Maintenance strategies after first-line oxaliplatin plus fluoropyrimidine plus bevacizumab for...
15
www.thelancet.com/oncology Published online September 9, 2015 http://dx.doi.org/10.1016/S1470-2045(15)00042-X 1 Articles Lancet Oncol 2015 Published Online September 9, 2015 http://dx.doi.org/10.1016/ S1470-2045(15)00042-X See Online/Comment http://dx.doi.org/10.1016/ S1470-2045(15)00125-4 *Contributed equally. HOPE—Practice for Oncology, Hamburg, Germany (Prof S Hegewisch-Becker MD); Kliniken Maria Hilf GmbH, Department of Hematology, Oncology and Gastroenterology, Mönchengladbach, Germany (U Graeven MD); Practice for Oncology, Münster, Germany (C A Lerchenmüller MD); Lahn-Dill-Kliniken, Department of Hematology/ Oncology, Wetzlar, Germany (B Killing MD); Practice for Oncology, Gütersloh, Germany (R Depenbusch MD); MVZ Hematology/Oncology, Stade, Germany (C-C Steffens MD); KrankenhausNordwest, UCT University Cancer Center, Frankfurt, Germany (Prof S-E Al-Batran MD); AsklepiosKlinikum, Department for Hematology/ Oncology, Weißenfels, Germany (Prof T Lange MD); KlinikumBietigheim, Department of Gastroenterology/ Hematology/Oncology, Bietigheim-Bissingen, Germany (G Dietrich MD); Institut für Tumorgenetik, Bonn, Germany (Prof J Stoehlmacher MD); Institute for Pathology, Ruhr-University, Bochum, Germany (Prof A Tannapfel MD); St Joseph Hospital, Ruhr University, Bochum, Germany (Prof A Reinacher-Schick MD); University Medical Center Hamburg-Eppendorf, Maintenance strategies after first-line oxaliplatin plus fluoropyrimidine plus bevacizumab for patients with metastatic colorectal cancer (AIO 0207): a randomised, non-inferiority, open-label, phase 3 trial Susanna Hegewisch-Becker*, Ullrich Graeven*, Christian A Lerchenmüller, Birgitta Killing, Reinhard Depenbusch, Claus-Christoph Steffens, Salah-Eddin Al-Batran, Thoralf Lange, Georg Dietrich, Jan Stoehlmacher, Andrea Tannapfel, Anke Reinacher-Schick, Julia Quidde, Tanja Trarbach, Axel Hinke, Hans-Joachim Schmoll, Dirk Arnold Summary Background The definition of a best maintenance strategy following combination chemotherapy plus bevacizumab in metastatic colorectal cancer is unclear. We investigated whether no continuation of therapy or bevacizumab alone are non-inferior to fluoropyrimidine plus bevacizumab, following induction treatment with a fluoropyrimidine plus oxaliplatin plus bevacizumab. Methods In this open-label, non-inferiority, randomised phase 3 trial, we included patients aged 18 years or older with histologically confirmed, previously untreated metastatic colorectal cancer, Eastern Cooperative Oncology Group (ECOG) performance status of 0–2, adequate bone marrow, liver, and renal function, no pre-existing neuropathy greater than grade 1, and measurable disease, from 55 hospitals and 51 private practices in Germany. After 24 weeks of induction therapy with either fluorouracil plus leucovorin plus oxaliplatin or capecitabine plus oxaliplatin, both with bevacizumab, patients without disease progression were randomly assigned centrally by fax (1:1:1) to standard maintenance treatment with a fluoropyrimidine plus bevacizumab, bevacizumab alone, or no treatment. Both patients and investigators were aware of treatment assignment. Stratification criteria were response status, termination of oxaliplatin, previous adjuvant treatment with oxaliplatin, and ECOG performance status. At first progression, re-induction with all drugs of the induction treatment was a planned part of the protocol. Time to failure of strategy was the primary endpoint, defined as time from randomisation to second progression after maintenance (and if applicable re-induction), death, or initiation of further treatment including a new drug. Time to failure of strategy was equivalent to time to first progression for patients who did not receive re-induction (for any reason). The boundary for assessment of non-inferiority was upper limit of the one-sided 98·8% CI 1·43. Analyses were done by intention to treat. The study has completed recruitment, but follow-up of participants is ongoing. The trial is registered with ClinicalTrials.gov, number NCT00973609. Findings Between Sept 17, 2009, and Feb 21, 2013, 837 patients were enrolled and 472 randomised; 158 were randomly assigned to receive fluoropyrimidine plus bevacizumab, 156 to receive bevacizumab monotherapy, and 158 to receive no treatment. Median follow-up from randomisation is 17∙0 months (IQR 9∙5–25∙4). Median time to failure of strategy was 6∙9 months (95% CI 6∙1–8∙5) for the fluoropyrimidine plus bevacizumab group, 6∙1 months (5∙3–7∙4) for the bevacizumab alone group, and 6∙4 months (4∙8–7∙6) for the no treatment group. Bevacizumab alone was non-inferior to standard fluoropyrimidine plus bevacizumab (hazard ratio [HR] 1∙08 [95% CI 0·85–1∙37]; p=0∙53; upper limit of the one-sided 99·8% CI 1·42), whereas no treatment was not (HR 1∙26 [0∙99–1∙60]; p=0∙056; upper limit of the one-sided 99·8% CI 1·65). The protocol-defined re-induction after first progression was rarely done (30 [19%] patients in the fluoropyrimidine plus bevacizumab group, 67 [43%] in the bevacizumab monotherapy group, and 73 [46%] in the no treatment group. The most common grade 3 adverse event was sensory neuropathy (21 [13%] of 158 patients in the fluoropyrimidine plus bevacizumab group, 22 [14%] of 156 patients in the bevacizumab alone group, and 12 [8%] of 158 patients in the no treatment group). Interpretation Although non-inferiority for bevacizumab alone was demonstrated for the primary endpoint, maintenance treatment with a fluoropyrimidine plus bevacizumab may be the preferable option for patients following an induction treatment with a fluoropyrimidine, oxaliplatin, and bevacizumab, as it allows the planned discontinuation of the initial combination without compromising time with controlled disease. Only a few patients were exposed to re-induction treatment, thus deeming the primary endpoint time to failure of strategy non-informative and clinically irrelevant. Progression-free survival and overall survival should be considered primary endpoints in future trials exploring maintenance strategies. Funding RochePharma AG and AIO Studien gGmbH.
-
Upload
wolfgang-maier -
Category
Documents
-
view
3 -
download
0
Transcript of Maintenance strategies after first-line oxaliplatin plus fluoropyrimidine plus bevacizumab for...

www.thelancet.com/oncology Published online September 9, 2015 http://dx.doi.org/10.1016/S1470-2045(15)00042-X 1
Articles
Lancet Oncol 2015
Published OnlineSeptember 9, 2015http://dx.doi.org/10.1016/S1470-2045(15)00042-X
See Online/Commenthttp://dx.doi.org/10.1016/S1470-2045(15)00125-4
*Contributed equally.
HOPE—Practice for Oncology, Hamburg, Germany (Prof S Hegewisch-Becker MD); Kliniken Maria Hilf GmbH, Department of Hematology, Oncology and Gastroenterology, Mönchengladbach, Germany (U Graeven MD); Practice for Oncology, Münster, Germany (C A Lerchenmüller MD); Lahn-Dill-Kliniken, Department of Hematology/Oncology, Wetzlar, Germany (B Killing MD); Practice for Oncology, Gütersloh, Germany (R Depenbusch MD); MVZ Hematology/Oncology, Stade, Germany (C-C Steff ens MD); KrankenhausNordwest, UCT University Cancer Center, Frankfurt, Germany (Prof S-E Al-Batran MD); AsklepiosKlinikum, Department for Hematology/Oncology, Weißenfels, Germany (Prof T Lange MD); KlinikumBietigheim, Department of Gastroenterology/Hematology/Oncology, Bietigheim-Bissingen, Germany (G Dietrich MD); Institut für Tumorgenetik, Bonn, Germany (Prof J Stoehlmacher MD); Institute for Pathology, Ruhr-University, Bochum, Germany (Prof A Tannapfel MD); St Joseph Hospital, Ruhr University, Bochum, Germany (Prof A Reinacher-Schick MD); University Medical Center Hamburg-Eppendorf,
Maintenance strategies after fi rst-line oxaliplatin plus fl uoropyrimidine plus bevacizumab for patients with metastatic colorectal cancer (AIO 0207): a randomised, non-inferiority, open-label, phase 3 trialSusanna Hegewisch-Becker*, Ullrich Graeven*, Christian A Lerchenmüller, Birgitta Killing, Reinhard Depenbusch, Claus-Christoph Steff ens, Salah-Eddin Al-Batran, Thoralf Lange, Georg Dietrich, Jan Stoehlmacher, Andrea Tannapfel, Anke Reinacher-Schick, Julia Quidde, Tanja Trarbach, Axel Hinke, Hans-Joachim Schmoll, Dirk Arnold
SummaryBackground The defi nition of a best maintenance strategy following combination chemotherapy plus bevacizumab in metastatic colorectal cancer is unclear. We investigated whether no continuation of therapy or bevacizumab alone are non-inferior to fl uoropyrimidine plus bevacizumab, following induction treatment with a fl uoropyrimidine plus oxaliplatin plus bevacizumab.
Methods In this open-label, non-inferiority, randomised phase 3 trial, we included patients aged 18 years or older with histologically confi rmed, previously untreated metastatic colorectal cancer, Eastern Cooperative Oncology Group (ECOG) performance status of 0–2, adequate bone marrow, liver, and renal function, no pre-existing neuropathy greater than grade 1, and measurable disease, from 55 hospitals and 51 private practices in Germany. After 24 weeks of induction therapy with either fl uorouracil plus leucovorin plus oxaliplatin or capecitabine plus oxaliplatin, both with bevacizumab, patients without disease progression were randomly assigned centrally by fax (1:1:1) to standard maintenance treatment with a fl uoropyrimidine plus bevacizumab, bevacizumab alone, or no treatment. Both patients and investigators were aware of treatment assignment. Stratifi cation criteria were response status, termination of oxaliplatin, previous adjuvant treatment with oxaliplatin, and ECOG performance status. At fi rst progression, re-induction with all drugs of the induction treatment was a planned part of the protocol. Time to failure of strategy was the primary endpoint, defi ned as time from randomisation to second progression after maintenance (and if applicable re-induction), death, or initiation of further treatment including a new drug. Time to failure of strategy was equivalent to time to fi rst progression for patients who did not receive re-induction (for any reason). The boundary for assessment of non-inferiority was upper limit of the one-sided 98·8% CI 1·43. Analyses were done by intention to treat. The study has completed recruitment, but follow-up of participants is ongoing. The trial is registered with ClinicalTrials.gov, number NCT00973609.
Findings Between Sept 17, 2009, and Feb 21, 2013, 837 patients were enrolled and 472 randomised; 158 were randomly assigned to receive fl uoropyrimidine plus bevacizumab, 156 to receive bevacizumab monotherapy, and 158 to receive no treatment. Median follow-up from randomisation is 17∙0 months (IQR 9∙5–25∙4). Median time to failure of strategy was 6∙9 months (95% CI 6∙1–8∙5) for the fl uoropyrimidine plus bevacizumab group, 6∙1 months (5∙3–7∙4) for the bevacizumab alone group, and 6∙4 months (4∙8–7∙6) for the no treatment group. Bevacizumab alone was non-inferior to standard fl uoropyrimidine plus bevacizumab (hazard ratio [HR] 1∙08 [95% CI 0·85–1∙37]; p=0∙53; upper limit of the one-sided 99·8% CI 1·42), whereas no treatment was not (HR 1∙26 [0∙99–1∙60]; p=0∙056; upper limit of the one-sided 99·8% CI 1·65). The protocol-defi ned re-induction after fi rst progression was rarely done (30 [19%] patients in the fl uoropyrimidine plus bevacizumab group, 67 [43%] in the bevacizumab monotherapy group, and 73 [46%] in the no treatment group. The most common grade 3 adverse event was sensory neuropathy (21 [13%] of 158 patients in the fl uoropyrimidine plus bevacizumab group, 22 [14%] of 156 patients in the bevacizumab alone group, and 12 [8%] of 158 patients in the no treatment group).
Interpretation Although non-inferiority for bevacizumab alone was demonstrated for the primary endpoint, maintenance treatment with a fl uoropyrimidine plus bevacizumab may be the preferable option for patients following an induction treatment with a fl uoropyrimidine, oxaliplatin, and bevacizumab, as it allows the planned discontinuation of the initial combination without compromising time with controlled disease. Only a few patients were exposed to re-induction treatment, thus deeming the primary endpoint time to failure of strategy non-informative and clinically irrelevant. Progression-free survival and overall survival should be considered primary endpoints in future trials exploring maintenance strategies.
Funding RochePharma AG and AIO Studien gGmbH.

Articles
2 www.thelancet.com/oncology September 9, 2015 http://dx.doi.org/10.1016/S1470-2045(15)00042-X
Department of Oncology, Haematology, Bone Marrow
Transplantation with Section Pneumology; Hubertus Wald
Tumorzentrum, University Hospital Eppendorf, Hamburg,
Germany (J Quidde MD); iOMEDICO AG, Freiburg,
Germany (T Trarbach MD); WiSP Wissenschaftlicher Service
Pharma GmbH, Langenfeld, Germany (A Hinke PhD);
Department of Hematology/Oncology, University Hospital,
Halle (Saale), Germany (Prof H-J Schmoll MD); and Klinik für Tumorbiologie,
Freiburg, Germany (Prof D Arnold MD)
Correspondence to:Prof Susanna Hegewisch-Becker,
HOPE—Practice for Oncology, Eppendorfer Landstrasse 42,
20249 Hamburg, [email protected]
IntroductionThe defi nition of an optimum duration of fi rst-line treatment for metastatic colorectal cancer is complex; treatment duration correlates with cumulative toxicity, potentially impairing quality of life and increasing treatment cost, but longer duration of treatment is associated with a longer progression-free survival and potentially increases overall survival.1
Since the establishment of standard combination chemotherapy regimens, diff erent treatment strategies have been explored, including those with a combination treatment used as induction followed by a planned de-escalation of at least part of the chemotherapy backbone, treatment-free drug holidays, or so-called stop-and-go strategies (intermittent treatment with all drugs). For oxaliplatin-containing regimens, the sequence defi nition is of high importance because of the dose-related cumulative occurrence of neuropathy. Use of a fl uoropyrimidine as single drug maintenance following an oxaliplatin plus fl uoropyrimidine combination was established as a result of the OPTIMOX trials.2,3
The addition of bevacizumab to a fl uoropyrimidine plus oxaliplatin combination resulted in a prolongation of progression-free survival in a pivotal phase 3 trial.4
However, this strategy will increase the cumulative dose of oxaliplatin, and therefore neurotoxicity, if it is continuously administered. Therefore, the continued administration of fl uoropyrimidines plus bevacizumab until progression, while withholding oxaliplatin, was the protocol-defi ned standard. Although the median treatment duration in this trial was only about 6 months, the patient subgroup that
followed this per-protocol management suggestion showed a longer progression-free survival.4
We aimed to investigate whether after a 24-week standard induction with any fl uoropyrimidine in combination with oxaliplatin and bevacizumab, either a complete treatment stop or the continuation with bevacizumab as a single drug were non-inferior to the standard arm, which was continuation of any fl uoropyrimidine plus bevacizumab.
MethodsStudy design and participantsIn this open-label, randomised, multicentre phase 3 trial (AIO 0207), patients were eligible if they had histologically confi rmed adenocarcinoma of the colon or rectum with at least one measurable metastatic lesion according to Response Evaluation Criteria in Solid Tumors (RECIST; version 1.1); were aged 18 years or older; had an Eastern Cooperative Oncology Group (ECOG) performance status of 0–2; adequate renal, hepatic, and haematological function; an estimated life expectancy of greater than 3 months; no previous therapy with bevacizumab; and no previous chemotherapy for metastatic colorectal cancer, unless it was previous neoadjuvant chemotherapy that was fi nished more than 6 months before starting study treatment.
Patients were ineligible if they had previously received anti-angiogenic therapy; inadequately controlled hyper-tension; a serious non-healing wound or active ulcer; a history of nephrotic syndrome, hypertensive crisis, hypertensive encephalopathy, bleeding diathesis, clinically relevant coagulopathy, or grade 3 or 4 venous
Research in context
Evidence before this studyThroughout the writing process and most recently on April 1, 2015, we searched PubMed for articles published in English and ClinicalTrials.gov for any phase 3 trials, and congress abstracts from the yearly meetings of the American Society of Clinical Oncology and the European Society for Medical Oncology (without restriction in publication dates). Search terms were “colorectal cancer”, “maintenance therapy”, and “bevacizumab”. Planned de-escalation as a part of a treatment strategy has been investigated in other advanced colorectal cancer trials. Our search identifi ed fi ve phase 3 trials, none of which are using athree-arm design or similar trial concept.However, in view of the heterogeneity in initial treatment combinations, de-escalation strategies (including defi nition of the de-escalation before treatment start, maintenance therapy with parts of the induction therapy, and drug holidays), and clinical endpoints, these studies did not allow defi nitive conclusions regarding standard maintenance options.
Added value of this studyTo our knowledge, this study provides mature data for the largest registered cohort so far, and is the only trial comparing
standard de-escalation to a fl uoropyrimidine plus bevacizumab combination with two other de-escalation maintenance strategies. The timepoint of randomisation (after induction) and the limitation of maintenance to patients suitable for this approach develops the “induction–maintenance” concept as a new treatment paradigm with maintenance as a stand-alone treatment line. Furthermore, to our knowledge, it is the only trial investigating RAS/RAF mutational status in this setting.
Implications of all the available evidenceWe noted no clinically meaningful diff erences in time to failure of strategy between treatment groups. Acceptance of the strategy of immediate re-induction after fi rst progression was low and this should be considered when designing future trials. Any active treatment during maintenance resulted in signifi cant prolongation of progression-free survival compared with that for no treatment. This is in concordance with other randomised trials for de-escalation maintenance after induction with combination chemotherapy and bevacizumab. Median overall survival was acceptable in all groups, suggesting that within the context of further treatment options, diff erent maintenance strategies following induction do not compromise overall survival.

Articles
www.thelancet.com/oncology Published online September 9, 2015 http://dx.doi.org/10.1016/S1470-2045(15)00042-X 3
thromboembolism; a history of myocardial infarction, unstable angina, signifi cant vascular disease, gastro-intestinal perforation, abdominal fi stula, intra-abdominal abscess, or active gastrointestinal bleeding within 6 months preceding study treatment; a major surgical procedure within 28 days preceding study treatment with the only exception of a high tumour load in case of synchronous metastases in just resected colorectal cancer (in such a case, treatment could be initiated as early as 2 weeks after surgery without addition of bevacizumab at the fi rst and eventually second administration); evidence of spinal cord compression or brain metastases; pre-existing peripheral neuropathy greater than grade 1; or known dihydropyrimidine dehydrogenase defi ciency. Patients were also ineligible if they had inadequate bone marrow function (absolute neutrophil count <1·5 × 10⁹ cells per L, platelet count <100 × 10⁹ platelets per L, or haemoglobin <90 g/L [transfusion or approved haemopoietic growth factors allowed]), hepatic function (serum total bilirubin >1·5 × institution upper limit of normal [ULN], aspartate aminotransferase and alanine aminotransferase >2·5 × ULN or >5 × ULN for patients with liver metastases), renal function (serum creatinine concentration >1·5 × ULN, creatinine clearance <50 mL/min calculated according to Cockcroft-Gault equation, urine dipstick for proteinuria greater than 1 + unless 24-h urine collection showed ≤1 g protein), or coagulation parameters (international normalised ratio >1·5 except for patients receiving anticoagulation treatment at a stable dose for ≥2 weeks and with coagulation monitoring within local therapeutic limits, activated partial thromboplastin time >1·5 × ULN within 7 days before the fi rst study dose).
All patients provided written informed consent. The study was done in full accordance with Good Clinical Practice guidelines and the Declaration of Helsinki. Independent ethics committees at all participating sites approved the protocol and all modifi cations. An independent data monitoring committee undertook ongoing review of all safety data and effi cacy.
Randomisation and maskingEligible patients were registered for the trial before starting an induction treatment with any fl uoropyrimidine (infusional fl uoropyrimidine or capecitabine), oxaliplatin, and bevacizumab; choice of a standard protocol (ie, FOLFOX, capecitabine plus oxaliplatin and bevacizumab [ for treatment protocols see appendix]) was at the treating physician’s discretion. Those patients without progression and without option for resection after 24 weeks were centrally randomly assigned (1:1:1) to either the standard maintenance group with any fl uoropyrimidine and bevacizumab, the bevacizumbab alone group, or the no treatment group (fi gure 1).
The randomisation result was retrieved for every individual patient via an online system (iOMINT randomisation version 1.2; iOMEDICO, Freiburg, Germany; WiSP, Langenfeld, Germany), which assured
concealment. The treatment allocation was done with a standard minimisation algorithm implementing a random component. Stratifi cation factors at the time of randomisation were stable disease versus partial or complete response; treatment with oxaliplatin stopped (eg, due to neurotoxicity) before termination of induction treatment versus oxaliplatin ongoing until end of induction phase; previous adjuvant treatment with oxaliplatin versus adjuvant treatment without oxaliplatin versus no adjuvant treatment; and ECOG performance status 0–1 versus 2.
Participants, investigators, the radiologists assessing the outcome, and the statistician were not masked to group assignment.
ProceduresAt registration, investigators selected the induction chemotherapy from prespecifi ed standard protocols of fl uoropyrimidines with oxaliplatin plus bevacizumab. Investigators assessed tumour response by CT or MRI scans at weeks 12 and 23 according to RECIST version 1.0. Randomised patients received continuation of any fl uoropyrimidine (either via infusion every 2 weeks [appendix pp 26–28]; or capecitabine every 3 weeks in standard dosages [appendix pp 26–28]; the fl uoropyrimidine could be changed between induction and maintenance treatment) plus bevacizumab (7∙5 mg/kg every 3 weeks, or 5 mg/kg every 2 weeks), bevacizumab alone (same doses), or no treatment.
Maintenance treatment was continued until disease progression, unacceptable toxicity, surgical resection, other ablative treatment, at patient’s request, or physician’s decision. If either bevacizumab or the fl uoropyrimidine was discontinued before progression the other drug was continued as monotherapy in the fl uoropyrimidine plus bevacizumab group.
Figure 1: Treatment schedules*Any fl uoropyrimidine in a standard protocol (see appendix pp 26–28 for details). †Time to failure of strategy=times to fi rst progression for patients not receiving re-induction.
Fluoropyrimidine*plus bevacizumabplus oxaliplatin
Fluoropyrimidine*plus bevacizumab
Any fluoropyrimidine*+/– bevacizumab+/– oxaliplatin
Bevacizumab
No treatment
Progression-free survival
Enrolment
1st p
rogr
essio
n
2nd
prog
ress
ion
Induction 24 weeks
Re-induction
Maintenance:non-progressivedisease
Time to failure of strategy
Time to failure of strategy†
Randomisation
Patients with complete response,partial response,or stable disease
See Online for appendix

Articles
4 www.thelancet.com/oncology September 9, 2015 http://dx.doi.org/10.1016/S1470-2045(15)00042-X
At fi rst progression, re-induction with at least part of the induction treatment (addition of oxaliplatin in the fl uoropyrimidine plus bevacizumab group; addition of fl uoropyrimidine and oxaliplatin in the bevacizumab alone group; and re-induction of all drugs for the no treatment group; appendix 26–28) was protocol-defi ned. Re-induction included all drugs that were components of the initial treatment except for those that could not be used because of persistent toxicity or contraindications.
Dose modifi cations of chemotherapy during induction, maintenance, and re-induction were allowed according to protocol-defi ned criteria. No recommendations to reduce the bevacizumab dose were made, although treatment could be delayed in the event of related grade 3 toxicities. A full set of dose modifi cation criteria is provided in the appendix (p 4).
During the maintenance and re-induction phases, CT or MRI scans and a standard clinical laboratory work-up were done every 6 weeks. A consistent imaging technique was used throughout the study for every patient. Laboratory assessments were done locally. Adverse events were recorded continuously from registration to the end of the fi nal study visit and were classifi ed and graded according to the National Cancer Institute Common Terminology Criteria for Adverse Events (NCI CTCAE) version 3.0.
Patient-reported outcomes were assessed with the European Organisation for Research and Treatment of Cancer (EORTC) Quality of Life Questionnaire-C30 (version 3), the colorectal cancer module EORTC CR29, and other instruments, to be completed at screening and then every 6 weeks during the induction and maintenance phase to a minimum of 24 weeks after randomisation independently from treatment and response. Questionnaires were answered at home strictly every 6 weeks independently from treatment delay, treatment change or response assessment, also beyond treatment failure. Sending and collecting the questionnaires was organised centrally by an independent site management organisation of the clinical research organisation. Detailed patient-reported outcome results will be reported separately.
Patients could withdraw from the trial at any time or be withdrawn at the discretion of the investigator if detrimental adverse events occurred. Patients could also be withdrawn for protocol violations, withdrawal of consent after start of induction, and loss to follow-up, and for administrative or safety reasons.
Central pathology testing was done by the Institute for Pathology (Ruhr-University Bochum, Germany). For mutational analysis of KRAS, NRAS, and BRAF, formalin-fi xed paraffi n-embedded tissue was microdissected and sectioned. DNA was extracted with a DNA Purifi cation Kit (Promega, Madison, WI, USA). Mutational analysis for all three genes was done stepwise using a pyrosequencing technique (Q24; Qiagen, Hilden, Germany). The mutation status of KRAS codons 12 and 13 was determined in step 1, and the mutation status of NRAS codons 59, 61, 117, and 146, and mutation hotspots in exons 2–4 were analysed in step 2 (p.G12, p.G13, p.A59, p.Q61, p.K117, and p.A146). For BRAF, we assessed the V600E mutation.
OutcomesTime to failure of strategy was chosen as the primary endpoint because the de-escalation of an induction treatment combination does not imply that the patient is refractory to this strategy, and they could be retreated with all components of the initial combination (re-induction) after fi rst progression. As discontinuation of active compounds before progression could result in a shorter time to fi rst progression, but also preserve the option of a re-induction of the active component, re-induction was
Figure 2: Trial profi le*Violation of major selection criteria: palliative pretreatment; interval since adjuvant chemotherapy too short; no evaluable metastatic lesion; inappropriate diagnostic procedures; major delay after end of induction; high GOT >5 × UNL or bilirubin >1·5 × UNL; or previous other malignancy.
158 received fluoropyrimidineplus bevacizumab
147 assessed for time to failureof strategy and progression-free survival anaylsis
156 assessed for overall survivalanalysis
156 received bevacizumabmonotherapy
472 eligible and randomised
825 eligible and started induction
837 selected
12 major protocol violations*
15 excluded due to late retractions(eg, consent withdrawn)
852 assessed for eligibility
153 assessed for time to failureof strategy and progression-free survival analysis
156 assessed for overall survivalanalysis
158 received no treatment
353 not randomised128 progression
44 metastatic resection52 unacceptable toxicity54 serious adverse events51 patient’s wish33 investigator decision29 death22 other
More than one reason could be reported
154 assessed for time to failureof strategy and progression-free survival anaylsis
158 assessed for overall survivalanalysis

Articles
www.thelancet.com/oncology Published online September 9, 2015 http://dx.doi.org/10.1016/S1470-2045(15)00042-X 5
part of the treatment strategy. Therefore, time to failure of strategy represents the clinically relevant period from randomisation to the start of a real second-line treatment, including at least one new drug.5,6 Time to failure of strategy was defi ned as time from randomisation to either: second progression (after maintenance and re-induction after fi rst progression); the beginning of another treatment (including a new drug) for any reason; no further treatment after fi rst progression; or death. Metastasis resection events were not included within the defi nition of treatment failure. Time to failure of strategy was regarded as equal to progression-free survival if patients did not receive re-induction (for any reason).
Secondary endpoints among others included were time to failure of strategy from enrolment, progression-free survival (time to disease progression or death from any cause), and overall survival (time to death from any cause) from randomisation and from enrolment (appendix p 16). We assessed reasons for discontinuation of treatment, safety (NCI CTCAE version 3.0), and quality of life (diff erence between treatment groups in the mean value of the general health status and quality of life score). Preplanned exploratory subgroup analyses included the eff ect of oxaliplatin dose reduction, response to induction treatment, and RAS mutational status on time to fi rst progression, progression-free survival, and overall survival.
Statistical analysisTwo primary hypotheses were independently assessed: (1) the non-inferiority of no treatment versus the standard maintenance (fl uoropyrimidine plus bevacizumab), and (2) the non-inferiority of bevacizumab alone versus standard maintenance with time to failure of strategy as the primary outcome parameter. The non-inferiority design was chosen because at the time the study was designed, active maintenance refl ected common practice, as it had been used in the pivotal NO16966 trial4 and was therefore regarded as a standard.
Due to multiple group comparisons, the one-sided type I error level was adjusted to 1·25%, according to Bonferroni and provided 1·43 as the upper limit of the one-sided 98·8% CI as the decisive boundary for the assessment of non-inferiority. A third formal hypothesis, comparing the bevacizumab alone group with the no treatment group for superiority, was to be assessed, hierarchically ordered, if and only if both null hypotheses of inferiority had been rejected. To confi rm non-inferiority, based on a clinically irrelevant diff erence in time to failure of strategy of less than 1·5 months (ie, assumed 5 months in fl uoropyrimidine plus bevacizumab group vs 3∙5 months in the bevacizumab alone group or the no treatment group), corresponding to a hazard ratio [HR] of 1∙43, a total of 448 events had to be occur to achieve a power of 80%.
Protocol-defi ned interim analyses were done after the observation of 100 and 200 events, based on a group
sequential design to be able to stop the trial in case of early proven superiority of the standard group. Further exploratory analyses were done after closure of randomisation and when at least 90% of the patients had completed protocol-defi ned treatment. As of Oct 12, 2014, it became evident that the expected number of time to failure of strategy events could not be reached within a reasonable timeframe because of losses to follow-up and an overall more favourable disease course than anticipated. Therefore, the steering committee decided
Fluoropyrimidine plus bevacizumab (n=158)
Bevacizumab (n=156)
No treatment (n=158)
Age (years) 64 (25–82) 65 (32–82) 66 (32–82)
Sex
Male 106 (67%) 106 (68%) 99 (63%)
Female 52 (33%) 50 (32%) 59 (37%)
ECOG performance score
0–1 151 (96%) 150 (96%) 151 (96%)
2 7 (4%) 6 (4%) 7 (4%)
Site
Colon 102 (65%) 95 (61%) 100 (63%)
Rectum 56 (35%) 61 (39%) 58 (37%)
Number of metastatic sites
1 71 (45%)* 68 (44%) 60 (38%)*
>1 86 (54%)* 88 (56%) 97 (61%)*
LDH
Normal 68 (43%) 79 (51%) 88 (56%)
Abnormal 70 (44%) 59 (38%) 55 (35%)
Not reported 20 (13%) 18 (12%) 15 (9%)
CEA at registration (ng/mL) 46 (6·9–170·9) 55 (13·2–615·2) 80 (12·7–477·9)
CEA at randomisation (ng/mL) 4·8 (2·4–15·0) 6·7 (3·0–34·2) 10·1 (3·6–39·7)
Stage of disease
Synchronous 126 (80%) 129 (83%) 131 (83%)
Metachronous 32 (20%) 27 (17%) 27 (17%)
Previous (neo)adjuvant chemotherapy 19 (12%) 18 (12%) 16 (10%)
Primary tumour resected 118 (75%) 120 (77%) 111 (70%)
Synchronous, resected 86/126 (68%) 93/129 (72%) 84/131 (64%)
Oxaliplatin dose <75% of plan 40 (25%) 42 (27%) 41 (26%)
Best response to induction treatment
Stable disease 64 (41%) 63 (40%) 65 (41%)
Partial or complete response 94 (59%) 93 (60%) 93 (59%)
Induction regimen plus bevacizumab
FOLFOX4 52 (33%) 49 (31%) 49 (31%)
FOLFOX4 modifi ed 26 (16%) 30 (19%) 36 (23%)
FOLFOX4 simplifi ed 12 (8%) 16 (10%) 12 (8%)
FOLFOX6 32 (20%) 32 (21%) 34 (22%)
FOLFOX7 modifi ed 3 (2%) 2 (1%) 4 (3%)
CAPOX 8 (5%) 9 (6%) 2 (1%)
XELOX 25 (16%) 18 (12%) 21 (13%)
Data are median (range), n (%), or median (IQR), unless otherwise indicated. For treatment protocols, please see appendix pp 26–28. *In one patient of each, the available information was insuffi cient for a valid categorisation. ECOG=Eastern Cooperative Oncology Group. LDH=lactate dehydrogenase. CEA=carcinoembryonic antigen.
Table 1: Baseline characteristics

Articles
6 www.thelancet.com/oncology September 9, 2015 http://dx.doi.org/10.1016/S1470-2045(15)00042-X
to close the database for the fi nal analysis (except overall survival) on Dec 20, 2014.
The primary hypotheses were evaluated with HRs and corresponding one-sided CIs derived from Cox proportional hazard models. In general, the log-rank test and Cox regression were used for time-to-event endpoints estimated with Kaplan-Meier curves, which were also used in subgroup and prognostic analyses. The t test was applied for group comparisons of quality-of-life data. All effi cacy analyses were based on the intent-to-treat population. Quality-of-life analysis was based on the randomised population who had at least one evaluable questionnaire during maintenance treatment. Except for the prospectively defi ned hypotheses, all p values shown are two-sided. Within the framework of exploratory analyses, p values of less than 0·05 was termed as signifi cant.
Data were analysed with SPlus (version 6.2), R (version 3), and Testimate (version 6.5).
The trial is registered with ClinicalTrials.gov, number NCT00973609.
Role of the funding sourceThe legal funder according to German regulations (Arzneimittelgesetz) is the AIO Studien gGmbH (Berlin, Germany). The AIO Studien gGmbH funded the trial and supplied human resources and administrative support. Roche Pharma AG provided the study drug and supported the trial through a clinical research grant awarded to AIO-Studien-gGmbH. Randomisation, monitoring, and data management and analysis were provided by a contract research organisation (iOMEDICO, Freiburg, Germany; WiSP, Langenfeld, Germany). The fi nancial supporters of the study had no role in study design, data collection, data analysis, data interpretation, or preparation of the clinical study report. The funder and Roche Pharma AG reviewed the manuscript before journal submission. SH-B, UG, AH, TT, and DA had full access to all the data. The corresponding author had the fi nal responsibility to submit for publication.
ResultsBetween Sept 17, 2009, and Feb 21, 2013, 837 patients were enrolled from 106 German institutions (55 hospitals and 51 private practices; appendix). Of those, 472 were randomised and eligible for maintenance treatment (fi gure 2): 158 received fl uoropyrimidine plus bevacizumab, 156 received bevacizumab monotherapy, and 158 received no treatment.
Stratifi cation parameters and patient characteristics were balanced between the treatment groups (table 1). At the time of this analysis, median follow-up from randomisation was 17∙0 months (IQR 9∙5–25∙4). 13 patients are still on treatment; six in maintenance phase and seven in re-induction phase. Median time to failure of strategy from randomisation was 6∙5 months (95% CI 5∙9–7∙2) for all
Figure 3: Kaplan-Meier estimates of time to failure of strategy (A), progression-free survival (B), and overall survival (C) from randomisation by treatment group
Number at riskFluoropyrimidineplus bevacizumab
Bevacizumab aloneNo treatment
Fluoropyrimidine plus bevacizumabBevacizumab aloneNo treatment
129145145
Events Median (95% CI)
6·9 months6·1 months6·4 months
(6·1–8·5)(5·3–7·4)(4·8–7·6)
147
153154
83
7777
38
3634
15
2414
7
14 4
5
92
2
51
1
10
147
153154
76
5340
34
246
14
152
6
101
4
71
1
31
1
10
156
156158
129
147141
113
119113
85
9686
59
7061
35
4938
26
2727
12
1414
6
86
6
32
0
01
0
20
40
60
80
100
Tim
e to
failu
re o
f str
ateg
y (%
)
Number at riskFluoropyrimidineplus bevacizumab
Bevacizumab aloneNo treatment
0
20
40
60
80
100
Prog
ress
ion-
free
surv
ival
(%)
Number at riskFluoropyrimidineplus bevacizumab
Bevacizumab aloneNo treatment
0
20
40
60
80
100
Ove
rall
surv
ival
(%)
0 5 10 15 20 25 30Months from randomisation
35 40 45 50 55
0 3
Log-rank test: p=0·13
Log-rank test: p<0·0001
Log-rank test: p=0·77
6 9 12 15 18 21 24 27 30 33 36 39 42 45
0 3 6 9 12 15 18 21 24 27 30 33 36 39 42 45
Fluoropyrimidine plus bevacizumabBevacizumab aloneNo treatment
131149150
Events Median (95% CI)
6·3 months4·6 months3·5 months
(5·8–7·6)(4·0–5·3)(2·9–4·1)
Fluoropyrimidine plus bevacizumabBevacizumab aloneNo treatment
98104
91
Events Median (95% CI)
20·2 months21·9 months23·1 months
(17·7–24·3)(18·7–26·9)(19·2–27·3)
A
B
C

Articles
www.thelancet.com/oncology Published online September 9, 2015 http://dx.doi.org/10.1016/S1470-2045(15)00042-X 7
patients and 6∙9 months (95% CI 6·1–8·5) in the fl uoropyrimidine plus bevacizumab group, 6∙1 months (5·3–7·4) in the bevacizumab alone group, and 6∙4 months (4·8–7·6) in the no treatment group (fi gure 3A). The pairwise comparison of each of the experimental groups to the standard fl uoropyrimidine plus bevacizumab group shows that for the bevacizumab alone group, non-inferiority can be claimed (HR 1∙08 [95% CI 0∙85–1∙37]; p=0∙53). After adjustment of the α error level the upper limit of the one-sided 98·8% CI of 1·42 did not exceed the predefi ned boundary. By contrast, the no treatment group failed to show non-inferiority to the standard treatment as the upper level of non-inferiority exceeded the predefi ned decisive boundary (HR 1∙26 [95% CI 0∙99–1∙60]; p=0∙056; upper limit of one-sided 98∙8% CI 1∙65). Median time to failure of strategy from enrolment was 12·4 months (95% CI 11·5–13·8) in the fl uoropyrimidine plus bevacizumab group, 11·4 months (10·6–12·9) in the bevacizumab alone group, and 11·6 months (10·1–12·9) in the no treatment group.
170 (36%) of 472 patients underwent a re-induction treatment after maintenance treatment. The proportion was lower in the fl uoropyrimidine plus bevacizumab group (30 [19%] of 158) than in both the experimental groups (67 [43%] of 156 in the bevacizumab alone group and 73 [46%] of 158 in the no treatment group). Reasons for not proceeding to re-induction were heterogeneous, with patient’s and investigator’s decision being the most frequent (table 2).
Progression-free survival from randomisation is shown in fi gure 3B and median time to fi rst progression was 4∙5 months (95% CI 4∙1–5∙2) for all patients. The pairwise comparison between treatment groups showed signifi cantly better progression-free survival in the more active group in each comparison: bevacizumab alone versus fl uoropyrimidine plus bevacizumab (HR 1∙34 [95% CI 1∙06–1∙70]; p=0∙015); no treatment versus fl uoropyrimidine plus bevacizumab (HR 2∙09 [95% CI 1∙64–2∙67]; p<0∙0001); and no treatment versus bevacizumab alone (HR 1∙45 [95% CI 1∙15–1∙82]; p=0∙0018).
From enrolment, median time to fi rst progression for all patients was 10 months (95% CI 9·6–10·6). Median time to fi rst progression was 11∙7 months (95% CI 10∙8–13∙2) for the fl uoropyrimidine plus bevacizumab group, 10∙0 months (9∙4–10∙6) for the bevacizumab alone group, and 9·0 months (8∙4–9∙6) for the no treatment group.
Overall survival data have low power, and an update is planned. With 293 (62%) events available to date, median overall survival was 21∙9 months (95% CI 19∙8–23∙8) from randomisation, without relevant diff erences between treatment groups (global log-rank test p=0∙76; fi gure 3C).
Analyses of pre-planned exploratory subgroups including demographics, laboratory results, and disease-related or treatment-related characteristics were restricted to time to fi rst progression (fi gures 4–6) and
overall survival (appendix pp 1–3) endpoints, because the low re-induction rates meant that the time to failure of strategy endpoint was non-informative.
Response to induction treatment at randomisation (complete or partial response vs stable disease) was a prognostic factor for both time to fi rst progression (5∙0 vs 4∙0 months; p=0∙016) and overall survival (23∙7 vs 8∙5 months; p=0∙00033) in a univariate analysis. In the subgroup analyses, the diff erences in time to fi rst progression between the randomisation groups remained signifi cantly diff erent both in patients with complete and partial responses (p<0∙0001) and those with stable disease (p=0∙0030) as best response in a univariate analysis.
Subgroup analyses according to other prognostic factors or patient characteristics (fi gures 4–6; appendix pp 1–3) did not show major diff erences to the progression-free and overall survival fi ndings in the total population.
Results for all RAS (KRAS exons 2, 3 and 4, and NRAS exons 2, 3, and 4) and BRAF (V600E) mutations were available for 565 (68%) of all 825 registered patients, of whom 221 (39%) had no mutation (all wild-type), 291 (52%) had any RAS mutation, and 53 (9%) had a BRAF mutation (table 3). The frequency of specifi c RAS mutations in our study was as follows (based on the 565 patients for which RAS analysis was available): KRAS exon 3: 13 (2%), KRAS exon 4: 17 (3%), NRAS exon 2: 14 (3%), NRAS exon 3: 12 (2%), and NRAS exon 4: none. The distribution of mutation frequencies in randomised patients was balanced between treatment groups (table 3).
Patients with RAS/RAF mutations showed a signifi cantly shorter median time to fi rst progression: 6∙0 months (95% CI 4∙5–7∙1) for patients with wild-type tumours, 4∙3 months (4∙0–5∙8) for patients with any RAS mutation, and 3∙9 months (3∙2–4∙8) for patients with a BRAF mutation (p<0·0001, log-rank test, overall comparison). Overall survival was signifi cantly diff erent for patients with diff erent RAS/RAF mutational status: median overall survival for patients with wild-type
Fluoropyrimidine plus bevacizumab (n=125)
Bevacizumab (n=89)
No treatment (n=83)
Investigator decision 25 (20%) 25 (28%) 20 (24%)
Patient wish, informed consent, withdrawn, or non-compliance
25 (20%) 15 (17%) 17 (20%)
Neuropathy 14 (11%) 13 (15%) 11 (13%)
Death 12 (10%) 7 (8%) 7 (8%)
Tumour resection 10 (8%) 4 (4%) 8 (10%)
Adverse event other than neuropathy 4 (3%) 7 (8%) 3 (4%)
Oxaliplatin intolerance 3 (2%) 1 (1%) 3 (4%)
Local therapy 5 (4%) 2 (2%) 2 (2%)
Other 27 (22%) 15 (17%) 12 (14%)
Data are n (%).
Table 2: Reasons for not proceeding to re-induction

Articles
8 www.thelancet.com/oncology September 9, 2015 http://dx.doi.org/10.1016/S1470-2045(15)00042-X
tumours, those with RAS mutations, and those with BRAF mutations was 28∙4 months (95% CI 24∙0–31∙7), 20∙3 months (18∙8–24∙9), and 9∙4 months (5∙3–17∙8), respectively (p<0∙0001).
Patients with wild-type RAS/RAF status in the bevacizumab alone and fl uoropyrimidine plus bevacizumab groups had longer time to fi rst progression compared with those in the no treatment
group (fi gure 7A), whereas patients with tumours carrying any RAS or RAF mutation, time to fi rst progression was longer in patients in the doublet treatment group compared with patients in the other two groups (fi gure 7B). The pairwise comparison between treatment groups in the all wild-type subgroup showed an HR of 2∙21 (95% CI 1∙38–3∙52; p=0∙00067) for no treatment versus bevacizumab alone. The
Figure 4: Forest plots of progression-free survival by patient subgroups—bevacizumab alone versus fl uoropyrimidine plus bevacizumabHR=hazard ratio. ECOG=Eastern Cooperative Oncology Group. LDH=lactate dehydrogenase. CEA=carcinoembryonic antigen.
HR (95% CI)Events (n/N)
Fluoropyrimidineplus bevacizumab
Bevacizumab
Sex
Male
Female
Age (years)
<70
≥70
ECOG performance score
0
1–2
Site
Colon
Rectum
Number of metastatic sites
1
>1
LDH concentration
Normal
Elevated
CEA before induction therapy
≤20 ng/mL
>20 ng/mL
CEA at randomisation
≤5 ng/mL
>5 ng/mL
Oxaliplatin dose intensity
≥75%
<75%
Metastasis
Synchronous, resection
Synchronous, no resection
Metachronous
Best response to induction therapy
Complete response/partial response
Stable disease
Mutation
RAS/RAF wild-type
Any mutation
Overall
89/101
42/46
98/110
33/37
63/73
60/65
84/95
47/52
55/64
75/82
56/64
59/64
43/49
76/83
49/56
43/46
99/112
32/35
67/78
37/39
27/30
88/98
43/49
39/45
49/58
131/147
103/105
46/48
98/100
51/53
72/75
69/70
92/94
57/59
62/65
87/88
76/77
56/58
36/39
97/98
48/50
69/69
108/112
41/41
89/91
35/36
25/26
90/93
59/60
43/45
59/61
149/153
7·3 (5·9–8·5)
6·0 (4·4–6·9)
6·6 (5·8–7·8)
6·2 (4·2–13·4)
7·3 (5·7–9·3)
6·0 (3·9–7·3)
5·9 (4·6–8·1)
6·8 (6·1–8·3)
8·3 (6·9–11·7)
5·2 (4·3–6·4)
5·9 (4·6–9·0)
6·9 (5·2–8·1)
9·4 (5·9–15·1)
5·8 (4·3–7·1)
8·0 (5·8–11·8)
5·8 (4·1–6·8)
6·8 (5·8–8·1)
5·8 (4·5–8·0)
6·7 (5·2–8·3)
5·8 (4·3–7·6)
7·1 (5·9–15·2)
6·6 (5·2–8·1)
6·1 (4·0–8·1)
8·1 (6·3–15·2)
6·4 (4·5–8·3)
6·3 (5·8–7·6)
4·3 (3·6–5·1)
5·3 (4·0–8·1)
4·3 (3·5–5·3)
5·3 (4·1–6·7)
4·4 (3·9–5·8)
5·1 (4·1–7·1)
4·4 (4·0–5·3)
5·0 (3·6–7·1)
5·3 (4·5–7·2)
4·1 (3·0–5·0)
5·8 (4·2–7·1)
3·2 (2·4–4·4)
6·0 (4·7–13·3)
4·1 (3·5–4·8)
6·0 (4·7–9·2)
4·0 (2·8–4·6)
4·6 (4·0–5·3)
4·4 (2·5–6·8)
4·4 (3·9–5·8)
4·3 (2·0–5·9)
5·4 (4·1–22·5)
5·3 (4·4–6·1)
4·0 (2·9–4·6)
6·2 (4·3–10·6)
4·1 (3·2–5·3)
4·6 (4·0–5·3)
1·62 (1·22–2·15)
0·88 (0·57–1·35)
1·34 (1·01–1·78)
1·42 (0·91–2·23)
1·59 (1·13–2·24)
0·97 (0·68–1·38)
1·39 (1·03–1·87)
1·27 (0·86–1·87)
1·24 (0·85–1·79)
1·44 (1·05–1·97)
1·14 (0·81–1·62)
1·85 (1·27–2·70)
1·06 (0·68–1·66)
1·43 (1·06–1·94)
1·15 (0·77–1·72)
1·53 (1·04–2·25)
1·40 (1·07–1·85)
1·20 (0·75–1·91)
1·52 (1·10–2·09)
1·63 (1·01–2·65)
0·76 (0·42–1·38)
1·22 (0·91–1·64)
1·55 (1·04–2·32)
1·07 (0·69–1·67)
1·51 (1·03–2·22)
1·34 (1·06–1·70)
Median (95% CI) (months)
Fluoropyrimidineplus bevacizumab
Bevacizumab
0·5 0·7 1·0 1·5 2·0
Favoursbevacizumab
Favoursfluoropyrimidineplus bevacizumab

Articles
www.thelancet.com/oncology Published online September 9, 2015 http://dx.doi.org/10.1016/S1470-2045(15)00042-X 9
corresponding comparison for patients with tumours harbouring any mutation showed an HR of 1∙19 (95% CI 0∙84–1∙70; p=0∙33).
For overall survival, the RAS/RAF mutation subgroup analyses do not show any interaction with the maintenance treatment groups (appendix).
Because of cumulative toxicity, oxaliplatin dose had to be reduced or suspended during induction in 123 (26%)
of 472 treated patients, and therefore these patients received an oxaliplatin dose lower than 75% of the originally intended dose. However, oxaliplatin dose reduction did not aff ect time to fi rst progression or overall survival, regardless of the maintenance strategy (appendix pp 4–9). The safety profi les in the three maintenance groups were consistent with the known side-eff ects of the individual drugs. The incidence of
HR (95% CI)Events (n/N)
Fluoropyrimidineplus bevacizumab
No treatment
Sex
Male
Female
Age (years)
<70
≥70
ECOG performance score
0
1–2
Site
Colon
Rectum
Number of metastatic sites
1
>1
LDH concentration
Normal
Elevated
CEA before induction therapy
≤20 ng/mL
>20 ng/mL
CEA at randomisation
≤5 ng/mL
>5 ng/mL
Oxaliplatin dose intensity
≥75%
<75%
Metastasis
Synchronous, resection
Synchronous, no resection
Metachronous
Best response to induction therapy
Complete response/partial response
Stable disease
Mutation
RAS/RAF wild-type
Any mutation
Overall
89/101
42/46
98/110
33/37
63/73
60/65
84/95
47/52
55/64
75/82
56/64
59/64
43/49
76/83
49/56
43/46
99/112
32/35
67/78
37/39
27/30
88/98
43/49
39/45
49/58
131/17
93/96
57/58
98/100
54/54
60/62
79/81
95/97
55/57
57/58
92/95
82/84
53/55
41/42
96/98
38/40
74/75
109/113
41/41
79/82
45/45
26/27
102/105
48/49
44/46
65/67
150/154
7·3 (5·9–8·5)
6·0 (4·4–6·9)
6·6 (5·8–7·8)
6·2 (4·2–13·4)
7·3 (5·7–9·3)
6·0 (3·9–7·3)
5·9 (4·6–8·1)
6·8 (6·1–8·3)
8·3 (6·9–11·7)
5·2 (4·3–6·4)
5·9 (4·6–9·0)
6·9 (5·2–8·1)
9·4 (5·9–15·1)
5·8 (4·3–7·1)
8·0 (5·8–11·8)
5·8 (4·1–6·8)
6·8 (5·8–8·1)
5·8 (4·5–8·0)
6·7 (5·2–8·3)
5·8 (4·3–7·6)
7·1 (5·9–15·2)
6·6 (5·2–8·1)
6·1 (4·0–8·1)
8·1 (6·3–15·2)
6·4 (4·5–8·3)
6·3 (5·8–7·6)
3·7 (2·8–4·5)
3·3 (2·8–4·1)
3·5 (2·8–4·1)
4·0 (2·7–5·6)
3·7 (2·8–5·0)
3·1 (2·7–4·1)
3·5 (2·8–4·2)
3·5 (2·9–4·6)
4·1 (3·5–6·1)
3·0 (2·6–4·1)
4·1 (3·3–4·5)
2·9 (1·7–4·1)
5·5 (4·1–8·2)
2·9 (2·7–3·8)
6·4 (4·3–7·5)
2·7 (2·2–3·5)
3·6 (2·9–4·1)
3·0 (2·7–4·4)
3·8 (2·9–5·0)
3·0 (2·2–4·1)
3·9 (2·6–7·0)
3·9 (3·0–4·6)
2·9 (2·6–4·1)
3·9 (2·7–5·7)
3·7 (2·8–5·1)
3·5 (2·9–4·1)
2·13 (1·57–2·88)
2·00 (1·32–3·04)
2·14 (1·60–2·86)
2·14 (1·38–3·64)
2·47 (1·70–3·59)
1·74 (1·23–2·46)
1·97 (1·46–2·66)
2·46 (1·61–3·76)
2·42 (1·64–3·59)
1·89 (1·38–2·58)
1·74 (1·23–2·47)
2·89 (1·92–4·35)
1·78 (1·15–2·77)
2·31 (1·67–3·18)
1·99 (1·26–3·14)
2·12 (1·43–3·14)
2·16 (1·63–2·87)
1·84 (1·14–2·96)
1·93 (1·39–2·70)
2·53 (1·58–4·07)
2·20 (1·24–3·90)
2·10 (1·56–2·82)
2·06 (1·34–3·17)
3·00 (1·86–4·86)
1·89 (1·29–2·75)
2·09 (1·64–2·67)
Median (95% CI) (months)
Fluoropyrimidineplus bevacizumab
No treatment
0·5 0·7 1·0 1·5 2·0
Favoursno treatment
Favoursfluoropyrimidineplus bevacizumab
Figure 5: Forest plots of progression-free survival by patient subgroups— no treatment versus fl uoropyrimidine plus bevacizumabHR=hazard ratio. ECOG=Eastern Cooperative Oncology Group. LDH=lactate dehydrogenase. CEA=carcinoembryonic antigen.

Articles
10 www.thelancet.com/oncology September 9, 2015 http://dx.doi.org/10.1016/S1470-2045(15)00042-X
grade 3 adverse events was low and similar in all groups (table 4; appendix p 17). The most frequent grade 3 adverse event was sensory neuropathy (21 [13%] of 158 patients in the fl uoropyrimidine plus bevacizumab group, 22 [14%] of 156 patients in the bevacizumab alone group, and 12 [8%] of 158 patients in the no treatment group). 52 (33%) of 158 patients in the fl uoropyrimidine plus bevacizumab group and 25 (16%) of 156 patients in the bevacizumab alone group required
at least one dose reduction of either fl uoropyrimidine (48 [30%] of 158 patients) or bevacizumab (19 [12%] of 158) during maintenance treatment. No patients had to discontinue treatment permanently for drug-related toxicity. No treatment-related deaths occurred during the study; three patients (one infection not further specifi ed in the fl uoropyrimidine plus bevacizumab group, and two septic complications in the no treatment group died of infection.
HR (95% CI)Events (n/N)
Bevacizumab No treatment No treatment
Sex
Male
Female
Age (years)
<70
≥70
ECOG performance score
0
1–2
Site
Colon
Rectum
Number of metastatic sites
1
>1
LDH concentration
Normal
Elevated
CEA before induction therapy
≤20 ng/mL
>20 ng/mL
CEA at randomisation
≤5 ng/mL
>5 ng/mL
Oxaliplatin dose intensity
≥75%
<75%
Metastasis
Synchronous, resection
Synchronous, no resection
Metachronous
Best response to induction therapy
Complete response/partial response
Stable disease
Mutation
RAS/RAF wild-type
Any mutation
Overall
103/105
46/48
98/100
51/53
72/75
69/70
92/94
57/59
62/65
87/88
76/77
56/58
36/39
97/98
48/50
69/69
108/112
41/41
89/91
35/36
25/26
90/93
59/60
43/45
59/61
149/153
93/96
57/58
98/100
54/54
60/62
79/81
95/97
55/57
57/58
92/95
82/84
53/55
41/42
96/98
38/40
74/75
109/113
41/41
79/82
45/45
26/27
102/105
48/49
44/46
65/67
150/154
4·3 (3·6–5·1)
5·3 (4·0–8·1)
4·3 (3·5–5·3)
5·3 (4·1–6·7)
4·4 (3·9–5·8)
5·1 (4·1–7·1)
4·4 (4·0–5·3)
5·0 (3·6–7·1)
5·3 (4·5–7·2)
4·1 (3·0–5·0)
5·8 (4·2–7·1)
3·2 (2·4–4·4)
6·0 (4·7–13·3)
4·1 (3·5–4·8)
6·0 (4·7–9·2)
4·0 (2·8–4·6)
4·6 (4·0–5·3)
4·4 (2·5–6·8)
4·4 (3·9–5·8)
4·3 (2·0–5·9)
5·4 (4·1–22·5)
5·3 (4·4–6·1)
4·0 (2·9–4·6)
6·2 (4·3–10·6)
4·1 (3·2–5·3)
4·6 (4·0–5·3)
3·7 (2·8–4·5)
3·3 (2·8–4·1)
3·5 (2·8–4·1)
4·0 (2·7–5·6)
3·7 (2·8–5·0)
3·1 (2·7–4·1)
3·5 (2·8–4·2)
3·5 (2·9–4·6)
4·1 (3·5–6·1)
3·0 (2·6–4·1)
4·1 (3·3–4·5)
2·9 (1·7–4·1)
5·5 (4·1–8·2)
2·9 (2·7–3·8)
6·4 (4·3–7·5)
2·7 (2·2–3·5)
3·6 (2·9–4·1)
3·0 (2·7–4·4)
3·8 (2·9–5·0)
3·0 (2·2–4·1)
3·9 (2·6–7·0)
3·9 (3·0–4·6)
2·9 (2·6–4·1)
3·9 (2·7–5·7)
3·7 (2·8–5·1)
3·5 (2·9–4·1)
1·22 (0·92–1·62)
2·07 (1·36–3·14)
1·43 (1·07–1·91)
1·45 (0·98–2·15)
1·36 (0·96–1·93)
1·67 (1·19–2·33)
1·34 (1·00–1·79)
1·64 (1·11–2·42)
1·68 (1·15–2·46)
1·29 (0·96–1·73)
1·53 (1·11–2·10)
1·19 (0·81–1·74)
1·57 (0·99–2·51)
1·47 (1·11–1·97)
1·51 (0·96–2·37)
1·38 (0·99–1·92)
1·42 (1·08–1·86)
1·51 (0·96–2·38)
1·23 (0·90–1·66)
1·69 (1·06–2·68)
2·15 (1·15–4·02)
1·56 (1·17–2·09)
1·33 (0·90–1·95)
2·21 (1·38–3·52)
1·19 (0·84–1·70)
1·45 (1·15–1·82)
Median (95% CI) (months)
Bevacizumab
0·5 0·7 1·0 1·5 2·0
Favoursno treatment
Favours bevacizumab alone
Figure 6: Forest plots of progression-free survival by patient subgroups—no treatment versus bevacizumab aloneHR=hazard ratio. ECOG=Eastern Cooperative Oncology Group. LDH=lactate dehydrogenase. CEA=carcinoembryonic antigen.
Articles
www.thelancet.com/oncology Published online September 9, 2015 http://dx.doi.org/10.1016/S1470-2045(15)00042-X 11
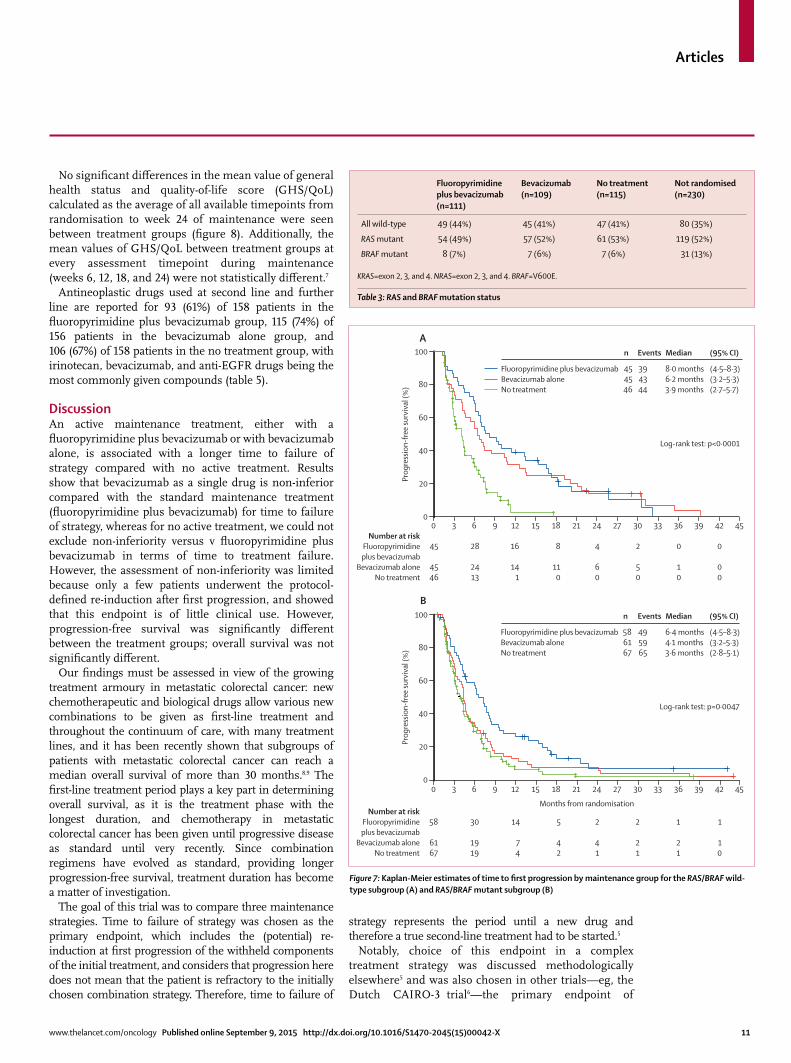
No signifi cant diff erences in the mean value of general health status and quality-of-life score (GHS/QoL) calculated as the average of all available timepoints from randomisation to week 24 of maintenance were seen between treatment groups (fi gure 8). Additionally, the mean values of GHS/QoL between treatment groups at every assessment timepoint during maintenance (weeks 6, 12, 18, and 24) were not statistically diff erent.7
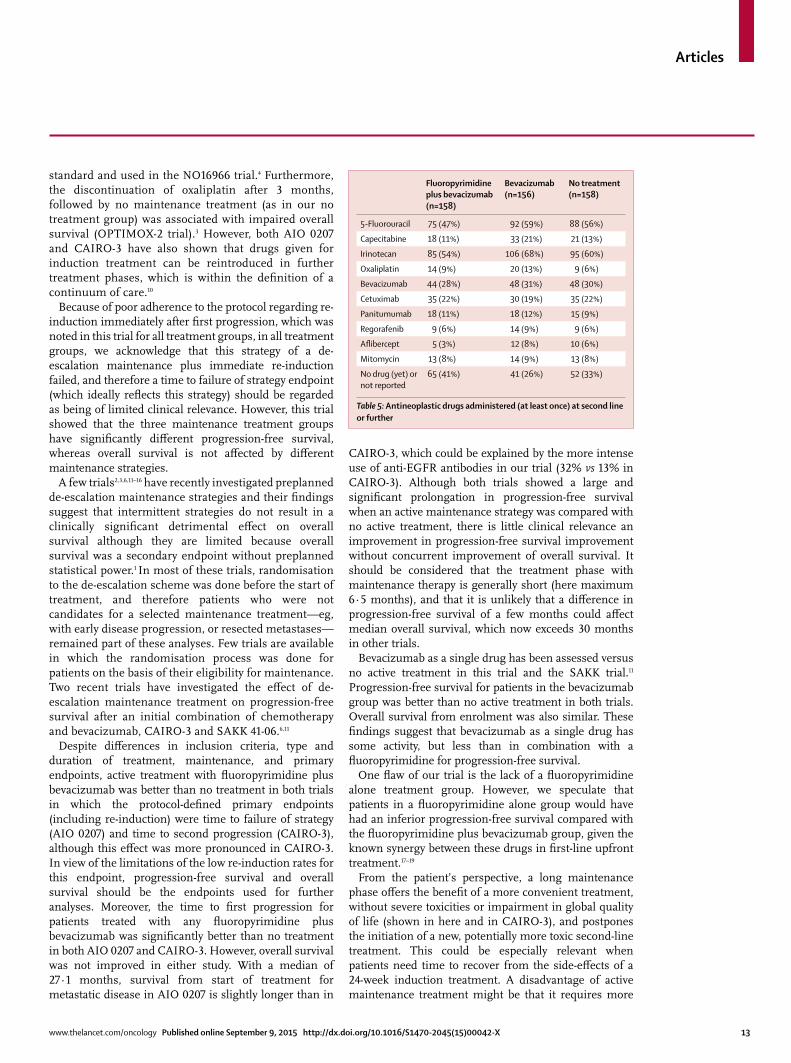
Antineoplastic drugs used at second line and further line are reported for 93 (61%) of 158 patients in the fl uoropyrimidine plus bevacizumab group, 115 (74%) of 156 patients in the bevacizumab alone group, and 106 (67%) of 158 patients in the no treatment group, with irinotecan, bevacizumab, and anti-EGFR drugs being the most commonly given compounds (table 5).
DiscussionAn active maintenance treatment, either with a fl uoropyrimidine plus bevacizumab or with bevacizumab alone, is associated with a longer time to failure of strategy compared with no active treatment. Results show that bevacizumab as a single drug is non-inferior compared with the standard maintenance treatment (fl uoropyrimidine plus bevacizumab) for time to failure of strategy, whereas for no active treatment, we could not exclude non-inferiority versus v fl uoropyrimidine plus bevacizumab in terms of time to treatment failure. However, the assessment of non-inferiority was limited because only a few patients underwent the protocol-defi ned re-induction after fi rst progression, and showed that this endpoint is of little clinical use. However, progression-free survival was signifi cantly diff erent between the treatment groups; overall survival was not signifi cantly diff erent.
Our fi ndings must be assessed in view of the growing treatment armoury in metastatic colorectal cancer: new chemotherapeutic and biological drugs allow various new combinations to be given as fi rst-line treatment and throughout the continuum of care, with many treatment lines, and it has been recently shown that subgroups of patients with metastatic colorectal cancer can reach a median overall survival of more than 30 months.8,9 The fi rst-line treatment period plays a key part in determining overall survival, as it is the treatment phase with the longest duration, and chemotherapy in metastatic colorectal cancer has been given until progressive disease as standard until very recently. Since combination regimens have evolved as standard, providing longer progression-free survival, treatment duration has become a matter of investigation.
The goal of this trial was to compare three maintenance strategies. Time to failure of strategy was chosen as the primary endpoint, which includes the (potential) re-induction at fi rst progression of the withheld components of the initial treatment, and considers that progression here does not mean that the patient is refractory to the initially chosen combination strategy. Therefore, time to failure of
strategy represents the period until a new drug and therefore a true second-line treatment had to be started.5
Notably, choice of this endpoint in a complex treatment strategy was discussed methodologically elsewhere5 and was also chosen in other trials—eg, the Dutch CAIRO-3 trial6—the primary endpoint of
Fluoropyrimidine plus bevacizumab (n=111)
Bevacizumab (n=109)
No treatment (n=115)
Not randomised (n=230)
All wild-type 49 (44%) 45 (41%) 47 (41%) 80 (35%)
RAS mutant 54 (49%) 57 (52%) 61 (53%) 119 (52%)
BRAF mutant 8 (7%) 7 (6%) 7 (6%) 31 (13%)
KRAS=exon 2, 3, and 4. NRAS=exon 2, 3, and 4. BRAF=V600E.
Table 3: RAS and BRAF mutation status
Number at riskFluoropyrimidineplus bevacizumab
Bevacizumab aloneNo treatment
Fluoropyrimidine plus bevacizumabBevacizumab aloneNo treatment
394344
Events
454546
n Median (95% CI)
8·0 months6·2 months3·9 months
(4·5–8·3)(3·2–5·3)(2·7–5·7)
45
4546
28
2413
16
141
8
110
4
60
2
50
0
10
0
00
58
6167
30
1919
14
74
5
42
2
41
2
21
1
21
1
10
0
20
40
60
80
100
Prog
ress
ion-
free
surv
ival
(%)
Number at riskFluoropyrimidineplus bevacizumab
Bevacizumab aloneNo treatment
0
20
40
60
80
100
Prog
ress
ion-
free
surv
ival
(%)
Months from randomisation
0 3
Log-rank test: p<0·0001
Log-rank test: p=0·0047
6 9 12 15 18 21 24 27 30 33 36 39 42 45
0 3 6 9 12 15 18 21 24 27 30 33 36 39 42 45
Fluoropyrimidine plus bevacizumabBevacizumab aloneNo treatment
495965
Events
586167
n Median (95% CI)
6·4 months4·1 months3·6 months
(4·5–8·3)(3·2–5·3)(2·8–5·1)
A
B
Figure 7: Kaplan-Meier estimates of time to fi rst progression by maintenance group for the RAS/BRAF wild-type subgroup (A) and RAS/BRAF mutant subgroup (B)

Articles
12 www.thelancet.com/oncology September 9, 2015 http://dx.doi.org/10.1016/S1470-2045(15)00042-X
CAIRO-3 was identical to that used here. Both trials also have in common that for patients that do not receive re-induction, this endpoint is equivalent to time to fi rst progression, and the use of another drug that was not part of the induction treatment, and death, were both considered events. Diff erences in defi nitions could exist in relation to the assessment of treatment
discontinuation or no further treatment before fi rst progression, and the method of censoring patients. This censoring is explicitly defi ned in the AIO 0207 protocol, whereas no information from CAIRO-3 is available in the manuscript.
The low frequency of re-induction (170 [36%] of 472 patients in total, and only 30 [19%] of 158 after fl uoropyrimidine plus bevacizumab maintenance) suggests that re-induction after fi rst progression, and therefore time to failure of strategy, was generally not accepted as a treatment strategy; investigator’s decision, patient’s wish, and non-compliance were the most frequently named reasons for not proceeding to re-induction. These fi ndings are consistent with those from the CAIRO-3 trial, in which only 60% (observation group) and 47% (capecitabine plus bevacizumab maintenance group) underwent an immediate, protocol-defi ned re-induction of the discontinued combination.6 Both trials have in common that the re-induction rates were signifi cantly lower in patients receiving fl uoropyrimidine plus bevacizumab maintenance than in those receiving no treatment. This fi nding probably refl ects patients’ and physicians’ distrust in the effi cacy of oxaliplatin or toxicity concerns in this setting. We have to acknowledge that an immediate re-induction of the initially selected protocol is mostly not pursued in routine practice. The higher rates of re-inductions in the CAIRO-3 trial compared with this trial could be related to the duration of the induction treatment phase in this trial. From the perspective of current clinical knowledge, we would conclude that a 24-week induction period is too long. However, at the time the trial was initiated, the continuous use of oxaliplatin until occurrence of toxicity (neuropathy) or progression was regarded as a
Fluoropyrimidine plus bevacizumab (n=158)
Bevacizumab (n=156) No treatment (n=158)
Grade 1–2 Grade 3 Grade 4 Grade 1–2 Grade 3 Grade 4 Grade 1–2 Grade 3 Grade 4
Sensory neuropathy 49 (31%) 21 (13%) 0 91 (58%) 22 (14%) 0 100 (63%) 12 (8%) 0
Diarrhoea 23 (15%) 3 (2%) 0 17 (11%) 0 0 12 (8%) 0 0
Hand-foot skin reaction 14 (9%) 4 (3%) 0 8 (5%) 1 (1%) 0 8 (5%) 1 (1%) 0
Hypertension 16 (10%) 5 (3%) 0 25 (16%) 2 (1%) 1 (1%) 13 (8%) 2 (1%) 0
Fatigue 39 (25%) 5 (3%) 0 25 (16%) 2 (1%) 1 (1%) 31 (20%) 0 0
Thrombosis 2 (1%) 2 (1%) 1 (1%) 1 (1%) 1 (1%) 0 1 (1%) 2 (1%) 0
Bleeding 13 (8%) 0 0 14 (9%) 0 0 10 (6%) 1 (1%) 0
Gastrointestinal perforation 0 1 (1%) 0 0 0 0 0 0 0
Neutropenia 3 (2%) 2 (1%) 1 (1%) 5 (3%) 3 (2%) 1 (1%) 1 (1%) 1 (1%) 0
Any infection 19 (12%) 2 (1%) 0 15 (10%) 3 (2%) 0 4 (3%) 2 (1%) 0
Nausea 20 (13%) 1 (1%) 0 14 (9%) 1 (1%) 0 13 (8%) 0 0
Vomiting 7 (4%) 0 0 4 (3%) 0 0 3 (2%) 0 0
Hair loss, alopecia 13 (8%) 0 0 15 (10%) 0 0 12 (8%) 0 0
Data are n (%). Two patients (one in the fl uoropyrimidine plus bevacizumab group, and one in the no treatment group) died of infection while on study.
Table 4: Adverse events relevant to treatment during maintenance
Fluoropyrimidine plusbevacizumab
Bevacizumab aloneNo treatment
Fluoropyrimidine plus bevacizumabBevacizumab aloneNo treatment
OverallGHS/QoL
0 6 12Week
18 24
55·0 (20·8)58·0 (18·0)57·5 (18·6)
Fluoropyrimidine plus bevacizumab vs bevacizumab: p=0·198Fluoropyrimidine plus bevacizumab vs no treatment: p=0·296
Bevacizumab vs no treatment: p=0·820
57·2 (20·9)
54·3 (22·8)55·1 (19·1)
58·5 (22·4)
59·0 (20·1)58·3 (19·4)
54·1 (23·3)
58·3 (20·1)58·5 (22·0)
56·7 (23·3)
58·0 (21·1)58·7 (22·9)
56·3 (21·6)
55·4 (20·7)57·0 (23·4)
0
40
50
60
70
80
Mea
n gl
obal
hea
lth a
nd q
ualit
y-of
-life
scor
e
Figure 8: Mean global health status and quality-of-life (GHS/QoL) score at maintenance assessment timepointsAll data are mean (SD). p values calculated with two-sided t test for the average of all available timepoints from randomisation to week 24 of maintenance. Overall GHS/QoL mean value calculated as the average of all available timepoints from randomisation to week 24 of maintenance.
Articles
www.thelancet.com/oncology Published online September 9, 2015 http://dx.doi.org/10.1016/S1470-2045(15)00042-X 13
standard and used in the NO16966 trial.4 Furthermore, the discontinuation of oxaliplatin after 3 months, followed by no maintenance treatment (as in our no treatment group) was associated with impaired overall survival (OPTIMOX-2 trial).3 However, both AIO 0207 and CAIRO-3 have also shown that drugs given for induction treatment can be reintroduced in further treatment phases, which is within the defi nition of a continuum of care.10
Because of poor adherence to the protocol regarding re-induction immediately after fi rst progression, which was noted in this trial for all treatment groups, in all treatment groups, we acknowledge that this strategy of a de-escalation maintenance plus immediate re-induction failed, and therefore a time to failure of strategy endpoint (which ideally refl ects this strategy) should be regarded as being of limited clinical relevance. However, this trial showed that the three maintenance treatment groups have signifi cantly diff erent progression-free survival, whereas overall survival is not aff ected by diff erent maintenance strategies.
A few trials2,3,6,11–16 have recently investigated preplanned de-escalation maintenance strategies and their fi ndings suggest that intermittent strategies do not result in a clinically signifi cant detrimental eff ect on overall survival although they are limited because overall survival was a secondary endpoint without preplanned statistical power.1 In most of these trials, randomisation to the de-escalation scheme was done before the start of treatment, and therefore patients who were not candidates for a selected maintenance treatment—eg, with early disease progression, or resected metastases—remained part of these analyses. Few trials are available in which the randomisation process was done for patients on the basis of their eligibility for maintenance. Two recent trials have investigated the eff ect of de-escalation maintenance treatment on progression-free survival after an initial combination of chemotherapy and bevacizumab, CAIRO-3 and SAKK 41-06.6,11
Despite diff erences in inclusion criteria, type and duration of treatment, maintenance, and primary endpoints, active treatment with fl uoropyrimidine plus bevacizumab was better than no treatment in both trials in which the protocol-defi ned primary endpoints (including re-induction) were time to failure of strategy (AIO 0207) and time to second progression (CAIRO-3), although this eff ect was more pronounced in CAIRO-3.In view of the limitations of the low re-induction rates for this endpoint, progression-free survival and overall survival should be the endpoints used for further analyses. Moreover, the time to fi rst progression for patients treated with any fl uoropyrimidine plus bevacizumab was signifi cantly better than no treatment in both AIO 0207 and CAIRO-3. However, overall survival was not improved in either study. With a median of 27·1 months, survival from start of treatment for metastatic disease in AIO 0207 is slightly longer than in
CAIRO-3, which could be explained by the more intense use of anti-EGFR antibodies in our trial (32% vs 13% in CAIRO-3). Although both trials showed a large and signifi cant prolongation in progression-free survival when an active maintenance strategy was compared with no active treatment, there is little clinical relevance an improvement in progression-free survival improvement without concurrent improvement of overall survival. It should be considered that the treatment phase with maintenance therapy is generally short (here maximum 6∙5 months), and that it is unlikely that a diff erence in progression-free survival of a few months could aff ect median overall survival, which now exceeds 30 months in other trials.
Bevacizumab as a single drug has been assessed versus no active treatment in this trial and the SAKK trial.11 Progression-free survival for patients in the bevacizumab group was better than no active treatment in both trials. Overall survival from enrolment was also similar. These fi ndings suggest that bevacizumab as a single drug has some activity, but less than in combination with a fl uoropyrimidine for progression-free survival.
One fl aw of our trial is the lack of a fl uoropyrimidine alone treatment group. However, we speculate that patients in a fl uoropyrimidine alone group would have had an inferior progression-free survival compared with the fl uoropyrimidine plus bevacizumab group, given the known synergy between these drugs in fi rst-line upfront treatment.17–19
From the patient’s perspective, a long maintenance phase off ers the benefi t of a more convenient treatment, without severe toxicities or impairment in global quality of life (shown in here and in CAIRO-3), and postpones the initiation of a new, potentially more toxic second-line treatment. This could be especially relevant when patients need time to recover from the side-eff ects of a 24-week induction treatment. A disadvantage of active maintenance treatment might be that it requires more
Fluoropyrimidine plus bevacizumab (n=158)
Bevacizumab (n=156)
No treatment (n=158)
5-Fluorouracil 75 (47%) 92 (59%) 88 (56%)
Capecitabine 18 (11%) 33 (21%) 21 (13%)
Irinotecan 85 (54%) 106 (68%) 95 (60%)
Oxaliplatin 14 (9%) 20 (13%) 9 (6%)
Bevacizumab 44 (28%) 48 (31%) 48 (30%)
Cetuximab 35 (22%) 30 (19%) 35 (22%)
Panitumumab 18 (11%) 18 (12%) 15 (9%)
Regorafenib 9 (6%) 14 (9%) 9 (6%)
Afl ibercept 5 (3%) 12 (8%) 10 (6%)
Mitomycin 13 (8%) 14 (9%) 13 (8%)
No drug (yet) or not reported
65 (41%) 41 (26%) 52 (33%)
Table 5: Antineoplastic drugs administered (at least once) at second line or further

Articles
14 www.thelancet.com/oncology September 9, 2015 http://dx.doi.org/10.1016/S1470-2045(15)00042-X
Pfi zer. JQ has received honoraria for speaker activities from Roche. TT has received honoraria and travel support from Merck, Sanofi -Aventis, Amgen, Lilly, and Novartis, has received research support from Roche, and is an employee of iOMEDICO. H-JS has received honoraria for participation in advisory boards from Roche. DA has received honoraria for speaker activities and participation in advisory boards from Roche, and honoraria from Sanofi -Aventis, Amgen, Merck, and Bayer. CAL, BK, RD, GD, TL, AT, and AH declare no competing interests.
AcknowledgmentsWe thank all the patients who agreed to take part in the trial. We also thank the investigators and the study teams who participated. We thank the members of the independent data monitoring committee: Andreas Hochhaus, (Jena, Germany), Jörg Thomas Hartmann (Bielefeld, Germany), and Gunter Schuch (Hamburg, Germany).
References1 Berry SR, Cosby R, Asmis TR, et al. Continuous versus
intermittent chemotherapy strategies in metastatic colorectal cancer: a systemic review and meta-analysis. Ann Oncol 2015; 26: 477–85.
2 Tournigand C, Cervantes A, Figer A, et al. OPTIMOX1: a randomized study of FOLFOX4 or FOLFOX7 with oxaliplatin in a stop-and-go fashion in advanced colorectal cancer–a Gercor study. J Clin Oncol 2006; 24: 394–400.
3 Chibaudel B, Maindrault-Goebel F, Lledo G, et al. Can chemotherapy be discontinued in unresectable metastatic cancer? The GERCOR OPTIMOX2 study. J Clin Oncol 2009; 27: 5727–33.
4 Saltz LB, Clarke S, Diaz-Rubio E, et al. Bevacizumab in combination with oxaliplatin-based chemotherapy as fi rst-line therapy in metastatic colorectal cancer: a randomized phase III study. J ClinOncol 2008; 26: 2013–19.
5 Chibaudel B, Bonnetain F, Shi Q, et al. Alternative end points to evaluate a therapeutic strategy in advanced colorectal cancer: evaluation of progression-free survival, duration of disease control, and time to failure of strategy—an aide et Recherche en Cancérologie Digestive Group study. J Clin Oncol 2011; 29: 4199–204.
6 Simkens LHJ, van Tinteren H, May AM, et al. Maintenance treatment with capecitabine and bevacizumab in metastatic colorectal cancer (CAIRO3): a phase 3 randomised controlled trial of the Dutch Colorectal Cancer Group. Lancet 2015; 385: 1843–52.
7 Quidde J, Arnold D, Hegewisch-Becker S, et al. Quality of life (QoL) in patients with metastatic colorectal cancer (MCRC) receiving maintenance therapy after fi rst-line inductive treatment: a QoL sub-analysis of the AIO KRK 0207 phase III trial. Ann Oncol 2014; 25: 522P (abstr).
8 Heinemann V, Fischer von Weikersthal L, Decker T, et al. FOLFIRI plus cetuximab versus FOLFIRI plus bevacizumab as fi rst-line treatment for patients with metastatic colorectal cancer (FIRE-3): a randomised, open-label, phase3 trial. Lancet Oncol 2014; 15: 1065–75.
9 Lenz H, Niedzwiecki D, Innocenti F, et al. CALBG/SWOG 80405: Phase III trial of irinotecan/5-FU/leucovorin (FOLFIRI) or oxaliplatin/5-FU/leucovorin (mFOLFOX6) with bevacizumab (BV) or cetuximab (CET) for patients (pts) with expanded ras analyses untreated metastatic adenocarcinoma of the colon or rectum (mCRC). Ann Oncol 2014; 25: 501O (abstr).
10 Van Cutsem E, Cervantes A, Nordlinger B et al. Metastatic colorectal cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow up. Ann Oncol 2014; 25: iii1–iii9.
11 Koeberle D, Betticher DC, Von Moos R, et al. Bevacizumab continuation versus no continuation after fi rst-line chemo-bevacizumab therapy in patients with metastatic colorectal cancer: a randomized phase III non-inferiority trial (SAKK 41/06). Ann Oncol 2015; 26: 709–14.
12 Johnsson A, Hagman H, Frödin J-E, et al. A randomized phase III trial on maintenance treatment with bevacizumab alone or in combination with erlotinib after chemotherapy and bevacizumab in metastatic colorectal cancer: the Nordic ACT trial. Ann Oncol 2013; 24: 2335–41.
13 Tournigand C, Chibaudel B, Samson B, et al. Bevacizumab with or without erlotinib as maintenance therapy in patients with metastatic colorectal cancer (GERCOR DREAM; OPTIMOX3): a randomised, open-label, phase 3 trial. Lancet Oncol 2015; (in press).
frequent visits to medical care institutions, infusions, and so on. However, the fi ndings of this trial and CAIRO-3 suggest that overall survival is not signifi cantly diff erent among diff erent maintenance strategies, which allows treatment intensity to be adapted to patient preferences. Unfortunately, we failed to identify parameters that could clearly predict a benefi t for any strategy for any patient groups. Although our exploratory analysis of the results according to RAS/BRAF mutational status suggest that patients with wild-type status could be treated with less intensive maintenance treatment compared with patients with mutant status, these fi ndings are at best hypothesis generating and require confi rmation.
The strategy of a non-toxic, moderate intensity mainten ance treatment is currently being assessed. First, so-called switch maintenance trials have evaluated combinations of bevacizumab with erlotinib12,13 and more of these so-called moderate intensity maintenance regimen are currently being evaluated in clinical trials and platforms.14 Another option could be the early integration of irinotecan or anti-EGFR antibodies to complex treatment algorithms, but that has not yet been investigated in clinical trials.
The patient-oriented approach of an induction-maintenance treatment sequence, with maintenance intensity related to clinical situation, patient preference, and (in the future) molecular profi les, represents a new step into the future treatment of metastatic colorectal cancer, and establishes maintenance treatment as a separate treatment phase. Active maintenance treatment with a fl uoropyrimidine plus bevacizumab could be regarded as the preferred treatment option for patients following induction treatment with a fl uoropyrimidine, oxaliplatin, and bevacizumab, as it allows the planned discontinuation of the initial treatment combination and provides the longest progression-free survival. This active maintenance treatment phase provides a benefi t on its own by maintaining disease control and quality of life without relevant toxicity.ContributorsSH-B and UG contributed equally to the trial. SH-B, UG, DA, H-JS, and AH were responsible for the fi nal study design. SH-B, UG, CAL, BK, RD, C-CS, S-EA-B, TL, GD, JS, AT, AR-S, JQ, and DA collected the data and recruited patients. SH-B, UG, DA, TT, and AH analysed the data. S-HB, UG, DA, and AH wrote the report. All authors participated in data interpretation, and revision and fi nalisation of the report for submission.
Declaration of interestsSH-B has received honoraria for participation in advisory boards from Roche, Merck, Amgen, and Lilly. UG has received honoraria for speaker activities and participation in advisory boards from Roche, Sanofi , Amgen, Bayer, Merck, Lilly, Hexal, Falk Foundation, Celgene, Mologen, GlaxoSmithKline, and MSD Sharp Dohme, and research support from Roche and AIO Studien gGmbH. C-CS has received honoraria for participation in advisory boards from Roche, GlaxoSmithKline, Sanofi -Aventis, and Lilly. SEA has received honoraria for participation in advisory boards and research support from Roche. JS has received research support from Roche. AR-S received honoraria for participation in advisory boards from Merck, Roche, Sanofi -Aventis, and Celgene, and honoraria for speaker activities or travel grants from Merck, Roche, Amgen, and Celgene

Articles
www.thelancet.com/oncology Published online September 9, 2015 http://dx.doi.org/10.1016/S1470-2045(15)00042-X 15
14 Arnold D, Zurlo A, Salazar R, et al. Immunomodulary maintenance therapy with TLR-9 agonist MGN 1703 in patients with metastatic colorectal carcinoma—the randomized phase 3 IMPALA study. Ann Oncol 2014; 25: 1077 (abstr).
15 Diaz-Rubio E, Gomez-Espana A, Massuti B, et al. First-line XELOX plus bevacizumab followed by XELOX plus bevacizumab or single-agent bevacizumab as maintenance therapy in patients with metastatic colorectal cancer: the phase III MACRO TTD study. Oncologist 2012; 17: 15–25.
16 Yalcin S, Uslu R, Dane F, et al. Bevacizumab and capecitabine as maintenance therapy after initial bevacizumab+XELOX treatment in previously untreated patients with metastatic colorectal cancer: Phase III stop and go study result—a Turkish Oncology Group trial. Oncology 2013; 85: 328–35.
17 Hurwitz H, Fehrenbacher L, Novotny W, et al. Bevacizumab plus irinotecan, fl uorouracil, and leucovorin for metastatic colorectal cancer. N Engl J Med 2004; 350: 2335–42.
18 Cunningham D, Lang I, Marcuello E, et al. Bevacizumab plus capecutabine versus capecitabine alone in elderly patients with previously untreated metastatic colorectal cancer (AVEX): an open-label, randomised phase 3 trial. Lancet Oncol 2013; 11: 1077–85.
19 Tebbutt NC, Wilson K, Gebski VJ, et al. Capecitabine, bevacizumab, and mitomycin in fi rst-line treatment of metastatic colorectal cancer: results of the Australasian Gastrointestinal Trials Group Randomized Phase III MAX Study. J Clin Oncol 2010; 28: 3191–98.