Integrated Care System Chairs Applicant Information Pack
53
North West Region - Integrated Care System C hairs Applicant Information Pack Cheshire & Merseyside Integrated Care System Chair Greater Manchester Integrated Care System Chair For an informal discussion, please email [email protected] or [email protected] or call 0161 498 3413 to speak with Gillian Powell or Peter Mason. Page 1
-
Upload
khangminh22 -
Category
Documents
-
view
6 -
download
0
Transcript of Integrated Care System Chairs Applicant Information Pack

North West Region - Integrated
Care System Chairs
Applicant Information Pack
Cheshire & Merseyside Integrated Care System Chair
Greater Manchester Integrated Care System Chair
For an informal discussion, please email [email protected] or [email protected] or call 0161 498 3413 to speak with
Gillian Powell or Peter Mason.
Page 1

Contents
The Opportunity and Role Description 3 Background Information on the Cheshire and Merseyside ICS 12 Background Information on the Greater Manchester ICS 38 How to Apply 53
We value and promote diversity and are committed to equality of opportunity for all. We believe that the best boards are those that reflect the
communities they serve.
We prioritise Equality, Diversity and Inclusion, team health and wellbeing and the principles of kind leadership in our 'ways of working'. All
postholders will have a key role in nurturing this culture.
Our recruitment processes are conducted in accordance with the principles of Cabinet Office The Governance Code for Public Appointments to ensure that they are made on merit after a fair and open process so that the best
people, from the widest possible pool of applicants, are appointed.
Page 2

1. The opportunity Integrated care systems (ICSs) are partnerships of health and care organisations, local government and the voluntary sector. They exist to improve population health, tackle health inequalities, enhance productivity and help the NHS support broader social and economic development. They will take on statutory form following the implementation of proposed legislation from April 2022 and will comprise an Integrated Care Board (ICB) which will take on CCGs’ functions and broader strategic responsibility for setting healthcare strategies for the system. The ICB will work with an Integrated Care Partnership (ICP) committee formed jointly with Local Authority Partners. Together the ICP and ICB will become the ICS. We are looking for candidates who will develop these systems, first as the chair of the non-statutory ICS, and later as chair of the statutory ICB, and, subject to legislation, support the proposed establishment of each system’s new statutory arrangements. Originally created as part of the NHS’s NHS Long Term Plan, there are 42 ICSs covering the whole of England, each serving between 500,000 and three million people. Each will hold substantial budget for commissioning high quality patient care and driving health and care improvements for their communities. The chair will lead a unitary board which will bring together leaders from across all parts of the NHS, local government, social care and the voluntary, community and social enterprise sector. 2. Role priorities, accountabilities, responsibilities and competencies Please note: the following Role Description is dependent on legislation. Appointees will be taken on in the first instance as Independent Chair of the current Integrated Care System (ICS) and designate Chair of the anticipated NHS Integrated Care Board (ICB). Final appointment to the role of Chair of the ICB, as described below, would be dependent on the passage of the Health and Care Bill, and any potential amendments made to that Bill. Indication is given where the role is initially for the ICS and anticipated to become for the ICB. Priorities The Chair is accountable for ensuring there is a long-term, viable strategy in place for the delivery of the functions, duties and objectives of the Integrated Care System / Integrated Care Board and for the stewardship of public money. The Chair champions action to help meet the four core purposes of Integrated Care Systems; to improve outcomes in population health and healthcare; tackle inequalities in outcomes, experience and access; enhance productivity and value for money and help the NHS support broader social and economic development. The Chair is an ambassador for and champion of effective partnership working with local government and NHS bodies, collaborative leadership and new governance arrangements across the Integrated Care System. Accountabilities Independent, non-executive Chair of the ICS/ICB and accountable to the NHS England Regional Director for the development and delivery of the plan of the ICS/ICB. The Chair would ensure the ICB is properly constituted and focused on improving outcomes in population health and healthcare, and encouraging greater partnership,
Page 3

integration and collaboration; both within the NHS and between the NHS and local government. The Chair would have a responsibility to establish and lead the unitary board of the ICB; which has joint collective and corporate accountability for the performance of the organisation, ensuring its functions are effectively and efficiently discharged and for NHS resources deployed to other organisations. The Chair provides strong leadership on issues that impact upon organisations and workforce across the ICS, including integration, the People agenda, Digital transformation, Emergency Preparedness, Resilience and Response (EPRR) and Covid-19 challenges. They will play a key role during 2021 / 2022 in preparing for the anticipated new statutory arrangements, with a view to ensuring that the ICB would meet its statutory duties, build strong partnerships and governance arrangements with system partners and take on commissioning functions from CCGs and NHS England. Roles and responsibilities / competencies Strategy and transformation • Leads the board in setting a vision, strategy and clear objectives for the ICS/ICB in
delivering on the four core purposes of the ICS, the triple aim and the body’s regulatory responsibilities.
• Holds the ICS Leader / ICB Chief Executive to account for delivery of the strategy of the ICS/ ICB, the plan for the delivery of health services for the population and effective stewardship of public money.
• Works with Local Government partners to establish the Integrated Care Partnership, establishing a strong relationship between the Board and the Partnership, and a dynamic which encourages a strong focus on health and care outcomes for the population.
Partnerships and communities • Is an ambassador for system working and collective accountability, building strong
partnerships and promoting effective dialogue across the ICS, with local government, NHS England and broader partnerships including the voluntary sector, to ensure joint planning and delivery, working through potential conflicts of interest.
• Engages Chairs and NEDs in partners across the system to work in a collaborative manner and build consensus.
• May act as the ICS Partnership Chair in addition to ICB Chair role. Otherwise, works with the ICS Partnership Chair to shape the new ICS Partnership and align the work of the ICB, with local government through the ICB.
• Establishes shared strategic priorities within the NHS in partnership with local government to tackle population health challenges and enhance services across health and social care.
Social justice and health equalities • Advocates and champions for diversity, health equality and social justice. Fosters
strong partnership arrangements with local government and wider partners to deliver these aims.
Page 4

• Ensures the ICS is responsive to people and communities – and that public, patient and carer voices are embedded in all of the ICS’s/ICB’s plans and activities.
• Promotes the values of the NHS Constitution a and role models the behaviours embodied in Our People Promise and forthcoming Leadership Way to ensure a collaborative, inclusive and productive approach across the system.
Sustainable outcomes • Leads the system through aligning partners in the implementation of the Long Term
Plan a and the People Plan, overseeing progress against their objectives. • Oversees the purposeful arrangements for effective clinical and professional care
leadership throughout the ICS. • Fosters a culture of research, innovation, learning and continuous improvement, to
support the delivery of high quality services for all. • Ensures the NHS plays its part in social and economic development and achieving
environmental sustainability, including the Carbon Net Zero commitment. Governance and assurance • Responsible for leading the board and ensuring it has the necessary constitutional
and governance arrangements and committee structures in place to ensure its effectiveness.
• Leads and supports a constructive and inclusive dynamic within the board, bringing independent and respectful challenge to the work programme and prioritisation.
• Actively brings in a range of voices to discussions, ensuring decisions take full account of perspectives from across the health and care system.
• Acts as the guardian of effective system governance; establishing strong place-based arrangements together with local government and dynamic joint working and governance with local partners, championing subsidiarity of decision making.
• Promotes open and transparent decision-making processes that facilitate consensus and manages areas of disagreement to deliver exceptional outcomes.
People and culture • Responsible for appointing the ICS Leader / ICB Chief Executive and independent
Non-Executive Directors (NEDs) with approval from NHS England, and ensuring they are supported and developed to maximise their contribution. Responsible for approving nominated ICB Partner member appointments.
• Together with the ICS Leader / ICB Chief Executive, provides visible leadership in developing a healthy and inclusive culture for the organisation which promotes diversity, encourages and enables system working and which is reflected and modelled in their own and the board’s behaviour and decision-making.
• Responsible for ensuring all members of the board, including the Partner members, comply with the Nolan Principles of Public Life and meet the Fit and Proper Persons test..
• As the ICS matures, the Chair would be expected to be actively engaged in NHS provider Chair and CEO appointments.
Scope and Scale Information specific to each NHS region and individual ICS Chair vacancy are included in the individual ICS Locality Pack
Page 5

4. Person Specification This section may be subject to change due to development of legislation. In order to be considered for this role, you should have the following attributes: Knowledge • Extensive knowledge of the health, care and local government landscape • An understanding of different sectors, groups, networks and the needs of diverse
populations • A deep understanding of the NHS triple aim (of improved population health, quality of
care and cost- control), the Kark review, and commitment to the values of the NHS Long Term Plan, the NHS
• People Plan, Nolan principles and the Standards for members of NHS Boards and Governing
• Bodies in England • An awareness and appreciation of social justice and how it might apply within an ICS • Sound understanding of good corporate governance as well as the difference
between governance and management Experience • Extensive experience of providing compassionate and inclusive leadership in a role
such as a Chair or Non-executive Director, at board or equivalent level in a complex public sector organisation such as; an NHS provider, Local Authority or CCG or have suitable leadership experience independent of the system
• Comprehensive experience of chairing complex professional meetings at a very senior level in a collaborative, efficient and effective manner
• Considerable experience of navigating politically sensitive situations and environments
• Significant experience of working with different sectors, groups, networks and building teams to deliver major transformation of public services
• Broad experience of working across agency and professional boundaries, collaboratively with the board and other stakeholders to oversee services and consult on transformation initiatives
• Experience of providing leadership and governance of a board, to identify and address issues, including underperformance and balance the competing objectives of quality, operational performance, and finance
• Track record of promoting Equality Diversity and Inclusion in leadership roles at board level and across systems
Skills • The ability to lead and build strong relationships across different sectors, and to
adapt to changing situations • Exceptional communication skills and be comfortable presenting in a variety of
contexts, with experience of dealing with the media and / or politicians on topics of healthcare or other public sector activities
• Ability to remain independent and neutral to provide independent and unbiased leadership of the board with a high degree of personal integrity
• Highly developed interpersonal and influencing skills, with the ability to lead in a creative environment which enables people to thrive and collaborate
Page 6

• Problem solving skills and the ability to identify issues and areas of risk, leading stakeholders to effective resolutions and decisions
• The ability to thrive and innovate in a complex and politically charged environment of change and uncertainty
• Confidence in constructively challenging information and explanations provided by others and negotiating when needed
• Understanding of your own strengths and the strengths of others, and where these are best deployed to solve challenges
Values • Demonstrates respect and adopts a compassionate and inclusive leadership style
with a demonstrable commitment to equality, diversity and inclusion (in respect of boards, patients and staff).
• Creates and lives by the values of openness and transparency • Works to espouse the values set out in the NHS People Plan, Nolan Principles and
soon to be published Leadership Way. • Demonstrate a strong commitment to public sector and NHS values Key Competencies Outlined above in the roles and responsibilities / competencies section are the six competency domains that illustrate some of the key behaviours we expect an ICS Chair to exhibit. The ICS Chair role and person specification have been agreed nationally and will provide a consistent framework for assessment based around the emerging Leadership Competency Framework. A summary person specification included as a graphic below groups the knowledge, experience, skills and values criteria within the competencies outlined above for ease of reference.
Page 7

Page 8

Page 9

Page 10

Eligibility The successful applicants will not have an ongoing leadership role at an organisation within the same ICS footprint. Applicants will need to stand down from such a role if appointed to the ICB Chair role. Elected officials including MPs and members of councils are excluded from the NHS ICB chair role. Applicants should have strong connections with the area served by the ICS. Given the significant public profile and responsibility members of NHS Boards hold, it is vital that those appointed inspire confidence of the public, patients and NHS staff at all times. NHS England / NHS Improvement makes a number of specific background checks to ensure that those we appoint are “fit and proper” people to hold these important roles. More information can be found on our website. Applications will be assessed on merit, as part of a fair and open process, from the widest possible pool of candidates. The information provided by applicants will be relied on to assess whether sufficient personal responsibility and competence have been demonstrated in previous/other roles, to satisfy the experience, skills and values being sought. We value and promote diversity and are committed to equality of opportunity for all. We believe that the best boards are those that reflect the communities they serve. • 50% of the working age population and 77% of the NHS workforce are women • 14% of the working age population and 23% of the NHS workforce are from ethnic
minorities • 16% of working age population and 5% of the NHS workforce are disabled • 2% of the population over 16 and 3% of the NHS workforce identify as LGB • 82% of working age adults and 79% of the NHS workforce are under 551
We want to increase the diversity of our NHS leadership and encourage applications from groups we know are all under-represented in these important roles. We prioritise Equality, Diversity and Inclusion, team health and wellbeing and the principles of kind leadership in our 'ways of working'. The successful applicants will have a key role in nurturing this culture. Terms of appointment This section may be subject to change due to development of the legislation. • The remuneration for this role will be competitive with reference to other such senior
roles in the NHS. • Initial term of appointment as current ICS chair and designate ICB chair until the
establishment of the ICB. The subsequent term of office as ICB chair would be confirmed if and when the legislation is in place and would be in accordance with the provisions of the constitution of the ICB.
• You will have considerable flexibility to decide how you manage the time needed to undertake this role.
• On average, it will require a minimum 2.5 to 3 days a week, including preparation time, the occasional evening engagement and events designed to support your continuous development.
Page 11

OFFICIAL-SENSITIVE
Cheshire and Merseyside
Chair Appointment
Page 12

OFFICIAL-SENSITIVE
Cheshire and Merseyside Footprint Overview
• Population of approx. 2.6 million • The STP/ ICS area is the 2nd largest footprint in England*• Complex system and late developer in ICS terms • 17 Providers** • 9 CCGs• 9 Local Authorities • 9 Places
*Taken from 2016 Sustainability and Transformation Plan ** And NWAS
Page 13

OFFICIAL-SENSITIVE
All Current C&M HCP Organisations
Key
Clinical Commissioning Group (CCG)
Local Authority
Liverpool City Council
Sefton Council
Wirral Metropolitan Borough Council
Trust
The Clatterbridge Cancer Centre NHS FT (CCC)
Wirral University Teaching Hospital NHS FT (WUTH)
NHS Wirral CCG
Wirral Community Health and Care NHS FT (WCHC)
NHS South Sefton CCG
NHS Southport and Formby CCG
Southport and Ormskirk Hospital NHS Trust (S&O)
Mid-Cheshire Hospital NHS FT
Cheshire East Council
East Cheshire NHS Trust
Warrington Borough Council
NHS Warrington CCG
St Helens and Knowsley Teaching Hospitals NHS Trust (STHKTH)
Mersey Care NHS FT
St Helens Council
NHS St Helens CCGNHS Knowsley
CCG
Cheshire West and Chester Council
Countess of Chester Hospital NHS FT (COCH)
Cheshire and Wirral Partnership NHS FT (CWP)
Alder Hey Children’s NHS FT
NHS Cheshire CCG
Liverpool University
Hospitals NHS FTLiverpool Heart and Chest NHS FT (LHCH)
Bridgewater Community Healthcare NHS FT (BCH)
Warrington and Halton Hospitals NHS Trust (WHH)
Knowsley Council
NHS Halton CCG
Halton Council
Liverpool Women’s
NHS FT
NHS Liverpool CCG
The Walton Centre NHS FT
Page 14

OFFICIAL-SENSITIVE
Cheshire and Merseyside Footprint Overview• 2.6 million people• Similar age structure to England
• More young people in Liverpool• More older people in Sefton and Cheshire East
• Deprivation levels vary significantly across the sub-region
https://www.cheshireandmerseysidepartnership.co.uk/wp-content/uploads/2021/03/Ethnicity-profiles-in-Cheshire-Merseyside.pdf
Page 15

OFFICIAL-SENSITIVE
Why the ICS opportunity is important to us• We need to collectively respond to the needs of our population and communities:
• High indices of deprivation • Complexity and variety of individual need • Inequalities of access and outcomes
• There is now pan system recognition and will for a system-wide step change - responding to shared challenges across health and care but ALSO beyond
• We need a framework which allows us to capitalise upon and embed increased democratic linkages and clear connections with communities
• We need a financially sustainable system that can respond to and support the system’s infrastructure needs
• There is growing international evidence that the only effective way to address these problems is through collaboration and integration
Page 16

OFFICIAL-SENSITIVE
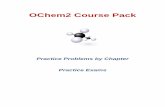
Life expectancy
Page 17

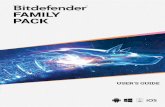
OFFICIAL-SENSITIVE
Why the gap• Causes of death in the North
West
• Causes of death and disability combined (DALYs) in the NorthWest
Page 18

OFFICIAL-SENSITIVE
Why are we doing this?• The NHS has been largely organized to provide episodic treatment for acute
illness• However it now needs, more than ever to deliver joined up support for
increasing numbers of older people and those living with chronic conditions• There continues to be an unacceptable inequality in the health of our
population and life expectancy is stalling• The wider determinants of health are well known but often tackled in silos • The integration of health and care has the potential to drive improvements in
population health by reaching beyond the NHS to involve local authorities and other agencies to tackle the wider determinants of health that drive longer term health outcomes and inequalities.
Page 19

OFFICIAL-SENSITIVE
HCP Vision, Mission and AimsVision:
• We want everyone in Cheshire and Merseyside to have a great start in life and get the support they need to stay healthy and live longer
Mission:
• We will tackle health inequalities and improve the lives of our poorest fastest. We believe we can do this best by working in partnership
Aims:
• Improve the health and wellbeing of local people• Shift from an illness focus to a health and wellbeing model
• Provide better joined up care, closer to homePage 20

OFFICIAL-SENSITIVE
Page 21

OFFICIAL-SENSITIVE
How we see that collaboration can occur
Page 22

OFFICIAL-SENSITIVE
Our emerging system
Page 23

OFFICIAL-SENSITIVE
C&M ICS Programme Overview
Page 24

OFFICIAL-SENSITIVE
Cheshire and Merseyside Overview
Table from Designing integrated care systems (ICSs) in England
Primary Care Networks
Place
C&M HCP
91
51
Page 25

OFFICIAL-SENSITIVE
Our Places or ICPs • Clinical care redesign (including (simplifying and standardising care pathways)
• Forming provider partnerships and alliances (including GPs) to redesign and integrate services
• Developing new provider models
• Joining up council/ hospital/ community services
• Closer working with LA and VCS partners on prevention and health inequalities
• Population health management
Integrated Place Based Care• Planning, managing and delivering services together for our populations in our neighbourhoods would enable us to
focus on need be that a health need or a wider determinant of health need• Linking education, employment and service delivery in a Place/Borough enables us to shape our workforce and build
resilience and opportunity in communities• Linking health skills and knowledge with housing and care across our neighbourhoods enables us to support our
families in need or at risk of harm
How• Will involve local discussion, influence or decision making• Alignment with appropriate governance structures – statutory roles like HWBB and OSCs but also decisions • Some local choices – our place development priorities are summarized within the annex
Page 26

OFFICIAL-SENSITIVE
Provider CollaborativesPreferred approach:
• Two provider collaboratives: one for acute and specialist services and one for mental health, learning disability and community services. Each to have a lead
• The groups should be convened under a single provider collaborative ‘partnership’ where there are issues to be addressed that require all providers to be engaged
• Initial priorities to be established Q2 onward 21/22
• Development of culture, infrastructure and shared decision making principles need to align to development of priorities
• Collaboration should support efficiency, improved quality and the closer system working with opportunity to delegate
Page 27

OFFICIAL-SENSITIVE
Annexes
Page 28

OFFICIAL-SENSITIVE
Key Reference Documents• Integrating care: Next steps to building strong and effective integrated care
systems across England• Integration and innovation: working together to improve health and social
care for all• FRC guidance on Board Effectiveness
https://www.frc.org.uk/getattachment/61232f60-a338-471b-ba5abfed25219147/2018-Guidance-on-Board-Effectiveness-FINAL.PDF
• Recast ICS Strategy 2021-25• Health and Care Partnership Memorandum of Understanding1
• Cheshire and Merseyside People Plan • Getting under the skin research and BAME action plan11 Supplied upon request
Page 29

OFFICIAL-SENSITIVE
Our Place & Place Priorities HCP is committed to devolved decision making. Taking decisions closer to populations but also supporting integration around neighbourhoods and with local partners where appropriate. Responsibilities, teams and decisions will be established at a system level where it makes sense to do so and the greatest potential for improvement can be achieved. This means we need to be focused on developing our places as well as our ICS system:
1) Integrated Care Partnership (ICP) Governance: clearly defined formal arrangements for place partners to meet and work together to deliver outcomes set by the Health & Wellbeing Board (HWB) and ICS.
2) ICP nominated ‘Place Lead’ with remit for integrated working who will connect with ICS3) Shared vision and plan for reducing inequalities and improving outcomes of local people approved
by HWB (underpinned by local population health and socio-economic intelligence)4) Agreed ICP development plan5) Defined footprints (e.g. neighbourhoods) for delivery of integrated care, clinically led by PCNs
working with social care, community, mental health, public health and other community groups. 6) Programme of ongoing public and wider stakeholder engagement at place
Places will be expected to develop an integrated approach to commissioning between health and local authority (such as shared posts, joint teams and pooled budgets) to underpin and support the work of
the ICPPage 30

OFFICIAL-SENSITIVE
20 |
Political Make up of C&M Councils
Presentation title
Council Political Make Up Next ElectionLiverpool City Labour (maj) May 2022Halton Labour (maj) May 2022Sefton Labour (maj) May 2022St Helens Labour (maj) May 2022Knowsley Labour (maj) May 2022Cheshire West and Chester NOC (Labour min) May 2023Cheshire East NOC (Labour and Ind) May 2023Warrington Labour (maj) May 2024Wirral NOC (Lab min) May 2022
Page 31

OFFICIAL-SENSITIVE
21 |
• Chris Matheson (City of Chester, Lab)
• Fiona Bruce (Congleton, Con)
• Kieran Mullan (Crewe & Nantwich, Con)
• Edward Timpson (Eddisbury, Con)
• Justin Madders (Ellesmere Port & Neston, Lab)
• Derek Twigg (Halton, Lab)
• David Rutley (Macclesfield, Con)
• Esther McVey (Tatton, Con)
• Charlotte Nichols (Warrington North, Lab)
• Andy Carter (Warrington South, Con)
• Mike Amesbury (Weaver Vale, Lab)
• Mick Whitley (Birkenhead, Lab)
List of Cheshire and Merseyside MPs
Presentation title
• Peter Dowd (Bootle, Lab)
• Maria Eagle (Garston & Halewood, Lab)
• George Howarth (Knowsley, Lab)
• Kim Johnson (Liverpool Riverside, Lab)
• Dan Carden (Liverpool Walton, Lab)
• Paula Barker (Liverpool Wavertree, Lab)
• Ian Byrne (Liverpool West Derby, Lab)
• Bill Esterson (Sefton Central, Lab)
• Damien Moore (Southport, Con)
• Conor McGinn (St Helens North, Lab)
• Marie Rimmer (St Helens South & Whiston, Lab)
• Angela Eagle (Wallasey, Lab)
• Alison McGovern (Wirral South, Lab)
• Margaret Greenwood (Wirral West, Lab) Page 32

OFFICIAL-SENSITIVE
Place, CCG & Local Authority ContinuityLocal Authority CCG
Wirral Council Wirral CCG
Cheshire West and Chester CouncilCheshire CCG
Cheshire East Council
Halton Council Halton CCG
Warrington Council Warrington CCG
Liverpool City Council Liverpool CCG
St Helen’s Council St Helens CCG
Knowsley Council Knowsley CCG
Sefton CouncilSouth Sefton CCG
Southport & Formby CCG
Page 33

OFFICIAL-SENSITIVE
23 |
C&M Trusts Most Recent CQC Rating Trust Rating & Date
Alder Hey Children's NHS Foundation Trust Good (April 2021)
Bridgewater Community Healthcare NHS Foundation Trust Requires Improvement (December 2018)
Cheshire and Wirral Partnership NHS Foundation Trust Good (June 2020)
Clatterbridge Cancer Centre NHS Foundation Trust Good (April 2019)
Countess of Chester Hospital NHS Foundation Trust Countess of Chester: Requires Improvement (May 2019)
East Cheshire NHS Trust Good (October 2019)
Liverpool Heart and Chest Hospital NHS Foundation Trust Outstanding (July 2019)
Liverpool University Hospitals NHS Foundation Trust Good (January 2021)
Liverpool Women's Hospital NHS Foundation Trust Good (April 2020)
Mersey Care NHS Foundation Trust Good (April 2019)
Mid Cheshire Hospitals NHS Foundation Trust Good (April 2020)
North West Ambulance Service NHS Trust Good (June 2020)
Southport and Ormskirk Hospital NHS Trust Requires Improvement (November 2019)
St Helens and Knowsley Teaching Hospitals NHS Trust Outstanding (March 2019)
The Walton Centre NHS Foundation Trust Outstanding (August 2019)
Warrington and Halton Hospitals NHS Foundation Trust Good (July 2019)
Wirral Community Health & Care NHS Foundation Trust Requires Improvement (July 2018)
Wirral University Teaching Hospital NHS Foundation Trust Requires Improvement (April 2021)
Page 34

OFFICIAL-SENSITIVE
24 |
Alder Hey Children’s Hospital NHS FT Louise Shepherd CEO [email protected]
Bridgewater Community Healthcare NHS FT Colin Scales CEO [email protected]
Cheshire and Wirral Partnership NHS FT Sheena Cumiskey CEO [email protected]
Countess of Chester NHS Foundation Hospital Dr Susan Gilby CEO [email protected]
Clatterbridge Cancer Centre NHS Foundation Truts
Liz Bishop CEO [email protected]
East Cheshire NHS Trust John Wilbraham CEO [email protected]
Liverpool University Foundation Trust Steve Warburton CEO [email protected]
Liverpool Heart and Chest Hospital NHS Foundation Trust
Jane Tomkinson CEO [email protected]
Liverpool Women’s Hospital NHS Foundation Trust
Kathryn Thompson CEO [email protected]
Mersey Care NHS Foundation Truts Joe Rafferty CEO [email protected]
Mid Cheshire Hospital NHS Foundation Trust James Sumner CEO [email protected]
Southport and Ormskirk NHS Trust Trish Armstrong-Child CEO [email protected]
St Helens and Knowsley Hospitals NHS Trust Ann Marr CEO [email protected]
Warrington and Halton Hospitals NHS Foundation Trust
Dr Simon Constable CEO [email protected]
Wirral Community Health and Care NHS FT Karen Howell CEO [email protected]
Wirral University Hospital Trust Janelle Holmes CEO [email protected]
The Walton Centre NHS Foundation Trust Jan Ross CEO [email protected]
NHS Provider contacts
Page 35

OFFICIAL-SENSITIVE
25 |
NHS Liverpool CCG Jan Ledward AO [email protected]
NHS Southport /Sefton CCG’s Fiona Taylor AO [email protected]
NHS St Helens CCG Mark Palethorpe AO [email protected]
NHS Cheshire CCG Clare Watson AO [email protected]
NHS Warrington CCG/ NHS Halton CCGs Andrew Davies AO [email protected]
NHS Knowsley CCG Dianne Johnson AO [email protected]
NHS Wirral CCG Simon Banks AO [email protected]
CCG Contacts
Page 36

OFFICIAL-SENSITIVE
26 |
St Helens Council Kath O’Dwyer CEO Katho’[email protected]
Warrington Council Steven Broomhead CEO [email protected]
Sefton Council Dwayne Johnson CEO [email protected]
Knowsley Council Mike Harden CEO [email protected]
Halton Council David Parr CEO [email protected]
Liverpool Council Tony Reeves CEO [email protected]
Wirral Council Paul Satoor CEO [email protected]
Cheshire West and Chester Council Andrew Lewis CEO [email protected]
Cheshire East Council Lorraine O’Donnell CEO Lorraineo’[email protected]
Local Authority Contacts
Page 37

NHS England and NHS Improvement
Chair Appointments – Greater Manchester ICS
Page 38

2 |
Map of Area –Greater Manchester
AND GLOSSOP
Greater Manchester
Population size 2, 732,900
(2014)
2021 Estimated:
2, 846, 901
#Trusts 10
#CCGs 10
#Providers 21
Page 39

3 |
CCGs and the Local Authorities
CCG Local Authority (LA)
NHS Bolton Clinical Commissioning Grouphttps://www.boltonccg.nhs.uk/
Bolton Councilhttps://www.bolton.gov.uk/
NHS Bury Clinical Commissioning Group https://www.buryccg.nhs.uk/
Bury Councilhttps://www.bury.gov.uk/
NHS Heywood, Middleton and Rochdale Clinical Commissioning Grouphttps://www.hmr.nhs.uk/
Rochdale Borough Councilhttp://www.rochdale.gov.uk/
NHS Manchester Clinical Commissioning Grouphttps://www.mhcc.nhs.uk/
Manchester City Council https://www.manchester.gov.uk/
NHS Oldham Clinical Commissioning Group http://www.oldhamccg.nhs.uk/
Oldham Council https://www.oldham.gov.uk/
NHS Tameside and Glossop Clinical Commissioning Grouphttps://www.tamesideandglossopccg.org/
Tameside Metropolitan Borough Council - https://www.tameside.gov.uk/
NHS Trafford Clinical Commissioning Group https://www.traffordccg.nhs.uk/Home.aspx
Trafford Council https://www.trafford.gov.uk/Home.aspx
NHS Salford Clinical Commissioning Group https://www.salfordccg.nhs.uk/
Salford Council https://www.salford.gov.uk/
NHS Stockport Clinical Commissioning Group https://www.stockportccg.nhs.uk/
Stockport Council https://www.stockport.gov.uk/
NHS Wigan Borough Clinical Commissioning Group https://healthierwigan.nhs.uk/
Wigan Council https://www.wigan.gov.uk/
Page 40

4 |
Providers and CQC Ratings
• Providers• CQC
Provider Current CQC rating and year of most recent inspection
The Pennine Acute Hospitals NHS Foundation Trusthttps://www.northerncarealliance.nhs.uk/
Good -2019
Manchester NHS Foundation Trust https://mft.nhs.uk/
Good - 2019
Salford Royal NHS Foundation Trusthttps://www.northerncarealliance.nhs.uk/
Outstanding -2018
The Christie NHS Foundation Trust https://www.christie.nhs.uk/
Outstanding – 2018
Greater Manchester Mental Health Foundation Trust https://www.gmmh.nhs.uk/
Good – 2019
Pennine Care NHS Foundation Trust https://www.penninecare.nhs.uk/
Requires Improvement – 2018
Tameside and Glossop Integrated Care NHS Foundation Trusthttps://www.tamesidehospital.nhs.uk/
Good - 2019
Stockport NHS Foundation Trusthttps://www.stockport.nhs.uk/
Requires Improvement – 2020
Bolton NHS Foundation Trust https://www.boltonft.nhs.uk/
Good – 2019
Wrightington, Wigan and Leigh Foundation Trust https://www.wwl.nhs.uk/
Good – 2019
Page 41

5 |
Existing Organisations and Accountable officers (CCGs & Providers)
CCG Chair Accountable Officer
NHS Bolton Clinical Commissioning Group
Dr NirubanRatnarajah
Susan Long
NHS Bury Clinical Commissioning Group
Dr Jeffrey Schryer Geoff Little
NHS Heywood, Middleton and Rochdale Clinical Commissioning Group
Dr Chris Duffy Steve Rumbelow
NHS Manchester Health and Care Commissioning
Dr Ruth Bromley Ian Williamson
NHS Oldham Clinical Commissioning Group
Majid Hussain Dr Carolyn Wilkins OBE
NHS Tameside and Glossop Clinical Commissioning Group
Dr Asad AliCo-Chair Dr Ashwin Ramachandra
Steven Pleasant MBE
NHS Trafford Clinical Commissioning Group
Dr Muhammad Imran
Sara Radcliffe Gareth James
NHS Salford Clinical Commissioning Group
Dr Tom Tasker Steve Dixon
NHS Stockport Clinical Commissioning Group
Dr Cath Briggs Andrea Green
NHS Wigan Borough Clinical Commissioning Group
Dr Tim Dalton Professor Craig Harris
Provider Name Chair CEO
Bolton NHS Foundation Trust
Donna Hall CBE Fiona Noden
The Christie NHS Foundation Trust
Chris Outram MBE Roger Spencer
Greater Manchester Mental Health Foundation Trust
Rupert Nichols Neil Thwaite
Manchester NHS Foundation Trust
Kathy Cowell OBE Sir Michael Deegan CBE
The Pennine Acute Hospitals NHS Foundation Trust
Chris Outram MBE Patrick Crowley
Pennine Care NHS Foundation Trust
Evelyn Asante-Mensah OBE
Claire Molloy
Salford Royal NHS Foundation Trust
Professor Michael Luger
Raj Jain
Stockport NHS Foundation Trust
Tony Warne Karen James OBE
Tameside and Glossop Integrated Care NHS Foundation Trust
Jane McCall Karen James OBE
Wrightington, Wigan and Leigh Foundation Trust
Robert Armstrong Silas Nicholls
Page 42

6 |
Local Authority Accountable officers
LA Leader Chief Exec DASS DPHBolton Council David Greenhalgh Tony Oakman Rachel Tanner Dr Helen LoweyBury Council Eamonn O'Brien Geoff Little Adrian Crook Lesley JonesRochdale Borough Council
Neil Emmott Steve Rumbelow Claire Richardson Andrea Fallon
Manchester City Council Sir Richard Leese Joanne Roney OBE Bernie Enright David ReganOldham Council Arooj Shah Dr Carolyn Wilkins OBE Mark Warren Katrina StephensTameside Metropolitan Borough Council
Brenda Warrington Steven Pleasant MBE Stephanie Butterworth Jeanelle De Gruchy
Trafford Council Andrew WesternSara Todd Diane Eaton Eleanor Roaf
Salford Council Paul Dennett Tom Stannard Cath Gormally Muna Abdul AzizStockport Council Elise Wilson Pam Smith Mark Fitton Jennifer ConnollyWigan Council David Molyneux Alison McKenzie-Folan Stuart Cowley Kate Ardern
Greater Manchester Combined Authority
Elected Mayor Andy Burnham
Chief Exec EamonnBoylan
Page 43

Greater Manchester Healthand Social Care Partnership
GM - CONFIRMED VISION, OBJECTIVES & PRIORITIESThe GMHSC Partnership review reaffirmed our original vision & objectives
which we are guided by.
To improve the health and wellbeing of all the residents of Greater Manchester .
-To use social value to tackle the inequalities around us and create lasting benefits for the people of GM, improve the local economy, whilst positively contributing (or at least minimising damage) to the environment;-To close the health inequalities gap within GM and between GM and the rest of the UK faster;- To deliver effective & efficient integrated health and social care across GM;-To continue to redress the balance of care to move it closer to home where possible;- To strengthen the focus on wellbeing, including greater focus on prevention and population health;-To ensure equality, diversity and inclusion are reflected in our leadership and guide our priorities and all areas of our work- To harness the breakthrough opportunities of digital technology for enhancing existing services and crafting novel services to give better outcomes to citizens and improved value for money;- To secure clinical & financial sustainability across the whole of the health and social care landscape;- To contribute to growth and connect people to growth and maximise impact from health innovation and digital;- To further develop our partnership between the NHS, local government, universities and science and knowledge industries for the benefit of the population.
1. Tackling inequalities and transforming population health
2. Guaranteeing Constitutional Standards and eliminating unwarranted variation in care
3. Connect health, social care, academia and industry to discover, develop and deploy innovation at pace and scale
4. Achieve comprehensive system Sustainabilityacross health and social care for the long term.
We have reaffirmed and refreshed our original objectives set out in Taking Charge and the MoU.
In doing so we have identified 4 main priorities
Page 44

Greater Manchester Healthand Social Care PartnershipGM ICS PROGRAMME OVERVIEW
March 2021 March 2022
GM Model Development Programme
GM Model DesignGM & Locality approach to Functions,
Governance & Accountability
Financial FlowsPeople & Culture
GM and Place Based Provider Collaboratives
GM Model Implementation
OD & Change Transition (aligned
workstreams)
GM & Local (ICS) Establishment & Safe transfer of functions
HR & safe transition of our people
Transformation of functions & services
GM Operating Model
GM System Partnerships,
Communications & Engagement
Learning & Insight
1. Tackling inequalities and transforming population health
2. Guaranteeing Constitutional Standards and eliminating unwarranted variation in care
3. Develop and deploy innovation at pace and scale
4. Achieve system Sustainabilityacross health and social care for the long term.
Priorities:
Health Innovation,
Digital & Data
Page 45

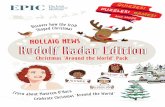
GM Health & Social Care Partnership Governance*
GM Combined Authority and GM Mayor
GM Reform Board GM Health and Care Board
Joint Commissioning Board
Provider Federation Board
Primary Care Advisory Board
LCO Network
Finance Executive Group
Performance and Delivery Board Quality Board
ProgrammeCo-ordination
Group
Programme Governance
Children’s Health and Wellbeing Baord
Health Innovation Manchester
Digital Collaborative
Workforce Collaborative
Strategic Estates Board
GM HSC Partnership Executive Board
* Governance currently under review as part of ICS Development
Page 46

Greater Manchester Healthand Social Care Partnership
ORGANISATIONAL STRUCTURE – GM HEALTH & SOCIAL CARE PARTNERSHIP
GM Strategies
Chief Officer
Executive Lead: Finance and Assurance
Executive Lead: Strategy &
Programmes
Executive Lead: Workforce, OD &
System Leadership
Medical Executive
Executive Lead: Commissioning & Population Health
Page 47

Greater Manchester Healthand Social Care Partnership
LINKS TO GREATER MANCHESTER STRATEGIES
GM Strategies
Taking Charge – the Next Five Years – Our Prospectus: https://www.gmhsc.org.uk/wp-content/uploads/2019/03/GMHSC-Partnership-Prospectus-The-next-5-years-pdf.pdf
Our People, Our Place – the Greater Manchester Strategy: https://www.greatermanchester-ca.gov.uk/media/1084/greater_manchester_summary___full_version.pdf
The Greater Manchester Model – Our White Paper on Unified Public Services for the People of Greater Manchester :https://www.greatermanchester-ca.gov.uk/media/2302/gtr_mcr_model1_web.pdf
Page 48

12 |
Whole region picture – North West
Page 49

13 |
North West Region Mission Statement
Page 50

15 |
North West Business Plan Summary
Page 52

More information The Government's White Paper on health and care reform place ICSs at the heart of the NHS. The four core purposes of an ICS are laid out in Integrating care: Next steps to building strong and effective integrated care systems across England, namely to improve outcomes in population health and healthcare; tackle inequalities in outcomes, experience and access; enhance productivity and value for money and help the NHS support broader social and economic development, all rooted in underlying principles of subsidiarity and collaboration. Support in preparing your application: • Building your application • Onboarding support, sources of information, useful reading • How we will handle your application and information • View all current chair and non-executive vacancies • Sign up to receive email alerts on the latest vacancies
NHS England / NHS Improvement respects your privacy and is committed to protecting your personal data. We will only use personal data where we have your consent or where we need to comply with a legal or statutory obligation. It is important that you read this information together with our privacy notice so that you are fully aware of how and why we are using your data Making an application For more information, you can get in touch with:
• Our advisors at Odgers Berndtson for an informal and confidential discussion about the ICS Chair role. Please email [email protected] or [email protected] or call 0161 498 3413 to speak with Gillian Powell or Peter Mason.
• Our Non-executive Talent and Appointments Team – for general enquiries about the
selection process contact the team at [email protected] If you wish to be considered for one of the roles please provide: • Confirmation of the ICS Chair role you are applying for. You may apply for more than one role if you meet the criteria, but we strongly advise that you tailor and submit individual applications to be competitive • a CV that includes your address and preferred contact details, highlighting and explaining any gaps in your employment history • a supporting statement that highlights your skills and experience and allows insights on your values and motivations for applying for the role. You should outline your personal responsibility and achievement within previous roles that demonstrates you have the knowledge, skills and competencies to deliver this role, as outlined in the person specification (max 2,000 words)
Page 53

• the names, positions, organisations and contact details for three referees. Your referees should be individuals in a line management capacity (or senior stakeholders), and cover your most recent roles and employer, any regulated health or social care activity or where roles involved children or vulnerable adults. Your references will be taken prior to interview and may be shared with the selection panel • a completed monitoring information form which accompanies this pack • a completed self-declaration form confirming that you do not meet any of the criteria that would disqualify you from appointment • tell us about any dates when you will not be available for the selection process This information should be emailed to [email protected] quoting “ICS Chair application” in the subject line and the reference number quoted in the individual ICS Locality Pack. Preliminary selection: information provided by applicants will be relied on to assess whether sufficient personal responsibility and competence have been demonstrated in previous/other roles, to satisfy the experience, skills and values outlined in the person specification. Long-listed applicants may be invited for a preliminary interview. Feedback from any preliminary assessment will be given to the selection panel who will agree the applicants invited to interview. Shortlisting: the selection panel will use the information provided by the applicants and feedback from any preliminary assessment to agree applicants invited to interview. Assessment will be based on merit against the competencies experience, skills and values outlined in the person specification. Stakeholder event: shortlisted applicants will be expected to participate in a stakeholder engagement event or events to meet groups of key stakeholders. Feedback from these sessions will be shared with the selection panel. Further details and dates are included in the individual ICS Locality Pack on the website Interviews: applicants will be asked to make a 5 -10 minute presentation to help the selection panel draw out the competencies, experience, skills and values outlined in the person specification. The formal interview will be 45 mins to an hour of open questions from the selection panel to showcase past experience and explore applicant’s values, motivations, creativity and ability. Appointment: Selection panels will be asked to identify appointable candidates based on merit against the competencies experience, skills and values outlined in the person specification. The preferred candidate will be presented to NHS England and Improvement for appointment and the Secretary of State for Health for final approval of appointment.
Page 54