Planning the diffusion of a neck-injury prevention programme among community rugby union coaches
10
Planning the diffusion of a neck-injury prevention programme among community rugby union coaches Alex Donaldson, 1 Roslyn G Poulos 2 1 Australian Centre for Research into Injury in Sport and its Prevention (ACRISP), Monash Injury Research Institute (MIRI), Monash University, Melbourne, Victoria, Australia 2 School of Public Health & Community Medicine, The University of New South Wales, Sydney, NSW, Australia Correspondence to Dr Alex Donaldson, Australian Centre for Research into Injury in Sport and its Prevention (ACRISP), Monash Injury Research Institute (MIRI), Monash University, Clayton, Melbourne, VIC 3800, Australia; alex.donaldson@ monash.edu Received 5 July 2012 Revised 19 September 2012 Accepted 9 November 2012 To cite: Donaldson A, Poulos RG. Br J Sports Med Published Online First: 10 December 2012 doi:10.1136/bjsports-2012- 091551 ABSTRACT Background This paper describes the development of a theory-informed and evidence-informed, context- specific diffusion plan for the Mayday Safety Procedure (MSP) among community rugby coaches in regional New South Wales, Australia. Methods Step 5 of Intervention Mapping was used to plan strategies to enhance MSP adoption and implementation. Results Coaches were identified as the primary MSP adopters and implementers within a system including administrators, players and referees. A local advisory group was established to ensure context relevance. Performance objectives (eg, attend MSP training for coaches) and determinants of adoption and implementation behaviour (eg, knowledge, beliefs, skills and environment) were identified, informed by Social Cognitive Theory. Adoption and implementation matrices were developed and change-objectives for coaches were identified (eg, skills to deliver MSP training to players). Finally, intervention methods and specific strategies (eg, coach education, social marketing and policy and by-law development) were identified based on advisory group member experience, evidence of effective coach safety behaviour-change interventions and Diffusion of Innovations theory. Conclusions This is the first published example of a systematic approach to plan injury prevention programme diffusion in community sports. The key strengths of this approach were an effective researcher–practitioner partnership; actively engaging local sports administrators; targeting specific behaviour determinants, informed by theory and evidence; and taking context-related practical strengths and constraints into consideration. The major challenges were the time involved in using a systematic diffusion planning approach for the first time; and finding a planning language that was acceptable and meaningful to researchers and practitioners. BACKGROUND The merits of strategically planning how to trans- late research evidence, policy decisions and safety programmes into practice, to achieve sustained population health improvements, have been debated for some time. 1–3 However, sports-injury prevention translation research has only recently received attention 4–7 and there are few published examples of sports injury implementation and effectiveness studies. 8 The Australian Rugby Union (ARU) introduced the Mayday Safety Procedure (MSP) in an attempt to achieve a nationally recognised call and response to potentially dangerous scrum situations. The MSP encourages a quick release of pressure in a ‘standing’ scrum and a controlled ‘unpacking’ of the scrum to avoid flexion or rotation of the neck of the potentially injured player. It was developed in consultation with medical, exercise physiology, rugby coaching and biomechanics experts 9 and is included in ARU medical and safety recommenda- tions 10 and compulsory coach and referee training. 11 Community rugby union (hereafter referred to as rugby) coaches know about the MSP but they do not have a good written recall of the key criteria nor do they regularly train or assess player compe- tency in it. 12 The challenge of translating rugby safety policy into changes in coach and player behaviour is not limited to the MSP nor to Australia. 13–16 The two authors (AD and RP) worked closely with two ARU representatives responsible for administering rugby in a single region in regional New South Wales, Australia, to develop a theory-informed and evidence-informed, context- specific diffusion plan to encourage and support coaches to train their players in the MSP. This paper describes the development of that diffusion plan. METHODS The Intervention Mapping (IM) health promotion programme planning protocol 17 includes a step (Step 5) dedicated to planning programme transla- tion. It comprises of seven tasks and is operationa- lised through six core processes ( figure 1). IM Step 5 was used in this project to plan improved diffu- sion of the ARU MSP policy. When applying the IM protocol, it is important to distinguish between the programme (to be adopted and implemented) and the intervention (to facilitate programme adoption and implementa- tion). In this project, the programme was defined as ‘training rugby players in the MSP’ and the inter- vention was ‘the planned activities undertaken to enhance the likelihood that rugby players would be trained in the MSP’. The tasks undertaken by the project team (the two authors and two ARU community-level admin- istrators) following the IM Step 5 protocol and how they were applied in this project are outlined in table 1. The project team undertook tasks 1–5. The advis- ory group established in task 2 reviewed and pro- vided advice on the work of the project team, and participated actively in tasks 6 and 7. The core pro- cesses of IM (see figure 1) were applied throughout, particularly during tasks 4 and 6 (table 2). This was the first time that the ARU had applied the IM protocol. To ensure that the process was manageable, the intervention was targeted on one Donaldson A, et al. Br J Sports Med 2012;0:1–9. doi:10.1136/bjsports-2012-091551 1 Original article BJSM Online First, published on December 11, 2012 as 10.1136/bjsports-2012-091551 Copyright Article author (or their employer) 2012. Produced by BMJ Publishing Group Ltd under licence. group.bmj.com on December 12, 2012 - Published by bjsm.bmj.com Downloaded from
-
Upload
federation-au -
Category
Documents
-
view
3 -
download
0
Transcript of Planning the diffusion of a neck-injury prevention programme among community rugby union coaches

Planning the diffusion of a neck-injury preventionprogramme among community rugby union coachesAlex Donaldson,1 Roslyn G Poulos2
1Australian Centre for Researchinto Injury in Sport and itsPrevention (ACRISP), MonashInjury Research Institute (MIRI),Monash University, Melbourne,Victoria, Australia2School of Public Health &Community Medicine, TheUniversity of New South Wales,Sydney, NSW, Australia
Correspondence toDr Alex Donaldson, AustralianCentre for Research into Injuryin Sport and its Prevention(ACRISP), Monash InjuryResearch Institute (MIRI),Monash University, Clayton,Melbourne, VIC 3800,Australia; [email protected]
Received 5 July 2012Revised 19 September 2012Accepted 9 November 2012
To cite: Donaldson A,Poulos RG. Br J Sports MedPublished Online First:10 December 2012doi:10.1136/bjsports-2012-091551
ABSTRACTBackground This paper describes the development ofa theory-informed and evidence-informed, context-specific diffusion plan for the Mayday Safety Procedure(MSP) among community rugby coaches in regional NewSouth Wales, Australia.Methods Step 5 of Intervention Mapping was used toplan strategies to enhance MSP adoption andimplementation.Results Coaches were identified as the primary MSPadopters and implementers within a system includingadministrators, players and referees. A local advisorygroup was established to ensure context relevance.Performance objectives (eg, attend MSP training forcoaches) and determinants of adoption andimplementation behaviour (eg, knowledge, beliefs, skillsand environment) were identified, informed by SocialCognitive Theory. Adoption and implementation matriceswere developed and change-objectives for coaches wereidentified (eg, skills to deliver MSP training to players).Finally, intervention methods and specific strategies (eg,coach education, social marketing and policy and by-lawdevelopment) were identified based on advisory groupmember experience, evidence of effective coach safetybehaviour-change interventions and Diffusion ofInnovations theory.Conclusions This is the first published example of asystematic approach to plan injury prevention programmediffusion in community sports. The key strengths of thisapproach were an effective researcher–practitionerpartnership; actively engaging local sports administrators;targeting specific behaviour determinants, informed bytheory and evidence; and taking context-related practicalstrengths and constraints into consideration. The majorchallenges were the time involved in using a systematicdiffusion planning approach for the first time; andfinding a planning language that was acceptable andmeaningful to researchers and practitioners.
BACKGROUNDThe merits of strategically planning how to trans-late research evidence, policy decisions and safetyprogrammes into practice, to achieve sustainedpopulation health improvements, have beendebated for some time.1–3 However, sports-injuryprevention translation research has only recentlyreceived attention4–7 and there are few publishedexamples of sports injury implementation andeffectiveness studies.8
The Australian Rugby Union (ARU) introducedthe Mayday Safety Procedure (MSP) in an attemptto achieve a nationally recognised call and responseto potentially dangerous scrum situations. TheMSP encourages a quick release of pressure in a‘standing’ scrum and a controlled ‘unpacking’ of
the scrum to avoid flexion or rotation of the neckof the potentially injured player. It was developedin consultation with medical, exercise physiology,rugby coaching and biomechanics experts9 and isincluded in ARU medical and safety recommenda-tions10 and compulsory coach and refereetraining.11
Community rugby union (hereafter referred to asrugby) coaches know about the MSP but they donot have a good written recall of the key criterianor do they regularly train or assess player compe-tency in it.12 The challenge of translating rugbysafety policy into changes in coach and playerbehaviour is not limited to the MSP nor toAustralia.13–16
The two authors (AD and RP) worked closelywith two ARU representatives responsible foradministering rugby in a single region in regionalNew South Wales, Australia, to develop atheory-informed and evidence-informed, context-specific diffusion plan to encourage and supportcoaches to train their players in the MSP. Thispaper describes the development of that diffusionplan.
METHODSThe Intervention Mapping (IM) health promotionprogramme planning protocol17 includes a step(Step 5) dedicated to planning programme transla-tion. It comprises of seven tasks and is operationa-lised through six core processes (figure 1). IM Step5 was used in this project to plan improved diffu-sion of the ARU MSP policy.When applying the IM protocol, it is important
to distinguish between the programme (to beadopted and implemented) and the intervention (tofacilitate programme adoption and implementa-tion). In this project, the programme was defined as‘training rugby players in the MSP’ and the inter-vention was ‘the planned activities undertaken toenhance the likelihood that rugby players would betrained in the MSP’.The tasks undertaken by the project team (the
two authors and two ARU community-level admin-istrators) following the IM Step 5 protocol andhow they were applied in this project are outlinedin table 1.The project team undertook tasks 1–5. The advis-
ory group established in task 2 reviewed and pro-vided advice on the work of the project team, andparticipated actively in tasks 6 and 7. The core pro-cesses of IM (see figure 1) were applied throughout,particularly during tasks 4 and 6 (table 2).This was the first time that the ARU had applied
the IM protocol. To ensure that the process wasmanageable, the intervention was targeted on one
Donaldson A, et al. Br J Sports Med 2012;0:1–9. doi:10.1136/bjsports-2012-091551 1
Original article BJSM Online First, published on December 11, 2012 as 10.1136/bjsports-2012-091551
Copyright Article author (or their employer) 2012. Produced by BMJ Publishing Group Ltd under licence.
group.bmj.com on December 12, 2012 - Published by bjsm.bmj.comDownloaded from

geographical region where the competition was administered by,and all clubs were affiliated to, a single regional governing body.Diffusion planning was done during October 2010–February2011 with the aim of undertaking intervention activities duringthe 2011 rugby season.
The University of New South Wales Medical and CommunityHuman Research Ethics Advisory Panel approved the study.
RESULTSThe outcomes of undertaking the seven tasks of IM step 5described in table 1 are presented below.
Task 1The project team identified the regional rugby association,regional rugby referees’ association, individual referees, clubadministrators, coaches and players as potential programmeadopters and implementers. Coaches of senior rugby teamswere identified as the primary focus of intervention activitiesbecause of their influence on player safety and training attitudesand behaviours,18–21 and their role in training players insafety.22
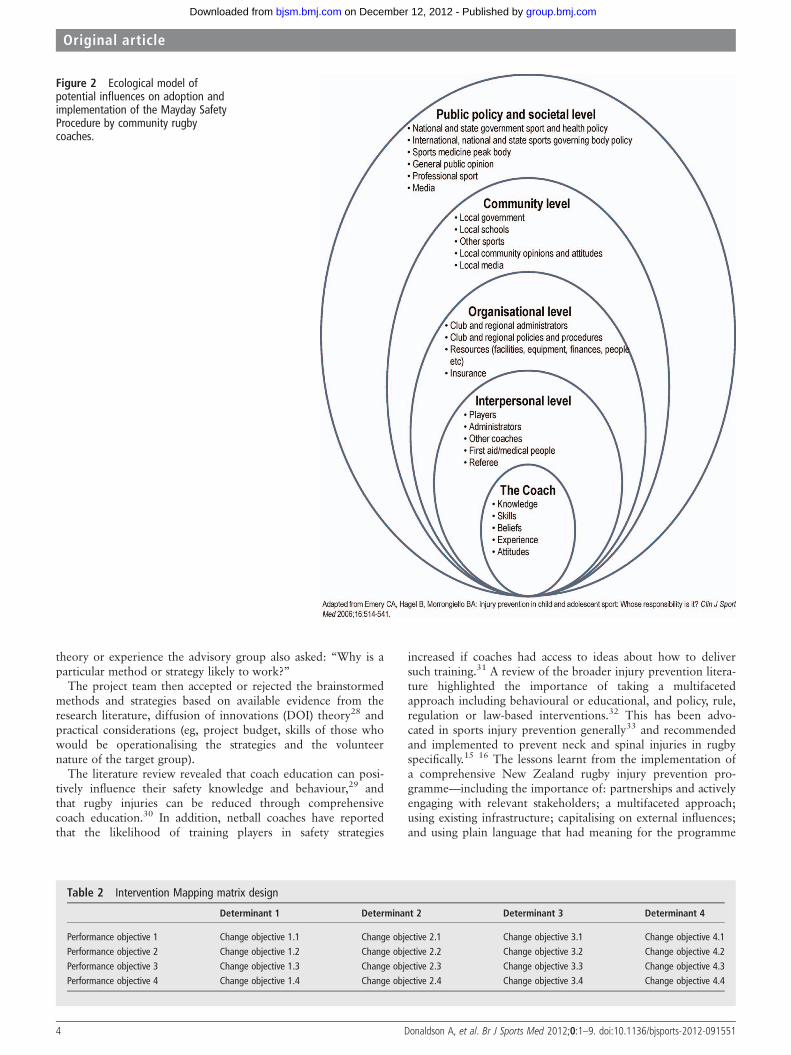
Other potential programme users and gatekeepers (eg,players, referees, first-aid providers and club and regional associ-ation administrators) were considered only in relation to theirinfluence on the coaches’ MSP decisions and actions. Figure 2provides an ecological or systems overview of programme adop-tion and implementation from the perspective of the coach asthe primary adopter or implementer.
Task 2The project team did not actively engage with the range ofpotential programme adopters and implementers at various eco-logical or system levels until the end of task 5. This was becausethe identified people were nearly all volunteers with limited cap-acity to participate in this project and it was agreed that the
most valuable contribution that they could make would be intasks 6 and 7 (figure 1). Also, the ARU representatives on theproject team were extremely knowledgeable about, and experi-enced in community rugby administration, coaching andplaying, and it was believed that they could represent the viewsof these groups during the initial diffusion planning tasks.Influential organisations (eg, regional rugby and referee associa-tions) were informed of project progress and knew that theycould actively participate in the later tasks.
During task 2, the project focused on the individual, interper-sonal and organisational ecological levels only (figure 2), as theyrelated to coaches. This kept the scope within one geographicalregion and within the management jurisdiction of the ARUadministrators on the project team. This approach reflected thesignificant role that local context plays in sports policy interpret-ation and implementation.23–25
Task 3Adequate programme adoption and implementation, based onthe experience of the ARU representatives on the project team,was defined as coaches delivering “at least four MSP trainingsessions to players before the start of the 2011 season (ie, in thepreseason),” and “at least one MSP practice opportunity every4 weeks during the season,” respectively.
Programme use outcomes and programme adoption andimplementation performance objectives were identified byasking “What do coaches need to do to constitute programadoption or adequate program implementation?”
The expected programme outcomes were that coaches would(1) decide to deliver MSP training to their players (adoption)and (2) actually deliver MSP training to their players(implementation).
The specific performance objectives describing what coachesneeded to do to adopt and implement the programme are listedin the left-hand columns of the matrixes in tables 3 and 4,
Figure 1 Intervention Mapping Step 5 tasks and core processes.17
2 Donaldson A, et al. Br J Sports Med 2012;0:1–9. doi:10.1136/bjsports-2012-091551
Original article
group.bmj.com on December 12, 2012 - Published by bjsm.bmj.comDownloaded from

respectively. Performance objectives for programme adoptionrevolved around coaches becoming aware of the need to trainplayers in the MSP and coaches themselves attending trainingon how to deliver MSP training to players (table 3). Programmeimplementation performance objectives (table 4) reflected thattraining players in the MSP would require coaches to scheduleand deliver the appropriate number of MSP training sessionsand practice opportunities to players in the preseason andregular season.
Task 4The determinants of coach programme adoption and implemen-tation were specified by asking “What is likely to influencewhether coaches adopt and implement the program?” Thepotential influences on coaches were explored using IM coreprocesses (figure 1). After brainstorming a list of answers to thequestion and considering existing coach MSP-related knowledgeand practices,12 it was concluded that coach programme adop-tion and implementation behaviours could be influenced by per-sonal and individual factors (knowledge, beliefs, skills, etc) andby social, environmental or organisational factors (resources,policies, training, time, etc). This is consistent with SocialCognitive Theory (SCT) and the idea that an individual’s behav-iour is dynamic and is simultaneously and continuously influ-enced by the person and the environment.26
When working in partnerships it is important to learn to‘speak each other’s language’.27 It became clear during projectteam discussions that some of the language of the SCT(eg, reciprocal determinism, expectancies, self-efficacy, etc) wasnot meaningful in the community sports sector. As a result,
significant effort was made to ensure that the language used waseasily understood by the end-users while still adequately reflect-ing the underlying SCT constructs. The broad determinants ofknowledge, skills, beliefs and environment were identified askey influences of coach programme adoption and implementa-tion behaviour that reflected several key ideas underpinningSCT (table 5).
The results of tasks 3 and 4 were then used to construct amatrix which served as a template for completing Task 5.
Task 5Specific programme adoption and implementation change objec-tives to be achieved by coaches are contained in the cells oftables 3 and 4, respectively. Conceptually, these represent amechanism for creating changes in both the personal (eg, coachknowledge, skills and beliefs) and environmental factors thatwill influence coach behaviour.
Tasks 6 and 7After the project team completed the programme adoption andimplementation matrices, the advisory group—comprised of aRegional Rugby Union Association (RRUA) representative(employed administration officer), a Referees’ Board representa-tive (also an active referee), a coach, a player and a club adminis-trator—reviewed the matrices and approved the changeobjectives. They then brainstormed potential methods and strat-egies to facilitate coaches achieving the identified change objec-tives by asking: “What could be done to help, support orencourage coaches to achieve the agreed change objectives?” Toensure that the suggested strategies had some basis in evidence,
Table 1 Tasks involved in Intervention Mapping step 5 and how they were applied in the Mayday Safety Procedure diffusion planning project
Intervention Mapping step 5 task PurposeApplication in Mayday Safety Procedure diffusionplanning project
Task 1 Identify potential programme adoptersand implementers
Identify organisations and individuals that would beinvolved in, or would influence, programmeadoption and implementation
Context in which the programme was to be adopted andimplemented was considered including individual,organisational and societal influences on programmeadoption and implemenation.7
Task 2 Establish a programme adoption andimplementation planning group
Link programme developers to programme adoptersand implementers
‘Advisory group’ established including representatives of thetwo stakeholder groups—ARU and community rugbycoaches—and ‘change agents’ who could influenceprogramme adoption and implementation
Task 3 State programme use outcomes andspecify adoption and implementationperformance objectives
Describe what intervention would accomplish andwho had to do what for the programme to beadopted and implemented
Asked: What do coaches need to do to constituteprogramme adoption and implementation?
Task 4 Specify determinants of programmeadoption and implementation
Identify what will influence whether or notprogramme adopters and implementers performedthe actions needed to accomplish the performanceobjectives
Asked: “What is likely to influence whether coaches adoptand implement the programme?”
Task 5 Create matrices of change objectives forprogramme adoption andimplementation
Link programme adoption and implementationperformance objectives (task 3) and determinants(task 4) to create change objectives
Separate programme adoption and implementation matricescreated (see table 2 for a generic example). Each cellassessed to judge whether the determinant was likely toinfluence accomplishment of the performance objectives.Asked: “What is it about the determinant that needs tochange for coaches to achieve the performance objectives?”
Task 6 Select theory-informed methods andpractical applications to enhanceprogramme adoption andimplementation
General methods and specific strategies to achievethe change objectives
Change objectives reorganised according to determinantsand ecological or system levels. Theory andevidence-informed methods or strategies selected based onperceived capacity to create change in the determinants
Task 7 Design interventions for programmeadoption and implementation
Develop and produce materials and resources tooperationalise methods and strategies
Generated a coherent set of activities and resources thatreflected thinking and planning done in tasks 1–6 that,when undertaken, should lead to improved programmeadoption and implementation by community rugby coaches
ARU, Australian Rugby Union represented by regional development staff.
Donaldson A, et al. Br J Sports Med 2012;0:1–9. doi:10.1136/bjsports-2012-091551 3
Original article
group.bmj.com on December 12, 2012 - Published by bjsm.bmj.comDownloaded from
theory or experience the advisory group also asked: “Why is aparticular method or strategy likely to work?”
The project team then accepted or rejected the brainstormedmethods and strategies based on available evidence from theresearch literature, diffusion of innovations (DOI) theory28 andpractical considerations (eg, project budget, skills of those whowould be operationalising the strategies and the volunteernature of the target group).
The literature review revealed that coach education can posi-tively influence their safety knowledge and behaviour,29 andthat rugby injuries can be reduced through comprehensivecoach education.30 In addition, netball coaches have reportedthat the likelihood of training players in safety strategies
increased if coaches had access to ideas about how to deliversuch training.31 A review of the broader injury prevention litera-ture highlighted the importance of taking a multifacetedapproach including behavioural or educational, and policy, rule,regulation or law-based interventions.32 This has been advo-cated in sports injury prevention generally33 and recommendedand implemented to prevent neck and spinal injuries in rugbyspecifically.15 16 The lessons learnt from the implementation ofa comprehensive New Zealand rugby injury prevention pro-gramme—including the importance of: partnerships and activelyengaging with relevant stakeholders; a multifaceted approach;using existing infrastructure; capitalising on external influences;and using plain language that had meaning for the programme
Figure 2 Ecological model ofpotential influences on adoption andimplementation of the Mayday SafetyProcedure by community rugbycoaches.
Table 2 Intervention Mapping matrix design
Determinant 1 Determinant 2 Determinant 3 Determinant 4
Performance objective 1 Change objective 1.1 Change objective 2.1 Change objective 3.1 Change objective 4.1Performance objective 2 Change objective 1.2 Change objective 2.2 Change objective 3.2 Change objective 4.2Performance objective 3 Change objective 1.3 Change objective 2.3 Change objective 3.3 Change objective 4.3Performance objective 4 Change objective 1.4 Change objective 2.4 Change objective 3.4 Change objective 4.4
4 Donaldson A, et al. Br J Sports Med 2012;0:1–9. doi:10.1136/bjsports-2012-091551
Original article
group.bmj.com on December 12, 2012 - Published by bjsm.bmj.comDownloaded from
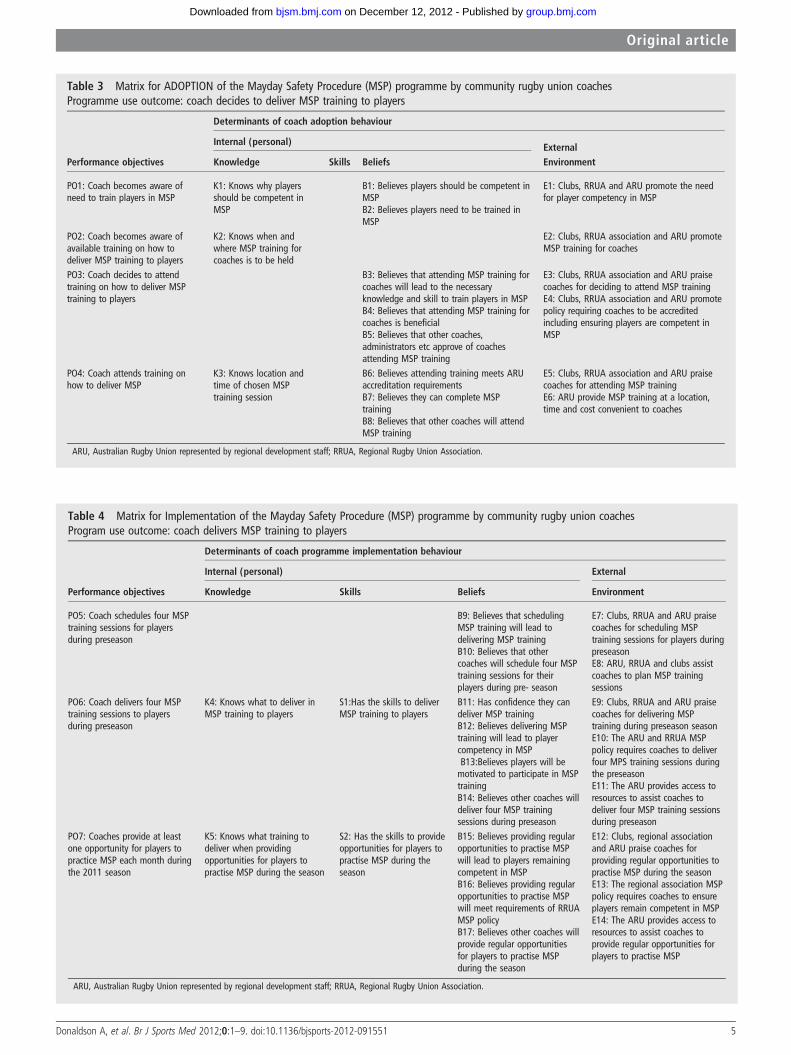
Table 4 Matrix for Implementation of the Mayday Safety Procedure (MSP) programme by community rugby union coachesProgram use outcome: coach delivers MSP training to players
Determinants of coach programme implementation behaviour
Internal (personal) External
Performance objectives Knowledge Skills Beliefs Environment
PO5: Coach schedules four MSPtraining sessions for playersduring preseason
B9: Believes that schedulingMSP training will lead todelivering MSP trainingB10: Believes that othercoaches will schedule four MSPtraining sessions for theirplayers during pre- season
E7: Clubs, RRUA and ARU praisecoaches for scheduling MSPtraining sessions for players duringpreseasonE8: ARU, RRUA and clubs assistcoaches to plan MSP trainingsessions
PO6: Coach delivers four MSPtraining sessions to playersduring preseason
K4: Knows what to deliver inMSP training to players
S1:Has the skills to deliverMSP training to players
B11: Has confidence they candeliver MSP trainingB12: Believes delivering MSPtraining will lead to playercompetency in MSPB13:Believes players will bemotivated to participate in MSPtrainingB14: Believes other coaches willdeliver four MSP trainingsessions during preseason
E9: Clubs, RRUA and ARU praisecoaches for delivering MSPtraining during preseason seasonE10: The ARU and RRUA MSPpolicy requires coaches to deliverfour MPS training sessions duringthe preseasonE11: The ARU provides access toresources to assist coaches todeliver four MSP training sessionsduring preseason
PO7: Coaches provide at leastone opportunity for players topractice MSP each month duringthe 2011 season
K5: Knows what training todeliver when providingopportunities for players topractise MSP during the season
S2: Has the skills to provideopportunities for players topractise MSP during theseason
B15: Believes providing regularopportunities to practise MSPwill lead to players remainingcompetent in MSPB16: Believes providing regularopportunities to practise MSPwill meet requirements of RRUAMSP policyB17: Believes other coaches willprovide regular opportunitiesfor players to practise MSPduring the season
E12: Clubs, regional associationand ARU praise coaches forproviding regular opportunities topractise MSP during the seasonE13: The regional association MSPpolicy requires coaches to ensureplayers remain competent in MSPE14: The ARU provides access toresources to assist coaches toprovide regular opportunities forplayers to practise MSP
ARU, Australian Rugby Union represented by regional development staff; RRUA, Regional Rugby Union Association.
Table 3 Matrix for ADOPTION of the Mayday Safety Procedure (MSP) programme by community rugby union coachesProgramme use outcome: coach decides to deliver MSP training to players
Determinants of coach adoption behaviour
Internal (personal) ExternalPerformance objectives Knowledge Skills Beliefs Environment
PO1: Coach becomes aware ofneed to train players in MSP
K1: Knows why playersshould be competent inMSP
B1: Believes players should be competent inMSPB2: Believes players need to be trained inMSP
E1: Clubs, RRUA and ARU promote the needfor player competency in MSP
PO2: Coach becomes aware ofavailable training on how todeliver MSP training to players
K2: Knows when andwhere MSP training forcoaches is to be held
E2: Clubs, RRUA association and ARU promoteMSP training for coaches
PO3: Coach decides to attendtraining on how to deliver MSPtraining to players
B3: Believes that attending MSP training forcoaches will lead to the necessaryknowledge and skill to train players in MSPB4: Believes that attending MSP training forcoaches is beneficialB5: Believes that other coaches,administrators etc approve of coachesattending MSP training
E3: Clubs, RRUA association and ARU praisecoaches for deciding to attend MSP trainingE4: Clubs, RRUA association and ARU promotepolicy requiring coaches to be accreditedincluding ensuring players are competent inMSP
PO4: Coach attends training onhow to deliver MSP
K3: Knows location andtime of chosen MSPtraining session
B6: Believes attending training meets ARUaccreditation requirementsB7: Believes they can complete MSPtrainingB8: Believes that other coaches will attendMSP training
E5: Clubs, RRUA association and ARU praisecoaches for attending MSP trainingE6: ARU provide MSP training at a location,time and cost convenient to coaches
ARU, Australian Rugby Union represented by regional development staff; RRUA, Regional Rugby Union Association.
Donaldson A, et al. Br J Sports Med 2012;0:1–9. doi:10.1136/bjsports-2012-091551 5
Original article
group.bmj.com on December 12, 2012 - Published by bjsm.bmj.comDownloaded from

adopters and implementers16—also informed method and strat-egy selection.
Although the idea of using theories and frameworks toinform the planning of programme implementation and dissem-ination activities can be daunting for those in non-academic set-tings,25 their use can enhance implementation anddissemination activities.34 DOI28 was identified as an appropri-ate theoretical framework to guide intervention strategy selec-tion and planning in this project because of its application inprevious health promotion programme diffusion and dissemin-ation research.35 36 In addition, preliminary project team discus-sions identified that DOI was meaningful for both the academicand practitioner team members. The particular aspects of DOIthat were applied to the selection, assessment and modificationof intervention strategies included the continuum of innovationand stages of adoption principles, multiple communication
channels, perceived programme characteristics (eg, compatibility,relative advantage, trialability, observability and complexity) andopinion leaders or change agents. The specific intervention strat-egies developed to support programme adoption and implemen-tation among coaches in this study, and how DOI was used toinform these strategies are outlined in tables 6 and 7.
DISCUSSIONAchieving widespread implementation of injury research out-comes or centrally developed safety policies and programmes incommunity sports is challenging.13 15 16 23 24 37 However,despite the use of dissemination and implementation theoriesand frameworks being recommended as a way of improving theuptake of evidence-based interventions, examples oftheory-informed attempts to address this problem in communitysports safety are not readily available. Although some studieshave developed sports-safety interventions using health promo-tion planning frameworks, including IM,15 38 39 we believe thisis the first study to focus specifically on planning the diffusionof a sports-safety programme within a sporting organisation.
The main strength of the process outlined above was that itinvolved a structured approach underpinned by a combinationof behaviour change theory and published evidence, comple-mented by an in-depth knowledge of the programme and inter-vention implementation context. Furthermore, it divided theprogram diffusion planning process into manageable and prag-matic steps based on answers to the straightforward questionsoutlined in table 8.
Anecdotally, community sports administrators have reportedfrustration with usual or traditional programme and policy dif-fusion strategies used by international, national, state andregional governing bodies and government departments (health,sport and recreation and local government). Typically, thesetend to jump directly from identifying what programme
Table 6 Evidence and theory informed, context-specific strategies developed to enhance the ADOPTION of the Mayday Safety Procedure(MSP) among community rugby coaches
Diffusion stage: adoptionPerformance objectives: PO1–PO4
Change objectives Intervention strategiesDiffusion of innovations construct used to inform strategydevelopment
Knowledge: K1–K3Beliefs: B1–B8Environment: E1–E6
▸ ARU develop MSP training package and incorporates packageinto existing coach accreditation training course
▸ ARU secure and promote RRUA support for MSP training▸ ARU liaise with RRUA and clubs to develop calendar of coachtraining events
▸ ARU and clubs use traditional and innovative methods to invitecoaches to attend MSP training
▸ ARU deliver coach MSP training courses using opinion leaders▸ ARU work with RRUA to develop and disseminate MSP policyand amend RRUA by-laws to require player MSP competency andincorporate the role of referees in monitoring player competency
▸ ARU work with RRUA to develop and disseminate Club SafetyCoordinator position description
▸ Compatibility: link coach MSP training to SmartRugby accreditationand current coaching ideas
▸ Multiple communication channels: use multimedia and inter-personalcommunication channels to disseminate MSP information andencourage coaches to attend MSP training
▸ Relative advantage: identify and promote relative advantage ofcoaches attending MSP training (eg, accreditation, developknowledge and skills to ensure player safety, learn skills to motivateplayers and work with small groups)
▸ Complexity: ensure it is easy for coaches to attend and participate inMSP training
▸ Opinion leaders: target high profile and respected clubs and coachesto participate in early coach MSP training sessions; identify andemploy high profile coach trainer to deliver MSP training
▸ Trialability and observability: ensure coach training includes severalopportunities to try and observe peers delivering MSP training
▸ Continuum of innovativeness: use different strategies to promoteattendance at MSP training to different levels of adopters
▸ Use of Change Agent: ARU development officer and club safetychampions liaise with RRUA, clubs and coaches about coach MSPtraining
ARU, Australian Rugby Union represented by regional development staff; RRUA, Regional Rugby Union Association.
Table 5 Determinants of coach adoption and implementation ofthe programme and the associated Social Cognitive Theory26
constructs
Determinants of programme adoptionand implementation identified in thisstudy
Social Cognitive Theoryconstruct incorporated
Knowledge Behavioural capability; situationBeliefs Self-efficacy; expectations,
expectancies; situationSkills Behavioural capability;
self-control; emotional copingresponses
Environment Environment; observationallearning; reciprocal determinism
Programme use outcome: coach delivers MSP training to players
6 Donaldson A, et al. Br J Sports Med 2012;0:1–9. doi:10.1136/bjsports-2012-091551
Original article
group.bmj.com on December 12, 2012 - Published by bjsm.bmj.comDownloaded from

adopters and implementers need to do, to implementing strat-egies to enhance adoption and implementation without askingand answering the other questions highlighted in table 8. Thiscould be described as a ‘miracle’ diffusion plan (figure 3) oftenoverly reliant on information dissemination, education andawareness raising as behaviour change strategies and a top-downcommunication process.
Understanding the implementation context and the perspec-tive of the intervention end-users are integral to the successfultranslation of sports injury prevention research.37 40 In thisproject, an ‘adoption and implementation planning group’ wasestablished with representation from all ecological or systemlevels of rugby considered likely to influence coach behaviour.This helped to ensure that the final diffusion plan was ‘owned’
by those who would ultimately implement it and that theactions and strategies included were likely to be doable and sus-tainable within the constraints and context of the region’s rugbyadministration beyond the life of the funded research project.
The diffusion plan development process and outcomesdescribed here were facilitated by the fact that the problemaddressed was identified by the ARU, and they actively contribu-ted to the development of a context-specific solution. This, inconjunction with a strong researcher–practitioner partnershipand a structured method of engaging with the programmeend-users, enabled the development of a diffusion plan thatmight bridge the gap between research (top-down) and commu-nity (bottom-up) driven programme implementation pro-cesses.33 41 In this case study, the application of the IM Step 5protocol facilitated an effective working partnership betweensports injury prevention scientists and community sports devel-opment experts, linking theoretical understandings of imple-mentation and behavioural science with a comprehensiveunderstanding of the programme implementation context.
Research translation models have been criticised as being toocomplex, academic or time consuming for application in real-world contexts.25 Following the IM Step 5 protocol for the firsttime was certainly time consuming and the language of behav-iour change theory and health promotion planning was challen-ging for researchers and practitioners alike. It took more timeand a different way of thinking compared with how communitysports administrators would normally plan the diffusion of asafety programme. However, it would be reasonable to expectthat this process would be much more efficient when under-taken again. In addition, a strength of IM is that the first twocore processes (figure 1)—posing planning problems as
Table 7 Evidence and theory informed, context-specific strategies developed to enhance Implementation of the Mayday Safety Procedure(MSP) among community rugby coaches
Diffusion stage: implementationPerformance objectives: PO5–PO7
Change objectives Intervention strategiesDiffusion of innovations theory construct to inform strategydevelopment
Knowledge: K4, K5Skills: S1, S2Beliefs: B9–B17Environment:E7–E14
▸ ARU works with the RRUA to create and implement monitoringsystems including team sheet noting of MSP incidents andpre-game referee auditing process for team MSP proficiency
▸ ARU and RRUA develop and disseminate clear statement of coachobligation (code of conduct/duty of care) and other supportmaterials including coaching resources, MSP poster and MSPwallet card
▸ ARU and RRUA develop and use creative/soft MSP reminders (eg,emails and texts with preseason message ‘Have you trained yourplayers in the Mayday Safety Procedure?’, ‘Are you SmartRugbyqualified?’ with details of available course dates and venues. Alsoin-season message: ‘Have your players practised Mayday thismonth?’, ‘A safe scrum is Mayday ready’ and ‘Can your playersanswer the Mayday call?’ Reminder email or text in early, mid andlate season: ‘Are your players Mayday competent?’ and ‘Are allnew players Mayday competent?’
▸ RRUA arrange for MSP demonstration by regional representativeteam early or through the season
▸ Multiple communication channels: use multimedia andinter-personal communication channels to disseminate informationencouraging coaches to schedule and deliver MSP training toplayers
▸ Compatibility: link coach delivery of MSP training to players withusual practise and current drills for practicing scrummaging
▸ Relative advantage: identify and promote relative advantage ofcoaches delivering MSP training to players (eg, duty of care, ensureplayer safety, build team morale, improve image of club and sport)
▸ Complexity: ensure it is easy for coaches to deliver MSP trainingand for referees to monitor and report player competency
▸ Opinion leaders: target high profile and respected coaches andteams to demonstrate delivering training and practising MSP. Useas case studies or testimonials
▸ Trialability: ensure resources include several short and easyopportunities to try delivery of MSP training to players
▸ Observability: eEnsure coaches are exposed to several examples ofothers delivering MSP training to, and providing practiseopportunities for players
▸ Continuum of innovativeness : use different strategies to promotedelivery of MSP training to different levels of adopters
▸ Use of Change Agent: ARU development officer and club safetychampions liaise with RRUA, clubs and coaches about coachdelivering MSP training to players
ARU, Australian Rugby Union represented by regional development staff; RRUA, Regional Rugby Union Association.
Table 8 Questions to ask and answer when planning the diffusionof a sports-safety programme
Question 1 Who will adopt and implement the program?Question 2 How can they be involved in the adoption and implementation
planning process?Question 3 What specific behaviours or actions will they need to do to adopt
and implement the program?Question 4 What knowledge, skills, beliefs and environmental support do
they need to undertake the required behaviours and actions?Question 5 What strategies can be put in place to influence these things?Question 6 What evidence or theory suggests that these strategies will work?Question 7 What specifically needs to be done to put these strategies in
place?
Donaldson A, et al. Br J Sports Med 2012;0:1–9. doi:10.1136/bjsports-2012-091551 7
Original article
group.bmj.com on December 12, 2012 - Published by bjsm.bmj.comDownloaded from
questions and brainstorming answers using current planninggroup knowledge—are not overly academic, and a participatoryplanning group and linkage system is established early in theprocess. This helps to ensure that the needs and capacities ofthe end-users and the complexities of the implementationcontext are considered from the start of the implementationplanning process. Programme impact and outcome is a functionof programme effectiveness and implementation.17 42
Therefore, although it may initially seem time consuming andcostly, investing in planning the implementation of evidence-based sports-safety programmes and using recognised imple-mentation planning frameworks, will probably improve theirimpact significantly.
Timing is crucial when developing and implementing newways of planning injury prevention programmes,16 and a senseof urgency is required to facilitate significant change withinsystems and organisations.43 We believe that the timing wasright and there was sufficient urgency for the ARU to committhe necessary resources to testing the new program diffusionplanning process described here. Not only was there new evi-dence highlighting the lack of success in translating organisa-tional safety policy into practice within community rugby,13 butthere was also anecdotal evidence of rugby administrator frustra-tion based on their experience of disseminating policies and
programmes to clubs and coaches, only to see very little changein behaviour and practice. We also believe that the ARU admin-istrators who invested in this project could see the long-termbenefits associated with improving programme diffusion pro-cesses within their organisation, above and beyond the immedi-ate improvement in player MSP competence.
CONCLUSIONThere is a growing awareness that sports-safety and injury pre-vention programme outcomes are determined by both theeffectiveness of the programme and the effectiveness of itsimplementation. The IM Step 5 protocol is a practical anduseful process that, if used creatively and flexibly, can lead tothe development of theory-informed, evidence-based andcontext-specific program diffusion plans. IM stresses the import-ance of researcher, practitioner and community end-user collab-oration early in the planning process. It also encourages the useof processes that place equal value on the knowledge, skills andexperience that these different groups bring to the diffusionplanning process.
Currently, we are evaluating the outcome of implementingthis diffusion plan in a single region during the 2011 rugbyseason to see if investment in the strategic planning process fordiffusion of the MSP was warranted.
Figure 3 A miracle approach toprogramme diffusion.ScienceCartoonsPlus.com
8 Donaldson A, et al. Br J Sports Med 2012;0:1–9. doi:10.1136/bjsports-2012-091551
Original article
group.bmj.com on December 12, 2012 - Published by bjsm.bmj.comDownloaded from
What are the new findings?
▸ This is the first published, detailed example of theapplication of a strategic process to plan the diffusion ofsports-safety intervention in a community sports setting.
▸ Step 5 of the Intervention Mapping health promotionprogramme planning protocol is a useful framework to planinterventions to facilitate the adoption and implementationof sports injury prevention programmes.
▸ Researcher–practitioner partnerships are a cornerstone toadoption and implementation planning to ensure theory,evidence and implementation context are all givenappropriate consideration.
▸ Finding a language that is meaningful to all stakeholders inan implementation planning partnership is a key challenge.
Acknowledgements The authors wish to thank Mr John Searl and Mr MatthewJohnston for their assistance in developing and implementing the diffusion plan, andfor helpful advice during the preparation of this paper. We also thank the rugbyreferees, coaches, players and administrators who participated in this study.
Contributors Both the authors (AD and RGP) made substantial contributions tothe conception and design of the study; the acquisition, analysis and interpretationof data; and drafting and revising the manuscript. Both the authors have given finalapproval of the version to be published.
Funding This research was funded by the NSW Sporting Injuries Committee.
Competing interests None.
Ethics approval The Medical and Community Human Research Ethics AdvisoryPanel at the University of New South Wales.
Provenance and peer review Not commissioned; externally peer reviewed.
REFERENCES1 King L, Hawe P, Wise M. Making dissemination a two-way process. Health Promot
Int 1998;13:237–44.2 Caburnay CA, Kreuter MW, Donlin MJ. Disseminating effective health promotion
programs from prevention research to community organizations. J Public HealthManag Pract 2001;7:81–9.
3 Glasgow RE, Vogt TM, Boles SM. Evaluating the public health impact of healthpromotion interventions: the RE-AIM framework. Am J Public Health1999;89:1322–7.
4 Finch CF. No longer lost in translation: the art and science of sports injuryprevention implementation research. Br J Sports Med 2011;45:1253–7.
5 Finch CF. Implementation and dissemination research: the time has come! Br JSports Med 2011;45:763–4.
6 Hanson D, Allegrante JP, Sleet AD, et al. Research alone is not sufficient to preventsports injury. Br J Sports Med Published Online First: 21 July 2012 doi:10.1136/bjsports-2012-091434
7 Finch CF, Donaldson A. A sports setting matrix for understanding theimplementation context for community sport. Br J Sports Med 2010;44:973–8.
8 Klugl M, Shrier I, McBain K, et al. The prevention of sport injury: an analysis of12 000 published manuscripts. Clin J Sport Med 2010;20:407–12.
9 Milburn PD. Biomechanics of rugby union scrummaging. Technical and safetyissues. Sports Med 1993;16:168–79.
10 Australian Rugby Union. Australian Rugby Union medical and safetyrecommendations for players, coaches, administrators & match officials, 2010.http://www2.rugby.com.au/LinkClick.aspx?fileticket=Bbng2ZhdFeM%3d&tabid=1950 (accessed Sept 2012).
11 Australian Rugby Union. SmartRugby Program. http://www.rugby.com.au/tryrugby/Coaching/Courses/SmartRugby.aspx (accessed Sept 2012)
12 Poulos RG, Donaldson A. Is sports safety policy being translated into practice: whatcan be learnt from the Australian Rugby Union Mayday procedure? Br J Sports Med2012;46:585–90.
13 Hollis SJ, Stevenson MR, McIntosh AS, et al. Compliance with return-to-playregulations following concussion in Australian schoolboy and community rugbyunion players. Br J Sports Med 2012;46:735–40.
14 Boffano P, Boffano M, Gallesio C, et al. Rugby players’ awareness of concussion. JCraniofac Surg 2011;22:2053–6.
15 Viljoen W, Patricios J. BokSmart—implementing a national rugby safety programme.Br J Sports Med 2012;46:692–3.
16 Chalmers DJ, Simpson JC, Depree R. Tackling rugby injury: lessons learned from theimplementation of a 5-year sports injury prevention program. J Sci Med Sport2004;7:74–84.
17 Bartholomew LK, Parcel GS, Kok G, et al. Planning health promotion programs. AnIntervention Mapping approach. 3rd edn. San Francisco: Jossey-Bass,2011:461–507.
18 Borkowski RP. The football coach and football safety. ASTM Special TechnicalPublication 1997;1305:167–71.
19 Emery CA, Hagel B, Morrongiello BA. Injury prevention in child and adolescentsport: whose responsibility is it? Clin J Sport Med 2006;16:514–41.
20 Finch CF, White P, Twomey D, et al. Implementing an exercise-training programmeto prevent lower-limb injuries: considerations for the development of a randomisedcontrolled trial intervention delivery plan. Br J Sports Med 2011;45:791–6.
21 Pinto D, Gomes H, Santos L, et al. Influence of presence of the coach on thebehaviour of the athlete in training. Br J Sports Med 2011;45:A4.
22 Hendricks S, Lambert M. Tackling in rugby: Coaching strategies for effectivetechnique and injury prevention. Int J Sports Sci Coach 2010;5:117–35.
23 Skille E. Understanding sport clubs as sport policy implementers: a theoreticalframework for the analysis of the implementation of central sport policy throughlocal and voluntary sport organizations. Int Rev Sociol Sport 2008;43:181–200.
24 Donaldson A, Leggett S, Finch CF. Sports policy development and implementation incontext: researching and understanding the perceptions of community end-users. IntRev Sociol Sport 2012;47:743–60.
25 Glasgow RE, Green LW, Taylor MV, et al. An evidence integration triangle foraligning science with policy and practice. Am J Prev Med 2012;42:646–54.
26 Baranowski T, Perry C, Parcel G. How individuals, environments, and healthbehavior interact. Social Cognitive Theory. In: Glanz K, Rimer B, Marcus Lewis F,eds. Health behavior and health education: theory, research and practice. 3rd edn.San Francisco: Jossey-Bass, 2002:165–84.
27 Miller AL, Krusky AM, Franzen S, et al. Partnering to translate evidence-basedprograms to community settings. Health Promot Pract 2012;13:559–66.
28 Rogers E. Diffusion of innovations. 5th edn. New York: Free Press, 2003:219–65.
29 Gianotti S, Hume PA, Tunstall H. Efficacy of injury prevention related coacheducation within netball and soccer. J Sci Med Sport 2010;13:32–5.
30 Gianotti SM, Quarrie KL, Hume PA. Evaluation of RugbySmart: a rugby unioncommunity injury prevention programme. J Sci Med Sport 2009;12:371–5.
31 Saunders N, Otago L, Romiti M, et al. Coaches’ perspectives on implementing anevidence-informed injury prevention programme in junior community netball. Br JSports Med 2010;44:1128–32.
32 Gielen AC, Sleet D. Application of behavior-change theories and methods to injuryprevention. Epidemiol Rev 2003;25:65–76.
33 Donaldson A. The development of preventive measures—the pragmatic approach.In: Verhagen E, van Mechelen W, eds. Methodology in sports injury research.Oxford: Oxford University Press, 2009:139–56.
34 Tabak RG, Khoong EC, Chambers DA, et al. Bridging research and practice: modelsfor dissemination and implementation research. Am J Prev Med 2012;43:337–50.
35 Nutbeam D, Harris E. Theory in a nutshell: a practical guide to health promotiontheories. 2nd edn. Sydney: McGraw Hill, 2004:23–7.
36 Owen N, Glanz K, Sallis J, et al. Evidence-based approaches to dissemination anddiffusion of physical activity interventions. Am J Prev Med 2006;31:S35–44.
37 Finch C. A new framework for research leading to sports injury prevention. J SciMed Sport 2006;9:3–9.
38 Collard DCM, Chinapaw MJM, Mechelen WV, et al. Design of the iPlay study:systematic development of a physical activity injury prevention programme forprimary school children. Sports Med 2009;39:889–901.
39 Simpson J, Chalmers D, Waller A. The New Zealand Rugby Injury and PerformanceProject: developing ‘Tackling Rugby Injury’, a national injury prevention program.Health Promot J Austr 2002;13:44–50.
40 Donaldson A, Finch C. Planning for implementation and translation: seek first tounderstand the end-users’ perspectives. Br J Sports Med 2012;46:306–7.
41 Layde PM, Christiansen AL, Peterson DJ, et al. A model to translate evidence-basedinterventions into community practice. Am J Public Health 2012;102:617–24.
42 Durlak J, DuPre E. Implementation matters: a review of research on the influence ofimplementation on program outcomes and the factors affecting implementation. AmJ Community Psychol 2008;41:327–50.
43 Kotter JP. Leading change: why transformation efforts fail. Harv Bus Rev1995:59–67.
Donaldson A, et al. Br J Sports Med 2012;0:1–9. doi:10.1136/bjsports-2012-091551 9
Original article
group.bmj.com on December 12, 2012 - Published by bjsm.bmj.comDownloaded from
doi: 10.1136/bjsports-2012-091551 published online December 11, 2012Br J Sports Med
Alex Donaldson and Roslyn G Poulos rugby union coachesprevention programme among community Planning the diffusion of a neck-injury
http://bjsm.bmj.com/content/early/2012/12/10/bjsports-2012-091551.full.htmlUpdated information and services can be found at:
These include:
References http://bjsm.bmj.com/content/early/2012/12/10/bjsports-2012-091551.full.html#ref-list-1
This article cites 33 articles, 13 of which can be accessed free at:
P<P Published online December 11, 2012 in advance of the print journal.
serviceEmail alerting
the box at the top right corner of the online article.Receive free email alerts when new articles cite this article. Sign up in
Notes
(DOIs) and date of initial publication. publication. Citations to Advance online articles must include the digital object identifier citable and establish publication priority; they are indexed by PubMed from initialtypeset, but have not not yet appeared in the paper journal. Advance online articles are Advance online articles have been peer reviewed, accepted for publication, edited and
http://group.bmj.com/group/rights-licensing/permissionsTo request permissions go to:
http://journals.bmj.com/cgi/reprintformTo order reprints go to:
http://group.bmj.com/subscribe/To subscribe to BMJ go to:
group.bmj.com on December 12, 2012 - Published by bjsm.bmj.comDownloaded from