
Magnetoencephalography: applications in psychiatry
11
REVIEW Magnetoencephalography: Applications in Psychiatry Martin Reite, Peter Teale, and Donald C. Rojas Magnetoencephalography (MEG) measures the extracra- nial magnetic fields produced by intraneuronal ionic current flow within appropriately oriented cortical pyra- midal cells. Based upon superconducting quantum inter- ference device technology operating at liquid helium temperatures (4 K), MEG offers excellent temporal and spatial resolution for selected sources, and complements information obtained from electroencephalograms and other functional imaging strategies. Current instrumenta- tion permits recording up to several hundred channels simultaneously with head-shaped dewars, although the cost of such systems is high. The fact that magnetic fields fall off with the square of the distance from the source is both a benefit (when separating activity in the two hemi- spheres) and a limitation (when attempting to record deep sources). The lack of skin contact facilitates using MEG to record direct current and very high frequency (.600 Hz) brain activity. The clinical utility of MEG includes pre- surgical mapping of sensory cortical areas and localiza- tion of epileptiform abnormalities, and localization of areas of brain hypoperfusion in stroke patients. MEG studies in psychiatric disorders have contributed materi- ally to improved understanding of anomalous brain later- alization in the psychoses, have suggested that P50 ab- normalities may reflect altered gamma band activity, and have provided evidence of hemisphere-specific abnormal- ities of short-term auditory memory function. Biol Psy- chiatry 1999;45:1553–1563 © 1999 Society of Biological Psychiatry Key Words: Magnetoencephalography, electroencepha- lography, schizophrenia, auditory evoked fields, somato- sensory evoked fields, magnetic source imaging, bipolar disorder, schizoaffective disorder, psychoses Introduction T he first human magnetoencephalogram (MEG) was reported by David Cohen in 1968 (Cohen 1968). Cohen placed a 1 million turn coil of fine 44-gauge wire next to the back of the heads of volunteer subjects sitting in a magnetically shielded chamber at the Massachusetts Institute of Technology, and averaging the output of the coil with a computer using an electroencephalogram (EEG) alpha wave as trigger, saw evidence of alpha frequency magnetic fields. Several years later, using a superconducting quantum interference device (SQUID)- based sensor developed, named, and provided by James E. Zimmerman, then at the Ford Motor Company, Cohen demonstrated the first human MEG recorded with a superconducting sensor (Cohen 1972). Since that time, significant advances have been made in the superconduct- ing technology used to record MEG, and in human clinical applications of MEG. This paper provides a brief review of the generation of magnetic fields in the brain, the instrumentation available for their recording, and the findings that have emerged to date, emphasizing MEG correlates of brain function in mental illness. Magnetic Fields of the Brain High school physics taught us that a current-carrying conductor produces magnetic fields that emerge from the conductor expanding with the speed of light, and follow- ing the right hand rule. Grasping the conductor with the right hand, with the thumb pointing in the direction of the current (positive charge flow), the magnetic field encircles the conductor in the direction of the closed fingers. Assuming now that the current(s) are the intraneuronal flow of charged ionic particles in the proximal dendritic segments of appropriately oriented cortical pyramidal cells (which are not necessarily firing, but whose membrane potentials are being modulated with resultant time varying intra- and extraneuronal current flow), such neurons also produce magnetic fields. The current density is highest intraneuronally; thus, these currents are most effective in producing coherent magnetic fields that exit the head. The extraneuronal return currents are equal, but widely distrib- uted, producing net magnetic fields that likely cancel or close intracerebrally, and are not well seen outside the head. It is these extraneuronal currents, however, that may be best seen by EEG. It has been estimated that about 50,000 similarly ori- ented cortical pyramidal cells modulated in unison will produce a magnetic field that can be recorded extracere- brally with contemporary SQUIDs (Okada 1993). In physical model situations, MEG and EEG electrocorticog- raphy (not scalp-recorded EEG) demonstrate similar lo- calization accuracy (1.5 mm versus 1.8 mm mean error, respectively), although the error in the electrical localiza- From Biomagnetic Imaging Laboratory, Department of Psychiatry, University of Colorado Health Sciences Center, Denver, Colorado, USA (MR) Address reprint requests to Martin Reite, MD, University of Colorado Health Sciences Center, Department of Psychiatry, Box C268-68, 4200 East Ninth Avenue, Denver, CO 80262. Received May 14, 1998; revised March 1, 1999; accepted March 3, 1999. © 1999 Society of Biological Psychiatry 0006-3223/99/$20.00 PII S0006-3223(99)00062-1
Transcript of Magnetoencephalography: applications in psychiatry

REVIEW
Magnetoencephalography: Applications in Psychiatry
Martin Reite, Peter Teale, and Donald C. Rojas
Magnetoencephalography (MEG) measures the extracra-nial magnetic fields produced by intraneuronal ioniccurrent flow within appropriately oriented cortical pyra-midal cells. Based upon superconducting quantum inter-ference device technology operating at liquid heliumtemperatures (4 K), MEG offers excellent temporal andspatial resolution for selected sources, and complementsinformation obtained from electroencephalograms andother functional imaging strategies. Current instrumenta-tion permits recording up to several hundred channelssimultaneously with head-shaped dewars, although thecost of such systems is high. The fact that magnetic fieldsfall off with the square of the distance from the source isboth a benefit (when separating activity in the two hemi-spheres) and a limitation (when attempting to record deepsources). The lack of skin contact facilitates using MEG torecord direct current and very high frequency (.600 Hz)brain activity. The clinical utility of MEG includes pre-surgical mapping of sensory cortical areas and localiza-tion of epileptiform abnormalities, and localization ofareas of brain hypoperfusion in stroke patients. MEGstudies in psychiatric disorders have contributed materi-ally to improved understanding of anomalous brain later-alization in the psychoses, have suggested that P50 ab-normalities may reflect altered gamma band activity, andhave provided evidence of hemisphere-specific abnormal-ities of short-term auditory memory function.Biol Psy-chiatry 1999;45:1553–1563 ©1999 Society of BiologicalPsychiatry
Key Words: Magnetoencephalography, electroencepha-lography, schizophrenia, auditory evoked fields, somato-sensory evoked fields, magnetic source imaging, bipolardisorder, schizoaffective disorder, psychoses
Introduction
The first human magnetoencephalogram (MEG) wasreported by David Cohen in 1968 (Cohen 1968).
Cohen placed a 1 million turn coil of fine 44-gauge wirenext to the back of the heads of volunteer subjects sittingin a magnetically shielded chamber at the MassachusettsInstitute of Technology, and averaging the output of the
coil with a computer using an electroencephalogram(EEG) alpha wave as trigger, saw evidence of alphafrequency magnetic fields. Several years later, using asuperconducting quantum interference device (SQUID)-based sensor developed, named, and provided by James E.Zimmerman, then at the Ford Motor Company, Cohendemonstrated the first human MEG recorded with asuperconducting sensor (Cohen 1972). Since that time,significant advances have been made in the superconduct-ing technology used to record MEG, and in human clinicalapplications of MEG. This paper provides a brief reviewof the generation of magnetic fields in the brain, theinstrumentation available for their recording, and thefindings that have emerged to date, emphasizing MEGcorrelates of brain function in mental illness.
Magnetic Fields of the Brain
High school physics taught us that a current-carryingconductor produces magnetic fields that emerge from theconductor expanding with the speed of light, and follow-ing the right hand rule. Grasping the conductor with theright hand, with the thumb pointing in the direction of thecurrent (positive charge flow), the magnetic field encirclesthe conductor in the direction of the closed fingers.Assuming now that the current(s) are the intraneuronalflow of charged ionic particles in the proximal dendriticsegments of appropriately oriented cortical pyramidal cells(which are not necessarily firing, but whose membranepotentials are being modulated with resultant time varyingintra- and extraneuronal current flow), such neurons alsoproduce magnetic fields. The current density is highestintraneuronally; thus, these currents are most effective inproducing coherent magnetic fields that exit the head. Theextraneuronal return currents are equal, but widely distrib-uted, producing net magnetic fields that likely cancel orclose intracerebrally, and are not well seen outside thehead. It is these extraneuronal currents, however, that maybe best seen by EEG.
It has been estimated that about 50,000 similarly ori-ented cortical pyramidal cells modulated in unison willproduce a magnetic field that can be recorded extracere-brally with contemporary SQUIDs (Okada 1993). Inphysical model situations, MEG and EEG electrocorticog-raphy (not scalp-recorded EEG) demonstrate similar lo-calization accuracy (1.5 mm versus 1.8 mm mean error,respectively), although the error in the electrical localiza-
From Biomagnetic Imaging Laboratory, Department of Psychiatry, University ofColorado Health Sciences Center, Denver, Colorado, USA (MR)
Address reprint requests to Martin Reite, MD, University of Colorado HealthSciences Center, Department of Psychiatry, Box C268-68, 4200 East NinthAvenue, Denver, CO 80262.
Received May 14, 1998; revised March 1, 1999; accepted March 3, 1999.
© 1999 Society of Biological Psychiatry 0006-3223/99/$20.00PII S0006-3223(99)00062-1

tions may increase more than magnetic localizations withincreasing source depths) (Gharib et al 1995).
One major advantage magnetic fields have over electri-cal potentials is that, once generated, they are relativelyinvulnerable to intervening variations in the media theytraverse (i.e., tissues and fluids of various types, and air).Additionally, they are absolute measurements and requireno reference. Thus, MEG avoids the disadvantages ofscalp-recorded EEG, including the electrode–skin inter-face, smearing of potential topography caused by conduc-tive differences of the skin, scalp, skull, and cerebrospinalfluid (CSF) intervening between source and electrode, andthe obligate referential requirement of potential record-ings. They also fall off in amplitude with the square of thedistance, which can be either an advantage (e.g., whentrying to separate activity in the two hemispheres), ordisadvantage (e.g., when trying to examine deep brainsources).
A representative illustration of the steps involved inMEG recording and magnetic source imaging (MSI) areillustrated in Figure 1.
The orientation of a cohort of physiologically entrainedpyramidal cells with respect to the inner skull surface isimportant in MEG recordings. Cells oriented in such amanner that their long axes are parallel to the plane of thetangent to the above surface will produce fields (remem-bering the right hand rule) that emerge from the conductor(brain) and cut the plane of the sensing coil, and theirfields will be “visible.” Such orientations are termedtangential. Cells whose long axes are radial to the surfaceof the brain will produce magnetic fields that surround thecells and are exactly cancelled by the action of theassociated volume currents; these orientations are termedradial, and they are essentially invisible to the magneticsensor. If the magnetic sensor is replaced by an EEGelectrode, the relative visibility of the two cellular orien-tations is reversed. Radial orientations are best seen withthe EEG electrode, as maximum electrical positivity ornegativity will be directed at the electrode. Cells withtangential orientations will not be seen as well by the EEGelectrode, for their plane of maximum potential lies at aright angle to the electrode. The implication of thisrelationship is that the scalp surface topography for mag-netic field and electric potential representations of thesame source will be orthogonal. That this is in fact trueoperationally is illustrated in Figure 2, which illustrates the100-msec latency auditory evoked field (EF) componentM100 and the comparable EEG evoked potential (EP)N100 recorded from the right hemisphere of the samesubject (using a localized very high spatial density elec-trode array for the EEG), with the corresponding neuralsource estimates located on the right superior temporalgyrus (STG).
In this illustration, the MEG and EEG inverse solutionsresult in sources very close to each other (mean vectordistance 1.6 cm) in the STG. Neurons oriented at random(i.e., in subcortical nuclei) will produce magnetic fieldsthat cancel, and will be largely invisible to MEG sensors,although a representation of their net extraneuronal currentflow may be visible with EEG, as for example with brainstem auditory-evoked potentials.
Instrumentation
Extracranial neuromagnetic signals are typically in therange of 50–500 femto Tesla (fT), which is about 1028 to1029 of the earth’s magnetic field, necessitating SQUID-superconducting technology as well as some degree ofmagnetic shielding for their successful identification (seeHamalainen et al, 1993, for a comprehensive review of thetopic).
The fact that all contemporary commercially availableinstrumentation for recording MEG is based on supercon-ducting technology operating at 4 K (liquid helium tem-perature) adds significantly to its cost and complexity. Theso-called high Tc (hTc) technology, based on supercon-ductors operating at higher temperature such as that ofliquid nitrogen (77 K) remains too noisy for use inmagnetoencephalography, although magnetocardiogramscan be recorded using hTc technology. Recording systemshave in common sensing coils of various geometriescoupled to a SQUID, both operated at 4 K, either sub-mersed in liquid helium, or in the case of new BiomagneticTechnologies, Inc. (BTi, San Diego, CA) instrumentation,contained within the vacuum space. All systems require alarge vacuum bottle or dewar (named after Sir JamesDewar, the Scottish chemist and physicist who invented it)to contain the liquid helium.
Most systems must also be operated in a magneticallyshielded room to screen out competing fields from theearth, sun, and magnetic noise in the environment. Excep-tions are those made by CTF Systems (Vancouver, BC,Canada), which manufactures MEG systems that can beoperated without shielding, utilizing instead additionalsensing coils to monitor environmental fields and softwareto provide cancellation, in effect resulting in an estimationof the third-order magnetic gradient. Most magneticallyshielded rooms are constructed from a combination ofaluminum and high permeability iron (mu metal). Thealuminum provides an eddy current shielding effect, inwhich impinging magnetic fields produce eddy currentswithin the aluminum that tend to cancel the impingingfields. The mu metal, placed either outside or inside thealuminum (or both), provides a low reluctance path for theexternal flux, essentially rerouting it around and awayfrom the interior of the shielded area. Conventional
1554 M. Reite et alBIOL PSYCHIATRY1999;45:1553–1563

radiofrequency (RF) shielding as is sometimes used forEEG or electrophysiological recordings is inadequate foruse in magnetic recordings.
Although it is possible to use a SQUID machinedfrom solid niobium as the actual magnetic sensor (Reiteet al 1981), more typically a coil located at the base ofthe dewar serves as sensor, which is coupled to a
SQUID. Sensing coil geometry can range from singleloops (magnetometers—measuring the total fluxthrough the coil—requiring exceptionally good shield-ing) to two or more loops wound in opposition (gradi-ometers—which discriminate against distant sources[more uniform fields] and favor the local [brain] sourc-es). Coils can be physically wound using niobium wire
C
A
B
Figure 1. Illustration of steps involved in magnetic source localization. (A) Left hemisphere recording of somatosensory responses toright median nerve stimulation (not shown) using BTI Magnes I 37 channel neuromagnetometer. (B) Somatosensory waveforms inlower half with time on thex axis (stimulus delivery at time zero), and strength in fempto Tesla on they axis. The upper waveformillustrates normalized error of the model fit versus poststimulus latency. (C) The 20-msec latency somatosensory source (green square)superimposed on the magnetic resonance image. Yellow dots indicate high proton density capsules attached to head.
MEG: Applications in Psychiatry 1555BIOL PSYCHIATRY1999;45:1553–1563

on quartz or similar material cores, or can be manufac-tured on thin film substrates.
For the past 15 years, we have seen MEG technologyevolve from single channel systems to multichannel sys-tems of various designs, to the present-day whole headsystems that can monitor well over 100 channels simulta-neously in a helmet-shaped dewar. The relatively high costof large multichannel systems has to date limited theirutilization, and cost has also been a rate-limiting step inadvancing basic knowledge in the field.
MEG and Magnetic-Evoked Fields
When written out on an inkwriter, the raw MEG looksstrikingly similar to the EEG. Posterior dominant alphaactivity is seen that blocks normally (Reite et al 1976);wicket or mu rhythms are prominent over sensorimotorcortex (Tiihonen et al 1989); and an 8–10-Hz magnetic taurhythm has been described over auditory cortex that isblocked by auditory stimulation (Tiihonen et al 1991).Alpha, mu, and tau rhythms may all reflect the idling stateof primary sensory cortex, which “block” (suppress withactivation) with specific sensory stimulation. To date itappears that MEG, because of its greater capability forspatial localization, may be of greater utility in isolating
such rhythms than EEG. For example, Kaufman andcolleagues have used MEG recordings to quantify block-ing of alpha activity from auditory cortical regions byspecific Sternberg-based tonal memory tasks as a measureof cortical activation accompanying short-term memorysearch and retrieval (Kaufman et al 1992). Such spatialprecision in EEG recordings has yet to be reported.
MEG recorded during sleep demonstrates waveformssimilar to those of sleep EEG, including delta activity,sleep spindle, and K complexes (Hughes et al 1976; Lu¨ STet al 1992), but comprehensive studies of sleep have yet tobe reported. Magnetic-evoked fields, like EEG-evokedpotentials, can be recorded to all types of sensory stimuli.
With few exceptions (Lewine and Orrison 1995;Makela et al 1998), the clinical interpretation of rawmultichannel MEG, as is done with EEG, is normally notpart of a MEG study, and thus its potential value remainslargely unknown. Similarly, although the statistical com-putations that form the basis for so called “computerized,”“quantified,” or “QEEG” (quantitative electroencephalog-raphy) could be performed with multichannel MEG data,such have not yet been reported.
Two special properties of MEG—the lack of an elec-trode–skin interface and the relative transparency of vary-ing conductivity tissues to magnetic fields—have facili-
Figure 2. M100 evoked field (EF) topography (left panel) compared with N100 evoked potential (EP) topography (right panel). In theleft panel, outgoing magnetic fields are shades of red, ingoing fields are shades of blue. In the right panel, scalp positivity is shownin shades of red, scalp negativity is shown in shades of blue. Field and potential topographies are essentially orthogonal, as would bepredicted. The magnetoencephalography (MEG) EF topography was obtained by plotting field values obtained from 91 coil locations(dots) at the time point 93 msec poststimulus, using 80-dB SPL, 1-kHz, 25-msec duration tone pips with 1.8 sec as the interstimulusinterval. Values were averages of 100 responses. Electroencephalogram EP topography obtained from a 16-electrode array indicatedby dark dots arranged in a “Star of David” configuration with inter-electrode distance of 2 cm. The same stimuli and analysisprocedures were used as in MEG. Underlying source location superimposed upon the right superior temporal gyrus indicated by whitedots (magnetic source in left panel; electrical source in right panel). Source locations differ by 16 mm, primarily in thex (medio-lateral)dimension. (Data from Teale P, Wang J, Reite M, Sheeder J, Nunez P Auditory source localization with MEG and EEG. Presented atthe 8th World Congress of the International Society for Brain Electromagnetic Topography, Zurich, March 1997.)
1556 M. Reite et alBIOL PSYCHIATRY1999;45:1553–1563

tated studies of very low frequency (or direct current[DC]) and very high frequency activity that is difficult torecord electrically. Tepley has used DC magnetic record-ings to study stroke, migraine, and head trauma patients,permitting investigation of possible spreading corticaldepression (Tepley et al 1996).
Several studies have examined higher frequency com-ponents in the MEG. Ribary and colleagues used a strategytermed magnetic field tomography (MFT) to examine theorigin of coherent 40-Hz gamma band magnetic activitythought to represent recurrent thalamocortical oscillation,and found evidence of abnormalities in Alzheimer’s pa-tients (Ribary et al 1991). These investigators estimatedthat MFT is able to provide temporal resolutions of,1msec with spatial accuracy of 2–5 mm at the level of thecortex, degrading to 1–3 cm at depths.6 cm. Thefrequency of sensory cortical MEG gamma band activitymay be a function of stimulus modality (and corticalregion), with spectral peaks between 30 and 40 Hz in theauditory system, between 45 and 55 Hz in the somatosen-sory system, and between 100 and 110 Hz in the visualsystem (Pantev et al 1995). Some evidence suggestssensory (auditory) stimuli may reset ongoing gamma bandactivity, possibly reflecting the temporal binding of sen-sory stimuli (Joliot et al 1994).
It is also possible to record much higher frequencyMEG activity (.600 Hz) elicited in the context of somato-sensory processing, which has been implicated as reflect-ing repetitive spike volleys conducted along the terminalsegments of somatotopically arranged thalamocortical ax-ons, or early intracortical spike activity (Curio et al 1997).Hashimoto has suggested such activity might reflect theactivity of intracortical GABAergic inhibitory interneu-rons (Hashimoto et al 1996). Pulvermuller and colleagueshave suggested that widely dispersed and bilateraltranscortical cell assemblies may represent elements ofhigher cortical processing and that the activities of suchassemblies may be reflected in higher frequency gammaband MEG (and EEG) activity (Pulvermuller et al 1995;Pulvermuller and Mohr 1996).
Most MEG studies have emphasized source localization,sometimes termed MSI, of either spontaneous (i.e., epilepti-form or pathological slow wave activity) or sensory-evokedmagnetic activity. The fundamental principal of localizingthe putative source of either spontaneous or evoked magneticactivity depends on several basic assumptions. First, that it isreasonable to consider a single, or relatively few, discretesources for the phenomena in question that can be appropri-ately mathematically modeled. Second, that sufficient basicneurophysiological and neuroanatomical information isavailable to provide the initial constraints for the localizationof such sources. We would not expect to localize primarysensory sources extracerebrally, or in white matter distant
from primary sensory cortex. Such assumptions are implicitin source localization.
The construct of the equivalent current dipole (ECD) iscentral to the principal of source localization. A knownsingle ECD in the brain (which is unlikely to actually existphysiologically) will produce one and only one clearlydefined magnetic field topography over the surface of thescalp. The identical surface topography, however, could intheory be produced by an infinite number of sourceconfigurations, thus necessitating intelligent constraints.Given a surface field topography (field strength in femtoTeslas from multiple sensors, which includes both positive[outgoing field] and negative [ingoing field] values), it ispossible to estimate the most likely source responsible forthis surface field distribution, includingx, y,andz location(usually with respect to “fiduciary points” on the skull orscalp), as well as source orientation and source strength.Usually a so-called “goodness of fit” calculation is in-cluded, which reflects the agreement between the knownsurface topography such a source would produce as afunction of the ideal mathematical “forward solution” andthe actually measured field pattern.
It has been gratifying to observe that many early(latency up to approximately 100 msec poststimulus)sensory evoked fields have a high goodness of fit to asingle ECD model, and that when such sources aremapped onto the corresponding magnetic resonance (MR)anatomy, the locations are found to fall within the appro-priate sensory cortex. This model provides face validity tothe source localization of such phenomena. This is lesslikely to be true for later (longer latency) evoked fieldscomponents that likely involve widely distributed cogni-tive processing that cannot be reasonably modeled with asingle or simple set of sources. Although it might bemathematically possible to calculate the inverse solutionin such cases, and even sometimes find a relatively highgoodness of fit, one should retain a high level of skepti-cism as to whether the solution is correct, and that a likelycomplex and widely distributed activity can be reasonablyreduced to a simple solution.
The availability of large array and whole head systemshave permitted the application of more sophisticatedmodeling procedures that appear capable of locating sev-eral widely distributed sensory sources at least in thevisual domain, (e.g., see Aine et al 1996). Novel methodsfor processing somatosensory EFs such as “signal spaceprocessing” with magnetic resonance imaging (MRI)-based source location constraints have been used toestimate thalamic contributions to extracranial field topog-raphy (Tesche 1996). Resolution using this method isestimated to be on the order of centimeters.
The mathematical modeling of multiple simultaneoussources is a field that, while progressing, remains
MEG: Applications in Psychiatry 1557BIOL PSYCHIATRY1999;45:1553–1563

immature but with very significant potential. It shouldbe understood that all such methods are dependent onthe model used to estimate the physiological locus ofprocessing and thus constrain the inverse solution.Unlike anatomical and functional MRI, and other im-aging techniques such as positron emission tomography(PET) and single photon emission computed tomogra-phy (SPECT), in which the raw data can directlyrepresent the structure (anatomy) or location of function(e.g., blood flow related signal changes), the MEGsignal can be interpreted only in the context of theparticular model being specified. EEG is also subject tothe same limitation. This limitation has complicated theinterpretation of MEG data and physiologically moremeaningful multi-source models individually separablein space and time have yet to be perfected.
Clear benefits of MEG stem from improved spatialresolution of certain sources complemented by the factthat fields fall off rapidly (1/r2) with distance, permittingimproved separation of activity in left and right hemi-spheres of the brain. The value of this improved accuracyof source localization is demonstrated by the ability ofMEG to map the tonotopic organization of the humanauditory cortex (Pantev et al 1988; Yamamoto et al 1992),the reorganization of digit representation in the motorcortex of violin players (Elbert et al 1995), and thereorganization of cortex observed in individuals afteramputations (Elbert et al 1997). Similarly, the clearseparation of activity in the two hemispheres permits thestudy of the independent development of electrophysio-logical activity in left and right hemispheres of children(Rojas et al in press) and the studies of anomalous cerebrallateralization and possible cortical reorganization inschizophrenia or the psychoses to be described below.
Clinical Utility of MEG Recordings
Perhaps the two most common clinical uses of MEG todate are in localization of epileptiform activity andpresurgical mapping of sensory cortex prior to neuro-surgical procedures. Neuroanatomically constrained ep-ileptiform sources can produce extracranial magneticfields whose topography and amplitude can be used toestimate the source of the abnormality, which can thenbe mapped onto anatomy by coregistration with MRIanatomical data. MEG recordings have been shown tobe capable of comparable accuracy to direct corticalEEG recordings (Nakasato et al 1994; Ebersole 1997),and may sometimes provide localization informationnot available with conventional EEG or MRI (Smith etal 1994; Knowlton et al 1997). When recorded simul-taneously, MEG and EEG sometimes appear to bemeasuring somewhat different current sources, suggest-
ing that both contain valuable but nonidentical data(Merlet et al 1997).
Similarly evoked sensory activity in the somatosensoryand auditory regions can be used presurgically to locateprimary sensory cortical areas to be avoided during surgicalprocedures. Hund et al (1997) used preoperative MEGmapping of sensory and motor sources in conjunction withMRI anatomical data in 40 candidate neurosurgical patientsand found the MEG source localizations to be of value indetermining whether operative or nonoperative approacheswere indicated. Rezai and colleagues described a methodwhereby functional MEG data can be integrated with CTscans, MRI data, and digital angiography within a stereotaxicdatabase that can be used interactively during computer-assisted stereotaxic volumetric resections for lesions involv-ing the sensorimotor cortex (Rezai et al 1996). These authorsasserted that the real-time availability of functional datatended to reduce surgical risk as well as functional morbidity(Rezai et al 1997).
In patients with cerebral infarcts, MEG slow waveactivity has been localized to tissue areas exhibiting mildreductions in N-acetyl levels and increases in lactatethought to reflect areas of hypoperfusion surroundinginfarcted areas (Kamada et al 1997).
MEG Studies in Psychiatric Disorders
The published literature on MEG in psychiatric disordersis increasing rapidly, but the absolute number of studies isnot yet large. Nonetheless, MEG studies to date havecontributed to our knowledge of:
1. disturbances in cerebral lateralization in psychoses,2. short-term auditory sensory memory abnormalities
in schizophrenia,3. possible cortical reorganization in schizophrenia,
and4. the possible role of gamma band generators in P50
abnormalities in schizophrenia.
Additionally, special characteristics of MEG recordingssuggest their potential value in examining early sensorycortical function, including the establishment and mainte-nance of memory trace, and in examining high frequencycortical activity reflecting both gamma band-like phenom-ena and very high frequency cortical activity possiblyrepresenting inhibitory interneuronal activity. As suchareas are developed, their relevance to the major mentaldisorders should prove to be substantial.
Disturbances in Cerebral Lateralization inPsychosis
The brain is not bilaterally symmetrical, and the hemi-spheres differ markedly in terms of both structure (Gala-
1558 M. Reite et alBIOL PSYCHIATRY1999;45:1553–1563
burda et al 1978; Weinberger et al 1982; Willerman et al1992; Galaburda 1995) and function (Gevins et al 1983;Sholl and Kim 1990; Davidson and Hugdahl 1995). Thereis also a long history relating possible disturbance incerebral lateralization to the psychoses, initially empha-sized by the work of Flor-Henry (1969) and Gruzelier andHammond (1980), and recently reviewed by Lohr andCaligiuri (1997). Crow has suggested that the psychoticillnesses, perhaps especially schizophrenia, are related todisturbances in the development of cerebral lateralization(Crow and Harrington 1994), and that they may representa continuum rather than discrete entities (Crow 1995).
MEG evidence of disturbed cerebral lateralization in thepsychoses have been described in both auditory andsomatosensory domain.
Auditory System in Schizophrenia
The magnetic counterpart of the auditory 100-msec la-tency EP complex N100 has been studied extensively innormal subjects using MEG recordings, in which it hasbeen variously termed the M100 or N100m. The M100appears to be generated in or near Heschl’s gyrus (Pantevet al 1988; Reite et al 1994), demonstrates a sex specificinterhemispheric asymmetry being relatively further ante-rior in the right hemisphere of males (Reite et al 1989;Nakasato et al 1995), and less so in females (Scheunemanet al 1991) and male homosexuals (Reite et al 1995).Functionally, the M100 complex may index echoic mem-ory (Lu Z-L et al 1992).
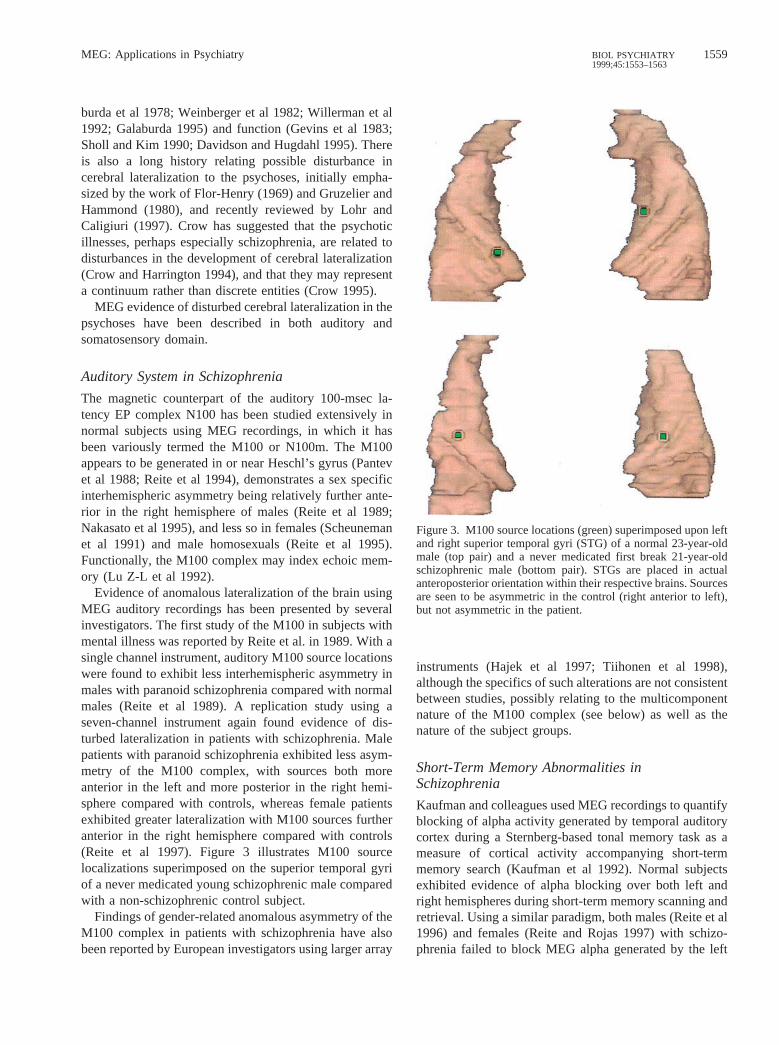
Evidence of anomalous lateralization of the brain usingMEG auditory recordings has been presented by severalinvestigators. The first study of the M100 in subjects withmental illness was reported by Reite et al. in 1989. With asingle channel instrument, auditory M100 source locationswere found to exhibit less interhemispheric asymmetry inmales with paranoid schizophrenia compared with normalmales (Reite et al 1989). A replication study using aseven-channel instrument again found evidence of dis-turbed lateralization in patients with schizophrenia. Malepatients with paranoid schizophrenia exhibited less asym-metry of the M100 complex, with sources both moreanterior in the left and more posterior in the right hemi-sphere compared with controls, whereas female patientsexhibited greater lateralization with M100 sources furtheranterior in the right hemisphere compared with controls(Reite et al 1997). Figure 3 illustrates M100 sourcelocalizations superimposed on the superior temporal gyriof a never medicated young schizophrenic male comparedwith a non-schizophrenic control subject.
Findings of gender-related anomalous asymmetry of theM100 complex in patients with schizophrenia have alsobeen reported by European investigators using larger array
instruments (Hajek et al 1997; Tiihonen et al 1998),although the specifics of such alterations are not consistentbetween studies, possibly relating to the multicomponentnature of the M100 complex (see below) as well as thenature of the subject groups.
Short-Term Memory Abnormalities inSchizophrenia
Kaufman and colleagues used MEG recordings to quantifyblocking of alpha activity generated by temporal auditorycortex during a Sternberg-based tonal memory task as ameasure of cortical activity accompanying short-termmemory search (Kaufman et al 1992). Normal subjectsexhibited evidence of alpha blocking over both left andright hemispheres during short-term memory scanning andretrieval. Using a similar paradigm, both males (Reite et al1996) and females (Reite and Rojas 1997) with schizo-phrenia failed to block MEG alpha generated by the left
Figure 3. M100 source locations (green) superimposed upon leftand right superior temporal gyri (STG) of a normal 23-year-oldmale (top pair) and a never medicated first break 21-year-oldschizophrenic male (bottom pair). STGs are placed in actualanteroposterior orientation within their respective brains. Sourcesare seen to be asymmetric in the control (right anterior to left),but not asymmetric in the patient.
MEG: Applications in Psychiatry 1559BIOL PSYCHIATRY1999;45:1553–1563

temporal lobe during this task, although right temporallobe alpha appeared to block normally.
To date, replication studies have not been reported, norhave there been reports of similar findings using EEGrecordings. It is possible that EEG may not providesufficient spatial resolution of STG alpha activity topermit this type of study, although increased spatialsampling might obviate this concern.
Interestingly, this left temporal impairment of alphablocking appeared to be independent of underlying volu-metric abnormalities, insofar as that we and others (Shen-ton et al 1992) have found evidence of decreased STGvolume in the left hemisphere of males with schizophre-nia, whereas females with schizophrenia do not appear toexhibit smaller left STG (Reite et al 1997).
The M100 component is thought by some investigatorsto index the echoic memory trace (Lu Z-L et al 1992).MEG-based measures of short-term memory functioninclude determining the time constant (t) of the decay rateof the echoic trace, which, although reported in normals,has yet to be reported in subjects with mental illness.Similarly, the MEG analog of EEG mismatch negativity,which has been found to be abnormal in schizophrenia(Javitt et al 1993), has yet to be reported in the literature.
Recent evidence suggests the M100 may actually consistof two independent subcomponents separated temporally byabout 25 msec. Source locations appear similarly in the leftSTG, but the later source is further anterior in the right STGby about 8–9 mm (Teale et al 1998). Each source mayinvolve a different aspect of echoic memory, and severalinvestigators have suggested that the early source maypreferentially index stimuli with shorter interstimulus inter-vals (ISI), and the later (and more anterior in the righthemisphere) source stimuli with longer ISI (Sams et al 1993;Loveless et al 1996). Recent findings from our laboratorysuggest neither source is lateralized in subjects with schizo-phrenia or schizoaffective disorder (data not shown). Allprevious published studies of the M100 in schizophrenia(Hajek et al 1997; Reite et al 1997; Tiihonen et al 1998) usedfiltering and analytic methods that tended to combine bothsources into an apparently unitary M100.
Studies of Somatosensory System in AffectivePsychoses
Electrical stimulation of the median nerve at the wristresults in a prominent series of EF components recordedfrom the contralateral somatosensory cortex. The 20-mseclatency component, termed the M20, is generated in area3b of the postcentral gyrus (Kamada et al 1993;Kawamura et al 1996), and in normal individuals exhibitsinterhemispheric asymmetry, being further anterior in theright hemisphere (Wikstrom et al 1997).
We examined the M20 component in 16 patients withDSM-IV schizoaffective disorder, and found that it wasreverse lateralized, compared with 16 control subjects(Reite et al in press a). That is, in the right hemisphere ofschizoaffective patients, the M20 was relatively furtherposterior compared with the left hemisphere source loca-tion (data not shown).
Another study examined the M20 source localization in12 normals and 21 individuals with bipolar I disorder, 9 ofwhom had never been psychotic, and 12 of whom hadbeen psychotic in the past during their mood episodes.None were psychotic at the time of the study. Bipolar Isubjects who had exhibited evidence of psychosis hadreversed lateralization of the M20 source (right posteriorto left), whereas bipolar I subjects who had not beenpsychotic were lateralized similarly to controls (rightanterior to left) (Reite et al in press b).
Both the above studies support the notion of alteredcerebral lateralization being associated with psychoses,but the additional implication is that there may be arelative anatomical displacement of the postcentral gyrus(right posterior to left) in the affective psychoses.
Evidence for Possible CorticalReorganization in Schizophrenia
The finding that the auditory M100 component exhibitsrelatively different source locations in the left and righthemispheres of subjects with schizophrenia could beexplained by either a shift in the anatomical location ofHeschl’s gyri, thought to be its generator site (Pantev et al1990; Reite et al 1994) or, alternatively, the componentcould be generated by a different region of cortex, imply-ing some degree of cortical reorganization. Rojas andcolleagues compared M100 source localizations with thevolume centroids of Heschl’s gyri in 24 controls and 21patients with paranoid schizophrenia (Rojas et al 1997).They found that the anomalous localization of the M100 inschizophrenia could not be explained by an anatomicalshift in Heschl’s gyri, which suggested a possible gender-specific functional reorganization of the auditory cortex inschizophrenia. Once again, however, in this study theM100 was conceptualized as a unitary component.Whether the evidence of cortical reorganization would beobtained by independently examining the early and laterM100 subcomponents remains to be determined.
Another method for addressing the problem of possiblecortical reorganization in schizophrenia would be to examinetonotopic organization of the auditory cortex in normalsubjects compared with subjects with schizophrenia. Thisfunctional organization can then be mapped onto underlyingneuroanatomical structures. As mentioned previously, MEGrecordings have demonstrated evidence of tonotopic organi-
1560 M. Reite et alBIOL PSYCHIATRY1999;45:1553–1563

zation in normals (Elberling et al 1982; Romani et al 1982;Pantev et al 1995). Yet to be reported in schizophrenia, suchstudies are now in progress in our laboratory.
Gamma Band Generators and the P50
The auditory P50 evoked potential component has been ofinterest in schizophrenia, apparently indexing a measure ofdisturbed habituation in the conditioning-testing paradigm(Adler et al 1982). The source of the P50 has beenvariously attributed to auditory cortex (Wood and Wolpaw1982), hippocampus (Goff et al 1980), or reticular struc-tures (Erwin and Buchwald 1986). Examining the mag-netic counterpart of the P50, termed the M50, Reite et alfound that inverse solution was compatible with a sourcein the superior temporal planum in the region of theauditory cortex (Reite et al 1988). The fact that themagnetic source localizes to the STG does not precludeother deeper sources from contributing to the vertex-recorded EP component, but to date, MEG evidence ofsuch activity has not been described. Recently, Clementzand collaborators have utilized MEG recordings to inferthat the P50 component may represent a subcomponent ofthe gamma band response, and the observed poor suppres-sion of P50 in schizophrenia might reflect an abnormalityin production of gamma band activity (Clementz et al 1997).
Summary
MEG is at a relatively early stage of development, andprogress has been limited by both the complexity andexpense of the technology and the advent of a number ofadditional new structural and functional imaging strategiesthat allow visualization of the brain in a manner notimaginable several decades ago. Nonetheless, MEG hasexcellent resolution in the temporal domain, and is oftensuperior to EEG in the spatial domain. MEG is the onlytechnique available that directly indexes intraneuronalcurrents. Promising contributions to our understanding ofthe psychotic disorders have resulted from MEG-baseddemonstrations of alterations in cortical reorganization,memory function, and brain lateralization, and expandedinterpretation of experimental findings from other meth-odologies. Anomalous lateralization and cortical reorgani-zation both imply a prenatal developmental disturbance,although disease-related mechanisms cannot yet be ex-cluded; additional data on specifics of such abnormalitiesmay permit a more accurate assessment of the timing ofthe processes involved. Future efforts at developing morecomprehensive models, data analytic strategies, and para-digms targeted to emphasize the strengths of MEG shouldpay rewards, as should the integration of MEG with otherfunctional and structural imaging technologies.
Supported by USPHS Grants no. MH47476 and MH56601.
ReferencesAdler L, Pachtman E, Franks R, Pecevich M, Waldo M,
Freedman R (1982): Neurophysiological evidence for a defectin neuronal mechanisms involved in sensory gating in schizo-phrenia.Biol Psychiatry17:639–654.
Aine CJ, Supek S, George JS, Ranken D, Lewine J, Sanders JA, etal (1996): Retinotopic organization of human visual cortex:departures from the classical model.Cereb Cortex6:354–361.
Clementz BA, Blumenfeld LD, Cobb S (1997): The gamma bandresponse may account for poor P50 suppression in schizo-phrenia.NeuroReport8:3889–3893.
Cohen D (1968): Magnetoencephalography: evidence of mag-netic fields produced by alpha-rhythm currents.Science161:784–786.
Cohen D (1972): Magnetoencephalography: detection of thebrain’s electrical activity with a superconducting magnetom-eter.Science175:664–666.
Crow TJ (1995): A continuum of psychosis, one human gene,and not much else—the case for homogeneity.Schizophr Res17:135–145.
Crow TJ, Harrington CA (1994): Etiopathogenesis and treatmentof psychosis.Annu Rev Med45:219–234.
Curio G, Mackert BM, Burghoff M, Neumann J, Nolte G, SchergM, et al (1997): Somatotopic source arrangement of 600 Hzoscillatory magnetic fields at the human primary somatosen-sory hand cortex.Neurosci Lett234:131–134.
Davidson RJ, Hugdahl K (1995):Brain Asymmetry.Cambridge,MA: MIT Press.
Ebersole JS (1997): Magnetoencephalography/magnetic source im-aging in the assessment of patients with epilepsy.Epilepsia38:S1–5.
Elberling C, Bak C, Kofoed B, Lebech J, Saemark K (1982):Auditory magnetic fields: source location and tonotopicorganization in the right hemisphere of the human brain.Scand Audiol11:61–65.
Elbert T, Pantev C, Wienbruch C, Rockstroh B, Taub E (1995):Increased cortical representation of the fingers of the left handin string players.Science270:305–307.
Elbert T, Sterr A, Flor H, Rockstroh B, Knecht S, Pantev C, et al(1997): Input-increase and input-decrease types of corticalreorganization after upper extremity amputation in humans.Exp Brain Res117:161–164.
Erwin RJ, Buchwald JS (1986): Midlatency auditory evokedresponses: differential recovery cycle characteristics.Electro-encephalogr Clin Neurophysiol64:417–423.
Flor-Henry P (1969): Psychosis and temporal lobe epilepsy: acontrolled investigation.Epilepsia10:363–395.
Galaburda AM (1995): Anatomic basis of cerebral dominence.In: Davidson RJ, Hugdahl K, editors.Brain Asymmetry.Cambridge, MA: MIT Press, pp 51–73.
Galaburda AM, Lemay M, Kemper TL, Geschwind N (1978):Right-left asymmetries in the brain.Science199:852–856.
Gevins AS, Schaffer RE, Doyle JC, Cutillo BA, Tannehill RS,Bressler SL (1983): Shadows of thought: shifting lateraliza-
MEG: Applications in Psychiatry 1561BIOL PSYCHIATRY1999;45:1553–1563

tion of human brain electrical patterns during brief visuomo-tor task.Science220:97–99.
Gharib S, Sutherling WW, Nakasato N, Barth D, Baumgartner C,Alexopoulos N, et al (1995): MEG and ECoG localizationaccuracy test.Electroencephalogr Clin Neurophysiol94:109–114.
Goff WR, Williamson PD, Vangilder JC, Allison T, Fisher TC(1980): Neural origins of long latency evoked potentialsrecorded from the depth and from the cortical surface of thebrain in man.Prog Clin Neurophysiol2:126–145.
Gruzelier J, Hammond NV (1980): Lateralized deficits and druginfluences on the dichotic listening of schizophrenia patients.Biol Psychiatry15:759–779.
Hajek M, Huonker R, Boehle C, Volz HP, Nowak H, Sauer H(1997): Abnormalities of auditory evoked magnetic fields andstructural changes in the left hemisphere of male schizophren-ics—a magnetoencephalographic-magnetic resonance imag-ing study.Biol Psychiatry42:609–616.
Hamalainen M, Hari R, Ilmoniemi RJ, Knuutila J, LounasmaaOV (1993): Magnetoencephalography—theory, instrumenta-tion, and applications to noninvasive studies of the workinghuman brain.Rev Mod Phys65:413–497.
Hashimoto I, Mashiko T, Imada T (1996): Somatic evokedhigh-frequency magnetic oscillations reflect activity of inhib-itory interneurons in the human somatosensory cortex.Elec-troencephalogr Clin Neurophysiol100:189–203.
Hughes JR, Hendrix DE, Cohen J, Duffy FH, Mayamn CI, SchollML, et al (1976): Relationship of the magnetoencephalogramto the electroencephalogram normal wake and sleep activity.Electroencephalogr Clin Neurophysiol40:261–278.
Hund M, Rezai AR, Kronberg E, Cappell J, Zonenshayn M, RibaryU, et al (1997): Magnetoencephalographic mapping: basic of anew functional risk profile in the selection of patients withcortical brain lesions.Neurosurgery40:936–942.
Javitt DC, Doneshka P, Zylberman I, Ritter W, Vaughan HGJ(1993): Impairment of early cortical processing in schizo-phrenia: an event-related potential confirmation study.BiolPsychiatry33:513–519.
Joliot M, Ribary U, Llinas R (1994): Human oscillatory brainactivity near 40 Hz coexists with cognitive temporal binding.Proc Natl Acad Sci USA91:11748–11751.
Kamada K, Oshiro O, Takeuchi F, Kuriki S, Houkin K, Iwasaki Y,et al (1993): Identification of central sulcus by using somatosen-sory evoked magnetic fields and brain surface MR images: threedimensional projection analysis.J Neurol Sci116:29–33.
Kamada K, Saguer M, Moller M, Wicklow K, Katenhauswer M,Kober H, et al (1997): Functional and metabolic analysis ofcerebral ischemia using magnetoencephalography and protonmagnetic resonance spectroscopy [see comments].Ann Neu-rol 42:554–563.
Kaufman L, Curtis S, Wang J-Z, Williamson SJ (1992): Changesin cortical activity when subjects scan memory for tones.Electroencephalogr Clin Neurophysiol82:266–284.
Kawamura T, Nakasato N, Seki K, Kanno A, Fujita S, Fujiwara S,et al (1996): Neuromagnetic evidence of pre- and post-centralcortical sources of somatosensory evoked responses [see com-ments].Electroencephalogr Clin Neurophysiol100:44–50.
Knowlton RC, Laxer KD, Aminoff MJ, Roberts TP, Wong ST,Rowley HA (1997): Magnetoencephalography in partial epi-lepsy: clinical yield and localization accuracy.Ann Neurol42:622–631.
Lewine JD, Orrison WWJ (1995): Magnetic source imaging:basic principles and applications in neuroradiology.AcadRadiol 2:436–440.
Lohr JB, Caligiuri MP (1997): Lateralized hemispheric dysfunc-tion in the major psychotic disorders: historical perspectivesand findings from a study of motor asymmetry in olderpatients.Schizophr Res27:191–198.
Loveless N, Levanen S, Jousmaki V, Sams M, Hari R (1996):Temporal integration in auditorysensory memory: neuromagneticevidence.Electroencephalogr Clin Neurophysiol100:220–228.
Lu ST, Kajola M, Joutsiniemi SL, Knuutila J, Hari R (1992):Generator sites of spontaneous MEG activity during sleep.Electroencephalogr Clin Neurophysiol82:182–196.
Lu Z-L, Williamson SJ, Kaufman L (1992): Behavioral lifetimeof human auditory sensory memory predicted by physiolog-ical measures.Science258:1668–1670.
Makela JP, Salmelin R, Hokkanen J, Launes J, Hari R (1998):Neuromagnetic sequelae of herpes simplex encephalitis.Elec-troencephalogr Clin Neurophysiol106:251–258.
Merlet I, Paetau R, Garcia-Larrea L, Uutela K, Granstrom ML,Mauguiere F (1997): Apparent asynchrony between interictalelectric and magnetic spikes.NeuroReport8:1071–1076.
Nakasato N, Fujita S, Seki K, Kawamura T, Matani A, TamuraI, et al (1995): Functional localization of bilateral auditorycortices using an MRI-linked whole head magnetoencepha-lography (MEG) system.Electroencephalogr Clin Neuro-physiol94:183–190.
Nakasato N, Levesque MF, Barth DS, Baumgartner C, Rogers RL,Sutherling WW (1994): Comparisons of MEG, EEG, and ECoGsource localization in neocortical partial epilepsy in humans.Electroencephalogr Clin Neurophysiol91:171–178.
Okada Y (1993): Neurogenesis of evoked magnetic fields. In:Williamson SJ, Romani GL, Kaufman L, Modena I, editors.Biomagnetism: An Interdisciplinary Approach.New York:Plenum Press, pp 399–408.
Pantev C, Bertrand O, Eulitz C, Verkindt C, Hampson S,Schuierer G, et al (1995): Specific tonotopic organizations ofdifferent areas of the human auditory cortex revealed bysimultaneous magnetic and electric recordings.Electroen-cephalogr Clin Neurophysiol94:26–40.
Pantev C, Hoke M, Lehnertz K, Lutkenhoner B, Anogianakis G,Wittkowski W (1988): Tonotopic organization of the humanauditory cortex revealed by transient auditory evoked magneticfields. Electroencephalogr Clin Neurophysiol69:160–170.
Pantev C, Hoke M, Lehnertz K, Lutkenhoner B, Fahrendorf G,Stober U (1990): Identification of sources of brain neuronalactivity with high spatiotemporal resolution through combi-nation of neuromagnetic source localization (NMSL) andmagnetic resonance imaging (MRI).Electroencephalogr ClinNeurophysiol75:173–184.
Pulvermuller F, Lutzenberger W, Preissl H, Birbaumer N(1995): Spectral responses in the gamma-band: physiolog-ical signs of higher cognitive processes?NeuroReport6:2059 –2064.
Pulvermuller F, Mohr B (1996): The concept of transcortical cellassemblies: a key to the understanding of cortical lateraliza-tion and interhemispheric interaction.Neurosci Biobehav Rev20:557–566.
Reite M, Adams M, Simon J, Teale P, Sheeder J, Richardson D,
1562 M. Reite et alBIOL PSYCHIATRY1999;45:1553–1563

et al (1994): Auditory M100 component 1: relationship toHeschl’s gyri.Cog Brain Res2:13–20.
Reite M, Rojas D (1997): MEG correlates of psychoses:anomalous lateralization and abnormal memory function.In: Witte H, Zwiener U, Schack B, Doering A, editors.Quantitative and Topological EEG and MEG Analysis.Erlangen, Germany: Druckhaus Mayer Verlag GMBHJena, pp 150 –154.
Reite M, Sheeder J, Richardson D, Teale P (1995): Cerebrallaterality in homosexual males: a preliminary communica-tion. Arch Sex Behav24:587–595.
Reite M, Sheeder J, Teale P, Adams M, Richardson D, Simon J,et al (1997): Magnetic source imaging evidence of sexdifferences in cerebral lateralization in schizophrenia.ArchGen Psychiatry54:433–440.
Reite M, Teale P, Goldstein L, Whalen J, Linnville S (1989):Late auditory sources may differ in the left hemisphere ofschizophrenic patients: a preliminary report.Arch Gen Psy-chiatry 46:565–572.
Reite M, Teale P, Rojar DC, Sheeder J, Arciniegas D (in press a):Schizoaffective disorder: Evidence for reversed cerebralasymmetry.Biol Psychiarty.
Reite M, Teale P, Rojas DC, Arciniegas D, Sheeder J (in pressb): Bipolar disorder: anomalous brain asymmetry associatedwith psychosis.Am J Psychiatry.
Reite M, Teale P, Sheeder J, Rojas DC, Schneider EE (1996):Magnetoencephalographic evidence of abnormal early audi-tory memory function in schizophrenia.Biol Psychiatry40:299–301.
Reite M, Teale P, Zimmerman JE, Davis K, Whalen J (1988): Sourcelocation of a 50 msec latency auditory evoked field component.Electroencephalogr Clin Neurophysiol70:490–498.
Reite M, Zimmerman JE, Edrich J, Zimmerman JT (1976): Thehuman magnetoencephalogram: some EEG and related correla-tions.Electroencephalogr Clin Neurophysiol40:59–66.
Reite M, Zimmerman JT, Zimmerman JE (1981): Magneticauditory evoked fields: interhemispheric asymmetry.Electro-encephalogr Clin Neurophysiol51:388–392.
Rezai AR, Hund M, Kronberg E, Zonenshayn M, Cappell J,Ribary U, et al (1996): The interactive use of magnetoen-cephalography in stereotactic image-guided neurosurgery.Neurosurgery39:92–102.
Rezai AR, Mogilner AY, Cappell J, Hund M, Llinas RR, Kelly PJ(1997): Integration of functional brain mapping in image-guidedneurosurgery.Acta Neurochir (Wien)68(suppl):85–89.
Ribary U, Ioannides AA, Singh KD, Hasson R, Bolton JP, LadoF, et al (1991): Magnetic field tomography of coherentthalamocortical 40-Hz oscillations in humans.Proc Natl AcadSci USA88:11037–11041.
Rojas D, Sheeder J, Teale P, Walker J, Robertson BA, Selig S, et al(in press): MEG measurement of auditory sensory memorypersistence via the M100 in children and adults. In: Aine C,Okada Y, Stroink G, Swithenby S, Wood C, editors.Advances inBiomagnetism Research: Biomag96.New York: Springer-Verlag.
Rojas DC, Teale P, Sheeder J, Simon J, Reite M (1997):Sex-specific expression of Heschl’s gyrus functional andstructural abnormalities in paranoid schizophrenia.Am JPsychiatry154:1655–1662.
Romani GL, Williamson SJ, Kaufman L (1982): Tonotopic orga-nization of the human auditory cortex.Science216:1339–1340.
Sams M, Hari R, Rif J, Knuutila J (1993): The human auditorysensory memory trace persists about 10 sec: neuromagneticevidence.J Cognitive Neurosci5:363–370.
Scheuneman D, Teale P, Linnville S, Goldstein L, Reite M(1991): Magnetic auditory M100 source location in normalfemales.Brain Res Bull26:747–751.
Shenton M, Kikinis R, Jolsz FA, Pollak SD, Lemay M, WibleCG, et al (1992): Abnormalities of the left temporal lobe andthought disorder in schizophrenia. A quantative magneticresonance imaging study.N Engl J Med327:604–612.
Sholl SA, Kim KL (1990): Androgen receptors are differentiallydistributed between right and left cerebral hemispheres of thefetal male rhesus monkey.Brain Res516:122–126.
Smith JR, Gallen C, Orrison W, Lewine J, Murro AM, King DW,et al (1994): Role of multichannel magnetoencephalographyin the evaluation of ablative seizure surgery candidates.Stereotact Funct Neurosurg62:238–244.
Teale P, Sheeder J, Rojas D, Walker J, Reite M (1998):Sequential source of the M100 exhibits inter-hemisphericasymmetry.NeuroReport9:2647–2652.
Tepley N, Bowyer S, Clifton Y, Saligram U (1996): A techniquefor sequential measurements of DC neuromagnetic fields.Electroencephalogr Clin Neurophysiol99:16–18.
Tesche CD (1996): MEG imaging of neuronal population dy-namics in the human thalamus.Electroencephalogr ClinNeurophysiol47(suppl):81–90.
Tiihonen J, Hari R, Kajola M, Karhu J, Ahlfors S, Tissari S(1991): Magnetoencephalographic 10-Hz rhythm from thehuman auditory cortex.Neurosci Lett129:303–305.
Tiihonen J, Kajola M, Hari R (1989): Magnetic mu rhythm inman.Neuroscience32:793–800.
Tiihonen J, Katile H, Pekkonen E, Jaaskelainen IP, HuotilainenM, Aronen HJ, et al (1998): Reversal of cerebral asymmetryin schizophrenia measured with magnetoencephalography.Schizophr Res30:209–219.
Weinberger D, Luchins D, Morihisa J, Wyatt R (1982): Asym-metrical volumes of the right and left frontal and occipitalregions of the human brain.Ann Neurol11:97–100.
Wikstrom H, Roine RO, Salonen O, Aronen HJ, Virtanen J,Ilmoniemi RJ, et al (1997): Somatosensory evoked magneticfields to median nerve stimulation: interhemispheric differ-ences in a normal population.Electroencephalogr Clin Neu-rophysiol104:480–487.
Willerman L, Schultz R, Rutledge JN, Bigler ED (1992):Hemisphere size asymmetry predicts relative verbal andnonverbal intelligence differently in the sexes: An MRI studyof structure–function relations.Intelligence16:315–328.
Wood C, Wolpaw J (1982): Scalp distribution of human auditoryevoked potentials. 2. Evidence for overlapping sources andinvolvement of auditory cortex.Electroenceph Clin Neuro-physiol54:25–38.
Yamamoto T, Uemura T, Llinas R (1992): Tonotopic organiza-tion of human auditory cortex revealed by multi-channelSQUID system.Acta Otolaryngol (Stockh)112:201–204.
MEG: Applications in Psychiatry 1563BIOL PSYCHIATRY1999;45:1553–1563




















