
Pastoral Care in the event of attempted suicide
34
ABSTRACT The research assignment looks at the issues and characteristics surrounding suicide and attempted suicide and presents a pastoral care plan for an individual who has attempted to do so. It begins by speaking of the necessity for pastoral carer’s to take care of their own well-being, and understanding when they need to refer the individual for professional counselling, therapy, or medical treatment. The paper also speaks of the importance of the carer in understanding and researching the issues surrounding suicide that way they are in a better position to offer care. It explains that the individual, their family and friends and also their communities are affected by suicide, and therefore care must be given in varying degrees to all affected. The paper addresses the stigma often attached and to offers brief Biblical arguments and examples which seek to change Christian attitudes toward suicide. The physical, emotional and spiritual aspects of caring for a person in this situation are addressed and are later incorporated into the pastoral care plan. Often through the paper, and in particular the first half, references made to the ‘Pastor’ also refers to any person who engages in pastoral care. An appendix is attached which has statistical information from the Australian Bureau of Statistics website, other relevant resources and useful information, as well as links to websites intended to help those who are facing this issue.
-
Upload
morlingcollege -
Category
Documents
-
view
2 -
download
0
Transcript of Pastoral Care in the event of attempted suicide
ABSTRACT
The research assignment looks at the issues and characteristics surrounding suicide and attempted suicide and presents
a pastoral care plan for an individual who has attempted to do so. It begins by speaking of the necessity for pastoral
carer’s to take care of their own well-being, and understanding when they need to refer the individual for professional
counselling, therapy, or medical treatment. The paper also speaks of the importance of the carer in understanding and
researching the issues surrounding suicide that way they are in a better position to offer care. It explains that the
individual, their family and friends and also their communities are affected by suicide, and therefore care must be given
in varying degrees to all affected. The paper addresses the stigma often attached and to offers brief Biblical arguments
and examples which seek to change Christian attitudes toward suicide. The physical, emotional and spiritual aspects of
caring for a person in this situation are addressed and are later incorporated into the pastoral care plan. Often through
the paper, and in particular the first half, references made to the ‘Pastor’ also refers to any person who engages in
pastoral care. An appendix is attached which has statistical information from the Australian Bureau of Statistics
website, other relevant resources and useful information, as well as links to websites intended to help those who are
facing this issue.
Providing pastoral care in the event of an attempted suicide must take into consideration a number of aspects
starting with the relevant pastoral issues attached with offering care, and then also the spiritual, physical and emotional
dimensions of the people involved. In order to be better informed on how to handle the situation relevant scriptures
will be used to attempt to alleviate the stigma attached to suicide, and also to help shape the attitudes of both the
pastoral carer and the people affected.
Firstly, carer’s must be aware of their own well-being when seeking to care for someone who has attempted suicide.1
The situation can easily overcome and swamp the very person who is seeking to bring healing and restoration. The
pastoral carer must realise that they are not the sum total of all the person’s needs, and that they do not have the
ability alone to “fix” them. Care should be offered with the understanding that the final outcome of the situation is
always the decision of the person for whom they are caring. They must be aware of when they are out of their depth as
far as the support they can offer and be quick to refer the person to qualified counsellors, psychologists, physicians etc.,
and, in addition they should be conscious of their own motivations. As a result of their spiritual authority and privileged
access into people’s lives, pastors have a considerable power and influence which could lead to them using the
relationship to serve their own need of value, worth, identity etc.2 For this reason, it is a good idea for the pastoral
carer to regularly meet with a supervising mentor who they can be honest with and to whom they are accountable.
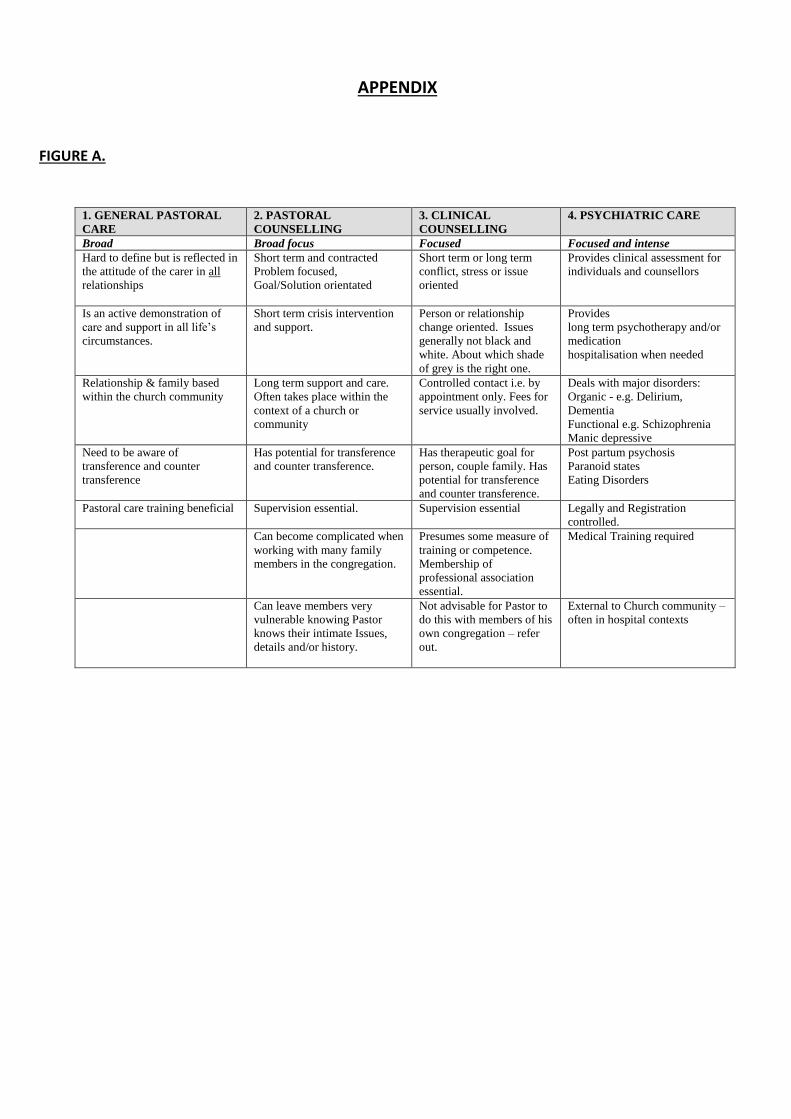
There also needs to be awareness of the difference between Pastoral Care, and Pastoral Counselling. Pastoral care is
generally much broader in focus and in the number of those for whom care is provided, whereas Counselling becomes
much more limited in the scope of people being cared for, and much more focused in the issues being dealt with, (See
Figures A3 and B4 in the Appendix).
1 On The Line, "Supporting Someone after a Suicide Attempt," http://suicideline.org.au/worried-about-someone/supporting-someone-after-a-suicide-attempt., Peter Brain, Going the Distance (Kingsford, NSW: Matthias Media, 2006).258, Wayne Cordeiro, Leading on Empty : Refilling Your Tank and Renewing Your Passion (Minneapolis, Minn.: Bethany House, 2009).183-202 2 Howard John Clinebell and Bridget Clare McKeever, Basic Types of Pastoral Care & Counseling : Resources for the Ministry of Healing and Growth, Updated and rev. / Bridget Clare McKeever. ed. (Nashville: Abingdon Press, 2011).461-77 3 Morling College lecture notes PC403/603 & MCO503 Week 1 Semester 2 – 24.07.2014 Page 7 4 Peter Janetzki, "Clarifying the Roles of Pastoral Care & Counselling within the Care Ministry of the Church.," http://www.peterj.com.au/wp-content/uploads/2013/03/Journal-Article.pdf.
Secondly, it is important that the pastor is informed about the issues surrounding suicide. By doing some research on
the topic, it will give insight into things such as the prevalence of the problem in society, common causes leading to
suicide, the demographic of people most at risk, and the warning indicators that an individual is thinking of taking their
own life. For example a quick look on the Australian Bureau of Statistics will show that the most suicides for men and
women occur in people aged between 35 and 44 years old. This is consistent across all states in Australia with the
exception of two states/territories – one being the Northern Territory whose most suicides occur for those aged
between 15-24 years of age. (See Tables 5.1 and 5.2 in Appendix). Therefore whilst for most states the age group most
at risk is 35 to 44 years old, there seems to be some reason why (for instance things like: drug/alcohol abuse, sexual
abuse, lack of employment etc etc.), in the Northern Territory the trend is different. So whilst not telling us everything
about the situation, these resources do provide valuable information. Closer research will give the carer even further
insight such as the fact that although men have higher rates of suicide, women actually have higher rates of attempted
suicide.5 As Howard Clinebell states, “Pastor’s need to know how to prevent suicide and to have enough information to
make quick evaluations of the likelihood that people in different categories – age, gender, suicidal thinking, life crises, or
levels of depression – will act on their suicidal threats or impulses.”6 Being armed with this kind of information will
assist the pastor to know if a person who has attempted suicide is planning to do so again. It is helpful for the carer to
try and understand the “head space” of the person who is thinking of or has attempted suicide. Psychologist Edwin
Shneidman, a leading authority on suicide, highlights ten characteristics that are commonly associated with suicide.7
(See Apendix Figure C.)8 Being aware of these will give insight into the possible thought patterns of those who are
affected.
Thirdly, the pastor should provide care for the individual directly, and also by providing the support needed to enable
their family, friends and community to assist. Although the main priority is to care for the person who has attempted
suicide, the effects of suicide or attempted suicide extend well beyond the individual. For this reason it is necessary that
pastoral care is provided to the person’s community, friends and family who are likely to be having feelings such as:
anger, shame, guilt, and fear, or who may be avoiding, minimising or simply pretending the problem doesn’t concern
5 D. Geldard and K. Geldard, Basic Personal Counseling: A Training Manual for Counselors, 5th ed. (Frenchs Forest, NSW: Prentice Hall / Pearson Learning Australia, 2005)., Clinebell and McKeever, Basic Types of Pastoral Care & Counseling : Resources for the Ministry of Healing and Growth.148 6 Basic Types of Pastoral Care & Counseling : Resources for the Ministry of Healing and Growth.148 7 Edwin Shneidman, Definition of Suicide (Jason Aronson, Incorporated, 1977).121-49, 8 AIPC (Australian Institute of Professional Counsellors), "Suicide: Statistics, Characteristics and Myths," AIPC Article Library, no. June 14, 2012 (2012).
them.9 In addition, seeing as the suicide of a friend or family member has been recognised as a contributing factor to
further suicides10, creating an environment where people feel safe to talk about it, is of the utmost importance.
Knowing and providing access to government and community resources and services designed to help prevent suicide is
one of the simple ways to initiate the conversation. (See Figure D, in Appendix for some resources).
There has traditionally been, and still exists, stigma attached to suicide in Christian communities.11 Much of this
stems from the 4th century AD when Augustine strongly pronounced against suicide in The City Of God, claiming it was a
type of murder.12 During the 16th and 17th centuries in England people such as, George Abbot, Anthony Anderson,
Thomas Beard, Bishop Lancelot Andrews and John Abernethy spoke so strongly against suicide that they went as far as
saying that those who committed this heinous act would be eternally condemned.13 Others such as James Gustafson,
claim that suicidal thoughts or actions stem from a poor spiritual state. In essence they say that if a person’s spiritual
walk with God is healthy, they would not be tempted to take their own life.14 Unfortunately, these attitudes can
sometimes still be expressed towards the person and the family of a person who has attempted suicide. These attitudes
only serve to further isolate them and thus aggravate the problem instead of bringing healing.
In response to the attitude above, it is worth noting that the Bible clearly says that there is only one unforgivable sin,15
and this is not the taking of one’s own life. Secondly there are examples recorded in scripture of prophets or people
who are regarded as heroes of the faith, who have despaired of life. For instance, the author of Ecclesiastes came to a
point of hating life,16 Jonah, although a prophet sent by God, reached a point where he preferred to die than live.17
Elijah wanting to die, prayed that God would take his life,18 as did Moses who came to a point where he was being
overwhelmed by the burden placed upon him,19 and the Apostle Paul speaks of being subjected to such intense pressure
9 On The Line, "Suicide Call Back Service," https://www.suicidecallbackservice.org.au/concerned-about-someone/supporting-someone-after-a-suicide-attempt. 10 Geldard, Basic Personal Counseling: A Training Manual for Counselors., Jack Wellman, "Suicidal Thoughts: 7 Biblical Tips," Telling Ministries LLC, http://www.whatchristianswanttoknow.com/suicidal-thoughts-7-biblical-tips/. 11 Kathy McKay and Jann E Schlimme, "Making Sense of Suicide," (2011). 12 Elizabeth K. Hunter, "'Between the Bridge and the Brook'," Reformation & Renaissance Review: Journal of the Society for Reformation Studies 15, no. 3 (2013).241 13 Ibid.238 14 Charles W. Stewart, "What Does the Bible Say About Suicide," Journal of Pastoral Care 45, no. 1 (1991).88-9 15 Matthew 12:31-32 16 Ecclesiastes 2:17 17 Jonah 4:3 18 1 Kings 19:4 19 Numbers 11:11-15
that he despaired of life itself.20 What this shows is that as humans we are all subject to times of weakness and intense
suffering which at times seems greater than we can bear, not to mention those who suffer mental illnesses, which come
with all their complexities. All people, given the right circumstances, are potentially susceptible and at risk of self harm.
In contrast, the Bible sympathises with those who suffer and records the cries and complaints of those who endured the
darkest of times. Psalm 69 gives a great example of ongoing suffering – to the point where the Psalmist is weary of
calling for help (vs3), and Psalm 88 ends so bleakly that the final words of the psalmist are ‘darkness is my closest
friend’. When attempting to care for someone who has attempted suicide it helps to remove the stigma by showing
that many others are going through similar struggles and that they are not alone. The scriptures provide some of the
most assuring passages that simply give ‘permission’ for the person to feel the way they are without compounding their
problem by added the further burden of guilt and shame upon them.
Scriptures provide a great spiritual source of strength for someone who has attempted suicide. The Bible affirms that
they have Christ as a mediator who is able to empathize with their weaknesses, and who offers grace and help in their
time of need.21 Through scripture they can be affirmed of their worth, value and position in Christ22, they are assured
that God is close to them23, that God has a plan and a good future for them24, and that they are able to overcome their
struggle through the strength they receive from Christ.25 Care should be used with passages that may often be quoted
with intentions to comfort, such as 1 Corinthians 10:13 because it may cause a person to feel as though they failed
when they should have found the way out, and thus have a negative impact. However, speaking the truth of God in
scriptures is a great way to provide the spiritual care they need. Other ways in which they will need to be cared for
spiritually is through ongoing prayer, through fellowship, through music and meditation on God, and through helping to
redirect their mind on all of God’s blessings in order to rediscover the joy, hope and peace they have in Christ.26
Nurturing a person’s spirit as a means to help recover from attempted suicide is recommended on suicide prevention
20 2 Corinthians 1:8 21 Hebrews 4:14-16 22 Psalm 139, John 3:16, Galatians 3:26, 1 John 3:1-2 23 Psalm 34:11 24 Jeremiah 29:11 25 Philippians 4:12-13 26 Philippians 4:4-9

websites for even those who do not necessarily profess a Christian faith, therefore consider how much more beneficial
it is for those who cry out to the one true God.27
To look after the emotional well-being of someone who has attempted suicide required regular contact in their
presence. They should also always have people who love and care for them around them for support. They will need to
be able to talk honestly and frankly about their thoughts and feelings with someone who they trust, and they will also
need the company, interaction and emotional support of friends and family who are happy just to be a part of their life
and participate in regular fun and light hearted activities with them. The carer should try and understand their
perspective and feelings and to seek the root causes that led to them attempting suicide in order to then put a plan in
place to prevent the same from re-occurring. It is imperative that they immediately seek professional help from a
counsellor or psychiatrist.28 The person should be encouraged to take as much responsibility for their own welfare as
they are capable of at that time, therefore by helping them to write out a safety plan in the event that they feel suicidal
again, or even getting them to sign a ‘Life Contract’29 in the presence of a witness, can assist them to do so.30
The physical ways in which care can be shown to someone who has attempted suicide is firstly to ensure that they
are safe and no longer in danger. They may need hospitalisation or medication that may help with the situation, and
therefore a visit to their General Practitioner may be what they require. The carer should ensure that all the means by
which they could plan to end their life are removed. This may include things like removing pills, razors, rope, poison etc.
Ensuring they are getting proper and regular sleep and that they are not using drugs or alcohol is important as a lack of
sleep or the use of drugs and alcohol can impair their ability to think clearly and logically. Encouraging them to do some
kind of exercise can also help to clear their mind, as well as provide them with a general sense of well-being. Depending
on what physical and emotional state they are in, they may also need assistance in completing everyday regular errands
27 David Horgan, "Body, Mind, Spirit... Tips," http://suicideprevention.com.au/body-mind-spirit-tips-2/. 28 Clinebell and McKeever, Basic Types of Pastoral Care & Counseling : Resources for the Ministry of Healing and Growth.148-51 29 A life contract is a simple form which states something like: “I will agree not to harm myself and if I do have suicidal thoughts, I agree that I will contact one of the following people….family member, friend, doctor, counsellor, help line etc.” 30 Suicide Call Back Service, "Supporting Someone after a Suicide Attempt," https://www.suicidecallbackservice.org.au/concerned-about-someone/supporting-someone-after-a-suicide-attempt.
and duties such as house-keeping, grocery shopping, washing and cooking etc., and they may also not be able to work
and therefore be struggling financially. The carer ought to keep these things into consideration and seek to help in
these areas also, therefore they may be required to organise a few people who can commit to provide meals, or they
may need to contact financial institutions for assistance etc.
Below I have created an example pastoral care plan that could be used for people who have attempted suicide.
Please not that this may not be applicable in all cases, and is intended primarily as a template to be used should the
need arise.
Pastoral Care Plan
Person’s situation: Ali has attempted suicide by jumping off a high bridge. Luckily his fall was broken by a stray
sheep which gave it’s life to save his, however still leaving him with two broken legs, a cracked rib and significant
bruising. He is 37 years old and owns a dairy farm in Tilba Tilba on the south coast of NSW, about a 5 hour drive from
Sydney. He lives on the farm with his wife Fatima and their three children Muhammed – 11 years old, Rasha – 9, and
Christian – 5. Profits have been low due to the farm being affected by a long drought, and they recently had to lay off
several of their employees. Muhammed is about to start high school but the nearest school is very far and would
require him to board. Given their current financial situation, Ali and Fatima cannot afford to send him to boarding
school and were considering studying by correspondence. Meanwhile, Christian is also about to start school. Fatima
wants to return to Sydney to live close to her family, who said they would provide temporary financial support and
housing on the condition that she and her family convert back to Islam. Ali has been disowned by his entire family, who
live in the neighbouring town 20km away, after his conversion to Christianity 8 years ago.
Major needs for the person:
Physical
- Ongoing medical care (doctor’s visits, getting medication etc)
- Mobility (general everyday actions ie. bathroom visits, showering, ‘walking’ around the farm)
- Worker to continue every day running of the farm
- Money
Social/Relational
- Regular Interaction with friends, family and church members
- Non-judgemental support
- Support for his immediate family
- Safety plan
Emotional/Mental
- Counselling/Psychological Therapy
- Self worth
- Love, Acceptance, Hope
- Family counselling
- Accountability Partner (someone he can talk to if he is feeling suicidal again)
Spiritual
- Prayer
- Fellowship/Church Family
- Comfort/Encouragement through scripture
- Faith strengthening support for him and his family
Support Network:
Pastor – Pastoral Care, Emotional Support, Spiritual Guidance, Fellowship, Accountability
Counsellor/Psychologist – Emotional Support, Accountability, Mental Support
Doctor – Physical healing, referral to other professionals
Wife – Physical support (helping him with bathroom visits, mobility, farm work etc), emotional support
Church Community/Friends – Emotional support, ongoing social interaction and visits, spiritual support,
financial support, help with work on the farm, prayer support, non-judgemental acceptance, support for his
family’s emotional and physical needs eg. cooking meals, cleaning house, helping to bathe and dress Ali,
people willing to listen and talk with wife and children.
Major Overall Objectives for Pastoral Care Plan:
- To prevent further suicide attempts by helping Ali to see hope and a realistic positive way forward
- To provide emotional, spiritual, social, and physical support for his immediate family
- To provide emotional and spiritual support for the church community and friends affected
- To create an environment of love and acceptance for him and his family
- To help ease the factors which led to his attempted suicide
Length of Plan and How It Will Be Reviewed:
This plan will last one year with reducing intensity based on how well Ali responds. There is a possibility of extension if
recovery takes longer than anticipated.
The plan will be reviewed after 1 month, 3 months, 7 months, and 12 months of activation. At each interval of the plan
some of the more demanding aspects of caring will be discontinued. For example, after 3 months his legs and rib should
have healed, therefore he may no longer need someone to help him bathe, and after 1 month he may no longer need
constant regular visits. This is designed to slowly and gently allow him to return to his position of self-sufficiency
without becoming disempowered and overly dependent, nor feeling neglected or abandoned.
Assessment in the reviews will be based on: whether there have been additional suicide attempts or ideation,
doctor/counsellor/psychologist recommendation, the needs of Ali and his family as expressed by them directly, and the
ability of church members and friends to continue providing care without them feeling overburdened. The effectiveness
will also be measured by the general well-being and stress levels of Ali and his family.
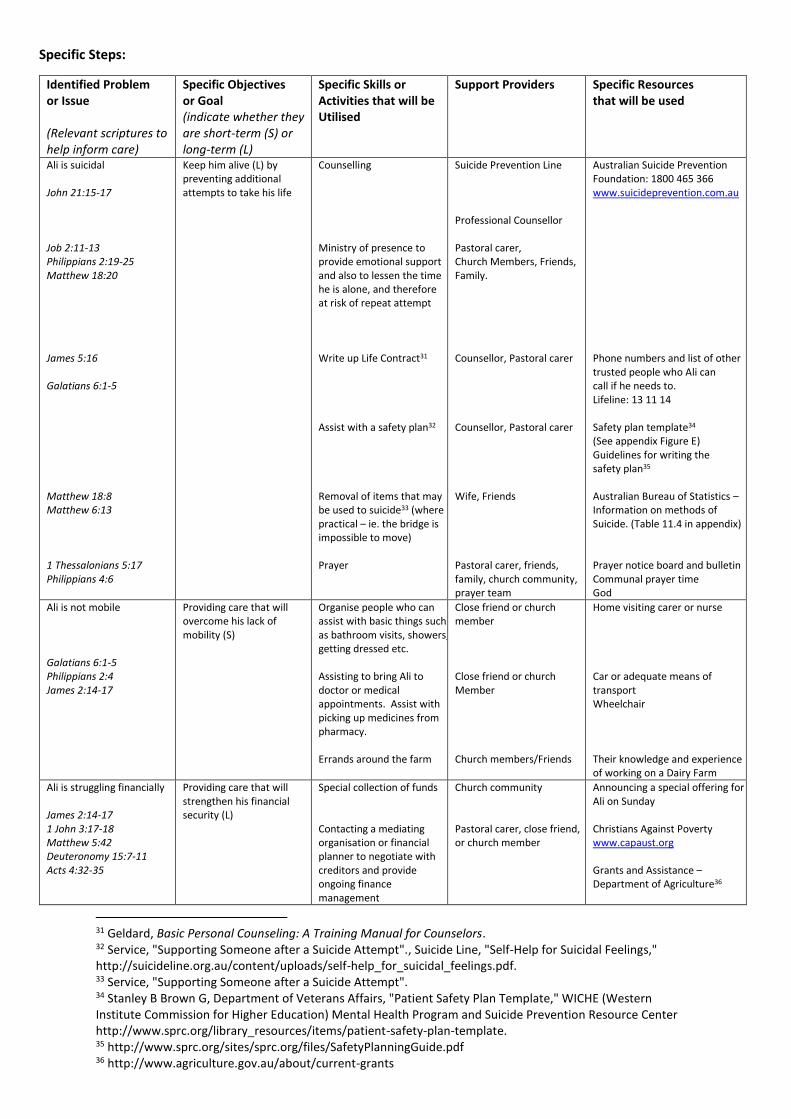
Specific Steps:
Identified Problem or Issue (Relevant scriptures to help inform care)
Specific Objectives or Goal (indicate whether they are short-term (S) or long-term (L)
Specific Skills or Activities that will be Utilised
Support Providers Specific Resources that will be used
Ali is suicidal John 21:15-17 Job 2:11-13 Philippians 2:19-25 Matthew 18:20 James 5:16 Galatians 6:1-5 Matthew 18:8 Matthew 6:13 1 Thessalonians 5:17 Philippians 4:6
Keep him alive (L) by preventing additional attempts to take his life
Counselling Ministry of presence to provide emotional support and also to lessen the time he is alone, and therefore at risk of repeat attempt Write up Life Contract31 Assist with a safety plan32 Removal of items that may be used to suicide33 (where practical – ie. the bridge is impossible to move) Prayer
Suicide Prevention Line Professional Counsellor Pastoral carer, Church Members, Friends, Family. Counsellor, Pastoral carer Counsellor, Pastoral carer Wife, Friends Pastoral carer, friends, family, church community, prayer team
Australian Suicide Prevention Foundation: 1800 465 366 www.suicideprevention.com.au Phone numbers and list of other trusted people who Ali can call if he needs to. Lifeline: 13 11 14 Safety plan template34 (See appendix Figure E) Guidelines for writing the safety plan35 Australian Bureau of Statistics – Information on methods of Suicide. (Table 11.4 in appendix) Prayer notice board and bulletin Communal prayer time God
Ali is not mobile Galatians 6:1-5 Philippians 2:4 James 2:14-17
Providing care that will overcome his lack of mobility (S)
Organise people who can assist with basic things such as bathroom visits, showers, getting dressed etc. Assisting to bring Ali to doctor or medical appointments. Assist with picking up medicines from pharmacy. Errands around the farm
Close friend or church member Close friend or church Member Church members/Friends
Home visiting carer or nurse Car or adequate means of transport Wheelchair Their knowledge and experience of working on a Dairy Farm
Ali is struggling financially James 2:14-17 1 John 3:17-18 Matthew 5:42 Deuteronomy 15:7-11 Acts 4:32-35
Providing care that will strengthen his financial security (L)
Special collection of funds Contacting a mediating organisation or financial planner to negotiate with creditors and provide ongoing finance management
Church community Pastoral carer, close friend, or church member
Announcing a special offering for Ali on Sunday Christians Against Poverty www.capaust.org Grants and Assistance – Department of Agriculture36
31 Geldard, Basic Personal Counseling: A Training Manual for Counselors. 32 Service, "Supporting Someone after a Suicide Attempt"., Suicide Line, "Self-Help for Suicidal Feelings," http://suicideline.org.au/content/uploads/self-help_for_suicidal_feelings.pdf. 33 Service, "Supporting Someone after a Suicide Attempt". 34 Stanley B Brown G, Department of Veterans Affairs, "Patient Safety Plan Template," WICHE (Western Institute Commission for Higher Education) Mental Health Program and Suicide Prevention Resource Center http://www.sprc.org/library_resources/items/patient-safety-plan-template. 35 http://www.sprc.org/sites/sprc.org/files/SafetyPlanningGuide.pdf 36 http://www.agriculture.gov.au/about/current-grants
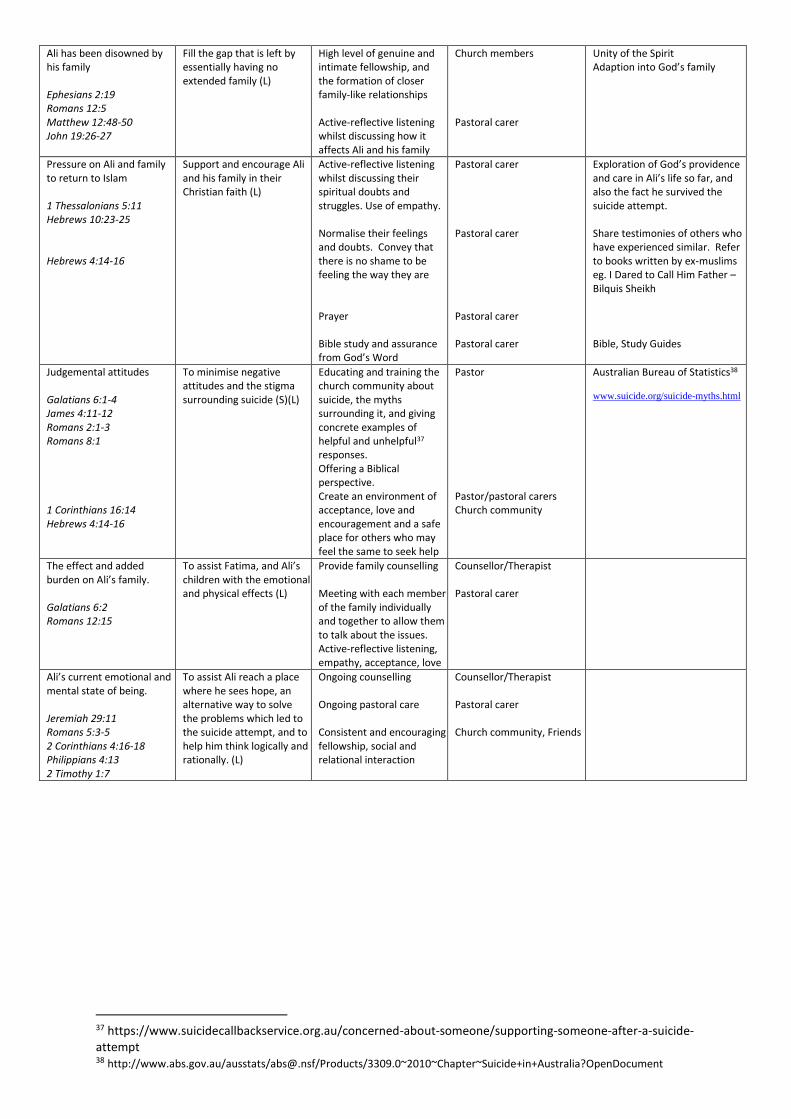
Ali has been disowned by his family Ephesians 2:19 Romans 12:5 Matthew 12:48-50 John 19:26-27
Fill the gap that is left by essentially having no extended family (L)
High level of genuine and intimate fellowship, and the formation of closer family-like relationships Active-reflective listening whilst discussing how it affects Ali and his family
Church members Pastoral carer
Unity of the Spirit Adaption into God’s family
Pressure on Ali and family to return to Islam 1 Thessalonians 5:11 Hebrews 10:23-25 Hebrews 4:14-16
Support and encourage Ali and his family in their Christian faith (L)
Active-reflective listening whilst discussing their spiritual doubts and struggles. Use of empathy. Normalise their feelings and doubts. Convey that there is no shame to be feeling the way they are Prayer Bible study and assurance from God’s Word
Pastoral carer Pastoral carer Pastoral carer Pastoral carer
Exploration of God’s providence and care in Ali’s life so far, and also the fact he survived the suicide attempt. Share testimonies of others who have experienced similar. Refer to books written by ex-muslims eg. I Dared to Call Him Father – Bilquis Sheikh Bible, Study Guides
Judgemental attitudes Galatians 6:1-4 James 4:11-12 Romans 2:1-3 Romans 8:1 1 Corinthians 16:14 Hebrews 4:14-16
To minimise negative attitudes and the stigma surrounding suicide (S)(L)
Educating and training the church community about suicide, the myths surrounding it, and giving concrete examples of helpful and unhelpful37 responses. Offering a Biblical perspective. Create an environment of acceptance, love and encouragement and a safe place for others who may feel the same to seek help
Pastor Pastor/pastoral carers Church community
Australian Bureau of Statistics38
www.suicide.org/suicide-myths.html
The effect and added burden on Ali’s family. Galatians 6:2 Romans 12:15
To assist Fatima, and Ali’s children with the emotional and physical effects (L)
Provide family counselling Meeting with each member of the family individually and together to allow them to talk about the issues. Active-reflective listening, empathy, acceptance, love
Counsellor/Therapist Pastoral carer
Ali’s current emotional and mental state of being. Jeremiah 29:11 Romans 5:3-5 2 Corinthians 4:16-18 Philippians 4:13 2 Timothy 1:7
To assist Ali reach a place where he sees hope, an alternative way to solve the problems which led to the suicide attempt, and to help him think logically and rationally. (L)
Ongoing counselling Ongoing pastoral care Consistent and encouraging fellowship, social and relational interaction
Counsellor/Therapist Pastoral carer Church community, Friends
37 https://www.suicidecallbackservice.org.au/concerned-about-someone/supporting-someone-after-a-suicide-attempt 38 http://www.abs.gov.au/ausstats/[email protected]/Products/3309.0~2010~Chapter~Suicide+in+Australia?OpenDocument
APPENDIX
FIGURE A.
1. GENERAL PASTORAL
CARE
2. PASTORAL
COUNSELLING
3. CLINICAL
COUNSELLING
4. PSYCHIATRIC CARE
Broad Broad focus Focused Focused and intense
Hard to define but is reflected in
the attitude of the carer in all
relationships
Short term and contracted
Problem focused,
Goal/Solution orientated
Short term or long term
conflict, stress or issue
oriented
Provides clinical assessment for
individuals and counsellors
Is an active demonstration of
care and support in all life’s
circumstances.
Short term crisis intervention
and support.
Person or relationship
change oriented. Issues
generally not black and
white. About which shade
of grey is the right one.
Provides
long term psychotherapy and/or
medication
hospitalisation when needed
Relationship & family based
within the church community
Long term support and care.
Often takes place within the
context of a church or
community
Controlled contact i.e. by
appointment only. Fees for
service usually involved.
Deals with major disorders:
Organic - e.g. Delirium,
Dementia
Functional e.g. Schizophrenia
Manic depressive
Need to be aware of
transference and counter
transference
Has potential for transference
and counter transference.
Has therapeutic goal for
person, couple family. Has
potential for transference
and counter transference.
Post partum psychosis
Paranoid states
Eating Disorders
Pastoral care training beneficial Supervision essential.
Supervision essential Legally and Registration
controlled.
Can become complicated when
working with many family
members in the congregation.
Presumes some measure of
training or competence.
Membership of
professional association
essential.
Medical Training required
Can leave members very
vulnerable knowing Pastor
knows their intimate Issues,
details and/or history.
Not advisable for Pastor to
do this with members of his
own congregation – refer
out.
External to Church community –
often in hospital contexts
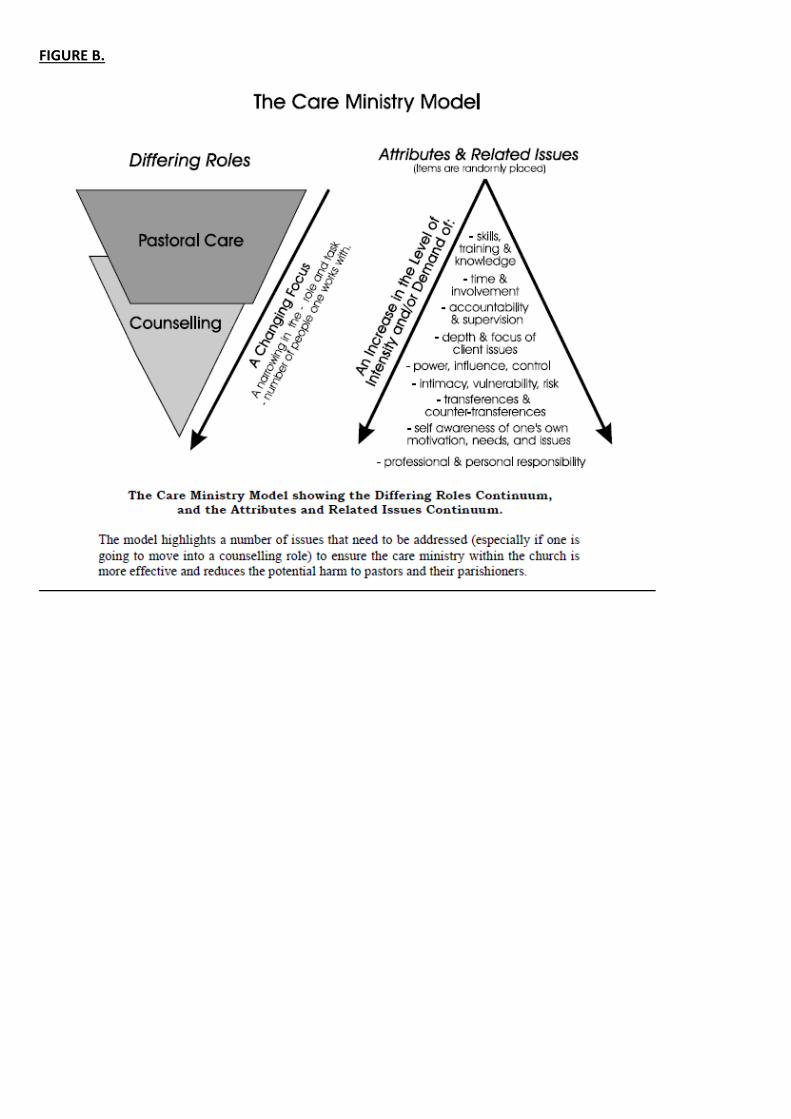
FIGURE B.
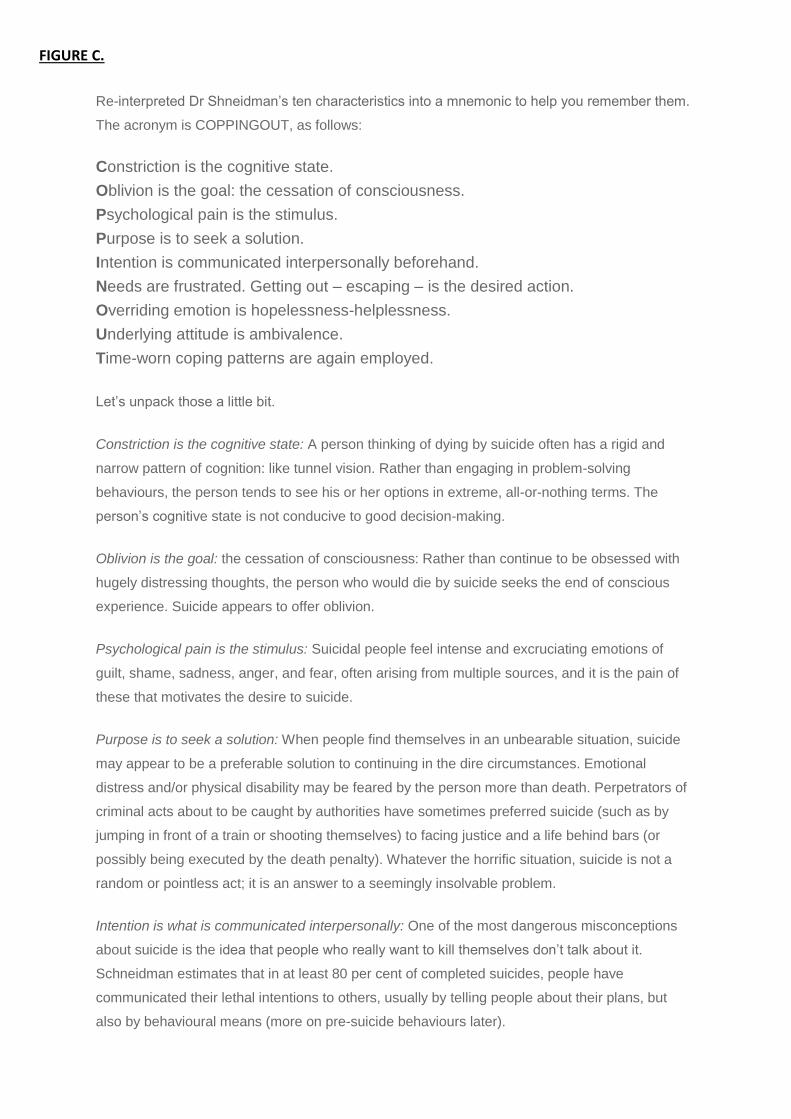
FIGURE C.
Re-interpreted Dr Shneidman’s ten characteristics into a mnemonic to help you remember them.
The acronym is COPPINGOUT, as follows:
Constriction is the cognitive state.
Oblivion is the goal: the cessation of consciousness.
Psychological pain is the stimulus.
Purpose is to seek a solution.
Intention is communicated interpersonally beforehand.
Needs are frustrated. Getting out – escaping – is the desired action.
Overriding emotion is hopelessness-helplessness.
Underlying attitude is ambivalence.
Time-worn coping patterns are again employed.
Let’s unpack those a little bit.
Constriction is the cognitive state: A person thinking of dying by suicide often has a rigid and
narrow pattern of cognition: like tunnel vision. Rather than engaging in problem-solving
behaviours, the person tends to see his or her options in extreme, all-or-nothing terms. The
person’s cognitive state is not conducive to good decision-making.
Oblivion is the goal: the cessation of consciousness: Rather than continue to be obsessed with
hugely distressing thoughts, the person who would die by suicide seeks the end of conscious
experience. Suicide appears to offer oblivion.
Psychological pain is the stimulus: Suicidal people feel intense and excruciating emotions of
guilt, shame, sadness, anger, and fear, often arising from multiple sources, and it is the pain of
these that motivates the desire to suicide.
Purpose is to seek a solution: When people find themselves in an unbearable situation, suicide
may appear to be a preferable solution to continuing in the dire circumstances. Emotional
distress and/or physical disability may be feared by the person more than death. Perpetrators of
criminal acts about to be caught by authorities have sometimes preferred suicide (such as by
jumping in front of a train or shooting themselves) to facing justice and a life behind bars (or
possibly being executed by the death penalty). Whatever the horrific situation, suicide is not a
random or pointless act; it is an answer to a seemingly insolvable problem.
Intention is what is communicated interpersonally: One of the most dangerous misconceptions
about suicide is the idea that people who really want to kill themselves don’t talk about it.
Schneidman estimates that in at least 80 per cent of completed suicides, people have
communicated their lethal intentions to others, usually by telling people about their plans, but
also by behavioural means (more on pre-suicide behaviours later).
Needs are frustrated: Frustrated psychological needs make someone more vulnerable to suicidal
ideation. People who have very high standards and expectations can feel especially disappointed
when progress towards their goals is thwarted. If they attribute the failure or disappointment to
their own shortcomings, they may come to see themselves as worthless, unlovable, or
incompetent: a perfect set-up for suicide. For young people, particularly, career/employment
issues, family conflict, and other interpersonal frustrations can precipitate suicide. Similarly,
studies have found that, in periods of high unemployment, suicide rates go up (Yang, B.,
Motohashi, Y., & Lester, D., 1992).
Getting out – escaping – is the desired action: Suicide seems to provide a way out of painful self-
awareness and/or intolerable circumstances: a definite way out.
Overriding emotion is hopelessness-helplessness: Even more central to predicting suicidal
behaviour than intense negative emotions (such as fear, anger, or sadness), is the pervasive
sense that the future is hopeless, and that no one can do anything to help. Pessimism breeds
suicide.
Underlying attitude is ambivalence: For all the intensity of negative emotion and sincere desire to
die, however, there is simultaneously in most suicides an equally strong wish to find a way out of
the dilemma. Thus, suicide contemplation is about intense ambivalence. The skilled social
support person can tap into this ambivalence, helping the person to swing to the “want to find a
way out of the dilemma” pole.
Time-worn coping patterns are again employed: Not surprisingly, people thinking about killing
themselves generally use the same patterns of thought and ways of coping to deal with the
current crisis as they have always used. If someone is habitually a loner, refusing to ask others
for help or believing that no one can help, that person is likely to act from a stance of isolation in
the lead-up to the suicide as well (Oltmanns & Emery, n.d.).
FIGURE D.
Crisis helplines
Lifeline: 13 11 14
Suicide Call Back Service: 1300 659 467
Kids Helpline (for young people aged 5 to 25 years): 1800 55 1800
Suicide Line: 1300 651 251
Australian Suicide Prevention Foundation: 1800 465 366
Websites
www.suicidecallbackservice.org.au
www.suicideline.org.au
www.kidshelp.com.au
www.lifeline.org.au
www.suicideprevention.com.au
www.suicidepreventionaust.org
www.jigsaw.ontheline.org.au

FIGURE E.

INFORMATION FROM THE AUSTRALIAN BUREAU OF STATISTICS
OVERVIEW
In 2010, a senate inquiry (The Hidden Toll: Suicide in Australia) highlighted the potential costs of suicide to individuals,
families and communities. Suicide can be defined as the deliberate taking of one's life (Butterworths Concise Australian
Legal Dictionary, 1997, Butterworths Sydney). To be classified as a suicide, a death must be recognised as being due to
other than natural causes. Detailed information on how deaths are classified as suicide by the ABS can be found in
Explanatory Notes 92-94.
This chapter contains summary statistics on suicide deaths registered in Australia, where the underlying cause of death
was determined as Intentional self-harm (suicide (X60-X84, Y87.0)). Further information on suicides is presented in the
data cubes associated with this publication.
External causes of death are required to be examined by the coroner, who investigates both the mechanism by which a
person died, and the intention of the injury (whether accidental, intentional self-harm or assault). For a death to be
determined a suicide, it may be established by coronial inquiry that the death resulted from a deliberate act of the
deceased with the intention of ending his or her own life (intentional self-harm). In addition to coroner-determined
suicides, deaths may also be coded to suicide following further investigation of information on the NCIS. For further
information on how a death may be coded to suicide, see Explanatory Note 94.
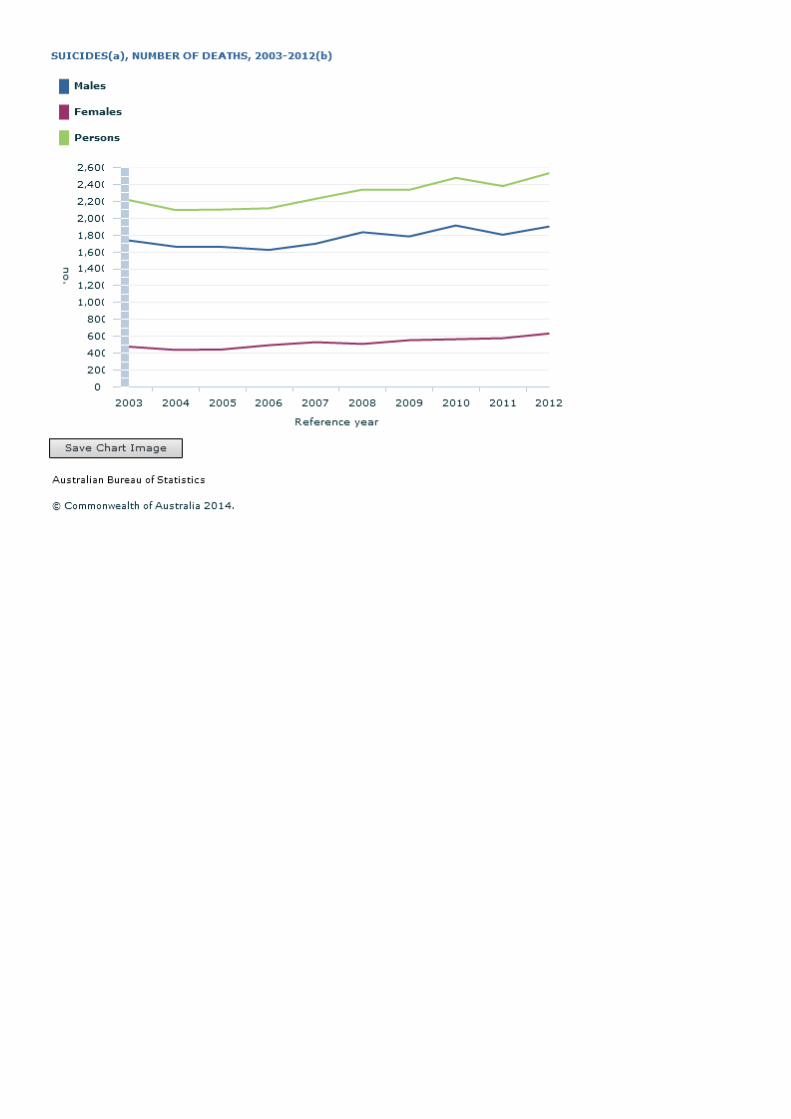
KEY CHARACTERISTICS
There were 2,535 deaths from Intentional self-harm (suicide, (X60-X84, Y87.0)) in 2012, resulting in a ranking as the 14th
leading cause of all deaths. Three-quarters (75.0%) of people who died by suicide were male, making suicide the 10th
leading cause of death for males. Deaths due to suicide occurred at a rate of 11.0 per 100,000 population in 2012.
AGE
Median age
The median age at death for suicide in 2012 was 44.6 years for males, 42.8 years for females
and 44.1 overall. In comparison, the median age for deaths from all causes in 2012 was 78.6
years for males, 84.6 years for females and 81.7 years overall.
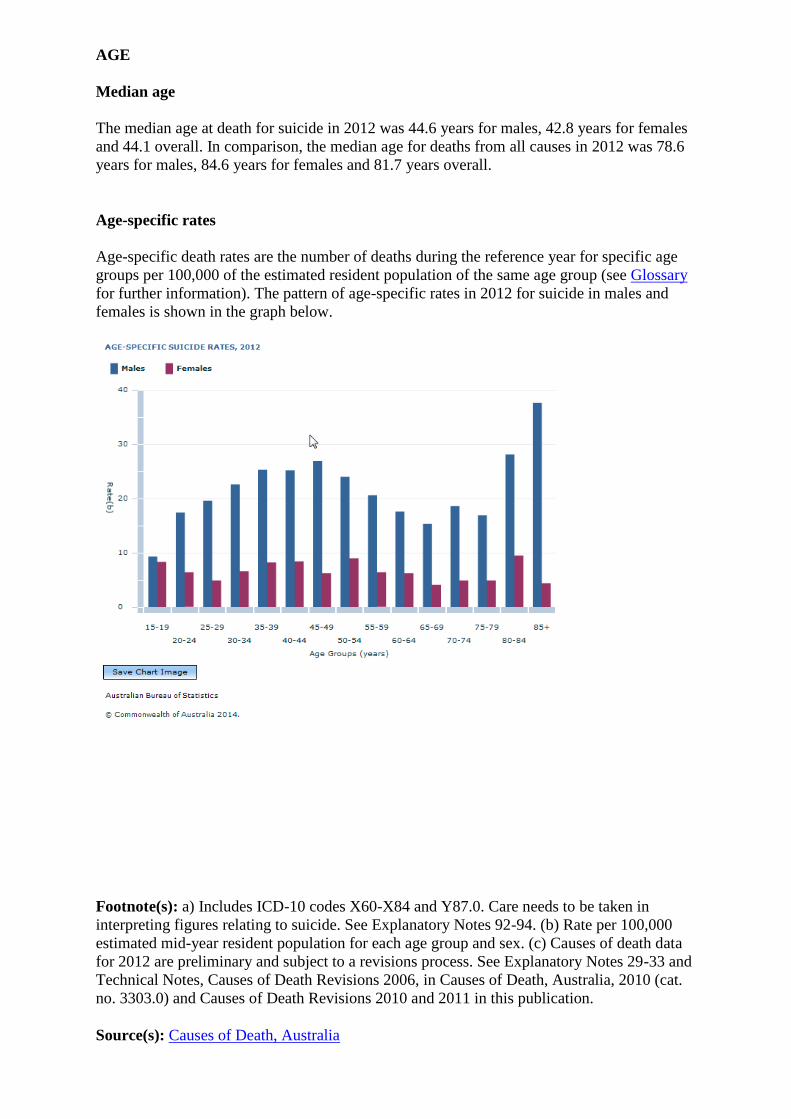
Age-specific rates
Age-specific death rates are the number of deaths during the reference year for specific age
groups per 100,000 of the estimated resident population of the same age group (see Glossary
for further information). The pattern of age-specific rates in 2012 for suicide in males and
females is shown in the graph below.
Footnote(s): a) Includes ICD-10 codes X60-X84 and Y87.0. Care needs to be taken in
interpreting figures relating to suicide. See Explanatory Notes 92-94. (b) Rate per 100,000
estimated mid-year resident population for each age group and sex. (c) Causes of death data
for 2012 are preliminary and subject to a revisions process. See Explanatory Notes 29-33 and
Technical Notes, Causes of Death Revisions 2006, in Causes of Death, Australia, 2010 (cat.
no. 3303.0) and Causes of Death Revisions 2010 and 2011 in this publication.
Source(s): Causes of Death, Australia
The highest age-specific suicide death rate for males in 2012 was observed in the 85 years
and over age group (37.6 per 100,000 males). As a proportion of total male deaths in this age
group, suicide deaths represented 0.3%. The second highest age-specific suicide rate was
observed in the 80-84 year age group, with 28.1 suicide deaths per 100,000 males. Suicide as
a proportion of total male deaths for this age group was 0.4%. Excluding the 0-14 year age
group, the age-specific suicide rate for males was lowest in the 15-19 year age group (9.3
deaths per 100,000), however, this represented over a fifth of all deaths in this age group
(21.9%).
For females the highest age-specific suicide death rate in 2012 was observed in the 80-84
year age group, with 9.5 deaths per 100,000. Outside of the 0-14 year age group, the lowest
age-specific death rate for female deaths was in the 65-69 year age group (4.1 deaths per
100,000).
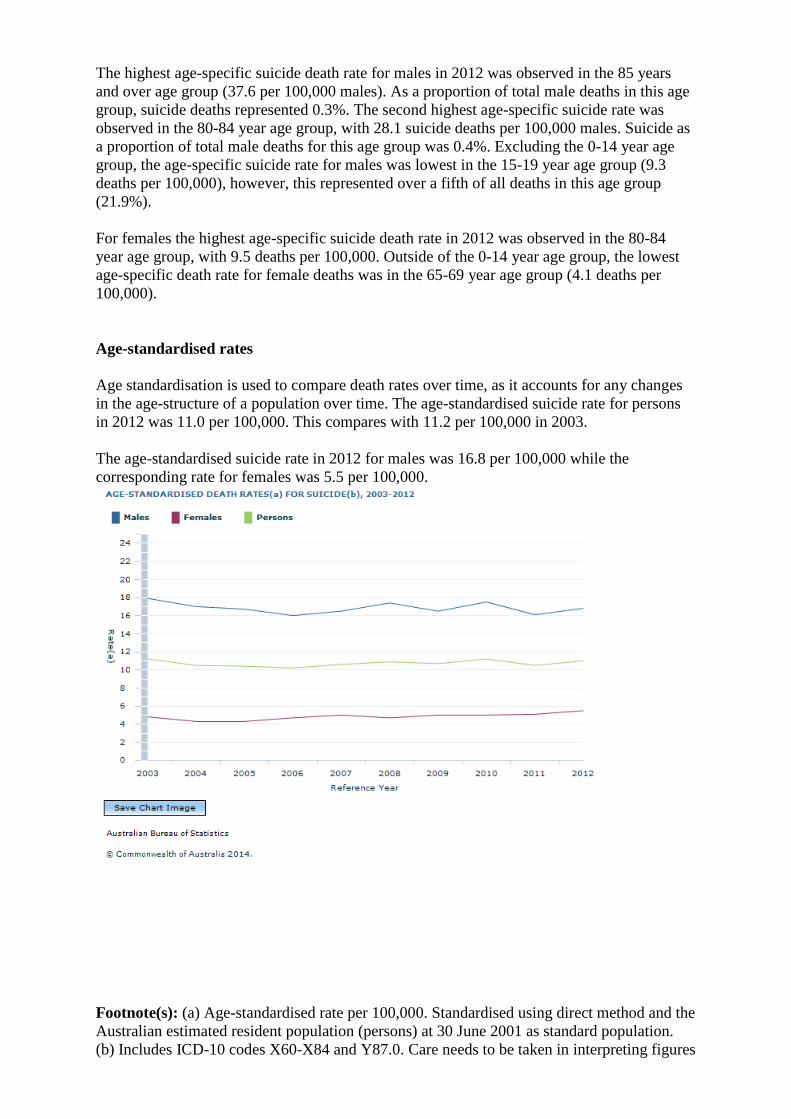
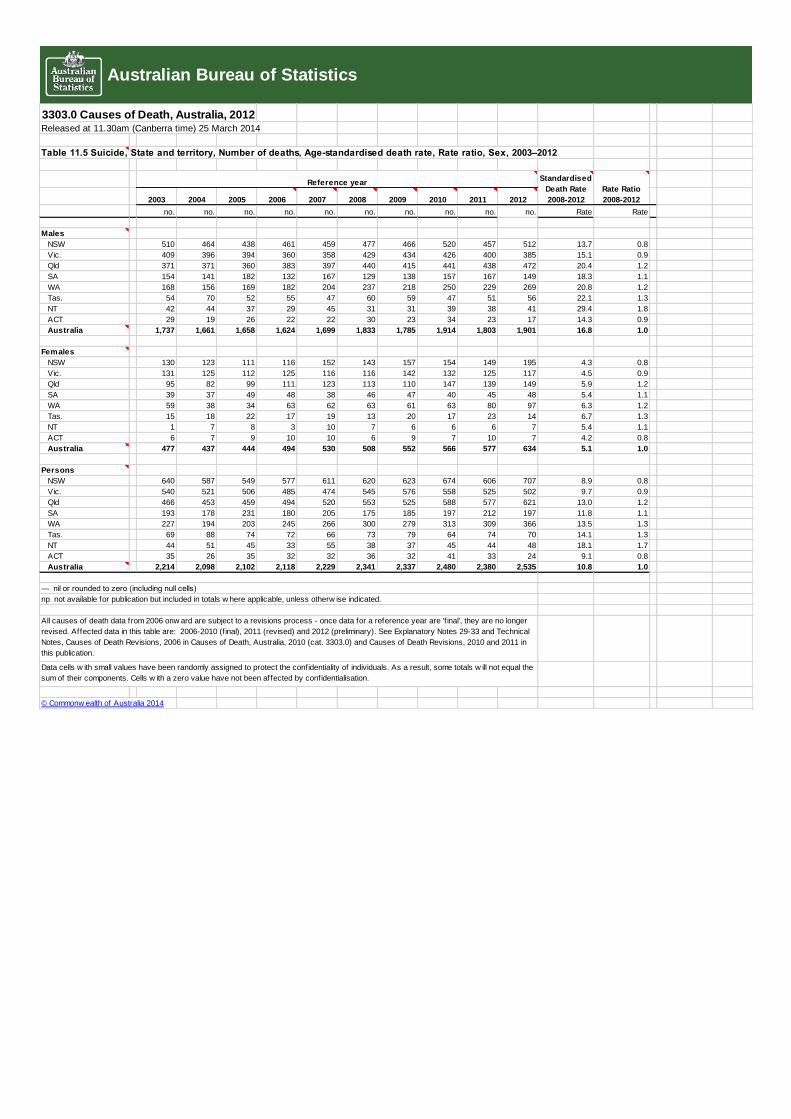
Age-standardised rates
Age standardisation is used to compare death rates over time, as it accounts for any changes
in the age-structure of a population over time. The age-standardised suicide rate for persons
in 2012 was 11.0 per 100,000. This compares with 11.2 per 100,000 in 2003.
The age-standardised suicide rate in 2012 for males was 16.8 per 100,000 while the
corresponding rate for females was 5.5 per 100,000.
Footnote(s): (a) Age-standardised rate per 100,000. Standardised using direct method and the
Australian estimated resident population (persons) at 30 June 2001 as standard population.
(b) Includes ICD-10 codes X60-X84 and Y87.0. Care needs to be taken in interpreting figures
relating to suicide. See Explanatory Notes 92-94. (c) All causes of death data from 2006
onward are subject to a revisions process - once data for a reference year are 'final', they are
no longer revised. Affected data in this table are: 2006-2010 (final), 2011 (revised), 2012
(preliminary). See Explanatory Notes 29-33 and Technical Notes, Causes of Death Revisions,
2006 in Causes of Death, Australia, 2010 (cat. 3303.0) and Causes of Death Revisions, 2010
and 2011 in this publication.
Source(s): Causes of Death, Australia
Suicide by year of occurrence
Sections 1-7 (including this section on suicide deaths) of the Causes of Death, Australia
publication are based on year of registration data (e.g. when the death was registered).
Section 8 is based on year of occurrence (e.g. the year the death actually occurred).
For the 2012 reference year, 10.3 of deaths had a year of occurrence prior to 2012. This
compares with the 2011 reference year where 7.0% of deaths occurred prior to 2010, and the
2010 reference year where 9.1% of deaths occurred prior to 2010.
The number of deaths that are registered in any year will be different to the number of deaths
that actually occurred in that year. Counts of specific causes of death (including suicide)
based on year of occurrence are available for 2002-2011 in the Year of Occurrence datacube.
The proportion of suicide deaths that occur in a previous reference period can impact the
overall count of suicide deaths, along with coronial investigations not being finalised and the
revisions process undertaken by the ABS.
Suicide deaths of children and young people under the age of 15
The number of suicide deaths of children and young people under the age of 15 is small, but
is significant in terms of the proportion of all deaths within this age group. The tables
provided below show aggregate data for the 5 year period from 2008-2012. The age group
published is for persons 5 to 14 years of age. This aligns with standards used elsewhere in the
Cause of Death release and with those used by the World Health Organisation (WHO). The
ABS is not aware of any recorded suicide deaths of children under the age of 5.
Deaths of children by suicide is an extremely sensitive issue. The number of deaths of
children attributed to suicide can be influenced by coronial reporting practices. Reporting
practices may lead to differences in counts across jurisdictions and this should be taken into
account when interpreting these data. For more information on issues associated with the
compilation and interpretation of suicide data, see Explanatory Notes 92-94.
The following two tables present the number of deaths from suicide by age group for the
2008-2012 reference period. Table 5.1 shows the number of deaths from suicide and age-
specific death rates by age group and sex. Table 5.2 shows the number of deaths from suicide
by age group and state or territory of usual residence.
It is recognised that the death rate from suicide differs between Aboriginal and Torres Strait
Islanders and non-Indigenous Australians. While not separately tabulated, it should be noted
that of the 57 deaths by suicide of children and young people under the age of 15, 15 deaths
(26.3%) were of Aboriginal and Torres Strait Islander Australians. The remaining deaths
were of non-Indigenous persons or persons for whom Indigenous status was not stated.
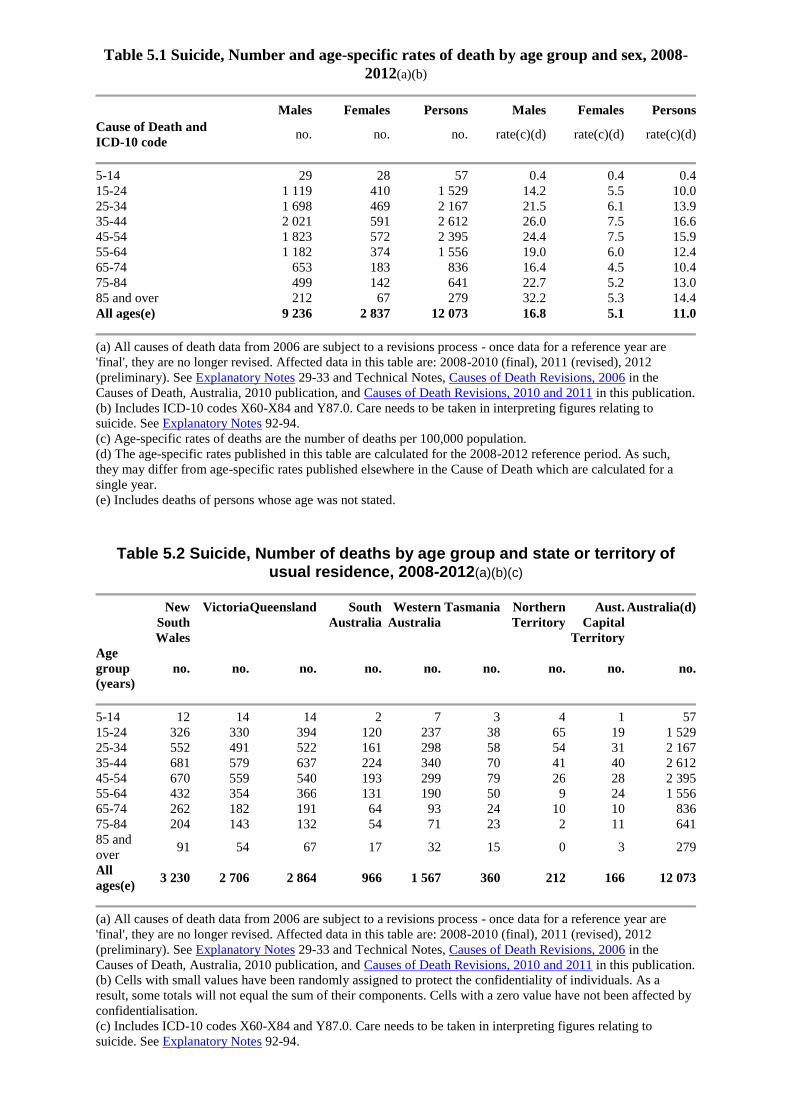
Table 5.1 Suicide, Number and age-specific rates of death by age group and sex, 2008-
2012(a)(b)
Males Females Persons Males Females Persons Cause of Death and
ICD-10 code no. no. no. rate(c)(d) rate(c)(d) rate(c)(d)
5-14 29 28 57 0.4 0.4 0.4 15-24 1 119 410 1 529 14.2 5.5 10.0 25-34 1 698 469 2 167 21.5 6.1 13.9 35-44 2 021 591 2 612 26.0 7.5 16.6 45-54 1 823 572 2 395 24.4 7.5 15.9 55-64 1 182 374 1 556 19.0 6.0 12.4 65-74 653 183 836 16.4 4.5 10.4 75-84 499 142 641 22.7 5.2 13.0 85 and over 212 67 279 32.2 5.3 14.4 All ages(e) 9 236 2 837 12 073 16.8 5.1 11.0
(a) All causes of death data from 2006 are subject to a revisions process - once data for a reference year are
'final', they are no longer revised. Affected data in this table are: 2008-2010 (final), 2011 (revised), 2012
(preliminary). See Explanatory Notes 29-33 and Technical Notes, Causes of Death Revisions, 2006 in the
Causes of Death, Australia, 2010 publication, and Causes of Death Revisions, 2010 and 2011 in this publication.
(b) Includes ICD-10 codes X60-X84 and Y87.0. Care needs to be taken in interpreting figures relating to
suicide. See Explanatory Notes 92-94.
(c) Age-specific rates of deaths are the number of deaths per 100,000 population.
(d) The age-specific rates published in this table are calculated for the 2008-2012 reference period. As such,
they may differ from age-specific rates published elsewhere in the Cause of Death which are calculated for a
single year.
(e) Includes deaths of persons whose age was not stated.
Table 5.2 Suicide, Number of deaths by age group and state or territory of usual residence, 2008-2012(a)(b)(c)
New
South
Wales
Victoria Queensland South
Australia Western
Australia Tasmania Northern
Territory Aust.
Capital
Territory
Australia(d)
Age
group
(years) no. no. no. no. no. no. no. no. no.
5-14 12 14 14 2 7 3 4 1 57 15-24 326 330 394 120 237 38 65 19 1 529 25-34 552 491 522 161 298 58 54 31 2 167 35-44 681 579 637 224 340 70 41 40 2 612 45-54 670 559 540 193 299 79 26 28 2 395 55-64 432 354 366 131 190 50 9 24 1 556 65-74 262 182 191 64 93 24 10 10 836 75-84 204 143 132 54 71 23 2 11 641 85 and
over 91 54 67 17 32 15 0 3 279
All
ages(e) 3 230 2 706 2 864 966 1 567 360 212 166 12 073
(a) All causes of death data from 2006 are subject to a revisions process - once data for a reference year are
'final', they are no longer revised. Affected data in this table are: 2008-2010 (final), 2011 (revised), 2012
(preliminary). See Explanatory Notes 29-33 and Technical Notes, Causes of Death Revisions, 2006 in the
Causes of Death, Australia, 2010 publication, and Causes of Death Revisions, 2010 and 2011 in this publication.
(b) Cells with small values have been randomly assigned to protect the confidentiality of individuals. As a
result, some totals will not equal the sum of their components. Cells with a zero value have not been affected by
confidentialisation.
(c) Includes ICD-10 codes X60-X84 and Y87.0. Care needs to be taken in interpreting figures relating to
suicide. See Explanatory Notes 92-94.

(d) Includes 'other territories'.
(e) Includes deaths of persons whose age was not stated.
Crisis helplines
Lifeline: 13 11 14
Suicide Call Back Service - 1300 659 467
Kids Helpline (for young people aged 5 to 25 years): 1800 55 1800
This page last updated 24 March 2014
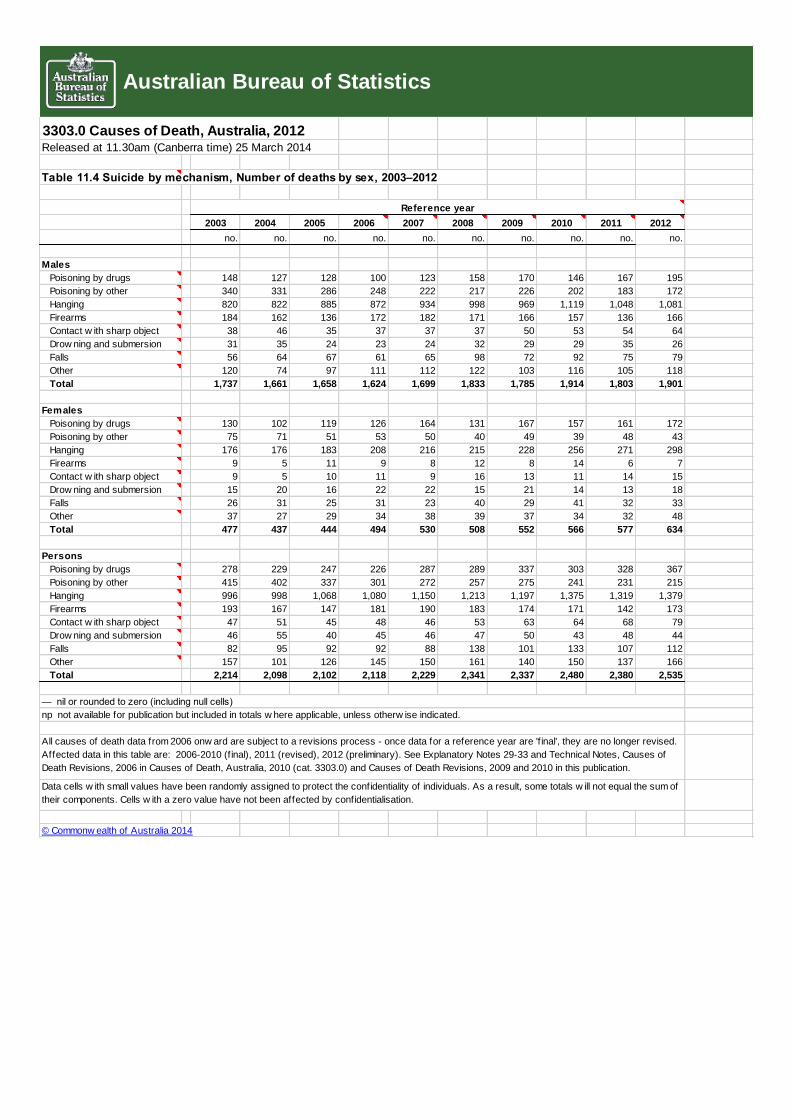
METHOD OF SUICIDE
In 2012, the most frequent method of suicide was hanging, strangulation and suffocation
(X70), a method used in more than half (54.4%) of all suicide deaths. Poisoning by drugs
(X60-X64) was used in 14.5% of suicide deaths, followed by poisoning by other methods
(X65-X69) including by alcohol and motor vehicle exhaust (8.5%). Methods using firearms
(X72-X74) accounted for 6.8% of suicide deaths. The remaining suicide deaths included
deaths from drowning, jumping from a high place, and other methods.
Mechanism By Intent - Selected Causes
Coronial processes to determine the intent of a death (whether intentional self-harm,
accidental, homicide, undetermined intent) are especially important for statistics on suicide
deaths because information on intent is necessary to complete the coding under ICD-10
coding rules. Coroners' practices to determine the intent of a death may vary across the states
and territories. In general, coroners may be reluctant to determine suicidal intent (particularly
in children and young people). In some cases, no statement of intent will be made by a
coroner. The reasons may include legislative or regulatory barriers, sympathy with the
feelings of the family, or sensitivity to the cultural practices and religious beliefs of the
family. For some mechanisms of death where it may be very difficult to determine suicidal
intent (e.g. single vehicle accidents, drownings), the burden of proof required for the coroner
to establish that the death was suicide may make a finding of suicide less likely.
The table below presents selected external causes of death by mechanism and intent. It is
possible that additional suicide deaths are contained within the Intent categories of Accidental
and Undetermined Intent, particularly for the mechanisms of poisoning and hanging, see
Explanatory Notes 92-94.
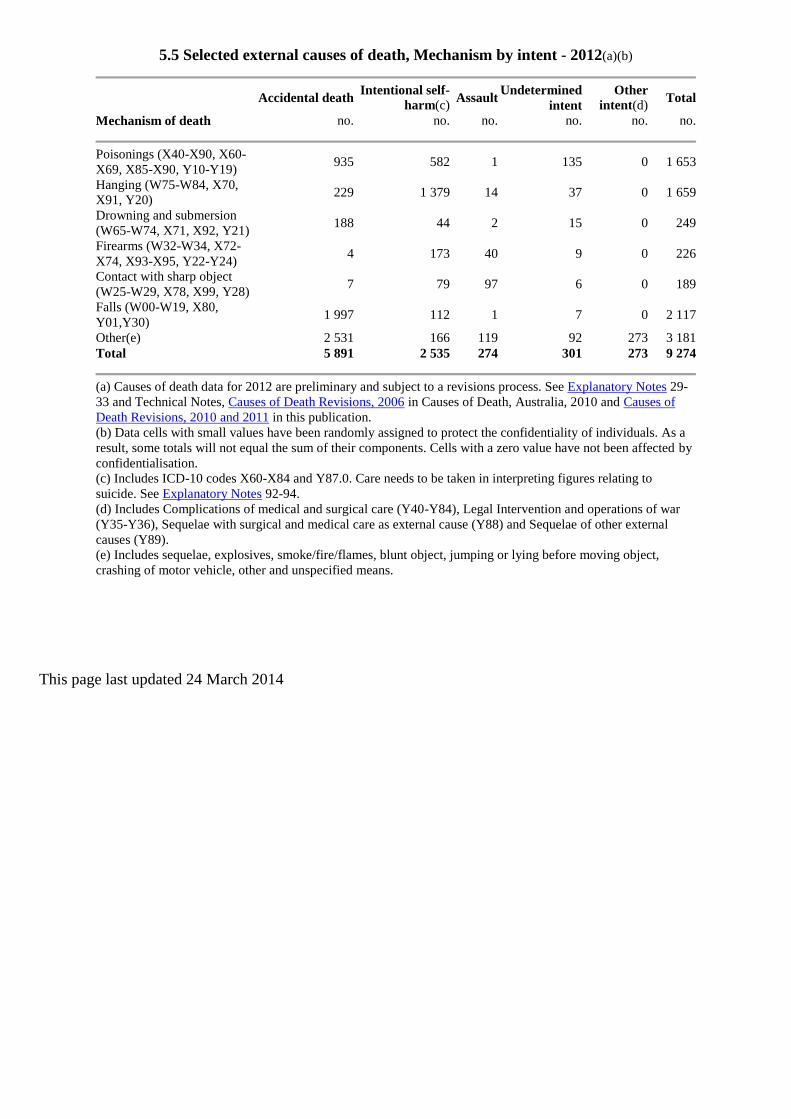
5.5 Selected external causes of death, Mechanism by intent - 2012(a)(b)
Accidental death Intentional self-
harm(c) Assault
Undetermined
intent Other
intent(d) Total
Mechanism of death no. no. no. no. no. no.
Poisonings (X40-X90, X60-
X69, X85-X90, Y10-Y19) 935 582 1 135 0 1 653
Hanging (W75-W84, X70,
X91, Y20) 229 1 379 14 37 0 1 659
Drowning and submersion
(W65-W74, X71, X92, Y21) 188 44 2 15 0 249
Firearms (W32-W34, X72-
X74, X93-X95, Y22-Y24) 4 173 40 9 0 226
Contact with sharp object
(W25-W29, X78, X99, Y28) 7 79 97 6 0 189
Falls (W00-W19, X80,
Y01,Y30) 1 997 112 1 7 0 2 117
Other(e) 2 531 166 119 92 273 3 181 Total 5 891 2 535 274 301 273 9 274
(a) Causes of death data for 2012 are preliminary and subject to a revisions process. See Explanatory Notes 29-
33 and Technical Notes, Causes of Death Revisions, 2006 in Causes of Death, Australia, 2010 and Causes of
Death Revisions, 2010 and 2011 in this publication. (b) Data cells with small values have been randomly assigned to protect the confidentiality of individuals. As a
result, some totals will not equal the sum of their components. Cells with a zero value have not been affected by
confidentialisation. (c) Includes ICD-10 codes X60-X84 and Y87.0. Care needs to be taken in interpreting figures relating to
suicide. See Explanatory Notes 92-94. (d) Includes Complications of medical and surgical care (Y40-Y84), Legal Intervention and operations of war
(Y35-Y36), Sequelae with surgical and medical care as external cause (Y88) and Sequelae of other external
causes (Y89). (e) Includes sequelae, explosives, smoke/fire/flames, blunt object, jumping or lying before moving object,
crashing of motor vehicle, other and unspecified means.
This page last updated 24 March 2014
3303.0 Causes of Death, Australia, 2012Released at 11.30am (Canberra time) 25 March 2014
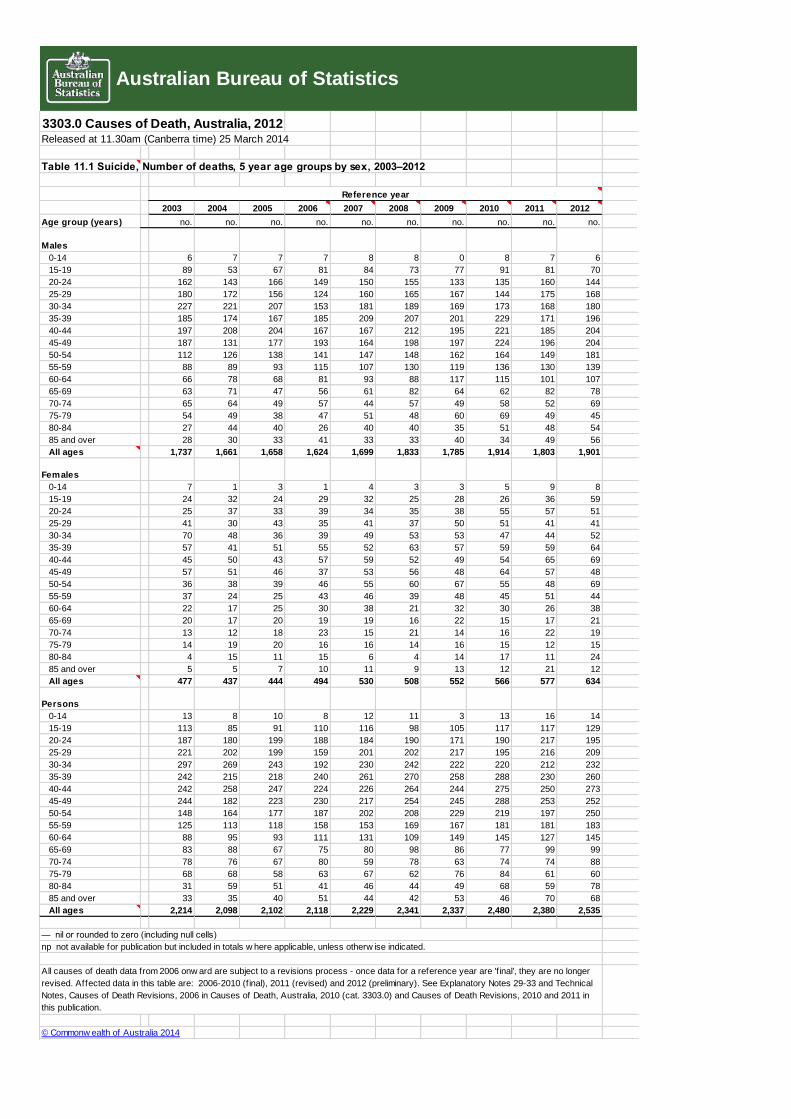
Table 11.1 Suicide, Number of deaths, 5 year age groups by sex, 2003–2012
2003 2004 2005 2006 2007 2008 2009 2010 2011 2012
Age group (years) no. no. no. no. no. no. no. no. no. no.
Males
0-14 6 7 7 7 8 8 0 8 7 6
15-19 89 53 67 81 84 73 77 91 81 70
20-24 162 143 166 149 150 155 133 135 160 144
25-29 180 172 156 124 160 165 167 144 175 168
30-34 227 221 207 153 181 189 169 173 168 180
35-39 185 174 167 185 209 207 201 229 171 196
40-44 197 208 204 167 167 212 195 221 185 204
45-49 187 131 177 193 164 198 197 224 196 204
50-54 112 126 138 141 147 148 162 164 149 181
55-59 88 89 93 115 107 130 119 136 130 139
60-64 66 78 68 81 93 88 117 115 101 107
65-69 63 71 47 56 61 82 64 62 82 78
70-74 65 64 49 57 44 57 49 58 52 69
75-79 54 49 38 47 51 48 60 69 49 45
80-84 27 44 40 26 40 40 35 51 48 54
85 and over 28 30 33 41 33 33 40 34 49 56
All ages 1,737 1,661 1,658 1,624 1,699 1,833 1,785 1,914 1,803 1,901
Females
0-14 7 1 3 1 4 3 3 5 9 8
15-19 24 32 24 29 32 25 28 26 36 59
20-24 25 37 33 39 34 35 38 55 57 51
25-29 41 30 43 35 41 37 50 51 41 41
30-34 70 48 36 39 49 53 53 47 44 52
35-39 57 41 51 55 52 63 57 59 59 64
40-44 45 50 43 57 59 52 49 54 65 69
45-49 57 51 46 37 53 56 48 64 57 48
50-54 36 38 39 46 55 60 67 55 48 69
55-59 37 24 25 43 46 39 48 45 51 44
60-64 22 17 25 30 38 21 32 30 26 38
65-69 20 17 20 19 19 16 22 15 17 21
70-74 13 12 18 23 15 21 14 16 22 19
75-79 14 19 20 16 16 14 16 15 12 15
80-84 4 15 11 15 6 4 14 17 11 24
85 and over 5 5 7 10 11 9 13 12 21 12
All ages 477 437 444 494 530 508 552 566 577 634
Persons
0-14 13 8 10 8 12 11 3 13 16 14
15-19 113 85 91 110 116 98 105 117 117 129
20-24 187 180 199 188 184 190 171 190 217 195
25-29 221 202 199 159 201 202 217 195 216 209
30-34 297 269 243 192 230 242 222 220 212 232
35-39 242 215 218 240 261 270 258 288 230 260
40-44 242 258 247 224 226 264 244 275 250 273
45-49 244 182 223 230 217 254 245 288 253 252
50-54 148 164 177 187 202 208 229 219 197 250
55-59 125 113 118 158 153 169 167 181 181 183
60-64 88 95 93 111 131 109 149 145 127 145
65-69 83 88 67 75 80 98 86 77 99 99
70-74 78 76 67 80 59 78 63 74 74 88
75-79 68 68 58 63 67 62 76 84 61 60
80-84 31 59 51 41 46 44 49 68 59 78
85 and over 33 35 40 51 44 42 53 46 70 68
All ages 2,214 2,098 2,102 2,118 2,229 2,341 2,337 2,480 2,380 2,535
© Commonw ealth of Australia 2014
Australian Bureau of Statistics
Reference year
— nil or rounded to zero (including null cells)
np not available for publication but included in totals w here applicable, unless otherw ise indicated.
All causes of death data from 2006 onw ard are subject to a revisions process - once data for a reference year are 'f inal', they are no longer
revised. Affected data in this table are: 2006-2010 (f inal), 2011 (revised) and 2012 (preliminary). See Explanatory Notes 29-33 and Technical
Notes, Causes of Death Revisions, 2006 in Causes of Death, Australia, 2010 (cat. 3303.0) and Causes of Death Revisions, 2010 and 2011 in
this publication.
3303.0 Causes of Death, Australia, 2012Released at 11.30am (Canberra time) 25 March 2014
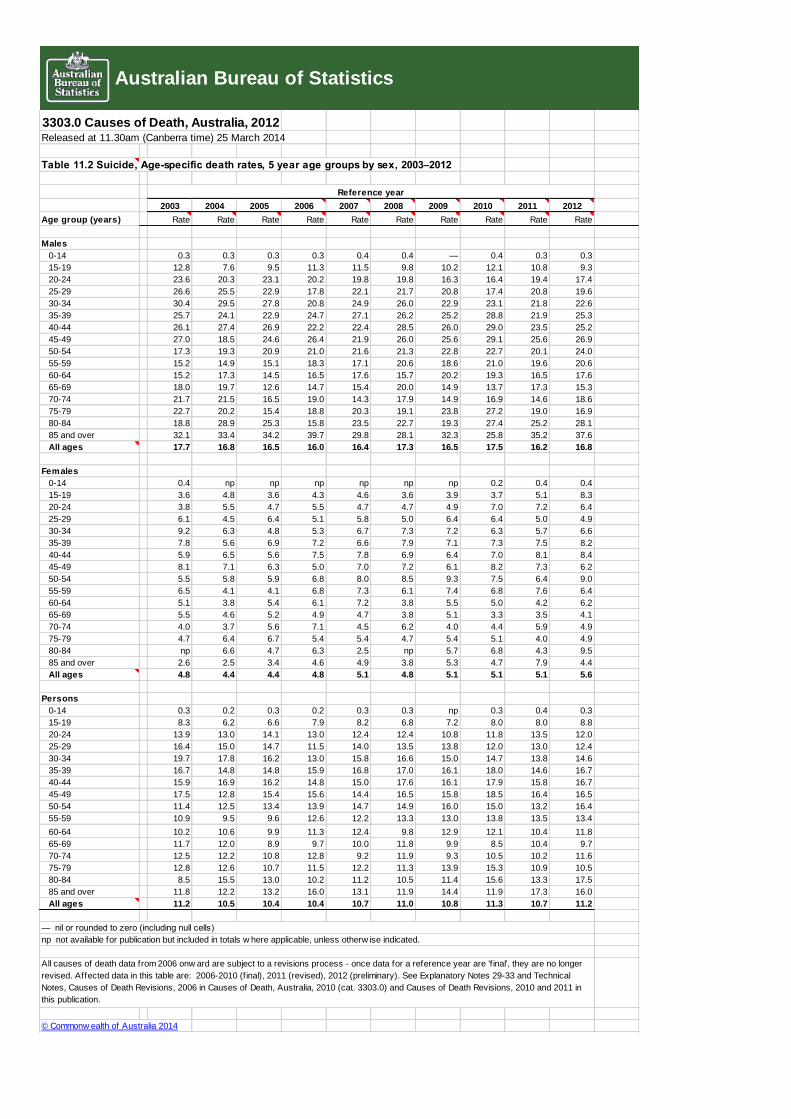
Table 11.2 Suicide, Age-specific death rates, 5 year age groups by sex, 2003–2012
2003 2004 2005 2006 2007 2008 2009 2010 2011 2012
Age group (years) Rate Rate Rate Rate Rate Rate Rate Rate Rate Rate
Males
0-14 0.3 0.3 0.3 0.3 0.4 0.4 — 0.4 0.3 0.3
15-19 12.8 7.6 9.5 11.3 11.5 9.8 10.2 12.1 10.8 9.3
20-24 23.6 20.3 23.1 20.2 19.8 19.8 16.3 16.4 19.4 17.4
25-29 26.6 25.5 22.9 17.8 22.1 21.7 20.8 17.4 20.8 19.6
30-34 30.4 29.5 27.8 20.8 24.9 26.0 22.9 23.1 21.8 22.6
35-39 25.7 24.1 22.9 24.7 27.1 26.2 25.2 28.8 21.9 25.3
40-44 26.1 27.4 26.9 22.2 22.4 28.5 26.0 29.0 23.5 25.2
45-49 27.0 18.5 24.6 26.4 21.9 26.0 25.6 29.1 25.6 26.9
50-54 17.3 19.3 20.9 21.0 21.6 21.3 22.8 22.7 20.1 24.0
55-59 15.2 14.9 15.1 18.3 17.1 20.6 18.6 21.0 19.6 20.6
60-64 15.2 17.3 14.5 16.5 17.6 15.7 20.2 19.3 16.5 17.6
65-69 18.0 19.7 12.6 14.7 15.4 20.0 14.9 13.7 17.3 15.3
70-74 21.7 21.5 16.5 19.0 14.3 17.9 14.9 16.9 14.6 18.6
75-79 22.7 20.2 15.4 18.8 20.3 19.1 23.8 27.2 19.0 16.9
80-84 18.8 28.9 25.3 15.8 23.5 22.7 19.3 27.4 25.2 28.1
85 and over 32.1 33.4 34.2 39.7 29.8 28.1 32.3 25.8 35.2 37.6
All ages 17.7 16.8 16.5 16.0 16.4 17.3 16.5 17.5 16.2 16.8
Females
0-14 0.4 np np np np np np 0.2 0.4 0.4
15-19 3.6 4.8 3.6 4.3 4.6 3.6 3.9 3.7 5.1 8.3
20-24 3.8 5.5 4.7 5.5 4.7 4.7 4.9 7.0 7.2 6.4
25-29 6.1 4.5 6.4 5.1 5.8 5.0 6.4 6.4 5.0 4.9
30-34 9.2 6.3 4.8 5.3 6.7 7.3 7.2 6.3 5.7 6.6
35-39 7.8 5.6 6.9 7.2 6.6 7.9 7.1 7.3 7.5 8.2
40-44 5.9 6.5 5.6 7.5 7.8 6.9 6.4 7.0 8.1 8.4
45-49 8.1 7.1 6.3 5.0 7.0 7.2 6.1 8.2 7.3 6.2
50-54 5.5 5.8 5.9 6.8 8.0 8.5 9.3 7.5 6.4 9.0
55-59 6.5 4.1 4.1 6.8 7.3 6.1 7.4 6.8 7.6 6.4
60-64 5.1 3.8 5.4 6.1 7.2 3.8 5.5 5.0 4.2 6.2
65-69 5.5 4.6 5.2 4.9 4.7 3.8 5.1 3.3 3.5 4.1
70-74 4.0 3.7 5.6 7.1 4.5 6.2 4.0 4.4 5.9 4.9
75-79 4.7 6.4 6.7 5.4 5.4 4.7 5.4 5.1 4.0 4.9
80-84 np 6.6 4.7 6.3 2.5 np 5.7 6.8 4.3 9.5
85 and over 2.6 2.5 3.4 4.6 4.9 3.8 5.3 4.7 7.9 4.4
All ages 4.8 4.4 4.4 4.8 5.1 4.8 5.1 5.1 5.1 5.6
Persons
0-14 0.3 0.2 0.3 0.2 0.3 0.3 np 0.3 0.4 0.3
15-19 8.3 6.2 6.6 7.9 8.2 6.8 7.2 8.0 8.0 8.8
20-24 13.9 13.0 14.1 13.0 12.4 12.4 10.8 11.8 13.5 12.0
25-29 16.4 15.0 14.7 11.5 14.0 13.5 13.8 12.0 13.0 12.4
30-34 19.7 17.8 16.2 13.0 15.8 16.6 15.0 14.7 13.8 14.6
35-39 16.7 14.8 14.8 15.9 16.8 17.0 16.1 18.0 14.6 16.7
40-44 15.9 16.9 16.2 14.8 15.0 17.6 16.1 17.9 15.8 16.7
45-49 17.5 12.8 15.4 15.6 14.4 16.5 15.8 18.5 16.4 16.5
50-54 11.4 12.5 13.4 13.9 14.7 14.9 16.0 15.0 13.2 16.4
55-59 10.9 9.5 9.6 12.6 12.2 13.3 13.0 13.8 13.5 13.4
60-64 10.2 10.6 9.9 11.3 12.4 9.8 12.9 12.1 10.4 11.8
65-69 11.7 12.0 8.9 9.7 10.0 11.8 9.9 8.5 10.4 9.7
70-74 12.5 12.2 10.8 12.8 9.2 11.9 9.3 10.5 10.2 11.6
75-79 12.8 12.6 10.7 11.5 12.2 11.3 13.9 15.3 10.9 10.5
80-84 8.5 15.5 13.0 10.2 11.2 10.5 11.4 15.6 13.3 17.5
85 and over 11.8 12.2 13.2 16.0 13.1 11.9 14.4 11.9 17.3 16.0
All ages 11.2 10.5 10.4 10.4 10.7 11.0 10.8 11.3 10.7 11.2
© Commonw ealth of Australia 2014
np not available for publication but included in totals w here applicable, unless otherw ise indicated.
Australian Bureau of Statistics
Reference year
— nil or rounded to zero (including null cells)
All causes of death data from 2006 onw ard are subject to a revisions process - once data for a reference year are 'f inal', they are no longer
revised. Affected data in this table are: 2006-2010 (f inal), 2011 (revised), 2012 (preliminary). See Explanatory Notes 29-33 and Technical
Notes, Causes of Death Revisions, 2006 in Causes of Death, Australia, 2010 (cat. 3303.0) and Causes of Death Revisions, 2010 and 2011 in
this publication.
3303.0 Causes of Death, Australia, 2012Released at 11.30am (Canberra time) 25 March 2014
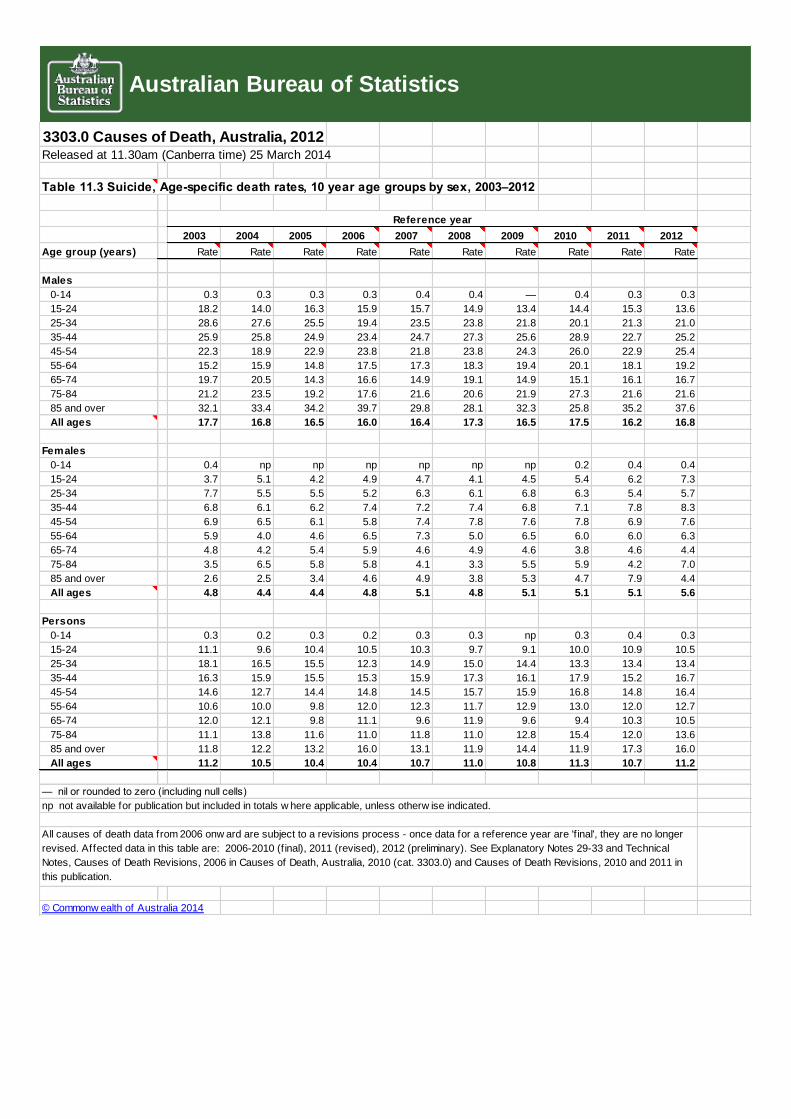
Table 11.3 Suicide, Age-specific death rates, 10 year age groups by sex, 2003–2012
2003 2004 2005 2006 2007 2008 2009 2010 2011 2012
Age group (years) Rate Rate Rate Rate Rate Rate Rate Rate Rate Rate
Males
0-14 0.3 0.3 0.3 0.3 0.4 0.4 — 0.4 0.3 0.3
15-24 18.2 14.0 16.3 15.9 15.7 14.9 13.4 14.4 15.3 13.6
25-34 28.6 27.6 25.5 19.4 23.5 23.8 21.8 20.1 21.3 21.0
35-44 25.9 25.8 24.9 23.4 24.7 27.3 25.6 28.9 22.7 25.2
45-54 22.3 18.9 22.9 23.8 21.8 23.8 24.3 26.0 22.9 25.4
55-64 15.2 15.9 14.8 17.5 17.3 18.3 19.4 20.1 18.1 19.2
65-74 19.7 20.5 14.3 16.6 14.9 19.1 14.9 15.1 16.1 16.7
75-84 21.2 23.5 19.2 17.6 21.6 20.6 21.9 27.3 21.6 21.6
85 and over 32.1 33.4 34.2 39.7 29.8 28.1 32.3 25.8 35.2 37.6
All ages 17.7 16.8 16.5 16.0 16.4 17.3 16.5 17.5 16.2 16.8
Females
0-14 0.4 np np np np np np 0.2 0.4 0.4
15-24 3.7 5.1 4.2 4.9 4.7 4.1 4.5 5.4 6.2 7.3
25-34 7.7 5.5 5.5 5.2 6.3 6.1 6.8 6.3 5.4 5.7
35-44 6.8 6.1 6.2 7.4 7.2 7.4 6.8 7.1 7.8 8.3
45-54 6.9 6.5 6.1 5.8 7.4 7.8 7.6 7.8 6.9 7.6
55-64 5.9 4.0 4.6 6.5 7.3 5.0 6.5 6.0 6.0 6.3
65-74 4.8 4.2 5.4 5.9 4.6 4.9 4.6 3.8 4.6 4.4
75-84 3.5 6.5 5.8 5.8 4.1 3.3 5.5 5.9 4.2 7.0
85 and over 2.6 2.5 3.4 4.6 4.9 3.8 5.3 4.7 7.9 4.4
All ages 4.8 4.4 4.4 4.8 5.1 4.8 5.1 5.1 5.1 5.6
Persons
0-14 0.3 0.2 0.3 0.2 0.3 0.3 np 0.3 0.4 0.3
15-24 11.1 9.6 10.4 10.5 10.3 9.7 9.1 10.0 10.9 10.5
25-34 18.1 16.5 15.5 12.3 14.9 15.0 14.4 13.3 13.4 13.4
35-44 16.3 15.9 15.5 15.3 15.9 17.3 16.1 17.9 15.2 16.7
45-54 14.6 12.7 14.4 14.8 14.5 15.7 15.9 16.8 14.8 16.4
55-64 10.6 10.0 9.8 12.0 12.3 11.7 12.9 13.0 12.0 12.7
65-74 12.0 12.1 9.8 11.1 9.6 11.9 9.6 9.4 10.3 10.5
75-84 11.1 13.8 11.6 11.0 11.8 11.0 12.8 15.4 12.0 13.6
85 and over 11.8 12.2 13.2 16.0 13.1 11.9 14.4 11.9 17.3 16.0
All ages 11.2 10.5 10.4 10.4 10.7 11.0 10.8 11.3 10.7 11.2
© Commonw ealth of Australia 2014
Australian Bureau of Statistics
Reference year
— nil or rounded to zero (including null cells)
np not available for publication but included in totals w here applicable, unless otherw ise indicated.
All causes of death data from 2006 onw ard are subject to a revisions process - once data for a reference year are 'f inal', they are no longer
revised. Affected data in this table are: 2006-2010 (f inal), 2011 (revised), 2012 (preliminary). See Explanatory Notes 29-33 and Technical
Notes, Causes of Death Revisions, 2006 in Causes of Death, Australia, 2010 (cat. 3303.0) and Causes of Death Revisions, 2010 and 2011 in
this publication.
3303.0 Causes of Death, Australia, 2012Released at 11.30am (Canberra time) 25 March 2014
Table 11.4 Suicide by mechanism, Number of deaths by sex, 2003–2012
2003 2004 2005 2006 2007 2008 2009 2010 2011 2012
no. no. no. no. no. no. no. no. no. no.
Males
Poisoning by drugs 148 127 128 100 123 158 170 146 167 195
Poisoning by other 340 331 286 248 222 217 226 202 183 172
Hanging 820 822 885 872 934 998 969 1,119 1,048 1,081
Firearms 184 162 136 172 182 171 166 157 136 166
Contact w ith sharp object 38 46 35 37 37 37 50 53 54 64
Drow ning and submersion 31 35 24 23 24 32 29 29 35 26
Falls 56 64 67 61 65 98 72 92 75 79
Other 120 74 97 111 112 122 103 116 105 118
Total 1,737 1,661 1,658 1,624 1,699 1,833 1,785 1,914 1,803 1,901
Females
Poisoning by drugs 130 102 119 126 164 131 167 157 161 172
Poisoning by other 75 71 51 53 50 40 49 39 48 43
Hanging 176 176 183 208 216 215 228 256 271 298
Firearms 9 5 11 9 8 12 8 14 6 7
Contact w ith sharp object 9 5 10 11 9 16 13 11 14 15
Drow ning and submersion 15 20 16 22 22 15 21 14 13 18
Falls 26 31 25 31 23 40 29 41 32 33
Other 37 27 29 34 38 39 37 34 32 48
Total 477 437 444 494 530 508 552 566 577 634
Persons
Poisoning by drugs 278 229 247 226 287 289 337 303 328 367
Poisoning by other 415 402 337 301 272 257 275 241 231 215
Hanging 996 998 1,068 1,080 1,150 1,213 1,197 1,375 1,319 1,379
Firearms 193 167 147 181 190 183 174 171 142 173
Contact w ith sharp object 47 51 45 48 46 53 63 64 68 79
Drow ning and submersion 46 55 40 45 46 47 50 43 48 44
Falls 82 95 92 92 88 138 101 133 107 112
Other 157 101 126 145 150 161 140 150 137 166
Total 2,214 2,098 2,102 2,118 2,229 2,341 2,337 2,480 2,380 2,535
© Commonw ealth of Australia 2014
Data cells w ith small values have been randomly assigned to protect the confidentiality of individuals. As a result, some totals w ill not equal the sum of
their components. Cells w ith a zero value have not been affected by confidentialisation.
Australian Bureau of Statistics
Reference year
— nil or rounded to zero (including null cells)
np not available for publication but included in totals w here applicable, unless otherw ise indicated.
All causes of death data from 2006 onw ard are subject to a revisions process - once data for a reference year are 'f inal', they are no longer revised.
Affected data in this table are: 2006-2010 (f inal), 2011 (revised), 2012 (preliminary). See Explanatory Notes 29-33 and Technical Notes, Causes of
Death Revisions, 2006 in Causes of Death, Australia, 2010 (cat. 3303.0) and Causes of Death Revisions, 2009 and 2010 in this publication.
3303.0 Causes of Death, Australia, 2012Released at 11.30am (Canberra time) 25 March 2014
Table 11.5 Suicide, State and territory, Number of deaths, Age-standardised death rate, Rate ratio, Sex, 2003–2012
2003 2004 2005 2006 2007 2008 2009 2010 2011 2012
no. no. no. no. no. no. no. no. no. no. Rate Rate
Males
NSW 510 464 438 461 459 477 466 520 457 512 13.7 0.8
Vic. 409 396 394 360 358 429 434 426 400 385 15.1 0.9
Qld 371 371 360 383 397 440 415 441 438 472 20.4 1.2
SA 154 141 182 132 167 129 138 157 167 149 18.3 1.1
WA 168 156 169 182 204 237 218 250 229 269 20.8 1.2
Tas. 54 70 52 55 47 60 59 47 51 56 22.1 1.3
NT 42 44 37 29 45 31 31 39 38 41 29.4 1.8
ACT 29 19 26 22 22 30 23 34 23 17 14.3 0.9
Australia 1,737 1,661 1,658 1,624 1,699 1,833 1,785 1,914 1,803 1,901 16.8 1.0
Females
NSW 130 123 111 116 152 143 157 154 149 195 4.3 0.8
Vic. 131 125 112 125 116 116 142 132 125 117 4.5 0.9
Qld 95 82 99 111 123 113 110 147 139 149 5.9 1.2
SA 39 37 49 48 38 46 47 40 45 48 5.4 1.1
WA 59 38 34 63 62 63 61 63 80 97 6.3 1.2
Tas. 15 18 22 17 19 13 20 17 23 14 6.7 1.3
NT 1 7 8 3 10 7 6 6 6 7 5.4 1.1
ACT 6 7 9 10 10 6 9 7 10 7 4.2 0.8
Australia 477 437 444 494 530 508 552 566 577 634 5.1 1.0
Persons
NSW 640 587 549 577 611 620 623 674 606 707 8.9 0.8
Vic. 540 521 506 485 474 545 576 558 525 502 9.7 0.9
Qld 466 453 459 494 520 553 525 588 577 621 13.0 1.2
SA 193 178 231 180 205 175 185 197 212 197 11.8 1.1
WA 227 194 203 245 266 300 279 313 309 366 13.5 1.3
Tas. 69 88 74 72 66 73 79 64 74 70 14.1 1.3
NT 44 51 45 33 55 38 37 45 44 48 18.1 1.7
ACT 35 26 35 32 32 36 32 41 33 24 9.1 0.8
Australia 2,214 2,098 2,102 2,118 2,229 2,341 2,337 2,480 2,380 2,535 10.8 1.0
© Commonw ealth of Australia 2014
Australian Bureau of Statistics
Reference year
Data cells w ith small values have been randomly assigned to protect the confidentiality of individuals. As a result, some totals w ill not equal the
sum of their components. Cells w ith a zero value have not been affected by confidentialisation.
All causes of death data from 2006 onw ard are subject to a revisions process - once data for a reference year are 'f inal', they are no longer
revised. Affected data in this table are: 2006-2010 (f inal), 2011 (revised) and 2012 (preliminary). See Explanatory Notes 29-33 and Technical
Notes, Causes of Death Revisions, 2006 in Causes of Death, Australia, 2010 (cat. 3303.0) and Causes of Death Revisions, 2010 and 2011 in
this publication.
— nil or rounded to zero (including null cells)
np not available for publication but included in totals w here applicable, unless otherw ise indicated.
Standardised
Death Rate
2008-2012
Rate Ratio
2008-2012
3303.0 Causes of Death, Australia, 2012Released at 11.30am (Canberra time) 25 March 2014
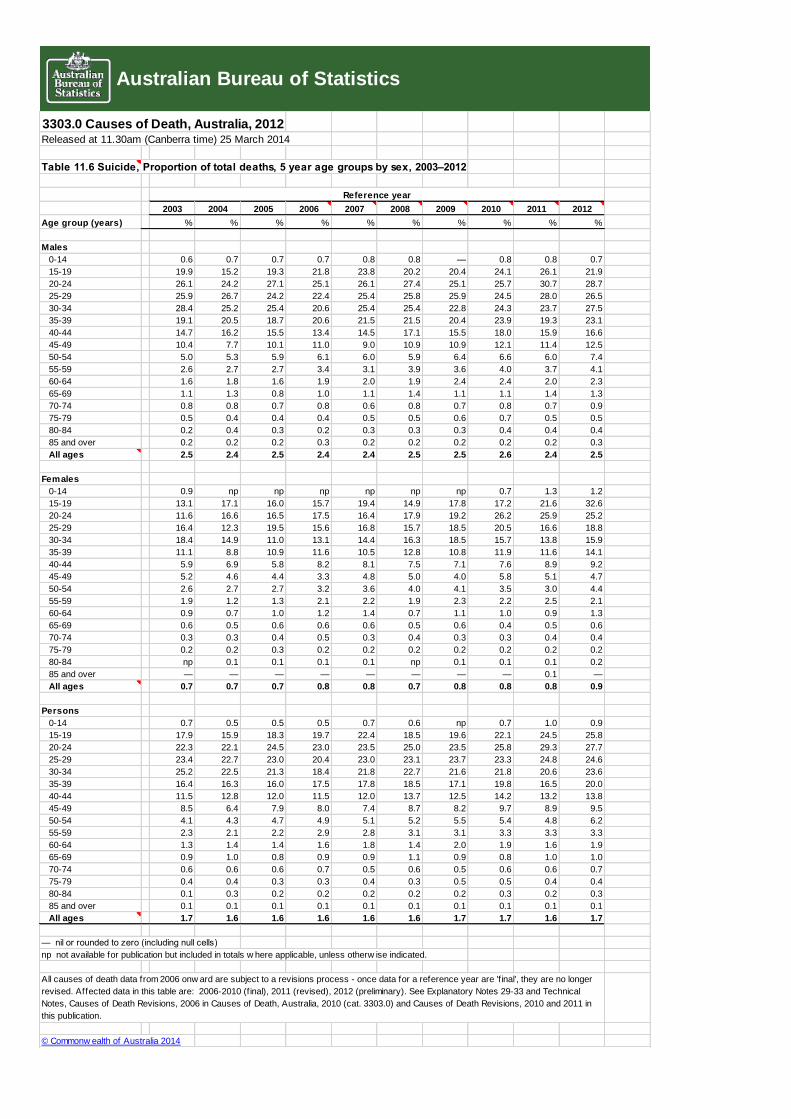
Table 11.6 Suicide, Proportion of total deaths, 5 year age groups by sex, 2003–2012
2003 2004 2005 2006 2007 2008 2009 2010 2011 2012
Age group (years) % % % % % % % % % %
Males
0-14 0.6 0.7 0.7 0.7 0.8 0.8 — 0.8 0.8 0.7
15-19 19.9 15.2 19.3 21.8 23.8 20.2 20.4 24.1 26.1 21.9
20-24 26.1 24.2 27.1 25.1 26.1 27.4 25.1 25.7 30.7 28.7
25-29 25.9 26.7 24.2 22.4 25.4 25.8 25.9 24.5 28.0 26.5
30-34 28.4 25.2 25.4 20.6 25.4 25.4 22.8 24.3 23.7 27.5
35-39 19.1 20.5 18.7 20.6 21.5 21.5 20.4 23.9 19.3 23.1
40-44 14.7 16.2 15.5 13.4 14.5 17.1 15.5 18.0 15.9 16.6
45-49 10.4 7.7 10.1 11.0 9.0 10.9 10.9 12.1 11.4 12.5
50-54 5.0 5.3 5.9 6.1 6.0 5.9 6.4 6.6 6.0 7.4
55-59 2.6 2.7 2.7 3.4 3.1 3.9 3.6 4.0 3.7 4.1
60-64 1.6 1.8 1.6 1.9 2.0 1.9 2.4 2.4 2.0 2.3
65-69 1.1 1.3 0.8 1.0 1.1 1.4 1.1 1.1 1.4 1.3
70-74 0.8 0.8 0.7 0.8 0.6 0.8 0.7 0.8 0.7 0.9
75-79 0.5 0.4 0.4 0.4 0.5 0.5 0.6 0.7 0.5 0.5
80-84 0.2 0.4 0.3 0.2 0.3 0.3 0.3 0.4 0.4 0.4
85 and over 0.2 0.2 0.2 0.3 0.2 0.2 0.2 0.2 0.2 0.3
All ages 2.5 2.4 2.5 2.4 2.4 2.5 2.5 2.6 2.4 2.5
Females
0-14 0.9 np np np np np np 0.7 1.3 1.2
15-19 13.1 17.1 16.0 15.7 19.4 14.9 17.8 17.2 21.6 32.6
20-24 11.6 16.6 16.5 17.5 16.4 17.9 19.2 26.2 25.9 25.2
25-29 16.4 12.3 19.5 15.6 16.8 15.7 18.5 20.5 16.6 18.8
30-34 18.4 14.9 11.0 13.1 14.4 16.3 18.5 15.7 13.8 15.9
35-39 11.1 8.8 10.9 11.6 10.5 12.8 10.8 11.9 11.6 14.1
40-44 5.9 6.9 5.8 8.2 8.1 7.5 7.1 7.6 8.9 9.2
45-49 5.2 4.6 4.4 3.3 4.8 5.0 4.0 5.8 5.1 4.7
50-54 2.6 2.7 2.7 3.2 3.6 4.0 4.1 3.5 3.0 4.4
55-59 1.9 1.2 1.3 2.1 2.2 1.9 2.3 2.2 2.5 2.1
60-64 0.9 0.7 1.0 1.2 1.4 0.7 1.1 1.0 0.9 1.3
65-69 0.6 0.5 0.6 0.6 0.6 0.5 0.6 0.4 0.5 0.6
70-74 0.3 0.3 0.4 0.5 0.3 0.4 0.3 0.3 0.4 0.4
75-79 0.2 0.2 0.3 0.2 0.2 0.2 0.2 0.2 0.2 0.2
80-84 np 0.1 0.1 0.1 0.1 np 0.1 0.1 0.1 0.2
85 and over — — — — — — — — 0.1 —
All ages 0.7 0.7 0.7 0.8 0.8 0.7 0.8 0.8 0.8 0.9
Persons
0-14 0.7 0.5 0.5 0.5 0.7 0.6 np 0.7 1.0 0.9
15-19 17.9 15.9 18.3 19.7 22.4 18.5 19.6 22.1 24.5 25.8
20-24 22.3 22.1 24.5 23.0 23.5 25.0 23.5 25.8 29.3 27.7
25-29 23.4 22.7 23.0 20.4 23.0 23.1 23.7 23.3 24.8 24.6
30-34 25.2 22.5 21.3 18.4 21.8 22.7 21.6 21.8 20.6 23.6
35-39 16.4 16.3 16.0 17.5 17.8 18.5 17.1 19.8 16.5 20.0
40-44 11.5 12.8 12.0 11.5 12.0 13.7 12.5 14.2 13.2 13.8
45-49 8.5 6.4 7.9 8.0 7.4 8.7 8.2 9.7 8.9 9.5
50-54 4.1 4.3 4.7 4.9 5.1 5.2 5.5 5.4 4.8 6.2
55-59 2.3 2.1 2.2 2.9 2.8 3.1 3.1 3.3 3.3 3.3
60-64 1.3 1.4 1.4 1.6 1.8 1.4 2.0 1.9 1.6 1.9
65-69 0.9 1.0 0.8 0.9 0.9 1.1 0.9 0.8 1.0 1.0
70-74 0.6 0.6 0.6 0.7 0.5 0.6 0.5 0.6 0.6 0.7
75-79 0.4 0.4 0.3 0.3 0.4 0.3 0.5 0.5 0.4 0.4
80-84 0.1 0.3 0.2 0.2 0.2 0.2 0.2 0.3 0.2 0.3
85 and over 0.1 0.1 0.1 0.1 0.1 0.1 0.1 0.1 0.1 0.1
All ages 1.7 1.6 1.6 1.6 1.6 1.6 1.7 1.7 1.6 1.7
— nil or rounded to zero (including null cells)
np not available for publication but included in totals w here applicable, unless otherw ise indicated.
© Commonw ealth of Australia 2014
Australian Bureau of Statistics
Reference year
All causes of death data from 2006 onw ard are subject to a revisions process - once data for a reference year are 'f inal', they are no longer
revised. Affected data in this table are: 2006-2010 (f inal), 2011 (revised), 2012 (preliminary). See Explanatory Notes 29-33 and Technical
Notes, Causes of Death Revisions, 2006 in Causes of Death, Australia, 2010 (cat. 3303.0) and Causes of Death Revisions, 2010 and 2011 in
this publication.
3303.0 Causes of Death, Australia, 2012Released at 11.30am (Canberra time) 25 March 2014
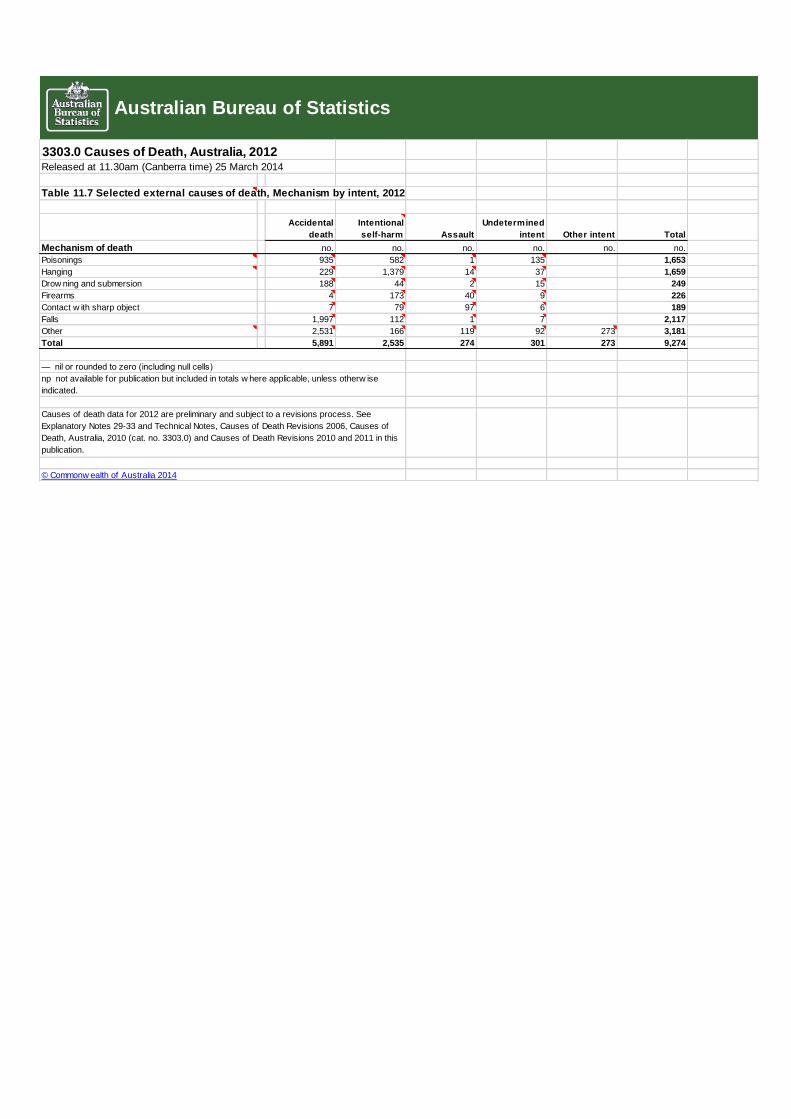
Table 11.7 Selected external causes of death, Mechanism by intent, 2012
Accidental
death
Intentional
self-harm Assault
Undetermined
intent Other intent Total
Mechanism of death no. no. no. no. no. no.
Poisonings 935 582 1 135 1,653
Hanging 229 1,379 14 37 1,659
Drow ning and submersion 188 44 2 15 249
Firearms 4 173 40 9 226
Contact w ith sharp object 7 79 97 6 189
Falls 1,997 112 1 7 2,117
Other 2,531 166 119 92 273 3,181
Total 5,891 2,535 274 301 273 9,274
© Commonw ealth of Australia 2014
Australian Bureau of Statistics
— nil or rounded to zero (including null cells)
np not available for publication but included in totals w here applicable, unless otherw ise
indicated.
Causes of death data for 2012 are preliminary and subject to a revisions process. See
Explanatory Notes 29-33 and Technical Notes, Causes of Death Revisions 2006, Causes of
Death, Australia, 2010 (cat. no. 3303.0) and Causes of Death Revisions 2010 and 2011 in this
publication.

BIBLIOGRAPHY
Brain, Peter. Going the Distance. Kingsford, NSW: Matthias Media, 2006. Brown G, Stanley B, Department of Veterans Affairs. "Patient Safety Plan Template." WICHE
(Western Institute Commission for Higher Education) Mental Health Program and Suicide Prevention Resource Center http://www.sprc.org/library_resources/items/patient-safety-plan-template.
Clinebell, Howard John, and Bridget Clare McKeever. Basic Types of Pastoral Care & Counseling : Resources for the Ministry of Healing and Growth. Updated and rev. / Bridget Clare McKeever. ed. Nashville: Abingdon Press, 2011.
Cordeiro, Wayne. Leading on Empty : Refilling Your Tank and Renewing Your Passion. Minneapolis, Minn.: Bethany House, 2009.
Counsellors), AIPC (Australian Institute of Professional. "Suicide: Statistics, Characteristics and Myths." [In English]. AIPC Article Library, no. June 14, 2012 (2012).
Geldard, D. Geldard and K. Basic Personal Counseling: A Training Manual for Counselors. 5th ed. Frenchs Forest, NSW: Prentice Hall / Pearson Learning Australia, 2005.
Horgan, David. "Body, Mind, Spirit... Tips." http://suicideprevention.com.au/body-mind-spirit-tips-2/.
Hunter, Elizabeth K. "'Between the Bridge and the Brook'." Reformation & Renaissance Review: Journal of the Society for Reformation Studies 15, no. 3 (2013): 237-57.
Janetzki, Peter. "Clarifying the Roles of Pastoral Care & Counselling within the Care Ministry of the Church." http://www.peterj.com.au/wp-content/uploads/2013/03/Journal-Article.pdf.
Line, On The. "Suicide Call Back Service." https://www.suicidecallbackservice.org.au/concerned-about-someone/supporting-someone-after-a-suicide-attempt.
———. "Supporting Someone after a Suicide Attempt." http://suicideline.org.au/worried-about-someone/supporting-someone-after-a-suicide-attempt.
Line, Suicide. "Self-Help for Suicidal Feelings." http://suicideline.org.au/content/uploads/self-help_for_suicidal_feelings.pdf.
McKay, Kathy, and Jann E Schlimme. "Making Sense of Suicide." (2011). Service, Suicide Call Back. "Supporting Someone after a Suicide Attempt."
https://www.suicidecallbackservice.org.au/concerned-about-someone/supporting-someone-after-a-suicide-attempt.
Shneidman, Edwin. Definition of Suicide. Jason Aronson, Incorporated, 1977. Stewart, Charles W. "What Does the Bible Say About Suicide." Journal of Pastoral Care 45, no. 1
(1991): 85-92. Wellman, Jack. "Suicidal Thoughts: 7 Biblical Tips." Telling Ministries LLC,
http://www.whatchristianswanttoknow.com/suicidal-thoughts-7-biblical-tips/.




















