On the Diffusion of Buddhist-Mindfulness in Psychiatry in Thailand and the United States
94
i ON THE DIFFUSION OF BUDDHIST-MINDFULNESS IN PSYCHIATRY IN THAILAND AND THE UNITED STATES Thesis submitted by Nicholas Roberts October 2007 In partial fulfilment of the requirements for the Degree of Bachelor of Arts (Honours) in the School of Anthropology, Archaeology and Sociology at James Cook University
Transcript of On the Diffusion of Buddhist-Mindfulness in Psychiatry in Thailand and the United States
i
ON THE DIFFUSION OF BUDDHIST-MINDFULNESS
IN PSYCHIATRY IN THAILAND
AND THE UNITED STATES
Thesis submitted by Nicholas Roberts
October 2007
In partial fulfilment of the requirements
for the Degree of Bachelor of Arts (Honours)
in the School of Anthropology, Archaeology and Sociology
at James Cook University
ii
Statement of Access
I, the undersigned, the author of this thesis, understand that James Cook
University will make the thesis available for use within the University Library
and, by microfilm, photographic or digital means, allow access to users in other
approved libraries. All users consulting the thesis will have to sign the following
statement:
“In consulting this thesis, I agree not to copy or closely paraphrase it in
whole or in part without the written consent of the author: and to make
proper written acknowledgement for any assistance that I have obtained
from it”
Beyond this, I do not wish to place any restriction on access to this thesis.
………………………………. .…………………………….
Nicholas Roberts (Date)
iii
Statement on Sources
Declaration
I declare that this thesis is my own work and has not been submitted in any
form for another higher degree or diploma at any university or other institution
of tertiary education. Information derived from the published or unpublished
work of others has been acknowledged in the text and a list of references is
given.
………………………………. .…………………………….
Nicholas Roberts (Date)
iv
Acknowledgements
This thesis is the result of many people, and not just the effort that I have
made to complete it. I have thoroughly enjoyed writing this thesis and I could
not have accomplished it without the following support:
Dr Robin Rodd for his indefatigable support, contribution, and friendship in
personally supervising this thesis; Mr Tom Ryan (Barrier Reef TAFE) for
bequeathing his experience about Buddhist-Mindfulness; Dr Sharn Rocco (JCU)
for initial communiqué on topics. To Dr Rosita Henry, Dr Nigel Chang & Dr
Marcus Barber for their assistance and efforts when called upon. To other
lectures, staff (including Library Staff and Copy Services Staff), and friends who
I have shared time with, thank you. Special mention to Joe, Chris, and Ali for
your warm and integral friendships. Credit and gratitude to those authors and
scholars whose work I have utilised in this thesis.
To my family: my mother Sue, for her interminable love and devotion
throughout my life - I love you Mum; Peter the J for his support and belief; my
father Kerry and family - Francis, Kieran, Thea and Natalie; my b.brother
Andrew, my complimentary contrary - ‘long may you run’; to Jane Sr. & Gwen,
Glen, Michelle Z&A, Gizmo folk and Tracy kin – love & devotion always.
Most importantly, to my inner circle – we intimately traversed this journey
together. Jane, you have been the roots of my tree and its foliage through this
process. Your constant supply of love sustained and sheltered me through the
vicissitudes of this year. We have weathered many seasons together, and in
keeping with life, we shall weather many more. To Joshua and Xy, the flowers
and fruit of my tree. You are my love and dedication manifest, and you return
these qualities to me as you grow through life. May you mature into healthy
trees yourselves, receiving nurturance through generating love and kindness.

5
There is a sociological fact that
must be taken into account in any
understanding of cultural integration.
This is the significance of diffusion.
Ruth Benedict, Patterns of Culture, 1946, p210.
Abstract
In Thailand and the United States Buddhist-Mindfulness is being diffused in
psychiatry as a method and process. In each context, Buddhist-Mindfulness is
diffused to improve the efficacy of psychiatric treatment of mental illness. A
cultural contextualisation of Buddhist-Mindfulness and the psychiatric process
has taken place through the process of diffusion, altering the practice of
Buddhist-Mindfulness and the process of psychiatry. Research in Thailand
highlights how Euro-American psychiatric and mental health aetiology,
nosology, and treatment protocols have been replaced with Buddhist
determinants of health. In the United States, Buddhist-Mindfulness is becoming
‘operationalised’ through diffusion into the Empirical Clinical Psychiatric
Practice, reflecting the dominance of this process over Buddhist aetiology and
nosology of mental illness. Analysis using the notion of habitus and theory of
practice reveal why Buddhist-Mindfulness is diffused differently in each
context. I argue that cultural ontological and cosmological logic is utilised in
each context revealing the different form, function, and meaning of Buddhist-
Mindfulness. The motivation by practitioners in Thailand and the United States
to utilise cultural ontology/cosmology is to balance and restore meaning and
social stability because of rapid social change and the crisis it is presenting
taken-for-granted life-ways in Thailand and the United States.
6
7
Contents
List of Figures/Tables………………………………………………….……………………9
Glossary……….………………………………………………………………………………….10
Introduction………………………………………………………………………………………13
1. The Diffusion of Buddhist-Mindfulness into Psychiatry in
Thailand and the United States: Two Case Studies……………16
Buddhist-Mindfulness: a Definition………………………………………………………………………………………17
Case Study 1: Buddhist Counselling for Patients with Anxiety. Rungreangkulkij, S &
Wongtakee, W (2006)……………………………………………………………………………………………………………19
Case Study 2: An Open Trial of an Acceptance-Based Behaviour Therapy for Generalised
Anxiety Disorder. Roemer, L & Orsillo, S (2007)………………………………………….………………………21
Discussion………………………………………………………………………………………………………………….……….…23
Buddhist-Mindfulness-Based Psychiatry………………………………………….……………………………………26
2. Diffusion & Cultural Change………………………..…………………28
Diffusion: Definition, Application, and Research in the Social Sciences………………………….…29
Method & Process…………………………………………………………………………………………….……………………32
Cultural Change & Revitalisation: Ontology, Habitus & Ideology……………………….………………33
The Social & Historical Praxis of Suffering……..……………………………………………………………………38
3. Diffusion, Health-Seeking & Culture Change in Northeast
Thailand………………………………………………………………………………40
Buddhism, Health & Culture Change……………………………………………………………………………………41
Healthcare in Northeast Thailand……………………………………………………………………………..…………44
Health-Seeking in Macro-Cosmic Context…………………………………………………….………………………49
Medical Pluralism in Northeast Thailand: Form & Function…………………………………………………52
8
4. Diffusion, Health-Seeking & Culture Change in the United
States……………………………………………………………………….…………55
Scientific Crisis & the ‘Operational’ Status of Buddhist-Mindfulness…………………..……………56
Medicalisation & Capitalism in the United States…………………………………………….…………………59
Health-Seeking in Macro-Cosmic Context……………………………………………………………………………62
Medical Pluralism in the United States: Form & Function………………………….………………………66
5. Cultural Change, Psychiatry & Diffusion……………..…………68
On the Diffusion of Buddhist-Mindfulness in Psychiatry……………………….……………….……………69
Cultural Crisis & the Collective Past……………………………………………….………………………..…………74
Conclusion…………………………………………………………………………………………75
References…………………………………………………………..……………………………77
9
List of Figures
Figure 1. Diffusion as a Process of Communication…………………………29 Figure 2. Use of Ontology & Cosmology in Modern Culture Change………………………………………………………………….……..……36 Figure 3. Buddhist Aetiology of Suffering & the Liberation from Suffering……….……………………………………………………….…….……43 Figure 4. Identified Diagnostic Options in Northeast Thailand..….…46 Figure 5. Identified Causes of Illness & Suffering in Northeast Thailand……………………………………………………………………….……48 Figure 6. Psychiatric Aetiology of Mental Illness…………………………….57 Figure 7. Consequences, or Differences in Form, Function & Meaning to Buddhist-Mindfulness through Diffusion….……71 Figure 8. Worldviews Influencing the Consequences to Buddhist- Mindfulness…………………………………………………………….…………72
10
Glossary of Terms & Abbreviations
Pali (P), Sanskrit (S) & Thai (T)
anapan-sati (S) meditation technique: Mindfulness of Breathing.
annáta (P) no-self; knowledge that the self is constructed and is
impermanent and transcendent; Universal Law
anníca (P) impermanence; knowledge that all phenomena is
subject to change; Universal Law
aviccha (P) ignorance; attachment
baap (P) positive merit; good social action or intentions that
are karmically reciprocal
baan (T) literally meaning ‘village’ or ‘community’
bun (P) negative merit; like baap, but harmful social action
dukkha (P) suffering; conflict of conditioned existence; Universal
Law
karma (S) [kam (T)] actions that are morally, socially, ethically relevant;
universal law of cause and effect
kwan (T) one of two souls the body contains; can be lost or
11
stolen; retrieved through ritual means
Mahayána (S) northern school of Buddhism
marga (P) eightfold noble path; leads towards nibbána
metta (P) loving-kindness; meditation technique that aims to
generate kindness and acceptance of all life
mor lam song (T) spirit medium; shaman
nibbána (P) [nirvána (S)] ultimate and final goal on Buddhist Path; release
from, and cessation of suffering
niróda (P) attainment of cessation of mental activity
pánna (P/S) wisdom; awareness of Universal Laws
phi (T) generic for a variety of helpful and malevolent
spirits; cultic like following and worship
samsára (S/P) the wheel of birth and death; law of being and
becoming
sati (S) mindfulness; clear awareness of activity
samudayá (P) realisation of the origin of suffering
tahná (P/S) craving; attachment
Theraváda (S) southern school of Buddhism
12
ti-lakkhána (P/S) three Universal Laws; philosophical teachings about
dukkha and how to attain cessation from dukkha
upadána (P/S) clinging; attachment
wat (T) buddhist temple
vipassana-bhavana insight meditation; stronger path to achieve
mindfulness and mental awareness
Abbreviations
AABT Acceptance-Based Behavioural Therapy
ACT Acceptance and Commitment Therapy
CAM Complimentary and Alternative Medicines
CBT Cognitive-Behavioural Therapy
DBT Dialectical-Behavioural Therapy
GAD Generalised Anxiety Disorder
ECPS Empirical Clinical Psychiatric Standards
MBCT Mindfulness-Based Cognitive Therapy
MBSR Mindfulness-Based Stress Reduction
13
Introduction
The diffusion of innovations occurs in all domains of global social and cultural
life, from within or without. The diffusion of innovations is a two-way flow
between cultures. Importantly, diffusion is a fundamental process of socio-
cultural adaption (Weinstein 2005). Contemporarily, the process of
globalisation is speeding up the process of diffusion between Euro-American
and non-Euro-American cultures (Hunter & Whitten 1976; Strinati 1995). In the
United States, ethnomedical and religious practices form the basis for current
paradigmatic shifts in science and medicine and are becoming increasingly
incorporated as therapeutic interventions. This application is highlighted by
efficacious results in treating states of ill health. Acupuncture, Indian
Ayurveda, Naturopathy, Shamanism, and Tibetan medicine are among a number
of ethnomedicines or religious traditions that are becoming incorporated with
or complementing existing biomedical and psychiatric services. In Thailand, the
same phenomenon is taking place. Traditional forms of medical and ritual
practice (Buddhism, spirit mediumship, exorcism) are being diffused with
biomedicine and psychiatry. In each context, cultural change and the lack of
meaning given to modern illness experience has motivated a retreat into
historical culture to affirm identity and balance biopsychosocial needs.
Psychiatry in the United States is currently incorporating Buddhist-Mindfulness
into practice. The diffusion of Buddhist-Mindfulness reveals what Dawson
(2006) describes as the ‘Western habitus’. Here, the “technologized
conceptualizations of the self, a depersonalized view of the cosmos, and a
metaphorization of the modern cultural field” have developed (Dawson 2006,
p1) historical and distinct ‘ways of seeing’ states of illness and illness
experience. Current shifts in scientific medicine and psychiatry in the United
14
States utilise ‘Eastern’ religion and other Complementary and Alternative
Medicines (CAM), ‘operationalising’ them into existing paradigms.
‘Operationalising’ is a process of experiment and abstraction that excludes
non-definable or non-experimental aspects of practices, distancing these
practices from their cultural origins (Moreland 1989). Dawson (2006) interprets
this as a “Westernisation of Eastern themes”, a process “structured along
enduring paradigms” (Boehnlein 2006, 644). This highlights an inability of social
institutions in the United States, including education, biomedicine, and
psychiatry to truly accept and embrace cross-cultural religion as religion
(Wallace 2007). Further, the rise and penetration of capitalism into social
institutions and social values (Harvey 2000), and the growing uncertainty in the
United States surrounding the efficacy of modern medicine to deliver adequate
healthcare (Bates 2002) has assisted in the development of CAM.
In Northeast Thailand, the diffusion of Buddhist-Mindfulness into psychiatry has
also transpired. Thailand is a Buddhist Kingdom that has remained relatively
isolated and insulated in Buddhist Southeast Asia for 500 years. Buddhism
represents a textual institutional and structural (Keyes 1984; Kirsch 1985;
Reynolds & Reynolds 1982) command over Thai society, and as a result has
been used to legitimate change and development for centuries. Medical
practice in Northeast Thailand is plural, and reflects a history of diffusion of
ethnomedical practices. The penetration of Thailand by Euro-American values,
institutions, and discourse over the last 150 years has dislocated many of the
traditional medical and transpersonal practices of Buddhism in Thailand.
Scientific medicine and psychiatry, which maintain high symbolic status in
Thailand are prominent examples, and have become part of the thriving
medical plurality here. However, Buddhism provides a philosophical and
practical dialogue on everyday experience in Thailand (Harvey 1990). Suffering
(dukkha) and the release from suffering (nibbána) are central aspects of
Buddhist philosophy and practice that combine with broader narratives linking
person-society-cosmos. Buddhist-Mindfulness is an integral cultural praxis
15
situated in a wider dialogue with Buddhist philosophy and personal lifeways in
Thailand. This is illustrated through the diffusion of Buddhist-Mindfulness into
psychiatry.
In this thesis I aim to determine why Buddhist-Mindfulness has been taken up in
each psychiatric context by examining the macro-global and local-social forces
that motivate this process. This thesis is based on a critical literature review.
The quality of ethnographic data permits an excellent ability to generate sound
conclusions on this topic. I define Buddhist-Mindfulness as a Buddhist practice
(that examines experience), and psychiatry as a socio-cultural system (that
treats mental illness). I argue that each is positioned in a critical engagement
with their larger socio-historical and cultural cosmological contexts. Chapter 1
presents one case study from each location (Thailand and the United States) to
emphasise how Buddhist-Mindfulness is applied in psychiatry through the
diffusion process. Chapter 2 explains the theoretical framework for the thesis.
Bourdieu’s (1977) theory of habitus and practice are employed to understand
why cultures are resistant to change and how culture reacts to change/crisis.
Kapferer’s (1988) theory of cultural ontology/cosmology utilisation to
legitimate change/crisis is employed to illustrate why the form, function, and
meaning of Buddhist-Mindfulness is different in Thailand and the United States.
Chapters 3 and 4 draw on ethnographic and historical data to analyse the
diffusion of Buddhist-Mindfulness into psychiatric practices in Thailand and the
United States respectively. Chapter 5 is a synopsis of the comparative
contextualisation of the diffusion of Buddhist-Mindfulness. Buddhist-
Mindfulness is incorporated in psychiatry in Thailand as a Buddhist practice and
in the United States as a scientific and medical process. I argue that prevailing
worldviews are ideologically recalled to legitimate social change and crisis,
change that ruptures the habitus, motivating a retreat to ontology/cosmology.
This process generates the distinct alteration of consequences that Buddhist-
Mindfulness receives through the process of diffusion in Thailand and the
United States.
16
Chapter 1
Buddhist-Mindfulness in Psychiatric Application:
Case Studies from Thailand
and the United States:
This chapter will highlight how Buddhist-Mindfulness is applied in psychiatry in
the United States and Thailand as a therapeutic intervention. Buddhist-
Mindfulness based psychiatric therapy is very popular in the United States.
However, only one therapeutic trial in Thailand has been located. This chapter
examines two case studies that utilise Buddhist-Mindfulness in clinical
psychiatry for the treatment of anxiety disorders. Rungreangkulkij &
Wongtakee’s (2006) pilot study of a Buddhist-Mindfulness based psychiatric
therapy in Northeast Thailand, and Roemer & Orsillo’s (2007) open trial of a
Buddhist-Mindfulness based behavioural therapy in the United States will be
examined to highlight the different application of Buddhist-Mindfulness in each
context. There are significant variations in the application of Buddhist-
Mindfulness as psychiatric therapy in each location. This is illustrated by
examining each case study individually to highlight the similarities and
differences in application in form, function, and meaning. Changes to Buddhist-
Mindfulness via the diffusion process are revealed through the trial aims, the
trial structure, and methods and terminology employed in the diagnostic,
therapeutic, and evaluative processes. This examination provides the
developmental basis for analysis in the following chapters.
17
Buddhist-Mindfulness: a Definition
Buddhist-mindfulness is a textual, philosophical, and cosmological aspect of
Buddhism. ‘Mindfulness’ (sati) is a cultivated state of mental awareness. It is
the human capacity to be aware and act upon this awareness. ‘Mindfulness’ is a
core and fundamental aspect of the Buddha’s thesis on suffering (dukkha),
providing philosophical and practical dialogue on suffering (dukkha) and the
release from suffering. ‘Mindfulness’ was developed by the Buddha 2500 years
ago following his liberation from suffering (nirvana), and has since been refined
in both the Mahayana (Northern School) and Theravada (Southern School)
Buddhist Traditions. The practice of ‘Mindfulness’ has flourished throughout
Buddhist culture in Asia. In many schools “it has become elevated to the hub of
the teachings (Titmuss 1998, p48). The aim of ‘Mindfulness’ and meditation
practice is to liberate people from physical and psychological suffering.
‘Mindfulness’ is directed towards cultivating awareness and acceptance of life
as-it-is-experienced (that is, Right Mindfulness). It is the most positive step
towards the liberation from ignorance, craving, and desire, the causes of
suffering (Titmuss 1998).
‘Mindfulness’ is the practice of focusing attention on the present moment of
experience, being non-judgemental and not striving towards solutions or goals,
accepting experiences, as they are experienced. To Buddhists, the mind is
cultivatable, and ‘Mindfulness’ is the most effective method to “bring the
different aspects of our being into focus” (Rinpoche 1992, p61). Buddhists
conceive of two minds: the everyday mind (illusory) and the nature of mind
(universal reality). The aim of ‘Mindfulness’ practice is to go beyond the
‘everyday mind’. Proper application of ‘Mindfulness’ can reveal the true
‘nature of mind’, as stated in various Buddhist texts, surpassing all ignorance
and craving to attain true awareness and insight into universal reality. On its
own ‘Mindfulness’ lacks the ability to cultivate deep wisdom. ‘Mindfulness’
must encompass meditation to enable correct cultivation of concentration,
18
awareness, and observation, factors that are crucial to successful meditation
and the attainment of the ‘universal mind’ (Harvey 1990; Rinpoche 1994).
‘Mindfulness’ is practised in congruence with meditative processes. Practice of
meditation and its incorporation with ‘Mindfulness’ is essential to achieving
true concentrated awareness in meditation. Effective practice aims to enable
‘Mindfulness’ to become a meditation in everyday life experiences. Two
examples of meditation are Loving-Kindness (metta) and Mindfulness of
Breathing (anapan-sati) meditation (Harvey 1990). Nhat-Hahn (1994) describes
how application of Mindfulness of Breathing (anapan-sati) is applicable as a
mediative practice in sitting or walking postures and in our interactions and
activities in day-to-day life. He decrees, “insight is not just knowledge but true
understanding” (Nhat-Hahn 1994, p101). The application of ‘Mindfulness’ as
waking-meditation promotes non-judgemental awareness and eventually
transcendence of suffering and illusory states of mind. The ultimate goal is the
liberation from suffering, or the achievement of enlightenment (nibbána) and
cessation of rebirths (samsára) in the various realms proscribed by Buddhist
cosmology (Griffiths 1986).
A recent explosion of Buddhist-Mindfulness (based) healthcare has occurred in
the United States. While Buddhism has been practised in a variety of ways in
the U.S since the 1950’s, modern psychiatry in the U.S has incorporated
Buddhist-Mindfulness into therapy. Psychiatric therapies based on Buddhist
paradigms of suffering (dukkha) are replacing and fusing with existing
cognitive-behavioural models. Buddhist-Mindfulness therapies promote
awareness and acceptance of pathological behaviour and experience avoidance
(Fronsdal 1999). Since the 1970’s, Buddhist-Mindfulness based programs have
operated in hospitals, clinical, workplace, and school settings in the United
States. John Kabat-Zinn, arguably the pioneer in the field of Buddhist-
Mindfulness based clinical intervention in the United States, opened a Stress
Reduction Clinic through the University of Massachusetts Medical Clinic. Self-
19
developed ‘Mindfulness Based Stress Reduction’ (MBSR) courses began here in
1979. MSBR is based on Buddhist-Mindfulness techniques and incorporates
Theravada Buddhist Insight (vipassana-bhavana) and mindfulness of breathing
(anapan-sati) mediation and Indian Hatha Yoga (Kabat-Zinn 1982; 2000; 2003).
A multitude of other programs have also been borne out of the original MSBR
program in the last decade, including Acceptance and Commitment Therapy
(ACT), Mindfulness Based Cognitive Therapy (MBCT), and Dialectical Behaviour
Therapy (DBT) (Baer 2003). The present aim is to ‘operationalise’ Buddhist-
Mindfulness as an Empirical Psychiatric method to treat and overcome mental
illness.
Case Study 1:
Buddhist Counselling For Patients With Anxiety.
Rungreangkulkij, S & Wongtakee, W (2006).
The aim of Rungreangkulkij & Wongtakee’s (2006) study is to determine the
efficacy of Individual Buddhist Counselling for Thai patients suffering diagnosed
anxiety disorders. Rungreangkulkij & Wongtakee (2006, p1) identify anxiety as
prevalent in Thailand, where 9.5% of the population is affected. They highlight
how socio-cultural change in Thailand has influenced anxiety levels. Socio-
cultural change has also altered the way Thai people seek medical treatment
and are inturn treated. Biomedical/psychiatric treatment is more widely
accessed than traditional medicines. Symptoms of anxiety are not always
detectible by psychiatric or General Practitioners. Physiological symptoms are
misdiagnosed as anxiety, while they are most probably a form of somatoform
disorder (see Okasha 2003). However, due to misdiagnosis (due to the similarity
of symptom to anxiety), patients are prescribed anti-anxiety medications.
Pharmaceutical addiction is a common problem in Thailand that has resulted
from anxiety disorder misdiagnosis.
20
Rungreangkulkij & Wongtakee (2006, p6) chose to incorporate Buddhist
discourse and practices into the counselling process “because it fits with the
clients’ belief and worldview”. They utilise the Buddhist concept of suffering
(dukkha), applying it in the therapeutic processes because it is relevant to the
process of healing. Another factor that influenced the use of Buddhist-
Mindfulness were trials in America, Europe, and Australia (Rungreangkulkij &
Wongtakee 2006, p2). Buddhism is already established throughout the health
system in Thailand, a fact that the authors express motivated them to
incorporate Buddhist discourse and practice into therapy. The goals of
Rungreangkulkij & Wongtakee’s (2006) study are to reduce or prevent mental
illness (anxiety), and to provide a framework of Buddhist/Mindfulness practice
for future psychiatric treatment.
The study was set in Northeast Thailand. The study was undertaken over a one-
month period. 21 patients/participants who had been treated for anxiety at
the local community hospital (30 beds) were involved. All patients were
Buddhists. All patients/participants were taking medication at the time of the
study. Demographic data (age, gender, religion, marital status, income,
occupation), anxiety measures (STAI: State-Trait Anxiety Inventory), and
participant diary and meditation logbooks were used to determine the efficacy
of the counselling process. The counselling process was on a practitioner/client
interaction. The practitioner is trained in counselling/psychiatry and
meditation (by a monk) and is a practising Buddhist and meditator. The
counselling process involves an initial 60-90 minute session and a follow-up
session one month later. Both counselling sessions had four structured phases:
1) Develop rapport between practitioner and patient. 2) Educate client about
symptoms, emotion, and suffering. Application of Buddhist philosophy (Three
Universal Laws; Four Noble Truths; Eightfold Noble Path) and mindfulness
meditation is introduced as the way to overcome suffering. 3) Practice of
21
mindfulness meditation and assessment of practice. 4) Session completion
through assessment of the patients’ understanding of their problems.
Data was analysed through a variety of statistical means (descriptive and non-
parametrical) and formulated into tables. Results considered demographic
data, contents of patient’s diaries, and the patients’ prescribed dosage of
medication. All subjects reported feeling calmer from the therapy, particularly
those who practised Mindfulness-meditation regularly. Two patients completely
stopped their medication, and fifteen patients required less medication than
before. Rungreangkulkij & Wongtakee (2006) concluded from this study that
Buddhist counselling has the ability to reduce levels of anxiety. They argue that
Buddhist counselling has the ability to change maladaptive behaviour and
habits through application of Buddhist principles (Three Universal Laws; Four
Noble Truths; Eightfold Noble Path; Mindfulness-meditation) into daily life.
They argue that their results prove this (Rungreangkulkij & Wongtakee 2006,
p5). Limitations are that the study was not a randomised trial. They call for
further studies to gain better understanding of the efficacy of Buddhist-
Mindfulness counselling of mental health disorders in Thailand.
Case Study 2:
An Open Trial of an Acceptance-Based Behaviour Therapy
for Generalised Anxiety Disorder.
Roemer, L & Orsillo, S (2007).
The aim of Roemer & Orsillo’s (2007) study was to test the efficacy of an
Acceptance-Based Behavior Therapy (ABBT) treating Generalised Anxiety
Disorder (GAD). Roemer & Orsillo (2007) acknowledge that GAD is the least
successfully treated anxiety disorder. The authors argue that previous
treatments, such as Cognitive-Behavioral Therapy (CBT) do not provide
22
adequate techniques to treat GAD. This conclusion warranted them to apply
new treatment (psychosocial) to assess GAD. ABBT is a modification of CBT.
The difference lies in the acceptance (Buddhist-Mindfulness) aspect of therapy
that centres this therapy on personal awareness of present cognitive
experience and experience avoidance. In CBT, purposeful change of cognitive
experience is the critical process of the therapy. In ABBT, cognitive experience
is accepted and made aware of unconditionally without any attempt to change
these experiences. Roemer & Orsillo (2007, p73-74) cite numerous studies and
authors who attest to the efficacy of integrating Buddhist-Mindfulness into GAD
therapy. The authors claim that ABBT is congruent with other Buddhist-
Mindfulness based therapies.
The trial was conducted at the Centre for Anxiety and Related Disorders and
Boston University, Boston, U.S.A over a three-month period. These included
pre, post, and follow up assessments of the clients. The authors and therapists
treated 16 clients in the ABBT trial. All patients were taking medication to deal
with anxiety and comorbid symptoms. Patients were initially assessed using
DSM-IV Anxiety Disorders Interview Schedule. Patients were also assessed
through various clinically applied measures to assess symptoms associated with
GAD. “Fear and avoidance of internal sensations” (Roemer & Orsillo 2007, p76)
were the main symptoms the authors posited to be significant aspects of GAD.
Treatment (following informed consent) consisted of individual therapy
comprising 16 sessions (first four at ninety minutes; following twelve at sixty
minutes; final two were tapered). Sessions 1-4 introduced clients to concepts
of ‘habit forming’ and ‘experience avoidance’ through handouts, presentations,
demonstrations, and finally through discussion.
In session 2, Buddhist-Mindfulness strategies were introduced. Clients were
encouraged to practice a variety of Buddhist-Mindfulness techniques, such as
breathing, muscle relaxation, and meditation. These practices were
incorporated from the beginning to the end of the sessions. Clients were

23
informed that Buddhist-Mindfulness techniques must be practised at home and
during the course of the client’s life for adequate changes to occur. “Clients
are taught that mindfulness is a skill and a process, rather than a desired end
state” (Roemer & Orsillo 2007, p79). Keeping a journal and writing about their
experiences was required throughout therapy to aid clients in clearly viewing
their avoidance and habitual tendencies, assessing their own emotional state
daily. The aim was for clients to live mindfully and become self-critical of their
actions towards their experiences. In this way the person becomes responsible
for their actions and illness.
Post-treatment assessment revealed significant reductions in fear, avoidance,
depressive and anxiety related symptoms. Two clients reduced their
medication, and two clients discontinued their medication altogether. A three-
month follow-up of the study (12 clients) showed one more client had
discontinued medication and an overall reduction in symptoms (worry, anxiety,
stress) and experiential avoidance from clients. Interestingly, depressive
symptoms were still prevalent after the three-month follow-up. Roemer &
Orsillo (2007) suggested that, overall, these findings indicate the potential for
ABBT and other Buddhist-Mindfulness based therapies to treat GAD. They agree
that further trials and more research are needed to clarify and determine if
their findings constitute significant changes in the treatment of GAD and other
associated disorders.
Discussion
Rungreangkulkij & Wongtakee’s (2005) pilot study of a Buddhist-Mindfulness
based therapeutic intervention in Northeast Thailand and Roemer & Orsillo’s
(2007) open trial of Mindfulness-Acceptance Based Behavioral Therapy in
America show considerable similarities and differences in the definition and
application of Buddhist-Mindfulness. Both studies applied Buddhist-Mindfulness
into the psychiatric process and cite its transformative potential in treating
24
anxiety disorders. Analysis of the trials’ aims, the trials’ structure, methods
and terminology employed in the diagnostic, therapeutic, and evaluation
processes of each trial reveals the different application of Buddhist-
Mindfulness. The form, function, and meaning of Buddhist-Mindfulness applied
in the two localities are dissimilar. This reveals a significant cultural-contextual
difference in the application of Buddhist-Mindfulness.
The function of applying Mindfulness-based intervention was comparable in
both trials. Each trial highlighted the potential efficacy of integrating Buddhist-
Mindfulness to treat anxiety. Each trial diagnosed and assessed patients
through standard psychiatric nomenclature. The aim of both trials was to
develop a more efficacious technique to alleviate completely or prevent
anxiety disorders. Previous research and application of Buddhist-Mindfulness
based therapy in the United States and Australia provided clinical evidence and
motivation for the application of Buddhist-Mindfulness into psychiatry in each
case. Buddhist-Mindfulness was defined by the two trials in a similar manner,
describing it as present-moment awareness, a non-judgemental acceptance of
life as it is experienced. Each trial highlights the importance of applying the
therapeutic process in the client’s life during treatment and by the client after
treatment to alleviate or prevent anxiety symptoms.
The aim of applying Buddhist-Mindfulness in each trial was to cure or prevent
anxiety. This aim was commensurable in both trials. However, the application
of Buddhist-Mindfulness was distinct. Rungreangkulkij & Wongtakee (2005, p2)
applied Buddhist-Mindfulness by utilising a Buddhist aetiology of suffering
(dukkha). While they modelled their therapy according to other Buddhist-
Mindfulness based therapies employed in the U.S and Australia, they structured
sessions around the Buddha’s thesis on suffering (dukkha) and the path to the
liberation from suffering. These were “the philosophical underpinnings of the
counselling sessions” (Rungreangkulkij & Wongtakee’s 2005, p2). Roemer &
Orsillo (2007) also apply Buddhist-Mindfulness in a manner built upon CBT and
25
other Buddhist-Mindfulness based therapies existing in the United States. In
contrast, however, there was no use of any Buddhist themes or any association
with Buddhism in their therapeutic application of Buddhist-Mindfulness, even
though their application of Buddhist-Mindfulness is derived from textual and
Theravada Buddhist philosophy and meditation practice (Roemer & Orsillo
2007, p75).
Each study contained explanation sessions between patients and practitioners.
The sessions functioned as an introduction to concepts and explanations of the
relationship between habit, behaviour, and anxiety. Rungreangkulkij &
Wongtakee (2005) applied the Buddha’s Three Universal Laws (ti-lakkhana);
impermanence (annicca), suffering (dukkha), and no-self (anatta); and the
concept of suffering (dukkha). This application was a Buddhist explanation of
the nature of suffering as habitual mental activity, describing how and why a
person suffers, and how a person can be liberated from suffering. Roemer &
Orsillo (2007) follow a very similar format to Rungreangkulkij & Wongtakee
(2005). They highlight the habitual, emotional, and behavioural actions
associated with anxiety, and introduce Buddhist-Mindfulness techniques to
patients to manage their anxiety. However, Roemer & Orsillo (2007) do not
associate any Buddhist relationship in anxiety aetiology nor do they apply
Buddhist philosophy or theory in this part of the therapeutic process.
The application of Buddhist-Mindfulness in each trial was to develop
acceptance of situations and experiences as they occur, without judgement or
expectation. Buddhist Mindfulness and Meditation techniques (Loving-Kindness
[mettá], Mindfulness of Breathing [ánápána-sati], and Insight [vipassaná]
Meditation {Harvey 1990}) were applied in each trial. These meditation
techniques are associated with Buddhist-Mindfulness and are consistent with
those practiced in traditional Theravada Buddhism. Rungreangkulkij &
Wongtakee (2005) apply Mindfulness Meditation in conjunction with The Three
Universal Laws (ti-lakkhana) (to teach that life is impermanent [annicca], that
26
suffering [dukkha] is an actuality of life, and that no-self [anatta] exists or is
attached to a body), The Four Noble Truths (patients can remedy their
suffering by becoming mindful of why they are suffering and what the causes of
their suffering are), and The Eightfold Noble Path (which leads on from the
Fourth Noble Truths and is the process to the liberation from suffering).
Conversely, Roemer & Orsillo (2007, p75) apply Buddhist-Mindfulness and other
Buddhist meditation techniques to treat anxiety from the format devised by
Kabat-Zinn (2003) in other Mindfulness/ acceptance therapies. This process
does not apply any Buddhist association.
The meaning of the application of Buddhist-Mindfulness is also distinct in each
trial. Application of Buddhist-Mindfulness in therapy could be described as
culturally consonant with the aetiological and philosophical delineation of
disease in each context respectively. Each application is consonant with its
cultural worldview in which it is practised. Thailand is a Buddhist Kingdom.
Rungreangkulkij & Wongtakee (2005, p6) argue that the Buddha’s teaching will
fit “with the client’s belief and worldview”. They contend that the application
of Buddhist-Mindfulness will prove efficacious and “increase compliance with
therapeutic instruction” (Rungreangkulkij & Wongtakee 2005, p2). While they
associate anxiety in Thailand as an effect of social and cultural change, the
meaning of anxiety and its treatment are presented as an exegesis of Buddhist
cosmological and existential philosophy regarding suffering and the human
condition. Roemer & Orsillo (2007) apply Buddhist-Mindfulness with no trace of
any religious, philosophical, or cultural association. Mindfulness is therapeutic
process that utilises Buddhist meditation and other Buddhist beliefs and
philosophy, but the contextual origins and meanings of this praxis are absent.
27
Buddhist-Mindfulness Based Psychiatry
Rungreangkulkij & Wongtakee’s (2005) pilot study of Buddhist mindfulness
based psychiatric therapeutic intervention in Northeast Thailand and Roemer &
Orsillo’s (2007) open trial of (Buddhist-Mindfulness) Acceptance-Based
Behavioral Therapy in the United States highlight how Buddhist-Mindfulness is
diffused into the psychiatric process. Both trials proved efficacious in
generating considerable reduction in symptoms associated with anxiety. Both
processes were therefore therapeutically successful because they improved
upon the previous methods used to explain and treat anxiety. However, the
application of Buddhist-Mindfulness was distinct in each trial. The diffusion of
Buddhist-Mindfulness in each context appears to be culturally and contextually
bound. This is clearly represented through the distinct medical aetiology
(methodological and theoretical guidelines) that each cultural context applies
to the practice of Buddhist-Mindfulness based psychiatry. Further analysis of
these distinctions will provide insight into the influence that culture has on the
diffusion of Buddhist-Mindfulness into psychiatry in Thailand and the United
States.

28
Chapter 2
Diffusion & Cultural Change
The diffusion of Buddhist-Mindfulness into psychiatry in Thailand and the
United States, as illustrated through the case studies in Chapter 1, are
contextually constrained and influenced by culture. Micro-cultural influence is
an important factor affecting the form, function, and meaning that Buddhist-
Mindfulness takes through diffusion in each cultural context. However, macro-
social processes motivate why the diffusion process occurs. A Macro-social
explanation will highlight why Buddhist-Mindfulness is being diffused in
psychiatry and what motivates this change. Each trial identified that socio-
cultural change, and the failure of the present psychiatric paradigm to treat
mental illness efficaciously, determined why the diffusion of Buddhist-
Mindfulness is taking place in Thailand and the United States. In this chapter I
explore why psychiatry in Thailand and the United States each incorporeate
Buddhist-Mindfulness differently. I do this by examining the contextual
difference that is located in the amalgamation of socio-historical ontological
and cosmological factors. Ontology and cosmology are history made meaningful
in the present by ideology, and the process of ontology/ideology incorporation
is to construct and interpret experience, and to maintain order. The
incorporation of ontology/ideology is motivated by change or the threat of
change to the existing social order or habitus. These are the conceptual
foundations employed to understand the contextual diffusion of Buddhist-
Mindfulness. Change motivates a drive to restore social order in a rapidly
changing world, to diffuse. And ontology/cosmology are utilised as the process
that gives meaning to and makes sense of change.
29
Diffusion: Definition, Application & Research in the Social Sciences
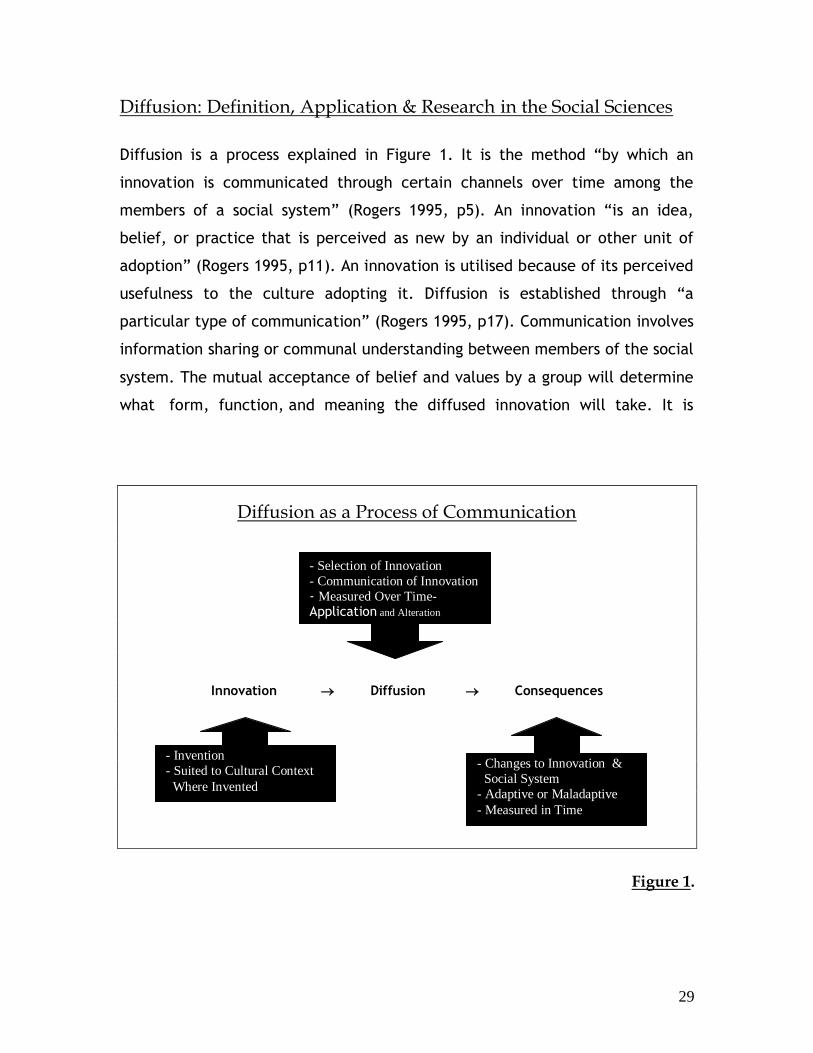
Diffusion is a process explained in Figure 1. It is the method “by which an
innovation is communicated through certain channels over time among the
members of a social system” (Rogers 1995, p5). An innovation “is an idea,
belief, or practice that is perceived as new by an individual or other unit of
adoption” (Rogers 1995, p11). An innovation is utilised because of its perceived
usefulness to the culture adopting it. Diffusion is established through “a
particular type of communication” (Rogers 1995, p17). Communication involves
information sharing or communal understanding between members of the social
system. The mutual acceptance of belief and values by a group will determine
what form, function, and meaning the diffused innovation will take. It is
Diffusion as a Process of Communication
Innovation Diffusion Consequences
Figure 1.
- Selection of Innovation
- Communication of Innovation
- Measured Over Time- Application and Alteration
Over Time
- Invention
- Suited to Cultural Context
Where Invented
- Changes to Innovation &
Social System
- Adaptive or Maladaptive
- Measured in Time

30
commonly accepted amongst diffusion researchers that innovations will change
and be reinterpreted in their new context through the process of diffusion
(Barnard 2000; Kroeber 1948 [1923]; Winthrop 1991). The socio-cultural system
will also change due to the diffusion of an innovation. Diffusion of innovations
tends to be top-down and do not always create benefit to all. Diffusion often
has extreme consequences to social and environmental health and the severity
will be different in each cultural context (McElroy & Townsend 1989).
The process of interpreting diffusion is not straightforward. This is due to the
socio-cultural differences inherent in each social context under examination.
Why the diffusion process occurs and what consequences to the social system
and the innovation result from diffusion continue to challenge researchers
(Rogers 1995). This fact is also compounded by the variety of research
traditions and research methodologies applied to study diffusion and resultant
culture change. Medical anthropology (McElroy & Townsend 1985), sociology
(Rogers 1971), and psychology (Berry 1990) represent a number of modern
diffusion research traditions. These traditions focus on how various aspects of
diffusion affect and are affected by various social and cultural factors including
art (Morphy 1994), foreign aid and development (Escobar 1995), health
(McElroy & Townsend 1989), migration, and religion (Mills 1997). Research
traditions that focus on cultural change through diffusion (and acculturation)
are often critical of the historical and modern studies of diffusion. Reynolds
(1971) highlights the need to increase the understanding of acculturation and
diffusion processes to create a useful and relevant theory. His work on religious
diffusion in the Philippines aimed to clarify current terminology for
acculturation/diffusion. Rogers (1995) explains the inability of diffusion
researchers and cultural-development agents to research the consequences of
the diffusion process, the third and arguably most important aspect of diffusion
research. This inability, he argues, rests with those who propose and enact
development projects, and with the researchers that fail to develop sufficient
long-term methodological and research-based projects into consequences of
31
diffusion cross-culturally. Sam & Berry (2006) highlight the inability of the
social sciences to adequately define the meaning and operation of
acculturation and diffusion as it is applied as a discursive and methodological
tool in psychology.
Within anthropology, de Sardan (2005) considers the need to develop an
‘Anthropology of Innovation’. de Sardan aims to clarify and unite the variety of
research methodologies and interpretations social scientists employ in
diffusion, acculturation, and innovation research. de Sardan’s (2005) critique of
the anthropological and sociological research traditions on diffusion,
acculturation, innovation, and the consequences of diffusion is timely. It
illustrates the need to make commensurate the various disciplinary concepts
into a methodologically precise and accurately defined approach to diffusion
research. What he articulates in his movement towards an ‘Anthropology of
Innovation’ resonates with Reynolds (1971), Rogers (1995), and Sam & Berry
(2006). It is clear that there is ambiguity regarding not only precise
interdisciplinary definition for diffusion (and acculturation), but also how to
study these phenomena as a process. de Sardan (2005) argues that there is
epistemological commensurability among these disciplines and a ‘reworking’ of
the various methodological and research objectives that these traditions have
applied to diffusion and acculturation research can be achieved within the field
of anthropology.
The amalgamation of various methodologies that focus on diffusion,
acculturation, and innovation would be an appropriate refinement considering
the broad research traditions with equally broad research basis. The
theoretical ‘reworking’ outlined by de Sardan (2005) would provide a baseline
that competently defines not just innovation, but the diffusion of innovations
(as designated by Rogers 1995). This would be a processual method, and all the
preceding and anteceding sub-processes of the diffusion process must be taken
into account. This would provide a transition beyond the methodological

32
limitations and departmental particularities that modern diffusion research
traditions exhibit. But this is not a straightforward task, considering the variety
of research traditions in existence. However, as Marcus and Fischer (1986, p8)
explain, there has been a “crisis of representation” within the social sciences
for the better part of their existence. They determine a need to examine the
various levels and domains of influence that are an effect of culture, inclusive
of scholarly theoretical and methodological predisposition. From the
perspective of Marcus and Fischer (1986) and de Sardan (2005), what is
important in this discussion is not a ‘shift’ but a necessary ‘clarification’ of the
diffusion of innovations in definition and process within Anthropology. With this
in mind, I do not attempt to clarify or resolve in totality the issues relating to
diffusion that I have raised in this thesis. I will examine what motivates the
diffusion of innovation in respect to socio-cultural history and a globalised
modernity.
Method & Process
In this thesis I propose to answer two questions. What are the macro-forces
that motivate the process of diffusion of Buddhist-Mindfulness into psychiatry
in Thailand and the United States? What are the mcro-social, cultural, and
historical driving mechanisms that influence the form, function, and meaning
of Buddhist-Mindfulness in each psychiatric application? I aim to explore this
problematic by utilising a theory of diffusion of innovation following de Sardan
(2005) and Rogers (1971; 1995), and Kapferer’s (1988) application of ontology
and cosmology to interpret social change and contextual meaning involved in
change. I define diffusion as the process of willing change; innovation as
borrowing a practice to control change; communication as the social movement
towards making change meaningful; and consequences as the new form of the
diffused innovation. A minimal theoretical framework will be utilised. I will
examine the diffusion of Buddhist-Mindfulness into psychiatry in the United
33
States and Thailand through the social incorporation of ontology and ideology,
whereby history is made meaningful in the present through rational action in
practice to construct and interpret experience and maintain order. This
method will suit an analysis of diffusion because diffusion is a socially adaptive
process that aims to maintain order when change or the threat of change/crisis
to the existing social order arises. I argue that the ideology to engage in
Buddhist-Mindfulness utilises cultural ontologies and cosmologies that will
create specific consequences to Buddhist-Mindfulness in each respective
context.
By examining the diffusion of Buddhist-Mindfulness into psychiatry in Thailand
and the United States, this comparative analysis will illustrate how macro-
global factors motivate micro-cultural action. This analysis will also highlight
the consequences to the innovation being diffused. Consequences are
determined as the changes to the form, function, and meaning of Buddhist-
Mindfulness through the diffusion process. I aim to illustrate the consequences
to Buddhist-Mindfulness that result from its diffusion. This is a movement from
traditional studies outlined by Rogers (1971; 1995), who defines consequences
in socio-cultural terms only. I argue that this examination of consequences will
highlight the difference in worldviews. Belief constrains and influences
ideological incorporation of ontology/cosmology in culture. This is the major
factor influencing the form, function, and meaning of Buddhist-Mindfulness in
the process of diffusion in psychiatry.
Cultural Change & Revitalisation: Ontology, Habitus & Ideology
To explain the diffusion of Buddhist-Mindfulness into psychiatry in Thailand and
the United States, three issues must be raised. What is ontology and cosmology
and why are they employed to maintain order and meaning in culture change
situations? What is ideology what is its role in engaging cultural ontologies
34
when habitus is ruptured? What relationship do ontology and ideology have with
health-seeking behaviour? To begin this analysis I situate this problematic with
a quote from Schutz (1970). He states:
“Man is born into a world that existed before his birth; and this world
is from the outset not merely a physical, but also a socio-cultural one.
The latter is a preconstituted and preorganised world whose particular
structure is the result of an historical process and is therefore different
in each culture and society” (Schutz 1970, p79)
From Schutz’ (1970) perspective, the present social world is historical, and
human beings in their present socio-cultural circumstances take their present
social world for granted. How people generate meaning and conclusions
regarding the universe and their place in it are determined by historically or
ontologically posited socio-structural and material culture.
Any analysis of reason and rationality in culture must primarily take into
account the role of ontology. Ontology is inquiry into the nature of being.
Cultural ontologies are “prior to deliberate conscious articulation” and form a
“preconscious orientation” (Bastin 2001, p23) to the world. Ontology
“describes the fundamental principles of a being in the world and the
orientation of such a being toward the horizons of its experience” (Kapferer
1988, p79). Ontologies inform social action. This makes the analysis of ontology
important, because of the role ontologies have in orientating social action,
intention, and experience. Importantly, ontologies are more often than not
undisclosed or unassumed by members of a culture. Cultures have multiple
ontologies that are mythical, textual, and topographic. These are accessible
through ideological processes. Kapferer (1988, p80) explains ideology as the
“selective cultural construction” of ontology or various ontologies, usually
“made in the circumstances of political or social action”. Ontologies are full of
35
potential, but their capacity is realised and manifest only when ideological
meaning is applied to them. This is the same for cosmologies. Ontologies and
cosmologies cannot exert meaning or force on their own, but must have
meaning and intention applied to them in practice to become emergent as a
social force. Ideology imparts meaning and intention to ontology and
cosmologies by applying a schematic structure to them, determined through
practice in the present social world.
Ontology is a vital part of the taken-for-granted or habitual aspect of self and
cultural construction and experience. Ontologies most commonly exist as
cultural practices, commonly identified as habitus. Habitus is defined by
Bourdieu (1977) as a structural and taken-for-granted modus operandi that
cultures and members of cultures generate and regenerate through practice in
fields of social action. Habitus represents the ontological aspect of culture in
practice. Bourdieu (1999, p109) explains habitus as the “internalisation of
externality” through a “dialect between habitus and institutions” (Bourdieu
1999, p111). Due to the persistence of a practice or set of practices over time,
and the construction of socio-structural and material structures in society
“property appropriates its owner, embodying itself in the form of a structure
generating practices perfectly conforming to its logic and its demands”
(Bourdieu 1990, p57). The socio-structural, material, and topographic aspects
of culture generate the successful performance of practice over generations.
This provides the taken-for-granted position where “that what has proved to be
valid up till now will continue to be so” (Schutz 1970, p80).
Habitus (or ontology for that matter) is not static. An inconsistent factor in
diffusion research applied by Rogers (1971; 1995) has been to postulate that a
form of cultural homeostasis or dynamic equilibrium can be constantly
achieved. Habitus is open to change from within or without, and is routinely
transforming. Change commonly occurs through events that result from
actions. Bastin (2001) explains that often events from outside the control of a
36
group propel them into action. In-group reaction to outside change is
ideological, a product of resistance of the group being acted upon. Ideology, as
previously stated, is a determined course of action that is based on ontological
reasoning. “Change”, explains Bastin (2001, p30), “provoke[s] repetition
through a retreat into tradition”. A retreat that Bourdieu (1999, p115)
substantiates “contains the solution to objective meaning without subjective
intention”. Social change pressures cultural reasoning to renegotiate personal
and social identity and meaning (Connor & Samuel 2001). A ‘retreat into
tradition’ to deal with these changes to make meaningful sense of them is a
common reaction when change and crisis threatens the established and taken-
for-granted social order. Meaning, as a social and collective notion, can be
rallied in times of change to legitimise action. Shared meaning constitutes an
integral aspect of the process whereby a collective past is made meaningful in
the present.
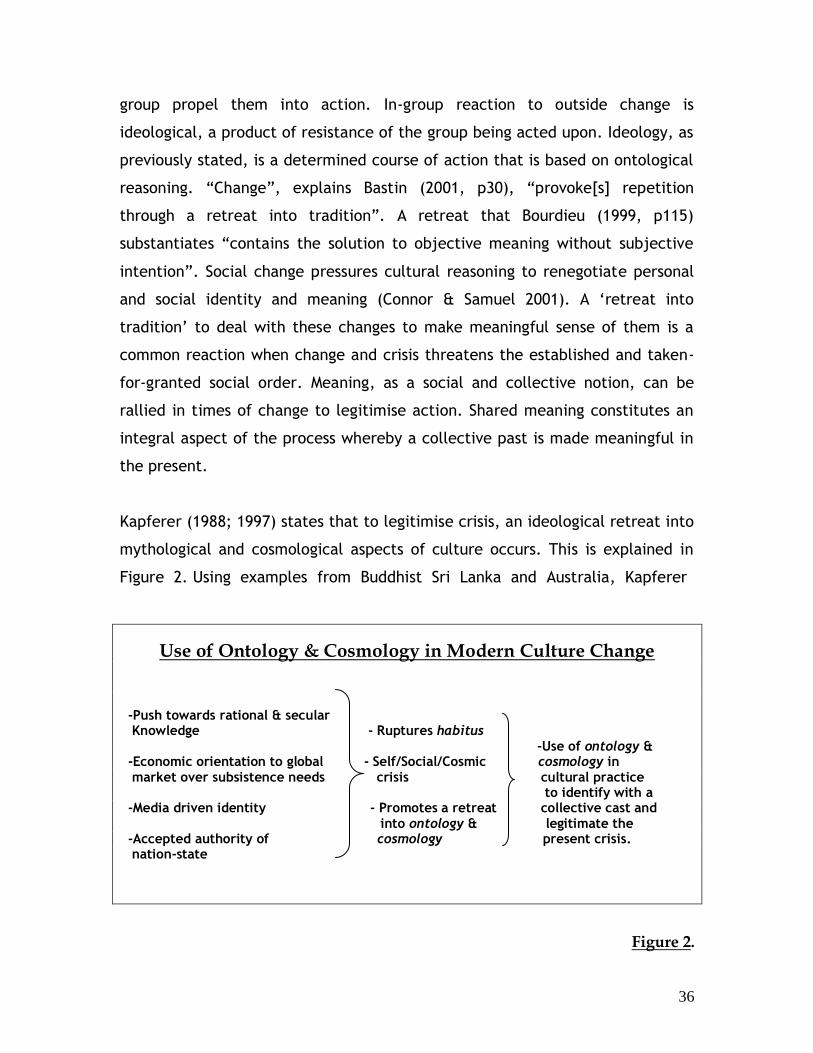
Kapferer (1988; 1997) states that to legitimise crisis, an ideological retreat into
mythological and cosmological aspects of culture occurs. This is explained in
Figure 2. Using examples from Buddhist Sri Lanka and Australia, Kapferer
Use of Ontology & Cosmology in Modern Culture Change
-Push towards rational & secular Knowledge - Ruptures habitus -Use of ontology & -Economic orientation to global - Self/Social/Cosmic cosmology in market over subsistence needs crisis cultural practice to identify with a -Media driven identity - Promotes a retreat collective cast and into ontology & legitimate the -Accepted authority of cosmology present crisis. nation-state
Figure 2.
37
(1988; 1997; 2001) illustrates the role ideology plays in legitimising ontological
and cosmological sources by reinterpretating them to motivate social action in
the present. This use of ideology in healing rituals and disputes regarding
nationalism aims to counter challenge to the social status quo. The chronicling
of Sinhalese Buddhist textual and mythic history is explained by Kapferer
(1988; 2001) as an example of ideological use of ontology for purposes of
legitimising violence and political aspirations against the Tamils. In these
instances, mythical deeds of monks and deities are reinterpreted and applied
to justify present action. Another common example throughout Buddhist
political history is where ‘sacred kingship’ has been used to authenticate and
legitimate political decisions in Buddhist terms (Hallisey 2006). In Australia,
Kapferer (1988) identifies similar tendencies as Sri Lanka, where the ANZAC
legends are used to legitimate social action when threats to the national
identity occur. Australian nationalism must embody individual and egalitarian
tendencies of persons, as ANZAC legends state, to maintain the moral order
and reconstitute social powers.
The ideology of ontology and cosmology is a characteristic of medical processes
and rituals that are Buddhist. From an ethnomedical perspective, Obeyesekere
(1985, p141) explains how Sri Lankan Buddhism “provides special occasions for
ontological reflections on despair”. Buddhist textual and visual meanings to
suffering (dukkha) are applied to interpret and explain illness experience. This
is also the case in Thailand. Examples reveal that lay explanation for
biomedical germ-theory and the genetic basis of diabetes contraction have
become ritually and mythically meaningful through situating new aetiological
and nosological categories to longstanding beliefs in sorcery, spirit
malevolence, and karma (Golomb 1988; Naemiratch & Manderson 2007).
Medical plurality affords Tibetan exiles in India “an infinite strategic resource”,
when modern values and pressures come to compete with existing medical
systems (Prost 2006, p126). In Japan, traditional therapies are incorporated
38
into psychiatric nosology and as aetiology for the treatment of mental illness.
Morita Therapy, an indigenous therapy of Japan, are inspired by
Buddhist/Shinto belief and are designed to address a culture specific illness,
taijin kyofusho (Nuckolls 2006). Ideology of ontology and cosmology are
utilised, as these examples reveal, because of challenges to the habitus that
disrupt the person-society-cosmos relationship. History is employed to amend
these ruptures to the taken-for-granted. Biomedical and psychiatric nosology
and aetiology are inadequately able to capture not only the experience, but
also the meaning of trauma and disorders in other cultural contexts (Hinton et
al 2007). This prompts a ‘retreat into tradition’ in response to the inability to
locate meaning in social and embodied terms in these cases.
The Social & Historical Praxis of Suffering
Ideological action, as it has been shown, engenders meaning to the present
when moments of crisis and change arise. By employing cultural ontologies and
cosmologies, a history that is collective in social memory and meaning
emerges. This is a dynamic relationship that is recreated mythically and
ritually, and where “the order of the body is identified and produced within
the order of the state” (Kapferer 1988, p78). When the habitus or the taken-
for-granted mode of cultural action is challenged during times of crisis or
change, there is a need to re-legitimate the ascribed social order. This occurs
through ideological reapplication of past mythical, cosmological, and textual
aspects of culture in practice. This is a process that has been proven valid and
successful throughout time, otherwise it would not be practised (Kapferer
1988; Schutz 1970). Importantly, the cultural field and its practices are not
static, but are dynamic and fluid. Habitus is not static and is constantly
changing and altering through the need to reincorporate ontology and
cosmology because of social change.

39
The diffusion of Buddhist-Mindfulness into psychiatry in Thailand and the
United States is interpreted by the conceptual theoretical foundation I have
outlined. The stimulus to incorporate Buddhist-Mindfulness in each context is
motivated by social change and the need to restore balance. This is articulated
through culturally specific meanings and practises. I argue that a microanalysis
of these cultural processes, positioned in macro-global context, will reveal
exactly why differences in form, function, and meaning occur. Macro-
motivation for diffusion in each context motivates the need to maintain order
in changing and uncertain times. The micro-cultural representation illustrates
the unique means by which people in Thailand and the United States negotiate
self and society in modernity. The diffusion of Buddhist-Mindfulness in each
context is the result of conscious (ideology) and non-conscious (ontology)
action in each context. The function of institutions, patterns of culture, and
their meaning is motivated by unique histories and worldviews that create the
differentiation revealed in the two case studies examined. These socio-
historical, material, and topographic social structures constrain and motivate
the form, function, and meaning of Buddhist-Mindfulness in each cultural
context.
40
Chapter 3
Diffusion, Health-Seeking & Culture Change
in Northeast Thailand
This chapter examines the diffusion of Buddhist-Mindfulness in psychiatry in
Thailand. I argue that this diffusion complements the plural nature of medicine
in Northeast Thailand. Moreover, it illustrates the importance of ‘Mindfulness’
as a Buddhist practice that examines experience, providing meaning to
personal and social illness experience. Medical plurality in Northeast Thailand
incorporates historical traditions that bear significant influence on
contemporary health-seeking behaviour. Northeast Thailand has a well-
established plural medical system that resembles an historical admixture of
therapies and discourses from ethnic Tai, India, and China. Buddhist
determinants of health, particularly through the concept of suffering (dukkha),
hold significant status among Thai people and umbrella other techniques. Euro-
American medicines have been utilised in Thai society for nearly two centuries.
Euro-American ethnomedicines are utilised as part of a plurality and not
exclusively for treatment. Therefore, health-seeking behaviour in Northeast
Thailand represents a history of diffusion of ethnomedicines. The current
assemblage of available services reflects the diffusive history of Thai medicine
where plural determinations of health preside. The incorporation of Buddhist-
Mindfulness to psychiatry is determined to represent another stage in the
process of Thai medical pluralism, and can only be understood when examined
within the matrix of health-seeking behaviour and medical practice.
41
Buddhism, Health & Culture Change
Northeast Thailand is geographically isolated from ‘modern’ Thai society. The
region suffers from a lack of access to and underdevelopment of resources and
infrastructure including education, medicine, and technological services. The
area has become dependant on the global market economy, mainly industrial
agricultural production, for employment and nutrition (Hoare 2004). The social,
cultural, and economic changes of industrialisation and modernity were
compounded by the 1997 financial crisis, generating undesirable health
consequences for the region. Primary health problems like malnutrition and
diseases such as respiratory, digestive system, infections and parasites are a
common form of pathology (Kauffman & Myers 1997). Many of these health
problems are avoidable. They are the result of inadequate infrastructure and
funding by the centralised Thai polity (Ionesgu-Tongyonk 1977; Rungreangkulkij
& Wongtakee 2006; Suwana 1969). Public and Private Health Clinics have been
common in Northeast Thailand since the 1980’s, and health professionals who
have been trained in appropriate biomedical and psychiatric diagnostic criteria
and terminology identify pathology and provide treatment for ailments.
However, social uncertainty and lack of money often inhibit people from
utilising these resources.
Biomedical and psychiatric diagnoses do not always correspond to, or are not
always commensurate with, lay determinants of health and illness (King &
Wilder 2003). This is a well-documented fact about psychiatry in its cross-
cultural application (Henningson 2003; Kirmayer 2006; Kleinman 1980, 1988;
Pilowsky 1997). People of Northeast Thailand rely on both Euro-American and
Traditional Thai medicine and practitioners when seeking treatment. In
Thailand “a tremendous diversity of diagnostic and therapeutic procedures”
exists, and “multiple aetiologies for a single illness” are commonplace (Golomb
1988[b], p761). Buddhism crosscuts all institutions and practices in
Northeastern Thai society and is entwined as part of a larger medico-religious
42
tradition that utilises various traditional medical techniques. Indian and
Chinese humoral and herbal theory (Naemiratch & Manderson 2007), ethnic Tai
belief’s in spirits, ghosts, witches, sorcery (Formoso 1996), and Euro-American
biomedical and psychiatric medicine are utilised to explain and reduce
suffering. In Northeast Thailand, health-seeking behaviour utilises traditional
medical practices and rituals more so than Euro-American ones. However, a
number of therapeutic methods may be employed at once where various
practitioners are sought by a person to obtain cures and meaning to illness
(Lyttleton 1996).
King (1999, p 221) highlights that “many South-East Asians have accepted the
technology of these [Euro-American] curative practices, but not their
premises”. The medico-religious aspect of Buddhism and its incorporation with
other beliefs and practices intertwine to explicate meaning and provide
techniques for the remedy of illness and misfortune. Meaning is acknowledged
as a substantial aspect of the diagnostic and healing process in Northeast
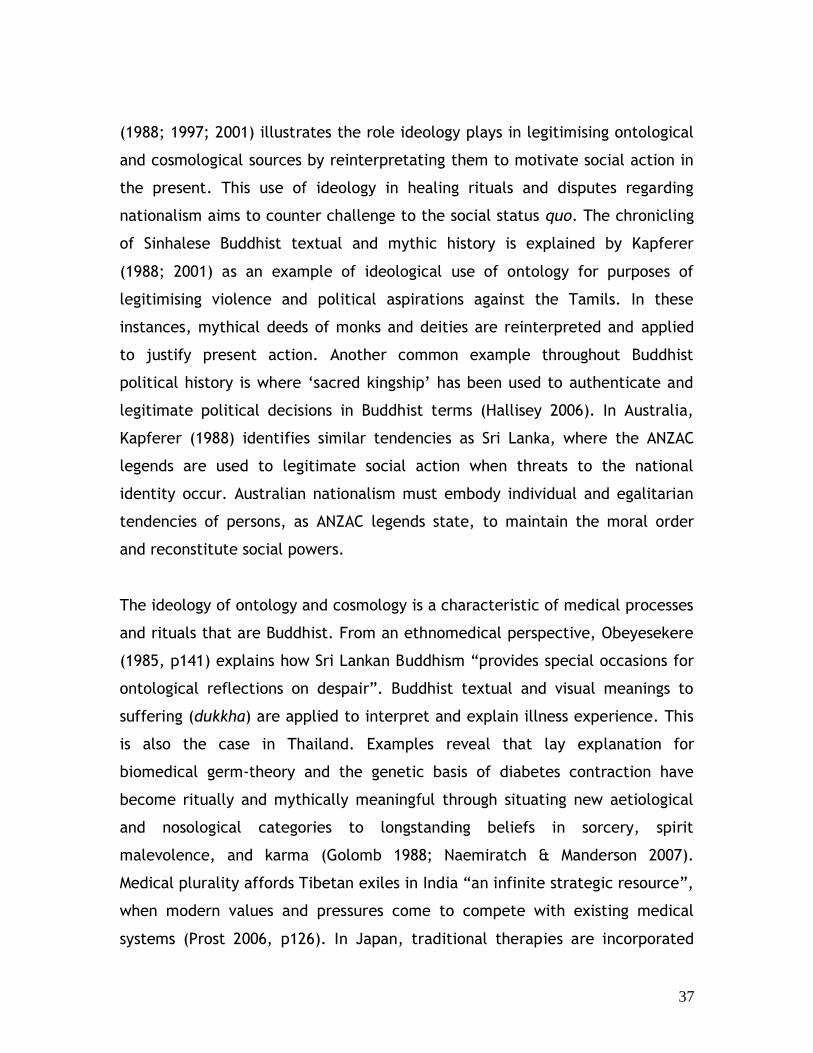
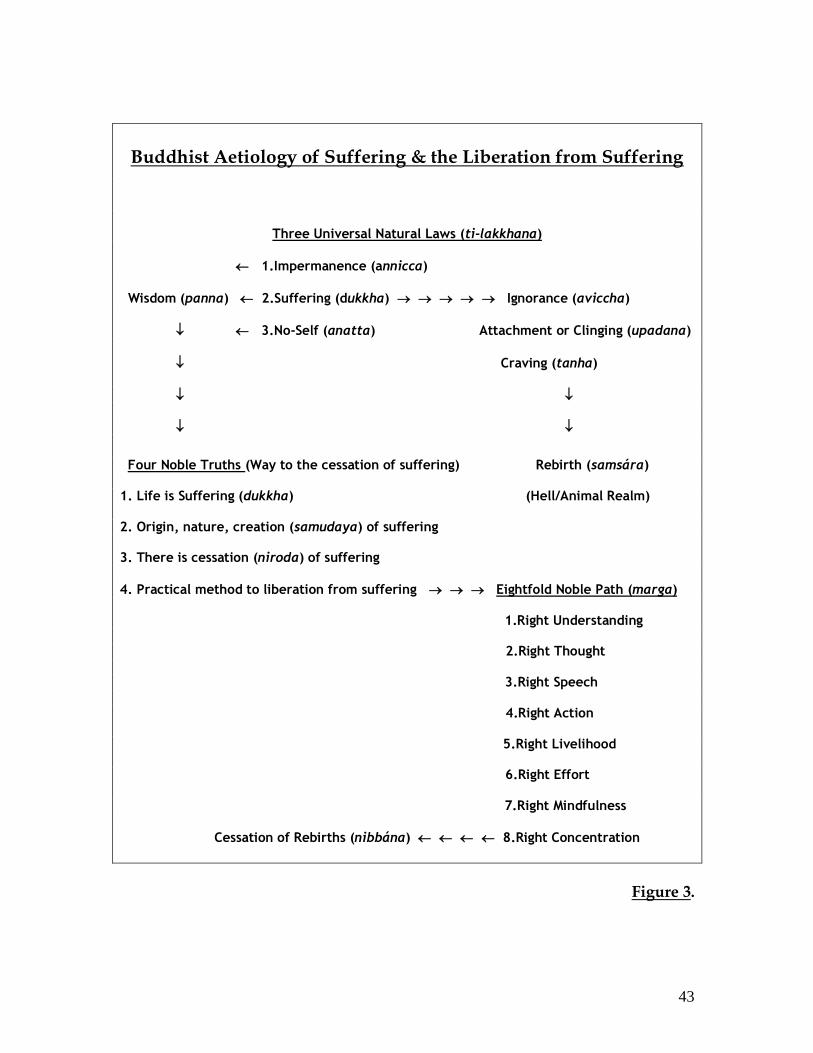
Thailand. Buddhism deals specifically with illness through the concept of
‘suffering’. Chen-kuo (1997, p298) maintains that suffering (dukkha) is a
fundamental edict of Buddhism, in which “the core of Buddhist practice
consists in meditating on the cause of suffering in order to overcome it”,
explained in Figure 3. Suffering (dukkha) in a Buddhist context is both
metaphysical and experiential. It includes the concepts of karma (kam) and
rebirth (samsára) as these concepts relate to text, cosmology, and the
vicissitudes of daily life (Harvey 1990). Buddhist beliefs freely interact with
aetiologies of fortune/misfortune and health/illness that involve spirit (phi)
malevolence, soul (kwan) loss, and possession or infliction by a sorcerer
(Golomb 1988).
43
Buddhist Aetiology of Suffering & the Liberation from Suffering
Three Universal Natural Laws (ti-lakkhana)
1.Impermanence (annicca)
Wisdom (panna) 2.Suffering (dukkha) Ignorance (aviccha)
3.No-Self (anatta) Attachment or Clinging (upadana)
Craving (tanha)
Four Noble Truths (Way to the cessation of suffering) Rebirth (samsára) 1. Life is Suffering (dukkha) (Hell/Animal Realm) 2. Origin, nature, creation (samudaya) of suffering 3. There is cessation (niroda) of suffering
4. Practical method to liberation from suffering Eightfold Noble Path (marga)
1.Right Understanding
2.Right Thought
3.Right Speech
4.Right Action
5.Right Livelihood
6.Right Effort
7.Right Mindfulness
Cessation of Rebirths (nibbána) 8.Right Concentration
Figure 3.
44
While modern medicine and medical facilities have penetrated Northeastern
Thailand, geographical isolation has facilitated the situation whereby
traditional Buddhist and animistic beliefs and practices remain strongly intact.
(Hoare 2004). Buddhism in Northeast Thailand associates a microcosmic/
macrocosmic relationship with the explanation and meaning of illness. The
body is positioned in relation to the cosmic order, and maintenance of this
relationship is vital in the construction, reconstruction, and maintenance of
self and society in a person-community-cosmos tripartite relationship. The
symbolism of the macrocosm/ microcosm is engendered as a curative element
in healing practice (Tambiah 1970; 1977; Whittaker 2002). In the process of
healing, the enactment of myths through this process of ritual is pertinent.
Taking this into account, I argue that ethnomedical resilience in Northeast
Thailand is the result of its relative geographical isolation where the practice
of Buddhism (and animism) as a ‘social-existential’ embodied culture is
occurring. Practice occurs on a needs basis to maintain order and security in
out-of-habitus-times. Analysis of the two case studies presented in Chapter 1, I
contend, will reveal how each of these phenomena unites to enable a
persistent traditional ethnomedical practice. This will illustrate why Buddhist-
Mindfulness was diffused with psychiatry as constituted in a Buddhist
framework.
Healthcare in Northeast Thailand
Several scholars have commented on Northeast Thailand’s geographic isolation
from centralised, urbanised and cosmopolitan Thailand. This focus has often
described rates and level of diffusion of modern health institutions and
discourse and how this has come to affect Northeast Thai society. More often
than not, these accounts paint a negative picture (Krongkaew 1995; McVey
2000). Research has revealed how isolation from the central bureaucracy has
established disadvantageous social, health, and economic disparities. Being
subordinate to the centralised polity, rural health development is often in the
45
hands of the Thai Government or NGO’s, and while local determinants of
health and healthcare is considered in development projects, change is usually
imposed from without (King 1999). Van Esterik (1998) maintains that this
attitude in Thailand is the result of a history of developmental ideology, the
perceived efficacy of Euro-American ‘scientific’ medicine, and the social status
of such medical practice.
Social perceptions of Euro-American medicine and meanings attributed to
specific diseases have filtered through to the village level via development
programs, NGO groups, the media, and word of mouth from patients. While
highlighting current determinants and levels of social health in Northeast
Thailand, these analyses have failed to show why multiple health care options
are accessed and utilised by people of Northeast Thailand, rather implying that
they simply do exist. As Lyttleton (1995) explains, modern illnesses,
particularly HIV/AIDS, are entwined with traditional meaning and causes of
illness. Why traditional beliefs regarding illness, and practices to explicate
illness, persist even though biomedical and psychiatric intervention is
commonplace, are not revealed by many analyses of Northeast Thailand.
Initial investigation reveals a well-established traditional medical system
already in place in Northeast Thailand. A thriving medical pluralism exists
between traditional Thai and Euro-American medicine (biomedical and
psychiatric), highlighted in Figure 4. Research from other regions of Thailand
suggests similar conclusions to those revealed in the Northeast (Golomb 1988;
Muecke 1976; Weisberg 1982). Patients are acknowledged to have a high
degree of autonomy and agency selecting services and treatments, and are
highly conscious about what types of therapy to utilise for which ailments.
Choice in health-seeking appears to be based on a set of selective criteria that
involves personal and social components relative to modern and historical
considerations and the array of therapeutic options available. Lyttleton (1996)
locates personal agency within the broader framework of embedded social
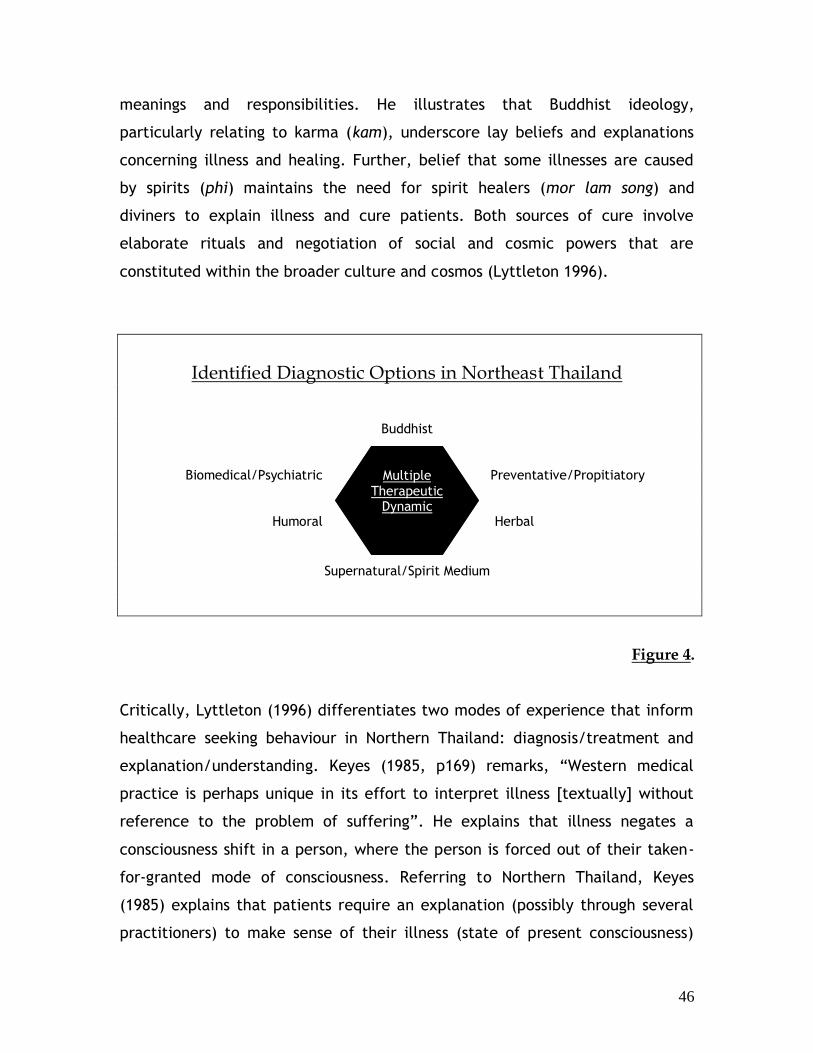
46
meanings and responsibilities. He illustrates that Buddhist ideology,
particularly relating to karma (kam), underscore lay beliefs and explanations
concerning illness and healing. Further, belief that some illnesses are caused
by spirits (phi) maintains the need for spirit healers (mor lam song) and
diviners to explain illness and cure patients. Both sources of cure involve
elaborate rituals and negotiation of social and cosmic powers that are
constituted within the broader culture and cosmos (Lyttleton 1996).
Identified Diagnostic Options in Northeast Thailand
Buddhist
Biomedical/Psychiatric Preventative/Propitiatory
Humoral Herbal
Supernatural/Spirit Medium
Figure 4.
Critically, Lyttleton (1996) differentiates two modes of experience that inform
healthcare seeking behaviour in Northern Thailand: diagnosis/treatment and
explanation/understanding. Keyes (1985, p169) remarks, “Western medical
practice is perhaps unique in its effort to interpret illness [textually] without
reference to the problem of suffering”. He explains that illness negates a
consciousness shift in a person, where the person is forced out of their taken-
for-granted mode of consciousness. Referring to Northern Thailand, Keyes
(1985) explains that patients require an explanation (possibly through several
practitioners) to make sense of their illness (state of present consciousness)
Multiple Therapeutic
Dynamic
47
and provide a course of action to achieve balance (commonsense perspective)
once again. It is well documented that in Northeast Thailand meanings of
illness go beyond purely medical textual interpretation, to religious and
cosmological explanations and interpretation of illness experience (Keyes 1985;
Tambiah 1977; Whittaker 2002). The utilisation of traditional medicine,
traditional medical practitioners, and traditional medical beliefs by patients is
for explicitly other reasons that the utilisation of Euro-American medicine
cannot address.
These modes of experience (diagnosis/treatment - explanation/understanding)
evidence themselves in health-seeking behaviour, experience of illness by
patients, and in the practitioner’s personal determination of their therapeutic
role. For example, psychiatric patients often cite possession, attack by spirits
and ghosts, or bad karma (kam) as the cause of diagnosed mental illness
(Burnard, Naiyapatana & Lloyd 2006). In some instances, diagnosed psychiatric
patients who believe they are possessed (and communicate with their spirit)
are treated reverently by other patients and even doctors, particularly if their
spirit is well known and powerful (Lyttleton 1996). Yet at the same time, Thai
psychiatric patients who link spirit possession to their symptoms can be
diagnosed as hypochondriacs or have convulsive or conversion disorders
(Kasantikul & Kanchanatawan 2007). Patients considered psychosomatic are
generally referred by medical practitioners to spirit mediums or monks for
treatment, or they chose personally to seek treatment with these traditional
practitioners because their initial consultation with Euro-American medicine
failed. This is a common trend when patients chose Euro-American medicine as
the first course of care and where traditional therapy and practitioners provide
a ‘second opinion’ when/if the initial consultation proves unsuccessful. Success
is relative to the patient’s perspective (Lyttleton 1996).
Euro-American and traditional Thai medical institutions and practitioners
exhibit various explanatory models for illness treatment and modes of
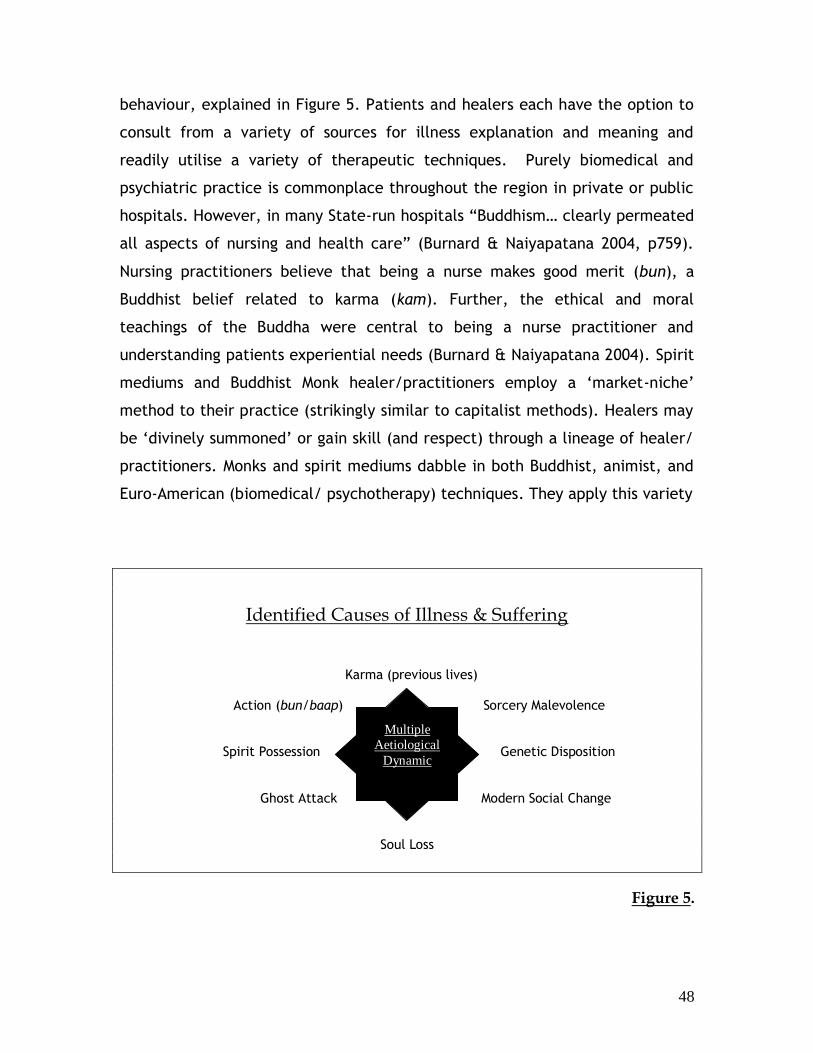
48
behaviour, explained in Figure 5. Patients and healers each have the option to
consult from a variety of sources for illness explanation and meaning and
readily utilise a variety of therapeutic techniques. Purely biomedical and
psychiatric practice is commonplace throughout the region in private or public
hospitals. However, in many State-run hospitals “Buddhism… clearly permeated
all aspects of nursing and health care” (Burnard & Naiyapatana 2004, p759).
Nursing practitioners believe that being a nurse makes good merit (bun), a
Buddhist belief related to karma (kam). Further, the ethical and moral
teachings of the Buddha were central to being a nurse practitioner and
understanding patients experiential needs (Burnard & Naiyapatana 2004). Spirit
mediums and Buddhist Monk healer/practitioners employ a ‘market-niche’
method to their practice (strikingly similar to capitalist methods). Healers may
be ‘divinely summoned’ or gain skill (and respect) through a lineage of healer/
practitioners. Monks and spirit mediums dabble in both Buddhist, animist, and
Euro-American (biomedical/ psychotherapy) techniques. They apply this variety
Identified Causes of Illness & Suffering
Karma (previous lives)
Action (bun/baap) Sorcery Malevolence
Spirit Possession Genetic Disposition
Ghost Attack Modern Social Change
Soul Loss
Figure 5.
Multiple
Aetiological
Dynamic
49
of ritual techniques to combat supernatural malevolence and sorcery
accusations and guard their skills and clientele resolutely (Golomb 1986).
Healer status is achieved through healing efficacy, usually obtained through
community acknowledgement of the practitioners’ healing ability (Golomb
1986; 1988).
Health-Seeking in Macro-Cosmic Context
Thailand exhibits a history of various socio-culturally embedded philosophies
and practices that inform health-seeking behaviour. Nonetheless, scholars have
long acknowledged Buddhism as the major socialising agent in Thai society.
Kirsch (1975, p181) explains, “the Buddhist worldview… provides a general
paradigm for all human life”. Keyes (1984, p226) iterates that “Buddhist
values…constrain and motivate” the roles of men and women within Thai
society. Socialisation in Thailand begins in childhood, where personal and social
praxis are instilled. The impression of social values traverses a person’s
lifetime. Access to material and spiritual resources is gendered, and age and
gender determine social responsibility and etiquette (Lyttleton 2002). Various
stages of importance (rites of passage) are marked by ritual events. As
Whittaker (2002, p32) declares, the construction of personhood is embodied
through these rituals, where “inscription of ideological values structuring
social, economic, and moral power relations” take place.
Buddhist precepts of karma (kam) and merit (bun/baap) are intimately
immersed in the ritual and social processes of Northeast Thailand. These
precepts define personal and social action, responsibility, and access to
material and spiritual resources (Ingersol 1975). Defined social roles and
obligations are informed through textual, mythological, and cosmological
traditions, “traditions [that] have expressed and nurtured Thai universalism
one the one hand, and Thai Buddhist particularism on the other” (Reynolds
50
1978, p195). Buddhist text, myth, and cosmology have become relatively
inseparable over the centuries through their diffusion as social action. The
elementary and foundational concepts of Buddhism (karma, samsára, dukkha,
and nirvana) can all be determined through a cosmological exegesis when
interpreted in context (Tambiah 1970). These concepts have been incorporated
into the pantheon of Buddhism and are articulated in social contexts as sacred
art and architecture (Hall 1998; Paul 1976; Tambiah 1970).
A symbolic microcosmic/macrocosmic connection permeates through to
Buddhist concepts of the self. The relationship between body, society, and
cosmos function as the integrative component between the personal, the
social, and universal laws/processes in village and national life (Laughlin,
McManus & d’Aquili 1990). Architectural and artistic structures in Thai society
reflect these social and political objectives. In Thailand, the concepts of
rebirth, karma, and suffering have been fused into a cosmological discourse,
‘The Sermon of the Three Worlds ’, and the admixture of religious and artistic
tradition (Khmer, Burmese, Chinese, and Euro-American) represent the
diffusive history of Thailand. Over five centuries of diffusion of other-cultural
beliefs, practices, and stylistic representation (including Euro-American)
permeates traditional and modern Thai structural design. Architectural
symbolism is a social organizational agent. It motivates village and temple
design and location, informs processes of ritual, and social action (Reynolds &
Reynolds 1982) in both village and urban contexts throughout Thailand. Askew
(2002, p220) explains that Buddhist architecture of the village (baan) and
temple (wat) have been utilised throughout history, and into the present as “a
site for the reproduction of key traditions associated with place and also life
cycle”.
Cosmological symbolism has functioned as a form of social organisation and
integration in Thailand since Sukhothai in the 14th century (Jackson 1989; Ray
2006). A ‘galactic polity’ has endured in Thai political and social structure
51
since Sukhothai in the 14th century, where the development of a ‘cosmological
topography’, featuring a central administration and hierarchically based social
structure and organization, circumnutating a centralised ‘sacred kingship’
(Reynolds & Reynolds 1982; Tambiah 1976). Social structure; between person,
village and state, reflects the Buddhist cosmology. This cosmology, interpreted
as “biological-organic” (King 1983, pxi), accepts that all phenomena are
interconnected and are conditioned through subjugation to universal laws of
cause and effect. Various universes exist, and are recognised as a “living body”
that is cyclical and infinite in both temporal and spatial demarcation, and
where human “existence is set” and is regulated by inherent cosmic laws (King
1983, pxii). The cosmic laws of Buddhism are causal and are regulated through
action. These laws vary and relate to psychological, physiological, biological,
moral, and spiritual conduct and action.
The law of Karma (kam) [moral/ethical causation] is the most pertinent
Buddhist cosmic law, and the “knowledge of this moral law enables us to
discover the cause of suffering and the release from it” (Ratanakul 2002).
Suffering (dukkha) and the removal of suffering is the central thesis of the
Buddha. The explanation for suffering and the way to be liberated from
suffering is outlined and explained in The Four Noble Truths (and The Eightfold
Noble Path), which the Buddha recognised through his enlightenment
experience (Harvey 1990). The Buddhist path is distinctly concerned “with a
[search for] truth that can have a practical effect in the release from
suffering” (Ratanakul 2002, p117). Karma (kam) is used to explain suffering,
and also fortune/misfortune, health/illness, or social status among other
existential and social problems in Buddhist society (Spiro 1967; 1971). More
importantly, it explains on a metaphysical level rebirth (samsára) and a
person’s past lives, all of which predicate one’s present karma, and which are
the result of ones action in their past lives (Ingersol 1975). Rebirth (samsára) is
the process of being and becoming; it is the cycle of lives that all beings
undertake until their liberation through enlightenment. Rebirth is significantly
52
cosmological as it describes the universe and the various levels of existence
that one can be born into. The type of rebirth one receives is predicated upon
action, or the law of Karma. A person’s Karma (kam) determines the rebirth
received, determining the level of suffering a person receives.
Personal social action is determined as good (bun) and bad (baap), usually
defined as ‘merit making’. The role of merit and merit making is a highly
esteemed and exercised practice in Thailand. Tambiah (1970, p53) decrees
that merit (bun) and de-merit (baap) making has developed into an institution
in Northeast Thailand “by which villagers conceptualise, evaluate, and explain
behaviour”. Merit is a Buddhist based tradition that exists at a public and
private level and concerns the individual, village, and national government
(Mulder 1969). Ingersol (1975) identifies that merit and identity are intricately
connected, and that making and storing merit is a multifarious aspect of Thai
village life. You are born with amounts of merit, you can make merit, store
merit, give merit, and lose merit. Merit is both obligatory and selective, and is
used to gain personal and social value in this life, and implicates the type of
rebirth received in the next life. Merit and Karma are intricately connected.
Merit is action in this life that is socially and cognitively contingent in this life.
More importantly, it will affect a person’s rebirth, thus level of suffering, in
their next life.
Medical Pluralism in Northeast Thailand: Form & Function
The preservation and perseverance of traditional Buddhist values in
Notheastern Thailand is obvious. Medical plurality is not diminished by Euro-
American diagnosis and treatment measures, but is maintained by the lack of
psychosocial meaning they apply. This is particularly due to the focus on
biological theory as the determinate of ill health. However, as Reynolds (1998,
53
p116) explains, “it has become increasingly difficult to speak of the country as
remote”. This is a geographical and religious statement. While Buddhism
penetrates the various levels of therapeutic process in Northeastern Thailand,
impregnating illness experience and healthcare seeking motivations with
meaning (particularly in regards to the discourse on suffering [dukkha], karma
[kam], and merit [bun/baap]), modern values are influential. None the less,
the meaning and the motivation behind personal action is the direct result of a
Buddhist socialisation process in Northeastern Thailand that has been occurring
for centuries. A person is defined by their karma (kam), a phenomenon that is
at the same time a priori and teleological. A person is bound by their past, but
can be liberated by their present action (bun/baap), as explicated in the
universal laws (Ratanakul 2002). Cosmologically speaking, a person has freedom
to act, and these actions can determine why they suffer now, and how much
they will suffer in their next life.
Notwithstanding, how a person acts is clearly articulated by social rules and
obligations that are both traditional and modern. As a result personal
existential needs are more often than not subjugated by social ordinations.
However, this does not remove personal agency from people. On the contrary,
health-seeking behaviour in Northeast Thailand reveals that while social rules
obligate people to behave in particular fashion, these requirements also
provide the means by which personal agency can be utilised to gain control of
‘suffering’ within the social and universal order. The incorporation of modern
Euro-American institutions and values has not altered this practice, but has
challenged these longstanding patterns of culture to adapt to them. The
diffusion of Buddhist-Mindfulness in psychiatry signifies that when “practical
meaning that cannot be obtained from those steeped in medical texts alone” is
sought after by patients seeking explanation for ‘suffering’ (Keyes 1985, p169).
This represents the process whereby Buddhist ontological and cosmological
concepts, particularly the discourse on suffering (dukkha), are applied to give
54
greater meaning the mental illness experience. The diffusion of Buddhist-
Mindfulness as a Buddhist practice is integral to the maintenance of the
personal and social order within the cosmos, and reflects the need for a
Buddhist cosmological significance to illness experience.
55
Chapter 4
Diffusion, Health-Seeking & Culture Change
in the United States
This chapter examines the diffusion of Buddhist-Mindfulness in psychiatry in the
United States. This is illustrated through analysis of modern and historical
socio-cultural influences that I argue motivate and drive this diffusion. This
analysis is similar in format to Chapter 3. Health seeking behaviour is explained
to illustrate how illness is experienced and made meaningful in the United
States. Following Hahn & Kleinman (1983), I define psychiatry and biomedicine
as Euro-American ethnomedicines. As ethnomedicines, they are also a
sociocultural system; they interact and reflect a larger socio-historical and
cultural cosmological context through critical engagement with the wider
macro-society. I situate Buddhist-Mindfulness among a number of other
Complementary and Alternative Medicines (CAM) and religious traditions that
are currently being diffused into United States society. Their diffusion reflects
the socio-historical structures of Christianity, science, and capitalism,
structures that make up the habitus and worldview of the United States, and
motivate why Buddhist-Mindfulness is diffused in psychiatry differently than it
is in Thailand.
56
Scientific Crisis & the ‘Operational’ Status of Buddhist-Mindfulness
Science and medicine in the United States are currently experiencing a
paradigm shift. The model of the universe, how it works, and how humans can
work within the universe is being amended (Ratanakul 2002). This
transformation is influenced by ‘Eastern’ concepts of reality, and subsequently
‘Eastern’ discourses of health/ill health experience have entered into medicine
and psychiatry. This new paradigm is described as the “rediscovery of Asian
philosophy, particularly the Buddhist tradition”, and is depicted as “the second
renaissance in the cultural history of the West” (Varrela, Thompson & Rosch
1993, p22). From a macro-perspective, the diffusion of non-Euro-American
ethnomedical and religious traditions is another ‘patch-up’ to manage the
current crisis that the Euro-American worldview faces (Holbrook 1981). In
micro-context, this involves the integration of medicine and psychiatry with
various ethnomedical and religious traditions (including Buddhist-Mindfulness)
in clinical and theoretical contexts. CAM’s are determined to share “common
threads” with Euro-American medicine, a view that supports their merger
(Arond 2006, p1450). While branches of scientific medicine and psychiatry in
the United States have been diffusing CAM into existing psychiatric and medical
programs for decades, the current diffusion is taking place at an increasing rate
(Baer 2005).
Buddhist-Mindfulness is the most popular of the CAM repertoire. Empirical
clinical scientific studies identify Buddhist-Mindfulness as a ‘breakthrough’ in
theoretical and clinical studies. Psychiatric application of Buddhist-Mindfulness
still utilises traditional aetiology (as Figure 6 reveals), but has merged and/or
annexed Buddhist theory with existing cognitive (Varrela, Thompson & Rosch
1993), consciousness (Burton 2005), and neuropsychologically based (Newberg
& Iversen 2003) research. Clinical application has provided therapeutic relief
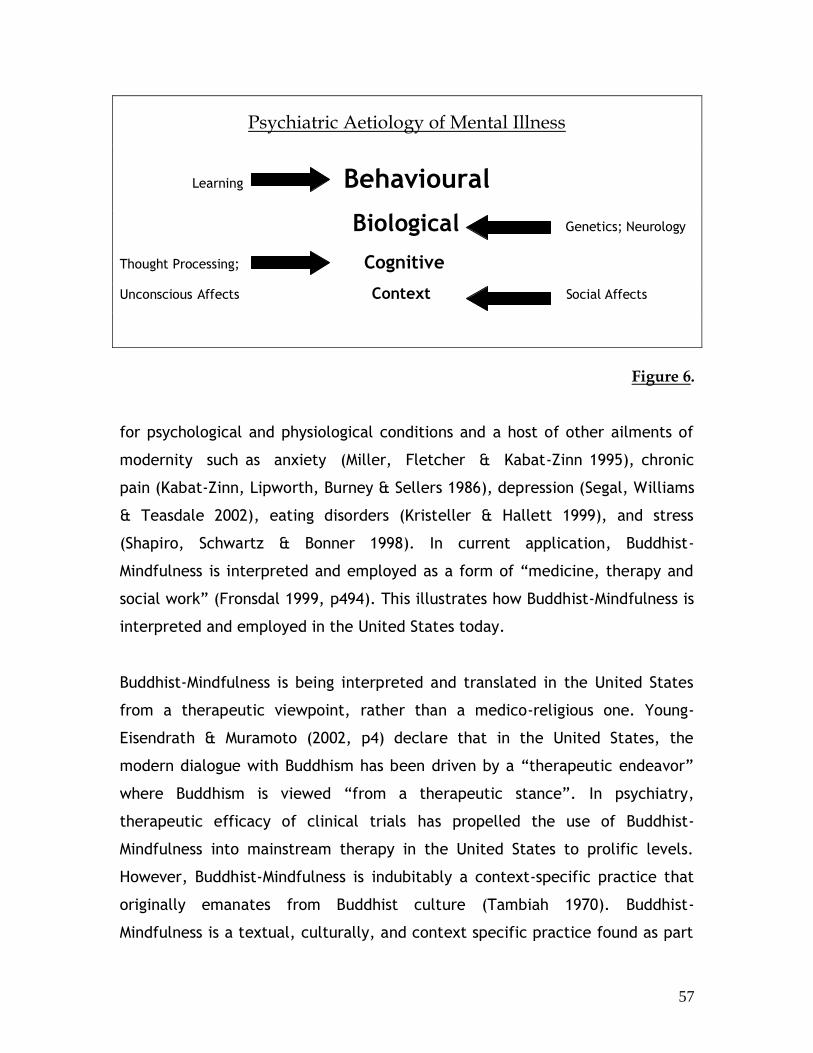
57
Psychiatric Aetiology of Mental Illness
Learning Behavioural
Biological Genetics; Neurology
Thought Processing; Cognitive
Unconscious Affects Context Social Affects
Figure 6. for psychological and physiological conditions and a host of other ailments of
modernity such as anxiety (Miller, Fletcher & Kabat-Zinn 1995), chronic
pain (Kabat-Zinn, Lipworth, Burney & Sellers 1986), depression (Segal, Williams
& Teasdale 2002), eating disorders (Kristeller & Hallett 1999), and stress
(Shapiro, Schwartz & Bonner 1998). In current application, Buddhist-
Mindfulness is interpreted and employed as a form of “medicine, therapy and
social work” (Fronsdal 1999, p494). This illustrates how Buddhist-Mindfulness is
interpreted and employed in the United States today.
Buddhist-Mindfulness is being interpreted and translated in the United States
from a therapeutic viewpoint, rather than a medico-religious one. Young-
Eisendrath & Muramoto (2002, p4) declare that in the United States, the
modern dialogue with Buddhism has been driven by a “therapeutic endeavor”
where Buddhism is viewed “from a therapeutic stance”. In psychiatry,
therapeutic efficacy of clinical trials has propelled the use of Buddhist-
Mindfulness into mainstream therapy in the United States to prolific levels.
However, Buddhist-Mindfulness is indubitably a context-specific practice that
originally emanates from Buddhist culture (Tambiah 1970). Buddhist-
Mindfulness is a textual, culturally, and context specific practice found as part
58
of a larger system of philosophy, myth, ritual, and religious Buddhist practice
throughout Asia (Harvey 1990). However, in recent decades, both Buddhists
and psychiatrists express that Buddhist-Mindfulness can be used therapeutically
in a non-religious way (Kabat-Zinn 2003; Rinpoche 1992; Rinpoche 1994). This is
because Buddhist-Mindfulness emanates from a textual tradition in Buddhism
where it has a “non religious, non philosophical” context (Titmuss 1998, p8).
From this rationale, a purely textual interpretation of Buddhist-Mindfulness has
become acceptable. This therapeutic application overtly reflects a non-cultural
context specific interpretation of Buddhist-Mindfulness by Euro-American
practitioners, Buddhists, and the lay population.
From analysis of a variety of medical research using Buddhist-Mindfulness, a
contextualisation of Buddhist-Mindfulness as therapy is taking place in the
United States. In science, as in psychiatry, the crisis of an outdated paradigm is
driving this. Subsequently, there is enormous pressure on Buddhist-Mindfulness
to conform to strict clinical scientific standards. The process of
‘operationalisation’ is reducing Buddhist-Mindfulness to a purely pragmatic
form to conform to the definitions and standards of scientific empiricism
(Kabat-Zinn 2003). This process could be described as supercilious. One
psychiatrist claims, “if religious and spiritual traditions are to enter empirical
clinical psychology, they must be ours” (Hayes, 2002, p105). Mindfulness-based
(and other CAM) intervention in psychiatry must “be free of the cultural,
religious, and ideological factors associated with Buddhist origins of
mindfulness” (Kabat-Zinn 2003, p149) before it can be accepted into clinical
practice. This is the process of converting Buddhist-Mindfulness to its
‘operational’ form. Kabat-Zinn (2000; 2003) and other Buddhist-Mindfulness
practitioners have begun to distance Buddhist-Mindfulness from their original
Buddhist context. Interestingly however, they still associate Buddhist
philosophy, concepts, and semantics with the methods they use and the results
one should expect in therapy, something they claim not to be doing.
59
The current “working [operational] definition of mindfulness” (Kabat-Zinn
2003, p145), while applying the central principles and practice of Theravada
Buddhist-Mindfulness, is isolated from the philosophical, cultural, and
cosmological framework in clinical application. Not only is Buddhist-Mindfulness
being converted to an ‘operational’ form, psychotherapists are instructing
Buddhists on what is missing in their understanding of subjectivity and mental
health (Rubin 1999). Titmuss (1998, p5) is critical of this kind of arrogance on
the behalf of psychiatry, declaring, “a tradition that is barely a century old
cannot expect to have the same depth of experience and realisation as a
tradition 2,500 years old”. Many centuries of clinical distance have been placed
between religious and scientific determinants of health in the United States,
disassociation through “ideological and institutional barriers” (Levin 1994,
1475) to socio-cultural and psychosocial determinants of mental health.
Interestingly, Newberg & Lee (2005) illustrate that Buddhist-Mindfulness,
among other ‘subjective’ based consciousness, religious, and ethnomedical
practices are not entirely reducible or ‘operational’ due to problems with
definition and objectivity in scientific standards. The problem of adequately
defining and measuring Buddhist-Mindfulness still plague its ‘operational’ status
(Brown & Ryan 2004; Hayes & Shenk 2004; Roemer 2003). The clinical
application of Buddhist-Mindfulness is in its genesis, and it can be expected
that more modification to this practice will occur in the attempt to
‘operationalise’ it and apply it within clinical standards.
Medicalisation & Capitalism in the United States
The ‘subjective’ problem encountered in ‘operationalising’ CAM and other
religious practices in scientific disciplines in the United States is a problem at
the core of science and medicine as disciplines. Subjective reality, as argued
by science, is not definable. The inability to define subjectivity has led to a
modern subjectivity in the United States based on scientific materialism and
medical rationalism (Good 1994; Wallace 2007). Anthropologists recognise a
60
macro-societal discourse in all societies. A ‘top-down’ effect impacts on local
socio-institutional and individual interpretation and experience of illness (Baer
2005). Foucault (1975) most prominently posited a social hierarchical
relationship between people and power in Euro-American societies. He
proposed that a culturally constructed and constituted ‘medicalisation’ has
resulted from Euro-American medical, particularly clinical, history. The process
of secularisation in society initiated “a transfer of moral regulation” (Turner,
1992, p22) to science and medicine from religion. Foucault (1972: 49) argued
that a medico-scientific ‘gaze’ has resulted, where “practices…systematically
form the objects of which they speak”. Foucault insinuated this
‘medicalisation’ of human society, particularly between the populace and the
state, as a result of the ‘gaze’. Human bodies and behaviour have become
classified and controlled through a medical ethos.
Porter (2006, p7) argues with Foucault, alleging that modern scientific
medicine has “driven itself to medicating normal life events”. This results from
a need by modern medicine to redefine itself and an overabundant social
acceptance of medicine, science, and technology. Furedi (2004, p12) claims
that modern medical institutions and science are cultivating vulnerability,
declaring, “people’s experience is interpreted through the medium of the
therapeutic ethos”. Subjectivity in the United States, they iterate, is being
managed and/or controlled by organisations and governments who are reliant
on and promote science and technology. Modern subjectivity is being
channelled in a medical direction, largely focused on the body. The processes
used to manoeuvre subjectivity are scientific and technological. Socially
subjective manipulation of bodies and minds also intertwines with capitalistic,
media, and market oriented process. Harvey (2000, 294) argues that the
current identity crisis afflicting many people in the United States propels
people to consume and remodify their bodies in a response to the “time-space
compression” that capitalism has created. This crisis of identity is of the self,
particularly as self-concepts relate to body image and social expectations. The
61
current crisis also affects science, medicine, and psychiatry, creating a vacuum
that is being filled by non-Euro-American ethnomedicines, religions, and
philosophies (Rindfleish 2007). A ‘spiritual revolution’ is argued to be beginning
in the wider society within the United States, highlighted by various forms of
religious movements and CAM utilised by the lay population (Tacey 2003).
A new form of medical plurality is occurring in the United States. This involves
the utilisation of multiple health aetiologies to cure and provide meaning to
illness. Plurality in health seeking behaviour is not new to the United States.
However, the social conditions that engender and motivate plurality in medical
care are. Attention is predominantly focusing away from Euro-American
medicines towards other cultural ethnomedinces (Rindflesh (2007). The ‘new’
link between religion and health, and the accepted inadequacy of Euro-
American medicines to provide meaning to illness experience perpetuates many
medical fields and social institutions in the United States, including psychiatry
(Galanter 2005; Johanson 2006). The term ‘spirituality’ has taken over from
‘religion’ because spirituality allows “the freedom to create one’s own notion
of the sacred or ultimate reality” (Hartz 2005, p4), that is meaningful,
transcendental, and loving. However, the paradigmatic shift in the United
States regarding the role of religion and spirituality in medicine and illness
experience is largely ideological and is still governed by a prevailing habitus,
motivated by a worldview that clearly aims to dominate and regulate new
enterprises. Consequently, materiality retains a stronghold over the
transcendental (Hartz 2005). Even though newly diffused ethnomedical or
religious traditions accommodate a meaningful and transcendental philosophy,
this is ‘watered down’ through its ideological interpretation and incorporation
with a pre-existing social discourse on ‘what is religion/spirituality?’ and ‘what
is health in relation to religion?’.
Ethnomedical and religious/spiritual traditions can only be described as being
modified by pre-existing paradigms on religion and health, and for general
62
consumption for people of the United States. Faldon (2004) argues that the
‘domestication’ of ethnomedicines and religious traditions enables a working-
with scenario for existing medical, scientific, and lay practice in the United
States. Domestication involves “a process by which the foreign is rendered
familiar and palatable to local tastes” (Faldon 2004, p72), and where “Eastern
themes are adapted for Western consumption (Dawson 2006, p8). Brazier
(2001, p80) insists, “Buddhism is being retailed to the Western world as a quest
for enlightenment”. This quest for enlightenment in the United States is not of
the transcendental ‘self’, but of an immortal ‘body’. The ideation of
immortality (not a new belief) contemporarily embraces a scientific and
technological thesis of the body as manipulable and transformable through
medical intervention. Genetic and neurobiological bases for disease and
consumer capitalism, when set against the historical backdrop of a lineal,
individual, and progressive worldview, fuels the acceptance of a society
comfortable with body manipulation. A spiritual-medical view of reality,
focused on the ‘body’ and the ‘image’ of the body constrain how contemporary
health seeking behaviour in the United States functions, influenced by a variety
of forces like science and consumer capitalism. Modern body image and ideals
are motivated by classical art, scientific and medical discourses and
commercial interests like fashion, fitness, and celebrity media (Urla &
Swedlund 2007). Gendered norms and influences of popular culture are
motivating people to act out phantasmagoric bodily and social roles like that of
‘Barbie’. These social discourses iterate an ideology of perfection and
chameleon-like possibilities of the body, driven by a consumer culture that has
come to be imbued with a medical ethos.
Health Seeking in Macro-Cosmic Context
Modern discourses of the body, medicine, and the cultural-other are
legitimated and transmitted through the accepted wisdom of science and
63
technology, an uncontrollable consumer society, and the power of modern
forms of media (Williams 2003). Set against the context of the body in history,
this is another process whereby human bodies are rendered meaningful by the
societal powers that govern them (Turner 1995). This concept is understood
more clearly when situated within the worldview of the United States. Dawson
(2006) argues that the overarching worldview in the United States and Europe
is encapsulated in the ‘Western habitus’. This habitus incorporates Christian,
scientific, technological, and capitalist influences. Dawson (2006, p2, 3) argues
that the ‘Western Habitus’ has developed through the combination of “multiple
fields of force (in space and time)…to constitute the modern Western
worldview”. He explains that this habitus comprises a “technologized
conceptualization of the self, a depersonalized view of the cosmos, and a
metaphorization of the modern cultural field” (Dawson 2006, p1). This habitus
has naturalised the tendency to diffuse or selectively adopt and modify
‘Eastern’ traditions. Diffusion of ‘Eastern’ practices by the United States is
constituted in the ‘Western Habitus’. Rather than accepting practices as they
are, a “Westernization of Eastern themes [rather] than an Easternisation of the
Western paradigm” occurs (Dawson 2006, p3). “Eastern themes” are “adapted
for Western consumption” explains Dawson (2006, p8), through “selective
appropriation and subsequent tailoring” that identifies with, correspond to,
and affirm “established predilections of the Western aesthetic”.
The Euro-American worldview is conditioned by an ontological and cosmological
logic. By cosmology I refer to be a culturally conditioned account of the
universe and Man’s place in it, not the cosmology of physics (however the role
of scientific practices like physics is imperative to this determination). Euro-
American cosmology is described as “mechanical” (King 1983, px). The
‘mechanical’ universe is understood as a process, lineal and limited, and the
laws that govern the universe are determined to be discoverable and
harnessed. King (1983, pxvi) notes that this cosmic view structures and
motivates Euro-American thought and action. It has generated a modern

64
society that has become “scientifically-technologically orientated”. Science-
based technology has been argued to be a religion in the United States, with
science as the religious form, and technology as its discourse (Roy 2005).
However, the application of a ‘total scientific cosmology’ has been criticised as
inadequate as a total representation of culture in the United States. This is
“through the inadequacy of modern science to provide meaning” (Laughlin,
McManus & d’Aquili 1990, p233). “Science provides a view of the world…that is
intentionally disconnected from the direct, everyday experience of people”
(Laughlin, McManus & d’Aquili 1990, p234), a worldview that has undoubtedly
abstracted human knowledge from experience. Many science-based disciplines
accept this, and it has been highlighted as a prominent reason for the present
paradigm shift in Euro-American science and medicine towards ‘Eastern’
concepts of reality (Ratanakul 2002; Varrela, Thompson & Rosch 1993).
A variety of beliefs and practices inform the United States worldview. The
insufficiency of science (and technology) to generate a total worldview has
been filled by the diffusion cosmologies and worldviews of non-United States
cultures and Indigenous Indian nations for centuries. Christianity (in its variety
of forms), science, technology, and capitalism are the most significant. Modern
science and medicine dominate the modern worldview of the United States.
Science and medicine are an extension of Ancient Greek, Renaissance,
Enlightenment, and modern physics rationale. Logic and reasoning of Ancient
Greece (Roninson & Groves 1999; Kenny 1993), Descartes Cartesian dualism
(Strathern 1996), Newtonian mechanics, Galileo’s physics (Coles 2000), the rise
of clinical medicine (Foucault 1975), and Einstein’s theory of general relativity
(Coles 2000) are major rationales that have been the influenced major
paradigmatic shifts in Euro-American scientific/medical theory and practice.
Tambiah (1991) explains that since the Enlightenment, European thought
pursued speculative and intellectual commentary on religion (including
Buddhism and Christianity). Enlightenment rationale is manifested in
contemporary scientific/medical rationalism in the United States, and has
65
come to dictate the way people experience illness (Tambiah 1991).
Contemplation created a gulf between religion and science, one that had by all
rights begun with the partitioning of physis and logos in Ancient Greece (aided
by the Renaissance re-discovery of Greek knowledge).
The modern worldview in the United States is still heavily symbolised by a
Christian theistic and scientific subject/object dualistic interpretation of
reality (e.g., good verse evil) (King 1983). However, centuries of dualistic
thinking and a rationalistic attitude based on empiricism of scientific method
influences modern ideology in the United States (Foucault 1975; Nuland 2000;
Scheper-Hughes & Lock 1987). This reveals how disease/illness reality is
constructed, enacted, and experienced in modern United States society.
Christianity and science have shared a history of united ideas and practice
together (Imperato 2002; McGrath 1999), however science and religion divided
during the Enlightenment in Europe due to the scientific focus on naturalism
(and refusal of supernaturalism). European and United States society became
secularised, a revolution apparent in the education system where science and
religion have become separate domains and are often at odds with each other
(Butts 1950; Wallace 2007). Contemporary public education in the United
States confirms this reality through science and religion, where science is
edified as ‘fact’, and religion as ‘belief’ (Wallace 2007).
Capitalism can be described as an essential component of the ‘Western
habitus’, refining what science had begun before its entrance on the social
platform and total-global dictator for life as a mode-of-production. The rise of
capitalism 300 years ago in industrial Europe, and its more recent post WWII
expansion, has had a substantial impact on the United States (Ganbmann 2006).
Preston (1979) highlights how capitalism has generated a “stress on personal
freedom, often expressed in the term individualism has been such a potent
force in our culture in the last three centuries” in the United States. More
recently, Harvey (2000) discerns that capitalism has become a metaphor for

66
modernity, defining sociality and selves in individual, lineal, progressive, and
modifiable terms. Marx initially highlighted the role capitalism played in
“continual revolutionizing of the methods of production” through its “intimate
connection with science and technology as a major productive force”
(Bottomore 2006, p61). Science and technology supported the capitalist
revolution in Europe and the United States from the 18th century, continuing to
support each other producing a capitalist ethos to modern society. Capitalism
has influenced the secularisation of science and raised it above status of
Christianity and other religious or cultural knowledge globally. It was an
influential factor in the colonial period and has continued into modern age,
motivating the desire to produce and attain wealth, particularly at the expense
of others.
Medical Pluralism in the United States: Form & Function
This chapter has revealed that scientific and medical institutions in the United
States are appropriating other cultural determinants and beliefs about the
universe. This process involves the ideological incorporation of a variety of
ontological and cosmological logics. This is driving how Buddhist-Mindfulness is
diffused into psychiatry in the United States. Psychiatry, as a branch of medical
science, applies an ‘operational’ logic to develop practices. Psychiatry employs
this mechanistic, biologically focused, and socially void interpretation of
reality, as does general science. As a result, Buddhist-Mindfulness is being
diffused through the practice of psychiatry (and medicine) without any
Buddhist connection. The diffusion of this and other CAM and religious
traditions into scientific medicine and psychiatry imply a paradigm shift in
modern scientific medicine and psychiatry, one that is experimenting with
‘Eastern’ interpretations of the universe. The United States exhibits historical
process by science and medicine to amend failing paradigms by diffusing other
cultural beliefs and practices. This highlights the ontological and cosmological
67
factors that are employed through ideological reasoning by science and
medicine in the diffusion of other cultural practices.
Diffusion of Buddhist-Mindfulness in psychiatry, along with the ‘domestication’
of CAM and religious traditions involves a scientific, medical, and capitalistic
drive that intentionally transforms these practices. There is a specific forces on
the body and its plasticity, one that correlates to the manipulation of CAM by
science and medicine. The matrix of medical practices and modern health-
seeking behaviour in the United States is a direct representation in micro-
context of a bricolage United States worldview. Consumer capitalism,
marketing of CAM, and their bodily consumption by people of the United States
is a major feature that contributes to the separation of health and religion, and
the confusion over determinants of illness between health and religion. The
present diffusion of Buddhist-Mindfulness and other CAM is not a new practice
in the United States. CAM and other religious traditions are interpreted as
medical/scientific practices, and are deprived of their original cultural milieu.
CAM and religious traditions are determined and applied as observable material
reality only. Through the process of ‘operationalism’ by scientific institutions in
the United States, the cultural and historical content is lost and their original
meaning is subverted.
68
Chapter 5
Cultural Change, Psychiatry & Diffusion
This chapter compares and contrasts the diffusion of Buddhist-Mindfulness in
Thailand and the United States. Examination of the diffusion of Buddhist-
Mindfulness in the psychiatric process in Thailand and the United States reveals
how cultural factors influence the process of diffusion, particularly the
consequences to Buddhist-Mindfulness. Each context has seen the diffusion of
Buddhist-Mindfulness in psychiatry to improve the efficacy of mental health
treatment. Each context has utilised Buddhist concepts of mental health,
causes of mental illness and the remedy of mental illness. Through comparison
it emerges that while each application of Buddhist-Mindfulness share the same
aim, the form, function, and meaning is distinct in each context. Each context
utilises the same practise (Buddhism/Psychiatry) for the same purpose
(reduce/cure mental illness), just in different ways. This is precisely due to the
influence of the prevailing worldview that informs culture-specific response
and action in each context. This reveals that it is necessary for each context to
maintain its original discourse on, and practice of medicine, and sees the
diffusion of the new medical system into an existing medical paradigm. I argue
that this process is adaptive and is essential to the maintenance of traditional
social order in times of change.
69
On the Diffusion of Buddhist-Mindfulness in Psychiatry
“Modernity”, as explained by Tanabe & Keyes (2002, p7), “entails an
irrevocable rupture with a habitus rooted in an unquestioned cosmology”. This
fissure of the taken-for-granted in Thailand and the United States has
prompted the diffusion of Buddhist-Mindfulness in psychiatry in each context.
The consequences to Buddhist-Mindfulness through the process of diffusion are
the result of a retreat into historical dimensions of culture. I argue that
cultural histories are employed ideologically in the process of modern identity
construction and negotiation. Through ethnographic analysis of Thailand and
the United States, this thesis has revealed the increasing importance placed on
social re-construction because of the constant need to renegotiate identity in a
modern and rapidly changing society. As Kapferer (1988, p85) articulates, “the
ideology of ontology is most evident in times of crisis”. Each context, Thailand
and the United States, produces and displays culturally and context-specific
historical dimensions of sociality regarding health. These elements configure
the different cultural praxis and consequences that Buddhist-Mindfulness
enjoys through its diffusion in psychiatry.
I argue that the macro-level motivation for the diffusion of Buddhist-
Mindfulness into psychiatry in Thailand and the United States is motivated by
global social change that is the effect of local social changes. Moreover, there
is a strong need for the illness experience to have meaning, which is not
provided for by psychiatry in either context. Modern social change and the
need for meaning in illness experience have been central themes running
through this thesis. These themes have been illustrated in the case studies and
were subsequently revealed through ethnographic analysis of health-seeking
behaviour and the social regulation of illness experience in Thailand and the
United States. Analysis of ethnographic data in Thailand has revealed that
modern globalised social change affects mental illness. Psychiatry (and
70
biomedicine), as agents to the globalising process (Kirmayer 2006), have
dislocated local understanding of health and illness, and also failed to provide
adequate meaning to the illness experience in each context. In Thailand, this
has enabled the practise of medical pluralism to proliferate. As a result,
health-seeking behaviour has continued along traditional channels, utilising
Euro-American medicine as part of the medical matrix there. In the United
States, the redevelopment of existing scientific and medical paradigms, and
the inclusion of CAM into the medical market, is generated by the failure of
current medical paradigms to supply adequate meaning in illness experience
and the existential crisis this has created. The social-wide desire for meaning,
driven distinctly by the lack of meaning in people’s lives, is directed towards
scientific and medical institutions. Accordingly, the ‘medicalisation’ of United
States society is prompting people to find meaning in medical and scientific
institutions and values.
The consequences of the diffusion of Buddhist-Mindfulness are remarkably
different in form, function, and meaning. This is explained in Figure 7. The aim
of diffusing Buddhist-Mindfulness in psychiatry in Thailand and the United
States was to develop a mental health practice and process that will improve
existing methods and treatment of mental illness. It has been discovered
through this thesis through careful examination that the diffusion of Buddhist-
Mindfulness in Thailand and the United States are distinctly different.
Remarkably, each context finds the utilisation of Buddhist-Mindfulness Based
Psychiatry for exactly the same purpose but with different therapeutic
methods, practises, and meaning. This has generated unique consequence to
Buddhist-Mindfulness. In the United States the practice of Buddhist-Mindfulness
has been manipulated by being ‘operationalised’ to suit Empirical Clinical
Psychiatric Standards (ECPS). The result is a form of ‘Mindfulness’ that is void
of any cultural/religious cosmological or existential significance, conforming to
psychiatric aetiology and nosology of mental illness. In Thailand, the
application of Buddhist philosophy and practice has superseded the

71
conventional (ECPS) psychiatric process. Buddhist aetiology and nosology of
suffering (dukkha) has replaced the psychiatric specifications of mental illness
aetiology and nosology.
Consequence, or Differences in Form, Function & Meaning
to Buddhist-Mindfulness through Diffusion
Thailand United States
Form - Buddhist-Mindfulness & Meditation used - Buddhist-Mindfulness & Meditation used in
in accordance with Theravada Buddhist ‘Operational’ status in accordance with
Tradition in Thailand was applied to the Empirical Clinical Psychiatric Standards
Standard Clinical Psychiatric Process was applied to the Standard Clinical
Psychiatric Process
Function - Treatment of anxiety - Treatment of anxiety (GAD)
Meaning - Removal of Suffering (dukkha) - Treatment of anxiety (GAD)
Figure 7.
Comparison of the diffusion of Buddhist-Mindfulness in Thailand and the United
States, with the ethnographic data, reveals that the diffusion of Buddhist-
Mindfulness in psychiatry in Thailand and the United States are influenced by
the habitus and its prevailing worldview in each context. The process of
diffusion has produced the culture-specific consequence to Buddhist-
Mindfulness revealed in this thesis. This is illustrated in Figure 8. Buddhist-
Mindfulness, and the cosmological and experiential notions of suffering
(dukkha) cannot be diffused in psychiatric practice in the United States without

72
a significant loss or alteration to them. Conversely, Euro-American psychiatric
practice and mental illness aetiology and nosology cannot be diffused without
difficulty in Northeast Thailand. Thus, the diffusion of Buddhist-Mindfulness in
psychiatry in Thailand in Buddhist form, and in the United States in scientific
form, disclose the foundational ontological and cosmological logic that informs
the habitus of each culture. I argue this is because each culture ideologically
employs unique aspects of ontology and/or cosmology to maintain cultural
identity during the changes that are affecting each context. Critically, I argue
that this process illustrates that it is necessary for Thailand and the United
States respectively to maintain their original and dominant paradigms on
mental illness and suffering during times of crisis. Buddhist-Mindfulness must
be diffused into the already existing and functional medical paradigm. This is
an adaptive process that I argue is essential to reinstating and maintaining the
social order and prevailing worldview.
Worldviews Influencing the Consequences to
Buddhist-Mindfulness
Thailand United States
- Polyphasic Consciousness - Monophasic Consciousness
- Biological/Organic Universe - Mechanistic Universe
- Interconnected - Individual
- Circular Time - Linear Time
- Spatially Infinite Universe - Spatially Finite Universe
- Reciprocal Role With the - Aim to Control the Forces Universe of the Universe
Figure 8.
73
Thailand and the United States each exhibit a distinct mental illness aetiology
and nosology. This is illustrated by the context-specific application of historical
aspects of culture to cope with or transcend illness experiences. Tyson &
Pongruengphant (2007, p1) explain that Buddhist “cosmology yields a
fundamental disagreement between Western psychological theory and
Buddhist’s conception of suffering”. The process of diffusing Buddhist-
Mindfulness in psychiatry in each context reveals that the United States
situates health on the level of the body and ego, and Thailand situates health
on a transcendent level of self and mind which can be eternally liberated.
These distinct processes of diffusion highlight that Thailand and the United
States utilise unique and pre-existing socio-cultural structures to explicate
health aetiology and treatment. In the United State, the refusal to apply
cultural significance to Buddhist-Mindfulness by psychiatry highlights the
dominance of the scientific paradigm in medicine. The ‘operationalising’ of
Buddhist-Mindfulness runs counter to current psychiatry and cognitive scientific
claims that these institutions are accepting a link between religion and health.
Buddhist–Mindfulness has consequently become a ‘medical’ practice, a cultural
terra nullius, tailored to the consumptive needs of a culture that seeks the
restoration of health/order in constant improvement of the body. Conversely,
in Thailand the total diffusion of Buddhist-Mindfulness in the Theravada
Buddhist format illustrates the cultural significance ‘Mindfulness’ and Buddhism
has in Thailand. Buddhist-Mindfulness retains its religious and cosmological
substance and is utilised as both a form of health care and as a guide and
process to eternal liberation from suffering (nibbána) in its psychiatric
application. This is a renegotiation of Euro-American values with Buddhist
values to deal with illness and misfortune as they iterate Buddhist concepts of
self, society, and cosmos in Thailand.
74
Cultural Crisis & the Collective Past
Through examination of the diffusion of Buddhist-Mindfulness in psychiatry, this
thesis has revealed that Buddhist-Mindfulness is manipulated in each context to
fit with the prevailing worldview. Health-seeking behaviour and discourse
about health is strongly conditioned by modern social and cultural-historical
forces. How people experience illness and the action selected to remedy illness
in Thailand and the United States are socially and historically regulated. As
Turner (1996, p214) declares, medical knowledge and practise “reflects the
overall patterns of values and institutions within a given society”. It has been
demonstrated in this thesis that the motivation to diffuse Buddhist-Mindfulness
in psychiatry in Thailand and the United States is an adaptive function to
restore order and balance to self and society in a modern and rapidly changing
global and local-social landscape. Additionally, the need for the illness
experience to be imbued with greater meaning, also prompted by social change
and the failure of psychiatric treatment has been shown to stimulate this
diffusion.
Contextual social and historical factors produce the consequences to Buddhist-
Mindfulness in each psychiatric application. This thesis has defined
consequences as any modifications to Buddhist-Mindfulness through the process
of diffusion. By analysing the contextual variations in the socio-cultural systems
and cultural histories of Thailand and the United States, the unique
transformations of Buddhist-Mindfulness in each context are established. The
theoretical and conceptual foundation utilised the concept of habitus and the
incorporation of ontology and cosmology to explain how and why meaning is
generated and legitimated. Social identity and solidarity has been revealed as a
critical aspect in culture during times of modern social change and crisis.
75
Conclusion
The diffusion of Buddhist-Mindfulness in psychiatry in Thailand and the United
States has been examined in this thesis to highlight how the process of
diffusion occurs and why innovations receive different consequences in
different cultural contexts. In this thesis I have determined why Buddhist-
Mindfulness has been diffused in each psychiatric context by examining the
macro-global and local-social forces that motivate this process. This thesis is
based on a critical literature review utilising quality ethnographic data that
permitted an excellent ability to produce sound conclusions on this topic.
In Chapter I it was established how Buddhist-Mindfulness was applied
differently in psychiatry in the United States and Thailand as a therapeutic
intervention. This was demonstrated through two case studies [Rungreangkulkij
& Wongtakee (2006) and Roemer & Orsillo (2007)] that applied Buddhist-
Mindfulness in clinical psychiatry for the treatment of anxiety disorders.
Chapter 2 provided the theoretical basis for this analysis. I argued that the
difference of each application of Buddhist-Mindfulness in psychiatry is affected
by culturally-contextualised socio-historical ontological and cosmological
factors. Consequences to Buddhist-Mindfulness are the result of the contextual
worldviews, and the need to maintain order and meaning in society. Chapter 3
revealed the dominance and persistence of Buddhism in historical and modern
Thai society, examining the Buddhist exegesis on suffering (dukkha) and the
role Buddhism plays in the construction of self and society in Thailand. Chapter
4 exposed the dominance of scientific and capitalistic discourse in the United
States. The ‘operationalising’ of Buddhist-Mindfulness revealed a history of
selective borrowing and modification by scientific and medical institutions.
Chapter 5 provided the final analysis of this thesis. Though examination of the
diffusion of Buddhist-Mindfulness in psychiatry in Thailand and the United
76
States, this thesis has revealed how ontology and cosmologies are used to
generate and legitimate meaning and certainty in times of social change and
crisis. The consequences to Buddhist-Mindfulness reflect these unique
worldviews. The institution of psychiatry, the psychiatric process, and the aims
of psychiatry are pliable when they are situated in different cultural contexts.
Analogously, the pliability of Buddhist-Mindfulness has also been revealed when
it is situated in psychiatry in another cultural context like the United States.
Long-term consequences to Buddhist-Mindfulness cannot be assessed in this
thesis. It is clear that the drive towards a global homogeneity of scientific,
technological, and consumptive cultural practice has the power to significantly
alter local medical and religious praxis. Further research into the processes of
diffusion is welcomed. In particular, why diffusion occurs and what
consequence innovations receive. Additional investigation into the diffusion of
Buddhist-Mindfulness and the modification of other ethnomedical and religious
practices will improve our understanding of the process of diffusion and the
consequential factors that diffusion to cultures and innovations.
77
References
Arond, D 2006, ‘Eye on religion: buddhism and medicine’, Southern Medical
Association, vol.99, no.12, pp.1450-1451.
Askew, M 2002, Bangkok: place, practice, and representation, Routledge,
London.
Baer, H 2001, The sociopolitical status of U.S naturopathy at the dawn of the
21st century, Medical Anthropology Quarterly, vol.15, no.3, pp.329-346.
- Baer, H 2005, ‘Trends in religious healing and the integration of
biomedicine and complementary and alternative medicine in the united
states and around the globe: a review’, Medical Anthropology
Quarterly, vol.19, no.4, pp.437-442.
Baer, R 2003, ‘Mindfulness training as a clinical intervention: a conceptual and
empirical overview’, Clinical Psychology: Science & Practice, vol.10, no.2,
pp.125-143.
Bates, D 2002, ‘Why not call modern medicine alternative’, The ANNALS of the
American Academy of Political and Social Science, vol.583, pp.12-28.
Barnard, A 2000, History and theory in anthropology, Cambridge University
Press, Cambridge.
Bastin, R 2001, Globalisation and conflict, Marga, Colombo
Benedict, R 1946, Patterns of culture, Mentor Books, New York.
78
Berry, J 1990, ‘Psychology of acculturation: understanding individuals moving
between cultures’, in Brislin, R (ed.), Applied cross-cultural psychology, Sage
Publications, London, pp.232-253.
Boehnlein, J 2006, ‘Religion and spirituality in psychiatric care: looking back,
looking ahead’, Transcultural Psychiatry, vol.43, no.4, pp.634-651.
Bottomore, T 2006, ‘Capitalism’, in Outhwaite, W (ed.), The blackwell
dictionary of modern social thought, Blackwell Publishing, London, pp.61-63.
Bourdieu, P 1977, An outline of theory as practice, Cambridge University Press,
London.
- 1990, The logic of practice, Stanford University Press, Stanford.
- 1999, ‘Structures, habitus, practices’, in Elliot, A (ed.), Contemporary
social theory, Blackwell, Massachusetts, pp.108-118.
Brazier, D 2001, The new buddhism, Robinson Press, London.
Brown, P 1998, Understanding and applying medical anthropology, Mayfield
Publishing Company, California.
Brown, K & Ryan, R 2004, ‘Perils and promise in defining and measuring
mindfulness: observations from experience’, Clinical Psychology: Science and
Practice, vol.11, no.3, pp.242-248.
Burnard & Naiyapatana 2004, ‘Culture and communication in thai nursing: a
report from an ethnographic study’, International Journal of Nursing Studies,
vol.41, pp.755-765.
79
Burnard, P, Naiyapatana, W & Lloyd, G 2006, ‘Views of mental illness and
mental health care in Thailand: a report of an ethnographic study’, Journal of
Psychiatric and Mental Health Nursing, vol. 13, pp. 742-749.
Burton, D 2005, ‘Unconscious beliefs in buddhist philosophy: a comparative
perspective’, Contemporary Buddhism, vol.6, no.2, pp.117-130.
Butts, R 1950, The american tradition in religion and education, The Beacon
Press, Boston.
Chen-Kuo, L 1997, ‘Metaphysics, suffering, and liberation: the debate between
two buddhisms’, in Hubbard & Swanson (eds.), Pruning the bodhi tree: the
storm over critical buddhism, University of Hawaii Press, Honolulu, pp.289-313.
Coles, P 2000, ‘Einstein and the birth of big science’, in Appignanesi, R (ed.),
Postmodernism and big science, Icon Books Ltd, Cambridge, pp.11-52.
Connor, L & Samuel, G (eds.) 2001, Healing powers of modernity: traditional
medicine, shamanism, and science in asian societies, Bergin & Garvey,
Westport.
Dawson, A 2006, ‘East is east except when it’s west: the easternization thesis
and the western habitus’, Journal of religion & society, vol.8, pp.1-13.
Davis, R 1984, Muang metaphysics: a study of northeast thai myth and ritual,
Pandora, Bangkok.
de Sardan, J-P 2005, Anthropology and development: understanding
contemporary social change, Zed Books, London.
80
Escobar, A 1995, Encountering development: the making and unmaking of the
third world, Princeton University Press, Princeton.
Faldon, J 2004, ‘Meridians, charkas and psycho-neuro-immunology: the
dematerialising body and the domestication of alternative medicine’, Body &
Society, vol.10, no.4, pp.69-86.
Ferudi, F 2004, Therapy culture: cultivating vulnerability in an uncertain age,
Routledge, London.
Formoso, B 1996, ‘Tai Cosmology and the Influence of buddhism’, Diogenes,
no.44, pp61-82.
Foucault, M 1972, The archaeology of knowledge. New York: Harper & Row.
- 1975 The birth of the clinic: an archaeology of medical perception
London: Tavistock Publications Ltd.
Fronsdal, E 1999, ‘Theravada spirituality in the west’, in Yoshinori, T (ed.),
Buddhist spirituality: later china, korea, japan, and the modern world, The
Crossroad Publishing Company, New York, pp.482-495.
Galanter, M 2005, Spirituality and the healthy mind: science, therapy, and the
need for personal meaning, Oxford University Press,Oxford.
Ganbmann, H 2006, ‘Capitalism’, in Harrington, A, Marshal, B & Muller, H-P
(eds.), Encyclopaedia of social theory, Routledge, London & New York, pp.44-
48.
Golomb, L 1986, ‘Rivalry and diversity among thai curer-magicians, Social
Science and Medicine, vol.22, no.6, pp.691-697.
81
- 1988(a), ‘Supernaturalist curers and sorcery accusations in
Thailand’, Social Science & Medicine, vol.27, no.5, pp.437-443.
- 1988(b), ‘The interplay of traditional therapies in south Thailand’,
Social Science & Medicine, vol.27, no.8, pp.761-768.
Good, B 1994, Medicine, rationality, and experience: and anthrpoplogical
perspective, Cambridge University Press, Cambridge.
Griffiths, P 1986, On being mindless: buddhist meditation and the mind-body
problem, Open Court, La Sale, Illinois.
Hahn, R & Kleinman, A 1983, ‘Biomedical practice and anthropological theory:
frameworks and directions’, Annual Review of Anthropology, vol.12, pp305-
333.
Hall, M 1988, Meditation symbols in eastern & western mysticism: mysteries of
the mandala, The Philosophical Research Society Ltd, Los Angeles.
Hallisey, C 2006, ‘Buddhism’, in Outhwaite, W (ed.), The blackwell dictionary
of modern social thought, Blackwell Publishing, London, pp.52-54.
Hartz, G 2005, Spirituality and mental health: clinical applications, The
Haworth Pastoral Press, New York.
Harvey, D 2000, ‘Capitalism: the factory of fragmentation’, in Roberts, J &
Hite, A (eds.), From modernisation to globalisation: perspectives on
development social change, Blackwell Publishers, Oxford, pp. 293-297.
82
Harvey, P 1990, An introduction to buddhism: teachings, history, and
practices, Cambridge University Press, Cambridge.
Hayes, S 2002, ‘Acceptance, mindfulness, and science’, Clinical Pychology:
Science & Practice, vol.9, pp.101-106.
Hayes, S & Shenk, C 2004, ‘Operationalizing mindfulness without unnecessary
attachments’, Clinical Psychology: Science and Practice, vol.11, no.3, pp.249-
254.
Helman, C 2000, Culture, health , and illness, Hodder Arnold, New York.
Henningsen, P 2003, ‘The body in the brain: towards a representational
neurobiology of somatoform disorders’, Acta Neuropsychiatrica, vol.15, pp157-
160.
Hinton, D, Nguyen, L & Pollack, M 2007, ‘Orthostatic panic as a key Vietnamese
reaction to traumatic events’, Medical Anthropology Quarterly, vol.27, no.1,
pp.81-107.
Hoare, T 2004, Thailand: a global studies handbook, ABD-CLIO, California.
Holbrook, B 1981, The stone monkey: an alternative chinese-scientific reality,
William Morrow and Company Inc, New York.
Hunter, D & Whitten, P 1976, Encyclopaedia of anthropology, Harper & Row,
New York.
Imperato, R 2002, Early and medieval Christian spirituality, University Press of
America, New York.
83
Ingersol, J 1975, ‘Merit and identity in village thailand’, in Skinner, W & Kirsch,
T (eds.), Change and persistence in thai society, Cornwell University Press,
London, pp219-251.
Ionesgu-Tongyonk, J 1977, ‘Transcultural psychiatry in Thailand: a review of
the last thirty years’, Transcultural Psychiatry, vol.14, pp-145-160.
Jackson, P 1989, Buddhism, legitimation and conflict, Institute of Southeast
Asian Studies, Singapore.
Janes, C 2002 ‘Buddhism, science, and the market: the globalisation of tibetan
medicine’, Anthropology & Medicine, Vol. 9, no. 3, pp 267-289.
Johanson, G 2006, ‘A survey of the use of mindfulness in psychotherapy’,
American Psychotherapy, summer annals, pp.15-24.
Kabat-Zinn, J, Lipworth, L, Burney, R & Sellers, W 1986, ‘Four year follow-up
of a meditation-based program for the self-regulation of chronic pain:
treatment outcomes and compliance’, Clinical Journal of Pain, vol.2, pp.159-
173.
Kabat-Zinn, J 1982, ‘An outpatient program in behavioural medicine for chronic
pain patients based on the practice of mindfulness meditation: theoretical
considerations and preliminary results’, General Hospital Psychiatry, vol.4,
pp.33-47.
- 2000, ‘Indra’s net at work: the mainstreaming of dharma practice
in society’, in Watson, G, Batchelor, S & Claxton, G (eds.), The
psychology of awakening: Buddhism, science, and our day-to-day
lives, Rider Books, London.
84
- 2003, ‘Mindfulness-based interventions in context: past, present,
and future’, American Psychological Association, vol.10, no.2,
144-156.
Kapferer, B 1988, Legends of people, myths of state: violence, intolerance,
and political culture in sri lanka and australia, Smithsonian Institute Press,
Washington.
- 1997, The feast of the sorcerer: practices of consciousness and
power, The University of Chicago Press, Chicago.
- 2001, ‘Globalization, the state, and civil violence in sri lanka’,
Bulletin of the Royal Institute for Inter-Faith Studies, vol.3, no.2,
pp.59-111.
Kasantikul, D & Kanchanatawan, B 2007, ‘Antipsychotic-induced tardive
movement disorders: a series of twelve cases’, Journal of the Medical
Association of Thailand, vol.90, no.1, pp.188-194.
Kauffman, K & Myers, D 1997, ‘The changing role of village health volunteers in
northeast thailand: and ethnographic field study’, International Journal of
Nursing Studies, vol.34, no.4. pp.249-255.
Kenny, A 1993 The oxford history of western philosophy. Oxford: Oxford
University Press.
Keyes, C 1984, ‘Mother or mistress but never a monk: buddhist notions of
female gender in rural thailand’, American Ethnologist, vol.11, no.2, pp.223-
241.
- 1985, ‘The interpretive basis of depression’, in Kleinman & Good
(eds.), Culture and depression: studies in the anthropology of
85
cross-cultural psychiatry of affect and disorder, University of
California Press, Berkley, pp.153-174.
King, V 1999, Anthropology and development in south-east asia: theory and
practice, Oxford University Press, Kuala Lumpur.
King, V & Wilder, W 2003, The modern anthropology of south-east asia: an
introduction, RoutledgeCurzon, London.
King, W, 1983, ‘Foreward’, in Nishtani, K, Religion and nothingness, University
of California Press, Berkley, pp.vii-xxii.
Kirmayer, L 2006, ‘Beyond the ‘new cross-cultural psychiatry’: cultural biology,
discursive psychology and the ironies of globalisation’, Transcultural
Psychiatry, vol.43, no.1, pp126-144.
Kirsch, T 1975, Economy, polity, and religion, in Skinner, W & Kirsch, T (eds.),
Change and persistence in Thai society, Cornwell University Press, London, pp
172-196.
- 1985, ‘Text and context: buddhist sex role/culture of gender
revisited’, American Ethnologist, vol.12, no.2, pp.302-320.
Kleinman, A 1980, Patients and healers in the context of culture, University of
California Press, Berkley.
- 1988, Rethinking psychiatry: from cultural category to personal
experience, The Free Press, New York.
86
Kristeller, J & Hallett, C 1999, ‘An exploratory study of a meditation-based
intervention for binge eating disorer’, Journal of Health Psychology, vol. 4,
pp.357-363.
Kreober, A 1948 [1923], Anthropology: race. Language, culture, psychology,
prehistory, Harcourt, Brace & Company, New York.
Krongkaew, M (ed.) 1995, Thailand’s industrialisation and its consequences,
Macmillan, New York.
Laughlin, C, McManus, J & d’Aquili, E 1990, Brain, symbol and experience,
Shambala, Boston.
Littlewood, R 2002, Pathologies of the west: and anthropology of mental
illness in Euro-America, Cornell University Press, New York.
Levin, J, 1994, ‘Religion and health: is there an association, is it valid, and is it
causal’, Social Science & Medicine, vol.38, no.11, pp.1475-1482.
Lyttleton, C 1995, ‘Storm warnings: responding to messages of danger in Isan’,
TAJA, vol.6, no.3, pp.178-196.
- 1996, ‘Health and development: knowledge systems and local
practice in rural Thailand’, Health Transmissions Review, vol.6,
pp.25-48.
- 2002, Magic lipstick and verbal caress: doubling standards in Isan
villages, in Manderson, L & Liamputtong, P (eds.), Coming of age
in south and southeast asia: youth, courtship and sexuality,
Curzon Press, Surrey, pp.165- 187.
87
Marcus, G & Fischer M 1985, Anthropology as cultural critique: an
experimental movement in the human sciences, University of Chicago Press,
Chicago.
McElroy, A & Townsend, P 1989, Medical anthropology in ecological
perspective, Westview Press, London.
McGrath, A 1999, Christian spirituality, Blackwell Publishers, Oxford.
McVey, R 2000, Money and power in provincial thailand, Silkworm Books,
Chaing Mai.
Miller, J, Fletcher. K & Kabat-Zinn, J 1995, ‘Three-year follow-up and clinical
implications of a mindfulness meditation-based stress reduction intervention in
the treatment of anxiety disorders’, General Hospital Psychiatry, vol.17, no.3,
pp.192-200.
Mills, M 1997, ‘Contesting the margins of modernity: women, migration and
consumption in thailand’, American Ethnologist, vol.24, no.1, pp. 37-61.
Moreland, J 1989, Christianity and the nature of science, Baker Book House,
Michigan.
Morphy, H 1994, ‘The anthropology of art’, in Ingold, T (ed.), Companion
encyclopedia of anthropology: humanity, culture and social life, Routledge,
London, pp.648-685).
Mueche, M 1976, ‘Health care systems as socialising agents: childbearing the
north thai and western ways’, Social Science & Medicine, vol.10, pp377-383.
88
Mulder, A 1969, Monks, merit and motivation, Centre for Southeast Asian
Studies, Illinois.
Naemiratch, B & Manderson, L 2007, ‘Lay explanations of type 2 diabetes in
Bangkok, thailand’, Anthropology & Medicine, vol.14, no.1, pp.83-94.
Nhat Hahn, T 1994, ‘look deep and smile’, in Batchelor, M & Brown, K (eds.),
Buddhism and ecology, Motilal Banarsidass Publishers, Delhi, pp.100-109.
Newberg, A & Iversen, J 2003, ‘The neural basis of the complex mental task of
meditation: neurotransmitter and neurochemical considerations, Medical
Hypotheses, vol.61, no.2, pp.282-291.
Newberg, A & Lee, B 2005, ‘The neuroscientific study of religious spiritual
phenomena: or why god doesn’t use biostatistics’, Zygon, vol.40, no.2, pp.469-
489.
Nisula, T 2006, ‘In the presence of biomedicine: medical integration and health
seeking in Mysore, South India’, Anthropology & Medicine, vol.13, no.3, pp.
207-224.
Nuckols, C 2006, ‘Ambivalence and anxiety in the psychiatric systems of the
united states and japan’, Anthropology and Medicine, vol.13, no.2, pp.173-186.
Nuland, S 2000, The mysteries within: a surgeon reflects on medical myths,
Simon & Schuster, New York.
Obeyesekere, G 1985, ‘Depression, Buddhism, and the work of culture in sri
lanka’, in Kleinman, A & Good, B (eds.), Culture and depression: studies in the
anthropology and cross-cultural psychiatry of affect and disorder, University of
California Press, Berkeley.
89
Okasha, A 2003, ‘Somatoform disorders revisited’, Acta Neuropsychiatrica,
vol.15, pp.161-166.
Paul, R 1976, ‘The sherpa temple as a model of the psyche’, American
Ethnologist, vol.3, pp.131-146.
Pilowski, Z 1997, Abnormal illness behaviour, John Wiley & Sons, Chichester.
Porter, R 2006 The cambridge history of medicine, Cambridge University Press,
Cambridge.
Preston, R 1979, Religion and the persistence of capitalism, SCM Press Ltd,
London.
Prost, A 2006, ‘Causation as strategy: interpreting humours among Tibetan
refugees’, Anthropology & Medicine, vol.13, no.2, pp.119-130.
Ratanakul, P 2002, ‘Buddhism and science: allies or enemies?’, Zygon, vol.37,
no.1, pp.115-120.
Ray, H, 2006, ‘The axial age in asia: the archaeology of Buddhism’, in Stark, M
(ed.), Archaeology of asia, Blackwell Publishing, Oxford, pp.303-323.
Reynolds, C 1998, ‘Globalisation and cultural nationalism in modern thailand’,
in Kahn, J (ed.), Southeast asian identities: culture and the politics of
representation in indonesia, malaysia, singapore ,and thailand, Institute of
Southeast Asian Studies, Singapore, pp.115-145.
90
Reynolds, F 1978, ‘Sacral kingship and national development’, in Smith, B (ed),
Religion and legitimation of power in thailand, loas, and burma, Anima Books,
USA, pp.100-110.
Reynolds, F & Reynolds, M 1982, The three worlds according to king ruang: a
thai Buddhist cosmology, Asia Humanities Press, Berkley.
Reynolds, H 1971, ‘Concepts of acculturation’, in Growing, P & Scott, W (eds.),
Acculturation in the philippines: essays on changing societies, New Day
Publishers, Philippines, pp.21-32.
Rindfleish, J 2007, ‘The “death of the ego” in east-meets-west spirituality:
diverse views from prominent authors’, Zygon, vol.42, no.1, pp.65-76.
Rinpoche, A 1994, Taming the tiger: Tibetan teachings for improving daily life,
Rider Books, London.
Rinpoche, S 1992, The Tibetan Book of Living and Dying, Rider Books, London.
Robinson, D & Groves, J 1999, Introducing philosophy, Allen & Unwin, Sydney.
Roemer, L 2003, ‘Mindfulness: a promising intervention strategy in need of
further study’, Clinical Psychology: Science & Practice, vol.10, no.2, pp.172-
178.
Roemer, L & Orsillo, S 2007, ‘An open trial of an acceptance-based behavior
therapy for generalized anxiety disorder’, Behavior Therapy, vol.78, pp.72-85.
Rogers, E 1971, Communication of Innovations, Free Press, New York.
- 1995, Diffusion of innovations, Free Press, New York.
91
Roy, R 2005, ‘Scientism and technology as religions’, Zygon, vol.40, no.4,
pp.835-844.
Rubin, J 1999, ‘Close encounters of a new kind: towards an integration of
psychoanalysis and buddhism’, The American Journal of Psychoanalysis, vol.59,
no.1, pp.5-24.
Rungreangkulkij, S & Wongtakee, W 2006 ‘Buddhist counselling for patients
with anxiety’, Unpublished Conference Paper, Bankok.
Sam, D & Berry, J (eds.) 2006, The cambridge handbook of acculturation
psychology, Cambridge University Press, Cambridge.
Scheper-Hughes, N & Locke, M 1987, ‘The mindful body: a prolegomenon to
future work in medical anthropology’, Medical Anthropology Quarterly, vol.1,
no.1, pp.6-41.
Schutz, A 1970, On phenomenology and social relations, University of Chicago
Press, Chicago.
Segal, Z, Williams, J & Teasdale, J 2002, Mindfulness-based cognitive therapy
for depression: A new approach for preventing relapse, Guilford Press, New
York.
Shapiro, S, Schwartz, G & Bonner, G 1998, ‘Effects of mindfulness-based stress
reduction on medical and premedical students’, Journal of Behavioural
Medicine, vol.21, pp. 581-599.
Spiro, M 1967, Burmese supernaturalism: on the explanation and reduction of
suffering,
92
- 1971, Buddhism and society, Allen & Unwin, London
Strathern, P 1996, Descartes in 90 minutes, Constable and Company Ltd,
London.
Strinati, D 1995, An introduction to theories of popular culture, Routledge,
London.
Suwana, A 1969, ‘Effect of cultural change on anxiety in women in Thailand’,
Autralian and New Zealand Journal of Psychiatry, vol. 2, no. 3, pp. 267-270.
Tacey, D 2003, The spiritual revolution: the emergence of contemporary
spirituality, HarperCollinsPublishers, Sydney.
Tambiah, S 1970, Buddhism and the spirit cults of north-east Thailand,
Cambridge University Press, Cambridge.
- 1976, World conqueror, world renouncer, Cambridge University
Press, Cambridge.
- 1977, ‘The cosmological and performative significance of a Thai
cult of healing through meditation’, Culture, Medicine &
Psychiatry, vol.1, pp97-132.
- 1991, Magic, science, religion, and the scope of rationality,
Harvard University Press, Cambridge.
Tanabe, S 2002, ‘The person in transformation: body, mind, and cultural
appropriation’, in Tanabe, S & Keyes, C (eds.) 2002, Cultural crisis and social
93
memory: modernity and identity in Thailand and Laos, RoutledgeCurzon,
London, pp. 43-67.
Tanabe, S & Keyes, C (eds.) 2002, Cultural crisis and social memory: modernity
and identity in thailand and laos, RoutledgeCurzon, London.
Titmuss, C 1998, Light on enlightenment, Shambhala Press, Boston.
Turner, B 1992, Regulating bodies: essays in medical sociology, Routledge,
London.
- 1995, Medical power and social knowledge, SAGE Publications,
London.
Tyson, P & Pongruengphant, R 2007, ‘Buddhist and western perspectives on
suffering, stress, and coping’, Journal of Religion & Health, vol.10, pp.1-7.
Urla, J & Swedland, A 2007, ‘The anthropometry of barbie: unsettling ideals of
the feminine body in popular culture’, in Douglas, J, Earle, S, Handsley, S,
Lloyd, C & Spurr, S (eds.), A reader in promoting public health: challenge and
controversy, Sage Publications, London, pp.123-132.
van Esterik, P 1998, ‘To strengthen and refresh: herbal therapy in southeast
Asia’, Social Science and Medicine, vol.27, no.8, pp.751-759.
Varella, F, Thompson, E & Rosch, E 1993, The embodied mind, The MIT Press,
Cambridge.
Wallace, A 2007, Contemplative science: where Buddhism and neuroscience
converge, Columbia University Press, New York.
94
Weinstein, J (ed.) 2005, Social and cultural change: social science for a
dynamic world, Rowman & Littleford Publishers Inc, Oxford.
Weisberg, D 1982, ‘Northern thai health care alternatives: patient control and
the structure of medical pluralism’, Social Science & Medicine, vol.16,
pp.1507-1517.
Whittaker, A 2002, ‘Water serpents and staying by the fire: markers of maturity
in a northeast thai village’, in Manderson, L & Liamputtong, P (eds.), Coming of
age in south and southeast Asia: youth, courtship and sexuality, Curzon Press,
Surrey, pp.17-41.
Williams, S 2003, Medicine and the body, Sage Publications, London.
Winthrop, R 1991, Dictionary of concepts in cultural anthropology, Greenwood
Press, New York.
Young-Eisendrath, P & Muramoto, S 2003, Awakening and insight: zen Buddhism
and psychotherapy, Taylor & Francis Inc, New York.