Ultrasound Lung Comets: A Clinically Useful Sign of Extravascular Lung Water

PRELIMINARY REPORT OF THE LUNG CANCER DETECTION PROGRAM IN NEW YORK
MYRON MELAMED, MD,* BETTY FLEHINCER, PHD,+ DANIEL MILLER, MD,* RAYMOND OSBORNE, MD,* MUHAMMAD ZAMAN, MD,* CAROLYN MCGINNIS, BA,*
AND NAEL MARTINI, MD*
The early lung cancer detection program in New York is described, and prelim- inary prevalence rate data are reported. Cigarette-smoking men over the age of 45, who are considered at high risk, are encouraged to enroll in the program and, to date, 6,612 have done so. These men receive P A and lateral chest x-rays annually, while a randomly selected sub-population of about half also have sputum cytology every four months. A controlled study of sputum cytology as an adjunct to the chest x-ray is now in progress. There were 15 cases of late lung cancer (pathologic stages I1 and 111) detected at the initial examination, and 11 early cases (pathologic stages 0 and I). In the population of 3,387 men who had x-rays alone there were three early lung cancers detected; in the population of 3,225 men who had both examinations four early cancers were detected by x- ray and four by cytology. In addition, three cases of larynx cancer were detected by cytology. The early lung cancers detected by x-ray were peripheral and most were bronchiolar or adenocarcinoma; the early cancers detected by cytology were central epidermoid carcinoma of major bronchi. No early carcinomas were detected by both techniques. These findings suggest that a combination of chest x-rays and sputum cytology can be more effective than either one alone in detecting early lung cancer.
Cancer 39:369-382, 1977.
YMPTOMATIC LUNG CANCER IS LATE LUNG CAN- S cer, and overall survival from the disease in this country is less than Once considered rare, it is now the most common cause of death from cancer in men, and the number of new cases each year is continuing to increa~e. '~~~' ' Except for oat celI carcinoma, the treatment of choice is surgical and the probability of survival is closely related to the stage of disease.' At present, two techniques are available for the detection of lung cancer at an early and poten- tially curable, asymptomatic stage-the chest
Presented in part at the 29th Annual hieeting of the Society of Surgical Oncology (James Ewing Society). April 1976.
* From the Cytology Service, Department of Pathology; Thoracic Surgical Service (Dr. Martini); and Department of Radiology (Dr. Osborne); Memorial Sloan-Kettering Can- cer Center, New York, New York; and ' IBM Thomas J . Watson Research Center, Yorktown Heights, New York; and 8 Preventive hledicine Institute-Strang Clinic, New York, New York.
Supported by Research Contract No. N-01-CN-45007 rrom the National Cancer Institute.
Address for reprints: Myron R. Melamed, M.D., 1275 York Avenue. New York, New York 10021.
We wish TO thank hlonica Grumberg and Mollie Colgan for their help in the program management and data han- dling, Joan Puccia for supervision of cytologic preparations and examinations, and ,Joan Rothman for supervision of radiologic examinations.
Received for publication October 15, 1976.
roentgenogram and sputum cytology. Mass sur- veys by chest x-rays alone have only slig tly
experience with sputum cytology in the detec- tion of early or unsuspected lung cancer-kas been largely anecdotal or limited to small col-
studies by a combination of roentgenologic and cytologic screening enhanced the number of cases detected, and drew attention to the com- plementary nature of the chest x-ray and spu- tum cytology. 10.14
In 1971, a program was undertaken by the National Cancer Institute to determine whether systematic, periodic examinations of sputum cy- tology, supplementing the chest x-ray, could lead to a significant reduction in the death rate from lung cancer in a selected population at high risk. Participants in the program, who have come to be called the "Cooperative Early Lung Cancer Group," now include the Mayo Founda- tion, Johns Hopkins University and Memorial Sloan-Kettering Cancer Center, with the Uni- versity of Cincinnati as statistical center. A de- tailed description of the program has been pub- lished by the group," and preliminary results of the study have been reported from the Mayo Foundation 83s,'5*33 and Johns Hopkins Univer- sity.3'16.L7This is a report of the program to date at Memorial Sloan-Kettering Cancer Center.
altered lung cancer mortality while t he
lected series of cases. 11,13.15.18.18.22.23.a1,32 Pilot
369

370 CANCER February 1977 Vol. 39
BIOSTATISTICAL RATIONALE
Among the general population the risk of lung cancer increases with increasing age, 20~2637~30 is greater in cigarette smokers than non- smokers,12*28.s4 and more frequent in men than
~.7,18,27.30 A population of men over 45 years of age who smoke at least one package of cigarettes daily is expected to have 3 to 4 cases of lung cancer per 1,000 man years,” a risk level that is felt to justify an effective screening pro- gram, and this population was chosen for screening by the three institutions.
We were interested in answering three specific questions: 1) Whether sputum cytology every four months, supplementing an annual PA and lateral chest x-ray, would lead to the earlier detection of lung cancer; 2) Whether the early cancers detected by cytology while still radio- logically occult can be consistently localized and treated; and, most important, 3) Whether the death rate from lung cancer can be reduced significantly by this type of screening program. Thus, all members of the population to be screened are randomly allocated into “A” and “B” groups of approximately equal size. The “A” group have sputum cytology every four months in addition to annual PA and lateral chest x-rays; the “B” group have only the an- nual chest x-rays.
The answer to question #3 will be obtained at the end of the study by comparing the number of deaths due to lung cancer in the two groups. I n planning the study, we were interested in find- ing whether there would be a difference in death rates, significant at the .05 level. We assumed that the death rate due to lung cancer for men screened by annual x-rays alone would be ap- proximately 3 per 1000 man years.” If the death rate is lowered by a factor of at least two by including sputum cytology examinations, then we want a .90 probability of detecting a signifi- cant difference in the two groups. Based on these considerations, we require 20,000 man years of observations on each group. The study is expected to go on for five to ten years, and 5,000 to 6,000 men are to be included in each group to allow for losses.
RECRUITMENT
A major effort and much of the cost of this program is devoted to recruitment and to main- taining compliance with the program.
The source of subjects recruited, or the mech- anism by which they were recruited, is listed in
Table 1. The initial, and still the largest single group, enrolled as a result of letters to sub- scribers of Group Health Inc. (G.H.I.) written by Dr. J. Allen Yager, Senior Vice President and Professional Services Coordinator for G. H.I., ex- plaining the program and its benefits to poten- tial participants. A second large group were New York City policemen who enrolled as a result of similar letters written to them by Police Commissioner Michael J. Codd. We also en- listed the aid of John 0. Moore, Director of Motor Vehicle Safety Program Coordination for New York State, to send letters explaining the program to registered motor vehicle operators in the metropolitan New York City area.
Other forms of recruitment included publicity and announcements by the New York City divi- sion of the American Cancer Society; paid no- tices in the New York newspapers, and in par- ticular in the New York Daily News; and reports of the study on local television and radio news and interview shows.
PHYSICAL FACILITIES
All subject-related physical facilities for the National Lung Program (NLP) are located in space that has been made available within the Strang-Preventive Medicine Institute in mid- Manhattan. It is easily accessible by subway and bus, and convenient to anyone working or shopping in New York City. The NLP occupies approximately 4000 square feet of space on the street level floor, divided into: a recep- tion/interview area; waiting area including dressing rooms; x-ray room; sputum induction cubicles; cytology preparation laboratory; stor- age and clerical area; and research laboratory for cytology specimen processing (Fig. I )
SCREENING PROGRAM
All subjects who are eligible for the program, and enter into it, do so on a voluntary basis. They are given specific appointments by mail or telephone. O n arriving, each man is referred to an interviewer who explains the program, rein- forces this with appropriate literature, and ad- vises him of our recommendation to stop smok- ing. He is then given a questionnaire to fill out, which provides us with the following informa- tion:
a) Name, age, date, home address, telephone number, social security number, and the name

No. 2 LUNG CANCER DETECTION Melamed et al. 371
FIG. 1. Floor plan of National Lung Program facility, designed to process a large number of subjects with minimum waiting time.
of a friend or relative who will always know of his whereabouts.
b ) Cigarette smoking history. c) Occupation and place of work. d ) Any known exposure to asbestos, arsenic,
chromium, nickel, iron oxides, chlormethyl ether, or radioactive materials.
e) Prior cancer. f ) Chronic cough; a recent cold, flu or pneu-
monia; asthma or hay fever; tuberculosis, asbes-
TABLE 1. Major Recruitment Sources
Number subjects enrolled
Group Health Incorporated New York City police Motor vehicle registrants Newspaper notices Television Radio Companies/unions Word of mouth and other
TOTAL
1,896 1,116 1,029
99 1 84 1 21 8 105 416
6,612
tosis, silicosis, emphysema; heart disease or high blood pressure.
g) Previous chest x-rays; when and where. h) Previous hospitalization for lung or chest
problem. i) Name and address of personal physician
(optional). Each applicant is also asked to sign a “con-
sent statement” indicating his understanding of the program and voluntary participation in it, and an authorization for release of any prior chest x-rays.
The data are immediately entered into the computer at a remote-entry terminal adjoining the interviewing area. Each individual is rando- mized by computer into “A” (x-ray and sputum cytology) or “ R ” (x-ray only) groups. The “A” subjects are screened by means of PA and lateral chest x-rays annually, induced sputum for cy- tology annually and spontaneous cough speci- mens for cytology mailed in from home three times a year. The “B” subjects are screened by means of PA and lateral chest x-rays annually,

372 CANCER February 1977 Val. 39
Group A Group B
PA & lateral chest x-ray Sputum induction Immediate Post-induction 3-day spontaneous sputum
mailed in 4 months 3-day spontaneous sputum
4 months 3-day spontaneous sputum
4 months PA & lateral r h w x-ray Sputum induction Repeat
mailed in
mailed in
Fic:. 2. Flow chart of screening procedures. Those pro- cedures requiring attendance at the National Lung Program facility, annually, are blocked in; everythins else is carried out at home and specimens are mailed in.
PA & lateral chest x-ray
12 months
PA & lateral chest x-ray
Repeat
without cytologic examinations. A flow chart to summarize the handling of both groups is dia- grammed in Table 1A.
Cytology Screening To obtain induced cough specimens of spu-
tum we now use an aerosol solution of 15% saline and 20% propylene glycol, heated to 63OC (vapor delivered at 45-50OC) in a nebulizer with heating unit (Inhalation Equipment Company, New York City). Each man is instructed to re- move any dentures prior to sputum induction,
TABLE 2. Occupations of Men Enrolled in the Study*
Group “A” Group “ B ” (70) (70 )
Professional/technical Managerial/administrative Sales Clerical Craftsmen Operative-non transport Operative-transport Service Laborers Other
19 16 10 6 4 1 4
26 13
2
20 16 9 6 4 1 4
25 14 3
* Occupational classification of the Social Security Administration.
clear his throat of any post-nasal secretions, and rinse his mouth with tap water five times. He is instructed to breath the vapor through a dis- posable mouthpiece for two minute intervals (with nose pinched closed), cough at the end of each interval, and repeat the procedure seven times. Cough specimens are collected directly into fixative.
Spontaneous cough specimens are collected over a three day period at home, and mailed back to the laboratory. The men are again in- structed on the importance of a deep cough specimen, particularly after arising in the morn- ing, and told to discard saliva and post-nasal material. The products of the cough are col- lected directly into fixative.
Sputum specimens received in the laboratory are processed by the Saccornanno “blending” technique, and four Papanicolaou stained slides are routinely prepared.24 Residual material is saved for at least four months and processed if any abnormality is found on that or subsequent specimens.
Cytology slides are taken by messenger, daily, to the Cytology Laboratory at Memorial Hospi- tal for screening and diagnosis by us. The qual- ity of each specimen is reported as excellent, good, fair, poor or unsatisfactory, largely ac- cording to the relative number of pulmonary histiocytes present. The diagnosis on each sample is coded as positive for malignant cells (CAN), suspicious (SUS), moderate atypia (MOD), slight atypia (SLI) or unsatisfactory (UNS). Specimens considered diagnostic of can- cer are reported “CAN,” and initiate immediate localization and treatment procedures. If there is real suspicion of carcinoma but cytologic evi- dence is too scanty for definite diagnosis, the specimen is reported “SUS,” and immediate re- peat is requested. If the repeat specimen is again “SUS,” localization procedures are initiated. The diagnostic category “MOD” is used to identify atypias thought not to be cancer, but requiring immediate repeat examination and possibly indicative of an early neoplastic poten- tial. Slight atypia (SLI) is considered to be unimportant at this time, and probably due to non-specific inflammatory processes. This diag- nosis generates no change in the routine exam- ination procedure.
Radiology Screening The screening chest x-rays are taken on the
premises of the NLP. We are using a newly installed General Electric 140 KVP machine with 10 foot distance and 6” air gap. The max-

No. 2 LUNG CANCER DETECTION Melamed et al. 373
imum, measured total dose of radiation for the combination of postero-anterior and lateral chest x-rays is 70 mrem-this is less than 1/7 the dose of a single dental film.
Following exposure the film is transported from the x-ray machine to a Sakura developer by means of an automatic conveyor that was spe- cially designed and constructed for us. This en- sures dust-free films, and minimizes artifacts that may arise from handling. The films are developed, dry and ready for inspection within two minutes after they are taken.
As part of our program, the x-ray tech- nologists are trained to examine and interpret these films, to repeat them if it is desirable tech- nically or to obtain additional views if some abnormality is found on preliminary exam- ination. The technologists record a “preliminary screening classification.” All films are sub- sequently re-examined and interpreted by radio- logists on the staff of Memorial Hospital, the double viewing being designed to prevent errors of omission by a single examiner.
The x-ray diagnoses are classified in two cate- gories, a primary diagnosis regarding the pres- ence or absence of lung cancer and secondary diagnoses regarding any other abnormalities. The primary diagnoses are “CAN,” “SUS” or “NEG.” “CAN” is used to indicate an abnor- mality that is probably lung cancer and requires immediate thoracic surgical consultation. “SUS ” designates an abnormality thought probably not lung cancer, but requiring further study to rule out that possibility. Chest x-ray findings that require review of old films, tomo- grams, special views or repeat examinations at an interval less than one year, but not requiring thoracic surgical consultation, are categorized as “SUS. ” Abnormalities such as emphysema, cardiomegaly, pulmonary inflammatory disease, etc., not indicative of lung cancer are classified “NEG” even though these films may indicate serious disease and require that the subject be referred for appropriate medical care.
Data Processing The interactive computer system was pro-
grammed by Shared Educational Computer System, Inc. (SECOS) to meet requirements specified by our group. Two terminals at NLP provide online access to an IBM 370-145 located in Manhattan at Cornell University Medical College.
The information obtained from question- naires, x-ray reports and cytology reports is en- tered into computer files as it is received. The
TABLE 3. Cigarette Smoking at Time of Enrollment
Number of cigarettes Group “A” Group “ B ” per day (70 men) (’70 men)
Recent ex-smokers 5 6 20 24 24 21-30 31 31 31-40 28 27 41 + 12 12
schedule of appointments and examinations for each patient is maintained and monitored in the computer, which reminds us when sputum bot- tles should be sent out, when the patient is due for an annual examination, and when he is delinquent in any activity. Lables for bottles, slides, x-rays, questionnaires and mailings are produced automatically. After each exam- ination, the computer checks to make sure all reports are filed and if there is no evidence of lung cancer, generates a postcard for the patient and a letter to his personal physician reporting those findings. Finally, the files may be queried to obtain information about individual patients and statistical data about any subset of patients at any time. Copies of the computer files are sent to the statistical center at the University of Cin- cinnati quarterly.
MANAGEMENT OF MEN WITH EVIDENCE OF LUNG CANCER
Radiologically Manifest Carcinoma The management of men with radiologic evi-
dence of lung cancer (CAN) is in accordance with generally accepted medical practice, and
NATIONAL LUNG PROGRAM
AGE DISTRIBUTION 7 inn , #”..
P
1000 900 = GROUP “A”
1-1 GROUP ”B“ 800
700
600
500
400
300
200
100
45-49 50-54 55-59 60-64 65-69 70-74 >75
Fic;. 3. Age distribution of subjects screened to date. Group “A” have had PA and lateral chest x-rays with sputum cytology; Group “B” have had chest x-ray only.

374 CANCER February 1977 V O l . 39
TABLE 4. Occupational Exposure to Possible Carcinogens’
Group “A” Group “B” (90 men) (70 men)
Asbestos 5.1 6.4 Arsenic 2.0 2.0 Chromium 0.8 1.2 Nickel 0.8 1.3 Iron oxides 3.1 3.7
Radioactive materials 0.9 1.2 Chlormethyl ether 0.9 1.1
* Some men reported exposure to two or more different carcinogens.
not unique to this study. Repeated sputum cy- tology (for “B” as well as “A” group men), additional radiologic studies, bronchoscopy, percutaneous needle aspirates and, in some cases, thoracotomy are carried out to confirm the diagnosis, evaluate the extent of disease and establish the histologic classification. Patients with A.J.C. stage I or I1 carcinoma are treated by surgical resection alone. Patients with A.J.C. stage 111, operable carcinoma are treated by surgery and irradiation; those with inoperable cancers are treated by radiotherapy and/or chemotherapy. All patients with T 3 or N2 carci- nomas receive intensive chemotherapy to toler- ance.
Radiologically Occult Carcinoma Detected by Cytology
When cancer cells are found by cytologic ex- amination of sputum and the chest roentgeno- gram is normal, a specific sequence of diagnostic procedures is initiated to identify the source of the cancer cells. This includes immediate repeat sputum cytology to confirm the diagnosis, and a careful head and neck examination with indirect laryngoscopy. If no upper respiratory tract le- sion is found, the patient is hospitalized and re- examined under anesthesia with direct lar- yngoscopy. Repeat examination of mouth, nasopharynx and upper airways is carried out, and any suspicious areas are biopsied. If this examination also is negative, a bronchoscopic study is performed.
Localization of radiologically occult, early lung cancer may be a difficult and trying experi- ence, and frequently is not possible with conven- tional bronchoscopic techniques. We perform both rigid and fiberoptic bronchoscopy on all patients, and use general anesthesia since the study often requires two or more hours. Rigid bronchoscopy is performed first. The trachea and main bronchi are inspected, and differential bronchial washings are collected for cytology
from the left and right sides in such a way as to assure that there is no cross-contamination be- tween specimens. For this purpose, the rigid bronchoscope is fitted with an inflatable cuff at its distal end. When this procedure is finished, the rigid bronchoscope is withdrawn and the patient intubated with an endotracheal tube that is fitted with a T-adapter, allowing simulta- neous general anesthesia and fiberoptic bron- c hoscop y.
The fiberoptic bronchoscopy permits vis- ualization of each bronchus and each pul- monary segment up to fifth and sixth generation bronchi. We carry out this examination and re- cord it in its entirety on color videotape for documentation and later review. If a tumor be- comes visible it is brushed for cytologic exam- ination and a biopsy obtained for histologic con- firmation. When no abnormality is seen, bronchial brushes are guided into each bron- chial segment under direct vision and brushings are obtained for cytology. This permits precise localization of the source of expectorated cancer cells, but requires meticulous collection and la- belling of material to ensure accurate local- ization and to avoid cross-contamination. Even so, precise localization may be difficult and in the absence of a visible lesion with biopsy con- firmation we require that localization by bron- chial brushing be confirmed on two separate occasions before recommending surgery.
If initial localizing attempts are unsuccessful re-examination is recommended in one month and at two monthly intervals thereafter until the case is resolved. Carefully performed broncho-
TABLE 5. Non-Neoplastic Radiologic Abnormalities on Initial Chest X-Rays*
Group “A” Group “B” no. men (’70) no. men (YO)
Marked emphysema 17 Bullae 53 Asbestosis 3 Marked fibrosis 7 Pleural effusion 1 Old inflam. dis. 337 Active inflam. dis. 12 Granulom. dis. 157 Vascular abnormality 32 1 Cardiac abnormality 115 Mediastinal abnormality 25 Accessorv lobe 31
0.5) 17 1.7) 62 0.1) 7 0.2) 7
0.4) 10
1 10.6) 386
4.9) 178 10.1) 386 3.6) 126
0.5) 1.8) 0.2) 0.2)
11.5) 0.3) 5.3)
11.5) 3.8)
0.8) 34( 1.0) 1.0) 25 ( 0.7)
Skeletal abnormality 556 (17.4) 539 (16.1) Pleural abnormality 516 (16.2) 505 (15.1) Diaphragmatic abnormality 40 ( 1.3) 48 ( 1.4) Soft tissue abnormality 108 ( 3.4) 121 ( 3.6) Previous surgery 53 ( 1.7) 40( 1.2)
* Some men had two or more abnormalities.
No. 2 LUNG CANCER DETECTION Melamed et al. 375
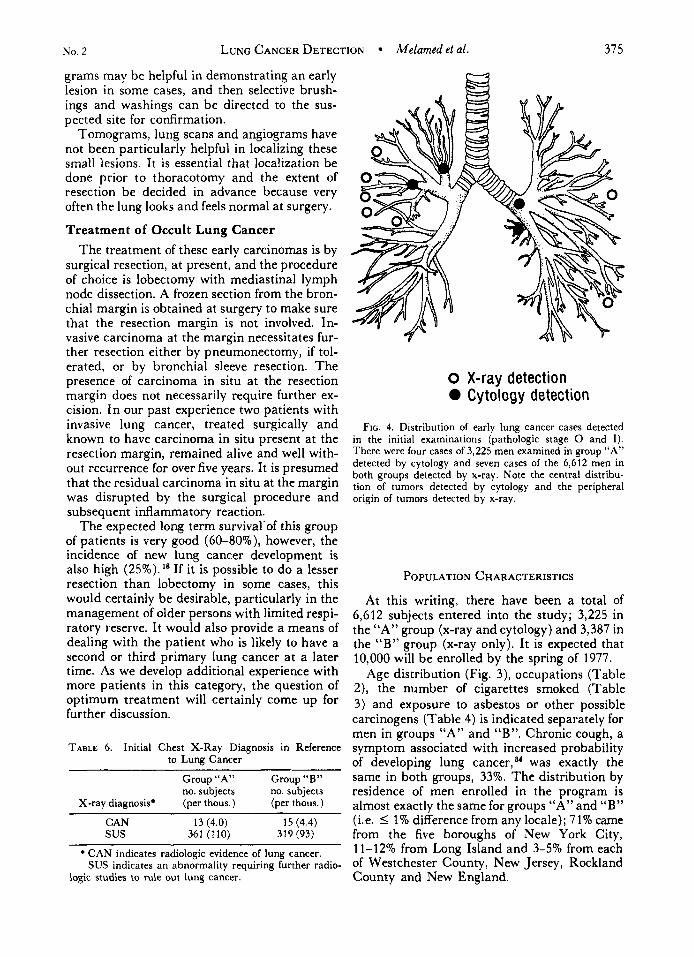
grams may be helpful in demonstrating an early lesion in some cases, and then selcctive brush- ings and washings can be directed to the sus- pected site for confirmation.
Tomograms, lung scans and angiograms have not been particularly helpful in localizing these small lesions. It is essential that localization be done prior to thoracotomy and the extent of resection be decided in advance because very often the lung looks and feels normal at surgery.
Treatment of Occult Lung Cancer The treatment of these early carcinomas is by
surgical resection, at present, and the procedure of choice is lobectomy with mediastinal lymph node dissection. A frozen section from the bron- chial margin is obtained at surgery to make sure that the resection margin is not involved. In- vasive carcinoma at the margin necessitates fur- ther resection either by pneumonectomy, if tol- erated, or by bronchial sleeve resection. The presence of carcinoma in situ at the resection margin does not necessarily require further ex- cision. In our past experience two patients with invasive lung cancer, treated surgically and known to have carcinoma in situ present at the resection margin, remained alive and well with- out recurrence for over five years. It is presumed that the residual carcinoma in situ at the margin was disrupted by the surgical procedure and subsequent inflammatory reaction.
The expected long term survival‘of this group of patients is very good (60-80%), however, the incidence of new lung cancer development is also high (25%). If it is possible to do a lesser resection than lobectomy in some cases, this would certainly be desirable, particularly in the management of older persons with limited respi- ratory reserve. It would also provide a means of dealing with the patient who is likely to have a second or third primary lung cancer at a later time. As we develop additional experience with more patients in this category, the question of optimum treatment will certainly come up for further discussion.
TABLE 6. Initial Chest X-Ray Diagnosis in Reference to Lung Cancer
Group “A” Group “B” no. subjects no. subjects
X-ray diagnosis* (per thous.) (per thous.)
CAN 13 (4.0) 15 (4.4) sus 361 (110) 319 (93)
* CAN indicates radiologic evidence of lung cancer. SUS indicates an abnormality requiring further radio-
logic studies to rule out lung cancer.
0 X-ray detection Cytology detection
FIG. 4. Distribution of early lung cancer cases detected in the initial examinations (pathologic stage 0 and I). There were four cases of 3,225 men examined in group “A” detected by cytology and seven cases of the 6,612 men in both groups detected by x-ray. Note the central distribu- tion of tumors detected by cytology and the peripheral origin of tumors detected by x-ray.
POPULATION CHARACTERISTICS
At this writing, there have been a total of 6,612 subjects entered into the study; 3,225 in the “A” group (x-ray and cytology) and 3,387 in the “B” group (x-ray only). It is expected that 10,000 will be enrolled by the spring of 1977.
Age distribution (Fig. 3), occupations (Table 2), the number of cigarettes smoked (Table 3) and exposure to asbestos or other possible carcinogens (Table 4) is indicated separately for men in groups “A” and “B”. Chronic cough, a symptom associated with increased probability of developing lung ~ a n c e r , ~ ‘ was exactly the same in both groups, 33%. The distribution by residence of men enrolled in the program is almost exactly the same for groups “A” and “B” (i.e. I 1% difference from any locale); 71% came from the five boroughs of New York City, 11-12% from Long Island and 3-5% from each of Westchester County, New Jersey, Rockland County and New England.

376 CANCER February 1977 Val. 39
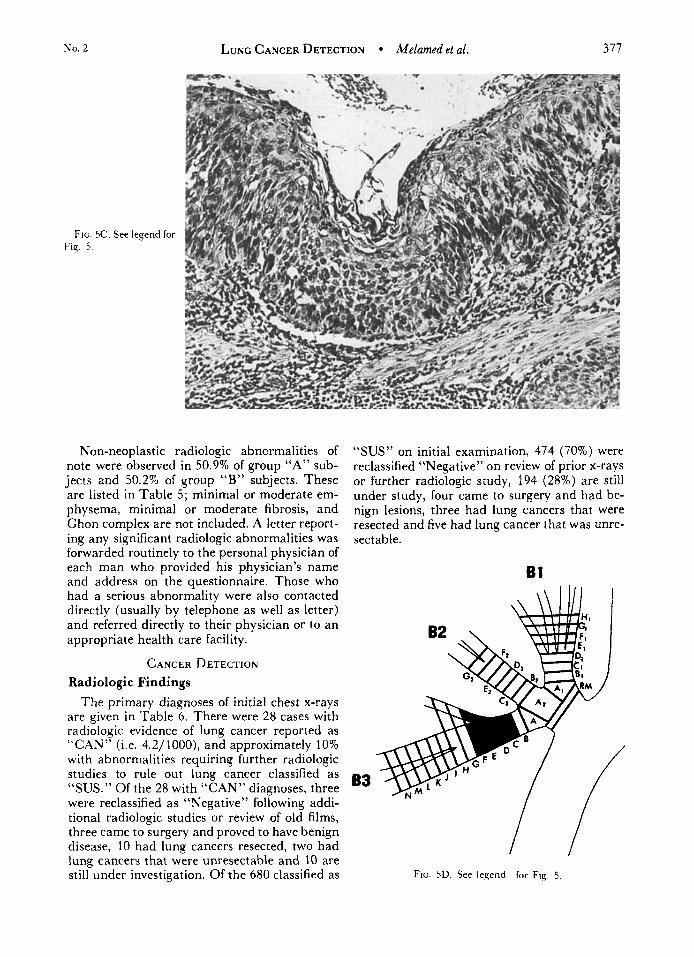
FIG 5. J.W., a 53-year-old man who was one of the four patients with early lung cancer detected by sputum cytology. Chest x-rays were normal, hut the initial sputum specimen contained desquamated cells of epidermoid carcinoma (i\-Papanicolaou stain X 350). T h e lesion which could not he visualized endoscopically, was localized to the anterior segmental bronchus of the right upper lobe by systematic fiberoptic bronchial brushing. Grossly the specimen was normal except for a slight. velvety thickening of mucosa coverine, a n area 1.0 X 0.6 cm in the anterior segmental bronchus (B) . The entire visible bronchial tree was step- sectioned. as is routine with these cases, and a well de- veloped epidermoid carcinoma in situ demonstrated (C-H & E. X 140), and mapped (D). There was bronchial gland involvement, but no invasion. Hilar and mediastinal lymph nodes were free of tumor This man is now three months postoperative, and well, with negative sputum cytology.
Fiti. 5B. See legend for Fig.. 5.
No. 2 LUNG CANCER DETECTION Melamed et al. 377
FIG. 5C. See legend for Fig. 5.
Non-neoplastic radiologic abnormalities of note were observed in 50.9% of group “A” sub- jects and 50.2% of group “B” subjects. These are listed in Table 5; minimal or moderate em- physema, minimal or moderate fibrosis, and Chon complex are not included. A letter report- ing any significant radiologic abnormalities was forwarded routinely to the personal physician of each man who provided his physician’s name and address on the questionnaire. Those who had a serious abnormality were also contacted directly (usually by telephone as well as letter) and referred directly to their physician or to an appropriate health care facility.
CANCER DETECTION Radiologic Findings
The primary diagnoses of initial chest x-rays are given in Table 6. There were 28 cases with radiologic evidence of lung cancer reported as “CAN” (i.e. 4.2/1000), and approximately 10% with abnormalities requiring further radiologic studies to rule out lung cancer classified as “SUS.” Of the 28 with “CAN” diagnoses, three were reclassified as “Negative” following addi- tional radiologic studies or review of old films, three came to surgery and proved to have benign disease, 10 had lung cancers resected, two had lung cancers that were unresectable and 10 are still under investigation. Of the 680 classified as
“SUS” on initial examination, 474 (70%) were reclassified “Negative” on review of prior x-rays or further radiologic study, 194 (28%) are still under study, four came to surgery and had be- nign lesions, three had lung cancers that were resected and five had lung cancer that was unre- sectable.
61
B3
FIG. 5D. See legend for Fig. 5

378 CANCER February 1977 Val. 39
Cytologic Findings The initial aerosol-induced cough specimen
and the immediately following 3-day spontane- ous cough specimen were together considered to be the initial cytologic examination; the higher diagnosis of the two was recorded as the initial cytologic diagnosis. A summary of those initial diagnoses is recorded in Table 7.
There were a total of 3,225 subjects examined, with eight reported as CAN (cancer cells pres- ent), seven reported as SUS (cancer suspected) and 23 showing moderate atypia (MOD). Over one-third had slight bronchial or squamous atypia (SLI).
Of the eight CAN cases, six now have proven
FIG. 6 . J.C., a 45-year-old man who was one of the seven patients with early lung cancer detected by x-ray. Sputum cytologv was normal The initial chest x-ray showed 1.0 cm shadow in the right mid-lung field, peripherally (A). Tomo- grams showed no calcification: there were no recent prior films available for comparison. Thoracotomy was performed and the nodule, which measured 0.9 cm in diameter, was re- moved from the superior segment of the right lower lobe by wedge resection (B). Frozen section showed a papillary bronchiolo-alveolar carcinoma. (C-H & E, X 140), and the lower lobectomy was completed. Lymph nodes were nega- tive. This man is now 17 months postoperative, and well.
lung cancer, including one with x-ray evidence of carcinoma; one has carcinoma of larynx; and one who refused treatment now has clinically evident carcinoma. Of the seven reported SUS, one subsequently had CAN cytology but is x-ray negative and under investigation; three had co- existing x-ray diagnoses of CAN and are there- fore included with the cases detected by x-ray and are now proven to have lung cancer; the remaining three have reverted to NEG, and are being followed. There were 23 cases reported MOD by cytology; one man who subsequently had “CAN” cytology, and another with two subsequent specimens reported SUS both proved to have larynx carcinoma. The remain- ing 21 have reverted to NEG.
TABLE 7. Initial Cytologic Diagnosis: Group “A” PREVALENCE OF LUNG CANCER CASES AND
MEANS OF DETECTION Cytologic diagnosis (see text) Number subjects (Per thous.)
CAN 8 (2 .5) Table 8 indicates the method of detection of s us 7 (2 .3) the confirmed cases of lung cancer. There were MOD 23 (7.2) 11 cases in group “B” detected by x-ray
(3.4/1000). In group “A” there were nine cases SLI 1329
TOTAL 3225 detected by x-ray (2.8/1000) and one case de-

No. 2 LUNG CANCER DETECTION iMelamed et al. 379
Fiti. 6B See legend for Fig-. 6.
tected by x-ray and cytology (0.3/1000). In the “A” group, five additional cases of lung cancer were detected by cytology (1.5/1000) in men without radiologic abnormalities. Since there are other cases still under study with abnor- malities that may prove due to lung cancer, these data represent minimum prevalence rates.
The cases with diagnoses still pending are recorded in Table IX. There are eight cases with abnormalities detected by x-ray in the “A” group (2.5/1000) and 10 cases in the “B” group (3.0/1000). One additional pending case in the “A” group is due to cytology (0.3/1000), and one due to both x-ray and cytology (0.3/1000). Thus, the final prevalence rate for lung cancer in the two groups should lie between 4.6-7.7/1000 in the “A” group and 3.4-6.4/1000 in the “B” group, the difference being due to cases detected by cytology.
PATHOLOGY OF CONFIRMED CASES OF LUNG CANCER
Table 10 indicates the pathologic stage of con- firmed lung cancer cases (i.e. A.J.C. post-surgi- cal staging’) according to the method of detec- tion. There is little difference in stage of the cases discovered by x-ray in group “A” (cy- tology and x-ray screening) compared with group “ B ” (x-ray screening only). However, five of the six cases in group “A” detected by cy- tology had no radiologic abnormalities, and four
FIG. 6C. See legend for Fig. 6.

380 CANCER February Vol. 39
T A B L ~ 8 Confirmed Cases of Lung Cancer According to Method of Detection
No. in No. in Group “A” (Per thous.) Group “B” (Per thous.)
Total no. subjects 3225 3387
Detected by : No. cases lung cancer 15 (4.6) I 1 (3.4)
X-ray 9 (2.8) 11 (3.4) Cytology 5 (1.5) X-ray and cytology 1 (0.3)
of the five were Stage 0 (i.e. in situ or super- ficially invasive epidermoid carcinoma, not in- vading through the bronchial wall; this differs from the A.J.C. Stage 0).
The histology of confirmed lung cancer cases and their site of origin is listed in Table 11, according to the means of detection.
Figure 4 shows the distribution of early lung cancers (Stage 0 and I), according to the method of detection. There were four early lung cancers detected by cytology in the 3,255 men of group “A” examined by this technique (Fig. 5 ) and seven early lung cancers detected by x-ray in the 6,612 men of both groups (Fig. 6). Thus, the early lung cancer case finding rate was very nearly the same by both techniques.
There are several points of interest in the pa- thology data. First, the cases detected early by cytology arise from lobar or segmental bronchi, or their first sub-segmental division; i.e. from relatively large and central bronchi; while the cases detected early by x-ray all arise pe- ripherally; i.e., from terminal tronchioles or bronchiolo-alvelolar epithelium. Furthermore, the cases detected by sputum are epidermoid carcinoma, most detected by x-ray are adeno- carcinomas or bronchiolo-alveolar carcinoma and, finally, there are relatively few cases de- tected simultaneously by both techniques. Thus, the radiologic and cytologic detection tech- niques complement each other very well; that is,
the central epidermoid carcinomas are first de- tected by cytology and peripheral bronchiolar carcinomas are first detected by x-ray.
Most of the late cases of cancer are first de- tected and most easily detected by x-ray, regard- less whether they have central or peripheral sites of origin (Fig. 7 ) , and cytology then became a confirming, diagnostic procedure.
TREATMENT
There were 11 patients with “early” lung can- cer, that is, stage 0 or stage I ; eight in group “A” (cytology and x-ray); and three in group “B” (x-ray only). All were operable and resect- able, and are now potentially cured. Eight of these patients had lobectomy, one required bilo- bectomy, one pneumonectomy and one with a small peripheral tumor was treated by wedge resection.
There were 15 patients with ‘‘late’’ lung can- cer, that is, stage I1 or 111; seven in group “A”; and eight in group “B”. Of these, only seven were operable and resectable, three others un- derwent thoracotomy and radio-isotope implan- tation, three were diagnosed by biopsy of distant metastases, one diagnosed by bronchoscopic biopsy was not operable, and one patient who sought treatment elsewhere was not operated and a confirming diagnosis was made at au- topsy.
TABLE 9. Cases Still Under Investigation According to Method of Detection
No. in No. in Group “A” (Per thous.) Group“B” (Per thous.)
Total no. subjects 3.225 3,387 No. cases pending diasnosis 10 (3.1) 10 (3.0) Detected by:
X-ray 8 (2.5) 10 (3.0) Cytolog-y 1 (0.3) X-ray and cytology 1 (0.3)

No. 2 LUNG CANCER DETECTION Melamed et al.
TABLE 10. Pathologic Stage of Confirmed Lung Cancers*
Group “A” Group “B” detected by detected by
Cytoloqy X-ray Both X-ray
Stage 0 4 Stage 1 4 3 Stage 2 2 Stage 3 1 5 1 6
* A.J.C. Post-Surgical Stage. ( I ) , determined at surgery and by examination of the pathologic specimen. Stage 0 is used here to mean carcinoma in situ in the bronchus or invading into the bronchial wall but not extending. outside the bronchus.
SUMMARY A N D CONCLUSIONS
The data presented in this report are the in- itial results of a controlled study of sputum cy- tology used as an adjunct to the chest x-ray in a lung cancer detection program. Prevalence rate data only are reported at this time, that is the results of the first examination, and the lung cancers detected are a mixture of cases that are early (pathologic states 0 and I ) and late (path- ologic states I1 and 111). All of the late cases except one (14 of 15) were visible and diagnosed by chest x-ray. There were three early lung can- cers detected by chest x-rays in the population of 3,387 men who had x-rays only; and in the 3,225 men who had both procedures there were four early lung cancers detected by x-ray and four detected by cytology. In addition, three cases of larynx cancer were detected by cytology. The early lung cancers detected by x-ray were pe- ripheral, and most were adenocarcinomas; while the early cancers detected by cytology were central, epidermoid carcinomas of major
38 1
0 X-ray detection 0 Cytology detection 0 Both
FIG 7. Distribution of late cases of carcinoma (Stage I1 and 1 1 1 ) found on initial examnation .All but one were ap- parent bv x-ray
bronchi. There were no early carcinomas de- tected by both techniques. These findings sug- gest that a combination of chest x-rays and spu- tum cytology can be an effective means of detecting early lung cancer. Regular, repeat ex- aminations are now being carried out on this population to determine whether a substantial proportion of the new lung cancers that develop after initial negative screening examinations can be detected in an early stage.
TABLE 11. Histology and Origin of Confirmed Lung Cancers
Cytology detection X-ray detection
Bronchiolar & Bronchiolar & Epid ca ad ca Epid ca ad ca
Lobar or segment broncus 4 Sub-segmental bronchus 1 Peripheral I *
2 1 0
~~ ~
* 1 case detected simultaneously by x-ray and cytology.
REFERENCES
I . American Joint Committee for Cancer Staging and
2. Axtell. L. M.. Cutler, S. J and hlyers. M. H.: End
results in cancer. Report No. 4, N.I.H. U.S. Dept. Health, Education and Welfare, 1972.
3. Baker, R. R. , Marsh. B R . , Frost, J. K., ef al.: The End Results Reporting. September 1973, Chicago.

382 CANCER February Val. 39
detection and treatment of early lung cancer. In Cancer of the Lung. G. F. Murray, Ed. New York, Stratton Inter- continental Medical Book Carp., 1976.
4 Boucot, K. R., Cooper, D. A., and Weiss, W.: The Philadelphia Pulmonary Neoplasm Research Project. M e d . Clzn. hbrih Am. 54:549-553, 1970.
5. Brett, G. 2.: Earlier diagnosis and survival in lung cancer. Br. M e d . 3. 4:260-262, 1969.
6 ’76 Cancer Facts and Figures. American Cancer Society, New York, 1975.
7. Cancer statistics, 1976. C A . 26: 14-29, 1976. 8. Fontana, R. S., Sanderson, D. R., Miller, W. E., ei a/.:
The Mayo Lung Project: Preliminary report of “early cancer detection” phase. Cancer 30: 1373- 1382, 1972.
9. Fontana, R. S., Sanderson, D. R., Woolner, L. B., e/ a/: The Mayo Lung Project for early detection and local- ization of bronchogenic carcinoma. A status report. Chest 67:511-522, 1975.
10. Grzybowski, S., and Coy, P.: Early diagnosis of carci- noma of the lung. Simultaneous screening with chest x-ray and sputum cytology. Cancer 25: 113-1 19, 1970.
11. Holman, C. W., and Okinaka, ,4.: Occult carcinoma of the lung. J . Thor. Cardiouasc. Surg. 47:466-471, 1964.
12. Kubik, A., Krivinka, R., Stasek, V., el a/ . : Screening for lung cancer high-risk groups. S c a d . 3. He~p. Dzs. 51 :290-300, 1970.
13. Lerner, hl. A , , Rosbach. H., Frank, H. A. , and Fleischner, F. G. : Radiologic localization and management of cytologically discovered bronchial carcinoma. N . Engl. 3. M e d . 264:480-485, 1961.
14. Lilienfeld. A., el al.: An evaluation of radiologic and cytoloqic screening for the early detection of lung cancer: A cooperative pilot study of the American Cancer Society and the Veterans Administration. Cancer Res. 26:2083-2121, 1966.
15. Manual of Procedures. National Cancer Institute Co- operative Early Lung Cancer Group Bethesda. Maryland, ,January 1975.
16. Marsh, B. R., Frost, J . K., Erozan. Y. S., and Carter. D.: Occult bronchogenic carcinoma. Cancer 30: 1348-1 352, 1973.
17. Marsh, 8. R.. Frost, J . K.. Erozan, Y . S.. el al.: Flexible fiberoptic bronchoscopy-its place in the search for lung cancer. Ann. Otol. Rhinol. Laryngol. 82:757-764, 1973.
18. Martini, N., Beattie, E. J., Cliffton, E. E., and Me- lamed, M. R: Radiologically occult lung cancer. Report of 26 cases. Surg. Clin. Yorth A m . 54:811-823. 1974.
19. Melamed, M. R., Koss, L. G., and Cliffton, E. E.: Roentgenologically occult lung cancer diagnosed by cy- tology. Cancer 16:1537-1551, 1963.
20. Miller, D.: Preventive medicine by risk factor analy- sis. J A M A 222:312-316, 1972.
21. Nash, F. A,, Morgan, J. M., and Tomkins, J. G.: South London Cancer Study. Br. Med. 3. 2:715-721, 1968.
22. Papanicolaou, G. A., and Koprowska, I . : Carcinoma in situ of right lower bronchus: case report. Cancer 4:141-146, 1951.
23. Pearson, F. G., and Thompson, D. W.: Occult carci- noma of the br0nchus.J. Can. Med. Assoc. 94:825-833, 1966.
24. Saccomanno, G., Saunders, R. P., Ellis, H., et a f . : Concentration of carcinoma or atypical cells in sputum. Acta L901. 7:305-310, 1963.
25. Sanderson, D. R., Fontana. R. S., Woolner, L. B., et al. : Bronchoscopic localization of radiographically occult lung cancer. Chest 65:608-612, 1974.
26. Schneiderman, M. A., and Levin, D. L.: Trends in lung cancer. Cancer 30: 1320-1325. 1973.
27. Schottenfeld, D.: Factors bearing on prognosis: A review of 3.124 cases. Chapter 2 I . In Lung Cancer. Watson, W . L., Ed. St. Louis, C. V. Mosby Co., 1968.
28. Smoking and Health: Report on the Advisory Com- mittee to the Surgeon General of the Public Health Service, L J . S Dept. of Health, Education and Welfare. Reprinted by the American Cancer Society, Inc.
29. Taylor, W: F., and Fontana, R. S.: Biometric design of the Mayo Lung Project for early detection and local- ization of bronchogenic carcinoma. Cancer 30: 1344-1347. 1972.
30. Third National Cancer Survey, 1969-71, National Cancer Institute, Biometry Branch, Bethesda, Maryland.
31 Woolner, L. B., Anderson, H. A,, and Bernatz, P. E.: Occult carcinoma of the bronchus: A study of 15 cases of in situ or early invasive bronchogenic carcinoma. Dis. Chesl 37:278-288, 1966.
32. Woolner. L. B., David, E., Fontana, R. S., Anderson, H. A. and Bernatz, P. E.: In situ and early invasive broncho- genic carcinoma: Report of 28 cases with postoperative sur- vival data. .7. Thor. Cardiouasc. Surg. 60:275-290, 1970.
33. Woolner, L. B., Fontana. R. S., and Bernatz, P. E.: Early bronchogenic carcinoma. problems in detection, local- ization and treatment. Surg. Clin. hhr ih Am. 53:761-768. 1973.
34. Wynder, E. L.: Etiology of lung cancer. Cancer 30.1332-1339. 1972.
Copyright © 2022 FDOKUMEN