process evaluation of nhif service provision in accredited ...
56
PROCESS EVALUATION OF NHIF SERVICE PROVISION IN ACCREDITED HEALTH FACILITIES: A CASE OF TEMEKE MUNICIPAL HEALTH FACILITIES
-
Upload
khangminh22 -
Category
Documents
-
view
2 -
download
0
Transcript of process evaluation of nhif service provision in accredited ...
1
PROCESS EVALUATION OF NHIF SERVICE PROVISION IN
ACCREDITED HEALTH FACILITIES:
A CASE OF TEMEKE MUNICIPAL HEALTH FACILITIES

2
PROCESS EVALUATION OF NHIF SERVICE PROVISION IN
ACCREDITED HEALTH FACILITIES:
A CASE OF TEMEKE MUNICIPAL HEALTH FACILITIES.
By
Rose Anthony Ntundu
A dissertation Submitted to the School of Public Administration and
Management (SOPAM) of Mzumbe University in the Partial Fulfilment of the
Requirement of the Award of Master Science in Health Monitoring and
Evaluation.
2015
i
CERTIFICATION
We, the undersigned, certify that we have read and hereby recommend for
acceptance by the Mzumbe University, a dissertation entitled “Process Evaluation of
NHIF Service Provision in Accredited Health Facilities: A Case of Temeke
Municipal Health Facilities” in partial Fulfilment of the Requirement of the Award
of Master Science Degree in Health Monitoring and Evaluation.
___________________________
Major Supervisor
___________________________
Internal Examiner
___________________________
External Examiner
Accepted for the Board of……………………
Signature
____________________________________________
DEAN/DIRECTOR, FACULTY/DIRECTORATE/SCHOOL/BOARD
ii
DECLARATION AND COPYRIGHT
I, Rose Anthony Ntundu, declare that this dissertation is my own original work and
that it has not been presented and will not be presented to any other university for a
similar or any other degree award.
Signature ___________________________
Date_______________________________
©
This dissertation is a copyright material protected under the Berne Convention, the
Copyright Act 1999 and other international and national enactments, in that behalf,
on intellectual property. It may not be reproduced by any means in full or in part,
except for short extracts in fair dealings, for research or private study, critical
scholarly review or discourse with an acknowledgement, without the written
permission of Mzumbe University, on behalf of the author.
iii
ACKNOWLEDGEMENT
This work would not have reached this stage, if it were not the effort and
contribution made by several people who gave their time and hard work. I thank all
of them for their assistance. Above all I thank God for keeping me healthy during
and throughout my study time at MU.
Firstly, I wish to express my sincere appreciation to my supervisors Mr. Amani Paul
and Dr Daudi Bunyinyiga for their constructive advice, criticism and corrections
right from the development of the proposal to the final stage of writing this report. I
also wish to extend my heartfelt gratitude and appreciation to the School of Public
Administration, Department of Health System Management for imparting to me the
knowledge and support during the entire period of my study.
Secondly, special thanks are extended to friends and mates for their constructive
ideas and advice towards the success of this work.
Thirdly, I am highly thankful to my employer for the permission to undertake this
study.
Lastly, I am grateful to all the respondents fromTemeke Municipal health facilities
for their cooperation and useful material they gave me during my data collection.
iv
DEDICATION
I dedicate this dissertation to my father Mr Anthony Jacob Ntundu, my husband Mr
Joseph Philip and my lovely daughters Winfrida and Faraja for their calmness,
patience, efforts and encouragement in the course of my studies at Mzumbe
University.
v
ABBREVIATIONS
AAR Africa Airway Rescue
AIDS Acquired Immune Disease Syndrome
CHF Community Health Fund
CHMT Council Health Management Team
CHSB Council Health Service Boards
DMHIS District-wide Mutual Health Insurance Schemes
DMO District Medical Officer
FBO Faith Based Organizations
FFS Fee-For-Service
GDP Gross Domestic Product
HFGC Health Facilities Governing Committees
HIV Human Immune-deficient Virus
HMO Health-Maintenance Organisation
HQ Headquarter
ILO International Labour Organization
MEDEX Medical Express
MOH Mutual Health Organization
MoHSW Ministry of Health and Social Welfare
NBS National Bureau Statistics
NHIF National Health Insurance Fund
vi
NHIS National Health Insurance Scheme
NGO Non-Governmental Organization
NSSF National Social Security Fund
PHC Primary Health Care
PhD Doctor of Philosophy
RHMT Regional Health Management Team
RMO Regional Medical Officer
SHI Social Health Insurance
SHIB Social Health Insurance Benefit
SHIS Social Health Insurance Scheme
SOPAM School of Public Administration and Management
SPSS Statistical Package for Social Science
TIKA Tiba Kwa Kadi
TIRA Tanzania Insurance Regulatory Authority
USD United States Dollar
WHO World Health Organization
vii
ABSTRACT
Background: Social Health Insurance Scheme is a health scheme insurance which
is provided by the governments to its employee. Tanzania introduced social health
insurance by establishment of the National Health Insurance Fund (NHIF) in 1999
with the objective of improving the quality and availability of health services to
Government employees (NHIF,2003). NHIF facilitates access of health care services
to its beneficiaries through a network of accredited health facilities countrywide. This
study evaluated NHIF service provision in accredited health facilities, challenges
encountered and improvement measures.
Methodology: The study was conducted in Dar es salaam, Temeke Municipal.
Facility based multiple case studies of both quantitative and qualitative nature was
carried to evaluate NHIF service provision in selected accredited health facilities. A
total of 80 respondents from 10 selected accreditted health facilities participated in
the study. The study population comprised of both male and female health workers
aged 18 to 60 years with the education level from secondary to university and above,
close to fifty percent (45%) had a working experience of more than ten years. Data
was processed and analyzed by using Microsoft excel and Statistical Package for
Social Sciences (SPSS) software.
Results: Over half of the respondents (51.3%) agreed that NHIF objectives were
achieved and there are several benefits gained by the beneficiaries and community
from accredited health facilities. Besides, a number of challenges were reported to
have been encountered by the accredited health facilities in the process of
implementing the NHIF service provision. For example, 41.3% mentioned low
Government health budget to the facilities as the main challenge and 36.3%
mentioned lack of active monitoring mechanism to ensure appropriate and timely
reimbursement of funds from NHIF. In addition, 20% recommended that
stakeholders‟ involvement in decision making is one of the strategies to improve the
NHIF service provision.
Conclusion: From these findings, the following recommendation can be drawn;
more effort is still needed to address the challenges encountered by accredited health

viii
facilities. These efforts include regural supportive supervisions to the facilities,
training to health workers, timely distribution of working tools and timely claims
reimbursement. However, measures to be taken to improve performance include;
active monitoring mechanism of NHIF funds, reviewed NHIF quarterly reports,
develop NHIF in charges at all facility levels, train NHIF coordinators, facilitate
head of departments and increase health budget. The information contained in this
evaluation is intended to create opportunities for multi-sectoral dialogue, to enhance
collaborative planning efforts, and ultimately to facilitate partnerships that lead to
increased health systems efficiencies and sustained health services.
ix
TABLE OF CONTENTS
CERTIFICATION ..................................................................................................... i
DECLARATION AND COPYRIGHT ................................................................... ii
ACKNOWLEDGEMENT ....................................................................................... iii
DEDICATION .......................................................................................................... iv
ABBREVIATIONS ................................................................................................... v
ABSTRACT ............................................................................................................. vii
LIST OF TABLES .................................................................................................. xii
LIST OF FIGURES ............................................................................................... xiii
CHAPTER ONE ....................................................................................................... 1
INTRODUCTION ..................................................................................................... 1
1.1 Study Overview ..................................................................................................... 1
1.1.1 Social Health Insurance Scheme in Tanzania .................................................... 1
1.2. Description of Program to be evaluated ............................................................... 2
1.2.1. Expected Program effects/objectives ................................................................ 2
1.2.2. Major strategies ................................................................................................. 3
1.2.3. Programme activities ......................................................................................... 3
1.2.4. Logic model ...................................................................................................... 4
1.2.5. Stakeholder analysis .......................................................................................... 4
1.3 Statement of the Problem ...................................................................................... 5
1.4 Objectives of the evaluation .................................................................................. 6
1.4.1 General objective ............................................................................................... 6
1.4.2 Specific objectives ............................................................................................. 6
1.5 Evaluation Questions ............................................................................................ 6
1.6 Significance of the Evaluation .............................................................................. 7
CHAPTER TWO ...................................................................................................... 8
LITERATURE REVIEW ......................................................................................... 8
2.1 Theoretical Literature Review............................................................................... 8
2.1.1 Programme evaluation ....................................................................................... 8
2.1.2 Health Insurance System in Tanzania ................................................................ 9
x
2.1.3 Types of Health Insurance ................................................................................. 9
2.1.4. National Health Insurance Fund...................................................................... 10
2.2 Empirical Literature Review ............................................................................... 10
2.3. Theoretical framework of the evaluation ........................................................... 12
CHAPTER THREE ................................................................................................ 14
EVALUATION METHODOLOGY ..................................................................... 14
3.1 Evaluation Approach ........................................................................................... 14
3.2 Evaluation Design ............................................................................................... 14
3.3 Evaluation Period ................................................................................................ 14
3.4. Description of the Study Area ............................................................................ 14
3.5. Study Population ................................................................................................ 15
3.6. Units of analysis ................................................................................................. 15
3.7. Variables and their measurements ..................................................................... 15
3.8. Sample size and sampling technique.................................................................. 16
3.9. Types and sources of data .................................................................................. 17
3.10. Data collection methods ................................................................................... 17
3.11. Validity issues .................................................................................................. 17
3.12. Data management and analysis methods.......................................................... 17
3.13 Ethical issues. .................................................................................................... 18
CHAPTER FOUR ................................................................................................... 19
PRESENTATION AND DISCUSSION OF EVALUATION FINDINGS ......... 19
4.1 Introduction ......................................................................................................... 19
4.2 Sample and its characteristics ............................................................................. 19
4.3 NHIF performance in compliance with accredited health facilities .................... 20
4.3.1 Responses on NHIF objectives achievement ................................................... 20
4.3.2 Responses on overall achievement of NHIF objectives. .................................. 21
4.3.3 Reasons for NHIF to initiate accredited health facilities ................................ 22
4.3.4 Benefits gained by the community from NHIF accredited health facilities .... 23
4.3.5 Attitude on NHIF services in accredited health facilities ................................ 24
4.4 To determine challenges faced by NHIF through accredited health facilities .... 25
xi
4.4.1 General challenges encountered in health facilities ......................................... 25
4.4.2 Factors hindering effective adherence to NHIF standards ............................... 27
4.5 Possible improvement measures on NHIF health service provision ................... 28
4.5.1 Strategies to improve NHIF service provision ................................................. 28
4.5.2 Ways to improve NHIF performance through accredited health facilities ...... 29
4.5.3 Perception on improvement measures on NHIF health service provision ....... 30
CHAPTER FIVE ..................................................................................................... 31
SUMMARY, CONCLUSION AND POLICY IMPLICATION ......................... 32
5.1 Summary ............................................................................................................. 32
5.2 Conclusion .......................................................................................................... 32
5.3 Policy implication ............................................................................................... 33
5.4 Areas for further evaluation ................................................................................ 33
REFERENCE .......................................................................................................... 33
APPENDICES ......................................................................................................... 37
xii
LIST OF TABLES
Table 1.1: Stakeholders Matrix ................................................................................... 5
Table 3.1: Variables and its measurements ............................................................... 16
Table 4.1: Demographic characteristics of the respondents...................................... 20
Table 4.2: Responses on NHIF objectives achievement ........................................... 21
Table 4.3: Responses on NHIF objectives achievement ........................................... 21
Table 4.4 Reasons for NHIF to initiate accredited health facilities .......................... 22
Table 4.5 Benefits community gain from accredited facilities ................................. 24
Table 4.6: Attitude on NHIF services in accredited health facilities ........................ 25
Table 4.7 Challenges encountered in accredited health facilities ............................. 26
Table 4.8 Factors hindering adherence of NHIF standards....................................... 28
Table 4.9 Strategies to improve NHIF service provision .......................................... 29
Table 4.10: Ways to improve NHIF performance .................................................... 30
Table 4.11: Perception on improvement measures on NHIF .................................... 31

xiii
LIST OF FIGURES
Figure 1.1 : Logic model of NHIF program at facility level ....................................... 4
Figure 2.1: Theoretical framework of the evaluation................................................ 13
Figure 4.1: Reasons for NHIF to initiate accredited health facilities ........................ 23
Figure 4.2: Benefits gained by the community from accredited health facility ........ 24
Figure 4.3 Challenges encountered in accredited health facilities ............................ 27
Figure 4.4 Factors hindering NHIF service provision .............................................. 28
Figure 4.5: Strategies to improve NHIF service provision ....................................... 29
1
CHAPTER ONE
INTRODUCTION
1.1 Study Overview
Social Health Insurance Scheme is a health insurance which is provided by
governments to its employees (Churchill, 2006). This type of insurance maintains a
risk pooling fund account into which contributions and other incomes are deposited.
Out of this account; the scheme makes reimbursement of medical costs to accredited
health facilities in respect of medical services provided to beneficiaries (Carrin and
James, 2002). The main objectives of Social Health Insurance are: “To provide
health care that avoids large out of pocket expenditure, to increase appropriate
utilization of health services and to improve health status” (ILO, 2008). .
The first Social Health Insurance Scheme was established by the Government of
Germany between 1883 and 1889 (Wagstaff, 2009). The beneficiaries of the scheme
access health services through accredited public and private facilities whereby the
accredited health facilities are being reimbursed by the insurance scheme (Wagstaff,
2009). The scheme set the standards which all accredited health facilities must
adhere to in order for their claims to be reimbursed, failure to do so, it resulted into
rejections of the claims (Churchill, 2006). The insurance scheme of Germany was
very successful, therefore it was a good example to other countries; by 1930s Social
Health Insurance had spread to Latin America, the United States and Canada
(Wagstaff, 2009). After the end of the second World War, Social Health Insurance
was introduced in many countries in Africa, Asia and the Caribbean area (Wagstaff,
2009). Currently a number of African countries are implementing Social Health
Insurance Scheme with different approaches, including Nigeria, Rwanda, Kenya,
Ghana and Tanzania (Wagstaff, 2009).
1.1.1 Social Health Insurance Scheme in Tanzania
The National Health Insurance Fund (NHIF) is the largest social health insurance
scheme in Tanzania; it was established by the Parliament Act number 8 of 1999
2
(NHIF, 2013). This was the outcome of 1990 -1992 study on long term options for
financing health services in Tanzania (MOH, 1994). The scheme started its
operations on 1st July 2001 by members and their respective employers starting to
contribute and beneficiaries started to access medical services from 1st October 2001
(NHIF, 2013). The scheme maintains a risk pooling fund account into which such
contributions and other incomes are deposited, out of this account, the scheme makes
reimbursement for medical costs to accredited health facilities in respect of medical
services provided to beneficiaries (NHIF, 2013).
1.1.2. NHIF Accredited Health Facilities
NHIF does not provide health care services to the beneficiaries directly in the sense
of ownership of health facilities; relatively, it facilitates access of health services
through a network of accredited health facilities (NHIF, 2013). Currently there are
5,840 accredited health facilities throughout the country; accredited Health Facilities
are classified as Government, Faith Based Organizations, NGO and Private health
facilities (NHIF, 2013). Accredited health facilities are required to provide quality
services to NHIF beneficiaries because the success of NHIF depends much on how
health care providers receive and treats NHIF beneficiaries (NHIF, 2013). Therefore,
an adherence to NHIF standards is very important to ensure that the facility gets high
reimbursement rate which will lead to improvement of services to NHIF
beneficiaries. In order for the accredited health provider to be reimbursed for the
services they provided to NHIF beneficiaries, they must adhere to NHIF guidelines
and standards, failure to which may result into adjustments or rejection of the amount
claimed.
1.2. Description of Program to be evaluated
1.2.1. Expected Program effects/objectives
NHIF has the following objectives:
(i) To avail necessary guidelines as per NHIF standards to every accredited
health facility, by the end of 2014.
3
(ii) Increase accessibility and quality of services to beneficiaries and providers
by 2015
(iii) Increase accreditation of health facilities from current average of 80% to
95% by 2015
(iv) To increase reimbursement rate from 60% to 90% in each health facilities
from year 2010 to 2015.
(v) To train 10,000 health professionals (clinicians) on NHIF matters at the end
of 2014.
(vi) To conduct supervision at accredited health facilities at least 2 times in
hospitals and at least once in health centre and dispensaries per year from
the year 2010 to 2014.
1.2.2. Major strategies
(i) Early reimbursement to the accredited health facilities
(ii) Training health workers in accredited health facilities in adherence to NHIF
standards
(iii) Feedback to the accredited health facilities by providing payment advice
letter that allows an assessment of performance for the health facilities
(iv) Distribution of guidelines, benefit package, price list, and disease code to
every accredited health facility.
(v) Ensure quality of services to members as per NHIF benefits package.
1.2.3. Programme activities
NHIF major activities of NHIF are:
(i) To register members and employers and issue identity cards to beneficiaries;
(ii) To accredit and inspect health service providers and avail a broader network
of health facilities for improving access to health services in the country
(iii) To undertake quality assurance processes of the claims from accredited
facilities;
(iv) To collect monthly contributions from employers;
4
(v) To provide health insurance education to the public with the aim of
marketing it and enhance public relations.
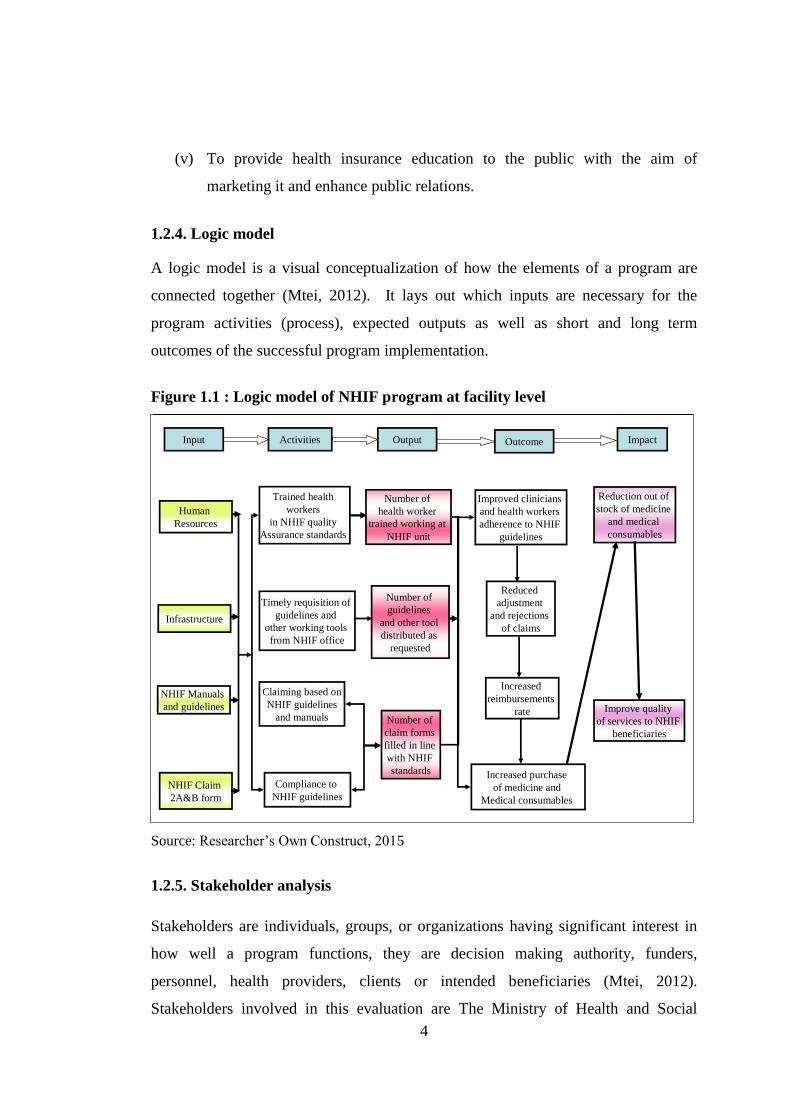
1.2.4. Logic model
A logic model is a visual conceptualization of how the elements of a program are
connected together (Mtei, 2012). It lays out which inputs are necessary for the
program activities (process), expected outputs as well as short and long term
outcomes of the successful program implementation.
Figure 1.1 : Logic model of NHIF program at facility level
Input OutputActivities ImpactOutcome
Human
Resources
Trained health
workers
in NHIF quality
Assurance standards
Timely requisition of
guidelines and
other working tools
from NHIF office
Compliance to
NHIF guidelines
Claiming based on
NHIF guidelines
and manualsImprove quality
of services to NHIF
beneficiaries
Number of
claim forms
filled in line
with NHIF
standards
Number of
guidelines
and other tool
distributed as
requested
Improved clinicians
and health workers
adherence to NHIF
guidelines
Infrastructure
NHIF Manuals
and guidelines
NHIF Claim
2A&B form
Reduction out of
stock of medicine
and medical
consumables
Number of
health worker
trained working at
NHIF unit
Increased purchase
of medicine and
Medical consumables
Increased
reimbursements
rate
Reduced
adjustment
and rejections
of claims
Source: Researcher‟s Own Construct, 2015
1.2.5. Stakeholder analysis
Stakeholders are individuals, groups, or organizations having significant interest in
how well a program functions, they are decision making authority, funders,
personnel, health providers, clients or intended beneficiaries (Mtei, 2012).
Stakeholders involved in this evaluation are The Ministry of Health and Social
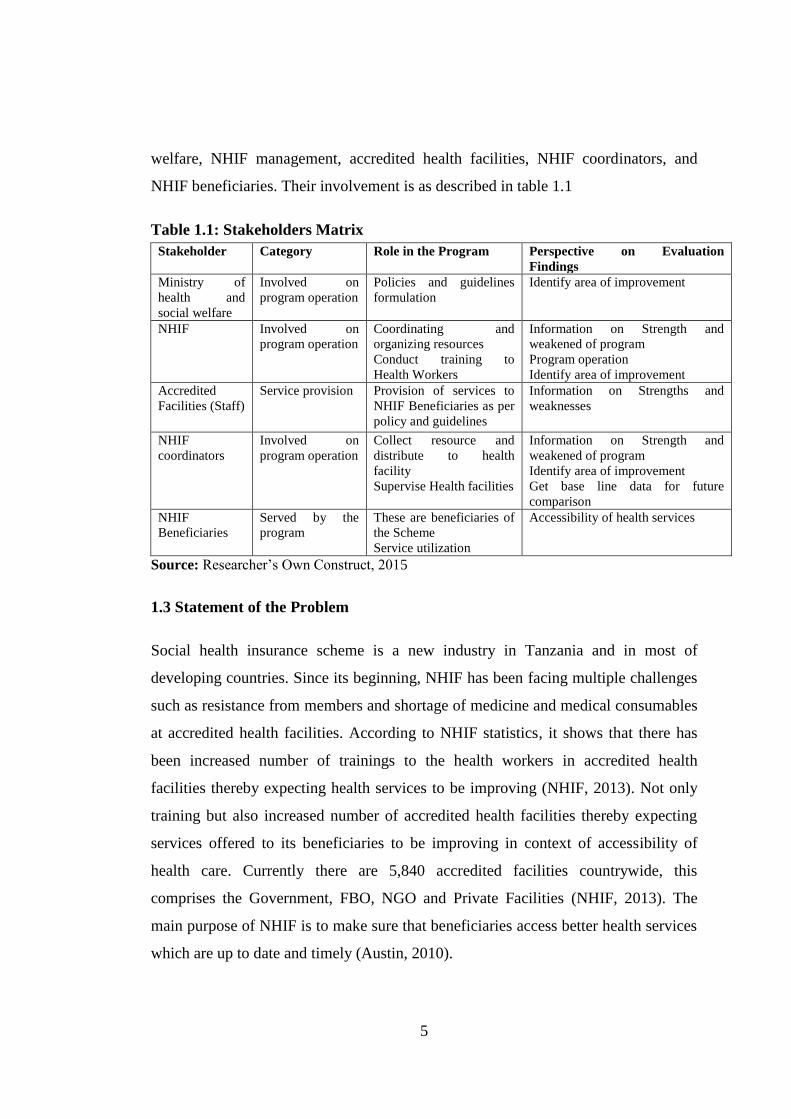
5
welfare, NHIF management, accredited health facilities, NHIF coordinators, and
NHIF beneficiaries. Their involvement is as described in table 1.1
Table 1.1: Stakeholders Matrix
Stakeholder Category Role in the Program Perspective on Evaluation
Findings
Ministry of
health and
social welfare
Involved on
program operation
Policies and guidelines
formulation
Identify area of improvement
NHIF Involved on
program operation
Coordinating and
organizing resources
Conduct training to
Health Workers
Information on Strength and
weakened of program
Program operation
Identify area of improvement
Accredited
Facilities (Staff)
Service provision Provision of services to
NHIF Beneficiaries as per
policy and guidelines
Information on Strengths and
weaknesses
NHIF
coordinators
Involved on
program operation
Collect resource and
distribute to health
facility
Supervise Health facilities
Information on Strength and
weakened of program
Identify area of improvement
Get base line data for future
comparison
NHIF
Beneficiaries
Served by the
program
These are beneficiaries of
the Scheme
Service utilization
Accessibility of health services
Source: Researcher‟s Own Construct, 2015
1.3 Statement of the Problem
Social health insurance scheme is a new industry in Tanzania and in most of
developing countries. Since its beginning, NHIF has been facing multiple challenges
such as resistance from members and shortage of medicine and medical consumables
at accredited health facilities. According to NHIF statistics, it shows that there has
been increased number of trainings to the health workers in accredited health
facilities thereby expecting health services to be improving (NHIF, 2013). Not only
training but also increased number of accredited health facilities thereby expecting
services offered to its beneficiaries to be improving in context of accessibility of
health care. Currently there are 5,840 accredited facilities countrywide, this
comprises the Government, FBO, NGO and Private Facilities (NHIF, 2013). The
main purpose of NHIF is to make sure that beneficiaries access better health services
which are up to date and timely (Austin, 2010).
6
However, despite all initiatives made by NHIF, beneficiaries are still complaining of
multiple problems in accredited facilities such as lack of medicine, lack of
laboratory services, inadequate accredited facilities and negative attitude of health
workers towards them at accredited facilities (NHIF, 2013).
Continuing with this current situation of multiple complains from beneficiaries in
turn inhibits the achievement of the goals of NHIF. Therefore need arises to evaluate
why despite NHIF efforts to achieve its goals towards accredited health facilities but
still there are persistent gaps. Furthermore, several studies on social health insurance
in Tanzania have been conducted in the focus of NHIF beneficiaries, therefore there
is a need to focus on health providers.
1.4 Objectives of the evaluation
1.4.1 General objective
The general objective of this study was to evaluate NHIF service provision in
accredited health facilities.
1.4.2 Specific objectives
(i) To assess service provision in NHIF accredited health facilities
(ii) To determine challenges faced by NHIF through accredited health facilities
(iii) To evaluate possible improvement measures on NHIF health service
provision
1.5 Evaluation Questions
(i) How are NHIF service provisions performed under accredited health
facilities?
(ii) What are the challenges faced by NHIF through accredited health facilities?
(iii) What are the possible improvement measures on NHIF health service
provision?

7
1.6 The Significance of the Evaluation
The justification of this process evaluation of NHIF service provision in accredited
health facilities is that, the main aim of NHIF is to increase access and quality of
service to its beneficiaries. If the reimbursement is low due to non-compliance to
NHIF standards therefore this goal will never be achieved. Therefore, findings from
this study are expected to reveal the achievement of NHIF, attitudes of health
workers towards NHIF, the challenges and measures to improve service provision in
accredited facilities. However, the findings of the evaluation may provide valuable
information to NHIF management and Ministry of Health and Social Welfare in
support of their decision making for the improving service provision in the health
facilities. Moreover, the successful completion of this study may lead to the award of
Master of Science in Health Monitoring and Evaluation of Mzumbe University.
8
CHAPTER TWO
LITERATURE REVIEW
2.1 Theoretical Literature Review
2.1.1 Program evaluation
According to Kolstad and Lindkvist (2013), evaluation is the periodic, in-depth
analysis of the programme performance by using indicators of the work plan. The
main purpose of evaluation is to assess overall achievements and performance,
therefore it helps an organization, program, project or any other intervention to
assess the progress and make decisions (Mtei, 2012).Evaluations usually focuses on
effectiveness, significance and impact, therefore it can be undertaken by programme
managers, supervisors, funders, external evaluators and beneficiaries (Mtei, 2012).
According to Bultman et al, (2012) there are three main designs of evaluation:
i. Goal based evaluation; Is the evaluation which takes place to determine the
actual outcome of a programme when compared to the goals/objectives of the
original plan (Bultman et al, 2012). Objectives are usually determined by the
people responsible for the funding or implementation of the programme
(Mtei, 2012).Therefore, this design of evaluation assists the organization to
further develop a successful process and either take out or reconfigure
unsuccessful goals.
ii. Process based evaluation; Is the evaluation which takes place while the
programme or project activities are in progress (Bultman et al, 2012).These
activities are assessed to date against the planned input and output, often
emphasizes on checking the progress of activity and applied to examine
reasons for the discrepancy of outputs of plans and suggest corrective
measures (Bultman et al, 2012). Therefore, this design of evaluation
examines operations of the programme and identifies strength, weakness and
areas that need improvement.
iii. Outcome based evaluation; Is the evaluation which takes place to assess
what occurred in the programme and whether the programme objectives has
9
been achieved (Bultman et al, 2012). It is used to assess the outcome of the
stated short-term, intermediate and long term programme objectives(Bultman
et al, 2012).Therefore, this design should be conducted when the programme
is matured enough to produce the intended outcome.
2.1.2 Health Insurance System in Tanzania
The Social Health Insurance in Tanzania is still at an infantry stage as compared to
other countries (NHIF, 2013). Up to 1990s the provision of health services was free
to all citizens and was financed by the government (NHIF, 2013). However, the
National Insurance Corporation (NIC) was providing voluntary Health Insurance
cover, very few people mainly businessmen and few others with fair income
managed to buy such premiums (NHIF, 2013). In the light of these factors, the
government made a health sector reform which initiated insurance schemes in the
country (NHIF, 2013). In 1997 the National Insurance Company established a health
insurance scheme known as Medicare for its members (Risha, 2002). In 1998 Igunga
Community Health Fund (ICHF) was established by the government in Tabora
(Risha, 2002). In 1999 NHIF was established by the government for formal sector
employees and CHF was established by parliamentary law no 8 in 2001 for informal
sector (NHIF, 2013).
2.1.3 Types of Health Insurance
There are three major types of health insurance which include: Social Health
Insurance; Private Health Insurance and Community Based Health Insurance (NHIF,
2013). Social Health Insurance is set by the government with clear benefits in return
for payment (NHIF, 2013). The main feature of this type of social insurance is that, it
is compulsory and mostly limited to those with salary stable wage earning
employment, normally referred in Tanzania as National Health Insurance (Ibrahim,
2001). Private health insurance normally covers groups or individuals through a
third party payer institution operating in the private sector (Ibrahim, 2001).
Community Based Health Insurance is normally voluntary and does not cover the
full cost of health care, contributions are collected when cash incomes are highest
10
and this helps to guarantee that the contributors have ongoing access to health care
(Ibrahim, 2001).
2.1.4. National Health Insurance Fund
The National Health Insurance Fund is a social health insurance scheme in Tanzania;
it was established by the Act number 8 of 1999 of Parliament (NHIF, 2013). This
was the outcome of 1990 -1992 study on long term options for financing health
services in Tanzania. The scheme started its operations on 1st July 2001 by members
and their respective employers starting to contribute and beneficiaries started to
access medical services from 1st October 2001 (NHIF, 2013). The scheme maintains
a risk pooling fund account into which such contributions and other incomes are
deposited, Out of this account, the scheme makes reimbursement for medical costs to
accredited health facilities in respect of medical services provided to beneficiaries
(NHIF, 2013).
2.2 Empirical Literature Review
Ghana National Health Insurance Scheme (NHIS) was established under the National
Health Insurance Act of 2003 and is based on District-wide Mutual Health Insurance
Schemes (DMHIS) which operate in all districts in the country (Slavea et al, 2009).
At the end of 2008, 61% of the population of Ghana was covered by the NHIS
(Slaves et al 2009). In 2009 an evaluation was conducted to evaluate the effects of
NHIS to service provider and beneficiaries of the scheme, data was collected using
closed and open ended questionnaires. The evaluation findings was that; there was
delays in insurance cards to beneficiaries, lack of motivation of DMHIS staff, lack
of understanding of the need for health insurance by community members and delays
in the reimbursement accredited health facilities (Slaves et al 2009). The authors
argued that delays in reimbursement soured relationship among service providers in
the district, who in some cases threatened to stop accepting insurance patients. The
study concluded that NHIS faced challenges which require Ghana Government to
use the findings of the study to improve the performance of NHIS by making
necessary reforms. However authors didn‟t point out the factors which contributed to
11
mentioned challenges especially the delays in the reimbursement process, therefore
this evaluation will look in the same scenario as Ghana but specifically on service
provision in accredited health facilities
In 2008 Mohammed et al, conducted an evaluation of NHIS in Zaria-Nigeria to
determine the enrolee‟s satisfaction with health service provision under a health
insurance scheme and the factors which influence the satisfaction. Mohammed et al
(2008) showed that Length of employment, salary income, hospital visits and
duration of enrolment slightly influenced satisfaction. Similarly, in 2012 Onyedibe et
al conducted a study to evaluate the level of enrolment of member to NHIS, the
results showed that the enrolment was very poor; authors pointed out that, the poor
enrolment was mainly contributed by dissatisfaction of health services offered to
NHIS beneficiaries. The authors concluded that the quality of the services was the
most important factor which influenced the enrolment of members to any insurance
scheme; therefore the Nigerian Government should use the evaluation findings to
improve the services in order to increase the enrolment. However, authors didn‟t
point out anything concerning the performance of the scheme in compliance with the
accredited health facilities, therefore this evaluation will evaluate the insurance
scheme in Tanzania but specifically on accredited health facilities.
According to Obonyo 1996, the Kenya National Health Insurance Fund (NHIF) has
been successful in implementing the scheme since 1966 to date, whereby the
coverage is 25% for the whole nation‟s population. The reason for their success is
that they have set a fee for services which is reasonable; hence health providers are
able to provide high quality health services (Obonyo, 1996.) Beneficiaries are
satisfied with the services and are fully utilizing them and have attracted even those
who are not compulsorily liable to join the scheme, such as self-employed people
and part-time workers who have joined the scheme as voluntary members (Obonyo,
1996). The second reason for Kenya‟s NHIF success is that it has the fund‟s
inspectorate unit, which inspects health providers regularly; they inspect their quality
of services and grade the providers according to score, they inspect drugs and
medical equipment availability and grade the facilities based on compliance with the
guidelines and standards. Thus, the author (Obonyo, 1996) presented utilization of
12
health insurance in Kenya and the factors that influence the utilization and how the
insurance inspects and grades the health providers. The author concluded that
inspection to the health providers is the key for improving the quality of NHIF
services. This evaluation will look on the same scenario but specifically for NHIF
accredited health facilities in the context of Tanzania.
In 2012 Musau et al conducted an evaluation on the health system of Tanzania,
specifically the National Health Insurance Fund. Data was collected using closed and
open ended questionnaires to NHIF beneficiaries and health workers in the
accredited health facilities. Authors pointed out that despite the significant effort in
developing insurance options; only13% of the population in Tanzania is currently
covered by health insurances (7.3%covered by NHIF). The study findings showed
that there was low member enrolment which was contributed by the health facilities
staff attitudes in treating NHIF patients, weakenesses of the public facilities
financially thus affects the services in terms of quality and availability. The authors
concluded that difficult reimbursement procedures done by NHIF is one of the factor
which led to poor services on accredited health facilities, therefore the Government
under MOHSW needs to review them in order to improve the performance of the
facilities. Therefore, this evaluation will specifically evaluate on service provision in
accredited health facilities.
2.3. Theoretical framework of the evaluation
The conceptual framework for this study assumes that NHIF health provision in
accredited health facilities (as a dependent variable) is determined by the following
(independent variables): knowledge of health workers, attitude of health workers
and compliance. Figure 2 shows conceptual framework for the roles played by health
workers in improving the service provision
13
Figure 2.1: Theoretical framework of the evaluation
Source: Researcher‟s Own Construct, 2015
Attitude of Health
workers on NHIF.
Knowledge of Health
workers on NHIF
services.
Compliance with NHIF
standards .
Improve NHIF
services provision
14
CHAPTER THREE
EVALUATION METHODOLOGY
3.1 Evaluation Approach
According to Patton (2012), formative evaluation is carried out in order to
understand what is going on with the implementation of the program, to find ways
and make recommendations on improving the program outcome. A formative
evaluation was conducted to assess the ongoing NHIF activities in order to provide
information that could be used for improvement.
3.2 Evaluation Design
An evaluation design is the arrangement of conditions for collection and analysis of
data in a manner that aims to combine relevance to the research purpose with
economy procedure (Kothari, 2010). There are several types of research designs such
as case study, survey and experimental. For the purpose of this study, facility based
multiple case studies of both quantitative and qualitative nature was carried out to
evaluate NHIF service provision in accredited health facilities.
3.3 Evaluation Period
The evaluation was conducted in four months. The work started on 1st February
2015 and it was completed on 31st May, 2015.
3.4. Description of the Study Area
Temeke Municipal
The process evaluation was conducted in Temeke Municipality, located in the south
of Dar es Salaam region, Tanzania. The municipality has estimated total population
of 1,368,881 whereby 669,056 are males and 699,825 are females with an estimated
area of 786.5 km2 and growth rate of 6.6% per year of (NBS, 2012). Temeke district,
is the largest of the three Dar es Salaam districts, to the north, it is bordered by Ilala
district: to the east by the Indian Ocean and to the South and West by the Coast
15
Region. It has an average temperature of 35OC and 1000mm of rainfall per year. The
district is administratively divided into three divisions with 24 wards. The
Municipality has an estimation of 4680 NHIF beneficiaries, there are 34 accredited
NHIF health facilities in the Municipality whereby 28 are public health facilities
(82.4%) while 6 facilities (17.6%) are private ones (NHIF, 2013).
3.5. Study Population
The population for this evaluation involved facility in-charges, doctors, nurses and
pharmacists working with NHIF accredited health facilities in the district. Facility in-
charges were intrviewed because of their roles as planners, decision makers and at
the same times are the most informed about health insurance operations. Also the
evaluator interviewed doctors, nurses and pharmacists since they are the ones who
attend NHIF beneficiaries.
3.6. Units of analysis
For the purpose of this assessment , the unit of analysis involved 80 respondents
from ten selected health facilities in Temeke Municial .
3.7. Variables and their measurements
In this evaluation study, a number of variables were involved as indicated in Table
3.1
16
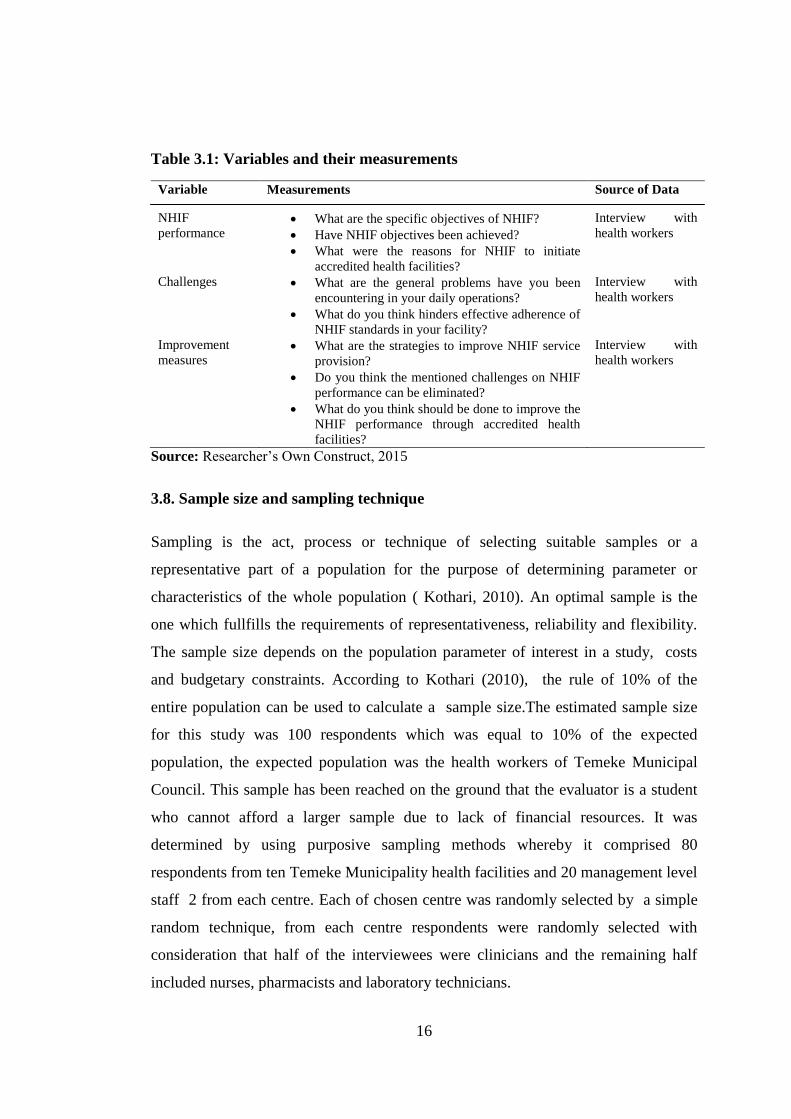
Table 3.1: Variables and their measurements
Variable Measurements Source of Data
NHIF
performance What are the specific objectives of NHIF?
Have NHIF objectives been achieved?
What were the reasons for NHIF to initiate
accredited health facilities?
Interview with
health workers
Challenges What are the general problems have you been
encountering in your daily operations?
What do you think hinders effective adherence of
NHIF standards in your facility?
Interview with
health workers
Improvement
measures What are the strategies to improve NHIF service
provision?
Do you think the mentioned challenges on NHIF
performance can be eliminated?
What do you think should be done to improve the
NHIF performance through accredited health
facilities?
Interview with
health workers
Source: Researcher‟s Own Construct, 2015
3.8. Sample size and sampling technique
Sampling is the act, process or technique of selecting suitable samples or a
representative part of a population for the purpose of determining parameter or
characteristics of the whole population ( Kothari, 2010). An optimal sample is the
one which fullfills the requirements of representativeness, reliability and flexibility.
The sample size depends on the population parameter of interest in a study, costs
and budgetary constraints. According to Kothari (2010), the rule of 10% of the
entire population can be used to calculate a sample size.The estimated sample size
for this study was 100 respondents which was equal to 10% of the expected
population, the expected population was the health workers of Temeke Municipal
Council. This sample has been reached on the ground that the evaluator is a student
who cannot afford a larger sample due to lack of financial resources. It was
determined by using purposive sampling methods whereby it comprised 80
respondents from ten Temeke Municipality health facilities and 20 management level
staff 2 from each centre. Each of chosen centre was randomly selected by a simple
random technique, from each centre respondents were randomly selected with
consideration that half of the interviewees were clinicians and the remaining half
included nurses, pharmacists and laboratory technicians.
17
3.9. Types and sources of data
Data are information, both qualitative and quantitative in nature, data for research
can be obtained through various sources. In this study the evaluator used both
primary and secondary sources. Primary data are those ones collected by the
researcher herself from the field, they are firsthand information and secondary data
are those which have been collected by other people or institutions but relevant to
your research. In this study, primary data were collected by administering
questionnaires to respondents. This method was used in order to gather the necessary
data and also to provide profound insight into the topic. The secondary data was
collected from different websites, reports, books, journals, and newspapers.
3.10. Data collection methods
Structured questionnaire with open and closed questions was used as data collection
tool in this study. The questinnaires was administered to individual respondents
through face to face interview. Data correctness was ensured by doing a data editing
and validation.
3.11. Validity issues
Validity refers to the quality that a procedure or an instrument used in the research is
accurate, true, meaningful and right (David, 2002). A measurement is valid when it
measures what is supposed be measure. The validity of data generated for this study
was ensured through comprehensive scrutiny of NHIF data by the evaluator.
Analysing the data descriptive statistical methods like tabulation, percentages and
frequencies were used.
3.12. Data management and analysis methods
The data has been analyzed by using both quantitative and qualitative methods with
assistance of SPSS software and microsofit word excel. After the completion of
questionnaires, data were coded, examined, compared and categorized based on the
18
evaluation questions. Throughout the analyzing process, comparison has been done
to find differences, similarities and meaning.
3.13 Ethical issues
Permission to conduct evaluation was obtained from the Director General of NHIF
and Temeke District Medical Officer (DMO). Each respondent was fully and clearly
informed about the aim of the evaluation and the confidentiality of the information.
Data security was ensured first and foremost by the principle for confidentiality. Data
collection instruments for the purpose of this evaluation were not constitute
personnel identifiers such as respondent‟s name.
19
CHAPTER FOUR
PRESENTATION AND DISCUSSION OF EVALUATION FINDINGS
4.1 Introduction
This chapter discusses the finding from the evaluation objectives. These were
understanding of the NHIF services provision in accredited health facilities,
determining challenges faced by NHIF through accredited health facilities, and
evaluation of possible improvement measures on NHIF health service provision.
Furthermore, the chapter puts into consideration the demographic information of the
respondents like their characteristics on sex,age and work experience.
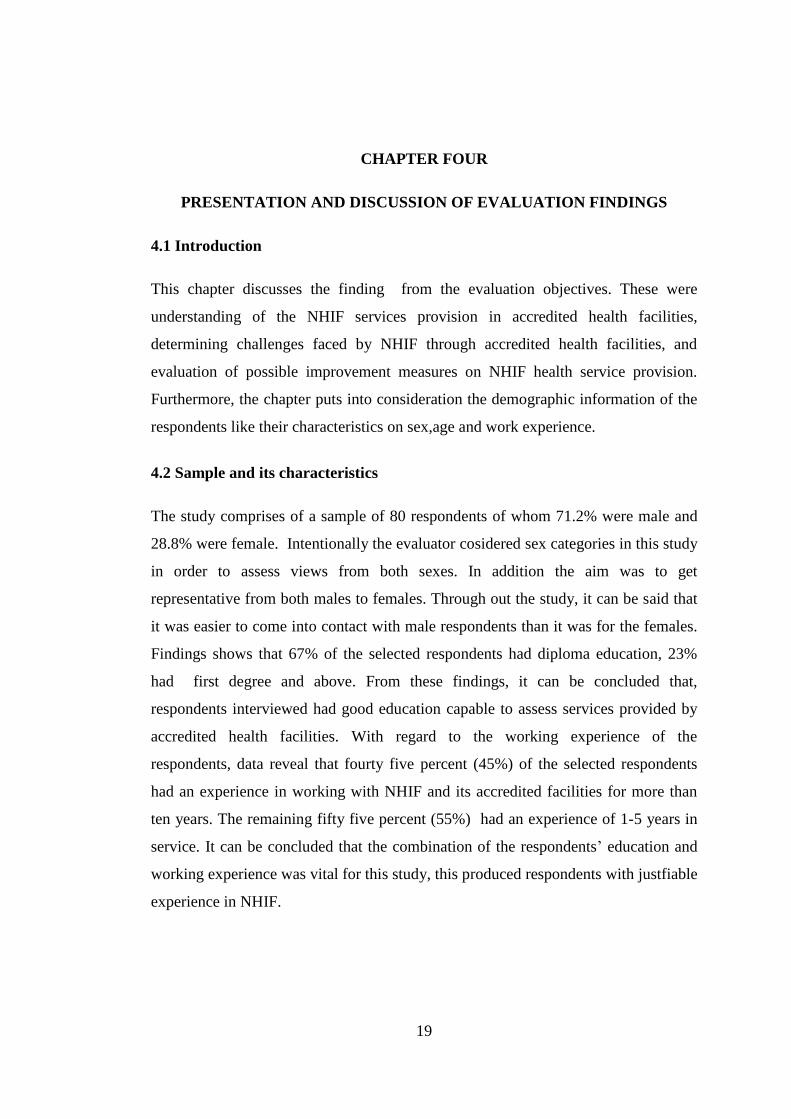
4.2 Sample and its characteristics
The study comprises of a sample of 80 respondents of whom 71.2% were male and
28.8% were female. Intentionally the evaluator cosidered sex categories in this study
in order to assess views from both sexes. In addition the aim was to get
representative from both males to females. Through out the study, it can be said that
it was easier to come into contact with male respondents than it was for the females.
Findings shows that 67% of the selected respondents had diploma education, 23%
had first degree and above. From these findings, it can be concluded that,
respondents interviewed had good education capable to assess services provided by
accredited health facilities. With regard to the working experience of the
respondents, data reveal that fourty five percent (45%) of the selected respondents
had an experience in working with NHIF and its accredited facilities for more than
ten years. The remaining fifty five percent (55%) had an experience of 1-5 years in
service. It can be concluded that the combination of the respondents‟ education and
working experience was vital for this study, this produced respondents with justfiable
experience in NHIF.
20
Table 4.1: Demographic characteristics of the respondents
Sn Variable Frequency Percentage
1 Sex of respondents
Male
Female
57
23
71.2%
28.8%
2 Education level Secondary
Certificate
Diploma
Degree and above
2
5
54
19
2.5%
6.3%
67.5%
23.8%
3 Working experience
Less than 1 year
1 to 5 years
6 to 10 years
More than 10 years
4
33
7
36
5.0%
41.3%
8.7%
45.0%
4 Age distribution
18-25 years
26-35 years
36-45years
46-55 years
56-60 years
11
24
16
15
14
13.8%
30.0%
20.0%
18.8%
17.5%
Source: Field data, 2015
4.3 NHIF service provision in accredited health facilities
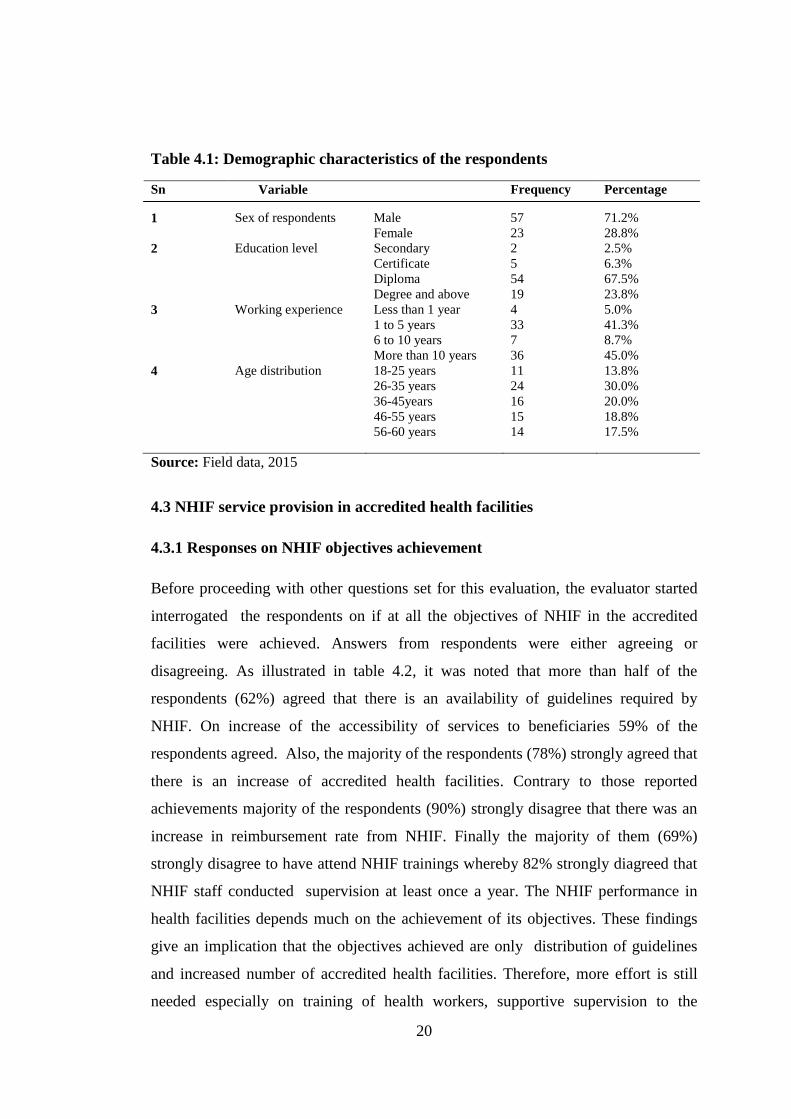
4.3.1 Responses on NHIF objectives achievement
Before proceeding with other questions set for this evaluation, the evaluator started
interrogated the respondents on if at all the objectives of NHIF in the accredited
facilities were achieved. Answers from respondents were either agreeing or
disagreeing. As illustrated in table 4.2, it was noted that more than half of the
respondents (62%) agreed that there is an availability of guidelines required by
NHIF. On increase of the accessibility of services to beneficiaries 59% of the
respondents agreed. Also, the majority of the respondents (78%) strongly agreed that
there is an increase of accredited health facilities. Contrary to those reported
achievements majority of the respondents (90%) strongly disagree that there was an
increase in reimbursement rate from NHIF. Finally the majority of them (69%)
strongly disagree to have attend NHIF trainings whereby 82% strongly diagreed that
NHIF staff conducted supervision at least once a year. The NHIF performance in
health facilities depends much on the achievement of its objectives. These findings
give an implication that the objectives achieved are only distribution of guidelines
and increased number of accredited health facilities. Therefore, more effort is still
needed especially on training of health workers, supportive supervision to the
21
facilities and increase of reimbursement rates in order for NHIF to achieve its
objectives as well as to improve service provision.
Table 4.2: Responses on NHIF objectives achievement
Statement Strongly
agree
Agree Uncertain Disagree Strongly
disagree
Availability of guidelines as per NHIF
standards in the facility
13.0% 62.0% 6.0% 13.0% 6.0%
There is increase of accessibility and
quality services to beneficiaries
10.0% 59.0% 15.0% 14.0% 2.0%
There is increase of accredited health
facilities
78.0% 20.0% 0.0% 1.0% 1.0%
There is increase of reimbursement in
facility from NHIF
0.0% 0.0% 5.0% 5.0% 90.0%
Attended training on NHIF matters 2.0% 18.0% 0.0% 11.0% 69.0%
Supervision conducted by NHIF at
least once per year
1.0% 0.0% 4.0% 13.0% 82.0%
Source: Field data, 2015
4.3.2 Responses on overall achievement of NHIF objectives
To check the overall achievement of NHIF, respondents were asked to agree or
disagree if at all the objectives of NHIF initiating accredited health facilities were
achieved. Table 4.3 shows that there are some achievements of NHIF objectives.
This is because only 51.3% of the respondents agreed that the objectives were
achieved. These results imply that respondents are aware of NHIF performances in
their health facilities.
Table 4.3: Responses on NHIF objectives achievement
Response Frequency Percent
Yes 41 51.3
No 8 10.0
Don‟t know 31 38.8
Total 80 100.0
Source: Field data, 2015
22
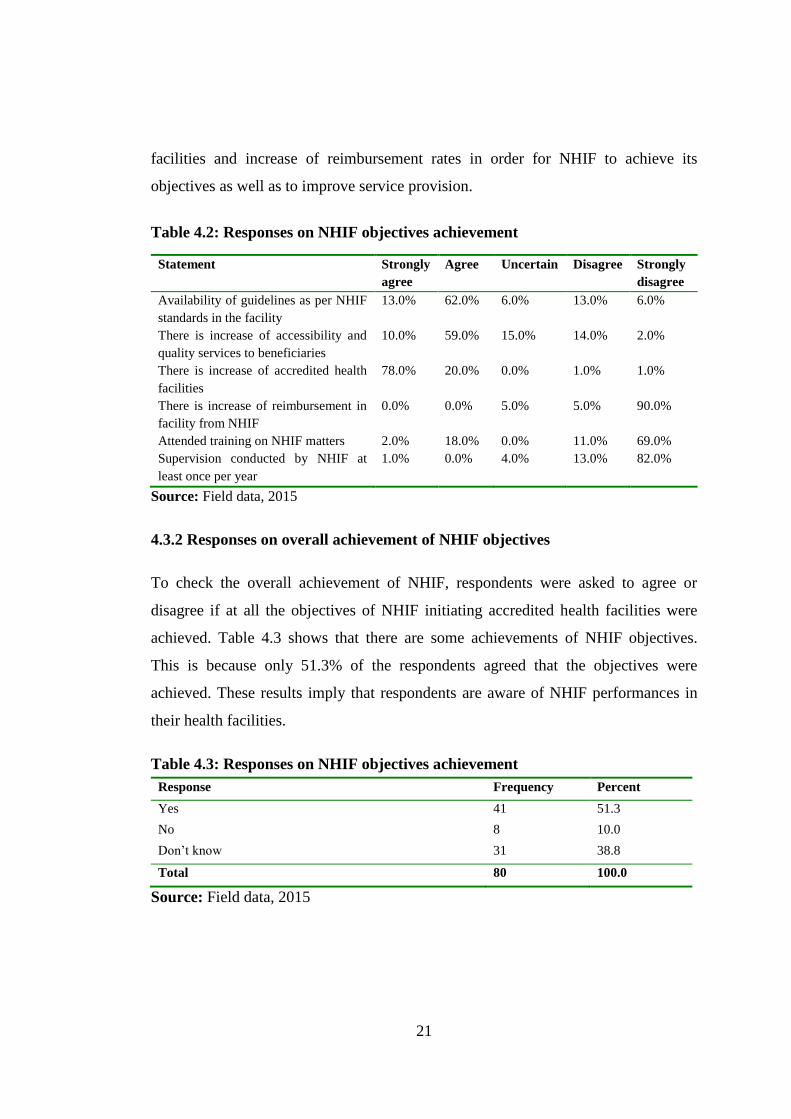
4.3.3 Reasons for NHIF to initiate accredited health facilities
In order to comply with NHIF in provision of services, health workers should be
aware of the reasons for NHIF to accredit health facilities. A question contained a list
of items that required each respondent to choose one. Table 4.3, shows that 32.5% of
the respondents said that it was primarily initiated to improve health services, while
others mentioned to speed up service provision (22.5%), These findings suggest that
health providers are aware of reasons of NHIF iniatiating accredited facilities. This
implies that NHIF has positively influenced health seeking behaviour and utilization
of healthcare services. Prepaid scheme has a potentiality of reducing out of pocket
payment for health services. Other respondents (21.3%) reported the reason was to
enable many people to get health services. In this report therefore NHIF should be
sustained to increase the affordability and access to heath services.This will improve
the performance and at the sametime promote universal coverage for the people of
Tanzania.
Table 4.4: Reasons for NHIF to initiate accredited health facilities
Reason Frequency Percent
To speed up service provision 18 22.5
To improve health service 26 32.5
To enable many people attend the service 17 21.3
To cover large areas 13 16.3
Not sure 6 7.5
Total 80 100.0
Source: Field data, 2015
23
Figure 4.1: Reasons for NHIF to initiate accredited health facilities
Source: Field data, 2015
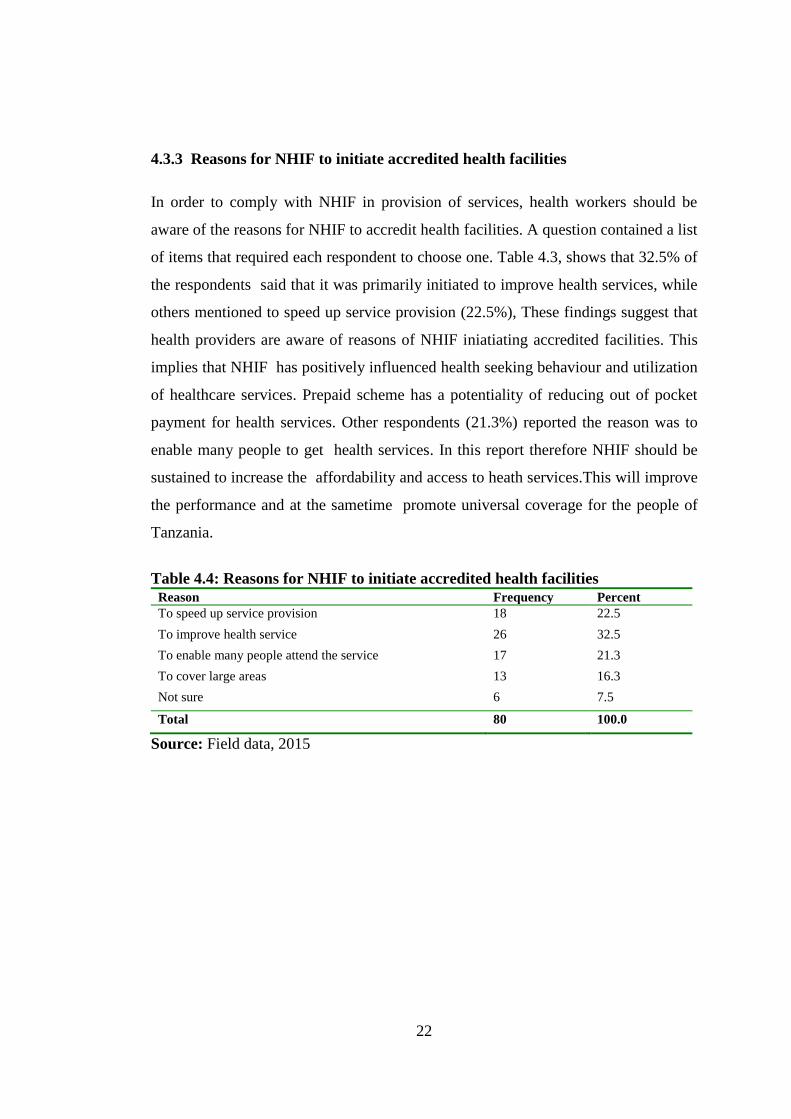
4.3.4 Benefits Gained by the Community.
Study findings has proved that accreditted health facilities are very important to
NHIF beneficiaries as well as to the community. During the study respondents were
asked to choose one benefit from the list, see figure 4.2, 38.8% of the respondents
stated that Primary Health Care (PHC) were more beneficial to communities. PHC
refers to essential health care that is based on scientifically sound and socially
acceptable methods and technology, which make universal health care, universally
accessible to individuals and families in a community (WHO, 2004). Therefore
NHIF needs to take a critical look in expanding primary health care geographically.
This will help to achieve universal health coverage. Also other 27.6% of respondents
mentioned large coverage was another benefit which the community gained from
these facilities. This implies that the beneficiaries have choice where to go for
services .i.e. Government, FBO or private for profit health facilities. The findings
generaly disclose that NHIF, has a significant influence on the use of health services
whereby beneficiaries are free to choose where to go for services, this is because
services are driven by quality consideration rather than cost and distance.
24
Table 4.5: Benefits community gain from accredited facilities
Benefit Frequency Percent
Primary Health Care 31 38.8
Access to medicines 9 11.3
Advice 7 8.8
Readily available health services 8 10.0
Large coverage 22 27.6
No benefits 3 3.8
Total 80 100.0
Source: Field data, 2015
Figure 4.2: Benefits gained by the community from accredited health facility
38.8
11.3
8.8
10
27.6
3.8
0 10 20 30 40 50 60 70 80 90 100
Primary care
Access to medicines
Advice
Readily available health services
Large coverage
No benefits
Percentages
Ben
efi
ts
Percent
Source: Field data, 2015
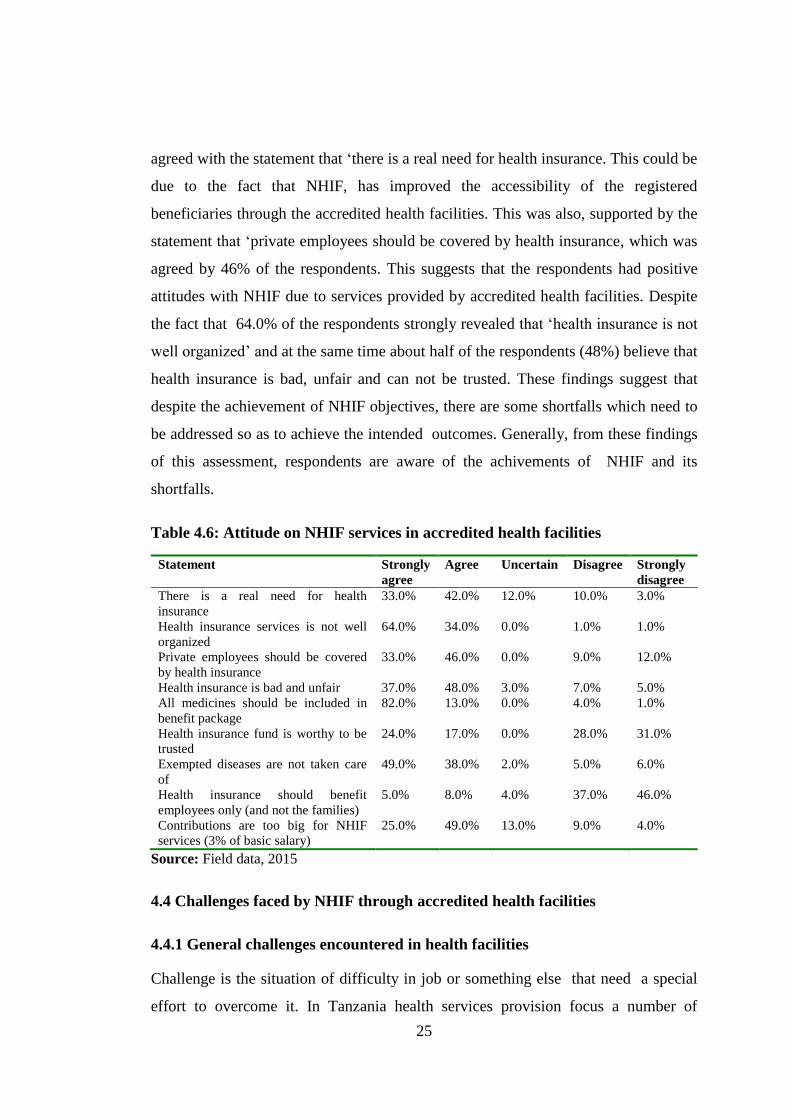
4.3.5 Attitude on NHIF services in Accredited Health Facilities
Attitudes is a mental position, which influence a person in regard to his/her feeling
or emotion toward the fact. Knowing health workers attitude toward NHIF, was of
great important in this assessment because workers attitude may affect the
organizational performance. A number of attitudinal statements were subjected, to
test the respondents‟ attitude on the performance of accredited health facilities under
NHIF. The information contained in table 4.5 shows that 42.0 % of respondents
25
agreed with the statement that „there is a real need for health insurance. This could be
due to the fact that NHIF, has improved the accessibility of the registered
beneficiaries through the accredited health facilities. This was also, supported by the
statement that „private employees should be covered by health insurance, which was
agreed by 46% of the respondents. This suggests that the respondents had positive
attitudes with NHIF due to services provided by accredited health facilities. Despite
the fact that 64.0% of the respondents strongly revealed that „health insurance is not
well organized‟ and at the same time about half of the respondents (48%) believe that
health insurance is bad, unfair and can not be trusted. These findings suggest that
despite the achievement of NHIF objectives, there are some shortfalls which need to
be addressed so as to achieve the intended outcomes. Generally, from these findings
of this assessment, respondents are aware of the achivements of NHIF and its
shortfalls.
Table 4.6: Attitude on NHIF services in accredited health facilities
Statement Strongly
agree
Agree Uncertain Disagree Strongly
disagree
There is a real need for health
insurance
33.0% 42.0% 12.0% 10.0% 3.0%
Health insurance services is not well
organized
64.0% 34.0% 0.0% 1.0% 1.0%
Private employees should be covered
by health insurance
33.0% 46.0% 0.0% 9.0% 12.0%
Health insurance is bad and unfair 37.0% 48.0% 3.0% 7.0% 5.0%
All medicines should be included in
benefit package
82.0% 13.0% 0.0% 4.0% 1.0%
Health insurance fund is worthy to be
trusted
24.0% 17.0% 0.0% 28.0% 31.0%
Exempted diseases are not taken care
of
49.0% 38.0% 2.0% 5.0% 6.0%
Health insurance should benefit
employees only (and not the families)
5.0% 8.0% 4.0% 37.0% 46.0%
Contributions are too big for NHIF
services (3% of basic salary)
25.0% 49.0% 13.0% 9.0% 4.0%
Source: Field data, 2015
4.4 Challenges faced by NHIF through accredited health facilities
4.4.1 General challenges encountered in health facilities
Challenge is the situation of difficulty in job or something else that need a special
effort to overcome it. In Tanzania health services provision focus a number of
26
challenges that need to be addressed. This would enable the program or organization
to improve the operating environments. In this regard, evaluation involved
determining the challenges encountered in NHIF accredited health facilities. Number
of challenges were noted from respondents point of view. 41.3% (figure 4.3 and
table 4.7) mentioned that low Government budget in health facilities is the leading
challenge in the facilities, followed by lack of modern technology (17.4%) and lack
of community awareness 16.3%. Other remaining problems are as shown in figure
4.3. These results suggest that NHIF performance in health facilities will be low and
the objective will never be achieved if the facilities will continue to face the
mentioned challenges. In conclusion NHIF in collaboration with other stakeholders
should increase public awareness and early reimbursement to health facilities in
order to increase performance in health delivery.
Table 4.7: Challenges encountered in accredited health facilities
Challenge Frequency Percent
Low government budget 33 41.3
Lack of community awareness 13 16.3
Lack of modern technology 14 17.5
Frail financial flow 12 15.0
Acceptance by the community 8 10.0
Total 80 100.0
Source: Field data, 2015
27
Figure 4.3: Challenges encountered in accredited health facilities
Source: Field data, 2015
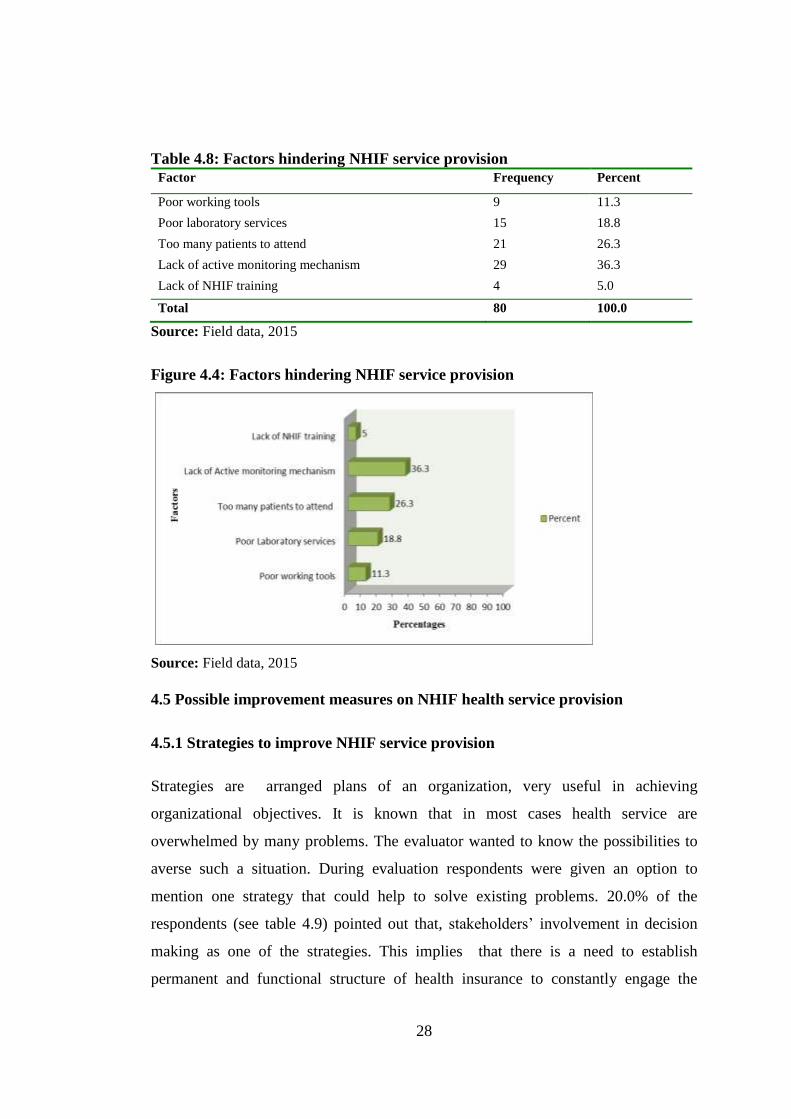
4.4.2 Factors for less adherence to NHIF standards
In regard to the operationalization of NHIF which has been in service for more than
ten years, the investigator felt it prudent to get an eyesight on reasons behind
unsatisfactory performance of NHIF. Analysing factors hindering NHIF service
provision, Most of respondents reported that (36.3%) it was due to lack of active
monitoring mechanism of NHIF funds (table 4.8). This is followed by respondents
(26%) who reported that overflow of attending NHIF clinics be a factor of poor
performance. Other factors are poor laboratory services (18%) and poor supply of
working tools(11.3%). View of this evaluation, NHIF, could achieve better
performance through effective monitoring claims and reimbursed funds. Referring to
a study conducted by Mtei (2012) pointed out that effective monitoring of claims and
funds improved the performance of private health insurance schemes in Tanzania.
Therefore, MOHSW and NHIF management should put more attention on the basic
requirements of the facilities to provide good working conditions for health workers.
This will motivate them to work hard as a result will promote the performance of
NHIF in health facilities.
28
Table 4.8: Factors hindering NHIF service provision
Factor Frequency Percent
Poor working tools 9 11.3
Poor laboratory services 15 18.8
Too many patients to attend 21 26.3
Lack of active monitoring mechanism 29 36.3
Lack of NHIF training 4 5.0
Total 80 100.0
Source: Field data, 2015
Figure 4.4: Factors hindering NHIF service provision
Source: Field data, 2015
4.5 Possible improvement measures on NHIF health service provision
4.5.1 Strategies to improve NHIF service provision
Strategies are arranged plans of an organization, very useful in achieving
organizational objectives. It is known that in most cases health service are
overwhelmed by many problems. The evaluator wanted to know the possibilities to
averse such a situation. During evaluation respondents were given an option to
mention one strategy that could help to solve existing problems. 20.0% of the
respondents (see table 4.9) pointed out that, stakeholders‟ involvement in decision
making as one of the strategies. This implies that there is a need to establish
permanent and functional structure of health insurance to constantly engage the
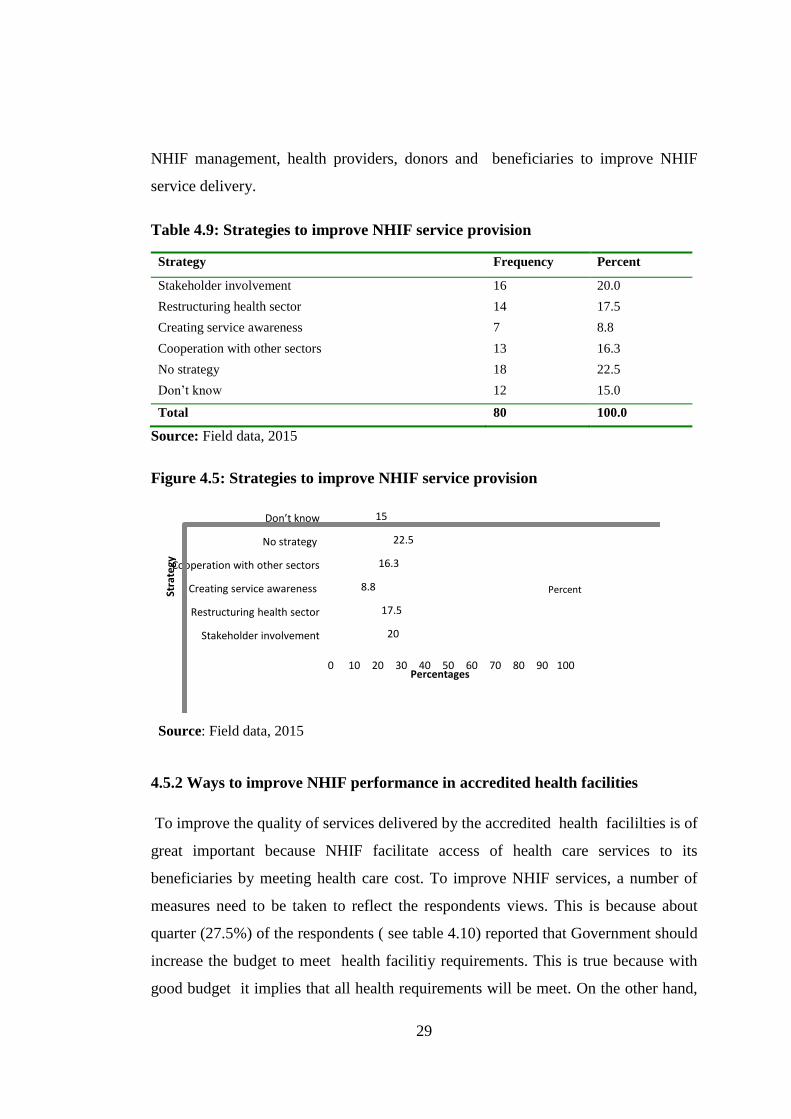
29
NHIF management, health providers, donors and beneficiaries to improve NHIF
service delivery.
Table 4.9: Strategies to improve NHIF service provision
Strategy Frequency Percent
Stakeholder involvement 16 20.0
Restructuring health sector 14 17.5
Creating service awareness 7 8.8
Cooperation with other sectors 13 16.3
No strategy 18 22.5
Don‟t know 12 15.0
Total 80 100.0
Source: Field data, 2015
Figure 4.5: Strategies to improve NHIF service provision
0 10 20 30 40 50 60 70 80 90 100
Stakeholder involvement
Restructuring health sector
Creating service awareness
Cooperation with other sectors
No strategy
Don’t know
20
17.5
8.8
16.3
22.5
15
Percentages
Strategy
Percent
Source: Field data, 2015
4.5.2 Ways to improve NHIF performance in accredited health facilities
To improve the quality of services delivered by the accredited health facililties is of
great important because NHIF facilitate access of health care services to its
beneficiaries by meeting health care cost. To improve NHIF services, a number of
measures need to be taken to reflect the respondents views. This is because about
quarter (27.5%) of the respondents ( see table 4.10) reported that Government should
increase the budget to meet health facilitiy requirements. This is true because with
good budget it implies that all health requirements will be meet. On the other hand,
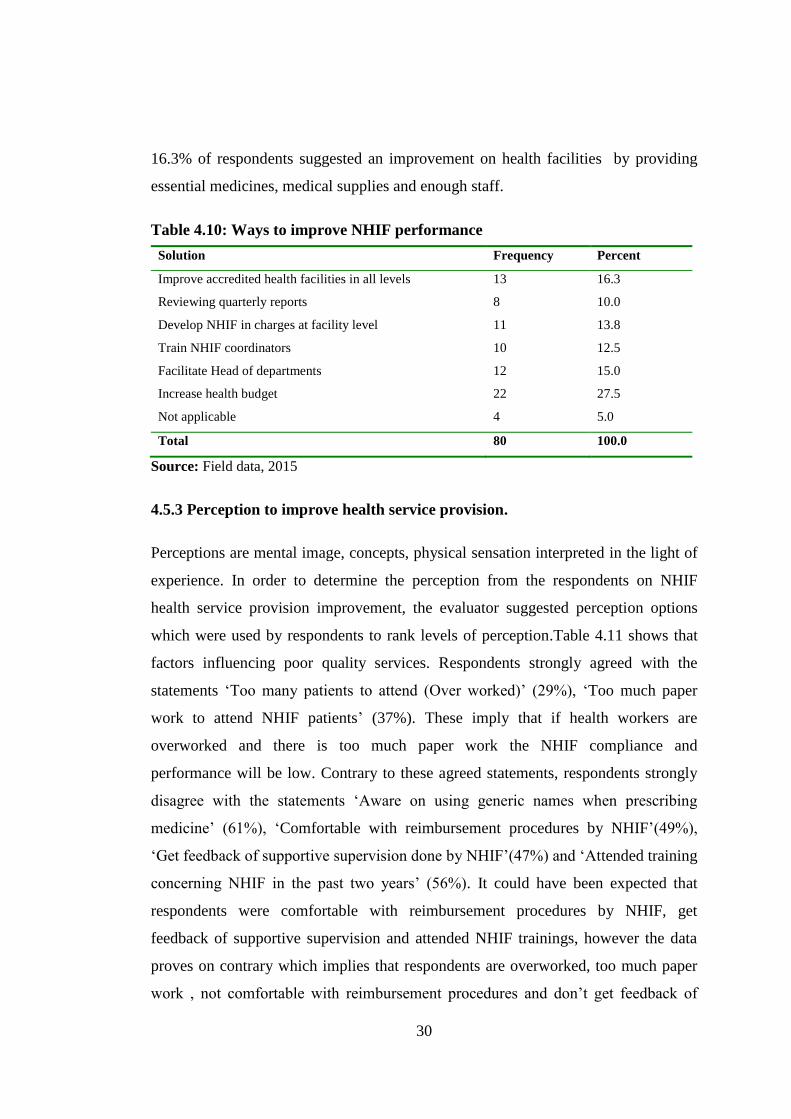
30
16.3% of respondents suggested an improvement on health facilities by providing
essential medicines, medical supplies and enough staff.
Table 4.10: Ways to improve NHIF performance
Solution Frequency Percent
Improve accredited health facilities in all levels 13 16.3
Reviewing quarterly reports 8 10.0
Develop NHIF in charges at facility level 11 13.8
Train NHIF coordinators 10 12.5
Facilitate Head of departments 12 15.0
Increase health budget 22 27.5
Not applicable 4 5.0
Total 80 100.0
Source: Field data, 2015
4.5.3 Perception to improve health service provision.
Perceptions are mental image, concepts, physical sensation interpreted in the light of
experience. In order to determine the perception from the respondents on NHIF
health service provision improvement, the evaluator suggested perception options
which were used by respondents to rank levels of perception.Table 4.11 shows that
factors influencing poor quality services. Respondents strongly agreed with the
statements „Too many patients to attend (Over worked)‟ (29%), „Too much paper
work to attend NHIF patients‟ (37%). These imply that if health workers are
overworked and there is too much paper work the NHIF compliance and
performance will be low. Contrary to these agreed statements, respondents strongly
disagree with the statements „Aware on using generic names when prescribing
medicine‟ (61%), „Comfortable with reimbursement procedures by NHIF‟(49%),
„Get feedback of supportive supervision done by NHIF‟(47%) and „Attended training
concerning NHIF in the past two years‟ (56%). It could have been expected that
respondents were comfortable with reimbursement procedures by NHIF, get
feedback of supportive supervision and attended NHIF trainings, however the data
proves on contrary which implies that respondents are overworked, too much paper
work , not comfortable with reimbursement procedures and don‟t get feedback of
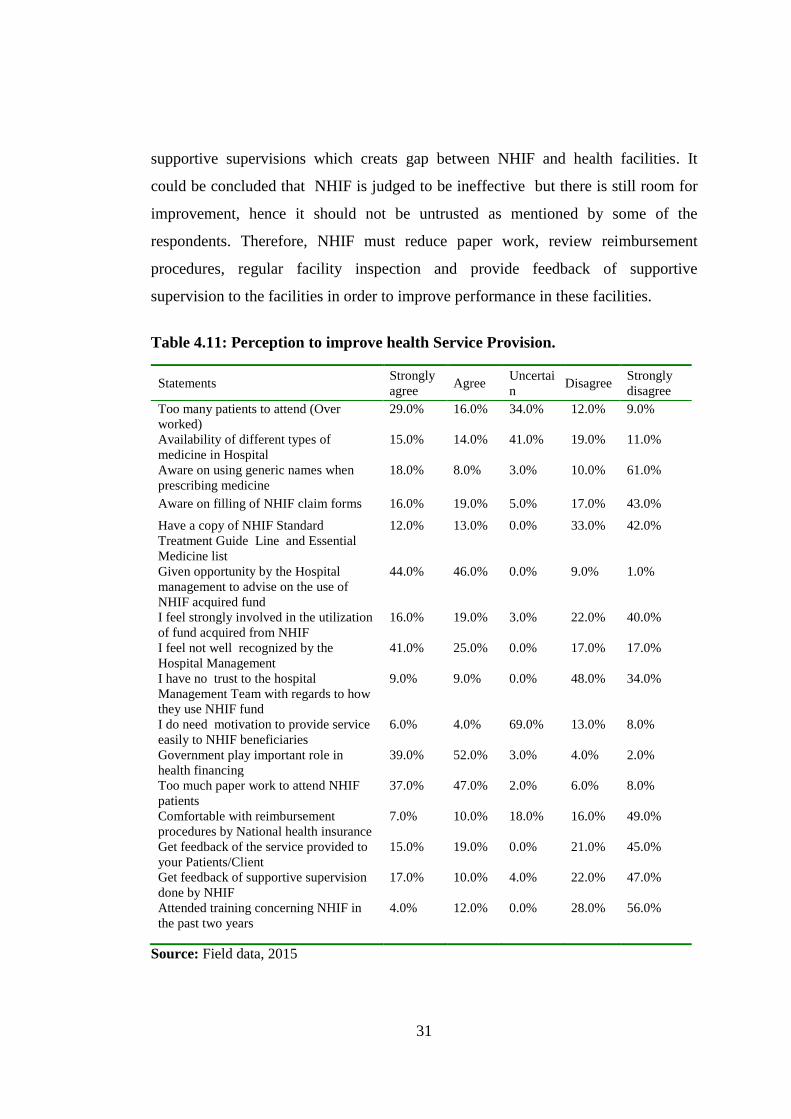
31
supportive supervisions which creats gap between NHIF and health facilities. It
could be concluded that NHIF is judged to be ineffective but there is still room for
improvement, hence it should not be untrusted as mentioned by some of the
respondents. Therefore, NHIF must reduce paper work, review reimbursement
procedures, regular facility inspection and provide feedback of supportive
supervision to the facilities in order to improve performance in these facilities.
Table 4.11: Perception to improve health Service Provision.
Statements Strongly
agree Agree
Uncertai
n Disagree
Strongly
disagree
Too many patients to attend (Over
worked)
29.0% 16.0% 34.0% 12.0% 9.0%
Availability of different types of
medicine in Hospital
15.0% 14.0% 41.0% 19.0% 11.0%
Aware on using generic names when
prescribing medicine
18.0% 8.0% 3.0% 10.0% 61.0%
Aware on filling of NHIF claim forms 16.0% 19.0% 5.0% 17.0% 43.0%
Have a copy of NHIF Standard
Treatment Guide Line and Essential
Medicine list
12.0% 13.0% 0.0% 33.0% 42.0%
Given opportunity by the Hospital
management to advise on the use of
NHIF acquired fund
44.0% 46.0% 0.0% 9.0% 1.0%
I feel strongly involved in the utilization
of fund acquired from NHIF
16.0% 19.0% 3.0% 22.0% 40.0%
I feel not well recognized by the
Hospital Management
41.0% 25.0% 0.0% 17.0% 17.0%
I have no trust to the hospital
Management Team with regards to how
they use NHIF fund
9.0% 9.0% 0.0% 48.0% 34.0%
I do need motivation to provide service
easily to NHIF beneficiaries
6.0% 4.0% 69.0% 13.0% 8.0%
Government play important role in
health financing
39.0% 52.0% 3.0% 4.0% 2.0%
Too much paper work to attend NHIF
patients
37.0% 47.0% 2.0% 6.0% 8.0%
Comfortable with reimbursement
procedures by National health insurance
7.0% 10.0% 18.0% 16.0% 49.0%
Get feedback of the service provided to
your Patients/Client
15.0% 19.0% 0.0% 21.0% 45.0%
Get feedback of supportive supervision
done by NHIF
Attended training concerning NHIF in
the past two years
17.0%
4.0%
10.0%
12.0%
4.0%
0.0%
22.0%
28.0%
47.0%
56.0%
Source: Field data, 2015
32
CHAPTER FIVE
SUMMARY, CONCLUSION AND POLICY IMPLICATION
5.1 Summary
This study evaluates NHIF service provision in accredited health facilities,.
Challenges encountered need a clear measures for improvement of health services.
This is because findings have revealed that NHIF objectives are not fully achieved
due to various factors. Also the evaluation noted a number of challenges facing
accredited health facilities.These challenges are manageable through good plan and
Government commitments.
5.2 Conclusion
NHIF facilitates access of health care services to her beneficiaries through a network
of accredited health facilities. Therefore, accredited health facilities are required to
provide quality services to NHIF beneficiaries. The success of NHIF depend on how
health care providers treat its client. The evaluation noted that, there are challenges
facing accredited health facilities in the country. The challenges encountered
included small health budget, poor financial flows, lack of community awareness,
lack of modern technology and low acceptance by the community. Also, other
factors are lack of active monitoring mechanism of NHIF and claims, poor laboratory
services, poor working tools, too many patients to attend and lack of training of
health facility staffs. The evaluation suggest that more effort is needed to improve
health services in accredited health facilies. These challenges need to be addressed in
order to promote performance as well as for the achievement of the objectives.
Measures to be taken include; improvement of accredited health facilities at all
levels, reviewing quarterly reports, Train all health facility incharges, train NHIF
coordinators and increase budget for health. Also NHIF can benefit from improved
data systems, supervision, and management support.
33
5.3 Policy implication
The essence of this study was to evaluate the health services in accredited health
facilities by the NHIF.The purpose of introducing NHIF is to support the government
in enhancing quality health service provision to the population of Tanzania. This
evaluation sought to provide a roadmap for optimizing health sector inputs within the
context of the overall health systems. The information contained in this evaluation is
intended to create opportunities for multi-sectoral dialogue, to enhance collaborative
planning efforts, and ultimately to facilitate partnerships that will lead to an
improved health systems. Tanzania has achieved much in this area, with support of
stakeholders from both public and private sectors. This has been possible due to
good policies toward public-private collaboration.
5.4 Areas for further evaluation
This evaluation study was not exhaustive since it covered few specific areas due to
financial limitations, specificity and many others. In this regard, further evaluation
could be considered to the following areas:
Financial contribution of the accredited health facilities to the National level
Contribution of accredited health facilities to the rural communities
The sustainability of accredited health facilities.
34
REFERENCE
Arhin-Tenkorang, D. (2001). Mobilizing resources for health, Paper presented 81
meeting of the health financing. University of Harvard. 2001.
Babbie, E. (2005). The basics of social research. 3rd
Edition. Toronto, Thomson.
Wadsworth.
(www.wadsworthmedia.com/marketing/sell_sheets/0534630367). [Visited on
12/4/2015].
Bethesda, M.D. (2011). Health Systems 20/20 project Report: Does the NHIS cover
the poor?
Bodenheimer, T.S. (2013). "Proposed Solutions to the physician shortage without
training more physicians". Health Affairs (Project Hope): 1881–1886.
Borghi, J., Maluka, S., Kuwawenaruwa, A., Makawia, S., Tantau, J., Mtei, G., Ally,
M. and Macha, J. (2013). Promoting universal financial protection: a case
study of new management of community health insurance in Tanzania.
Health research policy and systems / BioMed Central, 11.
Bultman, J., Kanywanyi, J. L., Maarifa, H. & Mtei, G. (2012). Tanzania Health
Insurance Regulatory Framework Review. Ministry of Health and Social
welfare and Social Security Regulatory Authority.
Carrin, G. and James, C. (2002). Reaching universal coverage via social health
insurance.
Churchill, C. (2006). An Investigation into the determinants of Customer
satisfaction. Journal of Marketing Research, Vol.19:491-504.
David, P. (2002). „‟Knowledge Management Research‟‟ Report Berg, L.B. (1989)
Qualitative research methodology for the social science, a division of Simon
and Schuster Needham heights, Massachusetts
35
De Vos, A.S. Delport, C.S.L. Fouchė, C.B. Strydom, H. (2005). Research at Grass
roots. For the social sciences and human service professions. Van Schaik
Publishers
Dill, M.J. (2012). "Survey shows consumers open to a greater role for physician
assistants and nurse practitioners". Health Affairs (Project Hope): 1135–
1142.
Furrow, B.R. (2013). Health law; Cases, materials, and problems. Upper Saddle
River: West Publishing Company.
Gravetter, F.J. & Forzano, L.B. (2003). Research methods for the behavioural
Sciences. Belmont: Wadsworth/Thomson Learning.
Humba, E. (2005). Social Health Insurance: Implementing social security health
care.
International Labor Organization. (2008). Protecting the poor.
Kolstad, J. R. and Lindkvist, I. (2013). Pro-social preferences and self-selection into
the public health sector: evidence from an economic experiment. Health
Policy Plan, 28, 320-7.
Kothari, C.R. (2010). Research Methodology Methods and techniques, 5nd
Ed,
Published by Wishwa Prakashan Division of New Age International (P)
Limited.
Mills, A., Ataguba, J. E., Akazili, J., Borghi, J., Garshong, B., Makawia, S., Mtei, G.,
Harris, B., Macha, J., Meheus, F. and Mcintyre, D. (2012). Equity in
financing and use of health care in Ghana, South Africa, and Tanzania:
implications for paths to universal coverage. Lancet, 380, 126-33.
Mouton, J. (2001). How to succeed in your Masters‟ & Doctoral Studies. A South
African Guide And Resource Book. (1st Ed.) Pretoria Van Schaik Publishers
36
Mtei, G. (2012). Who pays and who benefits from health care? An assessment of
equity in health care financing and benefit distribution in Tanzania. Health
Policy and Planning, 2012. 27(suppl 1): p. i23-i34.
National Bureau of Statistics, (2013).
National Health Insurance Fund, (2011). Corporate Plan, 2011 – 2015.
National Health Insurance Fund, (2013). Actuarial and Statistical Bulletin.
National Health Policy of Tanzania. (2007).
Nielsen, R.B. & Mayer, R.N. (2000). Why do people buy cancer insurance? An
exploratory study advancing the Customer Interest: A journal of Law,
policy and research.
Obonyo, A. (1996). National Hospital Insurance Fund in Kenya, Paper presented to
the National Health Insurance Workshop. CEDHA Arusha.1996.
Reeve, J; Paperboy, D. (2007). "Evaluating the evaluation: Understanding the utility
and limitations of evaluation as a tool for organizational learning". Health
Education Journal 66 (2): 120–131.
Svensson, I. and Palme, M.(1997). Social security, Occupational, Pension and
retirement, paper presented at the meeting of Health Occupational
conference. Sweden.
Waddington, C.J. and Enyimayew, K.A. (1990). “A price to pay, part 2: the impact
of user charges in the Volta region, Ghana”, International Journal of
Health Planning and Management, 5, 287-312
WHO, World Health Report (2010). Health System Financing: The Path to Universal
Coverage. 2010: Geneva
37
APPENDICES
Appendix 1: Questionnaire
A: Evaluator’s introduction
Dear Sir/Madam
I would like to introduce myself to you and the purpose for this study. I am a student
from Mzumbe University pursuing Master of Science in Health Monitoring and
Evaluation. My research title is „Evaluation of service provision in accredited health
facilities‟. I am conducting this study for academic purpose only and I will maintain
the confidentiality of the data which I am requesting from you all the time. Kindly I,
request your cooperation to fill this questionnaire, thanks in advance.
Thanks in advance
………………………… ………………..
Rose Anthony Ntundu Date
B: Socio- Demographic information of the respondents
1. Age
(a) 18-25 years
(b) 26-35 years
(c) 36-45 years
(d) 46-55 years ( )
(e) 56-60 years
2. Sex category
(a) Male
(b) Female ( )
38
3. Education level
(a) Secondary education ( )
(b) certificate
(c) Diploma
(d) Degree and above
4. Marital status
(a) Married
(b) Single
(c) Single parent ( )
(d) Widower
(e) Divorced
5. Working experience
(a) Less than 1 year
(b) 1 year to 5 years ( )
(c) 6 years to 10 years
(d) More than 10 years
C: To assess NHIF performance in compliance with accredited health facilities
6. What are the specific objectives of NHIF?
(a) Availability of guidelines as per NHIF standards in the facility
(b) There is an increase of accessibility and quality services to beneficiaries
(c) There is an increase of accredited health facilities [ ]
(d) There is an increase of reimbursement in facility from NHIF
(e) Attended training on NHIF matters
(f) Supervision conducted by NHIF at least once per year
7. Have the NHIF objectives been achieved?
(a) Yes
(b) No
(c) I Don‟t know [ ]
39
8. What were the reasons for NHIF to initiate accredited health facilities?
(a) To speed up service provision
(b) To improve health service
( c) To enable many people attend the service [ ]
(d) To cover large area
(e) Not sure
9. Indicate your attitude on the following statement pertaining to the accredited
health facilities
No Statement Strongly
agree Agree Uncertain Disagree
Strongly
disagree
1 There is a real need for health insurance
2 Expect good services with health insurance
3 NHIF is not well organized
4 Private employees should be covered by
health insurance
5 Health insurance is bad and unfair
6 All medicine should be included in benefit
package
7 Health insurance is worthy to be trusted
8 Exempted diseases are not taken care of
9 Health insurance should benefit employees
only (and not the families)
10 Contributions are too big for NHIF services
(3% of basic salary)
10. What benefits does the community gain from accredited health facility?
(a) Primary care
(b) Access to medicine
(c) Advice
(d) Readily available health services
(e) Large coverage
(f) No benefit [ ]
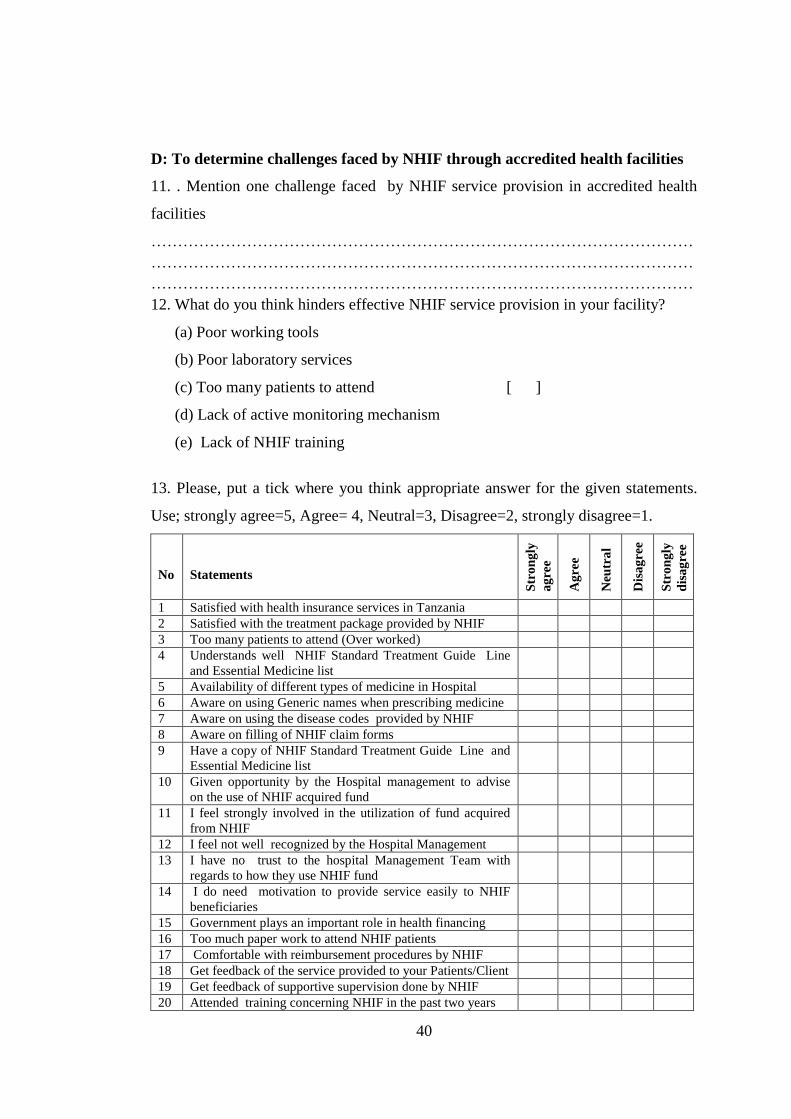
40
D: To determine challenges faced by NHIF through accredited health facilities
11. . Mention one challenge faced by NHIF service provision in accredited health
facilities
…………………………………………………………………………………………
…………………………………………………………………………………………
…………………………………………………………………………………………
12. What do you think hinders effective NHIF service provision in your facility?
(a) Poor working tools
(b) Poor laboratory services
(c) Too many patients to attend [ ]
(d) Lack of active monitoring mechanism
(e) Lack of NHIF training
13. Please, put a tick where you think appropriate answer for the given statements.
Use; strongly agree=5, Agree= 4, Neutral=3, Disagree=2, strongly disagree=1.
No
Statements
Str
on
gly
ag
ree
Ag
ree
Neu
tra
l
Dis
ag
ree
Str
on
gly
dis
ag
ree
1 Satisfied with health insurance services in Tanzania
2 Satisfied with the treatment package provided by NHIF
3 Too many patients to attend (Over worked)
4 Understands well NHIF Standard Treatment Guide Line
and Essential Medicine list
5 Availability of different types of medicine in Hospital
6 Aware on using Generic names when prescribing medicine
7 Aware on using the disease codes provided by NHIF
8 Aware on filling of NHIF claim forms
9 Have a copy of NHIF Standard Treatment Guide Line and
Essential Medicine list
10 Given opportunity by the Hospital management to advise
on the use of NHIF acquired fund
11 I feel strongly involved in the utilization of fund acquired
from NHIF
12 I feel not well recognized by the Hospital Management
13 I have no trust to the hospital Management Team with
regards to how they use NHIF fund
14 I do need motivation to provide service easily to NHIF
beneficiaries
15 Government plays an important role in health financing
16 Too much paper work to attend NHIF patients
17 Comfortable with reimbursement procedures by NHIF
18 Get feedback of the service provided to your Patients/Client
19 Get feedback of supportive supervision done by NHIF
20 Attended training concerning NHIF in the past two years
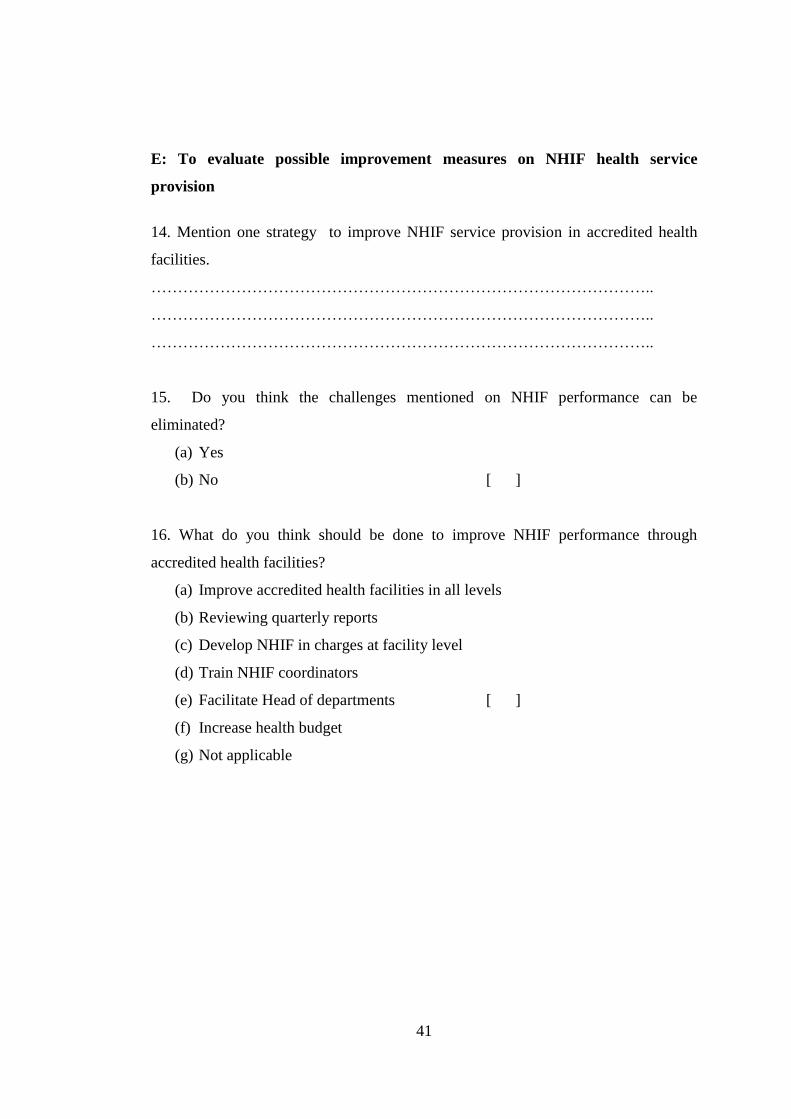
41
E: To evaluate possible improvement measures on NHIF health service
provision
14. Mention one strategy to improve NHIF service provision in accredited health
facilities.
…………………………………………………………………………………..
…………………………………………………………………………………..
…………………………………………………………………………………..
15. Do you think the challenges mentioned on NHIF performance can be
eliminated?
(a) Yes
(b) No [ ]
16. What do you think should be done to improve NHIF performance through
accredited health facilities?
(a) Improve accredited health facilities in all levels
(b) Reviewing quarterly reports
(c) Develop NHIF in charges at facility level
(d) Train NHIF coordinators
(e) Facilitate Head of departments [ ]
(f) Increase health budget
(g) Not applicable