IN SITU EXTRA CORPOREAL SHOCK-WAVE LITHOTRIPSY AS A PRIMARY TREATMENT FOR URETERAL STONES
7
1 IN SITU EXTRA CORPOREAL SHOCK-WAVE LITHOTRIPSY AS A PRIMARY TREATMENT FOR URETERAL STONES Mohamed Abol Saud M. Al-Hawary, Ayman Abdel Wahed Ahmed, Mohamed Abd Elmonem Abolnour AHMED MAHER TEACHING HOSPITAL (CAIRO) Abstract: The aim of the study was to evaluate the results of extracorporeal shock-wave lithotripsy (ESWL) as a primary treatment for ureteral calculi at different levels. Materials and Methods: We treated 166 consecutive patients with solitary ureteral stones (73 at the upper, 4 at the middle, and 89 at the lower ureter) by primary in situ ESWL on an outpatient basis. A maximum of three treatments were given individually before adopting ureteroscopy as an alternative treatment. The success rate was calculated on the basis of complete stone clearance and resolution of any associated obstruction. Re-treatment rates, complications and time to complete stone clearance were recorded. Results: Complete stone clearance was achieved in 152 patients (91.6%) after an average of 10.2 days (range 1-28). The average treatment rate was 1.3 sessions per patient. As whole groups, lower ureteral stones required more treatment sessions than those in the upper ureter, and the difference was statistically significant. However, the differences in the final success rate and time to stone clearance were statistically nonsignificant. When stratified according to size, the success rate was lowest for lower ureteral stones >1 cm in diameter. Conclusion: We believe ESWL is a safe and simple non-invasive option of choice for most ureteral calculi at different levels. Ureteroscopy represents an alternative choice in case of ESWL failure or in cases of larger stones in the lower ureter when it might be the first option. The natural evolution of ureteral calculi is their spontaneous passage. The adoption of a “watchful wait” involves uncertain occupational and medical outcome, especially in the military population. When a decision is made to treat this condition, most urologists offer either ESWL or ureteroscopy (URS) as primary therapy. Each of these techniques has its advantages and disadvantages, and should be considered complementary. 1 We report data from our institution using ESWL as a primary therapy for uretal stones at different levels. Materials and Methods We treated 166 consecutive patients (160 males and 6 females) with solitary ureteral stones at different levels by primary in situ ESWL. Characteristics of patient age, stone size and distribution are shown in Table 1. ESWL was performed on an outpatient basis using a Dornier Lithotripter S (Do Li S). The energy level of the machine is measured on a scale starting from 0.1 (9.5 KV), increasing by 0.1 increments up to 1.0 (13.4 KV), then by 0.5 increments to a maximum energy level of 9 (18.2 KV). Stone localization was done by using fluoroscopy, and intravenous contrast
-
Upload
independent -
Category
Documents
-
view
2 -
download
0
Transcript of IN SITU EXTRA CORPOREAL SHOCK-WAVE LITHOTRIPSY AS A PRIMARY TREATMENT FOR URETERAL STONES

1
IN SITU EXTRA CORPOREAL SHOCK-WAVE LITHOTRIPSY AS A PRIMARY TREATMENT FOR URETERAL STONES
Mohamed Abol Saud M. Al-Hawary, Ayman Abdel Wahed Ahmed, Mohamed Abd Elmonem Abolnour
AHMED MAHER TEACHING HOSPITAL (CAIRO)
Abstract: The aim of the study was to evaluate the results of extracorporeal shock-wave lithotripsy (ESWL) as a primary treatment for ureteral calculi at different levels.Materials and Methods: We treated 166 consecutive patients with solitary ureteral stones (73 at the upper, 4 at the middle, and 89 at the lower ureter) by primary in situ ESWL on an outpatient basis. A maximum of three treatments were given individually before adopting ureteroscopy as an alternative treatment. The success rate was calculated on the basis of complete stone clearance and resolution of any associated obstruction. Re-treatment rates, complications and time to complete stone clearance were recorded.Results: Complete stone clearance was achieved in 152 patients (91.6%) after an average of 10.2 days (range 1-28). The average treatment rate was 1.3 sessions per patient. As whole groups, lower ureteral stones required more treatment sessions than those in the upper ureter, and the difference was statistically significant. However, the differences in the final success rate and time to stone clearance were statistically nonsignificant. When stratified according to size, the success rate was lowest for lower ureteral stones >1 cm in diameter.Conclusion: We believe ESWL is a safe and simple non-invasive option of choice for most ureteral calculi at different levels. Ureteroscopy represents an alternative choice in case of ESWL failure or in cases of larger stones in the lower ureter when it might be the first option.
The natural evolution of ureteral calculi is their spontaneous passage. The adoption of a “watchful wait” involves uncertain occupational and medical outcome, especially in the military population. When a decision is made to treat this condition, most urologists offer either ESWL or ureteroscopy (URS) as primary therapy. Each of these techniques has its advantages and disadvantages, and should be considered complementary.1 We report data from our institution using ESWL as a primary therapy for uretal stones at different levels.
Materials and Methods
We treated 166 consecutive patients (160 males and 6 females) with solitary ureteral stones at different levels by primary in situ ESWL. Characteristics of patient age, stone size and distribution are shown in Table 1. ESWL was performed on an outpatient basis using a Dornier Lithotripter S (Do Li S). The energy level of the machine is measured on a scale starting from 0.1 (9.5 KV), increasing by 0.1 increments up to 1.0 (13.4 KV), then by 0.5 increments to a maximum energy level of 9 (18.2 KV). Stone localization was done by using fluoroscopy, and intravenous contrast

2
Table 1 – Patients’ age, stone size and location.Group No. of patients Age (years) Average stone size (mm)Upper ureter 73 35.1 8.2 (range 3-20)Middle ureter 4 34.5 13.8 (range 5-20)Lower ureter 89 38.9 8.7 (range 3-25)Total 169 37.1 8.6 (range 3-25)
was given when needed to aid localization of radiolucent or faintly opaque stones (6 cases). Patients with stones in the upper ureter were treated in the supine position, while a ventral prone position was used for middle and lower ureteral stones. Sedoanalgesia, using a bolus dose of pethidine (1 mg /kg body weight) with intravenous metoclopramide (10 mg), was given just before the start of lithotripsy. Treatment started at the lowest energy level with gradual increase according to the progress of fragmentation and patient tolerance, limiting the treatment to 4000 shocks per session. The bulk of cases were done by a single urologist.
Preoperative film of the kidneys, ureters and bladder and a sonogram were obtained for all patients, while intravenous urography (IVU) was done in selected cases to document the size and location of the stone, and evaluate the upper tract. Stone size was defined as the longest stone diameter as measured in the plain film of the abdomen. Patients were followed postoperatively with plain radiographs, sonograms and/or IVU on individualized intervals until they became stone free or received additional treatment. Treatment outcome was assessed by radiographic evidence of fragmentation, and success rate was calculated on the basis of complete disappearance of the stone and
resolution of any preoperatively associated obstruction. Failure was designated to cases that showed no effective fragmentation or failure to pass the stone fragments after a maximum of 3 ESWL treatments. Re-treatment rates, time interval to stone clearance, and complications were recorded. Failure cases were salvaged by ureteroscopic lithotripsy. Special care was taken to collect stone material which would be enough for analysis from these failed ESWL cases. The Z-test was used for the statistical analysis, with level of significance at a P value of > 1.9559.
Results
Table 2 summarizes the treatment results relative to the stone level and number of treatment sessions. Overall, complete stone clearance (success rate) was achieved in 152/166 patients (91.6%). Of the 152 patients, 8 required insertion of ureteral stents before treatment due to associated obstruction, 5 needed contrast injection at lithotripsy to help localization and 36 (21.7%) required 2 or 3 treatments before they became stone free. The average treatment rate for the whole group was 1.3 0.6 (range 1-3) sessions per patient; average power was 4.9 (15.7 KV) 1.8 (range 1-9) and the
3
Table 2 – Success rate in relation to the stone level and retreatments.Stone After 1 session After 2 session After 3 session Final success rate
LevelPatient
No.Success rate (%)
Patient no.
Success rate (%)
Patient no.
Success rate (%)
Patient no.
Success rate (%)
Upper 54/73 74 +11 89.1 +4 94.5 69/73 94.5Middle 3/4 75 - - - - ¾ 75Lower 60/89 67.4 +15 84.3 +5 89.9 80/89 89.9Total 117/166 70.5 +26 86.1 +9 91.6 152/166 91.6
Table 3 – Success rate in relation to stone level and size.
Level Upper ureteral stones Lower ureteral stones
Size ≤ 1 cm > 1 cm ≤ 1 cm > 1 cmNo. 57 16 77 12Success rate 55/57 14/16 72/77 8/12
96.5% 87.5% 93.5% 66.7%
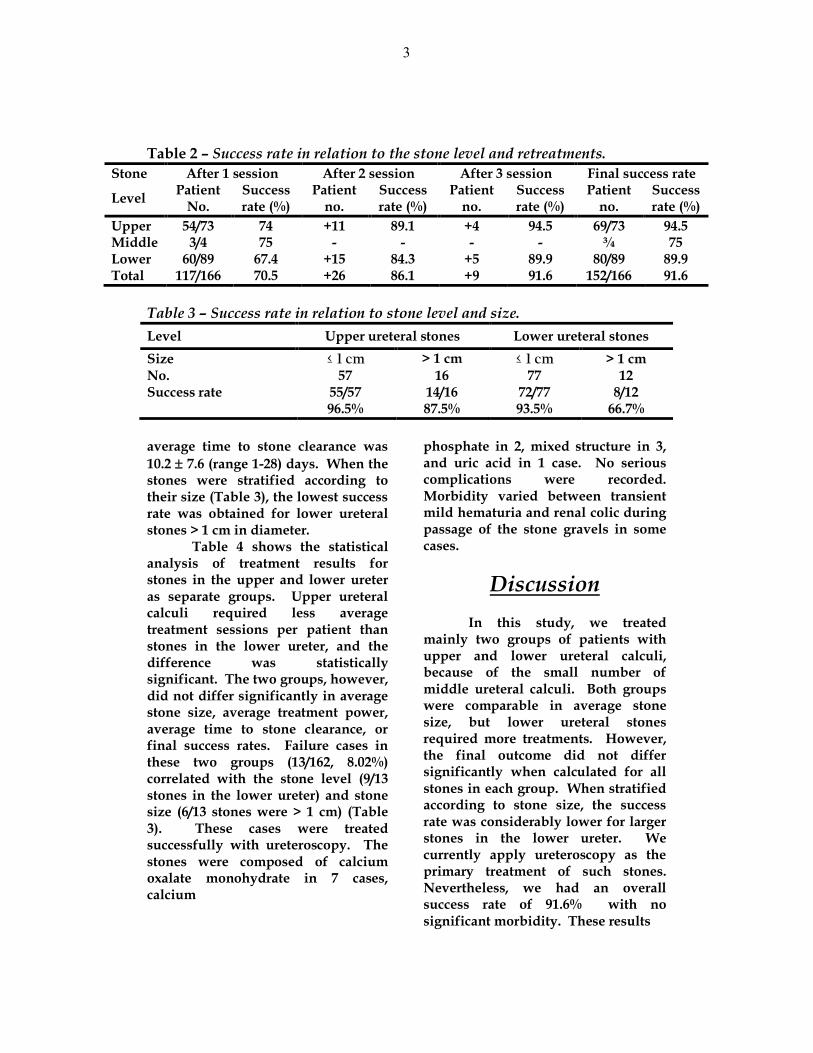
average time to stone clearance was 10.2 7.6 (range 1-28) days. When the stones were stratified according to their size (Table 3), the lowest success rate was obtained for lower ureteral stones > 1 cm in diameter.
Table 4 shows the statistical analysis of treatment results for stones in the upper and lower ureter as separate groups. Upper ureteral calculi required less average treatment sessions per patient than stones in the lower ureter, and the difference was statistically significant. The two groups, however, did not differ significantly in average stone size, average treatment power, average time to stone clearance, or final success rates. Failure cases in these two groups (13/162, 8.02%) correlated with the stone level (9/13 stones in the lower ureter) and stone size (6/13 stones were > 1 cm) (Table 3). These cases were treated successfully with ureteroscopy. The stones were composed of calcium oxalate monohydrate in 7 cases, calcium
phosphate in 2, mixed structure in 3, and uric acid in 1 case. No serious complications were recorded. Morbidity varied between transient mild hematuria and renal colic during passage of the stone gravels in some cases.
Discussion
In this study, we treated mainly two groups of patients with upper and lower ureteral calculi, because of the small number of middle ureteral calculi. Both groups were comparable in average stone size, but lower ureteral stones required more treatments. However, the final outcome did not differ significantly when calculated for all stones in each group. When stratified according to stone size, the success rate was considerably lower for larger stones in the lower ureter. We currently apply ureteroscopy as the primary treatment of such stones. Nevertheless, we had an overall success rate of 91.6% with no significant morbidity. These results
4
compare favorably with other reports even for stones in the lower ureter 2-5.
The clinical outcome of ESWL treatment of radiolucent stones did not appear to differ from that of radio-opaque ones. Intravenous contrast medium administration overcomes the problem of reduced visibility by indirectly depicting the localization of the stone. This same observation was found in other studies involving larger number of radiolucent stones 6.
ESWL treatment of lower ureter stones is cautioned in females in fertility age. We had six females among our patients, and two of them had lower ureteral stones. One of the two was beyond her fertility age, while the other referred to have ESWL rather than ureteroscopy despite our caution.
The ability to predict spontaneous passage of stones has improved over the years but remains imprecise. Whilst the range of therapeutic options continues to widen, most urologists recommend either ESWL or URS for treatment of ureteral stones. Different variables influence the results of ESWL treatment, including stone size and density, ureteral obstruction, and function of the renal unit. Fernandez-Rodriguez et al. 7 found only variables of size, obstruction and function of statistical significance. In addition, other studies correlated treatment failure with ESWL voltage and stone composition, but not location or inadequate treatment. 3, 8, 9 A subgroup of calculi less likely to succeed could thus be identified: calculi > 1 cm 2 , with severe uropathy and functional annulment or delay.
The major disadvantages of ESWL are the number of repetitions often required, and the long wait until the last fragment is passed. The greater strength of URS is that it can be resolved in just one episode in up to 95% of cases, avoiding the obstructive problems that can arise after ESWL. 1 However, the stone-free success rate with URS alone depends on the location of the ureteral stone. It is highest in the distal ureter, with lesser success in the middle and proximal ureter in that order. 8, 10
Although URS with holmium laser lithotripsy achieves excellent results for proximal ureteral stones 1 cm or larger, ESWL is equally efficient for stones less than 1 cm. 11
The consensus is that ESWL therapy should remain a first-line choice in upper ureteral stones, especially if it is less than 1 cm, keeping other modalities for unfragmented stones. 11,12 For distal ureteral calculi, ureteroscopy versus ESWL continues to be a topic of significant discussion. The success rate of ESWL for distal ureteral stones varies greatly in different reports, with stone-free rates from 53% -96% and retreatment rates of 10-30%. 2 The choice of URS as a first-line therapy for distal ureteral calculi relies on the higher success rate, less fluoroscopy time and time to achieve a stone-free state. 2, 4, 13, 14 Ureteroscopy is also less costly than ESWL for stones at all ureteral locations. 15 The high cost of purchasing and maintaining a lithotriptor is responsible for the high treatment cost associated with ESWL. However, cost is only one of a number of important factors that are considered when determining a treatment strategy. ESWL requires less

5
Table 4 – Statistical analysis: Z-test (Z critical two tail = 1.95996).Upper ureteral calculi Lower ureteral calculi
Mean SE SD Mean SE SD P – valueStone size (mm) 8.2 0.532 4.545 8.7 0.5555 5.2401 0.7244Treatment sessions 1.2 0.0584 0.4989 1.4 0.0671 0.6328 2.1116*Time to clearance (days) 9.4 0.8962 7.6575 11 0.7993 7.5408 1.3305Success 1.95 0.0268 0.2292 2.14 0.2278 2.1489 1.1470
SE = standard error, SD = standard deviation.
operating time, more often performed on outpatient basis, and shows a trend to less morbidity, fewer complications and quicker convalescence.16 Thus, it seems that the total expense of both approaches is similar. Such studies support proponents of ESWL as first choice treatment of ureteral calculi regardless the location, while saving URS as a first choice for distal obstructive calculi and those with difficult radiological study.3, 5, 8, 16
Although stones in the upper ureter might respond better to ESWL treatment than those in the lower ureter, the ultimate treatment results are comparable in both clinical settings. At an institution where ESWL and URS are equally available, ESWL is still a valid safe and simple non-invasive option of choice for most ureteral calculi at different levels. Ureteroscopy represents a second choice solution in case of failure of ESWL, except in larger stone sizes in the lower ureter where it might be the first choice option.
References
1. Gonzales-Enguita C, Sanches_Gomez J, Rodriguez-Minon-Cifuentes Jl, Carbera-Perez J, Calahorra-Fernandez FJ, Garcia-Cardoso J, et al. Lithiasis of the distal ureter: ESWL or URS. Actas Urol Esp 1998;22:735-42.
2. Turk TM, Jenkins AD. A comparison of ureteroscopy to in situ extracorporeal shockwave lithotripsy for the treatment of distal ureteral calculi. J Urol 1999; 161:45-7.
3. Strohmaier WL, Schubert G. Rosenkranz I, Weigl A. Comparison of extracorporeal shockwave lithotripsy and ureteroscopy in the treatment of ureteral calculi: a prospective study. Eur Urol 1999; 36:376-9.
4. Peschel R, Janetschek G, Bartsch G. Extracorporeal shock wave lithotripsy versus ureteroscopy for distal ureteral calculi: a prospective randomized study. J Urol 1999; 162:1909-12.
5. Kupeli B, AlKibay T, Sinik Z, Karaoglan U, Bozkirli I. What is the optimal treatment for lower ureteral stones larger than 1 cm2? Int J Urol 2000; 7: 167-71.
6. Buchholz NP, Van Rossum M. Shockwave lithotripsy treatment of radiolucent ureteric calculi with help of contrast medium. Eur Urol 2000; 9:200-3.
7. Fernandez-Rodriguez A, Mijan-Ortiz JL, Catero-Hinojosa J, Arrabal-Martin M, Dominguez-Molinero JF, Zuluaga-Gomez A. Determining factors in the success of treatment of ureteral lithiasis by ESWL. Actas Urol Esp 1997; 21:377-84.
8. Ganapragasam VJ, Ramsden PD, Murthy LS, Thomas DJ. Primary in situ extracorporeal shock wave lithotripsy in the treatment of ureteric calculi: results with a third generation lithotriptor. BJU Int 1999; 84:770-4.
9. Talic RF, Hassan SH, El Faqih SR, Attasi R, El Turaifi A, Neel KF, et al. Extracorporeal shockwave lithotripsy for ureterolithiasis in patients with urinary bilharziasis: efficacy and variables that influence treatment outcome. Eur urol 2000; 37: 26-9.
10. Fernandez De la Maza S. Noldus J, Huland H. Ureteroscopy (URS) in the treatment of ureteral calculi. I. Safety and effectiveness of URS as auxiliary treatment after ESWL. Urologe A 1999; 38:128-32.
11. Lam JS, Greene TD, Gupta M. Treatment of proximal ureteral calculi: Holmium: Yag laser ureterolithotripsy versus extracorporeal shock wave lithotripsy. J Urol 2002:167:1972-6.
12. Kupeli B, Biri H, Isen K. Onaran M, AlKibay T, Karaoglan U, et al. Treatment of ureteral stones: comparison of extracorporeal shock wave lithotripsy and endourologic alternatives. Eur Urol 1998; 34:474-9.
13. Bierkens AF, Hendrikx AJ, De La Rosette JJ, Stultiens GN, Beerlage HP, Arends AJ, et al. Treatment of mid-and lower ureteric calculi: extracorporeal shock-wave lithotripsy vs. laser ureteroscopy. A comparison of costs, morbidity and effectiveness. Br J Urol 1998; 81:31-5.

6
14. Yip SK, Lee FC, Tam PC, Leung SY. Outpatient treatment of middle and lower ureteric stones: extracorporeal shock wave lithotripsy versus ureteroscopic laser lithotripsy. Ann Acad Med Singapore 1998; 27:515-9.
15. Lotan Y, Gettman MT, Roehrborn CG, Cadeddu JA, Pearle MS. Management of ureteral calculi: a cost comparison and decision making analysis. J Urol 2002; 167:1621-9.
16. Pearle MS, Nadler R, Bercowsky E, Chen C, Dunn M, Figenshau RS, et al. Prospective randomized trial comparing shock wave lithotripsy and ureteroscopy for management of distal ureteral calculi. J Urol 2001; 166:1255-60.
7
Arabic summary
)لموجات التصادمیة كعالج لحصوات الحالب(
المشاركون في البحث:: مستشفى أحمد ماھر التعلیمي بالقاھرة*محمد أبوالسعود محمد الھواري/د) 1 أیمن عبدالواحد أحمد/د) 2 محمد عبدالمنعم أبوالنور /د) 3
میة كعالج أساسي لحصوات الحالب في الھدف من الدراسةھو تقییم الموجات التصاد.مستویات مختلفة89و , في وسط4, في أعلي73(مریض بحصوات حالب فردیة 166شملت الدراسة
).في أسفل الحالب
النتائج:یوم 28-1بعد حوالي % 91,6(مریض 152الزوال التام للحصوة تم إحرازه في )1
).جلسة للمریض1,3و حوالي حصوات أسفل الحالب إحتاجت ألي جلسات عالجیة أكثر و نجاح العالج كان ) 2
.سم1أقل في حالة الحصوات األكبر من
من خالل ھذه الدراسة یتضح أن الموجات التصادمیة عالج آمن وبسیط اإلستنتاج:اإلستعانة بمنظار الحالب یمثل إختیار . لمعظم حصوات الحالب بمستویاتھا المختلفة
ل في حالة فشل الموجات التصادمیة أو قد یكون اإلختیار األول في حاالت بدی.الحصوات الكبیرة بالحالب السفلي










![[Characteristics of encrustation of ureteric stents in patients with urinary stones]](https://static.fdokumen.com/doc/165x107/633645e7cd4bf2402c0b6fc8/characteristics-of-encrustation-of-ureteric-stents-in-patients-with-urinary-stones.jpg)