Insomnia With Objective Short Sleep Duration and Incident Hypertension: The Penn State Cohort *...
18
Antonio Vela-Bueno, Maria Basta and Edward O. Bixler Julio Fernandez-Mendoza, Alexandros N. Vgontzas, Duanping Liao, Michele L. Shaffer, State Cohort Insomnia With Objective Short Sleep Duration and Incident Hypertension : The Penn Print ISSN: 0194-911X. Online ISSN: 1524-4563 Copyright © 2012 American Heart Association, Inc. All rights reserved. is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Hypertension published online August 14, 2012; Hypertension. http://hyper.ahajournals.org/content/early/2012/08/14/HYPERTENSIONAHA.112.193268 World Wide Web at: The online version of this article, along with updated information and services, is located on the http://hyper.ahajournals.org/content/suppl/2012/08/15/HYPERTENSIONAHA.112.193268.DC1.html Data Supplement (unedited) at: http://hyper.ahajournals.org//subscriptions/ is online at: Hypertension Information about subscribing to Subscriptions: http://www.lww.com/reprints Information about reprints can be found online at: Reprints: document. Permissions and Rights Question and Answer this process is available in the click Request Permissions in the middle column of the Web page under Services. Further information about Office. Once the online version of the published article for which permission is being requested is located, can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Hypertension in Requests for permissions to reproduce figures, tables, or portions of articles originally published Permissions: at Milton S. Hershey Medical Center on August 22, 2012 http://hyper.ahajournals.org/ Downloaded from
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Insomnia With Objective Short Sleep Duration and Incident Hypertension: The Penn State Cohort *...
Antonio Vela-Bueno, Maria Basta and Edward O. BixlerJulio Fernandez-Mendoza, Alexandros N. Vgontzas, Duanping Liao, Michele L. Shaffer,
State CohortInsomnia With Objective Short Sleep Duration and Incident Hypertension : The Penn
Print ISSN: 0194-911X. Online ISSN: 1524-4563 Copyright © 2012 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Hypertension published online August 14, 2012;Hypertension.
http://hyper.ahajournals.org/content/early/2012/08/14/HYPERTENSIONAHA.112.193268World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://hyper.ahajournals.org/content/suppl/2012/08/15/HYPERTENSIONAHA.112.193268.DC1.htmlData Supplement (unedited) at:
http://hyper.ahajournals.org//subscriptions/
is online at: Hypertension Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer this process is available in the
click Request Permissions in the middle column of the Web page under Services. Further information aboutOffice. Once the online version of the published article for which permission is being requested is located,
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the EditorialHypertensionin Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
at Milton S. Hershey Medical Center on August 22, 2012http://hyper.ahajournals.org/Downloaded from

Insomnia With Objective Short Sleep Duration andIncident Hypertension
The Penn State Cohort
Julio Fernandez-Mendoza, Alexandros N. Vgontzas, Duanping Liao, Michele L. Shaffer,Antonio Vela-Bueno, Maria Basta, Edward O. Bixler
Abstract—Insomnia with objective short sleep duration appears to be a biologically more severe phenotype of the disorder.No longitudinal study to date has examined the association of this type of insomnia with incident hypertension usingpolysomnography. From a random, general population sample of 1741 adults of the Penn State Cohort, 1395 werefollowed-up after 7.5 years, and 786 did not have hypertension at baseline. Hypertension was determined by a self-reportof receiving treatment for high blood pressure. Chronic insomnia was defined as a complaint of insomnia lasting �1year, whereas poor sleep was defined as moderate-to-severe sleep difficulties. All of the subjects underwent 8-hourpolysomnography. Sleep-disordered breathing (SDB) was defined as an obstructive apnea/hypopnea index �5. We usedthe median polysomnographic percentage of sleep time to define short sleep duration (ie, �6 hours). We controlled forsex, race, age, caffeine, cigarettes and alcohol consumption, depression, sleep-disordered breathing, diabetes mellitus,obesity, and blood pressure in our analyses. Compared with normal sleepers who slept �6 hours, the highest risk forincident hypertension was in chronic insomniacs with short sleep duration (odds ratio, 3.8 [95% CI, 1.6–9.0]). The riskfor incident hypertension in poor sleepers with short sleep duration was significantly increased but became marginallysignificant after controlling for obesity (odds ratio, 1.6 [95% CI, 0.9 –2.8]). Chronic insomnia with short sleepduration is associated with an increased risk for incident hypertension in a degree comparable to sleep-disorderedbreathing. Objective short sleep duration in insomnia may serve as a useful predictor of the biological severity ofthe disorder. (Hypertension. 2012;60:00-00.) ● Online Data Supplement
Key Words: insomnia � polysomnography � hypertension � incidence
Approximately 30% of the US population has hyperten-sion, which is associated with significant morbidity and
increased mortality and great economic cost.1 A large amountof literature has linked sleep disorders, particularly sleep-disordered breathing (SDB), to hypertension.2–4 However,insomnia, which is the most prevalent sleep disorder,5 istraditionally associated with impaired occupational perfor-mance, increased work absenteeism, higher healthcare costs,and worse quality of life but not with significant cardiovas-cular morbidity, that is, hypertension risk. This leads someclinicians to view insomnia and the associated symptoms ofpoor physical health as obsessions of otherwise healthyindividuals.
Few studies that examined the association of insomniawith hypertension have reported modest and inconsistenteffects.6–11 More recent studies that used objective mea-sures of sleep have shown that insomnia with objective
short sleep duration is associated with significant morbid-ity, including hypertension,12 diabetes mellitus,13 neuro-cognitive deficits,14 and mortality,15 suggesting that objec-tive short sleep duration may be a marker of the biologicalseverity of the disorder16,17 and that insomniacs with shortsleep duration are at high risk for adverse medical out-comes. A limitation of these previous studies is that theywere cross-sectional and did not provide causality in termsof the direction of the association.
No study to date has examined whether insomnia withobjective short sleep duration is associated with the develop-ment of hypertension. To test this hypothesis, we examinedthe joint effect of the complaints of chronic insomnia andpoor sleep and objective sleep duration on the incidence ofhypertension in a large, random, general population sample.We hypothesized that chronic insomnia is associated with asignificant risk of incident hypertension and that the associ-
Received February 16, 2012; first decision March 11, 2012; revision accepted July 19, 2012.From the Sleep Research and Treatment Center, Department of Psychiatry (J.F.-M., A.N.V., E.O.B.), Department of Public Health Sciences (D.L.,
M.L.S.), Pennsylvania State University College of Medicine, Hershey, PA; Department of Psychiatry (A.V.-B.), School of Medicine, AutonomousUniversity, Madrid, Spain; Department of Psychiatry (M.B.), School of Medicine, University of Crete, Crete, Greece.
The online-only Data Supplement is available with this article at http://hyper.ahajournals.org/lookup/suppl/doi:10.1161/HYPERTENSIONAHA.112.193268/-/DC1.
Correspondence to Alexandros N. Vgontzas, Penn State University College of Medicine, Department of Psychiatry H073, 500 University Dr, Hershey,PA 17033. E-mail [email protected]
© 2012 American Heart Association, Inc.
Hypertension is available at http://hyper.ahajournals.org DOI: 10.1161/HYPERTENSIONAHA.112.193268
1 at Milton S. Hershey Medical Center on August 22, 2012http://hyper.ahajournals.org/Downloaded from

ation of chronic insomnia and incident hypertension is en-hanced by objective short sleep duration.
MethodsParticipantsThe data presented here were collected as part of a population-basedstudy of sleep disorders, which used a 2-phase protocol to recruitparticipants from various age groups.10,18–21 In the first phase of thestudy, telephone interviews were conducted with 4364 age-eligiblemen and 12219 age-eligible women residing in the sample house-holds, for a total sample of 16583, with response rates of 73.5% and74.1%, respectively. In the second phase of this study, a subsampleof 741 men and 1000 women, selected randomly from the first phase,were studied in our sleep laboratory, with response rates of 67.8%and 65.8%, respectively. After giving a complete description of thestudy to the subjects, written informed consent was obtained. Of the1741 subjects who completed the sleep laboratory evaluation, 1395subjects were followed up after an average duration of 7.5 years viatelephone interview. The response rate of the follow-up study was79.7%. After complete description of the follow-up study to thesubjects, verbal informed consent was obtained. The whole studyprocedure was approved by the university’s institutional reviewboard. Please see the online-only Data Supplement for details on thesampling procedure and the participant flow in the study.
Definition of Incident HypertensionFor the purpose of this study, the presence of hypertension atbaseline was defined by a self-report of receiving treatment for highblood pressure (BP), based on a standardized questionnaire com-pleted by the subjects on the evening of their sleep laboratory visit.Commensurate with the baseline definition, hypertension atfollow-up was defined by a self-report of receiving treatment forhigh BP. Of the 1395 subjects who were followed up, 786 did nothave hypertension at baseline and were selected for the presentstudy. A total of 191 subjects were incident cases of hypertension,whereas 595 did not have hypertension at follow-up. Twentysubjects had missing data on hypertension at follow-up.
Sleep Laboratory EvaluationAll of the subjects were evaluated for 1 night in the sleep laboratoryin sound-attenuated, light- and temperature-controlled rooms. Dur-ing this evaluation, each subject was continuously monitored for 8hours (fixed time period) using 16-channel polysomnography (PSG),including electroencephalogram, electrooculogram, and electromyo-gram. Bedtimes were adjusted to conform to subjects’ usual bed-times, and subjects were recorded between 10:00 PM to 11:00 PM and6:00 AM to 7:00 AM. The sleep recordings were subsequently scoredindependently, according to Rechtschaffen and Kales criteria.22 Thepercentage of sleep time is total sleep time divided by recorded timein bed and multiplied by 100. From the objectively recorded sleeptime data, we regrouped the entire study sample into 2 ordinalgroups, the top 50% of persons above the median percentage of sleeptime (“longer sleep duration group”) and the 50% of persons in thebottom half (“short sleep duration group”). We then rounded thecutoff point to meaningful numbers and thus created the following 2sleep duration groups: the longer sleep duration group consisted ofthose who slept �6 hours (ie, percentage of sleep time �75%) andthe short sleep duration group of those who slept �6 hours (ie,percentage of sleep time �75%). This cutoff point has been shownin previous cross-sectional studies to be predictive of significantmedical morbidity and mortality.12–15 Respiration was monitoredthroughout the night by use of thermocouples at the nose and mouthand thoracic strain gauges. All-night recordings of hemoglobinoxygen saturation were obtained with an oximeter attached to thefinger. For the purpose of this study, the presence of SDB wasdefined as an obstructive apnea/hypopnea index �5.18,19 Body massindex was based on measured height (in centimeters) and weight (inkilograms) during the subjects’ sleep laboratory visit. Furthermore,BP was measured in the evening, �2 hours before the start of the
sleep recording, using a pneumoelectric microprocessor-controlledinstrument with the appropriate-sized cuffs. The accuracy of thismonitor is reported to be �3 mm Hg; in addition, internal calibrationwas performed before each use, and the machine was checkedagainst a mercury sphygmomanometer at least annually. The re-corded BP was the average of 3 consecutive readings during a5-minute period after 10 minutes of rest in the supine position. Basedon these baseline BP measurements, a normal BP status was definedas systolic BP (SBP) �120 mm Hg and diastolic BP (DBP) �80 mmHg, a prehypertensive BP status as SBP �120 and �140 mm Hgand/or DBP �80 and �90 mm Hg, and a hypertensive BP status asSBP �140 mm Hg and/or DBP �90 mm Hg. BP measurementswere not taken at follow-up.
Insomnia and Other MeasurementsAs part of the standardized questionnaire, we also assessed thepresence of all sleep disorders. The presence of sleep difficulty wasestablished on 3 levels of severity. First, “chronic insomnia” wasdefined by a complaint of insomnia with a duration of �1 year.Second, “poor sleep” was defined as a moderate-to-severe complaintof difficulty falling asleep, difficulty staying asleep, early finalawakening, or nonrestorative sleep. Finally, “normal sleep” wasdefined as the absence of either of these 2 categories. To create 3mutually exclusive categories, none in the poor sleep group reportedhaving chronic insomnia, and none in the normal sleeping groupreported either chronic insomnia or poor sleep. Please see theonline-only Data Supplement for baseline characteristics of these 3groups.
Additional information obtained from the standardized question-naire included assessing other physical health conditions, depression,and substance use. The presence of diabetes mellitus at baseline wasdefined as a self-report of receiving treatment for diabetes mellitus orhaving a fasting blood sugar �126 mg/dL from blood drawn themorning after the subject’s PSG. We also ascertained at baselinewhether the respondent was currently treated for depression, includ-ing a history of suicidal thoughts or attempts. Participants’ dailyconsumption of caffeine (number of cups per day), tobacco (numberof cigarettes per day), and alcohol (number of drinks per day) wasalso assessed at baseline.
Follow-up measures taken through telephone interview includedthe standardized questionnaire that subjects completed at baselineduring their sleep laboratory visit. Physical health questions wereused to establish the presence of hypertension at follow-up.
Statistical AnalysesThe design of this study included oversampling of those at higherrisk for SDB and women with markedly higher body mass index toincrease the precision of the risk estimates. Because of this samplingstrategy, numeric sampling weights were developed for the analysisso that the estimates could be inferred to the original targetpopulation.18,19,21,23 We adjusted for the sampling weight in all ofour statistical analyses, including those estimating the rate ofincident hypertension. Please see the online-only Data Supplementfor details of the sampling weights.
Logistic regression models were used to assess the independentassociations of the 3-level sleep complaints and objective sleepduration with incident hypertension. The covariables that we ad-justed for included major confounding factors expected to affect thisrelation (ie, sex, race, age, caffeine, cigarettes and alcohol consump-tion, depression, SDB, diabetes mellitus, and obesity). We furthertested the interaction between sleep complaints and objective sleepduration using the likelihood ratio test in logistic regression models.Because of the significant interaction between sleep complaints andobjective sleep duration, we performed final logistic regressionmodels to include 5 dummy variables to represent all 6 possiblecombinations of sleep symptoms and objective sleep duration; weused normal sleepers with objective sleep duration �6 hours as acommon reference group. We calculated the odds ratios (OR) and the95% CIs from this model to estimate the risk of hypertensionincidence associated with different combinations of sleep complaintsand objective sleep duration, simultaneously adjusting for sex, race,
2 Hypertension October 2012
at Milton S. Hershey Medical Center on August 22, 2012http://hyper.ahajournals.org/Downloaded from
age, caffeine, cigarettes and alcohol consumption, depression, SDB,diabetes mellitus, obesity, and baseline SBP/DBP status. Please seethe online-only Data Supplement for more details. All of the analyseswere conducted with IBM SPSS version 20.0 for Windows.
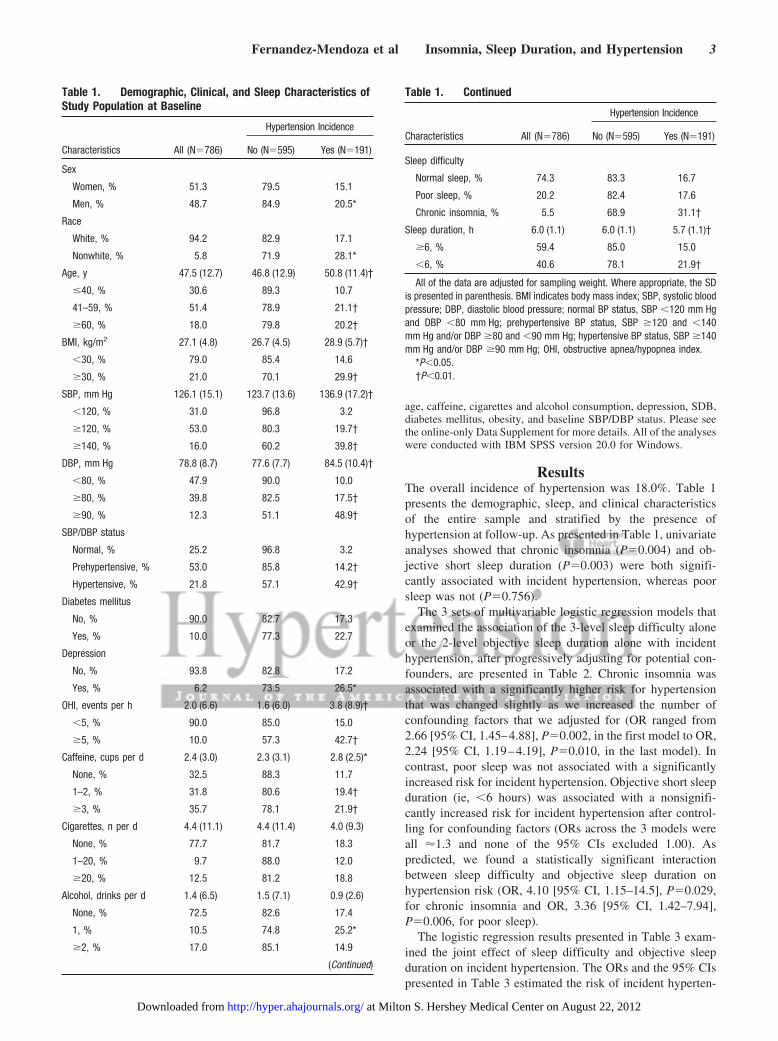
ResultsThe overall incidence of hypertension was 18.0%. Table 1presents the demographic, sleep, and clinical characteristicsof the entire sample and stratified by the presence ofhypertension at follow-up. As presented in Table 1, univariateanalyses showed that chronic insomnia (P�0.004) and ob-jective short sleep duration (P�0.003) were both signifi-cantly associated with incident hypertension, whereas poorsleep was not (P�0.756).
The 3 sets of multivariable logistic regression models thatexamined the association of the 3-level sleep difficulty aloneor the 2-level objective sleep duration alone with incidenthypertension, after progressively adjusting for potential con-founders, are presented in Table 2. Chronic insomnia wasassociated with a significantly higher risk for hypertensionthat was changed slightly as we increased the number ofconfounding factors that we adjusted for (OR ranged from2.66 [95% CI, 1.45–4.88], P�0.002, in the first model to OR,2.24 [95% CI, 1.19–4.19], P�0.010, in the last model). Incontrast, poor sleep was not associated with a significantlyincreased risk for incident hypertension. Objective short sleepduration (ie, �6 hours) was associated with a nonsignifi-cantly increased risk for incident hypertension after control-ling for confounding factors (ORs across the 3 models wereall �1.3 and none of the 95% CIs excluded 1.00). Aspredicted, we found a statistically significant interactionbetween sleep difficulty and objective sleep duration onhypertension risk (OR, 4.10 [95% CI, 1.15–14.5], P�0.029,for chronic insomnia and OR, 3.36 [95% CI, 1.42–7.94],P�0.006, for poor sleep).
The logistic regression results presented in Table 3 exam-ined the joint effect of sleep difficulty and objective sleepduration on incident hypertension. The ORs and the 95% CIspresented in Table 3 estimated the risk of incident hyperten-
Table 1. Demographic, Clinical, and Sleep Characteristics ofStudy Population at Baseline
Characteristics All (N�786)
Hypertension Incidence
No (N�595) Yes (N�191)
Sex
Women, % 51.3 79.5 15.1
Men, % 48.7 84.9 20.5*
Race
White, % 94.2 82.9 17.1
Nonwhite, % 5.8 71.9 28.1*
Age, y 47.5 (12.7) 46.8 (12.9) 50.8 (11.4)†
�40, % 30.6 89.3 10.7
41–59, % 51.4 78.9 21.1†
�60, % 18.0 79.8 20.2†
BMI, kg/m2 27.1 (4.8) 26.7 (4.5) 28.9 (5.7)†
�30, % 79.0 85.4 14.6
�30, % 21.0 70.1 29.9†
SBP, mm Hg 126.1 (15.1) 123.7 (13.6) 136.9 (17.2)†
�120, % 31.0 96.8 3.2
�120, % 53.0 80.3 19.7†
�140, % 16.0 60.2 39.8†
DBP, mm Hg 78.8 (8.7) 77.6 (7.7) 84.5 (10.4)†
�80, % 47.9 90.0 10.0
�80, % 39.8 82.5 17.5†
�90, % 12.3 51.1 48.9†
SBP/DBP status
Normal, % 25.2 96.8 3.2
Prehypertensive, % 53.0 85.8 14.2†
Hypertensive, % 21.8 57.1 42.9†
Diabetes mellitus
No, % 90.0 82.7 17.3
Yes, % 10.0 77.3 22.7
Depression
No, % 93.8 82.8 17.2
Yes, % 6.2 73.5 26.5*
OHI, events per h 2.0 (6.6) 1.6 (6.0) 3.8 (8.9)†
�5, % 90.0 85.0 15.0
�5, % 10.0 57.3 42.7†
Caffeine, cups per d 2.4 (3.0) 2.3 (3.1) 2.8 (2.5)*
None, % 32.5 88.3 11.7
1–2, % 31.8 80.6 19.4†
�3, % 35.7 78.1 21.9†
Cigarettes, n per d 4.4 (11.1) 4.4 (11.4) 4.0 (9.3)
None, % 77.7 81.7 18.3
1–20, % 9.7 88.0 12.0
�20, % 12.5 81.2 18.8
Alcohol, drinks per d 1.4 (6.5) 1.5 (7.1) 0.9 (2.6)
None, % 72.5 82.6 17.4
1, % 10.5 74.8 25.2*
�2, % 17.0 85.1 14.9
(Continued)
Table 1. Continued
Characteristics All (N�786)
Hypertension Incidence
No (N�595) Yes (N�191)
Sleep difficulty
Normal sleep, % 74.3 83.3 16.7
Poor sleep, % 20.2 82.4 17.6
Chronic insomnia, % 5.5 68.9 31.1†
Sleep duration, h 6.0 (1.1) 6.0 (1.1) 5.7 (1.1)†
�6, % 59.4 85.0 15.0
�6, % 40.6 78.1 21.9†
All of the data are adjusted for sampling weight. Where appropriate, the SDis presented in parenthesis. BMI indicates body mass index; SBP, systolic bloodpressure; DBP, diastolic blood pressure; normal BP status, SBP �120 mm Hgand DBP �80 mm Hg; prehypertensive BP status, SBP �120 and �140mm Hg and/or DBP �80 and �90 mm Hg; hypertensive BP status, SBP �140mm Hg and/or DBP �90 mm Hg; OHI, obstructive apnea/hypopnea index.
*P�0.05.†P�0.01.
Fernandez-Mendoza et al Insomnia, Sleep Duration, and Hypertension 3
at Milton S. Hershey Medical Center on August 22, 2012http://hyper.ahajournals.org/Downloaded from
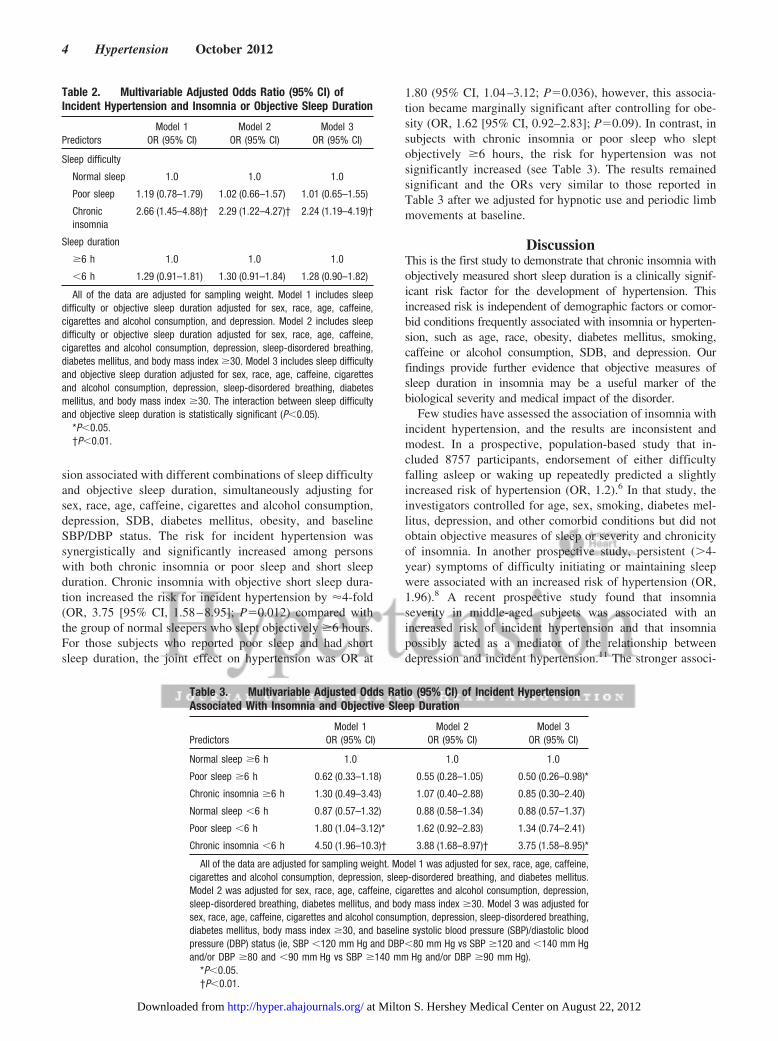
sion associated with different combinations of sleep difficultyand objective sleep duration, simultaneously adjusting forsex, race, age, caffeine, cigarettes and alcohol consumption,depression, SDB, diabetes mellitus, obesity, and baselineSBP/DBP status. The risk for incident hypertension wassynergistically and significantly increased among personswith both chronic insomnia or poor sleep and short sleepduration. Chronic insomnia with objective short sleep dura-tion increased the risk for incident hypertension by �4-fold(OR, 3.75 [95% CI, 1.58–8.95]; P�0.012) compared withthe group of normal sleepers who slept objectively �6 hours.For those subjects who reported poor sleep and had shortsleep duration, the joint effect on hypertension was OR at
1.80 (95% CI, 1.04–3.12; P�0.036), however, this associa-tion became marginally significant after controlling for obe-sity (OR, 1.62 [95% CI, 0.92–2.83]; P�0.09). In contrast, insubjects with chronic insomnia or poor sleep who sleptobjectively �6 hours, the risk for hypertension was notsignificantly increased (see Table 3). The results remainedsignificant and the ORs very similar to those reported inTable 3 after we adjusted for hypnotic use and periodic limbmovements at baseline.
DiscussionThis is the first study to demonstrate that chronic insomnia withobjectively measured short sleep duration is a clinically signif-icant risk factor for the development of hypertension. Thisincreased risk is independent of demographic factors or comor-bid conditions frequently associated with insomnia or hyperten-sion, such as age, race, obesity, diabetes mellitus, smoking,caffeine or alcohol consumption, SDB, and depression. Ourfindings provide further evidence that objective measures ofsleep duration in insomnia may be a useful marker of thebiological severity and medical impact of the disorder.
Few studies have assessed the association of insomnia withincident hypertension, and the results are inconsistent andmodest. In a prospective, population-based study that in-cluded 8757 participants, endorsement of either difficultyfalling asleep or waking up repeatedly predicted a slightlyincreased risk of hypertension (OR, 1.2).6 In that study, theinvestigators controlled for age, sex, smoking, diabetes mel-litus, depression, and other comorbid conditions but did notobtain objective measures of sleep or severity and chronicityof insomnia. In another prospective study, persistent (�4-year) symptoms of difficulty initiating or maintaining sleepwere associated with an increased risk of hypertension (OR,1.96).8 A recent prospective study found that insomniaseverity in middle-aged subjects was associated with anincreased risk of incident hypertension and that insomniapossibly acted as a mediator of the relationship betweendepression and incident hypertension.11 The stronger associ-
Table 2. Multivariable Adjusted Odds Ratio (95% CI) ofIncident Hypertension and Insomnia or Objective Sleep Duration
PredictorsModel 1
OR (95% CI)Model 2
OR (95% CI)Model 3
OR (95% CI)
Sleep difficulty
Normal sleep 1.0 1.0 1.0
Poor sleep 1.19 (0.78–1.79) 1.02 (0.66–1.57) 1.01 (0.65–1.55)
Chronicinsomnia
2.66 (1.45–4.88)† 2.29 (1.22–4.27)† 2.24 (1.19–4.19)†
Sleep duration
�6 h 1.0 1.0 1.0
�6 h 1.29 (0.91–1.81) 1.30 (0.91–1.84) 1.28 (0.90–1.82)
All of the data are adjusted for sampling weight. Model 1 includes sleepdifficulty or objective sleep duration adjusted for sex, race, age, caffeine,cigarettes and alcohol consumption, and depression. Model 2 includes sleepdifficulty or objective sleep duration adjusted for sex, race, age, caffeine,cigarettes and alcohol consumption, depression, sleep-disordered breathing,diabetes mellitus, and body mass index �30. Model 3 includes sleep difficultyand objective sleep duration adjusted for sex, race, age, caffeine, cigarettesand alcohol consumption, depression, sleep-disordered breathing, diabetesmellitus, and body mass index �30. The interaction between sleep difficultyand objective sleep duration is statistically significant (P�0.05).
*P�0.05.†P�0.01.
Table 3. Multivariable Adjusted Odds Ratio (95% CI) of Incident HypertensionAssociated With Insomnia and Objective Sleep Duration
PredictorsModel 1
OR (95% CI)Model 2
OR (95% CI)Model 3
OR (95% CI)
Normal sleep �6 h 1.0 1.0 1.0
Poor sleep �6 h 0.62 (0.33–1.18) 0.55 (0.28–1.05) 0.50 (0.26–0.98)*
Chronic insomnia �6 h 1.30 (0.49–3.43) 1.07 (0.40–2.88) 0.85 (0.30–2.40)
Normal sleep �6 h 0.87 (0.57–1.32) 0.88 (0.58–1.34) 0.88 (0.57–1.37)
Poor sleep �6 h 1.80 (1.04–3.12)* 1.62 (0.92–2.83) 1.34 (0.74–2.41)
Chronic insomnia �6 h 4.50 (1.96–10.3)† 3.88 (1.68–8.97)† 3.75 (1.58–8.95)*
All of the data are adjusted for sampling weight. Model 1 was adjusted for sex, race, age, caffeine,cigarettes and alcohol consumption, depression, sleep-disordered breathing, and diabetes mellitus.Model 2 was adjusted for sex, race, age, caffeine, cigarettes and alcohol consumption, depression,sleep-disordered breathing, diabetes mellitus, and body mass index �30. Model 3 was adjusted forsex, race, age, caffeine, cigarettes and alcohol consumption, depression, sleep-disordered breathing,diabetes mellitus, body mass index �30, and baseline systolic blood pressure (SBP)/diastolic bloodpressure (DBP) status (ie, SBP �120 mm Hg and DBP�80 mm Hg vs SBP �120 and �140 mm Hgand/or DBP �80 and �90 mm Hg vs SBP �140 mm Hg and/or DBP �90 mm Hg).
*P�0.05.†P�0.01.
4 Hypertension October 2012
at Milton S. Hershey Medical Center on August 22, 2012http://hyper.ahajournals.org/Downloaded from
ation found in these latter studies between insomnia andhypertension may be explained by the addition of severityand/or chronicity in their definition of insomnia. However, inthese studies, no polysomnographic measures were obtained,and, therefore, the potential confounder of SDB was notcontrolled for and the role of objective short sleep duration asa marker of the biological severity of the disorder was notexamined.
In our study, the group with chronic insomnia, that is, acomplaint of insomnia �1 year, was associated with asignificant risk for incident hypertension (OR, 2.2), whereasthe group with poor sleep, that is, moderate-to-severe insom-nia symptoms, was not associated with an increased risk forhypertension. When we introduced the criterion of objec-tively measured short sleep duration in the definition ofinsomnia, we showed a strong and significant joint effect onthe association of insomnia with the incidence of hyperten-sion. Chronic insomniacs who slept �6 hours had 3.8 higherodds of developing hypertension than subjects who slept �6hours and had no sleep difficulties. In contrast, chronicinsomniacs who slept �6 hours did not show an increasedrisk for incident hypertension compared with the controlgroup. Subjects with poor sleep had a significantly higher riskfor incident hypertension when they slept �6 hours (OR, 1.8)when compared with the control group; however, this in-creased risk became nonsignificant after controlling for obe-sity (OR, 1.6). Thus, both chronicity of the disorder andobjective short sleep duration, as a marker of a biologicallymore severe phenotype of insomnia, appear to have a strongeffect on the association between insomnia and the develop-ment of hypertension.
Our findings on the additive or synergistic effect ofinsomnia and objective sleep duration on incident hyperten-sion are consistent with previous reports that insomnia withshort sleep duration is associated with hypercortisol-emia,16,17,24 increased sympathetic activity (eg, increasedcatecholaminergic activity, 24-hour metabolic rate, heart rate,and impaired heart rate variability),25–29 and adverse impacton health (eg, hypertension, type 2 diabetes mellitus, neuro-cognitive deficits, and mortality).12–15 Also, a recent studyshowed that nighttime SBP was higher and day-to-night SBPdipping was lower in chronic insomniacs as compared withgood sleeper controls.30 Based on the data that insomnia isassociated with physiological hyperarousal,16,17,24–29 wespeculated in our previous cross-sectional study that the mostlikely direction was that insomnia leads to hypertension.12
This is consistent with previous longitudinal studies showingthat hypertension is not a significant risk factor for thedevelopment of insomnia.31,32 Thus, the results of the presentstudy further support the proposal that insomnia with objec-tive short sleep duration is a premorbid, modifiable risk factorfor hypertension.
In our study we found that chronic insomniacs or poorsleepers who slept �6 hours showed no or even a reducedrisk for incident hypertension. This finding is consistent withour recent findings, suggesting that poor sleep and chronicinsomnia with normal sleep duration are not associated withcardiometabolic morbidity or mortality.12–15
In our previous studies, PSG-measured sleep duration wasa strong predictor of hypothalamic-pituitary-adrenal axishyperactivity and medical morbidity among insomniacs.12–17
However, PSG involves significant expense and efforts, tendsto disturb a subject’s sleep (“first-night effect”), and, becauseof night-to-night variability of the subject’s sleep, multiplenight recordings are required to obtain a representativesample of an individual’s typical habitual sleep duration andpattern.33–35 More recently, night-to-night variability as-sessed with actigraphy for 1 to 2 weeks has been indicated asa very useful marker of the severity of insomnia, that is, thereis significant increase in the night-to-night variability amongchronic insomniacs than among the controls.36 There was alsoa significant adverse association between intraindividualvariability in sleep duration and fragmentation and psychos-ocial and physiological indices of stress, reflected as in-creased nighttime secretion of catecholamines.36,37 Thesestudies suggested the potential usefulness of other objectivemeasures of sleep, such as average sleep duration or night-to-night variability obtained with actigraphy for a period ofdays or weeks in the “habitual home environment,”38 whichis impossible with traditional PSG.
The data on the association of insomnia with hypertension,as well as previous reports on insomnia and the stresssystem16,17,24,25 and the autonomic system,26–29 provide thebasis for a meaningful phenotyping of chronic insomniabased on objective duration of sleep.39 One phenotype, themore biologically severe type of insomnia, is associated withphysiological hyperarousal, that is, short sleep duration,activation of the stress system, and significant medicalsequelae, for example, hypertension. The other phenotype, aless biologically severe form of insomnia, is not associatedwith physiological hyperarousal, that is, normal sleep dura-tion, normal activity of the stress system, and lack ofsignificant medical sequelae.
Some limitations should be taken into account wheninterpreting our results. First, incident hypertension wasdefined by self-report and not by BP measurements. How-ever, insomnia with objective short sleep duration remainedstrongly and significantly associated with incident hyperten-sion even after controlling for baseline prehypertensive andhypertensive BP status. Moreover, 2 sensitivity analyses wereperformed. We entered SBP and DBP in 2 separate models ascontinuous variables, and the pattern of associations (data notshown) was very similar to that reported in model 3. Also, weexcluded individuals with baseline SBP �140 mm Hg and/orDBP �90 mm Hg, and the pattern of associations (data notshown) remained very similar to that reported in model 3. Inaddition, other large epidemiological studies have used self-reports to ascertain incident hypertension.11 Thus, the consis-tency of the present findings with those of cross-sectionalstudies on the association of insomnia with objective shortsleep duration and hypertension12 and impaired heart ratevariability28,29 increases our confidence about the replicabil-ity of the present findings. Future studies should explore theassociation among insomnia, objective short sleep duration,and incident hypertension using BP monitoring at follow-up.Second, the objective sleep duration in this study was basedon 1 night of PSG, which may not be representative of the
Fernandez-Mendoza et al Insomnia, Sleep Duration, and Hypertension 5
at Milton S. Hershey Medical Center on August 22, 2012http://hyper.ahajournals.org/Downloaded from

subjects’ habitual sleep duration. However, in our previousstudies, the association between objective sleep duration andhypercortisolemia was based on a 4-consecutive-night sleeplaboratory protocol, which should represent better the typicalsleep profile of the subjects.16,17 The consistency of thefindings on the role of objective sleep duration in predictinginsomnia severity between these physiological studies withmultiple night recordings and the current epidemiologicalstudy based on a single night recording increases our confi-dence about the replicability and generalizability of thepresent findings. Future studies should explore the associa-tion among insomnia, sleep duration, and hypertension usingmultiple night recordings. Finally, we performed furtheranalyses to address the question of whether receiving treat-ment for hypertension at follow-up relatively improved thesleep of chronic insomniacs and perhaps decrease theirinsomnia-related cardiovascular risk (see the online-onlyData Supplement for details). In fact, we found that a higherpercentage of those who persisted with chronic insomniareported being treated for hypertension, which reinforces ourfindings that severe, persistent insomnia is a premorbid riskfactor for incident hypertension.
PerspectivesIn summary, insomnia with short sleep duration is associatedwith a high risk for the development of hypertension to adegree comparable with the other most common sleep disor-der, that is, SDB.2–4 Given the high prevalence of insomnia inthe general population and the widespread misconception ofa disorder of the “worried well,” its detection and diagnosisshould become the target of public health policy. It appearsthat insomnia with objective short sleep duration may repre-sent a biologically more severe phenotype of insomnia thatmay respond differentially to treatment. Finally, becausepolysomnographic measures of sleep are inconvenient andexpensive, there is a need for validation of practical, easy touse, inexpensive methods to measure sleep duration outsideof the sleep laboratory.
AcknowledgmentsThe work was performed at the Sleep Research and TreatmentCenter at the Penn State University Milton Hershey Hospital, and thestaff (C. Criley, P. Cain, S. George, and T. Miksiewicz) is especiallycommended for their efforts.
Sources of FundingThis research was in part funded by the National Institutes of Healthgrants R01 51931, R01 40916, and R01 64415.
DisclosuresNone.
References1. Writing Group Members, Roger VL, Go AS, Lloyd-Jones DM, Benjamin
EJ, Berry JD, Borden WB, Bravata DM, Dai S, Ford ES, Fox CS,Fullerton HJ, Gillespie C, Hailpern SM, Heit JA, Howard VJ, KisselaBM, Kittner SJ, Lackland DT, Lichtman JH, Lisabeth LD, Makuc DM,Marcus GM, Marelli A, Matchar DB, Moy CS, Mozaffarian D, MussolinoME, Nichol G, Paynter NP, Soliman EZ, Sorlie PD, Sotoodehnia N,Turan TN, Virani SS, Wong ND, Woo D, Turner MB, on behalf of theAmerican Heart Association Statistics Committee and Stroke Statistics
Subcommittee. Heart Disease and Stroke Statistics: 2012 update–a reportfrom the American Heart Association. Circulation. 2012;125:e2–e220.
2. Young T, Peppard P, Palta M, Hla KM, Finn L, Morgan B, Skatrud J.Population-based study of sleep-disordered breathing as a risk factor forhypertension. Arch Intern Med. 1997;157:1746–1752.
3. Bixler EO, Vgontzas AN, Lin HM, Ten Have T, Leiby BE, Vela-BuenoA, Kales A. Association of hypertension and sleep-disordered breathing.Arch Intern Med. 2000;160:2289–2295.
4. Nieto FJ, Young TB, Lind BK, Shahar E, Samet JM, Redline S,D’Agostino RB, Newman AB, Lebowitz MD, Pickering TG. Associationof sleep-disordered breathing, sleep apnea, and hypertension in a largecommunity-based study. JAMA. 2000;283:1829–1836.
5. National Institutes of Health. NIH state of the science statement onmanifestations and management of chronic insomnia in adults. J ClinSleep Med. 2005;1:412–421.
6. Phillips B, Mannino DM. Do insomnia complaints cause hypertension orcardiovascular disease? J Clin Sleep Med. 2007;3:489–494.
7. Phillips B, Bùzková P, Enright P, for the Cardiovascular Health StudyResearch Group. Insomnia did not predict incident hypertension in olderadults in the cardiovascular health study. Sleep. 2009;32:65–72.
8. Suka M, Yoshida K, Sugimori H. Persistent insomnia is a predictor ofhypertension in Japanese male workers. J Occup Health. 2003;45:344–350.
9. Janson C, Lindberg E, Gislason T, Elmasry A, Boman G. Insomnia inmen: a 10-year prospective population based study. Sleep. 2001;24:425–430.
10. Bixler EO, Vgontzas AN, Lin HM, Vela-Bueno A, Kales A. Insomnia incentral Pennsylvania. J Psychosom Res. 2002;53:589–592.
11. Gangwisch JE, Malaspina D, Posner K, Babiss LA, Heymsfield SB,Turner JB, Zammit GK, Pickering TG. Insomnia and sleep duration asmediators of the relationship between depression and hypertensionincidence. Am J Hypertens. 2010;23:62–69.
12. Vgontzas AN, Liao D, Bixler EO, Chrousos GP, Vela-Bueno A. Insomniawith objective short sleep duration is associated with a high risk forhypertension. Sleep. 2009;32:491–497.
13. Vgontzas AN, Liao D, Pejovic S, Calhoun S, Karataraki M, Bixler EO.Insomnia with objective short sleep duration is associated with type 2diabetes: a population-based study. Diabetes Care. 2009;32:1980–1985.
14. Fernandez-Mendoza J, Calhoun S, Bixler EO, Pejovic S, Karataraki M,Liao D, Vela-Bueno A, Ramos-Platon MJ, Sauder KA, Vgontzas AN.Insomnia with objective short sleep duration is associated with deficits inneuropsychological performance: a general population study. Sleep.2010;33:459–465.
15. Vgontzas AN, Liao D, Pejovic S, Calhoun S, Karataraki M, Basta M,Fernández-Mendoza J, Bixler EO. Insomnia with short sleep duration andmortality: the Penn State cohort. Sleep. 2010;33:1159–1164.
16. Vgontzas AN, Tsigos C, Bixler EO, Stratakis CA, Zachman K, Kales A,Vela-Bueno A, Chrousos GP. Chronic insomnia and activity of the stresssystem: a preliminary study. J Psychosom Res. 1998;45:21–31.
17. Vgontzas AN, Bixler EO, Lin HM, Prolo P, Mastorakos G, Vela-BuenoA, Kales A, Chrousos GP. Chronic insomnia is associated with nycto-hemeral activation of the hypothalamic-pituitary-adrenal axis: clinicalimplications. J Clin Endocrinol Metab. 2001;86:3787–3794.
18. Bixler EO, Vgontzas AN, Ten Have T, Tyson K, Kales A. Effects of ageon sleep apnea in men: I–prevalence and severity. Am J Respir Crit CareMed. 1998;157:144–148.
19. Bixler EO, Vgontzas AN, Lin HM, Ten Have T, Rein J, Vela-Bueno A,Kales A. Prevalence of sleep-disordered breathing in women: effects ofgender. Am J Respir Crit Care Med. 2001;163:608–613.
20. Waksberg J. Sampling methods for random digit dialing. J Am Stat Assoc.1978;73:40–46.
21. Kish L. Survey Sampling. New York, NY: John Wiley & Sons, Inc; 1965.22. Rechtschaffen A, Kales A. A Manual of Standardized Terminology,
Techniques and Scoring System for Sleep Stages of Human Subjects.Bethesda, MD: National Institutes of Health; 1968.
23. US Department of Health and Human Services (DHHS), National Centerfor Health Statistics. Third National Health and Nutrition ExaminationSurvey, 1988–1994. NHANES III Laboratory Data File. Hyattsville, MD:Centers for Disease Control and Prevention; 1996.
24. Rodenbeck A, Cohrs S, Jordan W, Huether G, Rüther E, Hajak G. Thesleep-improving effects of doxepin are paralleled by a normalized plasmacortisol secretion in primary insomnia. Psychopharmacology (Berl).2003;170:423–428.
6 Hypertension October 2012
at Milton S. Hershey Medical Center on August 22, 2012http://hyper.ahajournals.org/Downloaded from
25. Irwin M, Clark C, Kennedy B, Christian Gillin J, Ziegler M. Nocturnalcatecholamines and immune function in insomniacs, depressed patients,and control subjects. Brain Behav Immun. 2003;17:365–372.
26. Stepanski E, Glinn M, Zorick F, Roehrs T, Roth T. Heart rate changes inchronic insomnia. Stress Med. 1994;10:261–266.
27. Bonnet MH, Arand DL. 24-Hour metabolic rate in insomniacs andmatched normal sleepers. Sleep. 1995;18:581–588.
28. Bonnet MH, Arand DL. Heart rate variability in insomniacs and matchednormal sleepers. Psychosom Med. 1998;60:610–615.
29. Spiegelhalder K, Fuchs L, Ladwig J, Kyle SD, Nissen C, Voderholzer U,Feige B, Riemann D. Heart rate and heart rate variability in subjectivelyreported insomnia. J Sleep Res. 2011;20:137–145.
30. Lanfranchi PA, Pennestri MH, Fradette L, Dumont M, Morin CM,Montplaisir J. Nighttime blood pressure in normotensive subjects withchronic insomnia: implications for cardiovascular risk. Sleep. 2009;32:760–766.
31. Singareddy R, Vgontzas AN, Fernandez-Mendoza J, Liao D, CalhounS, Shaffer ML, Bixler EO. Risk factors for incident chronic insomnia:a general population prospective study. Sleep Med. 2012;13:346–353.
32. Fernandez-Mendoza J, Vgontzas AN, Bixler EO, Singareddy R, ShafferML, Calhoun SL, Karataraki M, Vela-Bueno A, Liao D. Clinical andpolysomnographic predictors of the natural history of poor sleep in thegeneral population. Sleep. 2012;35:689–697.
33. Buysse DJ, Ancoli-Israel S, Edinger JD, Lichstein KL, Morin CM. Rec-ommendations for a standard research assessment of insomnia. Sleep.2006;29:1155–1173.
34. Wohlgemuth WK, Edinger JD, Fins AI, Sullivan RJ. How many nightsare enough? The short-term stability of sleep parameters in elderlyinsomniacs and normal sleepers. Psychophysiology. 1999;36:233–244.
35. Scharf MB, Bixler EO, Kales A. Readaptation to the sleep laboratory.Psychophysiology. 1975;12:412–415.
36. Buysse DJ, Cheng Y, Germain A, Moul DE, Franzen PL, Fletcher M,Monk TH. Night-to-night sleep variability in older adults with andwithout chronic insomnia. Sleep Med. 2010;11:56–64.
37. Mezick EJ, Matthews KA, Hall M, Kamarck TW, Buysse DJ, Owens JF,Reis SE. Intra-individual variability in sleep duration and fragmentation:associations with stress. Psychoneuroendocrinology. 2009;34:1346–1354.
38. Lichstein KL, Steon KC, Donaldson J, Nau SD, Soeffing JP, Murray D,Lester KW, Aguillard RN. Actigraphy validation with insomnia. Sleep.2006;29:232–239.
39. Fernandez-Mendoza J, Calhoun SL, Bixler EO, Karataraki M, Liao D,Vela-Bueno A, Jose Ramos-Platon M, Sauder KA, Basta M, VgontzasAN. Sleep misperception and chronic insomnia in the general population:role of objective sleep duration and psychological profiles. PsychosomMed. 2011;73:88–97.
Novelty and Significance
What Is New?● Although insomnia is a highly prevalent sleep disorder, it has not been
consistently associated with significant cardiovascular morbidity.● There is a lack of longitudinal studies examining the association between
insomnia and incident hypertension, and none has included objectivemeasures of sleep to evaluate the biological severity of insomnia.
What Is Relevant?● Insomnia is highly prevalent in the outpatient practice of general
practitioners, such as family doctors, internists, and cardiologists.● Severe chronic insomnia is a risk factor for new-onset hypertension.
● Physicians should become aware that patients with hypertension mayexperience untreated severe chronic insomnia.
Summary
Insomnia with short sleep duration is associated with a high riskfor the development of hypertension to a degree comparable withthe other most common sleep disorder, sleep apnea. Given thehigh prevalence of insomnia in the general population, its earlydiagnosis and appropriate management should become a target ofpublic health policy in the prevention of hypertension.
Fernandez-Mendoza et al Insomnia, Sleep Duration, and Hypertension 7
at Milton S. Hershey Medical Center on August 22, 2012http://hyper.ahajournals.org/Downloaded from

ONLINE DATA SUPPLEMENTS INSOMNIA WITH OBJECTIVE SHORT SLEEP DURATION AND INCIDENT HYPERTENSION: THE PENN STATE COHORT Julio Fernandez-Mendoza, PhD;1 Alexandros N. Vgontzas, MD;1 Duanping Liao, MD;2 Michele L. Shaffer, PhD;2 Antonio Vela-Bueno, MD;3 Maria Basta, MD;4 Edward O. Bixler, PhD1
1 Sleep Research & Treatment Center, Department of Psychiatry, Pennsylvania State University
College of Medicine, Hershey, PA 2 Department of Public Health Sciences, Pennsylvania State University College of Medicine,
Hershey, PA 3 Department of Psychiatry, School of Medicine, Autonomous University, Madrid, Spain 4 Department of Psychiatry, School of Medicine, University of Crete, Crete, Greece
at Milton S. Hershey Medical Center on August 22, 2012http://hyper.ahajournals.org/Downloaded from

Insomnia, Objective Sleep Duration, and Incident Hypertension 1
ONLINE SUPPLEMENTAL METHODS Participants
The data presented here were collected as part of a population-based study of sleep disorders, which used a two-phase protocol in order to recruit participants from various age groups.1-3 In the first phase of the study, a sample of adult men and women (age ≥20 years) was randomly selected from local telephone households in two counties of Central Pennsylvania (Dauphin and Lebanon) using the Mitofsky-Waksberg two-stage random digit dialing procedure.4 A within-household selection procedure described by Kish5 was used to select the specific man or woman to be interviewed. Telephone interviews were conducted with 4,364 age-eligible men and 12,219 age-eligible women residing in the sample households, for a total sample of 16,583 with response rates of 73.5% and 74.1%, respectively. The questionnaire employed in this interview included basic demographic and sleep information. In the second phase of this study, a subsample of 741 men and 1,000 women, selected randomly from those subjects previously interviewed by telephone, were studied in our sleep laboratory. The response rates for this phase were 67.8% and 65.8% for men and women, respectively. After giving a complete description of the study to the subjects, written informed consent was obtained. We contrasted those subjects who were recorded in the laboratory with those who were selected but not recorded in terms of age, BMI, and prevalence of sleep disorders. There were no significant differences between these two groups on any of these variables.
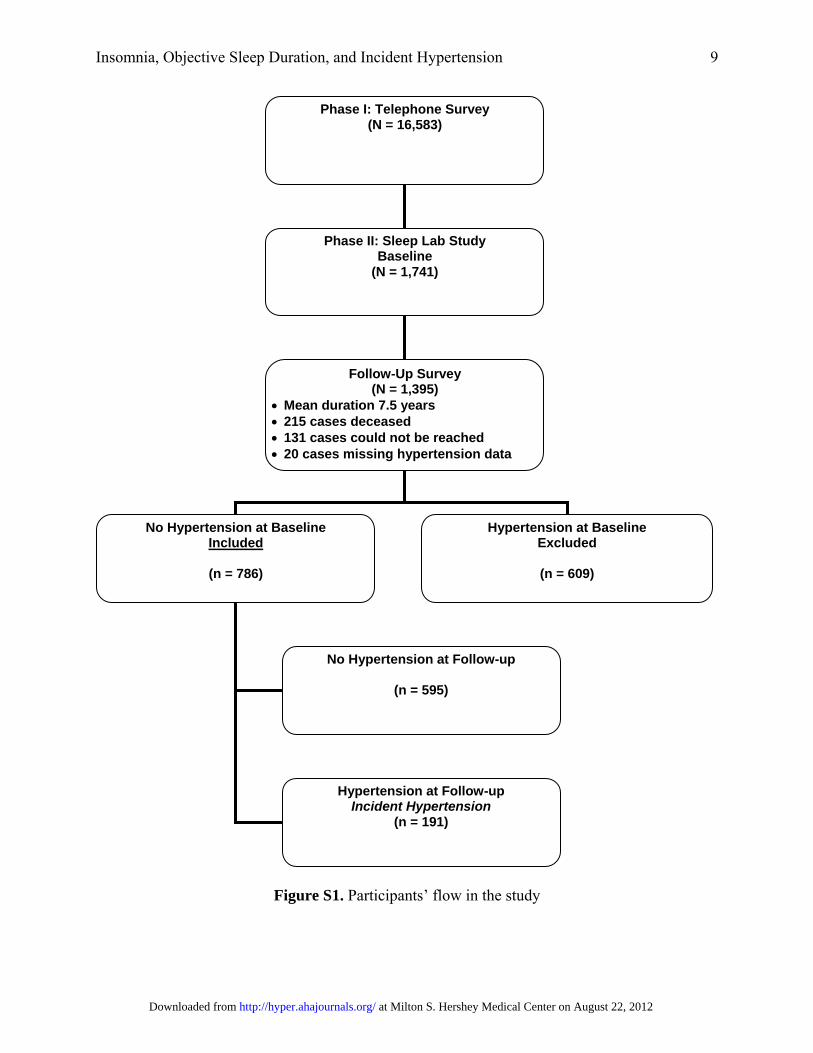
Of the 1741 subjects who completed the comprehensive sleep lab evaluation, 1395 subjects were followed up after an average duration of 7.5 years (mean duration of 4.5 years for women and 10.5 years for men) via telephone interview. In the Penn State Cohort Study, men were recruited first and women 5 years later. This explains the five-year difference in the follow-up period between men and women. The response rate of the follow-up study was 79.7%. However, if one considers that 215 subjects died between baseline and follow-up, then the response rate of those alive was 90.9%. After complete description of the follow-up study to the subjects, verbal informed consent was obtained. The whole study procedure was approved by the University’s Institutional Review Board. Figure S1 shows the participant flow in the study. Definition of Incident Hypertension
For the purpose of this study, the presence of hypertension at baseline was defined by a self-report of receiving treatment for high blood pressure, based on a standardized questionnaire completed by the subjects on the evening of their sleep laboratory visit. Commensurate with the baseline definition, hypertension at follow-up was defined by a self-report of receiving treatment for high blood pressure. Of the 1395 subjects who were followed-up, 786 did not have hypertension at baseline and were selected for the present study. A total of 191 subjects were incident cases of hypertension while 595 did not have hypertension at follow-up. Twenty subjects had missing data on hypertension at follow-up.
Sleep Laboratory Evaluation
Each subject selected for laboratory evaluation completed a comprehensive sleep history and physical examination. All subjects were evaluated for one night in the sleep laboratory in sound-attenuated, light- and temperature-controlled rooms. During this evaluation, each subject was continuously monitored for eight hours (fixed-time period) using 16-channel polysomnography (PSG) including electroencephalogram, electrooculogram, and
at Milton S. Hershey Medical Center on August 22, 2012http://hyper.ahajournals.org/Downloaded from
Insomnia, Objective Sleep Duration, and Incident Hypertension 2
electromyogram. Bedtimes were adjusted to conform to subjects’ usual bedtimes, and subjects were recorded between 22:00-23:00 and 06:00-07:00. The sleep recordings were subsequently scored independently, according to Rechtschaffen and Kales criteria.6 Percent of sleep time is total sleep time divided by recorded time in bed and multiplied by 100. From the objectively recorded sleep time data, we regrouped the entire study sample into two ordinal groups: the top 50% of persons above the median percent of sleep time (“longer sleep duration group”), and the 50% of persons in the bottom half (“short sleep duration group”). We then rounded the cutoff point to meaningful numbers and thus created the following two sleep duration groups: the “longer sleep duration group” consisted of those who slept ≥6 h (i.e., percent of sleep time ≥75%), and the “short sleep duration group” of those who slept <6 h (i.e., percent of sleep time <75%). This cutoff point has been shown in previous cross-sectional studies to be predictive of significant medical morbidity and mortality.7-10
Additional information obtained during the PSG included the assessment of sleep apnea. Respiration was monitored throughout the night by use of thermocouples at the nose and mouth and thoracic strain gauges. All-night recordings of hemoglobin oxygen saturation (SpO2) were obtained with an oximeter attached to the finger. Apnea was considered present if a breath cessation exceeded 10 seconds and each apnea was categorized in terms of obstructive (chest wall movement present) or central (chest wall movement absent). In addition, hypopnea was considered present when a reduction in airflow of approximately 50% was indicated at the nose or mouth and was associated with a reduction of 4% arterial blood oxygen saturation.2,3 For the purpose of this study, the presence of SDB was defined as an obstructive apnea/hypopnea index (OHI) ≥ 5. Body mass index (BMI) was based on measured height (cm) and weight (kg) during the subjects’ sleep laboratory visit. Furthermore, blood pressure (BP) was measured in the evening, about 2 hours before the start of the sleep recording, using a pneumoelectric microprocessor-controlled instrument with the appropriate sized cuffs. The accuracy of this monitor is reported to be ± 3 mm Hg; in addition, internal calibration was performed before each use, and the machine was checked against a mercury sphygmomanometer at least annually. The recorded BP was the average of 3 consecutive readings during a 5-min period following 10 min of rest in the supine position. Based on these baseline BP measurements, a normal BP status was defined as systolic BP < 120 mm Hg and diastolic BP < 80 mm Hg, a pre-hypertensive BP status as systolic BP ≥ 120 and < 140 mm Hg and/or diastolic BP ≥ 80 and < 90 mm Hg, and a hypertensive BP status as systolic BP ≥ 140 mm Hg and/or diastolic BP ≥ 90 mm Hg. BP measurements were not taken at follow-up.
Insomnia and Other Measurements
As part of the standardized questionnaire in our protocol we also assessed the presence of all sleep disorders, based on a standardized questionnaire completed by the subjects in the evening of their sleep laboratory visit. This questionnaire consists of 53 questions (7 demographic, 20 sleep-related, and 26 general health questions). In addition, women responded to 8 questions related to menstrual history, menopause, and hormone therapy. Sleep related questions were qualified in terms of severity on a scale of 0-3 (0 = none, 1 = mild, 2 = moderate, 3 = severe) and duration. The presence of sleep difficulty was established on three levels of severity. First, chronic insomnia was defined asy a complaint of insomnia (i.e., a positive response to the question “Do you feel you have insomnia?”) with a duration of ≥1 year. Second, poor sleep was defined as a moderate to severe complaint (based on a mild to severe scale) of difficulty falling asleep (“Do you have difficulty falling asleep?”), difficulty staying asleep (“Do
at Milton S. Hershey Medical Center on August 22, 2012http://hyper.ahajournals.org/Downloaded from
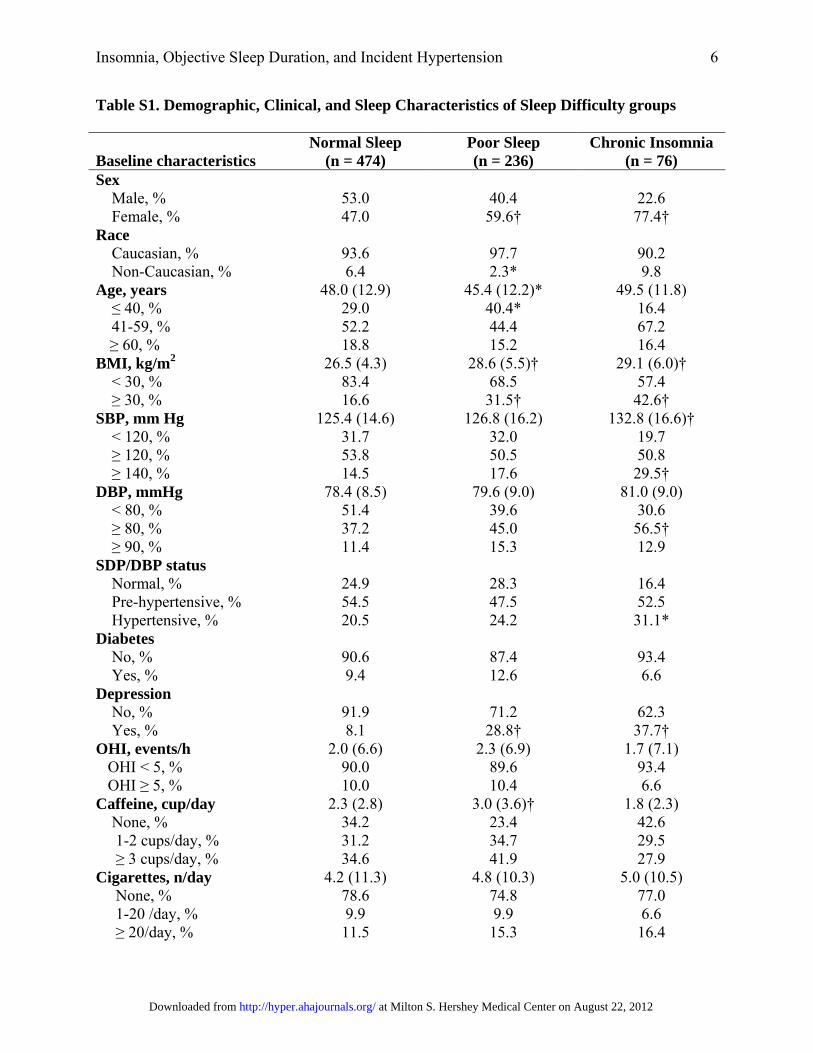
Insomnia, Objective Sleep Duration, and Incident Hypertension 3
you have difficulty staying asleep?”), early final awakening (“Do you wake up in the morning earlier than desired?”), or non-restorative sleep (“Do you still feel groggy and unrefreshed after morning awakening?”). Finally, normal sleep was defined as the absence of either of these two categories. In order to create three mutually exclusive categories, none in the poor sleep group reported having chronic insomnia and none in the normal sleeping group reported either chronic insomnia or poor sleep. Table S1 presents the characteristics of normal sleepers, poor sleepers, and chronic insomniacs at baseline.
Additional information obtained from the standardized questionnaire included assessing other physical health conditions, depression, and substance use. The presence of diabetes at baseline was defined as a self-report of receiving treatment for diabetes or having a fasting blood sugar ≥126 mg/dl from blood drawn the morning after the subject’s PSG. We also ascertained at baseline whether the respondent was currently treated for depression, including a history of suicidal thoughts or attempts. Participants’ daily consumption of caffeine (number of cups/day), tobacco (number of cigarettes/day), and alcohol (number of drinks/day) was also assessed at baseline.
Follow-up measures taken through telephone interview included the standardized questionnaire that subjects completed at baseline during their sleep laboratory visit. Physical health questions were used to establish the presence of hypertension at follow-up.
Statistical Analyses
The design of this study included oversampling of those at higher risk for SDB and women with markedly higher BMI to increase the precision of the risk estimates. Because of this sampling strategy, numeric sampling weights were developed for the analysis so that the estimates could be inferred to the original target population.2,3,11 Specifically, to improve the efficiency of subject identification and screening, compensatory weights were developed for the analysis to obtain estimates for the original target population of men and women in the two-county study area. Specifically, three weights were created for the men. First, in the telephone sample, 32 of the 963 clusters of phone numbers in the first stage were “exhausted” before the target sample size was obtained. A compensatory weight was computed which corrected for this problem. A second weight was computed because the within-household screening deliberately introduced unequal probabilities of selection across the three age groups in order to oversample the middle age group. The final weight for men was computed to account for the oversampling of subjects for the sleep laboratory study (Phase II); those with larger counts of the four possible risk factors, i.e., snoring, daytime sleepiness, obesity, and hypertension, had substantially higher probability of being selected. For women, the only weight required was to account for the oversampling of subjects for the sleep laboratory study. To eliminate any suggestion of possible sample bias, we calculated 32 unique weights for the women and 16 unique weights for the men corresponding to all possible combinations of the five risk factors for the women (menopause was the fifth risk factor) and four for the men. Any individual weight that had a cell size that was too small was combined with adjacent cells, so that <10% of the cells had a sample <25, and no cell had a size <10.5 As we began evaluating our sample of women, it appeared that the mean BMI was much higher than that of the national population. Because of the strong association between BMI and sleep apnea, it was felt that a post-stratification population control weight needed to be established to present a more accurate estimate of prevalence. We used the BMI and race distributions by age decade from the NHANES III laboratory data as the standard11 to adjust both the men and women in terms of BMI and race to be representative of the national
at Milton S. Hershey Medical Center on August 22, 2012http://hyper.ahajournals.org/Downloaded from
Insomnia, Objective Sleep Duration, and Incident Hypertension 4
population. Therefore, we adjusted for the sampling weight in all of our statistical analyses, including those estimating the rate of incident hypertension.
Logistic regression models were used to assess the independent associations of the three-level sleep complaints and objective sleep duration with incident hypertension. The covariables we adjusted for included major confounding factors expected to affect this relation (i.e., gender, race, age, caffeine, cigarettes, and alcohol consumption, depression, SDB, diabetes, and obesity). We further tested the interaction between sleep complaints and objective sleep duration using the likelihood ratio test in logistic regression models. Because of the significant interaction between sleep complaints and objective sleep duration, we performed final logistic regression models to include five dummy variables to represent all six possible combinations of sleep complaints and objective sleep duration; we used normal sleepers with objective sleep duration ≥ 6 h as a common reference group. We calculated the odds ratios (OR) and the 95% confidence intervals (95%CI) from this model to estimate the risk of hypertension incidence associated with different combinations of sleep complaints and objective sleep duration, simultaneously adjusting for gender, race, age, caffeine, cigarettes, and alcohol consumption, depression, SDB, diabetes, and obesity. Because incident hypertension was ascertained by self-report, we further adjusted for baseline SBP/DBP status, i.e., normal BP (SBP < 120 mm Hg and DBP < 80 mm Hg), pre-hypertensive BP (SBP ≥ 120 and < 140 mm Hg and/or DBP ≥ 80 and < 90 mm Hg), and hypertensive BP (SBP ≥ 140 mm Hg and/or diastolic BP ≥ 90 mm Hg). Moreover, two sensitivity analyses were performed. First, we entered SBP and DBP in two separate models as continuous variables and, secondly, we excluded individuals with baseline SBP ≥ 140 and/or DBP ≥ 90. The pattern of associations remained very similar to that reported in Table 3, Model 3 in the manuscript. All analyses were conducted with IBM SPSS version 20.0 for Windows. ONLINE SUPPLEMENTAL RESULTS Change in Sleep Difficulty from Baseline to Follow-up
In order to address the question whether individuals who started treatment for
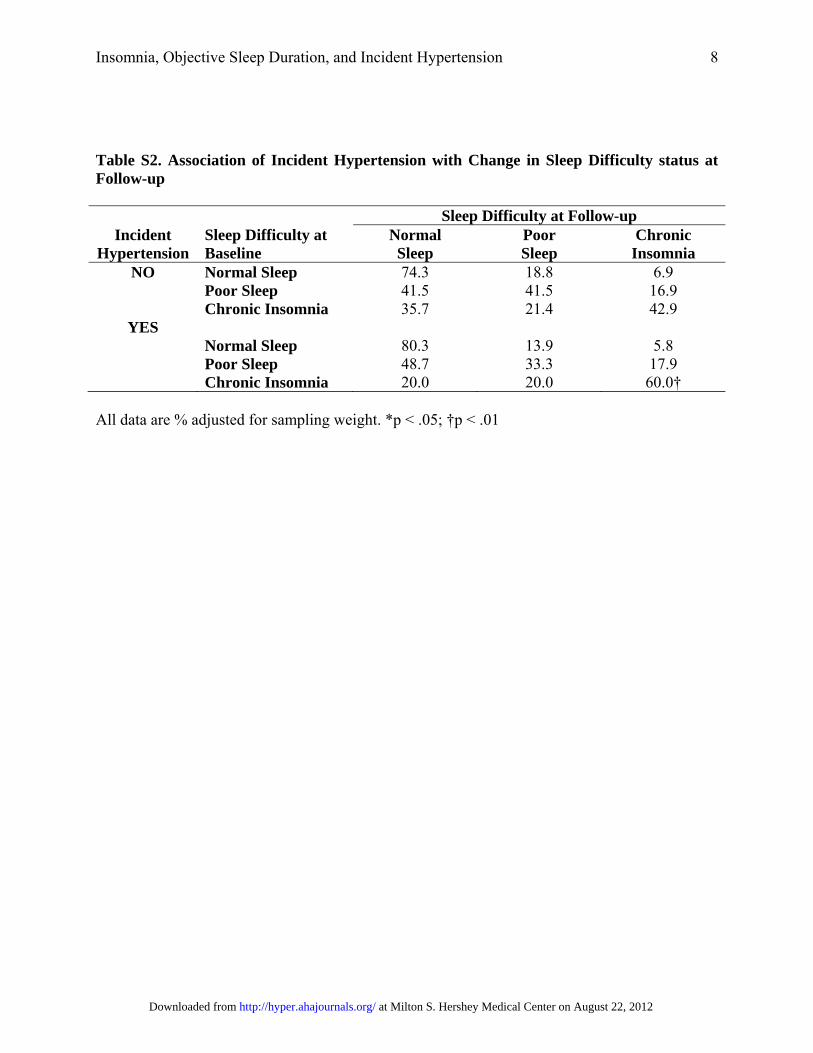
hypertension during the follow-up period have better subjective sleep compared with their baseline than did the control group (i.e., whether receiving treatment for hypertension at follow-up relatively improved their sleep and perhaps decrease their insomnia-related cardiovascular risk), Table S2 presents data on the association of incident hypertension with change in sleep difficulty status at follow-up in normal sleepers, poor sleepers, and chronic insomniacs.
In summary, when compared to those who did not report being treated for hypertension at
follow-up, insomniacs who did report being treated for hypertension over the follow-up did not have better subjective sleep at follow-up, i.e., normal sleep (20% vs. 35.7%) or poor sleep (20% vs. 21.4%). In fact, a higher percent of those who persisted with insomnia reported being treated for hypertension (60.0% vs. 42.9%), which reinforces our findings that severe, persistent insomnia is a premorbid risk factor for incident hypertension.
at Milton S. Hershey Medical Center on August 22, 2012http://hyper.ahajournals.org/Downloaded from
Insomnia, Objective Sleep Duration, and Incident Hypertension 5
REFERENCES 1. Bixler EO, Vgontzas AN, Lin HM, Vela-Bueno A, Kales A. Insomnia in Central
Pennsylvania. J Psychosom Res. 2002;53:589-592. 2. Bixler EO, Vgontzas AN, Ten Have T, Tyson K, Kales A. Effects of age on sleep apnea in
men: I. Prevalence and severity. Am J Respir Crit Care Med. 1998;157:144-148. 3. Bixler EO, Vgontzas AN, Lin HM, Ten Have T, Rein J, Vela-Bueno A, Kales A. Prevalence
of sleep-disordered breathing in women: effects of gender. Am J Respir Crit Care Med. 2001;163:608-613.
4. Waksberg J. Sampling methods for random digit dialing. J Am Stat Assoc. 1978;73:40-46. 5. Kish L. Survey sampling. New York: John Wiley & Sons, Inc, 1965. 6. Rechtschaffen A, Kales A. A manual of standardized terminology, techniques and scoring
system for sleep stages of human subjects. Bethesda, MD: National Institutes of Health, 1968.
7. Vgontzas AN, Liao D, Bixler EO, Chrousos GP, Vela-Bueno A. Insomnia with objective short sleep duration is associated with a high risk for hypertension. Sleep. 2009;32:491-497.
8. Vgontzas AN, Liao D, Pejovic S, Calhoun S, Karataraki M, Bixler EO. Insomnia with objective short sleep duration is associated with type 2 diabetes: A population-based study. Diabetes Care. 2009;32:1980-1985.
9. Fernandez-Mendoza J, Calhoun S, Bixler EO, Pejovic S, Karataraki M, Liao D, Vela-Bueno A, Ramos-Platon MJ, Sauder KA, Vgontzas AN. Insomnia with objective short sleep duration is associated with deficits in neuropsychological performance: a general population study. Sleep. 2010;33:459-465.
10. Vgontzas AN, Liao D, Pejovic S, Calhoun S, Karataraki M, Basta M, Fernández-Mendoza J, Bixler EO. Insomnia with short sleep duration and mortality: the Penn State cohort. Sleep. 2010;33:1159-1164.
11. U.S. Department of Health and Human Services (DHHS), National Center for Health Statistics. Third National Health and Nutrition Examination Survey, 1988-1994. NHANES III laboratory data file. Hyattsville, MD: Centers for Disease Control and Prevention, 1996.
at Milton S. Hershey Medical Center on August 22, 2012http://hyper.ahajournals.org/Downloaded from
Insomnia, Objective Sleep Duration, and Incident Hypertension 6
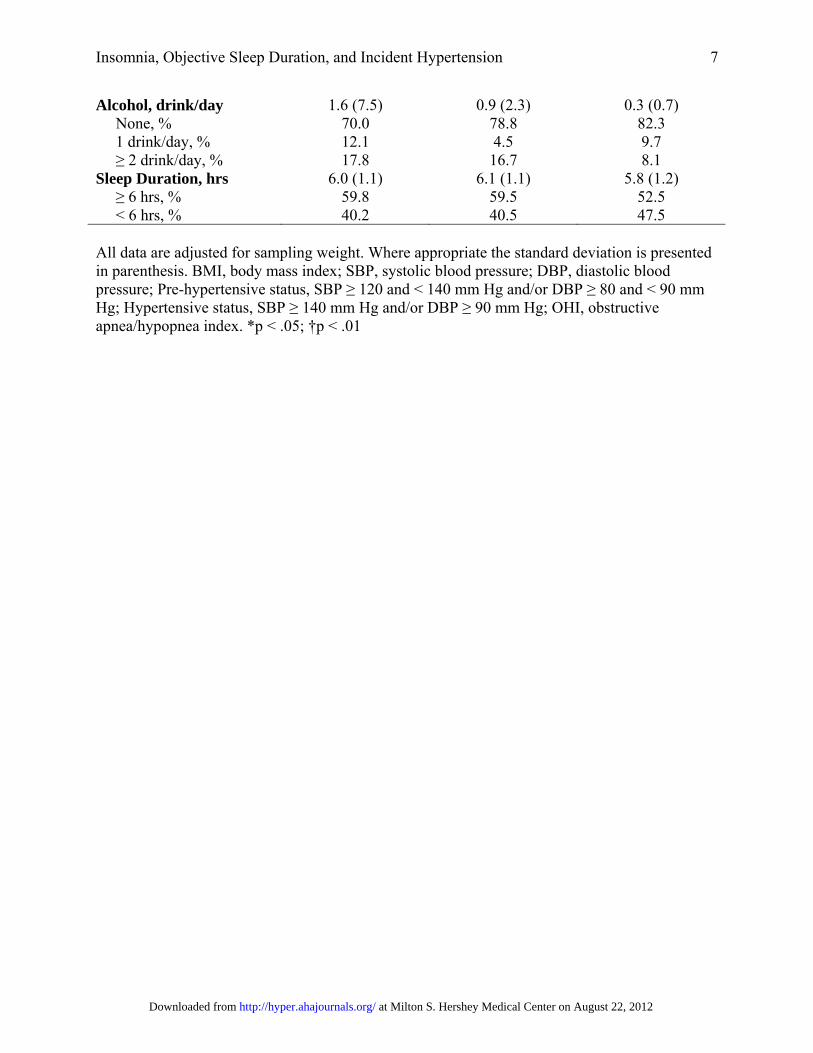
Table S1. Demographic, Clinical, and Sleep Characteristics of Sleep Difficulty groups
Baseline characteristics Normal Sleep
(n = 474) Poor Sleep (n = 236)
Chronic Insomnia (n = 76)
Sex Male, % 53.0 40.4 22.6 Female, % 47.0 59.6† 77.4† Race Caucasian, % 93.6 97.7 90.2 Non-Caucasian, % 6.4 2.3* 9.8 Age, years 48.0 (12.9) 45.4 (12.2)* 49.5 (11.8) ≤ 40, % 29.0 40.4* 16.4 41-59, % 52.2 44.4 67.2 ≥ 60, % 18.8 15.2 16.4
BMI, kg/m2 26.5 (4.3) 28.6 (5.5)† 29.1 (6.0)† < 30, % 83.4 68.5 57.4 ≥ 30, % 16.6 31.5† 42.6† SBP, mm Hg 125.4 (14.6) 126.8 (16.2) 132.8 (16.6)† < 120, % 31.7 32.0 19.7 ≥ 120, % 53.8 50.5 50.8 ≥ 140, % 14.5 17.6 29.5† DBP, mmHg 78.4 (8.5) 79.6 (9.0) 81.0 (9.0) < 80, % 51.4 39.6 30.6 ≥ 80, % 37.2 45.0 56.5† ≥ 90, % 11.4 15.3 12.9 SDP/DBP status Normal, % 24.9 28.3 16.4 Pre-hypertensive, % 54.5 47.5 52.5 Hypertensive, % 20.5 24.2 31.1* Diabetes No, % 90.6 87.4 93.4 Yes, % 9.4 12.6 6.6 Depression No, % 91.9 71.2 62.3 Yes, % 8.1 28.8† 37.7† OHI, events/h 2.0 (6.6) 2.3 (6.9) 1.7 (7.1) OHI < 5, % 90.0 89.6 93.4 OHI ≥ 5, % 10.0 10.4 6.6 Caffeine, cup/day 2.3 (2.8) 3.0 (3.6)† 1.8 (2.3) None, % 34.2 23.4 42.6 1-2 cups/day, % 31.2 34.7 29.5 ≥ 3 cups/day, % 34.6 41.9 27.9 Cigarettes, n/day 4.2 (11.3) 4.8 (10.3) 5.0 (10.5) None, % 78.6 74.8 77.0 1-20 /day, % 9.9 9.9 6.6 ≥ 20/day, % 11.5 15.3 16.4
at Milton S. Hershey Medical Center on August 22, 2012http://hyper.ahajournals.org/Downloaded from
Insomnia, Objective Sleep Duration, and Incident Hypertension 7
Alcohol, drink/day 1.6 (7.5) 0.9 (2.3) 0.3 (0.7) None, % 70.0 78.8 82.3 1 drink/day, % 12.1 4.5 9.7 ≥ 2 drink/day, % 17.8 16.7 8.1 Sleep Duration, hrs 6.0 (1.1) 6.1 (1.1) 5.8 (1.2) ≥ 6 hrs, % 59.8 59.5 52.5 < 6 hrs, % 40.2 40.5 47.5 All data are adjusted for sampling weight. Where appropriate the standard deviation is presented in parenthesis. BMI, body mass index; SBP, systolic blood pressure; DBP, diastolic blood pressure; Pre-hypertensive status, SBP ≥ 120 and < 140 mm Hg and/or DBP ≥ 80 and < 90 mm Hg; Hypertensive status, SBP ≥ 140 mm Hg and/or DBP ≥ 90 mm Hg; OHI, obstructive apnea/hypopnea index. *p < .05; †p < .01
at Milton S. Hershey Medical Center on August 22, 2012http://hyper.ahajournals.org/Downloaded from
Insomnia, Objective Sleep Duration, and Incident Hypertension 8
Table S2. Association of Incident Hypertension with Change in Sleep Difficulty status at Follow-up
Sleep Difficulty at Follow-up Incident
Hypertension Sleep Difficulty at Baseline
Normal Sleep
Poor Sleep
Chronic Insomnia
NO Normal Sleep 74.3 18.8 6.9 Poor Sleep 41.5 41.5 16.9 Chronic Insomnia 35.7 21.4 42.9
YES Normal Sleep 80.3 13.9 5.8 Poor Sleep 48.7 33.3 17.9 Chronic Insomnia 20.0 20.0 60.0†
All data are % adjusted for sampling weight. *p < .05; †p < .01
at Milton S. Hershey Medical Center on August 22, 2012http://hyper.ahajournals.org/Downloaded from
Insomnia, Objective Sleep Duration, and Incident Hypertension 9
Figure S1. Participants’ flow in the study
Phase I: Telephone Survey (N = 16,583)
Phase II: Sleep Lab Study Baseline
(N = 1,741)
Follow-Up Survey (N = 1,395)
Mean duration 7.5 years 215 cases deceased 131 cases could not be reached 20 cases missing hypertension data
No Hypertension at Baseline Included
(n = 786)
Hypertension at Baseline Excluded
(n = 609)
No Hypertension at Follow-up
(n = 595)
Hypertension at Follow-up Incident Hypertension
(n = 191)
at Milton S. Hershey Medical Center on August 22, 2012http://hyper.ahajournals.org/Downloaded from