Herbs Cultivation, Medicinal, Aromatic Plants cultivation ...
Upload
khangminh22Category
view
1download
0
MEDICINAL PROPERTIES OF SOME PLANTS USED FOR THE
TREATMENT OF SKIN DISORDERS IN THE O R TAMBO AND
AMATHOLE MUNICIPALITIES OF THE EASTERN CAPE PROVINCE,
SOUTH AFRICA
by
MAHACHI JOSIA
A dissertation submitted in fulfillment of the requirements for the degree of
MASTER OF SCIENCE (MSc): BOTANY
at
WALTER SISULU UNIVERSTY
SUPERVISOR: DR. L. KAMBIZI
SEPTEMBER 2013

ii
General Abstract
The use of medicinal plants for treatment of skin infections and improvement of skin tone
was assessed. The study covered Amathole and OR Tambo municipalities of the Eastern
Cape Province of South Africa. The study sought to identify and document some medicinal
plants which are used by the indigenous people on the skin, evaluate some biological
properties which attribute to their use for therapeutic use. This report provides
ethnobotanical data on some plant which were identified. Six medicinal plants (Kniphofia
drepanophylla, Gnidia capitata, Hypoxis hemerocallidea, Syzgium cordatum, Macaranga
capensis and Protorhus longifolia) which were implicated for treatment of skin diseases
were screened for their antibacterial and antioxidant properties.
Guided questionnaires were used to interview and gather ethnobotanical information
from the traditional healers. Members of the communities which were indicated to be
knowledgeable on use of medicinal plants in the areas were visited and interviewed. The
results revealed that a total of 45 plant species distributed in 41 Genera belonging to 28
Families are used for treatment of skin infections and improvement of skin texture. The
plant medicines were reported to be used as remedies against common skin problem
such as wounds, pimples, acnes and itches. Some were reported to have anti-
inflammatory effect on the skin while other were reported to oil dry skin and prevent skin
dryness and dry eczematous conditions. Others like Cassipourea flanaganii, and
Spirostachys africana were commonly used to enlighten skin and protect skin from ultra-
violet radiation. The most common mode of preparation of these medicinal plants was
pastes or decoctions. Sometimes crushed plant materials were put in bathing water or

iii
boiled and steamed on affected parts. It was reported that mixing pastes with oil, animal
fat and milk improve medicinal properties.
Water, methanol and acetone extracts of K. drepanophylla, G. capitata, H.
hemerocallidea, S. cordatum, M. capensis and P. longifolia were screened against five
strains of Gram negative bacteria. The results revealed that water extracts from five plant
species inhibited two or more strains of bacteria with the most common minimum
inhibitory concentrations (MICs) ranging between 5,0 to 10,0 mg/ml with the exception
of aqueous extracts of K. drepanophylla which failed to inhibit all strains of bacteria.
The screening of methanol extract of these plants for antioxidant and free radical activity
revealed a significant activity with 1, 1-diphenyl-2-picryl-hydrazyl (DPPH) free radical
(DPPH). The extracts of P. longifolia, G. capitata, M. capensis, S. cordutum and H.
hemerocallidea showed significantly higher free radical scavenging activity with IC50 of
ranging from about 11.0 to 41.2 µg/ ml while the IC50 value for K. drepanophylla could
not be determined at 100 µg/ ml.
Generally the study showed that medicinal plants still play a very important role in the
health care delivery system, especially in the O R Tambo and Amathole municipalities of
the Eastern Cape. Botanical medicine remains pivotal in the treatment of skin ailments
and improvement of the skin tone.

iv
Declaration of originality
I, Josia Mahachi, Student Number 209065494, solemnly declare that this dissertation entitled “Medicinal Properties of Some Plants Used for Treatment of Skin Disorders in the O R Tambo and Amathole Municipalities of the Eastern Cape Province, South Africa” is my original work. All sources used or quoted in the study have been
indicated and acknowledged by way of complete references.
MASTER’S CANDIDATE: MAHACHI JOSIA
SIGNATURE: ……………………………………..
DATE: ……………………………………..
SUPERVISOR: DOCTOR L. KAMBIZI
SIGNATURE: ……………………………………..
DATE: ……………………………………..
v
Plagiarism Declaration
(i) I am aware that plagiarism is defined at Walter Sisulu University (WSU) as the inclusion of another’s or other’s ideas, writing, works, discoveries and inventions from any source in an assignment or research output without the due, correct and appropriate acknowledgement to the author(s) in breach of the values, conventions, ethics and norms of different professional, academic and research disciplines and includes unacknowledged copying from intra- and internet and peers/fellow students.
(ii) I have duly and appropriately acknowledged references and confirmed to avoid plagiarism as defined by WSU.
(iii) I have made use of the citation and referencing style and stipulated by my supervisor.
(iv) This submitted work is my own. (v) I did not and will not allow anyone to copy my work and present it as his/her
own. (vi) I am committed to uphold academic integrity in the academic/ research activity. (vii) I am aware of the consequences of engaging in plagiarism.
…………………………………………… ……………………………
Signature Date
vi
Acknowledgement
Acknowledgements and thanks to:
To my supervisor Dr L. Kambizi for his expertise, excellent supervision and
mentorship which he provided during this study. Without his assistance it could
not have been possible to go through this research project;
Dr. D. Kamadyaapa and Mr. E.J. Ndebia for their technical support in performing
the antioxidant assays;
Dr. E. Immelman and Mr. E. Cleote for their assistance in the identification of
plants collected during the ethnobotanical survey;
Mr. D. Wopula for helping for social networking and conducting the ethnobotanical
survey;
Department of Physiology, Faculty of Health Science, Walter Sisisulu University for
allowing me to conduct antioxidant assays using its facilities;
Research Direcorate of Walter Sisulu University for funding this research;
National Research Foundation for funding this study;
Traditional practitioners and local people of Amathole and O R Tambo
Municipalities who provided ethnobotanical information on medicinal plants used
for treatment of skin ailments.

vii
Dedication
To my wife Tendayi Clarah Mahachi and my children Leo, Leon, Leonell and Leona who
endures the absence of their father during the period of this study and whose patience
and love is always beyond comprehension.
To my parents Leyo and Vongayi Mahachi who went through serious hardships for my
education.
To my late auntie Sosana Mahachi who took care of me during my childhood.

viii
LIST OF ABBREVIATIONS
AIDS Acquired Immune-Deficiency Syndrome
ARV Antiretroviral
DNA Deoxyribonucleic acid
DPPH 1, 1-diphenyl-2-picryl-hydazyl
HIV Human Immune-Deficiency Virus
MICs Minimum Inhibitory concentrations
S.A South Africa
UCHPP Walter Sisulu University Health Partnership Project
USA United State of America
WHO World Health Organization
WSU Walter Sisulu University

ix
Table of contents
General abstract ii
Declaration of originality iv
Plagiarism declaration v
Acknowledgements vi
Dedication vii
List of abbreviations viii
Table of contents ix
List of tables xiii
List of figures xiv
List of appendices xv
Chapter 1: Research problem 1
Introduction 1
Statement of the problem 2
Background of the problem 4
Objectives of the study 6
Significance of the study 6
Rationale of the study 9
Overview of Chapters 10
References 11
Chapter 2: Literature review 16
x
Skin disorders and infections 16
Inflammation and erythema 18
Hyperpigmentation and hypopigmentation 20
Psoriasis 21
Free radicals 22
Role of medicinal plants 23
Modern medicines from plants 25
Use of medicinal plants on the skin 27
Antimicrobial agents in plants 28
Anti-inflammatory and antierythema 30
Plant agents used against skin dryness and dry eczematous conditions 31
Antioxidant agents 31
References 33
Chapter 3: An ethnobotanical study of some medicinal plants
used for treatment of skin infection and improvement of skin
infections and improvement of skin tone in O R Tambo and
Amathole Municipalities
39
Abstract 39
Introduction 40
Materials and methodology 43
Ethnobotanical survey 44
Results 45
xi
Discussion 58
Conclusion 61
Acknowledgements 61
References 62
Chapter 4: Antibacterial activity of some plants used for
treatment of skin infections and disorders in O R Tambo and
Amathole Municipalities
66
Abstract 66
Introduction 67
Methodology 68
Results and Discussion 71
Acknowledgement 74
References 75
Chapter 5: In vitro antioxidant activity of some plants used for
treatment of skin problems in O R Tambo and Amathole
Municipalities
77
Abstract 77
Introduction 78
Materials and Methodology 80
Results and Discussion 82
Acknowledgement 86
References 87
xii
Chapter 6: General discussion 89
Discussion 89
Conclusions 93
Limitations 94
Recommendations 94
References 96
Appendices 98
Questionnaire respondent by traditional practitioners 98
Questionnaire respondent by local people 102

xiii
List of tables
Table No Title of table Page No
3.1 Ethnomedicinal plant species used for treatment and
improvement of skin in O R Tambo and Amathole
Municipalities
47
4.1 Antibacterial activity of some plants extracts used for
treatment of skin problems in O R Tambo and Amathole
Municipalities
73
5.1 1 In vitro antioxidant activity of methanol extracts of some
plants used for treatment of skin infections and disorders
84
xiv
LIST OF FIGURES
Figure No: Figure title: Page No:
2.1 Some conditions of the skin caused by infection 18
2.2 Erythema caused by mild sunburns 19
2.3 Erythema multicoforme complexes 20
2.4 Erythema multicoforme complexes 22
3.1 Map of Eastern Cape showing study area 44
3.2 Families of plant used for the treatment of skin disorders 53
3.3 Medicinal plants used for treatment and improvement 54
3.4 Type of medicinal plants used for treatment of skin
disorders
55
3.5 Mode of preparation of botanical medicines 55
3.6 M. capensis stem and leaves 56
3.7 H. hemerocallidea plant 56
3.8 K. drepanophylla underground parts 57
3.9 G. capitata plant 57
3.10 P. longifilia stem, leaves and a traditional practitioner 57
5.1 DPPH free radical activities of ascorbic acid and methanol
plant extracts
83

xv
List of Appendices
Questionnaire respondent by traditional practitioners 98
Questionnaire respondent by local people 102

1
Chapter 1: Research problem
INTRODUCTION
People on all continents have used hundreds to thousands of indigenous plants for the
treatment of ailments since prehistoric times (Acharya et al., 2008). In the Eastern Cape
Province of South Africa indigenous people have a long history of using phytotherapy for
the treatment of various diseases and ailments (Grierson and Afolayan, 1999; van Wyk,
et al., 1997) including various skin disorders. The use of medicinal plants is not something
of the past instead it is something essential for the future. Scientific literature indicated
that pathogens are increasingly becoming more resistant to antibiotics (Quave et al.,
2008). The evolution of highly resistant pathogenic microbial strains has compromised
the use of newer generation of antibiotics (Levy, 2002). The increase in resilience of
microbes to antibiotics threatens public health on global scale as it reduces the
effectiveness of treatment (Coastal et al., 1996) and increases morbidity, mortality and
health cost.
However, ethnomedicinal studies have shown that plant remedies are effective in spite
of the fact that they lack scientific justification (Jager et al., 1996; Fox, 1999; Kelmanson,
et al., 2000). Although the active phytochemicals may occur in lower concentrations,
medicinal plant extracts may be better sources of antimicrobial components than
synthetic drugs (Cox and Balick, 1994). It is believed that the phenomenon of synergism
is crucial in the efficacy of plant medicines (Kamatou et al., 2006). The development of

2
pathogenic resistance to synergistic drug combination such as those found in plants may
be slower than for single drug treatments (Quave et al., 2008).
Phytotherapy is a traditional medicinal practice based on the use of a wide variety of
plants, plant parts and plant extracts for prevention and treatment of diseases. Traditional
practitioners and herbalists use crude extracts from leaves, flowers, stems, berries, and
roots of plants to prevent, relieve, and treat illnesses. The World Health Organization
(WHO) estimates that about 80% of the population of most developing countries relies
on phytotherapy for their primary health care needs (Mukherjee and Wahil, 2006; de
Silva, 1997). It is important to note that out of the total 422,000 flowering plants reported
from the world (Govaerts, 2001) more than 50,000 are used for medicinal purposes
(Schippmann et al., 2002). That is, this great biodiversity of medicinal plants can be
utilized in scientific research for discovery of novel pharmaceuticals.
Phytotherapy depends on the ability of plants to synthesize chemical compounds that
help them defend against attack from a variety of predators such as insects, fungi and
herbivorous mammals (Wikipedia, 2010). Medicinal plants are biosynthetic factories of a
variety of chemical compounds such as phenols, aromatic substances or their oxygen
derivatives. About 11, 000 plant compounds have been isolated in recent years (Gupta,
1986). Although these compounds are toxic to plant predators and pathogens, by chance
some of these turn out to have beneficial effects when used to treat human diseases
(Wikipedia, 2010). Most of these plant compounds are taught to work in the same way
pharmaceuticals drugs used in mainstream healthcare system.

3
Statement of the Problem
Skin infections and disorders are commonly observed in local people in the O R Tambo
and Amathole Municipality Districts in the Eastern Cape Province of South Africa. They
took different forms like inflammation, erythema, ring worms, eczema, acne, insect bite
or skin pigmentation problems (hyperpigmentation and hypopigmentation). Skin
pigmentation can be a problem for all people with brown skin: people of African, Asian,
Latin and Native American background (Taylor, 2008). Hyperpigmention is caused by
ultraviolet radiation and is associated with conditions such as pregnancy, Addison’s
disease (decreased function of adrenal gland) and uses of drugs while hypopigmentation
is associated with vitiligo (an autoimmune disorder) and albinism (Levine, 2010).
Theseconditions often affect the people. In the Province, young boys undergo ritual
circumcision to be initiated into manhood. Every circumcision season the young boys
undergo advanced infections, severe blood loss and mutilation (Peltzer et al., 2008).
Plants and plant extracts have been used for the treatment of skin disorders and ailments
for centuries (Weckesser et al, 2007). As a result of increasing resistance to antibiotics of
many bacteria and fungi, plant extracts and plant compounds are of new interest as
antiseptics and antimicrobial agents in dermatology (Weckesser et al, 2007). There is an
increasing need for innovation in selecting therapeutical targets and finding leading plant
derived drugs (Bhagwandin, 2011) which are cheap and affordable to people. Most
African people still rely heavily on traditional medicine; traditional healers are often the
first and last line of defense against most diseases such as headaches, coughs, and
diarrhea, wound healing and skin diseases (Matsheta and Mulaudzi, 2008). Apart from

4
ethnobotanical property and primary health care system, medicinal plants were also the
alternate sources of income for the underprivileged communities (Dobriyal et al., 1997).
Background of the problem
The Walter Sisulu University Community Health Partnership Project (UCHPP) reported
that about 41 % diagnoses in the health centres in the Eastern Cape include injuries,
genital diseases and skin infections (Brueton et al., 2010). In this study about 10 % of
the complaints were skin infections, scabies and ascarisis. Although this significant
percentage of skin infections were reported in conventional health centres, direct
observation revealed that many cases of skin infections and disorders are not presented
to local clinics or hospitals. Instead, many people are topically using plant materials to
treat skin ailments and improve skin tone.
It is estimated that about twenty seven million South Africans use traditional medicine
because they consider pharmaceutical drugs expensive (Mander et al., 2007). Some
people live in remote locations where they do not have easy access to clinics and hospitals
and therefore, use traditional medicine as an alternative treatment (Mander et al., 1998).
It is worth to note that, about 33 % of phytotherapies in non-Western societies are used
for the treatment of skin problems (Mantle and Gok, 2001).
In the Eastern Cape Province, many people are exposed to high risks of skin infections
and skin problems. The risk factors include circumcision undertaken in non-clinical setting

5
(Peltzer et al., 2008), insect, tick, animal, and marine organism bites (Travel medicine,
2008) and exposure to ultra-violet light.
The main inhabitants of this Province, the Xhosa-speaking people, practice ritual
circumcision as a cultural institution. Every year, young abakwetha (Xhosa; initiates) are
circumcised, dressed and treated wounds using phyto-medicines. Medical circumcision
performed by health care professionals, who substitute traditional equipment and
dressing for medical ones are deemed meaningless. As a result of this cultural belief and
values many of the abakwetha go for initiation school.
In the scientific reports, there is a lot of literature depicting serious foreskin infection and
wounds from traditional circumcision generated from hospital records (Mayatula and
Mavundla, 1997; Meinjies, 1998) or circumcision/initiation school inspections. Peltzer et
al (2008) noted that pre-post intervention evaluation of 192 initiates physically examined
at the 14th day after circumcision by a trained clinical nurse 40 (20.8%) had mild delayed
wound healing, 31 (16.2%) had a mild wound infection and 22 (10.5%) mild pain. As a
result of the observed problems associated with this practice it leaves the efficacy of
botanical medicines questionable.
The districts of O R Tambo and Amathole are located along the coast and are sometimes
very hot as a result many people are observed swimming or navigating the sea shore.
This exposes them to marine hazards such as stingrays, jellyfish, and several species of
poisonous fish in the coastal waters (Travel medicine 2008). After swimming or
navigation of the sea shore many people would lay on beach sands warming themselves

6
in the sun. This exposes them to ultraviolet sun which may cause skin cancer and
hyperpigmentation. Other hazards include bites by snakes (cobras, mambas, adders,
vipers) and spiders (black and brown widow) as people camp in forests or visit game
parks (Travel Medicine, 2008).
Objectives of the study
The objectives of this study are to:
Identify and document some plant species used for the treatment of
dermatological infections and disorders in O R Tambo and Amathole
Municipality districts;
Evaluate antibacterial activities of some medicinal plants used for treatment
of skin infections and disorders;
Investigate antioxidant properties of some medicinal plants used for the
treatment of skin infections and disorders.
Significance of study
Phytotherapy has remained pivotal in the health care system of a large proportion of
people in the world. According to WHO, about 80 % of the world's population presently
uses phytotherapy for some aspect of primary health care needs. This is due to the fact
that pharmaceuticals are prohibitively expensive for most of the world's population (Edgar

7
et al., 2002), especially in South Africa where more than half of population lives below
the international established poverty datum line (Gutierrez, 2006). The Eastern Cape is
home to 6, 4 million [Statistics South Africa (SSA), 2004] and has the second highest
poverty levels in South Africa with 47 % households below the poverty line, which is
based on imputed monthly expenditure of less or equal R800 (SSA, 2004), combined with
the highest Provincial unemployment of 55 % in the country (SSA, 2004). This entails
that a significant population of the Province cannot afford the increasing pharmaceuticals
costs hence their natural resources especially medicinal plants play a very crucial role in
their health care system. This study attempts to identify and document some plant
species that are commonly used for the treatment of common skin infections and
disorders.
Documentation of ethnobotanical information is essential for understanding of human-
plant ecology. Indigenous knowledge on natural resource utilization of medicinal plants
not exceeding the resilience of the surrounding environment is an important measure of
sustainable plant biodiversity conservation (Kala, 2005). It is estimated that more than
700 hundred medicinal plants are being traded for medicinal purposes throughout the
country (Dold and Cock, 2001) resulting in the reserves and stocks of medicinal plants in
the country diminishing. In the Eastern Cape it was reported that 93 % of 116 plants are
harvested unsustainably for medicinal purposes (Cocks and MØller, 2002). A number of
these medicinal plants are endanger of extinct as a result of growing trade demands for
cheaper healthcare products and complacency to conservation. In addition, the
exploitation by the patent rights, communities and countries who invented the material

8
and the process, have been facing shortfall (Kingston et al., 2007) resulting in loss of
important information on medicinal plants and their use. Documenting the eroding plants
and associated indigenous knowledge can be used as a basis for developing management
plans for conservation and sustainable use of medicinal plants in the area.
Ethnobotanical data is very essential for discovery of novel plant derived drugs especially
where information is well evaluated. The traditional use of medicinal plants is recognized
as a way to learn more about future medicines. In 2001, researchers identified 122
compounds used as pharmaceutical drugs which are derived from “ethnomedical” plant
sources; 80 % of these compounds are used in the same way as they are used in the
traditional medicine (Fabricant and Farnsworth, 2001). There are over 750,000 plants on
earth relatively very few of them with healing properties have been studied scientifically
(Chong, 2004). The Eastern Cape Province is not an exceptional since it is endowed with
a diverse variety of medicinal plants which research has not yet translated into modern
pharmaceuticals.
Given the socio-economic standing of the people, the increasing costs of pharmaceuticals
and the great biodiversity of plant species, it is therefore, necessary to identify the some
plants and evaluate the medicinal properties of plants used for the treatment of skin
infections and disorders. This may be beneficial not only to the pharmaceutical industry
but also to the local people who are in need of the plant medicine.

9
Rationale of study
In the Eastern Cape approximately 70% of the physical related problems of an amaXhosa
family are managed using medicinal plants (Simon and Lamla, 1997). The wide spread
use of plant medicine among both urban and rural population in the Province is attributed
to cultural acceptability, efficacy against some types of diseases, physical accessibility
and economic affordability as compared to pharmaceuticals used in the mainstream
healthcare system. In addition, there are general claims that phytotherapy has no side
effects and therefore are safe to use as compared to synthetic medicines. Based on the
above arguments and low socio- economic position and inaccessibility of some health
centres to majority of people in the rural areas it is suggestive that many people use
medicinal plants to deal with health problems hence it is imperative and worth studying
the medicinal plants that are commonly used by local people.
The study of Eastern Cape medicinal plants has not been as fully realized as other
traditional communities elsewhere (Iwu, 1993). In the Province, though there has been
some organized ethnomedicinal studies, there is limited development of therapeutic
products. Generally, indigenous knowledge is getting lost owing to urbanization,
industrialization, rapid loss of natural habitats and changes in lifestyles (Teklehayamanot
and Giday, 2007). In the view of these facts documentation of the traditional medicinal
plants is of paramount importance for preservation of the indigenous knowledge and for
provision of baseline data for future pharmacological and phytochemical studies.

10
Overview of Chapters
The first chapter of this dissertation presents the research problem and its background.
The specific objectives are outlined in this chapter. In addition, the significance and
rationale for the study are described. Chapter 2 puts the problem into context by
providing the related literature. The ethnobotanical information on some plants used for
treatment of skin infections and disorders in O R Tambo and Amathole Municipalities of
Eastern Cape, South Africa are described in Chapter 3. This chapter presents an analysis
of ethnobotanical survey carried out in these two districts. From the survey six medicinal
plants namely Protorhus longifolia, Gnidia capitata, Macaranga capensis, Syzgium
cordutum and Hypoxis hemerocallidea were implicated for the treatment of skin infections
and disorders. Chapter 4 and chapter 5 report on the antibacterial activity and antioxidant
properties of these medicinal plants based on in vitro tests. The last chapter (6) provides
general discussion, limitations, and general conclusions to the study.

11
References
Acharya I, Deepak and Shrivastava A (2008). Indigenous Herbal Medicines: Tribal
Formulations and Traditional Herbal Practices, Aavishkar Publishers Distributor, Jaipur-
India: 440.
Bhagwandin W (2011). Medicinal Research Council. P.O. Box 19070, Tygerberg7505:
South Africa.1-2.
Brueton V, Yogeswaran P, Chandia, J, Mfenyana K, Modell B, Modell M, Nazareth
I (2010). Primary Morbidity in the Eastern Cape.Samj: South African Medical
Journal. 100 (5).
Chong’s Health Care Enterprise Inc (2004). Abstract.
Cock ML, MØller V (2002). Uses of and indigenized medicines to enhance personal
wellbeing: South African case study. Social Science Medicine 54. 384-389.
Coastal, J, Smith R, Miller M (1996) Superbug: should antimicrobial resistance be included
as a cost in economic evaluation? Health Economics.5:217-226.
Crowley IP, Kesner KM (1990). Ritual circumcision (Umkhetha) amongst the Xhosa of
Ciskei. BJU. 66: 318-321. [PubMed].
Deck AC, Dweck D (2002). Herbal Medicines for the skin –their Chemistry and Effects on
Skin and Mucous Membranes. Personal Care Magazine 3 (2): 19-20.
12
Dobriyal RM, Singh GS, Rao KS, Saxena, KG (1997). Medicinal plant resources in
Chhakinal Watershed in the north western Himalaya: traditional knowledge, economy and
conservation, Journal of Herbs, Spices and Medicinal Plants 5:15–27.
Dold T, Cock M (2001). The trade in medicinal plants in the Eastern Cape Province, South
Africa. Traffic Bulletin 19:11-13.
Edgar J. DaSilva, Elias B, Adnan B (2002). Biotechnology and developing world. Electronic
Journal of Biotechnology 5 (1).
Fabricant DS, Farnsworth NR (March 2001). The value of plants used in traditional
medicine for drug discovery. Environmental Health Perspective. 109 Supplementary 1:60-
75.
Farnsworth NR (1994). The role of Medicinal plants in drug development. In; Krogsgaard-
Larsen S, Brogger-Christensten S, Kofod H (Eds), Natural Products and Development,
Munkgaard, Copenhagen.
Fox, TR (1999). Aloe vera revered, Mystery Healer. Health Foods Business, 45-46.
Govaerts R (2001). How many species of seed plants are there? Taxon 50: 1085-1090.
Gupta R (1986). Integration of medicinal plants cultivation in forest and forest
plantations of northwestern Himalaya, Agroforestry Systems: A New Challenge, Indian
Society of Tree Scientists, Sloan, India. 59-67.
Guteierriez E (2006). Ecotourism and Biodiversity conservation. 597-607.

13
Questionnaire respondent by Iwu MM (1993). Handbook of African medicinal Plants. Boca
Raton: CRC Press.
Jager, AK, Hutching, A, van Staden J (1996). Screening of Zulu Medicinal plants for
prostaglandin-synthesis inhibitors. Journal of Ethnopharmacology.52; 95-100.
Kala, CP (2005). Ethnomedicinal botany of the Apatani in the Eastern Himalan region of
India. Journal of Ethnobiology and Ethnomedicine.1 (11).
Kamatau GPP, Viljoen AM, van Vuuren SF, van Zyl RL (2006). In vitro evidence of
antimicrobial synergy between Salvia chamelaeagnea and Leonnotis leonurus. South
African Journal of Botany. 72: 634-638.
Kelmanson JE, Jager AK, van Staden, J. (2000). Zulu medicinal plants with antibacterial
activity. Journal of Ethnopharmacology. 69; 241-246.
Kingston C, Jeeva S, Jeeva GM, Kiruba S, Mishara BP, Kannan, D (2007). Indigenous
knowledge of using medicinal plants in treating skin diseases in Kanyakumari district,
Southern India. Indian Journal of Traditional Knowledge.8 (2); 196-200.
Levine NMD (2010). Hyperpigmentation, hypopigmentation and your skin. WebMB:
Medical Reference.
Levy SB (2002). The antibiotic paradox: How the misuse of antibiotics destroys their
curative power. Perseus Publishing; Cambridge MA.
Mander M, Ntuli L, Diedericks N, Mavundla K (2007). South Africa’s Traditional Medicines
Industry. Department of Trade and Industry.

14
Matsheta MS, Mulaudzi FM (2008). The Perceptions of Traditional Healers of Cervical
Cancer Care at Ga Mothapo Village in Limpopo Province. Indilinga: African Journal of
Indigenous Knowledge Systems. 7:103–116.
Mayatula V, Mavundndla TR (1997). A review on male circumcision procedures among
South African blacks. Curationis. 20: 16-20.
Meintjies G (1998). Manhood at price; socio-medical perspectives on Xhosa traditional
circumcision. Institute of Social and Economic Research. Vol. 1.
Mentle D, Gok MA (2001). Adverse and beneficial effects of plants of extracts on skin and
skin disorders. Adverse Drug reactions and Toxicological Reviews. 20: 89-103.
Mukherjee PK, Wahil A (2006). Integrated approaches towards drug development from
Ayurveda and other Indian system of medicine, Journal of Ethnopharmacology103: 25-
35.
Peltzer K, Nqeketo A, Petros G, Kanta X (2008). Traditional circumcision during manhood
initiation rituals in the Eastern Cape, South Africa: a pre-post intervention evaluation.
BMC Public Health. 8: 64.
Quave CL, Plano LRW, Pantuso T, Bennett BC (2008). Effects of extracts from Italian
medicinal plants on plantonic growth, biofilm formation and adherence of methicillin-
resistant Staphylococcus aureus. Journal of Ethnopharmacol. 118 (3): 418-428.
Taylor S (2008). Skin pigmentation condition. Brownskin.net. 932 Pine Street,
Philadelphia, PA 19107.
15
Teklehaymanot T, Giday, M (2007). Ethnobotanical study of medicinal plants used by
people in Zegie Peninsula, Northwestern Ethiopia. Journal of Ethnobiology and
Ethnomedicine. 3.12.
Travel Medicine (2008). International Travel Guide.www.travmed.com.
“Traditional medicine”. http://www.who.int/mediacentre/factsheet/fs134/en/.
Simon C, Lamla M (1997). Merging pharmacopoeia; Understanding the origins of
incorporative pharmacopoeial processes among Xhosa healers in Southern Africa. J.
Ethnopharmacology. 33: 237-247.
Statistics South Africa (2004). Census 2001: Primary Tables Eastern Cape 2004. Pretoria.
Schippmann U, Cunningham AB, Leaman DJ (2002). Impact of cultivation and gathering
of medicinal plants on biodiversity: global trends and issues, Biodiversity and the
Ecosystem Approach in Agriculture, Forestry and Fisheries. Ninth Regular Session of the
Commission on Genetic Resources for Food and Agriculture, FAO Rome, Italy. 143–167
van Wyk, B, van Oudtshoorn, B, Gericke N (1997). Medicinal Plants of South Africa. Briza
Publications: Pretoria, South Africa.
Weckesser S, Engel K, Simon-Haarhaus B, Wittmer A, Pelz, Schempp (2007). Screening
of plant extracts for antimicrobial activity against bacteria and yeasts with dermatological
relevance. International Journal of Phytotherapy and Pharmacology.
Wikipedia (2010). Hebalism. The free encyclopaedia.

16
Chapter 2: Literature review
Skin disorders and infections
The human skin can show conditions ranging from simple dryness to severe erythema
and scaling. These indications are sometimes accompanied by pruritis, inflammation and
also may exhibit an associated oedema that further increases the discomfort (Dweck and
Dweck, 2002). In some cases binding of water in the stratum corneum can become
compromised and ineffective. This may result in skin dryness, desquamatory skin
conditions and dry eczematous conditions (Dweck and Dweck, 2002). Exposure to
ultraviolet light may present a problem of hyperpigmentation. The worst condition is when
there are injuries or damages to the skin and there are possibilities of wound infections
since this can turn even the simplest wound into a life-threatening condition (Dweck and
Dweck, 2002).
The skin is a haven for many microbes (Adeleye et al., 2003). The predominant ‘resident’
microorganisms of the skin include aerobic and anaerobic diptheroid bacilli such as
Corynebacterium, non-haemolytic aerobic staphylococci (S. epidermidis, Peptococcus),
Gram positive aerobic spore forming bacilli which are ubiquitous in the air, water and soil
namely: α-hemolytic Streptococcus (S. viridians) and Enterococci (S. faecallis), and gram
negative coliform bacilli and Acinetobacter (Jawets et al., 1978). Yeast and other forms
of fungi are often present in skin folds, while acid fast, non-pathogenic mycobacteria
occur in areas rich in sebaceous secretions (e.g. genitalia, outer ear) as normal skin flora
(Adeleye et al., 2003). These organisms are not harmful to the skin where they reside,

17
not until integrity of the skin is breached by trauma (injuries or surgical), burns, foreign
body or primary skin diseases (Badame, 1988).
The most common bacterial infections in the skin and soft tissue are Staphylococcus
aureus, Streptococcus pyogenes (Group A haemolytic Streptococcus), Clostridium
perfringes and the bacteriodes group (Adeleye et al., 2003). Others include
Mycobacterium tuberculosis, M. leprae, Neisseria gonorrhea, Pasturella tulurensis,
Bacillus antracis, Pseudomonas aeruginosa and many more factors other than trauma
and primary skin disease have been identified as contributory to skin infections (Adeleye
et al., 2003). However, some of these bacteria have evolved highly resistant strains which
have compromised the use of synthetic antibiotics (Levy, 2002). For example, many
strains of S. aureus a Gram-positive species carry resistant genes for penicillin antibiotics,
tetracyclines, methicillin and vancomycin (Quave et al., 2009). Therefore, the
development of new antiseptics and antimicrobial agents are of increasing interest.
Studies of some plant extracts and isolated plant compounds for antimicrobial activity
with dermatological relevance have shown that plant products may be essential for the
treatment of skin disorders like acne vulgaris and schorrhoic eczema (Weckesser et al.,
2007).
It was reported that biofilm-related infections caused by a staphylococci are among the
leading causes of nosocomial infections in the USA (Kong et al., 2006). Other skin
infections which are well documented are superficial fungal infection of the skin such as

18
Microsporium audounini, M. canis, M. fulum, Trychophyton tonsurans, T. scuneuleini, T.
mentagrophytes, T. rubrum, T. violaceum, Candida albicans, Epidermophyton flocossum,
Coccidiodes immitris, Cryptococcus neoformans, and Histoplasma capsulatums. Although
these infections are rare in man when they infect they may be chronic and resistant to
treatment (Adeleye et al., 2003).
Viral skin disease Disease of pigment Bacterial skin disease
Figure 2.1 Some conditions of the skin caused by infection: Adapted from
Medicine Net, 2011.
Inflammation and erythema
Inflammation and erythema are two conditions associated with the skin. Inflammation is
a protective tissue response to injury or destruction of tissues, which serves to destroy,
dilute, or wall off both the injurious agents and the injured tissues (Saunders, 2007). The
classical signs of acute inflammation are pain, heat, redness, swelling and loss of function.
The inflammatory response can be provoked by physical, chemical, and biologic agents
such as mechanical trauma, exposure to excessive amount of sunlight, X-rays, extreme
heat and cold, or by infectious agent like bacteria, viruses and other pathogenic
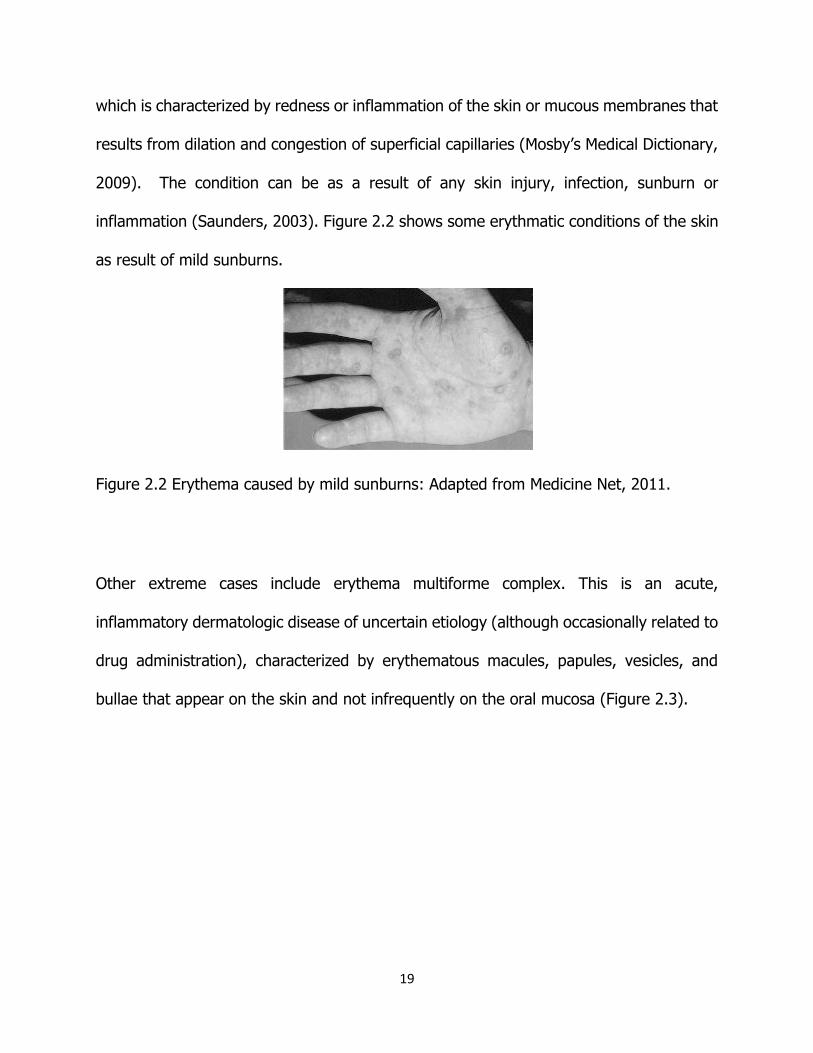
microorganisms (Saunders, 2003). Erythema on the other hand is a medical condition
19
which is characterized by redness or inflammation of the skin or mucous membranes that
results from dilation and congestion of superficial capillaries (Mosby’s Medical Dictionary,
2009). The condition can be as a result of any skin injury, infection, sunburn or
inflammation (Saunders, 2003). Figure 2.2 shows some erythmatic conditions of the skin
as result of mild sunburns.
Figure 2.2 Erythema caused by mild sunburns: Adapted from Medicine Net, 2011.
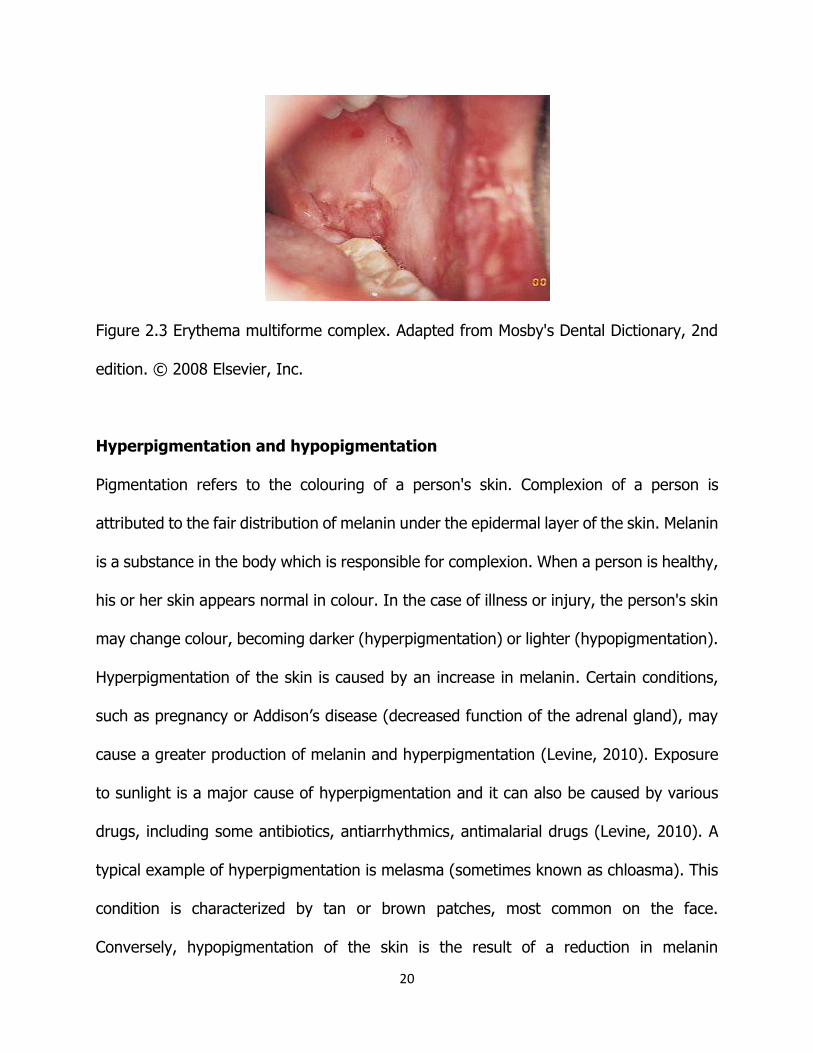
Other extreme cases include erythema multiforme complex. This is an acute,
inflammatory dermatologic disease of uncertain etiology (although occasionally related to
drug administration), characterized by erythematous macules, papules, vesicles, and
bullae that appear on the skin and not infrequently on the oral mucosa (Figure 2.3).
20
Figure 2.3 Erythema multiforme complex. Adapted from Mosby's Dental Dictionary, 2nd
edition. © 2008 Elsevier, Inc.
Hyperpigmentation and hypopigmentation
Pigmentation refers to the colouring of a person's skin. Complexion of a person is
attributed to the fair distribution of melanin under the epidermal layer of the skin. Melanin
is a substance in the body which is responsible for complexion. When a person is healthy,
his or her skin appears normal in colour. In the case of illness or injury, the person's skin
may change colour, becoming darker (hyperpigmentation) or lighter (hypopigmentation).
Hyperpigmentation of the skin is caused by an increase in melanin. Certain conditions,
such as pregnancy or Addison’s disease (decreased function of the adrenal gland), may
cause a greater production of melanin and hyperpigmentation (Levine, 2010). Exposure
to sunlight is a major cause of hyperpigmentation and it can also be caused by various
drugs, including some antibiotics, antiarrhythmics, antimalarial drugs (Levine, 2010). A
typical example of hyperpigmentation is melasma (sometimes known as chloasma). This
condition is characterized by tan or brown patches, most common on the face.
Conversely, hypopigmentation of the skin is the result of a reduction in melanin

21
production. Examples of hypopigmentation include vitiligo which causes smooth, white
patches on the skin and albinism which is inherited disorder caused by the absence of an
enzyme that produces melanin (Levine, 2010).
People with albinism should use a sunscreen at all times because they are much more
likely to get sun damage and skin cancer. In addition, pigmentation loss is as a result of
skin physical damage caused by infection, blisters, burns, or other trauma to the skin.
.
Psoriasis
Psoriasis is another condition which shows hyperpigmentation. Psoriasis is a non-
contiguous common skin condition that causes rapid skin cell reproduction resulting in
red, dry patches of thickened skin (William and Shiel, 2011). The disease is characterized
by dry flakes and skin scales resulting from the rapid buildup of skin cells. Psoriasis
commonly affects the skin of the elbows, knees, and scalp. Figure 2.4 shows the
conditions on the elbow. Psoriasis has many different indications including small flattened
bumps, large thick plaques of raised skin, red patches, and pink mildly dry skin to big
flakes of dry skin that flake off.

22
Figure 2.4 Psoriasis: Adapted from MedicineNet, 2011.
Free radicals
Free radicals are atoms or groups of atoms with an odd (unpaired) number of electrons
and can be formed when oxygen interacts with certain molecules in the body (NEJM,
1994). In living systems, free radicals are generated by cells as part of normal oxidative
respiration in the mitochondria of cells (Ara and Nur, 2009). Once formed these highly
reactive radicals can start a chain reaction in the cells providing the common pathway for
cancer, aging, and a variety of other degenerative diseases. The chief danger of free
radicals comes from the damage they can do when they oxidize important cellular
components such as proteins, lipids, nucleic acids such as DNA (Prakash, 2001). The free
radicals initiate peroxidation of lipids, which in turn stimulates glycation of proteins,
inactivation of enzymes and alteration in the structure and function of collagen basement
23
and membranes (Prior, 2003: Saha et al., 2008) resulting in poor functioning cell or death
of some cells. However, the amounts of the protective antioxidant principles present
under normal physiological conditions are sufficient only to cope with the physiological
rate of free radical generation (Haripyaree et al., 2010). It is, therefore, suggested that
any additional burden of free radical, either from environment or produced within the
body can disturb the free radical and antioxidant balance resulting to oxidative stress
(Sies, 1991). This subsequently results in tissue injuries and diseases.
The skin is one of the largest organs with billions of cells that are exposed to mitochondrial
oxidative respiration hence to free radical activity. Chemical mobilization of fats under
various conditions such as lactation, fever, infection, fasting and exercises enhances free
radical activity and damage in the skin and other organs (Ara and Nur, 2009). Studies
revealed that endurance exercises can increase oxygen utilization by a factor of 10 from
the resting state (Dekker et al., 1996). This increases the generation of free radicals,
raising concerns about increased damage on the skin, muscles and other tissues in
sporting people. To prevent free radical damage the body has a defense system of
antioxidants.
Role of Medicinal Plants
Plants were once a primary source of all the medicines in the world and they still continue
to provide mankind with new medicines (van Wyk et al., 2009). This traditional practice

24
is almost universal in non-industrialized communities (Barnes et al., 1998). In Africa,
medicinal plants play an important role in the treatment of infections and diseases
(Aboaba et al., 2006). In South Africa, a large part of the day-to-day medicine is still
derived from medicinal plants and large volumes of plant-derive medicines are sold in the
informal markets and commercial sectors of economy on daily basis (van Wky et al.,
2009). In the Eastern Cape, it is observed that majority of the people in the still rely on
the medicinal plants to manage their health problems.
Some drugs commonly used in the healthcare system today are of plant origin. It is
estimated that about 25% of the prescription drugs dispensed presently by physicians
contain at least one active ingredient derived from plant material (van Wyk et al., 2009;
Chong, 2003). Many drugs occur in the leaves, fruits, seeds, barks and roots of plants
(Kerrod, 1989). Some are made from plant extracts; others are synthesized to mimic a
natural plant compound (Chong, 2003). Some well-known plant-derived pharmaceuticals
are opium, aspirin, digitalis, quinine, codeine, taxol, atropine and vincristine. In the last
century, roughly 121 pharmaceutical products were formulated based on the traditional
knowledge obtained from various sources (Anesini and Perez, 1993). In recent times,
emphasis has been put on the use of these natural products for control and treatment of
various infections and diseases as they are considered having minimal side effects as
compared to synthetic drugs (Aboaba et al., 2006). It is important to note that there is
growing interest in natural and traditional medicines as source of new commercial
products (van Wyk et al., 2009).

25
In South Africa, it is estimated that there are about 200 000 traditional practitioners who
are dispensing plant derived medicines to about 60 % of the population usually in addition
to the mainstream medicine services (van Wyk et al., 2009). In rural communities, elderly
people who are knowledgeable about the use of medicinal plants play an important role
as first-aid healers with family repertoire of plant remedies (van Wyk et al., 2009). Thus
in this view medicinal plants form the first line of treatment.
Modern medicine from plants
Indigenous knowledge has provided the pharmaceutical industry with new novel
medicines. It is estimated that about 100 plant derived drugs were introduced in the USA
drug market during the period between 1950 and 1970 (Samy and Gopalakrishnakona,
2007). These include deserpidine, reseinnamine, reserpine, vinblastine and vincristine.
The same authorities noted that other plant based drugs like ectoposide, E-
guggulsterone, teniposide, nabilone, plaunotol, Z-guggulsterone, lectinan, artemisinin
and ginkgo ides were introduced between 1971 and 1990 and about 2 % of the drugs
(including paclitaxel, toptecan, gomishin, irinotecan) were also introduced during 1991-
1995.
Plant based drugs provide outstanding contribution to modern therapeutics (Samy and
Gopalakrishnakona, 2007); for instance taxol (isolated from Taxus baccata) is a highly
effective drug against breast cancer and ovarian cancer (van Wyk et al., 2009). Quinine
isolated from Cinchona species has been used as an effective remedy for malaria for more

26
than 300 years (van Wyk et al., 2009). Morphine (isolated from Papaver somniferum) is
a powerful analgesic, used for alleviation of intense pain. It is important to note that most
plant derived drugs came into use in the modern medicine through the uses of plant
material as indigenous cure in folklore or traditional systems of medicine (Samy and
Gopalakrishnakone, 2007). This system of medicine strengthens as scientific studies
investigate more medicinal properties of plants.
Chemical compounds from plants can work as growth hormones or antibiotics, nutrients,
and toxin neutralizers (Wikipedia, 2010). Others are used as laxatives, analgesics and
anti-inflammatory and even to improve appetite in sick people. Over the years medicinal
plants have been used to cure different ailments and conditions such as mental disorders,
tuberculosis, diabetes, malaria, headache, different kinds of cancers and skin diseases.
The ability of plant compounds to treat different conditions can be attributed to their
biological properties. Studies have revealed that some plant derived compounds have
antiviral, antibacterial, antifungal and anti-helminthes properties (Engel and Cindy, 2002).
In the human body, chemical compounds from plants mediate their effects by binding to
receptor molecules present in the body; such processes are identical to those already well
understood for pharmaceutical drugs and as such herbal medicines do not differ greatly
from conventional drugs in terms of how they work (Fabricant and Farnsworth, 2001).

27
Use of medicinal plants on the skin
The use of plants for the treatment of different ailments predates written human history.
However, the recorded knowledge in the care of the skin begins some 3 000 years before
the birth of Christ, when the Egyptians recorded in hieroglyphic plants form the care of
skin on temple wall paintings (Dweck and Dweck, 2002). Through the writings of some
great historic herbalists, like Pliny (Historia Naturalis), Pedanius Dioscorides (De Materia
Medica), Claudius Galenus or Galen (De Simplicibus), Abbess Hildergarde von Bingen
(numerous works), Theophrastus Bombastus von Hohenheim or Paracelsus (The Doctrine
of Signatures), Gerard, Culpeper, Turner, and Carolus Linnaeus, it is observed that there
is a pattern emerging of plants performing certain functions in phytotherapy (Dweck and
Dweck, 2002).
The use of plants to treat skin diseases and disorders is a common practice in most
cultures, although the causes of the conditions being treated are not always understood
(Grierson and Afolayan, 1999, Srinivasan et al., 2001). It is estimated that about 33% of
phytotherapy in non-Western communities are used for treatment of skin disorders,
wounds and infections (Mantle and Gok 2001). The topical application of medicinal plants
for the treatment of different skin conditions has proven effective due to biological
activities of the plant compounds such as antimicrobial, anti-inflammatory and anti-
erythema (Quave et al., 2009).

28
Antimicrobial agents in plants
Many plants possess antimicrobial agents and provide effective remedies for the
treatment of skin and soft tissue infections (Quave et al., 2009). The antimicrobial
properties of medicinal plants are a desirable tool for controlling and treatment of
infections. A large number of antimicrobial agents derived from traditional medicinal
plants are used for the treatment of various diseases caused by micro-organisms (Jain,
1994). They are used to eliminate the infecting micro-organisms (Bruneton, 1995; Samy
and Gopalakrishnakone, 2008); as antibacterial and antifungal plant derived agents are
useful for the treatment of dermatitis (Bruneton, 1995). Although the active constituents
may occur in low concentrations, plant extracts may be a better source of antimicrobial
compounds (Cox and Balick, 1994). One study has revealed that ethanol extracts from
78 traditional medicinal plants used to treat infectious diseases in India has antibacterial
and antifungal activity at 1, 6 mg/ ml (Valsaraj et al., 1997) while some antimicrobial and
phytochemical studies revealed that 45 medicinal plants from the same country are
effective against multi-drug resistant bacteria (Ahmad and Beg, 2001). The results of
these studies suggest the presence of anti-bacterial potency. It is important to note that
as a result of multi- drug resistance strains of infectious microbe screening of medicinal
plants has become a cost effective option for novel antibiotic protypes (Afolayan, 2003).
Medicinal plants have the ability to synthesize aromatic substances; most of them are
phenols or their oxygen derivatives (Geissman, 1963). Some of these plant derived
compounds serve as plant defense mechanism against micro-organisms, insects and
herbivores (Samy and Gopalakrishnakone, 2008). Plant extracts rich in polyphenolic
29
substances such as tannins, catechins, alkaloids, steroids and polyphenolic acids have
antibacterial activity (Samy and Gopalakrishnakone, 2008). Some examples of alkaloids
with antimicrobial activity include diterpenoid alkaloids isolated from Ranunculaceae
family, alkaloids pendulamine A, pendulamine B, and diterpenoid kolavenic cid and
azafluorene alkaloid isoursuline (Wanjala et al., 2002). Pyrolizidine alkaloids were also
reported to display antimicrobial activity against both fungi and bacteria (Craig, 1998).
Flavonoids are plant synthesized compounds which are also observed to have
antimicrobial activity (Dixion et al., 1983). Flavonoid, acacetin-7-o-β-D-galactopyranoside
was found to be active towards HIV (Hu et al, 1994). A wide variety of flavonoids,
sesquiterpenoid alcohols, triterpenoids and quinic acids caffeates from plants may be
useful antimicrobials (Hu and Chen, 1997).
Other plant derived compounds with antimicrobial activity include lectins, polypeptides,
polyphenols, phenolic, essential oils, terpenoids and tannins. Peptide called cathelicidins
was reported to provide protection against necrotic skin infection caused by
Streptococcus (Nizet et al., 2001). Phenolic compounds possessing a C3 side chain,
which are sometimes known as essential oils have antimicrobial activity (Samy and
Gopalakrishnakone, 2008). Tannins are water soluble polyphenol which are present in
medicinal plants and plant foods (Scalbert, 1991). The anti-microbial activities of tannins
are well documented (Samy and Gopalakrishnakone, 2008). Studies have shown that
tannins inhibit growth of many fungi, yeasts, bacteria and virus (Samy and
Gopalakrishnakone, 2008). Studies have revealed that tannins isolated from Carpobrotus
edulis (sour fig) inhibit the growth of phagocytized multi-drug resistant Mycobacterium

30
tuberculosis and methicillin-resistant Staphylococcus aureaus (van Wyk et al, 2009).
Polyphenols and many types of tannins are known for their anticarcinogenic properties
(Scalbert, 1991). The biological properties of tannins are associated with their ability to
form complexes with proteins such as digestive enzymes and fungal or viral toxins
(Bruneton, 1995) conferring antibacterial and antifungal activity.
Anti-inflammatory and antierythematic plant agents
Inflammation and erythema are skin conditions which can be treated using medicinal
plants. Studies have shown that some plants with high levels of flavonoids; those that
are used to firm and tone the skin are rich in tannins (Dweck and Dweck, 2002) and have
anti-inflammatory and antierythematic agents. Different studies have demonstrated that
flavonoids present at interesting levels have anti-inflammatory activity (Ferrandiz and
Alcaraz, 1991; Middleton, 1996). Tannins have a vasoconstrictor effect as result they
reduce fluid loss from wounds and burns thereby enhancing tissue regeneration
(Bruneton, 1995). German Chamomile (Matricaria recutita) and Roman Chamomile
(Anthemis nobilis) both of them in the family Compositae contain a flavonoid called
apigenin which have anti-inflammatory and antierythema qualities (Dweck and Dweck,
2002). The same authority noted that the extracts from these plant species have anti-
pruritic and as a result reduce itching and improve the speed at which wounds heal.
Medicinal plants such as Ginkgo biloba and Aesculus hippocastanum were reported to
contain Ginkgoide and eucibin which have antioedema properties (Dweck and Dweck,
2002. Other flavonoids which are thought to contain some anti-inflammatory and
antierythematic properties include quercetin, kaempferol, and delphinidin and

31
hyperocide. Studies have scientifically proven that some compounds from Aloe vera or
Aloe barbadensis, have healing properties to burn, be it radiation, thermal or solar (van
Wyk and Smith, 2004).
Plant agents used against skin dryness and dry eczematous conditions
When water protective ability of stratum corneum have been compromised and become
ineffective it may be beneficial to reduce the transepidermal water loss by topically
applying occlusive films (Dweck and Dweck, 2002). It is worth noting that some medicinal
plants synthesize compounds which give the skin smooth and moisturizing qualities that
are unsurpassed. Some of these medicinal plants provide a broad spectrum of oils with
fascinating fatty acids such as ricinoleic, oleic, linoleic, linoleic, arachidonic and erucic
(Dweck and Dweck, 2002). Clinical studies of some of these oils have demonstrated
cicatrizing activity and solutions to hyperpigmentation (Dweck and Dweck, 2002). Some
of them have skin hydrating and soothing properties.
Antioxidant agents
Antioxidants are molecules which can safely interact with free radicals and terminate the
chain reaction before vital molecules are damaged. Although there are several enzyme
systems within the body that scavenge free radicals, the principle micronutrient (vitamin)
antioxidants are vitamin E, beta-carotene, and vitamin C. Additionally, selenium, a trace
metal that is required for proper function of one of the body's antioxidant enzyme
systems, is sometimes included in this category (Ara and Nur, 2009). The body cannot

32
manufacture these antioxidants so they must be supplied in the diet or in medicines when
damage has been done.
Plants are chemical factories of some of these antioxidants. Several medicinal plants have
been reported to exhibit antioxidant activity (Ara and Nur, 2009). Most of these
antioxidant compounds from plants include flavonoids, isoflavones, flavones,
anthocyanins, coumarins, lignans, catechins and isocatechins (Aqil et al., 2006; Ara and
Nur, 2009). Antioxidant-based drug formulations are used for the prevention and
treatment of complex diseases like atherosclerosis, stroke, diabetes, Alzheimer’s disease,
cancer (Hennebelle et al., 2006; Augustin et al., 2005) and dermatitis. These conditions
tend to develop when the body has low antioxidant status. Antioxidants of external source
can prevent oxidative damage by inhibiting the generation of reactive species, scavenging
free radicals or raising the level of endogenous antioxidant defense (Haripyaree et al.,
2010). The effectiveness of these antioxidant formulations against chronic conditions has
increased interest into natural antioxidant from medicinal plants (Ara and Nur, 2009).
Studies on antioxidant properties of some medicinal plants have exhibited strong
anticancer, hepato-protective, anti-viral and other healing properties (Khalaf et al., 2008).
Some antioxidant formulations are known to form a protective layer on the skin and
mucosa, thereby enhancing tissue regeneration (Bruneton, 1995).
This chapter has discussed different types of skin disorders and the effects of free radicals
in the degeneration of the skin, the role of medicinal plants in the society and in modern
medicine. It has also discussed the importance of plant derived agents on the prevention
and treatment of skin diseases.

33
References
Aboaba OO, Smith SI, Olude FO (2006). Antibacterial effect of edible plant extracts on
Escherichia coli 0157:H7. Pakistan Journal of Nutrition 5(4): 325-327.
Ara N, Nur H (2009). In vitro antioxidant activity of methanolic leaves and flowers extracts
of Lippa alba. 4(1): 107-110.
Adeleye IA, Ogunniyi AA, Omoniggbehin EA (2003). Antimicrobial activity of some local
herbs on common skin pathogens. Bioscience Research Communications. 15 (3): 231-
236.
Afolayan AJ (2003). Extracts from the shoots of Artotis artotoides inhibit the growth of
bacteria and fungi. Pharmacology Biology. 41:22-25.
Ahmad I, Beg AZ (2001). Antimicrobial and phytochemical studies on 45 Indian medicinal
plants against multi-drug resistant human pathogen. Journal of Pharmacology. 72: 113-
123.
Andesine D, Perez JM (1993). In Samy RP, Gopalakrinakone, P (2007). Current status of
herbal and future perspectives. Nature Proceedings.
Augustin SM, Claudine M, Christine R, Christian R (2005). Dietary polyphenols and
prevention of diseases. Crit. Rev. Food Sciences. 45: 287-306.
Aqil F, Ahmed I, Mehmood Z (2006). Antioxidant and free radical scavenging properties
of twelve traditionally used Indian plants. Turkish Journal of Biology. 30: 177-183.
.Badame AI (1988). Incidence of skin diseases in rural Jamaica. International Journal of
Dermatology, 27, 109 – 111.

34
Barnes J, Ernst E (1998). "Traditional herbalists’ prescriptions for common clinical
conditions: A survey of members of the UK National Institute of Medical.
BBC NEWS, Medicinal plants ‘face extinction’: In Wikipedia (2010) Free Encyclopedia
Bruneton J (1995). Medicinal Plants. Pharmacognosy, Phytochemistry. Intercept,
Hampshire.
Craig WA (1998). Pharmacokinetics/pharmacodynamics parameters: rationale for
antibacterial dosing mice and men. Clinical Infectious Diseases. 26: 1-12.
Chong’s Health Care Enterprise, Inc. (2003).
Clinical Sciences (1991). Increased blood antioxidant systems of runners in response to
training load. Clinical Science .80: 611-618.
Cox PA, Balick MJ (1994). The ethnobotanical approach to drug discovery. Scientific
American. 270: 82-87.
Dekkers J, van Doornen L, Kemper H (1996). "The role of antioxidant vitamins and
enzymes in the prevention of exercise-induced muscle damage". Sports Medicine 21 (3):
213–38.
Dixion RA, Dey PM, Lamb CJ (1983). Phytoalexins: enzymology and molecular Biology.
Adv. Enzymol. 55: 1-69.
Dweck CA, Dweck D (200). Herbal medicine for Skin. Their chemistry and effects on skin
and mucous membranes. Personal Care Magazine. 3 (2): 19-21.

35
Engel, Cindy (2002). Wild Health: How Animals Keep Themselves Well and What We Can
Learn From Them. Houghton Mifflin.
Fabricant DS, Farnsworth NR (March 2001). "The value of plants used in traditional
medicine for drug discovery". Environment. Health Perspective. 109 Supplement 1: 69–
75.
Ferrandiz, M, Alcaraz (1991). Anti-inflammatory activity and inhibition of arachidonic acid
metabolism by flavonoids. Agents and Actions.32: 283-288.
Geissman TA (1963). Flavonoid compounds, tannins, lignins and related compounds. In;
Pyrrole Pigments, Isoprenoid Compounds and Phenolic Plant Constituents. Florkin M,
Stotz EH, eds. 9: New York: Elsevier, 2653.
Grierson DS, Afolayan AJ, (1999).Antibacterial activity of some indigenous plants used for
treatment of wounds in the Eastern Cape, South Africa. Journal of Ethnophamacology.
96: 429-444.
Haripyaree A, Guneshwor K, Damayanti M (2010). Evaluation of antioxidant properties of
some medicinal plants by sulfur free radical reactivity with curcumin as reference.
EJEAFChe 9 (2): 337-344.
Hennebelle TS, Sahpaz H, Joseph F, Bailleul F (2006). Phenolics and iridoids of Lippia
alba. Nat. Prod. Commin. 1: 727-730.
Hu CQ, Chen K, Shi, Q, Kilkuskie RE, Cheng YC, Lee KH (1994). Anti- AIDS agents, 10.
Acacetinin-7-o-β-D-galactopyranoside, an anti-HIV principle from Chrysanthemum
morifolium and a structure active correlation with some related flavonoids. J. Nat Prod.
57; 42-51.

36
Hu CQ, Chen Z (1997). Sesquiterpenoids from Chrysanthemum morifolium.
Phytochemisty. 44: 1287-1290.
Jain SK (1994). Ethnobotany and research on medicinal plants in India. Ciba Faoundation
Symposium. 185:153-164.
Jawetz E, Janet S, Nicholas L, Edwards E. (1978). Skin micro-organism. In: Medical
Microbiology. Lange International, N.Y., p. 25 – 27.
Khalaf NA, Shakya AK, Al-othman A, El-agbar Z, Farah H (2008). Antioxidant activity of
some common plants. Turkish Journal of Biology. 32: 51-55.
Kerrod R (Ed) (1989).The Plant World. Chicago; World Book Inc.:128
Samy RP, Gopalakrinakone, P (2007). Current status of herbal and future perspectives.
Nature Proceedings.
Saunders J (2007). Dorland's Medical Dictionary for Health Consumers: Elsevier.
Saunders J (2003). Miller-Keane Encyclopedia and Dictionary of Medicine, Nursing, and
Allied Health, Seventh Edition. Elsevier
Scalbert A (1991). Antimicrobial properties of tannins. Phytochemistry. 30: 3875-383.
Sies, H (ed.) (1990). Oxidative stress, oxidants and antioxidants. New York: Academic
Press. 105-107.
Srinivasan D, Nathan S, Suresh T, Permalsamy PL (2001). Antimicrobial activity of certain
Indian medicinal plants used in folkloric medicine. Journal of Ethnopharmacology. 74:
217- 220.
Kong KF, Vuong C, Otto M (2006). Staphylococcus quorum sensing in biofilm formation
and infection. International Journal of Medical Microbiology. 296: 133-139.

37
Levine, N (2010). WebMD Medical Reference. http://www.webmed.com/baby/default
htm.
Levy SB (2002). The antibiotic paradox: How the Misuse of antibiotic destroy the curative
power. Perseus Publishing; Cambridge.
Mentle D, Gok MA (2001). Adverse and beneficial effects of plants of extracts on skin and
skin disorders. Adverse Drug reactions and Toxicological Reviews. 20: 89-103.
Middleton, E (1996). Biological properties of plant flavonoids: An Overview. International
Journal of Pharmacol. 34: 344-348.
Mosby's Medical Dictionary (2009). 8th edition. Elsevier.
NEJM (1994). A Clinical Trial of Antioxidant Vitamins to Prevent Colorectal Adenoma
NEJM, 331 (3): 141-147.
Nizet V, Ohtake T, Lauth, X, Trowbridge J, Rudisill J, Dorscher RA, et al (2001). Innate
antimicrobial peptide protects the skin from invasive bacterial infection. Nature. 414: 454-
457.
Prakash A (2001). Antioxidant activity. Medallion Laboratories. Analytical Progress. 19
(2): 1-4.
Prior RL (2003). Fruits and vegetables in prevention of cellular oxidative damage.
American Journal of Clinical Nutrition. 78: 570S-578S.
Quave CL, Plano LRW, Pantuso T, Bennet BC (2009). Effects of extracts from Italian
medicinal plants on planktonic growth, biofilm formation and adherence of methicillin-
resistant Staphylococcus aureus. 118 (3):418-428.
38
Simon C, Lamla M (1991). Merging pharmacopoeia; Understanding the origins of
incorporative pharmacopoeial processes among Xhosa healers in Southern Africa. Journal
of Ethnopharmacology. 33: 237-247.
Srinivasan D, Nathan S, Suresh T, Permalsamy PL (2001). Antimicrobial activity of certain
Indian medicinal plants used in folkloric medicine. Journal of Ethnopharmacology. 74:217-
220.
Valsaraj R, Pushpangadan P, Smith UW, Adsersen A, Nyman U (1997). Antimicrobial
screening of selected medicinal plants from India. Journal of Pharmacology. 58: 75-83.
van Wyk B-E, Smith GF (2004). Guide to Aloe of South Africa.2edns. Braza Publications,
Pretoria.
van Wyk, B-E, van Oudtshoorn B, Gercke N (2009). Medicinal Plants of South Africa. Tien
Wah Press (Pte): Singapore.
Wanjala CC, Juma BF, Bojase G, Gashe, BA, Majinda RR (2002). Erythinaline alkaloids
and antimicrobial flavonoids from Erythrina latissima. Planta Medica 68: 640-642.
Weckesser S, Englel K, Simon-Haarhaus B, Wittmer A, Pelz K, Schempp (2007). Screening
of plant extracts for antimicrobial activity against bacteria and yeasts with dermatological
relevance. International Journal of Phytotherapy and Pharmacology.
Wikipedia (2010). Free Encyclopedia. Wikimedia Foundation Inc.
William C, Shiel Jr (2011). Get information on psoriasis treatment, symptoms, causes,
medication and types. Medicine Net

39
Chapter 3: An ethnobotanical study of some medicinal plants used
for the treatment and improvement of skin in the O R Tambo and
Amathole Municipalities, of the Eastern Cape, South Africa.
Abstract
Using ethno-direct methods, the medicinal plants used for the treatment and
improvement of skin texture were determined in O.R Tambo and Great Kei Municipal
Districts of the Eastern Cape. The ethnobotanical data were gathered from the Xhosa
speaking people using interviews, questionnaires and participatory rural appraisal from
March 2009 to November 2009. The informants were 37 local people among which 5
were tribal practitioners. They supplied consistent information concerning 45 plant
species distributed in 41 Genera belonging to 28 Families which are used for the
treatment of skin infections and improvement of its texture. Of these, 86.7 % (39 plants)
were used as remedies against common skin problem such as wounds, pimples, acnes
and itches, and 33% (15 plants) were reported to have anti-inflammatory effects on the
skin while about 28% (12) were reported to oil dry skin, enlighten skin and protect skin
from ultra-violet radiation. The medicinal plants used are listed with Latin names, local
names, parts used, uses, and mode of preparations.
Keywords: Anti-inflammatory, Ethno-direct methods, Medicinal plants, Skin problems,
Informants, Xhosa speaking people.
Introduction

40
Readily visible alterations of the skin surface have been recognized since the dawn of
history, with some being treated and some not. The use of medicinal plants against skin
infections is a common practice in many cultures, although the precise mechanism of
cure is not always understood (Grierson and Afolayan, 1999). It is estimated that about
33% of botanical therapies are used for the treatment of skin disorders and wounds
(Mantle and Gok, 2001). The topical application of many plant medicines for the treatment
of various skin conditions has proven effective due to the antimicrobial (Quave et al.,
2008) and antioxidant properties of plant secondary metabolites. The secondary
metabolites eliminate and inhibit the activity of the infecting pathogens (Samy and
Gopalakrishnakone, 2008). The plant antioxidants protect against the damaging effects
of free radicals generated under the skin by metabolic processes (Adedapo et al., 2008).
They react with these free radicals and neutralizing their damaging effect. The use of
plants with substantial antioxidants activity to afford protection against ultra-violet is
receiving attention (Katiyar et al., 2001). Some phytochemicals restrict diffusion of toxins
and lessen the adverse reaction to insect bites and stings (Finn, 2004). Furthermore, they
calm the effects of itching and irritated skin (Finn, 2004).
South Africa currently has the largest antiretroviral program in the world with half a million
people receiving antiretroviral (ARV) drugs (Avert organization, 2009). It is estimated that
about 50 000 people in the Eastern Cape are using ARV therapy (Nicolay, 2008), and the
government targets to increase the therapy by 80% of the HIV infected people by 2011
(Avert organization, 2009). The use of the first line of ARV like efavirenz, lamivudine and
stavudine has been characterized with hypersensitivity reactions resulting in skin and

41
subcutaneous tissue disorders (Ranbaxy (SA); 2006 Adcock Ingram, 2007). These
manifest as skin rashes and lesions, fungal dermatitis, eczema, itches, irritations and nail
disorders. Other adverse indicators which were reported include skin ulcer, skin nodules,
herpes simplex, herpes zoster, and pustular rash (Pharmacare limited, 2003). These
cause serious discomfort and post inflammatory hyperpigmentation in patients. In the
Eastern Cape, the amaXhosa, the inhabitants of the area use medicinal plants for the
treatment of skin diseases, ritual purposes, improvement of skin texture and complexion.
Medicinal plants like Cassipourea flanaganii were reported to be used by many people for
skin enlightening, reduction of blemishes, pimples, and increasing clarity of complexion
(Dold T, and Cocks, 2005).
Every year, young abakwetha (Xhosa initiates) are circumcised, dressed and treated
circumcision wounds using phyto-medicines. Medical circumcision performed by medical
practitioners who substitute traditional equipment and dressing of wounds for medical
ones are deemed meaningless (Stinson, undated).
People of the Eastern Cape Province have a great wealth of medicinal plants and an
ancestral tradition about their uses. The traditional knowledge of medicinal plants has
accumulated in the course of many centuries (Thirumalai et al., 2009). Local people who
include ordinary people, herbalists and traditional practitioners take advantage of this
knowledge to treat different ailments. Traditionally, this essential knowledge was passed
from generation to generation without documentation (Samy and Ignacimuthu, 2000).
The mode of transmission of knowledge could result in loss of treasure of knowledge.

42
Loss of such a treasure of knowledge may be detrimental to the healthcare system of
rural communities.
Ethnobotanical surveys have been found to be one of the reliable approaches to bio-
prospection of medicinal plants and their uses. Many plant medicines have been
incorporated in the mainstream of healthcare system. The pharmaceutical industries have
considered plant medicine as a source of bioactive agents that can be used in the
preparation of medicine (Aboaba et al., 2006). Many people believe phyto-medicines are
safe, this has been proven in the treatment of various ailments (Mitalaya et al., 2003).
Effective and inexpensive botanical remedies are gaining popularity equally among both
rural and urban areas (Katewa et al., 2004).
The objective of this study was to identify and document the medicinal plant species used
for the treatment of skin infections and improvement of skin texture by the Xhosa people.
The study is essential because it protects traditional knowledge from disappearing
(Grierson and Afolayan, 1999). This study may not be exhaustive however documenting
the indigenous knowledge through ethnobotanical studies is important for the
conservation of biological resources as well as their sustainable utilization (Igncimuthu,
et al., 2006; Revathi and Parimelazhagan, 2010).

43
Materials and methods
Study site
The Eastern Cape is a coastal province laying in the south-eastern South Africa. It is the
second largest province from Northern Cape with area of about 168 966 square
kilometres. O R Tambo and Amathole are two coastal municipal districts to the south-
east part of the province which are lined and lapped by the temperate Indian Ocean. The
coastal districts studied lay directly between Port St Johns and Cintsa East. In the North-
East along Wild Coast, towns like Port St. Johns, Mthatha, and East London experiences
long hot balmy conditions with mean summer temperatures between 16ºC and 26ºC and
mean winter temperatures between 7ºC and 20ºC and high rainfall
(southafrica.venues.com, 2009). The edapho-climatic conditions of the study area like
geographical location, topography, varied climate and fertile soils support high plant
diversity which includes temperate flora, grasslands, mangroves and dense green bushes
of the stretch.

44
Figure 3.1 Map of the Eastern Cape showing the study area. Adapted from
www.places.co.za.
Ethnobotanical survey
An ethnobotanical survey was conducted in several villages and forests around Bizana,
Port St Johns, Lusikisiki, Mt Allyff and Flagstaff areas in O R Tambo municipality district
and Cinsta, Mooiplas, and Glen Eden East Coast areas in Amathole municipality district
during March 2009 to November 2009 as phyto-medicinal wealth of the Xhosa speaking
Study Area
45
people. The study explored the traditional healthcare system of the communities for
treatment of skin problems and ailments. It included structured interviews with 37
inhabitants comprising of 21 female and 11 males of which 5 of them were traditional
practitioners (3 females and 2 males). Participatory rural appraisal was also utilized to
gather information. The participants were between the ages of 23 and 67 years. The
criteria for selection of informants were based on their knowledge of medicinal plants for
self-medication or treating others. Some informants were requested to show the plants
in the field using the local names. The species mentioned were collected and identified
taxonomically using facilities and help of staff of Walter Sisulu Herbarium. Some voucher
specimens of collected plants were prepared and deposited in the Kei Herbarium at Walter
Sisulu University.
Results
Through the survey a total of 45 plant species were recorded. These were distributed in
41 genera belonging to 28 families which are used by local people to either treat skin
ailments or improve skin texture. Thirty three percent (33 %) of the total plants are
represented by four families namely Asteraceae (5 species), Fabaceae (4 species),
Eurphobiaceae (3 species) and Solanaceae (3 species) while 22.2% is represented by 5
families which include Aloaceae, Asphodilaceae, Anacardiaceae, Asparagaceae and
Thymelaecae. The later families are each represented by 2 species. Other families which
were represented by a single species include Alliaceae, Asphodeaceae, Apiaceae,

46
Amarylliaceae, Caprifoliaceae, Curtiaceae Crussulaceae, Gunneraceae, Hypoxidaceae,
Lamiaceae, Misebembryantemaceae, Myrtaceae, Poaceae, Polygonaceae,
Plumbaginaceae, Pubiaceae, Rhizophoraceae and Verbanaceae. Figure 3.2 shows the
main families of plants used for the treatment and improvement of skin tone. Eight seven
percent (87%) of medicinal plants are used for the treatment of common skin problems
such as wounds, pimples, burns, itches, inflammations, acne and eczema, while 33% of
the plants are used as anti-inflammatory agents. About 31% of medicinal plants were
reported to improve skin texture by oiling, enlightening or protecting it from ultra-violet
rays. The main uses of medicinal plants on the skin are shown in Figure 3.3. Each use is
expressed as a percentage of the total number of the medicinal plants implicated for
treatment and improvement of the skin. Based on frequency of use by the amaXhosa
herbs are more preferred followed by trees and shrubs. Leaves, barks, roots and bulbs
are frequently used while seeds and twigs are rarely used. Figure 3.4 shows the growth
form analysis of medicinal plants used for the treatment or improvement of skin.

47
Table 3.1 Ethnomedicinal plant species used for the treatment or improvement skin
texture in O R Tambo and Amathole Municipal Districts.
Botanical name
Local name Part used Uses Mode of Preparations
Syzgium cordatum
Umswi Bark Blisters, pimples, inflammations, acne, and eczema.
Air dried bark paste is topically applied on affected part. Bark powder is mixed with cold water for 12-18 hours use to drink solution wash affected body parts.
Gnidia capitata Sisi dikili/ Umsila wengwe
Roots Wounds, burns, fractures, snake bites, sore throat, rashes, ringworm.
Decoction of air dried roots is used to wash affected parts twice daily. Burnt and ground small piece of root is applied on wound.
Gnidia anthyllides
Intozwane Roots Wounds, burns, snake bites, toothaches and earaches.
Burnt and ground small piece of root is applied on wound.
Protorhus longifolia
umhluthi/ ikhubalo
Bark Wounds, cuts, bruise and graze ringworm, acne, and eczema.
Decoction of air dried bark is used to wash affected parts twice daily.
Bulbine frutescens
Ithethe elimpofu
Leaves, or leaf gel
Wounds, herpes simplex, ringworm, insect bites, cuts and grazes, burns, sunburns, blister, itches, cracked lips, cold sores, pimples, mouth ulcers, rough skin, boils, stop bleeding.
Crush fresh leaf and apply on affected part. Apply gel from fresh leaf on affected.

48
Bulbine asphodeloide
Intelezi Leaves, or leaf gel
Wounds, itches, burns, sunburns, rough skin, insects’ bites and inflammation.
Fresh leaves are ground and paste applied on affected parts or fresh leaf is cut and gel is applied on affected parts.
Helichrysum petiolerare
Impepho Leaves Improves skin texture and beauty, wounds.
Decoction of fresh or air dried leaves are cooled and solution is used to drink and was affected parts or may steam on skin.
Helichrysum nudifolium
Indlebe zebhokwe/ Isicwe/ icholachola
Leaves and twigs
Wound and improves skin beauty.
Crushed fresh leave and twigs are used to bandage wound. Powder is topically applied on skin. Steaming of skin.
Cassipourea flanaganii
UmMemezi Bark Improves beauty and enlightens skin. Used as sunscreen.
Air dried bark powder is mixed with red oak in water. A paste is topically applied on the skin.
Spirostachys africana
Umthomb- othi
Bark Rashes on new born babies, nappy rashes, wounds and birth wounds, pimples.
Powder is allowed to stand for about 12 hours before solution is used to wash affected parts.
Sutherlandia frutescens
Unwele Leaves Wounds, inflammation of skin, herpes, cancer, chicken-pox, and eye infections.
Fresh leaves or air dried leaves are ground and are mixed with water or fresh milk and is applied on affected parts.
Aloe ferox Ikhala Leaves Wounds, dry skin, stop bleeding, removes post
Break fresh leaf and apply gel on

49
inflammatory spots, pimples and herpes.
affected part of body.
Aloe arborescens
Ingelwane Leaves or fresh gel
Pimples, dry skin, wounds, stops inflammation of skin and lighten skin.
Paste of air dried leaves is applied on affected parts.
Carpobrotus edulis
Igcukuma Leaves Sunburns, eczema, ringworms, nappy rash, dry skin, cuts and grazes, mosquito bites, stings sore throat, mouth infections.
Break leaf and rub the juice on affected part. Chew leaves and gaggle for sore throat.
Pentanisia prunelloides
Icimamlilo Roots Pains, wounds, cancer, corns.
Decoction of roots is used wash affected parts regularly.
Leonotis leonotis Umfinca- mfincane
Leaves Cancerous wounds. Air dried or fresh leaves are allowed to stand in cold water for 10 to 12 hours before drinking the solution three times a day.
Acacia karroo Umunga Bark, leaves Bumps on skin, boil, thrush.
Wet juice fibre used to tie together with splints on fracture. Boil fresh leaves and gaggle.
Miscanthus capensis
Umthala Roots Pimples, itches acne, eczema and wounds.
Decoction is used to steam the affected parts.
Gunnera perpensa
Iphuzilo- mlambo
Rhizomes Wounds, itches, eczema, inflammation and psoriasis.
Decoction of rhizomes is cool solution and drink.
Gerbera piloselloides(L) Cass
Umsa Roots Post inflammatory spots, pimples, wound hyperpigmentation, pimples and
Air dried roots are mix with oil or fresh milk and infusion is applied on affected parts.

50
improve skin texture.
Solanum incanum
Umthuma omncinci
Roots Ringworm, wounds, acne and eczema.
Air dried root are mix with water and chicken feaces. Paste is applied on affected parts.
Datura stramonium
Umhlavuthwa Leaves Wounds, boils abscesses and skin bumps.
Warm up leaf on hot plate. Apply it warm on affected part of body.
Cotyledon orbiculata
Imphewula Leaves Pimples, inflammation, genital warts, corns.
Fresh leaves crushed and rubbed on affected parts.
Kniphofia drepanophylla (Baker)
Ixonyi Rhizomes (root)
Ringworm, wounds, pimples, acne and eczema.
Dry, grind and mix with red oak or use alone in water. Apply on affected parts.
Macaranga capensis
Umpumelelo Bark Pimples, wounds eczema, and acne.
Decoction of air dried bark is allowed to cool. Solution is drunk while warm. Then induce vomit. Paste made of air dried bark and red oak is applied on affected part.
Curtisia dentana Umlahleni Roots Pimples, itches, rashes, acnes.
Decoction of roots is drunk twice a day.
Alepidea amaymbica(Ecl &Zeyh)
Umvuthuza Roots Pimples, lice on all hairy parts (head, armpits and genital area).
Decoction of roots is used to wash affected parts while cooled.
Eucomis automnalis
Umathunga Bulb Improves beauty, wounds, ulcer caused by STI and healing of fractures.
Dry or fresh bulbs are ground and mix with water and are then applied on affected part.

51
Hypoxis hemerocallidea
Inongwe/ Labatheka
Corm Pimples and improves beauty. Absorbs excess skin oils.
Dry the corm and rub it on stone, smear ground plant material on affected part.
Tulbaghia alliacea
Itswele lamlambo
Bulb Boils, wounds, pimples, eczema, herpes.
Squeeze, fresh bulb on affected part.
Euphorbia ingens
Umlonhlo Stem Skin rash, post inflammatory spots. Promote healing without hyper pigmentation.
Cut stem and apply milky fluid on affected parts.
Athrixia phylicoides
Icholocholo Leaf twigs, roots.
Wounds, boils, and septic wounds, stops bleeding.
Crush freshen parts of plant material are applied topically on affected parts.
Boobhone disticha
Icwadi/ Ishwadi
Bulb
Boils, cuts and grazes and wounds. ‘Suck’ pus from inflamed part skin.
Fresh leaf scales are used to dress circumcision cuts. Crush bulb. Apply on affected parts.
Withania somnifera
Ubuvuma Leaves Roots
Abscesses, septic wounds, cuts, bruise and inflammations. STI ulcers.
Air dried leaves or roots are mixed with animal fat then applied on affected parts.
Senecio speciosus
Ustukumbini Leaves Stems
Swellings, cuts, burns, and sores, inflamed gums.
Decoction of air dried leaves or stem are made into paste is applied on affected parts or affected parts may be steamed. Fresh leaves crushed and rubbed on affected parts.
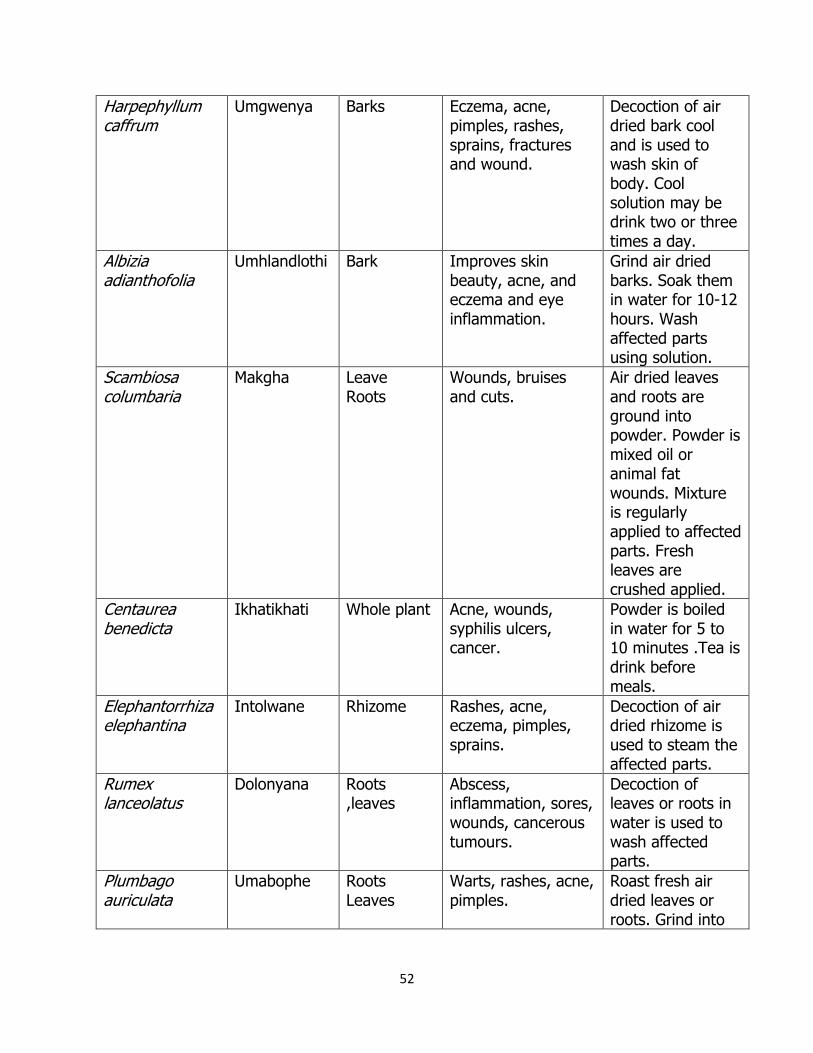
52
Harpephyllum caffrum
Umgwenya Barks Eczema, acne, pimples, rashes, sprains, fractures and wound.
Decoction of air dried bark cool and is used to wash skin of body. Cool solution may be drink two or three times a day.
Albizia adianthofolia
Umhlandlothi Bark Improves skin beauty, acne, and eczema and eye inflammation.
Grind air dried barks. Soak them in water for 10-12 hours. Wash affected parts using solution.
Scambiosa columbaria
Makgha Leave Roots
Wounds, bruises and cuts.
Air dried leaves and roots are ground into powder. Powder is mixed oil or animal fat wounds. Mixture is regularly applied to affected parts. Fresh leaves are crushed applied.
Centaurea benedicta
Ikhatikhati Whole plant Acne, wounds, syphilis ulcers, cancer.
Powder is boiled in water for 5 to 10 minutes .Tea is drink before meals.
Elephantorrhiza elephantina
Intolwane Rhizome Rashes, acne, eczema, pimples, sprains.
Decoction of air dried rhizome is used to steam the affected parts.
Rumex lanceolatus
Dolonyana Roots ,leaves
Abscess, inflammation, sores, wounds, cancerous tumours.
Decoction of leaves or roots in water is used to wash affected parts.
Plumbago auriculata
Umabophe Roots Leaves
Warts, rashes, acne, pimples.
Roast fresh air dried leaves or roots. Grind into

53
powder. Apply to affected parts.
Lippia javanica Inzinziniba Leaves, roots
Chicken pox, scabies and lice.
Decoction of fresh or air dried leaves used wash or steam the affected parts using solution.
Trichilia emetica Umkuhlu Leaves and seed.
Bruises, acne and eczema
Paste of air dried plant material applied to affected part.
Bowiea volubilis Umagaqana Bulb Pain killing effect in skin.
Rub crushed bulb on skin.
1
0
1
2
3
4
5
Number of species
A B C D E F G H I
Plant families
Figure 3.2 Families of plants used for treatment of skin disorders.
A Asteraceae
B Fabaceae
C Euphorbiaceae
D Solanaceae
E Aloceae
F Asphodalaceae
G Anacardiaceae
H Asparagaceae
I Thymelaeceae

54
About 95% of the local people reported that they get supplies of plant medicine from the
local forests. Few local people revealed that they have some few species they grow in
their homesteads.
The indigenous people were semi-skilled in identification and processing of medicinal
plants. Very often, medicinal plants are air dried in the sun before they are made into
paste or decoctions which are applied on affected parts. Juices, solutions, or burnt
products of plant material are used. It is interesting to note that most preparations are
made into concoctions although some plants are prepared singly. Most medicine
preparations are topically applied on the skin while some are orally taken as decoctions
or solutions.
87
33 31
0
50
100
Percentage of
Plant species
A B C
Medicinal uses
A Treatment of skin infections B Anti-inflammatory
C Improvement of skin texture
Figure 3.3 Medicinal plants used for treatment and skin improvement.

55
Figure 3.4 Types of plants used for treatment of skin disorders.
Herbs 37%
Trees 24%
Shrubs 24%
Grasses 13% Climbers 2%
Herbs
Trees
Shrubs
Grasses
Climbers
Paste 38%
Juices 12%
Warming 2% Burning 8%
Dissolution 10%
Decoction 30%
Paste
Decoction
Juices
Dissolution
Burning
Warming
Figure 3.5 Mode of preparation of herbal remedies.

56
Some medicinal plants identified as used for the treatment of skin infections.
Figure 3.6 M. capensis; stem and leaves.
Figure 3.7 H. hemerocallidea plant.

57
Figure 3.8 K. drepanophylla underground parts.
Figure 3.9 G. capitata.
Figure 3.10 P. longifolia stem, leaves and berries.

58
Discussion
Documentation of ethnobotanical data is pivotal in the understanding of human-plant
relationship and human-biodiversity relations (Ramakrishnappa, 2002). Bio-prospecting
of medicinal plants is an important tool in revealing plants with useful medicinal properties
(Balandrin et al., 1993). Based on the observations made during this study, the great
biodiversity of the Province remained a vast entity of unexploited medicinal plants which
could be transformed to important dermatological medicines and cosmetics. Recently,
screening of traditional medicinal plants has been the source of innumerable therapeutic
agents (Samy and Gopalakrishnakone, 2008), and future research may lead to discovery
of more new plant derived medicines. Indigenous medicinal plants are not only used to
meet primary health care needs but also in purging and cleansing of the body (Cocks and
Dold 2009). In addition, medicinal plants had developed economic significance in both
developing and developed countries since many are being traded in the informal and
formal markets. The over-exploitation of medicinal plants for commercial trade in South
Africa poses a threat to many species (Cocks and Dold, 2009). Ethnobotanical data is
essential for implementation of conservation policies and programmes by botanists,
conservationists and other stakeholders.
People in the study area were found to be sensitive to their natural wealth, since they
harvested and leave some parts for regeneration (Cocks and Dold, 2009). They have
many traditional norms which can be interpreted as means to prevent overexploitation of
their medicinal resources (van Wyk et al., 2009). For example, barks of trees such as
Protorhus longifolia and Syzgium cordatum are only harvested in the eastern and western

59
sides. Such norms prevent death of the trees due to desiccation by complete debarking
of the plant. When roots are harvested desiccation of the remaining underground parts
is prevented by replacing the soil on the hole. However, the increasing demand for
medicinal plants has threatened the sustainability of these plants. This was even revealed
by the local people when they indicated that plant species such as Hypoxis
hemerocallidea, Macaranga capensis, Cassipourea flanaganii, and Spirostachys africana
are now rare in their locality. Although the local people noted scarcity of these medicinal
plants, 95% of the respondents indicated that they walk for long distances to search for
these medicinal plants in the forest.
Ethnobotanical information revealed that the traditional knowledge on medicinal plants
is endowed in elderly people than in younger people. The latter had some difficulties in
identifying and describing how plant species work, therefore it can be assumed that in
future this treasure of knowledge may be lost. Poonam & Singh (2009) noted that the
other contributory factor to the loss of knowledge on medicinal plants is that local people
were hesitant to disclose their knowledge because they felt it provides them with
recognition and identity of society.
Pastes, decoctions, bathing and steaming were the most common form of use of
medicinal plants on the skin. Mixing pastes with oil, animal fat and milk is believed to
improve medicinal properties of the plant medicines by the local people (Poonam and
Singh, 2009). When the medicine is topically applied the active compound are absorbed
into the underlying tissues (van Wyk et al., 2009). For example, paste of Solanum
incanum and chicken feaces is topically applied for treatment of ringworm, pimples, acne

60
and eczema. Bathing and steaming under the blanket using plant medicinal preparations
are often used to maintain general skin health, to improve the tone by opening the pores
and stimulating cetaceous circulation and make the patient sweat (van Wyk et al., 2009).
Use of concoctions such as decoctions of Kniphofia drepanophylla and Gerbera
piloselloides are used for treatment of wounds, pimples, post inflammatory spots
(hyperpigmentation) and even improve skin texture. Mixture of different plant compounds
is believed to have synergistic effect that have vital role in the treatment of disease.
Volatile phytochemicals are administered by steaming affected parts under the blanket.
Helichrysum species and Senecio species are some of the medicinal plants that are
crushed, boiled and steamed to improve skin smoothness.
The study revealed that the method of preparation of plant medicine is critical, as it
determines the effectiveness of the ultimate plant medicine. Drying of the plant material
in the sun may cause some volatile phyto-chemicals to vaporize or initiate photochemical
reactions which may cause the medicine to be ineffective (Poonam and Singh, 2009). In
addition to appropriate volume of solvents such as water or alcohol and boiling for specific
time or partial burning serve to neutralize certain toxins (van Wyk et al., 2009). The local
people commonly use water as the solvent when preparing plant medicines while in some
cases saline sea water, milk and animal fat.
Diagnosis of skin problems was indicated to be critical for administration of correct plant
medicine by local people. Traditional practitioners use signs presented by patients and
symptoms told by patients as well as their personal experience in treating the skin
problem. They give specific prescriptions which they monitor if they suspect side effects.

61
They even strongly believe that some skin infections are as a result of wrong doings
which would have been done by the patient. In the latter, treatment would be done with
the guidance of a traditional practitioner who cleanses the family using medicinal plants
following specific rituals.
Conclusion
The results of the study revealed that plant medicines still play an integral role in the
treatment of skin ailments and improvement of skin texture. Women furnished novel data
on plants used for the improvement of the skin texture while men provided novel data
on treatment of skin conditions like wounds, ringworm and acne. The study documented
45 plant species of which an in depth biochemical and ethnopharmacological evaluations
may lead to discovery of drugs which may be used for the treatment of different skin
problems and cosmetics which may be used for improvement of the skin.
Acknowledgements
The research was supported by the Walter Sisulu University Research Centre. The author
is grateful for the assistances offered by the systematic personnel of the Department of
Biological Department of Walter Sisulu University. In addition, the provision of traditional
knowledge on plant medicine used to treat skin infections and improve skin by the people
of O R Tambo and Amathole districts is greatly appreciated.

62
References
Ababa OO, Smith SI, Olude FO (2006). Antibacterial Effect of Edible Plant Extract on
Escherichia coli 0157:h7.Pakistan Journal of Nutrition 5(4):325-7.
Adcock Ingram limited (2007). Instruction paper. William Nicolrylaan 3011, Bryanston,
Privaatsak X69, Bryanstan, 2021.
Adedapo AA, Jumoh FO, Kadura S, Afolayan AJ, Masika (2008). Antibacterial and
antioxidant properties of methanol extracts of leaves and stem of Calpurnia aurea.
Complementary and Alternative medicine
Avert organisation, (2009). AIDS, Fund rising, World AIDS Day, Help Advice. F:\History
of HIV and AIDS in South Africa.mht
Balandrin, MF, Kinghorn AD, Farnsworth NR (1993). Plant derived natural products in
drug discovery and development. In: Kinghorn, A.D and Balandrin, M.F. Editors, Human
Medicinal Agents from Plants, ACS Symposium series 534 American Chemical Society DC.
2-12.
Cocks ML, Dold AP (2009). Significance of plant diversity to rural households in the
Eastern Cape of South Africa. Forest, Trees and Livelihood. 13; 39-58.
Doled T, Cocks M (2005). Imbhola yesiXhosa Traditional Xhosa cosmetics. Veld and Flora.
123.
Finn, M. (2004) Affinity Lifestyleshttp://Iwouldbuy.com/manuka-oil.html
63
Grierson DS, Afolayan AJ. (1999). Antibacterial activity of some indigenous plants used
for treatment of wounds in the Eastern Cape, South Africa. Journal of
Ethnopharmacology, 66:103-106.
Ignacimuthu S, Ayyanar M, Sivaraman O.K. (2006). Ethnobotanical investigations among
tribes in Madurai District of Tamil Nadu (India). Journal of Ethnobiology and
Ethnomedicine.2:25.
Katewa SS, Chaudhary, BL, Anita, J (2004). Folk herbal medicine from tribal area of
Rajastan,India. Journal of Ethnopharmacology. 92: 41-6.
Katiyar SK, Afaqf, Perez A, Mukhtar H (2001). Green tea polyphenol (-)-epigallocatechin-
3-gallate treatment of human skin inhibits ultra-violet radiation induced by oxidative
stress. 22(2 ): 287-294.
Mantle D, Gok MA. (2001). Adverse and beneficial effects of plant extracts on skin and
skin disorders. Adverse Drug Reactions and Toxicological Reviews.77:89-103.
Nicolay N (2008). Metropolitan, South Africa.
Pharmcare limited (2003). Instruction paper. Building 12, Healthcare Park, Woodlands
Drive, Woodmead, Sandton, 2148.
Poonam K, Singh GS (2009). Ethnobotanical study of medicinal plants used by the
Taungya community in Terai Arc Landscape, India. Journal of Ethnopharmacology.123
(1): 16.

64
Ramakrishnappa K (2002). Impact of cultivation and gathering of medicinal plants on
biodiversity: case studies from India, Biodiversity and Ecosystem Approaches in
Agriculture, Forestry and Fisheries, Proceedings FAO, Inter-Departmental, Working
Group on Biological Diversity for Food and Agriculture, FAO Rome, Italy. 171-189.
Thirumalai T, Kelumalail B, Senthilkumar E, David E (2009). Ethnobotanical Study of
Medicinal Plants used by the Local People in Vellore District, Tamilnadu, India.
Ethnobotanical Leaflets 13: 1302-11.
Samy PR, Gopalakrishnakore, P (2008). Therapeutic Potential of Anti-microbial for Drug
Discovery.Evidence-based Complementary and Alternative Medicine.
Perumal Samy R, Ignacimuthu S (2000). Antibacterial activity of some folklore medicinal
plants used by tribals in Western Ghats of India. Journal of Ethnopharmacology. 73:63-
71.
Pharmcare limited (2003). Building 12, Healthcare Park, Woodlands Drive, Woodmead,
Sandton, 2148
Quave CL, Plano, LRW, Pantuso T, Bradley C (2008). Effects of extracts from Italian
medicinal plants on planktonic growth, biofilm and adherence of methicillin-resistant
Staphylococcus aureus. Journal of Ethnopharmacol.118 (3): 418-28.
Ranbaxy (SA) (PTY) LTD (2006). Third Floor, Outspan House, 1006 Lenchen Avenue
North, Centurion.
65
Revathi P, Parimelazhagan T (2010). Traditional Knowledge on Plants Used by the Irula
Tribe of Hasanur Hills, Erode District, Tamil Nadu, India. Ethnobotanical Leaflets 14:136-
60.
South Africa Meteorological Service (2009). southafrica.venues.com.
Stinson (undated). Male Circumcision in South Africa. How does it relate to Public Health?
van Wyk B, van Oudtshoorn B, Gericke N (2009). Medicinal Plants of South Africa. Briza
Publications: Pretoria, South Africa.

66
Chapter 4: Antibacterial activity of some medicinal plants used
for the treatment of skin infections and disorders in the O R
Tambo and Amathole of Municipalities of the Eastern Cape
Province, South Africa.
Abstract
The study aimed at evaluating the in vitro antibacterial activity of six medicinal plants
(Kniphofia drepanophylla, Gnidia capitata, Hypoxis hemerocallidea, Syzgium cordatum,
Macaranga capensis and Protorhus longifolia) used in O R Tambo and Amathole Municipal
Districts for the treatment of skin infections. Water, methanol and acetone extracts of
these medicinal plants were screened against five strains of Gram negative bacteria. The
results revealed that water extracts from five plant species inhibited two or more strains
of bacteria with the most common minimum inhibitory concentrations (MICs) ranging
between 5,0 to 10,0 mg/ml with the exception of aqueous extracts of K. drepanophylla
which did not inhibit all strains of bacteria. All methanol plant extracts were significantly
active against all strains of bacteria with MICs ranging from 0, 5 to 5, 0 mg/ml. Acetone
plant extracts were significantly active with most of them being able to inhibit at least
two or more strains of bacteria. However, all acetone extracts failed to inhibit Klebsiella
pneumoniae.
Keywords; antibacterial, gram negative bacteria, medicinal plants, Minimum inhibitory
concentration.
67
Introduction
Use of medicinal plants to treat diseases and complaints is universal among developing
nations (Edgar et al., 2002). In the Eastern Cape, plants have long played a pivotal role
in the lives of amaXhosa people, the inhabitants of the area (Keirungi and Fabricius,
2005). Approximately 70% of the physical related problems of an amaXhosa family are
managed using medicinal plants (Simon and Lamla, 1997). They use medicinal plants as
antiseptics, anti-inflammatory, blood clotting agents, to enlighten the skin or for
treatment of skin infections and to protect themselves from sun’s rays damaging effects.
In South Africa half the population lives below the international established poverty line
(Gutierrez, 2006). In the Eastern Cape, 49% of the population is unemployed and 41%
of the people dwell in the rural areas (South African Institute of Race Relations, 1999)
and are significantly poorer (Cock and MØller, 2002) and could not afford western
medicines. In recent years medical costs have generally increased beyond the rich of
many people. In some cases rural people live far away from clinics and hospitals for them
to easily access the needed medication. Their proximity of the forests and their richness
of medicinal plants and their vast experience in the use of use of medicinal plants enable
them to access readily available medicines.
The province’s plant biodiversity gives it a great potential to develop cheap and easily
accessible plant medicine, especially the coastal areas. Apparently plant resources are
the source of traditional medicines to about 80% of the continent’s population (Chibale,
68
2010). However, there is need to correct the perceived weaknesses of traditional plant
medicines by scientifically testing their efficacy and potency.
Amongst the plants used for treatment of skin infections and problems in O R Tambo and
Amathole municipal districts are Kniphofia drepanophylla, Gnidia capitata, Hypoxis
hemerocallidea, Syzgium cordatum, Macaranga capensis and Protorhus longifolia.
Ethnobotanical data collected from study area revealed that local people use these plants
for self-medication or are prescribed by either herbalists or traditional healers for the
treatment of skin diseases and other ailments. Therefore, this paper presents findings of
the antibacterial activities of these medicinal plants.
Materials and Methodology
Collection of plants and preparation of extracts
K. drepanophylla (rhizome), M. capensis (bark) and P. longifolia (bark) were collected in
Dimfi village near Lusikisiki, Mtambalala forest and Ntafufu village near Port St Johns in
O.R.Tambo districts while H. hemerocallidea (corm), G. capitata (roots) and S. cordatum
(bark) were collected in Glen Eden Far Resort Area and Ngxingxolo village respectively
during the period March 2009 and November 2009. They were air dried at room
temperature. Voucher specimens were prepared and deposited in the Kei Herbarium,
Walter Sisilu University.
Plant materials were crushed using a blender and were shaken in water, methanol, and
acetone for 24 to 36 hours. The extract solutions were decanted and filtered using
Whitman No.1 filter paper. Water filtrates were concentrated to dryness using a freeze

69
drier at reduced pressure and temperature. Methanol and acetone filtrates were
concentrated to dryness using a rotary evaporator at 40°C and 35°C, respectively. The
extracts were packed and closed in small sterile bottles under refrigerated conditions until
use.
Bacteria used in the study
The bacteria used in this study are not directly implicated to skin infections but they have
similar characteristics to those that cause skin infections (Masika and Afolayan, 2002).
The bacteria were selected on the basis of availability. Gram negative bacteria were used;
it was worth screening plant extracts against these bacteria because they may be
resistant to a wide range of antibiotics. The pathogenic capacity of Gram negative bacteria
is often associated with certain components of their cell wall particularly
lipopolysaccharides (Salton and Kim, 1996). One of the unique characteristics of the cell
wall being the ability to protect the bacteria from several antibiotics, dyes and detergents
that would damage the inner membrane or cell wall.
Preparation of agar plates
The dry plant extracts were re-dissolved in their respective solvents of extraction (water,
methanol and acetone) to make stock solutions of 50 mg/ml. Bio-kanamycin was also de-
ionized water to make a stock solution of 50 mg/ml. Nutrient agar (Oxoid) was prepared

70
in the usual way by autoclaving (Masika and Afolayan, 2002) and was allowed to cool to
45°C before mixing it with specific quantities of plant extracts drawn from stock solutions.
Nutrient agar was poured and plant extracts and bio-kanamycin were pipette and mixed
to make final concentrations of 0.5, 5.0, 7.0, and 10.0 mg/ml of respective plant extracts
in triplicate Petri dishes. Each mixture was swirled to spread evenly until it began to set.
Control plate containing 1.0 ml of water, methanol, acetone and bio-kanamycin were also
prepared in triplicate. Prepared plates were left for 12 hours to allow solvent to evaporate
before streaking with bacteria.
Antibacterial testing
Five Gram negative bacteria strains (Citrabacter freundii, Escherichia coli, Enterobacter
cloacae, Klebsiella pneumoniae, and Proteus mirabilis) obtained from the Nation of Health
Laboratory Services were used. Bacteria species were recovered for testing by growing
them in separate sterile Nutrient Broth (Oxoid) for 24 hours. Then each culture was
diluted hundred times in fresh nutrient broth. The bacteria were streaked in radial pattern
on the agar plates (Afolayan and Meyer, 1997). Radial pattern streaking enabled
management of more than one strain of organism in the same medium. The prepared
plates were incubated at 35°C for 24 hours before observation could be done.

71
Results and Discussion
Methanol extracts of all the plants in this study effectively inhibited all strains of bacteria
used with most common minimum inhibitory concentrations (MIC) ranging between 0, 5
and 10 mg/ml as revealed in the table 4.1. Inhibition of bacteria by methanol extracts
was observed in similar studies by (Rabe and van Staden, 1997; Grierson and Afolayan,
1999; Masika and Afolayan, 2002). Methanol extracts of K. drepanophylla was relatively
weak to K. pnuemoniae and E. coli. These strains of bacteria were inhibited at 7 mg/ml
and 10 mg/ml respectively.
The antibacterial assays of water extracts from five plant extracts in this study showed
inhibition of two or more strains of bacteria except of the extracts of K. drepanophylla
which was not active to all strains of bacteria. Both M. capensis and P. longifolia water
extracts inhibited K. pneumoniae at MIC of 5 mg/ml while other water extracts were
inactive to the same strain of bacteria. G. capitata, M. capensis and P. longifolia aqueous
extracts inhibited E. coli but the same strain of the bacteria was not inhibited by aqueous
extracts from the other plants. H. hemerocallidea corm aqueous extract only inhibited C.
freundii and P. mirabilis at 10 mg/ml.
Acetone extracts of all plants showed a significant inhibition of C. freundii and P. mirabilis
with MIC of 0, 5 mg/ml while they were inactive against E. cloaceae. M. capensis
consistently inhibited E. coli and K. pnuemoniae at 5 mg/ml while other five plant acetone
extracts were not active against the same strains of bacteria.

72
Traditionally, the local people prepared the plant medicines with water infusions or
decoctions. Based on the observation that some water and acetone extracts are inactive
it may be argued that traditional practitioners are unlikely to extract active components
of the medicinal plants; therefore it is recommendable to use methanol for extraction.
The ability of some water extracts to inhibit some strains justifies the use of the water
extracts by traditional practitioners.
Like bio-kanamycyin, some plant extracts inhibited some strains of bacteria tested at 0.5
mg/ml. Therefore, it can be argued that some of these plants extracts can be good
candidates for development of novel drugs. Bearing in mind that only crude preparation
showed a significant inhibition to some bacteria. If the active components are isolated,
purified and/ or modified they can go a long way in dealing with the health problems of
the local people and the world at large.

73
Table 4.1 Antibacterial activity of some plant extracts used for the treatment of skin
problems in O R Tambo and Amathole Districts.
Plant extracts (MIC or Na)
Solvents Bacteria Kd Gc Hh Sc Mc Pl Bio-K Control
Water
C.f Na 7.0 10.0 0.5 7.0 5.0 0.5 Na
E.c Na 5.0 Na Na 5.0 5.0 0.5 Na
E.cl Na 7.0 Na 5.0 5.0 5.0 0.5 Na
K.p Na Na Na Na 5.0 5.0 0.5 Na
P.m Na 7.0 10.0 1.0 5.0 5.0 0.5 Na
Methanol
C.f 5.0 0.5 5.0 0.5 0.5 0.5 Na
E.c 10.0 5.0 5.0 1.0 1.0 1.0 Na
E.cl 5.0 5.0 5.0 0.5 0.5 1.0 Na
K.p 7.0 5.0 5.0 1.0 0.5 1.0 Na
P.m 1.0 0.5 1.0 0.5 0.5 0.5 Na
Acetone
C.f 0.5 0.5 0.5 0.5 0.5 0.5 Na
E.c Na Na Na Na 5.0 Na Na
E.cl Na Na Na Na Na Na Na
K.p Na Na Na Na 5.0 Na Na
P.m 0.5 5.0 5.0 0.5 0.5 0.5 Na
Key Plants from which extracts were extracted; MIC: minimum inhibitory concentration (mg/ml) Kd: Kniphofia drepannophylla Na: Not active Gc: Gnidia capitata Bio-K: Bio-kanamycin Hh: Hypoxis hemerocallidea Sc: Syzgium cordatum Mc: Macaranga capensis Pl: Protorhus longifolia Bacteria on which extracts were tested; C.f: Citrabacter freundii

74
E.c: Escherichia coli E.cl: Enterobacter cloaceae K.p: Klebsiella pneumonia P.m: Proteus mirabilis
Acknowledgements
Great appreciation to National Research Foundation for funding this study, National
Health Laboratory Services for providing the bacteria used in this study, Department of
Health for providing bio-kanamycin, Mr. D. Wopula for his assistance in ethnobotanical
survey, Dr. K. L. Immelman and Mrs. E. Cloete for assistance offered in identification of
plants and the local people of the two districts studied for providing ethnobobatanical
information.

75
References
Afolayan AJ, Meyer JJM (1997). The antimicrobial activity of 3, 5, 7-trihydroxflavone
isolated from the shoots of Helichrysum aureonitenens. Journal of Ethnopharmacology.
57: 177-181.
Chibale K (2010). Discovery Africa’s drug potential Health. Integrating Modern and
traditional Medicines.
Cock ML, MØller V. (2002). Uses of and indigenized medicines to enhance personal
wellbeing: South African case study. Social Science Medicine. 54.387-397.
Edgar J, da Silva, Baydoun E, Badran A (2002). Biotechnology and the developing world.
Electronic J. of Biotechnology. 5:1.
Grierson DS, Afolayan AJ (1999). Antibacterial activity of some indigenous plants used for
treatment of wounds in the Eastern Cape, South Africa. Journal of Ethnopharmacology.
66: 103-106.
Gutierrez E (2006). Ecotourism and Biodiversity Conservation. 597-602 in Groom MJ,
Meffe GK, Carroll, CR. (Ed.). Principles of Conservation.
Keirungi J, Fabricius C (2005). Selecting medicinal plants for cultivation at Nqabara on
the Eastern Cape Wild Coast, South Africa. South African Journal of Science 101.
Masika PJ, Afolayan, AJ (2002). Antimicrobial activity of some plants used for the
treatment of livestocks in the Eastern Cape, South Africa. Journal of Ethnopharmacology.
83: 12.

76
Rabe T, van Stadens, J (1997). Antibacterial activity of Southern African plants used for
medicinal purposes. Journal of Ethnopharmacology. 56: 81-87.
Salton MJR, Kim, KS (1996). Structure in: Baron’s Medical Microbiology (Baron, S et al.,
Eds) (4th Ed). University of Texas Medical Branch.
Simon C, Lamla M (1997). Merging pharmacopoeia; Understanding the origins of
incorporative pharmacopoeial processes among Xhosa healers in Southern Africa. Journal
Ethnopharmacology. 33: 237-247.
South Africa Institute of Race Relations (1999). Fact 1, 1-2 Johannesburg.

77
Chapter 5: In Vitro Antioxidant activity of some plants used for
treatment of skin problems in O R Tambo and Amathole Districts
of the Eastern Cape Province, South Africa.
Abstract
The methanol extracts of some commonly used medicinal plants against skin infections
and disorders were screened for their antioxidant activity using ascorbic acid as standard
antioxidant. The free radical scavenging activity was evaluated using 1, 1-diphenyl-2-
picryl-hydrazyl (DPPH) free radical. The analysis was performed using a Phoenix-2000v
UV-VIS spectrophotometer. The methanol extracts of Protorhus longifolia, Gnidia
capitata, Macaranga capensis, Syzgium cordutum and Hypoxis hemerocallidea showed
significantly higher free radical scavenging activity than that of ascorbic acid while
Kniphofia drepanophylla showed very weak antioxidant activity. The IC50 of former plant
extracts were 11.5, 14.4, 14.6, 40.0, 41.2 and 44.0 µg/ml respectively while the IC50
value for K. drepanophylla could not be determined at 100µg/ml. The DPPH free radical
scavenging activity of the plant extracts increased with increasing concentration i.e. the
free radical activity was dose dependent. Generally, results revealed that these medicinal
plants are potential sources of natural antioxidant.
Keywords: Antioxidant, ascorbic acid, DPPH, free radical, scavenging activity.

78
Introduction
Many people worldwide are exposed to different stresses which result in the generation
of free radicals in biological systems. These include stresses from food toxins and food
adulteration, atmospheric pollution, exposure to ultraviolet radiation from the sun,
unhealthy lifestyles such as smoking and alcoholism. In addition, chemical mobilization
of fats under various conditions such as lactation, exercise, fever and infection can result
in high production of free radicals (Ara and Nur, 2009). Free radicals are molecule
fragments having one or more unpaired electrons; they are usually short-lived and highly
reactive (Chang and Cruickshank, 2005). Under both normal and pathological conditions
free radicals are produced in all cells by mitochondrial oxidative chain reaction (Ko and
Leung, 2007; Ara and Nur, 2009). Although oxidation reactions are crucial for life, they
can also be damaging; hence both plants and animals maintain complex systems of
multiple types of antioxidants, such as glutathione, ascorbic acid (vitamin C), tocopherol
(vitamin E) and antioxidant enzymes such as catalase, superoxide dismutase and various
peroxidases (Davies, 1995). Low levels of antioxidants, or inhibition of the antioxidant
enzymes, cause oxidative stress and may damage or kill cells resulting in development of
degenerative conditions such as heart diseases, ischemia, anemia, asthma, arthritis,
inflammation, neuro-degeneration, Parkinson’s disease, mongolism, cancer, aging and
dementias (Prakash, 2001; Ara and Nur, 2009).
Antioxidants are a diverse group of chemical compounds that are synthesized by plants.
As part of their adaptation from marine life, terrestrial plants began producing non-marine
antioxidants such as ascorbic acid (Vitamin C), polyphenols, flavonoids and tocopherols
79
(U.S. National Institute of Health, 2010). The main purpose of antioxidant in biological
systems is to scavenge and trap free radicals (Adedapo et al., 2008). They terminate
chain reactions which are responsible for oxidative stress by removing free radical
intermediates, and inhibit other oxidation reactions. Tutour (1990) noted that they have
an important role in protecting oxidative damage induced by highly reactive oxygen
species (ROS), in the cells and tissues. Thus an increase in the antioxidant reserves of
any organism can reduce oxidative stress (Ara and Nur, 2009). Furthermore, antioxidants
have been implicated in having a role in the proper functioning of the immune system,
which help to keep the body health including the skin. A significant number of plant
species have been reported to have extracts with antioxidant activity (Nooman et al.,
2008). The antioxidant and anti-radical properties of these plant products can be ascribed
to widely distributed secondary metabolites such as flavonoids, isoflavones, athocyanins,
coumarin, lignans, catechins and isocatechins (Ara and Nur, 2009). Most of these
antioxidants from plants are phenol and polyphenolic compounds (Prakash, 2001).
According to Hanson (2001) stratum corneum, the skins main protective barrier against
environmental assaults generates tremendous amounts of free radicals. This high
production of ROS increases the risk of oxidation of skin tissue resulting in dermatological
disorders. The ROS can initiate peroxidation of lipids, which in turn stimulates glycation
of proteins and alteration in structure and functions of collagen basement and other
membranes (Prior, 2003; Polterait, 1997; Saha et al., 2008;) and this play a role in the
development of long term complications (Lee et al., 2003; Prior, 2003) such as dementias,
quick aging of the skin, skin cancer, and skin inflammation. Therefore, it can be argued

80
that if these free radicals are left unchecked they can increase the risk for chronic and
oxidative diseases. Scientific evidence suggests that antioxidants reduce the risk for
diseases that are as a result of oxidative stress (Miller et al., 2000) and chronic diseases.
Over the past three decades antioxidant based formulations have played a major role in
chemo-prevention and treatment of pathological conditions caused by oxidative stress
(Prior, 2003; Khalaf et al., 2008; Hennebella, 2008). This resulted in a great deal of study
in natural antioxidant (Ara and Nur, 2009) in other parts of the world. In the Eastern
Cape, there is limited research in the field of antioxidants. Therefore, the present study;
evaluate the antioxidant activity of some plants used for the treatment of skin problems.
Medicinal plants which were investigated are Kniphofia drepanophylla, Gnidia capitata,
Hypoxis hemerocallidea, Syzgium cordatum, Macaranga capensis and Protorhus
longifolia.
Materials and methods
Collection of plant materials
Six plant species which were commonly implicated in the treatment of skin infections from
ethnobotanical data were selected for antioxidant evaluation. K. drepanophylla (rhizome),
M. capensis (bark) and P. longifolia were collected from O. R. Tambo district, at Dimfi
village near Lusikisiki, Mtambala forest and Ntafufu village near Port St Johns respectively.
H. hemerocallidea (corm), G. capitata (roots) and S. cordatum (bark) were collected from
Amathole District. The plant materials were collected between March 2009 and November

81
2009). They were air dried at room temperature. Voucher specimens were prepared and
deposited at Kei Herbarium, Walter Sisulu University.
Extraction of plant materials
Air dried plant materials were crushed using a blender and were extracted separately by
shaking approximately 100 g of each plant species in 95 % methanol for 24 to 36 hours.
The extracts were filtered using Whatman No.1 filter paper. The extract solutions were
concentrated to dryness using a rotary evaporator at 40 ⁰C under reduced pressure. The
extracts were packed and closed in sterile bottles and were refrigerated until use.
DPPH Radical Scavenging Activity
The free radical scavenging activity was evaluated in vitro using 1, 1-diphenyl-2-picryl
hydrazyl (DPPH) a known free radical. Both DPPH and methanol used were of analytical
grade. The method used by Ara and Nur (2009) and Khalaf et al. (2009) was adopted. A
0,004% w/v of DPPH was prepared in 99% methanol. Methanol stock solutions of 100
µg/ml of different plant extracts were prepared by dissolving 10 mg of each dry plant
extract in 100 ml of 99% methanol. From each stock solution 2 ml, 4 ml, 6 ml, 8 ml and
10 ml of solution were taken and poured into five test tubes. Each test tube was serially
diluted by topping up to 10 ml using 99 % methanol. As a result of this serial dilution
working solutions of concentrations 20 µg/ml, 40 µg/ ml, 60 µg/ ml, 80 µg/ ml and 100

82
µg/ ml established. From each of the working solution 2 ml of plant extract were added
to covet and to each covet 2 ml of DPPH was added. A control was made by adding 2 ml
of DPPH and 99 % methanol. A blank of 4 ml of methanol was used. They were prepared
in triplicates and were allowed to react in the dark for 15 minutes at room temperature.
The absorbance of mixtures was measured at 517 nm using a Phoenix-2000v UV-VIS
spectrophotometer. The mean absorbance of the triplicates was determined and the
scavenging of DPPH free radical was determined using the equation;
% DPPH radical scavenging = [(A –B)/A] x100
Where A =Absorbance of control and B =Absorbance of test sample.
Results and Discussion
DPPH is widely used to test the ability of plants extracts to act as free radical scavengers
or hydrogen donors (Prakash, 2001) and evaluate antioxidant activity of medicinal plants
extracts. The reaction of DPPH with numerous antioxidants has been reported (Miller et
al., 2000). The DPPH free radical scavenging activity of six indigenous plant species of
the Eastern Cape and ascorbic acid are presented in Figure 5.1. Availability of antioxidants
for reaction with DPPH depends on various factors such as solubility in the solvent of
extraction or whether antioxidants are bound to cell wall during extraction of plant
material. Based on these factors plant extracts may react with DPPH at different rates i.e.
differing kinetics and the reaction would sometimes not go into completion in some
reasonable assay time (Miller et al., 2000). Therefore, the sample size that scavenges

83
DPPH by 50 % (IC50 value) was chosen as the end-point for measuring the antioxidant
activity of the extracts. The in vitro antioxidant activities of methanol extracts are shown
in Table 5.1. Ascorbic acid was used as a frame of reference since it is a known antioxidant
which can scavenge DPPH and other free radicals.
0
20
40
60
80
100
120
0 20 40 60 80 100
% S
caven
gin
g o
f D
PP
H
Concentration (µ g/ ml)
Figure 5.1 DPPH free radical activity of Ascorbic Acid and Methanol Plant Extracts of some plants used for treatment
of skin infections and disorders.
Ascorbic acid
S. cordatum
H. hemerocallidea
M. capensis
P. longifolia
G. capitata
K. drepanophylla

84
Table 5.1 In vitro antioxidant activity of methanol extracts of some plants used for the
treatment of skin infections and disorders in the Eastern Cape.
Methanol plant extracts IC50 (µg/ml)
G. capitata 11.5
P. longifolia 14.4
M. capensis 14.6
S. cordatum 40.0
H. hemerocallidea 41.2
K.drepanophylla ***
Ascorbic acid 44.0
*** IC50 value not determined
As indicated in Figure 5.1, P. longifolia, G. capitata, M. capensis, S. cordutum and H.
hemerocallidea have proven to be effective antioxidant containing extracts compared to
the reference standard ascorbic acid. All these plant species extracts were observed to
have higher IC50 value as compared to Ascorbic acid as shown in Table 5.1. The IC50
values of these plant species were 11.5, 14.4, 14.6, 40.0, and 41.2 µg/ml respectively
while that of ascorbic acid was 44.0 µg/ml. The antioxidant activities of these medicinal
plants were dose dependent (Figure 5.1). As the concentration of these plants extracts
increases the antioxidant activity increased exponentially. The high scavenging activity of

85
these plant extracts against DPPH is of interests. As antioxidant-based formulations are
used for chemo-prevent and treatments of degenerative diseases like arthritis,
inflammation, neuro-degeneration, mongolism, aging process and dementias (Ara and
Nur, 2009). An antioxidant of external source can prevent oxidative damage by inhibiting
the generation of reactive species, scavenging free radicals or raising level of endogenous
antioxidant defense (Haripyaree et al., 2010). This result justifies the continual uses of
the medicinal plants for curing dermatological conditions by herbalist and traditional
healers. In addition, this explains why the local people of O R Tambo and Amathole
Districts still have strong belief in the efficacy and usefulness of the medicinal plants.
In contrary, to high antioxidant activity of the other five plant species K. drepanophlla
revealed a weak antioxidant activity as shown on Figure 5.1. This plant species could not
even achieve its IC50 value at the highest concentration of 100 µg/ ml used in this study.
The use of this plant species by herbalists and traditional practitioners for curing of
oxidative stresses is not justifiable. Perhaps if the use of this plant is justifiable the IC50
value of K. drepanophlla would be recognized at a higher concentration since increase in
concentration of the plant extract tend to increase the free radical activity of the plant
extracts.
Although these plant extracts revealed high antioxidant activity, there is need to
investigate the chemical constituents which are responsible for the antioxidant activity.
The possible constituents are flavones, isoflavones, flavonoids, tannins, glycosides and
many others. Many of these are potential antioxidant compounds synthesized by plants
(Lee et al., 2004). Some of them have been already isolated from plants and have been

86
tested in models for combating chronic diseases and their results revealed great potential
in controlling the conditions due to oxidative stresses (Prakash, 2001). This free radical
scavenging activity potential could be ascribed to natural antioxidant present in medicinal
plants. Isolation of the constituents could be critical in the development of antioxidant
therapy (Hasan et al, 2006; Erdemoglu et al., 2006).
Scientific evidence suggests that antioxidants reduce risk of oxidative conditions due to
free radicals (Prakash, 2001; Ara and Nur, 2009) and endogenous defense mechanisms
have evolved to offer protection against these conditions (Ara and Nur 2009). An increase
in the amount of the antioxidant reserves of an organism can be of great importance in
reduction of oxidative stress such as aging (Ara and Nur, 2009), inflammation, dementias
and other chronic diseases and treatment of these conditions. As revealed by this study,
G. capitata, P. longifolia, M. capensis, S. cordatum and H. hemerocallidea may be
considered as natural sources for antioxidant therapy and it is imperative to identify the
antioxidant molecules.
Acknowledgements
This research was supported by the Research Directorate of Walter Sisulu University and
the National Research Foundation of South Africa. Authors would like to thank Mr. E.J.
Ndebia and Dr. D. Kamadyaapa from Department of Physiology, Faculty of Health
Sciences, Walter Sisulu University for their technical support in the analysis of the results.

87
References
Adedapo AA, Jumoh FO, Koduro S, Afolayan AJ, Masika (2008). Antibacterial and
antioxidant properties of methanol extracts of leaves and stem of Calpurnia aurea.
Complementary and Alternative medicine.
Ara N, Nur H (2009). In Vitro Activity of Methanolic Leaves and Flowers Extracts of Lippia
alba. Res. J. of Med. and Med. Sc. 4(1):107-110.
Chang R, Cruickhank B (2005). Chemistry (8thed.). McGraw-Hill; New York; 968.
Davies K (1995). Oxidative stress; the paradox of aerobic life. Biochem. Soc. Symp. 61:1-
31.
Erdemoglu N, Taran NN, Cikici I, Sener BB, Aydin A (2006). Antioxidant Activities of Some
Lamiaceae Plant extracts. Phytotherapy research. 20:63-70.
Handson FG (2001). http//Iwouldbuy.com/manuka-oil.html.
Hasan MS, Ahmed MI, Mondal S, Uddin SJ, Masud MM, Sadhu SK, Ishibashi M (2006).
Antioxidant, antinociceptive activity and general toxicity study of Dendrophthoe falcate
and isolation of quertctrin as the major component. OPEM. 6: 355-60.
Haripyaree A, Guneshwor K, Damayanti M (2010). Evaluation of antioxidant properties
of some sulfur free radicals reactivity with curcumin as reference. EJEAFChe 9 (2): 337-
344.

88
Khalaf AN, Shakya AK, Al-othman A, El-agbar Z, Farah, H (2008). Antioxidant Activity of
Some Common Plants. Turkish Journal Biology 32:51-55.
Lee SE, Hwang HJ, Ha SJ (2003). Screening of medicinal plant extracts for antioxidant
activity. Life Sci. 73: 167-179.
Miller HE, Rigelhof F, Marquart L, Prakash A, Kanter M (2000). Cereal Foods World. 45(2):
59-63.
Polterait O (1997). Antioxidants and free radical Scavengers of Natural origin. Current
Org. Chem. 1: 415- 440.
Prakash A (2001). Antioxidant Activity. 19(2): 1-4.
Prior RL (2003). Fruits and vegetables in the prevention of cellular oxidative damage.
American Journal of Clinical Nutrition.78; 570S-578S.
Saha MN, Alam MA, Aktar R, Jahangir R (2008). In vitro free radical scavenging activity
of Ioxra coccinea L. Bang. Journal Pharmacology. 3: 90-93.
Tutour BL (1990). Antioxidant activities of algal extracts Synergistic effect with Vitamin
E. Phytochemistry. 29: 3759-3765.
U.S. National Institute of Health, Office of Dietary Supplements (2010). Antioxidant.
Wikimedia.

89
Chapter 6: General Discussion and Conclusions
DISCUSSION
The skin is frequently affected by diseases, whether as primary disease of the skin itself
or as a secondary effect of other conditions (DHB, 2011). The severity of the skin condition
varies enormously. At one extreme, there may be nothing more than a patch of redness
on the finger resulting from sensitivity to a particular metal in a ring. At the other extreme,
weeping blisters may cover an individual from head to foot, resulting in fluid loss to a
degree, which may be life threatening (DHB, 2011). Ethnobotanical information reveals
that bites, ringworm, boils, septic sores and burns were more common to children of less
than 15 years of age while other skin problems such as dryness eczema, acne, cancer,
hyperpigmentation and hypopigmentaion were reported in people of all age group
(Chapter 3). During the early 1990s the health transition in South Africa was characterized
by a very high in injury burden (Bradshaw et al., 2002).
The skin disorders were commonly reported in the rural area (Chapter 3) where the
majority of the population of Eastern Cape resides and where clinic and hospitals are
sparsely distributed (Cocks and Dold, 2000). In rural parts of the Eastern Cape, self-
medication is a common practice (Chapter 3) and wild medicinal plants are harvested and
used as initial response to illness (Dold and Cocks, 1997) including dermatological
problems (Chapter 3). In the case of severe skin disorders and other illness rural people
consult traditional herbalists and other knowledgeable people who live in their locality
(Chapter 3). It is of paramount importance to note that during both self-medication and

90
consultation of traditional practitioners, people take advantage of great biodiversity of
plant species in their proximity to cure disease and ailments (Ndubani and Hojer 1999).
For this reason, it was important to document information on the plant taxa that are used
to cure skin disorders before it is lost since it is transmitted from generation to generation
by unreliable oral means and in most cases the information is confined to traditional
practitioners and clan elderly people (Chapter 3).
Poor wound healing capacity in elderly and those with chronic skin diseases often makes
minor skin injuries or common skin diseases the precipitating event costly interventions.
In addition to adults and elderly people, many children suffer from inherited and acquired
skin diseases (Society for Investigative Dermatology, 2005). Chronic diseases of the skin,
hair and nail need fairly good treatment to maintain their functionality and to decrease
pain, severe itch and dependency. In the absences of complications, affected adults in the
study area are able to cope with skin diseases by topically applying botanical medicines
(Chapter 3). This study found that the use of juicy leaf medicinal plants such as Aloe
species, Bulbine species and Carpobrotus species for self-medication to treat minor skin
problems such as bruises, small wounds, itchy rash and corns is a common practice in
amaXhosa people in the study area (Chapter 3). This may be due to availability of
enormous knowledge on the use of plant preparations in traditional medicine and strong
belief in the effectiveness of these plant preparations (Chapter 3).
Ethnobotanical data obtained in this study can be very important to conservationist and
botanist who are interested in conversation of potentially useful plant species (Chapter 3).
While the in vitro antibacterial activity (Chapter 4) and in vitro antioxidant studies can be

91
used as baseline investigations by biologist, chemists and pharmacologist who may be
interested in the active ingredients of plants. There is growing interest in natural and
traditional plant medicine as a source of new commercial products (van Wyk, 2008).
Based on ethnobotanical data obtained in chapter 3, a judicious choice of 6 (Hypoxis
hemerocallidea, Gnidia capitata, macaranga capensis, Syziguim cordatum, Protorhus
longifolia and Kniphofia drepanophylla) out of 45 medicinal plants used for treatment of
skin disorders in O.R. Tambo and Amathole municipalities was done for further
investigation of medicinal properties of these plants. These plant species were selected
for further study because they were frequently implicated for use of treatment of skin
disorders in the study area (Chapter 3).
The in vitro antibacterial (Chapter 4) and antioxidant (Chapter 5) activities of these
medicinal plants (H. hemerocallidea, G. capitata, M. capensis, S. cordatum, P. longifilla)
were regarded effective in combating dermatological problems by most respondents.
Considering that some of these plant medicinal preparations were taken orally, traditional
practitioners and the local people ruled out any side effects when using these medicinal
plants (Nkomo, 2009).
Methanol, acetone and water extracts from H. hemerocallidae, G. capitata, M. capensis,
S. cordatum, and P. longifilia had significant antibacterial activity against Gram negative
bacteria used in this study. Conversely, methanol, acetone and water extract from K.
drepanophylla did not inhabit all strains of bacteria. However, there was a significant
difference in the antibacterial activity between extracts from different solvents (methanol,

92
acetone and water extracts). The methanol plant extracts were highly active against all
strains of bacteria with MICs raging from 0, 5 to 5, 0 mg/ml while other extracts were
less active. It can be argued that the type of solvent used for extraction is critical for
effective extraction of phytochemicals from the plant materials.
Despite the fact that water extracts have lesser activity than methanol extracts, their
significant antibacterial activity was of interest since water is the most common solvent
in the preparation of traditional botanical medicine. In most traditional preparations plant
materials are either crushed and mixed with water and boiled with water for a specific
length of time or macerated and allowed to stand for a specific length of time (Chapter
3). The antibacterial activity of the water extracts justifies their continual use in the
treatment of skin disorders and traditional practices (Chapter 3).
An antioxidant evaluation of the six medicinal plants based on ability of plants extract to
scavenge a standard free radical 1, 1-diphenyl-2-picryl-hydrazyl (DPPH) depicts that H.
hemerocallidea, G. capitata, M. capensis, S. cordatum, and P. longifilia have antioxidant
properties comparable to ascorbic acid except K. drepanophylla (Chapter 5). These plant
extracts had IC50 value less than that of ascorbic acid (IC50 value =44, 0 µg/ml) implying
that they have a higher antioxidant properties than that of ascorbic acid (Chapter 5). The
use of these external sources of antioxidants derived from medicinal plants can prevent
oxidative damage of free radicals in the body. This probably explains why plant derived
products are orally administered or topically applied to the body to combat skin diseases,
other diseases and ailments in traditional medicine (Chapter 3).

93
Participants in this study ranked the efficacy and effectiveness of medicinal plants very
high (Chapter 3). Based on both antibacterial and antioxidant properties of the
investigated medicinal plants (Chapter 4 and Chapter 5) it can be deduced that there are
phyto-chemicals in these plants responsible for healing process. It can be argued that if
these active ingredients are isolated and their toxicity is studied they can go a long way
in the treatment of skin diseases. Botanical medicines contain phyto-chemicals that act
directly or indirectly to prevent or treat diseases and maintain health (van Wyk et al,
2009).
CONCLUSION
From this study, it can be concluded that:
The usage of medicinal plants for the treatment of skin disorders and other
ailments among the amaXhosa in the O R Tambo and Amathole municipalities is
still pivotal for the primary health delivery system.
A variety of plants which include trees, shrubs, herbs, and grasses are used as
medicinal plants by amaXhosa in the study area.
Herbal medicines are cheaper than the mainstream drugs and can be afforded
easily and accessed by the majority of people in O R Tambo and Amathole
municipalities.
The people in O R Tambo and Amathole municipalities’ particularly in rural areas
still have a strong belief in the effectiveness and efficacy of their herbal remedies.

94
H. hemerocallidea, P. longifolia and K. drepanophylla are becoming scarce in the
natural forests.
Extracts of H. hemerocallidea, G. capitata, M. capensis, S. cordatum, and P.
longifilla have significantly high in vitro antibacterial activity against some Gram
negative bacteria and in vitro antioxidant activity on DPPH.
Methanol extracts of these plants have higher antibacterial and antioxidant
properties than water and acetone extracts.
Limitations
Gathering ethnobotanical information was a challenge since the local people were
conservative as regarding to their indigenous knowledge and most of them were reluctant
to give out information. However, persistence and patience of negotiating with the
intended respondents enable findings in this study. It was also a challenge to gather
information in sparsely populated and mountainous areas in the study area, but this meant
frequent trips and endurance.
RECOMMENDATIONS
Plants may be considered as good sources of natural antimicrobial and antioxidant for use
against diseases.
Further investigation on isolation and purification of active ingredients responsible for
the antimicrobial and antioxidant activities is recommended.
Further studies are suggested on the toxicity of these medicinal plants.

95
Based on the results of ethnobotanical studies there is need to establish medicinal
plant gardens for the propagation of much sought plant species yet under pressure
from harvesters as a conservation measure.

96
References
Bradshaw D, Schneider M, Dorrington R, Bourne D, Laubscher R (2002). South African
cause of death profile in transition – 1996 and future trends. South African Medicinal
Journal 92: 618-623.
Dold AP, Cocks M (1997). AmaYeza esiXhosa –an insight into Xhosa medicine. The
Phoenix, Eastern Cape Museum Magazine. 9, 2 & 3:4-5. Albany Museum, Graham’s town.
Cock ML, Dold AP (2000). The medicinal plants traded in the Eastern Cape Province.
Unpublished report, Department of Water Affairs and Forestry, Pretoria.
Disability Handbook (2011). DHB.
Ndubani P and Hojer B (1999). The traditional healers and treatment of sexually
transmitted illnesses in rural Zambia. Journal of Ethnopharmacology 67: 15-25.
Nkomo M (2009). Phytomedicinal studies of plants used in the treatment of dysmenorrhea
on O R Tambo Municipality. Unpublished report, Submitted in fulfiment of the requirement
of a Master degree of Science: Botany. Botany Department, Walter Sisisulu University:
Mthatha. 118-119.
Society for Investigative Dermatology (2005). Priority for Skin Biology and Disease
Research.
van Wky B-E (2008). Abroad review of commercially important South African medicinal
plants. Journal of Ehnopharmacol. 119: 342-355.

97
van Wky B-E, van Oudtshoorn B, Gericke N (2009). Medicinal plant of South Africa. Briza
Publications: Pretoria.

98
APPENDICES
Questionnaire respondent by traditional practitioners
ETHNOMEDICINAL OF STUDY OF SOME PLANTS USED FOR TREATMENT OF
SKIN INFECTIONS AND DISORDERS
Mahachi J is a student of Walter Sisulu University. He is carrying out a study to assess
and identify some medicinal plants used for treatment of skin infections and disorders
and improve the skin in the OR Tambo and Amathole Municipalities of the Eastern Cape.
This study will cover areas around Lusikisi, Flagstaff, Bizana and Port St. Johns in OR
Tambo and Mooiplas, Cinsta and Glen Eden Far Resort Area in the Great Kei sub- district
of Amathole Municipality. The results of this study will be made known to local people
and authorities as well to other interested parties. The purpose of this study is to find
enthomedical information of plants used for treatment of skin infections and improve the
skin.
1. Do you have people coming to consult you concerning treatment for skin diseases?
Yes No
2. What kind of skin problems do you normally have clients coming for treatment?
Wounds Ringworm itches Skin rashes psoriasis eczema Pigmentation
problems

99
3. Which plants do you use to use to prepare your medicines?
4. Which plant parts do you use to prepare the medicine?
5. How do you prepare you plant medicines?
6. How much of the plant material would need for each preparation?
7. What do you consider most important to prepare an effective medicine?
8. How do you know which plant species to use for treatment of a particular ailment
of the skin?

100
9. How is the medicine used by the patients?
Topical application Oral taken Steaming on affected
parts
10. How would you rank the efficacy of your plant medicines (Tick where appropriate).
Poor Fair Good Very good Excellent
11. Where do you get plant material which use to prepare your medicines?
12. How far are these plant materials from the place where you live?
13. Are the plants still in abundances?
Yes No

101
14. If yes: Which plant species are abundant?
15. If no: Which plants are rare?
16. May you assist by showing some plants which you use for medicines?

102
Questionnaire respondent by local people
ETHNOMEDICINAL OF STUDY OF SOME PLANTS USED FOR TREATMENT OF
SKIN INFECTIONS AND DISORDERS
Mahachi J is a student of Walter Sisulu University. He is carrying out a study to assess
and identify some medicinal plants used for treatment of skin infections and disorders
and improve the skin in the OR Tambo and Amathole Municipalities of the Eastern Cape.
This study will cover areas around Lusikisi, Flagstaff, Bizana and Port St. Johns in OR
Tambo and Mooiplas, Cinsta and Glen Eden Far Resort Area in the Great Kei sub- district
of Amathole Municipality. The results of this study will be made known to local people
and authorities as well to other interested parties. The purpose of this study is to find
enthomedical information of plants used for treatment of skin infections and improve the
skin.
1. Do you often use plant material as medicines on the skin?
Yes No
2. For what reasons do you use the plant material on the skin?
3. Which plants do you often use on the skin use on the skin?

103
4. Which plant parts do you use?
5. How do you prepare you medicine?
6. Where do you get plant material to prepare you medicines?
7. Do you still have these plants in abundances?
Yes No
8. If yes; which ones are still available easily?
9. If no; which ones are now rare?

104
10. Do you sometimes consult with the traditional practitioner for you to get the
plant medicines to use on the skin?
11. Which condition do you consult with traditional practitioner?
12. How do you rank the efficacy of the plant medicines? (Tick where appropriate).
Poor Fair Good Very good Excellent
13. Do you any plant materials that are used for treatment of skin problems or
improve the skin tone?
Yes No
14. If yes, which ones do you know?
15. What are these plants used for?
16. How are these plants prepared into medicine?

105
17. May you help me by showing me some of the plants which are used to treat
skin problems?

106
Copyright © 2022 FDOKUMEN