holidays.If you have chest pain or a life-threatening emergency you should always call 999.
Isle of ManGovernment
D EPA R T M EN T O F HEALTH A N D SO C IA L SECU RITY
I
I
I
I
I
I
I
I
I■
5 1 4 3 M a n x E m e r D o c t 8 / 7 / u j a : i o a m1 o no &cCXrv \f\-Qjr I S / 1 |0
Shirveishyn Slaynt
Public NoticeManx Emergency Doctor Service
Relocation of Surgery to new Hospital
This service will continue to be available when your doctor's surgery is closed.
If you have a medical condition that isn't life-threatening but cannot wait until the surgery opens, you should telephone your usual doctor's surgery and a recorded
message will inform you of the number to call to speak to the doctor on duty.
The duty doctor will:
• offer you medical advice over the telephone or
• advise you to attend a consultation at the out-of-hours surgery to which
directions will be given
• In exceptional circumstances, the doctor may arrange a home visit.
It is not a drop-in service and patients should note that they w ill not be seen by
the duty doctor without an appointment.
The service is available from 6pm to 8am Monday to Friday, with 24-hour cover
over weekends and bank holidays.
If you have chest pain or a life-threatening emergency you should always call 9 9 9 .
d o
is le o f M a nC a m i i iM t
DEPARTM ENT OF HEALTH AND SOCIAL SECURITYTEES
■ o-
H E A L T H S k R V I C E S
Shirveisbyn Slaynt
Public NoticeRamsey Minor Injury Unit
^Formerly the Accident, and Emergency Service]
The Department of Health and Social Security announce that following a decision by the Ramsey Group Practice to withdraw from the 24 hour emergency service at Ramsey and District Cottage Hospital, the following arrangements will be introduced with effect from 1st April 2003:-
GP led cover Monday to Friday 8.30 am to 6.00 pm Nurse led cover Monday to Friday 6.00 pm to 10.00 pm
Weekends and Bank Holidays 8.00 am to 10,00 pm
If you develop a medical condition outside these hours that isn't life-thneatening but cannot wait until either the Minor Injuries Unit or your CP’s surgery opens you should telephone your usual doctor's surgery. A recorded message will inform you of the number to call to speak to the ‘out-of-hours’ doctor on duty.
If you have chest pain or a life-threatening emergency you should always call 999 for which the ambulance service will continue to be provided 24hrs per day.
Isle of ManGovernment
DEPARTMENT OF HEALTH AND SOCIAL SECURITY
t\hcymt Slciynt as Slfickyrys )'T/tcuy
TSkirvetshyn S/aynt
Public NoticeEmergency Doctor Service
"»r.- • For the Health o f the Nation ~ Cour S la y n ty n - A s b q o n ^ ^ t ^ ^ ^ ^ ^ ^ ^ g ^ £ ^ s .
Wh ■ -C ■■;■■' ■ r'Mpurm&m **&:£ '" :'v:
The present emergency CP service will change in two respects from 1st April 2003.
First, the present service, which applies to the patients of all CPs except patients registered with the Ramsey. Laxey and Port Erin group practices, will be extended to include those patients and thus become an all-island service.
Second, responsibility for operating the service passes from MannDoc (a CP run co-operative) to the Primary Health Care Division of the Department of Health and Social Security.
The emergency CP service operates when your CP surgery is closed. If you have a medical condition that isn’t life-threatening but cannot wait until the surgery opens, you should telephone your usual doctor’s surgery and a recorded message will inform you of the number to call to speak to the doctor on duty.
The duty doctor will offer you medical advice over the telephone or advise you to attend a consultation at the out-of-hours surgery. In exceptional circumstances, the doctor may arrange a home visit. The out-of-hours doctor's surgery, based at Noble’s Hospital is not a drop-in service and patients should note that they will not be seen by the duty doctor without an appointment.
The service is available from 6pm to 8am Monday to Friday, with 24-hour cover over weekends and bank holidays.
If you have chest pain or a life-threatening emergency you should always call 999.
Isle of ManC o v rrn m c n i
D E P A R T M E N T O F H E A L T H A N D S O C I A L S E C U R IT Y I
H E A L T H S E R V I C E S
Shirveishyn Slaynt
Public NoticeRamsey Minor Injury Unit
(Formerly the Accident and Emergency Service)
The Department of Health and Social Security announce that following a decision by the Ramsey Group Practice to withdraw from the 24 hour emergency service at Ramsey and District Cottage Hospital, the following arrangements will be introduced with effect from 1st April 2003:-
GP led cover Monday to Friday 8.30 am to 6.00 pm Nurse led cover Monday to Friday 6.00 pm to 10.00 pm
Weekends and Bank Holidays 8.00 am to 10.00 pm
If you develop a medical condition outside these hours that isn’t life-threatening but cannot wait until either the Minor Injuries Unit or your GP’s surgery opens you should telephone your usual doctor’s surgery. A recorded message will inform you of the number to call to speak to the ‘out-of-hours’ doctor on duty.
If you have chest pain or a life-threatening emergency you should always call 999 for which the ambulance service will continue to be provided 24hrs per day.
Isle of ManGovernment
*,ll.r. til..DEPARTMENT OF HEALTH AND SOCIAL SECURITY
Rbevnn Siavnt as
Sbirprishyn SUyni
Changes in GP out of hours cover - your questions answeredFOR the past Tour years 57,000 people In various parts of the hie of Man - 75 per cent of the total population - have been successfully covered by a centralised Out-of-hours doctor servica.With the benefit of that experience, the system has now been developed to cover the whole island.The extended service Is supported by GP practices around the Island. Including those In Ramsey, laxey and Port Erin which previously provided local out-of-hours cover for their patients.The Department of Health and Social Seorlty recognises that the change from local to all-island cover In these three areas has caused public concern. The Department wishes to reassure the pub Sc that previous experience within the Island end elsewhere has shown that the system has worked satisfactorily.The Department does not believe the doctors Involved would be party to the extended service if they believed it exposed the public to real additional risk. However, e l with any new service Its Impact Is being ciosety monitored. The Department continues to be ccnvnftted to a high quality, comprehensive health service for all the people of the Isle of Man - a commitment demonstrated by our record of Investment in health over the years. In order to do this we have to recognise the changes nMch am taking place in the delivery of health care hi the wider NHS.We hope the following questions end answers will help to clarify the position. The questions end answers also address separata developments at Ramsay Cottage Hospital.
OUT-OF-HOURS DOCTORS Why have you changed the system?We need i d have competitive terms and conditions for our doctors if we hope to recruft them to work here in the future. There is an Insufficient number of CPs available to meet demand In the UK and GP nfgtrt services there are changing. We had to do some thing Similar.
How can e centralised out-of-hours doctor service based h Douglas provide adequate cover for Ihe whole o f the Island?The service provides one doctor on duty, hased at Nobles Hospital, with a second doctor on call, from 6pm to Bam the following morning seven days a week. Thera are two doctors Ml duty from Sam to Bpm on Saturdays. Sundays end Bank Holidays.This Is an improvement on the level of protection given to 75 per cent of the population lor the past four years under the successful 'Manndoc' centralised system, which provided ana duty doctor overnight but no doctor on call.The S7.D00 people covered by 'Manndoe' Included residents as Tar away from Douglas as fiushen. Dalby and Michael.The out-of -hours cover now given means that there are effectively two doctors available ror a population oT around 76,000 in an Island 33 miles long and 13 miles wtda. M s compares very favourably with arrangements acccpted hi the United Kingdom.
The experience gained in running the 'Manndoc' system has been useful in working out the level of cover considered appropriate for the all-Island service.
Whal about the fear that the out-of-hours doctors could be too far away to visit patients in the far north or south of the island In good time?The (ste of Man Is a relatively small place and nowhere is to far away that it cannot be reached In a time considered acceptable for s home v ijit by a GP. A car end driver are provided to convey the doctor speedily to the call-out destination.Homo visits are Just one part of the out-of-hourj service and only happen in exceptional circumstances - for example if a patient needs seeing and is unable to travel.In the first T3 days of the all-island service, which was Introduced on April i, the maximum number of home visits necessary overnight on weekdays - in the 14 hours from 6pm and flam - was three.The service also offers telephone advice and the opportunity to ettend the out-cf-hours surgery.
What If I haro no tnmsport7The doctor will take this into account In determining how to deal with your problem.REMEMBER - FOR LIFE-THREATENING EMERGENCIES THE AMBULANCE SERVICE IS AVAILABLE 24 HOUftS A DAY. SEVEN DAYS A WEEK. AND THESE ARRANGEMENTS ARE UNCHANGED.
When win an ambulance be based 24 hours ■ day In the south of the Ijlamf7The new ambulance station at Four Roads will become operational 24 hours a day by the Autumn.
Why can't tho Department Just pay to restore the local out-of- hours service* In Ramsey, Laxey and Port Erin?This is not a question of payment or funding. The atMsland service has been introduced, in cortfunalon with the doctors. Mowing the negotiation of a new contract Tor GPi relieving them of 24-hour responsibility for their patients.The new contract Is designed to improve the working fives of doctors and the Island would have great difficulty recruiting GPs in future If it maintained a requirement here that had been removed in the United Kingdom. Whether we tike It or not the profession expects improved working conditions today end we must recognise this If we want to attract doctors from a limited supply In competition with other areas, GPs are self-employed end cannot simply be directed by tha Department to provide certain services.
RAMSEY COTTAGE HOSPITAL Why ties the Department withdrawn out-of-hours cover a t the Minor InJtales Umt of Ramsey Cottage Hospttaf?THE DEPARTMENT HAS NOT DONE 50. Apart from being your GPs,
4 »IdeofMan
Gi n u h m U
Ramsey Group Practice has a separate contract to provide medical cover at tha Minor Injuries Unit and on 3rd March 2003 the Department received notice of its intention to withdraw from the out- of-hours aspect of the cant/act from Apr it 1 . The Department was disappointed by the decision coming as It did when changes were occurring in respect of GP night cover but had to recognise that this was entirely a matter Tor the Group Practice.Because of this the Minor Injuries Unit is now led by specially trained nurses, which is an established concept in tha United Kingdom and reflects the development of the nursing profession in recent years. The nurse-led service Is currently available during the busiest out-of-hours periods - up to 10pm at nights, and at weekends - and the effects of these changes are being closely monitored.
What about ambulance cover For Ramsey and tha north?An ambulance service continues to be based at Ramsey on a 24 hours a day, seven days a week basis. In addition. Ramsey has a 'first responder" on cell from 7pm to 7am seven days a week, comprising a paramedic with a suitably equipped vehicle.
Why has part of Ramsey Cottage Hospital been UVen enter for use « an NHS dental Clinic7An NHS dental clinic was needed for the people of Ramsey and tta north of the Island following the decision of the Ramsay dental practice to reduce Its NHS work. One of tha options was to convert a seven-bed unit at Ramsey Cottage Hospital, which was only in use one day every fortnight, and which could be utilised without detriment to existing services. This was the most cost-effective option and was the solution chosen by the Department which has a public duly to make the best possible use of the resources available for health care.Doesn't all this add up to a policy of running down Ramsey Cottage Hospital towards Its eventual closure?The Department has NO policy o f naming down or dosing Ramsay Cottage Hospital. More tKan £3 million in capital spending (including charitable donations) has been invested in the development of the hospital in recent years, and staffing levels have been maintained.The recent changes affecting the hospital have not bw n initial»«« hy the Oepam irent. but have been a case of the Department responding to decisions taken by other parties.The Department Q iJj appreciates the importance that is attached to Ramsey Cottage Hospital by the people of Ramsey and the north and Is proud of the standards of cars it delivers.
Win the Department consult the public over the future o f Ramsey Cottage Hospital?Yes. we ere consulting the public and interested parties over the present, medium and long-term policy for Ramsay Cottage Hospital. In line with a Tynwald resolution of March this year. Notices about this with further information are appearing In tho local press ertd you are Invited to take part in this exercise, visit: vmmt.gov.bn/dhst
AVkyrttt «rt ¿fitikyry* Y Utojy
Appendix 5.2
Statistical Summary of calls received by MEDS and their outcomes April 2003 to December 2003
Symbols used:
V = visit to patient’s home by the duty MEDS doctor.
apt = appointment made for patient to attend MEDS clinic at Nobles Hospital.
tel = telephone advise given
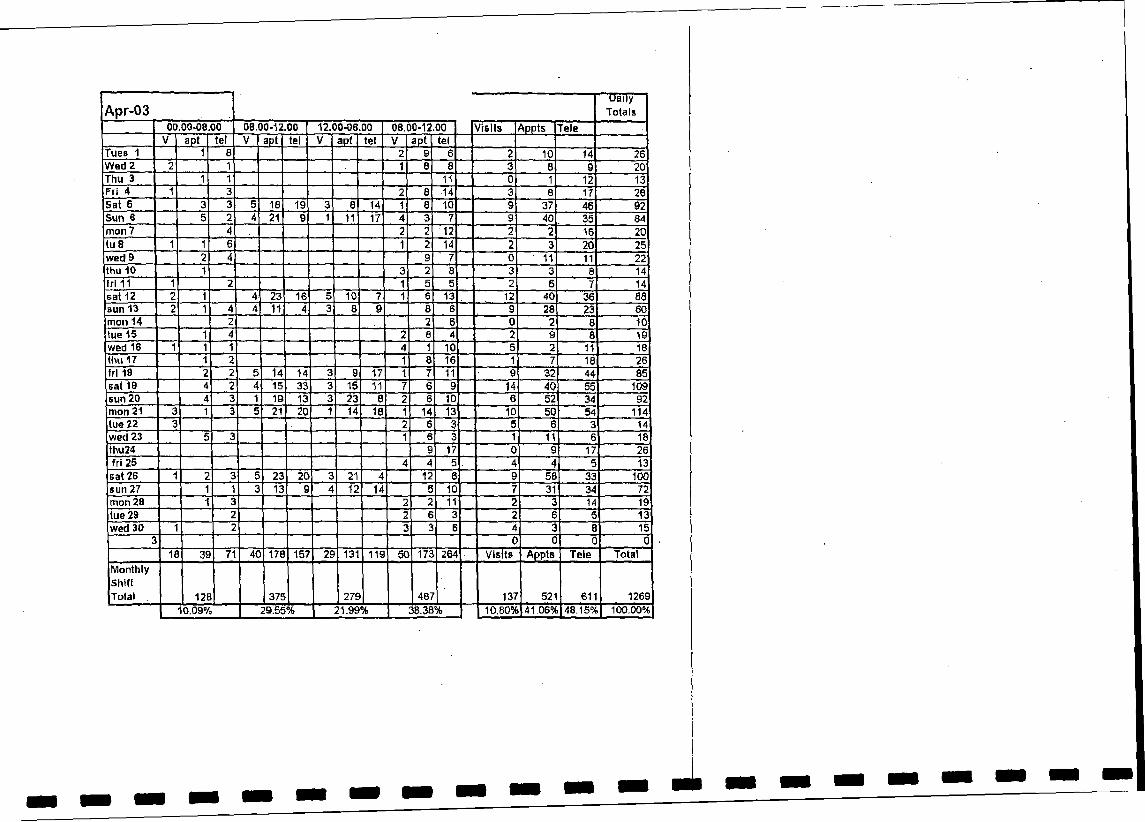
A p r - 0 3Daily
Totals00,00-08.00 08.00-12.00 12.00-06.00 08.00-12.00 Visits Appts Tele
V apt tel V apt tel V apt tel V apt telTues 1 1 8 2 9 6 2 10 14 26Wed 2 2 1 1 8 8 3 8 9 20Thu 3 1 1 11 0 1 12 13Fri 4 1 3 2 8 •14 3 8 17 28Sat 6 3 3 5 18 19 3 8 14 1 8 10 9 37 46 92Sun 6 5 2 4 21 9 1 11 17 4 3 7 g 40 35 84mon 7 4 2 2 12 ■ 2 2 16 20lu 8 1 1 6 1 2 14 2 3 20 25wed 9 2 4 9 7 0 ' 11 11 22thu 10 1 3 2 8 3 3 8 14frl 11 1 2 1 5 5 2 5 7 14sat 12 2 1 4 23 16 5 10 7 1 6 13 12 40 36 88sun 13 2 1 4 4 11 4 3 8 9 8 6 9 28 23 60mon 14 2 2 6 0 2 8 10tue 15 1 4 2 8 4 2 9 8 19wed 16 1 1 1 4 1 10 5 2 11 18thu 17 1 2 1 6 16 1 7 18 26frl 18 2 2 5 14 14 3 9 17 1 7 11 9 32 44 85sat 19 4 2 4 15 33 3 15 11 7 6 9 14 40 55 109sun 20 4 3 1 19 13 3 23 8 2 6 10 6 52 1 34 92mon 21 3 1 3 5 21 20 1 14 18 1 14 13 10 50 54 114I ue 22 3 2 6 3 5 6 3 14wed 23 5 3 1 6 3 1 11 6 18thu24 9 17 0 9 17 26fri 25 4 4 5 4 4 5 13sat 26 1 2 3 5 23 20 3 21 4 12 6 9 58 33 100sun 27 1 1 3 13 9 4 12 14 5 10 7 31 34 72mon 28 1 3 2 2 11 2 3 14 19tue 29 2 2 6 3 2 6 5 13wed 30 1 2 3 3 6 4 3 8 15
3 0 0 0 018 39 71 40 178 157 29 131 119 50 173 264 Visits Appts Tele Total
MonthlyShiftTotal 12B 375 279 487 137 521 611 | 1269
10.09% 29.55% 21.99% 38.38% 10.80% 41.06% 48.15%| 100.00%
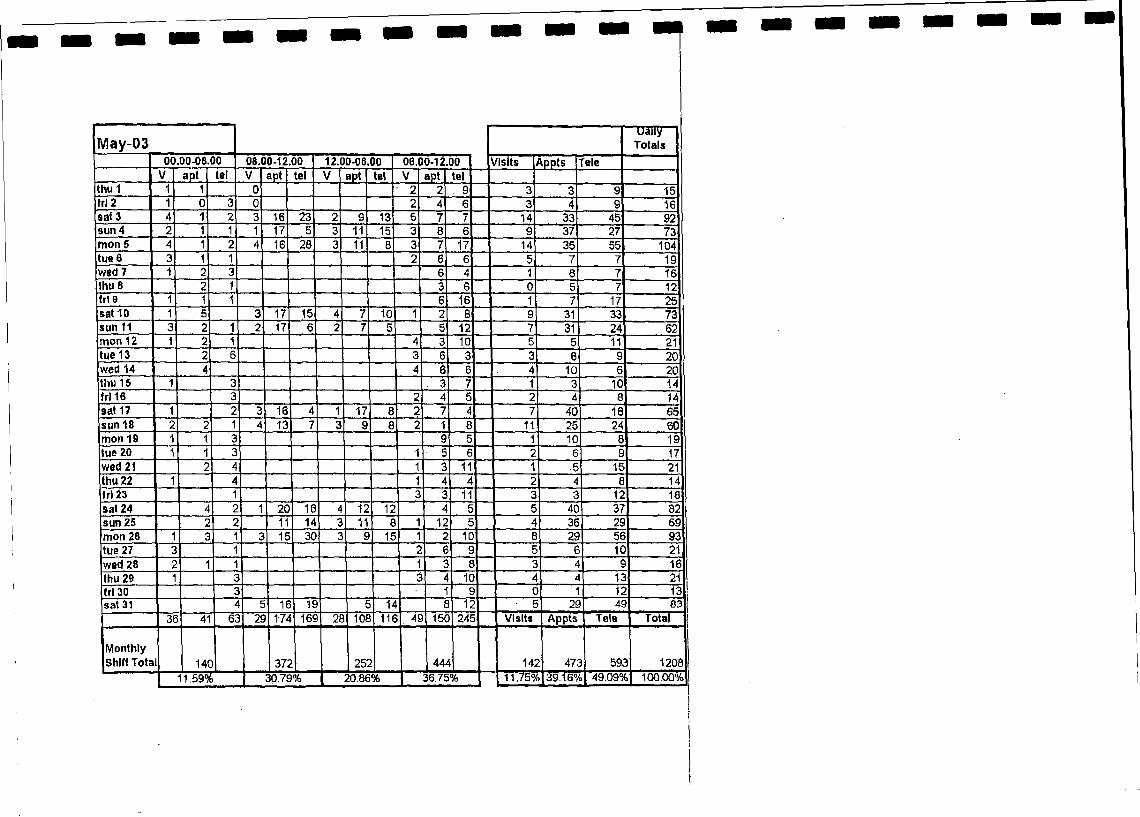
May-03uaiiy
Totals00.00-08.00 08.00-12.00 12.00-06.00 06.00-12.00 Visits ^ppts rele
V apt tel V apt tel V apt tel V apt telthu 1 1 1 0 2 2 . 9 3 3 9 15frl 2 1 0 3 0 2 4 6 3 4 9 16sat 3 4 1 2 3 16 23 2 9 13 5 7 7 14 33 45 92sun 4 2 1 1 1 17 5 3 11 15 3 8 6 9 37 27 73mon 5 4 1 2 4 16 28 3 11 8 3 7 17 14 35 55 104tue 6 3 1 1 2 6 6 5 7 7 19wed 7 1 2 3 6 4 1 8 7 16thu 8 2 1 3 6 0 5 7 12frl 9 1 1 1 . 6 16 1 7 17 25sat 10 1 5 3 17 15 4 7 10 1 2 8 9 31 33 73sun 11 3 2 1 2 17 6 2 7 5 5 12 7 31 24 62mon 12 1 2 1 4 3 10 5 5 '11 21tue 13 2 6 3 6 3 3 8 9 20wed 14 4 4 6 6 4 10 6 20thu 15 1 3 3 7 1 3 10 14frl 16 3 2 4 5 2 4 8 14sat 17 1 2 3 16 4 1 17 8 2 7 4 7 40 18 65sun 18 2 2 1 4 13 7 3 9 8 2 1 8 11 25 24 60mon 19 1 1 3 9 5 1 10 8 19tue 20 1 1 3 1 5 6 2 6 9 17wed 21 2 4 1 3 11 1 5 15 21thu 22 1 4 1 4 4 2 4 8 14Irt 23 1 3 3 11 3 3 12 18sat 24 2 1 20 18 4 12 12 4 5 5 40 37 82sun 25 2 2 11 14 3 11 8 1 12 5 4 36 29 69mon 26 1 3 1 3 15 30 3 9 15 1 2 10 8 29 56 93tue 27 3 1 2 6 9 5 6 10 21wed 28 2 1 1 1 3 8 3 4 9 16thu 29 1 3 3 4 10 4 4 13 21fr l 30 3 1 9 0 1 12 13sat 31 4 5 16 19 5 14 8 12 • 5 29 49 83
36 41 62 29 1-74 169 28 108 116 . 49 150 245 Visits Appts Tele Totai
M onthly Shift Tota 14C 37; 25: 44 A 142 472 592 1208
11.59% 30.79% 1 20.86% 1 36.75% 11.75^ 39.16°^ 49.09'H 100,00%
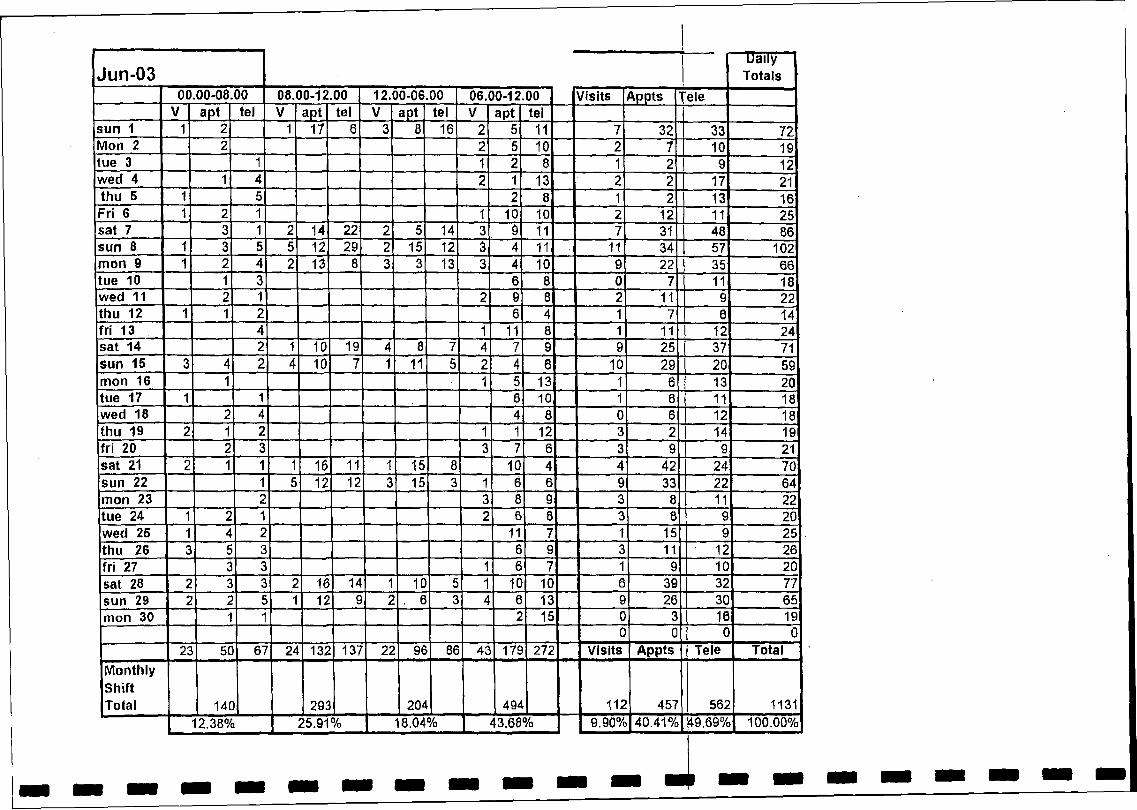
J u n - 0 3 |Daily
Totals00.00-08.00 08.00-12.00 12.00-06,00 06.00-12.00 Visits Appts 1ie le
V apt tel V apt tel V apt tel V apt tel Isun 1 1 2 1 17 6 3 8 16 2 5 11 7 32 I 33 72Mon 2 2 2 5 10 2 7 L 1Q 19tue 3 1 1 2 8 1 2 I 9 12wed 4 1 4 2 1 13 2 2 17 21thu 5 1 5 2 8 1 2 13 16Fri 6 1 2 1 1 10 10 2 12 11 25sat 7 3 1 2 14 22 2 5 14 3 9 11 7 31 48 86sun 8 1 3 5 5 12 29 2 15 12 3 4 11 11 34 57 102m on 9 1 2 4 2 13 8 3 3 13 3 4 10 9 22 35 66tue 10 1 3 6 8 0 7 11 18wed 11 2 1 2 9 8 2 11 9 22thu 12 1 1 2 6 4 1 7 6 14fri 13 4 1 11 8 1 11 12 24sat 14 2 1 10 19 4 8 7 4 7 9 9 25 37 71sun 15 3 4 2 4 10 7 1 11 5 2 4 6 10 29 20 59mon 16 1 1 5 13 1 6 13 20tue 17 1 1 6 10 1 6 11 18wed 18 2 4 4 8 0 6 12 18thu 19 2 1 2 1 1 12 3 2 14 19fri 20 2 3 3 7 6 3 9 9 21sat 21 2 1 1 1 16 11 1 15 8 10 4 4 42 24 70sun 22 ' 5 12 12 3 15 3 1 6 6 9 33 22 64mon 23 2 3 8 9 3 8 11 22tue 24 - 2 • 2 6 8 y 8 9 20wed 25 • 4 2 11 7 1 15 9 25thu 26 3 5 3 6 9 3 11 ' 12 26fri 27 3 3 1 6 7 1 9 10 20sat 28 2 3 3 2 16 14 ' 10 5 1 10 10 6 39 32 77sun 29 2 2 5 1 12 9 2 . 6 3 i. 6 13 9 26 30 65mon 30 - 2 15 0 3 16 19
0 0 0 023 50 67 24 132 137 22 96 86 43 179 272 Visits Appts Tele Total
MonthlyShiftTotal 14C 293 204 494 112 457 562 1131
12.38% 25.91% 18.04% | 43.68% 9.90%| 40.41 % \49.69% 100.00%
a
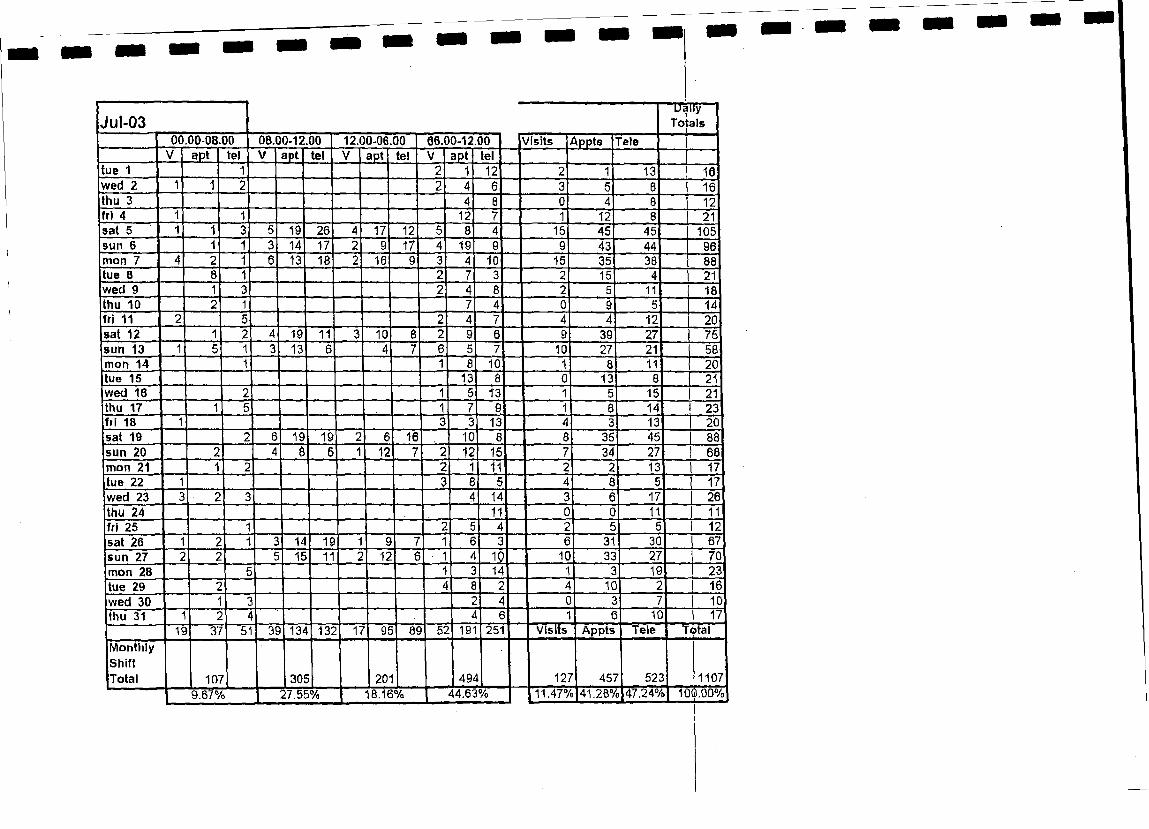
Jul-0300.00-08.00 08.00-12.00 12.00*06.00 06.00-12.00 V is its A p p ts Tele
Da ilyT o ta ls
V ap t te l V a p t te l V a p t te i V ap t te ltue 1 12 13 10wed 2 16thu 3 12fr i 4 12 12 21sa t 5 19 26 17 12 15 45 45 105sun 6 14 17 17 19 43 44 96m on 7 13 16 16 10 15 35 38 88tue 8 15 21w ed 9 11 18thu 10 14f r i 11 12 20sa t 12 19 11 10 39 27 75sun 13 13 10 27 21 58m on 14 10 11 20tue 15 13 13 21w ed 16 13 15 21thu 17 14 23f r i 18 13 13 20sa t 19 19 19 16 10 35 45 88s u n 20 12 12 15 34 27 68m on 21 11 13 17tue 22 17w ed 23 14 17 26thu 24 11 11 11fr i 25 12s a t 26 14 19 31 30 67s u n 27 15 11 12 10 10 33 27 70m on 28 14 19 23
tue 29 10 16w ed 30 10thu 31 6
■Visits10 17
Ïoïaî19 37 51 39 134 132 17 95 89 52 191 251 A p p ts Tele
M o n th lyS h iftT o ta l 107 305 201 494 127 457 523 1107
10^00%9.67% 27.55% 18.16% 44.63% 11.47% 41.2B%Ï47.24%
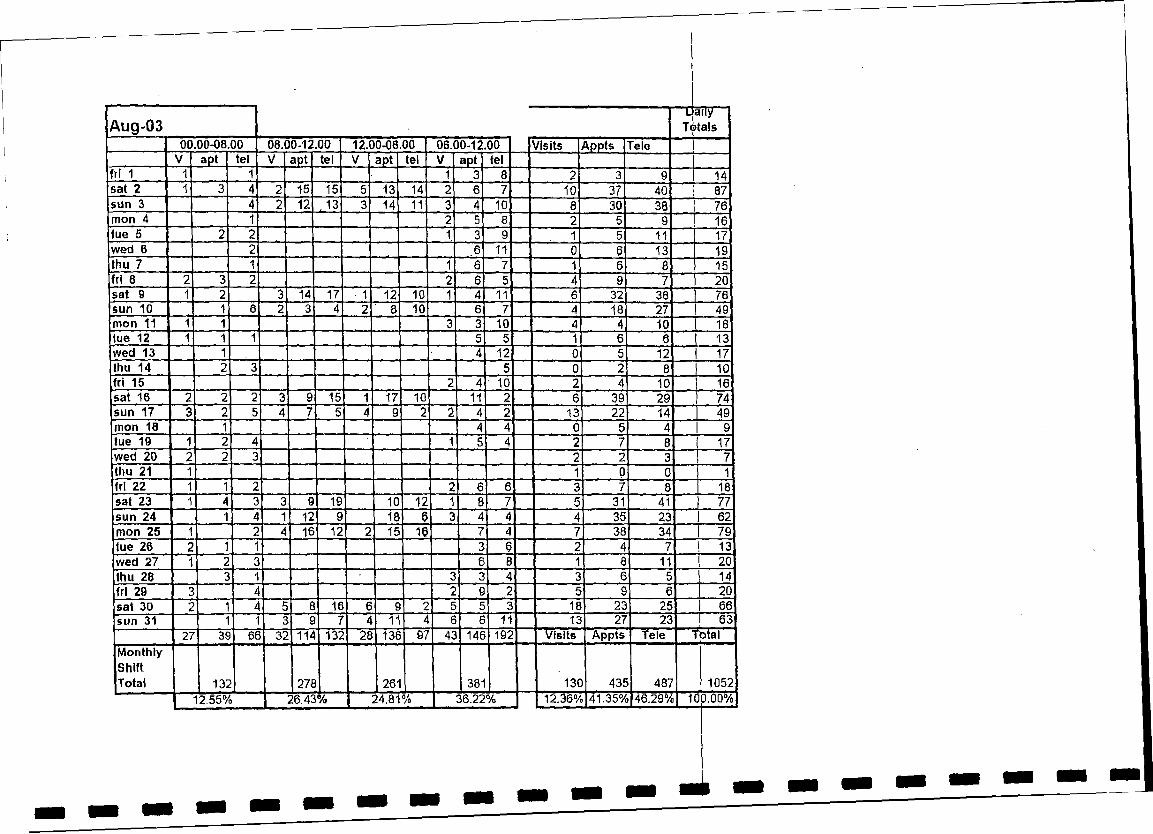
Aug-03Djail)/
T6 ta lsI00.00-08.00 08.00-12.00 12.00-06.00 06.00-12.00 V is its A ppts Tele )
V ap t te l V a p t te l V a p t te l V ap t te lfr i 1 1 1 1 3 8 2 3 9 14sa t 2 1 3 4 2 15 15 5 13 14 2 6 7 10 37 40 87s u n 3 4 2 12 ,1 3 3 14 11 3 4 10 8 30 38 76m on 4 1 2 5 8 2 5 9 16tu e 5 2 2 1 3 9 1 5 11 17w ed 6 2 6 11 0 6 13 19th u 7 1 1 6 7 1 6 8 15fr i 8 2 3 2 2 6 5 4 9 7 20s a t 9 1 2 3 14 17 1 12 10 1 4 11 6 32 38 76sun 10 1 6 2 3 4 2 8 10 6 7 4 18 27 49m on 11 1 1 3 3 10 4 4 10 I 18tue 12 1 1 1 5 5 1 6 6 I 13w ed 13 1 4 12 0 5 12 I 17thu 14 2 3 5 0 2 8 I 10f r i 15 2 4 10 r 2 4 10 ! 16s a t 16 2 2 2 3 9 15 1 17 10 11 2 6 39 29 74s u n 17 3 2 5 4 7 5 4 9 2 2 4 2 13 22 14 49m on 18 1 4 4 0 5 4 9tue 19 1 2 4 1 5 4 2 7 8 17w ed 20 2 2] 3 2 2 3 7thu 21 1 1 0 0 1f r i 22 1 1 2 2 6 6 3 7 8 18sa t 23 1 4 3 3 9 19 10 12 1 8 7 5 31 41 77sun 24 1 4 1 12 9 18 6 3 4 4 4 35 23 62m on 25 1 2 4 16 12 2 15 16 7 4 7 38 34 79fu e 26 2 1 1 3 6 2 4 7 ! 13w ed 27 1 2 3 6 8 1 8 11 ! 20thu 28 3 1 3 3 4 3 6 5 ! 14fr i 29 3 L 2 9 2 5 9 6 I 20s a t 30 2 • 4 5 8 16 6 9 2 5 5 3 18 23 25 1 66sun 31 1 1 3 9 7 4 11 4 6 6 11 13 27 23 1 63"
27 39 66 32 114 132 28 136 9 / 43 146 192 V is its A p p ts Tele T b ta l
M o n th lyS h iftT o ta l 132 270 261 381 130 435 487 1052
| 12.55% 26.43% 24.81% 36.22% 12.36% 41-35% 46.29% | U30.00%
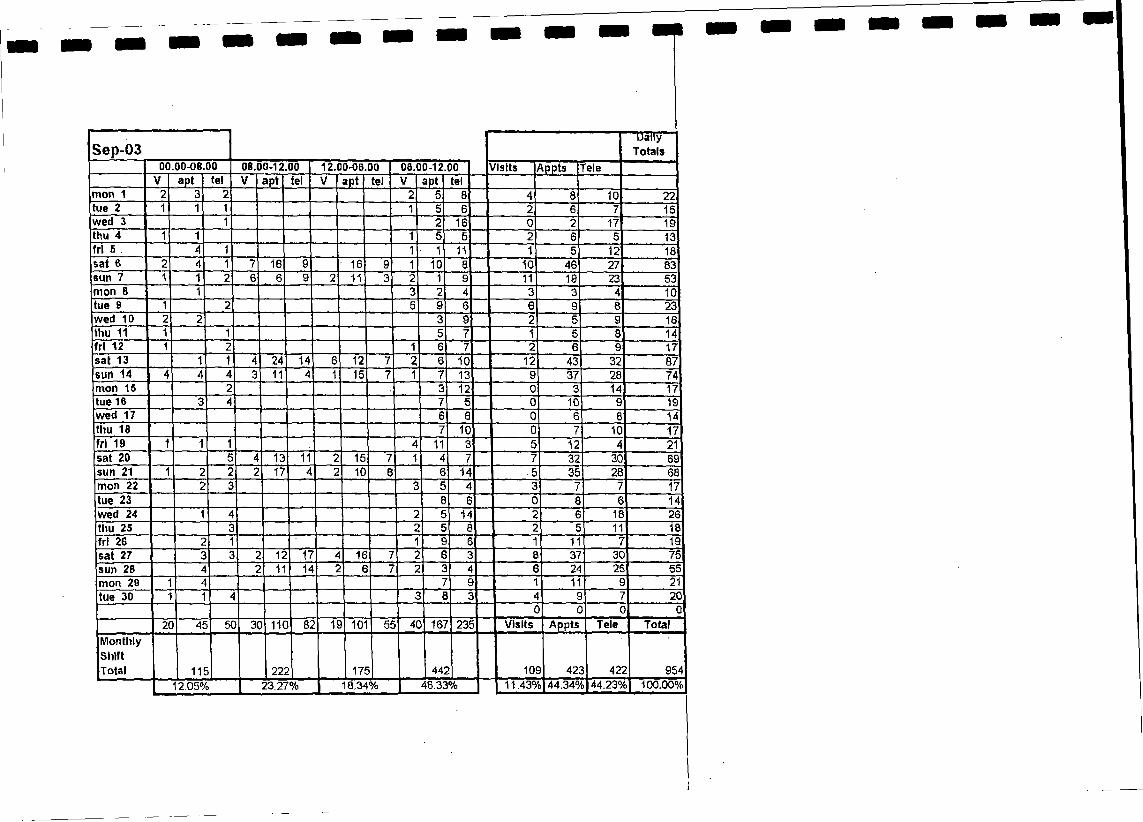
Sep-03D a llyTotals
00.00-08.00 08.00-12.00 12.00-06.00 00.00-12,00 /I sits ^ppts releV apt tel V apt tel V apt tel V apt tel
mon 1 2 3 2 2 5 8 4 8 10 22tue 2 1 1 1 1 5 6 2 6 7 15wed 3 1 2 16 0 2 17 19thu 4 1 1 1 5 5 2 6 5 13fr l 5 . 4 1 1 1 11 1 5 12 18sat 6 2 4 1 7 16 9 16 9 1 10 8 10 46 27 83sun 7 1 1 2 6 6 9 2 11 3 2 1 9 11 10 23 53mon 8 1 3 2 4 3 3 4 10tue 9 1 2 5 9 6 6 9 8 23wed 10 2 2 3 9 2 5 9 16thu 11 1 1 5 7 1 5 8 14fr l 12 1 2 1 6 7 2 6 9 17sat 13 1 1 4 24 14 6 12 7 2 6 10 12 43 32 87sun 14 4 4 4 3 11 4 1 15 7 1 7 13 9 37 28 74mon 15 2 3 12 0 3 14 17tue 16 3 4 7 5 0 10 9 19wed 17 6 Q 0 6 8 14thu 18 7 10 0 7 10 17fr l 19 1 1 1 4 11 3 5 12 4 21sat 20 5 4 13 11 2 15 7 1 4 7 7 32 30 69sun 21 1 2 2 2 17 4 2 10 6 6 14 .5 35 28 68mon 22 2 3 3 5 4 3 7 7 17tue 23 0 6 0 8 6 14wed 24 1 4 2 5 14 2 6 18 26thu 25 3 2 5 8 2 5 11 18fr l 26 2 1 1 9 6 1 11 7 19sat 27 3 3 2 12 17 4 16 7 2 6 3 8 37 30 75sun 28 4 2 11 14 2 6 7 2 3 4 6 24 25 55mon 29 1 4 7 9 1 11 9 21tue 30 1 1 4 3 8 3 4 9 7 20
0 0 G 020 45 5C 30 110 82 10 101 55 4C 167 235 Visits Appts Tele Total
M onthlyShiftTotal 11E 225 17E 442 10S 42C 42; 954
I 12.05% | 23.27% 18.34% | 46.33% 11.43°/ 44.34^ 44.23% 100.00%
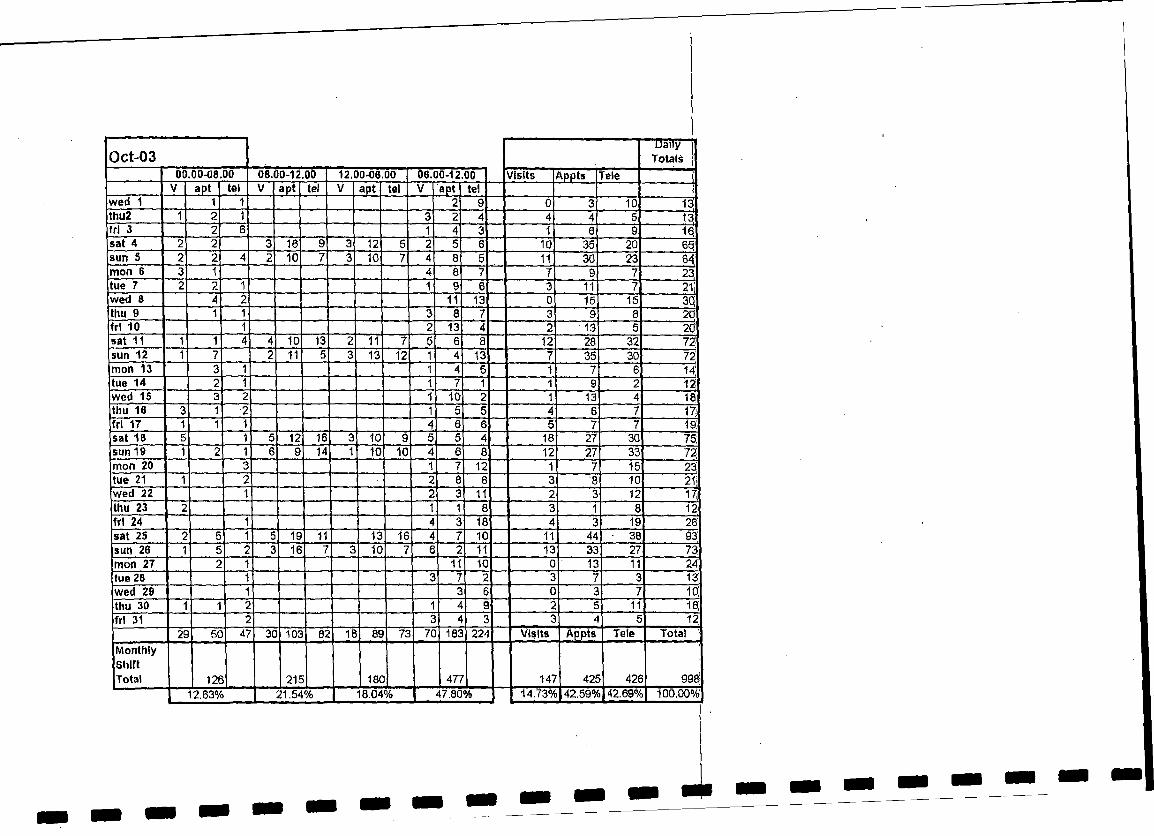
0ct-03Daily i
Totals |00.00-08.00 08.00-12.00 12.00-06.00 06.00-12.00 Visits ftppts Tele I
V apt tel V apt tel V apt tel V apt tel Iwed 1 1 1 2 9 0 3 10 13ithu2 1 2 1 3 2 4 4 4 5 13fr l 3 2 6 1 4 3 1 6 9 16.sat 4 2 2 3 16 9 3 12 5 2 5 6 10 35 20 65,sun 5 2 2 4 2 10 7 3 10 7 4 8 5 11 30 23 64,mon 6 3 1 4 8 7 7 9 7 23,tue 7 2 2 1 1 9 6 3 11 7 211wed & 4 2 11 13 0 15 15 3Qthu 9 1 1 3 8 7 3 9 8 20fr l 10 1 2 13 4 2 ■13 6 20,sat 11 1 1 4 4 10 13 2 11 7 5 6 8 12 28 32 72sun 12 1 7 2 11 5 3 13 12 1 4 13 7 35 30 72mon 13 3 1 1 4 5 1 7 6 r 14:tue 14 2 1 1 7 1 1 9 2 12wed 15 3 2 1 10 2 1 13 4 18’thu 16 3 1 2 1 5 5 4 6 7 17ifr l 17 1 1 1 4 6 6 5 7 7 19!sat 18 5 1 5 12 16 3 10 9 5 5 4 18 27 30 75:sun 19 1 2 1 6 9 14 1 10 10 4 6 8 12 27 33 72m on 20 3 1 7 12 1 7 15 23;tue 21 1 2 2 8 8 3 8 10 211wed 22 1 2 3 11 2 3 12 17|thu 23 2 1 1 8 3 1 8 12fr l 24 1 4 3 18 4 3 19 26'sat 25 2 5 1 5 19 11 13 16 4 7 10 11 44 • 38 93'sun 26 1 5 2 3 16 7 3 10 7 6 2 11 13 33 27 73;mon 27 2 1 11 10 0 13 11 24'tue 28 1 3 7 2 3 7 3 13wed 29 1 3 6 0 3 7 10;thu 30 1 1 2 1 4 9 2 5 11 10Efr l 31 2 3 4 3 3 4 5 12
29 50 47 30 103 02 18 89 73 70 183 224 Visits Appts Tele Total ’
M onthlyShiftTotal 126 216 18C 477 147 425 426 998
12.63% 21.54% 18.04% 47.80% 14.73% 42.59% 42.69% 100.00%;
1
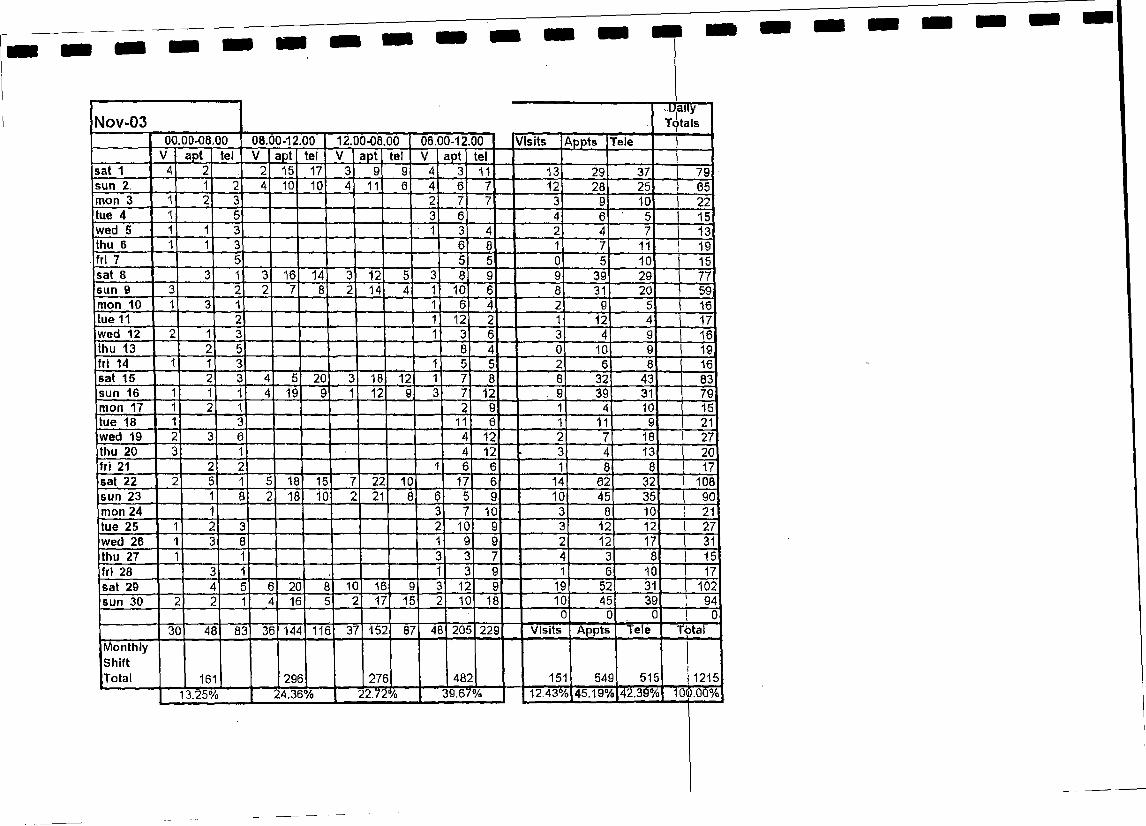
1
Nov-0300.00-08.00 08.00-12.00 12.00-06.00 06.00-12.00 V is its A p p ts Tele
.DailyT o ta ls
V a p t te l V ap t te l V a p t te l a p t te isa t 1 15 17 11 13 29 37 79sun 2. 10 10 11 12 28 25 65m on 3 10 22tue 4 15w ed 5 13thu 6 11 19fr i 7 10 15sa t 8 16 14 12 39 29 77
14 10 31 20 59m on 10 16tue 11 12 12 17w ed 12 16thu 13 10 19f r i 14 16sa t 15 20 18 12 32 43 83sun 16 19 12 12 39 31 79m on 17 10 15tue 18 11 11 21w ed 19 12 18 27thu 20 12 13 20f r i 21 17sa t 22 18 15 22 10 17 14 62 32 108sun 23 18 10 21 10 45 35 90m on 24 10 10 21tue 25 10 12 12 27w ed 26 12 17thu 27 15fr i 28 10 17sa t 29 20 10 16 12 19 52 31 102sun 30 16 17 15 10 18 10 45 39 94
30 48 83 36 144 116 37 152 87 46 205 229 V is its A p p t s Te le Tòta) -1 «■ ■M o n th lyS h iftT o ta l 161 296 276
13.25% I ' 24.38% | 22.72%482 151 549
12.43%|45.19%p[2.39%515 1215
"100.00%39.67%

Dec-03Daily
Totals00.00-08.00 08.00-12.00 12.00-06.00 06.00-12.00 Visits Appts Tele
V apt tel V apt tel V apt tel V apt telMon 1st 1 1 3 1 13 14 2 14 17 33Tues 2nd 2 2 11 8 4 11 8 23Wed 3rd 2 1 2 12 12 2 14 13 29Thurs 4th 3 12 15 0 12 18 30Frt 5th 2 2 10 11 2 10 13 25Sat 6th 5 2 26 23 16 18 3 1 11 10 43 52 105Sun 7th 2 3 2 5 14 5 3 18 6 2 8 18 12 43 31 86Mon 6th 2 3 3 9 9 3 11 12 26Tues 9th 2 4 1 9 14 1 11 18 30Weds 10th 1 1 1 7 12 1 8 13 22Thurs 11th 1 1 2 6 10 3 6 11 20Frl 12th 1 8 1 10 16 2 10 24 36Sat 13th 3 7 3 23 23 4 • 20 7 2 17 5 9 63 42 114Sun 14th 1 3 1 23 6 4 21 4 2 4 11 8 51 21 \ 80Mon 15th 3 1 1 4 6 9 7 7 10 24Tues 16th 4 1 2 4 10 4 8 11 6 25Wed 17th 2 4 2 6 5 2 8 9 19Thur 18th 1 7 1 7 7 2 14 7 23Fri 19th 2 1 3 8 5 2 9 8 19Sat 20th 6 2 5 21 19 4 19 11 6 7 8 15 53 40 108Sun 21st 1 5 7 15 12 2 12 14 2 2 6 12 29 37 78Mon 22nd 1 1 2 1 9 6 2 101 8 20Tues 23rd 2 2 3 7 7 6 9 9 24Weds 24th 4 1 1 10 6 2 14 7 23Thurs 25th 1 2 4 3 4 12 3 11 2 1 11 10 8 28 28 64Frl 26th 1 1 5 6 26 16 1 15 15 1 .10 6 9 52 42 103Sat 27th 1 1 49 41 2 31 18 4 9 17 7 90 76 173Sun 28th 2 2 2 8 28 5 3 16 11 4 7 8 17 53 26 96Mon 29th 2 1 2 11 9 2 13 10 25Tues 30th 3 4 3 3 5 6 3 9 18Weds 31st 1 3 4 4 3 5 4 6 15
40 50 76 40 229 162 26 179 106 65 256 287 Visits Appts tele Total
Monthly Shift Total 166 431 311 608 171 714 631 1516
| 10.95% 28.43% | 20.51% | 40.11% 1 i .28% 47.10% 41.62% 100.00%
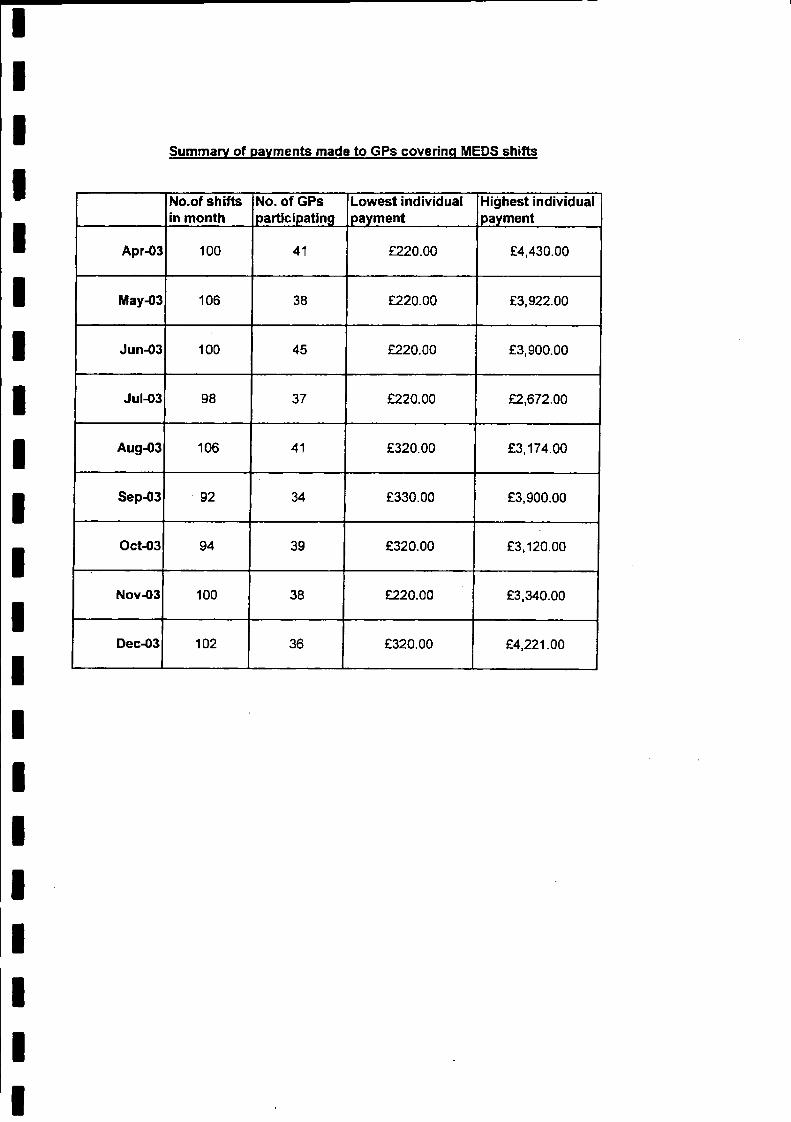
Summary of payments made to GPs covering MEDS shifts
No.of shifts in month
No. of GPs participating
Lowest individual payment
Highest individual payment
Apr-03 100 41 £220.00 £4,430.00
May-03 106 38 £220.00 £3,922.00
Jun-03 100 45 £220.00 £3,900.00
Jul-03 98 37 £220.00 £2,672.00
Aug-03 106 41 £320.00 £3,174.00
Sep-03 92 34 £330.00 £3,900.00
Oct-03 94 39 £320.00 £3,120.00
Nov-03 100 38 £220.00 £3,340.00
Dec-03 102 36 £320.00 £4,221.00
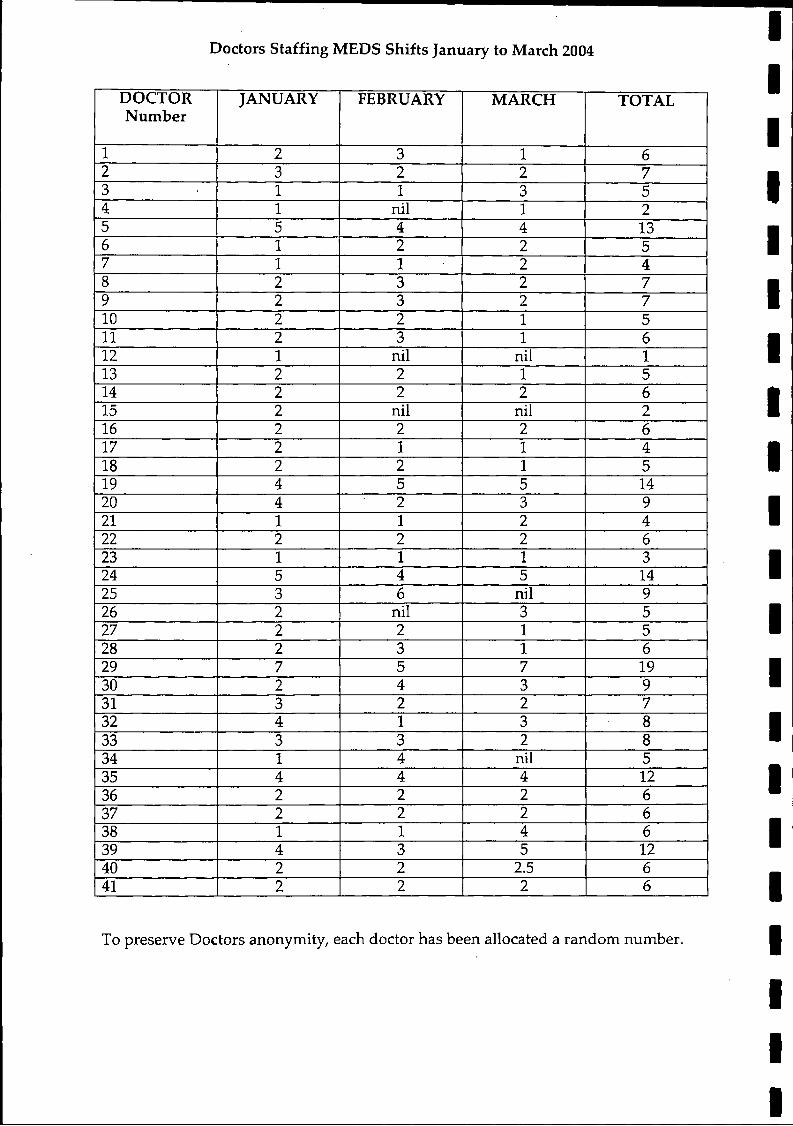
Doctors Staffing MEDS Shifts January to March 2004
DOCTORNumber
JANUARY FEBRUARY MARCH TOTAL
1 2 3 1 62 3 2 2 73 1 1 3 54 1 nil 1 25 5 4 4 136 1 2 2 57 1 1 2 48 2 3 2 79 2 3 2 710 2 2 1 511 2 3 1 612 1 nil nil 113 2 2 1 514 2 2 2 615 2 nil nil 216 2 2 2 617 2 1 1 418 2 2 1 519 4 5 5 1420 4 2 3 921 1 1 2 422 2 2 2 623 1 1 1 324 5 4 5 1425 3 6 nil 926 2 nil 3 527 2 2 1 528 2 3 1 629 7 5 7 1930 2 4 3 931 3 2 2 732 4 1 3 833 3 3 2 834 1 4 1 nil 535 4 4 4 1236 2 2 2 637 2 2 2 638 1 1 4 639 4 3 5 1240 2 2 2.5 641 2 2 2 6
To preserve Doctors anonymity, each doctor has been allocated a random number.
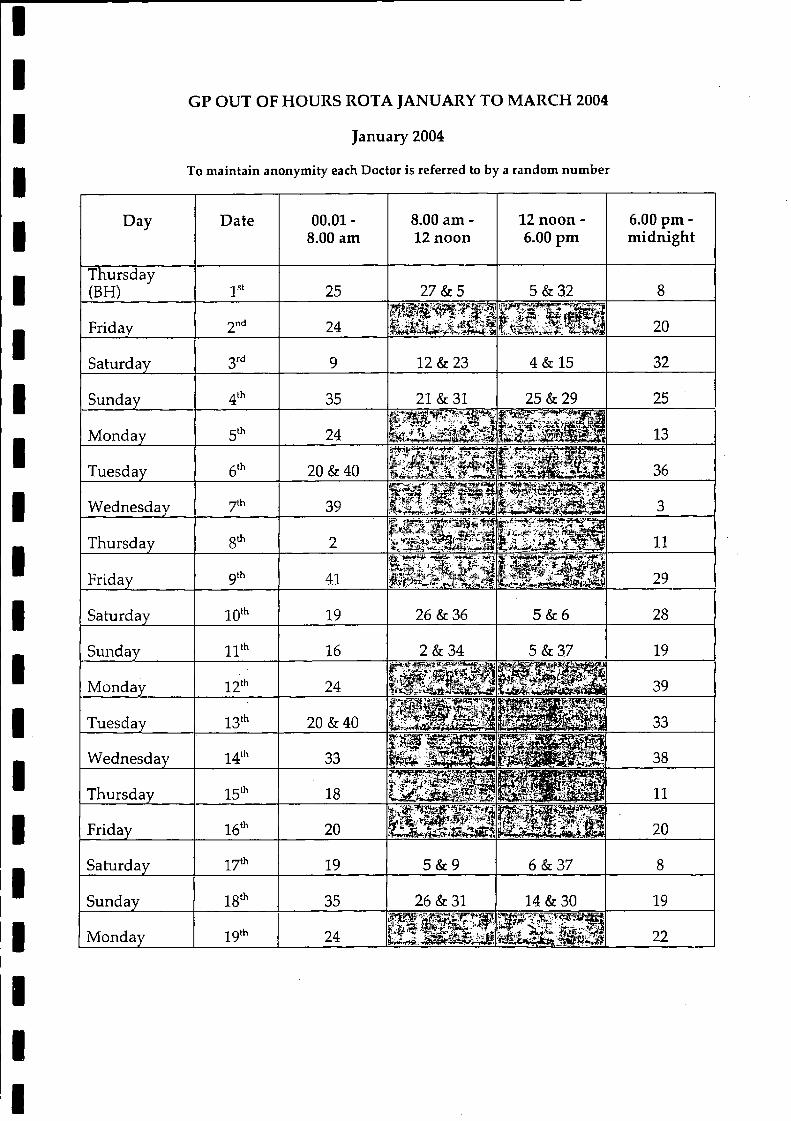
January 2004
To maintain anonymity each Doctor is referred to by a random num ber
GP OUT OF HOURS ROTA JANUARY TO MARCH 2004
Day Date 00.01 -8.00 am
8.00 am - 12 noon
12 noon - 6.00 pm
6.00 pm - midnight
Thursday(BH) 1st 25 27 & 5 5 & 32 8
Friday nd 24 S ll l l l l 20
Saturday 3rd 9 12 & 23 4 & 15 32
Sunday 4<h 35 21 & 31 25 & 29 25
Monday 5th 24 H H M 13
Tuesday 6th 20 & 40 TpSiiiSi vrc^*i . ■ -J> b lA j 36
Wednesday th 39 l\I ggSl3f 3
Thursday gth 2 11
Friday 9th 41 fife U mH M b 29
Saturday 10,h 19 26 & 36 5 & 6 28
Sunday 11th 16 2 & 34 5 & 37 19
Monday 12th 24 ISotslsilB llilllii 39
Tuesday 13th 20 & 40 h B H k i $ £ | 8 H B B 33
Wednesday 14lh 33 @ E £ B 3 i i l M H l 38
Thursday 15'h 18 IlilP lilll 11
Friday 16th 20 H H H 20
Saturday •yth 19 5 & 9 6 & 37 8
Sunday 18th 35 26 & 31 14 & 30 19
Monday 19th 24 US;isi &si¡ ¡ S ill 22
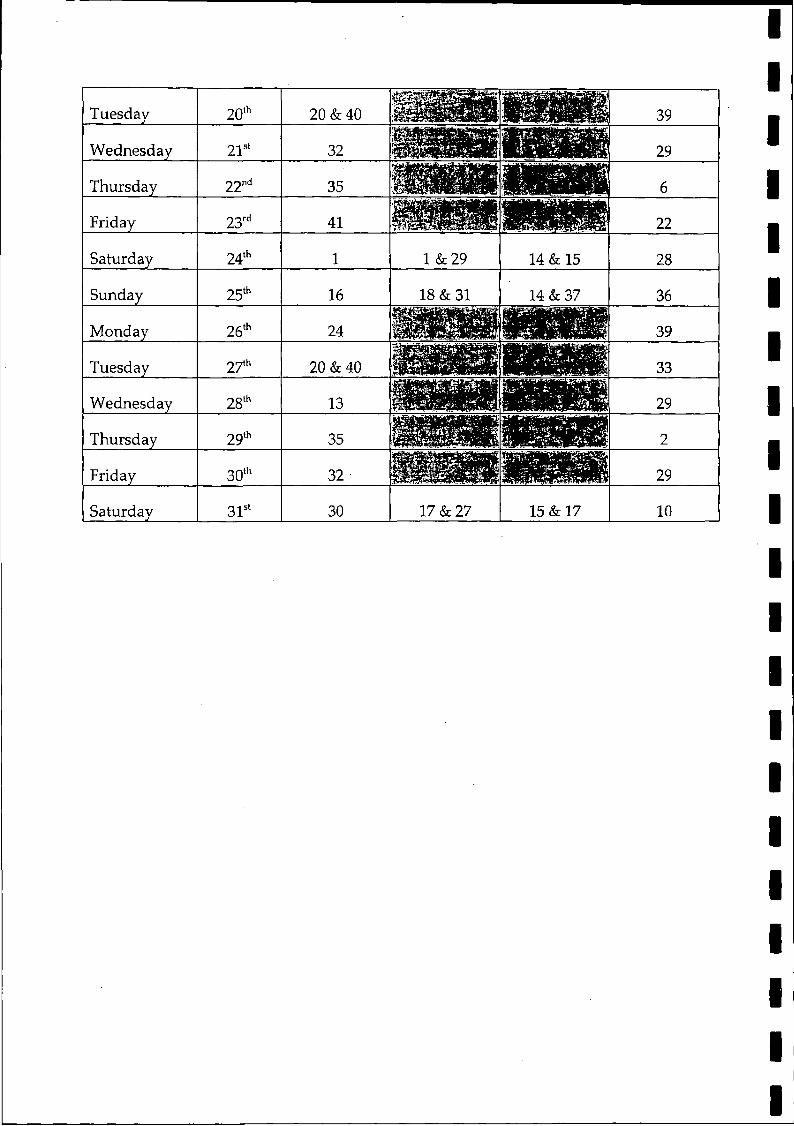
Tuesday 20th 20 & 40 39
Wednesday 21st 32 29
Thursday 22"d 35 M p i 6
Friday 23rd 41 22
Saturday 24th 1 1 & 29 14 & 15 28
Sunday 25th 16 18 & 31 14 & 37 36
Monday 26th 24 39
Tuesday 27th 20 & 40 33
Wednesday 28tl1 13 29
Thursday 29th 35 2
Friday 30th 32 29
Saturday 31st 30 17 & 27 15 & 17 10
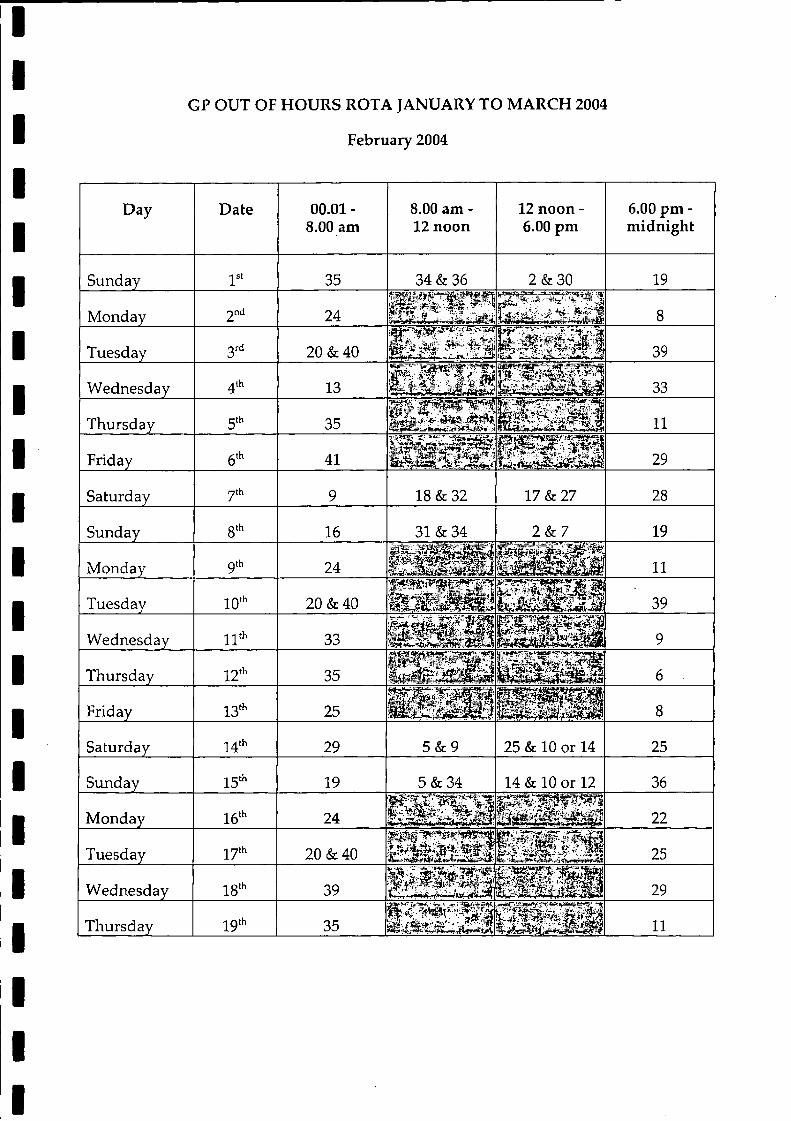
February 2004
GP OUT OF HOURS ROTA JANUARY TO MARCH 2004
Day Date 00.01 - 8.00 am
8.00 am - 12 noon
12 noon - 6.00 pm
6.00 pm - midnight
Sunday 1st 35 34 & 36 2 & 30 19
Monday 2nd 24 8
Tuesday 3rd 20 & 40 l l l t l l l l 39
Wednesday 4th 13 U W ^.iH TW !r 33
Thursday 5th 35 11
Friday 6th 41 29
Saturday yth 9 18 & 32 17 & 27 28
Sunday 8th 16 31 & 34 2 & 7 19
Monday 9 th 24 11
Tuesday lO“1 20 & 40 5 1 S I E I I 39
Wednesday 11th 33 I s l S f i S i s l I B 9
Thursday 12lh 35 6
Friday 13th 25 M B IjB f f 8
Saturday 14* 29 5 & 9 25 & 10 or 14 25
Sunday 15th 19 5 & 34 14 & 10 or 12 36
Monday 16'h 24 e s s s 22
Tuesday 2 yth 20 & 40 i f i S l l l i 25
Wednesday 18th 39 p # i # i l P r a 29
Thursday 19,h 35 mi^g^jai3Bs9m 11
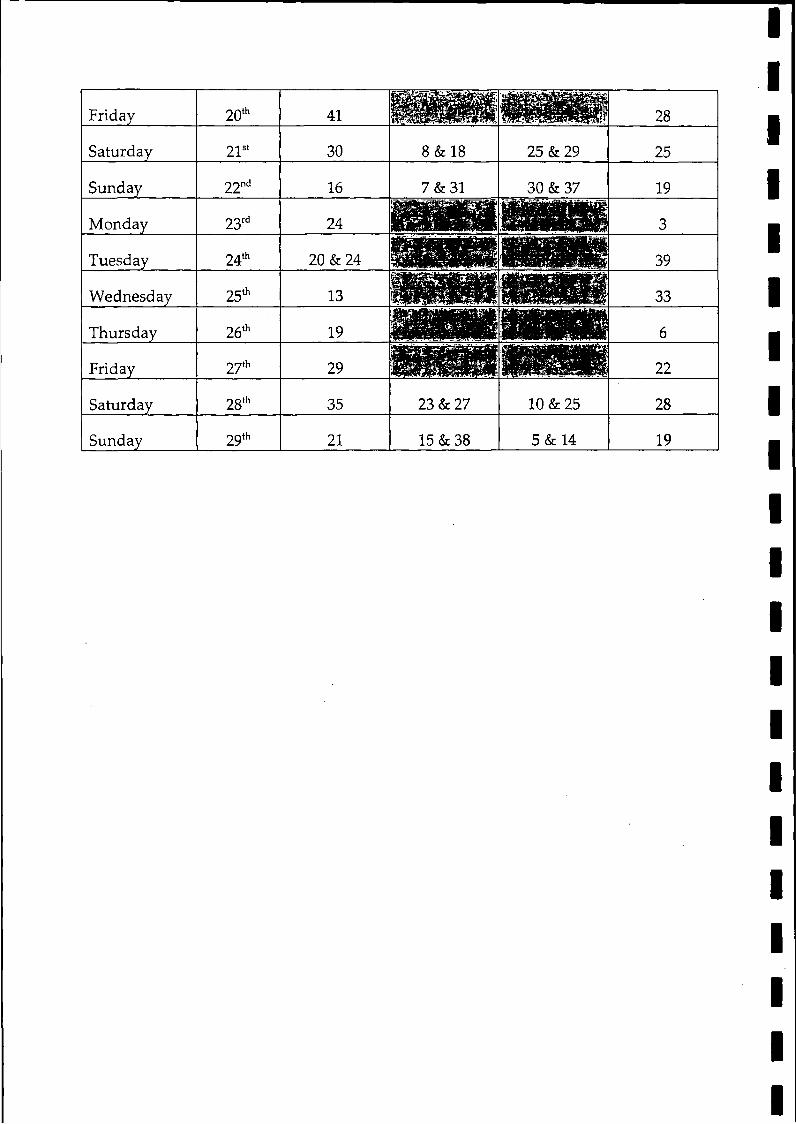
Friday 20th 41 28
Saturday 21st 30 8 & 18 25 & 29 25
Sunday 22nd 16 7 & 31 30 & 37 19
Monday 23rd 24 PIM P 3
Tuesday 24th 20 & 24 HMMKS 39
Wednesday 25th 13 w m u 33
Thursday 26th 19 6
Friday 27th 29 M W S IBBBB 22
Saturday 28th 35 23 & 27 10 & 25 28
Sunday 29th 21 15 & 38 5 & 14 19
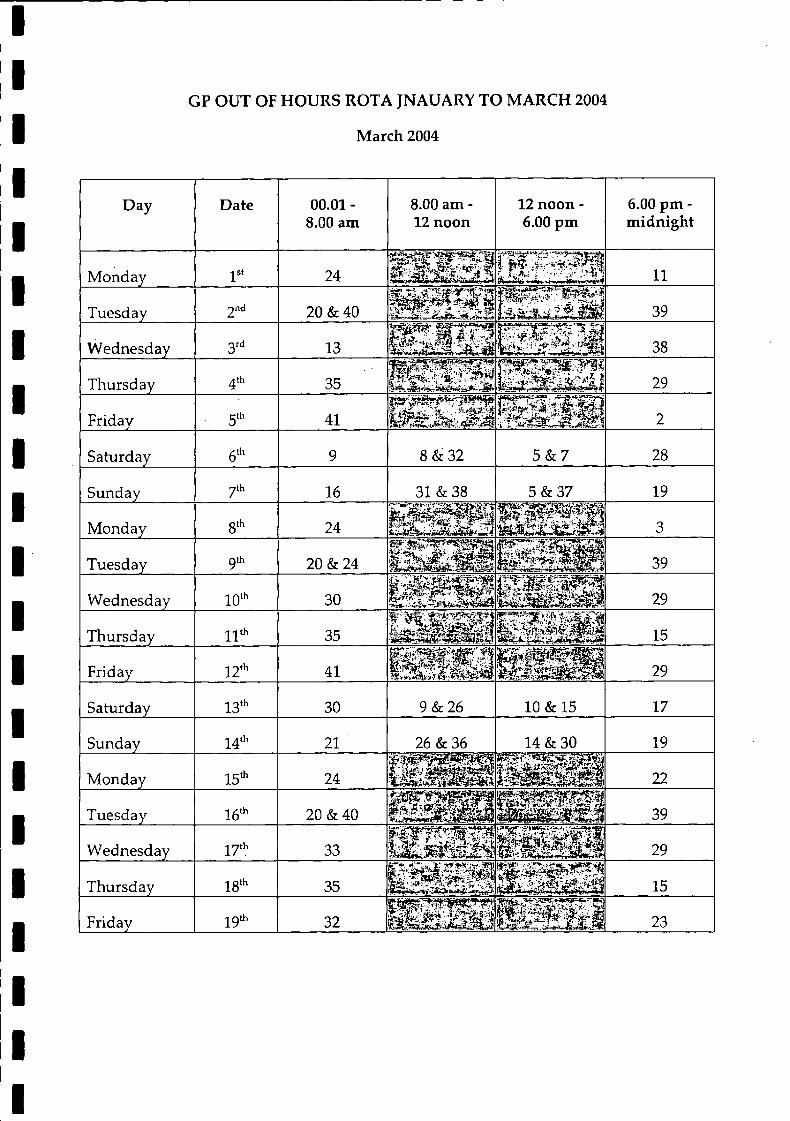
March 2004
GP OUT OF HOURS ROTA JNAUARY TO MARCH 2004
Day Date 00.01 - 8.00 am
8.00 am - 12 noon
12 noon - 6.00 pm
6.00 pm - midnight
Monday 1st 24 11
Tuesday 2nd 20 & 40 39
Wednesday 3rd 13 38
Thursday 35 29
Friday ■ 5th 41 2
Saturday 6th 9 8 & 32 5 & 7 28
Sunday y t h 16 31 & 38 5 & 37 19
Monday 8th 24 l i i l l l t i 3
Tuesday 9 th 20 & 24 39
Wednesday 10,h 30 B B B B i 29
Thursday 11th 35 w m m S Im 15
Friday 12th 41 M S Bp | | g g | 29
Saturday 13th 30 9 & 26 10 & 15 17
Sunday 14th 21 26 & 36 14 & 30 19
Monday 15th 24 22
Tuesday 16th 20 & 40 j H J M I 39
Wednesday 1 7 th 33 29
Thursday 18th 35ft*. mrsr- asti
l P i § l S | 15
Friday 19“’ 32 23
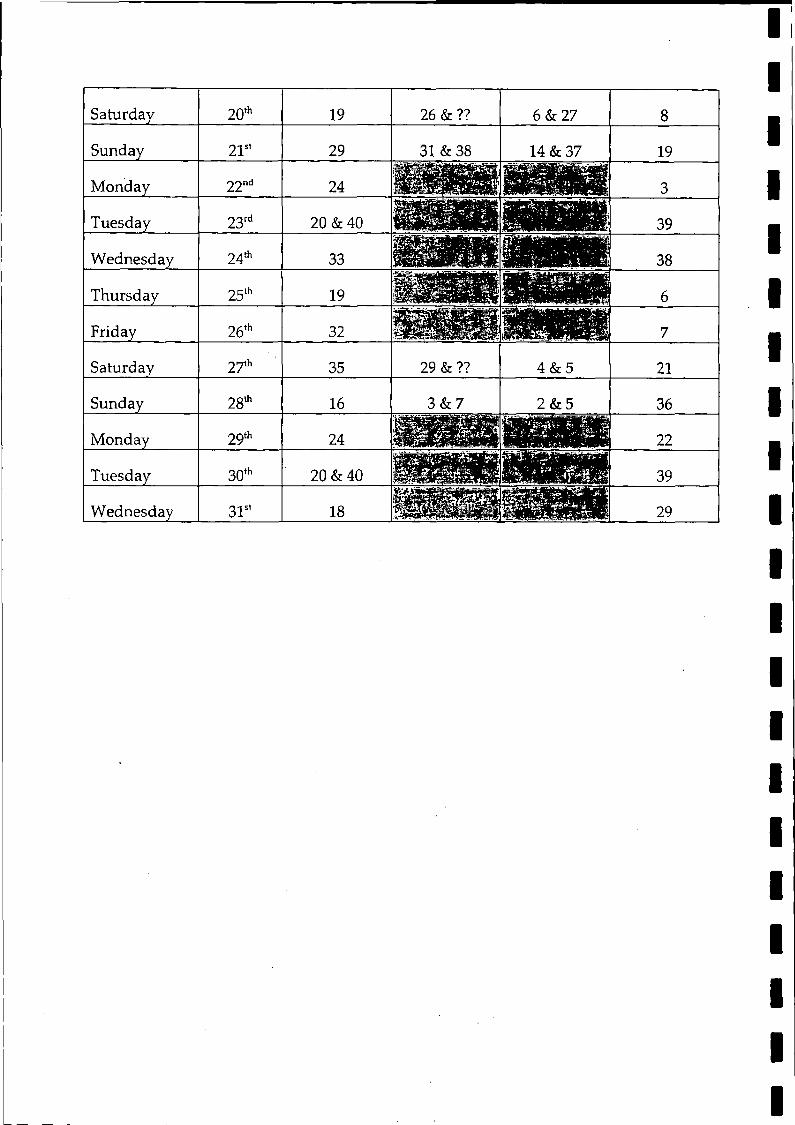
Saturday 20th 19 26 & ?? 6 & 27 8
Sunday 21st 29 31 & 38 14 & 37 19
Monday 22nd 24 3
Tuesday 23rd 20 & 40 39
Wednesday 24th 33 f G S H S H M H 38
Thursday 25th 19 6
Friday 26th 32 l a p p j M f f P p 7
Saturday 27th 35 29 & ?? 4 & 5 21
Sunday 28th 16 3 & 7 2 & 5 36
Monday 29th 24 22
Tuesday 30th 20 & 40 f f l M i l 39
Wednesday 31s' 18 I W — 29
Isle of ManG o vernm ent
Rn'/I ¿Him Vi*»/*
H E A L T H S E R V I C E S -
Shirveishyn Slaynt Primary Healthcare
Tel: (01624)642698 Fax: (01624) 642635
Mr P Lo BaoJoint Clerk to the CommitteeOffice of the Clerk of TynwaldLegislative BuildingsDouglasISLE OF MANI M I 3PW
Your ref:
Our ref: 4.1.2a
Date: 20 February 2004
Dear Mr Lo Bao
Re: Information requested by Select Committee of Tynwald on GP Services
I am writing with the Information requested by the Select Committee that is immediately available. I will need to follow up with some further information on the costs of MannDoc and the results of the survey of how practices handle the 8am "handover" but I enclose the following.
1. GPs undertaking hospital duties by specialty
AnaesthesiaEar, Nose and ThroatMedicine
Psychiatry GUM/Sexual Health
- Dr A Kelsey, Associate Specialist, Ramsey- Dr D M Bui), Clinical Assistant, Nobles- Dr A Blackman, Hospital Practitioner, Diabetes- Dr K Armour, Clinical Assistant, Care of the Elderly, Ramsey- Dr S Harris, Clinical Assistant, Drug and Alcohol- Dr 3 Hockings, Clinical Assistant, Nobles
2. Costs of MannDoc
I have the completed figures for the financial year 2001/2. The DHSS contributed £61,560 which pai^Tfor supporting staff and transport services and the participating GPs paid in £214,060 which, in turn, paid for the fees of those doctors who undertook to work in the service.
I will forward the completed figures for 2002/3 when they are available.
3. Relocation Scheme
I attach a copy of the relevant sections from the DHSS Relocation Scheme. It has been agreed with the GP negotiating committee that the DHSS will reimburse 90% of the costs involved up to a maximum amount to be set by the Department.
4. Statistics
I enclose monthly figures for MEDS for the months April 03-December 03 inclusive. As was stated when Mrs Duke and I attended the hearing, every contact comes via the telephone; those that are shown under
Health Services DivisionCrookall House. Demesne Road, Douglas, Isle of Man IM1 3QA
Website: www.gov.im/dhss
DEPARTMENT OF HEALTH AND SOCIAL SECURITY
Shickyrys Ÿ ffîê â fâ g } ¿ f e '
"tel" represent those contacts in which the sole contact is via telephone with no other action (ie a visit to the patient or an appointment for the patient to come to MEDS).
5. Range of income
I enclose a summary of payments made to doctors covering the MEDS shifts. The information shows the number of shifts, numbers of doctors participating and both the lowest and highest individual payment in that month to a particular doctor.
6. Frequency of standby callout
There was one occasion when the standby doctor was called in due to excessive workload and there have been four occasions (mainly over Christmas) when a doctor has extended his/her shift because of excessive workload.
7. Comments on the out of hours service
I enclose a copy of a letter received from the Ramsey District Nurses in May 2003. This letter gives a different view of the service from that presented in correspondence discussed when I attended the Committee hearing.
Yours sincerelv
Encs
Appendix 5
OFFICE OF THE CLERK OF TYNWALDLegislative Buildings, Douglas,
Isle of Man, British Isles, IMI 3PW
Our ref: C/G PS/02/plb
16th July 2003
Dr I H MacLean Director of Public Health Crookall House Demesne Road Douglas IMI 3QA
Dear Doctor MacLean
Select Committee of Tynwald on GP Services
I am writing to you at the request of the above Committee, to ask you to supply evidence, in writing, to the Committee concerning any observations you may have on the issue of provision of GP out of hours services and any changes that you may feel may be desirable in the future.
The Committee would be pleased to receive your views by Friday 12th September 2003. After it has examined the written evidence received, it may wish to call a number of experts to give oral evidence.
Please find attached a copy of the motion establishing the Committee.
Yours sincerely
Phil Lo BaoJoint Clerk to the Committee
DEPARTMENT OF HEALTH AND SOCIAL SECURITYHEAL TH SER VICES
MEMORANDUM
To: Select Committee of Tynwald on GP Services
From: Public Health Directorate
Date; 4 September 2003
Ref: PE/kg/Out of Hours
With reference to the letter of the 16th July 2003 from the Select Committee requesting evidence:
“Observations on the provision of GP out of hours services” and possible “changes that ... may be desirable in the future”
Foreword
The Public Health Directorate was represented at the contract negotiations which led to the establishment of the new model of out-of-hours service, MEDS (Manx Emergency Doctor Service) and fully supports the changes to date with a single proviso as recorded in the conclusion on page 9. The background and history up to the change to MEDS is laid out in a submission to the Committee by the Department of Health and Social Security and we will not repeat this in our evidence to the Committee but concur with that evidence as written.
Introduction
Public Health is interested in population health and disease and is traditionally tasked (among other issues) with promoting the improvement of health in a population and in tackling inequalities experienced by the same population. Public Health also traditionally advises officers of Health Departments on cost-effective and efficient methods of health service delivery in order to make “best use” of public resources. Thus we have an interest in establishing an out-of-hours service on the Isle of Man which delivers on the above principles. This is one of the reasons we were glad to participate in the GP Contract negotiations which led to the development of MEDS. Modernising our out-of-hours services requires a balancing act - making, services simpler, faster, more consistent and uniform for all patients, at the same time as reducing the burden of care on GPs.
Two basic principles are at the core of this new approach to out-of-hours service provision. Firstly, patient access to the service should be as simple and straightforward as possible - one telephone call, providing effective and timely advice and
Page 1 o f9Public Health Response
9 September 2003
where necessary, a face-to-face consultation at a time and place agreed with the patient, ie a prompt, professional and appropriate response to the myriad different needs of patients (and families) out-of-hours. Secondly, all those professionals involved in the delivery of care out-of-hours, regardless of the sector of the service in which they work, should work together co-operatively and collaboratively to deliver the best possible service to patients and to make the most effective use of resources.
We believe that MEDS on the Isle of Man delivers on both these principles.
In observing this new service or system it is useful to look at it from the perspective of users (patients), the GPs and the Department of Health and Social Security tasked with the responsibility to deliver health care.
1 . Patients
Any health service exists because of patient needs or demand. The reassurance and peace of mind that expert medical care (GP) is available outside normal surgery hours has been central to the public popularity of our primary care tradition. However, increasing demands for out-of-hours care (see Department of Health and Social Security submission) led to the establishment of MannDoc in 1998. These developments were only mirroring those happening in the United Kingdom where, by 1992, the majority of GPs had opted out of the individual responsibility for providing out-of-hours care. MannDoc was formed as a result of the crisis being experienced in GP services both locally and internationally. The old pattern of meeting the majority of patients’ requests for out-of-hours care by a home visit or face-to-face consultation by a GP disappeared in about 80% of England and 90% of the other UK areas from 1992 onwards. Since 1998 when MannDoc commenced on the Isle of Man to service 8 out of 11 GP practices, records show that only 10-15% of calls to GPs in MannDoc resulted in visits by the GP with about 50% of the callers accepting telephone advice. We are not aware of any formal complaints about the MannDoc quality of service since 1998 and the new model is virtually identical except that it is Island-wide. The needs of the majority of patients are now met safely and appropriately by a telephone consultation with a Nurse or a GP in many European Countries - including the UK, in New Zealand, Australia and many North American States.
There will always be a small minority of people whose clinical needs out-of-hours can only be met in their own homes and we believe the new system allows adequately for this situation.
All patients on the Isle of Man should have access to the same high quality, out-of- hours services regardless of the part of the Island in which they live or the particular GP practice with which they are registered. Before MEDS came into being in April 2003 this principle of equality was not present, with the type of service being reliant on the part of the Island in which one resided. Since April 2003 and into the future a uniform service has been provided which will be more easily monitored to ensure quality and “value for (public) money”.
Page'2 of 9Public Health Response
9 September 2003
Several large reviews of the demand for out-of-hours care from GPs in the UK have been published and we refer briefly to the results of these. Local Isle of Man data/information is lacking at present - indeed one of the significant improvements possible with the new model is that important information can be more easily collected and collated to effect change where necessary. From these reviews we know the following consistent findings emerge:-
a) There is a disproportionate number of calls from parents of children aged under 5 years of age, representing up,to a quarter of all out-of-hours calls.
b) These calls are most frequent in the evenings before 10 pm.
c) Call rates are lowest for older children and young adults and steadily rise with increasing age.
d) Calls about children more often result in telephone advice, whereas elderly patients are more likely to be visited.
e) More calls are received about female than male patients.
f) The most common reasons for calling were upper respiratory tract infections, diarrhoea and vomiting, childhood fevers and minor injuries.
g) More than 50% of all night calls occur before 1 am.
h) Call rates are higher on weekend nights than on weekday nights.
These findings allow GPs and Managers to plan the type of services required and define the training to be made available. We hope that the introduction of our new local service will be accompanied by the review of the way data is collected and the type of data collected for management purposes. The previous model did not permit easy data collection and analysis.
In a large study/survey in Denmark in 1992, following the introduction of a system similar to MEDS, it was found that the main cause of dissatisfaction with the new service was that the population had been given too little information about the background to the reforms and that politicians had failed to inform the public about the intentions of the new arrangement. It is suggested that we learn from this experience locally. In Denmark, it was found that, generally, patients adjusted quite easily to changes. A similar study in Leicester in the UK showed an overall patient satisfaction score of 72% (with the co-operative service, similar to MEDS).
The data from April to June 2003 indicates that only 1-2% of calls after hours are classified as urgent by the GPs and that 80-85% of calls are routine or non-urgent. This would suggest that GPs and health managers need to educate the public locally
Page 3 of 9Public Health Response
9 September 2003
as to the real function of out-of-hours service. About 10% of calls made during this period resulted in a visit by the GP. During this same period not a single written complaint has been made about MEDS. There have been press articles and phone complaints to the DHSS about MEDS and this is to be expected in any change to a popular service. While one accepts that complaints are a very crude indicator of patient satisfaction, nevertheless, we believe this data augurs well for the future as experience in other countries suggests that complaints are at their highest rates immediately after introducing a new service. This was the experience with MannDoc too.
In addition, the rate of calls per 1,000 patients in the Isle of Man suggests that demand locally is similar to that in the studies performed in the UK. This could be useful to planners as it allows us to look to experience in the UK, as our population appears to behave in a similar manner when contacting out-of-hours services.
2. General Practitioners (GPs)
All of our GPs have been recruited from regions of the UK and due to the professional Registration and Training regulations it is reasonable to assume that this scenario will continue. We would thus be foolish to ignore what is happening within general practice generally, and out-of-hours services in particular, in the UK. GPs are required within the terms of their contracts with the DHSS to maintain UK registration. This is essential if we are to expect a high quality of service to be maintained on the Island. Various statutory bodies such as the Scottish Executive, Audit Commission (UK) and the UK Royal College of General Practitioners (RCGP) together with the British Medical Association (BMA) have commissioned research and reports on the pressures, demands and workload issues faced by the GP body in Scotland, England, Wales and Northern Ireland. It was apparent before and during the negotiations between the DHSS and local GPs that the problems faced here are similar.
The recently published Strategy for Health for the Isle of Man and its acceptance by local politicians and senior officials of Government means that many of the initiatives that are ongoing in the UK will apply here on the Island - subject to local adaptation, e.g. National Service Frameworks (NSFs). These initiatives are mainly aimed at improving the quality of care but also at making care more uniform and cost effective. There will thus be an impact on all sectors of Island health care, including general practice, and we would do well to learn from and implement good practice coming out of experiences in the UK - as it is widely accepted in Health and Policy circles that the programme of change there is world class.
Although there is little hard evidence of a marked increase in general practice workload, there is evidence of a rise in the complexity of the GP workload and a marked rise in administrative workloads in the last decade. GPs work in an increasingly complex world with rapid advances in technology and clinical care, various policy initiatives and increased patient expectations. This has resulted in greater demands on staff. Examples of increasing demands are:-
Page 4 of 9Public Health Response
9 September 2003
a) The resident population as a whole is ageing over time and we know that the more elderly patients (aged 65 and over) tend to consult their GPs more often (six times a year compared with an average of four visits). Those aged over 75 years account for 40-50% of all GP home visits.
b) Changes in models of care have transferred the location of much healthcare from hospital to general practice; in particular, care of older people, mental health problems and cancer patients. The number of long-stay hospital beds has not increased along with the ageing population.
c) The average stay for ordinary hospital admissions is decreasing all the time as patients are discharged sooner after surgery or heart problems. This means more GP care.
d) The last 15 years have also seen dramatic changes in the management of chronic diseases due to a large number of better medications which can be delivered in primary care (GP),
e) Clinical staff, including GPs, are under greater scrutiny with new requirements for professional accountability and standards of care such as those in National Service Frameworks. This is to improve quality of care for patients but gives rise to increased stress levels.
f) The number of items being prescribed by GPs is increasing and this takes time and requires careful thought, eg cholesterol-lowering drugs in heart disease cases. Consultants in hospitals are asking GPs to take on more and more supervision and monitoring of complex drugs that were previously supervised in hospital clinics.
g) Patient expectations are rising all the time as greater access to information about health issues arises from the thousands of websites on computer systems.
The above are examples only but illustrate what one of our local GPs described ... “There’s a phenomenon called decision density where you've got to fit so many more decisions into an individual consultation now that it is difficult to remain the listening e a r and a common response in local meetings is along the lines of “Patients expect more ... they come in with their print-out from the internet and point to some piece o f information and query why they are not on such and such a drug or programme
A big factor in this changing workload for GPs is the shift from hospital to primary care which often is aimed at making the patient happier - and rightly so - but the impact on GPs has not really been measured objectively to assess the resources needed to compensate for this shift.
Page 5 of 9Public Health Response
9 September 2003
We have referred to some of the reasons for a more complex and busy day-time workload for GPs because these lead to the need to address the out-of-hours work. No reasonable employer or society can expect these professional people to work in an increasingly complex environment without looking for areas and ways of reducing the demands placed upon them. In all surveys and reviews we have looked at in the literature the common complaint from GPs has been the out-of-hours responsibility.
This was evident locally before and during the contract negotiations. We were given compelling evidence of the risk to our primary care services of not changing the previous “on call” system, namely early retirements and resignations.
Over 80% of the UK population is now covered by out-of-hours services which are very similar to our own MEDS and by December 2004 all the UK will have such a system in place in terms of the new UK GP Contract agreed and signed off in July 2003. As an Island community and Health Service we would be naive in the extreme to think that we could continue to attract GPs from the UK to the Isle of Man if the old system is continued. In a survey carried out by the Audit Commission (UK) in 2002 the “number one” burden on GPs was identified as night calls. It was clear to us at the negotiations that a similar situation existed on the Island and this was evidenced by the fact that the out-of-hours problem was one of the first items on the agenda of all meetings locally until the matter was resolved by agreeing to develop MEDS.
All sectors of the health community are insisting on a better balance between work, family life and social living. The increasingly complex daytime work (see above) of GPs makes it essential that a system is found to alleviate this workload and stressful environment and we believe the new model significantly addresses this issue. We have received evidence of increased morale among GPs since April 2003 due to MEDS. In the words of one of our GP representatives -“Night calls are a more important issue than pay rises”.
Recruiting and retaining our GPs will be at the heart of any successful delivery of service on the Island and in the opinion of the Public Health Directorate this will be extremely difficult - probably impossible - to do if our out-of-hours service is not at least as family-friendly as the model in the UK.
3. The DHSS
Throughout the process of agreeing upon the new model for the Isle of Man all parties to the negotiations looked to other working models in the UK and beyond, as well as drawing upon the experience of MannDoc locally. A review of the literature on out-of-hours care reveals that the vast majority of health services have developed or are progressing towards a model similar to MEDS. By December 2004 it is anticipated that the whole of England, Wales and Scotland will have such a system. Denmark and Germany have similar systems as do Australia, New Zealand and North American States. At present over 70% of the UK population (in excess of 40 million people) are served by a similar model.
Page 6 of 9Public Health Response
9 September .2003
The DHSS had to devise a system that would satisfy the high expectations of all of the Island community and the <aP expectations of a better life - work balance. The service has to be affordable but robust and deliverable bearing in mind recruitment and retention issues faced locally. The out-of-hours service in Primary Care should support, not detract from, the day-time service. We believe the new model is an early phase of what will become a system already in place in many other countries world-wide. We have thus witnessed the start of a “single point of access” to the DHSS out-of-hours (other than the “999” service).
MEDS will be uniform to all Island inhabitants, and the structure allows easy monitoring, control and change where necessary. We no longer have individual practices or small groups of practices offering different types of advice and service levels. If any person on the Island phones MEDS they will now be offered the same advice whether they live in Jurby or Port Erin or Douglas. This has obvious benefits in terms of quality control and clinical risk management for both DHSS management and the GP professional body. Uniform standardised training can thus be offered to all of our GP group. Another potential benefit is that data information about the service and types of call to it can be more easily collected for analysis as it will be available at a single source instead of the previous multiple sources. Complaints or problems will also become easier to manage as a result of this single access.
World-wide it is acknowledged that, to-date, the evaluation o f and research around the various out-of-hours services (including MannDoc) has been patchy and of poor quality. By introducing MEDS which is similar to most other models we can now benefit from any future research or evaluation done in other nations. This should benefit patients, GPs and DHSS Service Managers alike.
DHSS has a responsibility to deliver a high-quality service to the Island residents using public funds in the most cost-effective manner. This principle will be facilitated by creating a single access telephone service for the whole Island. In time, as experience in other areas confirms, we may well be able to utilise the considerable skills of specialist trained nurse practitioners to receive telephone calls, do triage for GPs and in certain cases be the person who visits patients. Studies carried out in England and the USA indicate that nurse specialists can perform on an equal footing or better to telephone consultations and certain treatment scenarios. The UK is rolling out the model of NHS Direct based on the findings of audit and research carried out over the last 4 years. By 2005 it is expected that this nurse-led service will be the first point of call to all NHS services (except “999” calls) in England, Scotland and Wales. The system established by MEDS will allow for this development once a decision to proceed on this route is taken at a senior management and political level.
There has been comment locally about a centralised service based in Douglas struggling to provide a quality service to Ramsey or Castletown areas. We have looked at the co-operative system in the UK and note that in many areas the same model (1 GP/1 Secretary with a back-up GP on call) services areas which are up to 10 times larger in area with up to 5 times the population size of the Island. As mentioned earlier in this commentary, when we review the calls made to MEDS since April, we note that the vast majority (85%-90%) of calls are dealt with
Page 7 of 9Public Health Response
9 September 2003
telephonically without need for a house visit. If the GP taking the call diagnoses a case of concern or genuine emergency, she/he will advise calling an Ambulance. MEDS has not detracted from the Isle of Man Ambulance Service which continues to deliver emergency care throughout the Isle of Man. It should be noted that extra paramedic and ambulance support has been posted in the North and South in case of need in an urgent or serious case.
From a Public Health perspective we are thus satisfied that the new service is well able to cope with whole-Island coverage (based on years of experience elsewhere); we believe that the new model permits a more appropriate use of health resource skills, and firmly believe that as a result of single-point access, better management control and audit can be achieved than was the case with the previous piece-meal system. There is no evidence from the literature that such a model impacts negatively on either the ambulance service or Hospital A&E Unit provided the public is aware o f the capabilities of each type of service.
Changes that may be desirable in the future - recommendations
Recommendation 1
We would support the plan to recruit one or two salaried GPs who would be employed by the DHSS to specifically work for MEDS. This would ease the pressures involved in searching for local GPs to be available on a rostered basis. Experience internationally, however, indicates that such work (full-time out-of-hours work) is only done by GPs nearing retirement or seeking a steady income for a short period. No GPs would make a career of this type of work due to the antisocial hours and the obvious lack of clinical challenges.
Recommendation 2
We would recommend that the Island moves towards a single telephonic access point answered by specialist-trained nurse practitioners and supervised by GPs, as is the case with NHS Direct (UK). We would suggest that if it is possible to link directly into the NHS Direct system then this should be actively explored. Advantages of using, a system that has been piloted, evaluated and audited over creating our own local system should be obvious in terms of risk management, quality control and recruiting of nurses.
Recommendation 3
Early evaluation of demand on MEDS should indicate the necessary adequate support personnel and resources required. This may or may not be adequate at present.
Recommendation 4
An exchange of data between MEDS, GP surgeries and other relevant DHSS care providers should be established as the Island considers its information
Page 8 of9Public Health Response
9 September 2003
needs. In the interim, all out-of-hours consultations to MEDS should be reported to the relevant GP by 9 am on the next normal working day.
Recommendation 5
MEDS should be delivered to standards agreed between GPs and DHSS. These standards could be the same as proposed for the UK to enable future audit and comparisons. This will mean that MEDS should be able to record:
a) the length of time taken to answer the call.b) all the communications that take place when the call is answered.c) accurate details of all clinical consultations recorded in an appropriate IT
clinical system.
Recommendation 6
Close collaboration between Ambulance/Paramedics, MEDS, minor injury units and the new Noble’s A&E Unit should be maintained and fostered.
Recommendation 7
Exploring the integration of MEDS with NHS Direct (UK) or, if this is not feasible, establishment of a similar model locally should be actively pursued. This will ease further the pressure on GPs and assist recruitment and retention. It is also a proven model for ensuring the more efficient use of valuable personnel skills at the correct level within a health service.
Conclusion
The Public Health Directorate supports the continuation and further development of MEDS for the reasons given above with the important proviso that, should it prove impossible for DHSS to staff the emergency MEDS roster, then the local GPs are held responsible in terms of their existing contractual obligations and until such time as a new Contract is implemented.
More active support should be encouraged from those politicians who are not opposed to the development. Our literature search indicates that political support for change to such a service is extremely effective.
The new service ensures equality of services to all Isle of Man residents and any fall-back to previous systems will be a retrograde step in our opinion.
Dr Paul EmersonConsultant in Public Health Medicine
FOR Dr Ian MacLeanChief Administrative Medical Officer / Director of Public Health
Page 9 of 9Public Health Response
9 September 2003
Appendix 5
Department of Health and Social SecurityRheynn Slaynt as Shickyrys Y Theay
AMBULANCE PARAMEDIC & PATIENT TRANSPORT SERVICE
Isle of M anGovernment
Rtftp flfen Vamtn
Ambulance HQ Ballakermeen Road Douglas Isle o f Man IM1 4QA
Telephone: 01624 642154Control Fax: 01624 642593Admin Fax: 01624 632711e-m ail: [email protected]
Mr Phil Lo BaoJoint Clerk to the CommitteeOffice of the Clerk of TynwaldLegislative BuildingsDouglasIsle of ManIM1 3PW
29th December 2003
Dear Mr Lo Bao
Re: Select Committee of Tynwald on GP Services
As promised please find enclosed figures that were requested by the members of the above committee in relation to work loads and performance statistics for our service.
The figures show the comparisons between April - November 2002 and the same period for 2003, again commencing in April 2003 when MEDS began operating. The forms are copies that we as a service submit to the Primary Health Care Manager who is responsible for the Ambulance Service.
The Activity report forms'show firstly the number of emergency calls we receive from each area followed by the total performance in relation to targets set.
The second part of the form is concerned with the Doctor Urgent Calls that we receive, these are calls received from GP’s around the Island usually requesting ambulance transport to one of the hospital’s, the performance target.for these calls relate to the time the Doctor wants the patient to be transported which is within 15 minutes of the time agreed 95% of the time. As you will see our performance results usually exceed the target of 95% and would be the envy of many other ambulance services that have had to sacrifice poor performance in this area to achieve their 999 call targets.
The final part of the form relates to the non-urgent patients that we transfer to and from the various treatment centres. The North, West and South relate to vehicles and not necessarily geographical areas of the Island, (for example the vehicle travelling from Ramsey may pick up patients in the Laxey or Onchan area before arriving at their destination which is usually Noble’s) but is commonly known as the North vehicle because it commences its journey from the North.
The pie charts enclosed show our performance in relation to the time taken on receipt of a call to having trained ambulance personnel at the side ill or injured person. As mentioned at the Public Committee in Ramsey, there are various performance targets and hopefully the colour coding on the pie charts together with the following explanation will aid understanding:
Areas of Red: Calls where trained staff are on scene within 8 minutes of any 999 call(a target of 75% is set for all 999 calls on the Island whereas in the UK with the exception of Staffordshire this target only applies to life threatening calls)
Areas of Blue: Calls where trained staff are on scene within 14 minutes of the 999 call.(a target of 95% is set for urban services such as London, West Midlands etc)
Areas of Green: Calls where trained staff are on scene within 19 minutes of the 999 call.(a target of 95% is set for rural services such as ours because of the geography)
Areas of Yellow: Calls where the above targets have not been met.
It is important to remember that the targets are for the whole geographical area as it would be impossible for any service to guarantee an 8 minute response in every location, especially in a rural setting like ours where sometimes it is difficult to get vehicles and equipment to those who are injured or ill in remote places that attract tourists.
As you will see from the pie charts enclosed there is slight variations in the performances in the North and East of the Island for the two years, the West of the Island still remains a problem for the 8 minute target, but as mentioned we are hoping to introduce first responders in the Peel area in conjunction with the Police which we hope, will improve the situation greatly. The main area the pie charts highlight is how the service has been improved to the population of the South of the Island since September of this year when the new Port Erin Station was opened and commissioned.
I hope the enclosed figures and charts give you the information you requested, but please feel free to contact me if either you require further information or explanations.
Yours sincerely
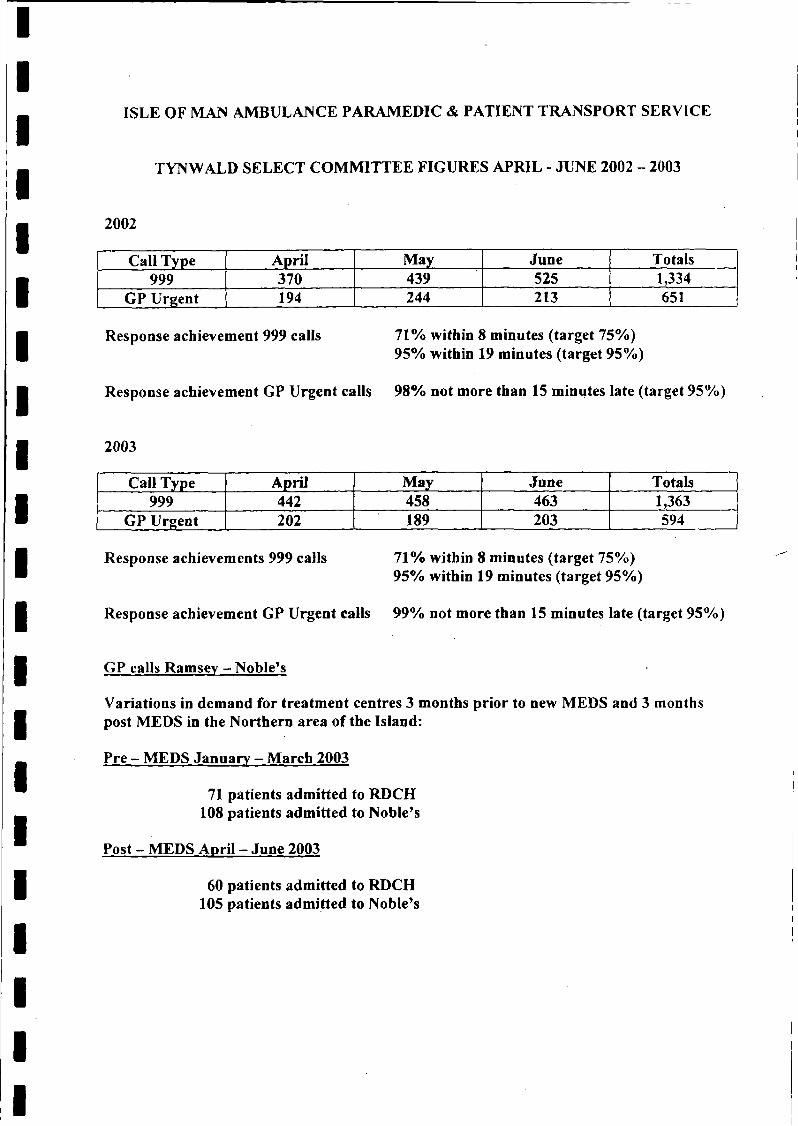
ISLE OF MAN AMBULANCE PARAMEDIC & PATIENT TRANSPORT SERVICE
TYNWALD SELECT COMMITTEE FIGURES APRIL - JUNE 2002 - 2003
2002
Call Type April May June Totals999 370 439 525 1,334
GP Urgent 194 244 213 651
Response achievement 999 calls 71% within 8 minutes (target 75%)95% within 19 minutes (target 95%)
Response achievement GP Urgent calls 98% not more than 15 minutes late (target 95%)
2003
Call Type April May June Totals999 442 458 463 1,363
GP Urgent 202 189 203 594
71% within 8 minutes (target 75%)95% within 19 minutes (target 95%)
99% not more than 15 minutes late (target 95%)
GP calls Ramsey — Noble’s
Variations in demand for treatment centres 3 months prior to new MEDS and 3 months post MEDS in the Northern area of the Island:
Pre - MEDS January - March 2003
71 patients admitted to RDCH 108 patients admitted to Noble’s
Post - MEDS April - June 2003
Response achievements 999 calls
Response achievement GP Urgent calls
60 patients admitted to RDCH 105 patients admitted to Noble’s
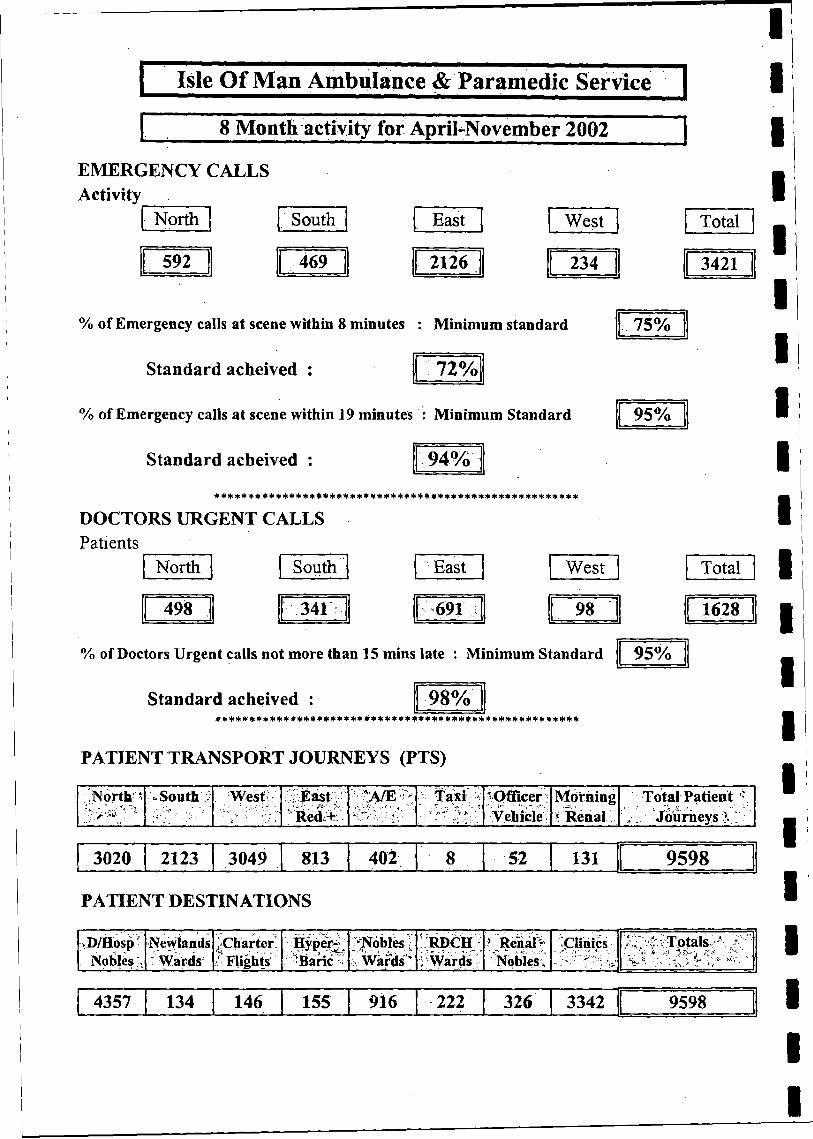
I Isle Of Man Ambulance & Paramedic Service
8 Month activity for April-November 2002
EMERGENCY CALLS Activity
North . South East West
592 469 2126 234
Total
3421 1
% of Emergency calls at scene within 8 minutes : Minimum standard
Standard acheived :
75%
72%
% of Emergency calls at scene within 19 minutes : Minimum Standard
Standard acheived :
95%
94%* * * * *** * ** * *** *** * ***** ******** * * * * ♦ ** * * ********** ** *
DOCTORS URGENT CALLS Patients
North South East
498 341 691
West Total]
98 1628
% of Doctors Urgent calls not more than 15 mins late : Minimum Standard 95%
Standard acheived : 98%* * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * *
PATIENT TRANSPORT JOURNEYS (PTS)
North * * South i . West " X Ë a st;/ ';.:"A/Ev> ta x i h ^Officer Morning Total Patient ** kedi+-’■
./••• r‘ .4, , '■ >’-»* v> Vehicle * Renal ' Journeys X
3020 2123 3049 813 402 y 8 52 131 9598
PATIENT DESTINATIONS
.D/Hosp Newlands ¿C h arte r Hyper- ‘ Nobles \ RDCH 5 Renài v Clinics í T o ta ls 1 • "•Nobles-. f W ards Í Flights Baric "•’ : W ards ' i W ards Nobles \
4357 134 146 155 916 222 326 3342 9598
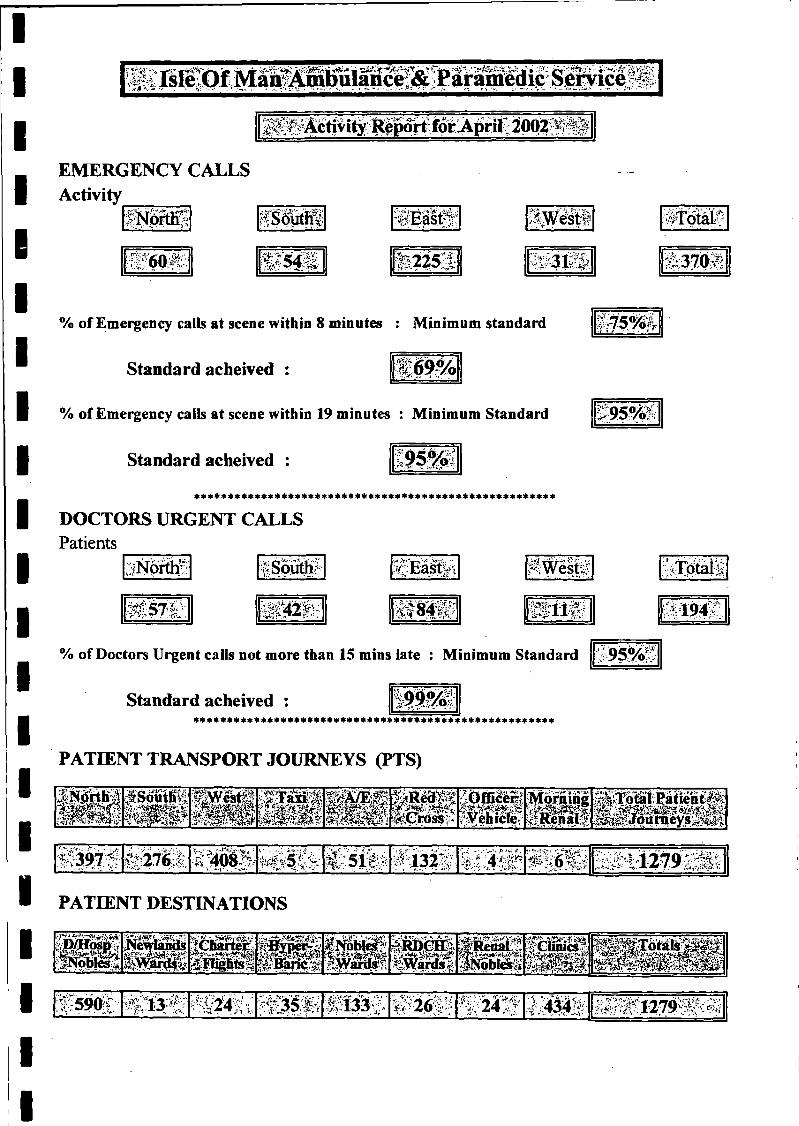
-s- «wÆSf j ¿S¿V^ïv'f>•■ -n A yrirni IflTIC^P ~‘ ^ ^ A « « n ^ >
 < ^ i t y ; ^ 2002
EMERGENCY CALLS Activity
*’l\|o r th ’
QyA.-'
ISSfitffi
® S $ Ä H ?2 5 :S " V 3 'f i ï
% of Emergency calls at scene within 8 minutes : Minimum standard
Standard acheived : ¡fgoy-
% of Emergency calls at scene within 19 minutes : Minimum Standard
Standard acheived :
>v
* * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * *
DOCTORS URGENT CALLS Patients
Ä §
I'TSiV*.-«u ■.
ISowtlK :*cEasty^
i^ 4 Ï W•iO r - ,3-, viSfi-f-i 5*: 1 9 4
% of Doctors Urgent calls not more than 15 mins late : Minimum Standard 95%!
Standard acheived :* * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * *
PATIENT TRANSPORT JOURNEYS (PTS)
f i i s s #^ F ä Ä i ¡ S p « W tèM S ïi
i e t ì ! *pfficëiïÜ Ü
,Tl Xfi'A T'V' ♦.¿fl'rMorning^R en aît
_;ÂTotalvÇâtient>M
:i W s $ ft:276-; Ì Ì 5 1 7 •> 132 - 4 ® > 4 t i 2 7 9 k ;ïi;
PATIENT DESTINATIONS
*-ppTosji\yW 0 m
NewlandsI s a r d s #
Seiwrï^tm f f î w m
f Â É fiw & Ê I.
z Nf. :< X_ÎTviftJRDÇHS;« g H
Ü elSKìÌÌióbIoiS
|fC MÇS |
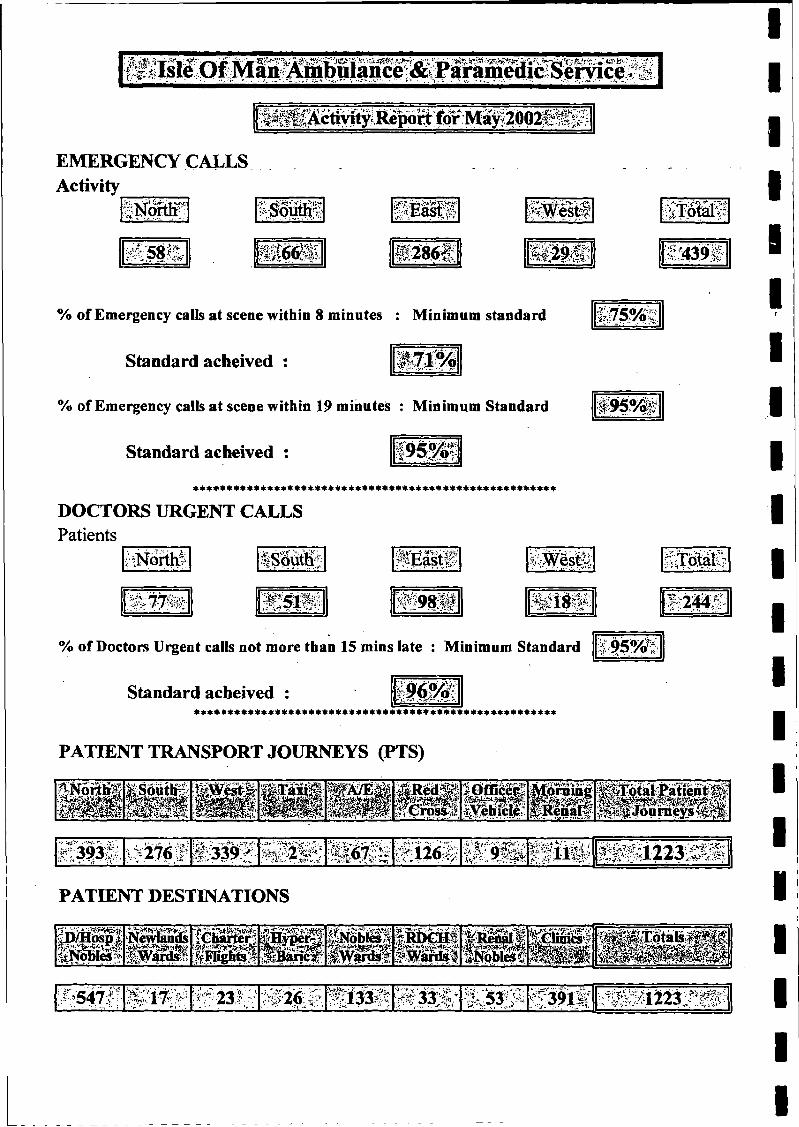
A*— A ’“k”iÄ— "Paramedic Service i
EMERGENCY CALLS Activity
¿NaM ? •>- ^.srLàst^
$ & g & S S f i Ä l M
% of Emergency calls at scene within 8 minutes : Minimum standard
Standard acheived : m S M
% of Emergency calls at scene within 19 minutes : Minimum Standard
Standard acheived :
® 9 5 ^
******************************************************
DOCTORS URGENT CALLS Patients
; {North? ¿y
IWt- S S 9 8 *
% of Doctors Urgent calls not more than 15 mins late : Minimum Standard
Standard acheived :******************************************************
PATIENT TRANSPORT JOURNEYS (PTS)
| j | | j | | | 9$ÊÊfiW M ¡Morning^Renaïtî8 ^ 8 N S @ ® I■
f^ 3 'S 2f339^.;ji. >■ 04Yifc$j ;■/■ j2 , 1Ï26Â s c i i
i/* ; - -* ‘ ' « •iÜ ; i i2 3 S I |
PATIENT DESTINATIONS
MßBNewitamls■feiuriri
Fl'igiW?ÊÉyêÊÈäNobliä! |10GBÌf-#anb-| rfptilcsC
CÜBic, M p E & S j
Wtäiir '-&26:'e ^ » •5 - ^ i t l c i-^K l223:^^
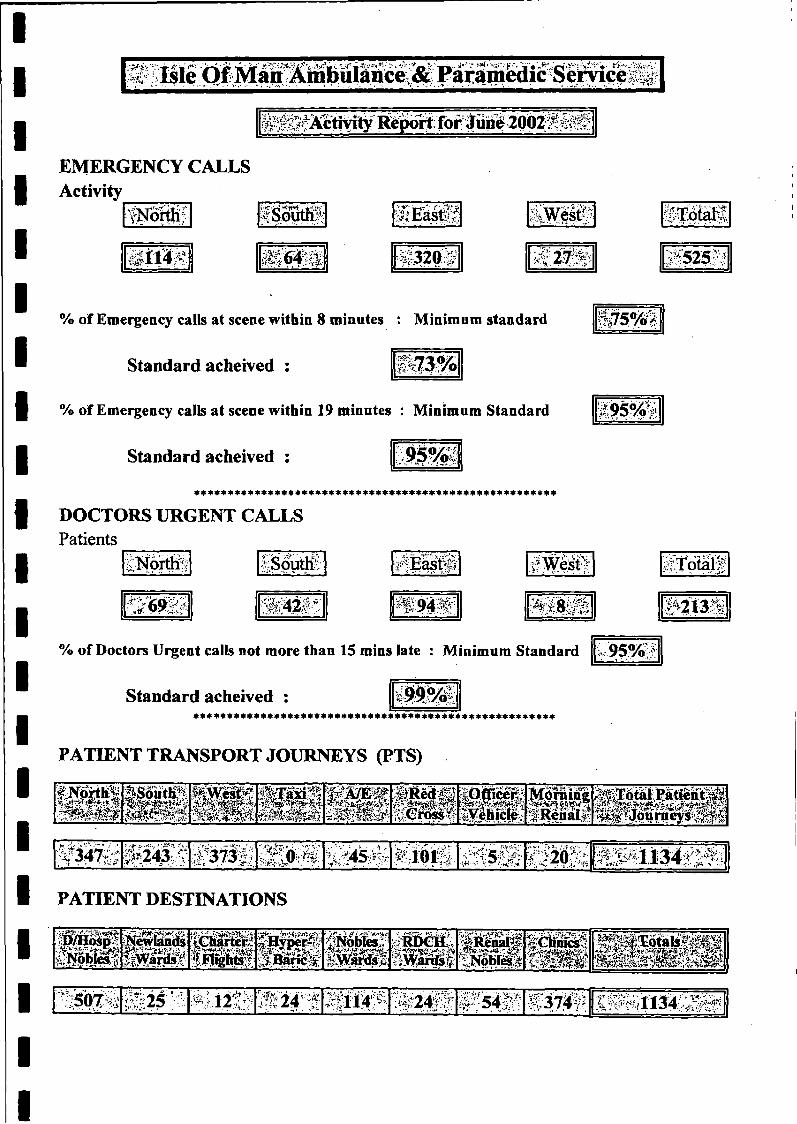
~pT -fü*'-AÆ ■■:-*? V -;•*-*£■;?A.V - ‘»<V.:;..:, J.-.'-:, jV„*' --------------
EMERGENCY CALLS Activity
tN oittif ;.-:a
$&■-
il^"6 3 2 m v • 27:';*v-
% of Emergency calls at scene within 8 minutes : Minimum standard
Standard acheived : •2*1
% of Emergency calls at scene within 19 minutes : Minimum Standard
Standard acheived :
* * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * *
DOCTORS URGENT CALLS Patients
Norths vSoutKi
;6 9 - » S i ? ®
% of Doctors Urgent calls not more than 15 mins late : Minimum Standard
Standard acheived : 1 9 9 % ’:******************************************************
PATIENT TRANSPORT JOURNEYS (PTS)
AV.
3 2 5 S
m im
S f S f B § 8 H tP ^ P h k m u a ®jH
I^Êictè,:MoraineS R filf A M I
'
l # P § É 2 4 & Î :#3Î7Ïlï / T,51V;, . . * -• 1. • k .f ë i ô t î l
•,«V» ’»•¡►.Ay *■>>’*C ï2 0 ^
PATIENT DESTINATIONS
ÂÉÉilpt¿.^obles,^
Newiäidsä w i ü
'iChàrterilflighte*r
:*%vne^t e p i l s ¿NpbiwiJ
.Iwâfdsï¿TffiêaS'âWards ;filili t p y SBMSSI
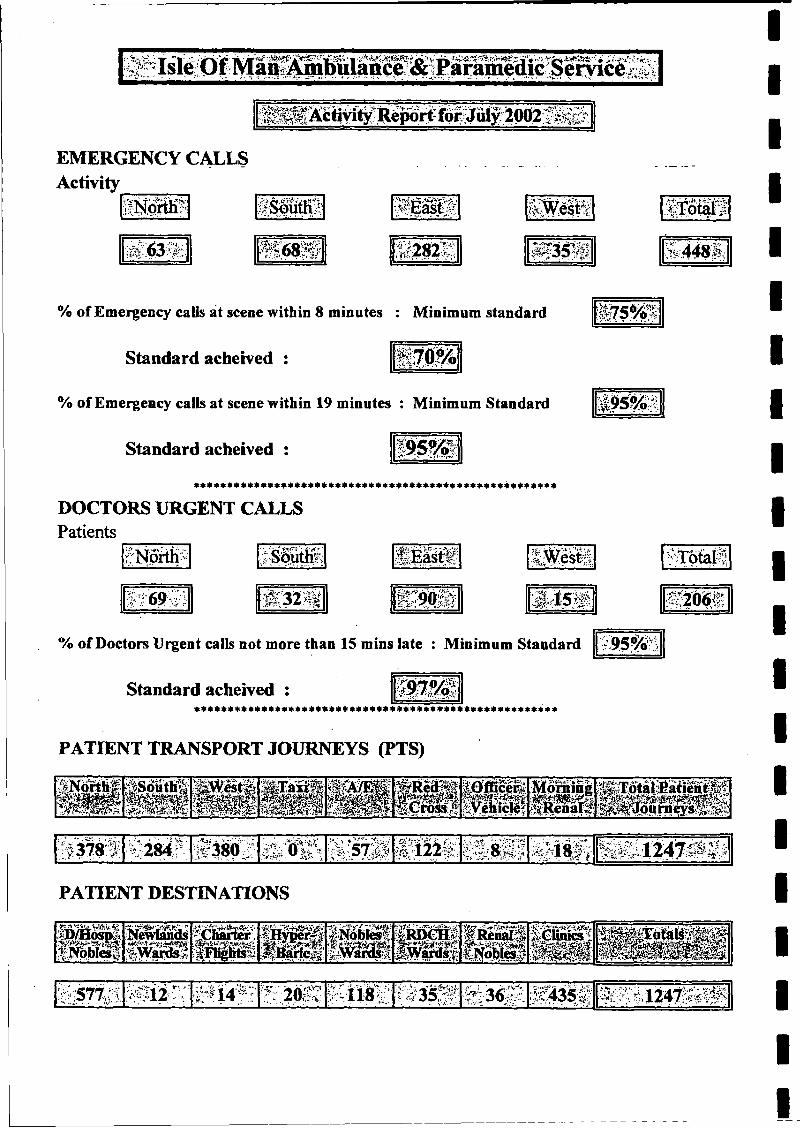
f t l ^ Activity- foporf
EMERGENCY CALLS Activity_______
«
« 282 5 © 3 5 Ä^ . • av1 4 48
% of Emergency calls at scene within 8 minutes : Minimum standard
Standard acheived
% of Emergency calls at scene within 19 minutes : Minimum Standard
Standard acheived :
* * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * *
DOCTORS URGENT CALLSPatients
SôîitKr
IT# /■ : r> ;2 0 6 «
% of Doctors Urgent calls not more than 15 mins late : Minimum Standard
Standard acheived : w M* * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * *
PATIENT TRANSPORT JOURNEYS (PTS)
9 5 %
;âSoÿtlt^' I $ P * 1 S iT a M i iM?»*m
|,öfßceife e
MorningM iP j j f e u n jiÓ ^ i y
I Î 3 7 8 Ï"V * ' ‘ * ? %\ •’
;%,284f:- ¿i C-' U' ' r '* • ^ 5 7 ^ .•122" :, £ k-Af. ■ LLvÌ?Ìf-'iSÄ f f l Ä J 2 4 7 I S #
PATIENT DESTINATIONS
^ 1 4 * 1 K i i s E :® M Ü 2.. - M 2 4 7 ; Ä ^
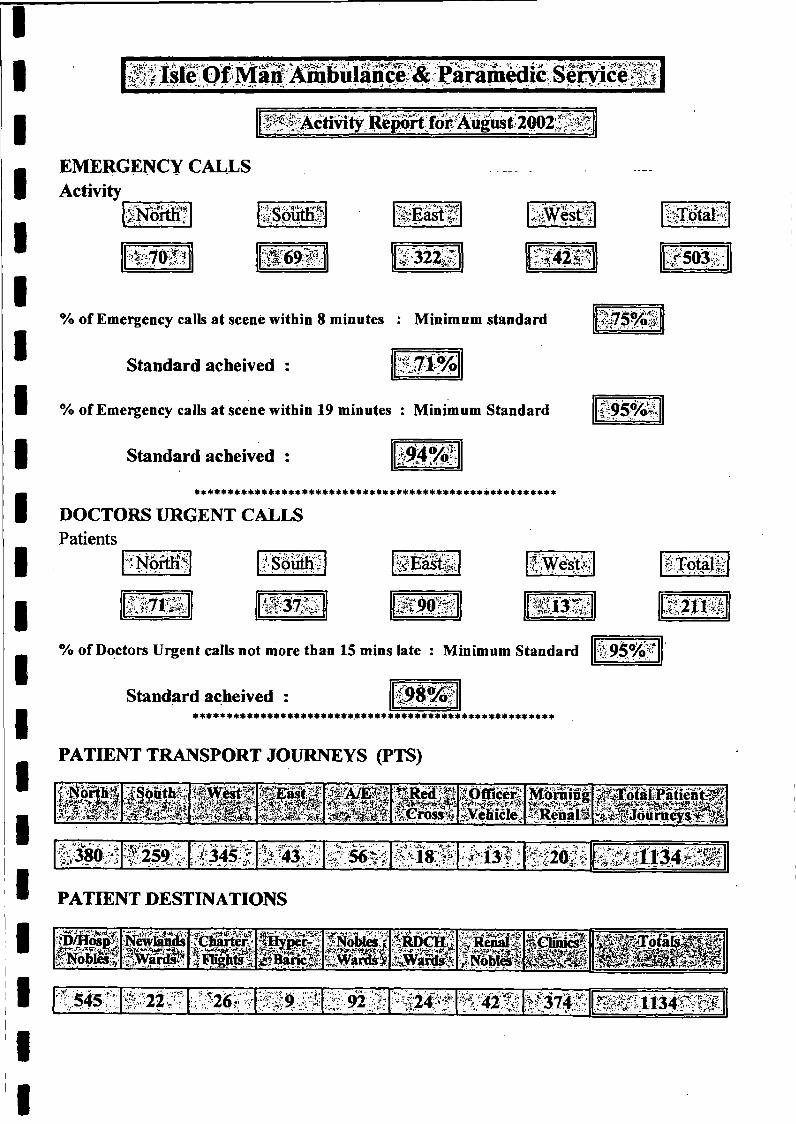
S I Ä
EMERGENCY CALLS Activity
!p£ im ÿffesfef
•Wfiû^SL Ì Ì 4 W #503
% of Emergency calls at scene within 8 minutes : Minimum standard
Standard acheived :
I M I
% of Emergency calls at scene within 19 minutes : Minimum Standard
Standard acheived :
* * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * *
DOCTORS URGENT CALLS Patients
l'N ortlil /Sôüth; ï iÉ a s t i
^v?*A’W1 ;^ ÎS 3 S ÿ § 1 9 ® ?
■¿V/'TJ I
% of Doctors Urgent calls not more than 15 mins late : Minimum Standard ¿ 9 5 % *
Standard acheived : vo:'* * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * *
1 5 2 «
PATIENT TRANSPORT JOURNEYS (PTS)
GrossoMi
f K&flgföVchicie
morning^RenalS
iT oialPatieù■. V V.V' iLX . rt W-t+üM -Ài :
I Ä f 259;-:A ..‘ - >'-C •v- ' • v
,-;•••?-•' -iv Ay‘ ' -**y- - •
•^13?; H m©
PATIENT DESTINATIONS
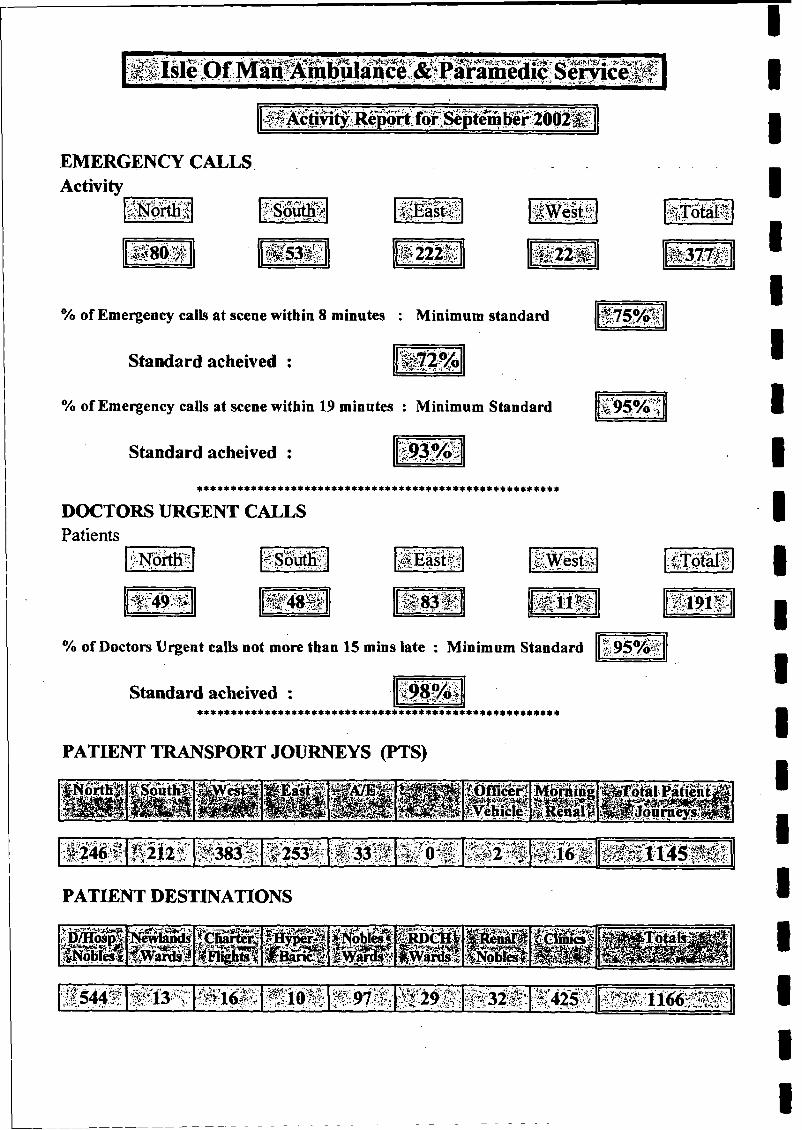
# f Activity Report forSeptem fóèr2002ti
EMERGENCY CALLS Activity
SNörtH! M E äsiS
Ä H 1 2 2 ® ; « i m A M m
% of Emergency calls at sceae within 8 minutes : Minimum standard
Standard acheived : w* *$£/ A /O
% of Emergency calls at scene within 19 minutes : Minimum Standard
Standard acheived :
I * * * * * * * * * : * : * * * * * * * * * : * * * * * : * * * * * * * * * * * * * : * * * : * * * * * : * * : : * « * * * : * *
DOCTORS URGENT CALLSPatients
Msft)rth -
1 f t (9 #
1 175?®
PI .£ $TÌ 7 0 ^ , /&*
g ® s Ä i p i f i
■r,
W 0 Ê
% of Doctors Urgent calls not more than 15 mins late : Minimum Standard im
Standard acheived : äs******************************************************
PATIENT TRANSPORT JOURNEYS (PTS)
fiËlii’WÊÊÊΡ¡¡¡SSWM9 H;|ÔfïÎceri<:Hot
■m ‘ir ? tìi.'"lì ''tZWrir-MorningîtsittliiÄ f o t a i P a tie n t^ Jou raeysf$ilf
:ll&f  212Ç . 0 2 5 3 ì f j : >v&> 8PI§i. Vt-r-'—'-'j--.y.-'-
_V-i J l JL. “ ‘i \
PATIENT DESTINATIONS
miê p n d sÜ 3 3 $
Ü ÜÌ P g h ^ ’p i l i
U * m,4rdchÎi S ft
ßSf
cSIl ^ lirn g -
':?|544ÿ: # l ^ v ‘•¿?s- < " r_ i'j-_ v
'••i ’ vW & M i W & Ê - K4$ê $.
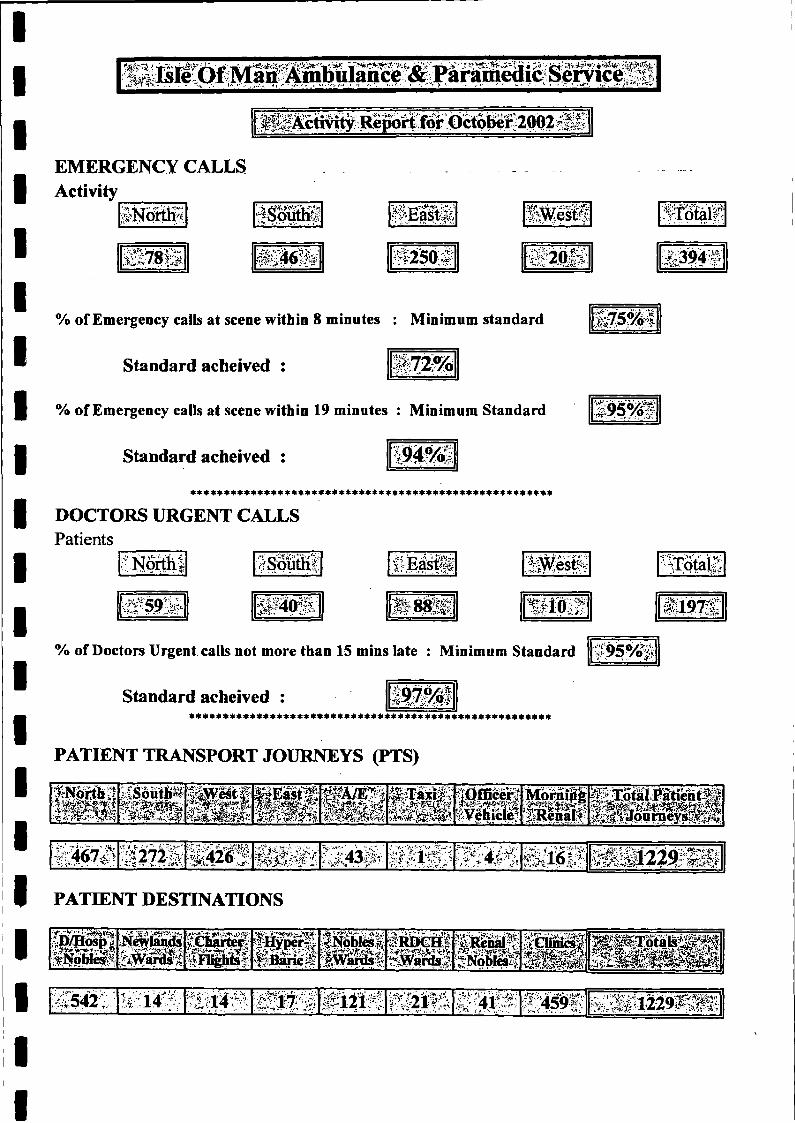
EMERGENCY CALLS Activity______
,;h>Tin©'C t
$S<jiiuh^
IO
l E a a f f
250 Í P 2 0 Í Í
% of Emergency calls at scene within 8 minutes : Minimum standard
Standard acheived :
% of Emergency calls at scene within 19 minutes : Minimum Standard
Standard acheived :
DOCTORS URGENT CALLSPatients
* * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * *
•'"North!
5 ^ ISWTS
% of Doctors Urgent calls not more than 15 mins late : Minimum Standard
Standard acheived :*********************************************
PATIENT TRANSPORT JOURNEYS (PTS)
95%O S
ÿNirth i S o ü t »
* fS S È
(Qffièër Mbrnípg¿íRenaR
v; '¡im tt lilfi ÎÏ4Â ’f1.--1* ■ - ■ ~C^ ' tíílll Ü Ü I
PATIENT DESTINATIONS
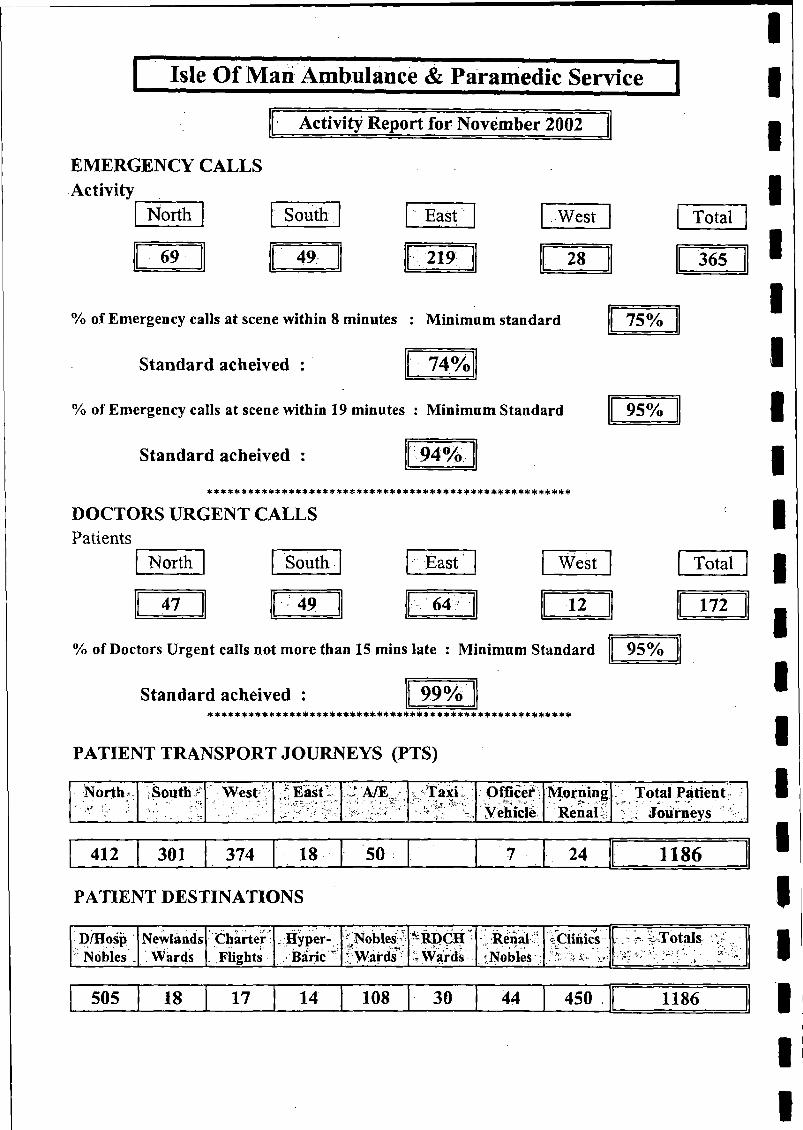
[ Isle Of Mari Ambulance & Paramedic Service |
Activity Report for November 2002
EMERGENCY CALLS Activity
North South East West
69 49 219 28
% of Emergeacy calls at scene within 8 minutes : Minimum standard
Standard acheived : 74%
% of Emergency calls at scene within 19 minutes : Minimum Standard
Standard acheived : 94%
DOCTORS URGENT CALLSPatients
North South East West
47 49 64 12
% of Doctors Urgent calls not more than 15 mins late : Minimum Standard
Standard acheived :*****!(:3»******* + *%***********#** + **#* + * + *+H(t****I)«**#* ***
PATIENT TRANSPORT JOURNEYS (PTS)
Total
365 [
75%
95%
Total
172
95%
North' South - West:V ,f: East a /e . Taxi Officer Morning ;V Total PatientK' ■ ■. ■ - ' ' •'* ' .It .T,; _vÿ/u « , '■i A Vehicle Renali :'U Journeys
412 301 374 18 50 24 1186
PATIENT DESTINATIONS
D/Hosp Nobles _
NewlandsWards
Charter . Flights
•Hyper- Baric '*
Nobles - Wardst
’ RDÇH •T Wards
. Reniai f : Nobles :
;r* • V • •¿Clinics > ¿ Totals .
505 18 17 14 108 30 44 450 1186
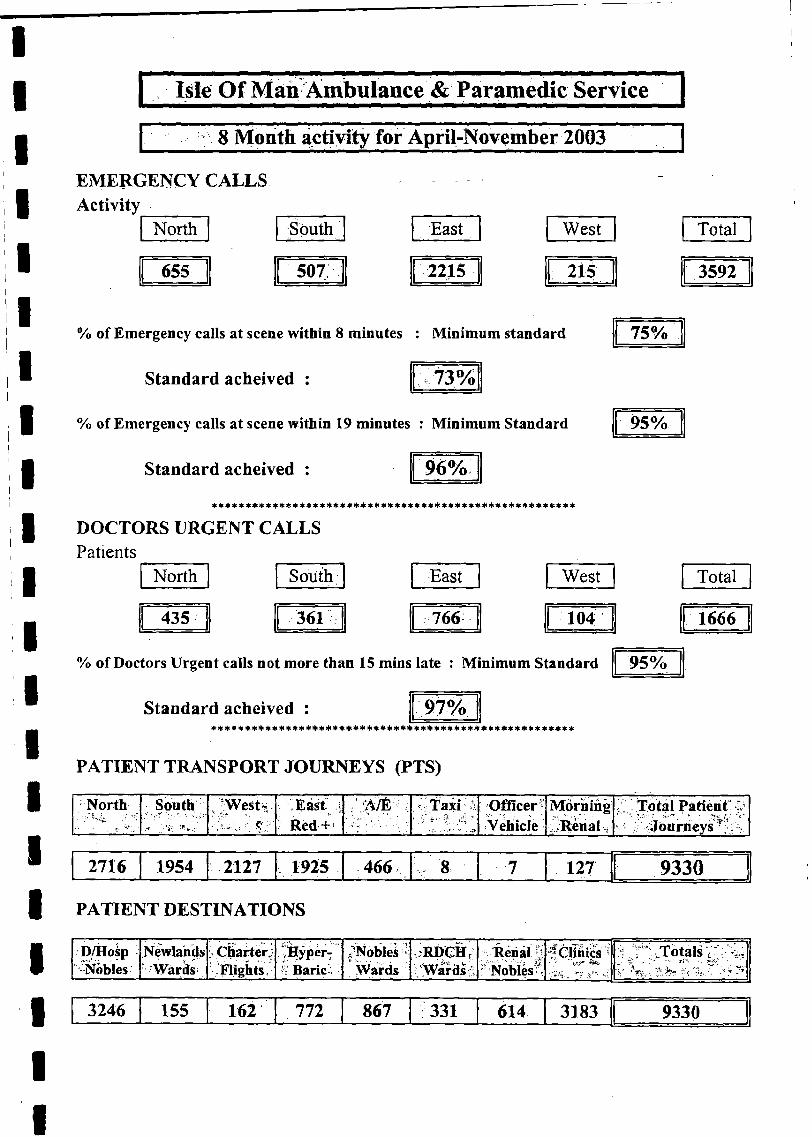
Isle Of Man Ambulance & Paramedic Service
8 Month activity for April-November 2003
EMERGENCY CALLS Activity
North South East West Total
655 507; 2215 215 3592
% of Emergency calls at scene within 8 minutes : Minimum standard
Standard acheived :
75%
73%
% of Emergency calls at scene within 19 minutes : Minimum Standard
Standard acheived :
95%
96%* * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * *
DOCTORS URGENT CALLS Patients
North South East West Total
435 361 766 104 1666
% of Doctors Urgent calls not more than 15 mins late : Minimum Standard 95%
Standard acheived :* * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * *
PATIENT TRANSPORT JOURNEYS (PTS)
North South , -West* . ■ East - ' À/É Taxi 1 Officer" Morning j " Tòtàl Patient' ^v •.*» ■■■.W' Î:: Red + '■&' -V • Vehicle Renal ^/Journeys
2716 1954 2127 1925 466 8 7 127 9330
PATIENT DESTINATIONS
D/Hosp Newlahds Charter,; ¡RÿPer:K Baric-;
<Nobleà * :RDCH? Renal ! .OlTÄics ' :f J -^ T o ta ls•Nobles Wards Flights Wards /Wards ' Noblest ---
3246 155 162 772 867 331 614 3183 9330
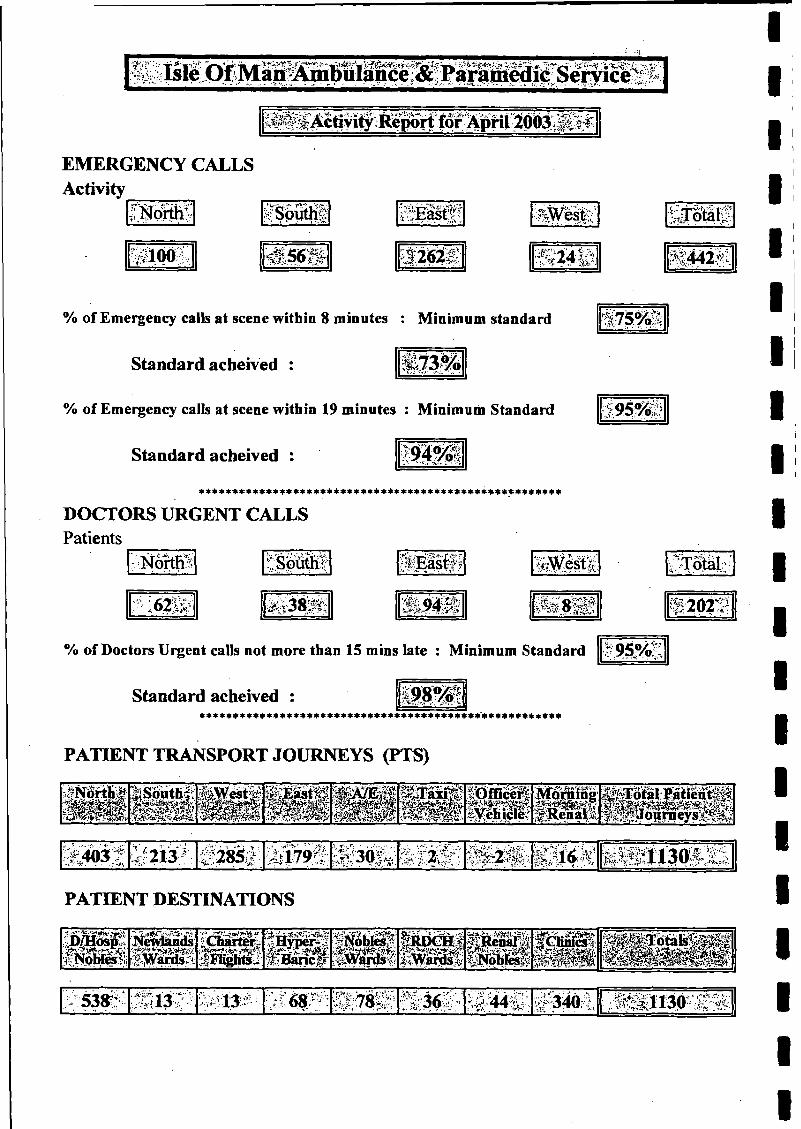
EMERGENCY CALLS Activity_______
Ÿ-'î'North
100 56^ '12621
% of Emergency calk at scene within 8 minutes : Minimum standard
Standard acheived :
% of Emergency calls at scene within 19 minutes : Minimum Standard ■J:.
Standard acheived : $ ■m
* * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * *
DOCTORS URGENT CALLSPatients
Norths Solitili » É S s t f l W M i-
’#Ér.Q#&b m m om s 202:5
% of Doctors Urgent calls not more than 15 mins late : Minimum Standard
Standard acheived* * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * *
95%!'
PATIENT TRANSPORT JOURNEYS (PTS)
Isäuthli: lÜfßcerf^Vehicle*
MorningSüll
^ 2 1 3 ^ ’; W 7 9 i £ I ? 3 # i:-V*. a •'• y "■ j-vjy .\ Sv •; 1 § 2 ; ;> ^ \ f r l l 3 0 ^ ; t S
PATIENT DESTINATIONS
K "538^ '0ïi$P iSÿ&tèU S £78|i Ü 3 ^ - • • V .-.J-340 \
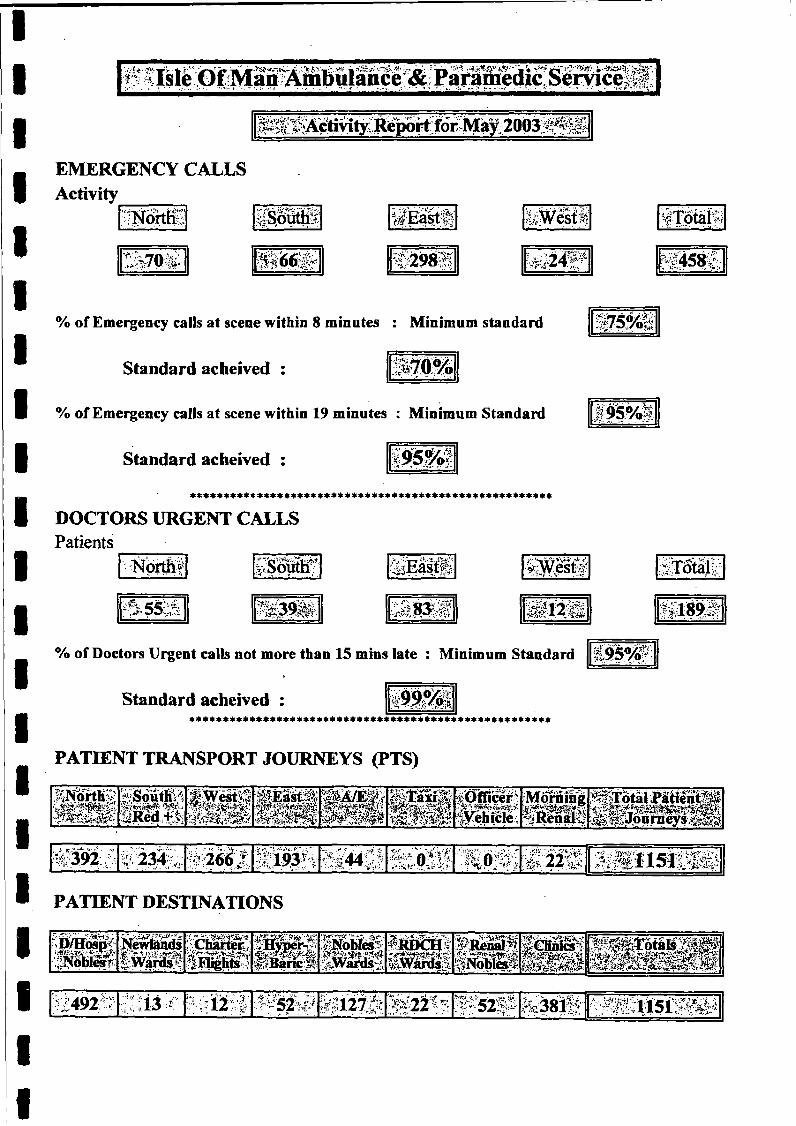
.ip*; 5.ÇÇ ^Actmiy;KeponioriYiay;ZUU<9 -T ‘
EMERGENCY CALLS Activity_______
I|§ouffii ÿEast;!' lÄesff; ÄTÖtaK
w m : t£983f S'458f:,
% of Emergency calls at scene within 8 minutes : Minimum standard
Standard acheived :
% of Emergency calls at scene within 19 minutes : Minimum Standard
Standard acheived :
* * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * *
DOCTORS URGENT CALLSPatients
North* V'Soüth? J-V t"'**
¿»•t CC': « 3 » 18ft
% of Doctors Urgent calls not more than 15 mins late : Minimum Standard $ 5 % ?
Standard acheived : %?X£/QI******************************************************
PATIENT TRANSPORT JOURNEYS (PTS)
M rtK ^ HSouthHiiiRèd
: iF .e it sIÉIÌM Ì'
S W eK8 8 S IIÌÌ
I S ^Officer-:>Yehicle;
Morning^RènalÇ
;feTo tal P atien t^ ^ § ^ o |ir n e y » ü ^
, ; *• '-*■ •* ■ •* , . 'V ^ • ' K •
" 1 9 3 h .Cf44Ç; • « ■•»-.. V ; ^ Î J i S â i s à î m
PATIENT DESTINATIONS
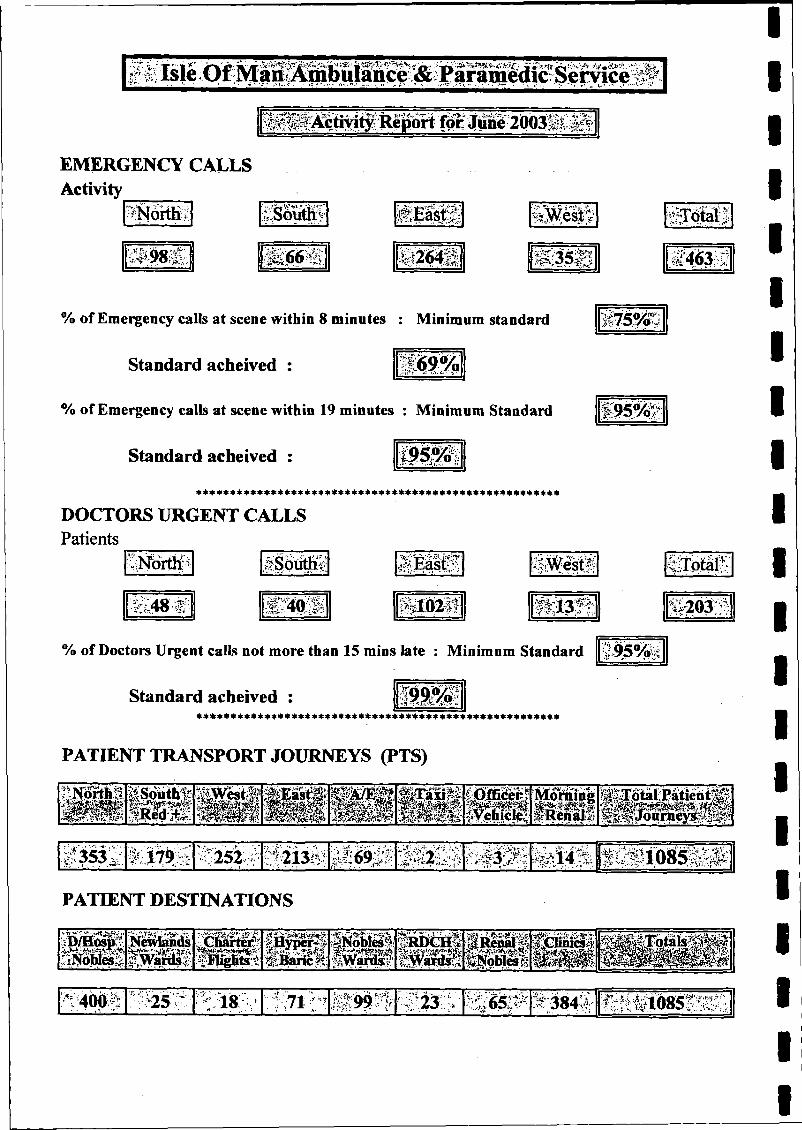
, v .*■r;. ’ V ?l'
>- .9 I ?*'’ TrTk *.¿4 ‘'■“j hinyityivepcinioc «lune
EMERGENCY CALLS Activity
?Nòith> iSoÏÏÉS' i l S i f 1
ÏS66®. %|264|| r-
1' :v
« i l
% of Emergency calls at scene within 8 minutes : Minimum standard
Standard acheived :
3$'
-m
% of Emergency calls at scene within 19 minutes : Minimum Standard
Standard acheived : i w m
* * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * *
DOCTORS URGENT CALLSPatients
Northi ÿSoiithÿ .TITT V|.'- ;'i ÏCki"
48 >i:V â i 4 0 è l â fc iifâ ¥ >;*>• 203
% of Doctors Urgent calls not more than 15 mins late : Minimum Standard 9 5 % i
Standard acheived : 'Vi*’TT -
* * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * *
PATIENT TRANSPORT JOURNEYS (PTS)
&South%?wtsitsmt1Ï8PliplpP S §PII; mng¡¡¡¡¡Siili#353§ ;f'25Ï:’Î H69§lï'1V- - t 4f2,„' ; ; 5- ¿ ¿5 '.-KT -£■*' f i l i l ö g s l l l i ;
PATIENT DESTINATIONS
së fflâ p ?, 1 el Jp a H é ii iH yper^l iSN oW «! f»SStt§ ItSenarftM B & 5\Wards-';. ■ifigìTts1 ® *iS f W M iS Ä
ÇÜiniâ§
^;40(1.5 i l t ^ l Ä ;3 8 4 ^ I S t t i O t ó S S Ì S ;
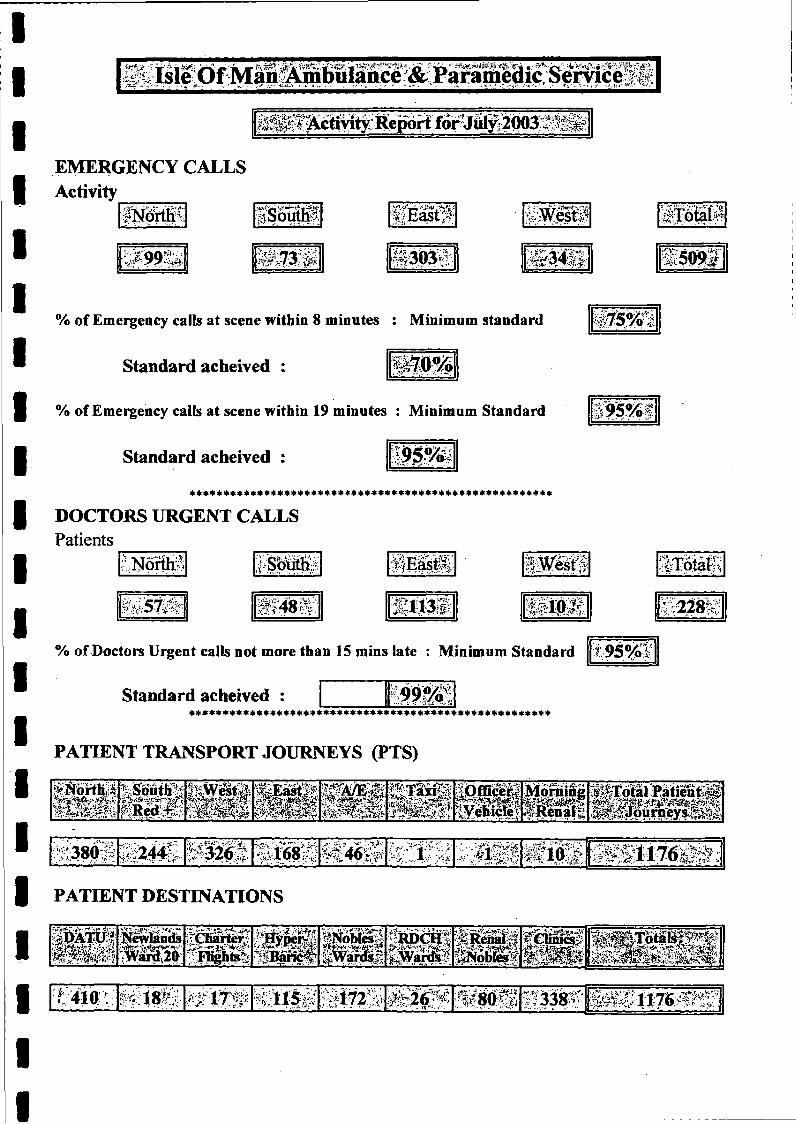
^ ¿ f c f ^ V ì f ^ , -ft*»-¿><':..» > A j/-., j - ' - y ' y J I ~~ “* 1 •• V/. I
_ _ _ - w ;Krv I<?\ yv TT. uï-':H<. V I
EMERGENCY CALLS Activity
ÿNorïm Ï S S i «•-'’ •-r— r-JH* ‘IM; ;^ fE a s t> ■IfTotaM
3 0 3 S iS O S f
% of Emergency calls at scene within 8 minutes : Minimum standard ¿75%-,:
Standard acheived : $æ7'
% of Emergency calls at scene within 19 minutes : Minimum Standard
Standard acheived
* * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * *
DOCTORS URGENT CALLSPatients
ÏM )rtte
i? 4 8 Ä . fr 228
% of Doctors Urgent calls not more than 15 mins late : Minimum Standard j,95°/o'S
Standard acheived : J S* * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * *
PATIENT TRANSPORT JOURNEYS (PTS)
l i l l l W W Èmimmm
S | p | f1®TS®8'H i t iYeKic]fé|
Morning^Renai
ÄEÄl^ilieniiäi#Jouraeys>fè§&
-ÎS24SI** W- P i ® . W M
4>- ::•'• > •-*'i ®
.Ä'.;«•$•I?,i-t.i* «.:• ¿4;*<
PATIENT DESTINATIONS
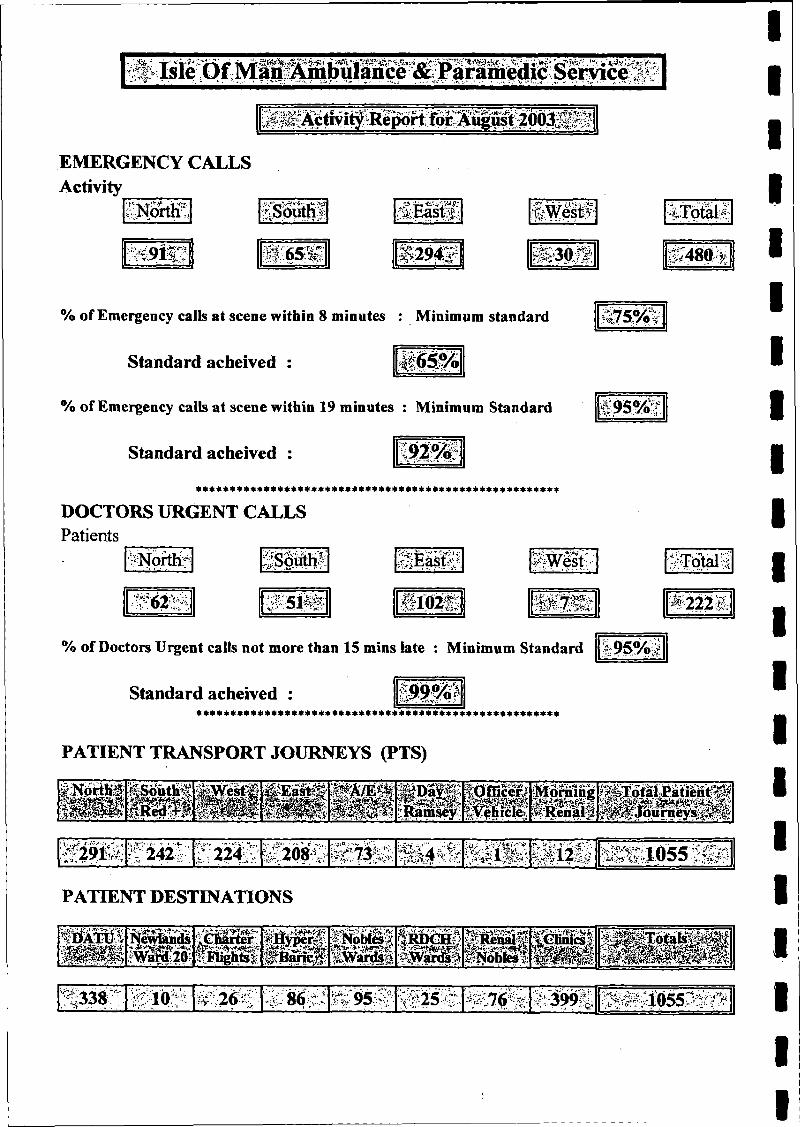
EMERGENCY CALLS Activity
South L-'SV
m m 1 Î 6 5 S :
't^Wèst?'
v ^ 3 0 ’ ■'■"V
% of Emergency calls at scene within 8 minutes : Minimum standard
Standard acheived :
% of Emergency calls at scene within 19 minutes : Minimum Standard
Standard acheived :
3a
* * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * *
DOCTORS URGENT CALLSPatients
'NortHr'-jf'J'i *# V
:5ÜS; 111 «2® i i l S l
480>
# 2 2 2 1 -
% of Doctors Urgent calls not more than 15 mins late : Minimum Standard
Standard acheived* * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * *
95%
PATIENT TRANSPORT JOURNEYS (PTS)
§.N0riB§ MSouttä ^EjastT ' Morning¡ M g
W i ? &-f -
r!-'242 l? 2 2 | iv § | ‘?3SR: i l # ® I P S : ÿ g t a 0 5 5 ‘Â
PATIENT DESTINATIONS
© P S ' ®26$' JÇ95# ÄSäfc “399%
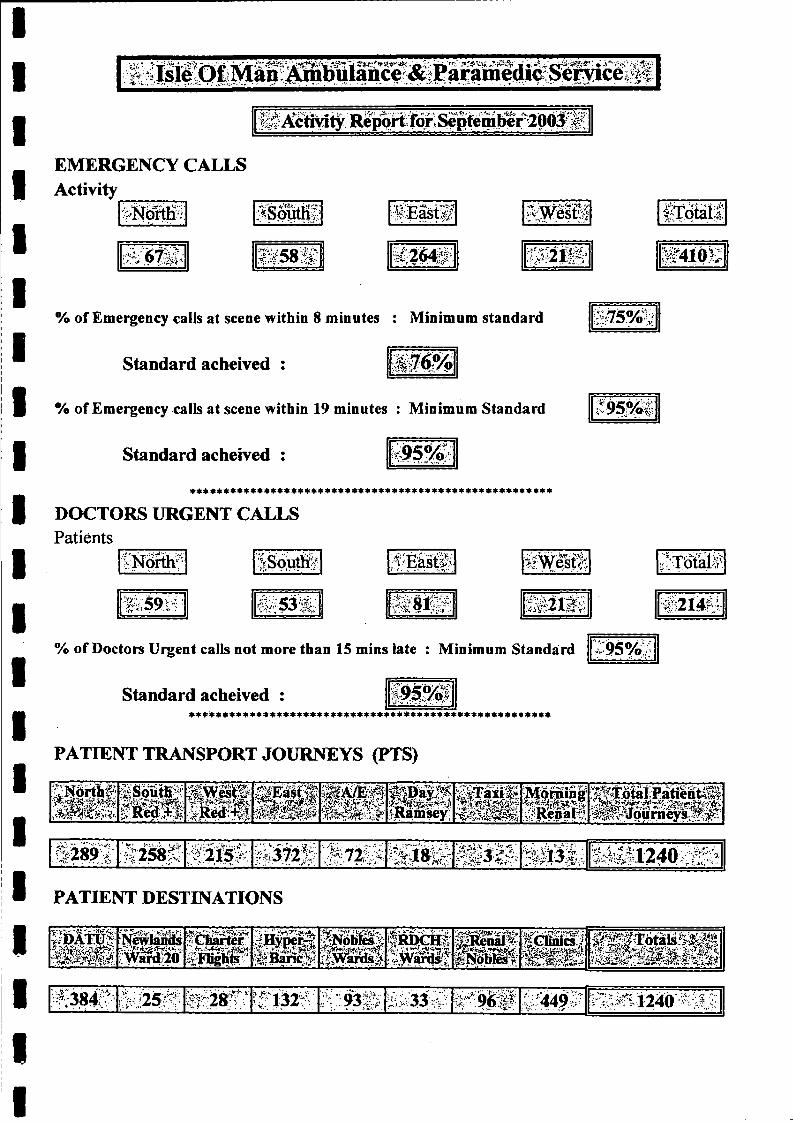
'T -p ^ ' - i 'm: • $ .♦ ■ ^ * '* ¿ 5 $ !
•17 A.Activity R e p o rt!^
EMERGENCY CALLS Activity
'Nörtffi SSoutHf 1 East!?
■W& S 1 5 8 Ä ■ }:' t? *"+*
% of Emergency calls at scene within 8 minutes : Minimum standard
Standard acheived : ' # 7 6 %
% of Emergency calls at scene within 19 minutes : Minimum Standard <V
Standard acheived :
* * * * * * * * * * * 4 * * * * * * * * * * * * * * * * * * * * * * * * * 4 * * * * * * * * * * * * * * * *
DOCTORS URGENT CALLSPatients
ÇNôrth? 7£. % >*• w es't% 'v\T^olÿ:
m r‘X ;,ir 53 <-V- Â 'S t^ Î* S§2li! ;# 2 J 4 S :
% of Doctors Urgent calls not more than 15 mins late : Minimum Standard 9 5 % :
Standard acheived :******************************************************
PATIENT TRANSPORT JOURNEYS (PTS)
3 Soutl|f§ ® »
m m m
m ffltè m Ê jS
§fMEÿ|Ramsey
' tTäxifi
l-S^ II
Iw
0.5 » M a i M t i l n ^ l lJ W W P w W i
>289;• *•• <c •>•!siZ58f- ;<:215V';. i iS f ö f g S . 7 Ì I I Ä l S p ;/sb’.\v É S iS 'ô s S é l l i 2 4 ô Â
PATIENT DESTINATIONS
p ïr ô ig !M s
Newlands «Charter:cv '
■«•wKfëS§ p s i
l iW n M -
S c S f f i
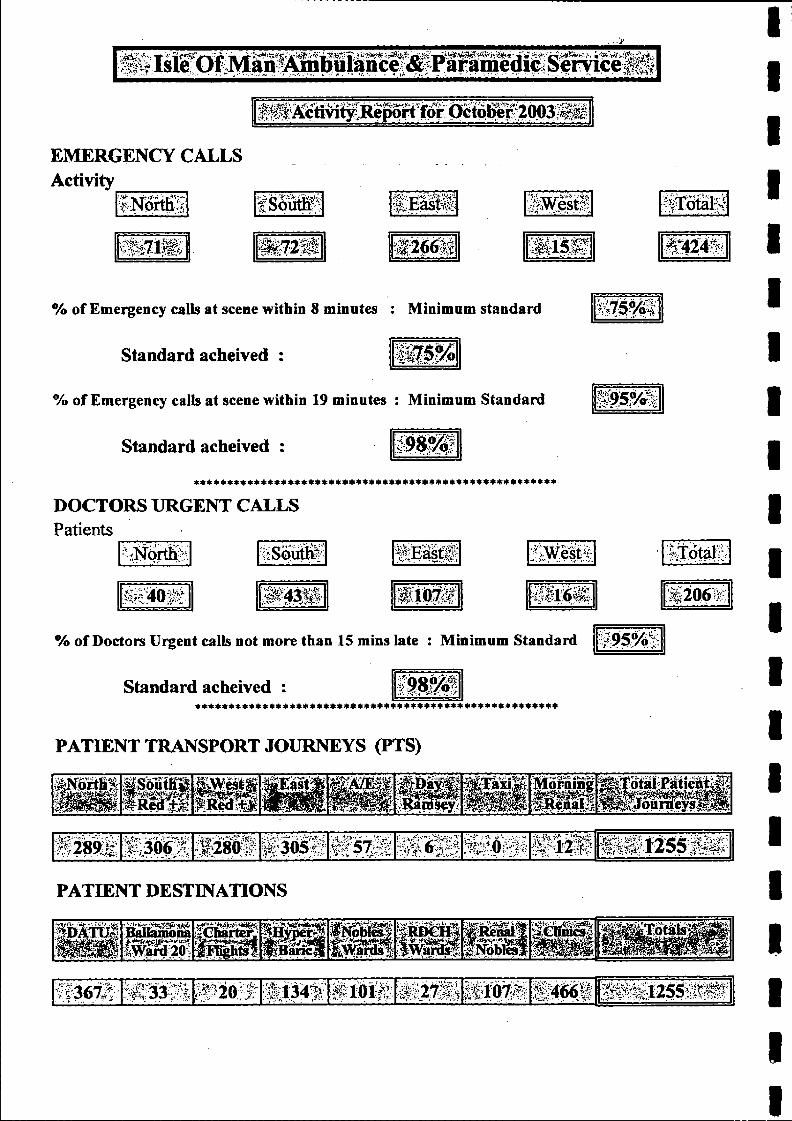
g g * iW K n f ii NlanÄmbulance^ Service
IjÀ^MfòìjlCR e p ^ 'iforì; OctóÌ>er2(K)3m i
EMERGENCY CALLS Activity______
■**■ ■> ■Yt t' -'j i^ r -
X- IScfflP ■3te Ü 1
« P f ® -?Kfer
% of Emergency calls at scene within 8 minutes : Minimum standard
Standard acheived : ■ m o m
% of Emergency calls at scene within 19 minutes : Minimum Standard
Standard acheived :
Igo-
»a****************************************************
DOCTORS URGENT CALLSPatients
^No rth^
■y&ì& "41
ISouthl- W 0 S
W^iivrMm iw m l ü l
% of Doctors Urgent calls not more than 15 mins late : Minimum Standard
Standard acheived : % ?♦♦♦♦»♦È***********************************************
PATIENT TRANSPORT JOURNEYS (PTS)
«2061
I f i if f É I H|||apat
W È Ê Ê È,'i*C W »V 'J1 Itp-. MiningSkeaaB
M W p M 1 1 3 ® ! f l lö l l t vi: 57-;;;; iV
MiP Ä’f 1 r „ 1 2 5 5 Ä F
PATIENT DESTINATIONS
BaUamonaÌ5w5:20!
fcËSiSgJTkICIIlS §
SHyperaj:fyBanc,it
j g g i S'ty ^ S a fc
ifiaëiâSäf 4»-w m m
;mjRenall.iPioblesï
¿jChnial^ p p | M Ì
W Ç Ï ïï: i C & i l M m fi- 134"/* Ï 10«/;; tf-'A h r r j Ä W is :ü s s 255ä ^

m T
'| ^ c tiv ity ;R e ^ r tfó r ;N o > ^ m b e r2 0 0 3
EMERGENCY CALLS Activity______
iN ortK r Y
S S 5 9 p •»i 51 {¿^264% I P ? » ÿ 4 0 d lÿ
% of Emergency calls at scene within 8 minutes : Minimum standard
Standard acheived :
% of Emergency calls at scene within 19 minutes : Minimum Standard $ 9 5 % $
Standard acheived :
4 4 4 4 * 4 * * * * * 4 4 4 4 * 4 * * 4 4 4 4 * 4 4 * 4 4 4 4 4 4 4 4 4 * 4 4 4 4 4 4 4 4 4 4 4 4 4 * * 4 4
DOCTORS URGENT CALLSPatients
4NoitH7 m § ë à
m m i - 202
% of Doctors Urgent calls not more than 15 mins late : Minimum Standard
Standard acheived :4 * * * * * * * * 4 4 4 4 4 4 * 4 4 * 4 * * 4 * * * * * * * 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 * 4 4 4 4 4
PATIENT TRANSPORT JOURNEYS (PTS)
r » • mJRêaÉË
H H Ä Mourning J i É » É a ï i ë n t ® ,
i m m ' g ï s s ÿ | | 7 5 # i --i-•V*-;V>Vvr'v/ ‘ v-i*? ,>
1 1 :2 8 ^ 1 * 2 3 8 * '
PATIENT DESTINATIONS
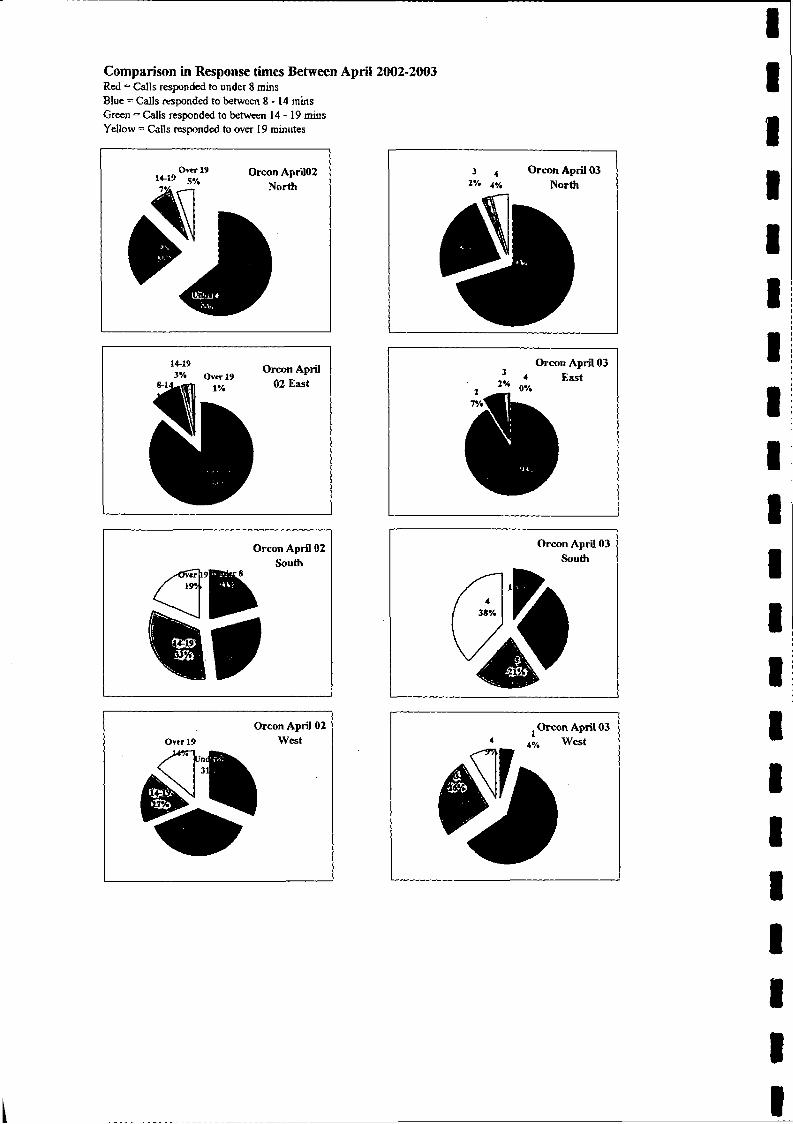
Comparison in Response times Between April 2002-2003Red = Calls responded to under 8 rains Blue = Calls responded to between 8 - 1 4 rains Green = Calls responded to between 1 4 - 1 9 mins Yellow = Calls responded to over 19 minutes
, . 10 ° ver 19 Orcon April0214-17 cm/______ North
3 4 Orcon April 03 I% 4% North
.. . Orcon April 3% Over 19
1% 02 East
Orcon April 03
2% 4 East , 2% 0%
Orcon April 02 South
/ 19H
I fOrcon April 03
South
(5 %Orcon April 02 Orcon April 03
4 UVtt
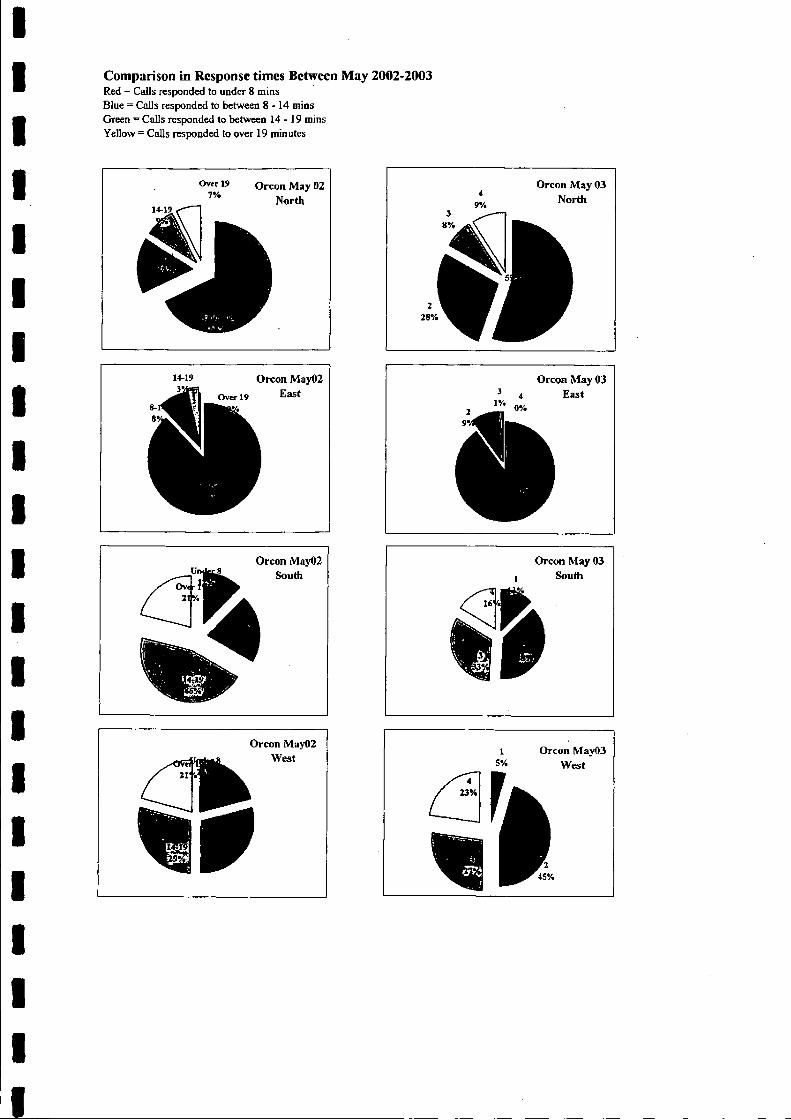
Comparison in Response times Between May 2002-2003Red = Calls responded to under 8 mins Blue = Calls responded to between 8 - 1 4 mios Green ~ Calls responded to between 14 - 19 mins Yellow = Calls responded to over 19 minutes
IV*
A
Orcon May 03 4 East
#%
Orcon May 03 i South
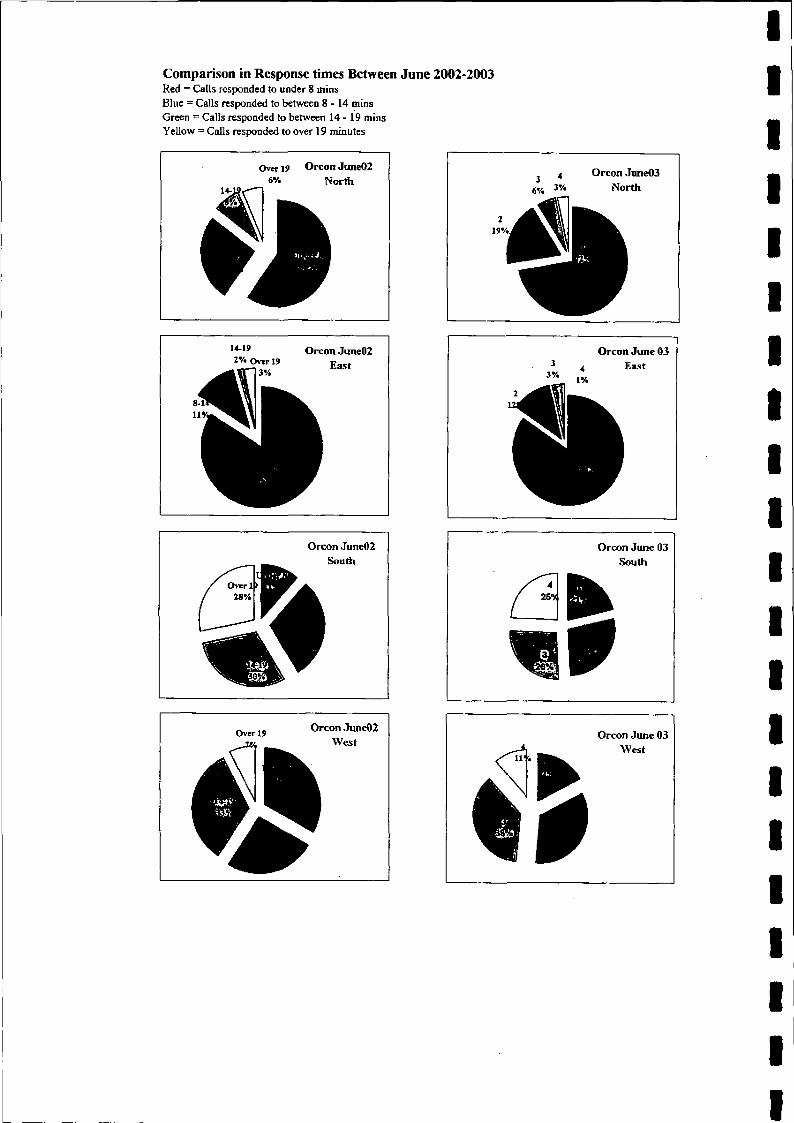
Comparison in Response times Between June 2002-2003Red = Calls responded to under 8 mins Blue = Calls responded to between 8 - 1 4 mins Green = Calls responded to between 1 4 - 1 9 mins Yellow = Calls responded to over 19 minutes
Over 19 Orcon Jime02 6% North
4 Orcon June03 3% North
Orcon June02 2%OverI 9 Easf
Orcon June 03 3 4 East
l%
Orcon June02
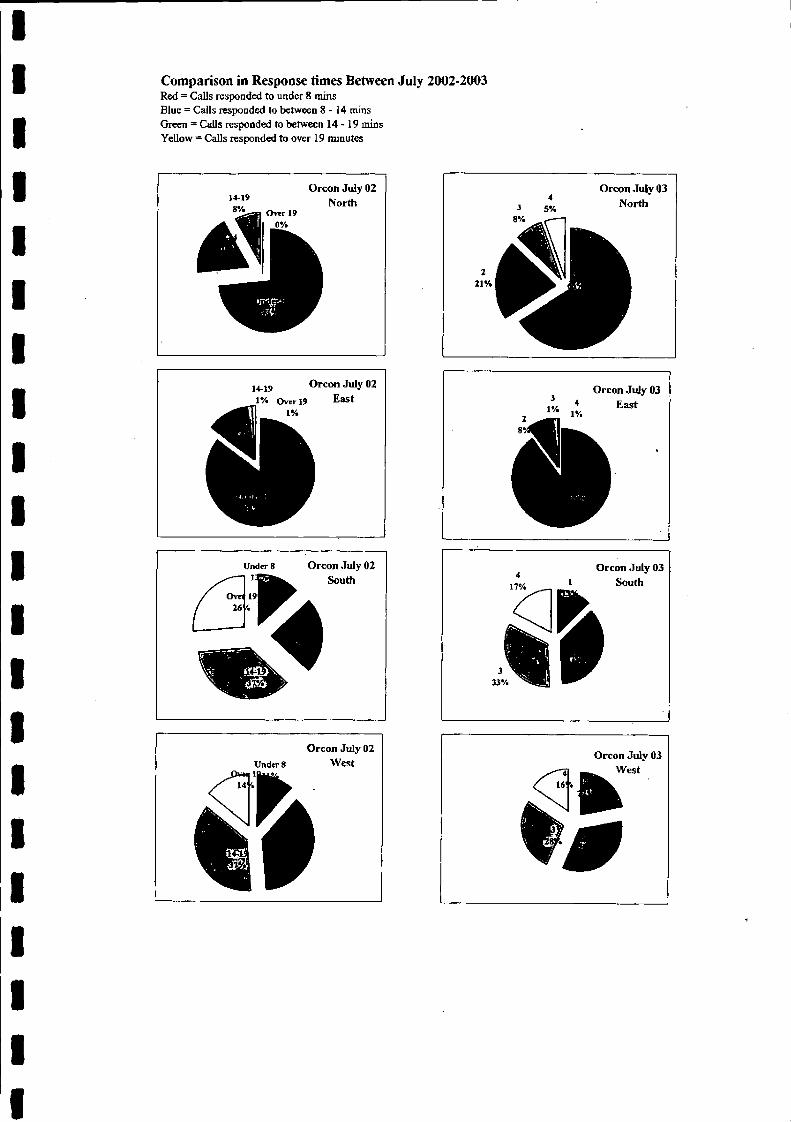
Comparison in Response times Between July 2002-2003Red = Calls responded to under 8 mins Blue = Calls responded to between 8 - 1 4 rains Green = Calls responded to between 14 - 19 mins Yellow = Calls responded to over 19 minutes
Orcon July 02West
K
i %
IOrcon July 03
East
17%
Orcon July 03 1 South
333%
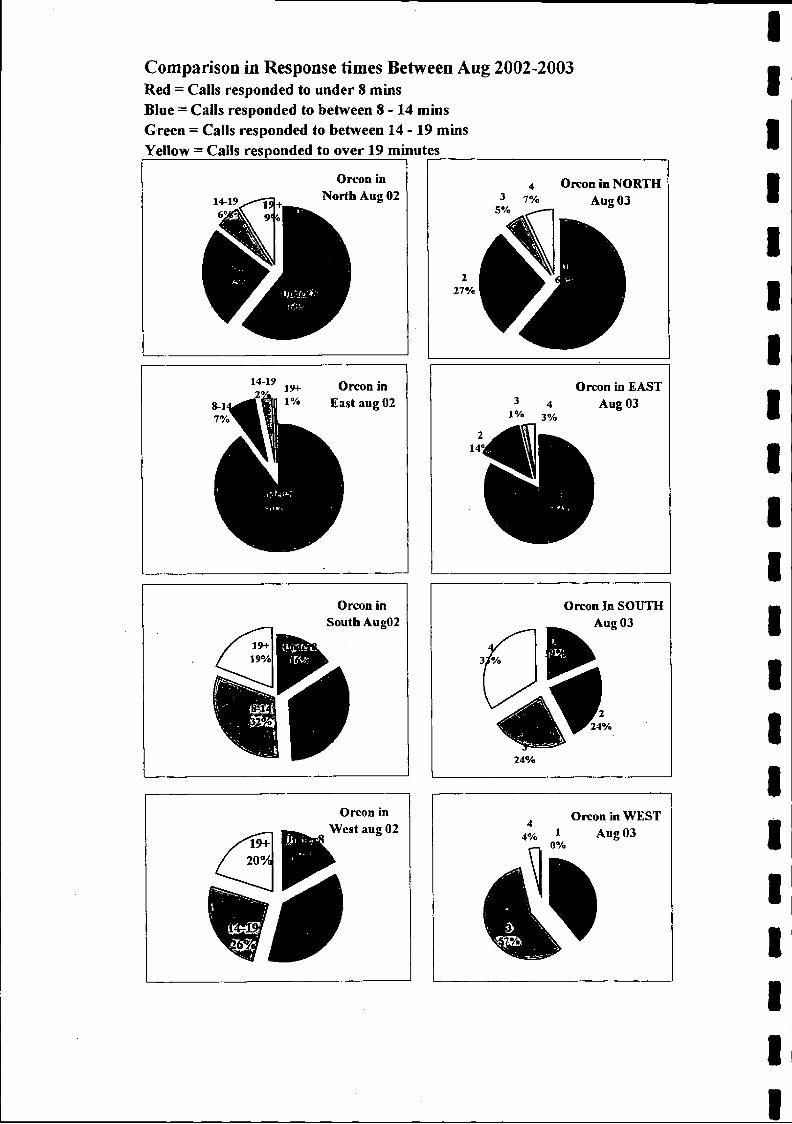
Comparison in Response times Between Aug 2002-2003Red = Calls responded to under 8 minsBlue = Calls responded to between 8-14 minsGreen = Calls responded to between 14 - 19 minsYellow = Calls responded to over 19 minutes_________________
14-19
Orton in North Aug 02
Orcon in NORTH Aug 03
27%
Orcon in East aug 02
Orcon in South Aug02
Orcon in EAST Aug 03
Orcon In SOUTH Aug 03
24%
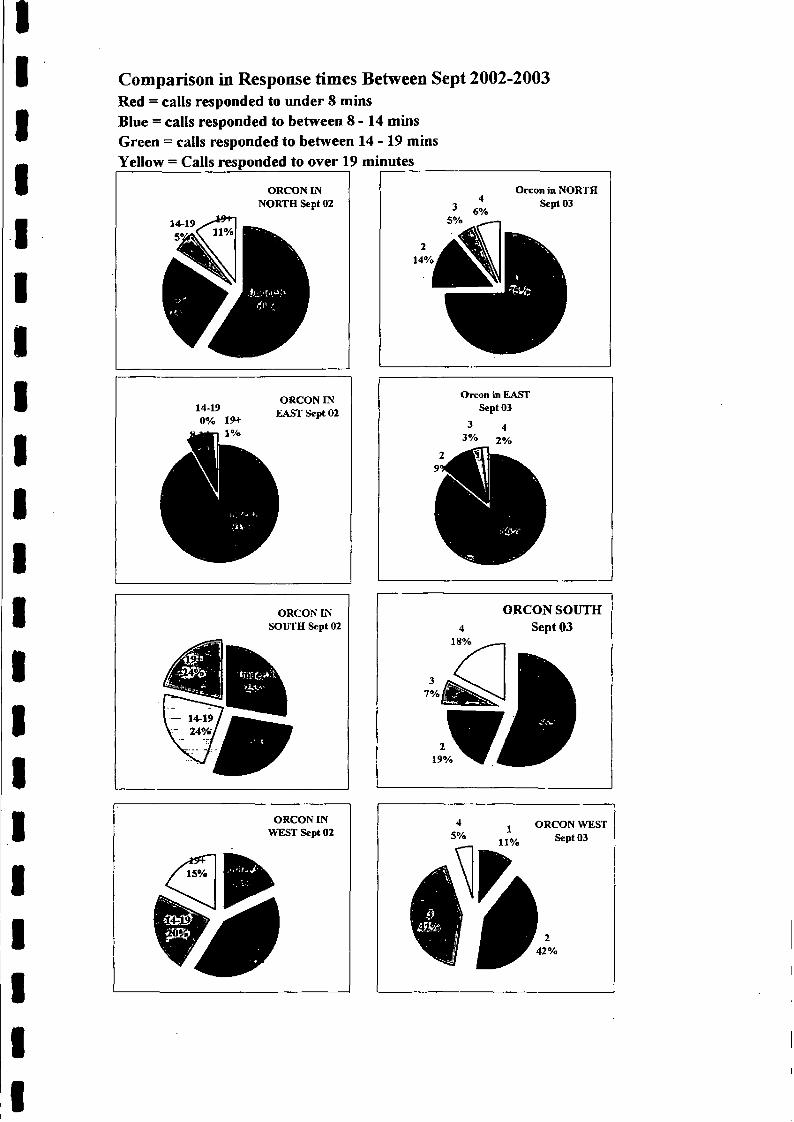
Comparison in Response times Between Sept 2002-2003Red = calls responded to under 8 minsBlue = calls responded to between 8-14 minsGreen = calls responded to between 14 - 19 minsYellow = Calls responded to over 19 minutes_________________
ORCON IN NORTH Sept 02
14-19 5% 6%
Orcon in NORTH Sept 03
14-19 0% 19+
1%
ORCON IN EAST Sept 02
Orcon in EAST Sept 03
ORCON IN SOUTH Sept 02
ORCON IN WEST Sept 02
* j ORCON WEST5% 11% ^P*03
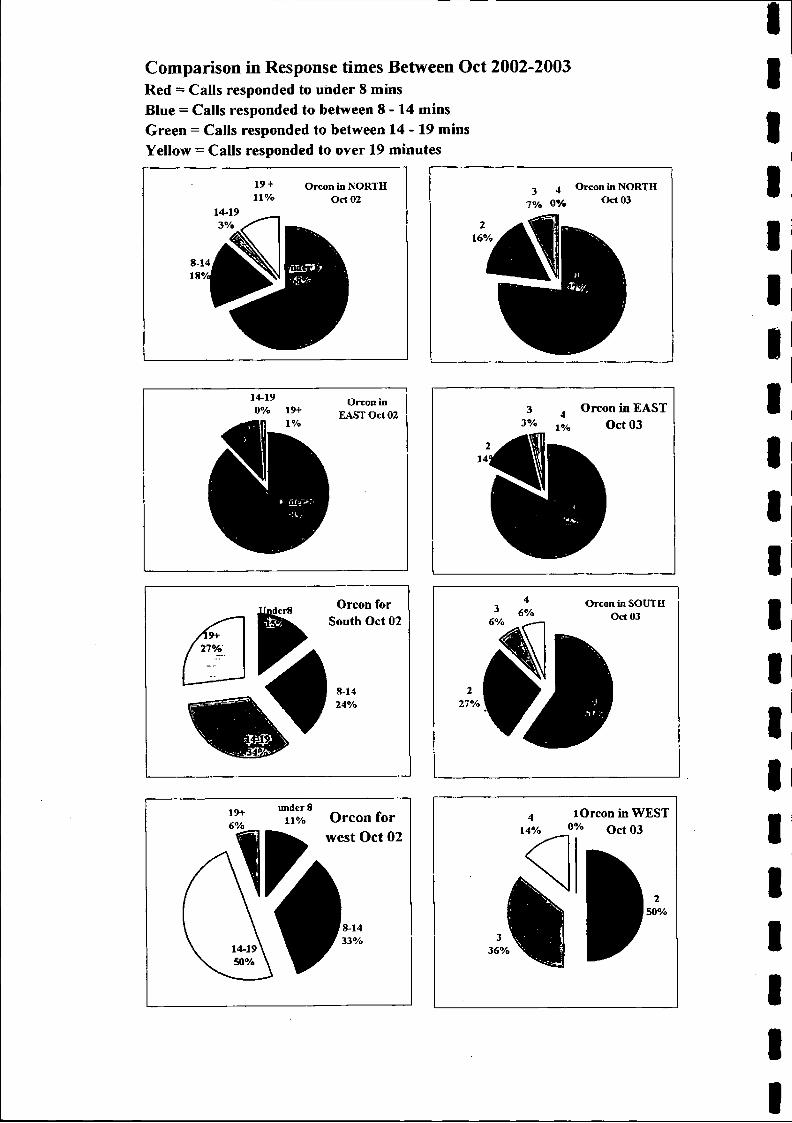
Comparison in Response times Between Oct 2002-2003Red = Calls responded to under 8 mins Blue = Calls responded to between 8 - 14 mins Green = Calls responded to between 14 - 19 mins Yellow = Calls responded to over 19 minutes
2 4 Orcon in NORTH
7% 0% 004 03
16%
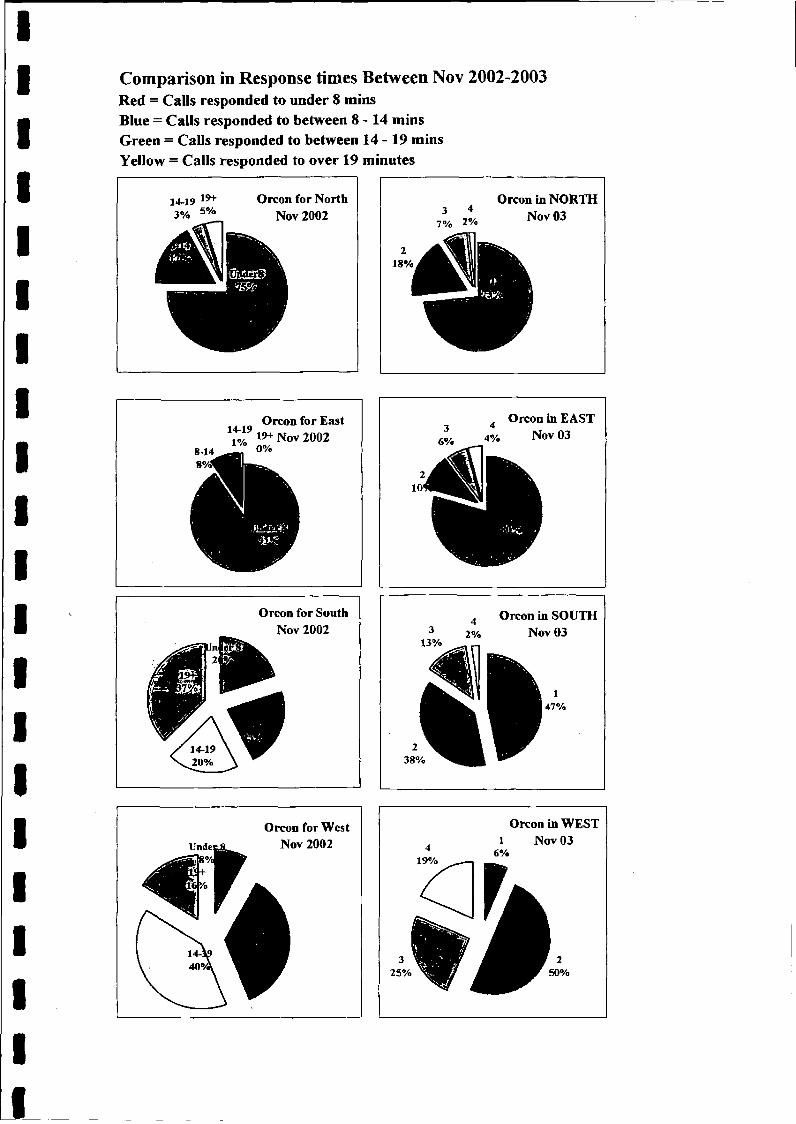
Comparison in Response times Between Nov 2002-2003Red = Calls responded to under 8 minsBlue — Calls responded to between 8-14 minsGreen = Calls responded to between 14 - 19 minsYellow = Calls responded to over 19 minutes
14-19 19+3% 5%
Orcon for North Nov 2002
18%
Orcon in NORTH Nov 03
14-19
8-14 - /0 0%8%<
Orcon for East 19+ Nov 2002
L Mm
w
Orcon in EAST Nov 03
Orcon for South Nov 2002
Orcon in SOUTH Nov 03
Orcon for West Nov 2002
Orcon in WEST l Nov 03
Isle of ManGovernment
to ltp Efton tom tr
Department of Health and Social SecurityRheynn Slaynt as Shickyrys Y Theay
AMBULANCE PARAMEDIC & PATIENT TRANSPORT SERVICE
Ambulance HQ Ballakermeen Road Douglas Isle o f Man IM1 4QA
Telephone: 01624 642154Control Fax: 01624 642593Admin Fax: 01624 632711e-m ail: [email protected]
Mr Phil Lo BaoJoint Clerk to the CommitteeOffice of the Clerk of TynwaldLegislative BuildingsDouglasIsle of ManDVfl 3PW
9th January 2003
Dear Mr Lo Bao
Re: Select Committee of Tynwald on GP Services
In response to your fax and letter dated today, please find the information requested for the periods January to March 2002 and January to March 2003.
After comparing March 2003 and April 2003 figures for the North area of the Island, I can quite understand Mr Singer’s concerns relating to what is a marked increase, double in fact, but that was due as you can see by a low March figure this year, compared with 2002 and a higher April figure this year than 2002 which can be misleading if viewed in isolation.
I hope the enclosed information is to your satisfaction, I will as requested fax the enclosed information to Mr L Singer MLC and should any members of the committee wish any further materials, please let me know.
Yours sincerely
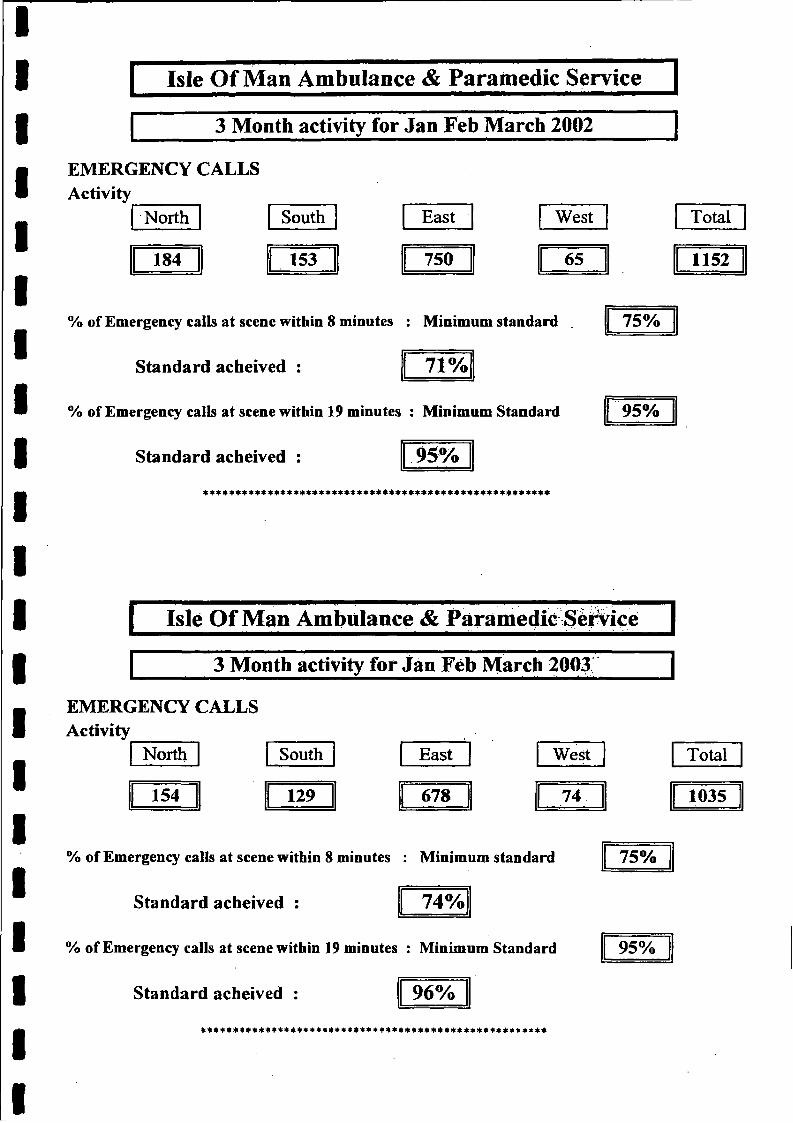
Isle Of Man Ambulance & Paramedic Service
3 Month activity for Jan Feb March 2002
EMERGENCY CALLS Activity
North South East
184 153 750
West
65
% of Emergency calls at scene within 8 minutes : Minimum standard
Standard acheived : 71%
% of Emergency calls at scene within 19 minutes : Minimum Standard
Standard acheived :
Total
1152
75%
95%
4444 4444 4* * * * * * * * * * * * * * * * 4 4 4 * 4 * 4 * 4 * 4 * 4 4 4 4 * 4141*
I Isle Of Man Ambulance & Paramedic Service |
3 Month activity for Jan Feb March 2003
EMERGENCY CALLS Activity
North South East West
154 129 678 74
% of Emergency calls at scene within 8 minutes : Minimum standard
Standard acheived : 74%
% of Emergency calls at scene within 19 minutes : Minimum Standard
Standard acheived : 96%* * * 44 * * * 4 * * 4* 4444444 * 44 * * * 4 * * * * 4* 4 * * 4 * 4* * 4* 44444*4 4*44
Total
1035
75%
95%
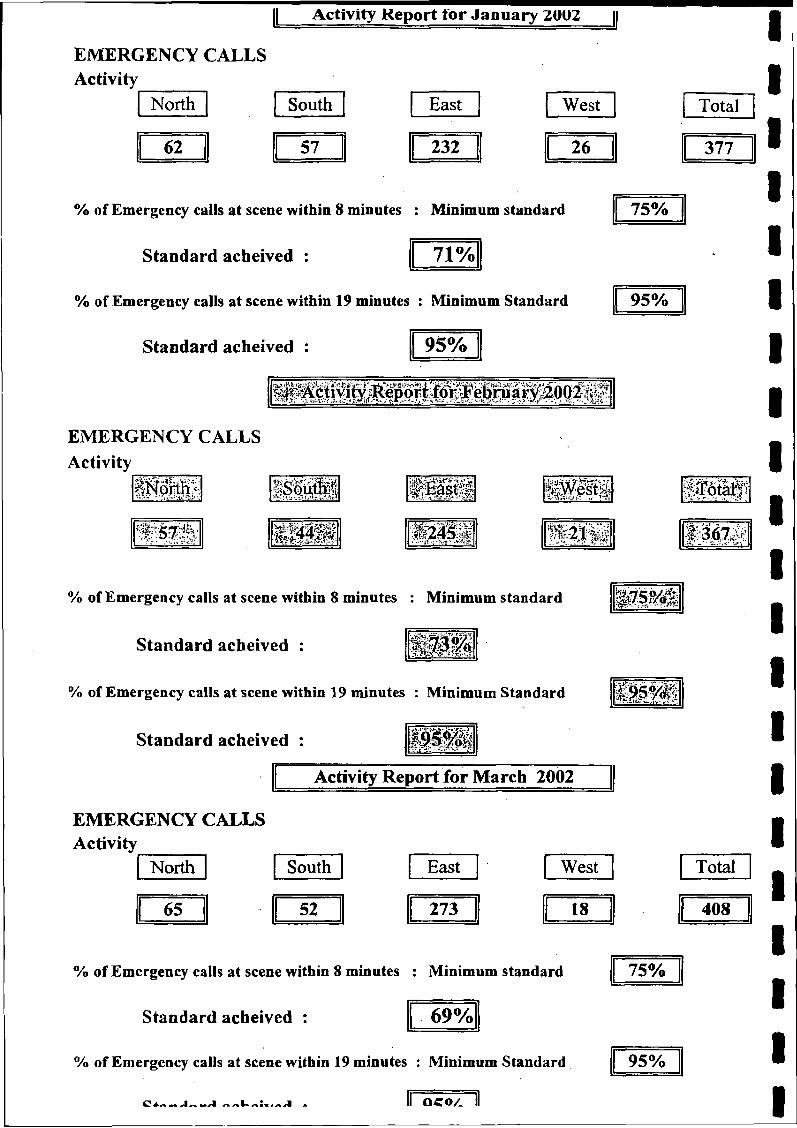
Activity Report tor January ZUOZ |
EMERGENCY CALLS Activity
North South East West
62 57 232 26
Total
377
% of Emergency calls at scene within 8 minutes : Minimum standard
Standard acheived : 71%
75%
% of Emergency calls at scene within 19 minutes : Minimum Standard 95%
Standard acheived : 95%
EMERGENCY CALLS Activity
XKîaïh* i.a - . ■ .1 ^ m m
U S
% of Emergency calls at scene within 8 minutes : Minimum standard P S ?/&
Standard acbeived : W O M
% of Emergency calls at scene within 19 minutes : Minimum Standard
Standard acheived :
Activity Report for March 2002
EMERGENCY CALLS Activity
North South East West T otal I
65 52 273 18 4 Ö O
% of Emergency calls at scene within 8 minutes : Minimum standard 75%
Standard acheived : 69%
% of Emergency calls at scene within 19 minutes : Minimum Standard 95%
OCO/_
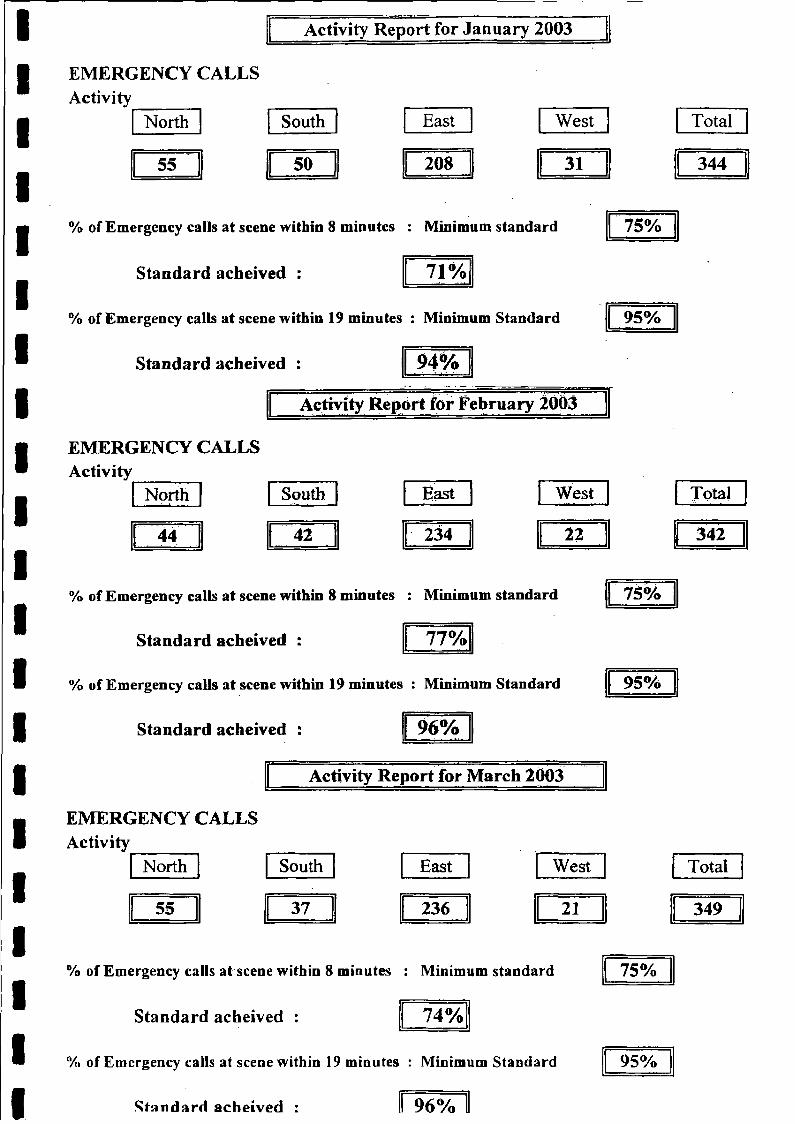
Activity Report for January 2003
EMERGENCY CALLSActivity
North South East West
55 50 208 31
% of Emergency calls at scene within 8 minutes : Minimum standard
Standard acheived : 71%
% of Emergency calls at scene within 19 minutes : Minimum Standard
Standard acheived : 94%
Activity Répòrt for February 2003
EMERGENCY CALLS
% of Emergency calls at scene within 8 minutes : Minimum standard
Standard acheived : 77%
% of Emergency calls at scene within 19 minutes : Minimum Standard
Standard acheived : 96%
Activity Report for March 2003
EMERGENCY CALLS Activity
North South East West
55 37 236 21
% of Emergency calls at scene within 8 minutes : Minimum standard
Stand ard acheived : 74%
% of Emergency calls at scene within 19 minutes : Minimum Standard
Standard acheived : ll 96%
Total
344
75%
95%
North South East West
44 4 1 234 22
Total
342
75%
95%
Total
349
75%
95%
Isle of ManGovernment
Department of Health and Social SecurityRheynn Slaynt as Shickyrys Y Theay
AMBULANCE PARAMEDIC & PATIENT TRANSPORT SERVICE
Eton v a n h
Ambulance HQ Ballakermeen Road Douglas Isle o f Man IM1 4QA
Telephone: 01624 642154Control Fax: 01624 642593Admin Fax: 01624 632711e-m ail: [email protected]
Mr Phil Lo BaoJoint Clerk to the CommitteeOffice of the Clerk of TynwaldLegislative BuildingsDouglasIsle of ManIM1 3PW
9th January 2003
Dear Mr Lo Bao
Re: Select Committee of Tynwald on GP Services
In response to your fax and letter dated today, please find the information requested for the periods January to March 2002 and January to March 2003.
After comparing March 2003 and April 2003 figures for the North area of the Island, I can quite understand Mr Singer’s concerns relating to what is a marked increase, double in fact, but that was due as you can see by a low March figure this year, compared with 2002 and a higher April figure this year than 2002 which can be misleading if viewed in isolation.
I hope the enclosed information is to your satisfaction, I will as requested fax the enclosed information to Mr L Singer MLC and should any members of the committee wish any further materials, please let me know.
Yours sincerely
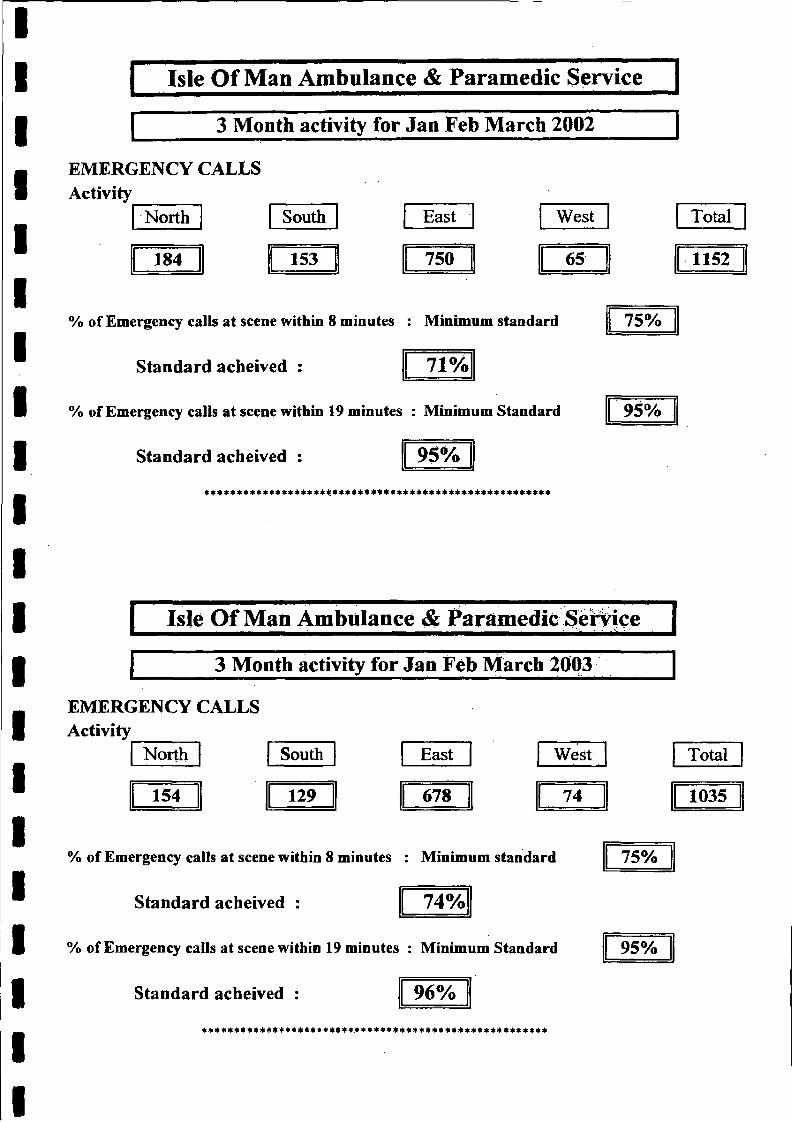
Isle Of Man Ambulance & Paramedic Service
3 Month activity for Jan Feb March 2002
EMERGENCY CALLS Activity
North South East West
184 153 750 65
Total
1152
% of Emergency calls at scene within 8 minutes : Minimum standard 75%
Standard acheived : 71%
% of Emergency calls at scene within 19 minutes : Minimum Standard 95%
Standard acheived : 95%*******************$***4******************************
I Isle Of Man Ambulance & Paramedic Service 1
3 Month activity for Jan Feb March 2003
EMERGENCY CALLS Activity
North South East West
154 129 678 74
Total
1035
% of Emergency calls at scene within 8 minutes : Minimum standard
Standard acheived : 74%
% of Emergency calls at scene within 19 minutes : Minimum Standard
Standard acheived : 96%
75%
95%
******************************************************
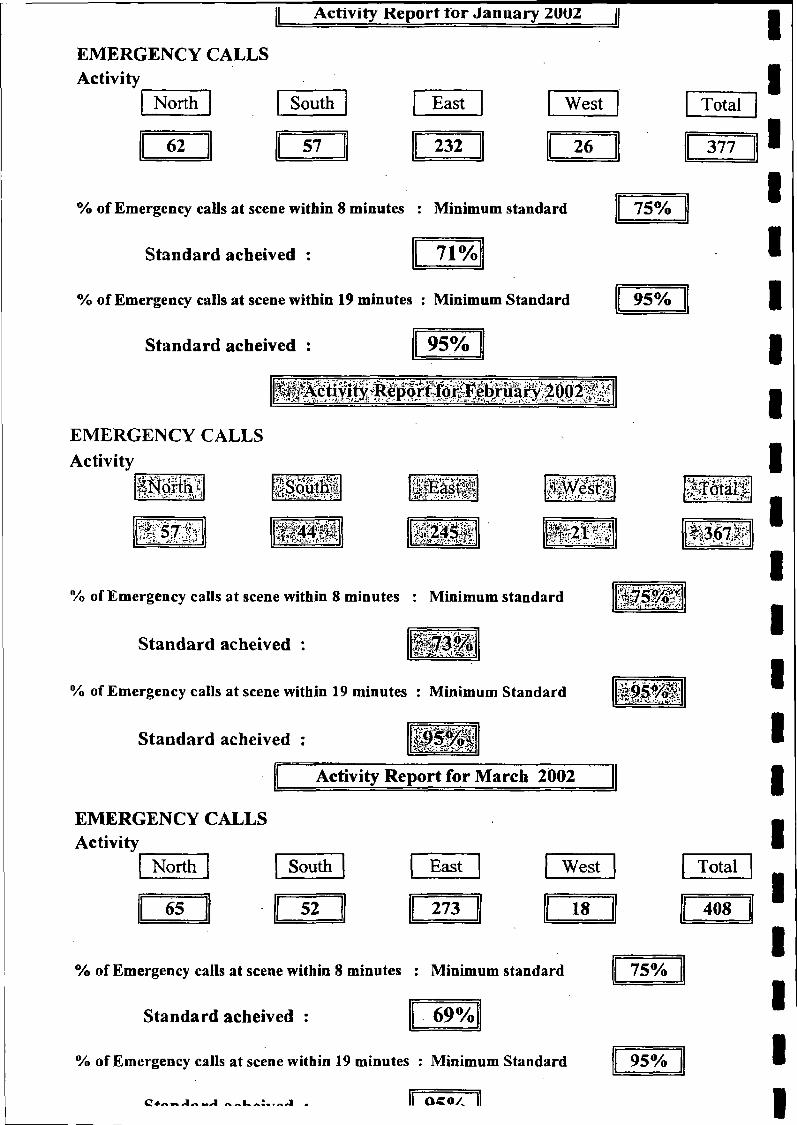
Activity Report for January 2UUZ
EMERGENCY CALLSActivity
North South East West
62 57 232 26
Total I
377 3% of Emergency calls at scene within 8 minutes : Minimum standard
Standard acheived :
75%
71%
% of Emergency calls at scene within 19 minutes : Minimum Standard
Standard acheived :
95%
95%
EMERGENCY CALLS Activity
' • •• • • Si! m §fEp|§| Ä f f t 1 P P 1
I P ÿ f ÿ Itili p 2 » 5 p•ft afri# WWiWSir £ J:: f§2®®' ||3<57|a|
% of Emergency calls at scene within 8 minutes : Minimum standard
Standard acheived :
^ 7 5 % ^
W ÿÊ$m .
% of Emergency calls at scene within 19 minutes : Minimum Standard
Standard acheived :
Activity Report for March 2002
EMERGENCY CALLS Activity
North South East West Total
65 52 273 18 408
% of Emergency calls at scene within 8 minutes : Minimum standard
Standard acheived :
75%
69%
% of Emergency calls at scene within 19 minutes : Minimum Standard
li o c o / ||
95%
—A n » k A: . r—i .
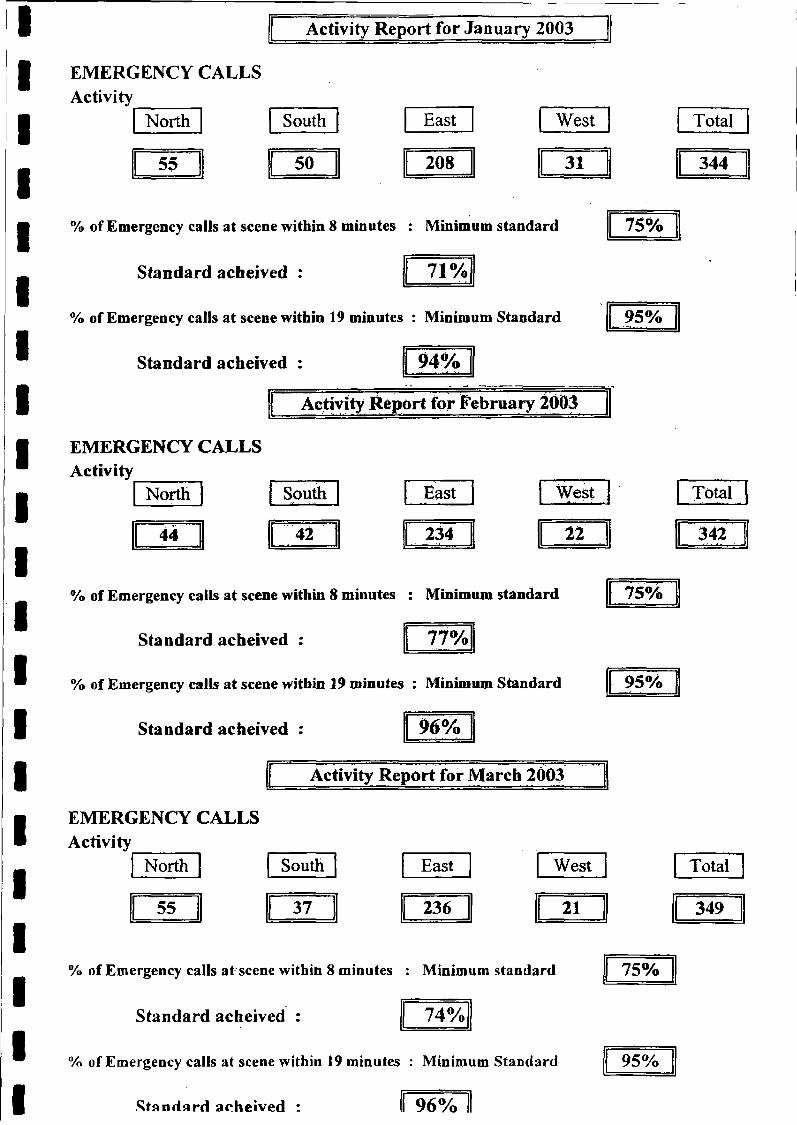
Activity Report for January 2003
EMERGENCY CALLSActivity
North South East West
55 50 208 31
Total
344
% of Emergency calls at scene within 8 minutes : Minimum standard
Standard acheived : 71%
% of Emergency calls at scene within 19 minutes : Minimum Standard
Standard acheived : 94%
Activity Report for February 2ÒQ3
EMERGENCY CALLS Activity
North South East West
44 42 234 22
75%
95%
Total
342
% of Emergency calls at scene within 8 minutes : Minimum standard
Standard acheived : 77%
% of Emergency calls at scene within 19 minutes : Minimum Standard
Standard acheived : 96%
Activity Report for March 2003
EMERGENCY CALLS Activity
North South East West
55 37 236 21
75%
95%
Total
349
% of Emergency calls at scene within 8 minutes : Minimum standard
Standard acheived : 74%
% of Emergency calls at scene within 19 minutes : Minimum Standard
Standard acheived : ll 96% 1
75%
95%
Isle of ManGovernment
Department of Health and Social SecurityRheynn Slaynt as Shickyrys Y Theay
AMBULANCE PARAMEDIC & PATIENT TRANSPORT SERVICE
Am bulance HQ Ballakerm een Road Douglas Is le o f Man IM l 4BR
Telephone: 01624 642154Control Fax: 01624 642593Adm in Fax: 01624 642711e-m a il: am bulancehq@ dhss.gov.fm
RECEIVED? 6 JUL 2001
OFFICE OF THE CLERK OF TYNWALD
Mr Phil Lo BaoClerk to the Committee of Tynwald on GP Services Office of the Clerk of Tynwald Legislative Buildings Douglas Isle of Man IMl 3PW
22nd July 2004
Dear Mr Lo Bao
Ref Your Letter Dated 19th June 2004
I will attempt to answer your question in relation to first responders and there use, but I must say from th’onset that this a very complex issue and if further clarification is needed I would be happy to answer an^questions that the Committee may have. I
Since the opening of the ambulance station in Port Erin last year together with the manning of the Ramsey ambulance station 24 hours per day the year before, we are in a position whereby we can now guarantee I ambulances on duty every night of the week 365 days of the year, this is instead of having 1 ambulance on duty for the Island and then two crews at home on standby who would need to respond to the station, meet ug with their partner before manning an ambulance and responding to an incident. |
Due to the opening of the station in Port Erin staff had to be re-located from the Douglas station to that of P o * Erin. These personnel obviously were given the usual protection in the form of mileage allowances an| guaranteed remuneration. However because of this move a problem was created whereby it was thought unfair and unrealistic that staff moving to Port Erin would also be expected to move homes so that they could be ott call for the area surrounding their station especially as before the opening of the Port Erin station this w ai resourced from Douglas. This was discussed and an agreement was reached that staff manning the Port Erin station would be able to offer their services as a first responder from their home and as the union pointed oifl this was stated in the Ambulance Whitley Terms & Conditions, apart from any new staff who were recruiteP or volunteered to work in Port Erin, who would be expected to live or reside in the area when conductin standby duties. I
IXT
What then followed was a joint staff grievance from the staff who had volunteered to work at Port Erin, an some of the Douglas and Ramsey staff who although worked at their respective stations were not allowed t conduct standby duties as it was considered that they lived too far from their stations (e.g Ramsey based sta living in Douglas). A meeting was called between the staffs union representative, a member of the Personnel Department, the late Mr Geoff Newbeiy and myself and it was agreed that due to the complexity of t h l situation both the union representative and myself should create a report that highlighted the differences between the staff side and ambulance management’s views. This was completed and together with a copy o^ the standby callout statistics submitted to the Primary Health Care manager. I
i
It was then decided back in March this year, that due to the fact that it was considered unreasonable to expect staff to move home or be confined to residing in an area where they worked when performing standby duties (1:8) that the boundaries that had existed should be removed and a six month trial should commence whereby staff would not be on standby for the catchment area for their station, but instead by on standby for the service as a whole, and therefore could conduct these duties from wherever they lived.
The Standby statistics showed that since the introduction of three ambulance being available every night the demand for standby staff had dropped dramatically 1 or 2 calls per month, and when these calls were studied further, an ambulance was either on scene at the same time or shortly after.
Due to this trial period that ends at the end of August the new control staff have been given guidance on how to move the three ambulances around the island to standby points when one or more are engaged on emergency or Doctor Urgent duties, this means that when the Douglas crew are busy a crew is called up to Ballasalla from Port Erin until the Douglas ambulance is free, likewise if the Ramsey ambulance is busy the Douglas ambulance moves to Cronk ny Mona to cover Douglas but is also ready to drive over the mountain to Ramsey if needed, if both Ramsey and Douglas are busy then the remaining crew from the South is repositioned to a central standby point which is the Douglas station.
During the trail period apart from enforcing the movement of vehicles to standby positions after reports were received that ambulances were not being moved and responses to patients were delayed, and some confusion shortly after the new control centre opened, there has not been any real problems, it is therefore expected that to revert back to expecting staff to live or reside in a certain area of the island could prove difficult.
However we will be looking at introducing volunteer first responder schemes around the Island which will involve members of the public and voluntary agencies undertaking training delivered by us and together with the provision of equipment will respond in their own community and stay with the patient until an ambulance arrives, as a trial later this year we will be working with the St John ambulance Brigade with the purpose of. them providing a service in the West of the Island, I am also interested in setting up schemes whereby off duty ambulance staff, nurses, first-aiders and Doctors who want to offer their services could also be on call for their community and I will be certainly offering my services as a paramedic and a trainer to my community in the North of the Island.
I hope this has answered your question, but as I have mentioned above this is a very complex matter and if you need further clarification, please feel free to contact me, or if you feel it would be better for me to attend in person, I would be happy to do so.
Yours sincerely
Steve SipHngActin^Chief Ambulance Officer
Appendix 6
T Y N W A L D C O U R T O F F I C I A L R E P O R T
R E C O R T Y S O I K O I L Q U A I Y L T I N V A A L
P R O C E E D I N G SD A A L T Y N
(HANSARD)
S E L E C T C O M M I T T E E ON GP O U T OF H O U R S S E R V I C E S
B I N G E R - L H E H M Y C H I O N E S H I R V E I S H Y N F I R - L H E E A Y N S O O R Y N S O C C A R A G H
Douglas, Thursday, 18th December 2003
Published by the Office of the Clerk of Tynwald, Legislative Buildings, Bucks Road, Douglas, Isle of Man. © Court of Tynwald, 2003 Printed by The Copy Shop Limited, 48 Bucks Road, Douglas, Isle of Man
2TGPS SELECT COMMITTEE, THURSDAY, 18th DECEMBER 2003
M e m b e rs P re se n t:
Hon. J A Brown SHK (Chairman)Mr D J Gelling MLC
Mr Q B Gill MHK Mr L I Singer MLC Mr G H Waft MLC
Clerk:Mr P Lo Bao, Third Clerk
B usiness tra n s a c te d
PageProcedural............................................................................................................................................................................................ 3
Mr S Sieling, Deputy Chief Ambulance Officer, & Mr R Beattie, Operations Manager Ambulance Service............... 3
Procedural....................................................................................... ...................................................................................................14
Dr Maska, Chair GP Subcommittee of IOM Medical Executive..................................................................................... 14
Procedural........................................................ ................................................................................................................................. 23
Mr & Mrs Penrose, Ramsey Cottage Hospital League of Friends....................................................................................23
Procedural..........................................................................................................................................................................................28
The Committee adjourned at 1.19 p.m.
Procedural.............................................................................................................. ........................................................................... 28
Mrs A V Craine M H K ....................................................... :...............................................................................................28
Procedural............................................................................. ................ ........................................................................................... 33
MrPAGawne M H K ........................................................................................................................................................... 33
Procedural......................................................................................................................................................................................... 37
Hon A R Bell M HK.............................................................................................................................................................. 37
Procedural..........................................................................................................................................................................................43
HonSCRodan MHK.......................................................................................................................................................... 43
Procedural......................................................................................................................................................................................... 47
The Committee sat in private at 5.05 p.m
Oral Evidence SELECT COMMITTEE, THURSDAY, 18th DECEMBER 2003 3TGPS
Tynwald Select Committee on GP Out of Hours Services
The Committee sat in public at 10.47 am. in the Conference Room,
Town Hall, Ramsey
[Mr Speaker in the Chair]
Procedural
The Chairman (The Speaker): Good morning, ladies and gentlemen.
Today the Select Committee, appointed by Tynwald in June 2003, with the remit - and I quote - to:
‘investigate the matter of the General Practitioner’ “Out of HoursServices" being provided throughout the Island',
has determined to come to Ramsey to take oral evidence and is holding its sitting here in Ramsey Town Hall. We extend our thanks and appreciation to the Ramsey Town Commissioners for the use of this facility.
We are here to take oral evidence from persons invited by the Committee, in relation to our remit, as approved by Tynwald. All proceedings will be officially recorded and, subsequently, a written record of our proceedings will be published.
The five members of the Committee appointed by Tynwald are: myself, Speaker of the House of Keys, and I am Chairman of the Committee; Mr Gelling MLC; Mr Gill MHK; Mr Singer MLC; and Mr Waft MLC. In attendance is our Third Clerk, Mr Lo Bao.
The Committee has received and considered a substantial amount of written evidence from across the Island. The Committee will make its report to Tynwald, when it has considered all the oral and written evidence put before it and finalised its considerations.
The procedures for today’s hearing follow the normal procedures of a select committee, and that is: we shall, initially, hear evidence from the persons who have been invited by the Committee to appear before us today. Therefore, in a moment, I will invite the first persons to appear before the Committee today to take their seats in front of us here, and then I will invite them to put forward their points, any points that they wish to put as a matter for consideration. The Committee may then ask questions of those individual persons who have been giving evidence.
Finally, there will be an opportunity for the persons giving evidence to make a closing statement, if they so wish. 1 hope everybody is clear on that. Thank you.
EVIDENCE OF MR S SIELING AND MR R BEATTIE
The Chairman: If I could, in starting our proceedings, invite Mr Sieling, Deputy Chief Ambulance Officer, and Mr Beattie, Operations Manager of the Ambulance Service,
who I understand are in the room. Would you like to take a seat, gentlemen?
Again, can I just read out the remit, so you are clear on what our remit is? It is to investigate the matter of the general practitioners' out-of-hours services being provided throughout the Island. Okay? So that you are clear, Tynwald has also given us powers under the Tynwald Proceedings Act 1876, sections 3 and 4, in relation to taking written and oral evidence, so we have powers that have been authorised by Tynwald.
You are going to introduce yourself first and then pass over to your colleague. I think that would be helpful, so, if you could first state your name and your position, Mr Sieling.
Mr Sieling: My name is Steve Sieling, Deputy Chief Ambulance Officer for the Isle of Man Ambulance Service, where I have been for 11 years.
The Chairman: Thank you.
Mr Beattie: My name is Ray Beattie. I am Operations Manager for the Isle of Man Ambulance Service and have been in post for the last seven years.
The Chairman: Now then, Mr Sieling, do you wish to give your evidence first to the Committee? I think if you can give your view on this issue, we will go from there. And, also, if I could ask you to speak up, because, otherwise, people may not be able to hear you, because, unfortunately, your backs are to them, so you will need to speak a little bit louder, if I could ask you to, please. Okay, so if I go over to you, Mr Sieling.
Mr Sieling: The first thing is probably to give you some brief outline of how the ambulance service works out of hours, so to speak, when the MEDS is working.
During the week, after six o’clock in the evening, we have three ambulances on duty, one based in Ramsey, one in Douglas and one in the south of the Island at Port Erin. In addition to those, we have a duty officer always on call for management queries and we also have, resources permitting, three first responders. We try to keep those in the areas, again, north, central and south.
We have looked at some of the figures for three months last year, before the MEDS service was introduced for the whole Island, and three months of this year, and we have not seen that much of a change in the figures, with regard to 999 calls or GP urgent calls. A 999 call is obviously a call that is responded to from a result of a 999 call, or at the scene of an emergency. A GP urgent call is one when we receive a call from a doctor and he actually specifies the time that the patient needs to be in hospital. As I say, looking at the figures so far, we have not seen a dramatic rise in either emergencies or doctors’ urgents.
The Chairman: You have not seen that?
Mr Sieling: No.
The Chairman: I think people are having a problem hearing. If anybody wishes to move forward, please do so now, because you might find it easier. So, if we just break there, if we may.
Is everybody alright? Right Anything else you wish to say, Mr Sieling?
ProceduralTynwald Select Committee on GP Out of Hours Services - Evidence of Mr S Sieling and Mr R Beattie
4TGPS SELECT COMMITTEE, THURSDAY, 18th DECEMBER 2003 Oral Evidence
Mr Sieling: I suppose what I am saying is we have not really seen that much of a change, with regard to the ambulance work, with the introduction of an all-island GP service, out of hours.
The Chairman: Would you like it if Mr Beattie now comes in and then we can start asking questions? Alright?
Mr Sieling: Yes.
The Chairman: Mr Beattie.
Mr Beattie: Yes, basically, I would just like to concur. As Mr Sieling has said, the figures themselves have not changed dramatically to cause any concern. There is nothing really much else I can add to that, to be honest.
The Chairman: That is fine. I think it best then, maybe, to ask questions and then we will see where we go from there. Okay?
Mr Beattie: Yes.
The Chairman: Could I see if any of my colleagues wish... Mr Gelling?
Mr Gelling: When you say the figures have not changed, is that in totality, or is it for specific 999 calls? In other words, evidence, perhaps, would suggest that ambulances are having to come from Ramsey through to Douglas for cases which normally would have been treated in Ramsey. Your figures are stating that, in fact, there is no change, which would dispel that, unless you are talking about a specific 999 call service, rather than the ambulance being called by a doctor or... Could you explain that?
Mr Sieling: Both sets of figures, the 999 calls and the ‘GP urgents’, as we call them - the doctor calls - have not really changed. We did expect, possibly, a rise in emergency calls initially because, like you say, some people may fear that they cannot get the GP quickly enough, so they are going to phone for our service. So, we were expecting that, but it did not actually happen.
If you are referring to the treatment in the Ramsey area, regarding the Minor Injuries Unit (MIU) - is that what you are saying? - there is, obviously, a difference there, whereby we are now taking more people down to Noble’s, but that is not really to do with the Manx Emergency Doctors Service (MEDS); it is to more to do with the local issues in Ramsey.
The Chairman: Mr Gelling.
Mr Gelling: Does that mean that the calls that you log and the figures you have produced... Is that because they are the ones that you have attended? Could there, perhaps, be calls that you have not been able to go to, where they have had to find other ways of getting to hospital, and they are not logged by yourself, because the ambulance was not available?
Mr Sieling: There has always been an ambulance available for calls that have been requested by a GP, or by an emergency, as far as I know. We have never had any
complaints to the contrary. Obviously, if the doctor has arranged other transport, we would not know that, but we certainly have not had a position, as far as I know - and Ray will back me up on this, I am sure - where we have not had an ambulance available to respond.
The Chairman: Mr Beattie.
Mr Beattie: Yes, I think I understand where Mr Gelling is coming from, in that, between the hours of six at night and eight in the morning, now, if we pick up a patient, that patient invariably will have to go to Noble’s, which means that the vehicle is not as available now as it was previously. Has that had a major effect on the ambulance service? No.
Mr Sieling: I think another point, if I may, is that, obviously, recently we have also introduced three vehicles at night, 24 hours, whereas, say, 18 months ago we only had one vehicle on duty up till midnight and then two vehicles at home on standby, where we used to call the staff from home. It was not planned, it was a coincidence that part of our business plan was to actually get more 24-hour vehicles on the road, and that happened recently. In the last 18 months: we have now got three vehicles 24 hours a day, which has helped us at night anyway.
The Chairman: Mr Gill.
Mr Gill: Thank you, Chairman.Could I ask a few questions, Mr Sieling? First of all,
the three-ambulance out-of-hours arrangement that you described: I think you said that was for weekdays. Is that for weekends also?
Mr Sieling: That is seven days.
Mr Gill: That is seven days?
Mr Beattie: That is 24/7.
Mr Gill: Right, thank you. What weaknesses have you experienced with this arrangement?
Mr Sieling: With the MEDS service?
Mr Gill: With the out-of-hours three-ambulancc arrangement that you have described.
Mr Sieling: We have not, really. Like I said, because ii coincides with us putting more vehicles, or more resources on at night, we are obviously providing a better service now than we were before. Our response times have... Oui Island target is to actually get a vehicle on scene withir eight minutes 75 per cent of the time. In the past we have been struggling to hit 70, but, since the introduction ol three vehicles at night, we are now hitting the 75 per cen target - not every month, but some months.
Mr Gill: Yes. Could I ask you: what would a typica travelling time be for an ambulance from Port Erin to Noble’: and from Ramsey to Noble’s?
Mr Sieling: I can get you some figures, but, off the tof of my head, it is about 20 to 25 minutes.
Tynwald Select Committee on GP Out of Hours Services - Evidence of M r S Sieling and M r R Beattie
Oral Evidence SELECT COMMITTEE, THURSDAY, 18th DECEMBER 2003 5TGPS
Mr Beattie: By the time you have decanted your vehicle, taken the patient to the ward and everything, you are approximately an hour and a half a round trip.
Mr Sieling: That is from beginning to end.
Mr Gill: And there would be circumstances where that would be extended, that time: bad weather, having to delay. So, what would your maximum time be, worst-case scenario?
Mr Beattie: The worst case scenario is TT, when the road is closed from the north. We are possibly envisaging maybe a two to three-hour turnaround time on a vehicle.
Mr Gill: And do you have any capacity to bring in an additional vehicle to cover that?
Mr Sieling: Like I said, what we normally do is move the three vehicles around to standby areas. The main area - because that is where the demand is - is Douglas, so we always make sure there is one vehicle in Douglas. If the Ramsey vehicle is coming down to Noble’s, we will move that Douglas vehicle towards Ramsey so it now covers Ramsey and Douglas. Likewise, we move the vehicle from Port Erin up to Santon. You have probably seen the vehicles standing by the roads. That is the reason: they can go either way then and cover. On top of that, out of hours, we have then, as I said, got three first responders, who are staff who take a vehicle home with them. It is not a full-sized ambulance, but what it does is allow them to respond directly from home and attend to an injured person, or an ill person, until an ambulance arrives,
Mr Gill: Could you just briefly describe the Joint Emergency Services’ Control Room and what effect that will have on your service, please, Mr Sieling?
Mr Sieling: It will have quite an effect, in that -
Mr Gill: Just for Hansard, could you tell us how you perceive the concept of it in practice?
Mr Sieling: Yes. The Joint Emergency Control Room is designed to actually receive calls for all three emergency services and despatch their resources. Lots of money is being put into the software and the technology. Part of that that we insisted on was software called Predictive Analysis, which allows the system itself to take in the information and tell us where we need to put the vehicles at certain times of the day, and have seasonal variations built into it as well. But, to be honest, because the Island is not that vast an area, it is not really rocket science to actually say, ‘Well, you do need an ambulance near your biggest demand area, which will always be Douglas, because of the population, which increases during the day. ’ But that was the idea of the concept of the joint control room: that all three services would be serviced by one despatch centre.
Mr Gill: And what changes do you anticipate that will have on your service?
Mr Sieling: It has taken our control away from us, if you like. We are losing control of our control of the ambulances;
we are relying on another service to actually do that for us. Obviously, we are heavily involved with the project, as it is, and we will continue to be involved with it after it starts going live on 5 th April, because we do anticipate that there have got to be teething problems and there will be policies and procedures that need to be written to cover over areas that have been highlighted.
The Chairman: Mr Singer.
Mr Singer: I have got a few questions, Mr Chairman.You have got three ambulances, one for Ramsey, one for
Douglas and one for Port Erin; I take it these are all manned by paramedics?
Mr Sieling: There is a paramedic and an ambulance technician on each vehicle.
Mr Singer: Can I ask you about these first responders? They will go out when there is no ambulance available immediately. Are they qualified paramedics?
Mr Sieling: They could either be a paramedic or an ambulance technician.
Mr Singer: So, if it is an ambulance technician, they are there just to do what? They cannot, obviously, undertake a paramedic’s duties.
Mr Siding: I suppose the best way to answer that would be that the difference between a paramedic and an ambulance technician’s training is that a paramedic can give a wider range of drugs, but they are limited to what they can do working on their own. So an ambulance technician’s skills now have been brought up sufficiendy to provide on-scene or on-site emergency aid, such as defibrillation, using a... You have seen on the telly, on Casualty probably, the electric shocks for the heart. All technicians can do that. All technicians can give drugs for diabetes. They can give advanced airway support, so they can actually manage a patient who is in an emergency situation until an ambulance arrives. A paramedic, yes, can then continue that care by giving more drugs. The technician is still not... They are a lot more trained than just basic first aid,
Mr Singer: Can I ask: what difference has it made to the ambulance service now that they cannot have the choice of going to Ramsey Cottage Hospital, which they had before, and they have got to go down to Douglas? What difference has that made to the service that is offered and the times, collection times, getting to people?
Mr Sieling: What it does mean - and obviously your question is referring to the MTU, I take it, yes - is that, now, if we pick someone up after 6 p.m. in the evening and we know that they need emergency treatment the MIU cannot offer, then we have to take them to Noble’s. That means, for the service, we then have to move, like I have said earlier, a vehicle from Douglas closer to Ramsey to cover both areas, until that vehicle is back in its own area, and possibly call on a first responder.
Mr Singer: That is because, I Understand, you have requested access to equipment at Ramsey Cottage Hospital
Tynwald Select Committee on GP Out of Hours Services - Evidence of Mr S Sieling and M r R Beattie
6TGPS SELECT COMMITTEE, THURSDAY, 18th DECEMBER 2003 Oral Evidence
and that was refused during those hours. Is that correct?
Mr Sieling: We have asked to go in there for certain conditions. If we had a cardiac arrest, what we have asked to do is actually go in there and treat someone in there, in their setting, because it is obviously more beneficial to a patient than actually trying to work in the back of an ambulance, especially if there is some query about the delay of the journey getting over the mountain.
Mr Singer: So that is one disadvantage, obviously, of the Cottage Hospital not being available to the ambulancemen: they do not have the choice. I understand - I think we all understand - that, in the case of a heart attack or a coronary, there is the specific time to treat people. If you cannot get into Ramsey Cottage Hospital and you have got to take people over the mountain, what effect could that have on the patient? And let me add to that: if the mountain road is shut and the coast road can be shut, what difference does it make to the ambulance service?
Mr Beattie: It is an added burden, but I think what you are getting at is the potential outcome for the health of that patient. That I do not think is our remit; I think that is more of a clinical decision to be able to say, on a time factor or a delay of treatment, what that potential outcome would be., We are not qualified to make that kind of comment
Mr Singer: But that must be a concern to you.
Mr Sieling: Obviously, what we are looking at at the moment is contingency, I have to say, because we are coming into the months now where the roads could be blocked.
Mr Singer: Can I ask you: on moving the ambulances now, if the northern ambulance has gone down to Noble’s, you say you would move - and we have seen them - the ambulances up to the Bungalow. Surely - and this is, I think, a main contention of everybody - if the weather is bad - and it can be bad at any time of the year - or the road is closed, what are the response times going to be, if the ambulance is even parked at the Bungalow, to get up to Bride? How are you going to do them in the times?
Mr Sieling; You cannot achieve the eight minutes then. It would be extended; there is no doubt about that.
Mr Singer: The service then, obviously, would be poorer.
Mr Sieling: I think what you have got to consider, though, is that, like I said earlier, up until 18 months ago you only had one ambulance on duty for the whole Island, and that was based in Douglas and that was covering the whole Island from midnight until six o’clock the following morning.
Mr Singer: At one time - isn’t it true? - we used to have an ambulance in Ramsey that was not a 24-hour ambulance, but the ambulance was permanently here, and whilst it might have taken five minutes to get the person who was going to run the ambulance to the ambulance, they could then go out in a much shorter time than if it was coming, say, from Douglas and getting people back to the hospital.
Mr Sieling: That is what we have replaced now with the ambulance being there 24 hours a day. It is the same crews, but they are now there on station, so they can respond direct, as well as having the third member at home on standby.
Mr Singer: You said there was no obvious increase in emergency calls. Is that correct?
Mr Sieling: There is a steady increase throughout the service, but we have not seen -
Mr Singer: Would I be wrong in saying the increase in emergency calls for the whole Island since the introduction of MEDS was 35 per cent, and, for the North, is about 80 per cent of the figures that you have got, in comparative terms?
Mr Sieling: The figures that we have got do not show that.
The Chairman: Would you like to give us those figures, please, read them out? I think it would be helpful if you could read out the figures.
Mr Sieling: Yes. The figure for the 999 calls - this was for 2002, and we have just taken a snapshot period of April to June, which is three months, but I can give you more figures if you wish later on - was 1,334.
The 999 calls for the same period this year, after MEDS took on the new service, was 1,363. So, as you can see, that is a rise of 29 calls - emergency calls, that is.
GP urgents, where a doctor has called us out: for 2002 there were 651 calls, and, in 2003, it actually dropped to 594. This is all-island; we have not broken it down into north or south.
The Chairman: And is that a like-for-like period (Mr Sieling: Yes.) or are you comparing a full year against... Have you got copies there?
Mr Sieling: 1 have, yes.
The Chairman: I think it would be helpful if, maybe, if it is possible, you could get us a breakdown on that (Mi Sieling: Yes.) and if you could forward that to our Clerk, please.
Mr Sielmg: No problem, yes. Will do.
The Chairman: We will get them circulated now.
Mr Singer: Could I ask you: when you pick up a patienl and go down to take them to the hospital, is it normal practice for the ambulance to have to turn back and go back and pick up another person, as has been happening since MEDS, and, therefore, be taking two people down to Noble’s? Is this within your accepted practice?
Mr Sieling: Sorry, an ambulance leaving the north oi the Island?
Mr Singer: Or wherever. It has picked somebody up and then it has to go and pick somebody else up before it can gc on to the hospital.
Tynwald Select Committee on GP Out of Hours Services - Evidence of Mr S Sieling and M r R Beattie
Oral Evidence SELECT COMMITTEE, THURSDAY, 18th DECEMBER 2003 7TGPS
Mr Sieling: Only if the crew themselves feel that they can do that. If they have picked someone up with, perhaps, a wrist injury or something... You know, I am just thinking of the times I have seen it come up in the control room, where someone has picked up someone as a low demand, such as a wrist injury or whatever, and then been asked to pick up someone else with, again, not an emergency, or they may be asked to attend an emergency until an ambulance arrives. But it is not normal practice, no. It is not done every day.
Mr Singer: Is it acceptable practice?
Mr Sieling: It is acceptable providing the crew... The crew themselves are practitioners in their own right, so, if the patient that they have already got on board is being treated by the paramedic and technician, and they are comfortable that there is no danger to the patient, then, yes.
Mr Singer: So if a person is, say, not too far from Ramsey - or it can be anywhere - and a call comes through for another emergency, they will then turn back and pick up the other person and delay the first person getting to hospital?
Mr Sieling: They could do, yes.
Mr Singer: And they make a judgement?
Mr Sieling: Yes, because the second person they go to, obviously, may be, like you say, someone not breathing o r -
Mr Singer: So, if the first person has something serious and they are on the way to Douglas, say - it may be over the mountain - and then they get another coronary or something similar, what happens then? How long would it take an ambulance to come back?
Mr Sieling: They will not turn back. They would cany on down.
Mr Singer: So, how long would it, then, take an ambulance to come from somewhere else?
Mr Sieling: Providing the control staff have followed our plan, then the next ambulance should be, at the furthest, say at the Creg ny Baa, but if it is out of hours, there will also be a first responder, resources permitting. We cannot guarantee this every night of the week but, resources permitting, there will be a first responder in the north of the Island who can respond while the ambulance is actually backing them up.
Mr Singer: So, would you feel that, in that sort of case, it would be advantageous to have availability at Ramsey Cottage Hospital to use the emergency resuscitation equipment that is there? Particularly — and I am talking, Mr Chairman, from the north, obviously (The Chairman: Yes.) - would it be to your advantage to have that hospital open, so it would be quicker to get people in?
Mr Sieling: Yes, it would be, and if you are asking my personal opinion, it would also be advantageous to have the MIU open, where they can take the people that are not quite so injured, so that they can treat them and so that it does
relieve the ambulance, then, to stay in the area and not have to go down to Noble’s.
Mr Singer: Can I ask you about inappropriate referral forms? You obviously have these. Have a number of these inappropriate referral forms... These are filled in by the ambulancemen, aren’t they, when they are called out and they feel it inappropriate? How has this changed since the MEDS service has come in?
Mr Sieling: The reason staff themselves actually led this idea was to actually bring in or raise matters where they feel the MIU could have, perhaps, dealt with a patient and they have not been; they have been asked to take them to Noble’s. So, the crew themselves - this is again only applying to the north of the Island, so it is not Island-wide - would have said, ‘Normally we would have been able to take this to Ramsey Cottage Hospital, but, on this occasion, we were told to go to Noble’s.’
Mr Singer: Is that because the hospital was shut, if it was after ten o’clock at night, or during the weekend?
Mr Sieling: It is when usually a doctor was not available to -
Mr Beattie: It is to do with the doctor’s hours, basically. It is about the appropriate treatment of the patient and whether the skill level at the MIU was of a high enough standard to be able to deliver that care needed.
Mr Sieling: That is no contradiction of the MIU staff themselves; it is just the regulations and the rules they are working under. There are certain patients that they just cannot take in.
The Chairman: Can I just ask: is that unusual to the MEDS system, bepause MEDS has come in, that apparently that has changed?
Mr Beattie: Yes.
Mr Sieling: And withdrawal of the doctor -
Mr Beattie: Yes. Because the doctor is not there... Basically, a nurse would always get the guidance from a doctor on how they were going to treat that patient. Once that facility was no longer there, they were given strict guidelines under the RCN of their practice and how they can administer care and what their limitations are.
The Chairman: And can you advise me on the withdrawal of that facility that was there before? Who made that decision? Do you know?
Mr Sieling: It was the DHSS.
Mr Beattie: That is about the withdrawal of the doctor?
The Chairman: Yes.
Mr Beattie: Yes.
Mr Sieling: As far as we know, yes.
Tynwald Select Committee on GP Out of Hours Services - Evidence of Mr S Sieling and M r R Beattie
8TGPS SELECT COMMITTEE, THURSDAY, 18th DECEMBER 2003 Oral Evidence
The Chairman: Mr Singer.
Mr Singer: Are you aware of the views of the ambulancemen who actually work from the north of the Island, as to the change in... They have actually given evidence to this Committee, and I wondered whether you agreed they... And I appreciate the fact that they have actually taken it upon themselves to feel that it is necessary to bring to the attention of the Committee various matters. They talk about resuscitation:
‘Performed in a stable environment, a resuscitation room, cardiopulmonary resuscitation is only 30 per cent effective of normal cardiac output. Bearing in mind this statement, 30 per cent optimum effectiveness cannot be achieved in the back of a moving ambulance. At present running times from Ramsey to Noble’s average 25 minutes; obviously, this time will be extended during the winter months. In order to give the patient the best chance, surely, we should all be morally and legally aiming to provide the four links which make up the chain of survival, which are: early access to emergency services, eaily basic life support, early defibrillation and early advanced life support in a resuscitation room.'
With a note that:
‘Defibrillation: for each minute’s delay, the chances of successful outcome fall dramatically by 7 to 10 per cent’
So, we know, as you have said, that it would be that you really believe you should have access, for those very reasons, to the emergency equipment at Ramsey. Would you, therefore, agree with everything that is being said there?
Mr Sieling: Yes. I mean, the defibrillation part can be a bit misleading, because they do, obviously, carry defibrillators in the vehicles, so they can give that early shock on scene, but I think it is more the case of if you have got someone in that situation of cardiac arrest, where, clinically, they are dead and you are trying to revive them, the more facilities you have got the better» so the better working environment, as well as additional help. If you go into a larger hospital, you have a full cardiac arrest team, so more people working round a patient has got to be better than two - and I can understand where they are coming from - whereas, before, they could go into Ramsey and District Cottage Hospital (RDCH) and actually have the assistance of doctors and nurses to help in resuscitating a patient.
Mr Singer: Then they also say all the changes that have taken place have led to a sustained increase in the number of call-outs from the solo responder, who produces basic life support, while waiting for back-up. Is that... You seem to say they were not these extra figures.
Mr Beattie: We have been looking into the standby call-out figures in the last three to four months, and I think there were six call-outs in the first three months - this is only off the top of my head and these are not accurate figures - whereas, obviously, prior to the ambulances available at night, the call-out figures were far higher. Those six call-outs were Island-wide. How many of them were for the north of the Island I do not know, but what I can say is the majority of them were for the north of the Island.
The Chairman: Can you provide us with that information, please?
Mr Beattie: Yes.
The Chairman: If you would forward that to the Third Clerk.
Mr Beattie: Okay.
Mr Singer: I am also slightly contradicting what you said originally: they say - and they are the people who are doing the work - there has been a large increase in transportation of patients from the North to Noble’s Hospital who could effectively be treated at Ramsey and District Cottage Hospital prior to the changes.
Mr Sieling: I think there are definitely more patients, obviously, going to Noble’s now than there were going to RDCH for the emergency side of things, because now we cannot take them into the MIU, because -
Mr Singer: So you are having to take cases of people - drunks or whatever - down to Noble’s now, (Mr Sieling: Yes.) who would normally -
Mr Sieling: Out of hours.
Mr Singer: - out of hours, yes - have gone into hospital here? So, there could be somebody seriously ill here, whilst you are taking a drunk or someone with a cut knee, a child with a cut knee, down to - (Mr Sieiing: Yes.) Thank you.
The Chairman: Mr Waft.
Mr Waft: Thank you, Mr Chairman.The situation that you arc in, from the ambulance service
point of view: do you subscribe to a professional body which looks after your interests and your work levels and the situations where you have to make decisions? Is there a professional body which you subscribe to which stipulates that?
Mr Sieling: It is the Ambulance Service Association. It was first founded by the Chief Ambulance Officers' Association and then changed, and also the Institute of Healthcare and Development (IHCD) - that is the medical side of it.
Mr Waft: Do you have a responsibility to report to that Association if there has been a problem, as you see it, with regard to the service, a decrease, or, perhaps, people are more at risk than they were previously? Would you notify your Association that there is a problem, or do you not think it would be necessary?
Mr Sieling: We are very lucky on the Island, I suppose. In fact, we use the Ambulance Service Association and the IHCD to actually give us our performance targets, both for training and the medical side, as well as responding tc emergencies. The position we are in at the moment is that we far exceed a lot of what the UK are achieving, anyway, so they would see us as being better than what they are doing over there, anyway.
Mr Waft: Would you say that the present situation, as
Tynwald Select Committee on GP Out of Hours Services - Evidence of M r S Sieling and M r R Beattie
Oral Evidence SELECT COMMITTEE, THURSDAY, 18th DECEMBER 2003 9TGPS
opposed to the previous situation, has got better or worse from a patient point of view?
Mr Sieling: From an ambulance point of view, we are better now in responding to emergencies. We can get there more quickly because of the extra vehicles we have got on board. From the point of actually getting treatment on site, then, obviously, that has deteriorated, not necessarily to the patient’s condition, but because they cannot now go into the MTU, which used to be an urgent treatment centre. They are now having to travel down to Noble’s.
Mr Waft: When you get a 999 call, to whom does that 999 call... To whom is it directed specifically? Who makes the decision on the call-out?
Mr Sieiing: It usually goes to Manx Telecom first, obviously. They ask them which service they need and then it gets passed through to us, if it is an ambulance.
Mr Waft: You would respond to 999 calls, irrespective of from whence they came?
Mr Sieling: Yes.
Mr Waft: Is there a filter by which attendance of an ambulance to a specific site... Is there anybody that filters that at all?
Mr Sieling: No. The control staff themselves use a system known as Medical Priority Despatch. What that does is it takes the caller through a sequence of questions and it then categorises the call into A, B, C or D, D being the most life-threatening.
In the UK they actually use this to categorise calls and they only set the eight-minute response target for category D, which is the life-threatening ones. For other calls, they allow the ambulance to get there within 19 minutes. On the Island we do not do that; we use it to actually give first aid advice over the phone to the caller while the ambulance is arriving, but we do not actually categorise the calls and say, ‘Well, Ds should get eight minutes and Bs and Cs should get 19 minutes.’ We say that if anyone rings 999, they should all get the same treatment and the same sort of level of service.
Mr Waft: Is there any situation where the ambulance crew, or the ambulance supervisor, would say, ‘You contact your GP in those circumstances’?
Mr Sieling: They have, yes. If they go into someone’s house and they feel that the patient would better benefit from a visit from a GP, then they can do a referral. It has to be recorded through our control room, though, to make sure.
Mr Waft: I mean prior to the visitation of the ambulance. You would not advise them to see a GP first?
Mr Sieling: No.
Mr Beattie: No.
Mr Waft: You respond to all 999 calls?
Mr Sieling: Yes.
Mr Waft: But provided they fill the criteria of what is expected for your ambulance despatch?
Mr Sieling; No. Even if we know that we are going to something that is not really an emergency, we still attend, just in case.
Mr Waft: Right. Thank you, Mr Chairman.
The Chairman: If I could just ask a couple of questions, if I may, and then I will go back to my colleagues.
Mr Sieling, in your evidence, you said there were three ambulances on duty, if I have picked it up right, and three first responders - they are now available - and the ambulances are one Douglas, one South and one North, and that is 24 hours a day?
Mr Sieling: Yes.
The Chairman: Yes. Could you just advise me how it used to be prior to this change? In other words, what was available?
Mr Sieling: Yes. What we had were two ambulances in Douglas. One of them was 24 hours a day and the second vehicle started at 8.30 in the morning until 8.30 in the evening. They then had a vehicle in Ramsey that started at... 7.00 in the morning?
Mr Beattie: It was 07.30.
Mr Sieling; Yes, 07.30 in the morning, and finished at midnight. So, what that meant was that after midnight - well, after half past eight in the evening - you would be down to two ambulances. After midnight you were down to one for the whole Island, but you did have two crews then at home that you could call in on standby, as Mr Singer mentioned earlier. They would then respond to the station, pick up a vehicle and then go on to the emergency.
The Chairman: And what about first responders? There were no first responders, so they came into being when?
Mr Sieling: When we put three vehicles on nights.
The Chairman: Which was what date?
Mr Beattie: It was 1st September.
Mr Sieling: Yes, 1st September this year.
The Chairman: In 2003?
Mr Sieling: Yes.
The Chairman: Right, okay. Just so we are clear on that. That is fine, thank you. Could you just explain to me who determines and how they determine - in other words, the criteria - when to call out the first responders?
Mr Sieling: It is the Ambulance Control Assistants, really. It is their remit that, if it is life-threatening... So if, for instance, you are saying that the vehicle has got to come
Tynwald Select Committee on GP Out of Hours Services - Evidence of Mr S Sieling and Mr R Beattie
10 TGPS SELECT COMMITTEE, THURSDAY, 18th DECEMBER 2003 Oral Evidence
from Douglas to the North or from Douglas to the South and if we know it is a life-threatening emergency, it is category D, then they will call out the first responder for that area, who will attend until the ambulance arrives.
The Chairman: And the first responders, you said, operate from home. Where do they live?
Mr Sieling: Probably, at the moment, the majority of people who work in the Ramsey area live in the north of the Island. Where we have now moved half the staff from Douglas to service the Port Erin station, obviously some of them still live in Douglas. So, unfortunately, on some nights you will have a person on standby for the first responder duties who, although he is connected to the Port Erin station, is actually living in Douglas. So, there will be nights where there is no first responder for the Port Erin station. The control staff will obviously plan their vehicles accordingly then; they know then not to ring the Port Erin vehicle up, obviously, unless it is a last resort.
The Chairman: And if a first responder was called out, what is the sort of time span... I mean, do you monitor how quickly they get to incidents?
Interjection by Mr Beattie.
Mr Sieling: We do, yes, There is a -
The Chairman: Sorry, please answer whoever feels most appropriate.
Mr Sieling: Yes, there are response times, but for people coming from home there is no set-down time.
The Chairman: So you do not monitor how they respond?
Mr Sieling: We do monitor, yes.
The Chairman: What would be an average? Do you know?
Mr Beattie: It depends on the location of the call to the person’s home address. Our targets are eight-minute responses; that is the best that we aim for, a government figure. If the person, fortunately, might be next door to where the call comes in, therefore they respond to that within that eight minutes. We do achieve response calls from home within eight minutes. It depends on the time of the day and the location from the responder’s address to the incident address.
Mr Sieling: Yes. The other thing you have got to weigh up is that if you do cover the first responder - the control staff would be considering this, obviously - the ambulance may actually head out before the first responder actually arrives, because, if it is the early hours of the morning, you have got to expect the person to get out of bed, get dressed and then get in the vehicle to go.
The Chairman: Right. So, it would not be unusual to say to a first responder that there is a call and also send the ambulance?
Mr Beattie: There is always an ambulance despatched to back up a first responder.
Mr Sieling: Oh, yes.
The Chairman: That is fine. Could I just ask: you said that, of the eight-minute response time, which is your target, 75 per cent of the time is achieved. How many of the 25 per cent of calls that are not achieved relate to calls outside of the Douglas area?
Mr Sieling: I think it is important to tell you there are two response targets: one is the 75 per cent within eight minutes, and then the remainder must be responded to within 19 minutes 95 per cent of the time.
The Chairman: So it is in 19 minutes?
Mr Sieling: Yes, 95 per cent of the time.
The Chairman: Of that 19, of that 25 per cent, 95 per cent have to reach the -
Mr Sieling: Yes. It is still that target amount, really.
Mr Singer: Do you reach that level?
Mr Sieling: Sony?
Mr Singer: Do you reach that level?
Mr Sieling: We do, yes. We actually exceed it, usually.
Mr Singer: Is that split, though, between different areas?
Mr Sieling: We can do it in different areas, but we have to do it as a service. Like other services report back, it is the whole-service percentage. So, if you looked at areas, then, obviously, you could say you have not got a station in Peel, so you know you are not going to achieve eight minutes in Peel, because the nearest ambulance is Douglas. We can get there within' 13 or 14 minutes from Douglas on a good day, but this is common sense that you have not got a station in Peel, but, looking at the calls, you look at 15 or 20 emergency calls a month for Peel, which is not to say that they should not deserve a station; it is just that we are looking at other ways of actually bridging that gap.
The Chairman: You say that there is an ambulance normally situated in the Douglas area, south and north. Can you tell me: with the new system, clearly, if there is an incident and, say, the north ambulance is already at an incident in the north and another incident was to occur in the north, presumably you would despatch the Douglas one? Has there been any knock-on effect, then, in terms not only of servicing out of Douglas, but inside Douglas, because of how the ambulances may have been called? Do you know if that has caused any problems?
Mr Sieling: As soon as the north vehicle is despatched, we move the Douglas vehicle to the Creg ny Baa. If that is then dispatched, or used either in‘Douglas, or in the north of the Island, we bring up the Port Erin vehicle to Douglas.
Tynwald Select Committee on GP Out of Hours Services - Evidence of M r S Sicling and Mr R Beattie
Oral Evidence SELECT COMMITTEE, THURSDAY, 18th DECEMBER 2003 11TGPS
It is a bit like a game of chess, I suppose, in a way, but, no, we have not seen it because it has always been better than what we have had before.
The Chairman: So, the ambulance service you now have is, in your opinion, better than what was there prior to September this year?
Mr Sieling: Yes, and that was part of our plan, to put more vehicles on 24 hours; it was not, really, a result of anything else.
The Chairman: Could you give any information on the type of patients that the ambulance service has started to deal with in terms of: has there been a change, since the introduction of MEDS, in the type of people who are now calling for the ambulance service, or has it, basically, stayed thè same?
Mr Beattie: There is nothing that stands out, that I could say there is any change in the type of client.
The Chairman: So, you have not seen people calling the ambulances for more minor sorts of issues?
Mr Sieling: No. Like I say, we expected that initially, because we thought people were fearing that they could not get a GP quickly enough and they may call us, but that did not come about.
The Chairman: Could I ask - and then I will go back to my colleagues: in terms of any problems that you have, could you explain your reporting procedures, how to get improvements to the system if there is a problem? In other words, what is your authority to implement that, and, if it is above you, in terms that you need more resource, or you need whatever it may be, how do you progress that through the system?
Mr Sieling; Obviously, we report back to Primary Healthcare; they are our managers, if you like - Geoff Newbery. What we do every year is we put a plan together. We have the five-year ongoing business plan. We look at the statistics, and, if we can see a marked increase in demand, then we put that forward as a bid to Primary Healthcare, who then put it through to the Health Services Division and so on.
The Chairman: Right. So, if you saw something happening in your statistics that was causing concern, and you felt it was quite urgent, how quickly could you get a response to dealing with that? Is it waiting for another six months or a year, or can you actually respond more quickly than that to get the additional resource, if the Department - ?
Mr Sieling: We do not have authority to do that; no; we have to go through Primary Healthcare. All we can do is put our case forward and stress how important it is, if you like.
The Chairman: So, you are then reliant on Primary Healthcare to make a case to the Department?
Mr Sieling: Yes.
The Chairman: Okay, and if there was a matter causing you serious concern, how do you leave it? Do you just leave it with Primary Healthcare or do you pursue it?
Mr Sieling: We just have to leave it with Primary Healthcare; that is our ‘command structure’, if you like. We are not allowed to leap-frog over our General Manager, which is -
The Chairman: No, that is fine. How much do you cajole, push, pressure?
Mr Sieling: Oh, we do put quite a bit... Yes, we do sort of fight our comer.
The Chairman: You do not just sit and wait?
Mr Sieling: No, we do fight our comer quite well, yes.
The Chairman: Okay, that is fine. Mr Gill. Thank you.
Mr Gill: Thank you. I am just conscious of the clock, so I will be brief.
Given that the remit of the Committee is an all-island brief, not just specifically the North, I will ask you a couple of southern questions, if I may. What complementary role does the Rushen Ambulance Service provide?
Mr Sieling: It does not, to be honest with you. We have tried. We have worked with Martin Benson from the Rushen Ambulance Service for many years and we have tried to get them involved with first responding for the area, especially as, like I said earlier on, some of our staff have moved from Douglas to the Port Erin station, so they cannot provide this first responder duty, actually, in the southern area. So, we thought the Rushen Ambulance Service would be ideal for that. We have offered them training and we have offered them anything to come on board with us, but, unfortunately, we still wait for their reply.
Mr Gill: But that is ongoing?
Mr Sieling: Yes.
Mr Gill: Okay. Secondly, you have described the circumstances that are consequent on the closure of the MIU in the North. Given that this is the situation we have got now and that we have never, in the South, enjoyed an MIU, would you say, broadly, the North and the South now have pretty much the same cover?
Mr Sieling: Yes. We do not get quite so many calls for the South of the Island as we do for the North, but yes, you have now got the 24-hour ambulance, apart from, as I say, at the moment this problem with the transitional period where the staff who man the station live in Douglas, so the first responder duties are limited.
Mr Gill: I think you mentioned previously that, in your opinion, the MIU would be a facility'you would like to see in the North?
Tynwald Select Committee on GP Out of Hours Services — Evidence of M r S Sieling and M r R Beattie
12 TGPS SELECT COMMITTEE, THURSDAY, 18th DECEMBER 2003 Oral Evidence
Mr Sieling; Yes. Well, the MIU would be a service we could actually take patients into, yes.
Mr Gill: So would that be a fair extension to say that that would be mirrored in the South, that would be the same benefit?
Mr Sieling: Yes. One of the things that we are looking at at the moment and closely monitoring is what is.. . I know we do not follow what the UK do, and a good example of that is our response times. We decided to do better, and, on top of that, we are looking very closely at what the ambulance Service is now providing in the community over there, which is that they are actually manning MIU centres in certain areas of their counties with paramedics. While they are on station they can provide two services: one is the emergency service for the ambulance, but also they can actually respond when people come into a ‘one-stop shop’, I believe they call it now, and they actually prescribe.
Mr Gill: Just finally, can you tell us: the three-ambulance cover system you have described - how does that compare in cost terms? Is that more expensive than the previous system?
Mr Sieling: No. What we have done is actually restructured the ambulance service itself. We have moved the people from Douglas down into Port Erin, and, to bridge the gap, we have actually brought in some outside services to do some of our lower demand work, which is the Patient Transport Service (PTS), people bringing people into Noble’s and Ramsey for out-patient appointments and such. That is now done by the Red Cross, which has relieved us of human resources, so we can actually then place the resources, highly trained as they are, down into Port Erin to man the station.
Mr Gill: Thank you.
The Chairman: Mr Singer.
Mr Singer: One point: are you aware of the ambulance ever turning up at the MIU and being refused admission with a patient? And, secondly, as a general point of view, from an ambulance service point of view - and probably you might want to take the north, centre and the south separately - what improvements would you like to see in the provision of out-of-hours patient care in the Island, from an ambulance point of view, in the three areas? What would you like to sec, ideally?
Mr Sieling: In no special order, I know there were some problems initially when the RDCH went down to an MIU, and that was to do with timings and communication between us and them, I think, in some ways. We have improved that now and the actual crews have got mobile phones in the vehicles and they can ring directly into the MIU to: firstly, tell them what they have got, to see if the MIU can actually deal with it; and, secondly, to forewarn them that they are actually coming in, so it helps them prepare as well. But, initially, there were problems with communication, yes, where ambulances would turn up and there was no-one there to receive, perhaps, the patient.
Mr Singer: And as it is Christmas, what would you like to see, (Laughter) from your ambulance point of view, to
improve the out-of-hours patient care on the Island?
Mr Sieling: The out-of-hours? If you are talking about ambulance services, or you are talking about -
Mr Singer: Yes, from your -
Mr Sieling: From the ambulance service? The ambulance services would like something in the west of the Island, whether it be something working in conjunction with the doctors’ surgery there and, like I said, if we had some sort of Minor Injuries Unit in the North of the Island, I would obviously like something down in the South as well, which, perhaps, again we could be involved with and partly man, providing we are obviously given the resources to man it.
Mr Singer: A 24-hour service, or just-
Mr Sieling: Yes, 24 hours.
The Chairman: Okay? Mr Waft.
Mr Waft: Could I ask: what have you lost in the presenl changes that have taken place that you think is important?
Mr Sieling; What have we lost? If you are, again, referring to the MEDS service, I do not think we have lost; we are the same as what we were. If you are asking specifically about the MIU, we have lost the facility whereby we could turn our vehicles round more quickly in depositing patients -
Mr Waft; Just a minor... Just a clarification for the people listening: what is an MI Unit? What does it actually do?
Mr Sieling: Minor Injuries Unit. They deal with things like -
Mr Beattie: Very minor injuries -
Mr Sieling: Very minor injuries, yes.
Mr Beattie: They can suture. That has taken a little while to put in place, but they are limited in what they can suture, so, again, it is... Sutures mean stitching, so it depends, again, on the severity of the wound as to whether they can deal with that or not,
Mr Waft: Do you have to do that?
Mr Beattie: No. They will assess the patient as tc whether they can deal with the patient or not and, depending on what their criteria are based against, then we might have to transfer that patient down to Noble’s for the appropriate treatment.
Mr Waft: If it is not there, you would have had to dc that? It would not be direct, would it?
Mr Beattie: Yes. If there is a facility there, then obviousl> you can use that facility.
Mr Waft: What else would that facility provide?
Tynwald Select Committee on GP Out of Hours Services - Evidence of M r S Sieling and M r R Beattie

Oral Evidence ' SELECT COMMITTEE, THURSDAY, 18th DECEMBER 2003 13 TGPS
Mr Beattie: As an MIU, they have their criteria. I could not really teil you off the top of my head. There are a lot of areas that they can cover. They can administer antibiotics to a certain level. {Interjection) They cannot?
Mr Singer: I know that from experience.
Mr Beattie: Right. I thought that they could, so, again, am I wrong in that aspect. They have got a guideline book that they work to. You would probably be better off getting a copy of that and then you could see exactly what they can and what they cannot deal with.
Mr Waft: Could I ask... The situation with regard to Geoff Newbery and the Primary Care to which you refer any problems that you have from an ambulance point of view: do you take into account the demographic changes that take place within the Island and do you submit that sort of information? Say, for instance, there is a problem, perhaps, for you or for your side of it when there is a large housing estate going in the Peel area and having two or three hundred houses; that would have an input, would it, into your considerations?
Mr Sieling: Yes, it would do, yes. It would add weight to any bids that we had got in for something in the west of the Island, if it was Peel you are talking about, yes.
Mr Waft: Would you also take into consideration the geographical problem of outlying districts of the Island as well? That has a bearing on your decision?
Mr Sieling: It does, yes. We have already got first responders within the service. One of our other things for the future is to actually get groups of people who live in these remote communities to actually operate a first responder scheme themselves, which is where we thought Rushen would be the first ones, perhaps, to come on board. It is not necessarily groups of people who would, maybe... People who are also members of the fire service, retained fire service, or local policemen in police stations... (Mr Beattie: Yes.) So, we are hoping to get them on board to actually bridge the gap until the ambulance gets there.
Mr Waft: Thank you, Chairman.
The Chairman: Mr Gelling.
Mr Gelling: I am very conscious of the time, Mr Speaker, but I am intrigued, really, about the strategy of the ambulances and I was, of course, clicked on when you said if the northern ambulance designated was already running someone, the Douglas one would come up to Creg ny Baa, and then if that one was taken, the one from Port Erin would come in, so the South was left with no ambulance, basically. One of the questions Mr Gill has already asked, and that was: what part should the Rushen ambulance be playing? Jt used to play a very important part, and what I am coming to is, whether it be perception or comfort, it gave a comfort to the people in that area that there was an ambulance there, standing by, and people relaxed a little more, because they knew that they could be attended to very quickly. Basically, now that you have moved and you have got these ambulances strategically positioned, I know at Santon, of course, we
have become very privileged, because I have an ambulance at the top of my road, and when you are over 65 (Laughter) that is a great comfort.
However, I am coming to the practicalities. You have got men and ladies sitting in an ambulance at the side of the road. Now the practicalities of that: is that not something that needs attention, inasmuch as should you not now have decided to have a depot there? Should the ambulance not be plugged into the mains electricity? I am thinking: engines running, keeping them warm. They have to go to the loo. How is that going to progress? Is that something where, now you have had a trial run, you should have a depot at wherever it is, the Bungalow and Santon, or wherever? It just seems that it is a loose arrangement, in my mind, in the practicalities.
Mr Sieling: We do rely heavily on our colleagues from the Education Department for Santon, because we have got Santon School, so we can actually park the vehicle there, or, if they are going to be there for some time, they can use the facilities there, such as toilets, and there are also tea-making facilities, so they can have a brew.
The Bungalow is a different scenario, because, at the moment, we have not got any access, but we are hoping, seeing what is going on, the new development up at the Bungalow, to tie in with that, so we can actually use some of their facilities, perhaps. But, in the winter, also we use Laxey, and we have now got the new GP surgery in Laxey, and we have been promised accommodation there if we need it.
Mr Gelling: Just one more, Mr Speaker. Have you made this request through the normal channels, through to the DHSS from the ambulance scrvice, that this is something that needs serious consideration, having permanent places at your strategic positions?
Mr Sieling: Yes. We have brought it up at Primary Healthcare level, yes, because that is how we got permission to use, obviously, the GP surgery in Laxey. Also Primary Healthcare then contacted the Education Department at Santon. We have not approached them yet about the Bungalow, to be fair.
Mr Gelling: Thank you.
The Chairman: I think, mainly, I have just the one question: I just want to ask you, maybe, to give some view and answer whether or not you have an emergency procedure in place in relation to inclement weather. As we are all aware, the North, because of the mountain road, can be hit quite hard, and also, of course, it can be hit hard through the Kirk Michael area. It is not unusual, if we do have snow, that those two areas actually get snow that blocks them off. Could I ask: do you have any emergency procedures in place in that sort of circumstance? How do you deal with it?
Mr Sieling: We do work closely with the fire brigade, who have got vehicles that can actually get in and out better than ours. We have had to use the Pinzgauers in the past, to actually transport patients to a road that is clear. In a dire emergency, obviously, at the very worst, we could always use the RAF, through the Coastguard, but we are also looking at the moment, in discussions with Ramsey Cottage Hospital, specifically for the north of the Island, if we cannot get down to Noble’s, at a contingency whereby it is opened, or
Tynwald Select Committee on GP Out of Hours Services - Evidence of M r S Sieling and M r R Beattie
14TGPS SELECT COMMITTEE, THURSDAY, 18th DECEMBER 2003 Oral Evidence
it is upgraded for an emergency, as they do and help us out for the TT.
The Chairman: So, it is an issue that is current? (Mr Sieling: Yes.) I think that is fine.
First, I would just thank you very much for the evidence you have given and would say that we may wish to speak with you again, so, if we do, we will be in contact. And there were two issues: one was the breakdown of calls in terms of North, South and so on - if you could forward that to us - and also the breakdown of the calls for the first response times.
Okay. Thank you very much.
unfortunate because we have never used this room before, so we do not know and it is quite difficult. Right. Okay? If we are all happy, that is fine.
Thank you, Dr Maska, for coming this morning. Can I just read out the remit which we are working to, so that you are aware of it? The remit that Tynwald has given this Committee is to investigate the matter of the general practitioners’ out- of-hours services being provided throughout the Island. As a Select Committee, we received written correspondence from you and also we felt it would be helpful to have the opportunity to hear oral evidence from you. So, first, if you would like to do some form of introduction and then we will take it from there and ask questions. Okay?
Dr Maska was called at 11.44 a.m.
Procedural
The Chairman: Right. If I can invite Dr Maska, Chair of the GP Subcommittee of the Isle of Man Medical Executive, to come forward, please.
A Member of the Public: I am sorry, we cannot hear. Are we meant to hear? (Laughter)
The Chairman: You are meant to hear, but we did invite people to move forward, because it is a problem -
A Member of the Public: It is still impossible to hear. (Interjections by other members o f the public)
Dr Maska: Sitting at the back, it was virtually impossible to hear what was said.
The Chairman: Unfortunately, the acoustics are not the best and we cannot do an awful lot about that, I am afraid, but if you want to move forward again, all we can do is -
(Interjections) As long as it does not cause problems for the equipment. It will not, as long as we do not pull wires out.
Really, if those asking questions — and we apologise if we have not asked loudly enough - and those responding can speak up, that will be fine, but if we can move that table slightly around, I do not know if that will help. (Interjection)
Dr Maska: Would it help if I pulled that thing closer?
The Chairman: No. We had better let our technician, our Hansard people, deal with that. Can I just say that if you cannot hear, just indicate with your hand and we will just ask people to speak up. Alright? It is just unfortunate, because the room is actually a different shape than where we usually use and, of course, it is not too bad to hear in there. Also, this has got a system that blows air, so it is making a background noise, which is not helping. I do not know if the press want to turn their table around a bit, because I think you are having difficulty as well, aren’t you?
Dr Maska: We will try not to ignore Mr Gelling, but we will ignore the press! (Interjection and laughter)
The Chairman: As you will appreciate, it is just
EVIDENCE OF DR M MASKA
Dr Maska: My name is Marius Maska. I am currently a GP Principal at the Ramsey Group Practice and have been there for some 10 years now. Prior to that, I was also a GP Principal in Canada for some two years. Currently, for my sins, I sit as Chair of the GP Group, which is an informal talk-shop which represents GPs’ views via the Isle of Man Executive, which is the negotiating body for both GPs and consultants on the Island and represents their views to whichever Department wishes a view from doctors. That is it in a nutshell, or quite simply. (The Chairman: Right.)
Let me think. Can I just ask: have any of you gentlemen heard of the ‘red book’?
The Chairman: I certainly have not. (Dr Maska: Right.) Not the little red book; the little black book. (Laughter and interjections)
Dr Maska: It is, basically, to know at what level to pitch my answers, because the red book is a book that was started in the mid-1960s when a GP contract was first mooted then, arid it is, basically, a book that sets out terms and conditions for general practitioners in the UK. It is the book that we have followed on the Isle of Man, with one or two minoi exceptions at the end of the day. The book sets out currenl terms and conditions and it is partly important, in that the new GP contract which comes out in the UK, as of April next year, really dispenses with the red book completely.
Can I also ask: have any of you gentlemen received a copy of a DoH document dated October 2000 which is the Department of Health response to the independent review oi GPout-of-hours services in England: ‘Raising standards foi patients: new partnerships in out-of-hours care’?
The Chairman: I think we have, actually. Just bear with us; we have had quite a lot, so I am sure we have. Yes, we have, from the DHSS. That is fine. Thank you.
Dr Maska: Right. I will just say that the remit thai I thought the Group... You know I am here to represem ‘GPs - Isle of Man’ and not particularly Ramsey Group Practice, nor the Ramsey Cottage Hospital, because Tynwald has asked for a further report with regard to the Cottage Hospital, which is separate.
The Chairman: Yes, that is fine. Is there anything -
Tynwald Select Committee on GP Out of Hours Services - Evidence of M r S Sieling and M r R BeattieProcedural
Tynwald Select Committee on GP Out of Hours Services - Evidence of Dr M Maska
Oral Evidence SELECT COMMITTEE, THURSDAY, 18th DECEMBER 2003 15TGPS
(Interjection) Sorry, I think it would be helpful if you gave background as to how the GPs on the Island see the new system, where they may or may not see problems, any benefits, just as a general broad brush, really, to give us some information on it.
Dr Maska: Taking it as a general broad brush, the GP out-of-hours is just part of, basically, looking at how we recruit and retain GPs to the Island. In the UK there is a big problem with general practice. I have a little snippet from The Telegraph dated from October of this year
‘Vacant GP posts rise by 33 per cent.’
They are not my statistics; they came from The Telegraph. The Isle of Man, basically, does not produce GPs; it is virtually entirely reliant on the UK for its workforce. How do we, as an Island, turn around and compete with the UK? At the moment we have been lucky on the Island, in that we do not have shedloads of GP posts vacant, like other parts of the United Kingdom.
There are areas of the United Kingdom... I gave the reference of a chap from Peterborough Primary Care Trust (PCT), quite a nice part of England; he had been advertising for GPs for 12 months. It was not a case that he had interviewed anyone; it was a case of no-one had even applied, or even rung up to ask what the job was all about. TTiat tells you the scale of it.
A counterpart of his in Lincolnshire was predicting that, within 18 months, he would have no GPs left in East Lincolnshire, and there are various factors for that: one, there is a bulge of GPs at the moment who are on the cusp of retirement, and it is, sort of, like that on the Isle of Man. If you look theoretically, 25 per cent of GPs on the Isle of Man could retire in the next five years. If you are looking, perhaps, a little bit long term, virtually 50 percent of us could go in 10 years, if we wanted. So, although we have not got a problem at the moment, it is a case of: how do we pre-empt the problem? It is nicer to turn around and say that we have been pre-emptive, rather than reactive.
There is also, sort of a... Although the UK Government says the number of doctors in training has gone up, that is a little bit of a false premise, because over 50 per cent of the intake of medical schools is female. Now, no offence to the ladies, but they do not tend to, as a whole, want to work full-time and they want, basically, hours that are family friendly, and that roughly translates that they do not want to do out-of-hours work. So, most of your GPs that are being trained now are female. To train one full-time partner, you are more or less having to train two or three people. And, again, it is not just female doctors; a lot of male doctors are now wanting to work three-quarter time - nine to five hours, or nine to five Monday to Friday. So, there is a problem, and there are posts within the UK, salaried posts, that fulfil the requirements of those people. So, we have to find ways of somehow competing.
GP out-of-hours: even when I was a trainee, going back 15 years, large areas were already covered by co-ops to, basically, ease the burden. It took a long time to establish the old Manndoc service on the Island, and really MEDS is bringing us into a situation where we have just really caught up with the UK. The days of GPs... Other than the ones who are really in the far flung spots of the Highlands and Islands of Scotland, who did their own on-call; they are
very few and far between the numbers of GPs who now do their own on-call.
If you turn around and say, ‘What is every chief executive of every PCT in the country doing at the moment for Christmas?’, the answer is that they are pulling their hair out, because they do not know how, of April next year, they are going to cover the out-of-hours. The BBC surveyed that eight out of 10 GPs were not going to do any out-of-hours, and, under the new contract, the default position for GPs with regard to out-of-hours is to do none. You have to vote into the service, not vote out of it.
For a change, on the Isle of Man, I would say we are a year ahead. We have sorted that. We have got a decent deputising service, so, for a change, we have actually been pre-emptive. With Mr Tomlinson, Mr Killip, the GPs who have negotiated this, Mr Newbury, Mr Wilson and Mr Jones, we have actually got a set-up now which I use, my family use, my relatives use, my friends use, and if it was not safe, if something was going to be put on the Island, I would be after Leonard and kicking him all over the place to sort it out, so -
Mr Singer: It is not me any more.
Dr Maska: I think the service that has been put in is extremely good, when you compare it to co-ops in the UK - and several of us visited the Preston co-op. If you look at overall staffing levels within it, it is actually quite generous, and, if you look to the equivalent of how you would staff the Island on a Preston basis, you would have a third of the number of GPs.
I will make a comment about the biggest problem with access, and if you want to write it down, if you are going to ban it, it is called the TT and the Manx Grand Prix. They have been the single two factors that have prevented access. I cannot remember who it was who mentioned - whether it was yourself - road closures in winter.
I have been here 10 years and I do not think I have seen the roads totally closed, where we could not get anywhere, and if it is at that level that patients cannot get there, I am not going to get there either. We have already had a MEDS vehicle off the mountain road in the last week in the fog.
So, basically, there are problems with regard to recruitment and retention of GPs to the Island, and this is just one way of trying to even up the playing field. If you are going to say, ‘You have to do more on-call than the UK’, you are going to be like that guy in Peterborough, where no-one is going to apply.
As part of the reference, I did pull classified ads out of the British Medical Journal (BMJ) and, in my letter .explained that, for virtually all the posts, there was no on- call commitment with them, or, basically, most of these jobs implied that there was a co-op in place. So, the advent of MEDS has really not been a quantum leap by UK standards - and even on the Island standards - because Manndoc already covered the vast majority of the Island. It has not made huge amounts of difference.
If you are going to look at the Ramsey perspective, there was a lot of wild rumour initially, like: the ambulance station was closed; there were no GPs available, full stop, after 6 o’clock; and that you could not get hold of a doctor after six. Largely that hullabaloo has died down. Certainly, looking at the service that the Group‘Practice offered at the weekend, I think that MEDS provides a better service than
Tynwald Select Committee on GP Out of Hours Services - Evidence of Dr M Maska
16TGPS SELECT COMMITTEE, THURSDAY, 18th DECEMBER 2003 Oral Evidence
we did because, as GPs, we spent most Saturday mornings scurrying around the Cottage Hospital, which meant that you were very lucky if you ever got visited before midday, whereas now, with MEDS, most people get visited within half an hour, which has actually bettered the situation.
I can quote Mrs Brew from Ballacob, because she has allowed me to use her name. She used the service at the weekend and said it was absolutely fantastic, and that has generally been the flavour of things that have come across to me. Speaking to Mr Bell at the Cottage Hospital buffet last week, he, basically, has not heard of any complaints within the Ramsey area about the new MEDS service. Yes, I can understand that any change brings a certain amount of anxiety, and I think some of that was probably engendered by the Ramsey rumour mill, as well, but, once people have got the correct information as to how to access the service, what to expect from the service, most people have been extremely happy with it, and I do not know of any formal complaints made against MEDS at all.
So, I think the system that we have got allows us, as GPs, to basically compete on a more comparable level with our UK counterparts and allows that, perhaps, when GPs start retiring, we can attract people here. There was certainly one practice that spent two years advertising for a partner, and it would be nice that we had managed to keep ahead of the game.
The service that is in place, I think, works very well. The GPs like working for it. It has opened it up also to non- principals, as well, to a small number of non-principals who work on the Island, and long may it continue. Those GPs who have wished to cut down their out-of-hours commitments have been allowed to do so, and it has made a difference to certain partners within our practice, one of whom, with a recent illness, did not feel that she would be able to continue with out-of-hours. We may well have lost one of our best partners within the practice; they have managed to get around that. I included, again, a resignation letter from one of the Douglas GPs. He has, basically, stayed on, again because he has been allowed to cut his out-of-hours commitment. So, some of your most senior GPs, the people that you value the most, have decided to continue. Talking to colleagues across, they are very envious of what we have managed to achieve here.
If you are going to say, ‘What pitfalls? What would you like to see on your Christmas shopping list?’, I would like to see purpose-built premises for the out-of-hours service, because, at the moment, we are based in the fracture clinic, which was designed as a fracture clinic and make no bones about it: when the new hospital was designed, there was no wind of Primary Care health services being held within it. Again, with the Preston set-up, there is a nice big red entrance with ‘A & E\ Fifty feet down the road is a nice big entrance for Primary Care. It is. the same with Holton. It has been mirrored up and down the country, and, certainly, it would be nice to have purpose-built premises which are more designed for the needs of examining patients within Primary Care, rather than with broken legs per se. You have it in a nutshell.
The Chairman: Okay, thank you for that. Just before I go to my colleagues, could I just ask a question? Partly, you may have hinted at it, in that part of your evidence was that there seems to be a misunderstanding or preconception that the system is not very good, and so on and so on.
Have you - when I say ‘you’, I mean you are representing the GPs - a concern about the lack of effective publicity, promotion, information, advice to the general public, which is causing a lot of misunderstandings? And, in fact, it may well be that it is only when they experience the service that they actually see whether or not it is what they fear.
Dr Maska: You say ‘causing’ ; I would have said ‘caused at the time’. I think that, because the negotiations went down to a fine wire, there was not a huge amount of time available to publicise the changes. In hindsight, yes, you would have liked to have given more public warning of that Whether that would have changed the anxiety of people... As I was saying before, any change causes a certain amount of anxiety. Whether that would have changed things, I am not certain. I think a lot of the fallacies and rumours that went around initially have been laid to rest, and I think, now, the information that is... People have now got used to the service; it has been running for over six months. Largely it is not particularly an issue now; I think people know how to access it.
The Chairman: Have you any information as to the amount, either in numbers or percentages, of people who experience the new system and who are, in fact, unhappy with it, as against those who are content with it?
Dr Maska: As far as I am aware - and I do not have written figures, I am only going off what I have had verbally from Mr Newbery - there have been no formal complaints with regard to the MEDS service.
The Chairman: That would not necessarily be unusual. I was really looking to when the GP arrives, or -
Dr Maska: I have not heard of any particular grumbles. I do not, personally, keep those statistics because I am not there all the time. The system is now administered by Primary Care.
The Chairman: But, on the ‘coal face’, to use this term, the GPs -
Dr Maska: No. I think the vast majority of people are extremely happy with it. Most of the time you get people who phone up - ‘Oh, I saw Dr So-and-So’ - and it is anecdotal evidence from, say, the receptionist staff that ‘Oh, can you pass a message on to Dr So-and-So? So-and-So phoned back. They were extremely happy with the service.’ My gut feeling is that there has been a lot more of that kind of saying than someone who has phoned up saying, ‘Well, that was a bag of old whatever. ’
The Chairman: So, when people are expressing concern, presumably they would do that when the doctor is actually with them, because of whatever? Is there a general trend in what that is?
Dr Maska: I think that is fairly minimal. I think most people are quite happy with the service. Ones that are sometimes not too happy with thé service are where, perhaps, it is not what is regarded as an emergency by the doctor and there is a difference in views as to whether that person should have been attending there in the first place. You certainly do
Tynwald Select Committee on GP Out of Hours Services - Evidence of Dr M Maska
Oral Evidence SELECT COMMITTEE, THURSDAY, 18th DECEMBER 2003 17 TGPS
get a certain number of people who are out for the second opinion out of hours. They have seen the doctor during the day or during the week, and, really, you get the impression that what they are asking is a second opinion. It is not really an emergency out-of-hours call, or what they are asking is not realistic.
I will give you an instance: someone phoned one particular doctor at four in the morning, asking if they could expedite their eye appointment with Mr Travers. Is that really appropriate? No.
The Chairman: But presumably they are pretty rare?
Dr Maska: They are not as rare as you would like to think.
The Chairman: Just my last one for now, before I go over to my colleagues: in terms of the GPs who are working with the people directly out of hours, do you have a system within your organisation to feed back information which then can be passed onto Primary Care, where there are concerns, or where there are improvements, so that there is, actually, a realistic picture being portrayed?
Dr Maska: There is at the moment an Out-of-hours Committee, which comprises GPs, Geoff Newbery from Primary Care, Sally Duke, who oversees the running of the MEDS service, and everyone there... Again, there are some people from the hospital side, as well, there - Mr Inman sat in on a couple of those meetings. I have yet to meet Mr Phillips himself, but he was invited to the last meeting that we had this week. We look at all-encompassing issues: how the service is performing, crude statistics on numbers, whether there are problems elsewhere, accessing hospital services. It, basically, looks at the whole running of the out-of-hours service.
I must say that, for Primary Care - because they have never, actually, physically had to run that kind of service - yes, they are coming up to running speed. I think, six months down the road, it seems to be working better. There are still issues with more or less portering within the hospital, which are not really particularly the GP/patient care side of things, and facilities offered to GPs within the hospital.
The Chairman: Okay. Mr Singer and then Mr Gelling.
Mr Singer: Dr Maska, I do not think anybody, really, is complaining that the doctors have decided, ‘We do not wish to do out-of-hours any more’; what they are concerned about is what has replaced the fact that their general practitioners are no longer available overnight And I must say that, whilst you say there have been no formal complaints, I think that many people would say a lot of people do not make formal complaints about the doctor, because they are afraid that the doctor can turn around and strike them off their list, so I am asking this question a little in trepidation, I think.
Dr Maska: I won’t mention anything to Dr Brownsdon!
Mr Singer: Our evidence that we have got - and the evidence is here and I think there is probably as much evidence for this Committee as any - splits clearly into two
lots of evidence.On this hand, you have the doctors, who are all saying,
as you have said, ‘We no longer want to work these long hours, but we think the MEDS service is working very, very well’, and there is a complete split from the other side, the evidence from people, who are saying, ‘We are worried, as patients, that we are not getting the service, for various reasons, that we feel we should get.’ A lot of it is, maybe, perceived, but also we have lists of letters here - while there is no complaint from people giving actual instances of things that they have complained about - and some of those will be printed in the final evidence. But can you tell me: is there any financial consideration in the fact that the doctors have given up the night cover?
Dr Maska: There are two bits. To give up the night cover was costing GPs £6,000 a year per person. There is a fee schedule within what MEDS pays doctors, which... If you work for MEDS, then some of that cost is offset If you do not work, you lose six grand. For us in Ramsey there is a bigger cost, because we no longer cover the casualty either, so we have lost the payment for that. So, as a Ramsey GP, I lose a lot more, but that is purely Ramsey.
As general GPs, it has been set at £6,000. That was the figure that was set by the UK Government, as to how much opting out of out-of-hours would cost a general practitioner. So, we, basically, sat down and roughly divided the number of sessions by the number of GPs and came up with a fee schedule, that if you did a couple of sessions in MEDS a month, it would more or less get you back that £6,000. That was just shared within the 42 GPs that are on the Island.
Mr Singer: How many of the GPs on the Island have now given up the night cover because they wanted to work fewer hours are actually taking part within the MEDS system?
Dr Maska: It is difficult for me to give you a categorical figure, because -
Mr Singer: Most of them.
Dr Maska: No, most of them do work; most of them do contribute.
There were certainly two GPs, who, at the onset of MEDS, said they were not going to do the out-of-hours, full stop. Other GPs... It depends on the individual, and you would end up... You can ask me, but I can only speak for myself. I do not mind doing a couple of sessions. Some of my partners do not do any sessions; some do more.
It is the same with the Douglas GPs and the Port Erin GPs. It is up to the individual. If they do not want to work, they do not have to work. If they want to work, it is up to them. It is a personal decision.
Mr Singer: The fact is, though, that anybody who chooses to work only has to do a few sessions per annum to recover what they were paid for covering all the time.
Dr Maska: Yes. That is part of it, but, historically, what was paid for under this red book was basically peanuts, absolutely peanuts. I have deliberately kept a little snippet that came out of The Times a year or so ago, and it sort of started on about rates that varied from between £60 to £80 an hour and then went up to £140 per hour. That was for
Tynwald Select Committee on GP Out of Hours Services - Evidence of Dr M Maska
18TGPS SELECT COMMITTEE, THURSDAY, 18th DECEMBER 2003 Oral Evidence
London plumbers, and we are still not paid... It is still more lucrative to be a London plumber out of hours on an hourly rate. (Interjection by Mr Singer) Yes.
Mr Singer: Could I just put together a little scenario for you, really?
We have evidence presented that the GPs’ lists are greater than anywhere in the UK - we have got those figures today - although I know it must change between doctors. We also have patients saying - and they have said - that it is difficult, generally, for them to get an appointment to see the doctor, and yet we have GPs who are doing other work. I think it is known that Doctor Blackman, for example, works two days in the Diabetic Clinic.
The suggestion is that, for example, if we talk about up here, the Ramsey Cottage Hospital would return to the umbrella of Isle of Man Hospitals and the doctors should be recruited via Noble’s Hospital in the normal manner. They would then look after the in-patients and all-night cover, so that would release you from your responsibility of having to look at the hospital. It would improve the service to the people in the north of the Island. It would give you more time to look after your patients and everybody else more time to look after their patients. Don’t you think that would be an improvement of service to the patients, as I say, while leaving GPs purely to concentrate, as you seem to want to, on your own patients and give more time, maybe, to see those patients generally and to have more appointments available?
Then we have full-time cover in the Ramsey Cottage Hospital for the north, with doctors -
Dr Maska: Full-time cover in the north is completely irrelevant if you are a Port Erin GP -
Mr Singer: No, but if you do -
Dr Maska: GP out-of-hours, Leonard, is not the Cottage Hospital -
Mr Singer: No, but if you had the full cover here, then you and the people who want to do the MEDS would then be able to concentrate on the rest of the Island, but we have still got an urgent treatment and release return here, rather than a minor injuries unit which is shut for about two thirds of the time.
Dr Maska: Right. With regard to numbers of GPs, basically within the UK - a little snippet - half of all PCTs... PCTs are Primary Care Trusts; they are basically the people who run a local hospital and primary care within the UK now - just to explain to everyone what these organisations are. They have, more or less, taken over from the local health authorities, and they encompass primary care and secondary care.
If you look at figures, they have come out with a figure that, basically, says that there should be roughly 55.5 GPs per 100,000 population. Now, there is a difference between the census population and the registered population of the Isle of Man. It is a contentious issue,.but, basically, all those characters who were away in Tenerife for 3 months do not fill in the census, nor do Afghan refugees in London, which is part of the reason why the UK’s registered population is far bigger than the census population. When you look at that level, then we, basically... Yes, we do have fewer GPs than
the UK counterpart.If you look at overall list sizes, certainly compared to
Scotland, Wales and Ireland, we are on a rough par, perhaps, with some of... Well, we are definitely way ahead of that. We are fairly comparable with England, with some parts of England. So, our list sizes are higher.
Doctor Blackman is a part-time GP. What she does in her own free time is up to her.
Mr Singer: She cannot complain of overwork, which she does do. (Interjection)
Dr Maska: That is something you would have to ask her, and again it is... She is overworked during the time that she is actually a GP. Very few... It is a gripe of many part-time GPs that, in practice, they do not end up half-time; they end up three-quarter time. So, it is not really a particularly fair question.
We deliberately - in Ramsey - when we appointed Dr Allinson, basically to cover the extra workload, and because this was not an option to us at the time, basically increased by half a partner, which cost us financially. All practices are run as businesses. We are self-employed individuals; we are not employees of the Department, and that, again, cost us financially to, basically, try and make our workloads a little saner.
The anecdotes about alcoholic doctors and all the rest of it: there are a fair number around that I have come across, and it is about workload pressures. If you actually ran an occupational health service for GPs, with the criteria that we use to sign off certain people you would probably sign off half the GPs in the Isle of Man at a stroke and probably have them on permanent sick when you look at them.
Workloads have gone up. We have become a dumping ground for everyone. Everyone. Let us get a check from the GP for x, y and z. So, workloads have increased incredibly. People’s expectations of the Health Service have increased exponentially. So, our workload has... What we can achieve for people has increased, so I think it is a little bit of a red herring, particularly when you are dealing with GP out-ofhours. Again, I would say I am not...
Is it really the remit of the Committee to be talking about the Cottage.Hospital as such? (Interjection by Mr Singer) You might say Ramsey, but the same applies to Port Erin, really,
Mr Singer: Yes, of course, it does.
The Chairman: I think that -
Dr Maska: Traditionally, Ramsey is basically... If you look at the level of service that has been offered in Ramsey, there are very few parts of the United Kingdom which have had that level of service. It has been a very enviable service; particularly people in the south of the Island think they are damned lucky. They are very lucky and continue to be lucky that they have got an MIU on the doorstep, as well, which covers the vast majority of problems.
The Chairman: 1 think, just on the issue - if you like, call it partially - of the Ramsey Cottage Hospital, as it is difficult to avoid it, because it is part of the out-of-hours - or has been - 1 am just conscious of time, because we are behind on what we are, and I would make the point that, if necessary, we can always invite you back to speak to as, Dr Maska.
Tynwald Select Committee on GP Out of Hours Services — Evidence of Dr M Maska
Oral Evidence SELECT COMMITTEE, THURSDAY, 18th DECEMBER 2003 19 TGPS
Can I move on to my colleagues and we will endeavour to, maybe, work until around half past twelve to leave it quarter of an hour late.
Mr Gelling.
Mr Gelling: We have come down to questions. The first one: I was very interested when you asked if we are conversant with the red book. We are not; the red book has gone. I have put down that that was obviously the bible for GPs. So the bible has gone out through the window and now we have got a contract. That is a modem way of doing things.
Could you tell me who took that initiative? I am all for being proactive, getting something done before it is absolutely required, but did the initiative come from our DHSS, or did it come from the GPs?
Dr Maska: It was sort of a bilateral process. If your yardstick, the red book, is going out the window, you have got to look at: what are we going to replace it with? You cannot reinvent the wheel within general practice. General practice is pretty similar - or its overall similarities are similar - in the Isle of Man, the UK and Canada that I have had experience in. General practice is fairly similar. So, it is a case of how you remunerate GPs, what terms and conditions you put in place, and it did not really make a lot of sense to us to go wildly different from the UK, particularly as your GPs are going to be trained within the United Kingdom.
Again, most of the benchmarks for quality are set within the United Kingdom, and, again, the new contract... The quantum leap there is that it is a quality-based contract. For the first time, GPs are going to be paid for on outcomes, to a certain extent, rather than just purely ‘bums on seats in surgeries’. That is a big change for the public; that is a big, positive change for the public. It did not really make sense for us to go wildly trying to reinvent the wheel. Again, most of the computer systems that we use within the practice are based on UK models. It would be very difficult for us to, somehow, get a supplier in to do something completely different.
So, on a practical basis, yes, we can tweak certain things in the Isle of Man and, again, my name appeared in the medical press because we have gone away from this target pay. Target payments for MMR, the measles, mumps and rubella: certain GPs within the UK were throwing people off lists because *1 am not going to meet my target by 0,1 per cent. If I wing that family off, I will meet that target.’ We have done the sensible thing in the Isle of Man, saying, ‘Well, if someone is a conscientious objector, does not wish to take up that particular vaccination, even though it has been offered, it is not me that is being financially penalised’ and, therefore, no one can turn around and say, ‘The GP has put pressure on me to have it because he has got a financial incentive.’
That is just a sensible way of tweaking that contract. So, we have not followed it completely wholesale; we have adapted certain bits of it, and again 1 think we have been pre-emptive in that.
Mr Gelling: Can I just follow that, Mr Speaker? (The Chairman: Yes.) Therefore, I think, taking the Island as a whole, we in the south are very envious of the situation in the north, (Dr Maska: Yes.) and I think we were led to believe, in the early stages, that the strategy would have been
to actually recreate the Ramsey Cottage in the South, and, suddenly, that all disappeared and this came into being.
So, it would be fair to say that, in the rest of the Island, we have been following what was the old system, now changed, so we are used to it. You made the statement ‘People do not like change’, and I accept that.
The thing that would appear as an all-island problem, not a Ramsey or a north problem, is the times for appointments, and what runs through your mind is: do these long days - in fact, sometimes a week - between an appointment request and an appointment given generate more emergency cases because they are not seen? In other words, I know we are unique, we are different, and I hope we always will be different and I always hope our DHSS will be better than the UK and I do not want to pitch ourselves to the UK, but I just wonder whether that is a problem.
Dr Maska: We deliberately looked at that. We wondered whether the MEDS service... Certain GPs within MEDS do have the option of saying, 'Right. No, MEDS is not really the appropriate place for you to be seen. You have an ongoing problem. You should make a GP appointment.’
We, deliberately, with Ramsey, altered some of our appointments and actually made more appointments available. It has not really transpired that there has been any great increase in workload.
More interestingly, if you walk into the Ramsey Group Practice, there is aboard there: 200 people last month did not pitch up for their appointments. That is 200 appointments; that is not an insubstantial number.
Again - and it is one of my personal bugbears - people make appointments to request sick notes for illnesses that last less than one week. The Department policy for years has been that these people should self-certify, and I must admit that the actual Government is one of the biggest transgressors, in that it insists that its employees get a sick note. That is a waste of a GP appointment, it is a waste of that person’s time because they are away from work yet again and not doing anything, and it is a waste for the employer. If we could, basically, get the message across - yes, self-certify if you are less than a week - again that would free up appointments.
I think emergency appointments, certainly within the Group Practice... If you need to speak to someone - and I can only talk about the Group Practice as that is the only practice I work in on the Island - you will get to speak to the GP, you will get to speak to one of our practice nurses, who can deal with a whole range of more minor complaints, you can get to see the practice nurse who will deal with the complaint. Most emergencies will be seen within 24 hours, if it is a true emergency.
Fine, you might not necessarily be able to pick your appointment for 3.30 this afternoon with Dr Maska because it suits you, but, if you have need, you will be seen by someone within that practice, or you will have access to a healthcare professional and you will be offered the appropriate advice.
Mr Gelling: Just one more, Mr Speaker.In the general concept of the Island’s GP services, is
it a general thing, for argument’s sake, that now Saturday mornings seem to have disappeared...? I am now talking from an employer/employee relationship - it was the very time when somebody would be off work and could pop into
Tynwald Select Committee on GP Out of Hours Services - Evidence of Dr M Maska
20 TGPS SELECT COMMITTEE, THURSDAY, 18th DECEMBER 2003 Oral Evidence
the surgery. It seems to have gone. You have got Saturday and Sunday now, which is fairly long, you know, two days where there is not an appointment available.
Dr Maska: Under the red book regulations, there was never an obligation for practices to be open on Saturday. Basically, most practices did open, as a way of managing some of the emergency calls on a Saturday, but they were meant to be for emergencies.
Fine, some people swung the system, saying, ‘Well, I work nine to five, Monday to Friday’ and were, basically, using it as a routine appointment, which was inappropriate. Certainly, within Northern Ireland, Dr Armour informed me that, for as long as he has ever known general practice in Northern Ireland, GPs in Northern Ireland have never offered Saturday morning surgeries. So, there was never any obligation and, again, under the new contract, that is just spelt out more in black and white.
Mr Gelling: Thank you, Mr Speaker.
The Speaker: Mr Gill.
Mr Gill: Some of the questions have been covered, Dr Maska, but just three briefly. You used the phrase ‘non-principals’ -
Dr Maska: These are people who are not GP principals within an actual general practice.
Some of you may have heard of Ben Harris, who is the Hospice doctor. His wife is vocationally trained, does locums for practices, but is not actually a full-time general practitioner, so there are several individuals like that on the Island, or several people who have spouses who are GP- trained, (Interjection by Mr Gill) but they are not employed full-time by a practice. They are employed, perhaps, on a locum basis, so that they help out.
Mr Gill: Okay. So could I ask you: what would the maximum those non-principals, or yourself, or your colleagues as principals...? A typical Saturday night, last-minute arrangements to be made: what would be the maximum amount that that doctor could expect to be paid?
Dr Maska: I think it is about £90 an hour. Do not quote me, because I have not got the schedule in front of me. I think it is about £90 an hour for the top shift. There is also a certain amount of a retainer, just in case. It might happen that the doctor went off the road with the driver and was injured, so, basically, they had to call a second on it, and there is a retainer fee which, I think, sits around about £10 an hour.
Mr Gill: That is for a shift of how long?
Dr Maska: The shifts vary. During Monday to Friday, there is a shift that starts at six in the evening and goes on until 12 midnight. Then there is another doctor who starts at midnight and carries on until eight in the morning. A slight difference there: there are no back-up reception staff after midnight; it is the doctor who acts as receptionist.
During the weekends the shifts are, again, split slightly differently: yes, there are the existing six to midnight shift and midnight to 8 a.m., but, during the day, you have two
doctors on on a Saturday morning, who work from eight until twelve and then there are two doctors who work from twelve until six, and, generally, what tends to happen is one of those doctors tends to mop up most of the visits, whilst the other one sits at MEDS seeing to people who come in. Fine, if they are quieter, then both of them will be seeing patients at MEDS. After six it is the one doctor.
Mr Gill: In relation -
Dr Maska: They also provide verbal advice to the MIU in Ramsey.
Mr Gill: Right. In relation to Ramsey Cottage Hospital, what sort of remuneration would GPs get for covering that, annually?
Dr Maska: The contract again is split into various parts. There is the contract for running the day-to-day basis of the beds in the Cottage Hospital, in-patient care, and that is currently run on what is called the points system. The points system is a way of performance-related pay, if you want to look at it that way. You are paid so much per patient on a sliding scale over a month. So, there is no vestige in using the Cottage Hospital as, basically, a nursing home. It is not cost effective. It is a way of trying to get people back into the community, which is the aim of it. GPs in Ramsey still cover that 24 hours a day, seven days a week, 365 days a year. That bit has not changed.
The bit that has changed is where we cover the MIU. We cover the MIU from eight in the morning now until six in the evening, giving back-up to the nursing staff. So it gives the MIU staff the option of those patients they have seen at night and who require a further review coming back, say the following morning.
If I have got to talk about the MIU, then, basically, if you look at what the MIU sees out of hours, we were always hampered in what we dealt with after hours, anyway. We do not have X-ray there at weekends generally, apart from the Saturday mornings, and we generally did not have it out of hours, which meant, again, that some cases that you would, perhaps, if you had seen them at eleven in the morning, have treated in Ramsey tended to go up to Douglas at the weekends. So, if you are looking at overall changes, fine. The more minor injury stuff: really, people in Ramsey have not seen a change with that. The MIU closes, at the moment, at 10 o’ clock in the evening. When you look at overall figures, the demand for the MIU was always relatively small after that time, anyway.
Mr Gill: I would just go back to the question of the remuneration for the bed-cover points: what would that be in the region of?
Dr Maska: Currently it stands - and it has not been changed in the last two years and again is being looked at by the BMA - at, I think, £1,40 a point. We are not on the full rate for that at the moment. The Department has gradually staged the introduction of that system, so we are not on the full rate.
Mr Gill: Just very briefly, is there a gap between eight and eight thirty in the morning in the MEDS system?
Dr Maska: There should not be. Basically what happens
Tynwald Select Committee on GP Out of Hours Services — Evidence of Dr M Maska
Oral Evidence SELECT COMMITTEE, THURSDAY, 18th DECEMBER 2003 21 TGPS
is practices should take their calls from eight o’ clock. Most practices have it that they will not take appointments before half past eight in the morning, but if you need to access a doctor, then there has to be a system. If you are having problems, then say so, because your practice is not doing what it should do. MEDS does not cover you between eight and half past eight.
Mr Gill: Thank you.
The Chairman: Mr Waft.
Mr Waft: Yes, thank you, Mr Speaker.Could I just clarify the situation? You began talking to us
about the hullabaloo that took place at the time - your own words - over the possibility that you could not get a GP after 6 p.m. That sort of thing was... Would you like to explain in your own words what has changed from that time until now? Has there been... Were they totally wrong? Were they partly wrong? Or were they right in some ways?
Dr Maska: It is like all Chinese whispers. Someone says something, someone tells you nine tenths of it, it then gets passed on down the line and what comes out, like in most Chinese whispers, is totally unrelated to what actually was said in the first place.
I think people did get the wrong end of the stick with certain parts of it. Some people understood some parts of the system. As I have quoted, some people were under the apprehension that there was no ambulance service in the north of the Island, whereas when you explain there is now a 24-hour service, which is actually better than it used to be because it used to, more or less, have a cut-off at midnight, your service is actually better.
And, again, just accessing the service people: what they thought was happening was that you could not call the GPat all and, if you are elderly, that is a worry, but now that they know there still is someone at the end of that phone that will answer, deal with it for you, they have been reassured. It is just learning how to access the system.
Mr Waft: Could you clarify, for myself particularly, with regard to MEDS and emergency admissions there: what computerised records do you have available to you? For instance, if you had somebody brought in unconscious or whatever, who would not be able to tell you what drugs they were on, what their situation was, what computer records would you have that would give you something?
Dr Maska: Right. If they were unconscious, basically they would not be coming to us.
Basically, most chest pains, most emergency things, should not really be coming through to GPs. We do not, basically, do the hands-on stuff such as Raymond and Steve Sieling, who are here. It is far better that you have a trained paramedic service to get them to Noble’s to be thrombalised. Whether they get shipped to Liverpool after that... Treatment of those kinds of things has changed and we do not subscribe to it in Ramsey any more. It is basically specialist care now, so those kinds of patients would not come to us.
It has always been a problem, if you have never seen that particular... You may well have not seen that patient for donkey’s years. Not everyone can necessarily tell you what drugs they are on. It does not matter whether it is
someone from your own practice, or from another practice; you generally never have access to the full medical record, as such. So, to say, ‘Is there any computerised access at MEDS?’, the answer is no, but there never has been, really, with any service. You rely on the patient.
Mr Waft: So, within MEDS, you are not hooked up to the latest blood reports on a certain patient? (Dr Maska: No.) You would not know what was happening, really. (Dr Maska: No.) It is purely that they are in off the street and you have to assess them.
Dr Maska: And, generally, if you are requiring that level of detail on a patient, you are going to be putting them into the hospital scenario if you are that worried about them. It is a bit like running the AA. You have got a choice: you can either fix it at the roadside or tow it off to Noble’s, and that is your choice, really.
Mr Waft: Somebody mentioned striking patients off lists. How does that happen? Who authorises that and is there any appeal?
Dr Maska: There are very few patients who are struck off lists. The only one that I have ever booted off my list was someone who threatened to biff me -
Mr Singer: It was not me!
Dr Maska: And it was not him. (Laughter) But there are very few instances where patients are struck off lists. It is not done at the drop of a hat and, usually, it is a complete and irretrievable breakdown of the doctor/patient relationship for some reason. It is not a big issue, really. It happens very seldom and it is usually that someone has been extremely violent and abusive.
Mr Waft: Where would they go, then?
Dr Maska: They are allocated, at the moment.Within Ramsey, unfortunately, they still wind up with us
in the Group Practice, so they may well have changed their GP, but, unfortunately, you still may well end up seeing them. In Douglas they will be allocated to another practice, and, again, allocations... I will mention that because, again, if you now try and register in Douglas, there is only one practice that is open for new patient registrations.
Lots of people get allocated within the Douglas area. It is not a case that you can pitch up at Kensington and Palatine; their books are full. So, people have problems in registering with GPs in the Douglas area particularly.
Mr Waft: So, I take it you have no concerns with the changes that have taken place? (Dr Maska: No.) At the moment there has been no reduction in the amount of service to the people of the North?
Dr Maska: I still think that the level of service, particularly with the MIU for minor injuries, that people get in Ramsey most people in the United Kingdom and the south of the Island would be very jealous of and continue to be very jealous of. It is a level of service that very few parts of the country actually have.
Mr Waft: Thank you, Mr Speaker.
Tynwald Select Committee on GP Out of Hours Services - Evidence of Dr M Maska
22 TGPS SELECT COMMITTEE, THURSDAY, 18th DECEMBER 2003 Oral Evidence
The Chairman: Mr Singer.
Mr Singer: Can I ask one final question? It is picking up partly on what Mr Waft said about the safety of the MEDS service, somebody picking up the phone, and I have got in front of me the General Medical Council guidelines on providing advice and medical services on-line or by telephone, which is dated November 1998, but is still on the official website. I assume it is still current.
‘Giving advice by telephone is part of many doctors' day-to-day .relationship with our patients. In some circumstances providing advice by telephone or computer link may be essential, for example where patients are geographically isolated from their doctor. However, the use of phone or e-mail should not diminish the quality of care patients receive. Consultations and prescribing by phone or e-mail may seriously compromise standards of care where: the patient is not previously known to the doctor;’
- MEDS -
‘no examination can be provided;’
- MEDS -
'there is little or no provision for appropriate monitoring of the patient or follow-up care.’
- MEDS -
‘Doctors who wish to provide telephone or on-line services should consider carefully whether such a service will serve their patient’s interests and, if necessary, seek advice from their professional association or medical defence society.’
So, the obvious question is: what is MEDS - ? (Interjection by Dr Maska) MEDS is not complying with any of those three main points. They are giving advice over the phone - and wc know they are giving advice over the phone - and people ring you and tell you that, sometimes, one might get what they feel is inappropriate advice. They have no knowledge of what that person’s medication is, no knowledge of what that person’s history is, yet they are saying, ‘Take two aspirins and ring your doctor in the morning.’
Dr Maska; You say they have no knowledge.
Mr Singer: Very little.
Dr Maska: I fully subscribe to that. That is very true. There are a lot of pitfalls and dangers with offering telephone advice.
The on-line bit is a slightly different issue, because you... Just like chatrooms and paedophiles, you do not know who is on the other end of the line. Basically, there is no on-line service on the Isle of Man, so that is one issue we can put to one side, mainly because you do not know who the hell you are talking to.
Telephone service: NHS Direct. What do they offer? They are going to be - or the UK Government would like them to be - basically the first port of call for all access to healthcare within the United Kingdom, and the vast majority of what they do is telephone triage. Yes, you have to be certain that you know what you are dealing with over the phone. If you are uncertain, then you really do have a duty to actually see that person, and that is where the difference lies.
I subscribe to that document completely. Most doctors offering advice carefully assess the situation. Advice can be something as simple as, ‘Can I give CalpoF - which is a paracetamol - ‘with a certain brand of antibiotic?’ You do not, really, need to see the patient for that, and you would subscribe to that as a pharmacist. A lot of advice that we give over the phone is of that nature, people uncertain: ‘What should I do? I have dropped this tablet. I have taken it too early.’ There is a lot of out-of-hours advice that comes into that domain, a lot of appropriate advice. A lot of people phone up without having really done anything themselves. They are ringing the doctor because they want to make sure: ‘Can I take a paracetamol for my headache? I am on drug such-and-such.’ A lot of it is that advice. It is simple, straightforward stuff. Certainly, where there is doubt, I think any GP who does not want to see the patient is treading on thin ice there.
But, certainly, telephone triage has established itself throughout the United Kingdom. Even before NHS Direct, large... Something that we actually wanted to try and run in Ramsey at one stage was a service that was offered in Swanage and which was based in a cottage hospital that, basically, had nurse triage. So, basically, telephone advice is a well-established, proven and safe way of offering advice to patients, offering a service to patients.
Mr Singer: As long as the doctor says, ‘I will come and see you, if necessary’, because what is happening... I can tell you what is happening: doctors have said, ‘I am not coming to Ramsey. You have to come down and see me’ to people who have got no cars, people out in Jurby who have got no cars. They have got young children and they have said that they have not been able to get down, and I have got cases -
Dr Maska: That is the difference between offering telephone advice and offering a service -
Mr Singer: This is what is happening -
The Chairman: I am sony Could you respond to that, please?
Dr Maska: That is the difference between offering telephone advice and offering for that patient to basically come down to MEDS and visit.
Mr Singer: And if they cannot?
Dr Maska: There are very few patients who, these days, cannot make it.
I am sorry, Leonard, I will go back to Canada. (Interjection by Mr Singer) Take things back to the Canadian principle. I did two house visits in two years in Canada. Canadians are not physiologically different to the UK population. Why is that? There is just a certain ethos about ‘Oh, traditionally we have had the doctor visit’, and it is tradition. Now, really, GP guidelines state that house visits are for those people who are truly bed-bound and who are terminally ill. Those are the two groups that really should be visited. Most people, other than that, are fit to travel.
The Chairman: Could I just ask, then, just to follow that through: if they are unable to get to MEDS because they
Tynwald Selcct Committee on GP Out of Hours Services - Evidence of Dr M Maska
Oral Evidence SELECT COMMITTEE, THURSDAY, 18th DECEMBER 2003 23 TGPS
have no transportation, they have no-one to call upon, it may be in the middle of the night or whatever, they cannot get a taxi, what is the situation?
Dr Maska: Most will get visited, as far as I am aware. You have to make a... It is difficult to give you a categorical answer because every set of circumstances is slightly different.
The Chairman: So, do you monitor... If people express concern about that, what happens? Who deals with that? Is that the Primary Care people or is that yourselves?
Dr Maska: That would be the Primary Care people.
The Chairman: That is something we, maybe, need to ask. Okay. Thank you, Dr Maska. Is there anything you wish to finally wind up on or... (Dr Maska: No.) Right.
Dr Maska: I have covered the issues.
The Chairman: Thank you very much. I would just thank you again for your time and say that we may well wish to speak to you again. If we do, we will be in touch. Thank you very much.
Dr Maska: Thanks.
Mr and Mrs Penrose were called at 12.49 p.m.
Procedural
The Chairman: Ladies and gentlemen, we are, as you understand, slightly behind time, but I think it is important to have the opportunity for comments to be made and questions to asked, so we are going to continue. If I could ask Mr and Mrs Penrose, Ramsey Cottage Hospital League of Friends, if they would like to come and take a seat, please.
Again, could I welcome you both - and please feel relaxed. (Laughter)
Mr Singer: May I record, for Hansard, Mr Speaker, that I am actually Chairman of the League of Friends, but I have stood back from any of the matters since I was appointed to this Committee.
The Chairman: That is fine, thank you.Again, can I just remind you of the remit? The remit that
was given to the Committee was to investigate the matter of the general practitioners’ out-of-hours services being provided throughout the Island, and that was the remit given to us by Tynwald in June 2003.
And, again, just to say - because I know you have been in - first is the opportunity for you to make a statement, in other words to put forward the points of concern that you may have - and how you do that between the two of you is a matter for yourselves - and then we will ask questions. Again, whoever feels easy to answer them or both, then that is fine. Then we will give you an opportunity just to say any final comments that you wish to say. Okay?
So, if I can really go over to you both. I do not know
who wishes to start first.
Mrs Penrose: Ask the question and we will sort it out.
The Chairman: Well, I think the main point is if you wish to make an opening statement on behalf of the League. If you would do that, that is fine.
Mr Penrose, please.
EVIDENCE OF MR AND MRS H PENROSE
Mr Penrose: I have been favoured with being Treasurer of the League of Friends for the past 26 years. We have worked tirelessly for the Hospital and provided over £500,000 worth of equipment for the Hospital, and the public in Ramsey approach us, as part of the League of Friends, and say, ‘Will you do so-and-so?’ or ‘Will you put up this argument?' or ‘We have problems. Will you take it up for us?’
We can only go so far with that, but someone had to stand up and be counted, and it, unfortunately, fell to me. Well, I do not mind. It has to come from me, and that is about all we can say.
The Chairman: So, would you like to, maybe, just give a brief overview of the reaction you have had, the concerns that have been expressed to you from the people in general terms, very specifically about the out-of-hours, if you can?
Mr Penrose: Yes, well, generally the worries that we have are from the elderly, the young people with children and the people who live on their own, where they feel that, without doctor coverage, they are cut off from the necessary medical supervision that they think they should be able to take - as it was before - from the Hospital.
The Chairman: Have you had any concerns expressed to you about lack of service, people’s reactions once they have had the service, whether they feel it is better?
Mr Penrose: There have been several recently where we have had people complaining to us that they have not had the service that they think they should have had.
The Chairman: Does that relate to - ?
Mr Penrose: That relates to the MEDS.
The Chairman: Right, but does it relate to what they see as the lack of the hospital aspect being available in the north, or just generally?
Mrs Penrose: They are very angry about the complete change of status of the Hospital. It is now primary, where it was a full working hospital, which all of them... The whole district was very proud of Ramsey Cottage Hospital. That is why we have been able to help so much, because everybody is so keen to keep the thing going.
As these emergency... Usually the complaints we get are an emergency type, like a cardiac arrest or stroke - probably, maybe, even a suspicion of one, but so badly that they did not know if they had got a heart problem or not, but they had
ProceduralTynwald Select Committee on GP Out of Hours Services - Evidence of Mr and Mrs H Penrose

24 TGPS SELECT COMMITTEE, THURSDAY, 18th DECEMBER 2003 Oral Evidence
the pains in the chest - and they have had to travel all the way to Noble’s, which, in the condition they were in, they did not feel they were fit to do.
The Chairman: Could I just ask then, if I may, just on that: prior to this change from acute, basically, to primary, if a person had that sort of problem, were they always taken to Ramsey Cottage Hospital?
Mrs Penrose: Yes, and dealt with. Oh, yes.
Mr Penrose: Yes, they would be taken either by ambulance or by their own friends to the Hospital. Doctors would see them. It would then be assessed as to whether they would be taken to Noble’s. If they were in need of stabilising, they would be stabilised at Ramsey before they went over the mountain, which I think is a big thing in the care that should be taken with the patients.
The Chairman: Over to Mr Gill.
Mr Gill: Yes, Mr Penrose, could I ask: if you go back to the meeting that was in Ramsey with the march and the protest, (Mr Penrose: Yes.) one of the Ramsey GPs, I think, made a statement to the effect that this is not a problem that you can throw money at to solve. What is your reaction to that? (Interjection) I think that was in relation to GPs' unwillingness to work out of hours, as we have just heard from Dr Maska.
Mrs Penrose: Well, you can solve it with money, then, can’t you? Because we just need a replacement of medical doctors after six.
Mr Penrose: We do.
Mrs Penrose: And for the bank holidays and weekends.
Mr Gill: Could you detail that a bit?
Mr Penrose: Really, what we feel should happen is that the DHSS should employ - themselves, not by contract, employ them by themselves - doctors to cover Ramsey Hospital. That would completely solve, I think, the problems in the north of the Island. It would open up the A&E or the Urgent Treatment Centre, which would relieve a lot of problems with the MEDS. It would allow resuscitation to take place immediately it was required, not having to be done in the back of an ambulance, and it would lead to an uplift in the general welfare of the people of Ramsey and the north of the Island. It would alleviate a lot of the fear that is in the north of the Island.
Mrs Penrose: Yes, there is tremendous fear. We should also.,. We have lost... We have been slowly weakened - the Hospital - over, say, the last five years. We have been slowly losing. The X-ray department, for example, cannot work after six o’ clock unless there is a doctor on the premises. The resuscitation room is closed after six, so that has to be done on the ambulance for the same reason: no doctor.
What is the third thing? There is something else, isn’t there? There is another facility that we have lost as well, but
all of these facilities... Those are the ones we know of. There may be ones we do not know of, but that is all because there is no doctor on the premises. The facilities are there to be used, but that is the reason given: ‘No doctor, so I am sorry. ’ That means you have to go to Noble’s or -
The Chairman: Could I ask: after six o’ clock in the evening, then, or whatever time - ?
Mrs Penrose: Yes, after six.
The Chairman: So the difference, then, was that, of course, the GP could be called in. (Mr Penrose: Yes.) That was the difference. (Mr Penrose: Yes.) Okay, Mr Waft.
Mr Waft: I just wanted to... You say there has been a slow-down, an eroding, (Mrs Penrose: Yes.) of the facilities within Ramsey Cottage Hospital. Do you think that has been done purposely to run down the Hospital and actually achieve the situation we are in now?
Mrs Penrose: Yes, we feel so.
Mr Penrose: Well, actually, I think the situation we are in now has accelerated the problem. Before, we lost the X- ray, it was out of action for two years before we were told about it, but immediately we were told about it, the League of Friends sported £60,000 to re-equip it. (Mrs Penrose: Yes.) There are several things like that which were a weakening of the patient care in the Hospital, not care inasmuch as it affects the patient, but the number of facilities that can be used for -
Mrs Penrose: Were lost.
Mr Waft: Have there been any figures to justify the need for that erosion of the facilities as being available?
Mr Penrose: Not at that time, no. It was a -
Mrs Penrose: It has been very slow.
Mr Penrose: It has been very slow -
Mrs Penrose: Well, the name. We were called... It went from... What were we called?
Mr Penrose: It went from ‘A&E* to ‘Urgent Treatment Centre*. We now have a Minor Injuries Unit, which...
There was a comment made a little earlier as to what the Minor Injuries Unit does, and it is: minor cuts or wounds, sprain or strain, soft tissue injury/bruising, bite/sting, minor eye problems, wound infection, pulled elbows, uncomplicated head injury, small abscesses, minor bums and scalds.
Mr Singer: Could I come in, Mr Speaker, to explain to Mr Waft the difference? There was a big blurb in 2001: Ramsey and District Cottage Hospital Urgent Treatment Centre. They then said there was no longer Accident and Emergency - legally, it could not be - but this was what they were going to do - this is only July 2001:
*a 24-hour facility available to residents and visitors to the north of the
Tynwald Select Committee on GP Out of Hours Services - Evidence of M r and Mrs H Penrose
Oral Evidence SELECT COMMITTEE, THURSDAY, 18th DECEMBER 2003 25 TGPS
Island provided by nursing staff supported by general practitioners, all of whom have the knowledge, skills and experience to care for people with: minor trauma; sprains and strains; simple head injuries; certain fractures; joint injuries; bums and scalds; wounds and lacerations; fits, faints and falls; acute abdominal pain; chest pain and suspected cardiac conditions; other acute pain; pyrexia; asthma; uncomplicated eye problems; accidental or deliberate overdoses.’
It also was to:
‘provide a comprehensive service with minor injuries or sudden onset illnesses and the interim treatment of people with more serious injuries or conditions, prior to transfer elsewhere, and interim treatments for persons whose injuries are not considered minor and who require management at another establishment e.g. Noble’s Hospital.'
And it was also, very importantly, supposed to be in support of Noble’s Hospital, as required by the Major Incident Policy. (Mr Penrose: Yes.) So that is why people have felt this sudden change. Only two years ago, that is what they said - ‘This is what we are going to do from this Hospital’ - and suddenly we are doing bandages.
The Chairman: Again, we do not want to be too much leading the issue, but we are here to try and find out. But in fairness to that statement, which was made in July 2001, is it not correct that the change happened because the GPs withdrew their service for the Ramsey Cottage Hospital?
Mr Penrose: Yes, but to answer that, I think the DHSS knew this change was coming and it was incumbent on the DHSS to replace the doctor coverage at Ramsey so there was no hiccup, if you like, in the system.
The Chairman: Okay. We can ask the Department that question when we have the Minister before us.
Mr Waft: What I was leading up to were the facilities that you did have and the facility that you have now. With the facilities that you offer now, do you have a qualified nurse in place at the Ramsey Cottage Hospital until 10 p.m.?
Mr Penrose: There are nurse practitioners - or they are termed ‘nurse practitioners’. I do not know how the situation is, but, as I have been told by people off-Island, a nurse practitioner has to sit various examinations and it is a two-year course. Whether that happened on the Island, I do not know, but if they are not qualified, they cannot be called nurse practitioners.
Mr Waft: But if they did have a problem with someone that they, perhaps, could not see, who would they ring in that circumstance?
Mrs Penrose: Only ambulancemen, usually.
Mr Penrose: It would be MEDS. It would, definitely. It would be MEDS.
Mrs Penrose: And they would go to Noble’s.
Mr Waft: Okay, thanks.
Mrs Penrose: And the big worry from the people is the time. The ambulance can be somewhere off-station and take an hour to get back to Ramsey, where the patient is
waiting, and then if they have to have treatment, they have to pull the ambulance. As we understand it - this is what we are told - the ambulance has to pull off the street to give injections or whatever treatment the person needs before they can carry on any further.
Mr Penrose: As was said to me not so very long ago, if I am coming up the Jurby road with a patient in the ambulance and he has a cardiac arrest on the comer of Jurby road, where do I go? Do I pull in and try and treat him there, or do I go straight through to Douglas?
Mrs Penrose: When the Hospital is just up the road.
Mr Penrose: Yes.
The Chairman: Mr Gelling.
Mr Gelling: Yes, I would like, if I could, first of all, to say I think you have done a marvellous job up here, because the late Norman Radcliffe was the Chairman for many years -
Mrs Penrose: Yes, he was.
Mr Gelling: — and he used to keep informing me of the huge amounts of money that you raised for the Hospital. I already have said we were looking, certainly, for a level playing-field and we liked what you had up here and we would have loved to have had it. We appear to have got a level playing field, but it is by decreasing what you have got to what we have always had. (Mr Penrose: Yes.) That is just really an initial remark.
What I want to just concentrate on is: what is your opinion of the statement by the good doctor who gave us evidence that, in fact, a GP - right, I am just coming to the point - is not the person that you should be seeing if you had a cardiac arrest or chest pains and that a paramedic and Noble’s - in other words, in that order - is where you want to be? So I am trying to get, in my own mind: what really is the Ramsey Cottage Hospital future? Is it to deal with minor injuries and accidents to save people going to Ramsey? And taking the gentleman’s remark - if he was coming down the Jurby road, where would he go? - after listening to the good doctor, I would say, ‘Straight to Noble’s’ because his emphasis was ‘You want to be in there, where they have got the apparatus, and the paramedics are’ - I think I wrote down - ‘better equipped than a GP.’ I am a little concerned, then, when Ramsey Cottage was run by the GPs -
Mrs Penrose: Yes, all these years.
Mr Gelling: - as to how that actually divides. Would that be the place to take them - Ramsey Cottage - or would you not head straight over the road to Ramsey?
Mrs Penrose: If we had GPs in service in Ramsey Cottage, to my mind that would be the best place to go direct, so that that patient could be assessed as to whether they could stay for two or three days in that Hospital and, maybe... You do not know the degree of that heart attack, whether it is a minor one or a very serious one, but if they were in the Hospital there with a doctor, the doctor could then assess that situation -
Mr Penrose: Yes, certainly.
Tynwald Select Committee on GP Out of Hours Services - Evidence of M r and Mrs H Penrose
26 TGPS SELECT COMMITTEE, THURSDAY, 18th DECEMBER 2003 Oral Evidence
Mrs Penrose: - and say, ‘Well, maybe three days and if you have recovered, you can go home' or ‘I am soiry, maybe a couple of days here and when you are fit or slightly better, then you go to Nobles.’ He is the man with experience.
Mr Penrose: Or, straightaway, resuscitation to the degree where they are fit to stand the journey across the mountain. (Mrs Penrose: Stabilised.) As a matter of fact, I would love to ask the gentlemen of the Committee whether they have ever been in the back of an ambulance at speed over the mountain.
A Member: No, I have not.
Mr Penrose: Well, I would suggest that you, one of these days, do it for the experience.
Mrs Penrose: Yes, it would be -
The Chairman: I might delegate that to one of our Committee members. (Laughter and interjections) Right, okay.
Mr Singer: Just briefly - and I know I have really got two hats on here - is it not a fact, though, that the situation of getting the patient to the Ramsey Cottage Hospital is for that assessment and that the League have spent thousands of pounds on equipment, on having a hospital, in order for the doctors to be able to make that assessment as to whether the person should be treated initially there or stabilised and whether they are fit enough to go over to the hospital? Would you agree with that?
Mrs Penrose: Yes, absolutely.
Mr Penrose: The amount of cardiac equipment that we have bought for monitoring cardiac arrest for the hospital: in the last two years we have bought two machines costing £7,500 apiece, which will actually monitor closely thé patient’s heart attack and, if needs be, will relay the information down the telephone line.
Mr Singer: Can I just ask you: you heard what the ambulancemen said about their figures - no increases. Have you - ?
Mr Penrose: I am sorry* I do not agree with it.
Mrs Penrose: I do not agree with it, no.
Mr Penrose: The number of urgent calls up to March was about 150. We have now gone up to 256, so you have got, basically, nearly an 80 per cent rise.
The Chairman: Well,, we have asked for those figures» so, once we get (Mr Penrose: Yes.) the breakdown, we will be able to assess that.
Mr Gelling.
Mr Gelling: Can I come back in, Mr Speaker?Coming back to the funds you raise, I well remember - 1
think it was - an extension or a refurbishment of an operating theatre down here -
Mr Penrose: That’s right.
Mrs Penrose: Yes.
Mr Gelling: - and it was a large amount of money. (Mr Penrose: Yes.) And I remember very well a caveat being put into that by the DHSS Minister of the day, and that was: this is all very well, it is all very nice, but we cannot promise to be able to resource it with doctors and so on. So, all of what you have now given and produced, has that been done in conjunction with the DHSS or the GPs, and have they gone along and encouraged you to do it?
Mr Penrose: No, it has been done in association with the Hospital. We will not supply any equipment that the Hospital does not ask for. If the Hospital asks for equipment, it is there.
Mrs Penrose: Yes, or a building.
Mr Penrose: And in the particular instance you are talking about, there was a very generous anonymous donor who provided the money to build a new operating theatre. After a while someone asked the question, ‘Why isn’t it open?’ ‘Oh, we haven’t got a recovery room. ’ So, the League of Friends stumped up £62,000 for the recovery room, and then we were told, ‘Oh, it won’t be used because it is being mothballed. It is being mothballed to be available, should anything happen at Noble’s.’
Fortunately, there are day operations done and there are also some endoscopy operations done now in the main theatre, but this has been a long time coming.
Mrs Penrose: Yes. We had to kick up a fuss.
Mr Penrose: We did.
Mr Gelling: Thank you.
The Chairman: Mr Gill.
Mr Gill: Just lastly, and I will ask you first Mr Penrose, because I will ask the same question of both of you, and if you disagree with your wife, you will be in trouble when you get out that door. (Laughter)
A Member: He is always in trouble.
Mr Gill: On a sliding scale of one to ten, one being ‘not reassured’ and ten being ‘totally reassured’, from the evidence that you have heard from Dr Maska and the Ambulance Service officers, how reassured are you by what they have told you?
Mrs Penrose: Not at all.
Mr Penrose: Not at all. Zero, sorry.
Mrs Penrose: Yes, exactly.
The Chairman: Mr Waft.
Mr Waft: Yes, just to clarify the point with regard to the future of Ramsey Cottage Hospital, that is not our remit. It is the after-hours GP services, allied to, if you like, the reduction of services at Ramsey Cottage, but it is not the
Tynwald Select Committee on GP Out of Hours Services - Evidence of M r and Mrs H Penrose
Oral Evidence SELECT COMMITTEE, THURSDAY, 18th DECEMBER 2003 27 TGPS
future of Ramsey Cottage Hospital; it is what has been put in its place and whether that is satisfactory or not.
Mr Singer: And if not, what you do.
Mr Penrose: Could I just read you something which I wrote out and which will give some idea of the development in Ramsey which is coming? And it is coming very quickly.
‘What must be taken into consideration is that we are, at Ramsey and in the North, to see shortly the following developments; the building of 150 houses at Pooyldooie; 74 apartments at the Premier Road site; 60 apartments at the Queen’s Hotel site; a major Government development at Jurby; more industry at Jurby; developments at Kirk Michael; and last, but not least, the new prison at Jurby. All of these developments require the services of a modem hospital within easy access, and Ramsey is ideally situated to cover these developments. You have, in Ramsey Cottage Hospital, a hospital of which we are all justly proud, and any visitors who are unfortunate to require the services are full of praise for the nursing staff and the care and attention they are given.'
That is looking forward as to what -
Mr Waft: Okay. What you are saying is that the population is increasing,
Mr Penrose: It is going to increase, yes.
Mr Waft: I do not want to put words in your mouth, but, perhaps, in view of the way things are going, not only in the Island, but internationally, with these MEDS services, would you like to see MEDS services in place in Ramsey Cottage Hospital?
Mrs Penrose: Only if it restored the Hospital’s status. (Mr Penrose: Yes.) If they just came in the evening and sat there and sent everybody off to Noble’s and nothing altered, no.
Mr Penrose: Unfortunately, the MEDS service cannot admit patients to Ramsey. At the present moment they cannot admit patients to Ramsey, which is one of the problems.
Mr Waft: It is a purely hypothetical question. We cannot a decision on that-
Mrs Penrose: No.
Mr Penrose: No, certainly not.
Mr Waft: - but it is the way things are going.
Mr Penrose: But what I would really like to see - we are going to the south of the Island and also the west of the Island - is the establishment of 24-hour GP clinics in all of the major population areas on the Island, including Port Erin, Port St Mary, Castletown and Peel, with a doctor available in each. Ramsey has already got a model hospital in situ, which is essential because of the terrain, and Douglas and Onchan are already very well served by Noble’s. So, if we could push that along slightly, more for the south, more for the west, I think it would be a way out of it. It runs along similarly to what Dr Maska was saying.
Mrs Penrose: In emergencies, which... In all the
conversations there have been today, to my mind it was not talking about emergencies, the sudden strokes and heart attack, or child meningitis; with those things, time is of the essence.
Mr Penrose: Oh, yes, most certainly.
Mrs Penrose: And in that case Noble’s, where it is, is no use to us. And that, I think, applies to you down south, everywhere. People must have 24-hour access to a doctor for those emergency problems.
The Chairman: I think, in fairness to that, if I can just comment, we are mainly examining GP out-of-hours services, and I think it is fair to say what we were endeavouring to get from the ambulance service was how the overall emergency service applies throughout the Island, and that is different to GP services.
There are two different issues there. I think it is worth just making that point, because I think it is important. It is difficult for us to keep in mind, but it is important for us to keep in mind. Okay? And I think, if I may say, there tend to be two issues from you, if I am right: one is returning the status -
Mr Penrose: Here they are linked; there is no other way you can look at it.
The Chairman: No, but there are two issues, I think, which are coming out from you: one is that you wish to see the status of the Hospital at Ramsey here reinstated, and then there is the out-of-hours service that you see as being -
Mrs Penrose: The two, really, in the case of the North here, are inextricably linked.
Mr Penrose: If you have doctors in the Hospital here, you have established medical coverage for the whole of the north of the Island, 15,000 people, 24 hours a day.
The Chairman: Okay. Is there anything you wish to say finally, just before I close the proceedings?
Mr Penrose: I believe it is pretty well covered.
Mrs Penrose: I think so, except if you would take up our suggestion: put yourself in one of our ambulances at Ramsey, belt in, like the patient does, and imagine you are having a heart attack and in bad pain, and then when you are at Noble’s, believe me .. .
The Chairman: Well, I can tell you that I have had the experience of travelling in the Ramsey Cottage Hospital ambulance about 25 or 26 years ago after I had had an accident, but that was on the southern roads, which I hasten to add are not necessarily better than the northern roads, (Laughter and interjections) and so I had the joy of that, with all the sirens going and everything. So, anyway -
Mr Gill: I think we know who you are going to volunteer, as well, Mr Chairman. (Laughter)
The Chairman: Actually, I was looking for somebody older, so we are alright! (Laughter)
Tynwald Select Committee on GP Out of Hours Services - Evidence of Mr and Mrs H Penrose
28 TGPS SELECT COMMITTEE, THURSDAY, 18th DECEMBER 2003 Oral Evidence
Right, anyway, can I thank you both for coming along and thank you for putting forward your points of view so clearly, and if we need any further information or advice, we will certainly contact you again.
Mr Penrose: Thank you very much.
at the end of it, I will then invite the person who is giving evidence to wind up and make any final statement they wish to make.
So, that is how the proceedings will go, and our first person that has been invited is Mrs Craine MHK. Over to you, Mrs Craine, if you would like to make your opening remarks and then we will take it from there.
Procedural
'The Chairman: Can I just advise everybody that the Committee will now adjourn. We will resume at 2.30 this afternoon, and we are going to have evidence from Mrs Craine MHK, Mr Gawne MHK, Mr Bell MHK and Mr Rodan MHK. So. our proceedings will start again at 2.30.
Thank you all very much.
The Committee adjourned at 1.19 p.m. and resumed its sitting at 2.36 p.m.
Procedural
The Chairman: For any of you who were not here this morning, just to advise you that this is a Select Committee appointed by Tynwald in June 2003 and the remit of the Committee is - and I quote
‘io investigate (he matter of the general practitioners* out-of-hoursservices being provided throughout the Island’.
The Committee consists of: myself, as Chairman and Speaker of the House of Keys; Mr Gill MHK; Mr Singer MLC; Mr Waft MLC; and Mr Gelling MLC. The Clerk is Mr Lo Bao, the Third Clerk of Tynwald, and then we also have our Hansard Office, who are recording the proceedings.
All the proceedings this afternoon, as is normal practice with select committees, will be recorded and eventually they will be published through the Hansard Office as official records of the proceedings.
We have a number of people who we have invited to give evidence this afternoon. Can I just say that we do apologise that there is a slight problem with this room, in that the acoustics are not very good and we also have the background noise of the heating/freezing system, whichever way it works, depending on the time of the year, which is also causing a slight problem for everybody to hear, but if you will just bear with us.
If you find that you cannot hear, please just move forward closer to the front, and if you still cannot hear, if you just indicate to me by putting your hand up, we will try and endeavour to catch you and then ask whoever is speaking to speak up a bit. But we will do our best, so if you just bear with us on that.
The persons that we have invited to give evidence this afternoon are: Mrs Craine MHK; Mr Gawne MHK; Mr Bell MHK; and Mr Rodan MHK. They will be invited to give evidence at the appropriate time. First there will be an opening statement by them if they so wish, adding to evidence that they may have already put in in writing, and then the Committee will, if they wish, ask questions, and,
EVIDENCE OF MRS A V CRAINE MHK
Mrs Craine: Thank you, Mr Speaker.I would, first of all, like to thank the Committee for
the opportunity of making this verbal presentation this afternoon. As you know, the submission that I made was written in September and so, even in that time, some things have moved on.
If I could start off by saying that, when this problem first erupted, it was at a time that I was canvassing to become a Member of the House of Keys, and I would like to state that, without any exception, every house that I went to during my canvassing - and that was a considerable amount of canvassing that I did - wanted to stop and discuss this matter which was of such importance to them. It has struck a fear within the community, and I do not restrict that fear just particularly to the elderly, or to those with young children, but to all categories of the community.
I would like to also say that I understand that you have been to Ramsey Cottage this morning or at lunchtime and you will, therefore, appreciate that there has been enormous community investment in this Cottage Hospital, and so we are not talking about something that is of standard Health Service delivery; we are talking about something in which the people in this community have a vested investment, and I would like you to bear those things in mind.
Whilst it is accepted that the GPs effectively have withdrawn their contract, the reasoning for this is not for me to go over here. It is historical and I know you have it in all of your papers. However, I would think that it is worth saying that there is a balance to be wrought, and whilst we accept that some people’s expectations may have been too high and have, therefore, spoilt the delivery of service by the GPs wishing to remove their service, there.are other cases that are genuinely of concern and do require the attendance of a GP without delay. And so there is a balance to be wrought in this matter.
We are geographically isolated here, as... I know it trips easily off the tongue when you say that, but, historically, the positioning of Ramsey over these hills does make us in a position of isolation, does put us into certain isolation. We do also have a larger number of elderly people living within our community than in other areas of the Island, and I believe that is an historic fact that we live with.
If I could say that, when I made my submission, or when I was first considering this matter, I thought that there were three ways of remedying the situation. I thought that we could split the present MEDS service between the north and south. I thought that, as Ramsey Group Practice already service their in-patients during the night, we may be able, through the emergency nurse practitioners, to call on their goodwill to be able to attend the hospital after a filtering by the emergency nurses.
However, on that score, I have been made well aware
Procedural: Procedural Tynwald Select Committee on GP Out of Hours Services — Evidence of Mrs A V Craine MHK
Oral Evidence SELECT COMMITTEE, THURSDAY, 18th DECEMBER 2003 29 TGPS
that that would not be acceptable to the GPs, that they, in no circumstances, are prepared to offer their out-of-hours services to this community again.
1 did also make a suggestion that we should remove the Ramsey GPs from the hospital altogether and that we should have some satellite arrangement with Accident and Emergency at Noble’s. I made that suggestion because the GPs are on a standard GP contract. They are on another contract for attending the hospital during the day and they are on a further contract for their in-patients at night, and so it seemed a little like having their cake and eating it that they were able to pick and choose as to which contracts they chose to service.
More recently I have become aware that the contracts that the GPs are able to receive from the Health Services for their work at Ramsey Cottage Hospital in fact subsidise their ability to have more than the quota of GPs on their practice. Therefore, that leaves this community in something of a cleft stick: if we take them out of the hospital altogether, we have fewer GPs.
There are many instances - and I have cited two in my written evidence - that are of concern. We have had cases... I think the situation that we have is one whereby, at the moment, our people of the north are attending Noble’s and are accessing the medical services through the MEDS service. We had an instance, last week, of a child who suffers from severe asthma and who rang to receive information from the MEDS service and asked for a call-out. Having already been up to the Cottage Hospital, the child was going downhill pretty rapidly.
The doctor was in Ballaugh, but could not detour to Glen Auldyn. I am told that there was no back-up doctor to fulfil any call-out up there and I would like clarification, through the Committee, of the arrangement for the MEDS service. I understood that when one doctor goes on call-out, another one automatically comes in behind, but that does not appear to be happening.
I think that the situation where we, at the present time, are subject to GPs being able to make admissions to the Hospital, but not emergency practice nurses, is unacceptable. In fact, I should state that the whole situation of the Hospital being closed during night hours is unacceptable, entirely unacceptable, to the whole of this community. I do think that we should have an ability for the emergency nurse practitioners to be able to make admissions if they feel it necessary.
There is also an issue about the Ambulance Service and the ability that they have to be able to make their own judgement about whether it is best to take a patient into Noble’s or directly to the Cottage Hospital for stabilisation before they go to Noble’s, and that is a grey area that I think is of immense importance for us to establish. They are in an untenable situation at the present time. It is just unacceptable for them to be refused admittance at Ramsey Cottage Hospital when they know that the patient’s best chance is admission - and, in some cases, perhaps, that is the patient’s only chance of survival. We have a facility there. It is wrong to be driving past the door to have to go and use Noble’s, however good it is. I am not saying that we should not be going to the best place for the best treatment; I am saying that there are issues and problems that can be dealt with in Ramsey and that we should be dealing with in Ramsey.
I would just like to conclude, Mr Speaker. Perhaps you have questions for me, but I would like to say that I know
that I wrote some recommendations in my submission and I would like to add to those submissions, or to clarify them if they are already in. I would like to state, categorically, that this hospital needs to be open 24 hours a day. If that entails additional recruitment or development of nurses to become emergency nurse practitioners, then so be it.
I believe that we should have a ‘TeleMEDS’ service that can be accessed by the emergency nurse practitioners. In the instance of severe laceration, instead of having to entail people in driving to Douglas, it could be viewed and the advice confirmed by a GP in Douglas that we can make the diagnosis come right in Ramsey, deal with it here. I believe that there should be the ability for the ambulance to come to Ramsey Cottage Hospital, for cardiac problems particularly.
I believe that in the new tranche of contracts that will be negotiated with future consultants it must be written in that they should come to Ramsey to use the facilities here, and, in the event of patients having to be transferred to Douglas, or advised to go to Douglas, whether it be by the MEDS service or if it was by the Hospital, it would be probably taken by the Ambulance Service, both going and returning. I believe that there is a case for the provision of free transport. Our doctors are still signing up for the MEDS service, but not all of them are, and I believe that, in the case of GPs who were able to do a night service in Ramsey and now find that they are willing to do one in Douglas for a fair consideration, this should not be an option; it should be compulsory.
And I think, Mr Speaker, that there should be no misunderstanding when I say that the GPs may say otherwise, but they need to understand that patients in Ramsey and the north are dissatisfied with the present arrangement.
Thank you.
The Chairman: Thank you, Mrs Craine.Mr Singer.
Mr Singer: Mrs Craine, it was said this morning about doctors, that they were not aware that there were any complaints being made, now that things have settled down. It was also alleged that all this that they have tended to call lhype’ at the very beginning was from misinformation and misunderstanding. From your experience, as you say, of knocking on the doors and talking to people, would you say, first of all, that people were only complaining because they misunderstood or were misinformed, and do you believe, having said, just now, that you have had previous complaints, that the whole thing has settled down and people are - well, whatever word you would like to use - resigned to the service as it is now, or are happy with the service? It appears, from some views, that people are now happy now that they understand what service they are getting.
Mrs Craine: Thank you.If I could refer to the second part of your question first, Mr
Singer, the allegation that people’s concerns were whipped up through hype: if I could just comment there that I do think that, in the very first instance, the Department of Health did not conduct this exercise with the greatest sensitivity to this community, and I would have to say that, in terms of public relations, a lot was left to be desired. I think that they then tried to put things right, but there were silly mistakes and those aggravated people’s feelings; things like distributing a leaflet stating ‘here for an improved service’ did nothing to
Tynwald Select Committee on GP Out of Hours Services - Evidence of Mrs A V Craine MHK
30 TGPS SELECT COMMITTEE, THURSDAY, 18th DECEMBER 2003 Oral Evidence
enhance people’s feelings about the matter at the time.There was also the situation of where we were told that
if you need a doctor in the night, then you must contact the surgery telephone number and you will be transferred to another number, and why that message came out I do not understand. If those leaflets came out to everybody, then they could have easily have been distributed with the right number in the first place. Okay, there could have also been the facility of accepting that, if you cannot remember the new number, ring the old one and we will transfer you, but to save time just give them the new number. And so, I do think that there was misinformation at that time, which did nothing to enhance the feeling of the people of Ramsey.
On the issue of complaints, I would like to comment - and I am sure that the Committee has been made aware in the submissions that you have received - that Ramsey Town Commissioners did a pro-forma form for people to fill in, and it is my understanding that the Clerk of Tynwald’s Office have asked people to confirm if they are prepared to allow their evidence to go in writing, as would be normal in a select committee of this sort. It is my understanding that many ppople have written back and said, no, they do not wish their evidence to be confirmed in writing, and that refusal emanates from fear of repercussion.
If there is that degree of fear of repercussion from their GPs, then it is no surprise to me that the GPs are unaware of the complaints that are being bandied around. I carry with me a number of formal complaint procedures for the Hospital for people to be able to make their complaints in formal style, because that is the only way in which they are going to get dealt with. However, people are not prepared to put their complaints in writing.
The Chairman: Could I just clarify that, in the responses we have had, the majority of people have, in fact, agreed that their complaints can go as part of the report. (Mrs Craine: Good.) So it is a minority who have actually said that they did not wish to. Just to clarify that.
Mrs Craine: Thank you for that. I think that, with the minority, that would be the reason for their reluctance.
The Chairman: I think that we accept that there are people who would be concerned about their name being in the public arena. Anyway -
Mrs Craine: But, far from this issue going away, there is genuine concern and fear still within the community.
Mr Singer: So, just to pick up the point which I asked you first - I suppose the answer was that it should have come last - in your opinion and in your experience, because there are not marches and ‘hullabaloos’, as the word was used this moming, do you feel, from what you have heard, that things have settled down, that people are accepting the position, or do you think that they are still very adamant that they wish to see the kind of service return to the Hospital that they had before?
Mrs Craine: I think that they are still very adamant that they wish to see the level of service that we enjoyed before returned, but becoming realistic that that may not be able to be serviced by our GPs. Having said that, I still believe that there are many people who are still very worried and do not
accept the situation that we are in at the present time.
The Chairman: Mr Waft
Mr Waft: Thank you.Mrs Craine, have you seen any figures with regard to the
situation ‘before and after’, as it were, with regard to the need to continue as it was and, perhaps, the need to have another MEDS situation in the north of the Island? That seems to be the in thing at the moment: having this MEDS facility, rather than a GP on call. What are your views on that?
Mrs Craine: I have not seen any figures of the before and after scenario, except those that we received in Tynwald in the very first instance about the number of GPs who had signed up to the MEDS service. Those were the only figures that I have been able to look at. You referred to a MEDS service in the north; I think that that could only be operated, providing it was made compulsory for those doctors to sign up to, and I do not know that there is the willingness on the part of GPs to make that commitment.
I think it would be a very difficult contract to negotiate. That is why I have been looking at, within my submission, alternative arrangements, but the bottom line is'that, whether there is a MEDS service here or in Douglas, we have to have doctors available to come out on call, and that is why I believe that there should be a continuous fall back on the rota for GPs within the MEDS service.
Mr Waft: You mentioned the problem that GPs have with regard to the future. One of the problems being expressed to us is that there is a lack of parity with the United Kingdom, which is, if you like, the area from where we do get our GPs, albeit that it some of our local Manx people go over there to train and we have Manx GPs here. There still is, nevertheless, a recruitment problem in the future, perhaps because of this problem of out-of-hours work. How would you respond to that situation?
Mrs Craine: To be glib for a moment, I think if GPs are not careful, they will find that there is no job to do, because people will find ways around needing to use them. They seem to be doing themselves out of a job with the withdrawal of so many of their services, but, on a serious note, I do believe that it is difficult to recruit GPs and it is preferable, within the Isle of Man, to have GPs that are not recruited from foreign parts, because people have a fear of not being able to understand their GPs and that, I believe, is a genuine concern. I know that we have to recruit from within the UK by and large and, because of that, I accept that we cannot easily manage to recruit GPs here.
I think that is why we have to be looking at alternatives to just a straight GP service. Whether we can afford the luxury of having a north/south MEDS service, I do not know.
Mr Waft: With regard to the future, then, how would you view the situation?
Mrs Craine: I would like to see an increase in emergency nurse practitioners developed and I would like them to have the ability to make admissions into Ramsey Cottage Hospital. I would like them to have the availability of a ‘TeleMEDS’ service and the ability to call out a doctor when they needed one.
Tynwald Select Committee on GP Out of Hours Services - Evidence of Mrs A V Craine MHK
Oral Evidence SELECT COMMITTEE, THURSDAY, 18th DECEMBER 2003 31TGPS
Mr Waft: The situation that you found at the time: it has been said that a hullabaloo took place and, perhaps, there was some misinformation. Do you think that the complaints that you receive now are at the same level as the situation then, or has it decreased or increased, or is it the same?
Mrs Craine: The number has decreased. The seriousness of the complaints that I now receive has not altered and I would say that those people who have a genuine case - that is not to say that there are not those who are not genuine, but those who have the more serious concern - are those who will come forward and let me know, and there have been instances that make uncomfortable listening to.
Mr Waft: And you have relayed those worries to the Department concerned at the time?
Mrs Craine: Yes. There was one this week; I have not referred that yet.
Mr Waft: Right. Thank you, Mrs Craine.
The Chairman: Mr Gelling,
Mr Gelling: Yes, thank you, Mr Speaker.I was interested in a statement made by Mrs Craine:
‘remove the GPs from the Hospital’. Having just been up at Ramsey Cottage Hospital and had a look around, as a Committee, it is very impressive what is there and how the community have actually helped in funding a lot of the equipment that is there, but this morning we heard very clearly from a GP representative - not representing just Ramsey, but representing all the GPs in the Island - putting forward the case that we are about 12 months ahead of the game, ahead of the UK, inasmuch as we are being proactive rather than reactive to keeping a service for the people and our community. He put forward a case whereby, because they get paid so much per bed and looking after wards and visiting the hospital, it enables them to have income with which then they can employ or have more partners in the practice.
If GPs were, therefore, removed from the Hospital, they would have a loss of income. You would probably find that you would lose three GPs from your practice because they could not afford to pay them and then put three into the Hospital. Are you putting forward a scenario that that would be preferable to having the GPs trying to look after the Hospital, not being able to give 24-hour cover, and that, if it was separated and had dedicated doctors at the hospital, that would be something that, in your travels around about this area, would be more acceptable?
Mrs Craine: No, sir. When I referred to that possibility that was in my initial thinking - and I did go on to say that I had become aware more recently that that was the case and, in fact, that that does present us with something of a cleft stick - what I should have clarified was that, when I referred to removing the GPs from the Hospital, that was really to be able to sever their contracts with the Hospital. I would not wish to see the Hospital, obviously, without any medic or doctor cover, because then we could not function at all. So, the suggestion there with removing GPs from the Hospital would be to replace them with other medics who were permanently based at the Hospital.
However, as you rightly point out, it would mean that
the extra income that they earn to service additional GPs would be removed and, no, sir, I do not believe that that is an option for this community. And as much as it might gall some of us, I think that we have to accept that the GPs do receive additional moneys for their contracts and service the Hospital at the same time.
Mr Gelling: Through Mr Speaker, that was what, really, I was envisaging, maybe three doctors being permanently at Ramsey Cottage Hospital, but then you would lose three GPs because the income that would normally have been paid to them would be paid, obviously, to resource the permanent doctors - let us call them doctors - at Ramsey Cottage.
Mrs Craine: It does beg the question, Mr Speaker, that if our GPs are so reliant on the contracts with the Hospital, I wonder how GPs in other areas of the Island sustain their service on their standard pay.
The Chairman: Mr Singer.
Mr Singer: Just briefly to take up on that point, the average number of GPs and patients per GP on the Island is slightly higher than the UK, but the contract to the other doctors in Douglas is purely for their own practice. Now, our doctors - and I am not sure - I think have a smaller number of patients per doctor, but they have an income of about £180,000 coming in to them for the surgery, for going to the Hospital eight till six doing the minor operations and coming in occasionally at night to see a patient
Do you not think that, if the doctors were taken away from the Hospital, they would have more time to see the patients in the practice? One of the complaints is, ‘We cannot get an appointment’, and that money could then go to be invested into having permanent doctors in the Hospital, who would look after not only the in-patients but the emergency service and the night service as well.
Mrs Craine: I think that is an interesting point, Mr Speaker, because, whilst it is evident that the... One of the reasons given by the GPs for the removal of the service was that they were tired, and we can accept that However, their patient or their surgeiy hours have not increased since the withdrawal of night service to the Hospital, and I think it is pertinent that we do pay our GPs additionally for the contracts in the Hospital.
One thing would concern me that Mr Singer has raised, and that is that, if we did remove them altogether from the Hospital contract and, therefore, their salary would be reduced... I think that we had always thought in Ramsey that having the Hospital was an additional dimension and that most GPs enjoyed the ability to have a cottage hospital to operate, in addition to a general practice. If we were to make ours a standard service, I would fear that we would not be able to recruit GPs very satisfactorily.
The Chairman: Mr Gill.
Mr Gill: You have spoken, Mrs Craine, understandably but exclusively, pretty much about the north, (Mrs Craine: Yes.) but this, of course, is an all-island remit the Committee has, as you will be aware. Just on that last point, you seem to be saying that we cannot take the doctors out of the surgery because we would not be able to replace them. Is that what you are saying?
Tynwald Select Committee on GP Out of Hours Services - Evidence of Mrs A V Craine MHK
32 TGPS SELECT COMMITTEE, THURSDAY, 18th DECEMBER 2003 Oral Evidence
Mrs Craine: I think that that is a genuine fear. I think Mr Waft referred to that earlier on. As I say, the extra dimension of having the Cottage Hospital available for the GPs to go and provide the service there has proved - or we thought proved - to be an extra attraction to recruiting doctors in Ramsey. But what I am talking about now is: if we do remove that, then we do find ourselves in a cleft-stick position and we would be in a situation where we would, I think, find it difficult to recruit GPs. I think that comes back to Mr Waft’s point: it is difficult to recruit GPs throughout the Isle of Man as a whole and throughout the United Kingdom.
Mr Gill: Yes. So that would be the situation in the south and the west?
Mrs Craine: Yes.
Mr Gill: Right. So, on that basis, the north actually currently enjoys a better service than other regions of the Island?
Mrs Craine: We do, and I accept that, to that degree, but I would emphasise the fact that we have a hospital here. It might be to your regret, Mr Gill, that you do not have one in the south, and I am sorry about that, but the fact is that we do have one here and we should not be trying to level down the service; we should be trying to upgrade it.
Mr Gill: Right. You mentioned your theory that we could oblige specialists to, contractually, through contracts, work in the Hospital. How would you reconcile that if the clinical risk assessment was to the contrary?
Mrs Craine: Obviously, if the clinical risk assessment was to the contrary, then we would have to abide with that. However, it does, at the present time, seem to be very much at the behest of the personal decision of the consultants whether they all choose to come to Ramsey or not, and there are procedures that have been carried out in the past in Ramsey that could be carried out again. And let us not forget that, whilst we do have a splendid new hospital at Noble’s, it will be worthwhile retaining our theatre facilities in Ramsey in the case of an emergency.
The Chairman: I think that is fine. I think we are getting too close into the actual operation of Ramsey Cottage Hospital as against out-of-hours services, so I would just...
Mr Gill: Just one more then, Mr Speaker. You mentioned - and 1 am sure Mr Gawne, in his role in the DHSS, will be able to advise us on this - that free transport should be provided. (Mrs Craine: Yes.) Well, there is nothing free. Who would pay for it?
Mrs Craine: What we have been told is that the withdrawal of the GP services has not been made with a financial consideration. I believe that, yes, there does have to be a refocusing of finances within the Health Services. I am aware that the Health Services themselves are looking into all of this issue at the moment and 1 believe that for... And I know that the Treasury Minister later will probably argue that there is no money in the budget, but let us face the fact that, if you are taken to hospital with something serious suspected in the middle of the night by ambulance and you
find yourself then discharged because you are not as ill as they thought you were going to be, you might be facing a £36 or £40 taxi ride home. Now, that is not acceptable. I do not believe that people, for the sake of goodwill, should have to accept that. It is not going to be an instance that happens on a continual basis - it is not going to happen ten times a night - and whilst you might say, ‘Okay, within a certain radius, maybe, we would give you an allowance to get yourself home, or you can make a claim’, but I do think that it would be a facility that at least would reinstate some of the goodwill that is required towards the community.
The Chairman: Mrs Craine, just a question: in your evidence you talk quite a bit about the actual operation of Ramsey Cottage Hospital and its future and so on and the views that you have received from the public and, naturally, the concerns within the community. Could I ask: is it difficult, or has it been clear for you, to distinguish between people’s concerns about the potential reducing of the status of the Ramsey Cottage Hospital, potential fears that it will go altogether, and then, separately, the out-of-hours services? In fact, have they become confused?
Mrs Craine: I think that there is a blending of the issues. I would say that there is. Certainly the...
It was said to me, only yesterday, that, of course, this whole thing precipitates the closure of Ramsey Cottage Hospital and we need to instill some major form of confidence that that is not going to happen. I know that that is not going to happen, but the public at large are not convinced, or not comforted, by that. They need evidence that that is not going to be an issue. When you refer to the two issues becoming clouded, I think... There is the situation that affects Ramsey Cottage Hospital; there is also the situation that people are not receiving adequate service from the MEDS service when they need it.
The Chairman: Right And just the other one: you said you would like to see the Hospital open 24 hours a day, 7 days a week, which, of course, in recent times it has been - for out-patients, anyway. That operates throughout the week. So, you see that as, in fact, developing it further than it is now?
Mrs Craine: I do, sir. I think that we need what used to be the Accident and Emergency Minor Injuries Unit. I believe that we need to have that reopened, reinstated, 24 hours a day.
The Chairman: Okay. We finally go to Mr Gelling.
Mr Gelling: Thank you, Mr Speaker.I do not want to put you on the spot, but I am going to.
(Laughter) You said, if you removed the services of the GPs from the Hospital, it would become unattractive. Can I put you on the spot and ask you: is that unattractive because they wish to carry out minor operations and they liked the Hospital, or is it financially attractive?
Mrs Craine: Both, sir.
Mr Gelling: A true politician. (Laughter).
The Chairman: Thank you, Mrs Craine.
Mr Waft: Could I just ask one last thing of Mrs Craine,
Tynwald Select Committee on GP Out of Hours Services - Evidence of Mrs A V Craine MHK
Oral Evidence SELECT COMMITTEE, THURSDAY, 18th DECEMBER 2003 33 TGPS
which she may know, just to clarify the position for me? If the patient, for instance, is in Ramsey Cottage Hospital and they get a problem in the Hospital after ten o’clock, they get in touch with that patient’s GP. Correct?
Mrs Craine: They get in touch, not with that patient’s GP, but one who is on call that night, out of the practice.
Mr Waft: Not that patient’s GP?
Mrs Craine: No.
Mr Waft: All right, thank you.
Mrs Craine: It is my understanding that they operate a rota arrangement for their in-patients throughout the night, so you would not necessarily get your own GP, but it would be one of the practice.
The Chairman: That is over and above MEDS? That is their contract?
Mrs Craine: Yes, that is purely for in-patients in the Hospital and on a separate contract to the GP service.
The Chairman: Thank you very much, Right, then, Mrs Craine, I do not know if you want to say anything finally?.
Mrs Craine: No, sir, just thank you again for your time and trouble in coming to Ramsey, and I wish you all a very happy Christmas.
The Chairman: Thank you very much, Mrs Craine. I do apologise, but, as inevitably happens on occasions like this, our time slips a little bit behind, but I think most important is that we have the opportunity to hear the evidence given to us.
Mr Gawne was called at 3.18 p.m.
Procedural
The Chairman: I now invite Mr Gawne MHK to come to the front, please.
Mr Singer: Welcome to Ramsey.
Mr Gawne: Thank you very much.
The Chairman: Can I, in welcoming you, Mr Gawne, just really cover the remit again, so we are all clear? The remit of the Committee, which was given by Tynwald, is to investigate the matter of the general practitioners’ out-of- hours services being provided throughout the Island. If I can invite you to make any opening remarks .. .
EVIDENCE OF MR PA GAWNE MHK
Mr Gawne: Thank you very much for giving me the opportunity to add to my written submission and also giving
me the opportunity to get some Christmas shopping done in Ramsey! I will not go through the written submission that I have already made. There were a few points worth highlighting, I think, though, particularly subsequent to -
The Chairman: Can you speak up a little bit. I think people are having difficulty at the back.
Mr Gawne: Sorry.Particularly subsequent to making the written submission,
there are a few issues that have arisen and generally a few things I would like to point out. Certainly, having sat there and listened to Mrs Craine, I am very much minded that I probably would have made a very similar submission myself, had I not been appointed to the Department of Health and Social Security.
Obviously, I have been, and I do see now some of the difficulties that, perhaps, are not as clear to people who are not on that Department. But I am not here as a member of the Department of Health and Social Security. When I joined the Department it was made very clear to me that, bearing in mind my position on this issue was made prior to joining the Department, that was respected and I would not have to change my position to fit in with the Department.
I certainly do not envy the Committee as, to do the job properly, you really will have to have the wisdom of Solomon. It has been mentioned that what we need is this, and we need that, and this should be introduced and that should be introduced, and I am quite sure that, when the Treasury Minister comes along, he will tell you there is no money to do it, so you have to make a decision: do you want to close a wing of an old folks’ home down, do you want to cut a benefit, or do you want to have the improved service, or return to the service that we had before? It is a difficult issue, and I am glad that I was not the person who had to make the original decision.
Again, there has been talk about whipping up frenzies and hype and all the rest of it. In my position, going round knocking on doors for the by-election in Rushen, it was made very clear to me that this was a significant problem. I did not whip up people. I did not go and approach them and say, ‘Have you heard about this? Isn’t it dreadful?’ They said to me, ‘This is a problem. We do not like what is happening here. We do not want this change to happen.’ So I think that charge is, perhaps, a'little bit disingenuous. It is important for politicians to reflect what their people are saying, and this is what was being said. It is not a cheap shot at the Department of Health and Social Security.
1 think, as I outiined in my written submission, there are two significant problems with the whole MEDS service. TTie first one was the way it was introduced, which I do not feel was particularly good, and also the service does not meet the actual medical needs of the people in the north and the south, and I think that is again important. It is easy to focus, particularly sitting here in Ramsey, on the needs of the people in the north, but the people in the south are also affected by this and I hope that by being here I am making that clear.
Since I have joined the Department - and I am not saying this is down to me - I think the Department of Health and Social Security has actually addressed some of the issues; particularly, I think, the ambulance paramedic service based full-time now in Port Erin - although I am sure Mr Speaker would prefer it in Castletown - is a significant step forward. The phone access, again, has been improved. I understand
Tynwald Select Committee on GP Out of Hours Services - Evidence of Mrs A V Craine MHKProcedural
Tynwald Select Committee on GP Out of Hours Services - Evidence of M r P A Gawne MHK
34 TGPS SELECT COMMITTEE, THURSDAY, 18th DECEMBER 2003 Oral Evidence
now that if you ring up your GP, you are automatically transferred through to the MEDS service, whereas, in the early stages of the service, you received a recorded message with a telephone number which you then had to go and ring up, so that is an improvement. Also, I know that the Department has been monitoring the service and it claims that it has had few complaints, but I would say that this is a little bit like if you have got a bus service, for example, from Port Erin to Castletown. You cut the service and you introduce a service from Cregneash to Ronague. The service runs from Cregneash to Ronague perfectly well. You do not get any complaints, but the problem is that people want to travel from Castletown to Port Erin; they do not want to go from Cregneash to Ronague. So, whilst there are not that many significant complaints about the MEDS service, I think it is more to do with the underlying worries and fears that people have about the service as it is being introduced and the perceived failings in that service.
I mentioned the way that the service was introduced.I think it was rushed through. It was not particularly well advertised. I think there were particular reasons why this happened. I am not saying that to justify the Department’s position, but it certainly was a problem, I noted from the Public Health Directorate’s written submission to your Committee that there was a survey undertaken in Denmark in 1992 which showed that a similar system to MEDS had been introduced and, generally, had worked very well, but too little information had been given about the background, the reasons for introduction, how the system would work.
Bearing in mind that that information was available to the Department, I think they should have taken far more heed of it at the time the service was being introduced, I think it would help if the Department had been a lot more open with the problems that it faces over this issue. It would have been much more helpful for them to explain in detail the financial constraints, the difficulties, the problems with the doctors’ contracts. I think that would have really helped for people to actually understand what the significant issues are surrounding this introduction. So, certainly more information should have been available, and I still think that more information is needed on how the MEDS service works and where it is located in the new Noble’s Hospital. Those sorts of things are required.
Also I think the costs were mentioned of travelling in and out. I think this, again, is probably the most significant underlying problem and fear that the people feel. They are reluctant to ring the MEDS service because they feel that if they are told to go into Douglas, they will not be able to afford to. That is a big problem and I do not feel that Department officials actually recognise that as being significant enough at the moment. I do understand, however, that there is available some form of subsidy or grant for travel for particularly hard-up cases, but, again, I do not think that is particularly well advertised or promoted by the Department.
More or less drawing to a close on this bit for me, the nurse-led services have been mentioned for Ramsey. I think, if such a thing was introduced in Ramsey, a similar provision could easily be provided by using DHSS premises in the south.
Going again at the business of the payment to doctors, whether GPs are getting sufficient money for doing their out-of-hours cover, again there was a quote in the Public Health Directorate’s submission in which - in the words of one of our GP representatives -
‘night calls are a more important issue than pay rises’.
It is not about money; it is about the hours that they work. This seems to be the significant problem. This is the problem which the Department was trying to address. Whether it has addressed it well or not is down to you, as a Committee, to decide.
The only other thing I think I would like to add is that I was a little bit disappointed with the submission from the Health Division, that there was no mention of the two petitions and the march which were basically highlighting people’s fears, as I felt that these were very much at the heart of the problem which this Committee has been set up to address. Certainly, with my petition that I organised in the south, which was addressed to the Minister - and I understood the Minister was the Department - I was very surprised there was no reference to the 2,000 signatures that we received in the south calling for reinstatement of a similar level of provision to that which we had had before.
So, I think that is as much as I can add. Thank you very much.
The Chairman: Thank you, Mr Gawne.Mr Waft.
Mr Waft: You mentioned that it was not a financial problem and it was purely down to the quality of life of the GPs and the way they see their situation now, perhaps their job satisfaction and their family life. Do you think that there is not a problem there with regard to recruitment in the future, and how do you think the DHSS will approach that, given the problems that have arisen because of that decision? Is there any other way - ?
Mr Gawne: The decision is really based, as far as I understand... Again, I am not here to answer for the Department, as I think that is for them to do and they will be doing so in January, I understand, but, as I understand it, the GP contract has been negotiated in the UK - they are finally being completed, I think - and that lays down very specific guidelines, conditions of contract and the like. Certainly the very strong message which is coming out of this is that, in particular, GPs are not interested in more money, but they are interested in having better working conditions.
Unfortunately we do not produce enough doctors in the Isle of Man to run our own system. We do not have the training hospitals and we do not have the facilities to train up doctors in the Isle of Man and set up our own system. We do seem to feel that the UK system is the best one to follow and, consequently, we are very limited in the actions we can take in terms of GP contracts.
Mr Waft: I know you are not speaking on behalf of the Department, but, in view of the concerns that have been filtering through over the last 12 months, and with the situation with regard to MEDS, do you see any difference there for the future of MEDS and out-of-hours? We had a report of the MEDS section being under a different area of the hospital that was not built for that, if you like; they are just adapting something else.
Mr Gawne: Again I am not really in a position to speak directly on what the internal operation of the MEDS service is going to be. I do not think that the newly-negotiated UK
Tynwald Select Committee on GP Out of Hours Services - Evidence of M r PA Gawne MHK
Oral Evidence SELECT COMMITTEE, THURSDAY, 18th DECEMBER 2003 35 TGPS
GP contract is going to significantly affect the way in which the MEDS service has been set up because, effectively, we were pre-guessing the new contract and establishing what we felt were going to be the guidelines under which we would have to work. So, I think the MEDS service, as is, is very much based on the currently now agreed contract.
Mr Waft: With regard to the level of complaints and the number of complaints you personally have received with regard to your area - because we are dealing with an all- island situation from a Committee point of view - has the level of complaints gone up or down, or stayed as it is?
Mr Gawne: I think people are becoming resigned to what has been put in place.
I think there is still a very large degree of concern about the service, about the accessibility of the service in particular, and again, going back to the issue of transport, a number of people have certainly spoken to me and said that they are reluctant to ring up the MEDS service because they feel that they will not be able to afford to get to use it, they will not be able to afford the journey in and out of Douglas to use the service. It does appear that MEDS only actually go out where they feel there is an emergency now, so if you are in one of those grey areas, not quite an emergency but significantly ill enough to want to see a doctor, you will have to pay to get in and out of Douglas.
As I say, there is the facility to reclaim that money if you are on income support or whatever - and I am not sure what the exact criteria are - but it has not been particularly well promoted and certainly people are still very concerned about that.
Mr Waft: Have you had personal knowledge of somebody actually using the MEDS situation and complaining to you?
Mr Gawne: Yes, a few niggly complaints about things, but particularly, I think, cases where, again, it is not so much the emergency issues. The emergency issues tend to be dealt with reasonably well, although, again, there was one situation where an ambulance had to be called out and the ambulance from Port Erin was not in Port Erin - it had to move off to somewhere else - and, consequently, the person who needed the ambulance did not get the ambulance for some very considerable time afterwards.
There are also cases where parents or grandparents who were looking after children were asked to bring their children, who were vomiting and had diarrhoea, in to the MEDS service. They could not find the MEDS service when they eventually got into Douglas. These sorts of things are the kind of tales that you pick up as you are going around constituents.
Mr Waft: The reason I asked is I believe it has been placed in the fracture clinic at the hospital. (Mr Gawne: Right.) I just wondered what the Department was doing to, perhaps, make it more available, signage et cetera.
Mr Gawne: I am afraid you would need to ask the Department that.
Mr Waft: So the level of complaints: did you say they were still coming in?
Mr Gawne: I think yes, oh, yes, they are still coming in and, as I say, particularly the perception of how the service is going to work, that is the thing that really I find most, that people are anxious to use the service because they feel that they will not be able to afford to get in and out of town.
Mr Waft: To what level do you think it is perception, rather than actual problems?
Mr Gawne: Well, I think it is a real significant problem for people who cannot afford to just pay out £40 on a taxi, or however much it is going to be. TTiat is a real problem. It is not a perceived problem; it is a real issue. There are, I think, ways in which, as I mentioned, perhaps people could get around that problem, but it is... No, I think it is a genuine concern for people.
Mr Waft: It seems to be a dilemma from the perceived problem, the actual problem, and the needs of the GPs for future recruitment, and where is that dividing line?
Mr Gawne: That is, fortunately, not for me to find out. (Laughter) I know it is a difficult one.
The Chairman: Mr Gelling.
Mr Gelling: Yes, Mr Gawne is from the south and not long having fought an election and he has given us the benefit of the up-to-date information, but certainly this morning we were given, in public session, the view that we have to change, that the old idea of calling the doctor and expecting him or her to arrive at your house is not something that we should continue to think is the norm. Therefore, I know in your written submission you put a lot of emphasis on the cost of getting there and coming back, which would not only be for the out-of-hours, but would be for the ordinary time, going to a doctor.
And then it was stated that a cardiac arrest or chest pains are better dealt with by a paramedic and going straight into the Noble’s Hospital, where the unit is to look after you. We have had conflicting information, then, from this end of the Island, whereby Ramsey Cottage is there and it is very close and this is the emergency that should go there, and ! just wondered, with the experience in the south, where we have had what is now the norm for the whole Island for quite some time: do you get any complaints from that area in respect of a GP looking after someone who has had a chest pain or a cardiac, or are they satisfied that they are taken immediately to Noble’s?
Mr Gawne: I think now, particularly that we have got the paramedic ambulance service, there is a lot more reassurance in the south about that particular issue.
Mr Gelling: So, it is confidence that they feel comfortable that they are going to be treated? (Mr Gawne: Yes.)
Could I just ask then, Mr Speaker: what about the Rushen ambulance? That used to have a tremendous following, volunteers, and they used to run people in from the south. That, a few years ago now, was dropped out of the strategy and yet it would appear that that was a similar thing. It was a very good service operated by volunteers, voluntary money et cetera. Does that play any part in the future of the coverage from the Island? Again I just refer to what we heard this
Tynwald Select Committee on GP Out of Hours Services - Evidence of M r PA Gawne MHK
36 TGPS SELECT COMMITTEE, THURSDAY, 18th DECEMBER 2003 Oral Evidence
morning about the northern ambulance: if it is called out, the Douglas ambulance comes up to take over the north and that means Douglas is not covered, and the south ambulance comes into Douglas, so the south has got no ambulance.
Mr Gawne: Certainly, I think Government’s obsession with regulations and red tape seems to come in when it comes to the Rushen ambulance. It seems that, because of the nature of the Ambulance Service being a voluntary service, it is all but impossible for the volunteers who crew the ambulance to actually undertake sufficient training to be registered and to be used by the Department for emergencies, which seems like a very crazy situation that the world has developed into.
Mr Gelling: Just one more, Mr Speaker.Therefore, does that mean that, in the south, we were
seeing this change happen a number of years ago because normally the group practice in the south, the GP, would, maybe, have attended that patient and called out the Rushen ambulance? So, you have got the immediate medical care and decision and they are sent off. (Mr Gawne: Yes.) So, in other words, what you are saying is it is something that has been happening through evolution for a little while,
Mr Gawne: Yes, certainly the Southern Group Practice, I understand, were still using the Rushen ambulance, but the MEDS service does not.
Mr Gelling: Thank you, Mr Speaker.
The Chairman: Mr Singer.
Mr Singer: Thank you.Mr Gawne, you were present at the march and the
meeting and I think you would have heard the Chief Minister address the meeting, but afterwards he said that he was not influenced by demonstration. I think he said that within Tynwald, although he did not dare say that to the audience he addressed.
You said that the doctors were not particularly interested in more money, but how do you balance that against the fact that the majority of doctors who have given up the night cover and have given up £6,000 a year are all members of the MEDS - or most of them are members of MEDS - and can earn up to £500 per session? It does not take many sessions to make up that £6,000, so would you still say they are not interested in the money? (Laughter)
Mr Gawne: I think what 1 was trying to point out was that, in terms of the actual contract negotiations, this was being pushed as the main consideration. It was not necessarily about the money; it was about working hours and conditions. It does seem very clear to me that doctors are still getting an awful lot of money and this is, perhaps, why they do not see money as being the most significant problem.
Mr Singer: In your evidence you made one comment that you were made aware of the widespread anxieties and concerns of Rushen constituents, as the MEDS service was introduced a few days after you began your election campaign and you estimated that 80 to 90 per cent of constituents that you spoke to expressed anger and worries. And then you also said, ‘I have continued to receive calls from constituents expressing their concerns over the service.’
Did you say before that you are still getting those complaints, and what do those complaints actually say? For example, are they saying that doctors are refusing to visit, that people are too ill to visit the doctor and are unable to make the journey to Douglas, or they cannot find a taxi from your area to get there at three o’clock in the moming?
Mr Gawne: Yes, primarily, it is about the transport issue.I have to say I have not received very many complaints recently about significant problems with doctors refusing to attend in cases of real emergency, although it is quite clear now that emergency patients are the only patients that doctors will go to see. They will not go to see - as I think I have mentioned earlier- that kind of grey area where we are not quite sure whether it was an emergency or not.
So, I think, for people contacting me, the major issue overwhelmingly is the issue of transport, of whether they are actually going to be able to get in and how they are going to be able to get the taxi, how much it is going to cost. There is a big fear there that people’s spending money for the rest of the week could be wiped out on a trip into the MEDS service.
The Chairman: Okay? Mr Gill.
Mr Gill: Can I just ask you: in fairness to Mr Waft and Mr Singer’s question about the concerns you have raised subsequently, do you have any instances of people in the south actually stating that they are satisfied with the MEDS service?
Mr Gawne: Yes, certainly. A number of people have said that. I would not say it is anywhere near the number compared with those who are not satisfied, but certainly there are people who say that they are satisfied with the service.
The Chairman: Thanks.Mr Gawne, in your submission - 1 think this was prior to
you going on the Department - you made the point that you felt that the most significant move in relation to alleviating people’s concerns would be for MEDS to be manned by three or four doctors instead of one and one in reserve and that, of course, has an implication on funding and manpower. Do you still think that is the way forward for MEDS and do you think that would alleviate, if not all, most concerns?
Mr Gawne: I think it would certainly help, but again, whatever Department you are a member of, you have officers and the officers give you their best advice, and when the best advice is that the current service is as good as we feel is necessary, and to improve that service would be to require quite substantial increases in funding, then it is very difficult to argue against those officers. Indeed, there would be a number of people who would take great pleasure in criticising you if you did introduce what could be described as a wasteful service, a service which affected people was wasting taxpayers’ money. You are going against the advice of your officers, who are supposedly the people who know about these areas.
The Chairman: And I think you have partly answered this: you mentioned the point about concerns, complaints really, MEDS versus Manndoc, because Port Erin did not have Manndoc, whereas the rest of the south did. And then
Tynwald Select Committee on GP Out of Hours Services - Evidence of Mr P A Gawne MHK
Oral Evidence SELECT COMMITTEE, THURSDAY, 18th DECEMBER 2003 37 TGPS
MEDS came into it, which brought in the whole of the Island.
In those concerns, am I clear you are saying most of those are to do with transportation, not the service provided by the doctors?
Mr Gawne: Yes, I think overwhelmingly it is down to the transport issue. There are a few other things - 1 think I mentioned problems with the actual service itself - but most people are concerned about how they can get in. I suppose, in a way, that is down to the MEDS service, in that previously their doctor would have visited them, so it is related to the MEDS service certainly, but the concern overwhelmingly is about transport.
The Chairman: And is that concern, based on what you have heard, based on reality, or perception of a concern, because they think that could be a problem?
Mr Gawne: I think it is a real problem. Exactly how the Department’s grant assistance or... I am not quite sure exactly what the arrangement is, but I do know there is this arrangement whereby people can reclaim some of the money. Now, exactly what that is... As I say, I am on the Department and I do not really understand the full ins and outs of that I think that is probably an area that really should be better addressed, but, again, the more that that is highlighted, the more money will have to go out of that budget, and, currently, as I am sure Members will know, there is not an awful lot of money sloshing around in Departments.
The Chairman: But the point I am trying to get at really is: when you have had people expressing concern about that, which you say is the biggest issue, is that because of their own experience, or is that because they perceive that to be a problem. In other words they have not experienced it yet, but they think it is going to be the problem?
Mr Gawne: A bit of both.
The Chairman: Right, thanks. Mr Gill.
Mr Gill: I will quite understand if you do not know the answer, but do you know if the Department could help people get to the MEDS occasionally?
The Chairman: One for the Department, I think. (Laughter)
Mr Gawne: I think that is probably best. Yes, leave that to the Department, I think. I know there is a fairly comprehensive system of recording being undertaken on these things, but I think you had better ask the Department.
The Chairman: Right, thank you, Mr Gawne.Is there anything you would like to wind up with or are
you content?
Mr Gawne: No, I just wish the Committee all the best for Christmas, obviously, but also on your deliberations. I th'^k we are going to need an awful lot of wisdom to come
. vith a solution which suits everybody and does not cost any money.
The Chairman: Maybe that is why we have three MLCs on! (Laughter) Right, thank you for that. Thank you, Mr Gawne.
Mr Bell was called at 3.49 p.m.
Procedural
The Chairman: Can I invite Mr Bell MHK to come forward, please? Good afternoon, Minister.
Mr Bell: Good afternoon, gentlemen.Welcome to Ramsey.
The Chairman: Thank you, Mr Bell, for coming along to give some oral evidence. We have had written evidence from you. Can I just remind you the remit of the Committee, which was given to us by Tynwald - that is to investigate the matter of the general practitioners’ out-of-hours services being provided throughout the Island. That is where we start from.
I am going to invite you, really, to make any introductory comments you wish and then we will ask you questions, if we have any.
EVIDENCE OF HON. A R BELL MHK
Mr Bell: Thank you for that, Mr Chairman.As you say, I have sent in a brief written outline of my
views on that, and I would not particularly want to go through that in any detail, but I think I would just like to comment on two or three areas which are of genuine concern. Your remit, I know, is to look at the out-of-hours GP services for the whole Island and I recognise that. There are two areas, really, that I would want to comment on there.
But, first of all, at the outset, I recognise - and I think, to be fair, although it did not happen in the early days, now most people recognise - that the changes have been brought about not necessarily by policy changes in the DHSS but by the change in the GPs’ contract and that contract negotiated in the United Kingdom and washing over into the Isle of Man. It is unfortunate and people do not like change, but I think we do need to recognise that change is with us and we now have to accept that and find the best way possible to improve the service, or deliver the best possible service that we can.
My two concerns, really, at the outset are from the doctors’ point of view. One which surprised me, I have to say, was that when the changes took place - on 1 st April, I think it was - I was shocked to learn that the contract was only on four weeks’ notice. The whole of the medical service on the Isle of Man, the GPs’ service, was subject to four weeks’ notice of withdrawal of contract. To begin with, whatever new contract we end up with in relation to GPs, there has to be some hard look at that. We cannot have the health of our people put at risk on a four-week contract in future.
My second point, and I think the one which has caused probably more concern and problems than anything else, was that when the new scheme was brought in - and I think
Tynwald Select Committee on GP Out of Hours Services - Evidence of M r P A Gawne MHKProcedural
Tynwald Select Committee on GP Out of Hours Services - Evidence of Hon. A R Bell MHK
38 TGPS SELECT COMMITTEE, THURSDAY, 18th DECEMBER 2003 Oral Evidence
Dne or two of the people who have given you evidence today nave commented on that - the PR from the Department was absolutely appalling. I think that, had they made more of an effort to explain to people the circumstances why the contract was being renegotiated, why the changes were coming in, what the implications were and what the new solutions were proposed to be, then I think there would have been a wider acceptance of the necessity for change, albeit reluctant acceptance. That was a singular total failure on the part of the Department and they do deserve criticism for that, I think.
Unfortunately, as a result of that, because of the lack of a clear explanation from the Department, a great deal of confusion and misinformation circulated, which has caused fear, genuine fear, I think, in a lot of people, particularly elderly people, who obviously look on their GPs for security from a health point of view. So, I think if anything like this were to happen again, it is most important that the Department look at this side of things.
I think there is another issue here which I do not know whether it is possible to get around, really. It has been stated that the change is not financial, and I accept that in the main, although there could be arguments that finances do come into it, but, perhaps, that is more of a peripheral matter. On my discussion - I have spoken to a number of GPs - their real concern is that the hours that some of them have been putting in have actually led to a diminution in the quality of the service they feel they are able to give to patients because they are tired, they are not spending as much time on the patients as, perhaps, they would like to do, and this new contract would help them to do that So, it is not just a financial issue.
I think, though, we also need to look at one other aspect of that and that is that, I do believe, the attitude to the GPs is very much a generational thing. The older GPs - and many of them are now coming up to retirement, and I think something like a third of Manx GPs are retiring in the next 5 or 6 years - have been brought up in the National Health Service ethos and have, in the past, been willing to work long hours and accept difficult conditions, perhaps, in some cases. What I am finding, talking to people now - and I do not think this is just with GPs, I have certainly found it in the dental services as well - is that the new generation of GPs coming in are not as committed to the Health Service in the same way as their forebears were. They are in it as a career. They want the same sort of lifestyle, hours, salary and rewards as their equivalents in the private sector, and so, I think, you have got this strain between the generations, that the older ones are happy to work with the old system, or happier to work with the old system, but the new ones will not. And, therefore, I think that the thought of, perhaps, trying to wind the clock back and get ourselves into a situation where we get back again the level of service or the type of service which prevailed before 1st April is unrealistic and I do not think we are going to make any progress on that. As I say, we have exactly the same problem with dental services as we do with the GPs.
As far as the other point I was going to make is concerned, I know you are talking about GP services for the whole of the Island and I accept that. In Ramsey, though, in the north of the Island, it is virtually impossible to separate the out-of-hour GP services from the operation of the Hospital and the level of service that the people have had there. As a southerner, you might say, ‘Well, the north of the Island
has been spoilt in the past.’ We have had good service. The Hospital has been a huge asset to the north of the island. It has helped our people over generations. That has provided virtually 24-hour medical cover in the north and has been well used. The fact that the south or Douglas has not had this service is no reason to assume that the north should accept a dilution of service; what we should be aiming to do is bring the rest of the Island up to what is an acceptable level of service, rather than take away from what is available at the moment.
I do not want to stray into the argument about the future of the Cottage Hospital because I know there is another committee looking into that, but I think that, when you are gathering your thoughts on this, you must bear in mind the special situation of Ramsey and the north in relation to the Hospital and the extra level of service we have had from there, and so you can imagine the shock that occurred in the north of the Island when not only did we lose the out-of-hours GP service, but the GPs also then ended their contract with the Hospital for night cover and the accident and emergency hours reduced et cetera. All this coming at the same time, without it being properly explained, as you might expect, has caused considerable anger and frustration in the north of the Island, as well as quite a degree of fear. So, you need to bear that in mind, even though it may not be part of your remit.
The other thing I think you need to also bear in mind is that by extending the old Manndoc service now to cover the whole of the Island with, in effect, the same level of resource, you are not only diminishing the level of service that is available for Ramsey and the north; you are also diminishing what was available in the rest of the Island, because that resource is now spread over somewhere like another 20,000 people. You have now got one doctor covering the whole of the Island; as opposed to the 50,000, perhaps, you were covering before, you are now covering 75,000. So, in reducing the north and extending it to the north, you are actually reducing the service to the rest of the Island too, so I think that needs to be bome in mind.
One of the major concerns I have had expressed to me, probably more frequently than anything in the early days, was the impact on the Ambulance Service. I have to say that that situation has improved considerably, because we now have the third ambulance. Again’ 1 talk on a number of occasions to the ambulance operators in the north and they say that their early concerns now have been allayed and the problems that they did experience in the early days, by and large, now have subsided.
Overall the number of complaints I have now are considerably less than what I had in the early days. That is not to say that I do not get them still, although I have to say that, in the last couple of weeks, for the first time, I have started to get compliments about the system. So, whether things are turning around or not, I do not know.
There is one thing - 1 do not know, but I would imagine it has been brought in - really, which I think does need to be bome in mind where the provision of service to the north is concerned. The service has worked reasonably well, I think, over the last few months and that is, perhaps, a seasonal thing. The weather has been fine up until now, but the north of the Island is very dependent on the mountain road and access to facilities via that route. Frequently, from this period onwards, the mountain road can be closed because of snow, bad weather or fog. We have a large stretch of quite fast
Tynwald Select Committee on GP Out of Hours Services - Evidence of Hon. A R Bell MHK
Oral Evidence SELECT COMMITTEE, THURSDAY, 18th DECEMBER 2003 39 TGPS
road going through Ramsey which is frequently the source of accidents and, therefore, the roads can be blocked.
We do have a particular problem, I think, in the north of the Island in terms of access - or speed of access, shall we say - to Noble’s Hospital, which other parts of the Island do not suffer from. So, I think, when you are looking at the type of service provision up here, you need to bear in mind that that particular problem does arise from time to time, which, as I say, does not happen anywhere else.
I am trying, Mr Chairman, not to duplicate what has already been said unnecessarily. Again I do not know if it has been raised earlier, but an issue which has caused problems - or more concerns, shall we say — in the north of the Island than elsewhere is that, demographically, although I have not got the figures to hand, there is a higher proportion of elderly people in the north of the Island than the rest. That is traditional; it has been something that has grown up over the last 30 or 40 years. Therefore, the fear that has existed and the need, I think, for an efficient service can be explained by the fact that we do have so many elderly people here who may well be in need of help from time to time.
In particular - I think, again, it has been raised by one or two people and it is certainly raised with me on a number of occasions - probably the main one is the cost of getting home from the Noble’s. If they have to be taken into Noble’s Hospital, they are left then, as I understand it, more or less to find their way home. A lot of these people are elderly, they are frail and may not always have someone to go in with them, and, of course, there is the cost of then finding their own way back afterwards, and if you are an elderly person disturbed in the middle of the night, the likelihood is you are going to be quite confused, and with all this extra worry on top of it, I think this is actually causing some real concerns.
So, I was interested to hear the previous contributor say that there is some reimbursement scheme available. I have to say I was not aware of that and so, if it is available, it is clearly not being advertised very widely, because certainly no-one I have spoken to appears to have been aware of it and no-one from the DHSS has said anything to me about it So, if it is there, it is a very well-kept secret, and it is nothing to do with Treasury» I can tell you!
The Chairman: I can assure you it is there.
Mr Bell: Right, I accept that, but that, clearly, is not well known and it is a regular comment which is made to me.
I do not want to go through it all again, Mr Chairman, but, perhaps, if I could leave it there, just my few comments, and then answer any questions you might have.
The Chairman; Okay, thank you, Mr Bell.Mr Gelling.
Mr Gelling: Yes. We kept away from finance quite well there. (Laughter)
Really two things, which were changing direction completely in one, and that is we have had information and written complaints with regard to the problem that has also arisen since the change, and I just wondered whether you had anything in the north, because certainly it is the one that I get in the south and in the middle of the Island, and that is the difficulty when someone has died, either at home, or in a home, and again the availability of a doctor to certify death at a very traumatic time, a very sensitive time. Is that
something that you have had in the north as a difficulty? We have had one or two submissions from this area that that is something that has caused them problems.
Mr Bell: It has not been brought to me as a major problem, but it has been mentioned to me. It was some little while ago now and I am just a bit vague on the details. I cannot remember quite what the set of circumstances were, but I certainly have had a comment, I think on two occasions, where there were difficulties in getting GPs to come out in those circumstances, yes.
Mr Gelling: And the only other one was, really, a comment: we have weather problems - I am dealing now with the north - but we also have self-inflicted closures of the mountain road and the Kirk Michael Road through here, which probably amount to more than what the weather causes the north. Have you a comment as to some improvement that could be reached in that direction?
Mr Bell: (Laughter) You are talking about the speed limits. Yes, you have the TT races, obviously, and you have the Grand Prix races, so the roads are closed for a month a year, anyway, on and off.
It is tradition now with the police, which never really used to be quite as much before, that when there is a serious accident now, whereas before it would, really, just be put to one side of the road, the road now is almost automatically closed off, and that can lead to several hours of closure in some circumstances and that obviously causes great concerns as well.
Ramsey covers this from Kirk Michael right up to almost Creg ny baa, so there is quite a long stretch that Ramsey is covered with. There is a very high instance... The highest instance, I think, of accidents on the Island is over that stretch and, therefore, clearly the potential for delays in transport into Douglas at what will be, obviously, critical times, because they realise that they are only going to be taken into hospital if they believe there is a serious emergency. They are not going to be brought in for minor issues. So, if you have got the threat of these road closures all the time, then I think the concerns are going to build up.
My own view - and I have still, in spite of what the previous speaker has said, got to be convinced that I am wrong on this one - is that the present system would be more effective if there was a doctor based in Ramsey, so that there was one in Noble’s and one in Ramsey, the one in Ramsey perhaps covering as far as Peel, if you wanted to extend that to make it more effective.
So, we would have at least one part of the MEDS system covering the north of the Island over to the west, and then Douglas to the south, covering the west, and that would cut out the concerns over the central bit with the mountain being closed under the possibility of lots of these accidents. So, I think if we looked at it from that point of view, yes, there would be an extra cost, but I think there would be much greater reassurance amongst the public to know that we had our own doctor based in the north of the Island for this type of emergency, and, of course, that would also then improve the quality of availability of the remaining doctor based in Douglas for the rest of the Island. So, by putting a doctor based in the north, that would help the whole Island, not just Ramsey and the genera! area.
Mr Gelling: Thank you.
Tynwald Select Committee on GP Out of Hours Services - Evidence of Hon. A R Bell MHK
40 TGPS SELECT COMMITTEE, THURSDAY, 18th DECEMBER 2003 Oral Evidence
The Chairman: Okay. Mr Singer.
Mr Singer: You did actually touch, Mr Bell, on part of your initial letter, where you talked about this doctor now covering an extra 20,000 people, the Manndoc:
‘Obviously, as Treasury Minister and a Member of Keys, I would bepleased to see the expansion in the north...out in Jurby, the expansionof homes and industry and the prison; the expansion in Michael.. .Thereare several hundred houses forecast for Ramsey.’
Does this, therefore, strengthen your view that there should be some service, out of hours, permanently from Ramsey Cottage Hospital, whether it is MEDS or permanent doctors?
Mr Bell: Yes, I do and again, really, it builds on the point I was just making. There needs to be a facility, I believe, based...
We have got the perfect facility in Ramsey Cottage Hospital. It is a superb hospital. We have got all the equipment that would be required for most emergencies. Even in the past, the most severe emergencies went into Noble’s anyway, so we are not talking about every case here; wc are only talking up to a certain level. But the Cottage Hospital is well equipped, it is a very modem hospital. We have superb staff up there and, therefore, I think it is quite logical to have a doctor or a medical facility based in that hospital, covering the north of the Island and, as I say, possibly across to Peel as well, if you wanted to make it more cost effective.
Mr Singer: How do you equate that with the policy of...? It has been complained about by the ambulancemen in the north; we heard today from Mr Sieling of the Ambulance Service that they thought everything was going well, but the ambulancemen of the north have written to us and said that they are very concerned they are denied access to Ramsey Cottage Hospital - outside the hours of 8 to 6 - to the resuscitation equipment. They have no judgement now as to whether they can actually... If they wish to take people there, maybe to treat them, or just to stabilise them, they cannot get in there.
Mr Bell: Well, I have spoken to the ambulancemen only fairly recently. I do keep in close contact with them and they have indicated to me that the situation has been improving. 1 cannot really comment on that: this issue has not been raised with me as a problem, but if that is a problem, then it is a very serious problem and it is also a totally illogical situation.
If you have resuscitation equipment close at hand, it should be available for the ambulance and the paramedics to use, not to say, ‘Right, because of our rules we cannot use that; we have got to go into Douglas instead. ’ That does not make sense from anyone’s point of view, I would have thought, but I have to say I cannot comment on it, because that has not been raised with me and the only comment I have had is that things have been improving.
The Chairman: Thank you.Right, Mr Gill.
Mr Gill: Just one question, Mr Bell: in your Government role, as much as your Ramsey MHK role, do you think the EU directives on working restrictions, the length of time
people can work, would have any significant effect?
Mr Bell: I think we are in a time of change generally on these issues. It is not just in the medical profession; I think we will start to see some changes coining in right across the board over the next few years in attitudes to working practices, the time that people work.
Whether or not Government adopts all of these, of course, is for the individual Departments to look at and see what would be appropriate. In the main, Government usually does follow those directives, because... Certainly, if we are looking at the medical side of things, we are very, very heavily dependent on employees coming from the United Kingdom, whether they be doctors, or nurses, or dentists, or whatever they might be, and, if we were to offer a set of working conditions in the Isle of Man which was less attractive than what they would normally expect in the United Kingdom, then, frankly, we are not going to get them coming here.
As I say, the generation where you got total commitment to the National Health Service, I believe, has gone and the younger people coming through... It is not a criticism that they are anti-National Health; it is just that they are now growing up with a different attitude and, therefore, they are not prepared to make the same level of sacrifices, I do not believe, of their own lives, their social lives, their family lives et cetera that the previous generation would and they will be looking to achieve the same level of working conditions in the Isle of Man, at least to what they would be used to expecting in the United Kingdom.
I think we need to bear in mind very much here that, in all the areas we are talking about now, as I say, whether they are GPs, dentists - dentists are a good example - nurses, there is a national shortage, a UK national shortage, and that is why they are so heavily dependent on overseas professionals coming in to fill the gaps there, so they actually have a whip hand. They can choose now where they go to work and, therefore, if they are not getting the conditions they want here, they will simply go to somewhere where they can and that would be an even worse situation than we are in at the moment.
The Chairman: Thank you.
Mr Singer: With Treasury hat on, (Laughter) you probably heard the Minister say at the public meeting and at other times - and I think you did touch on it - finance is not the problem; it is the recruitment of GPs.
Would you agree with me that the DHSS do not seem to have any difficulty recruiting GPs for Noble’s Hospital - they use agencies - but it is the doctors here who are saying they do their own recruiting and have the difficulty? Would you not think, therefore, it might be useful to recruit doctors for the Hospital through the normal Noble’s channels and then bring those doctors to this Hospital?
Mr Bell: That might be a way of looking at it. I have deliberately tried not to stray into the operation of the Hospital here, but I know the argument has been put forward, and it might bear some consideration at least, for the overall management of the Cottage Hospital to come under the Noble’s wing and, therefore, the same employee availability would then apply for Ramsey, as well as Noble’s and, therefore, you would not have fhe separate recruiting issue.
Tynwald Select Committee on GP Out of Hours Services - Evidence of Hon. A R Bell MHK
Oral Evidence SELECT COMMITTEE, THURSDAY, 18th DECEMBER 2003 41 TGPS
I do know that the availability of the Ramsey Cottage Hospital has been a big attraction, and all the doctors I have spoken to about this agree that it has been a major attraction in bringing people to Ramsey because they like the broader experience of working in a cottage hospital, as opposed to simply being in a GP situation. So, in that sense, the Hospital has some attractions from a recruitment point of view, but without pre-empting what the other committee is doing, I do think that, perhaps, the time has come for, at least, a reassessment of the management of the Cottage Hospital to see if we can get better facilities into Ramsey on the back of the changes on that.
The Chairman: Mr Waft.
Mr Waft: Thank you.Just taking the line of another GP to cover the problem
area, as you see it, at night, are you thinking along the lines of another MEDS in Ramsey, as well as centrally?
Mr Bell: Yes, that was really what I have been thinking for some time, really right from the outset of this, that a lot of the problems that we have had, the fear that has undoubtedly existed over the last few months... And.you cannot ignore2,000 people marching on a very wet day in Ramsey, without accepting there is concern and fear, and I do not know whether that public demonstration has been fully appreciated yet in Douglas. You have got that fear there and... I am sorry. I have just lost the... What was the. ..
Mr Waft: I asked about a similar situation with MEDS in the north.
Mr Bell: Oh, sorry. Yes, I do see that as being the way forward. I think it would reassure the people in the north of the Island and, undoubtedly, it would improve the quality of the service in the north.
As I said, if you split the Island in two - we are not just thinking about Ramsey, although I know Ramsey is obviously very important to us up here - with Ramsey and the west and Douglas and the south, I think the level of service availability, then, for the whole of the Island would be far more acceptable to people, not just up here, but in the south as well. They are suffering a diminution of their service as well because, as I said earlier, the doctor now is having to cover Ramsey as well.
So, my view would be that we would have one based in Ramsey, based at the Hospital, and one based in Noble’s, with a doctor on call, covering so that the Island is split in two, and I think that would go probably 90 per cent of the way to resolving a lot of people’s fears and concerns.
Mr Waft: What somebody has said about the possibility of a young mother who has got two or three children and one of them, usually the youngest, gets earache or severe headache in the middle of the night and she rings in and she is told to get them into the MEDS service, and she has got to bring them all in because she is on her own (Mr Bell: Yes.): what is the situation with regard to finding them a taxi at that time in the morning?
Mr Bell: In the north of the Island, I would think that is impossible. It is very, very difficult, certainly, to get taxis late on at night here. I do not know what the availability...
Douglas might be a bit different, but, certainly, I would imagine the south is very much the same - and the west, indeed - as the north.
Outside the weekend period, it is very rare to be able to get taxis freely in the middle of the night, and, of course, when you have emergencies like this it does not choose its time very carefully and it is usually in the middle of the night when it happens, and it is natural, isn’t it, that the mother with the family round her are going to be very upset, very stressed, by a situation like that, if it is deemed to be an emergency? And if you have got the added problem, then, of trying to find taxis and, of course, possibly in some cases, £40 for a taxi back again afterwards if they are going up to Douglas...
Mr Waft: There is apparently a criterion by which an ambulance can be sent, I think. An ambulance can be sent in emergency cases, but there is always that problem of ‘Is it an emergency? Isn’t it an emergency?’ and it is down to the officer of the day.
Mr Bell: Yes, but, of course, if you have a sick child at 3 o’clock in the morning, it is an emergency, isn’t it, in their eyes? That is the way they would look at it.
Mr Waft: But the geography of the area... Some of the numbers here give voice for a facility in the north.
Mr Bell: I think so, and I think most people in Ramsey and the north believe that, as well. And, indeed, experience shows it: I use the road every day, as you know, and frequently, from now on, the road can be blocked because of snow. The Highway Board policy has changed over the years: in the past, as soon as it snowed, they used to have the gritters out and the snow would be gone, but now it is left to its own devices. It has been shut for weeks, sometimes, in bad weather, I remember last winter, coming back from Douglas, the mountain road was closed and I got caught in a blizzard on the coast road on the way back. It took me over two hours to get back from Douglas to Ramsey, because there was no other way of getting back at the time. If you are in an ambulance in an emergency situation, we are stuck.
Mr Waft: The residential increase in the Isle of Man, when I say ‘generally’, is increasing steadily. Has there been a levelling off or are there increases, say, more so in Peel than Ramsey and Castletown?
Mr Bell: Well, in Peel, of course, the population is growing faster. They have just built 200 new houses in Peel and I think are building a lot more as well, so the population is increasing very fast in the west of the Island. It has increased in the north, although probably not at the same rate, because Ramsey at least has not had the same level of residential development, although it is continuing elsewhere.
There are proposals for a new village, if not a new town, at Jurby to be developed over the next few years. We are in the process of building the new water treatment plant at Sulby, which will then give the north of the Island a boost over the rest of the Island, in the sense that there will be available pure water to enable developments to take place, so it could well be that, over the next few years, the north of the Island, if not Ramsey itself, will see a considerable increase in population if the economy continues to grow.
Tynwald Select Committee on GP Out of Hours Services - Evidence of Hon. A R Bell MHK
42 TGPS SELECT COMMITTEE, THURSDAY, 18th DECEMBER 2003 Oral Evidence
So, there are a number of factors there now which I think would indicate that we do need to look again at the level of emergency provision.
Mr Waft: There is always a hypothetical emergency situation you can dream up where... It is very difficult, but from a Minister’s point of view, we must look at the Island as a whole within the whole of our service. If you were to put her hat on, perhaps, what would you advise?
Mr Bell: I would advise her to take my advice (Laughter) and have someone based in Ramsey and someone based in Douglas, and I think that would cover it. Do not forget: whilst the population in the north of the Island is increasing, the population elsewhere is increasing as well. There are developments in the south of the Island now; even Castletown has got development, after many years of waiting. Douglas is still growing, (A Member: Yes.) so the population down there is growing as well and, therefore, if you keep the level of provision at the same level as it is now, with one person based in Douglas, then that person inevitably, regardless of any other changes that take place, is going to be stretched more and more thinly, because the population is creeping up all the time. So, by doing it this way, splitting it, one in Ramsey, one in Douglas, it covers the whole Island and it also gives a fresh impetus to the use of the Hospital and the emergency facilities which we have there, which, as I say, are first class and are being under-utilised at the moment.
The Chairman: Right, Mr Gill.
Mr Gill: You mentioned the difficulties in getting a taxi to get to Douglas. What difference would it make if Ramsey Cottage was open in those circumstances, when it is the same problem getting two miles as 22 miles?
Mr Bell; Well, yes, there is an element of truth in that. It would depend on where you are coming from. Of course, it is a fair comment. Perhaps you would get neighbours more inclined to pop into Ramsey Cottage Hospital than going all the way to Douglas, so I really would not like to comment on that.
The Chairman: Okay, just a couple of questions if I can, Mr Bell, in relation to the issue... And I think we need to be careful not to give a wrong impression out, but I think, generally, my understanding is that if a person has a problem getting a GP or whatever, then the advice from the Department is to dial 999 and ask for an ambulance -
Mr Bell: Yes, I think that is an extreme -
The Chairman; - and I think we should just make sure that it is not picked up that there is nothing you can do, because there clearly is.
Mr Bell: Yes, sorry, on that point, though, I have not heard it so much lately, but, certainly, in the early days, when there was a concern whether they would get a doctor or not, I know a number of people were actually dialing 999, whether it was an emergency or not, because that way they could be sure of getting an ambulance coming along. That was causing chaos with the ambulance service here, because they were being called out for someone with a cut finger, as
opposed to someone who, perhaps, might be sitting at home with a heart attack waiting to happen.
The Chairman: I appreciate that, but I think it is important that that is still there, and I think that was the advice from the Department in the early days when this started up and there was a problem: it had that impact, but when it settles down, hopefully it does not. (Mr Bell: Yes.)
I just wondered what your views were on the situation that if money is not a problem and if we all said yes, we would like to see an improvement in the service that we are talking about, so the Isle of Man Government goes down that road to promote \i, makes the money available, but the stumbling-block is there just are no GPs, we cannot attract them to the Isle of Man. How do you see us dealing with the issue? We are stuck where we are.
Mr Bell: Yes. I guess the only way round that, then, would be to enhance the reward for GPs ahead of the United Kingdom, so that the Isle of Man, once again, becomes an attractive place to move to.
There is a shortage and all the information I have is that that shortage is likely to continue for some time yet. There is not a wave of eager new GPs just about to burst onto the marketplace and I think the big concern - and it is most certainly true in the Isle of Man, but I think it is also true in the UK, from the figures I have seen - is that the situation, in terms of availability of GPs, is actually likely to get worse over the next five or six years, because a large number of GPs are retiring and I think, as I say, something like a third of the Isle of Man GPs are retiring over the next five or six years, so that is a lot of GPs you have got to produce just to stand still. That is apart from enhancing the service.
I do not think you are going to be able to persuade the GPs to work longer hours, so we are going to have to find other ways of making the Isle of Man more attractive. That might mean finance may come in at that point, where, perhaps, we have to pay our GPs a higher rate over here. I do not know. I am not on the DHSS, so I do not know the options that would be available for them, but, certainly, it is vitally important that the Island.provides an acceptable level of health service for our people. That is the least people expect from us and we have to find mechanisms to achieve that.
The Chairman: So, if the Government is aware that this situation is likely to get worse, are you aware of whether or not Government is actually looking to see if it can combat this issue by starting now, so that it does not actually get to a stage which is even worse than we have today?
Mr Bell: I cannot be specific, because I am not on the DHSS, so I do not know the details of what they are looking at, but I know they are aware of the concerns, and they have been looking at options as to what they are. You would have to ask the DHSS Minister. (The Chairman: Okay.) I cannot help you on that one.
The Chairman: Thank you, Mr Bell. Is there anything you wish to say in closing, or are you happy?
Mr Bell: No, I do not think so. I would like to thank you, like the others, for taking the time to come up to Ramsey. It is greatly appreciated, not just because it is nice to see
Tynwald Sclect Committee on GP Out of Hours Services — Evidence of Hon. A R Bell MHK1
Oral Evidence SELECT COMMITTEE, THURSDAY, 18th DECEMBER 2003 43 TGPS
people from the south of the Island sometimes up here, but also, really, just to reinforce the very real concern there is and has been amongst the people of Ramsey and the north over this change which has taken place.
As I said, right at the outset, there was very, very poor PR to begin with, and I think there needs to be an effort to reassure people, in Ramsey and the north of the Island that the quality of service that they have enjoyed previously is not going to be diluted and that the fears that have existed there are unfounded and people can retain or maintain their faith in the Manx National Health Service.
The Chairman: Right, I would just add to that, that, of course, that can be done without any action by this Committee, as you -
Mr Bell: Oh, I appreciate that, yes, but as you are doing the job, I am blaming you for it, sir. (Laughter)
The Chairman: I hope the Government will wait until we report. Thank you, Mr Bell.
Mr Rodan was called at 4.26 p.m..
Procedural
The Chairman: Right, now if I can invite Mr Rodan. Apologies for the delay. Good afternoon, Mr Rodan.
Mr Rodan: Good afternoon.
The Chairman: Welcome to our deliberations, and apologies for the delay but, as you appreciate from being on this side as well, it sometimes becomes a problem and the important thing is to let people have the opportunity to have their say (Mr Rodan: Indeed) and to take the opportunity to question.
Again, just to remind you of the remit, the Committee is to investigate the matter of the general practitioners’ out- of-hours services being provided throughout the Island. We did receive a written submission from yourself, 1 think, in relation to this issue and we had comments on that in terms that we have them available. Really it is just a matter of inviting you to make your submission and then we will go from there.
EVIDENCE OF HON. S C RODAN MHK
Mr Rodan: Well, thank you, Chairman, and thank you for this opportunity. I hope my observations might be helpful to the Committee.
I am the representative of persons, of course, in the constituency of Garff, which ranges from Baldrine in the south to the borders of Ramsey at Ballure and takes in Maughold.
The majority of the people I represent, I think, as patients, have been in a pretty well unique situation up until April of this year, as compared with patients in the rest of the Island, the vast majority of whom have had their primary healthcafe GP out-of-hours requirements met by a centralised Manndoc
system - I think there has been one practice in the south, similarly, that was not in the Manndoc system - and what I mean by that is this: many of my constituents have been well served by the Laxey GP practice, which was, as I say, until April one of the few which operated a system of rota-based out-of-hours and night visits direct to the patient in the home, and, secondly, my constituents in Maughold, in common with, I think, the great majority of patients in Ramsey, had their out-of-hours GP requirements met through the Ramsey GP practice, largely based on the Ramsey Cottage Hospital for night cover and out-of-hours cover.
In respect of the first group of patients, these people have, for many years, enjoyed very high standards of medical care, delivered in a home setting by a GPfrom their own practice. In fact, in the case of the Laxey practice, there was a one- in-four chance that the doctor visiting the home at night would be their own doctor, and they were understandably concerned that, following the introduction of a centralised service, the standards of care would go down. Doctors visiting would be unknown to the patient. They would not necessarily know the medical history. They would not be able to find the house. These were concerns that were voiced to me earlier in the year.
I think, in reality, after the introduction - and I am talking about my constituents in the Laxey and Lonan part of Garif - they found that those fears were not realised and thè emergency doctor service delivered from Douglas was relatively speedy and the anticipated problems of slower service or inferior standards were not experienced, generally speaking. I have had one or two instances quoted to me which were quite the opposite, and there was some dissatisfaction, particularly when patients were invited to attend at Noble’s to the emergency doctor service and were not getting the standard of care they felt they were entitled to, but there were particular issues that, perhaps, are outwith the concern of this Committee.
The disadvantages of having a centralised emergency doctor system, I think, from the NHS point of view, are that it costs, from the figures I have seen, around twice as much as the previous system, certainly the rota-based system, and GPs who visit are having to work from first diagnostic principles because they do not have access to case histories and there are issues to do with other medication that the patient may be on that the doctor is not aware of. As time goes on and technology advances, and with us entering an era of paperless practices and centralised computer records, I think a lot of those problems will not appear quite so much in the future, and with access to details of records - allergic reactions, past medical history and this sort of thing - any disadvantages that there are at the moment will disappear with the advent of technology in the future.
I think, very importantly, a point I would like to make is that what we will have in the NHS under this new regime will be doctors on duty because they want to be on duty and not because they have to be on duty, or feel some compulsion to deliver what is an old-fashioned, but very good level of service of home visits. I think there is every reason to believe that a centralised service will become more sophisticated and more tuned to the patients1 requirements, and, certainly, there can be no going back if the Isle of Man wants to be an attractive place in terms of recruitment of GPs in the future. The young generations of doctors will simply not tolerate, I think, what the older generation of doctors were expected to endure in terms of anti-social hours and night service.
Tynwald Select Committee on GP Out of Hours Services - Evidence of Hon. A R Bell MHK1Procedural
Tynwald Select Committee on GP Out of Hours Services - Evidence of Hon. S C Rodan MHK
44TGPS SELECT COMMITTEE, THURSDAY, 18th DECEMBER 2003 Oral Evidence
I understand operational guidelines are in place for this emergency doctor service. The intention is that standards are kept high, but I am sure the Committee will want to check for itself that this is indeed so. All I can say, from the point of view of patients who were previously served by the rota- based GP service, is that night visits to their home do not appear to me, judging by the level of comment I have had, to have been disadvantaged under the new arrangements from April.
I cannot say the same of those of my constituents in Maughold, in particular, who, along with residents of Ramsey, have experienced a significant change to the levels of service - high levels of service - which they enjoyed previously, and the reason, of course, is that the Ramsey Cottage Hospital facilities were made available previously, in effect, for out-of-hours consultation, with Ramsey GPs providing a quasi-emergency service in a hospital environment. Other practices never had that available to the GPs and, in the case of Ramsey, the Hospital was used effectively as a much valued out-of-hours ‘super-waiting room’ or a ‘super-surgery’ type of arrangement delivered by GPs. Ramsey Cottage has never been an acute general hospital with specific accident and emergency facilities; it had a very valuable minor injuries unit serviced by the Ramsey GPs and available to their patients. But we have to accept that the loss of these excellent facilities, out of hours, was inevitable the moment the Ramsey GPs, like everyone else on the Island, moved towards a centralised system of provision, a system based in Douglas with GPs on call, visiting from Douglas.
I think it is not surprising that, in the case of Ramsey and Maughold patients, they have, very understandably, been expressing great concern about a lower standard of service in terms of speed of attendance by the GPs visiting from Douglas. If there is a requirement to attend, which there often is, then there is a lengthy journey to Douglas, and we have heard from other evidence about the potential problems that this would present in terms of delays, adverse weather conditions and all the rest of it. And, consequently, there has been a severe loss of confidence on the part of patients in the north of the Island due to there being a facility there which is not, apparently, available any longer for the high standards of out-of-hours care that was previously available, i.e. a 24-hour doctor-led service. That is certainly a regrettable situation, and the Department’s response to that, of having an extended nurse-led provision for part of those out-of-hours periods, I think can only partially remedy that situation.
I believe that the standard that is provided is of a high professional standard and I am not aware of complaints, as far as the service provided by the nurses primarily is concerned. The complaint remains that there is no on-call medical cover. As we know, of course, there is accident and emergency cover and 24-hour medical care available at Noble’s, but, of course, what we do not have in Ramsey, I do not think, is a hospital service that is fully integrated into the NHS, from a clinical management point of view. It is a very convenient facility that Ramsey GPs traditionally used to see their patients in out of hours and there were high standards of facility on tap, as it were. That is no longer the situation.
So we have a combination of accident and emergency delivered by Noble’s being available and Ramsey Cottage Hospital not being fully realised, and we have, therefore, a somewhat confused situation, where Ramsey Cottage
Hospital, which was never an acute facility, was always part of the primary healthcare available to patients in a way that was never available in primary healthcare to anyone else, to patients of other GPs. But, for very understandable reasons, people in the north had enjoyed a level of care and had grown accustomed to a level of care and continue to believe, rightly, that they are entitled to at least the same standard of care.
So, in conclusion, Chairman, I would say that there are some major issues in respect of what Ramsey Cottage Hospital can be expected to deliver out of hours. It is a facility that is here, it is not being used to its full advantage out of hours the way it previously was, and I am sure the Committee will want to look at the alternatives available. I have suggested, in my written evidence, that the Department really ought to - for a trial period, perhaps 18 months, perhaps 2 years - have a fully salaried medical service as part of Ramsey Cottage Hospital, evaluate that after the trial period in terms of its effectiveness in providing local healthcare, primary healthcare, assess that against the accident and emergency service, assess it against the visiting emergency doctor service and reassess it then and assess the costs of doing that, because I very much suspect, with you having had evidence about the cost of providing GP-led cover in the Hospital, that that cost, if applied to a fully salaried service at Ramsey Cottage Hospital, could give the community the level of service that it previously enjoyed.
The Chairman: Okay, thank you, Mr Rodan. Thank you for that.
Mr Gill.
Mr Gill: Could I just pick up on your last point, Mr Rodan? Are you saying that, because of history, Ramsey and the north previously enjoyed a superior service to other regions of the Island and that should continue to be the case?
Mr Rodan: I think what is indisputable is that, in terms of primary healthcare, because of the arrangements that were entered into by the Ramsey GPs, whereby they were able to see patients out of hours in a hospital setting, and GPs and other practices would make home visits on a rota basis, yes, the patients got a very high level of service. Having had that high level of service, I do not see why they should be expected to have a lesser level of service. The nature of the service will have, of course, changed and it has changed, but 1 think what we must endeavour to do is to ensure that the standard of service is as high as it has been. We should not have a decrease in the level of service. The means of delivering it, though, is bound to be quite different.
Mr Gill: So, are you saying we should have a two-tier system, Ramsey and other regions, or are you saying other regions should enjoy the same as Ramsey?
Mr Rodan: I do not see how other regions could enjoy the same level of service as Ramsey unless they had a cottage hospital situation in their locality, but what I think they are entided to expect is a level of service that is as high there as it is in Ramsey, and anywhere in the Island should have a high level of out-of-hours provision.
Mr Gill: You mentioned the perceived loss of confidence
Tynwald Select Committee on GP Out of Hours Services - Evidence of Hon. S C Rodan MHK
Oral Evidence ' SELECT COMMITTEE, THURSDAY, 18th DECEMBER 2003 45 TGPS
in people of the north of your constituency, in Maughold and Ramsey. Is that actually based on direct experience, or would you describe that as a perception?
Mr Rodan: You are asking me what evidence I have to make that statement? (Mr Gill: Yes.) Well, I think, certainly, the evidence of loss of confidence is there for all to see. What 1 think the Committee may well want to test and assess is the experience since April, such that that loss of confidence is warranted. In other words, what has been the experience on the ground of the emergency doctor service as the alternative to patients in the Ramsey area? I have not had a larger number of comments one way or the other since the changes came in April, so I am not able to say whether that loss of confidence is justified, but I certainly do know that it is there.
Mr Gill: Finally, if I could, you mentioned that, with this new service, that would fall back on first diagnostic principles. Would that have been the case with the Manndoc system?
Mr Rodan: Oh, absolutely. They are in the same situation, and what I am saying is that those who enjoyed a GP home-visit service were expressing genuine concerns and fears to me that they would be visited by doctors who would not know them, not know their case histories, allergies and so on. I can say that my experience since April of that situation is that those fears were largely unjustified, as I am sure would have been the case when patients elsewhere in the Island some years ago moved onto the Manndoc system. I cannot comment on those having had the Manndoc system and what their experiences were with the new emergency doctor system.
The Chairman: Mr Singer.
Mr Singer: Could you explain that a little bit further? Whoever visits them - whether it is a Manndoc system or under this new MEDS system - a strange doctor visits a patient, they do not know the patient’s history at ail, they do not know the patient, so when you seem to say they are more satisfied with the service, they still do not have that information to treat the patient.
Mr Rodan: No, I think what I said was that the concerns and the fears of moving from a visit by a GP, either their own GP or one of the other GPs in that practice, and the concerns over having visits from a doctor who would not know them or their medical history, in my experience, have not really been bome out in practice.
Mr S ingen There must still be those same concerns and the same fears, but they have had to accept it. They have got no other choice.
Mr Rodan: That may well be. I would also suggest that, at three o’clock in the morning, if you are in pain, you just want to see a doctor and you are not particularly bothered if it is a doctor visiting from Douglas or your own GP. I think that would be fair comment.
Mr Singer: Can I go on to... You talked about going, in Ramsey, to a fully salaried service, even on a provisional basis. Did you mean the fully salaried service to actually cover the whole Hospital for looking after in-patients,
looking after the Hospital at night and looking after the emergency service and taking that service away from the Ramsey doctors, taking that part of the contract away, and that £180,000 they are going to save going to this salaried service, or did you just mean for out-of-hours service?
Mr Rodan: What I am referring to is out-of-hours service. If the means of achieving that, in fact, is to revisit all the contractual arrangements of the Ramsey GPs, I would say: let that review take place. There are various models of how it can be done. Ramsey GPs are contractually obligated to attend patients out of hours who may be in-patients in the Hospital. Whether we enter into a contract to make medical care available to out-patients as well I think is a matter for very careful assessment by the Department, bearing in mind that it is not a fully... It is a very good hospital with good, high standards of equipment, but it is not a fully equipped accident and emergency situation, as I understand it, and I think very careful assessment would need to be made. It would also need to be assessed whether a fully salaried service was justified in economic terms, bearing in mind that the call on those medical services during out of hours might be very rare, which is why I have said, ‘Let us test it.’ I do not know - and I suspect the Department will have a better idea than I do - but, really, until we have a trial to fully assess it, we cannot say one way or the other.
The Chairman: Okay. Mr Gelling.
Mr Gelling: Yes, I was quite impressed with the positive way in which you responded in your written submission -
‘The MEDS service will help secure future recruitment of GPs to theIsle of Man’
- so I am thinking, ‘Mr Rodan is all for the new system.’ And then another quote:
‘I cannot accept that Maughold patients now enjoy a similar tevel ofservice from MEDS that they previously enjoyed from their GPs.’
Then:
‘The disadvantages of a centralised out-of-hours system are that it iscosting more to run than the previous system.'
So, I was very interested to see your article in the press about removing the GPs out of the Hospital, having a - following on from Leonard - Hospital set-up, putting our own DHSS people in there. This morning we heard evidence whereby we were told that the fact that they get paid for looking after the Hospital during daytime helps them employ more people; I think it was eight that are in the practice now. So, I am just trying, now, to test your ingenuity in this plan you had, this marvellous plan that... How would that... Would that follow the system whereby we would actually take the money from the GPs and put three into the Hospitals - it would take three to do a 24-hour cover in the Hospital, not just the one - and how did that scenario work from the fact that... I am trying to separate the two. You think it is the way forward - we were told this moming it is the only way forward to keep GPs coming to the Island - and yet Maughold people are not getting the same service.
Mr Rodan: I think I am just stating the situation and facts, which are there for all to see. The historical situation
Tynwald Select Committee on GP Out of Hours Services - Evidence of Hon. S C Rodan MHK
46 TGPS SELECT COMMITTEE, THURSDAY, 18th DECEMBER 2003 Oral Evidence
has been a very particular one in the north because of the Cottage as a local hospital, as a local facility, and I do not think there is anything contradictory in the statements and those quotations you made. If we are to ensure, in the general sense, recruitment to the Isle of Man of qualified GPs and to have a fully resourced and staffed primary healthcare service, it is inexorable that we have to go down this route of a centralised emergency doctor service for out of hours or we will not be able to recruit anybody. So, I do not think that there is any dispute about that and I support that and I have argued that that system has met reasonably well, as far as I can tell, the fears of those who are used to a home visit system from their GPs in the Laxey area.
In the north it has been different: they have had a service that has been delivered by their GPs, not just in a home setting but in a fully equipped hospital setting, which ensured high levels of service. It gave great confidence to people- particularly, as has been said, to many elderly people in the North for whom transport might be a problem - to know that there is a hospital environment that can attend to their needs. I think what has happened and what has grown up is this hybrid situation, where we have primary healthcare being delivered in a secondary setting. So, we have Ramsey Cottage Hospital, which is neither fish nor fowl: it is not a GPs’ surgery and it is not a fully serviced acute general hospital. It is a cottage hospital, and cottage hospitals, I think, over the past 100 years, or since the early years of the 20th century, have been a feature of many rural areas of Great Britain and had roles appropriate to their era. We have moved on from that and I think thé challenge for the Department is to give the Ramsey Cottage Hospital a full working hospital role that will improve on this hybrid primary healthcare role delivered by GPs, who are there for primary healthcare in the first instance and are not hospital doctors. So -
Mr Singer: So, we should basically go back to what it was before -
Mr Rodan: Well, not necessarily go back, but acknowledge the fact that we have got a médical facility here that is of great value, it is resourced, but I do not think we are getting the best out of it. And, in clinical management terms, I am pretty sure we are not getting the best out of it. We cannot admit people there out of hours with confidence because there is no medical provision 24 hours and the GPs do not want to attend out of hours for out-patients, understandably - and I think the system has changed and they ought not to be obliged to - so the Department is going to have to use this very good facility, resourced by the taxpayer, to the maximum effect.
The Chairman: Mr Waft.
Mr Waft: Thank you. Can you explain to me, Minister, how you can use the Ramsey Cottage to the maximum effect if you are not having a GP actually either on site or on call for that situation?
Mr Rodan: Well, I have suggested salaried doctor medical cover 24 hours, and I suspect that may not be particularly cost effective. I think - and I am aware the Department are looking at options for Ramsey Cottage Hospital, and I am not sure the extent to which you are investigating that - having a salaried medical service would restore confidence that there was a doctor there, but, by
nature, that doctor is going to be of a general discipline and there are not going to be specialist services available 24 hours, such as there are at Noble’s.
So, I think, in practice, it is going to be fairly difficult to achieve a full working 24-hour hospital with medical cover.I do not have the answer to it; I have just offered up a way of maintaining, as far as possible, the standards of medical care that were available in the north and are no longer available. Trial a salaried doctor service, see how it compares with a visiting emergency doctor service and see how it compares against accident and emergency provision to Noble’s through the ambulance service.
Mr Waft: If you have not had any figures as to the situation before what happened took place and after, there is no real comparison there, is there?
Mr Rodan: I am not aware of that. I do not know what sort of records the Department has of the type of cases that were out-patients at Ramsey Cottage Hospital out of hours. I am not aware of that. I would very much hope they did have it so an assessment could be made. I suspect they do not.
Mr Waft: Whilst you gave mention to how good it is to have a GP who knows you, or knows the family, or somebody within that practice to be on call during the night, would you accept the fact that, if you have an emergency situation, any doctor would do, actually, to try and get you over that period until the morning?
Mr Rodan: Yes, and I think I said that, at three in the morning, you arc just pleased to see any doctor at all. Without repeating myself unnecessarily, I think, while the ideal would be a doctor that knows you and your case history to visit, or at least a doctor from the same practice to do so, when they might well have access to medical notes, that is the ideal, but those days have gone and they are not likely to return.
Mr Waft: Have you had, personally, any knowledge of any increase in problems arising because of the situation?
Mr Rodan: No, I have not been made aware of problems because of the new system, as compared with the GP visiting system.
Mr Waft: So they have not been increasing, then?
Mr Rodan: Not that 3 am aware of. I am aware of particular issues and particular instances with patients under the new emergency doctor service, but I would not like to quote those as being illustrations of some defect in the system.
Mr Waft: Are you aware of any recompense of the transport costs from the DHSS?
Mr Rodan: No, I have no knowledge on that whatsoever.
Mr Waft: Thank you.
The Chairman: Mr Gelling.
Mr Gelling: I am just interested in, perhaps, a personal opinion. The original strategy of an acute hospital, as you
Tynwald Select Committee on GP Out of Hours Services - Evidence of Hon. S C Rodan MHK
Oral Evidence SELECT COMMITTEE, THURSDAY, 18th DECEMBER 2003 47 TGPS
might recall, was a cottage hospital, of which we have the model, in Ramsey, a cottage hospital in the south and one actually in Douglas, in the central part of Douglas. Where would you have thought the pressure came from to actually get to where we are today when, in fact, that strategy was to have those three satellite cottage hospitals and then one an acute hospital? Do you believe that it, perhaps, was the lobby from the GPs that they did not want to lose a lucrative income, or do you think it was that the GPs thought this would be too much work, or... I just wondered where you think that, possibly, we arrived at a situation where we have not got what we originally set out to try to achieve.
Mr Rodan: I would like to think that the Island’s healthcare needs were being viewed objectively overall and that a place had been envisaged for a community hospital- type of operation to supplement the high standards of an acute general hospital, which is why I assume the strategy of community hospitals in Douglas, Ramsey and the south was always part of this strategy. Now we have drifted away from that entirely. Whether it was the GPs putting particular pressure on for their own financial reasons, I could not comment on that. 1 would like to think it was because of the success of a cottage hospital-type of arrangement in the south, where patients could be seen and looked after in a hospital setting and the value of that was recognised and identified as being, ideally, part of the Health Service of the future.
The Chairman: Mr Gill.
Mr Gill: Thank you, Chairman.The practice you described of trialling this doctor service:
1 think you described it as non-cost effective. Is that a practice you have seen elsewhere in Government?
Mr Singer: It is everywhere.
Mr Rodan: I am sorry. I could not quite understand... Sorry.
Mr Gill: What we are actually saying is that we should have a trial, even though it will not be cost effective?
Mr Rodan: I think the trouble is we are, quite often, very ready to take up positions and jump to conclusions before we have got any evidence, and I am just trying to make a suggestion of a way of getting the evidence. I suspect it might not be cost effective. What it will do, I think, is restore a level of medical service in that hospital setting that was available until April of this year.
Therefore, if you are going to radically change, especially when you are obliging people to accept a system that they perceive as being less than what they had become accustomed to, I think it is reasonable to phase in such a change, and I would certainly have... If you are going to... You were always going to have to, in April, change the doctors’ contract, but what you could also have done was phase in the other aspects to this, i.e. the 24-hour medical cover available from the local cottage hospital, assess it, trial it and then make your decision.
The Chairman: Okay. Thank you very much. Anything else you wish to add, Mr Rodan?
Mr Rodan: No, thank you very much for the opportunity. I am not sure that this is the first time a select committee has met outside of Douglas. 1 - (Interjection) Oh, the second.
The Chairman: The first since 1977.
Mr Singer: And we will soon be working out of hours! (Laughter)
Mr Rodan: Well, I hope you will put in your claim.
The Chairman: We certainly hope to be home before midnight. Right, thank you, Mr Rodan.
Procedural
The Chairman: Can I just advise the public that the next public sitting of the Committee to take oral evidence will take place on Wednesday, 28th January 2004, starting at 9.40 a.m., and that will take place in the Millennium Conference Room in the Tynwald Precinct in Douglas. We will be taking evidence from Mr Cannan MHK, Mr Quine MHK and Mrs Christian MLC, Minister for Health and Social Security - and she will be accompanied by Mr Killip, the Chief Executive of the DHSS - and we will also be taking evidence from Mr Newbery, the General Manager for Primary Healthcare Services, and Mrs Duke of MEDS, the administrator of MEDS. Also we expect to be taking evidence from Ramsey Town Commissioners.
That concludes the public session. We are now going into private, so if I can ask everyone to make their way out. Thank you.
The Committee sat in private at 5.05 p.m.
Tynwald Select Committee on GP Out of Hours Services - Evidence of Hon. S C Rodan MHKProcedural
Appendix 7

T Y N W A L D C O U R T O F F I C I A L R E P O R T
R E C O R T Y S O I K O I L Q U A I Y L T I N V A A L
P R O C E E D I N G SD A A L T Y N
(HANSARD)
S E L E C T C O M M I T T E E ON GP OUT OF HOURS S E R V I C E S
B I N G E R - L H E H M Y C H I O N E S H I R V E I S H Y N F I R - L H E EA Y N S O O R Y N S O C C A R A G H
Douglas, Wednesday, 28th January 2004
Published by the Office of the Clerk of Tynwald, Legislative Buildings, Bucks Road, Douglas, Isle of Man. © Court of Tynwald. 2004 Printed by The Copy Shop Limited, 48 Bucks Road, Douglas, Isle of Man
Price Band E
50 TGPS SELECT COMMITTEE, WEDNESDAY 28th JANUARY 2004
Members Present:
Hon. J A Brown SHK (Chairman)Mr D J Gelling MLC Mr Q B Gill MHK Mr LI Singer MLC Mr G H Waft MLC
Clerk:Mr P Lo Bao, Third Clerk
Business transacted
PageProcedural.............................................................. ...................................................................... ..........................................51
Evidence of Mr J D Q Cannan MHK............................................................................................................................... ..51
Procedural...............................................................................................................................................................................55
Evidence of Mr R E Quine MHK....................................................................................................................................... 55
Procedural........................................ ......................................................................................................................................60
Evidence of Hon. C M Christian MLC and Mr D Killip..................... ............................................................................60
The Committee adjourned at 1 2.17 p.m.
Procedural............................................................................. ......................... ........................................................................71
Evidence of Mr G Newbury and Mrs S Duke................................................................................................................... 72
Procedural................... ........................................................................................................................................................... 85
Evidence of Mr P Radcliffe and Mr P Whiteway............................................................................................................ 85
The Committee sat in private at 4.23 p.m
Oral Evidence SELECT COMMITTEE, WEDNESDAY 28th JANUARY 2004 51 TGPS
Tynwald Select Committee on GP Out of Hours Services
The Committee sat in public at 9.40 a.m. in the Millennium Conference Room,
Legislative Buildings, Douglas
[THE SPEAKER in the Chair]
Procedural
The Chairman (Mr Speaker): Good morning, everyone. Could I invite Mr Cannan to come forward, please? Good morning, Mr Cannan.
You know all the members of the Committee, so I do not think we need to introduce, unless you specifically want. Can I welcome you and thank you for the evidence that you have provided? We are pleased to give you the opportunity to submit evidence directly to us.
Just to remind you, the Select Committee was appointed by Tynwald to investigate the matter of the general practitioners’ out-of-hours services being provided throughout the Island, with the power to take written and oral evidence pursuant to sections 3 and 4 of the Tynwald Proceedings Act of 1876, and to report.
So, I am sure you are clear oh our remit, being part of the decision-makers on that, and, really, it is a matter, if 1 may, of handing over to you to submit your evidence to us.
EVIDENCE OF MR J D Q CANNAN MHK
Mr Cannan: Well, thank you very much, Chairman.As your members will be aware, I represent the
constituency of Michael on the north-west of the Island, and 75 per cent of that constituency are serviced by the Ramsey Group Practice and Ramsey Cottage Hospital. The other 25 per cent are serviced by the Peel Group Practice, and, therefore, those patients go to Noble’s Hospital.
The Committee will be aware that the strong feeling in the north of the Island culminated in a protest march of over2,000 people in May last year, expressing their great concern at the out-of-hours service, and part of the loss of that out-of- hours service was the loss of the facility of Ramsey Cottage Hospital. The discontent in the community is as strong as ever, based on the lack of being able to call the duty doctor of the Ramsey Group Practice or, alternatively, being taken to Ramsey Cottage Hospital and knowing that there was a doctor on duty.
The community, I think, fully appreciate that the doctors want their weekends off and fewer commitments in the evenings, but, to balance that, they believe it is the duty of the Health Service to make alternative arrangements, and in my letter to the Committee on 18th August last, I wrote:
.'Numerous complaints have been received from persons resident inthe northern parishes for the failure of the GPout-of-hours service and
the resulting non-availability of a doctor at Ramsey Cottage Hospitalto provide a satisfactory healthcare service.’
Nursing and residential homes can no longer have the comfort of knowing a doctor will visit out of hours to attend an emergency. There are, as you appreciate, in the north of the Island, based in Ramsey and outside Ramsey, nursing homes, care homes, who have* since their establishment, relied upon the fact that there is a doctor available in the north of the Island if they so need it, and they have benefited, like the community, from the fact that a doctor is based in Ramsey, part of the Group Practice, and will visit these care and residential homes as and when required. And being care and residential homes, I am sure that you will appreciate there are no flippant or unnecessary call-outs of a doctor. They have responsible staff and will call a doctor when they think it is necessary. As you will appreciate, now they have to ring up Manndoc and get instructions down the telephone, which is not the same as the doctor seeing the patient, and, no matter how good you are - medically qualified - as a nurse or duty nurse, it is not quite the same as the doctor actually seeing the patient face to face or the requirements.
A GP also will not attend out of hours at a sudden death at a private home. Instead, the police have to call out a police doctor to certify death, and that is another, not so much lack of service, but a charge to the Government. The Home Affairs Department have submitted evidence to your Committee, Chairman, fairly long evidence, setting out the reasons. And when there is a death in the community, in the parish and so on, at home, the person who was living in the house with the deceased had the comfort of knowing that a doctor would come from the Group Practice to see and handle matters. Instead, there may be some time before a police doctor had to be called out.
There are other examples of problems relating to healthcare caused by the introduction of the GPs’ out-ofhours service. You will have had many examples in your evidence, and I am not going to be repetitive of complaints of people trying to get a doctor, trying to get an ambulance going to the hospital - not available. A very recent complaint to me - and it is only ‘third-hand’, so to speak - is that a football player on a Saturday was injured on a playing field in Ramsey and they had to wait three-quarters of an hour to get even an ambulance, whereas, previously, one had the confidence of knowing that the ambulance was up in the Cottage Hospital and was whipped down and you were into the Cottage and so on. And I have seen many cases of that, watching sport, both rugby and football and other sports in Ramsey, where somebody is injured - or, indeed, outside Ramsey, in the football fields of die parishes - an ambulance is called and comes, or a doctor is called and so on. So, there is general dissatisfaction in the community in that respect.
Also, I have come to make enquiries as to who has a duty of care for the patients in Ramsey Cottage Hospital, and those who have the duty of care to the patients in Ramsey Cottage Hospital, as I understand it, for the whole 24 hours, seven days a week, are the doctors of the Ramsey Group Practice. And I have enquired of the Health Services Department and I have been advised by the Chief Executive that the Ramsey Group Practice are remunerated in the sum of £160,000 a year for the care of their patients in Ramsey Cottage Hospital. But they are not caring for them - or are they caring for them? I have not really been able to find out- during those hours when they are hot able to care for the rest of their patients in out-of-hours service.
ProceduralTynwald Select Committee on GP Out of Hours Services - Evidence of Mr JD Q Cannan MHK
52 TGPS SELECT COMMITTEE, WEDNESDAY 28th JANUARY 2004 Oral Evidence
I say this as part of my submission: what should be done to benefit those patients in the north of the Island - and that represents 75 per cent of my constituents, who are in the Ramsey medical care area - is that Ramsey Cottage Hospital should be transferred from the responsibility of the Primary Healthcare Division of the DHSS to Isle of Man Hospitals, and, therefore, the patient, when it goes into Ramsey Cottage Hospital, is the responsibility of Isle of Man Hospitals, just the same as a patient who goes into Noble’s Hospital.
The moment you go into Noble’s Hospital, you cease to be under the duty of care of the Group Practice. So there seems to be an anomaly here now. Up to 1st April, the Ramsey Group Practice had a duty of care for all the patients in the hospital and a duty of care for the whole of the north of the Island, 24 hours a day, seven days a week. They do not have a duty of care now outside the new hours, but who has a duty of care for patients in the Ramsey Cottage Hospital? I believe that this situation can be regularised by saying that the Cottage Hospital becomes a cottage hospital providing the same measure of care as it did prior to 1 st April by putting it under Isle of Man Hospitals and that it would not be any greater significant burden to the taxpayer by having a doctor from Isle of Man Hospitals on a rota basis or if they have a resident doctor there, especially for cover in the evenings and out-of-hours service in the north, based on the hospital and with a duty of care to the nursing homes and the hospital area. There would be a saving, on the one hand, of £160,000, which is the current estimate which I have had submitted to me by the DHSS, and that would be used to offset the cost of a doctor covering the north of the Island on the full seven days a week.
The basis of my submission is that there is discontent. You will be receiving many letters, and I am not going to be repetitive. The nursing and residential homes no longer have the comfort of knowing a doctor will visit out of hours. There is no doctor now to certify death at home when somebody just dies at home; the police have to be called, a police doctor has to be called to certify death. And I believe that much of this can all be reorganised if the Ramsey Cottage Hospital is transferred to Isle of Man Hospitals, a doctor is on duty there, and that the costs will be offset against the costs of the savings for Ramsey Cottage Hospital to have the duty of care of the patients in the Hospital.
The Chairman: Thank you, Mr Cannan. Anything else? That’s fine for now, is it?
Mr Cannan: Unless you have some questions. I may enlarge on whatever your questions are, Chairman.
The Chairman: I did not know if you were pausing, or I was interrupting. (Mr Cannan: No.) That was all.
Mr Singer.
Mr Singer: Mr Cannan, whilst you have been concentrating on the area that you represent, this Subcommittee is looking into the changes in GPs* services throughout the whole of the Island, and there are changes down in the south of the Island. Have you, particularly, any opinion on the effect that this has had on the people of the south of the Island, deleterious or otherwise, the fact that similarly their doctors have withdrawn services?
Mr Cannan: I am aware that their doctors have
withdrawn services. I am only aware in terms of hearsay that they are dissatisfied in the south of the Island, but what I have tried to put over to you is that I have first-hand knowledge, because they are my constituents and they are doing it... And those who may not live in Ballaugh, Jurby or half of Kirk Michael have their relations living in Bride, Andreas, Lezayre, Maughold - you know, in the greater area served by the Ramsey Cottage Hospital - so, I am aware, on a hearsay basis, of the problems in the south of the Island.I am fully conversant with what is happening in the north of the Island.
Mr Singer: Can I ask one more question?
The Chairman: Mr Singer.
Mr Singer: It is now nearly nine months since the service was changed. Would you say that there are fewer actual people protesting, that it has reduced the amount of people actually protesting? Would you put that down to people getting tired of protesting and saying, *Oh, we have got to accept it’, or that they perceived that there was a problem and there is no longer a problem, or do you find that you are still getting the same number of complaints from people on an individual basis when they come up against this problem of not being able to find a doctor or an ambulance?
Mr Cannan: The public view is that they have made their protest, they have had their marches, they have been shouting and shouting about it. They know the Select Committee is on. It has been well advertised. They are relying now on the members to do something about it, but that does not stop them actively complaining about the cases that go on.
I mentioned the football case - 1 think it was the weekend before last, maybe. I gave you that one. Then there is an uproar, and there are other numerous cases. There was a recent death in one of the villages I represent, a home death. I will not go into details, obviously, but there are complaints. To begin with, there was the general complaint, of everybody complaining against it who had not actually experienced it, because they knew the service was being withdrawn. Now you are getting the actual complaints that, a year ago this, that and the other could have happened.
The Chairman: Now it is actually happening.
Mr Cannan: Now it has actually happened, where everybody before knew what was going to happen and now we see what is going to happen. As I say, the football case is...
The Chairman: Okay. Mr Gelling.
Mr Gelling: Actually following on directly from Mr Singer, inasmuch as I think you are in a unique position because you straddle from the Peel area practice, if you like, which tends to some of your constituents, to the north. So you will have experienced the Pee! practice dealing with your constituents - and I tend to remember that you have been complaining about the attention even to your constituents in your area from the Peel practice - would you say that there has been a change of attitude of GPs, in general, to the way in which they look after their patients from, say, outwith the north, that is the Peel end? That was the first question, really.
Tynwald Select Committee on GP Out of Hours Services - Evidence of M r J D Q Cannan MHK
Oral Evidence SELECT COMMITTEE, WEDNESDAY 28th JANUARY 2004 53 TGPS
And did they come to terms with it, or is it just the case that they have become complacent?
The othef question, really, is that which you raised about the death: is that another complaint as a constituent representative that you get not just the certification of death, but also the whole what appears now to be strung-out way of not just the certificate of death but then getting the release of the body for funerals? Funerals that used to be in three days are now a fortnight. Generally, is that another problem you are finding in your particular area?
Mr Cannan: That has all been drawn to ray attention by people concerned about the general service that they are providing. 1 have even had a formal complaint from an undertaker in the north about not being able to get bodies released, which was causing distress to the families. .
If it is general GP service... The Peel practice, as you know, has closed down the branch surgery in Kirk Michael, and I can assure you that there is complete discontent - and the strongest possible discontent. I think it was only in October that I had a public meeting in Kirk Michael about three matters - coastal erosion, the bypass and the medical centre - and there was, as reported on the radio and in the press, a unanimous vote from a packed hall, an absolutely packed hall, against the withdrawal of the medical facility from Kirk Michael and the requirement for a resident doctors’ surgery and community medical centre.
As politicians, you are aware of all that and the grievance felt that, whilst people are delighted that Laxey, Castletown, Ballasalla and Rushen have all had brand new surgeries and brand new medical facilities, this one part of the Island is being denied this facility. I have drawn it to the attention of the consultant reviewing the Ramsey Cottage Hospital- not a medical consultant, you know, the administrative consultant - and the development of Jurby and the coming of the prison, the requirements of a prison doctor and so on. All these matters have been forcibly expressed by me to the relevant authorities and the DHSS.
But there is no complacency in Kirk Michael about the lack of a medical facility, elderly people having to travel on a bus late at night, on a black winter’s night, and struggle up a hill in Peel - I suppose the residents of Peel have to struggle up a hill, too - to the doctors* surgery. There is general discontent, and they feel that the community, which had a branch surgery ever since I can remember... And I was bom in the village and recall going there at the age of four or five or six, or whatever, with my mother, you-know - my mother taking me to see the doctor, Doctor JrO y Z C l— and suddenly it is withdrawn.
Mr Gelling: Just one more. Again, I am looking at where you represent. Where would be the demarcation line to call when the Ramsey Cottage Hospital was available to you? Would someone in Michael, for argument's sake, call the Ramsey Cottage Hospital, and would south of Michael call for an ambulance from Noble’s? Where was, would you suggest, the dividing line in your constituency where that perhaps would have happened?
Mr Cannan: My constituency consists of the parishes of Kirk Michael, Ballaugh and Jurby. Ballaugh and Jurby are 100 per cent under the control of the Ramsey Group Practice. Half of the residents of Kirk Michael -48 per cent or whatever, as near as damn half - are under the Ramsey Group Practice, and the other half under the Peel practice.
Some years ago, the Ramsey Group Practice, because of its increasing size, stopped taking any further patients from Kirk Michael, so that number is withering on the vine, and all new residents to Kirk Michael have to go to Peel. Previously, in- if I could say - the good old days, if there was an accident in Kirk Michael, you did not sort of look over and say, ‘Hello, fellow. Are you from Ramsey or are you from Douglas?’; you just called an ambulance and it came -
Mr Gelling: Would it be Ramsey?
Mr Cannan: It would generally be Ramsey, but you did not stand and look over the injured body in the middle of the road and try to find out...
Mr Gelling: Thank you.
The Chairman: Mr Gill.
Mr Gill: Thank you, Chairman.Mr Cannan, you have spoken at length about the concerns
in the north, and you have touched on the hearsay awareness that you have of the south. Can I put the question 1 put to your colleagues, who voiced the same sorts of issues: Is the effect of what you are saying that you would support a two- tier system for the regions, one for Ramsey and a different system for the other regions?
Mr Cannan: I understood, some years ago, when I was voting for the health centre in Rushen, that we were voting for a cottage hospital for the south of the Island. The goal posts seemed... Either I was not paying attention to what I was voting, or the goalposts have moved, and I suggest, Chairman - and you have been in Tynwald as long as I have- that the goalposts have moved. (Interjections) So that answers your question.
Mr Gill: No, it does not, with respect. If the goalposts have moved -
Mr Cannan: Not by my -
Mr Gill: No, but nonetheless, if we accept that the goalposts have moved, is the net effect that you would support a two-tier system?
Mr Cannan: I suggest that the goalposts be reinstated to where I originally gave my vote. I gave my vote some five or six years ago, whenever we voted for the health centre, that that was to be a cottage hospital for the south. I stand corrected by those members who were there, but that was the... And nothing to do with Tynwald, but purely executive decisions by the DHSS have changed the goalposts. I was never asked, or concurred, to change the goalposts, and my view is exactly the same.
Mr Gill: Secondly, you touched on the issue that your constituents, you say, had a complaint that either they could not be sure of seeing a Ramsey Group Practice doctor or they could not be sure of seeing a doctor from either the Ramsey practice or somewhere else at the Cottage Hospital. Is that the essence of the complaint?
Mr Cannan: No. There is no doctor at the Cottage Hospital.
Tynwald Select Committee on GP Out of Hours Services - Evidence of M r J D Q Cannan MHK

54TGPS SELECT COMMITTEE, WEDNESDAY 28th JANUARY 2004 Oral Evidence
Mr Gill: Oh, no. That was the complaint: that there is none. Am I right?.
Mr Cannan: There is no doctor at the Cottage Hospital after 6 o’clock or at weekends.
Mr Gill: And is that the essence of the complaint of your constituents: that either they cannot see their own Group Practice doctor or, failing that, they cannot see any doctor?
Mr Cannan: There are two issues for your question. Prior to 1 st April, they went to the Cottage Hospital, and there was a duty doctor, who was the duty doctor for the whole of the north of the Island. So, if your child fell over and had needed a few stitches, you whipped him in the car and you took him to the Ramsey Cottage Hospital at 8 o’clock on a summer’s evening or whatever, and the whole matter was dealt with. You cannot do that now. Also, if your child took seriously ill or quite ill in the evening, you rang and the doctor came to see your child. I am not talking about trivia, but, you know... That does not happen now, because there was a member of the Ramsey Group Practice, which has eight doctors, and one doctor was on duty the whole time.
The Chairman: Could I just -
Mr Cannan: I am trying to answer Mr Gill, Chairman, but what I am trying to say is that the complaint is that there is not a doctor on duty for the north of the Island,
The Chairman: Can I just follow that on, if I may, at this stage, because it ties in. Part of the evidence you have given, Mr Cannan, is that, in fact, the view of your constituents is that, whilst that service had been removed by the GPs, the DHSS should provide a similar service out of hours by having a doctor at the Ramsey Cottage Hospital.
Mr Cannan: Yes, but what I am trying to say is that they can either provide the out-of-hours doctor and keep the care of the patients during the other hours under the Ramsey Group Practice or have the Ramsey Group Practice withdraw from the Cottage, so that the duty of care for the patients the moment they went into Ramsey Group Practice was under Isle of Man Hospitals.
The Chairman: Okay. Thank you. Mr Waft.
Mr Waft: Thank you.Mr Cannan, we have heard evidence from DrMaska with
regard to the problem of attracting GPs to the Island and the possibility of 50 per cent of our present GPs going within 10 years. With regard to the problem of attracting doctors per se to the Island and the concerns that the DHSS have with recruitment, have you any sort of crumb of comfort or way forward for them, given the circumstances that they face with regard to recruitment and the problem that GPs these days are not keen on taking out-of-hours service under their remit of work? Have you anything to suggest on that?
Mr Cannan: In my campaign for a proper doctors’ surgery and medical centre for Kirk Michael, Ballaugh and Jurby, I was told by the DHSS that there were no doctors available and there was no possibility of getting doctors, to which I was happy to respond that a young man from Kirk
Michael, who was a GP in his mid-thirties in Merseyside, and his wife, who was also a GP, were very, very anxious to return home to the Isle of Man, and I think that is the benefit, to establish the doctors’ surgery to serve Kirk Michael, Ballaugh and Jurby, which actually put the DHSS in a state of panic, because they had told me there were no such doctors available.
The doctor and his wife have now taken a short-term contract with a practice in the Isle of Man, still hoping that a proper surgery will be established in the north-west of the Island which he can man. So, every so often these kites are flown: we cannot get doctors. And, with that response to the DHSS, I just rest my case.
The Chairman: Okay. Mr Gill.
Mr Gill: So, on that anecdotal basis, you do not accept -
Mr Cannan: It is not anecdotal. I know the doctor. (Mr Gill: Yes.) He was at school with my sons. His mother lives in Kirk Michael.
' Mr Gill: On that example, you would say that there is no crisis, there is no difficulty increasing GPs -
Mr Cannan: I am not saying that, but, perhaps, if they went out and looked a bit harder - (Mr Gill: Right.) They were telling me there were no doctors available, to which I was cheerfully able to respond that here was a doctor who was anxious, and had already made inquiries before that, of the DHSS.
I understand it is not for the DHSS to recruit doctors but the practice, and the practice may or may not wish to recruit doctors because, as you know, the more doctors, the more dilution of income.
The Chairman: Okay. Mr Waft.
Mr Waft: The practice which Dr Maska is a member of has said there is a problem with recruitment of GPs to the Island - 1 am only going on what he tells me.
Mr Cannan: I do not wish to disclose a confidence, but perhaps the doctor I mentioned did actually ring up Ramsey doctors to find out whether there was a vacancy.
Mr Waft: Given the situation with regard to Manndoc- it is now MEDS - have you any problems with that when it is working? Have you had anybody who has had experience of having to travel in the night to get -
Mr Cannan: Oh, certainly, they have. They have been up. They have been treated at Noble’s and told to go home at four o’clock in the morning. Could not get a taxi to get back to Kirk Michael. Told to go home at 4 o’clock in the morning after the necessary treatment, and they had to ring up a family member from somewhere, because the wife was not able to drive, or the husband had been up for an aneurysm. I can recite these cases that are brought to my attention.
The Chairman: Could I just ask, then, Mr Cannan, on that: are you saying that that did not happen when the Ramsey Cottage Hospital was available? In other words, they would not have sent them home at four in the morning?
Tynwald Select Committee on GP Out of Hours Services - Evidence of M r J D Q Cannan MHK
Oral Evidence SELECT COMMITTEE, WEDNESDAY 28th JANUARY 2004 55 TGPS
Mr Cannan: No, they left them in a bed. They made a bed available. There was a certain ‘care’, you know.
The Chairman: The important issue: that did not happen before?
Mr Cannan: I cannot say it did not happen before, (The Chairman: Right.) but it was never drawn to my attention before, because if you went where there was a culture of care in Ramsey Cottage Hospital, there always has been a culture of care, and if you were there at 4 o’clock in the morning and if there was no real facility, they just said, ‘Well, you rest in bed. ’
The Chairman: That is fine, Mr Singer.
Mr Singer: Mr Cannan, you were present, obviously, as I was, at that meeting in Ramsey when the Minister of Health addressed the meeting. One of the things she said, and which I believe she repeated in Tynwald, was that finance was not a problem; it was recruiting doctors. But on the finance position, if finance is not important, would you, therefore, be happy if the Department of Health and Social Security actually employed MEDS doctors to be placed in Ramsey Cottage Hospital and possibly in Port Erin?
One of the things that you have said - and I have heard the same - is that if the doctors at Ramsey no longer had anything to do with the hospital, as, for example, the doctors in Douglas, there would be a saving of between £160,000 and £180,000, which would finance doctors through the Health Service. But if the Minister did not want to do that, would you be equally happy for the Minister to say, ‘Well, I will place MEDS doctors in adequate numbers at the hospital’ and what is now the ‘out-of-hours’ would still be covered?
Mr Cannan: Absolutely, and for the south, too. I am concerned for the north, but, as I have already said, I voted for the cottage hospital for the south.
The Chairman: Okay, thank you. (Interjection) That is fine.
Thank you, Mr Cannan. Is there anything you wish to say to wind up your evidence?
Mr Cannan: Just to say - quoting Mr Singer now- that Mrs Christian said at the meeting at Ramsey, which culminated at the end of the big march, that finance was no problem and doctors were a problem. Well, we have two doctors for the surgery for the north-west of the Island; the only problem is that the Minister is unwilling to finance it We are not asking for capital expenditure; we are just asking them to pay the rent, just as they are paying the rent for somebody else’s capital expenditure in Ballasalla.
The Chairman: Okay. Thank you, Mr Cannan, for coming along to give evidence.
Mr Cannan: Thank you.
Mr Quine was called at 10.16 a.m.
Procedural
The Chairman: Thank you, Mr Quine. Thank you for
coming along.
Mr Quine: Thank you, Mr Speaker.
The Chairman: As you know, the Select Committee was set up by Tynwald to investigate the matter of the general practitioners’ out-of-hours services being provided throughout the Island, with power to take written and oral evidence pursuant to sections 3 and 4 of the Tynwald Proceedings Act of 1876, and to report.
You have made representation to the Committee, and we are pleased to invite you to give evidence. I think the best way is to go over to you and ask you to present your evidence, please.
Mr Quine: Yes, thank you.
The Chairman: You know all the members of the Committee, so we do not need to introduce them,
Mr Quine: I do indeed.
The Chairman: Right, thank you.
EVIDENCE OF MR R E QUINE MHK
Mr Quine: Well, thank you. As you said, I have made a written submission to the Select Committee, but I am grateful, of course, for the opportunity to amplify some of the matters in that written evidence and, indeed, to add in some additional points.
I should say, at the outset, that I attached to my submission- not just attached to it, but I sent in, I think, as a second bite of the cherry - some more correspondence from my constituents, and I am sure that is before the Committee, but I think there are a number of very important points made in that correspondence. I know the Select Committee will be looking at that, but I just want to draw attention to that.
The situation, as I see it, with the Department of Health and Social Security is a difficult one, and I will say, at the outset, that I understand the position with which they are faced. But, that said, the situation is not one that has come about ovemijght; issues have been allowed to drag on for an inordinate period of time. Our reliance on the United Kingdom as a source from which to recruit doctors and the ‘benchmarking’, so to speak, in terms of standards, remuneration and conditions of service: I recognise that, too. I know where we are coming from in that respect, but that is not to say that different and more attractive arrangements, if that be needed, do not remain an option, and I would have to say that, as I see it, part of the problem is an element of inept management by the DHSS.
I will just give one small example here, but I can give you others if you so wish. The example I will give you is that the DHSS should be party to a contract with the Ramsey Group Practice for out-of-hours cover which had a provision in it for one month’s notice for the contract to be cancelled. 1 think that illustrates the point: for such a vital service to be subject to cancellation at one month’s notice, I think, is a ludicrous situation for the DHSS to place themselves in. That is a specific point. It was a poirit which was made by the Minister at the public meeting in Ramsey, and I sincerely
Tynwald Select Committee on GP Out of Hours Services - Evidence of M r J D Q Cannan MHKProcedural
Tynwald Select Committee on GP Out of Hours Services - Evidence of M r R E Quine MHK
56 TGPS SELECT COMMITTEE, WEDNESDAY 28th JANUARY 2004 Oral Evidence
trust that it is not common to other contracts in respect of the delivery of vital health services.
Assuredly, Mr Speaker, we do not want overworked GPs. That would not be in their interests. It would not be in the community’s interest. At the same time, there are unsocial aspects attached to various professions, and many of us have served in those professions. If you go into that vocation, you expect the unsocial aspects that attach to those duties. Call it a job, call it a vocation, but it is not unexpected; it is attached to the job. Inevitably, there is an element of compensation built into remuneration and conditions which compensates for that to a very large extent.
Another element of the GPs’ complaint, as I understand it - and I have certainly read it in some of the documentation- is that additional work is being placed on the shoulders of the GPs. It is not just the question of the extended hours that they have to work, but the work in totality that is being placed upon them. Having read some other literature here from the Republic of Ireland, I notice that there is a different split between the discharge of medical functions as between those two jurisdictions, certainly, and it seems to me that there is an issue to be considered as to whether or not certain primary care services could be undertaken in community hospitals and removed from the GPs, in order to ease that burden. It is a matter which, clearly, calls for study, and it is not a study that I have undertaken. I am just saying that that would appear to be something that needs to be examined, and I am just dealing with the generalities of the medical service here before I go on to the situation in the north.
While dealing with the general situation, I would say that we should be seeking a balance and seeking to bring about a restructuring of arrangements, but the bottom line must surely be that the service the public receives must not become worse, nor more difficult to obtain, and it is quite clear - indeed, it is a matter of fact - that the medical services involved here are worse, certainly in the north of the Island, and they are more difficult to access. So, I think, as a Government, we have failed in that respect. There has been this slippage. As one of my constituents put it to me, how can it be otherwise when we have chemists, nurses and paramedics having to perform duties appropriate to doctors and previously done by doctors? Personally, I take no comfort at all from the DHSS information centre, which has pushed out publicity saying that all of this that we have seen taking place in recent years represents an improved service. I think that is an absolutely ludicrous statement to make. If that is not spin, what is?
In considering the situation that has developed with GPs, I think we should not overlook the position in relation to dentists. It is all part of these medical services, and I would invite Hon. Members to examine the figures produced by the DHSS in response to my written question at the October 2003 sitting of Tynwald. I have a copy here, but I am sure the Clerk will have got those figures for you anyway. I would just draw attention on my reading of certain figures in that question. In the year ending March 2001,48,467 patients were registered with NHS general dental practitioners. At March 2002 and March 2003, the figures had already started to slip: it was 44,861, and then, in 2003, it was 27,689. So, the registered patients were slipping - in fact, cut by half, basically. Patients registered with NHS salaried dental practitioners, which, of course, was the element that was brought in to try to compensate for this, at March 2003 was 6,868 and, at June -just a quarter later, but I am giving you both the figures - it
was 8,520, according to this answer to the written question. So, it seems to me that over the last two years some 10,000 patients have been lost or, I think, to be more precise - and what is more likely - they have been pushed into the arms of the private sector. That is not right, either.
If I move on now more specifically to the north of the Island, there has been a downgrading of medical and dental services, and that is clear for all to see, but this is not exclusively related to changes in the GP arrangement- in large part it is, but not exclusively. There is no longer an accident and emergency facility. It became arf urgent treatment centre and now it is a Minor Injuries Unit, so it is downgrade, downgrade. Access to this unit - call it what you will - on a seven-day-a-week, 24-hour basis, which was stated by the DHSS as recently as July 2001 as something that was going to be retained - this was another part of the blurb that came out from the information centre - has been abandoned, and that was only July 2001 when they reaffirmed that it would be kept on that basis.
The severe limitation on admission to Ramsey Cottage Hospital is a matter of very considerable importance. Indeed, it can be a matter, I would suggest, of life and death. The paramedics point out that it means that, in some instances, they are denied access, because they are denied access to the hospital, to important equipment for what they consider to be essential emergency treatments. The importance of direct access to Ramsey Cottage Hospital has been explained to me by one of the professionals, in the context of what has been referred to as a ‘chain of survival’. It has been suggested to me that there are at least four elements in this vital chain of survival in terms of emergency response: the first thing that is needed is, it has been put to me, early access to emergency services; secondly, early basic life support; thirdly, early defibrillation; and fourthly, early access to resuscitation facilities. In many instances, of course, you can add to that that there is also the matter of early pain relief prior to transportation to Douglas, which takes a considerable period of time. It can but be a matter of time before a life is needlessly lost by what amounts to bypassing Ramsey Cottage Hospital en route to Douglas.
With the limited hours of operation of the Minor Injuries Unit, the Ramsey-based ambulance, of course, is widely used as a taxi to convey persons to Douglas for relatively minor treatments, and the two that have been quoted to me by ambulance drivers here are instances of cut fingers and a stitch. The first-response unit from Ramsey is no substitution for the loss of the first-call ambulance. It does not have the same facilities. The Ramsey Group Practice, in common with many north-side people - indeed, the great majority oi north-side people - themselves advocate a 24-hour-a-day seven-day-a-week nurse-led Minor Injuries Unit as theii bottom line, and they are the people who have, in part, moved out and created this situation.
If we take these ambulance timings... And I must say I take no comfort whatsoever from the figures I have in 2 letter from the DHSS to me saying that 75 per cent of the response time is eight minutes. If you set that in the context of Bride and Andreas and the Lhen, that is fallacious, but il we take Ramsey-Bride-Ramsey as a run, from the time oi a call to getting back to Ramsey Cottage Hospital, where hitherto there was more competent and qualified treatmeni available, we are talking of a 20-minute run. If we take Douglas-Bride-Douglas as a run, then it is over an hour and that is what I mean about it being only a matter of time
Tynwald Select Committee on GP Out of Hours Services - Evidence of M r R E Quine MHK
Oral Evidence SELECT COMMITTEE, WEDNESDAY 28th JANUARY 2004 57 TGPS
before bypassing Ramsey is going to be directly attributed to a loss of life. Should the mountain road not be available, then the time is significantly greater, and this presupposes that the Douglas ambulance drivers can immediately find the address down the north, and that is proven not to be the case. In fact, that has been a cause of two complaints that I have received, where time was spent where they were trying to find an address.
Ambulance drivers are forced, unnecessarily, into some critical decisions, which I would suggest are decisions that, given the proper arrangement, they should not be called upon to make. And they are very competent people, the nurses are very competent, but recently a man in his nineties who collapsed was left sitting in an ambulance outside Ramsey Cottage Hospital, waiting for the doors to open. The crew- probably quite rightly - calculated that the run to Douglas would have taken longer than the time that would lapse before the doors opened, and so he was left sitting in an ambulance outside Ramsey Cottage Hospital, a ninety- year-old man.
And there is something illogical about the restricted access to Ramsey Group Practice doctors. People in the north of the Island can access their Ramsey Group Practice doctors - and these are figures that are in a letter which has been sent in to you - under the new arrangements for 50 hours a week. For the other remaining 118 hours, they are reliant on the MEDS doctors based in Douglas, and the irony of the situation is that, when they get to Douglas, they may be attended to in Douglas by a Ramsey doctor on MEDS rota.
I find some difficulty also in reconciling the demand by the Ramsey Group Practice doctors that their hours of work be reduced, given their retention of the contract for Ramsey Cottage Hospital out-of-hours ward coverage, and I must say it is with some disdain that I read the DHSS commentary on the MEDS system, coupled with advice to patients - and, again, I have the copies of these documents here.
Is it right that a patient in need of medical treatment should be asked to self-diagnose his complaint and for him to decide whether it is life-threatening and take a decision based on that as to what he does? I would suggest that it is not. I would suggest that, in some instances, they are not in a position to do that. Of course, he can always say, ‘Well, when in doubt, dial 999’, but if we were falling back on a system that is as hit or miss as that, then there is, quite clearly, something wrong. And then, in the same documentation, the DHSS advise that if it is his conclusion that it is not life- threatening, then he should seek to hang on until the next morning and seek an appointment with his doctor - and that, of course, is assuming that the next morning is not a weekend or a public holiday, because for three or four days he may not be able to see his own doctor.
I find it deplorable that we should adopt a system necessitating such inadequate practices. We are down to telephone advice, diagnosis over the telephone, self- diagnosis. That type of thing, given the Island’s situation, where we are really in quite a different setting... But if you look at it in the cold light of day, those sorts of practices, it smacks more of the Australian outback than it does of the Isle of Man.
The Minister has pointed out that there has been some £3 million capital investment in Ramsey Cottage Hospital. She omitted to say, of course, that most of this sum was raised by the League of Friends. However, be that as it may,
the point that I would like to make is that such expenditure makes the case for greater use of the facilities, not less. It does not make a case for running down Ramsey Cottage Hospital; it makes a case for greater utilisation of Ramsey Cottage Hospital.
I think a balance has to be struck in a restructuring of arrangements, but the bottom line has got to be that the service the public receives must be no worse and no more difficult to access than before the recent changes. As far as the people of the north of the Island are concerned, the people that I represent, the feedback I am getting, very strongly, from those people - and they speak virtually as one voice in this matter - is that their expectation, which is manifestly reasonable, is that we need to at least revert to a situation where we have a seven-day, 24-hour locally-based doctor cover and a seven-day, 24-hour admission to Ramsey Cottage Hospital and, of course, to the Minor Injuries Unit as well. These steps, which amount essentially to what was previously in place, would resolve the ambulance problem in itself, but we would be back to where we essentially started.
The Minister has said that money is not the issue. I think that is a somewhat embracing statement, but that is what she is on record as saying. I would simply state that if the two requirements that I have mentioned here are to be met, then, quite clearly, there is an additional cost. There is a new financial equation to be drawn up, and that equation should take into account the DHSS Ramsey Group Practice contract for out-of-hours ward cover. That should be reviewed as part of a new financial equation in new financial arrangements for the funding of services.
I think that is it, Mr Speaker. Thank you.
The Chairman: Thank you, Mr Quine.Mr Gelling.
Mr Gelling: Could I ask Mr Quine: in Mr Cannan’s evidence this morning, we were talking about the situation with Ramsey, very much followed by yourself in a very similar vein. I was probably quite concerned to hear evidence in Ramsey from the doctor who was representing, not just the GPs but the GPs generally of the Island, where we were trying to explore the difference between what it was and what it is now and the absence of Ramsey Cottage Hospital out of hours for emergency cases now. You have said there will be a case where a loss of life will -
Mr Quine: I am sure.
Mr Gelling: Right. We were told that, in fact, for a heart attack or chest pains, going to Ramsey Cottage Hospital to see a GP is not the answer and was never the answer, that that would be a waste of time and that it is an ambulance with a paramedic you need, because they know what they are doing. How have you found your constituents’ attitude to that? Is that a fact that your constituents feel that, or is this a doctor who is saying that, quite honestly, that is the best solution, the quickest is to get that person to Douglas with a paramedic, because they are well equipped to do that job, and Ramsey, in fact, would have been a hindrance?
Mr Quine: I suppose the short answer is that is a matter for independent medical advice, but the position that has been given to me by the ambulance drivers - the people who
Tynwald Select Committee on GP Out of Hours Services - Evidence of M r R E Quine MHK
58 TGPS SELECT COMMITTEE, WEDNESDAY 28th JANUARY 2004 Oral Evidence
obviously witness what you are referring to - is that, seeking to pass on the parcel t o . i t is important to get early treatment en route to Douglas, and that does not mean... There is a gap. This patient who has something, as I read it, of a heart attack living down in Cranstal: it is going to be an hour before he is into Douglas. There are certain treatments which he can be given in the ambulance en route by paramedics, but the paramedics argue there are other matters that can be dealt with to increase the chances of the patient surviving that attack if they had access to Ramsey Cottage Hospital, where there is equipment. You will see that there is a letter attached to the correspondence I sent in. I think it is signed by three paramedics, and they make that point quite strongly.
Mr Gelling: Right. Just one, if I might, Mr Chairman.
The Chairman: Mr Gelling.
Mr Gelling: You quoted a time of - 1 think it was - July 2001, where the Department was still saying the accident- (Mr Quine: Yes.) Right, OK. Would you have any comment on the fact that you have been in the House quite a long time and the strategy was that we would have a main hospital which was an acute hospital and we would have the Ramsey Cottage Hospital and something similar in the south? Do you believe, in fact, that we now have a situation where we have not anything in the south and that strategy might have been changed, along with the withdrawal by the GPs because of a change of attitude of the GPs? I know that, in the south, that was also, I think, one of the questions: would the GPs do the same in the south as they are doing in the north? Would you have any comment on the fact that, perhaps, the withdrawal of the Ramsey facilities is something to equalise the Island out, rather than enhance the south to meet what has been a wonderful arrangement in the north which, probably, everybody was jealous about?
Mr Quine: 1 suspect that the answer... I cannot see that. There is no rationale for that sort of reasoning. 1 was in the Health Department going back ~ I do not know, too many years now -12 years or more than that, going back 15 years, I suppose, and, indeed, in the very early health strategy that was put together, the object of the exercise was to move the facilities up and provide the south with a community hospital and provide Douglas with a community hospital.
The idea was we would have Ramsey, we would have a community hospital down south and we would have a community hospital in Douglas, which was going to be, at that time, Ballamona, if I remember rightly: three community hospitals. The idea was not to run it down. This is something that has crept in. If that is the current thinking, then it represents a substantial change in the line of thought over what was there in the late 1980s.
Mr Gelling: Thank you.
The Chairman: Mr Waft.
Mr Waft: Yes, thank you, Mr Chairman.Thank you, Mr Quine. You have mentioned that unsocial
aspects are often attached to any job. I know, being in the nursing profession in the past, that you did not say, ‘Well, you come to start work and you can knock off at five o’clock.1 That was never envisaged. However, given supply and
demand these days, and the recruitment problems within the DHSS and, indeed, practices to obtain more general practitioners and the recognition in the United Kingdom that, perhaps, this way of either Manndoc or MEDS, whatever they call it, has taken a hold, do you think that, perhaps, the Isle of Man, given its geographical position, especially with regard to the north of the Island and Ramsey Cottage Hospital, is a special case and should be treated differently by anyone else?
Mr Quine: It is certainly different. I do not think you need to be the brain of the month to realise that there is a material difference in try ing to service the north of the Island in terms of the services we are discussing and servicing those around Douglas and the central valley. That is different.
I think the differences arc certainly less discernible if you take the south as against the north, but there is still one important factor, and that is getting over that mountain. You have got to get over or around that mountain, and that is materially different.
The other difference, I think, is also that we are talking, in terms of Ramsey, of a hospital that is already in being. It has been there for years and years and years, essentially out of moneys raised in the north of the Island, initially by Mr Noble, but it has been added to in large sums through local fund-raising over the years. It is there, it is in being, the system was there, the people were relatively happy with that system, and what appears to have happened is that the Department has been led along, whatever the pressures, by the medical profession to enforce changes without any consultation, without any reference to the people of the north, changes which do represent a downgrading of these services. Clearly they represent a downgrading of the services, and to chum out the sort of material that we have in at least two ol these documents here, I think it is an insult to injury.
Mr Waft: We have heard evidence previously that we are going to lose 50 per cent of the GPs, perhaps, in the next 10 years. You did mention, with regard to the present situation with general practitioners, that you feel that different and more attractive conditions of service might encourage people to come to the Island. Would you like to elaborate on that?
Mr Quine: I said two things, basically. I said that, reading the literature, some of which is from the UK, and more recently I was looking at the position in the Republic oi Ireland, there seems to be a different split between some oi the duties that are carried out in GPs' surgeries, as opposed to what is carried out in hospital, and, perhaps, there is an area to be looked at in terms of whether all the duties that are being placed upon the GPs at this time need to be carried out through the GP practices. It might be tidy, it might fit in with Markwell House philosophy, but is it essential? Is it possible to move some of those over to the community hospital and lighten the load in that way?
And the other thought is that, certainly if you take Ramsey and what we now call the ‘Minor Injuries Unit’, if we talk about 24-hour ward coverage, it should be perfectly feasible - because we are not talking about GPs - to staff Ramsey Cottage Hospital with at least doctors to provide those services, which lightens the load again on the Ramsey Cottage Hospital, presumably eases their burden in terms of recruitment and filling posts. That is the line of thought that I was putting across there.
Tynwald Select Committee on GP Out of Hours Services - Evidence of M r R E Quine MHK
Oral Evidence SELECT COMMITTEE, WEDNESDAY 28th JANUARY 2004 59 TGPS
Mr Waft: You did not mention chemists, nurses and paramedics perhaps having to do the work of doctors.
Mr Quine: They are. If you look at the literature, there is one directive that advises the public to use them.
Mr Waft: Thank you.
The Chairman: Mr Singer.
Mr Singer: After the public meeting, there was obviously a lot of comment in the newspapers and the radio et cetera, and, over the last nine months, that has tended to die down, in that we are not seeing those letters in newspapers any more. Would you say that it was people getting tired of protesting because they say there is no action, or would you say that people are now accepting the position, saying that, overall, this new arrangement is OK, or that the problems were more perceived than actual? How would you sum it up in your particular area?
Mr Quine: It is a very live issue as far as the north of the Island is concerned, but I think this is a lull in the proceedings, so to speak.
It is a lull in the sense that they are aware that there is a Select Committee sitting, and I think there is a view that ‘they have a job to do, and wait and let us see what the Select Committee produce’. Of course, they have been told again that there is a review being carried out by the DHSS through independent consultants. I am very sceptical about that, because, if you hire your own consultant, you can produce whatever document you want, but the public understand that that is being done, so there is this feeling abroad that there is something happening to find a solution to the problem this time.
I think, as you said, that there are two or three other contributing factors as well, but I think the predominant one at the moment is that they are greatly disturbed with having to work with this system and they believe that something constructive is being done to try to find an answer to that. The majority of people say, ‘Right. Let this exercise run and see if something can be produced*, but I do not think there is any war weariness. I am quite convinced we will see a resurgence, rather than any slippage, in terms of the response of the people of the north if there is not a solution found. I have no doubt whatsoever that that will be the case.
The Chairman: OK. Mr Gill.
Mr Gill: Thank you, Mr Chairman. If I could ask the same question I have asked your political colleagues from the north, Mr Quine. You introduced your evidence with general comments about the medical services, and then you moved on to the specifics of the north. Notwithstanding what you were saying about the goalposts being moved with the southern community hospital - I think the comment was ‘Now we have nothing in the south’ - would that lead you to say that you would still be arguing for a two-tier system effectively, one for the north and one for the other regions?
Mr Quine: My views have not changed. You will probably say, perhaps, that is to be expected, as 1 was author to the earlier arrangement, but I think it is logical and sensible that that is what we should have, that there should be one for
the south, one for the north and, obviously, one for Douglas and the central area. That was all thrashed out, Tynwald approved all of that - 1 am going back now, shall we say, to the late 1980s - and I see no reason to change that. I think that if you are talking of dragging everybody into the centre for two-thirds of the time rather than working through their own GPs, that is a retrograde step. That is retrograde.
Mr Gill: Secondly, I think the figures are £160,000 to £180,000, part of which is in relation to the Ramsey Group Practice cover for the beds in the Cottage Hospital. You would support the idea that that should be renegotiated to actually provide a service and that service would be solely based at Ramsey Cottage - or would that be an all-island service?
Mr Quine: No. The DHSS would have to look at this Island-wide. I accept that. The point I was making is that if we have to come up with a restructuring of arrangements and there are additional costs attached to those, then one would expect the DHSS to look at the total financial equation. If, for example, you are going to be putting doctors into Ramsey Cottage Hospital to provide the 24-hour doctor coverage, if that is the solution that is going to come up - and that is the one that seems the most obvious one to define and to implement - then you have to look at this contract .which I understand is in being between Ramsey Group Practice and the DHSS in respect of out-of-hours ward coverage, because you cannot leave the cat there with all the cream. It has got to make sense across the board financially.
Mr Gill: Thank you, Chairman.
The Chairman: Thank you. Could I just ask, Mr Quine: could you, maybe, just cover... I think you have slightly touched on it, but it may be helpful if you could give your view, and that of your constituents, those who have spoken to you, about how they have seen the changes since the introduction of MEDS in terms of the out-of-hours service. In other words, has it been totally that people are not happy with it, or have there been some who have said they have been surprised how it has been good, or whatever it may be? Have you had feedback on that?
Mr Quine: Oh, yes, I have had feedback. I have had one family who wrote to me and said that their experience was good, and that is fair enough. In their case, it all clicked and that particular family said that it was good. That is the only instance I have got of anybody supporting the MEDS. I have had numerous complaints about it, numerous complaints..
The attitude seems to be - in the north now - that the whole approach is to filter you out from getting to the doctor, either to your own doctor or to the MEDS doctor, and if you must see a doctor, then you have to get yourself from Bride up to Douglas. And I have had this experience recently within the family. It was made quite clear that, as far as they were concerned, you get yourself up to Douglas, and, in one instance, this was not possible. There was a difference of opinion between the MEDS doctor and the family, because the lady and the family felt that she was far too ill to travel by car. There was a delay because of this difference of opinion. Eventually the family held their ground and an ambulance was sent - a delay, I would suggest, of about two and a half hours. Now that lady has unfortunately passed on, she has
Tynwald Select Committee on GP Out of Hours Services - Evidence of Mr R E Quine MHK
60 TGPS SELECT COMMITTEE, WEDNESDAY 28th JANUARY 2004 Oral Evidence
left this world, and I am not suggesting that there is any immediate or direct connection between the two things, but it has left a very sour taste in the mouths of all the members of that family.
And the other thing in this particular case was that, given a person who was considered by the family to be in too much pain and too difficult to move by car to Douglas, where did the ambulance take them? Up through Tholt-y- Will, because it was the shortest distance. They were not local ambulance people. It is impersonal. It is a ‘patch-and- make-do* arrangement.
The Chairman: Thank you, Mr Quine. Thank you very much for your evidence. Thank you.
Mr Quine: Thank you very much for your time.
Mrs Christian and Mr Killip were called at 11.00 a.m.
Procedural
The Chairman: Now then, we are slightly behind our schedule. We are at 11 o’clock. If I can invite the Minister and the Chief Executive of the DHSS to come forward, please.
Good morning, Minister, and good morning, Mr Killip. I do not think we really need to introduce ourselves, so that will save a bit of time. I am sure you all know us. Thank you for the written submissions that we have received from you, as the Department. We are pleased to give the opportunity to give evidence to the Committee orally, and I think the easiest way, Minister, would be if you would like to present, if you like, an opening statement, in the Department’s view, of the situation we have.
If I can just remind you so that everybody is clear, the Committee was set up by Tynwald, and its remit was to investigate the matter of the general practitioners’ out-of- hours services being provided throughout the Island, with power to take written and oral evidence pursuant to sections 3 and 4 of the Tynwald Proceedings Act 1876, and to report. So, we are all clear on the remit.
I think it would be helpful, maybe, as I say, Minister, if you would like to give an opening statement.
EVIDENCE OF HON. C M CHRISTIAN MLC AND MR D KILLIP
Mrs Christian: If I may, Chairman, give an opening statement, you have had our documentation on the issue, and I will simply take you back to the concerns that the Department has in the longer term of sustaining GP services in the Island. I think that is the fundamental matter which is driving the changes that we have experienced.
Members will know from what we have submitted that there has been a move in the United Kingdom to remove emergency out-of-hours services from GP cover. They have effected that in practical terms themselves by setting up co-operatives to reduce their 24-hour responsibility in the past, but the change currently being negotiated and taking place in the United Kingdom, as well as here, is to remove the contractual obligation to provide that 24-hour
responsibility.You will be aware, as has been said by people giving
previous evidence or, I think, by one of your Committee members, that, looking at the age profile of our own GPs, in the next few years a number will be retiring and, therefore, we are going to have to replace them - not only that, there are pressures from GPs to change the nature of their contract and to reduce their list sizes, which means that we would need more GPs to carry out the current workload. So, we need to have an attractive contract to bring GPs to work in the Isle of Man. There is evidence to suggest that GPs have had less response to their advertisements in recent times than used to be the case when it was riot difficult to attract people here. However, if we are not going to sustain our contract at least on a par with the United Kingdom provisions, it is going to be difficult for us to sustain GP practices in general.
With regard to the cover out of hours, I can very well understand the reaction of people who see this as a major change and regard it perceptually as a deterioration in service. Indeed, when I first was aware of it, I too was concerned about that. And there has been comment about cost. The current service has cost us more money. To double that service and have a two-centre GP provision out of hours would obviously incur further cost - not only that, it would require us to recruit more GPs, and this is more the crux of the matter, the availability of GPs to undertake those tasks.
In this first year, we have been monitoring the response to the MEDS service and the demands on the MEDS service, and I think it is important that we do, after a period of time, evaluate the numbers of calls, the demands on the service and the way in which they have responded to the public, and consider and review whether or not that service is proving to be satisfactory from a medical point of view. If one had infinite resources, one could place services north, south, in the middle and in the west, but we do not have infinite resources, and what we have to be very conscious of is making optimum use of those services which we do provide, within the budgets that we have at our disposal.
The service, as you will recall, had been operating in a MEDS-type manner for several years before the final three practices came into it last April. There was no response from the public or from Members at that time to the change. It worked very smoothly and satisfactorily. However, when we have taken it wider, there has clearly been a very strong public reaction. There is confusion in the north between the hospital service and the GP services, and I understand your remit is to look at GP out-of-hours services. Because of the way the GP practice in the north delivered its GP services, very often in the hospital, there is confusion in the minds of the people of the north as to what the GP service was and what the hospital service was, and I can understand that But, in terms of GP services, the Isle of Man is not unique in going down this road.
In terms of its geographical area, I understand the concerns that have been expressed, but we have also monitored the demands on the ambulance service during this period to make sure that they are adequately staffed for the job, and I believe that you have had statistics on the ambulance responses and so on.
What also needs to be borne in mind is that, before this change, there were protocols about where ambulances took people, whether they took them to Ramsey or to Douglas, and those protocols clearly take into account medical opinion as to what is the best thing to do in respect of the patient. There
Tynwald Select Committee on GP Out of Hours Services — Evidence of M r R E Quine MHKProcedural
Tynwald Select Committee on GP Out of Hours Services - Evidence of Hon. C M Christian M LC and Mr D Killip
Oral Evidence SELECT COMMITTEE, WEDNESDAY 28th JANUARY 2004 61 TGPS
are those who, maybe, disagree with that medical opinion, but, nevertheless, those decisions are based on medical opinion, and, indeed, we have had our services reviewed by risk managers to ensure that we are doing the appropriate thing, again, in terms of patient care and litigation.
Mr Chairman, there are many areas I could cover, but perhaps I could stop there and respond to questions. It might be the easiest way of coming to the points that you wish to extract from the Department.
The Chairman: That is fine. Thank you, Minister.Is Mr Killip willing to contribute at this stage or happy
to respond to questions?
Mr Killip: Thank you for the invitation, Chairman, but I will defer comment until questions, if that is OK.
The Chairman: Mr Gill.
Mr Gill: Mrs Christian, in the spring by-election campaign in Rushen, you will remember that Mr Gawne, who was subsequently elected, had a petition raising some concerns. Could you tell us what the subject of those concerns was in that petition?
Mrs Christian: The principal concerns were: not being able... Not to see their own doctor, the difficulty with ambulance cover and actually getting to the service in Douglas were some of the main concerns. I think, in both the petitions which the Department received, it was a perception that people would, somehow, be exposed to greater risk by being treated through the MEDS service than they were through their own GP services.
Mr Gili: So what response, given that opinion, has the Department made to the petitioners or the people organising the petition?
Mrs Christian: In terms of the southern petition, we have strengthened the ambulance service in the south and, as you are aware, we have opened the ambulance station at Southlands now. That has reflected in much better response times from the south, as will be shown in the documentation you have had from the ambulance service. They are now meeting the ORCON standards more effectively than they were before, and I think it is fair to say that, probably, it is the west of the Island now which needs attention in terms of cover by ambulance or paramedics.
Mr Gill: For the sake of consistency, Mrs Christian, could I ask you the same question I have asked others? Does your Department feel that there is any situation where you would support or administer a service that was effectively a two-tier service, so Ramsey Cottage Hospital might have one service for people that it serves and other regions in the Island would have a different service?
Mrs Christian: I think that we have got to be careful not to mix up GP services and hospital services. Ramsey Cottage Hospital is there, and we need to make best use of it in terms of today’s delivery of medical services. It depends how far you refine these issues down. I do not want to deliver different services to different parts of the Island. In terms of the GP service, it is now an all-island service. Obviously,
those a little bit north of Ramsey have further to travel than anyone else to get to Douglas, and they will argue, then, I think, that that makes a difference to their case. If you take the Isle of Man situation and transfer it to a rural area in the United Kingdom, you would find that very, very much greater areas are being served by MEDS services.
We are conscious that there are major changes going on here. There are changes going on in the way in which healthcare is delivered. Nurses are taking a much more developed role than they were in the past. Paramedics are taking on new responsibilities, and, as we review what is happening here and go forward and await with interest the results of your deliberations, as well as considering the review for Ramsey, then all of these issues will be taken into account in the way in which we develop our services into the future. I think that the only thing we can guarantee is change. There will always be change in the Health Services.
To come back to your original question, there is no justification for different levels of GP service across the Island.
Mr Gill: Thank you.
The Chairman: Mr Gelling.
Mr Gelling; Could I ask, Minister what is the DHSS’s recognised or accepted patient per doctor? What is the number that you would accept as being acceptable for a doctor per population?
Mrs Christian: We know that the average in the United Kingdom is about 1,800. We know that our own practices now are exceeding that figure on average, and, therefore, we are already underpressure in respect of GP services. Clearly, we would wish to, in our priorities somewhere, deal with the issue of numbers on lists, and that is one of the issues that are being negotiated in the GP contract, which is, as you are aware, under discussion at the present time.
Mr Gelling: The reason 1 asked the question is I was quite concerned to hear a figure expressed recently at a public opening of a medical centre - which we do appreciate in the south - that in 1997 there were 2,400 patients in a practice where you had two full-time doctors: Now there are 4,700 where you have got three doctors, but two are working part- time, because they work in the hospital at other times, and I just wondered whether that was an area in which you would intervene, as the DHSS, and say, ‘Well, I am sorry, but you are the ones responsible’, because, of course, they are. The practice brings on board more doctors. Does there not come a time when, perhaps, the DHSS would say to a practice, ‘I am sorry, but you cannot be giving the care, because your ratio has gone too far the other way’? You have said you are concerned; is it something in which you would intervene?
Mrs Christian: You are quite right, in that GPs are self-employed people. They establish their practices, and, to a degre.e they can decide when they will take on another partner. One recognises that taking on another partner means a dilution, unless they increase their numbers, of the return to the practice. So, we have to have concerns about the standards of care that are being delivered, and I think, under the new contract, those are issues which will be much better defined than they are under the present contract. Also, I think
Tynwald Select Committee on GP Out of Hours Services - Evidence of Hon. C M Christian MLC and M r D Killip
62 TGPS SELECT COMMITTEE, WEDNESDAY 28th JANUARY 2004 Oral Evidence
that, whilst we recognise there have been increases in lists, there have been changes in the way practices operate, for example by taking on practice nurses who carry out some of the tasks that, perhaps, hitherto the GPs would have done themselves. So, you have to take those sorts of changes into account as well, but I think the new contract will look at service level more closely than in the past.
The Chairman: Could I just follow through on that, if I may, Mr Gelling. So, how does the Department see the situation where, on one hand, following the situation described by Mr Gelling of the service provided at GP level, on the other hand, it is then employing the same GPs to work within its hospital, which, of course, the DHSS does control? Does it have to satisfy itself that the actual GP service is not suffering because of them working in two venues? Is that not an issue that you would take on board?
Mrs Christian: Yes, I think that has to be recognised, but I think there are fewer GPs doing hospital work now than there used to be.
The Chairman: Right, but if it is causing a problem, say, in an area - if it is - would the DHSS take a view on that?
Mrs Christian: Well, we would have to, yes. I think we would take a view in terms of the service that is being delivered by the practice. They have, perhaps, more authority to do that under the new contract.
The Chairman: And where would your priority be: the GP service or the hospital service? I think that is a fair question.
Mrs Christian: We would have to look at the service they were delivering in the hospital and find the right balance in those areas. It might be that if they are working in a hospital, they have a specialism. It might be easier to replace them with locum cover in their own practices as GPs than to replace them in the hospital.
The Chairman: But that would cost them at their own GP level, wouldn’t it? The contract -
Mrs Christian: But then they are earning more by doing the other contract in the hospital.
The Chairman: So the question is: if that happens, does the Department put pressure on the GP service, then? I suppose that is the question I am trying to get to.
Mrs Christian: If the Department became concerned, I am sure they would put pressure on the GP practice to ensure that the GP coverage was adequate.
The Chairman: Right, okay. Mr Gelling. Thank you.
Mr Gelling: Do you still have a Medical Practitioners Board within the DHSS?
Mrs Christian: There is a committee: the Medical Services Committee. I think, perhaps, that is the committee that the -
Mr Gelling: Does that then consider... If a group
practice decides to engage more doctors, do they approach that particular division or committee and have to request that and who that person might be and they are then vetted? Is that still the -
Mrs Christian: That is how it works, but that is subject to change because, as you know, we have a new NHS Act, and the way in which those matters are going to be handled in future will be changing, but we need to bring new regulations to Tynwald in order to deal with those issues.
Mr Gelling: So the Island, therefore, is divided up by the way it is in the evolution. The different group practices have different areas from which they, I suppose, bring in their patients, but patients then travel from many other different parts of the Island. If the DHSS were convinced, or persuaded, that it would be in the best interest of persons in a certain area of the Isle of Man that another practice be created- not an extension of a practice, another practice - would that be something that, in fact, you, as the DHSS, would have to appoint, and would that be within the contract of perhaps some of the adjoining practitioners’ groups? Would they be able to protest against that or would that be something that you could actually create?
Mrs Christian: We can create a new practice. In fact, we have it in our plans to do so. The situation with regard to other practices may well be that they would be reluctant, because they might be losing income under the present structures. I think under the new structures the situation may change somewhat in those terms. Apart from that, the doctors are arguing that they want to have lower numbers on their lists, so one would expect that they would not protest too much if they lost some of the patients off the lists.
Mr Gelling: Yes, so the last question in that series is: therefore, if you were persuaded that the eight-person group practice in Ramsey could not cope and cover, for argument’s sake, the Ramsey Cottage Hospital as well, it would be within your powers to actually create a new group of whatever they might have been, GPs who do out-of-hours service or under a hospital situation where there would be doctors within your control? That would be something you would have power to do?
Mrs Christian: Chairman, through you, I think the Hon. Member is coming to a situation where he is asking, ‘Could you put GPs into the hospital for 24 hours a day or maybe establish a new group practice in that area?’ We could do both. What you have to bear in mind is that even establishing a new group practice is not significantly going to affect the availability of practitioners to go on the out-of-hours rota, because the number of hours out of hours and the number of sessions out of hours require a considerable number of doctors to fulfil those out-of-hours services. So, one or two more GPs is not going to make a significant difference.
If you were to staff the hospital full-time with GPs, 24 hours, seven hours a day, you would probably find that they became deskilled. That is another element of this equation which is not in the perception of the public, but it is an important one, both in terms of risk management and professional achievement, if you like, or professional maintenance of standards. So, you have got to balance all of those things up in looking for ways forward.
Tynwald Select Committee on GP Out of Hours Services - Evidence of Hon. C M Christian M LC and M r D Killip
Oral Evidence SELECT COMMITTEE, WEDNESDAY 28th JANUARY 2004 63 TGPS
I can see that people come forward with things that they think are solutions to these problems, but you have to take into account professional bodies’ expectation for the type of work that their practitioners are going to do. Those practitioners now have to prove that they are maintaining standards and doing practice of certain kinds on a regular basis, and we have to have risk managers look through our hospitals to ensure, from an insurance perspective and a medico-legal perspective, that we have people who are skilled and that they have not become deskilled because they are not doing enough of a particular task. So, while the answer is ‘Yes’, there are some caveats that must be added to that.
Mr Gelling: Thank you, Mrs Christian.
The Chairman: Mr Waft.
Mr Waft: Thank you, Mr Chairman.Minister, you mentioned the standards of care and how
responsible the Department is to acknowledge the standards of care and perhaps keep them up to date. With regard to the changes that have taken place within Ramsey Cottage Hospital and the GP services out of hours in the north and the expressions of concern that happened at that time, was there any particular reason why that was done so suddenly, which caused quite a problem for the people in the north of the Island and concern to the people who lived in those areas?
Mrs Christian: Yes, there is.First of all, your statement indicates the general thinking
that the two are linked. They were not directly linked. The GP contract is to do with GP cover out of hours. The Ramsey Group Practice, along with all the other practices who had been outside of Manndoc, were opting, because of the change in the GP contract in the UK which was to be coming into effect in the Isle of Man, to get out of their out-of-hours responsibilities. They had a GP contract with us and wanted to be included with the rest of the Island in removing their out-of-hours responsibility from their contract. That is their GP contract.
They had a separate Hospital contract, and this is where people get confused about it. They had a separate contract with the Hospital - a number of contracts, actually - to provide care in Ramsey Cottage Hospital to in-patients. When they had decided that they wanted to opt out of their GP emergency responsibility, they, at the same time, notified the Department that they wished to opt out of one element of their Hospital contract, that is the night-time Hospital contract in the Minor Injuries Unit. We did not provoke that or indeed expect it, but they are self-employed people, and they decided that they wished to change the contract and opted out. We were then left with the task of replacing them in the hospital in the Minor Injuries Unit in some way.
The Chairman: Could I just ask, then, Minister - sorry to interrupt - what they were paid for that part of the contract to provide the out-of-hours service for the Hospital? Do you know?
Mrs Christian: The Minor Injuries... The total for Ramsey Cottage Hospital, I think, is of the order of £180,000 to £190,000, which was split into three payments. One'was for the in-patients in the Hospital. They have retained that
contract, and they are prepared to get up in the night to go to those patients, but they are no longer prepared to admit patients at night-time, and, in fact, they rarely get called out at night. As has been said before, as we go forward, all of these issues are going to need consideration by the Department.
They had a payment for the Minor Injuries Unit - I am not sure that it is sub-divided - I think of the order of £30,000 -
The Chairman: Would you be able to try to find that and come back to us? If necessary, you could write to us on that, (Mrs Christian: Indeed.) but if you could find it today it would be -
Mrs Christian: I am sure this afternoon, when you are taking evidence from Mr Newbury, he will be able to provide you with the breakdown in that contract. In fact, I probably do have it here. The doctors clearly wanted to forego the remuneration for providing that service, and one can see the thinking: ‘If I am not going to have to get up every night now, or I am not going to have to be on call as a GP, I do not want to be on call for.the Minor Injuries Unit either’. Partly that is because, in Ramsey, they had clearly confused the two roles, because, very often, they would get a call, as a GP, and they would say to their patients, ‘I will treat you if you pop into the Minor Injuries Unit. I will meet you in Ramsey Cottage Hospital’, whereas any GP anywhere else would say, ‘Come to the surgery.’ They substituted Ramsey Cottage Hospital for their surgery with their GP hats on, partly because they had this other contract for the Minor Injuries Unit, and that is where the whole thing is confused in the thinking of the population of the north, and I can understand that they have seen that as the way the service has been delivered in the past.
The Chairman: Thank you. Mr Waft.
Mr Killip: Could I just (The Chairman: Sorry.) endeavour to give an interim answer, Chairman. You asked specifically about the payments to the Ramsey Group Practice for serving the Minor Injuries Unit in the Hospital.
I would invite the Committee to seek elaboration on this this afternoon from the Primary Care director, but it seems that that is in the order of about £28,500 per annum at present. It is formed from two component parts: one is a flat-rate allowance, and the substantially greater part is what is referred to as a ‘sessional7 allowance. So, in terms of the overall payments made to the Ramsey Group Practice for their hospital work, the Minor Injuries Unit accounts for about £28,500 of a total in the order of £190,000. The larger slab, therefore the majority payment, is for providing in-patient treatment and care of people in Gardner House.
The Chairman: Right, so if I can just ask, then, in relation to them providing the MEDS system, presumably they get a payment for that from the system?
Mr Killip: Yes, MEDS is remunerated independently of the contractual payments.
The Chairman: Still by the Department?
Mr Killip: Yes.
The Chairman: Have you any idea what that value is to them?
Tynwald Select Committee on GP Out of Hours Services - Evidence of Hon. C M Christian MLC and Mr D Killip
64TGPS SELECT COMMITTEE, WEDNESDAY 28th JANUARY 2004 Oral Evidence
Mr Killip: At this moment I cannot answer that for you.I am sorry.
Mrs Christian: I can answer you that. GPs used to be paid an allowance in respect of their lists, and they were called for call-outs at night. When they gave up their 24- hour responsibility, on average they sacrificed £6,000 each. Whether or not they make that up depends on whether they now participate in the MEDS contract, which is quite separate. Some of them make it up and plus, and others perhaps do not make it up, depending on how much they want to participate in that programme.
The Department clearly drew back the money that they used to pay for the night cover, but is now spending it on the MEDS service. The distribution of that funding is not across the board; it is according to what sessions any individual doctor does on the MEDS service, and there are different rates of pay for different hours of the day and night.
The Chairman: Right. Mr Gelling.
Mr Gelling: Just following that, while we have that trend, I was not aware that there was a split, but I was quite interested in you saying that they wanted to hold on to, if you like, the clinic in the Hospital, the emergency. Is that because they have not got the facilities in their GP practice, so it would obviously be very attractive to them to keep, I suppose... When we were down there it was called ‘the dirty theatre’ - which I thought was quite alarming, that there was a ‘clean theatre’ and a ‘dirty theatre’ - and that was where... Is that because they have not the facilities, so, therefore, it is attractive for them to hang on to that particular part? In other words, it is cherry picking, perhaps?
Mrs Christian: Well, I think if one looks at other GP practices, the sort of minor surgery that they could do probably could be done somewhere in the surgery - whether they have outgrown it, I do not know - but if the hospital is next door, I suppose one would see it as logical to use the facilities which are there. So, it is not surprising, in many ways, that they do use the facilities that are there. In fact, I think other GPs are free to come and use the facilities at Ramsey for minor surgery if they wanted to. .
The Chairman: Okay. Mr Waft.
Mr Waft: Carrying on from where I left off, the Minor Injuries Unit then, for the sake of clarification - because you said there was confusion in the minds of the people in the north - and the out-of-hours services are the main withdrawals of service?
Mrs Christian: Yes.
Mr Waft: But they have kept on the out-of-hours ward coverage?
Mrs Christian: Yes.
Mr Waft: That is correct. Right. Now can I ask about transport with regard to the MEDS services? We have heard this morning that, at 4 a.m., people have been told to go home, and to get a taxi at that hour in the morning is not very easily done.
Mrs Christian: No.
Mr Waft: With regard to a hypothetical situation, where you have a family in the north at that hour of the morning and they need transport to the MEDS when they say, 'Come down and see us’, is there a finite line when you say, ‘Well, you get yourself down here’, and you have to find a neighbour or something, and if they have got children... Is there a possibility of them using the ambulance service in that situation?
Mrs Christian: The ambulance service should only be used for emergencies. When the doctor gets the call, they log the calls - and you may want to have the statistics and so on from the Department. When they get the call, the doctor makes a clinical judgement as to whether or not they should visit, whether they should ask the patient to attend, or whether they can simply resolve the matter by giving telephone advice.
They categorise each of the calls as urgent, routine, emergency, or low priority, and even if, perhaps, they have decided to make a visit, they will record at the end of the day whether it was .. It might, in fact, turn out to be a routine matter, notwithstanding the fact that they have visited.
To go back to the transport issue, the doctor should take into consideration all the circumstances in coming to the decision that they come to. I am conscious that there are some cases where people feel that the transport issues were difficult, and I think that, as we review the way this is developing, transport will be something that we will have to look at carefully in terms... or at least accessibility to somebody, whether that be a paramedic visiting or a nurse visiting. There are different models in the United Kingdom of how people handle these issues, and when the review has finished by the Select Committee and when we consider that, along with our own Ramsey Cottage Hospital review, I am sure that new models will be evolving out of this as to how to best make use of the facilities that we have in the north and, indeed, for the Island as a whole.
Mr Waft: There was a mention about the signage to actually get to the MEDS services at the hospital. Has that been a problem -
Mrs Christian: It was an issue with someone. I think that they confused... Obviously, there can be a difficulty where a doctor talks to someone who is not very well and they, perhaps, do not pick up the message quite accurately. We have had a circumstance where someone went to the main entrance instead of to the A&E We have taken steps to improve the signage, and I am not aware of any recent issues being raised with regard to signage.
Mr Waft: There are obviously legal consequences to the Department with regard to any change of service for whatever reason, and you say you have had advice with regard to the legal consequences, that you must always act within certain criteria of degree of risk management, as it were. Did you use an outside source for that?
Mrs Christian: We used the Medical Defence Union, who do risk management in these situations and advised the Department on those issues. As far as the parameters which guide the doctors in how they respond to the phone calls
Tynwald Select Committee on GP Out of Hours Services - Evidence of Hon. C M Christian MLC and M r D Killip
Oral Evidence SELECT COMMITTEE, WEDNESDAY 28th JANUARY 2004 65 TGPS
are concerned, there are protocols laid down to which they work, which are generally accepted throughout the medical profession in the NHS, and every doctor is responsible for the decision that they make. That was true before this change, and it continues to be true now, so that where people feel that the doctor made the wrong decision, he probably would have made the same decision before there was a MEDS service. The issues, I suppose, are perceptions of whether or not the distances add greater concern to people, but, in emergencies, the ambulance responds in the same way as it always did, and the same protocols applied before as do now, although protocols are changing from time to time.
Mr Waft: There was a thought, perhaps, that with regard to the recruitment problem, as has been said, 50 per cent are going to go within the next 10 years - GPs - and to try to attract people in, the change of conditions of service might be looked at, perhaps. There was a concern also that general practitioners were able to change their contract with a month’s notice. Maybe that could be looked at as well for future situations when that arises.
Mrs Christian: Can 1 comment on that, Chairman?
The Chairman: Yes.
Mrs Christian: It is true that at Ramsey Cottage Hospital the period of notice was limited, and I understand the concerns about that. With regard to the GP contract, that had been in negotiation for some time but was only finally concluded a short time before the implementation date, and I think the Department has acknowledged that it did not handle that very well from a PR perspective.
Mr Waft: Given the problem with recruitment et cetera, I think someone mentioned that, perhaps, you could recruit, particularly, purely for out-of-hours service and not be involved in the rest of it. Have you any thoughts on that?
Mrs Christian: That has happened in some places. They are not very common, doctors who simply want to do night duties, given that the demands at night are not high, and they are generally, perhaps, younger GPs who want do this for a short spell of time. The remuneration can be quite good, but it is not something that goes on for ever. We had considered that. We do not believe that we could recruit enough GPs to provide a MEDS service in its entirety without recourse to our GP body in the Island, but a slight change has occurred since last April, in that when we started off the MEDS service most of our general practitioners were involved in the rota. Since that time, we have involved qualified doctors who are not practising GPs, but who are qualified to do sessions on the MEDS service.
Mr Waft; I appreciate the situation with the extended role of the nurses, but at the same time there is a problem with recognition from the public that a doctor is necessary in certain circumstances. Have you any problems with that?
Mrs Christian: I hope we have defined what the Minor Injuries Unit can do and what nurses can do. I think that, going forward, we have clearly changed some of our legislation in recent times, which will allow nurses to take on a more active role. Clearly, there we are going to have
to do a job in informing the public about how the nurse’s role is changing.
Mr Waft: Thank you, Chairman.
The Chairman: Okay. Mr Singer.
Mr Singer: Thank you.Minister, in July 2001 the Department issued a statement,
a news release, about Ramsey Cottage Hospital, that instead of Accident and Emergency it was going to become an Urgent Treatment Centre. There was a document released which gave quite a lot of different treatments that were available, and the intention was that the aim was to provide a comprehensive service to persons with minor injuries, or sudden onset illnesses/conditions, and the interim treatment of people with more serious injuries or conditions prior to transfer elsewhere. That has now changed to be a Minor Injuries Unit, because a doctor was on call then 24 hours.
Has that change from an Urgent Treatment Centre to a Minor Injuries Unit come about because of the withdrawal of the doctors’ services out of hours at the Cottage Hospital, or was it planned to do that, anyway?
Mrs Christian: First of all, I do not think that is an issue which impinges on the GPout-of-hours; it is quite a separate issue. The withdrawal of the doctors from Ramsey is nothing to do with the GP out-of-hours service.
However, in response to your question, the Department always has to be mindful of the changing definitions that are currently clinically acceptable in terms of treatment for people. The Minor Injuries Unit is a Minor Injuries Unit even with GPs there. The GPs are there during the day; they still function in the Minor Injuries Unit. The situation at Ramsey, like in other places, is that we have to carry out risk assessments from time to time and determine, in the light of current medical knowledge, what are the best ways of delivering care in any particular situation. We have an A&E consultant, we have the Medical Defence Union giving us advice and protocols are drawn up to establish what is appropriate in a community hospital.
Ramsey Cottage Hospital is a community hospital, but, in many terms, it does more than many community hospitals do, but we still are within the parameters which were set in 1991 in terms of what it was envisaged Ramsey would ' have and do.
Mr Singer: It does say, Minister, here:
‘Objectives: to provide facilities for a 24-hour service for persons whohave suffered a minor injury or required urgent medical treatment forother reasons*.
If the GPs were still complying or still had their agreement for out-of-hours service, that would still be available, would it not? But now, in fact, it is not available because the GPs will not go there between 10 o’clock at night -
Mrs Christian: Yes, that is clear. It is not available 24 hours a day. You asked whether the change in name was because the doctors had not provided their service.
Mr Singer: But a lot of it is because the doctors are not there, otherwise some of these things would be able to be done.
Tynwald Select Committee on GP Out of Hours Services - Evidence of Hon. C M Christian MLC and M r D Kiilip
66 TGPS SELECT COMMITTEE, WEDNESDAY 28th JANUARY 2004 Oral Evidence
Mrs Christian: Yes, the doctors are not there, but the ‘Minor Injuries Unit’ definition, like any other medical practice, is changing all the time.
Mr Singer: So it has changed quite dramatically in two years. Certainly with regard to these things that were listed as being
'treatable at the Hospital, provided by nursing staff supported by generalpractitioners, all of whom have the knowledge, skills and experienceto care for people w ith ...’ ,
they have no longer got that ability to care for many of these treatments that were available to the general public in 2001.
Mrs Christian: I think it would be helpful, perhaps, if we sent some evidence in to the Committee of what changes there have been in respect of what could or could not happen in the Minor Injuries Unit, and why.
Mr Singer: And the difference between when there is a doctor there and when, there is not a doctor there.
Mrs Christian: And when there is not. Indeed.
Mr Singer: Thank you. Can I ask you: through the ability to recruit doctors - and we are told that the doctors are talking now about the unsociable aspects of the job - when doctors were with Manndoc before the MEDS, were they paid the same per session as they are now paid under MEDS?
Mrs Christian: The Manndoc service was organised by the doctors themselves; it was not funded by the Department. The Department paid, as I indicated to you before, a GP call*out fees for night visits and their capitation fees. What they did was organise themselves into a co-operative and use their own funding to pay each other. I am not party to what they paid each other for that service. As far as what we pay them now for the MED service is concerned, clearly there are parameters and scales which are established in other places and which the doctors have used to negotiate their fees here.
Mr Singer: So, is it a fact that, in some of the sessions, depending on when it is - during the day or the week or the weekend or whenever - doctors can earn between £400 and £500 for a session which is consisting of up to eight hours?
Mrs Christian: I think the maximum payment - and I would stand correction here, because I am doing this from memory - is £90 an hour
Mr Singer: And the sessions can last how long?
Mrs Christian: The session can last eight hours, yes.
Mr Singer: So that is £700 for an evening’s work.
Mrs Christian: Well, most doctors would do one session from, say, midnight until 8 o’clock. That is the most expensive session.
Mr Singer: That is £90 an hour?
Mrs Christian: I think so.
Mr Singer: I am not holding you directly to that figure. So when the doctors turn round and say, ‘We do not wish to do any unsociable hours, and we are actually giving up £6,000 a year each because we are no longer looking after people at night’, it is a fact, is it not, that the majority of doctors do take part in MEDS - 1 am saying majority - and that, maybe, some of them, within very few sessions, will soon recoup the money that they are saying they have lost, the £6,000?
Mrs Christian: Yes, that is true. What they do not have to do now is as many on-calls as they did before. We have been concerned that, maybe, a doctor would do a huge amount of sessions out of hours and that could be detrimental for their daytime delivery of care, but I think the evidence shows that there is no real abuse of the system in that way. Undoubtedly, those who are prepared to do the night-time sessions are making more money than they might have done under the old regime, but not all of them want to do that, and, clearly, that is the reason why they have got out of their overnight obligations. Indeed, the fact is that, when we started this, we had to put some pressure on to make sure that we sustained our rota, because they clearly wanted tc reduce their obligations. Now the rota, as I say, includes not only our GPs, but other practitioners who can take up sessions in the rota, which further reduces the need for the GPs to be involved in this service.
Mr Singer: But whilst most people would recognise unsociable hours as being hours, say, between 12 o’clock al night and 8 o’clock in the morning, the doctors are calling unsociable hours working Saturdays and Sundays as well. Is that not true?
Mrs Christian: In the sense that they are now part of the emergency hours, yes. But then, of course, Saturdays and daytime hours are paid at different rates.
Mr Singer: But we permitted the doctors to come to Ramsey to retain their contract, by which they attend the Hospital to see any patient or any person who wishes tc see them between 8 o’clock in the morning and 6 o’clock at night, and they will still come out at night if one of theii patients happens to be in the Hospital, to see them, which must be very occasionally, and, for that, they are remunerated at about £160,000 a year. Is that correct?
Mrs Christian: Yes, of that order.
Mr Singer: So really, my opinion — and I do not know if you would agree - is that they are - 1 think that the word that was used before was - ‘cherry-picking’, because in facl attending the Hospital is only during their normal surgery hours, so they are working a 40-hour week, plus occasionally going into the Hospital.
Mrs Christian: Yes. I think that is correct. They were cherry-picking, and as we go forward and review all of this, one would have to... Well, we have been looking at various scenarios of how we deliver care in the future, but you cannot run the Hospital with the services it is providing withoul
Tynwald Select Committee on GP Out of Hours Services - Evidence of Hon. C M Christian M LC and Mr D Killip
Oral Evidence SELECT COMMITTEE, WEDNESDAY 28th JANUARY 2004 67 TGPS
some cover, and if you withdraw that payment to them, you certainly have to find some other cover. Whether we can do it more economically can be explored, certainly.
Mr Singer: Would you answer this question, Minister? There have been various suggestions for the way it could be done. Have you looked, within the Department, at any other methods of... Because, first of all, you did say at one time that finance was not a problem, it was recruitment. Have you -
Mrs Christian: I was slightly misquoted on that. I said that finance was not the main issue, I think. It is always a problem -
Mr Singer: Right. Finance was not the main issue. You have got the possibility here of saying, for example, to the doctors at Ramsey, ‘You will undertake the same type of contract as they have, maybe, in Douglas, where they are just within their surgery and finish. They just look after their surgery, and you would have a saving there of, now, possibly, £160,000 to put into some other service. Have you looked at the possible way of providing any other service at Ramsey Cottage Hospital?
Mrs Christian: Chairman, I make the point that this Committee is about GP out-of-hours services but, in respect of Ramsey Cottage Hospital, we have, as you know, just had a review of the whole of the structures of Ramsey and its potential for the future, and those issues are considered in that review.
Mr Singer: Could I ask more specifically: are you looking within that other suggestion that there be cover going back to Isle of Man Hospitals, rather than under Primary Care?
Mrs Christian: The remit of the independent consultants was to look at all of those issues as to whether or not Primary Care or the Hospital secondary care structures were the most appropriate for the future, so that is covered in this report.
Mr Singer: Thank you. Can you tell me how you recruit doctors for the Isle of Man hospitals? How do you recruit them?
Mrs Christian: We advertise in the medical journals.
Mr Singer: Do you use agencies?
Mrs Christian: We use agencies, I think, only for locums - 1 would have to stand correction on this - but I do not think that they generally use agencies for recruitment purposes.
Mr Singer: Are there any problems recruiting doctors for Isle of Man hospitals because they will not do what are called ‘unsociable hours’? Is that the next step, that doctors in hospitals turn round and say, ‘We will not do unsociable hours’?
Mrs Christian: Indeed it may very well be.
Mr Singer: But that is not the situation at the moment?
Mrs Christian: At the moment, naturally, because the Island is an island, there are pressures on consultants in terms of their out-of-hours cover. They may be one-in-two or one-in-three, which is a fairly onerous responsibility, and I dare say that consultants everywhere will be looking to redress the balance a bit.
Mr Singer: I was talking more about the doctors in Accident and Emergency, recruitment for them.
Mrs Christian: Recruitment for A&E?
Mr Singer: Yes.
Mrs Christian: I think that they would be on shifts and, therefore, would expect -
Mr Singer: Unsociable shifts.
Mrs Christian: Well, indeed.
Mr Singer: But they do not say, ‘Well, we are not going to come to the Isle of Man, because we do not want to work certain hours’?
Mrs Christian: I have not been aware of that problem at all. I think it is recognised that, on A&E, it is a 24-hour service.
Mr Singer: Therefore, if you were to recruit doctors for the emergency service through that same system, would you be more likely to recruit doctors, rather than leaving it to the GPs to recruit GPs?
Mrs Christian: I am confused about the question, Chairman. Is this to do with respect to Ramsey and the -
Mr Singer: No, generally. For the MEDS -
Mrs Christian: For the MEDS service, sorry.
Mr Singer: It depends whether we have a MEDS service or we keep the MEDS service in the south and centrally and have doctors.in Ramsey Cottage Hospital. But from what you are saying, it -
Mrs Christian: The MEDS service is a GP service; it is not an A&E service.
Mr Singer: But an alternative might be recruiting people in the same methods through the hospital services, doctors who would expect to work some out-of-hours time. We are told that GPs cannot do it.
Mr Killip: If I may, Minister, (Mrs Christian: Yes.) I think there is a distinction here between the kinds of medical services being provided. As the Minister has said, MEDS is a GP service, and you would not recruit a hospital doctor to deliver an out-of*hours GP service. I think, to a degree, there is a distinction between, as it were, the kinds of doctor that you are talking about.
And also a point the Minister made earlier: would it - I think the question was posed - be possible to recruit GPs only to work out of hours and effectively have a core of
Tynwald Select Committee on GP Out of Hours Services - Evidence of Hon. C M Christian MLC and Mr D Killip
68 TGPS SELECT COMMITTEE, WEDNESDAY 28th JANUARY 2004 Oral Evidence
GPs providing that service? It may be possible, though, of course, one would need a fairly substantial number of them to provide the requisite out-of-hours service because, as the Minister said, the core of out-of-hours GPs is drawn broadly from those that we already have.
But a further difficulty that one would encounter, and which is being found in the UK, is that merely to be an out-of-hours emergency GP, whilst in short bursts probably financially attractive, is most certainly not attractive in terms of the development of a career, because one is not seeing an adequate spread of patients with particular medical need. One is not becoming experienced at long-term delivery of treatment to particular patients; it is all the short, sharp hit of delivering somebody who is unwell at, for argument’s sake, 1 a.m. So, one has to be aware of the nature of the service that one is providing and the evolution of a medical career, or the type of doctor that one is proposing to involve in the delivery of the service.
Mr Singer: What is the difference between going down to the MEDS service and seeing your GP in the middle of the night, and going to the A&E and seeing a doctor there in the middle of the night? You have still got your GP to see the following day or whatever. What is the difference in seeing them at those particular out-of-hours unsociable times?
Mr Killip: There is no difference in terms of the exposure there of the patient. If you turn up at A&E, you will receive medical treatment according to your need, as you would if you were visited by the GP. But I think the point you were making is: can we not recruit hospital-type doctors and use them to deliver the out-of-hours service?
Hospital doctors are, of course, pursuing a career that is not general practice and are progressing through the various career structures, getting exposure to particular elements of medical care, and most probably endeavouring to develop their career in a speciality to obtain, as they would aspire to, I imagine, a consultant post, and you will not be able to achieve that if you are only dealing with emergency cases.
Mr Singer: One of the suggestions which I hope you are looking at is that, under Isle of Man Hospitals, you recruit doctors, maybe through the hospital service, put die Ramsey Cottage Hospital under the hospital service, and then you can have them - with this money you are saving, this £160,000- you have already got a pot of money there - based 24 hours, doing all the jobs within the Ramsey Cottage Hospital, even looking after the patients. And once they are within the Isle of Man Hospitals, they can then be easily rotated through Noble’s et cetera to get all the experience, and yet you have got the 24-hour cover at Ramsey Cottage Hospital. I hope this is something of a possibility -
Mr Killip: It certainly is a possibility, and the latter point you make is a very important one, that there would have to be a recognition of the need to maintain the medics’ exposure to a full cross-section of medical circumstances, which, by retaining individuals exclusively in Ramsey, they almost certainly would not get.
Mr Singer: It would be to the advantage of everybody, patients and doctors, to do it on a rotation.
The Chairman: Just before you do... 1 think it may be
of help, so hopefully we will be as clear as we can. The issue that has been put to us is that if Ramsey Cottage Hospital- and I know we are not specifically looking at that, we are looking at the out-of-hours, but it is linked, because it has provided that and there is the GP link - came under the Isle of Man Hospitals and, therefore, was open 24 hours a day, seven days a week, provided with a doctor or doctors who were there in those out-of-hours times, when MEDS were called, if there was a case where somebody required hospital treatment that could be made available at Ramsey, because it was open 24-7 with a doctor there, they may, in fact, be able to get that treatment there, whereas at the moment they have to go through to Noble’s. That was the point that was put to us.
Mrs Christian: That is a fair enough point. I think, again, I do not want to get into developing the argument or the other aspects of the case -
The Chairman: I just wanted to be clear that that was the point.
Mrs Christian: Certainly the review of Ramsey has asked them to look at the whole global thing and bring forward suggestions for the future, but you have to bear in mind the scale of Ramsey and remember that our GPs at th« moment are doing their GP job as well and that the demands in Ramsey are, of necessity, limited.
The Chairman: But it relates to this bit that Ramsey is shut at certain hours now, so everybody has to go tc Douglas, and this is a view that has been put to us: could that not happen?
Mrs Christian: Yes, but I think we need to look at the statistics to see how many people actually have to go tc Douglas, or whether most of the calls are dealt with by waj of advice. The numbers of calls are not huge through the night, and I think it would be useful for the Committee tc consider the workload.
The Chairman: Yes. I just wanted to be clear on wh> that point is really being put. Mr Singer.
M r Singer: Just a couple more questions, Mi Chairman.
Can I talk to the Minister about the problem that people feel that there is in ringing up a doctor and a strange doctoi picks up the other end of the phone and makes a clinical judgement over the phone and is expecting the patient, whc may be sick, who may be old, who may have a young child, to give a self-diagnosis, before they make the decision or whether they should say to them over the phone, ‘Go anc see your doctor in the morning’, ‘Come down here1, ‘Take two aspirins’, whereas before, certainly within the Ramsej area - and I should imagine it was within the south as well- when you rang up the doctor and you said to the doctor. ‘Can you call?’, there was a tendency for the doctor tc say, ‘Yes, I will call’, because the doctor was only a few minutes away? Taking into account what I have said, and the GMC guidelines, which we have mentioned and certainl} mentioned in recent days - that they do not advise diagnosis and advice for treatment over the phone - can you put thai into your perspective?
Tynwald Select Committee on GP Out of Hours Services - Evidence of Hon. C M Christian MLC and Mr D Killip
Oral Evidence SELECT COMMITTEE, WEDNESDAY 28th JANUARY 2004 69TGPS
Mrs Christian: Yes. With regard to the first point you make about people being concerned, I think we have to recognise that, for the vast majority of the population, the Manndoc service has been doing that for years, and it is obviously clearly the same practice that happens over the whole of the United Kingdom through their night service. Indeed, before our own GPs in the north or the south came into the MEDS service, you would not be guaranteed to get to your own doctor, because they shared the night duties. You might get someone whose face you recognised, but you would not necessarily get someone who was au fait with your particular circumstances, so there is not anything new about that.
With regard to the GMC guidelines, clearly our doctors work within the GMC guidelines, and I think that comment through the media has rather cherry-picked from that document. There is nothing ‘abnormal’, shall we say, or out of line in respect of our own practitioners doing this; it is common practice within emergency cover for doctors to give advice over the phone. One can see in the United Kingdom the whole development of NHS Direct, with nursing advice and triage' being given over the phone.
So, it is not unusual, nor is it out of line, and one has to bear in mind also that the guidelines say that it also depends on resource availability. With regard to risk, the Department is very conscious of risk as to where its service is provided and the extent of that service, and so one should not assume that we are not conscious of risk and have not made an assessment of risk.
Mr Singer: But isn’t the argument here that we are not part of the United Kingdom and that, up to the change in these arrangements, the local doctor in Ramsey, or in Port Erin, or wherever, was within ten minutes of where the person lived, which is not the case in the United Kingdom? When it was Manndoc, probably the majority of people covered by Manndoc were within 10 minutes of where the doctor was, and it was that much easier for the doctor when they said, ‘Doctor, I would like to see you.’ The doctor got in his car and went 10 minutes to that person.
Mrs Christian: Chairman, the majority of people are still within 10 minutes of MEDS, and that is a geographical fact. As far as Manndoc was concerned, it extended quite extensively across the Island. Many of the Peel Group Practice people live in Michael, and Michael has been covered by Manndoc before this service came in, and so on down through towards the south of the Island. (Interjection by Mr Singer)
Chairman, we, indeed, are not part of the United Kingdom, but we recruit primarily from the United Kingdom, and our GPs are expected to meet the requirements of the United Kingdom for their registration purposes. We cannot but at least equal the terms and conditions of the United Kingdom if we want to remain competitive. If we want to be more competitive, then we have to better those terms and conditions, but we have to weigh that up within the whole of our resource, which I can tell you, in the future, this year and going forward, is not going to be easy.
Mr Singer: You must be aware, Minister, that, with all that, there are people who have telephoned for the doctor, asked the doctor to come out, and the doctor has not come
out and has said, ‘You come in here’, and the people have not been able to come in here. I am aware of a case of a child who, the following day, saw the doctor and was immediately rushed into hospital.
Mrs Christian: Right, well ~
Mr Singer: So, you would admit, therefore, that diagnosis over the phone and the doctor’s judgement within the risk assessment may be acceptable if only a 1 per cent risk, but it still affects people?
Mrs Christian: Can I say, Chairman, that that situation has not changed because of MEDS. When you rang your doctor before, if it was your local GP, he made the same judgements as apply to MEDS.
Mr Singer has indicated that people feel that their doctors went to visit them at home more frequently when they were dealing with their own group practice. That probably stands scrutiny in terms of the statistics, but that is one of the concerns of the doctors, that they felt that they were being put under too much pressure to respond when they did not really feel that there was a need, and they feel that they can now better exercise their clinical judgement without those kinds of pressures. But it is, at the end of the day, a matter for clinical judgement, and the doctor has to stand by his decision, in any case. In some cases, one can accept that they have got it wrong - doctors are not immune to making mistakes any more than anybody else is - but they have to be responsible for their decisions.
Mr Singer: Can I now refer to the ambulance position- not the positioning of the ambulance, but the ambulance position - in that we have heard that ambulances have been denied access to Ramsey Cottage Hospital on request? In fact, I did see a fax from Ramsey Cottage Hospital, saying that on no account were the ambulances to come at any time out of the hours their hospital was open to knock on the door.
Minister, you were talking about the judgement of the ambulance drivers. Is it not true, though, that if their judgement is npw that they should be able to go into Ramsey to get to the resuscitation equipment, that is being denied them? Is anything being done about that? And are you aware of the letter that actually came from some of the northern drivers to this Committee, very worried about the situation that they were being placed in?
Mrs Christian: 1 am not aware of their letter. I am aware of their concerns. I have discussed it with some of the Ramsey ambulance drivers and, as a layperson, wondered why it could not be made possible for them to access Ramsey. I do not know the date of the fax you referred to, but I suspect it was possibly early on in the development of the new service.
Mr Singer: It was.
Mrs Christian: Since that time, there have been multi- disciplinaiy discussions and meetings between the ambulance service, the management at Ramsey, the nursing provision, the A & E consultant and staff at Noble’s to determine what the protocol should be in respect of taking patients to Noble’s, and the overall view of that multi-disciplinary group is that
Tynwald Select Committee on GP Out of Hours Services - Evidence of Hon. C M Christian MLC and Mr D Killip
70 TGPS SELECT COMMITTEE, WEDNESDAY 28th JANUARY 2004 Oral Evidence
the protocols which now apply are in the best interests of the patient, notwithstanding the fact that there may be some ambulancemen who do not agree with it.
Mr Singer: A final question, and I would like you to answer ‘Yes’ or ‘No\ but I do not think, Minister, you will probably give me a ‘Yes’ or ‘No’. Would you say to people generally throughout the Island and to the people of the north that their worries are unfounded, that they have the wrong perception that the change has put them and their family at any greater risk than they were before the changes last April?
Mrs Christian: I believe that the GPs are making the same clinical judgements that they were before. In an emergency situation, the ambulance services are as they were before and applying protocols which are in the best interests of the patient - indeed, the ambulance services in the south have been strengthened.
In respect of perception, I think there has been quite a lot of concern about the availability, or the ability, to get to the doctor in an emergency situation in the night. I think that, so far, our statistics show - and you may have had complaints, but we have monitored complaints directly to the Department, and they have been limited - that the service is working. If we had infinite resources, we could put A&E north, south, east and west, but we have not, and we have not only resource considerations to take into account but we have to have the ability to recruit the professionals in this equation as well, and it is not a simple solution that we can reach.
Mr Singer: So, it is not a ‘Yes’ and it is not a ‘No’. (Laughter)
Mrs Christian: It involves perception. I believe the service is effective.
The Chairman: In fairness, I think the Minister has answered it. When you ask a complicated question, you do not necessarily get a ‘Yes or ‘No’.
Mrs Christian: Can I say that nobody, in any circumstance, can ever rule out risk. (The Chairman: Absolutely.) Life is not without risk.
The Chairman: Okay. Thank you. Mr Gill.
Mr Gill: Thank you. Just two questions, please, Minister.
When can we hope to see the review into Ramsey Cottage Hospital?
Mrs Christian: The Department has recendy received that. It will be considered by the Health Division now, and I am hoping to table it, possibly at the February sitting of Tynwald, but we might not make that. I will need to consider it first, but we probably will try to get it to February, because we feel it is not for us necessarily to come to a conclusion on it before it has gone to Tynwald, and you may well want to look at it in terms of your own considerations. I think the Department certainly would wish to consider that report in conjunction with your own findings.
Mr Gill: And, finally, the current MEDS-GP arrangement
in existence now: is that 24-hour cover?
Mrs Christian: No. MEDS does not operate in the daytime hours, except at weekends and on bank holidays.
Mr Gill: No, between the two of them, between the GPs and the MEDS service.
Mrs Christian: Oh yes.
Mr Gill: Right. So, just to be absolutely clear, there is no break in that cover between 8 a.m. and 9 a.m.?
Mrs Christian: No.
Mr Singer: There should not be.
Mr Gill: Thank you.
The Chairman: Okay. Mr Waft.
Mr Waft: Just, broadly speaking, Minister, would you say you were following the United Kingdom with regard to MEDS and Manndoc purely because of the problems with the GPs wanting a better quality of life and having to build the medical services around that, and that is why you have reached the position you are in?
Mrs Christian: Yes, indeed, I think it is to look ahead and see what the recruitment issues are in the years ahead, to recognise that the GPs were putting us - and they were certainly putting us - under pressure to renegotiate their contracts, and the first item on the agenda for renegotiation was that out-of-hours service. If we had not had to do it, I do not suppose we would have done, we would have left things as they were before, but we are in a negotiating situation and have to have an eye to the future.
Mr Waft: Thank you.
The Chairman: Thank you, Minister. I just have a couple of questions, just really following that.
So, categorically, we can say that the whole change thal has happened has been GP led, not Department led?
Mrs Christian: The Department did not resist the renegotiation of the contract, because it recognised that il had to get involved in those negotiations -
The Chairman: But it was a GP initiative.
Mrs Christian: - but I think it started off with a GF initiative, pointing out to us that this is coming up.
The Chairman: That is fine. Could you just go back tc the issue of this problem that has been raised with us aboui the lack of availability of people interested, as in GPs, tc come to the Isle of Man? The only evidence we have got, really, is the GPs’ group saying this and you indicating thal you endorse that. In other words, you have been advised oi that and that is it.
Could I ask: have you, as a Department, tried to tesi the theory? In other words, have you placed adverts to see if there is a problem? Have you tried to identify what ii
Tynwald Select Committee on GP Out of Hours Services - Evidence of Hon. C M Christian MLC and Mr D Killip
Oral Evidence SELECT COMMITTEE, WEDNESDAY 28th JANUARY 2004 71 TGPS
the problem? Is it just a lack of numbers, or is it a lack of incentive to come here?
Mrs Christian: I think there are a number of issues. There is, we know, a shortage of GPs across the UK. There are 1,000 or 2,000 or so vacancies, maybe in one particular area, I read recently. So, across the UK there are several thousand vacancies, I suspect. You could probably get accurate figures on that from Geoff Newbury. So, first of all, there is not the pool there to recruit from.
We have not tested it, because it is the GPs themselves who have been recruiting at this point. We have not been in a position to establish a new practice ourselves. We are working towards that at the moment. So, it has not been for us to test We do not want to advertise for people we cannot employ or give a practice to. So, we have been reliant on the GPs, but we are aware of how many applicants they have had, because our Medical Services Committee has to approve any appointments or changes to practices. So, the numbers of applicants have decreased substantially.
I think the only thing I can say in respect of the Department’s experience is in relation to our wish to appoint a GP to act as a locum across the Island to assist practices when they are invited to send representatives to departmental meetings or to take up training or to have leave. We have tried to recruit a GP for that purpose. It may be that it is a particular kind of person who wants that peripatetic work, but we had to advertise three times before we were able to make an appointment.
The Chairman: And are you aware of the package that the individual practice would put out in terms of trying to attract a GP to the Isle of Man? One could say that if they just put a general advert in the general practitioners’ magazine saying, ‘Come to the Isle of Man and be a GP’ and, on the face of it, it just sounds the same as if they were in the UK, that would not necessarily attract someone to say, ‘Oh, yes, I will move to the Isle of Man.’
Mrs Christian: I have to say I do not think we have been involved in the methods of their advertising.
The Chairman: So, could I say that, in the evidence we were given on behalf of the GPs, this was seen to be quite a critical issue, in terms of them saying this is going to be a big problem. If that is the case, then there is a clear responsibility on them, and presumably with you, to try and see how we are going to combat this, as an Island, in the future. At the moment, it seems very much that they are left on their own to try and deal with it, and I was really just trying to find out how serious a problem it is. The Isle of Man is an attractive place to come to. I am sure the pressures will be slightly different than in some parts of the United Kingdom. I suppose we find it difficult to accept that there is very little interest in coming to the Isle of Man, and the basis of that may well be how the jobs are promoted.
Mrs Christian: The basis of that, in the recent past, has been the out-of-hours service, because in most areas of the United Kingdom they have out-of-hours services. Notwithstanding the fact that their contract had not changed, most areas had moved to separate out-of-hours services over the last decade. So, there were not many areas of the UK which did not have a specific out-of-houre service, and so
inviting them to come here and to continue with 24-hour cover was not attractive.
The Chairman: So that may have -
Mrs Christian: That is certainly the case that has been put to us, that that is not attractive when you are trying to recruit new partners.
The Chairman: You mentioned the GP practices and the numbers exceeding 1,800 patients. Do you have figures on how many practices exceed that figure?
Mrs Christian: Yes. I do not know whether I have the averages here. Have you got your averages, David?
Mr Killip: No, I have not got the averages. I can fairly readily get the average per practice to you.
The Chairman: I think the Committee would be interested to know how many GP practices throughout the Island are employing below that standard In other words, if it is 1,800 that is seen as the standard number of patients per GP, how many are actually exceeding that? So, if you could provide that it would be helpful.
Mrs Christian: Yes. We can certainly get that information for you. I have the figures for total patient numbers, and then we have got the numbers of practitioners. I can do a quick calculation, but it will probably hold you up.
The Chairman: As long as you can provide it for us, that would be helpful, and that is fine. And the other one is: how many of your GPs are actually working in the hospital service, over and above their GP?
Mrs Christian: We will get you that information.
The Chairman: If you could provide that, that would be helpful. Thank you. If you would just bear with me, I will just check my notes to make sure I have not missed anything.
Mrs Christian: We will, of course, provide any other information if you would like to contact us.
The Chairman: I appreciate that. I think that is all I have, Minister. Thank you very much for your time, and Mr Killip, and thank you for providing the evidence you have.
That concludes the public sitting for this morning - or early afternoon, as it is now. We will resume at 2.30 p.m. for the public sitting. Thank you very much.
The Committee adjourned at 12.17 p.m. and resumed its sitting at 23 0 p.m.
Procedural
The Chairman: Good afternoon, Mr Newbury and Mrs Duke. Can I introduce you to the members of the Select Committee: myself as Chairman, Speaker of the House of Keys; to my right is Mr Waft MLC; next to him is Mr Gill
Tynwald Select Committee on GP Out of Hours Services - Evidence of Hon. C M Christian MLC and Mr D KillipProcedural

72 TGPS SELECT COMMITTEE, WEDNESDAY 28th JANUARY 2004 Oral Evidence
MHK; and then to my left is Mr Singer MLC. We have apologies from Mr Gelling MLC, who is unfortunately tied up and cannot attend this afternoon, and then the Third Clerk to Tynwald is Mr Lo Bao, who is at the end of the table. Okay?
The Select Committee, as you may be aware, was set up by Tynwald, and there were five members appointed. Our remit is to investigate the matter of the general practitioners’ out-of-hours services being provided throughout the Island, with power to take written and oral evidence pursuant to sections 3 and 4 of the Tynwald Proceedings Act of 1876, and to report.
We have had information from you in terms of the general workings of the system and the general practitioners, and, really, it is an opportunity for us to question you, naturally, but before we do that, you are quite welcome to make any opening statement that you may wish. I do not know whether you want to work as a team or whether you wish to submit any evidence individually. That is a matter for yourselves, but, maybe, Mr Newbury, if you would like to start?
EVIDENCE OF MR G NEWBURY AND MRS S DUKE
Mr Newbury: Yes. We are planning to work as a team, and we have not prepared any particular opening statement. We are quite happy to use the full time available to answer any questions you have.
The Chairman: Right, so you have no opening remarks that you wish to make. Okay. That is fine.
Generally, what we are endeavouring to do, as I am sure you are aware, is to try and find out about the out-ofhours services in relation to the Island - GP services, that is- where we have had concerns expressed to us, try to collate information and really develop a picture of what is actually happening and where there may or may not be problems.
Mr Singer: Could I possibly ask Mrs Duke to explain what her position is within the Health Services as Family Practitioner Services Manager? Could you tell us what your duties are within the -
Mrs Duke: In relation to MEDS, we run the service from day to day, ensuring the rota is filled, and maintaining the service, watching the staff.
Mr Singer: Do you work within the Family Practitioner Section of the Government?
Mrs Duke: That is right, yes, and Mr Newbury is my line manager.
The Chairman: I think that would be helpful for the record and, again, at least we know the basis of what your role is, so that is fine.
I think the main point is trying to ascertain as best we can, really, what is happening to the service, where there are problems - if there are any - how the new system has bedded in as far as you are concerned, in relation to any link you have with it, and if there are concerns, what they may or may not be in terms of the service generally for the public.
Maybe, to just help the ball roll, I suppose: we have had some views expressed to us - and part of this is linked to the Ramsey Cottage Hospital in terms of its out-of-hours service, which was GPorientated and which has ceased now, after hours, in that there is GP cover but not the hospital availability - and one of the issues that was put to us was the possibility of having the Hospital transferred to the hospital service so that it could then provide medical cover 24 hours a day, seven days a week, for emergency cover in terms of out of hours, where the GPs then could refer people to if there was a problem in the north of the Island and it may be beneficial to take somebody directly there.
I do not know whether you have any comments on that, but, for example, we have had it said to us that, on one occasion, an ambulance had picked up a patient and they actually waited outside the Ramsey Cottage Hospital until it opened, because that was actually beneficial to the patient and, in fact, I think, quicker than driving through to Douglas because of the time span.
I just wondered if you had any comment on that, because we understand that, in that circumstance, they cannot actually get into the Hospital with the patient. They have to wait until the Hospital opens. I just wondered if, maybe, to start the ball rolling, you had any comment on that, if that is a point you would like to cover.
Mr Newbury: Yes, I am happy to talk about Ramsey, because it does form part of my management area at the moment, although what we are then talking about, I have to make clear, are hospital services and not GP services.
The Chairman: Can I just make it clear that we are relating to what was the GP out-of-hours service that was accommodated at the Hospital.
Mr Newbury: Yes, I -
The Chairman: It is a very fine line, but it is quite different, and we are trying to keep that difference if we can, but, naturally, it does overlap a bit.
Mr Newbury: Right, I accept that. I think the issues that we have to take on board in regard to Ramsey and out of hours are the fact that there are obviously still in-patients there 24 hours a day and the medical cover for those is provided by the GPs, but in a hospital doctor capacity, sc the reduction in service has been for the Minor Injuries Unit only.
If you were looking at providing a hospital-based service 24 hours a day, seven days a week, from the in-patieni viewpoint you would be replacing what is already there - ii happens to be GPs who provide that service. If the GPs did not, some other doctor would have to provide the care foi the in-patients, and the issue there for starters is: would thal be a job that would prove attractive to anybody in terms oi the very limited career development and medical experience that it would offer? Because of the nature of a cottage hospital, the range of patients who can be cared for there is limited and the range of conditions is limited. That bring! into question issues of the recognition of that post by the Royal Colleges and, from my personal view, it is unlikely that such a post would be recognised for future training, sc any doctor who had career aspirations would not be attractec to that sort of post.
ProceduralTynwald Select Committee on GP Out of Hours Services - Evidence of Mr G Newbury and Mrs S Duke
Oral Evidence SELECT COMMITTEE, WEDNESDAY 28th JANUARY 2004 73 TGPS
So, while it is, theoretically, an option, you have to look at it in practical terms as to whether it is an achievable way of providing the medical cover for the in-patients.
The Chairman: Mr Singer and then Mr Gill.
Mr Newbury: Sorry, I -
The Chairman: Mr Singer.
Mr Singer: I understand what you are saying about just recruiting a doctor, or whatever, through Primary Care and putting that doctor into the Hospital, instead of the GPs, but what if you were to - and I know it is taking it away from you - take the Hospital out of Primary Care and put it back where it was within Isle of Man Hospitals and then say to the doctors, ‘Like every other doctor in Douglas, you finish at the door of your surgery’? Then doctors are recruited through the Isle of Man Hospitals service and, as in the normal methods they do, you then put doctors into the Ramsey Cottage Hospital who could, well, because it is an Isle of Man service, rotate with Noble’s, so that they are getting the experience and providing a 24-hour service, including the patients. In doing that, you take the doctor’s responsibility for the Hospital, which they have now from eight until six, away from them - and, at night, when they are occasionally visiting - and, by that, you save up to, possibly, £160,000 or £180,000, which you then put into this service to provide the doctors through the Isle of Man Hospitals.
Mr Newbury: To revert to what I was saying, the issue there, even if you had doctors on rotation, would be whether the experience that they would be gaining by working at Ramsey and District Cottage Hospital, as opposed to in an acute setting in the Hospital, would be classed as appropriate for the recognition for that post.
Mr Singer: But they would be doing, wouldn’t they, because you would have the ability to move them around? The doctors would do some time in Ramsey and they would do some time in Douglas at Noble’s. In fact, they would get other experiences, extra experiences, by being in a cottage hospital. It would add to their experience, not detract from it, I would say.
Mr Newbury: That is arguable, and you would heed to take advice from organisations, such as the Royal College of Physicians, who actually give the approval for jobs for training purposes.
Mr Singer: So you don’t have an opinion on that?
Mr Newbury: I do have an opinion. It is an opinion based on my own experience, but I would advise you that if you are going into that area, there are other people who have a better understanding of the requirements for a modem junior doctor in their training, and you would need to seek those.
So, do not take my opinion as gospel, but I am pointing it out as, if you like, an area of risk in that proposal, because, even though the doctors are on rotation, what the Royal Colleges will look at is the totality of experience that is delivered in a job. Their standards are continually reviewed, and, for any such proposal, their advice would need to be sought to see if it was viable.
Mr Singer: Okay.
The Chairman: Mr Gill.
Mr Gill: Mr Newbury, when we were previously touching on the viability of a stand-alone system at Ramsey for the out-of-hours cover that you were describing, you were speaking about the difficulties that you have elaborated on about recruiting and the career development difficulties that might follow, but if we can just come back to that stand-alone position, it would not be one post you would be seeking to recruit, would it? How many would you envisage would be required for that?
Mr Newbury: If we are just talking about the 24-hours- a-day, seven-days-a-week in-patient care, a rule of thumb is that, to have somebody on duty 24 hours a day, seven days a week, that is actually five posts. That is not exact, but it is a rule of thumb to cover for all the hours and different shifts and holidays and sickness and such like.
The Chairman: Could I just ask you: if you split the Island into four components - north, south, east and west- in terms of primary care and the relationship with the GPs’ services, what are the problems in terms of providing cover on a 24-hour basis? Are there any?
Mr Newbury: For GP services?
The Chairman: From where you sit, in terms of ensuring that the people who you are responsible for get a good service.
Mr Newbury: From where I sit, there are no substantial problems. The only issues that we are tackling at the moment, in terms of GP availability for their normal services, is the fact that the population in Douglas and Onchan is growing faster than in the rest of the Island, and that is putting more of a pressure on the GP practices in Douglas, but that is for their day-to-day general practice work.
The Chairman: But the DHSS could develop and open up a new practice.
Mr Newbury: Which is what we are planning to do.
The Chairman: Right. And based on the numbers we were advised this morning, something like 1,800 patients per doctor is a basic rule of what is an acceptable level.
Mr Newbury: That is the average list size for the Isle of Man, which equates very closely to the average list size in England. The average list size in Scotland is lower, but then they have very much larger geographical areas to cover, so you do have some practices with very small list sizes. In terms of practice by practice and the list size per doctor, the lowest in one practice is 1,641 per doctor and the highest is 2,124 per doctor. As I say, if you put all those together, the average is 1,852..
The Chairman: Right. And is there anywhere within that average that stands out as a potential problem in terms of numbers?
Mr Newbury: As I have said, the higher list sizes, because
Tynwald Select Committee on GP Out of Hours Services - Evidence of Mr G Newbury and Mrs S Duke
74 TGPS SELECT COMMITTEE, WEDNESDAY 28th JANUARY 2004 Oral Evidence
of the growth in population, tend to be in Douglas.
Mr Singer: Can you tell us what the Ramsey levels are, please?
Mr Newbury: Ramsey is 1,682 patients per GR
Mr Singer: Right. But, on top of that - sorry, can I just clear this up? - they get paid per patient? Is that correct?
Mr Newbury: Under the present system, yes.
Mr Singer: And then they get paid, now, this £160,000 to £180,000 a year between eight and six to go to the Hospital to see patients in the Minor Injuries Unit, and if they are called out to one of their patients in the Hospital at night? And that is on top of their GP salaries.
Mr Newbury: Just hang on; I brought some figures with me. At least, I hope I brought some figures with me. Here we are.
Darting back and forward a bit, but still: the present remuneration for the Ramsey GPs. What I have brought with me is information on their hospital remuneration. I have brought no information on their GP remuneration. For their hospital remuneration, for their in-patient work, which is obviously 24 hours a day, we estimate that that costs £160,000. The reason I sayvwe ‘estimate’ is that they are paid on a points system, and each patient earns them so many points, depending on how long they are in hospital, so we cannot tell you what the actually expenditure will be until the end of the year.
The Chairman: In the region.
Mr Newbury: In the region of £160,000. For their work at present in minor injuries, they are paid a fiat rate of £2,493 and a sessional allowance that amounts to £25,805. So, those are their incomes for their work in the Hospital,
The Chairman: So that is over -
Mr Singer: £190,000.
Mr Newbury: Yes. That is their income. Don't get too technical. The cost to the Department is slightly higher, because we would add on national insurance and superannuation, but -
The Chairman: But that is the basic.
Mr Newbury: That is what they would take home.
The Chairman: Right. Could I ask: generally, then, throughout the Island, we have a number of GPs who also work in the Hospital doing special work. Do you know the numbers on those at all?
Mr Newbury: I am afraid I don’t know. 1 could get that information. So, that is people who are working in Noble’s doing sessions and -
The Chairman: Yes, as long as they are a GP and, if you have the information, whether they are full-time undertaking
their GP work, as well as working within the Hospital.
Mr Newbury: Yes. I think all of them do the majority of their work as GPs and then do one or two sessions a week in various specialities, but I can get -
The Chairman: If you could provide that to MrLoBao, that would be helpful.
Mr Newbury: - that information for you, certainly.
The Chairman: Thank you. Mr Waft.
Mr Waft: You mentioned, Mr Newbury, the lack of training facilities and the recognition of Ramsey Cottage Hospital as being a training facility for training purposes for furthering their career. Is it not a fact that geriatricians, once they have been qualified as a geriatrician, would be quite happy to work amongst geriatrics and would be expected, possibly, to do so?
Mr Newbury: Yes, but you are talking about consultants who have completed their training. I was making reference to the more junior grades who are having to complete their training.
Mr Waft: What would you say Ramsey Cottage Hospital is, then?
Mr Newbury: I would say Ramsey Cottage Hospital is a mixture of, if you like - this is not a proper classification- the lower level of acute illness and some rehabilitation.
Mr Waft: It has been given to us over and over about the number of general practitioner vacancies in the UK and the problems of getting general practitioners over to the Island and their quality of life and how they do not want to work after 5 o’clock and all weekends and all that sort of thing. Could you give us your view on the situation with regard to the Island and its ability to attract general practitioners and the situation they expect to have on the Island as in the UK? Could you explain that?
Mr Newbury: Yes. We basically recruit from the UK. There is one exception to that at the moment on the Island- there is one doctor who is Spanish by background - but, basically, we recruit from the UK. Certainly, there have been problems for some time in the UK in the filling of vacancies. When I worked in the UK, certainly the number of doctors who were applying when a practice vacancy came up was reducing significantly, and there are areas where it is almosi impassible to recruit. Some of those are to do with the socioeconomic conditions in some parts of the UK, which do noi replicate here.
In terms of the practices on the Island, there are nc vacancies at the moment, but certainly, when practices have advertised a vacancy, the numbers of applications are arounc the one/two/three level - a very small pool to choose frorr- and there have been occasions when, from those, they have not made an appointment and have had to re-advertise. So, ii is not easy for practices to select people whom they would regard as suitable to work with them in practices, so we are in the same position as the UK.
The Chairman: Could I just follow up on that, if I may
Tynwald Select Committee on GP Out of Hours Services - Evidence of Mr G Newbury and Mrs S Duke
Oral Evidence SELECT COMMITTEE, WEDNESDAY 28th JANUARY 2004 75 TGPS
George? Just to ask the question: when they advertise - it is a question I have tried to get some answers to this morning, and they said you are the best person to ask, which is a good answer, isn’t it? - do you know the basis of the advert? Is it just a general advert which would replicate what would happen in the UK or do they actually promote the Isle of Man as being a place to come and live and so on and so on? And do we know why there is a reluctance to move here? Is it a lack of GPs, or is it other factors that tend to put them off coming to the Island?
Mr Newbury: Certainly, the adverts we have seen - and we have made some financial contribution towards them— do, as far as they can, advertise the Island, and we make information that we produce for recruitment packs available for them to use when sending out, which saves the practices the job of doing it.
It is difficult to generalise, because different practices have different characteristics and a doctor who may be acceptable in one practice might not be in another. Personalities do come into it. The majority of people we recruit tend to have some connection with the Island. That is not an absolute, but some sort of connection with the Island is attributable in most cases - either they have got family connections here, or they have been here a number of times, and they know something about it There is, if you like, a distance factor that comes into play. Moving 70 miles across the Irish Sea is not the same as moving 70 miles from somewhere in England to somewhere else. There are communication issues. There are people who find that difficult and do not settle, or decide that they cannot cope with that sort of separation.
So, that is the best answer I can give from the limited number of vacancies that I have had information on.
Mr Singer: Is there less difficulty in recruiting for the hospital service?
Mr Newbury: I honestly don’t know. I am not involved in that at all.
The Chairman: And do you keep in contact with the GPs if there seems to be a problem?
Mr Newbury: Yes.
The Chairman: So are the DHSS, through you, endeavouring to assist to try and, if you like, generate more interest?
Mr Newbury: Yes. We have also talked about other resources that we can make available, such as housing assistance when people move across, because that is an additional extra cost of moving across here, and that is now part of the new contract deal.
Mr Waft: You mentioned communication issues when you mentioned the UK, We seem to have our own communication issues here on the Island with regard to the way this situation evolved within the north, and it has been stated that there is certainly confusion about GP services and hospital services.
In hindsight, do you think that there is anything that could possibly have been done to make it clearer to the residents of the north as to exactly what was happening and why it
was happening?Mr Newbury: I think that, with hindsight, you can
always look back and look at things that you could have improved. Yes, I think there are very few things where you do look back and say, ‘No, that was perfect.’ Whether it would have substantially altered the perception of people in relation to the services at Ramsey, I really do not know.
Mr Waft: It seems to be far from perfect when there was a rally down there of nearly 2,000 people, I think, that presented themselves and a big public meeting taking place. Perhaps you do not think there was any big problem arising down there?
Mr Newbury: I am not saying that there was not a problem; I am saying that, with hindsight, you can always look to do things better. I still repeat, though: whether it would have made any difference, I am not so sure.
When I worked in North Yorkshire, we undertook a review - not a change in service, but a review - of two community hospitals of a very similar nature to Ramsey and District Cottage Hospital, one in Whitby and one in Malton, and, in both cases, even though there was only a review taking place, there were public meetings held with similar numbers of attendants.
Mr Waft: If I could go to the MEDS now and the situation there, there seem to be some communication problems with the transport of people to and from that facility when there is a problem, perhaps, that is not serious enough for an ambulance to arrive on the doorstep, but serious enough to get them into the MEDS situation. Is there any facility for transport arrangement in those situations?
Mr Newbury: We do not provide any facility at the moment It is an issue that has been raised elsewhere, and I think it is one that we should look at in the light of our experiences.
Mr Waft: There has been concern, also, about the lack of signage in the area. I understand that is being cleared up. Is it going to be addressed?
Mrs Duke: There were some problems in patients not being given clear instruction on where MEDS was once they reached the new hospital. At the time, as well, the new Hospital was very new and people were not sure of the layout of the Hospital itself.
The receptionists now do give very clear instructions, and we have not had any recent problems at all relating to people actually getting there. I think, initially, we did have somebody who had gone to the front of the hospital, rather than the A&E entrance, but that does not seem to be happening now.
Mr Waft: We seem to have two facilities right alongside one another - am 1 wrong? - with regard to the MEDS facility and the out-patients and general hospital that is there 24 hours a day anyway. One is staffed by the GPs providing the doctors and the out-patients are staffed by other doctors. Is that not the case?
Mrs Duke: Yes. I think A&E was always going to be sited... This is before my time, but that is the siting of A&E.
Tynwald Select Committee on GPOut of Hours Services - Evidence of Mr G Newbury and Mrs S Duke
76 TGPS SELECT COMMITTEE, WEDNESDAY 28th JANUARY 2004 Oral Evidence
MEDS is almost next door by default, because it is the accommodation that was offered for MEDS availability. It was all that we could find that was suitable at that time for siting MEDS. But they are two separate services. They do different things.
Mr Waft: But you have doctors alongside one another all night?
Mrs Duke: Yes, but A&E staff and GPs are slightly different.
The Chairman: Mr Singer.
Mr Singer: When Manndoc was formed, that was formed by the doctors as a co-operative, wasn’t it, when they decided to give up attending their own patients from their own surgeries and they formed Manndoc and they financed it themselves? Do you know why, when the doctors now in Ramsey and the south of the Island did the same thing- decided to give up their responsibilities - they did not, in fact, go into the Manndoc system, self-financing rather than... Why did the Department have to bring all the doctors under the MEDS system under the Department? Why could it not have remained within the Manndoc system itself?
Mr Newbury: The first point to make about the Manndoc system is that that system did receive financial assistance from the Department. It was not totally self-funding by the doctors. We provided most of the additional costs, in terms of reception and practice management staffing, and transport in terms of the car that takes the doctors out, so there was an input from the Department.
The reasons for three practices not being in Manndoc, I think, are individual to each of those three practices, and I will now do the cop-out of ‘it happened before 1 arrived’. I think in Ramsey, certainly, there was still some concern around how they would match that with their work in the Hospital, and that was one of the reasons why they decided not to enter at that time. The reasons for the other two practices, I think, are bound up in the personalities of the doctors in those two practices. When it was agreed, as part of the implementation of the new GP contract, that doctors would be able to opt out of their out-of-hours commitment, each practice had the option, if they wished to, to continue to undertake their own out-of-hours commitment, and it was at that point that the three remaining practices, Ramsey, Laxey and Port Erin, decided that they would wish to opt out and, therefore, be covered by whatever system was put in its piace.
The Chairman: Could I just ask, then, why - (Interjection by Mr Singer) Sorry, if I could just ask this, and you can come back? Could you explain the reasoning why the Department found it necessary to provide funds, financial assistance and other things for Manndoc?
Mr Newbury: Why did we provide it for Manndoc?
The Chairman: As the responsibility was for the GPs to provide a service.
Mr Newbury: Yes, because there was provision within the then terms of service for GPs in England - as in the Isle
of Man, because we follow the same terms of service - to provide assistance where GPs come together to form a cooperative, and that was done to assist the development of the co-operative, again on the basis that we try and provide and match the sort of service development that takes place in England.
The Chairman: And what would have been the outcome, do you think, if you had not provided that assistance?
Mr Newbury: I think it may have been more difficult for a GP co-op to have developed and to have provided a service.
The Chairman: And what would have happened to the service, do you think, the general service that patients were enjoying up to that period? Manndoc was self-funding, was it not?
M r Newbury: No. Manndoc was funded partly by the Department and partly by GPs, but from payments they received from the Department.
The Chairman: Whereas MEDS is funded differently.
Mr Newbury: MEDS is funded totally by the Department, but you could argue that Manndoc was funded all by the Department, because we were making payments to the GPs and they were using that money to fund Manndoc. It is all coming from the same source.
The Chairman: Right. So, in the funding that you are now giving to MEDS, what influence do you have over the service that is provided by the GPs?
Mr Newbury: We clearly have been in discussion with them as to what service and what staffing we would have and what operational policies we would wish to see followed.
The Chairman: And if they do not meet them?
Mr Newbury: Then we will have to review how that service is provided, but it has not, as yet, happened that they have not met those service standards.
The Chairman: Okay. Mr Singer.
Mr Singer: The doctors say that they have given up £6,000 per annum by opting out of providing an out-of-hours service, so how much money, then, taking into account the £6,000 for each doctor who was in Manndoc plus what the Department put in with the extra services, the car, did Manndoc cost annually?
Mr Newbury: I would have to come back on that.
The Chairman: If you could provide that information at least -
Mr Singer: Because I want to compare that with the amount that MEDS is now costing annually.
The Chairman: Okay. Mr Waft.
Mr Waft: Who does provide the equipment at MEDS?
Tynwald Select Committee on GP Out of Hours Services - Evidence of Mr G Newbury and Mrs S Duke
Oral Evidence SELECT COMMITTEE, WEDNESDAY 28th JANUARY 2004 77 TGPS
Mr Newbury: We provide the equipment, with some exceptions. (Interjections)
Mrs Duke: In the main, things like defibrillators, nebulisers, everything that you would not expect a doctor to carry on his own, is provided by the Department. Doctors bring their own stethoscopes and ‘carryable’ things that they have in their bags. We have a small drugs supply at MEDS for use by the doctors there, although some of them do bring their own. The Department provides the car.
Mr Waft: If the - for want of another word - ‘client’ finds he has a complaint, who would he go to then, the DHSS or the GP service?
Mrs Duke: A complaint about MEDS?
Mr Waft: Yes.
Mrs Duke: We would encourage them to come back to the Department so that we could deal with that.
Mr Waft: To the Department?
Mr Newbury: Yes.
Mr Waft: I understand, from information from others, that it was designated originally as a plaster-cast room. Is that correct?
Mr Newbury: The area that the MEDS operates from is the fracture clinic, which is a series of rooms where patients who have experienced some form of fracture either come for initial treatment or review treatment. That is what it is used for during the day.
Mr Waft: Right. Is that satisfactory?
Mr Newbury: I think it is broadly satisfactory, but we are in discussion with the doctors as to what improvements we could make, or whether some alternative would be an improvement. The one issue with the facility is that it is a shared facility, and where you have different users- (Interjection by the Chairman and laughter) Sorry. Where was I? Yes, where you have some users using a facility during the day and then a completely different group of staff using it during the evening, from time to time that causes operational issues. The advantages of it are that it is located within the hospital, so there is security, and, in terms of patients who then have to be admitted — because sometimes a patient comes to MEDS with a complaint and the doctor decides that they do need to be admitted - they are already in the hospital building and the transfer is easier.
So, if we were looking at an alternative, all those pros and cons would have to be taken into consideration, but the doctors have asked us to see whether there is something that could be self-contained and their own, but we are looking at the options at the moment.
Mr Waft: So you are not moving anywhere else at the moment?
Mr Newbury: Not at the moment, no.
Mr Waft: Not at the moment, okay. Can I ask about the
information that you have when you get somebody in at 3 o’clock in the morning? What information has the GP that is doing the MEDS services that evening? Does he have access to computerised records, for instance, from the different areas of the Island or does he just go into it cold, as it were?
Mr Newbury: He has to go into it on the basis of what the patient says. He will not have access to the patient’s notes. (Interjection by Mr Waft) No.
Mr Singer: So, how does he know, when he speaks to a patient over the phone who is ill, or has a sick child, or is old, that the answers he is getting to his questions are either incorrect or have serious omissions? Is this not against the GMC guidelines not to prescribe over the phone?
Mr Newbury: You have used the word ‘prescribe’, and -
Mr Singer: Consult.
Mr Newbury: ‘Consult’ is slightly different from ‘prescribe’, because he would have difficulty prescribing over the phone to an individual at 3 o’clock in the morning, anyway.
Mr Singer: But they say, Take two paracetamols and see a doctor in the morning’? That is prescribing.
Mr Newbury: I would call that ‘advice’, but will not get into the semantics of it, because you are a pharmacist and I am not. You were referring to GMC guidance, or instruction,
. or what? Any particular guidance? Any guidance that you were referring to?
The Chairman: I think it is the one in November 1998: providing advice and medical services on line or by telephone, (Mr Newbury: Right.) if you have got that. I do not know if you have.
Mr Newbury: I have a piece of guidance that is dated November 1998. If I quote from it, because I presume this is what you have been given:
‘Consultation and prescribing by phone or e-mail may seriouslycompromise standards o f care where’
- and you have to read all these three together -
‘ the patient is not previously known to the doctor’
and
‘no examination can be provided’
and
'there is little or no provision for appropriate monitoring o f the patientor follow-up care.’
What that guidance is saying is: think carefully about telephone consultation. But the fact remains that a significant amount of consultation does take place, and has taken place for some years, by telephone, by GPs. So, I think you really need to address questions of GMC guidance to doctors.
I am again expressing my opinion, because I have not
"tynwald Select Committee on GP Out of Hours Services - Evidence of Mr G Newbury and Mrs S Duke
78 TGPS SELECT COMMITTEE, WEDNESDAY 28th JANUARY 2004 Oral Evidence
discussed these with the doctors, but even when there were the days when each practice undertook its own out-of-hours service, the initial out-of-hours contact with a doctor would be by telephone, and the initial consultation would be by telephone. The only difference is that the doctor may have had a better knowledge of that patient, but then, in a practice of seven or eight GPs and 13,000 patients, even that would not have been guaranteed, because it would have been a long, long time since you would have been speaking to the one and only doctor in the practice who would always have known you. So, telephone consultation is not a new thing. It has happened for many years, well before the development of co-ops.
Mr Waft: Are the telephone calls that the public make in the middle of the night to their GP - and they are obviously transferred to MEDS - automatically transferred, or do some of them say, ‘I am afraid you will have to ring such-and-such a number’?
Mrs Duke: In two instances, calls are automatically transferred from the doctor’s surgery. We use the doctor’s telephone number as the first point of contact, because we maintain that is the number that a patient will most likely remember in case of emergency. Two of the practices actually divert the calls directly to MEDS, but the others all have an answer machine message, advising people that if they have a life-threatening emergency, they should dial 999 straight away, or giving them the MEDS number if they cannot wait until their own GP’s surgery opens at the next available opportunity- So, they then -
The Chairman: Could you just speak up slightly, please? (Mrs Duke: Sorry.) We can hear you, but the microphone is not picking your voice up very clearly. I am sorry.
Mrs Duke: Sorry, but yes, they then are given the MEDS number to contact.
Mr Waft: It would not have been too much of a problem to ask those who have that service to have an automatic transfer to the MEDS services?
Mrs Duke: We are actually looking at a new system of diverting calls. We particularly wanted to keep die voice message, so that people were advised that if it was life- threatening, they should phone 999 - that is important - but also to advise them of what was happening. We are looking at a system now whereby, rather than them actually having to put the telephone down and redial MEDS, they could just simply press a button and be diverted automatically to MEDS, which will cut out, then, any problems that there might be in remembering the number or misdialling at getting through.
Mr Waft: Right. Thank you.
Mr Singer: Could I ask some questions on MEDS?
The Chairman: Well, can 1 -
Mr Singer: I am sorry.
The Chairman: - just go to Mr Gill, because he has
been waiting for a while, and then we will come back to it. Okay? Mr Gill.
Mr Gill: Thank you, Chairman.Mr Newbury, just to come back to the housing allowance
you touched on, would it be possible for you to send us the details of that and the criteria and the rationale behind your considerations for that?
Mr Newbury: Sorry, housing?
Mr Gill: Yes, did you mention a relocation allowance for GPs -
Mr Newbury: Oh, sorry. I was thinking of benefits. Yes, sorry. Relocation scheme.
The Chairman: It is the package, really. We are interested in the package.
Mr Newbury: Yes.
Mr Gill: If that is not the proper title -
Mr Newbury: We call it ‘relocation’.
The Chairman: Yes, that is fine.
Mr Gill: Secondly, could I ask: on the point about the GMC criteria, with the GPs’ side of the negotiations reaching the settlement that they have with you, would that be theii responsibility to bear in mind the GMC requirements and making sure that their members were acting within that?
Mr Newbury: Yes.
Mr Gill: Not yours?
Mr Newbury: No, although there are... Telephone consultations take place during normal general practice anyway, and it would clearly be their responsibility tc have that awareness, and that, if you like, carries over. There are standards of service for, at the present, GP cooperatives in England, which we are now looking at to see how far MEDS measures up to that and whether there are other improvements we should make, and I think there is something in there about the use of the telephone, but it is a standard thing for GPs, anyway.
Mr Gill: And could I turn to you, Mrs Duke, if I may, and ask just a few questions? First of all, could you explain to the Committee the administrative system used to get doctors tc fill the slots in the MEDS programme, the MEDS rota?
Mrs Duke: The rota. Basically, we produce a blank rota, and we ask the doctors to fill in which shifts they are available to do and would like to do.
Mr Gill: When you say 'the doctors’, you mean those who have indicated a willingness to be considered?
Mrs Duke: Yes. Those, yes.
Mr Gill: Okay. And second, do you have any problems
Tynwald Select Committee on GP Out of Hours Services - Evidence of Mr G Newbury and Mrs S Duke
Oral Evidence SELECT COMMITTEE, WEDNESDAY 28th JANUARY 2004 79 TGPS
finding doctors to fill all the slots on the rota?
Mrs Duke: On occasion, we have had some difficulty. August last year was a problem, because we believe the shortened school holidays meant that more of the GPs were taking holidays at one time than we had predicted, and odd shifts we do have difficulty filling. We have never not managed to fill one, and we simply contact the MEDS GPs and ask them until somebody comes forward and fills the shift.
Mr Gill: And the nearer to that shift it gets, does the cost of filling that slot go up?
Mrs Duke: No. They have a set price for each -
Mr Gill: Okay, but you have answered my other question: there has never been an occasion where there has been a failure, there has been a gap, in the MEDS system?
Mrs Duke: No.
Mr Gill: Just a couple more very specific points. On week days, we were led to understand that there might be a gap between 8 and 8.30 or 8 and 9 a.m. between the MEDS service and the GP services taking over. Can you give us any reassurance that that is not the case?
Mr Newbury: I think 1 had better deal with that one. The MEDS service runs until 8 o’clock in the morning, and it is very clear to all practices that they take responsibility for their patients from 8 a.m. in the morning until 6 p.m. in the evening. That does not necessarily mean that all practices open at 8 in the morning, but they have to have a system in place whereby, if at one minute past eight a patient has a problem and contacts the practice, they deal with it.
The Chairman: Could I just follow that up, then? If somebody rings up the surgery, there is an answerphone on which it says, ‘In an emergency, ring 999, or ring this number’, which happens to be MEDS, because nobody will have gone into the surgery, presumably, to switch that off. How do you deal with that?
Mr Newbury: The practice have to have a system in place whereby that does not happen.
The Chairman: And are you satisfied that does not happen?
Mr Newbury: Satisfied in the sense that I have not had any complaint around that area.
The Chairman: But you have not checked whether or not the transfer over between one service and the other actually is happening smoothly?
Mr Newbury: No, but then I have not had cause to check, either
Mr Singer: Would you like to check?
The Chairman: I suppose that leads me into a question, if I may, and I will go back to Mr Gill.
Mr Newbury: I do not want to lose Mr Singer’s point.
The Chairman: That leads me into questions. How does the Department monitor the effectiveness of the MEDS system for its patients? On what regular basis do you do it? Monthly reports, or what? You do not wait for complaints, surely.
Mr Newbury: No, we do not wait for complaints. We have a regular report, which I get, on the usage of the service, which is base-line statistical information, but it would indicate whether there were problems with particular shifts, or workloads, or such like, if they are particularly high or particularly low.
We have, through the receptionists, a system - although we do need to enhance this - of reporting any exceptional incidents. I am not talking about complaints now, but if there was a problem, if there was an aggressive patient, or if there was some other difficulty in providing a service, they can be picked up when they happen. And I have regular contact with a group of GPs who have, between them, agreed to be a joint working group on the MEDS service, both in terms of the facilities that we offer and also in terms of how the service itself is performing.
The Chairman: You would not pick up from that, though, whether or not the answerphone was turned off or the message altered at 8 o’clock in the moming. You would not pick that up from that.
Mr Newbury: I would not specifically pick that up, no - i f it is a problem-but I have already agreed with Mr Singer that we will do a particular survey of that issue.
The Chairman: Yes, 1 appreciate that, but it is not something... What we are trying to get at is: how is the system monitored to make sure, from your responsibilities, which are looking after primary care, that, in fact, the primary care is effective and there aren’t these gaps without, in other words, waiting for complaints? We all learn from complaints, but we do not always wait for them.
Right, Mr Gill.
Mr Newbury: That is a fair point.
The Chairman: Thank you. Mr Gill.
Mr Gill: What, would happen - and I appreciate you having to talk to this point - if you were in the unhappy situation of being unable to fill a slot? What would happen?
Mr Newbury: If that absolute crisis happened, then we would have to rely on the Accident and Emergency service for patients who could present themselves, and we would have to see what other arrangements we could make in terms of people who were unable to attend and who required a visit.
Mr Gill: Right. And then, finally, Chair, for me: from your different experiences, or your shared experience, what improvements to the MEDS system would you like to see?
Mr Newbury: There are certain areas that we can
Tynwald Select Committee on GP Out of Hours Services - Evidence of Mr G Newbury and Mrs S Duke
80 TGPS SELECT COMMITTEE, WEDNESDAY 28th JANUARY 2004 Oral Evidence
certainly examine. One is the use of nurses to provide advice initially, because, again, from experience in England, there are a range of conditions and calls where the nurse can actually take the call and provide advice, but that would be in the aim of reducing the dependence upon doctors, although it could also be seen partly as an enhancement of the service.
There are some parts of the country where they have made more use of paramedics in terms of going out to visit and providing first-line treatment in an out-of-hours service beyond the way the ambulance service operates at the moment.
So, I am not saying we would do those things, but there are certainly other extensions of the service that we would look at in our context and see whether they would be beneficial.
Mr Gill: Okay.
The Chairman: Could I just ask a couple of questions, and then I will go back to my colleagues again? Telephone access to MEDS: certainly when Manndoc set up, there were some problems with access - in other words, not enough phone lines. Are there any problems with MEDS on that, in terms of people saying that they ring up, and ring up, and ring up and are having difficulty getting an answer? And if there are, what are you doing about it with MEDS?
Mrs Duke: That has been an issue because of the heightened number of calls, and what we are doing is monitoring the numbers, because, on occasion, you might not get a call at MEDS for four hours. So, the problem with the telephone lines is not just bringing more lines in, but having more people to answer them, and what we do not want to happen is people having lots of numbers to ring but not being responded to in that way. So, we are monitoring statistics on that to see how that can be improved.
1 think that, at the moment, we are doing quite well, and if we know that there is a period where things are going to be busy... For example, at Christmas, though we did not bring more lines in, we made use of extra lines, so, -as somebody telephoned, we brought more receptionists in and calls were transferred, and that did prove quite reasonably... We were pleased with the way that that worked.
The Chairman; So, can you give an indication of how many calls a week are going to MEDS? Any idea? Or a day- or a night, I should say?
Mrs Duke: I do have some statistics. We do keep a breakdown of the statistics, so I can give you -
The Chairman: Yes, please, if you could send a copy
Mrs Duke: Yes, certainly. I think that would be the sensible thing to do.
The Chairman: Right. Have you any indication, just as an example?
Mrs Duke: Just because this is... Probably 1st April last year was not such a good time to go from. 1 will pick October, because this is what I have opened it on. On Wednesday 1st
October, there were 13 contacts, so that was... Ten of them were dealt with over the telephone - advice - and three of them were appointments, and that covered shifts from midnight to 8 of that morning.
M r Singer: Excuse me. When you say three were appointments, that was people coming down to MEDS?
Mr Newbury: Yes. MEDS.
Mrs Duke: To MEDS, yes.
Mr Singer: That night, the doctors did not go out -
Mrs Duke: No, they did not.
Mr Singer: - and they did not send any ambulances out?
Mrs Duke: No, but -
Mr Singer: Right, okay.
Mrs Duke: - they may have sent an ambulance out. That would actually be counted as a telephone advice, because the doctor did not actually attend.
Mr Singer: They did not go out.
Mrs Duke: Yes, that is right.
The Chairman: And are those calls monitored? In other words, can you say how many calls there were between 12 and 1, and 1 and 2, so you know where they are peaking? At certain times of night -
Mrs Duke: We can. As each call comes in, it is logged, (The Chairman: Right) so we know exactly when a call was received. For statistical purposes, we break them down into shifts, because that is the easiest.
The Chairman: I appreciate that, but you actually can monitor (Mr Newbury: Yes.) where there is a peak. In othei words, let us say, for example, Saturday night, 12 to 1, could be a popular time for MEDS being contacted. (Mrs Duke: Yes.) You would be able to identify that if it was a problem' (Mr Newbury and Mrs Duke: Yes.) And if it was a problem, you would then take action, presumably, to deal with that?
Mr Newbury: Yes, I mean -
The Chairman: If a pattern was to develop, presumably you are going to take action on that?
Mr Newbury: Yes. As things stand at the moment, the staffing that we are provided deals with the patterns except, as we said, at Christmas, because we knew frorr experience from Manndoc that, particularly when you have got Christmas Day, Boxing Day and then a weekend- whichever way it goes, you get four-day weekends - those will be peak periods.
The Chairman: I think what I am trying to get frorr you, really, is that if a pattern develops and it is causing i
Tynwald Select Committee on GP Out of Hours Services - Evidence of Mr G Newbury and Mrs S Duke
Oral Evidence SELECT COMMITTEE, WEDNESDAY 28th JANUARY 2004 81 TGPS
problem, then there is no reluctance by the Department to deal with it?
Mrs Duke: Oh, no.
Mr Newbury: Oh, no. We are still learning from this.
The Chairman: I appreciate that.
Mr Newbury: Come the end of March, we will have a whole 12 months’ pattern to look at.
The Chairman: Okay.
Mr Singer: Can I? Of those 10 where it was just down that it was consultation over the phone, does it indicate to you whether the doctor said to that person, ‘I think you should come into Douglas’ and the person said, ‘I cannot come into Douglas’?
Mrs Duke: No. The information I have here is simply the number of calls that were made.
Mr Singer: So, you do not really know what the conversation was about or why the end product was just a consultation?
Mrs Duke: We do have that information, because, as they speak to a patient and the information is taken from that patient, the doctors note on the contact sheet what happened. The doctors generally note if somebody has made a comment like that. If an appointment is offered and it has been declined, they will actually note that on the sheet.
Mr Singer: And if the person says, *1 think you need to come out to see me, because I cannot get in and somebody is ill\ will the doctor put that down?
Mrs Duke: They normally make a note of anything that comes up in the conversation, yes.
The Chairman: And that would come into your monitoring, then, and identify if there was a problem of a pattern of, for example, the GPs not responding in a way you would expect? Is that right? (Mr Newbury: Yes.) Right.
So, could I just say, so I do not forget: when you do the survey on the answerphones, could you let us have the results of that? As we have raised it, I think it would be handy to know what you found out. Okay, Mr Newbury?
Mr Newbury: Sorry, just to check, do you specifically want information on patients who were offered an appointment, but could not come in, or are you looking at just generally what -
The Chairman: I was just talking about when Mr Singer said to you, ‘Wouldn’t you like to do a survey?’, the point about the answerphone between 8 to 8.30, and you said you would do a survey on that. Could you let us have the results so we know what you found out?
Mr Newbury: Oh, yes, sorry. I was intending to do that, anyway.
The Chairman: That is fine. Just so that is not forgotten, okay?
There is one other area I would just like to cover, and then I will go to my colleagues, because they were getting more questions in than I am, but that does not matter, as long as we get the questions in. There is just one issue I would like to cover, and that is in relation to primary care and an issue that has been raised with us, which is about attendance of doctors at sudden deaths. There seems to be a problem there. We understand the Department of Home Affairs have raised this issue, in terms that GPs now do not go out to those. Have you any information on that or any advice you can give us as to what is happening?
Mr Newbury: There has been some discussion involving the coroner, because I think this arose from a particular incident where the Coroner made some comment in the newspaper - which, as it happens, related to Ramsey - and, subsequent to that, there has been some discussion between the Coroner and Doctor Armour, who initially took it up on behalf of the Ramsey Group Practice, but, actually, he is now taking it on on behalf of the Isle of Man Medical Society, so it is not just a Ramsey issue.
The discussion was around the circumstances under which a GP should come out and the circumstances under which it would be not appropriate for them to do. At that discussion, the initial discussion, there was nobody from the police service present. I spoke to Dr Armour about this, and there was a subsequent meeting held, but I am told by Dr Armour that the police officer who attended was not fully briefed on the subject and it was not a particularly conclusive meeting. As far as Dr Armour is concerned, he is still waiting for a further representation from the police so that the discussions can be completed.
The Chairman: Right, okay. So that is in hand. Thank you. Mr Singer.
Mr Singer: Mr Gill covered a few of these. It was really statistics I was asking for. Mr Gill covered a few before. Can you tell me the number of GPs in practice on the Island?
Mr Newbury: There are 44.75 whole-time equivalents. I think that actually equates to about 46 actuals.
Mr Singer: Okay. And can you tell me the percentage of doctors that take part in the MEDS?
Mr Newbury: I do not know if we can do that straight off or whether we would have to do a count, because it will vary from month to month, because there may be a month when -
Mr Singer: What I mean is those who have actually taken part in the MEDS over -
Mrs Duke: I think it was 40.
Mr Singer: So there are six who have not.
Mrs Duke: Yes, it was 40.
Mr Singer: Right, so 40 have taken part. So there are only six who have not. And can you tell me of the lengths of the sessions? We know there is a 12 till 8, isn’t there? What are the other sessions?
Tynwald Select Committee on GP Out of Hours Services - Evidence of Mr G Newbury and Mrs S Duke
82 TGPS SELECT COMMITTEE, WEDNESDAY 28th JANUARY 2004 Oral Evidence
Mrs Duke: The sessions that they do are midnight to 8 a.m., and 6 p.m. to midnight on weekdays... Sorry, 6 p.m. to midnight, midnight to 8 a.m., and at weekends - and there are the bank holidays - there is an 8 a.m. to 12 noon shift and a 12 noon to 6 p.m. shift.
Mr Singer: And can you tell me... We know from a Minister this morning - 1 do not know whether she took the figure off the top of her head, whether it was exactly accurate, but she said - £90 an hour was the maximum payment, and I suppose that was the worst shift.
Mr Newbury: That is correct.
Mrs Duke: Yes.
Mr Singer: What is the minimum payment?
Mr Newbury: The minimum is £42.
Mr Singer: Can you give us any examples of income that doctors have, over the nine months, received by taking part in the sessions? Some doctors take part in more than others. So, the doctors who take part in the most sessions: how much will they have earned in the year, compared to a doctor who only does one or two sessions?
Mrs Duke: I have not got any of those figures -
Mr Newbury: Again, we do collect that, so we could give you a range -
Mr Singer: Because somebody could earn up to £700 for a session. (Mr Newbury: Okay.) So, is eveiy session for 365 days a year between 12 midnight and 8 in the morning paid at £90 a session?
The Chairman: It is important to get these figures right, so if you have not got them, then we would prefer to have them provided, but if you have them, it would be helpful.
Mr Newbury: Sorry, no. I stand corrected by my staff- which happens more often than I would like, but still. The £90 an hour is for midnight on Sunday until 8 a.m. on Monday, but that is the only shift that is paid at £90 an hour.
Mr Singer: What is then the shift pay below that?
Mr Newbury: On Sundays, the other shifts are paid at f R0 an hour.
Mr Singer: And those are eight-hour shifts?
Mr Newbury: No, all the shifts on a Sunday, whichever duration, are £80 an hour.
Mr Singer: And shifts are six hours, is that correct, on a weekend?
Mr Newbury: Well, on a Sunday, the shortest shift is four hours. There are two of six hours. There is one of eight hours. But no-one, to my knowledge, has ever worked all those shifts.
The Chairman: Okay?
Mr Singer: But the doctors talk to us about having given up their cover at nights because of unsocial hours. Does it not appear, though, that the money makes the hours less unsociable? How can ‘unsociable hours’ be during the day on Saturday and Sunday? Is that unsociable?
Mrs Duke: I think the difference is that they can choose. Rather than before, where they were obliged to cover their patients out of hours, here they choose what they want to do.
Mr Singer: And 46 doctors have chosen to take part. Can you tell me what time the receptionist is on till?
Mrs Duke: They work up until midnight.
Mr Singer: So what happens for someone who wants a doctor between midnight and 8 o’clock, if the doctor is out?
Mrs Duke: The calls are transferred to a mobile phone, to the doctor. The doctor answers the phone directly.
Mr Singer: Fine. So, the doctor could be down in the south of the Island and somebody wants a doctor in the north of the Island, so what would the doctor say to them, then? He cannot say, ‘Come down to the hospital1, because he is not there.
Mrs Duke: Well, he could. The doctor would decide, obviously based on what he was doing at that time, what the best course of action was. What they very often do is, rather than say, ‘Come down straight away’, they will give somebody an appointment time. So, that doctor may say, ‘Well, I am actually in Port Erin at the moment but will be back in Douglas in an hour. I will meet you there’, and by the time the person has got themselves ready and come down from Ramsey, they would be there.
Mr Singer: But if that doctor in Port Erin has to travel to the north of the Island, is that not making an unacceptable risk to that patient?
Mrs Duke: That is a medical opinion, and it would be dependent on what the patient was presenting with.
The Chairman: So what would happen if it was serious, but not serious enough for an ambulance, but needed a doctor? Can he not contact another doctor to go?
Mrs Duke: We have a second on call. For the shifts where there is only one duty doctor working, we have a second on call, who is available to be called in if the duty doctor feels that there is a need. The duty doctor would weigh up all the circumstances around what was happening at that time and could then call in the second on call if they chose to do that.
Mr Singer: How does the Department judge risk? What is acceptable risk and what is not acceptable risk?
Mr Newbury: The Department has judged the risks
Tynwald Select Committee on GP Out of Hours Services — Evidence of Mr G Newbury and Mrs S Duke
Oral Evidence SELECT COMMITTEE, WEDNESDAY 28th JANUARY 2004 83 TGPS
attached to the out of hours by quite lengthy discussions with the doctors who have been operating oat of hours in the past and using their experience.
Mr Singer: Fine. So they will accept a risk. We have talked about risk assessment et cetera before. If there is a risk, whether it is a 1 per cent risk or 2 per cent risk, the person who is included within that 1 per cent risk is the one who may well suffer because of that 1 percent risk. So, to them it is a 100 per cent risk, but the Department is happy to accept that risk when, perhaps, it could be reduced in bringing in a different kind of system, a better system?
Mr Newbury: You can go on reducing risk to an infinitely small level by putting more and more and more resources into that service, but the Department does have to make a judgement as to the effectiveness of the use of those resources as against other uses that may be put by those resources for other problems we are facing. In the world of economics, you eventually get to diminishing marginal return, in that you could double the amount of money we were putting into MEDS, but you would not get double the service, and you would not reduce the risk necessarily by half.
Mr Singer: Would you say that there is no greater risk to a patient now living out in Bride or in Port Erin, now that there is a MEDS service, there is no greater risk to that person’s health than there was when there was a local doctor who they could ring up?
Mr Newbury: I can see no evidence that there is any greater medical risk in that situation.
The Chairman: So you monitor that risk through your consultations?
Mr Newbury: Through the continued discussions with the doctors who are undertaking the service and-looking at the conditions that they are dealing with.
The Chairman: How regularly do you meet with the GPs on this issue?
Mr Newbury: I meet with the Chairman of the GP Subcommittee on a monthly basis, dealing with other matters as well. but we have the opportunity to discuss that. I attend the GP Subcommittee when it meets - which, I have to say, is not a regular pattern - and we have had meetings, probably on a quarterly basis, of the group that is looking at MEDS.
Mr Singer: We have snow today. The mountain road is shut. It is possible, maybe later or sometime, that the coast road will be impassable, so an ambulance cannot get through. Because we are talking about the mountain here, if the doctor was Ramsey based and could go and see the patient and take them to Ramsey Cottage Hospital, there is no greater risk to the patient under the present system?
Mr Newbury: You are assuming that the patient would then be appropriately cared for and would have a condition that would be appropriately cared for in Ramsey and District Cottage Hospital under those circumstances.
Mr Singer: Is it not better to go to Ramsey Cottage
Hospital than not being able to get to them at all?
Mr Newbury: Again, I think you are straying into areas where you would need medical advice on what you are discussing.
Mr Singer: It is not medical advice you actually need -
The Chairman: Just in primary care terms, which is what we are really looking at - and I accept the medical side, but from your point of view, which is to safeguard the public interest through the Department, to ensure there are adequate services - if I put the question another way: if the weather conditions were so adverse that the mountain road and the coast road from the north - or, for that matter, from anywhere else, but in this case from the north - were blocked off, you have a Ramsey Cottage facility there, albeit a limited facility in terms of what it can provide. If a patient was serious in their terms of illness, they needed certain care, or they needed to have certain treatment, how would you deal with that in certain conditions, with the weather adverse? We are talking about adverse conditions.
Mr Newbury: I thought we would get round to weather today eventually.
The Chairman: It is a good day, with the snow -
Mr Newbury: It is a good day, yes. Obviously, in extraordinary circumstances, we would have to take extraordinary measures, and we do have a 24-hour ambulance service in Ramsey now, and it is supported by a standby paramedic, who has a four-wheel drive vehicle available. And if all roads were blocked and there was absolutely no possible passage, then we may - this is obviously looking at the extremes - have to use an ambulance in circumstances when we normally would not, and we may have to use Ramsey Hospital in circumstances when we normally would not, but those are extraordinary circumstances, and then you use what facilities you have available.
The Chairman: And may that include using an emergency helicopter facility?
Mr Newbury: We do not have an emergency helicopter facility.
The Chairman: But we have access to it? (Mr Ne wbuiy: No.) Not through the RAF or -
M r Newbury: Well, that would be through the coastguard.
The Chairman: But you would have access to it through them, presumably?
Mr Newbury: I have never had cause to, so 1 have to say I do not actually know whether we could use it for those purposes or not, but that is out of ignorance.
The Chairman: Right. You have not been here when it has snowed heavily yet, then?
Mr Newbury: Not as heavily as when I lived in West
Tynwald Select Committee on GP Out of Hours Services - Evidence of Mr G Newbury and Mrs S Duke
84 TGPS SELECT COMMITTEE, WEDNESDAY 28th JANUARY 2004 Oral Evidence
Yorkshire or on the east coast of Scotland.
The Chairman: We have had our moments like that.
Mr Newbury: So I am told.
The Chairman: Okay. Mr Waft, and then Mr Gill.
Mr Waft: I am just interested in the situation where you feel there has been no reduction in the service to the people of the north resulting from the closure of Ramsey Cottage Hospital.
Mr Newbury: Sorry? Is that... Whether -
Mr Waft: Did you say there was no reduction in the service for the people of the north of the Island because of the inability to gain access to Ramsey Cottage Hospital in the evening?
Mr Newbury:. I actually thought I was being asked a question about GP out-of-hours services and whether there had been any reduction, or whether the service was still appropriate as before, so my answer was in relation, I understood, to GP out-of-hours services.
The Chairman: But part of the normal GP out-of-hours service has been the use of Ramsey Cottage out of hours, so it is linked, and that has now ceased. That is, I think, the question that Mr Waft is -
Mr Newbury: If you are roping Ramsey Hospital back into GP out-of-hours, then I have to say that, from all the information I have received, I am satisfied with the level of service that is available out of hours,
Mr Waft: Irrespective of the fact that they have not got access to Ramsey Cottage Hospital after hours?
Mr Newbury: Yes.
Mr Singer: And where the ambulancemen have written to this Committee, expressing their concern that they do not have a choice, that there are times when they would wish to have access to the resuscitation equipment in Ramsey?
Mr Newbury: I think it would have been helpful if the ambulancemen who wrote that letter had sent a copy to me as well.
Mr Singer: They have not. They have written to us, to Members, and it will be in the information at the back of the report.
The Chairman: I think, in fairness to Mr Newbury, you are not aware of that. That is what you are saying.
Mr Newbury: I am not aware of that letter, but if it is an issue and if it comes out in the report, I would be happy to look at it.
The Chairman: Okay. Mr Singer will have a look while Mr Gill asks a question.
Mr Newbury: I am happy for it to come out in the report, and 1 -
The Chairman: Yes. Mr Gill.
Mi* Gill: Thank you, Chair. Just two things. Perhaps Mrs Duke could tell us: how often has the second doctor, the standby doctor that you described, been required to be called out?
Mrs Duke: I do not have the definitive number. I know there were two occasions over Christmas where the second on call was actively called out, and I do know of one incident before Christmas, but I can check that for you and let you know.
Mr Newbury: But it is unlikely to be more than four or five. Yes, we will give you a definitive figure, certainly.
Mr Gill: And then, finally, from me: we have heard a lot about the north and a lot less about - the remit is the all-island out-of-hours GP services - the west or the south. From your professional primary healthcare perspective- not political or wherever you happen to live, but just from your professional perspective - would you feel it would be appropriate if we had a two-tier system, where Ramsey was served by one arrangement and the south and the west had a different arrangement?
Mr Newbury: I think the best way for the Island is to have a universal service so that everybody is served in the same way. At the moment, that is by a single base in Douglas, and my opinion is that that is the most appropriate way for it to be delivered. If you start to, if you like, fragment that service, you would have to fragment it equally around the Island.
Mr Gill: Thank you.
The Chairman: Okay. Mr Waft, anything else? (Mr Waft: No.) Right. Mr Singer.
Mr Singer: I have got the letter. I realise you have not got it. Can I just tell you something of what it says? It says:
‘As members o f the emergency services, we would like to express our personal objections to the current level o f healthcare provision as a result o f the changes affecting the north o f the Island.'
This was not April; this was September, so it was not as it happened.
‘Ambulance staff have asked for a local agreement for support provided by hospital on-call GPs incases out o f hours. It was refused. Performed in a stable environment - a resuscitation room - cardio-pulmonary resuscitation is only 30 per cent effective o f normal cardiac output. Bearing in mind this statement, 30 per cent optimum effectiveness cannot be achieved in the back o f a moving ambulance. At present, running times from Ramsey to Noble’s average 25 minutes. Obviously, this time will be extended considerably during the winter months.’
They then give a chain of survival, which I am sure you are aware of, with a note saying:
‘Defibriilation: with each minute delay, the chances o f successful outcome fall dramatically by 7 to 10 per cent.’
They are saying that when they would wish to go into to Ramsey, they cannot go into Ramsey, and that is of concern to them.
Tynwald Select Committee on GP Out of Hours Services - Evidence of Mr G Newbury and Mrs S Duke
Oral Evidence SELECT COMMITTEE, WEDNESDAY 28th JANUARY 2004 85 TGPS
Can I also ask you: we had a letter from one of the local homes, again complaining because of the changes - this was from Ramsey - and no GP being available out of hours. They are complaining:
'W e endeavour to have high standards and good practice through training and expertise. However, we have no-one on site qualified as nurses, paramedics or doctors, and we do not hold specialised hospital equipment Our current status dictates our staffing levels, which fall into two duty staff and... ’‘A s this is the absolute minimum requirement for this establishment at any given time, it was never an option for one o f these three people who are on call, working at that time, to leave the building to transport a sick or injured resident anywhere, even the short distance to Ramsey Cottage Hospital prior to the introduction o f Manndoc.’
I think they mean MEDS, but never mind, because now it becomes Noble’s:
‘We have heavily relied on the assistance, advice and expertise o f both on-call local doctors and staff at Ramsey Cottage Hospital, including ambulance crew and paramedics, who had access to vital client history and condition as well as personal knowledge. Response time was so minimal it was never an issue. Good relations were held all round, and co-operation and goodwill went without saying. Everyone felt secure. Since the introduction, we now have on-call doctors ranging from those known, those helpful and those who attend, to the total opposite, where advice is difficult to obtain, or outright refusal to attend. We have even been left with instructions to wait a bit longer until normal working hours.’
This is in an old people’s home. They are obviously very unhappy at the change. Do you find that that is acceptable? They say:
'Hours have been wasted on the phone, leaving us exasperated.’
The Chairman: Okay. Mr Newbury.
Mr Newbury: Yes. Again, I have not seen that either, and you are asking me to respond in public to something I have not seen. Clearly, if there is a specific complaint or complaints that that home has and they wish to make the details available, I would be very happy to look into them.
Mr Singer: This is not specifics; this is an overall picture.
Mr Newbury: You are quoting a letter, Mr Singer.
The Chairman: Right. Okay? The letter is a specific, from an individual, and I appreciate that. 1 think the point is what it demonstrates is... Partly because we advertised for anybody with any views, we are bound to get letters that you have not had, so that is what happened. I think what we are trying to do is highlight that these are problems that have been identified, and you have said you have not had them, so we were trying to identify if you had had them and if anything was being done. Okay. That is fine.
Right. I think that is fine. Have you anything, Mr Newbury or Mrs Duke, that you wish to say to wind up your evidence?
Mr Newbury: No. Thank you for the opportunity to come and talk to you.
The Chairman: Thank you both for answering the
questions so openly, and we appreciate your time. Thank you.
Mr Newbury: And we will try and talk more loudly next time!
The Chairman: That is all right. Not all ladies have a quiet voice, do they?
Mrs Duke: I have never been accused of being quiet before.
Mr Newbury: First time ever, (Laughter)
The Chairman: Thank you very much.
Mr Radcliffe and Mr Whiteway were called at 3.48 p.m.
Procedural
The Chairman: Can I invite the representatives from Ramsey Town Commissioners to come forward, please?
Good afternoon, gentlemen. Can I ask you both to advise us of your positions? We know, I think, one. I am not sure about the other, except you are a Commissioner.
Mr Radcliffe: That is right. I am Richard Radcliffe, member of the Town Commission.
Mr Whiteway: Peter Whiteway, the Town Clerk for Ramsey Town Commissioners.
The Chairman: Thank you.Can I just remind you of the remit of the Committee?
As you know, the Committee was set up by Tynwald Court, and they appointed five members. Mr Gelling unfortunately is unable to attend this afternoon. You know the rest of the Committee, I think. If you do not know any member, please indicate and I will introduce them. Our remit, which was given to us by Tynwald, is to investigate the matter of the general practitioners’ out-of-hours services being provided throughout the Island, with power to take written and oral evidence pursuant to sections 3 and 4 of the Tynwald Proceedings Act 1876, and report. So, that is the basis of what our remit is.
Understandably, because of the unique situation of the Ramsey Cottage Hospital, in that it was part of that out-of- hours service, it has been quite obvious in the evidence we have received that there has been that link with it We have, I think, in fairness, given some flexibility to that, but, basically, we are endeavouring to deal with the out-of-hours service of that, and I would really just invite yourselves... 1 do not know, Mr Radcliffe, whether it is you or the Town Clerk who is going to start, but over to whoever wishes to.
EVIDENCE OF MR R RADCLIFFE AND MR P WHITE WAY
Mr Radcliffe: Mr Whiteway will start proceedings, and
Tynwald Select Committee on GP Out of Hours Services - Evidence of Mr G Newbury and Mrs S DukeProcedural
Tynwald Select Committee on GP Out of Hours Services - Evidence of Mr Radcliffe and Mr P Whiteway
86 TGPS SELECT COMMITTEE, WEDNESDAY 28th JANUARY 2004 Oral Evidence
we would like to thank you for the opportunity to come here and present evidence, Mr Chairman.
The Chairman: Okay. So, Mr Whiteway.
Mr Whiteway: Thank you, Mr Chairman.. I open by thanking the Select Committee for the
opportunity to come today and present evidence in addition to the written evidence the Commissioners have already submitted, more particularly because of the strong feelings that are expressed by the people of the north of the Island in relation to the changes that have occurred to doctors’ services over the past year.
Whilst we recognise the Committee’s remit relates to GP services, it is clear from what was said this morning and also to the northern residents that this has historically been linked to the Cottage Hospital. It has raised a considerable amount of comment, and although I suppose, to a degree, it could be argued that things might have gone quiet, it is something that has been in the minds of the Commissioners over the recent months and, in fact, they have been watching the progress of the Committee and did consider last week who should attend and what should be said when we got here.
As far as the service issue is concerned, the position is one which should be of concern to everybody on the Island. It is not just a north problem; it does, in our opinion, occur as an issue which has the same implications for people in the south of the Island. It is about remoteness and access. It is accepted, from what the Minister has said today, that change is going to occur, but the extent of change which has occurred in the last 12 months is considered to be quite excessive. I apologise if this seems like a Ramsey approach, but, to put it in context, the access level to GPs has been reduced from ‘24/7’, to use the common parlance, to 40 hours a week, which is effectively a reduction in service of over 75 per cent. The position of the GPs is appreciated- obviously, they have contractual obligations, and they have to be prepared to work hours which are acceptable to them as individuals - but it should not diminish the responsibility the Department of Health and Social Security to provide adequate and appropriate emergency access to doctors’ services on the Island.
The Committee is aware of the advice from the GMC, which was publicised last week from the Town Commissioners, and I believe it was raised with the Committee previously when they met in Ramsey. This morning we were accused of cherry-picking, but I think the Minister referred to it and Mr Newbury referred to it earlier. I will leave a copy in case the Members have not got it, anyway, but it is quite specific and it is important to read what it says. It says:
‘G iving advice by telephone is part o f many doctors' day-to-day relationships with their patients.’
- the emphasis on the word ‘their’ -
‘In some circumstances, providing advice by telephone or computer link may be essential, for example where patients are geographically isolated from their doctor. However, use o f phone or e-mail should not diminish the quality o f care patients receive. Consultations and prescribing by phone or e-mail may seriously compromise standards o f care w h ere ...’
and then it gives the three examples which Mr Newbury quoted and identifies that there is a risk of compromised
care.The Minister said this morning that the same level of
clinical judgement is made now as was made previously. However, looking through other documents which are issued by the General Medical Council on GMP - Good Medical Practice - and particularly the Good Medical Practice document issued to all doctors in May 2001, one of the requirements for clinical care is that, again, in each case, an adequate assessment of the patient’s condition, based on history and symptoms and, if necessary, an appropriate examination, has been provided. So, it reinforces what the good practice is and the risk assessment attached to telephone consultations. It says - and it is not just an isolated item, but it is something that is written throughout GMC good practice notes -
‘Statistically, the Island as a whole may meet all the service level indicators for comparable U K areas. It does not mean, however, that the standard is consistent between Douglas/Onchan and the north, the south and the west o f the Island/
It is ironic today that the Committee is taking evidence when the mountain road is closed. I travelled to Douglas this morning, mid morning. It took about 45 minutes to get into Douglas itself. Travel times will take over an hour at certain times of the day, and getting through town to the hospital could take even longer. And this applies equally to the south of the Island: I have had experience recently of trying to get through the Quarterbridge in the morning, and the traffic banks up there as badly as it banks up from the north. The removal of the GP input to the Cottage has resulted in a greatly reduced service. It is compounded by the ability of the Ambulance Service to deal with the requirement to use Noble’s following the removal of availability of services at Ramsey.
UK service standards for ambulance responses are: 14 minutes for urban areas; 17 minutes for rural areas; and 19 minutes for Wales, for some strange reason. These are service standards, and, obviously, their performance is assessed against a proportion of visits that are achieved in that time. But today I had a phone call, before I arrived, from someone in the town, drawing attention to an incident where a footballer waited 48 minutes, with a broken leg, for an ambulance to attend. A week before, a rugby player- unfortunately, both sporting injuries - waited over an hour for the ambulance to attend, and, in both cases, obviously, they then have to be taken to Noble’s Hospital. If it is a straightforward break, then that is not a problem, but if it is a complicated break, then an hour-plus getting back to the Hospital could present really serious problems in terms oi their recovery and the ability to be treated adequately.
That same difficulty applies to people who visit MEDS. The previous witnesses made reference to the supply of equipment for the MEDS doctors’ defibrillators. It is again ironic. There seems to be a suggestion that Ramsey is confused by the services, how they were provided, and that it is mixed up, and yet the MEDS doctors are provided with facilities which you would expect to find in an A&E, or in a hospital: a defibrillator. So, there are still some grey areas there. They are not just providing GP services; they are actually providing other services, more acute services, where required.
In summary, the issue is about service levels. The policy of the DHSS to encourage care in home, the rising average ages on the Island, longevity of life, and reduced family
Tynwald Select Committee on GP Out of Hours Services - Evidence of Mr Radcliffe and Mr P Whiteway

Oral Evidence SELECT COMMITTEE, WEDNESDAY 28th JANUARY 2004 87 TGPS
unit sizes all provide greater numbers of people who are unable to deal adequately with the MEDS service. They have difficulty getting access to the service because of availability of transport, because of age, or because they may be single parents with one or two children and either have not got transport or cannot leave the second child, and all these things should be looked at and be considered in determining what level of service/access to doctors should be provided on the Island.
I would leave it at that. Thank you.
The Chairman: Thank you, Mr Whiteway.Mr Radcliffe, do you wish to add anything to that?
Mr Radcliffe: I have nothing to add to that. Thank you, Chairman.
The Chairman: Mr Gill,
Mr Gill: You started with almost a headline figure there, that there had been a 75 per cent reduction in GP access in Ramsey. Is that right?
Mr Whiteway: If you take the 24/7 approach, which is what was available one way or the other, and then calculate out the 5 days a week, assuming 40 hours a week and bank holidays, that is what you are looking at: over 75 per cent.
Mr Gill: Is that accurate, though? I am just thinking that if you have... Or should it really be that access to a Ramsey Group Practice GP is reduced by 75 per cent in 20 per cent of cases, if we assume that all 8 GPs in Ramsey are part of the 40 that are on the... I am not being pedantic, but.that is the point.
Mr Whiteway: If you multiply the access... It is the access time which was looked at, rather than the number of doctors.
Mr Gill: There is still, perhaps crucially, access to a GP. It just might not be a Ramsey Group Practice GP.
Mr Whiteway: It certainly will not be in the Ramsey area.
Mr Gill: Are any of the Ramsey Group Practice GPs on the MEDS list?
Mr WTiiteway: Yes, but they are based in Douglas.
Mr Gill: Yes, but at some time -
Mr Whiteway: At some time you could meet your own doctor, yes.
Mr Gill: But there will still be access to a GP 24/7 through the MEDS service.
Mr Whiteway: Through the MEDS service, yes.
Mr Gill: As far as access to a GP is concerned, which is what you were leading with, that has not actually diminished; it is the access to a Ramsey Group Practice GP.
Mr White way: To a local GP.
Mr Gill: Yes. Thank you.
Mr Singer: Is it not also relevant that it is the speed of access which is totally different, as well?
Mr Whiteway: It is the isolation, yes. It is how quickly you can get access to them, as well, which is the issue.
Mr Singer: Could I be a little pedantic? On the first statement, on the interpretation, when it says, ‘For example, where parents are geographically isolated from their doctor -
Mr Whiteway: Patients, yes.
Mr Singer: Patients. Do you think it would be an argument that could be put by people to say, ‘Well, if you are in Ramsey and the doctor on duty is in Douglas, then they are geographically isolated’?
Mr Whiteway: Not all year, certainly, no, but I think if weather conditions or prevailing weather conditions are such that access to Douglas is difficult, or the time which it would take to get to Douglas is extensive, then that would be applicable.
Mr Radclifte: Does that not relate to a doctor who has a rural practice, such as in Wales, where he is actually isolated from his own patients, rather than dealing with the patients of another practice?
Mr Singer: Yes. This is just the argument that may well be put.
The Chairman: Can I just follow on the point about the access to a GP? 1 think it is important. You were making the point, and you have clarified the issue about the Ramsey- based GPs. In your answer, though, you then indicated that it is because people from the north now have to ring MEDS, where the Ramsey GP may be, or it may be another GP. Do I take it from that that you are saying that previously the Ramsey practice GPs did not give telephone advice? So, eveiybody, actually, had a call from their doctor?
Mr WTiiteway: No, they were available on a -
The Chairman: They are still available, in theory -
Mr Whiteway: In theory, yes.
The Chairman: - and can be available. So, I just want to get to the issue: in other words, is it right to say that people in the north of the Island, on occasions, received telephone advice, the same as they do now?
Mr Whiteway: Yes, and they would also -
The Chairman: Or maybe a different doctor?
Mr Whiteway: - be able to meet the doctor, either at the practice or at the Hospital, who wouid have access to their case history and notes -
Tynwald Select Committee on GP Out of Hours Services - Evidence of Mr Radcliffe and Mr P Whiteway
88 TGPS SELECT COMMITTEE, WEDNESDAY 28th JANUARY 2004 Oral Evidence
The Chairman: But not always?
Mr Whiteway: Not always. If necessary, they -
The Chairman: If I understand a GP practice - and in Ramsey there were eight - people would be linked to a doctor, but they might not always get that doctor if they go to the surgery. So, it might be another doctor who is not the one they usually deal with, dependent on their circumstances.
Mr Whiteway: One doctor in the practice.
The Chairman: Right. And this is not just Ramsey; this is throughout the Island, and we are looking at the whole Island, but you have raised the issue. So, it would be fair to say that it is not unusual that a person might have a doctor within the practice but does not always get to see that doctor, depending on when they want the advice or the help. Is that fair?
Mr Whiteway: That is not unusual, but, in those cases, the doctor would always have the benefit of the patient notes and history.
The Chairman: ‘May’, because if on call, under the old system, it might not have been your doctor on call, even in the Ramsey area. It might have been one of the others, who might still have given advice over the phone. Is that not correct?
Mr Whiteway: No, because it was a group practice. Doctors who provided that -
The Chairman: But he still might be giving the advice from his home.
Mr Singer: They always had the option -
The Chairman: It is not for you to answer the questions. (Laughter)
Mr Whiteway: In certain cases, they would give advice from home, yes.
The Chairman: Righi. I am just trying to get to the fairness of this. Therefore, it is fair to say that a patient could have rung - we will use the Ramsey one - the Ramsey on-call GP -
Mr Whiteway: And received advice -
The Chairman: - and received advice not from their doctor, but from a doctor within the practice who was at home and did not have their records. Right. So, in that aspect, that has not changed, but it could be now that it could be a doctor who is not even from Ramsey. Okay. I just want to... I think it is important to get the perception right.
Mr Whiteway: No, that is right.
The Chairman: Could I just ask, then, on the delay: you mentioned the incident at the football match, and I think you said a rugby match as well, and there was a delay of 40 to 45 minutes?
Mr Whiteway: I was told this morning that it took 48 minutes from the call for the ambulance to attend.
The Chairman: Right. Could I ask the question of both of you, really, because I do not know who may be able to answer this, if you can: from that, do I take it that that, in itself, is an unusual incident? In other words, are you indicating from that message, if you like, that, in fact, that would never have happened when there was a Ramsey Cottage Hospital ambulance available?
M r Radcliffe: My experience from refereeing football matches is that the response time was very much shorter than that.
The Chairman: But are you saying -
Mr Radcliffe: And also when there were motorcycle races on the Ramsey circuit, it was five minutes’ response time.
The Chairman: Right, but could we guarantee that? I suppose that is the question I am asking.
M r Radcliffe: I can only tell you what my experience is. Obviously, nothing is able to be guaranteed, because -
The Chairman: The Ramsey Cottage Hospital often used to take people through to Noble’s, (Mr Radcliffe: Yes.) so if an incident happened in those circumstances, presumably wouldn’t that be an ambulance then despatched from Noble’s, because the Ramsey one was taking somebody already to Noble’s? It is a coincidence how it would have all linked up. Again, all I am trying to get to is: yes, it has occurred, or we understand it has occurred, and yes, that might not be something we all like to see happen, but can we say, because of the change of the system, that, in fact, thal has resulted in this circumstance? Or could it have happened under the old system?
Mr Radcliffe: Presumably it could have happened, but my experience, as 1 have said before, is that it did nol happen before, (The Chairman: Right.) so it is a reasonable assumption that it has something to do with the change in service levels.
The Chairman: Okay. Mr Singer.
Mr Singer: Whilst we were talking before about the access of the Ramsey doctor to their patient previously, although it was not the same doctor, is it not a fact, would you not agree, that that doctor then had the choice, if he felt, tc go to the surgery, open up the surgery and find that patient’s records, where now there is no access to the doctor who ii speaking from the MEDS to get into those records?
Mr Radcliffe: Yes, that is absolutely right, and thai certainly increases the risk to the patient and is contrary tc the advice that is from the GMC.
Mr Singer: And, on the ambulance situation, which yoi have just been talking about now, would you not agree it was a fact that if the ambulance was in Ramsey, it came down, as you say, within 5 to 10 minutes, but if it had to come frorr
Tynwald Select Committee on GP Out of Hours Services - Evidence of Mr Radcliffe and Mr P Whiteway
Oral Evidence ' SELECT COMMITTEE, WEDNESDAY 28th JANUARY 2004 89TGPS
Douglas because that Ramsey ambulance was already going to Douglas, it might take the 25 to 30 minutes, but they then had the opportunity to take that person to Ramsey Hospital either to be stabilised and to see a doctor -
Mr Radcliffe: That was actually the normal situation -
Mr Singer: - before they sent them off over the mountain?
Mr Radcliffe: Yes.
The Chairman: Okay. Mr Waft.
Mr Waft: WTiat sort of warning did you get prior to the notification that the facility at Ramsey Cottage Hospital was going to be withdrawn at night and the out-of-hours GP service was going to be taken over by MEDS?
Mr Radcliffe: You mean official notification?
Mr White way: I am not 100 per cent certain. I seem to recall there might have been a press notice, a public notice given in the paper, maybe a matter of weeks -
Mr Waft: Nobody mentioned it to the Commissioners at all?
Mr Whiteway: No.
Mr Waft: The facility at Ramsey Cottage Hospital at night is one of the main thrusts of your argument - or is it the fact that you should have an out-of-hours GP in the northern area anyway? Or is it both?
Mr Whiteway: 1 think, in the main, it is access to a doctor. I do not think people are concerned whether it is a GP or a hospital doctor, as long as they can get a reasonable level of access to a doctor in the situations where they need to get that access. So, whether it is provided through the GPs, or whether it is provided through a hospital service, I think it is just the access to the doctor that is the concern.
Mr Gill: And the point of access.
Mr Whiteway: And the point of access in the locality, reasonable access to a doctor.
Mr Waft: Have you had complaints with regard to people who have actually used the MEDS service?
Mr Whiteway: We do not receive complaints from people about the MEDS service. We are not the type of body who would receive them, anyway. I would assume that if someone had a complaint about MEDS, they would write to the DHSS. We occasionally get comments given by people, members of the public, that they have concerns, and you hear tales which go round the town, but we do not record it in any way.
Mr Waft: The Commissioners, as a body, have not received complaints about -
Mr Radcliffe: I have. I have had telephone complaints
from numerous people in the last couple of days, one from a bedridden lady who phoned the MEDS service and, basically, was told, ‘You will have to suffer until your own doctor can see you, if you cannot get yourself to Noble’s.’ That is somebody who is bedridden. Obviously, her home help is not going to come out in the middle of the night to help, and that was the advice she was given. There was another of parents who were visiting the Island, who had a 10-day-old baby. The MEDS service refused to come, and the father had to struggle to Douglas at 12.45 a.m. It is a very welcoming Island. That sends out the wrong message.
Mr Gill: And do you know, Mr Radcliffe, have both those cases led to formal complaints or -
Mr Radcliffe: I am unaware. All I know is that the two people concerned telephoned me in order that I could be aware of the situation, as they knew I was coming here today.
The Chairman: Mr Gill.
Mr Gill: Mr Radcliffe, could you tell us a bit about the questionnaire that the Commissioners organised and what your interpretation of that is?
Mr Radcliffe: The reason that was circulated was that people are quite happy to join a march and make their feelings known, but actually setting out a letter, a lot of them would probably feel intimidated with that, so the whole point of the questionnaire was to give them the basis of a letter that they could send in and make their views known. You do find that people are much more likely to respond to a questionnaire than they are to start with a blank sheet of paper and set their views out.
Mr Gill: How many questionnaires did you send out?
Mr Whiteway: Hundreds. There were getting near to 200. I am not sure. We actually had them available in the Town Hall, so people could just come in and collect them. We know that some people actually took a copy and photocopied it themselves, and we e-mailed copies out, where requested. In doing the questionnaire, what we sought to do - and it may not have been as professional as might have been able to be done - was not to try and put in questions which were seen as leading, but to put in questions regarding the basis of the level of service and give ¿hem the opportunity to submit views on top of that, if they wished to do so.
Mr Gill: What would your interpretation... What kind of response level did you get, and what was the content of those responses?
Mr Whiteway: We did not analyse the responses; we forwarded them directly to the Committee, because, effectively, what we did not want to do was to try and put forward a submission that analysed people’s views, but to give people the opportunity to submit something to the Committee themselves.
Mr Gill: Thank you, Chairman.
The Chairman: Mr Singer.
Tynwald Select Committee on GP Out of Hours Services - Evidence of Mr Radcliffe and Mr P Whiteway
90 TGPS SELECT COMMITTEE, WEDNESDAY 28th JANUARY 2004 Oral Evidence
Mr Singer: It is a bit difficult, maybe, to say, but I am sure you would agree with me that those of us who live in the north feel that we have been very fortunate, over the last 90 years, to have a hospital, and obviously we regret that there is not one elsewhere. But the fact is we have got the Hospital, and the Hospital has been the centre of the community.
But times are changing in Ramsey, and would you like to give some details to the Committee of the expansion that is taking place in Ramsey? I would feel personally - 1 will say ‘personally’ - that a hospital and a doctor are getting more and more needed there because of the expansion. Would you like to outline what is going on in Ramsey as an expansion and the number of extra people that are going to come et cetera?
Mr Radcliffe: It depends, obviously, on planning permission for the West Ramsey plan, but there is a huge area there to be developed, which could have 400 more houses. If you say three people a house, that is another 1,200 residents, plus the areas on the Peveril plot, which, again, could be developed for fiats, bringing another 500 people into the town. Again, pressure on the services, but, again, as we have said, it is not just a Ramsey problem; population is increasing everywhere.
I work with people from Douglas and the south of the Island, and they have all said that they want 24/7 access to local GPs. They are most unhappy with ringing Manndoc and being, most of the time, fobbed off. The doctors seem very reluctant to leave the base, and there is great unhappiness, not just in the north of the Island; it is an all-island problem. But, certainly, in Ramsey, the people of Ramsey and the north are seeing a reduction in standards of medical care. Surely we should be trying to improve at all times, not reduce levels of service to people.
The Chairman: Sorry, just clarify it there: we are talking about MEDS now, aren’t we, not Manndoc?
Mr RadclifTe: Yes, quite.
The Chairman: Just so we are right, we are on the right thing. I know it is easy to make a mistake, because we do, but just so we are clear.
Mr Waft.
Mr Waft: Given the problems that the Minister finds- and, indeed, the information from the GP services themselves - with regard to recruitment to attract GPs to the Island and greater expectations of quality of life, better than their previous incumbency of those positions, what do you feel could be done to, perhaps, attract GPs to the service at the moment?
Mr Radcliffe: Well, why do GPs go in there? Presumably, they want to provide a service to the people. They have been able to provide that since the National Health Service started, I see no justification for reducing the service. We do not hear the police saying that they want to work 9 to 5, Monday to Friday, nor do we hear that from the fire service. I do not see that doctors are any different. If they are properly remunerated, then they will provide the service.
The Chairman: But aren’t doctors different because they are self-employed, whereas the police are not? They
are under a contract; they are not employed by the DHSS, so there is a difference. Just to throw back at your answer, (Mr Radcliffe: Yes.) does that not make a difference?
Mr Radcliffe: No. If people are properly remunerated, they will provide the service that you want. It is up to the Department to negotiate the contracts, in order that it can provide the service that people want.
The Chairman: So, can I take it from there that you feel, as Commissioners, that the doctors are not properly remunerated?
Mr Radcliffe: What would appear to be the problem, from what has emanated from the doctors, is that they feel that, number 1 in the north - I have not spoken to doctors elsewhere - it was due to the pressure of having to cover the Hospital, as well as providing out-of-hours service for their own patients. There is a solution with regard to the doctors providing service at the Hospital, which is to transfer it to Isle of Man Hospitals and staff it through there. That would remove their necessity to provide cover at Ramsey Cottage Hospital and free up significant time for them.
The Chairman: The reason I asked that is because I understood, from the evidence given to us here in Ramsey, that, in fact, money was not the problem; it was quality of life for themselves. Is that not correct?
Mr Radcliffe; That was alluded to, but if you remove the pressure from them, providing cover for Ramsey Cottage Hospital, then that improves the quality of life, reduces their working time -
The Chairman: So, just based on this morning -
Mr Radcliffe: - but these doctors also have signed up for Manndoc, which tends to weaken their argument that it was to do with quality of life.
The Chairman: But also this morning, we were given evidence that said that the doctors, the GPs in Ramsey themselves, had determined to terminate one of their contracts in relation to the services they provide at the Hospital, and I think it was eight they retained or something like that. Therefore, they seem content with providing the link with the Hospital during the daytime. The only area that they had a concern about was providing the night-time service seven days a week and a weekend service, which was outside that daytime normal service. So, they made a conscious decision, and my understanding of that, based on the evidence we were given in Ramsey, was because the GPs themselves wanted to improve their quality of life. Is that not a fair assumption of what they said?
Mr Whiteway: With respect, Mr Chairman, the GPs have retained their contract to provide in-patient 24-houi cover -
The Chairman: But not out-patients.
Mr Whiteway: But not out-patients, although, as the Minister points out, they are -
The Chairman: They made that decision to terminate that contract?
Tynwald Select Committee on GPOut of Hours Services - Evidence of Mr Radcliffe and Mr P Whiteway
Oral Evidence SELECT COMMITTEE, WEDNESDAY 28th JANUARY 2004 91 TGPS
Mr Whiteway: They did. They have made the decision to terminate the out-patient one for the A&E, or the Minor Injuries Unit, but they have retained the in-patient 24-hour cover, although, as the Minister says, they are infrequently called out.
The Chairman: So, does that not tell us something? In other words, they know that is infrequent, as against the other one, which was giving them more work. I am, really, just coming back to the point Mr Radcliffe made. I am just trying to put another argument, in a way, to try and get out of you how you think about that, in that it was not just about money and it was more about the fact that they were having to be called upon seven nights a week, weekends, for the out-patient issue side, which was the one that was putting the pressure on them. So, it wasn’t about money as such.
Mr Radcliffe: No, but there are ways of reducing their hours of work. It seemed to be the total amount of hours that they felt they were obliged to work that were the problem. There are methods by which the amount of hours can be reduced, (Interjection by the Chairman) but, perhaps, if the doctors are self-employed, if competition between practices was introduced, they would then provide the 24-hour service that vets, who are obliged to compete, already provide.
The Chairman: I am not being funny; I am just trying to work round this issue, because it is an important issue, because we, as lay people, are trying to work out what has happened. But in that they work those hours by agreement, which is their contract, within the Ramsey Cottage Hospital it has been a special contract - 1 think it was eight components- and the only component they have stepped out of has been the night cover and weekend cover for out-patients, and they made that decision, not the DHSS. So, it is not a matter of money; it seems to be an issue, from the doctors’ point of view, of what they see as their quality of life, having free time. Is that not a reasonable assumption?
Mr Radcliffe: It may well be a reasonable assumption, yes.
The Chairman: Right So money wouldn’t necessarily answer the problem? That is what I am trying to say.
Mr Radcliffe: It tends to reduce arguments.
Mr Singer: Would you not agree, though, that if the doctors will not say, ‘We want to give up our night-time, roing occasionally to see our patients, and go to the Hospital between 8 and 6’, the reason they are not giving that up is because it gives them £25,000 a year each, so it is not one they are going to give up?
The Chairman: Okay. Mr Gill.
Mr GiU: At the march and then the subsequent meeting in Ramsey, which I, because it is an all-island issue, was anxious to attend, just for clarity, can I recall - and you can indicate if this is an accurate recall - I think it was Dr Fenton - certainly it was one of the Ramsey GPs, who was clearly held in great regard by everybody present and was very experienced - made the quote... Are you nodding, Mr
Radcliffe? It was Dr Fenton?
Mr Radcliffe: It was Graham Wilson.
Mr Gill: Wilson, right. Sorry, I do not know all the doctors individually, but he made the comment - which nobody queried -
‘This is not a problem you can solve by throwing money at it.’
Is that an accurate recall?
Mr Whiteway: I have to admit I never actually got into the church on the day. The place was too busy. (Laughter) I listened to it outside, and I did not manage to catch everything that was said.
Mr Gill: I am not casting an opinion over that; I am just trying, for clarity, to determine that that was an accurate view. Two things then briefly, if I could: first of all, could I confirm that you are speaking with the unanimous concurrence of the whole of the board?
Mr Radcliffe: Yes, of the Commissioners, yes.
Mr Gill: Thank you. Finally, then, just for clarity again, could you briefly tell us what role the Commissioners would like to see Ramsey Cottage Hospital fulfilling in the out-of- hours care?
Mr Radcliffe: Ideally, we would like it back to providing the A&E that it once did provide for the immediate assessment of cases and stabilisation, particularly with heart attack cases.
The Chairman: So, if the GPs from the group practice in Ramsey are not willing to provide that, how could it be provided?
Mr Radcliffe: We have already put in our submission that we believe that the responsibility should be transferred to Isle of Man Hospitals and it is staffed appropriately by Isle of Man Hospitals, as opposed to the current system.
The Chairman: And do you see that being staffed by a GP or a consulting doctor?
Mr Radcliffe: By a house doctor.
The Chairman: A house doctor. Okay. Mr Waft.
Mr Waft: There was a problem there, elucidated by, especially, Mr Newbury, with regard to staffing it with a doctor 24/7, because there is a certain lack of training in that facility to ensure a constant supply of medics in that area. Have you any comment on that one?
Mr Whiteway: I listened to what Mr Newbury said. I suppose, to an extent, you could argue that was the case if you employed purely in Ramsey. I think, if you look at it as an Island problem, there is probably a similar need in the south of the Island, the Southern Community Centre, and if employment was undertaken through Ramsey, through Noble’s Hospital, I would not have thought it would be too
Tynwald Select Committee on GP Out of Hours Services - Evidence of Mr Radcliffe and Mr P Whiteway
92 TGPS SELECT COMMITTEE, WEDNESDAY 28th JANUARY 2004 Oral Evidence
difficult, with the numbers of staff they can call upon and with the range of other duties that they have available in the Hospital, to rota it so that a reasonable level of variety of casework could be dealt with by doctors who may spend a time in Ramsey, a time in the south and a time in Noble’s Hospital.
Mr Waft: Okay. Thank you.
The Chairman: Anything' you would like to say in closing, Mr Radcliffe or Mr Whiteway?
Mr Whiteway: Only, I think, in short, to thank the Committee for the opportunity again to appear today.
As a final thought, just probably more from myself than from the Commissioners, on the doctors’ service or GPs’ service: access to doctors is not comparable with a clerical function or a bank; it is something which impacts upon people during the full time of their life, not just between 9 and 5 on a Monday to Friday. I think that needs to be borne
in mind when deciding what level of service should be provided through doctors, and if it is not possible to provide an appropriate service using GPs, then other options of providing that level of service should be investigated.
The C hairm an: Thank you. Can I thank the Commissioners for their assistance, on behalf of their community, in collating information which we have found interesting and, in some cases, quite helpful. I would also just put on the record our thanks to the Commissioners for the use of the Town Hall the last time we had our public sitting and the facilities, and especially the Town Clerk.
Mr Whiteway: You are very welcome, Mr Speaker.
The Chairman: Thank you very much, everyone.That concludes the public proceedings of the Committee.
Thank you very much.
The Committee sat in private at 4.23 p.m.
Tynwald Select Committee on GP Out of Hours Services - Evidence of Mr Radcliffe and Mr P Whiteway
TGPS, No. 3
L y v94rw*v
T Y N W A L D C O U R T O F F I C I A L R E P O R T
R E C O R T Y S O I K O I L Q U A I Y L T I N V A A L
P R O C E E D I N G SD A A L T Y N
(HANSARD)
SELECT COMMITTEE ON GP OUT OF HOURS S E R V I C E S
B I N G E R - L H E H M Y C H I O N E S H I R V E I S H Y N F I R - L H E EA Y N S O O R Y N S O C C A R A G H
Douglas, Friday, 7th May 2004
2004
Published by the Office o f the Clerk o f Tynwald, Legislative Buildings, Bucks Road, Douglas, Isle o f Man. © Court of Tynwald, 2004 Printed by The Copy Shop Limited, 48 Bucks Road, Douglas, Isle o f Man
Price Band B
94 TGPS SELECT COMMITTEE, FRIDAY, 7th MAY 2004
Members Present:
Hon. J A Brown SHK (Chairman) Mr D J Gelling MLC
Mr Q B Gill MHK Mr L I Singer MLC
Clerk:Mr P Lo Bao, Third Clerk
Business transacted
Page
Procedural..........................................................................................................................................................................................95Committee remit............................. ....................................... .......................................................................................................... 95
Evidence of Mr John Wilson, Head of Health Services Divisionand Mr A Jones, Acting Manager, Primary Health Care Services......................................................... ..........................95
The Committee sat in private at 3.55 p.m.
Oral Evidence SELECT COMMITTEE, FRIDAY, 7th MAY 2004 95 TGPS
Tynwald Select Committee on
GP Out of Hours Services
The Committee sat in public at 2.15 p.m. in the Millennium Conference Room,
Legislative Buildings, Douglas
[THE SPEAKER in the Chair]
Procedural
The Chairman (The Speaker): Good afternoon, Mr Wilson, Mr Jones, and everyone who is here.
As you are aware, I think you know everybody on the panel and the names are in front of us. We have apologies from one of our Members, who is off the Island, Mr Waft; otherwise we are complete, and we have our Secretary of the Committee, Mr Lo Bao, who is there, of course, to take notes, and the Hansard, which will record the proceedings, which I am sure you are well used to.
Can I just say that when we are questioning you, we will come to you. If you have anything to answer or wish to say, then catch my eye and I will invite you to speak, okay?
Committee remit
The Chairman: Can I just read out the remit of the Committee, so that you are clear on what the Committee’s remit is: it is a Select Committee of five Members and we were appointed to investigate the matter of the general practitioners’ out-of-hours service, which is being provided throughout the Island, with power to take written and oral evidence, pursuant to sections 3 and 4 of the Tynwald Proceedings Act 1876 and to report.
So, that is the basis of what we are here for. I am sure you are well aware of the investigation we are undertaking and can I just thank you for coming along this afternoon.
EVIDENCE OF MR J WILSON AND MR A JONES
The Chairman: To start, the issue for which we have invited you in today, Mr Wilson and Mr Jones, is in relation to the GP contracts and how that related to the out-of-hours service. Our understanding is based on information we have got, and what we wish to get further clarification on is that the old GP contract was in place up until 31 st March 2004, and then a new GP contract was effective from 1 st April 2004; but the MEDS came into effect on 1st April 2003, and that provided for the new out-of-hours service. It is that aspect, how that inter-relates to the old and the new contract really, that we wish to specifically cover and the indications that
we have from the Department in correspondence, and in the evidence that we received previously was that, in fact, the Department was under pressure to introduce the MEDS system, and that this was being introduced with some sort of pressure on, in terms of getting it in, because there was a concern there would be no out-of-hours GP service for the Island.
The issue, initially, that we invite you to respond to, is that, if this is correct, then how does that relate to the original GP contract that was effective up to 31st March 2004, which, in fact, specifically allowed for an out-of-hours service and required the GPs to provide that service? Therefore, as that was in being until 31st March 2004, why was there what seems to have been a rush to bring in the MEDS system, to secure the out-of-hours service a year earlier?
That is an issue that we would like to have clarified, so Mr Wilson, I do not know if you, John, want to respond to that first.
Mr Wilson: Thank you, sir.I should say at the beginning, I have asked Mr Jones along
with me this afternoon, as he is acting for Primary Healthcare, following the sad death of Mr Newbery last month, and he is here to provide help and support to me, in issues and detail which may be helpful to the Committee.
The basis of the way in which GPs have provided services was based on the 1978 regulations. Details of those regulations were submitted to the Committee in the evidence we, the Department, provided at the beginning of this enquiry. Under those old regulations, GPs were responsible for their patients, seven days a week, 24 hours per day, full responsibility. They were entitled, under the regulations, to have that cover provided by other doctors, as, clearly, it would be impractical for a doctor to cover 24 hours a day, 7 days a week for all of their patients, all the time.
So, they were entitled under the regulations to pass that responsibility on to colleagues or other doctors, but they retained full responsibility, even in circumstances where that responsibility was passed on. So, if there was a problem with a particular service, then the GP with whom the patient was registered, would still retain full responsibility for them.
In a letter dated November 2001, the GP group of the Isle of Man Medical Executive wrote to the Chief Minister. Again, this letter is enclosed in the evidence which I previously provided to the Committee. The letter is signed by Dr M Maska, Chairman of the GP Sub-Committee to the Isle of Man Medical Executive and, in that letter, the GP group expressed concerns over the increasing difficulties they were having, in managing what was becoming a very onerous workload. They set out for the Chief Minister, in some detail, the basis of those concerns.
The main concern, or the first concern, and I quote from the letter, was titled, ‘Appropriate and central funding for out-of-hours provision’, and the GPs were making the point very seriously to the Department that the current arrangements, under which they had this 24 hours, 7 days a week responsibility, was such that it could no longer, in their view, be sustained. In presenting that evidence, in that letter, they made reference to negotiations that were taking place in the United Kingdom on the introduction of a new GP contract. It was early days, at that stage, with regard to the new GP contract, but the point was very clearly made to us that the work that had been going on in the UK was likely to result in a situation where GPs would be relieved
Procedural Committee remit
Tynwald Select Committee on GPOut of Hours Services - Evidence o fM rJ Wilson and Mr A Jones
96 TGPS SELECT COMMITTEE, FRIDAY, 7th MAY 2004 Oral Evidence
in the new contract of 24-hour responsibilities.So, we were aware at that stage, in November 2001 „ that
the then situation, where GPs had this full responsibility would, under the new contract, be changed. It was at that time, and bearing in mind the issues which were raised by them in the letter to the Chief Minister, that we started to talk with the profession, to see how best we could address their concerns, bearing in mind that the new contract provision in relation to out of hours was going to change, anyway.
At that time, and again in the evidence that you already have available to you, a number of practices on the Island had already entered into an arrangement called Manndoc, under which they had joined as a consortium, as it were, to ensure that a doctor representing those practices - and I think there were eight of them - would cover out of hours for all the practices. They include every practice, with the exception of Ramsey, Port Erin and Laxey, and that situation with Manndoc had, in fact, been running for four and a half years.
When we started talking to them, subsequent to 2001, it became apparent to us that one way of addressing this situation with regard to out of hours, was perhaps to look at extending the Manndoc service into an all-island service. Not only would that meet the concerns of the three practices who were then outside of Manndoc, but it would also go a long way to addressing what we knew was likely to be the position in the new contract, i.e. the release of GPs from their 24-hour cover.
Those negotiations became advanced and, eventually, concluded with the development of the Manx Emergency Doctor Service (M EDS), replacing Manndoc, but incorporating all practices on the Island, including those three practices which were then outside the system, and that new service came into being on 1st April 2003, even though the regulations still required GPs to cover their own patients, at that time, and, indeed, for the remaining year- 1st April2003, when the MEDS system came in, up until 31st March2004, when the new contract came in. Even though we were operating a MEDS service,, it was still a responsibility of all GPs to look after their own patients.
So, if there were any problems with a patient being managed under MEDS during that period, then responsibility for that still fell back on the GP with whom the individual patient was registered. The new contract came in, in the UK on 1st April this year.
The Department has been working with the profession for the last 12 months in relation to that contract and, as had been predicted, the main plank of the new contract was, in fact, to statutorily remove responsibility from GPs for patients on a 24-hour, 7-days-a- week basis.
So, in fact, the Department had anticipated the new contract in introducing the MEDS services on 1st April 2003. There was no statutory requirement for us so to do in April 2003, but because of the concerns being expressed by the profession, which were many and, in particular, related to our ability to recruit doctors to the Island, we felt it was appropriate to move ahead of the UK, and did so, knowing very well that from 1st April this year, statutorily, the legislation would change and that responsibility would be relieved of them.
So, we have moved ahead of the United Kingdom in this system, and from discussions I had with the late Primary Healthcare Manager, I can advise the Committee that a number of Primary Care Trusts in the UK had been looking
at the system that we had introduced on the Island, as : model which they could adopt and, perhaps, use in areas ii the UK, where responsibility changed on 1st April this yeai under the new contract.
That is the situation and why we acted ahead of thi legislation itself, which as you say, sir, changcd on 1st Apri this year.
The Chairman: Thanks, Mr Wilson.If I can just follow up, first, on the points you have made
I think it is quite clear that we understand the difficult} the Department has, in terms of the knowledge and trying to provide the Committee with the evidence, due to th< unfortunate circumstances that have arisen.
Taking that on board and based on what you have saic and the information that would be available to you - anc there is no problem, l am sure from the Isle of Man saying ‘Yes, where we can, we should go in advance of the UK because we may be able to do it’, or whatever, I do not think any of us would criticise that at all, especially if it was ar improvement in service - but, a number of the issues that certainly, seem to have come out in evidence are that then was a rush to provide appropriate facilities for MEDS tc operate from, and I do not know if you can advise us on that, what you may know about that.
We visited the MEDS centre and there is no doubt it if not really adequate for long-term operation of the facility, in that it is a shared facility and, therefore, equipment and stufl has to be moved in and out, and so on. So, by advancing il quickly, it seems, on the surface, that, in fact, the Department was not ready itself, in terms of facilities to be available foi the operation of MEDS. I do not know if that is correct, but I would like you to comment on that.
The other one is, if you would, you said that even though MEDS came in prior to the new GP contract becoming effective in April 2004, that the responsibility for the patients still lay with the GP, and I think we can all understand that. But, of course, if then a patient was trying to contact their GP, they were being directed to MEDS and if they were having a problem getting service from MEDS, they could not get hold of their GP, so whereas in theory it seems that there was still a responsibility on the individual GP, they had actually abrogated that to MEDS, or it was not possible for patients to contact their own GP if they needed them.
So, would you like to comment on that, and what the Department’s view is on that, if you know what it is?
Mr Wilson: Yes, in terms of the MEDS accommodation, one has to recognise that, prior to MEDS coming in, Manndoc was in place, and Manndoc was based in accommodation run by the Manndoc service in the old hospital. When MEDS began on 1st April 2003, they simply assumed the accommodation, which was previously used by Manndoc.
It is certainly tme to say, that there was no planning for a purpose-built MEDS unit and, in fact, since the old hospital has closed and the new hospital has opened, it did put the Department in a difficult situation, because the planning of the new hospital did not take account of a requirement for an out-of-hours GP unit, because when the planning of the hospital was taking place, that was not a consideration.
Therefore, when the Manndoc extended into MEDS, and the move to the new hospital took place, we were at the beginning, using accommodation which was not purpose built and, therefore, by virtue of that, one has to accept is not ideal.
Tynwald Select Committee on GP Out of Hours Services - Evidence of Mr J Wilson and Mr A Jones
Oral Evidence SELECT COMMITTEE, FRIDAY, 7th MAY 2004 97 TGPS
The Chairman: Could I just follow through on that? If that was known, then why did the Department agree, a year in advance of what it had, to introduce, or allow the introduction of MEDS? There were financial implications, there were accommodation implications and, clearly, from what you have said, they had not been prepared for the operation of a system that was going suddenly to get up and running. Presumably, the Department was aware of that, and I just wondered why the Department still felt it was appropriate to advance this by a year, when, in fact, they did not have to, when it could be argued that, in fact, they were not ready to.
Mr Wilson: I am not sure it is fair to say that the Department... I would suggest - no higher than that- the Department had concerns and did not take those into account.
I think there was an assumption that the Manndoc accommodation would be satisfactory for the extended MED Service.
The point I was making, really, I think, is accepting the point in relation to the new hospital: as I said before, planning for the new hospital did not take into account a requirement for a MEDS unit, which would be purposely provided and, therefore, more satisfactory than using accommodation which is used for other purposes.
The Chairman: Did the Department not envisage that the MEDS would have to come out of the old Noble’s site?
Mr Wilson: I think it was recognised, at that stage, that, as Manndoc was based at the old hospital, it was a fairly good position for it in a hospital, because if someone has a problem in MEDS, then it is easier to transfer that individual into the hospital. So, I think it was always recognised that, having established Manndoc at the old hospital, that we would have to be looking at some stage, to move it into the new hospital, but there was no final decision made on that There was no great discussion or consideration given to it.
Whilst there are benefits of having the Manndoc or the MEDS service in the hospital, it is not specifically required: it could be based somewhere else. It is just from a logistical point of view, it is probably better, and we take this view now: it is probably better for it to be in the new hospital.
I have to say there are different views on that, and there are some views which suggest that the MEDS service can be located elsewhere. The Department and the medical staff in the hospital - and I am not saying these views are necessarily shared by medical staff in general practice - but the view of the hospital is that it was better located in a hospital environment, for the reasons I have given.
If an individual patient attended a MEDS unit located away from the hospital, and an admission at the hospital is required, then, obviously, that would require an ambulance lO be called, and the patient transferred from the unit into the hospital. If the unit is based in the hospital, then, clearly, that would not be necessary.
So the view, strongly, of the Department at the moment is, that the MEDS unit is best placed in the hospital, although I repeat the Department accepts the accommodation in the new hospital is not purpose built and, therefore, is not totally ideal. The Department is looking at that currently, and is trying to address those concerns, which a number of people have raised.
Mr Jones: Can I just say, sir, it is probably fair to say that, had MEDS not been introduced on 1 st April 2003, then the accommodation issues we were faced with, we would have been faced with anyway, with Manndoc. It was an extension from Manndoc into MEDS, rather than introducing a brand new service, so Manndoc would have continued. We would have moved up to the new hospital, and we would still have decisions to make as how best to accommodate whatever out-of-hours service we were going to be providing.
The Chairman: But Manndoc, of course, was only a smaller group of GPs, as against all of the GPs.
Mr Jones: Of course.
The Chairman: Therefore covering a smaller area of the Island.
Mr Jones: A smaller area, yes, but with the similar size of accommodation.
The Chairman: Thanks for that Mr Jones.Could I take you back to the question about GPs’
responsibilities, please, Mr Wilson.
Mr Wilson: As I indicated previously, despite the fact that MEDS came in on 1st April 2003 in advance of the new contract, individual GPs remain responsible for their patients during that period up until 1 st April 2004, and that was full, total responsibility for them.
Responsibility means that if there is a problem with a service provided by a locum GP, or one of the MEDS or Manndoc doctors, then responsibility for that, in terms of action, would revert back to the GP with whom the patient was registered.
Now, GPs accept that, that is part of their terms and conditions of service. They accepted that was the case at that time. From 1st April this year, responsibility for the service in relation to a GP is that of the MEDS doctor. I am sure that answers the...
The Chairman: Well, it still leaves the issue of people trying to contact their own GP, if they have a problem with MEDS.
Mr Jones: Can I just say, sir?
The Chairman: Mr Jones, yes.
Mr Jones: MEDS, in terms of what we are saying and the responsibility of doctors, was a continuation of Manndoc, in that, under the Manndoc arrangements, an individual GP would have 24-hour responsibility for his patients, albeit he would have made arrangements for someone else to attend to that patient in certain circumstances.
That continued under MEDS: the doctor continued to have 24-hour responsibility, there was not any change in that respect The only difference, perhaps, was that there would be a greater number of GPs who might be acting on his behalf or her behalf when attending to a patient. The main difference from 1st April 2003 is not in the responsibility of the GP, but in the way the service was administered, and the fact that it was administered under a separate contract, whereas, previously, it had been administered under the same General
Tynwald Select Committee on GP Out of Hours Services - Evidence of Mr J Wilson and Mr A Jones
98 TGPS SELECT COMMITTEE, FRIDAY, 7th MAY 2004 Oral Evidena
Medical Services (GMS) contract as the doctor carried out all his other responsibilities under.
The Chairman: Thank you. Can I now go to Mr Gill to ask some questions.
Mr Gill: So, during that period between 1st April 2003 to April of this year, would the doctors have been receiving payments for a 24-hour cover which they were not providing?
Mr Jones; No, sir, they would be getting paid under a separate contract for the work they carried out as individuals, as part of the new out-of-hours service.
Mr Gill: -Thank you. Mr Wilson, you said a few things, that there was no planning for the MEDS facilities -
Mr Wilson: In the new hospital.
Mr Gill: - in the new hospital. The new hospital had no planned facilities for any out-of-hours GP services. Also, you felt, or the predominant view in the service is, that it is better to have Manndoc or MEDS service located within the hospital?
Mr Wilson: Yes, sir.
Mr Gill: So, does that indicate a lack of foresight?
Mr Wilson: Well, as I said earlier, MEDS does not necessarily have to be in the hospital. It is only by experience, really, that we found that is preferable to be there. One can accept that, knowing that the changes were being introduced under a new contract, it would have been better had something been planned for the new hospital; but the new hospital planning, of course, goes back to 1993, and by the time the Manndoc and MEDS changes were taking place, the planning of the new hospital was at a fairly advanced stage.
Mr Gill: I am not trying to be clever with hindsight, (Mr Wilson: No.) because I appreciate that that was a consideration you had. Would that additional year that you could have chosen, to defer adopting the MEDS system until this year, have given you more breathing space to have addressed some of those issues, though?
Mr Wilson: I have to say, I do not think so: bearing in mind the new hospital opened on 14th July 2003 and was in the commissioning stage at that date, that year would not have been particularly beneficial, in terms of locating MEDS within purpose-built accommodation.
Mr Gill: You also mentioned, Mr Wilson that, in fact, there were UK Health Authorities or Trusts who were impressed with the MEDS system here, and they were going to adopt it themselves, with a view to adopting it themselves. Are you aware, given the contract changes in the UK, of whether that has happened?
Mr Wilson: The new arrangements for out-of-hours services are now in place in the United Kingdom. The comments I have made are based on information I had
received from the late Primary Healthcare Manager, whc indicated to me that he had verbal contacts from forme! colleagues - he was a former primary healthcare managei in the UK - who are interested in what we are doing here and were looking to adopt some of the practices that w< had introduced.
Mr Gill: Finally, if I cant we have heard the concern that you initially outlined about the onerous workload a; the GPs described it in 2001 and some of the issues. One 01
those, I think we have heard, was about the work-life balance they were concerned about. Is this MEDS system from youi perspective, more driven by a value for money or a quality service perspective, or are you trying to marry the two?
Mr Wilson: My own view is that it has significan; benefits for patients. I know that is not the popular perceptior of the service, but in this way, under an arrangement where GPs had responsibilities for patients all the time and, in fact were called out regularly, for out-of-hours commitments then, clearly, that was putting them in a very difficult positior. to run surgeries the following day.
If you speak to GPs - and I am sure you have, the Committee has, in fact, spoken to GPs - you will not« that their life has transformed, and they feel that they are providing a much better service during the day time, tc the patients that they are seeing, in the sense that they are no longer tired and worn out from being up half the night previously.
From a patient perspective point of view, there is a feeling that the benefits to GPs have had a significant benefit also tc the patients they are responsible for.
The Chairman: Can I just bring Mr Gelling in, because I know he wants to ask a question. Mr Gelling?
Mr Gelling: I just want to follow up, if I could, Mi Wilson, inasmuch as I can understand points you made in your first presentation, about the concern. The first question, really, was to lead into it. Why was the letter, which sel this ail off, sent .to the Chief Minister? Is the contract nol with the Health Service and, therefore, would you not have expected that to have gone to the Health Minister or to the Administrator. Was it to raise the political profile of this?
M r Wilson: Well, that question I think is more appropriately addressed to the author of the letter.
The only comment I would make is that the letter, which is of November 2001, was somewhat in advance of the new contract itself, and the details of the new contract were nol specifically known at that stage. There were indications, certainly, in the medical press, that the out-of-hours service would be changing, but there was little detail at that stage as to what those changes would be.
Now, one can speculate as to the reasons why they wrote to the Chief Minister, but I would imagine that the one you have made reference to is probably not far from the truth.
Mr Gelling: I also took note: from what you said, the concern from the doctors was over work overload and not having a quality of life, and I can understand that, but with evidence that we have - obviously, we have noted on your MEDS - how many local GPs actually are on the MEDS. Would you not, therefore, have concern that, if they are doing
Tynwald Select Committee on GP Out of Hours Services - Evidence of Mr J Wilson and Mr A Jones
Oral Evidence SELECT COMMITTEE, FRIDAY, 7th MAY 2004 99 TGPS
their GP work and also on duty in MEDS, it is defeating the whole object of giving them the leisure time and the quality time, because if they are on MEDS, they will not be able to run the surgery the next morning. Does this concern you as an administrator of the hospital that, in fact, they are moonlighting in your hospital, and, therefore, not really carrying out their duty under contract, which is a GP?
Mr Wilson: Well, two comments to that. Mr Jones, I think, will give you some idea as to the involvement of existing GPs in the MEDS out-of-hours arrangements. It is patchy: some GPs will provide more commitment to the new service than others will.
One has to remember, of course, that one or two GPs are now covering the whole of the Island, and, therefore, the best slots within the cover are fairly well spread. It is not a commitment every week or every two days; it can vary quite considerably. There may be some GPs more than others who are involved, and, yes, if it became apparent that a GP was putting in a huge commitment to MEDS, then we would probably want to know the basis upon which that has been provided, and whether, in fact, it is impacting upon their normal responsibilities.
Mr Gelling: This is something you are keeping an eyeon?
Mr Wilson: Indeed.
Mr Gelling: Had you anticipated that, because the 24- hour responsibility of the GP has now been removed from the patient, have you anticipated that there are patients who now, very readily, use MEDS as a second opinion, because they get far quicker response, they do not have to wait days for an appointment, they get immediate attention?
So, therefore, is there not a likelihood that you will actually do the total reverse, and have to boast up your MEDS and, therefore, do away with GPs altogether? In fact, you could run the whole business yourselves, if you are running it for half the time, anyway. Why do you not run the whole business of GP cover from the DHSS?
Mr Wilson: One has to distinguish sir, between General Medical Services (GMS) and what are out-of-hours services. Out-of-hours services are, essentially, emergency services where an individual has a problem. General Medical Service, on the other hand, is a service which is available to the whole of the population, which would not really be classed an emergency service, at all.
So, I do not think that the proposition that you put to me would, in fact, be appropriate. The out-of-hours service is being managed, we feel, reasonably well, but it does not compare with the numbers of patients which are going through general practice, on a daily basis. In fact, I think the last figures I looked at, there were something like half a million GP attendances on the Island every year. So, that is significant: the numbers going through MEDS are very minuscule, compared to what goes through GP surgeries in the daytime.
Mr Gelling: Just following that up, because John has not quite answered the question about the increase that I am told is happening, that people are .finding MEDS is a very good way of getting a second opinion, and they reply
to you urgently: do you not see that that perhaps is going to be something that will grow? In fact, have you any evidence that it is growing?
Mr Wilson: Mr Jones has got some information data, which you might be able to -
Mr Jones: We do not have data in terms of the type of consultation: that is not readily available. I cannot comment, really, on what you say, sir, but we could certainly look at that. There is no evidence that has come forward, at the moment, to say that those sorts of enquiries are increasing.
It is difficult to comment without any information.
Mr Wilson: I think there is some anecdotal evidence that an individual who would otherwise have to make an appointment and attend a GP practice, could be seen more quickly if they contacted the out-of-hours service. Whether that is translated into a significant workload on the out-of- hours service, which may grow, again, we could speculate on, and the Department is closely monitoring the attendances. If that turned out to be the situation then, clearly, we would have to address it, and understand precisely why people are attending MEDS.
We must remember that the MED service is, essentially, a telephone contact, initially, and if the GP who answers the phone, feels that it is not appropriate to see that individual patient, then, clearly, they would ask them to attend their GP practice the next day. They would not be seeing patients simply because a patient wants to see the GP; they would enquire what the circumstances were and whether a contact was necessary.
The Chairman: Mr Gill.
Mr Gill: Just a couple of points, please. If we just go back to the issue about 24-hour GP cover, that would actually be a practice cover, wouldn’t it, rather than an individual GP? So, for example, I have the privilege of living in the south, if my wife had a GP and I had a different GP in the same practice, we would not be calling each of those out in the middle of the night; if we were in - ?
Mr Wilson: No, you would be calling the practice, and the on-call doctor for that practice would be responding to you as a patient.
Mr Gill: So, for a larger practice you will be dividing that responsibility by the number of people who would be available.
Mr Wilson: Absolutely.
Mr Jones: I think just to clarify, the 24-hour cover is 24-hour responsibility to make sure something is in place for that doctor’s patient to be seen, not 24 responsibility to attend to that patient.
Mr Gill: But if attendance was required, that would be one of those people covered within that practice?
Mr Wilson: Yes.
Mr Gill: So, there is no certainty that GPs have their own list?
Tynwald Select Committee on GP Out of Hours Services - Evidence of Mr J Wilson and Mr A Jones
100 TGPS SELECT COMMITTEE, FRIDAY, 7th MAY 2004 Oral Evidenct
Mr Wilson: No.
Mr Gill: Secondly, you were kind enough to relate your understanding of the response of GPs now, to the arrangements, feeling that their quality of life had improved. But the question I have asked was: from your service perspective, when you anticipated the UK’s contractual changes and you introduced a year ahead of them, and the deadline, effectively, for yourselves, is that about value for money or is that about a service quality improvement for yourselves?
Mr Wilson: I would not want to suggest, in any way, that the arrangements which have been made, in relation to MEDS were, in any way, connected with financial considerations; they were not.
The decision to introduce the MED service reflected the concerns that the profession and, indeed, the Department had, in maintaining existing GP services on the Island. Therefore, when one mentions value for money, one always feels there is a connotation that this is being done because of costs, and so on. That was never a consideration in relation to the new service.
Mr Gill: So, it was professional service/advantage to the patient? (Mr Wilson: Yes.) Thank you.
The Chairman: Could I just, before you go on, follow that up, if I may, Mr Wilson? What you have said about the cost: are you, and is the Department, satisfied that in not restricting it down to a cost base, to say, ‘That is all you can have’, that, in fact, what is being paid is value for money?
Mr Wilson: The Department feels that the current arrangements are certainly providing value for money. The point I was making, sir, was: saving money is the suggestion that is often made, ‘this has been done as a cost cutting exercise’ and so on, could not be further from the truth. In fact, the new service is costing the Department increased funding.
The Chairman: The increased funding: you are satisfied it is necessary to provide and secure the service.
Mr Wilson: Yes, exactly, so increasing money is necessary for that purpose. The out-of-hours is only one part of the new GP contract, it is only a part of it; there are a lot of other parts to it.
By way of an example, the Department, in an attempt to assist GPs, has introduced additional support for practice staff, nursing staff, for example, in order to relieve GPs of work which, clearly, they do not need to be concerned with, they can be managed by nursing staff. Now, full 100 per cent funding is provided, through the contract for, for example, practice nurses, with the sole intention of trying to ensure that GPs are doing work which they are best at, i.e. dealing with the clinical and medical needs of their patients.
The Chairman: That is fine, thank you.
Mr Gill: Can I just make clear: I am not trying to suggest for a moment that there is any suggestion of doing things on the cheap or cost saving, and what you have just described is value for money.
Mr Wilson: Yes, sir.
The Chairman: Mr Singer.
Mr Singer: It was said, earlier on, that Manndoc wher into MEDS which we all know, but is there not a majoi difference between the running of Manndoc and the running of MEDS, in that with Manndoc, that was a doctor’s choice and they financed it, basically, themselves, but the DHSS ha: now chosen to fully fund MEDS? So, can you tell me: wha was the cost to the DHSS, when Manndoc was in force, anc what is the annual cost now that MEDS is in force?
Mr Jones: Well, the overall cost, now that MEDS ii in force, during the year ended March 2004, was just ovei £500,000. But that is not all additional money: prior to the introduction of MEDS, even though they were operating i Manndoc service, GPs were getting paid out-of-hours fee'- annual fees, plus night visit fees. It was that money thai they were using, mainly, to fund the Manndoc service. ] have not got those figures in front of me, but I can certainl) get them for you.
But the total cost of just over £500,000 will need to bi compared to what the total cost previously was, in othei ways, in items of service fees, which were paid to GPs, which ceased on the 1st April 2003. In other words, when you saj the GPs were funding Manndoc, which they certainly were they were utilising their item service fees that they got frorr the Department, to provided an out-of-hours service toward« the cost of Manndoc.
Mr Singer: That was £6,000 per head, wasn’t it, pei doctor, for those who were in it?
Mr Jones: No. There were two fees: the night visit fees, which were based on every visit that was paid or every patiem that was seen out of hours; and then there was the out-ofhours set amount. They would have to be added together and calculated, which, as I say, I have not got the figures in from of me, but I can certainly get them for you.
Mr Gill: It would be helpful, if you can.
Mr Singer: I seem to recall Doctor Maska saying to us. when he gave evidence, that doctors were giving up £6,000 a year from that particular part of their contract. So, I assume that, similarly, any doctor who worked on Manndoc was getting £6,000 a year and putting that into finance the other doctors who were doing the out-of-hours service.
Mr Jones: Yes, doctors, regardless of whether they were operating within Manndoc or not, all got an out-of-hours payment. But the doctors who were in Manndoc were using that payment to help towards the funding of the Manndoc arrangements: in other words, paying the people who were acting on their behalf.
Mr Singer: So, if there were, say, 30 doctors in the original Manndoc, they were putting in £5,000 each, which is £150,000 a year, plus, I believe, the Department put in about £50,000, didn’t they, to finance the use of the car and a driver?
Mr Jones: That is right.
Tynwald Select Committee on GP Out of Hours Services - Evidence of Mr J Wilson and Mr A Jones
Oral Evidence SELECT COMMITTEE, FRIDAY, 7th MAY 2004 101 TGPS
Mr Singer: So, from £150,000 a year, it was suddenly now costing £500,000 a year.
Mr Jones: No, that would be excluding the night visit fees. I would have to get the figures, but I think we would find that the night visit fees, which were paid per patient seen, together with the set sum that was paid a year, would need to be calculated.
Mr Singer: A GP in a practice that was not in Manndoc would have received £6,000 a year, that part of the contract, for 24-hour cover. Did they then also receive a fee every time they were called out to a patient?
Mr Jones: Yes.
Mr Singer: How much was that?
Mr Jones: I think it was in the region of £2 to £3, but I would have to check with that.
Mr Singer: £2 to £3?
Mr Jones: Yes, but I would have to check with that: I have not got the figures in front of me. It is fees that are part of the comprehensive statement of fees and allowances paid to GPs, as one aspect of that.
The Chairman; I think, we would welcome it, if you could clarify that.
Mr Jones: I will do, yes, sir.
Mr Sjnger: It is only in a short time, in particular, today, that it has been confirmed to us that the GPs’ contract actually went on until 31st March 2004.1 do not know whether you are of the same opinion, but, certainly, the DHSS, last year, seemed to imply that the doctors were withdrawing their cover from March 31st 2003, because they said, *We have had a lack of time to do proper publicity’, but, in fact, it was the DHSS themselves who decided that the doctors would not be asked to complete their contract to 2004, but because the doctors were shouting, they said, ‘Okay we will let you finish on 31 st March 2003\
Mr Wilson: I think, with respect, there is a confusion here. The first point I would like to make, though: you say, sir, that this is the first indication that you had, today, with regard to the responsibility up to the 1 st April 2004. That information was, certainly, set out in a letter to the Committee, dated 25th March, by Mr Newbery, and I would refer you to that (Interjections by Mr Jones and Mr Singer) Very well, I just make the point that it was set out in that letter.
The confusion I think arises by the erroneous, but understandable, link with the services and the minor injuries unit at Ramsey Cottage Hospital. The Department has been negotiating with GPs with regard to out-of-hours services for nearly two years, as I say, since the letter to the Chief Minister from Doctor Maska.
The target date of the 1st April 2003 was part of those negotiations. The confusion, I think, with respect - 1 am not saying in the minds of the Committee, but it is certainly in the minds of some media coverage which we are aware of
- relates to the notice given by the Ramsey Group Practice to reduce their commitment to the Ramsey Cottage Hospital’s out-of-hours service, which, in fact, was a month’s notice.
So, I do not think it is fair to say that the GPs gave the Department some sort of ultimatum, or that there was a short period of notice. The decision to target the 1st April 2003 as the implementation date for the introduction of the MED Service was a negotiated agreement between the Department and the profession.
Mr Singer: So, if the Department had decided that, in order to make better arrangements for the MED Service, they were not going to actually introduce the MED Service until the new contract 1 st April 2004, would the doctors have been obliged to have completed their contract, with the 24-hour cover?
Mr Wilson: Yes, sir.
Mr Singer: We talked, before, about the amount of time that doctors are putting into the MED Service, and I think it was said that you would be looking at whether a doctor had a high input, and, if the doctor was putting in a high input, you would be asking why. What would you consider a high input?
Mr Wilson: Difficult to answer that question, but if it became clear that an individual full-time practising GP was providing out-of-hours service on a regular basis - and ‘a regular basis’ is a bit subjective, I accept - then the Department would need to be satisfied that that individual was able so to do, at the same time as honour his commitments to his general practice during the daytime.
I do not think I could comment, specifically. I think the Department has set an indicator, a line, if you like, over which, if a doctor provided two night’s service, then we would question him; it would be something we would be looking at over a period of time, perhaps a few months, and if that became obvious that there was a total commitment there, then we would perhaps want to have a look at that.
But I would just comment on this point to you, and it is: one should not imagine that it is particularly easy to recruit doctors to provide out-of-hours services; it is not. GPs, by and large, are interested in some of the slots, but the more unsocial hours’ slots are not easy to fill.
It is often an issue for Department officers to be contacting GPs quite late, in terms of the arrangements need to be made, in order to fill slots, which previously were vacant. We have done a lot of work on that, and we have a rota in place, now, which I think extends for a 12-month period ahead -
Mr Jones: I have heard it is up till March next year.
Mr Wilson: - until March next year. But in early days, particularly, there were significant problems in actually filling some of the more unsocial hours, nature of the out- of-hours GP...
So, I do not want to give the impression that GPs are falling over themselves to provide the service.
Mr Singer: We are now 12 months later, though, and the rotas are all filled.
Mr Jones: No, sir. They are not filled, no. There are gaps
Tynwald Select Committee on GP Out of Hours Services-Evidence of Mr J Wilson and Mr A Jones
102TGPS SELECT COMMITTEE, FRIDAY, 7th MAY 2004 Oral Evidenci
which are continually monitored, and on occasion, as Mr Wilson has pointed out, the manager in charge of the rota will have to ring round and fill those gaps.
For example, I got a copy of this rota in the last couple of days, and there are presently gaps on Saturday afternoon- 22nd and 29th May - which are not filled at all, and need to be filled by two doctors; and Bank Holiday Monday, 31st May, afternoon. They will be filled, but they are not filled easily, and they are not filled immediately.
Mr Singer: But we do know that there are doctors who are running a GP practice, they are working on MEDS, they have got further employment, separate to contracts within the Health Service. How do you ensure that there first priority is to their patients as a GP? Where do you draw the line there?
Mr Wilson: As I indicated to an earlier question, this is a difficult issue to address. The Department, as I have said, previously, cannot be specific. We chase a certain amount of work and you cannot work beyond that.
There will be occasions where GPs and, indeed, doctors generally, are providing a more onerous commitment than we wish them to do so. The Department’s first concern is to its patients, and, indeed, the service’s first concern is the patients. So, it will be, occasionally, necessary for an individual to provide a service, or fill a service, because of the absence of someone else so to do, in circumstances where preferably we would prefer someone else could do it.
But I cannot be precise, a doctor does 40 hours and, therefore, cannot do any more than this. This is a huge issue within the Health Service, as to the extent of work doctors can do.
There is some guidance being made available, and which the Committee may be aware about, under something called the European Working Time Directive, which attempts to place a limit on the number of hours that individual commissions can work, beyond which they require a specified period of time off - rest period, as it is described- after they have worked that specific amount of time. This is particularly relevant in areas like junior doctors’ cover, in hospitals overnight. All staff will be subject to this European Working Time Directive, and, I suppose, if one is looking for a guidance as to when an individual is more committed than is good for him or his patients, then reference to the Working Time Directive is likely to be the benchmark that Departments will be having to look at in the future.
The Chairman: Could I just come in, just follow up the issue of the work of the GPs. One of things that we have identified in evidence, which it would be helpful if you could comment on, is that we have been told by the GPs and by their association, and in writing and orally, that, in fact, the pressures they have at work and the long hours are telling on them, and they do not want to work these long hours. Yet, on the other hand, we have evidence of GPs who are working long hours out of their own choice, and, in fact, 1 would like to, maybe, ask you to explain: how does the Department see, for example, when we have GPs who are spending half their week, or less than half their week, working within the hospital system providing services as well as being a GP, and yet the Department has a difficulty and the GP surgeries, the practices, have a difficulty getting enough GPs to provide the service to the public at the ground level, in terms of through
their GP surgeries.So, we have a situation where some of those GPs art
doing quite long hours working within the hospital system Why does the Department allow that to happen,, whilst then is pressure on the GP service? Is there a conftision? Is it i matter of necessity? And how does the Department see tha in the arguments being put forward to yourselves, as the) have been, and have been put forward to us, that, in fact one of the problems is the amount of long hours the GPs ar< doing, and yet, they are consciously some of them taking those long hours on, doing a different job, if you like, b) working within the hospital system.
Mr Wilson: In attempting to respond to that, one ha! to recognise that it has always been a tradition within the National Health Service that GPs do take up what are callec ‘clinical assistance roles’ in hospitals. This tends to be ir specialist areas where they feel that to gain a knowledge i; helpful to them and their ordinary patients.
For example, we have had clinical assistance provided b) GPs in area like obstetrics and gynaecology, diabetes, ENT but, in recent years, that sort of commitment has, in fact reduced. We have far less clinical assistance in our hospitals than we had previously, and I have been there long enough to see this happen: there has been a reduction.
One has to bear in mind that, if a GP is working in i hospital, performing a clinical assistant role, it is normall) for a small number of sessions: something like one to twc sessions a week, a session being half a day. So, it is no! a significant commitment that GPs have, in working ir. hospitals. It tends to be, as I say, one half day or maybe twc half days a week and in so doing, they are actually doing ii at a time when otherwise they would be working in genera] practice.
So, clinical assistants have not tended to be working as GPs full-time in their practices, and then beyond thai working in hospitals. They tend to be working in hospitals as part of. their normal working week: in other words, the practice has agreed that one of the partners, every Thursday afternoon, attends the hospital to provide a clinical assistani role in ENT, for example.
So, I think it would be wrong to suggest that where GPs do carry hospital commitments, they are not doing it, necessarily, on top of a full-time GP responsibility. They tend not to be doing that; they would be doing it within their normal working week.
The Chairman: So could I ask: how does the Department monitor that to ensure, that, in fact, what you are saying, in terms of what are the sessions, is actually controlled. For example, would the Department find it acceptable if any ol the GPs were working say three days in their surgery and two full days in the hospital?
Mr Wilson: As I say, I do not think there are any GPs currently working two or three days in hospital. The clinical assistant tends to be one half day a week or perhaps one day a week.
The Chairman: And do you monitor that in the Department?
Mr Wilson: When posts are available they are advertised, it is during that interview for the post that the panel which
Tynwald Select Committee on GP Out of Hours Services - Evidence of Mr J Wilson and Mr A Jones
Oral Evidence SELECT COMMITTEE, FRIDAY, 7th MAY 2004 103 TGPS
consists generally of Health Service managers would want to be satisfied that an individual is capable and able to carry out that hospital commitment, bearing in mind that they are also full-time GPs. So, the monitoring is done at the appointment. It would not be appropriate to appoint a GPto, as you suggest, a three-day week in the hospital, if he had a full-time GP responsibility: it just would not be appropriate to do so.
So, we at the panel and, indeed, the practice and the other partners in the practice, would need to be satisfied that one of their partners was providing this role, bearing in mind they had a full-time GP role, as well.
There may be, and I cannot say that there may not be, concerns in some areas, and I am speaking generally. But generally speaking, that issue has not arisen.
Mr Jones: In terms of the out-of-hours rota, sir, if I just make it clear: there are a number of GPs in GP practice, who choose not to participate in the out-of-hours rota, and there are some GPs who, perhaps, participate very infrequently. There are qualified doctors not operating as GPs who do sessions, as well.
It would be very unusual - and I just had to confirm this to myself, looking at the rota - to have any GP doing more than one session a week - very unusual, indeed.
The Chairman: This is the MEDS?
Mr Jones: This is the MEDS, yes. I am aware of particular GPs who choose sessions - maybe an evening session - when they know they are off a halfday the following morning, and they do so, intentionally.
The Chairman: We were provided with a copy of the... to show a pattern of how it works. One thing that we did notice was that, in fact, some GPs were content to regularly take what I suppose would be classed as the ‘prime spots’ in the rota. As it is self pleasing, in a way, they decide what they want, does that not cause any concern? In other words, the most lucrative payments for certain MEDS sessions tend to go to one or two of the GPs?
Mr Wilson: Well, to be fair, that may reflect the fact that sometimes the lucrative ones, as you describe them, are the ones that are most difficult to fill, which is why the rates are perhaps slightly higher than at other times of the week.
It is difficult to say. There are sessions which are attractive to GPs either because of the fee or they are attractive to GPs because it is a part of the week that suits the rest of their working week. It may be attractive to GPs because it is particularly quiet or particularly busy, so it is difficult to say what attracts a GP to a particular session.
The Chairman: I suppose the point I am getting at is: is the Department, which is ultimately responsible for the service, satisfied that a regular pattern does not affect the good operation of the GP surgery, because of the operation of a doctor being in MEDS at certain times, regularly. And if you are not sure, do you have a system to monitor it?
Mr Wilson: We have no evidence sir - and that is the best answer I can give - that, in fact, the commitment GPs are giving to the out-of-hours’ service is affecting the service they are providing in general practice.
The Chairman: Okay. Mr Gelling, then.
Mr Gelling: Could I just go onto something entirely new, actually. I listened very carefully this morning to a radio broadcast about a new Bill - a Health Service (Amendment) Bill - which was going to make; the Isle of Man much more attractive to GPs to come to serve here. Are you in position to perhaps give the Committee some indication of what that might be, or is there a copy available?
Mr Wilson: A copy of the Bill? (Mr Gelling: Yes.) Yes, there are copies of the Bill, certainly. I think it was at its First Reading last week.
The new Bill, in essence - and I am not prepared, I have not got that information with me, but to my knowledge of it - I believe, will change the way in which GPs - well, Primary Care Services generally, not just GPs - are managed, switching from a management by regulation to management by contract.
So, in the future the Primary Care Services will be based very much on a contractual agreement, rather than by formal regulations. That is my understanding of it.
Now, to go on to take the second point of that question, then: if it is established by contract rather than by regulation, then it is in line with what will be the situation in the United Kingdom, as a result of the new contract, and it is providing services on the same basis as is available in the United Kingdom, we feel will allow us to compete in attracting practitioner services to the Island, because they will be employed in - 1 was going to say ‘looser’ way, but it gives the wrong connotation - in a more flexible way than they are currently managed, which, as I say, is very much by legislation.
Mr Gelling: I apologise, Mr Chairman, for the question, but, of course, you must appreciate that on this Committee there are three hard-working Members of the Legislative Council, who are not in the Keys, so, therefore, we have not been party to the Bill. The positive spin on this morning was that it was something new for the Isle of Man, but, in fact, it is only a copy, really, of the United Kingdom scheme.
Mr Wilson: It follows what is taking place in the United Kingdom.
Mr Jones: What it does, if I could just explain is: it introduces a degree of flexibility, in terms of having contracts with individual practices, which allows doctors who have a particular expertise in an area, or are able to provide a particular service, as what is termed an ‘enhanced’ service, which the Department may wish to be provided to the patients of the Isle of Man, to enable them to do that in negotiation. So, it widens from, perhaps, a more rigid system of regulation to allow that flexibility to take place.
The Chairman: 1 think we have to stop that subject there, because it is a Bill before the Keys, and it is really not appropriate for us to investigate it too much. Mr Singer.
Mr Singer: I have two points, just following on what I was asking before. You talked about the fact that the MEDS is more expensive than Manndoc, and there was not a cost restriction, MEDS had come in because of the service that the Department wanted to introduce. Would you agree or confirm
Tynwald Select Committee on GP Out of Hours Services - Evidence of Mr J Wilson and Mr A Jones
104 TGPS SELECT COMMITTEE, FRIDAY, 7th MAY 2004 Oral Evidena
that, in fact, even now, there is no cost restriction on MEDS, if it was found that it could provide a more comprehensive and better service than it is providing now?
Mr Wilson: The Department, within its business planning, has identified additional costs* which will be necessary, in order to fund the new contract. Therefore, the new contract requirement for GPs will be significantly more costly than the existing arrangements. But they do bring with them a high degree of reform in the way in which services are being provided, with a much heavier emphasis towards quality, as opposed to simply paying GPs for the amount of patients on their list, which is the existing arrangement or was the existing arrangement prior to 31st March this year.
So, yes, there will be increased cost, they have been identified but they reflect what the new contract’s aims are, and that has introduced much higher quality services. Mr Jones has mentioned, for example, the potential for introducing enhanced services by various GP groups, which currently may or may .not be available to their patients.
Tony, would you like to give an example of an enhanced service which might be possible?
Mr Jones: Yes. Enhanced service may well be services which are provided on a limited basis at the moment, but not in any structured way, and they could involve direct access which sets down criteria, in terms of the access a patient has to his or her doctor, within certain time periods, and there will need to be procedures put into place.
There is provision for minor injuries in certain outlying areas, which will require specific designated rooms to be set to one side, but may take pressure off the A & E Department. There is a lot of emphasis on these enhanced services of shared care with the secondary service. It is not just a case of introducing something separate; it is trying to decide where is the most appropriate place for these services to be provided.
There are a number of enhanced services, some of them nationally recognised, and others which will be up for local negotiation.
Mr Singer: If you could find you could produce an enhanced service for out-of-hours provision, is there a cost restriction on that?
Mr Wilson: All Departments, as you will appreciate sir, are subject to the budgets which are being made available to them, and, therefore, the Department of Health and Social Security like any other Department has to work within those constraints.
The out-of-hours service is now totally separate from the GP contract - totally separate - and, therefore, the Department has decided on the current arrangements as being the most appropriate within the resources available to us - and when I say ‘resources’, I do not just mean financial resources, but also within our ability to recruit and retain professionals to provide that service.
Mr Singer: Finally, Mr Wilson, can you therefore confirm to me that it was the Department’s intention and commitment to introduce the MED Service on April 1st 2003, a year before the new contract, and it was not introduced because of any threat from the doctors to withdraw their cover; it was an actual Department decision to introduce it?
Mr Wilson; It was a recognition that doctors wen having serious concerns in their ability to continue to providt services, in the way they had traditionally and historicall; been providing services. Therefore, the decision to move t( the 1st April 2003 was one taken jointly by the Departmen and the profession.
The Chairman: Can I just read a minute, if I may jus interject, then I want to go on to Mr Gelling: in a letter 25tl March 2004 from Mr Newbery, on the second page, there is; paragraph there which is about the working group’s meeting that was held on the 17th April 2002. It relates to the recordet matter about the separate contract, and in there it says, anc I am quoting from the latter part of that:
‘Mention was made that GPs currently have to pay more to be par o f Manndoc than they are paid by the Department for out-of-hour cover’ .
He then goes on in his letter, to say, in the paragraph undei that, and I quote again:
‘From this meeting, a decision is taken to move to extend the out of-hours service to include all GP practices, with ad m in istrate responsibility passing to the Department. It was also decided to changi the name o f the service to M ED S, with implementation dates set t< bethe 1 st April 2003 ’ .
The difficulty I have, in reading that, is that, in one meeting, it seems, it was mentioned there was a problem ol cost to the GPs for the operation of Manndoc, and at the ver> same meeting it was determined to transfer everything ovei to the Department, from the 1st April 2003, call it MEDS. and the Department would take over substantial proportion of the cost.
From a political point of view, it seems a very efficient meeting, that at that one meeting, when suddenly it was. as recorded, ‘mentioned’ that a decision was actually determined. I just wonder if you are able to comment on that. I am not sure whether Mr Wilson or Mr Jones, either of you, are on that working group or whether you have background knowledge to be able to respond to that, but I just wondei if you are able to.
Mr Jones: Well, I think all we can say is that, from our involvement in it, the decision regarding the ongoing provision of out-of-hours services, as with all the other services that were being negotiated, was taken over a prolonged period of time, in negotiation with the profession.
I can understand your view, reading that, but if that is indicating that all the decision and all the discussion regarding this took place at one meeting, it is misleading.
The Chairman: But that is what it says.
Mr Wilson: I’ll read the quote.
The Chairman: Okay.
Mr Singer: In that quote, Chairman, it says that Manndoc had been a helpful step away from providing practices with their own out-of-hours cover, GPs thought it was a heavy workload to undertake - they found Manndoc heavy. Does that mean they found Manndoc heavy to undertake or just the out-of-hours cover?
Tynwald Select Committee on GP Out of Hours Services - Evidence of Mr J Wilson and Mr A Jones
Oral Evidence SELECT COMMITTEE, FRIDAY, 7th MAY 2004 105 TGPS
Mr Wilson: Well, 1 am reading the quote. I think the quote says:
‘Although Manndoc had been a helpful step away from practiccsproviding their own out-of-hours cover, GPs felt that it was a heavyworkload to undertake as well as full-time general practice’ .
Mr Singer: Taking that into account, and the fact that whilst we have now gone to MEDS and there is a pool of more doctors, in fact, the Ramsey doctors in January, February and March only undertook 6 per cent of the total cover. So, basically, the GPs who were in Manndoc are having the same load on them now, except they are getting paid a lot more money; would you agree?
Mr Jones: No. I think it is fair to point out that there are a number of doctors who previously were not involved in Manndoc, beyond those who were in general practice outside of Manndoc, who are now covering a lot of the sessions. So, the impact on individuals because of that, in the main, is far less than it was when they were operating Manndoc.
The Chairman: Mr Gelling.
Mr Gelling: Taking your point, Mr Speaker, I do not wish to raise anything that is’before the House of Keys. However, could I just put it to you that you did mention that doctors are under regulation; in future, they will be under contract, and could I take it, from what you have said, that each contract could, in fact, be a bespoke service for different practices?
Does that, therefore, not mean that, perhaps, taking Mr Jones’s point that - let us take Ramsey - in fact, the Ramsey Group Practice, with their specialities, could, in fact, have a contract which would be totally outwith the contract of, perhaps, a Douglas practice, that is adjacent to the acute hospital, and that they could, in fact, go and have a contract that would completely, once again, restore a 24-hour practice - 1 am only saying this as a point - and that MEDS, therefore, is only an interim measure, until that contract has been, in fact, negotiated? And, can I say, before that, that the same thing could happen in the south, in the Southlands area?
Mr Jones: As far as the out-of-hours specifically is concerned, the new GP contract allows practices to opt out of their out-of-hours’ arrangements. It also, by definition, allows them to opt in. So, if Ramsey GPs or southern GPs, for example, wish to continue to provide their own out-ofhours, as a practice, then there would be nothing to stop them doing that.
As far as a bespoke contract is concerned, the basis... and we have to remember this is a general practitioner contract, not just a contract which may take on board anything outside of general practice. The main contract will be similar for all practices, but there will be add-ons, there will be slight variations, depending on the types of enhanced services, particularly, that that practice will want to provide.
The Chairman: Thank you. Right. Mr Singer.
Mr Singer: Can we change the subject a little?
Mr Gill: Can I - ?
The Chairman: Same subject? (Mr Gill: Yes.) Right,
we first go to Mr Gill. I want to try and wind up now, so, Mr Gill, I know you want to raise some other questions.
Mr Gill: Could I ask: how do these bespoke contract arrangements that Mr Gelling has touched on and you have just advised us, Mr Jones, reconcile with the DHSS policy of providing a uniform service across the Island?
Mr Jones: The uniform service will be the main basis of every contract. If there is a bespoke contract, it will be over and above that, to reflect any particular expertise an individual practitioner might have, that he may wish to contract, or negotiate with the Department, to provide such things as enhanced services. There will be a quality contract which applies to all practices.
Mr Wilson: I would just give you an example of that, by saying that if a practice had, in their area, a nursing or residential home which they felt they would like to provide some services beyond normal general medical services, then that would be an issue that the practice could raise with the Department, and an enhanced arrangement could be made, to pay for that additional service. So, you see, you can bespoke, in the words of Mr Gelling, a service to a particular area and a particular practice.
Mr Singer: Could I ask you on recruitment of doctors: could you tell me how doctors are recruited as GPs, and how doctors are recruited for the Isle of Man hospitals? What is the difference?
Mr Wilson: Taking the hospitals first, they are subject to the regulations called the Appointment of Specialist Regulations, and consultant staff would have to apply for a vacant post and be interviewed, under those Regulations. The regulations are fairly comprehensive, are consistence with appointment of specialist regulations elsewhere, i.e. in the United Kingdom, and require, for example, the normal checks on registration and bona fides, and the appointment panel would include on it an external assessor, generally from the Royal College* to assess the competence and appropriateness of the person who is applying for that post.
So, hospital staff are employees, in other words, and they are appointed in a very similar way to most employees in secondary care.
Mr Singer: That is consultants; what about general doctors, A & E, et cetera?
Mr Wilson: Consultants and the non career grade staff i.e. staff grade posts, associate specialist posts and the like, would be appointed under those same arrangements. Junior staff, on the other hand, are generally appointed under an arrangement the Department has with a UK university and through the Merseyside Deanery, and they would be generally appointed under that arrangement, and cooperation with university concerned.
GPs, on the other hand, are self employed, and, therefore, they are not, by definition, employees of the Department, and we would expect the individual practices to be responsible for appointing their own partners. Each GP who would then be appointed would have to apply to be included on what used to be the medical list - it has now changed to the -
Tynwald Select Committee on GP Out of Hours Services-Evidence of Mr J Wilson and Mr A Jones
106 TGPS SELECT COMMITTEE, FRIDAY, 7th MAY 2004 Oral Evidenc
Mr Jones: Yes - performers list
Mr Wilson: - ‘performers’ list’, and they would then be appointed to this performers’ list which would entitle them to work as GPs on the Island.
But the responsibility, essentially, for appointing and selecting to GP practices rests with the practice themselves.
Mr Jones: There are just one or two exceptions to that, if I might say so. One, perhaps, does not apply so much now; in the case of a single-handed practice, which we do not have any more, it would be the responsibility of the Department to appoint a replacement to a single-handed practice. In addition, if we were setting up a new practice which, in fact, we are doing at the moment in Douglas, then it is the responsibility of the Department to appoint, as we have done, a lead GP to start that practice off. He would then be responsible for interviewing and appointing his associates, as partners.
Mr Singer: When you appoint people to the hospital, are you quite sure you just rely on a UK university? Do you not use agencies when you want doctors or housemen, or agencies to recruit on your behalf in the UK?
Mr Wilson: Junior doctors would not be: junior doctors are appointed through the deanery, and they come for fixed stints of time - sue months, 12 months, fixed-term contracts. Everyone other than junior doctors would be appointed through, possibly, by agencies or the assistance of agencies, but also by direct adverts by the Department in the normal medical journals, and so on.
Mr Singer: We hear, they talk about, there may be difficulties in recruiting GPs et cetera, what is the position with recruiting hospital doctors? Do you have great difficulty or are people happy to come here for experience?
The Chairman: Sorry, can I just interject: I am just a bit concerned we are drifting away, unless there is a reason for it.
Mr Singer: Yes, there is a reason, Chairman. It is just - we were talking about recruiting doctors, generally - whether we can, in fact, recruit doctors, in a GPs’, or people to do out-of-hours or to be replacement GPs in hospitals, who are not necessarily GPs, but are doctors. It is a case of, if we can get a service for recruiting people for the out-of-hours service, or even to replace doctors back in Ramsey, and take away the GPs away from that hospital, whether it is difficult in recruiting doctors generally.
Mr Wilson: It is patchy is the answer. Some specialties are. extremely hard to recruit to, others less so. So, it is not possible to be specific.
I can give you an example: consultant psychiatrists are extremely difficult to recruit, as, indeed, are consultant paediatricians. On the other hand, the evidence suggests, currently, that there is less problem in appointing, for example, consultant obstetricians and gynaecologists. So, it is patchy.
A large degree of the problem we are facing at the moment is that, in recent years, there has been a very high
level of specialism. You cannot get generalists any more You cannot get a general surgeon; you get a surgeon wh is a vascular surgeon, or an urologist. Generalists are ver rare these days, and, in some of the sub-specialties, they ar extremely hard to recruit posts.
Mr Singer: No problem with doctors at A & E and junia doctors and housemen?
Mr Wilson: A & E is not a particularly easy post t< appoint to, I have to say.
Mr Singer: Can I turn to the ambulance service? Can yoi tell me how the service works and how the paramedics ari intended to work as the first responders, if an ambulance i: away from an area? What is expected of a first responder?
Mr Wilson: You will have to forgive me: I am not ai expert in ambulance services. My understanding is that a firs responder paramedic, by definition, again, would assess th( nature of the casualty that he or she comes across, and makt a judgement as to whether or not treatment can be providec there and then, or whether alternative services would be necessary, by a follow-up ambulance with a full team.
Mr Singer: So, if an ambulance is not there, a firsi responder would be sent out to assess until the ambulance arrives?
Mr Wilson: Indeed, that is my understanding.
Mr Singer: Well, I understand - perhaps Mr Jones may be able to confirm this - that now the situation is that a first responder does not necessarily have to be or live near the station from which they are responding. And I understand- perhaps, you could confirm this or deny it - that it is possible - and it does happen - that the first responder for, say, Ramsey or for Port Erin, can live in Douglas.
Mr Jones: I am certainly not aware of that, I have not got that information. I can neither confirm it or deny it I am afraid. Again, it is something I shall make enquiries about.
Mr Singer: So, who would be responsible for approving... surely it must be the Health Services somewhere, who would approve this as permissible or not? Because, obviously, the worry is that if you have somebody, say, in the north and the ambulance is in the south, and you send out a first responder, that first responder can take 30 or 40 minutes to get to this patient, if they are permitted to live in Douglas.
Mr Jones: My understanding is, and I would need to check, that the first responder in Ramsey who would respond in the absence of the ambulance because it is called elsewhere, would be a person who lives in Ramsey area.
Mr Singer: Well, can I tell you that I have had a letter from people in ah ambulance who are saying that it is not the fact, and I would like you to have a look at that; they are saying that in an evening during the week all three first responders to the Island can all be based in Douglas.
Mr Jones: Can I ask, sir, if you could let us have a copy of that?
Tynwald Select Committee on GP Out of Hours Services - Evidence of Mr J Wilson and Mr A Jones
Oral Evidence SELECT COMMITTEE, FRIDAY, 7th MAY 2004 107 TGPS
Mr Singer: No, sir, I cannot let you have a copy. I have got it here, but it is confidential and I do not want to reveal...
The Chairman: Could I just clarify the basis of the questioning is because: the out-of-hours’ GP service, if there is a difficulty in getting a GP, they might then ring up for an ambulance and the first responder is then elsewhere, and takes too long to get there... so, there is a link, albeit quite loose, but it does all interrelate to the out-of-hours’ service, hence the question.
So, 1 think if you are clear on the points that are raised, Mr Jones, then we will move on, okay? And you may wish to respond back to the Committee, if you would please.
Mr Jones: I will do.
The Chairman: Mr Gill, any final questions?
Mr Gill: Yes, please.If a GP accepts a place on the out-of-hours rota, and then
has to withdraw, or chooses to withdraw for whatever reason, do they have to justify that? Do they have to arrange cover or is that responsibility on the Division?
Mr Wilson: No, the full responsibility now for the out- of-hours’ MED Service rests with the Division, and it would be our responsibility to find a replacement for that individual who withdrew for whatever reason.
Mr Gill: And with those out-of-hours places being allocated on a volunteer basis, effectively, would that be accurate? (Mr Wilson: Yes.) That is accurate. Is that a positive development, would you say?
Mr Wilson: Well, one can always construct a case for appointing full-time doctors to run the out-of-hours service, but I am not sure that is a practical proposition, frankly, and we are really relying on existing GPs and others to provide us with this service.
I know there has been some work done on the possibility of appointing the odd GP on a full-time basis, who would be willing to do this. But, I have to say, it is a very unattractive post for an individual to take on - full-time out-of-hours cover for seven days a week! It is hardly practical, I would suggest.
Mr Jones: We have, obviously, looked at the options- many .options. It is estimated that there would need to be a minimum of six full-time doctors to man the out-of-hours
Mr Singer: How much would that cost?
Mr Jones: That would cost probably in the region of £600,000, but that is only an estimate in terms of the negotiations as to how much they would be expecting to be paid for working such unsocial hours.
Mr Gill: The worrying contingency that must have crossed your mind is that if, for whatever reason, either an individual GP says, ‘yes, I’ll cover at the eleventh hour, I’ll cover a particular shift or shifts, but it will cost you five times the going rate’ , or, indeed, if there is a corporate
group of GPs who say, ‘We’ll continue this arrangement, but the prices have doubled’. That is a concern you must have addressed.
Mr Wilson: Oh absolutely, the basis of the current payments to out-of-hours doctors is a negotiated settlement. There is no guidance available as to what you pay people to provide this service. It is a market place issue, frankly, and we are aware that other parts of the United Kingdom are paying significantly higher rates for out-of-hours cover than we have negotiated on the Island.
Mr Gill: I would hope that we could depend on the service ethic of our GPs, and I would not anticipate that they would succumb to such behaviour.
Mr Wilson: The indications are that the payments that are being made, currently, on the Island are within the broad parameters of what is being paid elsewhere.
Mr Gill: Mr Chairman, if I may, you mentioned your Department business planning and the need to, or your wish to, incorporate optimisation of the enhanced services that could be available, and as part of that you mentioned, I think, the Department’s intention, you described it, to provide minor injuries units around thé Island.
Mr Jones: Well, what, sony, perhaps I was misunderstood: that is one of the enhanced services that might be able to be provided in negotiation. It is one of the list of national enhanced services that could be available, and there has been an initial interest from a number of practices outside of the Douglas area in providing that. But there are laid down criteria, as I pointed out before: it has to be a designated room in a practice, it has to be available at all times and the intention would be to provide immediate treatment for minor accidents, to take pressure off the A & E Department. We have not actually negotiated any enhanced services of that nature at the moment.
Mr Gill: Just from the southern prospective, we are not in the fortunate position that we are with the MED Service, with the hospital not being planned into that, will you be bearing this in mind when you are looking at, say, the development of the old Southlands building that a minor injuries unit should be incorporated into that facility?
Mr Wilson: Yes, the old Southlands building is something that the Department is looking at currently, and there are a number of calls on the accommodation within that building. Clearly, whilst I could not commit the Department to providing a service in the way you described, that must be a possibility for the future.
I would, though, mention, talking about minor injuries units, provided by GPs, does not necessarily translate into a 24-hour minor injuries facility. A minor injuries facility of a room in a GP practice is to deal with it on a normal day basis. I cannot imagine there would be any circumstances where a practice would be prepared to provide a 24-hour facility for the population in that particular practice.
Mr Gill: But possibly an out-of-hours service
Mr Wilson: Again, as I said, out-of-hours is now totally
Tynwald Select Committee on GP Out of Hours Services - Evidence of Mr J Wilson and Mr A Jones
108 TGPS SELECT COMMITTEE, FRIDAY, 7th MAY 2004 Oral Evidence
separate from the contract, but if it was ever suggested or proposed by a practice that they would wish to talk to us about that then, clearly, we would be willing to do so.
Mr Singer: But the Department is not prepared then, or is not looking at putting a minor injuries unit into other areas than the one that is at Ramsey now.
Mr Wilson: No, sir.
The Chairman: Right, can I just then: two final points from myself, if I may.
Would it be a fair statement to make that since 2003, when the new MEDS came into operation, to date, that, in fact, the remuneration of the GPs has substantially increased for fewer hours?
Mr Jones: The cost of providing an out-of-hours service has increased to the Department. Who is in receipt of those payments varies compared to who was in receipt of the payments previously.
The Chairman: But prior to the 2003 agreement, the GPs had to provide the out-of-hours services as part of their regional contract for either small payments, you could argue - it depends on the context you put that into but, a reasonable payment may be a better word to use: We now have a situation where that has changed and the taxpayer, through the Department, is now paying substantially more for a service that is, or could be said to have been, reduced on what used to be available throughout the Island. Is that correct?
Mr Jones: I do not believe that is justified, sir.
The Chairman: Or would you not accept, in terms of there are now fewer GPs available at night time out of hours than used to be throughout the whole Island and, therefore, the population relies now on two GPs, whereas previously it relied on, I think, quite a larger number of GPs, because each practice, accepting that - I’ve forgotten the name of the one now that used to be - (Laughter) Manndoc (Mr Wilson: Manndoc.) - had grouped together one group, so in other words we now have normally two GPs available - one on duty, one on call. Is that right? For MEDS ?
Mr Jones: Yes, two on duty at certain times of the week.
The Chairman: Whereas before they would be on duty throughout all different practices.
Mr Jones: No, apart from Laxey, Southern and Ramsey- they would all be part of Manndoc, apart from Laxey, Southern and there would only be one GP on.
The Chairman: But there were more GPs available.
Mr Jones: Throughout the Island there would be, yes.
The Chairman: So we are paying more for less GPs out-of-hours? Is that fair? A fair statement?
Mr Jones: I am not sure where we link into that the
service that is provided.
The Chairman: I suppose that comes down to whether the Department has got in place ways of auditing the services that is being provided to the public for what the Department is paying to those who provide the service, and that is an issue I am sure, I would hope, that the Department has very much got in hand, because you must be able to assess the effectiveness of the service that you are now substantially paying more for.
Mr Jones and Mr Wilson: Yes.
The Chairman: Is that an issue the Department is dealing with?
Mr Jones: Well it is, but going back to what you said, 1 think it may be simplifying it by saying that you are paying more for fewer GPs. There, certainly, in an Island-wide situation, there are fewer GPs available; but it is what they are providing, I think, and who they are providing it to thal we need to look at.
The Chairman: Yes, but I mean the Department is nol monitoring it, yet
Mr Jones: Well, we are certainly monitoring the services being provided by MEDS on an ongoing basis.
Mr Wilson: Absolutely.
The Chairman: And there is a system in place then foi the Department to keep itself advised on the effectiveness and appropriateness of the service?
Mr Wilson: There is a number of ways in which the Department would monitor this service, and, indeed other services, and this Select Committee enquiry (Laughter), foi example, would be one way in which we would - because, clearly, you will have taken evidence from people who may have concerns on the basis, and we will need to evaluate what those concerns are, and will do so.
There is also the normal issue of complaints about the service, and we will need to explore the basis of those complaints, and whether they are a direct result, or otherwise, of the new arrangements.
The evidence we have available to us now, and we are now 12 months into the MED Service, the evidence that we have that the concerns which perhaps were initially being voiced have not proved to be as difficult as perhaps they might have been.
And, indeed, the same applies to the Manndoc service. 1 mean, there were concerns when Manndoc was introduced, as to whether they would be capable on the basis of one GP covering those eight practices to be providing the same level of service as previously was the case when the practice itself was covering its own patients, and let us remember the Manndoc service was covering not just one part of the Island, it was covering 75 per cent of the Island’s population, including areas as far away, if I may say, as Peel to Douglas and more to the south. Yet those concerns at that stage, and it ran for four and a half years, with Manndoc covering that three quarters of the population, seemed to have bedded in quite well.
Tynwald Select Committee on GP Out of Hours Services - Evidence of Mr J Wilson and Mr A Jones
Oral Evidence SELECT COMMITTEE, FRIDAY, 7th MAY 2004 109 TGPS
Now, there will always be concerns of a patient who calls a GP and finds that the response is not as good as they would have hoped, but, frankly, those concerns applied previously when individual practices were covering their own patients.
I mean, the Department has a very comprehensive complaints service in place, and I think the number of complaints that we have been handling in the last 12 months are... certainly, there is no indication they are anything significantly greater than they were previous to that.
So, in terms of monitoring, that is the best way to monitor services, i.e. listen to what patients and the public say about the service, and by and large, whilst there will be individual cases raised from time to time, which we need to address seriously, and establish why what is claimed to have happened has happened, to pretend that everything in place, previously, was superb and there were never any complaints is frankly not the case.
The Chairman: I am sure we recognise that. 1 think the main point I was trying to get over was that we now are paying substantially more, in terms of the service for out- of-hours, now, that we have.
Mr Wilson: Yes, I think I will just qualify that, we will be, we are paying significantly more for the new contract. The
new contract has introduced significantly extra costs, but, again, people have said before, that new contract is aimed at providing better quality services, so there is a high element of reform in the way in which services are being provided, in the future, but yes, the costs are increased.
The Chairman: And, presumably, with that is a procedure for the Department to effectively monitor the new contract
Could I just ask on that, we do not seem to have a copy of the new contract: could you forward one to the Secretary of the Committee, please? Okay? Right, Mr Gill, have you any last questions?
Right, can I then thank you both gentlemen very much for your time, and for being so open and frank in responding to our questions and we appreciate the difficulty that you have been under, in terms of personnel problems, and we appreciate your time. Thank you very much.
Mr Wilson and Mr Jones: Thank you.
The Chairman: Right, that concludes the public session, thank you very much.
The Committee sat in private at 3.55 p.m.
Tynwald Select Committee on GP Out of Hours Services - Evidence of Mr J Wilson and Mr A Jones
Appendix 8

Department of Home AffairsRheynn Cooishyn Sthie
Isle of Man■ Government
t i l t y * E t I o n V a n n i n
Administration, Legislation & Gambling Section “Homefield”88 Woodboume Road Douglas Isle of Man IM2 3APTelephone (01624) 623355 Ex 211Fax (01624) 621298e-mail [email protected] Site . www.gov.iro
Date: 11* September 2003
Mr M Comwell-Kelly Clerk of Tynwald Legislative Buildings DOUGLAS IMI 3PW
Dear Mr Comwell-Keliy
I write on behalf of the Department of Home Affairs to the Tynwald Select Committee currently examining the provision of General Practitioners Services.
The Department of Home Affairs is currently in discussions with the Department of Health and Social Services in regard to problems that have arisen concerning the certification of death in sudden or unexpected cases.
In this connection at a recent Department meeting the Minister Hon R P Braidwood MHK agreed that a report should be prepared on the issue and submitted to the Tynwald Select Committee on the basis that these problems were related to the issue of the provision of General Practitioners Services.
I would, therefore, be grateful if you could ensure the attached report, which explains the issues involved, is provided for information of the Select Committee.
Thank your for your assistance in regard to this matter
S C Lalor-Smith Administrator
cc Hon R. P Braidwood MHK, Hon C M Christian MLC, J D Q Cannan MHK, Q B Gill MHK, Mr W Greenhow and Mr D Killip.
DEPARTMENT OF HOME AFFAIRS
REPORT TO THE TYNWALD SELECT COMMITTEE EXAMINING THE PROVISION OF GENERAL PRACTITIONERS SERVICES
ON THE CERTIFICATION OF DEATH IN SUDDEN OR UNEXPECTED CASES
1. Introduction
1.1 This report sets out the role of the Isle of Man Constabulary in cases of sudden or unexpected death. It seeks to explain the situation before the introduction of the Manndoc system; it details the changes that have arisen as a result of that system and it makes suggestions for improvements.
2. The Role of the Coroner and The Coroner*» Officer
2.1 The Coroner of Inquests is responsible for investigating the cause of all sudden or unexpected deaths. In an average year around 170 such deaths are reported by Doctors, either General Practitioners, Hospital Doctors or Police Surgeons.
2.2 It is the responsibility of the Coroner to inquire into the circumstances of each death and, acting upon the advice of a Medical Practitioner, determine the cause of death. In cases where death is found to have been due to natural causes the Coroner may be content for a Doctor to sign a Death Certificate allowing the death to be treated as if it had been expected.
2.3 In a minority of cases the Coroner may request that a Post Mortem and, occasionally, an Inquest be held. In the latter circumstances this judicial process will determine the identity of the deceased, where and when they died and the cause of death. In reaching such a verdict, the Coroner may be assisted by a Jury.
2.4 Sudden or unexpected deaths are reported to the Coroner via the Police. In most cases this is done via the Coroner’s Officer, a specially trained Police Officer, whose duty it is to investigate all such deaths. The Coroner’s Officer carries out a number of functions, including acting as line of communication between the Coroner and the Medical Practitioner.
2.5 In an average year around 170 sudden deaths are reported to the Coroner. Of these, around 150 require the attendance of a Medical Practitioner at the scene of the death. Such locations can range from fetal road traffic collisions to the deceased’s own home. In all other cases death has occurred at a Hospital
2.6 Around 30 of the 170 deaths would initially be deemed to be suspicious in nature, in which case the Police would ensure that the scene (or the body, if death occurred at a Hospital) is visited by a Police Surgeon. Other than in the case of road deaths, the vast majority of these deaths are found not to have been as a result of third party action.
1
3- The Rok of the Medical Practitioner
3.1 In simple terms, the Medical Practitioner attending a death has two distinct functions
(a) to pronounce life extinct; and
(b) where possible, to determine the cause of death.
In the Isle of Man, the Coroner requires the former function to be conducted by a suitably qualified Medical Practitioner (Doctor). In some other jurisdictions, including parts of the United Kingdom, this function can be carried out by other professionals such as Paramedics. Where this occurs, their actions are often subsequently confirmed by a Medical Practitioner.
3.2 In ideal circumstances, the deceased’s own General Practitioner would be called to the death. This would then allow that Doctor to pronounce life extinct and, if they were able to do so, determine the cause of death. Where a General Practitioner has treated the deceased within the past month, he or she may determine the cause of death without recourse to a Post Mortem examination. In all other cases the Coroner will order such an examination to determine the cause of death.
3.3 Doctors are required to report all sudden or unexpected deaths using a form widely known as the 'blue form’. Usually the Doctor passes this form, to the Coroner’ s Officer. It is not unusual for a Doctor to complete only that part of the form relating to the identity of the deceased and where and when life was pronounced as extinct.
4. Suspicious Deaths
4.1 As can be seen at paragraph 2.6 above, comparatively few deaths are suspicious. It is for the police to determine whether a death is suspicious in nature and, naturally, this forms a part of ongoing Police training processes. From time to time General Practitioners may be called to an apparently routine death only to find that there are suspicious circumstances. In such cases the death would then be reported to the Police.
4.2 Police Surgeons are retained by the Department of Home Affairs to provide a number of different services. In broad terms their duties comprise of three main functions:
(a) provision of medical services to detained people;
(b) examination of victims of violent or sexual offences;
(c) attending suspicious deaths.
To allow them to fulfil their functions, Police Surgeons are given specialist training in forensic medicine.
2
4.3 At the present time there are four Police Surgeons, who provide all of the functions set out in paragraph 4.2 above. From time to time specialist Surgeons are employed to deal with female or child victims of sexual abuse. Police Surgeons are paid an annual retainer and they subsequently receive payment for all the services that they conduct. This includes travel cost; fees for specific functions such as determining whether a detained person is fit to he detained; examining victims of crime; writing reports and certifying death. The fees are determined by the Department of Home Affairs.
5. Pre-2003
5.1 Prior to changes to the General Practitioner service in the Isle of Man very few problems were encountered in respect of sudden or unexpected deaths. As fer as possible the deceased's own General Practitioner would attend the death, pronounce life extinct and, when it was possible to do so, provide a cause of death. Where the deceased’s own General Practitioner could not attend, the attending Doctor would almost invariably be from the same medical practice.
5.2 The involvement of Police Surgeons was limited to those deaths considered to be suspicious in nature or, in a very limited number of cases, where the deceased's own General Practitioner could not be contacted or, indeed, actually identified.
6. 2003
6.1 Changes to the provision of General Practitioner services in the Isle of Man have had a significant impact upon the pronouncement of life extinct and the certification of death. The effects have ranged from causing genuine and unnecessary distress to grieving relatives to the transfer of the cost of death certification from the Department of Health and Social Security to the Department of Home Affairs.
6.2 Case Study - 'Mrs IC
(a) The issue of non-attendance at sudden deaths first appeared on 03 May 2003, which ironically was the day in which several thousand people protested in Ramsey at the reduction in services at the town's Cottage Hospital.
(b) Mrs K, a 44 years old woman, was found dead in bed by her husband at approximately 7.30a.m. His call to the Manndoc service was answered by a General Practitioner from the Ramsey Group Practice, where Mrs K was a patient. Thé Doctor was unable to attend and asked that a Police Surgeon be asked to attend. A Police Officer attended and saw that, other than the deceased’s age, there was nothing suspicious about her death. The duty Police Surgeon, Dr Philip Christian, spent the morning at Police Headquarters examining victims of crime and detained persons. (This is normal for a Saturday morning) He was only able to attend Mrs K’s home at 11.40a.m. This meant that her family had bad to wait for four hours simply for a Doctor to pronounce life extinct. Obviously a General Practitioner would have attended promptly.
3
(c) The failure of a General Practitioner to attend the scene was new. The Isle of ManConstabulary had not been informed that changes to the General Practitioner services would lead to such an outcome. No consultation had taken place at operational or strategic levels. So concerned was the Force that a letter of Complaint was sent to the Coroner of Inquests, bringing to his attention the implications of the change, especially for grieving relatives.
6.3 Since the case of 'Mrs K\ the situation has remained difficult and, in many cases, uncertain. In most cases of sudden death, when the circumstances have not been suspicious, Police Surgeons have been required to attend. Where deaths have take place during surgery hours, a General Practitioner has attended, but such cases have been a minority. In four cases a Doctor from the Manndoc service has attended but this was clearly the exception, rather than the norm.
6.4 (a) On average the cost to the Isle of Man Constabulary of a Police Surgeon attending a non- suspicious death is just over £100. The Police Surgeon budget for the Force stands at £82,900 this budget certainly does not cater for the attendance at non-suspicious sudden deaths.
(b) Police surgeons face very heavy demands. It is evident that there is no spare capacity. In the longer term use of police surgeons to carry out routine death certification will be unsustainable. The individuals concerned cannot be expected to carry such heavy workloads over a long period of time.
6.5 The greatest impact of the changed procedure has been on the relatives of the deceased. Delays are now common and Police Officers have struggled to provide explanations that would assuage the feeling of people who have been suddenly - and often- unexpectedly bereaved. Such people cannot understand why their own Doctor cannot attend; they also struggle to appreciate that ambulances do not remove corpses. This is done by a contractor retained for the purpose by the Coroner.
6.6 On occasions, an informal, yet illogical compromise has been found. In many cases relatives will ring for an ambulance to report, for example, that they have found a relative apparently dead in bed. In most, but not all of these cases, an ambulance will be dispatched and a paramedic will attend. Upon determining that the person is dead, the paramedic will leave and ask that the Police deal with the matter. Sometimes people ring the Police direct and an Officer will attend the scene. In such cases an ambulance would not be dispatched. In any event grieving relatives find it difficult to understand that a tragic yet simple set of circumstances can be handled in an apparently callous way. Indeed, this is before any delays in obtaining the attendance of a Doctor.
7. Conclusion and Suggestions for Improvement
7.1 Changes to the involvement of General Practitioners in attendance at scenes of sudden or unexpected deaths came without prior consultation with the Police, or with Police Surgeons.
7.2 As a result of the changes the service provided to members of the public at a difficult and traumatic time has deteriorated Considerably.
7.3 In most cases, the Isle of Man Constabulary (and by implications, the Department of Home Affairs) now carries the cost of funding a General Practitioner to attend routine, non-suspicious sudden deaths.
4
7.4 Suggestions for the future include:
(a) Clear definition to be given to the role of the Manndoc service in regard to thepronouncement of life extinct and the certification of death.
(b) Such definition should determine that Police Surgeons need only attend at suspiciousdeaths.
(c) Financial responsibility for the issue of attendance at sudden deaths to be clarified andresolved. If the responsibility for attendance at sudden deaths is to be transferred from the Department of Health and Social Security to the Department of Home Affairs then there should be a transfer of the appropriate budgetary provisioa
(d) Discussions are necessary between the Coroner, the Department of Health and Social Security, the Department of Home Affairs and the Police about alternative methods of operating. These might include paramedics being given the authority to pronounce life extinct and remove bodies to the Noble’s Hospital Mortuary where death could formally be certified by a duty accident and emergency Doctor.
Issued by the Department of Home Affairs on 11th September 2003
5
Department of Home AffairsRheynn Cooishyn Sthie Administration, Legislation & Gambling Section
“HomefielcT 88 Woodbourae Road Douglas Isle of Man LM2 3APTelephone (0 1624) 623355 E x 2 1 1Fax (0 1624) 621298e-mail julian. IaIor-amith@dha. gov. imWeb Site www.gov.im
R e i \ i y s E l i a n V a n « / n
Date: 22* July 2004
Mr P Lo BaoThird Clerk of Tynwald and Clerk AdministratorClerk of Tynwald’s OfficeLegislative BuildingsDOUGLASIMI 3PW
Dear Mr Lo Bao
I write with reference to your recent letter in regard to the Tynwald Select Committee which has been examining the provision of General Practitioners Services.
In this connection I have consulted with the Isle of Man Constabulary and understand that Chief Inspector Gary Roberts has met with representatives of the ambulance service and the Medical Association.
As a result of this meeting and with the consent of the Coroner new protocols were established. I also understand that these protocols seem to be working, substituting as they do paramedics for surgeons on most occasions. The protocols are as follows
Where an ambulance has been called:
Paramedic will request police attendance via ESJCR (Emergency Services Joint Control Room). Paramedics will attempt to contact GP, if known.GP will decide whether or not to attend.Ambulance crew will remain on scene until police arrival. If another emergency occurs nearby then all steps must be taken to ensure urgent police response.Paramedic will pronounce life extinct and complete relevant parts of the blue form.Police will then deal with the matter under normal protocols: removal of body after permission from coroner etc.
Where Police need to force an entry to a property or where a body is found in a public place:
If any doubt exists that the person is dead, then an ambulance will be called.In all other cases a police surgeon will be called.
RECEIVED? 6 JUL 2004
C 'VIZ;' OF THE CLERK OF TYNWALD
Isle of ManGovernment
Suspicious Deaths:
Even if a paramedic has been in attendance a police surgeon will still be called.
Expected deaths in nursing homes and similar establishments:
Discussions are taking place with a view to existing practices being rationalised.
In connection with the above matter I would be grateful if you would pass on the Department’s appreciation to the Committee for the opportunity to have an input in the Committee consideration of these issues.
Yours^neerelyours tfis
J C Lalor-Smith Administrator
DEPARTMENT OF HEALTH AND SOCIAL SECURITY MANX EMERGENCY DOCTOR SERVICE
CONFIRMATION AND CERTIFICATION OF DEATH
Expected deaths of patients
At Home
If the death occurs in the patient's own home, and the relative or friend requests the attendance of a doctor from MEDS, the doctor will attend as soon as the urgent needs of living patients permit. It is possible that the doctor from MEDS may not be able to attend and arrangements may have to be made with the medical practice who attended the deceased for a doctor to attend.
If the relative or friend is content to make arrangements with an undertaker, without the doctor attending, then MEDS will inform the medical practice with whom the deceased was registered as soon as possible.
In a residential or nursing home
If the death occurs in a residential or nursing home it is appropriate for the GP who attended the patient during the last illness to attend when practicable and issue a death certificate. The doctor on call will almost certainly not be the one who has been attending the deceased person during their last illness, and cannot therefore initiate the death certification process. The MEDS doctor will only attend an expected death during the out of hours period where there is a genuine doubt as to whether the person is dead
Where an expected death occurs in a residential or nursing home it is recommended that the home contacts the undertaker if they wish the body to be removed and ensures that the medical practice with whom the patient was registered is notified as soon as practicable.
Sudden or unexpected deaths
A call from a relative or a nursing or residential home, about a patient who has been found to be dead, unexpectedly, but apparently in circumstances which are not suspicious. The doctor should respond as quickly as the urgent needs of their living patients permit. It is possible that the doctor from MEDS may not be able to attend and arrangements may have to be made with the medical practice who attended the deceased for a doctor to attend.
Where a request is received from the police or ambulance service that the doctor should attend upon a body found in a public place, a deserted building or as the result of a road or other form of accident or other situation. Callers will be advised to obtain the services of a retained police surgeon.
April 2004Drafted by Michael Morrison
Parliamentary Copyright
available from:
The Tynwald LibraryLegislative BuildingsDOUGLASIsle of Man IMI 3PWBritish IslesTel: 01624 685520Fax: 01624 685522e-mail [email protected]
November 2004
Price: £8.00




















