
Psychotraumatology in antiquity
11
Stress and Health 26: 21–31 (2010) © 2009 John Wiley & Sons, Ltd. 21 RESEARCH ARTICLE Psychotraumatology in Antiquity Philippe J. Birmes* † , Eric Bui, Rémy Klein, Julien Billard, Laurent Schmitt, Charlotte Allenou, Nicolas Job & Christophe Arbus Laboratoire du Stress Traumatique (JE 2511) Université de Toulouse & CHU de Toulouse, Toulouse, France Summary From antiquity onwards, chroniclers have reported cases of agitation or stupor sometimes associated with terrifying nightmares. Responses during the impact of a traumatic experience have attracted attention: terror, confusion and disorganized behaviour during the fire of Rome; the numbness of Patroclus, and loss of bowel and bladder control among warriors. The same applies to the most obvious post-traumatic responses: the recurrent and intrusive dis- tressing recollections of Gilgamesh, the dreams of battle in De Natura Rerum and the dissociative episodes concern- ing Marius. Although symptoms of re-experience are perfectly described, the long-term dissociative symptoms and their somatic components are also the object of unequivocal anecdotes. The scientific reading of the historical studies of a clinical and seemingly isolated fact contributes towards the establishment of modern psychotraumatol- ogy. Copyright © 2009 John Wiley & Sons, Ltd. Received 16 October 2007; Accepted 28 November 2008 Keywords antiquity; somatic symptoms; dissociation; psychotraumatology; traumatic stress *Correspondence Philippe J. Birmes, Laboratoire du Stress Traumatique (JE 2511), Université de Toulouse & CHU de Toulouse, Hôpital Casselardit Psychiatrie, 170, av. de Casselardit, TSA 40031, 31059 Toulouse Cedex 9, France. † Email: [email protected] Published online 15 January 2009 in Wiley InterScience (www.interscience.wiley.com) DOI: 10.1002/smi.1251 tology. According to the Diagnostic and Statistical Manual of Mental Disorders, 4th edition, text revision (DSM-IV; APA, 2000), acute stress disorder (ASD) and post-traumatic stress disorder (PTSD) are anxiety dis- orders that can develop following a trauma or a life- threatening event. Such stressful events may occur in particular during natural disasters or wars. As battles and wars were part of everyday life in ancient times, it is likely that psychotraumatology was not infrequent in antiquity. However, despite references to warriors, enemies and foes in ancient texts such as ‘Various Dreams’ in the complete works of Hippocrates (1849), the ‘father of medicine’, (ca 460–370 bc), medical trea- tises by famous figures such as Celsus, Galen, Oribasius and Pliny the Elder show no trace of psychotraumatic Introduction Over the past two decades, the scientific work in the field of traumatic stress to a large extent has been inspired by the interest aroused in the United States by the veterans of the Vietnam War. The concept had developed gradually, evolving around three main steps: (1) a scientific interest awakened by clinical case reports; (2) the integration of repeatedly observed symptoms into a syndrome using reliable criteria; and (3) the individualization of an etiopathogenic specific- ity corroborating clinical observations (Birmes, Hatton, Brunet, & Schmitt, 2003). Throughout this process, the scientific reappraisal of historical reports has contributed to the rise of modern psychotrauma-
-
Upload
chu-toulouse -
Category
Documents
-
view
2 -
download
0
Transcript of Psychotraumatology in antiquity

Stress and Health 26: 21–31 (2010) © 2009 John Wiley & Sons, Ltd. 21
RESEARCH ARTICLE
Psychotraumatology in AntiquityPhilippe J. Birmes*†, Eric Bui, Rémy Klein, Julien Billard, Laurent Schmitt, Charlotte Allenou, Nicolas Job & Christophe Arbus
Laboratoire du Stress Traumatique (JE 2511) Université de Toulouse & CHU de Toulouse, Toulouse, France
Summary
From antiquity onwards, chroniclers have reported cases of agitation or stupor sometimes associated with terrifying
nightmares. Responses during the impact of a traumatic experience have attracted attention: terror, confusion and
disorganized behaviour during the fi re of Rome; the numbness of Patroclus, and loss of bowel and bladder control
among warriors. The same applies to the most obvious post-traumatic responses: the recurrent and intrusive dis-
tressing recollections of Gilgamesh, the dreams of battle in De Natura Rerum and the dissociative episodes concern-
ing Marius. Although symptoms of re-experience are perfectly described, the long-term dissociative symptoms and
their somatic components are also the object of unequivocal anecdotes. The scientifi c reading of the historical
studies of a clinical and seemingly isolated fact contributes towards the establishment of modern psychotraumatol-
ogy. Copyright © 2009 John Wiley & Sons, Ltd.
Received 16 October 2007; Accepted 28 November 2008
Keywords
antiquity; somatic symptoms; dissociation; psychotraumatology; traumatic stress
*Correspondence
Philippe J. Birmes, Laboratoire du Stress Traumatique (JE 2511), Université de Toulouse & CHU de Toulouse, Hôpital Casselardit Psychiatrie,
170, av. de Casselardit, TSA 40031, 31059 Toulouse Cedex 9, France.†Email: [email protected]
Published online 15 January 2009 in Wiley InterScience (www.interscience.wiley.com) DOI: 10.1002/smi.1251
tology. According to the Diagnostic and Statistical
Manual of Mental Disorders, 4th edition, text revision
(DSM-IV; APA, 2000), acute stress disorder (ASD) and
post-traumatic stress disorder (PTSD) are anxiety dis-
orders that can develop following a trauma or a life-
threatening event. Such stressful events may occur in
particular during natural disasters or wars. As battles
and wars were part of everyday life in ancient times, it
is likely that psychotraumatology was not infrequent
in antiquity. However, despite references to warriors,
enemies and foes in ancient texts such as ‘Various
Dreams’ in the complete works of Hippocrates (1849),
the ‘father of medicine’, (ca 460–370 bc), medical trea-
tises by famous fi gures such as Celsus, Galen, Oribasius
and Pliny the Elder show no trace of psychotraumatic
Introduction
Over the past two decades, the scientifi c work in the
fi eld of traumatic stress to a large extent has been
inspired by the interest aroused in the United States by
the veterans of the Vietnam War. The concept had
developed gradually, evolving around three main steps:
(1) a scientifi c interest awakened by clinical case
reports; (2) the integration of repeatedly observed
symptoms into a syndrome using reliable criteria; and
(3) the individualization of an etiopathogenic specifi c-
ity corroborating clinical observations (Birmes,
Hatton, Brunet, & Schmitt, 2003). Throughout this
process, the scientifi c reappraisal of historical reports
has contributed to the rise of modern psychotrauma-

Psychotraumatology in Antiquity P. J. Birmes
22 Stress and Health 26: 21–31 (2010) © 2009 John Wiley & Sons, Ltd.
symptoms. The answer to this inconsistency may lie in
these symptoms being considered as normal emotional
responses to stress at the time. Indeed, although absent
from the medical textbooks of antiquity, evidence of
psychotraumatology is to be found in the historical
accounts of chroniclers who, for example, reported
cases of agitation or stupor sometimes associated with
terrifying nightmares (Birmes et al., 2003).
A historical review in search of symptoms induced
by trauma may therefore retrospectively uncover DSM
symptoms, but may also illustrate raw trauma responses,
which could enhance our current traumatology per-
spectives. A comparison between ancient accounts of
post-traumatic responses and modern diagnoses of
psychotraumatology could reveal symptoms over-
looked by current classifi cations. The aim of our study
is therefore to review the texts that date back to antiq-
uity in search of psychological and somatic symptoms
that might have occurred in the aftermath of traumatic
events in order to compare them to DSM criteria.
Method
We have conducted a review of literature dating back
to antiquity in search of all events that might have
accounted for stress-related symptoms: mass violence,
war, combat and disasters. A computerized search
(using MEDLINE, PILOTS and GALLICA) identifi ed
English- and French- language articles. PILOTS is a bib-
liographical database covering published international
literature on traumatic stress, and GALLICA is an
Internet server covering the digitized collections of the
Bibliothèque Nationale de France. We then selected
historical accounts and observations on the basis of
their descriptive power and extracted stress-related psy-
chological and somatic symptoms.
Results
Trauma-related psychological and somatic symptoms
highlighted by our search followed two main patterns:
(1) acute reactions; and (2) post-traumatic and long-
term responses.
(1) Acute reactions
Acute reactions found in the aftermath of mass vio-
lence, disasters and combats encompass two main types
of symptoms: panic and terror on the one hand, and
stupor and dissociation on the other.
Panic and terror
In mass violenceThe destruction of the city of Ur in the days of King
Ibisin (2026–2003 bc) and the death in battle of King
Urnamma (2111–2094 bc) help shed light on the per-
ception of trauma in antiquity (Ben-Ezra, 2004). Ur
was a city in ancient Sumer and was considered sacred
by the god Nanna. The ‘Lamentation for the destruc-
tion of Ur’ refers to traumatic events:
The righteous house they break up with pickaxe;
the people groan. The city they make into ruins;
the people groan. Its lady cries: ‘Alas for my city,’
cries: ‘alas for my house’. In its lofty gates, where
they were wont to promenade, dead bodies were
lying about; in its boulevards, where the feasts
were celebrated, scattered they lay. In all its
streets, where they were wont to promenade,
dead bodies were lying about. In its places, where
the festivities of the land took place, the people
lay in heaps. (Kramer, 1969)
In the same manner, the account of the death of
Urnamma contains an explicit description of the trau-
matic event, however this time, followed by a reference
to panic experienced by the inhabitants:
From the [. . . , the . . .] was [. . .] evenly in/on
the land. [The . . .] struck, the palace(s) was col-
lapsed. [The . . .] spread panic rapidly among its
Black-headed who dwelt there. [The . . .] estab-
lished its abandoned places in Sumer. In its vast
[. . .] cities are destroyed, the people are seized
with panic. Evil came upon Ur. (Fluckiger-
Hawker, 1999)
In disastersAs for civilian disasters, in his Annals, Tacitus (ca
56–117 ad), a senator and a historian of the Roman
Empire, describes the behaviour of the inhabitants
during the Great Fire of Rome (64 ad) (Crocq, 2004):
Added to this were the wailings of terror-stricken
women, the feebleness of age, the helpless inex-
perience of childhood, the crowds who sought to
save themselves or others, dragging out the
infi rm or waiting for them, and by their hurry in
the one case, by their delay in the other, aggravat-
ing the confusion. At last, doubting what they

Stress and Health 26: 21–31 (2010) © 2009 John Wiley & Sons, Ltd. 23
P. J. Birmes Psychotraumatology in Antiquity
should avoid or whither betake themselves, they
crowded the streets or fl ung themselves down in
the fi elds, while some who had lost their all, even
their very daily bread, and others out of love for
their kinsfolk, whom they had been unable to
rescue, perished, though escape was open to
them. (Tacitus, 1996)
This great civilian disaster gives insight into the
crowd’s terror, confusion and the desperate behaviour
that sometimes emerges among victims.
In combatsThe Second Punic War, referred to as ‘The War
Against Hannibal’, lasted from 218 to 201 bc and
involved combatants in the Western and Eastern Medi-
terranean area. It was the second of three major wars
between Carthage and the Roman Republic. In the
depiction of the Roman defeat at the lake of Trasimene,
Livy (59 bc to 17 ad), a Roman historian who wrote a
monumental history of Rome, reported clashes that
appeared unequalled:
In such a thick fog ears were of more use than
eyes; the men turned their gaze in every direction
as they heard the groans of the wounded and the
blows on shield or breastplate, and the mingled
shouts of triumph and cries of panic. (Livy, 1972)
Here again, the traumatic event is followed by a state
of panic among victims.
In a letter written 3000 years ago, a veteran of the
Pharaoh named Hori thus questioned a young and
inexperienced offi cer (Dyer, 2004):
You determine to go forward, though you don’t
know the way. Shuddering seizes you, the hair of your
head stands on end, your soul lies in your hand. Your
path is full of boulders and shingle, there is no passable
track, for it is all overgrown with thorns, neh-plants and
wolf ’s-pad. The ravine is on one side of you, the moun-
tain rises on the other. On you go, and guide your
chariot beside you, and fear that the horse will fall. The
sky is open, and you imagine that the enemy is behind
you. (Cottrell, 1968)
Sennacherib (705–681 bc), the King of Assyria,
relates his enemies’ terror following a massacre (Dyer,
2004):
The commander-in-chief of the King of Elam,
together with his nobles. I cut their throats like sheep.
As to the Sheiks of the Chaldeans, panic from my
onslaught overwhelmed them like a demon. They aban-
doned their tents and fl ed for their lives, crushing the
corpses of their troops as they went. [In their terror]
they passed scalding urine and voided their excrement
in their chariots. (Saggs, 1984)
Thus, in the aftermath of mass violence, combats and
disasters, feelings of panic, terror and helplessness have
been described in antiquity. Furthermore, disorganized
behaviour produced by such states of mind have also
been reported among the victims and witnesses of trau-
matic events.
Stupor and dissociation
Two other types of acute post-traumatic reactions
brought forward by our review are stupor and dissocia-
tion. Acute dissociative symptoms are included in the
ASD criteria: subjective sense of numbing, detachment,
absence of emotional responsiveness, reduction in
awareness of one’s surroundings, derealization, deper-
sonalization and dissociative amnesia (see Table I).
In disastersPliny the Younger, a lawyer, author and natural phi-
losopher of ancient Rome, recorded the reactions of
panic observed during the eruption of the Vesuvius (24
August 79 ad):
We were followed by a panic-stricken mob of
people wanting to act on someone elses’s deci-
sion in preference to their own (a point in which
fear looks like prudence), who hurried us on our
way by pressing hard behind a dense crowd. You
could hear the shrieks of women, the wailing of
infants, and the shouting of men; some were
calling their parents, others their children or
their wives. People bewailed their own fate or
that of their relatives, and there were some who
prayed for death in their terror of dying. (Pliny
the Younger, 1969)
Furthermore, he described his reaction while exposed
to danger while the walls of his house were splitting
apart:
We sat down in the forecourt of the house. I
don’t know whether I should call this courage or
folly on my part (I was only seventeen at the
Psychotraumatology in Antiquity P. J. Birmes
24 Stress and Health 26: 21–31 (2010) © 2009 John Wiley & Sons, Ltd.
time) but I called for a volume of Livy and went
on reading as if I had nothing else to do. Up came
a friend. When he saw us sitting there and me
actually reading, he scolded us both -me for my
foolhardiness and my mother for allowing it.
Nevertheless, I remained absorbed in my book.
(Pliny The Younger, 1969)
He did not feel that he was part of what was going
on: a state of total passivity that could be a result of
absence of emotional response.
In combatIn the Iliad (8th century bc), one of two ancient
Greek epic poems, with the Odyssey traditionally
attributed to Homer, the author relates the story of
Patroclus, close friend of Achilles, who helped lead the
battle against the Trojans. In the midst of battle he was
struck with what appears to be stupor:
Not only that, but the long-shadowed spear,
huge, thick and heavy with its head of bronze,
was shattered in Patroclus’ hands; the tasselled
shield with its baldric fell from his shoulder to
the ground; and King Apollo Son of Zeus undid
the corslet on his breast. Patroclus was stunned;
his shapely legs refused to carry him; and as he
stood there in a daze, a Dardanian called Euphor-
bus came close behind and struck him with a
sharp spear midway between the shoulders.
(Homer, 1950)
Here the decreased awareness of his surroundings
(e.g. ‘being in a daze’) might indicate a dissociative
reaction. Plutarch (46–120 ad), a Greek historian, biog-
rapher and essayist (with Roman citizenship), reported
the reactions of terror observed during the siege of
Syracuse by the Romans (213 bc): ‘When the Romans
fi rst attacked by sea and land, the Syracusans were
struck dumb with terror and believed that nothing
could resist the onslaught of such powerful forces’
(Plutarch, 1965). The besieged inhabitants experienced
a state of dumbness, which may also be a sign of
dissociation.
These passages suggest that symptoms that may refer
to acute traumatic reactions, such as being dazed or
feeling alienated from what was going on at the time,
were described in texts dating back as far as antiquity.
(2) Post-traumatic and long-term responses
Re-experiences are by far the most widely described
symptoms, doubtless because they are the most obvious
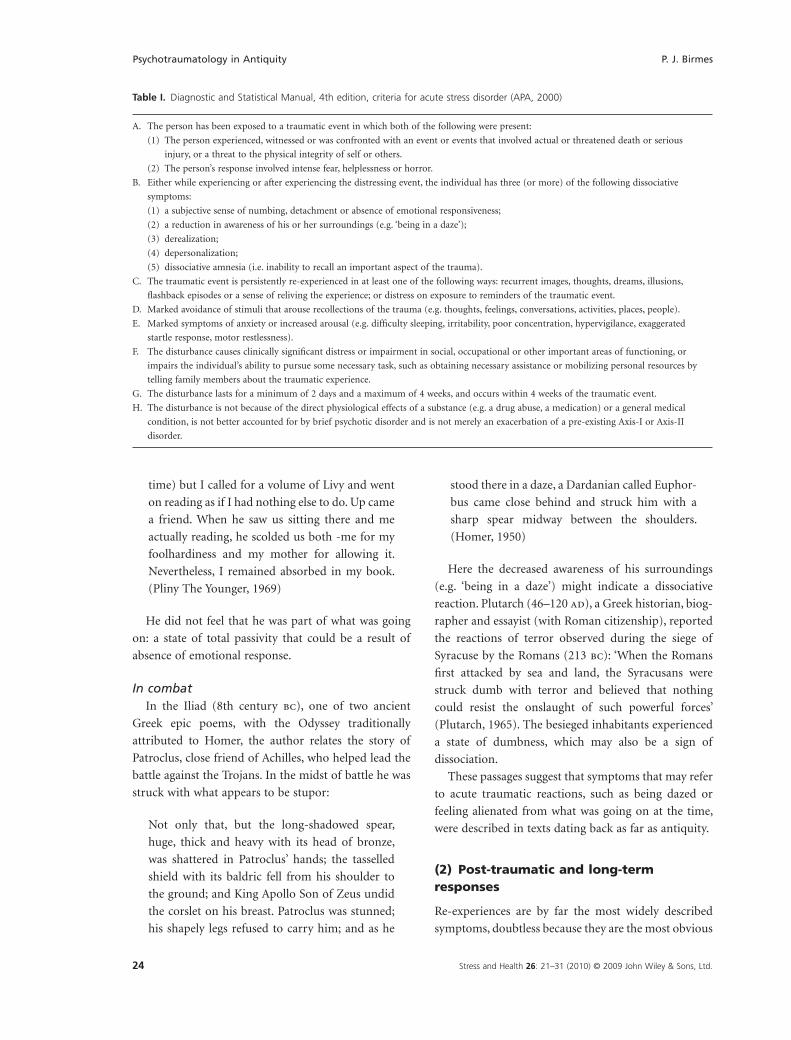
Table I. Diagnostic and Statistical Manual, 4th edition, criteria for acute stress disorder (APA, 2000)
A. The person has been exposed to a traumatic event in which both of the following were present:
(1) The person experienced, witnessed or was confronted with an event or events that involved actual or threatened death or serious
injury, or a threat to the physical integrity of self or others.
(2) The person’s response involved intense fear, helplessness or horror.
B. Either while experiencing or after experiencing the distressing event, the individual has three (or more) of the following dissociative
symptoms:
(1) a subjective sense of numbing, detachment or absence of emotional responsiveness;
(2) a reduction in awareness of his or her surroundings (e.g. ‘being in a daze’);
(3) derealization;
(4) depersonalization;
(5) dissociative amnesia (i.e. inability to recall an important aspect of the trauma).
C. The traumatic event is persistently re-experienced in at least one of the following ways: recurrent images, thoughts, dreams, illusions,
fl ashback episodes or a sense of reliving the experience; or distress on exposure to reminders of the traumatic event.
D. Marked avoidance of stimuli that arouse recollections of the trauma (e.g. thoughts, feelings, conversations, activities, places, people).
E. Marked symptoms of anxiety or increased arousal (e.g. diffi culty sleeping, irritability, poor concentration, hypervigilance, exaggerated
startle response, motor restlessness).
F. The disturbance causes clinically signifi cant distress or impairment in social, occupational or other important areas of functioning, or
impairs the individual’s ability to pursue some necessary task, such as obtaining necessary assistance or mobilizing personal resources by
telling family members about the traumatic experience.
G. The disturbance lasts for a minimum of 2 days and a maximum of 4 weeks, and occurs within 4 weeks of the traumatic event.
H. The disturbance is not because of the direct physiological effects of a substance (e.g. a drug abuse, a medication) or a general medical
condition, is not better accounted for by brief psychotic disorder and is not merely an exacerbation of a pre-existing Axis-I or Axis-II
disorder.

Stress and Health 26: 21–31 (2010) © 2009 John Wiley & Sons, Ltd. 25
P. J. Birmes Psychotraumatology in Antiquity
and the easiest to express and to objectify for the victims
and the witnesses.
Re-experiences
The most famous work of Mesopotamia, the Epic of
Gilgamesh, which dates back to the third millennium
bc, relates the journey of Gilgamesh, the renowned
King of Uruk in Mesopotamia. On witnessing the death
throes of his companion Enkidu, he sensed a profound
feeling of despair (Tomb, 1994):
I wept for him seven days and nights till the
worm fastened on him. Because of my brother I
am afraid of death, because of my brother I stray
through the wilderness. His fate lies heavy upon
me. How can I be silent, how can I rest? He is
dust and I too shall die and be laid in the earth
forever. I am afraid of death. (Sandars, 1972)
These intrusions may have persisted long after the
traumatic event for his friend’s death was to become an
impetus for his lifetime quest for eternal life. Some of
Plutarch’s works consist of biographies of famous men
or ‘Parallel Lives’. According to Tomb (1994), we dis-
cover that Gaius Marius (157–86 bc), a Roman general
and politician elected consul for an unprecedented
seven times during his career, presented traumatic
recollections:
But Marius himself, now worn out with toils,
deluged, as it were, with anxieties, and wearied,
could not sustain his spirits, which shook within
him as he again faced the overpowering thought
of a new war, of fresh struggles, of terrors known
by experience to be dreadful, and of utter weari-
ness. (Plutarch, 1973)
Plutarch also reported recurrent nightmares:
Tortured by such refl ections, and bringing into
review his long wandering, his fl ights, and his
perils, as he was driven over land and sea, he fell
into a state of dreadful despair, and was prey to
nightly terrors and harassing dreams. (Plutarch,
1973)
More painful recollections also appeared during a
highly agitated moment of delirium during which he
suffered from illusions:
Some, however, say that his ambitious nature
was completely revealed during his illness by
his being swept into a strange delusion. He
thought that he had the command in the
Mithridatic war, and then, just as he used to do
in his actual struggles, he would indulge in all
sorts of attitudes and gestures, accompanying
them with shrill cries and frequent calls to battle.
(Plutarch, 1973)
In ‘The Lament for Ur’, nightmares and dreams as a
response to the traumatic event (i.e. the destruction of
Ur) are also mentioned (Ben-Ezra, 2004):
At night a bitter lament having been raised unto
me, I, although, for that night I tremble, fl ed not
before that night’s violence. The storm’s cyclone
like destruction—verily its terror has fi lled me
full. Because of it’s [affl iction] in my nightly
sleeping place, in my nightly sleeping place verily
there is no peace for me; nor, verily, because of
its affl iction, has the quiet of my sleeping place,
the quiet of my sleeping place been allowed me.
(Kramer, 1969)
In the Iliad, Achilles falls prey to recollections con-
cerning his friend Patroclus who has been killed in
combat. These recollections are recurrent and cause
very agitated sleep:
But Achilles went on grieving for his friend,
whom he could not banish from his mind, and
all-conquering sleep refused to visit him. He
tossed to one side and the other, thinking always
of his loss, of Patroclus’s manliness and
spirit . . . of fi ghts with the enemy and adven-
tures on unfriendly seas. As memories crowded
in on him, the warm tears poured down his
cheeks. (Homer, 1950)
Homer dramatically conveys Achilles’s grief by enu-
merating his actions such as self-mutilation, weeping
and loss of appetite, and by describing his thoughts of
self-reproach and intrusive memories of the dead (Shay,
1994).
De Natura Rerum, literally meaning ‘On the Nature
of Things’, is an epic poem written around 50 ad by the
Roman poet and philosopher Lucretius (ca 99–55 bc)
in which traumatic dreams are also mentioned:

Psychotraumatology in Antiquity P. J. Birmes
26 Stress and Health 26: 21–31 (2010) © 2009 John Wiley & Sons, Ltd.
Whatever employment has the strongest hold on
our interest or has last fi lled our waking hours,
so as to engage the mind’s attention, that is what
seems most often to keep us occupied in dreams.
Generals lead their troops into action. Sailors
continue their pitched battle with the winds.
Very similar as a rule is the behaviour in sleep of
human minds, whose mighty machinations
produce massive feats. Kings take cities by storm,
are themselves taken captive, join in battle and
cry aloud as though their throats were being
slit—and all without stirring from the spot.
(Lucretius, 1994, p. 120)
Numbing and hyperarousal
Even if re-experiences are the most recurrent symp-
toms of post-traumatic responses found in texts dating
back to antiquity, others are also mentioned although
less frequently. Following the death of Enkidu, Gil-
gamesh embarked on a long period of wandering,
searching for everlasting life:
Siduri said to him why are your cheeks so starved
and why your face so drawn? Why is despair in
your heart and your face like the face of one who
has made a long journey? Yes, why is your face
burned from heat and cold, and why do you
come here wandering over the pastures in search
of the wind? (Sandars, 1972)
His feeling of helplessness and his aimless roaming
are at the forefront. Gilgamesh may indeed have been
suffering from a numbing of his general reactivity.
Finally, according to Plutarch, tormented by night-
mares and racked by insomnia, Marius drank heavily
in an attempt to fi nd sleep. It could be said that in this
case, alcohol abuse appeared as a consequence of his
trauma-induced hyperarousal: ‘And since above all
things he dreaded the sleepless nights, he gave himself
up to drinking-bouts and drunkenness at unseasonable
hours and in a manner unsuited to his years, trying thus
to induce sleep as a way of escaping his anxious
thoughts’ (Plutarch, 1973).
Dissociative symptoms
Lastly, dissociative symptoms are also found to be
a long-term consequence of traumatic events in
antiquity.
The Greek historian Herodotus (ca 484–425 bc)
describes a case of psychic traumatic blindness in an
Athenian warrior following the fear and terror he expe-
rienced during the battle of Marathon:
Epizelus, the son of Cuphagoras, an Athenian soldier,
was fi ghting bravely when he suddenly lost the sight in
both eyes, though nothing had touched him anywhere
neither sword, spear, nor missile. From that moment
he continued blind as long as he lived. I have heard that
in speaking about what happened to him he used to say
that he thought he was opposed by a man of great
stature in heavy armour, whose beard overshadowed
his shield; but the phantom passed him by, and killed
the man at his side. (Herodotus, 1996)
While Herodotus does not describe all of the
symptoms necessary for a diagnosis of PTSD under
DSM criteria, Epizelus has a lifetime sequelae (blindness)
as a consequence of exposure to combat at the Battle of
Marathon (Hudson, 1990).
A separate place must be given to the tragic end of a
hero in the Trojan war, ‘Ajax the Great’. Deprived of
the Arms of Achilles in favour of Ulysses, and over-
whelmed by rage, Ajax tried to slaughter the Greek
leaders he accused of deceit. However, in a bout of
‘madness’ sent by Athena, he slaughtered a fl ock of
sheep instead. Upon recovering his senses, he then
committed suicide (Sophocles, 1953). According to
Tritle (2000), Ajax could be described as suffering from
PTSD. Furthermore, references to the slaughtering of
animals and the ‘madness’ indicate a possible dissocia-
tive fl ashback.
Several anecdotes clearly present symptoms that are
greatly evocative of post-traumatic symptoms, some of
which are currently defi ned, as well as others that seem
to have been ‘overlooked’ by international classifi ca-
tions. Although devoid of any reference to medicine,
such disorders were already identifi ed and meticulously
described.
Discussion
We have reviewed ancient texts dating back to antiquity
in search of trauma-related psychological and somatic
reactions. Extracting psychiatric syndromes from
ancient anecdotes would not have been possible, yet
isolated and sometimes specifi c symptoms have been
pinpointed. Our search has yielded two types of symp-
toms: acute reactions on the one hand (panic, terror,
stupor and dissociation) and post-traumatic reactions

Stress and Health 26: 21–31 (2010) © 2009 John Wiley & Sons, Ltd. 27
P. J. Birmes Psychotraumatology in Antiquity
(re-experiences, numbness, hyperasousal, insomnia
and dissociative symptoms) on the other.
Acute reactions and ASD symptoms
The fi rst acute reactions highlighted by our search were
panic and terror, as in the destruction of Ur, after the
death of King Urnamma, during the Roman defeat at
lake Trasimene and other combat settings, and during
the Great Fire of Rome. An anthropological content
analysis of Homer’s ‘Iliad’ and ‘Odyssey’, considered to
be the staple text for the descriptions of ancient battles,
revealed the large number and variety of words used to
evoke fear (‘dread’, ‘terror’, ‘panic’, ‘alarm’, ‘anxiety’,
‘horror’, ‘fright’, ‘anguish’, ‘trembling’, ‘fear’, ‘scare’,
‘obsessive fear’, ‘apprehension’, ‘worry’, ‘shuddering’)
(Zaborowski, 2002), thus confi rming the importance of
such acute reactions in contexts of wars. With regard
to current classifi cations, these feelings of ‘panic’ or
‘terror’ fall under DSM criterion A2 (‘the person’s
response involved intense fear, helplessness, or horror’,
APA, 2000; see Table I). Reactions described by
Sennacherib (disorganized fl eeing and loss of sphincter
control on his enemies’ part) and Tacitus (Romans
fl eeing the Great Fire in confusion) may point to
peritraumatic distress. Peritraumatic distress describes
the emotional distress and physical symptoms of fear
and anxiety felt during a traumatic event: negative
emotions (fear, horror, etc.), perception of a life-
threatening element and bodily arousal (feelings of
personal life threat, loss of bowel and bladder control)
(Brunet et al., 2001). The DSM insists upon the impor-
tance of the immediate emotional impact (responses of
intense fear, helplessness or horror) as being an essen-
tial peritraumatic condition to the development of
PTSD. A growing number of investigators however
have argued that the current criterion A (2) is too nar-
rowly defi ned and should be expanded to include other
heightened negative emotions (e.g. anger, shame, grief)
and diminished emotional responses such as numbness
or shock (Weathers & Keane, 2007). Peritraumatic dis-
tress, including emotional distress and physical symp-
toms of anxiety (bodily arousal) experienced during a
traumatic event, signifi cantly related to PTSD measures
(Birmes, Daubisse, & Brunet, 2008; Jehel, Brunet,
Paterniti, & Guelfi , 2005; Simeon, Greenberg, Nelson,
Schmeidler, & Hollander, 2005).
Secondly, our review uncovered evidence of dissocia-
tion and stupor in the immediate aftermath of a trau-
matic event (Patroclus in combat or Syracuse’s
inhabitants during the Roman siege, and possibly Pliny
the Younger faced with the eruption of Vesuvius). Peri-
traumatic dissociation represents moments during
which the victim looses track of time or blanks out,
fi nding himself acting on ‘automatic pilot’, of not being
aware of things that happened during the event, and
confusion and disorientation were experienced during
exposure (Marmar, Weiss, & Metzler, 1998). These acute
dissociative experiences are also included in the current
DSM criterion B ‘dissociative symptoms’ for ASD (Table
I). There is a stongly signifi cant and relevant relationship
between peritraumatic dissociation and the development
of PTSD symptoms later on in life. Although this
outcome suggests that experiencing dissociation during
or shortly after a potentially traumatizing event increases
the probability of PTSD later on in life, this should not
be interpreted as proof of a causal relationship (Ben-
Ezra, Essar, & Saar, 2006; Birmes, Arrieu, Payen, Moron,
& Schmith, 1998; Lensvelt-Mulders et al., 2008; Panase-
tis & Bryant, 2003; Zoellner, Alvarez-Conrad, & Foa,
2002).
PTSD symptoms
The most frequent post-traumatic and long-term reac-
tions highlighted by our review are re- experiences: rec-
ollections of a friend’s death for Gilgamesh and Achilles,
and of war and mass violence for Marius and the inhab-
itants of Ur. These re-experiences are threefold: intru-
sive memories (Gilgamesh, Marius, Achilles), traumatic
nightmares (Marius, the inhabitants of Ur) and illu-
sions during a state of delirium (Marius). These symp-
toms clearly fi t the DSM criterion B for PTSD (APA,
2000; see Table II). The second set of post-traumatic
symptoms highlighted in our historical review involves
the modifi cation of general reactivity. Gilgamesh’s
aimless roaming suggests a numbness of his general
reactivity as described in the DSM criterion C for PTSD
(Table II). On the other hand, post-traumatic hyper-
arousal is also mentioned in texts dating back to antiq-
uity. Marius’ ‘anxious thoughts’ and ‘sleepless nights’
are indeed highly evocative of the criterion D for PTSD
(Table II). Lastly, it can be argued that Ajax’s dissocia-
tive fl ashback also fi ts the re-experience criterion of
the DSM-IV (criterion B). The main advantage of PTSD
symptoms is that all clinicians now acknowledge them.
When a patient consults following exposure to a trau-
matic event, few physicians omit to ask about

Psychotraumatology in Antiquity P. J. Birmes
28 Stress and Health 26: 21–31 (2010) © 2009 John Wiley & Sons, Ltd.
possible re-experiences and pathognomonic symptoms.
Although a minority of authors continue to question
their validity, the fact that Man started to write about
them as soon as he was able to describe his feelings or
observations following a traumatic experience should
contribute towards giving them strong substance. Yet,
on the one hand, some clinical forms appear more
complex than the standard triptych of re- experiences/
avoidance/hyperarousal, and on the other hand, for a by
no means insignifi cant number of victims, other catego-
ries of real post-traumatic symptoms may be expressed
and should also be recognized.
Other post-traumatic symptoms
Although these extracts of literature dating back to
antiquity reveal very characteristic ASD or PTSD symp-
toms, several reactions do not clearly fall under PTSD
DSM criteria.
Epizelus’ blindness of psychological origin suggests
hysterical or dissociative symptoms. Although dissocia-
tion and somatoform disorders do not belong to the
DSM criteria for PTSD, some authors have proposed a
specifi c clinical entity called complex PTSD (Herman,
1992; Shay, 2002) or disorders of extreme stress not oth-
erwise specifi ed (Pelcovitz et al., 1997; Roth, Newman,
Pelcovitz, Van der Kolk, & Mandel, 1997), and have
argued that many features of complex PTSD are mani-
festations of dissociation. Van der Hart, Nijenhuis, and
Steele (2005) thus described negative PTSD dissociative
symptoms (numbness, loss of perceptual or motor
functions, etc.) and positive PTSD dissociative symp-
toms (traumatic memories and nightmares that have
cognitive and somatosensory components, sensory dis-
tortions, etc.). Long-term dissociative symptoms and
their somatic components raise the question of their
inclusion in the diagnosis of PTSD. Van der Kolk et al.
(1996) showed that subjects who currently suffer from
Table II. Diagnostic and Statistical Manual, 4th edition, criteria for post-traumatic stress disorder (APA, 2000)
A. The person has been exposed to a traumatic event in which both of the following have been present:
(1) The person experienced, witnessed or was confronted with an event or events that involved actual or threatened death or serious
injury, or a threat to the physical integrity of self or others.
(2) The person’s response involved intense fear, helplessness or horror. Note: In children, this may be expressed instead by disorganized or
agitated behaviour.
B. The traumatic event is persistently re-experienced in one (or more) of the following ways:
(1) recurrent and intrusive distressing recollections of the event, including images, thoughts or perceptions. Note: In young children,
repetitive play may occur in which themes or aspects of the trauma are expressed;
(2) recurrent distressing dreams of the event. Note: In children, there may be frightening dreams without recognizable content;
(3) acting or feeling as if the traumatic event were recurring (includes a sense of reliving the experience, illusions, hallucinations and
dissociative fl ashback episodes, including those that occur upon awakening or when intoxicated). Note: In young children, trauma-
specifi c re-enactment may occur;
(4) intense psychological distress at exposure to internal or external cues that symbolize or resemble an aspect of the traumatic event;
(5) physiological reactivity on exposure to internal or external cues that symbolize or resemble an aspect of the traumatic event.
C. Persistent avoidance of stimuli associated with the trauma and numbing of general responsiveness (not present before the trauma), as
indicated by three (or more) of the following:
(1) efforts to avoid thoughts, feelings or conversations associated with the trauma;
(2) efforts to avoid activities, places or people that arouse recollections of the trauma;
(3) inability to recall an important aspect of the trauma;
(4) markedly diminished interest or participation in signifi cant activities;
(5) feeling of detachment or estrangement from others;
(6) restricted range of affect (e.g. unable to have loving feelings);
(7) sense of a foreshortened future (e.g. does not expect to have a career, marriage, children or a normal lifespan).
D. Persistent symptoms of increased arousal (not present before the trauma), as indicated by two (or more) of the following:
(1) diffi culty falling or staying asleep;
(2) irritability or outbursts of anger;
(3) diffi culty concentrating;
(4) hypervigilance;
(5) exaggerated startle response.
E. Duration of the disturbance (symptoms in criteria B, C and D) is more than 1 month.
F. The disturbance causes clinically signifi cant distress or impairment in social, occupational or other important areas of functioning.

Stress and Health 26: 21–31 (2010) © 2009 John Wiley & Sons, Ltd. 29
P. J. Birmes Psychotraumatology in Antiquity
PTSD have signifi cantly increased rates of dissociation
and somatization symptoms compared with those who
no longer met criteria for PTSD. It must be said that
for some authors, such as Shay (2002), ‘complex PTSD
is a simple PTSD plus the destruction of the capacity
for social trust’, a fact that seems to have been con-
fi rmed by the return of veterans from the most recent
confl icts (Friedman, 2005).
Gilgamesh is described as showing ‘cheeks so starved’:
a sign of severe weight loss. It has been argued that
trauma late in life might lead to the onset of anorexia
nervosa in hypomanic- functioning subjects (Tobin,
Molteni, & Elin, 1995), or that eating disorders can be
the manifestations of an underlying PTSD (Torem &
Curdue, 1988). But the best explanation for weight loss
might also be a mood disorder. Apart from Gilgamesh’s
weight loss, references are also made in several anec-
dotes to feelings of ‘despair’ (Marius, Gilgamesh) or
grief (Achilles’, ‘tears poured down [his] cheeks’). In
these cases, several symptoms or modes of behaviour
can fi nd their origin in a mood disturbance such as
complicated bereavement or depression. Depression
may develop as a complication of PTSD and its
associated impairment. On the other hand, some
trauma victims develop PTSD, whereas others develop
major depression or substance use disorder, depending
on their pre-existing vulnerabilities (Breslau, 2002).
Marius suffered from alcohol abuse if not addiction.
Use of alcohol or drugs to relieve the distressing
symptoms of PTSD may increase the likelihood of
dependence. Previous research among Vietnam combat
veterans and civilian victims of traumatic events
generally found considerably stronger associations
between trauma exposure and alcohol use disorder
when PTSD was present than when it was absent
(Breslau, 2002).
Limits
PTSD symptoms thus seem to be present in antiquity.
However, we are unable to confi rm a ‘full PTSD diag-
nosis’ because authors were not likely to assess all DSM
criteria among their contemporaries. Our retrospective
diagnoses are based on historical evidence, and there-
fore inevitably biased. As we mentioned earlier, fi rstly,
several descriptions are not unequivocal and might
indicate other symptoms such as bereavement or a
depressive disorder for example. Secondly, a stylistic
bias might also have been introduced by the authors:
they may have exaggerated the symptoms to emphasize
the drama of their heroes’ lives. Even if causality
between trauma and ASD or PTSD symptoms seems
obvious in the presented anecdotes, our review has not
been able to establish any relationship between acute or
peritraumatic symptoms and later PTSD.
Little reference is made to Tritle’s (2000) ‘From
Melos to My Lai: War and survival’ in our review. In
his extensive work on war, Tritle does indeed argue that
Xenophon’s (soldier and a contemporary of Socrates,
ca 431–355 bc) portrayal of the Spartan Clearchus
(Xenophon, 2007) ‘provides us with the fi rst known
historical case of PTSD’. However, instead of referring
to DSM criteria, Tritle defi nes PTSD using criteria that
are not included in international classifi cations: ‘persis-
tent mobilization of the body and the mind for lethal
violence, with the potential for explosive danger’, ‘sui-
cidality’, etc. This could represent a clinical form of
complex PTSD, but the triptych of re-experiences/
avoidance/hyperaousal is not described.
Conclusion
Our historical survey shows that, even from the begin-
ning of antiquity, psychological responses to extreme
trauma have been the source of phenomenological
interest. Intrusive memories and arousal seem to have
been known always to follow exposure to traumatic
events (Weisaeth, 2002). These symptoms are notable
and attract attention because of what one experiences
when facing death. While confi rming the importance
of the specifi city of traumatic stress in chronological
clinical forms (peritraumatic, ASD and PTSD), we have
offered clinical descriptions that are previous to con-
temporary nosologies and could enhance our current
psychotraumatology perspectives. The clinical value of
the symptoms described lies in their great detail and the
pre cision of the historical anecdotes, and thus high-
lights their perfect overlap with modern psychotrauma-
tology. Thus, alongside the immediate reaction of
intense fear and horror, and the standard triptych of
re-experiences, avoidance and hyperarousal, the signs
of grief, despair, passivity, hysterical blindness and
other somatic and affective reactions should remind us
that the human responses to trauma remain varied and
complex, and necessitate great perspicacity on the clini-
cian’s part.

Psychotraumatology in Antiquity P. J. Birmes
30 Stress and Health 26: 21–31 (2010) © 2009 John Wiley & Sons, Ltd.
REFERENCES
American Psychiatric Association (APA) (2000). Diagnos-
tic and statistical manual of mental disorders, 4th edition,
text revised. Washington, DC: APA.
Ben-Ezra, M. (2004). Trauma in antiquity: 4000 year
old post-traumatic reactions? Stress and Health, 20,
121–125.
Ben-Ezra, M., Essar, N., & Saar, R. (2006). The association
between peritraumatic dissociation and acute stress
reactions among rescue personnel 36–48h after a gas
pipe explosion in Tel-Aviv: A preliminary report. Stress
and Health, 22, 197–201.
Birmes, P., Arrieu, A., Payen A., Moron, P., & Schmitt, L.
(1998). Catastrophe aérienne de Tambacounda: accueil
des blessés au CHU de Toulouse. Annales Médico-
psychologiques, 156, 41–45.
Birmes, P., Daubisse, L., & Brunet, A. (2008). Predictors
of enduring PTSD after an industrial disaster. Psychiat-
ric Services, 59, 116.
Birmes, P., Hatton, L., Brunet, A., & Schmitt, L. (2003).
Early historical literature for post-traumatic symptom-
atology. Stress and Health, 19, 17–26.
Breslau, N. (2002). Epidemiologic studies of trauma,
posttraumatic stress disorder, and other psychiatric
disorders. Canadian Journal of Psychiatry, 47, 923–929.
Brunet, A., Weiss, D.S., Metzler, T.J., Best, S.R., Neylan,
T.C., Rogers, C., Fagan, J., & Marmar, C.R. (2001). The
Peritraumatic Distress Inventory: A proposed measure
of PTSD criterion A2. American Journal of Psychiatry,
158, 1480–1485.
Cottrell, L. (1968). The warrior Pharaohs. London: Evans
Brothers.
Crocq, L. (2004). Historique des catastrophes urbaines et
industrielles. Revue Francophone du Stress et du Trauma,
4, 55–64.
Dyer, G. (2004). War. The lethal custom. New York: Carrol
& Graf Publishers.
Fluckiger-Hawker, E. (1999). Urnamma of Ur in Sumerian
literary tradition. Guttingen, Germany: University Press
Fribourg.
Friedman, M.J. (2005). Veterans’ mental health in the
wake of war. The New England Journal of Medicine, 352,
1287–1290.
Herman, J.L. (1992). Complex PTSD: A syndrome in sur-
vivors of prolonged and repeated trauma. Journal of
Traumatic Stress, 5, 377–392.
Herodotus. (1996). Book six. In A. De Sélincourt, revision
by J.M. Marincola (Eds), The Histories (trans.) (pp.
325–371). London: Penguin Books.
Hippocrates. (1849). Livre Quatrième ou des Songes. In E.
Littré (Ed.), Œuvres Complètes, Vol. VI (trans.) (pp.
638–663). Paris: JB Baillière.
Homer. (1950). The Iliad (translated by E. Rieu). London:
Penguin Books.
Hudson, C.J. (1990). The fi rst case of battle hysteria? The
British Journal of Psychiatry, 157, 150.
Jehel, L., Brunet, A., Paterniti, S., & Guelfi , J.D. (2005).
Validation of the Peritraumatic Distress Inventory’s
French translation. Canadian Journal of Psychiatry, 50,
67–71.
Kramer, S.N. (1969). A Sumerian lamentation. In J.B.
Pritchard (Ed.), Ancient near eastern texts: Relating to the
Old Testament (pp. 455–463). Princeton, NJ: Princeton
University Press.
Lensvelt-Mulders, G., Van der Hart, O., Van Ochten, J.M.,
Van Son, M.J., Steele, K., & Breeman, L. (2008). Rela-
tions among peritraumatic dissociation and posttrau-
matic stress: A meta-analysis. Clinical Psychology Review,
28, 1138–1151.
Livy. (1972). Book 22: Lake Trasimene. In B. Radice (Ed),
The war with Hannibal (trans) (p. 99). London: Penguin
Books.
Lucretius. (1994). Book Four: Sensation and Sex. In R.E.
Latham, revision by J. Godwin (Eds), On the nature of
the universe (trans.) (pp. 95–128). London: Penguin
Books.
Marmar, C.R., Weiss, D.S., & Metzler, T. (1998). Peritrau-
matic dissociation and posttraumatic stress disorder. In
J.D. Bremner, & C.R. Marmar (Eds), Trauma, memory,
and dissociation (pp. 229–252). Washington, DC:
American Psychiatric Press.
Panasetis, P., & Bryant, R.A. (2003). Peritraumatic versus
persistent dissociation in acute stress disorder. Journal
of Traumatic Stress, 16, 543–566.
Pelcovitz, D., Van der Kolk, B.A., Roth, S.H., Mandel, F.S.,
Kaplan, S.J., & Resick, P.A. (1997). Development of a
criteria set and a structured interview for disorders of
extreme stress (SIDES). Journal of Traumatic Stress, 10,
3–16.
Pliny The Younger. (1969). To Cornelius Tacitus. In B.
Radice (Ed.), The letters of the Younger Pliny (trans.) (pp.
170–173). London: Penguin Books.
Plutarch. (1965). Marcellus. In I. Scott-Kilvert (Ed.),
Makers of Rome (trans.) (pp. 85–118). London: Penguin
Books.
Plutarch. (1973). Fall of the Roman republic. Six lives,
Marius, Sulla, Crassus, Pompey, Caesar, Cicero (trans-
lated by R. Warner). London: Penguin Classics.
Roth, S., Newman, E., Pelcovitz, D., Van der Kolk, B.A., &
Mandel, F.S. (1997). Complex PTSD in victims exposed
to sexual and physical abuse: Results from the DSM-IV
fi eld trial for posttraumatic stress disorder. Journal of
Traumatic Stress, 10, 539–556.
Saggs, H. (1984). The might that was Assyria. London:
Sidgwick & Jackson.

Stress and Health 26: 21–31 (2010) © 2009 John Wiley & Sons, Ltd. 31
P. J. Birmes Psychotraumatology in Antiquity
Sandars, N.K. (1972). The search for everlasting life. In
N.K. Sandars (Ed.), The epic of Gilgamesh (pp. 97–107).
London: Penguin Books.
Shay, J. (1994). Achilles in Vietnam: Combat trauma and
the undoing of character. New York: Atheneum.
Shay, J. (2002). Odysseus in America: Combat trauma and
the trials of homecoming. New-York: Scribner.
Simeon, D., Greenberg, J., Nelson, D., Schmeidler, J., &
Hollander, E. (2005). Dissociation and posttraumatic
stress 1 year after the World Trade Center disaster:
Follow-up of a longitudinal survey. The Journal of Clini-
cal Psychiatry, 66, 231–237.
Sophocles. (1953). Ajax. In E.F. Watling (Ed.), Electra and
other plays (trans.) (pp. 19–20). London: Penguin
Books.
Tacitus. (1996). The Burning of Rome. In M. Grant (Ed.),
The annals of Imperial Rome (trans.) (pp. 362–363).
London: Penguin Classics.
Tobin, D.L., Molteni, A.L., & Elin, M.R. (1995). Early
trauma, dissociation, and late onset in the eating dis-
orders. International Journal of Eating Disorder, 17,
305–308.
Tomb, D.A. (1994). The phenomenology of post-
traumatic stress disorder. The Psychiatric Clinics of
North America, 17, 237–250.
Torem, M.S., & Curdue, K. (1988). PTSD presenting as an
eating disorder. Stress Medicine, 4, 139–142.
Tritle, L.A. (2000). Clearchus’ story: The heroic ideal
transformed. In L.A. Tritle (Ed.), From Melos to My Lai:
War and survival (pp. 55–78). London; New York:
Routledge.
Van der Hart, O., Nijenhuis, E.R.S., & Steele, K. (2005).
Dissociation: An insuffi ciently recognized major feature
of complex posttraumatic stress disorder. Journal of
Traumatic Stress, 18, 413–423.
Van der Kolk, B.A., Pelcovitz, D., Roth, S., Mandel, F.S.,
McFarlane, A., & Herman, J.L. (1996). Dissociation,
somatization, and affect dysregulation: the complexity
of adaptation to trauma. The American Journal of Psy-
chiatry, 153 (Festschrift Supplement), 83–93.
Weathers, F.W., & Keane T.M. (2007). The Criterion A
problem revisited: Controversies and challenges in
defi ning and measuring psychological trauma. Journal
of Traumatic Stress, 20, 107–121.
Weisaeth, L. (2002). The European history of psychotrau-
matology. Journal of Traumatic Stress, 15, 443–452.
Xenophon. (2007). Characters of the fi ve generals. In R.
Warner (Ed.), The Persian expedition (trans.) (pp. 130–
135). London: Penguin Classics.
Zaborowski, R. (2002). Fear and Bravery in the Iliad and
Odyssey. Lexico-graphical contribution to the Homeric
psychology of emotions. Warsaw, Poland: Stakros.
Zoellner, L.A., Alvarez-Conrad, J., & Foa, E.B. (2002). Peri-
traumatic dissociative experiences, trauma narratives,
and trauma pathology. Journal of Traumatic Stress, 15,
49–57.




















