A study of the enablers and challenges in the implementation ...
1
We’re here to support carers: Barriers
and enablers for Carers Leeds to attract
carers to the service in Primary and
Secondary care.
Authors
Mike Jestico, Dr. Penny Wright
and Professor Anna Madill
2
Table of Contents
Authors 3
Introduction 3
Aim 5
Method 5
The Setting 5
Participants 6
The Interviews 6
Analysis 7
Results 8
Participants 8
Analysis of barriers and Enablers 8
Working with the Integrated Teams 9
Working in primary Care 14
Dementia Support in primary Care 16
Hospital based Support Worker 18
The influence of the attitudes and beliefs of carers 21
Plans for the future 26
Recommendations 27
References 31
Appendix 1 32
Appendix 2 34
3
Authors
Mike Jestico is a PhD student at the University of Leeds researching Health Psychology.
Dr Penny Wright is Associate Professor in Psychosocial Cancer Care, Leeds Institute of Cancer
and Pathology.
Professor Anna Madill is Chair in Qualitative Inquiry and Deputy Head of the School of
Psychology at the University of Leeds.
Introduction
The population of the U.K. over the age of 65 has risen from 9.3 million in 2001 to 10.3 million in
2011 (ONS, 2011). This is projected to rise to 16.8 million by 2050 (Rutherford, 2012). Frailty
develops with age, with between a quarter and a half of those over the age of 85 estimated to be
frail (Clegg, Young Illife, Rikkert & Lockwood, 2013). Frailty is a state of increasing vulnerability with
age leading to major poor outcomes from minor stressors. This often leads to periods of disability
and incapacitation requiring care from others. People with long-term conditions are living longer
too requiring more care.
Although the NHS and Social Care services provide care for those in need, the majority of care is
performed unpaid by relatives and friends. This unpaid care if performed by professionals would
cost an estimated £119 billion in 2011, more than the cost of the NHS (£98.8 billion) for that year
(Carers UK, 2011). These 6 million unpaid carers are crucial in caring for ill or disabled loved ones,
providing medication, ensuring they attend NHS appointments and often providing 24 hour care
involving personal care to those who are bed ridden.
When those they care for are in hospital, the carers can feel ignored and excluded from the caring
process even though they are the experts in caring for that person (Carers UK, 2008). Carers are
twice as likely to be permanently sick or disabled compared to the general population and often
neglect their own health to focus on those they care for.
The carer population is changing all the time with just over 2.1 million people in the UK becoming
carers each year and just under 2.1 million people find their caring role comes to an end (Carers UK,
4
2014). Many people do not seek help when they are carers, mainly because they do not know help
is out there or they find the role of caring too time consuming to navigate the complex health, social
care and benefits systems.
The Carers Trust (2012) defines a carer as anyone who cares, unpaid, for a friend or family member
who due to illness, disability, a mental health problem or an addiction cannot cope without their
support. The last census in 2011 identified 6.3 million people who saw themselves as carers in Great
Britain with 71,500 of those in Leeds. This number may be under represented as it does not include
those who do not identify themselves as carers. In response to this growing need the
Transformation Project was set up in 2013 to improve and reduce costs for NHS services in Leeds
(http://www.leedspft.nhs.uk/about_us/change/Transformationproject). This was primarily aimed at
the top two percent users of the NHS who are adults with long term conditions. These patients
often have multiple health conditions such as chronic obstructive pulmonary disease, heart
conditions, diabetes, dementia, and drug and alcohol abuse. This group also includes the frail
elderly. Two of the aims of the Transformation Project were to release more time for staff to care
and to develop a new care pathway so that people can be cared for in their own home rather than
hospital. The document outlining the aims of the project said that it aimed to give a better
experience for people who use services, their families and carers (identifying need earlier, reducing
the number of different professionals involved, giving greater choice and supporting people to stay
at home for longer). Twelve new integrated adult health and social care teams were established
across the city. These were set up to provide integrated care in the community, reduce the burden
on hospitals and provide a more joined up service for patients. These teams include community
matrons, district nurses, social workers, occupational therapists, physiotherapists and dementia
workers. Each team had a different make up depending on services and location.
Carers Leeds, a Leeds based charity, applied for funding from the Clinical Commissioning Group
(CCG) in charge of the Transformation Project and received money for two posts, initially for one
year, later extended to two, to start in October 2013. The remit of these posts was to work with the
5
twelve new integrated adult health and social care teams. The two support workers from Carers
Leeds were appointed to promote the services Carers Leeds provides to the members of these
teams so that if they visited a patient and there was a carer present, they would refer the carer to
Carers Leeds. Carers Leeds would then support carers sufficiently to enable them to live a better life
and reduce the cost to the NHS, thus fulfilling the aims of the Transformation Project.
Aim
The aim of this research was to provide Carers Leeds with information on their effectiveness in
working with the newly set up integrated adult health and social care teams and identifying barriers
and enablers for identifying carers. Additionally, there was an opportunity to understand barriers
and enablers for identifying carers in the work Carers Leeds undertakes with GP surgeries and other
areas. This information will give Carers Leeds the opportunity help develop their effectiveness in
attracting and supporting carers and to provide additional information to their already well
developed internal communication channels.
Method
Ethical approval was received from the University of Leeds School of Psychology ethics committee,
Ethics reference: 14-0089.
The setting
Carers Leeds is a third sector organisation based in Leeds city centre. They provide a range of
services for carers over the age of 18 including advice, home visits, wellbeing sessions for carers and
social events. They also send out a bi-monthly newsletter to all carers registered at Carers Leeds.
The staff organisational structure is quite complicated as there are people from other organisations
working under the Carers Leeds name (appendix 1). The paid staff are supplemented by many

6
volunteers who allow Carers Leeds to achieve far more than they could with the funding they
receive. Carers Leeds has agreement with all GP surgeries in the Leeds area to use the Yellow Card
system for referring carers identified by the surgeries to Carers Leeds. GPs are encouraged to
identify carers and keep a note of them. Yellow Cards are an A5 yellow leaflet, distributed to all GP
practices in Leeds. Identified carers are asked by the GP practice to complete the details on the
Yellow Card asking about their caring responsibilities, which the practice makes a note of, and carers
have the option to allow their details to be forwarded on to Carers Leeds for contact.
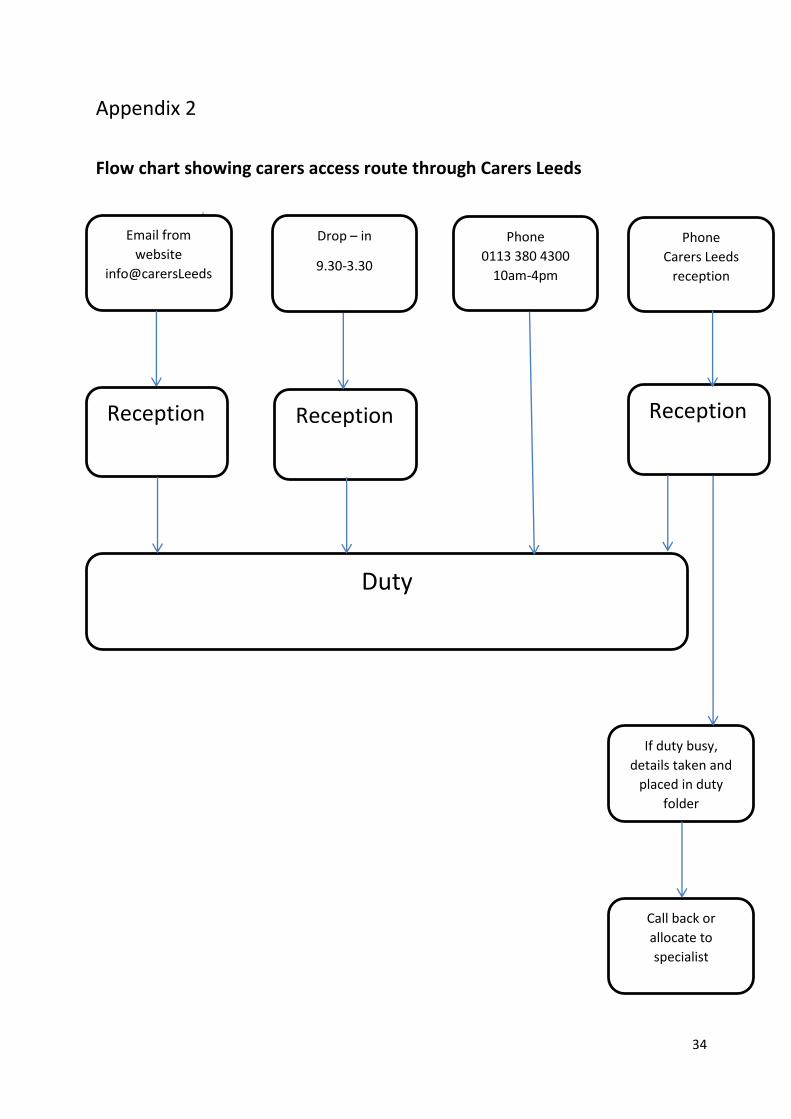
The good work Carers Leeds performs has recently been given recognition with the contract and
funding for the Combined Carers Service and phone number. This brings together five organisations
under one banner supporting carers in Leeds. The pathway for carers using the new service at
Carers Leeds in shown in Appendix 2.
Participants
Participants were staff working for Carers Leeds. They were specifically selected for their knowledge
of the area researched. All participants were recruited at a staff meeting at Carers Leeds. They were
all given participant information sheets and given the opportunity to ask any questions they wished
prior to giving informed consent. All participants were reminded of this prior to their individual
interviews to check if they had any questions and were still willing to participate. Participants were
informed they could refuse to participate, refuse to answer any specific question and withdraw their
data at any time up to the first reports produced.
The interviews
All interviews took place between June and October 2014. Six of the nine interviews took place at
the Carers Leeds offices, one at the support workers office in hospital and two at the researcher’s
place of work. Participants were asked to describe their role and how they perceived the impact of
7
the major changes on the organization. They were also asked about barriers and enablers for their
role.
Individual interview schedules were devised for each participant based on knowledge gained from
previous interviews and the specific nature of their job role. Interviews were audio-recorded and
transcribed by an external resource previously used and approved by the University of Leeds.
All electronic data is kept in a secure folder on the University of Leeds computer hard drive. All hard
copies of anonymised transcripts were kept in a locked filing cabinet in MJs home. All signed
consent forms were kept securely at the School of Psychology, University of Leeds. On study
completion these data were removed from the home of MJ and archived in secure University of
Leeds electronic and hard copy filing systems.
Analysis
Transcripts were analysed using Content and Thematic Analysis (Braun & Clarke, 2006), undertaken
by MJ and discussed at project management meetings with AM and PW as the work progressed. .
8
Results
Participants
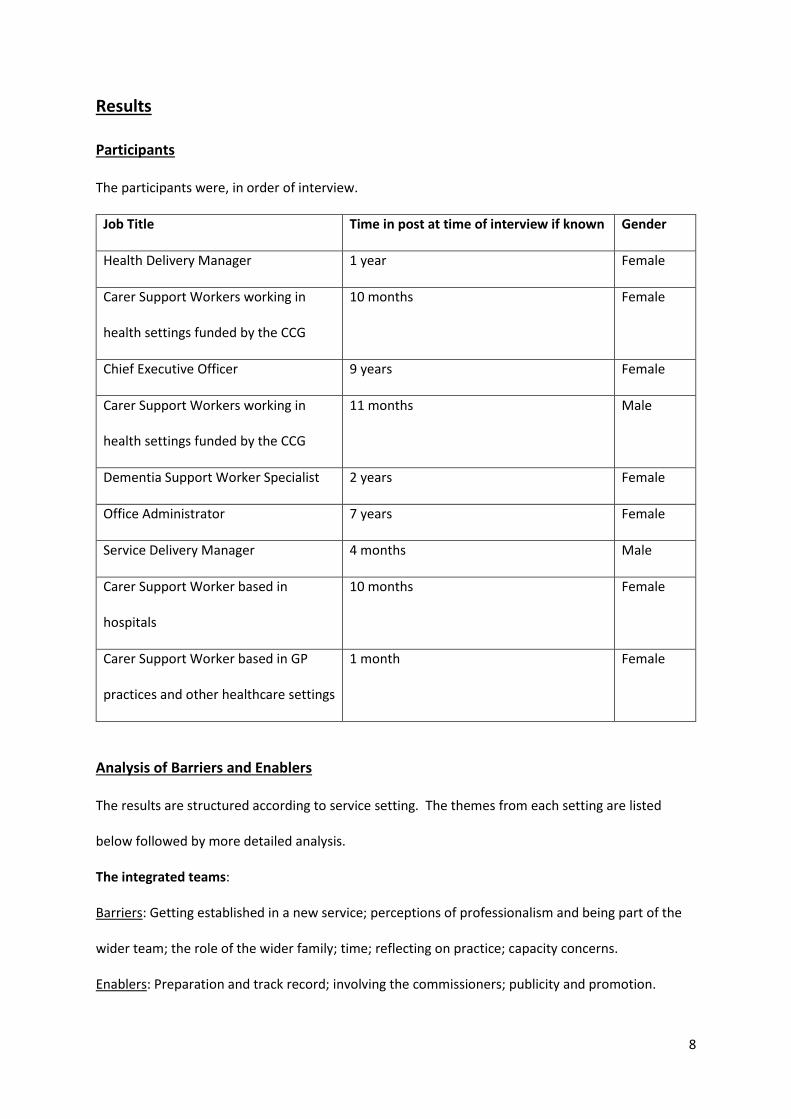
The participants were, in order of interview.
Job Title Time in post at time of interview if known Gender
Health Delivery Manager 1 year Female
Carer Support Workers working in
health settings funded by the CCG
10 months Female
Chief Executive Officer 9 years Female
Carer Support Workers working in
health settings funded by the CCG
11 months Male
Dementia Support Worker Specialist 2 years Female
Office Administrator 7 years Female
Service Delivery Manager 4 months Male
Carer Support Worker based in
hospitals
10 months Female
Carer Support Worker based in GP
practices and other healthcare settings
1 month Female
Analysis of Barriers and Enablers
The results are structured according to service setting. The themes from each setting are listed
below followed by more detailed analysis.
The integrated teams:
Barriers: Getting established in a new service; perceptions of professionalism and being part of the
wider team; the role of the wider family; time; reflecting on practice; capacity concerns.
Enablers: Preparation and track record; involving the commissioners; publicity and promotion.
9
Working in primary Care:
Barriers and Enablers: Building on established practice; space and costs.
Dementia Support in Primary care:
Enablers: Learning from the integrated support workers experience; working with supportive GPs.
Barriers: Lack of easy to use and user friendly systems; competing interests.
Hospital based support worker:
Enablers: NHS status; publicity and accessibility; networking; Working between two organisations:
Carers Leeds and the Leeds Hospitals NHS Trust.
Barriers: Competing interests, priorities and spreading the word; communication with Carers Leeds.
The influence of the attitudes and beliefs of carers:
Barriers: Defining themselves as carers; striving for dignity and independence; stigma; accessing
support; funding; synthesising evidence
Enablers: Publicity; relationships; product; internal; funding
Working with the integrated teams
Barriers
Getting established in a new service
The two support workers from Carers Leeds first approached the integrated teams as they were
being set up. They encountered two barriers at this point. Firstly, that the integrated teams were
going through a process of major change and were working out how to work efficiently together.
There was also a sense of tension as different internal parts of the Health and Social Care teams
were working out internal politics and how to refer to each other within the teams.
Support worker
“that was quite interesting because they’re adapting to a new way of working and
health and social care are very different and there’s lots of problems within that
10
as well, and then as well there’s myself and the other Support Worker that are
outside again so there’s all these different layers so it’s quite interesting.”
Secondly, there were many other Third Sector organizations pitching their services to the integrated
teams and the Carers Leeds message was effectively lost in the noise.
Perceptions of professionalism and being part of the wider team
Once the initial teething problems for the integrated teams had calmed down, the two support
workers found further barriers in gaining referrals from the teams. One support worker said that
Carers Leeds was seen as Third sector, as a Charity or a voluntary organisation and that Carers Leeds
staff were not seen as part of the Health and Social Care team, and not professional like staff who
work for the NHS. The point that anyone not working for the NHS was not professional was
emphasised by the support worker.
Support worker
“oh well, we’re NHS, you know, we’re professional”
This means that the Third Sector is not in the thoughts of the integrated teams as they do their job
and it takes real effort to get the members of the Integrated teams to realise what Carers Leeds have
to offer. Two of the integrated teams blocked all outside agencies from attending meetings despite
the CCG funding of the two support workers. These issues were in the process of being resolved at
time of interview.
The role of the wider family
This lack of acknowledgement of what Carers Leeds can offer was summed up when a manager said
that everyone thinks that carers do a wonderful job and their services would cost “another NHS
altogether”. However, although the enormous contribution made by carers was mentioned by the
Health Delivery Manager, Carers Leeds described it feeling like lip service and the real issues carers
face are not understood. There appeared to be blindness from the teams to what Carers Leeds
could offer. The integrated teams provide a very comprehensive package of care and could not see
that there is anything else to offer. This broader point about who the health service serves, the
11
patient or the wider family and support network is picked up later in the report. The staff on the
integrated teams were not buying into wanting to help carers. The Carers Leeds staff had to
undertake a lot of work to educate the integrated teams about the needs of carers and the benefits
to the cared for. This was not helped by not being known by the teams so time was taken to build
relationships with the teams to gain rapport.
Time
Building rapport was difficult however, as the support workers were given a five minute slot at the
beginning or the end of the integrated team’s hour long meeting. This gave a feeling that the service
Carers Leeds provides was not very important and just an add-on. The members of the integrated
teams have limited time when visiting patients in their own homes and can be task driven. This
means that they do not see the patient’s wider environment and those that might need support in
caring for the patient. Due to the lack of time, they might not want to start asking questions as they
know this could create more work if an issue was raised. This lack of time meant that the integrated
team members might not want to spend the time it takes generating a referral for Carers Leeds and
this issue was acknowledged by the Carers Leeds support workers.
Reflecting on practice
Another issue raised by both support workers and their manager was that there was no formal way
to share best and worst practice within Carers Leeds. This meant that no-one was sure about what
was working to generate referrals and what was not. There were informal chats but no formal
process that could reflect on what was happening.
Capacity concerns
The final potential barrier was a possible capacity issue if a lot of referrals started coming in. The
two support workers also perform case work with the new referrals and if there were more referrals
than capacity for casework then there would not be the time to visit the integrated teams as often
to keep the Carers Leeds message in the minds of the teams.
12
Support worker
“Because I mean there are twelve neighbourhood teams, soon to be thirteen and
if they all start referring at least two then we’re going to be pretty full soon and
be having waiting lists and at which point we’ll need to look at well how do we
work it.”
Enablers
Preparation and track record
Several factors enabled a smooth start to the meetings with the integrated teams. Firstly the teams
had been informed that Carers Leeds were going to be visiting their meetings and this meant the
support workers were expected and welcomed. Secondly, the good work that Carers Leeds has
done in the past with GPs and the Yellow Cards meant that the support workers could ‘get a foot in
the door’.
Support worker
“at least you can say “I’m from Carers Leeds”, “oh I’m not sure”, “well we’ve got
the yellow cards”, “oh yes, the yellow card”, so you’ve got kind of, you’ve got a
good foot in the door with that because they are well-known for doing good work
so that is good.”
This was particularly apparent in Middleton as the community staff nurses on the integrated teams
were linked to a surgery who are frequent users of the Yellow Card. This meant successful referrals
from this team from an early stage. This idea of using reputation was used to sell the service to the
integrated teams. One of the support workers said it was better to talk about what they have done
rather than what they can do.
Involving the commissioners
Initially, there was not much interest from the integrated teams in referring carers to the support
workers. This issue was raised at Carers Leeds and a meeting was set up between the support
workers, their manager and members of the CGG who commissioned the service. This meeting was
13
extremely useful in lots of ways. The commissioners fed back to the integrated teams that they
needed to refer carers to Carers Leeds. The support workers learnt a lot about what the
commissioners expected from the funding and from the integrated teams without the message
being diluted through layers of management.
Support worker
“And that’s been really good actually just to see where the commissioners are
coming from and what their ideas are pitted against our own”
The support workers could see how much the commissioners wanted it to work and how hard they
were pushing the service. Pushing the service at all levels of the NHS gets different levels talking
about the services Carers Leeds can provide and ingrains it in the culture. The other benefit to the
support workers from attending the meeting with the commissioners was that they networked other
people in the NHS they would otherwise not have had access to. One support worker said they met
someone from the Leeds Community Healthcare Communications team who showed how to better
promote the service with the integrated teams.
Support worker
“whether it’s sending a text message or something to, you know, that kind of that
you wouldn’t really think of beforehand”
Both support workers said that the relationship with the team coordinators proved to be the most
productive as they referred the most carers. This could be that they have more time than the
patient-facing staff to do this. The other main point of referral was the dementia leads on the
teams. Possibly as they have a different focus in the team or that the people that they see are more
likely to have a carer.
Publicity and promotion
To gain access and promote themselves to the integrated teams, the support workers have invited
themselves to meetings and produced a range of publicity materials. These have included leaflets,
14
posters and a small card for the members of the teams to carry in their diaries to remind them to
think about carers.
Support worker
“we took some flyers and things to them, a week later they rang up and said “oh
we’ve got a referral for you””
The support workers found that being at the meetings together meant that one person could fill in
for the other if necessary and both people with the same message appeared to be more persuasive.
The other thing that appeared to make a difference at meetings was listening to questions and
answering them rather than just talking at the teams. The support workers have been using the
teams that do refer carers as a model to promote the service to other teams, however at the time of
the interviews it was not possible to say whether this was making a difference. To enable them to
know what has been said at each team meeting a chronology for each team was kept by one of the
support workers so that they were not repeating themselves at meetings. This also will enable the
support workers to see which approaches generated the most referrals. Again, at the time of
interview, there was no data on the whether this was a success. Finally the support workers
reported that people tended to carry on referring if they’ve had a successful referral. However, it
was always the same people referring, for others, referring carers was not on their agenda. This
follows Rogers (2002) Theory of Innovation; people take time to adopt new ideas. He says 2.5% of
people are very receptive to new ideas and will take to them quickly. Another 13.5% of people are
the next group of people to adopt new ideas. These are the most important of all the people who
adopt the new idea as they are often the opinion leaders in any organisation. These are the people
to use to promote the service to their peers (see recommendations).
15
Working in primary care
Barriers and Enablers (these are combined in this case as the barriers and enablers are entwined)
Building on established practice
A Yellow Card system for carer referrals is in place in all GP surgeries in Leeds. Talks are also
available from Carers Leeds to staff at GP surgeries about Carers Leeds and carer’s issues. Referrals
do not come in from all surgeries however, as some GPs don’t see the point of the Yellow Cards or
the benefit to the surgery. Within surgeries that do refer, it is only certain staff that are doing the
referring. When these staff leave the surgery, the referrals stop.
Health Development Manager
“what’s been interesting is that often it’s particular GPs for example, or particular
people in the staff team who refer people into the clinic so it’s often not the
whole staff team”
In the period while the two support workers were waiting for referrals from the integrated teams,
they worked in GP surgeries to create referral pathways. This work was reduced when the referrals
came in from the integrated teams but was still done to a lesser extent in surgeries that sent
referrals.
An example of a high referring surgery is Lingwell Croft in Middleton. The support worker has
attended team meetings, the head GP had driven the need for referrals and allowed the support
worker to email staff with reminders about the service and why it is a benefit to them. This process
takes time and the communication must be kept going as people do forget about the service.
Space and costs
There were problems setting up clinics in GP surgeries, some because they were too small and had
no spare space, others because they wanted to charge for the service. The issues around charging
were mostly ironed out by the support workers manager. When the clinics were set up, they often
filled up quite quickly, showing there is a need for this service within GP surgeries. This model could
be used for further funding for this service. The clinics also made life easier for the reception staff at
16
the surgery as all they had to do was fill in a room booking for a referral rather than filling out the
Yellow Card.
Dementia support in primary care
During the period of the research, funding for two new posts was received by Carers Leeds from the
Leeds West Clinical Commissioning Group. These were aimed at increasing referrals of carers of
people with memory problems or a diagnosis of dementia from the thirty eight GP practices in Leeds
West and other healthcare settings such as the Leeds Community Healthcare Trust and the various
teams that work within that. One of the support workers had been in post for a month when
interviewed, the other had not yet been appointed. The remit of this role was still to be finalised by
the CCG at the time of the interview, with only one of the two support workers in post by the time of
the study close. However, it had been agreed that the post would aim to enable more carers to
know about support in a timely fashion rather than when it reaches crisis point. This would then
hopefully reduce the amount of genuine and inappropriate visits a day by the carer and the person
they care for to the GP. This will be achieved by looking at educating them around the effects of a
UTI or a chest infection. How to manage them without going to the GP or A&E in the first instance.
Hopefully reducing carer stress which leads to things like insomnia, stomach upsets and headaches,
these are a big part of why carers present to GP practices. The support workers will be working with
carers to reduce the impact on GP practices and other healthcare services.
Enablers
Learning from the integrated support workers experience
The two support workers in place working with the integrated teams have given the new GP support
worker lots of contacts to start the process quickly, rather than the slow start they encountered.
GP Support Worker
“They’ve had some really good contacts within the neighbourhood teams that I’ve
been able to use as well that have got me into different places”
17
They also gave the new support worker a good idea about what to expect with the job from the
perspective of home visits. These were unexpected for the new support worker and enabled them
to be more flexible with their work planning.
Working with supportive GPs
As a trial of possible future ways of identifying carers, the new support worker gathered data from
one GP about patients with dementia and wrote directly to all those patients with the header ‘Please
give to your family member’. To date, four responses have been received from carers, none of
whom were registered at the GP or known to Carers Leeds. They have been registered at the GP as
carers. The support worker has also been trying to discover why these carers were unknown to the
GP surgery.
Barriers
Lack of easy to use and user friendly systems
At the surgery that supplied the data about patients with dementia, the GP support worker did a
spot check on their carers’ database and checked if they were known to Carers Leeds. The majority
were not. If the Yellow Card referral scheme was working effectively then it might be predicted that
there would be a higher proportion on the GP database known to Carers Leeds. Other GPs have
been quite receptive but again they feel it’s just another thing for them to do when they’ve already
got so many other targets and pressures. A barrier seen by the GP support worker was that that
there is not a referral form on the systems that they use. Another project funded by the same CCG
at the same time has got on their system with a referral form.
Competing interests
Trying to get into the GP meetings is quite difficult, the GP support worker had only attended two so
far and at one, they were co-presenting with another project which was the baby of one of the GPs.
Some of the Practice Managers are business partners and have been commenting that they are
running a business but the CCGs keep funding different things but not telling the organisations about
each other. The day that the GP support worker attended the surgery, another project from a
18
completely different organisation had been presented to the surgery that morning. The practice
manager queried why the CCGs were expecting the GP practices to do the extra work and give
rooms to these funding streams when they weren’t getting anything in return. They cannot see the
immediate financial benefit from a business point of view. The CCGs are not communicating
effectively with the GPs or those that they are funding to create a more joined up way of delivering
services.
Hospital based support worker
One member of Carers Leeds staff is based at St. James’s University Hospital in their own office close
to the older person’s wards. They had been in post for ten months at time of interview. They
promote Carers Leeds to anyone in all the Leeds hospitals. The funding and the main focus of their
role is for dementia patients in the hospitals but will refer or advise anyone in the hospital who is a
carer or being cared for including staff. The role was initially purely for carers supporting someone
with dementia but it became easier for Carers Leeds if anyone over the age of 65 was referred to the
hospital support worker and Carers Leeds took care of the rest. If Carers Leeds become aware of a
carer in hospital, the support worker can be with them within the hour.
Enablers
NHS status
The support worker has an honorary contract with the NHS allowing them access to the systems and
wards so carers can be identified quickly. The ward patient notes are marked with the dementia
forget-me-not flower for easy identification. The main purpose is to make sure the person in
hospital is getting the right care package and that the carer knows what is going on with the person
they care for as often they do not. The ward staff will only refer to the support worker if the patient
mentions the word carer. The support worker said they were trying to get the Triangle of Care
(Carers Trust, 2013) up and running within the Trust, or at least the parts of it applicable to their
role. It is acknowledged as best practice in dementia care by the Carers Trust and the Royal College
19
of Nursing. Leeds and York NHS Trusts have signed up to the scheme but do not currently
implement it. The best time to be there for the carer is when the patient is discharged. This is when
they will have questions about what happens next for them and the person they care for. When the
carer visits the patients at other times, they are not thinking ahead, only of the here and now.
Publicity and accessibility
The hospital support worker has used a huge number of methods to raise awareness for their role:
stalls in reception, being part of newsletters, speaking at nursing conferences, being part of
dementia training sessions, and is written into the process triggered when a patient over 75 with
memory problems is identified. There is also a page on the Trust intranet and the role publicised on
computer screen savers at every hospital in the Trust. There are regular drop in sessions advertised
for carers to attend. Visiting the wards is good for referrals but is not viable time wise as nothing
else would get done.
Networking
The support worker has set up links with many ‘allies’. These are people from other organisations
who also work with a similar demographic at the same hospital or others. When a person is
identified as being in need of help from other organisations, these referral pathways are triggered
and the allies refer people to each other.
Hospital Support Worker
“Seacroft Hospital has an eye clinic which there’s a lady from a charity who does a
similar role to me but in terms of sight and we’ve got a referral pathway set up so
people going to her outpatient clinic she sends over to me, and anyone I get who’s
got eyesight problems I send over to her”
The support worker also talked about getting a volunteer to help and what a difference this would
make as the support worker could achieve so much more.
20
Working between two organisations: Carers Leeds and the Leeds Hospitals NHS Trust.
The support worker works personally with some carers if referring to Carers Leeds office means
duplication of work and then tries to stay in touch with these carers. This means they sometimes
are in contact with post hospital discharge problems. This ensures a seamless service and helps the
support worker feel connected post discharge.
The support worker said how comfortable they felt contacting Carers Leeds with any concerns they
had or sorting out problems. They also said how much they enjoyed going to Carers Leeds for the
Monday meeting and how supportive their manager was with all issues carer related. The support
worker also said how much they enjoyed being autonomous at the hospital and the freedom to try
new things and doing their own thing which seems to work.
Barriers
Competing interests, priorities and spreading the word
Despite the huge publicity for the hospital support workers role and many staff knowing about the
role and support worker, the staff do not refer as much as they could. The support worker said
there were too many other agendas that staff needed to focus on and their role was forgotten. The
support worker said that they rely on the wards with older people to remember about the service
and this does not always happen. Similar to the situation in GP practices, there was a time when
there were two ward sisters who would refer all the time to the service, however, when they left
their posts, the referrals dried up and the process of building relationships began again.
Hospital Support Worker
“when I started I had certain ward sisters who consistently referred and would
send me, pretty much everyone with dementia they would refer to me so I could
just check it out, make sure the carer was okay, that was, but they both left and
that was really hard because then it was trying to rebuild those relationships”
The support worker is based at St James’s hospital and also deals with referrals from Leeds General
Infirmary who have an orthopaedic ward. There have been very few referrals as the support worker
21
has had difficulties getting embedded at that unit. The support worker has received little interest in
their work at the orthopaedic unit to date.
Communication with Carers Leeds
The support worker also said that there has been a lack of understanding at Carers Leeds of their
role. This has led to staff either referring people to the support worker inappropriately, for things
that should not be done in hospital or forgetting that the support worker is based in the hospital and
dealing with things they do not understand. The support worker said that they publicise their role
within Carers Leeds to try and overcome this.
The influence of the attitudes and beliefs of carers
Although no carers were interviewed as part of this project many of the staff interviewed mentioned
the importance of the carers’ perception of their role.
Barriers
Defining themselves as carers
People don’t know that they are carers. They could have a continuation of looking after a relative or
friend who has a short term condition that stretches into a long term one or a condition that is
followed by another condition. This is often the case with people who have dementia. Alternatively,
they do not recognise themselves as carers; they see themselves as father, wife or friend.
Service Delivery Manager
“so when you’re actually saying, “we’re here to support carers”, it might not really
be relevant to people if they don’t actually have some sort of connection with that
term, and often it is people don’t see themselves as carer”
Carers Leeds wish to empower carers, however, the label carer can mean to people that they are
they are unable to cope. To accept that label means that within the relationship, it is no longer
22
husband/wife or mother/daughter but carer/cared for. This can be hard to accept and can lead to
carers rejecting the label and not seeking a support as a result.
Striving for dignity and independence
People may feel that they do not need support or they are too proud to ask for help; they are able to
cope on their own. Carers hide problems from their families; they do not want the family to know
there is a problem. Partly to prevent the family from worrying and partly to prevent the family
intervening. This links into carers not wanting things to change at home or their control of the
situation taken away or their partner taken into care. If carers rely on someone else to provide care
for their partner, then their relationship will change forever, they will feel side-lined and much less
involved. Talking to someone else about the problems encountered while caring could be seen as a
betrayal of the relationship, seen as talking behind their partners back. People who become carers
become socially isolated as the care can be all consuming. Despite this, carers do not want strangers
in their own home. This links to the point about becoming side-lined within the relationship.
Partners need to be needed even though the care is all consuming.
Stigma
If the cared for has dementia, there is still stigma amongst older people around dementia and
mental health issues.
Dementia Support Worker
“we don’t really like the word Alzheimer’s and we certainly don’t like dementia or
senile dementia but we can talk about memory problems which is fine”
This may prevent them from wanting to talk about it or admitting that their partner is suffering
mental health problems.
Accessing support
If people recognise that they need help, there are other barriers to accessing support. Carers might
not know that there is support or if they do where to go for it. Carers who have very busy lives may
not have the time to access support. Care is often kept within families until there is a crisis. At this
23
point family members are less able to engage with outside services. When outside services do
become involved, the relationships between carers and public health workers can be difficult. Who
are the workers there for? The cared for or the family who has cared up to this point? If there is no
engagement by the health workers with the carer, then the carer can feel very alone and unable to
speak out. These problems can be exacerbated by the carer not understanding NHS terminology or
about mental health issues if appropriate. This situation can be made worse if the carer has a
different first language or culture from those providing the care.
Funding
Within Carers Leeds, other barriers were identified around the short term funding implicit in third
sector organisations. Opportunity funding means that sometimes the money for a service arrives
before plans are in place to use it efficiently. The planning is then not thought through thoroughly
and the service provided may not be the most efficient way of spending the money. At the end of
the funding, a service can end with nothing to take its place. This can leave people with needs
without a service to support them. The GP support worker was very clear in their mind that they
were involved in a short term project and was giving their and the Carers Leeds phone number to
everyone. The NHS has fads and phases. Carers Leeds needs to be seen as more than just a fad by
being seen as something permanent.
Synthesising evidence
The final barrier within the organisation is not being sure what makes a difference to carers. It is
obvious from the reactions from the carers that Carers Leeds makes a difference to their lives. This
has, however, never been qualified or quantified, therefore it is difficult to isolate what is good and
bad about the service and improve the service in specific areas. Carers Leeds has a database on
which their activities are recorded. However, to get the most out of this system Carers Leeds needs a
fulltime IT person rather than short term input on which it has to rely on currently. This would allow
for routine reports to be generated from database extracts rather than the bespoke reports that
have to be ordered. Having access to this type of evidence might help with their responses to
24
calls from a target of a funding stream making it easier to demonstrate their interventions are
making a difference.
Enablers
Publicity
Carers Leeds is very effective at publicising its services. The staff believe in the product they are
promoting, this helps with getting the message across. The organisation is outward looking and
pushes the service at every opportunity and at every level of organisation they encounter. This drive
comes from the Chief Executive who does not miss an opportunity to promote Carers Leeds to
whoever she meets and at whatever event she attends.
Health Delivery Manager
“we do have a Chief Executive who is excellent at being a figurehead for this
organisation and promoting this service really well and who absolutely has no
hesitation at approaching, you know, Chief Executives and Directors of health and
social care services, and saying, “Look, this is what we’re doing,” so as a
consequence our profile has grown and risen significantly over the last four or five
years particularly I think”
The publicity is information giving and awareness raising about the good news stories that come
from the successes in service and training provision. Carers Leeds are very community focused, with
stalls, community events and social events for carers. This community networking pushes up self-
referrals. Finally, word of mouth publicises the service. If the carers get a good service, they will pass
this message on and promote the service themselves.
Relationships
From all the interviews, the most important enabler that keeps on coming up is building
relationships. These relationships can be with statutory organisations, fellow third sector
organisations, individuals and carers. Carers Leeds has a limited capacity to promote the service,
25
however, by building relationships and networking, all these other people and organisations can
refer carers and pass the message on.
Working in partnership is also seen as a very important enabler. It is better economically for all the
partners and breaks down the ‘we do this and you do that culture’. It means that Carers Leeds can
get so much more done and learn new skills.
Carers Leeds is able to understand NHS politics and funding opportunities to make the most of who
has influence and money to continue to gain funding opportunities for the organisation. It is the
third sector organisation on some committees and working groups and very clearly has a voice about
what’s happening in terms of carers support across the city. This shows that Carers Leeds is seen as
a really serious partner in health and social care. However, this perception may only be clear at the
top of organisations and not so clear where support workers are trying to promote the service to the
integrated teams and at GP surgeries.
Product
The contract to hold the new combined carers phone number has shown that Carers Leeds is
considered the best organisation in Leeds to support carers. This perception comes from the ethos
at Carers Leeds that carers come first and no one is ever turned away, no matter how busy it is. At
Carers Leeds, people can ring up, they can drop in and see someone the same day, and they can see
people with different experiences and specialities.
Dementia Support Worker
“The Chief Executive’s ethos is carers always come first, if they come in at
lunchtime they come in at lunchtime, if they drop in they drop in, they will be
seen, if it’s a staff meeting and somebody drops in on a Monday because it’s not a
drop-in day, they won’t be turned away, they should never be turned away.”
The diversity of support at Carers Leeds has increased since the new combined phone number has
been introduced. Carers Leeds provides direct support, information, advice, emotional support to
26
carers and is raising awareness among the health and social care providers. How they can support
carers through training, information stalls and better relationships with their referrers.
Being a non-statutory organisation, allows people who use Carers Leeds services to be more honest
than when they think what they say will be recorded and reported. This allows a deeper level of
service to be offered where carers can be honest and receive the appropriate care package.
The dementia carers training has been extremely popular with each training session oversubscribed.
This can allow carers an anonymous way of accessing services and raise awareness of the
organisation at the same time.
Internal
Carers Leeds has a Chief Executive that is excellent at being a figurehead and promoting the
organisation, so the profile has grown over the years. However, the structures are in place within
the organisation for it to continue without the Chief Executive if necessary without everything falling
apart. The leadership from the Chief Executive has allowed Carers Leeds to manage change very
effectively by using positive management to drive changes through. This has been especially useful
in the recent major changes to the way Carers Leeds operates.
Within the organisation, one of the support workers reported that her colleagues and manager were
really supportive. The support worker also reported that Carers Leeds has a really nice atmosphere
and they felt they could ask anything.
Funding
If short term funding becomes permanent, it gives Carers Leeds more flexibility around how they
deliver services.
Plans for the future
One of the managers said that following upon referrals at some point in the future and whether
Carers Leeds had made any impact and been beneficial to carers would help inform the service. This
was expanded in a later interview with another manager where the idea of using the Carers Star
27
(Outcomes star 2012) was put forward. This would be used to measure the quality of difference to
carer’s lives. This would ask carers what key areas are important to them and what sort of things
would make a difference? It is visual and collaborative, a way to develop an action plan and has
consistency of use by all. There is a need to move away from instant action only, long term results
are needed, approximately 3-6 months. It will be used by support workers who have a relationship
with carers. This will also ask carers, ‘How was it for you? How can we improve?’ Services are
usually led by resources but the service needs to be needs led, by what carers feel that they want. A
good holistic assessment reveals needs but how does Carers Leeds go about providing that?
Competent and skilled staff are needed to be able to deliver this. Although there are lots of
administrative tasks to be undertaken currently, these need to be reduced so staff can spend more
time with carers. Also, making referrals fast and accessible with a quick response and making sure
that responses are personal to that carer.
Recommendations
Most of the recommendations come from staff members at Carers Leeds but some are the
researchers’ observations.
1. Referral and carer contact
a. To embed the message about carers with the Neighbourhood teams, a support worker
should be included in all meetings with all the teams. This would enable them to be seen as
part of the team and professional and remove some of the negative connotations involved
with being a third sector partner. The precedent for this is the hospital based support
worker who has an honorary contract with the NHS. Whether this is possible or not, the
teams should be questioned about what prompted them to refer a carer when visiting
patients at home. This could be collated and presented to the teams as a model of best
practice for them to follow. This could also be supplemented by a regular push from the
CCG to make sure the message is coming from all directions. This approach could be used
28
for all funded projects where the message is pushed at all levels to make Carers Leeds in
everyone’s mind at all times.
b. One of the Neighbourhood team support workers said that they were designing all their own
literature for use in presenting to the teams or for use as reminders. They also said they had
designed a blue card to go in the diaries of the Neighbourhood team members as a reminder
of carers Leeds while out on calls. Should these blue cards be Yellow to keep a corporate
identity with the NHS? Would it also be possible for all literature used by anyone promoting
the service to be centrally designed or have some guidelines for designs that conform to a
corporate identity that keeps the message uniform and consistent?
c. As services regularly change both internally and externally, there should be a referral
pathway form for use by all staff in contact with carers. This would make sure nothing was
missed when considering options for signposting or support. This would be regularly
updated as new services come in and old ones are phased out. The new and old services
could include start and finish dates to accurately guide.
d. Rogers Theory of Innovation (2002) could be used to create change faster. Use the first 16%
of those who refer carers in any context as opinion leaders for the rest. Rogers says these
opinion leaders influence those who are not initially receptive the new ideas. The message
here is to keep pushing the message even when it feels like people are not listening as it
takes time for people to come round to new ideas. When change starts to happen, use
those that change as opinion leaders to persuade the rest faster.
e. To build on the enablers identified in this report and use them to aid identifying carers. To
acknowledge barriers to referrals wherever they occur and challenge them as much as
possible as the carer always comes first.
2. Future use of data
a. The link between referrals and outcomes from the neighbourhood teams and other projects
could be of benefit for future funding proposals. For example, ‘there were 100 referrals in
29
seven months from the Neighbourhood teams the outcomes for these referrals were…..’
This could highlight the excellent work that Carers Leeds does for carers and even highlight
some estimated savings for the NHS in terms of reduced usage of the NHS by carers and
cared for. This data could also be used to present to the Neighbourhood teams and
commissioners about the effectiveness of Carers Leeds.
b. Within the database, the Carers Star data could be used as an outcome marker at regular
intervals to highlight when data needs to be gained from Carers and to make data easier to
collate. This could then be used a service wide link between referrals and outcomes of
different types.
3. Other recommendations
a. A street view shop for drop in. Somewhere visible from the street, it would draw more
people in and be hugely beneficial in terms of publicity as it would be visible from all the
buses that travel up and down the Headrow.
b. A new group name for organisations that are funded by the NHS to carry out non statutory
work. Carers Leeds has employees and volunteers and is not a charity and the term ‘third
sector’ does not convey the value of the work that it does. A name for the organisations
that allows them to be seen as an equal partners with the NHS.
c. Is it better to wait until major change occurs to introduce smaller changes at the same time?
The benefits would be that staff would be more receptive to the smaller changes at a time of
change. They would also have periods of few changes providing a more stable environment.
d. The final recommendation is the largest. Carers Leeds is asking those caring for others to
change the perception of themselves from being relative or friend to that of carer with the
connotations mentioned earlier in the report. There should be an attempt to change how
society thinks about carers and acknowledges them in a similar way that society thinks
differently now about dementia. This could be done through information, relationships and
policy where working carers are recognised by employers and non-working carers are

30
recognised by the government to bring the debate about carers into the public
consciousness.
e. The integrated community teams should record how many times they refer to Carers Leeds,
and make it one of their service outcomes.
31
References
Braun, V., & Clarke, V. (2006). Using thematic analysis in psychology. Qualitative Research in psychology, 3(2), 77-101.
Carers Trust. (2012). What is a Carer? Retrieved Jan 7, 2015, from http://www.carers.org/what-carer Carers Trust. (2013). The Triangle of Care. Carers included: A guide to best practice for Dementia
Care. London: Carers Trust. Carers UK. (2008). Spotlight on… Carers and the NHS. Manchester: Carers UK. Carers UK. (2011). Unpaid carers save £119 billion a year. Retrieved Dec 28, 2014, from:
http://www.carersuk.org/northernireland/news-ni/unpaid-carers-save-119-billion-a-year Carers UK. (2014). Carers UK. Need to know: Transitions in and out of caring: the information challenge. Carers UK. Clegg, A., Young, J., Iliffe, S., Rikkert, M. O., & Rockwood, K. (2013). Frailty in elderly people. The
Lancet, 381,9868, 752-62. Office for National Statistics. (2011). 2011 Census: Population Estimates for the United Kingdom, 27
March2011. London: Office for National Statistics Outcomes Star (2012) Retrieved Dec 28, 2014, from http://www.outcomesstar.org.uk/carers-star/ Rogers, E. M. (2002). Diffusion of preventative Innovations. Addictive Behaviors, 27, 989-993. Rutherford, T. (2012). Population ageing: statistics. House of Commons library. Retrieved Dec 28,
2014, from: www.parliament.uk/topics/PopulationArchive
32
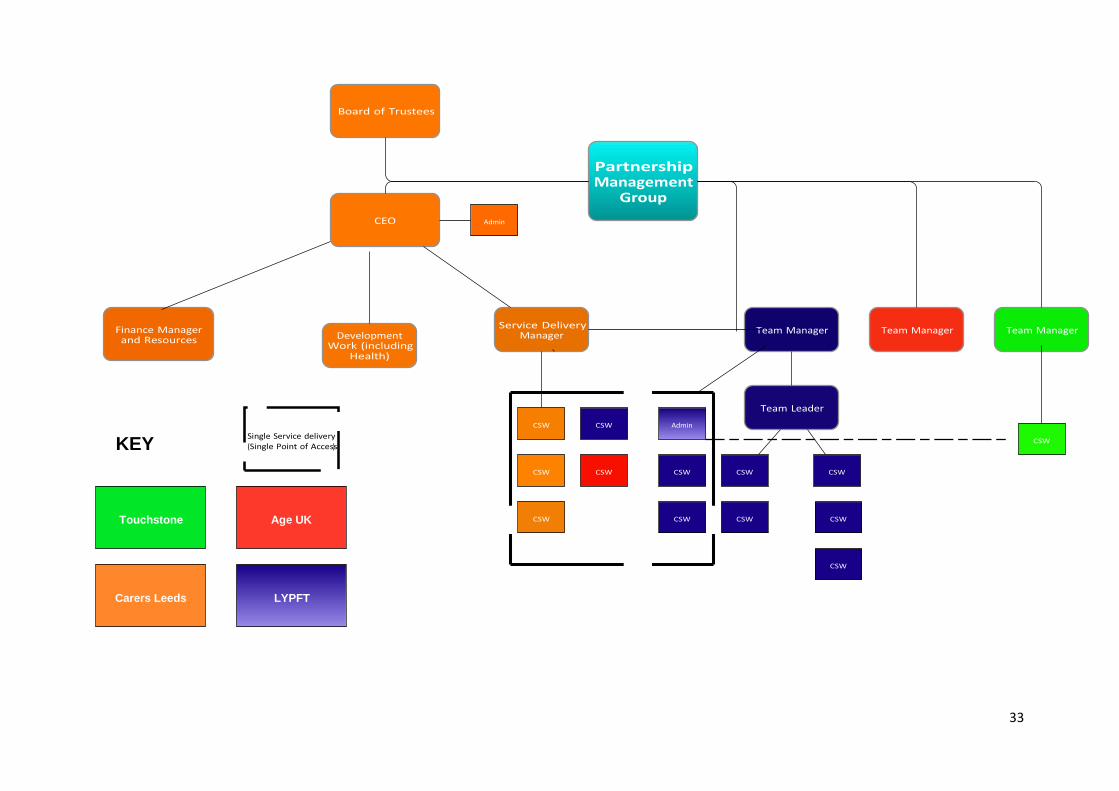
Appendix 1
Carers Service: Organisation Structure
Key:
CEO – Chief Executive Officer
CSW – Carers Support Worker
LYPFT – Leeds and York Partnership Foundation Trust
33
LYPFT Carers Leeds
Age UK Touchstone
KEY
34
Appendix 2
Flow chart showing carers access route through Carers Leeds
113 380 4300
Email from
website
info@carersLeeds
Duty
Reception Reception
Drop – in
9.30-3.30
Reception
Phone
0113 380 4300
10am-4pm
If duty busy,
details taken and
placed in duty
folder
Call back or
allocate to
specialist
Phone
Carers Leeds
reception
Copyright © 2022 FDOKUMEN