
High carrier prevalence of combinatorial CYP2C9 and VKORC1 genotypes affecting warfarin dosing
8
PERSONALIZED MEDICINE IN A CTION 10.2217/17410541.5.3.225 © 2008 Future Medicine Ltd ISSN 1741-0541 Personalized Medicine (2008) 5(3), 225–232 225 part of High carrier prevalence of combinatorial CYP2C9 and VKORC1 genotypes affecting warfarin dosing Gualberto Ruaño 1† , Paul D Thompson 2 , David Villagra 1 , Bruce Bower 1 , Mohan Kocherla 1 , Golriz Yazdanpanah 1 , Richard L Seip 1,2 , Andreas Windemuth 1 , C Michael White 2 , Jorge Duconge 3 , Theodore R Holford 4 & Alan HB Wu 5 † Author for correspondence 1 Genomas, Inc., 67 Jefferson St., Hartford CT 06106, USA Tel.: +1 860 545 4574; E-mail: g.ruano @genomas.net 2 Department of Cardiology, Hartford Hospital, Hartford, CT 06102–5037 USA 3 School of Pharmacy, University of Puerto Rico, San Juan, PR 00936–5067, Puerto Rico 4 Department of Biostatistics, Yale University School of Medicine, New Haven, CT, USA 5 University of California, San Francisco, Department of Laboratory Medicine, Clinical Chemistry Laboratory, San Francisco General Hospital; 1001 Portero Avenue, San Francisco, CA 94110, USA Keywords: adverse drug reaction, Coumadin ® , CYP2C9, genotyping, personalized medicine, single nucleotide polymorphisms, VKORC1, warfarin Background: Polymorphisms in the cytochrome P450 2C9 (CYP2C9) and vitamin K epoxide reductase complex subunit 1 (VKORC1) genes significantly alter the effective warfarin dose. The CYP2C9*2 (430C>T), CYP2C9*3 (1075A>C) and VKORC1 -1639 G>A polymorphisms affect warfarin dose through altered metabolism (CYP2C9) and sensitivity (VKORC1). Objective: We determined the frequencies of SNPs in the CYP2C9 and VKORC1 genes in a clinical outpatient population and the carrier prevalences for a variety of genotype combinations to gauge the impact of these polymorphisms on warfarin dosage using published algorithms. Method: A total of 127 patients from an outpatient clinic at Hartford Hospital (Hartford, CT, USA) were genotyped for five SNPs in the CYP2C9 gene and seven SNPs in the VKORC1 gene using Luminex ® technology. Results: The polymorphism frequencies were 10.2, 7.9 and 37.4% for the functionally deficient CYP2C9*2, CYP2C9*3 and VKORC1 -1639 G>A polymorphisms, respectively. Combining prevalence of combinatorial genotypes, 18% were carriers of both CYP2C9 and VKORC1 polymorphisms, 13% were CYP2C9 polymorphism carriers only, 42.5% were VKORC1 carriers only, and the remaining 27% were noncarriers for either gene. Based on published warfarin dosing algorithms, carriers of 1, 2, 3 and 4 functionally deficient polymorphisms predict reductions of 1.0 to 1.6, 2.0 to 2.9, 2.9 to 3.7, and 3.6 to 4.4 mg/day, respectively, in warfarin dose. Conclusion: Overall, 73% of the population carried at least one polymorphism predicting deficient warfarin metabolism or responsiveness and 18% were carriers for polymorphisms in both genes studied. Combinatorial genotyping of CYP2C9 and VKORC1 can allow for individualized dosing of warfarin amongst patients with gene polymorphisms potentially reducing the risk of accentuated responses and bleeding. Warfarin is the most commonly prescribed oral anticoagulant in the USA, with over 19.5 mil- lion prescriptions written in 2006 [1]. Dosing remains a challenging task, as anticoagulation therapy using warfarin is influenced by many factors, both physiological and genetic. For instance a patient’s International Normalized Ratio (INR) varies with Vitamin K intake [2], age [3] and body size and gender [4]. Common polymorphisms in two genes, cyto- chrome P450 2C9 (CYP2C9) and vitamin K epoxide reductase complex subunit 1 (VKORC1), affect warfarin dose through differ- ent mechanisms. Polymorphisms of CYP2C9 include *2 and *3 which are associated with a decrease in enzyme activity to approximately 70 and 5% of the normal level, respectively [5–9]. The result is excess warfarin accumulation, ele- vated INR (>4.0) and possible hemorrhagic complications [10]. The variants have a significant impact on the body’s ability to metabolize war- farin in Swedish, Japanese, Italian, North Ameri- can, British Caucasian and Hong Kong Chinese populations [6,8,11–18]. The CYP2C9 status by itself accounts for approximately 15–20% of the variance in warfarin dose [13,18,19]. Warfarin exerts an anticoagulant effect through its inhibition of the vitamin K epoxide reductase multiprotein complex (VKOR), part of which is subunit 1, encoded by VKORC1 [20,21]. VKOR is responsible for con- verting vitamin K epoxide to vitamin K hydro- quinone, which is an essential cofactor required for the carboxylation of clotting factors II, VII, IX and X [22]. A common polymorphism of the VKORC1 promoter sequence (-1639 G>A) results in decreased vitamin K epoxide reduc- tase enzyme activity as shown by in vitro pro- moter luciferase activity assays [23]. Patients who are carriers of this polymorphism require a lower warfarin maintenance dosage. In addi- tion, six rare coding sequence mutations result in syndromes of warfarin resistance [20,24]. In patients requiring anticoagulant therapy, the -1639 genotype can independently determine 20–25% of warfarin dose variance [18,24].
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of High carrier prevalence of combinatorial CYP2C9 and VKORC1 genotypes affecting warfarin dosing

PERSONALIZED MEDICINE IN ACTION
High carrier prevalence of combinatorial CYP2C9 and VKORC1 genotypes affecting warfarin dosing
Gualberto Ruaño1†, Paul D Thompson2, David Villagra1, Bruce Bower1, Mohan Kocherla1, Golriz Yazdanpanah1, Richard L Seip1,2, Andreas Windemuth1, C Michael White2, Jorge Duconge3, Theodore R Holford4 & Alan HB Wu5†Author for correspondence1Genomas, Inc., 67 Jefferson St., Hartford CT 06106, USATel.: +1 860 545 4574;E-mail: [email protected] of Cardiology, Hartford Hospital, Hartford, CT 06102–5037 USA3School of Pharmacy, University of Puerto Rico, San Juan, PR 00936–5067, Puerto Rico4Department of Biostatistics, Yale University School of Medicine, New Haven, CT, USA5University of California, San Francisco, Department of Laboratory Medicine, Clinical Chemistry Laboratory, San Francisco General Hospital; 1001 Portero Avenue, San Francisco, CA 94110, USA
part of
Keywords: adverse drug reaction, Coumadin®, CYP2C9, genotyping, personalized medicine, single nucleotide polymorphisms, VKORC1, warfarin
10.2217/17410541.5.3.225 © 2
Background: Polymorphisms in the cytochrome P450 2C9 (CYP2C9) and vitamin K epoxide reductase complex subunit 1 (VKORC1) genes significantly alter the effective warfarin dose. The CYP2C9*2 (430C>T), CYP2C9*3 (1075A>C) and VKORC1 -1639 G>A polymorphisms affect warfarin dose through altered metabolism (CYP2C9) and sensitivity (VKORC1). Objective: We determined the frequencies of SNPs in the CYP2C9 and VKORC1 genes in a clinical outpatient population and the carrier prevalences for a variety of genotype combinations to gauge the impact of these polymorphisms on warfarin dosage using published algorithms. Method: A total of 127 patients from an outpatient clinic at Hartford Hospital (Hartford, CT, USA) were genotyped for five SNPs in the CYP2C9 gene and seven SNPs in the VKORC1 gene using Luminex® technology. Results: The polymorphism frequencies were 10.2, 7.9 and 37.4% for the functionally deficient CYP2C9*2, CYP2C9*3 and VKORC1 -1639 G>A polymorphisms, respectively. Combining prevalence of combinatorial genotypes, 18% were carriers of both CYP2C9 and VKORC1 polymorphisms, 13% were CYP2C9 polymorphism carriers only, 42.5% were VKORC1 carriers only, and the remaining 27% were noncarriers for either gene. Based on published warfarin dosing algorithms, carriers of 1, 2, 3 and 4 functionally deficient polymorphisms predict reductions of 1.0 to 1.6, 2.0 to 2.9, 2.9 to 3.7, and 3.6 to 4.4 mg/day, respectively, in warfarin dose. Conclusion: Overall, 73% of the population carried at least one polymorphism predicting deficient warfarin metabolism or responsiveness and 18% were carriers for polymorphisms in both genes studied. Combinatorial genotyping of CYP2C9 and VKORC1 can allow for individualized dosing of warfarin amongst patients with gene polymorphisms potentially reducing the risk of accentuated responses and bleeding.
Warfarin is the most commonly prescribed oralanticoagulant in the USA, with over 19.5 mil-lion prescriptions written in 2006 [1]. Dosingremains a challenging task, as anticoagulationtherapy using warfarin is influenced by manyfactors, both physiological and genetic. Forinstance a patient’s International NormalizedRatio (INR) varies with Vitamin K intake [2],age [3] and body size and gender [4].
Common polymorphisms in two genes, cyto-chrome P450 2C9 (CYP2C9) and vitamin Kepoxide reductase complex subunit 1(VKORC1), affect warfarin dose through differ-ent mechanisms. Polymorphisms of CYP2C9include *2 and *3 which are associated with adecrease in enzyme activity to approximately 70and 5% of the normal level, respectively [5–9].The result is excess warfarin accumulation, ele-vated INR (>4.0) and possible hemorrhagiccomplications [10]. The variants have a significantimpact on the body’s ability to metabolize war-farin in Swedish, Japanese, Italian, North Ameri-can, British Caucasian and Hong Kong Chinese
populations [6,8,11–18]. The CYP2C9 status byitself accounts for approximately 15–20% of thevariance in warfarin dose [13,18,19].
Warfarin exerts an anticoagulant effectthrough its inhibition of the vitamin K epoxidereductase multiprotein complex (VKOR), partof which is subunit 1, encoded byVKORC1 [20,21]. VKOR is responsible for con-verting vitamin K epoxide to vitamin K hydro-quinone, which is an essential cofactor requiredfor the carboxylation of clotting factors II, VII,IX and X [22]. A common polymorphism of theVKORC1 promoter sequence (-1639 G>A)results in decreased vitamin K epoxide reduc-tase enzyme activity as shown by in vitro pro-moter luciferase activity assays [23]. Patients whoare carriers of this polymorphism require alower warfarin maintenance dosage. In addi-tion, six rare coding sequence mutations resultin syndromes of warfarin resistance [20,24]. Inpatients requiring anticoagulant therapy, the-1639 genotype can independently determine20–25% of warfarin dose variance [18,24].
008 Future Medicine Ltd ISSN 1741-0541 Personalized Medicine (2008) 5(3), 225–232 225

PERSONALIZED MEDICINE IN ACTION – Ruaño, Thompson, Villagra et al.
226
Together, the CYP2C9 and VKORC1 combina-torial genotypes may explain up to 45% ofwarfarin response variability [12,13,19,24].
In August 2007, the US FDA revised the war-farin label to include a pharmacogenomic sub-section in which the metabolic impact of theCYP2C9 and VKORC1 gene polymorphisms isoutlined [25]. The CYP2C9 and VKORC1 poly-morphisms are additionally referenced in the‘Precautions and Dosage’ and ‘Administration’sections of the label, noting that the presence ofpolymorphisms in those two genes may lead tothe need for more frequent INR monitoring andreduced warfarin doses [25].
Given the narrow therapeutic range of theINR among patients receiving warfarin therapy,dose estimate empiricism is risk prone. The con-sequences of over- or under-anticoagulation canbe serious, ranging from life-threatening bleed-ing to cerebrovascular emboli, and require inten-sive treatment. Major and fatal bleeding eventsoccur at rates of 7.2 and 1.3 per 100 patientyears, respectively, according to a meta-analysisof 33 studies [26]. If DNA typing were performedbefore warfarin is prescribed, an estimated85,000 serious bleeding events and 17,000strokes could be avoided annually in the USAalone, saving over US$1 billion in healthcarespending [27]. The USA National Heart, Lung,and Blood Institute is currently sponsoring aprospective genotype-guided warfarin dosingprotocol [28].
The goals of our study were to determine thefrequencies of SNPs in the CYP2C9 andVKORC1 genes in a cardiovascular populationand the carrier prevalences for their combina-torial genotypes, and to gauge the impact ofthese polymorphisms on warfarin dosage usingpublished algorithms.
Materials & methodsPatient cohortAs part of a study of dyslipidemias, outpatientsat Hartford Hospital (Hartford, CT, USA) wererecruited and provided written consent asapproved by the Institutional Review Board [29].All patients were adults and unrelated. Agesranged from 28 to 88 years, with an average ageof 67 years. The ethnicities of the surveyed pop-ulation were obtained from each participant’sself-report at recruitment. The ethnic composi-tion of the survey obtained was 80% Caucasian,10% African–American, 9% Hispanic and1% Asian.
Laboratory analysisA 5–10 ml blood sample treated with ethylenedi-aminetetraacetic (EDTA) was obtained at thetime of routine lipid collection for each patient.DNA samples were extracted from whole bloodusing QIAamp DNA Blood Midi Kit (Qiagen,CA, USA) following the manufacturers protocol.Extracted DNA was stored at -80ºC in trishy-droxymethylaminomethane (TRIS)-EDTA (TE)buffer. Quantification of DNA was performed byfluorescent staining of double-stranded DNA(PicoGreen® dsDNA Quantitation Kit, Molecu-lar Probes, OR, USA). Fluorescent intensity wasmeasured using a fluorescent micro-titer platereader (POLARstar OPTIMA, BMG LABTECHGmbH, Offenburg, Germany).
DNA typing of the CYP2C9 and VKORC1genes at 12 variable sites, five SNPs in CYP2C9(Table 1) and seven SNPs in VKORC1 (Table 2), wasperformed at the Laboratory of PersonalizedHealth (LPH), a division of Genomas Inc. (Hart-ford, CT, USA). The LPH is a high-complexityclinical DNA testing center licensed by the Con-necticut Department of Health (CL-0644) andcertified by the Centers for Medicare and Medic-aid Services (ID# 07D1036625) under ClinicalLaboratory Improvement Amendments (CLIA).The Tag-It™ Mutation Detection assays(Luminex Molecular Diagnostics, Toronto, Can-ada) were utilized for DNA typing [30]. Theseassays employed PCR to amplify selectively thedesired genes without co-amplifying pseudogenesor other closely related sequences.
The kits use multiplexed allele-specificprimer extension (ASPE) to identify smallnucleotide variations including single basechanges and deletions. In brief, a PCR-derivedtarget DNA with two universally-tagged allele-specific primers whose 3´ ends define the alleleswas used for each variation tested. A thermo-philic DNA polymerase was used for primerextension and biotin-deoxycytidine triphos-phate (dCTP) label incorporation. Because thetagged allele-specific primers overlap the SNPsite in the target DNA, only the correctlyhybridized primers were extended to generatelabeled products. Single-tagged ASPE primerswere used to detect the presence of unique PCRfragments generated for the deletion and dupli-cation gene rearrangements. Following ASPE,tagged, extended products labeled with biotinwere captured by their tag complements (anti-tags), which had been chemically coupled tospectrally addressable polystyrene microspheres.
Personalized Medicine (2008) 5(3) future science groupfuture science group

Combinatorial genotypes & warfarin dosing – PERSONALIZED MEDICINE IN ACTION
future science groupfuture science group
Table 1. CYP2C9 alle
Allele
*1
*2
*3
*4
*5
*6
Those observed among n =AA: Amino acid.
Table 2. VKORC1 all
Allele
Reference
-1639
85
121
134
172
1331
3487
Those observed in n = 254 AA: Amino acid.
A fluorescent reporter molecule (streptavidin-phycoerythrin) was used to detect incorporatedbiotin. The fluorescent reporter signals gener-ated for each bead population was measured onthe Luminex xMAP™ system. (Luminex®
Corp., TX, USA).
Statistical analysisTo explore the population-wide impact of thepolymorphisms on warfarin dose, we classifiedpatients by VKORC1 and CYP2C9 combinato-rial genotypes. We calculated the expected reduc-tion in dose for each combination, using theequations of Sconce et al. [13] and Zhu et al. [12].First, warfarin dose was estimated for each com-binatorial genotype, assuming a reference personof age 60 years and height 165 cm, weight68.1 kg for a female, and height 177 cm, weight78.3 kg for a male. The algorithms of Sconceet al. [13] and Zhu et al. [12] account for body sizethrough inclusion of height and body weight,respectively. In our analysis, four values weregenerated for each combinatorial genotype: twovalues for the Sconce et al. [13] algorithm incor-porating the reference male and female heights,and two values for the Zhu et al. [12] algorithmincorporating the respective weights.
The reduction in dose for each combinatorialgenotype was calculated as the differencebetween the dose predicted for that combinato-rial genotype and the dose predicted for the ref-erence genotype CYP2C9 *1/*1, VKORC1 GG.The dose reductions for the reference man andwoman were averaged separately within eachcombinatorial genotype for Zhu et al. [12], andfor Sconce et al. [13] The Zhu et al. [12] algo-rithm predicts a systematically greater warfarindose reduction across combinatorial genotypescompared with Sconce et al. [13].
ResultsSurvey results for the CYP2C9 SNPs are shownin Table 1. The frequency of the alleles *2 and *3were 10.2 and 7.9%, respectively. With respectto warfarin metabolism, the *3 allele is deemed‘highly deficient’, having a metabolic functionof only 5% relative to the normal level. Table 2
presents the SNP frequencies for the VKORC1gene. The LPH tests for seven differentVKORC1 SNPs, but only the -1639A promoterallele was observed, at 34.7% frequency.
The carrier prevalence for our 127-patient sur-vey, combining polymorphisms in both CYP2C9and VKORC1 genes is shown in Figure 1. Patient
les.
DNA change AA change Frequency (%) Allele count
Reference Reference 81.9 208
430C>T Arg 144 Cys 10.2 26
1075A>C Ile 359 Leu 7.9 20
1076T>C Ile 359 Tyr 0 0
1080C>G Asp 360 Glu 0 0
818delA Frameshift 0 0
254 alleles from 127 individuals are shown in bold.
eles.
DNA change AA change Frequency (%) Allele count
Reference Reference 62.6 159
G>A Promoter 37.4 95
G>T Val 29 Leu 0 0
G>T Ala 41 Ser 0 0
T>C Val 45 Ala 0 0
A>G Arg 58 Gly 0 0
G>A Val 66 Met 0 0
T>G Leu 128 Arg 0 0
alleles from 127 individuals of the present study are shown in bold.
227www.futuremedicine.com
PERSONALIZED MEDICINE IN ACTION – Ruaño, Thompson, Villagra et al.
228
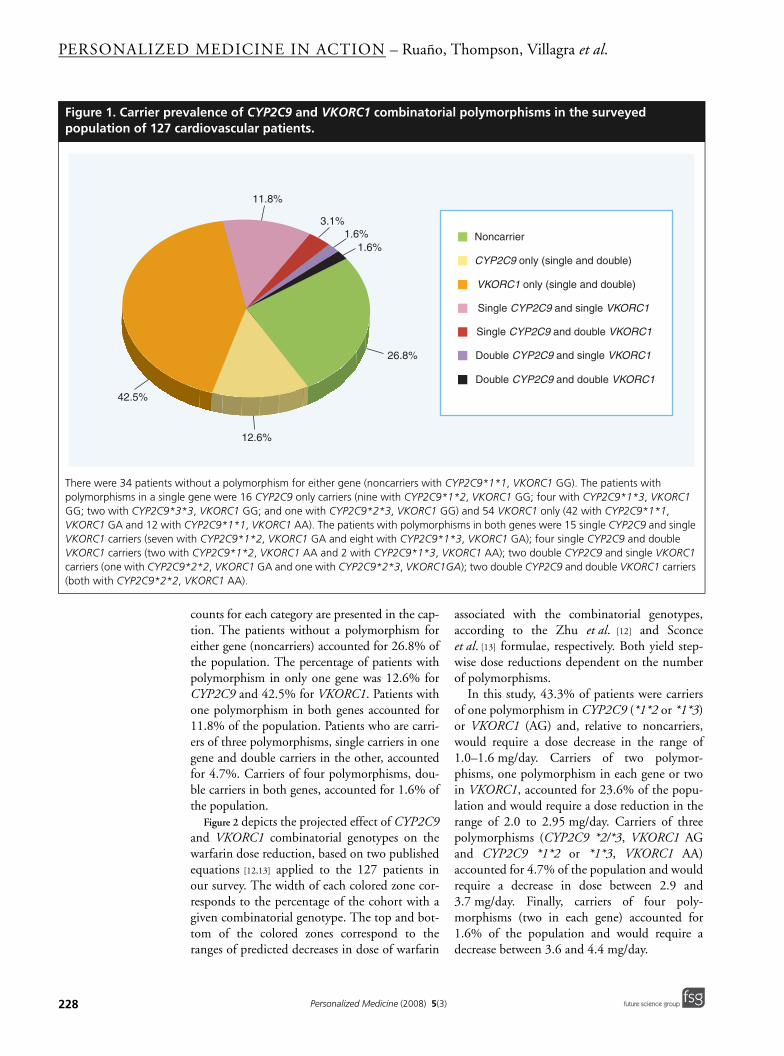
Figure 1. Carrier prepopulation of 127 c
There were 34 patients wpolymorphisms in a singlGG; two with CYP2C9*3VKORC1 GA and 12 withVKORC1 carriers (seven wVKORC1 carriers (two wicarriers (one with CYP2C(both with CYP2C9*2*2
42.5%
counts for each category are presented in the cap-tion. The patients without a polymorphism foreither gene (noncarriers) accounted for 26.8% ofthe population. The percentage of patients withpolymorphism in only one gene was 12.6% forCYP2C9 and 42.5% for VKORC1. Patients withone polymorphism in both genes accounted for11.8% of the population. Patients who are carri-ers of three polymorphisms, single carriers in onegene and double carriers in the other, accountedfor 4.7%. Carriers of four polymorphisms, dou-ble carriers in both genes, accounted for 1.6% ofthe population.
Figure 2 depicts the projected effect of CYP2C9and VKORC1 combinatorial genotypes on thewarfarin dose reduction, based on two publishedequations [12,13] applied to the 127 patients inour survey. The width of each colored zone cor-responds to the percentage of the cohort with agiven combinatorial genotype. The top and bot-tom of the colored zones correspond to theranges of predicted decreases in dose of warfarin
associated with the combinatorial genotypes,according to the Zhu et al. [12] and Sconceet al. [13] formulae, respectively. Both yield step-wise dose reductions dependent on the numberof polymorphisms.
In this study, 43.3% of patients were carriersof one polymorphism in CYP2C9 (*1*2 or *1*3)or VKORC1 (AG) and, relative to noncarriers,would require a dose decrease in the range of1.0–1.6 mg/day. Carriers of two polymor-phisms, one polymorphism in each gene or twoin VKORC1, accounted for 23.6% of the popu-lation and would require a dose reduction in therange of 2.0 to 2.95 mg/day. Carriers of threepolymorphisms (CYP2C9 *2/*3, VKORC1 AGand CYP2C9 *1*2 or *1*3, VKORC1 AA)accounted for 4.7% of the population and wouldrequire a decrease in dose between 2.9 and3.7 mg/day. Finally, carriers of four poly-morphisms (two in each gene) accounted for1.6% of the population and would require adecrease between 3.6 and 4.4 mg/day.
valence of CYP2C9 and VKORC1 combinatorial polymorphisms in the surveyed ardiovascular patients.
ithout a polymorphism for either gene (noncarriers with CYP2C9*1*1, VKORC1 GG). The patients with e gene were 16 CYP2C9 only carriers (nine with CYP2C9*1*2, VKORC1 GG; four with CYP2C9*1*3, VKORC1 *3, VKORC1 GG; and one with CYP2C9*2*3, VKORC1 GG) and 54 VKORC1 only (42 with CYP2C9*1*1, CYP2C9*1*1, VKORC1 AA). The patients with polymorphisms in both genes were 15 single CYP2C9 and single ith CYP2C9*1*2, VKORC1 GA and eight with CYP2C9*1*3, VKORC1 GA); four single CYP2C9 and double
th CYP2C9*1*2, VKORC1 AA and 2 with CYP2C9*1*3, VKORC1 AA); two double CYP2C9 and single VKORC1 9*2*2, VKORC1 GA and one with CYP2C9*2*3, VKORC1GA); two double CYP2C9 and double VKORC1 carriers , VKORC1 AA).
11.8%
3.1%1.6%
1.6%
26.8%
12.6%
Noncarrier
CYP2C9 only (single and double)
VKORC1 only (single and double)
Single CYP2C9 and single VKORC1
Single CYP2C9 and double VKORC1
Double CYP2C9 and single VKORC1
Double CYP2C9 and double VKORC1
Personalized Medicine (2008) 5(3) future science groupfuture science group

Combinatorial genotypes & warfarin dosing – PERSONALIZED MEDICINE IN ACTION
future science groupfuture science group
DiscussionThe results from this study in Figure 1 demonstratethat 73.2% of the patients in our population werecarriers of one or more CYP2C9 or VKORC1polymorphisms resulting in deficient warfarinmetabolism (CYP2C9) or sensitivity (VKORC1).Frequencies for each polymorphism are consistentwith published literature values. Since onlyapproximately a quarter of our study population isnot a carrier of CYP2C9 or VKORC1 poly-morphisms, the potential need for genotype-guided warfarin dosing in all cardiovascularpatients can be discerned. Carriers of three or fourpolymorphisms accounted for 1.6% of the popu-lation. Remarkably, even with 127 patients in thestudy, two subjects were found to be carriers offour polymorphisms, with double polymorphismsin both CYP2C9 and VKORC1 genes.
The CYP2C9 and VKORC1 genes map tochromosomes 10q24 and 16p11.2, respectively.Hence, their polymorphisms would be expectedto segregate independently in populations. Ourresults establish this independent assortment tobe the case. The combined frequency of CYP2C9*1*2 or *1*3 and VKORC1 GA for example,could be calculated to be [(18/127 + 14/127)X59/127], or 0.117, which is in agreement withthe observed carrier prevalence of 15/127, or0.118, for the combinatorial genotype CYP2C9*1*2 or *1*3, VKORC1 GA. While these combi-natorial genotypes can be calculated, indepen-dent segregation should be confirmed, as eachallele combination has a different effect on dosageadjustment. Our survey documents the existinghigh prevalence of combinatorial genotypesaffecting warfarin dosing.
Figure 2. Predicted mean decreases in warfarin dose (mg/day) in the 127 patients from the surveyed population with reference to carrier status for polymorphisms in the CYP2C9 and VKORC1 genes.
The decreases were calculated as described in the methods using published formulae [12,13] that employ age, gender, weight, height, CYP2C9 genotype and VKORC1 genotype. The colored areas indicate ranges of predicted dose reductions. The top and bottom of the coloured zones represents the reductions according to the formulae of Zhu et al. [12] and Sconce et al. [13], respectively. The carrier prevalences and their respective combinatorial genotypes were: 26.8% noncarriers; 43.3% carriers of one polymorphism (33.1% with CYP2C9*1*1, VKORC1 GA and 10.2% with CYP2C9 either *1*2 or *1*3, VKORC1 GG); 23.6% carriers of two polymorphisms (11.8% with CYP2C9 either *1*2 or *1*3, VKORC1 GG; 9.4% with CYP2C9*1*1, VKORC1 AA; 2.4% with CYP2C9 either *2*2 or *2*3, VKORC1 GG); 4.7% carriers of three polymorphisms (3.1% with CYP2C9 either *1*2 or *1*3, VKORC1 AA; 1.6% with CYP2C9 either *2*2 or *2*3, VKORC1 GA); and 1.6% carriers of four polymorphisms (CYP2C9*2*2, VKORC1 AA).
5
4
3
2
1
0Pre
dic
ted
dec
reas
e in
war
fari
n d
ose
(m
g/d
ay)
Cumulative percentage of the population
25 50 75 100
Noncarriers
*1*1,GA
*1*2,GG*1*3,GG
*1*2,GA*1*3,GA
*1*1,AA*2*3,GG*3*3,GG
*1*2,AA*1*3,AA*2*2,GA*2*3,GA
*2*2,AA
229www.futuremedicine.com

PERSONALIZED MEDICINE IN ACTION – Ruaño, Thompson, Villagra et al.
230
As shown quantitatively in Figure 2, whenapplied to dosing algorithms, the combinatorialgenotypes shed valuable information on the fre-quency and magnitude of potential genotype-guided adjustments in a typical population ofcardiovascular patients. To estimate the effect ofthese genotypes on clinical dosing practices, wecalculated the warfarin dosage for each patientbased on CYP2C9 *2/*3 and VKORC1-1639G>A alleles, age, gender and physicalattributes using the published algorithms ofZhu et al. [12] and Sconce et al. [13]. Clearly, thepatients who stand to benefit most from geno-typing are those found to have the greatest num-ber of deficient polymorphisms. Enrichment forrisk-associated combinatorial genotypes may beexamined in patients with reported adverseevents. Recent studies demonstrate that carriersof a combination of CYP2C9 and VKORC1polymorphisms have a significantly increasedrisk of severe over-anticoagulation when com-pared with patients who carry polymorphismsin only a single gene [31,32].
For the present cohort, the potential impactof the genotype test results on the populationburden of anticoagulation therapy risk can beseen in Figure 2. As the beginning of a practicalmnemonic, it can be appreciated that eachpolymorphism in CYP2C9 and VKORC1 forwhich the patient is a carrier entails an approx-imately proportional dose reduction. We foundthe dose reductions to be in excellent agree-ment with those derived for patients aged 60years from a recently published nomogram,which predicted effective warfarin dose rangesfor combinatorial genotypes for the VKORC16853 G>C SNP and CYP2C9 *2/*3 in patientsaged 40–85 years [33]. The VKORC1 SNPs at -1639 and 6853 are in linkage disequilibrium,serving as equivalent markers for the VKORC1haplotypes A and B [24]. In the present studyand that of Caldwell et al. [33], the reductionsin warfarin dose for carriers of one, two andthree polymorphisms compared with noncarri-ers were in the ranges 15–29%, 34–47% and55–62%, respectively.
Discrepancies in warfarin management fromthe genotype-guided doses may increase the riskof overdosing and bleeding complications [34,35],especially during the initiation of warfarin ther-apy [36,37]. Studies in Caucasian populationsshow that the CYP2C9 polymorphisms are asso-ciated with a two- to three-fold increased risk ofbleeding during warfarin induction [9,10,38,39],but not during long-term therapy [40].
This study has some limitations. The uni-verse of alleles for CYP2C9 and VKORC1 genescontinues to expand with genomic sequencingefforts in various populations. Nevertheless, webelieve our multiplexed panel of five and sevenalleles for CYP2C9 and VKORC1, respectively,addresses common and clinically relevant allelesfor these genes. Another limitation is the lack ofdosing algorithms applicable to ethnogeograph-ically diverse urban populations. We are cur-rently pursuing targeted recruitment anddosing algorithm development for the Hispanicpopulation. A recent study in African–Ameri-cans has demonstrated increased risk of hemor-rhage during long-term therapy in patients withCYP2C9 minor variants [36]. In Asian popula-tions, where VKORC1 polymorphisms are morefrequent than in Caucasians [41,42], genotype-guided warfarin dosing may also be clinicallyvaluable [37].
DNA typing for CYP2C9 and VKORC1 poly-morphisms has the potential to enhance thestandard of care in warfarin management. Web-sites and other portals now facilitate the applica-tion of a warfarin dosing algorithm byphysicians, taking into account the CYP2C9 andVKORC1 genotypes as well as age, gender, smok-ing history and concomitant medications [43].Warfarin dosing represents a current workingmodel for the practice of personalized healthcareincreasingly dependent on DNA typing andmanaging therapy according to combinatorialgenotype. DNA-guided pharmacotherapy holdsgreat potential to enhance patient safety basedon each individual’s innate drug metabolism andsensitivity [101].
AcknowledgementsThe authors roles in this work are listed in order to clarifypossible conflicts of interest: GR conceived of the study, andparticipated in its design and in drafting the manuscript;PDT and AHBW participated in the design and conduct ofthe study; MK and GY performed DNA analysis; AW per-formed statistical analyses; DV, RLS, JD, and BB preparedthe manuscript; and TRH and CMW participated in datainterpretation. We thank Darrin D’Agostino, D.O., for hiscontributions to the manuscript.
Financial & competing interests disclosureThis research was funded by grants from the Hartford Hospi-tal Research Administration and by Genomas internalresearch and development funds. All work, including the con-ception and design of the study, the collection of the biologicalsamples from patients, DNA typing and writing of the manu-script, was completed at Hartford Hospital and Genomas,
Personalized Medicine (2008) 5(3) future science groupfuture science group

Combinatorial genotypes & warfarin dosing – PERSONALIZED MEDICINE IN ACTION
future science groupfuture science group
Executive summary
• In August 2007, the Uconsequences of CYP
• There is a need to trapredicting dose adjus
• 127 outpatients with warfarin therapy, wer
• The individual gene alG>A VKORC1 polymo
• The combinatorial genwere carriers of one ppolymorphisms. Compublished algorithms.
• A dosing profile constwarfarin dose reducti
• This population dosinpotential benefits of g
Inc. The following relevant conflicts of interest exist: GR isfounder and President of Genomas, Inc., AW and MK areemployees and GY is a former employee of Genomas Inc. RLSand TRH are consultants for Genomas, Inc. The authorshave no other relevant affiliations or financial involvement
with any organization or entity with a financial interest in orfinancial conflict with the subject matter or materialsdiscussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production ofthis manuscript.
S FDA revised the warfarin label to include pharmacogenomic information on prescription and clinical 2C9 and VKORC1 gene polymorphisms.
nslate this guidance into public health impact based on the prevalence of combinatorial genotypes tments in substantial segments of the population with cardiovascular morbidity.
dyslipidemia, a diagnosis that places them at risk for cardiovascular disease and raises the potential for e genotyped for five DNA sequence variants in the CYP2C9 gene and for seven in the VKORC1 gene.
lele frequencies were 10.2, 7.9 and 37.4% for the functionally deficient *2 CYP2C9, *3 CYP2C9 and -1639 rphisms, respectively.
otype analysis revealed that 26.8% of the population had one or more polymorphisms: 43.3% of patients olymorphism, 23.6% were carriers of two, 4.7% were carriers of three and 1.6% were carriers of four
binatorial genotypes predict step-wise reductions ranging from 1.0 to 4.4 mg/day in warfarin dose based on
ructed for this dyslipidemic population illustrated the large segments of the population potentially requiring ons according to the prevalence of CYP2C9 and VKORC1 combinatorial genotypes.
g profile enables the projection of the present therapeutic risks of standard warfarin therapy and of the enotype-guided warfarin dosing.
BibliographyPapers of special note have been highlighted as either of interest (•) or of considerable interest (••) to readers.1. The top 200 generic drugs in 2006 (by
units). Drug Topics 151, 25 (2007).2. Couris R, Tataronis G, McCloskey W et al.:
Dietary vitamin K variability affects International normalized ratio (INR) coagulation indices. Int. J. Vitam. Nutr. Res. 76, 65–74 (2006).
3. Hylek EM: Oral anticoagulants. Pharmacologic issues for use in the elderly. Clin. Geriatr. Med. 17, 1–13 (2001).
4. Absher RK, Moore ME, Parker MH: Patient-specific factors predictive of warfarin dosage requirements. Ann. Pharmacother. 36, 1512–1517 (2002).
5. Kamali F, Pirmohamed M: The future prospects of pharmacogenetics in oral anticoagulation therapy. Br. J. Clin. Pharmacol. 61, 746–751 (2006).
6. Linder MW, Looney S, Adams JE III et al.: Warfarin dose adjustments based on CYP2C9 genetic polymorphisms. J. Thromb. Thrombolysis 14, 227–232 (2002).
7. Rettie AE, Wienkers LC, Gonzalez FJ, Trager WF, Korzekwa KR: Impaired (S)-warfarin metabolism catalysed by the R144C allelic variant of CYP2C9. Pharmacogenetics 4, 39–42 (1994).
8. Scordo MG, Pengo V, Spina E, Dahl ML, Gusella M, Padrini R: Influence of CYP2C9 and CYP2C19 genetic polymorphisms on warfarin maintenance dose and metabolic clearance. Clin. Pharmacol. Ther. 72, 702–710 (2002).
9. Voora D, Eby C, Linder MW et al.: Prospective dosing of warfarin based on cytochrome P-450 2C9 genotype. Thromb. Haemost. 93, 700–705 (2005).
10. Higashi MK, Veenstra DL, Kondo LM et al.: Association between CYP2C9 genetic variants and anticoagulation-related outcomes during warfarin therapy. JAMA 287, 1690–1698 (2002).
11. Reynolds KK, Valdes R Jr, Hartung BR, Linder MW: Individualizing warfarin therapy. Personalized Med. 4, 11–31 (2007).
•• Comprehensive and well-illustrated review of warfarin dosing algorithms from development to clinical translation.
12. Zhu Y, Shennan M, Reynolds KK et al.: Estimation of warfarin maintenance dose based on VKORC1 (-1639 G>A) and CYP2C9 genotypes. Clin. Chem. 53, 1199–1205 (2007).
• Recent study that predicts warfarin dosing regimen based upon age, gender, body mass, CYP2C9 and VKORC1 genotype.
13. Sconce EA, Khan TI, Wynne HA et al.: The impact of CYP2C9 and VKORC1 genetic polymorphism and patient characteristics upon warfarin dose requirements: proposal for a new dosing regimen. Blood 106, 2329–2333 (2005).
• Pivotal study developing and confirming a warfarin dosing regimen based upon an algorithm that takes into account genetic and physical factors, including age, height, CYP2C9 and VKORC1 genotype.
14. Wu AH: Use of genetic and nongenetic factors in warfarin dosing algorithms. Pharmacogenomics 8, 851–861(2007).
15. Mushiroda T, Ohnishi Y, Saito S et al.: Association of VKORC1 and CYP2C9 polymorphisms with warfarin dose requirements in Japanese patients. J. Hum. Genet. 51, 249–253 (2006).
16. Wadelius M, Sorlin K, Wallerman O et al.: Warfarin sensitivity related to CYP2C9, CYP3A5, ABCB1 (MDR1) and other factors. Pharmacogenomics J. 4, 40–48 (2004).
17. Wadelius M, Chen LY, Downes K et al.: Common VKORC1 and GGCX polymorphisms associated with warfarin dose. Pharmacogenomics J. 5, 262–270 (2005).
18. Wadelius M, Chen LY, Eriksson N et al.: Association of warfarin dose with genes involved in its action and metabolism. Hum. Genet. 121, 23–34 (2007).
231www.futuremedicine.com

PERSONALIZED MEDICINE IN ACTION – Ruaño, Thompson, Villagra et al.
19. Hillman MA, Wilke RA, Caldwell MD, Berg RL, Glurich I, Burmester JK: Relative impact of covariates in prescribing warfarin according to CYP2C9 genotype. Pharmacogenetics 14, 539–547 (2004).
20. Rost S, Fregin A, Ivaskevicius V et al.: Mutations in VKORC1 cause warfarin resistance and multiple coagulation factor deficiency Type 2. Nature 427, 537–541 (2004).
21. Li T, Chang CY, Jin DY, Lin PJ, Khvorova A, Stafford DW: Identification of the gene for vitamin K epoxide reductase. Nature 427, 541–544 (2004).
22. Suttie JW: The biochemical basis of warfarin therapy. Adv. Exp. Med. Biol. 214, 3–16 (1987).
23. Yuan HY, Chen JJ, Lee MT et al.: A novel functional VKORC1 promoter polymorphism is associated with inter-individual and inter-ethnic differences in warfarin sensitivity. Hum. Mol. Genet. 14, 1745–1751 (2005).
24. Rieder MJ, Reiner AP, Gage BF et al.: Effect of VKORC1 haplotypes on transcriptional regulation and warfarin dose. N. Engl. J. Med. 352, 2285–2293 (2005).
• Retrospective study of patients receiving long-term warfarin therapy, in which multiple linear regression analysis determined that VKORC1 haplotype groups (low and high-dose) account for 25% of the variance in warfarin dose.
25. Bristol-Myers Squibb Pharma Company: Coumadin Label. Bristol-Myers Squibb Pharma Company Princeton, NJ, USA, August 16, (2007).
26. Linkins LA, Choi PT, Douketis JD: Clinical impact of bleeding in patients taking oral anticoagulant therapy for venous thromboembolism: a meta-analysis. Ann. Intern. Med. 139, 893–900 (2003).
27. McWilliam A, Lutter R, Nardinelli C: Health care savings from personalized medicine using genetic testing: the case of
warfarin. Working Paper 06–23. AE1-Brookings Joint Center for Regulatory Studies (2006).
28. Rosenberg Y: Rationale and outline of an NHLB/NIH Initiative for a large, multicenter randomized trial of genotype-guided dosage of warfarin therapy. Slide presentation from the NHLB/NIH workshop (2006).
29. Ruano G, Thompson PD, Windemuth A et al.: Physiogenomic analysis links serum creatine kinase activities during statin therapy to vascular smooth muscle homeostasis. Pharmacogenomics 6, 865–872 (2005).
30. Gordon J, Merante F, Weiss S, Zastawny R: Pharmacogenetic P-450 screening using the Tag-it universal bead-based array platform. In: Pharmacogenomics and Proteomics: Enabling The Practice of Personalized Medicine. Wong SH, Linder MW, Valdes R, (Eds). AAC Press, Washington, DC, USA (2006).
31. Schalekamp T, Brasse BP, Roijers JF et al.: VKORC1 and CYP2C9 genotypes and acenocoumarol anticoagulation status: interaction between both genotypes affects overanticoagulation. Clin. Pharmacol. Ther. 80, 13–22 (2006).
32. Schwarz UI, Stein CM: Genetic determinants of dose and clinical outcomes in patients receiving oral anticoagulants. Clin. Pharmacol. Ther. 80, 7–12 (2006).
33. Caldwell MD, Berg RL, Zhang KQ et al.: Evaluation of genetic factors for warfarin dose prediction. Clin. Med. Res. 5, 8–16 (2007).
• Recent survey of the field including clinically useful nomograms for genotype-guided warfarin dosing.
34. Sanderson S, Emery J, Higgins J: CYP2C9 gene variants, drug dose, and bleeding risk in warfarin-treated patients: a HuGEnet systematic review and meta-analysis. Genet. Med. 7, 97–104 (2005).
35. Lindh JD, Lundgren S, Holm L, Alfredsson L, Rane A: Several-fold increase
in risk of overanticoagulation by CYP2C9 mutations. Clin. Pharmacol. Ther. 78, 540–550 (2005).
36. Limdi NA, McGwin G, Goldstein JA et al.: Influence of CYP2C9 and VKORC1 1173C/T genotype on the risk of hemorrhagic complications in African–American and European–American patients on Warfarin. Clin. Pharmacol. Ther. 83, 312–320 (2007).
37. Gage BF, Lesko LJ: Pharmacogenetics of warfarin: regulatory, scientific, and clinical issues. J. Thromb. Thrombolysis 25, 45–51(2007).
38. Visser LE, van Vliet M, van Schaik RH et al.: The risk of overanticoagulation in patients with cytochrome P450 CYP2C9*2 or CYP2C9*3 alleles on acenocoumarol or phenprocoumon. Pharmacogenetics 14, 27–33 (2004).
39. Margaglione M, Colaizzo D, D'Andrea G et al.: Genetic modulation of oral anticoagulation with warfarin. Thromb. Haemost. 84, 775–778 (2000).
40. Taube J, Halsall D, Baglin T: Influence of cytochrome P-450 CYP2C9 polymorphisms on warfarin sensitivity and risk of over-anticoagulation in patients on long-term treatment. Blood 96, 1816–1819 (2000).
41. Veenstra DL, You JH, Rieder MJ et al.: Association of Vitamin K epoxide reductase complex 1 (VKORC1) variants with warfarin dose in a Hong Kong Chinese patient population. Pharmacogenet. Genomics 15, 687–691 (2005).
42. Cho HJ, Sohn KH, Park HM et al.: Factors affecting the interindividual variability of warfarin dose requirement in adult Korean patients. Pharmacogenomics 8, 329–337 (2007).
43. Ruano G: Quo Vadis personalized medicine? Personalized Med. 1, 1–7 (2004).
Website101. Warfarin Dosing. Barnes-Jewish Hospital,
Washington University Medical Center www.warfarindosing.org/Source/Home.aspx
232 Personalized Medicine (2008) 5(3) future science groupfuture science group




















