
Medical Negligence :Law and practice in Bangladesh
108
Research on Medical Negligence Law & Practice in Bangladesh International Islamic University , Chittagong Presented by Akther Jahan ID No : LM-131214 Course Code: Submission Date: 20- 4-2014 Submitted to: Adv. Anjuman Ara Begum Assistant Professor Law Department Supervisor of the concerned thesis 1
Transcript of Medical Negligence :Law and practice in Bangladesh

Research onMedical Negligence
Law & Practice in Bangladesh
International Islamic University , Chittagong
Presented by Akther Jahan
ID No : LM-131214
Course Code:
Submission Date: 20-4-2014
Submitted to: Adv. Anjuman Ara Begum
Assistant Professor
Law Department
Supervisor of the concerned thesis
1
Preface
In the name of ALLAH, the Most Beneficial,the Most Merciful.
This Research Monograph is submitted in partial fulfillmentof the requirement for the degree of Bachelor of laws. Thecourse teacher gave two options for research. I have chosenthis topic for research due to my interest and strongcuriosity regarding this topic.
In writing this Research paper , I have taken help frommany books, journals and internet. freely used these booksfrom Noshirvan H. Jhabvala’s “The Law of Torts”25th Edition, Markesan’s and Deakin’s “Tort Law” 5th edition,Dr. Durga Das Basu’s “The Law of Torts”’ 11th Edition, andAin O Salish Kendra’s “Chikitshai Obohela”. Beside thesealso I have taken the help of some websites and journals. Iam grateful to the learned authors and to the editors ofthese books and websites and journals.
I would like to give special thanks to honorable supervisorAdv Anju Maan Ara Begum Department of Law, InternationalIslamic University Chittagong, for her motivation. Beingaware of limitations, I discussed this subject with all ofmy teachers. I am grateful to all my learned courseteachers for discussing the complicated issues with me andfor giving valuable suggestions and advice.
2
Acknowledgement
This research paper is made possible through the help and
support from everyone, including: parents, teachers, family,
friends, and in essence, all sentient beings. Especially,
please allow me to dedicate my acknowledgment of gratitude
toward the following significant advisors and contributors.
First and foremost, I would like to thank Adv .Taslima
Khannum and Adv. Anju maan Ara begum for their most support
and encouragement. They kindly have read my paper and
offered invaluable detailed advices on grammar,
organization, and the theme of the paper
.Second, I would like to thank all the respective teachers of
Law department, who longed to read my thesis and to provide
valuable advices, 3

Finally, I sincerely thank to my parents, family, and
friends, who provided the advice and financial support. The
product of this research paper would not be possible without
all of them.
Thank You
Akther Jahan
Abbreviations
ASK……………………. ..Ain o Salish Kendra
BMA………………………Bangladesh Medical Association
BMDC…………………… Bangladesh Medical and Dental Council
CEDAW………………….. Convention on Elimination of All forms of
Discrimination against Women
CPC ……………………..Code of Civil Procedure, 1908
CRC ……………………...Child Rights Convention
CrPC ………………………Code of Criminal Procedure, 1898
4
ICESCR ……………………International Covenant on Economic, Social
and Cultural
Rights
NHP ………………………..National Health Policy
NWDP ……………………...National Women Development Policy
UDHR………………………. Universal Declaration of Human Rights
UN…………………………… United Nations
WHO …………………………World Health Organization.
PIL…………………………….Public Interest Litigation.
List of Instruments and Laws The Constitution of Bangladesh, 1972
The Penal Code, 1860
The Vaccination Act, 1880
5
The Code of Criminal Procedure, 1898
The Code of Civil Procedure, 1908
The Drugs Act, 1940
The Eye Surgery (Restriction) Ordinance, 1960
The Pharmacy Ordinance, 1976
The Drug (Control) Ordinance, 1982
The Medical Practice and Private Clinics and Laboratories
(Regulation)
Ordinance, 1982
The Bangladesh Unani and Ayurvedic Practitioners Ordinance,
1983
The Transplant of Organ in Human Body Act, 1999
The Safe Blood Transfusion Act, 2002
The Consumer Rights Protection Ordinance, 2008
The Bangladesh Medical and Dental Council Act, 2010
The National Child Policy, 1994
The National Health Policy, 2011
The National Women Development Policy, 2011
The Code of Medical Ethics, adopted by the Bangladesh
Medical and
Dental Council
6
Table of Contents
Preface…………………………………………………………………………….1
Acknowledgement………………………………………………………………..2
Chapter 1:Introductory Chapter
1.1 Introduction…………………………………………………………………….....9
1.2 Aims and Objectives of Research………………………………………………...10
1.3 Nature and Scope…………………………………………………………………10
1.4 Research Methodology…………………………………………………………...10
1.5 Limitation of Research………………………………………………………….. 11
Chapter 2: Conceptual Analysis of Medical Negligence
2.1 Definition Of Negligence………………………………………………………… 6
2.2 Reasonable Man……………………………………………………………………8
7
2.3 Professional Negligence……………………………………………………………8
2.4 Essential of a suit for Negligence…………………………………………………..9
2.5 Negligence by Medical Professional……………………………………………...10
2.5.1 Definition of Medical Negligence………………………………………………..11
2.5.2 Essential of a suit for Medical Negligence………………………………………11
2.6 Defenses to an action of Negligence………………………………………………..12
2.6.1 Vis Major………………………………………………………………………….12
2.6.2 Inevitable Accident………………………………………………………………..13
2.6.3 Contributory Negligence…………………………………………………………..13
Chapter 3 Principles of Negligence and Burden of Proof
3.1 Contributory Negligence…………………………………………………………. 14
3.2 Contributory Negligence by
Children………………………………………………..16
3.3 Burden of Proof………………………………………………………………………16
3.4Doctrine of identification……………………………………………………………..17
3.5 Res Ipsa Loquitor…………………………………………………………………….18
3.6 Burden of proof of Negligence…………………………………………………….. .19
8
Chapter 4 Places of Medical Negligence and Consequence of
Medical Negligence
4.1 Medical Negligence by Public Hospitals…………………………………………20
4.2 Medical Negligence by Private Hospitals…………………………………………
21
4.3 Medical Negligence by Private Clinic…………………………………………….23
4.4 Consequences of Medical Negligence…………………………………………….25
Chapter 5 Liability And Victim
5.1 Persons liable for Medical Negligence………………………………..……………
26
5.1.1 Doctor…………………………………………………………………………….26
5.1.2 Nurse………………………………………………………..…………….………27
5.1.3 Staffs of the Hospitals………………………………………….…………..…….27
5.2 Victims of Medical Negligence
5.2.1 Women………………………………………………………………………......28
5.2.2 Children………………………………………………………………………..29
5.2.3 Students……………………………………………………………..…………30
9

5.2.4 Politicians and Others… ……………………………………………..……….30
Chapter 6 Rights and Duties of Doctor and Patient
6.1 Rights of the patients…………………………….…………………………...…31
6.2 Duties of the Patient…………………………….……………….…………..…..33
6.3 Rights of the Doctor…………………………..…………………………..……..39
6.4 Duties and liabilities of Doctor………………………………………………….39
6.5 Duties of Doctor in general………………………………………………………39
Chapter 7 Real condition of the Health Sector in Bangladesh
7.1 State of our Health sector………………………………………………………....41
7.1.1 Hospitals ,Doctors and Health
Care……………………………………………..41
7.1.2 Melamine in Milk……………………………………………………………..…43
7.1.3 Chart of Health Condition In
Bangladesh………...........................………… …..44
Chapter 8 Remedies under the Law of Bangladesh
8.1 constitutional remedies………………………………………………………….…..47
8.2 Human Rights Law………………………………………………………………….48
8.3 Departmental Remedies………………………………………………….………….49
8.4 Statutory Remedies…………………………….………………………………..…..51
8.4.1 Civil Remedies………………………………………………………….………....51
8.4.2 Criminal Remedies………………………………………………..……………….52
10
Chapter 9 Recommendation
9.1 Statutory Recommendations ………………………………………………………..57
9.2 Other Recommendations……………………………………………………………..58
9.3 Recommendation by Government…………………………………………………59
9.4 Recommendation BMDC………………………………………………………….60
Chapter 10 Concluding Chapter
10.1 Findings
10.2 Statutory Limitations
10.3 Procedural Limitation
10.4 Obstruction on Remedy
Appendix A
Appendix B
References
11
Abstract
The prime objects of this paper are to undertake stock of the laws that are
in practice in Bangladesh, to guide the healthcare service providers and
users, policy formulators and legislators. Towards these objects the
researcher h a s u n d e r t a k e n d e t a i l e d l i t e r a t u r e s u r v e y ,
d i s c u s s e d i n g r o u p s w i t h practicing doctors specializing in
Healthcare Administration, attended s e m i n a r s a n d f o r l a t e s t
d a t a s e a r c h e d t h r o u g h a p p r o p r i a t e i n t e r n e t addresses. The
researcher has addressed the Healthcare Rights under Bangladesh
Constitution, Laws for Medical Negligence & Legal Remedies, Health Policy, , and
a number o f re l evant i s s ues and fi n a l l y , made a nu mber o f
recommend at ions to comply with the original research objectives.
Historically, the standard of care in medical negligence provided considerable
scope for external evaluation of clinical judgment. Under the Bolam test,
however, determining the standard was seen by the courts as essentially a
matter for the medical profession, to be resolved by expert testimony with
minimal court scrutiny. In recent years, courts have become more willing to
probe such testimony and challenge the credibility of medical experts, although
they would very rarely override clinical judgment
12
Key words: Court, Hospitals , Negligence, Medical
Negligence, Doctors and other staffs, Rights and Duties,
Reasonable Man, Judgment, Laws
Chapter One
Introductory Chapter
1.1: Introduction
For a patient, the doctor is like God. And, the God is
infallible. But that is what the patient thinks. In reality,
doctors are human beings. And, to err is human. Doctors may
commit a mistake. Doctors may be negligent. The support
staff may be careless. Two acts of negligence may give rise
to a much bigger problem. It may be due to gross negligence.
Anything is possible. In such a scenario, it is critical to
determine who was negligent, and under what circumstances.
13
In a country committed to the rule of law, such matters are
taken to the court and judges are supposed to decide.
Negligence by doctors is difficult to be determined by
judges as they are not trained in medical science. Their
decisions are based on experts’ opinion. Judges apply the
basic principles of law in conjunction with the law of the
land to make a decision. Reasonableness and prudence are the
guiding factors.
However, Medical negligence mainly concerns negligent or
rash act of medical professionals causing any injury to the
patient. Medical negligence is a kind of professional
misconduct on the part of a medical practitioner. In a
strict sense the term, medical negligence, may not include
professional misconduct or malpractice of other kinds such
as fraudulent misrepresentation regarding eligibility or
qualification, prescribing unnecessary drugs or tests for
undue profit, taking undue advantage of the patient’s
situation etc. But, while addressing medical negligence from
a human rights perspective, the whole range of medical
malpractice and misconduct including the professional
negligence of medical professionals, has to be taken into
consideration. Because, all these vices have one thing
common in consequence; they cause serious violation of right
to health and access to medical care. More importantly,
these issues have a nexus at their origin and coexistence.
Therefore, while dealing with medical negligence and right
14
to health care, it is also essential to consider these
aspects of medical services in order to make a comprehensive
assessment.
We would like to go through these principles in the light of
some court judgments and try to understand as to what is
expected from a doctor as a reasonable person. As these
issues are at the core of medical profession and hospitals
are directly affected by new interpretation of an existing
law regarding medical professionals, it is pertinent to deal
with them at the individual level of the doctor, and also at
the employer’s level i.e., hospital.
1.2: Aims and Objectives of the Research
The present study aims at ascertaining the legal status of
medical negligence and fraudulent practice of private
clinics on review of existing laws and policies of
Bangladesh. It should be noted that the first part of the
title of the study ‘Medical Negligence’ refers to the
overall situation of medical negligence and malpractices
existing in both public and private sector, while the latter
part ‘Fraudulent Practice in Private Clinics’ refers to the
fraudulent practice of private clinics to signify a special
emphasis on that particular phenomenon. This study also aims
to identify the gaps and inconsistencies in the existing
15

laws and policies to ensure accountability of health care
service providers and to protect the right to health care of
the citizens. The study finally attempts to make certain
recommendations as to law and policy reform concerning
medical negligence and malpractice. The ambit of the study
is limited to the assessment of the relevant laws and
policies of Bangladesh. It also relies on a number of
previous works and publications, including some of ASK’s own
studies and publications.
After completing the Research Paper in fruitful manner we
shall be able to find out the doctors negligence on medical
treatment and also be able to take a legal action against
the doctor’s medical malpractice. We shall also be able to
find out the doctors rights and duties towards the patients
and the rights and duties of the patients to their surgeons
and when a doctor fails to provide proper care to his
patient then what will be its consequences and what remedies
are available for a victim of medical negligence. In a
nutshell we shall able to know details about medical
negligence of which the Patients are the victims of Death.
1.3: Nature and Scope of the Research
Every Research paper has nature and scope. So my Research
paper is not beyond the nature and scope. As selected topic
for Research is “Medical Negligence: Law and practice in
16

Bangladesh”, so it is related with analytical, historical,
scientific, historical and systematical methods. The
assigned topic is an important and a demandable topic for
law students. Especially for those who wants to spend theirs
life in human rights sector.
1.4: Research Methodology
This assigned topic is very important one in our legal
sector. This thesis has been done and published with more
reference from books, journals, and internet and from some
articles. This thesis paper is tort and human rights related
subject matter. When I started this research paper, I always
looked for strong references and correct information. I have
tried to enrich this Research paper by providing all
necessary information. The scheme has also been improved and
has been made much more methodical, analytical, historical,
scientific
This study is mainly based on analysis of the existing laws
and policies relating to medical services and medical
malpractice. It relies on a number of previous reports,
publications, laws and policies. The study also attempts a
17
comparative analysis of other countries’ experiences in
legislations and litigations involving medical negligence,
such as India, Nepal, Malaysia and South Africa.
This study makes a comprehensive assessment of the legal
regime of Bangladesh concerning medical negligence. Starting
from constitutional safeguards in favor of right to health
care, it analyzes the different aspects of policy
statements of the Government that have been reflected in the
National Health Policy of 2011 and other two policies on
development of women and children. The study examines a
series of statutes which are relevant to medical services.
The statutes reviewed in this study include:
. The statutes reviewed in this study include:
• The Vaccination Act, 1880 • The Drugs Act, 1940 • The Eye Surgery (Restriction) Ordinance, 1960 • The Pharmacy Ordinance, 1976 • The Drug (Control) Ordinance, 1982 • The Medical Practice and Private Clinics and Laboratories (Regulation) Ordinance, 1982 • The Bangladesh Unani and Ayurvedic Practitioners Ordinance, 1983 • The Transplant of Organ in Human Body Act, 1999 • The Safe Blood Transfusion Act, 2002 • The Consumer Rights Protection Ordinance, 2008 • The Bangladesh Medical and Dental Council Act, 2010
18
On identifying the gaps in the legal regime, this report
cites some statutory/legal arrangement of some other
countries in providing remedy against medical negligence.
1.5: Limitation of the Research
Every research study has some limitations. So this researchmonograph is not the exception of this limitation andreduced the scope of the study. The main limitation toprepare this thesis is time limitation. To make a fulfillthesis the time period is not sufficient. Another problem isthat every body talks, write articles on “MedicalNegligence” but there is no book from where we can informedabout “Medical Negligence. By going to make a research on“Medical Negligence: Law and Practices in Bangladesh” I haveto face some medical term which are totally unknown to me.Beside these, there are also some negligible problems tomake this thesis fruitfully.
19
Chapter Two
Conceptual Analysis of Medical Negligence
2.1: Definition of Negligence
It is very difficult to define negligence, however,
the concept has been accepted in jurisprudence. The
authoritative text on the subject in India is the ‘Law of
Torts’ by Ratanlal and Dhirajlal.Negligence has been
discussed as:
Negligence is the breach of a duty caused by the
omission to do something which a reasonable man, guided
by those considerations which ordinarily regulate the
conduct of human affairs would do, or doing something which
a prudent and reasonable man would not do. Actionable
negligence consists in the neglect of the use of ordinary
care or skill towards a person to whom the defendant owes
the duty of observing ordinary care and skill, by which
neglect the plaintiff has suffered injury to his
person or property.
20
The definition involves three constituents of negligence:
(1) A legal duty to exercise due care on the part of the
party complained of towards
the party complaining the former's conduct within the scope
of the duty;
(2) breach of the said duty; and
(3) consequential damage.
Cause of action for negligence arises only when damage
occurs; for, damage is a necessary ingredient of this tort.
Thus, the essential components of negligence are three:
'duty', 'breach' and 'resulting damage'
1. Austin defines negligence thus – “In case of negligence, a
party performs not an act to which he is obliged; he breaks
a positive duty.[1]”
2. Actionable negligence consists in the neglect of the use of
the ordinary care or skill towards a person to whom the
defendant owes the duty of observing ordinary care and
skill, by which neglect the plaintiff has suffered injury to
his person or property.[2]
21
3. Salmond considered ‘negligence’ as state of mind which was an
element for liability for torts, in general, as an
alternative to ‘intention’. It is, however, established that
negligence is a specific tort if the following conditions
are present, which must be established by the plaintiff-
(i) That the defendant was under a duty to take care towards
the plaintiff to avoid the damage complained of;
(ii) That there was a breach of that duty on the part of the
defendant; and
(iii) That the plaintiff has suffered actual damage and that
the breach was the direct and proximate cause of the damage
complained of.[3]
Thus, if a man walks across a crowd of people, carrying
sharp edged tools in his hand, he is under a duty to ensure
that he does no injury to those around him. Will have to be
more careful than a man who merely carries an umbrella (even
though this is nearly as bad in crowded cities today). –
And, of man with the umbrella would have to be more careful
than a man who carries nothing at all.
2.2 The ‘Reasonable Man’
It has been held by the courts that the test of
reasonableness is that of the ‘ordinary man’ or also called
22
as the ‘reasonable man’. In Bolam case, it was discussed
that:
In an ordinary case it is generally said you judge
it by the action of the man in the street. He is the
ordinary man. In one case it has been said you judge it by
the conduct of the man on the top of a Clapham omnibus. He
is the ordinary man.
2.3: Essentials of a Suit for Negligence
The burden of proving negligence is on the part of the
plaintiff who alleges it. In order to succeed in an action
for negligence, the plaintiff must prove the following five
things:
1. That the defendant was under a legal duty to exercise due
care and skill, – as there cannot be any liability for
negligence unless there is a breach of some legal duty.
2. That the duty was towards the plaintiff.
3. That, in the circumstances of the case, the defendant
failed to perform that duty, i.e. the duty to exercise due
care and skill.
4. That the breach of such duty was the causa causans, i.e.
the direct and proximate cause, of the damage complained of.
If the causal connection between the negligent act and the
23
damage is not direct, the damage is too remote, for which
there is no remedy
5. That the damage was caused on account of this breach of
duty. The Bombay High Court has laid down that in an action
for negligence against a doctor, the plaintiff has to prove
three things, viz.-
(i) That the doctor was under a duty to take reasonable care
towards the plaintiff, to avoid the damage complained of, or
not to cause damage to the patient by failure to use
reasonable care;
(ii) That there was a breach of such duty on the part of the
doctor; and
(iii) That such breach of duty was the real cause of the
damage complained of, and such damage was reasonably
foreseeable.[4]
2.4 Professional
According to the English language, a professional is a
person doing or practicing something as a full-time
24
occupation or for payment or to a make a living;
and that person knows the special conventions, forms
of politeness, etc. associated with a certain
profession. Professional is contrasted with amateur – a
person who does something for pleasure and not for payment
Negligence by professionals
The Supreme Court of India discussed the conduct of
professionals and what may amount to negligence by
professionals in Jacob Mathew’s case:
In the law of negligence, professionals such as lawyers,
doctors, architects and others are included in the category
of persons professing some special skill or skilled persons
generally. Any task which is required to be
performed with a special skill would generally be
admitted or undertaken to be performed only if the person
possesses the requisite skill for performing that task. Any
reasonable man entering into a profession which requires a
particular level of learning to be called a professional of
that branch, impliedly assures the person dealing with
him that the skill which he professes to possess
shall be exercised and exercised with reasonable
degree of care and caution….
He does not assure his client of the result…A physician
would not assure the patient of full recovery in every case.
25
A surgeon cannot and does not guarantee that the result of
surgery would invariably be beneficial, much less to
the extent of 100% for the person operated on…
…Judged by this standard, a professional may be held liable
for negligence on one of two findings: either he was not
possessed of the requisite skill which he professed to have
possessed, or, he did not exercise, with reasonable
competence in the given case, the skill which he did
possess. The standard to be applied for judging,
whether the person charged has been negligent or not,
would be that of an ordinary competent person
exercising ordinary skill in that profession. It is
not necessary for every professional to possess the highest
level of expertise in that branch which he practices.
…A highly skilled professional may be possessed of better
qualities, but that cannot be made the basis or the
yardstick for judging the performance of the
professional proceeded against on indictment of negligence.
2.5: Negligence by Medical Professionals
In Jacob Mathew case, the Supreme Court of India
has gone into details of what is the meaning of
negligence by medical professionals.
26
Negligence in the context of medical profession necessarily
calls for a treatment with a difference. To infer rashness
or negligence on the part of a professional, in particular a
doctor, additional considerations apply.
A case of occupational negligence is different from one of
professional negligence. A simple lack of care, an error of
judgment or an accident, is not proof of negligence on the
part of a medical professional. So long as a doctor follows
a practice acceptable to the medical profession of that
day, he cannot be held liable for negligence merely
because a better alternative course or method of
treatment was also available or simply because a more
skilled doctor would not have chosen to follow or resort to
that practice or procedure which the accused followed.
When it comes to the failure of taking precautions
what has to be seen is whether those precautions
were taken which the ordinary experience of men has
found to be sufficient; a failure to use special or
extraordinary precautions which might have prevented
the particular happening cannot be the standard for
judging the alleged negligence.
So also, the standard of care, while assessing the practice
as adopted, is judged in the light of knowledge available
at the time of the incident, and not at the date
of trial. Similarly, when the charge of negligence27

arises out of failure to use some particular
equipment, the charge would fail if the equipment was not
generally available at that particular time (that is, the
time of the incident) at which it is suggested it should
have been used.
2.5.1: Definition of Medical Negligence
Medical negligence is a species of professional negligence
and, as such, forms part of the law of tort. Medical
negligence, or clinical negligence as it is more commonly
known today, is concerned with claims for damages for
injuries suffered by patients (and others) at the hands of
doctors and other health care professionals. Unlike in other
professional contexts, the law of contract plays little or
no part in medical law. Other than in situations where the
seeks treatment privately, patients do not enter into
contracts with their doctors.[5] or,
Medical malpractice is professional negligence by act or
omission by a health care provider in which care provided
deviates from accepted standards of practice in the medical
community and causes injury or death to the patient.[6] Or,
Failure of a physician or other medical personnel to meet
the standards of conduct for duties relating to the medical
profession. Those standards are based on what a reasonable
28

person with the requisite knowledge and skills would or
would not do.[7]
2.5.2: Essentials of a Suit for Medical Negligence
A person who alleges negligent medical malpractice must
prove four elements:
(1) A duty of care was owed by the physician;
(2) The physician violated the applicable standard of care;
(3) The person suffered a compensable injury; and
(4) The injury was caused in fact and proximately caused by
the substandard conduct.
The burden of proving these elements is on the plaintiff in
a malpractice lawsuit.
2.6: Defences to an action for negligence
The following three defences can be raised in an action for
negligence, viz
(A) Vis major,
(B) Inevitable accident, and
(C) Contributory negligence of the plaintiff.
2.6.1: Vis Major
29

Vis Major (or act of God) is such a direct, violent, sudden,
and irresistible act of nature as could not, by any amount
of human foresight, have been foreseen, or, if foreseen,
could not, by any amount of human care and skill, have been
resisted. Thus, acts which are occasioned by the elementary
forces of nature, unconnected with the agency of man or
other cause, will come under the category of acts of God.
E.g. storm, tempest, lightning, extraordinary fall of rain,
extraordinary high tide, extraordinary severe frost. Etc.[8]
The defendant had a series of artificial lakes on his land,
in the construction or maintenance of which there had been
no negligence. Owing to a most unusual fail of rain, so
great that it could not have been reasonably anticipated
some of the reservoirs burst and carried away four country
barges. It was held that the defendant was not liable
inasmuch as the water escaped by an act of God.[9]
2.6.2: Inevitable accident
The second defense in an action for negligence is that of
inevitable accident. Thus, A is lying drunk on a roadway. B
approaches in a motor car round a bend in the road, but just
before he reaches the point at which, under ordinary
circumstances, he would first see a, sheet of newspaper is
blown by the wind against his windscreen and materially
obscures his view. He runs over A, and injures him. Here, A
30

cannot succeed, it being a case of inevitable accident or
misfortune.[10]
X was on a golf course as a spectator, and Y, who was not
striking the ball in a game of golf, but was merely
demonstrating a stroke to S’s brother, negligently struck X
in the face with the golf club. In a suit by X against Y for
damages, Y contended that by going to the golf course, X
took the risk of such an accident. It was held that X was
entitled to damages. This is not a case of sport or a game,
but a regular business.[11]
2.6.3: Contributory negligence of the plaintiff
The third defence to an action for negligence is that of the
contributory negligence of the plaintiff himself.
Contributory negligence has been defined as “negligence in
not avoiding the consequence arising from the negligence of
some other person, when means and opportunity are afforded
to do so”. The term negligence in this context does not,
ordinarily, mean any breach of duty to another, but only
failure to take reasonable care of one’s own self. Every man
has a duty to look after himself, and he will have no remedy
for injuries which he might have a voided by the use of
reasonable care. As stated in an old case, “One person being
in fault will not dispense with another’s using ordinary
care of himself”[12]
31

Chapter Three
Principles of Negligence and Burden of Proof
3.1: Contributory Negligence
Contributory negligence has been defined as “negligence in
not avoiding the consequence arising from the negligence of
some other person, when means and opportunity are afforded
to do so”. The term negligence in this context does not,
ordinarily, mean any breach of duty to another, but only
failure to take reasonable care of one’s own self. Every man
32
has a duty to look after himself, and he will have no remedy
for injuries which he might have a voided by the use of
reasonable care. As stated in an old case, “One person being
in fault will not dispense with another’s using ordinary
care of himself”[13]
More recently, Lord Denning has distinguished ‘negligence’
and ‘contributory negligence’ as follows:
“Negligence depends on a breach of duty, whereas
contributory negligence does not, Negligence is a man’s
carelessness in breach of duty to others. Contributory
negligence is a man’s carelessness in looking after his own
—safety”.[14]
1. The principle underlying the doctrine has been stated to
application of the maxim “In pari delicto potior est condition
defendantis”, which means that when both parties are equally
to blame, neither can hold the other liable.
But the more accepted view is that it is an application of
the rule as to remoteness of damage.
2. At common law, contributory negligence of the plaintiff
is a complete defence to an action for damages for
negligence of the defendant, the burden of establishing it
being on the defendant.
33
3. Contributory negligence is, however, no defence where the
plaintiff was not bound to take such care as the defendant
contends but has a right to assume that the defendant had
done all things rightly and carefully.
4. Again, contributory negligence of the plaintiff is no
defence if the defendant had a later opportunity than the
plaintiff of avoiding the accident by reasonable care.
5. The soundness of the last opportunity test founded on
Davles. Mann has, however, been questioned by the House of
Lords in Admiralty Commissioner v. North of Scotland .Their
Lordships quoted with approval the statement of the Law
Revision Committee, 1939.
“In truth, there is no such rule – the question, as in all
questions of liability for a tortuous act, is, not, who had
the last opportunity of avoiding the mischief, but whose act
caused the wrong”.[15]
6. Another controversial topic relating to contributory
negligence is whether the existence of a duty is necessary
to raise the plea. The position has been authoritatively
summarized by the Privy Council thus.[16]
(i) When negligence is alleged, as the basis of an
actionable wrong, a necessary ingredient in the conception
is the existence of a duty owed by the defendant to the
34
plaintiff to take due care. But when contributory negligence
is set up as a defence, its existence does not, generally
depend on any duty owed by the injured party to the party
sued and all that is necessary to be shown in order to
establish such defence is that the inured party did not in
his own interest take reasonable care of himself and
contributed, by his want of care, to his own injury. The
principle underlying the defence of contributory negligence
is that where a man is part author of his own injury, he
cannot call on the other party to compensate him in full.
(ii) In cases relating to ‘running down accidents’, however,
the question of duty to take care in relation to the other
party does, in fact, come in. The general principle in such
cases is: “When two parties are so moving in relation to one
another as to involve risk of collision, each owes a duty to
the other to move with due care, and this is true whether
they are both in control of vehicles, or both proceeding on
foot, or whether one is on foot and the other controlling a
moving vehicle.
7. In England, the doctrine of contributory negligence has
undergone a great shock by the passing of the Law Reform
(Contributory Negligence) Act, 1945, which has introduced
the principle of apportionment of liability in all cases of
contributory negligence, which was before this Act confined
to Admiralty proceedings only- After the passing of this
35
Act, the common law rule which applied before, viz, that
parties guilty of negligence had no claim has disappeared,
and the Court has to assess the liability of both parties,
and apportion the damages accordingly.[17]
3.2: Contributory Negligence of Children
The defence of contributory negligence is more difficult to
make out against a child than against an adult. When the
plaintiff is a child, he will not be disentitled to relief
merely because he has failed to show as much care as a
person of, mature age. Allowance must be made for his
inexperience and infirmity of judgment [18]. This rule is
sometimes expressed in the form ‘contributory negligence of
is no defence. This rule however is not to be literally
accepted, but only as meaning that what amounts to
contributory negligence in a grown-up person may not be so
in a child of tender years.[19] Hence the age and mental
development of the child becomes relevant.
3.3: Burden of proof of Contributory Negligence
The onus of proving affirmatively that there was
contributory negligence on the part of the person inured
rests, in the first instance, upon the defendant, and in
absence of evidence tending to that conclusion, the
plaintiff is not bound to prove its non existence. If the
Court finds itself unable to discover to what extent the
36
negligence of the plaintiff or that of the defendant
contributed to bring about the accident, the defendant is
entitled to succeed, for in pari delicto potiorest conditio defendants.
[20]
A few decided cases on the doctrine of contributory
negligence are given below. A police constable seeing the
door of the defendant’s warehouse open after dark, and in
order to see that everything was right, and in the execution
of his duty, entered the warehouse and injured himself by
falling into an unfenced sawpit inside.[21]
It was held that he had no legal right to enter, being
neither a licensee nor an invitee, but that even assuming he
had, the defendant was under no duty to make the place safe
for him or to warn him of the danger.[22]
3.4: Doctrine of Identification
The doctrine of identification can be explained thus: Where
a child is in the actual custody of an adult at the time of
the accident, the contributory negligence of the adult will
disentitle the child from recovering damages, because the
child is so identified with the adult that his negligence
would amount to the negligence of the child. So, a special
application of the doctrine of identification is to be met
with where an infant, who is incapable of taking care of him
and is in charge of an adult, suffers injury owing to the
37
negligence of the third person, as well as the contributory
negligence of the custodian.[23]
At one time, it was though that the contributory negligence
of an adult having actual custody of a child at the time of
the accident would be a bar to an action by the child
against the other party whose, negligence helped to bring
about the accident. A child of five under the control of its
grand mother was inured by a train owing to the contributory
negligence of the grandmother. It was held that the child
had to be identified with its grandmother, and so had no
right of action against the company.[24]
But the doctrine of identification laid down in this case
has been overruled since the decision in Mills v. Armstrong.
An infant, of four years old, was crossing a road under the
care of his grand father. He was struck by a motor omnibus
and received permanent injuries to his left hand. The infant
sued the Omnibus Company for damages sustained by him
through the negligent driving of the omnibus belonging to
the company for damages sustained by him through the
negligent driving of the omnibus belonging to the company.
The jury found that the accident occurred through the
negligence of the driver of the omnibus and the contributory
negligence of the grand father. It was held that,
nevertheless, the infant could recover damages.[25]
38
3.5: Res Ipsa Loquitur
The rule that in action of negligence, the plaintiff must
affirmatively prove negligence may cause hardship in cases
where the plaintiff can prove the accident, but cannot show
how it happened, the fact being solely outside his knowledge
and within the knowledge of the defendant who causes it. In
such cases, it is sufficient for the plaintiff to prove the
accident and nothing more – for there is a presumption of
negligence according to the maxim. “Res ipsa loquitur (the thing
speaks for itself). Such a presumption, arises when the
cause of the mischief was apparently under the control of
the defendant or his servants. The accident itself
constitutes reasonable avoidance of negligence in the
particular circumstances.
The application of the maxim “Res ipsa loquitur” has been
explained thus: “Where the thing is shown to be under the
management of the defendant or his servants, and the
accident in such as, in the ordinary course of things, does
not happen, if those who have the management use proper
care, it affords reasonable evidence. In the absence of
explanation by the dependant that the accident arose from
want of care.[26]
Thus, the following are the three essential requirements of
the application of the maxim:
39
(i) The accident must be such as would not, in the ordinary
course of things, have happened without negligence.
(ii) The accident must be such as would not, in the ordinary
course of things, have happened without negligence.
(iii) There must be no evidence of the actual cause of the
accident.[27]
3.6: Burden of proof of Negligence
As a rule, the onus of proving negligence is on the
plaintiff. He must not merely establish the facts of the
defendant’s negligence and of his own damage, but must show
that the one was the effect of the other
First, where there is no contract, the plaintiff must prove
facts inconsistent with due diligence on the defendant’s
part. Where the balance is even as to which party is in
fault, the one who relies on the negligence of the other is
bound to turn the scale.
Secondly, where there is a contract or personal undertaking,
the plaintiff must prove such contract or undertaking, and
also injury to himself. The mere fact of an injury
happening, if unexplained, is evidence of negligence. It is
for the defendant to prove that he himself was exercising
due care.
40
-Thirdly, under certain circumstances, the mere happening of
an accident will afford prima facie evidence that it was the
result of not taking due care; res ipsa loquitur (the thing
speaks for itself). This is so when –
(i) The injurious agency was under the management or control
of the defendant; and
(ii) The accident is such as, in the ordinary course of
things, does not happen if those who have the management use
proper care.
Thus, in cases involving res ipsa loquitur, there is a
presumption of negligence, and it is for the defendant to
rebut it.[28]The Rajasthan High court has held that, in a
case against a doctor for damages, if the plaintiff shows
that the doctor was in fact negligent, but fails to prove
that any loss or injury was caused to him by such
negligence, he cannot be awarded any damages, and his claim
will be dismissed. [29]
Chapter Four
Places of Medical Negligence and Consequence of Medical
Negligence
Medical malpractice is professional negligence by act or
omission by a health care provider in which care provided
deviates from accepted standards of practice in the medical
41
community and causes injury or death to the patient.
Standards and regulations for medical malpractice vary by
country and jurisdiction within countries. Medical
negligence may take place in public hospitals, or in a
private hospital or in a private clinic etc. a nut shell
medical negligence may took place in any place of a country
where there is an arrangement for medical treatment.
4.1: Medical Negligence in public Hospital
A public hospital or government hospital is a hospital which
is owned by a government and receives government funding.
This type of hospital provides medical care free of charge,
the cost of which is covered by the funding the hospital
receives. Most hospitals worldwide are public.
As most of the people of this country are poor and their
economic condition is not good. So for taking treatment they
depend on public hospital. But the condition of the public
hospitals is not good. The doctors, nurse and the stuffs of
the public hospital, all are involved in corruption. They do
not do their duty properly. That means the doctors of the
public hospitals are not found in their duties. The nurses
are also not attentive in their duties. The stuffs are not
also do their duty properly .The want money or Brive from
the patients. Particularly the surgeons always neglect the
patients. Some surgeon tells their patient to go his private
chamber.42
The doctors of the public hospital do not think the patients
as human. They always neglect the patient. For example, Omar
Faruk, 24, son of Abdul Zabbar of Bazuriya village under
Bochaganj upazila of Dinajpur, died due to alleged
negligence of doctors at Dinajpur Medical College and
Hospital. Faruk was admitted to the hospital on Thursday
evening as he took poison. Faruk relatives alleged he died
at about 4:30pm yesterday due to the negligence of the
doctors.[30]
This is not a single example of the doctor’s medical
negligence in public Hospital. There are thousands of
examples which shows the prove of medical negligence of the
doctors in public hospital.
4.2: Medical Negligence in Private Hospital
A private hospital is a hospital owned by a for-profit
company or a non-profit organization and privately funded
through payment for medical services by patients themselves,
by insurers, or by foreign embassies. The citizens of this
country who have not confidence in public hospitals of this
country and want a better service from a surgeon, they only
go to a private hospital. But the conditions of the private
hospitals are not good. The doctors, nurse and the stuffs of
the public hospital, all are involved in corruption. They do
not do their duty properly. That means the doctors of the
private hospitals are not taking care of their patients43

properly. The nurses are also not attentive in their duties.
The stuffs are not also do their duty properly .The want
money or Bribe from the patients i.e. Baksheesh. That’s why
the V.I.P and the people who has a lot of money for a better
treatment they go to abroad.
In private hospitals, though the patients expend their
pocket money but are not getting proper service from their
surgeons. In this stage, a true fact will say about the
medical negligence in Bangladesh.
On October 29, 2007, when Bangladeshi software engineer
Masum P. Mohammad, flew back to Bangladesh to see his ill
father struggling for life at the Central Care Unit (CCU) of
Lab Aid Cardiac Hospital, he was in shock.[31]
Masum alleges that when he saw his father lying on a bed,
full of blood. Then he asked the nurse to show him where he
was operated, and he was speechless to see the unhygienic
condition where his father was put in. He stood there for
the longest moment, not knowing what to say.
Masum’s father Late A.K.M Fazlum Haq was admitted at Lab Aid
on October 25 under the treatment of Dr Prof. Baren
Chakraborty, after he was struck by a sudden chest pain.
After Haq had a massive heart attack on October 26, he was
given injection and later a ring was put around his heart on
44

October 27. Later that week, Haq’s chest x-ray revealed dark
areas over the lung, after which Prof. Ali Hossain was
involved for the lung treatment. ‘On November 2 that day,
Hossain told to Masum that, food was stuck in the patient’s
lung and he wants a Bronchoscope immediately.’[32]
After the Bronchoscope Prof. Hossain provided cough samples
for the Tuberculosis (TB) test in two different diagnostic
centers-one in Lab Aid, and another in Monowara Diagnostic,
at Panthopath, Dhaka. Three days later the result was
completely different in the two hospitals. Masum alleges
that the Lab Aid results showed that his father has not have
TB, and the Monowara Diagnostic test result showed that the
report was actually positive!.[33]
Masum explains that later they also learnt that his father
had suffered from massive brain injury right after being
admitted to the hospital, which was not detected by any of
the doctors. ‘When he had a heart attack earlier, blood was
stuck in his brain. So, he was not being treated for his
brain injury during all these days.[34]
Masum says that his father’s TB test was sent on November 3,
2007. He asked that why did it take so long to send the TB
test for diagnostic, and why did it take so long to detect
this TB? Masum also alleged that even the TB diagnosis
result was wrong.
45
Masum also told when his father was given a medication; his
father could not recognize them anymore. At that time they
requested Prof. Chakraborty to call a neurologist to check
his father’s brain, but again he did not bother to listen to
him. Two days later, on November 11, his father was
announced dead.[35]
‘Masum’s story is nothing exceptional,’[36] says Dr
Quamruzzaman who heads the Dhaka Community Hospital in
Malibagh and has himself been a victim of medical negligence
through which he lost a perfectly-functioning kidney. ‘We
have countless other cases of medical negligence and
ignorance. But, it is important to realize that one of the
biggest flaws of our health care system is that we have no
accountability what so ever.’
Indeed, Masum’s case is not an isolated one. According to an
investigation of a Dhaka-based NGO, Ain-o-Shalish Kendra,
between January to October 2007 alone, there were over 76
death cases reported to be caused by medical negligence.[37]
4.3: Medical Negligence in Private Clinic, etc.
In Bangladesh, clinical negligence is a regular phenomenon.
Every year hundreds of people die due to clinical negligence
in Bangladesh. Most of them are child and woman. As, it
takes much expense to treat in private clinic and as the
public hospitals are not providing well services in our
46
country. So for getting a better service the people of this
country, by finding no other alternatives are bound to go to
a nearest private clinic. But in spite of great expense the
people of this country are becoming the victims of medical
negligence. The surgeons, the nurses and the stuffs of the
hospitals are mainly liable for clinical negligence.
In this stage, referring a true fact about medical
negligence in private clinic of Bangladesh. This fact fact
will say about the clinical medical negligence in
Bangladesh.
A Pregnant housewife Nayan Begum from Chanpur village of
Bhairab upazila was rushed to the Sadek Medical Hall in
Bhairab town with severe pain in her stomach. On her arrival
at the hospital, they were relieved to find that the owner
of the clinic ‘Doctor Sadek’ was one of the attending
doctors. Insisted that she deliver the baby immediately.
‘Without any proper investigation of what the cause of the
pain might be,’ he told the victim that he will have to
deliver the baby, dismissing our suggestions that perhaps he
should do an ultrasound,’ says Nayan’s daughter Mili Begum,
a third honors student at Dhaka’s Eden College.[38]
She was instantly taken to a dirty, dark room in the medical
facility used for delivery purposes. The doctor insisted
that none of her female relatives who accompanied her to the
hospital be in the operating theatre with her. She was47
already very nervous. Mili says that when she was wheeled
inside, she was asked to close her eyes and not given any
anesthetics or pain killers to ease her delivery process.
Mili also told that initially, doctor Sadek had tried to use
his spiritual powers to deliver the baby. But when his
spiritual powers were of no use and ma’s situation was
getting worse, he made a forced delivery attempt on her. In
trying to forcefully deliver the baby, he caused severe head
injuries to the fetus using a sharp blade. My mother was
screaming in pain as she was subject to blade swipes on her
internal organs by an unskilled hand. My mother also started
to bleed profusely.[39]
When Nayan’s family discovered her in such dire condition,
they immediately rushed her to a hospital in Dhaka. On April
19, the baby died at a hospital in Dhaka. Luckily, Nayan had
escaped with her life. Mili said that her mother was in a
crazed state when she had recovered always asking about the
baby. The baby was a boy and my mother kept on asking every
one where her son was.[40]
In this stage, referring another true fact about medical
negligence in private clinic of Bangladesh. This fact fact
will say about the clinical medical negligence in
Bangladesh.
Khokan is an inhabitant of Dinajpur, who admit his wife at
Janata Clinic, Dinajpur on 14th October. His wife was a48
patient of fiver. He was informed from clinic that his wife
is attacked by typhoid. She was under treatment at that
hospital for 5 days. On 18th October she felled oxygen
problem. But at that clinic, oxygen was not available. The
duty nurses of the clinic make a communication with Dr.
Saidur Rahman. Then Mr. Rahman instructs them to send her at
the Dinajpur Medical College for removing her oxygen
problem. At about 8.00 pm in the way of hospital.[41]
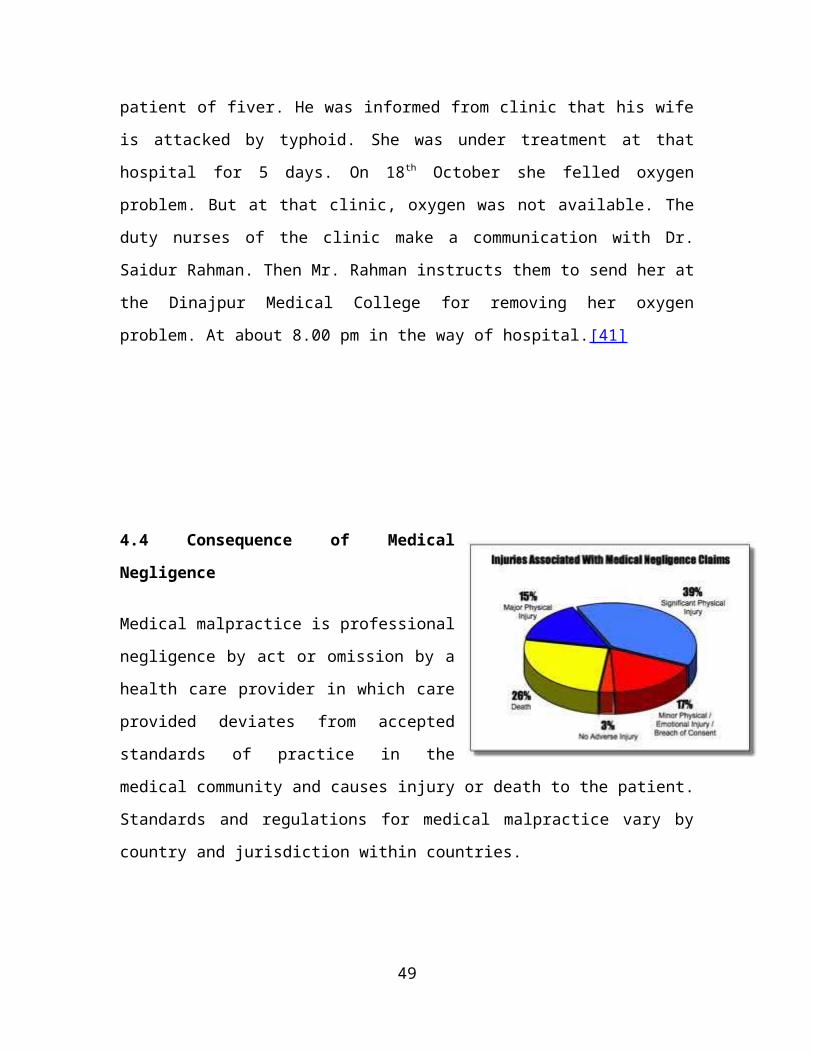
4.4 Consequence of Medical
Negligence
Medical malpractice is professional
negligence by act or omission by a
health care provider in which care
provided deviates from accepted
standards of practice in the
medical community and causes injury or death to the patient.
Standards and regulations for medical malpractice vary by
country and jurisdiction within countries.
49
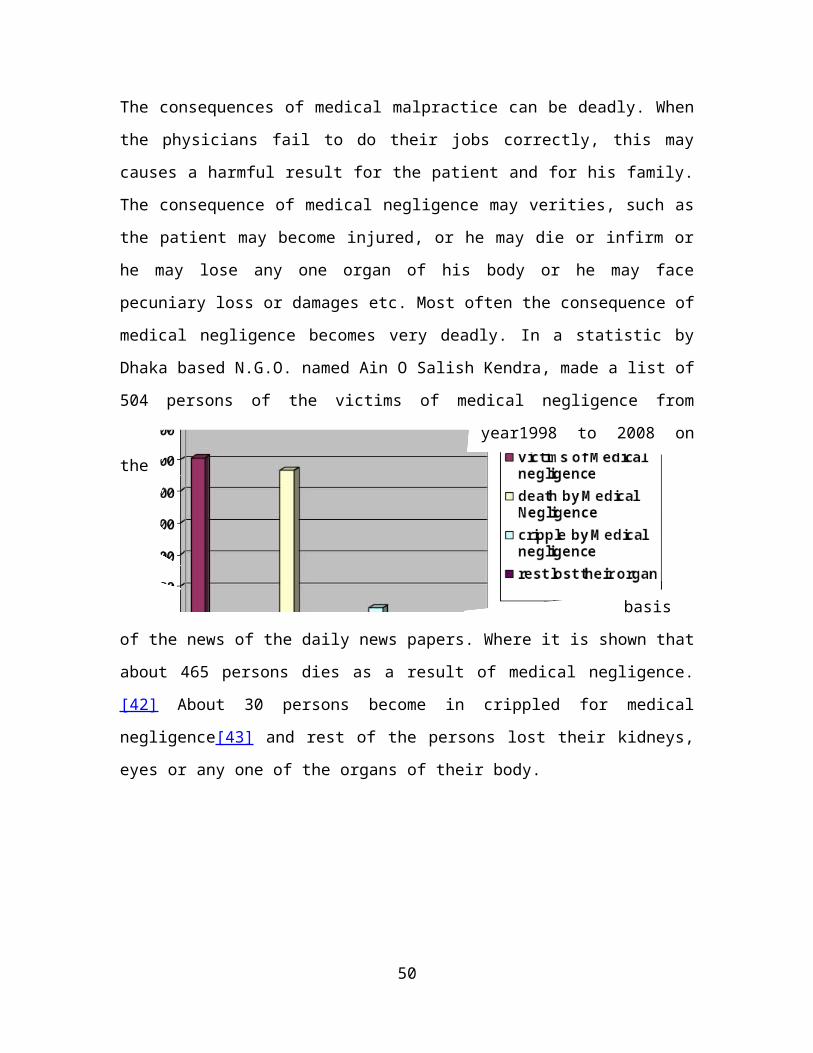
The consequences of medical malpractice can be deadly. When
the physicians fail to do their jobs correctly, this may
causes a harmful result for the patient and for his family.
The consequence of medical negligence may verities, such as
the patient may become injured, or he may die or infirm or
he may lose any one organ of his body or he may face
pecuniary loss or damages etc. Most often the consequence of
medical negligence becomes very deadly. In a statistic by
Dhaka based N.G.O. named Ain O Salish Kendra, made a list of
504 persons of the victims of medical negligence from
year1998 to 2008 on
the
basis
of the news of the daily news papers. Where it is shown that
about 465 persons dies as a result of medical negligence.
[42] About 30 persons become in crippled for medical
negligence[43] and rest of the persons lost their kidneys,
eyes or any one of the organs of their body.
50

Chapter Five
Who are liable for Medical Negligence and who are victims of
it?
5.1: The persons who are liable for Medical Negligence
Medical malpractice is professional negligence by act or
omission by a health care provider in which care provided
deviates from accepted standards of practice in the medical
community and causes injury or death to the patient.
Standards and regulations for medical malpractice vary by
country and jurisdiction within countries. All the persons
who are involved in treatment matters are liable for medical
negligence. Particularly the doctors, nurses, stuffs of the
hospitals, hospital management or authority etc. are liable
for medical negligence. In short, those persons who do not
care a patient in times of his disease are liable for
medical negligence. In this chapter I’ve tried to make a
list of the persons who are liable for medical negligence
and are the victims of medical negligence.
5.1.1: Doctor
51
Mainly the doctors or surgeons are liable for medical
negligence. They do not do their duty properly. Every year
hundreds of people become the victim of medical negligence
by the surgeons. In a statistic by Dhaka based N.G.O. named
Ain O Salish Kendra, made a list of 504 persons of the
victims of medical negligence from year1998 to 2008 on the
basis of the news of the daily news papers. Where it is
shown that about 492 persons dies as a result of medical
negligence of the surgeons.[44] Doctor’s medical negligence
may take place in any public or private hospitals of
Bangladesh even in the house of the patient or in the
chamber of a doctor. Most often, medical negligence take
place in public hospitals of Bangladesh.
5.1.2: Nurse
Not only the doctors of our country are liable for medical
negligence but also the stuffs of the hospitals of our
country are also equally liable for medical negligence. Most
of the time the nurses remain in the hospitals to do their
duty. They act in place of the doctors. They are engaged to
take care of a patient. They have to give medicine to a
patient regularly. But most of the nurse does not do their
duty properly. When a patient needs a nurse in the time of
taking medicine, they are not found. Without money they are
not interested to serve the patients properly. They want
extra money from the patients.
52
In a statistic by Dhaka based N.G.O. named Ain O Salish
Kendra, made a list of 504 persons of the victims of medical
negligence from year1998 to 2008 on the basis of the news of
the daily news papers. Where it is shown that about 8
persons dies as a result of medical negligence of the
surgeons.[45]
5.1.3: Stuffs of Hospitals, etc.
Not only the doctors and the nurses of our country are
liable for medical negligence but also the stuffs of the
hospitals of our country are also equally liable for medical
negligence. The maximum stuffs of the country are corrupted.
They do not do their duties properly. Their manner of
speaking to the patients is not also good. Most of the
stuffs want extra money from the patients. Without money
they are not interested to serve the patients properly. In a
statistic by Dhaka based N.G.O. named Ain O Salish Kendra,
made a list of 504 persons of the victims of medical
negligence from year1998 to 2008 on the basis of the news of
the daily news papers. Where it is shown that about 4
persons dies as a result of medical negligence of the
medical stuffs.[46]
Tajnin Sultana who is a baby of one and half years old. Her
parents admitted her at that hospital for a surgery in her
mouth as she is a patient of talukata. On 07/11/2010[47] her
parents admitted her at that hospital for the purpose of53
operation. They have come from Brahman Baria. During time of
admission, as whole environment of the hospital was unknown
to her, the baby started crying. At that time the stuffs of
the hospital made a rough conduct with her even with her
parents. They also threatened the innocent baby. It is also
mentionable here that the hospital treat the babies without
any cost who are the patients of talukata. But the baby’s
parents paid 60,000 tk. for her operation. In spite of
paying tk. they did not get redeem from their rough conduct.
This is a glorious example of the negligent of the Hospitals
stuffs.[48]
5.2: Victims of Medical Negligence
One who is harmed or killed by a doctor or a surgeon or by a
nurse or by a stuff of the hospital or by the management of
the hospital is called a victim of a medical negligence.
That’s means whoever become an injured person by aforesaid
persons shall be treated as a victim of medical negligence.
The victims of the medical negligence may be a woman, the
children, the students, the politicians, the lawyers, the
businessman, the teachers, the journalists, the actors, the
actress and the painters etc. In short, those who take
medical treatment from hospital or from any other places may
be the victim of medical negligence. But in most cases,
women and the children becomes the victim of medical
negligence.
54

0
100
200
300
400
500
600
Dow rydispute
DomesticViolence
Raped andKilled
Victim ofMedical
Negligence
Dow ry dispute
Domestic violence
Raped and Killed
Victim of MedicalNegligence
5.2.1: Women
For the reason of socioeconomic condition of Bangladesh the
Women of this
country are treated
weak and dependant
to others. That’s
why they are
becoming oppressed
in every sectors of
the country. In
2008, there were 518 cases of violence against women in
Bangladesh, according to a report released by Ain O Salish
Kendra, a human rights organization. Of the victims, 172
women were killed over dowry disputes and 246 through
domestic violence, while 83 were killed after being raped.
The list includes 17 female domestic helpers. Furthermore,
367 more women were raped and eight of them committed
suicide during the one-year period. Two domestic helpers
also committed suicide. Also, 20 women fell victim to
punishment according to Fatwa, or religious edicts by
religious village leaders.[49] Medical sector is not
exception to this. Large number women are becoming the
victim of medical negligence. In a statistic by Dhaka based
N.G.O. named Ain O Salish Kendra, made a list of 504 persons
of the victims of medical negligence from year1998 to 2008
on the basis of the news of the daily news papers. Where it
55
0
100
200
300
400
500
600
victim by medicalnegligence
children being thevictim of MedicalNegligence
victim by medicalnegligencechildren being the victimof Medical Negligence
is shown that about 165 woman dies as a result of medical
negligence of the surgeons of Bangladesh. Maximum medical
negligence occurred with the women in times of delivery. A
glorious example of medical negligence is given here where
the victim is a woman.[50]
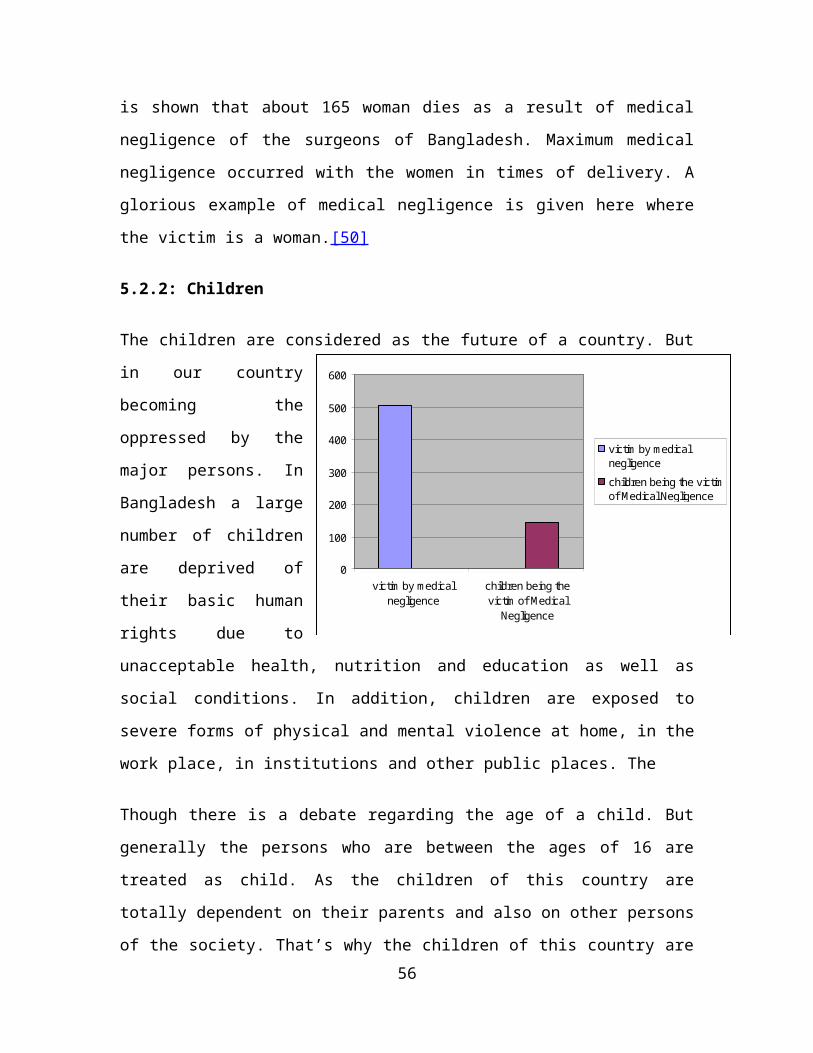
5.2.2: Children
The children are considered as the future of a country. But
in our country
becoming the
oppressed by the
major persons. In
Bangladesh a large
number of children
are deprived of
their basic human
rights due to
unacceptable health, nutrition and education as well as
social conditions. In addition, children are exposed to
severe forms of physical and mental violence at home, in the
work place, in institutions and other public places. The
Though there is a debate regarding the age of a child. But
generally the persons who are between the ages of 16 are
treated as child. As the children of this country are
totally dependent on their parents and also on other persons
of the society. That’s why the children of this country are56
0
100
200
300
400
500
600
victim of M edicalNegligence
Student being the victimof M edical Negligence
victim of M edicalNegligenceStudent being the victim ofM edical Negligence
becoming the victim in every sphere of the society. In a
statistic by Dhaka based N.G.O. named Ain O Salish Kendra,
made a list of 504 persons of the victims of medical
negligence from year1998 to 2008 on the basis of the news of
the daily news papers. Where it is shown that about 146
children dies as a result of medical negligence of the
surgeons.[52].
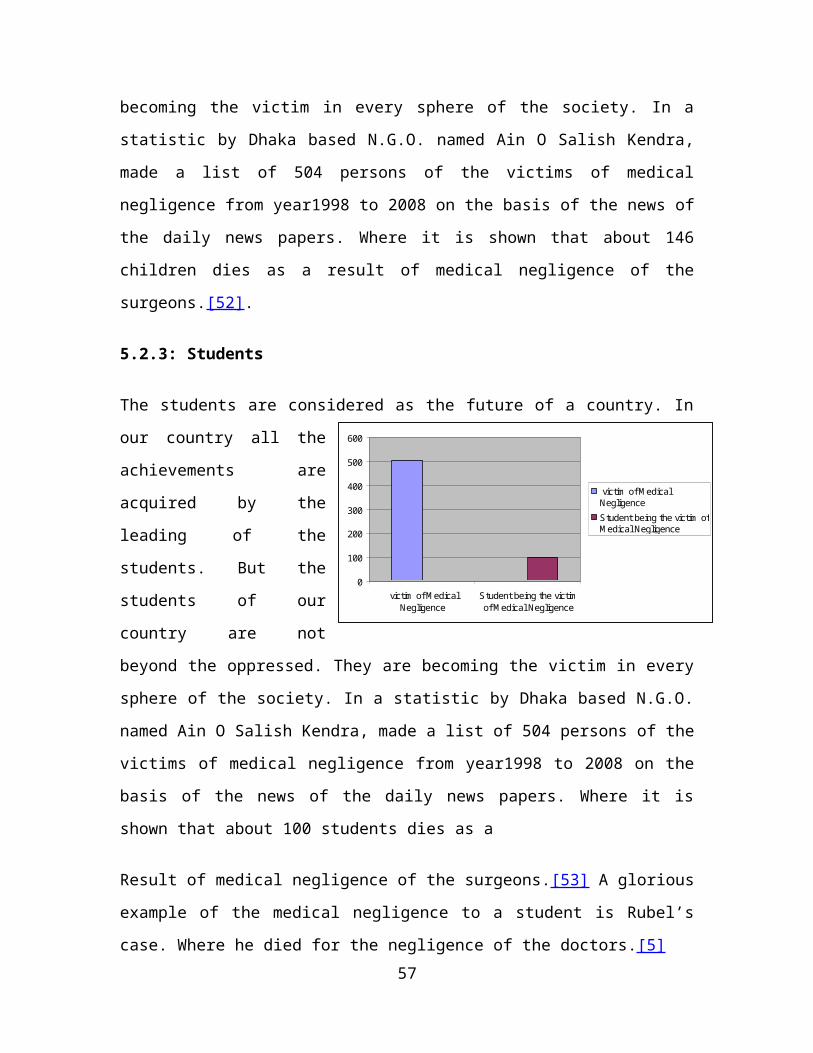
5.2.3: Students
The students are considered as the future of a country. In
our country all the
achievements are
acquired by the
leading of the
students. But the
students of our
country are not
beyond the oppressed. They are becoming the victim in every
sphere of the society. In a statistic by Dhaka based N.G.O.
named Ain O Salish Kendra, made a list of 504 persons of the
victims of medical negligence from year1998 to 2008 on the
basis of the news of the daily news papers. Where it is
shown that about 100 students dies as a
Result of medical negligence of the surgeons.[53] A glorious
example of the medical negligence to a student is Rubel’s
case. Where he died for the negligence of the doctors.[5]57
5.2.4: Politicians, etc.
The politicians play a vital role in a country. They are the
social reformist in a society. But they are also not the
beyond the medical negligence. Every year a numerable
politician for the fear of medical negligence is going to
abroad for taking treatment. As they do not believe the
surgeons of our country. In a statistic by Dhaka based
N.G.O. named Ain O Salish Kendra, made a list of 504 persons
of the victims of medical negligence from year1998 to 2008
on the basis of the news of the daily news papers. Where it
is shown that about 10 politicians dies as a result of
medical negligence of the surgeons.A film star named Manna
died for the medical negligence on 17th February in 2008 at
United Hospital Dhaka on Sunday afternoon. He was also a
member of Zia Shangskritic Sanghatan.[55]
Chapter Six
Rights and Liabilities of Doctors and Patients
6.1: Rights of the Patients
A patient’s rights occur at many
different levels, and in all
specialties. When a patient goes to a
doctor or a hospital there arise some
58
rights of the patient. In 2003 a lift let is published by
the Ministry of Health and Family Welfare. In that lift let
the following rights were include as the right of the
patient.
1. The right to receive information from physicians about
the services
2. The right to safe and continuity of health care
3. The right to confidentiality
4. Right to get respect and dignity
5. Right to share idea
6. Right to get redress
7. Right to inform the highest authority when the rights are
violated.
8. Right to choice treatment and the method of family
planning
9. Right to get all documents relating to treatment
10. Right to receive all information about the treatment[56]
59

Generally all states have recognized these rights as the
right of the patient. For example, The American Medical
Association (AMA) outlines fundamental elements of the
doctor-patient relationship in their Code of Medical Ethics.
These rights include the following:
1. The right to receive information from physicians and to
discuss the benefits, risks, and costs of appropriate
treatment alternatives
2. The right to make decisions regarding the health care
that is recommended by the physician
3. The right to courtesy, respect, dignity, responsiveness,
and timely attention to health needs
4. The right to confidentiality
5. The right to continuity of health care
6. The basic right to have adequate health care.
Patient’s Bill of Rights
The Consumer Bill of Rights and Responsibilities was adopted
by the US Advisory Commission on Consumer Protection and
Quality in the Health Care Industry in 1998. It is also
60
known as the Patient’s Bill of Rights. The summary of The
Patient’s Bill of Rights is given bellow:
The Patient’s Bill of Rights was created to try to reach 3
major goals:
1. To help patients feel more confident in the US health
care system; the Bill of Rights:
Assures that the health care system is fair and it
works to meet patients’ needs
Gives patients a way to address any problems they may
have
Encourages patients to take an active role in staying
or getting healthy
2. To stress the importance of a strong relationship between
patients and their health care providers
3. To stress the key role patients play in staying healthy
by laying out rights
6.2: Duties of the Patients
1. Duty to uphold his own health:The patient should
preserve and promote his own health and well-being so
far as is reasonably opens to him to do so. For
instance, he should follow a responsible lifestyle that
does not put his health avoidably at significant risk;
61
he should follow health promotion guidelines; he should
take account of the risk factors affecting him,
including what he can reasonably know of his own family
history.
2. Duty to protect the health of others: The patient
should avoid being a source of ill health for others
within the same health jurisdiction. He should promote
the health and well-being of his own dependants and he
should not engage in, promote, or needlessly tolerate
practices that are harmful to health.
3. Duty to seek and access healthcare responsibly: The
patient should act responsibly regarding when and how
he seeks healthcare. For instance, general practice
surgeries already expect that patients with non-urgent
conditions should accept the need to wait for an
initial primary care appointment on a later day. If it
is feasible for him to present himself at the surgery,
he should not request a home visit. The patient also
has a duty to be courteous and tolerant when attending
healthcare institutions, including accident and
emergency departments, as part of taking responsibility
for the reasonableness of his own expectations of care.
4. Duty of truthfulness: The patient should be truthful
during the consultation and history-taking, thereby
inter-alias helping the achievement of a realistic
62

diagnosis. For instance, he should divulge everything
that is relevant, and he should avoid embellishment and
evasion.
5. Duty of compliance: The patient should comply with his
clinical management and medication unless he has good
reason to think that these have not been properly
arrived at .[57]
6. Duty of recovery or maintenance: During and after
treatment, the patient should wherever possible promote
his own recovery or, where this is unrealistic (for
instance, in the case of chronic illness), try to
maintain a reasonable quality of life.
6.3: Rights of the Doctors
A doctor has the following rights:
1. Right to privacy
2. To know about the patients life-
style, particularly if it has an
impact on your SCI or complications from the injury, or
proposed treatment.
3. To withdraw from giving treatment to a patient if-
a) the doctor himself is not well or free.
63
b) the doctor has had a bad experience in the past.
c) He cannot be compelled to treat a patient in odd hours.
d) There is no legal obligation to answer a call to visit
the patient at his or her place of residence.
e) Doctor treats a patient in emergency on ethical grounds.
It does not mean that he has accepted the patient.
f) If a patient does not agree with the method of treatment
g) In his honest opinion, if a doctor feels that he is not
in a position to treat a patient because of non availability
of certain facilities, instruments, medicines, staff etc. he
may refer the patient to a suitable place.
Besides a Doctor have the following general rights. These
rights of doctor’s are shortly described here:[58]
Selection of drugs
In some diseases, more than one
medicines are effective and the
decisions as to which of them
should be prescribed is the
absolute right of the doctor. Here
doctor applies his own knowledge,
experience and skill, over and above giving consideration to
theoretical effects of the medicine.
64

Selection of method
In medical science, more than one type of
treatment are approved and available for
a particular disease. A doctor may adopt
any one of th em. For example, the
removal of gall bladder (cholecystectomy)
can be performed through various
incisions, with the choice of incision depending on the
doctor based on his experience. Moreover, in a surgery, from
anesthesia to stitch thread, everything is to be decided by
the surgeon only.
Investigation
it is not always possible for a doctor to make certain
diagnosis only from clinical examination of the patient.
Additional laboratory tests, X-ray, sonography etc., may be
required. The doctor is the best judge to decide about
number and type of investigations to be carried out.
65
Some doctors insist for a particular laboratory or X-ray
clinic as in his opinion their reports are perfect and
reliable. Of course patient might take it the other way, so
a doctor may insist but should not over insist. In
emergencies, the doctor has wider discretion about the
treatment.
6.4: Duties and Liabilities of the Doctors
By International Code of Medical Ethics of the World Medical
Association – 1949 the following duties has been included as
the duties of a doctor. The duties of a doctor are:
6.4.1: Duties of Doctors in General
1. A doctor must always maintain the highest standards of
professional conduct.
2. A doctor must practice his profession uninfluenced by
motives of profit.
The following practices are deemed unethical:
a. Any self advertisement except such as is expressly
authorized by the national code of medical ethics;
b. Collaborate in any form of medical service in which the
doctor does not have professional independence;
66
Receiving any money in connection with services rendered to
a patient other than a proper professional fee, even with
the knowledge of the patient.
Chapter Seven
Real conditions of the Health Sector and the Hospitals of
Bangladesh
7.1: The state of our health sector
The term ‘health’ does not just mean absence of illness or
disease. It also includes physical and mental well—being.
However, given the state of our health service delivery
system, even physical and mental well—being is adversely
affected – if not the patients’, then their family member’s.
7.1.1: Hospitals, doctors and health care
According to statistics, there is one hospital bed available
per 2,732 persons and one doctor per 3,125 persons according
to the Bangladesh Bureau of Statistics. The quality of
medicine has gone down and adulterated food, drink and
medication has created a negative impact all over the
67
country. For example, in 2008, the disease Kala zar struck
45 districts and it was reported that 7 persons had died
after taking the medicine Miltefosin. The medicine was
tested in a WHO approved laboratory—and found to be
inadequate. Again, in the early 1990’s infants in Bangladesh
were falling grievously ill due to adulterated Paracetamol-
based medication and on June 5, UNB reported from Faridpur
that ‘some 150 children aged between six months and five
years reportedly fell sick day before after taking Vitamin A
capsules and deforming tablets at Charshalipur village in
Charbhadrashan upazila’. On June 9 The New Age reported,
‘Another child reportedly died of complications from Vitamin
A plus capsule and antihelminthic or deforming tablet in
Munshiganj on Sunday night raising the number of such deaths
to two and several thousand children across the country fell
sick in the last three days after taking the medicine.’
Health services are delivered by specialized personnel. When
one thinks of health and well being, one of the first images
that come to mind is that of a doctor. However, given the
poor state of our health services, it is safe to say that
some doctors are involved in contributing to the terrible
state of things. The health ministry established a
Monitoring and Supervisory Committee on August 31, 2008, in
response to the reports of appalling health care conditions
published in newspapers. In September that year, it was
reported that 104 personnel in several government hospitals
68
were found to be responsible for mismanagement and
corruption, and were penalized. Between January and October
2007 alone, there were over 76 death cases reported to be
caused by medical negligence, according to an investigation
of a Dhaka-based NGO, Ain-o-Shalish Kendra.
Again, between January and September 2008, press reports
indicate that some 52 persons had allegedly died due to
medical negligence. Malpractice cases are numerous, and even
affect some of the country’s senior-most and reputed doctors
because they treat scores of patients daily, giving each
little time or thought, points out Dr Quazi Quamruzzaman of
Dhaka Community Hospital. ‘It’s just that the whole system
that needs to be fixed.’
According to Dr Mohammad Saiful Islam, pediatric surgeon and
dean of surgery, BSMMU, one of the biggest flaws in
Bangladesh’s medical system is that there is no monitoring
mechanism which checks whether doctors are administering
wrong treatment resulting deaths. ‘The organization that is
to oversee such cases of negligence, the Bangladesh Medical
and Dental Council, is now dead. While an alarming number of
cases go unreported, the issue of accountability is hardly
on the agenda of health care sector in Bangladesh.
Again, our country’s numerous private clinics need close
monitoring. Many of such clinics are nothing but money—
making ventures, paying little regard to human life. In the69
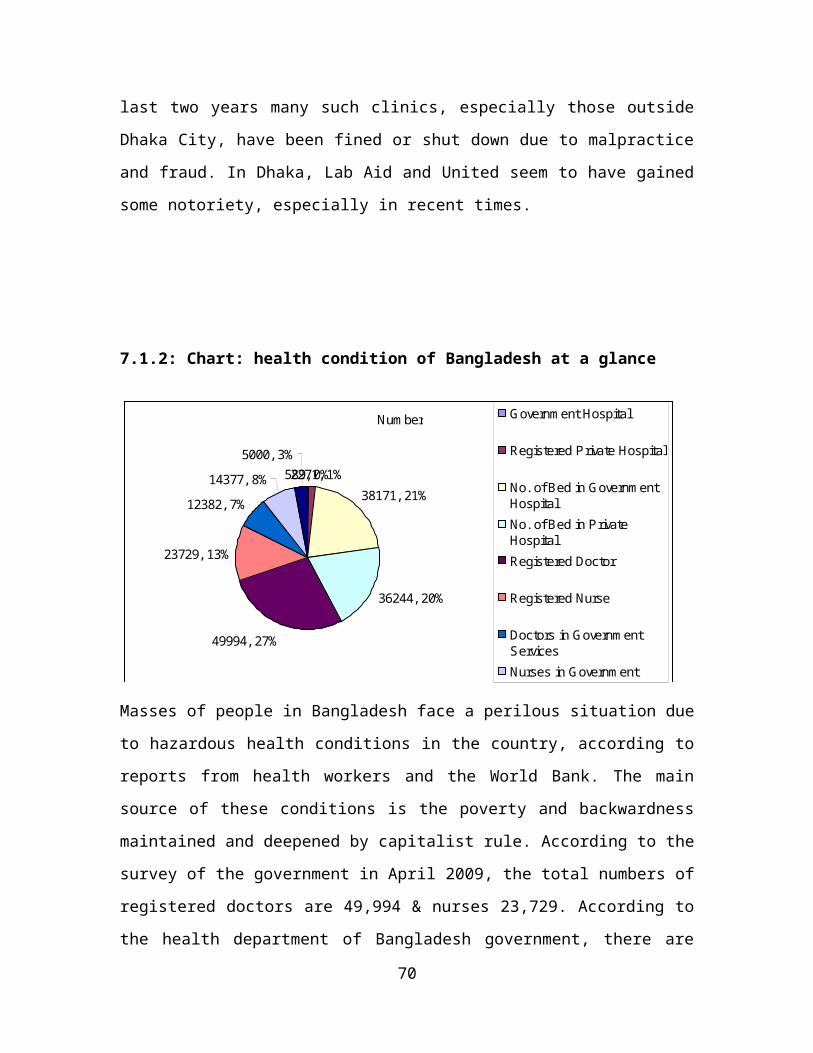
Num ber
589, 0%2271, 1%38171, 21%
36244, 20%
49994, 27%
23729, 13%
12382, 7%14377, 8%
5000, 3%
Governm ent Hospital
Registered Private Hospital
No. of Bed in Governm entHospitalNo. of Bed in PrivateHospitalRegistered Doctor
Registered Nurse
Doctors in Governm entServicesNurses in Governm entServicesTrained M idwives
last two years many such clinics, especially those outside
Dhaka City, have been fined or shut down due to malpractice
and fraud. In Dhaka, Lab Aid and United seem to have gained
some notoriety, especially in recent times.
7.1.2: Chart: health condition of Bangladesh at a glance
Masses of people in Bangladesh face a perilous situation due
to hazardous health conditions in the country, according to
reports from health workers and the World Bank. The main
source of these conditions is the poverty and backwardness
maintained and deepened by capitalist rule. According to the
survey of the government in April 2009, the total numbers of
registered doctors are 49,994 & nurses 23,729. According to
the health department of Bangladesh government, there are
70

estimated one doctor for every 2860 people and one nurse for
every 5720 people. According to the public health
specialists, one doctor required 3 nurses and 5 assistants.
The proportion is 1:3:5. But in Bangladesh the proportion
is1: .54: .27. According to the WHO the estimation of doctor
and nurse for every 10,000 people in South Asian countries
are as follows
Country Doctor Nurse
Bangladesh 3 3
India 6 13
Srilanka 6 17
Pakistan 8 5
This summary states that our work force in health sector is
very poor. According to the health department, 12,382
doctors and 14,377 nurses are working in government health
sectors. They are serving in 589 government establishments
71
including Thana Health Complex, District Hospital, Medical
College Hospital, Specialized Hospital and Research
Institute. The most pathetic information is that maximum
portions of these 12,382 are serving in cities, metropolitan
towns or areas alongside the towns. Therefore, the sceneries
of rural areas are more formidable. In some areas there,
only one doctor runs a total health complex or hospitals. He
has to manage about 300-400 patients everyday. A report in
Prothom Alo states that there is only one doctor in
Sadullapur health complex of Gaibandha. There total posts
for doctor are 20. But government appointed only five. Among
them two went to deputation, one went to abroad for higher
studies and the remaining one is busy with government
duties. So there is only one doctor to look after the whole
health complex.
According to health department, 6861 posts of doctor and
16707 posts of nurse & medical assistants are still empty.
The reason behind this is most of the doctors are interested
to practice privately. On the other hand, every year
thousands of ill Bangladeshis go abroad in the hope of
getting better; in spite of huge costs of travel, hospital
care & surgery. This large-scale exodus of patients reflects
the dismal condition of health care in Bangladesh. Wrong
diagnosis & medical negligence are rampant even in the most
prestigious hospitals. This has led to a deterioration of
public trust in medical professionals. Many patients
72
complain that doctors refuse to talk to them properly or
explain what their ailment is or how they will be treated.
Those who can afford it & those who manage to scrape up
their savings or use whatever source of funding they have
opt for going thousands of miles away where they believe
they will get the proper treatment.
At a glance these are the conditions of our health sectors.
The government should take appropriate measures for removing
these problems of our Health Sector.
7.2 Causes of Medical Negligence and Medical Wrong
In course of providing the aforesaid services, medical
negligence is a common phenomenon. Numbers of such
incidents are unknown in Bangladesh, as there is no
accurate data recording system. However, i n t h e
n e w s p a p e r s , a l m o s t e v e r y d a y , t h e r e i s n e w s o n
m e d i c a l negligence of a kind or the other. In
microscopic level, legal actions are seen to be taken for
wrong diagnosis, Wrong prescription, wrong doses of
medicine, Wrong or faulty medical equipments , lack
of maintenance, Prescribing extra medicine with
business i n t e r e s t , M e d i c a l C o r r u p t i o n , O u t -
d a t e d m e d i c i n e s , M e d i c a l Malpractice, Breach of
Confidence by the Doctors and Nurses, False Medical
Certificates, Lack of quality Care
73
Chapter Eight
Remedies under the law of Bangladesh for Medical Negligence
Medical negligence is such act which a health care provider
is bound to provide but he has failed to provide it. On the
other hand, malpractice is such a things where the health
care provider has done some wrong act and during doing so he
ought to know that he has done wrong. But in practice, these
are so related that in case of filing a suit these must
consider together. For medical negligence the remedies which
are available are mainly tortuous remedies. That means, to
make good. Besides, there are also available remedies
regarding medical negligence these are Departmental remedy
and Professional remedy. For instance, the Ministry of
74
Health and Family welfare can take a departmental remedy
against the doctors of Public Hospital for the allegation of
medical negligence. On the other hand, the BMDC gives
license to the doctors. BMDC can cancel license of a doctor
if the allegation is proved. Another remedy is available
here, i.e. filing a suit under criminal law. These remedies
are shortly described here.
8.1: Constitutional Remedies
The Constitution of Bangladesh has recognized to promote and
protection of Human Rights. In the Constitution of
Bangladesh Civil and Political Rights are included as the
fundamental rights. But the right to get Medical treatment
is not included as the fundamental rights.
Article 8 speaks of social justice
Article 11 of the Constitution of Bangladesh that the
Republic shall be a democracy in which fundamental
human rights and freedoms and respects for the dignity
and worth of the human person shall be guaranteed. The
provision of the basic necessities of life, including
food, shelter, education and medical care.[60]
Article 16 of the Constitution of Bangladesh that the
state shall adopt effective measures for the
improvement of public health. Again in Article 18 it is
mentioned that the state shall regard the raising of
75
the level of nutrition and the improvement of public
health as among primary duties and in particular it
shall adopt effective measures for medical care.
Article 19 of the Constitution it is also said that
the state shall adopt effective measures to remove
social and economic inequality between man and man.
Lastly by Article 32 the right to life is recognized
as fundamental right. So the Constitution has
recognized the right to healthy life by getting medical
facilities.
Besides, according to Article 21(2) of the Constitution,
‘Every person in the service of the Republic has a duty to
strive at all times to serve the people.’ So in the light of
this provision it is possible to make liable all the doctors
and all other employee of the Public Hospitals on the ground
of negligence in the duty. And in this circumstance it is
possible to get redress by filling a writ petition in higher
court.
For example, in a case filed by the Ain O Salish Kendra, the
High Court Division of the Supreme Court of Bangladesh has
promulgated a rule nisi directing to the concerned authorities
to provide the citizens proper and sufficient health service
by abiding the provisions of law.
76

8.2: Remedies under Human Rights Law
Human right to health is now widely recognized in numerous
international instruments. Universal Declaration of Human
Rights
• Article 25( basic necessities)
‘Everyone has the right to a standard of living adequate
for the health of himself and of his family, including
food, clothing, housing and medical care and necessary
social services.’
International Covenant on Economic, Social and Cultural
Rights 1996
• Article 12( enjoyment of the highest attainable
standard of physical and mental health’ )
Right to health is also recognized in the following
conventions
• International Convention on the Elimination of All
Forms of Racial Discrimination of 1965 (Article 11)
77
• Convention on the Elimination of All Forms of
Discrimination against Women of 1979 (Article 12)
• Convention on the Rights of the Child of 1989 (Article
24)
• European Social Charter of 1961 (Article 11)
• African Charter on Human and Peoples’ Rights of 1981
(Article 16)
• and the Additional Protocol to the American Convention
on Human Rights in the Area of Economic, Social and
Cultural Rights of 1988 (Article 10).
Similarly, the right to health has been proclaimed by the
Commission on Human Rights, as well as in the Vienna
Declaration and Programs of Action of 1993 and other
international instruments.
8.3: Departmental Remedies
Departmental remedies means to take a step by the higher
authority against the liable doctors and employees. Some
mentionable regulatory statutes to control the doctors and
hospitals or clinics in Bangladesh are:
1. BDMC Code of Ethics,
78

2. Medical Practice and Private Clinics and Laboratories
(Regulation) Ordinance, 1982 and
3. Drag (Control) ordinance, 1982 etc.[61]
In these statutes some measures has been included for the
protection of the interests of the patients and some measure
has taken to make liable the doctors, employees and stuffs
for their negligence in their service. But the uses of these
statutes are so limited and these are not so familiar to the
people.
According to the Medical and Dental Council Act, 1980 the
Bangladesh Medical and Dental Council may refuse to permit
the registration of any person or direct the removal
altogether or for a specified period from the Register of
the name of any registered medical practitioner or
registered dentist who has been convicted of any such
offence as implies in the opinion of the Council a defect of
character or who, after any inquiry at which opportunity has
been given to such person to be heard in person or through
advocate, has been held by the Council as guilty of infamous
conduct in any professional respect or who has shown himself
to be unfit to continue in practice on account of mental ill
health or other grounds.
But till December 2007 there is not found any single prove
that such measures has been taken against any doctor. At
present how much allegation is deposited in BMDC and what is79

present situation of these allegations, there is no
information about these.
There is a lot of power in the hands of the Director General
of the Ministry of Health and Family Planning. He can take
measure against any doctor, hospital, clinic etc. of
Bangladesh. The office of the Director General, Can suo moto
make inquiry against any hospital and clinic. If the alleged
hospital or clinic is found guilty then he can take any
legal action against these hospitals or clinics. But such
actions are quite administrative, such as cancellation of
the license of the alleged hospital or clinic, imposing fine
etc. But such statutory measures can not bring good result
for the victim or for his family. But these can be more
effective for the prevention of future event.
8.4: Statutory Remedies
There are two statutory remedies are available in
Bangladesh. These are shortly described here.
8.4.1: Civil Remedies
Tort laws have not developed in Bangladesh still now. That’s
why there is no effective remedy for the event of
80

negligence. There exist 45 civil statutes relating to health
affairs. Among these: Vaccination Act, 1880 Pharmacy
Ordinance, 1976 Medical Practice and Privet Clinics
and ;laboratory (Regulation) ordinance, 1982 Medical and
Dental Council Act,1980 Safe Blood Transfusion Act,2002
Privet Health Service Act, 2005 etc.
If a victim wants then he can take a step by the help of the
aforesaid statutes. But the main problems of the civil suit
are-
1. The victim should pay advalurem court fee under the
Court Feed Act, 1887. For the incapability to pay court
fees maximum victims cannot file a suit in the court
for proper remedy.
2. As the civil case takes much time so the victims or
their families are undesired to file a suit in the
court for proper remedy.
3. For the corruption, bribe etc. of the courts Clark,
employees or stuffs of the hospitals the victims are
not interested to file a suit in the court.
4. For much cost of the suit the victims are not
interested to file a suit in the court.[8
For the aforesaid reasons a victim party is interested to
file a civil suit. Besides, in some cases the doctor or
hospital authorities come to a solution by way of
negotiation with the poor victims. These negotiations may81
take place before the trial or when the suit is pending in a
court.
8.4.2: Criminal Remedies
Many lawyers believe that under existing criminal laws the
remedies for medical negligence can be affordable. According
to them, if the sections of the Penal Code can change to
some extend then the remedies will available under existing
law. Now we will discuss the sections of the Penal Code by
which are related to criminal remedies.Sections 269 and
270 covers punishments for negligent
Section 275 of the Penal Code, 1860 deals with Sale of
adulterated drugs.
“Which states that whoever, knowing any drug or medical
preparation to have been adulterated in such a manner as to
lessen its efficacy, to change its operation, or to render
it noxious, sells the same, or offers or exposes it for
sale, or issues it from any dispensary for medicinal
purposes as unadulterated, or causes it to be used for
medicinal purposes by any person not knowing of the
adulteration, shall be punished with imprisonment of either
description for a term which may extend to six months, or
82
with fine which may extend to one thousand taka, or with
both.”
The offence under this section consists in selling, or
offering or exposing for sale, or issuing from any
dispensary, an adulterated drug as unadulterated. This
section prohibits its sale and also its issue from any
dispensary. This section should be read along with section
521 CrPC.[62]
. There are some materials, though these are used as
medicine, but under Section 275 these will treated as
medicine. For example, there are some Unani Surgeons who use
kerosene as medicine. But under this section, kerosene will
not be called as medicine. Those things are used as medicine
only these are treated as medicine not other things.
Under this section the following things must be proved:
1. That the drug has been adulterated.
2. That the adulteration was such as to lessen its
efficacy or change its operation, or renders it
noxious.
3. That the accused sold, or offered or exposed, such
drug for sale; or that he issued it from a
medicinal dispensary; or that he caused it to be
83
used from a medicinal dispensary; or that he
caused it to be used for medicinal purpose.
4. That he sold, or issued such drug as an
unadulterated drug; or caused it to be used by a
person who did not know of such adulteration.
5. That he knew that such drug was so adulterated
when he sold, etc.[63]
Section 284 of the Penal Code deals with negligent conduct
with respect to poisonous substance which states that
whoever does, with any poisonous substance, any act in a
manner so rash or negligent as to endanger human life, or to
be likely to cause hurt or injury to any person, or
knowingly or negligently shall be punished with imprisonment
of either description for a term which may extend to six
months, or with fine, which may extend to one thousand taka,
or with both.
Section 304A of the Penal Code, 1860 deals with causing
death by negligence.
“Whoever causes the death of any person by doing any rash or
negligent act not amounting to culpable homicide shall be
punished with imprisonment of either description for a term
which may extend to five years, or with fine, or with both.”
84
Under this section, Criminal rashness is hazarding a
dangerous or wanton act with the knowledge that it is so,
and that it may cause injury, but without intention to cause
injury, or knowledge that it will probably be caused. When a
doctor by his busyness gives to his patient a toxic medicine
in replace of good one. Here, offence under section 304A has
been committed.
Though, criminal rashness and criminal negligence is used
for same meaning, but there are differences between these.
Criminal rashness is hazarding a dangerous or wanton act
with the knowledge that it is so, and that it may cause
injury, but without intention to cause injury, or knowledge
that it will probably be caused. On the other hand, criminal
negligence is acting without the consciousness that the
illegal and mischievous effect will follow, but in
circumstances which show that the actor has not exercised
the caution incumbent upon him, and that if he had, he would
have had the consciousness.[According to section 304A, both
are equal offence.
Whether there exists a rashness or negligent in an act, may
be proved by the following two ways.
Firstly, the amount of care and cautions which a reasonable
person deemed sufficient and
85

Secondly, whether such act was done with due thought and
caution or not.
Under this section the following things must be proved:
1. The death of the person in question
2. That the accused caused such death
3. That such act of the accused was rash or negligent,
although it did not amount to culpable homicide.
Where the negligence is mot directly related to the death of
the deceased person, then the accused person is entitled to
get facilities. For example- When a contractor of a bus dies
from the Patatan of that bus, then the driver of that bus
could not be liable. In this case, if it is claimed that the
driver of that bus has driven the bus by shaking is not
cognizable.
Section 316 of the Penal Code deals with causing death of
quick unborn child by act amounting to culpable homicide.
“Which provides that whoever does any act under such
circumstances, that if he thereby caused death he would be
guilty of culpable homicide, and does by such act cause the
death of a quick unborn child, shall be punished with
imprisonment of either description for a term which may
extend to ten years, and shall also be liable to fine.”
86
For example, A, knowing that he is likely to cause the death
of a pregnant woman, does an act which, if it caused the
death of the woman, would amount to culpable homicide. The
woman is injured but does not die; but the death of an
unborn quick child with which she is pregnant thereby
caused. A is guilty of the offence defined in this section.
This section is only applicable in case of an unborn quick
child. But when the pregnant woman dies then this section
will not applicable.[64]
Under this section the following things must be proved:
1. That the woman was pregnant
2. That the accused did an act to cause the death of the
child.
3. That the circumstances under which the act was done was
such as to make the accused guilty of culpable homicide
if death has been caused.
4. That such act caused the death of the quick unborn
child.
87
Chapter Nine
Recommendations
The following recommendations may be consider for proper
remedy of medical negligence.
9.1: Statutory Recommendations
For removing the aforesaid statutory and procedural
limitations, the following reforms should be taken. If it is
possible to legislate a different statute for medical
negligence, then it will be more efficacious. In the
proposed law there shall be a definition chapter where the
definition of medical negligence and the detailed
88
description of medical negligence and its kind will
described. The trial and investigating procedure must be
include in that Act for medical negligence. Besides, there
must ensure that during the treatment period, there must not
make an unreasonable obstruction to the doctors. It also be
remember that the safety measures must be adaptable with
real situations. Sometimes it has been observed that by the
help of safety measures all the criminals are saved. So, all
these things must be deeply think at the time of
legislation.
Above all, it is not possible to change the present
situation of our health sectors by a night only. So, to
prevent medical negligence and to provide legal remedy to
the victims the following recommendations may be consider.
1. Some sub-sections may include for medical negligence
with the existing sections (337,338, 304A) of the Penal
Code.[65]
2. With these inclusions, the definition of medical
negligence, its types and its scale must be clearly
mentioned.
3. In case of medical negligence, all the procedural
complication must be removed.
89
4. In case of medical negligence, all the lump sum inquiry
procedure must be removed. As these procedures of
inquiry extends the time of the suits.
5. The Police must be well trained for investigating the
matters of medical negligence. As they have no concept
about medical negligence. Particularly, their corrupted
mental tendency must be changed.Sometimes it is seen
that they are helping the offenders to move openly in
spite of committing an offence. The offenders stop the
mouth of police by giving bribe. So the corrupted mind
of police must be changed for establishing rule of law
in the society.
6. According to the Medical Practice and Private Clinics
and Laboratories (Regulation) Ordinance, 1982, there
must take a measure for the inspection of the private
clinics. As under the Ordinance there is no scope of
inspection of the Private Clinics of our country. As in
the Ordinance there is not strict provision of
punishment for the violation of the Ordinance. So for
taking an action against such violation there must be a
provision of punishment for violation of the Ordinance.
7. By amending the Medical Practice and Private Clinics
and Laboratories (Regulation) Ordinance, 1982,
accountability of the inspecting authority must be
ensured.
90
8. The private clinics or hospitals must have sufficient
treatment facilities, appropriate medical equipment and
adequate sitting arrangements for patient visitors to
receive license.
9. There must take appropriate measures for fixing fees
for private clinic and private laboratories for
surgical operations, medical examinations and services,
including pathological and radiological examinations,
and maintenance of patient’s records.[66]
9.2: Other Recommendations
The following recommendations may also be considered.
9.3: Recommendations for Government
1. There must take a consciousness program by the government
for the rights which are available for a patient i.e. the
right to receive information from physicians about the
services, the right to safe and continuity of health care,
the right to confidentiality, right to get respect and
dignity, right to share idea, right to get redress, right to
inform the highest authority when the rights are violated,
91
right to choice treatment and the method of family planning,
right to get all documents relating to treatment etc.[67]
2. The govt. should form an information store from village
to capital for the purpose of preservation of all supporting
information’s relating to health affairs. Where all
supporting documents and the problems of the public and
private hospitals and health care centers will be preserved.
If it is required, their must be a measure for supplying
information.[68]
3. In Upazila Health Complex, there must be improvement
regarding equipment, manpower and infrastructure. In every
health centre there should be hang a list about what kind of
health facilities are available and how much the price of
these services are. The proportion of doctor and patient
must be reduced by taking effective measures.
4. An awareness program may be taken for the nurse and ward
boy of the hospitals, clinics and for all institutions
relating to health care regarding the rights of the
patients. A training program should also be taken for all.
5. A cautious measure should be taken in case of writing
medical records and of its preservation. If it is required a
different training program may be taken.
6. Unwanted political interfere should be reduced.
92
7. The budget for health sector should be increased and
proper use of such budget must be ensured.
8. The government should establish a separate Food, Health,
Cosmetics and Consumer Tribunal.[69]
9.4: Recommendations for Bangladesh Medical and Dental
Council
The BMDC may consider the following recommendations for the
control the medical Colleges and existing hospitals of
Bangladesh.
1. The BMDC should make as an institution which will free
from political power and shall be people’s representative,
impartial and effective
2. During the renewal of the doctors registration there
should a measure for the reevaluation.
3. The environment of the hospitals should make as the
patient intensive.[
4. The accountability of the management of the hospitals
must be ensured.
5. The tribunal of the BMDC should make active.[70]
93
Chapter Ten
Concluding Chapter
10.1: Findings
There is no separate law in Bangladesh regarding medical
negligence. When any one become infirmed or injured
physically, then he should get the help of the sections 337
and 338 of the Penal Code for proper remedy. Besides,
section 304A includes the provision for causing death by
negligence. In Bangladesh, When any one wants to get remedy
then he should take the help of the aforesaid sections. But
these sections have some limitations. These are shortly
described here.
10.2: Statutory Limitations
94
The aforesaid sections of the Penal Code have some
salutatory limitations. In these sections it is said about
general negligence. As the medical negligence is a special
negligence and it was necessary to specify those negligence
for bring it as the criminal negligence. But in this case it
is absent. Though in section 304B of the Penal Code there is
a provision of punishment for rash or negligent driving of
any vehicle, but there is no special section regarding
medical negligence.
Medical negligence is one kind of professional negligence.
The persons who are specialized in a work, their act of
negligence and the negligence of the general people are not
the same thing. Here the proof of the act of negligence lies
on the expected degree of care, which is quite different
from general negligence and professional negligence. But in
this Act there is no explanation or illustration regarding
this.
Generally the patient or his kin could not make a demand
that for the surgeon had the intention to kill him or his
kin. In case of criminal liability it is a sin qua non that
there must be an intention that for committing an offence.
But the word itself speaks that the act is not by
intentionally but lack of due care.
95

10.3 Procedural Limitations
There exist some procedural limitations in our statutes:
1. At first, when a victim wants to file a suit against
the medical negligence or against the doctor, the
police station is not interested to take the case. Even
the Magistrates are also not showing their interest to
take suit.
2. Against the negligence of public hospitals though a
case is taken, when after prima-facie inquiry it is
found that the alleged doctors are guilty then the
permission of the Ministry of Health affairs is
required. This is very time consuming process and also
creates secretariat complications.
3. In these suits, the current process of collecting
evidence is a lengthy process and in some cases
irrational and unnecessary. In any case the cases of
death are referred for post mortem report and for
surothal. In present situation when a case is referred
for a post mortem report or for a surothal report ,
then the process of the suit will pending for a long
period. The customary processes of inquiry hamper and
obstruct the main suit.
96
4. Fourthly, there exists lack of experience in criminal
inquiry. Generally, Criminal investigation is done by
police. The police investigations present process is
not sufficient for the medical investigation. The
Bangladesh police have not sufficient knowledge and
capability to investigate like the matters of medical
negligence.
These are the limitations of the criminal laws regarding
negligence. Besides section 312, 313, 314, 315 & 316 of the
Penal Code are related with abortion and the death of unborn
child. These sections are not directly to medical negligence
besides the doctors there may involve any other authority
for negligence.
10.4: Obstructions on Criminal Remedy
In case of criminal offence the following three obstructions
creates an obstruction from getting proper remedy.
10.4.1: Mens Rea
In case of criminal trial mens rea is an important thing. The
offence which has already been committed, whether there was
an intention of the doer, the judge of a case find out by
97

records and evidence. If it is proved, that offender has not
any intention to do the offence then the amount of his
punishment is also reduced. For example, when a man is
charged for an offence and if it is proved that he has done
the act for his self defense, then it will deem that he has
not committed an offence. Because he has not any intention
for committing the offence. So in case of medical
negligence, it is difficult to prove mens rea.
10.4.2: Relation between negligence and injury
There should be a direct relation between injury and
negligence. If there is no direct relation between injury
and negligence then the accused person shall not be liable
for negligence.
10.4.3: Good Faith
In case of criminal cases, particularly, in negligence suit,
good faith is widely used. The accused surgeons show plea of
good faith for their self defense. The Penal code also does
the offences as offence which are directly relate with good
faith. For example,
Surgeon, knowing that a particular operation is likely to
cause the death of Z, who suffers under the painful
complaint, but not intending to cause Z’s death, and
intending, in good faith, Z’s benefit, performs that
98
operation on Z, with Z’s consent. A has committed no
offence.
It is said in section 89 of the Code, that nothing-which is
done in good faith for the benefit of a person under twelve
years of age, or of unsound mind, or by consent, either
express or implied, of the guardian or other person having
lawful charge of that person, is an offence by reason of any
harm which it may cause, or be intended by the doer to cause
or be known by the doer to be likely to cause to that
person. For example,
A, in good faith, for his child’s benefit without his
child’s consent, has his child cut for the stone by a
surgeon knowing it to be likely that the operation will
cause the child’s death, but not intending to cause the
child’s death. A is within the exception, in as much as his
object was the cure of the child.
10.4.4: Other obstructions
Besides the aforesaid obstructions, there are also some
obstructions. These obstructions play a vital rule in case
of criminal suit. For example,
1. Corruption in the different field of Police and
government.
99
2. Investigating officers has lack knowledge and technical
ability in case of dealing of a case.
3. Destroy of the evidence as a result of delay.
4. Lack of Knowledge of the lawyers and the judges
regarding this matter.
5. It is difficult to collect medical records, witness,
etc.
6. Lack of the provision for taking technical opinion.
Bibliography
Books Name
1. Ain O Salish Kendra, “Chikitshai Obohela”, December, 2008
2. Durga Das Basu, ‘The Law of Torts’ 11th Edition
3. Gazi Shamsur Rahman, Dandabidhir Vashya, 6th Edition
(amended), July 2001, Re-printed2007
100
4. Msrkesinis and Dekinn, “Tort Law”, 5th Edition
5. Noshirvan H. Jhabvala, “The Law of Torts”, 25th Edition
6. Ratanlal Ranchhodas and Dhirajlal Keshavial Thakore,
“The Indian Penal Code” 28th Edition
7. Zahirul Huq, The Penal Code, 4th Edition 2001
Journals
1. Daily New age, 11th may 2007, Xtra Cover
2. Daily Prothom Alo
3. Daily Star
4. Pakistan Criminal Law Journal 1970, Page-1159
5. . Pakistan Criminal Law Journal 1985, Page-813(Lahore)
6. World Medical Association Bulletin, vol. no.1, 3rd
October 1949
Websites
1. http//cancer.org/Treatment/
FindingandPayingforTreatment/
UnderstandingFinancialandLegalMatters/patients-bill-of-
rights
101
2. www.california-personal-injuuy.com/medical-malpractice-
legal-glossary/ medical- malpractice-legal-
glossarym.html
3. http:// www.Emedicinehealth.com/patients_rights
/article_em.htm
4. en.wikipdia.org/wiki/Medical_negligence
5. http://www.expresshealthcaremgmt.com/20021231/
focus4.shtml
6. http://www.highbeam.com/doc/1G1-174942758.html
7. http://jme.bmj.com/content/33/12/689.full
http://www.newagebd.com/2009/jul/05/edit.html
8. http://www.newagebd.com/2008/feb/29/feb29/
xtra_cover.html
9. http://www.newagebd.com/2007/may/11/may11/
xtra_cover.html
10. http://www.odhikar.org/report/pdf/child.pdf
http://www.thedailystar.net/newDesign/news-details.php?
nid=143251
http://www.upiasia.com/Blogosphere/williamgomes/2009022
2/victims_of_brutality_women_in_bangladesh/.
[1] Noshirvan H. Jhabvala, “The Law of Torts”, 25th
Edition ,
102
[2] Heaven vs. Pender, 1883 11 Q.B.D.507.
[3] Ibid
[4] Philips India Ltd. V. Kunju Punnu, (1974), B.L.R. 337.
[5] Pfizer Corp vs. Ministry of Health 1965 AC 512.
[6] Available on: en.wikipdia.org/wiki/Medical_negligence;
last accessed on: 18/11/2013
[7] Available on:
www.california-personal-injuuy.com/medical-malpractice-
legal-glossary/ medical-
malpractice-legal-glossarym.html; last accessed on:
18/11/2013
[8] Noshirvan H. Jhabvala, “The Law of Torts”, 25th
Edition ,
[9] Niochls v. Marsland, L.R. 2 Ex. Div. 1.
[10] Noshirvan H. Jhabvala, “The Law of Torts”, 25th Edition
,
[11] Cleghorn v. Oldham, (1927) W.N. 147.
[12] Butterfield v. Forrester, (1809), 11 East 90
1. Butterfly v. Forrester, (1809) 11 East 90.
103
2. Froom vs. Butcher, (1975) 3 All E.R. 520 (524) C.A.
[15] Boy Andrews v. St. Rongvald, (1947) 2 A.E.R. 350(H.L).
[16] Nance v. British Columbia Ry. Co. (1951) 2 All E.R. 448
(P.C).
[17] . Durga Das Basu, ‘The Law of Torts’ 11th Edition,
[18] Lynch vs. Nurdin, (1841) 1 Q.B. 29.
[19] Glasgow Corporation vs. Taylor, (1922) 1 A.C. 44.
[20] Noshirvan H. Jhabvala, “The Law of Torts”, 25th Edition
[21] GREAT CENTRAL RLY.v. BATES (1921) 3 K.B. 578.
[22] Ibid
[23] Noshirvan H. Jhabvala, “The Law of Torts”, 25th Edition
,
[24] White v. N.e. Rly, (1888) E.B. &E. 719.
[25] Mills v. Armstrong, (1888) 12 App. Cas.1.
[26] Noshirvan H. Jhabvala, “The Law of Torts”, 25th Edition
[27] Ibid,
[28] Noshirvan H. Jhabvala, “The Law of Torts”, 25th
Edition,
104
[29] Sidhraj Dhadda v. State of Rajastan, A.I.R. 1994 Raj.
68;
[30] Available on:
http://www.thedailystar.net/newDesign/news-details.php?
nid=143251, last accessed on: 02/11/2013
[31] Available on:
http://www.newagebd.com/2008/feb/29/feb29/xtra_cover.html;
last Accessed on: 21/11/2013
[32] Ibid
[33] Ibid
[34] Daily New age, 11th may 2007, Xtra Cover; Ref:
http://www.newagebd.com/2008/feb/29/feb29/xtra_cover.html
[35] Ibid
[36] Ibid
[37] Ibid
[38] Available
on:http://www.newagebd.com/2007/may/11/may11/xtra_cover.html
; last Accessed on:21/11/2013
[39] The Daily New Age, 11th May, 2007, Xtra cover
[40] Ibid
105

[41] Chikitshai Obohela, Ain O Salish Kendra , December,
2008,
[42] Chikitshai Obohela, Ain O Salish Kendra , December,
2008.
[43] Ibid
[44] Chikitshai Obohela, Ain O Salish Kendra , December,
2008.
[45] Chikitshai Obohela, Ain O Salish Kendra , December,
2008.
[46] Ibid
[47] A case study conducted at the City Hospital on:
07/11/2010
[48] Ibid
[49] http://www.upiasia.com/Blogosphere/williamgomes/
20090222/victims_of_brutality_wome n_in_bangladesh/; last
Accessed on: 23/11/2013
[50] Ibid
[51] Available on: http://www.odhikar.org/report/pdf/child.pdf;last Accessed on: 09/11/2010
[52] Chikitshai Obohela, Ain O Salish Kendra , December, 2008
106
[53] Chikitshai Obohela, Ain O Salish Kendra, December,2008
[54] Ibid,
[55] Ibid
[56] https://www.samedical.org/drs-patients-rights.html
[57] https://www.samedical.org/drs-patients-rights.html
[58] https://www.samedical.org/drs-patients-rights.html
[60] Constitution of Bangladesh.
[61] Chikitshai Obohela Ain o Salish kendro
[62] Zahirul Huq, The Penal Code, 4th Edition 2001,
[63] ibid
[64] ibid
[65 ] Chikitshai Obohela, Ain O Salish Kendra, December,
[66] ibid
[67] ibid
[68] ibid
[69] ibid
[70] ibid
107
108




















