iCAN Self-Management Technology: Helping Patients Adhere to Medical Appointments
21
Imperial College London iCAN SelfManagement Technology: Helping Patients Adhere to Medical Appointments CID: 00884448 Word Count: 3,711 May 5, 2014
Transcript of iCAN Self-Management Technology: Helping Patients Adhere to Medical Appointments
I m p e r i a l C o l l e g e L o n d o n
iCAN Self-‐Management Technology: Helping Patients Adhere to Medical Appointments
08 Fall
CID: 00884448
Word Count: 3,711 May 5, 2014
2
Table of Contents
Abstract ....................................................................................................................... 3
Introduction ................................................................................................................ 3 Missing Appointments Economical Burden ................................................................................................... 3 Reasons for Missing Appointments in the UK ............................................................................................... 4
Background ................................................................................................................. 5 Existing Interventions To Tackle DNAs ........................................................................................................... 5 Successes & Limitations of Skype ....................................................................................................................... 5 Building social capital: Community & networking ...................................................................................... 5 Internet For Health Care Delivery ....................................................................................................................... 5
Bridging The Gap ........................................................................................................................................................ 6 Rationale ..................................................................................................................... 7 The Role of Disruptive Innovation in Cutting Costs .................................................................................... 7 Behavioral Change: Nudge Theory & MIND SPACE Framework ........................................................... 8 Patient-‐Centered Design ......................................................................................................................................... 9
The Intervention ........................................................................................................ 11 Aim & Objectives ..................................................................................................................................................... 11 iCAN Framework ..................................................................................................................................................... 11
Design and Delivery ................................................................................................... 12 Target population ................................................................................................................................................... 12 iCAN Components: Telemedicine & mHealth ............................................................................................. 12
Implementation and Resources ................................................................................. 13 Costs ............................................................................................................................................................................. 13 Timeline ...................................................................................................................................................................... 14
Monitoring & Evaluation ........................................................................................... 14 Limitations of Evaluation .................................................................................................................................... 15
Study Limitations & Discussion .................................................................................. 16 Availability, Accessibility, & Acceptability ................................................................................................... 16 Recommendations .................................................................................................................................................. 16 Conclusion ................................................................................................................. 17
Appendix A: ............................................................................................................... 18
References ................................................................................................................ 19

3
Abstract In the UK missing medical appointments result in huge financial losses in the NHS. Reasons behind missed appointments are varied and include patient forgetfulness, confusion, commitments, fear, and lack of clear communication on the part of healthcare providers. This report will explore the aforementioned reasons as symptoms of patients’ disengagement with their own health. Not only do these symptoms hinder patients from attending their medical appointments, but they also impede adherence to their treatment. By critically investigating these complex interacting symptoms, the report will highlight the need for a structural intervention to provide an empowering environment for diabetic outpatients to self-manage their care, gain ownership and control over their health, and ultimately adhere to their medical appointments. The proposed environment will be a patient-centered software building on the Skype platform and tailored to meet diabetic outpatients needs. iCAN is a self-management technology that will seek to use a combination of novel theories and frameworks, such as Nudge Theory for behavioral change and MINDSPACE to Immerse patients, help them take Control of their health, Adhere to their appointments and encourage them to Network with their GP and other diabetics.
Introduction Missing Appointments Economical Burden Missing appointments pose significant burdens on health care providers, both in terms of financial cost and time lost (George and Rubin, 2003). Missed appointments disrupt the flow of operations and interfere with the continuity of healthcare in acute and chronic conditions, leading to medical and administrative waste of resources (Perron et al., 2010). Cost increases in two ways: directly through the underutilization of administrative resources, and indirectly by increasing hospital readmission rate (Lynn A Nuti et al., 2012). In addition, ‘Did not attends’ (DNAs) have significant impact on waiting lists (Nichol, 2014). Failure to attend the appointments increases the time other patients must wait to see a hospital specialist, which leads to underutilization of labor force and equipment (MRCP et al., 2002). DNAs affect all specialties: medicine, surgery, general practice (GP) and dentistry (MRCP et al., 2002). Reasons for DNAs have been widely assessed and include factors such as forgetfulness, feeling better or worse, transport problems, time commitment, lack of control, fear and confusion about the content and the time of appointment (WM, 1980, Mahvash Hussain-Gambles et al., 2004, MRCP et al., 2002, Neal et al., 2005). See table 1 and figure 1.

4
Reasons for Missing Appointments in the UK
Table 1: Responses to statements about the specific missed appointment (Neal et al., 2005)
In 2009 the BBC reported that ‘missing appointments cost the National Health Service (NHS) above £600 million per year, enough to run two medium-size hospitals’ (BBC, 2009). In 2012, 6.7million UK patients did not attend their medical appointments (Nichol, 2014). Health care professionals believe patient DNAs will cost around £100 per appointment (Nichol, 2014, BBC, 2009). The national rate of non-attendance in the UK is around 12% (NHS 1995). Figures from UK health departments revealed that young men in their twenties are among the highest non-attenders, as compared to elderly patients who are the most conscientious (BBC, 2009).
Fig. 1: Main reasons stated by respondents for not attending their appointment (William Hamilton et al., 2002)

5
Background
Existing Interventions To Tackle DNAs Several interventions have been proposed to reduce the number of missed appointments. Among the most successful and cost-effective are: telephone reminders in the form of short message services (SMS), phone calls, and postal reminders (Perron et al., 2010, Hasvold and Wootton, 2011, F Dockerya et al., 2001). On the other hand some interventions, such as overbooking and fining, have been deemed problematic or less successful. Overbooking is inefficient because of the possibility that, if all the patients showed up, some would be turned away, and if none showed up doctors and medical equipment would be wasted. Similarly, fining patients for not showing up was unsuccessful. Absent patients were fined a trivial amount of £10 (MRCP et al., 2002). This approach was ineffective not only because it failed to deter people from missing appointments, but also because it proved difficult to determine whether or not people had reasonable excuses for not attending. Furthermore, the costs of collecting the money may be higher than any amount refunded (Jones, 2013). The most recent intervention being tested in the UK, and which is seeing promising results in reducing the number of missed appointments, is a combination of webcam appointments via Skype and SMS reminders (Smith, 2012).
Successes & Limitations of Skype
Building social capital: Community & networking “Social relationships, or the relative lack thereof, constitute a major risk factor for health—rivaling the effect of well established health risk factors such as cigarette smoking, blood pressure, blood lipids, obesity and physical activity.” (House et al., 1988). Evidence shows that better-connected people take better care of their health and have a better survival rate than isolated ones. A meta-analysis carried by Holt-Lunstad J et al. showed that there was a 50% increased probability of survival as a function of stronger social relations. Measures of social integration and isolation were powerful predictors of mortality. The effect remained consistent across age, sex, initial health status, follow-up period, and cause of death (Holt-Lunstad et al., 2010). Raynold et al similarly showed that the absence of perceived sources of emotional support was most consistent predictor of survival (P Reynolds et al., 1994).
Internet For Health Care Delivery Internet use among people of all ages has increased significantly over the past decade. More and more services are finding internet platforms to reach their customers, and this trend has paved the way for health services to build on (Hall et al., 2012). Sutcliffe et al. fifteen studies systematic review showed that communication technologies increased
6
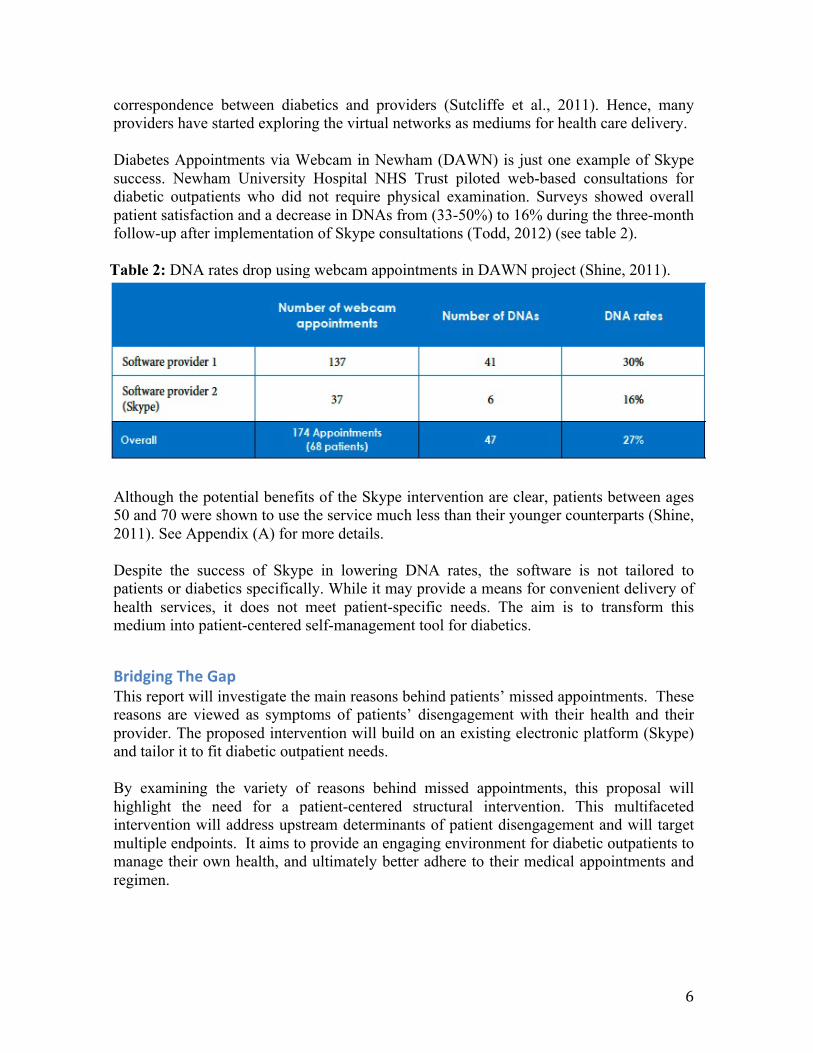
correspondence between diabetics and providers (Sutcliffe et al., 2011). Hence, many providers have started exploring the virtual networks as mediums for health care delivery. Diabetes Appointments via Webcam in Newham (DAWN) is just one example of Skype success. Newham University Hospital NHS Trust piloted web-based consultations for diabetic outpatients who did not require physical examination. Surveys showed overall patient satisfaction and a decrease in DNAs from (33-50%) to 16% during the three-month follow-up after implementation of Skype consultations (Todd, 2012) (see table 2).
Table 2: DNA rates drop using webcam appointments in DAWN project (Shine, 2011).
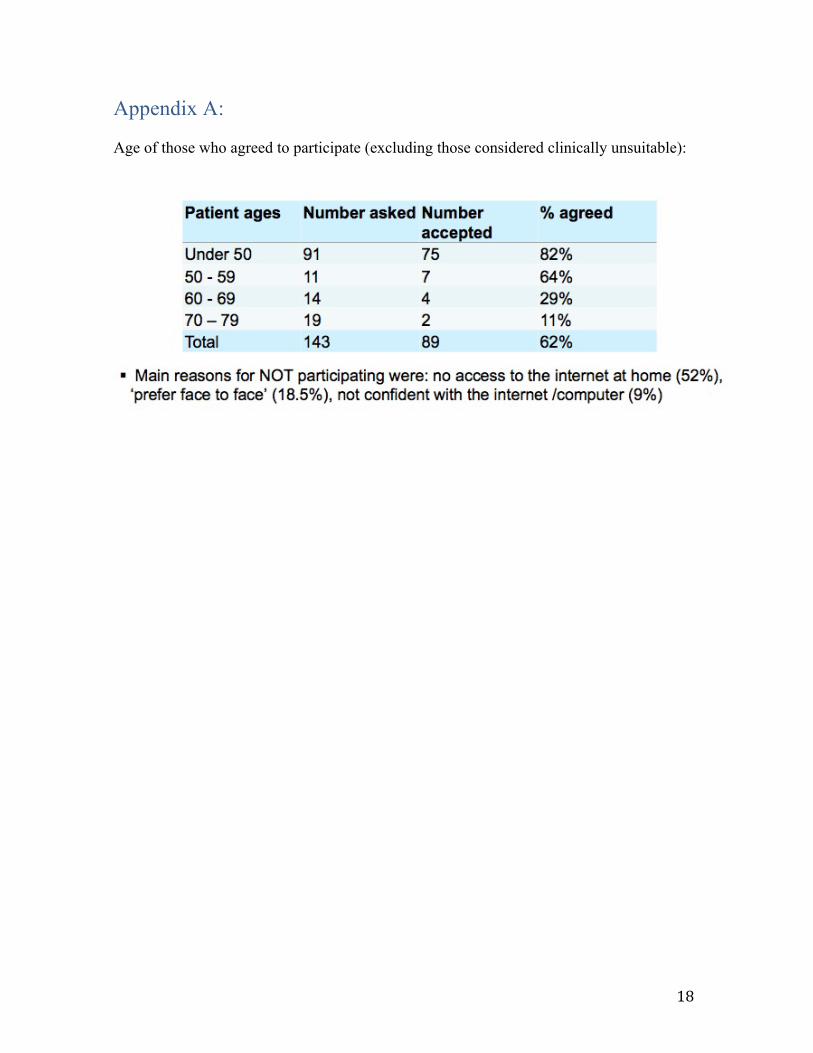
Although the potential benefits of the Skype intervention are clear, patients between ages 50 and 70 were shown to use the service much less than their younger counterparts (Shine, 2011). See Appendix (A) for more details. Despite the success of Skype in lowering DNA rates, the software is not tailored to patients or diabetics specifically. While it may provide a means for convenient delivery of health services, it does not meet patient-specific needs. The aim is to transform this medium into patient-centered self-management tool for diabetics.
Bridging The Gap This report will investigate the main reasons behind patients’ missed appointments. These reasons are viewed as symptoms of patients’ disengagement with their health and their provider. The proposed intervention will build on an existing electronic platform (Skype) and tailor it to fit diabetic outpatient needs. By examining the variety of reasons behind missed appointments, this proposal will highlight the need for a patient-centered structural intervention. This multifaceted intervention will address upstream determinants of patient disengagement and will target multiple endpoints. It aims to provide an engaging environment for diabetic outpatients to manage their own health, and ultimately better adhere to their medical appointments and regimen.
7
Specifically the paper will propose a versatile electronic platform that utilises video conferencing, electronic forums, health promotion links and chat rooms to engage and immerse diabetics in their health. The rationale for the project is based on the success of Skype and SMS reminders, which proved effective in promoting adherence at reduced costs. The intervention will use self-management, behavioral change frameworks − Nudge Theory, MIND SPACE, and patient-centered design − to tackle some of the factors deterring patients from adhering to their appointments.
Rationale The Role of Disruptive Innovation in Cutting Costs Faced with longer life expectancies and decreased fertility rates, developed countries will inevitably confront an increasing ageing population. OECD elderly populations will need extensive long-term care. This increased dependency will further lead to increase in the utilization of health care workers, expensive technologies and surgeries, and ultimately to a tremendous increase in health care expenditure. Disruptive innovation through self-management is an important way to tackle the rising costs of non-communicable diseases like diabetes. We are in need of simple and convenient innovations that are affordable and accessible to most of the population. Figure 2, below, shows the necessity for disruptive innovations that shift the complexity/cost curve down by investing more in primary care, nurses, and patient self-management. Task-shifting to allow specialists to focus on the sickest, giving nurses and allied healthcare workers more complex jobs than what they were previously allowed to do, and finally educating patients to self-manage their health, are all necessary for cutting costs and coping with current epidemiological transition (Christensen, 2000).

8
Fig. 2: ‘Will Disruptive Innovations Cure Healthcare?’ Harvard Business Review (Christensen, 2000)
Behavioral Change: Nudge Theory & MIND SPACE Framework “It turns out that the environmental effects on behaviour are a lot stronger than most people expect.” Daniel Kahneman. As mentioned previously, fines and potentially overburdening the healthcare system have proved ineffective. Incentives and promotions are frequently used to change behaviour but evidence shows that people do not always respond in the most rational way. New approaches based on changing contexts or environments in which we operate (‘Nudging’) are likely to make significant impacts in reforming our behavior and decision-making at cheaper costs (Dolan et al., 2009). This project will use technology to support the behavioral change through mHealth, reminders, telehealth, and forums. Research has shown that technology helps support behavioral changes. One UK study shows that smoking cessation was twice as successful if participants received supporting text messages (Free et al., 2011). The MINDSPACE (Messenger, Incentives, Norms, Defaults, Salience, Priming, Affect, Commitment and Ego) framework provides a brief overview of some of the most powerful effects on behaviour, which can be used as tools for behaviour change (Dolan et al., 2009). MINDSPACE targets ‘inflection points’ (see Table 3) in influencing behaviour. These

9
principles are underpinned by laboratory and field research from social psychology, cognitive psychology and behavioural economics (Dolan et al., 2009).
Table 3: MIND SPACE Framework (Dolan et al., 2009)
The intervention will adopt the MINDSPACE model for behavioral change. Further details are provided in ‘iCAN Framework’ and ‘Design & Delivery’ sections.
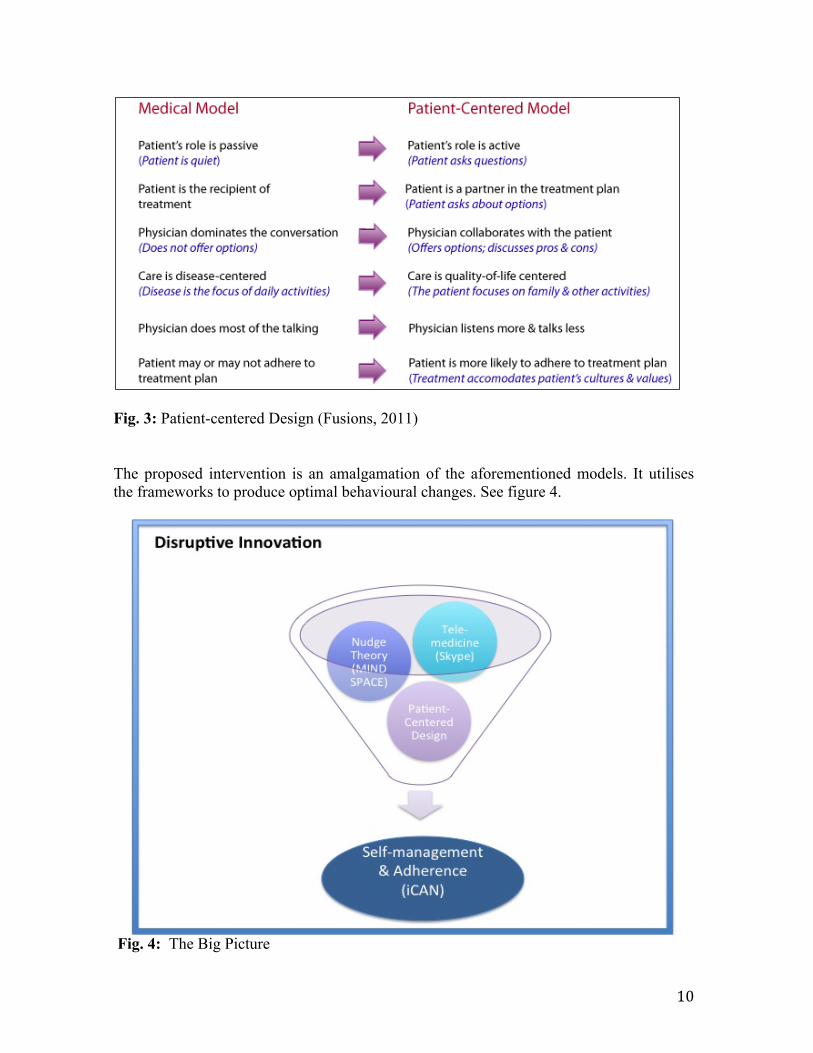
Patient-‐Centered Design A patient-centered health system supports patients to make their own educated decisions and equips them with the tools to successfully manage their own health (Silva, 2014). This intervention will give patients these tools and shift the focus towards self-managed health care. It will include informative links to educate the patients about their condition and the importance of appointments. Patients will also be able to exchange knowledge through chat rooms and forums. See figure 3 for a detailed explanation of patient-centered models and figure 5 for iCAN User Interface.
10
Fig. 3: Patient-centered Design (Fusions, 2011) The proposed intervention is an amalgamation of the aforementioned models. It utilises the frameworks to produce optimal behavioural changes. See figure 4.
Fig. 4: The Big Picture
11
The Intervention
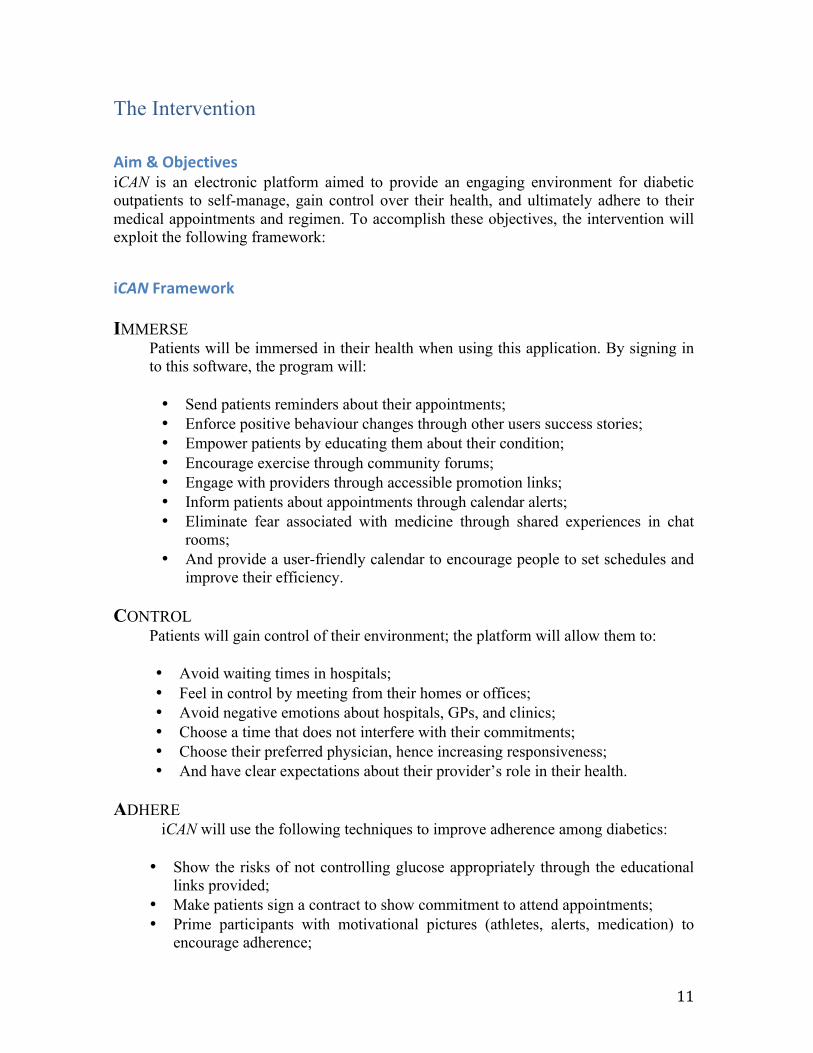
Aim & Objectives iCAN is an electronic platform aimed to provide an engaging environment for diabetic outpatients to self-manage, gain control over their health, and ultimately adhere to their medical appointments and regimen. To accomplish these objectives, the intervention will exploit the following framework:
iCAN Framework
IMMERSE Patients will be immersed in their health when using this application. By signing in to this software, the program will:
• Send patients reminders about their appointments; • Enforce positive behaviour changes through other users success stories; • Empower patients by educating them about their condition; • Encourage exercise through community forums; • Engage with providers through accessible promotion links; • Inform patients about appointments through calendar alerts; • Eliminate fear associated with medicine through shared experiences in chat
rooms; • And provide a user-friendly calendar to encourage people to set schedules and
improve their efficiency.
CONTROL Patients will gain control of their environment; the platform will allow them to:
• Avoid waiting times in hospitals; • Feel in control by meeting from their homes or offices; • Avoid negative emotions about hospitals, GPs, and clinics; • Choose a time that does not interfere with their commitments; • Choose their preferred physician, hence increasing responsiveness; • And have clear expectations about their provider’s role in their health.
ADHERE
iCAN will use the following techniques to improve adherence among diabetics: • Show the risks of not controlling glucose appropriately through the educational
links provided; • Make patients sign a contract to show commitment to attend appointments; • Prime participants with motivational pictures (athletes, alerts, medication) to
encourage adherence;

12
• And show success stories of patients who are leading healthy lives.
NETWORK The software will foster networking by enabling patients to:
• Communicate with other patients and share concerns; • Learn new methods to cope with appointments and medication; • Organize socials events and perhaps exercise with each other; • Network and exchange useful links and articles; • And motivate each other to take challenges.
Design and Delivery
Target population This intervention will target diabetics, specifically T2DM outpatients in clinics who do not require physical examination of all age groups.
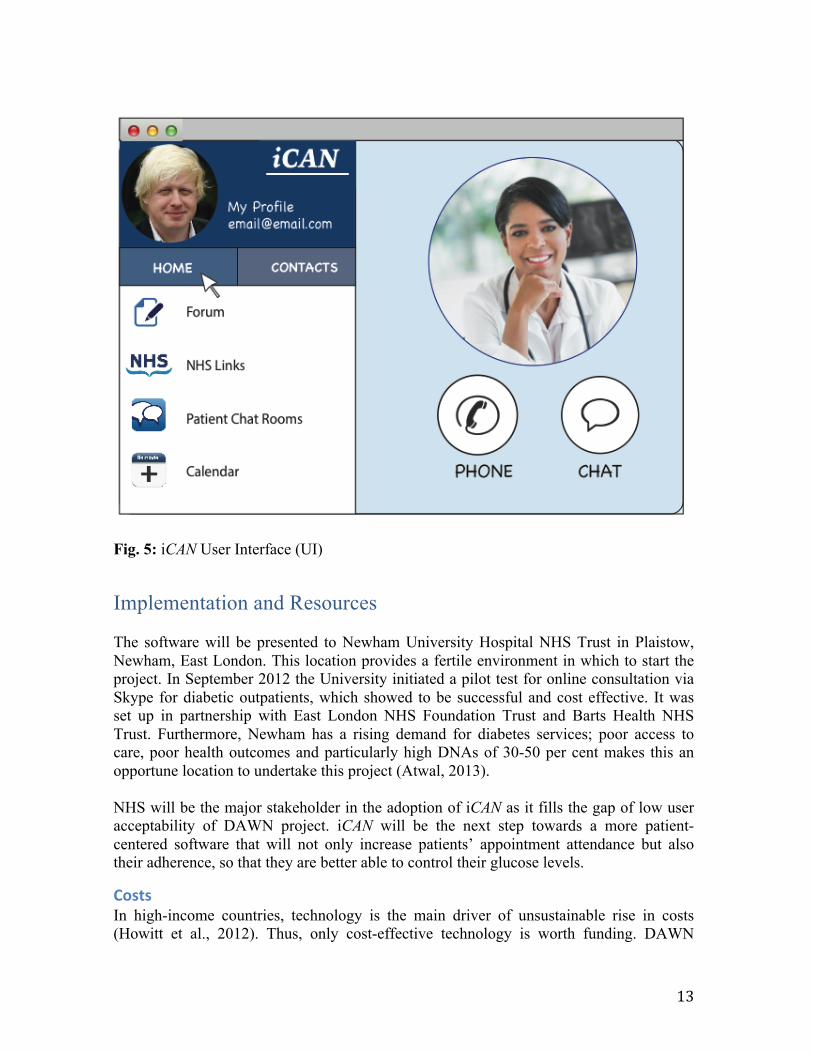
iCAN Components: Telemedicine & mHealth The bifurcated design of this intervention will include synchronous telemedicine; appointments will be in the form of a real-time videoconference between patients and GPs. This will be accompanied with mHealth component, which is composed of calendars, reminders, forums, and useful links. iCAN software will be similar to Skype user interface (UI) and user experience (UX) mainly in its user-friendly and familiar style. However, it will be adjusted based on user complaints and will be geared to fit patients needs. Legends will be added, fonts and buttons will be larger to aid older users. In addition, adding contacts including GPs should be more intuitive (Liam, 2013). Although users report liking the Skype UI, ratings are low for its UX. Adding text labels underneath icons will make it easier for older users to navigate (Jimmy, 2013). More tabs will also be added to link patients to NHS Q&A pages relevant to their conditions and allow them to create their own forums where they can exchange ideas within the diabetic community. Patients will be able to voice their concerns, ask each other questions and encourage one another to exercise, helping them to develop a healthy lifestyle. These forums will be under the supervision of a moderator who will monitor the forum daily in case of fraud or inappropriate answers. Users will be able to post links and articles to share with other patients. Users can video-chat with their GP after scheduling appointments using the built-in calendar. They will be sent reminder notifications the night before the appointment and an hour preceding it. These reminders will be accompanied with information explaining reasons for the appointment, expectations, and a reminder of the signed consent. There will also be tutorials available for patients and providers detailing how to use the software during initiation. See figure 5 for iCAN UI.
13
Fig. 5: iCAN User Interface (UI)
Implementation and Resources The software will be presented to Newham University Hospital NHS Trust in Plaistow, Newham, East London. This location provides a fertile environment in which to start the project. In September 2012 the University initiated a pilot test for online consultation via Skype for diabetic outpatients, which showed to be successful and cost effective. It was set up in partnership with East London NHS Foundation Trust and Barts Health NHS Trust. Furthermore, Newham has a rising demand for diabetes services; poor access to care, poor health outcomes and particularly high DNAs of 30-50 per cent makes this an opportune location to undertake this project (Atwal, 2013). NHS will be the major stakeholder in the adoption of iCAN as it fills the gap of low user acceptability of DAWN project. iCAN will be the next step towards a more patient-centered software that will not only increase patients’ appointment attendance but also their adherence, so that they are better able to control their glucose levels.
Costs In high-income countries, technology is the main driver of unsustainable rise in costs (Howitt et al., 2012). Thus, only cost-effective technology is worth funding. DAWN

14
project reported modest short-term savings of about 3,290/yr per hospital and 1,646/ yr per hospital due to reduction in avoidable A&E attendance. However, long-term savings are promising. Decreased demand for other complimentary services accompanied by reduction in cost of transport, hospital staffing, and health promotion constitute large savings (Shine, 2011) . Another example is pediatric telehealth in Brisbane, Australia. Telepediatrics was cheaper to deliver outpatient services when workload exceeded 774 consultations (Smith et al., 2007). Breakdown of costs is shown in table 4. Table 4: Cost of Tele-Health vs. Conventional Health in Brisbane Tele-pediatrics (Smith et al., 2007)
Timeline For the purpose of this 12-month pilot study, 50 patients will be selected to participate in the project. The planned change will be cyclical and iterative in nature. Plan-Do-Study-Act (PDSA) model will be used. Three months will be dedicated for each of the four stages: Plan: Gather a team that has knowledge of DNAs, and then describe the Aim Statement. Do: Start implementing the action plan. Collect data to assist in evaluation. Study: Assess improvement using the evaluation indicators discussed in the following section. Act: If the pilot is successful, then scale up, if failure, then try different approach (MDH, 2014).
Monitoring & Evaluation The project will be evaluated using a formative evaluation. An adequacy evaluation will assess if expected change has occurred. This evaluation will not require a comparator or a
Expenditure Tele-appointents1(A$) Tele-appointents1(£) Conventional1outpatients1(A$) Conventional1outpatients1(£)
FIXED1COSTSEquipment*(5-year*total*annuatized*cost) 128,191 70,527.47 0 0
ISDN*installation 2655 1,460.71 0 0ISDN*line*rental 32,400 17,825.67 0 0Coordinators*salaries 475,000 261,333.07 0 0
Sub1total1638,246VARIABLE1COSTSTelecommunications*ISDN*Line*charges 65,400 35,981.44 0 0
Staff*salaries:RCH*Consultants*($200*per*h) 109,000 59,969.06 109,000 59969.063RCH*Nursing/Allied*Health*($50*per*h) 27,250 14,992 27,250 14,992.27
RCH*Admin*Support*($30*per*h) 0 0 16,350 8995.359Regional*presenter*($150*per*h) 81,750 44,976.80 0 0Regional*admin*support*($30*per*h) 16,350 8,995.36 0 0
Patient*travel*subsidy*scheme:Travel 0 0 1,391,670 765,661.89Accommodation 0 0 8,994 4,948.27Project*costs 18,000 9,903.15 0 0
Sub1total1317,750 174,818.07 1,553,264 854,566.85Total1cost1955,996 525,964.99 1,553,264 854,566.85

15
control group but rather a set criteria (JP Habicht et al., 1999). For example: to show that 70% of users are satisfied. The evaluation will target two major indicators: utilization and impact. To estimate utilization, qualitative research design will be used to measure two outcomes: patient use and satisfaction by online surveys, interviews and focus groups. To estimate impact, number of DNAs pre/post intervention will be measured. The project will also use quasi-experimental design to measure HA1c levels. Each of these measurements will be taken while the project is being implemented to allow immediate feedback (see table 5).
Table 5: iCAN Methods of Evaluation.
Limitations of Evaluation While assessing utilization, it is reasonable to attribute an observed success to the intervention. For example, it is easy to ascribe patient satisfaction to the use of iCAN. However, when measuring impact it will be difficult to attribute change to the intervention alone since there is no control group to ensure change is not due to chance or other unobserved factors. In this case to measure impact it will be necessary to use an analytical design and go beyond simply observing the patients (Marris and King, 2007). To measure the impact of iCAN, levels of HA1C, quasi-experimental design could be used where a
Indicators Outcome Method Time
Every&3&Months&(Follow&up&for&a&year)
Patient&Use
Patient&Satisfaction
Every&3&Months&(Follow&up&for&a&year)
Every&Month&(Repeated&for&a&year)Utilization
&Surveys,&online&questionnaires&for&feedback,&focus&groups,&interviews,&&(qualitative&
research)
Impact
Number&of&DNAs
Pre/Post&Intervention&design,&OXO&,&O=&Observation,&X=&Intervention.&Count&number&
of&DNAs&Pre&and&Post&intervention&via&Electronic&Health&Records&&&iCAN$database&
Ha1c&Levels
QuasiS&experimental&design:&Two&groups,&one&uses&iCAN&software&and&one&that&uses&
traditional&way.&Both&groups&are&measured&at&the&same&time&before&and&after&iCAN&
introduction.

16
group of patients are non-randomly assigned to use iCAN while others use traditional method. Nonetheless, risk of contamination is possible as some users might use both services. For example a patient assigned online consultation visits her GP or vice versa, which may lead to biased estimation of effect size. In terms of ethics, participants will be assigned the intervention based on their preference followed by consent (Peter Craig et al., 2008). The evaluation will follow CES guidelines for ethical conduct (Marris and King, 2007).
Study Limitations & Discussion
Availability, Accessibility, & Acceptability In order to scale up a technology it needs to be available, accessible, and acceptable (Howitt et al., 2012). In terms of accessibility and equity, iCAN is designed for developed OECD countries, specifically the UK. This is because its cost and quality resonates with the UK standards. In the UK, NICE guidelines for health technology evaluation are unable to evaluate technologies that are ‘inferior’ to incumbent ones. Despite the fact that NHS can afford this intervention, this does not guarantee equal accessibility in the country. Deprivation is widespread and many households do not have internet, smart phones, or lack the confidence to use this technology. One cannot deny the fact that technology is not available for the most people who need it. Despite the substantial use of technology in health care systems in developed countries, deprived areas within the same countries lack fundamental devices like personal computers (Howitt et al., 2012). Further, the availability and accessibility of a technology does not guarantee its acceptance. Although this intervention is convenient and aims to make patients feel in control, many patients and providers prefer face-to-face interaction. Moreover, patients particularly in developed countries value their confidentiality. iCAN do use chat rooms and participants can use nicknames but identity could be revealed. Both reasons could hamper the acceptability of the proposed intervention.
Recommendations Many successful multi-faceted interventions have not been widely adopted because they are resource-intensive and may require specialized infrastructure. Thus, there is an urgent need to develop and test simple scalable improvement techniques in real-world settings. Leveraging current technology and investing in cheaper or frugal technologies is essential to cope with the increasing demand in healthcare.

17
Conclusion The proposed intervention builds on the success of Skype and social networking in promoting patients’ adherence to medical appointments and treatment. iCAN is a self-management tool tailored to meet patient needs, particularly T2DM outpatients who do not need physical examination. Those needs were extracted from current literature on reasons for DNAs in the UK. Upon analyzing these needs, it was determined that patients disengagement with their own health was a determining factor in missing appointments. iCAN is a patient-centered platform. It is designed using cutting-edge technologies and frameworks including telemedicine, Nudge theory for behavioral change, and MINDSPACE. It aims to Immerse patients, help them take Control over their health, Adhere to their appointments, encourage them to Network with their GP and other diabetic patients. As Dr. Duffy accentuated: ‘A massive surge in digital health investing reflects how rapidly confidence in this space is growing. We can clearly see a future where a doctor’s prescription sends you to an immersive online experience as often as it does to a pharmacy’(Duffy, 2014).
18
Appendix A: Age of those who agreed to participate (excluding those considered clinically unsuitable):
19
References ATWAL, K. 2013. Newham project’s award for helping diabetics to have appointments
on Skype [Online]. Newham Recorder. Available: http://www.newhamrecorder.co.uk/news/newham_project_s_award_for_helping_diabetics_to_have_appointments_on_skype_1_2920173?usurv=skip [Accessed 1/5/2014.
BBC. 2009. 'No shows' cost the NHS millions BBC News, 19/4/2014. CHRISTENSEN, C. 2000. Will Disruptive Innovations Cure Healthcare? [Online].
Harvard Business Review. Available: http://hbr.org/web/extras/insight-‐center/health-‐care/will-‐disruptive-‐innovations-‐cure-‐health-‐care-‐sb2 [Accessed 1/5/2014.
DOLAN, P., HALLSWORTH, M., HALPERN, D., KING, D. & VLAEV, I. 2009. MIND SPACE: Influencing behaviour through public policy. UK: Institute For Government.
DUFFY, S. 2014. What If Doctors Could Finally Prescribe Behavior Change? [Online]. Forbes. Available: http://www.forbes.com/sites/sciencebiz/2014/04/17/what-‐if-‐doctors-‐could-‐finally-‐prescribe-‐behavior-‐change/ [Accessed 2/5/2014.
F DOCKERYA, C RAJKUMARA, C CHAPMANA, C BULPITTA & NICHOLLB, C. 2001. The effect of reminder calls in reducing non-‐attendance rates at care of the elderly clinics. Postgrad Med J, 77.
FREE, C., KNIGHT, R., ROBERTSON, S., WHITTAKER, R., EDWARDS, P., ZHOU, W., RODGERS, A., CAIRNS, J., KENWARD, M. G. & ROBERTS, I. 2011. Smoking cessation support delivered via mobile phone text messaging (txt2stop): a single-‐blind, randomised trial. Lancet, 378, 49-‐55.
FUSIONS, I. D. 2011. Patient-‐centered care [Online]. Instructional Design Fusions. Available: http://instructionaldesignfusions.wordpress.com/2011/03/10/patient-‐centered-‐care/ [Accessed 2/5/2014.
GEORGE, A. & RUBIN, G. 2003. Non-‐attendance in general practice: a systematic review and its implications for access to primary health care. Fam Pract, 20, 178-‐84.
HALL, N., YOUNG, C. & WILKINS, A. 2012. Digital First The delivery choice for Englands's population Department of Health NHS.
HASVOLD, P. E. & WOOTTON, R. 2011. Use of telephone and SMS reminders to improve attendance at hospital appointments: a systematic review. J Telemed Telecare, 17, 358-‐64.
HOLT-‐LUNSTAD, J., SMITH, T. B. & LAYTON, J. B. 2010. Social relationships and mortality risk: a meta-‐analytic review. PLoS Med, 7, e1000316.
HOUSE, J. S., LANDIS, K. R. & UMBERSON, D. 1988. Social relationships and health. Science, 241, 540-‐5.
HOWITT, P., DARZI, A., YANG, G. Z., ASHRAFIAN, H., ATUN, R., BARLOW, J., BLAKEMORE, A., BULL, A. M., CAR, J., CONTEH, L., COOKE, G. S., FORD, N., GREGSON, S. A., KERR, K., KING, D., KULENDRAN, M., MALKIN, R. A., MAJEED, A., MATLIN, S., MERRIFIELD, R., PENFOLD, H. A., REID, S. D., SMITH, P. C.,
20
STEVENS, M. M., TEMPLETON, M. R., VINCENT, C. & WILSON, E. 2012. Technologies for global health. Lancet, 380, 507-‐35.
JIMMY. 2013. Feedback on UI design of Skype for Windows 8 [Online]. the Skype community. Available: http://community.skype.com/t5/Modern-‐Windows-‐from-‐Windows/Feedback-‐on-‐UI-‐design-‐of-‐Skype-‐for-‐Windows-‐8/td-‐p/1783460 [Accessed 1/5/2014.
JONES, C. 2013. Fining patients for missing hospital appointments should be last resort, says Derbyshire doctor. Derby Telegraph, 19/4/2014.
JP HABICHT, CG VICTORA & VAUGHAN, A. J. 1999. Evaluation designs for adequacy, plausibility and probability of public health programme performance and impact. International Epidemiological Association, 28.
LIAM. 2013. A few questions for the user interface design team [Online]. the Skype community. Available: http://community.skype.com/t5/Mac/A-‐few-‐questions-‐for-‐the-‐user-‐interface-‐design-‐team-‐at-‐Skype/td-‐p/1517097 [Accessed 1/5/2014.
LYNN A NUTI, MARK LAWLEY, AYTEN TURKCAN, ZHIYI TIAN4, LINGSONG ZHANG, KAREN CHANG, DEANNA R WILLIS & SANDS., A. L. P. 2012. No-‐shows to primary care appointments: subsequent acute care utilization among diabetic patients. BMC Health Services Research, 304.
MAHVASH HUSSAIN-‐GAMBLES, RICHARD D NEAL, OWEN DEMPSEY, LAWLOR, D. A. & HODGSON, A. J. 2004. Missed appointments in primary care: questionnaire and focus group study of health professionals. British Journal of General Practice, 54.
MARRIS, B. V. & KING, B. 2007. Evaluating Health Promotion Programs. University of Toronto.
MDH. 2014. PDSA: Plan-‐Do-‐Study-‐Act [Online]. Minnesota Department of Health. Available: http://www.health.state.mn.us/divs/opi/qi/toolbox/pdsa.html [Accessed 5/5/2014.
MRCP, A. M. M., MRCP, C. R. M., BA, H. L. & FRCP, T. C. K. T. M. 2002. Why do patients not keep their appointments? Prospective study in a gastroenterology outpatient clinic. J R Soc Med, 95.
NEAL, R. D., HUSSAIN-‐GAMBLES, M., ALLGAR, V. L., LAWLOR, D. A. & DEMPSEY, O. 2005. Reasons for and consequences of missed appointments in general practice in the UK: questionnaire survey and prospective review of medical records. BMC Fam Pract, 6, 47.
NICHOL, S. 2014. The huge £24m burden of missed appointments by patients in the North East Chroniclelive, 19/4/2014.
P REYNOLDS, P T BOYD & R S BLACKLOW 1994. The relationship between social ties and survival among black and white breast cancer patients. National Cancer Institute Black/White Cancer Survival Study Group. Cancer Epidemiol Biomarkers Prev, 3.
PERRON, N. J., DAO, M. D., KOSSOVSKY, M. P., MISEREZ, V., CHUARD, C., CALMY, A. & GASPOZ, J. M. 2010. Reduction of missed appointments at an urban primary care clinic: a randomised controlled study. BMC Fam Pract, 11, 79.

21
PETER CRAIG, PAUL DIEPPE, SALLY MACINTYRE, SUSAN MICHIE, IRWIN NAZARETH & MARK PETTICREW 2008. Developing and evaluating complex interventions: the new Medical Research Council guidance. BMJ, 337.
SHINE. 2011. Newham University Hospital NHS Trust: Web based outpatient consultations in diabetes [Online]. The Health Foundation: Inspiring Improvement Available: http://www.health.org.uk/areas-‐of-‐work/programmes/shine-‐eleven/related-‐projects/newham-‐university-‐hospital/ [Accessed 1/5/2014.
SILVA, D. D. 2014. Helping measure person-‐centred care. The Health Foundation. SMITH, A. C., SCUFFHAM, P. & WOOTTON, R. 2007. The costs and potential savings of
a novel telepaediatric service in Queensland. BMC Health Serv Res, 7, 35. SMITH, R. 2012. Skype and text to avoid patients missing appointments NHS told. The
Telegraph 19/4/2014. SUTCLIFFE, P., MARTIN, S., STURT, J., POWELL, J., GRIFFITHS, F., ADAMS, A. & DALE, J.
2011. Systematic review of communication technologies to promote access and engagement of young people with diabetes into healthcare. BMC Endocr Disord, 11, 1.
TODD, R. 2012. Newham Skype pilot cuts DNAs [Online]. E-‐Health Insider. Available: http://www.ehi.co.uk/news/acute-‐care/8031/newham-‐skype-‐pilot-‐cuts-‐dnas [Accessed 1/5/2014.
WILLIAM HAMILTON, BARNFIELD HILL SURGERY, MANJO LUTHRA, SMITH, T. & EVANS, A. P. 2002. Non-‐attendance in general practice: a questionnaire survey. Primary Health Care Research and Development, 3.
WM, B. 1980. Failed appointments. Who misses them, why they are missed, and what can be done. Prime Care, 4.