Microsoft Office HTML Example
321
P 1 Comparison of Detrusor-Sphincter Dyssynergia in the SCI and Non-Neurogenic Bladder: Preliminary Study Sung Woon Baik 1* , Gi Wook Kim 1,2 , Yu Hui Won 1,2 , Sung Hee Park 1,2 , Myoung Hwan Ko 1,2 , Myung Ki Kim 3 , Jeong Hwan Seo 1,2† Department of Rehabilitation Medicine, Chonbuk National University Hospital 1 , Biomedical Research Institute of Chonbuk National Universitiy Hospital,Research Institue of Clinical Medicine of Chonbuk National University 2 , Department of Urology, Chonbuk National University Hospital 3 Objective The urinary bladder function of storing and voiding urine is controlled by central and peripheral nervous systems. The pathophysiology of detrusor-sphincter dyssynergia (DSD) in neurogenic bladder is represented by disruption of spinobulbospinal tract between the pontine micturition center and Onuf’s nucleus. However, dyssynergic sphincter activity can be seen in non- neurogenic etiology. In this retrospective study, we aimed to find out the differences of dyssynergic sphincter activity patterns and urodynamic parameters in the spinal cord injured and the non-neurogenic dysfunctional bladder. Methods Seventy-eight patients of dysfunctional voiding with urodynamic study reports were enrolled. They were divided into spinal cord injured group or non-neurogenic group by reviewing the medical records. We categorized the urodynamic study findings into 6 types according to dyssynergic sphincter activities. Type 1-3 belonged to true DSD and the other types to pseudo-DSD. And we also analyzed their urodynamic parameters such as bladder capacity, compliance, detrusor leak point pressure, peak detrusor pressure (PdetQmax), post-void residual urine volume and electromyographic activity of the sphincter. Results About 16% (8 patients out of 48 patients) of non-neurogenic group and 86.7% (26 patients out of 30 patients) of cord injury group showed dyssynergic sphincter activity, respectively. There were significant differences in bladder capacity (t=2.537, p<0.05) and compliance (t=3.364, p<0.05) between true DSD patients and pseudo-DSD patients. There were significant difference in peak detrusor pressure at maximal urinary flow rate (t=2.489, p<0.05) between cord injured group and non-neurogenic group. There were no significant difference in other urodynamic parameters such as bladder capacity (t=1.844, p=0.099), compliance (t=0.727, p=0.477), DLPP (t=0.322, p=0.752), PVR (t=1.036, p=0.314) when compared dyssnergic sphincter activity patients in each two groups. Conclusion Detrusor-sphincter dysfunction was not infrequent in patients with non-neurogenic bladder. And those who have dyssynergic sphincter activity had higher bladder capacity and compliance tendency. Also, cord injury group had higher peak detrusor pressure at maximal urinary flow rate during voiding than that of non-neurogenic bladder group. Further study with more patients is necessary.
-
Upload
khangminh22 -
Category
Documents
-
view
3 -
download
0
Transcript of Microsoft Office HTML Example

P 1
Comparison of Detrusor-Sphincter Dyssynergia in the SCI and Non-Neurogenic Bladder: Preliminary Study
Sung Woon Baik1*
, Gi Wook Kim1,2
, Yu Hui Won1,2
, Sung Hee Park1,2
, Myoung Hwan Ko1,2
, Myung Ki Kim3, Jeong Hwan Seo
1,2†
Department of Rehabilitation Medicine, Chonbuk National University Hospital1, Biomedical Research Institute of Chonbuk National
Universitiy Hospital,Research Institue of Clinical Medicine of Chonbuk National University2, Department of Urology, Chonbuk
National University Hospital3
Objective The urinary bladder function of storing and voiding urine is controlled by central and peripheral nervous systems. The pathophysiology of detrusor-sphincter dyssynergia (DSD) in neurogenic bladder is represented by disruption of spinobulbospinal tract between the pontine micturition center and Onuf’s nucleus. However, dyssynergic sphincter activity can be seen in non-neurogenic etiology. In this retrospective study, we aimed to find out the differences of dyssynergic sphincter activity patterns and urodynamic parameters in the spinal cord injured and the non-neurogenic dysfunctional bladder. Methods Seventy-eight patients of dysfunctional voiding with urodynamic study reports were enrolled. They were divided into spinal cord injured group or non-neurogenic group by reviewing the medical records. We categorized the urodynamic study findings into 6 types according to dyssynergic sphincter activities. Type 1-3 belonged to true DSD and the other types to pseudo-DSD. And we also analyzed their urodynamic parameters such as bladder capacity, compliance, detrusor leak point pressure, peak detrusor pressure (PdetQmax), post-void residual urine volume and electromyographic activity of the sphincter. Results About 16% (8 patients out of 48 patients) of non-neurogenic group and 86.7% (26 patients out of 30 patients) of cord injury group showed dyssynergic sphincter activity, respectively. There were significant differences in bladder capacity (t=2.537, p<0.05) and compliance (t=3.364, p<0.05) between true DSD patients and pseudo-DSD patients. There were significant difference in peak detrusor pressure at maximal urinary flow rate (t=2.489, p<0.05) between cord injured group and non-neurogenic group. There were no significant difference in other urodynamic parameters such as bladder capacity (t=1.844, p=0.099), compliance (t=0.727, p=0.477), DLPP (t=0.322, p=0.752), PVR (t=1.036, p=0.314) when compared dyssnergic sphincter activity patients in each two groups. Conclusion Detrusor-sphincter dysfunction was not infrequent in patients with non-neurogenic bladder. And those who have dyssynergic sphincter activity had higher bladder capacity and compliance tendency. Also, cord injury group had higher peak detrusor pressure at maximal urinary flow rate during voiding than that of non-neurogenic bladder group. Further study with more patients is necessary.

P 2
Correlation between Fiber Tractography and Clinical Status in Patients with Spinal Cord Injury
Kyung Cheon Seo1*
, Seong Jae Lee 1, Jung Keun Hyun
1,2, Tae Uk Kim
1, Seo Young Kim
1†
Department of Rehabilitation Medicine, Dankook University Hospital1, Department of Nanobiomedical Science & WCU Research
Center, Dankook University2, Institute of Tissue Regeneration Engineering (ITREN), Dankook University
3
Objective
To delineate the usefulness of diffusion tensor imaging (DTI) and tractography by analyzing correlation with the neurological and
functional status in patients with spinal cord injury (SCI)
Methods
We recruited 34 patients with spinal cord injury who performed diffusion tensor tractography initially. Imaginary fiber numbers at
each cervical level from C3 to C7 level and crossing fiber numbers from C3 to C5, C6, or C7 were calculated. Neurological status
including the International Standards for Neurological Classification of Spinal Cord Injury (ISNCSCI) and functional status including
Functional Independence Measurement (FIM), and Korean modified Barthel index (K-MBI) were reviewed at admission and after 4
weeks. We assessed the statistical correlation between fiber numbers and neurological and functional scores. Eight patients who
performed follow-up diffusion tensor tractography after cervical spine operation were also evaluated the statistical correlation
between the changes of fiber numbers and that of neurological and function recovery.
Results
The K-MBI score (p = 0.038) and self-care score of FIM (p = 0.046) were significantly associated with the crossing fiber numbers from
C3 to C6 at admission. Also, the K-MBI score (p = 0.044), transfer/locomotion of FIM (p = 0.014) and total FIM score (p = 0.046) were
also significantly associated with the crossing fiber numbers from C3 to C7 at admission. The changes of light touch sense score of
upper extremities (p = 0.029) was significantly associated with the imaginary fiber numbers at C4 level. The change of motor score
of Lt. upper extremity was significantly associated with the imaginary fiber numbers at the C7 level. (p = 0.024). All follow-up
imaginary fiber numbers and crossing fiber numbers were less than those at admission. However, there were strongly positive
correlations between the changes of the imaginary fiber numbers and the gain of transfer/locomotion score of FIM (p = 0.042, r =
0.829) and the changes of the crossing fiber numbers from C3 to C5 and gain of self-care score of FIM (p = 0.036, r = 0.841).
Conclusion
The imaginary fiber numbers at each cervical level and fiber numbers crossing the cervical lesion are associated with the
neurological and functional status. Although follow-up DTI did not well reflect the neurologic and functional status because of the
surgery, the changes in DTI data might help predict the prognosis of functional status.

P 3
Optimal Needle Placement for Electromyography of the Teres Minor Muscle: A Cadaveric Investigation.
Mee Gang Kim1*
, Eun Ah Hong2, Yong Seok Nam
2, Jong In Lee
1†
Department of Rehabilitation Medicine, Seoul St. Mary’s Hospital, College of Medicine, The Catholic University of Korea1,
Department of Anatomy, Institute for Applied Anatomy, College of Medicine, The Catholic University of Korea2
Introduction
The teres minor is one of the four boundaries of the quadrilateral space, and it functions as an external rotator of the shoulder.
The axillary nerve passes through the quadrilateral space and innervates to the deltoid and the teres minor. It is important to
accurately sample the teres minor for the diagnosis of axillary neuropathy by needle electromyography. However, as the teres
minor is relatively small in size and acts as an external rotator of the shoulder, it may be difficult to distinguish it from the
infraspinatus. The purpose of this study is to propose the optimal needle insertion point of the teres minor for needle
electromyography and to compare the accuracy with the conventional method.
Materials and methods
28 shoulders of 14 fresh cadavers were dissected. The relation of the muscle to nearby muscular and bony structures was
measured in the prone position with the shoulder abducted at 90 degrees. The length of the reference line from the acromion to
the inferior angle of the scapula (AA-IA) was measured (T). The reference line crossed the teres minor muscle, and the mean
distance from the acromion to the proximal (P) and the distal (D) crossing points were measured respectively. We hypothesized
the midpoint (X) of proximal and distal crossing points would be the optimal target point for needle insertion (Figure 1). We
calculated the mean proportion of X to T (X/T) and simplified it to propose a new target point. As the conventional method by
Perotto and Delagi suggested the upper one-third of AA-IA (1/3 T) was the target point of needle insertion in the teres minor, we
compared the probabilities that the new target point (simplified mean X/T) and the conventional target point (1/3 T) would be
inside the teres minor, between the proximal and distal crossing points.
Results
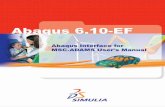
The mean T was 152.51mm. The mean P was 52.82mm, and the mean D was 88.42mm. The mean X was 70.62mm. The mean X/T
was 0.46, and we simplified the proportion to 0.5. We set a new target point of the teres minor as 1/2 T, and compared it to 1/3 T,
which was the conventional target point. The probability that 1/2 T would reside between P and D was 24 out of 28 (85.71%). In
the rest 4 shoulders, 1/2 T was distal than D, which is assumed to be inside the teres major or the latissimus dorsi. The probability
for 1/3 T was 11 out of 28 (39.29%). In the rest 17 shoulders, 1/3 T was more proximal than P, which is assumed to be inside the
infraspinatus or the deltoid (Table 1).
Discussion
We proposed a new target point of the teres minor (the midpoint of AA-IA) by dissecting and measuring cadaveric shoulders using
surface landmarks and compared the accuracy with the conventional needle insertion method by calculating measured values. The
accuracy of the new method seemed relatively high (85.71%), compared to that of the conventional method (39.29%). However,
further study to prove the accuracy by actual needle insertion will be needed.
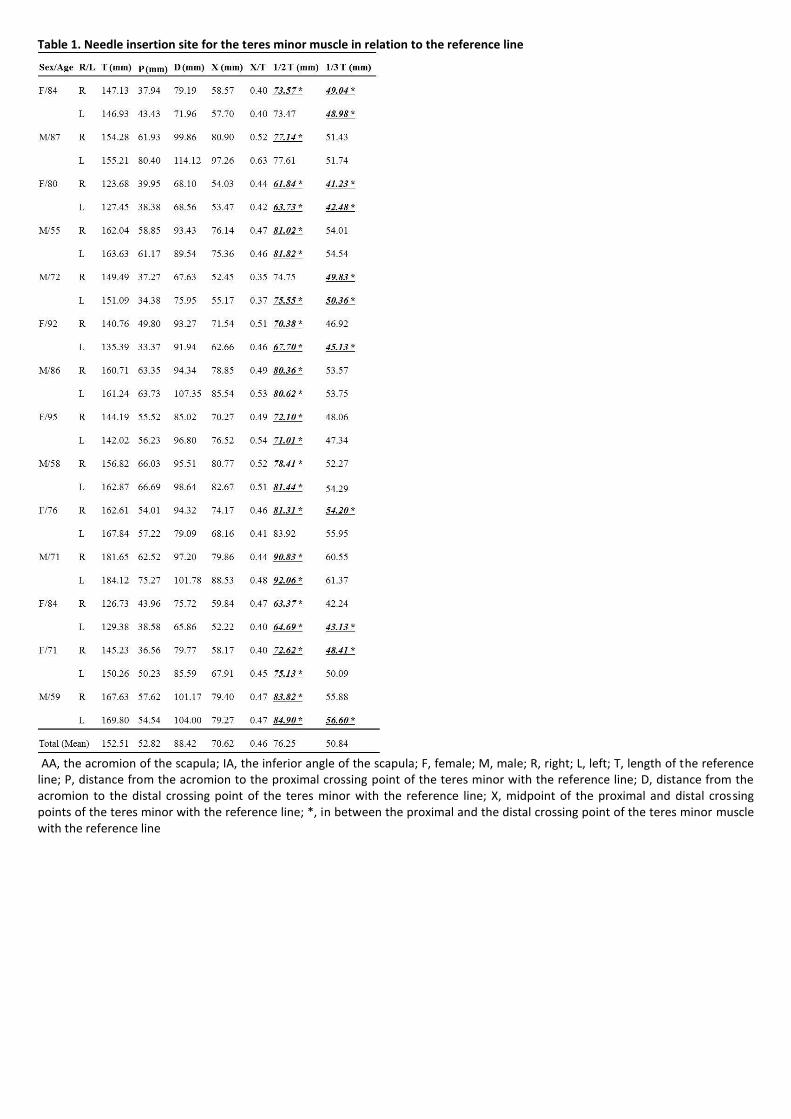
Table 1. Needle insertion site for the teres minor muscle in relation to the reference line
AA, the acromion of the scapula; IA, the inferior angle of the scapula; F, female; M, male; R, right; L, left; T, length of the reference line; P, distance from the acromion to the proximal crossing point of the teres minor with the reference line; D, distance from the acromion to the distal crossing point of the teres minor with the reference line; X, midpoint of the proximal and distal crossing points of the teres minor with the reference line; *, in between the proximal and the distal crossing point of the teres minor muscle with the reference line

Figure 1. Topographic anatomy of the teres minor in relation to the reference line AA, the acromion of the scapula; IA, the inferior angle of the scapula; T, length of the reference line from the acromion to the inferior angle of the scapula; P, distance from the acromion to the proximal crossing point of the teres minor with the reference line; D, distance from the acromion to the distal crossing point of the teres minor with the reference line; X, midpoint of the proximal and distal crossing points of the teres minor with the reference line; *, in between the proximal and the distal crossing point of the teres minor muscle with the reference line.

P 4
Tracheostomies in infants can hamper head control development
Hyun Iee Shin1*
, Hyung Ik Shin1†
Department of Rehabilitation Medicine, Seoul National University Hospital1
Background
It has been widely known that in normal developmental milestones, head control precedes rolling. However, infants with
tracheostomies may show different developmental process with different muscle activation process due to environmental factors.
Tracheostomy tube on the ventral side of neck and frequently with devices such as ventilators, infants with tracheostomies may
show different developing pattern, especially in head control.
Objective
By analyzing the scores of Gross Motor Function Measure (GMFM-88) in lying and rolling dimension of infants with tracheostomies,
and comparing them with control group of infants without tracheostomies, the authors attempt to evaluate the sequence of head
control and rolling in patients with tracheostomies.
Methods
The medical records and GMFM of infants who visited the division of Pediatric Rehabilitation between March, 2012 and February,
2018 were retrospectively reviewed. Finally, 21 patients with tracheostomies and 141 patients without tracheostomies were
extracted by matching gestational age and body weight at birth. Scores of GMFM, especially those of head control in prone and
rolling were compared. To evaluate relationships among each index, multinomial logistic regression analysis were performed.
<br>Results : Among many factors that affect development, the corrected age of patients when the test was performed and
necrotizing enterocolitis (NEC) were significantly different between groups (Table 1). GMFM scores of head control and in prone
were significantly different between two groups (Table 2). When multinomial logistic regression analysis was performed as head
control being dependent variable, the corrected age of patients when the test was performed, brain injury, and tracheostomy were
significantly important (p=0.05, p=0.011, p=0.027, respectively). Tracheostomy is found to be the significant influencing factor for
the development of head control in the study group. Moreover, 8 out of 29 patients in the study group, rolling preceded head
control. On the other hand, none in the control group had this sequence. (Figure 1)
Conclusion
Infants with tracheostomies have aberrant course of development, and are especially vulnerable to late head control. This finding
should help clinicians to establish rehabilitation plans for this patient group.

Table 1. Characteristics of participants.
Data are presented as n (%), except for gestational age, body weight, corrected age at GMFM, which are presented as mean standard deviation. p-values less than 0.05 are marked with asterisks*. GMFM; Gross Motor Function Measure, BPD; Bronchopulmonary Dysplasia, ROP; Retinopathy of Prematurity, NEC; Necrotizing Entero-Colitis. HIE; Hypoxic Ischemic Encephalopathy. Table 2. GMFM scores of subjects according to each function.
P-values less than 0.05 are marked with asterisks*. Data are presented as n (%)
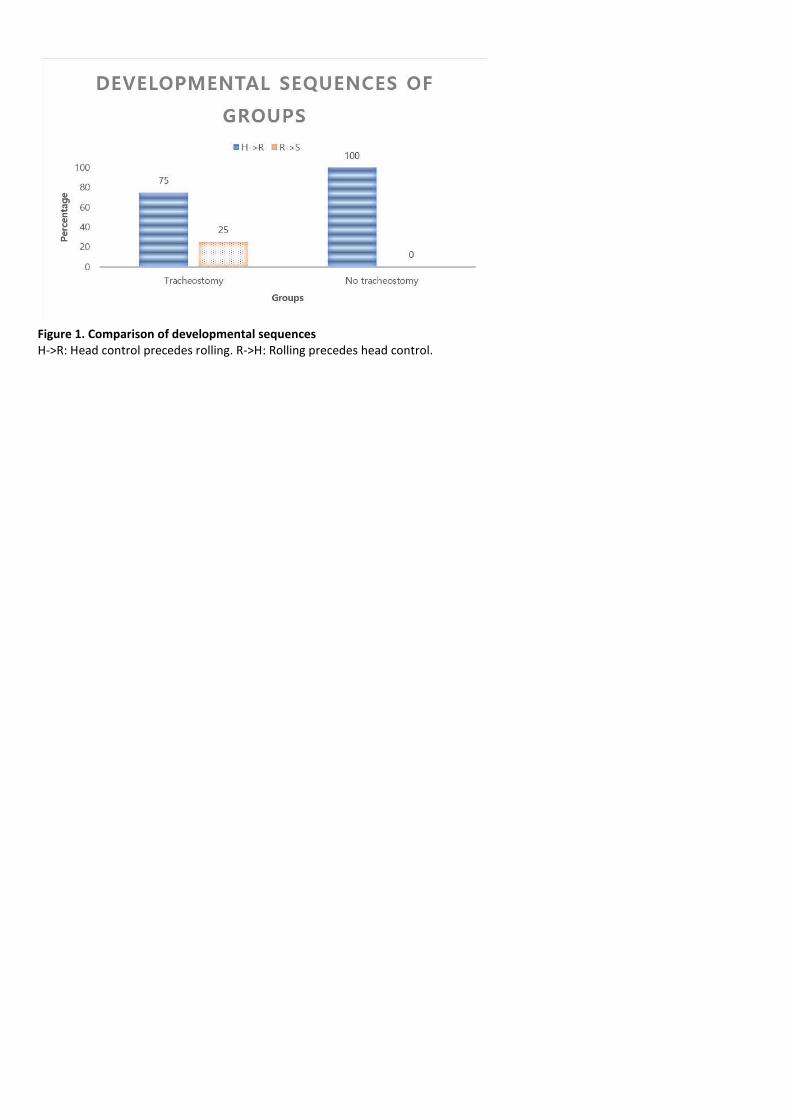
Figure 1. Comparison of developmental sequences H->R: Head control precedes rolling. R->H: Rolling precedes head control.

P 5
Safety and efficacy of platelet-rich plasma for the treatment of chronic plantar fasciitis
Jihye Park1*
, Hyun Mi Oh2, Yujung Seo
1, Young-Jin Ko
1†
Department of Rehabilitation Medicine,St. Paul Hospital, The Catholic University of Korea1, Department of Rehabilitation
Medicine,Incheon Hospital, Korea Workers’ Compensation and Welfare Service2, Department of Rehabilitation Medicine,National
Traffic Injury Rehabilitation Hospital3, Department of Rehabilitation Medicine,The Catholic University of Korea Seoul St. Mary`s
Hospital 4
Objectives
Plantar fasciitis (PF) is the most common cause of heel pain. The aim of this study was to evaluate the efficacy and safety of PRP for
patients who were resistant to conservative management of PF.
Methods
Fifty-five chronic plantar fasciitis patients nonresponding to conservative management were included. 33 patients received
ultrasound-guided 3ml autologous PRP injection and 22 patients received exercise education. All participants were encouraged to
exercise for plantar fascia. Clinical outcome were evaluated by AOFAS hindfoot score, a visual analogue scale (VAS), 5-likert scale at
3 and 6months, and plantar fascia thickness using ultrasonography at 6months. The primary outcome was AOFAS hindfoot score at
3 months. Statistical analysis was done using SPSS version 24.0 software.
Results
In baseline analysis of the patients in the two groups, there was no difference in age, gender, body mass index, duration of
symptoms, and location of symptoms between the two groups. But the AOFAS hindfoot score, VAS, 5-Likert scale and tendon
thickness were significantly different, indicating that the symptoms of patients in PRP group were severe (Table 1). In the primary
outcome, the AOFAS hindfoot score in the PRP group increased from 70.56 ± 10.04 to 82.26 ± 8.58 with statistically significant
improvement, while the score in the exercise group increased from 79.75 ± 8.8 to 82.25 ± 12.2 without statistical difference (Table
2). In the secondary outcome, there were significant improvement in VAS and 5-Likert scale at 3 months in both groups. At 6 months,
the AOFAS hindfoot score, VAS and 5-Likert scale were significantly improved in both groups compared with baseline. The thickness
of the plantar fascia was significantly decreased from 0.61 ± 0.82 cm to 0.40 ± 0.21 cm in the PRP group over 6 months. However,
the thickness of the exercise group decreased from 0.53 ± 0.09 to 0.51 ± 0.09 cm without significant difference. There was no
serious adverse events in both groups.
Conclusion
We concluded that autologous PRP injection is safe and has a long term effect for improving pain and function in chronic plantar
fasciitis. PRP injections can be recommended as a treatment option for patients with chronic recalcitrant plantar fasciitis.
Acknowledgment: This research was supported by the 'Conditional Approval System of Health Technology’ funded by the Ministry of
Health and Welfare.

Table 1. Baseline values of PRP and control groups (based on the patients who visited at 3 months)
Table 2. Clinical results of PRP and control groups at 3 months.

P 6
Biomechanical Influence of Spinal Stenosis on Knee Joint: Kinematic & EMG analysis
Jin Ju Kim1, Han Cho
1, Yulhyun Park
2, Hong Joong Jung
2, Min Yong Lee
3, Ju Seok Ryu
2*†
Department of Medicine,Seoul National University1, Department of Rehabilitation Medicine,Seoul National University Bundang
Hospital2, Department of Rehabilitation Medicine,Seoul National University Hospital
3
Objective
The objective of this study was to determine the effect of lumbar spinal stenosis (LSS) on gait pattern (stride width and femorotibial
angle) and hip abductor surface electromyography in varied stride widths of LSS patients compared with healthy individuals.
Design
Prospective experimental study
Participants
Seventeen LSS patients and 20 healthy individuals without LSS symptoms (numbness or tingling in the lower extremities) were
enrolled.
Interventions
Each participant completed three gait assessments in their usual, adducted, and abducted stride widths.
Main Outcome Measure(s)
Stride width during usual gait was evaluated using a force plate. The femorotibial angle (FTA) was measured by Bluetooth sensors
using elastic straps. Surface electromyography (sEMG) signals were obtained from the bilateral gluteus medius (GMe), tensor faciae
latae (TFL), and quadriceps femoris (QF) muscles. Visual analog scale (VAS) was used to quantify the degree of discomfort in the
gluteal area and medial side of the knee.
Results
The average stride width, normalized by height, was slightly higher in the LSS patients (4.11%) compared with the control group
(4.07%), but without statistical significance. The sEMG signals of LSS patients’ QF were significantly lower than those in the control
group during normal gait (P-value<0.001); when the hip abductors’ sEMG signals were normalized by QF, LSS patients showed
significantly higher activation ratios throughout all gait patterns (P-value<0.05). Generally, sEMG signals and ratios were significantly
higher during abducted gait compared with a normal gait. QF of the control group was the only exception, which significantly
decreased during abducted gait (P-value<0.05). FTA became closer to the varus in healthy individuals during abducted gait (P-
value<0.05). When FTA during normal gait was compared between the two groups, LSS patients exhibited FTA significantly closer to
the varus (P-value<0.05). VAS scores were higher in the patient group and during abducted gait (P-value<0.05).
Conclusion
Wider stride widths indicated increased relative activation of the hip abductors, closer proximity between FTA and varus, and
increased VAS scores for discomfort. The same tendency was observed in LSS patients compared with healthy individuals. Widening
of stride width in LSS patients despite abductor weakness suggests that additional muscle recruitment may be needed to maintain
balance. Furthermore, such distinctive gait pattern exerts increased loading on the medial knee, relating to the escalated risk of
degenerative knee osteoarthritis.
Acknowledgment: This research was supported by a grant of the Korea Health Technology R&D Project through the Korea Health
Industry Development Institute (KHIDI), funded by the Ministry of Health & Welfare, Republic of Korea (grant number : HI18C1169)

. These figures show the evaluation method. (A) Step width during normal gait. Step width was measured using the force plate (FreeStep). Participants were instructed to walk end-to-end for 4 times. The first 2 trials were regarded as familiarization trials and the outcomes from the last 2 trials were obtained for step width analysis. (B) Three gait patterns. First, the participants were instructed to walk in their normal pace (“Normal gait”). Then, they were asked to walk with their medial boarders of feet touching each other (“Adduction gait”). Finally, they were told to walk with their feet approximately 40cm apart (“Abduction gait”). (C) Surface electromyography (sEMG) analysis. sEMG was measured using BTS FREEEMG 1000 with EMG-BTS EMG-Analyzer®. (D) Gait analysis in coronal plane. The femorotibial angle (FTA) was measured using Human Track® (Gait & Motion Analysis System).

. This figure shows the results of Femorotibial angle (FTA). The FTA was changed to varus angle during abducted gait in the both groups (p<.05 only in control). During normal gait, LSS group’ FTA was significantly closer to varus than the control group (p<.05). (Right)
These figures show the results of sEMG analysis of gluteus medius, tensor fasciae and latae and quadriceps femoris muscles. (A) RMS of gluteus medius and tensor fasciae latae were significantly increased during abducted gait than the normal gait. However, in case of QF, the control group showed a decrease in amplitude while LSS group showed an increase (p-value < .05). (B) The peak values are consistent to the results of the RMS.

P 7
Long-term outcome of Extracorporeal Shock Wave Therapy for Painful Plantar Fibromatosis
Jin Tae Hwang1*
, Kyung Jae Yoon1, Jong Geol Do
1, Kun Woo Kim
1, Jae Hyeoung Choi
1, Yong Taek Lee
1†
Department of Rehabilitation Medicine, Kangbuk Samsung Medical Center1
Introduction
Plantar fibromatosis is uncommon proliferative disease in plantar fascia that is often associated with palmar and penile fibromatosis.
Symptoms include the pain, tenderness and palpable lump in the foot sole, which can lead to walking disability. Previous studies
have shown that extracorporeal shock wave therapy (ESWT), which is commonly used as an effective therapeutic option for chronic
plantar fasciitis, can be also applied therapeutically to various forms of fibromatosis such as palmar and penile fibromatosis. The
purpose of this study is to evaluate the long-term therapeutic effect of ESWT in plantar fibromatosis and to compare its result with
plantar fasciitis.
Methods and Materials
Medical charts of 170 patients (198 feet) with plantar fibromatosis or plantar fasciitis confirmed by ultrasonography (US) were
reviewed. Subsequently, total 84 feet (16 feet for plantar fibromatosis; 68 feet for plantar fasciitis) who underwent ESWT for lasting
pain more than 3 months and “Poor” or “Fair” grade in Roles-Maudsley score (RMS) despite the conventional conservative
treatment were included. A maximum of 12 sessions of ESWT (0.10-0.14 mJ/mm2; 900 shocks, weekly) was conducted until the RMS
reached “Good” or “Excellent” grade. Numeric rating sacle (NRS) and RMS were evaluated at short-term follow-up (one week after
all ESWT sessions) and long-term follow-up (mean 35 months after ESWT). In plantar fibromatosis group, follow-up US was
conducted at long-term follow up. A more than 50% reduction in the NRS and “good” or “excellent” in RMS were regarded as
treatment success.
Results
Repeated measures ANOVA demonstrated that NRS and RMS point improved with time after ESWT up to long-term follow-up (time
effect, p<.001). On the other hand, the group interaction was not significant, which means there was no significant difference of the
therapeutic effect for pain reduction and functional improvement between two groups (p=0.828 for NRS; 0.923 for RMS). The
success rate was 68.8% (11 feet) at short-term and long-term follow-up in the plantar fibromatosis group, and 63.2% (43 feet) at
short-term follow-up and 75% (51 feet) at long-term follow-up in plantar fasciitis group. In long-term follow-up US, mean thickness
of fibromas was significantly reduced from 4.1±1.2 mm to 2.8±1.2 mm while there was no significant change in mean length
(12.9±4.7 mm; 12.7±4.7 mm) and width (8.9±4.0 mm; 8.4±3.4 mm).
Conclusion
Low-energy ESWT appears to have a long-term effect for subjective pain and performance in the plantar fibromatosis equivalent to
plantar fasciitis. In terms of morphologic change of fibroma, long-term follow-up US showed no definite change except the
reduction of thickness.

Fig 1. Flow chart of the study
Fig 2. Outcomes of subjective pain and function (NRS and RMS)
Fig 3. Morphologic change of fibroma (length, width and thickness)

P 8
Spinal stabilization exercise with Direct Vibration in patients with non-specific chronic low back
Soo Hoon Yoon1*
, Sang Heon Lee1, Nack Hwan Kim
1†
Department of Rehabilitation Medicine, Korea University Anam Hospital1
Introduction
Spinal stabilization exercise has become a well-known therapeutic modality commonly used in clinical practice. Various studies
assessing long-term outcomes showed that stabilization exercise as a single or combined modality could improve pain intensity and
disability and prevent recurrent episodes of chronic low back pain (CLBP). Physical exercise through vibration application was
previously studied based on the reflex modification mechanism by improving neural adaptation. However, no studies have reported
on clinical trials of the spinal stabilization with direct vibration application to the paraspinal muscles. This study investigated the
clinical effect of localized and direct vibration to the trunk muscles during spinal stabilization exercise in patients with non-specific
CLBP.
Methods
Design: A pilot randomized controlled trial. Setting: Outpatient clinic. Participants: Sixty-two participants with non-specific CLBP
were randomly assigned to two groups: conventional stabilization exercise (CSE) or vibration stabilization exercise (VSE).
Interventions: The groups performed 12 sessions of the spinal stability exercise program over 4 weeks. Objective outcome measures:
Trunk muscle thickness and activity were determined of the following muscles using ultrasonography and surface electromyography
(sEMG), respectively: transverse abdominis (TrA), external oblique (EO), internal oblique (IO), rectus abdominis (RA), lumbar
multifidus (LM), and lumbar erector spinae (LES). Each Ultrasound and sEMG were perfomed at T0 and T1. Subjective outcome
measures: Pain intensity was measured using a VAS. CLBP related functional disability was evaluated using the Oswestry Disability
Index (ODI). Pain and disability were assessed at T0, T1, and T2.
Results
The ultrasonographic examination revealed the increased ratio of the muscle thickness to the muscle contraction and relaxation
after the training of the TrA and LM muscles in the CSE group and the TrA, LM, and IO muscles in the VSE group. The sEMG
evaluation resulted in statistical increases in the post-treatment activities of the EO, IO, and LM muscles in the CSE and the TrA, IO,
and LM muscles in the VSE group. The ratio of muscle activity also revealed statistical increases: the IO/RA ratio in the CSE group
and the IO/RA, TrA/RA, and LM/LES ratios in the VSE group. After the exercise, the VAS and ODI showed statistically significant
clinical improvement in both groups that were maintained after 8 weeks. There were no significant intergroup differences.
Conclusions
Simultaneously with the voluntary contraction of the trunk muscles, direct vibration can be used as an adjunct to enhance the effect
25 of core stabilization exercises in patients with non-specific CLBP.

Flow chart showing subject recruitment and randomization. CLBP: chronic low backpain; CSE: conventional stabilization exercise; VSE: vibration stabilization exercise; VAS: visual analog scale; ODI: Oswestry Disability Index; sEMG: surface electromyography.
Spinal stabilization exercise program consisted of five different exercises: upper-body extension (A), alternate arm and leg lift (B), alternate arm and leg extension (C), diagonal curl up (D), and curl-up (E).
The conceptual design (A) and actual picture (B) of the applied vibration device.

P 9
Long-term outcome of high intensity interval training in patients with acute myocardial infarction.
Geon Sang Lee1*
, Soo-Hyun Soh1, Ji Hee Kim
1†
Department of Rehabilitation Medicine, Wonkwang University, School of Medicine1
Objective
To compare the effect of high intensity interval training (HIIT) and moderate continuous training (MCT) in patients with acute
myocardial infarction (AMI) after 1 year.
Method
This study was designed as a retrospective study. A total of 28 participants who experienced AMI were recruited from March 2014.
Among them, 14 subjects performed HIIT, and 14 subjects performed MCT. Both groups conducted cardiac rehabilitation (CR)
exercise training for 6 to 8 weeks. Exercise tolerance test was executed to compare the effects of CR, and outcome measures were
evaluated at the baseline (T0), 3 months after the baseline (T1), and 1 year after the baseline (T2).
Result
After CR, various parameters including resting heart rate (HRrest), peak metabolic equivalent (METpeak), peak oxygen uptake
(VO2peak) were significantly improved over time in both group. VO2peak significantly improved from 24.20±5.03ml/kg/min at
baseline to 28.90±3.54ml/kg/min at T1 (p=0.03), and 30.64±5.96ml/kg/min at T2 (p=0.001) in the HIIT group. Also, VO2peak
significantly improved from 26.66±3.90ml/kg/min at baseline to 29.89±4.49ml/kg/min at T1 (p=0.035), and 28.41±3.10ml/kg/min at
T2 (p=0.003) in the MCT group. And there was significant time and group interaction effect on VO2peak (F2, 33=8.167, p=0.008).
Conclusion
Aerobic capacity improved after HIIT and MCT, and the effect sustained after 1 year. However, HIIT increased cardiorespiratory
fitness more effectively than MCT. Therefore, HIIT is recommended for cardiac rehabilitation in patients with acute myocardial
infarction.

P 10
Predictive Factors of Deep Vein Thrombosis in Gynecologic Cancer Survivors
Jong Hyuk Choi1, Seunghun Park
1, Jung Joong Kang
1, Dong Kyu Kim
1†, Tae Hee Kim
1, Jungin Kim
1*
Departments of Rehabilitation Medicine, School of Medicine, Konkuk University1
Objective
To examine predictive factors of the deep vein thrombosis (DVT) and to propose an algorithm-based approach in making a
differential diagnosis of the lower extremity edema (LEE) from lymphedema in gynecologic cancer survivors.
Methods
In this single-center, retrospective study, a total of 63 eligible patients include 16 patients with DVT and 47 without DVT. They were
therefore divided into two groups: the DVT group (n=16) and the non-DVT group (n=47). Then, baseline and clinical characteristics
of the patients were compared between the two groups.
Results
By the location of the DVT, there were five cases in the iliac vein, four cases in the femoral vein, three cases in the popliteal vein,
three cases in the peroneal vein and one case in the inferior vena cava. In our series, the incidence of DVT had no significant
correlation with the treatment modalities and co-morbidities. In addition, there were no significant differences in the circumference
of the lower extremity, regional lymph node involvement and D-dimer levels between the two groups. But the distal organ
metastasis and advanced-stage cancer were significantly more prevalent in the DVT group as compared with the non-DVT group
(56.8% vs. 32.9%, p=0.03 and (62.33% vs. 36.3%, p=0.01, respectively).
Conclusion
In conclusion, our results indicate that it is necessary to consider the possibility of LEE arising from DVT in gynecologic cancer
survivors with advanced-stage cancer as well as distant organ metastasis.
Table 1. Baseline characteristics of the patients

Table 2. Patient characteristics in each group.
Table 3. Predictive factors of the deep vein thrombosis
.

P 11
Effect of EMG biofeedback-based mobile game for upper limb rehabilitation in stroke patients
Hyoseon Choi1, Joon Woo Kim
1*, Seung Eui Lim
2, Hyunmi Lim
2, Jeonghun Ku
2, Youn Joo Kang
1†
Department of Rehabilitation Medicine,Eulji Hospital, Eulji University1, Department of Biomedical Engineering,College of medicine,
Keimyung University2
Introduction
Electromyographic (EMG) biofeedback induces the motions necessary for rehabilitation through the feedback of the EMG signal.
However, the rehabilitation program using EMG biofeedback has limitations in utilizing and attracting the interest of stroke patients.
Therefore, a new EMG biofeedback rehabilitation program is needed, which is more therapeutically accessible and increases
patient's interest and participation. The purpose of this study was to investigate the effects of a new rehabilitative program,
integrating a mobile game and a wearable device based on EMG biofeedback and motion sensing, on the recovery of upper limb
function in stroke patients.
Methods
The mobile game was designed to enable rehabilitative training through games reflective of flexion, extension, abduction, and
adduction identified by motion sensors along with grasping motions recognized by EMG signals measured by the wearable device.
Twenty-two participants with upper extremity motor impairment within 3months after stroke were included in this study.
Participants were randomized to either the intervention group or the control group. The intervention group (n=12) received 30 min
of conventional occupational therapy (OT) and 30 min of the EMG biofeedback-based mobile game training. The control group
(n=10) received conventional OT alone for 1 h per day. Rehabilitation consisted of 10 sessions of therapy, 5 days per week, for 2
weeks. The outcome measures were Manual Function Test (MFT), Fugl−Meyer Assessment (FMA), Box and block test (BBT), Manual
Muscle Testing (MMT), and modifed Barthel index (MBI). Participants were assessed before treatment (pre), after 2 weeks of
treatment (post), and at 1 month (2 weeks after the end of treatment, 1mo). Statistical analysis was performed using independent
sample t-tests and repeated measures ANOVA.
Results
The baseline characteristics showed no significant differences between the two groups. Both groups showed significant within-
group improvement in the MFT, BBT, MMT and MBI after treatment and at 1month (p<0.05). The FMA scores increased significantly
in the intervention group after treatment and at 1month (p<0.05), but not in the control group. There was a significant interaction
effect in MFT (p<0.05), but not in other measures. Changes in the MFT (pre vs. 1 mo and post vs. 1 mo) were significantly greater in
the intervention group than in the control group (p<0.05).
Conclusion
This EMG biofeedback-based mobile game was more effective in improving upper limb function than the conventional OT in the
stroke patients. This game appears to be feasible and can be used as an alternative to standard rehabilitation.
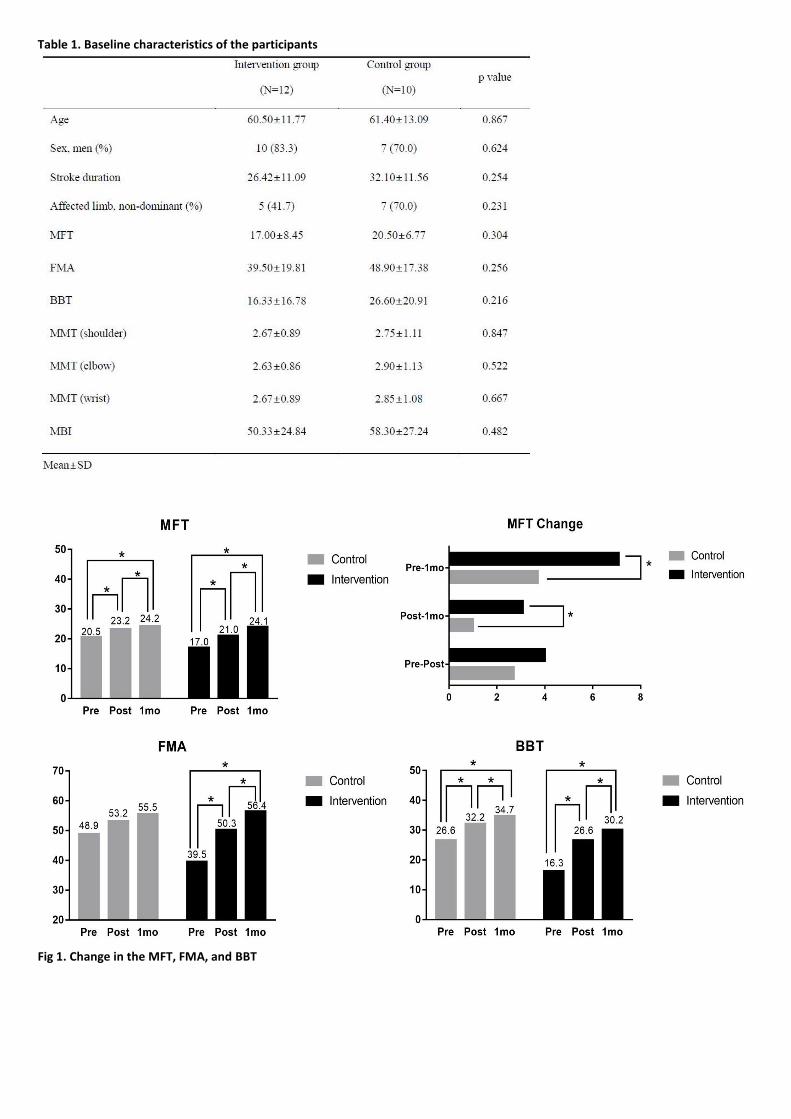
Table 1. Baseline characteristics of the participants
Fig 1. Change in the MFT, FMA, and BBT

Fig 2. Change in the MMT (shoulder, elbow, wrist) and MBI

P 12
Near-Infrared Spectroscopy during Complex Cognitive Function Tasks in Mild Cognitive Impairment
Da Hwi Jung1*
, Ra Yu Yun1, In Joo Kong
2, JongKwan Choi
2, Ji Yeong Baek
3, Eun Joo Kim
4, Yong-Il Shin
5, Myoug-Hwan Ko
1, Yong Beom
Shin1, Myung Jun Shin
1, Jin A Yoon
1†
Department of Rehabilitation Medicine,Pusan National University Hospital1, Inc.,OBELAB
2, Department of Neurology,Pusan
National University Hospital3, Department of Rehabilitation Medicine,Pusan National University Yangsan Hospital
4, Department of
Physical Medicine and Rehabilitation,Chonbuk National University Hospital5
Objective
The present pilot study aimed to conduct a comparative analysis of the level of activation in the prefrontal cortex among a normal
elderly group and amnestic and non-amnestic mild cognitive impairment (MCI) groups, and investigate the presence of neural
compensatory mechanisms according to types of MCI and different cognitive tasks.
Method
We performed functional near-infrared spectroscopy (fNIRS) along with cognitive tasks, including two-back test, Korean color word
Stroop test and semantic verbal fluency task (SVFT), to investigate hemodynamic response and the presence of neural
compensation and neuroplasticity in the prefrontal cortex of patients with amnestic and non-amnestic MCI compared with a healthy
elderly group. (Fig. 1, 2)
Result
During two back test, there was showed no significant difference in bilateral region-of interest analysis (ROI) in three groups. (Fig. 3)
During Stroop test, right sided hyperactivation compared to the left side during task was shown in non-amnestic MCI and normal
group with statistical significance. (Fig. 4) Mean acc∆〖 HbO〗 _2 on the right side was highest in non-amnestic MCI group (0.30 uM)
followed by normal group (0.07 uM) and amnestic MCI group (-0.10 uM). Otherwise, inter group ROI analysis of acc∆〖 HbO〗 _2 in
these activated right sides showed no significant difference. During VFT test, there was showed no significant difference in bilateral
region-of interest analysis in three groups. The highest mean acc∆〖 HbO〗 _2 was showed in normal group (0.79 uM) followed by
non-amnestic MCI group (0.52 uM) and amnestic MCI group (0.21 uM). Otherwise, there was no significant difference between
groups. (Fig. 5)
Discussion
Although the neuroplasticity of the right prefrontal cortex in MCI has been described earlier, this is the first study to compare its
effect between amnestic and non-amnestic MCI groups preforming various cognitive tasks. According to the results of our study, the
neuroplasticity of the right prefrontal cortex during Stroop test was preserved only in the non-amnestic MCI group. First, Stroop test
might be a sensitive tool to evaluate cognition flexibility impairment, which has shown strong relationship with episodic memory in
a previous study. Our finding of hypoactivation in the amnestic MCI group and compensatory hyperactivation in the non-amnestic
MCI group on the right prefrontal cortex can be explained with this approach. The cognitive flexibility impairment could sufficiently
be compensated for in the non-amnestic MCI group but not in the amnestic MCI group. Stroop test could be used for evaluating
cognitive control and preservation of neural compensatory mechanisms in MCI.
Conclusion
The hemodynamic response during fNIRS showed different findings according to MCI types and cognitive tasks. Among the three
tasks, Stroop test showed results that were suggestive of neural compensatory mechanisms in the prefrontal cortex in non-amnestic
MCI.

Figure 1. Cognitive task protocol used for the NIRSIT system. K-CWST, Korean color word Stroop test; SVFT, semantic verbal fluency task
Figure 2. Arrangement of sources and detectors, and location of region of interest channels

Figure 3. Activation map during two-back test in three groups showing no significant difference between groups. MCI, mild cognitive impairment

P 13
Insufficient physical activity after stroke and its association with mortality and recurrence
Seong-Min Kang1*
, Sun-Hyung Kim1, Kyung-Do Han
2, Nam-Jong Paik
1, Won-Seok Kim
1†
Department of Rehabilitation Medicine,Seoul National University Bundang Hospital1, Department of Biostatistics,The Catholic
University of Korea College of Medicine2
Background and Purpose
Sufficient physical activity (PA) is highly recommended for better prognosis after stroke. But there have been few studies on changes
in physical activity level before and after stroke, and its association with post-stroke hard outcomes, especially stroke recurrence.
The purpose of this study is to identify the changes in physical activity level before and after ischemic stroke, and to find out their
associations with adverse outcomes including mortality, myocardial infarction (MI), and stroke recurrence.
Methods
This observational retrospective cohort study was performed on the basis of the Nationwide Health Insurance Service (NHIS)
database in South Korea. A total number of 55,759 subjects between the ages of 20 to 80, who had an ischemic stroke from 2010 to
2013 were included. Ischemic stroke was confirmed by the ICD code I63 or I64 with hospitalization and claim for computed
tomography (CT) or magnetic resonance imaging (MRI). Subjects who got disability grading from 1 to 3 (who could not walk) were
excluded. Subjects were divided into subgroups according to PA level (sufficient vs. insufficient) before and after stroke using
questionnaire responses during the health check-up. Hard outcomes including mortality, MI (ICD code I21) and stroke recurrence
(re-admission for ICD code I63 or I64 and claim for CT or MRI) were collected after stroke. Multivariate Cox proportional regression
analysis was performed to identify the benefit for sufficient PA to reduce the adverse outcomes after ischemic stroke, with adjusting
for possible confounders.
Results
Of the 55,759 subjects with ischemic stroke, only 22,737 (40.8%) participated in sufficient PA after stroke. Among subjects who
showed insufficient PA (n=32,591), only 10,159 (31.2%) changed their PA to sufficient level after stroke. Forty-five percent of
subjects became inactive after stroke among subjects who showed sufficient PA level (n=23,168) before stroke. Subjects who
changed their PA level from insufficient to sufficient level after stroke showed lower risk of adverse hard outcomes (mortality:
HR=0.659 (95% CI: 0.597-0.727), MI: HR=0.897 (95% CI: 0.763-1.055), stroke recurrence: HR=0.820 (95% CI: 0.751-0.895)) than those
who maintained insufficient PA level. Subjects who maintained sufficient PA level after stroke showed significantly lowest risk for all
adverse hard outcomes (mortality: HR=0.571 (95% CI: 0.513-0.634), MI: HR=0.643 (95% CI: 0.537-0.711), stroke recurrence:
HR=0.691 (95% CI: 0.631-0.757) than those who maintained insufficient PA level after stroke.
Conclusion
Achieving sufficient PA level after ischemic stroke reduces adverse major events including mortality, MI and stroke recurrence.
However, even in patients with ischemic stroke who might walk, changing to or maintaining sufficient PA level are difficult.
Systematic rehabilitation strategies to improve the PA level after mild to moderate ischemic stroke is urgently required.

P 14
Clinometric Gait Analysis Using Smart Insoles in Post Stroke Hemiplegia
Ra Yu Yun1*
, Myung Hun Jang1, Min-seok Seo
2, Myung Jun Shin
1†
Department of Rehabilitation Medicine, Pusan National University Hospital1, Biomedical Research Institute,Pusan National
University Hospital2
Background
For effective rehabilitation after stroke, it is essential to conduct an objective assessment of the patient’s functional status. Several
stroke severity scales have been used for this purpose, but such scales have various limitations. Gait analysis using Smart Insole
technology can be applied continuously, objectively and quantitatively, thereby overcoming the shortcomings of other assessment
tools.
Methods
To confirm the reliability of gait analysis using Smart Insole technology, normal healthy controls wore insoles in their shoes during
the timed up-and-go (TUG) test. (Fig. 1) The gait parameters were compared with the manually collected data. To determine the gait
characteristics of patients with hemiplegia due to stroke, they were asked to wear insoles and take the TUG test: gait parameters
were calculated and compared with those of control subjects. To investigate whether the gait analysis accurately reflected the
patients’ clinical condition, we analyzed the relationships of 22 gait parameters on four stroke severity scales.
Results
The Smart Insole gait parameter data were similar to those calculated manually. Among the 22 gait parameters tested, 14 were
significantly effective at distinguishing patients from healthy controls. The Smart Insole data revealed that the stance duration on
both sides was longer in patients than controls, which has proven difficult to show using other methods. Furthermore, the
unaffected side in patients showed a markedly longer stance duration. Regarding swing duration, that of the unaffected side was
shorter in patients than controls, whereas that of the affected side was longer. (Fig. 2, 3) We identified 10 significantly correlated
gait parameters on the stroke severity scales. Notably, the difference in stance duration between the right and left sides (%) was
significantly correlated with the Fugl-Meyer Assessment (FMA) lower extremity score. (Fig. 4)
Conclusions
This study confirmed the feasibility and applicability of the Smart Insole as a device to assess the gait of patients with hemiplegia
due to stroke. In addition, we demonstrated that the FMA score was significantly correlated with the Smart Insole data. Further
studies are required to assess the clinical effectiveness of the Smart Insole for rehabilitation and long-term monitoring of patients
with hemiplegia due to stroke.

Figure 1. Dividing swing / stance phase 1) The swing phase corresponded to a sum of pressure sensor value of 0, while the stance was represented by non-zero values. 2) If both sides are in Stance state, it is treated as double support. If only one side is in stance state, it is treated as single support.
Figure 2. Swing and stance duration distribution of affected and sound side 1) The patients showed a shorter swing duration on the sound side than the control subjects, whereas that on the affected side was longer. 2) While the patients showed a longer stance duration on both sides compared to the control subjects, the sound side showed a markedly longer duration.
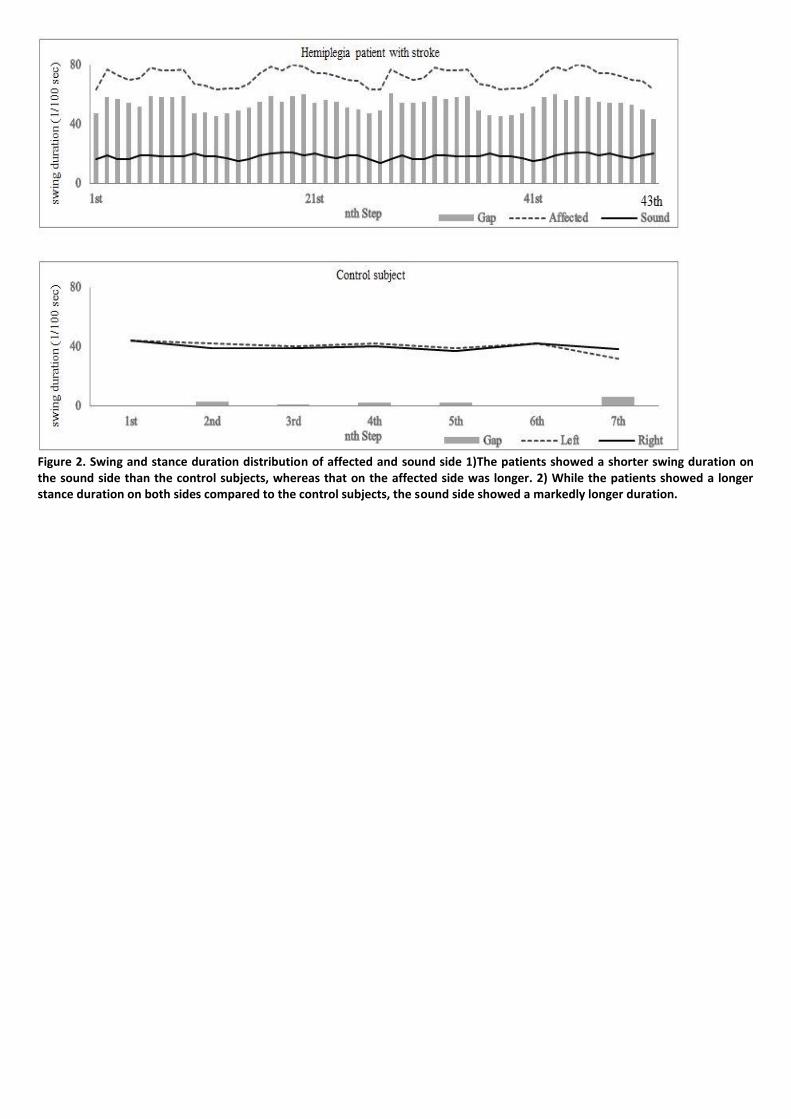
Figure 2. Swing and stance duration distribution of affected and sound side 1)The patients showed a shorter swing duration on the sound side than the control subjects, whereas that on the affected side was longer. 2) While the patients showed a longer stance duration on both sides compared to the control subjects, the sound side showed a markedly longer duration.
P 15
Predictability of AF and ILF on Language Recovery in Aphasia after Stroke
Jun Soo Noh1*
, Yoonhye Na3, Sekwang Lee
3, Minjae Cho
3, Yu Mi Hwang
2, Woo-Suk Tae
2, Sung-Bom Pyun
1,2†
Department of Physical Medicine and Rehabilitation, Korea University College of Medicine1, Brain convergence research
center,Korea University2, Department of Biomedical Sciences,Korea University
3
Objectives
This study aims to investigate the predictability of 6-month language function in patients with aphasia (PWA) using parameters of
diffusion tensor tractography (DTT) of arcuate fasciculus (AF) and inferior longitudinal fasciculus (ILF) utilizing machine learning
classification.
Methods
We collected data of PWA after stroke from the hospital. Thirty-five stroke patients were included for analysis who had 1) left
hemispheric stroke, 2) performed diffusion tensor image (DTI), 3) evaluated language function after onset and 6 months poststroke
using Korean version of western aphasia battery (K-WAB). We classified the language outcome at 6 months of PWA either favorable
or poor recovery using three cutoff values of aphasia quotient (AQ); 1) 61.6 points (50 percentile), 2) 75.0 points (3rd quartile), 3)
80.3 points (cutoff value of normal in K-WAB). AF and ILF was reconstructed by DTIstudio and ratio of fractional anisotropy (FA)
between two hemispheres (DTT index) was calculated in two tracts. Group classification was conducted with machine learning
method and the input value of initial FA of AF and ILF separately or both tracts utilizing support vector machine (SVM) algorithm.
And the results were compared with the clinical classification based on three cutoff values.
Results
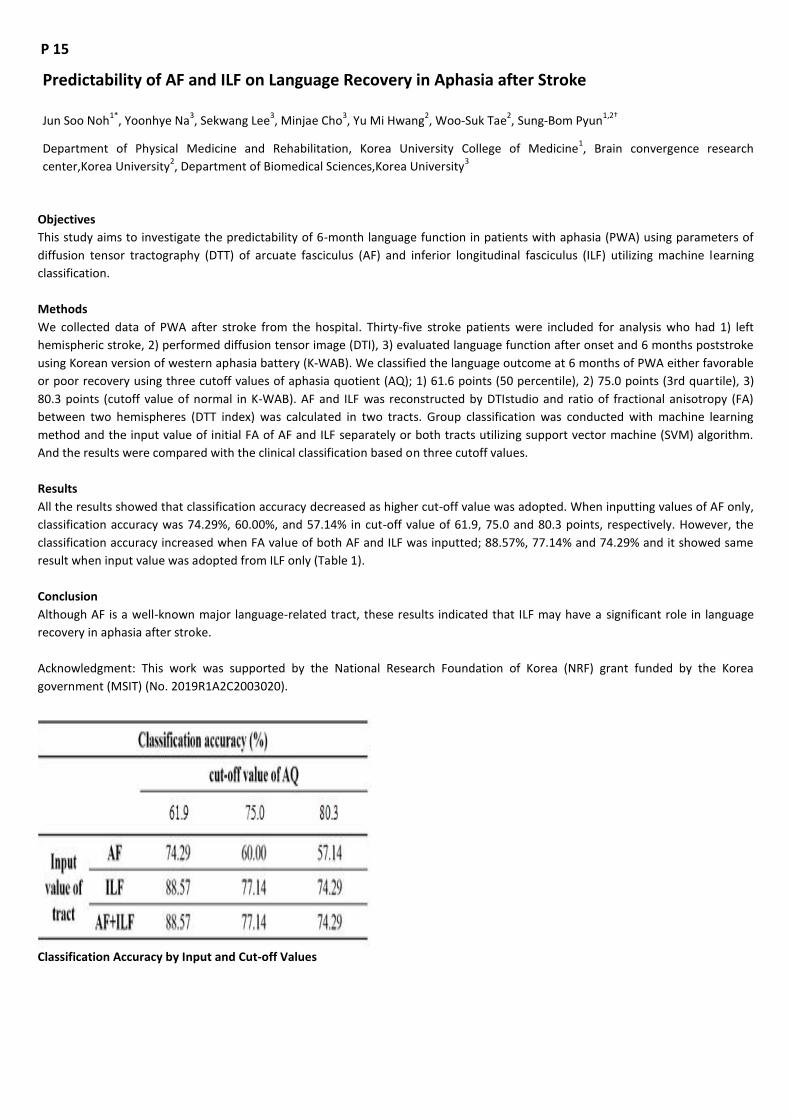
All the results showed that classification accuracy decreased as higher cut-off value was adopted. When inputting values of AF only,
classification accuracy was 74.29%, 60.00%, and 57.14% in cut-off value of 61.9, 75.0 and 80.3 points, respectively. However, the
classification accuracy increased when FA value of both AF and ILF was inputted; 88.57%, 77.14% and 74.29% and it showed same
result when input value was adopted from ILF only (Table 1).
Conclusion
Although AF is a well-known major language-related tract, these results indicated that ILF may have a significant role in language
recovery in aphasia after stroke.
Acknowledgment: This work was supported by the National Research Foundation of Korea (NRF) grant funded by the Korea
government (MSIT) (No. 2019R1A2C2003020).
Classification Accuracy by Input and Cut-off Values

P 16
Factors associated with improvement or decline in cognitive function after hemorrhagic stroke
Ji Hong Min1*
, Ju Hyun Son1, Deog Young Kim
2, Min Kyun Sohn
3, Jongmin Lee
4, Sam-Gyu Lee
5, Yang-Soo Lee
6, Eun Young Han
7, Min
Cheol Joo8, Gyung-Jae Oh
8, Junhee Han
9, Won Hyuk Chang
10, Yun-Hee Kim
10, Yong-Il Shin
1†
Department of Rehabilitation Medicine,Pusan National University Yangsan Hospital1, Department of Rehabilitation
Medicine,Severance Hospital2, Department of Rehabilitation Medicine,Chonnam National University Hospital
3, Department of
Rehabilitation Medicine,Konkuk University Medical Center4, Department of Rehabilitation Medicine,Chonnam National University
Hospital5, Department of Rehabilitation Medicine,Kyungpook National University Hospital
6, Department of Rehabilitation
Medicine,Jeju National University Hospital7, Department of Rehabilitation Medicine,Wonkwang University School of Medicine &
Hospital8, Department of Statistics,Hallym University
9, Department of Rehabilitation Medicine,Samsung Medical Center
10
Objective
To identify the prevalence of delayed cognitive impairment; patients progress to either converter, stable, or reverter group after
hemorrhagic stroke and clinical and demographic factors associated with improvement or decline in cognitive function between 3
months and 12 months after hemorrhagic stroke.
Methods
We analyzed the cognitive assessments of total patients and patients older than 65 years separately. All patients with an
hemorrhagic stroke were divided into normal cognitive group (NCG) and impaired cognition group (ICG) by using a cutoff score on
the Korean Mini-Mental State Examination (K-MMSE). Patients were additionally classified into 3 subgroups according to the
changes in their K-MMSE scores between 3 and 12 months: Stable group with K-MMSE scores changes ranging from −2 to +2 points
(−2 ≤ △MMSE ≤ +2); converter group with increase more than 3 points (3 ≤ △MMSE); and reverter group with decrease more than
3 points (−3 ≤ △MMSE). We also analyzed factors affecting cognitive change from 3 months to 12 months among the 3 groups
including baseline medical record, stroke and treatment characteristics, and various functional assessments after 3 months.
Results
This study included 603 patients with the first time hemorrhagic stroke. Among these patients, 446 (74.0%) were classified as NCG,
while 157 patients (26.0%) were belonged to the ICG at 3 month. Within the NCG, 372 patients (82.4%) were stable group, 26
patients (5.4%) were converter group, and 48 patients (12.2%) were reverter group at 12 months onset. Within the ICG group, 66
patients (53.0%) were stable group, 64 patients (36.1%) were converter group, and 27 patients (10.9%) were reverter group. When
different factors were investigated, the three subgroups in NCG and ICG showed a few different factors affecting cognitive function
from 3 to 12 month.
Conclusions
The prevalence of cognitive impairment showed little difference between 3 and 12 months after hemorrhagic stroke. By
investigating the influencing factors from each group, the factors associated improvement or decline in cognitive function after
hemorrhagic stroke were the age and sex factor in ICG of older patients, and the history of coronary heart disease and early GCS
scores in ICG of total patients.

P 17
Lumbar paraspinal muscle morphometry in patients with hemiplegia
Wookyung Park1*
, Geonho Yoon1, Mi Ri Suh
1,2, Jong Moon Kim
1,2, MinYoung Kim
1,2, Kyunghoon Min
1,2†
CHA University School of Medicine, Department of Rehabilitation Medicine,CHA Bundang Medical Center1, Rehabilitation and
Regeneration Research Center,CHA University2
Objective
Patients with hemiplegia usually have impaired trunk control. Trunk balance influences the selective movements of upper and lower
limbs. Loss of trunk control results in a negative influence on the posture and functional activities. Spinal muscles are considered to
be one of the spinal stabilizing systems with neural control unit and spinal column. Although the causal link between lumbar muscle
morphology and low back pain is not clear, there are several studies on paraspinal muscle morphology in patients with low back
pain (LBP). Paraspinal muscles are significantly smaller in patients with chronic LBP. In stroke, there are several changes in the
muscles, such as decreased muscle mass and decreased muscle fiber length. This study aims to identify the asymmetry of paraspinal
muscles using functional cross-sectional areas on magnetic resonance imaging (MRI) in patients with hemiplegia.
Methods
The medical records and lumbar MRI of subjects with hemiplegia who visited hospital between April 1, 2013 and May 1, 2018 were
reviewed. Demographics and clinical features were acquired with etiology of hemiplegia. Inclusion criteria were history of
hemiplegia and lumbar MRI performed after stroke. Subjects were excluded if they were quadriplegia or did not have any symptoms
of weakness. Total cross-sectional area (CSA) and functional cross-sectional area (FCSA), defined as fat-free muscle mass,
measurements of the multifidus muscle and the erector spinae muscle at L4-L5 level, bilaterally, were directly obtained for each
subject using ImageJ (Figure, version 1.52, National Institutes of Health, Bethesda, Maryland). Independent t-test and Mann-whitney
test were used to compare the parameters between the affected and unaffected sides. Differences were considered significant
when the p-value was less than 0.05.
Results
Characteristics of subjects are described in Table 1. There were no significant differences in CSA of multifidus and erector spinae
muscles between affected side and unaffected side. However, FCSA of the affected side of multifidus and erector spinae muscles
was significantly small as compared with the unaffected side (p=0.049 and p=0.036, respectively). FCSA/CSA of multifidus muscle
was significantly low as compared with the unaffected side (p=0.006) but not in erector spinae muscle. The results are summarized
in the Table 2.
Conclusion
FCSA of affected side of paraspinal muscle is smaller than the other side in patients with hemiplegia. Fat infiltration is also increased
in affected side of paraspinal in patients with hemiplegia. Asymmetric paraspinal muscles might be associated with trunk imbalance.
Furthermore, the association of such morphological asymmetry and functional parameters such as postural stability and activities of
daily living (ADL) should be further studied.
Acknowledgment: This research was supported by a grant of the Korea Health Technology R&D Project through the Korea Health
Industry Development Institute (KHIDI), funded by the Ministry of Health & Welfare, Republic of Korea (grant number : HI16C1559)

Table 1. Baseline characteristics of subjects
Table 2. Bilateral paraspinal muscle measurements at L4-L5 level
Figure. Measurement of total cross-sectional area of left multifidus muscle at L4–L5 (Left). Lean muscle functional cross-sectional area (FCSA) of the muscle using a threshold method is represented by the area not highlighted in green (Right).

P 18
Psychometric validation of the Korean version of Rehabilitation Complexity Scale version 1
Tae-Woo Kim 1,2†
, Hoo Young Lee1,2*
, Seong Hoon Lim3, Hyung-Ik Shin
4, Jeehyun Yoo
5, Sun Im
6, Myung Eun Chung
7, Soon Yong
Kwon8, Hyun-Mi Oh
1,2, Jihye Park
7, Hyo Eun Kim
9, Da Ban Lim
10, Si Young Park
10, Ji-Yeon Lee
10
TBI rehabilitation center,National Traffic Injury Rehabilitation Hospital1, Department of Rehabilitation Medicine,The Catholic
University of Korea Seoul St. Mary`s Hospital 2, Department of Rehabilitation Medicine,The Catholic University of Korea St.
Vincent`s Hospital 3, Department of Rehabilitation Medicine,Seoul National University Hospital
4, Department of Rehabilitation
Medicine,Inje University Ilsan Paik Hospital5, Department of Rehabilitation Medicine,The Catholic University of Korea Bucheon St.
Mary`s Hospital 6, Department of Rehabilitation Medicine,St. Paul Hospital, The Catholic University of Korea
7, Department of
Rehabilitation Medicine,Bobath Memorial Hospital8, Department of Nursing,National Traffic Injury Rehabilitation Hospital
9, Traffic
Injury Rehabilitation Research Institute,National Traffic Injury Rehabilitation Hospital10
Background and aim
To establish a rehabilitation medical delivery system according to the circumstances in Korea, existing Korean Rehabilitation Patient
Group Version 1.1 (KRPG v1.1) alone is insufficient to embrace complex rehabilitation needs because it solely depends on the
diagnosis, age, and physical and mental function. Therefore, it is necessary to complement the KRPG v1.1 and develop the
comprehensive and feasible rehabilitation patient classification system that assess the complexity of rehabilitation needs. The aim
of this study was to translate and cross-culturally adapt the RCS-E (13th version) to provide Korean version of the RCS(K-RCS), to
report on the key clinimetric properties of the K-RCS, and to investigate its performance in a sample of patients in the subacute
post-injury phase with highly complex rehabilitation needs. We also explored its dimensionality and relationship with the other
functional outcome measures in order to evaluate its potential as a measure of caseload complexity in complex neurological
rehabilitation settings. Furthermore, we quantified the predictive validity of the K-RCS on length of stay (LOS) and allocation of
rehabilitation resources by R squared and compared with KRPGv1.1.
Methods
We translated, cross-culturally adaptd the RCS-E (13th version) to provide K-RCS and explored content and face validity. KRPGv1.1
and K-RCS data were collected for a total of 430 patients (234 males and 196 females) with complex neurological or musculoskeletal
disabilities, mainly following acquired brain injury, from six designated rehabilitation institutions during a 8-month period from 1
January to 31 August 2018. K-RCS ratings of the level of medical (M), nursing (N), care(C), therapy (Ti for intensity and Td for
disciplines), and equipment (E) were examined for dimensionality, repeatability, reliability, validity, responsiveness, explained
variance and compared with the KRPGv1.1.
Results
Content Validity Index was >0.8. The test-retest reliability confirmed the RCS to be repeatable (spearman’s rho 0.69 to 0.86).
Cronbach-α was 0.63. Item-total correlations were >0.50 for M, N, C, Ti with moderate to high loadings on the first principal
component. Factor analysis revealed two clear factors (‘M/N,’ and ‘C/Td/Ti/E’). Comparative fit index was 0.871. MMSE-KC, MBI,
MMT correlated well with N, C, and total score (Spearman rho 0.368~0.495). K-RCS was superior to KRPGv1.1 in predictive validity.
R-squared measures were 13.6%, 20.3%, 13%, 38% for total, medical, rehabilitative therapy costs, and LOS, respectively, and were
higher than each R-squared measure of KRPGv1.1.
Conclusion
The K-RCS provides a sensitive and reliable tool that appears to be suitable for measuring clinical complexity in Korean rehabilitation
hospitals. Its psychometric validation may have an important impact on guiding the patient’s assignment to the rehabilitation
setting that best suit their specific needs.
Acknowledgment: This research was supported by the R&D grant (No. 5-2018-A0024-00001) on rehabilitation by Korea National
Rehabilitation Center Research Institute, Ministry of Health & Welfare.

The Korean version of Rehabilitation Complexity Scale version 1
R-squared measures for explained variance of K-RCS and KRPGv1.1

Multiple regression analysis of K-RCS on rehabilitation resource and length of stay

P 19
The impact of sarcopenic obesity on physical function in the elderly
Hyun Ho Kong1*
, Won Kim2†
, Han Gyeol Cho1
Department of Rehabilitation Medicine, Chungbuk National University Hospital1, Department of Rehabilitation Medicine,Asan
Medical Center2
Introduction
It is known that sarcopenia (age-associated loss of muscle mass) and obesity (high percentage body fat in body composition
regardless of the decrease in muscle mass) are associated with decreased physical function in the elderly. Sarcopenic obesity, which
is a condition of coexistence of sarcopenia and obesity, is expected that cause a synergistic effect on a deterioration of physical
function, but the research on this is still limited.
Objective
This study aimed to investigate the impact of sarcopenic obesity on physical function in the elderly. <br> <br>Methods <br>This is a
cross-sectional study using the Korean Frailty and Aging Cohort Study (KFACS) database for the elderly living in a community (1131
males and 1265 females) in the 70-84 age group. Appendicular skeletal muscle mass was measured by dual-energy X-ray
absorptiometry and sarcopenia is defined as the lower 20% of the value measured by the appendicular skeletal muscle mass divided
by height squared (kg/m²). Obesity was defined as a male with an abdominal circumference greater than 90 cm and a female
greater than 85 cm. Physical function was measured by grip strength, timed up and go (TUG) test, and short physical performance
battery (SPPB).
Results
When divided into four groups according to muscle mass and abdominal circumference, the proportions of males and females were
normal (39.5% vs. 26.4%), obesity (40.5% vs. 53.8%), sarcopenia (16.1% vs. 13.1%) and sarcopenic obesity (3.9% vs. 6.7%),
respectively. In men, the sarcopenic obesity had significantly lower grip strength and total score of SPPB compared to the
normal/obesity (p < 0.05), but not significantly different from the sarcopenia (p > 0.05). In women, grip strength was the same result
as for men, but the TUG test was significantly slower for the sarcopenic obesity than for the sarcopenia. In the total score of SPPB,
the sarcopenic obesity was significantly lower than the other three groups (p < 0.05). In logistic regression analysis after adjusting
for age, demographic and cardiovascular risk factors to observe the association between scores of SPPB and body composition, men
with sarcopenic obesity had greater odds to belong to a lower score category of SPPB than normal (OR 2.02, 95% CI = 1.01 - 4.04).
This tendency was more prominent in women (OR 3.82, 95% CI = 2.04 - 7.16).
Conclusion
Sarcopenic obesity is associated with decreased physical function in elderly men and it appears to be a synergistic impact on the d
eterioration of physical function especially in elderly women.

Table 1. Characteristics of study participants and physical functions according to groups in elderly men
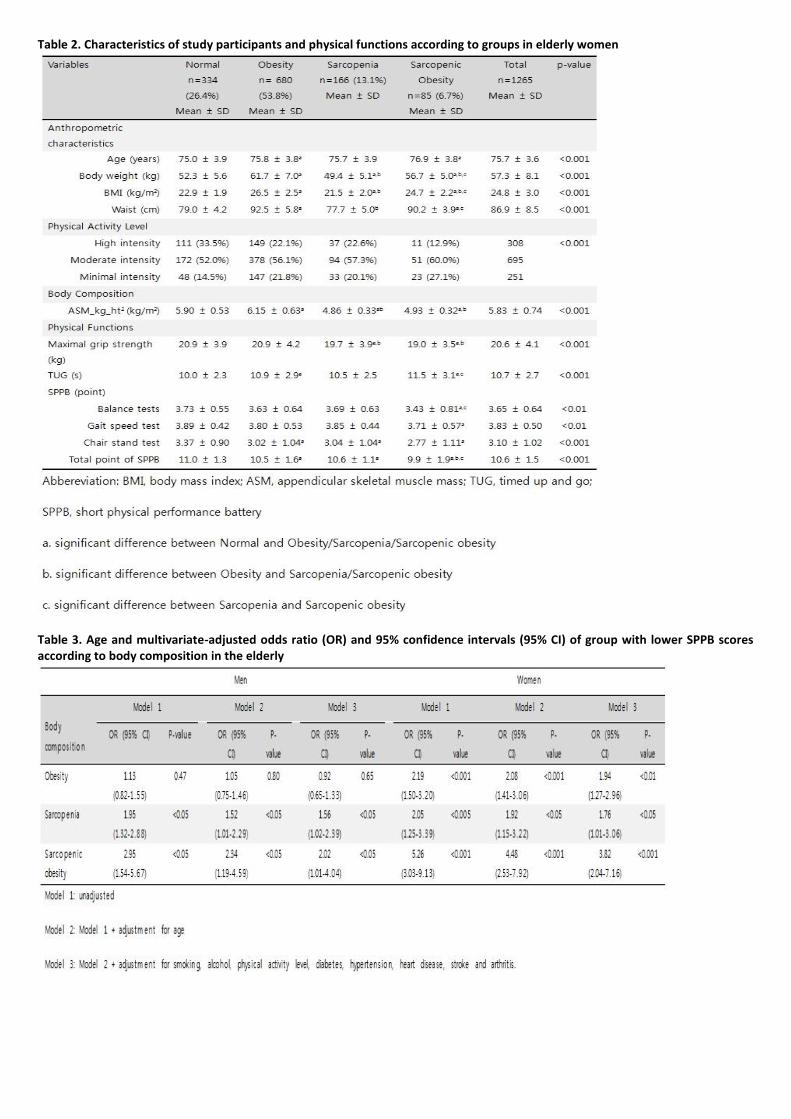
Table 2. Characteristics of study participants and physical functions according to groups in elderly women
Table 3. Age and multivariate-adjusted odds ratio (OR) and 95% confidence intervals (95% CI) of group with lower SPPB scores according to body composition in the elderly

P 20
Efficiency of Injury Prevention Program for Short Track Skaters on Non-contact Injury Incidence
Hokyung Choi1,1
, Eunkuk Kim1,1*†
Department of Physical Education, Korea National Sport University1
This study aimed firstly to identify the efficiency of short track-related sports injury prevention program on the non-contact sports
injury incidence, and secondly to assess the characteristics of subjective symptoms from sports injuries in ankle, knee joints and low
back. Twenty-five short track skaters participated in this study from Nov. 2017 to Jul. 2018. Information on their non-contact injuries
developed during the period were collected and injury prevention program which consisted of 8 different exercises developed
based on the short track skating motion focusing on muscle strength and neuromuscular training was implemented in their daily
warm-up exercise sessions and competitions. (Fig 1) The main outcome measures were the change in incidence rate which was
expressed as the number of injuries caused by athletes participating in 1000 h of exposure in short track training and competitions
using the formula; [(total number of injuries occurred / total time of participation) × 1000]. Post-intervention interview using a
questionnaire (7 questions with a 5-point Likert Scale), OSTRC Overuse Injury Questionnaire for a low back and knee joint, and
Cumberland ankle instability tool for ankle joint were also measured for subjective symptoms. The post-intervention incidence rate
was 2.79 injuries/1,000 h, which was lower than pre-intervention incidence rate (3.04 injuries/1,000 h). (Fig 2) The changes in
subjective symptom levels were significantly reduced in all three measures (Table 1) In conclusion, implementation of specific injury
prevention program exerted beneficial influence on the non-contact sports injury incidence as well as skaters's subjective symptoms
suffering from various sports injuries.
Acknowledgment: This research was supported by Sports Scientification of Convergent R&D Program through the National Research
Foundation of Korea (NFR) funded by the Ministry of science, ICT and Future Planning (NRF-2014M3C1B1033324)
Fig 1 Short track skating specific injury prevnetion program

Fig 2. Sports injury incidences in pre-and post-implementation of injury prevention program
Table 1Changes in subjective symptoms in ankle, knee and low back

P 21
Young-Ah Choi1, Dae-Hyun Jang
1†, Dong-Woo Lee
1, Jaewon Kim
1*, Geun-Young Park
2
Department of Rehabilitation Medicine,Incheon St. Mary’s Hospital, College of Medicine, The Catholic University of Korea1,
Department of Rehabilitation Medicine,Bucheon St. Mary’s Hospital, College of Medicine, The Catholic University of Korea2
Introduction
To Date, a total of eight families and five pathogenic variants related hereditary sensory and autonomic neuropathy (HSAN) 2B due
to RETREG1 mutation have been reported since Kurth et al. first reported four families in 2009. HSAN 2B is characterized by
progressive sensory deficit, and variable autonomic and motor involvement. Because the reported RETREG1 mutations are rare,
there is no clear description of the phenotype of HSAN 2B. Here, we describe a novel frameshift mutation
(c.765dupT/p.Gly256TrpfsTer7) of the RETREG1 and paternal uniparental isodisomy 5 in a patient diagnosed as having HSAN 2B.
Case
The proband was a 22-year-old female who visited our clinic for evaluation because of a sensory disturbance on both lower
extremities and unstable gait. The patient is from a non-consanguineous Korean family and there was no familial history of
hereditary disorders. She had a normal birth history and developmental milestone. Her symptoms had begun around ten years of
age and gradually progressed. The patient exhibited a decreased pain, temperature, touch, vibration and position sense on the both
lower extremities, and an ulcer on left toe which lasted more than a year and healed recently (Fig 1-A). She had mild lower
extremities distal motor weakness (MRC 4), spasticity, and increased deep tendon reflex on the both lower extremities. She had
normal intelligence and no autonomic symptoms. Nerve conduction study showed a sensory more than motor axonal
polyneuropathy and sympathetic skin response was impaired on both sole. The multi-gene panel study related with neuromuscular
disorders which was previously reported by us was performed. We found a frameshift homozygous variation in the patient’s
RETREG1: c.765dupT/p.Gly256TrpfsTer7, which is a novel variation. However, of patient’s parents, only the father was identified as
carrier for the variation on the Sanger sequencing tests (Fig 1-B). Furthermore, SNP array was performed in the patient and her
parents, revealed a paternal uniparental disomy 5. (Fig 1-C and D)
Discussion
We have summarized the clinical features of our case and all the families reported previously in table 1. All cases have similar
characteristics which are early onset (1st - 2nd decade), progressive sensory disturbance, distal motor weakness, skin ulcer, and/or
spasticity, variable autonomic involvement. We reported a case with the patient diagnosed as having HSAN 2B caused by a novel
frameshift mutation (c.765dupT/p.Gly256TrpfsTer7) of the RETREG1 and paternal uniparental isodisomy 5 in a non-consanguineous
family. Clinicians should be aware that autosomal recessive disorders can be occurred by uniparental disomy in a non-
consanguineous family.
Acknowledgment: This work was supported by the National Research Foundation of Korea (NRF) grant funded by the Korea
government (MSIT) (No. 2017R1C1B5014840) This research was supported by a Grant of Translational R&D Project through Clinical
Research Laboratory, Incheon St. Mary's Hospital.

Fig 1. (A) Left toe ulcer, (B) Chromotographies of RETREG1 gene, (C) SNP array, (D) Pedigree Table 1. Clinical features of our case and all the families with HSAN 2B reported previously

P 22
Hyun Sung Lee1*
, Chang hwan Kim1†
, Chang Beom Kim1, Chan Hyuk Park
1, Han Young Jung
1, Kyung Lim Joa
1, Myeong-Ok Kim
1
Department of Rehabilitation Medicine, Inha University Hospital1
Introduction
Diabetic amyotrophy (DA) also known as, diabetic lumbosacral radiculoplexus neuropathy (DLRPN), has been considered to be an
often asymmetric, relatively acute, painful neuropathy dominated by proximal lower-limb muscle weakness. Painless DA, considered
as a variant of DLRPN, is characterized by subacute or chronic and more symmetric distal lower limbs weakness. However, we
experienced a patient who presented with acute pattern of painless DA. Appropriate treatment in early stage is important and
expected to reduce permanent disability. We report a case of painless DA showing a rapid recovery through early steroid treatment.
Case report
A 28-year-old man with diabetes mellitus (DM) type 1 over 10 years ago, admitted to our hospital because of progressive lower
limbs weakness, difficulty climbing stairs over 2 months. A week after hospitalization, he felt sudden severe lower extremities
weakness without pain and accompanied by mild weakness of upper extremities. Physical examination revealed upper limbs- MRC
grade 4/5, lower limbs- MRC grade 1~2/5, and stocking pattern of sensory impairment existed. Tendon reflexes of the ankles and
knees were absent. Pathologic reflexes were negative. Laboratory findings such as CBC, ESR and CRP level were within normal limits,
and ANCA test was negative. Nerve conduction study demonstrated no response in lower limb sensory and motor nerves, except for
relatively reduced motor amplitude of left femoral nerve. Electromyography (EMG) showed denervation potential in lower limbs
and lumbar paraspinal muscles. These findings were compatible with bilateral lumbosacral radiculoplexopathy with underlying
length dependent pattern diabetic polyneuropathy (Table 1a, 1b). Pelvic plexus MRI showed diffuse enlargement and high signal
intensity of the femoral, genitofemoral and sciatic nerves and lumbosacral trunk and sacral plexus, symmetrically (Fig. 1). We
started intravenous high dose steroid therapy. The weakness was recovered dramatically (MRC grade of 4/5 bilateral) only after a
week of steroid therapy. After 1 month, he can walk without assistance, and berg balance scale’s score was elevated from 14 to 36.
Conclusion
DLRPN showed a spectrum of disorders exhibiting several clinical presentations. The painless DLRPN has been known to be a slowly
progressive course. However, we experienced a case with acute exacerbation form of the painless DLRPN. The early recognition and
following an immunomodulatory therapy would be a good choice for the neurologic improvement.
*: Abnormal data, Lat: latency, Amp: amplitude, CV: conduction velocity, Amplitude (mV) in motor conduction study, Amplitude (uV) in sensory conduction study, MUPs: motor unit potentials, Fibs: fibrillation potentials, PSW: positive sharp waves, Poly: polyphasia, Amp: amplitude, Dur: duration, R: recruitment, S: silent, LFCN: Lateral femoral cutaneous nerve, NE: Not evoked, LA: large amplitude, LD: long duration, VM: Vastus medialis, TA: Tibialis anterior, PL: Peroneus longus, GCM: Gastrocnemius medial head, PVM: paravertebral muscle
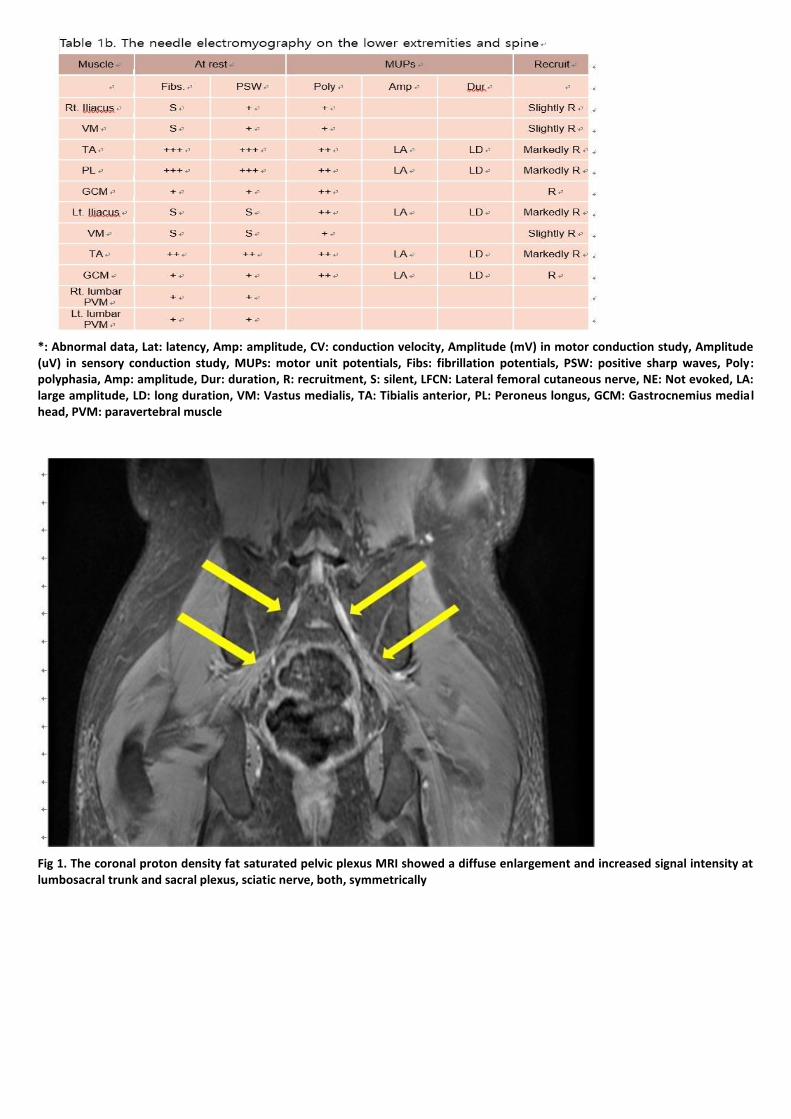
*: Abnormal data, Lat: latency, Amp: amplitude, CV: conduction velocity, Amplitude (mV) in motor conduction study, Amplitude (uV) in sensory conduction study, MUPs: motor unit potentials, Fibs: fibrillation potentials, PSW: positive sharp waves, Poly: polyphasia, Amp: amplitude, Dur: duration, R: recruitment, S: silent, LFCN: Lateral femoral cutaneous nerve, NE: Not evoked, LA: large amplitude, LD: long duration, VM: Vastus medialis, TA: Tibialis anterior, PL: Peroneus longus, GCM: Gastrocnemius medial head, PVM: paravertebral muscle
Fig 1. The coronal proton density fat saturated pelvic plexus MRI showed a diffuse enlargement and increased signal intensity at lumbosacral trunk and sacral plexus, sciatic nerve, both, symmetrically

P 23
ANCA-associated vasculitis with concomitant mononeuritis multiplex in a stroke patient
Dong Min Kim1*
, Young Mo Kim1, Jae Hyeok Chang
1, Jin A Yoon
1†
Department of Rehabilitation Medicine, Pusan National University Hospital1
Introduction
Antineutrophil cytoplasmic antibody associated vasculitis (ANCA-associated vasculitis; AAV) is a group of rare autoimmune diseases
that show typical characteristic inflammatory cell infiltration and blood vessel wall necrosis. This vascular damage can occur in many
parts of the body, resulting in serious kidney failure, skin lesions and respiratory distress. In some cases, AVV affects the brain. Here,
we report a rare patient who presented with AAV and concomitant mononeuritis multiplex.
Case Report
A 63-year-old man was admitted for fever of unknown origin for two months. He also experienced weight loss and motor weakness
of his left upper and lower extremities. During the effort to find the cause of the fever, the patient was diagnosed with AVV in a
blood test and biopsy. While the patient was treated with steroid therapy, sudden dysarthria and motor weakness of the left upper
and lower extremities occurred. Magnetic resonance imaging (MRI) revealed acute cerebral infarction on the right corona radiata,
putamen and external capsule with hemorrhagic transformation. After 2 weeks later, sudden weakness of the right upper extremity
was noted. Imaging study revealed intracerebral hemorrhage in the left basal ganglia. The patient did not have any stroke risk
factors such as old age (>65), hypertension, diabetes, cardiovascular problems, dyslipidemia, smoke and drink except sex (male). On
the 14 days of onset, muscle strength of both upper and lower extremities were good (G) grade on manual muscle test except his
hand grip was poor (P) grade on the right side and the left ankle dorsiflexion, great toe extension, ankle plantarflexion were zero (Z)
grade on manual muscle test with focal decreased deep tendon reflex. To diagnose the cause of his motor weakness of distal part of
extremities an electromyography was done and bilateral median, left ulnar, common peroneal nerve and tibial nerves lesions were
found. These findings were compatible with mononeuritis multiplex. His motor strength showed recovery on his ankle plantarflexion
from Z to poor (P) grade on discharge, but ankle dorsiflexion was still Z grade. To overcome imbalance caused by his left foot drop,
the ankle-foot-orthosis was prescribed for gait training.
Conclusion
AVV rarely involves the central nervous system (CNS). Vasculitis associated with CNS lesion should be suspected if patients have
neurological manifestations consistent with CNS involvement, particularly if they have evidence of disease activity elsewhere, and if
imaging study shows ischemic or haemorrhagic lesions on brain. In addition, our patient showed asymmetric progression of
revealed concomitant peripheral nervous system (PNS) lesion showing focal lower motor neuron signs including foot drop which is
characteristically seen in vasculitic polyneuropathy. Therefore, it is important to conduct detail physical examination not to overlook
complex CNS and PNS lesions associated with this autoimmune diseases.
Fig 1. Brain CT

Table 1. Findings of nerve conduction study
Table 2. Findings of needle electromyogram

P 24
Successfully Managed Respiratory Insufficiency in a Patient with BMPER Gene Mutation : A Case Report
Ho Eun Park1*
, Ji Won Hong1, Youngha Lee
2, Jin A Yoon
1, Yong Beom Shin
1†
Department of Rehabilitation Medicine, Pusan National University Hospital1, Department of Biomedical Sciences, College of
Medicine, Seoul National University2
Introduction
Diaphanospondylodysostosis (DSD) is an extremely rare and fatal disease that can occur as a phenotype of the BMPER gene
mutation. We report a patient diagnosed with DSD and describe a successful management of respiratory insufficiency by chest
retraction through non-invasive ventilator (NIV).
Case Report
The female patient was born at 40 weeks with a birth weight of 2600g by Cesarean section. Since birth, she revealed several
abnormal morphologies (Fig. 1). Brain and spinal magnetic resonance image, electrodiagnostic study, creatinine phosphokinase, a
chromosome study, GDF and SMN gene test were performed, but no significant abnormal findings were found. During the follow-up
visit to our clinic, the patient complained of mild respiratory distress that occurred when she was 12 years old. Pulmonary function
test showed a pattern of restrictive lung disease due to thoracic deformity and encouraged air stacking exercise with bag valve mask.
From the age of 14, she used NIV only at night with concern of hypoventilation during sleep. At the age of 15 years, she suffered
from upper respiratory infection and visited the emergency room with dyspnea. Arterial blood gas analysis showed marked carbon
dioxide retention upto 73 mmHg of arterial partial pressure of carbone dioxide (pCO2). According to history taking, she had not
been able to apply the NIV for the past month because of poor compliance. With appropriate adjustment of NIV, PCO2 was lowered
to 48 mmHg within one week of hospitalization and she discharged to home on the 9th day, maintaining NIV application at night.
We suspected DSD in this patient with respiratory insufficiency, and other characteristic morphologic features including axial
skeletal anomaly and diagnosed by confirming BMPER mutation through Sanger sequencing (Figure 2, 3, Table 1, 2).
Discussion
DSD is a rare, fatal disease with little known disease progression or prognosis. According to previous reports, long term progression
of DSD is affected by renal function due to renal disease, and we suggest the possibility that respiratory insufficiency due to chest
deformity may also affect the course of the disease. Therefore, we recommend early pulmonary rehabilitation for chest expansion
and NIV training to improve quality of life, reduce hospital stay, delay disease progression. In patients with DSD, axial skeletal
development is abnormal, whereas appendicular skeletal development is relatively normal. In this case, however, symmetrical
muscle wasting was observed in the both upper and lower extremities. This may be due to the extremely rare reports of DSD and
the possibility that the life span of the patient was so short that we could not fully see the course of the disease. Future research is
needed to determine the role of pulmonary rehabilitation as a disease modifying therapy for DSD patients and to determine
whether the decline in muscle wasting in extremities is present.

Figure 1. Characteristic morphologic features (A) Short neck and stature, protruded abdomen, bell shaped thorax (B) Three dimensional computer tomography (CT) of whole spine shows multiple anamaly at spine and sacrum; Fusion of C2/3, C4/5 vertebra; C5, C6, C7 butterfly vertebra; C1, C5, C6, T8 dysraphism; Hypogenesis of sacrum (C) Severe scoliosis of Cobb angle of 62 degrees, lung hypoplasia, decreased number of ribs, downward tilt of ishchiopubic rami
Figure 2. Family pedigree and Sanger sequencing traces confirming the compound heterozygous variants in BMPER gene.
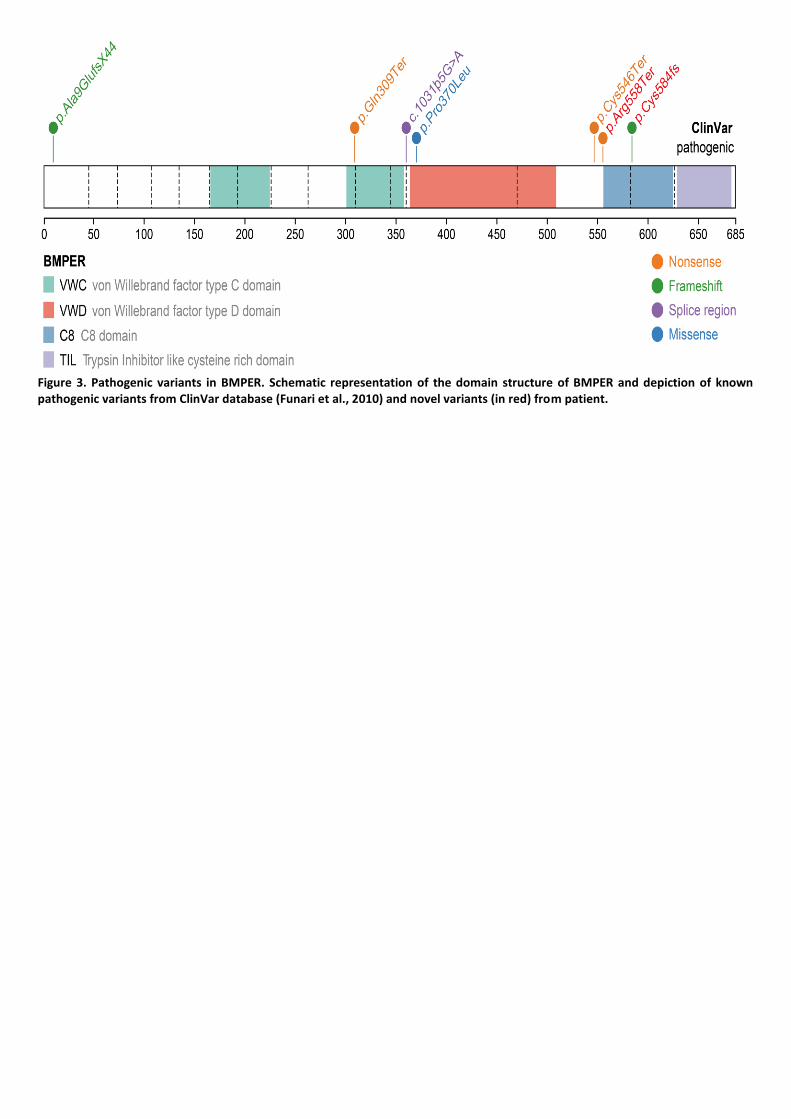
Figure 3. Pathogenic variants in BMPER. Schematic representation of the domain structure of BMPER and depiction of known pathogenic variants from ClinVar database (Funari et al., 2010) and novel variants (in red) from patient.

P 25
Factors Related to Reversal of Developmental Milestones in Rolling in Korean Infants
Ho Eun Park1*
, Mi-Kyung Cho1, Yong Beom Shin
1, Je-Sang Lee
2†
Department of Rehabilitation Medicine, Pusan National University Hospital1, Department of Rehabilitation Medicine, East Gimhae
Hospital, Gimhae, Korea2
Introduction
The Back-to-Sleep campaign, which began in the United State in 1992, is known as a groundbreaking event that lowered the rate of
sudden infant death syndrome. However, since the campaign spread negative perceptions of the prone position, parents have
started to maintain their babies in the supine position while the babies are awake or babies are older than 2 months. Also, previous
studies revealed that the campaign increased the incidence rates of brachycephaly and plagiocephaly; particularly, the incidence
rate of plagiocephaly in the US was one out of 300 prior to 1992 but dramatic increase of up to 600% for plagiocephaly was reported.
This study is aimed to confirm the incidence of reversed sequence of prone-to-supine and supine-to-prone rolling in Korean infants
and to investigate the caregivers' awareness of developmental milestones for rolling. Through a comparison between the two
groups, deformational plagiocephaly (DP) and normocephaly, in which the developmental order of rolling was different, we
investigated the cause of the different developmental sequence and whether there was a relationship with the incidence of skull
deformities.
Method
A questionnaire survey was conducted among total of 120 persons, who visited our clinic from January 2018 to May 2018 (Fig. 1). Of
the children surveyed, most visited the hospital for confirmation of the plagiocephaly. Group of children with plagiocephaly is
mentioned as ‘Group P’ and that of children with normocephaly is mentioned as ‘Group N’. Group of children flipped supine-to-
prone firstly is mentioned as ‘Group STP’, and the opposite is mentioned as ‘Group PTS’. Statistical analysis was performed using
SPSS, and paired t-test and chi-square test were used for comparison of parameters with differences between groups.
Result
According to Table 1, the order of rolling-over in the development of Korean children is totally reversed, and pandemic
misperception of development is present. Table 2 shows the comparison between Group P and Group N. The proportion of
caregivers who answered that the child rolled over supine-to-prone first showed statistically significant differences between the two
groups. According to table 3, the proportion of caregivers who answered that the child with DP showed statistically significant
differences between two groups. Also, caregiver perception of the rolling-over order showed significant difference between the two
groups.
Conclusion
In this study, the reversal of the order of rolling is confirmed to be associated with an increase in the prevalence of plagiocephaly.
The pandemic phenomenon of reversed sequence of gross motor development in Korea stems from a lack of awareness in
caregivers. So, it is necessary to advertise that the prone position should be recommended during hours when infants are awake
and supervised.

Table 1. Demography of the subjects
Table 2. Comparison of parameters between Group P and Group N

Table 3. Comparison of parameters between Group STP and Group PTS

P 26
Checking serum testosterone level in patient with CVD who presents symptoms of hypogonadism.
Han Gyeol Cho1*
, Goo Joo Lee 1†
Department of Rehabilitation Medicine, Chungbuk National University Hospital1
Introduction
There is a debate in effect of testosterone on cardiovascular disease. The combination of the male preponderance of coronary
artery disease, the protective effects of estrogen in premenopausal women, and the increased incidence of coronary vascular death
in men abusing anabolic steroids led to the belief that testosterone is deleterious to the male heart. Contrary, there are recent
studies that normal physiologic levels of testosterone are beneficial to the male cardiovascular system and that testosterone
deficiency is associated with increased coronary disease risk
Case report
A 49 year old male with history of multiple cardiovascular events, hypertension, diabetes mellitus came to our outpatient clinic for
cardiac rehabilitation. According to his medical report, First myocardial infarction was in 2010 and he received PCI at left circumflex
artery, right coronary artery. Second event was in 2013. Third event was in 2015 and he received proximal segment of left anterior
descending artery, plain old balloon angioplasty for ramus intermedius. Last event was in 2016 and he received PCI for proximal
right coronary artery. He participated in 3-week inpatient cardiac rehabilitation program. After cardiac rehabilitation program, he
showed improvement in maximal oxygen consumption, but he presented exercise intolerance, fatigue in addition to erectile
dysfunction and depression. We did laboratory testing including early morning of serum testosterone. Testosterone level was 1.63
ng/mL (normal range: 2.20-7.16 ng/mL). After consultation to urologist, he received testosterone replacement therapy and he
participated in 8 more sessions of cardiac rehabilitation program. After hormonal replacement and rehabilitation program,
testosterone elevated to 3.59(ng/mL) and showed further improvement in maximal oxygen consumption. In addition
symptoms\ related to testosterone deficiency improved.
Discussion
At the present time, the issue of the cardiovascular safety of testosterone remains controversial. But considering recent studies that
testosterone may have a role in treating angina/myocardial ischemia, we think is worth to check serum testosterone if patient with
cardiovascular disease presents symptoms related with testosterone deficiency and consider testosterone treatment.
Result of exercise tolerance test

P 27
Unfavorable Functional Outcomes of Subacute Combined Degeneration from Nitrous Oxide Inhalation
Seungbeen Hong1*
, Junghyun Park2†
, Jinyoung Park2, Sangwon Hwang
1
Department of Rehabilitation Medicine, Severance Hospital1, Department of Rehabilitation Medicine, Gangnam Severance
Hospital2
Introduction
Subacute combined degeneration (SCD) is a myelopathy caused by demyelination of dorsal and lateral spinal cord. The most
common cause of SCD is vitamin B12 deficiency, which is usually associated with pernicious anemia or severe malnutrition. Nitrous
oxide (N2O), better known as “Laughing gas” or “Happy Balloon gas”, is commonly used as sedative agents by pediatric dentists,
which allows a feeling of euphoria. However, massive inhalation of N2O can cause SCD. The aim of this study is to report the
prognosis of SCD due to N2O inhalation.
Case Reports
This study was conducted on 3 patients who were diagnosed with subacute combined degeneration from with laughing gas
inhalation history. The “inverted V sign”, bilateral high-intensity T2 signal within the posterior column of spinal cord, was found in
magnetic resonance imaging (MRI) of C-spine MRI in all three patients. Patient 1 was a 30-year-old woman who presented with
progressive paresthesia and weakness in her legs. She inhaled “laughing gas” more than 100 times for 1 year. A neurological
examination revealed decreased proprioception and bilateral weakness of both lower extremities. When she was transferred to
department of rehabilitation, she couldn’t stand or walk independently. After 4 weeks of rehabilitation, she is still unable to walk
without holding bar. Patient 2 was a 24-year-old woman who presented with progressive paresthesia and weakness in her arms and
legs. She inhaled N2O gas for once but she ate only one meal for weight reduction about 3 months. A neurological examination
revealed decreased proprioception. When she was transferred to department of rehabilitation, she was able to stand alone and
walk with one hand support. After 10 months, she still requires assistance for walking. Patient 3 was 22 years old when she started
to inhale N2O gas. She felt weakness in bilateral legs after using it every weekend for 2 months. When she was transferred to
department of rehabilitation, she could not stand alone and required wheelchair to move. She recovered rapidly during
rehabilitative therapy and independent standing was available after 1 week. Now she walks independently after 1–year follow–up
but she still shows impaired standing balance.
Discussion
N2O gas is a safe analgesic substance, however, massive consumption of N2O gas could be hazardous to cause SCD. In addition, it is
necessary to mention that only one time exposure to N2O gas can cause SCD if someone has a predisposing factor such as anorexia
nervosa, pernicious anemia or chronic vitamin B deficiency. Early differential diagnosis of SCD and proper treatment including
medication and rehabilitation could be crucial to a favorable outcome. It is recommended not to be exposed to N2O gas since full
recovery may not be achieved.

Figure 1. C-spine MRI of Patient 2 showing T2-hyperintensity involving the posterior column of the cervical spinal cord sagittal view (A) and “inverted V sign” on T2-weighted transverse image (B, arrow)

P 28
Treatment of Central Hyperthermia with Sub-acute Pontine Hemorrhage-A Care Report-
Soo In Yun1*
, Ah Ra Cho1†
Department of Rehabilitation Medicine, St. Paul Hospital, The Catholic University of Korea1
Introduction
Central thermoregulation dysfunction is a very rare symptom that may occur after subarachnoid hemorrhage, brain damage, and
stroke. If the temperature is higher than 41 ° C, or if there is fever more than 39 ° C within 6 hours after stroke, or if there is severe
fluctuation within 1 month, the mortality rate is 70%. Therefore, early diagnosis and treatment of central hyperthermia are
important after brain damage, and are discussed in a few case reports. However, there are no reports of patients with central
thermoregulation dysfunction persisted until the sub-acute phase. In this case report, we report the pattern and treatment of
central hyperthermia in a patient with sub-acute phase after pontine hemorrhage.
Case Report
A 37-year-old man was hospitalized with acute pontine hemorrhage. The size of hemorrhage was 3.8x1.5x2.0cm in brain computed
tomography (CT) and he took the non-surgical treatment (figure 1). The fever developed on the day of the cerebral hemorrhage and
prolonged despite of the termination of treatment for the infectious disease. Two months after pontine hemorrhage, he was
hospitalized again with a recurrent intermittent fever over 38°C. Body temperature changed from 36.3 to 40.3°C. He had alert
consciousness at normal body temperature but showed drowsiness at high temperature. Initial evaluation was performed two
months after hemorrhage and his Korean version of Mini-Mental State Exam (K-MMSE) was zero. All infectious diseases were
excluded and diagnosed as central thermoregulation dysfunction. The over 38.3 degrees of body temperature persisted despite
taking the medication as follows; acetaminophen 3600 mg, naproxen 1000 mg, baclofen 60 mg. So, bromocriptine 5 mg was added
and after 3 days the dose was increased to 10 mg. After adding bromocriptine, the body temperature was maintained within the
normal range, and baclofen was reduced to 10 mg over 10 days. Hyperthermia again occurred and baclofen was increased to 20 mg.
Thereafter, his body temperature remained normal range and he was able to participate in rehabilitation program. His K-MMSE
score was improved to 13/30, and simple communication was possible.
Discussion
It is known that high fever is highly likely to cause neurological deficits and deterioration of cognitive function. In this case, the
patient’s participation in rehabilitation program was limited due to low consciousness accompanied with high fever and after
control of thermoregulation, his neurological recovery could be expected. The possibility of central thermoregulation dysfunction
should be considered in patients with recurrent hyperthermia also in the sub-acute phase after stroke, and the treatment may have
an impact on prognosis.
Figure 1. Initial brain computed tomography (CT)
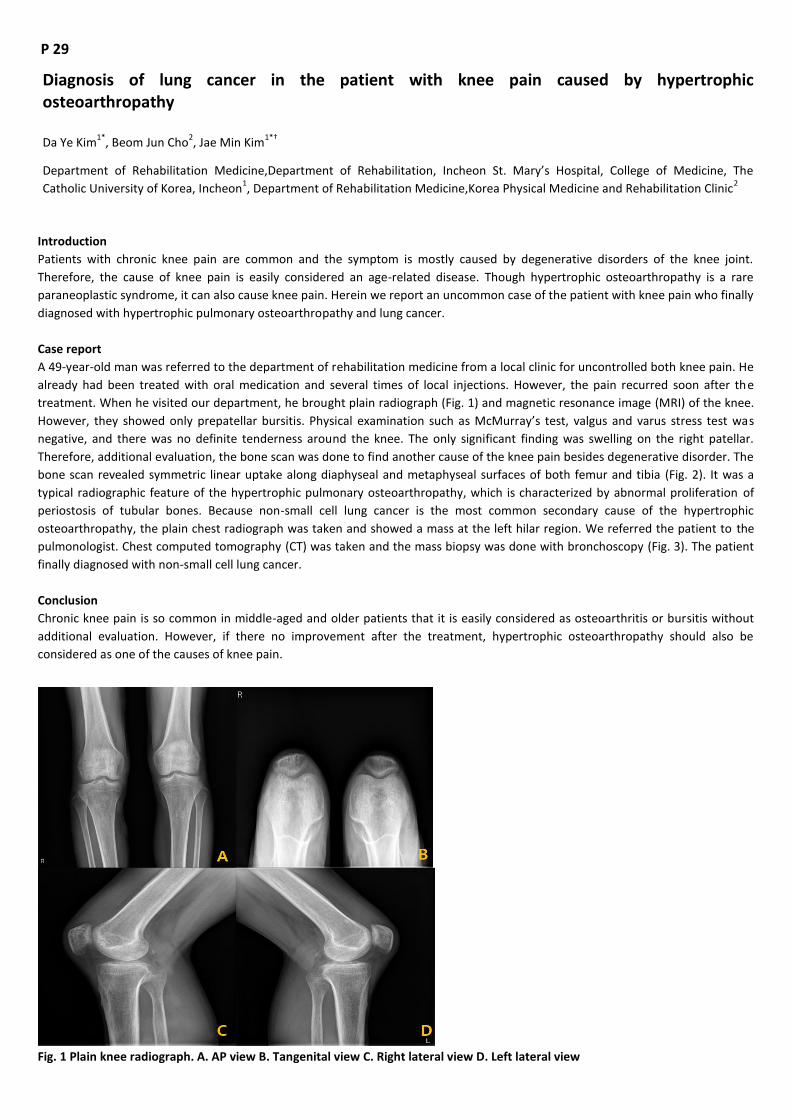
P 29
Diagnosis of lung cancer in the patient with knee pain caused by hypertrophic osteoarthropathy
Da Ye Kim1*
, Beom Jun Cho2, Jae Min Kim
1*†
Department of Rehabilitation Medicine,Department of Rehabilitation, Incheon St. Mary’s Hospital, College of Medicine, The
Catholic University of Korea, Incheon1, Department of Rehabilitation Medicine,Korea Physical Medicine and Rehabilitation Clinic
2
Introduction
Patients with chronic knee pain are common and the symptom is mostly caused by degenerative disorders of the knee joint.
Therefore, the cause of knee pain is easily considered an age-related disease. Though hypertrophic osteoarthropathy is a rare
paraneoplastic syndrome, it can also cause knee pain. Herein we report an uncommon case of the patient with knee pain who finally
diagnosed with hypertrophic pulmonary osteoarthropathy and lung cancer.
Case report
A 49-year-old man was referred to the department of rehabilitation medicine from a local clinic for uncontrolled both knee pain. He
already had been treated with oral medication and several times of local injections. However, the pain recurred soon after the
treatment. When he visited our department, he brought plain radiograph (Fig. 1) and magnetic resonance image (MRI) of the knee.
However, they showed only prepatellar bursitis. Physical examination such as McMurray’s test, valgus and varus stress test was
negative, and there was no definite tenderness around the knee. The only significant finding was swelling on the right patellar.
Therefore, additional evaluation, the bone scan was done to find another cause of the knee pain besides degenerative disorder. The
bone scan revealed symmetric linear uptake along diaphyseal and metaphyseal surfaces of both femur and tibia (Fig. 2). It was a
typical radiographic feature of the hypertrophic pulmonary osteoarthropathy, which is characterized by abnormal proliferation of
periostosis of tubular bones. Because non-small cell lung cancer is the most common secondary cause of the hypertrophic
osteoarthropathy, the plain chest radiograph was taken and showed a mass at the left hilar region. We referred the patient to the
pulmonologist. Chest computed tomography (CT) was taken and the mass biopsy was done with bronchoscopy (Fig. 3). The patient
finally diagnosed with non-small cell lung cancer.
Conclusion
Chronic knee pain is so common in middle-aged and older patients that it is easily considered as osteoarthritis or bursitis without
additional evaluation. However, if there no improvement after the treatment, hypertrophic osteoarthropathy should also be
considered as one of the causes of knee pain.
Fig. 1 Plain knee radiograph. A. AP view B. Tangenital view C. Right lateral view D. Left lateral view

Fig. 2 Bone scan shows linear uptake along diaphyseal and metaphyseal surfaces of both femur and tibia (arrow)
Fig. 3 Chest plain radiography(A) and chest computed tomography(B) demonstrate mass(arrow) at the left hilar region.

P 30
Applying body-powered, 3D printed prostheses in finger amputation patients: Case series Study
Seung Hak Lee1*
, Ja-Ho Leigh2,3
, Hyung Seok Nam2,3
, Hwang eun young2, Lee Jung Yeon
2, Gangpyo Lee
2†
Department of Rehabilitation Medicine,Asan Medical Center1, Department of Rehabilitation Medicine,Incheon Workers
Compensation Hospital2, Department of Rehabilitation Medicine,Seoul National University Hospital
3
Introduction
Finger amputations are the most common work-related amputation in Korea. Even through amputated fingers can be functional
when more than half of the proximal phalanx is preserved, it has negative impacts of the patient's hand function, quality of life, and
self-esteem. Recently, 3D-printed prostheses has been gaining attention in various levels of upper limb amputation due to its low
cost, onsite fabrication, and easy customization. In this study, we reports two cases of work-related finger amputation patients who
received body-powered, 3D-printed finger prostheses and underwent sufficient prosthetic training.
Cases
The first patient was a 25 year old female who had a second, third, and fourth finger amputation due to blender injury in the
workplace. Her fourth finger was replanted but second and third finger was amputated at proximal interphalangeal level. We
created body-powered prostheses that mimicking DIP joint motion through MCP joint motion using 3D printer (Cubicon, Single plus,
Korea) for the second and third fingers. The source code was the Knick Finger downloaded from e-NABLE and the material used ABS
resin for the hard part and TUP resin for the soft part. During the assembly, fishing line and rubber strings were used and the total
cost was about 30,000 won. The patient was trained for two weeks on the use of prostheses and she was very satisfied. (Figure 1)
The second patient was a 25 year old male who had left second finger PIP disarticulation during plumbing work. We created body-
powered prosthesis using similar method and principle. Jebsen Taylor Hand Function Test results were increased from 65 points
before wearing prosthesis to 85 points after wearing. And he said that prosthesis is especially useful when typing on a
computer.(Figure 2)
Conclusion
Body-powered, 3D-printed finger prosthesis is feasible and can be applied quickly and easily for finger amputation patients
Acknowledgment: This work was supported by a grant of the Research Center for Innovation in Medical Rehabilitation, funded by
the Korea Workers' Compensation and Welfare Service.
Case 1


Case 2

P 31
Which approach was most appropriate assessment for dysphagia in patients with dementia?
Yeun Jie Yoo1*
, Jae Won Kim2, Joon Sung Kim
2, Bo Young Hong
2, Kyoung Bo Lee
2, Seong Hoon Lim
2†
Department of Rehabilitation Medicine, The Catholic University of Korea Yeouido St. Mary`s Hospital 1, Department of
Rehabilitation Medicine, The Catholic University of Korea St. Vincent`s Hospital 2
Purpose
Dysphagia is an important causative factor of aspiration pneumonia for elderly, especially in patients with dementia. However, the
relation of cognitive function for swallowing function was not well uncovered. Thus, we investigated the effect of cognition on
swallowing function in patients with dementia.
Methods
Twenty subjects with dementia were recruited. The swallowing function of all subjects were evaluated by videofluoroscopic
swallowing study (VFSS) with dysphagia outcome and severity scale (DOSS), modified of Mann assessment of swallowing ability
(mMASA), muscle activity with surface EMG on suprahyoid and infrahyoid muscles, the strength of lip and tongue with the Iowa Oral
Performance Instrument® (IOPI) system. The cognitive function was evaluated by mini–mental state examination (MMSE), Montreal
cognitive assessment (MoCA), global deterioration scale (GDS), and clinical dementia rating (CDR). Logistic regression test were
performed among swallowing function and cognition.
Results
The values of mMASA were correlated with the score of MMSE, MoCA, GDS and CDR (all P<0.05). The values of DOSS were
correlated with the score of GDS and CDR (P<0.05). The values for muscle activity of suprahyoid and infrahyoid muscles, the
strength of lip and tongue with IOPI did not correlate with the score of MMSE, MoCA, GDS and CDR. <br>Conclusion: The
assessment with mMASA for dysphagia may be reflected with the cognitive function and swallowing function rather than DOSS of
VFSS. Other parameters for muscle strength did not correlated with level of cognition in patients with dementia. These results may
be useful for planning rehabilitation strategies for dysphagia in patients with dementia.
Acknowledgment: This research was supported by Basic Science Research Program through the National Research Foundation of
Korea (NRF) funded by the Ministry of Science and ICT (grant number: 2017R1E1A1A01074324)
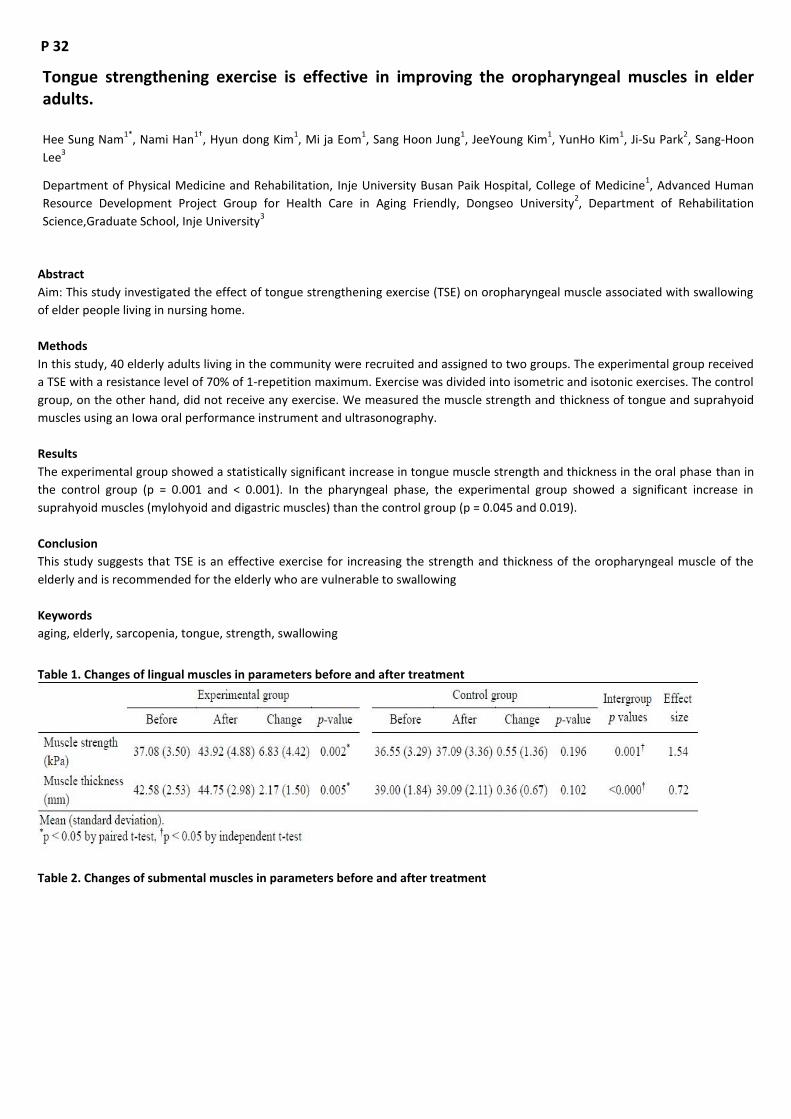
P 32
Tongue strengthening exercise is effective in improving the oropharyngeal muscles in elder adults.
Hee Sung Nam1*
, Nami Han1†
, Hyun dong Kim1, Mi ja Eom
1, Sang Hoon Jung
1, JeeYoung Kim
1, YunHo Kim
1, Ji-Su Park
2, Sang-Hoon
Lee3
Department of Physical Medicine and Rehabilitation, Inje University Busan Paik Hospital, College of Medicine1, Advanced Human
Resource Development Project Group for Health Care in Aging Friendly, Dongseo University2, Department of Rehabilitation
Science,Graduate School, Inje University3
Abstract
Aim: This study investigated the effect of tongue strengthening exercise (TSE) on oropharyngeal muscle associated with swallowing
of elder people living in nursing home.
Methods
In this study, 40 elderly adults living in the community were recruited and assigned to two groups. The experimental group received
a TSE with a resistance level of 70% of 1-repetition maximum. Exercise was divided into isometric and isotonic exercises. The control
group, on the other hand, did not receive any exercise. We measured the muscle strength and thickness of tongue and suprahyoid
muscles using an Iowa oral performance instrument and ultrasonography.
Results
The experimental group showed a statistically significant increase in tongue muscle strength and thickness in the oral phase than in
the control group (p = 0.001 and < 0.001). In the pharyngeal phase, the experimental group showed a significant increase in
suprahyoid muscles (mylohyoid and digastric muscles) than the control group (p = 0.045 and 0.019).
Conclusion
This study suggests that TSE is an effective exercise for increasing the strength and thickness of the oropharyngeal muscle of the
elderly and is recommended for the elderly who are vulnerable to swallowing
Keywords
aging, elderly, sarcopenia, tongue, strength, swallowing
Table 1. Changes of lingual muscles in parameters before and after treatment
Table 2. Changes of submental muscles in parameters before and after treatment
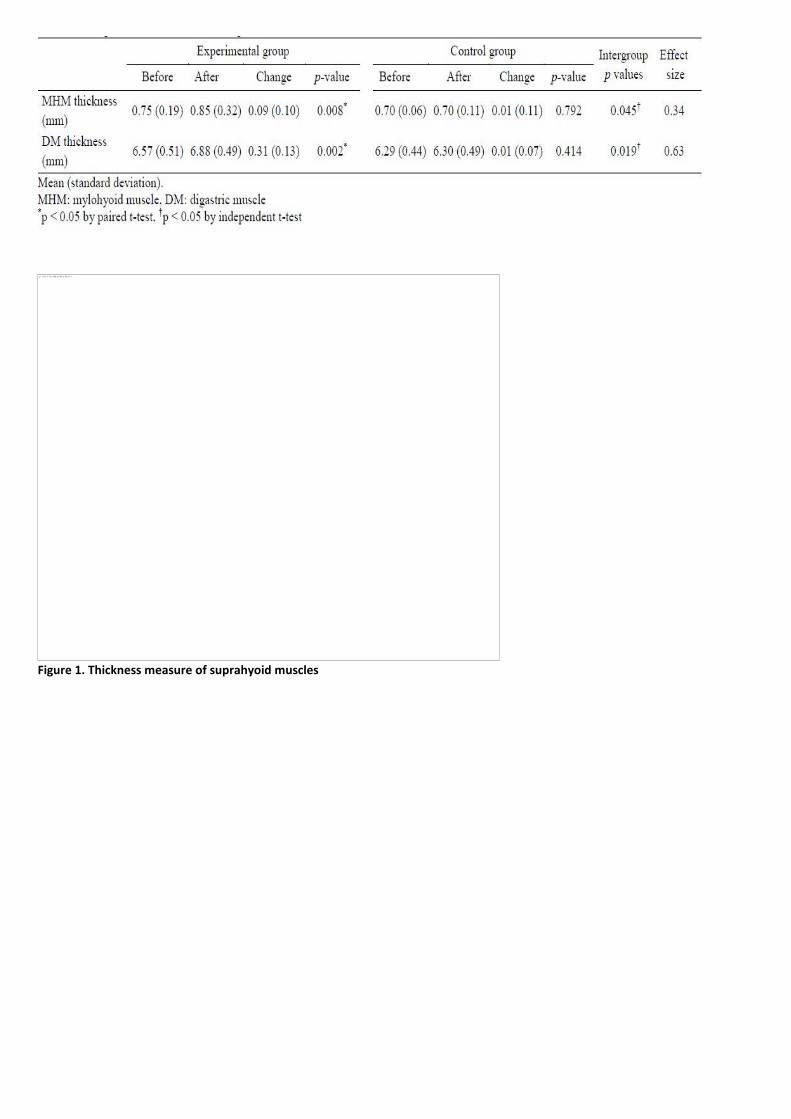
Figure 1. Thickness measure of suprahyoid muscles

P 33
The Functional Outcomes of FIRM in Sarcopenic Patients after Hip Fracture: a 6 month of follow-up
Seung-Kyu Lim1*
, Jae-Young Lim2†
1. Department of Physical Medicine and Rehabilitation,Gyeongsang National University Changwon Hospital, Gyeongsang National
University School of Medicine1, Department of Rehabilitation Medicine,Seoul National University Bundang Hospital, Seoul National
University College of Medicine2
Objectives
To compare the change of functional levels for 6 months in both patients with sarcopenia and without sarcopenia who received
FIRM after HF surgery, and to identify variables influencing independent ambulation at 6 months after HF
Methods
A prospective observational study was conducted with 80 patients older than 65 years of age who had undergone surgery for HF
and followed by multidisciplinary rehabilitation. Sarcopenia was defined according to the Asian Working Group for Sarcopenia
criteria. Functional outcomes were measured at rehabilitation admission, at discharge, at 3 months and 6 months after surgery.
Main measures were ambulatory function (KOVAL, Functional Ambulatory Category (FAC) and the possibility of independent
ambulation (IA) at 6 months after surgery. Other secondary functional outcomes for mobility, balance and fall risk, cognitive
function, mood, activities of daily living, frailty and handgrip strength were measured.
Results
Thirty-five patients (43.8%) satisfied the criteria for sarcopenia. KOVAL and FAC improved in all time course by significant time main
effect (p<0.001). There were no significant group by time interaction (KOVAL: p=0.889, FAC: p=0.702), and no group main effect
(p=0.162) in KOVAL, which means no significant difference in the time course of improvement between groups. Other secondary
functional outcomes showed similar improvement patterns in both groups, either. There was no significant difference on the final
functional status (6 months) after FIRM compared to non-sarcopenia group in all functional measures. IA before fracture (OR: 4.055)
and age (≥80 years) (OR: 0.313) were independent predictors and Sarcopenia was not a predictor for the possibility of IA at 6-
months after surgery.
Conclusions
We found that FIRM was effective for functional recovery in older patients with fragility HF even with sarcopenia. Sarcopenia did not
affect the possibility of independent ambulation at 6-months after surgery for patients after FIRM. These findings will provide
evidence for strong need for comprehensive and integrated rehabilitation management in fragility fracture care to increase
functional recovery in patients with sarcopenia.
Acknowledgment :This research was supported by a grant of the Korea Health Technology R&D Project through the Korea Health
Industry Development Institute (KHIDI), funded by the Ministry of Health and Welfare, Republic of Korea (Grant Number:
HC15C1189).

Time dependent changes of a) KOVAL and b) FAC between gourps after inpatient rehabilitation (FIRM). Data are means ± standard error. P-values were determined by Two-way repeated measures Two-way ANOVA (treatment and time). * Significant difference between groups by Bonferroni post-hoc test.
Time dependent changes of a) MRMI, b) BBS, c) MBI, d) MMSE, e) EQ5D, f) KIADL, g) GDS, h) KFRAIL and i) Handgrip strength between gourps after inpatient rehabilitation (FIRM). Data are means ± standard error. P-values were determined by Two-way repeated measures ANOVA (treatment and time). * Significant difference between groups by Bonferroni post-hoc test
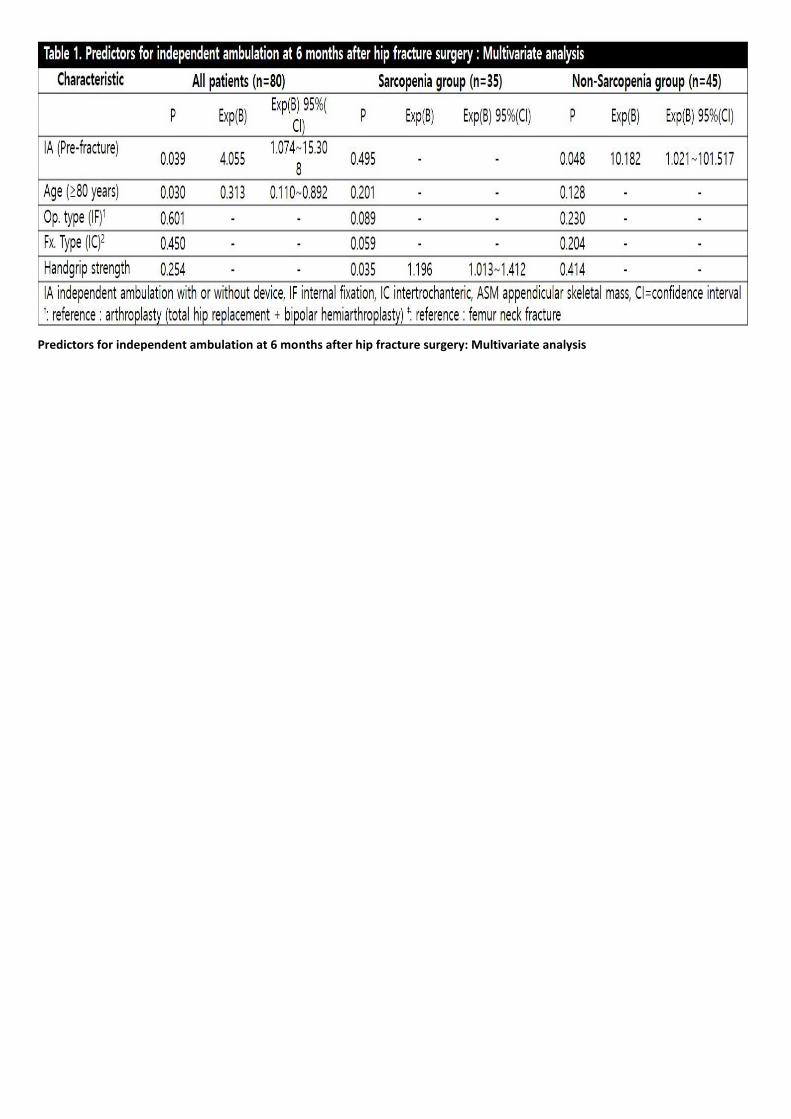
Predictors for independent ambulation at 6 months after hip fracture surgery: Multivariate analysis

P 34
Difference of the Application for Dementia Special Grade According to Regional and Education Level
Han Eol Cho1*
, Wooin Choi2, Seung Nam Yang
3, Jong Hun Kim
4, Hyun Sun Lim
5, Hyoung Seop Kim
2†
Department of Rehabilitation Medicine,Gangnam Severance Hospital, Yonsei University College of Medicine1, Department of
Rehabilitation Medicine,National Health Insurance Service Ilsan Hospital2, Department of Rehabilitation Medicine,Guro Hospital,
Korea University3, Department of Neurology, Dementia Center,National Health Insurance Service Ilsan Hospital
4, Research and
analysis team,National Health Insurance Service Ilsan Hospital5
Introduction
We analyzed the long-term care insurance service (LTCI) in Korea to investigate whether the timing of the application for Dementia
Special Grade (DSG) is different according to socioeconomic status (SES) such as regional differences and education level.
Methods
We collected DSG data from 2014 to 2016. The DSG patients were classified into two categories according to their residence, urban
and countryside. We also examined patients who has received treatment for dementia for more than 6 months and those who have
received anti-dementia medication in order to confirm the treatment of dementia by region. In addition, we divided the level of
patients’ education into five categories: illiteracy, only literacy without formal education, 1-6 years, 6-12 years, and more than 12
years of formal education. Alzheimer's and vascular dementia were sub-grouped to identify differences by dementia type.
Results
A total of 27,611 patients were treated for dementia for more than 6 months. Of these patients, 56.56% (15618) were living in the
city and 43.44% (11993) were living in the country side. Of the 41728 patients who received anti-dementia medication, 55.87%
(23313) were living in the city, and among the people living in the city, 44.13% (18415) were diagnosed with dementia and at DSG
approval. Urban residents were diagnosed and approved DSG significantly earlier than rural residents (Figure 1). We found that the
age at the time of dementia diagnosis and the time of DSG application were faster as the education level was higher. Similar results
were obtained in the sub-group of Alzheimer’s dementia and vascular dementia (Figure 2).
Discussion
1) To apply for DSG, medical staffs with professional training for the diagnosis of dementia with advanced diagnostic tools such as
MRI are necessary. If there are hospitals that specializes in dementia, people can easily get tested for dementia. Therefore, it can be
assumed that people living in large cities with hospitals specializing in dementia have an inclination towards earlier diagnosis of
dementia. 2) Our results were in conflict with the previous study which states that lower level of education is correlated with higher
risk of dementia. We considered few possible explanation for this conflict. First, the higher the level of education, the easier it will
be for the patients to discover their abnormal symptoms that occur with the onset of dementia. In other words, the patients with
higher the level of education will have greater functional status, so the caregivers could be more sensitive to detect cognitive
decline. Second, it might be due to cognitive reserve. Many studies have shown that the patients with greater cognitive reserve
capacity shows faster cognitive decline after the onset of dementia. Patients with high levels of education may have more rapid
cognitive decline after the onset of dementia.

Figure 1. Difference between urban and rural area
Figure 2. Age at the diagnosis of dementia and application of DSG according to education level
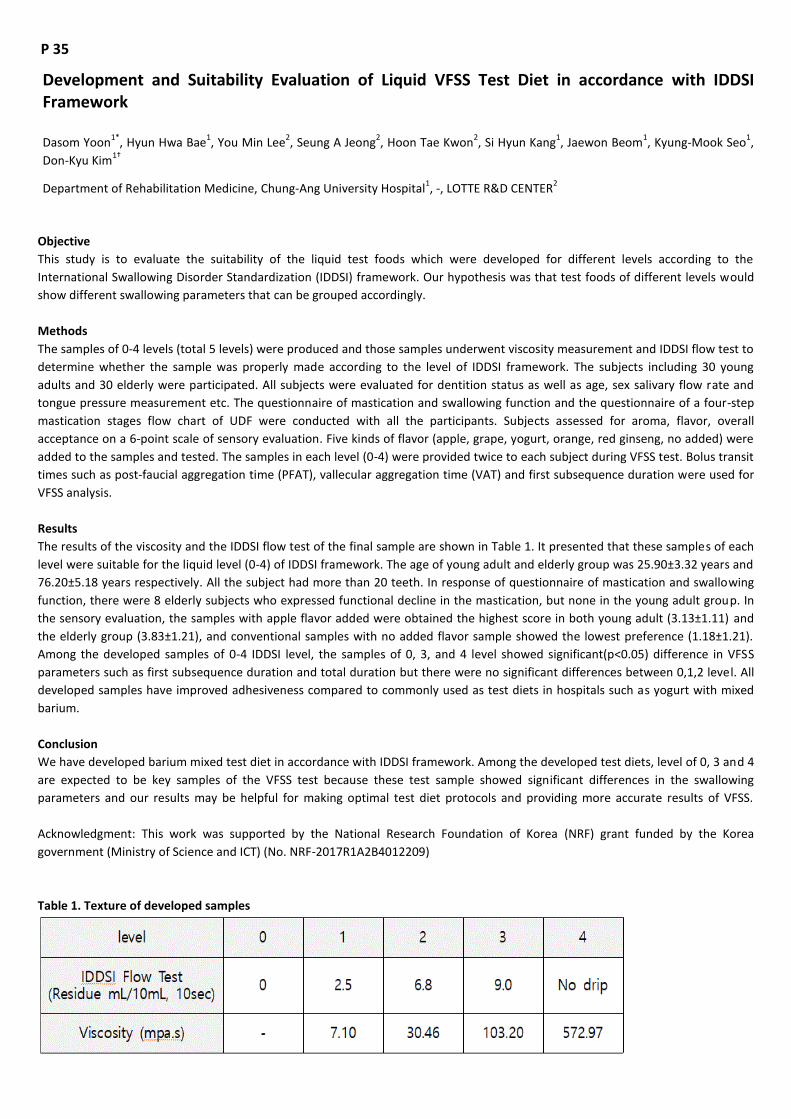
P 35
Development and Suitability Evaluation of Liquid VFSS Test Diet in accordance with IDDSI Framework
Dasom Yoon1*
, Hyun Hwa Bae1, You Min Lee
2, Seung A Jeong
2, Hoon Tae Kwon
2, Si Hyun Kang
1, Jaewon Beom
1, Kyung-Mook Seo
1,
Don-Kyu Kim1†
Department of Rehabilitation Medicine, Chung-Ang University Hospital1, -, LOTTE R&D CENTER
2
Objective
This study is to evaluate the suitability of the liquid test foods which were developed for different levels according to the
International Swallowing Disorder Standardization (IDDSI) framework. Our hypothesis was that test foods of different levels would
show different swallowing parameters that can be grouped accordingly.
Methods
The samples of 0-4 levels (total 5 levels) were produced and those samples underwent viscosity measurement and IDDSI flow test to
determine whether the sample was properly made according to the level of IDDSI framework. The subjects including 30 young
adults and 30 elderly were participated. All subjects were evaluated for dentition status as well as age, sex salivary flow rate and
tongue pressure measurement etc. The questionnaire of mastication and swallowing function and the questionnaire of a four-step
mastication stages flow chart of UDF were conducted with all the participants. Subjects assessed for aroma, flavor, overall
acceptance on a 6-point scale of sensory evaluation. Five kinds of flavor (apple, grape, yogurt, orange, red ginseng, no added) were
added to the samples and tested. The samples in each level (0-4) were provided twice to each subject during VFSS test. Bolus transit
times such as post‐faucial aggregation time (PFAT), vallecular aggregation time (VAT) and first subsequence duration were used for
VFSS analysis.
Results
The results of the viscosity and the IDDSI flow test of the final sample are shown in Table 1. It presented that these samples of each
level were suitable for the liquid level (0-4) of IDDSI framework. The age of young adult and elderly group was 25.90±3.32 years and
76.20±5.18 years respectively. All the subject had more than 20 teeth. In response of questionnaire of mastication and swallowing
function, there were 8 elderly subjects who expressed functional decline in the mastication, but none in the young adult group. In
the sensory evaluation, the samples with apple flavor added were obtained the highest score in both young adult (3.13±1.11) and
the elderly group (3.83±1.21), and conventional samples with no added flavor sample showed the lowest preference (1.18±1.21).
Among the developed samples of 0-4 IDDSI level, the samples of 0, 3, and 4 level showed significant(p<0.05) difference in VFSS
parameters such as first subsequence duration and total duration but there were no significant differences between 0,1,2 level. All
developed samples have improved adhesiveness compared to commonly used as test diets in hospitals such as yogurt with mixed
barium.
Conclusion
We have developed barium mixed test diet in accordance with IDDSI framework. Among the developed test diets, level of 0, 3 and 4
are expected to be key samples of the VFSS test because these test sample showed significant differences in the swallowing
parameters and our results may be helpful for making optimal test diet protocols and providing more accurate results of VFSS.
Acknowledgment: This work was supported by the National Research Foundation of Korea (NRF) grant funded by the Korea
government (Ministry of Science and ICT) (No. NRF-2017R1A2B4012209)
Table 1. Texture of developed samples

Figure 1. First subsequence duration for each sample of the elderly group

P 36
The effect of IT convergence gamification training in community-dwelling older people (RCT)
Da Hwi Jung1*
, Lee Eun Lee1, Byeong-Ju Lee
1, Myung Jun Shin
1†, Myoung-Hwan Ko
2
Department of Rehabilitation Medicine, Pusan National University Hospital1, Department of Rehabilitation Medicine, Chonbuk
National University Hospital2
Background
For the elderly, the reduction of motor function is natural phenomena, but requires a variety of concerns about how to slow down
the rate of decline. Therefore, it is necessary to expand the exercise facilities or welfare facilities for the elderly, but the reality is
suffering from space, cost problem and compliance. In the case of elderly people, the social exercise and the medical exercise
therapy should be distinguished, but the boundary is usually ambiguous. Furthermore, exercise for the elderly, whether preventive
or therapeutic, should be provided as a public service, but this is also difficult. So we tried to approach exercise therapy for
improvement of elderly physical function such as walking, balance and flexibility etc. through gamification exercise equipment
(Men&Tel, Korea, Balpro110, Model No. SBT 110).
Methods
This study is a multicenter randomized controlled trial. The elderly between 60 and 85 years of age were divided into 20 people
conventional exercise group (group 1) and 20 people Balpro110 group (Group 2). Both group were trained for 8 weeks (30
minutes/3 times/week) and the functional assessment was evaluated before starting of training(pre-evaluation), after training of 8
weeks and after 4 weeks of rest.
Results
There were functional improvements in both Group. After 8 weeks of training, five time sit-to-standing test, berg balance score,
timed-up and go test and 10 meter walking test and KFES-I(Korean version of falls efficacy scale-international) were statistically
significantly improved (Table 1). Although there were no significant differences in between groups in the pre-evaluation, 8weeks,
12weeks. There was no significant statistical difference but showed a tendency to increase further in group 2 than group 1. In
addition, when comparing the results of functional assessment after 8 weeks of training and after 4weeks of rest, group 2 showed a
tendency for the training effect to persist (Figure 1).
Conclusion
The results of this study suggest that the information technology convergence gamification device will be a supplementary tool for
the exercise of the next generation elderly population and at the same time provide an opportunity to think about the future
direction.
Acknowledgment: 본 연구는 보건복지부의 재원으로 한국보건산업진흥원의 보건의료기술연구개발사업 지원에 의하여
이루어진 것임(과제고유번호: HI15C1529).
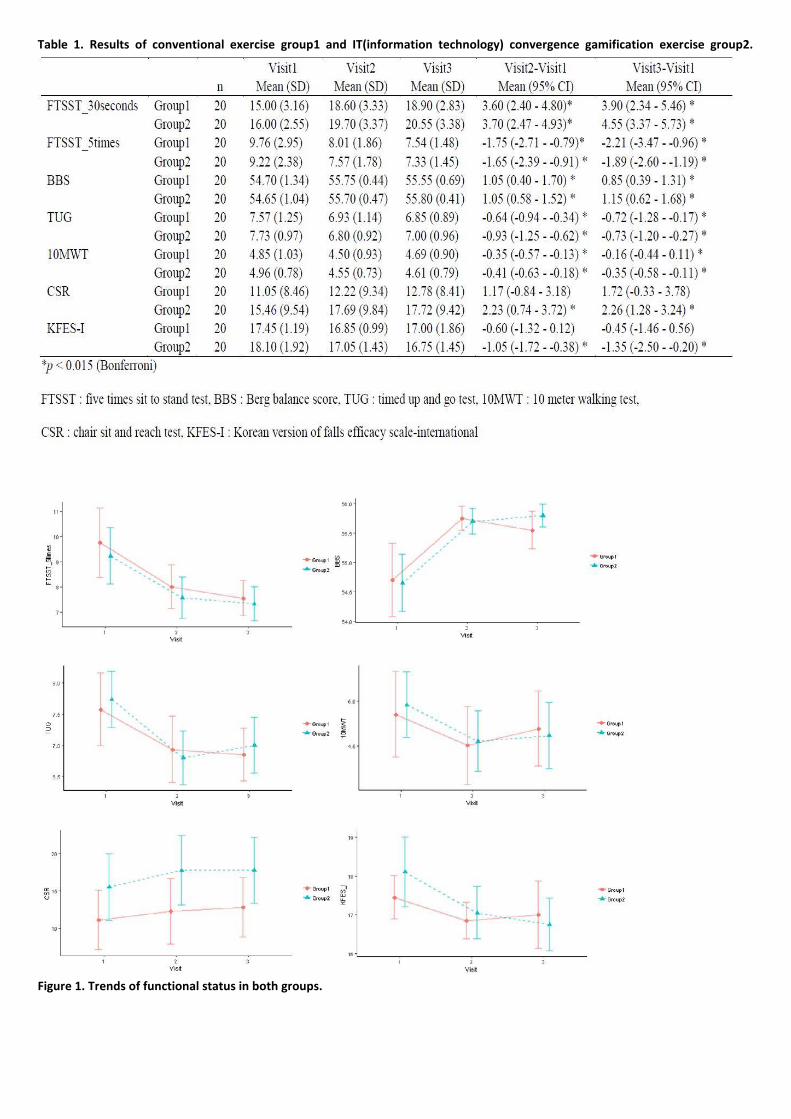
Table 1. Results of conventional exercise group1 and IT(information technology) convergence gamification exercise group2.
Figure 1. Trends of functional status in both groups.

P 37
Development of an Aquatic Performance Measure for Rehabilitation Therapy
You Gyoung Yi2,3*
, Hyung-Ik Shin1,2†
, Jung Woo Kim1, Wamulwange Lieto
2, Sung Eun Hyun
1, Lee Jong Hyuk
3
Department of Rehabilitation Medicine ,Seoul National University Hospital1, Department of Rehabilitation Medicine ,Seoul National
University College of Medicine2, Department of Rehabilitation Medicine,Veterans Health Service Medical Center
3
Background
Aquatic therapy is reported to have positive effects on mobility in persons with disabilities. However, there is no validated tool for
assessment of aquatic performance that can be compared with physical function on land. This study aimed to develop an aquatic
performance measure for rehabilitation therapy based on Water Orientation Test Alyn (WOTA), which was developed for both
swimming activity and aquatic rehabilitation therapy. We also investigated the validity of the new scale in comparison with on-land
activities.
Methods
Patients with brain lesions (traumatic brain injury and stroke) and spine injuries (spinal cord injury, spine fracture, and cauda equina
syndrome), who underwent aqua therapy and WOTA assessment, were retrospectively reviewed. Twenty-one WOTA items,
excluding 16 items related to swimming activities, were categorized through exploratory factor analysis (EFA). Confirmatory factor
analysis (CFA) was performed to evaluate the validity of the structure of the new functional evaluation tool. Spearman’s correlation
analyses were completed with the Medical Research Council (MRC) sum score and modified Barthel index (MBI) score.
Results
Ninety-five patients (mean age: 53.4 years, range: 27–73 years) were included in the analysis. WOTA items were classified into 3
categories through EFA: altering the center of gravity (9 items), basic functional activity (8 items), and progressive basic functional
activity (4 items). Convergence and discrimination validity of the measurement model for all 3 factors were established through CFA.
The total scores of the new functional evaluation tool for aquatic performance showed a strong correlation with the MBI score (r =
0.636, p < 0.001) and correlated with the MRC sum score (r = 0.298, p = 0.01).
Conclusion
The new functional evaluation tool for aquatic performance presented herein has adequate validity with physical function on land,
suggesting the possibility of using this tool for functional assessment during aquatic rehabilitation therapy.
Acknowledgment: This study was funded by Korea Workers' Compensation and Welfare Service.

Table 1. Aquatic Performance Measure for Rehabilitation Therapy
Table 2. Correlation between aquatic performance measure for rehabilitation therapy and MRC sum score, MBI score
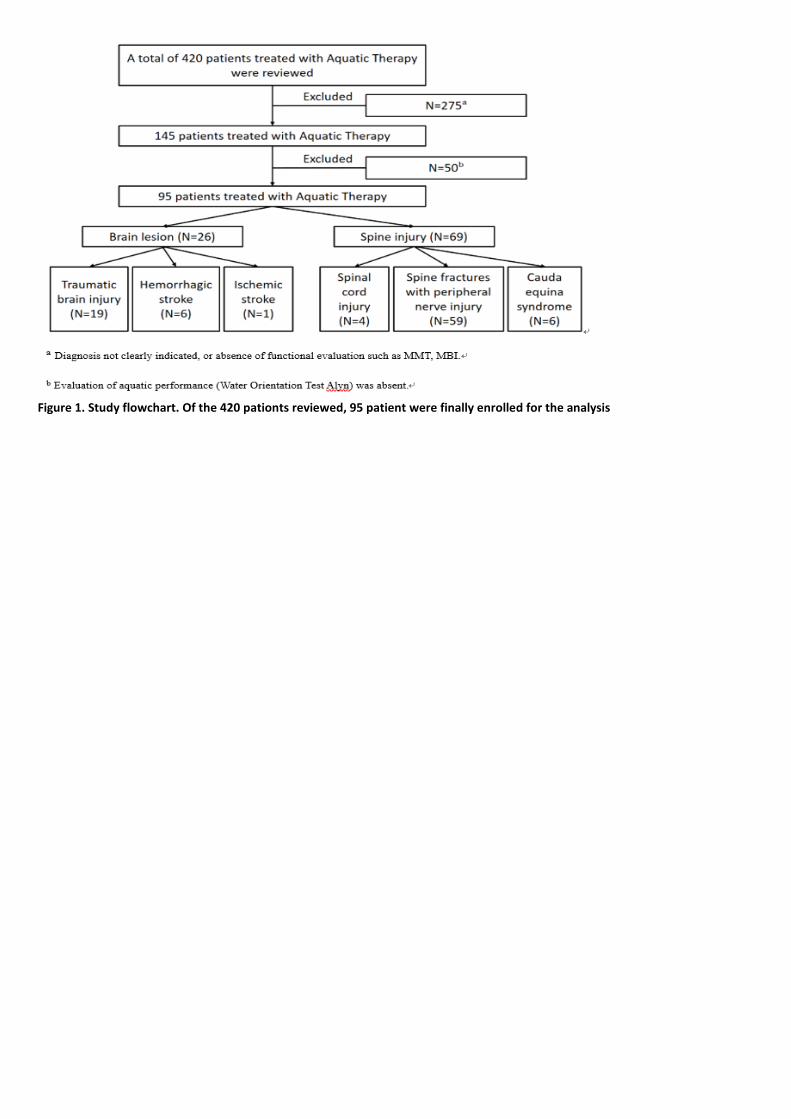
Figure 1. Study flowchart. Of the 420 pationts reviewed, 95 patient were finally enrolled for the analysis

P 38
The effect of graded motor imagery on motor function of upper limb in chronic stroke patients: A RCT
Seong Hoon Lim1*†
, Eun Kyu Ji1, Hae Hyun Wang
1, Sung June Jung
1, Joon Sung Kim
1, Bo Young Hong
1, Kyoung Bo Lee
1, Hyehoon
Choi1
Department of Rehabilitation Medicine, The Catholic University of Korea St. Vincent`s Hospital1
Purpose
Although several occupational therapy for the motor recovery of upper limb in patients with chronic stroke have been investigated,
most of all treatments might be focused on treatment of hospital or clinic setting. Thus, we investigated the effect of graded motor
imagery (GMI) training on motor recovery of upper limb and activities of daily living (ADL) in patients with stroke, as home exercise
program with randomized controlled trial.
Methods
Forty subjects with chronic stroke, over than 3 months after onset, by supratentorial first-ever stroke, were recruited. A total of 8
weeks of GMI program with 30 min at home was educated and was done by himself at home for intervention group. All patients in
intervention or control groups, had been taken conventional occupational therapy (OT) for 1 hour, twice per week throughout all
intervention period. The primary outcome measure was the change of motor function, assessed by manual function test (MFT),
Fugl-Meyer assessment (FMA) from baseline to 8 weeks. Secondary outcome measure was the changes of ADL, assessed by
modified Bathel Index (MBI).
Results
Of the 40 subjects, 37 completed the 8-week follow-up (17 in the GMI group and 20 in the control group). All subjects showed
significant improvement for MFT, FMA and MBI with time and conventional OT (p<.05). The improvement of total score for MFT,
FMA and MBI in GMI group did not differ from those in control group. The score of proximal upper limb of intervention group was
significantly improved than control group (p<.05).
Conclusion
The home exercise program with GMI induced the improvement for proximal muscle function of upper limb in patients with chronic
stroke, over than 3 months after onset. The GMI home program may be an adjunctive treatment with conventional rehabilitation
treatment for chronic stroke. These results may be useful for planning rehabilitation strategies for motor function of upper limb in
patients with chronic stroke.
Acknowledgment: This research was supported by Basic Science Research Program through the National Research Foundation of
Korea (NRF) funded by the Ministry of Science and ICT (grant number: 2017R1E1A1A01074324)

P 39
Structural and functional connectivity correlates with motor impairment in chronic stroke
Jang Ho Lee1*
, Dae Hyun Kim1†
Department of Physical Medicine and Rehabilitation, Veterans Health Service Medical Center, Seoul1
Objective
To identify differences in structural and functional brain connectivity between post-stroke mild and severe motor impairment.
Methods
Twenty-four chronic stroke patients, who underwent diffusion tensor imaging and resting state functional magnetic resonance
image, were retrospectively included. All patients were classified into two groups (mild motor impairment: 11 patients and severe
motor impairment: 13 patients) according to their Fugl-Meyer motor assessment score. Tract-based spatial statistics and group
independent component analyses were applied to investigate between-group differences in structural and functional connectivity,
respectively.
Results
The fractional anisotropy values of motor-related brain regions in the affected hemisphere were significantly higher in mild motor
impairment than in severe motor impairment (corrected P < 0.05). The inter-network functional connectivity between: 1. the
supplementary motor area and primary motor cortex in the affected hemisphere, 2. the supplementary motor area and dorsolateral
prefrontal cortex in the unaffected hemisphere, and 3. the ischemic lesion and primary motor cortex in the unaffected hemisphere
was significantly higher in mild motor impairment than in severe motor impairment (PFWE < 0.05).
Conclusion
Better motor recovery after stroke could be facilitated by means of treatments aimed at enhancing structural and functional
connectivity among motor-related brain regions such as noninvasive brain stimulation and neurodevelopmental therapy.
Acknowledgment: This work was supported by the National Research Foundation of Korea (NRF) grant funded by the Korea
government (MSIT) (No. 2017R1C1B1003)
Fig 1. Lesion maps in mild (a) and severe (b) groups.

Fig 2. Tract-based spatial statistics differences between mild and severe chronic stroke patients.
Fig 3. Inter-network functional connectivity differences between the mild (a) and severe (b) groups.
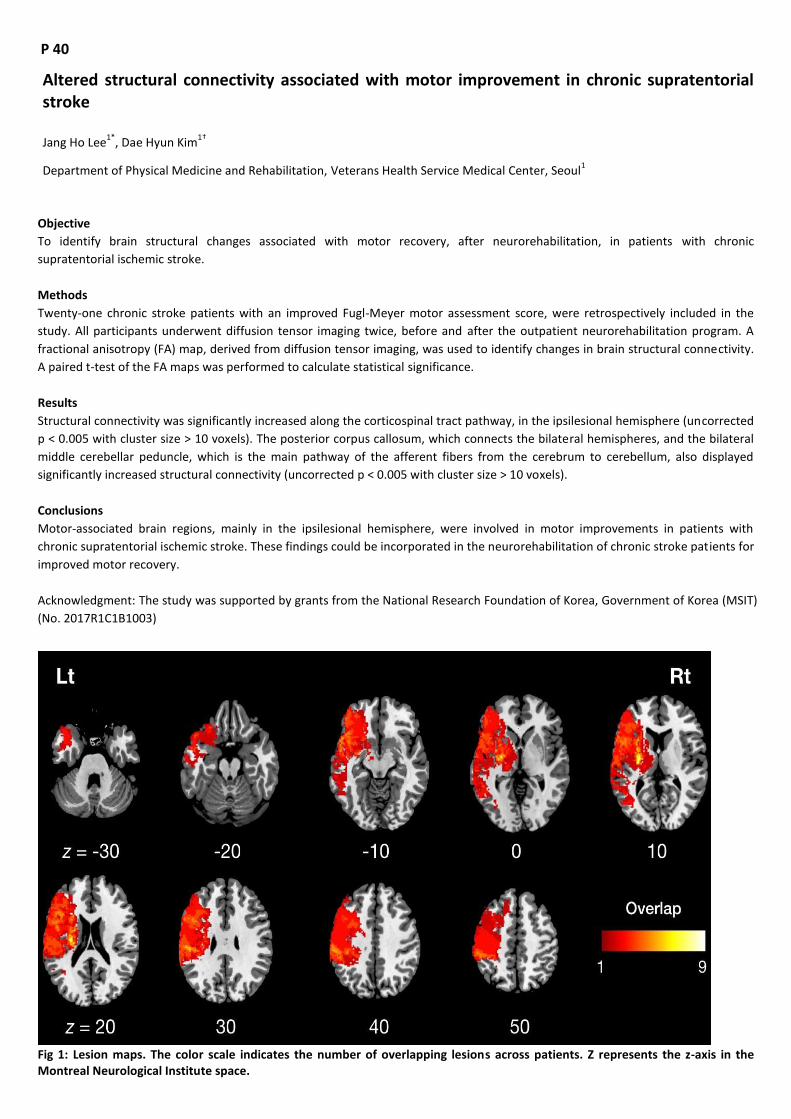
P 40
Altered structural connectivity associated with motor improvement in chronic supratentorial stroke
Jang Ho Lee1*
, Dae Hyun Kim1†
Department of Physical Medicine and Rehabilitation, Veterans Health Service Medical Center, Seoul1
Objective
To identify brain structural changes associated with motor recovery, after neurorehabilitation, in patients with chronic
supratentorial ischemic stroke.
Methods
Twenty-one chronic stroke patients with an improved Fugl-Meyer motor assessment score, were retrospectively included in the
study. All participants underwent diffusion tensor imaging twice, before and after the outpatient neurorehabilitation program. A
fractional anisotropy (FA) map, derived from diffusion tensor imaging, was used to identify changes in brain structural connectivity.
A paired t-test of the FA maps was performed to calculate statistical significance.
Results
Structural connectivity was significantly increased along the corticospinal tract pathway, in the ipsilesional hemisphere (uncorrected
p < 0.005 with cluster size > 10 voxels). The posterior corpus callosum, which connects the bilateral hemispheres, and the bilateral
middle cerebellar peduncle, which is the main pathway of the afferent fibers from the cerebrum to cerebellum, also displayed
significantly increased structural connectivity (uncorrected p < 0.005 with cluster size > 10 voxels).
Conclusions
Motor-associated brain regions, mainly in the ipsilesional hemisphere, were involved in motor improvements in patients with
chronic supratentorial ischemic stroke. These findings could be incorporated in the neurorehabilitation of chronic stroke patients for
improved motor recovery.
Acknowledgment: The study was supported by grants from the National Research Foundation of Korea, Government of Korea (MSIT)
(No. 2017R1C1B1003)
Fig 1: Lesion maps. The color scale indicates the number of overlapping lesions across patients. Z represents the z-axis in the Montreal Neurological Institute space.

Fig 2: Results of paired t-test between pre- and post-treatment with chronic stroke patients. Red areas show FA values significantly increased in post-treatment as compared with pre-treatment (uncorrected p value < 0.005 and cluster size > 10 voxels).
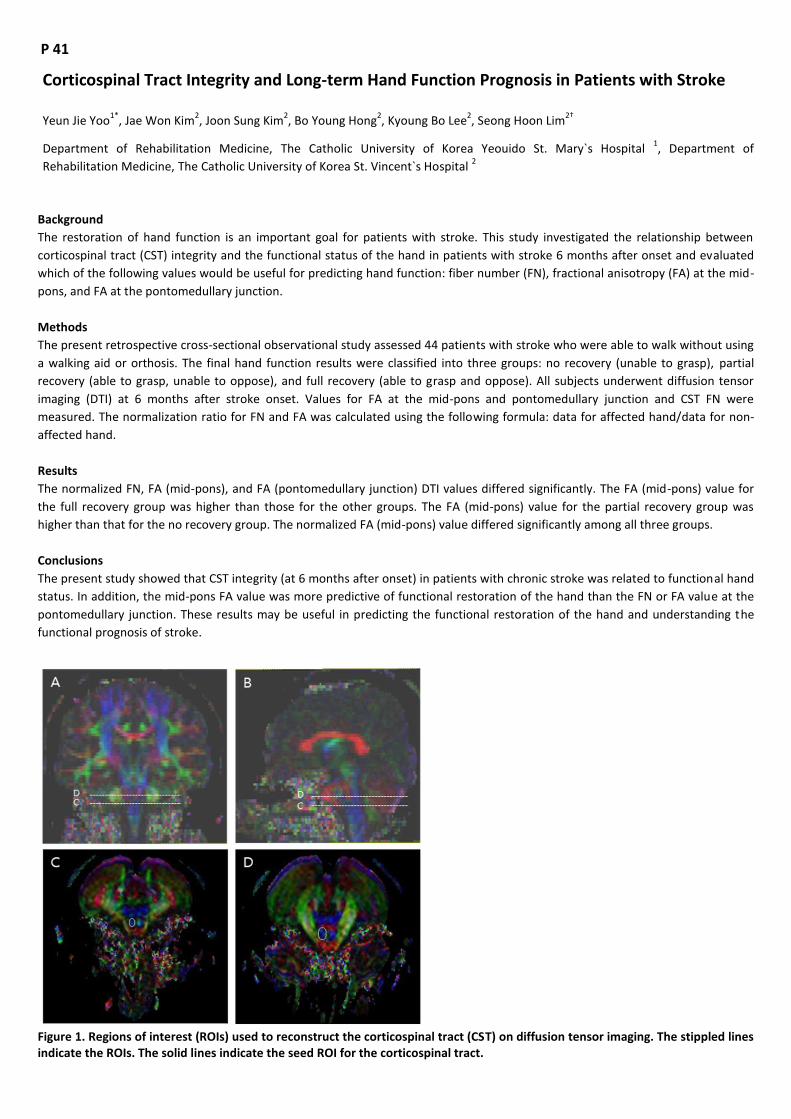
P 41
Corticospinal Tract Integrity and Long-term Hand Function Prognosis in Patients with Stroke
Yeun Jie Yoo1*
, Jae Won Kim2, Joon Sung Kim
2, Bo Young Hong
2, Kyoung Bo Lee
2, Seong Hoon Lim
2†
Department of Rehabilitation Medicine, The Catholic University of Korea Yeouido St. Mary`s Hospital 1, Department of
Rehabilitation Medicine, The Catholic University of Korea St. Vincent`s Hospital 2
Background
The restoration of hand function is an important goal for patients with stroke. This study investigated the relationship between
corticospinal tract (CST) integrity and the functional status of the hand in patients with stroke 6 months after onset and evaluated
which of the following values would be useful for predicting hand function: fiber number (FN), fractional anisotropy (FA) at the mid-
pons, and FA at the pontomedullary junction.
Methods
The present retrospective cross-sectional observational study assessed 44 patients with stroke who were able to walk without using
a walking aid or orthosis. The final hand function results were classified into three groups: no recovery (unable to grasp), partial
recovery (able to grasp, unable to oppose), and full recovery (able to grasp and oppose). All subjects underwent diffusion tensor
imaging (DTI) at 6 months after stroke onset. Values for FA at the mid-pons and pontomedullary junction and CST FN were
measured. The normalization ratio for FN and FA was calculated using the following formula: data for affected hand/data for non-
affected hand.
Results
The normalized FN, FA (mid-pons), and FA (pontomedullary junction) DTI values differed significantly. The FA (mid-pons) value for
the full recovery group was higher than those for the other groups. The FA (mid-pons) value for the partial recovery group was
higher than that for the no recovery group. The normalized FA (mid-pons) value differed significantly among all three groups.
Conclusions
The present study showed that CST integrity (at 6 months after onset) in patients with chronic stroke was related to functional hand
status. In addition, the mid-pons FA value was more predictive of functional restoration of the hand than the FN or FA value at the
pontomedullary junction. These results may be useful in predicting the functional restoration of the hand and understanding the
functional prognosis of stroke.
Figure 1. Regions of interest (ROIs) used to reconstruct the corticospinal tract (CST) on diffusion tensor imaging. The stippled lines indicate the ROIs. The solid lines indicate the seed ROI for the corticospinal tract.

Figure 2. Representative diffusion tensor tractography images of the corticospinal tract in typical subjects from the three groups.
Figure 3. The normalized fiber number (FN), fractional anisotropy (FA) at the mid-pons, and FA at the pontomedullary junction of the corticospinal tract in all groups. The median values are shown as dots. For all values, the error bar shows the interquartile range between the first and third quartiles.

P 42
Clinical Factors related to DVT in Patients Suspected of Thromboembolism after Cerebral Infarction
Su Hwan Bae1*
, Dae Yul Kim1†
Department of Rehabilitation Medicine, Asan Medical Center, University of Ulsan College of Medicine1
Purpose
The purpose of study was to determine association between the occurrence of thromboembolism and the characteristics of cerebral
infarction lesion (vascular territory location, etiology, size), rehabilitative evaluation outcomes when patients suspected of
thromboembolism in rehabilitation setting after cerebral infarction.
Methods
This study was retrospective, cross-sectional study of admissions after cerebral infarction from January 2012 through April 2017.
Patients who were suspected of thromboembolism and underwent evaluation were included in analyses. We divided patients into
two groups: Patients who were normal or negative for evaluation (DVT (-) group) and patients who were diagnosed with DVT or PTE
(DVT (+) group). For clinical variables with significant differences between two groups, logistic regression analysis was used to
ascertain how the identified clinical variables were associated with the occurrence of thromboembolism.
Results
Total 27 patients (2.95%) were diagnosed with thromboembolism. Patients in DVT (+) group were more likely to have higher ratio of
women, previous DVT history, MCA infarction, large arterial disease, mRS 5, abnormal speech and higher D-dimer than DVT (-) group.
In multivariate logistic regression analysis, female gender, MCA infarction and mRS 5 were significantly associated with the
occurrence of thromboembolism when patients were suspected of thromboembolism. In contrast, other rehabilitative evaluation
outcomes, cerebral infarction etiology (TOAST classification) and infarct volume were not associated with the occurrence of
thromboembolism.
Conclusion
Female gender, MCA infarction and mRS 5 could be the potential risk factors for thromboembolism in rehabilitation patients after
cerebral infarction. For this work, further large-scale studies that compare thromboembolism group and non-thromboembolism
group in cerebral infarction patients will be necessary.
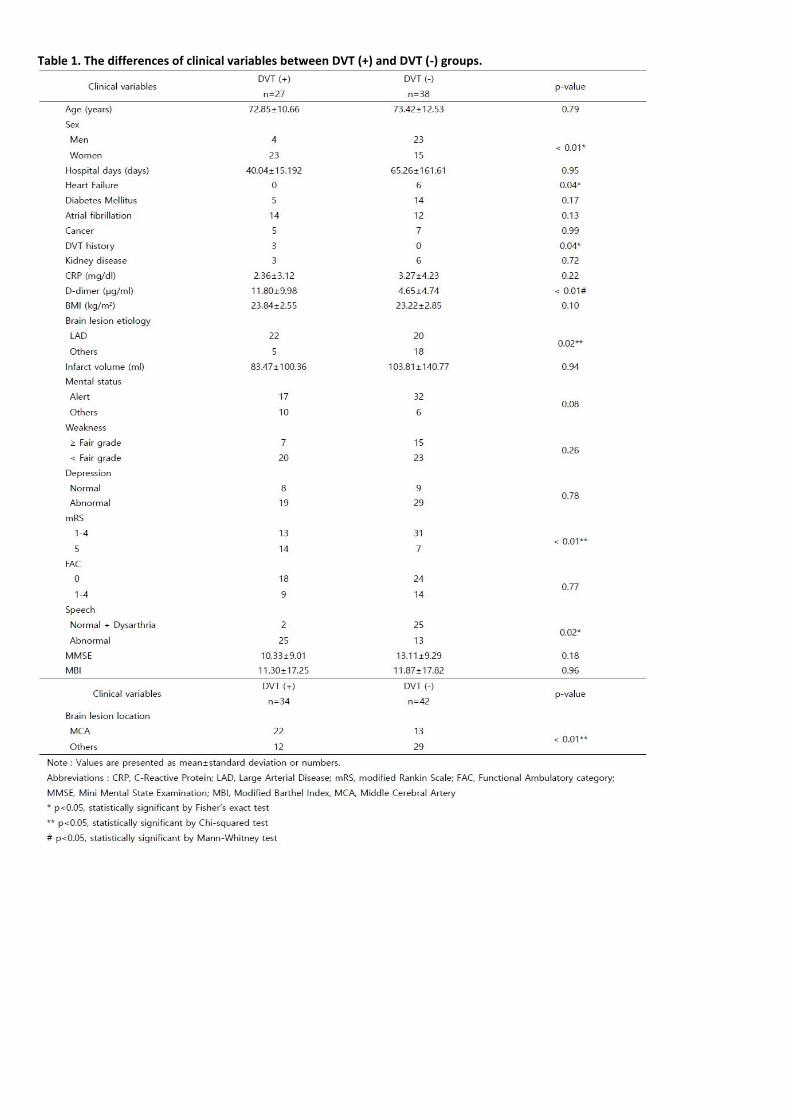
Table 1. The differences of clinical variables between DVT (+) and DVT (-) groups.
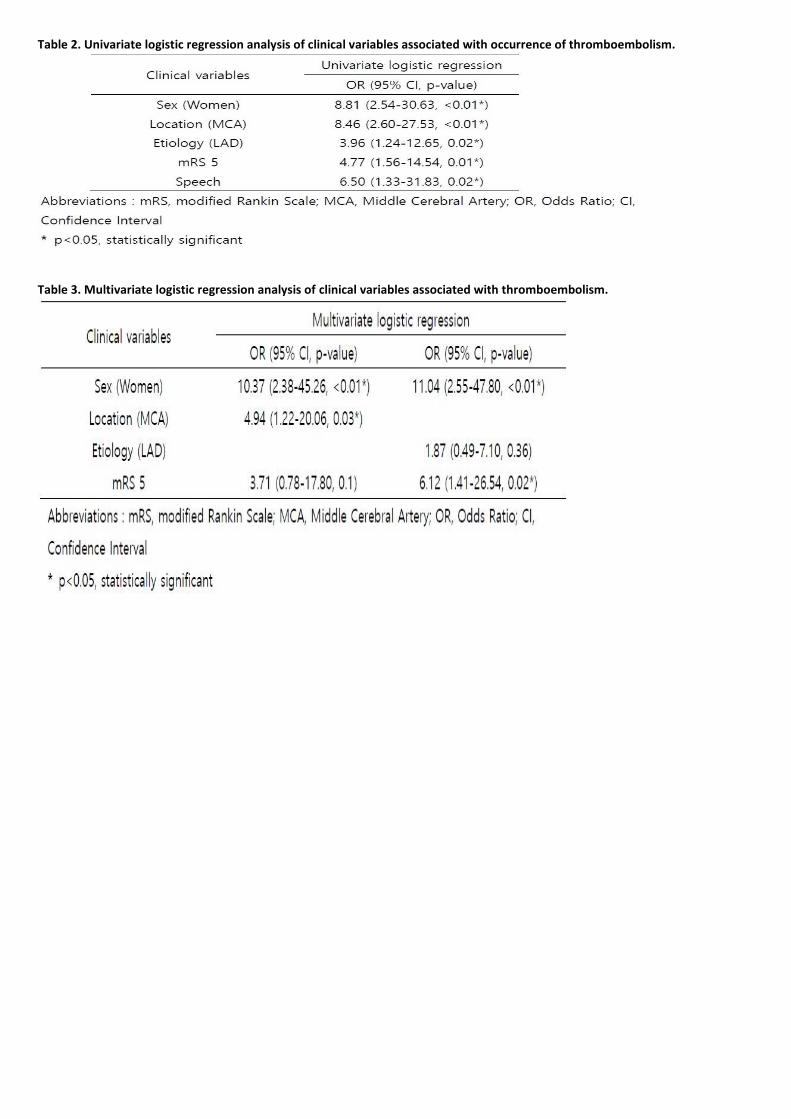
Table 2. Univariate logistic regression analysis of clinical variables associated with occurrence of thromboembolism.
Table 3. Multivariate logistic regression analysis of clinical variables associated with thromboembolism.

P 43
Comparison of the ACC-AHA and the ATP-III Guidelines for Cardiovascular Disease Prevention in Korea
Jong Weon Lee1*
, Hun Sun Lim2, Jong Hun Kim
3†, Hyoung Seop Kim
1†
Department of Physical Medicine and Rehabilitation,National Health Insurance Service Ilsan Hospital1, Research and Analysis
Team,National Health Insurance Service Ilsan Hospital2, Department of Neurology,National Health Insurance Service Ilsan Hospital
3
Objective
The 2013 American College of Cardiology and the American Heart Association (ACC-AHA) released new guidelines to replace the
Third Adult Treatment Panel (ATP-III) guidelines for cholesterol management. In order to better prevent cardiovascular diseases, the
ACC-AHA guidelines expanded the indications for statin therapy by lowering the threshold to a 7.5% 10-year atherosclerotic
cardiovascular disease (ASCVD) risk. Application of the new guidelines, however, has not been thoroughly studied in non-US
population. Therefore, we aim to reveal clinical efficacy of the ACC-AHA guidelines, as compared with the ATP-III guidelines, in a
large-scale Korean cohort.
Materials and Methods
Using the National Health Insurance Service–National Sample Cohort (NHIS-NSC) from 2009-2013, we analyzed proportions of
participants for whom statin therapy would be recommended using both guidelines. Baseline characteristics and risk factor profiles
of the study participants were also collected. Cumulative incidences of major adverse cardiovascular events (MACE; including
cardiovascular disease mortality, fatal or non-fatal myocardial infarction, and stroke) were the main outcome measures during the
follow-up. Hazard ratios of MACE in both guidelines were calculated using univariable and multivariable analysis.
Results
During the mean follow-up of 4.6 years, 338,332 participants of age 40 to 75 years were included in this study. 69,163 participants
(20.4%) were already on statin therapy. Under the ACC-AHA guidelines, 111,600 participants (33.0%) would be additionally eligible
to receive statin, as compared with 50,023 participants (14.8%) according to the ATP-III guidelines. The ACC-AHA guidelines showed
the largest increase of statin recommendation in participants who were eligible due to the 7.5% 10-year cardiovascular disease risk
(n = 74,826, 22.1%). In the statin-recommended groups, participants with previous CVD showed the highest incidence of MACE in
both guidelines; 5.0% (n = 863) in the ACC-AHA guidelines and 4.8% (n = 580) in the ATP-III guidelines. Participants who were statin
eligible by the ACC-AHA guidelines had higher and statistically significant HR of MACE when compared with those eligible by the
ATP- III guidelines: 1.28 (95% CI 1.18-1.39) vs. 1.06 (95% CI 0.99-1.14). Among many causes of MACE, stroke showed statistically
significant HR of 1.24 (95% CI 1.13-1.36) according to the ACC-AHA guidelines only.
Conclusion
The 2013 ACC-AHA guidelines for the management of blood cholesterol increase the number of statin-eligible patients in Korean
population. This result is concordant with NHANES and ARIC studies performed in the US adult population. By implementing statin
therapy to more people at risk of future cardiovascular diseases, we can efficiently reduce the incidence of MACE, especially stroke
among other causes.

P 44
Different brain regions affecting language function in patients with subacute and chronic stroke
Hee Dong Shin1*
, Dae Hyun Kim1†
Department of Physical Medicine and Rehabilitation, Veterans Health Service Medical Center1
Objectives
The present study aimed to identify the brain regions involved in language function in subacute and chronic phase after stroke.
Methods
40 patients with left hemisphere stroke with aphasia were included and divided into two groups (17 patients in subacute and 23
patients in chronic groups). The mean ages in subacute and chronic groups were 74.5 and 65.0 years respectively. The average
duration from stroke onset in two groups were 43 and 2236 days respectively. Fractional anisotropy (FA) mapping using diffusion
tensor imaging and language evaluation, including aphasia quotient, scores of spontaneous speech, comprehension, repetition and
naming in the Korean version of Western Aphasia Battery were used for examinations. Linear regression analyses were conducted
with the FA map as a dependent variable, each score of language evaluation as an independent variable, and patient age as a
covariate.
Results
FA in the posterior limb of internal capsule and corpus callosum of the left hemisphere, bilateral frontal lobe were positively
associated but FA in superior longitudinal fasciculus of the left hemisphere was negatively associated with aphasia quotient in acute
group. FA in bilateral frontal lobe was positively associated with spontaneous speech and FA in superior temporal gyrus of the left
hemisphere was positively associated with comprehension in acute group. FA in corpus callosum, frontal lobe of the left hemisphere
were negatively associated with repetition in acute group. FA in left midbrain, superior longitudinal fasciculus and inferior parietal
lobule of the right hemisphere were negatively associated with naming in acute group. However, FA in the splenium of corpus
callosum of the right hemisphere was only negatively associated brain region with comprehension in chronic group (corrected p <
0.05).
Conclusions
Multiple bilateral brain regions positively and negatively influence the language function in subacute phase but not in chronic phase
after stroke.
Acknowledgment: This work was supported by the National Research Foundation of Korea (NRF) grant funded by the Korea
government (MSIT) (No. 2017R1C1B1003).
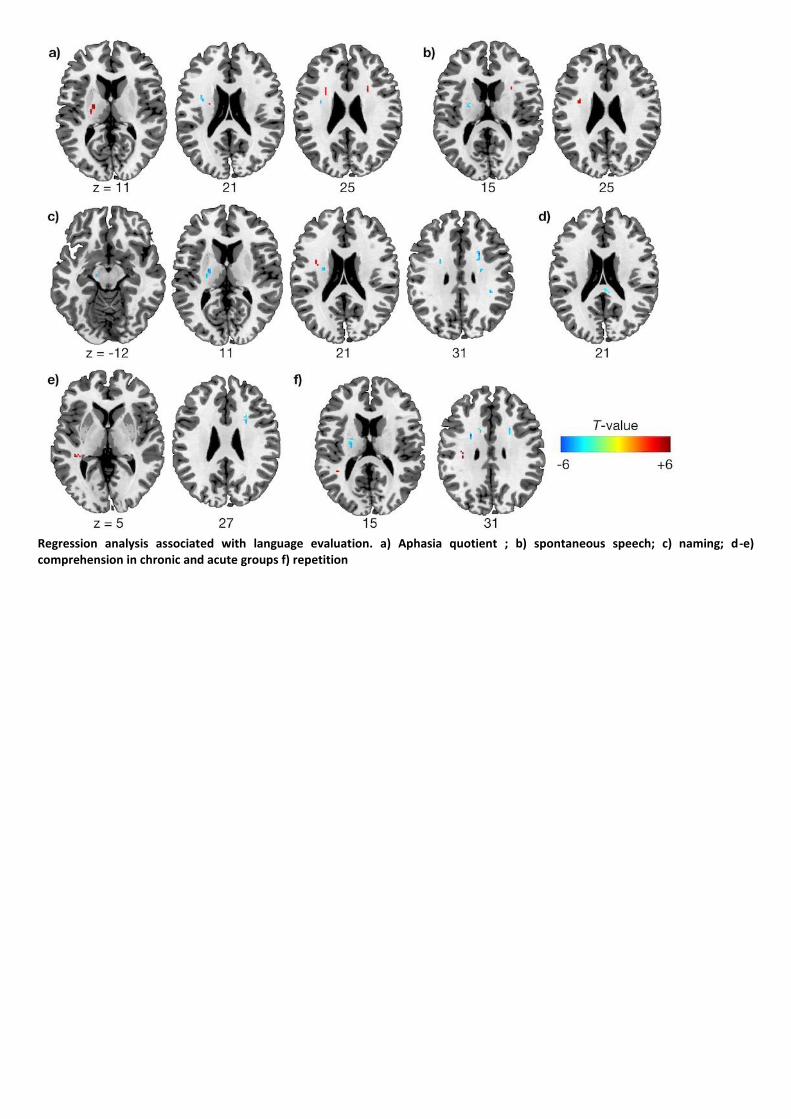
Regression analysis associated with language evaluation. a) Aphasia quotient ; b) spontaneous speech; c) naming; d-e) comprehension in chronic and acute groups f) repetition

P 45
Usefulness of goal attainment scale in inpatient rehabilitation of subacute stroke patients
Youngsu Jung1,2*
, Byungtae Ahn1, Eunyoung Park
1, Jinsoo Yoon
1, Jong Moon Kim
1,2, MinYoung Kim
1,2†
Department of Rehabilitation Medicine, CHA Bundang Medical Center1, Rehabilitation and Regeneration Research Center,CHA
University2
Introduction
The Goal attainment scale (GAS) is an assessment tool that is set individually according to the patient's condition and the therapists.
The GAS is appropriate for evaluating rehabilitation outcome without floor or ceiling effect, and it is also helpful in communication
and collaboration between medical staff. In addition, the patient can be enrolled in the course of the treatment, and it is
advantageous to be able to achieve the proper motivation. The purpose of this study is to introducing the usefulness of GAS in
intensive inpatient rehabilitation of subacute post-stroke patients.
Method
From January 2015 to December 2018, we collected data of stroke patients who were hospitalized at one rehabilitation center
retrospectively. Patients of 15 to 90 days after stroke onset, who had undergone rehabilitation for more than 4 weeks and had both
initial and follow up evaluation were included. Poor communication and poor cognition cases in the initial evaluation were excluded.
In physical therapy (PT), three specific goals were selected in the mobility (home, community), and body function (pain, posture)
areas. Also in occupational therapy (OT), three specific goals in the area of upper limb function, activities of daily living. All goals
were determined through active communication between patients and caregivers and medical staff. The goal attainment scale was
evaluated on a 5-point scale after 4 weeks of rehabilitation. A score of 0 indicates the expected level of achievement; +1 and +2 are
'slightly' and 'much’ better than expected; -1 and -2 represent ‘slightly’ and ‘much’ lower than expected level of achievement. We
analyzed whether the effects of rehabilitation treatment before (2015) and after (2016, 2017, 2018) introducing GAS were different.
To confirm the usefulness of GAS, we also checked the correlation with the changes in other evaluations and the questionnaire with
13 therapists.
Result
The data before the introduction of GAS (2015) (n = 58) and the data after the introduction of GAS (2016, 2017, and 2018) (n = 141)
showed no significant difference in baseline characteristics. There was no difference in improvement after rehabilitation treatment
between the patients before and after the introduction of GAS (Table 1). However, most therapists answered positively about the
quality of treatment and the increased participation of patients in treatment according to a questionnaire survey of therapists
(Table 2). In the PT (Figure (A)) and OT (Figure (B)), the GAS standard score showed a statistically significant positive correlation with
the change in ADL outcome.
Conclusion
Goal attainment scaling is a useful tool for evaluating the functional improvements of post-stroke patients in subacute period.
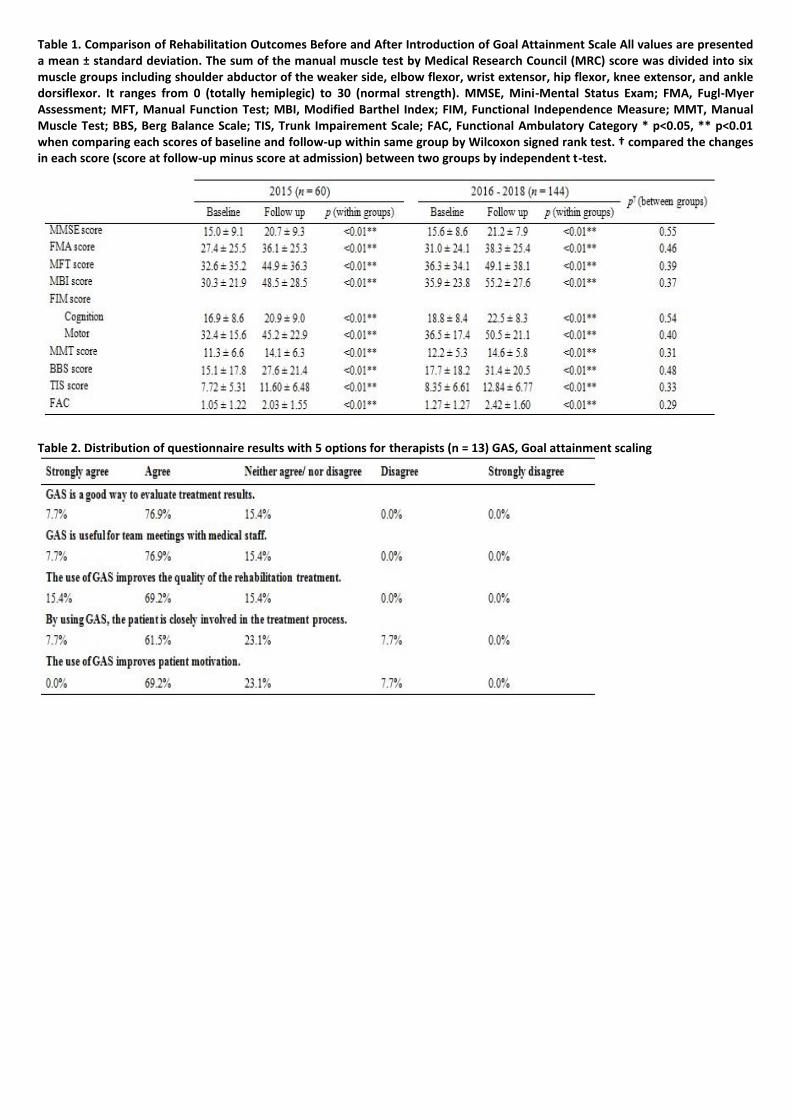
Table 1. Comparison of Rehabilitation Outcomes Before and After Introduction of Goal Attainment Scale All values are presented a mean ± standard deviation. The sum of the manual muscle test by Medical Research Council (MRC) score was divided into six muscle groups including shoulder abductor of the weaker side, elbow flexor, wrist extensor, hip flexor, knee extensor, and ankle dorsiflexor. It ranges from 0 (totally hemiplegic) to 30 (normal strength). MMSE, Mini-Mental Status Exam; FMA, Fugl-Myer Assessment; MFT, Manual Function Test; MBI, Modified Barthel Index; FIM, Functional Independence Measure; MMT, Manual Muscle Test; BBS, Berg Balance Scale; TIS, Trunk Impairement Scale; FAC, Functional Ambulatory Category * p<0.05, ** p<0.01 when comparing each scores of baseline and follow-up within same group by Wilcoxon signed rank test. † compared the changes in each score (score at follow-up minus score at admission) between two groups by independent t-test.
Table 2. Distribution of questionnaire results with 5 options for therapists (n = 13) GAS, Goal attainment scaling

Figure. Correlation between GAS T score and conventional ADL outcome measurements A) Correlation between GAS T score of physical therapy and FIM - cognition, FIM - motor, and MBI B) Correlation between GAS T score of occupational therapy and FIM - cognition, FIM - motor, and MBI The standard score = 50 + {(10Σ(wixi))/(0.7Σwi2 + 0.3(Σwi)2)½} All the assigned weights (wi) were treated the same PT, Physical therapy; OT, Occupational therapy; ADL, Activities of daily living; GAS, Goal Attainment Scale; FIM, Functional Independence Measure; MBI, Modified Barthel Index

P 46
The efficacy of combination tDCS and TENS in stroke patients
Jun Hyun Choi1*
, Won Jae Jo1, Jong Hoo Lee
1†
Department of Physical Medicine and Rehabilitation and Medical Device Clinical Trial Center, Presbyterian medical center1
Objective
Transcranial direct current stimulation (tDCS) and sensory stimulation via transcutaneous electrical nerve stimulation (TENS) have
been reported to be effective in improving motor function in stroke patients. We investigate the effects on combination of tDCS and
TENS on upper extremity function in stroke patients.
Methods
Patients with post-stroke paralysis and upper limb dysfunction were randomly assigned to one of two groups. Only TENS
(Modulated frequency: 70-130Hz, 5 second cycle, 20 minutes) via a conductive glove was applied with the control group. Study
group applied tDCS and TENS concurrently. 8 stroke patients in each group were enrolled and received therapies for 4 weeks.
Manual muscle test, modified Ashworth scale, box and block test, 9 hole peg test, Fugl-Meyer Assessment and somatosensory
evoked potential were used to evaluate the effects of the treatment
Results
Both groups improved in upper limb function score after 4 weeks of treatment. By comparing the two groups, the study group
showed more significant improvement than the control group in box and block test, 9 hole peg test and Fugl-Meyer Assessment
(p<0.05)
Conclusion
It was found that combination of tDCS and TENS is more effective treatment compared to TENS only. We recommend to use both
tDCS and TENS. Thus, we suggest to apply the combined therapy to the stroke patients.
P 47
Factors Affecting Keep in Employment Status after Return to Work in Persons with Stroke
So Jung Kim1*
, Hae In Lee2, Ji Hong Min
1, Junhee Han
3, Deog Young Kim
4, Min Kyun Sohn
5, Jongmin Lee
6, Sam-Gyu Lee
7, Gyung-Jae
Oh8, Yang-Soo Lee
9, Min Cheol Joo
10, Eun Young Han
11, Won Hyuk Chang
12, Yun-Hee Kim
12, Yong-Il Shin
1,2†
Department of Rehabilitation Medicine,Pusan National University Yangsan Hospital1, Department of Rehabilitation Medicine, Pusan
National University School of Medicine2, Department of Statistics,Hallym University
3, Department and Research Institute of
Rehabilitation Medicine,Yonsei University College of Medicine4, Department of Rehabilitation Medicine,Chungnam National
University School of Medicine5, Department of Rehabilitation Medicine,Konkuk University School of Medicine
6, Department of
Physical and Rehabilitation Medicine,Chonnam National University Medical School7, Department of Preventive
Medicine,Wonkwang University School of Medicine8, Department of Rehabilitation Medicine,Kyung-pook, National University
College of Medicine9, Department of Rehabilitation Medicine,Wonkwang University School of Medicine
10, Department of
Rehabilitation Medicine,Jeju University Hospital, University of Jeju College of Medicine11
, 2Department of Physical and
Rehabilitation Medicine, Center for Prevention and Rehabilitation, Heart Vascular and Stroke Institute, Samsung Medical Center,
Sungkyunkwan University School of Medicine12
Objective
To investigate the rate of return to work and identify the key factors affecting return to work between 3 months and 2 years after
stroke.
Design
Prospective cohort study.
Setting:
The Korean Stroke Cohort for Functioning and Rehabilitation (KOSCO) in Korea.
Participants
A total of 193 first-ever stroke who reported working status at 3 months after stroke.
Outcome measures
Baseline characteristics were collected from medical records. Functional assessments and an enumeration survey were performed
using previously validated instruments.
Results
Overall, 145 (75.1%) persons with stroke of the ‘Continuously Employed’ group and 48 (24.9%) persons with stroke of the
‘Employed-Unemployed’ group returned to work between 3 months and 2 years after stroke. Multivariate logistic analysis
demonstrated that characteristics of persons with stroke, including age, the Psychosocial Well-being Index-Short Form (PWI-SF)
score, and caregiver characteristics, including age, sex (female), and living status, were significantly associated with return to work
between 3 months and 2 years after stroke.
Conclusion
The age and PWI-SF score of persons with stroke as well as the age, sex and living status of caregivers are the key factors affecting
return to work, which is important for the well-being of persons with stroke.

P 48
Therapeutic mechanisms of repetitive transcranial magnetic stimulation
Sung Hoon Kim1†
, Jun Young Park1*
, Ji Hyun Kim1, Sang Yeol Yong
1, Sung-Rae Cho
3, Ahreum Baek
1,2, Ji Yoon Jang
1, Ji Sun Hong
1, Min
Woo Kim1
Department of Rehabilitation Medicine,Yonsei university Wonju College of medicine1, Department of Global Medical
Science,Yonsei University Wonju Colleage of Medicine2, Department and Research Institute of Rehabilitation Medicine,Yonsei
University College of Medicine3
Introduction
Repetitive transcranial magnetic stimulation (rTMS) is a nonaggressive therapy that can be used to diagnose and treat many
neurological disorders. It is well known that high-frequency (> 3 Hz) stimulation generally results in facilitation, while low-frequency
(< 1 Hz) rTMS induces reduction of synaptic efficiency. Although rTMS has been the neurobiological mechanisms underlying the
effects of rTMS remain unclear. Therefore, the current study examined the differential effects of rTMS depending on frequencies in
both in vitro and in vivo experimental models.
Materials and methods
Mouse neuroblastoma cells were randomly divided into three groups—sham, low-frequency (0.5 Hz) and high-frequency (10 Hz)
groups—and were stimulated over three days. In high-frequency group, cell proliferation was increased via up-regulation of
neurotrophic factors. Then, low-frequency and high-frequency groups were characterized by RNA-seq transcriptome analysis.
Among several pathways, long-term potentiation pathway is an enriched significant pathway. Furthermore, high-frequency group
induced phosphorylation of cAMP-response element binding protein (CREB), brain-derived neurotrophic factor (BDNF) transcription
via activation of calcium (Ca2+)-/calmodulin-dependent protein kinase II (CaMKII)-CREB pathway. Next, cells were differentiated
with retinoic acid and established for the in vitro oxygen glucose deprivation/reoxygenation (OGD/R) condition. After OGD/R injury,
cells were randomly divided into three groups—OGD/R+sham, OGD/R+low-frequency and high-frequency groups—and were
stimulated with rMS on day 1. High-frequency group increased cell proliferation and reduced apoptosis in OGD/R injured cells.
Furthermore, high-frequency group increased BDNF expression and synaptic plasticity via activation of Ca2+-CaMKII-CREB signaling
pathway in OGD/R injured cells.
Results
Eight-week Sprague-Dawley rats were unilaterally injected with 6-hydroxydopamine (6-OHDA) into the right striatum. High-
frequency of rTMS (10 Hz) was treated during four weeks in the PD rats. High-frequency of rTMS improved motor functions and
preserved dopaminergic neurons from damages in the substantia nigra pars compacta and striatum by 6-OHDA administration.
Furthermore, neurotrophic growth factor expression was increased in high-frequency rTMS-treated PD rats, suggesting a potential
for rTMS treatment in the PD.
Conclusion
Taken together, these studies will provide a better understanding of the therapeutic mechanisms of rTMS. These mechanisms may
also be applicable in neural stem cells and patient-derived induced pluripotent stem cells for future studies.

Expression of neurotrophic/growth factors increase after repetitive magnetic stimulation in neuroblastoma cells
Effect on the proliferation of neuroblastoma cells treated with repetitive magnetic stimulation

P 49
Dysphagia-related Health Information Improved Consumers’ Acceptability of Thickened Beverages
Sang Hun Kim1*
, Myung Jun Shin1, Jihye An
2, Jeehyun Lee
2, Jin A Yoon
1†
Department of Rehabilitation Medicine,Pusan National University Hospital1, Department of Food Science and Nutrition & Kimchi
Research Institute,Pusan National University2
Introduction
Dysphagia refers to symptoms that are difficult or inconvenient to swallow bolus. Patients with dysphagia require dietary
modification by increasing the viscosity of foods and beverages. This study was conducted to investigate changes in sensory
perception of consumers before and after providing dysphagia-related health information using thickened beverages.
Method
The total number of participants was 120, consisting of 60 young consumers aged between 19 and 39 and 60 middle-aged
consumers aged between 40 and 65. Experiments were conducted twice at one week interval. The first session proceeded without
any information, and the second session provided information about the dysphagia and needs of diet modification before
evaluation. All processes were the same except providing information. Three beverages (orange juice, red bean water, and sports
drink) were used with nectar-like (51 to 350 cP) and honey-like (351 to 1750 cP) stages. And also, original beverage samples (0%)
were used as a control. Consumers were asked about acceptability, flavor liking, intensity, and General Health Interest (GHI) (Table
1).
Result
Data analysis was done using analysis of variance that showed the change of flavor and acceptance from the uninformed session to
informed session. Although there were differences between the samples by age groups, the thickened beverages showed increased
acceptability after information was provided. Acceptance of their characteristics (swallowing, viscosity, and mouthfeel) also changed
a after providing information (Table 2). There were no significant differences for 0% samples. The mean of GHI for the youth group
was 3.97±0.85 and that for the middle age group was 4.81±0.68. GHI was divided into High GHI and Low GHI groups using their
average value. High GHI groups showed significant acceptability for the informed evaluation but Low GHI group were not influenced
by the dysphagia information.
Discussion
This study examined the use of thickened beverages to see whether information provision affects people's acceptability. The
provision of information on dysphagia affects preference in beverages with increased viscosity. It was also found that swallowing,
viscosity, and taste of mouthfeel were also affected. The mean value of GHI was different according to the age, and was divided into
High GHI and Low GHI groups accordingly. According to the GHI, the degree of preference was also changed. In addition, it is
necessary to verify whether the experiment that ordinary people did can replace the experiment for patients. It needs consumer
acceptance test for dysphagia patients who are prescribed a viscosity enhancer by doctor. And it should be considered suitability of
samples to replenish the patient’s water supply and to ensure long-term use. Also, the preference test should be extended to the
patient experiment by judging suitability for dysphagia patients using other types of beverages, liquid diet and solid diet further.

Table 1. The information and viscosity of samples
Table 2. Mean acceptability of swallowing, viscosity, and mouthfeel characteristics of thickened beverages

P 50
Secretome from neural precausor cells attanuated neuronal injury in pMCAO rat model
Ji Yoon Jang1*
, Ji Hyun Kim1†
, Ji Yong Lee2, Han-soo Kim
3, Jun Yoon Park
1, Ji Seon Hong
1
Department of Rehabilitation Medicine,Wonju Severance Christian Hospital1, Department of Anatomy,Yonsei University Wonju
College of Medicine2, Department of Biomedical Sciences,Catholic Kwandong University College of Medicine
3
We previously showed that the transplantation of pluripotent stem cell-derived neural precursor cells (NPCs) improve functional
outcomes in a rat model of ischemic stroke. NPCs exerted the beneficial effects, in part, through paracrine mechanism. In this study,
we investigated the ability of NPC secretome to improve behavioral function in a rat stroke model. Data showed that rats
administrated with NPC secretome are superior to those treated with blank in behavioral function throughout time points. To
investigate its underlying events, immunohistochemical (IHC) analysis was performed on rat ischemic brains. IHC analyses showed
that NPC secretomes reduced inflammation, enhanced angiogenesis with increased endogenous neurogenesis in rat injured brain.
In conculsion, NPC secretome promotes the functional recovery of damaged stroke brain via modulation of anti-inflammation,
angiogenesis and neurogenesis. Thus, NPC secretome closely recapitulateds the effects seen upon NPC transplantation
Acknowledgment: Granat supported by the National Research Foundation, MSIP, 2017M3A9B4042583

P 51
Determining the peak cough flow values to predict dysphagia in stroke patients
Hyunhwa Lee MD.1*
, Yeonjae Han MD.1, Geun-Young Park MD, Ph.D.
1, Sun Im MD, Ph.D.
1†
The Catholic University of Korea, Department of Rehabilitation Medicine,Bucheon, St. Mary’s Hospital, College of Medicine1
Objective
Cough failure in patients may be a life-threatening condition leading to aspiration pneumonia. Ineffective cough production is
associated with a higher prevalence of respiratory complications in stroke. In our study, to determine the diagnostic parameters and
appropriate cut-off values of the cough strength, we assessed, the maximal inspiratory and expiratory pressures and peak cough
flow to determine which parameter could accurately screen presence dysphagia in stroke patients.
Method
Retrospective analysis of a prospectively maintained database was done. in a single university affiliated hospital. Patients with first-
ever diagnosed dysphagia attributable to cerebrovascular disease, prospectively performed spirometry measurements for the
voluntary peak cough flow and respiratory pressure meters were recruited. These values were compared to patients with no
evidence of dysphagia after stroke. Primary outcome measures were peak cough flow (L/min) during voluntary coughing and
maximal pressure meter (cmH22O)).
Results
Total eligible patients (N=237) with 163 patients who were diagnosed with dysphagia related to stroke were recruited. A final 163
patients had full medical records with 6-month follow-up. Receiver operating curve analysis showed that peak cough flow cut-off
values set at 151 L/min were significantly associated with presence of dysphagia with sensitivity levels of 0.72 (0.66-0.79) and
specificity levels of 0.78 (0.69-0.88) [area under the curve (AUC) 95% confidence interval (CI)=0.81 (0.76-0.87)] [fig.1]. In contrast,
the cut-off values set at 20 and 38 for the MIP and MEP showed lower sensitivity levels (0.49, 0.58) with lower AUC values of
0.65(0.58-0.72) and 0.70(0.64- 0.77).Peak cough flow, as an independent predictor of dysphagia in stroke patients, could
significantly predict the presence of dysphagia with an adjusted odds ratio of 4.12 (2.20-8.69, p<0.001) in a multivariate logistic
regression analysis [fig.2].
Conclusions
Among the various respiratory parameters, the peak cough flow cut-off values of the voluntary cough flow set at 151 L/min can
significantly indicate the presence of dysphagia. Results advocate the objective measurement of peak cough flow from voluntary
coughing to be used as part of the formal assessment those with post-stroke dysphagia. Our results indicate that among the various
respiratory parameters, objective strength measurement of the peak cough flow could help screen those with dysphagia.
Fig. 1 Peak cough flow cut-off values set at 151 L/min were associated with presence of dysphagia [area under the curve (AUC) 95% confidence interval (CI) = 0.81 (0.76–0.87)]

Fig. 2 Peak cough flow, as an independent predictor of dysphagia in stroke patients, could significantly predict the presence of dysphagia in a multivariate logistic regression analysis

P 52
Degeneration of Corticobulbar tract in patients with Poststroke Dysphagia
Youngkook Kim1*†
, Sun Jae Won1, Yeun Jie Yoo
1, DaYe Kim
1*, Mi-Jeong Yoon
1
Department of Rehabilitation Medicine, Yeouido St. Mary’s Hospital1
Introduction
The aim of our diffusion tensor tractography study was to determine whether degeneration of the corticobulbar (CBT) is associated
with the presence of poststroke dysphagia in patients with middle cerebral artery (MCA) infarction.
Material & Methods
Seventeen patients with dysphagia after unilateral MCA infarction were enrolled. We reviewed Videofluoroscopic Swallowing Study
(VFSS) findings performed in the subacute rehabilitation of stroke, and the severity of dysphagia was evaluated using the dysphagia
outcome and severity scale (DOSS). Probabilistic tractography was performed using FSL's ProbtrackX program. The two regions of
interest (ROIs) were placed over cortex and brainstem to reconstruct the CBT. The seed ROI was located on the lip and tongue
representing area corresponding to Homunculus from axial slices. The way ROI was located where the corticobulbar tract lies at
mid-pontine level. Tract volume was calculated by multiplying the voxel volume by the number of traced voxels during fiber tracking.
Comparison between the affected and unaffected CBT volume were conducted to explore the role of CBT on poststroke dysphagia.
Correlation analysis was conducted to determine the association between the DOSS and the integrity of CBT.
Results
Demographic characteristics were as follows; mean age, 65.6 ± 12.5 years; time to VFSS, 22.7 ± 15.5 days, time to DTI acquisition,
32.9 ± 17.1 days, mean DOSS, 4.2 ± 1.8. The volume of affected CBT was smaller than those of unaffected one (affected vs.
unaffected CBT, 2774 ± 3839 vs 8029 ± 6090 mm3, p = 0.005). No significant correlation was found between the DOSS and the
affected CBT volume.
Conclusions
Degeneration of the affected CBT may be associated with poststroke dysphagia in patients with MCA infarction. The integrity of the
affected CBT was not associated with the severity of dysphagia.
Acknowledgment: N/A

P 53
The effect of sensory deficit on gait and balance of supratentorial stroke patients after acute phase
Minsun Kim, MD1*
, Hyun Haeng Lee1, Jongmin Lee
1†
Department of Rehabilitation Medicine, Konkuk University Medical Center and Konkuk University School of Medicine1
Objective
Sensory deficit is common in patients with stroke and seems to be related to balance and ambulation. Previous studies which have
shown the association between sensory impairment and balance evaluated the integrity of sensory system by using clinical scoring
system. The aim of the present study was to determine the relationship between parameters of somatosensory-evoked potential
(SSEP) as quantitative measure and stability of gait and balance in supratentorial hemiplegic stroke patients after acute phase.
Method
We retrospectively reviewed the medical records for stroke patients who were admitted to the department of rehabilitation
medicine from January 1, 2006 to February 28, 2019. Inclusion criteria were as follows: 1) patients with only supratentorial stroke; 2)
interval between stroke onset and SSEP > 2 weeks; 3) MRC grade 4 or higher on hemiplegic lower extremities including hip flexor,
knee extensor and ankle dorsiflexor; 4) independent gait before onset of stroke. We excluded 1) patients with a previous stroke,
visual field defect, hemineglect, spasticity; 2) those with peripheral polyneuropathy of lower extremities confirmed by
electrophysiologic study; 3) those with SSEP abnormalities at non-hemiplegic side. We divided 69 enrolled patients into two
subgroups according to SSEP abnormalities of hemiplegic side (Figure 1). The criteria for abnormality of SSEP were delayed latency
more than 43.9 msec and amplitude (P39-N50) less than 0.5uV.
Results
The mean age of patients was 50.94, with 30 men and 47 ischemic stroke, and 11 patients had thalamic lesions. The mean score of
BBS and FAC was 37.29 and 3.52 score, respectively. The mean latency and amplitude of SSEP at hemiplegic side was 44.05 and 2.29
respectively and mean of side-to-side difference was 3.38. The mean latency and amplitude of SSEP at non-hemiplegic side was
41.02 and 2.61, respectively (Table 1). Among 69 enrolled patients, 17 patients had the abnormalities of SSEP at hemiplegic side.
The mean BBS scores of each subgroup was 38.50 and 33.59, and mean FAC scores was 3.67 and 3.06, respectively. In the group
with abnormalities of SSEP, the score of BBS and FAC tended to be low, without reaching statistical significance (Table 2).
Conclusion
The dysfunction of balance and gait in hemiplegic patients with supratentorial stroke tended to be more severe in the group with
abnormalities of SSEP compared to the group without abnormalities, albeit without statistical significance. The results were
probably due to small sample size of enrolled patients and insensitivity of reference value of SSEP.
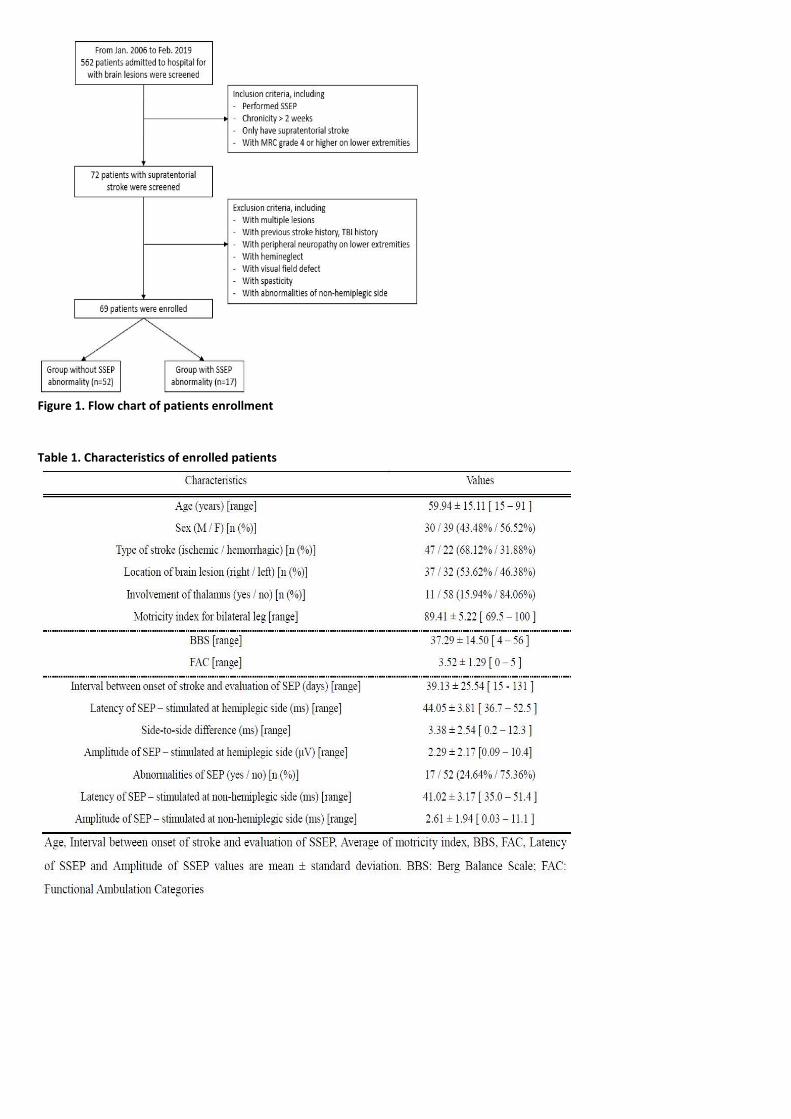
Figure 1. Flow chart of patients enrollment
Table 1. Characteristics of enrolled patients
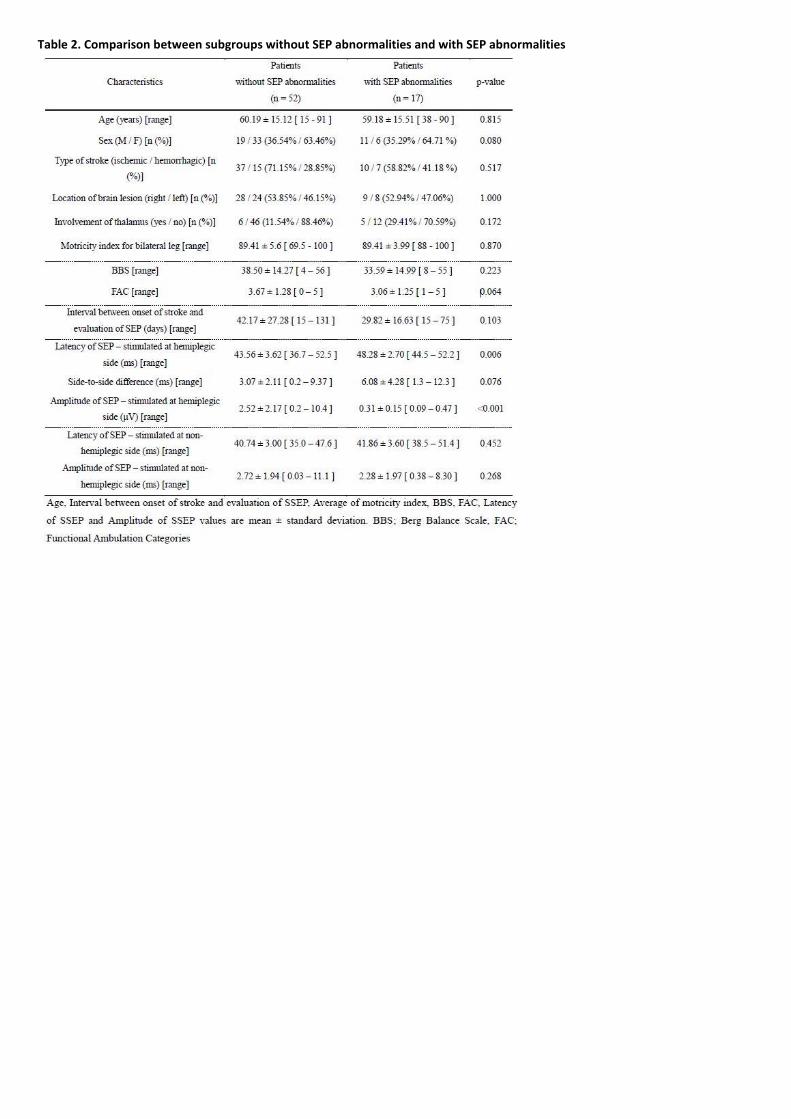
Table 2. Comparison between subgroups without SEP abnormalities and with SEP abnormalities

P 54
Effect of Body Mass Index on Recovery of Chronic Stroke Patients with Sarcopenia
Ho Joong Jung1*
, Hyng Haeng Lee1, Jongmin Lee
1†
Department of Rehabilitation Medicine, Konkuk University Medical Center1
Background
Sarcopenia is characterized by decreased muscle mass, muscle strength, and physical performance. Previous studies suggest that
sarcopenia as well as body mass index (BMI) associated with post-stroke functional outcome. However, the effect of BMI in chronic
post-stroke patient with sarcopenia has not been studied. In this study, we analyzed the association between BMI and functional
outcome in chronic stroke patients with sarcopenia.
Methods
Patients with history of neuropathy or myopathy, and severe medical comorbidities were excluded. Sarcopenia was diagnosed with
criteria of Asian Working Group for Sarcopenia consisting of decreased skeletal muscle index (SMI) of bioelectrical impedance
analysis, hand grip strength and 4-m gait speed. BMI, motricity index, Fugl-Meyer Assessment (FMA), Modified Barthel Index (MBI),
Berg Balance Scale (BBS), and Functional Ambulatory Category (FAC) were measured at admission and discharge. Patients were
divided into 2 groups according to BMI; underweight group (<18.5kg/m2) and normal group (18.5 to 25 kg/m2). The difference of
outcome measures between two subgroups at initial, discharge and the change were analyzed.
Results
We enrolled fifteen first-ever chronic stroke patients (interval between onset of stroke and enrollment; >6 months) with sarcopenia
(six females; mean age of 69.5 years). We found no significant difference of age, gender, and chronicity of stroke between two
subgroups (Table 1). The mean interval between initial and follow-up evaluation was 28.4 days. The FMA measured on the affected
and unaffected side did not show significant difference in initial and discharge, but the significant difference was found in change of
FMA, which was attributed to noticeable change of upper extremities FMA (Table 2). We also found that MBI, BBS, FAC, and
motricity index had no significant difference between 2 subgroups.
Conclusion
In this study, we found that under-BMI affected negatively neurological recovery of upper extremities in chronic post-stroke
patients with sarcopenia significantly. Therefore, we postulate that state of sarcopenia with under-BMI impede recovery of chronic
post-stroke patient. Further study with larger sample size should be performed to prove the hypothesis.
Table 1. Demographics of enrolled patients
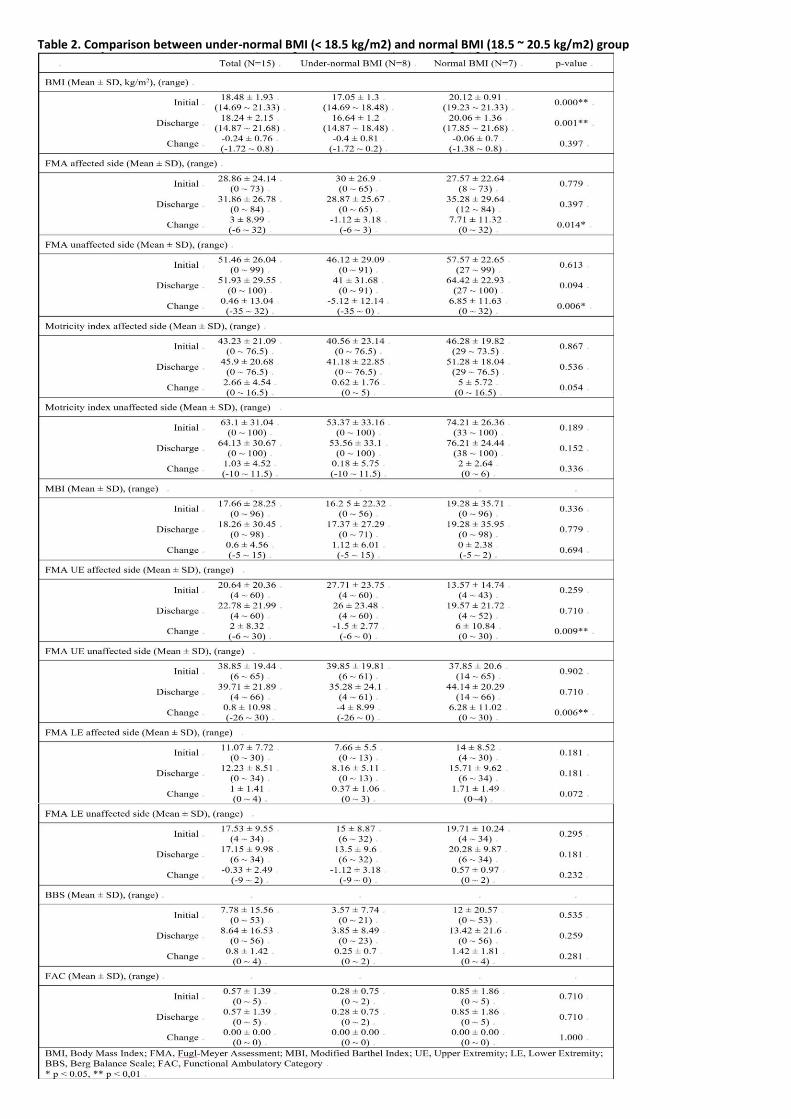
Table 2. Comparison between under-normal BMI (< 18.5 kg/m2) and normal BMI (18.5 ~ 20.5 kg/m2) group

P 55
Gait analysis of Parkinson’s Disease and Multiple Systemic Atrophy: Preliminary Study
Chang Hoon Bae1*
, Hye Won Jung1, Ji Young Yun
2, Jeong Eun Lee
3, Soo Jeong Han
1†
Department of Rehabilitation Medicine,Ewha Womans University Mokdong Hospital1, Department of Neurology,Ewha Womans
University Mokdong Hospital2, Department of Rehabilitation Medicine,Seoul Medical Center Seonam Hospital
3
In Parkinson’s disease (PD), gait disturbance is one of the most disabling characteristics of the disease since the quality of life
diminishes with increasing fall frequency; the overall quality of life diminishes with developing gait disturbance. It is estimated that
more than 70% of patients fall during the course of the disease and such events often result in fractures, often leading to another
morbidity. Along with the classical PD, there are other diseases with similar characteristics observed in the PD: atypical Parkinsonian
disorders (APD). Popular APDs are multiple system atrophy (MSA), progressive supranuclear palsy, corticobasal syndrome, etc. The
diseases are commonly referred to as Parkinsonism, despite of differences in etiology and treatment plans. Although the PD has the
clinical features commonly associated with Parkinsonism, there is a broader spectrum of disease represented by a collection of
phenotypically-similar neurodegenerative conditions that mimic core features of PD, including gait pattern. Thus, it is a challenge to
distinguish a specific disease among various diseases with similar clinical presentation. In this study, we have tried to find difference
in similar gait patterns displayed by between the PD group and the MSA group. From September 2016 to August 2018, 76 patients
were selected among those who visited the hospital for evaluation of Parkinsonism. We evaluated the patients’ gait patterns using
Zebris® gait analysis system (Fig. 1). The spatiotemporal parameters of gait were estimated from the vertical pressures measured on
a force platform housed within a treadmill. The patient pool was filled as the diagnosis was given; 11 patients without clear
diagnosis were excluded, then the patients diagnosed with non-Parkinsonism, such as syphilis and depression, and the patients with
diagnosis other than PD and MSA were excluded. Total of 17 PD patients and 17 MSA patients were recruited for the study, but 6
patients from each group were excluded due to severe gait disability with gait velocity slower than 1.0km/hr. We gathered and
analyzed step length, difference in step length, stride length, step width, stance phase percentage, swing phase percentage,
cadence, lateral symmetry, and double stance phase percentage. The statistical analysis is made via Mann-Whitney U-test, using
SPSS 21.0 In this study, there was a statistically significant difference in lateral symmetry between the PD group and the MSA group
(Table 1), indicating that the PD patients had more deviated center of gravity than the MSA patients at the time of initial evaluation
of the disease (Fig. 2); median values with standard deviation are 16.51±11.24 for PD and 2.31±9.23 for MSA. This study indicates
that there may be differences in gait pattern between Parkinson’s disease and multiple systemic atrophy patient groups, which may
be extended to further research to help distinguish a specific disease among various Parkinsonian diseases.
Fig. 1 Gait analysis by Zebris® system used for the study

Fig. 2 Stem-and-Leaf Plot for Lateral Symmetry for PD and MSA. The median value with standard deviation are indicated: 16.51 ± 11.24 for PD and 2.31 ± 9.23 for MSA Table 1. Statistical Analysis for PD and MSA using Mann-Whitney U Test. The analysis results indicate that only the lateral symmetry measured from the gait analysis platform has a statistically significant difference between the PD and the MSA groups with U-value = 24.000, p-value 0.017, suggesting that the PD patients had more deviated center of gravity than the MSA patients at the time of initial evaluation of the disease

P 56
The clinical efficacy and safety of Information and Communication Technology (ICT)-based system
Jong Min Kim1, Donghwi Park
1, Byung Joo Lee
1, Lee Hyomin
1, Ju Young Cho
1, Hyunseok Moon
1, Sungwon Park
1, Zeeihn Lee
1†, Kwang
Jae Yu1*
Department of Rehabilitation Medicine, Daegu Fatima Hospital1
Background
Currently, as our society enters the aging society, the population of the elderly, particularly the elderly living alone, is increasing.
And these elderly people are usually accompanied by chronic diseases and need long-term medication. In these elderly people,
however there are many problems in using pills safely and regularly. Patients with dementia, especially Alzheimer’s disease, often
forget to take medicine because of memory impairment, or even take medicine duplicately. So, it is difficult to take medication
regularly in patients with AD.
Objective
The purpose of this study was to investigate the effectiveness and safety about the drug compliance when using ICT-based systems
with smart drug kit, including the function of patient identification, of recording the scene of taking medicine for confirming an
accurate medication, of informing caregivers and medical staffs if the medicine is not applied.
Subjects and Methods
108 patients with mild dementia who were diagnosed by Diagnostic and statistical manual of mental disorder-IV, and who were
taking or are expected to take an acetylcholine esterase initiator are recruited prospectively. And these subjects randomly were
distrubuted in a 1:1 ratio to clinical trial groups using ICT-based systems with smart drug kit (Group A) and control groups (Group B).
To evaluate the efficacy of ICT-based systems with smart drug kit, the drug compliance, changes in cognitive function and ADL were
investigated. And each evaluation was conducted at 12 weeks and 24 weeks after starting the medication.
Results
In the result, the drug compliance assessment (taking compliance, timing compliance, and drug holiday) in the group A was
significantly lower than that of the Group B (control group). However, there were no significant differences between the two groups
in an investigation of a medication, and no significant differences in K-MMSE, CDR, CDR-SB, Barthel ADL and IADL. In addition, there
were no significant difference in the degree of changes between the time of visit. There was no significant difference in GDS
between the two groups, but there was a statistically significant improvement of the visit points in both groups. In the satisfaction
survey of group A, satisfaction of ICT was 35.81 ± 5.24. The safety assessment analysis found that 28 cases of adverse events were
reported in the group A, 37 reported in the group B. However, there was no significant difference between the two groups and no
adverse event directly related to the study.
Conclusion
In this study, there was no statistically significant difference in the drug compliance between the two groups. However, clinically
there was a significant improvement in the drug compliance, and safety of ICT-based systems with smart drug kit was confirmed in
this study. Therefore, in the future, clinical applications of ICT-based systems with smart drug kit may be useful in increasing the
drug compliance in patients with mild dementia.

P 57
Correlation with stroke patients' ADL and oral health
Geun Su Lee1*
, Ji Hong Cheon1, Na Na Lim
1, Won Ki Hong
1, Hyun Kyung Lee
1†, Sung Hoon Lee
1, Eun Young Kang
1, Youn Kyung Jo
1
Department of Rehabilitation Medicine, Kwangju christian hospital1
Correlation between ADL score and oral health status in chronic stroke patients
Objective
As acute stroke management and stroke rehabilitation have developed, the survival rate of acute stroke patients and the lifespan of
stroke patients with disability have been increased. Stroke patients have disabilities, such as limited mobility, ADL dependence and
dysphagia. Deterioration of the oral health status is also common in stroke patients. This study aims to evaluate oral health status of
chronic stroke patients and to analyze correlation between ADL score and oral health status.
Methods
Twenty stroke patients were hospitalized in Kwangju Christian Hospital. Twenty patients in chronic phase were classified as
independent ADL (> K-MBI 70), maximal ADL (< K-MBI 47). The divided groups were evaluated by a dentist using 'The Oral Health
Assessment Tool'
Results
The statistically significant correlation has observed between ADL score and oral health status. The lower ADL score, the higher 'The
Oral health assessment tool' score. (table1)
Conclusion
These results suggest that chronic stroke patients with low ADL score have low oral hygiene. So we need to focus on improving ADL
independence to maintain oral health status of patients with chronic stroke.
Table 1. ADL (K-MBI) and the oral health assessment tool in chronic group. Data are presented as mean

P 58
Objective Assessment and Therapeutic Effect of rTMS in mild Traumatic Brain Injury with Central Pain
Dong-Ha Kang1*
, Yu Hui Won1,2
, Sung-Hee Park1,2
, Myoung-Hwan Ko1,2
, Jeong-Hwan Seo1,2
, Gi-Wook Kim1,2†
Department of Rehabilitation Medicine ,Chonbuk National University Hospital1, Biomedical Research Institute of Chonbuk National
University Hospital,Research Institute of Clinical Medicine of Chonbuk National University2
The mechanism and treatment of the mild Traumatic Brain Injury (TBI) with central pain has been studied, but it has not been
clarified yet. The aim of this study was to investigate the therapeutic effect of repeated transcranial magnetic stimulation therapy
(rTMS) in mild TBI with central pain and the changes in the objective evaluations of central pain before and after rTMS. Subjects of
this study are the patients with mild TBI who complained of pain but had no specific findings on neurological examination and brain
magnetic resonance (MR) – fluid attenuated inversion recoveryimaging. We have attempted to perform various objective
evaluations related to central pain on subjects such as physical examination (perception of pain, temperature, crude touch, and
pressure sensation), Visual Analogue Scale (VAS), Quantitative Sensory Test (QST), Sympathetic Skin Response (SSR) and Fractional
Anisotropy (FA) test of spinothalamic tract using brain diffusion tensor MRI. Patients who were included in this study were in car
traffic accidents, all of which were side-impacts resulting in vehicle rotation.The pain that patients complained is whole body pain
below neck area, with more severe symptoms on either the left or right side than another side. And there is difference in perception
of temperature sensation compared one side with another.We applied rTMS to patients for treatment using 8-shaped coil and we
determined the cortical site at which single pulse TMS evoked a contralateral motor evoked potential of maximal amplitude in a
hand muscle. The study comprised two separate rTMS sessions. Each sessionincluded five rTMS per week for three weeks, total 15
treatments.In first session, we applied rTMS on M1 cortex area contralateral to painful side and subjects received 10 consecutive
trains of 200 stimuli pulses at a frequency of 20Hz. And in second session, rTMS was applied to the contralateral side. Physical
examination, VAS, QST, SSR, and brain diffusion tensor MRI were performed again after treatment. All treatments and pre- and
post-treatment evaluations according to the plan described above were only completed in three patients. All three patients showed
improvement in physical examination and VAS and there is decreased amplitude of SSR after rTMS. And two patients showed
improvement in FA value of spinothalamic tract on brain diffusion tensor MRI.The QST did not show any significant difference
between the right and left side beforerTMS, and there was no change before and after rTMS. In this study, we found that the pain
patterns of three TBI patients with central pain changed from neurogenic pain to musculoskeletal pain after rTMS.And we were able
to identify the evaluation showing changes of assessment of central pain before and after rTMS.In the future, further studies
involving more patients will be needed to establish an objective evaluation and treatment system for mild TBI patients with central
pain.

P 59
Psychometrics of the Functional Oral Intake Scale for Infants
You Gyoung Yi1,3*
, Hyung-Ik Shin1,2†
, Ju Chan Kim2, Hee Dong Shin
3
Department of Rehabilitation Medicine,Seoul National University College of Medicine1, Department of Rehabilitation
Medicine ,Seoul National University Hospital2, Department of Rehabilitation Medicine ,Veterans Health Service Medical Center
3
Objective
The aim of this study was to investigate the reliability and validity of functional oral intake scale (FOIS) for infants.
Methods
We included infants younger than one year of age who underwent videofluorscopic swallowing study (VFSS). Based on nutrition
records at the time of VFSS, two raters separately evaluated five-point scale FOIS for infants and applied the FOIS levels 1, 2, and 3
as defined for adults. However, we divided full oral feeding (FOF) into two categories: (1) achievement of oral diet expansion, the
initiation of pureed foods before 9 months, and the initiation of mashed foods and those with soft lumps before 12 months as
normal developmental stages; and (2) no achievement of this oral diet expansion. Cross-validity was estimated by comparing the
infantile FOIS scores to the categorical ratings of swallowing impairment and aspiration severity and the presence of swallowing
impairment and aspiration determined by the VFSS.
Results
A total of 201 infants were evaluated. Interrater reliability of FOIS for infants was high with 95.5 % absolute agreement. Significant
associations were identified between the FOIS for infants and aspiration severity in VFSS. Seven of 33 infants with both oral and
tube feeding (partial oral feeding, POF) continued POF after one year, and their mean caloric contribution of oral feeding was 6.00
(SD: 5.45) % while that of infants who acquired FOF after one year (n=26) was 28.46 (SD: 22.79) %.
Conclusions
The five-point scale FOIS for infants which reflects expansion of oral diet as they grow had adequate reliability and validity. Caloric
contribution in addition to consistency of oral feeding could be considered to distinguish FOIS level 2 and 3, both of which
correspond to POF status in infants.
Acknowledgment: This study was funded by Seoul National University Hospital (assignment number: 0420180810).
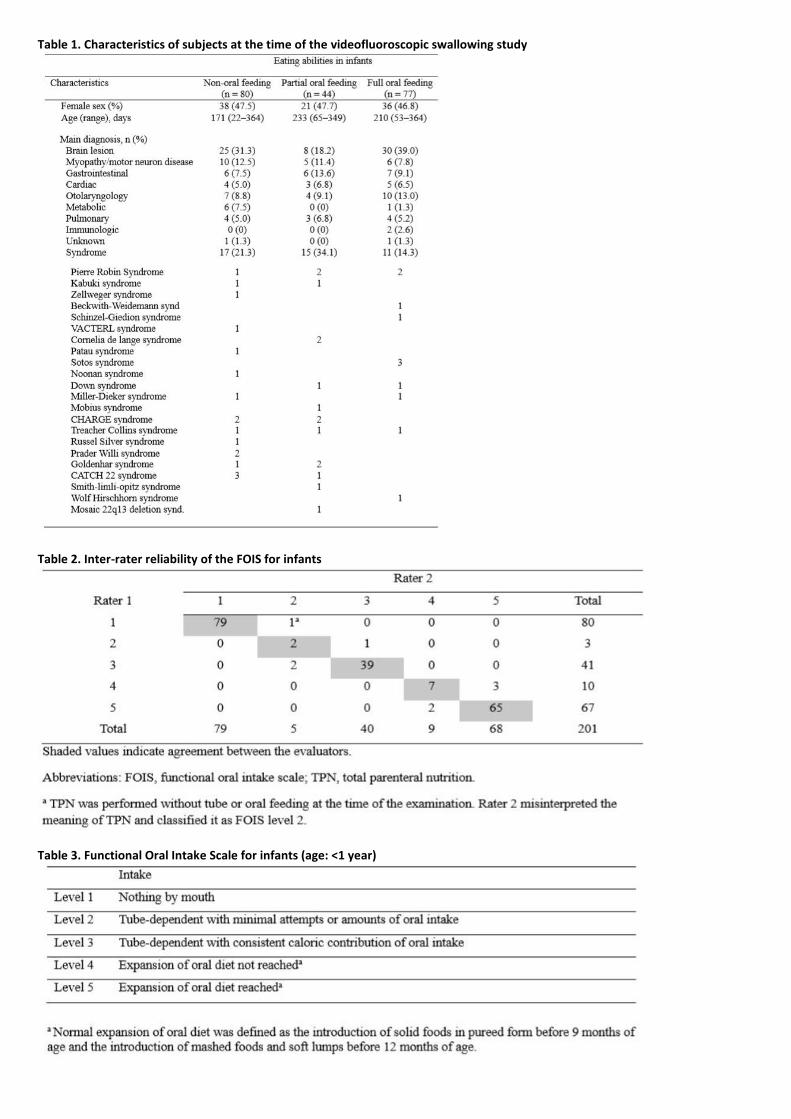
Table 1. Characteristics of subjects at the time of the videofluoroscopic swallowing study
Table 2. Inter-rater reliability of the FOIS for infants
Table 3. Functional Oral Intake Scale for infants (age: <1 year)

P 60
Effects of tDCS on cognition and language in children with cerebral palsy with cognitive dysfunction
Su Hwan Bae 1*
, In Young Sung 1†
, Eun Jae Ko 2, Mi Jin Hong
3, Jin Sook Yuk
4
Department of Rehabilitation Medicine,Asan Medical Center, University of Ulsan College of Medicine1, Department of Physical
Medicine and Rehabilitation,Ulsan University Hospital, University of Ulsan College of Medicine2, Department of Rehabilitation
Medicine,Konyang Medical Center, University of Konyang College of Medicine3, Department of Rehabilitation Medicine,Asan
Medical Center4
Introduction
There have been studies about noninvasive brain stimulation in cognitive development in recent 30 years, however, there are not
many studies discussing the effect of transcranial direct current stimulation (tDCS) in children. Furthermore, studies of tDCS in
children with cerebral palsy (CP) were targeting at motor function, not cognition nor language. Therefore, the aim of this study was
to evaluate the effect of tDCS on cognition, activities of daily living (ADL), and language in children with CP associated with cognitive
impairment.
Method
This is a preliminary report of prospective, randomized, double blinded study. Thirteen children with CP whose cognitive age under
42 months were randomly assigned to tDCS (n = 8, active tDCS and cognitive training, DC-Stimulator Plus (neuroConn, Germany),
1mA, 20 min/session, total 20 sessions, anode electrode placed over the more involved side of the dorsolateral prefrontal cortex,
cathode electrode placed over the contralateral supraorbital region) and control (n = 5, sham tDCS and cognitive training) groups.
Mental scale of Bayley Scales of Infant Development II (BSID II), Pediatric Evaluation of Disability Inventory (PEDI),
interest/persistence domain of the Laboratory Temperament Assessment Battery (Lab-TAB), Early Childhood Behavior
Questionnaire (ECBQ), Korean version of MacArther-Bates Communicative Development Inventories (M-B CDI-K), and the
Sequenced Language Scale for Infants (SELSI) or the Preschool Receptive-Expressive Language Scale (PRES) were evaluated.
Results
There was no significant difference between the two groups when comparing the baseline characteristics, including age, sex, GMFCS
level, side of anodal stimulation, and all outcome measurements (Table 1). After 12 weeks of intervention, the tDCS group showed
significant improvements in all measurements (p<0.05) except grammar domain of M-B CDI-K, whereas the control group only
showed significant improvements in manipulation domain of LAP-TAB, attentional shifting domain of ECBQ, and comprehension
domain of M-B CDI-K (Table 2). When comparing the degree of improvements after intervention, the differences was not
statistically significant (p>0.05) (Table 3). Total 13 caregivers of the children participated in the questionnaire regarding symptoms
and side effects after tDCS. Only one caregiver replied that the child had a moderate degree of mood change after tDCS, and the
rest of the 12 caregivers replied that there was no symptoms or side effects after tDCS.
Conclusion
Application of tDCS showed improvements in cognitive function, ADL, and language in children with CP associated with cognitive
dysfunction.

Table 1. Comparison of Baseline Characteristics between the tDCS and the Control Groups
Table 2. Comparison of Outcome Measurements Before and After Treatment in Each Group

Table 3. Comparison of Improvements of Outcome Measurements between Two Groups
P 60
Safety and efficacy of allogenic umbilical cord blood therapy for global development delay
Hyunseok Kwak1*
, Joonhyun Park1, Shinyoung Kwon
1, Mi Ri Suh
1,2, MinYoung Kim
1,2†
CHA University School of Medicine, Department of Rehabilitation Medicine,CHA Bundang Medical Center1, Rehabilitation and
Regeneration Research Center,CHA University2
Introduction
Global developmental delay (GDD) can be defined as a clinical presentation that has a various etiologic profile and is a subset of
developmental disabilities defined as significant delay in two or more of the following developmental domains; gross/fine motor,
speech/language, cognition, social/personal behavior, and activities of daily living. As most GDD patients have limited improvements
with conventional treatments, stem cell therapy can be an emerging therapeutic option. This study aims to determine the efficacy
and safety of allogenic umbilical cord blood (UCB) therapy for children with GDD.
Materials and Methods
We conducted a prospective study including total of 13 children with GDD. Allogenic UCB units were selected from UCB bank of our
organization. The conditions for UCB selection were at least 4 out of 6 matching HLA typing for A, B, and DRB1 antigens.
Cyclosporine was administered orally from 3 days before to 13 days after allogenic UCB injection. After thawing and washing
according to our protocol, UCB was infused intravenously. Raw scores of Bayley scales of infant development-II (BSID-II) were
followed at baseline, 3, 6, and 12 months. Secondary outcomes such as gross motor function measure, (GMFM) and Wee Functional
Independent Measure (WeeFIM) were also evaluated at the same period. Adverse events were recorded through the whole study
period.
Results
The demographics of 13 eligible patients are described in Table 1. No adverse events were reported during 1 year follow-up. BSID-II
was improved significantly at 3, 6 and 12 months after UCB injection for mental score (p=0.005, 0.003 and 0.003, respectively) and
motor score (p=0.038, 0.005, and 0.005, respectively). Also GMFM revealed significant improvements at 6 and 12 months after
treatment (p=0.006 and 0.009, respectively). Wee-FIM also showed improvements respectively in motor, cognitive and total score
at 6 months (p=0.027, 0.041, and 0.027 for motor, cognitive and total WeeFIM, respectively) and 12 months (p=0.011, 0.015, and
0.011 for motor, cognitive and total WeeFIM, respectively) after treatment.
Conclusion
Allogenic UCB therapy is a safe and effective treatment option for children with GDD.
Acknowledgment :This research was supported by a grant of the Korea Health Technology R&D Project through the Korea Health
Industry Development Institute (KHIDI), funded by the Ministry of Health & Welfare, Republic of Korea (grant number : HI16C1559)
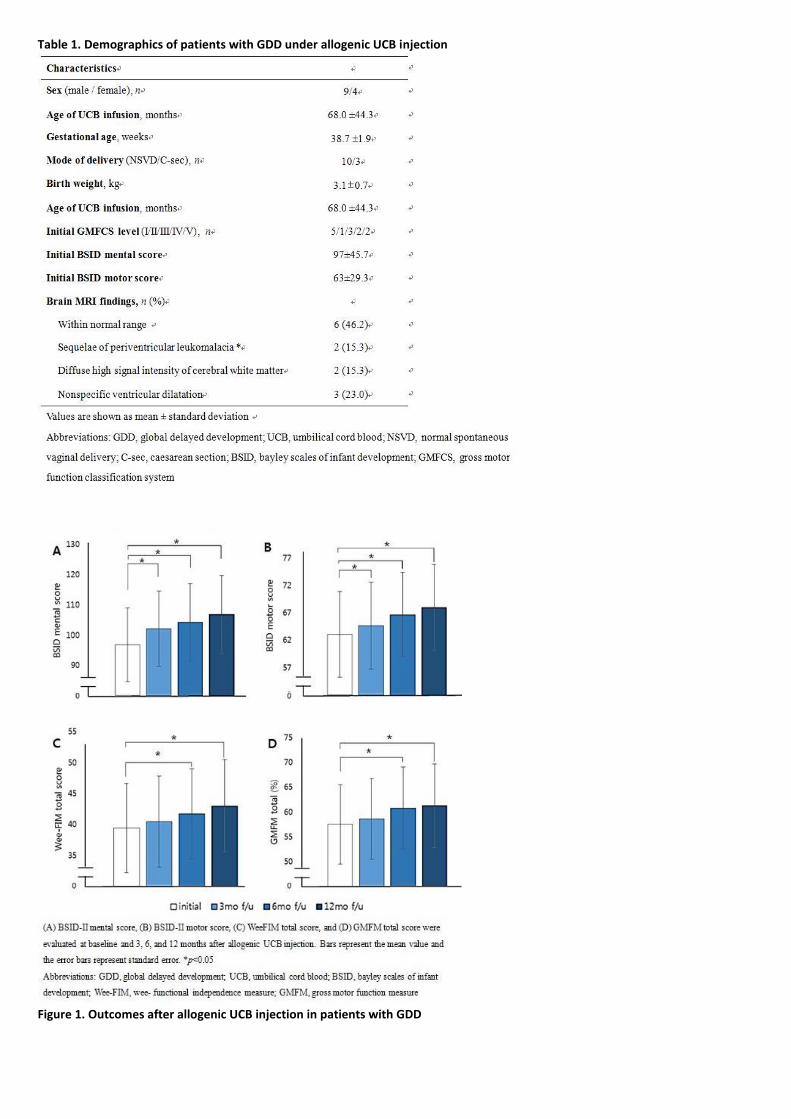
Table 1. Demographics of patients with GDD under allogenic UCB injection
Figure 1. Outcomes after allogenic UCB injection in patients with GDD
P 62
Effect of robot-assisted gait training in children with cerebral palsy
Min Kyun Sohn1†
, Shingseung Yang1*
, LIhua JIn1, Jayoung Choi
1, Dongmin Hwang
1, Sehi Kweon
1
Department of Rehabilitation Medicine, Chungnam National University Hospital1
Background
Partial weight support gait training is known to be an effective therapy. Likewise, robot-assisted gait training enables children to
have effective gait training as it partially supports body weight and to walk longer. Robot-assisted gait training is established as a
treatment option, but the clinical evidence on the neurologic recovery or musculoskeletal system is rare. So we assessed the impact
of robot-assisted gait training on motor function and body composition in children with cerebral palsy by comparing the functional
change of usual care period and robotic therapy period.
Study Design
Single-blinded, randomized, cross-over trial
Participants and settings
A total of 20 children diagnosed with spastic cerebral palsy pf GMFCS II~IV were recruited in the tertiary educational rehabilitation
hospital. The inclusion criteria are like as follow; Children (1) diagnosed with spastic cerebral palsy(3~12 years-old); (2) gross motor
function classification system Level II~IV ; (3) height of 98 ~ 160 centimeters; (4) follow the instructions and communicate if they feel
pain or discomfort; We excluded patients with any of the following ; (1) cognitive impairment so that each assessment cannot be
performed properly ; (2) history of neurosurgery or orthopedic surgery operated on limbs ; (3) severe joint contracture (knee joint :
more than 20 degrees flexion contracture, hip joint more than 40 degree contracture).
Materials and Methods
Children were randomized into two groups; Group 1 (Robotic Training - Usual Care), Group 2 (Usual Care-Robotic training). Group 1
had got the robot-assisted gait training (RT) 3 times a week in addition to the usual care for 6 weeks and then had got the routine
physical therapy for 6 weeks of usual care (UC). Group 2 had got the therapy in the opposite order. For the primary outcome, gross
motor function measure (GMFM-88) score, functional independence measure (WeeFIM) score was measured, and the manual
muscle power, the range of motion (ROM), modified Ashworth scale (MAS) were assessed before and after each treatment periods
for secondary outcome. The motor evoked potential (MEP), balance function, body composition were assessed before and after RT
period. Delta value for each period was compared by paired T-test.
Results
The means age, GMFCS level, height, weight, and BMI of the two groups were not significantly different. The improvement of C and
D dimension of GMFM-88 score of RT period was higher than that of UC period (p<0.05). Changes of manual muscle power, ROM,
MAS, and weeFIM scores were not different between the RT period and UC period. Latencies of MEP, balance function were not
changed, but skeletal muscle mass increased in GMFCS level 2-3 group after RT (p<0.05).
Conclusion
Robot-assisted gait training has the favorable effect not only on the recovery of motor function but also on body composition in
children with cerebral palsy.
Acknowledgment: This study was supported by the Translational Research Center for Rehabilitation Robots (#NRCTR-EX18010),
National Rehabilitation Center, Ministry of Health and Welfare, Korea.
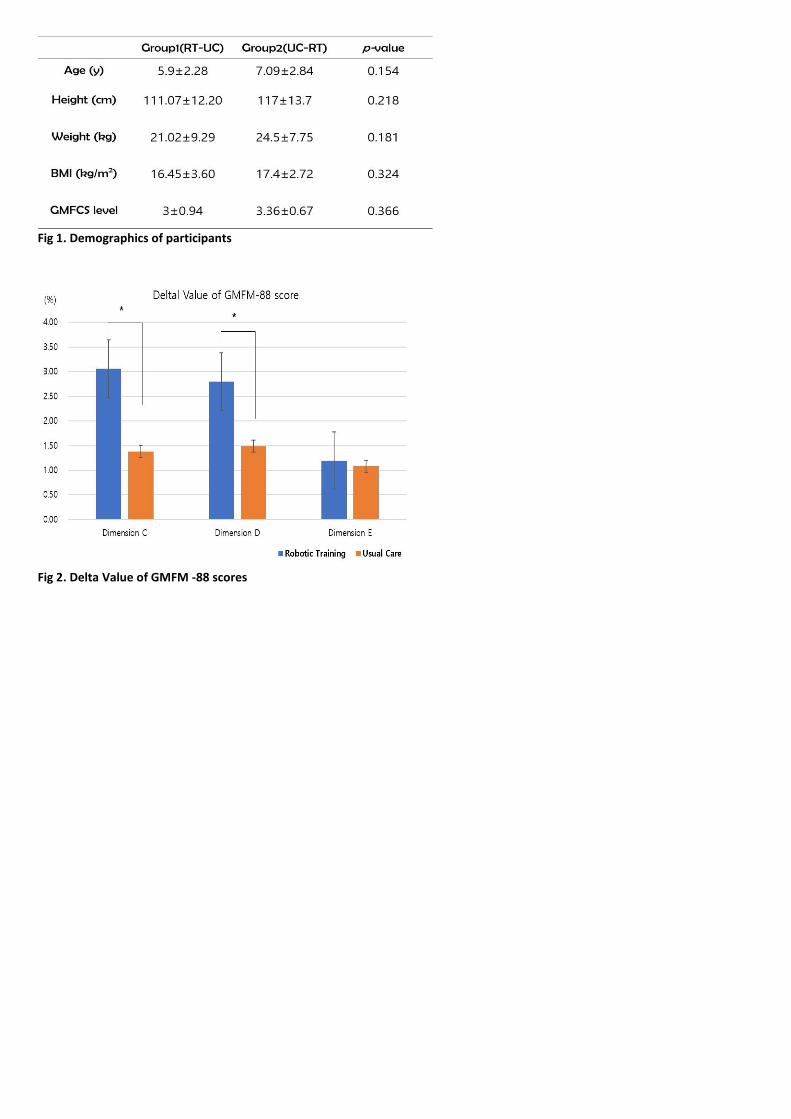
Fig 1. Demographics of participants
Fig 2. Delta Value of GMFM -88 scores

P 63
Factors associated with gait outcomes in patients with traumatic lumbosacral plexus injuries
Yeo Hyung Kim1*
, Jung Soo Lee1†
Department of Rehabilitation Medicine,College of Medicine, The Catholic University of Korea, Seoul, Republic of Korea1
Purpose
Lumbosacral plexus injuries usually occur in patients with severe, multiple traumas requiring intensive care, affecting gait function.
The purpose of the present study was to identify the initial factors associated with gait outcome in lumbosacral plexus injuries
caused by traumas.
Methods
We retrospectively identified 664 patients with pelvic fractures caused by trauma between 2006 and 2017. The lumbosacral plexus
injuries were electrodiagnostically confirmed in 30 patients (4.5%). Demographic, injury-related, fracture-related and
electrodiagnostic factors were compared between patients with long-term unassisted gait outcomes to those with assisted gait
outcomes, with an average of 27 months elapsing after the trauma.
Results
Eleven patients (36.7%) remained in the assisted gait group during the follow-up period. Complex pelvic trauma, rather than the
severity of trauma to the entire body, was associated with a poor gait outcome. Among the various causes of injury, pedestrians
struck by vehicles were associated with assisted gait outcomes. The number of anatomic locations involved in pelvic fractures, pelvic
ring instability by Tile classification, and the proportion of unstable sacral fractures were higher in patients with assisted gait
outcomes compared with those having unassisted gait outcomes. Weaknesses in the initial hip extensor, knee flexor, ankle
dorsiflexor and ankle plantar flexor were observed significantly more often in patients with assisted gait outcomes. The Dumitru and
Wilbourn's scale of the anterior and posterior sacral plexus was significantly higher in the assisted gait group.
Conclusions
Gait outcome after lumbosacral plexus injury is associated with the range and stability of the pelvic fracture and the severity of the
anterior and posterior sacral plexus injury. Poor gait outcome was associated with the severity of the trauma to the pelvis rather
than that to the entire body.

P 64
Walking downhill slope with “Walker with Non-Powered Automatic Velocity Controlled Wheel"
Eunsil Cha1*
, Jimin Song1, Wonil Kang
1, Kwang-Ik Jung
1, Woo-Kyoung Yoo
1, Suk Hoon Ohn
1†
Department of Physical Medicine and Rehabilitation, Hallym University College of Medicine1
Objective
After hip fracture, walking aids are usually provided for effective muscle training and ambulation. Although the rolling walker, which
is widely used nowadays, makes the move and turn easier, it can rather increase the risk of fall at downhill ramp due to unskilled
control. As a result, the fear of falling increases, which can hinder proper rehabilitation and functional recovery. Therefore, we
developed the world’s first “walker with non-powered automatic velocity controlled wheel”(ORBITN, SEOUL, KOREA) according to
the necessity of walking aids satisfying the efficiency, safety and convenience of walking, and we aimed to verify the effect of this
walker using surface electromyography (sEMG).
Methods
Seven patients who are using rolling walker after surgery on unilateral femur fracture were enrolled. We excluded patients who
cannot walk with walker, already have gait disturbance caused by other causes, and have history of surgery on lower limbs. Patients
walked a 5-degree downhill ramp using conventional “4-wheel rolling walker” and newly devised “walker with non-powered
automatic velocity controlled wheel”(fig 1). Patient walked ramp three times for each walker and had 5-minute rest periods
between each test so that previous experiment did not affect the following experiment. Surface electrodes were placed over the
Tibialis anterior (TA), Gastrocnemius (GCM), Vastus medialis (VM), Biceps femoris (BF) muscles of bilateral legs, and we measured
average root mean square (RMS) values per one gait cycle to quantify muscle contraction. Also we measured highest RMS value,
normalized to maximum voluntary isometric contraction (MVC) data obtained in trials prior to gait acquisitions. Subjective
satisfaction and fatigue degree of patients were recorded using a 10-point scale. The Wilcoxon signed-rank test was used for
statistical analysis.
Results
Four patients underwent hemiarthroplasty and three patients had intramedullary nailing. Patients participated in the experiment
58.9±73.4 days after surgery. Average RMS values per one gait cycle of GCM and BF muscle in the affected side were significantly
larger when the participants were using “walker with non-powered automatic velocity controlled wheel”. They reported similar
safety and fatigue when using both walking aids.
Conclusions
The contraction of GCM and BF muscles were stronger when the participants were using “walker with non-powered automatic
velocity controlled wheel”. This result suggests that the patients could perform more powerful toe-off with “walker with non-
powered automatic velocity controlled wheel” when walking downhill slope.
Acknowledgment: This work was supported by the Technology development Program (S2410642) funded by the Ministry of SMEs
and Startups (MSS, Korea)

Fig 1. The patient walking downhill ramp with “walker with non-powered automatic velocity controlled wheel”

P 65
Polysomnography in Myotonic Muscular Dystrophy versus Duchenne Muscular Dystrophy
Mi Ri Suh1,2*
, Won Ah Choi3,4
, Seong-Woong Kang3,4†
Department of Rehabilitation Medicine,CHA Bundang Medical Center, CHA University School of Medicine1, Rehabilitation and
Regeneration Research Center,CHA University2, Department of Rehabilitation Medicine and Pulmonary Rehabilitation
Center,Gangnam Severance Hospital, Yonsei University College of Medicine 3, Rehabilitation Institute of Neuromuscular
Disease,Yonsei University College of Medicine4
Introduction
Sleep-related disorders, such as obstructive sleep apnea associated with sleep hypoxia and hypercapnia, rapid eye movement sleep
dysregulation, and diurnal somnolence are commonly reported in patients with myopathies. We aimed to analyze polysomnography
data and ventilation monitor of myotonic muscular dystrophy (MMD), and compared them with that of duchenne muscular
dystrophy (DMD) to compare the different characteristics of apnea patterns in different myopathies at similar ventilatory status.
Materials and Methods
We retrospectively collected and analyzed polysomnographic data and overnight ventilation monitoring parameters among the
patients with MMD and DMD, who were admitted for evaluation of respiratory failure from January, 2012 until August, 2017 and
underwent ventilation monitoring and polysomnography at the same time. Ventilation parameters such as overnight partial
pressure of transcutaneous carbon dioxide (tcpCO2) and oxygen saturation (SaO2), and polysomnographic parameters such as total
apnea-hypopnea index (A-HI), apnea index, hypopnea index, obstructive apnea index, central apnea index, and mixed apnea index
were collected. Mean values of each parameter were compared using independent t-test and spearman correlation test was
performed to find the relationship between the different parameters.
Results
Twenty-five patients with MMD and 41 patients with DMD were included in the study. All of the patients with MMD were with sleep
apnea, where nearly half of them (12/25, 48.0%) were with severe type of sleep apnea. On the other hand although 34 patients with
DMD (34/41, 82.9%) were with sleep apnea, only 1 was with severe type of sleep apnea. Also, all the polysomnographic parameters
showed significant difference between the two groups. The average SaO2 and the lowest SaO2 during the night were significantly
lower in MMD (p=0.011 and p=0.001, respectively), while mean tcpCO2 and maximal tcpCO2 during the night were similar among
the two groups. In patients with DMD, A-HI showed negative correlation with average SaO2 (r=-0.450, p=0.001) and the lowest SaO2
(r=-0.405, p=0.004), while it showed negative correlation with average SaO2 (r=-0.453, p=0.012) and positive correlation with mean
tcpCO2 (r=0.386, p=0.035) in patients with MMD. In patients with MMD, A-HI also showed strong positive correlation with
obstructive apnea index (r=0.704, p=0.002) and central apnea index (r=0.526, p<0.001) while it only showed weak positive
correlation with obstructive apnea index (r=0.457, p=0.002).
Conclusion
Among the patients with MMD and DMD, severity of apnea was much more severe and proportion of central apnea was higher in
patients with MMD at similar tcpCO2 level.
Table 1. Polysomnographic parameters and overnight ventilation monitor in DM1 and DMD. data are shown as mean±standard deviation. †p value < .05. *Shows severity of apnea according to apnea-hypopnea index – none, fewer than 5 events/h; mild, 5-14 events/h; moderate, 15-29 events/h and severe, 30 or more events per hour. Abbreviation : DM1, myotonic muscular dystrophy type1; DMD, duchenne muscular dystrophy; tcpCO2, partial pressure of transcutaneous carbon dioxide; SaO2, oxygen saturation
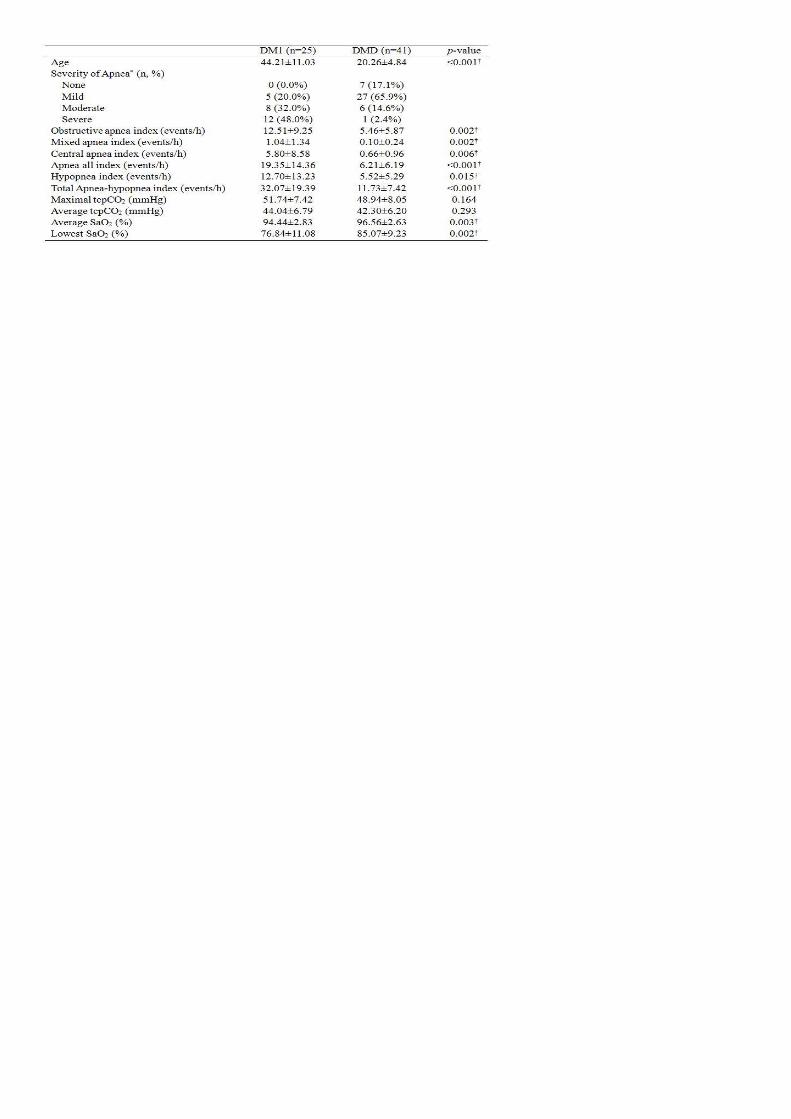

P 66
The Relationship between PNTML and Diebetes Mellitus
Seunghee Han1*
, Gayang Shim1, Jongkyu KIM
1†
Department of Physical Medicine & Rehabilitation, Seoul Medical Center1
Introduction
PNTML (Pudental nerve terminal motor latency) is one of the major methods for evaluating fecal incontinence with anorectal
manometry and can measures damages of pudendal motor nerves associated diabetic peripheral polyneuropathy. The aim of this
study was to evaluate the relationship between PNTML and Diebetes mellitus.
Method
Data was collected for patients who admitted to the Department of Physical Medicine and Rehabilitation and Colorectal surgery for
fecal incontinence between March 2014 and December 2018. Patients were evaluated for PNTML and anorectal manometry. For
these people, we found the records of PNTML, Resting anal pressures, Squeeze anal pressures. Mann-Whitney U tests were done
using IBM SPSS 23.0.
Result
31 patients with fecal incontinence were included. Demographic features were noted in Table 1. They showed differences between
normal PNTML and delayed PNTML for mean and maximal squeeze anal pressure. (Table 2) There is no difference between Diabetes
mellitus and non-Diabetes mellitus for the gains. (Table. 3) The period of Diabetes mellitus was not significantly associated with
latency of PNTML. (Table. 4)
Conclusion
There seem to be no differences in latency of PNTML between diabetic and non-diabetic patients with fecal incontinence.
Table 2. Difference in anorectal manometry in patients with normal PNTML and delayed PNTML
Table 3. Difference in PNTML and anorectal manometry in patients with Diabetes mellitus and non-Diabetes mellitus
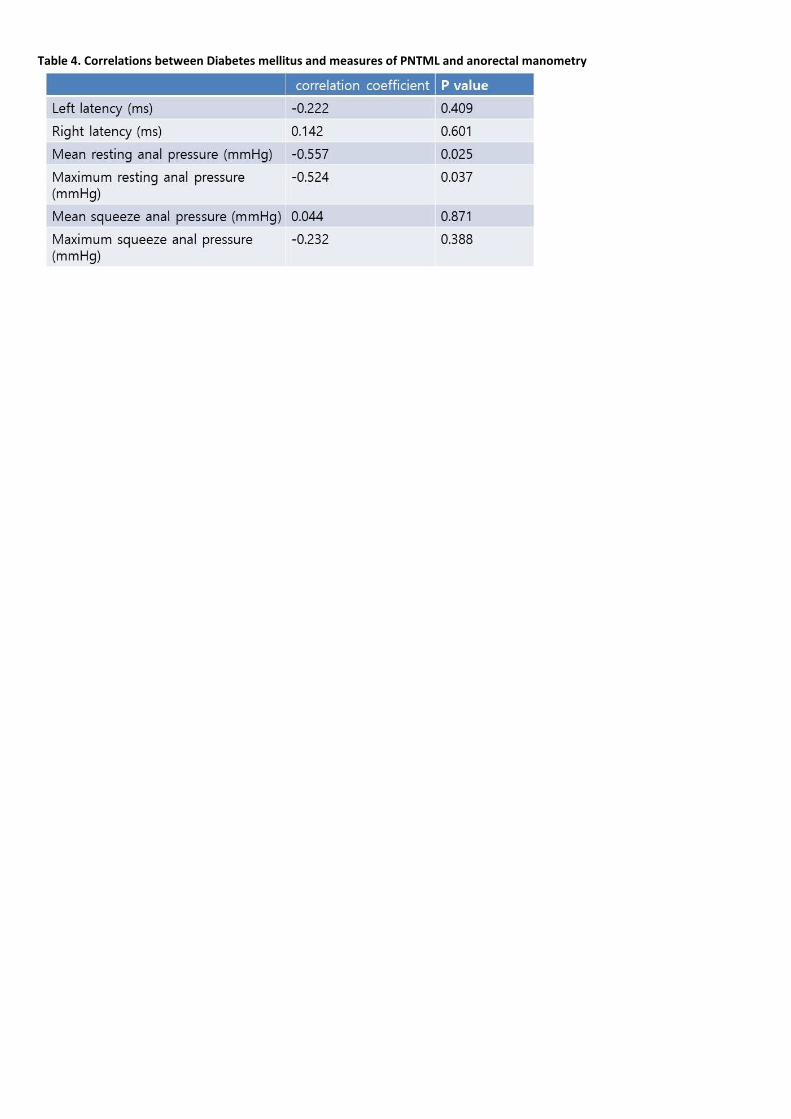
Table 4. Correlations between Diabetes mellitus and measures of PNTML and anorectal manometry

P 67
Prediction of stroke after intracranial aneurysm surgery using intraoperative EP monitoring
Jihye Park1*
, Jung-Jae Lee2, Young-Jin Ko
2†
Department of Rehabilitation Medicine,St. Paul Hospital, The Catholic University of Korea1, Department of Rehabilitation
Medicine,The Catholic University of Korea Seoul St. Mary`s Hospital 2
Objective
Although the application of evoked potential (EP) in intracranial aneurysm surgery has been well demonstrated, the relationship
between the duration of EP deterioration and postoperative neurological deficits (PNDs) is still not clear. The objectives of this study
were (1) to evaluate the sensitivity, specificity, and predictive value of intraoperative somatosensory evoked potential (SSEP) and
motor evoked potential (MEP) monitoring for predicting postoperative stroke after intracranial aneurysm surgery; (2) to detect the
relationship between the EP deterioration duration and PND.
Methods
We reviewed the results of intraoperative SSEP and MEP monitoring in 728 patients who underwent intracranial aneurysm neck
clipping between June 2013 and December 2018. Postoperative stroke was diagnosed using a medical record about the motor and
sensory deficit, aphasia and mental status.
Results
The mean age of the 728 patients was 59.7 years and consisted of 485 women (66.6%). Subarachnoid hemorrhage were 42 cases
and non-ruptured aneurysm were 686 cases. The change of SSEP occurred in 9 out of 728 cases (1.24%), and the change of MEP in
14 out of 728 cases (1.92%). The sensitivity, specificity, PPV and NPV were 38.5%, 99.4%, 55.6% and 98.9%, respectively when there
was only SEP change, and 46.2%, 98.9%, 42.9%, 99.0%, respectively when there was only MEP change. We analyzed data from 23
patients with EP deterioration. Four patients presented irreversible change and 19 patients presented reversible change. In the
patients with deteriorated SSEP, 5 patients had PNDs and the mean SSEP deterioration duration was 48 ± 43 min (mean standard
deviation, here and elsewhere). Four patients did not have PNDs, and mean SSEP deterioration duration was 6 ± 4 min. In the
patients with deteriorated MEP, there were 6 patients with PNDs and the mean duration of MEP deterioration was 63 ± 39 min.
Eight patients had no PNDs, and mean MEP deterioration duration was 24 ± 30 min. There was no statistically significant difference
between the patients with and without PND (p-value=0.30), but the MEP deterioration duration showed statistical difference
between patients with and without PND (p-value=0.05). The optimal cut-off value of MEP change duration avoiding PND was 14 min
(area under the curve = 0.867, sensitivity 100%, specificity 66.7%).
Conclusion
Intraoperative MEP monitoring can provide higher sensitivity for postoperative stroke than SSEP monitoring. We can conclude that
the duration of MEP deterioration is important to postoperative neurological function, and in order to avoid PND, the MEP
deterioration duration must not exceed 14 min.
Fig 1. ROC curve of MEP deterioration duration in predicting PND. The area under the curve (AUC) is 0.87.

Fig 2. Summary of 728 patients who underwent clipping of cerebral aneurysms with intraoperative EP monitoring.

P 68
Correlation of Bone Mineral Density with Pulmonary Function in Advanced Duchenne Muscular Dystrophy
Justin Byun1*
, Jang Woo Lee2, Han Eol Cho
1,3, Won Ah Choi
1,3, Seong-Woong Kang
1,3†, Mi Ri Suh
4, Soojin Choi
2
Department of Rehabilitation Medicine and Rehabiliation Institute of Neuromuscular Disase,Gangnam Severance Hospital1,
Department of Physical Medicine and Rehabilitation,National Health Insurance Service Ilsan Hospital2, Pulmonary Rehabiliation
Center,Yonsei University College of Medicine3, Department of Physical Medicine and Rehabilaition,Bundang CHA
4
Objective
The purpose of the study is to determine whether pulmonary function, including respiratory muscle strength is related to bone
mineral density (BMD) in advanced Duchenne muscular dystrophy (DMD) patients.
Materials and Methods
This single-center, cross-sectional study aimed to determine whether pulmonary function, including respiratory muscle strength, is
related to BMD in patients with advanced DMD. All patients included in the study were over 20 years of age and admitted to the
Gangnam Severance Hospital from March 2013 to June 2017. They were nonambulatory and supported by mechanical ventilators.
The patients’ age, weight, and pulmonary function as well as the BMD of the first and the fourth lumbar vertebra were assessed. A
bivariate correlation for BMD and other parameters was calculated, and hierarchical regression analysis was used to determine
predictors of spine Z-score.
Results
The decrease of BMD of spine was not significantly correlated with age. However, body mass index (BMI) and the parameters of
pulmonary function such as forced vital capacity (FVC), maximal insufflation capacity (MIC), unassisted and assisted peak cough flow
(UPCF and APCF), maximal expiratory pressure (MEP) and maximal inspiratory pressure (MIP) were correlated with BMD.
Hierarchical regression analysis showed BMI, MIC, UPCF and APCF were powerful predictors of spine BMD.
Conclusion
The BMD of lumbar spine correlated with BMI and some parameters of pulmonary function in DMD patients with advanced stage.
Acknowledgment: This study supported by Rehabilitation Institute of Neuromuscular Disease, Yonsei University College of Medicine
research grant.

P 69
Reliability of the portable dynamometer anchoring system in critically ill patients
Min Yong Lee1*
, hyung-suk Ham1, Kwan-Sik Sung
1, You Gyoung Yi
3, Hyung-Ik Shin
1,2†
Department of Rehabilitation Medicine,Seoul National University Hospital1, Department of Rehabilitation Medicine,Seoul National
University College of Medicine2, Department of Rehabilitation Medicine,VHS Medical Center
3
Introduction
It is well known that hospitalization has detrimental physiologic effects on muscle strength and function. In addition, in patients in
intensive care unit (ICU), ICU-acquired weakness (ICUAW) may develop. However, because most of them cannot ambulate
independently, it is difficult to measure strength, objectively. Therefore, for the use on a hospital bed, we developed a portable
dynamometer anchoring system that can measure knee extensor strength in a supine position (Figure 1). In the previous study, for
39 healthy people, we confirmed that this portable dynamometer anchoring system was a reliable and valid tool. In the present
study, we aimed to investigate the reliability of knee extensor strength measurement using a portable dynamometer anchoring
system in a supine position in critically ill patients.
Methods
The patients admitted in Seoul National University Hospital, who can obey command 3 steps and cannot ambulate independently
with age above 18 years were included. Three trials of three contractions were assessed by two raters using the portable
dynamometer anchoring system while the participant was in the supine position. After the measurement, one investigator assessed
the Medical Research Council (MRC) sum score and de Morton Mobility Index (DEMMI) for evaluating their functional status. The
intraclass correlation coefficient (ICC) and 95% limits of agreement (LOA) for intra- and inter-rater reliability were obtained.
Results
The mean age of analyzed subjects (n = 33, 18 male and 15 female) is 69.24 ± 13.91 years old. The ICC for intra-rater reliability was
0.974 for the maximum measurements of knee extensor strength (95% confidence interval [CI]: 0.948–0.987) and 0.959 (95% CI:
0.917–0.980) for inter-rater reliability (Table 1). The mean difference (%) between the maximum knee extensor strength
measurements of each trial was 2.51% (LOA range: -19.79 to 24.81%) for intra-rater and 7.81% (LOA range: -21.45 to 37.07%) for
inter-rater measurements, respectively (Figure 2).
Conclusions
The portable dynamometer anchoring system is a reliable for measuring isometric knee extensor strength in a supine position in
critically ill patients.
Acknowledgment: This work was funded by Korea Workers’ Compensation and Welfare Service.
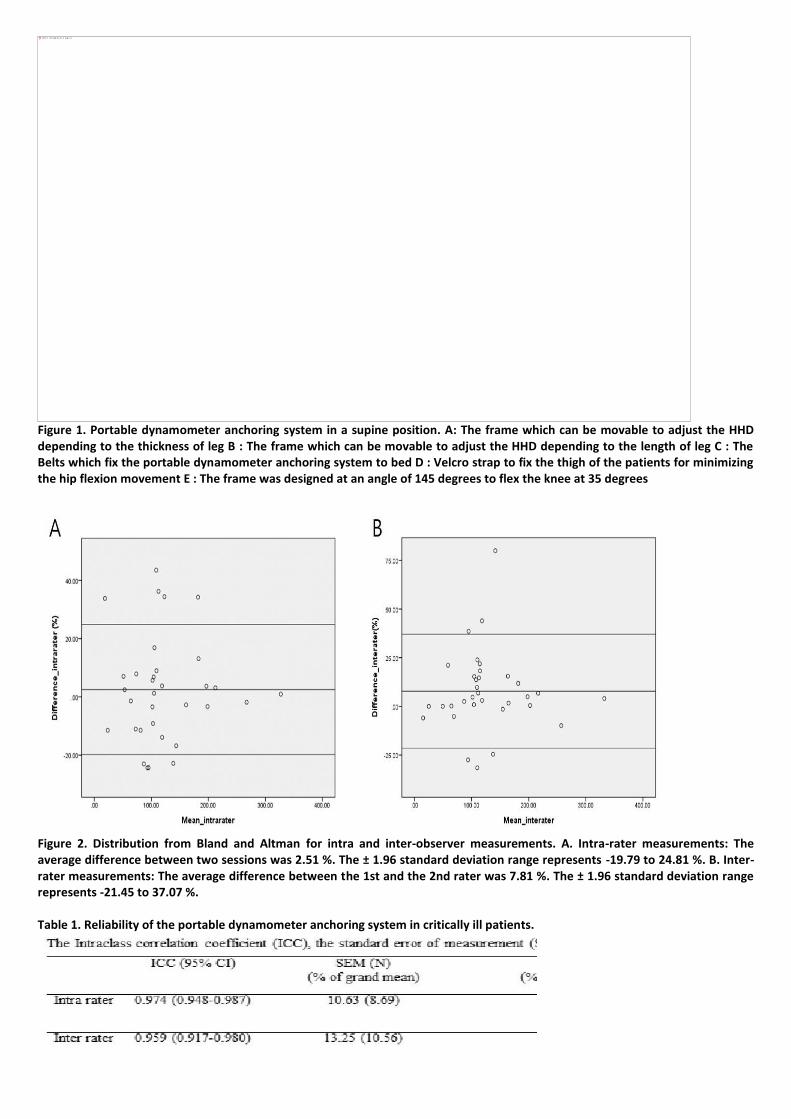
Figure 1. Portable dynamometer anchoring system in a supine position. A: The frame which can be movable to adjust the HHD depending to the thickness of leg B : The frame which can be movable to adjust the HHD depending to the length of leg C : The Belts which fix the portable dynamometer anchoring system to bed D : Velcro strap to fix the thigh of the patients for minimizing the hip flexion movement E : The frame was designed at an angle of 145 degrees to flex the knee at 35 degrees
Figure 2. Distribution from Bland and Altman for intra and inter-observer measurements. A. Intra-rater measurements: The average difference between two sessions was 2.51 %. The ± 1.96 standard deviation range represents -19.79 to 24.81 %. B. Inter-rater measurements: The average difference between the 1st and the 2nd rater was 7.81 %. The ± 1.96 standard deviation range represents -21.45 to 37.07 %. Table 1. Reliability of the portable dynamometer anchoring system in critically ill patients.
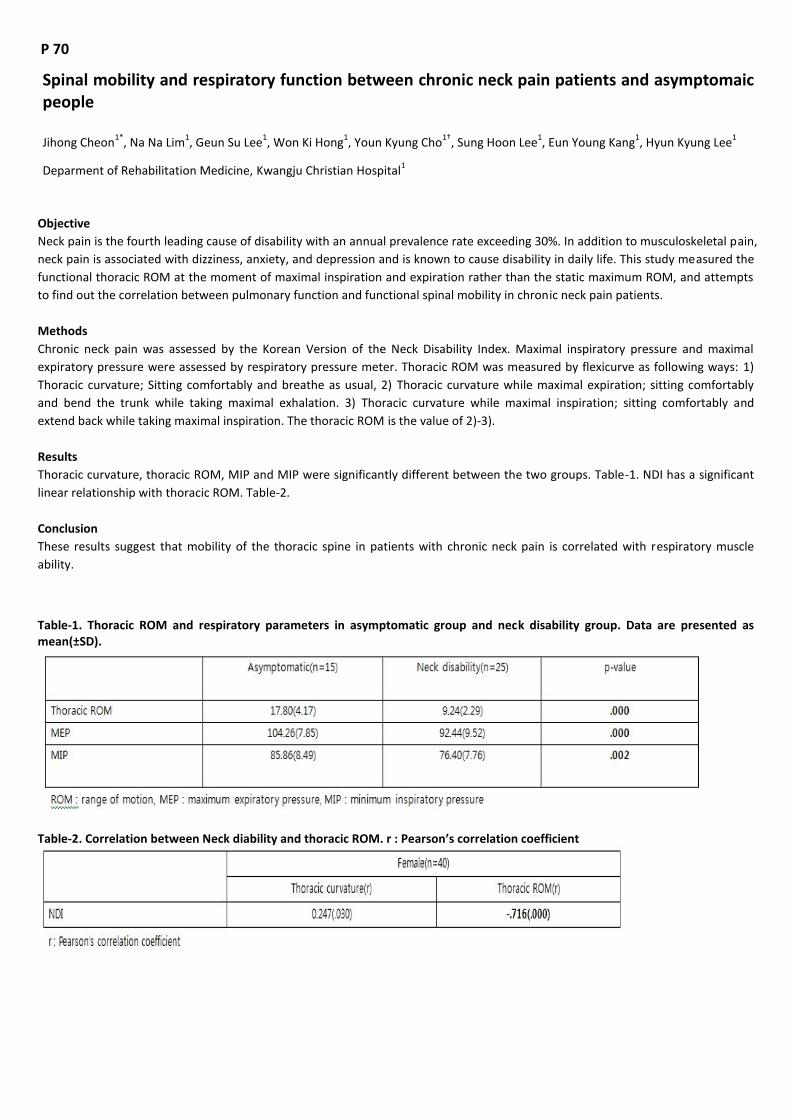
P 70
Spinal mobility and respiratory function between chronic neck pain patients and asymptomaic people
Jihong Cheon1*
, Na Na Lim1, Geun Su Lee
1, Won Ki Hong
1, Youn Kyung Cho
1†, Sung Hoon Lee
1, Eun Young Kang
1, Hyun Kyung Lee
1
Deparment of Rehabilitation Medicine, Kwangju Christian Hospital1
Objective
Neck pain is the fourth leading cause of disability with an annual prevalence rate exceeding 30%. In addition to musculoskeletal pain,
neck pain is associated with dizziness, anxiety, and depression and is known to cause disability in daily life. This study measured the
functional thoracic ROM at the moment of maximal inspiration and expiration rather than the static maximum ROM, and attempts
to find out the correlation between pulmonary function and functional spinal mobility in chronic neck pain patients.
Methods
Chronic neck pain was assessed by the Korean Version of the Neck Disability Index. Maximal inspiratory pressure and maximal
expiratory pressure were assessed by respiratory pressure meter. Thoracic ROM was measured by flexicurve as following ways: 1)
Thoracic curvature; Sitting comfortably and breathe as usual, 2) Thoracic curvature while maximal expiration; sitting comfortably
and bend the trunk while taking maximal exhalation. 3) Thoracic curvature while maximal inspiration; sitting comfortably and
extend back while taking maximal inspiration. The thoracic ROM is the value of 2)-3).
Results
Thoracic curvature, thoracic ROM, MIP and MIP were significantly different between the two groups. Table-1. NDI has a significant
linear relationship with thoracic ROM. Table-2.
Conclusion
These results suggest that mobility of the thoracic spine in patients with chronic neck pain is correlated with respiratory muscle
ability.
Table-1. Thoracic ROM and respiratory parameters in asymptomatic group and neck disability group. Data are presented as mean(±SD).
Table-2. Correlation between Neck diability and thoracic ROM. r : Pearson’s correlation coefficient

P 71
Long-Term Outcomes of Cardiac Rehabilitation in DM and Non-DM Patients With Myocardial Infarction
Ji Woo Park1*
, Na Ri Yun1, Ji Hee Kim
1†
Department of Rehabilitation Medicine, Wonkwang University School of Medicine & Hospital1
Objective
To investigate the long-term outcomes of cardiac rehabilitation (CR) on exercise capacity in diabetic (DM) and non-diabetic (non-DM)
patients with myocardial infarction (MI).
Methods
Of the MI patients who received hospital-based CR from November 2012 to December 2018, we retrospectively reviewed the
medical records of the patients who continued follow-up through the outpatient clinic and community-based self-exercise after CR.
A total of 28 patients (12 with DM and 16 without DM) were included in this study. Exercise capacity was measured by symptom-
limited exercise tests before hospital-based CR (T0) and 1 year (T1) and 2 year (T2) after the onset of MI.
Results
After the CR, both groups showed significant improvement in their cardiopulmonary factors over time (p<0.001). Mean exercise
time of the DM group increased significantly from 769.8 at T0 to 1017.8 at T2 (p<0.001), and the mean exercise time of the non-DM
group increased significantly from 875.7 at T0 to 1022.4 at T2 (p<0.001). In addition, peak oxygen consumption (VO2peak) of the
DM group increased significantly from 24.4 ± 4.8 at T0 to 29.7 ± 7.6 at T2 (p<0.001), and the VO2peak of the non-DM group
increased significantly from 22.9 ± 4.5 at T0 to 29.5 ± 5.6 at T2 (p<0.001). However, no significant time and group interaction effects
were observed in the DM and non-DM groups.
Conclusion
As a result of continued follow-up through an outpatient clinic and community-based self-exercise after hospital-based CR in
patients with MI, both DM and non-DM groups were significantly improved in cardiopulmonary factors over time and had similar
exercise capacity 2 year after the onset of MI. But both groups maintained their improved exercise capacity following hospital-based
CR. This suggests the importance of long term CR in DM patients.

P 72
The Relationship between Body Muscle Mass and Respiratory Muscle Strength after Lobectomy Patients
Ra Yu Yun1*
, Myung Jun Shin1, Byeong-Ju Lee
1, Sang Hun Kim
1, Je-Sang Lee
2†, Bo-Hyeon Kim
3, Jong-Hwan Park
3, Jeong Su Cho
4, Hyo
Yeong Ahn4
Department of Rehabilitation Medicine,Pusan National University Hospital1, Department of Rehabilitation Medicine,East Gimhae
Hospital2, Biomedical Research Institute,Pusan National University Hospital
3, Department of Thoracic and Cardiovascular
Surgery,Pusan National University Hospital4
Introduction
The purpose of this study was to compare the body composition, cardiopulmonary function, pulmonary function and respiratory
muscle strength of lung cancer patients of pre and post lobectomy, and showed following result in relation of removed lung volume
with muscle mass, lung function and respiratory muscle strength.
Methods
The present study was approved by the Institutional Review Board (IRB) at B Hospital. Recruitment notices were posted at the
thoracic surgery and rehabilitation medicine clinic at B Hospital to recruit patients scheduled to undergo video-thoracoscopic
lobectomy for lung cancer. Before lobectomy, the patients underwent computed tomography (CT), cardiopulmonary exercise
testing (CPET), pulmonary function test, Inbody dual energy X-ray absorptiometry (DEXA), whole body DEXA, and grip strength
measurements. These tests were repeated four weeks after surgery. One week after surgery, all tests except CT, CPET, and whole
body DEXA were performed. All evaluations were performed by a single skilled physician. Thirteen patients with lung cancer were
enrolled in this study. Their mean age was 65±6.84 years, with 9 men and 4 women.
Result
The maximum oxygen uptake per body weight was significantly decreased from 26.34±6.98 ml/kg/min to 23.13±4.66 ml/kg/min
after 4 weeks (p<.01). Forced vital capacity (FVC) and forced expiratory volume in one second (FEV1) showed significant differences
between pre-operation, 1 week and 4 weeks of operation. Maximal inspiratory pressure (MIP) was significantly different between
the periods (p<.05). Peak expiratory flow (PEF) was also significantly different between the periods (p<.001). The correlation
between muscle mass and MIP, muscle mass and PEF is shown in <Fig 1> and <Fig 2>. Muscle mass and MIP showed significant
correlation between the spearman correlation(r=.521, p=.013) and partial correlation coefficient(r=.517, p=.023). Muscle mass and
PEF showed significant correlation between the spearman correlation(r=.500, p=.018) and partial correlation coefficient(r=.473,
p=.018). The correlation between muscle mass, respiratory muscle strength, pulmonary function according to pre and post-
operative lung volume is shown in <Table 1>. Spearman correlations were used to calculate coefficients of correlation among delta
lung volume and skeletal muscle mass, respiratory muscle, pulmonary function. Statistical analysis was conducted by using partial
correlation, adjusted for age, BMI, gender. Differences in lung volume before and after surgery showed significant correlation by
appendicular lean mass (ALM) (r=.690, p=.001), MIP(r=.403, p=.043), PEF(r=.413, p=.045), FVC(r=.705, p=.001), FEV1(r=.484, p=.022).
Conclusion
In conclusion, the increase in muscle mass due to lung volume difference in lung cancer patients will have positive effect on survival
rate, respiratory muscle strength and lung function and therefore have positive result to viability and quality of life of the patients.

Figure 1. The relationship between MIP and total lean mass in patients with lung cancer.
Figure 2. The relationship between PEF and total lean mass in patients with lung cancer
Table 1. The correlation between delta lung volume and skeletal muscle mass, respiratory muscle strength, pulmonary function in patients with lung cancer
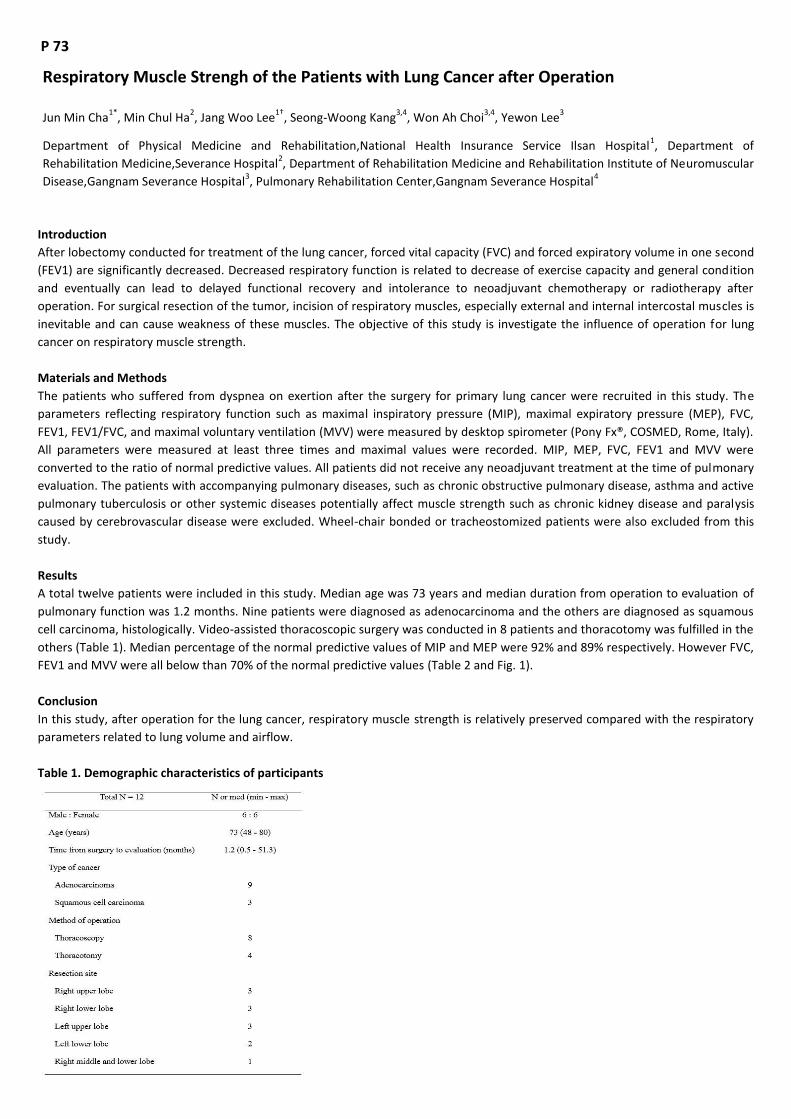
P 73
Respiratory Muscle Strengh of the Patients with Lung Cancer after Operation
Jun Min Cha1*
, Min Chul Ha2, Jang Woo Lee
1†, Seong-Woong Kang
3,4, Won Ah Choi
3,4, Yewon Lee
3
Department of Physical Medicine and Rehabilitation,National Health Insurance Service Ilsan Hospital1, Department of
Rehabilitation Medicine,Severance Hospital2, Department of Rehabilitation Medicine and Rehabilitation Institute of Neuromuscular
Disease,Gangnam Severance Hospital3, Pulmonary Rehabilitation Center,Gangnam Severance Hospital
4
Introduction
After lobectomy conducted for treatment of the lung cancer, forced vital capacity (FVC) and forced expiratory volume in one second
(FEV1) are significantly decreased. Decreased respiratory function is related to decrease of exercise capacity and general condition
and eventually can lead to delayed functional recovery and intolerance to neoadjuvant chemotherapy or radiotherapy after
operation. For surgical resection of the tumor, incision of respiratory muscles, especially external and internal intercostal muscles is
inevitable and can cause weakness of these muscles. The objective of this study is investigate the influence of operation for lung
cancer on respiratory muscle strength.
Materials and Methods
The patients who suffered from dyspnea on exertion after the surgery for primary lung cancer were recruited in this study. The
parameters reflecting respiratory function such as maximal inspiratory pressure (MIP), maximal expiratory pressure (MEP), FVC,
FEV1, FEV1/FVC, and maximal voluntary ventilation (MVV) were measured by desktop spirometer (Pony Fx®, COSMED, Rome, Italy).
All parameters were measured at least three times and maximal values were recorded. MIP, MEP, FVC, FEV1 and MVV were
converted to the ratio of normal predictive values. All patients did not receive any neoadjuvant treatment at the time of pulmonary
evaluation. The patients with accompanying pulmonary diseases, such as chronic obstructive pulmonary disease, asthma and active
pulmonary tuberculosis or other systemic diseases potentially affect muscle strength such as chronic kidney disease and paralysis
caused by cerebrovascular disease were excluded. Wheel-chair bonded or tracheostomized patients were also excluded from this
study.
Results
A total twelve patients were included in this study. Median age was 73 years and median duration from operation to evaluation of
pulmonary function was 1.2 months. Nine patients were diagnosed as adenocarcinoma and the others are diagnosed as squamous
cell carcinoma, histologically. Video-assisted thoracoscopic surgery was conducted in 8 patients and thoracotomy was fulfilled in the
others (Table 1). Median percentage of the normal predictive values of MIP and MEP were 92% and 89% respectively. However FVC,
FEV1 and MVV were all below than 70% of the normal predictive values (Table 2 and Fig. 1).
Conclusion
In this study, after operation for the lung cancer, respiratory muscle strength is relatively preserved compared with the respiratory
parameters related to lung volume and airflow.
Table 1. Demographic characteristics of participants
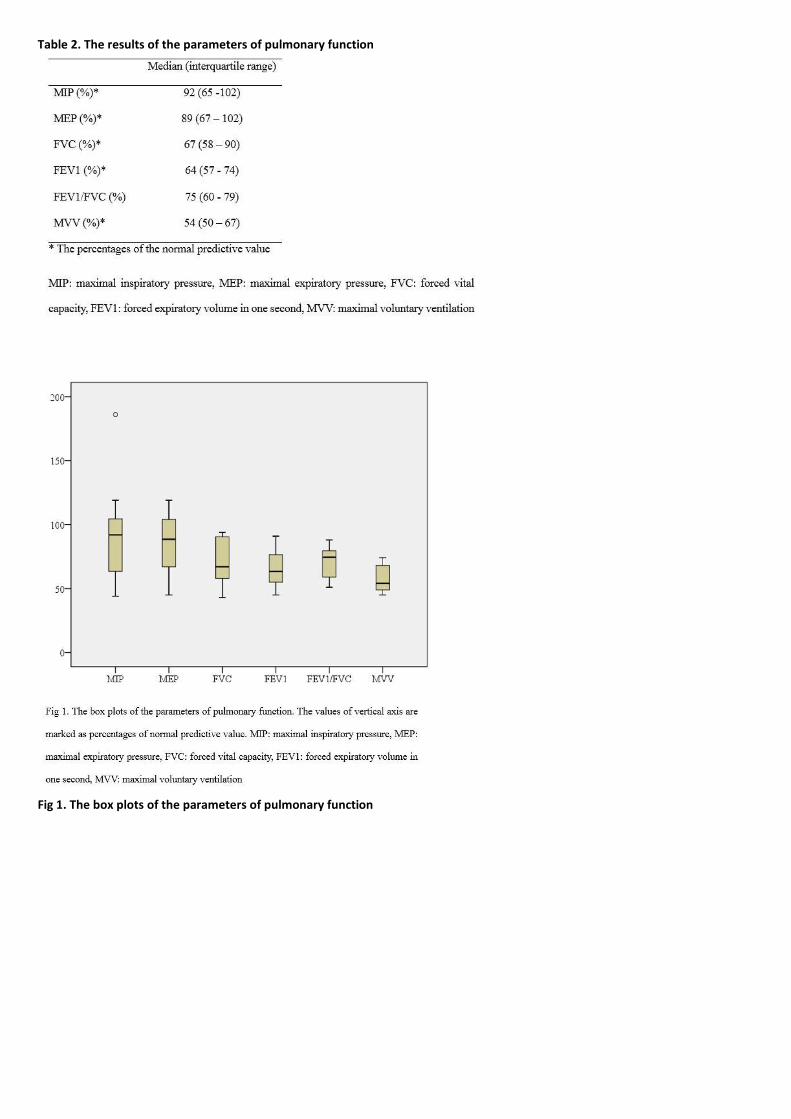
Table 2. The results of the parameters of pulmonary function
Fig 1. The box plots of the parameters of pulmonary function

P 74
The Lower extremity kinematics during ascending and descending stair according to height of stair.
Aeri Jang1*
, Hasuk Bae1†
Department of Rehabilitation Medicine, Ewha Womans University Mokdong Hospital1
Background
It is important to training stairs because ascending and descending stairs are commonly encountered in activities of daily living. The
purpose of this study was to present reference data by comparing the difference of lower extremity kinematics with stairs of
different height when ascent and descent stairs.
Methods
Twenty-five healthy indivisuals (12 males, 13 females) participated in this study. They ascent and descent the standard (15cm) and
low (7.3cm) height stair of 5 steps with attaching inertial measurement unit (IMU). Lower extremity kinematics were evaluated
using markerless motion capture system, IMU technology. First, IMU sensor provided to patients’abdomen, both thigh, shank and
foot dorsum. And next, patients climbed up and down the stair of standard and low height. During ascending and descending the
stair, degrees of hip, knee joint and ankle joints are detected. The difference between ascending and descending stair and the
difference between the height of stairs were analyzed by paired sample t-test, using SPSS. Statistical significance was defined as
P<0.05.
Results
Data were expressed as mean and standard deviation for angles, respectively. When ascending the stair, there was a significant
difference between the standard and low height stair in followings: hip flexion-extension peak angle and range of motion (ROM), hip
adduction-abduction peak angle and ROM, hip internal-external rotation peak angle, knee flexion-extension peak angle and ROM,
ankle dorsiflexion peak angle and ROM, ankle inversion-eversion peak angle, Table 1. And when descending the stair, there was a
significant difference between the height of stairs in followings: hip flexion-extension ROM, hip internal-external rotation ROM,
knee flexion-extension peak angle and ROM, knee internal-external rotation peak angle and ROM, ankle dorsiflexion ROM, ankle
inversion-eversion peak angle and ROM, Table 2. Regardless of the height of the stair, subjects demonstrated greater flexion-
extension peak angle and ROM, hip adduction-abduction peak angle and ROM, hip internal-external rotation ROM during stair
ascent compared to descent. But ankle dorsiflexion ROM, ankle inversion-eversion ROM and ankle internal rotation peak angle were
greater during stair descent compared to ascent, Table 3.
Conclusion
When comparing the differences according to the height of the stair, there was a significant difference mainly in hip joint on
ascending stairs, while knee joints show those on descending stairs. Furthermore, ankle joints showed significant differences
according to the height of the stair on both ascending and descending. Regardless of the height of the stair, subjects required
greater angle of hip joint during stair ascent compared to descent but subjects used more the ankle joint to descent the stair
compared to ascend. This study presents a normative database which could be used as reference data for gait rehabilitation training
for stair.

Table 1. Comparison of lower extremity kinematics during ascending standard-height and low-height stairs.
Table 2. Comparison of lower extremity kinematics during descending standard-height and low-height stairs.

Table 3. Comparison of lower extremity kinematics during ascending and descending the stair.

P 75
The prevalence and incidence of chronic diseases before and after disability registration
Rhee Seung Yeon1*
, Jeon Ha Ra1†
, Kim Seong Woo1, Chae Min Ji
1
Department of Physical Medicaine and Rehabilitation, NHIS Ilsan Hospital1
Introduction
The number of persons with disabilities in Korea increased from 1,134,177 in 2001 to 2,511,051 in 2016. The proportion of disabled
people is also reported to have increased from 2.4% to 4.9%, which has more than doubled over the past 15 years. In addition, there
are some studies that the prevalence of chronic diseases is higher in disabled people than in non-disabled people. The disabled
people are more likely to have secondary health problems. However, there are few studies that mentioned the temporal
relationship between disability and health status and they have limitations that they are based on the questionnaire or limited to a
certain period. In this study, we aimed to investigate the prevalence and incidence of chronic diseases in the persons with physical
disability or brain lesion disability.
Materials & Methods
We enrolled persons with disability who have been registered first into the physical disability and brain lesion disability from 2009 to
2011. From 2002 to 2016, the data were analyzed based on the cohort data of the National Health Insurance Corporation. We
considered that the subjects who were taking hypertension, diabetes, or dyslipidemia medicine have these chronic diseases. Also,
we assumed that it is the time of occurrence of disease when the subjects have started to take medicines.
Results
The prevalence of chronic diseases increased dramatically for three years before and after the time of disability registration. The
prevalence of hypertension, diabetes, and dyslipidemia increased gradually until two years before disability registration. The
prevalence of hypertension, diabetes, and dyslipidemia gradually increased until two years before the time of disability registration,
and then rapidly increased until the time of disability registration. After the time of the disability registration, it gradually increased
again. The incidence of chronic diseases of hypertension, diabetes, and dyslipidemia increased sharply from two years before the
disability registration to one year after the disability registration.
Conclusion
The prevalence and incidence of chronic diseases such as hypertension, diabetes, and dyslipidemia were significantly increased
around the time of disability registration in the persons with physical disability or brain lesion disability. Considering the process for
registration of disability in Korea, it can be considered that the incidence of chronic diseases are increased around the time of
disability registration. Therefore, active health care is needed in the persons with disabilities.
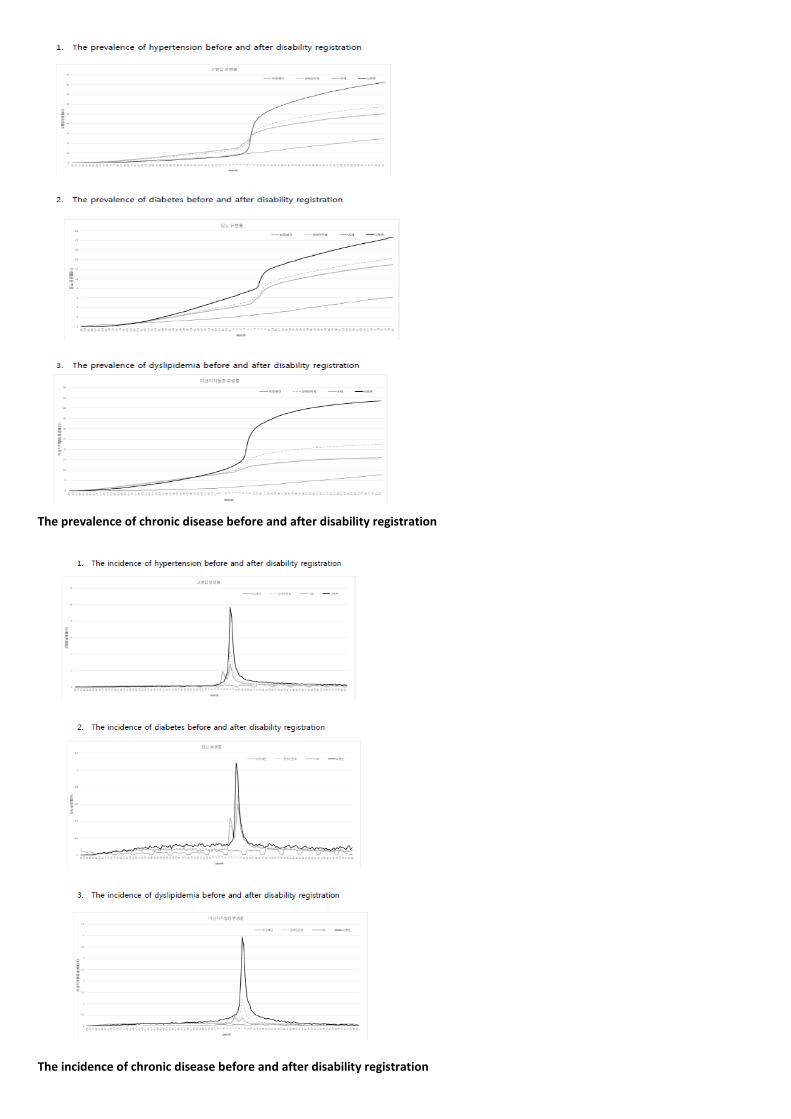
The prevalence of chronic disease before and after disability registration
The incidence of chronic disease before and after disability registration

P 75
Medical care utilization status before and after disability registration in the disabled persons
Rhee Seung Yeon1*
, Jeon Ha Ra1†
, Kim Seong Woo1, Chae Min Ji
1
Department of PHysical Medicine and Rehabilitation, NHIS Ilsan Hospital1
It is reported that the rate of national health screening of disabled people is lower than that of non-disabled people, and the
medical cost of disabled people is increasing every year. As such, people with disabilities are vulnerable to social, economic, and
medical problems. It is considered that there are differences medical care utilization before and after disability registration. The
purpose of this study was to investigate the medical care utilization status of the disabled people before and after the disability
registration through the rate of national health screening, medical costs, the number of hospital visits, and monthly hospitalization
rate in the persons with physical disability or brain lesion disability. We enrolled persons with disability who have been registered
first into the physical disability and brain lesion disability from 2009 to 2011. From 2002 to 2016, the data were analyzed based on
the cohort data of the National Health Insurance Corporation. Among the medial records the rate of national health screening, total
medical costs, the number of hospital visits, and the monthly hospitalization rate were compared before and after the disability
registration. The average daily medical expenses in the non-disabled people were maintained at a certain level. However, the daily
average medical expenses in the disabled people increased sharply from the disability registration to the one year after the disability
registration. The number of hospital visits in the non-disabled people increased gradually, but the number of hospital visits in the
disabled people sharply increased and then decreased from the time of the disability registration to the one year after the disability
registration. The monthly hospitalization rate in the non-disabled people were maintained at a certain level. However, the monthly
hospitalization rate in the disabled people sharply increased and then decreased from the time of the disability registration to the
one year after the disability registration. The rate of national health screening gradually increased in the non-disabled people. The
rate of national health screening in the disabled people was maintained at a certain rate until the time of the disability registration,
but gradually decreased from the point of 2 years after the disability registration. The medical costs, the number of hospital visits,
and monthly hospitalization rate in the persons with physical disability or brain lesion disability sharply increased and then
decreased from the time of the disability registration to the 1 year after disability registration. The rate of national health screening
in the disabled people gradually decreased from the time of 2 years after the disability registration. This suggests that healthcare
after disability is difficult to manage as before disability and the burden of medical costs increases after disability. Therefore active
health care policy is needed to support the disabled people.
The medical costs, monthly hospitalization rate and the rate of national health screening before and after disability registration

P 77
The Effectiveness of Regional Rehabilitation Center for Children with Disabilities
Sehee Kim1*
, Joon-Sung Kim2, Seong Hoon Lim
2, Bo Young Hong
2†
Department of Rehabilitation Medicine,Seoul St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, Seoul ,
Republic of Korea1, Department of Rehabilitation Medicine,St. Vincent’s Hospital, College of Medicine,The Catholic University of
Korea, Suwon, Republic of Korea2
Introduction
The International Classification of Functioning, Disability and Health-Children and Youths (ICF-CY) defines that the decline in physical
functioning caused by illness or health problem can lead to limitations of activity and restrictions on participation, which is also
influenced by social and environmental impacts. Therefore, there is a need to revitalize support for rehabilitation treatment of
children and adolescents with disabilities. Hwaseong City, which is located in Gyeonggi Province, has been operating rehabilitation
centers for children with disabilities for twelve years. The purpose of this study was to investigate the objective benefits of
community-based disability child rehabilitation center in addition to improving human rights. We also tried to confirm the user
satisfaction of the service provided.
Method
The movement time calculation was made using the navigation program. We confirmed the travel time to places where pediatric
rehabilitation is available such as the clinic, welfare center, and rehabilitation center from 9 locations in Hwaseong City several times,
at 02:00 pm on Wednesday. User satisfactions were surveyed.
Results
Table 1 shows that the minimum time required to reach the treatment facility. We compared the time difference between when
there was a center and when there was no center operated by Hwaseong City. The time difference with the center was the biggest
difference at the Songsan-myeon office, about 30 minutes by a car and 80 minutes by public transportation. This only measured the
vehicle travel time so the actual travel time will be longer. Figure 1 clearly shows the traffic time difference between with the
rehabilitation center by Hwaseong City and without the rehabilitation center by a car (Figure 1). User satisfaction points was 4.12
points out of 5 points (Table 2).
Conclusion
In this study, we confirmed the effectiveness of the Rehabilitation Center for Children with Disabilities operated by local
government. Shortening the travel time for treatment will contribute to the quality of life of the child and the caregiver. Also, user
satisfaction was 4.12 points out of 5 points, which shows relatively high satisfaction of users. The rehabilitation center operated by
the local government will contribute to the improvement of the quality of life of the disabled child and family by shortening the
travel time for the treatment when the supply of the place where pediatric rehabilitation treatment is available is less than the
demand.

Table 1. Minimum time required to arrive at a place where children can receive pediatric rehabilitation treatment
Table 2. The result of user satisfaction survey
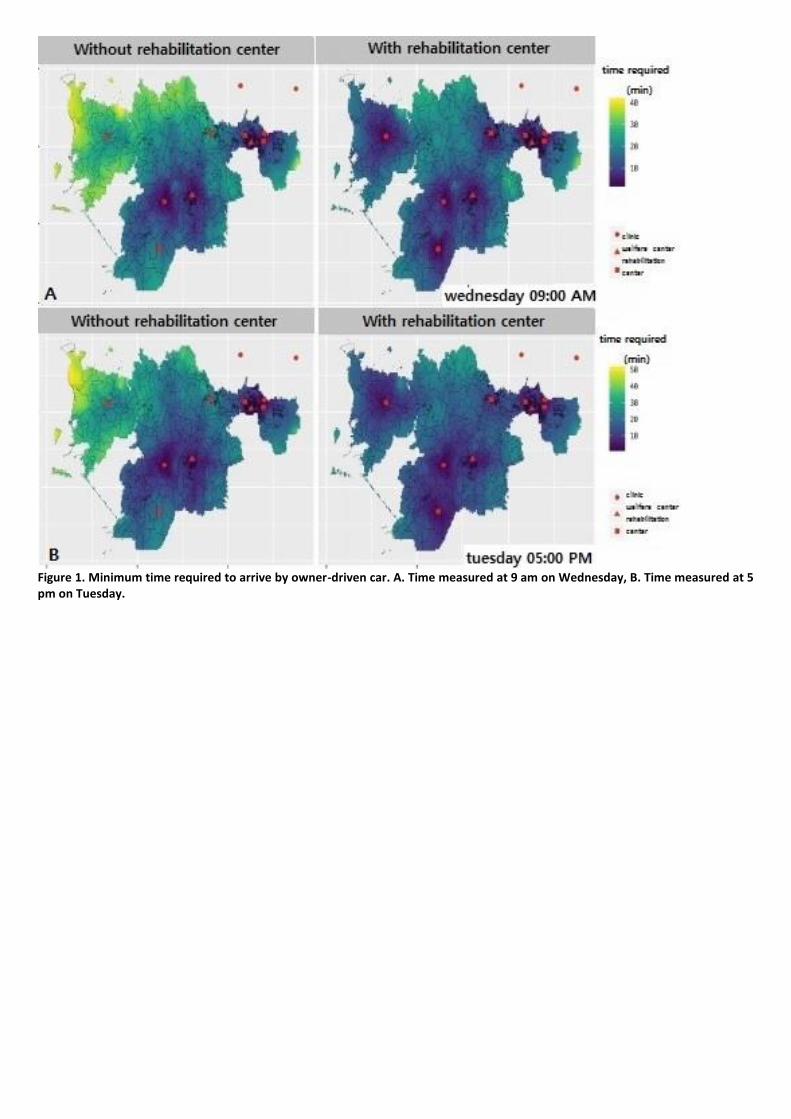
Figure 1. Minimum time required to arrive by owner-driven car. A. Time measured at 9 am on Wednesday, B. Time measured at 5 pm on Tuesday.

P 78
Incidence Estimation and Severity Determinants of Traumatic Spinal Cord Injury in Korean Military
Jeong-Gil Kim, M.D., MPH.1*†
Department of Rehabilitation Medicine, Armed Forces Daejeon Hospital1
Background
Traumatic spinal cord injury is a catastrophic disease that affects individuals and society due to persistent sequela. For this reason,
overseas researches about traumatic spinal cord injuries have been actively reported at the national or regional level, but there are
no epidemiological studies conducted on specific population groups in Korea yet.
Purpose
The purpose of this study was to evaluate the incidence and severity determinants of traumatic spinal cord injuries by reviewing the
medical records of all patients with traumatic spinal cord injuries registered in the N-DEMIS (New Defense Medical Information
System).
Methods
From May 2012 to December 2017, a total of 3,011 patients with a diagnosis of traumatic spinal cord injury registered on N-DEMIS
were listed and duplicate patients were eliminated. Then, 89 patients with traumatic spinal cord injuries who finally meet the
definition of American Spinal Injury Association (ASIA) were reviewed by a rehabilitation specialist.
Results
The average incidence of traumatic spinal cord injury in the study was 24.99 per 1 million people per year. The military officers were
19 (21.3%), NCOs (non-commissioned officers) 30 (33.7%), soldiers 38 (42.7%), and cadets 2 (2.25%). And army (86.5%), navy (7.9%)
and air force (5.6%) were identified and the mean age at injury was 29.82 (± 9.99) years. According to the common classification
criteria of overseas researches, 37 cases (41.6%) suffered traumatic spinal cord injury due to falls, 16 cases (18.0%) were injured by
motor vehicles accidents, There were 14 (15.7%) injuries during the military training, 11 (12.4%) sports injuries, 7 (7.9%) diving
injuries and 4 (4.5%) other injuries. There were 64 patients (71.9%) of cervical spinal cord injuries, 9 patients (10.1%) of thoracic
spinal cord injuries, and 16 patients (18.0%) of lumbosacral spinal cord injuries. The degree of impairment was classified as AIS (ASIA
Impairment Scale). Twenty four patients had complete paralysis which made of AIS A grade 19 (21.3%) and AIS B grade 5 (5.6%). On
the other hand, patients with incomplete paralysis were 65 (73.0%), consisted with AIS C grade 14 (15.7%), AIS D grade 51 (57.3%),
respectively. When the severity of traumatic spinal cord injury was classified as 'complete paralysis' and 'incomplete paralysis', the
shorter the military career and the younger age at the time of injury, the more significant correlation was found with the severity of
traumatic spinal cord injury. This is the first study to present the incidence of traumatic spinal cord injuries in military by
epidemiological method and this study is the first to analyze the incidence of specific population in Korea.

P 79
A pediatric case of central cord syndrome relevant to infarction in conus medullaris
Sungchul Huh1*
, Eun-Ho Yu1, Hyun-Yoon Ko
1†
Department of Rehabilitation Medicine, Pusan National University Yangsan Hospital1
INTRODUCTION
Pediatric non-traumatic spinal cord infarction is very uncommon condition and difficult to diagnose. The spinal cord infarction can
be either ischemic or hemorrhagic. There are some etiologic causes for non-traumatic spinal cord infarction such as cardiovascular
cause, thrombosis or embolism, infection, and vascular inflammation. The reporting case is about pediatric non-traumatic spinal
cord infarction and following successful rehabilitation process.
CASE REPORT
A 12-year-old female began to feel abrupt low back pain for two days and subsequent weakness and pain of both lower extremities.
She was not able to stand independently and voided unintentionally. She previously had upper respiratory infection with cough and
rhinorrhea a month before the symptoms onset. She had no genetic family history or previous medication history. Initial physical
examination at first visit to hospital indicated weak motor grades as poor grades in hip flexors, both knee extensor and ankle
dorsiflexors, but normal sensory. Bilateral knee jerks and ankle jerks were hypoactive, however there was no pathologic reflex
elicited in both legs. She underwent an extensive work-up for infection diseases and demyelinating diseases. Lumbar puncture study
was unremarkable. With a presumptive diagnosis of either transverse myelitis or acute inflammatory demyelinating polyneuropathy,
pediatric neurologist started methylprednisolone pulse therapy for three days. Following MR imaging study revealed T2
hyperintensity with diffusion restriction in T12 to conus medullaris which indicated spinal cord infarction in high probability (Fig 1.
and Fig 2.). After 26 days after admission to the clinic, she was transferred to rehabilitation unit. Follow-up motor grades of both
legs were as follows: L2 3/3, L3 3/3, L4 4/4, L5 3/4 and S1 1/1. Anal sense was positive bilaterally, but voluntary anal contraction was
absent. Neither anal reflex nor clitocavernous reflex were absent. Neurologic level of injury was L3 paraplegia AIS D. Urodynamic
study revealed acontractile detrusor function, and the patient start intermittent catheterization for void (Fig 3.). She discovered
newly onset of neuropathic pains of both legs, which were well controlled with low dose of gabapentin. Calcaneal gait pattern was
obvious, and the rehabilitation was focus on gait training with strengthening of both lower extremities. With rapid recovery, she
uses walking aids, walker or bilateral Lofstrand crutches, for ambulation.
COMMENTS
Although average prognosis of spinal cord infarction is very severe, pediatric spinal cord infarction seems to be quite reversible on
account of unknown reason. Plasticity after infarction might give a rough explanation.

Fig 1. MR L-spine shows Ill-defined hyperintensity involving T12 level to conus medullaris of the spinal cord and subtle leptomeningeal and intramedullary enhancement.
Fig 2. MR diffusion restriction image at T12 vertebral level.

Fig 3. Acontractile detrusor function at urodynamic study.

P 80
Prevalence of Autonomic Dysreflexia and Orthostatic Hypotension in Patients With Spinal Cord Injury
Na Ri Yun1*
, Min Cheol Joo1†
Department of Rehabilitation Medicine, Wonkwang University School of Medicine1
Objectives
To investigate the prevalence of autonomic dysreflexia (AD), orthostatic hypotension (OH) and circadian changes in blood pressure
after spinal cord injury (SCI).
Methods
Eighty-five patients diagnosed with SCI were enrolled. 24-hour ambulatory blood pressure monitoring (ABPM) was utilized to assess
AD. Using ABPM, systolic blood pressure (SBP), diastolic blood pressure (DBP), and heart rate (HR) were measured at 30-minute
intervals at day-time and 60-minute interval at night-time. AD was defined as SBP 20 mmHg higher than basal SBP. OH was
evaluated using head up tilt test (HUTT). OH was defined as a decrease in SBP of ≥20 mmHg or a decrease in DBP of ≥10 mmHg after
3 minutes in the 60° angle of tilt test.
Results
The study included 60 men and 25 women with a mean age of 57.8±13.5 years. Regarding the cause of SCI, 64 and 21 patients had
SCI due to trauma and non-trauma, respectively. Mean duration after SCI was 29.0 ± 64.3 months. Regarding the level of injury, 47
patients had cervical SCI and 28 patients had thoracic SCI and 10 patients had lumbar SCI. With respect to SCI severity, 18 patients
were classified as having motor complete SCI (AIS grades A and B) and 67 patients were classified as having motor incomplete SCI
(AIS grades C and D). According to the ABPM, AD occurred in 41 patients (48%) and OH occurred in 29 patients (76%). In subacute
and motor complete group, the night-time mean SBP appeared to be 2.6mmHg, 3.9mmHg higher than day-time mean SBP,
respectively. These findings show reverse-dipper BP pattern, suggesting the loss of nocturnal dipping in SCI patients (Table 1). There
was also a significant increase in OH prevalence in subacute and motor complete group compared to chronic and motor incomplete
group (Table 2). <br>When comparing the result according to the injury level, average day-time and night-time SBP were 121.1±16.2
mmHg and 124.8±18.1 mmHg, in above T6 group. And the night-time mean SBP appeared to be 3.7mmHg higher than day-time
mean SBP, suggesting the loss of nocturnal BP dipping. However, this phenomenon did not appear in the below T6 group (Table 3).
In above T6 group, AD and OH prevalence were significantly higher than below T6 group (Table 2). In the below T6 group, 24hr mean
SBP was 126.7±11.7 mmHg, which was higher than the above T6 group (121.8±16.1) (Table 3).
Conclusions
AD and OH were highly prevalent in SCI patient, especially in above T6 level. In addition, there was the loss of nocturnal BP dipping
in SCI patients. These results suggest the necessity of proper diagnostic and therapeutic interventions for managing AD and OH.

Table 1. Comparison of ABPM values in SCI patients
Table 2. Prevalence of AD and OH in SCI patients
Table 3. Comparison of ABPM values between above T6 and below T6 groups

P81
Relationship between LEMS and Mobility score of K-SCIM in Patient with Cauda equina syndrome
Howook Kim1*
, Chang-Won Moon1, Il-Young Jung
1, Kang Hee Cho
1†
Department of Rehabilitation Medicine, School of Medicine, Chungnam National University1
Objective
Understanding mobility of patients with Cauda equina syndrome is important because it can predict the patient's functional
outcome. If the level of mobility can be predicted early, appropriate individual rehabilitation treatment can be provided at the
earliest possible time. To investigate the relationship between the lower extremity motor score (LEMS) and the mobility score of
Korean Version of Spinal Cord Independence Measure (K-SCIM) to predict the patient's level of mobility.
Subjects & Methods
We retrospectively reviewed 42 patients with cauda equina syndrome who were admitted to our rehabilitation center from March
2015 to February 2019. For a diagnosis of cauda equina syndrome, one or more of the following must be present: (1) Neurologic
deficit in the lower limb (motor/sensory loss, reflex change), (2) Bladder and/or bowel dysfunction, and (3) Reduced sensation in the
saddle area. We excluded patients with any of the following: (1) a diagnosis of cerebral infarction or hemorrhage in the brain by CT
or MRI, (2) complete or incomplete limb paralysis due to spinal cord injuries, (3) a history of traumatic brain damage or brain tumor,
(4) presence of neuromuscular diseases (e.g., amyotrophic lateral sclerosis and myasthenia gravis), and (5) unstable medical
condition. Demographic characteristics and clinical characteristics were analyzed to identify factors influencing the lower extremity
motor scores. Patients were divided into three groups according to age, and the correlation between LEMS and K-SCIM was
analyzed. The lower extremity motor score is a sum of assessed voluntary muscle strength of 5 key muscles (hip flexor, knee
extensor, ankle dorsiflexor, long toe extensor, ankle plantarflexor). We classified the three groups according to age and the lower
extremity motor scores and the mobility score of K-SCIM were analyzed to compare the relationship between strength of lower
extremities and mobility of patients.
Results
Forty- two patients with cauda equine syndrome were analyzed for data (22 male and 20 female patients). Subject ages ranged from
21 to 85 years with a mean of 62.0±16.5 years. The mean <br>LEMS was 35.5±8.2 points on the basis of a total of 50 points. And,
the mean LEMS-HE was 42.3±9.8 points on the basis of a total of 60 points. The mean mobility score of K-SCIM was 4.2±2.2 points
on the basis of a total of 8 points (Table 1). The correlation between LEMS or LEMS-HE and mobility score of K-SCIM was evaluated,
and LEMS was found to have a significant effect on mobility score of K-SCIM in all groups. Comparing LEMS and LEMS-HE, LEMS-HE
had a higher coefficient of determination, which tended to increase with age (Table 2).
Conclusion
There was a significant correlation between LEMS or LEMS-HE and mobility score of K-SCIM in patients with cauda equina syndrome,
especially LEMS-HE statistically significant and high coefficient of determination. In patients with cauda equina syndrome, the level
of mobility of p
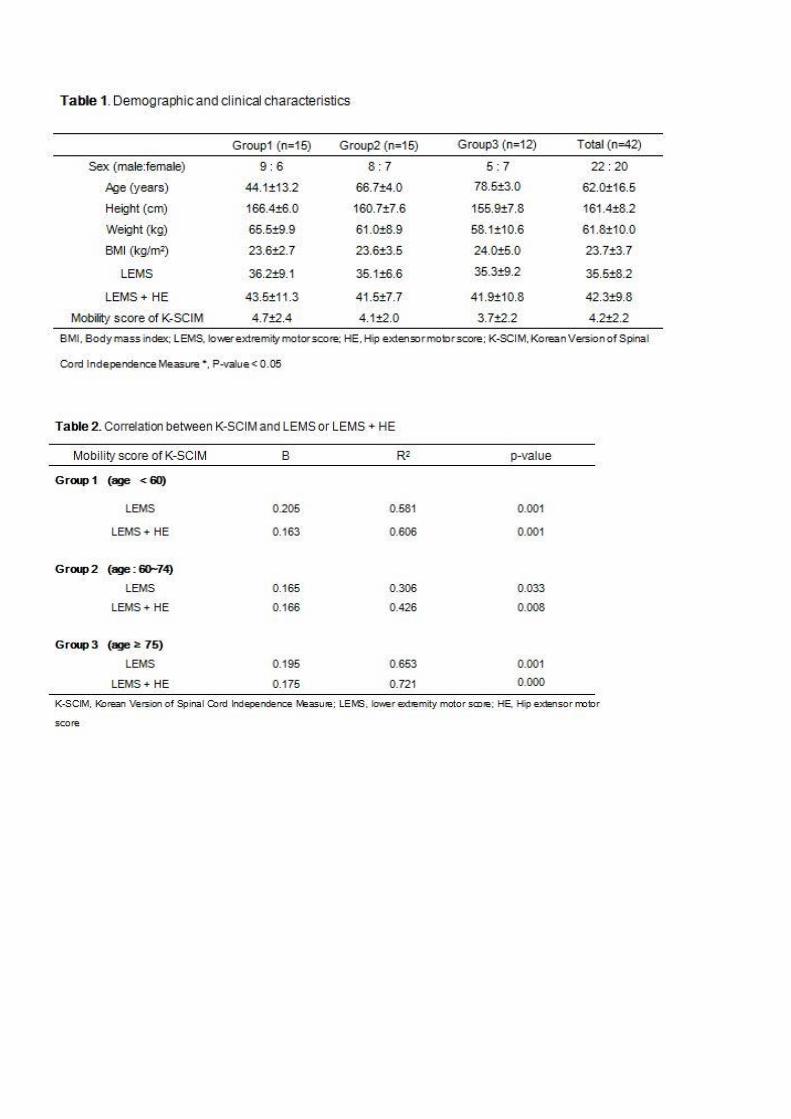

P 82
Modified Clinical Test of Sensory Integration and Balance in the Patient with Incomplete SCI
Mi-Kyung Cho1*
, Dong Min Kim1, Tae Sung Park
2, Myung-Jun Shin
1, Sang Hun Kim
1†
Department of Rehabilitation Medicine, Pusan National University Hospital1, Biomedical Research Institute, Pusan National
University Hospital2
Background
Falls in the elderly can cause serious complications and accelerate deterioration of physical function. Even if walking is possible, in
persons with incomplete tetraplegic spinal cord injury (SCI), the balance ability abruptly decreased than before. This study is a
preliminary study to determine what results are obtained in patients with incomplete spinal cord injury using Fall Risk Assessment
(FRA, InBody®, Republic of Korea) system that can measure modified clinical test of sensory integration and balance (m-CTSIB) more
specifically and quantitatively.
Method
12 male participants with AIS D SCI who could walk 10 meters independently without walking aid were recruited. The m-CTSIB
consists of the following four conditions (Table 1). 14 normal male elderly are also recruited as a control group. Mean age of each
group are 65.00±4.26 and 71.14±1.40 respectively. The output of this test is sway index of gravity center. Using the FRA system, we
could easily quantify the value of the gravity center in the X-Y axis and the degree of sway in centimeters.
Results
The m-CTSIB is designed to evaluate the interaction of multiple sensory systems in elderly. The mean sway indexes of each stage are
shown in the Table 2 and Figure 1.
Conclusion
Somatosensory impairment is often associated with incomplete SCI patients who can walk independently. The sway indexes of SCI
group are worse than the normal elderly in the condition 2, 3 and 4. By comparing the condition 1 and 2, we can estimate the
degree of enhancing effect of vision for balance. The m-CTSIB via FRA has the advantage of being able to obtain simply clear and
objective results. In addition, FRA might be useful as a tool for evaluating the risk of falls and prescribing proper walking aids in
these patients.
Figure 1. Mean difference of sway index between two groups

Table 1. m-CTSIB in FRA system
Table 2. Mean differences of sway index between two groups

P 83
Spinal cord infarction with antiphospholipid syndrome; literature review
Kiyeun Nam1†
, Jeonghwan Lee2, Ho Jun Lee
1, Jin-Woo Park
1, Bum Sun Kwon
1, Yongjin Cho
1*
Department of Rehabilitation Medicine, Dongguk University Ilsan Hospital1, Department of Rehabilitation Medicine, Dongguk
University Gyeongju Hospital2
Background
Spinal cord infarction is a rare but often devastating disorder caused by a wide array of pathologic states. Patients typically present
with acute paraplegia or quadriplegia, depending on the level of the spinal cord involved. The diagnosis is generally made clinically,
with neuroimaging to confirm the diagnosis and exclude other conditions. <br>Antiphospholipid (aPL) syndrome (APS) is a systemic
autoimmune disorder associated with hypercoagulability and aPL antibodies, and it can occur in isolation (primary APS) or can
accompany other systemic autoimmune disorders, such as SLE (secondary APS). There are few report APS as an etiologic factor for
spinal cord infarction.
Methods
We performed a search for clinical studies of spinal cord infarction with antiphospholipid syndrome published up to Feb. 2019. We
placed no restrictions on language or year of publication in our search, and we searched the following keywords: spinal cord
infarction, antiphospholipid syndrome, anterior spinal artery syndrome, posterior spinal artery syndrome, paraplegia, quadriplegia.
Results
We identified 3 cases of SCI induced by APS. We added up to our case and confirmed four cases in total. Two cases were ASIA-A at
thoracic level and our cases were ASIA-B and T5 / T5. In all 4 cases, APS was diagnosed with anti-cardiolipin antibody and no
abnormality of coagulation factor was observed. We did not know if the rehabilitation protocol was performed, but there was no
motor improvement in two cases and a 10% motor improvement in one case.
Conclusions
APS is quite rare as an etiologic factor for spinal cord infarction. It is difficult to diagnose APS induced SCI definitively due to its rarity
and MRI findings that are detected over time. This study noted that in patients with spinal cord infarction, APS should also be
considered as an evaluation. In patients with acute spinal cord infarction, there is no space occupying lesion on neurologic imaging,
and patients with coagulopathy symptoms should suspect APS. In three cases, SCI induced by APS showed no motor improvement
or motor improvement as low as 10%. Perhaps acute complete artery occlusion may be the cause, but more research will be done.

Table 1. Spinal cord infarction with antiphospholipid syndrome

P 84
Factors affecting psychological distress of SCI patients in inpatient rehabilitation settings
Chul Jung1*
, Jong Yoon Yoo1†
Department of Rehabilitation Medicine, Asan Medical Center1
OBJECTIVE
To assess the presence of psychological distress including anxiety and depression among adults with spinal cord injury in inpatient
rehabilitation settings and to investigate the association with sociodemographic and injury characteristics.
METHODS
This study was conducted through retrospective review of medical records and it included 133 spinal cord injury patients
hospitalized for rehabilitation from January, 2016 to December, 2018. Sociodemographic characteristics including age, sex, place of
residence, education level, marital status, religion and caregiver information were collected. Injury characteristics were also
collected including injury level, severity, etiology, time since injury, Spinal Cord Independence Measure (SCIM), and so on.
Depression and anxiety was assessed using Beck Depression Inventory (BDI) and Stait-Trait Anxiety Inventory-X-I (STAI-X-I)
respectively. The patients were divided into subgroups: patients with BDI ≥ 14 were classified as depressive group and STAI ≥ 52
were classified as anxious group.
RESULTS
51 and 37 of total 133 patients included in this study were classified as depressive group and anxious group, respectively. (Table 1)
In addition, there were no significant difference in depression and anxiety scores according to sociodemographic and injury
characteristics. (Table 2) Among the characteristics, only SCIM showed significant difference between non-depressive group and
depressive group. (p=0.014) (Table 3) In depressive group, SCIM was significantly lower than non-depressive group. There was no
characteristics showing significant difference between non-anxious group and anxious group.
CONCLUSION
It was found that spinal cord injury patients showed high prevalence of depression and anxiety. Also, most sociodemographic and
injury characteristics except SCIM did not affect depression and anxiety significantly. Compared with low SCIM scores, SCI patients
with high SCIM scores showed lower risk of depression. Therefore, it should be taken care of depression especially in SCI patients
showing low independence in activity of daily living.

Table 1. Sociodemographic and injury characteristics of patients
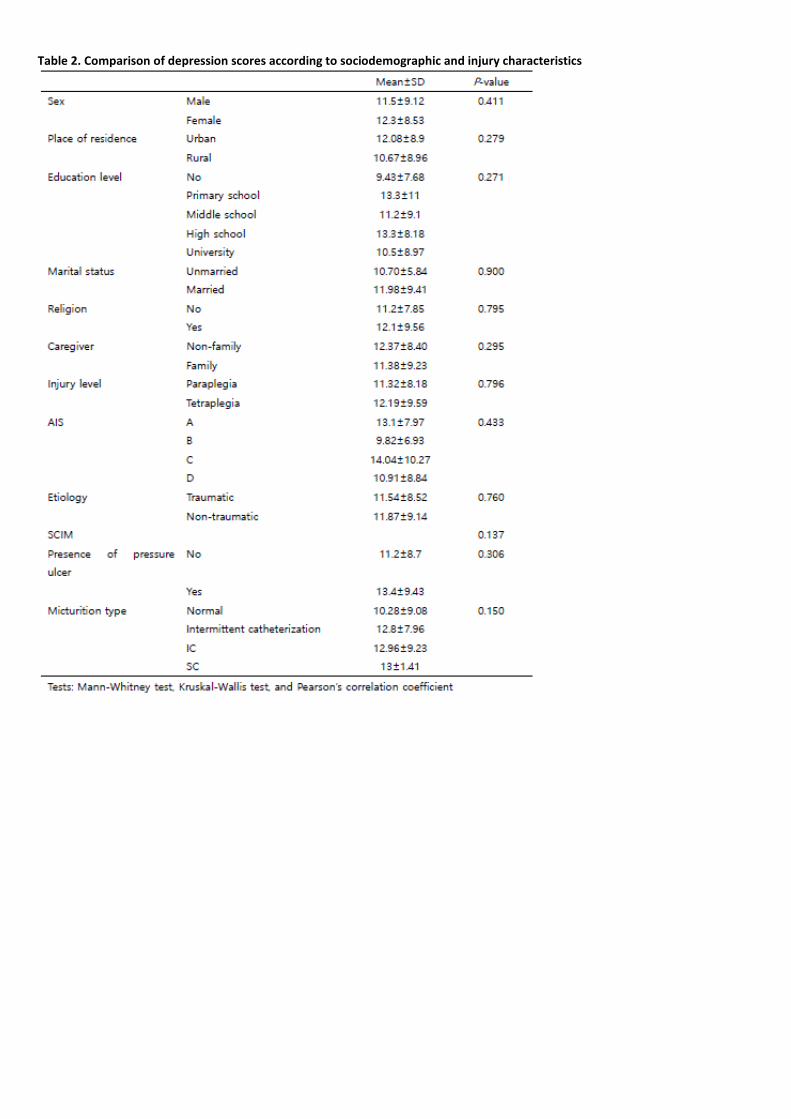
Table 2. Comparison of depression scores according to sociodemographic and injury characteristics
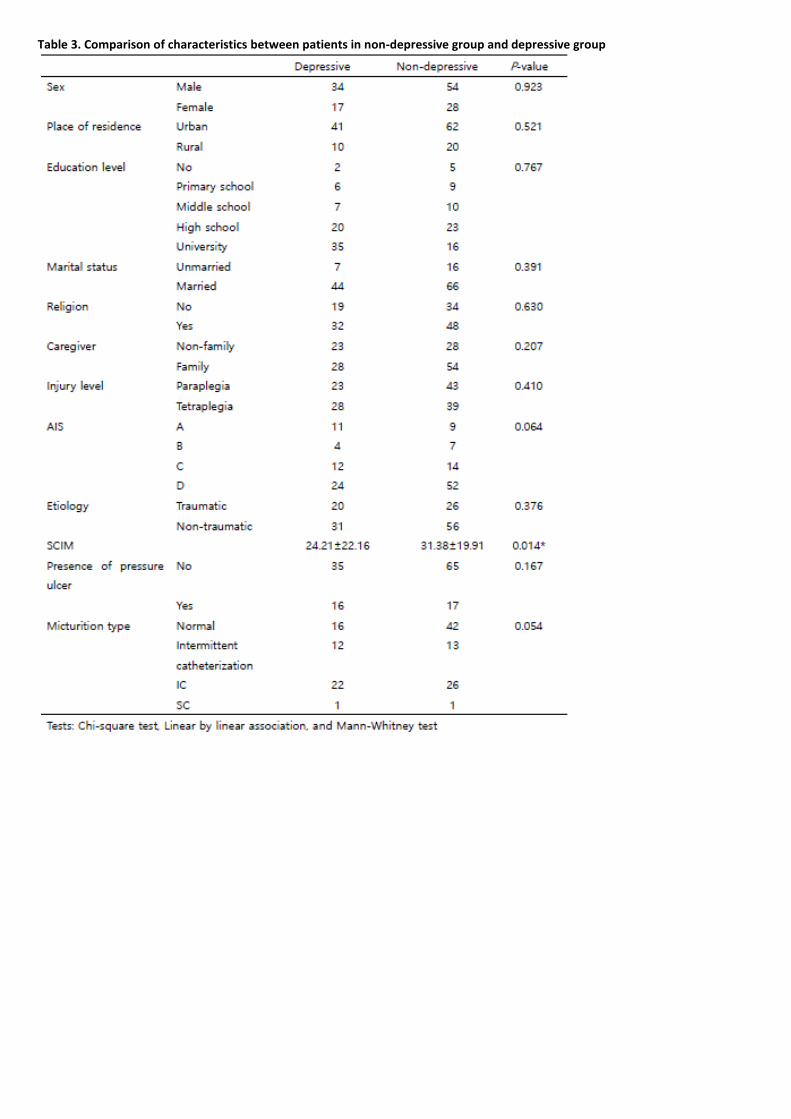
Table 3. Comparison of characteristics between patients in non-depressive group and depressive group
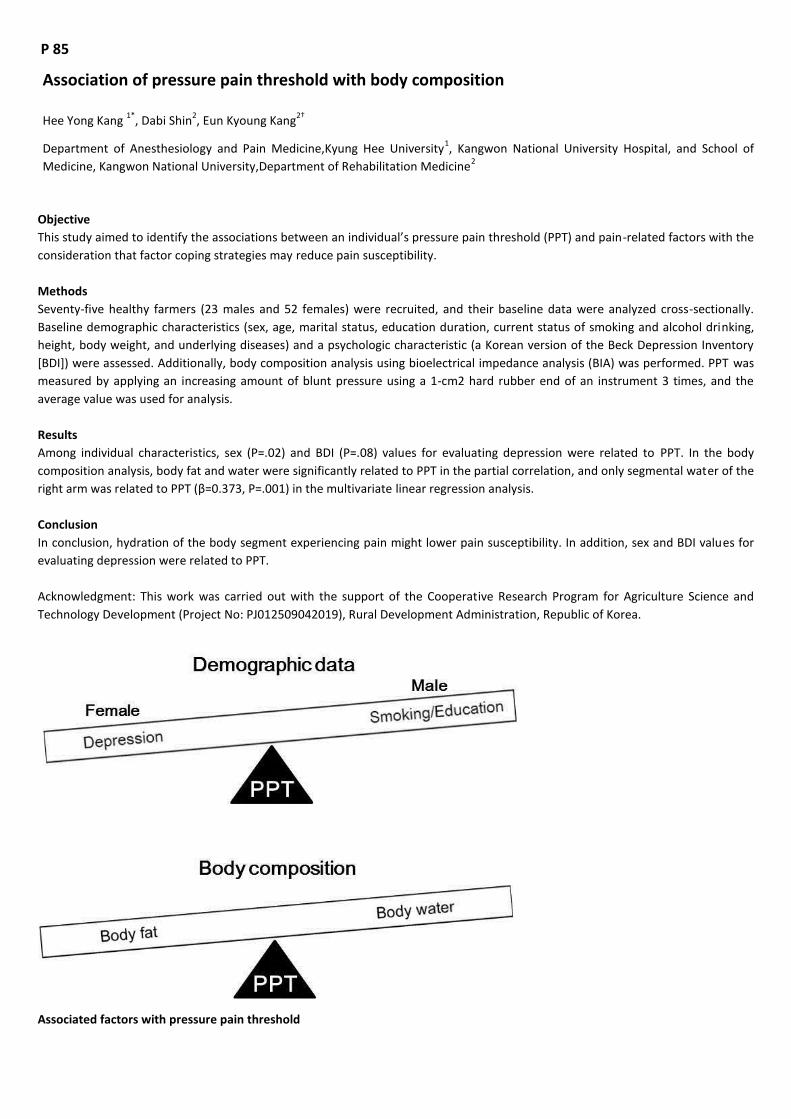
P 85
Association of pressure pain threshold with body composition
Hee Yong Kang 1*
, Dabi Shin2, Eun Kyoung Kang
2†
Department of Anesthesiology and Pain Medicine,Kyung Hee University1, Kangwon National University Hospital, and School of
Medicine, Kangwon National University,Department of Rehabilitation Medicine2
Objective
This study aimed to identify the associations between an individual’s pressure pain threshold (PPT) and pain-related factors with the
consideration that factor coping strategies may reduce pain susceptibility.
Methods
Seventy-five healthy farmers (23 males and 52 females) were recruited, and their baseline data were analyzed cross-sectionally.
Baseline demographic characteristics (sex, age, marital status, education duration, current status of smoking and alcohol drinking,
height, body weight, and underlying diseases) and a psychologic characteristic (a Korean version of the Beck Depression Inventory
[BDI]) were assessed. Additionally, body composition analysis using bioelectrical impedance analysis (BIA) was performed. PPT was
measured by applying an increasing amount of blunt pressure using a 1-cm2 hard rubber end of an instrument 3 times, and the
average value was used for analysis.
Results
Among individual characteristics, sex (P=.02) and BDI (P=.08) values for evaluating depression were related to PPT. In the body
composition analysis, body fat and water were significantly related to PPT in the partial correlation, and only segmental water of the
right arm was related to PPT (β=0.373, P=.001) in the multivariate linear regression analysis.
Conclusion
In conclusion, hydration of the body segment experiencing pain might lower pain susceptibility. In addition, sex and BDI values for
evaluating depression were related to PPT.
Acknowledgment: This work was carried out with the support of the Cooperative Research Program for Agriculture Science and
Technology Development (Project No: PJ012509042019), Rural Development Administration, Republic of Korea.
Associated factors with pressure pain threshold

P 86
Hydraulic distension with pumping technique for treating frozen shoulder: A Case-Controlled Study
Sang Hoon Shin1*
, Yong Wook Kim1, Won Hyuk Jang
2, Sang Chul Lee
1†, Sang Chul Lee
1†
Yonsei University College of Medicine, Seoul, Republic of Korea,Department of Rehabilitation Medicine and Research Institute1,
Center for Prevention and Rehabilitation, Heart Vascular Stroke Institute, Samsung Medical Center, Sungkyunkwan University
School of Medicine, Seoul, Republic of Korea,Department of Physical and Rehabilitation Medicine2
Objective
To determine effect of capsule-preserving hydraulic distension using a pumping technique compared to that of capsule-preserving
hydraulic distension without the pumping technique on frozen shoulder.
Subject & Method
This study included outpatients with frozen shoulder who underwent hydraulic distension in the outpatient clinic of department of
rehabilitation medicine of a single university hospital between March 2013 and October 2018. Patients (N = 47) with frozen shoulder
who were treated with capsule-preserving hydraulic distension were assigned into the pumping group (N = 24) and the non-
pumping group (N = 23). Capsule-preserving intra-articular hydraulic distension was performed on the affected shoulders for all
patients with or without the pumping technique. Using aseptic technique, a 6-cm, 23-gauge needle was placed in the glenohumeral
joint with verification of intra-articular position under ultrasonography. A mixture of 1 mL of triamcinolone (40 mg), 10 mL of local
anesthetic (1% lidocaine), and 19 mL (0.9% NaCl) of normal saline solution (30 mL total) was prepared. The mixture solution was
divided into three 10-mL syringes. For the first syringe, 40 mg triamcinolone was added before the injection. The mixture of 30 mL
was injected into the joint slowly with pressure while monitoring by ultrasonography to preserve the joint capsule and maximize the
injected volume. With the pumping technique the regurgitation occurred into the syringe as a result of increased intra-articular
pressure during the procedure, the back flowed solution was pushed into the joint and the syringe was held for 10 seconds followed
by regurgitation. The investigator repeated the same procedure 10 times. These injections were repeated a total of five times in
two-week intervals. Individual range of motion (ROM) values in three shoulder joint directions (forward flexion, abduction, and
external rotation) and their total sum, shoulder pain and disability index (SPADI), and visual analogue scale (VAS) scores were
assessed on seven occasions (five times pre-procedurally and twice post-procedure at three and six months).
Results
Significant improvement of total ROMs, abduction, flexion, and external rotation were observed from the timepoint of the 2nd
injection in each group. There were significant differences in total passive ROMs, abduction, and flexion between the two groups
and external rotation was significantly higher in the pumping group. Significant improvement of SPADI was observed in each group
and there was significant difference in the disability domain of SPADI between the two groups. Significant improvement of VAS was
observed in each group.
Conclusion
While the effect on pain reduction was excellent in both groups, the superiority of the new pumping technique was demonstrated
by reduction of SPADI disability subscale score and improvement of ROM of the shoulder compared to the non-pumping technique.
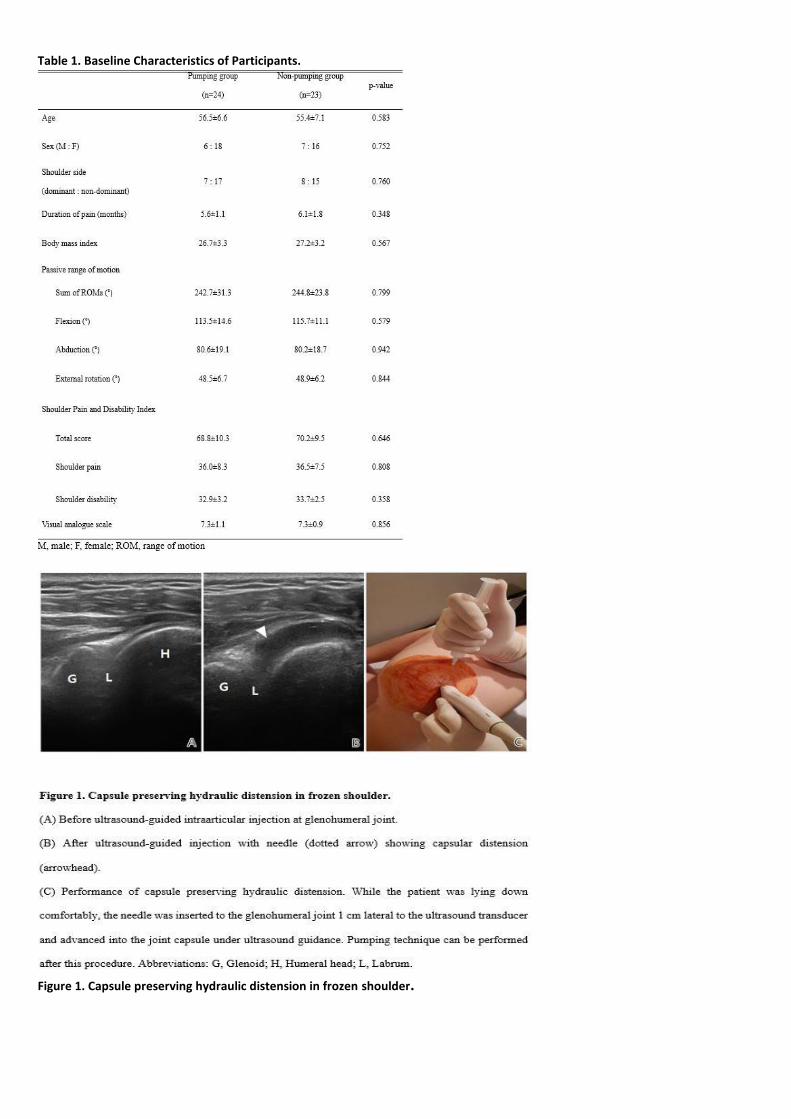
Table 1. Baseline Characteristics of Participants.
Figure 1. Capsule preserving hydraulic distension in frozen shoulder.

Figure 2. Outcomes change from baseline to each assessment and between-group differences.

P 87
Effects of Mesenchymal Stem Cells on Tendon Disorders: A Meta-Analysis of Clinical Studies
Woo Sup Cho1*
, Sun Gun Chung1, Won Kim
2, Chris H. Jo
3, Shi-Uk Lee
4, Sang Yoon Lee
4†
Department of Rehabilitation Medicine,Seoul National University Hospital1, Department of Rehabilitation Medicine,Asan Medical
Center2, Department of Orthopedic Surgery,SMG-SNU Boramae Medical Center
3, Department of Rehabilitation Medicine,SMG-SNU
Boramae Medical Center4
Objectives
Although several animal studies have reported the effects of mesenchymal stem cells (MSCs) for tendon regeneration, little is
known about the efficacy and safety of MSCs in human tendon disorders. Furthermore, a number of clinical studies used not pure
MSCs but bone marrow aspirates or stromal vascular fractions cells. Thus, we performed an update meta-analysis of prospective
clinical studies to evaluate the efficacy and safety of MSCs therapy in patients with tendon disorders.
Methods
Four randomized controlled trials investigating the effect of MSCs on tendon disorders were retrieved (Table 1) from a PubMed,
Embase, and Cochrane Library search. We performed a pairwise meta-analysis using fixed- or random-effects models.
Results
MSCs showed a significant overall effect size (overall Hedge’s g pooled standardized mean difference (SMD) = 1.868; 95%
confidence interval [CI], 1.274–2.462; P < 0.001) (Figure 1). Pain, functional scores, radiologic parameters (magnetic resonance
image or ultrasonography), and arthroscopic findings all improved with MSCs treatment. In meta-regression analysis, there was a
significant cell dose-dependent responses in pain relief (Q=9.06, P = 0.029) (Figure 2). While three studies reported mild adverse
events after MSCs injection, these were not severe and spontaneously relieved.
Conclusion
Our meta-analysis revealed that MSCs therapy can improve pain, functions, radiologic and arthroscopic parameters in patients with
tendon disorder. Due to the small sample size in this meta-analysis and considering the increasing MSCs applications, there is a need
for large-scale randomized controlled trials to confirm the long-term functional improvement and adverse effects of MSCs on
tendon disorders.
Table 1. Characteristics of included individual studies

Figure 1. Forest plot of the overall effect size of mesenchymal stem cells on tendon disorders determined by a fixed-effects meta-analysis. Effect sizes are indicated as Hedges’ g standardized mean differences and 95% confidence intervals.
Figure 2. Meta-regression of the standardized mean differences in means for cell dose. The area of the circles is proportional to the studies’ weights in the regression.

P 88
Correlation between the shoulder pain and disability index and EMG in rotator cuff tear
Seunghun Park1*
, Jung Joong Kang1, Jungin Kim
1, Dong Kyu Kim
1, Tae Hee Kim
1†
Departments of Rehabilitation Medicine, School of Medicine, Konkuk University1
Objective
To analyze electromyographic (EMG) activities of shoulder muscles in patients with a unilateral, partial-thickness tear of
supraspinatus.
Methods
We evaluated a total of nine patients with a unilateral, partial-thickness supraspinatus tear. We analyzed the correlation between
EMG activities of shoulder muscles, such as the upper trapezius, lower trapezius, lateral deltoid and posterior deltoid muscles,
during shoulder range of motions exercise, such as flexion, abduction, scaption, shrugging, flexion with resistance, abduction with
resistance, scaption with resistance and shrugging with resistance and the Shoulder Pain and Disability Index (SPADI) scores. To do
this, we classified total SPADI scores into two categories based on a cut-off value of 50 points; the patients were subdivided into two
subgroups: the higher SPADI score group (SPADI >50 points) and the lower SPADI score group (SPADI <50 points).
Results
The EMG amplitude of the upper trapezius was significantly higher after the abduction, scaption, abduction with resistance and
scaption with resistance on the affected side as compared with the non-affected one (p<0.05). In addition, the higher SPADI score
group (SPADI >50 points) had a significantly longer amplitude after shrugging, flexion with resistance, abduction with resistance,
scaption with resistance and shrugging with resistance on the affected side as compared with the non-affected one (p<0.05).
Conclusion
In conclusion, our results indicate that the Korean version 49 of the SPADI is a valid, reliable <br>
Table 1. Baseline characteristics of the patients (n=9).

Table 2. Amplitude of electromyographic activity of the upper trapezius on the affected and non-affected side.
Table 3. Correlation between amplitude recovery time and the Shoulder Pain and Disability Index scores.
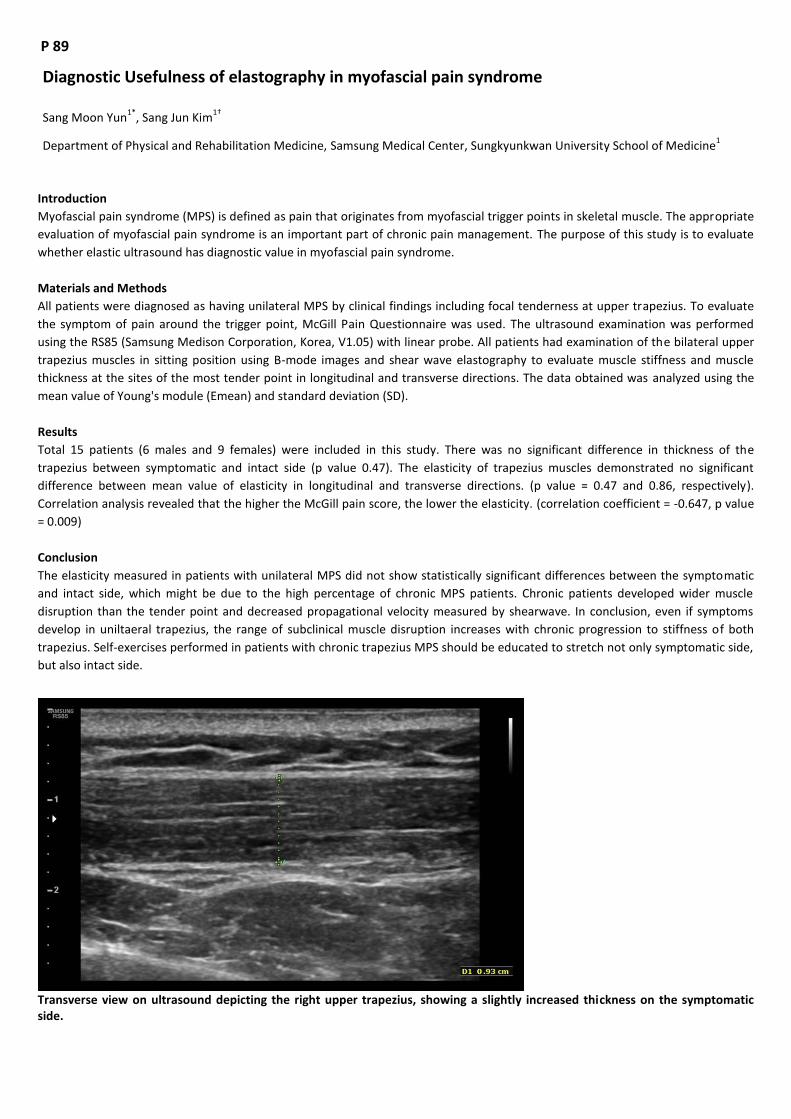
P 89
Diagnostic Usefulness of elastography in myofascial pain syndrome
Sang Moon Yun1*
, Sang Jun Kim1†
Department of Physical and Rehabilitation Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine1
Introduction
Myofascial pain syndrome (MPS) is defined as pain that originates from myofascial trigger points in skeletal muscle. The appropriate
evaluation of myofascial pain syndrome is an important part of chronic pain management. The purpose of this study is to evaluate
whether elastic ultrasound has diagnostic value in myofascial pain syndrome.
Materials and Methods
All patients were diagnosed as having unilateral MPS by clinical findings including focal tenderness at upper trapezius. To evaluate
the symptom of pain around the trigger point, McGill Pain Questionnaire was used. The ultrasound examination was performed
using the RS85 (Samsung Medison Corporation, Korea, V1.05) with linear probe. All patients had examination of the bilateral upper
trapezius muscles in sitting position using B-mode images and shear wave elastography to evaluate muscle stiffness and muscle
thickness at the sites of the most tender point in longitudinal and transverse directions. The data obtained was analyzed using the
mean value of Young's module (Emean) and standard deviation (SD).
Results
Total 15 patients (6 males and 9 females) were included in this study. There was no significant difference in thickness of the
trapezius between symptomatic and intact side (p value 0.47). The elasticity of trapezius muscles demonstrated no significant
difference between mean value of elasticity in longitudinal and transverse directions. (p value = 0.47 and 0.86, respectively).
Correlation analysis revealed that the higher the McGill pain score, the lower the elasticity. (correlation coefficient = -0.647, p value
= 0.009)
Conclusion
The elasticity measured in patients with unilateral MPS did not show statistically significant differences between the symptomatic
and intact side, which might be due to the high percentage of chronic MPS patients. Chronic patients developed wider muscle
disruption than the tender point and decreased propagational velocity measured by shearwave. In conclusion, even if symptoms
develop in uniltaeral trapezius, the range of subclinical muscle disruption increases with chronic progression to stiffness of both
trapezius. Self-exercises performed in patients with chronic trapezius MPS should be educated to stretch not only symptomatic side,
but also intact side.
Transverse view on ultrasound depicting the right upper trapezius, showing a slightly increased thickness on the symptomatic side.

Transverse B-mode image (left) shows symptomatic upper trapezius muscle. Corresponding color elastogram (right) shows homogeneous blue color elasticity signal (blue ROI; Mean 26.1kPa, Diameter 0.3cm, RMI 0.8)
Correlation between McGuill Pain Questiaonnaire and SWV (Shear Wave Velocity)

P 90
Correlation between Facet Tropism and Discogenic Pain: A Pilot Study
Jae ik Lee1*
, Hae In Lee1, Nack Hwak Kim
1†, Sang Heon Lee
1†
Department of Rehabilitation Medicine, Korea University Anam Hospital1
Facet tropism is defined as the angular asymmetry between left and right facet joint orientation. Several studies attempted to clarify
the correlation between facet tropism and degenerative spondylolisthesis and disc herniation. Although there is no defined
consensus, these studies suggest facet tropism is related to increased risk of degeneration and disc herniation. In our study, we
attempt to explicate the correlation between facet tropism and discogenic pain. 30 patients with low back pain and/or lower
extremity radiating pain who visited our spine clinic from 2015 to 2018 were included. Each patient received provocative
discography in one or more lumbar levels. The targeted discs were as followings: L2/3 in one patient, L3/4 in six patients, L4/5 in 18
patients and L5/S1 in 12 patients. Discogenic pain was considered positive if the patient felt the same pain he suffered when the
relevant intervertebral disc was irritated. Facet joint angles were measured using axial magnetic resonance images that were taken
before provocative discography. In patients with positive results in provocative discography, correlation between age and tropism
was noted: the younger the patient, the greater the tropism. We divided the patients into six groups according to their age. Facet
angle differences increased from 0.29 in patients over 70 to 5.34 in patients under 30. However, in patients with negative results in
provocative discography or with axial low back pain, no positive association was found. Facet angle differences were similar in all
age groups, from 4.64 to 8.53. Nonparametric regression analysis was used for statistical measures. According to our study,
correlation between facet tropism and discogenic pain is noted, especially in younger patients. Thus, chronic discogenic pain
diagnosed by provocative discography has more diagnostic value in younger patients as they are more influenced by mechanical
factors.

P 91
Effectiveness of Lymphaticovenous Anastomosis in Patients with Lymphedema
Junhee Lee1*
, Hasuk Bae1†
Department of Rehabilitation Medicine, Ewha Womans University Mokdong Hospital1
Introduction
The gold standard treatment with patients in reductive (phase 1) and maintenance (phase 2) phase is complex decongestive therapy.
In addition, recent days, surgical treatment, especially micro-surgical treatment has been issued. Lymphaticovenous Anastomosis
(LVA) involves the creation of connections between the lymphatic system and the venous system in the distal or proximal extremity.
It has been concerned that supermicrosurgery (anastomosis less than 0.8 mm vessels) is used in this technique, in which lymphatic
vessels and adjacent venules are anastomosed, mostly in an end-to-end fashion
Purpose
The purpose of this study was to assess the effectiveness of LVA in Patients with Lymphedema by using ultrasonography.
Methods
The study was retrospective study which included the data of 36 patients (man 1, women 35) with International Society of
Lymphography stage 1 or 2 upper or lower extremity lymphedema (upper 18, lower 18), who underwent LVA between July of 2018
and February of 2019. All patients were examined at 4 point of period; pre-operation, follow up after surgery at 1week after
operation, 4weeks after operation and 3months after operation. Several measurement were gathered with time flow, at same
location: above 10cm and below 10cm of elbow or knee level of affected and unaffected side. Outcome measures were consisted
with circumference and ultrasonographic findings, such as skin thickness, subcutaneous thickness and elastocity. Also, pre-operative,
post-operative (4weeks after operation) evaluation of Lymphedema Qualitiy of Life (LYMQOL) and SF-36 test were done. By using
repeated measurements, the effect of time and operation (on lesion side) was evaluated with Mixed-linear model. For making a
decision on final model of each measurement, Akalike Information Criterion was considered. For statistical analyses, SPSS Version
25.0 KO for Windows (SPSS Korea Data Solutions Inc, Seoul, South Korea) was utilized. For all tests, statistical significance was set at
0.05.
Results
As a result, skin thickness above 10cm and subcutaneous thickness above 10cm of elbow and knee showed significance(P<0.05).
Also, subcutaneous thickness below 10cm of elbow and knee showed borderline significance (P=0.067). In addition, there was a
tendency of improvement in score of LYMQOL and SF-36 test. The limitation of this study includes the followings. First, the ecruited
amount of case was small, therefore, the statistical significance was too hard to get. Second, all patients data was not complete, so,
e incomplete data was included on statistical analyses.
Conclusion
This study shows not only the effectiveness of LVA in patients with Lymphedema, but also the usefulness of utilizing
ultrasonography on following up evaluation. Through LVA, the pressure maybe controlled, therefore, skin and subcutaneous
thicknesses are decreased along the time. Further follow up study is needed for interpretation the progress of lymphedema.
Table 1. Baseline characteristics

Figure 1. Example of US evaluation
Table 2. Results with significance

P 92
Efficacy of Limb Cyclical Pressure Device on Pain and Edema in Long-Standing Worker
Da-Sol Kim1,2*
, Gi-Wook Kim1,2
, Sung-Hee Park 1,2
, Myoung-Hwan Ko1,2
, Jeong-Hwan Seo1,2
, Dong Hyun Kim3, Yu Hui Won
1,2†
Chonbuk National University Medical School,Department of Physical Medicine and Rehabilitation1, Biomedical Research Institute of
Chonbuk National University Hospital,Research Institute of Clinical Medicine of Chonbuk National University2, Hallym University
College of Medicine,Kangdong Sacred Heart Hospital3
Introduction
In this study, we aim to evaluate the efficacy and safety of limb cyclical pressure device (LUXURY-ZAM) in healthy working people
with long-standing posture for relief of leg pain and swelling.
Methods
This study is designed to compare the treatment effect of LUXURY-ZAM. All subjects had no known acute and chronic disease and
had to participate in three sessions: 1) natural resting, 2) sequential pressure mode and 3) cyclical pressure mode with LUXURY-ZAM.
Before these sessions, the subject visited after long-standing work, and measured outcome parameters at 0min (T1) before
intervention, 30min (T2) after intervention. During the natural resting session, the subjects rested in supine position without any
therapeutic intervention, although both sequential and cyclical pressure session treated with LUXURY-ZAM for 30 min. The
difference between the sequential and cyclical pressure method is whether the initial chamber, which there have five chambers,
continue or decrease its pressure after the next chamber is operated. In the cyclical pressure method, the pressure sustain until the
last chamber is operated. We measured leg pain with visual analogue scale (VAS) as a primary outcome, and leg circumference (cm)
and volume (ml) were evaluated as a secondary outcome.
Results
Total twenty healthy adults were enrolled and mostly were women (95%), mean age of 37.8, working as a nurse or nurse’s aide
(75%). VAS in all three sessions was improved 30 min after working significantly, but the therapeutic groups of cyclical and
sequential pressure mode decreased the 3 times more score (p<0.001) (Table 1). Similarly, the mean value of leg volume after
resting, cyclical and sequential treatment significantly decreased in all subjects after 30 minutes of intervention, however difference
from T1 to T2 among groups was not significant (Table 2). The leg circumference also declined noticeably, and these therapeutic
effects in both sequential and cyclical sessions were superior to resting session (Table 3). In the post-hoc analysis, the differences
between resting and cyclical mode, and between resting and sequential mode were statistically significant in VAS and leg
circumferences, although the comparison between sequential and cyclical mode did not show significant difference.
Conclusion
In this study, LUXURY-ZAM can consider as an efficient and safe therapeutic option for relief of leg pain and edema in healthy adults.
However, there were no significant differences between sequential and cyclical mode.
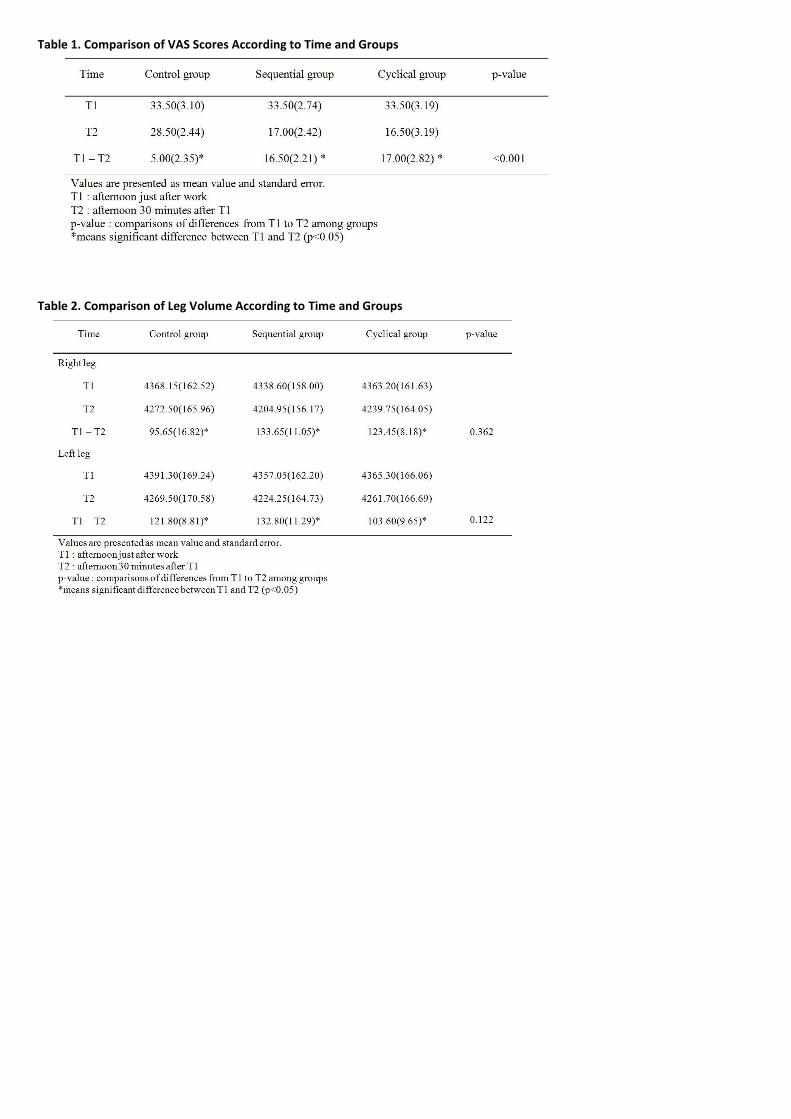
Table 1. Comparison of VAS Scores According to Time and Groups
Table 2. Comparison of Leg Volume According to Time and Groups

Table 3. Comparison of Leg Circumferences According to Time and Groups

P 93
Effectiveness of ETOIMS on Muscular Pain after Open Abdominal Surgery
Jinyoung Park1*†
, Hyung Sun Kim2, Joon Seong Park
2†, Jung Hyun Park
1, Sanghoon Shin
3, Jae Eun Park
3, Sangwon Hwang
3, Do Young
Kim1
Department of Rehabilitation Medicine,Gangnam Severance Hospital, Rehabilitation Institute of Neuromuscular Disease, Yonsei
University College of Medicine, Seoul, Republic of Korea1, Pancreatobiliary Cancer Clinic, Department of Surgery,Gangnam
Severance Hospital, Yonsei University College of Medicine, Seoul, Republic of Korea2, Department and Research Institute of
Rehabilitation Medicine,Yonsei University College of Medicine, Seoul, Republic of Korea3
Objective
Pylorus preserving pancreaticoduodenectomy (PPPD) is a treatment for the resectable tumor or cancer in pancreaticoduodenal
system. Although laparoscopic PPPD has been limitedly performed, open surgery is currently the main trend. In open surgery,
incision and suture of the abdominal muscles cause the inflammatory changes, strain, and contraction in the skeletal muscles, and
consequently elicit muscular pain which deteriorates the quality of life. We therefore suggest electrical twitch obtaining
intramuscular stimulation (ETOIMS) as a new treatment modality for pain control after PPPD.
Methods
Between June 2018 and January 2019, among the patients who underwent PPPD in Department of Surgery, participated 45 patients
were randomly assigned to two groups. The Group 2 received ETOIMS right after surgery under the general anesthesia. ETOIMS was
conducted on each patient using Clavis (Alpine Biomed ApS, Denmark). Aseptic monopolar needle electrode was inserted into the
transverse abdominis muscle under ultrasound guidance. The stimulations were delivered with 2-mA intensity, 0.2-ms pulse
duration, and 1-Hz frequency with unipolar negative square waves for 5 seconds at each stimulation point, which induced muscle
twitching. The 14 dermatomal points, 2 cm bilaterally apart from the incision line were stimulated (Figure 1). The pain score (visual
analogue scale, VAS), peak cough flow (PCF), gait speed were compared with proportion to the preoperative values. Pain score was
taken 13 times; a day before surgery, post-operative day (POD) 0~9, discharge day, and 3 weeks after discharge in outpatient clinic.
The PCF and gait speed were measured 5 times; a day before surgery, POD 2, 7, discharge day, and 3 weeks after discharge. The
independent T test, chi-square test were applied to analyze the basic characteristics. The 3 main outcomes were analyzed by linear
mixed model or repeated measures ANOVA using SPSS 23.0.
Results
With 7 dropouts, total 38 patients’ data were analyzed. The basic characteristics including age, sex, height, weight, body mass index,
preoperative pain score and PCF were not significantly different, where the gait speed was faster in Group 1 (P = 0.03) (Table 1). The
pain score was highest on the day of surgery (Group 1: 6.5 ± 2.2, Group 2: 5.5±1.9, P = 0.17) and decreased gradually. Through the
course of pain relieving, the pain scores were significantly lower in Group 2 after PPPD (P = 0.01) (Figure 2A). Although the PCF at
each measuring time points didn’t show the group difference (P = 0.20), the improved PCF from the second day of surgery to
discharge was greater in Group 2 (P = 0.02) (Figure 2B). Although the gait speeds at each time point were not significantly different,
the time course of improving was significantly faster in Group 2 (P < 0.01) (Figure 2C).
Conclusion
The ETOIMS is helpful in fast reducing postoperative somatic pain developed after PPPD, and also helpful in fast improvement of
PCF and gait speed.

Table 1. Basic characteristics
Figure 1. Stimulating points of ETOIMS
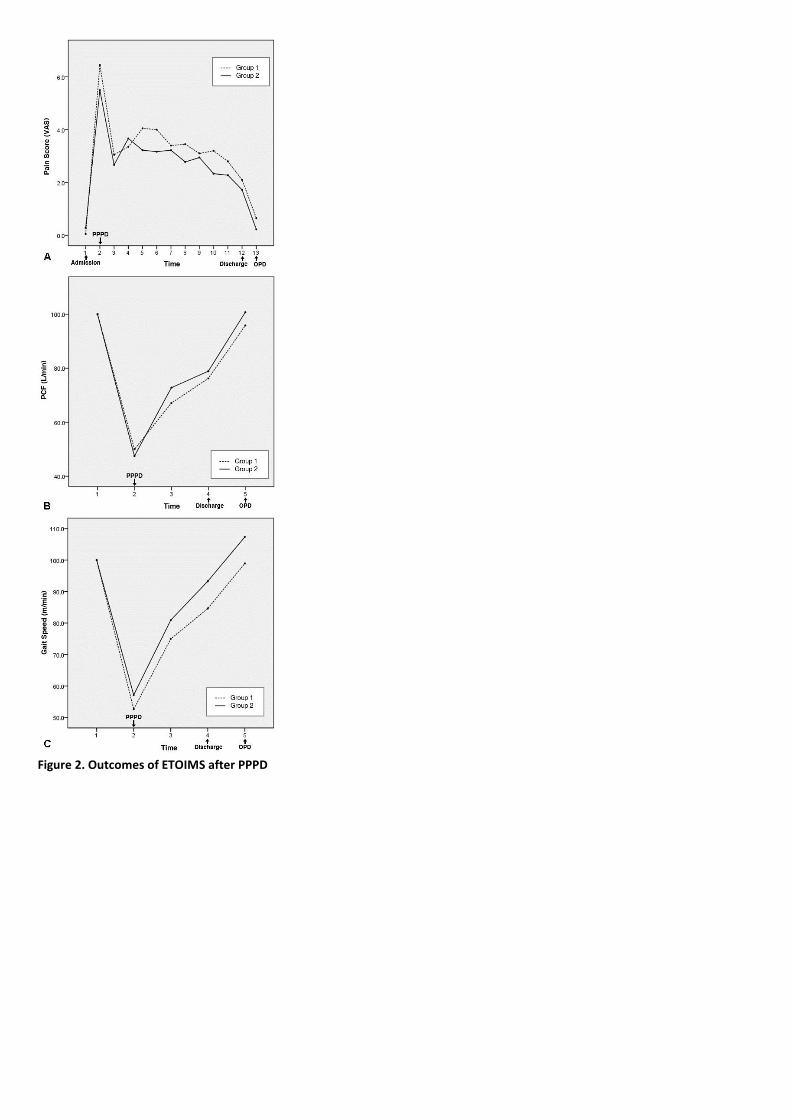
Figure 2. Outcomes of ETOIMS after PPPD

P 94
Changes in Body Composition and Proinflammatory Marker Levels in Ovariectomized Rats
Mi-Kyung Cho1*
, Young Mo Kim2, Young Joo Lee
3, Byung-Joo Lee
4, In-Joo Kim
5, Seong-Jang Kim
4, Kyoungjune Pak
6, Yun Kyung Jeon
7,
Ji Min Kim7, Jeong Hun Kim
1, Myung Jun Shin
4, Yong Beom Shin
1, Keunyoung Kim
1, Jin A Yoon
1†
Department of Rehabilitation Medicine,Pusan National University Hospital1, Department of Obstetrics and Gynecology,Pusan
National University Hospital2, Department of Otorhinolaryngology,Pusan National University Hospital
3, Department of Nuclear
Medicine,Pusan National University Hospital4, Department of Nuclear Medicine,Pusan National University Yangsan Hospital
5,
Department of Internal Medicine-Endocrine,Pusan National University Hospital6, Pusan National University Medical Research
Institute,Pusan National University Hospital7
Introduction
This study examined the effect of TSH-suppressive dose of levothyroxin (LT4) on changes in body composition and pro-inflammatory
markers in ovariectomized rats.
Method
Bilateral ovariectomy (OVX) and sham operations (Sham) were performed in female Sprague-Dawley virgin rats at 7 weeks of age.
Rats were divided into four experimental groups of Sham, Sham+LT4, OVX, and OVX+LT4. Eight weeks after surgery, the body
composition was analyzed using dual-energy X-ray absorptiometry (DXA), along with measurements of serum levels of pro-
inflammatory parameters.
Result
The amount of weight gain was significantly higher in the OVX than in the Sham groups (median: 104.6; IQR: 91.27-116.8 vs. median:
66.4; IQR: 61.5-71.2, P=0.001), and administration of LT4 did not have an effect on body weight in either group. (Fig. 1.) The fat mass,
but not lean mass, was significantly increased in the trunk area of rats in the OVX group compared with control group, regardless of
LT4 treatment. (Fig. 2.) Among the pro-inflammatory cytokines, the serum level of C-reactive peptide, interleukin (IL)-6, and IL-10
was significantly increased in the OVX group, and only IL-6 could be further increased upon additional treatment with LT4. (Table 1.)
Discussion
Nowadays, a concept of the combination of reduced muscle mass and increased fat volume, known as obesity-related sarcopenia or
sarcopenic obesity (SO) has emerged. The reduced lean body mass and increased fat mass in OVX rats indicates that menopause
induces obesity-related sarcopenic changes. In our study, the weight gain due to increased fat mass in trunk area was different
between ovariectomized rats and controls, regardless of the TSH suppressive therapy. Although total mass increased, we did not
find a significant change in the lean body mass, and the decreasing trend of lean mass in the trunk area due to TSH suppressive LT4
treatment was similar in both OVX and Sham groups. Reduced and weakened muscle quality in OVX is inevitable because estrogen
functions to resolve the inflammatory response and to accelerate muscle healing through proliferation and activation of the muscle
fiber satellite cells. In accordance with previous reports, our findings showed that the change in body composition, characterized as
a combination of reduced muscle mass and excess body fat, was associated with elevated inflammatory markers, CRP and IL-6, but
not TNF-α, which was associated with SO‐related phenotypes in postmenopausal women. In addition, Further, the elevated level of
inflammatory cytokines in OVX+LT4 group indirectly suggests that menopause and TSH suppressive therapy might raise the risk of
cardiovascular disease.
Conclusion
The results of our study have clinical implications for considering TSH suppressive therapy as a latent risk factor for overall survival.
We propose that body composition and muscular function should be evaluated in menopausal patients being considered for long-
term TSH-suppressive therapy.
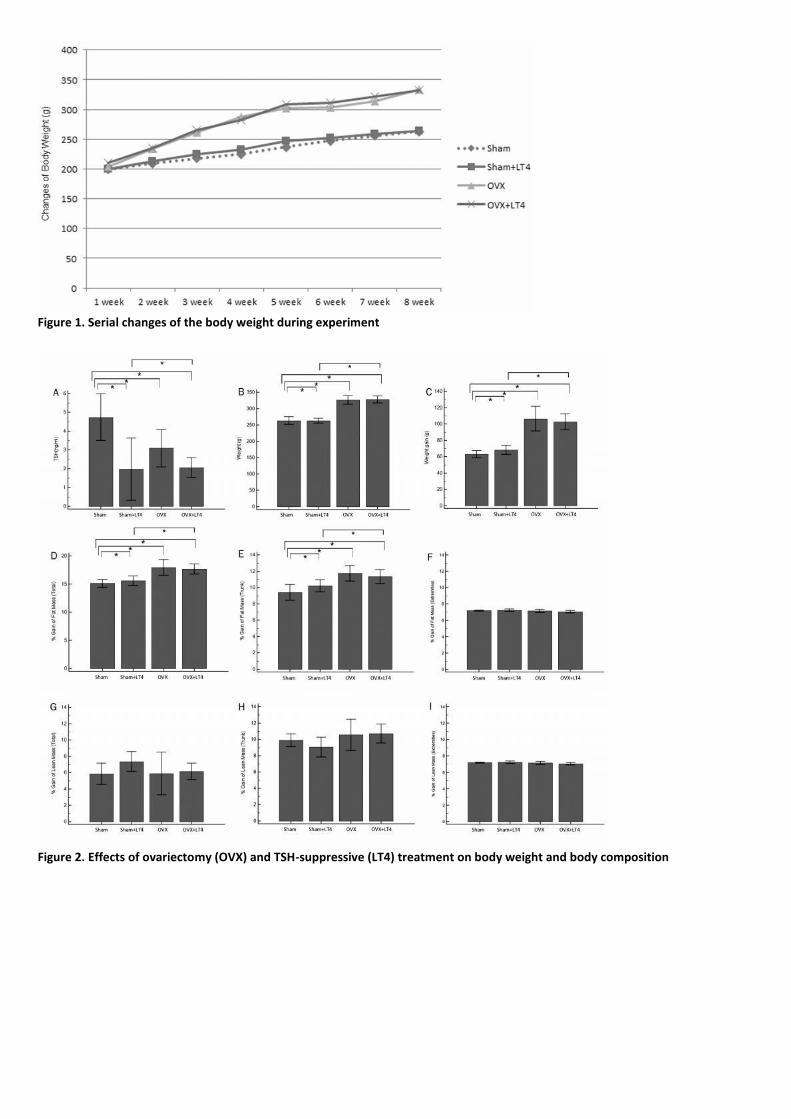
Figure 1. Serial changes of the body weight during experiment
Figure 2. Effects of ovariectomy (OVX) and TSH-suppressive (LT4) treatment on body weight and body composition

Table 1. Effects of ovariectomy and LT4 treatment on cholesterol level and proinflammatory markers

P 95
The association between sagittal plane alignment and disc height changes of lumbar spine
Ki Hoon Park1,2*
, Sora Baek1,2†
Department of Rehabilitation Medicine, Kangwon National University School of Medicine1, Center for Farmers’ Safety and Health,
Kangwon National University Hospital2
Objectives
Decreased lumbar lordosis is known to be associated with lumbar spinal stenosis and low back pain. Increased lordosis was
associated with increased subsidence and less favorable outcome after spinal fusion operation. We aimed to investigate whether
the lumbar lordosis, lumbar segmental lordosis, and sacral slope are related with lumbar disc height changes.
Study design:
Total 590 farmers in Gangwon-do, South Korea were recruited. Twenty-one subjects were excluded due to history of spine surgery,
569 farmers were included in final analysis. The average age of subject was 58 years old, and the average period of agriculturing was
26 years. The percentage of people with back pain was about 75%.
Methods
Spine radiograph was obtained in standing posture. A disc height change (DHC) was defined if there is a difference of 25% or more,
with compare to two adjacent discs. We defined 1) lumbar lordosis (LL) as the angle between the cranial end plate of L1 and the
cranial end plate of S1, using Cobb’s method in the neutral position of lumbar X-ray; 2) lumbar segmental lordosis (LSL) as angle
from the cranial endplates of adjacent vertebrae using Cobb’s method, described as L1-2, L2-3, L3-4, L4-5, and L5-S1, respectively; 3)
sacral slope (SS) as the angle between the horizontal line and the cranial sacral end plate tangent.
Results
Lumbar DHCs were most frequently observed in L5-S1 (69.6%) and L4-5 (45.7%). DHCs in L1-4 was 55 (9.7%) in L1-2, 79 (13.9%) in
L2-3, and 35 (23.7%) in L3-41. The average of LL was 49.8 degree. The largest proportion of LL was L5-S1 LSL, which was 20.4 degree
(41% of LL), and the second largest lordosis was in L4-5, which is 12.6 degree (25% of LL). Thus L4-S1 accounted for a total of 66% of
LL. The average of SS was 34 degree. In the presence of DHC at any level between L1-S1, LL and SS was statistically significant
decreased compared to not having DHC (p<0.05). In the presence of L1-2 DHC, LSL was significantly decreased at L1-2, L2-3, L3-4,
and L4-5 LSL, with the largest change in L1-2 (Δ3.99). In the presence of L2-3 DHC, LSL was significantly decreased at L1-2, L2-3, L3-4,
and L4-5 LSL with the largest change in L2-3 (Δ3.31). In the presence of L3-4 DHC, LSL was significantly decreased at L3-4 and L4-5
LSL with the largest change in L3-4 (Δ2.87). In the presence of L4-5 DHC, LSL was significantly decreased at L4-5 and L5-S1 LSL with
the largest change in L4-5 (Δ3.31) while L1-2 LSL was increased inversely (Δ-0.75). In the presence of L5-S1 DHC, LSL was significantly
decreased at L5-S1 LSL (Δ4.44) while L2-3 LSL was increased contrarily (Δ-0.94).
Conclusions
Lumbar lordosis was occurred about 66% at L4-5, L5-S1 level. Lumbar DHC was also most commonly observed at that two lower
levels. In the presence of DHC, both LL and SS were decreased. The decrease of lordosis was mostly occured around the level of DHC.
In contrary, LSL at distant level was increased in the presence of L4-5 and L5-S1 DHC.
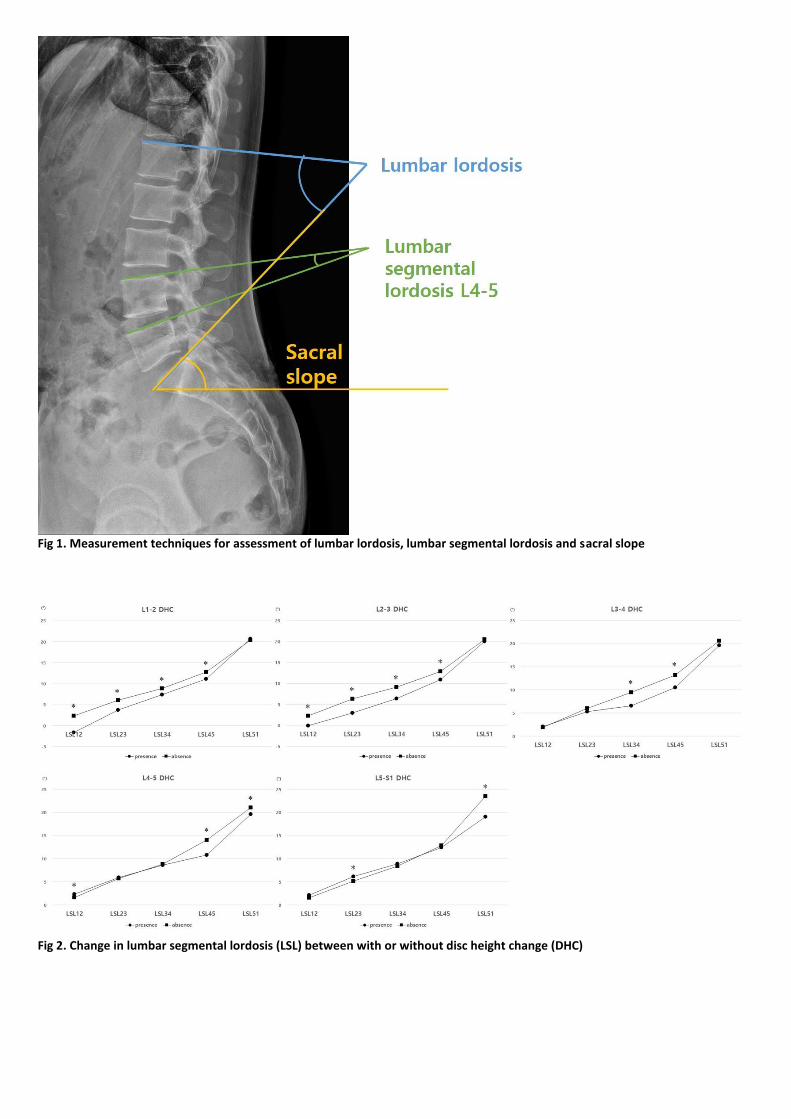
Fig 1. Measurement techniques for assessment of lumbar lordosis, lumbar segmental lordosis and sacral slope
Fig 2. Change in lumbar segmental lordosis (LSL) between with or without disc height change (DHC)
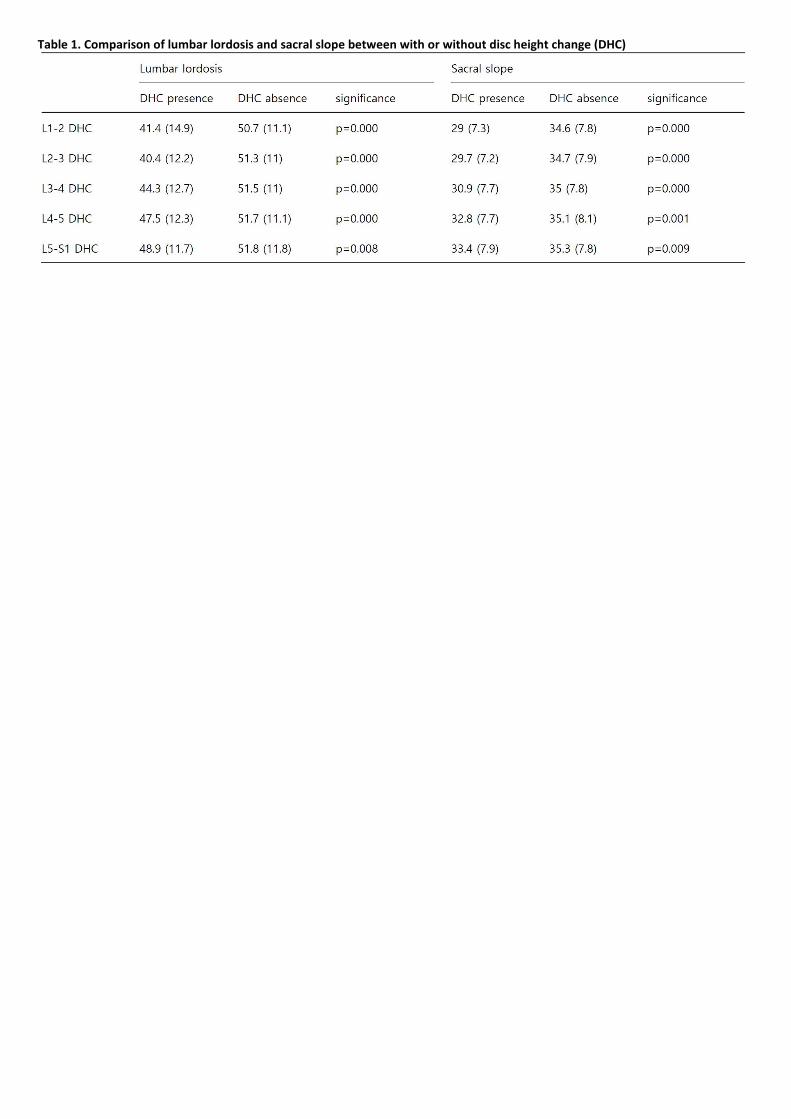
Table 1. Comparison of lumbar lordosis and sacral slope between with or without disc height change (DHC)

P 96
Automatic Cervical Spine Detection in Videofluoroscopic Images by Machine Learning Software
Joo Young Ko1*
, Jung Keun Hyun1,2
, Seo Young Kim1, Sang Il Choi
4, Hyun Il Kim
5, Seong Jae Lee
1†
Department of Rehabilitation Medicine,Dankook University Hospital1, Department of Nanobiomedical Science & BK21 PLUS NBM
Research Center for Regenerative Medicine,Dankook University2, Institute of Tissue Regeneration Engineering (ITREN),Dankook
University3, Department of Applied Computer Engineering,Dankook University
4, Department of Software Engineering,Dankook
University5
Objective
Over the past few decades, medical imaging techniques have been used for the early detection, diagnosis, and treatment of
diseases. Conventionally, those images are interpreted by human experts such as radiologists and physicians. However, given wide
variations in pathology and the potential fatigue of human experts, researchers and doctors have begun to benefit from computer-
assisted interventions. Videofluoroscopic swallowing study (VFSS), which is one of the radiologic studies that demands high
concentration and fatigue of reading physicians, could be a good candidate. We aimed to make a deep learning program that can
automatically detect cervical spines from VFSS images, as a first step in development of VFSS reading system.
Methods
From 195 VFSS video files, images were separated in 24 frame per second. Images most distinct cervical spine in each file were
selected and calibrated via contrast limited adaptive histogram equalization (CLAHE) technique. After creating a ground truth for
each image based on manual annotation of vertebrae boundaries, image patches of 120 x 120 pixel size centered on ground truth
were extracted following Gaussian distribution. Image patches overlapping with ground truth by 45% or more were defined as
positive samples, and those overlapping less than 25% were treated as negative samples. Samples overlapping 25-45% were
excluded because they were likely to act noise. Through this procedure, about total 69,400 samples were obtained. Machine
learning was performed by three models of convolution neural network (one conventional machine learning model (support vector
machine with histogram of oriented gradient (Hog + SVM)) and two deep learning models (Alexnet, and Resnet 50)) and the
accuracy was compared.
Results
Cervical detection rate of each model delineated as following order (SVM, Alexnet, Resnet50). Accuracy was 92%, 96%, and 99%,
recall was 94%, 95%, and 99%, Precision was 90%, 98%, and 99%, respectively.
Conclusion
By deep learning, computer can detect cervical spine accurately from videofluorospic images without any manual intervention.
Resnet 50 showed best result among the models used in this study. Authors believe that the results of this study will contribute to
development of automatic reading program for VFSS.
Acknowledgment: “This research was supported by Basic Science Research Program through the National Research Foundation of
Korea (NRF) funded by the Ministry of Education (grant number: 2018R1D1A3B07049300)”

Table 1. Cervical detection rate of each model
Fig 1. Example of cervical detection of each model
P 97
The Effects of ESWT on Physical Function in Preradiographic Knee Osteoarthritis patients.
Min-Ji An1*
, Woo-Yong Shin1, Nam-Kyu Lim
1, Kyung-rok Oh
1, Yuri Choe
1, Su-Ra Ryu
1, Seo-Ra Yoon
1†
Department of Rehabilitation Medicine, Gwangju Veterans Hospital1
Objective
The aim of this study is to investigate the effect of Extracorporeal Shock Wave Therapy (ESWT) on pain and decrease in pain can
improve physical function in patients with pre-radiographic knee osteoarthritis.
Subjects and Methods
We enrolled 20 patients with knee pain belonging to K-L grade 0 or 1 on radiological examination, from December 2017 to
December 2018. Patients were randomly assigned to the ESWT group (Group I) and the controlled group (Group II). The Group I
(n=10) were treated once a week for 3 consecutive weeks using low energy ESWT (1000 shock wave and with low energy level of
0.04mJ/mm2, Dornier AR2®) with medical therapy, and the Group II (n=10) received only conventional medical therapy. The focus of
shockwave treatment was 0.5cm below the medial tibia plateau in anteroposterior view and 0.5cm from the skin edge in lateral
view. Pain and physical functional outcome was assessed by visual analogue scale (VAS), Western Ontario and McMaster
Universities Osteoarthritis Index (WOMAC) score, Timed Up and Go (TUG) test and 6-minute walk test (6MWT). All outcome
measurements were assessed at baseline, and at 1 and 4 weeks after the treatments were completed.
Results
There are no significant differences in the baseline characteristics and initial values between the two groups. The ESWT group
showed significant improvement in VAS score and 6MWT. But, no significantly improvement in the WOMAC and TUG score.
Conclusion
Our result showed that low energy ESWT may be effective for patients with pre-radiographic knee osteoarthritis. The most
important finding of the study was that a significantly improvement of ESWT in the long distance walking in patients with pre-
radiographic knee OA. Therefore, ESWT can be another useful treatment option for them.

P 98
Back muscle workload in static work analyzed using surface electromyography
Sora Baek1,2†
, Gowun Kim1,2*
Department of Rehabilitation Medicine, Kangwon National University School of Medicine1, Center for Farmers’ Safety and Health,
Kangwon National University Hospital2
Objective
Work-related musculoskeletal disorder is rapidly growing every year. Maintaining an inappropriate posture for a long time is a cause
of musculoskeletal disorders and such a static posture may be maintained in an industrial field and daily life. The purpose of this
study was to investigate the effects of the back muscle workload in variable static work.
Method
Sixteen male participated in the study. We performed test to subjects keeping continuous posture for 10 minutes. Seven different
postures were tested. 1) Standing; upright standing posture, 2) Twist; trunk axial twisting posture, 3) Reaching, 60º; upright standing
with arm flexion, 60º between arm and trunk, 4) Reaching, 120º; upright standing with arm flexion, 120º between arm and trunk, 5)
Stoop, 20º; stooped posture with 20º trunk flexion in sagittal plane, 6) Stoop, 40º; stooped posture with 40º trunk flexion in sagittal
plane, 7) Stoop, 60º; stooped posture with 60º trunk flexion in sagittal plane. Back muscle workload was studied using surface
electromyography (sEMG) at lumbar multifidus, longissimus thoracis, iliocostalis lumborum, quadratus lumborum, latissimus dorsi,
external oblique, internal oblique and rectus abdominis muscles from each subject during the whole task. Portable respiratory gas
analyzer was used to measure the physiological response and the quantitative oxygen consumption in a static posture. Rating of
Perceived Exertion (RPE) and Numeric Rating Scale (NRS) were used to monitor exercise intensity and pain.
Result
Root mean square (RMS) of sEMG data was calculated using initial 204 seconds from 16 subjects. NRS was significantly increased in
each posture and the highest in the 40 degree stooped posture (7.4 ± 1.02, P < 0.001)). NRS difference between pre- and post-test
was also greatest in the 40 degree angle stooped posture (5.7 ± 1.66, P < 0.001). (Table 1) In 120 degree (between body and arm)
reaching posture, mean RPE was the highest (17.7 ± 1.49, P < 0.001) and the posture holding time was the shortest (351.9 ± 111.22
seconds, P < 0.001). The RMS has a positive correlation with NRS and RPE among back muscle, it was most relevant in lumbar
multifidus (r=0.478, P < 0.001) and latissimus dorsi muscle (r=0.256, P < 0.05), respectively. (Table 2) Both VO2 and VCO2 showed
significant differences in all postures (P < 0.001) and the highest value in 60º stooped posture. In stooped posture, VO2 and VCO2
were higher in stooped angle of 40 and more degree than less than 40 degree. (Table 3)
Conclusion
The posture associated with back pain was the 40 degree stooped posture. Among back muscle, activity of lumbar multifidus muscle
was related with back pain and stooped posture. Maintaining a posture bent 40 and over degrees may cause back pain and
workload can be increased.
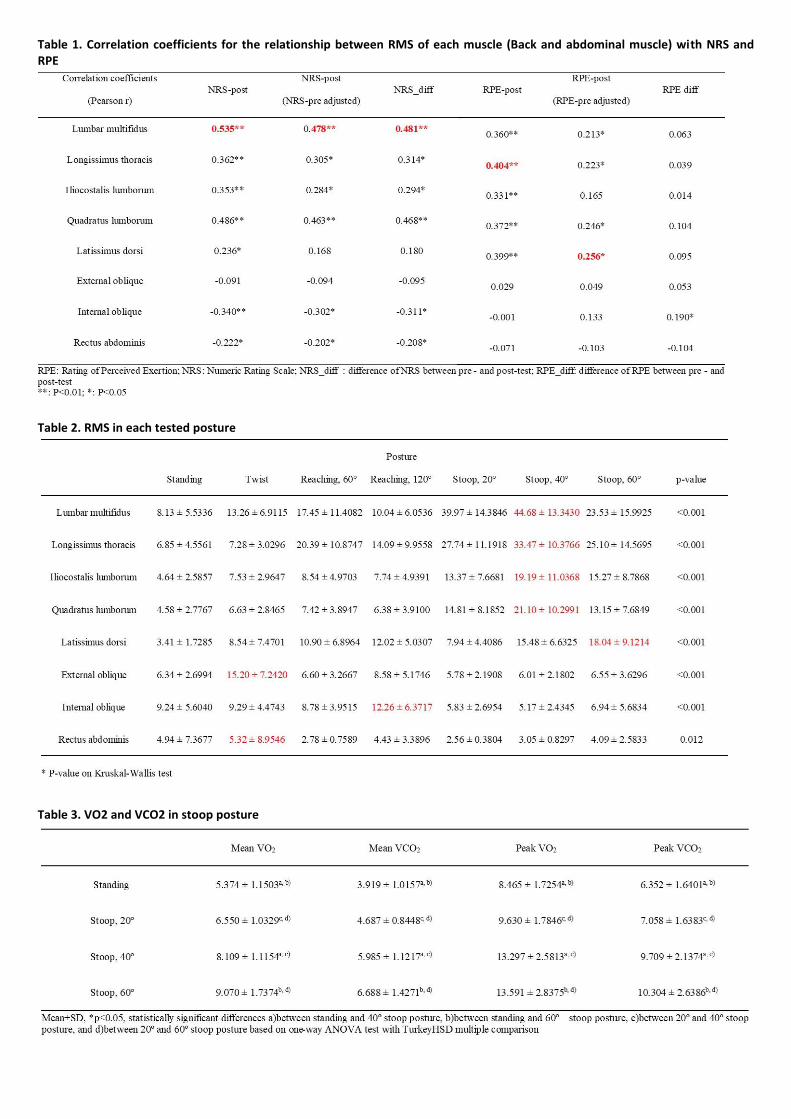
Table 1. Correlation coefficients for the relationship between RMS of each muscle (Back and abdominal muscle) with NRS and RPE
Table 2. RMS in each tested posture
Table 3. VO2 and VCO2 in stoop posture

P 99
Effects of core muscle strengthening exercise on discogenic low back pain
Dahn Kim1*
, Nack-Hwan Kim1†
, Sang-Heon Lee1
Department of Rehabilitation Medicine, Korea University Anam Hospital1
Objective
To examine the effects of core muscle strengthening exercise on discogenic low back pain patients.
Subjects and Method
Total 270 patients suffered from low back pain only were enrolled retrospectively in the study. The low back pain patients received
provocative manual discography for the diagnosis of discogenic low back pain (DLBP). Those patients of the positive provocative
manual discography were selectively had intradiscal injection with mixture of steroid and local anesthetics medicine. The patients’
pain responses were checked in numeric rating scale (NRS) over time: baseline, 1 day, 1 month, 3 months, 6 months after the
injection. One day after the intradiscal injection, the patients were categorized into 2 groups according to their pain response: >50%
pain relief group (=positive response, PR); ≤50% pain relief group (=negative response, NR). The patients of the both groups were
categorized into 2 subgroups depending on the core muscle strengthening exercise application more than 1 month: core muscle
exercise subgroup(=PT subgroup); non-exercise subgroup(=NPT subgroup). The baseline and follow-up NRS of each group were
compared. Intergroup differences in demographic and clinical data were assessed using Mann-Whitney test. ANOVA tests were
performed to compare the NRS changes between each group. The “IBM SPSS Version 25.0” software package was used for the
analysis.
Results
Overall, 131 DLBP patients were eligible for the 6-month follow-up period. Among those 131 DLBP patients, 75 patients reported
reduced NRS more than 50% compared to the baseline NRS, which were allocated to PR group while the others were allocated to
NR group. PR and NR groups were not significantly different in baseline characteristics according to Mann-Whitney analysis. Both PR
and NR groups showed significant time-related NRS decrease. In NR group, the patients showed significant difference in the NRS at 6
months after the intradiscal injection between PT subgroup and NPT subgroup. This tendency of the NRS difference at 6 months
after the intradiscal injection between PT and NPT subgroups were also proved in PR group.
Conclusion
The core muscle strengthening exercise could be applied to DLBP patients for supportive treatment especially for the patients
whose analgesic intradiscal injections were not effective. The core muscle strengthening exercise can make difference on pain relief
effect at 6 months after the intradiscal injection. Further studies for the relationship of DLBP pathophysiology and core muscle
strengthening exercise are expected.
Acknowledgment: N/A


P 100
Relationship between NRA Sign, MRI Findings and Clinical Symptoms of Lumbar Spinal stenosis
In-Sik Lee1†
, Seunghwan Lee1*
Department of Rehabilitation Medicine, Konkuk University Medical Center and Konkuk University School of Medicine1
Objective
In this study, we investigated the relationship between the Nerve Root Aggregation (NRA) sign and clinical symptoms in patients
with Lumbar Spinal Stenosis (LSS). Moreover we identified the correlation between the Proportion of Area of Nerve Root to Dural
Sac (PANRDS) and NRS sign.
Methods
This retrospective study involved 19 patients diagnosed with lumbar spinal stenosis at the L4-5. We assessed the NRA sign and
measured the PANRDS on T2-weighted axial images of MRI at the lower margin of the disc space just proximal to the level of LSS. In
order to evaluate the NRA sign quantitatively, we measured the area of the nerve root and the dural sac divided into right and left
and then calculating the ratio. Clinical symptoms included the intensity of lower extremity pain and degree of claudication. The AP
diameter of the spinal canal at the most stenotic level was also measured to identify the association with the severity of LSS.
Results
In the positive NRA sign group, the PANRDS was found to be significantly higher than the negative NRA sign group. Also, interval
between onset of symptoms and MRI evaluation in the positive NRA sign group was significantly longer than the negative. Diabetes
mellitus was more prevalent in the positive NRA sign group, albeit without significance. However, there was no statistically
significant association between NRA sign and clinical symptoms of LSS.
Conclusion
The positive NRA sign had a statistically significant relationship with PANRDS and interval between onset of symptoms and MRI
evaluation. However, no statistical significance was found between NRA sign and clinical symptoms of LSS.
Keywords
lumbar spinal stenosis, nerve root aggregation sign, Magnetic reasonance imaging, clinical symptoms, proportion of area of nerve
root to dural sac

Table 1. Characteristics of patients
Table 2. Characteristics of patients according to the NRA sign
Figure 1. T2-weighted axial image of MRI. Blue line: area of dural sac, Red line: area of nerve root
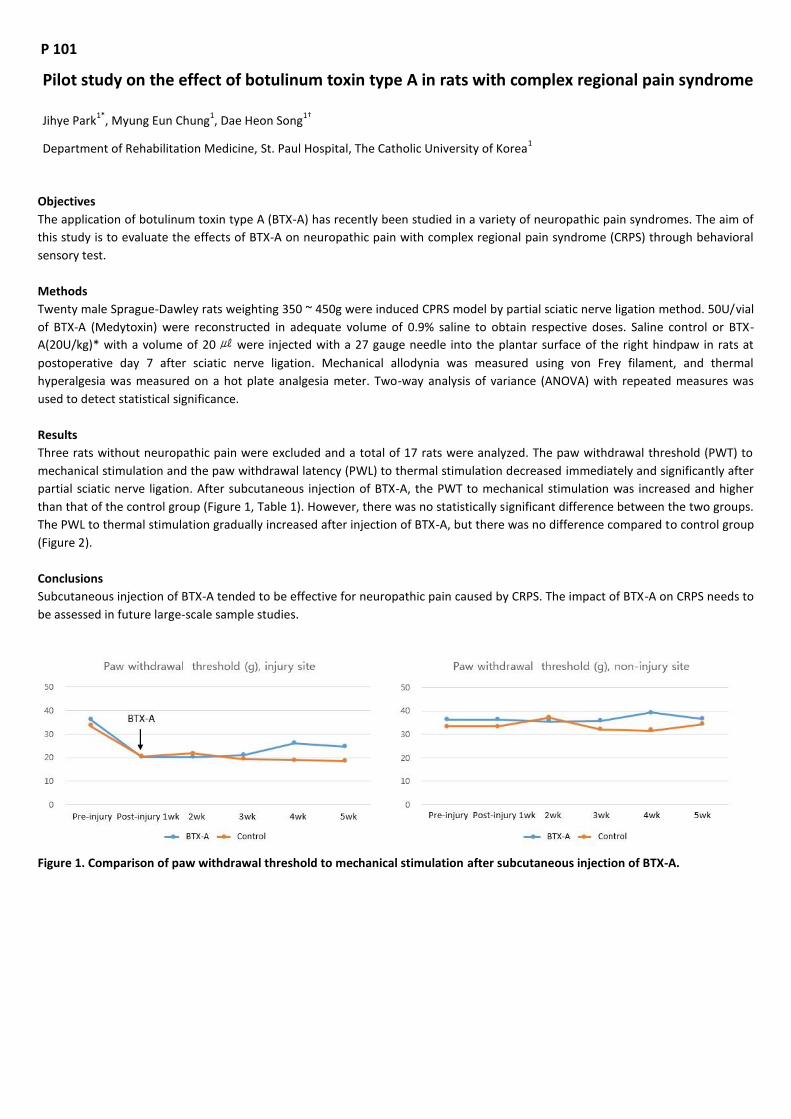
P 101
Pilot study on the effect of botulinum toxin type A in rats with complex regional pain syndrome
Jihye Park1*
, Myung Eun Chung1, Dae Heon Song
1†
Department of Rehabilitation Medicine, St. Paul Hospital, The Catholic University of Korea1
Objectives
The application of botulinum toxin type A (BTX-A) has recently been studied in a variety of neuropathic pain syndromes. The aim of
this study is to evaluate the effects of BTX-A on neuropathic pain with complex regional pain syndrome (CRPS) through behavioral
sensory test.
Methods
Twenty male Sprague-Dawley rats weighting 350 ~ 450g were induced CPRS model by partial sciatic nerve ligation method. 50U/vial
of BTX-A (Medytoxin) were reconstructed in adequate volume of 0.9% saline to obtain respective doses. Saline control or BTX-
A(20U/kg)* with a volume of 20㎕ were injected with a 27 gauge needle into the plantar surface of the right hindpaw in rats at
postoperative day 7 after sciatic nerve ligation. Mechanical allodynia was measured using von Frey filament, and thermal
hyperalgesia was measured on a hot plate analgesia meter. Two-way analysis of variance (ANOVA) with repeated measures was
used to detect statistical significance.
Results
Three rats without neuropathic pain were excluded and a total of 17 rats were analyzed. The paw withdrawal threshold (PWT) to
mechanical stimulation and the paw withdrawal latency (PWL) to thermal stimulation decreased immediately and significantly after
partial sciatic nerve ligation. After subcutaneous injection of BTX-A, the PWT to mechanical stimulation was increased and higher
than that of the control group (Figure 1, Table 1). However, there was no statistically significant difference between the two groups.
The PWL to thermal stimulation gradually increased after injection of BTX-A, but there was no difference compared to control group
(Figure 2).
Conclusions
Subcutaneous injection of BTX-A tended to be effective for neuropathic pain caused by CRPS. The impact of BTX-A on CRPS needs to
be assessed in future large-scale sample studies.
Figure 1. Comparison of paw withdrawal threshold to mechanical stimulation after subcutaneous injection of BTX-A.

Figure 2. Comparison of paw withdrawal latency to thermal stimulation after subcutaneous injection of BTX-A.
Table 1. Effects of BTX-A on pain threshold in CRPS rat model.

P 102
Aerobic Capacity Correlates with Health Related Quality of Life after Breast Cancer Surgery
Doo Young Kim1*
, Jae-Hyung Kim1, Si-Woon Park
1†
Department of Rehabilitation Medicine, Catholic Kwandong University International St Mary’s Hospital1
Objective
To investigate the relation of physical functions to health related quality of life (HRQOL), physical activity and fatness of patients
during breast cancer treatment within one year after surgery
Methods
We retrospectively reviewed the patients with breast cancer at the cancer rehabilitation clinic within one year after surgery.
Physical function assessment included aerobic capacity, muscle strength, flexibility and edema. Physical activity was assessed using
the International Physical Activity Questionnaire-Short Form and HRQOL was assessed using the European Organization for Research
and Treatment of Cancer Quality of Life Questionnaire Core 30. Stepwise multivariate linear regression analysis was used to find the
association factors.
Results
Of the physical functions in subjects, aerobic capacity was 88.64% compared to predictive value. The mean overall QOL was
60.82±20.98. The mean physical activity was 2245.49±3687.66MET/week and 39 patients (41.5%) were inactive. As the results of
stepwise multivariate linear regression analysis, aerobic capacity was a significant factor of HRQOL and physical activity.
Conclusion
The impairment of physical functions affects the HRQOL of patients within one year after breast cancer surgery. Among the physical
functions, the decrease in aerobic capacity was significantly associated with the decrease in the overall QOL of the patients.

P 103
The Quantitative Parameters of Lymphoscintigraphy for the Evaluation of Mild Lymphedema
Ji Won Hong1*
, Da Hwi Jung1, Myung Jun Shin
1, Jin A Yoon
1†
Department of Rehabilitation Medicine, Pusan National University Hospital1
Background
We aimed to evaluate the potential role of quantitative method of lymphoscintigraphy for the assessment of severity of
lymphedema post-operative patients with breast cancer who did not show definite dermal backflow (DB) activity on the
lymphoscintigraphy.
Method
We evaluated 49 mild lymphedema patients with International Society of Lymphology Classification of limb volume difference
minimal (5% to 10%) and mild (10% to 20 %). The patients received a mastectomy and axillary dissection or sentinel lymph node
dissection for invasive ductal carcinoma of the breast. A round ROI of axillary lymph node activity & Squared ROIs of arms drawn for
the acquisition of the tracer uptake and for the calculation of quantitative asymmetry indices (QAI) for evaluate the asymmetric
uptake was shown in Figure 1. The QAI of both arms were calculated at axilla, upper arm, fore arm and total arm. The QAI was
defined as the radiopharmaceutical uptake ratio of affected side to the unaffected side. Arm circumference was measured at four
locations per arm to identify the maximal circumference difference (MCD) between affected and unaffected sides. The ratio of
measured circumference was also used for the analysis.
Results
The representative examples of lymphangiography without dermal backflow includes delayed flow and decreased activity of axillary
lymph node (Figure 2A) or collateral lymph node activity, such as subclavian lymph node (Figure 2B). Among total patients, 21
patients showed minimal degree and 28 patients showed mild degree of lymphedema. There was weak correlation between QAIs
and circumference difference in total and segmental analysis (Table 1). QAIs of forearm (QAI-F) and whole arm (QAI-T) showed
significant difference between two groups (Figure 3).
Discussion
In our study, quantitative lymphangiography showed low correlation with MCD in mild lymphedema. Although the quantitative
analyses are a useful lymphedema assessment tool, it showed less feasibility to distinguish the degree of circumference difference
between affected and unaffected limb in these patients. Otherwise, to divide the patients by volume difference, whole arm and
forearm QAI were significant values for the evaluation of the severity of lymphedema and may have potential to work as an
objective tool for the assessment of mild lymphedema without dermal backflow.

Figure 1. An example of the region of interest (ROI) for quantification
Figure 2. Representative example of lymphedema without dermal backflow

Figure 3. Comparison of QAIs of forearm (QAI-F), upper arm (QAI-U) and whole arm (QAI-T)

P 104
Factors affecting physical activity in patients with prostate cancer
Sehee Kim1*
, Kyung Eun Nam1, Jong-in Lee
1†
Department of Rehabilitation Medicine, Seoul St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, Seoul,
Korea1
Introduction
According to national cancer registration statistics in 2013, prostate cancer is the fifth most common cancer among men in Korea.
Prostate cancer has the highest relative survival rate over 5 years after surgery compared with other cancers. Postoperative
complications such as urinary incontinence, urinary retention, cystitis and erectile dysfunction may occur. Androgen deprivation
therapy (ADT) decreases muscle mass resulting in a decrease in exercise capacity. In many studies, exercise has been studied as an
effective intervention for reducing side effects of cancer treatment and improving quality of life.
Objective
In this study, we compared the general demographics and physical status, including weight, body mass index (BMI), and
appendicular skeletal muscle mass (ASM) of patients with prostate cancer patients according to the degree of physical activity
measured by International physical activity questionnaire(IPAQ) in patients diagnosed with prostate cancer and to elucidate the
factors affecting physical activity.
Method
Patient enrollment was conducted from August 2015 to January 2016. The inclusion criteria were (1) 50 years of age or older, (2)
histologically confirmed prostate adenocarcinoma, and (3) treatment with radical prostatectomy, radiation therapy, or ADT. A total
of 95 patients were enrolled. Muscle mass was measured using a direct segmental multifrequency bioelectrical impedance analysis
system. ASM was calculated as the sum of arm and leg skeletal muscle. 2-minute walking test performed and handgrip strength was
assessed using a hand-held dynamometer. Patients were divided into 2 groups based on the physical activities measuring by IPAQ,
one group was defined as 'inactive' and the other group was defined as 'minimally active or health enhancing physical activity (HEPA)
active' groups. A Student’s t- test was done to determine statistical differences of physical activities and general demographics
between two groups.
Results
The mean age of 95 patients was 69.24 ± 7.29 years and mean body mass index was 24.25 ± 2.56 (Table 1). 65 patients were
classified as inactive group and the remaining 30 were classified as 'minimally active' or 'HEPA active' groups. BMI, 4m gait speed
and lower extremity 1RM showed statistically significant difference between the two groups. In this study, we elucidate that lower
BMI, smaller low extremity 1RM, and slower gait speed are associated with lower physical activity (Table 2).
Discussion
Physical activity has been shown to be related to quality of life and lower fatigue symptom in cancer patients. In this respect, the
American Cancer Society guidelines recommend regular physical activity of at least 150 min of moderate intensity or 75 min of
vigorous intensity each week. Knowing the factors that affect physical activity will allow physicians to encourage more exercise for
patients who are expected to have less physical activity.

Table 1. General demographics
Table 2. Comparison between the groups classified by IPAQ

P 105
The cause of respiratory arrest later diagnosed as presbyesophagus by VFSS: A case report
Yong Sung Jeong1*
, Jong Keun Kim1, Jin Seok Bae
1, Hyo Sik Park
1, Kang Jae Jung
1, Jong Youb Lim
1†
Department of Rehabilitation Medicine, Eulji University Hospital1
Introduction
The gastrointestinal tract undergoes changes with aging, and the esophagus is not exempt from those changes. Presbyesophagus is
the term used to describe the age-related changes in the esophagus, including decreased lower esophageal sphincter relaxation,
incomplete dilatation of the esophagus, decrease in esophageal peristaltic pressure, abnormal esophageal contractions and delayed
emptying of the esophagus. Adverse effects of aging likely contribute to the increased reports of choking spells and aspiration. Here
we report a case of respiratory arrest of old woman after femur fracture operation, the cause of which was later diagnosed as
presbyesophagus by VFSS.
Case report
An 88-year-old woman with a medical history of diabetes mellitus visited emergency room. She slipped down at home and she was
diagnosed as a femur fracture. She was admitted to Orthopedic Surgery Department and received operation. She had no special
complications related to the operation on that day. The next day she showed cyanosis during the meal. There was a pulse, but no
breathing was found, and immediately the airway was opened and oxygen was supplied. After that, breathing was returned and she
was transferred to the intensive care unit. There was no definite cause to cause respiratory arrest. So, the patient was referred to
Rehabilitation Medicine Department for the evaluation of the cause of aspiration. On video fluoroscopic swallowing study (VFSS),
there were no particular findings on the oral phase and the pharyngeal phase. On the esophageal phase, delayed emptying of the
esophagus, abnormal esophageal contraction, and dilatation of the esophagus were found. The patient was referred to
Gastroenterology Department to rule out presbyesophagus, achalasia, and abdominal masses. On endoscopy, there was dilatation
of the esophagus, but lower esophageal tone was not increased. On esophagography, the esophagus did not show abnormal filling
defects or barium collections. And there was delayed relaxation of the lower esophageal sphincter. Presbyesophagus was confirmed
and the patient was recommended to start with liquid diet with the dyspepsia medicine. The patient had no special symptoms
hospitalization, and was discharged to home.
Conclusion
We report a patient presenting respiratory arrest caused by presbyesophagus. Dysphagia has been reported in about 28.2% of the
old people over 85 years. Dysphagia due to presbyesophagus, might become more severe after events such as surgery that could
worsen general conditions. Any old people even without poor general conditions, we have to pay attention to dysphagia and further
evaluation is warranted.

Fig. 1. VFSS showed delayed emptying of the esophagus.
Fig. 2. Esophagography showed delayed relaxation of the lower esophageal sphincter.

P 106
A case report of dysphagia caused by post radiation therapy related tracheo-esophageal fistula
Yeon Jae Han1*
, Sun Im1, Geun Young Park
1, Dong Gyun Sohn
1†
Department of Rehabilitation Medicine, The Catholic University of Korea Bucheon St. Mary`s Hospital 1
Introduction
Progressive dysphagia following chemoradiation therapy is the most common complaint of esophageal cancer patients. Common
causes for acquired TEF in adults include trauma, prolonged endotracheal intubation, and malignancy. There are sparse data on
incidence of acquired malignant TEF as it is very rare. In few studies, incidence of TEF following primary esophageal cancer and lung
cancer was reported at 4.5% and 0.3%, respectively. In this case, we report a patient in which distal TEF may have been missed
during conventional Videofluroscopic Swallowing Study (VFSS) but was diagnosed only after sequential cup drinking of liquid brim.
Case
67-year-old man was reffered for dysphagia and newly diagnosed as esophageal cancer. He took Ivor-Lewus operation
(Esophagectomy and esophagogastrostomy) on October, 2017 and due to anastomtic site leakage, endoscopic foam packing was
done. He had been eating soft diet after operation and had no difficulty in swallowing. He readmitted for CCRT to paraesophageal
region, regional recurrence and finished RT on July, 2018. At that point, the patient complained of coughing in liquids, especially
when he drank in large amounts. A neurological exam showed no abnormalities in this cranial nerve system. At the same time he
was diagnosed with aspiration pneumonia and was kept nil per mouth until the cause of aspiration was confirmed. He was referred
to our department to find the cause of aspiration pneumonia. A standardized VFSS following the Logemann protocol was performed.
He swallowed spoons of liquid barium, subsequent bolus introduction with nectar thin jelly followed by soft and hard solid bolus
showed no evidence of oropharyngeal dysphagia. Before leaving, He was asked to swallow a cup of liquid drinking in a sequential
manner and after swallowing the liquid barium, he suddenly coughed out the barium liquid that was previously seen to go through
the esophagus with no evidence of entrance past the glottis. A scanning of the esophageal and bronchial levels showed barium
radiocontrast on his whole trachea and whole brochus. A post VFSS Abdomen showed presence of most barium that the patient had
swallowed during the exam. However, a high suspicion of TEF was made. Further evaluation revealed presence of TEF through both
chest CT and bronchoscopy. We suspect that due to the small size of the TEF, no aspiration was detected during small amounts of
liquid or other thicker boluses and that it was only entrance past TEF during cup drinking that showed the presence of aspiration
past TEF.
Conclusion
Patient with esophageal cancer, especially after radiation therapy, may complain of dysphagia related to post radiation changes of
the pharyngoesophageal walls. Physicians should be aware of possibility of hidden structural abnormality like TEF when a
standardized swallowing protocol of the VFSS failed to capture any positive findings, despite event suspicious symptom of dysphagia.

Figure 1. VFSS finding showing normal passage of liquid barium (#1~4) without aspiration, and delayed regurgitation of the swallowed liquid barium via trachea (#5~8). Post VFSS chest and abdomen x-ray findings showing increased haziness in RMLF and RLLF and gastric contents of swallowed barium (A~B).
Figure 2A. Broncoscopy finding showing fistula opening around surgical metal clip lesion proximal to right lower bronchus. 2B. CT scan showing a few tiny air bubbles around the right mainstem (circle), abutting the surgical clippings.

P 107
Improvement of dysphagia in neurovascular compression due to trauma patient: A Case Report
Jung Hyun Cha1*
, Yong Kyun Kim1†
, Yong Seob Jo1, Yun Jung Lee
1
Department of Rehabilitation Medicine, MyongJi Hospital1
Neurovascular compression syndrome is known to be an uncommon condition that involves mechanical irritation caused by direct
contact of the cranial nerve with blood vessels. Trigeminal neuralgia, hemifacial spasm, vestibulocochlear neuralgia are the most
prevalent symptoms to occur, and dysphagia due to CN IX and X invasions have rarely been reported.
The Glossopharyngeal nerve provides taste sensation and sensory information from the posterior one-third of the tongue, while the
Vagus nerve is responsible for sensation and motor function of the soft palate, pharynx, larynx, and esophagus. Thus, neuritis of
these two nerves can result in dysphagia.
On April 12, 2018, a 75-year-old female patient had head trauma by falling down forwards inside her house and after the incident,
dysarthria and dysphagia consecutively occurred. The patient was sent to the emergency room via 119 and was transferred to the
neurology department. Enhanced ICA MRI results taken on April 15, 2018, indicated neurovascular compression. The radiograph
showed neuritis involving the left cranial nerve complex 9 to 11 with perineural inflammation of left distal vertebral artery appeared
to be tortuous and in contact with the exit root zone of the left lower cranial nerve. 25mg of Solondo was initiated and was tapered
by 5mg a week and discontinued after 5 weeks.
Due to unsolved dysphagia, the patient was admitted to our Department of Rehabilitation Medicine on July 14, 2018, in a
nasogastric feeding state. Cranial nerve exam indicated left uvular deviation and impaired gag reflex. The oral phase showed to be
intact on a VFSS performed on 17, July 2018. In the semisolid bolus swallow test, the initial remnant was 40% of the bolus, which
was nearly cleared after multiple swallowing and without aspiration. Liquid cup swallows were also successful with no aspiration.
Thereafter, nasogastric tubing was successfully removed, and the patient proceeded to dysphagia diet level I with no occurrence of
aspiration. To evaluate the presence of vocal cord palsy, we consulted to the otorhinolaryngology department and verified the
bilateral vocal cord mobility to be intact, and then continued rehabilitation with rehabilitative balloon swallowing treatment
included. At a follow-up VFSS on August 2, 2018, the initial post-swallow remnant of semisolid bolus improved to 5%, which allowed
dietary build-up adjustments to dysphagia diet level II and eventual discharge.
The patient was admitted to the hospital with dysphagia after neurovascular compression resulted in neuritis in cranial nerves 9 to
11 due to head trauma. This is known to be a rare condition, which usually demands drug therapy or surgical treatment in severe
cases.
However, after active ballooning treatment and removing the nasogastric tube, the patient recovered quickly, and resulted in the
pharyngeal remnant from 40 to 5 percent. Therefore, it may be necessary to consider rehabilitation first rather than surgical
treatment.
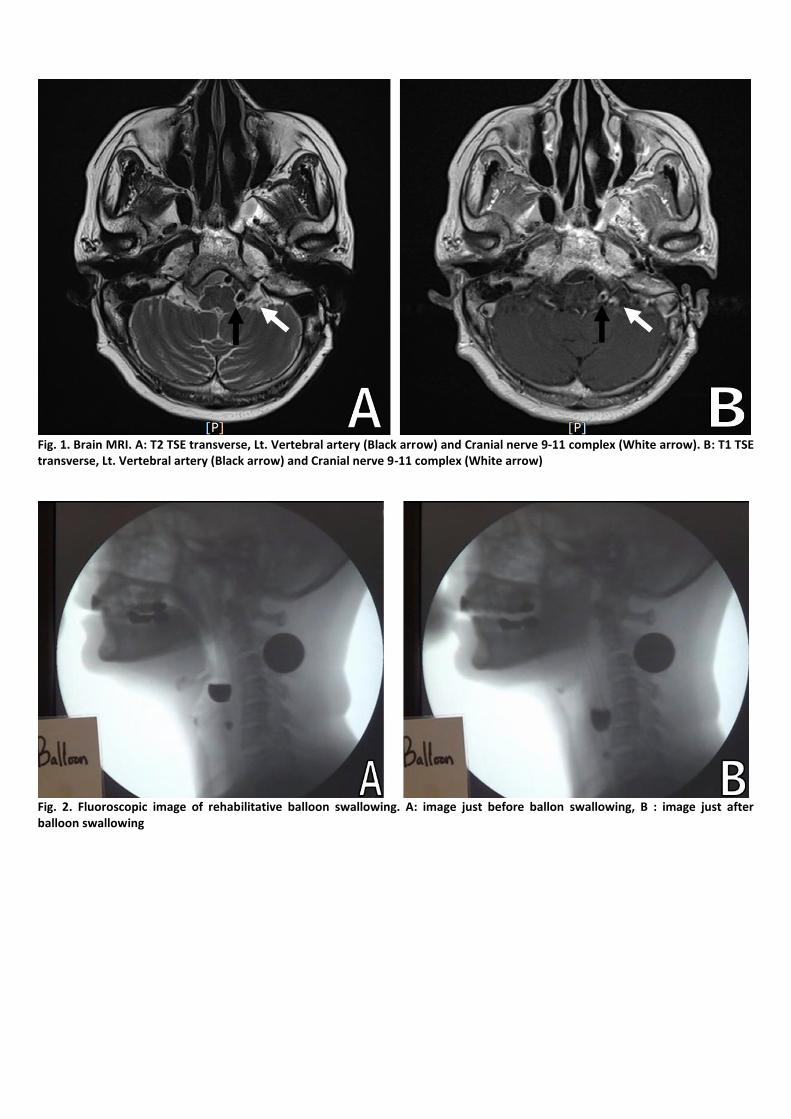
Fig. 1. Brain MRI. A: T2 TSE transverse, Lt. Vertebral artery (Black arrow) and Cranial nerve 9-11 complex (White arrow). B: T1 TSE transverse, Lt. Vertebral artery (Black arrow) and Cranial nerve 9-11 complex (White arrow)
Fig. 2. Fluoroscopic image of rehabilitative balloon swallowing. A: image just before ballon swallowing, B : image just after balloon swallowing

P 108
Foix-Chavany-Marie syndrome secondary to right corona radiata infarction: Case Report
Young Hwan Yoo1*
, Ju young Lim1, Su Hong Kim
1, Chang-Hwan Kim
1, Myeong Ok Kim
1, Han Young Jung
1, Kyung Lim Joa
1†
Department of Physical and Rehabilitation Medicine, Inha University School of Medicine1
Bilateral anterior opercular syndrome is also known as Foix-Chavany-Marie syndrome (FCMS). FCMS is characterized by a loss of
voluntary control of facial, lingual, pharyngeal and masticatory muscles, in the presence of preserved reflexive and automatic
functions (automatic-voluntary dissociation) of the same muscles. The lesions are usually located at the anterior part of the
operculum. Here, we report the case of a patient in whom FCMS developed following right putamen and corona radiata stroke.
Case report
A 62 - year old man with manifesting left hemiparesis, anarthria and hypomimia visited our clinic. He had a past history of
hospitalization with left basal ganglia infarction in same year. Understanding of spoken and written language was preserved and
there were no apraxia or agnosia. The mouth was closed, but the patient could open his mouth about 2 finger breath. On neurologic
examination, corneal reflex was preserved. There was no limitation of eyeball movement, but he could not completely close his
both eyes. Bilateral facial paralysis was observed, severe in the left side, but sensory of face was preserved. The gag reflex was
diminished, and he was unable to initiate swallowing due to severe clumsiness of tongue. On the other hand, swallowing reflex was
preserved. The tongue was immobile, did not show fibrillate, with slightly right side deviation. He had a severe left upper and lower
limb paresis (upper - MRC grade 1/5, lower- MRC grade 2/5). He had a generalized hyperreflexia in left upper and lower limb, and
Babinski reflex was not observed. He had bilateral lip, tongue, and pharyngeal weakness with automatic-voluntary dissociation of
the lower face.
These symptoms were the hallmark of FCMS and also referred to as bilateral opercular syndrome. Brain MRI performed on the day
of symptom onset showed acute cerebral infarction in the right putamen and corona radiata and encephalomalacia due to old
infarct in left putamen and corona radiata. The subcortical lesion causes an automatic-voluntary dissociation because the
corticobulbar tract from the fronto-parietal cortex passes through the corona radiata and posterior limb of internal capsule. This
suggests that the subcortical lesion could lead to FCMS due to the failure of the connection between cortical and subcortical
structures.
Conclusion
In this case, the brain MRI finding did not demonstrate bilateral opercular lesions. We suggest that a unilateral corona radiata lesion
may lead to FCMS in a patient who already has contralateral subcortical dysfunction although bilateral opercular lesions is the main
etiology of FCMS.

Fig. 1. Brain MRI images demonstrate acute infarction in right putamen and corona radiate on diffusion-weighted images and old infarction in left putamen and corona radiata on T2-weighted images.

P 109
Progressive multifocal leukoencephalopathy in Systemic Lupus Erythematosus
Chang woo Kim1*
, Young Sook Park1†
, Hyun Jung Chang1, Eun sol Cho
1, Jae Sam Seo
1, Kyo Hun Ku
1
Dapartment of Physical Medicine & Rehabilitation, Samsung Changwon Hospital, Sungkyunkwan University school of Medicine1
Progressive multifocal leukoencephalopathy (PML) is rare and serious demyelinating disease characterized by progressive damage in
the white matter of a brain. PML occurs to patients with severe immune deficiency and most commonly to those infected by the
human immunodeficiency virus (HIV). We present a rare case of PML in systemic lupus erythematosus (SLE). A 21-year-old SLE
woman visited our outpatient clinic for left ankle motor weakness. For evaluation of peripheral neuropathy, nerve conduction study
was done but result was normal. For evaluation of neuropsychiatric SLE like cerebrovascular disease, evoked potential study was
carried out. There was dysfunction of motor evoked potential on her left abductor hallucis muscle recording. A brain MRI was done
and it showed a manifestation of non-enhancing and non-territorial localized confluent hyper-intensities in her right corona radiate
and fronto-parietal lobe. To treat the neuropsychiatric SLE, steroid pulse therapy put in place, using 1000mg of methylprednisolone
for 5 days, but the left ankle motor was gradually deteriorating. We transferred the patient to the rheumatology department of
Samsung Seoul Medical Center for additional studies. In cooperation with neurology, a CSF study was undertaken and a brain biopsy
was performed. The JC virus was detected by polymerase chain reaction (PCR) in the CSF study, and SV 40 (polyomavirus) was found
in viral particles in her brain tissue. PML was confirmed. Currently, she is in a general ward with a stupor mental state and is
undergoing a palliative treatment. This suggests that PML may be underdiagnosed in patients with SLE. A possibility of PML must
therefore be considered when undertaking a differential diagnosis of SLE patients who demonstrate unexplained neurologic
symptoms or signs.

P 110
Psychosis Caused by Limbic disconnection
Youngkook Kim1*†
, Sun Jae Won1, Yeun Jie Yoo
1*, DaYe Kim
1, Mi-Jeong Woon
1
Department of Rehabilitation Medicine, Yeouido St. Mary’s Hospital1
Background
Injury to the limbic system can result in amnesia, language difficulties, behavioral abnormalities, and psychological disorders. We
present a patient who suffered psychosis related to disconnection of the limbic system after intraventricular and orbitofrontal
hemorrhages following removal of a sellar meningioma.
Case Description
A 23-year-old male presented with left homonymous hemianopia and underwent a brain MRI that revealed a sellar meningioma. He
underwent a craniotomy with tumor removal via a subfrontal transbasal approach. However, a postoperative intraventricular
hemorrhage involving lateral ventricle accompanying a left orbitofrontal hemorrhage occurred 1 day later. After 4 weeks,
unexpected bizarre behaviors and hallucinations were emerged on the recovery course of cognitive dysfunction. Diffusion tensor
tractography was performed to evaluate the entire limbic system for the differential diagnosis of psychosis caused by organic brain
injury. The tractography results showed degeneration of the fornix, left cingulum, mammillothalamic tract and uncinate fasciculus.
These findings were corresponded to the manifestations of psychosis, anterograde amnesia, and anomic aphasia. The follow-up
tractography revealed the regenerating limbic tracts that coincided with the recovery of clinical symptoms after 14 weeks.
Conclusions
The neuropsychiatric problems could result from disconnection of the limbic system following a postoperative intraventricular
hemorrhage. Diffusion tensor tractography was valuable for evaluating the integrity of the injured limbic tracts and determining the
regeneration of tracts corresponding to neuropsychiatric recovery
Acknowledgment: n/a

P 111
A Multimodal therapy to delayed encephalopathy following carbon monoxide poisoning: A Case Report
Su Hong Kim 1*
, Chan Hyuk Park 1, Kyung Lim Joa
1, Myeong Ok Kim
1, Chang Hwan Kim
1, Han Young Jung
1†
Department of Rehabilitation Medicine, Inha University Hospital1
Introduction
Delayed encephalopathy can occur after 2 to 4-week asymptomatic period following clinical remission of acute carbon monoxide
(CO) poisoning. The patient with delayed encephalopathy suffered from serious disabilities including cognitive impairment,
psychiatric symptoms and gait impairment. Up to the present time, there have not been effective treatments in delayed
encephalopathy, so the prognosis is poor. We report a case about nearly complete recovery of delayed encephalopathy with
multimodal therapy.
Case Report
A 39-year-old man was admitted to the acute local hospital after attempting suicide using burning artificial coal. Upon admission,
the patient was diagnosed with acute CO poisoning and had been treated with hyperbaric oxygen (HBO) therapy. He was discharged
8 days later without any disturbance of consciousness, cognition and movement disorders.
About 20 days after discharge from acute local hospital, he began to experience amnesia, cognition deficit, and balance impairment,
which worsened within a few days. He was hospitalized again to our department at 38 days after the CO poisoning. On examination,
he demonstrated a retardation of thought, irrelevant thinking and cognitive impairment and also cannot walk independently. He
had a Mini-Mental State Examination (MMSE) score of 8/30 and an intelligence quotient (IQ) score of 41. He exhibited akathisia, and
balance impairment with Berg balance scale score of 36/56. Sensory disturbance and muscle weakness were not detected. Brain
MRI showed high-intensity lesions in the white matter of the frontal, temporal, and parietal lobes on a T2-weighted image (T2WI)
and a diffusion-weighted image (DWI) (Fig. 1).
The patient was administered initially high dose steroid, and cerebrolysin for about three weeks and maintained with memantine
and vitamins. HBO therapy (1.5 atm, 60 minutes, every day) was administered concurrently and continued over 21 subsequent
sessions. However, these therapeutic regimens appeared only mild or transient effects. After cessation of steroid therapy, he has
been treated with a repetive-transcranial magnetic stimulation (rTMS) (to left prefrontal cortex facilitation, 5 days a week) therapy.
After the multimodal therapy, he showed improvement of cognition (MMSE score 21) and also improvements in gait disturbance
(Berg balance score 54) at discharge. <br> One month later from discharge (4months after acute CO poisoning), he could perform
nearly complete ADL independently and return to work with good cognitive function (IQ score of 98) and normal gait (berg balance
scale 56). Follow up Brain MRI showed much disappearance of high intensity areas on frontal, parietal, and also temporal areas. (Fig.
2)
Conclusion
We report a patient with great improvement as a result of multimodal therapy on delayed encephalopathy following CO poisoning.
Further investigation would be needed on the mechanism associated with these improvements

Fig. 1 Brain MRI after 38 days (severe cognition deficit) from CO exposure
Fig. 2 Brain MRI after 6 months from CO exposure

Fig. 3 time table with cognition and balance score and treatment

P 112
Effect of cerebrolysin on disorders of consciousness secondary to Intracranialhemorrhage: A casestudy
Nayeon Ko 1*
, Hyun Haeng Lee1, Jongmin Lee
1,2†
Department of Rehabilitation Medicine, Konkuk University Medical Center1, Center for Neuroscience Research, Institute of
Biomedical Science & Technology, Konkuk University2
Introduction
Cerebrolysin, which consists of peptides and amino acids and is extracted from pig brain tissue, is a nootropic drug with
neuroprotective and neurotrophic properties. It was reported to improve the neurological outcomes of stroke. However, the effect
of cerebrolysin on disorders of consciousness (DOC) is still unknown. Here, we show a case suggesting effect of cerebrolysin on DOC
secondary to intracranial hemorrhage (ICH).
Case
A 41-year-old man who had no medical history did not wake up in the morning with vestige of vomiting around him on Sep 23, 2018.
He was found to be in stuporous condition responding only to painful stimuli. He was diagnosed with an intracranial hemorrhage in
the left frontal lobe combined with subarachnoid hemorrhage secondary to rupture of left posterior communicating artery
aneurysm. He underwent coil embolization and surgery of craniectomy and hematoma evacuation at the day of onset. After
postoperative monitoring in the intensive care unit, he was transferred to the Department of Rehabilitation Medicine (RM) for
comprehensive rehabilitation therapy days after the onset of the illness. On the day of transfer to RM (Oct 25, 2018), the total score
of CRS-R was 8 (auditory function scale-2, visual function scale-2, motor function scale-2, oromotor/verbal function scale-0,
communication scale-1, and arousal scale-1), which meant that he was barely able to fixate eyes on target. He also showed definite
sleep cycle. Keppra 500mg was administered as anti-epileptics twice a day. On the 38th day after onset (Oct 30, 2018), Cerebrolysin
(2.152g/10ml) twice a day (at 6AM and 6PM) started to be administered intravenously. Three days after the initiation of
Cerebrolysin treatment, he began to raise his hands up to his head, which had not been observed before. On the 7th day of
Cerebrolysin administration, he started to reach objects purposefully with his arms (total score of CRS-R was 15 (auditory function
scale-3, visual function scale-4, motor function scale-3, oromotor / verbal function scale-1, communication-1, arousal scale-3). On
the 14th day, he started to use the objects functionally, which meant that he had emerged from minimally conscious state. On the
25th day of drug administration, the total score of CRS-R went up to 20 (auditory function scale-4, visual function scale-4, motor
function scale-6, oromotor/verbal function scale-1, communication-1, arousal scale-3). He was transfered to Department of
Neurosurgery and underwent Cranioplasty surgery on 68th day after onset (Nov 29, 2018). He was transferred to RM on 40th day of
Cerebrolysin administration (Dec 08, 2018) and showed the MMSE (MiniMental Status Exam) score 11. On 43th day of Cerebrolysin
administration (Dec 11, 2018), MMSE score 12. The patient was discharged and transferred to another hospital on Dec 24th, 2018.
Conclusion
Cerebrolysin could be potent agent with significant effect on DOC secondary to ICH.

Left: Brain CT taken at 2018.9.23 (the day of illness onset), Right : Brain CT taken at 2018.10.22 (day 30 after onset and surgery)

P 113
Improvement of Drooling with Daily Neuromuscular Electrical Stimulation in a child: A Case Report.
Hyehoon Choi1*
, JungGeun Park1, Seong Hoon Lim
1, Joon Sung Kim
1, BoYoung Hong
1†
Department of Rehabilitation Medicine, St. Vincent’s Hospital, College of Medicine, The Catholic University of Korea, Republic of
Korea1
Introduction
Drooling do harms on basic function and social relationship even in children. Diseases affecting the facial and oromotor muscles
such as cerebral palsy, myopathy, and several genetic disorders could cause drooling. There are a variety of methods to manage
drooling such as oral myofunctional therapy, behavior-modifying techniques, medication, botulinum toxin injection and surgical
methods. We report a case in which drooling was improved by neuromuscular electrical stimulation in a child with muscular
dystrophy.
Case presentation
A 4-year-old girl with muscular dystrophy had severe drooling. Twenty-eight to 30 scarf bibs were needed daily due to her
overflowing saliva. She could maintain sitting but was not able to change her position. Muscle tone was generally hypotonic
including all extremities and facial muscles. Her buccinator and hyoid muscles were stimulated with VitalStim® five times a week. No
other dysphagia therapy was performed except to give a cue to swallow saliva. Drooling had gradually decreased so the scarf bib
was not needed on weekdays in the fourth week of the neuromuscular electrical stimulation treatment. However, she still needed
4-5 scarf bibs on weekends without rehabilitation. In the sixth week, the drooling improved so that scarf bibs were not needed even
on the weekend. As drooling improved, electrical stimulation was ceased. However, drooling increased again since the third week of
discontinuation.
Conclusion
Several studies have shown that muscular strength can be maintained or improved when long-term neuromuscular electrical
stimulation is applied to patient with muscular dystrophy. According to our case, applying neuromuscular electrical stimulation to
the buccinator and hyoid muscles could be effective in the management of drooling for a short-term. However, the efficacy does not
maintain after the discontinuation.

P 114
Rehabilitation of an Infant with Pelizaeus-Merzbacher Disease: A Case Report
Ki-Hong Kim1*
, Min-Keun Song1†
, Hyeng-Kyu Park1, Jae-Young Han
1, In-Sung Choi
1
Department of Physical & Rehabilitation Medicine, Chonnam National University Hospital1
Objective
Pelizaeus-Merzbacher disease (PMD) is a rare X-linked recessive disorder caused by mutations in the PLP1 gene. It causes severe
demyelination in the central nervous system in infancy and early childhood. The typical symptoms of PMD are hypotonia, nystagmus,
and delayed development of motor skills. As the child gets older, spasticity, ataxia, and choreiform movements develop. The
prevalence of PMD is estimated to be approximately 1.45 in 100, 000 live births in Japan and 0.13 in 100, 000 live births in Germany.
The average life span of PMD patients is approximately 30 years. No cure for PMD is known yet, nor does it have a standard course
of treatment. We aimed to report functional improvement of a child with PMD after rehabilitation treatment.
Case description
A 12-month-old boy with PMD visited our children’s hospital rehabilitation center for comprehensive pediatric rehabilitation. His
brain MRI (Figure 1) showed total demyelination in the bilateral white matter. He had nystagmus, decreased truncal tone with
ataxia. His consciousness was clear and the muscle strength of all four limbs was measured grade 3 (normal grade 5). Muslce stretch
reflex was increased in both lower limbs and Babinski reflex was positive in both sides. Spascity was not observed. Gross Motor
Function Classification System (GMFCS) was checked level V and Gross Motor Function Measure (GMFM) was scored 19. On
developmental assessment, gross motor was measured 5 months, fine motor 7 months, social 7 months, and language 10 months.
Comprehensive rehabilitation was performed for 3 months. The first and the last one month of 3 months were through inpatient
rehabilitation and he received inpatient rehabilitation at another hospital during the second month. After 3 months of rehabilitation,
there was no difference in physical examination such as consciousness, mucle strength, muscle stretch reflex, and Babinski reflex.
However, GMFCS, developmental assessment and GMFM showed some improvement. GMFCS was checked level IV. Gross motor
was measured 6 months, fine motor 10 months, social 9 months, and language 12 months. GMFM scored 51; the score improved 17
to 36 in lying & rolling, 2 to 12 in sitting, and 0 to 3 in crawling & kneeling probably because of the improvement of truncal tone and
ataxia (Table 1).
Conclusion
We report an infant with PMD who underwent comprehensive rehabilitation for 3 months. After rehabilitation treatment, GMFCS,
GMFM and developmental assessment improved. Comprehensive pediatric rehabilitation would help children with rare PMD
achieve their maximal functional ability.
Key Words: Pelizaeus-Merzbacher disease, congenital disease, ataxia, rehabilitation
Acknowledgment: This study was supported by the Rehabilitation Research & Development Support Program (NRC RSP-2019001),
National Rehabilitation Center, Ministry of Health and Welfare, Korea.

Figure 1. Brain MRI image
Table 1. Functional neuromuscular evaluation

P 115
Allogeneic umbilical cord blood stem cell therapy in Mowat-Wilson syndrome: a case report
Joonhyun Park1*
, Wookyung Park1, Jaehoon Sim
1, Mi Ri Suh
1,2, MinYoung Kim
1,2†
Department of Rehabilitation Medicine,CHA Bundang Medical Center, CHA University School of Medicine1, Rehabilitation and
Regeneration Research Center,CHA University2
Introduction
Mowat-Wilson syndrome (MWS), also known as Hirschsprung disease-intellectual disability syndrome, is a rare genetic disorder
caused by heterozygous pathogenic variants or deletions in ZEB2. There is yet no specific treatment, for ZEB2 gene mutation affects
the early stages of embryonic neural crest formation in MWS. In this report, we present a case of MWS with improved functional
outcome after umbilical cord blood (UCB) stem cell therapy.
Case report
A 10-month-old female infant was referred to our department. She was born with a full-term pregnancy, however could not creep
or crawl until 10 months. She also had calyceal diverticulum, small ventricular septal defect and chronic constipation. Physical exam
showed thumb-in-palm posture and spasticity of bilateral ankles. A brain MRI shows dilated ventricles with decreased white matter
volume and thin corpus callosum. Under the interim diagnosis of cerebral palsy, she was enrolled in an allogeneic UCB
transplantation trial. Unrelated allogeneic UCB units were selected from UCB bank of our organization. The conditions for UCB
selection were at least 4 out of 6 matching HLA typing for A, B, and DRB1 antigens. For allogeneic UCB injection, cyclosporine was
administered intravenously for 1 week and orally for 3 weeks. After thawing and washing according to our protocol, UCB was
infused intravenously at age of 13 months. Side effects associated with immune rejection were not observed during the hospital
stay and no adverse effect related to neoplasm was reported. ZEB2 gene mutation in exon 5, c.502C>T was found by exon
sequencing and confirmed the diagnosis of MWS five years after the UCB injection. Figure 1 shows the results of the functional
assessment. She was in GMFCS IV at the initiation of PT. The GMFM score increased gradually until the 26th month of age, which
was 1 year after cord blood transplantation. During that period, GMFCS remained improved to III for approximately 1.5 years.
Improvement was also observed in the BSID-II both in mental and motor scores. Epilepsy is known as a major manifestation of MWS,
and the prevalence of epilepsy in MWS is about 70-75%. In one study, and the median age at seizure onset was 14.5 months. In this
case, the first seizure episode occurred at the age of 3 years and there was no seizure event for 2 years after the injection. Diffuse
tensor images in magnetic resonance imaging were taken 3 months before and 6 months after the procedure (Figure 2). The
hypogenesis of corpus callosum was continuously observed, but the fiber density of both hemispheres including the corpus callosum
increased at 6 months after injection.
Conclusion
In this MWS case, UCB stem cell injection was performed without significant side effects, and seemed to be effective. This suggests
that the stem cell therapy may be considered as a therapeutic option in inherited neural developmental disorders.
Acknowledgment: This research was supported by a grant of the Korea Health Technology R&D Project through the Korea Health
Industry Development Institute (KHIDI), funded by the Ministry of Health & Welfare, Republic of Korea (grant number : HI16C1559)
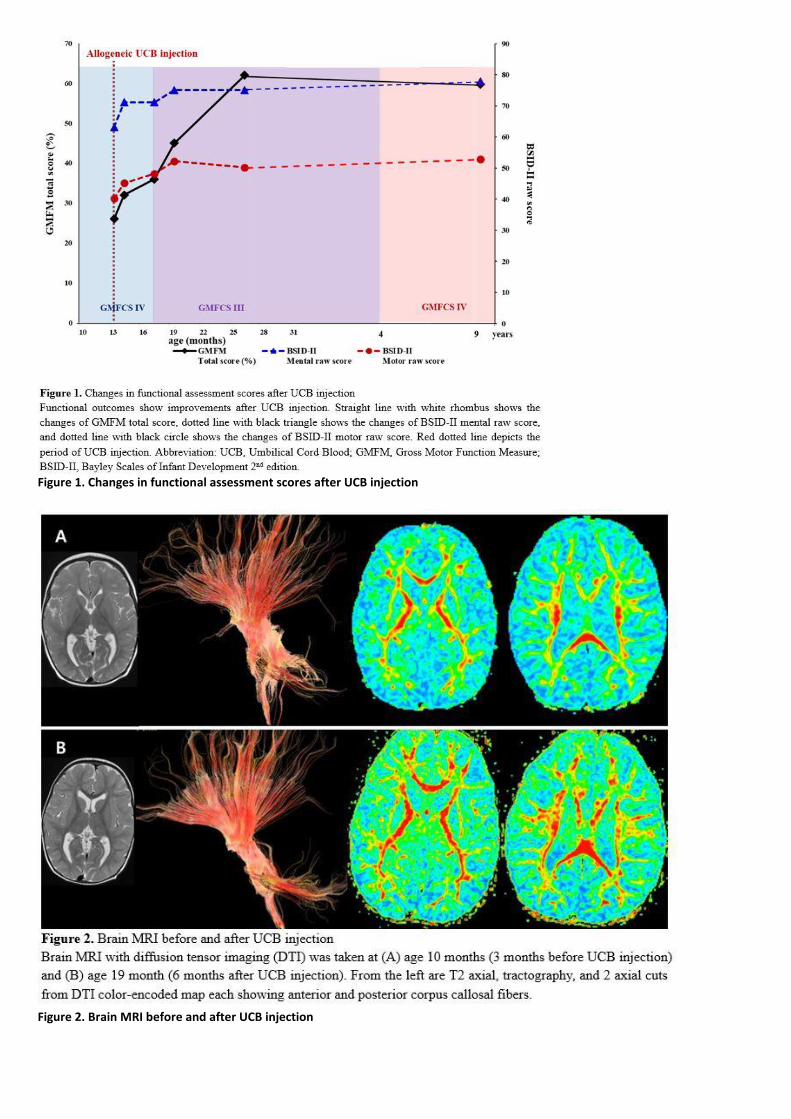
Figure 1. Changes in functional assessment scores after UCB injection
Figure 2. Brain MRI before and after UCB injection

P 116
Evaluating the Usefulness of Smart Naso for Nasalance Measurement in Cleft Palate Patients
Nguyen Phuoc Minh Tam1,3*
, Xiaopeng Yang2, Gi-Wook Kim
1,3, Yu Hui Won
1,3, Sung-Hee Park
1,3, Jeong-Hwan Seo
1,3, Seung-O Ko
3,4,
Jin-A Baik3,4
, Heecheon You2, Myoung-Hwan Ko
1,3†
Department of Physical Medicine and Rehabilitation,Chonbuk National University Medical School1, Department of Industrial &
Management Engineering,Pohang University of Science and Technology2, Biomedical Research Institute of Chonbuk National
University Hospital,Research Institute of Clinical Medicine of Chonbuk National University3, Chonbuk National University,Dental
School4
Objective
Previous worldwide popular Nasometer (such as Nasometer II 6450) requires tight contact between the plate and the philtrum of
patient that restricts natural oral movement. The Smart Naso was developed with the desiration to provide clinician with more
comfortable and affordable device. Therefore, the present study was conducted to evaluate the usefulness of this new device.
Methods
Two cleft palate patients were measured nasalance using both Nasometer II 6450 and Smart Naso. Besides, repetitive
measurements with one-week interval and by two examiners were performed for Smart Naso to assess its intra-rater and inter-rater
reliability. Speech materials including /a/, /i/, /papapapapapa/, /mamamamamama/, and oral phrase were used. Nasalance results
measured using two devices, by two examiners and two measurements with one-week interval were compared each other.
Results
Applying Smart Naso for nasalance measurement in two patients showed similar results to Nasometer II 6450 (First patient: 12.5
and 11 for /a/, 13.5 and 14 for /i/, 11.5 and 12 for /papapapapapa/, 30.5 and 40 for /mamamamamama/, 15.6 and 10 for oral
phrase; Second patient: 60.5 and 61 for /a/, 74.4 and 93 for /i/, 53.9 and 62 for /papapapapapa/, 72.2 and 68 for
/mamamamamama/, 62 and 74 for oral phrase). Repetitive measurement with one-week interval by the same examiner using Smart
Naso showed similar scores (First patient: 12.7 and 12.5 for /a/, 25.8 and 13.5 for /i/, 11 and 11.5 for /papapapapapa/, 22.1 and 30.5
for /mamamamamama/, 17.2 and 15.6 for oral phrase; Second patient: 73.5 and 60.5 for /a/, 62.4 and 74.4 for /i/, 69.6 and 53.9 for
/papapapapapa/, 76 and 72.2 for /mamamamamama/, 69.7 and 62 for oral phrase). There were also similarity between results of
two examiners using Smart Naso (First patient: 12.5 and 12.3 for /a/, 13.5 and 17.5 for /i/, 11.5 and 6.3 for /papapapapapa/, 30.5
and 23.9 for /mamamamamama/, 15.6 and 15.8 for oral phrase; Second patient: 60.5 and 62.4 for /a/, 74.4 and 70.4 for /i/, 53.9
and 56.5 for /papapapapapa/, 72.2 and 65.9 for /mamamamamama/, 62 and 62.6 for oral phrase).
Conclusions
The developed Smart Naso showed similar nasalance results to Nasometer II 6450. There were similarity in results of repetitive
measurements with one-week interval and by two examiners using Smart Naso. More cleft patients are needed to assess the
reliability and validity of this new device in nasalance measurement.
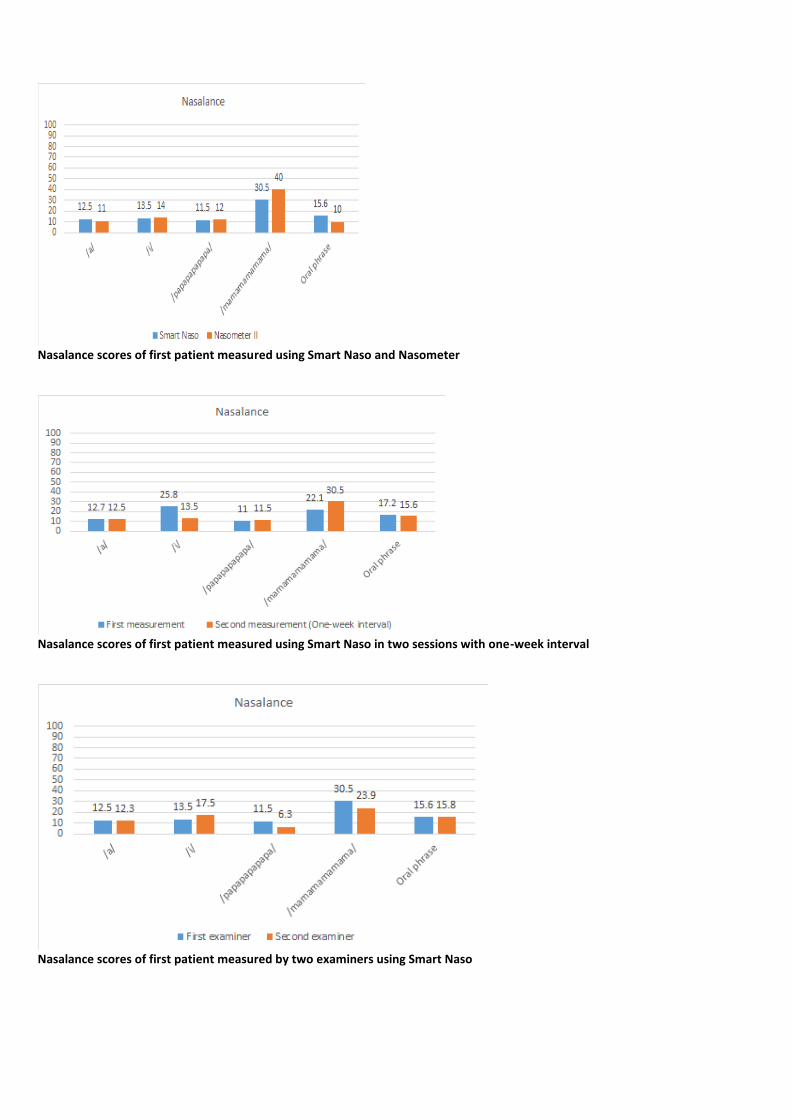
Nasalance scores of first patient measured using Smart Naso and Nasometer
Nasalance scores of first patient measured using Smart Naso in two sessions with one-week interval
Nasalance scores of first patient measured by two examiners using Smart Naso

P 117
Visual assessment of Healthy Infants Under 24-months Using PreViAs Questionnaire
Jungjae Lee1*
, Hae yeon Park1, Kyung Eun Nam
1, Eunhee Kim
2, Joo Hyun Park
1†
1Department of Rehabilitation Medicine,Seoul St. Mary’s Hospital, College of Medicine, The Catholic University of Korea1,
Department of Pediatrics,Areumdri Pediatric Clinic2
Visual difficulties in infancy is not limited to ophthalmologic problems such as visual field loss and visual acuity. It has been known
that cortical visual impairment is involved in visual behaviors. Early visual approach willhelp screen high-risk infant and predict their
neurological and cognitive development, including visual impairment. The Preverbal Visual Assessment (PreViAs) questionnaire
designed by V. Pueyo et. al, is a useful tool for assessing visual integrative functions in infants under 24 months either healthy
children or outside the range of normality. PreViAs questionnaire is easily performed by primary caregiver. All 30 questions can be
answered within a short period of time, and each item is related to one or more of four domains (visual attention, visual
communication, visual–motor coordination, and visual processing). (Table 1). This tool was developed in Spanish and validated on a
Spanish speaking population. Normal references in full term infants were obtained by the authors and internal consistency was
verified. But there are yet no reports of normal reference data in Korea. We collected normative data in healthy infants without
known visual symptoms. The Preverbal Visual Assessment (PreViAs) questionnaire were administered to full term infants who
visited a local pediatric clinic for under 24 months. The caregivers of 97 patients have completed the questionnaire. None of the
children had brain MRI assessments, and one child with brain sonography was normal. The age of infants were divided into 6 groups:
birth to 3.99 months, 4 to 7.99 months, 8 to 11.99 months, 12 to 15.99 months, 16 to 19.99 months, 20 to 23.99 months (Fig. 1).
Each domains were added up by items corresponding to each visual function. The average scores for each domain were shown.
(Table 2). The PreViAs questionnaire is a simple and useful tool for assessing the visual performance. This normal reference data will
be the basis of further studies for high-risk infants including premature babies with cortical visual impairment.
Table 1. The Preverbal Visual Assessment (PreViAs) questionnaire

Table 2. The mean scores of each visual domain for each age group.
Fig 1. Distribution of the infant age groups.

p 118
Two novel mutations in WDR62 gene in a patient with autosomal recessive primary microcephaly
Jaewon Kim1*
, Dae-Hyun Jang1†
, Dong-Woo Lee1
Department of Rehabilitation Medicine, Incheon St. Mary’s Hospital, College of Medicine, The Catholic University of Korea1
Introduction
Autosomal recessive primary microcephaly is a condition in which infants are born with a very small head and a small brain.
Autosomal recessive primary microcephaly causes intellectual disability, which is typically mild to moderate and does not become
more severe with age. Most affected individuals have delayed speech and language skills. As the advanced genetic technologies, the
underlying molecular causes of autosomal recessive primary microcephaly have been recently elucidated. We here report a case of
primary microcephaly with two novel mutations in WDR62 gene
Case
A 6-year-old girl was referred in the outpatient rehabilitation clinic because of microcephaly and delayed development. The patient
had been born at 36+4 weeks of gestation by caesarean section. The birth weight was 1800g (<1st percentile). On the prenatal
course, intrauterine growth restriction was detected on ultrasonography test. The patient had one older sibling, who has no
microcephaly and developmental abnormality. On the examination, delayed speech development and microcephaly with
occipitofrontal head circumference of 43.5cm (< -3SD, Fig 1) was noted. Her gross and fine motor development was normal. On
Preschool Receptive-Expressive Language Scale (PRES), expressive and receptive language of 41 months was revealed. Korean-Leiter
International performance Scale - Revised (K-LIP-R) examination, IQ was 43 (<0.1 percentile), which indicate the level of 27-month-
old. Social maturity scale was 35.5 (SQ=76.92). Brain CT and MRI was unremarkable. The laboratory findings including organic acids
were normal. In chromosomal study, karyotype of 46, XX, inv (9) (p12q13) was revealed, which was benign. Microdeletion syndrome
study (Multiplex ligation-dependent probe amplification technique) showed no abnormality. Chromosomal microarray (Affymetrix
Cytoscan 750K array, genome build: Hg19 method) was normal. In clinical exome sequencing test, heterozygous two novel variants
were found in the WDR62 gene at 2 different sites: in exon 8 (NM_001083961.1: c.883-4_890del) from mother and in exon 13
(NM_001083961.1: c.1684C>G) from father. In addition, patient’s parents were identified as heterozygous carriers for each variation
which occurs in trans. Each variation was confirmed by conventional Sanger sequencing. These two novel variations have not been
reported in control databases such as the 1,000 Genomes Project, Exome Aggregation Consortium, gnomAD and the dbSNP
Database. The proband was diagnosed as autosomal recessive primary microcephaly type 2 based on clinical and molecular findings.
Occipitofrontal head circumference of the proband

P 119
A case with GNAO1 gene mutation misdiagnosed as dyskinetic cerebral palsy
Jaewon Kim1*
, Dae-Hyun Jang1†
, Dong-Woo Lee1
Department of Rehabilitation Medicine, Incheon St. Mary’s Hospital, College of Medicine, The Catholic University of Korea1
Introduction
Cerebral palsy (CP) represents a group of chronic and non-progressive disorders secondary to brain dysgenesis or injury. It is
characterized by significant impairment in movement and posture that begins during infancy or early childhood. Dyskinetic CP is
characterized by abnormal movements, with fluctuating patterns of tone and posture. Because the diagnosis of cerebral palsy is
performed through clinical aspects, primary dystonia due to genetic cause is often misdiagnosed as dyskinetic cerebral palsy. We
report a case with primary dystonia due to GNAO1 gene mutation who was diagnosed dyskinetic cerebral palsy previously.
Case
A 7-month-old girl was referred to the outpatient rehabilitation clinic because of delayed development. The patient had been born
at 38 weeks of gestation by vaginal delivery. The prenatal and perinatal course was non-specific. There was no family history of
delayed development or other known hereditary diseases. The patient had one older sibling, who has no developmental
abnormality. The birth weight was 2800g (16th Percentile). On the examination, there was increased muscle tone and primitive
reflexes, with grossly hypertonic posture, extension tendency of all extremities, and extensor thrust. Head control was poor. She
showed excessive involuntary movements on bilateral upper and lower limbs. The electrodiagnosic study, brain MRI and neonate
screening test for metabolic disorders were normal. Chromosomal abnormality was not seen. At that time, she was diagnosed
dyskinetic cerebral palsy. At 36-month-old, Bayley Scales of Infant and Toddler Development showed below 0.1 percentile of
development in all domains (cognitive development 3 month 20 days, receptive communication 4 month 10 days, expressive
communication 2 month 20 days, fine motor development 3 month 10 days, and gross motor development 1 month of age). At 4-
year-old, follow-up brain MRI was showed no abnormality. She was referred to the genetic clinic to assess hereditary dystonia. The
multi-gene panel study related with primary dystonia which was developed by us was performed (Table 1). We found a
heterozygous variation in the patient’s GNAO1: c.607G>A (p.Gly203Arg), which is related with a neurodevelopmental disorder with
involuntary movements. Clinicians should be cautious that patients diagnosed with cerebral palsy in full-term births without specific
MRI findings may have genetic diseases masquerading as cerebral palsy.
Acknowledgment: This study was supported by a Chyung Ki Lee research grant of Korean Academy of Rehabilitation Medicine for
2018

Table 1. Primary dystonia gene panel
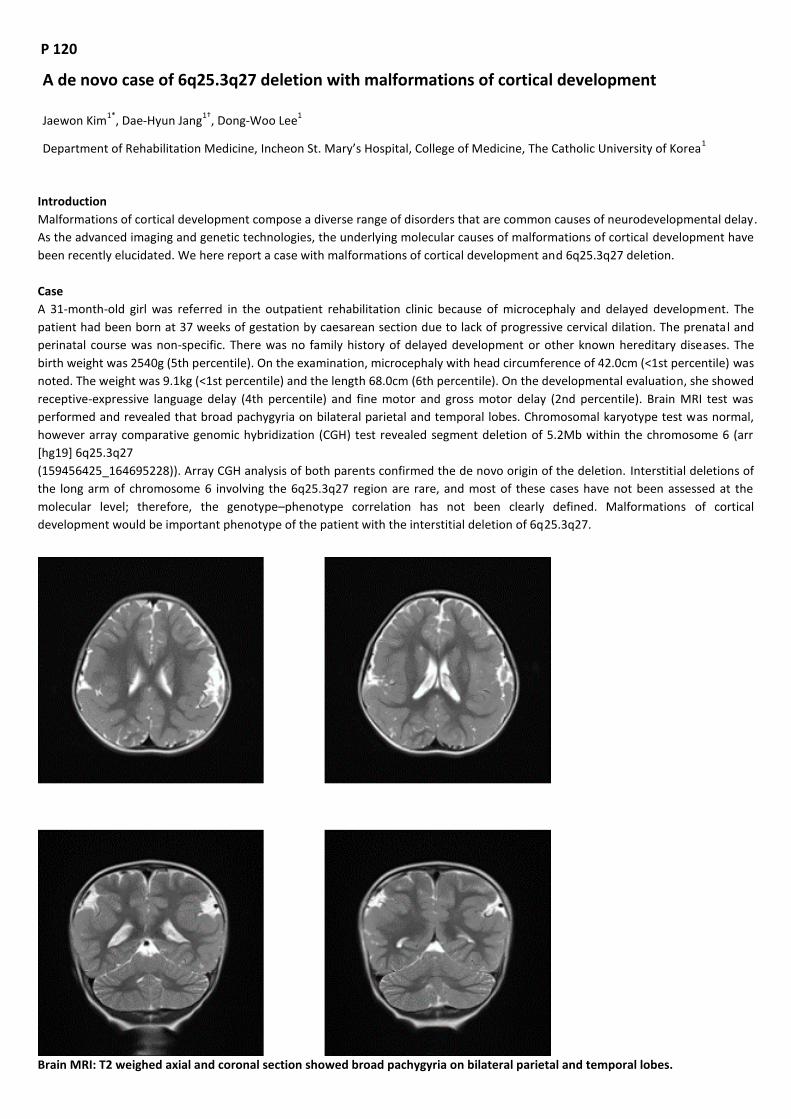
P 120
A de novo case of 6q25.3q27 deletion with malformations of cortical development
Jaewon Kim1*
, Dae-Hyun Jang1†
, Dong-Woo Lee1
Department of Rehabilitation Medicine, Incheon St. Mary’s Hospital, College of Medicine, The Catholic University of Korea1
Introduction
Malformations of cortical development compose a diverse range of disorders that are common causes of neurodevelopmental delay.
As the advanced imaging and genetic technologies, the underlying molecular causes of malformations of cortical development have
been recently elucidated. We here report a case with malformations of cortical development and 6q25.3q27 deletion.
Case
A 31-month-old girl was referred in the outpatient rehabilitation clinic because of microcephaly and delayed development. The
patient had been born at 37 weeks of gestation by caesarean section due to lack of progressive cervical dilation. The prenatal and
perinatal course was non-specific. There was no family history of delayed development or other known hereditary diseases. The
birth weight was 2540g (5th percentile). On the examination, microcephaly with head circumference of 42.0cm (<1st percentile) was
noted. The weight was 9.1kg (<1st percentile) and the length 68.0cm (6th percentile). On the developmental evaluation, she showed
receptive-expressive language delay (4th percentile) and fine motor and gross motor delay (2nd percentile). Brain MRI test was
performed and revealed that broad pachygyria on bilateral parietal and temporal lobes. Chromosomal karyotype test was normal,
however array comparative genomic hybridization (CGH) test revealed segment deletion of 5.2Mb within the chromosome 6 (arr
[hg19] 6q25.3q27
(159456425_164695228)). Array CGH analysis of both parents confirmed the de novo origin of the deletion. Interstitial deletions of
the long arm of chromosome 6 involving the 6q25.3q27 region are rare, and most of these cases have not been assessed at the
molecular level; therefore, the genotype–phenotype correlation has not been clearly defined. Malformations of cortical
development would be important phenotype of the patient with the interstitial deletion of 6q25.3q27.
Brain MRI: T2 weighed axial and coronal section showed broad pachygyria on bilateral parietal and temporal lobes.
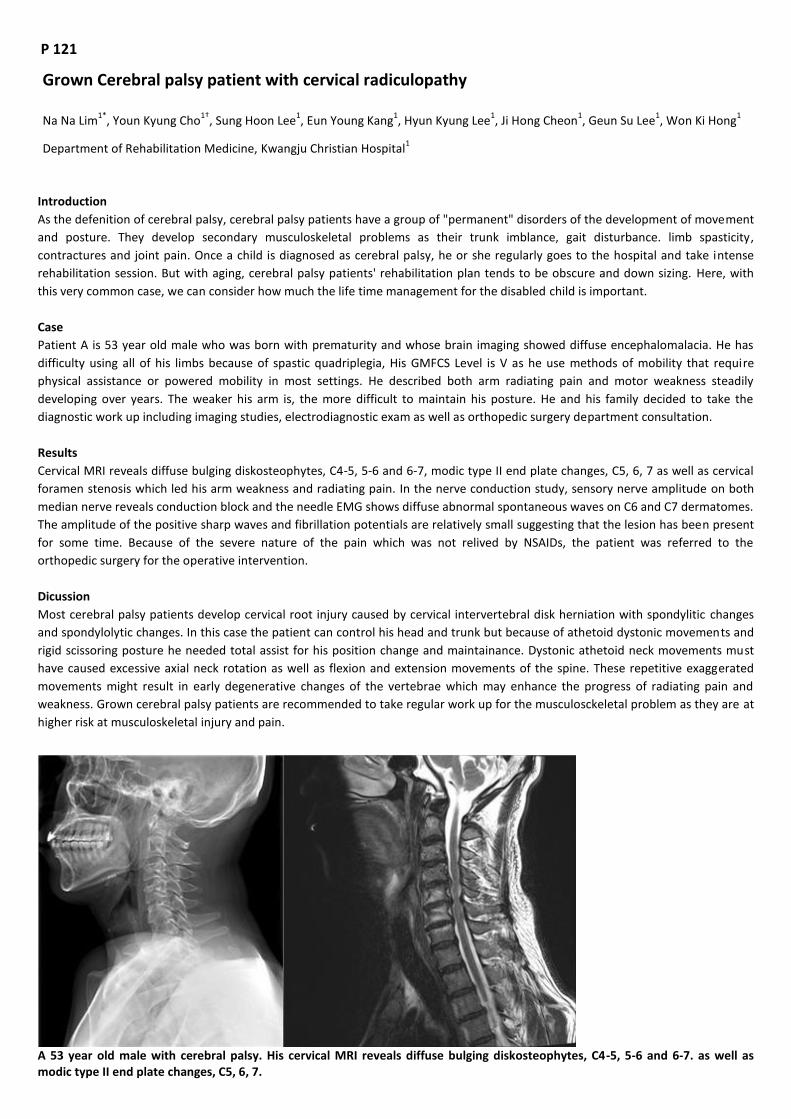
P 121
Grown Cerebral palsy patient with cervical radiculopathy
Na Na Lim1*
, Youn Kyung Cho1†
, Sung Hoon Lee1, Eun Young Kang
1, Hyun Kyung Lee
1, Ji Hong Cheon
1, Geun Su Lee
1, Won Ki Hong
1
Department of Rehabilitation Medicine, Kwangju Christian Hospital1
Introduction
As the defenition of cerebral palsy, cerebral palsy patients have a group of "permanent" disorders of the development of movement
and posture. They develop secondary musculoskeletal problems as their trunk imblance, gait disturbance. limb spasticity,
contractures and joint pain. Once a child is diagnosed as cerebral palsy, he or she regularly goes to the hospital and take intense
rehabilitation session. But with aging, cerebral palsy patients' rehabilitation plan tends to be obscure and down sizing. Here, with
this very common case, we can consider how much the life time management for the disabled child is important.
Case
Patient A is 53 year old male who was born with prematurity and whose brain imaging showed diffuse encephalomalacia. He has
difficulty using all of his limbs because of spastic quadriplegia, His GMFCS Level is V as he use methods of mobility that require
physical assistance or powered mobility in most settings. He described both arm radiating pain and motor weakness steadily
developing over years. The weaker his arm is, the more difficult to maintain his posture. He and his family decided to take the
diagnostic work up including imaging studies, electrodiagnostic exam as well as orthopedic surgery department consultation.
Results
Cervical MRI reveals diffuse bulging diskosteophytes, C4-5, 5-6 and 6-7, modic type II end plate changes, C5, 6, 7 as well as cervical
foramen stenosis which led his arm weakness and radiating pain. In the nerve conduction study, sensory nerve amplitude on both
median nerve reveals conduction block and the needle EMG shows diffuse abnormal spontaneous waves on C6 and C7 dermatomes.
The amplitude of the positive sharp waves and fibrillation potentials are relatively small suggesting that the lesion has been present
for some time. Because of the severe nature of the pain which was not relived by NSAIDs, the patient was referred to the
orthopedic surgery for the operative intervention.
Dicussion
Most cerebral palsy patients develop cervical root injury caused by cervical intervertebral disk herniation with spondylitic changes
and spondylolytic changes. In this case the patient can control his head and trunk but because of athetoid dystonic movements and
rigid scissoring posture he needed total assist for his position change and maintainance. Dystonic athetoid neck movements must
have caused excessive axial neck rotation as well as flexion and extension movements of the spine. These repetitive exaggerated
movements might result in early degenerative changes of the vertebrae which may enhance the progress of radiating pain and
weakness. Grown cerebral palsy patients are recommended to take regular work up for the musculosckeletal problem as they are at
higher risk at musculoskeletal injury and pain.
A 53 year old male with cerebral palsy. His cervical MRI reveals diffuse bulging diskosteophytes, C4-5, 5-6 and 6-7. as well as modic type II end plate changes, C5, 6, 7.
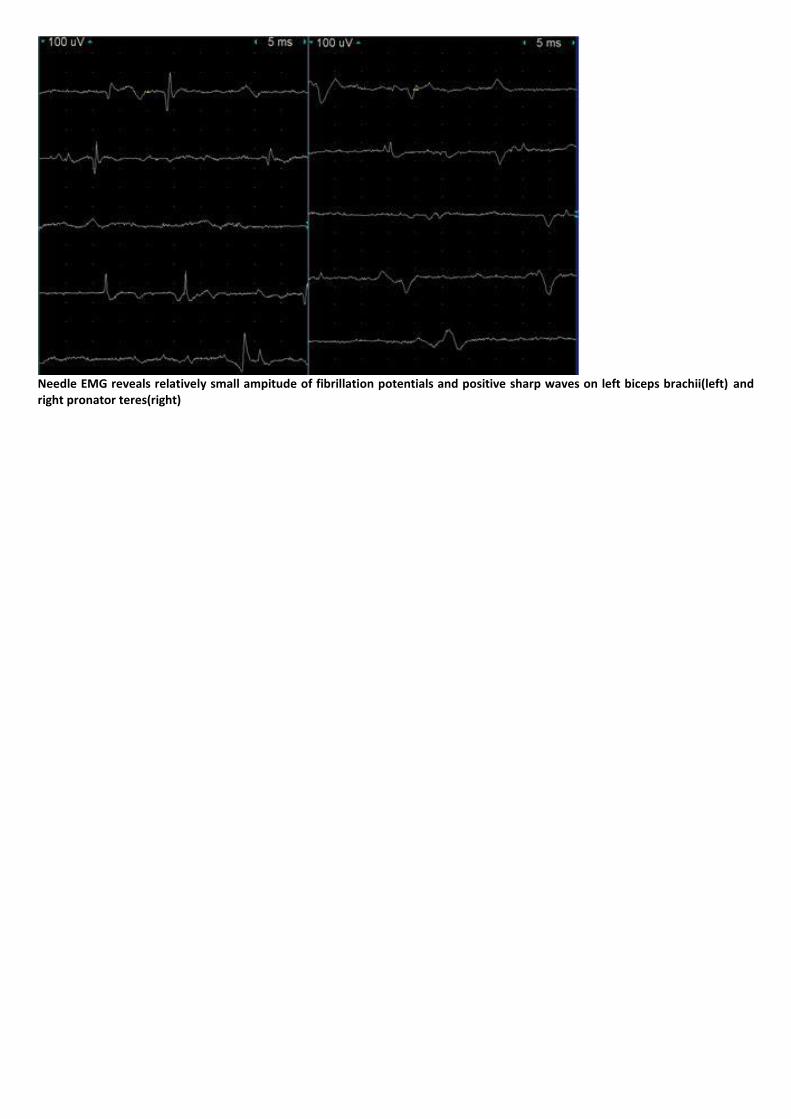
Needle EMG reveals relatively small ampitude of fibrillation potentials and positive sharp waves on left biceps brachii(left) and right pronator teres(right)

P 122
Therapeutic effect of tibia counter-rotator in in-toeing gait of the patient with rickets
Ju Young Cho1*
, Jong Min Kim1, Donghwi Park
1, Byung Joo Lee
1, Kwang Jae Yu
1, Hyunseok Moon
1, Sungwon Park
1, ZeeIhn Lee
1†
Department of Rehabilitation Medicine, Daegu Fatima Hospital1
Introduction
In hypophosphatemic rickets, softening and weakening of the bone causes bending deformities in long bone (e.g. genu varum or
genu valgum) in response to weight-bearing. And affected child often walks with waddling gait due to coxa vara and/or in-toeing
gait secondary to internal tibial torsion. Internal tibial torsion is a variation of normal anatomy and is caused partially by intrauterine
position, sleeping in the prone position after birth, and sitting on the feet. It is the most common cause of in-toeing gait in children
between the ages of 2-4 years. Examining a child with internal tibial torsion with the patella straight, there will be medial rotation of
the feet. Internal tibial torsion gradually resolves on its own by the time the child reaches eight years of age. Despite adequate
medical treatment, some patients with hypophosphatemic rickets are left with residual skeletal deformities and these skeletal
deformities may require surgical correction when growth has ceased. Therefore, we tried to treat internal tibial torsion in patient
with hypophosphatemic rickets using orthotic device (e.g. tibia counter-rotator (TCR) that can correct the tibial torsion by gradually
adjusting the angle of shoe rotation) before invasive surgical treatment.
Case
The patient is 12-year-old female who diagnosed as hypophosphatemic rickets at the age of 2. After diagnosis, treatment was
started with supplementation of phophate as Joulie`s solution and oral calcitriol was also given. The dose of the drug was adjusted
based on regular blood tests and she is still taking medication continuously. At the age of 10, the patient visited our clinic and
complained about in-toeing gait. On physical examination, right genu varum, left genu valgum and in-toeing gait pattern were seen.
TMA measured by gravity goniometer was -34 degree on the right side and -17 degree on the left side. On low extremity CT,
Femoral anteversion angle was 7.2 degree on the right side and 12 degree on the left side. And tibial torsion angle was -8 degree on
the right and -3 on the left side. Then, we applied the right TCR and biomechanic foot orthosis (BFO). 6 months after applying
orthosis, we found that TMA was improved with -14 degree on the right side and -1 degree on the left. And 18 months after the
treatment, TMA was measured at 6 degree on the right and 12 degree on the left and in-toeing gait pattern was significantly
improved as well.
Conclusion
There is controversy about the effectiveness of orthotic devices in treating patients with in-toeing gait caused by internal tibial
torsion, but patients with rickets, whose skeletal deformities is only treated by invasive treatments such as surgery, could try the
TCR for in-toeing gait before considering surgery.
P 123
GAIT REHABILITATION USING LOWER LIMBS ROBOT ASSISTED TRAINING SYSTEM ON PATIENTS WITH BURN
So Young Joo1*
, Seung Yoel Lee2, Yoon Soo Cho
1, Cheong Hoon Seo
1†
Department of Rehabilitation Medicine, Hangang Sacred Heart Hospital1, Department of Rehabilitation Medicine, Soonchunhyang
University Bucheon Hospital2
Introduction
Gait enables human beings to move forward, and most people consider gait to be natural skill. But gait disturbances are very
prevalent to the the patients with burn injury. A major cause of functional impairment including pain and joint contractures.
Contractures at the lower extremities such as the hip, knee and ankle significantly limit gait. Recent attention of the application of
artificial intelligence in rehabilitation, in particularly lower limbs robot assisted rehabilitation has become a hot issue of studies. This
study is purposed to find the efficacy and study the mechanism of motor recovery after robot assisted gait training on patients with
lower extremity burn.
Method
7 patients with lower extremity burn were included. All patients received 4 weeks robot assisted training. Functional scores of
functional ambulation category (FAC) and 6-minute walking distances, and pain score of visual analog score (VAS) during robot
assisted gait training were measured.
Results
FAC and VAS scores after training were better than the scores before training. 6-min walking distance after training were
significantly increased than the measure before training (p<0.05). Lower limbs robot assited rehabilitation training improves
patient’s pain, and increases walking speed on patients with lower extremity burn.
Conclusion
Lower limbs robot assited rehabilitation improves the walking speed, and prolongs their walking distances. The use of robot assisted
rehabilitation may facilitate early recovery from burn injury.

P 124
Lipomatosis of median nerve mimicking carpal tunnel syndrome: A Case Report
Hae-Yeon Park1*
, Jungjae Lee1, Jong In Lee
1†
Department of Rehabilitation Medicine, Seoul St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Seoul1
Introduction
Median neuropathy above wrist level is uncommon when compared with the median entrapment neuropathy at the wrist.
Differentiating between median neuropathy at the wrist and above wrist level may be difficult when relying only on physical
examination, so electrodiagnostic study is important tool in localizing the lesion in proximal median neuropathy. Here, we present a
case report of lipomatosis of median nerve mimicking carpal tunnel syndrome, in which electrodiagnostic study played an important
role in diagnosis.
Case report
A 38-year-old woman visited our institution presenting symptoms of hypoesthesia and paresthesia at right thumb and index finger,
which started 6 months ago. During 6 months, she had visited local clinics and received injection therapy under impression of
cervical radiculopathy and carpal tunnel syndrome. Because the symptoms persisted despite of the therapy, she visited our
institution and was referred to rehabilitation department for electrodiagnostic evaluation. On physical examination, there was no
motor weakness at both upper extremities, but light touch sensation of right thumb and 2nd finger was decreased. Tinel sign at
wrist was positive at right side, but other physical examination showed no significant findings. Cervical spine x-ray showed
degenerative change with cervical straightening.
On the nerve conduction study (NCS), the right median sensory NCS in the digit III was normal, but the right median sensory NCS in
the digit II and thumb showed decreased amplitudes when compared with the left side. The right median motor NCS to abductor
pollicis brevis muscle showed conduction block and decreased conduction velocity between wrist and elbow segment. The right
median motor NCS to pronator quadratus muscle showed no abnormal findings (Table 1). On needle electromyography, abnormal
spontaneous activities were noted in the right abductor pollicis brevis, flexor pollicis brevis, and opponens pollicis muscles (Table 2).
The patient was diagnosed with right median neuropathy above the wrist level. Magnetic resonance imaging (MRI) of right wrist was
done, and collection of slightly enlarged nerve fascicles along the course of median nerve was surrounded by high signal fat, which
showed spaghetti-like appearance (Figure 1). With the diagnosis of lipomatosis of median nerve, she underwent the surgery of
median nerve neurolysis wih lipoma excision.
Conclusion
Lipomatosis of peripheral nerve is rare disorder involving diffuse infiltration of peripheral nerves with fibrous and adipose tissues.
When involving median nerve, clinical symptoms may be similar to those of carpal tunnel syndrome, and may lead to different
treatment. Electrodiagnostic study is one of the useful diagnostic tools in localizing the lesion, and can lead to proper management.
Table 1. Sensory and Motor Nerve Conduction Study

Table 2. Needle Electromyography Study
Figure 1. Magnetic resonance imaging (MRI) of right wrist. (A) Coronal T2-weighted image of right wrist. (B) Axial T2-weighted image of right wrist. Collection of slightly enlarged nerve fasicles along the course of median nerve is surrounded by high signal fat, showing spaghetti-like appearance.
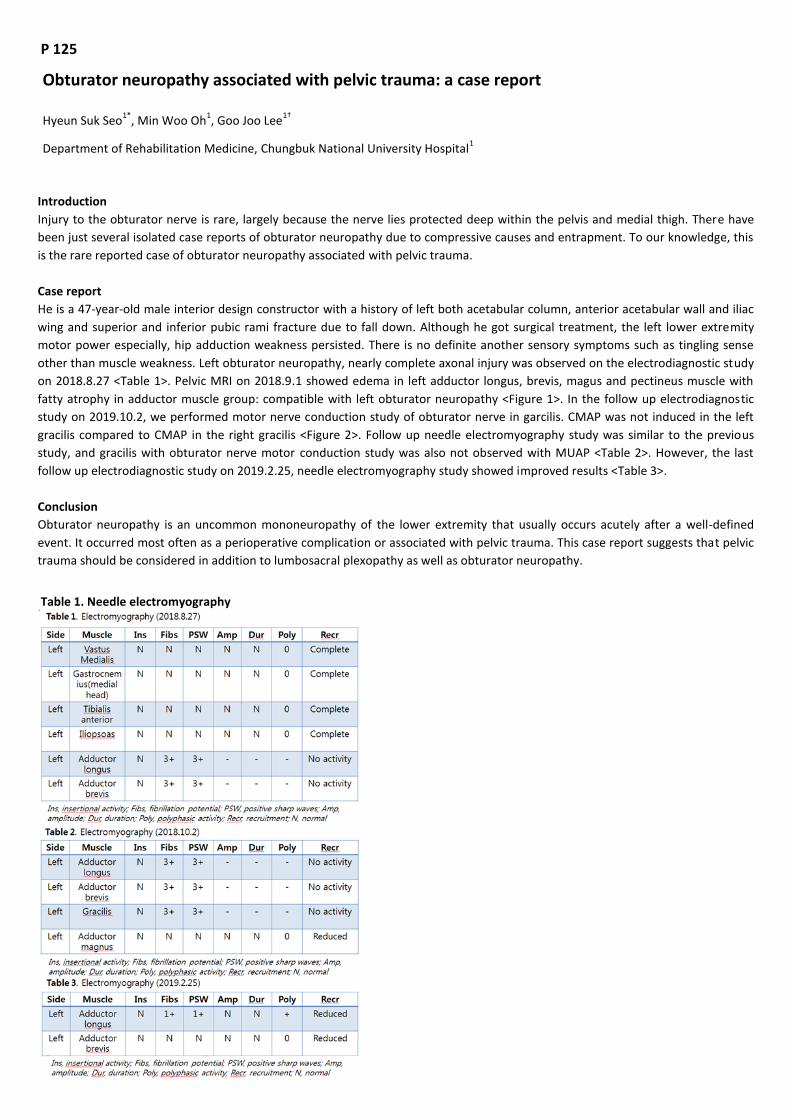
P 125
Obturator neuropathy associated with pelvic trauma: a case report
Hyeun Suk Seo1*
, Min Woo Oh1, Goo Joo Lee
1†
Department of Rehabilitation Medicine, Chungbuk National University Hospital1
Introduction
Injury to the obturator nerve is rare, largely because the nerve lies protected deep within the pelvis and medial thigh. There have
been just several isolated case reports of obturator neuropathy due to compressive causes and entrapment. To our knowledge, this
is the rare reported case of obturator neuropathy associated with pelvic trauma.
Case report
He is a 47-year-old male interior design constructor with a history of left both acetabular column, anterior acetabular wall and iliac
wing and superior and inferior pubic rami fracture due to fall down. Although he got surgical treatment, the left lower extremity
motor power especially, hip adduction weakness persisted. There is no definite another sensory symptoms such as tingling sense
other than muscle weakness. Left obturator neuropathy, nearly complete axonal injury was observed on the electrodiagnostic study
on 2018.8.27 <Table 1>. Pelvic MRI on 2018.9.1 showed edema in left adductor longus, brevis, magus and pectineus muscle with
fatty atrophy in adductor muscle group: compatible with left obturator neuropathy <Figure 1>. In the follow up electrodiagnostic
study on 2019.10.2, we performed motor nerve conduction study of obturator nerve in garcilis. CMAP was not induced in the left
gracilis compared to CMAP in the right gracilis <Figure 2>. Follow up needle electromyography study was similar to the previous
study, and gracilis with obturator nerve motor conduction study was also not observed with MUAP <Table 2>. However, the last
follow up electrodiagnostic study on 2019.2.25, needle electromyography study showed improved results <Table 3>.
Conclusion
Obturator neuropathy is an uncommon mononeuropathy of the lower extremity that usually occurs acutely after a well-defined
event. It occurred most often as a perioperative complication or associated with pelvic trauma. This case report suggests that pelvic
trauma should be considered in addition to lumbosacral plexopathy as well as obturator neuropathy.
Table 1. Needle electromyography
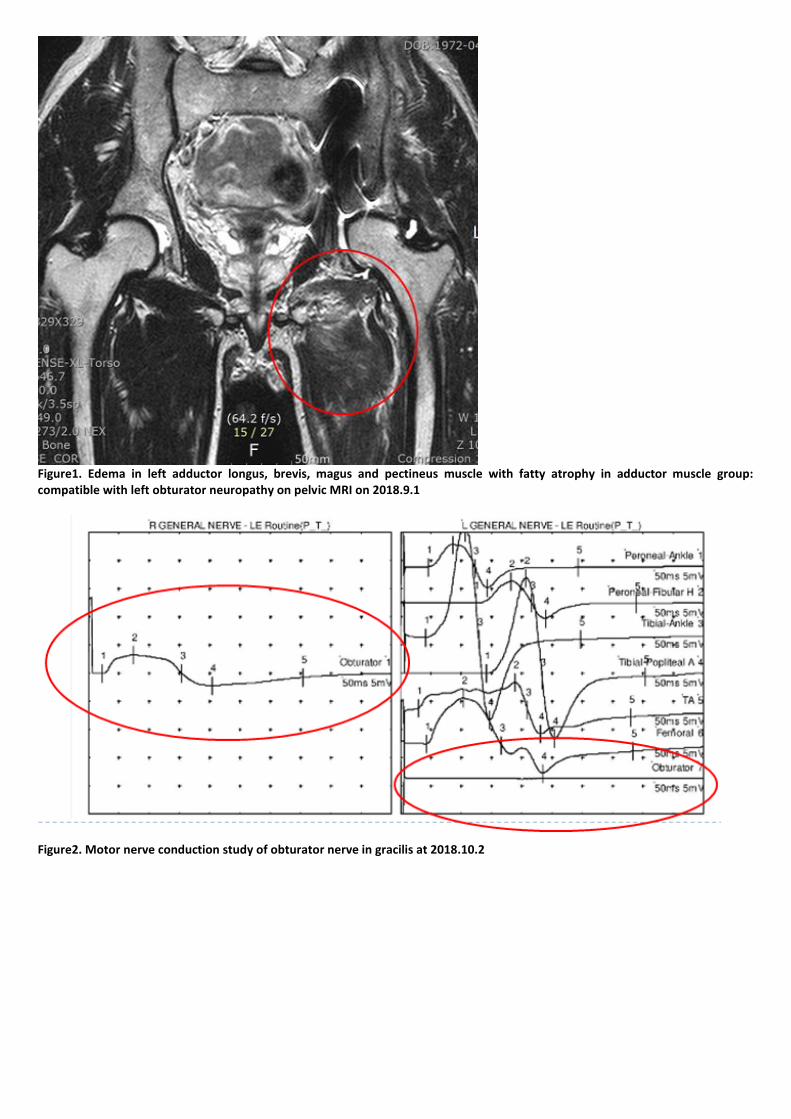
Figure1. Edema in left adductor longus, brevis, magus and pectineus muscle with fatty atrophy in adductor muscle group: compatible with left obturator neuropathy on pelvic MRI on 2018.9.1
Figure2. Motor nerve conduction study of obturator nerve in gracilis at 2018.10.2

P 126
Sciatic Nerve Injury Caused by Streching for the Adductor muscle – Case report
Min Woo Oh1*
, Goo Joo Lee1†
, Hyeun Suk Seo1
Department of Rehabilitation Medicine, Chungbuk National University Hospital1
Introduction
The sciatic nerve is the largest nerve in the human body and primary continuation of the sacral plexus, which contains nerve fibers
from L4 - S3. The usual causes of sciatic nerve injury are fractures (Pelvic, Acetabular, Femoral), and the other lesion is intramuscular
injection, and neoplasm and laceration, compression (external or internal), ischemia. Sciatic nerve injury casued by hyperstretching
is an extremely rare mechanism
Case report
An 14-year-old female patient who had performed ballet training presented with left foot drop. Based on initial physicial
examination, strength was grade 4 in the left knee flexion and 1 in the left ankle dorsiflexion and long toe extensor. The sensation
was dimished to pinprick and light touch on the left antero-lateral aspect of lower leg. Eighteen days ago she stretched when she
practiced ballet. The posture is the act of stretching both legs apart while lying down and is known as the stretching method of the
adductor. The electrodiagnostic nerve conduction studies were performed in both lower limbs. The superficial peroneal, sural and
deep peroneal sensory nerve action potentials (SNAP) were absent on the left side. The amplitude of compound muscle action
potentials (CMAP) of the deep peroneal motor action potential was markedly decreased than the right side. And its motor
conduction velocity was also lower than the right side. When compared with the right side, the amplitude of CMAP on the left tibial
nerve was less than half. Moving on to the needle elctromyographic examination, left tibialis anterior, peroneus longus,
gastrocnemius (medial head), biceps femoris (short head) showed abnormal spontaneous activity. This electrophysiologic study is
compatible with left sciatic neuropathy, partial axonal injury (more severely involved peroneal portion than tibial portion). Magnetic
resonance imaging (MRI) studies of the lower legs showed signal change at left common peroneal nerve below obturator internus
and it was a suspicious finding to sciatic nerve injury. After the diagnosis, she underwent steroid pulse therapy, EST therapy and
conservative rehabilitation. Follow up EMG at 4 and 7 months after injury showed an increase in peroneal and tibial CMAP. 13
monts after ionjury, electric potential was induced in the sural sensory nerve and we confirmed that abnormal spontaneous activity
disappeared in tibialis anterior and peroneus longus.
Discussion
Hyperstretching is an extremely rare mechanism of sciatic nerve injury. Most of the previous case reports concerning stretch related
injury involved compression and hyperstretching over a long period (ex. lithotomy position for more than 2 hours). Althoug the
exact caus is not yet known, when the sciatic nerve in the gluteal region is damaged, the peroneal division is damaged much more
frequently than the tibial division, like this case. In this case, we can identify sciatic nerve injury due to excessive stretching of the
adductor muscle.

Fig 1. Magnetic resonance imaging (MRI) studies of the left lower legs Table 1. Nerve conduction study
Table 2. Needle electromyography

P127
Suprascapular nerve injury induced by shoulder subluxation: A case report
Hyo Sik Park1*
, Jong Keun Kim1, Jin Seok Bae
1, Yong Sung Jeong
1, Kang Jae Jung
1, Jong Youb Lim
1†
Department of Rehabilitation Medicine, Eulji University Hospital1
Introduction
The suprascapular nerve originates from the upper trunk of the brachial plexus. Suprascapular neuropathy may be caused by
repetitive use, direct trauma, transverse scapular ligament injury, tumors or massive retracted rotator cuff tears. However, it is a
rare conditions that suprascapular nerve damage induced by shoulder subluxation. We report a patient with suprascapular nerve
injury following a shoulder subluxation.
Case report
A 38-year-old man referred to the Department of the Rehabilitation Medicine to evaluate his right shoulder pain. In his past medical
history, he underwent surgery for the right shoulder instability in 2000. The patient slipped down and hit his right shoulder. He felt
right shoulder pain and felt discomfort when moving the glenohumeral joint. He performed a closed reduction immediately. After
closed reduction, he felt discomfort when he raised up his right shoulder and he felt weakness on his right shoulder. On Manual
muscle strength testing, abduction, flexion and external rotation of the right glenohumeral joint were moderately weak. On physical
examination the apprehension test and sulcus test for shoulder joint instability were positive. MRI images showed Bankart fractures
and Hill-Sachs lesions. For further evaluation, we performed electromyography to evaluate weakness of the right shoulder. During
needle electromyography, abnormal spontaneous activities were observed only in the supraspinatus, infraspinatus, deltoid and
teres minor muscle. On the motor nerve conduction test, the right axillary nerve showed reduced compound muscle action
potential (CMAP). The patient underwent open reduction and internal fixation in the Department of Orthopedic surgery. After
surgery, the patient was discharged without complications.
Conclusion
Clinically, injury of the suprascapular nerve may be overlooked at the shoulder subluxation However, through accurate physical
examination and interview with the patient, we performed additional EMG and confirmed suprascapular nerve injury. A function of
the shoulder was significantly impaired in patients with injury of the suprascapular nerve. Therefore, it is important to confirm the
lesion of the suprascapular nerve at the shoulder subluxation.

P 128
Suspected the posterior interosseous nerve injury induced by blind TPI: A case
Hyo Sik Park1*
, Jong Keun Kim1, Jin Seok Bae
1, Yong Sung Jeong
1, Kang Jae Jung
1, Jong Youb Lim
1†
Department of Rehabilitation Medicine, Eulji University Hospital1
Introduction
Myofascial trigger point injections are frequently indicated for myofascial pain syndrome and are performed as blind procedures.
Although these injections are usually safe and effective, complications resulting in pneumothorax, epidural abscess, skeletal muscle
toxicity, intrathecal injection, and nerve injury has been reported. We report a patient with radial nerve injury after blind myofascial
trigger point injection.
Case report
A 53-year old man referred to the Department of Rehabilitation Medicine to evaluate his left wrist drop. He has no significant past
medical history. He visited a local clinic to manage his left shoulder pain. He was given an injection on his shoulder. But the pain
continued, and he underwent a blind myofascial trigger point injection on his left shoulder, elbow, forearm, and hand. Since then,
the left wrist drop has appeared. On manual muscle strength testing, abduction of left 5th finger, radial deviation of the 2nd finger
and finger extension were severely weak but extension and flexion of wrist, supination, and pronation of forearm and extension of
the elbow were normal. There were no hypesthesia, tingling sensation. On physical examination, there were no tinel's sign at wrist,
elbow and radial nerve. For further evaluation, we performed electromyography to evaluate the injury of the left radial nerve.
During needle electromyography, abnormal spontaneous activities were observed in the extensor indicis proprius and extensor
digitorum communis. Triceps brachii, extensor carpi radialis longus, and brachioradialis muscle were normal. On the motor nerve
conduction study, the left radial nerve showed low compound muscle action (CMAP) and slow conduction velocity. On the sensory
nerve conduction study, the superficial radial sensory nerve action potential (SNAP) was normal. After the electromyography, the
symptom improved mildly and he has undergone medication and joint exercises to prevent the complication.
Conclusion
Clinically posterior interosseous neuropathy (PIN) usually occurs as an entrapment under the tendinous Arcade of Froshe. Rarely
other mass lesions result in PIN. In this case, we suspect a nerve injury by injection. Therefore, although blind myofascial trigger
point injection is known to be relatively safe, we advise performing ultrasound-guided injection to prevent complications.

P 129
Isolated unilateral cranial XI nerve palsy after traumatic brain injury: a case report
Jae Joon Lee1*
, Yunsoo Soh1†
, Hee-Sang Kim1, Jong Ha Lee
1, Dong Hwan Yun
1, Jinmann Chon
1, Yong Kim
1, Myung Chul Yoo
1
Department of Rehabilitation Medicine,Kyung Hee University Medical Center1
There have been several reports of various traumatic lower cranial nerve injury that usually followed a fracture through the jugular
foramen or occipital condyle fracture (OCF). Thus, the anatomical location can account for the frequent occurrence of lower cranial
nerve deficits following these fractures but only a few cases are reported and isolated single nerve palsy is extremely rare. We
report a case of skull base fracture near pars vascularis of right jugular foramen, which was clinically associated with isolated cranial
nerve XI palsy with shoulder weakness as the chief complaint.
A 60-year-old male was sent to the emergency department after falling from 3m height during roof repair. He had no particular
history of underlying deseases. He slowly recovered his consciousness after two months of inpatient treatment. According to the
patient, he started noticing weakness in right shoulder movement after the recovery. The symptoms worsened and he visited
rehabilitation unit two months later for further evaluation of the symptoms. On initial assessment, he had difficulty at shrugging and
abduction of right shoulder. At right side, lateral winging scapula and trapezius muscle atrophy was also observed. Other clinical
signs of lower cranial neuropathy (hoarseness, dysarthria, difficulties swallowing) did not appear and no sensory symptoms was
involved.
Brain CT taken at the time of the accident had contusional hemorrhage of the right anterior temporal fossa and subarachnoid
hemorrhage, and fracture of the base of skull extending to the jugular foramina. No abnormal findings were observed on cervical
spine X-ray. Electromyography study revealed positive sharp waves and fibrillation potential in the right trapezius muscle and
positive sharp waves in the right SCM muscle. The interference pattern showed discrete at both trapezius and SCM muscles. Right
cranial XI palsy was confirmed based on the collective findings.
The patient underwent physical therapy for right shoulder weakness. The patient had education for stretching and strengthening
exercises. At three month follow-up, clinically right shoulder weakness and range of motion improved and electromyography
revealed mild improvement with no abnormal spontaneous activity in trapezius, SCM muscles.
Since patients traumatic brain injury could be affected, skull fracture should be considered in patients with isolated cranial XI nerve
injury.

P 130
Popliteal Entrapment Syndrome after Isolated Popliteus Muscle Overuse Injury: Case Report
Miryeong Yang1*
, Jong Ha Lee1†
, Hee Sang Kim1, Dong Hwan Yun
1, Jinmann Chon
1, Yunsoo Soh
1, Yong Kim
1, Myung Chul Yoo
1
Department of Rehabilitation Medicine, Kyung Hee University Medical Center1
Entrapment of the proximal tibial nerve in popliteal fossa is rare in clinical practice, compared to distal tibial neuropathy in the tarsal
tunnel syndrome. We present a case of isolated popliteal muscle injury causing proximal tibial neuropathy.
A 75-year-old man visited our hospital for his left foot pain and weakness started about four months ago. Before the pain started, he
played “Jegi-chagi”, a Korean traditional game, for one week with his left leg. After kicking “Jegi” for one week, he had a left
popliteal painful swelling. He took medication for popliteal painful swelling, and then the symptom subsided. However, pain at left
plantar foot started around one month later. He had no other history of trauma to the knee and foot. At the time of his visit to our
hospital, the left calf was generally soft and had no tenderness. Left plantar foot pain scored 7 in visual analog scale. The sensation
was diminished to light touch on the plantar area of his left foot. He had 4 of 5 strength of big toe dorsiflexion and 2 of 5 strength of
2nd to 5th toes flexion and abduction. Knee stability testing showed negative results. Magnetic resonance imaging of left knee
showed edema and enlargement of the left popliteus muscle with diffuse high signal intensity at T2-weighted fat suppression image.
Nerve conduction study showed decreased compound muscle action potential (CMAP) amplitude and delayed CMAP latency in the
left tibial nerve. The amplitude of sensory nerve action potential was unobtainable in the left medial plantar nerve and lateral
plantar nerve. The needle electromyography study showed abnormal spontaneous activities and discrete recruitment patterns at
left abductor digiti quinti, abductor hallucis and tibialis posterior. Under the basis of these results, we confirmed his diagnosis with
proximal tibial neuropathy caused by isolated popliteus muscle injury.
Isolated popliteus injury is uncommon. It typically occurs after a traumatic event, such as external rotation of slightly flexed knee or
a twisting injury. Playing “Jegi-chagi” consists of repetitive motion of internal rotation of the tibia on the femur. It might cause
overuse of popliteus muscle. Our case is rare and unique in that proximal tibial neuropathy was caused by compression related to
mass effect from the enlarged popliteus muscle.

P 131
Esophagostomy, an alternation of PEG or PRG for dysphagia in muscular dystrophy : A case report
Jin Seok Bae1*
, Jong Keun Kim1, Yong Sung Jeong
1, Hyo Sik Park
1, Jong Youb Lim
1, Kang Jae Jung
1†
Department of Rehabilitation Medicine, Eulji University Hospital1
Introduction
The muscular dystrophy is a group of disease that causes weakness and loss of mass. Progressive mobility impairment and
dysphagia may limit the ability of the patient with a myopathy to self-feed. When feeding becomes insufficient to meet the patient’s
needs, a discussion should address treatment strategies including the placement of a gastrostomy tube. We report that performed
other methods, esophagostomy when we were unable to do gastrostomy.
Case Report
A 40-year-old man known as muscular dystrophy admitted to the Department of Rehabilitation Medicine to perform gastrostomy
tube for deteriorated dysphagia. He applied a home ventilator for all day long. The patient could not use a nasogastric tube because
he applied a mask. Also, it was difficult to perform endoscopic gastrostomy, so we planned radiologic gastrostomy. He took chest
and abdomen radiograph for further evaluation.
Abdomen radiograph showed paralytic ileus. Radiologic gastrostomy or jejunostomy was considered to be high risk because
transverse colon was located on the stomach and jejunum. Therefore, there was no space for entering gastrostomy or jejunostomy.
By using an orogastric and rectal tube, abdominal decompression was performed. However, paralytic ileus did not improve. Finally,
we consult the Department of Radiology to perform fluoroscopy guided esophagostomy. After esophagostomy, there was no
complication. The patient could get sufficient nutritional support by esophagostomy tube. After 2 weeks, the patient was able to
oral feeding.
Conclusion
In severe myopathies, individuals may develop nutritional inadequacy as their disease progress. When feeding becomes insufficient
to meet the patient’s needs or the time and effort required for consuming meals negatively impacts the quality of life, a discussion
should address treatment strategies. Esophagostomy can be a good treatment option that can be performed in patients who do not
undergo percutaneous endoscopic gastrectomy or jejunostomy.

Figure 1. Simple x-ray showed Esophagostomy tube.
Figure 2. CT showed colonic gas in front of stomach.

P 132
Peroneal nerve compression secondary to weight loss : slimmer’s paralysis
Ji Hong Min1*
, Eun-Ho Yu1, Hyun-Yoon Ko
1, Soo-Yeon Kim
1†
Department of Rehabilitation Medicine, Pusan National University Yangsan Hospital1
Peroneal neuropathy is the most frequent mononeuropathy encountered in the lower limb, resulting in foot drop. We reports a
case of the unilateral peroneal neuropathy after weight reduction.
A 39-year-old women complained weakness on her left foot for two weeks. She had lost 16kg within a month. She had no
comorbidity. She was, then, referred to our electromyography (EMG) laboratory. She had habitual leg crossing and weakness of the
left ankle dorsiflexion and eversion (2/5) and weakness of the left toe extension (2/5). The strength of other muscles was normal.
She had also hypoesthesia at the dorsum of the left foot. Deep tendon reflexes on upper and lower extremities were normal.
Pathologic reflex was not elicited. The laboratory findings and imaging findings were normal. The compound muscle action potential
(CMAP) was recorded with a surface electrode placed on extensor digitorum brevis muscle (EDB) for deep peroneal nerve motor
conduction study. The supramaximal stimulation was done at ankle, above, and below the fibular neck. The motor conduction
velocity at the left fibular head were slowed (left: 30.0 m/s, right: 59.0m/s, normal: >40 m/s). The CMAP amplitude loss about 91%
was observed at the left fibular head. Sensory nerve action potential (SNAP) showed reduced amplitudes in the left superficial
peroneal sensory nerve conduction study. Other nerve conduction studies were within normal limits. Abnormal spontaneous
activities were observed on needle EMG of the left tibialis anterior and peroneus longus muscles. Reduced recruitment of motor
unit potentials were seen in tibialis anterior and peroneus longus muscle. Needle EMG studies of the other muscles in lower
extremities were normal. These findings were compatible with conduction block and partial axonal loss of peroneal nerve around
the left fibular head.
Our case report demonstrating peroneal neuropathy caused by weight loss. Many cases have been published about the correlation
between peroneal neuropathy and weight loss, such as diets, malnutrition, anorexia, and severe diseases including malignant
diseases, but, there have been published reports rarely in Korea. Physicians need to be alert about peroneal neuropathy which
develops after weight loss.

P 133
Intrathecal Baclofen Trial in Stiff Person Syndrome
Young Je Kim1*
, Yongmin Choi1, So Young Lee
1, Du Hwan Kim
1†
Department of Rehabilitation Medicine, Keimyung University Dongsan Medical Center1
Introduction
Stiff Person Syndrome (SPS) is a rare neuroimmunological disorder characterized by progressive and fluctuating muscular rigidity
and painful spasm affecting both the axial and peripheral musculature. A large proportion of SPS patients report difficulty
performing activities of daily living independently and requiring an assistive device for safe ambulation. Treatments such as long
acting benzodiazepine, antispasmodic agents, intramuscular botulinum toxin A are used to symptomatic therapy. Recently,
immunomodulating agents and intrathecal baclofen (ITB) have been described in the management of SPS. ITB achieves therapeutic
cerebral spinal fluid levels with much smaller doses compared to oral medications while reducing systemic side effects. We
introduce a case of ITB trial in SPS.
Case report
A 36-year-old woman presented with 1-year progressive rigidity and pain in her proximal upper and lower limbs. On physical
examination, generalized rigidity and spasm were noted in the proximal upper and lower extremities. Electromyography (EMG)
revealed continuous motor unit activity in the agonist and antagonist muscles. Brain magnetic resonance image (MRI) was normal.
Based on the clinical features and typical EMG finding, she was diagnosed as having SPS. <br>We attempted to administer oral
diazepam, intravenous steroid and intravenous immunoglobulin (IVIG), but only transient improvement of muscle rigidity and pain
was observed in IVIG treatment. Because her symptoms worsened despite continued treatment attempts, we tried intrathecal
baclofen by other treatment option.
She was underwent three times of test injection to find optimal doses (6.25, 12.5 and 18 micrograms). Assessments include
modified Ashworth scale (MAS) for evaluation of rigidity, gait speed, and gross photo for muscle bulk evaluation at baseline, 2, 4,
and 8 hours after the procedure. The most effective dose was 12.5 mcg considering improved walking speed and improved muscle
stiffness. At 12.5 mcg dose, the decrease in muscle mass was prominent at 4 hours and 8 hours after the procedure. (Figure 1) The
gross changes and stiffness of upper extremity muscle did not change before and after the procedure in all trials.
Discussion
SPS management is challenging when there are no effective oral medication and injectable agents. ITB is an effective therapy for
refractory spasticity of cerebral or spinal origin. Several case reports and one case series have examined ITB usage in SPS. We
confirmed effectiveness of ITB in SPS also. ITB usage may be another treatment option for SPS patients who have less effect in
primary and secondary treatment.
Fig 1. Inspection of the both proximal leg. (A) The patient’s both quadriceps and adductor muscles during rest was prominent at the baseline. (B)(C)(D) Muscle mass was reduced at the 1 hours, 4 hours, and 8 hours after intrathecal baclofen injection. (At 12.5 mcg dose)

P 134
Mononeuropathy multiplex associated with livedoid vasculopathy : A case report
Dongwoo Lee1*
, Minsuk Kang1, Dae-Hyun Jang
1†
Department of Rehabilitation Medicine,Incheon St. Mary’s Hospital, College of Medicine, The Catholic University of Korea,
Incheon;1
Introduction
Livedoid vasculopathy is a chronic, painful, thrombo-occlusive cutaneous vasculopathy that involves the lower extremities. It is a
rare disease that has the clinically characteristic clinical features of livedoid skin changes (linear or angular, erythematous nodules),
atrophie blanche (smooth, ivory-white plaques), and recurrent painful ulceration. It is most common in young to middle-aged
women, and the course seems to be chronic with seasonal exacerbations.
The pathogenesis of livedoid vasculopathy is controversial and the disorder can be a primary or a secondary manifestation of
inflammatory and hypercoagulation disorders. The diagnosis of this disease relies on clinical features and skin biopsy.
Systemic involvement is not common and clinical symptoms of this disease are mainly limited to skin. Peripheral nervous system
involvement may occur due to multifocal thrombosis and ischemia of the vasa nervorum, but such cases are rare. So, we report a
patient presenting with mononeuropathy multiplex combined with livedoid vasculopathy, which was confirmed by
electrophysiological and pathological studies.
Case report
A 46-year-old woman visited our clinic complaining of left leg pain and foot drop in in February 2019. She had suffered from
radiating pain in left lower extremity three months ago. She was diagnosed with livedoid vasculopathy in 1996 and was taking
medication at another hospital.
On admission, neurological examination showed severe weakness in left ankle dorsiflexion and great toe extension (grade 0) and
mild weakness in left ankle eversion, inversion, and plantarflexion. There was no sensory loss or pathologic reflex, and tendon reflex
was normal. The patient had ulcerative skin lesions with livedo reticularis and multiple purpuric patches at the both ankles and distal
lower legs. There were also painful chronic ulcerations in left foot with fibrosclerotic white scars.
Nerve conduction study showed axonal injury of both sensory and motor fibers nerve and sural nerves (table 1). In needle
electromyography, there was no motor unit action potential in left tibialis anterior muscle, and no abnormal findings were found in
other sampled muscles. This supported a diagnosis of mononeuropathy multiplex. At this stage, sural nerve biopsy was performed
on the left sural nerve. Microscopic pathological examination represented asymmetric loss of myelinated fibers both within and
between fascicles. There were hyalinized dermal blood vessels with intravascular thrombosis in the perineurium and extensive
infarct of the peripheral nerve and Schwann cells. Perivascular mononuclear cell infiltrates were rarely observed.
This patient was diagnosed with ischemic neuropathy associated with livedoid vasculopathy and treated with enoxaparin and oral
methylprednisolone. Five days after the start of treatment, enoxaparin was converted to rivaroxaban. After a follow-up period of 2
weeks, neurological symptoms had considerably improved.

Fig 1. Sural nerve biopsy. (A) hyalinized dermal blood vessels with intravascular thrombosis (B) Severe loss of myelinated fibers and some axonal degeneration due to ischemic necrosis (paraffin section, hematoxylin–eosin staining, ×100).

Table 1. Nerve conduction study. (A) Sensory nerve conduction study. (B) Motor nerve conduction study.
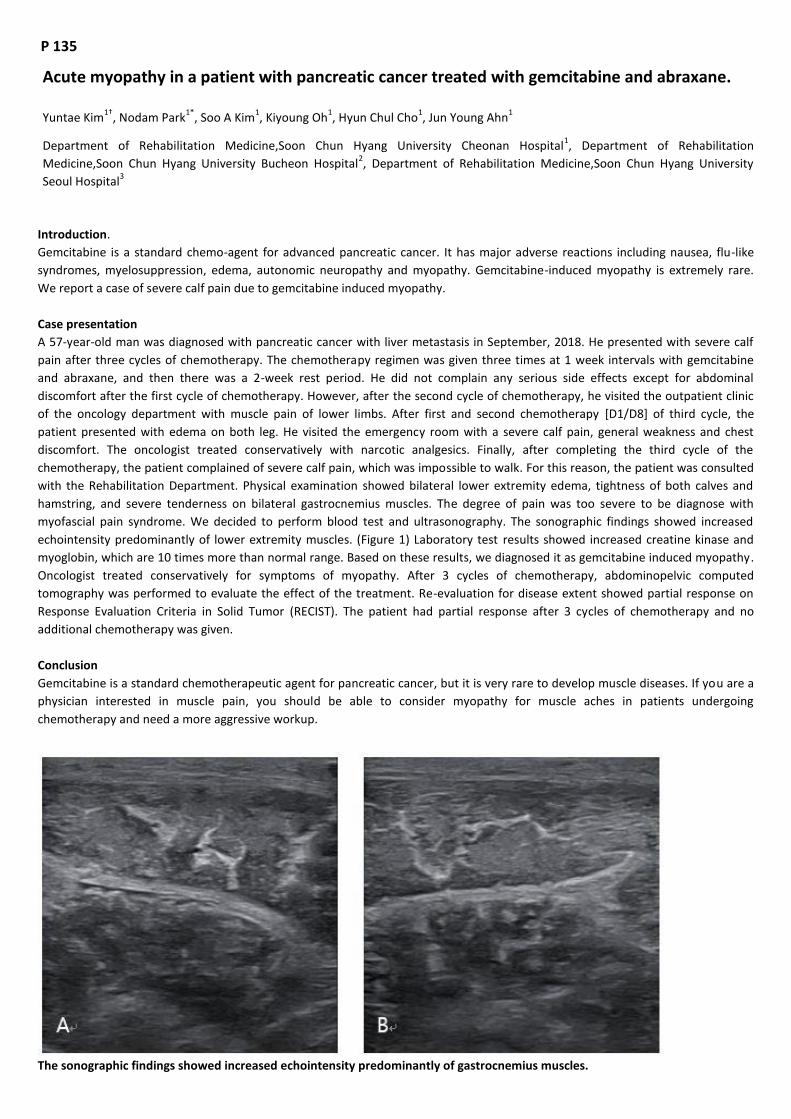
P 135
Acute myopathy in a patient with pancreatic cancer treated with gemcitabine and abraxane.
Yuntae Kim1†
, Nodam Park1*
, Soo A Kim1, Kiyoung Oh
1, Hyun Chul Cho
1, Jun Young Ahn
1
Department of Rehabilitation Medicine,Soon Chun Hyang University Cheonan Hospital1, Department of Rehabilitation
Medicine,Soon Chun Hyang University Bucheon Hospital2, Department of Rehabilitation Medicine,Soon Chun Hyang University
Seoul Hospital3
Introduction.
Gemcitabine is a standard chemo-agent for advanced pancreatic cancer. It has major adverse reactions including nausea, flu-like
syndromes, myelosuppression, edema, autonomic neuropathy and myopathy. Gemcitabine-induced myopathy is extremely rare.
We report a case of severe calf pain due to gemcitabine induced myopathy.
Case presentation
A 57-year-old man was diagnosed with pancreatic cancer with liver metastasis in September, 2018. He presented with severe calf
pain after three cycles of chemotherapy. The chemotherapy regimen was given three times at 1 week intervals with gemcitabine
and abraxane, and then there was a 2-week rest period. He did not complain any serious side effects except for abdominal
discomfort after the first cycle of chemotherapy. However, after the second cycle of chemotherapy, he visited the outpatient clinic
of the oncology department with muscle pain of lower limbs. After first and second chemotherapy [D1/D8] of third cycle, the
patient presented with edema on both leg. He visited the emergency room with a severe calf pain, general weakness and chest
discomfort. The oncologist treated conservatively with narcotic analgesics. Finally, after completing the third cycle of the
chemotherapy, the patient complained of severe calf pain, which was impossible to walk. For this reason, the patient was consulted
with the Rehabilitation Department. Physical examination showed bilateral lower extremity edema, tightness of both calves and
hamstring, and severe tenderness on bilateral gastrocnemius muscles. The degree of pain was too severe to be diagnose with
myofascial pain syndrome. We decided to perform blood test and ultrasonography. The sonographic findings showed increased
echointensity predominantly of lower extremity muscles. (Figure 1) Laboratory test results showed increased creatine kinase and
myoglobin, which are 10 times more than normal range. Based on these results, we diagnosed it as gemcitabine induced myopathy.
Oncologist treated conservatively for symptoms of myopathy. After 3 cycles of chemotherapy, abdominopelvic computed
tomography was performed to evaluate the effect of the treatment. Re-evaluation for disease extent showed partial response on
Response Evaluation Criteria in Solid Tumor (RECIST). The patient had partial response after 3 cycles of chemotherapy and no
additional chemotherapy was given.
Conclusion
Gemcitabine is a standard chemotherapeutic agent for pancreatic cancer, but it is very rare to develop muscle diseases. If you are a
physician interested in muscle pain, you should be able to consider myopathy for muscle aches in patients undergoing
chemotherapy and need a more aggressive workup.
The sonographic findings showed increased echointensity predominantly of gastrocnemius muscles.

P 136
Gluteal Nerve Injury after Radical Hysteretomy ; A Case Report
Da Hwi Jung1*
, Ji Won Hong1, Sang Hun Kim
1, Yong Beom Shin
1†
Department of Rehabilitation Medicine, Pusan National University Hospital1
Introduction
Gluteal nerve consists of superior gluteal nerve and inferior gluteal nerve. Superior gluteal nerve, derives from L4 to S1, involves in
hip abduction. Inferior gluteal nerve arising from L5 to S2, mainly innervates gluteus maximus and extends the hip. Both nerves are
part of lumbosacral trunk and escapes pelvic cavity through greater sciatic foramen and runs under the pyriformis muscle. Gluteal
nerve injury usually occurs at hip arthroplasty, which approach on the lateral or posterior side of the hip. On contrast, hysterectomy,
which approach pelvic cavity anteriorly and rarely damages the gluteal nerve.
In this case report, the patient demonstrates weak right hip abduction and flexion after radial hysterectomy. The symptom was
revealed as a result of gluteal nerve and femoral nerve injury. This unusual case of gluteal nerve injury after hysterectomy was
diagnosed by electromyogram (EMG).
Case Report
The 66-year-old female patient complained of right thigh and buttock pain with motor weakness of the proximal part of right leg
after hysterectomy. She was diagnosed as cervical cancer and underwent the radical hysterectomy with bilateral salpingo-
oophorectomy with bilateral pelvic lymphadenectomy and paraaortic lymph node dissection. After surgery, she exhibited gait
abnormality with motor weakness of her right lower extremity: right hip flexor and abductor were poor (P) grade on manual muscle
test (MMT). Excessive right hip external rotation was noted at swing phase of gait (Fig. 1.). To diagnose the cause of her motor
weakness, EMG was done at the Department of Rehabilitation 43 days after the surgery (Table 1.). The needle EMG performed on
right gluteus medius and maximus, tensor fascia lata and iliacus muscle revealed increased insertional activity and some abnormal
fibrillations (Fibs) and positive sharp waves (PSWs) at rest and reduced recruitment of motor units on volition and decreased
interference on full volition. Hence, right superior and inferior gluteal nerve lesions with right femoral nerve injury were diagnosed.
On follow-up examination 81 days after the surgery, she showed improvement of muscle strength: right adductor and hip flexor
were fair (F) grade on MMT compared to P grade at first. Follow-up EMG done on the same day showed improvement of gluteal
nerve injury: interference improved from 25% to 75% and normalized spontaeous activity and recruitment ratio were noted (Table
2.).
Discussion
Nerve injury during hysterectomy may occur by malpositioning of retractor, prolonged lithotomy position and by surgical incision.
Since neuropathy after hysterectomy has low prevalence, it is difficult to diagnose motor weakness or pain after the surgery.
Therefore, surgeons should keep in mind that any nerve injury during pelvic cavity operation is possible and it can be prevented by
correct positioning and nerve-sparing surgical technique.

Figure 1. Gait pattern of the patient: Excessive external rotation of right hip during the swing phase of gait
Table 1. Findings of needle electromyogram 43 days after the surgery
Table 2. Findings of needle electromyogram on 81 days after surgery


P 137
Winged scapula due to congenital abnormalities of scapular without neurological injury
So Yeon Jun1*
, Seong Hoon Lim2, Bo Young Hong
2, Joon Sung Kim
2†
Department of Rehabilitation Medicine,Seoul St. Mary's Hospital, College of Medicine, The Catholic University of Korea1,
Department of Rehabilitation Medicine,St. Vincent’s Hospital, College of Medicine, The Catholic University of Korea2
Introduction
A winged scapula is a skeletal problem in which the shoulder bone protrudes from a person’s back as a faulty position. Though the
most common causes of a winged scapula is due to serratus anterior palsy, and less commonly trapezius and rhomboid palsy.
Electrodiagnostic study is important tool in differentiating those neuropathies. Also these needs to be considered the other
situation like structural abnormalities such as the injury of scapulothoracic muscles. Here, we introduce a case report of young
patient with winged scapula due to congenital scapular abnormalities without neurological injury
Case report
A 20 year old man visited our clinic referred from orthopedics department for electrodiagnostic exam for winged scapula on right
side (Figure 1). There was no specific finding in the birth or growth periods and there was no particular problem in doing daily life.
However, after enlistment in the army, he felt the discomfort with a heavy backpack. He didn’t know the exact onset time for that
symptom. On physical examination, there was weakness of the abduction or flexion of right shoulder compared to left side as grade
fair. There was no sensory change and deep tendon reflex was normoactive in bilateral upper extremities. Cervical spine x-ray
showed just narrowing of neural foramina, left side of C4/5 and C5/6. On the nerve conduction study (NCS), normal range of peak
latencies, amplitudes of SNAPs and onset latencies, amplitudes of CMAPs in all sampled nerves including accessory, axillary, long
thoracic, musculocutaneous and suprascapular nerves in bilateral sides (Table 1). On needle electromyography, there was no
abnormal spontaneous activities were noted in the all sampled muscles with normal configuration of MUAPs on minimal volition.
Just only reduced interferential patterns on maximal volition in bilateral serratus anterior and right upper trapezius muscles were
showed (Table 2). In magnetic resonance imaging of right shoulder there were partial tears at superior tendinous portion of right
subscapularis and supraspinatus muscles. On the image of computed tomography of upper extremities, only minimal instability was
suspected with slight deformed contour in the sternoclavicular joint. With these findings we considered the congenital
abnormalities of scapula without nerve injury for the reasons of those symptoms.
Conclusion
Long thoracic neuropathy is major cause of winged scapula. In cases without nerve injury, there were some reports about the
causes of winged scapula was related to a lengthening or weakness of serratus anterior muscle. In our case the patient also showed
the weakness of serratus anterior muscle power compared to another side. On the physical exam, the asymmetry of both clavicle
and scapulothoracic joints was also showed. Therefore, we should be interested in not only the presence of nerve injury but also the
structural asymmetry of the joint in the patients with winged scapula.
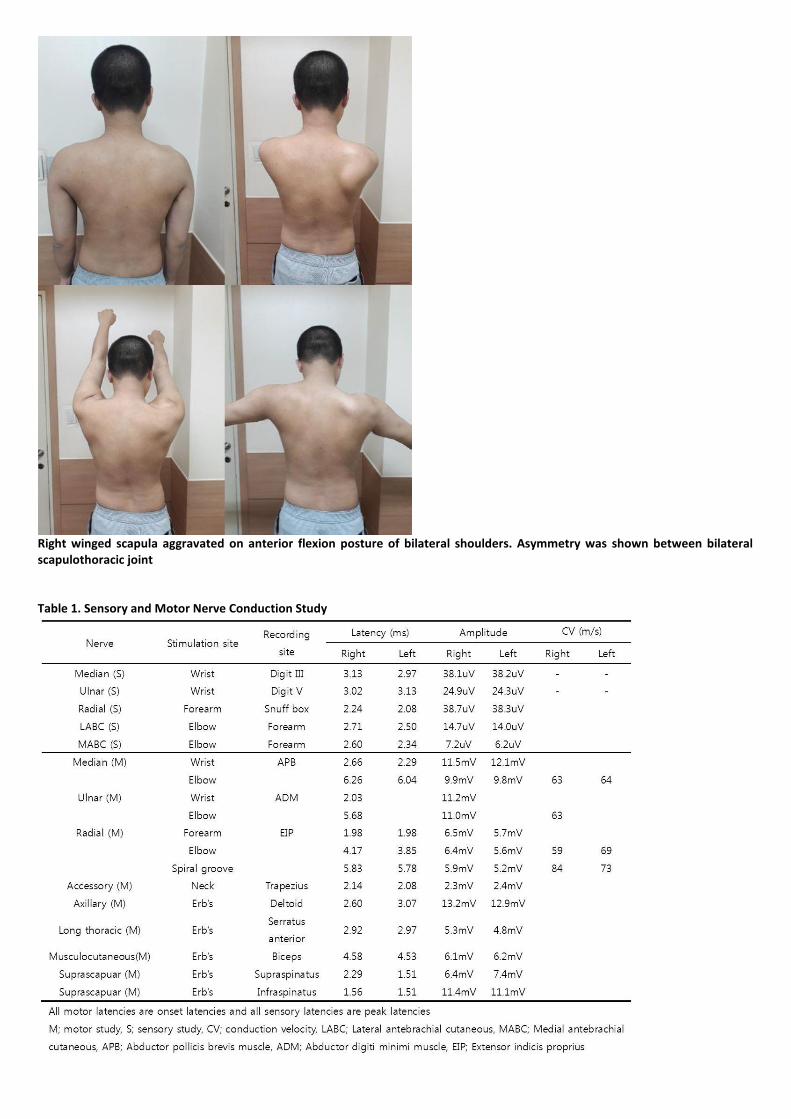
Right winged scapula aggravated on anterior flexion posture of bilateral shoulders. Asymmetry was shown between bilateral scapulothoracic joint Table 1. Sensory and Motor Nerve Conduction Study

Table 2. Needle Electromyography Study

P 138
Mononeuritis multiplex misdiagnosed as Lumbosacral Radiculopathy
Yun jeong Jang1*
, Chang Han Lee1, Min Kyun Oh
1, Eun Shin Lee
1, Hee Suk Shin
1, Chul Ho Yoon
1†
Department of Rehabilitation Medicine, Gyeongsang National University School of Medicine and Gyeongsang National University
Hospital1
Introduction
Vasculitis means damage to the blood vessel wall due to the infiltration of inflammatory cells. Clinical symptoms are associated with
ischemic injury to the organ receiving blood supply by damaged blood vessels. Peripheral nervous system involvement is common in
systemic vasculitis and is sometimes the first symptom of systemic vasculitis. Vasculitic neuropathy manifests in form of
mononeuritis multiplex but in some patients it may occur in form of symmetric sensory motor neuropathy involving the distal part.
We report a case of mononeuritis multiplex that was misdiagnosed as lumbosacral radiculopathy in a patient with rheumatoid
arthritis.
Case presentation
In this case report, a 71-year-old female patient presented with severe back pain, symmetrical distal lower limb weakness and
sensory abnormalities in her distal lower limbs for 2 months. Initially this was thought to be the result of lumbar radiculopathy or
peripheral polyneuropathy. Electrodiagnosis was performed and then diagnosed as lumbosacral radiculopathy and peripheral
polyneuropathy (Table 1). After about 10 to 14 days, motor weakness and sensory loss in the lower extremities worsened,
accompanied with severe pain. Mononeuritis multiplex was diagnosed on a follow – up electrodiagnosis (Table 2). The evidence of
progressive peripheral polyneuropathy over the distal limbs was observed compared with the previous study. The nerves that were
involved were both the tibial, common peroneal, median and ulnar nerves. Thereafter, the patient was transferred to rheumatology
department for treatment on the vasculitis and mononeuritis multiplex. Steroid pulse therapy was attempted, however, due to large
amount of rectal bleeding after the first session, the treatment was not completed. After 10 months, the patient still had symptoms
of distal limb weakness and sensory loss but the severity of the pain was greatly reduced.
Conclusion
Patients in the early stages of vasculitic neuropathy may present with features of lumbosacral radiculopathy. The diagnosis of
vasculitic neuropathy can be made through continuous checks on the progress of the symptoms occurring within a short period of
time and by conducitng serial electrodiagnosis. In the case of this patient, prognosis would be good if early treatment was possible
with rapid diagnosis. Proper early diagnosis enables early treatment and reduces complications and mortality.
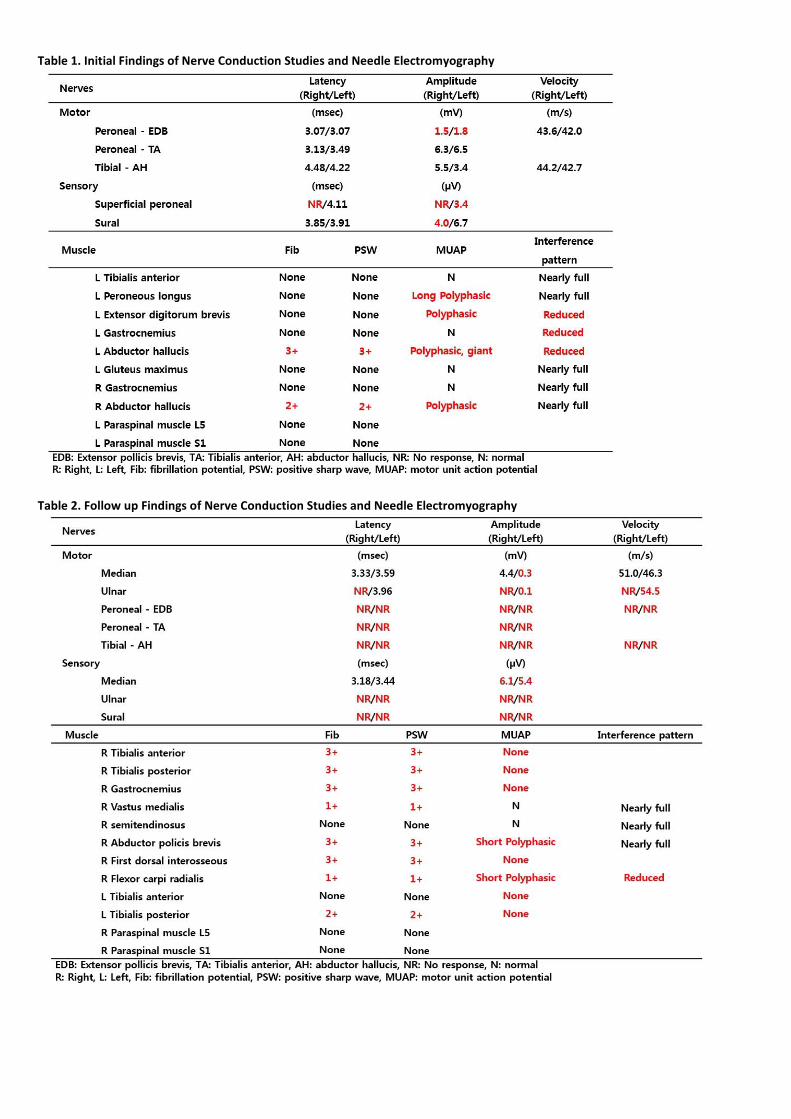
Table 1. Initial Findings of Nerve Conduction Studies and Needle Electromyography
Table 2. Follow up Findings of Nerve Conduction Studies and Needle Electromyography

P 139
T1 spinal nerve schwannoma presenting as a lung mass : Case Report
Joung Hyun Doh1*
, Yuntae Kim1†
, Soo A Kim1, Ki Young Oh
1, Jin Young Kim
2, Sang Hoon Lee
3
Department of Physical Medicine & Rehabilitation,Soonchunhyang University College of Medicine, Cheonan, Korea1, Department of
Physical Medicine & Rehabilitation,Soonchunhyang University College of Medicine, Bucheon, Korea2, Department of Physical
Medicine & Rehabilitation,Soonchunhyang University College of Medicine, Seoul, Korea3
Introduction
Schwannoma is nerve sheath tumor composed of Schwann cells, which normally produce the insulating myelin sheath covering
peripheral nerves. Large schwannoma in the spine are relatively rare, usually expand into the mediastinum and retroperitoneum
and can reach considerable size before they become symptomatic. The patients mostly complain of nerve compression symptoms
during the growth of the mass, with numbness and pain in the corresponding limb. In this case, we present a patient with painless,
isolated mass on right mediastinum.
Case presentation
A 33-year-old woman showing suspicious lung mass in chest x-ray was admitted to hospital at pulmonology department for the
evaluation. The patient had no specific past medial history and did not show any symptoms. The lung mass was in RUL, and after
bronchoscopy and PTNB, the result of immunohistochemical stain showed S-100 protein (+), Ki-67 (+), SMA, Desmin, CD34 (-),
revealed the mass as schwannoma. The mass was 3cm sized, well-marginated extrapleural mass of the pleural wall located in Right
upper hemithorax. She was admitted to hospital again at cardiovascular surgery department for ‘Resection of mediastinal mass via
VATS’. During the operation the mass was found close to subclavian vessels and had adhesions with small vessels. 1 month after
surgery, she complained weakness in hand intrinsic muscles, and hypoesthesia on right upper arm and forearm, and hypohidrosis on
right hand, axillar, and face. The follow up chest CT showed remnant post-op. granulation tissue with calcification in right apex, but
other than that no abnormality was found. So she was referred to physical medicine and rehabilitation department for evaluation of
the symptoms. After close physical examination, weakness was showed in right abductor pollicis brevis and abductor digiti minimi
muscles, and hypoesthesia was showed in medial antebrachial cutaneous and medial brachial cutaneous nerve. We performed
electromyography on right upper extremity and found out the amplitude of sensory nerve action potential of right medial brachial
cutaneous nerve, and abnormal spontaneous activity was showed in abductor pollicis brevis and first dorsal interossei muscles. So
we concluded as injury of T1 spinal nerve lesion. Two months after surgery, her symptoms improved and only numbness on right
MBC and MABC areas was remained.
Conclusion
We report a case of T1 spinal nerve schwannoma which first presented as a lung mass. Primary benign spinal neoplasm and lung
cancer require different surgical strategies and treatment, so we must consider the possibility of malignant neoplasm when
confronted by single spinal mass. Large benign schwannomas are rare. But in most cases it can be treated through one surgical
approach such as complete resection, and expecting a good postoperative prognosis. Although we should always be aware of the
possible recurrence of spinal schwannomas, and a long-term follow-up is recommended.
Fig1. X-ray and Chest CT images, showing lung mass in Rt. Apex., coronal / axial/ sagittal view(A, B, C)

Fig2. X-ray image of the chest, 2 weeks after the surgery (A), Chest CT image, 1 month after the removal of mass showing granulation tissue with calcification (B)

P 140
A Case of a Patient with Guillain-Barre Syndrome with Severe Sensory Impairment
Chang Bae Lee1*
, Eun Jae Ko1†
Department of Rehabilitation Medicine, Ulsan University Hospital1
Introduction
Guillain-Barre syndrome (GBS) is a rapid-onset muscle weakness cause by the immune system damaging the peripheral nervous
system. The initial symptoms are typically changes in sensation or pain along with muscle weakness, beginning in the feet and hands.
We report a rare case of a patient with GBS who mainly had a symptom of severe sensory impairment.
Case
A 40-year-old man without any past medical history and infection history had tingling sensation of both hands one month ago, and
the symptom progressed to both feet. Afterward, he began to have some difficulty of sit to stand independently. He was admitted
to the Department of Neurology for evaluation. Initial physical examination of the patient revealed muscle weakness at fingers,
ankles, and big toe grade 3. He appealed reduced sensation at both hands and feet. In detail, pain and temperature was check 6-7
out of 10, and touch and vibration was 5-6 out of 10. Deep tendon reflex was hyporeflexic, and there is no facial palsy. Brain MRI
was normal, and there is no signal intensity change in spinal cord, small central herniated disc, C5/6, C6/7, and central extruded disc
L5/S1 in spine MRI. NCS results on 1st and 23rd day of admission are presented in Table 1. Decreased CMAP was checked in both
studies, which showed mild improvement on 23rd day compared to the 1st day. Both studies showed no sensory nerve action
potential and no F-wave in both peroneal and Lt. tibial nerves, and increased latency in Rt. tibial nerve. Needle EMG done on 23rd
day of admission confirmed abnormal spontaneous activity and reduced recruitment and polyphasic MUAP in Lt. abductor pollicis
brevis, Lt. 1st dorsal interossei, Rt. Gastrocnemius, and Rt. Peroneus longus muscles. Cerebrospinal fluid test showed normal.
Enzyme-linked immunosorbent assay for IgG and IgM antibodies against GM1, GD1b, GQ1b were negative. In laboratory test, HBsAg,
anti-HBs, anti-HAV, anti-HCV were negative, and increased AST/ALT (293/293) was checked. Result of abdomen US was moderate
fatty liver, mild splenomegaly. Based on clinical features, laboratory findings, and electrophysiologic investigation, the patient was
diagnosed the acute motor sensory axonal neuropathy (AMSAN), one of the subtype of GBS. He was treated with intravenous
immunoglobulin for 5 days. He was transferred to the Department of Rehabilitation on 10th day of admission. He could gait with
minimal assist, however, he had severe sensory impairment at both hands and feet (Table 2). After 3 weeks of the physical and
occupational therapies including sensory stimulation and sensory integration, he could gait with supervision, but his sensory
impairment did not improve much (Table 2). K-MBI score was 92, and AST/ALT level became normalized.
Conclusion
This case shows a rare case of a patient with GBS who mainly had a symptom of severe sensory impairment which did not improve
much. The long term follow up of the patient is needed for evaluation of prognosis.
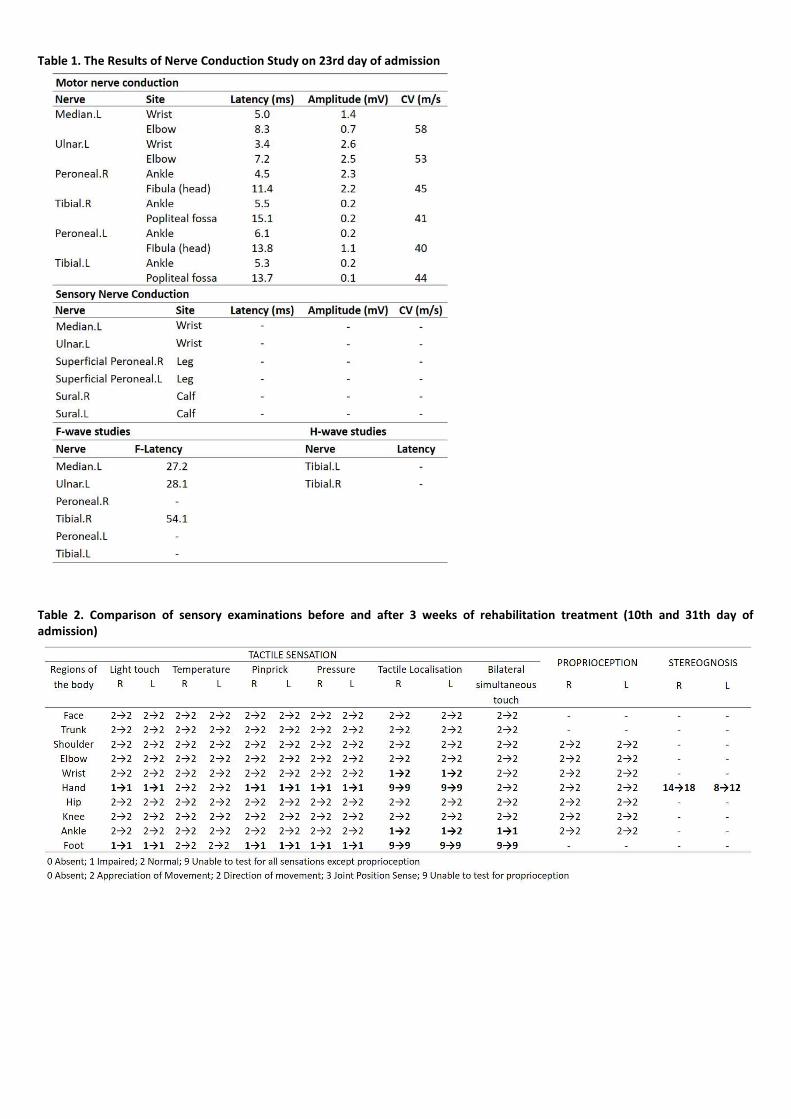
Table 1. The Results of Nerve Conduction Study on 23rd day of admission
Table 2. Comparison of sensory examinations before and after 3 weeks of rehabilitation treatment (10th and 31th day of admission)

P 141
Emery-Dreifuss muscular dystrophy due to SYNE2 gene mutation: A case report
Sook Joung Lee1*
, Eun-Seok Choi1†
, Sang Ji Lee1, Mi Kang Kim
2, Saerom Kang
1
Department of Rehabilitation Medicine, The Catholic University of Korea Daejeon St. Mary`s Hospital 1, Department of
Rehabilitation Medicine,The Catholic University of Korea Bucheon St. Mary`s Hospital 2
Emery-Dreifuss muscular dystrophy (EDMD) is a rare, a genetic disorder which presents slowly progressive skeletal muscle weakness.
Most EDMD is inherited as an X- linked, and rarely inherited as an autosomal dominant (AD) disease. Mutations in six genes (EMD,
LMNA, SYNE1, SYNE2, FHL1 and TMEM43) are associated with the EDMD.
We report a patient who showed AD inheritance EDMD due to SYNE2 gene mutation. Interestingly, different from other muscular
dystrophy, he showed neuropathic pattern in electrodiagnostic study.
Case report
55 years old male was visited to the outpatient department of rehabilitation to get a medical certificate for applying social welfare
services. He was diagnosed as a progressive muscular disorder when he was 23 years old (nearly 30 years ago) in another hospital
through the electrodiagnostic study. At that time, his social economic status was low and he couldn’t evaluate for his exact diagnosis.
This time, he wants to know his exact diagnosis, because his only son showed progressive muscle weakness like the patients. His
Next-Generation Sequencing showed that mutation of SYNE2 gene which is related to EDMD.
The patient was normal at birth and healthy until 8 years old. When he was nine, he showed waddling gait and suffered frequent
ankle inversion event. When he was twenty, muscle power of lower extremities showed progressively weakness and both calf
muscle start to atrophy. When he was 30 years old, both upper extremities weakness and hand intrinsic muscle atrophy was also
started, and his gait function was progressively decrease and he only could indoor gait with cane. When he was 40 years old, his
upper and lower muscle weakness and atrophy were aggravated, and he could not gait et al, and he had to use wheelchair for
ambulation.
In the physical Examination, motor power was decreased on both upper and lower extremities, proximal weakness was
predominant (shoulder and hip girdle: trace, elbow, wrist, hand, and ankle: trace to poor). He has multiple joint contractures on
both hip, shoulder, ankle, and hand joints. And he showed muscle atrophy on all extremities. Deep tendon reflex showed hypoactive,
and no pathologic reflex was checked. Laboratory test showed normal CK level (102 IU/L) and cardiac markers (CK-MD, Troponin,
ProBNP). Echocardiogram showed normal function, and ejection pressure of LV was 63.2%. His pulmonary function test revealed
mild restrictive lung defect, and functional vital capacity was 2.41 Liter (55% of estimated level).
In his familial history, his parents were healthy but died when the patients visit our clinic, and his siblings were all healthy. His only
son was affected when he was 15 years old.
Electrodiagnostic study showed generalized sensorymotor neuropathy. Motor and Sensory nerve conduction study showed delayed
latency and decreased amplitude in all extremities (Fig.2). Needle EMG showed abnormal spontaneous activity and large amplitude
long duration MUAP in all extremities (Fig.3)
Fig 1. Pedigree analysis of the proband (arrow) with de nove mutation in SYNE2 gene

Fig 2. Nerve conduction study of the patient
Fig 3. Needle EMG of the patient

P 142
So youn Chang1*
, Sang jee Lee1†
Department of Rehabilitation Medicine,Daejeon St. Mary’s Hospital, The Catholic University of Korea1, Department of
Rehabilitation Medicine,Daejeon St. Mary’s Hospital, The Catholic University of Korea2
Introduction
One of the most common injury from deadlifting is back strain or hamstring injury. We report a rare case of sciatic nerve injury only
involving tibial component during deadlifting.
Case
A 68-year-old man visited our clinic with left thigh pain. A month ago, while lifting 30 kg barbell, he happened to lost his balance and
supported on left leg. At that time, he felt extremely sharp radiating pain to left calf. The pain was so severe that it was hard to walk
without crutch for a week. On physical examination, left posterior calf and lateral foot areas’ sensation was slightly decreased. There
was no weakness of hip, knee, ankle and great toe. Deep tendon reflex and pathologic reflex were intact. The spine and pelvis
radiograph study showed no abnormality. He had no evidence of other combined injury of spine or muscle. Electrodiagnostic
findings were compatible with left sciatic neuropathy mainly involving tibial component. Nerve conduction study showed no
abnormal finding at lower extremity. H-reflex at left tibial nerve stimulation was not evoked. In needle electromyography study,
Abnormal spontaneous activities at rest were shown in left long head of biceps femoris, semitendinosus, semimembranosus, medial
head of gastrocnemius and soleus muscles. No denervation potentials were detected in left short head of biceps femoris innervated
by the peroneal portion of sciatic nerve and lumbosacral paraspinal muscles. We performed ultrasound study for identifying the
condition of left sciatic nerve. On longitudinal view, there were some loss of axonal continuity at far lateral side of sciatic nerve at
greater trochanteric level.
Conclusion
We report a rare case of injury of the tibial portion of sciatic nerve with describing the detailed electrodiagnostic study and
ultrasound. It is likely that far lateral side of sciatic nerve was selectively stretched from simultaneous back and leg extension during
deadlifting. It is less common because peroneal fascicles of sciatic nerve which they are medially located are more vulnerable to
traction injury of thigh.
Table 1. Needle electromyographic study

Figure 1a. Left sciatic nerve on greater trochanteric level - longitudinal view of sciatic nerve at medial side
Figure 1b. Left sciatic nerve on greater trochanteric level - longitudinal view of sciatic nerve at lateral side

P 143
The effect of exercise-based cardiac rehabilitation in patients with heart failure
Yong Seob Jo1*
, Yong Kyun Kim1†
, Jung Hyun Cha1
Department of Rehabilitation Medicine, MyoungJi Hospital1
Introduction
Heart failure is commonly referred to the state that the heart is no longer pumping enough amount of blood to meet the need of
body organs, causing dysfunction of multi-organ systems. The biggest problem of patients with heart failure is the reduced cardiac
output, so cardiac rehabilitation would be considered as one of the effective treatments for these patients. The case is a patient
with cardiac failure who presented edema in the lower extremities even after pharmaceutical treatment with diuretic. The cardiac
function of the patient was greatly improved after the cardiac rehabilitation, and the patient eventually stopped taking diuretics at
the time of discharge.
Case presentation
A 81 year old male patient developed dyspnea, thus was admitted in our hospital from November 27, 2018. Echocardiography that
was performed on November 28, 2018 showed ejection fraction that is equal to 26%. In December 20, 2018, the patient was
additionally prescribed with Lasix 40mg#1 and Aldactone 25mg#1 for the edema on both lower extremities, but the dose of Lasix
and Aldactone were subsequently increased to 80mg#1, 50mg#1 due to worsening of symptom on January 5, 2019. The patient
showed improvement in edema of lower extremities after intake of increased dose of medication, but diuretics were stopped
shortly after January 9, 2019 due to hyponatremia. Cardiac rehabilitation were started to control the above symptoms after
diuretics were stopped. Cardiac rehabilitation was started from January 9, 2019. At the point of beginning the cardiac rehabilitation,
patient was evaluated, and showed Peak VO2/HR 4.5(mL/beat), maximal PetCO2 28(mmHg), and VE/VCO2 39.6, thus the patient
started training of bicycle ergometer with exercise load of 5-10Watt for 3 cycle intervals. Also, the patient's edema was evaluated
using total of 7 different levels to diagnose the degree of edema on lower extremities.(Figure 1) In January 21, 2019, there was
improvement in the patient's edema on lower extremities(Figure 2); hence the patient's cardiac function was re-evaluated where
the result showed as Peak VO2/HR 4.6(mL/beat), maximal PetCO2 30(mmHg), and VE/VCO2 32.1.(Table 1) The patient was
discharged without prescription of diuretics.
Conclusion
As a result of comparing the results of the first and last cardiac rehabilitation evaluation of the patient, patient showed the
improvement in VE/VCO2 which is a marker of severity of heart failures, Peak VO2/HR which is a peak cardiac output parameter,
and PetCO2 which reflects the cardiac performance. There was no recurrence of edema due to improvement in the fundamental
cardiac function. Therefore, Cardiac rehabilitation can be actively considered as one of treatment options that can effectively
improve cardiac output since biggest problem of the patient with chronic heart failure is the reduced cardiac output.
Figure 1. 7 Different levels to diagnose the degree of edema on lower extremities

Figure 2. Comparison patient's edema on lower extremities before and after cardiac rehabilitation
Table 1. Comparison patient's cardiac function values before and after cardiac rehabilitation
P 144
Necessity of Guideline for Regular Pulmonary Monitoring in Patients with Prader-Willi Syndrome
Eu-Deum Kim1,2*
, Gi-Wook Kim1,2
, Sung-Hee Park1,2
, Myoung-Hwan Ko1,2
, Jeon-Hwan Seo1,2
, Yu Hui Won1,2†
Department of Physical Medicine and Rehabilitation,Chonbuk National University Hospital1, Research Institute of Clinical Medicine
of Chonbuk National University - Biomedical Research Institute ,Chonbuk National University Hospital2
Introduction
Children with Prader-Willi syndrome (PWS) often have sleep disordered breathing (SBD) and develop respiratory failure. They are at
increased risk for SDB due to hypotonia and facial dysmorphism. We report case series of PWS showing dyspnea and cyanosis in
daytime and treated successfully with noninvasive ventilation (NIV) during night.
Case report
Case 1 A 11-year-old boy with PWS (body mass index, BMI 30.2) showed dyspnea, orthopnea, excessive sleepiness, sweating and
cyanosis at daytime 5 months after scoliosis surgery. Sleep O2 and CO2 monitoring revealed severe hypoxia and hypercapnia.
Minimum and mean SpO2 were 50% and 89%, respectively during sleep. Maximum and mean transcutaneous CO2 were 71.6mmHg
and 62.6mmHg, respectively. Polysomnography (PSG) showed severe obstructive sleep apnea (OSA) (apnea / hypopnea index, AHI
91.2). Pulmonary hypertension was detected on echocardiography. Nasal noninvasive ventilation with bi-level positive airway
pressure (BiPAP) was initiated. We used ventilator settings with an inspiratory positive airway pressure (IPAP) of 20cmH2O and
expiratory positive airway pressure (EPAP) 5 cmH2O, and respiratory rate (RR) of 18. The symptoms were improved after use of
overnight NIV.
Case 2 A 18-year-old girl with PWS with a history of scoliosis correction at 12 was hospitalized due to daytime somnolence, hypoxia,
cyanosis, and syncope. The patient showed severe obesity of BMI 49.2, also, hypoventilation, severe resting pulmonary
hypertension, and cor pulmonale. PSG showed moderate obstructive sleep apnea (AHI 15.8, mean SaO2 89%, minimal SaO2 50%).
After 18-days of critical care, obesity related hypoventilation was improved with use of NIV via oronasal mask (BiPAP, IPAP =
20mH2O, EPAP = 5mH2O, RR 16) 10-hours during sleep.
Case 3 A 13- year-old boy with PWS developed exertional dyspnea after 6 months of scoliosis correction surgery (BMI 43.3). The
results of sleep monitoring and PSG showed severe hypoxia, hypercapnea and severe OSA (AHI 33.9), and symptoms improved after
use of NIV via oronasal mask during sleep. NIV setting was synchronized intermittent mandatory ventilation with pressure (P-SIMV)
mode, IPAP = 10mH2O, EPAP = 5mH2O, RR 16, and pressure support at 6cm H2O.
Discussion
When detectable symptoms of hypoventilation appear during daytime, the advanced respiratory failure already occurred in patients
with PWS, especially after scoliosis operation and with obesity. However, it is challenging to evaluate respiratory status with
pulmonary function test because of patient’s poor cooperation. Therefore, specific guideline of pulmonary evaluations such as
routine PSG for PWS patients will be needed.
Acknowledgment :1 Department of Physical Medicine & Rehabilitation, Chonbuk National University Hospital 2 Research Institute of
Clinical Medicine of Chonbuk National University - Biomedical Research Institute of Chonbuk National University Hospital

P 145
Incidental Diagnosis of Coronary Artery Disease in Lung Cancer Patient by Preoperative CPET
Young Mo Kim1*
, Ho Eun Park1, Dong Min Kim
1, Sang Hun Kim
1†
Department of Rehabilitation Medicine, Pusan National University Hospital1
Introduction
By American college of chest physician guideline, calculating predicted postoperative lung functions before lung resection surgery in
lung cancer patients without cardiac problems is known to be an important predictor of postoperative mortality. Here, we report a
rare case that in cardiopulmonary exercise testing (CPET) as preoperative assessment before lung cancer resection surgery found
severe coronary artery obstructive disease (CAOD) and the surgery was postponed.
Case report
A 68 year-old male visited department of pulmonary medicine complaining dyspnea on exertion for 3 months. He had history of
hypertension, 9 pack-years of smoking and quit 30 years ago. On chest computed tomography revealed 1.4 cm-sized nodule at the
left posterior basal segment, and he was referred to the department of thoracic surgery and planned for surgical approach. For
taking preoperative assessment, he was referred to the department of rehabilitation medicine. Pulmonary function test showed
mild obstructive pattern, suggesting chronic obstructive pulmonary disease (COPD). In 6 minute walk test, he walked for 490 m, 78%
of predicted value. He was admitted the day before surgery and took CPET for the last preoperative assessment. The test was
performed under modified Bruce protocol. From stage 3, he complained intermittent chest discomfort and systolic blood pressure
was decreased by 10 mmHg, in stage 4. From stage 4, ST depression was noted by 1.5 to 1.8 mm at V4 to V6 lead with horizontal
and down sloping. In stage 5, patient complained dyspnea and severe chest discomfort, and the test was suspended after 1 minute
and 20 seconds elapsed. In recovery stage, his uncomfortable symptoms gradually disappeared (Table 1). According to the result of
preoperative CPET, we recommended that previous surgical plan should be held immediately and the confirmation for the coronary
artery problem was needed by cardiologist. Coronary angiography revealed discrete 95% of stenosis on descending right coronary
artery and percutaneous coronary intervention was performed with drug-eluting stent, taking dual antiplatelet therapy (Fig. 1).
After 4 weeks, he got left lower lobe lobectomy safely without concern of CAOD.
Conclusion
According to preoperative algorithm of cardiac evaluation by European respiratory society, he had no risk of cardiac problem and
there was no need for further evaluation such as CPET due to small resection area. Because it is difficult to distinguish coronary
artery problem by routine preoperative examinations, we need to consider the importance of CPET as preoperative assessment
before lung cancer resection surgery such as this rare case. In addition, it should be remembered that CPET is a useful test to
distinguish dyspnea on exertion from angina in patients with COPD or healthy persons.
Figure 1. Coronary angiography with percutaneous coronary intervention: stenosis on descending right coronary artery

Table 1. Cardiopulmonary exercise testing under modified Bruce protocol

P 146
Cardiac Rehabilitation Concept for the Patient with Spinal Cord Infarction due to Aortic Dissection
Doyoung Kim M.D.1*
, Juntaek Hong M.D.2, Jun Min Cha M.D.
3, Jinyoung Park M.D.
1†, Junghyun Park M.D. , Ph.D
1†
Department of Rehabilitation Medicine,Gangnam Severance Hospital, Rehabilitation Institute of Neuromuscular Disease, Yonsei
University College of Medicine1, Department and Research Institute of Rehabilitation Medicine,Yonsei University College of
Medicine, Severance Hospital2, Department of Physical Medicine and Rehabilitation,National Health Insurance Service Ilsan
Hospital3
Introduction
Individuals survived from aortic dissection often have questions about regarding lifestyle, return to normal physical activity, and
even exercise. The optimal dose of exercise in patients after aortic dissection still remains unclear. The goal of exercise is a reduction
in resting blood pressure and improved cardiovascular health, while possibly minimizing the risk of aortic dissection. In this report,
we present a case of paraplegia patient with spinal cord infarction due to aortic dissection and its 2-month follow-up after
rehabilitation program.
Case report
A 69-year-old woman visited our hospital with lower extremities weakness. Three months ago, she felt severe back pain and lower
extremities weakness developed. After the admission to the local hospital clinic, she was diagnosed with aortic dissection and
intramural hematoma by computed tomography (CT) (Figure 1). The magnetic resonance imaging (MRI) on T2WI showed increased
signal intensity in the spinal cord (T11 to L1 level), such as spinal cord infarction (Figure 2). She was transferred to our hospital for
comprehensive rehabilitation and appropriate exercise intensity settings. The initial manual muscle test showed trace to fair grade
in lower extremities (Table 1). She could sit to stand and stand alone. But she could not gait independently, so need wheelchair for
ambulation. Goal of physical activity in post-aortic dissection is decreasing the risk of future aortic complications by aerobic exercise.
To set the exercise intensity of aerobic exercise, VO2 max monitoring is needed. However, this patient was unable to walk and could
not measure VO2 max in the conventional manner. Therefore, exercise intensity was set indirectly by checking METs and blood
pressure. A MET is defined as oxygen uptake in ml/kg/min with one MET equal to the oxygen cost of sitting quietly, equivalent to 3.5
ml/kg/min. In another study, aerobic activity at an intensity of 3 to 5 metabolic equivalents (METs) may lower resting blood pressure
by a greater amount and reduce the chance of aortic complication. Our target parameters as rehabilitation program are Borg scale
10-11, target blood pressure below 146~160 mmHg according to METs intensity, maximal heart rate below 83~105 per minute by
Karoven formular. After 2-month rehabilitation program, manual muscle test showed improved grade in lower extremities in
compared with initial status (Table 1). Functional level also improved, this patient could gait with mono-cane and showed increase
endurance of gait to 30 min. No serious complications occurred during rehabilitation.
Discussion
Our report shows that beneficial impact and safety of physical activity on post-aortic dissection patients. Alteration of aerobic
capacities in paraplegic patient also needed considering functional capacity and habitual physical activity. Further studies are
necessary to investigate the intensity of rehabilitation program and the target parameter during exercise.
Table 1. 2-month follow up of manual muscle test (MMT) on lower extremities

Figure 1. Initial aorta CT shows type A intramural hematoma (white arrow) and bilateral pleural effusion.
Figure 2. Initial spine MRI shows increased T2 signal intensity in spinal cord, T11 to L1 level.

P 147
The effect of customized electric wheelchair control device aids made by 3D scanning technology
Da Hyun Ahn1*
, Hee Seung Yang1†
Department of Rehabilitation Medicine, Veterans Health Service Medical Center, Seoul1
BACKGROUND
Several disabled patients employ electric wheelchairs for daily activities and ambulation. Since tetraplegia (quadriplegia) patients
suffer from severe hand dysfunction, an electric wheelchair cannot aid them completely. Electric wheelchair joysticks are often
available as standardized ready-made products. Consequently, there are certain limitations to providing different complementary
features for each patient’s hand dysfunction. However, owing to advancements in science and technology, the 3D scanning and
printing technology can overcome such limitations.
AIM
The objective of this study is to develop customized electrical wheelchair joysticks that aid tetraplegia patients with severe hand
dysfunction, whereby patients’ driving performance with electrical wheelchairs can be improved.
METHOD
During the period of September 1, 2018 to December 31, 2018, five tetraplegia patients using electric wheelchairs but not content
with the original joysticks participated in this study. Patients' discomfort and issues regarding previously used wheelchair joysticks
were individually identified. Through 3D scanning and modeling, customized electrical wheelchair joysticks were designed and
developed. After using the customized joysticks for two weeks, the patients’ driving abilities and satisfaction with the electric
wheelchairs were evaluated. Modified power-mobility indoor driving assessment (PIDA), National Aeronautics and Space
Administration task load index (NASA-TLX), and psychosocial impact of assistive devices scale (PIADS) were employed for evaluation.
RESULTS
Results for one of the five patients are excluded owing to the patient’s medical issues. Case 1 (KDH), Case 2 (LYH), and Case 3 (HDY):
Modified PIDA scores have the highest values (patients can follow instructions easily, accompanied by a safe and successful first trial)
in the pre-test and post-test. Modified PIDA time measurements indicate time reduction in the post-test as compared to the pre-
test. NASA-TLX and PIADS values indicate greater satisfaction through usage of customized joysticks in the post-test. Case 4 (PIS):
Modified PIDA score has a higher value in the post-test (mean-value=4) as compared to the pre-test (mean-value=3.33). Modified
PIDA time measurement indicates time reduction in the post-test as compared to the pre-test. NASA-TLX and PIADS values indicate
greater satisfaction through usage of customized joysticks in the post-test.
DISCUSSION AND CONCLUSION
By using customized joysticks, patients can improve their electric wheelchair driving abilities and can thereby experience greater
satisfaction.

Figure 1. KSH(Case 1) 환자와 IYH(Case 2) 환자의 조이스틱 전/후
Figure 2. PIS(Case 3) 환자와 HDY(Case 4) 환자의 조이스틱 전/후

P 148
A New Simple Orthosis Solves a Problem in a Patient with Adult-onset Primary Focal Foot Dystonia
Yong Min Lee1*
, Kyeong Eun Uhm1, Joingmin Lee
1†
Department of Rehabilitation Medicine, Konkuk University Medical Center and Konkuk University School of Medicine, Seoul, Korea1
Introduction
The foot or lower extremity is rarely the initial site in adult-onset dystonia, and isolated lower extremity dystonia in adults is rarely
on a primary basis. Botulinum toxin injections have been reported as beneficial in treatment of limb dystonia. In this report, we
describe a case of primary focal foot dystonia which showed further improvement after applying a new simple ankle-foot orthosis.
Case report
A 58-year-old female was referred to the Department of Rehabilitation for the left toe curling movement while walking. It began 2
years ago when she had a minor trauma of left foot. When she visited our clinic, she complained abnormal curling movement of all
left toes while walking and limited walking distance due to foot pain. In detail, toe curl amount decreased during stance phase when
walking with usual speed, and toe curl was observed at swing phase. And walking in slow speed, there was no curl in stance phase,
but toe curl was observed in swing phase. Neurological examination was otherwise unremarkable, and no joint contracture was
noted. There were no significant abnormalities in MRI of foot and brain, electrophysiological study and all laboratory studies. It was
concluded that the patient had a rare case of primary adult-onset primary focal foot dystonia. The patient was initially prescribed
baclofen and clonazepam with limited success. She received the botulinum toxin (BTX) injections five times under EMG guidance in
the left tibialis posterior, flexor digitorum longus, and flexor halluces longus muscles. At first time, she showed immediate
improvement of dystonic movement and pain after the BTX injection. But, the 5th injection was less effective than the previous. At
the follow up visit, surprisingly, she found that the toe clawing was reduced when she clang a jumping rope on her big toe during
walking. We planned to create an ankle-foot brace (Figure 1) that could force the big toe in the direction of extension using ankle
straps. With this new ankle-foot orthosis, there was no dystonic movement at any speed.
Conclusion
This case demonstrates that adult-onset primary focal foot dystonia can be managed by using the new orthosis we suggest. We
believe that this new orthosis seems to be effective in suppressing the initiation of dystonic movement by providing extension
moments to the big toe.
Keywords: Dystonia; Focal; Foot; Adult-onset; Orthosis;
Fig 1. This new ankle-foot brace could provide extension moments to the big toe.

P 149
Case Report : Myelopathy Caused by Spinal Dural Arterio-Venous Fistula
Jaehoon Sim1*
, Mi Ri Suh1,2
, Jong Moon Kim1,2
, MinYoung Kim1,2
, Kyunghoon Min1,2†
Department of Rehabilitation Medicine,CHA Bundang Medical Center, CHA University School of Medicine1, Rehabilitation and
Regeneration Research Center,CHA University2
Introduction
Spinal dural arteriovenous fistula (SDAVF) is one of the most common spinal vascular malformations. However its diagnosis can be a
challenge with the risk of delayed treatment.
Case report
A 56-year-old male patient had suffered from gradual weakness of the bilateral lower extremities and gait disturbance for 3 months.
After taking an magnetic resonance image (MRI) of the lumbar spine, he was referred with the impression of acute transverse
myelitis. At that time, his leg strength was grade IV accompanied by tingling sensation below his both thighs. Despite of steroid
pulse therapy there was no significant improvement. The MRI was carried again and it showed diffuse intramedullary T2 high signal
intensity from T8 to conus medullaris and suspicious of engorged pial vessels in spinal dura (Fig. 1). Spinal angiography confirmed
SDAVF at L5 level that supplied by left T11 intercostal artery and anterior spinal artery, and drained to anterior spinal vein (Fig. 2).
His symptoms got worse and the motor weakness of lower extremities deteriorated to grade III. He had difficulty with walking
without assist. He underwent surgical ligation of SDAVF. After the operation, he received rehabilitation. His leg strength was
improved and he became able to ambulate under supervision.
Conclusion
The prognosis of neurological recovery could be more favorable if the SDAVF was diagnosed earlier. This case showed that it is
important for physicians to understand the disease and to consider it as a differential diagnosis especially when engorged vessels
are identified on MRI. If there are vessel engorgement on MRI (Fig. 1), spinal angiography should be performed to confirm the vessel
malformation.
Figure 1. Sagittal T2-weighted magnetic resonance image of the thoracolumbar spine showing diffuse intramedullary T2 high SI from T8 to conus medullaris (white arrow) and engorged pial vessels (white arrow head) suggestive of a spinal dural arteriovenous fistula with myelopathy

Figure 2. Spinal angiogram showing a arteriovenous fistulous connection (white arrow) at L5, which was supplied by left T11 intercostal artery and anterior spinal artery (white arrow head), and drained to anterior spinal vein.

P 150
Spinal cord compression with foot drop in neurofibromatosis type 1: A case report
Kiyeun Nam1†
, Jeonghwan Lee2, Ho Jun Lee
1, Jin-Woo Park
1, Bum Sun Kwon
1, Taeyeon Kim
1*
Department of Rehabilitation Medicine, Dongguk University Ilsan Hospital1, Department of Rehabilitation Medicine, Dongguk
University Gyeongju Hospital2
Background
Spinal cord compression represents an important clinical problem in patients with neurofibromatosis type 1, but is rarely described.
Case
A 22-year-old woman with no past medical history visited the hospital with gait abnormality. One year prior to presentation, she
developed right ankle weakness. She tended to fall forward when walking. However, gait endurance or speed was in the normal
range without an assistive device or assistant. Physical examination revealed café-au-lait spots and right-sided foot drop.
Neurological examination presented increased both ankle reflexes; positive Babinski sign; positive ankle clonus; Modified Ashworth
Scale 0; manual muscle testing grades 4/5 weakness of right ankle dorsiflexor. Initial Modified Barthel Index score was 100 points.
Electromyography showed findings of a mixed axonal and demyelinating sensory polyneuropathy, and right L5 radiculopathy with
evidence of ongoing denervation in the L5-innervated muscles. Sensory evoked potential was recorded as normal on both tibial
nerve studies. Magnetic resonance imaging showed multiple intradural extramedullary masses with severe cord compression at C1-
2, C2-3, C3-4, T10-11 and cauda equina compression at L4-5, and L5-S1 levels. The patient underwent surgical excision of masses at
posterior column of cervical and thoracic level. Pathologic findings were consistent with neurofibromas. After surgical management,
walking was difficult without walker due to impaired proprioception and severe degree of spasticity (Modified Ashworth Scale 3),
but with preservation of muscle strength, temperature and pain sensation. Rehabilitation included walker gait training, both
quadriceps co-contraction training and activities of daily living training. At six weeks of rehabilitation, Botulinum toxin injections
were performed, because ankle clonus was persisted and ankle dorsiflexion was limited due to spasticity, which aggravated genu
recurvatum. Eight weeks after rehabilitation, endurance of gait with walker increased from 3m to 30m and 10m walk test showed
speed improvement from 1minute 50seconds to 1minute 10seconds. The Modified Barthel Index score improved from 60 points to
74 points and Berg Balance Scale was 12 points.
Conclusion
In our case, the patient who had gait abnormality was diagnosed with neurofibromatosis type 1 and underwent surgical excision of
neurofibromas with severe cord compression. Unfortunately, after surgical management, walking was difficult for the patient due to
impaired proprioception and severe degree of spasticity. This was thought to be posterior cord syndrome which have poor
prognosis for ambulation. Actually, despite rehabilitation treatment, the patient’s overall scores for evaluation improved, but it was
difficult to return to the pre-operative state. In conclusion, we recommend conservative treatment rather than surgical intervention
for neurofibromatosis type 1 patients with spinal cord compression at posterior column.

P 151
Cauda Equina Syndrome after Alcohol Sclerotherapy due to misdiagnosed Talov Cyst : A case report.
Kiyeun Nam1†
, Jeonghwan Lee2, Ho jun Lee
1, Jin-Woo Park
1, Bum sun Kwon
1, Shengshu KIM
1*
Department of Rehabilitation Medicine, Dongguk University Ilsan Hospital1, Department of Rehabilitation Medicine, Dongguk
University Gyeongju Hospital2
Cauda Equina Syndrome after Alcohol Sclerotherapy due to Misdiagnosed Talov Cyst: A case report.
BACKGROUND
Tarlov cyst (TC) as known as perineural cyst are usually found in the sacral region, asymptomatic and incidental findings. Endopelvic
extension of TC is rare and can be misdiagnosed for adnexal mass.
CASE
We report a TC misdiagnosed to adnexal cyst in a 38-year-old woman. She was visited to local gynecology hospital for regular
checkup. Pelvic ultrasonography finding was left 6cm ovarian cyst incidentally and treated by alcohol sclerotherapy (100% alcohol
irrigation, 20cc). After that, she presented both lower leg weakness and left leg radiating pain. In manual muscle test, muscular
weakness was observed in both lower limbs : hip flexor 3+/3 (right/left), knee extensor 3+/3, ankle dorsi flexor(ADF) 3+/3, hallucis
extensor 3+/3, and ankle plantar-flexor(APF) 3+/3 grades. The patient had sensory change below L4 dermatome. The
bulbocavernosus reflex (BCR) was absent. The anal tone was decreased. Patient had anal sphincter weakness and neurologic
bladder symptom of incontinence, nocturia. Ankle clonus and Babinski sign were negative. Lumbar spine MRI finding was 6.5*5.0cm
sized anechoic cyst in perineurium of sacrum extension to pelvic cavity with bony erosion. In motor and sensory nerve conduction
study, both common peroneal, tibial, superficial peroneal and sural nerve conduction was normal. In needle electromyography
(EMG) 3month after sclerotherapy, left tibialis anterior, gastrocnemius, vastus medialis, tensor fascia lata, gluteus maximus and S1
paraspinal muscle presented abnormal spontaneous activity (ASA), normal motor unit action potential (MUAP) and reduced single
recruitment pattern. Left peroneus longus and biceps femoris presented ASA and polyphasic MUAP, reduced single recruitment
pattern. Both external anal sphincter muscle presented ASA. Left external anal sphincter presented polyphasic MUAP, reduced
complete recruitment pattern. In somatosensory evoked potential test (both tibial nerve), left side latency was more delayed and
waveform was more attenuated than right side. In H-reflex, delayed latency was presented on left side. BCR latency test was no
response. Those EMG findings were corresponding with cauda equina sydrome (CES). In isokinetic test, difference of right and left
ADF peak torque was 78.0%. In balance test, overall balance index was 10.7°. Electric stimulation therapy, strengthening, gait
exercise and stretching was done 3 times per week. After 6 months, weakness, radiating pain, incontinence, anal sphincter
weakness and sensory change were improved. In follow-up EMG, CES was partially improved state. In follow-up Isokinetic test,
difference of right and left ADF peak torque was 14.3% (Left side was better). In follow up balance test, overall balance index was
6.7°.
CONCLUSION
This is very rare report of recovery of iatrogenic chemical CES in patient with tarlov cyst

P 152
Ischemic colitis of spinal cord injury : case report
Cheon Ji Kang1*
, Jong Yoon Yoo1†
Department of Rehabilitation Medicine, Asan Medical Center1
Introduction
Ischemic colitis is uncommon in the general papulation. Hypoperfusion of the colon contributes to the pathogenesis of ischemic
colitis. The risk factor of ischemic colitis is known 65 years and older, irritable bowel syndrome and chronic obstructive pulmonary
disease. But in a patient of the spinal cord injury (SCI), ischemic colitis is not much known. The aim of this study is to report a case of
diagnosed with ischemic colitis in SCI and illustrates management and outcomes.
Case
A 48 years old previously healthy man got a traffic accident. After a few hours later, he got a lower extremities weakness and
numbness sensation. He presented with a zero grade lower extremity weakness, loss of sensory up to the level C5. But voluntary
anal contracture and deep anal sensation were preserved. He was prescribed high dose steroid therapy. Magnetic resonance
imaging (MRI) demonstrated high signal intensity in C2-4 level of spinal cord and low signal intensity hemorrhage in C3-4 disc level
on T2 weighted images. He was diagnosed the spondylotic myelopathy due to ossification of posterior longitudinal ligament, C3-4.
He underwent an anterior cervical discectomy with fusion. He was transferred to a rehabilitation medicine. He had daily defecation
but need clean intermittent catheterization. He took medicine of gastrointestinal regulator and laxative for bowel management.
Three weeks later, he complained of pain in the suprapubic area. Despite urination with a nelaton, the pain persisted. Rather, pain
developed at the RLQ area of the abdomen. On abdomen X-ray, the ileus was observed. The pain was exacerbated, abdominal
computed tomography (CT) was taken. There was fecal stasis with small and large bowel dilatation. Glycerin enema was performed
and a small amount of fresh blood was mixed in the stool. Next day, he underwent sigmoidoscopic exam from an anal verge (AV) to
AV 70cm. The mucosa of the colon was relatively normal below AV 7cm. However, severe mucosal edema, erythema and ulcer were
continuously observed in AV 70cm ~ AV 7cm. No endoscopic findings were found other than atrophic gastritis. He took a supportive
care including bowel rest and antibiotics. After 4 days, the diet was tried, but the hematochezia recurred and high-spike fever
occurred. Then, NPO was maintained. After two weeks, there was still linear or geographic ulceration in the follow-up
sigmoidoscopy, but some improvement was seen. Three days later, the diet proceeded without hematochezia and fever.
Conclusion
The upper motor neurogenic bowel of SCI tends to have slower transit time throughout the colon and could result in severe
constipation. Decreased sensation below the injury level aggravates this tendency. It makes the patient with SCI more susceptible to
ischemic colitis than the general population. And they have a higher severity of ischemic colitis. Careful attention to the neurogenic
bowel and management of fecal incontinence are required.

P 153
Incidental finding of esophageal cancer with VFSS performed due to postoperative dysphagia
Yong Seob Jo1*
, Yong Kyun Kim1†
, Jung Hyun Cha1
Department of Rehabilitation Medicine, MyongJi Hospital1
Introduction
Dysphagia is generally known as one of the most common postoperative complications following Anterior cervical dissectomy &
fusion (ACDF) surgery. Therefore, it is easy to zero in on surgery as the cause of dysphagia when dysphagia occurs after surgery. It is,
however, important to rule out all possible causes of dysphagia that might be attributed to patient's dysphagia. Hence, it is always
necessary to rule out the additional causes of patient's dysphagia in the course of tests. This is a case of a patient who underwent
VFSS (Videofluoroscopic swallowing test) due to difficulty of swallowing that occurred after ACDF surgery, and incidentally found to
have esophageal cancer on esophagogastroduodenoscopy(EGD) that was performed to rule out mechanical obstruction.
Case presentation
In December 21, 2018, a patient with a history of hypertension and thyroid cancer came to the emergency department of the
hospital with forehead injury after falling forward. Several diagnostic tests were ordered, and found ankylosing spondylitis with C4/5
Fracture, thus the patient was admitted to the neurosurgery department for C4/5 ACDF with C3-6 anterior plating. In December 24,
2018, the patient underwent C4/5 total laminectomy & C3-7 posterior fusion. <br>VFSS was conducted on January 17, 2019 due to
dysphagia after operation, and as a result of a measurement, 15% remnant with no aspiration in semisolid 4/8cc, 60% remnant with
no aspiration in Solid 4/8cc, and positive penetration with no aspiration in liquid 4/8cc and cup drinking were observed. Due to the
great amount of remnant observed in solid, patient underwent EGD to check the possibility of mechanical obstruction. (Figure 1) In
the course of the test, there was incidental finding of esophageal cancer which is blocking 1/4 of the esophageal lumen. (Figure 2)
The patient was then referred to a hemato-oncology department where PET-CT was ordered. (Figure 3) Additional tissue biopsy and
plan to proceed for chemo-radiation therapy are currently on work.
Conclusion
When VFSS was first performed in this patient, the cause of dysphagia could be simply considered as postoperative dysphagia after
ACDF surgery. However, there was great amount of remnant found in VFSS with solid components. To rule out the mechanical
obstruction, EGD was ordered and eventually found an esophageal cancer in the patient. Thus, even if dysphagia after surgery is a
common complication, it is necessary to carefully examine and approach the patients with complaint of dysphagia after surgery,
using VFSS to rule out other possible causes of dysphagia. In addition, there is a need to perform EGD for the patients presenting
great amount of remnant in solid components, to measure the cause of mechanical obstruction.
Figure 1. Videofluoroscopic swallowing test result with solid 8cc component

Figure 2. Esophageal cancer on esophagogastroduodenoscopy (EGD)
Figure 3. PET-CT performed to confirm the location of esophageal cancer

P 154
Spontaneous Spinal Epidural Hematoma due to venous malformation in a child : A Case Report
Chang Beom Kim1*
, Kyung Lim Joa1, Chang Hwan Kim
1, Han Young Jung
1, Myeong Ok Kim
1†
Department of Physical and Rehabilitation Medicine, Inha University School of Medicine1
Introduction
Spontaneous spinal epidural hematoma (SSEH) is a rare disease. The incidence of SSEH is 0.1 patients per 100,000 per year. It has
been reported to occur in all age groups, and very rarely in children. While the lesion is located in the thoracolumbar lesion in older
patients, the cervicothoracic site is more common in children. We report the case of a child who presented with acute onset of
progressive weakness of his upper and lower limbs without any trauma history, to the point of being unable to stand or walk. <
Case Report
A 14-year-old, previously healthy boy was admitted to our hospital with a chief complants of progressive weakness of his upper and
lower limbs (upper - Medical Research Council (MRC) grade 3/5, lower- MRC grade 0/5) without trauma history. The pediatrician
suspected Guillain-Barre syndrome early. MRI of the brain was normal. And MRI of the whole spine revealed posterior epidural
hematoma from C5-6 to T5 level and abnormal T2 high signal at the anterior spinal cord at C6-7 levels (Fig.1). After transferred to
the department of Neurosurgery, he underwent C7 to T3 laminectomy with hematoma removal. During surgery, vein engorgement
was observed near the hematoma. After 2 weeks, he was referred to the rehabilitation unit. At that time, MRC grade 0/5 in the right
leg, 2/5 in the left leg and 3/5 in the both arm. On sensory examination, there was diminished sensation to light touch and pinpricks
below C7 on the both. His ASIA impairment scale (AIS) was C and neurologic level was C7. The walking index spinal cord injury
(WISCI) level was 0/20. The spinal cord independence measure (SCIM) was 10/100. Clean intermittent catheterization was
performed for incomplete voiding. After the urodynamic study, he was diagnosed as a neurogenic bladder with characteristic
detrusor hyperreflexia. Somatosensory evoked potentials (SEP) study showed delayed latency in right posterior tibial nerve. And
motor evoked potentials (MEP) of the both lower extremities is not evoked (Table 1). The patient was performed all rehabilitation
modalities. After two months, it revealed improvement in left leg MRC Grade 3-4 and in right leg MRC Grade 1-2 (Table 2). And
upper extremity muscle strength improved to MRC Grade 4. Sensory examination showed decreased sensation to light touch and
pinpricks below T4 on the both side. His AIS improved to D and neurologic level was C7. He could walk with the aid of walker. WISCI
improved to 13/20 and SCIM improved to 51/100.
Conclusion
The SSEH is extremely rare in children. In children with non-traumatic motor weakness, this condition should be considered a
differential diagnosis through spine/brain MRI. Although his disease was initially suspected of Guillain-Barre syndrome, he was
diagnosed with SSEH in a spine MRI. After emergency surgery and early rehabilitation, his symptoms recovered quickly. So, we
report this case to emphasize that rapid diagnosis and treatment are helpful for recovery.
Fig. 1. Whole spine MRI revealed abnormal T2 high signal at the anterior spinal cord at C6-7 levels. (a) T2 high-resolution axial weighted image at C7 level (b) T2 high-resolution sagittal weighted image at C7 level

Table 1. Somatosensory evoked potentials (SEP) study and motor evoked potentials (MEP) study
Table 2. Changes in lower extremity motor MRC grade on initial and 2 months follow up

P 155
Traumatic spinal cord injury without abnormal findings on MRI : A Case Report
Won Jae Jo1*
, Eun Sil Kim1†
, Seung bok Lee1
Department of Rehabilitation Medicine, Presbyterian medical center (Jesus hospital)1
Introduction
Traumatic spinal cord injury can manifest as a wide variety of clinical syndromes resulting from damage to the spinal cord or its
surrounding structures. Magnetic resonance imaging (MRI) has become the gold standard for imaging neurological tissues including
the spinal cord due to high sensitivity for detection of acute soft tissue and cord injuries.
Case reports
A 34-year-old female patient presented to our clinic with symptoms of both upper and lower limbs weakness, hypoesthesia below
the C4 dermatome level and voiding difficulty about 2months after car accident. At that time of the accident, she was pregnant and
had an abortion with vaginal bleeding after the accident. Cervical spine MRI, lumbar spine MRI and whole spine T2 saggital MRI
revealed no abnormal findings with the exception of C6-C7 central disc protrusion and L4-L5 central spinal stenosis. Brain MRI was
performed, but it did not reveal any abnormal findings. Voiding cystourethrography and urodynamic tests were also performed
owing to subjective reports of persistent dysuria. Hyposensitive, hypotonic, and areflexic bladder findings were confirmed and clean
intermittent catheterization regimen was prescribed to promote optimal bladder emptying. Electromyographic findings were left C7,
C8, L5 and S1 dermatome somatosensory pathway dysfunction. The patient's deep tendon reflex was hyperreflexic and the
symptoms of motor weakness and hypoesthesis gradually worsened, especially on the left side. International standards for
neurological classification of spinal cord injury by American Spinal Injury Association/International Spinal Cord Society (ASIA/ISCOS)
revealed a neurologically incomplete spinal cord injury. ASIA impairment scale was D and neurological level of injury was C4. The
presenting clinical signs were suspicious of an underlying traumatic spinal cord injury. However, there were no objective evidence of
spinal cord injury on MRI.
Discussion
The patient's symptoms were more severe on the left side, suggesting that there was more damage in the left side of the spinal cord.
MRI over time has become a valuable diagnostic tool in diagnosing spinal cord injury in both pediatric and adult patients. The
imaging technique offers a superior ability in identifying soft tissue lesions including cord edema, hematomas and transections, and
disco-ligamentous injuries that may not be visualized by plain radiography and CT imaging. However, despite the lack of any
evidence of spinal cord injury on MRI, injury cannot be completely ruled out.
Conclusion
We observed a patient who was suspected to have a traumatic onset cervical level spinal cord injury following a motor vehicle
accident. There were no abnormal findings on MRI to support our clinical suspicion. Despite the negative test results by imaging, we
concluded that an underlying spinal cord injury should not be ruled out strictly by the lack of abnormal findings on MRI.

P 156
Therapeutic approach at tibial nerve entrapment point in chronic plantar fasciitis.
Jong Burm Jung1*
, Yuntae Kim1†
, Soo A Kim1, Ki Young Oh
1, Sung Jae Lee
2, Kyudong Noh
3
Department of Physical Medicine & Rehabilitation,Soonchunhyang University Cheonan Hospital1, Department of Physical Medicine
& Rehabilitation,Soonchunhyang University Seoul Hospital2, Department of Physical Medicine & Rehabilitation,Soonchunhyang
University Bucheon Hospital3
Introduction
Plantar heel pain is well-known in orthopedics, and usually caused by plantar fasciitis. Untreated plantar fasciitis can lead to chronic
heel pain. We report a case of intractable heel pain that was diagnosed as plantar fasciitis, and was successfully treated with 4
injections of normal saline within the soleus.
Case presentation
A 43-year-old healthy male patient with right inferior heel pain for 5 years was diagnosed with plantar fasciitis at an orthopedic
clinic. His heel pain was aggravated when taking the first barefoot steps in the morning. In addition, he complained of burning pain
in his heel area while resting. He had been receiving conservative treatments, such as nonsteroidal anti-inflammatory drugs,
physical therapy, extracorporeal shockwave treatment, and wearing custom-made orthotic shoes for plantar fasciitis. However,
there was no pain improvement, and surgery was finally recommended, which he refused. Plain radiography revealed nonspecific
findings. Physical examination revealed tenderness of the right medial calcaneal tubercle region, and compared with the opposite
side, there was severe tenderness over the medial flexor retinaculum and soleus regions near the soleus tendinous arch. Thus, we
hypothesized that the tenderness point of the soleus was tibial nerve entrapment point (NEP), and the entrapped tibial nerve at the
soleus tendinous arch stimulated the medial calcaneal nerve originating from the tibial nerve, which caused the chronic heel pain.
He was diagnosed with tibial nerve entrapment syndrome within the soleus. As a therapeutic intervention, to release the tibial NEP
within the soleus, 4 mL of normal saline was injected at approximately the point of proximal 1/4th of the lower leg—the most
tender region—under ultrasound guidance. The injection was repeated at 1, 3, and 6 weeks after the first injection. Before the first
treatment, the baseline Foot and Ankle Ability Measure–activities of daily living subscale (FAAM-A), numeric pain rating scale (NPRS),
and percent pain intensity difference (PPID) scores were 52, 7, and 100 points, respectively. At 1-week follow-up after the first
treatment, they improved to 65, 4, and 60 points, respectively, and further improved to 75, 1, and 20 points, respectively, at 6
months after the first injection (Figure 4). At 6 months, the patient reported comfort without wearing the custom-made orthotic
shoes. He had no adverse effects.
Conclusion
This report is meaningful because it describes the case of intractable heel pain in a healthy adult male for 5 years that was
diagnosed as plantar fasciitis, and was successfully treated with 4 injections of normal saline into the soleus. This case suggests the
importance of detailed history and physical examination before initiating treatment. Furthermore, normal saline injection at NEP of
the soleus could be considered in chronic unhealed plantar heel pain, including plantar fasciitis, to release the entrapped tibial nerve.
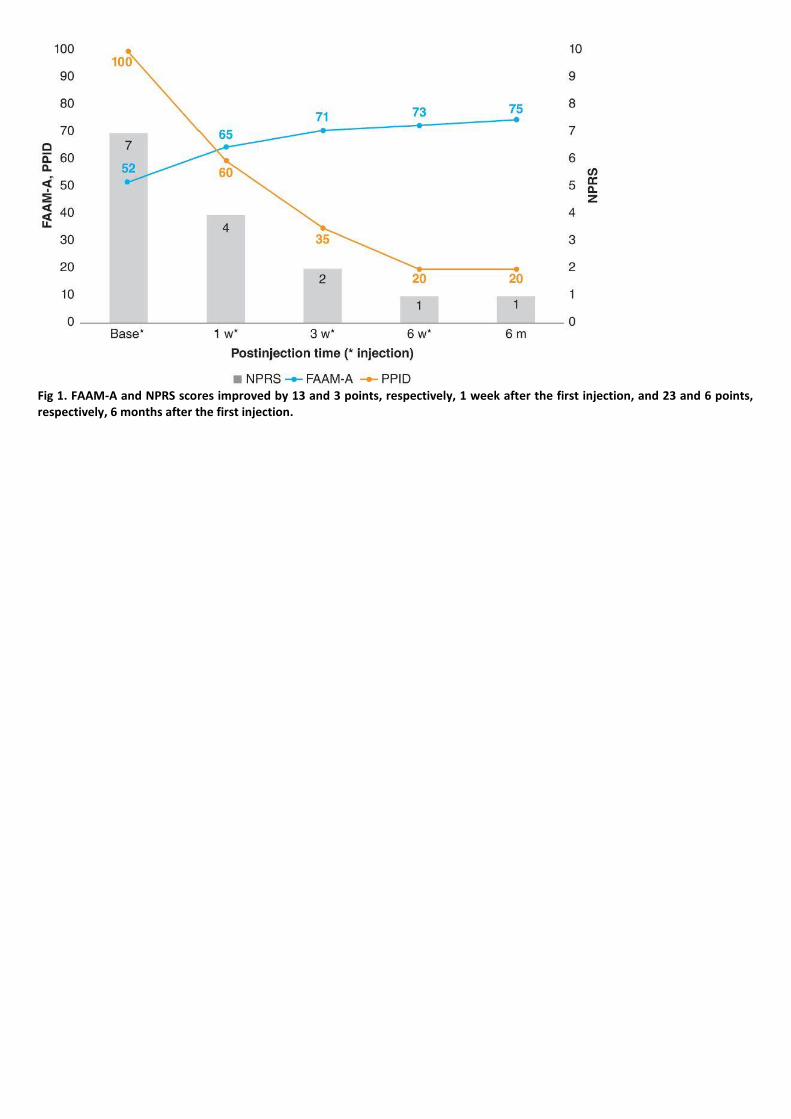
Fig 1. FAAM-A and NPRS scores improved by 13 and 3 points, respectively, 1 week after the first injection, and 23 and 6 points, respectively, 6 months after the first injection.

P 157
Discography negative discogenic pain confirmed by displacement and reposition of intradiscal device
Soonwoo Kwon1*
, Nackhwan Kim1†
, Sang Heon Lee1†
Department of Physical Medicine and Rehabilitation, Korea University Medical Center1
Low back pain is highly prevalent in general population of all ages and its etiology seems to be multifactorial. The diagnosis of
discogenic back pain is based on the typical symptoms, physical examination, imaging study and discography. Discography is known
as the main diagnostic tool and also a therapeutic tool. However, it is reported that there are some patients who present with
symptoms of discogenic pain and also have the abnormal discs in MRI but showed negative discography.
We report a case of a 56-year-old, male with a history of axial low back pain and both inguinal pain which persisted and worsened
for several years. The patient presented with probable symptoms of discogenic pain and had obvious pathological changes on MRI
at L4/L5 and L5/S1 level disc. The electrodiagnostic studies showed no definite evidence of lumbosacral radiculopathy. Discography
performed at L3/L4, L4/L5, L5/S1 level discs were negative. Conservative treatment including intradiscal steroid injection and
percutaneous disc decompression and ablation with L’DISQ device was unsuccessful with re-occurrence of similar pain few days
after the treatment. Consequently, he was transferred to neurosurgery department and discharged with a relief of the symptom
after having ‘posterior screw fixation on L4/L5, L5/S1 disc level and oblique lumbar interbody fusion with cage inserted at L4/L5,
L5/S1 disc’ done. However, although there was a pain relief for 6 weeks post-surgery, the disabling symptom re-ocurred and he was
admitted for further evaluation. The groin pain worsened with Valsalva maneuver and coughing but pathologic lesions were not
noted in evaluation by urology and colorectal specialists. Plain films of lumbar spine showed the cage of L5/S1 disc was displaced
anteriorly over the anterior edge of the vertebral body. So the patient had revisional cage reposition operation. Postoperatively, the
disabling pain relieved and was able to walk.
Diagnosis of discogenic pain is known to be difficult and the reliability of the diagnostic tools including discography has been
controversial. This is a case of a patient with probable discogenic pain but was negative in discography. In consideration of patients’
typical symptom of discogenic low back pain and pathological findings on lumbar spine MRI, conservative treatment targeting
discogenic origin was performed but wasn’t effective. The patient re-visited and re-admitted for the reoccurring disabling pain. So
the patient willingly wanted to have the surgery as the last resort. Although the discography did not provoked the concordant pain,
the displacement and and reposition of surgically inserted intradiscal device provoked and also relieved the symptom. This may
explain the origin of this disabling but undiagnosed pain could be from intradiscal lesion. Therefore it is important not to exclude the
diagnosis of discogenic pain even though the discography was negative.
Acknowledgment: none

Fig 1. T2-weighted magnetic resonance imaging (A, B) of lumbar spine. Mid-saggital view (A) and transverse view (B) of L5/S1. Disc bulging and degeneration with annular fissures at L4/5 and L5/S1 is noted.
Fig 2. Intra-discography images (A, B). Coronal (A) and saggital (B) intra-discography images. The L4/5 and L5/S1 disc had a damaged annulus that permitted contrast extravasation. The patient expressed pain among the exam but showed no concordant pain.

Fig 3. Plain radiographs of lumbar spine (A, B). Anterior displacement of the L5/S1 intradiscal device (A) and surgically repositioned intradiscal device (B).

P 158
Rapid Functional Enhancement of Ankylosing Spondylitis with Severe Hip Joint Involvement
Sangwon Hwang1*
, Jinyoung Park2†
, Jung Hyun Park2, Doyoung Kim
2
Department of Rehabilitation Medicine and Research Institute,Yonsei University College of Medicine, Seoul, Korea1, Department of
Rehabilitation Medicine,Gangnam Severance Hospital, Rehabilitation Institute of Neuromuscular Disease, Yonsei University College
of Medicine, Seoul, Korea2
Objective
Spondyloarthritis (SpA) is a group of diseases, characterized by the chronic inflammatory reaction of the axial skeleton or peripheral
joint. There are several previous reports that the concomitant bilateral hip joint arthritis deteriorates the quality of life in ankylosing
spondylitis (AS) patients. This is the first report of rapid functional enhancement that the range of motion (ROM) of hip joints
doubled, which were severely limited within 2 weeks by multimodal therapies.
Methods
1. Patient A 20-year-old young man visited the Department of Orthopedic Surgery of a tertiary hospital for limitation of ROM and
pain (Numeric Rating Scale, NRS 4) in bilateral hip joints, and gait disturbance. He was diagnosed as AS by 5 years of low back pain,
grade III sacroiliitis by simple plain images, and positive HLA B27. MRI confirmed synovitis in bilateral hip joints, inflammatory
changes in right gluteus minimus, medius, and maximus muscles. Even after 6 months of pharmacologic treatment, the ROM still
severely limited to use bilateral crutches, where NRS was 0. On the day of admission to the Department of Rehabilitation Medicine,
total ROM of the bilateral hip joints was 140°. Bath Ankylosing Spondylitis Metrology Index (BASMI) score was 2.2 (maximal
intermalleolar distance; 7.0 cm). Bath Ankylosing Spondylitis Disease Activity Index (BASDAI) score was 7.0.
2. Procedure First, to resolve the synovitis, ultrasonography-guided intra-articular injection on each hip joint was done with
corticosteroid (20 mg) and hyaluronic acid (20 mg). Second, to release the tight gluteal muscles, multimodal therapy was done
including 10 sessions of manual therapy (soft tissue technique, articulatory treatment, direct myofascial release), 2 session of
electrical twitch obtaining intramuscular stimulation on bilateral gluteus maximus, gluteus medius, quadratus lumborom, and lower
lumbar multifidus (L4-S1) muscles, 1 sessions of extracorporeal shock wave therapy on gluteus maximus and medius muscles, ICT,
ultrasound, and hot pack were applied on quadratus lumborum, multifidus (L4-S1) muscles (Table 1).
Results
By 10 days of multimodal rehabilitation program, the total ROM of bilateral hip joints was doubled to 280° (Figure 1). BASMI score
was 1.8 (maximal intermalleolar distance has increased to 31.0 cm, a 443% improvement) (Figure 2). BASDAI score was improved to
3.2. Finally, he came to be able to walk independently.
Conclusion
In this case, as peri-articular inflammatory process, the shortened and tight hip girdle muscles also caused functional decrement.
The management should focus on the muscle relaxation as well as the direct control of intra-articular or inflammation. Even in short
period, rapid functional regain is possible by enhancing the ROM of hip joints by multimodal therapy.

Table 1. Multimodal treatment for ankylosing spondylitis with severe hip joint involvement
Figure 1. Comparison of bilateral hip range of motion among hospital days

Figure 2. Comparison of BASMI assessment between initial evaluation and 10 days later

P 159
Calcific tendinitis of the longus colli muscle: a case
Kwang Jae LEE1,2*†
, Yong-Soon Yoon1,2
, Jung-Hoo Lee1,2
, Won-Jae Jo1, Jun-Hyun Choi
1, Yumi Kim
1
Department of Rehabilitation Medicine, Presbyterian Medical Center1, Medical Device Clinical Trial Center, Presbyterian Medical
Center2
Calcific tendinitis of the longus colli muscle (CTLC) is an inflammatory or granulomatous response to the deposition of calcium
hydroxyapatite crystals and has been reported as an unusual cause of neck pain and dysphagia. It is usually involves the superior
oblique fibers of that muscle from C1-3 levels and diagnosed by calcification in prevertebral space on radiograph, CT or MRI. We
report a case of CTLC located on the C4-5 level of the neck, which was detected accidentally by ultrasound during SGB guidance for
right upper extremity pain for 2 years after right humeral shaft fracture by motor vehicle accident, but had no neck pain or
dysphagia. This present case shows that we have to consider CTLC if we find calcification in prevertebral area during ultrasound
examination, and that CTLC can exist usually at C1-3 but down to C4-5 and C5-6 level.

P 160
Skeletal muscle metastasis from advanced gastric cancer presenting with severe buttock pain
Jae Hyeong Choi1*
, Kun Woo Kim1, Jin Tae Hwang
1, Kyun Jae Yoon
1, Yong Taek Lee
1, Jong Geol Do
1†
Department of Rehabilitation Medicine, Kangbuk Samsung Medical Center1
Introduction
Gastric cancer is one of the most common malignancy, but reported cases of skeletal muscle metastases from gastric carcinoma are
extremely rare. We report here a case of a 60-year-old female patient with skeletal muscle metastasis from advanced gastric cancer.
Case report
A 60-year-old woman presented with a right buttock pain for 2 months. She had been suffering from a pain in the right buttock area
after she walked down from the 15th floor. Two years earlier, she was diagnosed with gastric cancer and had undergone total
gastrectomy with lymph node dissection, splenectomy and colon segmental resection. The pathologic diagnosis was poorly
differentiated adenocarcinoma with signet ring cell accompanied by lymph nodes but no any other distant organ metastases. She
had undergone adjuvant chemotherapy with capecitabine and oxaliplatin. At follow-up, 1 year after surgery, a peritoneal metastasis
was found and the patient received chemotherapy again. Her right buttock pain was aggravated by activities such like walking and
squatting. On physical exam, she had tenderness at right buttock area and positive Patrick’s sign was observed. But, muscle
weakness and sensory deficit were not observed. In laboratory test, white blood cell count was 5670 /mm³, percentage of
segmented neutrophil was 74%, C-reactive protein was 0.38 mg/dL, creatine kinase was 41 IU/L, and lactate dehydrogenase was
177 IU/L. No bony abnormality was observed in X-ray. Under suspicion of gluteus muscle strain, oral analgesic was prescribed. As
her right buttock pain had not subsided, we performed a comprehensive radiologic evaluation. In whole body bone scan, mild
diffusely increased uptake was observed in right ilium (figure 1). Contrast-enhanced pelvic bone MRI revealed diffuse muscle
swelling and high signal intensity change along both hip muscles in contrast enhanced T1 weighted image and peri-neural
inflammation observed around the bilateral sciatic nerve in T2 weighted image. (figure 2). On PET-CT scan, right gluteus muscle
swelling was observed but, FDG uptake (max SUV = 2.4 < 2.5) was not obviously increased in right buttock muscle (figure 3). To
differential diagnosis of myositis, primary soft tissue sarcoma, and metastatic carcinoma, muscle biopsy was performed. Pathologic
examination showed metastatic adenocarcinoma from stomach origin. The patient commenced on chemotherapy with paclitaxel
and ramucirumab, the swelling and pain in right buttock are progressively improving.
Discussion
Skeletal muscle metastases reported to be approximately 0.8 - 16% in autopsy study and 1.2% in clinical study. The skeletal muscle
metastases is challenging to diagnosis. The diagnosis of skeletal muscle metastases should be considered in the differential
diagnosis of painful condition in advanced cancer patients.

Figure 1. Whole body bone scan
Figure 2. Contrast enhanced pelvic bone MR

Figure 3. PET-CT scan

P 161
The Nonoperative Treatment in the C2-3 Disc Herniation: A Follow up Study
Dong Seok Yang1†
, Ki Hyun Byun 1*
, Son Seong Wook 1
Department of Rehabilitation Medicine, Ulsan University Hospital1
Although disc herniation disc at C2-C3 level (C2-3) is very rare, it resultS in severe neurological symptoms. The exact diagnosis for
upper cervical disc level is difficult to clarify depending on clinical examination and presentations. Until now, there is no report
about non-operative treatment of C2-3 despite the fact is nonoperative treatment for the herniation disc is one of the best option.
We report successfully management on a patient with C2-3 and also shown serial imaging study.
Case report
A 68-year old male visited emergent clinics due to severe dizziness and headache for one day. After 7 days at headache clinic, he
had complained intractable pain of numbness and dysesthesia on right upper face and at the occipital area. Post-onset 12 days he
referred to our department to control his pain. Physical examination disclosed positive spurling sign and the pain was provoked on
the usual sites, mainly C2 and C3 dermatomes, The patient’s sensation was decreased on C2, C3 and C4 dermatomes. At neck
extension the pain became worse. But there is no abnormal of upper motor neuron signs like increased on deep tendon areas,
Hoffman’s and Babinski’ signs. His past medical history included a hypertension, chronic obstructive lung disease and left
nephrectomy due to renal stone. Sagittal and axial Magnetic resonance (MR) images showed that 5 X5 X 4 mm, soft disc materials
was close to the right of para-median site on C2-3 level [Figure 1. A and B]. We did not perform operation due to his medical
condition and expected the spontaneous regression of the soft disc. Therefore, we treated him with 8mg of methylprednisolone
twice daily for five days, amitriptyline 5mg and pregabalin 75mg, once daily, 5mg buprenorphine patch weekly. Eight day after
medications, his pain was improved by 80%. Two months later, he said that replied to pain survey that he is rare discomfort; pain
intensity, VAS 3, 3-4 times during 10-15 sec at day. He only is taking amitriptyline 5mg and aceclofenac 100mg daily. Serial MR
images three months after initial MR showed absorption of disc particle on C2-3 level [Figure 1. C and D].
Conclusion
Nonoperative treatment with steroid may be a very useful method for upper cervical disc herniation, which is high possibility of
spontaneous regression overtime.
Acknowledgment: This research was supported by Basic Science Research Program through the National Research Foundation of
Korea funded by the Ministry of Education (No. 2013R1A1A4A01013178)
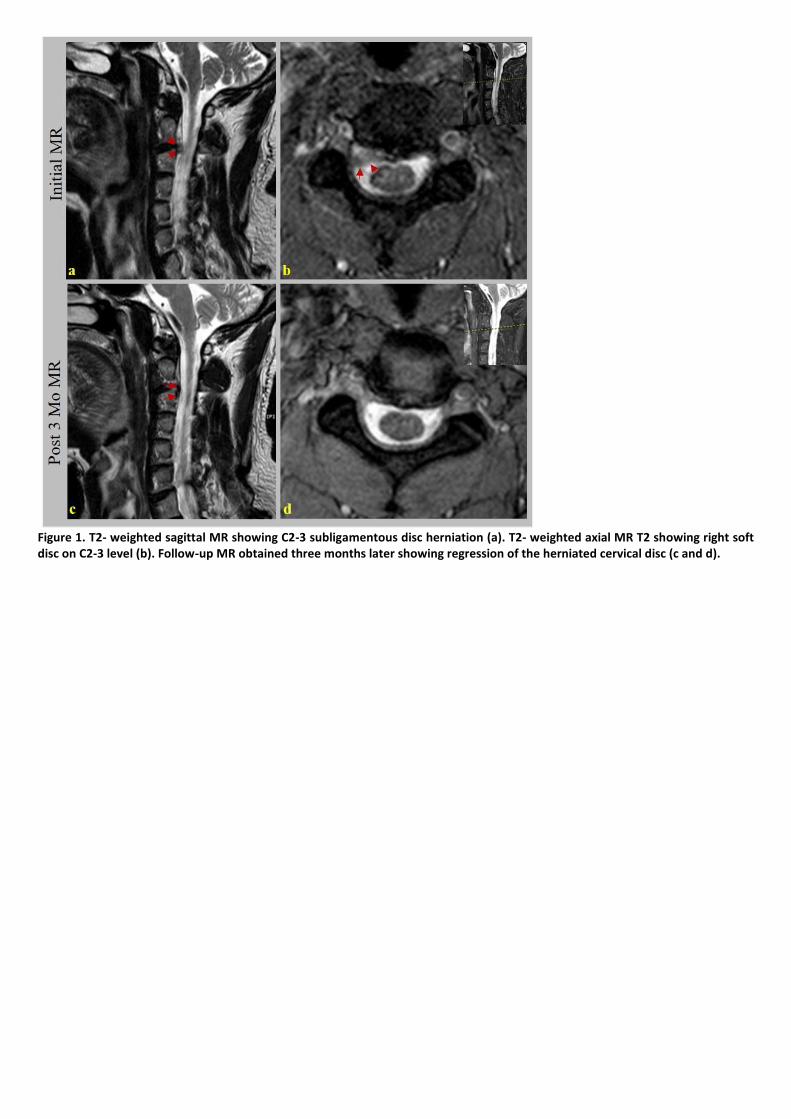
Figure 1. T2- weighted sagittal MR showing C2-3 subligamentous disc herniation (a). T2- weighted axial MR T2 showing right soft disc on C2-3 level (b). Follow-up MR obtained three months later showing regression of the herniated cervical disc (c and d).

P162
The botulinum toxin injection as a treatment for peripheral polyneuropathy related pain
Hyo Joon Jin1*
, Yong Min Choi1†
, Du Hwan Kim1, So Young Lee
1, Chang Gyu Jung
2
Department of Rehabilitation Medicine,Keimyung University Dongsan Medical Center1, Department of Internal Medicine,Keimyung
University Dongsan Medical Center2
Introduction
Polyneuropathy related pain (PP) is often encountered problem. Despite many medications, it is challenging to the treat PP. <br>Of
the existing methods, sympathetic ganglion block (SGB) is known to reduce pain. But blocking effect is temporary in most patients.
By repeating SGB or using neurodestructive material can make effect longer. However, complications can occur. Not like
neurodestructive material, botulinum toxin (BT) inhibits the release of acetylcholine from cholinergic nerve endings and typically
used for dystonia. Sympathetic blocking effect can be obtained by directly inject BT at the sympathetic ganglion. Also there are
several reports about prolonged sympathetic blocking effect of SGB using BT. So we hypothesized that if patients have effect of SGB
with local anesthetics and steroid, SGB with BT can relief PP much longer.
Case report
A 48 years old man with Eosinophilic Granulomatous polyangitis (EGPA) was referred to our Department about both feet tingling
sensation for 1 month. Both feet pain was started with both leg edema and purpura, without trauma. Pain was tingling nature [VAS
8]. After admission, he was diagnosed with EGPA. Also they did Nerve Conduction Velocity test (NCV) and findings are suggesting
bilateral peroneal and tibial neuropathy. Despite the use of steroid, gabapentin and pregabalin, both feet pain didn’t subside and he
can’t walk and sleep. After referred to us, we assumed that his foot pain can be improved by Lumbar SGB (LSGB). So we did Both L2
LSGB with steroid and local anesthetics. After both LSGB, both feet pain was improved but didn’t last long. So 2 weeks later, we did
both LSGB with BT 50units on each side. After injection, both feet pain and neuropathic pain were decreased from vas 8 to 3 and
maintained for a month.
Discussion
PP is challenging to the treat. If PP didn’t relived by medications, sympathetic block can be helpful. There are several studies
reporting pain relieving effect of SGB. But the blocking effect is temporary in most case. Repeating SGB with local anesthetics or
neurodestructive procedures can be a option for longer effect. BT is commonly used for focal dystonia. BT can block releasing
acetylcholine at pre-synaptic nerve terminals. Recently many studies report SGB with BT can relief various kind of pain and also
effect last for at least 1 month. In this case report, patients have intractable both feet pain despite using various medications. So we
did both LSGB with local anesthetic agent and steroid, and pain was improved but after 1 week, pain recurred. For longer effect, we
did Both LSGB with BT and effect both feet pain and neuropathic pain were decreased from vas 8 to 3 and maintained for a month.
According to this case, We report that SGB using BT could be helpful if PP caused by EGPA has not improved despite drug use.
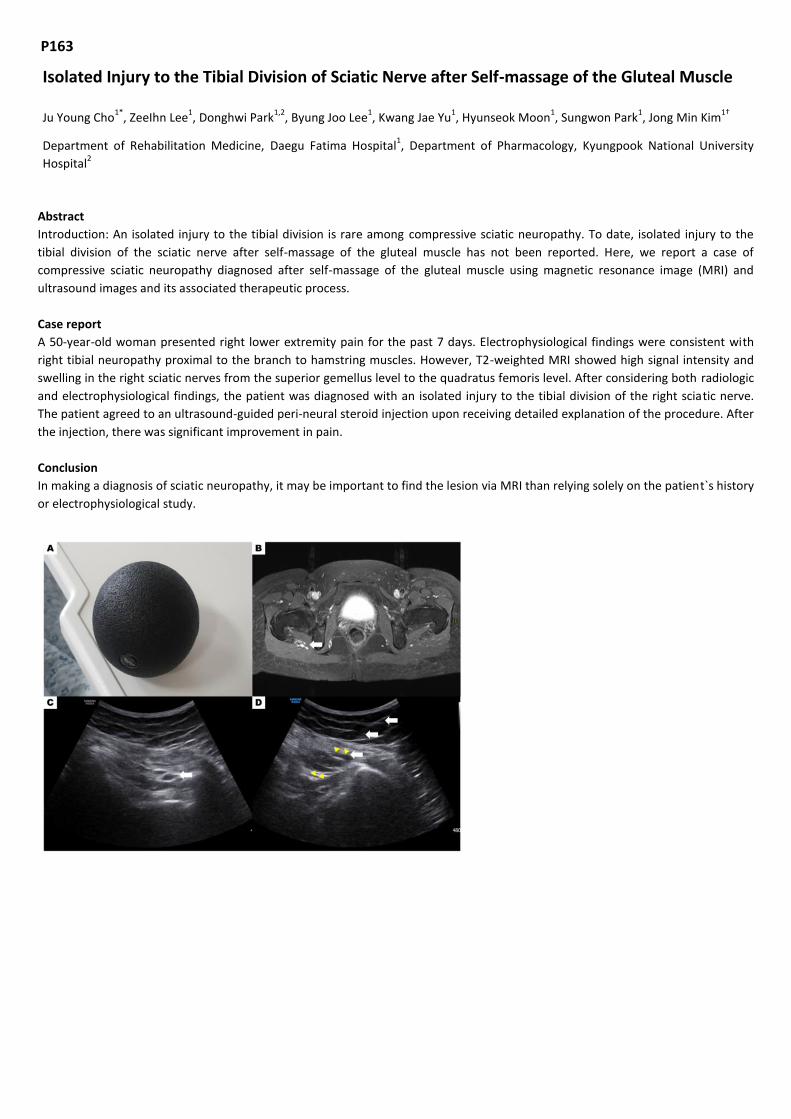
P163
Isolated Injury to the Tibial Division of Sciatic Nerve after Self-massage of the Gluteal Muscle
Ju Young Cho1*
, ZeeIhn Lee1, Donghwi Park
1,2, Byung Joo Lee
1, Kwang Jae Yu
1, Hyunseok Moon
1, Sungwon Park
1, Jong Min Kim
1†
Department of Rehabilitation Medicine, Daegu Fatima Hospital1, Department of Pharmacology, Kyungpook National University
Hospital2
Abstract
Introduction: An isolated injury to the tibial division is rare among compressive sciatic neuropathy. To date, isolated injury to the
tibial division of the sciatic nerve after self-massage of the gluteal muscle has not been reported. Here, we report a case of
compressive sciatic neuropathy diagnosed after self-massage of the gluteal muscle using magnetic resonance image (MRI) and
ultrasound images and its associated therapeutic process.
Case report
A 50-year-old woman presented right lower extremity pain for the past 7 days. Electrophysiological findings were consistent with
right tibial neuropathy proximal to the branch to hamstring muscles. However, T2-weighted MRI showed high signal intensity and
swelling in the right sciatic nerves from the superior gemellus level to the quadratus femoris level. After considering both radiologic
and electrophysiological findings, the patient was diagnosed with an isolated injury to the tibial division of the right sciatic nerve.
The patient agreed to an ultrasound-guided peri-neural steroid injection upon receiving detailed explanation of the procedure. After
the injection, there was significant improvement in pain.
Conclusion
In making a diagnosis of sciatic neuropathy, it may be important to find the lesion via MRI than relying solely on the patient`s history
or electrophysiological study.

P 164
Idiopathic hypertrophy of the first dorsal interosseous presenting as a mass: A Case Report
Kun-Woo Kim1*
, Jin-Tae Hwang1, Jae-Hyung Choi
1, Jong-Geol Do
1, Kyung Jae Yoon
1, Yong-Taek Lee
1†
Department of Rehabilitation Medicine, Kangbuk Samsung Hospital, Sungkyunkwan University, School of Medicine1
Introduction
Anomalous muscle conditions in the hand can be categorized into three types: hypertrophy, accessory muscle, and abnormal distal
extension of proximal muscle. Among them, accessory abductor digiti minimi is the most common and its prevalence has been
reported up to 24%. However, idiopathic hypertrophy of the first dorsal interosseous is extremely rare. It was first described in 1988
and only few cases have been published since then. To our knowledge, in Korea, there is no reported case of this condition. Here,
we report the first case of an idiopathic first dorsal interosseous hypertrophy in Korea, presented as a mass lesion of non-dominant
hand and diagnosed by ultrasonography and magnetic resonance imaging.
Case Description
A 36 year-old man presented with a mass in his left hand at the first web space. The man reported that he had noticed the mass 3
weeks ago, but the exact onset was uncertain. He had no pain or any other symptoms, such as functional restriction of hand. The
patient was right handed and worked as an office worker. There was no reported history of trauma or other activities that would
predispose the patient's hand to be swollen. On inspection, there was a mass-like lesion at the dorsal aspect of the first web space
(Figure 1). The mass was soft on palpation, and there was no tenderness, heating sensation or redness at the site. Muscle strength,
sensation and range of motion of hand were normal. Plain radiography showed no bony abnormality. Ultrasonography (US) on the
dorsal aspect of first web space revealed a hypertrophy of the first dorsal interosseous in left hand. The US image of the muscle
showed normal muscular echotexture with hyperechoic fibroadipose septa separating the hypoechoic muscle bundles. The maximal
thicknesses of left and right first dorsal interosseous on the long axis view were 10.5 mm and 7.7 mm, respectively (Figure 2). To rule
out pathologic conditions such as soft tissue tumor, magnetic resonance imaging (MRI) were conducted. MRI demonstrated
hypertrophy of the left first dorsal interosseous muscle with normal signal intensity. In the contrast enhanced T1-weighted images,
abnomally enhanced lesion was not observed (Figure 3).
Figure 1. Picture of the patient’s both hand. Mass-like lesion of the left first dorsal web space is shown.

Figure 2. Ultrasonography of (A) left and (B) right first dorsal interosseous in the long axis view. The maximal thicknesses of left and right first dorsal interosseous were 10.5 mm and 7.7 mm, respectively. Asterisk, first metacarpal bone; FDI, first dorsal interosseous.
Figure 3. Magnetic resonance imaging of left hand: (A) Coronal view of proton density-weighted image, Axial view of (B) T1-weighted image and (C) contrast enhanced, fat suppressed, T1-weighted image. Hypertrophied left first dorsal interosseous muscle with normal signal intensity is shown.

P 165
A rare case with lymphedema tarda of unilateral upper limb
Cheolhwan Hyun1*
, Kyeong Eun Uhm1, Jongmin Lee
1†
Department of Rehabilitation Medicine, Konkuk University Medical Center1
Introduction
Primary lymphedema is generally classified into congenital, praecox and tarda by onset age. In particular, primary lymphedema
occur frequently in the lower limb, and unilateral arm swelling is rarely reported. In this report, we present a patient with
lymphedema tarda of the unilateral upper limb.
Case report
An 89-year-old female was referred to the Department of Rehabilitation for the evaluation of progressive left arm swelling for 3
months. She has no history of trauma, surgery and cancer treatment. On physical examination, firm pitting edema was palpated on
left whole arm including hand dorsum. Difference of circumference was 5.5cm at upper arm and 6.6cm at forearm. There was no
abnormalities in the right arm and legs. Laboratory investigations were performed, and complete blood counts, electrolytes,
creatinine, D-dimer and acute phase reactants were within normal limits. Contrast-enhanced computed tomography scans of the
chest and abdomen did not show specific findings. RI lymphoscintigraphy showed the lymphatic flow of the left upper limb was
slower than that of the right upper limb. The left axillary lymph nodes were observed late and activity was lower than right. A
dermal backflow was also observed in the left forearm. To exclude the hidden malignancy such as breast cancer, she was referred to
the Department of Breast Surgery. Breast ultrasonography revealed no specific findings except for a left axillary lymph node
enlargement. Fine Needle Aspiration (FNA) biopsy was performed for that lymph node, and results showed numerous
polymorphous lymphoid cells consistent with a reactive lymph node. Finally, she was diagnosed as lymphedema tarda occurred in
unilateral upper limb, and managed with compressive garment and flavonoid.
Conclusion
Primary lymphedema isolated on unilateral upper limb is a rare presentation of lymphedema. In this case, we could diagnose the
lymphedema tarda after exclude secondary causes by laboratory and imaging studies

P 166
Injury of medial antebrachial cutaneous nerve after axillary lymph node dissection in breast cancer
Dong-Ha Kang1*
, Gi-Wook Kim 1,2
, Sung-Hee Park1,2
, Myoung-Hwan Ko1,2
, Jeong-Hwan Seo1,2
, Yu Hui Won1,2†
Department of Rehabilitation Medicine ,Chonbuk National University Hospital1, Biomedical Research Institute of Chonbuk National
University Hospital,Research Institute of Clinical Medicine of Chonbuk National University2
Introduction
Complications after mastectomy with axillary resection in patients with breast cancer are most commonly associated with
lymphedema, as well as peripheral nerve injury and surgical site infection, and so on. Based on previous reports, it is known that the
injury of the intercostobrachial nerve (ICBN) account for largest part of the peripheral nerve injury after breast surgery, followed by
medial brachial cutaneous nerve (MBCN) of the arm. Here, we present the rare case who suffered from an injury to the medial
antebrachial cutaneous nerve (MACN) of forearm after breast cancer surgery.
Case presentation
A 49 years old woman, on April 2018, accidentally noticed palpable mass in her left breast. The patient underwent various breast
evaluations and diagnosed with invasive ductal carcinoma (pT2N1). Partial mastectomy with axillary lymph node dissection (ALND)
level 1, 2 was done on May 24, 2018. Patient was supine with arm extension positioned during surgery and skin incision type was
radial linear incision. On the 12th postoperative day, the patient complained of numbness in the medial area of left forearm with
overall edema of the left arm. Peripheral nerve injury in the left arm was suspected, and left MACN lesion was detected on nerve
conduction study, which showed right MACN of forearm with onset latency of 2.05ms, amplitude of 12.3mV, and left MACN of
forearm with onset latency of 1.75ms, amplitude of 4.3mV(Table 1, Fig 1-A). The amplitude of left MACN nerve was 34.9% of the
amplitude of right MACN. The patient was done with rehabilitative treatment for lymphedema and nerve injury and discharged on
23 May, 2018. She had finished chemotherapy for about 5 months after discharge, and she was feeling pain in her left forearm even
more aggravated compared with the time of admission (VAS 7). Follow up electrophysiologic study was performed approximately 9
months after the previous one, and left MACN lesion was still detected and there was no interval change. The result of nerve
conduction study was onset latency of 1.60ms, amplitude of 15.9mV with right MACN of forearm, and onset latency of 2.20ms,
amplitude of 5.2mV with left MACN of forearm, which showed still 32.7% of right MACN amplitude (Table 1, Fig 1-B). After taking
medication and rehabilitation for about 2 months, she felt mild improvement of the pain (VAS 7→5).
Conclusion
Nerve injuries as following complication of breast surgery with ALND are common in ICBN and MBCN, but MACN damage can also
occur considering its anatomic course. The MACN of forearm runs in parallel with the ICBN and MBCN in the lateral area and passes
through the axillary area. There are studies that mentioned about ICBN dividing proximally to give a contribution to the MACN and
about great variation of MACN. If patients who underwent breast cancer surgery with axillary dissection uncommonly complain of
sensory symptoms in the forearm, we need to consider injury of MACN and carry out a check on it.
Table 1. Sensory nerve conduction study
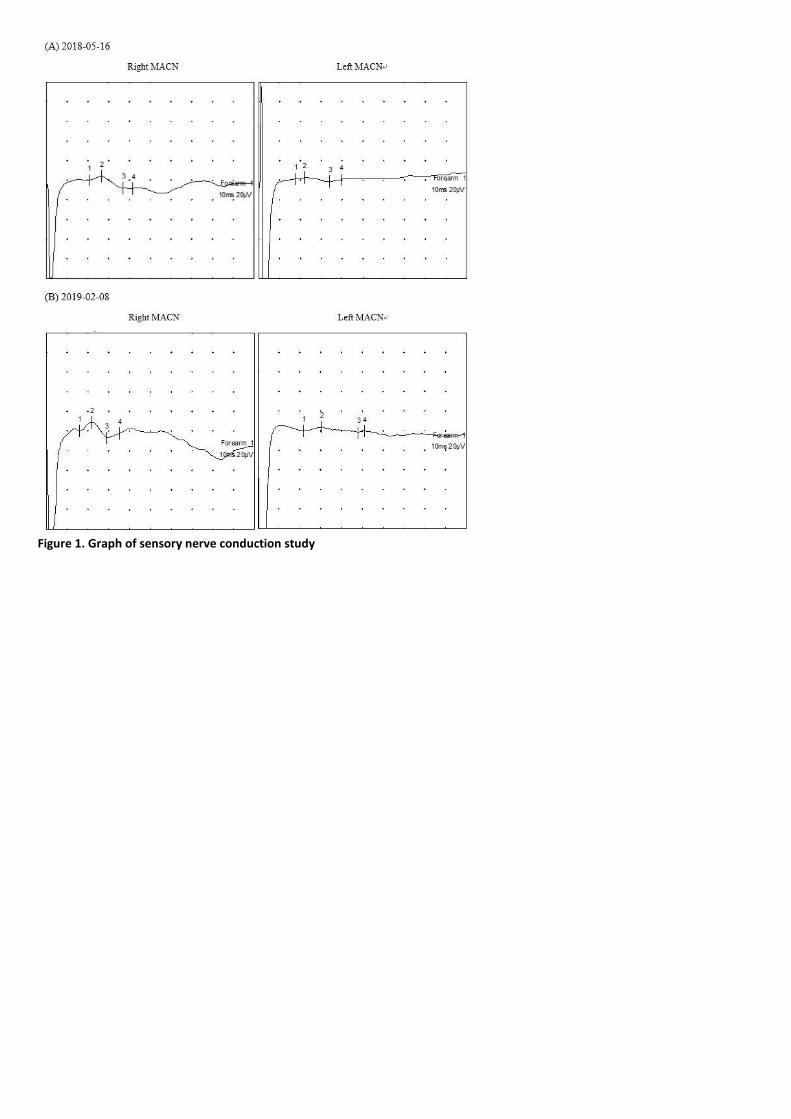
Figure 1. Graph of sensory nerve conduction study

P 167
Predicting the Effect of Stellate Ganglion Block on Lymphedema Using Cold Immersion Test
Hyo Joon Jin1*
, Soyoung Lee1†
, Du Hwan Kim1, Yong Min Choi
1, Seung Wook No
1
Department of Rehabilitation Medicine, Keimyung University Dongsan Medical Center1
Introduction
Cervical cancer related lymphedema is caused by damaged lymphovascular system. Also autonomic system regulate lymphatic
transfer by regulating lymphatic vessel which collects and discharges waste debris and fluid from the superficial lymphatic system
into the systemic circulation. But for now, there is no screening tool for autonomic dysfunction of cervical cancer related
lymphedema. Cold immersion test (CIT) is economic, non invasive and simple test for checking autonomic disturbance. We
hypothesized that we could use CIT as a screening test for evaluating autonomic function of cervical cancer related lymphedema
and if the patient has abnormal autonomic system, sympathetic ganglion block (SGB) would be effective.
Case
A 61 years old woman, with cervical cancer related lymphedema for 6 years, was referred to our out-patients clinic. She was
diagnosed with cervical cancer 15 years ago and did total abdominal hysterectomy with bilateral salpingo-oophorectomy and
radiotherapy. We managed her with complex decongestive physical therapy including compression bandage and stocking for 6 years.
But her symptom has fluctuated and the compliance with treatment was not good. We were planning to do SGB and tested her
autonomic function with CIT. The result of the CIT was abnormal on both lower extremities (Figure 1). We did Lt. lumbar SGB 2 times
every two weeks. Her subjective and objective symptom was much improved after lumbar SGB and made a very good progress
(Table 1).
Conclusion
According to this preliminary report, we can assume that lumbar SGB will improve not only swelling but also heaviness in cervical
cancer related lymphedema patients who have abnormal CIT. And there should be continuous research for the effect of SGB in the
lymphedema patient with abnormal autonomic regulatory system in the future.
Figure 1. Abnormal cold immersion test of both lower extremity

Figure 2.ymphscintigraphy before lumbar sympathetic ganglion block
Table 1. Change of the left leg girth and heaviness

P 168
Suicidal attempts after spinal cord injury
Jun-Il Park 1*
, Hanbit Ko1, Chang-Won Moon
1, Il-Young Jung
1, Kang Hee Cho
1†
Department of Rehabilitation Medicine, School of Medicine, Chungnam National University Hospital1
Introduction
Depression is not simply limited to the mood disorder, but it is less amenable to treatment, including rehabilitation. This leads to
deterioration of patients’ recovery, disagreement with caregivers, and long-term hospital days. In extreme case, suicidal attempts
may occur. We present two cases with suicidal attempt after spinal cord injury because we need to be alert and educate patients
and caregivers.
Case Presentation
Case I A 71-year-old man who underwent surgical decompression surgery due to muscle weakness caused by cervical spinal stenosis
was found unconscious on a winter morning in his room where there were remnants of burned-out charcoal briquettes. After
Receiving ICU care for CO intoxication, he was transferred for rehabilitation. His initial mini mental state examination (MMSE) score
27/30, motor power was grade 4/4 in the upper extremity and grade 3~4/3~4 in the lower extremities. During hospitalization, the
patient’s memory deficiency and cognitive impairment gradually deteriorated. The last mini mental state examination (MMSE) score
4/30, motor power was weakened. After Brain MRI follow-up, the patient was diagnosed with delayed encephalopathy. The
cognitive and functional improvement, which was our rehabilitation goal, was not achieved.
Case II A 75-year-old man admitted our hospital with a back pain, left lower limb weakness (grade IV), which began in February 2018,
and underwent surgical decompression under spinal stenosis diagnosis. In April 2018, he was transferred for rehabilitation because
bilateral lower limb weakness persisted (grade IV/IV). In October 2018 midnight, he wasn’t confirmed in his bed, and was found
hanging with electric wire in the restroom of other floor in hospital and CPR was performed, but expired. During the hospitalization
period, the patient was consistently dissatisfied with lower limb weakness after surgery and told his family that he wanted to die
occasionally, and there also contained a negative mention in nursing record.
Discussion
Patients with spinal cord injuries are often accompanied by depression, and occasionally suicide attempts may occur as in these
cases. Not only just because of suicidal attempt post SCI, but also because depression itself adversely affects patient’s recovery,
participation in rehabilitation, and quality of life, the screening for depression in SCI patients is very important. In our hospital,
screening for depression is performed by Beck Depression Inventory (BDI) and Beck Hopelessness Scale (BHS) test for patients with
SCI, and if the BHS is above 10 points, it is known to be closely related to suicidal attempt. The depression screening tests that can
be conducted in rehabilitation medicine are self-report-type depression. So there is a limit to believing in them. Therefore, we need
to regularly check patients' caregivers and families to see if they have any negative thoughts or comments about life at home during
their hospitalization period.

BHOP