Harvest of Superficial Layers of Fat With a Microcannula and Isolation of Adipose Tissue-Derived...
14
http://aes.sagepub.com/ Aesthetic Surgery Journal http://aes.sagepub.com/content/early/2014/03/28/1090820X14528000 The online version of this article can be found at: DOI: 10.1177/1090820X14528000 published online 31 March 2014 Aesthetic Surgery Journal Gabriele Toietta Angelo Trivisonno, Giuliana Di Rocco, Claudio Cannistra, Valerio Finocchi, Sebastian Torres Farr, Massimo Monti and and Vascular Cells Derived Stromal - Harvest of Superficial Layers of Fat With a Microcannula and Isolation of Adipose Tissue Published by: http://www.sagepublications.com On behalf of: American Society for Aesthetic Plastic Surgery can be found at: Aesthetic Surgery Journal Additional services and information for http://aes.sagepub.com/cgi/alerts Email Alerts: http://aes.sagepub.com/subscriptions Subscriptions: http://www.sagepub.com/journalsReprints.nav Reprints: http://www.sagepub.com/journalsPermissions.nav Permissions: What is This? - Mar 31, 2014 OnlineFirst Version of Record >> at Istituto Regina Elena on April 1, 2014 aes.sagepub.com Downloaded from at Istituto Regina Elena on April 1, 2014 aes.sagepub.com Downloaded from
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Harvest of Superficial Layers of Fat With a Microcannula and Isolation of Adipose Tissue-Derived...

http://aes.sagepub.com/Aesthetic Surgery Journal
http://aes.sagepub.com/content/early/2014/03/28/1090820X14528000The online version of this article can be found at:
DOI: 10.1177/1090820X14528000
published online 31 March 2014Aesthetic Surgery JournalGabriele Toietta
Angelo Trivisonno, Giuliana Di Rocco, Claudio Cannistra, Valerio Finocchi, Sebastian Torres Farr, Massimo Monti andand Vascular Cells
Derived Stromal−Harvest of Superficial Layers of Fat With a Microcannula and Isolation of Adipose Tissue
Published by:
http://www.sagepublications.com
On behalf of:
American Society for Aesthetic Plastic Surgery
can be found at:Aesthetic Surgery JournalAdditional services and information for
http://aes.sagepub.com/cgi/alertsEmail Alerts:
http://aes.sagepub.com/subscriptionsSubscriptions:
http://www.sagepub.com/journalsReprints.navReprints:
http://www.sagepub.com/journalsPermissions.navPermissions:
What is This?
- Mar 31, 2014OnlineFirst Version of Record >>
at Istituto Regina Elena on April 1, 2014aes.sagepub.comDownloaded from at Istituto Regina Elena on April 1, 2014aes.sagepub.comDownloaded from

Aesthetic Surgery Journal 1 –13© 2014 The American Society for Aesthetic Plastic Surgery, Inc.Reprints and permission: http://www .sagepub.com/journalsPermissions.navDOI: 10.1177/1090820X14528000www.aestheticsurgeryjournal.com
Research
Since isolating multipotent cells from human lipoaspirates1— referred to as adipose-derived stromal and stem cells (ADSC)2—became possible, plastic surgeons have begun to consider adipose tissue not only for lipofilling proce-dures but also for sourcing progenitor cells with unique regenerative, anti-inflammatory, and immunomodulatory properties. With collagenase digestion and differential cen-trifugation,3 it is possible to isolate from adipose tissue a heterogeneous population of stromal vascular fraction (SVF) cells, including circulating blood cells, fibroblasts,
528000AESXXX10.1177/1090820X14528000Aesthetic Surgery JournalTrivisonno et alresearch-article2014
Dr Trivisonno is a plastic surgeon in private practice in Rome, Italy; Dr Trivisonno is also a PhD student and Professor Monti is Director of the Interdisciplinary Operative Unit of General and Reconstructive Surgery in the Department of Surgical Science F. Durante, Policlinico Umberto I, University of Rome La Sapienza, Rome, Italy. Dr Di Rocco and Dr Toietta are research fellows in the Department of Experimental Oncology, Regina Elena National Cancer Institute IRCCS, Rome, Italy. Dr Cannistra is a staff physician in the Department of General Surgery, Bichat C. B. University Hospital, Paris, France. Dr Finocchi is a resident in the Department of Plastic and Reconstructive Surgery, Università Cattolica School of Medicine, Rome, Italy. Dr Torres Farr is a plastic and maxillofacial surgeon in private practice in Catania and Rome, Italy.
Harvest of Superficial Layers of Fat With a Microcannula and Isolation of Adipose Tissue–Derived Stromal and Vascular Cells
Angelo Trivisonno, MD; Giuliana Di Rocco, PhD; Claudio Cannistra, MD; Valerio Finocchi, MD; Sebastian Torres Farr, MD; Massimo Monti, MD; and Gabriele Toietta, PhD
AbstractBackground: Adipose tissue is a source of stromal and vascular cells suitable for regenerative medical applications. Cell recovery depends on several factors, including the characteristics of the cannula used to harvest tissue.Objectives: The authors assess whether aspiration of superficial layers of adipose tissue performed with a microcannula, rather than a standard cannula, allows for improved isolation of stromal and vascular cells, and they evaluate the angiogenic potential of the isolated cells in vitro and in vivo.Methods: Adipose-derived stromal and stem cells (ADSC) were collected from the lipoaspirate of the abdomen and hip regions of 6 healthy female donors. For adipose tissue harvest, several options were compared: (1) a rounded-tip cannula with a length of 170 mm, a diameter of 3 mm, and a single elliptic suction port on the side near its distal end (port diameter: 3 × 9 mm) or (2) a rounded-tip infiltration cannula with a length of 170 mm, a diameter of 2 mm, and 5 round ports placed spirally along the sides of the distal cannula shaft (each port diameter: 1 mm) (Shipper Medical Technologies Corporation, Centennial, Colorado). Isolated cells were characterized for (1) expression of the endothelial specific marker CD31 by immunohistochemical and cytofluorimetric analyses and (2) tubular-like structure formation using a 3-dimensional angiogenesis assay on Matrigel. Human ADSC were transduced to express firefly luciferase as a marker suitable for bioluminescent tracking and transplantation studies into immunosuppressed mice were performed.Results: ADSC yield was determined to be significantly higher in samples collected with the microcannula (P = .04). Moreover, isolated cells acquired typical endothelial-like morphology in vitro, formed capillary-like structures, and expressed the distinctive endothelial cell marker CD31. Cells implanted into immunosuppressed mice persisted for several weeks in areas undergoing neovascularization.Conclusions: These results suggest that aspiration of adipose tissue with a microcannula can be a minimally invasive method to obtain clinically relevant numbers of stromal and vascular cells useful for autologous transplant procedures and for promoting tissue regeneration and neovascularization.
Keywordsresearch, adipose-derived stromal cells, lipoaspirate, liposuction, tissue regeneration, autologous fat transfer, endothelial cells, microcannula, stromal vascular fraction
Accepted for publication August 29, 2013.
INTE
RNAT
IONAL CONTRIBUTION
Aesthetic Surgery Journal OnlineFirst, published on March 31, 2014 as doi:10.1177/1090820X14528000
at Istituto Regina Elena on April 1, 2014aes.sagepub.comDownloaded from

2 Aesthetic Surgery Journal
pericytes, and preadipocytes. Moreover, mature endothe-lial cells (EC)4,5 and EC precursors,6-8 which are able to incorporate into vessels and promote postischemic neovas-cularization, can also be purified from adipose tissue. This method of isolation is expensive and time-consuming (1-2 hours in addition to surgery), and to comply with legal restrictions, the procedure must be performed intraopera-tively. Therefore, the need exists to find alternative tech-niques for higher yield isolation of ADSC with minimal manipulation and costs.
The yield of ADSC isolated from human lipoaspirate is influenced by several factors, including patient-to-patient variability, harvest site, collection system, lipoaspirate storage duration, cell isolation method, extent of collage-nase digestion, and centrifugation protocol.9-16 Recent evi-dence suggests that ADSC originate from perivascular cells localized around blood vessels.7,17,18 In keeping with this, it has been demonstrated that the number of isolated ADSC correlates with blood vessel density in adipose tissue.19 On the other hand, variations in blood vessel density have been observed in different subcutaneous adipose tissue layers.20 Therefore, superficial liposuction, which removes fat from the more vascularized hypodermic layer,21 may lead to improved recovery of ADSC compared with con-ventional suction-assisted liposuction, which removes fat from a deeper layer. Liposculpture can be performed more superficially with less risk of producing skin irregularities by using multiple-holed cannulae with reduced diameters, which can be inserted and positioned within the tissue with greater accuracy.
According to Klein’s definition,22 a microcannula has an inside diameter of 2.0 mm or less. Recently, a closed syringe microcannula system for performing fat grafting has been described.23 In the present study, we evaluated, for fat aspiration, the use of a microcannula originally designed as an infiltration cannula for liquid solution. We examined whether the design and reduced size of the microcannula could confer an advantage in reducing the harvest of well-organized fat, which is mostly composed of mature adipocytes, and improving the collection of more superficial layers of adipose tissue, which are associated with a higher percentage of ADSC.
Methods
Adipose Tissue HarvestLipoaspirates were obtained from the abdomen and hip regions of 6 healthy female donors after acquiring their
written informed consent in accordance with the standards of the Institutional Ethical Committee. Each procedure was performed under local anesthesia. Collection sites were infiltrated with tumescent solution through small inci-sions, as described by Klein.24 For adipose tissue harvest, we compared (1) a rounded-tip cannula with a length of 170 mm, a diameter of 3 mm, and a single elliptic suction port on the side near its distal end (port diameter: 3 × 9 mm) and (2) a rounded-tip infiltration cannula with a length of 170 mm, a diameter of 2 mm, and 5 round ports placed spirally along the sides of the distal cannula shaft (each port diameter: 1 mm) (Shipper Medical Technologies Corporation, Centennial, Colorado) (Figure 1). The can-nulae were both connected by a Luer-Lok to a 5- or 10-mL syringe and pushed through the site of access at the most superficial level considered necessary. Negative pressure was then applied manually to the syringe, and fat was har-vested by aspiration.25
ADSC IsolationA volume of physiological solution equal to the volume of the collected lipoaspirate was added, and the samples were centrifuged for 2 minutes at 300g. Adipose tissue was col-lected, and its volume and weight were determined. Subsequently, an equal volume of digestion solution con-taining 2 mg/mL collagenase A dissolved in phosphate-buffered saline (PBS) solution was added (eg, 10 mL of collagenase solution plus 10 mL of lipoaspirate collected after the washing step in physiological solution), and digestion was performed in agitation at 37°C for 30 min-utes. After tissue disaggregation, 1 volume of PBS was added, and the solution was filtered through a 40-µm cell strainer. Stromal cells were collected by centrifugation at low speed (500g) for 5 minutes and then washed twice in PBS and cultured as previously described.26
Total Count and Cell Viability DeterminationCell counts were performed using the automated cell coun-ter ADAM-MC (NanoEnTek, Inc, Seoul, Korea) and 2 fluo-rescence dye staining solutions containing propidium iodide (PI): the Accustain Solution T (PI/lysis solution) (NanoEnTec, Inc)—which permeabilizes the plasma mem-branes of all cells and stains the nuclei, allowing for total cell number counts—and the Accustain Solution N (PI/PBS) (NanoEnTec, Inc)—which exclusively stains the
Corresponding Author:Dr Gabriele Toietta, Department of Experimental Oncology, Regina Elena National Cancer Institute, Via delle Messi d’Oro 156, 00158 Rome, Italy. E-mail: [email protected]
at Istituto Regina Elena on April 1, 2014aes.sagepub.comDownloaded from

Trivisonno et al 3
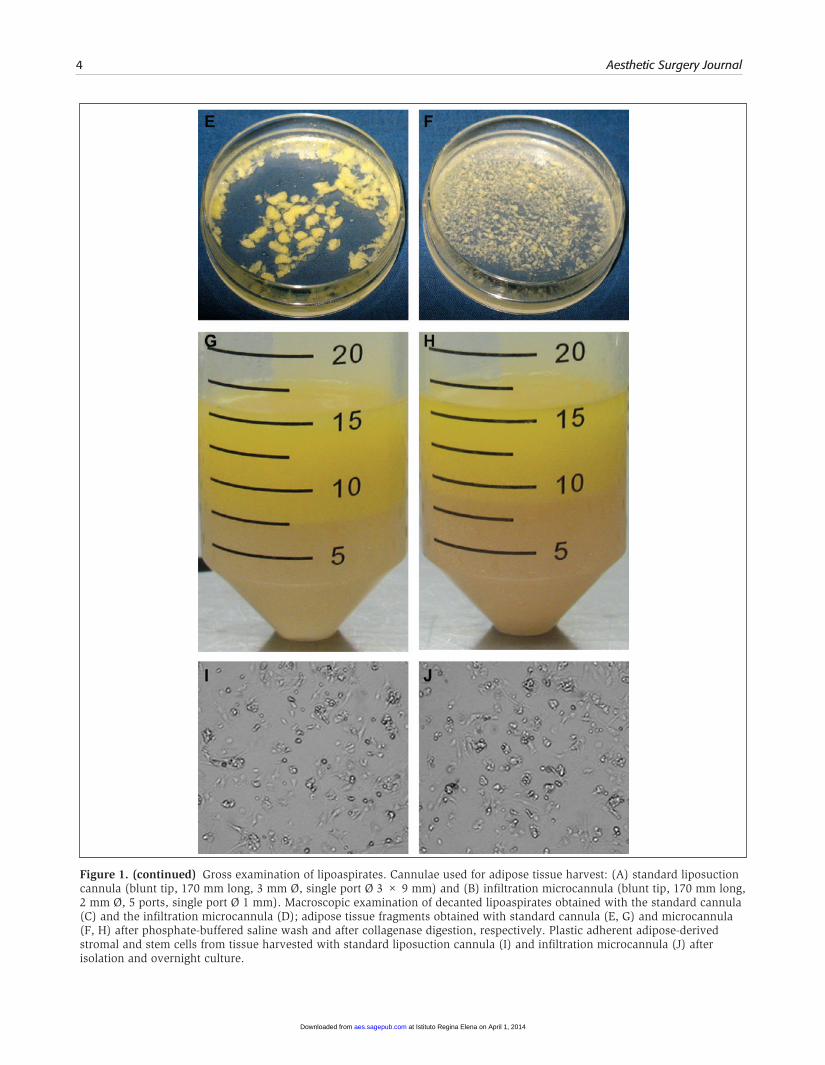
Figure 1. Gross examination of lipoaspirates. Cannulae used for adipose tissue harvest: (A) standard liposuction cannula (blunt tip, 170 mm long, 3 mm Ø, single port Ø 3 × 9 mm) and (B) infiltration microcannula (blunt tip, 170 mm long, 2 mm Ø, 5 ports, single port Ø 1 mm). Macroscopic examination of decanted lipoaspirates obtained with the standard cannula (C) and the infiltration microcannula (D); adipose tissue fragments obtained with standard cannula (E, G) and microcannula (F, H) after phosphate-buffered saline wash and after collagenase digestion, respectively. Plastic adherent adipose-derived stromal and stem cells from tissue harvested with standard liposuction cannula (I) and infiltration microcannula (J) after isolation and overnight culture.
at Istituto Regina Elena on April 1, 2014aes.sagepub.comDownloaded from
4 Aesthetic Surgery Journal
Figure 1. (continued) Gross examination of lipoaspirates. Cannulae used for adipose tissue harvest: (A) standard liposuction cannula (blunt tip, 170 mm long, 3 mm Ø, single port Ø 3 × 9 mm) and (B) infiltration microcannula (blunt tip, 170 mm long, 2 mm Ø, 5 ports, single port Ø 1 mm). Macroscopic examination of decanted lipoaspirates obtained with the standard cannula (C) and the infiltration microcannula (D); adipose tissue fragments obtained with standard cannula (E, G) and microcannula (F, H) after phosphate-buffered saline wash and after collagenase digestion, respectively. Plastic adherent adipose-derived stromal and stem cells from tissue harvested with standard liposuction cannula (I) and infiltration microcannula (J) after isolation and overnight culture.
at Istituto Regina Elena on April 1, 2014aes.sagepub.comDownloaded from

Trivisonno et al 5
nucleus of nonviable cells, allowing for determination of cell viability. With this procedure, cell counts were repro-ducible and not influenced by contaminant red blood cells. Cellular yield was calculated as the number of cells obtained per milliliter of processed lipoaspirate.
ADSC and Adipose Tissue Endothelial Cells (AT-EC)ADSC collected as detailed above were plated at 2.5 × 104 cells/cm2 on tissue culture dishes in maintenance medium (Dulbecco’s modified Eagle’s medium [DMEM; Gibco, Life Technologies, Carlsbad, California] supplemented with 20% fetal bovine serum, 2 mM L-glutamine, 100 U/mL penicillin, and 100 U/mL streptomycin) or endothelial basal medium (endothelial basal medium 2 [EBM-2] supplemented with human epidermal growth factor, vascular endothelial growth factor, basic fibroblast growth factor, insulin-like growth factor 1, hydrocortisone, heparin, ascorbic acid, gentamicin, ampho-tericin B, 2% fetal bovine serum [endothelial growth medium, EBM-2 Bulletkit, Lonza, Walkersville, Maryland], 100 U/mL penicillin, and 100 U/mL streptomycin) and placed overnight at 37°C with 5% CO
2 in a humidified incubator. Following
incubation, dishes were washed with PBS to remove residual nonadherent cells, media were replaced, and cells were allowed to grow until they reached approximately 80% con-fluence. Cells were then subcultured at a 1:3 ratio. Morphologic changes were monitored by an inverted microscope.
In Vitro Angiogenesis AssayA 200-µL aliquot of Cultrex reduced growth factor basement membrane extract (Trevigen, Inc, Gaithersburg, Maryland) was added to each well of a 24-well tissue culture plate and allowed to solidify. ADSC maintained in EBM-2 for 7 days were trypsinized, and 6.0 × 104 cells were suspended in 1 mL of EBM-2, plated onto the gel matrix, cultured for approxi-mately 18 hours, and analyzed for formation of capillary-like structures. Human umbilical vein endothelial cells and ADSC maintained in DMEM were used as controls.
ImmunofluorescenceCells were rinsed twice with PBS, fixed for 10 minutes with 4% paraformaldehyde, and washed several times. For immu-nofluorescence, the following antibodies at 1:100 (volume/volume) dilution were used: anti-CD31 (platelet endothe-lial cell adhesion molecule, PECAM-1) (Santa Cruz Biotechnology, Santa Cruz, California) and α–smooth muscle actin (α-SMA) (Abcam, Cambridge, United Kingdom). Alexa Fluor 594–labeled anti–mouse immunoglobulin G (Molecular Probes, Carlsbad, California) was used as a secondary antibody.
Flow Cytometric AnalysisCells were resuspended in 100 µL of PBS containing 0.5% bovine serum albumin and incubated with mouse anti–human CD31 monoclonal antibodies at a 1:20 dilution. As a secondary antibody, anti–mouse fluorescein isothiocyanate–conjugated antibodies (Becton Dickinson, Franklin Lakes, New Jersey) were used. Negative controls without antibod-ies or with isotype controls were included. Cells were ana-lyzed on an FACSCalibur fluorescence-activated cell sorter (Becton Dickinson) using CellQuest software (Becton Dickinson).
Lentiviral-Mediated Gene Transfer Into ADSCCreation of a third-generation self-inactivating lentiviral vector (LV)–expressing firefly luciferase has been described in the literature.27 Recombinant vesicular stomatitis virus–pseudotyped LV were produced by transient transfection of 293 T cells. Viral supernatants were collected 48 hours after transfection, filtered through 0.22-µm pore nitrocel-lulose filters, concentrated by ultracentrifugation at 50,000g for 140 minutes at room temperature, and stored at –80°C. Titers were determined by serial dilution on HeLa cells.28 ADSC were transduced with 10 TU/cell of LV stocks in the presence of 6 µg/mL Polybrene (Santa Cruz Biotechnology). Assessment of luciferase activity was performed 72 hours after gene transfer.
In Vivo Gel Plug AssayThe subcutaneous gel plug assay in mice is the method of choice for in vivo testing for angiogenesis. The assay, based on the implant of Matrigel plugs29 (Becton Dickinson), was performed as previously described.26 According to this assay, test cells were introduced into cold liquid gel and injected subcutaneously in mice using a 1-mL syringe. After implantation, gel solidified to form plugs, which were removed, examined for formation of new blood ves-sels, and processed for ex vivo bioluminescence imaging (BLI). In typical gel plug in vivo angiogenesis assays, plugs are removed 7 to 21 days after implantation.29 Formation of vessel-like structures by ADSC in Matrigel plugs has been observed 14 days after implantation.6 In this study, the per-sistence of administered luciferase-positive cells in the plugs was determined by BLI at several time points (0, 3, 7, 11, 14, 18, 21, 25, and 28 days), and the animals were sacrificed 28 days after implantation to collect data on the kinetics of engraftment of the implanted ADSC. Animals used were immunocompetent FVB mice (n = 4), immuno-suppressed by intraperitoneal administration of 20 mg/kg/day cyclosporin A (Novartis, Basel, Switzerland). All experimental procedures were performed according to the
at Istituto Regina Elena on April 1, 2014aes.sagepub.comDownloaded from

6 Aesthetic Surgery Journal
guidelines of the National Institutes of Health and were approved by the Institutional Animal Care and Use Committee.
Optical Bioluminescence ImagingTo detect ADSC expressing firefly luciferase, BLI analysis was performed using the IVIS Lumina equipped with Living Image software (Caliper Life Sciences, Hopkinton, Massachusetts) for data quantification. For ex vivo imag-ing, ADSC and gel plug explants containing luciferase-expressing cells were placed into clear-bottomed tissue culture dishes and incubated in a saline solution contain-ing 150 µg/mL D-luciferin (Caliper Life Sciences) before analysis. For in vivo analysis, mice were anesthetized with tribromoethanol and D-luciferin dissolved in PBS (150 mg/kg body weight), which was administered by intraperito-neal injection 10 minutes before analysis. Photons emitted from luciferase-expressing ADSC transplanted into the ani-mals were collected with final accumulation times of 5 minutes.
Statistical AnalysisResults were expressed as means ± standard error of the mean. Data analysis and comparisons between groups were done with INSTAT software (GraphPad Software, San Diego, California). The significance of differences was assessed with a 2-tailed Student t test for unpaired data; statistical significance level was set at P < .05.
Results
Effect of Harvesting Cannula on Isolation Yield of ADSC From Human LipoaspiratesRecovery rate of ADSC from human donor lipoaspirates is dependent on the cannula used for tissue aspiration.9 We evaluated the recovery of ADSC from lipoaspirates collected using both a standard 3-mm cannula and a rounded-tip 2-mm infiltration microcannula, currently used for infiltration pro-cedures (Figure 1A,B). We isolated adipose tissue from 6 female white donors with an average age of 36.8 years (range, 25-56 years). From each donor, lipoaspirates were collected
using the 2 cannulae. At macroscopic evaluation, samples collected using the microcannula contained finely minced tis-sue fragments (Figure 1D,F) smaller than those collected with the larger diameter cannula (Figure 1C,E). At the end of the collagenase treatment, samples were completely dissociated, and no macroscopic differences were evident (Figure 1G,H). From an equal volume of freshly isolated lipoaspirate, the total number of cells isolated from the samples collected with the microcannula was significantly higher (approximately 2-fold) than the number isolated from samples collected with the standard cannula (P = .04) (Table 1). We did not detect any significant difference in cell viability (Table 1), which suggests that the increased shear force manually applied dur-ing liposuction with the smaller diameter cannula equipped with multiple smaller ports did not significantly affect the viability of the recovered ADSC.
Cells were then cultured, and plastic-adherent adipose tissue–derived stromal cells were isolated. At this stage, ADSC obtained with the 2 harvesting cannulae were simi-lar in terms of morphology and proliferation capacity (Figure 1I,J). These results indicate that it is possible to improve the isolation yield of ADSC by using a microcan-nula for fat harvest.
Adipose Tissue–Derived Endothelial Cell Expansion and CharacterizationFreshly isolated ADSC were cultured in EBM-2. Within 5 days, these cells assumed the cobblestone phenotypic mor-phology distinctive of endothelial cells, while cells cultured in maintenance medium retained their typical fibroblastic shape (Figure 2). A fraction of the cells expanded in EBM-2 was positive for PECAM-1 (a typical endothelial marker also referred to as CD31) expression, as assessed by immu-nohistochemistry analysis (Figure 2D). This is in accor-dance with recent evidence describing fat as a source of vascular cells referred to as adipose tissue endothelial cells (AT-EC).5,30 By fluorescence-activated cell sorting (FACS) analysis, we determined that the presence of CD31-positive cells in cultures obtained from microcannula-harvested fat was approximately 3 times higher than in cultures obtained from standard cannula–harvested fat. In cells grown in maintenance medium, we detected, by immunohistochem-istry, cells positive for α-SMA, a stromal marker expressed in smooth muscle cells and pericytes (Figure 2B).17,31
Table 1. Adipose Tissue–Derived Stromal Vascular Fraction Cell Isolation Yield (Expressed as Nucleated Cell Number/mL of Lipoaspirate)
Standard Cannula Infiltration Microcannula P Value
Number of samples 6 6
Total cells/mL ± SE 1.38 × 105 ± 3.28 × 104 2.91 × 105 ± 6.87 × 104 .04
Vitality (%) ± SE 70 ± 4 71 ± 3 .91
at Istituto Regina Elena on April 1, 2014aes.sagepub.comDownloaded from

Trivisonno et al 7
The functional properties of AT-EC were determined by an in vitro angiogenesis Matrigel assay that tested the ability of cells to form 3-dimensional (tubular-like) struc-tures when cultured on an appropriate extracellular matrix substrate. Cells expanded in vitro for 1 week in EBM-2 were able to organize capillary-like tubular struc-tures when seeded on basement membrane extract, while cells grown in maintenance medium were not (Figure 3). Cells from samples harvested with the microcannula
resulted in improved formation of capillary-like struc-tures compared with samples collected with the 3-mm diameter cannula, as determined by the number of branching points (Figure 3A).
Moreover, comparing the number of cells derived from collagenase digestion of the same amount of lipoaspirate, after 1 week of culture, we obtained 1.5 times more cells cul-tured in EBM-2 from samples harvested with the smaller diameter cannula.
Figure 2. Cultured adipose tissue–derived cell characterization. Adult stem stromal and cells from adipose tissue isolated with the microcannula were cultured for 1 week in (A, B) maintenance medium (Dulbecco’s modified Eagle’s medium) or (C, D) endothelial basal medium 2. (A, C) Bright-field microscopic analysis and immunofluorescence analysis (green) using (B) anti–human α–smooth muscle actin antibody and (D) anti–human CD31 antibody. Hoechst was used to visualize nuclei (blue). Original magnification ×40.
at Istituto Regina Elena on April 1, 2014aes.sagepub.comDownloaded from

8 Aesthetic Surgery Journal
Persistence of AT-EC Implanted Into Basement Membrane Matrix Plugs In VivoIt has been demonstrated that transplant of ADSC in combi-nation with EC results in organization of a functional vascular network in vivo.32-34 We assessed the in vivo persistence of
AT-EC in an angiogenesis basement membrane extract plug assay to determine the role of AT-EC in promoting vascular regeneration. ADSC cultured in EBM-2 underwent lentiviral-mediated firefly luciferase gene transfer to track human cells expressing luciferase by BLI analysis upon in vivo administra-tion. Approximately 7 × 105 cells were then resuspended in 200 µL of PBS, added to 400 µL of Cultrex, and implanted into
Figure 3. In vitro angiogenesis basement membrane matrix assay. (A) Adipose tissue–derived cells grown for 1 week in maintenance medium (Dulbecco’s modified Eagle’s medium [DMEM]) or in endothelial basal medium 2 (EBM-2) were seeded on Cultrex (Trevigen, Inc, Gaithersburg, Maryland) substrate. Capillary-like structure quantification in cells isolated from samples collected with the 2 different cannulae seeded on basement membrane matrix for 18 hours. Values are expressed as mean ± standard error of the mean; asterisk represents a statistically significant difference between the 2 EBM-2 groups (P < .05). Representative images of capillary-like network formation by cells isolated from samples harvested with the microcannula grown (B) in maintenance medium and (C) in EBM-2 five days after seeding on the Cultrex matrix.
at Istituto Regina Elena on April 1, 2014aes.sagepub.comDownloaded from

Trivisonno et al 9
Figure 4. Kinetics of engraftment of administered cells by bioluminescence imaging (BLI) analysis. Human adipose tissue endothelial cells expressing luciferase were implanted in Cultrex (Trevigen, Inc, Gaithersburg, Maryland) matrix into immunosuppressed FVB mice. (A-I represent time points: 0, 3, 7, 11, 14, 18, 21, 25, and 28 days after implantation, respectively) BLI analysis of 1 representative animal at several time points after implant; quantification of BLI signals’ intensity was performed on fixed regions of interest (depicted in red) and expressed in photons/s/cm2/sr. Color bar: minimum (blue) 3 × 103 to maximum (red) 3 × 104 photons/s/cm2/sr. (J) Values are expressed as mean ± standard error of the mean indicated by error bars; n = 4.
at Istituto Regina Elena on April 1, 2014aes.sagepub.comDownloaded from

10 Aesthetic Surgery Journal
immunosuppressed FVB mice. Persistence of luciferase-expressing cells was determined by BLI at several time points after gel plug implant (Figure 4). Since luciferin metabolism performed by luciferase-expressing cells requires adenosine triphosphate, BLI signal strictly correlates with implanted live cells. Therefore, with this tracking system, we were able to determine the biodistribution and the kinetics of survival of administered cells at different time points after transplanta-tion. We detected the presence of luciferase-expressing human ADSC for up to 1 month after gel plug implantation, indicating survival of administered cells (Figure 4). Quantification of BLI signal indicated maximal levels 3 days after transplant, then a decrease, suggesting that only a por-tion of implanted cells survived. Early cell death after trans-plant is a common observation in cell therapy studies and is, at least in part, a result of apoptosis and lack of oxygenation due to delayed revascularization at the transplantation site.35 BLI levels at day 7 were maintained for up to 3 additional weeks, indicating survival of administered cells (Figure 4J).
Four weeks after implant, animals were sacrificed, gel plugs were explanted, and BLI was performed ex vivo (Figure 5). BLI signal was determined in the presence of the vascular network in the Cultrex gel implant (Figure 5), suggesting that the implanted cells may play a role in vascular remodeling in vivo through cell differentiation or proangiogenesis mediated by paracrine effects.
discussionIn the present study, we determined that, compared with fat harvested with a conventional 3-mm diameter cannula, adipose tissue aspiration performed with a microcannula can confer an advantage in harvesting superficial layers of fat and improving ADSC isolation yield. Moreover, in lipoaspirates collected with an infiltration microcannula, we established the presence of a higher fraction of vascular cells that acquire typical endothelial-like morphology in vitro, are able to form capillary-like structures in a
Figure 5. In vivo angiogenesis basement membrane matrix assay. Analysis of 1 representative animal 4 weeks after implantation of Cultrex (Trevigen, Inc, Gaithersburg, Maryland) containing 7 × 105 luciferase-expressing adipose tissue endothelial cells. Vessels were visible in the gel plug region both during (A) in vivo macroscopical analysis and (C) after dissection. The same area was positive by bioluminescence analysis in vivo (B) and ex vivo (D).
at Istituto Regina Elena on April 1, 2014aes.sagepub.comDownloaded from

Trivisonno et al 11
basement membrane matrix assay, and express CD31. Cell-tracking studies demonstrated that those cells support neo-vascularization upon transplant in a murine model.
Adipose tissue is a relevant source of stromal and vas-cular cells suitable for clinical approaches to tissue regen-eration mediated by cell transplant.36 Currently, clinical trials are being used to investigate both the use of freshly isolated ADSC and in vitro–expanded mesenchymal cells.37,38 Before full clinical exploitation of cell therapy approaches using ADSC, there should be further consider-ation of issues such as how to easily harvest adipose tissue noninvasively, effectively isolate cells, and differentiate cells in vitro, as well as how transplanted cells engraft in the regenerating tissue.39
Isolation of ADSC involves tissue harvest, decantation, collagenase disaggregation, filtration, and multiple differ-ential centrifugation steps. Donor variability and differ-ences in some parameters of harvesting and isolation procedures may influence the recovery yield of ADSC iso-lated from human lipoaspirates. Using a 3-mm cannula for tissue harvest, we isolated approximately 1.4 × 105 cells/mL of lipoaspirate, which is comparable to the value described by several authors using a similar procedure.9,30,40 Adipose tissue—harvested using an infiltration microcan-nula from the same donors and processed in parallel—resulted in more than a 2-fold increase in recovery yield.
The existence of progenitor cell reserves in the area sur-rounding capillaries, veins, and arteries has been postu-lated.7,17,18 The use of a microcannula may facilitate the harvest of more superficial layers of adipose tissue, which is more vascularized. In addition, we determined that by using a microcannula, it is possible to isolate an increased number of cells that acquire endothelial-like morphology and express endothelial marker CD31 when cultured in endothelial basal medium. These cells are able to organize a vascular-like network both in vitro and in vivo and can persist for several weeks upon transplant in animal mod-els, presumably taking part in vascular regeneration.
Recently, human adipose tissue has been shown to rep-resent a source of cells suitable for vascular application.5,41 In particular, it has been determined that, from a small liposuction (approximately 10-50 mL of lipoaspirate), after 1 week of culture, it would be possible to isolate enough vascular cells to create a tissue-engineered graft suitable for therapeutic use.30 This approach requires extensive ex vivo manipulation and cell culture expansion to be carried out in authorized facilities according to Good Manufacturing Practice regulations. Based on the current data, we suggest that adipose tissue harvest with a Klein-type microcannula can further facilitate the availability of clinically relevant numbers of vascular cells suitable for clinical use in the timeline of a single surgical procedure, reducing the costs and risks of chromosomal instability associated with exten-sive ex vivo cell manipulation.
Concurrent transplantation of aspirated fat and ADSC, a procedure referred to as cell-assisted lipotransfer (CAL),42 improves fat grafting in soft tissue augmentation proce-dures such as breast enhancement and facial recontour-ing.43,44 Fat harvested with the infiltration microcannula contained finely minced tissue, which can be easily infil-trated in lipofilling and CAL procedures. Therefore, adi-pose tissue harvested with an infiltration cannula might be used as a source of cells for regenerative purposes, as shown in the current study, and as a filler—even in fibrotic tissue or areas with very thin tissue layers, such as the periorbital region.
Aspiration of fat with a microcannula yields smaller vol-umes of aspirated tissue with each stroke and has longer sampling times compared with aspiration with a standard cannula. Adipose tissue harvest with a smaller cannula is more time-consuming (approximately 2 times slower com-pared with manual suction with the larger cannula). We calculated the time required to collect 5 mL of lipoaspirate and found that a 5-mL syringe can be filled in approxi-mately 2 minutes (range, 120-180 seconds) with the micro-cannula and in about 1 minute (range, 40-70 seconds) with the larger cannula.
On the other hand, the microcannula may have multiple advantages. Tissue harvested with the microcannula is associated with a higher number of stromal and vascular cells (resulting in improved yield of ADSC isolation), is finely minced (facilitating collagenase disaggregation), and is suitable for lipofilling procedures. Use of the micro-cannula also reduces patient discomfort and trauma; facili-tates the removal of adipose tissue in more superficial, localized areas (reducing the risk of skin irregularities); and minimizes the risk of vascular injury due to multiple reduced-size ports. Because the insertion is more precise and requires less force, the microcannula allows for more accurate control during liposuction, more superficial removal of fat (reducing the risk of accidental penetration of deeper tissues), more overall fat removal despite the small volume of collection per stroke, and faster healing due to the microincisions required.
Taking into account basic, translational, and clinical studies performed in the past decade, possible applica-tions of ADSC in tissue regeneration have been recently reviewed.36 The same review also contains an exhaustive list of the cell surface expression markers (including, for instance, CD54 and CD90 as positive markers and CD14 and CD45 as negative markers) for phenotypic character-ization of human ADSC.36 Based on the data presented in this study, which was limited to the endothelial-specific marker CD31, we are using FACS analysis to evaluate pos-sible phenotypic differences between cells isolated with the different cannulas. Moreover, we are assessing an originally designed, custom-made microcannula (round tip, 2 mm diameter, with 5 small holes placed in line) for
at Istituto Regina Elena on April 1, 2014aes.sagepub.comDownloaded from

12 Aesthetic Surgery Journal
the harvest of hypodermic adipose tissue. We are also evaluating the injection of autologous fat tissue harvested with a microcannula in wound beds to promote the heal-ing of chronic diabetic ulcers and burn lesions. Preliminary results suggest that the procedure may be useful to sup-port and promote angiogenesis and granulation tissue formation.
conclusionsCell therapy and cell-assisted lipotransfer are innovative approaches for the treatment of some acute and chronic soft tissue degenerative conditions. Adipose tissue repre-sents an easily accessible source of stromal and vascular cells suitable for regenerative medical applications. New avenues to obtain a number of cells suitable for clinical use with minimal manipulation are needed. We described a procedure for adipose tissue removal from superficial lay-ers. From harvested fat, we isolated a population of cells able to acquire endothelial-like morphology, express the CD31 endothelial-specific marker, form vascular-like net-works in vivo and in vitro, and persist for several weeks upon transplant in animal models. This procedure allows for a significant improvement in the recovery of stromal and vascular cells, which are useful for autologous trans-plant procedures and for promoting tissue regeneration and neovascularization.
Authors’ noteAngelo Trivisonno and Giuliana Di Rocco contributed equally to this work.
AcknowledgmentsThe authors are grateful for the support of the Department of Experimental Oncology, Istituto Nazionale dei Tumori Regina Elena IRCCS, Rome, Italy.
disclosuresS. Torres Farr is an advisor of Shippert Medical Technologies Corporation, Centennial, Colorado. The company is the manu-facturer of the microcannula used in the current article. The company did not provide financial support for the work. All other contributors do not have conflicts of interest to disclose.
FundingPartial funding for this research was provided by the Ministero della Salute, Italy.
ReFeRences 1. Zuk PA, Zhu M, Ashjian P, et al. Human adipose tis-
sue is a source of multipotent stem cells. Mol Biol Cell. 2002;13:4279-4295.
2. Bourin P, Bunnell BA, Casteilla L, et al. Stromal cells from the adipose tissue–derived stromal vascular frac-tion and culture expanded adipose tissue–derived stro-mal/stem cells: a joint statement of the International Federation for Adipose Therapeutics and Science (IFATS) and the International Society for Cellular Therapy (ISCT). Cytotherapy. 2013;15:641-648.
3. Schaffler A, Buchler C. Concise review: adipose tissue–derived stromal cells—basic and clinical implications for novel cell-based therapies. Stem Cells. 2007;25:818-827.
4. Kern PA, Knedler A, Eckel RH. Isolation and culture of microvascular endothelium from human adipose tissue. J Clin Invest. 1983;71:1822-1829.
5. Szoke K, Beckstrom KJ, Brinchmann JE. Human adipose tissue as a source of cells with angiogenic potential. Cell Transplant. 2012;21:235-250.
6. Planat-Benard V, Silvestre JS, Cousin B, et al. Plasticity of human adipose lineage cells toward endothelial cells: physiological and therapeutic perspectives. Circulation. 2004;109:656-663.
7. Zannettino AC, Paton S, Arthur A, et al. Multipotential human adipose-derived stromal stem cells exhibit a peri-vascular phenotype in vitro and in vivo. J Cell Physiol. 2008;214:413-421.
8. Madonna R, De Caterina R. In vitro neovasculogenic potential of resident adipose tissue precursors. Am J Physiol Cell Physiol. 2008;295:C1271-C1280.
9. Aust L, Devlin B, Foster SJ, et al. Yield of human adipose-derived adult stem cells from liposuction aspi-rates. Cytotherapy. 2004;6:7-14.
10. Oedayrajsingh-Varma MJ, van Ham SM, Knippenberg M, et al. Adipose tissue–derived mesenchymal stem cell yield and growth characteristics are affected by the tissue- harvesting procedure. Cytotherapy. 2006;8:166-177.
11. Jurgens WJ, Oedayrajsingh-Varma MJ, Helder MN, et al. Effect of tissue-harvesting site on yield of stem cells derived from adipose tissue: implications for cell-based therapies. Cell Tissue Res. 2008;332:415-426.
12. Galie M, Pignatti M, Scambi I, et al. Comparison of differ-ent centrifugation protocols for the best yield of adipose-derived stromal cells from lipoaspirates. Plastic Reconstr Surg. 2008;122:233e-234e.
13. Fraser JK, Wulur I, Alfonso Z, et al. Differences in stem and progenitor cell yield in different subcutaneous adi-pose tissue depots. Cytotherapy. 2007;9:459-467.
14. Padoin AV, Braga-Silva J, Martins P, et al. Sources of pro-cessed lipoaspirate cells: influence of donor site on cell concentration. Plastic Reconstr Surg. 2008;122:614-618.
15. Conde-Green A, de Amorim NF, Pitanguy I. Influence of decantation, washing and centrifugation on adipocyte and mesenchymal stem cell content of aspirated adipose tis-sue: a comparative study. J Plast Reconstr Aesthetic Surg. 2010;63:1375-1381.
16. Alharbi Z, Oplander C, Almakadi S, et al. Conventional vs. micro-fat harvesting: how fat harvesting technique affects tissue-engineering approaches using adipose tis-sue–derived stem/stromal cells. J Plast Reconstr Aesthetic Surg. 2013;66(9):1271-1278.
at Istituto Regina Elena on April 1, 2014aes.sagepub.comDownloaded from
Trivisonno et al 13
17. Cai X, Lin Y, Hauschka PV, et al. Adipose stem cells origi-nate from perivascular cells. Biol Cell. 2011;103:435-447.
18. Corselli M, Chen CW, Crisan M, et al. Perivascular ances-tors of adult multipotent stem cells. Arterioscler Thromb Vasc Biol. 2010;30:1104-1109.
19. da Silva Meirelles L, Sand TT, Harman RJ, et al. MSC frequency correlates with blood vessel density in equine adipose tissue. Tissue Eng. 2009;15:221-229.
20. El-Mrakby HH, Milner RH. Bimodal distribution of the blood supply to lower abdominal fat: histological study of the microcirculation of the lower abdominal wall. Ann Plast Surg. 2003;50:165-170.
21. Gasperoni C, Gasperoni P. Subdermal liposuction: long-term experience. Clin Plast Surg. 2006;33:63-73, vi.
22. Klein JA. Tumescent technique chronicles: local anesthesia, liposuction, and beyond. Dermatol Surg. 1995;21:449-457.
23. Alexander RW, Harrell DB. Autologous fat grafting: use of closed syringe microcannula system for enhanced autolo-gous structural grafting. Clin Cosmet Investig Dermatol. 2013;6:91-102.
24. Klein JA. The tumescent technique: anesthesia and modified liposuction technique. Dermatol Clin. 1990;8:425-437.
25. Rodriguez RL, Conde-Green A. Quantification of negative pressures generated by syringes of different calibers used for liposuction. Plastic Reconstr Surg. 2012;130:383e-384e.
26. Di Rocco G, Gentile A, Antonini A, et al. Enhanced healing of diabetic wounds by topical administration of adipose tissue–derived stromal cells overexpressing stromal-derived factor-1: biodistribution and engraft-ment analysis by bioluminescent imaging. Stem Cells Int. 2010;2011:304562.
27. Di Rocco G, Gentile A, Antonini A, et al. Analysis of bio-distribution and engraftment into the liver of genetically-modified mesenchymal stromal cells derived from adipose tissue. Cell Transplant. 2012;21:1997-2008.
28. Tiscornia G, Singer O, Verma IM. Production and purifica-tion of lentiviral vectors. Nat Protocols. 2006;1:241-245.
29. Passaniti A, Taylor RM, Pili R, et al. A simple, quantita-tive method for assessing angiogenesis and antiangiogenic agents using reconstituted basement membrane, heparin, and fibroblast growth factor. Lab Invest. 1992;67:519-528.
30. Harris LJ, Zhang P, Abdollahi H, et al. Availability of adi-pose-derived stem cells in patients undergoing vascular surgical procedures. J Surg Res. 2010;163:e105-e112.
31. Traktuev DO, Merfeld-Clauss S, Li J, et al. A population of multipotent CD34-positive adipose stromal cells share
pericyte and mesenchymal surface markers, reside in a periendothelial location, and stabilize endothelial net-works. Circ Res. 2008;102:77-85.
32. Traktuev DO, Prater DN, Merfeld-Clauss S, et al. Robust functional vascular network formation in vivo by cooperation of adipose progenitor and endothelial cells. Circ Res. 2009;104:1410-1420.
33. Merfeld-Clauss S, Gollahalli N, March KL, et al. Adipose tissue progenitor cells directly interact with endothelial cells to induce vascular network formation. Tissue Eng. 2010;16:2953-2966.
34. Saif J, Heeschen C, Aicher A. Add some fat to vascular progenitor cell therapy. Circ Res. 2009;104:1330-1332.
35. Smith MK, Peters MC, Richardson TP, et al. Locally enhanced angiogenesis promotes transplanted cell sur-vival. Tissue Eng. 2004;10:63-71.
36. Zuk PA. Adipose-derived stem cells in tissue regenera-tion: a review. ISRN Stem Cells. 2013;2013:713959.
37. Wilson A, Butler PE, Seifalian AM. Adipose-derived stem cells for clinical applications: a review. Cell Prolif. 2011;44:86-98.
38. Gimble JM, Guilak F, Bunnell BA. Clinical and preclinical translation of cell-based therapies using adipose tissue-derived cells. Stem Cell Res Ther. 2010;1:19.
39. Ogawa R. The importance of adipose-derived stem cells and vascularized tissue regeneration in the field of tissue transplantation. Curr Stem Cell Res Ther. 2006;1:13-20.
40. Mojallal A, Lequeux C, Shipkov C, et al. Influence of age and body mass index on the yield and proliferation capac-ity of adipose-derived stem cells. Aesthetic Plast Surg. 2011;35:1097-1105.
41. Marchal JA, Picon M, Peran M, et al. Purification and long-term expansion of multipotent endothelial-like cells with potential cardiovascular regeneration. Stem Cells Dev. 2012;21:562-574.
42. Sterodimas A, de Faria J, Nicaretta B, et al. Cell-assisted lipotransfer. Aesthetic Surg J. 2010;30:78-81.
43. Matsumoto D, Sato K, Gonda K, et al. Cell-assisted lipo-transfer: supportive use of human adipose-derived cells for soft tissue augmentation with lipoinjection. Tissue Eng. 2006;12:3375-3382.
44. Mizuno H, Hyakusoku H. Fat grafting to the breast and adipose-derived stem cells: recent scientific consensus and controversy. Aesthetic Surg J. 2010;30:381-387.
at Istituto Regina Elena on April 1, 2014aes.sagepub.comDownloaded from