Effects of Smoking Cessation on Lung Function and Airway Inflammation in Smokers with Asthma
Upload
khangminh22Category
view
0download
0
Primary Care Asthma
Program
Spirometry Manual
Version 2020

Primary Care Asthma ProgramSPIROMETRY MANUAL TABLE OF CONTENTS
PCAP SPIROMETRY MANUAL: TABLE OF CONTENTS Version: August 2020
1.0 Introduction/Background
Primary Care Asthma Program (PCAP) Background-Spirometry - 1 page
2.0 PCAP Policy & Procedures
PCAP Spirometry Policy and Procedures (Aug 2020) - 10 pages
PCAP Medical Directive for Performing Spirometry Pre & Post Bronchodilator at a Primary Care Site
(Aug 2020) – 4 pages
Sample of a Spirometry Requisition Order Form
Sample of a Spirometry Report Form (From Coates AL et al. Spirometry in Primary Care. Can Respir
J 2013; 20(1); 13-20) – 1 page
3.0 Spirometry Practicum
The Lung Health Foundation Spirometry Interpretation Guide - 1 page
PCAP Spirometry Operator Checklist Tool (August 2020) – 2 pages
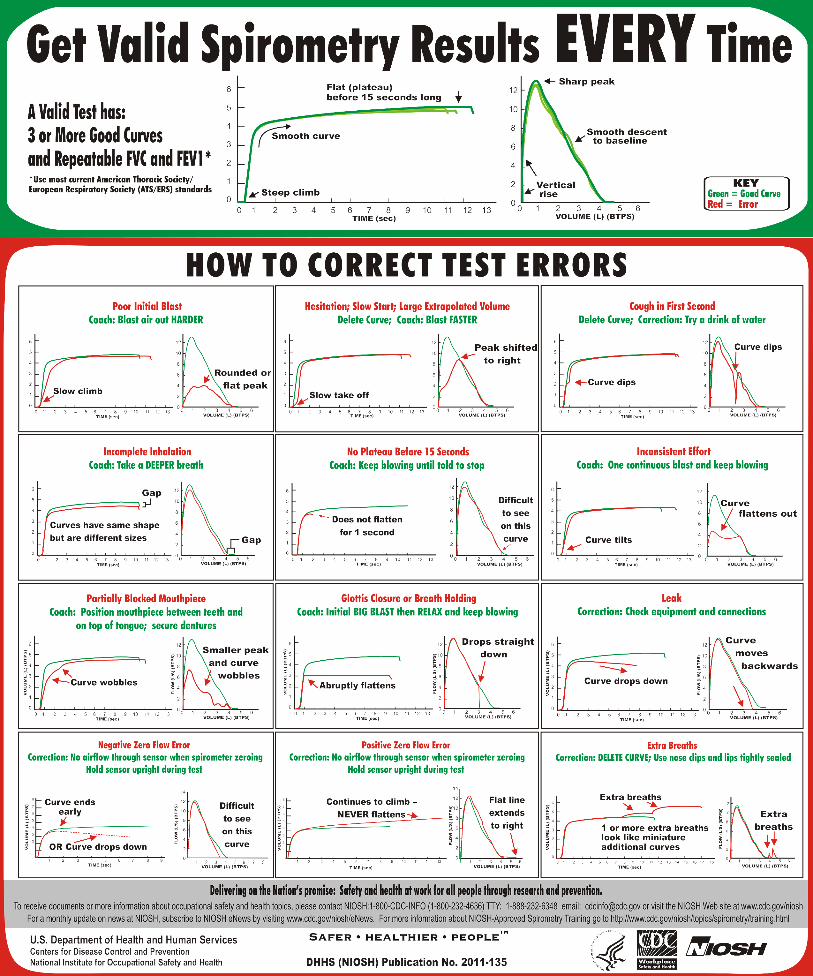
Get Valid Spirometry Results Every Time (From U.S. Department of Health and Human Services :Centers for Disease Control and Prevention National Institute for Occupational Safety and Health(NIOSH)) – 1 page
4.0 Standards/References
ATS Standardization of Spirometry 2019 Update – 19 pages
CTS 2013 Spirometry in Primary Care – 10 pages
ATS/ERS Recommendations for a Standardized Pulmonary Function Report – 9 pages
PCAP Resource Links for Standards in Spirometry (Aug 2020) – 1 page

Primary Care Asthma Program SPIROMETRY MANUAL
PCAP Spirometry Manual Version: August 2020 Page 1 of 1
Introduction/Background
The Primary Care Asthma Program (PCAP) is an evidence-based asthma and COPD
program intended to provide primary care providers with decision aids to support best
practice regarding asthma and COPD assessment, diagnosis and management. The
Ministry of Health currently supports and funds PCAP as part of Ontario’s Asthma and
COPD Program.
Currently, PCAP is delivered within a multi disciplinary team of primary care providers
with the support of a Certified Asthma/Respiratory Educator (CAE/CRE). The CAE/CRE
assists with program implementation, mentoring, education of patients and staff and
ensuring the ongoing sustainability of the program. The program is modeled on
fostering patient and family self-management.
Key to the success of this primary care program is the expertise of the educator who
provides current evidence-based knowledge and assists with on-site objective
measurements via spirometry (please see policy and procedures in the manual for who
can conduct spirometry and who can interpret spirometry). Spirometry, in accordance
with American Thoracic Society/European Respiratory Society (ATS/ERS) Standards,
will be used as the primary objective measure for the confirmation of the diagnosis of
asthma and as the objective measure for the monitoring of clients who are capable of
performing this test.
This Spirometry Manual was developed by the PCAP coordinator group for health care
providers in the primary care setting. The purpose of the manual is to promote quality
spirometry in primary care.

Section 2: Policy and
Procedure

Primary Care Asthma Program SPIROMETRY MANUAL
Page 1
PCAP Spirometry Policy and Procedures FINAL Aug 2020
2.1 Primary Care Asthma Program (PCAP) Spirometry Policy and Procedures
Purpose: To assist “PCAP” primary care providers with policies and procedures for performing spirometry testing in accordance with current American Thoracic Society/European Respiratory Society (ATS/ERS) Standardization of Lung Function Testing (1,14) as well as the Canadian Thoracic Society (CTS) guidelines for Spirometry in Primary Care (2).
Policy: Spirometry is a non-invasive, diagnostic test that measures ventilatory capacity as a function of time, reflecting the flow resistive properties of the airways. Spirometry, pre- and post-bronchodilator, in accordance with ATS/ERS standards, will be used as the primary objective measure for clients who are able to perform the test for the confirmation of the diagnosis of asthma and COPD and as an objective measure of lung function for the monitoring of asthma and COPD clients. Refer to PCAP Generic Program Standards (GPS) # 5. (3)
Procedure: Instrumentation, calibration, hygiene, infection control, performance of the test to meet criteria for acceptability and repeatability, reporting results for interpretation, and spirometry training recommendations are essential elements of performing spirometry that can have a significant impact on the quality/accuracy of the test and the appropriate interpretation of the results.
2.1.1 Instrumentation
Spirometer equipment recommendations apply to all spirometers and are minimal requirements. Instrumentation
recommendations should be followed to provide accurate data and information that is comparable from laboratory
to laboratory and from one time period to another. The accuracy of a spirometry system depends on the
characteristics of the entire system, from the volume or flow transducer and the use of an in-line filter, to the
recorder, display or processor. Changes in any aspect of the equipment or errors at any step in the process can
affect the accuracy of the results. All spirometry should be reported at BTPS (Body Temperature and Pressure
Saturated) by any method (measuring temperature and barometric pressure). When a subject performs an FVC
maneuver into a spirometer, the air leaving the lungs is approximately 33ºC-35ºC and saturated with water vapour.
If the expired gas is assumed to be at BTPS, an error of ~1% will occur. Most volume-type spirometers assume
instant cooling of the gas but this is not always the case. If the flow sensor is located further from the mouth, such
as adding an in-line filter, more cooling will occur allowing for more errors. For example, if the BTPS correction
factor is wrong, an accurately measured FVC will be incorrectly reported (1).
Flow-Sensing Spirometers – currently the most widely used instruments
Utilizes a sensor that measures flow as the primary signal and calculates volume by electronic (analog)
or numerical (digital) integration of the flow signal producing a FLOW-VOLUME curve
Most commonly used flow sensors detect and measure flow from: the pressure drop across a resistance
(pneumotach); cooling of a heated wire; or by electronically counting the rotation of a turbine blade
General Considerations (2,14):
All spirometers must meet ISO 26782 standards, with a maximum permissible error of +/-2.5% for
accuracy, linearity and repeatability when tested with a 3L calibration syringe.
Exhalation-only spirometers are not recommended (e.g. Spirometers where the patient inhales to
maximal lung volume, then while holding their breath, places mouth on mouthpiece and does a forced
exhalation into the spirometer). This is because it requires more coordination from the patient and can

Primary Care Asthma Program SPIROMETRY MANUAL
Page 2
PCAP Spirometry Policy and Procedures FINAL Aug 2020
cause inaccurate measurement due to leakage that occurs between the time when the patient reaches
maximal lung volume and when the patient places their mouth on the mouthpiece. It is recommended
that the spirometer chosen allows the patient to take tidal breaths with their mouth on the mouthpiece
prior to the FVC maneuver. This allows for the person conducting the test to evaluate a proper seal
around the mouthpiece and the nose clip is functioning properly. Any leakage that occurs at maximal
lung volume will be captured and will be used to determine whether the test meets ATS/ERS standards.
Display (2):
The Display must show both the flow-volume loop and the volume-time curve real time with sufficient
resolution so that the person conducting the testing can determine whether test results have met the
ATS/ERS standards (see page 6 of this Policy and Procedure)
It should be possible for the person conducting the spirometry testing be able to observe both the
display and the patient effort allowing for instant coaching and for the person conducting the spirometry
testing to terminate the test early if the test is unacceptable
The spirometer should be able to analyze each maneuver to determine whether each effort meets
ATS/ERS standards (acceptability and repeatability) and provide “warning messages” to indicate if the
maneuver was not acceptable (e.g. “end of test criteria not met – blow out longer”) This should be
recognized by the person conducting the spirometry testing and an effort will be repeated even if the
computerized system has accepted the test. Note: Most of the ATS/ERS standards are based on the
adult population and many children can meet requirements with submaximal efforts and poor quality
tests. Information about special considerations in children are available at the end of this document.
2.1.2 Calibration Attention to equipment quality control and calibration is an important part of good laboratory practice, necessary for valid reliable results. At a minimum, the requirements are as follows:
(Refer to Appendix 1: PCAP Spirometry Operator Checklist)
A Spirometer should have a Calibrating syringe. ATS/ERS standards specify that a 3L syringe be usedfor checking and calibrating a spirometer daily.
A simple leak test (to test if there is a leak in the calibration syringe) using a stopper in the calibrationsyringe should be done monthly by pushing or pulling the syringe (2)
Spirometers using pre-calibrated inserts must still be checked daily for accuracy using a 3L calibrationsyringe. (2)
Daily calibration log should be maintained for all equipment requiring calibration;
Room temperature, Barometric Pressure and Relative Humidity should be measured, not estimated. If abarometer is unavailable, pressure reported from a nearby weather station can be accessed from theEnvironment Canada website: http://weather.gc.ca/canada_e.html and must be corrected for altitude:http://www.engineeringtoolbox.com/air-altitude-pressure-d_462.html (3)
Calibration should be conducted with mouthpiece/filter in-line with the calibration syringe;
Monthly normal biological tests (e.g. perform spirometry on a staff member (with no underlying lungcondition) on all spirometers in the clinic on a monthly basis for comparison (must be within 150mL ofeach other)
Documentation of repairs or other alterations which return the equipment to acceptable operation; &preventative maintenance, corrective actions;
Dates of computer software and hardware updates or changes; and
If equipment is changed or relocated (e.g. industrial surveys), calibration checks and quality-controlprocedures must be repeated before further testing begins.

Primary Care Asthma Program SPIROMETRY MANUAL
Page 3
PCAP Spirometry Policy and Procedures FINAL Aug 2020
Follow manufacturer’s manual for complete calibration procedures. While manufacturers are responsible for demonstrating the accuracy and reliability of the systems that they sell, it is the user who is responsible for ensuring that the equipment’s measurements remain accurate (1).
2.1.3 Hygiene and Infection Control Each site is responsible to follow their site specific infection control policy. Each site will establish specific responsibilities and guidelines related to spirometry for their site safety and the prevention of infectious disease transmission. The goal of infection control is to prevent the transmission of infection to patients and staff during spirometry testing. Indirect transmission of aerosol droplets generated by the patient blowing into the pneumotach can be blown into the atmosphere. It is recommended that the operator follow local public health and infectious disease recommendations for testing (e.g., appropriate PPE, hand hygiene, ventilation, etc.). Please note that these recommendations can change to respond to local/regional policies and should be reviewed regularly.
2.1.4 Performing the Spirometry Test
Who Can Conduct Spirometry? By a trained and qualified personnel in a setting with a regular quality assurance program (e.g. Trained
health care professionals who are Registered Respiratory Therapist (RRT) or Registered Cardio-pulmonary Technologist, RCPT(P) or
other regulated health care professionals who received formal training which included studies in anatomy and physiology of the cardiorespiratory system and who successfully completed a recognized spirometry training course, and other trained health care technologists who successfully completed a recognized spirometry training course (please refer to section 2.1.8 of this document for training programs) (2).
Reference Values: Performing the test not only includes attention to the instrumentation, calibration and infection control but also to how the test is performed and attention to the quality of the measurements produced. All measurements are expressed as litres (L) or litres/second (L/s) and as % predicted, with the predicted values being derived from standardized data sets. Predicted values should reflect the patient population of your clinic. The current CTS guidelines recommend the use of Lower Limit of Normal (LLN). The Lower Limit of Normal (LLN) is defined as the 5th percentile (i.e. the value that marks the lower 5th percentile of the normal population). The 5th percentile is considered the threshold below which a value is considered to be abnormal. The Global Lung Function Initiative (GLI) recommends the all-age spirometry values developed by Quanjer et al. be used as reference values (age 3.5 - 90yrs). Most major spirometers have committed to implementing the Quanjer et al. reference values. Another choice of reference equations is the National Health and Nutrition Examination Survey (NHANES III) for Caucasian, African-American and Hispanics between 8-80 years of age. These equations should not be used outside this age range. This set is contained in almost all current spirometry systems. There are no reference equations for the Canadian Aboriginal population and therefore, spirometry tests involving this population should be interpreted with caution using the Caucasian reference values (2). More recently, the Canadian Health Measurement Survey (CHMS) provides reference values for the Canadian Caucasian population from 6 to 79 years of age and guidelines to approximate correction for other ethnic groups (12). Clinics may want to align with labs in their geographical region using the same reference sets understanding that if different reference sets are used only the patient’s absolute values can be compared between tests. Predicted values take into account height, age, gender, ethnic origin. Weight is normally recorded for monitoring but is not in the equation for predicted spirometry values. The height should not be estimated but measured using a measuring tape (attached to the wall) with the patient standing without shoes with his/her back flat against the wall with a right angle device making contact with the top of the head and the measuring tape. When height cannot be measured using this method (e.g. chest wall deformities) arm span (middle finger tip to middle finger tip) can be used as an approximate (2).

Primary Care Asthma Program SPIROMETRY MANUAL
Page 4
PCAP Spirometry Policy and Procedures FINAL Aug 2020
The spirometer selected must have specific sets of normal reference values, both adult and pediatric, pre-programmed into its software. If it does not, insist that they be installed prior to purchase (2)
Reference values must be appropriate for the age and ethnicity of the population and be able to provide the Lower Limit of Normal (LLN) (2). It is recommended that you inquire about a software update to obtain the LLN with your spirometer equipment if not already available.
The interpretation of spirometry tests should be based on the LLN (2)
Indications for Spirometry (14):
Diagnosis
To evaluate symptoms, signs, or abnormal laboratory results
To measure physiologic effect of disease or disorder
To screen individuals at risk or having pulmonary disease
To assess preoperative risk
To assess prognosis
Monitoring
To assess response to therapeutic intervention
To monitor disease progression
To monitor patients for exacerbations or disease and recovery from exacerbations
To monitor people for adverse reactions to drugs with known pulmonary toxicity
Disability/impairment evaluations
To assess patients as part of a rehabilitation program
To assess risks as part of an insurance evaluation
To assess individuals for legal reasons
Other
Research and clinical trials
Epidemiological surveys
Derivation of reference equations
Pre-employment and lung health monitoring for at-risk occupations
To assess health status before beginning at-risk physical activities
Table 1: Terminology and Definitions
Measurement Abbreviation Definition
Forced Vital Capacity (L) FVC Maximum volume of air that can be expired as
forcefully, quickly and completely as possible
following a complete inspiration
Forced Expiratory Volume in FEV1 Volume of air expired in the first second of the FVC -
Used to assess airflow
1 second (L/sec)
Ratio of FEV1 to FVC % FEV1/FVC Used for the assessment of airflow obstruction
Peak Expiratory Flow (L/sec) PEF The maximum flow rate at the onset of the FVC
maneuver – judges max effort
Forced Expiratory Flow 25- FEF 25-75 The average flow rate during the middle half of
75% (L/Sec) the FVC maneuver – reflects airflow *FEF50/FIF50 = The ratio of flow at 50% of expiration and flow at 50% inspiration (Maximum flow at 50% that can be inspired as
forcefully, quickly and completely as possible following a complete exhalation). Recognizing that the inspiratory loop is not always done in
primary care, this loop might be useful in evaluating any upper airway obstruction (UAO). FEF50/FIF50 = 1 in fixed UAO, FEF50/FIF50 >
1 in variable extrathoracic UAO and FEF50/FIF50 < 0.3 in variable intrathoracic UAO (13)

Primary Care Asthma Program SPIROMETRY MANUAL
Page 5
PCAP Spirometry Policy and Procedures FINAL Aug 2020
There are two types of graphs that are commonly displayed for Spirometry: the Flow Volume loop and the Volume Time curve. Your spirometer may be formatted to print out both curves.
Figure 1: Flow Volume loop - This is a record of how fast the air flows in/out (Flow) versus the
amount (Volume) of air exhaled or inhaled within a certain time (8).
Flow (Y) versus Volume (X)
FIF 50
Figure 2: Volume time curve - This is a record of the expired volume in relation to time (8).
Volume (Y) versus Time (X)

Primary Care Asthma Program SPIROMETRY MANUAL
Page 6
PCAP Spirometry Policy and Procedures FINAL Aug 2020
Table 2: Test Procedures for the Forced Vital Capacity maneuver (Flow-Volume loop) (2,14) Preparation
Ensure the spirometer has daily calibration performed
Contraindications should be listed on the spirometry order requisition form or checklist form
Activities that should preferably be avoided prior to lung function testing
Smoking and/or vaping and/or water pipe use within at least 1 h of testing (to avoid acute bronchoconstriction due to smoke inhalation)
Consuming intoxicants within 8 h of testing (to avoid problems in coordination, comprehension and physical ability)
Performing vigorous exercise within 1h of testing (to avoid potential exercise-induced bronchoconstriction)
Wearing clothing that substantially restricts full chest and abdominal expansion (to avoid external restrictions on lung function)
Eating a large meal within 2 h of testing
Inhaler Medication (Refer to Medication Section: Post Bronchodilator Testing to withhold prior to spirometry testing)
Wash hands (or use an approved hand sanitizer)
Prepare the patient
Dispense hand sanitizer for patient
Confirm patient identification, age, birth sex, ethnicity, etc.
Measure weight and height without shoes
Ask the patient about:
o Smoking/vaping
o Recent illness
o Inhaler/ medication use
Instruct and demonstrate the test to the subject
Position the mouthpiece and nose clip
correct posture and head slightly elevated
Inspire rapidly until completely full
Expire with maximal effort until completely empty
Inspire with maximal effort until completely full
Confirm that the patient understands the instructions and is willing to comply
Test Performance
Perform maneuver Have subject assume the correct seated posture (a chair without wheels, feet flat on the ground)
Attach nose clip*, place mouthpiece in mouth and close lips around the mouthpiece, perform 2-4 tidal breaths
Inhale completely and rapidly with a pause of ≤2 s at TLC
Exhale forcefully and rapidly until no more air can be expelled while maintaining upright posture
Repeat instructions as necessary
Repeat for a minimum of three maneuver, usually no more than eight for adults
Check FEV1 and FVC repeatability and perform more maneuvers as necessary
*Recommendation is to use Nose Clips or manual occlusion of the nares, to avoid leaks, especially for nose
breathers. People must mouth breathe during the procedure

Primary Care Asthma Program SPIROMETRY MANUAL
Page 7
PCAP Spirometry Policy and Procedures FINAL Aug 2020
Post Bronchodilator Spirometry/Flow-volume loop (for bronchodilator responsiveness testing): Spirometry testing and the administration of bronchodilators, requires a signed requisition from the Physician or a verbal or standing order as per site specific Medical Directives and provincial regulations that should indicate whether post bronchodilator testing is requested, and which bronchodilator is to be administered for the testing and how much bronchodilator should be given for testing
Medication to withhold prior to spirometry testing
The decision to avoid bronchodilators before testing is dependent on the reason for the test. If post bronchodilator testing is to be performed to diagnose an underlying lung condition, the patient may/should withhold the following medication prior to spirometry testing: Note: It is important to tell the patient that if they need to use their rescue inhaler for symptoms, they can do so and not withhold it for the test.
Inhaled bronchodilators (14) Medication Withholding time prior to Spirometry Testing Short-Acting Beta2 Agonist (SABA) e.g., albuterol or salbutamol
4 - 6 Hours
Short-Acting Muscarinic Antagonist (SAMA) e.g., ipratropium bromide
12 Hours
Long-Acting Beta2 Agonist (LABA) e.g., formoterol or salmeterol)
24 hours
Ultra-long acting beta2 agonist (ultra-LABA) e.g., indacaterol, vilanterol or oladaterol
36 hours
Long-Acting Muscarinic Antagonist (LAMA) e.g., tiotropium, umeclidinium, aclidinium or glycopyrronium)
36-48 hours
Other medications to withhold: Theophylline: 48 hours (7), LTRA 24 hours (2)
Antihistamines and steroids (oral and inhaled) do not need to be withheld
Note: if the test is to determine the response to a medication, then the referring physician may choose not to
withhold the medication prior to testing. The spirometry requisition order form should indicate whether to withhold a medication before testing and specify which medication to withhold
To standardize bronchodilator reversibility testing: Short Acting Beta Adrenergic (SABA) medications are the most commonly used bronchodilator, other
drugs can be used (e.g. Short-Acting Muscarinic Antagonist (SAMA) such as Ipratropium Bromide) After the pre-bronchodilator test, administer SABA –
4 separate doses* of 100mcg each, Total of 400 mcg salbutamol, or 4 separate doses* of 40mcg each, Total of 160mcg of Ipratropium Bromide
*Inhale separate doses from a valved holding chamber device 30 seconds apart (7) Perform post-bronchodilator testing 15 minutes post for SABA and 30 minutes post for SAMA
Note: ATS does not currently specify any recommendations for the pediatric population.

Primary Care Asthma Program SPIROMETRY MANUAL
Page 8
PCAP Spirometry Policy and Procedures FINAL Aug 2020
2.1.5 Acceptability and Repeatability Test Criteria (14) Acceptability criteria:
Previously, the term “end of test (EOT) criteria” was used to denote the end of forced expiration. Now the standards stress the importance of maximal inspiration following the forced expiration. Therefore, EOT criteria terminology has changed to End of Forced Expiration (EOFE)
There is no longer a minimum expiratory time (previously 6 seconds was the threshold for adults)
Must have BEV ≤5% of FVC or 100mL, whichever is greater
Must have no evidence of a faulty zero-flow setting
Must have no cough in the first second of expiration*
Must have no glottis closure within the first sec of expiration*
Must have no glottis closure after 1 sec of expiration
Must achieve one of these three EOFE indicators; 1. Expiratory plateau (≤0.025L in the last 1 sec of expiration) 2. Expiratory time ≥15 sec 3. FVC within repeatability tolerance of or is greater than the largest prior observed FVC
Must have no evidence of obstructed mouthpiece or spirometer
Must have no evidence of a leak
If the maximal inspiration after EOFE is greater than FVC, then FIVC – FVC must be ≤100mL or 5% of FVC, whichever is greater
*For children <6 years of age, must have at least 0.75 sec of expiration without glottis closure or cough

Primary Care Asthma Program SPIROMETRY MANUAL
Page 9
PCAP Spirometry Policy and Procedures FINAL Aug 2020
Repeatability:
Age >6 years
The difference between the two largest FVC values must be ≤150mL, and the difference between the two largest FEV1 values must be ≤150mL
Age ≤6 years
The difference between the two largest FVC values must be ≤100mL or 10% of the highest value, whichever is greater, and the difference between the two largest FEV1 values must be ≤100mL or 10% of the highest value, whichever is greater
Figure 3: Flow chart on application of Acceptability & Repeatability criteria (14)

Primary Care Asthma Program SPIROMETRY MANUAL
Page 10
PCAP Spirometry Policy and Procedures FINAL Aug 2020
2.1.6 Reporting Results (3)
When considering a spirometer, consider whether it is compatible with your Electronic Medical Record (EMR)
Flow and volume measures are reported at body temperature and pressure saturated with water vapor (BTPS)
The largest FVC and FEV1 from acceptable maneuvers is reported, even though the values may not come from the same maneuver
Largest PEF is reported All other flows i.e. FEF25-75% are reported from the “best curve” (defined as the maneuver with the
largest sum of FVC and FEV1) Final reports should include the technologist’s comments regarding the patient performance, recent
use of bronchodilators, quality of testing and whether or not the results were acceptable and reproducible (e.g. Patient had good effort, results reproducible, unable to perform reproducible curves, unable to attain residual volume, etc.)
Note: Please refer to Appendix A in this spirometry manual for what a sample report (2) should look like. Who Can Interpret Spirometry?
Primary Care physicians and Nurse Practitioners who interpret spirometry should have completed a spirometry interpretation course or specific training in spirometry interpretation (2). Please refer to Page 11 of this policy and procedure for recommended courses.
2.1.7 Technical Support (2):
A spirometer must be sufficiently robust to be unaffected by drops or bumps. If a spirometer is dropped, a calibration check is recommended before continuing testing
Ensure the vendor who provided you with the spirometer provide sufficient training initially in the use of a spirometer. They should also be able to provide technical support for addressing problems with the operation of the spirometer. If your spirometer needs to be checked, request a loaner device. There should be regular notification of any software upgrades and the spirometer should be thoroughly checked on a regular basis for any upgrades.
2.1.8 Training Recommendations for Performing Spirometry Purpose:
This policy will provide guidelines on the minimum criteria and core components of training based on the ATS/ERS/CPSO guidelines for personnel with regards to performing spirometry. Policy: The following minimum criteria are recommended by ATS/ERS to establish competency in spirometry testing:
Knowledge of theory and practical aspect of applied techniques, measurements, calibrations, hygiene, quality control, basic background in lung physiology and pathology;
Introduction to the standards of spirometry, review of spirometry role in the diagnosis, management of asthma and assess contraindications;
Test performance: Proper technique for performing spirometry including how to coach for best results (practical workshop or hands on training);
Discuss predicted values and actual/absolute values; Review reporting process.

Primary Care Asthma Program SPIROMETRY MANUAL
Page 11
PCAP Spirometry Policy and Procedures FINAL Aug 2020
Spirometry training can be attained through an accredited Institution. Recommended institutions: Certification in conducting spirometry:
“SpiroTrec” (Lung Association of Saskatchewan National program: http://www.resptrec.org/)
Additional Supports:
The Lung Health Foundation Spirometry Interpretation workshop and e-modules Workshops: https://hcp.lunghealth.ca/workshops/
e-modules: https://hcp.lunghealth.ca/e-modules/
Job shadowing with a local/regional expert can enhance practical training objectives. This can be
available but limited according to resources. Please contact PCAP Provincial Coordinator for more
information https://hcp.lunghealth.ca/clinical-programs/
*Please Note:
Permission and proper acknowledgement is required in any modification of the PCAP tools as per the PCAP process
Primary Care Asthma Program SPIROMETRY MANUAL
Page 12
PCAP Spirometry Policy and Procedures FINAL Aug 2020
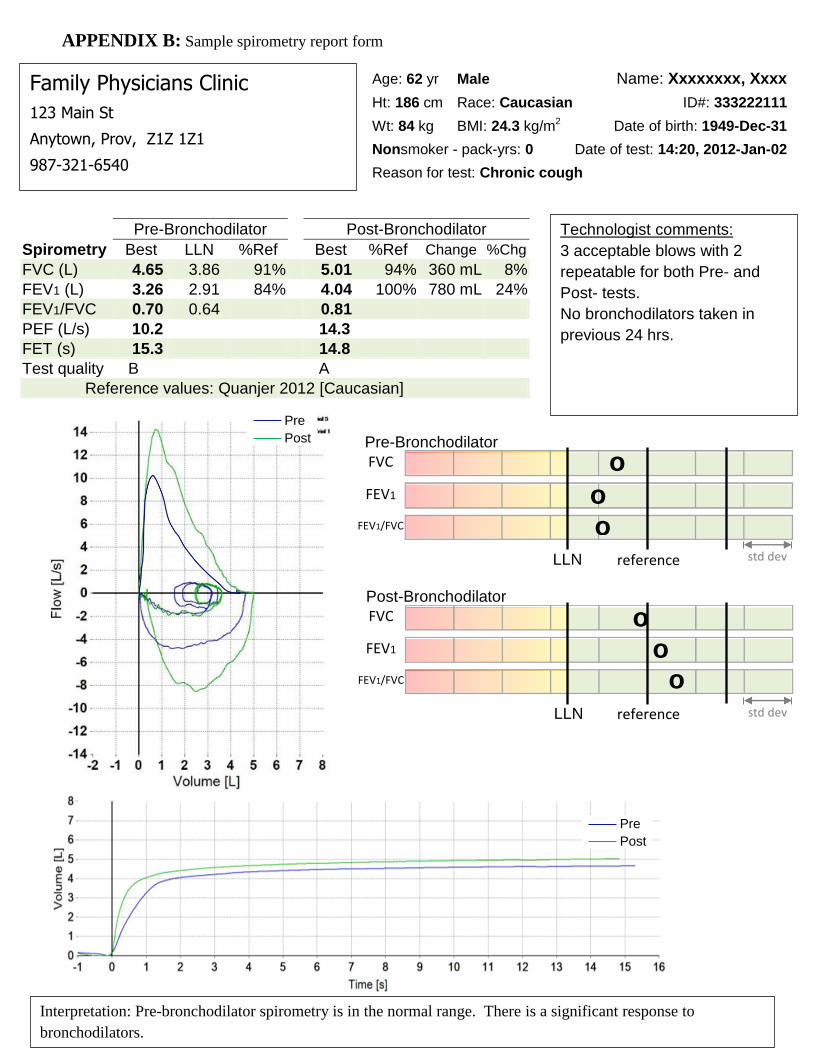
APPENDIX 1: PCAP SPIROMETRY OPERATOR CHECKLIST (Page 1)
Barometric Pressure, Relative Humidity and Temperature updated daily
Daily calibration performed according to manufacturer’s and ATS/ERS Standards
Relative Contraindications (Refer to the list on the reverse side of this page)
Minimum of three acceptable FVC performed, with two repeatable maneuvers, maximum eight performed (ATS/ERS 2005)
Assess Patient Performance: (Acceptability)
o Maximum peak effort o Must have BEV ≤5% of FVC or 100mL, whichever is greater o Must have no evidence of a faulty zero-flow setting o Must have no cough in the first second of expiration* o Must have no glottis closure within 1 sec of expiration* o Must have no glottis closure after 1 sec of expiration o Must achieve one of these three EOFE indicators; o Expiratory plateau (≤0.025L in the last 1 sec of expiration) o Expiratory time ≥15 sec o FVC within repeatability tolerance of or is greater than the largest prior observed FVC o Must have no evidence of obstructed mouthpiece or spirometer o Must have no evidence of a leak o If the maximal inspiration after EOFE is greater than FVC, then FIVC – FVC must be ≤100mL or 5%
of FVC, whichever is greater
Assess Measurements: (Repeatability)
Age >6 years
o The difference between the two largest FVC values must be ≤150mL, and the difference between the two largest FEV1 values must be ≤150mL
Age ≤6 years
o The difference between the two largest FVC values must be ≤100mL or 10% of the highest value, whichever is greater, and the difference between the two largest FEV1 values must be ≤100mL or 10% of the highest value, whichever is greater
Technical comments recorded on spirometry report

Primary Care Asthma Program SPIROMETRY MANUAL
Page 13
PCAP Spirometry Policy and Procedures FINAL Aug 2020
APPENDIX 1: PCAP SPIROMETRY OPERATOR CHECKLIST (Page 2)
Relative Contraindications for Spirometry (14)*
Due to increases in myocardial demand or changes in blood pressure
Acute myocardial infarction within 1 week
Systemic hypotension or severe hypertension
Significant atrial/ventricular arrhythmia
Noncompensated heart failure
Uncontrolled pulmonary hypertension
Acute cor pulmonale
Clinically unstable pulmonary embolism
History of syncope related to forced expiration/cough
Due to increases in intracranial/intraocular pressure
Cerebral aneurysm
Brain surgery within 4 weeks
Recent concussion with continuing symptoms
Eye surgery within 1 week
Due to increases in sinus and middle ear pressures
Sinus surgery or middle ear surgery or infection within 1 week Due to increases in intrathoracic and intraabdominal pressure
Presence of pneumothorax
Thoracic surgery within 4 weeks
Abdominal surgery within 4 weeks
Late-term pregnancy
Infection control issues
Active or suspected transmissible respiratory or systemic infection, including tuberculosis
Physical conditions predisposing to transmission of infections, such as hemoptysis, significant secretions, or oral lesions or oral bleeding
*It is recommended that the decision to conduct spirometry testing should be made on a case by case basis in
consultation with the primary care provider Please note:
Permission & Proper acknowledgement is required in any modification of the PCAP Tools as per PCAP process.

Primary Care Asthma Program SPIROMETRY MANUAL
Page 14
PCAP Spirometry Policy and Procedures FINAL Aug 2020
References
1. American Thoracic Society /European Respiratory Society Task Force: Standardization of Lung
Function Testing: Standardization of Spirometry. Eur Respir J 2005;26: 319-338 http://www.thoracic.org/statements/
2. Coates AL et al. Spirometry in Primary Care. Can Respir J 2013; 20(1): 13-20.
3. Primary Care Asthma Program, Generic Program Standards, PCAP Group, June 2013
4. American Thoracic Society /European Respiratory Society Task Force: Standardization of Lung
Function Testing: General considerations for lung function testing. Eur Respir J 2005;26: 153-161 http://www.thoracic.org/statements/
5. American Thoracic Society/ European Respiratory Society Task Force: Standardization of Lung Function
Testing: Interpretative strategies for lung function tests. Eur Respir J 2005; 26: 948-968 http://www.thoracic.org/statements/
6. American Association for Respiratory Care- AARC Clinical Practice Guideline, Spirometry, 1996 Update,
Respir Care 1996; 41(7):629–636 http://www.rcjournal.com/cpgs/spirupdatecpg.html
7. College of Physicians and Surgeons of Ontario (CPSO) Independent Health Facilities (IHF)- Clinical Practice Parameters and Facility Standards for Diagnostic Spirometry & Flow Volume Loop Studies – 4th edition http://www.cpso.on.ca/CPSO/media/documents/CPGs/IHF/Pulmonary-Function-Studies.pdf
8. The Provincial Infection Diseases Advisory Committee, Infection Prevention and Control for Clinical
Office Practice, June 2013; Revised April 2015 (116 pages) http://www.publichealthontario.ca/en/eRepository/IPAC_Clinical_Office_Practice_2013.pdf
9. Ruppel, G. Manual of Pulmonary Function Testing. Seventh Edition. St. Louis, MO, the C.V. Mosby
Company, 1997.
10. NIOSH, Spirometry Training Guide 2003 http://www.cdc.gov/niosh/docs/2004-154c/
11. Coates, A.L. Wong, S.L., Tremblay, C., Hankinson, J.L. Reference Equations for Spirometry in the Canadian Population. Ann Am Thorac Soc 2016 Vol 13, No 6 pp 833-841
12. Hankinson, J.L. Odencrantz, J.R. Spirometric Reference Values from a Sample of the General U.S. population, American Journal of Respiratory and Critical Care Medicine 1999 Vol 159 p179-187 http://www.ndd.ch/UserData/Download_00141_00.pdf
13. Karkhanis VS, Joshi JM. Spirometry in Chronic Obstructive Lung Disease (COPD). Supplement to
JAPI 2012; 60: 22-26
14. American Thoracic Society: Standardization of Spirometry 2019 Update. Am J Respir Crit Care Med Vol 200, Iss 8, pp e70-e88, Oct 15, 2019

Page 1 of 5 PCAP Medical Directive on Spirometry Pre & Post Bronchodilator (Sample)
FINAL August 2020
[NAME OF PRIMARY CARE SITE]
Medical Directive: Administration of Salbutamol Sulfate Beta-2
Agonist during the Spirometry Pre and Post Testing Procedure
Approval Date: __________________
Review Date: ____________________
Background Information
The Primary Care Asthma Program (PCAP) is an evidence-based asthma
and COPD program intended to provide primary care providers with
decision aids to support best practice regarding asthma and COPD
assessment, diagnosis and management.
Spirometry is part of PCAP offered at [site name]. Although it is not a
controlled act, it is practice to include spirometry within the directive of
administering an inhaled substance during the post testing spirometry
procedure.
Spirometry, when indicated for the diagnosis and monitoring of respiratory
conditions, requires the administration of a beta-2 agonist bronchodilator,
followed by post spirometry testing. This post testing is performed both on
initial visits to assist with confirming a diagnosis and also during follow up
visits to assist in monitoring the clients respiratory status.
Setting where medical directive to be Implemented:
In house spirometry testing at ________ [site name].
Professional Staff covered by the Directive: Authorized staff that have
been observed and trained to perform spirometry according to American
Thoracic Society/European Respiratory Society (ATS/ERS) guidelines
under ____________ [site name] quality assurance and quality control
policies for spirometry testing and that the undersigned presently holds the
designation and college certification in good standing as within their
respective regulated health colleges.
Indications:
To perform pre and post-spirometry testing which involves administration of
a beta-2 agonist to primary care clients during the initial and follow-up visits

Page 2 of 5 PCAP Medical Directive on Spirometry Pre & Post Bronchodilator (Sample)
FINAL August 2020
with the PCAP program to determine whether there is any reversible lung
function and to monitor respiratory status.
Contraindications:
Relative Contraindications for administrating salbutamol sulfate beta-2
agonist:
Hypersensitivity to any component of the medication being
administered
History of any adverse effects to the medication being administered
Relative Contraindications for spirometry: Due to increases in myocardial demand or changes in blood pressure
Acute myocardial infarction within 1 week
Systemic hypotension or severe hypertension
Significant atrial/ventricular arrhythmia
Non-compensated heart failure
Uncontrolled pulmonary hypertension
Acute cor pulmonale
Clinically unstable pulmonary embolism
History of syncope related to forced expiration/cough
Due to increases in intracranial/intraocular pressure
Cerebral aneurysm
Brain surgery within 4 weeks
Recent concussion with continuing symptoms
Eye surgery within 1 week
Due to increases in sinus and middle ear pressures
Sinus surgery or middle ear surgery or infection within 1 week
Due to increases in intrathoracic and intraabdominal pressure
Presence of pneumothorax
Thoracic surgery within 4 weeks
Abdominal surgery within 4 weeks
Late-term pregnancy
Infection control issues
Active or suspected transmissible respiratory or systemic infection, including
tuberculosis
Physical conditions predisposing to transmission of infections, such as hemoptysis,
significant secretions, or oral lesions or oral bleeding

Page 3 of 5 PCAP Medical Directive on Spirometry Pre & Post Bronchodilator (Sample)
FINAL August 2020
Clinical Criteria:
1. The client must be rostered with [site name] with a documented
referral for pre/post spirometry. A physician or NP must be on site
during the conducting of a spirometry test in case of a medical
emergency arising from the test.
2. Informed verbal consent for the test is obtained from the client or the
legal guardian.
3. A list of medication to be put on hold prior to testing is provided to
the patient in advance of testing
4. No contraindication for testing.
Process:
1. Review chart to confirm spirometry order
2. Explain the purpose of spirometry, how the test will be performed,
contraindications, and obtain client’s consent.
3. Inform client of the following potential side effects of the beta-2
agonist that will be administered:
a. Increased heart rate (palpitations)
b. Tremors of extremities lasting approximately 30 minutes
c. Headaches
4. If the client has an allergy to salbutamol sulfate or refuses to take
salbutamol sulfate then the PCAP staff must stop the procedure and
refer back to the primary care provider for an alternative
bronchodilator.
5. Perform spirometry correctly as per the latest ATS/ERS/CTS
guidelines
6. Administer salbutamol sulfate HFA (100mcg) via metered dose
inhaler and spacer:
a. Adult: 4 puffs
b. Pediatric: >6 years: 4 puffs
7. If any of the above side effects are noted, stop any further administration
of the beta-2 agonist and do not perform post spirometry testing. Document
the side effects in the EMR and notify the client’s primary care provider.
Documentation and Communication
The performance of spirometry by the PCAP educators through this medical
directive will be documented in the EMR in accordance with the College of
“________” of Ontario Documentation Standards. The PCAP educator will
ensure the following is documented in the EMR:
1. Verbal consent was obtained from the client or legal guardian

Page 4 of 5 PCAP Medical Directive on Spirometry Pre & Post Bronchodilator (Sample)
FINAL August 2020
2. Side effects of the beta-2 agonist were reviewed with the client or legal
guardian.
3. The number of doses given to client of the beta-2 agonist, the method of
delivery and if the medication was delivered properly to the client.
4. Document in the EMR, any side effects the client may have experienced,
if the test was stopped and that the primary care provider was notified.
Review and Quality Monitoring
1. All delegators and implementers will maintain their professional
competence with their regulatory college.
2. All delegators and implementers will participate in educational
opportunities to maintain/update their knowledge on any new beta-2
medications and the skill of delivering these medications.
3. All delegators and implementers will participate in peer evaluations and
chart audit practices.
4. All delegators and implementers will document the performance and
results of all
spirometry that they have performed and will document any client
concerns in the EMR.
5. All delegators and implementers agree to consult with and communicate
any significant changes in the client’s condition with the client’s primary
care provider as soon as possible.
Signatures:
The physician(s) and nurse practitioners indicated below delegate the order
to perform pre and post spirometry and administer beta-2 agonist to the
PCAP educator who is working at [site name] when all conditions are met.
Physician/NP authorizing delegation for ___________ [Site name] :
_______________________________ Date: ____________________
Executive Director:
_______________________________ Date: ____________________
List of Authorized Staff for the Medical Directive
Ordering and performing pre/post bronchodilator Spirometry Testing

Page 5 of 5 PCAP Medical Directive on Spirometry Pre & Post Bronchodilator (Sample)
FINAL August 2020
Name Date Certified Review Date_______
References:
1. Coates AL et al. Spirometry in Primary Care. Can Respir J 2013;
20(1): 13-20. 2. American Thoracic Society: Standardization of Spirometry 2019
Update. Am J Respir Crit Care Med Vol 200, Iss 8, pp e70-e88, Oct 15, 2019

1
Adapted from the Sample Spirometry Requisition Form from Appendix A of CTS Spirometry in Primary Care (Coates AL et al. Spirometry in Primary Care. Can Respir J 2013; 20(1): 13-20)
Sample Spirometry Requisition Form
Requisition for Spirometry
Primary Care Clinic 123 Main St Anytown, Prov Z1Z 1Z1 Tel (987) 321-6540 Fax (987) 321-1234
Patient Name:_________________________ Patient ID#:___________________________ Referring Primary Care provider:__________________________ Primary care Provider Signature:_________________________ Date:______________ Tel:________________
Reason for Test
Diagnosis__________________________________________________________
Follow-up__________________________________________________________
Other_____________________________________________________________
Previous Test at this clinic? Yes No
Clinical Diagnosis: ________________________________________________________________
Smoking History: Current smoker Former smoker Never smoker No. of pack years: _________
Spirometry requested
Pre-bronchodilator Post-bronchodilator (400mcg salbutamol)
Relative Contraindications:
Acute myocardial infarction within 1 week
Systemic hypotension or severe hypertension
Significant atrial/ventricular arrhythmia
Non-compensated heart failure
Uncontrolled pulmonary hypertension
Acute cor pulmonale
Clinically unstable pulmonary embolism
History of syncope related to forced expiration/cough
Cerebral aneurysm
Brain surgery within 4 weeks
Recent concussion with continuing symptoms
Eye surgery within 1 week
Sinus surgery or middle ear surgery or infection within 1 week
Presence of pneumothorax
Thoracic surgery within 4 weeks
Abdominal surgery within 4 weeks
Late-term pregnancy
Active or suspected transmissible respiratory or systemic infection, including tuberculosis
Physical conditions predisposing to transmission of infections, such as hemoptysis, significant secretions, or oral lesions or oral bleeding
Respiratory Medications: ________________________________________________________________________________________________________________________________________________________
Appointment Date: ________________________________ Time: ______________________

2
Adapted from the Sample Spirometry Requisition Form from Appendix A of CTS Spirometry in Primary Care (Coates AL et al. Spirometry in Primary Care. Can Respir J 2013; 20(1): 13-20)
Instructions to Provide to the Patient:
Depending on the reason for doing the test, the patient should be instructed whether or not medications are to be withheld prior to testing, and if so, precisely which medications be withheld and for how long. It is important to instruct any patient withholding medications that, if needed for symptom relief, a rescue inhaler should be used and the time of use noted so that it can be reported to the technologist conducting the test.
Withhold medications? Yes No List medications to withhold: _____________________________________________________________
Short-Acting Beta2 Agonist (SABA) e.g., albuterol or salbutamol 4 - 6 Hours
Short-Acting Muscarinic Antagonist (SAMA) e.g., ipratropium bromide 12 Hours
Long-Acting Beta2 Agonist (LABA) e.g., formoterol or salmeterol) 24 hours
Ultra-long acting beta2 agonist (ultra-LABA) e.g., indacaterol, vilanterol or oladaterol
36 hours
Long-Acting Muscarinic Antagonist (LAMA) e.g., tiotropium, umeclidinium, aclidinium or glycopyrronium)
36-48 hours
The patient should be instructed to avoid the following prior to testing:
Smoking and/or vaping and/or water pipe use within at least 1 h of testing (to avoid acute bronchoconstriction due to smoke inhalation)
Consuming intoxicants within 8 h of testing Performing vigorous exercise within 1h of testing Wearing clothing that substantially restricts full chest and abdominal expansion Eating a large meal within 2 h of testing
Pre-Bronchodilator Post-Bronchodilator
Spirometry Best LLN %Ref Best %Ref Change %Chg
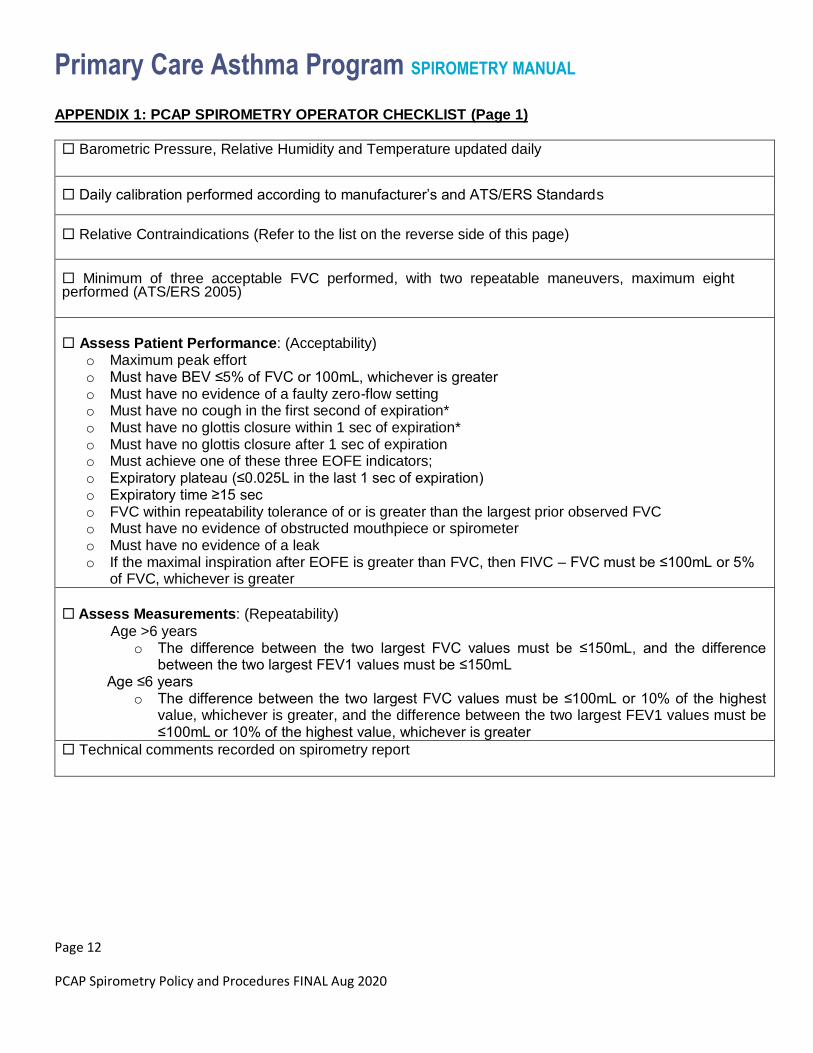
FVC (L) 4.65 3.86 91% 5.01 94% 360 mL 8%
FEV1 (L) 3.26 2.91 84% 4.04 100% 780 mL 24%
FEV1/FVC 0.70 0.64 0.81
PEF (L/s) 10.2 14.3
FET (s) 15.3 14.8
Test quality B A
Reference values: Quanjer 2012 [Caucasian]
Family Physicians Clinic
123 Main St
Anytown, Prov, Z1Z 1Z1
987-321-6540
Age: 62 yr Male Name: Xxxxxxxx, Xxxx
Ht: 186 cm Race: Caucasian ID#: 333222111
Wt: 84 kg BMI: 24.3 kg/m2 Date of birth: 1949-Dec-31
Nonsmoker - pack-yrs: 0 Date of test: 14:20, 2012-Jan-02
Reason for test: Chronic cough
Interpretation: Pre-bronchodilator spirometry is in the normal range. There is a significant response to
bronchodilators.
Physician: Dr. Blow Hard
FVC
FEV1
FEV1/FVC
LLN reference
o
o
o
FVC
FEV1
FEV1/FVC
LLN reference
Pre-Bronchodilator
Post-Bronchodilator
o
o o
Pre
Post
Pre
Post
Technologist comments:
3 acceptable blows with 2
repeatable for both Pre- and
Post- tests.
No bronchodilators taken in
previous 24 hrs.
std dev
std dev
APPENDIX B: Sample spirometry report form

Section 3: Spirometry
Practicum

FVC Normal ≥ LLN 4
Spirometry Interpretation Guide
Consistent
with COPD
Consider
methacholine
challenge
No
Adapted and revised with permi ssion from Primary Care Respiratory Alliance of Canada (PCRAC)
hcp.lunghealth.ca/clinical-tools
Pre ß2-agonist
FEV1 / FVC Ratio
Reduced: < LLN
(or <0.70)5
ß2-agonist
FEV1 / FVC Reduced
< LLN (or <0.70)5,6
FEV1 / FVC Normal
≥ LLN (or ≥0.70)5,6
Improved FEV1
12% and 200mL1
Improved FEV1
12% and 200mL1
Consistent with Asthma
or COPD or Asthma
COPD Overlap (ACO)
LLN=Lower Limit of Normal
(Consider patient history in all interpretation decision making)
Consistent
with Asthma
1. 200mL criteria only necessary for adults and children ≥ 12 years
2. Reversibility criteria not met. May occur with chronic asthma - consider methacholine challenge or referral
3. Normal Spirometry: in the context of persistent symptoms consider further clinical testing i.e. methacholine challenge
4. LLN may not be available on outdated systems – use 80% predicted
5. If the LLN is not available use 0.70 in an adult if COPD is suspected and 0.80 in a child
6. If FVC < LLN (or < 80%) predicted, consider hyperinflation/gas trapping. If post-BD FVC remains < LLN (or < 80%) predicted, consider combined obstructive and restrictive defect and full PFT.
Note: Recommended reference equations: GLI, CHMS, and NHANES III
(not consistent
with COPD)
Normal: ≥ LLN
(or ≥0.70)5
ß2-agonist
Improved FEV1 12%
and 200mL1
NoYes
Improved FEV1 12%
and 200mL1
Normal
Spirometry2,3
NoYes
Consider FULL
PFT (+/- referral to
specialist)
Suspect
Asthma
(Consistent with restriction)
Yes
Suspect
Asthma
YesYes No
No
(Consistent with obstruction)
© 2018 Ontario Lung Association
Ontario Lung Association is a registered charity operating as the Lung Health Foundation
Primary Care Asthma Program Spirometry Operator’s Checklist
1
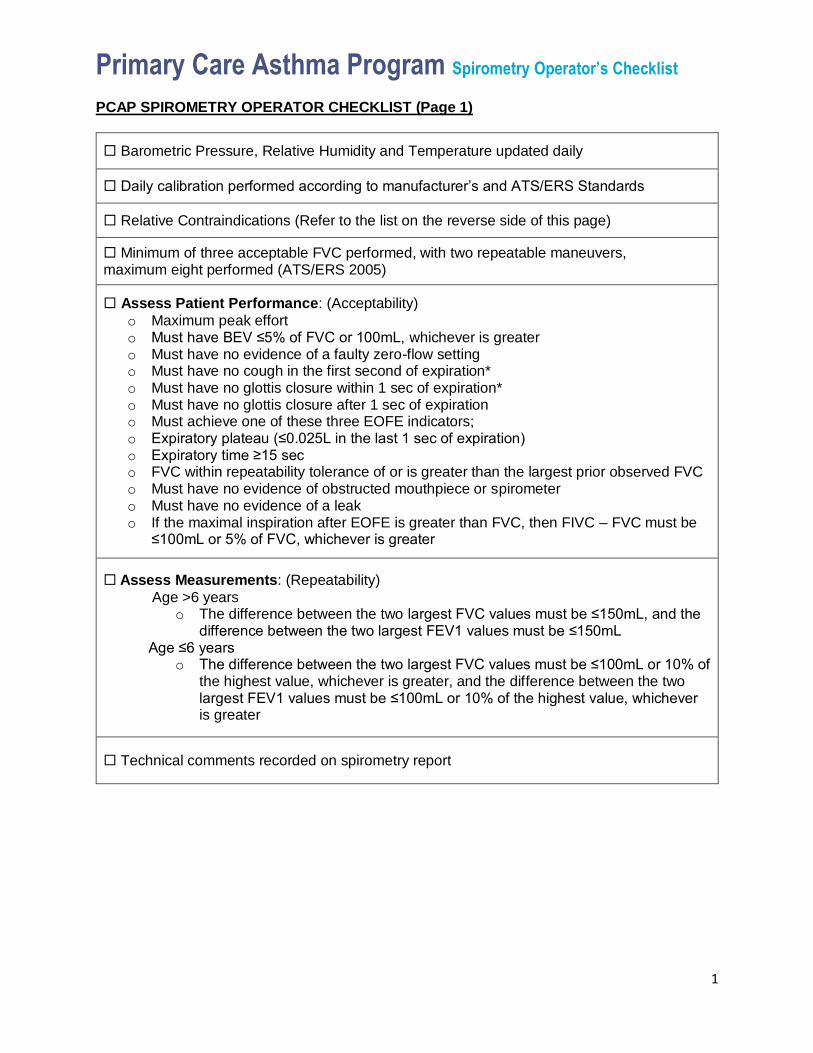
PCAP SPIROMETRY OPERATOR CHECKLIST (Page 1)
Barometric Pressure, Relative Humidity and Temperature updated daily
Daily calibration performed according to manufacturer’s and ATS/ERS Standards
Relative Contraindications (Refer to the list on the reverse side of this page)
Minimum of three acceptable FVC performed, with two repeatable maneuvers, maximum eight performed (ATS/ERS 2005)
Assess Patient Performance: (Acceptability)
o Maximum peak effort o Must have BEV ≤5% of FVC or 100mL, whichever is greater o Must have no evidence of a faulty zero-flow setting o Must have no cough in the first second of expiration* o Must have no glottis closure within 1 sec of expiration* o Must have no glottis closure after 1 sec of expiration o Must achieve one of these three EOFE indicators; o Expiratory plateau (≤0.025L in the last 1 sec of expiration) o Expiratory time ≥15 sec o FVC within repeatability tolerance of or is greater than the largest prior observed FVC o Must have no evidence of obstructed mouthpiece or spirometer o Must have no evidence of a leak o If the maximal inspiration after EOFE is greater than FVC, then FIVC – FVC must be
≤100mL or 5% of FVC, whichever is greater
Assess Measurements: (Repeatability)
Age >6 years o The difference between the two largest FVC values must be ≤150mL, and the
difference between the two largest FEV1 values must be ≤150mL
Age ≤6 years o The difference between the two largest FVC values must be ≤100mL or 10% of
the highest value, whichever is greater, and the difference between the two largest FEV1 values must be ≤100mL or 10% of the highest value, whichever is greater
Technical comments recorded on spirometry report

Primary Care Asthma Program Spirometry Operator’s Checklist
2
PCAP SPIROMETRY OPERATOR CHECKLIST (Page 2)
Relative Contraindications for Spirometry*
Due to increases in myocardial demand or changes in blood pressure
Acute myocardial infarction within 1 week
Systemic hypotension or severe hypertension
Significant atrial/ventricular arrhythmia
Noncompensated heart failure
Uncontrolled pulmonary hypertension
Acute cor pulmonale
Clinically unstable pulmonary embolism
History of syncope related to forced expiration/cough
Due to increases in intracranial/intraocular pressure
Cerebral aneurysm
Brain surgery within 4 weeks
Recent concussion with continuing symptoms
Eye surgery within 1 week
Due to increases in sinus and middle ear pressures
Sinus surgery or middle ear surgery or infection within 1 week
Due to increases in intrathoracic and intraabdominal pressure
Presence of pneumothorax
Thoracic surgery within 4 weeks
Abdominal surgery within 4 weeks
Late-term pregnancy
Infection control issues
Active or suspected transmissible respiratory or systemic infection, including tuberculosis
Physical conditions predisposing to transmission of infections, such as hemoptysis,significant secretions, or oral lesions or oral bleeding
*It is recommended that the decision to conduct spirometry testing should be made on a case
by case basis in consultation with the primary care provider

Section 4:
Standards/References

AMERICAN THORACIC SOCIETYDOCUMENTS
Standardization of Spirometry 2019 UpdateAn Official American Thoracic Society and European Respiratory SocietyTechnical StatementBrian L. Graham, Irene Steenbruggen, Martin R. Miller, Igor Z. Barjaktarevic, Brendan G. Cooper, Graham L. Hall,Teal S. Hallstrand, David A. Kaminsky, Kevin McCarthy, Meredith C. McCormack, Cristine E. Oropez,Margaret Rosenfeld, Sanja Stanojevic, Maureen P. Swanney†, and Bruce R. Thompson; on behalf of the AmericanThoracic Society and the European Respiratory Society
THIS OFFICIAL TECHNICAL STATEMENT WAS APPROVED BY THE AMERICAN THORACIC SOCIETY AND THE EUROPEAN RESPIRATORY SOCIETY SEPTEMBER 2019
Background: Spirometry is the most common pulmonaryfunction test. It is widely used in the assessment of lung functionto provide objective information used in the diagnosis of lungdiseases andmonitoring lung health. In 2005, theAmerican ThoracicSociety and the European Respiratory Society jointly adoptedtechnical standards for conducting spirometry. Improvements ininstrumentation and computational capabilities, together withnew research studies and enhanced quality assurance approaches,have led to the need to update the 2005 technical standards forspirometry to take full advantage of current technicalcapabilities.
Methods: This spirometry technical standards document wasdeveloped by an international joint task force, appointed by theAmerican Thoracic Society and the European Respiratory Society,with expertise in conducting and analyzing pulmonary function tests,laboratory quality assurance, anddeveloping international standards.
A comprehensive review of published evidence was performed. Apatient survey was developed to capture patients’ experiences.
Results: Revisions to the 2005 technical standards for spirometryweremade, including the addition of factors that were not previouslyconsidered. Evidence to support the revisions was cited whenapplicable. The experience and expertise of task force members wereused to develop recommended best practices.
Conclusions: Standards and consensus recommendations arepresented for manufacturers, clinicians, operators, and researcherswith the aims of increasing the accuracy, precision, and quality ofspirometric measurements and improving the patient experience. Acomprehensive guide to aid in the implementation of these standardswas developed as an online supplement.
Keywords: spirometry; spirometer; pulmonary function; technicalstandards
ContentsOverview
Key Updates
IntroductionMethodsThe Patient Experience
IndicationsRelative ContraindicationsLaboratory Details
†Deceased February 17, 2019.
ORCID IDs: 0000-0003-1794-7682 (I.S.); 0000-0001-9971-5759 (M.R.M.); 0000-0002-8096-0858 (I.Z.B.); 0000-0003-0785-1038 (B.G.C.);0000-0002-6217-9494 (G.L.H.); 0000-0002-5059-6872 (T.S.H.); 0000-0002-6515-8023 (D.A.K.); 0000-0003-1702-3201 (M.C.M.);0000-0001-7931-8051 (S.S.); 0000-0002-5885-0652 (B.R.T.).
Supported by the American Thoracic Society and the European Respiratory Society.
An Executive Summary of this document is available at http://www.atsjournals.org/doi/suppl/10.1164/rccm.201908-1590ST.
You may print one copy of this document at no charge. However, if you require more than one copy, you must place a reprint order. Domestic reprint orders:[email protected]; international reprint orders: [email protected].
Correspondence and requests for reprints should be addressed to Brian L. Graham, Ph.D., Division of Respirology, Critical Care and Sleep Medicine, Universityof Saskatchewan, 103 Hospital Drive, Saskatoon, SK, S7N 0W8 Canada. E-mail: [email protected].
This article has an online supplement, which is accessible from this issue’s table of contents at www.atsjournals.org.
Am J Respir Crit Care Med Vol 200, Iss 8, pp e70–e88, Oct 15, 2019
Copyright © 2019 by the American Thoracic Society
DOI: 10.1164/rccm.201908-1590ST
Internet address: www.atsjournals.org
e70 American Journal of Respiratory and Critical Care Medicine Volume 200 Number 8 | October 15 2019

Hygiene and Infection ControlEquipment
DisplayBTPS Adjustment
Device Quality AssuranceOperator DetailsPatient Details
Patient Preparation
FEV1 and FVC ManeuverTest ProcedureWithin-Maneuver EvaluationBetween-Maneuver EvaluationMaximum Number of Maneuvers
Bronchodilator ResponsivenessTesting
Test Procedure
Reported ValuesOther Derived Indices
Grading the Quality of the Test SessionVC and Inspiratory Capacity Maneuver
EquipmentTest Procedure
Further StudiesOther Potential Analyses
Overview
This document is an update of the 2005American Thoracic Society (ATS) andEuropean Respiratory Society (ERS)standardization of spirometry (1), whichin turn built on a wealth of previous work(2–6). Additional standards have beendeveloped for occupational surveillance(7) and for preschool children (8).Improvements in instrumentation andcomputational capabilities, together withnew research studies and enhanced qualityassurance approaches, have led to the needto update the 2005 technical standards forspirometry to take full advantage of currenttechnical capabilities and evolving bestpractices. This technical report coversdefinitions, equipment specifications,patient-related procedures, quality control,and data reporting. A comprehensive guideto aid in the implementation of thesestandards was developed as an onlinesupplement. A summary of the primarychanges in this update is provided inTable E1 in the online supplement.
Key Updatesd A new list of relative contraindicationswas added.
d Spirometers are now required to meetInternational Organization forStandardization (ISO) 26782 standards,but with a maximum permissibleaccuracy error of 62.5%.
d Device quality assurance procedures wereupdated.
d Operator training as well as attainmentand maintenance of competency wereaddressed.
d The list of activities that patients shouldavoid before testing was updated.
d There is a focus on the use of devicesthat measure both expiration andinspiration.
d Maneuver acceptability and repeatabilitycriteria were updated. The end of forcedexpiration (EOFE) was redefined.
d Requirements for spirometry systems toprovide uniform cues and feedback to theoperator were added.
d New withholding times forbronchodilators before bronchodilatorresponsiveness testing were developed.
d A new grading system for assessment ofspirometry quality was developed.
d Standardized operator feedback optionsthat promote synoptic reporting weredeveloped.
d Preliminary findings derived from aninternational patient survey were presented.
Introduction
Spirometry is a physiological test that measuresthemaximal volumeof air that an individual caninspire and expire with maximal effort. Theprimary signal measured in spirometry is eithervolume or flow as a function of time. The mostrelevant measurements discussed in thisdocument are the FVC, which is the volumedelivered during an expiration made asforcefully and completely as possible startingfrom full inspiration, and the FEV1, which is theexpiratory volume in the first second of an FVCmaneuver. These standards also apply tomeasurements of FEV1 in airwayresponsiveness testing and exercise testing.Other spirometric variables derived from theFVC maneuver are also addressed, as well asthe measurement of VC from a slowmaneuver.
In this document, the “operator” is theperson conducting the test; the term“patient” is used for the person beingtested, recognizing that not all persons willbe patients; and “maneuver” is the termused for the inspiratory and expiratory VCexcursions. The term “must” is used toindicate a requirement for meeting thestandards, and “should” is used to indicateactions that may not be mandatory but areconsidered to be best practices.
These standards are the minimumcriteria that must be met for clinicalspirometry, whichmay not be sufficient for all
settings, such as research or occupationalsurveillance (7). The spirometry facilitymanager is also responsible for following localregulations, which may have additionalrequirements. As manufacturers continueto improve spirometric instrumentation andas new technology is implemented, it isexpected that new systems will meet and,in many cases, exceed these new standards.Standards that are developed and updatedfrom time to time should not limit the questfor continual improvement in the quality oflung function measurements and innovationin applying new technology (9).
This revision also includes updates ofapplicable sections of the 2005 ATS/ERSgeneral considerations for lung functiontesting document (10). Although thesestandards apply in primary care, somestudies have shown that standards are oftennot met in primary care (11, 12). However,in studies of patients with asthma and/orchronic obstructive pulmonary disease(COPD), office spirometry was accurateand reliable when compared with laboratory‐based spirometry (13–15), demonstrating thatcompetent operators using equipment thatmeets ATS/ERS standards can meet thespirometry acceptability criteria in theprimary care setting.
Methods
An application was submitted for a jointATS and ERS task force to update the 2005spirometry standards (1). The task forcemembership and co-chairs were approvedby the ATS and the ERS. Task forcemembers were scientists and physicianswith experience in international guidelinesand standards; clinical experience inroutine lung function testing; and specialistknowledge of spirometry, includingresearch publications. All potential conflictsof interest were disclosed and managedaccording to the rules and procedures of theATS and the ERS. A search in the
AMERICAN THORACIC SOCIETY DOCUMENTS
American Thoracic Society Documents e71

MEDLINE database (using PubMed) forpublications containing various termsrelated to spirometry published from 2004to 2018 yielded 23,368 citations (searchterms listed in Section E3). Task forcemembers reviewed the abstracts andidentified 190 as directly relevant to theproject and a further 382 as potentiallyrelevant. New publications were monitoredafter the initial search, and twelve 2018 and2019 references are included. Allmanufacturers of spirometry equipmentwere sent a survey requesting equipmentspecifications. The task force also reviewedequipment specifications published on themanufacturers’ websites. An internationalsurvey of patients was conducted throughthe European Lung Foundation to elicittheir experience in spirometry testing.Using the 2005 standards as the basedocument, revisions and additions weremade on a consensus basis. Therecommendations in this documentrepresent a consensus of task forcemembers in regard to the evidenceavailable for various aspects of spirometricmeasurement (as cited in the document)and otherwise reflects the expert opinionof the task force members for areas inwhich peer-reviewed evidence was eithernot available or incomplete. Constraints onthe development of these standards arelisted in Section E12.
The Patient Experience
To gather information regarding patients’experiences and to identify problems facedby patients who have performedspirometry, an online survey completed by1,760 spirometry patients from 52 countrieswas conducted in August and September2018 by the European Lung Foundation.Patients reported the need for moreinformation about spirometry before thetest, including medication withholding.Eighty percent of respondents found thedegree of difficulty to be mostly acceptableor completely acceptable. Even so, 31%considered the statement “To keep blowingeven though you do not feel anything iscoming out” to describe a moderate orserious issue. This could be addressed byhaving an analog or digital display of flowin ml/s on the screen to give patientsfeedback on their expiratory rate during themaneuver. Key messages from the surveyare provided in Section E4. Full results of
the survey will be forthcoming in a futurepublication.
Indications
Spirometry is fundamental in theassessment of general respiratory health.Spirometry enables measuring the effect of adisease on lung function, assessing airwayresponsiveness, monitoring disease courseor the result of therapeutic interventions,assessing preoperative risk, and determininga prognosis for many pulmonary conditions.Spirometry is a valuable tool that providesimportant information to clinicians which isused together with other physical findings,symptoms, and history to reach a diagnosis.Common indications for spirometry aregiven in Table 1.
Relative Contraindications
Performing spirometry can be physicallydemanding. The forced expiratorymaneuver used in spirometry increasesintrathoracic, intraabdominal, andintracranial pressures (16–20). Potentialrisks of spirometry are primarily related tomaximal pressures generated in the thoraxand their impact on abdominal andthoracic organs, venous return andsystemic blood pressure, and expansion ofthe chest wall and lung. The physical effortrequired can increase myocardial demand.Caution must be used for patients withmedical conditions that could beadversely affected by these physiologicalconsequences (Table 2). Although suchrisks are likely to be minimal for spirometryin most patients (21), the potential risksassociated with testing should always beweighed against the benefit of obtaininginformation about lung function (16, 17,22). Spirometry should be discontinued ifthe patient experiences pain during themaneuver. Patients with potentialcontraindications that would preventtesting in the primary care setting may betested in a pulmonary function laboratorywhere operators are more experienced andthere may be access to emergency care ifneeded. Furthermore, because spirometryrequires the active participation of thepatient, inability to understand directionsor unwillingness to follow the directionsof the operator will usually lead tosubmaximal test results.
A 20-year review of 186,000 pulmonaryfunction tests in a tertiary institution foundthat patient safety incidents occurred in 5 ofevery 10,000 routine pulmonary functiontests (excluding exercise and provocationtests) with generally low risk of harm (21).Cardiopulmonary incidents, primarilysyncope, were the most common finding. Astudy found that 10% of patients havingmaximal cardiopulmonary exercise testshad simple, self-limited arrhythmiasinduced by spirometry (23). No adverseeffects were reported in spirometryconducted in studies of 56 and 230 (24, 25)patients with abdominal aortic aneurysmsfrom 5 to 13 cm in size and in 519 patientswith thoracic aortic aneurysms from 5 to 8cm in size (26).
Laboratory Details
Ambient temperature, barometric pressure,and time of day must be recorded.Temperature is an important variable inmost pulmonary function tests and issometimes measured directly by theinstrument. The way in which it is measuredand used may vary from instrument toinstrument (e.g., a simple thermometer oran internal thermistor). Regardless of themethod used, the operator should confirmthe accuracy of temperature measurements,and the manufacturer should describe orprovide a clear mechanism for checking theaccuracy of instrument temperaturemeasurements. Spirometers that require abarometric pressure measurement shouldhave a barometric pressure sensor or theability to calculate mean barometricpressure using altitude above sea level (27).
Testing should preferably occur in aquiet and comfortable environment that isseparated from the waiting room and otherpatients being tested. Drinking water shouldbe available. Tissues or paper towels shouldbe offered to help patients deal withsecretions. The patient should be seatederect, with shoulders slightly back and chinslightly elevated. A chair with arms (toprevent falling sideways should syncopeoccur), without wheels, and with a heightadjustment so that the feet are flat on thefloor should be used. A smaller chair or araised footstool should be provided forchildren and small adults. For themaneuvers described below, a noseclip ormanual occlusion of the nostrils should beused. If testing is undertaken with the
AMERICAN THORACIC SOCIETY DOCUMENTS
e72 American Journal of Respiratory and Critical Care Medicine Volume 200 Number 8 | October 15 2019

patient in another position, this must bedocumented in the report. Tests done whilestanding are similar to sitting in studies ofadults (28), obesity (29), and children (30).Fowler’s position (elevated head and torso)yields higher values than supine or Crook’sposition (knees raised) (31). In most studiesinvolving healthy subjects or patients withlung, heart, neuromuscular disease, orobesity, FEV1 and FVC were higher in moreerect positions, whereas for subjects withtetraplegic spinal cord injury, FVC and FEV1
were higher in supine than while sitting (32).
Hygiene and InfectionControl
The goal of infection control is to preventthe transmission of infection to patients andstaff during pulmonary function testing (33,34). The number of documented cases ofinfection transmission is very small, butthe potential is real. Infection can betransmitted by direct contact with surfacessuch as mouthpieces, noseclips, handheldspirometers, chair arms, and immediateproximal surfaces of valves or tubing.Indirect transmission occurs by aerosoldroplets generated by the patient blowinginto the equipment but also expelled intothe air of the testing room betweenmaneuvers.
The operator must wash her or hishands or use an approved hand sanitizerbefore contact with each new patient (35).Additional steps may be required by localinfection control policies. Using disposablegloves does not eliminate the need for handwashing or sanitizing, but if gloves are used,a new pair is required for each patient. Thepatient should be given an approved handdisinfectant gel or wipe upon first entryinto the testing station, because patientswill be touching various surfaces, and manyspirometers are handheld.
The use of disposable, in-line filters forspirometers has become standard practice inmost facilities. Furthermore, the mouthpieceis usually an integral part of the filter andwill reduce contamination of the spirometer.All disposable items, including filters,mouthpieces, noseclips, and gloves, must bedisposed of at the end of the testing session.
To avoid operator exposure and cross-contamination, hands must be washedimmediately after direct handling ofmouthpieces, tubing, breathing valves,or interior spirometer surfaces. Glovesshould be worn when handling potentiallycontaminated equipment and/or if the operatorhas any open cuts or sores on his or her hands.
Manufacturers must explicitly describeacceptable methods of cleaning anddisinfecting their equipment, includingrecommended chemicals and
concentrations, as well as safety precautionsfor the operator. Local infection controlrequirements, especially for at-riskpopulations such as patients with cysticfibrosis (36), may supersede bothmanufacturers’ recommendations andthose in this document.
Extra precautions should be taken forpatients with, or suspected of having,tuberculosis, hemoptysis, oral lesions, orother known transmissible infectiousdiseases. Possible precautions includereserving equipment for the sole purpose oftesting infected patients or testing suchpatients at the end of the workday to allowtime for spirometer disassembly anddisinfection and/or testing patients in theirown rooms with adequate ventilation andappropriate protection for the operator.Hygiene processes are described in moredetail in the ATS Pulmonary FunctionLaboratory Management and ProcedureManual (37).
Equipment
Manufacturers must ensure that allspirometers meet the standards containedin the current update of ISO 26782 (38).The current update is ISO 26782:2009,last reviewed in 2016 and scheduled to bereviewed next in 2021. Although notexplicitly stated in ISO 26782, it is notpermissible to recalibrate a spirometerbetween the individual test profiles ofAnnex C of ISO 26782. Notwithstandingthe ISO 26782, Section 7, performancerequirements of being within 63.0% foraccuracy, linearity, and repeatability,spirometric equipment must have amaximum permissible error of 62.5%when tested with a 3-L calibration syringeand when using the test profiles of ISO26782, Section 7, Annex C. If future ISO26782 revisions specify a maximumpermissible error less than 62.5%, then thelower value must be used. A 2018 survey ofspirometer manufacturers worldwidefound that 17 of 19 respondents reportedthat the accuracy of their products waswithin 62%. A study of 7,497 calibrationverifications of volume spirometersdemonstrated the need for more stringentstandards (39). Thirteen of 19 manufacturersresponding to the survey were compliantwith ISO 26782:2009. A study has questionedwhether the previously recommended ATSstandard waveforms were sufficient (40). For
Table 1. Indications for Spirometry
DiagnosisTo evaluate symptoms, signs, or abnormal laboratory test resultsTo measure the physiologic effect of disease or disorderTo screen individuals at risk of having pulmonary diseaseTo assess preoperative riskTo assess prognosis
MonitoringTo assess response to therapeutic interventionTo monitor disease progressionTo monitor patients for exacerbations of disease and recovery from exacerbationsTo monitor people for adverse effects of exposure to injurious agentsTo watch for adverse reactions to drugs with known pulmonary toxicity
Disability/impairment evaluationsTo assess patients as part of a rehabilitation programTo assess risks as part of an insurance evaluationTo assess individuals for legal reasons
OtherResearch and clinical trialsEpidemiological surveysDerivation of reference equationsPreemployment and lung health monitoring for at-risk occupationsTo assess health status before beginning at-risk physical activities
AMERICAN THORACIC SOCIETY DOCUMENTS
American Thoracic Society Documents e73

digitization of the flow or volume signal,the sampling rate must be >100 Hz (41)with a minimum resolution of 12 bits. TheERS/ATS standards for diffusing capacity(42) specify a volume accuracy of 62%,but the flow range required for thediffusing capacity maneuver is smaller thanthat for spirometry, and the systemsmeasuring diffusing capacity primarily usehigher-grade instrumentation. Therefore,laboratories using such equipment areexpected to exceed accuracy requirementsfor spirometry.
DisplayFor optimal quality control, bothvolume–time and flow–volume real-timedisplays are required, and operators mustvisually inspect the performance of eachmaneuver for quality assurance beforeproceeding with another maneuver. Forthe flow–volume graph, expiratory flowmust be plotted upward, and expiratoryvolume must be plotted toward the right.A 2:1 aspect ratio must be maintainedbetween the flow and volume scales; that
is, 2 L/s of flow and 1 L of volume mustbe the same distance on their respectiveaxes.
Displays of flow versus volume providemore detail than volume–time graphs forthe first 1 second of the FVC maneuver.Because this portion of the maneuver,particularly the peak expiratory flow (PEF),is correlated with the pleural pressureduring the maneuver, the flow–volumegraph is useful to assess the magnitude ofeffort during the initial portions of themaneuver. The ability to overlay a seriesof flow–volume graphs registered at thepoint of maximal inspiration may behelpful in evaluating repeatability anddetecting submaximal efforts. However, ifthe point of maximal inspiration variesbetween maneuvers, then the interpretationof these results is difficult because the flowsat identical measured volumes are beingachieved at different absolute lung volumes.In contrast, display of the FVC maneuver asa volume–time graph provides more detailfor the latter part of the maneuver. In adisplay of multiple trials, the sequencing of
the maneuvers should be apparent to theoperator.
For the start of test display, thevolume–time graph must begin at the pointof maximum inspiration or 1 second beforeTime 0 (defined below), whichever occursfirst. The display of the maneuver shouldcontinue to the end of the plateau (definedbelow) or the beginning of inspiration.
BTPS AdjustmentAll spirometry outcomes must be reportedat BTPS (body temperature, ambientbarometric pressure, saturated with watervapor). The ambient temperature mustalways be recorded with an accuracyof 618C. In situations when the ambientair temperature is changing rapidly (.38Cin ,30 min), continuous temperaturecorrections may be necessary (Section E5).Operators should be aware of potentialproblems with tests performed outside therange of ambient temperatures andbarometric pressures specified by themanufacturer for their particularspirometer.
Changes in spirometer or flow sensortemperature can be a source of variability(43). Spirometer temperature should bemeasured and not assumed to be constant,even over the course of one testing session.For volume spirometers, errors up to 6%in FEV1 and FVC can occur if ambienttemperature is used instead of internaltemperature of volume spirometers (44).Therefore, when using volume spirometers,the temperature inside the spirometershould be measured for each breathingmaneuver.
Device Quality Assurance
Attention to equipment quality assuranceand calibration is an important part of goodlaboratory practice. The minimumrequirements are as follows: 1) maintenanceof a log of calibration results, 2)documentation of repairs or otheralterations that return the equipment toacceptable operation, 3) recording of datesof computer software and hardwareupdates or changes, and 4) recording thedates equipment is changed or relocated(e.g., industrial surveys). Calibrationverifications and quality control proceduresmust be repeated after any such changesbefore further testing begins. Key aspects of
Table 2. Relative Contraindications for Spirometry
Due to increases in myocardial demand or changes in blood pressureAcute myocardial infarction within 1 wkSystemic hypotension or severe hypertensionSignificant atrial/ventricular arrhythmiaNoncompensated heart failureUncontrolled pulmonary hypertensionAcute cor pulmonaleClinically unstable pulmonary embolismHistory of syncope related to forced expiration/cough
Due to increases in intracranial/intraocular pressureCerebral aneurysmBrain surgery within 4 wkRecent concussion with continuing symptomsEye surgery within 1 wk
Due to increases in sinus and middle ear pressuresSinus surgery or middle ear surgery or infection within 1 wk
Due to increases in intrathoracic and intraabdominal pressurePresence of pneumothoraxThoracic surgery within 4 wkAbdominal surgery within 4 wkLate-term pregnancy
Infection control issuesActive or suspected transmissible respiratory or systemic infection, including tuberculosisPhysical conditions predisposing to transmission of infections, such as hemoptysis,significant secretions, or oral lesions or oral bleeding
Spirometry should be discontinued if the patient experiences pain during the maneuver. Relativecontraindications do not preclude spirometry but should be considered when ordering spirometry.The decision to conduct spirometry is determined by the ordering healthcare professional on thebasis of their evaluation of the risks and benefits of spirometry for the particular patient. Potentialcontraindications should be included in the request form for spirometry.
AMERICAN THORACIC SOCIETY DOCUMENTS
e74 American Journal of Respiratory and Critical Care Medicine Volume 200 Number 8 | October 15 2019

equipment quality assurance aresummarized in Table 3.
A calibration procedure determines therelationship between flow or volumetransducer signals measured by the sensorand the actual flow or volume. In contrast, acalibration verification is the procedureused to validate that the device is withincalibration limits (i.e., 63% [accuracytolerance, 62.5% for spirometersplus 60.5% for calibration syringes]).Spirometry systems must include acalibration verification option using roomair at ambient conditions. If a device fails itscalibration verification (Table 4), then anew calibration procedure or equipmentmaintenance is required. Manufacturersmust provide an alert if the new calibrationfactor either varies by more than 62 SDsfrom the mean calibration factor or changesby more than 6% from the previouscalibration factor, because this may indicatethat the spirometer requires cleaning,maintenance, and/or repair. Calibrationverifications must be undertaken daily, ormore frequently if specified by themanufacturer. Precalibrated spirometerscannot be recalibrated by the operator butmust still undergo a calibration verification.Manufacturers must specify the action tobe taken if a precalibrated device failsthe calibration verification. Spirometrysoftware must include the ability togenerate a report of calibrations thatincludes the results of all verifications, thenumber of failed calibration verificationsin each session, and the changes incalibration factors. A warning should beissued if the calibration verification errordiffers from the historical mean calibrationverification error by more than 62 SDs(37, 39, 45, 46).
The spirometry system must determinethe zero-flow level with the spirometerblocked before calibration, calibrationverifications, and patient tests. If variableflow is detected during the zero-flow settingprocedure or if the zero level has changedsignificantly, the zero-flow setting proceduremust be repeated.
A 3-L syringe used to both recalibrateand verify the volume calibration ofspirometers must have an accuracyof 60.015 L or 60.5% of the full scale,and the manufacturer must providerecommendations concerning appropriateintervals between checks of the syringeaccuracy. The syringe must be kept at roomtemperature. Holding the syringe body to
steady the syringe during a calibrationverification can raise its temperature andcontribute to measurement error.Operators should be aware that a syringewith an adjustable or variable stop may beout of calibration if the stop is reset oraccidentally moved. Calibration syringesmust have a monthly leak test at more thanone volume up to their maximum; this canbe done by attempting to empty or fill themwith the outlet corked (47). A dropped ordamaged syringe should be considered outof calibration until it is checked.
Calibration verifications must beundertaken at least daily using a 3-L syringecycled at least three times to give a rangeof flows varying between 0.5 and 12 L/s(with 3-L injection times between 0.5 and6 s). If an in-line filter is used in spirometrytesting, then it must also be used duringrecalibrations and verifications. Themeasured volume at each flow must meetthe accuracy requirement of 63% for bothinspiration and expiration (or for expirationonly for volume-based spirometers). Fordevices using disposable flow sensors, anew sensor from the supply used for patienttests must be tested each day.
The ATS Pulmonary FunctionLaboratory Management and ProcedureManual (37) includes the option for abiological control: a healthy, nonsmokingindividual capable of performing veryrepeatable spirometry. A biological controlis not a substitute for the use of a calibrationsyringe. However, operators are encouragedto know their own usual FEV1 and FVC,which allows them to conduct a quick,rough check if they suspect a problem. Insome jurisdictions, including a biologicalcontrol in quality control reporting mayconstitute a breach of employee privacyprotection.
Operator Details
As Ruppel and Enright observed, “Thereare 3 key elements to obtain high qualitypulmonary function data: accurate andprecise instrumentation, a patient/subjectcapable of performing acceptable andrepeatable measurements, and a motivatedtechnologist to elicit maximum performancefrom the patient. In the realm ofstandardization, the technologist has receivedthe least attention” (48). The importance ofthe operator was also a key message derivedfrom the patient experience survey.
It is the responsibility of the operatorto observe and engage with the patient toachieve optimal results, which requires acombination of training and experience.Training courses for conducting qualityspirometry testing are available in manycountries, which has led to operatorsfollowing ATS/ERS standards (14, 15,49–51), but short-term follow-up andsupplementary training are important tomaintain quality (52, 53). Operator trainingand attainment and maintenance ofcompetency must be integrated in anyspirometry testing service (54).
Patient Details
The patient’s age, height, and weight(wearing indoor clothes and without shoes)are recorded. It is preferable to calculate ageusing the date of birth and the date of thetest, including in jurisdictions where birthdates may only be recorded to the nearestmonth. Age must be reported in years toone decimal place. Height in centimeters toone decimal place (55) and weight to thenearest 0.5 kg must be recorded; these mayalso be expressed in inches and poundson reports in jurisdictions still using thosemeasures. Body mass index should becalculated as kg/m2. The height must bemeasured without shoes, with the feettogether, standing as tall as possible withthe eyes level and looking straight ahead,and the back flush against a wall orstadiometer. For patients unable to standerect, height may be estimated using ulnalength (preferred for children) (56) or armspan (57) (see Section E6), recognizingthat there are sex, age, and ethnicdifferences in such estimates. Ulna lengthshould be measured with calipers to avoiderror introduced using a tape measure. Inpersons aged 25 years or older, for whom areliable height measurement has been madepreviously in the same facility, remeasuringheight at subsequent visits within 1 yearmay not be necessary.
Birth sex and ethnicity should beincluded in the patient information on thespirometry request. Otherwise, the operatorwill ask the patient to provide thisinformation. When requesting birth sexdata, patients should be given theopportunity to provide their gender identityas well and should be informed thatalthough their gender identity is respected, itis birth sex and not gender that is the
AMERICAN THORACIC SOCIETY DOCUMENTS
American Thoracic Society Documents e75

determinant of predicted lung size.Inaccurate entry of birth sex may lead toincorrect diagnosis and treatment. Similarly,patients should be informed of the need forreporting ethnicity (58). Ethnicitycategories for the Global Lung FunctionInitiative (GLI) reference values (59) arewhite (i.e., European ancestry), AfricanAmerican, Northeast Asian, SoutheastAsian, and other/mixed (Section E7). Ifbirth sex and/or ethnicity data are notdisclosed, the operator notes must alert theinterpreter of this omission and state whatdefault values were used for calculatingpredicted values.
Patient PreparationPatients should avoid the activities listedin Table 5 before testing, and theserequirements should be given to the patient
at the time of making the appointment. Onarrival, all of these points must be checked,and any deviations from them must berecorded.
Patients should be as relaxed as possiblebefore and during the tests. Patients shouldbe asked to loosen tight-fitting clothing.Well-fitting dentures are usually left inplace. A 2001 study found thatspirometry results are generally better withdentures in place (60), but a larger 2018study found that FVC was an average of0.080 L higher when dentures wereremoved (61).
The decision to withhold long- andshort-acting bronchodilators before testingis a clinical one determined by the referringhealthcare professional. If the study isperformed to diagnose an underlying lungcondition, then withholding bronchodilators
before testing is useful (see BRONCHODILATOR
RESPONSIVENESS TESTING). For studies todetermine a response to an existingtherapeutic regimen, bronchodilatormedications are generally not withheld.
Instructions on withholdingmedications should be given to the patient atthe time of making the appointment. Theoperator must record the type and dosage ofany inspired, oral, or injected medicationthat may alter lung function and when thedrugs were last administered. The operatorshould record observed signs or symptomssuch as cough, wheeze, dyspnea, or cyanosis.
FEV1 and FVC Maneuver
Test ProcedureFor spirometers that measure inspirationand expiration, there are four distinctphases of the FVC maneuver: 1) maximalinspiration, 2) a “blast” of expiration, 3)continued complete expiration for amaximum of 15 seconds, and 4) inspirationat maximal flow back to maximum lungvolume. Most of the variability in resultsobtained from spirometry relates toinadequate and variable inspiration toTLC, ending the expiration prematurely,and variable effort.
The operator must demonstratethe appropriate technique and follow theprocedure described in Table 6. Oncethe zero-flow level has been determined, thepatient should insert the mouthpiece andbe instructed to breathe normally or easily.The operator checks that the patient has theproper posture, the noseclip is in place, andthe lips are sealed around the mouthpiece.Patients unable to use a mouthpiece maybe able to use a face mask (62). In somecircumstances, such as patients withtracheostomy or nasal resection, noninvasiveadjustments such as a sealing face mask,tubing connectors, or occlusion valves canbe applied at the discretion of the operatorand must be recorded in the operator notes.
Maximal inspiration. Patients shouldbe informed that maximal inflation isunnatural; they may not have achieved itbefore, and it may seem somewhatuncomfortable. Reductions in PEF andFEV1 have been shown when inspirationis slow and/or there is a 4- to 6-secondpause at TLC before beginning expiration(63, 64). It is therefore important that thepreceding inspiration be rapid and anypause at full inspiration be minimal (<2 s).
Table 3. Equipment Quality Assurance (for Both Volume- and Flow-based Sensors)
Spirometerd Daily calibration verification at low, medium, and high flow: If the calibration verificationfails, check for and remediate problems (Table 4) and repeat calibration verification
d If an in-line filter is used in spirometry testing, then it must also be used duringrecalibrations and verifications
d Recalibrate the spirometer both after failed calibration verification and at intervalsspecified by the manufacturer
d If the change in calibration factor is >6% or varies by more than 62 SD from the mean,inspect and, if necessary, clean the spirometer according to the manufacturer’sinstructions; check for errors (Table 4) and recalibrate the spirometer
d Perform routine checks and maintenance at intervals specified by the manufacturer
3-L calibration syringed Daily inspection for displacement of the piston stopd Daily check for smooth operation of the syringe with no sticking or catchingd Accuracy of 60.015 L verified by manufacturer on delivery and at intervalsrecommended by the manufacturer
d Monthly syringe leak test
Documentationd A log of all quality control findings, repairs and adjustments, and hardware and softwareupdates
d Verification of reference value calculations after software updates
Table 4. Potential Reasons for Calibration Verification Failure
d A slight change in spirometer function that requires a subsequent recalibration procedureto adjust the calibration factor
d A leak in the connection of the spirometer to the calibration syringed Air flow through the spirometer during the zero-flow setting procedured Failure to fully fill and empty the calibration syringe in one smooth actiond Calibration syringe malfunction (e.g., piston leak or displacement of the piston stop orsyringe damaged by dropping)
d Spirometer blockage either by debris in the spirometer sensor or by the operator’s handwhile holding the spirometer in place
d Improper assembly of the sensor, mouthpiece, filter, and/or breathing tubed Differences between room temperature and calibration syringe temperatured Data entry errors in the ambient temperature and/or pressure
AMERICAN THORACIC SOCIETY DOCUMENTS
e76 American Journal of Respiratory and Critical Care Medicine Volume 200 Number 8 | October 15 2019

The operator should be in a position toview the patient and the display of thetesting device, but the major sign that thesubject has achieved full inflation will comefrom the patient. The patient’s head andface should be observed while thecommand to “inspire as deeply as possible”(not just “take in a deep breath”) is given.During the inspiration, the operatorshould coach the patient using phrases suchas “more, more, more.” Indicators ofmaximal inspiration include eyebrows raisingor eyes widening, and sometimes the headbegins to quiver. A patient who lookscomfortable is not likely to be at full inflation.
Maximal expiration. At full inflation,without hesitation, the patient should beprompted to “blast,” not just “blow,” the airfrom their lungs, and then he or she shouldbe encouraged to fully expire. Continuousand enthusiastic coaching of the patient isrequired throughout the maneuver, usingappropriate body language and phrasessuch as “keep going.” The operatorsimultaneously observes the patient and thecomputer display during the test to helpensure maximal effort. The spirometrysystem must signal the operator when aplateau has been reached or forcedexpiratory time (FET) reaches 15 seconds.Having an audio cue for end expirationpermits the operator to observe the patientmore closely. The patient survey indicatedthat many were concerned by being askedto keep blowing when they felt nothingmore was coming out. If the patient is ableto see a volume–time trace still moving asthey blow and/or a numeric or analogdisplay of flow in mL/s, this might helpmotivate them to keep blowing. Childrenmay benefit from incentive displays. Ifthe patient shows signs of syncope, themaneuver should be stopped. Reducing theeffort partway through the maneuver (after4 s) (65, 66) may give a higher expiratoryvolume in some patients and may preventglottic closure and avoid syncope, but then
it is no longer a true maximally forcedexpiration. Some patients with restrictivelung disease and young patients with highelastic recoil can empty their lungs quicklyand may not be able to hold an expiratoryplateau for 1 second. The operator needs torecognize the convex pattern of theflow–volume graph in such patients anddistinguish it from an early termination ofexpiration (Figure E2).
Maximal inspiration after forcedexpiration. Upon completing the forcedexpiration, the patient should remain on themouthpiece, and the operator should againcoach the patient to rapidly inspire to fullinflation. This will provide a measure offorced inspiratory VC (FIVC). It is amaximal effort to return to TLC to completethe flow–volume loop. Comparison of theFIVC with the FVC will provide feedbackto the operator on whether the patientbegan the forced expiration from fullinflation (67). It is important that theinspiration to full inflation before and afterthe forced expiration be coached with equalvigor so that a valid comparison can bemade.
With appropriate coaching, children asyoung as 2.5 years old with normal cognitiveand neuromotor function are able toperform acceptable spirometry (8, 59). Theoperators who are involved in thepulmonary function testing of youngchildren should be specifically trained andcompetent to work with this population. Achild-friendly environment is importantfor successful testing. Encouragement,detailed but simple instructions, lack ofintimidation, and visual feedback in theteaching are important in helping childrento perform the maneuver (8, 68). Even ifunsuccessful at the first session, childrenwill learn to be less intimidated, and theirperformance may improve in subsequentsessions. Testing children in “adult”laboratories requires extra time and effortto cater to the specific needs of the younger
patient (69). Other techniques such asraised volume rapid thoracic compressiontechnique that are used for infants (70) arenot included in this document.
For spirometers measuring expirationonly, the procedure is modified as follows.The patient first inspires rapidly to maximallung volume and then within 2 secondsinserts the mouthpiece, seals his or her lipsaround the mouthpiece, and initiatesmaximal expiration. Keeping the mouthopen until the mouthpiece is in place canhelp minimize air loss before sealing the lips.The mouthpiece is removed at EOFE.Regarding expiration-only maneuvers, astudy found that the use of noseclips did notaffect group mean performance (71).
Within-Maneuver EvaluationThe following criteria were developed asobjective measures to determine whether amaximal effort was achieved and acceptableFEV1 and/or FVC measurements wereobtained. However, in some cases,maneuvers that do not meet all of thecriteria may be the best that the patient isable to do on that occasion, and althoughthe FEV1 and/or FVC measurements arenot technically acceptable, they may beclinically useful (i.e., “usable”) (Table 7).
The start of forced expiration, for thepurpose of timing, is determined by theback-extrapolation method (Figure 1)(1, 38). At the point of PEF on thevolume–time graph, a tangent is drawnwith a slope equal to PEF, and itsintersection on the abscissa defines Time0, which becomes the start for all timedmeasurements. The back-extrapolatedvolume (BEV) is the volume of gas that hasalready been expired from maximal lungvolume to Time 0 and is included in theFEV1 and FVC measurements. To ensurethat the FEV1 comes from a maximal effort,the BEV must be ,5% of the FVC or 0.100L, whichever is greater (72, 73). The 0.100-Ltolerance is a reduction from the 0.150-Ltolerance in the 2005 standards (1). Thehesitation time, defined as the time fromthe point of maximal inspiration to Time 0,should be 2 seconds or less (Figure E13).FEV1 and FVC measurements from amaneuver with BEV exceeding the limit areneither acceptable nor usable. A large BEVwill usually result in an erroneously highFEV1 (74). Patients with upper airwayobstruction or neuromuscular disease areoften unable to initiate a rapid increase inflow, and the BEV limit may be exceeded.
Table 5. Activities That Should Be Avoided before Lung Function Testing
d Smoking and/or vaping and/or water pipe use within 1 h before testing (to avoid acutebronchoconstriction due to smoke inhalation)
d Consuming intoxicants within 8 h before testing (to avoid problems in coordination,comprehension, and physical ability)
d Performing vigorous exercise within 1 h before testing (to avoid potential exercise-inducedbronchoconstriction)
d Wearing clothing that substantially restricts full chest and abdominal expansion (to avoidexternal restrictions on lung function)
AMERICAN THORACIC SOCIETY DOCUMENTS
American Thoracic Society Documents e77

The operator must have the ability tooverride the BEV acceptability designationfor such patients.
The volume–time graph must include1 second before the start of forcedexpiration (Time 0) or begin before thepoint of maximum inspiration, whicheveroccurs first. The system should display theBEV value. Inspection of the flow–volumegraph may be added as a measure of thesatisfactory start of a test. PEF should beachieved with a sharp rise and occur closeto Time 0 as measured by the rise timefrom 10% to 90% of peak flow (75), whichshould be<150 ms but may be greater thanthis in a maneuver in a patient with upperairway obstruction.
End of forced expiration. Previousstandards used the term “end of test” and
the abbreviation “EOT” to denote end offorced expiration (EOFE). These standardsstress the importance of a maximalinspiration after the forced expiration. Assuch, the end of forced expiration is not theend of the maneuver, and hence the termEOFE is used.
Recognizing a satisfactory EOFE isimportant to ensure that a true FVC hasbeen achieved. Achieving one of thefollowing three recommended indicators ofEOFE is required (Figure 2):
1. There is less than a 0.025-L changein volume for at least 1 second (a“plateau”). This is the most reliableindicator of complete expiration. Thesystem must provide both an indicatoron the real-time display and an audioalert—a single beep—when this criterion
has been reached. Note that a closure ofthe glottis may prematurely terminate amaneuver, hence rendering it unacceptablefor FVC, even when the apparent durationof expiration is much longer.
OR2. The patient has achieved an FET of 15
seconds. The system must provide bothan indicator on the real-time display andan audio alert—a double beep—whenthis criterion has been reached. Forpatients with airway obstruction or olderpatients, longer FETs are frequentlyachieved; however, FETs .15 secondswill rarely change clinical decisions(1, 4). The 1994 ATS spirometrystandards used “forced exhalation is ofreasonable duration” as an indicatorof EOFE and suggested that 12–15seconds was sufficient (4). A study ofadults (mean age, 67 yr) found thatmore than 95% of obstructed patientshad an FET of ,15 seconds and that.95% of normal subjects had an FET of,11 seconds (76). Multiple prolongedexpirations are seldom justified andmay cause light-headedness, syncope,undue fatigue, and unnecessarydiscomfort.
OR3. The patient cannot expire long enough
to achieve a plateau (e.g., children withhigh elastic recoil or patients withrestrictive lung disease). In this case, themeasure of whether EOFE has beenreached is for the patient to repeatedlyachieve the same FVC. For within-maneuver acceptability, the FVC mustbe greater than, or within the repeatabilitytolerance (see below) of, the largest FVCobserved before this maneuver in thecurrent testing set. If the first maneuverof either the prebronchodilator testingset or the post-bronchodilator testing setdoes not have a plateau and FET ,15seconds, it provisionally meets thisEOFE criterion for acceptability, subjectto comparison with the FVC fromsubsequent maneuvers. It becomesacceptable if it is within the repeatabilitytolerance of, or is greater than, asubsequent FVC. Hence, for theprebronchodilator and post-bronchodilator testing sets analyzedseparately, all FVC values frommaneuvers without a plateau andFET ,15 seconds that are within therepeatability tolerance of the maximumFVC in that set are judged to have met
Table 6. Procedures for FVC Maneuvers
Wash hands* (or use an approved hand sanitizer)
Prepare the patientDispense hand sanitizer for the patientConfirm patient identification, age, birth sex, ethnicity, etc.Measure weight and height without shoesAsk about activities listed in Table 5, medication use, and any relative contraindicationsflagged on the requisition; note respiratory symptoms
Instruct and demonstrate the testPosition of the mouthpiece and noseclipCorrect posture with head slightly elevatedInspire rapidly until completely fullExpire with maximal effort until completely emptyInspire with maximal effort until completely fullConfirm that patient understands the instructions and is willing to comply
Perform maneuverHave patient assume the correct postureAttach noseclip, place mouthpiece in mouth, and close lips around the mouthpieceBreathe normallyInspire completely and rapidly with a pause of <2 s at TLCExpire with maximal effort until no more air can be expelled while maintaining anupright posture
Inspire with maximal effort until completely fullRepeat instructions as necessary, coaching vigorouslyRepeat for a minimum of three maneuvers, usually no more than eight for adultsCheck FEV1 and FVC repeatability and perform more maneuvers as necessary
Perform maneuver (expiration-only devices)Have patient assume the correct postureAttach noseclipInspire completely and rapidly with a pause of <2 s at TLCPlace mouthpiece in mouth and close lips around the mouthpieceExpire with maximal effort until no more air can be expelled while maintaining anupright posture
Repeat instructions as necessary, coaching vigorouslyRepeat for a minimum of three maneuvers, usually no more than eight for adultsCheck FEV1 and FVC repeatability and perform more maneuvers as necessary
*Additional steps may be required by local infection control policies. Using disposable gloves does noteliminate the need for hand washing or sanitizing, but if gloves are used, a new pair is required foreach patient.
AMERICAN THORACIC SOCIETY DOCUMENTS
e78 American Journal of Respiratory and Critical Care Medicine Volume 200 Number 8 | October 15 2019

the EOFE acceptability criterion.Although patients should be stronglyencouraged to achieve their maximaleffort, the operator should be alert toany indication that the patient isexperiencing discomfort and shouldterminate the maneuver if a patient issignificantly uncomfortable or isapproaching syncope.
Maneuvers that do not meet any of theEOFE acceptability criteria will not provideacceptable FVC measures. However, anacceptable FEV1 measurement may beobtained from a maneuver with earlytermination after 1 second. For childrenaged 6 years or younger, an acceptableFEV0.75 (the forced expiratory volume inthe first 0.75 s) may be obtained from amaneuver with early termination after0.75 seconds.
Note that there is no requirement for aminimum FET. Studies have shown thatpatients with airflow obstruction and elderlypatients may have difficulty meeting the
2005 ATS/ERS requirement of achieving aplateau (77–79), and the criterion results inthe exclusion of too many patients whilehaving minimal impact on predicted values(80). A large occupational health study inan older population (mean age, 63 yr)found that 53% of spirometry maneuversfailed to reach a plateau despiteencouragement by trained operators and longFETs (72). However, in another study, 90% ofpatients with severe lung functionimpairment were able to meet the criteria(81). Other large adult population studiesfound that more than 95% of subjects whoexpired for longer than 6 seconds achieved aplateau (82, 83). A large clinical trial usingwell-trained, supervised operators found that94% of patients with COPD were able tomeet the 1994 ATS spirometry standardsplateau criteria (4, 84).
The 2005 ATS/ERS requirement of aminimum FET (1) resulted in some validmaneuvers being classified as inadequate(77, 78, 85). In a study of 1,631 healthychildren aged 10–18 years, only 18% met
the 2005 minimum FET in maneuvers thatwere visually judged to be acceptable (73).However, because the requirement for aminimum FET has been eliminated,increased vigilance by the operator and theinterpreter is required in the assessment ofwhether expiration was complete or therewas early termination.
If the volume of the maximalinspiration (i.e., FIVC) after EOFE is greaterthan FVC, then the patient did not start themaneuver from TLC. FEV1 and FVCmeasurements from a maneuver withFIVC2 FVC. 0.100 L or 5% of FVC,whichever is greater, are not acceptable.
A cough during the first second of themaneuver can affect the measured FEV1
value, and the FEV1 from such a maneuveris neither acceptable nor usable. However,the FVC may be acceptable.
Glottic closure or early termination,such as inspiration or coming off themouthpiece, renders FVC unacceptable and,if it occurs in the first 1 second, rendersFEV1 unacceptable and unusable. A similar
Table 7. Summary of Acceptability, Usability, and Repeatability Criteria for FEV1 and FVC
Required for Acceptability Required for Usability
Acceptability and Usability Criterion FEV1 FVC FEV1 FVC
Must have BEV <5% of FVC or 0.100 L, whichever is greater Yes Yes Yes YesMust have no evidence of a faulty zero-flow setting Yes Yes Yes YesMust have no cough in the first second of expiration* Yes No Yes NoMust have no glottic closure in the first second of expiration* Yes Yes Yes YesMust have no glottic closure after 1 s of expiration No Yes No NoMust achieve one of these three EOFE indicators: No Yes No No1. Expiratory plateau (<0.025 L in the last 1 s of expiration)2. Expiratory time >15 s3. FVC is within the repeatability tolerance of or is greater than
the largest prior observed FVC†
Must have no evidence of obstructed mouthpiece or spirometer Yes Yes No NoMust have no evidence of a leak Yes Yes No NoIf the maximal inspiration after EOFE is greater than FVC, then
FIVC2FVC must be <0.100 L or 5% of FVC, whichever isgreater‡
Yes Yes No No
Repeatability criteria (applied to acceptable FVC and FEV1 values)Age .6 yr: The difference between the two largest FVC values must be <0.150 L, and the difference between the two largest FEV1 values
must be <0.150 LAge <6 yr: The difference between the two largest FVC values must be <0.100 L or 10% of the highest value, whichever is greater, and
the difference between the two largest FEV1 values must be <0.100 L or 10% of the highest value, whichever is greater
Definition of abbreviations: BEV=back-extrapolated volume; EOFE=end of forced expiration; FEV0.75 = forced expiratory volume in the first 0.75 seconds;FIVC= forced inspiratory VC.The grading system (Table 10) will inform the interpreter if values are reported from usable maneuvers not meeting all acceptability criteria.*For children aged 6 years or younger, must have at least 0.75 seconds of expiration without glottic closure or cough for acceptable or usablemeasurement of FEV0.75.†Occurs when the patient cannot expire long enough to achieve a plateau (e.g., children with high elastic recoil or patients with restrictive lung disease) or whenthe patient inspires or comes off the mouthpiece before a plateau. For within-maneuver acceptability, the FVC must be greater than or within the repeatabilitytolerance of the largest FVC observed before this maneuver within the current prebronchodilator or the current post-bronchodilator testing set.‡Although the performance of a maximal forced inspiration is strongly recommended, its absence does not preclude a maneuver from being judgedacceptable, unless extrathoracic obstruction is specifically being investigated.
AMERICAN THORACIC SOCIETY DOCUMENTS
American Thoracic Society Documents e79

termination in the first 0.75 secondsrenders FEV0.75 unacceptable and unusable.
There must be no leak at the mouth (4).Patients with difficulty making a sealaround the mouthpiece may require aflange-type mouthpiece or assistance fromthe operator to guarantee an adequate seal.
Obstruction of the mouthpiece (e.g., bythe tongue being placed in front of themouthpiece, by teeth in front of themouthpiece, or by distortion from biting)may affect the performance of either thedevice or the patient. Errors also occurbecause of obstruction of a handheldspirometer by improper hand placement.
Maneuvers conducted with anerroneous zero-flow level will either under-or overestimate FEV1 and FVC. Figure E13shows the effects of a faulty zero-flow setprocedure that renders both FEV1 and FVCneither acceptable nor usable.
Operator feedback. The spirometrysystem software must provide explicitfeedback to the operator indicating FEV1
and FVC acceptability at the completion ofeach maneuver. Sample warning messagesand suggested corrections are provided inSection E8. The operator must have theability to override the acceptabilitydesignation, because the operator may note
a leak, a cough, inadequate inspiration orexpiration, or a faulty zero-flow level thatwas not detected by the software.
Records of all maneuvers with FEV1
and/or FVC that are acceptable or usablemust be retained because, for somepatients, their best performance may yieldonly usable data that does not meetacceptability criteria. Examples ofacceptable and unacceptable volume–timecurves and corresponding flow–volumecurves are provided in Figures E1–E12.
Between-Maneuver EvaluationThe goal of each prebronchodilator testingset and post-bronchodilator testing set isto achieve a minimum of three acceptableFEV1 and three acceptable FVCmeasurements. Note that acceptable FEV1
and acceptable FVC measurements are notnecessarily from the same maneuver. Theoperator must ensure that sufficient timeis allowed between maneuvers for thepatient to sufficiently recover and agree toperform another maximal maneuver.FVC repeatability is achieved when thedifference between the largest and the nextlargest FVC is <0.150 L for patients olderthan 6 years of age (86) and <0.100 L or10% of largest FVC, whichever is greater,for those aged 6 years or younger (8, 87).For FEV1 repeatability, the differencebetween the largest and the next largestFEV1 is <0.150 L for those older than6 years of age and <0.100 L or 10% of thelargest FEV1, whichever is greater, forthose aged 6 years or younger. If thesecriteria are not met in three maneuvers,additional trials must be attempted, up toeight maneuvers in adults, although moremay be done in children (Figure 3).
Achieving repeatable results is the bestindicator that the patient performed themaximal FEV1 and FVC that she or hewas capable of doing. The degree ofrepeatability, which is quantified in thegrading system (see GRADING THE QUALITY OF
THE TEST SESSION), guides the confidencelevel in the interpretation of the results. Therepeatability criteria are used to determinewhen more maneuvers are needed. In manycases, patients can and will achieve closerrepeatability than these criteria. Studieshave found that most adults are able toachieve FVC and FEV1 repeatability towithin 0.150 L (82, 88) and that childrenare able to achieve repeatability within0.150 or 0.100 L (89).
Achieved an expiratory plateau( 25 mL in the last 1 s of expiration)?
no
yes*
yes
yes
no
no
Achieved expiratory time 15 s?
FVC is within the repeatabilitytolerance of, or is greater than, the
largest prior observed FVC?
FVC meets EOFEacceptability criteria
FVC may meet EOFEuseability criteria
Figure 2. Flowchart outlining the end of forced expiration (EOFE) acceptability criteria for FVC. *Ifthere are no prior observed FVC values in the current pre- or post-bronchodilator testing set, then theFVC provisionally meets EOFE acceptability criteria.
volu
me
(L)
time (s)
5
4
3
2
1
0321–1 0
BEV BEV
volu
me
(L)
time (s)
5
4
3
2
1
0321–1 0
Figure 1. Back-extrapolated volume (BEV). Time 0 is found by drawing a line with a slope equal topeak flow through the point of peak flow (red line) on the volume–time curve and setting Time 0 to thepoint where this line intersects the time axis. The BEV is equal to the volume of gas exhaled beforeTime 0 (inset), which, in these two examples from the same patient, is 0.136 L for the left panel(acceptable) and 0.248 L for the right panel (unacceptable). For this patient, the BEV limit is 5%FVC=0.225 L.
AMERICAN THORACIC SOCIETY DOCUMENTS
e80 American Journal of Respiratory and Critical Care Medicine Volume 200 Number 8 | October 15 2019

Maximum Number of ManeuversAlthough there may be some circumstancesin which more than eight consecutive FVCmaneuvers may be needed, eight is generallya practical upper limit for most adults(90, 91). After several forced expiratorymaneuvers, fatigue can begin to take its tollon patients, and additional maneuverswould be of little added value. In rarecircumstances, patients may show aprogressive reduction in FEV1 or FVC witheach subsequent maneuver. If the FEV1
from an acceptable test drops below 80% ofthe start value, the test procedure should beterminated in the interest of patient safety.When testing children, more than eightattempts may be required because eachattempt may not be a full maneuver.Children may benefit from practicing thedifferent phases of the maneuver beforeattempting a full maneuver. Operatorsshould be aware of the child’s enthusiasmand effort to avoid exhausting ordiscouraging the child from futuretesting.
BronchodilatorResponsiveness Testing
Previously, the term “reversibility testing”has been used, but the term“bronchodilator responsiveness testing” isused in these standards to avoid theunwarranted inference that “reversibility”
implies the complete elimination of airwayobstruction (92). Bronchodilatorresponsiveness testing is a determination ofthe degree of improvement of airflow inresponse to bronchodilator administrationas measured by changes in FEV1 and FVC.It is commonly undertaken as part ofspirometry testing. The choice ofbronchodilator, dose, and mode of deliveryis a clinical decision depending on what thereferring clinician wishes to learn from thetest.
If the aim of the test is to determinewhether the patient’s spirometric lungfunction can be improved with therapy inaddition to their regular treatment, then thepatient may continue with his or herregular medication before the test. If thetest is used for diagnosis or to determinewhether there is any change in spirometriclung function in response to bronchodilators,then the clinician ordering spirometrywill instruct the patient to withholdbronchodilators before baseline testing.Table 8 lists suggested withholding timesfor various bronchodilators. The withholdingtimes are based on studies of the lastingbronchodilator effects of the various agents(93, 94). Inhaled corticosteroids andleukotriene modifiers need not be withheld.It is important to notify and remind thepatient about withholding medicationsbefore the test and confirm withholding atthe time of the test (95).
Because normal baseline spirometrydoes not rule out a bronchodilator response,all initial spirometry done for diagnosticreasons should be performed before andafter bronchodilator administration.Thereafter the clinician may choose toperform spirometry without bronchodilatorresponsiveness testing, but it is important toconsider baseline variability in lung functionwhenmaking this decision. Monitoring lungfunction by serial spirometry, especially inpatients with obstructive lung disease, maybe more useful by following post-bronchodilator values (96).
Test ProcedureThe patient first performs prebronchodilatorspirometry to achieve three acceptableFEV1 and FVC measurements asdescribed previously. Next, thebronchodilator is administered in thedose and by the method specified in theprotocol for the spirometry facility(Section E9). Three or more additionalpost-bronchodilator acceptable FEV1
and FVC measurements are then obtainedafter the wait time specified in the facilityprotocol. Every facility conductingbronchodilator responsiveness testing musthave a written protocol for the test.
It is not uncommon for a post-bronchodilator maneuver to be erroneouslycoded as prebronchodilator, or the converse.The spirometry system must permit theoperator to change the designation of themaneuver from pre- to post-bronchodilator,and vice versa, so that a good maneuveris not lost and the patient is not requiredto perform an additional unwarrantedmaneuver.When the first post-bronchodilatormaneuver is initiated by the operator, thesystem must display the time elapsed sincethe last prebronchodilator maneuver. Ifthe elapsed time is less than the wait timefor the bronchodilator effect, then thesystem must provide a warning messageto the operator.
Reported Values
The following measurements are reportedseparately for the sets of prebronchodilatorand post-bronchodilator maneuvers(Table 9). The largest FVC and the largestFEV1 observed from all of the acceptablevalues are reported (or largest usable valuesif none are acceptable). Their ratio is usedfor FEV1/FVC, even though the largestFVC and the largest FEV1 may notnecessarily come from the same maneuver.If a bronchodilator is administered, boththe percentage change and the absolutechange in FEV1 and FVC compared withprebronchodilator values are reported.Recent studies showed that reporting thechange in FEV1 as a percentage of thepredicted FEV1 or as z-scores avoids sexand height bias in assessing bronchodilatorresponsiveness (97, 98).
FIVC is the largest inspiratoryvolume immediately after forced expirationfrom all of the maneuvers. PEF is the highestflow achieved from a maximum forcedexpiratory maneuver started withouthesitation from a position of maximal lunginflation. The largest value from maneuversmeeting the acceptability criteria for FEV1
in Table 7 is reported.FET is the time in seconds measured
from Time 0 to the end of the expiratoryplateau or the beginning of inspiration aftermaximal forced expiration, or the time thatthe patient comes off the mouthpiece,
Perform FVC maneuver
no
yes
yes
yes
no
no
Within-maneuver criteria met?
Achieved three acceptable FEV1 and
three acceptable FVC measurements?
Between-maneuver criteria met?
Determine largest FVC and largest FEV1
Determine other indices from maneuver
with largest sum of FVC + FEV1
Store data
Figure 3. Flowchart outlining application ofacceptability and repeatability criteria.
AMERICAN THORACIC SOCIETY DOCUMENTS
American Thoracic Society Documents e81

whichever is shortest. The FET does notinclude any period of zero flow at the end ofexpiration. The FET from the maneuverwith the largest FVC is reported. For patientswith airflow obstruction, the FVC maydepend on FET. The interpreter must beaware that an apparent change in FVC afterbronchodilator administration may be due toa change in FET.
FEVt is the maximal volume expiredby Time t seconds from Time 0 of a forcedexpiratory maneuver. Children aged 6 yearsor younger have relatively large airwayscompared with their lung volume and maycomplete expiration in ,1 second.Therefore, FEV0.75 and FEV0.5 have beenused. In children aged 6 years or younger,FEV0.75 was found to provide informationsimilar to that of FEV1 (99, 100). The
ATS/ERS statement on pulmonary functiontesting in preschool children states thatFEV0.75 and FEV0.5 should be reported(8). However, because GLI referencevalues for FEV0.75 (but not for FEV0.5) areavailable for ages 3–7 years (59), FEV0.75
should be reported for children aged 6 yearsor younger, and if FET is .1 second, thenFEV1 should also be reported.
The mean forced expiratory flow,midexpiratory phase (FEF25-75), may bereported from the maneuver with thelargest sum of FEV1 and FVC. It should benoted that FEF25-75 is highly dependent onthe validity of the FVC measurement andthe degree of expiratory effort. A volumeadjustment may be required whencomparing pre- and post-bronchodilatorFEF25-75 values (101).
Other Derived IndicesFEV1/FEV6 has been shown to be useful inthe diagnosis of airflow obstruction inadults (102, 103). Recording FEV6 has theadvantages of being more reproducible thanFVC, being less physically demanding forpatients, reducing the risk of syncope,and providing a more explicit EOFE(104–107). Appropriate reference values forFEV6 must be used (108–111). The ratioof FEF at 50% VC to forced inspiratory flowat 50% VC (FEF50/FIF50) is sometimesused as an indicator of upper airwayobstruction (112, 113). A table of all of themeasurements required to be availableand stored is provided in the onlinesupplement (Section E10).
The ATS standardized report form(114) should be the default report form forspirometry systems. The default set ofreference values for all ages should be theGLI reference equations (59), althoughother options may be provided. In additionto summary reports, the interpreter shouldhave access to a report of all maneuverswithin a testing session. The flow and/orvolume data from each test session must beavailable for export with adequateinformation for the facility manager toextract results and plot volume–time andflow–volume graphs of each maneuver(Section E10). The system should also havethe capability to export data to electronicmedical records, both as .pdf file copies ofthe printed report and as discrete data,using the Clinical Document ArchitectureRelease 2 standard of HL7 International(115) or Fast Healthcare InteroperabilityResources. Logical Observation IdentifiersNames and Codes should be used toidentify test data so that data captured inthe electronic health record can be accessedand understood universally. A workshop atthe ATS 2019 International Conferencebegan the process of developing aninteroperability roadmap to integratepulmonary function data in electronic healthrecords.
The date and time for each maneuvermust be recorded. Diurnal variations of 3%in FEV1 and 6% in PEF have been reported(116), with lower values noted in patientswith COPD in the afternoon comparedwith the morning (117). In addition, thetime data are useful for verifying pre- andpost-bronchodilator maneuvers.
Operator comments are a key part ofthe report. The system must permit theoperator to enter comments from a
Table 8. Bronchodilator Withholding Times
Bronchodilator Medication Withholding Time
SABA (e.g., albuterol or salbutamol) 4–6 hSAMA (e.g., ipratropium bromide) 12 hLABA (e.g., formoterol or salmeterol) 24 hUltra-LABA (e.g., indacaterol, vilanterol, orolodaterol)
36 h
LAMA (e.g., tiotropium, umeclidinium, aclidinium, orglycopyrronium)
36–48 h
Definition of abbreviations: LABA= long-acting b2-agonist; LAMA= long-acting muscarinicantagonist; SABA= short-acting b2-agonist; SAMA=short-acting muscarinic antagonist.Note: Withholding times for post-bronchodilator testing are shorter than those for methacholinechallenge testing (147) because the bronchoprotection provided by these agents lasts longer thantheir bronchodilation effects. In the case of dual bronchodilators, the withholding time for thelonger-acting bronchodilator is used.
Table 9. Measured Variables (Reported Separately for Pre- and Post-bronchodilatorTests)
Variable Units
FVC LitersFEV1 LitersFEV1/FVC Decimal fraction to two decimal placesPEF Liters per secondFET SecondsFIVC LitersFor children <6 yrFEV0.75 LitersFEV0.75/FVC Decimal fraction to two decimal places
Definition of abbreviations: FET= forced expiratory time; FEV0.75 = forced expiratory volume in the first0.75 seconds; FIVC= forced inspiratory VC; PEF=peak expiratory flow.Volumes in liters and PEF in L/s are reported to two decimal places at BTPS (body temperature,ambient barometric pressure, and saturated with water vapor). Spirometry systems must be capableof measuring these variables and reporting them as recommended in the American Thoracic Societystandardized format (114). Although FEV1, FVC, and FEV1/FVC are obligatory, the facility managermust have the ability to configure the report to include the other optional variables, such as FEV6,FEV1/FEV6, FEV0.5, and mean forced expiratory flow, midexpiratory phase (forced expiratory flowbetween 25% and 75% of the FVC).
AMERICAN THORACIC SOCIETY DOCUMENTS
e82 American Journal of Respiratory and Critical Care Medicine Volume 200 Number 8 | October 15 2019

dropdown menu as well as free text. Thefacility manager should have the ability toedit the list of menu options. A list ofstandard operator comments is given inSection E11.
Grading the Quality of theTest Session
Technical standards are designed to helpattain the best result possible for eachpatient. Spirometry results are verydependent on patient cooperation.Maneuvers done at maximal lung volumewith maximal effort are more repeatablethan maneuvers that are done at submaximallung volumes or with submaximal effort.Although there may be other indicators ofsubmaximal spirometry, in general, theacceptability and repeatability criteriaprovided in this document are validated andobjective (1, 86, 114, 118).
The grading system that isrecommended by the ATS for spirometryreporting (114), which is a modified versionof the system developed by Hankinson andcolleagues (80) and expanded to includeyoung children, should be used (Table 10).Grade “U” was added to denote “usable”values. FEV1 and FVC are graded separately.The grading applies to the set ofprebronchodilator maneuvers as a wholerather than individual maneuvers and isdetermined separately for the set of post-bronchodilator maneuvers.
This grading system informs theinterpreter about the level of confidence thatthe spirometry results represent the best thatthe patient was able to do at the time of the
test and the probability that an equivalentvalue would be achieved if the test were to berepeated. Some patients may not be able tomeet the criteria for acceptability andrepeatability that are necessary for grade A,but nevertheless, their results may beclinically useful. For example, thespirometry maneuver may trigger the coughreflex, and after the first one or twoattempts, the patient may not be able to doanother acceptable maneuver. In cases inwhich grades less than A are the best thatcan be achieved within the test session, theclinical judgment of the interpreter becomesa more important factor in theinterpretation of the results. Although somemaneuvers may be acceptable or usable atgrade levels lower than A, the overridinggoal of the operator must be to alwaysachieve the best possible testing quality foreach patient.
Patients who see the grade assigned totheir values might erroneously assume thatthe grade applies to the health of their lungs.The operator should inform the patient thatthe grade refers to the consistency of theirblows.
VC and Inspiratory CapacityManeuver
The VC is the volume change between TLCand residual volume (RV). The slow VC canbe derived in two ways. The expiratory VC(EVC) is the volume of gas slowly expiredfrom TLC to RV. The inspiratory VC (IVC)is the volume of gas slowly inspired from RVto TLC (Figure 4). These maneuvers areunforced, except at the point of reaching
RV or TLC, respectively, when extra effortis required (119).
Inspiratory capacity (IC) is the volumechange recorded at the mouth when taking aslow full inspiration with no hesitation,inspiring from a position of passive end-tidal expiration (i.e., FRC) to a position ofmaximum inspiration (i.e., TLC). IC is anindirect estimate of the degree of lunghyperinflation at rest and is useful to assesschanges in FRC with pharmacologicalinterventions and physical exercise(120–123).
EquipmentFor measurements of VC and IC, thespirometer must comply with therequirements for FVC maneuvers above.VC can be measured using conventionalspirometers or equipment used to measurestatic lung volumes and their subdivisions(124). Both inspiratory and expiratorymaneuvers must be included in the displayof the VC maneuver. Regardless of whetherthe inspiratory or expiratory maneuver isused for deriving measurements, a displayof the entire recorded VC maneuver mustbe provided to determine whether thepatient obtained a plateau in the expiratoryeffort.
Test ProcedureFor a slow VC, a maximum of eightmaneuvers is a practical upper limit. It ispreferable that VC maneuvers be performedbefore FVC maneuvers because of thepotential for muscular fatigue and volumehistory effects, whereby, after maximalinspiratory efforts, some patients withsevere airway obstruction return to a falsely
Table 10. Grading System for FEV1 and FVC (Graded Separately)
Grade Number of Measurements Repeatability: Age >6 yr Repeatability: Age <6 yr*
A >3 acceptable Within 0.150 L Within 0.100 L*B 2 acceptable Within 0.150 L Within 0.100 L*C >2 acceptable Within 0.200 L Within 0.150 L*D >2 acceptable Within 0.250 L Within 0.200 L*E >2 acceptable .0.250 L .0.200 L*
OR 1 acceptable N/A N/AU 0 acceptable AND >1 usable N/A N/AF 0 acceptable and 0 usable N/A N/A
Definition of abbreviation: N/A=not applicable.The repeatability grade is determined for the set of prebronchodilator maneuvers and the set of post-bronchodilator maneuvers separately. Therepeatability criteria are applied to the differences between the two largest FVC values and the two largest FEV1 values. Grade U indicates that only usablebut not acceptable measurements were obtained. Although some maneuvers may be acceptable or usable at grading levels lower than A, the overridinggoal of the operator must be to always achieve the best possible testing quality for each patient. Adapted from Reference 114.*Or 10% of the highest value, whichever is greater; applies for age 6 years or younger only.
AMERICAN THORACIC SOCIETY DOCUMENTS
American Thoracic Society Documents e83

high level of FRC or RV as a result of gastrapping or stress relaxation (4). The VCmaneuver may measure either IVC or EVC(Figure 4). Important differences between IVCand EVC maneuvers may be observed inpatients with airway obstruction (125–127).
Patients should be relaxed, seated erectwith a noseclip in place, and asked tobreathe normally until the end-expiratorylung volume is stable. Stability is defined ashaving at least three tidal breaths with end-expiratory lung volume within 15% of theVT. If this is not achieved within 10 breaths,the VC part of the maneuver may begin,but the IC will not be reliable. The patient isthen urged either 1) to take a deep breath toTLC with no hesitation and expire to RV or2) to breathe all the way out to RV and thentake a deep breath in to TLC, and thenbreathe normally (Figure 4).
The maneuver is not forced but isperformed in a relaxed manner, except nearend inspiration and end expiration. Theoperator should encourage the patient toreach maximal inspiratory and expiratoryvolumes with a relatively constant flow. Inhealthy patients, adequate maximalinspiratory and expiratory levels areachieved within 5–6 seconds. Patients withairway obstruction will take longer, butexpiration should be terminated after 15seconds. The expiration should not beexcessively slow, because this can lead tounderestimation of VC. Operators shouldobserve the patient carefully to ensure thathis or her lips are sealed around themouthpiece, nothing obstructs themouthpiece, the noseclip is in place with noleaks, and TLC and RV are reached. Thesystem must provide both a visual and anaudible signal (single beep) when a stableend-expiratory tidal lung volume is detected
or there have been 10 tidal breaths and, forexpiration to RV in either IVC or EVCmaneuvers, a double beep when a plateau isreached (,0.025 L in the last second) or theexpiration time reaches 15 seconds.
For within-maneuver evaluation, theremust be no leak at the mouth or nose andno obstruction of the mouthpiece. The ICmay be underestimated if the inspiratorymaneuver is too slow because of poor effortor hesitation or if there is premature closureof the glottis.
For between-maneuver evaluation, aswith forced maneuvers, a minimum of threeacceptable VCmaneuvers must be obtained.If the difference in VC between the largestand next largest maneuver is .0.150 L or10% VC, whichever is smaller, for patientsolder than 6 years of age or .0.100 L or10% VC, whichever is smaller, for thoseaged 6 years or younger, then additionaltrials should be undertaken. Meetingrepeatability criteria may requireperforming up to eight maneuvers, withsufficient rest time between the maneuversso that the operator and patient agree thatthe next maneuver may begin. Largevariability in this test is often due toincomplete inspiration. For VC, the largestvalue from at least three acceptable maneuversshould be reported. For maneuvers inwhich stable end-expiratory tidal lungvolume was not attained, IC is not reported.For IC, the average value from theacceptable maneuvers should be reported.
Further Studies
An analysis of BEV measures from bothchildren and adults is needed to developevidence-based criteria for acceptable BEV
limits. An analysis of FETs in patients withairflow obstruction is needed to determinebetter criteria for maneuver acceptabilityand the impact of shorter FETs in thesepatients on their diagnosis. Research isneeded to validate the EOFE plateaucriterion (<0.025 L in 1 s), which is basedon expert opinion dating back to 1979 (2).Other unknowns include the optimalresting time between maneuvers and theeffect of mouthpiece shape (round, oval,and flared). Updated standards are requiredfor unattended home monitoringspirometry (128–130) and peak flowmonitoring. A grading system for the slowVC needs to be developed and evaluated.Studies have shown that ongoingsupervised training using a telemedicinesystem is effective and valid for assessingand monitoring the quality of thespirometry tests performed in primaryhealth centers in a public health system(131, 132).
Other Potential AnalysesAlthough FEV1 and FVC are the primaryvariables measured in spirometry, there isfar more information contained in the flowand volume data. Continuing research oninnovative analyses that may improvediagnoses or lead to earlier diagnosis inat-risk persons is important, and newmethods of measuring volume and floware strongly encouraged.
Measures of curve shape using flow andvolume signal analyses have good agreementwith expert impression of expiratoryflow–volume curve concavity, which isuseful in assessing asthma and cysticfibrosis in children (133). The slope ratiomay be useful in mild COPD (134). Thecalculation of Time 0 may be improved bybreakpoint methods using a recursive,segmented linear regression technique(135).
More advanced analyses of the flow andvolume data have been proposed to assist inthe automation of spirometry qualityassessment (136–138) and to automaticallydetect errors in early termination, cough,extra breaths, and variable flow (139). Asystem developed using machine learningtechniques demonstrated a crediblepotential to differentiate acceptablemaneuvers from ones with poor quality,with performance rates near the level ofexperts (140).
A study found that an isolatedreduction of the FEV3/FVC ratio is an
EVCtidalbreathing
tidalbreathing
ERV ERV
FRC
RV
TLC
IVCIC
IC
Vol
ume
(1 L
grid
line
s)
Time (5 s grid lines)
Figure 4. Measurement of VC and IC. VC may be measured either as EVC (left panel) or IVC (rightpanel). In these examples, divisions on the volume axis are 1 L, and those on the time axis are 5seconds. ERV= expiratory reserve volume; EVC= expiratory VC; IC= inspiratory capacity;IVC= inspiratory VC; RV= residual volume.
AMERICAN THORACIC SOCIETY DOCUMENTS
e84 American Journal of Respiratory and Critical Care Medicine Volume 200 Number 8 | October 15 2019

indicator of mild lung injury (141), andreductions in FEV1/FEV6 (142) orFEV3/FEV6 (143) may have highersensitivity than FEV1/FVC for detectingearly airflow limitation. Lower limits ofnormal have been derived for FEV1/FEV6,
FEV3/FEV6, and FEV3/FVC (109).Estimating FVC using data from thefirst 2–3 seconds of expiration mightpotentially either assist in determiningwhether EOFE was attained or provide asurrogate for FVC when EOFE is not
attained (144, 145). Imaging technologyhas the potential to monitor spirometrywithout a direct connection to thepatient (146), permitting testing ofpatients unable or unwilling to use amouthpiece. n
This official technical statement was prepared by a joint ATS/ERS task force.
Members of the task force are as follows:
BRIAN L. GRAHAM, PH.D.1 (Chair)IRENE STEENBRUGGEN, R.P.F.T.2 (Co-Chair)IGOR Z. BARJAKTAREVIC, PH.D., M.D.3
BRENDAN G. COOPER, PH.D.4,5
GRAHAM L. HALL, PH.D.6,7
TEAL S. HALLSTRAND, M.D., M.P.H.8
DAVID A. KAMINSKY, M.D.9
KEVIN MCCARTHY, R.P.F.T.10
MEREDITH C. MCCORMACK, M.D., M.H.S.11
MARTIN R. MILLER, M.D.12
CRISTINE E. OROPEZ, M.D.13
MARGARET ROSENFELD, M.D., M.P.H.14
SANJA STANOJEVIC, PH.D.15
MAUREEN P. SWANNEY, PH.D.16
BRUCE R. THOMPSON, PH.D.17
1Respiratory Research Centre, Division ofRespirology, Critical Care and Sleep Medicine,University of Saskatchewan, Saskatoon,Saskatchewan, Canada; 2Department ofPulmonology, Isala Hospital, Zwolle, theNetherlands; 3Pulmonary and Critical CareMedicine, University of California, Los Angeles,Los Angeles, California; 4Lung Function & SleepDepartment, Queen Elizabeth Hospital,Birmingham, United Kingdom; 5UniversityHospitals Birmingham NHS Foundation Trust,Birmingham, United Kingdom; 6Children’s
Lung Health, Telethon Kids Institute, PerthChildren’s Hospital, Perth, Australia; 7School ofPhysiotherapy and Exercise Science, Faculty ofHealth Science, Curtin University, Bentley, Perth,Australia; 8Division of Pulmonary, Critical Careand Sleep Medicine, Department of Medicine,University of Washington, Seattle, Washington;9Pulmonary Disease and Critical Care Medicine,University of Vermont Larner College ofMedicine, Burlington, Vermont; 10ERT Inc.,Matthews, North Carolina; 11Pulmonary FunctionLaboratory, Pulmonary and Critical CareMedicine, Johns Hopkins University, Baltimore,Maryland; 12Institute of Applied Health Research,University of Birmingham, Birmingham, UnitedKingdom; 13Pulmonary Function and ExercisePhysiology Laboratory, Department of Medicine,University of Arizona, Tucson, Arizona; 14Divisionof Pulmonary and Sleep Medicine, Departmentof Pediatrics, University of Washington School ofMedicine, Seattle, Washington; 15TranslationalMedicine, The Hospital for SickChildren, Toronto, Ontario, Canada;16Department of Respiratory Medicine,Canterbury District Health Board, Christchurch,New Zealand; and 17Physiology Service,Department of Respiratory Medicine, The AlfredHospital and School of Health Sciences,Swinburne University of Technology,Melbourne, Australia
Author Disclosures: I.Z.B. served on anadvisory committee for GlaxoSmithKline; served
as a consultant for AstraZeneca, BoehringerIngelheim, CSL Behring, Fisher & PaykelHealthcare, GE Healthcare, Grifols, Mylan/Theravance, and Verona Pharma; and receivedresearch support from AMGEN, GEHealthcare, and Prolung. B.G.C. receivedresearch support from ndd MedicalTechnologies and MedChip. G.L.H. served onan advisory committee for and receivedresearch support from Vertex. D.A.K. servedas a speaker for MGC Diagnostics; served as aconsultant for Spiration; and served on a dataand safety monitoring board for Acorda. K.M.served as a speaker for Medical GraphicsCorporation and Genentech; and served on anadvisory committee for Genentech. M.C.M.received royalties from UpToDate; and servedon an advisory committee for GlaxoSmithKline.B.R.T. served as a consultant for BoehringerIngelheim, GlaxoSmithKline, and ndd MedicalTechnologies; served on an advisorycommittee for Bayer; received royalties fromUpToDate; and served on a data and safetymonitoring board for Faron and Ferring Labs.B.L.G., I.S., T.S.H., M.R.M., C.E.O., M.R.,S.S., and M.P.S. reported no relevantcommercial relationships.
Acknowledgment: The task force is grateful forthe support of the European Lung Foundation inthe design, implementation, and analysis of thespirometry patient survey.
References
1. Miller MR, Hankinson J, Brusasco V, Burgos F, Casaburi R, Coates A,et al.; ATS/ERS Task Force. Standardisation of spirometry. Eur RespirJ 2005;26:319–338.
2. American Thoracic Society. ATS statement: snowbird workshop onstandardization of spirometry. Am Rev Respir Dis 1979;119:831–838.
3. Statement of the American Thoracic Society. Standardization ofspirometry: 1987 update. Am Rev Respir Dis 1987;136:1285–1298.
4. American Thoracic Society. Standardization of spirometry, 1994 update.Am J Respir Crit Care Med 1995;152:1107–1136.
5. Quanjer PH. Standardized lung function testing: report working partystandardization of lung function tests. Bull Eur Physiopathol Respir1983;19(Suppl 5):1–95.
6. Quanjer PH, Tammeling GJ, Cotes JE, Pedersen OF, Peslin R, YernaultJC. Lung volumes and forced ventilatory flows. Eur Respir J 1993;6(Suppl 16):5–40.
7. Redlich CA, Tarlo SM, Hankinson JL, Townsend MC, Eschenbacher WL,Von Essen SG, et al.; American Thoracic Society Committee onSpirometry in the Occupational Setting. Official American ThoracicSociety technical standards: spirometry in the occupational setting.Am J Respir Crit Care Med 2014;189:983–993.
8. Beydon N, Davis SD, Lombardi E, Allen JL, Arets HG, Aurora P, et al.;American Thoracic Society/European Respiratory Society WorkingGroup on Infant and Young Children Pulmonary Function Testing. An
official American Thoracic Society/European Respiratory Societystatement: pulmonary function testing in preschool children. Am JRespir Crit Care Med 2007;175:1304–1345.
9. Graham BL. Pulmonary function standards: a work in progress. RespirCare 2012;57:1199–1200.
10. Miller MR, Crapo R, Hankinson J, Brusasco V, Burgos F, Casaburi R,et al.; ATS/ERS Task Force. General considerations for lung functiontesting. Eur Respir J 2005;26:153–161.
11. Hegewald MJ, Gallo HM, Wilson EL. Accuracy and quality of spirometryin primary care offices. Ann Am Thorac Soc 2016;13:2119–2124.
12. Schermer TRJ, Verweij EHA, Cretier R, Pellegrino A, Crockett AJ, PoelsPJ. Accuracy and precision of desktop spirometers in generalpractices. Respiration 2012;83:344–352.
13. Bambra G, Jalota L, Kapoor C, Mills PK, Vempilly JJ, Jain VV. Officespirometry correlates with laboratory spirometry in patients withsymptomatic asthma and COPD. Clin Respir J 2017;11:805–811.
14. Licskai CJ, Sands TW, Paolatto L, Nicoletti I, Ferrone M. Spirometryin primary care: an analysis of spirometery test quality in aregional primary care asthma program. Can Respir J 2012;19:249–254.
15. Epton MJ, Stanton JD, McGeoch GR, Shand BI, Swanney MP. Thedevelopment of a community-based spirometry service in theCanterbury region of New Zealand: observations on new servicedelivery. NPJ Prim Care Respir Med 2015;25:15003.
16. Cooper BG. An update on contraindications for lung function testing.Thorax 2011;66:714–723.
AMERICAN THORACIC SOCIETY DOCUMENTS
American Thoracic Society Documents e85

17. Coates AL, Graham BL, McFadden RG, McParland C, Moosa D,Provencher S, et al.; Canadian Thoracic Society. Spirometry inprimary care. Can Respir J 2013;20:13–21.
18. Vieira GM, Oliveira HB, de Andrade DT, Bottaro M, Ritch R. Intraocularpressure variation during weight lifting. Arch Ophthalmol 2006;124:1251–1254.
19. Tiller NB, Simpson AJ. Effect of spirometry on intra-thoracic pressures.BMC Res Notes 2018;11:110.
20. Boerrigter BG, Bogaard HJ, Vonk-Noordegraaf A. Spirometry in chronicobstructive pulmonary disease: a hemodynamic roller coaster? Am JRespir Crit Care Med 2012;186:e6–e7.
21. Roberts C, Ward S, Walsted E, Hull JH. Safety of pulmonary functiontesting: data from 20 years. Thorax 2018;73:385–387.
22. Garcıa-Rıo F, Calle M, Burgos F, Casan P, Del Campo F, Galdiz JB,et al.; Spanish Society of Pulmonology and Thoracic Surgery(SEPAR). Spirometry. Arch Bronconeumol 2013;49:388–401.
23. Araujo CG, Vianna LC. How often does spirometry testing inducecardiac arrhythmias? Prim Care Respir J 2009;18:185–188.
24. Zagami D, Wilson J, Bodger A, Sriram KB. Respiratory function testingis safe in patients with abdominal aortic aneurysms. VascEndovascular Surg 2014;48:522–523.
25. Goodyear SJ, Yow H, Saedon M, Shakespeare J, Hill CE, Watson D,et al. Risk stratification by pre-operative cardiopulmonary exercisetesting improves outcomes following elective abdominal aorticaneurysm surgery: a cohort study. Perioper Med (Lond) 2013;2:10.
26. Frost F, Peat R, McWean J, Shaw M, Field M, Nazareth D, et al.Pulmonary function testing is safe in patients with thoracic aorticaneurysms. Eur Respir J 2018;52:1800928.
27. Johns DP, Hartley MF, Burns G, Thompson BR. Variation in barometricpressure in Melbourne does not significantly affect the BTPScorrection factor. Respirology 2004;9:406–408.
28. Lalloo UG, Becklake MR, Goldsmith CM. Effect of standing versussitting position on spirometric indices in healthy subjects.Respiration 1991;58:122–125.
29. Gudmundsson G, Cerveny M, Shasby DM. Spirometric values in obeseindividuals: effects of body position. Am J Respir Crit Care Med1997;156:998–999.
30. Swamy K, Isroff C, Mhanna MJ, Chouksey AK. Effect of sitting vsstanding posture on spirometry in children. Ann Allergy AsthmaImmunol 2016;117:94–96.
31. Pal AK, Tiwari S, Verma DK. Effect of recumbent body positions ondynamic lung function parameters in healthy young subjects. J ClinDiagn Res 2017;11:CC08–CC10.
32. Katz S, Arish N, Rokach A, Zaltzman Y, Marcus EL. The effect of bodyposition on pulmonary function: a systematic review. BMC PulmMed 2018;18:159.
33. Kendrick AH, Johns DP, Leeming JP. Infection control of lung functionequipment: a practical approach. Respir Med 2003;97:1163–1179.
34. Rasam SA, Apte KK, Salvi SS. Infection control in the pulmonaryfunction test laboratory. Lung India 2015;32:359–366.
35. Pittet D, Allegranzi B, Boyce J; World Health Organization WorldAlliance for Patient Safety First Global Patient Safety Challenge CoreGroup of Experts. The World Health Organization guidelines on handhygiene in health care and their consensus recommendations. InfectControl Hosp Epidemiol 2009;30:611–622.
36. Saiman L, Siegel JD, LiPuma JJ, Brown RF, Bryson EA, Chambers MJ,et al.; Cystic Fibrous Foundation; Society for HealthcareEpidemiology of America. Infection prevention and control guidelinefor cystic fibrosis: 2013 update. Infect Control Hosp Epidemiol 2014;35(Suppl 1):S1–S67.
37. Wanger J, Mottram C. ATS pulmonary function laboratory managementand procedure manual, 3rd ed. New York: American ThoracicSociety; 2016.
38. International Organization for Standardization. ISO 26782. Anaestheticand respiratory equipment: spirometers intended for themeasurement of time forced expired volumes in humans. Geneva,Switzerland: International Organization for Standardization; 2016.
39. McCormack MC, Shade D, Wise RA. Spirometer calibration checks: is3.5% good enough? Chest 2007;131:1486–1493.
40. Lefebvre Q, Vandergoten T, Derom E, Marchandise E, Liistro G. Testingspirometers: are the standard curves of the American ThoracicSociety sufficient? Respir Care 2014;59:1895–1904.
41. Miller MR, Lloyd J, Bright P. Recording flow in the first second of amaximal forced expiratory manoeuvre: influence of frequencycontent. Eur Respir J 2002;19:530–533.
42. Graham BL, Brusasco V, Burgos F, Cooper BG, Jensen R, Kendrick A,et al. 2017 ERS/ATS standards for single-breath carbon monoxideuptake in the lung. Eur Respir J 2017;49:1600016.
43. Miller MR, Sigsgaard T. Prevention of thermal and condensation errorsin pneumotachographic recordings of the maximal forced expiratorymanoeuvre. Eur Respir J 1994;7:198–201.
44. Johnson LR, Enright PL, Voelker HT, Tashkin DP. Volume spirometersneed automated internal temperature sensors. Am J Respir Crit CareMed 1994;150:1575–1580.
45. Haynes JM, Ruppel GL. Should spirometer quality control be treatedlike other laboratory devices? ERJ Open Res 2019;5:00249-2018.
46. Westgard JO, Groth T, Aronsson T, Falk H, de Verdier CH. Performancecharacteristics of rules for internal quality control: probabilitiesfor false rejection and error detection. Clin Chem 1977;23:1857–1867.
47. Madsen F. Validation of spirometer calibration syringes. Scand J ClinLab Invest 2012;72:608–613.
48. Ruppel GL, Enright PL. Pulmonary function testing. Respir Care 2012;57:165–175.
49. Cooper BG, Steenbruggen I, Mitchell S, Severin T, Oostveen E, BurgosF, et al. HERMES spirometry: the European Spirometry DrivingLicence. Breathe (Sheff) 2011;7:258–275.
50. Steenbruggen I, Mitchell S, Severin T, Palange P, Cooper BG;Spirometry HERMES Task Force. Harmonising spirometryeducation with HERMES: training a new generation of qualifiedspirometry practitioners across Europe. Eur Respir J 2011;37:479–481.
51. Swanney MP, O’Dea CA, Ingram ER, Rodwell LT, Borg BM; ANZSRSSpirometry Training Course Working Group. Spirometry trainingcourses: content, delivery and assessment: a position statementfrom the Australian and New Zealand Society of Respiratory Science.Respirology 2017;22:1430–1435.
52. Borg BM, Hartley MF, Fisher MT, Thompson BR. Spirometry trainingdoes not guarantee valid results. Respir Care 2010;55:689–694.
53. Represas-Represas C, Botana-Rial M, Leiro-Fernandez V, Gonzalez-Silva AI, Garcıa-Martınez A, Fernandez-Villar A. Short- and long-termeffectiveness of a supervised training program in spirometry usefor primary care professionals. Arch Bronconeumol 2013;49:378–382.
54. Haynes JM. Quality assurance of the pulmonary function technologist.Respir Care 2012;57:114–122. [Discussion, pp. 122–126.]
55. Quanjer PH, Hall GL, Stanojevic S, Cole TJ, Stocks J; Global LungsInitiative. Age- and height-based prediction bias in spirometryreference equations. Eur Respir J 2012;40:190–197.
56. Gauld LM, Kappers J, Carlin JB, Robertson CF. Height prediction fromulna length. Dev Med Child Neurol 2004;46:475–480.
57. Quanjer PH, Capderou A, Mazicioglu MM, Aggarwal AN, Banik SD,Popovic S, et al. All-age relationship between arm span and height indifferent ethnic groups. Eur Respir J 2014;44:905–912.
58. Braun L, Wolfgang M, Dickersin K. Defining race/ethnicity andexplaining difference in research studies on lung function. Eur RespirJ 2013;41:1362–1370.
59. Quanjer PH, Stanojevic S, Cole TJ, Baur X, Hall GL, Culver BH, et al.;ERS Global Lung Function Initiative. Multi-ethnic reference values forspirometry for the 3–95-yr age range: the Global Lung Function 2012equations. Eur Respir J 2012;40:1324–1343.
60. Bucca CB, Carossa S, Colagrande P, Brussino L, Chiavassa G, Pera P,et al. Effect of edentulism on spirometric tests. Am J Respir Crit CareMed 2001;163:1018–1020.
61. Indrakumar HS, Venkatesh D, Adoni VV, Kashyap R, Jayanthi D,Prakash N. Spirometric assessment of impact of complete dentureson respiratory performance: an in vitro study. J Contemp Dent Pract2018;19:177–180.
62. Banerjee SK, Davies M, Sharples L, Smith I. The role of facemaskspirometry in motor neuron disease. Thorax 2013;68:385–386.
63. Wanger JS, Ikle DN, Cherniack RM. The effect of inspiratory maneuverson expiratory flow rates in health and asthma: influence of lungelastic recoil. Am J Respir Crit Care Med 1996;153:1302–1308.
AMERICAN THORACIC SOCIETY DOCUMENTS
e86 American Journal of Respiratory and Critical Care Medicine Volume 200 Number 8 | October 15 2019
64. D’Angelo E, Prandi E, Milic-Emili J. Dependence of maximal flow-volume curves on time course of preceding inspiration. J ApplPhysiol (1985) 1993;75:1155–1159.
65. Stoller JK, Basheda S, Laskowski D, Goormastic M, McCarthy K. Trialof standard versus modified expiration to achieve end-of-testspirometry criteria. Am Rev Respir Dis 1993;148:275–280.
66. Stoller JK, McCarthy K. Benefits of a modified spirometry technique.Eur Respir J 2007;30:813–814, author reply 814–815.
67. Haynes JM, Kaminsky DA. The American Thoracic Society/EuropeanRespiratory Society acceptability criteria for spirometry: asking toomuch or not enough? Respir Care 2015;60:e113–e114.
68. Kozlowska WJ, Aurora P. Spirometry in the pre-school age group.Paediatr Respir Rev 2005;6:267–272.
69. Seed L, Wilson D, Coates AL. Children should not be treated like littleadults in the PFT lab. Respir Care 2012;57:61–70. [Discussion, pp.71–74.]
70. American Thoracic Society; European Respiratory Society. ATS/ERSstatement: raised volume forced expirations in infants: guidelinesfor current practice. Am J Respir Crit Care Med 2005;172:1463–1471.
71. Newall C, McCauley TM, Shakespeare J, Cooper BG. Is it necessary touse a noseclip in the performance of spirometry using a wedgebellows device? Chron Respir Dis 2007;4:53–57.
72. McKibben JM, McKay RT, Freeman AG, Levin LS, Pinney SM, AlshaikhE. Redefining spirometry hesitating start criteria based on the ratio ofextrapolated volume to timed FEVs. Chest 2011;140:164–169.
73. Muller-Brandes C, Kramer U, Gappa M, Seitner-Sorge G, Huls A, vonBerg A, et al. LUNOKID: can numerical American ThoracicSociety/European Respiratory Society quality criteria replace visualinspection of spirometry? Eur Respir J 2014;43:1347–1356.
74. National Institute for Occupational Safety and Health (NIOSH).Spirometry quality assurance: common errors and their impact ontest results. Washington, DC: NIOSH; 2012 [accessed 2019 May 5]DHHS (NIOSH) Publication No. 2012-116. Available from:https://www.cdc.gov/niosh/docs/2012-116/pdfs/2012-116.pdf.
75. Miller MR, Pedersen OF, Quanjer PH. The rise and dwell time for peakexpiratory flow in patients with and without airflow limitation. Am JRespir Crit Care Med 1998;158:23–27.
76. Glover R, Cooper BG, Lloyd J. Forced expiratory time (FET) as anindicator for airways obstruction. Eur Respir J 2014;44:1819.
77. Giner J, Plaza V, Rigau J, Sola J, Bolıbar I, Sanchis J. Spirometricstandards and patient characteristics: an exploratory study of factorsaffecting fulfillment in routine clinical practice. Respir Care 2014;59:1832–1837.
78. Sumphao-Ngern P, Foocharoen C, Boonsawat W, Mahakkanukrauh A,Suwannaroj S, Sae-Oue U, et al.; Scleroderma Research Group.Causes and prevalence of inadequate pulmonary function testingamong patients with systemic sclerosis. Arch Med Sci 2015;11:1255–1260.
79. Czajkowska-Malinowska M, Tomalak W, Radliński J. Quality ofspirometry in the elderly. Pneumonol Alergol Pol 2013;81:511–517.
80. Hankinson JL, Eschenbacher B, Townsend M, Stocks J, Quanjer PH.Use of forced vital capacity and forced expiratory volume in 1second quality criteria for determining a valid test. Eur Respir J 2015;45:1283–1292.
81. Torre-Bouscoulet L, Velazquez-Uncal M, Garcıa-Torrentera R,Gochicoa-Rangel L, Fernandez-Plata R, Enright P, et al. Spirometryquality in adults with very severe lung function impairment. RespirCare 2015;60:740–743.
82. Enright P, Vollmer WM, Lamprecht B, Jensen R, Jithoo A, Tan W, et al.Quality of spirometry tests performed by 9893 adults in 14 countries:the BOLD Study. Respir Med 2011;105:1507–1515.
83. Tan WC, Bourbeau J, O’Donnell D, Aaron S, Maltais F, Marciniuk D,et al.; CanCOLD Collaborative Research Group. Quality assurance ofspirometry in a population-based study—predictors of goodoutcome in spirometry testing. COPD 2014;11:143–151.
84. Janssens W, Liu Y, Liu D, Kesten S, Tashkin DP, Celli BR, et al. Qualityand reproducibility of spirometry in COPD patients in a randomizedtrial (UPLIFT®). Respir Med 2013;107:1409–1416.
85. Tomalak W, Radliński J, Latawiec W. Quality of spirometricmeasurements in children younger than 10 years of age in the light of therecommendations [in Polish]. Pneumonol Alergol Pol 2008;76:421–425.
86. Hankinson JL, Bang KM. Acceptability and reproducibility criteria of theAmerican Thoracic Society as observed in a sample of the generalpopulation. Am Rev Respir Dis 1991;143:516–521.
87. Kirkby J, Welsh L, Lum S, Fawke J, Rowell V, Thomas S, et al.; EPICureStudy Group. The EPICure study: comparison of pediatric spirometryin community and laboratory settings. Pediatr Pulmonol 2008;43:1233–1241.
88. Enright PL, Beck KC, Sherrill DL. Repeatability of spirometry in 18,000adult patients. Am J Respir Crit Care Med 2004;169:235–238.
89. Gochicoa-Rangel L, Vargas-Domınguez C, Garcıa-Mujica ME,Bautista-Bernal A, Salas-Escamilla I, Perez-Padilla R, et al. Quality ofspirometry in 5-to-8-year-old children. Pediatr Pulmonol 2013;48:1231–1236.
90. Ferris BG Jr, Speizer FE, Bishop Y, Prang G, Weener J. Spirometry foran epidemiologic study: deriving optimum summary statistics foreach subject. Bull Eur Physiopathol Respir 1978;14:145–166.
91. Kanner RE, Schenker MB, Muñoz A, Speizer FE. Spirometry inchildren: methodology for obtaining optimal results for clinicaland epidemiologic studies. Am Rev Respir Dis 1983;127:720–724.
92. Barjaktarevic I, Kaner R, Buhr RG, Cooper CB. Bronchodilatorresponsiveness or reversibility in asthma and COPD: a need forclarity. Int J Chron Obstruct Pulmon Dis 2018;13:3511–3513.
93. Davis BE, Blais CM, Cockcroft DW. Methacholine challenge testing:comparative pharmacology. J Asthma Allergy 2018;11:89–99.
94. LaForce C, Korenblat P, Osborne P, Dong F, Higgins M. 24-Hourbronchodilator efficacy of single doses of indacaterol in patients withpersistent asthma: comparison with placebo and formoterol. CurrMed Res Opin 2009;25:2353–2359.
95. Jones TE, Southcott A, Homan S. Drugs potentially affecting the extentof airways reversibility on pulmonary function testing are frequentlyconsumed despite guidelines. Int J Chron Obstruct Pulmon Dis 2013;8:383–388.
96. Enright PL, Lebowitz MD, Cockroft DW. Physiologic measures:pulmonary function tests: asthma outcome. Am J Respir Crit CareMed 1994;149:S9–S18. [Discussion, pp. S19–S20.]
97. Ward H, Cooper BG, Miller MR. Improved criterion for assessing lungfunction reversibility. Chest 2015;148:877–886.
98. Quanjer PH, Ruppel GL, Langhammer A, Krishna A, Mertens F,Johannessen A, et al. Bronchodilator response in FVC is larger andmore relevant than in FEV1 in severe airflow obstruction. Chest 2017;151:1088–1098.
99. Crenesse D, Berlioz M, Bourrier T, Albertini M. Spirometry in childrenaged 3 to 5 years: reliability of forced expiratory maneuvers. PediatrPulmonol 2001;32:56–61.
100. Piccioni P, Borraccino A, Forneris MP, Migliore E, Carena C,Bignamini E, et al. Reference values of forced expiratory volumesand pulmonary flows in 3-6 year children: a cross-sectional study.Respir Res 2007;8:14.
101. Cockcroft DW, Berscheid BA. Volume adjustment of maximalmidexpiratory flow: importance of changes in total lung capacity.Chest 1980;78:595–600.
102. Swanney MP, Jensen RL, Crichton DA, Beckert LE, Cardno LA, CrapoRO. FEV6 is an acceptable surrogate for FVC in the spirometricdiagnosis of airway obstruction and restriction. Am J Respir CritCare Med 2000;162:917–919.
103. Vandevoorde J, Verbanck S, Schuermans D, Kartounian J, Vincken W.FEV1/FEV6 and FEV6 as an alternative for FEV1/FVC and FVC in thespirometric detection of airway obstruction and restriction. Chest2005;127:1560–1564.
104. Kainu A, Lindqvist A, Sarna S, Sovijarvi A. Intra-session repeatabilityof FET and FEV6 in the general population. Clin Physiol FunctImaging 2008;28:196–201.
105. Bellia V, Sorino C, Catalano F, Augugliaro G, Scichilone N, Pistelli R,et al. Validation of FEV6 in the elderly: correlates of performance andrepeatability. Thorax 2008;63:60–66.
106. Perez-Padilla R, Wehrmeister FC, Celli BR, Lopez-Varela MV,Montes de Oca M, Muiño A, et al.; PLATINO Team. Reliability ofFEV1/FEV6 to diagnose airflow obstruction compared withFEV1/FVC: the PLATINO longitudinal study. PLoS One 2013;8:e67960.
AMERICAN THORACIC SOCIETY DOCUMENTS
American Thoracic Society Documents e87

107. Akpinar-Elci M, Fedan KB, Enright PL. FEV6 as a surrogate for FVC indetecting airways obstruction and restriction in the workplace. EurRespir J 2006;27:374–377.
108. Hankinson JL, Odencrantz JR, Fedan KB. Spirometric referencevalues from a sample of the general U.S. population. Am J RespirCrit Care Med 1999;159:179–187.
109. Hansen JE, Porszasz J, Casaburi R, Stringer WW. Re-defining lowerlimit of normal for FEV1/FEV6, FEV1/FVC, FEV3/FEV6 and FEV3/FVCto improve detection of airway obstruction. Chronic Obstr Pulm Dis2015;2:94–102.
110. Marsh S, Aldington S, Williams M, Weatherall M, Shirtcliffe P,McNaughton A, et al. Complete reference ranges for pulmonaryfunction tests from a single New Zealand population. N Z Med J2006;119:U2281. [Published erratum appears in N Z Med J 120:U2551.]
111. Tian XY, Liu CH, Wang DX, Ji XL, Shi H, Zheng CY, et al. Spirometricreference equations for elderly Chinese in Jinan aged 60-84 Years.Chin Med J (Engl) 2018;131:1016–1022.
112. Raposo LB, Bugalho A, Gomes MJ. Contribution of flow-volumecurves to the detection of central airway obstruction. J BrasPneumol 2013;39:447–454.
113. Modrykamien AM, Gudavalli R, McCarthy K, Liu X, Stoller JK.Detection of upper airway obstruction with spirometryresults and the flow-volume loop: a comparison of quantitativeand visual inspection criteria. Respir Care 2009;54:474–479.
114. Culver BH, Graham BL, Coates AL, Wanger J, Berry CE, Clarke PK,et al.; ATS Committee on Proficiency Standards for PulmonaryFunction Laboratories. Recommendations for a standardizedpulmonary function report: an Official American Thoracic Societytechnical statement. Am J Respir Crit Care Med 2017;196:1463–1472.
115. Salas T, Rubies C, Gallego C, Muñoz P, Burgos F, Escarrabill J.Technical requirements of spirometers in the strategy forguaranteeing the access to quality spirometry. Arch Bronconeumol2011;47:466–469.
116. Goel A, Goyal M, Singh R, Verma N, Tiwari S. Diurnal variation in peakexpiratory flow and forced expiratory volume. J Clin Diagn Res2015;9:CC05–CC07.
117. Fregonezi G, Resqueti VR, Cury JL, Paulin E, Brunetto AF. Diurnalvariations in the parameters of pulmonary function and respiratorymuscle strength in patients with COPD. J Bras Pneumol 2012;38:257–263.
118. Johnston R. PFT blog: a modest proposal for a clinical spirometrygrading system. 2018 Sep 16 [accessed 2019 May 5]. Availablefrom: https://www.pftforum.com/blog/a-modest-proposal-for-a-clinical-spirometry-grading-system/#more-2420.
119. British Thoracic Society; Association of Respiratory Technology andPhysiology. Guidelines for the measurement of respiratory function:British Thoracic Society and the Association of RespiratoryTechnology and Physiology. Respir Med 1994;88:165–194.
120. Babb TG, Viggiano R, Hurley B, Staats B, Rodarte JR. Effect of mild-to-moderate airflow limitation on exercise capacity. J Appl Physiol(1985) 1991;70:223–230.
121. O’Donnell DE, Lam M, Webb KA. Spirometric correlates ofimprovement in exercise performance after anticholinergic therapyin chronic obstructive pulmonary disease. Am J Respir Crit CareMed 1999;160:542–549.
122. Pellegrino R, Rodarte JR, Brusasco V. Assessing the reversibility ofairway obstruction. Chest 1998;114:1607–1612.
123. Younes M, Kivinen G. Respiratory mechanics and breathing patternduring and following maximal exercise. J Appl Physiol 1984;57:1773–1782.
124. Wanger J, Clausen JL, Coates A, Pedersen OF, Brusasco V, Burgos F,et al. Standardisation of the measurement of lung volumes. EurRespir J 2005;26:511–522.
125. Brusasco V, Pellegrino R, Rodarte JR. Vital capacities in acute andchronic airway obstruction: dependence on flow and volumehistories. Eur Respir J 1997;10:1316–1320.
126. Hansen LM, Pedersen OF, Lyager S, Naerra N. Differences in vitalcapacity due to the methods employed. Ugeskr Laeger 1983;145:2752–2756.
127. Borg BM, Thompson BR. The measurement of lung volumes usingbody plethysmography: a comparison of methodologies. RespirCare 2012;57:1076–1083.
128. Russell AM, Adamali H, Molyneaux PL, Lukey PT, Marshall RP,Renzoni EA, et al. Daily home spirometry: an effective tool fordetecting progression in idiopathic pulmonary fibrosis. Am J RespirCrit Care Med 2016;194:989–997.
129. Wang W, Finkelstein SM, Hertz MI. Automatic event detection in lungtransplant recipients based on home monitoring of spirometry andsymptoms. Telemed J E Health 2013;19:658–663.
130. Murgia F, Bianciardi F, Solvoll T, Tagliente I, Bella F, Carestia A, et al.Telemedicine home program in patients with cystic fibrosis: resultsafter 10 years. Clin Ter 2015;166:e384–e388.
131. Burgos F, Disdier C, de Santamaria EL, Galdiz B, Roger N,Rivera ML, et al.; e-Spir@p Group. Telemedicine enhances qualityof forced spirometry in primary care. Eur Respir J 2012;39:1313–1318.
132. Marina Malanda N, Lopez de Santa Marıa E, Gutierrez A, Bayon JC,Garcia L, Galdiz JB. Telemedicine spirometry training and qualityassurance program in primary care centers of a public healthsystem. Telemed J E Health 2014;20:388–392.
133. Weiner DJ, Forno E, Sullivan L, Weiner GA, Kurland G. Subjective andobjective assessments of flow-volume curve configuration inchildren and young adults. Ann Am Thorac Soc 2016;13:1089–1095.
134. Dominelli PB, Foster GE, Guenette JA, Haverkamp HC, Eves ND,Dominelli GS, et al. Quantifying the shape of the maximal expiratoryflow-volume curve in mild COPD. Respir Physiol Neurobiol 2015;219:30–35.
135. Stuart-Andrews CR, Kelly VJ, Sands SA, Lewis AJ, Ellis MJ,Thompson BR. Automated detection of the phase III slope duringinert gas washout testing. J Appl Physiol (1985) 2012;112:1073–1081.
136. Anogeianaki A, Negrev N, Ilonidis G. Contributions of signal analysisto the interpretation of spirometry. Hippokratia 2007;11:187–195.
137. Lian N, Li L, Ren W, Jiang Z, Zhu L. Angle b of greater than 808 at thestart of spirometry may identify high-quality flow volume curves.Respirology 2017;22:527–532.
138. Melia U, Burgos F, Vallverdu M, Velickovski F, Lluch-Ariet M, Roca J,et al. Algorithm for automatic forced spirometry quality assessment:technological developments. PLoS One 2014;9:e116238.
139. Luo AZ, Whitmire E, Stout JW, Martenson D, Patel S. Automaticcharacterization of user errors in spirometry. Conf Proc IEEE EngMed Biol Soc 2017;2017:4239–4242.
140. Velickovski F, Ceccaroni L, Marti R, Burgos F, Gistau C, Alsina-RestoyX, et al. Automated spirometry quality assurance: supervisedlearning from multiple experts. IEEE J Biomed Health Inform 2018;22:276–284.
141. Morris ZQ, Coz A, Starosta D. An isolated reduction of theFEV3/FVC ratio is an indicator of mild lung injury. Chest 2013;144:1117–1123.
142. Bhatt SP, Kim YI, Wells JM, Bailey WC, Ramsdell JW, Foreman MG,et al. FEV1/FEV6 to diagnose airflow obstruction: comparisons withcomputed tomography and morbidity indices. Ann Am Thorac Soc2014;11:335–341.
143. Dilektasli AG, Porszasz J, Casaburi R, Stringer WW, Bhatt SP, Pak Y,et al.; COPDGene investigators. A novel spirometric measureidentifies mild COPD unidentified by standard criteria. Chest 2016;150:1080–1090.
144. Ioachimescu OC, Venkateshiah SB, Kavuru MS, McCarthy K, StollerJK. Estimating FVC from FEV2 and FEV3: assessment of a surrogatespirometric parameter. Chest 2005;128:1274–1281.
145. Miller MR, Grove DM, Pincock AC. Time domain spirogram indices:their variability and reference values in nonsmokers. Am Rev RespirDis 1985;132:1041–1048.
146. Liu C, Yang Y, Tsow F, Shao D, Tao N. Noncontact spirometry with awebcam. J Biomed Opt 2017;22:57002.
147. Coates AL, Wanger J, Cockcroft DW, Culver BH, Carlsen KH, DiamantZ, et al. ERS technical standard on bronchial challenge testing:general considerations and performance of methacholine challengetests. Eur Respir J 2017;49:1601526.
AMERICAN THORACIC SOCIETY DOCUMENTS
e88 American Journal of Respiratory and Critical Care Medicine Volume 200 Number 8 | October 15 2019

SERIES ‘‘ATS/ERS TASK FORCE: STANDARDISATION OF LUNGFUNCTION TESTING’’Edited by V. Brusasco, R. Crapo and G. ViegiNumber 2 in this Series
Standardisation of spirometryM.R. Miller, J. Hankinson, V. Brusasco, F. Burgos, R. Casaburi, A. Coates,R. Crapo, P. Enright, C.P.M. van der Grinten, P. Gustafsson, R. Jensen,D.C. Johnson, N. MacIntyre, R. McKay, D. Navajas, O.F. Pedersen, R. Pellegrino,G. Viegi and J. Wanger
CONTENTS
Background . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 320
FEV1 and FVC manoeuvre . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 321
Definitions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 321
Equipment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 321
Requirements . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 321
Display . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 321
Validation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 322
Quality control . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 322
Quality control for volume-measuring devices . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 322
Quality control for flow-measuring devices . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 323
Test procedure . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 323
Within-manoeuvre evaluation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 324
Start of test criteria. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 324
End of test criteria . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 324
Additional criteria . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 324
Summary of acceptable blow criteria . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 325
Between-manoeuvre evaluation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 325
Manoeuvre repeatability . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 325
Maximum number of manoeuvres . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 326
Test result selection . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 326
Other derived indices . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 326
FEVt . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 326
Standardisation of FEV1 for expired volume, FEV1/FVC and FEV1/VC . . . . . . . . . . . . . . . . . . . . 326
FEF25–75% . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 326
PEF . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 326
Maximal expiratory flow–volume loops . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 326
Definitions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 326
Equipment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 327
Test procedure . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 327
Within- and between-manoeuvre evaluation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 327
Flow–volume loop examples. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 327
Reversibility testing . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 327
Method . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 327
Comment on dose and delivery method . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 328
Determination of reversibility . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 328
VC and IC manoeuvre . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 329
Definitions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 329
AFFILIATIONS
For affiliations, please see
Acknowledgements section
CORRESPONDENCE
V. Brusasco
Internal Medicine
University of Genoa
V.le Benedetto XV, 6
I-16132 Genova
Italy
Fax: 39 103537690
E-mail: [email protected]
Received:
March 23 2005
Accepted after revision:
April 05 2005
European Respiratory Journal
Print ISSN 0903-1936
Online ISSN 1399-3003
Previous articles in this series: No. 1: Miller MR, Crapo R, Hankinson J, et al. General considerations for lung function testing. Eur Respir J 2005; 26:
153–161.
EUROPEAN RESPIRATORY JOURNAL VOLUME 26 NUMBER 2 319
Eur Respir J 2005; 26: 319–338
DOI: 10.1183/09031936.05.00034805
Copyright�ERS Journals Ltd 2005
c

VC and IVC . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .329
IC. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .329
Equipment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .329
Test procedure . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .329
VC . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .329
IC. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .330
Use of a nose clip . . . . . . . . . . . . . . . . . . . . . . . . . . .330
Within-manoeuvre evaluation . . . . . . . . . . . . . . . . . . . . .330
Between-manoeuvre evaluation . . . . . . . . . . . . . . . . . . .330
Test result selection . . . . . . . . . . . . . . . . . . . . . . . . . . .330
Peak expiratory flow . . . . . . . . . . . . . . . . . . . . . . . . . . .330
Definition . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .330
Equipment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .330
Test procedure . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .330
Within-manoeuvre evaluation . . . . . . . . . . . . . . . . . . . . .331
Between-manoeuvre evaluation . . . . . . . . . . . . . . . . . . .331
Test result selection . . . . . . . . . . . . . . . . . . . . . . . . . . .331
Maximum voluntary ventilation . . . . . . . . . . . . . . . . . . .331
Definition . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .331
Equipment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .331
Test procedure . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .331
Within-manoeuvre evaluation . . . . . . . . . . . . . . . . . . . . .331
Between-manoeuvre evaluation . . . . . . . . . . . . . . . . . . .331
Test result selection . . . . . . . . . . . . . . . . . . . . . . . . . . .331
Technical considerations . . . . . . . . . . . . . . . . . . . . . . . .331
Minimal recommendations for spirometry systems . . . . . .331
BTPS correction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .332
Comments . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .332
Test signals for spirometer testing . . . . . . . . . . . . . . . . .333
Method . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .333
Accuracy test . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .333
Repeatability test . . . . . . . . . . . . . . . . . . . . . . . . . . . .333
Test signals for PEF meter testing . . . . . . . . . . . . . . . . .333
Method . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .333
Accuracy test . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .333
Repeatability test . . . . . . . . . . . . . . . . . . . . . . . . . . . .334
Test signals for MVV testing. . . . . . . . . . . . . . . . . . . . . .334
Abbreviations. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .334
Appendix . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .335
KEYWORDS: Peak expiratory flow, spirometry, spirometry standardisation, spirometry technique, spirometry traning,
ventilation
BACKGROUNDSpirometry is a physiological test that measures how anindividual inhales or exhales volumes of air as a function oftime. The primary signal measured in spirometry may bevolume or flow.
Spirometry is invaluable as a screening test of generalrespiratory health in the same way that blood pressureprovides important information about general cardiovascularhealth. However, on its own, spirometry does not leadclinicians directly to an aetiological diagnosis. Some indica-tions for spirometry are given in table 1.
In this document, the most important aspects of spirometry arethe forced vital capacity (FVC), which is the volume deliveredduring an expiration made as forcefully and completely aspossible starting from full inspiration, and the forced expira-tory volume (FEV) in one second, which is the volumedelivered in the first second of an FVC manoeuvre. Otherspirometric variables derived from the FVC manoeuvre arealso addressed.
Spirometry can be undertaken with many different types ofequipment, and requires cooperation between the subject andthe examiner, and the results obtained will depend ontechnical as well as personal factors (fig. 1). If the variabilityof the results can be diminished and the measurementaccuracy can be improved, the range of normal values forpopulations can be narrowed and abnormalities more easilydetected. The Snowbird workshop held in 1979 resulted in thefirst American Thoracic Society (ATS) statement on thestandardisation of spirometry [1]. This was updated in 1987and again in 1994 [2, 3]. A similar initiative was undertaken bythe European Community for Steel and Coal, resulting in thefirst European standardisation document in 1983 [4]. This was
then updated in 1993 as the official statement of the EuropeanRespiratory Society (ERS) [5]. There are generally only minordifferences between the two most recent ATS and ERSstatements, except that the ERS statement includes absolutelung volumes and the ATS does not.
This document brings the views of the ATS and ERS togetherin an attempt to publish standards that can be applied more
TABLE 1 Indications for spirometry
Diagnostic
To evaluate symptoms, signs or abnormal laboratory tests
To measure the effect of disease on pulmonary function
To screen individuals at risk of having pulmonary disease
To assess pre-operative risk
To assess prognosis
To assess health status before beginning strenuous physical activity
programmes
Monitoring
To assess therapeutic intervention
To describe the course of diseases that affect lung function
To monitor people exposed to injurious agents
To monitor for adverse reactions to drugs with known pulmonary toxicity
Disability/impairment evaluations
To assess patients as part of a rehabilitation programme
To assess risks as part of an insurance evaluation
To assess individuals for legal reasons
Public health
Epidemiological surveys
Derivation of reference equations
Clinical research
STANDARDISATION OF SPIROMETRY M.R. MILLER ET AL.
320 VOLUME 26 NUMBER 2 EUROPEAN RESPIRATORY JOURNAL

widely. The statement is structured to cover definitions,equipment and patient-related procedures. All recordingdevices covered by this statement must meet the relevantrequirements, regardless of whether they are for monitoringor diagnostic purposes. There is no separate category for‘‘monitoring’’ devices.
Although manufacturers have the responsibility for producingpulmonary function testing systems that satisfy all therecommendations presented here, it is possible that, for someequipment, meeting all of them may not always be achievable.In these circumstances, manufacturers should clearly identifywhich equipment requirements have not been met. Whilemanufacturers are responsible for demonstrating the accuracyand reliability of the systems that they sell, it is the user who isresponsible for ensuring that the equipment’s measurementsremain accurate. The user is also responsible for followinglocal law, which may have additional requirements. Finally,these guidelines are minimum guidelines, which may not besufficient for all settings, such as when conducting research,epidemiological studies, longitudinal evaluations and occupa-tional surveillance.
FEV1 AND FVC MANOEUVREDefinitionsFVC is the maximal volume of air exhaled with maximallyforced effort from a maximal inspiration, i.e. vital capacityperformed with a maximally forced expiratory effort,expressed in litres at body temperature and ambient pressuresaturated with water vapour (BTPS; see BTPS correctionsection).
FEV1 is the maximal volume of air exhaled in the first secondof a forced expiration from a position of full inspiration,expressed in litres at BTPS.
EquipmentRequirementsThe spirometer must be capable of accumulating volume foro15 s (longer times are recommended) and measuring
volumes of o8 L (BTPS) with an accuracy of at least ¡3% ofreading or ¡0.050 L, whichever is greater, with flows between0 and 14 L?s-1. The total resistance to airflow at 14.0 L?s-1 mustbe ,1.5 cmH2O?L-1?s-1 (0.15 kPa?L-1?s-1; see Minimal recommen-dations for spirometry systems section). The total resistance mustbe measured with any tubing, valves, pre-filter, etc. includedthat may be inserted between the subject and the spirometer.Some devices may exhibit changes in resistance due to watervapour condensation, and accuracy requirements must be metunder BTPS conditions for up to eight successive FVCmanoeuvres performed in a 10-min period without inspirationfrom the instrument.
DisplayFor optimal quality control, both flow–volume and volume–time displays are useful, and test operators should visuallyinspect the performance of each manoeuvre for qualityassurance before proceeding with another manoeuvre. Thisinspection requires tracings to meet the minimum size andresolution requirements set forth in this standard.
Displays of flow versus volume provide more detail for theinitial portion (first 1 s) of the FVC manoeuvre. Since thisportion of the manoeuvre, particularly the peak expiratoryflow (PEF), is correlated with the pleural pressure during themanoeuvre, the flow–volume display is useful to assess themagnitude of effort during the initial portions of themanoeuvre. The ability to overlay a series of flow–volumecurves registered at the point of maximal inhalation maybe helpful in evaluating repeatability and detecting sub-maximal efforts. However, if the point of maximal inhala-tion varies between blows, then the interpretation of theseresults is difficult because the flows at identical measuredvolumes are being achieved at different absolute lungvolumes. In contrast, display of the FVC manoeuvre as avolume–time graph provides more detail for the latter partof the manoeuvre. A volume–time tracing of sufficientsize also allows independent measurement and calculationof parameters from the FVC manoeuvres. In a display ofmultiple trials, the sequencing of the blows should beapparent to the user.
For the start of test display, the volume–time display shouldinclude o0.25 s, and preferably 1 s, before exhalation starts(zero volume). This time period before there is any change involume is needed to calculate the back extrapolated volume(EV; see Start of test criteria section) and to evaluate effortduring the initial portion of the manoeuvre. Time zero, asdefined by EV, must be presented as the zero point on thegraphical output.
The last 2 s of the manoeuvre should be displayed to indicate asatisfactory end of test (see End of test criteria section).
When a volume–time curve is plotted as hardcopy, the volumescale must be o10 mm?L-1 (BTPS). For a screen display,5 mm?L-1 is satisfactory (table 2).
The time scale should be o20 mm?s-1, and larger timescales are preferred (o30 mm?s-1) when manual measure-ments are made [1, 6, 7]. When the volume–time plot is used inconjunction with a flow–volume curve (i.e. both displaymethods are provided for interpretations and no hand
������������ �������������
��������������� �
������� �� �
��������������� ������
������������ �������
�����������
�����������
������������������������ �
�����������������
��������������� �������� �� ������
FIGURE 1. Spirometry standardisation steps.
M.R. MILLER ET AL. STANDARDISATION OF SPIROMETRY
cEUROPEAN RESPIRATORY JOURNAL VOLUME 26 NUMBER 2 321

measurements are performed), the time scale requirementis reduced to 10 mm?s-1 from the usually required minimumof 20 mm?s-1 (table 2). The rationale for this exception isthat the flow–volume curve can provide the means forquality assessment during the initial portion of the FVCmanoeuvre. The volume–time curve can be used to evaluatethe latter part of the FVC manoeuvre, making the time scaleless critical.
ValidationIt is strongly recommended that spirometry systems should beevaluated using a computer-driven mechanical syringe or itsequivalent, in order to test the range of exhalations that arelikely to be encountered in the test population. Testing theperformance of equipment is not part of the usual laboratoryprocedures (see Test signals for spirometer testing section).
Quality controlAttention to equipment quality control and calibration isan important part of good laboratory practice. At a minimum,the requirements are as follows: 1) a log of calibration resultsis maintained; 2) the documentation of repairs or otheralterations which return the equipment to acceptable opera-tion; 3) the dates of computer software and hardwareupdates or changes; and 4) if equipment is changed orrelocated (e.g. industrial surveys), calibration checks andquality-control procedures must be repeated before furthertesting begins.
Key aspects of equipment quality control are summarised intable 3.
Calibration is the procedure for establishing the relationshipbetween sensor-determined values of flow or volume and theactual flow or volume.
A calibration check is different from calibration and is theprocedure used to validate that the device is within calibrationlimits, e.g. ¡3% of true. If a device fails its calibration check,then a new calibration procedure or equipment maintenance isrequired. Calibration checks must be undertaken daily, ormore frequently, if specified by the manufacturer.
The syringe used to check the volume calibration of spiro-meters must have an accuracy of ¡15 mL or ¡0.5% of the fullscale (15 mL for a 3-L syringe), and the manufacturer must
provide recommendations concerning appropriate intervalsbetween syringe calibration checks. Users should be awarethat a syringe with an adjustable or variable stop may be outof calibration if the stop is reset or accidentally moved.Calibration syringes should be periodically (e.g. monthly) leaktested at more than one volume up to their maximum; this canbe done by attempting to empty them with the outlet corked. Adropped or damaged syringe should be considered out ofcalibration until it is checked.
With regard to time, assessing mechanical recorder time scaleaccuracy with a stopwatch must be performed at leastquarterly. An accuracy of within 2% must be achieved.
Quality control for volume-measuring devicesThe volume accuracy of the spirometer must be checked at leastdaily, with a single discharge of a 3-L calibrated syringe. Dailycalibration checking is highly recommended so that the onset ofa problem can be determined within 1 day, and also to helpdefine day-to-day laboratory variability. More frequent checksmay be required in special circumstances, such as: 1) duringindustrial surveys or other studies in which a large number ofsubject manoeuvres are carried out, the equipment’s calibrationshould be checked more frequently than daily [8]; and 2) whenthe ambient temperature is changing (e.g. field studies), volumeaccuracy must be checked more frequently than daily and theBTPS correction factor appropriately updated.
The accuracy of the syringe volume must be considered indetermining whether the measured volume is within accep-table limits. For example, if the syringe has an accuracy of0.5%, a reading of ¡3.5% is appropriate.
The calibration syringe should be stored and used in such away as to maintain the same temperature and humidity of thetesting site. This is best accomplished by keeping the syringe inclose proximity to the spirometer, but out of direct sunlightand away from heat sources.
Volume-type spirometer systems must be evaluated for leaksevery day [9, 10]. The importance of undertaking this daily testcannot be overstressed. Leaks can be detected by applying aconstant positive pressure of o3.0 cmH2O (0.3 kPa) with thespirometer outlet occluded (preferably at or including themouthpiece). Any observed volume loss .30 mL after 1 minindicates a leak [9, 10] and needs to be corrected.
TABLE 2 Recommended minimum scale factors for time,volume and flow on graphical output
Instrument display Hardcopy graphical outputParameter
Resolution
required
Scale
factor
Resolution
required
Scale
factor
Volume# 0.050 L 5 mm?L-1 0.025 L 10 mm?L-1
Flow# 0.200 L?s-1 2.5 mm?L-1?s-1 0.100 L?s-1 5 mm?L-1?s-1
Time 0.2 s 10 mm?s-1 0.2 s 20 mm?s-1
#: the correct aspect ratio for a flow versus volume display is two units of flow
per one unit of volume.
TABLE 3 Summary of equipment quality control
Test Minimum interval Action
Volume Daily Calibration check with a 3-L syringe
Leak Daily 3 cmH2O (0.3 kPa) constant pressure
for 1 min
Volume linearity Quarterly 1-L increments with a calibrating syringe
measured over entire volume range
Flow linearity Weekly Test at least three different flow ranges
Time Quarterly Mechanical recorder check with stopwatch
Software New versions Log installation date and perform test using
‘‘known’’ subject
STANDARDISATION OF SPIROMETRY M.R. MILLER ET AL.
322 VOLUME 26 NUMBER 2 EUROPEAN RESPIRATORY JOURNAL

At least quarterly, volume spirometers must have theircalibration checked over their entire volume range using acalibrated syringe [11] or an equivalent volume standard. Themeasured volume should be within ¡3.5% of the reading or65 mL, whichever is greater. This limit includes the 0.5%accuracy limit for a 3-L syringe. The linearity check procedureprovided by the manufacturer can be used if it is equivalent toone of the following procedures: 1) consecutive injections of1-L volume increments while comparing observed volumewith the corresponding cumulative measured volume, e.g. 0–1,1–2, 2–3,…6–7 and 7–8 L, for an 8-L spirometer; and 2)injection of a 3-L volume starting at a minimal spirometervolume, then repeating this with a 1-L increment in the startposition, e.g. 0–3, 1–4, 2–5, 3–6, 4–7 and 5–8 L, for an 8-Lspirometer.
The linearity check is considered acceptable if the spirometermeets the volume accuracy requirements for all volumestested.
Quality control for flow-measuring devicesWith regards to volume accuracy, calibration checks must beundertaken at least daily, using a 3-L syringe discharged atleast three times to give a range of flows varying between 0.5and 12 L?s-1 (with 3-L injection times of ,6 s and ,0.5 s). Thevolume at each flow should meet the accuracy requirement of¡3.5%. For devices using disposable flow sensors, a newsensor from the supply used for patient tests should be testedeach day.
For linearity, a volume calibration check should be per-formed weekly with a 3-L syringe to deliver three relativelyconstant flows at a low flow, then three at a mid-range flowand finally three at a high flow. The volumes achieved at eachof these flows should each meet the accuracy requirement of¡3.5%.
Test procedureThere are three distinct phases to the FVC manoeuvre, asfollows: 1) maximal inspiration; 2) a ‘‘blast’’ of exhalation; and3) continued complete exhalation to the end of test (EOT).
The technician should demonstrate the appropriate techniqueand follow the procedure described in table 4. The subjectshould inhale rapidly and completely from functional residualcapacity (FRC), the breathing tube should be inserted into thesubject’s mouth (if this has not already been done), makingsure the lips are sealed around the mouthpiece and that thetongue does not occlude it, and then the FVC manoeuvreshould be begun with minimal hesitation. Reductions in PEFand FEV1 have been shown when inspiration is slow and/orthere is a 4–6 s pause at total lung capacity (TLC) beforebeginning exhalation [12]. It is, therefore, important that thepreceding inspiration is fast and any pause at full inspirationbe minimal (i.e. only for 1–2 s). The test assumes a fullinhalation before beginning the forced exhalation, and it isimperative that the subject takes a complete inhalation beforebeginning the manoeuvre. The subject should be prompted to‘‘blast,’’ not just ‘‘blow,’’ the air from their lungs, and then he/she should be encouraged to fully exhale. Throughout themanoeuvre, enthusiastic coaching of the subject using appro-priate body language and phrases, such as ‘‘keep going’’, is
required. It is particularly helpful to observe the subject withoccasional glances to check for distress, and to observe thetracing or computer display during the test to help ensuremaximal effort. If the patient feels ‘‘dizzy’’, the manoeuvreshould be stopped, since syncope could follow due toprolonged interruption of venous return to the thorax. This ismore likely to occur in older subjects and those with airflowlimitation. Performing a vital capacity (VC) manoeuvre (see VCand IC manoeuvre section), instead of obtaining FVC, may helpto avoid syncope in some subjects. Reducing the effort part-way through the manoeuvre [13] may give a higher expiratoryvolume in some subjects, but then is no longer a maximallyforced expiration. Well-fitting false teeth should not beroutinely removed, since they preserve oropharyngeal geome-try and spirometry results are generally better with them inplace [14].
With appropriate coaching, children as young as 5 yrs ofage are often able to perform acceptable spirometry [15].The technicians who are involved in the pulmonary functiontesting of children should be specifically trained to dealwith such a situation. A bright, pleasant atmosphere,
TABLE 4 Procedures for recording forced vital capacity
Check the spirometer calibration
Explain the test
Prepare the subject
Ask about smoking, recent illness, medication use, etc.
Measure weight and height without shoes
Wash hands
Instruct and demonstrate the test to the subject, to include
Correct posture with head slightly elevated
Inhale rapidly and completely
Position of the mouthpiece (open circuit)
Exhale with maximal force
Perform manoeuvre (closed circuit method)
Have subject assume the correct posture
Attach nose clip, place mouthpiece in mouth and close lips around the
mouthpiece
Inhale completely and rapidly with a pause of ,1 s at TLC
Exhale maximally until no more air can be expelled while maintaining an upright
posture
Repeat instructions as necessary, coaching vigorously
Repeat for a minimum of three manoeuvres; no more than eight are usually
required
Check test repeatability and perform more manoeuvres as necessary
Perform manoeuvre (open circuit method)
Have subject assume the correct posture
Attach nose clip
Inhale completely and rapidly with a pause of ,1 s at TLC
Place mouthpiece in mouth and close lips around the mouthpiece
Exhale maximally until no more air can be expelled while maintaining an upright
posture
Repeat instructions as necessary, coaching vigorously
Repeat for a minimum of three manoeuvres; no more than eight are usually
required
Check test repeatability and perform more manoeuvres as necessary
TLC: total lung capacity.
M.R. MILLER ET AL. STANDARDISATION OF SPIROMETRY
cEUROPEAN RESPIRATORY JOURNAL VOLUME 26 NUMBER 2 323

including age-appropriate toys, reading material and art, isimportant in making children feel at ease. Encouragement,detailed but simple instructions, lack of intimidation andvisual feedback in the teaching are important in helpingchildren to perform the manoeuvre. Even if unsuccessful atthe first session, children will learn to be less intimidatedand may perform far better in a subsequent session. Testingchildren in ‘‘adult’’ laboratories, where no effort is made tocater for the specific needs of the younger subjects, is to bediscouraged.
The use of a nose clip or manual occlusion of the nares isrecommended, and, for safety reasons, testing should bepreferably done in the sitting position, using a chair witharms and without wheels. If testing is undertaken with thepatient standing or in another position, this must bedocumented on the report.
Within-manoeuvre evaluationStart of test criteriaThe start of test, for the purpose of timing, is determined by theback extrapolation method (fig. 2) [1, 3, 9, 16]. The new ‘‘timezero’’ from back extrapolation defines the start for all timedmeasurements. For manual measurements, the back extrapola-tion method traces back from the steepest slope on thevolume–time curve [17]. For computerised back extrapolation,it is recommended that the largest slope averaged over an 80-ms period is used [18]. Figure 2 provides an example andexplanation of back extrapolation and the derivation of EV. Toachieve an accurate time zero and assure the FEV1 comes froma maximal effort curve, the EV must be ,5% of the FVC or0.150 L, whichever is greater. If a manoeuvre has an obviouslyhesitant start, the technician may terminate the trial early toavoid an unnecessary prolonged effort.
Rapid computerised feedback to the technician when the startcriteria are not met is strongly encouraged. In addition to theexpiratory manoeuvre, the volume-time curve display (graph)
should ideally include the whole preceding inspiratorymanoeuvre, but must include o0.25 s and preferably o1 sprior to the start of exhalation (time zero). The equipmentshould display the EV value. Inspection of the flow–volumecurve may be added as a measure of the satisfactory start oftest. PEF should be achieved with a sharp rise and occur closeto the point of maximal inflation, i.e. the start of exhalation (seeEquipment section).
End of test criteriaIt is important for subjects to be verbally encouraged tocontinue to exhale the air at the end of the manoeuvre to obtainoptimal effort, e.g. by saying ‘‘keep going’’. EOT criteria areused to identify a reasonable FVC effort, and there are tworecommended EOT criteria, as follows. 1) The subject cannot orshould not continue further exhalation. Although subjectsshould be encouraged to achieve their maximal effort, theyshould be allowed to terminate the manoeuvre on their own atany time, especially if they are experiencing discomfort. Thetechnician should also be alert to any indication that the patientis experiencing discomfort, and should terminate the test if apatient is becoming uncomfortable or is approaching syncope.2) The volume–time curve shows no change in volume(,0.025 L) for o1 s, and the subject has tried to exhale foro3 s in children aged ,10 yrs and for o6 s in subjects aged.10 yrs.
The equipment should signal to the technician if the plateaucriteria were not met. A satisfactory EOT may still have beenachieved, but an equipment alert will help the technician topinpoint where the subject may need more encouragement.It is of note that a closure of the glottis may prematurelyterminate a manoeuvre at ,6 s, even when the apparentduration of the blow exceeds 6 s.
For patients with airways obstruction or older subjects,exhalation times of .6 s are frequently needed. However,exhalation times of .15 s will rarely change clinical decisions.Multiple prolonged exhalations are seldom justified and maycause light headedness, syncope, undue fatigue and unneces-sary discomfort.
Achieving EOT criteria is one measure of manoeuvre accept-ability. Manoeuvres that do not meet EOT criteria should notbe used to satisfy the requirement of three acceptablemanoeuvres. However, early termination, by itself, is not areason to eliminate all the results from such a manoeuvre fromfurther consideration. Information such as the FEV1 may beuseful (depending on the length of exhalation) and can bereported from these early terminated manoeuvres.
Some young children may have difficulty meeting the ATSEOT criteria [3], although they may meet other repeatabilitycriteria [19]. Curve-fitting techniques [20] may prove useful indeveloping new EOT criteria specific for young children.
Additional criteriaA cough during the first second of the manoeuvre can affectthe measured FEV1 value. Coughing in the first second or anyother cough that, in the technician’s judgment, interferes withthe measurement of accurate results [3] will render a testunacceptable.
!"#
�$!"!
%"!
!"&
!"'
!"(
$ ���
�)
!"*!!"(*!"!!+�,���-��
.����
FIGURE 2. Expanded version of the early part of a subject’s volume–time
spirogram, illustrating back extrapolation through the steepest part of the curve,
where flow is peak expiratory flow (PEF), to determine the new ‘‘time zero’’. Forced
vital capacity (FVC)54.291 L; back extrapolated volume (EV)50.123 L (2.9% FVC).
-----: back extrapolation line through PEF.
STANDARDISATION OF SPIROMETRY M.R. MILLER ET AL.
324 VOLUME 26 NUMBER 2 EUROPEAN RESPIRATORY JOURNAL

A Valsalva manoeuvre (glottis closure) or hesitation during themanoeuvre that causes a cessation of airflow in a manner thatprecludes an accurate estimate of either FEV1 or FVC [3] willrender a test unacceptable.
There must be no leak at the mouth [3]. Patients withneuromuscular disease may require manual or other assistancefrom the technician to guarantee an adequate seal.
Obstruction of the mouthpiece, e.g. by the tongue being placedin front of the mouthpiece or by teeth in front of themouthpiece, or by distortion from biting, may affect theperformance of either the device or the subject.
Summary of acceptable blow criteriaThe acceptability criteria are a satisfactory start of test and asatisfactory EOT, i.e. a plateau in the volume–time curve. Inaddition, the technician should observe that the subjectunderstood the instructions and performed the manoeuvrewith a maximum inspiration, a good start, a smoothcontinuous exhalation and maximal effort. The followingconditions must also be met: 1) without an unsatisfactory startof expiration, characterised by excessive hesitation or falsestart extrapolated volume or EV .5% of FVC or 0.150 L,whichever is greater (fig. 2); 2) without coughing during thefirst second of the manoeuvre, thereby affecting the measuredFEV1 value, or any other cough that, in the technician’sjudgment, interferes with the measurement of accurate results[3]; 3) without early termination of expiration (see End of testcriteria section); 4) without a Valsalva manoeuvre (glottisclosure) or hesitation during the manoeuvre that causes acessation of airflow, which precludes accurate measurement ofFEV1 or FVC [3]; 5) without a leak [3]; 6) without an obstructedmouthpiece (e.g. obstruction due to the tongue being placed infront of the mouthpiece, or teeth in front of the mouthpiece, ormouthpiece deformation due to biting); and 7) withoutevidence of an extra breath being taken during the manoeuvre.
It should be noted that a usable curve must only meetconditions 1 and 2 above, while an acceptable curve must meetall of the above seven conditions.
It is desirable to use a computer-based system that providesfeedback to the technician when the above conditions are notmet. The reporting format should include qualifiers indicatingthe acceptability of each manoeuvre. However, failure to meetthese goals should not necessarily prevent reporting of results,since, for some subjects, this is their best performance. Recordsof such manoeuvres should be retained since they may containuseful information.
Between-manoeuvre evaluationUsing the previously described criteria, an adequate testrequires a minimum of three acceptable FVC manoeuvres.Acceptable repeatability is achieved when the differencebetween the largest and the next largest FVC is f0.150 Land the difference between the largest and next largest FEV1 isf0.150 L [21]. For those with an FVC of f1.0 L, both thesevalues are 0.100 L. If these criteria are not met in threemanoeuvres, additional trials should be attempted, up to, butusually no more than, eight manoeuvres. Large variabilityamong tests is often due to incomplete inhalations. Somepatients may require a brief rest period between manoeuvres.
Volume–time or flow–volume curves from at least the bestthree FVC manoeuvres must be retained. Table 5 gives asummary of the within- and between-manoeuvre evaluation.
Manoeuvre repeatabilityFor FVC measurements, acceptability must be determined byascertaining that the recommendations outlined previously onperforming the FVC test are met. The guidelines of the ATS [3]contain examples of unacceptable volume–time and corre-sponding flow–volume curves. Figure 3 shows a flow chartoutlining how the criteria for blow acceptability are appliedbefore those for repeatability.
The repeatability criteria are used to determine when morethan three acceptable FVC manoeuvres are needed; thesecriteria are not to be used to exclude results from reports or toexclude subjects from a study. Labelling results as beingderived from data that do not conform to the repeatabilitycriteria described previously is recommended. In addition, therepeatability criteria are minimum requirements. Many sub-jects are able to achieve FVC and FEV1 repeatability to within0.150 L. Manoeuvres with an unacceptable start of test or acough (unusable curve) must be discarded before applying therepeatability criteria and cannot be used in determining thebest values. Manoeuvres with early termination or a Valsalvamanoeuvre may be used for selecting the largest FVC andFEV1.
TABLE 5 Summary of within- and between-manoeuvreacceptability criteria
Within-manoeuvre criteria
Individual spirograms are ‘‘acceptable’’ if
They are free from artefacts [3]
Cough during the first second of exhalation
Glottis closure that influences the measurement
Early termination or cut-off
Effort that is not maximal throughout
Leak
Obstructed mouthpiece
They have good starts
Extrapolated volume ,5% of FVC or 0.15 L, whichever is greater
They show satisfactory exhalation
Duration of o6 s (3 s for children) or a plateau in the volume–time curve or
If the subject cannot or should not continue to exhale
Between-manoeuvre criteria
After three acceptable spirograms have been obtained, apply the following
tests
The two largest values of FVC must be within 0.150 L of each other
The two largest values of FEV1 must be within 0.150 L of each other
If both of these criteria are met, the test session may be concluded
If both of these criteria are not met, continue testing until
Both of the criteria are met with analysis of additional acceptable spirograms
or
A total of eight tests have been performed (optional) or
The patient/subject cannot or should not continue
Save, as a minimum, the three satisfactory manoeuvres
FVC: forced vital capacity; FEV1: forced expiratory volume in one second.
M.R. MILLER ET AL. STANDARDISATION OF SPIROMETRY
cEUROPEAN RESPIRATORY JOURNAL VOLUME 26 NUMBER 2 325

No spirogram or test result should be rejected solely on thebasis of its poor repeatability. The repeatability of resultsshould be considered at the time of interpretation. The use ofdata from manoeuvres with poor repeatability or failure tomeet the EOT requirements is left to the discretion of theinterpreter.
Maximum number of manoeuvresAlthough there may be some circumstances in which morethan eight consecutive FVC manoeuvres may be needed, eightis generally a practical upper limit for most subjects [22, 23].After several forced expiratory manoeuvres, fatigue can beginto take its toll on subjects and additional manoeuvres would beof little added value. In extremely rare circumstances, subjectsmay show a progressive reduction in FEV1 or FVC with eachsubsequent blow. If the cumulative drop exceeds 20% of startvalue, the test procedure should be terminated in the interestof patient safety. The sequence of the manoeuvres should berecorded.
Test result selectionFVC and FEV1 should be measured from a series of at leastthree forced expiratory curves that have an acceptable start oftest and are free from artefact, such as a cough (i.e. ‘‘usablecurves’’). The largest FVC and the largest FEV1 (BTPS) shouldbe recorded after examining the data from all of the usablecurves, even if they do not come from the same curve.
Other derived indicesFEVt
FEVt is the maximal volume exhaled by time t seconds (timedfrom the time zero defined by back extrapolation) of a forcedexpiration from a position of full inspiration, expressed in litresat BTPS. Very young children may not be able to produceprolonged expirations, but there is increasing evidence thatindices derived from blows with forced expiratory times of
,1 s may have clinical usefulness [19]. At present, there areinsufficient data to recommend the use of FEV0.5 or FEV0.75.
When the subject does not exhale completely, the volumeaccumulated over a shorter period of time (e.g. 6 s) may beused as an approximate surrogate for FVC. When suchsurrogates are used, the volume label should reflect the shorterexhalation time (e.g. FEV6 for a 6-s exhalation). FEV6 has beenincreasingly considered a reasonably reliable surrogate forFVC [24] and can be used for normalising FEV1 (e.g. FEV1/FEV6). Recording FEV6 seems to have the advantage of beingmore reproducible than FVC, being less physically demandingfor patients and providing a more explicit EOT. Confirmationfrom other studies is required.
Standardisation of FEV1 for expired volume, FEV1/FVC and FEV1/VCIn some patients, a slow or unforced VC or inspiratory vitalcapacity (IVC) manoeuvre (see VC and IC manoeuvre section)may provide a larger and more appropriate denominator forcalculation of the FEV1/VC%. Some investigators havereported that the VC is slightly higher than the FVC in normalsubjects [25].
FEF25–75%
The mean forced expiratory flow between 25% and 75% ofthe FVC (FEF25–75%) has also been known as the maximummid-expiratory flow. This index is taken from the blowwith the largest sum of FEV1 and FVC. The FEF25–75% mustbe measured with an accuracy of at least ¡5% of reading or¡0.200 L?s-1 whichever is greater, over a range of up to 7 L?s-1.It should be noted that it is highly dependent on the validity ofthe FVC measurement and the level of expiratory effort.
PEFPEF is usually obtained from flow–volume curve data. It is themaximum expiratory flow achieved from a maximum forcedexpiration, starting without hesitation from the point ofmaximal lung inflation, expressed in L?s-1. When PEF isrecorded using a patient-administered portable PEF meter, it isoften expressed in L?min-1. PEF is covered in more detail later.
Maximal expiratory flow–volume loopsThe shape of a maximum flow–volume loop (MFVL), whichincludes forced inspiratory manoeuvres, can be helpful inquality control and in detecting the presence of upper airwayobstruction. None of the numerical indices from a MFVL hasclinical utility superior to FEV1, FVC, FEF25–75% and PEF, andare not considered in detail here.
DefinitionsWith regard to instantaneous flows, the recommendedmeasure is the instantaneous forced expiratory flow whenX% of the FVC has been expired (FEFX%). The maximalinstantaneous forced expiratory flow when X% of the FVCremains to be expired (MEFX%) was the term previouslyrecommended in Europe.
Instantaneous forced inspiratory flow when X% of the FVC hasbeen expired (FIFX%) and mid-inspiratory flow when X% of theFVC has been expired refer to the flows measured onthe inspiratory limb of a flow–volume loop. FIF25–75%, also
/��� ���$���� �����
��,� ��0��� �����������������������1
�� ����� ��������������� ������1
����,������ �����������������������1
2����������3���$�������3����$%
�������� �����,� ���3����� ��$�4��$% �������� ���������
� ������������
5��
5��
5��
+
+
+
FIGURE 3. Flow chart outlining how acceptability and reapeatability criteria are
to be applied. FVC: forced vital capacity; FEV1: forced expiratory volume in one
second.
STANDARDISATION OF SPIROMETRY M.R. MILLER ET AL.
326 VOLUME 26 NUMBER 2 EUROPEAN RESPIRATORY JOURNAL

referred to as maximal mid-inspiratory flow, is analogous toFEF25–75% (see Other derived indices section).
EquipmentInstantaneous flows must be measured with an accuracy of¡5% of reading or ¡0.200 L?s-1, whichever is greater, over arange of -14–14 L?s-1. The level of minimum detectable flowshould be 0.025 L?s-1. When a maximum flow–volume loop isplotted or displayed, exhaled flow must be plotted upwards,and exhaled volume towards the right. A 2:1 ratio must bemaintained between the flow and volume scales, e.g. 2 L?s-1 offlow and 1 L of exhaled volume must be the same distance ontheir respective axes. The flow and volume scales, used inreviewing test performance, must be equivalent to that shownin table 2.
Test procedureThe subject has to make a full expiratory and inspiratory loopas a single manoeuvre. In many laboratories, this is theprimary manoeuvre for spirometry. The subject is asked totake a rapid full inspiration to TLC from room air through themouth, then insert the mouthpiece and, without hesitation,perform an expiration with maximum force until no more gascan be expelled, followed by a quick maximum inspiration. Atthis point, the manoeuvre is finished.
An alternative procedure is for the subject to insert themouthpiece while undertaking tidal breathing at FRC, andthen, in one continuous sequence, do the following: make aslow expiration to residual volume (RV); followed directly by aslow inspiration to TLC; follow this by a rapid full expirationwith maximal effort to RV; and followed by a rapid fullinspiration with maximal effort back to TLC.
This procedure is slightly more complicated and may not besuitable for all equipment, but it obtains a measurement of VCas well as FVC.
Within- and between-manoeuvre evaluationThese evaluations are the same as for FVC (see Within-manoeuvre evaluation and Between-manoeuvre evaluation sec-tions). Occasionally, a subject is unable to perform asatisfactory inspiratory limb immediately following a maximalforced expiratory manoeuvre. This is particularly common inthe elderly and the infirm. In these circumstances, it may benecessary for the subject to record an inspiratory manoeuvreseparately from the expiratory manoeuvre. Equipment shouldbe able to perform these separately and then present three ormore loops together on a graphical display or output.
Flow–volume loop examplesThe following figures (figures 4–10) give typical examples ofcommonly encountered flow–volume loop configurations. Theadvantages of visual pattern recognition from the MFVL canreadily be appreciated. The shapes of the manoeuvres must berepeatable (fig. 10) for any interpretation to be made. This isespecially true for the plateau effect on expiratory andinspiratory limbs of the manoeuvre found in upper airwayobstruction, as this can be mimicked by poor effort, which isusually variable from blow to blow. A further explanation isgiven in the ATS/ERS statement on lung function interpreta-tion [26].
Reversibility testingA determination of airflow-limitation reversibility with drugadministration is commonly undertaken as part of lungfunction testing. The choice of drug, dose and mode ofdelivery is a clinical decision depending on what the clinicianwishes to learn from the test.
If the aim of the test is to determine whether the patient’s lungfunction can be improved with therapy in addition to theirregular treatment, then the subject can continue with his/herregular medication prior to the test.
If the clinician wants to determine whether there is anyevidence of reversible airflow limitation, then the subjectshould undergo baseline function testing when not taking anydrugs prior to the test. Short-acting inhaled drugs (e.g. the b-agonist albuterol/salbutamol or the anticholinergic agentipratropium bromide) should not be used within 4 h of testing.Long-acting b-agonist bronchodilators (e.g. salmeterol orformoterol) and oral therapy with aminophylline or slow-release b-agonists should be stopped for 12 h prior to the test.Smoking should be avoided for o1 h prior to testing andthroughout the duration of the test procedure.
MethodThe following steps are undertaken. 1) The subject has threeacceptable tests of FEV1, FVC and PEF recorded as describedpreviously. 2) The drug is administered in the dose and by themethod indicated for the test. For example, after a gentle andincomplete expiration, a dose of 100 mg of albuterol/salbuta-mol is inhaled in one breath to TLC from a valved spacerdevice. The breath is then held for 5–10 s before the subjectexhales. Four separate doses (total dose 400 mg) are delivered at,30-s intervals. This dose ensures that the response is high onthe albuterol dose–response curve. A lower dose can be used ifthere is concern about any effect on the patient’s heart rate ortremor. Other drugs can also be used. For the anticholinergicagent ipratropium bromide, the total dose is 160 mg (4640 mg).
Three additional acceptable tests are recorded o10 min andup to 15 min later for short-acting b2-agonists, and 30 min laterfor short-acting anticholinergic agents.
%(
%!
#
&
'
(
!
0(
0'
0&
0#
�� ,)6�0%
! % ( 7 ' * &$ ����)
FIGURE 4. Flow–volume loop of a normal subject.
M.R. MILLER ET AL. STANDARDISATION OF SPIROMETRY
cEUROPEAN RESPIRATORY JOURNAL VOLUME 26 NUMBER 2 327

Comment on dose and delivery methodStandardising the bronchodilator dose administered isnecessary in order to standardise the definition of asignificant bronchodilator response. The rate of pulmonarydeposition of a drug with tidal breathing from an unventednebuliser will depend on drug concentration, rate ofnebuliser output, particle-size distribution, and the ratioof the time spent in inspiration over the total respiratorytime (ti/ttot) [27]. The fraction of the aerosol carried inparticles with a diameter of f5 mm that is expected todeposit in adult lungs if inhaled through a mouthpiece [28]is defined as the respirable fraction (RF). For example,2.5 mg of salbutamol (albuterol) in 2.5 mL of solution,placed in a Hudson Updraft II (Hudson RCI, Temecula,CA, USA) driven by a PulmoAide compressor (De Vilbiss,Somerset, PA, USA), would produce ,0.1 mg?min-1 in theRF. For a respiratory rate of 15 breaths?min-1 and a ti/ttot
of 0.45, this would give ,3 mg deposited in the lungs perbreath, or 45 mg?min-1. For adults using a metered dose
inhaler (MDI) with a valve-holding chamber (spacer),between 10 and 20% [29, 30] of a 100-mg ‘‘puff’’ (or ,15mg per activation) would be expected to be deposited inthe lung of an adult. Without a spacer, the deposition willbe less, and heavily technique dependent [31]. Pulmonarydeposition from dry-powder inhalers is device specific, andbreath-enhanced nebulisers deposit much more thanunvented ones [32, 33]. CFC-free MDIs produce a smallerparticle-size distribution and improved (up to 50% of dose)lung deposition compared with those with CFC propellant[34]. For children, pulmonary deposition is less than that inadults [35], possibly relating to the size of the upperairway. Each laboratory should be familiar with thepulmonary-deposition characteristics of the devices theyuse.
Determination of reversibilityThis aspect is covered in detail in the interpretative strategydocument of the ATS and ERS [26].
%(
%!
#
&
'
(
!
0(
0'
0&
0#
�� ,)6�0%
! % ( 7 ' * &$ ����)
FIGURE 5. Flow–volume loop of a normal sub-
ject with end expiratory curvilinearity, which can be
seen with ageing.
%(
%!
#
&
'
(
!
0(
0'
0&
0#
�� ,)6�0%
! % ( 7 ' * &$ ����)
FIGURE 6. Moderate airflow limitation in a
subject with asthma.
%(
%!
#
&
'
(
!
0(
0'
0&
0#
�� ,)6�0%
! % ( 7 ' * &$ ����)
FIGURE 7. Severe airflow limitation in a subject
with chronic obstructive pulmonary disease.
%(
%!
#
&
'
(
!
0(
0'
0&
0#
�� ,)6�0%
! % ( 7 ' * &$ ����)
FIGURE 8. Variable intra-thoracic upper airway
obstruction.
%(
%!
#
&
'
(
!
0(
0'
0&
0#
�� ,)6�0%
! % ( 7 ' * &$ ����)
FIGURE 9. Variable extra-thoracic upper airway
obstruction.
%(
%!
#
&
'
(
!
0(
0'
0&
0#
�� ,)6�0%
! % ( 7 ' * &$ ����)
FIGURE 10. Fixed upper airway obstruction
shown by three manoeuvres.
STANDARDISATION OF SPIROMETRY M.R. MILLER ET AL.
328 VOLUME 26 NUMBER 2 EUROPEAN RESPIRATORY JOURNAL

VC AND IC MANOEUVREDefinitionsVC and IVCThe VC is the volume change at the mouth between the positionof full inspiration and complete expiration, expressed in litres atBTPS. The slow VC can be derived in two ways. The expiratoryvital capacity (EVC) is the maximal volume of air exhaled fromthe point of maximal inhalation. The IVC is the maximal volumeof air inhaled from the point of maximal exhalation, achieved bya slow expiration from end-tidal inspiration. These manoeuvresare unforced, except at the point of reaching RV or TLC,respectively, where extra effort is required [36].
ICInspiratory capacity (IC) is volume change recorded at themouth when taking a slow full inspiration with no hesitation,from a position of passive end-tidal expiration, i.e. FRC, to aposition of maximum inspiration, expressed in litres at BTPS.IC is an indirect estimate of the degree of lung hyperinflation atrest, and is useful to assess changes in FRC with pharmaco-logical interventions and physical exercise [37–41].
EquipmentFor measurements of VC and IC, the spirometer or flow metermust comply with the requirements for FVC (as describedpreviously) and be capable of accumulating volume for o30 s.
Expiratory manoeuvres or, ideally, both inspiratory andexpiratory manoeuvres should be included in the display ofVC manoeuvre. Regardless of whether the inspiratory orexpiratory manoeuvre is used for deriving measurements, adisplay of the entire recorded VC manoeuvre must beprovided. The maximal expiratory volume must be assessedto determine whether the subject has obtained a plateau in theexpiratory effort. For display of the slow VC, the time scalemay be reduced to 5 mm?s-1.
Test procedureVCVC can be measured using conventional spirometers. It mayalso be recorded from equipment used to measure static lungvolumes and their subdivisions [42]. For slow VC, a maximumof four manoeuvres is a practical upper limit. It is preferablethat VC manoeuvres be performed before FVC manoeuvresbecause of the potential for muscular fatigue and volumehistory effects, where, after maximal inspiratory efforts, somepatients with severe airways obstruction return to a falselyhigh level of FRC or RV, due to gas trapping or stressrelaxation [3]. The VC manoeuvre may be considered either asan IVC, where the subject inhales completely from a position offull expiration, or as an EVC, where the subject exhalescompletely from a position of full inspiration. Figure 11 showsthe recording of IVC and figure 12 shows an EVC recording.Important differences between inspiratory (i.e. IVC) andexpiratory (i.e. EVC) manoeuvres may be observed in patientswith airways obstruction [43, 44].
The test is begun by instructing the subject in the VCmanoeuvre and demonstrating the appropriate technique. Itis important that subjects understand they must completely filland empty their lungs. The VC manoeuvre is performed withthe subject using a mouthpiece and wearing a nose clip. The
manoeuvre is not forced; it is performed in a relaxed manner,except near end-inspiration and end-expiration. The subjectexhales completely to RV, then inhales to TLC, and finallyexhales to RV again. The technician should encourage thesubject to reach maximal inhaled and exhaled volumes with arelatively constant flow. The exhalation should not be undulyslow, as this can lead to underestimation of VC. Techniciansshould observe the subject carefully to ensure that his/her lipsare sealed, nothing obstructs the mouthpiece, no leaks occur,and that TLC and RV are reached.
Alternatively, the subject inhales maximally, inserts themouthpiece just past his/her front teeth, seals his/her lipsaround the mouthpiece, and blows slowly and evenly untilthere is no volume change (,0.025 L) for a 1-s period (see Endof test criteria section). Patients with neuromuscular diseasemay need assistance in maintaining a tight seal at the mouth.The technician must observe the subject’s inhalation to ensure
.)�
8�
��$8$�
���
�$
.�������� ��3
8������� �
�9����� �
.���
FIGURE 11. Tracing of tidal breathing followed by an expiratory manoeuvre to
residual volume (RV), followed by a full inspiration to total lung capacity (TLC) to
record inspiratory vital capacity (IVC) and inspiratory capacity (IC). FRC: functional
residual capacity; ERV: expiratory reserve volume.
.�������� ��3
.)�
���
�$
8��$�
FIGURE 12. Tracing of tidal breathing followed by an inspiratory manoeuvre to
total lung capacity (TLC) to record inspiratory capacity (IC), followed by a full
expiration to residual volume (RV) to record expiratory reserve volume (EVC). FRC:
functional residual capacity.
M.R. MILLER ET AL. STANDARDISATION OF SPIROMETRY
cEUROPEAN RESPIRATORY JOURNAL VOLUME 26 NUMBER 2 329

that it is complete, and that air is not exhaled while themouthpiece is being inserted. The technician should assurethat the expiratory manoeuvre is not forced. In healthysubjects, adequate maximal inspiratory and expiratory levelsare achieved within 5–6 s.
ICSubjects should be tested in the seated position wearing a noseclip with no air leaks between the mouth and the mouthpiece.Subjects should be relaxed (shoulders down and relaxed) andasked to breathe regularly for several breaths until the end-expiratory lung volume is stable (this usually requires at leastthree tidal manoeuvres). They are then urged to take a deepbreath to TLC with no hesitation. Figure 12 shows a tracingfrom the recording of IC.
Use of a nose clipThe use of a nose clip is encouraged in VC measurements,since some people breathe through the nose when performinga slow VC manoeuvre. A nose clip must be used whenperforming inspiratory manoeuvres such as the IVC or IC.
Within-manoeuvre evaluationThese are the same as for FVC EOT criteria as describedpreviously. There must be no leak at the mouth, no hesitationduring the manoeuvre, and no obstruction of the mouthpiece(see Additional criteria section). The IC may be underestimatedif the inspiratory manoeuvre is too slow due to poor effort orhesitation, or if there is premature closure of the glottis.
Between-manoeuvre evaluationAs with spirometry, a minimum of three acceptable VCmanoeuvres must be obtained. If the difference in VC betweenthe largest and next largest manoeuvre is .0.150 L, additionaltrials should be undertaken. Meeting repeatability criteria mayrequire that up to, but usually no more than, four manoeuvresare performed, with a rest period of o1 min between themanoeuvres. Large variability in this test is often due toincomplete inhalations. Volume–time curves from the best twoVC manoeuvres must be retained. For the IC, at least threeacceptable manoeuvres should be performed. The meancoefficient of variation for IC in chronic airflow obstructionhas been found to be 5 ¡3% [39].
Test result selectionFor VC, the largest value from at least three acceptablemanoeuvres should be reported. For IC, the average of at leastthree manoeuvres should be reported.
PEAK EXPIRATORY FLOWStudies on the measurement of PEF are ongoing. Recentevidence has suggested that the previously applied standardsmay allow incorrect measurements to be made [45], and it ispossible that more stringent requirements may be required. Afurther statement will be made when the position on theclinical significance of this is clear. However, since PEFmeasurements are part of asthma-management programmes,the previous recommendations [3, 46] are reiterated here.
Other instantaneous flow measurements (e.g. FEF50%, FEF75%)are not proven to be superior to conventional spirometric
indices in a clinical setting, and, therefore, are not consideredfurther.
DefinitionPEF is the highest flow achieved from a maximum forcedexpiratory manoeuvre started without hesitation from a posi-tion of maximal lung inflation [46]. When it is obtained fromflow–volume curve data, it is expressed at BTPS in L?s-1. Thedefining characteristics of the flow–time curve, in relation toPEF, are the time taken for flow to rise from 10% of PEF to 90%of PEF, i.e. the rise time (RT), and the duration that flow is .90%of PEF, called the dwell time (DT). When PEF is obtained withportable monitoring instruments, it is expressed in L?min-1.
EquipmentIdeally, PEF should be recorded by an instrument thatprimarily records flow. Measuring PEF requires an instrumentthat has a flat frequency response (¡5%) up to 15 Hz [46].Although there is evidence of significant frequency content inPEF up to 20 Hz [47], it is recommended, at this stage, thatmanufacturers achieve a goal of recording fidelity up to 15 Hz.The PEF must be measured with an accuracy of ¡10%or ¡0.3 L?s-1 (20 L?min-1), whichever is the greater. Meaninstrument resistance measured across the range of theinstrument should be ,2.5 cmH2O?L-1?s-1 (0.25 kPa?L-1?s-1;table 6). PEF is sensitive to the resistance of the meter; forexample, a resistance of 0.25 kPa?L-1?s-1 decreases PEF by ,8%compared with PEF measured with a low-resistance pneumo-tachograph [48].
Intra-instrument repeatability must be ,5% or 0.150 L?s-1
(10 L?min-1), whichever is the greater. Inter-device reproduci-bility must be ,10% or 0.300 L?s-1 (20 L?min-1), whichever isthe greater. Calculating PEF by differentiating volume–timedata may introduce noise; hence, a parabolic-fitting algorithmmay be used [2] as a smoothing procedure.
Equipment validation is covered in the Test signals for PEFmeter testing section.
Test procedurePEF is dependent on effort and lung volume, with subjectcooperation being essential. PEF must be achieved as rapidlyas possible and at as high a lung volume as possible, in orderto obtain the maximum value [49]. The subject must beencouraged to blow as vigorously as possible. The neck shouldbe in a neutral position, not flexed or extended, and the subjectmust not cough. A nose clip is not necessary.
After the point of full lung inflation, the subject must deliverthe blow without any delay. Hesitating for as little as 2 s orflexing the neck allows the tracheal visco-elastic properties torelax and PEF to drop by as much as 10% [50]. Tonguing,spitting or coughing at the start of the blow may falsely raisethe recorded PEF in some devices.
In the laboratory, the subject must perform a minimum of threePEF manoeuvres. When PEF is a self-administered recording,it is important that the subject has been adequately taught howto perform the test, when to perform it and what action to takedepending on the resulting value obtained. Regular checks ofthe patient’s PEF technique and meter are an important part ofthe follow-up.
STANDARDISATION OF SPIROMETRY M.R. MILLER ET AL.
330 VOLUME 26 NUMBER 2 EUROPEAN RESPIRATORY JOURNAL
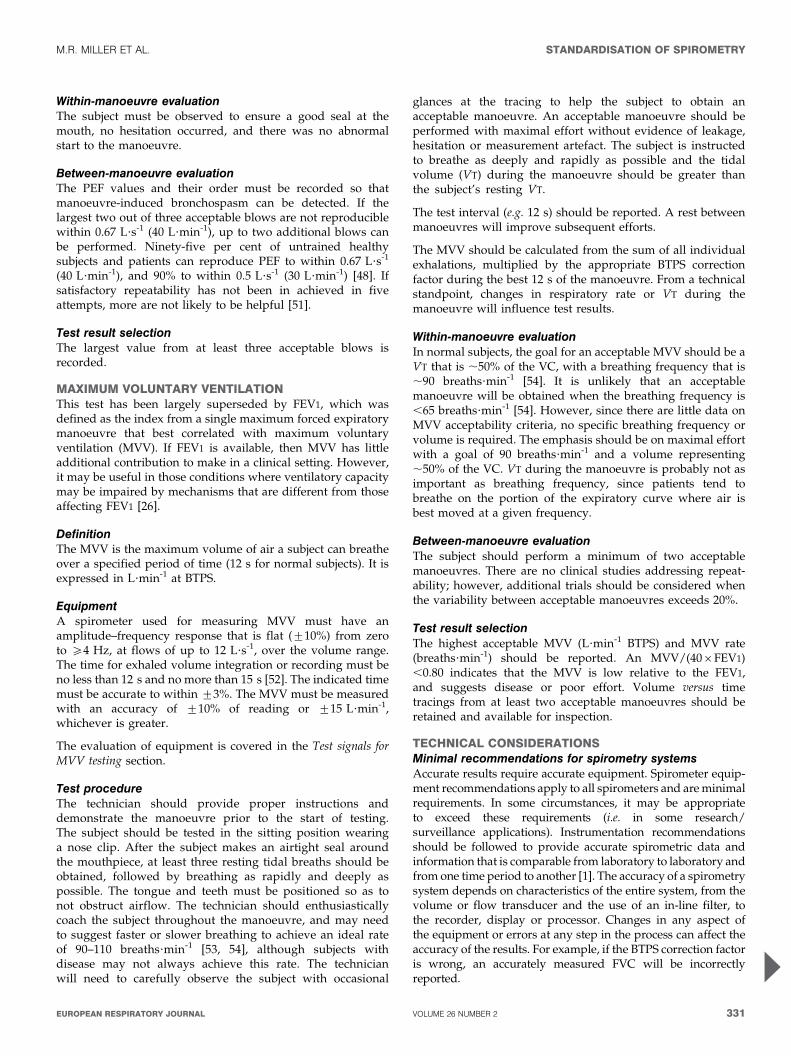
Within-manoeuvre evaluationThe subject must be observed to ensure a good seal at themouth, no hesitation occurred, and there was no abnormalstart to the manoeuvre.
Between-manoeuvre evaluationThe PEF values and their order must be recorded so thatmanoeuvre-induced bronchospasm can be detected. If thelargest two out of three acceptable blows are not reproduciblewithin 0.67 L?s-1 (40 L?min-1), up to two additional blows canbe performed. Ninety-five per cent of untrained healthysubjects and patients can reproduce PEF to within 0.67 L?s-1
(40 L?min-1), and 90% to within 0.5 L?s-1 (30 L?min-1) [48]. Ifsatisfactory repeatability has not been in achieved in fiveattempts, more are not likely to be helpful [51].
Test result selectionThe largest value from at least three acceptable blows isrecorded.
MAXIMUM VOLUNTARY VENTILATIONThis test has been largely superseded by FEV1, which wasdefined as the index from a single maximum forced expiratorymanoeuvre that best correlated with maximum voluntaryventilation (MVV). If FEV1 is available, then MVV has littleadditional contribution to make in a clinical setting. However,it may be useful in those conditions where ventilatory capacitymay be impaired by mechanisms that are different from thoseaffecting FEV1 [26].
DefinitionThe MVV is the maximum volume of air a subject can breatheover a specified period of time (12 s for normal subjects). It isexpressed in L?min-1 at BTPS.
EquipmentA spirometer used for measuring MVV must have anamplitude–frequency response that is flat (¡10%) from zeroto o4 Hz, at flows of up to 12 L?s-1, over the volume range.The time for exhaled volume integration or recording must beno less than 12 s and no more than 15 s [52]. The indicated timemust be accurate to within ¡3%. The MVV must be measuredwith an accuracy of ¡10% of reading or ¡15 L?min-1,whichever is greater.
The evaluation of equipment is covered in the Test signals forMVV testing section.
Test procedureThe technician should provide proper instructions anddemonstrate the manoeuvre prior to the start of testing.The subject should be tested in the sitting position wearinga nose clip. After the subject makes an airtight seal aroundthe mouthpiece, at least three resting tidal breaths should beobtained, followed by breathing as rapidly and deeply aspossible. The tongue and teeth must be positioned so as tonot obstruct airflow. The technician should enthusiasticallycoach the subject throughout the manoeuvre, and may needto suggest faster or slower breathing to achieve an ideal rateof 90–110 breaths?min-1 [53, 54], although subjects withdisease may not always achieve this rate. The technicianwill need to carefully observe the subject with occasional
glances at the tracing to help the subject to obtain anacceptable manoeuvre. An acceptable manoeuvre should beperformed with maximal effort without evidence of leakage,hesitation or measurement artefact. The subject is instructedto breathe as deeply and rapidly as possible and the tidalvolume (VT) during the manoeuvre should be greater thanthe subject’s resting VT.
The test interval (e.g. 12 s) should be reported. A rest betweenmanoeuvres will improve subsequent efforts.
The MVV should be calculated from the sum of all individualexhalations, multiplied by the appropriate BTPS correctionfactor during the best 12 s of the manoeuvre. From a technicalstandpoint, changes in respiratory rate or VT during themanoeuvre will influence test results.
Within-manoeuvre evaluationIn normal subjects, the goal for an acceptable MVV should be aVT that is ,50% of the VC, with a breathing frequency that is,90 breaths?min-1 [54]. It is unlikely that an acceptablemanoeuvre will be obtained when the breathing frequency is,65 breaths?min-1 [54]. However, since there are little data onMVV acceptability criteria, no specific breathing frequency orvolume is required. The emphasis should be on maximal effortwith a goal of 90 breaths?min-1 and a volume representing,50% of the VC. VT during the manoeuvre is probably not asimportant as breathing frequency, since patients tend tobreathe on the portion of the expiratory curve where air isbest moved at a given frequency.
Between-manoeuvre evaluationThe subject should perform a minimum of two acceptablemanoeuvres. There are no clinical studies addressing repeat-ability; however, additional trials should be considered whenthe variability between acceptable manoeuvres exceeds 20%.
Test result selectionThe highest acceptable MVV (L?min-1 BTPS) and MVV rate(breaths?min-1) should be reported. An MVV/(406FEV1),0.80 indicates that the MVV is low relative to the FEV1,and suggests disease or poor effort. Volume versus timetracings from at least two acceptable manoeuvres should beretained and available for inspection.
TECHNICAL CONSIDERATIONSMinimal recommendations for spirometry systemsAccurate results require accurate equipment. Spirometer equip-ment recommendations apply to all spirometers and are minimalrequirements. In some circumstances, it may be appropriateto exceed these requirements (i.e. in some research/surveillance applications). Instrumentation recommendationsshould be followed to provide accurate spirometric data andinformation that is comparable from laboratory to laboratory andfrom one time period to another [1]. The accuracy of a spirometrysystem depends on characteristics of the entire system, from thevolume or flow transducer and the use of an in-line filter, tothe recorder, display or processor. Changes in any aspect ofthe equipment or errors at any step in the process can affect theaccuracy of the results. For example, if the BTPS correction factoris wrong, an accurately measured FVC will be incorrectlyreported.
M.R. MILLER ET AL. STANDARDISATION OF SPIROMETRY
cEUROPEAN RESPIRATORY JOURNAL VOLUME 26 NUMBER 2 331
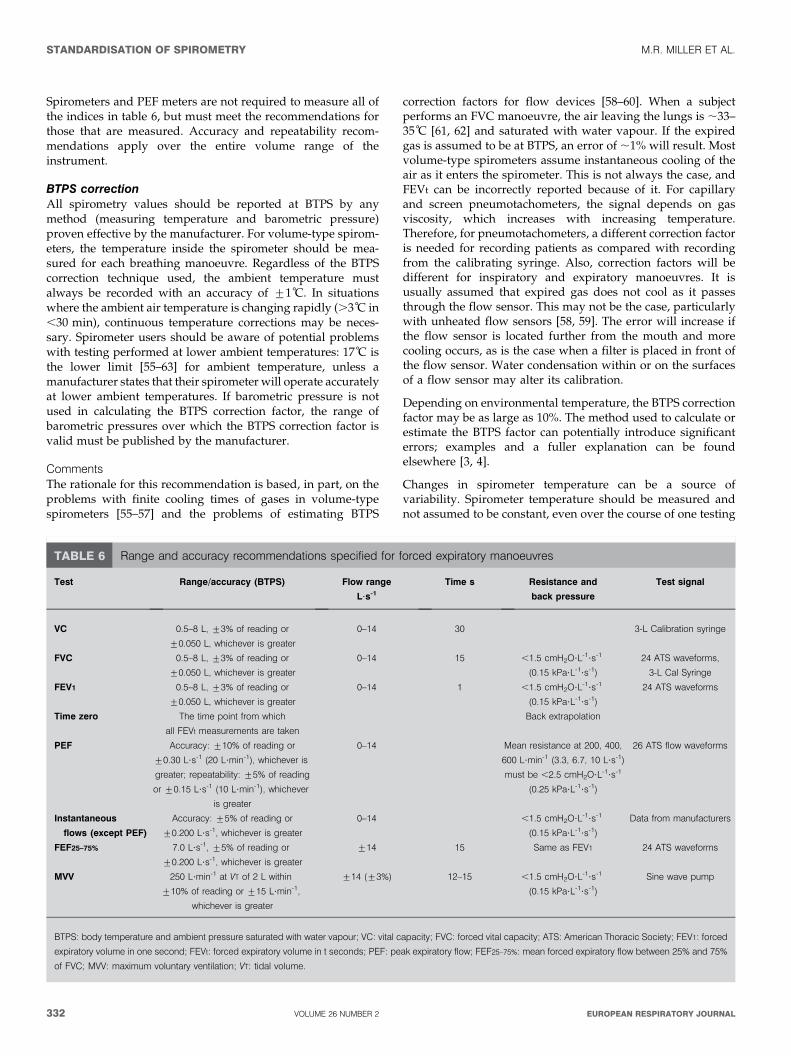
Spirometers and PEF meters are not required to measure all ofthe indices in table 6, but must meet the recommendations forthose that are measured. Accuracy and repeatability recom-mendations apply over the entire volume range of theinstrument.
BTPS correctionAll spirometry values should be reported at BTPS by anymethod (measuring temperature and barometric pressure)proven effective by the manufacturer. For volume-type spirom-eters, the temperature inside the spirometer should be mea-sured for each breathing manoeuvre. Regardless of the BTPScorrection technique used, the ambient temperature mustalways be recorded with an accuracy of ¡1 C. In situationswhere the ambient air temperature is changing rapidly (.3 C in,30 min), continuous temperature corrections may be neces-sary. Spirometer users should be aware of potential problemswith testing performed at lower ambient temperatures: 17 C isthe lower limit [55–63] for ambient temperature, unless amanufacturer states that their spirometer will operate accuratelyat lower ambient temperatures. If barometric pressure is notused in calculating the BTPS correction factor, the range ofbarometric pressures over which the BTPS correction factor isvalid must be published by the manufacturer.
CommentsThe rationale for this recommendation is based, in part, on theproblems with finite cooling times of gases in volume-typespirometers [55–57] and the problems of estimating BTPS
correction factors for flow devices [58–60]. When a subjectperforms an FVC manoeuvre, the air leaving the lungs is ,33–35 C [61, 62] and saturated with water vapour. If the expiredgas is assumed to be at BTPS, an error of ,1% will result. Mostvolume-type spirometers assume instantaneous cooling of theair as it enters the spirometer. This is not always the case, andFEVt can be incorrectly reported because of it. For capillaryand screen pneumotachometers, the signal depends on gasviscosity, which increases with increasing temperature.Therefore, for pneumotachometers, a different correction factoris needed for recording patients as compared with recordingfrom the calibrating syringe. Also, correction factors will bedifferent for inspiratory and expiratory manoeuvres. It isusually assumed that expired gas does not cool as it passesthrough the flow sensor. This may not be the case, particularlywith unheated flow sensors [58, 59]. The error will increase ifthe flow sensor is located further from the mouth and morecooling occurs, as is the case when a filter is placed in front ofthe flow sensor. Water condensation within or on the surfacesof a flow sensor may alter its calibration.
Depending on environmental temperature, the BTPS correctionfactor may be as large as 10%. The method used to calculate orestimate the BTPS factor can potentially introduce significanterrors; examples and a fuller explanation can be foundelsewhere [3, 4].
Changes in spirometer temperature can be a source ofvariability. Spirometer temperature should be measured andnot assumed to be constant, even over the course of one testing
TABLE 6 Range and accuracy recommendations specified for forced expiratory manoeuvres
Test Range/accuracy (BTPS) Flow range
L?s-1
Time s Resistance and
back pressure
Test signal
VC 0.5–8 L, ¡3% of reading or
¡0.050 L, whichever is greater
0–14 30 3-L Calibration syringe
FVC 0.5–8 L, ¡3% of reading or
¡0.050 L, whichever is greater
0–14 15 ,1.5 cmH2O?L-1?s-1
(0.15 kPa?L-1?s-1)
24 ATS waveforms,
3-L Cal Syringe
FEV1 0.5–8 L, ¡3% of reading or
¡0.050 L, whichever is greater
0–14 1 ,1.5 cmH2O?L-1?s-1
(0.15 kPa?L-1?s-1)
24 ATS waveforms
Time zero The time point from which
all FEVt measurements are taken
Back extrapolation
PEF Accuracy: ¡10% of reading or
¡0.30 L?s-1 (20 L?min-1), whichever is
greater; repeatability: ¡5% of reading
or ¡0.15 L?s-1 (10 L?min-1), whichever
is greater
0–14 Mean resistance at 200, 400,
600 L?min-1 (3.3, 6.7, 10 L?s-1)
must be ,2.5 cmH2O?L-1?s-1
(0.25 kPa?L-1?s-1)
26 ATS flow waveforms
Instantaneous
flows (except PEF)
Accuracy: ¡5% of reading or
¡0.200 L?s-1, whichever is greater
0–14 ,1.5 cmH2O?L-1?s-1
(0.15 kPa?L-1?s-1)
Data from manufacturers
FEF25–75% 7.0 L?s-1, ¡5% of reading or
¡0.200 L?s-1, whichever is greater
¡14 15 Same as FEV1 24 ATS waveforms
MVV 250 L?min-1 at VT of 2 L within
¡10% of reading or ¡15 L?min-1,
whichever is greater
¡14 (¡3%) 12–15 ,1.5 cmH2O?L-1?s-1
(0.15 kPa?L-1?s-1)
Sine wave pump
BTPS: body temperature and ambient pressure saturated with water vapour; VC: vital capacity; FVC: forced vital capacity; ATS: American Thoracic Society; FEV1: forced
expiratory volume in one second; FEVt: forced expiratory volume in t seconds; PEF: peak expiratory flow; FEF25–75%: mean forced expiratory flow between 25% and 75%
of FVC; MVV: maximum voluntary ventilation; VT: tidal volume.
STANDARDISATION OF SPIROMETRY M.R. MILLER ET AL.
332 VOLUME 26 NUMBER 2 EUROPEAN RESPIRATORY JOURNAL

session. For volume spirometers, errors up to 6% in FEV1 andFVC can occur if ambient temperature is used instead ofinternal spirometer temperature [64]. For volume spirometers,the temperature inside the spirometer should be measured foreach breathing manoeuvre.
Test signals for spirometer testingThe diversity of FVC manoeuvres encountered in clinicalpractice is currently best simulated by the 24 standard volume–time waveforms developed by the ATS [3] and HANKINSON andGARDNER [65]. These waveforms can be used to drive acomputer-controlled mechanical syringe, or its equivalent, fortesting actual hardware and software [66, 67], or, when put in adigital form, they can evaluate only the software. Computer-controlled mechanical syringes (i.e. pump systems) used forvalidation should be accurate within ¡50 mL, which is 0.5% oftheir full range up to 10 L for FVC and FEV1. Pump systemsmay have accuracy values better than this for many profiles,but reproduce less accurately those test profiles with short DTsand RTs to peak flow [68, 69]. The ATS spirometry statement[3] shows the measured values for each of the 24 standardwaveforms. On request, the ATS can provide these waveformsin an electronic format. Appropriate corrections for using gasat the ambient temperature and humidity instead of BTPS mayneed to be made for some mechanical syringe–spirometercombinations.
MethodA production spirometer is connected to the pump system fortesting, orientated as it would be to test human subjects.Connecting tubing must be kept to the minimum (,0.300 L)and must not be distensible. If an in-line filter is required fortesting human subjects, one must be included when theinstrument is tested. Each of the 24 ATS waveforms isdischarged into the spirometer five times under ambientconditions, and all of the readings are recorded.
BTPS conditions are simulated by discharging waveforms 1–4to the spirometer three times, using air heated to 37¡1 C andat .98% relative humidity. The time between each of the threetests should be ,2 min.
Accuracy testThe average of the five tests under ambient conditions iscompared with the standard value in the following way:
Deviation~average{standard ð1Þ
Percentage deviation~100|(average{standard)=standard ð2Þ
The accuracy validation limits for volumes, which include the
waveform-generator inaccuracy, are ¡3.5% of reading or
¡0.100 L, whichever is greater. An accuracy error occurs if
the deviation (for volumes ,2.857 L) or percentage deviation
(for volumes .2.857 L) exceed these limits. These limits
include the allowable inaccuracy of the pump system.
Acceptable spirometer performance is defined as fewer thanthree accuracy errors for either FVC or FEV1 across the 24waveforms (,5% error rate).
The average FVC and FEV1 values of the three tests simulatingBTPS conditions are compared with the standard values. The
validation limits for these tests under BTPS conditions are¡4.5% or 0.200 L, whichever is the greater, and these limitsinclude the allowable inaccuracy for the pump system.
Acceptable spirometer performance under BTPS conditions isdefined as the accuracy requirement being met for all of thefour profiles used.
Repeatability testThe FEV1 and FVC data from the accuracy test are used toderive the span of the five recordings:
Span~maximum�minimum ð3Þ
Percentage span~100|span=average ð4Þ
The repeatability validation limits for the volume measured atambient conditions are ¡3.5% or ¡0.100 L, whichever isthe greater, and, for BTPS conditions, ¡4.5% or ¡0.200 L,whichever is the greater. A repeatability error occurs if thespan (for volumes ,2.857 L at ambient or 4.444 L at BTPS) orpercentage span (for volumes above this) exceeds these limits.
Acceptable spirometer performance for repeatability underambient conditions is defined as fewer than three accuracyerrors for either FVC or FEV1 across the 24 profiles (,5% errorrate). For BTPS conditions, the acceptable spirometer perfor-mance for repeatability is defined as the accuracy requirementbeing met for all of the four profiles.
Test signals for PEF meter testingThe 26 flow–time ATS waveforms were chosen to represent arange of PEF profiles suitable for delivery by mechanicalsyringe or pump systems to test PEF meters [3]. The range ofprofiles and method of delivery may need to be revised, asresearch on PEF measurement continues [45]. The mechanicalsyringe or suitable pump system used to validate PEFmeasuring equipment must have an accuracy of ¡2% indelivering PEF. Pump systems may have difficulty meetingthis accuracy standard for profiles more demanding than theset of 26 [68, 69]. Recent evidence suggests that the frequencycontent in the first second of the blow that contributes to PEF ishigher [47] than previously determined [70, 71]. The 26waveforms may not cover the range of RT and DT found in,25% of the client population [72], and, hence, moredemanding test profiles may be required in future [45].
MethodTwo randomly chosen production models of the flow metersshould each have the 26 waveforms delivered to them fivetimes under ambient conditions and the readings recorded.Any waveforms with a PEF outside the meter’s statedoperational range would not be included in the testingsequence. Appropriate correction factors for testing underambient conditions should be applied as recommended by themanufacturer.
Accuracy testThe average reading for each of the two meters is comparedwith the standard, as for volumes.
The accuracy validation limits are ¡12% or ¡25 L?min-1,whichever is the larger, and these limits include the 2%inaccuracy limit for the waveform generator. An accuracy error
M.R. MILLER ET AL. STANDARDISATION OF SPIROMETRY
cEUROPEAN RESPIRATORY JOURNAL VOLUME 26 NUMBER 2 333

for a given meter and given waveform occurs if the deviationand percentage deviation exceed these limits.
Acceptable performance is defined as fewer than threeaccuracy errors out of the total of 52 tests (26 waveforms,two meters).
Repeatability testFlow waveforms 1, 4, 8 and 25 are discharged three times toeach of 10 production meters. The repeatability validationlimits are ¡6% or ¡15 L?min-1, whichever is the greater, andthese limits include 1% for waveform-generator variability. Arepeatability error occurs if the span and percentage spanexceed these limits.
Acceptable performance is defined as six or fewer errors in the120 tests (i.e. maximum error rate of 5%).
Test signals for MVV testingA spirometry system used to measure MVV should be testedunder ambient conditions with a pump producing a sinusoidalwaveform, with stroke volumes up to 2 L using the fourpatterns of delivery previously specified [3]. Testing at BTPS isnot required, and each pattern is tested twice. The accuracyvalidation limits of the spirometer used for measuring MVVwith flows up to 250 L?min-1 are ¡10.5% of reading or¡20 L?min-1, whichever is greater. The pressure at themouthpiece must not exceed ¡10 cmH2O (1 kPa) at any pointduring MVV testing. These requirements apply to volumespirometers throughout their volume range.
Acceptable performance is defined as no errors in the eighttests (four patterns, twice).
ABBREVIATIONSTable 7 contains a list of abbreviations and their meanings,which will be used in this series of Task Force reports.
TABLE 7 List of abbreviations and meanings
ATPD Ambient temperature, ambient pressure, and dry
ATPS Ambient temperature and pressure saturated with water vapour
BTPS Body temperature (i.e. 37 C), ambient pressure, saturated with
water vapour
C Centigrade
CFC Chlorofluorocarbons
cm Centimetres
COHb Carboxyhaemoglobin
DL,CO Diffusing capacity for the lungs measured using carbon
monoxide, also known as transfer factor
DL,CO/VA Diffusing capacity for carbon monoxide per unit of alveolar
volume, also known as KCO
DM Membrane-diffusing capacity
DT Dwell time of flow .90% of PEF
EFL Expiratory flow limitation
ERV Expiratory reserve volume
EV Back extrapolated volume
EVC Expiratory vital capacity
FA,X Fraction of gas X in the alveolar gas
FA,X,t Alveolar fraction of gas X at time t
FEF25-75% Mean forced expiratory flow between 25% and 75% of FVC
FEFX% Instantaneous forced expiratory flow when X% of the FVC has
been expired
FEV1 Forced expiratory volume in one second
FEVt Forced expiratory volume in t seconds
FE,X Fraction of expired gas X
FIFX% Instantaneous forced inspiratory flow at the point where X% of the
FVC has been inspired
FI,X Fraction of inspired gas X
FIVC Forced inspiratory vital capacity
FRC Functional residual capacity
FVC Forced vital capacity
H2O Water
Hb Haemoglobin
Hg Mercury
Hz Hertz; cycles per second
IC Inspiratory capacity
IVC Inspiratory vital capacity
KCO Transfer coefficient of the lung (i.e.DL,CO/VA)
kg Kilograms
kPa Kilopascals
L Litres
L?min-1 Litres per minute
L?s-1 Litres per second
lb Pounds weight
MEFX% Maximal instantaneous forced expiratory flow where X% of the
FVC remains to be expired
MFVL Maximum flow–volume loop
mg Milligrams
MIF Maximal inspiratory flow
mL Millilitres
mm Millimetres
MMEF Maximum mid-expiratory flow
ms Milliseconds
MVV Maximum voluntary ventilation
PA,O2 Alveolar oxygen partial pressure
PB Barometric pressure
PEF Peak expiratory flow
PH2O Water vapour partial pressure
PI,O2 Inspired oxygen partial pressure
h (theta) Specific uptake of CO by the blood
RT Rise time from 10% to 90% of PEF
RV Residual volume
s Seconds
STPD Standard temperature (273 K, 0 C), pressure (101.3 kPa,
760 mmHg) and dry
TB Tuberculosis
TGV (or VTG) Thoracic gas volume
tI Time taken for inspiration
TLC Total lung capacity
Tr Tracer gas
ttot Total time of respiratory cycle
VA Alveolar volume
VA,eff Effective alveolar volume
VC Vital capacity
Vc Pulmonary capillary blood volume
VD Dead space volume
VI Inspired volume
VS Volume of the expired sample gas
mg Micrograms
TABLE 7 (Continued)
STANDARDISATION OF SPIROMETRY M.R. MILLER ET AL.
334 VOLUME 26 NUMBER 2 EUROPEAN RESPIRATORY JOURNAL

APPENDIXProposal for a standard data format for spirometryThis proposal would not preclude the use of other dataformats, but would require that a spirometer should at least beable to output data in the required format. The advantage of astandard format is the ease of moving data into datarepositories, such as quality control, healthcare and researchdatabases. It should simplify and reduce the cost of datatransfer when users change instrument models and manufac-turers. Easier transfer of data into healthcare databases has thepotential for improving the utility of lung function by makingmore complete data readily available to clinicians andhealthcare researchers. In research and clinical settings, astandard data format should simplify and reduce the cost oftransferring data into quality control software and couldcontribute to improved overall test quality. Finally, it is timefor this change; pulmonary function is one of the last medicalarenas without a standard data format.
Proposed formatThe spirometry data file will consist of an American StandardCode for Information Interchange, comma-delineated file withvariable length records. Comma-delineated text files are easilygenerated and are standard import formats for severaldatabase programs. Although some redundancies will exist,each record shall represent one curve and will be terminatedwith a carriage return and line feed. The ATS will distributeexamples of this data format from their web site.
Table 8 shows a list of parameters that must be included inevery record. If a parameter is unavailable, the space mustremain blank (‘‘,,’’). The flow–time data points must beprovided with a sampling interval of 0.01 s (100 samples?s-1)in mL?s-1. If necessary, interpolation or other techniques must
TABLE 8 List of parameters#
ID (patient identification)
Patient name
Data type (SP followed by E5expiratory or I5Inspiratory, followed by S5single
or B5best curve)
Barometric pressure (mmHg)
Temperature ( C) used in BTPS calculation
Relative humidity (%)
FVC quality attribute (A, B, C, D or F)
FEV1 quality attribute (A, B, C, D or F)
Effort attribute (A, B, C, D or F)
Interpretation code (see ATS interpretation scheme)
Deleted manoeuvre (Y or N)
Acceptable manoeuvre (Y or N)
Technician quality control code (A, B, C, D or F)
Computer quality code (A, B, C, D or F)
Plateau achieved (Y or N)
Review (N or R for ‘‘needs review’’ or ‘‘was reviewed’’)
Date of review (DD/MM/YYYY)
Reviewer initials
BTPS factor (x.xxx)
Spirometer manufacturer
Spirometer model
Spirometer serial number
Spirometer type
Testing facility name
City
State/region
Zip/post code
Country
Phone number
Calibration date (DD/MM/YYYY)
Calibration time (HH:MM)
Calibration result (P or F for ‘‘passed’’ or ‘‘failed’’)
Date (DD/MM/YYYY)
Time (HH:MM)
Technician ID (technician identification code or initials)
Manoeuvre number
Age (integer years)
Height (cm)
Weight (kg)
Sex (M or F)
Race (2-character race code)
Date of birth (DD/MM/YYYY)
Reference values source (first author surname and date of publication, e.g.
‘‘Knudson 1983’’)
Reference values correction factor (x.xx, 1.00 for no correction)
Testing position (standing, sitting or supine)
Test type (pre-, post-, bronchodilator, methacholine concentration or dose)
FVC (mL)
Extrapolated volume (mL)
FEV1 (mL)
FEV6 (mL)
PEF (mL?s-1)
FEF25–75% (mL?s-1)
VC (mL)
Forced expiratory time (s)
Time to PEF (ms)
Predicted FVC (mL)
Predicted FEV1 (mL)
Predicted FEV6 (mL)
Predicted FEV1/FVC% (xxx.x%)
Predicted FEV1/FEV6% (xxx.x%)
Comments text
Original sampling interval (ms)
Blank 1 or FEF25%
Blank 2 or FEF50%
Blank 3 or FEF75%
Blank 4 or FEF90%
Blank 5
Blank 6
Blank 7
Blank 8
Blank 9
Blank 10
Number of data points
Flow data points (mL?s-1; variable number contained in number of data points)
Carriage return
Line feed
#: All text type variables should be enclosed with double quotes (‘‘) to prevent
confusion with control or data separator type characteristics.
TABLE 8 (Continued)
M.R. MILLER ET AL. STANDARDISATION OF SPIROMETRY
cEUROPEAN RESPIRATORY JOURNAL VOLUME 26 NUMBER 2 335
ACKNOWLEDGEMENTSM.R. Miller: University Hospital Birmingham NHS Trust,Birmingham, UK; J. Hankinson: Hankinson Consulting, Inc.,Valdosta, GA, USA; V. Brusasco: Universita degli Studi diGenova, Genova, Italy; F. Burgos: Hospital Clinic Villarroel,Barcelona, Spain; R. Casaburi: Harbor UCLA MedicalCenter, Torrance, CA, USA; A. Coates: Hospital for SickChildren, Toronto, ON, Canada; R. Crapo and R. Jensen:LDS Hospital, Salt Lake City, UT, USA; P. Enright: 4460E Ina Rd, Tucson, AZ, USA; C.P.M. van der Grinten:University Hospital of Maastrict, Maastricht, theNetherlands; P. Gustafsson: Queen Silvias Children’sHospital, Goteborg, Sweden; D.C. Johnson: MassachusettsGeneral Hospital and Harvard Medical School, Boston, MA,USA; N. MacIntyre: Duke University Medical Center,Durham, NC, USA; R. McKay: Occupational Medicine,Cincinnati, OH, USA: D. Navajas: Universitat de Barcelona- IDIBAPS, Barcelona, Spain; O.F. Pedersen: University ofAarhus, Aarhus, Denmark; R. Pellegrino: AziendaOspedaliera S. Croce e Carle, Cuneo, Italy; G. Viegi: CNRInstitute of Clinical Physiology, Pisa, Italy; J. Wagner:Pharmaceutical Research Associates, Inc., Lenexa, KS, USA.
REFERENCES1 Renzetti AD Jr. Standardization of spirometry. Am Rev
Respir Dis 1979; 119: 831–838.2 American Thoracic Society. Standardization of spirometry:
1987 update. Am Rev Respir Dis 1987; 136: 1285–1298.3 American Thoracic Society. Standardization of spirometry,
1994 update. Am J Respir Crit Care Med 1995; 152:1107–1136.
4 Quanjer PH, ed. Standardized lung function testing.Report Working Party Standardization of Lung FunctionTests. European Community for Coal and Steel. Bull EurPhysiopathol Respir 1983; 19: Suppl. 5, 1–95.
5 Quanjer PH, Tammeling GJ, Cotes JE, Pedersen OF,Peslin R, Yernault J-C. Lung volume and forced ventilatoryflows. Report Working Party Standardization of LungFunction Tests, European Community for Steel and Coal.Official Statement of the European Respiratory Society. EurRespir J 1993; 6: Suppl. 16, 5–40.
6 Morgan KC. The assessment of ventilatory capacity(committee recommendations). Chest 1975; 67: 95–97.
7 Gardner RM, Crapo RO, Billings RG, Shigeoka JW,Hankinson JL. Spirometry: what paper speed? Chest 1983;84: 161–165.
8 Gardner RM, Clausen JL, Crapo RO, et al. Qualityassurance in pulmonary function laboratories. Am RevRespir Dis 1986; 134: 626–627.
9 Morris AH, Kanner RE, Crapo RO, Gardner RM. Clinicalpulmonary function testing: a manual of uniform labora-tory procedures. 2nd Edn. Salt Lake City, UT,Intermountain Thoracic Society, 1984.
10 Townsend MC. The effects of leaks in spirometers onmeasurement of pulmonary function. J Occup Med 1984; 26:835–841.
11 Association for the Advancement of MedicalInstrumentation, Standard for spirometers (draft),October 1980. AAMI Suite 602, 1901 N. Ft. Myer Drive,Arlington, VA 22209–1699.
12 D’Angelo E, Prandi E, Milic-Emili J. Dependence ofmaximal flow-volume curves on time course of precedinginspiration. J Appl Physiol 1993; 75: 1155–1159.
13 Stoller JK, Basheda S, Laskowski D, Goormastic M,McCarthy K. Trial of standard versus modified expirationto achieve end-of-test spirometry criteria. Am Rev RespirDis 1993; 148: 275–280.
14 Bucca CB, Carossa S, Colagrande P, et al. Effect ofedentulism on spirometric tests. Am J Respir Crit CareMed 2001; 163: 1018–1020.
15 Eigen H, Bieler H, Grant D, et al. Spirometric pulmonaryfunction in healthy preschool children. Am J Respir CritCare Med 2001; 163: 619–623.
16 Smith AA, Gaensler EA. Timing of forced expiratoryvolume in one second. Am Rev Respir Dis 1975; 112:882–885.
17 Horvath EP Jr, ed. Manual of spirometry in occupationalmedicine. Division of Training and ManpowerDevelopment, National Institutes for Occupational Safetyand Health. Cincinnati, NIOSH, 1981.
18 Hankinson JL, Gardner RM. Standard waveforms forspirometer testing. Am Rev Respir Dis 1982; 126: 362–364.
19 Aurora P, Stocks J, Oliver C, et al. Quality control forspirometry in preschoolchildren with and without lungdisease. Am J Crit Care Med 2004; 169: 1152–1159.
20 Desmond KJ, Allen PD, Demizio DL, Kovesi T, Coates AL.Redefining end of test (EOT) criteria for pulmonaryfunction testing in children. Am J Respir Crit Care Med1997; 156: 542–545.
21 Hankinson JL, Bang KM. Acceptability and reproducibilitycriteria of the American Thoracic Society as observed in asample of the general population. Am Rev Respir Dis 1991;143: 516–521.
22 Ferris BG Jr, Speizer FE, Bishop Y, Prang G, Weener J.Spirometry for an epidemiologic study: deriving optimumsummary statistics for each subject. Bull Eur PhysiopatholRespir 1978; 14: 146–166.
23 Kanner RE, Schenker MB, Munoz A, Speizer FE.Spirometry in children: methodology for obtaining optimalresults for clinical and epidemiological studies. Am RevRespir Dis 1983; 127: 720–724.
24 Swanney MP, Jensen RL, Crichton DA, Beckert LE,Cardno LA, Crapo RO. FEV(6) is an acceptable surrogatefor FVC in the spirometric diagnosis of airway obstructionand restriction. Am J Respir Crit Care Med 2000; 162:917–919.
25 Paoletti P, Pistelli G, Fazzi P, et al. Reference values forvital capacity and flow-volume curves from a generalpopulation study. Bull Eur Physiopathol Respir 1986; 22:451–459.
be used to provide the 0.01-s sampling interval. The recordlength will vary, depending on the number of data pointspresent in the flow–time portions of the record. The curve datamust include o0.25 s of data points prior to the onset of theinspiratory or expiratory manoeuvre.
Volume–time curves may be calculated by adding the flow–time values (mL?s-1) and multiplying the sum by 0.01 s. Toobtain the highest precision, the sum of the flow values shouldbe calculated for each volume data point before multiplying by0.01 s.
STANDARDISATION OF SPIROMETRY M.R. MILLER ET AL.
336 VOLUME 26 NUMBER 2 EUROPEAN RESPIRATORY JOURNAL

26 Pellegrino R, Viegi G, Enright P, et al. Interpretativestrategies for lung function tests. Eur Respir J 2005 (Inpress).
27 Coates AL, Allen PD, MacNeish CF, Ho SL, Lands LC.Effect of size and disease on expected deposition of drugsadministered using jet nebulization in children with cysticfibrosis. Chest 2001; 119: 1123–1130.
28 Coates AL, Ho SL. Drug administration by jet nebulization.Pediatr Pulmonol 1998; 26: 412–423.
29 Newman SP, Clark AR, Talaee N, Clark SW. Pressurizedaerosol deposition in the human lung with and without an‘‘open’’ spacer device. Thorax 1989; 44: 706–710.
30 Tal A, Golan H, Grauer N, Aviram M, Albin D,Quastel MR. Deposition pattern of radiolabeled salbutamolinhaled from a meter-dose inhaler by means of a spacerwith mask in young children with airway obstruction. JPediatr 1996; 128: 479–484.
31 Newhouse MT. Asthma therapy with aerosols: arenebulizers obsolete? A continuing controversy. J Pediatr1999; 135: 5–8.
32 Coates AL, MacNeish CF, Lands LC, Meisner D,Kelemen S, Vadas EB. A comparison of the availability oftobramycin for inhalation from vented versus unventednebulizers. Chest 1998; 113: 951–956.
33 Devadason SG, Everard ML, Linto JM, LeSouef PN.Comparison of drug delivery form conventional versus‘‘Venturi’’ nebulizers. Eur Respir J 1997; 10: 2479–2483.
34 Leach CL, Davidson PJ, Hasselquist BE, Boudreau RJ.Lung deposition of hydofluoroalkane-134a beclometha-sone is greater than that of chlorofluorocarbon fluticasoneand chlorofluorocarbon beclomethasone: a cross-overstudy in healthy volunteers. Chest 2002; 122: 510–516.
35 Wildhaber JH, Devadason SG, Hayden MJ, Elber E,Summers QA, LeSouef PN. Aerosol delivery to wheezyinfants: a comparison between a nebulizer and two smallvolume spacers. Pediatr Pulmonol 1997; 23: 212–216.
36 Guidelines for the measurement of respiratory function.Recommendations of the British Thoracic Society and theAssociation of Respiratory Technicians and Physiologists.Respir Med 1994; 88: 165–194.
37 Babb TG, Viggiano R, Hurley B, Staats B, Rodarte JR. Effectof mild-to-moderate airflow limitation on exercise capa-city. J Appl Physiol 1991; 70: 223–230.
38 O’Donnell DE, Lam M, Webb KA. Spirometric correlates ofimprovement in exercise performance after cholinergictherapy in chronic obstructive pulmonary disease. Am JRespir Crit Care Med 1999; 160: 542–549.
39 Pellegrino R, Rodarte JR, Brusasco V. Assessing thereversibility of airway obstruction. Chest 1998; 114:1607–1612.
40 Pellegrino R, Brusasco V. Lung hyperinflation and flowlimitation in chronic airway obstruction. Eur Respir J 1997;10: 543–549.
41 Younes M, Kivinen G. Respiratory mechanics and breath-ing pattern during and following maximal exercise. J ApplPhysiol 1984; 57: 1773–1782.
42 Wanger J, Clausen JL, Coates A, Pedersen OF.Standardisation of the measurement of lung volumes.Eur Respir J 2005; (In press).
43 Brusasco V, Pellegrino R, Rodarte JR. Vital capacitiesduring acute and chronic bronchoconstriction: dependence
on flow and volume histories. Eur Respir J 1997; 10:1316–1320.
44 Hansen LM, Pedersen OF, Lyager S, Naerra N.[Differences in vital capacity due to the methodsemployed]. Ugerkr Laeger 1983; 145: 2752–2756.
45 Miller MR, Atkins P, Pedersen OF. Inadequate peakexpiratory flow meter characteristics detected by acomputerised explosive decompression device. Thorax2003; 58: 411–416.
46 Quanjer PH, Lebowitz MD, Gregg I, Miller MR,Pedersen OF. Peak expiratory flow: conclusions andrecommendations of the European Respiratory Society.Eur Respir J 1997; 10: Suppl. 24, 2s–8s.
47 Miller MR, Lloyd J, Bright P. Recording flow in the firstsecond of a maximal forced expiratory manoeuvre: influ-ence of frequency content. Eur Respir J 2002; 19: 530–533.
48 Pedersen OF, Rasmussen TR, Omland Ø, Sigsgaard T,Quanjer PH, Miller MR. Peak expiratory flow and theresistance of the mini-Wright peak flow meter. Eur Respir J1996; 9: 828–833.
49 Pedersen OF, Pedersen TF, Miller MR. Gas compression inlungs decreases peak expiratory flow depending onresistance of peak flow meter. J Appl Physiol 1997; 83:1517–1521.
50 Kano S, Burton DL, Lanteri CJ, Sly PD. Determination ofpeak expiratory flow. Eur Respir J 1993; 6: 1347–1352.
51 Ferris BG Jr, Speizer FE, Bishop Y, et al. Spirometry for anepidemiologic study: deriving optimum summary statis-tics for each subject. Bull Eur Physiopathol Respir 1978; 14:145–166.
52 Federal Register, 38:4265, Feb. 12, 1973, Section ofpulmonary function specifications. Washington, DC,United States Government Printing Office.
53 Bernstein L. The effect of the rate of breathing onmaximum breathing capacity determined with a newspirometer. Thorax 1952; 7: 255–262.
54 Miller WF, Johnson RL Jr, Wu N. Relationships betweenmaximal breathing capacity and timed expiratory capa-cities. J Appl Physiol 1959; 14: 510–516.
55 Hankinson JL, Viola JO. Dynamic BTPS correction factorsfor spirometric data. J Appl Physiol 1983; 44: 1354–1360.
56 Hankinson JL, Castellan RM, Kinsley KB, Keimig DG.Effects of spirometer temperature on FEV1 shift changes.J Occup Med 1986; 28: 1222–1225.
57 Pincock AC, Miller MR. The effect of temperature onrecording spirograms. Am Rev Respir Dis 1983; 128: 894–898.
58 Hankinson JL, Viola JO, Petsonk EL, Ebeling TR. BTPScorrection for ceramic flow sensors. Chest 1994; 105:1481–1486.
59 Miller MR, Pincock AC. Linearity and temperature controlof the Fleisch pneumotachograph. J Appl Physiol 1986; 60:710–715.
60 Perks WH, Sopwith T, Brown D, Jones CH, Green M.Effects of temperature on Vitalograph spirometer readings.Thorax 1983; 38: 592–594.
61 Cole P. Recordings of respiratory air temperature. JLaryngol 1954; 68: 295–307.
62 Madan I, Bright P, Miller MR. Expired air temperature atthe mouth during a maximal forced expiratory manoeuvre.Eur Respir J 1993; 6: 1556–1562.
M.R. MILLER ET AL. STANDARDISATION OF SPIROMETRY
cEUROPEAN RESPIRATORY JOURNAL VOLUME 26 NUMBER 2 337

63 Liese W, Warwick WJ, Cumming G. Water vapourpressure in expired air. Respiration 1974; 31: 252–261.
64 Johnson LR, Enright PL, Voelker HT, Tashkin DP. Volumespirometers need automated internal temperature sensors.Am J Respir Crit Care Med 1994; 150: 1575–1580.
65 Hankinson JL, Gardner RM. Standard waveforms forspirometer testing. Am Rev Respir Dis 1982; 126: 362–364.
66 Nelson SB, Gardner RM, Crapo RO, Jensen RL.Performance evaluation of contemporary spirometers.Chest 1990; 97: 288–297.
67 Gardner RM, Hankinson JL, West BJ. Evaluating commer-cially available spirometers. Am Rev Respir Dis 1986; 134:626–627.
68 Hankinson JL, Reynolds JS, Das MK, Viola JO. Method toproduce American Thoracic Society flow–time waveformsusing a mechanical pump. Eur Respir J 1997; 10: 690–694.
69 Miller MR, Jones B, Xu Y, Pedersen OF, Quanjer PH. Peakexpiratory flow profiles delivered by pump systems:limitations due to wave action. Am J Respir Crit Care Med2000; 162: 1887–1896.
70 Peslin R, Jardin P, Bohadana A, Hannhart B. Contenuharmonique du signal de debit pendant l’expiration forceechez l’homme normal [Harmonic content of the flow signalduring forced expiration in normal man]. Bull EurPhysiopath Respir 1982; 18: 491–500.
71 McCall CB, Hyatt RE, Noble FW, Fry DL. Harmoniccontent of certain respiratory flow phenomena of normalindividuals. J Appl Physiol 1957; 10: 215–218.
72 Miller MR, Pedersen OF, Quanjer PH. The rise and dwelltime for peak expiratory flow in patients with and withoutairflow limitation. Am J Respir Crit Care Med 1998; 158:23–27.
STANDARDISATION OF SPIROMETRY M.R. MILLER ET AL.
338 VOLUME 26 NUMBER 2 EUROPEAN RESPIRATORY JOURNAL

Primary Care Asthma Program SPIROMETRY MANUAL Resource Links:
ATS:
ATS Standardization of Spirometry 2019 Update:
https://www.atsjournals.org/doi/pdf/10.1164/rccm.201908-1590ST
ATS/ERS Task Force Standardisation of Lung Function Testing: Standardisation of spirometry (2005):
https://www.thoracic.org/statements/resources/pft/PFT2.pdf
ATS/ERS Task Force Standardisation of Lung Function Testing: General considerations for lung function
testing (2005): https://www.thoracic.org/statements/resources/pft/PFT1.pdf
ATS/ERS Task Force Standardisation of Lung Function Testing: Interpretative strategies for lung function
tests (2005): https://www.thoracic.org/statements/resources/pft/pft5.pdf
ATS/ERS Task Force Standardisation of Lung Function Testing: Standardisation of the measurement of
lung volumes (2005): https://www.thoracic.org/statements/resources/pft/pft3.pdf
ATS/ERS Recommendations for a Standardized Pulmonary Function Report (2017):
https://www.thoracic.org/statements/resources/pft/standardized-pulmonary-function-report.pdf
CPSO:
Independent Health Facilities: Assessment Protocol for Pulmonary Function Studies - Technologist
Assessor https://www.cpso.on.ca/CPSO/media/Documents/physician/your-practice/quality-in-
practice/clinic-inspections-special-programs/ihf-general-assessment-tools/pulmonary-function/ihf-
pulmonary-function-pft-checklist-tech.pdf
Independent Health Facilities Clinical Practice Parameters and Facility Standards: Pulmonary Function
Studies – http://policyconsult.cpso.on.ca/wp-content/uploads/2014/04/Final-Draft-February-2014.pdf
CTS:
Spirometry in Primary Care:
http://www.respiratoryguidelines.ca/sites/all/files/CTS_Spirometry_Primary_Care_2013.pdf
Practicum:
Lung Health Foundation Education Workshops, Events and E-Modules:
https://hcp.lunghealth.ca/events/
Resptrec Spirotrec course:
https://www.resptrec.org/course/spirometry.php?&currMenu=Spirometry
Copyright © 2022 FDOKUMEN