Maternal Infant Health Program (MIHP) Benefits Administered ...
Upload
independentCategory
view
1download
0
TITLE PAGE
HEALTH CARE DELIVERY AND THE PREVALENCE OF INFANT ANDMATERNAL MORTALITY IN JOS NORTH LOCAL GOVERNMENT.
BY
NUHU, KEFAS DALYOP
UJ/2007/SS/0614
A RESEARCH PROJECT SUBMITTED TO THE DEPARTMENT OF SOCIOLOGY,FACULTY OF SOCIAL SCIENCES, UNIVERSITY OF JOS, IN PARTIALFULFILLMENT OF THE REQUIREMENTS FOR THE AWARD OF BACHELOR OFSCIENCE (B. SC) DEGREE IN SOCIOLOGY.
NOVEMBER, 2012
1
APPROVAL PAGE
This research work has been read and approved as
meeting the requirements for the award of a Bachelor of
Science (B.Sc.) degree in Sociology in the Department of
Sociology, Faculty of Social Sciences, and University of
Jos.
--------------------------------- ------------------------------- Mr. P. N. Wika
Date Supervisor
---------------------------------- -------------------------------Professor E.G. Best
Date Head ofDepartment
2
---------------------------------- -------------------------------- External Examiner
Date
ATTESTATION
I, NUHU, KEFAS DALYOP with matriculation number
UJ/2007/SS/0614, hereby attest that besides the references
made in this research work, the ideas contained in this
project are solely mine and that the work is not copied,
neither has it been presented here in the University of Jos
or elsewhere for the award of a certificate.
3
---------------------------------------------------------------NUHU, KEFAS DALYOP
Date
DEDICATION
This project is dedicated to God Almighty, for His
mercies and grace upon my life. And also to my Mum, Dad and
my Siblings.
4

AKNOWLEDGEMENTS
5

I am highly indebted to Almighty God who in his
infinite mercy has spared my life thus far and in his wisdom
has granted me the inspiration to write this project, he is
the reason for my academic success today and without him,
this dream wouldn’t have come to reality. May his name be
praised and glorified forever (Amen).
I acknowledge with sincere thanks and gratitude my able
supervisor, Mr. P. N. Wika. Your constructive criticism,
endurance, patience and encouragement in the course of
supervising this project work have really made me proud,
your corrections have always brought me back on track
whenever I drifted, I also appreciate you a lot for
permitting me write on this topic, you made me discover the
academic potential in me. May God in his infinite mercy
reward you abundantly.
I wish to appreciate my level coordinator, Mrs. S.
Kumswa for her encouragement during the course of my
studies. My special appreciation goes to Prof. Ogoh Alubo
who have been my secret mentor academically and whose works
6
have inspired me to write on this topic, I also appreciate
him for giving me some of his materials which I used in this
study, may God bless you sir. My gratitude also goes to my
HOD Department of Sociology, Prof. E.G Best, may God bless
and reward you. My special appreciation also goes to all the
lecturers in the Department of sociology which I passed
through their able tutelage, Prof. Ibanga, Prof. Alubo, Prof
Adelakun, Prof. Ityavyar, Prof Alemika, Prof. Best, Prof.
Gofwen, Prof. Ejikeme, Prof. Idyorough, Dr. Ikoh, Dr.
Orisaremi, Dr. Olumodeji, Mrs. Plang, Mrs. K. C Best, Mr.
Wika, Mr. Gulleng, Mr. Abari, Mrs. Wuya, Mrs. Kumswa – you
people have change my thoughts and expose me to the reality
of the world and society we live in, may God bless you all.
My profound gratitude goes to my family especially my
lovely parents Mr. and Mrs. Nuhu B. Dalyop for their love,
care, prayers, encouragement and ultimately the financial
support given to me to make sure I become somebody in life.
I am highly indebted to you and promise not to let you down
and also ensure that your effort does not go in vein. May
God continue to bless and keep you. My gratitude also goes7

to my lovely siblings, Samuel Dalyop, Samson Nuhu, Comfort
Nuhu. Thanks to you guys for your support and encouragement.
And also to my Bigbros Gaius Nuhu and my Bigsis Salome Manji
and her husband, you people indeed have been great, thanks
for your prayers and encouragement which has always kept me
going. May God bless you all. I also acknowledge my uncles
Mr. Dauda B. Dalyop, Mr. Habila B. Dalyop, Mr. Dachollom and
to all my extended family, may god bless you all.
How can I forget my course mates and friends whom we
both passed through this tedious journey together, Abraham,
Patrick, Muhammed, Elijah, Nanpan, Monday, Jennifer, Fatima,
Anne and many others too numerous to mention, may God bless
you all. And to my close friends, Jaduk Mark, Kweng Danladi,
Peter Philip, Dalyop Dachollom, Matawal Jaja, Eric Innocent,
Kyermun Alpha, Jane Sunday, Jane and John Yusuf, Blessing
Sunday, Mafeng Peter and many others – indeed, you guys have
been friends. May God bless you all.
8
Finally, I am grateful to all the women that
participated in this research work and also to Samuel and
Chucks who helped in distributing my questionnaires.
TABLE OF CONTENTS
Title Page - - - - - - - - -i
Approval Page - - - - - - - - -ii
Attestation - - - - - - - - -iii
Dedication - - - - - - - - -iv
Acknowledgements - - - - - - - -v
Table of Contents - - - - - - - -vii
List of Tables - - - - - - - -- ix
Abstract - - - - - - - - - xi
CHAPTER ONE: INTRODUCTION
9

1.1 Background of the Study - - - - - -1
1.2 Statement of the Research Problem - - - -- 4
1.3 Research Questions - - - - - - -8
1.4 Research Objectives - - - - - -- 9
1.5 Significance of the Study - - - - -- 9
1.6 Definition of Key Concepts - - - - -- 10
CHAPTER TWO: LITERATURE REVIEW AND THEORETICALFRAMEWORK
2.1 Introduction - - - - - - - -12
2.2 The Concept of Health - - - - - -12
2.3 Factors Responsible for Infant and Maternal Mortality- - 17
2.3.1 Health Factors Responsible for Infant and MaternalMortality - 18
2.3.2 Non Health Factors Responsible for Infant andMaternal Mortality - 26
2.4 Theoretical Framework - - - - - -36
10
2.4.1 Medical Perspective - - - - - -- 36
2.4.2 Materialist Perspective - - - - -- 43
CHAPTER THREE: RESEARCH METHODLOGY
3.1 Introduction - - - - - - - -48
3.2 Method of Data Collection - - - - -- 48
3.3 Population and Sampling - - - - - -49
3.4 Method of Data Analysis - - - - - -50
3.5 Problems of Data Collection - - - - -- 50
CHAPTER FOUR: DATA PRESENTATION AND ANALYSIS
4.1 Introduction - - - - - - - -52
4.2 Personal Data of Respondents - - - - -53
4.3 Questions on Infant and Maternal Mortality - -- - 58
CHAPTER FIVE : SUMMARY, CONCLUSION AND RECOMMENDATIONS
5.1 Summary of Major Findings - - - - -- 68
11

5.2 Conclusion - - - - - - - -70
5.3 Recommendations - - - - - - -71
References - - - - - - - - -75
Appendix - - - - - - - - - 78
LIST OF TABLES
Table 4.1: Distribution of respondents by Age - -- - 53
Table 4.2: Distribution of Respondents by EducationalAttainment - 53
Table 4.3: Distribution of Respondents by Occupation- - - 54
Table 4.4: Distribution of Respondents by Monthly Income- - 55
Table 4.5: Distribution of Respondents by Number ofChildren - - 55
12

Table 4.6: Distribution of Respondents by Years ofMarriage - - 56
Table 4.7: Distribution of Respondents by Age they gotMarried - 57
Table 4.8: Distribution of Respondents on the Number ofChildren Lost during or after delivery - -
- - - - - 57
Table 4.9: Infant/Children born in poor families are athigher risk of mortality that those in richfamilies. - - - - - - 58
Table 4.10: Socio-economic Status of Parents influencesaccess to health care and infant/child nutrition
- - - - -- - 59
Table 4.11: Education attainment of a mother determinesaccess and quality of health care her child(ren)get - - - - - - 60
Table 4.12: A poor sanitary environment with non or poorsocial amenities increase the risk of infant/childillnesses and death - - - 61
Table 4.13: How effective is the service been rendered inthis hospital or health care centre with regardsto antenatal, natal and post natal care? -
62
Table 4.14: How will you rate the cost of service beenprovided in the hospital or health care centre?
- - - - - - 62
Table 4.15: Women from poor families are at a high riskof mortality during pregnancy, child birth andafter delivery - - - 63
13
Table 4.16: Mother’s socio-economic status is likelygoing to determine the kind of health care andnutrition she gets during pregnancy and afterdelivery -63
Table 4.17: Educational attainment of a mother is morelikely going to influence her decision to seekproper health care during pregnancy, child birthand after delivery - - - - - -
- 64
Table 4.18: A dirty or poor sanitary environment with nonor poor social amenities increase the risk ofmaternal illness and death - - 65
Table 4.19: Women awareness and empowerment and animprovement in their living standard will reducethe high risk or prevalence of infant and maternalmortality - - - - - - - 59
Table 4.20: A clean and healthy environment with theprovision of basic social amenities will ensuresafety infanthood and motherhood - 66
Table 4.21: Ways to reduce the causes and prevalence ofinfant and maternal mortality-67
14
ABSTRACT
The first five years of life are the most crucial to
the physical and intellectual development of children and
can determine their potential to learn and thrive for a
lifetime. For young children, every single day counts, ‘the
name of the child is today, tomorrow may be too late.
However, just as the first five years of life of a child are
crucial, so is the life of the mother during pregnancy,
child delivery and even after delivery, this is because
15

pregnancy outcomes rank among the most pressing reproductive
health challenges all over the world. Globally, an annual
estimate of 600,000 women of reproductive age died of
pregnancy with Nigeria accounting for well over 10 percent
of this figure, this is why Nigeria holds the enviable
second position of infant and maternal only behind India.
The challenges that we face regarding the health of Nigerian
infant/children and their mothers cannot be put off, and
they are insurmountable. The problem of infant and maternal
mortality in Nigeria is precarious, thus, the study was
embark upon to look into health care delivery and the
prevalence of infant and maternal mortality in Nigeria. The
study is intended to explore the conception of health and
the major factors or causes of infant and maternal mortality
in Nigeria with particular reference to Jos North LGA.
However, the study only intends to look at the non health
factors responsible for the prevalence of infant and
maternal mortality, this is because it is social and a
sociological research at such. Factors such as educational,
socio-economic and environmental accounts for infant and
16
maternal mortality in Nigeria, therefore, this study look at
ways in which these factors influence or determine the
prevalence of infant and maternal mortality and ways in
which infant and maternal mortality can be curbed or
curtailed. If the 4th and 5th millennium development goal are
to be achieved, then the government has to put more effort
and political will to curb this menace that has become a
public disgrace.
17
CHAPTER ONE
INTRODUCTION
1.1. BACKGROUND OF THE STUDY.
Infant mortality is defined as the number of infant
deaths (one year of age or younger) per 1000 live births
(WHO). Maternal mortality refers to the death of women while
pregnant or within fourty-two days after delivery or
termination of pregnancy excluding accidental causes of
death (WHO). For any woman who succumbs to maternal death,
many more will suffer injuries, infections and disabilities
18
brought about by complications such as obstetric fistula.
This is commonly known as vesico-virginal fistula (VVF), a
hole in the birth canal that allows leakage from the bladder
or rectum into the vagina which is a major complication from
pregnancy and childbirth. This is usually a problem of young
girls who marry early, often before their bodies are ready
for that function.
Just as the first five years of life are the most
crucial to the physical and intellectual development of
children and can determine their potential to learn and
thrive for a lifetime, the health of the mother is also of
utmost important. Even as available data indicates that
Nigeria’s child survival is precarious leading to huge
number of deaths particularly in the first month of life, it
also indicates that maternal mortality is exceedingly high
and nothing short of an obstetric carnage. For young
children and the mothers, every single day counts. The
challenges that we face regarding the health of Nigerian
children and mothers cannot be put off, and they are not
insurmountable. We have tools, resources, and knowledge to19

address our nation’s most critical infant and maternal
survival problems and build on the considerable achievements
that have been made since the world summit for Children in
1990. What is needed is urgent action and greater national
priority placed on children’s issues so that significant
gaps and the growing disparity in child health and survival
do not reverse the progress already made.
Nigeria’s estimated population of over 150 million
makes it the largest country in sub-Saharan Africa and the
tenth most populated country worldwide. Nigeria’s population
is largely rural, with 63.7 percent of the population living
in rural areas. Currently, about 45 percent of Nigeria’s
total population is less than age 15, with about 20 percent
(24million) under age five. The sheer numbers involved,
therefore, demand that child survival issues be placed in
the forefront of the national agenda.
Despite its wealth of human and natural resources,
Nigeria was ranked among the 13th poorest countries in the
world; two of every three Nigerians (66%) live below the
20

extreme poverty line of US$1 a day (World Bank, 2001).
Nigeria’s low Gross National Product (GNP) –per capita of
$310 in 1998 – is lower among people living in rural areas,
limiting their access to adequate nutrition, quality health
care, and other basic social services, especially among
vulnerable groups (women and children) (World Bank, 1999;
UNICEF, 1999). Less than one-half of the population has
access to safe water (40% in rural areas) and only 41
percent have access to adequate sanitation (32% in rural
areas). Overall , the adult literacy rate is 56 percent;
however, the rate for males (67%) is much higher than for
females (47%). These facts adversely affects the survival of
children and the reproductive health (RH) status of women in
general.
Infant and maternal survival in Nigeria is threatened
by nutritional deficiencies and illnesses, particularly
malaria, diarrheal diseases, Acute Respiratory Infections
(ARI), and Vaccine Preventable Diseases (VPD), which account
for the majority of morbidity and mortality. There is need
for an enabling environment through well-articulated21

policies, projects, and programmes’ to ensure wholesome
development of Nigerian infant/maternal and enhance the
guilty of life.
At the dawn of the twenty-first century, it is tragic
that one in seven Nigerian children die before his or her
fifth birthday (FOS/UNICEF, 2001). Infant and child
mortality rates are exceedingly high, and Nigeria ranks 15th
highest in the world among countries with high under-five
mortality (UNICEF,2001). With more than one million children
dying annually from preventable diseases, Nigeria is one of
the least successful of African countries in achieving
improvement in the past four decades, in spite of advances
in universal immunization and oral- rehydration therapy
(ORT) for diarrheal diseases, and the wealth of Nigeria’s
human natural resources.
Although the 1999 Nigerian Demographic and Health
Survey (NDHS) shows some improvement in Infant Mortality
Rate (IMR) and Under Five Mortality Rate (U5MR), these rates
still fall short of the World Summit for Children (WSC)
22

national goals for reducing IMR (50/60 per 1,000) and U5MR
(70/80 per 1,000) by one-third by 2006. The 1999 NDHS report
cautions, however, that its mortality rates are likely to be
underestimates. The huge variations in these rates among
different parts of the country, notably urban and rural
areas and north and south, are striking. UNICEF’s 1999
Multiple Indicator Cluster Survey (MICS) shows that U5MR was
almost 1.5 times higher in rural areas than urban areas and
that almost twice as many children died before their fifth
birthday in the northwest than in the southwest of Nigeria.
Maternal mortality in Nigeria is also high, varying
between 700 and 800 deaths per 100,000 live births with wide
geographical disparity ranging from 166 per 100,000 in the
Southeast to1,549 per 100,000 live births in the Northeast
(1999 NDHS). Nigeria contributes to 10 percent of worlds
maternal mortality deaths with an average of seven for every
1,00 births. With about 2.4 million live births annually,
about 17,000 Nigerian women die annually. Or put it another
way, one woman dies every 30 minutes from complications of
pregnancy and childbirth (NPC/UNICEF, 2001). These23

indicators have a negative impact on child survival, since
children who lose their mothers experience an increased risk
of death or other complications, such as malnutrition.
Studies have shown that children who lose their mothers
during childbirth, particularly female children, are 10
times more likely to die than those whose mothers survive
(Strong, 1992). For each woman who dies, approximately 20 –
30 others suffer short- and long-term disabilities from
complication of pregnancy and childbirth. Major causes of
maternal mortality are haemorrhage, infection, unsafe
abortion, hypertensive disease of pregnancy, and obstructed
labour.
1.2. STATEMENT OF THE RESEARCH PROBLEM.
Statistics from Save the Child organization (2011), an
international non- profit group, has revealed that almost
800,000 Nigerian children die every year before their fifth
birthday, making Nigeria the country with the highest number
of new born deaths in Africa. The statistics showed that
healthcare is under-funded, under-utilized, and irregular in
24

the country, resulting in high infant and child mortality
rates, particularly in the Northern states. Many rural
clinics lack structure, medical equipment, drugs and
qualified staff to provide quality health services.
Infant mortality is a dark spot on Nigeria’s health
profile. Available data indicates that Nigeria’s child
survival is precarious leading to huge number of deaths
particularly in the first months of life. The situation
which is much higher than the sub Saharan average of 175 per
100,000 is dire because:
Nigeria has been reported to have the worst U5MR[under five mortality rates] in Africa, rangingfrom 235 to 198 per 1000 live births in 1990 to2003 respectively… Four killer diseases in synergywith malnutrition still account for up to 90% ofchildhood deaths (Nigerian Health Review 2006;45).
The above passage confirms an earlier position that
under five mortality rates are higher than the average in
sub Saharan Africa (Federal Government of Nigeria 2004; 4).
Immunization which protect children from some
conditions has declined precipitously in Nigeria. The
federal government has acknowledged the precipitous
25

decline; “The routine immunization coverage that had reached
80% in the early 1990s has nosedived to an all time low by
2000” (Federal Government of Nigeria 2004:4). In 2004, many
states in the North rejected polio immunization alleging
that the vaccines contain anti-fertility agents (Yahaya
2007).
The major cause of childhood deaths are malaria, acute
respiratory infection, diarrhoea, and a host of diseases
such as measles, tetanus, tuberculosis, polio, diphtheria,
etc which are vaccine preventable. Those conditions act in
concert with poor “malnutrition, poor immunization status,
household poverty and food insecurity. Other factors are
maternal illiteracy, poor living conditions (housing, water
and sanitation) and poor home practices for childcare during
illness” (HERFON 2006:47).
The nutritional status of children is a most urgent
challenge all over the country, but particularly in the
northern regions, childhood malnutrition is a major crisis.
The child survival experiences show that at the base of the
26

problem is poverty. As Ogoh Alubo noted in his inaugural
lectures, series 41 titled “In sickness and in health:
Issues in the sociology of health in Nigeria”, up to 60
percent of Nigeria’s under five children are underweight,
stunted and manifest all visible signs of poor nutrition
such as protruding stomachs and shrivelled limbs.
Experiences show that many parents are unable to provide the
necessary diet, many fall back on carbohydrates such as
garri, tuwon masara and pure starch. Even when fluids are
provided, these do not go beyond akamu. The needed nuts and
pulses, proteins, vitamins and irons are deficient in these
foods and hence infants stay malnourished, underweight and
more prone to diseases. This situation is a further
manifestation of what is here called the social production
of sickness. The issue is about the structural location of
parents which divides the children, in the popular parlance,
into aje butter and aje kwaki. While many of children in latter
category present with kwashiorkor and stunted growth, some
in the former show childhood obesity (ibid).
27
The high infant mortality is also due to bout of
diarrhoea, most of it from contaminated water (Alubo and
Ibanga 1994). The factors driving the poor child survival
records point mostly to material poverty.
Just as infant mortality is one of the dark spot in
Nigeria’s health profile, so is maternal mortality, as the
two are different sides of a coin. The different sources
comes to one conclusion: maternal mortality is exceedingly
high and nothing short of an obstetric carnage. According to
the 2006 Nigeria Health Review,
Nigeria has one of the highest maternal mortalityratios in the world, contributing 10% of allmaternal deaths. WHO estimates that about 55,000Nigerian women who die annually from pregnancy andchildbirth complications, an average of 150 womenevery day, or one woman in every ten minutes(HEFRON 2006: 53-54).
The data show that one mother dies out of every 100
deliveries and another 20 may suffer long term complications
(Shiffman 2007, Federal Government of Nigeria 2004).
Nigeria’s maternal mortality experience is exceeding only by
28

India, Nigeria occupies the unenviable second position in
the world (Shiffman 2007:797).
The overall picture, bad as it is, however conceals
huge disparities between regions as well as between urban
and rural centres (Alubo 2010). The centre for reproductive
rights presents the situation in more clear terms:
A woman in Nigeria has 1-in-18 risk of dying inchildbirth or from pregnancy related causes duringher lifetime, which is higher than the overall 1-in-22 risk for women in Sub Saharan Africa. Therisk of maternal deaths are even greater forcertain Nigerian women without formal education.The MMR in the Northern region is consistentlyover 1000 per 100,000 live births, compared to MMRin the Southern region, which is frequently below300 per 100,000 live births. As at 2007, mostNorthern states had MMRs of about 1000 per 100,000live births. Meanwhile, some states in theSouthern region such as Ogun, have MMRs that areconsistently below 200 per 100,000 live birth andthat are progressively decreasing (Centre forReproductive Rights 2008:13).
According to Alubo (2010), if data were disaggregated
by socio-economic status, the differences between the
various strata would be no less striking. This is because
from the materialist point of view, the privations which
manifest as diseases and death are essentially indices of
29

poverty and one’s position within the socio-economic
structure. Thus, issues of early marriage, nutrition in
pregnancy, access to ante-natal services and adequate rest
during pregnancy are all conditions skewed against the poor.
Already, there are data to show that rising incidence of
poverty is the main factor in deteriorating maternal
mortality and morbidity. According to Harrison (1997), the
introduction of user fees and the over Structural Adjustment
of which it was a part, led to rapid decline in ante-natal
attendance on the one hand, and increases in maternal
mortality on the other. The situation also led to more
complications resulting in higher numbers of caesarean
sections as the poorer people who could not afford the new
charges paid with the lives of their mothers, wives and
sisters.
There is a great deal of issues surrounding infant and
maternal mortality in Nigeria, however, this research
intends to find out the relationship or the impact of health
care delivery and the prevalence of infant and maternal
30

mortality in Nigeria with a case study of Jos North Local
Government Area of Plateau State.
1.3. RESEARCH QUESTIONS.
This research work is set to asked questions such as:
I. What are the causes of infant and maternal mortality
in Jos North?
II. Does socio-economic status of parents have an
influence on infant and maternal mortality?
III. What is the relationship between educational
attainment of parents and health care delivery in
Jos North?
IV. Does environmental conditions have an impact on
infant and maternal mortality in Jos North?
1.4. RESEARCH OBJECTIVES.
a) General Objectives:
31

This research aims at investigating health care
delivery and the prevalence of infant and maternal mortality
in Jos North Local Government Area of Plateau state.
b) Specific objectives:
Specifically, the research aims at investigating the
following:
I. To assess the causes of infant and maternal
mortality in Jos North.
II. To establish the relationship between socio-economic
status of parents on infant and maternal mortality
in Jos North.
III. To analyse the relationship between educational
attainment of parents and health care delivery in
Jos North.
IV. To identify some environmental conditions and its
impact on infant and maternal mortality in Jos
North.
V. To proffer solutions to the problems that will be
identified in the course of this study.
32

1.5. SIGNIFICANCE OF THE STUDY.
Infant and maternal mortality is a dark spot on Nigeria’s
health profile, hence this research will serve the following
purposes:
i. It intends to serve as a document for policy framework
which can be used by government and other relevant
agencies.
ii. It aims at contributing to the existing
knowledge/literature on the subject matter of this
investigation.
iii. The research will help in proffering solutions to the
problems of infant and maternal mortality as identified
in this research.
1.6. DEFINITION OF KEY CONCEPTS.
Concepts are interpretive devices. In the social
sciences, they are used for the interpretation of phenomena,
since social science do not demand precise definitions as it
is the case with natural science. There arises the need
33
therefore, to use operational or conceptual definition of
the major concepts employed in this research.
Health care delivery: This refers to the extent to which
individuals who perceived themselves to be sick or have an
identified ill-health condition can be attended to at a
source known to offer reliable, safe and effective care.
This care should also be accessible, acceptable and
affordable. Also known as health services, deals with
anything that can be done to prevent the occurrence of
disease. Such things like environmental sanitation,
vaccination, provision of good water, cleaning of personal
effects like clothing’s, underwear’s, hair, etc. health
care or services can simply be termed as preventive actions
against diseases.
Infant mortality: This is defined as the number of infant
deaths (one year of age or younger) per 1000 live births.
simply put, it is the mortality of live-born infants in the
first year of life. Infant mortality has become a major
topic of discourse in recent times, this is because infants
34

have a slim chances of seeing their first birthday and
children their fifth birthday. Any death occurring before
the first and fifth birthday of infants and children is what
is termed infant/child mortality. This death can occur as a
result of complications during birth, disease that may occur
after birth and the health condition of the child.
Maternal mortality: Maternal mortality according to World
Health Organization (WHO) using the tenth revision of the
International Classification of Diseases (ICD-10) can be
defined as a death of a woman while pregnant or within 42
days of termination of pregnancy, irrespective of the site
or duration of pregnancy, from any cause related to, or
aggravated by the pregnancy or its management, but not from
accidental or incidental causes. Direct maternal deaths are
those resulting from complications of the pregnant state
(pregnancy, labour and puerperium), from interventions,
omissions, incorrect treatment, or from chain of events
arising from any of the above while indirect maternal death
are those due to previously existing disease or disease that
develop during pregnancy, and not due to direct obstetric
35
causes but which was aggravated by the physiological effects
of pregnancy.
CHAPTER TWO
LITERATURE REVIEW AND THEORETICAL FRAMEWORK
2.1 INTRODUCTION
The chapter review popular conceptions on health care
delivery and the prevalence of infant and maternal
mortality. The concept of health has become a major concern
36

to both government and the citizenry, even scholars in the
field of medicine, nursing, psychologist, education,
psychiatry, social work, sociology etc have for a long time
chosen it as a subject of academic discourse.
The research will explore the following
The concept of health
Factors responsible for infant and maternal mortality
Theories of health
2.2 THE CONCEPT OF HEALTH
The concept of health in modern societies is strongly
influenced by it in modern times. Explanations for events
such as illness are rarely understood, for example, in
religious terms, at least not by the majority of lay people
in countries such as UK and the USA, though such ideas may
be prevalent in particular communities. Medical information
is disseminated and available in numerous ways today,
especially through television, the Internet and other media.
If the development of an individualistic medical model has
shaped lay understanding and experience of health, then
37

modern cultures have been equally conducive to its
widespread acceptance. It would be surprising, under these
circumstances, to find an entirely separate system of ‘folk
beliefs’ about illness, shaped by a non-medical culture.
At the same time, enough has already been said to
indicate health, illness and medicine refer to a wide range
of events and experiences, and ideas about these are bound
to contain tensions and contradictions, as well as
ambivalence about the role of medical treatments in dealing
with them (William and Calnan, 1996). Sociological research
on lay concepts of health has provided important insight
into the complexity and sophistication of views about such
matters. Whilst this work has shown the widespread inclusion
of medical messages about health, it has also shown how this
is translated and reconciled with other areas of life, and
assessed against alternative sources of information. Modern
ideas about health and illness can also draw earlier
notions, such as the need for ‘balance’ in sustaining well-
being.
38
In the first place it need to be recognized that health
may be an overriding concern to health care professionals
and researchers, including medical sociologists, but not for
lay people in everyday life. Health, for many, and for most
of the time, is part of the ‘natural attitude’ to life, in
which taken-for-granted meanings are an essential background
and are unconsidered for much of the time. In his study of
risky behaviour and HIV, Bloor (1995), for example, drawing
on the writings of Alfred Schutz, distinguished between ‘the
world of routine activities’ and ‘a world of considered
alternatives and calculative action’ in interpreting how
health risks were perceived by his respondents. Bloor’s
study reinforces the view that daily life presupposes
health, unless it is threatened by events of information
that draw the people into considering alternatives. Health
risks vie with the routine nature of daily life, with its
own pressures and pleasures, constraints and potentialities.
As widely seen, only a minority of people are forced, or
choose, to abandon an assumption of health as a given. Those
concerned with health promotion (as opposed to the treatment
39

of illness) who wish to encourage people to become more
health-conscious have to face this issue in doing so. Health
is not necessarily a pressing and overriding value,
consciously considered on a daily basis. Information on
health risks is actively interpreted within specific social
contexts (Alaszweski and Horlick-Jones, 2003).
In addition to this, lay thinking about the causes and
origins of good and ill health has been found to be
characterized by complex considerations. Even if health is
often taken for granted, and only missed when it is felt to
be compromised, this does not mean that people lack clear
ideas about the relationship between health and illness. In
one of the earliest and most influential studies of lay
concepts of health, Herzlich (1973) showed how, among a
sample of 80 middle-class French respondents (mostly from
Paris) health was linked to the connection between
individuals and ‘the way of life’. Health beliefs, or the
‘representations of health’ as Herzlich called them, located
the source of illness in the character of urban living, with
its tendency to create stress, fatigue and nervous tension.40

This, it was felt, could ‘facilitate’ or ‘release’ forces
that could aid the development of illness. But such forces
could also ‘generate’ illness – that is, be more
pathological in their own right – and not just exacerbate
existing problems, for example, by making an infection
worse.
Positive health, on the other hand, was seen to be
inherent in the individual. The balance or ‘equilibrium’
between the healthy individual and illness could be upset by
a number of features of environment. Cancer was linked to
allergies, and to the nervous strain of city life and the
polluted atmosphere found there. Mental illness was linked
to the ‘restlessness’ of modern living and heart disease to
the ‘many worries which people live in a certain state of
anxiety’ (Herzlich, 1973: 22). Whilst the respondents in
this study recognized that individuals attributes to poor
health, these attributes were never seen as both necessary
and sufficient. The individual’s ‘nature’, heredity,
temperament and predisposition might make the individual
41

vulnerable, but the’ way of life’ remained crucial to the
development of poor health.
If Herzlich’s work set out to provide a framework for
understanding the links between way of life and the
individual in lay concepts of health, subsequent work has
explored their variation across different age and social
groups. In a study which build conceptually on Herzlich, but
draws on a large national study of health and lifestyle in
the UK, Blaxter (1990) has provided a detailed picture of
some of these variations. This study also shows that health
is not a single or unitary concept, but one that has a
number of dimensions as applied to different areas of life
and lifestyles (Blaxter, 2003, 2004).
However, there are two important additions to this
general picture. The first is that health has a moral
dimension, reflecting not only the adoption or maintenance
of a healthy lifestyle, but also how people respond to
illness and deal with its aftermath. Illness runs the risk
of devaluing a person’s identity, either because of
42

causation (e.g. smoking, sexual contact, failure to ‘keep
well’) or because of inappropriate behaviour in the face of
symptoms. Moral dimensions of health have found in a number
of other studies, such as Conrad’s (1994) study of students
in the USA and G. Williams’ (1984) study of middle-aged and
older people with arthritis in England. From this viewpoint
illness is not simply a deviation from biological norms, as
in the medical model, but a significant departure from
social norms.
Second, Blaxter shows that health, illness and disease
are not always mutually exclusive in lay thought.
Respondents in her study often reported that they saw
themselves as healthy despite having serious conditions such
as diabetes, this implies that it is possible to have a
disease and not be ill as well as being ill and not have a
disease. There is clearly a strong motivation towards
feeling and being seen to be healthy, if at all possible.
This issue becomes particularly salient when the question of
disability is considered, given the complex relationship
between health and a range of different disabling43

conditions. For individuals with stable disabilities, or
conditions that are not accompanied by generalized illness
or ‘malaise’, being healthy may be redefined to incorporate
how the person feels now, not in relation to the general
norm. adaptation to illness or disability alters the
baseline from which the individual judges the nature of
health and its implications.
While medical sociology has made an important
contribution to understanding the rationality, relevance and
socially contextualized nature of lay health belief, it is
important not to overstate the argument. Whilst individuals
have unique insights into their own situations, these cannot
be substituted for the expert knowledge in all and every
circumstance (Atkinson, 2003).
2.3 FACTORS RESPONSIBLE FOR INFANT AND MATERNAL MORTALITY.
Without healthy mothers, you cannot have healthy
children. The issue of maternal health actually begins with
44

the conception of the child in the mother’s womb. The health
of the baby within the mother, the circumstances and events
of her birth, her early infancy, childhood, adolescence,
early adulthood, her experiences as regards nutrition, child
care, education, physical, mental, intellectual and
emotional development; all have vital and independent roles
to play in what we term maternal health (Sariki, 2008). Also
children who are raised by physical and emotional nurturing
environment will be more likely to survive and less likely
to succumb to illness and disease.
UNICEF observes that infant/child and maternal
mortality have many triggers. Both direct and indirect.
Poorly funded and culturally inappropriate health and
nutrition services, food insecurity, inadequate feeding
practice and lack of hygiene are direct causes of mortality
in both children and mothers. The indirect causes may be
less obvious externally, but play just as large role in
mortality statistics. Female literacy adversely affects
maternal and child survival rates and is also linked to
early pregnancy. In many countries, especially where child45

marriage is prevalent, the lack of primary education and
lack of access to healthcare contribute significantly to
child and maternal mortality statistics. UNICEF also notes
that discrimination and exclusion of access to health and
nutrition services due to poverty, geographic and political
marginalization are factors in mortality rates as well
(Sariki, 2008).
The researcher has decided to categorized the factors
responsible for infant and maternal mortality into Health
and Non Health factors.
2.3.1 Health factors responsible for infant and
maternal mortality.
Nigeria’s maternal mortality is particularly dire as it
comprises only 1 percent of the world’s population but
accounts for 10 percent of maternal mortality (Alubo, 2012).
According to the 2010-2015 National Health Development Plan
(2010-2012), the main causes of maternal mortality are;
haemorrhage, infection, anaemia, obstructed labour, unsafe
46

abortion and enclampsia. These factors are briefly discussed
below.
Although specific studies on haemorrhage in Nigeria are
scanty, the contribution of postpartum haemorrhage to
maternal mortality is well documented. According to National
Health Development Plan, Haemorrhage accounts to 23% of
maternal mortality in Nigeria. According to Balachandran, in
the studies he conducted in Kaduna, Northern Nigeria
documented postpartum haemorrhage as the most common cause
of maternal mortality. In Nigeria, as in other countries of
the world, haemorrhage is most commonly cause by uterine
anatomy. Other most common causes include retention of the
placenta or placental fragments, trauma to the genital
tract, prolonged second stage of labour, multiple
gestations, past history of postpartum haemorrhage, ante
partum haemorrhage, uterine fibroids, mismanaged third stage
of labour, and caesarean section.
Infection is another factor that is the leading cause
of maternal mortality in women worldwide, especially in the
47

developing world, mainly by haemorrhage, and infection.
Though haemorrhaging will be hard to treat in areas of
limited resources, infection takes days to finally cause
death, and so is preventable. Infection is brought mainly by
preterm rupture of the amniotic membrane, and the prolonged
period before birth. The longer this period, the more likely
infection will set in and subsequent death. This can easily
be treated by administration of antibiotics, and sterile
delivery, the early antibiotics are taken, the higher the
survival rate and the lower the morbidity.
Iron deficiency and anaemia during pregnancy, two
nutritional disorders of public health importance, are
common in developing countries. Anaemia, defined as
haemoglobin concentration below 110g/1 has been recognised
as an important public health problem globally, with high
prevalence, especially among children and women of
childbearing age in developing countries. In Nigeria,
anaemia prevalence in pregnancy varies across regions. Iron
deficiency (believed to be the most common cause of anaemia
in pregnancy) like its anaemia has been recognised as the48
number one nutritional disorder in the world affecting
pregnant women in both developing and developed countries.
According to the National Food Consumption and Nutrition
Survey in 2003, 43.7% of pregnant women in Nigeria are iron
deficient. Animal and human studies have shown that iron
deficiency, anaemia as well as high haemoglobin
concentration during pregnancy is associated with adverse
pregnancy outcomes. Maternal iron deficiency and anaemia
during pregnancy is a product of many factors, such as
maternal malaria, intestinal parasitic infection, recurrent
infection, reduced dietary intakes and many others.
Obstructed labour is one of the most common preventable
causes of perinatal morbidity and mortality in developing
countries. It accounted for 11% of maternal deaths in
Nigeria in 1999 (FMOH,2004). Its occurrence is regarded as a
sign of poor level of obstetric practice in any environment,
because obstructed labour is due to mechanical difficulties
in labour, which takes place where access to proper
obstetric care might not be available or utilized. In booked
patients obstructed labour is prevented by elective49

caesarean section where dyscocia is anticipated and the use
of partogram in labour management with early recourse to
emergency caesarean section.
Abortion is also a leading cause of maternal deaths in
Nigeria. Abortion is illegal in Nigeria except to save a
woman’s life. it is also common, and most procedures are
performed under unsafe, clandestine conditions. In 1996, an
estimated 610,00 abortions occurred (25 per 1,000 women of
childbearing age), of which 142,000 resulted in
complications severe enough to require hospitalization. The
number of abortions is estimated to have risen to 760,000 in
2006 (Bankole et al, 2006). Unsafe abortions are a major
reason Nigeria’s mortality rate – 1,100 deaths per 100,000
live births – is one of the world’s highest (WHO, 2005).
According to conservative estimates, more than 3,000 women
die annually in Nigeria as a result of unsafe abortion
(Henshaw et al, 2008). Many researchers have consistently
shown that high rates of abortion reflects levels of
unintended pregnancy, and that is certainly the case in
Nigeria. Of the estimated 6.8 million pregnancies that occur50
annually in Nigeria, one in five is unplanned, and half of
these ends in induce abortion (Guttmacher Institute, 2008).
Unsafe abortion impacts every level of Nigerian society. It
comprises the health and well-being of women, thereby
compromising the well-being of their families and
communities. Nigerian women experience a variety of
complications from unsafe procedures of abortion; these
include retained pregnancy tissue, infection, haemorrhage,
septic shock, anaemia, intra-abdominal injury (including
perforation of the uterus and damage to the cervix or
bowels) and reactions to chemicals or drugs used to induce
abortion.
Enclampsia also, remains a complication of pregnancy
and a leading contributor to maternal and perinatal
morbidity and mortality in Nigeria. Worldwide it accounts
for 50,000 maternal deaths annually. In spite of several
global and regional interventions and initiatives from
government and other concerned agencies, maternal mortality
continue to rise in Sub – Saharan Africa with enclampsia as
a major cause. Over the last decade it remained the leading51

cause of maternal mortality in Nigeria. This picture could
even be worse especially in the north-eastern part of
Nigeria with so far the worst case fatality rate of 11.6%
(11,600/100,000) as reports in Gombe by Dr. Abubakar Ali
Kullima et al, of the department of Obstetrics and
Gynecology, Federal Medical Center, Nguru, Yobe State. In
their studies of maternal mortality associated with
enclampsia in tertiary institutions in Northern Nigeria in
2009. According to the report, during the first five years
of study period, out of the 224 cases of enclampsia, 52
maternal deaths were recorded, giving case fatality rate of
22.3%. Enclampsia no doubt contributes significantly to
maternal mortality in Nigeria.
The situation of infant mortality is equally dire as
child malnutrition results in the underweight and the
stunting of up to 54 percent of under-five children (Alubo,
2012). There is a clear class character to the epidemiologic
profile in general and infant mortality in particular. There
is evidence that:
52
Infant and child mortality rates are high... Atpresent, one out of every 8 children dies beforehis fifth birthday...child mortality in thecountry is slightly higher than what its incomeper capita would suggest...in the case of infantmortality, ...it is still lower than countrieswith similar income (National Strategic HealthPlan, (2004:24).
The major causes of under-five mortality are;
malnutrition, neonatal tetanus, malaria, diarrhoea,
pneumonia, and measles. These causes are also briefly
discussed below.
In Nigeria, more than 50% of childhood deaths have
under-nutrition as underlying factor (NPC/UNICEF, 1998).
According to the National Strategic Health Plan,
malnutrition in Nigeria accounts for 53% of infant and child
mortality. Progress in nutrition is assessed from indicators
of malnutrition, breastfeeding, sail iodisation, and
vitamin-A supplementation for children under five. The World
Health Organization and the United nation Children
Children’s Fund (1989) recommends that children be
exclusively breastfed for the first four to six months of
life, and thereafter introduced to appropriate and adequate
53

complementary foods along with breast milk. According to the
1999 National Demographic Health Survey, 96 percent of
mothers admitted to breastfeeding babies, and 86 percent of
children ages 12-23 months were still being breastfed.
Despite the slight improvement in the practice of exclusive
breastfeeding, available literatures have shown that
Nigerian infants are not getting maximum benefits of
exclusive breastfeeding, given that about 40 percent of
infant’s ages 2 – 3 months were already receiving
supplements, thus putting them at risk of diarrhoeal
infections, an underlying factor in malnutrition. For older
children, the problem is lack of adequate complementary
feeding. Adequate complementary foods must contain the
recommended dietary allowances for energy, measured by
caloric intake and protein. Majority of young children
receive more cereal and root based carbohydrates as opposed
to protein-rich foods. Nutritional indices for children
under age three are equally poor. According to National
Demographic Health Survey, almost 50 percent are stunted
indicating chronic malnutrition. In addition to adequate
54

protein and energy, intake of micronutrients, especially
vitamin A deficiency contributes to 25 percent of infant,
child and maternal mortality in Nigeria because of reduce
resistance to protein-energy malnutrition, Acute Respiratory
Infection, measles, malaria, and diarrhoea (UNICEF, 2002).
Neonatal tetanus is highly debilitating disease with
high rate of mortality. Global efforts at eliminating the
disease in developing countries yielded results but slower
than expected. The high case of fatality of neonatal tetanus
remains a therapeutic challenge to physicians and requires
continues evaluation. According to the World Health
Organization (WHO), tetanus accounts for 7% of neonatal
deaths globally, and up to 20% in Nigeria. Although only 5%
of neonatal tetanus cases are actually reported to health
services, the indices, the incidence of neonatal tetanus in
Nigeria ranges between 14.6 and 20 per 1,000 live births
(Onalo et al, 2011). Recent data revealed that Nigeria
contributes 16% of global neonatal tetanus. While the WHO
had planned to eliminate neonatal tetanus from Africa by
2005 (WHO/UNICEF, 2001), there has been report on the impact55

of the organization’s neonatal tetanus elimination in
Nigeria. According to Onalo et al of the department of
paediatrics, Ahmadu Bello University Teaching Hospital,
Zaria, in a research conducted on the prevalence and outcome
of neonatal tetanus in Zaria, North-western Nigeria reports
that, in the present study, traditional ovulectomy was the
suspected portal of entry in about two-thirds of cases
followed by the umbilical cord in one-tenth of the patients.
The local practice of cutting the uvula between the third
and seventh days of life as well as the unhygienic handling
of the umbilical cord may be among the factors contributing
to the persistence of neonatal tetanus in this locality and
will definitely require urgent dissuasive efforts to be
controlled. In their studies, it shows patients presented
within the first week of life had higher mortality rate than
those seen in the second and third week of life. This
outcome may be related to the relationship between the
response of the immune system and the toxin load at this age
compared to the one of older infants with more matured
immunity, in that the relativity immature immune systems of
56

newborns in the first week of life could be easily
overwhelmed by the toxin load.
Malaria is also a leading cause of infant/child death
in Nigeria. According to the National Strategic Health Plan
(2010: 28). Malaria is by far the most important cause of
morbidity and mortality in infants and young children as it
accounts to 53% of mortality. It also accounts for maternal
deaths, especially for first-time mothers. It contributes
largely to neonatal and perinatal mortality as well as
anaemia in young children, thus undermining their growth and
development. It is estimated that 50 percent of the
population has at least one episode of malaria each year,
whereas children less than age five suffer from two to four
attacks a year. In addition, malaria indirectly exacerbates
poverty by diminishing productivity and household income,
which further adversely affects child health and well-being.
Malaria has remained problematic because, like in most other
tropical countries, efforts to control malaria prior to Roll
Back Malaria (RBM) Initiative, failed to adopt and inter-
sectoral approach in considering the social and57

environmental factors sustaining disease. Victims were thus
dependent on home-based treatment and chloroquine.
Pneumonia is also a leading cause of infant mortality
in Nigeria. This has to do with Acute Respiratory Infection
which include a wide range of upper and lower respiratory
tract infections, commonly manifesting with cough, fever,
and rapid breathing. Pneumonia as another main cause of
infant and child mortality in Nigeria accounts for 20% of
mortality in infants and young children. Reports from the
1999 National Demographic Health Survey reveals that about
11 percent of infants less than three years of age had Acute
Respiratory Infections symptoms in two weeks of preceding
the survey; however, less than one-half were taken to health
facility for treatment. Although there was no urban – rural
differential in the prevalence of pneumonia, affected
children in urban areas were more likely to be taken to
health facility.
Diarrhoea is another most common cause of infant deaths
and under-five mortality as it accounts for 16% of infant
58
and child mortality (National Strategic Health Plan, 2010;
28). The World Bank (2001) reveals that Nigeria has lost 43
healthy years of life per 1,000 from diarrhoeal illnesses. A
comparison of data from the 1990 and 1999 National
Demographic Health Survey reveals appreciable improvement in
the treatment of diarrhoea by care-givers, indicating
significant progress in the past decades. The huge
investment of promoting Oral Rehydration Therapy (ORT),
embarked on in the 1980s by the government, has yielded
substantial results as depicted by an increase in the
proportion of children receiving ORT in the 1999 National
Demographic Health Survey compared with data from the 1990
NDHS. Hitherto, the response of parents and other care-
givers to diarrhoea have been to withhold fluids and foods.
The strategy employed to improve home based management of
diarrhoea placed heavy emphasis on the public education of
parents and caregivers vie commercial advertising and other
means of communication. These methods could be borrowed in
promoting other initiatives such as routine immunisation and
the use of insecticide treated nets for malaria control .
59

Measles is one of the leading causes of deaths among
young children even though a safe and effective vaccine is
available. In 2010, there were 139,300 measles deaths
globally – nearly 380 deaths every day or 15 deaths every
hour (WHO, 2010). According to UNICEF, more than 95% of
measles deaths occur in low-income countries with weak
health infrastructures. Measles is a highly contagious,
serious disease caused by a virus in the paramyxovirus
family. The measles virus normally grows in the cells that
line the back of the throat and lungs. Measles is a human
disease and not known to occur in animals. The first sign of
measles is usually a high fever, which begins about 10 to 12
days after exposure to the virus, and last for seven days. A
runny nose, a cough, red and watery eyes, and small white
spots inside the cheeks can develop in the initial stage. In
1980, before widespread vaccination, measles caused an
estimated 2.6 million deaths each year. It remains one of
the leading causes of death among young children globally,
despite the availability of safe and effective vaccination.
Severe measles is more likely among poorly nourished young
60

children, especially those with insufficient vitamin A, or
whose immune systems have been weakened by HIV/AIDS or other
diseases.
Thus from all the health factors responsible for
infant/child and maternal mortality, it can be said that
they are chiefly influenced or informed by the non health
factors which will be discussed below.
2.3.2 Non Health factors responsible for infant and
maternal mortality.
There are other factors responsible for the prevalence
of infant and maternal mortality in Nigeria that are not
directly related to health issues but determines the health
and survival of infants and mothers, these factors also to a
large extend determine the access to health care delivery,
thus, this research tend to lay more emphasis on the non-
health factors. These include:
Socio-economic factors.
61
Socio economic condition of people in society has a
strong impact on infant/child and maternal mortality. Access
to medical and health care is a class issue. While some can
afford the best centres within Nigeria, including elaborated
private hospitals; many more can only afford General
Hospitals, in fact, others can’t even afford any of the two.
Others attend the informal medical sources. These combined
sources apparently add up to 50% of Nigerian’s recorded as
accessing medical care. Many other Nigerians travel abroad
for medical care.
There are regular reports of VIPs visits to these
destinations as well as missions which are unsuccessful.
There is little doubt that overseas remains the last port
for the rich while the poor continue to anguish with
different degrees of illnesses as a result of poor health
and medical care. The deplorable condition in the health
services is due to long military usurpation of political
power and long period of mismanagement of public fund made
for the health sectors. Although, Nigeria National Health
Policy (NHP) was formulated in 1988 and revised in 2004 to62

bring about a comprehensive health care system based on
primary health care that is protective, preventive,
restorative and rehabilitative to every citizen of the
country within the available resources so that individuals
and communities are assured of social well-being and
enjoyment of living.
Despite this, health system in Nigeria still boils down
with chronic problems, such as inappropriate budgetary
allocation, poor infrastructure in the public health
facilities, lack of drugs, uneven distribution of health
facilities and lack of qualified medical personnel. This has
resulted in the increase in the use of private health
facilities which made the private sector provides 65.7
percent of health care delivery in Nigeria (UNICEF, 2001).
Presently, continued economic difficulties in Nigeria
have undermined the public health system with the
introduction of payment schemes based on selling of
essential drugs. This is one of the main reason of the
Bamako Initiative, according to which the income generated
63

would ensure reliable supply of drugs and would improve
other aspects of the quality of the services rendered. Thus,
quality improvements would compensate for the financial
barrier and as a result the utilization of public health
services would be increased or at least maintained. But
this, has led to the rise in the ‘informal’ private sector
like the traditional medicine healers, itinerant drug
peddlers and hawkers, mixed-trade dispensers, unlicensed
patent medicine dealers and injection doctors.
This sector, offer very low quality treatment
(treatment without laboratory diagnosis, making wrong
diagnosis, sale of drugs with little regard for dosage or
treatment regimen and the use of fake and expired drugs), it
is a more important source of disease treatment and
prevention for the poor. The frequent media advertisement of
traditional medicine healers, who openly challenge the
utility of western medicine, makes them very popular,
especially among the poor. Also, doctors in public services
are allowed to operate private clinics. Some of these
facilities are below standard (unregistered, poorly64

equipped, lack of diagnostic facilities, dirty premises,
employing auxiliaries to work as registered nurses,
dispensing medicines and irrational prescription).
In plateau state for example, the government set up a
committee recently to weed out unqualified and unregistered
private medical institutions in the state, this committee
has been able to identify and close down no fewer than 40
private health care centres. Most of these health facilities
are death traps for the poor who patronize them.
There is a synergic interrelationship between poverty,
poor health, malnutrition, and reduced child and maternal
survival, which is worsened by social exclusion and
political marginalization. A child born to a financially
deprive family is at risk of dying perinatally or within the
first month of life, since the mother was probably poorly
nourished during pregnancy, had little or no ante natal
care, and is unlikely to have delivered at health facility.
On surviving the first month of life, the child is been
exposed to increased risks of illnesses, such as malaria and
65

diarrhoea, due to poor living conditions, limited access to
safe water and inadequate sanitation, malnutrition from
household food, insecurity, or ignorance about good child
feeding practices.
Large family size (ignorance of and lack of access to
family planning) puts pressure on the mother to work in
order to provide for the family, thus leaving the child
quite possibly inadequately cared for. All these factors are
further aggravated by limited access to health services due
to poor income and low level of maternal education, often
leading to no-immunization of the child. Recent estimates
place about 70 percent of Nigerian population below the
poverty line (UNDP, 2001). It also shows that persons
earning less than 1$ a day were 9 percent less likely to use
insecticide treated nets, less able to perceive malaria as a
preventable disease, and less likely to have adequate
sanitation (refuse disposal).
66

Educational factors.
Women’s education has been reported as a key factor in
reducing infant/child and maternal mortality. The higher a
woman’s level of education, the more likely it is that she
will marry later, play a greater role in decision making,
and exercise her reproductive rights. Her children will tend
to be better nourished and enjoy better health. Data from
both the 1999 NDHS and the 1999 MICS reveal that lower
education levels among females was related to higher infant
and under-five mortality.
Both surveys highlighted female illiteracy and under-
five mortality being twice as high in the northern zones
than in the south. Similarly, rural areas had lower levels
of female literacy and consequently higher under-five
mortality than the urban areas.
The relationship between female literacy and child
survival is also clearly demonstrated when looking at
immunization coverage rates and treatment of diarrhoeal
illnesses. Timely and appropriate use of Oral Rehydration
67

Therapy (ORT) in the treatment of diarrhoeal illnesses (the
second main cause of under-five mortality after malaria)
reduces mortality outcomes. The 1999 NDHS reports that the
proportion of caregivers that use ORT progressively rises
with levels of education.
The same survey data also show that the proportion of
children not immunized at all decreases from 60 percent
among illiterate mothers to 24 percent among mothers with
primary education, before dropping to 10 percent among
mothers with secondary education. Some scholars have argued
that education is the most influenced factor in
differentiating infant and maternal mortality levels within
all other factors. Mother’s education seems to be directly
related with the health of a child. There is no doubt that
an educated mother can provide better care of child than a
mother with no education or lower level of education.
Education makes a mother socially advanced, free from
traditional values and changes her pattern of behaving and
attitude. Caldwell (1976) argued that other things being
equal, children of educated mothers experienced lower68

mortality than the children of uneducated mothers. Of course
educational attainment of parents or mother to be precise
may determine the kind of occupation she does. Mother’s
occupation is also associated with nutritional status of her
child(ren) and also her nutritional status during pregnancy
and after delivery.
Other than the intrinsic importance of education and
its important role in economic growth, a causal link has
been established between education and range of health
outcomes. One of the most consistent and powerful findings
in public health is strong association between mother’s
education and child mortality. Results of previous studies
have shown that a 1-year increment in the mother’s education
7-9% reduction in mortality in children younger than five
years and that child mortality rates among mothers with at
least 7 years of schooling were 58% lower than among those
without any education (Cleland and Ginneken, 1988).
In the past 30 years, many hypothesis have been
proposed for the mechanisms through which increased
69
education could lead to reduction in child mortality rates,
including individual level effects through improved use of
health services, economic advantages, empowerment and
independence of women, and community-level affect. Increased
in educational attainment are also strongly linked to
reduction in fertility, which contributes to reduced child
and maternal mortality rates (ibid). The commission on
Social Determinants of Health reinforced the importance
increasing educational attainment to reduce disparities in
health.
Environmental factors.
Globally the number of deaths among under five has
reduced from 12.4 million in 1990 to 8.1 million in 2009
(UNICEF, 2010) majorly due to interventions targeted at
communicable diseases such as malaria, measles, diarrhoea,
respiratory infections and other immunizable childhood
infections which have been major causes of child mortality.
However, these health gains were short lived especially in
70

Africa because disease oriented vertical program alone were
not effective (Mutunga, 2007).
Environmental, maternal and socio-economic factors were
acknowledged as additional important determinants of child
survival (Espo, 2002). Child mortality rates still remain
unacceptably high in sub-Saharan Africa despite the region
having only one fifth of the world’s children population
(Smith, 2010). For instance, in sub-Saharan Africa, 1 child
in 8 dies before age five – nearly 20 times the average of 1
in 167 in developed parts of the world (Ojikutu, 2008).
Similarly, UNICEF (2010) in the state of the world’s
children report noted that 8.1 million children across the
world who died in 2009 before their fifth birthday lived in
developing and died from disease or a combination of disease
that could easily have been prevented or treated.
It also noted that, half of these deaths occurred in
just five countries namely, India, Nigeria, the Democratic
Republic of Congo, Pakistan and China with India and Nigeria
both accounting for one third of the total number of under
71

five deaths worldwide. The report describes the declining
rate as disturbing and grossly insufficient to achieve the
MDG gaol by 2015 as only 9 out of the 64 countries with high
mortality rate are on track to meet the MDG goal. Though,
common causes of child mortality and morbidity include
diarrhoea, malaria, measles, and acute respiratory
infections, studies have shown that in Nigeria, many
children die mainly from malaria, diarrhoea, whooping cough,
tuberculosis and bronchopneumonia (Ogunlesi, 1961; Baxter-
Grillo & Leshi, 1964; Morley, 1973; Animashaun, 1977; Ayeni,
1980). Ogunjuyigbe (2004) viewed morbidity and mortality of
the child to be influenced by the underlying factors of both
biological and socio-economic that operates through
proximate determinants.
Jinadu et al. (1991), in a study, found dirty feeding
bottles and utensils, inadequate disposal of household
refuse and poor storage of drinking water to be
significantly related to the high incidence of diarrhoea.
Although, several studies by health actuaries exists on
child mortality, evidence on why the rates is still high in72
Nigeria in spite of various action plans and interventions
made remain sparse. Possibly, the cause of disease and death
over which not much controversies and uncertainties exists
is the total environment of man (Adeyemi et al. 2008).
Malaria, acute respiratory infections, measles, and
diarrhoea which are today major causes of mortality for
children under five are consequence of the built environment
of man. In developing countries like Nigeria, one in eight
children does not live to see their birthday due to
avoidable environmental threats, resulting into
approximately 11 million avoidable childhood deaths yearly
(WRI, 1999; World Bank, 2004).
According to World Bank (2001) in a recent study,
environmental risk factors were estimated to account for
about one-fifth of the total burden of disease in low income
countries. The WHO (2002) similarly, reported in Mutunga
(2007) that among the ten identified leading mortality risks
in high mortality developing countries, unsafe water,
sanitation and hygiene ranked second while smoke from solid
73

fuels ranked fourth. About 3% (1.7 million) of the resulting
deaths are attributable to environmental risk factors and
child deaths account for about 90% of the total. The
environmental burden of disease as noted by Listorti and
Douman (2001), in Adeyemi et al. (2008) was highest in sub-
Saharan Africa with 26.5% while the average for all less
developed countries was 18%.
Environmental health risks are broadly categorized into
two (Shyamsundar, 2002). The first are the traditional
hazard related to poverty and lack of development, such as
waste disposal, vector borne diseases, inadequate
sanitation, air pollution (indoor) and lack of safe water
while the second emanated from the modern hazards such as
rural air pollution and exposure to agro industrial chemical
and wastes, caused by development that lacks environmental
safeguards.
Many of the diseases that lead to increased morbidity
and mortality of children under five and their mothers are
largely related to the unavailability of safe water,
74

unhygienic behaviours, poor sanitary facilities, and poor
housing conditions. Acute Respiratory Infection (ARI), a
major killer of children under five, along with Vaccine
Preventable Diseases (VPD) such as measles, diphtheria, and
tuberculosis, are easily spread in poor overcrowded houses.
Also, increased prevalence of diarrhoeal disease, cholera,
and typhoid is seen in situations of unsanitary refuse,
excreta disposal, and use of unsafe drinking water. In
addition, inadequate drainage and accumulated waste water
encourage breeding of mosquitoes with increased malaria
attacks (the single most significant cause of death among
children). The 1999 MICS reports that 54 percent of the
population in Nigeria had access to safe drinking water (71%
and 48% in urban and rural areas, respectively). The
southeast is the worst hit region; only 39 percent of the
population get their drinking water from safe sources. Just
over one-half (53%) of the population live in households
with a sanitary means of excreta disposal (1999 MICS), a
situation which varies from 40 percent in the northeast to
75
58 percent in the southwest, and from 44 percent in rural
areas to 75 percent in urban areas.
A comparison of data from the 1990 and 1999 NDHS shows
improvement in access to safe water, the proportion of the
population collecting water from surface sources declined
from 52 to 38 percent, while the proportion of obtaining
water from ground sources such as boreholes and wells rose
from 35 to 44 percent between the two surveys. Poor access
to safe drinking water encourages the spread of certain
vector-borne illnesses: onchocerciasis (river blindness) and
dracunlliasis (guinea worm), which are transmitted by
vectors associated with water, causing more debilitating
illnesses than those listed above. In the 1990s, remarkable
progress was made in reducing guinea worm cases from 394,082
in 1990 to 13,237 in 1999, representing a 97 percent
reduction from efforts of the Nigeria Guinea Worm
Eradication Programme (NIGEP).
In 1999, only about eight states were reporting
significant numbers of cases. Poor coverage for water supply
76
and sanitation is linked with insufficient funding of
operations and maintenance, lack of capital to complete and
initiate water projects, and inadequacy of skilled labour
and management capacity. Compounding the lack of safe water
in the lack of awareness of the health consequences of
unhygienic behaviours, such as defecating and urinating in
bushes outside houses, poor refuse disposal, and infrequent
hand washing. Another problem is the use of the same water
source for bathing, washing, and feeding cattle.
Faced with this environmental health threats, and
coupled with the world desire to reduce child and maternal
mortality worldwide as reflected in the MDG, understanding
the factors responsible for high incidence of mortality is
expedient and prudent.
2.4 THEORETICAL FRAMEWORK
Health is a cherished but often misunderstood concept.
In health discourse in Nigeria the primary concern is often
about hospitals and drugs and rarely about the conditions
which make drugs and hospitals necessary. The Medical and
77

Materialist perspective of health are two contending
paradigms which address these issues and what can be done
about them.
2.4.1 Medical Perspective
Much of what contemporary populations think about
health and illness, and much of the focus of research –
including sociological research – is strongly influenced by
the prevailing medical model. In public debate, the medical
approach remains central.
It is said that the medical perspective of health is a
negative one: that is, that health is essentially the
absence of disease. Despite bold attempts by bodies such as
the World Health Organization (WHO) to argue for a
definition of health as ‘a state of complete physical,
mental and social well-being, and not merely the absence of
disease or infirmity’, most medically related thought
remains concerned the disease and illness. This is hardly
surprising, given the fact that people turn to medicine in
times of trouble, not when they are feeling well. It has
78

also been found that promotion of positive health, whether
by doctors or ‘health promoters’, competes with other valued
goals, for individuals and for societies as a whole. Matters
become even more complicated when it is realized that the
presence of ‘disease or infirmity’ does not, in any event,
mean that people always regard themselves as unhealthy. The
phrase ‘complete well-being’ remains elusive as it is
positive, and health, illness and medicine are related in
complex ways. The medical model of health, though often
charged with ‘reductionism’, at least has the attraction of
cutting through some of these knots.
As historians such as the late Roy Porter (2002a) have
pointed out, the medical perspective, as we now know it,
took on its main characteristics in the eighteenth and
nineteenth centuries. Prior to this date most medicine in
Western countries was committed to observation and the
exhaustive classification of symptoms. Although this
attachment to observation and entailed a rejection of
existing authorities (represented especially in Galen’s
writings) and was linked to reformist view of science and79

society, developments were not straightforward. For many
physicians in the seventeenth and eighteenth centuries,
emerging views concerning the nature of disease were
anathema. Physiology in French and chemistry in Germany were
bringing the laboratory sciences to bear on human health and
disease, and many thought this undermined the doctor’s
traditional role at the patient’s bedside. However, during
the nineteenth century, the development of bacteriology and
anatomy marked a major change in both thought and practice.
Doctors now claimed exclusive jurisdiction over health
and illness, the warrant of medical model of disease as
their support. This situation meant that modern citizens
were increasingly encouraged to see their health as an
individual matter, and their health problems as in need of
attention of a doctor. It is this Foucault (1973) saw as
constituting the ‘medical gaze’ which focused on individual
and on processes on inside the body – its ‘volumes and
spaces’.
80

This ‘gaze’ (extended in due course to health-related
behaviours) underpinned the development of the modern
‘doctor-patient’ relationship, in which all authority over
health matters was seen to reside in the doctors’ expertise
and skill, especially as show in diagnosis. This meant that
the patient’s view of illness and alternative approaches to
health were excluded from serious consideration. Indeed, the
patient’s view was seen as contaminating the diagnostic
process, and it was better if the patient occupied a passive
role. It is for this reason that the ‘medical model’ of
disease has been regarded critically in many sociological
accounts.
Health is frequently conceived as a medical issue and
reduced to provision of medical care. This paradigm comes
from development of bacteriology, especially the work of
Louis Pasteur with anthrax and cholera. The medical model
conceives health as a biophysical malfunctioning which
disrupts the body’s equilibrium. Such malfunctioning is
caused by germs and other bacteria (Rossdale, 1965; Turshen,
81

1977a; McKeown, 1979). The model has a machinelike image of
the human body and,
In terms of both diagnostics and therapy, the bodywas considered to be analogue to the machine thusallowing for instrumentalist approach to the body.Individual parts could be examined and treatedwithout the rest of the body being affected(Berliner, 1975:576).
In accordance with this conception, specializations in
medicine (such as ophthalmology, urology, Ear, Nose and
Throat, etc) began to concentrate on individual systems and
organs to the exclusion of the rest of the body (Navarro,
1980; Powles, 1973).
This conception of health was further reinforced by
restructuring of the medical education in the USA and Canada
about 1910-1915 (Brown 1979; Starr 1982) which stipulated
training in the laboratory based on sciences to be followed
by supervised clinical tutelage of unspecific content and
duration. The utility of medical practice was then limited
as the capacity to cause harm and heal were equal (Brown
1979; Starr 1982). Heroic medicine, as it was then called,
used procedures like purging, blistering and bleeding with
82

an instrument called the lancet. It is not accident that the
oldest and most respected medical journal in the world took
that name. This restructuring of medical curriculum
radically changed the situation which turned medicine from
craft to the profession of high status and income (Alubo,
2010). It pushed medicine beyond the poor both in terms of
opportunity for medical education and access to doctors’
services. This is the brand of medical training that was
imported into Nigeria and other developing countries. As
Alubo (2010) noted, that the internalization of the
curriculum has contributed to the respect for Nigerian
trained doctors but has also facilitated the brain drain.
It must be noted that continued reference to
Hippocrates as the intellectual; ancestor of modern medicine
(there is for example the Hippocratic Oath) is, in some
sense, contradictory. This is because the current
individualistic-mechanic conception is different from
Hippocrates’ who viewed health as a relationship between the
individual and the environment, including the political
economic (Alubo, 2010). According to Hippocrates:83

Health means a healthy mind in a health body andcan be achieved only by governing daily life inaccordance with natural laws which ensures anequilibrium between the forces of the organism andthose of the environment (Dubos 1965:323).
Through the medical conception, health care has become
equated with medical care and policies have stressed the
intensification of curative medical services (Alubo 1985a,
Erinosho, 1982). Other aspects of health such as preventive
and rehabilitative dimensions are ignored. Politicians are
comfortable with medical perspective and the policy thrust
has revolved around the following initiatives:
1. The training of more personnel to achieve a better
practitioner-patient ration. Nigeria’s various
governments have been proud of increases in both the
ratio and absolutely number of various cadres of
personnel trained.
2. Building of more clinics, hospitals and treating
centres and expanding existing ones. Even a situation
where existing facilities are in crisis and most have
atrophied, new ones are being built.
84
3. Procurement and better distribution of drugs equipments
and other materials (Federal Government’s in Nigeria
1981, 2005).
This conception of health neatly fits modernization
path to health care development especially that it creates
markets for drugs and equipment manufacturers.
The modernization path appears to be a universal
phenomenon in underdeveloped countries as:
The poorer... countries have tended to copy bothphilosophy and development priorities of thedeveloped world, even though problems andpopulation structures are different. In followingthe health delivery trends of the technologicallysophisticated societies, African countries have sofar failed to make their health system effective,let alone efficient. Clearly, the system does notfit the population (Mburu 1981:17).
There are hardly questions about the impact of this
perspective on health problems. At issue is how medical care
can solve problem whose root causes are political and
economic. The common diseases in Nigeria are nutritional
such as kwashiorkor and marasmus; parasitic like malaria and
water borne such as cholera and guinea worm, all of these
85

diseases have accounted to the high prevalence of infant and
maternal mortality in Nigeria. How can cure to these
conditions be achieved without attending to the root causes?
Better understanding of the root causes of these illnesses
which has to do with environment and health care in general
need to be given attention. These are the factors that
causes the high rate of mortality in any given society
especially Nigeria and most especially among
infants/children and nursing mothers, hence, attention
should be given to health care delivery instead of medical
care.
Equally important is the distinction between cure and
care, there is a huge imbalance in health investment in
favour of cure. This is a deliberate ideological strategy
for as Navarro and others (Kelman 1972, Turshen 1999) long
argued, reducing problems of political and economic origins
to medical problems of political and economic origins to
medical problems serves an important legitimacy function for
the capitalist system:- makes people believe that structural
problems can be resolved through the individualist86

approaches of modern medicine. It diverts attention from
poverty and deprivation, the resolution of which will pose
threats to the accumulation process. This is because,
By situating the diagnosis and treatment ofdiagnosis and treatment of disease at the level ofthe individual, (medicine) provided the rulingclass with a means of social control: patientswould fail to make common cause with each other orto protest the external, underlying conditionsthat make them ill. The effect is to depoliticizemalnutrition, alcoholism, drug addiction andmental illness defining them as medical problems(Turshen 1977:57)
Furthermore, there is a trained class bias in medicine
which also reflects and reinforces the system. Curative
medicine is only useful to the affluent and others whose
basic needs are guaranteed. Under such circumstances, the
medical magic unveiled. But for the majority of the people
whose material condition of existence are not secure,
medicine serves little purpose. Indeed as Versayer, a
Russian writer and physician, once noted “medicine is the
science of dealing with the treatment of the rich only. In
relation to everybody else, it is merely a theoretical
science dealing with how they would be cured if they were
87

rich” (quoted in Navarro 1977:19). It is therefore correct
that the medical conception of disease and treatment
“meet(s) the health needs of the bourgeoisie, not the entire
population” (Navarro 1977:46). Thus from the above, it is
visible that medical care hardly benefits the poor, this is
because medical care lay more emphasis on the building of
hospitals, only the rich can afford to pay for the services
in the hospitals. But if government attention is centred on
the provision of health care facilities such as potable
drinking water, good sanitary environment and improve the
living standard of the poor, the y won’t need to visit the
medical facilities frequently as there won’t be any or
minimal cause of falling ill from preventable diseases
The medical paradigm remains the guiding principle of
health which has informed Nigeria’s health care policy and
practice. There are regular references to health care
delivery, as if, in the words of Aron Wildavsky, “the
welcome wagon was supposed to roll up to the door and
deliver health wrapped in a neat package” (Wildavsky
1977:112). In the illusionary pursuit of health care88

delivery over 80 percent of health budgets has consistently
gone into curative medicine (Alubo 1985a). Whether such huge
investments yielded the desired outcome is immaterial –
perhaps because of the under the table payment which
accompany the investments in contracts for hospital
construction and supply for drug equipment.
Thus from the medical approach to health, it can be seen
that more emphasis is been laid on the provision of medical
health care (which is curative in nature) instead of health
care delivery (which is preventive in nature). This makes
government forget the root causes or the major factors
responsible for illness and rather pay more attention on
curing these illnesses that should have preventable. All
factors responsible for infant and maternal mortality in
Nigeria have been proven to have a direct link with the
environmental or and living standard of the society, but
government have decided to concentrate its energy and
resources on the building of medical centres such as
hospitals and the training of doctors, nurses etc to attend
89

to infant maternal related issues instead of providing the
basic necessities for the prevention of such diseases.
2.4.2 The Materialist Perspective.
The materialist perspective of health care is anchored on
this fundamental assumption: health is part and parcel of
society within which individual lives, has a being;
reproduces him/her self and relates to other human beings in
these processes health is experimental and holistic, rather
than being a commodity which can be bought and sold.
From the outset, the focus is holistic, total and
socio-political rather than mechanistic, individualistic or
biophysical. According to Sander Kelman (1977:8), the
materialist conception of health:
Begin(s) with the axiom that human beings are thebasis of both forces of production (physicalingredients of production , such as labour,resources and equipment) and the relations ofproduction (division of labour, legal property andsocial institution and practices) in any societyand therefore appropriate human organismicconditions (i.e. ‘health’) can only be understoodin the correct text of the particular mode oforganization of production and the dialectical
90

relationship between the productive forces andrelations (quoted in Alubo, 2010:13)
So conceived, health is inseparable from the political
condition under which people live, meet (or fail to meet)
their daily needs and reproduces life (Turshen 1977a;
Navarro 1976). Nor is health separable from such processes
as the rate of capital and profit accumulation,
privatization and deregulation, and other super structural
aspects of materialist basis in which the individual has
relative control over his/her existence in a purposeful and
meaningful way, devoid of overarching structures of
oppression, alienated and exploitation. Such existence must,
at the same time, be conducive to material and spiritual
wellbeing.
For this material conception, bio-physical malfunctions
are important not in their own rights, but for the politic-
economic contradictions they symptomatize. Kwashiorkor, for
instance, is only the bio-physical manifestation of the
contradictions in the same social relations of production
which cannot guarantee adequate nutrition. Similarly, worm
91
related infections and water-borne conditions are not really
the disease. The real problem is the nature of the society
and individual’s location within it. The diseases arises
from the political economy of reward structure which
benefits some while placing others at a disadvantage. Those
place at a disadvantage are left at the mercy of the rich,
hence making them more prone to high risk of mortality.
The materialistic conception of health is not new, it
is only long ignored (Alubo 2010). As far back as the 12th
century, long before the discovery of bacteria and its
derivation, the germ theory, the relationship between low
socio-economic status and low life expectancy for all
courses was observed (Syme and Berkman 1981:35).
Furthermore, Karl Marx and Friedreich Engels, jointly and
individually discussed how poor material conditions
predisposed people to disease in works like the Communist
Manifesto and the Conditions of the Working class in
England. Because of the obvious ideological implications,
this conception has remained ignored. An illustration of the
material interpretation provides the explanations not only92

for susceptibility to disease but to individuals’ responses.
The last point is starkly brought home in Earl Koos’ classic
book, The Health Regionville, which is a community reaction
to sickness and illness. Koos quoted a woman as saying ‘how
I wished I knew what you mean about being sick. She said she
sometimes felt she would curl up and die but cannot afford
the luxury to be sick because there was no money for the
doctor’ (quoted in Alubo, 2010). Her experience is shared by
many much as the women making akara by the street corner,
the motorcycle, taxi operators and many more who live from
hand to mouth. So being sick is itself a luxury that cannot
be afford, as members of the underclass drag themselves
until they are at the point of dropping dead.
Class and class relations bear on who becomes sick and
types of sickness: diabetes and gout are found more among
the middle and upper classes, just as kwashiorkor and
stunting are common among lower classes. Even malaria has a
class character because the mosquito vector is egalitarian
in biting the rich and the poor but the latter succumb more
93

frequently to malaria (Alubo 2010). Class or socio economic
status also determines access to available care.
This perspective shows the power play in the access to
health care. According to the Strengthening Health System
document “children and infants among the poorest 20% of the
population are about three times more likely to die than
among the riches 20%. The disparity is even greater for
under 5 mortality where the mortality is 87 per 1,000 among
the wealthiest population and staggering 219 per 1,000 among
the poorest” (Federal Ministry of Health, 2009:1). The
situation is blamed on the increasing poverty and weakness
of the ‘health care system’. It is here observed that what
is described as the health care system is essentially the
various levels of medical care system (Alubo, 2012). Most of
the causes of deaths and serious illnesses, which occur
among Nigerians, can be treated with simple remedies...
communicable disease are... often compounded by malnutrition
(Health Policy, 2006). Thus, this shows the power play
between the upper class even in terms of who get ill and
what kind of illness.94

Access of health care or medical care as the case may
be is now determined by the ability to pay and where various
Nigerians fit in the stratification order. The situation
speaks to the nature of wealth, power and privileges in
modern Nigeria where the structures created these processes
have replaced cordon sanitaire (the philosophy of physical
separation of colonialist from natives as a way of guarding
against possible spread of disease from the latter) of the
colonial period (Alubo, 2010). The materialistic conception
of health is about how people live, what facilities they
have and what essentials they are denied. This to a large
extent also determine who gets ill and who does not.
The materialistic conception classically explain the
dire situation of infant and maternal mortality in Nigeria,
as many researchers have shown that infant and maternal
mortality is high among the lower class (poor) than among
the upper class (rich), this is largely because they (the
rich) have more access to both medical and health care
services than the poor who barely have enough to afford
95

three square meal a day, not to talk of affording a balance
diet.
CHAPTER THREE
RESEARCH METHODOLOGY
96

3.1 INTRODUCTION
This chapter highlights how the researcher intends to
conduct the study by gathering necessary and valid data that
can be tasted and replicated. It specifies the method to be
used and way they are used in the study. Point of focus in
this chapter may include the method of data collection and
analysis, how the data will be analyzed and the instrument
that was employed and use in the study analysis. Finally,
these procedures will enable the researcher to make a fairly
convenient study from which readers can be assured of
reliability and validity.
3.2 METHOD OF DATA COLLECTION
The method of data collection used in this study is the
survey method. This is because of its explicit rules and
procedures in gathering information about a large
population. The primary source of data collection was use to
generate data from the study. The primary source of
collecting data involve a response from the respondents.
Questionnaires will be design especially for women and
97

health workers in a structured form, this is due to its
relative advantage in terms of time utilization, cost
involved in the gathering of information and its
reliability.
The questionnaire will consists of two parts. Part “A”
will consist of the socio-demographic characteristics or
bio-data of the respondents. Part “B” will consist of
questions that will be administered – the questionnaire is
structured in an open and close ended manner. An open ended
questions enable the respondents to give their own view
without options while in the close ended, options will be
given to the respondents to choose from them. It is believed
that responses from both women (who are/were mothers) and
health workers would guarantee effective representation of
their experiences and views on the research topic, journals
and textbooks will form part of the study as secondary
source of data.
3.3 POPULATION AND SAMPLING
98

According to Ibanga, (2006.11), a researcher would love
to study all cases he is confronted with in a given research
situation. However, certain constraints usually make such
design not more than a wish. In other words, it is quite
difficult to study every case in the population, thus, there
is the need for a researcher to use smaller proportion of
the population. For this research work however, the sample
size that will be use is two hundred (200) women or
respondents. Two hundred questionnaires will be administered
to respondents living within Jos metropolis. The
questionnaire will be administered in some of the private
hospitals within the area understudy. Private clinics and
hospitals will be used due to the fact that all the Primary
Health Care (PHC) centres in the state have been on strike
for a long time, thus have not been functioning. The
distribution of the questionnaires will be made during ante
natal days in those hospitals. The parts that will be
covered will include Tudun Wada, Angwan Rukuba, Nasarawa
Gwong, Jenta and other places. The respondents will cut
across the group comprising of the Hausa, Berom, Igbo,
99

Yoruba, Anagutas, among others. Their level of education and
age will also be considered in this research work. Random
sampling will be used for this purpose.
3.4 METHODS OF DATA ANALYSIS
The method that will be used in this research work will
be the statistical and arithmetic method. The use of simple
percentage will be used to calculate data and findings of
the research. Data will be assumed as the basis for making
deduction and reaching conclusions on one hand. Data on the
other hand will be referred to as actual figures or a body
of figures.
Statistical data are frequently arranged and presented
in form of tables to enable the reader have a good grasp of
the information which the researcher intends to convey with
a minimal effort.
Tabulation is the process of transferring data from
data gathering instruments to a tabular form. This makes it
possible to be systematically examined. Tabulations of data
also forms basis for reducing and simplifying the details
100
given in a mass data. It is for the above reason that the
tabulation method of data analysis shall be adopted in this
study.
3.5 PROBLEMS OF DATA COLLECTION
The researcher might encounter some problems during the
field work despite the benefits derived from adopting these
methods. The most prevailing among the problems that might
be encountered will be that of secrecy of the respondents.
Most of the respondents might feel that issues concerning
the death of children and their mothers should be kept
secret as any attempt to raise it up again may raise
emotions, most of the respondents may find it difficult in
providing information on infant/child and maternal mortality
especially those that concern them directly or indirectly,
this might made most of the respondents to hide some of the
important information required. Another problem that might
be encountered will be getting the attention of some of the
respondents who might perceived this process as time
consuming against their own activities as the questionnaires
101

will be administered during ante natal days in the hospitals
or health care centres as the case may be.
102
CHAPTER FOUR
DATA PRESENTATION AND ANALYSIS
4.1 INTRODUCTION
This chapter is mainly concerned with the presentation,
analysis and interpretation of research findings. This
chapter is designed in such a way that the presentation,
interpretation and analysis are guided by the research
problem and the objectives of the study.
Two hundred (200) questionnaires were administered
within the area coverage of the study, however, one hundred
and eighty four (184) questionnaires were filled and
returned, 84 of the other questionnaires were misplaced,
this was because the researcher distributed the
questionnaires in private health care centres during ante
natal, and some of the women forgot and left with the
questionnaires given to them. Therefore, the data
presentation, analysis and interpretation will be done base
103

on the number of questionnaires that were filled and
retrieved.
The responses from the questionnaires have been
tabulated showing the frequencies and percentage analysis.
The questionnaire is divided into two sections: Section ‘A’
is the bio data or socio-demographic characteristics of the
respondents, which is on the basis of age, education,
occupation monthly income, number of children, years of
marriage, age at which the respondents got married and the
number of children lost during or after delivery if any.
Section ‘B’ deals with the analysis of health care delivery
and the prevalence of infant and maternal mortality as
presented in the following tables.
4.2 PERSONAL DATA OF THE RESPONDENTS.
Table 4.1: Distribution Respondents by Age
Age in Years Frequency Percentage (%)18 – 24 35 1925 – 30 68 3731 – 35 44 2436 – 40 26 1440 – above 11 6Total 184 100Source: Field survey
104

Table 4.1: represents the distribution of respondents
by age. From the table above, it can be seen that most of
the respondents lies between age 25 – 30, with 37% of the
respondents (68) being within that range, this if followed
by those between age 31 – 35, accounting to 24% of the total
respondents. Others include those within the age range of 18
– 24, which are 35 and accounts to 19% of the total
respondents, those within the age range of 36 – 40 accounts
to 14% of the total respondents, and finally those within
the age range of 41 – above accounts to only 6% of the
total respondents. Thus, from the table, it can be seen that
a large percent of the total respondents and within child
bearing age.
Table 4.2: Distribution of Respondents by EducationalAttainment
Education Frequency Percentage (%)Primary 15 8Secondary 80 44Tertiary 85 46Non 4 2Total 184 100Source: Field survey
105
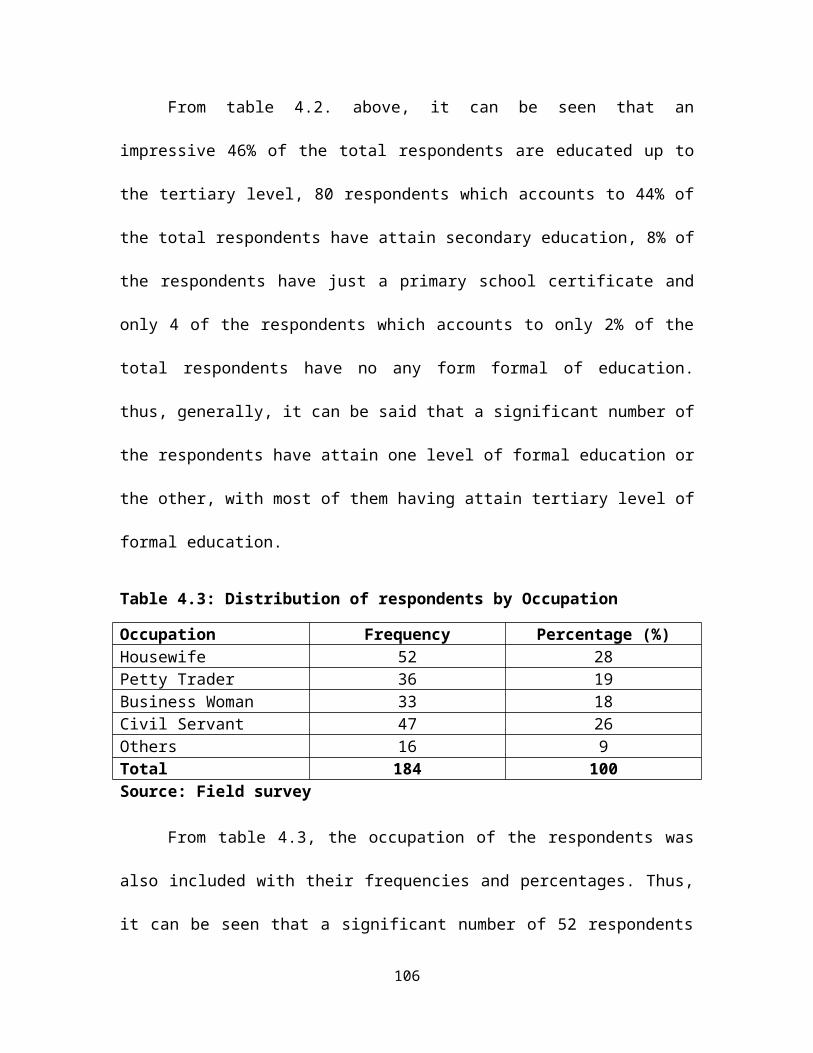
From table 4.2. above, it can be seen that an
impressive 46% of the total respondents are educated up to
the tertiary level, 80 respondents which accounts to 44% of
the total respondents have attain secondary education, 8% of
the respondents have just a primary school certificate and
only 4 of the respondents which accounts to only 2% of the
total respondents have no any form formal of education.
thus, generally, it can be said that a significant number of
the respondents have attain one level of formal education or
the other, with most of them having attain tertiary level of
formal education.
Table 4.3: Distribution of respondents by Occupation
Occupation Frequency Percentage (%)Housewife 52 28Petty Trader 36 19Business Woman 33 18Civil Servant 47 26Others 16 9Total 184 100Source: Field survey
From table 4.3, the occupation of the respondents was
also included with their frequencies and percentages. Thus,
it can be seen that a significant number of 52 respondents
106

which accounts to 28% are housewives, 47 respondents (26%)
are civil servants, 19% of the total respondents are petty
traders, 18% of the respondents are business women, while 16
respondents which accounts to 9% engage in other activities
for livelihood. However, despite the fact that an impressive
number of women (26%) from the above table are civil
servants, many more lies within the category of those who
are housewives (28%), business women (18%), and petty
traders ( 19%) who engage in petty trade to feed on in their
homes.
Table 4.4: Distribution of Respondents by Monthly Income
Income (N) Frequency Percentage (%)5,000 – 10,000 80 4411,000 – 20,000 48 2621,000 – 35,000 28 1536,000 – 50,000 15 850,000 – above 13 7Total 184 100Source: Field survey
107

Table 4.4 above shows the distribution of respondents
base on monthly income. It can be seen from the above table
that majority of the respondents (80) which accounts to 44%
of the total respondents earns a monthly income between
N5,000 – N10,000, this is largely due to the fact that most
of the respondents are either housewives or petty traders,
48 of the respondents which accounts to 26% of the total
respondents earns a monthly income ranging between N11,000 –
N20,000, 15% of the respondents earns a monthly income
between N21,000 – N35,000, 8% earns a monthly income of
between N36,000 – N50,000, and only a few 13 respondents
which accounts to 7% of the total respondents earns a
monthly income of between N51,000 – above. Thus, this
largely explains the poor socio-economic status of women
which to a large extend determines the prevalence of infant
and maternal mortality.
Table 4.5: Distribution of Respondents by Number of Children
Number of Children Frequency Percentage (%)1 – 3 86 444 – 6 66 36None 32 17Total 184 100
108

Source: Field survey
Table 4.5: shows the distribution of respondents by
number of children. Thus, it can be seen from the table
above that 47% of the total respondents have a number of
children that ranges between 1 – 3, this is due to the fact
that most of the respondents are at their early child
bearing, 66 of the respondents accounting to 36% of the
total respondents have a number of children ranging from 4 –
6, none of the respondents have children more than 6
children, and finally, 32 respondents which accounts to 17%
did not have any child or are yet to have children, probably
because they just had their first pregnancy and have not
delivered yet or have lost their child(ren).
Table 4.6: Distribution of Respondents by Years of Marriage
Years of Marriage Frequency Percentage (%)1 – 5 87 476 – 10 65 3511 – 15 20 1116 – above 12 7Total 184 100Source: Field survey
109
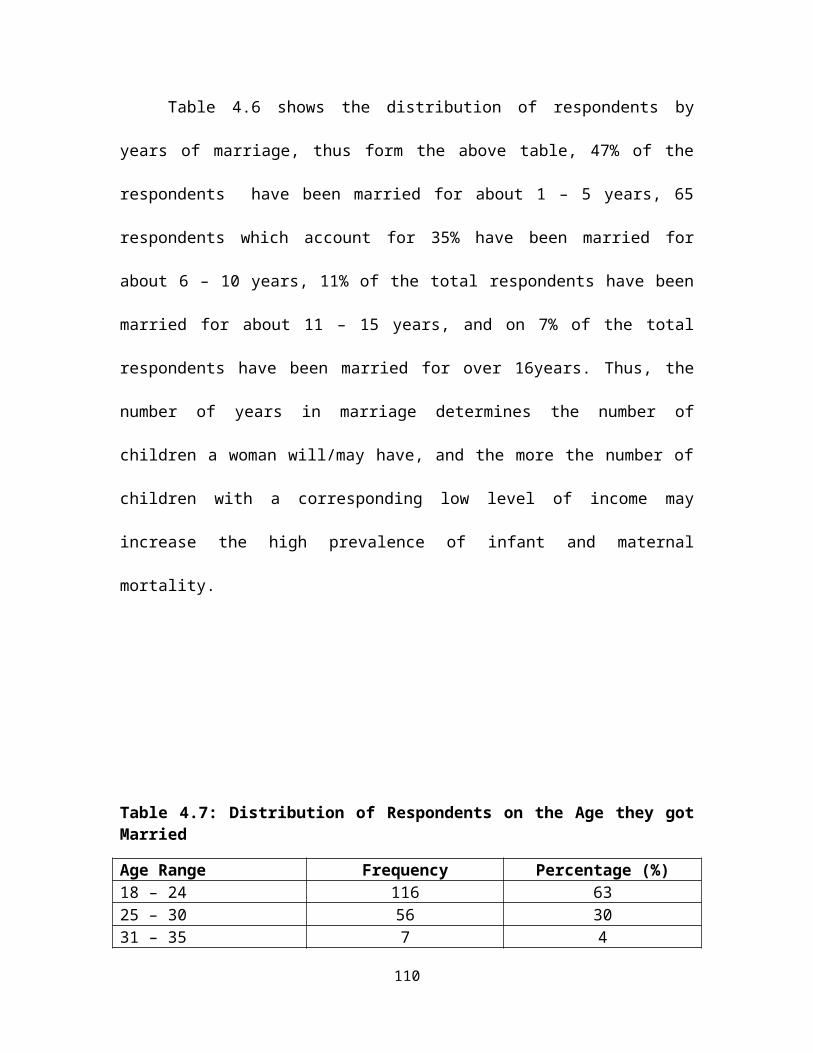
Table 4.6 shows the distribution of respondents by
years of marriage, thus form the above table, 47% of the
respondents have been married for about 1 – 5 years, 65
respondents which account for 35% have been married for
about 6 – 10 years, 11% of the total respondents have been
married for about 11 – 15 years, and on 7% of the total
respondents have been married for over 16years. Thus, the
number of years in marriage determines the number of
children a woman will/may have, and the more the number of
children with a corresponding low level of income may
increase the high prevalence of infant and maternal
mortality.
Table 4.7: Distribution of Respondents on the Age they gotMarried
Age Range Frequency Percentage (%)18 – 24 116 6325 – 30 56 3031 – 35 7 4
110

36 – above 5 3Total 184 100Source: Field survey
The table above also shows the distribution of
respondents on the age they got married, table 4.7: shows
that 116 respondents which represents a whopping 63%
accounts for those that got married between ages 18 – 24,
30% of the respondents got married between ages 25 – 30, 4%
of the respondents got married between ages 31 – 35, and
only 3% of the respondents got married between the ages of
36 – above. Thus, it can be seen that those that got married
between ages 18 – 24 has the highest number of respondent
(63%), this is largely because in Nigeria and other parts of
the country, the more conventional age of getting married
lies between that range, however, the early an individual
gets married, the more number of children he may have and
vice versa. Also, the situation can be explained because a
considerable number of the respondents have only a secondary
level of education, and this may push them into early
marriage between the age range of 18 – 24.
111
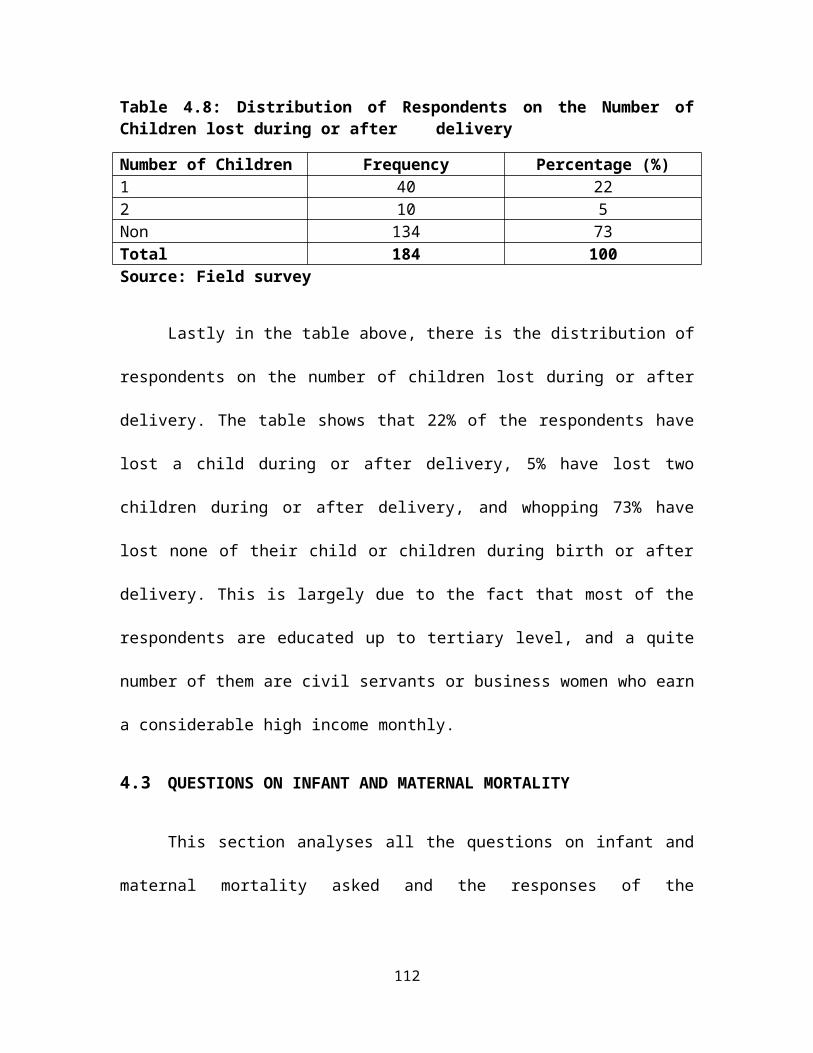
Table 4.8: Distribution of Respondents on the Number ofChildren lost during or after delivery
Number of Children Frequency Percentage (%)1 40 222 10 5Non 134 73Total 184 100Source: Field survey
Lastly in the table above, there is the distribution of
respondents on the number of children lost during or after
delivery. The table shows that 22% of the respondents have
lost a child during or after delivery, 5% have lost two
children during or after delivery, and whopping 73% have
lost none of their child or children during birth or after
delivery. This is largely due to the fact that most of the
respondents are educated up to tertiary level, and a quite
number of them are civil servants or business women who earn
a considerable high income monthly.
4.3 QUESTIONS ON INFANT AND MATERNAL MORTALITY
This section analyses all the questions on infant and
maternal mortality asked and the responses of the
112

respondents. The analysis of the data obtained is presented
below.
Infant mortality
Table 4.9: Infant/Children born in poor families are athigher risk of mortality than those in rich families.
Responses Frequency Percentage (%)Strongly Agree 89 48.4Agree 77 41.8Disagree 14 7.6Strongly Disagree 4 2.2Total 184 100Source: Field Survey
Table 4.9 above shows responses of respondents on the
question ‘infant/children born in a poor family are at a
higher risk of mortality than those from rich families’.
From the table, it can be seen that 48.4% which accounts for
89 of the total respondents strongly agree with the
statement or question, 41.8% agree, 7.6% of the total
respondents disagree, while 2.2% representing 4 of the total
number of respondents strongly disagreeing. Thus, to a large
extent, it can be said that infant/children born in a poor
family are at a higher risk of mortality than those born in
113

well-to-do families or rich families, this is because a
considerable number of the total respondents either strongly
agree or agree to this fact.
Table 4.10: Socio-economic status of parents influencesaccess to health care and infant/child nutrition.
Responses Frequency Percentage (%)Strongly Agree 112 61Agree 64 35Disagree 8 4Total 184 100Source: Field survey
From table 4.10 above, it shows that most of the
respondents strongly agreed that there is a relationship
between socio-economic status of parents on infant/child
mortality as seen from the table above, 61% of the
respondents strongly agreed of this relationship, 64
respondents which account for 35% of the total respondents
agree of the relationship, as only 8% of the total
respondents disagree of this relationship and none of the
respondents strongly disagree of the relationship.
Thus from the table, it shows that a strong
relationship exist between socio-economic status of parents
114

on infant/child mortality especially in Jos North, this is
because a mothers income or socio-economic status determines
the kind of nutrition she gets during pregnancy and even
after delivery, it also informs a choice of quality health
care.
Table 4.11: Educational attainment of a mother determinesaccess and quality of health care her child(ren) get.
Responses Frequency Percentage (%)Strongly Agree 89 48.4Agree 42 22.8Disagree 29 15.8Strongly Disagree 24 13Total 184 100Source: Field survey
Table 4.11: shows that educational attainment of mother
determines access and quality health care delivery for her
child or children. From the table, it can be seen that 48.4%
of the total respondents strongly agreed that there is a
relationship between the educational attainment of mother
and quality health care delivery her child(ren), 42 of the
respondents (22.8%) agreed to this relationship, 15.8%
115
disagree to this relationship while 13% of the total
respondents strongly disagree to the relationship between
educational attainment of parents and quality health care
delivery.
Thus, it can also be seen from the table presented
above that a relatively strong relationship exist between
educational attainment of parents and health care delivery,
this is because educated parents are not ignorant, and are
likely to attain ante natal during pregnancy and post natal
care even after delivery, as can also be seen in table 4.1
above, most educated women has a good occupation and a
considerable amount of higher monthly income than those with
little or no form of education, thus, this determines access
to health care services. Educated parents also know what to
do and what not to do during pregnancy and are likely to
give their infant or young children a good nutrition and an
exclusive breast feeding compared to those with little or no
form of education whom may be ignorant of those things.
116

Table 4.12: A poor sanitary environment with non or poorsocial amenities increases the risk of infant/childillnesses and death.
Responses Frequency Percentage (%)Strongly Agree 53 28.8Agree 102 55.4Disagree 18 9.8Strongly Disagree 11 6Total 184 100Source: Field survey
Table 4.12 shows the responses, frequency and
percentages of respondents on the impact of environmental
conditions on infant/child illnesses and mortality. From the
table above, 28.8% of the respondents strongly agree that a
poor sanitary environment have a great impact on infant
health and mortality in Jos North, 102 respondents which
accounts for 55.4% of the total respondents Agree to the
impact of environmental conditions on infant and maternal
mortality, 9.8 percent of the respondents Disagree, while 6%
of the total respondents strongly disagree that that a poor
sanitary environment can increase the risk of infant/child
illnesses and death .
117

Thus from the above table, it can be seen that a quiet
number of the respondents either strongly agreed or agreed
to the fact that environmental conditions such as unhealthy
environment with no or little social amenities such as
potable drinking water, stagnated water which breeds
mosquitoes that in turn becomes a major cause of infant
morbidity and mortality.
Table 4.13: How effective is the service been rendered inthis hospital or health care centre with regards toantenatal, natal and post natal care?
Cost Frequency Percentage (%)Very Costly 38 20.7Costly 83 45.1Not Costly 63 34.2Total 184 100Source: Field survey
The above table 4.14: shows one of the findings of this
study, from the table, 20.7% of the total respondents
believe that the cost of service (ante-natal, natal and
post-natal care) in the private hospitals is very costly, 83
118

respondents which represents 45.1% of the total respondents
are of the view that the service is costly, while 63
respondents (34.2%) believed that the service is not costly.
Thus, from the table, it can be seen that those who said the
services been rendered in the private clinics of health care
centres are higher compared to those of the view that the
services are not costly.
Table 4.14: How will you rate the cost of service beenprovided in the hospital or health care centre?
Effectiveness Frequency Percentage (%)Very Effective 56 30Effective 97 53Not Costly 31 17Total 184 100Source: Field survey
Also, concerning the effectiveness of the service, 30%
of the respondents said the service rendered in the private
health care centres is very effective, 53% of the
respondents argued that the service is effective, while 31
respondents (17%) are of the view that the service is not
effective. However, generally, it can be seen that a
significant number of respondents are of the view that the
119

service is either very effective or effective, this may be
due to the fact that the cost of service is high which may
correspond to the effectiveness of the service been
rendered, another explanation to this may be that the
questionnaires were only distributed in private health care
centres whose services over the years have been effective
but costly.
Maternal Mortality
Table 4.15: Women from poor families are at a high riskof mortality during pregnancy, child birth and afterdelivery.
Responses Frequency Percentage (%)Strongly Agree 104 56.5Agree 73 39.7Disagree 7 3.8Total 184 100Source: Field survey
From the table above, 104 of the total respondents
strongly agree to the fact that women from poor families are
at a high risk of mortality during pregnancy, child birth
and after delivery, 39.7% of the respondents agreed to this
fact, 3.8& disagree while none of the respondents strongly
disagreed. Thus, this indicates that most of the respondents
120

strongly agree or agreed to the fact that women from poor
families are at a high risk of mortality during pregnancy,
child birth and after delivery.
Table 4.16: Mother’s socio-economic status is likely goingto determine the kind of health care and nutrition she getsduring pregnancy and after delivery.
Responses Frequency Percentage (%)Strongly Agree 115 62.5Agree 61 33.2Disagree 8 4.3Total 184 100Source: Field survey
Table 4.16 shows the response, frequency and percentage
of respondents. 62.5% of the respondents strongly agree that
mother’s socio-economic status is likely going to determine
the kind of health care and nutrition she gets during
pregnancy and after delivery, 33.2% of the total respondents
agree, 8 of the total respondents which accounts for 4.3%
disagree while none of the respondents strongly agreed to
this fact. The above table thereby indicates that mothers
socio-economic status largely determine the kind of health
care and nutrition she gets during pregnancy and after
delivery.
121

Table 4.17: Educational Attainment of a mother is morelikely going to influence her decision to seek properhealth care during pregnancy, child birth and afterdelivery.
Responses Frequency Percentage (%)Strongly Agree 111 60Agree 70 38Disagree 2 1Strongly Disagree 1 1Total 184 100Source: Field survey
Table 4.17 above shows that educational attainment of a
mother is more likely going to influence her decision to
seek proper health care during pregnancy, child birth and
after delivery. This is because 111 of the total respondents
(60%) strongly agree to this fact, 38% of the respondents
agree, 1% of the respondents disagreed as well as 1%
strongly disagreed to this fact.
Table 4.18: A dirty or poor sanitary environment with non orpoor social amenities increases the high risk of maternalillness and death.
122
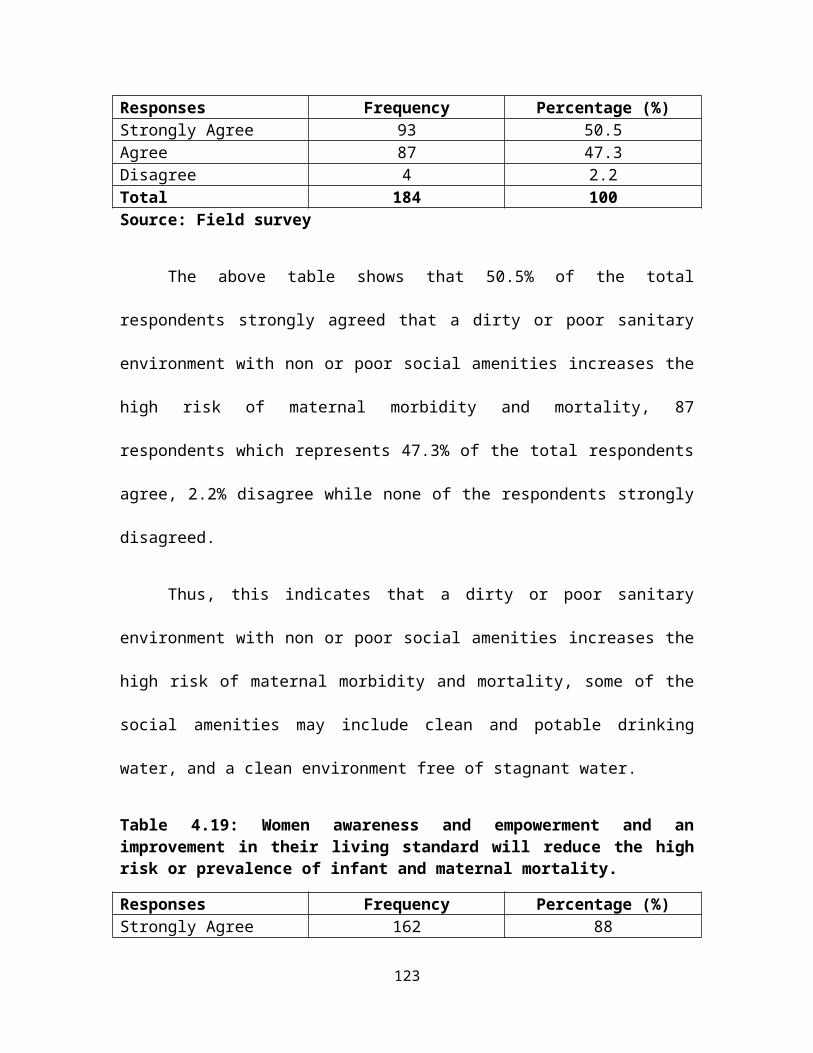
Responses Frequency Percentage (%)Strongly Agree 93 50.5Agree 87 47.3Disagree 4 2.2Total 184 100Source: Field survey
The above table shows that 50.5% of the total
respondents strongly agreed that a dirty or poor sanitary
environment with non or poor social amenities increases the
high risk of maternal morbidity and mortality, 87
respondents which represents 47.3% of the total respondents
agree, 2.2% disagree while none of the respondents strongly
disagreed.
Thus, this indicates that a dirty or poor sanitary
environment with non or poor social amenities increases the
high risk of maternal morbidity and mortality, some of the
social amenities may include clean and potable drinking
water, and a clean environment free of stagnant water.
Table 4.19: Women awareness and empowerment and animprovement in their living standard will reduce the highrisk or prevalence of infant and maternal mortality.
Responses Frequency Percentage (%)Strongly Agree 162 88
123

Agree 22 12Total 184 100Source: Field survey
In table 4.19, most of the respondents (88%) strongly
agreed that women awareness and an improvement in their
living standard will reduce the high risk or prevalence of
infant and maternal mortality, 12% of the respondents agreed
and none of the respondents either disagree or strongly
disagree. Thus this indicates that the high risk and
prevalence of infant and maternal mortality can be reduced
to the barest minimum only if women awareness and
empowerment and an improvement in their living standard is
ensured.
Thus, the above shows that women awareness and
empowerment and also an improvement in their living standard
will reduce the high risk or prevalence of infant and
maternal mortality.
Table 4.20: A clean and healthy environment with theprovision of basic social amenities will ensure safetyinfanthood and motherhood.
Responses Frequency Percentage (%)Strongly Agree 107 58
124

Agree 73 40Disagree 4 2Total 184 100Source: Field survey
Table 4.20 shows that 58% of the respondent strongly
agreed that a clean and healthy environment with the
provision of basic social amenities will ensure safety
infanthood and motherhood, 40% of the respondents which
accounts for 73 of the total respondents agree to this fact,
2% of the total respondents disagree while none of the
respondents strongly disagreed. This means that, to ensure
safety infanthood and motherhood, a clean and healthy
environment must be ensured.
Solutions to the Problems Identified
This study was able to get some possible solutions to
the problems of infant and maternal mortality in Jos North
from the respondents, table 4.6 below provide some of the
possible solutions.
Table 4.21: Ways to reduce the causes and prevalence ofinfant and maternal mortality.
Responses Frequency Percentage (%)
125

Free ante-natal andpost-natal care
76 41.3
Women Empowermentand Education
59 32.1
Building of Newhealth care centresand training ofpersonnel
23 12.5
Provision of BasicSocial Amenities.
26 14.1
Total 184 100Source: Field survey
From the above table 4.21, 76 respondents which
represents 41.3% of the total respondents are of the opinion
that if ante-natal and post-natal care is been made free in
all hospitals and clinics, it will go a long way in reducing
the prevalence of infant and maternal mortality in Jos
North, 32.1% of the total respondents advocate for women
empowerment and education, 12.5% of the respondents believed
that building new health care centres and the training of
health personnel like midwives will go a long way in curbing
the prevalence of infant and maternal mortality in Jos
North, however, 26 respondents (14.1%) are of the view that
the provision of basic social amenities will reduce the much
cases of infant and maternal mortality.126

From the above, it can be seen that a significant
number of the respondents are of the view that infant and
maternal mortality can be reduced if both private and public
hospitals render such services free to enable all women have
access to it.
CHAPTER FIVE
SUMMARY, CONCLUSION AND RECOMMENDATIONS
5.1 SUMMARY OF MAJOR FINDINGS
Infant and maternal mortality are one of the very dark
spots in Nigeria’s health profile. Major causes of death
among women in Nigeria are pregnancy-related. Information on
the extent to which women in Nigeria receive care during
pregnancy, during delivery, and a few weeks after delivery
presents a picture of the health care available to mothers
127

and the new born. Such care is also critical for the
survival and well-being of both mother and child.
The research work is carried out in Jos North Local
Government Area of Plateau State, it is aimed at looking at
health care delivery and the prevalence of infant and
maternal mortality in Nigeria, with this, the research
looked at the prevalence, factors, causes and possible
solutions of infant and maternal mortality.
The research finds out that most of the women or
respondent are either petty traders or housewives, hence
most of them have a monthly income of N5,000 – N10,000,
thus, this income is barely enough to enable them get
quality access to health care delivery and good nutrition
during pregnancy and after delivery, this in turn leave
their children malnourished and more prone to morbidity and
subsequent mortality.
In this study, it is seen that socio-economic status of
parents influence access to health care delivery and also
the type of nutrition a mother and her child get. This is
because of the cost involve in quality health care delivery
128

as argued by the respondents, thus it said that children
born in poor families are at high risk of morbidity and
mortality than those born in rich homes or families, also
mothers whose socio-economic status is high can afford the
basic nutrition needed during pregnancy and even after
delivery.
Another outstanding findings of this study is that the
educational attainment of a mother determines health care of
the mother and her child, this is because she is not
ignorant of what she ought to do during pregnancy and after
delivery. Educated mothers are more likely to visit the
hospital during pregnancy for ante natal, natal and post
natal care than those without any form of education. It is
also seen that the educational attainment of a mother to a
large extent determines her occupation and also her monthly
income. Therefore, the educational attainment of a mother is
a major factor in infant and maternal mortality.
Another finding of this study is that though the theirs
effectiveness in health care delivery, the cost implication
of such health care services is also high, thus most women
129

who are financially incapacitated prefer to deliver at home
than in the hospital, they only resort to the hospital when
there are complications during delivery and most of the time
becomes too late. However, the effectiveness and cost of
this health care services can be explained due to the fact
that the study centred in the private hospitals or health
care facilities.
Finally, this study was able to find out also the fact
that environmental factors also affects or influence infant
and maternal mortality. It is found out that a poor and
unhealthy environment with little or no access to social
amenities like potable drinking water will to a large extent
affect infant and maternal survival, this is because a dirty
and unhealthy environment is likely going to breed
mosquitoes, and malaria which is caused by mosquitoes have
been identified as one of the killer disease in
infant/children.
5.2 CONCLUSION
High infant and maternal mortality is a manifestation
of gross underdevelopment. Hence, permanent reduction
130
requires societal transformation. The prevalence of infant
and maternal mortality in Nigeria cannot be overemphasized,
hence this study is meant to help identify the causes and
factors responsible for infant and maternal mortality and
how those causes can be minimize to reduce the prevalent
cases of this menace which has become a national
embarrassment.
Infant and maternal mortality can be attributed to
factors such as educational, socio-economic and
environmental factors. This factors have been found to be
major causes of infant and maternal mortality in Jos North
and Nigeria in general, the study shows that most of the
women only have a secondary school certificate and most of
them are either housewives or petty traders, hence don’t
have the financial capacity to seek better health care
during pregnancy and after delivery and also cannot afford
the required nutrition needed for their children and
themselves after delivery.
Lack of access to available and better health care at a
cheaper rate have been identified as a factor that also
131

increases the high prevalence of infant and maternal
mortality in Nigeria. Women continue to become victims of
poor and dilapidated health facilities in the health care
centres that ordinary should have been created by any
responsible government, clean and healthy environment with
available of social amenities which ordinarily should be
provided by government has become an illusion, that is why a
women in Nigeria has 1-in-8 risk of dying in child birth or
from pregnancy related causes during her lifetime, which is
higher than the overall 1-in-22 risk for women in Sub
Saharan Africa.
The number of mothers in Nigeria who die in the cause
of pregnancy and childbirth is unacceptably high, as is the
number of infants born in Nigeria who do not live to their
first birthday. For the majority of these deaths, the
medical causes are well understood and there are effective
preventive strategies available. Urgent health system and
socio-economic interventions should therefore be put in
place to reduce maternal and infant mortality in Nigeria.
5.3 RECOMMENDATIONS
132

The following recommendations are derived from the
findings of this work and also from the responses of
respondents. The following are recommendation that if taken
into consideration, will reduce the prevalence of infant and
maternal mortality in Jos North and Nigeria at large.
i) Government should provide financial and technical
support for NGOs working on infant and maternal
mortality. Education programmes that stress the
prevention of infant and maternal mortality should be
introduced in schools, workplaces, churches/mosques,
and community groups.
ii) Women should be empowered economically in terms of
employment opportunities and also and material
empowerment to help them be able to seek quality
antenatal and post natal care during pregnancy and
after delivery.
iii) Both government and the NGOs should embark on media
campaigns using the print and electronic media to raise
awareness on the issues of infant and maternal
133

mortality, also public campaigns should be carried out
using posters, stickers, rallies and drama, etc.
iv) The Mother-Newborn-Child Continuum of care should be
adopted, this has to do with the core principle
underlying the strategies to develop maternal, newborn
and child care programmes. Care has to be provided as a
continuum throughout the lifecycle and in a seamless
continuum that spans the home, the community, the
health centre and the hospital. This will save lives of
many women, newborns and children.
v) There should be Increase effectiveness and utilization
of antenatal care, this is due to the importance of
Antenatal and post natal care which is a variable
package of screening (through clinical evaluation and
investigations) and treatment for pregnant women with
the prime objective of prevention, early detection and
treatment of complications in the mother and fetus, and
the ultimate goal of optimizing maternal and perinatal
health.
134

vi) It is however important to note that antennal and post
natal care as identified above should be made free of
charge in both private and public health care centres
and hospitals, and such services should also be
accessible to the general public or to all pregnant
women.
vii) Malaria in pregnancy is an important and critical
health concern in Sub-Saharan Africa, therefore, cost
effective interventions should be made available to
reduce the burden of malaria in pregnancy. Intense
public health education, advocacy and political will
are needed to scale up malaria in pregnancy.
viii) Government should provide a clean and healthy
environment, and also be able to provide basic social
amenities in all communities in country such as potable
drinking water, and also creating awareness on keeping
the environment clean and free from stagnated water
which may breed mosquitoes leading to other diseases.
ix) The presence of midwives and skilled birth attendant at
childbirths is a very effective intervention for
135

reducing maternal mortality and newborn mortality,
therefore, government should make a deliberate effort
in training and retraining of midwives and traditional
birth attendants which should be posted to every nook
and cranny of the country including rural areas for
effective delivery.
x) The need to address childhood and motherhood
malnutrition in a holistic sense, to positively affect
child and maternal survival and development as well as
eradicate childhood disease in a sustainable manner
cannot be overemphasized. Adequate childhood and
maternal nutrition should be seen as an outcome of
several related factors in the family, community and
society, not just a process in the child’s body. The
nutrition of the mother is also of utmost importance
for her
xi) If the 4th and 5th Millennium Development Goal are to be
attained and sustained, the structures on the
successful immunization programmes depend, chiefly the
primary health care system must be revitalized. There
136

is also a need to promote local research into the
demand-side of immunization services such as missed
opportunities, factors that affect uptake knowledge and
attitudes of community members to immunization.
xii) Maternal mortality cannot be reduced without some
degree of financial investment to bring the standard of
care to a minimum level. The issue of budgetary
allocation to health should be addressed. Strong
political will and commitment is required to sustain
the flow of financial resources in the long term.
xiii) A strong advocacy and awareness should be made on the
need for exclusive breastfeeding by mothers. Early
initiation and sustained exclusive breastfeeding are
proven, almost cost-free child survival strategies
whose benefits begin in the neonatal period and extend
well beyond infancy. Breastfeeding alone can save the
lives of thousands of babies.
137

REFERENCES
Alubo, S. O. (1985a). Underdevelopment and Health Care Crisis inNigeria. Medical Anthropology 9 (4): 319-335
Alubo, S. O. (1987). Power and Privileges in Medical Care: An Analysis of
Medical Care in Post-Colonial Nigeria. Social Science and
Medicine 24-5: 453-462138

Alubo, S. O (2010). In Sickness and in Health: Issues in the Sociology of
Health in Nigeria, University of Jos Inaugural Lecture
Series No. 41
Alubo, S. O, and Ibanga, A. (1994). Household Reactions to
Diarrhoea in Plateau State. Nigerian Journal of Pediatrics 21
(Suppl): 111-120
Alubo, S .O. and Franklin Vivekananda (1995). Beyond the
Illusion of Primary Health Care in an African Society, Stockholm:
Bethany Books.
Akpala, C. O. (1993). Perinatal Mortality in a Northern
Nigerian Rural Community”. Journal of the Royal Society for
Health 113(3).
Caldwell, J. C. (1979). Education as a Factor in Mortality Decline: An
Examination of Nigerian Data. Population Studies, 33(3),
395-413. http.//dx.doi.org/10.2307/2173888.
Erinosho, O. (1982). Health Planning in Nigeria, Nigerian
Journal of Sociology and Anthropology.
Espo, M. (2002). Infant Mortality and its Underlying Determinants of Rural
Malawi (Dissertation). University of Tampere Medical
School.
Federal Government of Nigeria. (1986). The National Policy and
Strategy to Achieve Health for All in Nigeria, Lagos Federal Ministry
of National Planning
139

Harrison, K. (1997). Maternal Mortality in Nigeria: The Real
Issues, African Journal of Reproductive Health, 1(1): 7-13.
HERFON. (2006). Nigeria Health Review 2006 Abuja: HERFON
Ibanga, U. A. (1992). Statistics for Social Sciences, Jos. Centre for
Development Studies University of Jos.
Jinadu, M. K., Olusi, S. O., Agun, J. I., & Fabiyi, A. K.
(1991). Childhood Diarrhoea in rural Nigeria:
Studies on Prevalence, Mortality and Socio-environmental
Factors. Journal of Diarrhoea Diseases Research, 9 (4), 323-327.
Koos, E. (1954). The Health of Regionville, What the people did about it,
New York: University Press
Mckeown, T. (1979). The Role of Medicine: Dream, Mirage or Nemesis New
Jersey: Princeton University Press.
Mutunga, C. J. (2007). Environmental Determinants of Child Mortality in
Kenya. UNU- WIDER Research Paper No. 2007/83. Helsinki:
United Nations University World Institute for
Development Economic Research.
NDHS. (2008). Nigerian Demographic and Health Survey.
Shiffman, J. (2007). Generating Political Priority for
Maternal Mortality Reduction in 5 Developing countries,
American Journal of Public Health 97(5): 796-803.
140

Strong, M. A. (1992). The Health of Adults in the Developing World: The
View from Bangladesh, Health Transition Review
2(2):215-224.
Starr, P. (1982), The Social Transformation of American Medicine, New
York: Basic Books
Turshen, M. (1977). The Political Ecology of Disease. Review of
Radical Political Economy 9(1): 45-60
UNICEF (2009). Maternal and Child Health: The Social Protection Dividends
in West and Central Africa, Briefing Paper/Social Policies,
UNICEF West and Central Africa Regional Office.
UNICEF. (2010). Levels and Trends in Child Mortality, Report 2010,
New York: UNICEF.
Wall, L. (1998). Death Mothers and Injured Wives: The Social Context of
Maternal Mortality in Northern Nigeria. Studies in Family
Planning.
Wildavsky, A. (1977). Doing Better and Feeling Worse: The Political
Pathology of Health Policy. P105-123 John Knowles (ed) Doing
Better and Feeling Worse New York: WW Nortion
William, G. H. (1984). The Determinant of Health: Structure, Context
and agency. School of Social Science, Cardiff University,
Wales.
World Bank. (2004). Health and Environment. Background paper for the
World Bank Environment Strategy, Washington, DC: World Bank.
141

World Health Organization. ( 2006). WHO Proposes Survival
For African Children. Retrieved from Wikipedia, the free
encyclopedia, 07/04/2010.
Yahya, M. (2007). Polio Vaccines – No, Thank you! Barriers to Polio
Eradication in Northern Nigeria. African Affairs.
APPENDIX A
QUESTIONNAIRE
Department ofSociology,
University of Jos,Nigeria
142

P.M.B. 2084,
Jos.
Dear Respondent,
I am a final year student of Sociology Department,
University of Jos, conducting a research on ‘healthcare
delivery and the prevalence of Infant and maternal mortality in Jos North
Local Government Area of Plateau State, Nigeria’. Your cooperation
in answering these questions is highly solicited. This
is purely an academic exercise; hence any information
given will be treated with utmost confidentiality and
respect.
Thanks for your cooperation.
Yours faithfully,
Nuhu, Kefas
Dalyop
143
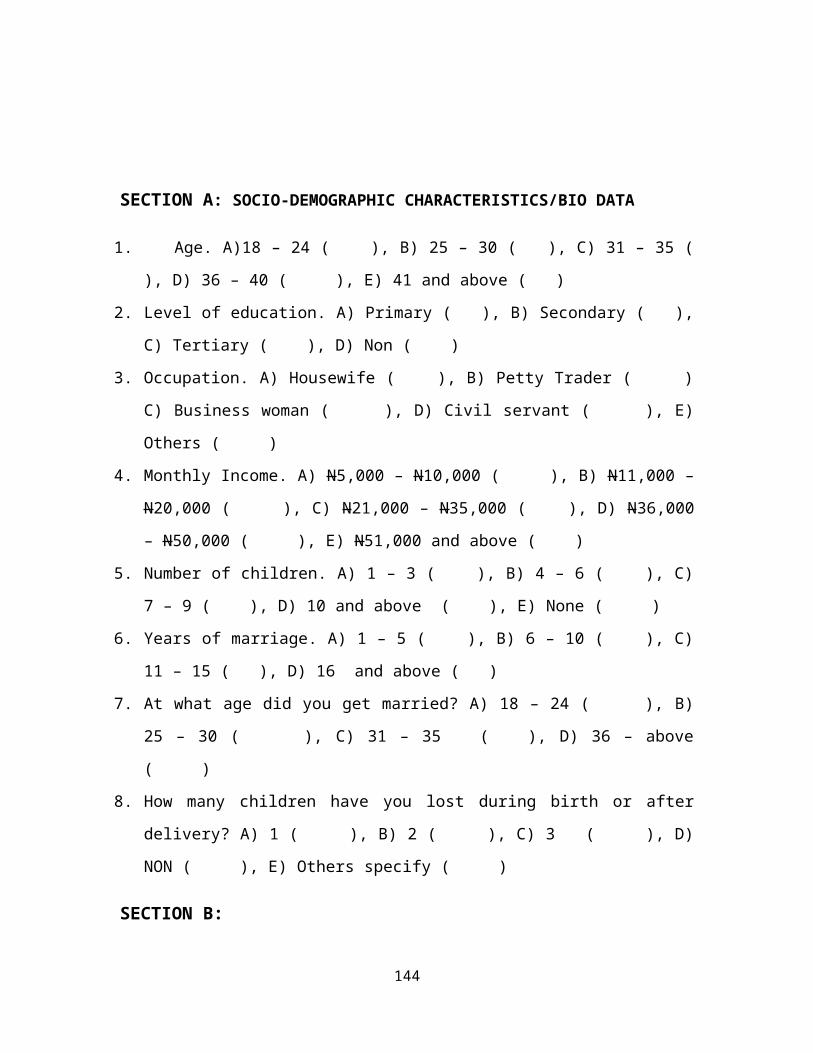
SECTION A: SOCIO-DEMOGRAPHIC CHARACTERISTICS/BIO DATA
1. Age. A)18 – 24 ( ), B) 25 – 30 ( ), C) 31 – 35 (
), D) 36 – 40 ( ), E) 41 and above ( )
2. Level of education. A) Primary ( ), B) Secondary ( ),
C) Tertiary ( ), D) Non ( )
3. Occupation. A) Housewife ( ), B) Petty Trader ( )
C) Business woman ( ), D) Civil servant ( ), E)
Others ( )
4. Monthly Income. A) N5,000 – N10,000 ( ), B) N11,000 –
N20,000 ( ), C) N21,000 – N35,000 ( ), D) N36,000
– N50,000 ( ), E) N51,000 and above ( )
5. Number of children. A) 1 – 3 ( ), B) 4 – 6 ( ), C)
7 – 9 ( ), D) 10 and above ( ), E) None ( )
6. Years of marriage. A) 1 – 5 ( ), B) 6 – 10 ( ), C)
11 – 15 ( ), D) 16 and above ( )
7. At what age did you get married? A) 18 – 24 ( ), B)
25 – 30 ( ), C) 31 – 35 ( ), D) 36 – above
( )
8. How many children have you lost during birth or after
delivery? A) 1 ( ), B) 2 ( ), C) 3 ( ), D)
NON ( ), E) Others specify ( )
SECTION B:
144

INFANT/CHILD MORTALITY
9. Infants/children born in a poor family are at a higher
risk of mortality than those in rich families. A)
Strongly Agree ( ), B) Agree ( ), C) Neutral
( ), D) Disagree ( ), E) Strongly
Disagree ( )
10.Socio-economic status of parents influence access to
health care and infant/child nutrition. A) Strongly
Agree ( ), B) Agree ( ), C) Neutral ( ), D)
Disagree ( ), E) Strongly Disagree ( )
11.Educational attainment of determine access and quality of
health care her child(ren) get. A) Strongly Agree (
), B) Agree ( ), C) Neutral ( ), D) Disagree (
), E) Strongly Disagree ( )
12.A poor sanitary environment with non or poor social
amenities such as safe and potable water increases the
risk of infant/child illness and death. A) Strongly
Agree ( ), B) Agree ( ), C) Neutral ( ), D)
Disagree ( ), E) Strongly Disagree ( )
13.How effective is the services been rendered in this
hospital or health care centre with regards to Ante
natal, natal and post natal care. A) Very Effective (
), B) Effective ( ), C) Neutral ( ),
D) Not Effective ( )
14.How will you rate the cost of service been provided in
this hospital or health care centre. A) Very Costly (
145

), B) Costly ( ), C) Neutral ( ), D) Not Costly (
)
MATERNAL MORTALITY
15.Women from poor families are at a high risk of mortality
during pregnancy, child birth and after birth. A)
Strongly Agree ( ), B) Agree ( ), C) Neutral (
), D) Disagree ( ), E) Strongly Disagree ( )
16.Mother’s socio-economic status is likely going to
determine the kind of health care and nutrition she gets
during pregnancy and after delivery A) Strongly Agree (
), B) Disagree ( ), C) Neutral ( ), D) Disagree
( ), E) Strongly Disagree ( )
17.Educational attainment of a mother is more likely going
to influence her decision to seek proper health care
during pregnancy, child birth and after delivery. A)
Strongly Agree ( ), B) Agree ( ), C) Neutral (
), D) Disagree ( ), Strongly Disagree ( )
18.A dirty or poor sanitary environment with non or poor
social amenities such as safe and potable water increases
the high risk of maternal illness and death. A) Strongly
Agree ( ), B) Agree ( ), C) Neutral ( ), D)
Disagree ( ), E) Strongly Disagreed ( )
19.Women awareness and empowerment and an improvement in
their living standard will reduce the high risk or
prevalence of infant and maternal mortality? A) Strongly
146

Agree, ( ), B) Agree ( ), C) Neutral ( ), D)
Disagree ( ), E) Strongly Agree ( )
20.A clean and healthy environment with the provision of
basic social amenities such as clean and potable water
will ensure safety infanthood and motherhood. A) Strongly
Agree ( ), B) Agree ( ), C) Neutral ( ), D)
Disagree ( ), Strongly Disagree ( )
21.What in your own opinion are some of the ways to reduce
the causes and prevalence of infant and maternal
mortality?
---------------------------------------------------------
---------------------------------------------------------
---------------------------------------------------------
---------------------------------------------------------
---------------------------------------------------------
---------------------------------------------------------
---------------------------------------------------------
--------------------
147
Copyright © 2022 FDOKUMEN