FORMULARY DECISIONS FROM JANUARY 2012 ONWARDS
148
FMG Minute ref Decision Medicine Restrictions /Indications Prescribers TLL Licensed? (Y/N) Guideline / place in therapy /rationale behind proposed change/comments (Amber shading = amendment to netFormulary required once further action completed) Restriction as it appears in Formulary entries only May 2013 onwards (Green = netFormulary updated) (Unshaded = netFormulary not yet updated) (Amber = clarification required) BNF category Decision date Dec 16.1 Add Degarelix 80mg, 160mg (Firmagon®) (injection) For treatment of advanced hormone-dependent prostate cancer in accordance with NICE TA 404. Degarelix will be reserved for patients with spinal metastases with / or impending spinal cord compression • Prescribing initiation by or consultant Oncologists, continuation by GPs once an amber guideline is in place Red Y • Prescribing initiation by consultant Oncologists, continuation by GPs once an amber guideline is in place • For treatment of advanced hormone-dependent prostate cancer in accordance with NICE TA 404. Degarelix will be reserved for patients with spinal metastases with / or impending spinal cord compression. • Degarelix will be used for the first three months of treatment, after which it will routinely be switched to an LHRA agonist (currently triptorelin three monthly). The first injection will be administered by the hospital followed by two monthly injections administered by the GP. Switch to LHRA agonist will take place after a review by the Specialist at three months. Restricted- prescribing initiation by consultant Oncologists only. For continuation by GPs once amber guideline is in place (guideline awaiting). For treatment of advanced hormone-dependent prostate cancer in accordance with NICE TA 404. Degarelix will be reserved for patients with spinal metastases with / or impending spinal cord compression. 8.3.4.2 (Gonadotrophin-releasing hormone antagonists) Dec-16 Dec 16.3 Add indication Nivolumab 10mg/ml (solution for infusion) 4ml, 10ml Treatment of previously treated advanced renal cell carcinoma, NICE TA 417 and NHSE SSC 1663, Oct 16 • Prescribing by Consultant Oncologists (Renal) only Red Y • Prescribing by Consultant Oncologists (Renal) only • For treatment of previously treated advanced renal cell carcinoma, NICE TA 417 and NHSE SSC 1663, Oct 16 FOR ALL PRESCRIBING - a completed and approved HIGH COST DRUG compliance form, via BLUETEQ, is required. 1. Restricted - prescribing by Consultant Oncologists (Melanoma) at OUH only in accordance with: i. NICE TA 384 for treating advanced (unresectable or metastatic) melanoma and in accordance with NHS England Specialised Services Circular (SSC 1617) ii. In combination with ipilimumab for treating advanced melanoma in accordance with NICE TA 400, Jul 16 and NHSE Letter ref 1640 from end Oct 2016. 2. Restricted- prescribing initiation by consultant Oncologists (Renal) only. For treatment of previously treated advanced renal cell carcinoma in line with NICE TA 417 and NHSE SSC 1663, Oct 16 8.1.5 Dec-16 Dec 16.4 Add Osimertinib 40mg, 80mg (Tagrisso®) (film- coated tablets) • For treatment of locally advanced or metastatic EGFR T790M mutation- positive non-small-cell lung cancer in accordance with NICE TA 416 and NHSE SSC 1660 consultant Oncologists (Lung) Red Y • Prescribing by consultant Oncologists (Lung) • For treatment of locally advanced or metastatic EGFR T790M mutation-positive non-small-cell lung cancer in accordance with NICE TA 416 and NHSE SSC 1660 FOR ALL PRESCRIBING - a completed and approved HIGH COST DRUG compliance form, via BLUETEQ, is required. Restricted - prescribing by Consultant Oncologists (Lung) in accordance with NICE TA 416 and NHSE SSC 1660 for treatment of locally advanced or metastatic EGFR T790M mutation-positive non-small-cell lung cancer. 8.1.5 (protein kinase inhibitors) Dec-16 FORMULARY DECISIONS FROM JANUARY 2012 ONWARDS - most recent decisions listed first FMG DECISIONS DECEMBER 2016
-
Upload
khangminh22 -
Category
Documents
-
view
5 -
download
0
Transcript of FORMULARY DECISIONS FROM JANUARY 2012 ONWARDS

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
De
c 1
6.1
Add Degarelix 80mg,
160mg (Firmagon®)
(injection)
For treatment of advanced
hormone-dependent
prostate cancer in
accordance with NICE TA
404. Degarelix will be
reserved for patients with
spinal metastases with / or
impending spinal cord
compression
• Prescribing initiation
by or consultant
Oncologists,
continuation by GPs
once an amber
guideline is in place
Re
d
Y
• Prescribing initiation by consultant Oncologists, continuation
by GPs once an amber guideline is in place
• For treatment of advanced hormone-dependent prostate
cancer in accordance with NICE TA 404. Degarelix will be
reserved for patients with spinal metastases with / or
impending spinal cord compression.
• Degarelix will be used for the first three months of treatment,
after which it will routinely be switched to an LHRA agonist
(currently triptorelin three monthly).
The first injection will be administered by the hospital followed
by two monthly injections administered by the GP. Switch to
LHRA agonist will take place after a review by the Specialist at
three months.
Restricted- prescribing initiation by consultant
Oncologists only. For continuation by GPs once amber
guideline is in place (guideline awaiting).
For treatment of advanced hormone-dependent prostate
cancer in accordance with NICE TA 404. Degarelix will
be reserved for patients with spinal metastases with / or
impending spinal cord compression.
8.3
.4.2
(G
on
ad
otr
op
hin
-re
lea
sin
g
ho
rmo
ne
an
tag
on
ists
)D
ec-1
6
De
c 1
6.3
Add
indication
Nivolumab 10mg/ml
(solution for infusion)
4ml, 10ml
Treatment of previously
treated advanced renal cell
carcinoma, NICE TA 417
and NHSE SSC 1663, Oct
16
• Prescribing by
Consultant
Oncologists (Renal)
only
Re
d
Y
• Prescribing by Consultant Oncologists (Renal) only
• For treatment of previously treated advanced renal cell
carcinoma, NICE TA 417 and NHSE SSC 1663, Oct 16
FOR ALL PRESCRIBING - a completed and approved
HIGH COST DRUG compliance form, via BLUETEQ, is
required.
1. Restricted - prescribing by Consultant Oncologists
(Melanoma) at OUH only in accordance with:
i. NICE TA 384 for treating advanced (unresectable or
metastatic) melanoma and in accordance with NHS
England Specialised Services Circular (SSC 1617)
ii. In combination with ipilimumab for treating advanced
melanoma in accordance with NICE TA 400, Jul 16 and
NHSE Letter ref 1640 from end Oct 2016.
2. Restricted- prescribing initiation by consultant
Oncologists (Renal) only. For treatment of previously
treated advanced renal cell carcinoma in line with NICE
TA 417 and NHSE SSC 1663, Oct 16
8.1
.5
De
c-1
6
De
c 1
6.4
Add Osimertinib 40mg,
80mg (Tagrisso®) (film-
coated tablets)
• For treatment of locally
advanced or metastatic
EGFR T790M mutation-
positive non-small-cell lung
cancer in accordance with
NICE TA 416 and NHSE
SSC 1660
consultant
Oncologists (Lung)
Re
d
Y
• Prescribing by consultant Oncologists (Lung)
• For treatment of locally advanced or metastatic EGFR T790M
mutation-positive non-small-cell lung cancer in accordance with
NICE TA 416 and NHSE SSC 1660
FOR ALL PRESCRIBING - a completed and approved
HIGH COST DRUG compliance form, via BLUETEQ, is
required.
Restricted - prescribing by Consultant Oncologists
(Lung) in accordance with NICE TA 416 and NHSE SSC
1660 for treatment of locally advanced or metastatic
EGFR T790M mutation-positive non-small-cell lung
cancer. 8.1
.5 (
pro
tein
kin
ase
inh
ibito
rs)
De
c-1
6
FORMULARY DECISIONS FROM JANUARY 2012 ONWARDS - most recent decisions listed first
FMG DECISIONS DECEMBER 2016

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
De
c 1
6.5
Add Certolizumab Pegol
200mg (Cimzia®)
(injection, prefilled
syringe
• Treatment rheumatoid
arthritis in adult patients
(monotherapy or in
combination with
methotrexate) in
accordance with NICE TA
415 and the Bucks
Biologics in Rheumatoid
arthritis algorithm
Consultant
Rheumatologists
Re
d
Y
• Prescribing by Consultant Rheumatologists
• Treatment rheumatoid arthritis in adult patients (monotherapy
or in combination with methotrexate) in accordance with NICE
TA 415 and the Bucks Biologics in Rheumatoid arthritis
algorithm
FOR ALL PRESCRIBING - NICE compliance form
required - see link from Formulary homepage. NICE
compliance to be verified if form not yet available.
NOTE: use restricted in BHT to patients with a low
number of co-morbidities and low risk of infection and is
subject to further audit.
Restricted - prescribing by Consultant Rheumatologists
only,
1. in accordance with Biologics for Rheumatoid Arthritis
guideline (BHTCG 749FM), NICE TA 375 and NICE TA
415.
2. as an alternative first line biologic treatment for
Psoriatic Arthritis in accordance with Biologics for
Psoriatic Arthritis guideline (BHTCG 740FM) and to be
used as described for other anti TNF treatments in
Etanercept, Infliximab and Adalimumab for the treatment
of Psoriatic Arthritis (NICE TA199)or Golimumab for
Psoriatic Arthritis (NICE TA220)
10
.1.3
(C
yto
kin
e m
od
ula
tors
)
De
c-1
6
Add Tocilizumab 162mg
(sub-cutaneous
injection, pre-filled
syringe)
Add Tocilizumab
80mg/4mL,
200mg/10mL,
400mg/20mL
(RoActemra®)
(concentrate for
intravenous infusion)
De
c-1
6
De
c 1
6.7
• Treatment for Takayasu
Arteritis (TAK) in adult in
accordance to criteria
defined in NHS England
Clinical Commissioning
Policy 16056/P
• Prescribing by
consultant
Rheumatologists
following approval by
Thames Valley
Specialised
Rheumatology
Network MDT
Re
d
Y
• Treatment for Takayasu Arteritis (TAK) in adult in accordance
to criteria defined in NHS England Clinical Commissioning
Policy 16056/P
• Prescribing by consultant Rheumatologists following approval
by Thames Valley Specialised Rheumatology Network MDT.
BHT Rheumatology consultants will prescribe as outreach to
the Specialist Centre delivered as part of a provider network.
Name of Specialist centre and clinician involved in MDT to be
communicated to Formulary Team prior to initiating treatment
at BHT
FOR ALL PRESCRIBING - NICE compliance form
required - see link from Formulary homepage. (NICE
compliance to be verified if NICE compliance form not
yet available)
1. Restricted - to Rheumatology consultant prescribing
only for treatment of rheumatoid arthritis, as an
alternative to tocilizumab IV recommendations in NICE
TA 247 and in accordance with Biologics for Rheumatoid
Arthritis guideline (BHTCG 749FM)
2. Restricted - consultant Rheumatologists following
approval by Thames Valley Specialised Rheumatology
Network MDT. For treatment for Takayasu Arteritis (TAK)
in adult in accordance to criteria defined in NHS England
Clinical Commissioning Policy 16056/P. BHT
Rheumatology consultants will prescribe as outreach to
the Specialist Centre delivered as part of a provider
network. Name of Specialist centre and clinician
involved in MDT to be communicated to Formulary Team
prior to initiating treatment at BHT
NOTE: Patients should use either IV or SC tocilizumab.
If they fail on either of the routes, they may not use the
alternative route.
10
.1.3
(C
yto
kin
e m
od
ula
tors
)

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
De
c 1
6.8
Add Rituximab
100mg/10mL,
500mg/50mL
(MabThera®)
(intravenous infusion)
• Treatment of ANCA-
associated vasculitis in
adults, NHSE Clinical
Commissioning policy
A13/P, Jan 15
• Prescribing by
consultant
Rheumatologists
following approval by
Thames Valley
Specialised
Rheumatology
Network MDT.
Re
d S
pe
c C
en
tre
Y
• Treatment of ANCA-associated vasculitis in adults, NHSE
Clinical Commissioning policy A13/P, Jan 15
• Prescribing by consultant Rheumatologists following approval
by Thames Valley Specialised Rheumatology Network MDT.
BHT Rheumatology consultants will prescribe as outreach to
the Specialist Centre delivered as part of a provider network.
Name of Specialist centre and clinician involved in MDT to be
communicated to Formulary Team prior to initiating treatment
at BHT
De
c-1
6
De
c 1
6.9
Add Rituximab
100mg/10mL,
500mg/50mL
(MabThera®)
(intravenous infusion)
• Treatment of
dermatomyositis and
polymyositis (adults),
NHSE SSC Policy 1636/P
,July 2016
• Prescribing by
consultant
Rheumatologists
following approval by
Thames Valley
Specialised
Rheumatology
Network MDT. R
ed
Y
• Treatment of dermatomyositis and polymyositis (adults),
NHSE SSC Policy 1636/P ,July 2016
• Prescribing by consultant Rheumatologists following approval
by Thames Valley Specialised Rheumatology Network MDT.
BHT Rheumatology consultants will prescribe as outreach to
the Specialist Centre delivered as part of a provider network.
Name of Specialist centre and clinician involved in MDT to be
communicated to Formulary Team prior to initiating treatment
at BHT
Add Carbocisteine
750mg/10ml oral
sachets
Gre
en
Y
As second line to carbocisteine capsules where
carbocisteine capsules cannot be swallowed
In secondary care restricted - Respiratory Team
In primary care review effectiveness after 2-4 weeks
3.7
(M
uco
lytics)
De
c-1
6
Delete Carbocisteine
250mg/5ml liquid
Bla
ck
Y
3.7
(M
uco
lytics)
De
c-1
6
FOR ALL PRESCRIBING - NICE compliance form
required - see link from Formulary homepage.
1. Restricted - to Rheumatology consultant prescribing
only, in accordance with Biologics for Rheumatoid
Arthritis guideline (BHTCG 749FM) and NICE TA 195.
2. Restricted - to consultant consultant Rheumatologists
prescribing following approval by Thames Valley
Specialised Rheumatology Network MDT for:
a. treatment of ANCA-associated vasculitis in adults,
NHSE Clinical Commissioning policy A13/P, Jan 15.
b. treatment of dermatomyositis and polymyositis
(adults), NHSE SSC Policy 1636/P ,July 2016.
BHT Rheumatology consultants will prescribe as
outreach to the Specialist Centre delivered as part of a
provider network. Name of Specialist centre and clinician
involved in MDT to be communicated to Formulary Team
prior to initiating treatment at BHT
see Section 8.2.3 (for Haematology)
10
.1.3
(C
yto
kin
e m
od
ula
tors
)
De
c 1
6.1
6
• Carbocisteine sachets are cheaper in hospital and primary
care than carbocisteine 150mg in 5mL solution,
• Carbocisteine sachets are much more expensive than
capsules in hospital and primary care.
• Delete carbocisteine 250mg in 5mL solution from the
formulary
• Add carbocisteine sachets as a second line to carbocisteine
capsules when carbocisteine capsules cannot be swallowed

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
De
c 1
6.2
2
Add Elsbavir 50mg/
grazopevir 100mg
(Zepatier®) (film-
coated tablets)
• Treatment of chronic
Hepatitis C in accordance
with NICE TA 413
• Prescribing by
Consultant
Gastroenterologists/H
epatologists and
Associate Specialist
(Gastroenterology),
as part of Thames
Valley ODN
Re
d
Y
• Treatment of chronic Hepatitis C in accordance with NICE TA
413
• Prescribing by Consultant Gastroenterologists/Hepatologists
and Associate Specialist (Gastroenterology), as part of Thames
Valley ODN
• Future new hepatitis C NICE TAs and NHSE policies and
circulars need to be noted at FMG but the consultant does not
need to be present
FOR ALL PRESCRIBING - a completed and approved
HIGH COST DRUG compliance form, via BLUETEQ, is
required.
Restricted- prescribing by Consultant
Gastroenterologists/Hepatologists and Associate
Specialist (Gastroenterology), as part of Thames Valley
ODN in accordance with NICE TA 413.
05
.03
.03
.02
De
c-1
6
De
c 1
6.2
3
Add Ivacaftor 150mg
(Kalydeco®) (film-
coated tablets)
Cystic Fibrosis in
accordance with NHSE
Clinical Commissioning
Policy A01/P/c and SSC
1541,Oct 2015
• Prescribing by
Respiratory and
Paediatric
consultants only after
initiation in a
Specialist Centre and
delivered as outreach
as part of a provider
network
Re
d S
pe
c C
en
tre
Y
• For Cystic Fibrosis in accordance with NHSE Clinical
Commissioning Policy A01/P/c and SSC 1541,Oct 2015
• Prescribing by Respiratory and Paediatric consultants only
after initiation in a Specialist Centre and delivered as outreach
as part of a provider network
• The name of the Specialist centre and consultant initiating
ivacaftor to be communicated to Pharmacy Formulary Team
prior to prescribing
Restricted- prescribing by Respiratory and Paediatric
consultants only after initiation in a Specialist Centre and
delivered as outreach as part of a provider network.
For Cystic Fibrosis in accordance with NHSE Clinical
Commissioning Policy A01/P/c and SSC 1541,Oct 2015.
The name of the Specialist centre and consultant
initiating ivacaftor to be communicated to Pharmacy
Formulary Team prior to prescribing 3.7
(M
uco
lytics)
De
c-1
6
Add Sildenafil 20mg, 25mg
tablet
Add Taladafil 20mg tablet
Add Bosentan 62.5mg,
125mg
(tablet)
Restricted- prescribing by Respiratory consultants only
after initiation in a Specialist Centre. May be continued in
BHT via shared care between Specialist centre and BHT
via a network model
For pulmonary arterial hypertension in accordance with
NHSE Specialised Commissioning Policy A11/P/b, June
2014: National policy for targeted therapies for the
treatment of pulmonary hypertension in adults
The name of the Specialist centre and consultant
initiating drug to be communicated to Pharmacy
Formulary Team prior to prescribing
See also 7.4.5 for use in erectile dysfunction
2.5
.1
De
c-1
6
Restricted- prescribing by Respiratory consultants only
after initiation in a Specialist Centre. May be continued in
BHT via shared care between Specialist centre and BHT
via a network model
For pulmonary arterial hypertension in accordance with
NHSE Specialised Commissioning Policy A11/P/b, June
2014: National policy for targeted therapies for the
treatment of pulmonary hypertension in adults
The name of the Specialist centre and consultant
initiating drug to be communicated to Pharmacy
Formulary Team prior to prescribingDe
c 1
6.2
3
Prescribing by
Respiratory
consultants only after
initiation by a
Specialist Centre.
May be continued in
BHT via shared care
between Specialist
centre and BHT via a
network model
Re
d S
pe
c C
en
tre
Y
For pulmonary arterial hypertension in accordance with NHSE
Specialised Commissioning Policy A11/P/b, June 2014:
National policy for targeted therapies for the treatment of
pulmonary hypertension in adults
• Prescribing by Respiratory consultants only after initiation by a
Specialist Centre. May be continued in BHT via shared care
between Specialist centre and BHT via a network model
• The name of the Specialist centre and consultant initiating
drug to be communicated to Pharmacy Formulary Team prior to
prescribing

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Add Ambrisentan 5mg
(tablet)
Add Macitentan 10mg (film-
coated tablets)
Add Iloprost
50micrograms/0.5mL
(injection)
Unlicensed - High Risk
1. Restricted - prescribing by Consultant vascular
surgeons, rheumatologists and dermatologists only.
See Iloprost Infusion Protocol (BHTCG 684)
2. Restricted- prescribing by Respiratory consultants
only after initiation in a Specialist Centre. May be
continued in BHT via shared care between Specialist
centre and BHT via a network model.
For pulmonary arterial hypertension in accordance with
NHSE Specialised Commissioning Policy A11/P/b, June
2014: National policy for targeted therapies for the
treatment of pulmonary hypertension in adults
The name of the Specialist centre and consultant
initiating drug to be communicated to Pharmacy
Formulary Team prior to prescribing
Add Iloprost 10
micrograms/mL
(Ventavis®) (nebuliser
solution)
Restricted- prescribing by Respiratory consultants only
after initiation in a Specialist Centre. May be continued in
BHT via shared care between Specialist centre and BHT
via a network model
For pulmonary arterial hypertension in accordance with
NHSE Specialised Commissioning Policy A11/P/b, June
2014: National policy for targeted therapies for the
treatment of pulmonary hypertension in adults
The name of the Specialist centre and consultant
initiating drug to be communicated to Pharmacy
Formulary Team prior to prescribing
2.5
.1
De
c-1
6
Restricted- prescribing by Respiratory consultants only
after initiation in a Specialist Centre. May be continued in
BHT via shared care between Specialist centre and BHT
via a network model
For pulmonary arterial hypertension in accordance with
NHSE Specialised Commissioning Policy A11/P/b, June
2014: National policy for targeted therapies for the
treatment of pulmonary hypertension in adults
The name of the Specialist centre and consultant
initiating drug to be communicated to Pharmacy
Formulary Team prior to prescribingDe
c 1
6.2
3
Prescribing by
Respiratory
consultants only after
initiation by a
Specialist Centre.
May be continued in
BHT via shared care
between Specialist
centre and BHT via a
network model
Re
d S
pe
c C
en
tre
Y
For pulmonary arterial hypertension in accordance with NHSE
Specialised Commissioning Policy A11/P/b, June 2014:
National policy for targeted therapies for the treatment of
pulmonary hypertension in adults
• Prescribing by Respiratory consultants only after initiation by a
Specialist Centre. May be continued in BHT via shared care
between Specialist centre and BHT via a network model
• The name of the Specialist centre and consultant initiating
drug to be communicated to Pharmacy Formulary Team prior to
prescribing

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Add Epoprostenol
500micrograms
(infusion)
1. Restricted - for use on NICU, ITU and SCBU only
2. Restricted- prescribing by Respiratory consultants
only after initiation in a Specialist Centre. May be
continued in BHT via shared care between Specialist
centre and BHT via a network model.
For pulmonary arterial hypertension in accordance with
NHSE Specialised Commissioning Policy A11/P/b, June
2014: National policy for targeted therapies for the
treatment of pulmonary hypertension in adults
The name of the Specialist centre and consultant
initiating drug to be communicated to Pharmacy
Formulary Team prior to prescribing
2.8
.1 (
Ep
op
roste
no
l)
Remove Lumacaftor/ivacaftor
200mg/125mg
(Orkambi®)
(Tablets)
Bla
ck
Y
Negative recommendation in NICE TA398 for treating cystic
fibrosis homozygous for the F508del mutation
Blacklist
3.7
De
c-1
6
Oct
16
.10
Add Belimumab 100mg,
400mg powder for
concentrate for
solution for infusion
Active autoantibody-
positive systematic lupus
erythematosus
• Initiation by
consultant
Rheumatologists
under shared care
with a Specialist
Centre. In BHT this is
generally OUH
Re
d S
pe
c C
en
tre
Y
• For treating active autoantibody-positive systemic lupus
erythematosus in accordance with NICE TA397
• Steroids, DMARDs doesn’t increase infections; maybe
regional guidelines re rel place in therapy, Centres
• Initiation by consultant Rheumatologists under shared care
with a Specialist Centre. In BHT this is generally OUH
FOR ALL PRESCRIBING - a completed and approved
HIGH COST DRUG compliance form, via BLUETEQ, is
required.
Restricted- prescribing by Consultant Rheumatologists,
under a shared care with a Specialist Centre. In BHT this
is generally OUH. Prescribing is in accordance with
NICE TA 397 and NHSE SSC 1705.
10
.1.3
De
c-1
6
Ju
n 1
6.3
Add Capsaicin 0.025%
(Zacin®)
(cream)
Gre
en
Y
• For the symptomatic treatment of osteoarthritis of the hand as
an adjunct to core treatments in line with a Bucks Osteoarthritis
treatment algorithm which needs to be developed
The algorithm should describe the following place in therapy for
capsaicin 0.025% cream::
• Step 1: Regular oral paracetamol
• Step 2: Regular oral paracetamol + topical NSAID*.
*First choice ibuprofen gel, 2nd choice diclofenac gel, 3rd
choice piroxicam gel.
After a trial of all THREE topical NSAIDs has failed due to
inefficacy, intolerance or CI
• Step 3: Regular paracetamol and oral NSAIDs
• Step 4: Regular paracetamol and codeine
• Step 5: Topical capsaicin only.when all of the above
treatments are unsuitable if
Capsaicin 0.025% cream should be prescribed for three months
maximum after which it should be stopped. It should not be
added as a repeat prescription on GP computer systems.
For the symptomatic treatment of knee and hand
osteoarthritis as an adjunct to core treatments in line
with Bucks Osteoarthritis treatment algorithm (BHTCG
819FM).
Capsaicin 0.025% cream should be prescribed for three
months maximum after which it should be stopped. It
should not be added as a repeat prescription on GP
computer systems.
10
.3.2
De
c-1
6D
ec-1
6
Prescribing by
Respiratory
consultants only after
initiation by a
Specialist Centre.
May be continued in
BHT via shared care
between Specialist
centre and BHT via a
network model
Re
d S
pe
c C
en
tre
Y
For pulmonary arterial hypertension in accordance with NHSE
Specialised Commissioning Policy A11/P/b, June 2014:
National policy for targeted therapies for the treatment of
pulmonary hypertension in adults
• Prescribing by Respiratory consultants only after initiation by a
Specialist Centre. May be continued in BHT via shared care
between Specialist centre and BHT via a network model
• The name of the Specialist centre and consultant initiating
drug to be communicated to Pharmacy Formulary Team prior to
prescribing

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Fe
b 1
5.5
Add Adapalene/Benzoyl
Peroxide 0.1%/ 2.5%
(Epiduo®) gel
Gre
en
Y
Epiduo® was approved for formulary inclusion as follows:
• Prescribing by all prescribers in hospital and primary care
(Green on the traffic light list)
• For the treatment of acne in line with BAD/ CKS guideline on
acne vulgaris and the Bucks acne treatments algorithm as a
second line topical fixed dose combined agent when first line
topical fixed dose combinations (Duac® or Isotrexin®) are
either ineffective or unsuitable
For use in accordance with the Bucks Acne Treatment
Algorithm.
13
.6.1
De
c-1
6
Fe
b 1
5.5
Add Benzoyl
Peroxide/Clindamycin
5%/ 1% (Duac® Once
Daily) gel
Gre
en
Y
For use in accordance with the Bucks Acne Treatment
Algorithm.
13
.6.1
De
c-1
6
Fe
b 1
5.5
Add Erythromycin/Isotretin
oin 2%/0.05%
(Isotrexin®) gel
Gre
en
Y
For use in accordance with the Bucks Acne Treatment
Algorithm.
13
.6.1
De
c-1
6
Fe
b 1
5.5
Reject Erythromycin/Tretinoi
n 0.025%/ 4%
(Aknemycin®) solution
Bla
ck
Y
Reviewed as part of acne treatment algorithm
13
.6.1
De
c-1
6
Fe
b 1
5.5
Reject Clindamycin/ Tretinoin
1%/0.025% (Treclin®)
gel
Bla
ck
Y
Reviewed as part of acne treatment algorithm
13
.6,1
De
c-1
6
De
c 1
6.2
5 Add Metolazone tablet
2.5mg Re
d
N
5mg tablet is formulary and 2.5mg is also in use. Both are
unlicensed and 2.5mg added to formulary already as result of
first unlicensed meeting.
2
De
c-1
6
Delete Streptokinase 250,000
iu Bla
ck
N
No longer available and not ordered for more than 2 years
De
c-1
6
Add Streptokinase 1.5MU
Re
d
N
In small but regular use. Movianto is supplier
De
c-1
6
DeletePhosphate buffered
0.83mmol/ml
bla
ck
N
No use in community
Not on JAC. Eastbourne DGH may manufacture but not
ordered in years.
9
De
c-1
6
• For the treatment of moderate acne at risk of scarring when
use of monotherapy (benzoyl peroxide or a retinoid) is
ineffective, in line with BAD/CKS guidance.
• Green on the traffic light list
• Joint second line options (after monotherapy with benzoyl
peroxide or a retinoid has been unsuccessful)
FORMULARY MEDICINES TRAFFIC LIGHT CLASSIFICATION DECEMBER 2016

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
TLL
Phosphate buffered
solution saline pH 7.4
inj
Re
d
N
All use in by Burns Unit and manufactured by Tayside
P'ceuticals.
20 issued per year
Special and needs risk assessment and updating of JAC
9
De
c-1
6
TLL
Phosphate Mixture (JR
formula) 527mmol/litre -
Unlicensed - low risk
Re
d
N
No use in community
70-90 per yr. £20.65 per 100mL. Virtually all use is by
Paediatrics/NICU 9
De
c-1
6
TLLCalcium acetate tablets
1g
AI
NRestricted - initiation in secondary care with continuation by
GPs. Unlicensed - low risk9
De
c-1
6
TLL
Cefuroxime 125/5
AR
an
d B
lack
N
£23.75 / 180 3 issued 15/16 and 10 to date 16/17 5
De
c-1
6
TLL
Cefuroxime 125mg,
250mg tabs AR
an
d
N
Agreed AR with CCG 5
De
c-1
6
TLL
Fusidic acid 250mg/5mL
AR
N
Agreed AR with CCG 5
De
c-1
6
TLL
Fusidic acid tablets
250mg
AR
N
Agreed AR with CCG 5
De
c-1
6
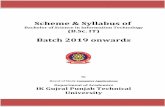
Revise
restriction
Clindamycin capsules
75mg, 150mg
Gre
en
N
Expand note on formulary for all regarding opening of capsules
and mixing with food/liquid in place of suspension. Primary
care already have this note and Micro suggested this when
Chapter 5 Traffic light classification was discussed.
In secondary care restricted - Microbiology approval
required for use in patients over 85 years of age, but
caution in prescribing for any patient over 65 years due
to increased risk of Clostridium difficile associated
diarrhoea
In primary care 2nd/3rd line choice in cellulitis and 2nd
line in dental abcesses. No other indications for use
identified in primary care antibiotic guidelines.
NOTE: If patient cannot swallow capsules they can be
opened, dispersed in water and administered.
5
De
c-1
6
FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Revise
restriction
Clindamycin suspension
75mg/5mL Re
d
N
NOTE: If patient cannot swallow capsules they can be opened
and dispersed in water and administered. Only prescribe
suspension if patient cannot swallow capsules or manage to
open and disperse contents of capsule.
Savings may be possible for BHT if stop using suspension
Unlicensed - Medium risk
In secondary care restricted - Microbiology approval
required for use in patients over 85 years of age, but
caution in prescribing for any patient over 65 years due
to increased risk of Clostridium difficile associated
diarrhoea. Use in accordance with Recommended
Empirical Antibiotic Regimens for Common Hospital
Infectious Conditions (BHTCG 279)
NOTE: If patient cannot swallow capsules they can be
opened and dispersed in water and administered. Only
prescribe suspension if patient cannot swallow capsules
or manage to open and disperse contents of capsule.
5
De
c-1
6
DELETEAlpha Tocoppheryl
Acetate tablets 50mg,
200mg
Bla
ck
N50mg not listed on JAC and not use of 200mg for several
years. Using licensed suspension in place
9
De
c-1
6
ADD Amylmetacresol/Dichlor
obenzyl lozenges
(Strepsils)
Re
d
Y
Missed being added to netFormulary at upload.
Formulary states: In community patients to purchase OTC
12
De
c-1
6
ADD Benzocaine/Cetylpyridin
ium chloride
10mg/1.4mg
(Merocaine) lozenge
Gre
en
Y
Added note to formular: yIn community encourage patient to
purchase OTC.
12
De
c-1
6
Revise Haloperidol
500micrograms
Gre
en
Y
Sometimes tablets are cheaper and other times capsules are
cheaper. Added option of tab or cap for the 500microgram.
4
De
c-1
6
Revise
restriction
Sotalol tablets 40mg,
80mg
AR
an
d B
lack Y Amber Recommendation - restricted to recommendation
by secondary care with continuation by GPs for anti-
arrhythmic treatment only.
Black - Not to be prescribed to treat hypertension
2
De
c-1
6
Agreed TLL
and
restriction
Naftidrofuryl capsules AI
Y Restricted - to be initiated in secondary care with
continuation by GPs in accordance with NICE TA223 for
the treatment of intermittent claudication in people with
peripheral arterial disease.
Agree with CCG as part of TLL/Unlic work
2
De
c-1
6
Delete Doxepin tablets
Bla
ck Y Not been used since 2012. Only appear in Ox Health formulary
under a Dermatology entry (Xepin), 5% cream.
4
De
c-1
6

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Delete Gabapentin suspension
250mg/5mL Bla
ck N Removed from formulary as licensed solution now available
from Rosemont p'ceuticals
4
De
c-1
6
Add Gabapentin solution
50mg/1mL
Gre
en Y Replaced unlicensed product with same restriction: May be prescribed generically (see link to MHRA
Epilepsy alert above)
Before prescribing, consider opening gabapentin
capsules (this is preferable and is more cost effective)
Restricted - only for use in patients who, cannot swallow
capsules and are unable to manage opening the
capsules.
4
De
c-1
6
Revise
restriction
Zuclopenthixol acetate
50mg/1mL, 100mg/2ml
Clopixol Acuphase
Re
d Y Restricted - initiation by Consultant Psychiatrist (Mental
Health Trust) only.
IMPORTANT NOTE:- when prescribing, dispensing or
administering, check that this is the correct preparation -
this preparation is usually used in hospital for an acute
episode and should not be confused with depot
preparations which are usually used in the community or
clinics for maintenance treatment.
4
De
c-1
6
Revise
restriction
Tuberculin 2u/0.1ml
Gre
en CCG requested addition of note to formulary stating:
"Public Health responsible for testing in Primary Care"
14
Revise
restriction
Tuberculin 10u/0.1mlG
reen CCG requested addition of note to formulary stating:
"Public Health responsible for testing in Primary Care"
14
TLL Lidocaine
HCl/adrenaline 2%/
1:80000 2.2mL cartridge
Re
d Y Injection - red
No use in community
15
TLL Lidocaine 0.5%, 10mL
amps Re
d Y Injection - red
No use in community
15
TLL Lidocaine HCl
2%/adrenaline
1:200,000 10ml vial
Re
d N Injection - red
No use in community
15
TLL Ethyl Chloride
Re
d Make red as not likely to be prescribed 15
Add Paraldehyde 50% in
olive oil
red N replacing paraldehyde in sunflower oil. Medium Risk Unlicensed- medium risk 4
Delete Paraldehyde 50% in
sunflower oil Bla
c N Not ordered for years by BHT 4
Delete Paraldehyde injection
Bla
ck N Only enema referred to in BHT CG 383 Epilepsy in Children.
No use at BHT in several years
4
Add Triclosan 1% surgical
scrub Re
d In regular use by theatres in Trust 13
De
c-1
6

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Add Hydrogen Peroxide
Sterile 10 volume 3%, Re
d N In regular use by theatres in Trust . Unlicensed - Low Risk Unlicensed- low risk 13
Add Lidocaine HCl
2%/adrenaline
1:200,000 20ml
multidose vial
Gre
en Y 10mL vial is unlicensed and used across BHT. Multidose
widely used by CCG. Add to formulary
15
Delete Povidone iodine 10%
alcoholic paint 8mL Bla
ck No longer available 13
Delete Furosemide solution
1mg/1mL Bla
ck N Removed when paediatric liquids reviewed by BHT. Unlicensed 2
DELETE Neostigmine tablets
15mg
Bla
ck? Y No longer unlicensed. Amend formulary to remove unlicensed
symbol and primary care comment regarding availability.
Check with ITU lead as to whether these should remain on
formulary as not ordered in many years (OCt12).
2
Delete Chloral hydrate
suppositories 60mg Bla
ck N No use in years. Retain 50mg as red and delete the 60mg 4
TLL Chloral hydrate
suppositories 50mg Re
d N 4
revise
restriction
Clonazepam
500micrograms, 2mg
tablets
gre
en Y Add note saying tablets disperse easily in water as a more cost
effective option if patients cannot swallow tablets. Info from MI
25Nov16 Clonazepam tablets disperse quite easily in water. If
giving down an NG tube, should be dispersed in about 30mL of
water before administration (the large volume of water is
necessary to stop the clonazepam from sticking to the feeding
tube)
Prescribing generically or by brand is discretionary
NOTE: tablets disperse quite easily in water and are a
more cost effective option for patients who cannot
swallow tablets. If giving down an NG tube, disperse in
30mL water before administration. The large volume of
water is to stop the clonazepam sticking to the NG tubing
4
revise
restriction
Clonazepam oral
solution
500micrograms/5mL
AI
Y Add note saying tablets disperse easily in water as a more cost
effective option if patients cannot swallow tablets.
Prescribing generically or by brand is discretionary
Restricted - initiation by Psychiatric team only for use
when patient cannot swallow tablets.
NOTE: Clonazepam tablets disperse easily in water and
are a more cost effective option for patients who cannot
swallow the tablets.
4
TLL Lidocaine 0.5%
/Adrenaline 1:200,000
10mL amps
Re
d N Injection - red
No use in community
15
De
c-1
6
TLL LidocaineHCl
1%/adrenaline
1:200,000 10ml
Re
d N Injection - red
No use in community
15
De
c-1
6
ADD Lidocaine HCl
2%/adrenaline
1:200,000 20ml
multidose vial
Gre
en Y Not currently on formulary but in regular use in community.
CCG agree green. Not currently in use at BHT.
15
De
c-1
6D
ec-1
6D
ec-1
6
FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
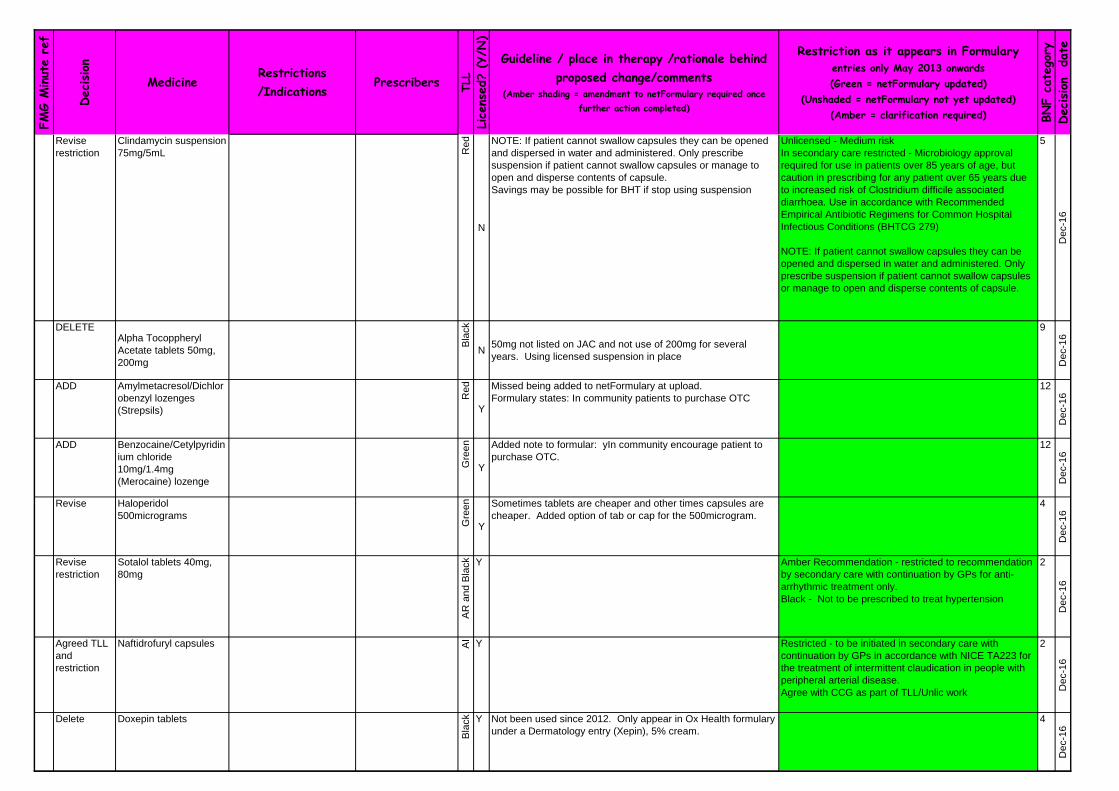
Delete Amobarbital sodium
200mg cap
Amobarbital
sodium/secobarbital
sodium caps
50mg/50mg
Butobarbital tablet
Bla
ck No longer in use 4
De
c-1
6
DELETE Lidocaine 0.5%
/Adrenaline 1:200,00
pre-filled syringe
Bla
ck Y No longer available. 15
De
c-1
6
Revise
restriction
Theophylline 60mg,
125mg, 250mg (Slo-
Phyllin) MR capsule Gre
en Y Add note to formulary: for patients who experience difficulty in
swallowing capsules, the contents of a capsule may be
sprinkled on to a spoonful of soft food, e.g. yoghurt.
NOTE: For patients who cannot swallow the capsules,
the contents of the capsule can be opened and sprinkled
onto a spoonful of soft food eg yoghurt.
3
De
c-1
6
Revise
restriction
Theophylline 200mg,
300mg, 400mg
(Uniphyllin Continus®)
(MR tablet)
Gre
en N Add note to formulary: Tablets should be swallowed whole and
not crushed or chewed.
3
De
c-1
6
Revise
restriction
Theophylline oral
solution 60mg/5mL
?? N 15 (15/16), 7 issued yr to date
Agree addition of note saying the capsules can be opened and
sprinkled on food.
Traffic light position still not agreed. Ideally if all patients were
on Slophyllin the capsules could be opened and sprinkled if
patient unable to swallow capsules. Further discussion/work
required on switching all patients to Slophyllin as more cost
effective and consistent levels.
Restricted - Phone Pharmacy to Order.
unlicensed - LOW risk
Named patient
NOTE: For patients who cannot swallow capsules, the
contents of the capsules (Slo-Phyllin®) can be opened
and sprinkled onto a spoonful of soft food eg yoghurt.
3
De
c-1
6
Revise
restriction
Indometacin 25mg/5ml
suspension Re
d N Propose addition of note to formulary suggesting Ibuprofen as a
liquid alternative if treatment with a liquid is to be continued in
the community. The unlicensed indometacin and naproxen are
very costly.
Need agreement from Rheumatology? Paeds?
10
De
c-1
6
Revise
restriction
Naproxen 125mg/5ml
suspension Re
d Y Propose addition of note to formulary suggesting Ibuprofen as a
liquid alternative if treatment with a liquid is to be continued in
the community. The unlicensed indometacin and naproxen are
very costly.
Need agreement from Rheumatology? Paeds?
When first discussed at FMG it was agree to hold at Red until
such time as it was needed or removed.
11Feb15 Sally Edmonds, Cons Rheu agreed that first
prescription to be written in secondary care. She would also be
happy with AR if GPs agree. Usage is virtually nil so AR not
really appropriate. No use in community at all. Keep as red for
now but consider removal from formulary once discussed with
Rheumatology and Paeds.
10
De
c-1
6

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Change from
Unlic to
Licensed
Cocaine 10% sterile
solution Re
d N 24Nov16 Change status on Formulary from unlicensed to
licensed. MI noted a licensed product is now available from
Martindale. Cease buying unlicensed from Huddersfield.
15
De
c-1
6
Revise
restriction
Spironolactone
suspension - all
strengths Gre
en N CCG have agreed all green but current formulary wording
states initiation in secondary care with continuation by GPs
which suggests amber initiation, therefore remove this wording
if green.
Note that it is more cost effective to crush the tablets is already
on the formulary.
2
De
c-1
6
ADD Spironolactone
suspension 10mg in
5mL Gre
en N In use in community and not at BHT. Paed Liq review for BHT
recently removed all strengths except the 25/5.
DT prices for 125mL are:
5/5 £51.86, (£2.07 per dose) 10/5 £58.58 ( £1.17 per 5mg
dose)
25/5 £39.24 (£0.31 per 5mg dose) 50/5 £62.51 (£0.25 per
5mg dose)
The 25/5 is significantly more cost effective than the 10/5
Note to crush tablets is already on formulary.
Note added to formulary: not in use in secondary care, primary
care use only.
2
De
c-1
6
Revise
restriction
Spironolactone
suspension 5mg in 5mL Bla
ck N Note to be added to formulary: not in use in secondary care,
primary care use only.
2
De
c-1
6
Revise
restriction
Spironolactone
suspensions
Gre
en Add a note to this entry saying that only the 25mg in 5mL is to
be used in secondary care.
Add second note labelling this as the most cost effective
formulation.
In primary care 44 issued in last year £3344
2
De
c-1
6
De
c 1
6.2
4 Add
restriction
Alpha Tocopheryl
Acetate 500mg/5mL
(Vitamin E)
Gre
en
Y
Super high doses are for metabolic disorders and require
specialist input
Dose according to specialist recommendation in Cystic
Fibrosis and RDA in other conditions (green on TLL)
9.6
.5
De
c-1
6
Add Alpha Tocopheryl
Acetate 500mg/5mL
(Vitamin E)
(suspension)
Re
d
N
As above Restricted- for treatment continuation in metabolic
disorders, only after initiation by tertiary specialist
centres (e.g. Oxford - John Radcliffe) .
9.6
.5
De
c-1
6
Change TLL Naltrexone
Hydrochloride 50mg
(tablet) Re
d
Y
Oxford Health have discussed and red-listed this (this is how it
appears on Oxford Health formulary)
Restricted - Initiation by Mental Health Trust physicians
only
4.1
0.3
De
c-1
6
unlicensed - Low risk
NOTE 1: before prescribing a suspension consider the
more cost effective option to crush the tablets.
NOTE 2: only 25mg/5mL in use in secondary care.
NOTE 3: 25mg/5mL liquid is the most cost effective of
the available liquid formulations.
BHT FORMULARY CHANGE TO NOTE Dec 2016

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Add Kerramax Care 20 cm
x 50 cm
Gre
en
Y
Available from ONPOS
19
.1.3
De
c-1
6
Add Nomegestrol acetate
2.5mg/ estradiol 1.5mg
tablets (Zoely®) Bla
ck
Y
New drug never discussed
7.3
.1
De
c-1
6
Add Ivermectin 10mg/g
cream
Bla
ck
Y
New drug never discussed
13
.6
De
c-1
6
Add Avanafil 50mg, 100mg,
200mg tablets
Bla
ck
Y
New drug never discussed
7.4
.5
De
c-1
6
Add Triamcinolone
acetonide 0.1%
oramucousal paste Bla
ck
Y
Discontinued
12
.3.1
De
c-1
6
Add Calipostriol
50micrograms/g /
Betametasone 0.5mg/g
cutaneous foam
(Enstilar®) Bla
ck
Y
New drug never discussed
13
.5.2
De
c-1
6
Add Chlorhexidine 2% in
70% IPA wipes (Sani-
Cloth®) Re
d
Y
New product following disinfectant products review in BHT.
Confirmed with Claire Brandish, anti-infectives pharmacist
Available via Supplies.
For peripheral line insertion, venepuncture and hub and
connection port cleaning.
13
.11
.3
De
c-1
6
Remove
brand name
Fludroxycortide
4micrograms/cm2
(Haelan®)
(tape)
Gre
en
Y
Note Branded haelan tape has been discontinued as of
Nov 2016. This is now available as generic
13
.4
De
c-1
6
Change TLL Hydrocortisone
2mg/mL
(suspension)
Bla
ck
Y
Current formulary states In primary care not recommended as a
pharmaceutical special, consider lozenges or a soluble steroid
tablet. In secondary care we never use this as mouthwash. Also
confirmed with paeds not used. 12
.3.1
De
c-1
6
Add note Hydrocortisone 2.5mg
(mucoadhesive buccal
tablet)
Gre
en
Y
In primary care hydrocortisone suspension is not
recommended as unlicensed, consider licensed
alternatives (e.g. lozenges or soluble steroid tablets)
12
.3.1
De
c-1
6
Add Hydrocortisone
1mg/mL
(suspension)
Gre
en
Y
Paeds pharmacists requested in the past.
Wanted the 5mg/5mL as that is what they use in Oxford and
often we get patients transferred across to us so it makes
sense from a continuity of care point of view. Hydrocortisone
tablets are very difficult to crush.
Risk assessed as LOW.
Restricted- for use in paediatrics.
6.3
.2
De
c-1
6

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Add ACD-A Anticoagulant
Citrate Dextrose
Solution
Re
d
Y
This is already stocklist in Wycombe theatres but not on
formulary. It is used for the cell saver machines which allow
theatres to give patients their own blood back. Theatres are
worried it would be a risk to use a bag of saline that you would
need to add heparin to rather than having a pre-made bag of
ACD which is easier to differentiate.
Restricted- for use in theatres for cell salvage
2.8
.1
De
c-1
6
Add
indication
Fibrin Sealant
(Tisseel®)
(Ready to use syringe)
Re
d
Y
Expected use is average of 2 packs per month. Cost agreed
with SDU
• Restrictions:
o Prescribing by Cardiology Consultant only
o For use in patients at increased risk of bleeds during device
implant or box change procedures
Restricted - for use by:
1. Spinal surgeons
2. Anterior segment procedures in Ophthalmology
3. Cardiology Consultant for use in patients at increased
risk of bleeds during device implant or box change
procedures
16
.1
De
c-1
6
Add note Moxifloxacin 400mg
tablets
AR Y
For use in accordance with BHT CG 133 Management and
antibiotic therapy for respiratory tract conditions in adults for
patients who are penicillin-allergic and with a CURB-65 score of
2.
In secondary care restricted:
1. for use in accordance with BHT CG 133 Management
and antibiotic therapy for respiratory tract conditions in
adults for patients who are penicillin-allergic and with a
CURB-65 score of 2
2. Ophthalmology patients.
For all other uses Microbiology approval required.
May be recommended by specialist in secondary care
with continuation by GPs
5.1
.12
De
c-1
6
Add note +
restriction
Moxifloxacin
400mg/250mL
(intravenous infusion)R
ed
Y
As above and IV is 3 x more expensive than oral. Oral
bioavailability is 92%
Restricted- only to be used if nil by mouth or nausea and
vomiting. Oral bioavailability is good.
For use in accordance with BHT CG 133 Management
and antibiotic therapy for respiratory tract conditions in
adults for patients who are penicillin-allergic and with a
CURB-65 score of 2.
For all other uses Microbiology approval required.
5.1
.12
De
c-1
6
Amend link Liraglutide 6mg/mL
(injection, 3mL
prefilled pen Am
be
r
Y
NICE TA 203 has been superseded by NICE NG28
6.1
.2.3
De
c-1
6
Amend link Exenatide 2mg
(Bydureon®)
(MR injection, vial and
pre-filled pen) Am
be
r
Y
NICE TA 203 has been superseded by NICE NG28
6.1
.2.3
De
c-1
6
Amend
licensed
status
Cocaine
Hydrochloride 10%
(topical sterile
solution)
Re
d
Y
There is now a licensed cocaine solution 10% which is made by
Martindale. Originally buying unlicensed preparation
15
.2
De
c-1
6

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Amend
restriction
Tacrolimus
500micrograms, 1mg,
5mg (Prograf®,
Adoport®)
(capsule)
Re
d
Y
Currently bullet point 2- formulary states for transplant patients
but not quite clear. Also it still states that patients under shared
care by GP would be transferred back to secondary care
prescribing by April 2016- which is passed the deadline.
1. Restricted - to prescribing by Consultant
Dermatologists (see Section 13.05.03)
2. Restricted - to prescribing by Consultant Renal
physicians and other consultants for transplant patients
after initiation by a Specialist Centre.
3. Restricted - to prescribing by Consultant
Gastroenterologists for autoimmune hepatitis following
initiation by a Specialist Centre
Oral Tacrolimus products should be prescribed and
dispensed by brand name only (MHRA drug safety
update, June 2012). Adaport® brand is the first choice.
8.2
.2
De
c-1
6
Amend
restriction
Tacrolimus
500micrograms, 1mg
(Progaf®, Adoport®)
(capsule)
Re
d
Y
Restricted - to prescribing by Consultant Dermatologists
Adaport® brand is the first choice. If changing brands,
monitoring is required.
Oral Tacrolimus products should be prescribed and
dispensed by brand name only (MHRA drug safety
update, June 2012)
see also Section 08.02.02
13
.5.3
De
c-1
6
Add link Prednisolone 1mg,
5mg, 25mg
(tablet)G
reen
Y
Add link to leaflet as prednisolone 5mg tablets can be
crushed
http://www.medicinesforchildren.org.uk/prednisolone-
asthma 6.3
.2
De
c-1
6
Add Riluzole 25mg/5ml
(liquid)
Re
d
Y
Confirmed with the neurologists that they are not stopping
riluzole when patients are NBM. They have requested to be
used for patients who are on PEG- which is not easy for
patients to manage in their own homes
Restricted to patients who cannot swallow riluzole tablets
4.9
.3
De
c-1
6
Add size Sodium Hyaluronate
10mg in 1ml pre-filled
syringe
Re
d
Y
Cheaper alternative brand available
11
.99
.99
.99
De
c-1
6
Oct
16
.3
Add
indication
Radium-223 dichloride
1000 kBq/ml (Xofigo®)
(solution for injection)
For treating hormone-
relapsed prostate cancer
with bone metastases in
accordance with NICE TA
412
OUH Oncologists
only
Re
d
Y
NICE TA 376 replaced with NICE TA 412 published September
2016.
Approved for:
• Prescribing by OUH Oncologists only
• For treating hormone-relapsed prostate cancer with bone
metastases in accordance with NICE TA 412
Restricted - prescribing by consultant oncologists at
OUH only for the treatment of hormone-relapsed
prostate cancer with bone metastases in accordance
with NICE TA 412
8.3
.4.2
Oct-
16
FMG DECISIONS OCTOBER 2016

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Oct
16
.4
Add
indication
Pemetrexed 500mg
(injection)
For maintenance treatment
for non-squamous non-
small-cell lung cancer after
pemetrexed and cisplatin in
accordance with NICE TA
402 and NHSE SSC 16 47
Consultant
Oncologist (Lung)
Re
d
Y
• For maintenance treatment for non-squamous non-small-cell
lung cancer after pemetrexed and cisplatin in accordance with
NICE TA 402 (Aug 2016) and NHSE SSC 16 47.
• Prescribing by consultant Oncologist (Lung)
FOR ALL PRESCRIBING: NICE compliance form
required - see link from Formulary homepage or via
Blueteq. NICE compliance to be verified if form not
available.
1. Restricted - Consultant Oncologist prescribing only in
accordance with NICE TA 181.
2. Restricted - prescribing by Oncologists only, in
accordance with NICE TA 190.
3. Restricted - prescribing by Oncologists only, in
accordance with NICE TA 135.
4. Restricted - prescribing by consultant Oncologists
(Lung) only. For maintenance treatment for non-
squamous non-small-cell lung cancer after pemetrexed
and cisplatin in accordance with NICE TA 402 and NHSE
SSC 16 47
8.1
.3
Oct-
16
Oct
16
.5
Add Crizotinib 250mg
capsules (Xalkori®)
For untreated anaplastic
lymphoma kinase-positive
advanced non-small-cell
lung cancer in accordance
with NICE TA 406
Consultant
Oncologist (Lung)
Re
d
Y
• for untreated anaplastic lymphoma kinase-positive advanced
non-small-cell lung cancer in accordance with NICE TA 406
• Prescribing by consultant Oncologist (Lung)
FOR ALL PRESCRIBING: NICE compliance form
required - see link from Formulary homepage or via
Blueteq. NICE compliance to be verified if form not
available.
Restricted - prescribing by consultant Oncologists (Lung)
only. For untreated anaplastic lymphoma kinase-positive
advanced non-small-cell lung cancer in accordance with
NICE TA 406
8.1
.5
Oct-
16
Oct
16
.6
Add Trifluridine-tipiracil
15mg/6.14mg,
20mg/8.19mg film-
coated tablets
(Lonsurf®)
For previously treated
metastatic colorectal
cancer in accordance with
NICE TA 405 and NHSE
SCC 1662
Consultant
Oncologists
Re
d
Y
• For previously treated metastatic colorectal cancer in
accordance with NICE TA 405 and NHSE SCC 1662
• Prescribing by consultant Oncologists
FOR ALL PRESCRIBING: NICE compliance form via
Blueteq required.
Restricted - prescribing by consultant Oncologists. For
previously treated metastatic colorectal cancer in
accordance with NICE TA 405 and NHSE SCC 1662
8.1
Oct-
16
Oct
16
.7
Add Talimogene
laherparepvec
solution for injection
(Imlygic®)
Treatiment of unresectable
metastatic melanoma.
NICE TA 410
OUH Consultant
Oncologists (Skin)
Re
d
Y
• Prescribing by OUH Consultant Oncologists (Skin)
• Treatiment of unresectable metastatic melanoma. NICE TA
410
Restricted - prescribing by OUH consultant Oncologists
(skin). For treatment of unresectable metastatic
melanoma in accordance with NICE TA 410. 8.2
.4
Oct-
16
Oct
16
.8
Add Bosutinib 100mg,
500mg film-coated
tablets (Bosulif®)
previously treated chronic
myeloid leukaemia in
accordance with NICE TA
401 and NHSE SCC 1661
Consultant
Haematologists
Re
d
Y
• for previously treated chronic myeloid leukaemia in
accordance with NICE TA 401 and NHSE SCC 1661
• prescribing by consultant Haematologists only
FOR ALL PRESCRIBING: NICE compliance form via
Blueteq required.
Restricted - prescribing by consultant Haematologists.
For previously treated chronic myeloid leukaemia in
accordance with NICE TA 401 and NHSE SSC 1661.
8.1
.5 (
Pro
tein
kin
ase
inh
ibito
rs)
Oct-
16

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Revise
restriction
Palivizumab 50mg,
100mg
(injection)
Use in accordance with
SSC 1646 Palivizumab (To
reduce the risk of RSV in
High Risk Infants) for the
2016 Vaccination Season
Consultant
Paediatricians
Re
d
Y
Amend entry to state Blueteq form required and in line with
SSC 1646
FOR ALL PRESCRIBING: NICE compliance form via
Blueteq required.
Restricted - prescribing by consultant Paediatricians. To
reduce risk of RSV in high risk infants, in accordance
with JCVI criteria and SSC 1646 palivizumab for the
2016 vaccination season.
5.3
.5
Oct-
16
Add Atarulen 125mg,
250mg, 1000mg
granules for oral
suspension
Use in accordance with
SSC 16 33 NICE HST3
Ataluren for treating
Duchenne muscular
dystrophy with a nonsense
mutation in the dystrophin
OUH Specialist
centre
Re
d
Y
• use in accordance with SSC 16 33 NICE HST3 Ataluren for
treating Duchenne muscular dystrophy with a nonsense
mutation in the dystrophin gene July 16 and NHSE Aug 16.
• Prescribable by OUH Specialist Centre only; not prescribable
by BHT
Restricted- prescribing by OUH specialist centre only,
not prescribable by BHT. For treatment of Ducehenne
muscular dystrophy with a nonsense mutation in the
dystrophin gene in accordance with SSC 16 33 NICE
HST3 and NHSE Aug 16.
10
.2.1
Oct-
16
Add Bedaquiline 100mg
tablets
Add Delamanid 50mg
tablets
Revise
restriction
Sofosbuvir/Ledipasvir
400mg/90mg
(Harvoni® )
(tablet)
FOR ALL PRESCRIBING - a completed and approved
HIGH COST DRUG compliance form, via BLUETEQ, is
required.
Restricted - prescribing by Consultant
Gastroenterologists/Hepatologists and Associate
Specialist (Gastroenterology), as part of Thames Valley
ODN in accordance with NICE TA 363 or NHSE
Commissioning Policy statement 1524, June 2015 -
Hepatitis C with cirrhosis and NHSE SSC 1615. All
patients will be discussed in the ODN MDT.
Revise
restriction
Daclatasvir 30mg,
60mg (Daklinza®)
(tablet)
FOR ALL PRESCRIBING - a completed and approved
HIGH COST DRUG compliance form, via BLUETEQ, is
required.
Restricted - prescribing by Consultant
Gastroenterologists/Hepatologists and Associate
Specialist (Gastroenterology), as part of Thames Valley
ODN in accordance with NICE TA 364 or NHSE
Commissioning Policy statement 1524, June 2015 -
Hepatitis C with cirrhosis and NHSE SSC 1615. All
patients will be discussed in the ODN MDT.
use in accordance with SSC 1645: Bedaquiline and Delamanid
for defined patients with Multidrug-Resistant/Extensively Drug-
resistant Tuberculosis (MDR/XDR-TB)
Prescribing by OUH Specialists in multiple resistant TB only -
not BHT, blueteq approval form required
FOR ALL PRESCRIBING: NICE compliance form via
Blueteq required.
Restricted- prescribing by OUH specialists only, not
prescribable by BHT. Use in multidrug-resistant TB in
accordance with NHSE SSC 1645.
5.1
.9
Oct-
16
Restricted -
prescribing by
Consultant
Gastroenterologists/H
epatologists and
Associate Specialist
(Gastroenterology),
as part of Thames
Valley ODN
Re
d
Y
Amend entry to include SSC 1615 implementation of NICE Tas
363, 364, 365
5.3
.3.2
Oct-
16
Oct
16
.12
use in accordance with
SSC 1645: Bedaquiline
and Delamanid for defined
patients with Multidrug-
Resistant/Extensively Drug-
resistant Tuberculosis
(MDR/XDR-TB)
Prescribing by OUH
Specialists in multiple
resistant TB only - not
BHT
Re
d
Y

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Revise
restriction
Viekirax
12.5mg/75mg/50mg
(tablet)
Contains: Ombitasvir/Paritaprevir/Ritonavir
FOR ALL PRESCRIBING - a completed and approved
HIGH COST DRUG compliance form, via BLUETEQ, is
required.
Restricted - prescribing by Consultant
Gastroenterologists/Hepatologists and Associate
Specialist (Gastroenterology), as part of Thames Valley
ODN in accordance with NICE TA 365 or NHSE
Commissioning Policy statement 1524, June 2015 -
Hepatitis C with cirrhosis and NHSE SSC 1615. All
patients will be discussed in the ODN MDT.
Add note Chapter 5.3.1
Re
d
Y
New NHSE Clinical Commissioning Policy F03/P/c • HIV
treatment as prevention in infection adults
Prescribing of all HIV medicines restricted to
Genitourinary (GUM) consultants only. Traffic light list:
Red
• HIV treatment as prevention in infection adults in
accordance to NHSE Clinical Commisioning Policy
F03/P/c 5.3
.1
Oct-
16
Remove
note
Fluphenazine
Decanoate 25mg/1mL
(injection (oily))
Remove
note
Fluphenazine
Decanoate
50mg/0.5mL,
100mg/1mL
(injection (oily))
Change TLL Mianserin
Hydrochloride 10mg,
30mg
(tablet)
Bla
ck
Y
Black on Oxford Health formulary no use in primary or
secondary care
4.3
.1
Oct-
16
Add
restriction
Tisseel Ready to use
(Baxter)
Spinal surgeons,
opthamologists
Re
d
Y
Currently on formulary for spinal use only. Opthamologists
proposed to use for gluing the conjunctival autograft after
pterygium excision. It has amazing results, both in terms of
postoperative inflammation (the lack of it with the use of glue as
opposed to sutures) and surgical time (shorter by about
20minutes).
Restricted- for use by:
1. Spinal surgeons
2. Anterior segment procedures in Ophthalmology
16
.1
Oct-
16
Restricted -
prescribing by
Consultant
Gastroenterologists/H
epatologists and
Associate Specialist
(Gastroenterology),
as part of Thames
Valley ODN
Re
d
Y
Amend entry to include SSC 1615 implementation of NICE Tas
363, 364, 365
5.3
.3.2
Oct-
16
Oct
16
.12
Oct-
16
Oct
16
.15
Am
be
r
Y
Stock now available from Sanofi Sep 16. Remove previous
notes stating that this was not available and then available
again
Protocol in development
4.2
.2

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Add note Dexamethasone
500micrograms, 2mg
(tablet)
Gre
en
Y
Add for 2mg: "use soluble tablets as they are currently cheaper
than plain tablets Oct 16"
Note for 2mg tablets: Use soluble 2mg tablets as they
are currently cheaper than plain 2mg tablets Oct 16
6.3
.2
Oct-
16
Add Dexamethasone 2mg
soluble tablets
Gre
en
Y
"soluble tablets are currently cheaper than plain tablets and are
therefore recommended for all uses Oct 16"
Note soluble tablets are currently cheaper than plain
2mg tablets and are therefore recommended for all uses
Oct 16
6.3
.2
Oct-
16
Ju
n 1
6.6
Add Medroxyprogesterone
acetate 104 mg in 0.65
mL subcutaneous
prefilled injector
device (Sayana
Press®) Gre
en
Y
• As an alternative to IM medroxyprogesterone acetate injection
for patients who wish to self administer (following training)
• Prescribable in primary or secondary care.
• As an alternative to IM medroxyprogesterone acetate
injection for patients who wish to self administer
(following training)
See video training links below for further information:
For Health Care Professionals:
https://www.youtube.com/watch?v=H_BH7RWfPWI
For patients:
https://www.youtube.com/watch?v=hi2o-mlQJjc
07
.03
.02
.02
Oct-
16
Ju
n 1
6.1
1a
Add Sacubitril/Valsartan
24mg/26mg
49mg/51mg
97mg/103mg
(tablet
For treating symptomatic
chronic heart failure with
reduced ejection fraction in
accordance with NICE TA
388
Initiation by
consultant
Cardiologists, dose
titration and
monitoring by the
heart failure team for
the first three months
prior to transfer to the
G
Am
be
rY
For treating symptomatic chronic heart failure with reduced
ejection fraction in accordance with NICE TA 388 in people
with:
• with New York Heart Association (NYHA) class II to IV
symptoms and
• with a left ventricular ejection fraction of 35% or less and
• who are already taking a stable dose of ACE inhibitors or
ARB.
Initiation by consultant Cardiologists, dose titration and
monitoring by the heart failure team for the first three months
prior to transfer to the GP in accordance with an amber
initiation guideline.
Restricted - initiation by Consultant cardiologists for
treating symptomatic chronic heart failure with reduced
ejection fraction in accordance with NICE TA388. Dose
titration and monitoring by the heart failure team for the
first three months prior to transfer to the GP in
accordance with Sacubitiril Valsartan for Symptomatic
Chronic Heart Failure - Secondary/ Primary Care
Guideline (BHTCG 817FM) 2.5
.5.2
Oct-
16
Oct
16
.15

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Ju
n 1
6.1
5
Add Insulin Glargine
300units/mL
(injection)
For treatment of type 1 or
type 2 diabetes in patients
who are already receiving
an optimised insulin
regimen AND:
• receiving basal analogue
insulin at a high dose
(more than 80 Units in a
single dose) in order to
reduce injection volume
OR
• receiving insulin glargine
100 Units/mL and
experiencing nocturnal
hypoglycaemia OR
requiring more flexibility in
injection timing
Prescribing initiation
by Consultant
Diabetologists or
Diabetes Specialist
Nurses only, dose
titration on the advice
of Diabetes Specialist
Nurses, continuation
by GPs
Am
be
r
Y
For treatment of type 1 or type 2 diabetes in patients who are
already receiving an optimised insulin regimen AND:
• receiving basal analogue insulin at a high dose (more than 80
Units in a single dose) in order to reduce injection volume OR
• receiving insulin glargine 100 Units/mL and experiencing
nocturnal hypoglycaemia OR
requiring more flexibility in injection timing
Prescribing initiation by Consultant Diabetologists or Diabetes
Specialist Nurses only, dose titration on the advice of Diabetes
Specialist Nurses, continuation by GPs
Initiation will also include GP practices’ who sign up to this
service (in due course once the “Direct Award” is developed
and agreed). This action should not prevent this drug
becoming available on the formulary.
Prescribing by brand name in accordance with MHRA advice
All discharge letters recommending a change to a high strength
insulin should highlight clearly the unusual strength in an effort
to reduce the risk of errors.
NOTE: Prescribe all insulins by brand
Toujeo (3mL prefilled disposable injection device)
Restricted- initiation by Consultant Diabetologists or
Diabetes Specialist Nurses only, dose titration on the
advice of Diabetes Specialist Nurses, continuation by
GPs. Initiation will also include GP practices’ who sign
up to this service (in due course once the “Direct Award”
is developed and agreed
For treatment of type 1 or type 2 diabetes in patients
who are already receiving an optimised insulin regimen
AND:
• receiving basal analogue insulin at a high dose (more
than 80 Units in a single dose) in order to reduce
injection volume OR
• receiving insulin glargine 100 Units/mL and
experiencing nocturnal hypoglycaemia OR
requiring more flexibility in injection timing
All discharge letters recommending a change to a high
6.1
.1.2
Oct-
16
Ju
n 1
6.1
6
Add Insulin Degludec
200units/mL
(injection)
For treatment of type 1 or
type 2 diabetes in patients
already receiving an
optimised insulin regimen
AND
• receiving basal analogue
insulin at a high dose
(more than 80 units in a
single dose) such that an
increase in dose would
require administration of an
extra injection OR
• receiving insulin glargine
100 Units/mL and
experiencing nocturnal
hypoglycaemia. In this
situation, insulin degludec
200 Units/mL Tresiba®
would be second line to
insulin glargine 300
Units/mL Toujeo®
Prescribing initiation
by Consultant
Diabetologists or
Diabetes Specialist
Nurses only, dose
titration on the advice
of Diabetes Specialist
Nurses, continuation
by GPs
Am
be
r
Y
Insulin degludec 200 Units/mL Tresiba® was approved for
formulary inclusion as follows:
For treatment of type 1 or type 2 diabetes in patients already
receiving an optimised insulin regimen AND
• receiving basal analogue insulin at a high dose (more than 80
units in a single dose) such that an increase in dose would
require administration of an extra injection OR
• receiving insulin glargine 100 Units/mL and experiencing
nocturnal hypoglycaemia. In this situation, insulin degludec 200
Units/mL Tresiba® would be second line to insulin glargine 300
Units/mL Toujeo®
Where more flexibility in injection timing is required
Prescribing initiation by Consultant Diabetologists or Diabetes
Specialist Nurses only, dose titration on the advice of Diabetes
Specialist Nurses, continuation by GPs
Initiation will also include GP practices’ who sign up to this
service (in due course once the “Direct award” is developed
and agreed). This action should not prevent this drug
becoming available on the formulary.
Prescribing by brand name in accordance with MHRA advice
• All discharge letters recommending a change to a
high strength insulin should highlight clearly the unusual
strength in an effort to reduce the risk of errors.
NOTE: Prescribe all insulins by brand
Tresiba (FlexTouch 3mL prefilled disposable injection
device)
Restricted- initiation by Consultant Diabetologists or
Diabetes Specialist Nurses only, dose titration on the
advice of Diabetes Specialist Nurses, continuation by
GPs. Initiation will also include GP practices’ who sign
up to this service (in due course once the “Direct award”
is developed and agreed).
For treatment of type 1 or type 2 diabetes in patients
already receiving an optimised insulin regimen AND
• receiving basal analogue insulin at a high dose (more
than 80 units in a single dose) such that an increase in
dose would require administration of an extra injection
OR
• receiving insulin glargine 100 Units/mL and
experiencing nocturnal hypoglycaemia. In this situation,
insulin degludec 200 Units/mL Tresiba® would be
second line to insulin glargine 300 Units/mL Toujeo®
where more flexibility in injection timing is required
All discharge letters recommending a change to a high
strength insulin should highlight clearly the unusual
strength in an effort to reduce the risk of errors.
See also above Guideline for Using High Strength
Insulins - Primary/Secondary Care Guideline (BHTCG
818FM)
6.1
.1.2
Oct-
16

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Ju
n 1
6.1
7
Add Insulin lispro 200
units/ml (injection)
• For treatment of type 1 or
type 2 diabetes in patients
receiving more than 60
units of prandial insulin as
a single dose in order to
reduce injection volume
• Prescribing initiation
by Consultant
Diabetologists or
Diabetes Specialist
Nurses only, dose
titration on the advice
of Diabetes Specialist
Nurses, continuation
by GPs
• For treatment of type 1 or type 2 diabetes in patients receiving
more than 60 units of prandial insulin as a single dose in order
to reduce injection volume
• Prescribing initiation by Consultant Diabetologists or Diabetes
Specialist Nurses only, dose titration on the advice of Diabetes
Specialist Nurses, continuation by GPs
• Initiation will also include GPs practices’ who sign up to this
service (in due course once the “Direct award” is developed
and agreed). This action should not prevent this drug
becoming available on the formulary. Prescribing by brand
name in accordance with MHRA advice
• All discharge letters recommending a change to a high
strength insulin should highlight clearly the unusual strength in
an effort to reduce the risk of errors.
NOTE: Prescribe all insulins by brand
Humalog® (Kwikpen 3mL prefilled disposable injection
device)
Restricted- initiation by Consultant Diabetologists or
Diabetes Specialist Nurses only, dose titration on the
advice of Diabetes Specialist Nurses, continuation by
GPs. Initiation will also include GPs practices’ who sign
up to this service (in due course once the “Direct award”
is developed and agreed).
For treatment of type 1 or type 2 diabetes in patients
receiving more than 60 units of prandial insulin as a
single dose in order to reduce injection volume
All discharge letters recommending a change to a high
strength insulin should highlight clearly the unusual
strength in an effort to reduce the risk of errors.
See also above Guideline for Using High Strength
Insulins - Primary/Secondary Care Guideline (BHTCG
818FM)
6.1
.1.2
Oct-
16
Ap
r 1
6.6
Add Fidaxomicin 200mg
film-coated tablets
(Dificlir®)
• Treatment of recurrent
Closridium difficile infection
(CDI) or for use in patients
at high risk (elderly
patients or those with
severe CDI) of recurrent
CDI.
• Prescribing on
Consultant
Microbiologist
recommendation onlyR
ed
Y
• Treatment of recurrent Closridium difficile infection (CDI) or for
use in patients at high risk (elderly patients or those with severe
CDI) of recurrent CDI.
• Prescribing on Consultant Microbiologist recommendation
only
Restricted- on Consultant Microbiologist
recommendation only
Treatment of recurrent Closridium difficile infection (CDI)
or for use in patients at high risk (elderly patients or
those with severe CDI) of recurrent CDI.
5.1
.7
Oct-
16
Abatacept 125mg
(Orencia®)
(sub-cutaneous
injection)
FOR ALL PRESCRIBING - NICE compliance form
required - see link from Formulary homepage. NICE
compliance to be verified if form not yet available.
Restricted - to prescribing by Consultant
Rheumatologists only for the treatment of rheumatoid
arthritis, as the preferred choice when abatacept IV is
recommended in accordance with Biologics for
Rheumatoid Arthritis guideline (BHTCG 749FM) and
NICE TA 375
NOTE If patients fail to respond to one route they may
NOT try the alternative route.
Ap
r 1
6.3
a
Amend
restriction
• For the treatment of
rheumatoid arthritis not
previously treated with
DMARDs or after
conventional DMARDs only
have failed, in accordance
with NICE TA 375
Consultant
Rheumatologists
Re
d
Y
• For the treatment of rheumatoid arthritis not previously treated
with DMARDs or after conventional DMARDs only have failed,
in accordance with NICE TA 375,
• NICE TA 375 supersedes and replaces the following NICE
TAs on the formulary:
o adalimumab, etanercept and infliximab for the treatment of
rheumatoid arthritis (TA130)
o certolizumab pegol for the treatment of rheumatoid arthritis
(TA186)
o golimumab for the treatment of methotrexate-naive
rheumatoid arthritis (TA224) and
o abatacept for treating rheumatoid arthritis after the failure of
conventional disease-modifying anti-rheumatic drugs (TA280).
• NICE TA 375 partially updates golimumab for the treatment of
rheumatoid arthritis after the failure of previous disease-
modifying anti-rheumatic drugs (TA225) and tocilizumab for the
treatment of rheumatoid arthritis (TA247).
10
.1.3
Oct-
16

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Abatacept 250mg
(Orencia®)
(intravenous infusion)
FOR ALL PRESCRIBING - NICE compliance form
required - see link from Formulary homepage
Restricted - to Rheumatology consultant prescribing
only, in accordance with Biologics for Rheumatoid
Arthritis guideline (BHTCG 749FM) and NICE TA 195
and NICE TA 375
Certolizumab Pegol
200mg (Cimzia®)
(injection, prefilled
syringe)
FOR ALL PRESCRIBING - NICE compliance form
required - see link from Formulary homepage. NICE
compliance to be very verified if form not yet available.
NOTE: use restricted in BHT to patients with a low
number of co-morbidities and low risk of infection and is
subject to further audit.
Adalimumab 40mg
(Humira®)
(injection, prefilled
pen or syringe)
FOR ALL PRESCRIBING - NICE compliance form
required - see link from Formulary homepage.
1. Restricted - to Rheumatology consultant prescribing
only, in accordance with Biologics for Rheumatoid
Arthritis guideline (BHTCG 749FM) and NICE TA 375
and TA 195.
2. Restricted - to Rheumatology consultant prescribing
only, in accordance with Biologics for Ankylosing
Spondylitis guideline (BHTCG 737FM) and NICE TA 143.
3. Restricted - to prescribing by Rheumatology or
Dermatology consultants only, in accordance Biologics
for Psoriatic arthritis guideline (BHTCG 740FM) and
NICE TA 199
See section 01.05.03 (Gastroenterology) and 13.05.03 Etanercept 25mg
(Enbrel®)
(injection)
FOR ALL PRESCRIBING - NICE compliance form
required - see link from Formulary homepage.
NOTE:
ALL prescribing of etanercept must include generic and
brand name.
Benepali® is first choice etanercept preparation for the
treatment of patients greater than 18 years with
Ap
r 1
6.3
a
Amend
restriction
• For the treatment of
rheumatoid arthritis not
previously treated with
DMARDs or after
conventional DMARDs only
have failed, in accordance
with NICE TA 375
Consultant
Rheumatologists
Re
d
Y
• For the treatment of rheumatoid arthritis not previously treated
with DMARDs or after conventional DMARDs only have failed,
in accordance with NICE TA 375,
• NICE TA 375 supersedes and replaces the following NICE
TAs on the formulary:
o adalimumab, etanercept and infliximab for the treatment of
rheumatoid arthritis (TA130)
o certolizumab pegol for the treatment of rheumatoid arthritis
(TA186)
o golimumab for the treatment of methotrexate-naive
rheumatoid arthritis (TA224) and
o abatacept for treating rheumatoid arthritis after the failure of
conventional disease-modifying anti-rheumatic drugs (TA280).
• NICE TA 375 partially updates golimumab for the treatment of
rheumatoid arthritis after the failure of previous disease-
modifying anti-rheumatic drugs (TA225) and tocilizumab for the
treatment of rheumatoid arthritis (TA247).
10
.1.3
Oct-
16
FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Etanercept 50mg
(Benepali®, Enbrel®)
(injection)
FOR ALL PRESCRIBING - NICE compliance form
required - see link from Formulary homepage.
NOTE:
ALL prescribing of etanercept must include generic and
brand name.
Benepali® is first choice etanercept preparation for the
treatment of patients greater than 18 years with
rheumatoid arthritis (NICE TA375), psoriatic arthritis
(NICE TA199) and ankylosing spondylitis (NICE TA383)
- as the first choice for new patients
- as an option in patients already established on
Enbrel®if the clinician decides that it is appropriate and
the patient consents to switching
Enbrel® brand is the treatment of choice for initiation in
patients who are less than 18 years of age, those with
juvenile idiopathic arthritis (JIA) and those requiring a
dose of 25mg
1. Restricted - to Rheumatology consultant prescribing
only in accordance with NICE TA 35.
2. Restricted - to Rheumatology consultant prescribing
only in accordance with Biologics for Ankylosing
Spondylitis guideline (BHTCG 737FM) and NICE TA 143.
3. Restricted - to prescribing by Rheumatology or
Dermatology consultants only, in accordance Biologics
for Psoriatic arthritis guideline (BHTCG 740FM) and
NICE TA 199.
4. Restricted - to Rheumatology consultant prescribing
only, in accordance with Biologics for Rheumatoid
Arthritis guideline (BHTCG 749FM) and NICE TA 375
and NICE TA 195.Golimumab 50mg
(Simponi®)
(injection, prefilled
pen or syringe)
FOR ALL PRESCRIBING - NICE compliance form
required - see link from Formulary homepage. NICE
compliance to be verified if form not yet available.
1. Restricted - to prescribing by Rheumatology or
Dermatology consultants only, in accordance Biologics
for Psoriatic arthritis guideline (BHTCG 740FM) and
NICE TA 220.
2. Restricted - to Rheumatology consultant prescribing
only, in accordance with Biologics for Rheumatoid
Arthritis guideline (BHTCG 749FM) and NICE TA 375.
3. Restricted - to Rheumatology consultant prescribing
only in accordance with Biologics for Ankylosing
Spondylitis guideline (BHTCG 737FM) and NICE TA 233.
Ap
r 1
6.3
a
Amend
restriction
• For the treatment of
rheumatoid arthritis not
previously treated with
DMARDs or after
conventional DMARDs only
have failed, in accordance
with NICE TA 375
Consultant
Rheumatologists
Re
d
Y
• For the treatment of rheumatoid arthritis not previously treated
with DMARDs or after conventional DMARDs only have failed,
in accordance with NICE TA 375,
• NICE TA 375 supersedes and replaces the following NICE
TAs on the formulary:
o adalimumab, etanercept and infliximab for the treatment of
rheumatoid arthritis (TA130)
o certolizumab pegol for the treatment of rheumatoid arthritis
(TA186)
o golimumab for the treatment of methotrexate-naive
rheumatoid arthritis (TA224) and
o abatacept for treating rheumatoid arthritis after the failure of
conventional disease-modifying anti-rheumatic drugs (TA280).
• NICE TA 375 partially updates golimumab for the treatment of
rheumatoid arthritis after the failure of previous disease-
modifying anti-rheumatic drugs (TA225) and tocilizumab for the
treatment of rheumatoid arthritis (TA247).
10
.1.3
Oct-
16

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Infliximab 100mg
(Inflectra, Remsima,
Remicade®)
(intravenous infusion)
FOR ALL PRESCRIBING - NICE compliance form
required - see link from Formulary homepage.
NOTE:
ALL prescribing of infliximab must include generic and
brand name.
Inflectra® is first choice infliximab biosimilar for all new
patients, with Remsima® second choice only when first
choice is more expensive or not available.
Infliximab biosimilars may be prescribed for patients
currently receiving Remicade® brand when considered
clinically appropriate by the relevant consultant and with
consent of the patient.
1. Restricted - to Rheumatology consultant prescribing
only, in accordance with Biologics for Rheumatoid
Arthritis guideline (BHTCG 749FM) and NICE TA 375
and 195.
3. Restricted - to prescribing by Rheumatology or
Dermatology consultants only, in accordance Biologics
for Psoriatic arthritis guideline (BHTCG 740) and NICE
TA 199.
see Section 1.5.3 (for Gastroenterology) and 13.5.3 (for
Dermatology)
De
c 1
5.1
8
Add brand Magnesium
Glycerophosphate
(Mg2+ 4mmol)
(tablet)
Initiation in secondary
care with continuation
by GPs
Am
be
r
N
• A less expensive unlicensed brand (YourMag®) has been
approved for use instead and this will lead to a saving of £1,000
in BHT and £20,000 in the community
- Maglyphos® tablets will continue to be the formulary oral
magnesium brand of choice for patients requiring less than
4mmol Magnesium and those for whom PEG and NG tube
administration is required. YourMag® tablets to be used for all
other patients.
Unlicensed - Low Risk
Restricted - to initiation in secondary care with
continuation by GPs.
Maglyphos® brand for patients requiring < 4mmol
magnesium and PEG/NG tube administration
YourMag® brand preferred for all other patients
In primary care these are a pharmaceutical special
Contains: Mg2+ 4mmol per tablet
9.5
.1.3
Oct-
16
Oct
16
.9
Add Secukinumab 150mg
(injection, prefilled
pen)
Treatment of active
ankylosing spondylitis in
adults in accordance with
NICE TA 407 as described
in Bucks Biologics in AS
algorithm. It will be used as
a first line biologic if there
are contraindications to an
antiTNF and as a second
line biologic after failure of
two anti TNFs.
Consultant
Rheumatologists
Re
d
Y
• Treatment of active ankylosing spondylitis in adults in
accordance with NICE TA 407 as described in Bucks Biologics
in AS algorithm. It will be used as a first line biologic if there are
contraindications to an antiTNF and as a second line biologic
after failure of two anti TNFs.
• Prescribing by consultant Rheumatologists only
FOR ALL PRESCRIBING - NICE compliance form
required - see link from Formulary homepage.
Restricted - to Rheumatology consultant prescribing
only, in accordance with Biologics in Ankylosing
Spondylitis algorithm and NICE TA 407.
See section 13.5.3 (for Dermatology)
10
.1.3
Oct-
16
Amend
restriction
• For the treatment of
rheumatoid arthritis not
previously treated with
DMARDs or after
conventional DMARDs only
have failed, in accordance
with NICE TA 375
Consultant
Rheumatologists
Re
d
Y
• For the treatment of rheumatoid arthritis not previously treated
with DMARDs or after conventional DMARDs only have failed,
in accordance with NICE TA 375,
• NICE TA 375 supersedes and replaces the following NICE
TAs on the formulary:
o adalimumab, etanercept and infliximab for the treatment of
rheumatoid arthritis (TA130)
o certolizumab pegol for the treatment of rheumatoid arthritis
(TA186)
o golimumab for the treatment of methotrexate-naive
rheumatoid arthritis (TA224) and
o abatacept for treating rheumatoid arthritis after the failure of
conventional disease-modifying anti-rheumatic drugs (TA280).
• NICE TA 375 partially updates golimumab for the treatment of
rheumatoid arthritis after the failure of previous disease-
modifying anti-rheumatic drugs (TA225) and tocilizumab for the
treatment of rheumatoid arthritis (TA247).

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Add Urgoclean 10cm x
10cm dressing
Gre
en
Restricted - only to be used in accordance with the Leg
Ulcer Treatment Pathway (Primary Care).
Available on ONPOS
In Secondary Care restricted to prescribing by Tissue
Viability only. Phone Pharmacy to Order
A5
.2
Add Urgostart 10cm x
10cm dressing
Gre
en
Restricted - only to be used in accordance with the Leg
Ulcer Treatment Pathway (Primary Care).
Available on ONPOS
In Secondary Care restricted to prescribing by Tissue
Viability only. Phone Pharmacy to Order
A5
.4.1
Delete Tegaderm Foam -
6.9cm x 6.9cm soft
cloth border
Bla
ck
Formulary states: Biatain Silicone is an appropriate alternative
A5
.2.5
Oct-
16
Delete Tegaderm Foam oval -
10cm x 11cm
Bla
ck
Formulary states: Biatain Silicone is an appropriate alternative
A5
.2.5
Oct-
16
Delete Mepilex Border Lite -
4cm x 5cm, 6cm x
8.5cm
Bla
ck
Formulary states: Biatain Silicone/Lite is an appropriate
alternative
A5
.2.3
Oct-
16
Delete Aquacel Foam Non
Adh - 10cm x 10cm,
15cm x 15cm
Bla
ck
Formulary states: Biatain Non-Adhesive is an appropriate
alternative
A5
.2.4
Oct-
16
revise
restriction
Aquacel Foam
Adhesive - 19.8cm x
14cm (Heel)
Gre
en
Formulary states: 2nd Choice if Tegaderm Heel not
working or contraindicated.
In Primary Care available on prescription only A5
.2.4
Oct-
16

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
revise
restriction
Aquacel Foam
Adhesive - 8cm x 8cm,
10cm x 10cm, 12.5cm
x 12.5cm, 17.5cm x
17.5cm, 10cm x 20cm
Gre
en
. 16.9cm x 20cm (sacral)(420626)
Sizes below are 2nd Choice if Biatain Silicone® not
appropriate or contraindicated.
8cm x 8cm (420804)(ONPOS)
10cm x 10cm (420680)(ONPOS)
19.8cm x 14cm (heel)(420625) 2nd Choice if
Tegaderm® Heel not working or contraindicated. (In
primary care available on prescription only)
12.5cm x 12.5cm (420619)(ONPOS)
17.5cm x 17.5cm (420621)(ONPOS)(in secondary care
may only be stocked in Spinal Outpatients)
In primary care available as stock through the On-line
Non-Prescription Ordering System (ONPOS) except
19.8cm x 14cm (heel) which is presciption only.
In secondary care all above, restricted to prescribing
only by TV Nurse, Dermatology, Burns and Plastics and
Spinal teams
A5
.2.4
Oct-
16
Add Aquacel Foam 10cm x
20cm
Gre
en
Included in above entry. New size approved for surgical
wounds.
A5
.2.4
Oct-
16
Delete Biatain Adhesive -
12.5cm x 12.5cm,
18cm x 18cmB
lack
Formulary states: Biatain Silicone is an appropriate alternative
A5
.2.5
Oct-
16
revise
restriction
Biatain Adhesive -
7.5cmx 7.5cm,
10cmx10cm, 18cm x
28cm
Gre
en
Fomulary states:
7.5cm 7.5cm (3462)
10cm x 10cm (3430)(this size not available in secondary
care)
18cm x 28cm (3426)
In primary care available as stock through the On-line
Non-Prescription Ordering System (ONPOS)
BNF A5.2.5
In secondary care obtain from Pharmacy
A5
.2.5
Oct-
16
Add Biatain Silicone -,
12.5cm x 12.5cm,
15cm x 15cm, 17.5cm
x 17.5cm
Gre
en
Formulary states:
12.5cm x 12.5cm (3436)
15cm x 15cm (3437)
17.5cm x 17.5cm (3438)
Available in primary care as stock through the On-line
Non-Prescription Ordering System (ONPOS)
BNF A5.2.5
In secondary care to be ordered through Pharmacy
A5
.2.5
Oct-
16

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Add Biatain Silicon Lite -
5cm x 5cm.
Gre
en
Formulary states:
5cm x 5cm (3452)
In secondary care - restricted for use by Dermatology
only or on Tissue Viability recommendation.
Available in primary care as stock through the On-line
Non-Prescription Ordering System (ONPOS)
BNF A5.2.5
In secondary care to be ordered through Pharmacy
A5
.2.5
Oct-
16
revise
restriction
Mepilex Border - 7 x
7.5cm, 10cm x 12.5cm,
15cm X 17.5cm, 17cm
x 20cm Re
d
Biatain Silicone is an appropriate alternative.
Restricted - to prescribing only on the Burns/Plastics or
Spinal wards/units. A5
.2.3
Oct-
16
Delete Aquacel Ag Burn
Bla
ck
This product was originally added to the formulary to be
evaluated. The evaluation was never completed and no
feedback was received from Burns to justify continued
inclusion in the formulary. There has been little use of
this product and Burns are using up the stock albeit
slowly. Pharmacy will not order more. Any further
request for use will need to be applied for through the
proper process for a new wound dressing.
?
Oct-
16
Delete Steripaste
Bla
ck
No longer available
A5
.8.9
Oct-
16
Add Viscopaste
Gre
en
Restricted - for use in eczema. NOT recommended for
leg ulcers as long term use may lead to the development
of sensitivity.
Available on ONPOS
BNF A5.8.9
In secondary care obtain from Pharmacy
A5
.8.9
Oct-
16
1st Choice Tegaderm Foal Heel
(13.9cmx 13.9cm)
Gre
en
Made 1st choice as Aquacel Foam heel is agreed 2nd Choice.
A5
.2.5
Oct-
16
FMG DECISIONS SEPTEMBER 2016

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Se
p 1
6.1
Add Cabazitaxel 60mg in
1.5ml concentrate for
infusion
In accordance with NICE
TA 391 and NHSE SSC 16
37
Consultant
Oncologists
(Prostate)
Re
d
Y
Treatment of hormone-relapsed metastatic prostate cancer
treated with Docetaxel in accordance with NICE TA 391 and
NHSE SSC 16 37
FOR ALL PRESCRIBING - a completed and approved
HIGH COST DRUG compliance form, via BLUETEQ, is
required.
Restricted - prescribing by Consultant Oncologists
(prostate) only
Treatment of hormone-relapsed metastatic prostate
cancer treated with Docetaxel in accordance with NICE
TA 391 and NHSE SSC 16 37.
8.1
.5
Sep-1
6
Se
p 1
6.2
Add Ceritinib 150mg
capsules
in accordance with NICE
TA 395 and NHSE SSC 15
38
Consultant
Oncologists (Lung)
Re
d
Y
As an option for treating advanced anaplastic lymphoma kinase
positive non small cell lung cancer in adults who have
previously had crizotinib in accordance with NICE TA 395 and
NHSE SSC 15 38
FOR ALL PRESCRIBING - a completed and approved
HIGH COST DRUG compliance form, via BLUETEQ, is
required.
Restricted - prescribing by Consultant Oncologists (lung)
only
As an option for treating advanced anaplastic lymphoma
kinase positive non small cell lung cancer in adults who
have previously had crizotinib in accordance with NICE
TA 395 and NHSE SSC 15 38 8.1
.5 (
pro
tein
kin
ase
inh
ibito
rs)
Sep-1
6
Add
indication
Nivolumab 10mg/1ml
(Injection)
In combination with
ipilimumab in accordance
with NICE TA 400, Jul 16
and NHSE Letter ref 1640
from end Oct 2016.
Consultant
Oncologists
(Melanoma) at OUH
only
Re
d
Y
Nivolumab in combination with ipilimumab was approved for
formulary inclusion as follows
• for treating advanced melanoma in accordance with NICE TA
400, Jul 16 and NHSE Letter ref 1640 from end Oct 2016.
FOR ALL PRESCRIBING - a completed and approved
HIGH COST DRUG compliance form, via BLUETEQ, is
required.
Restricted - prescribing by Consultant Oncologists
(Melanoma) at OUH only in accordance with:
1. NICE TA 384 for treating advanced (unresectable or
metastatic) melanoma and in accordance with NHS
England Specialised Services Circular (SSC 1617)
2. In combination with ipilimumab for treating advanced
melanoma in accordance with NICE TA 400, Jul 16 and
NHSE Letter ref 1640 from end Oct 2016. 8.1
.5 (
an
tin
eo
pla
stic d
rug
s)
Sep-1
6
Add
indication
Ipilimumab
50mg/10mL,
200mg/40mL
(concentrate for
intravenous infusion)
As above Consultant
Oncologists
(Melanoma) at OUH
only
Re
d
Y
Add note to Ipilimumab entry as above Restricted:
1. Prescribing by ORH Oncology consultants in
accordance with TVCN protocol and NICE TA 268
2. Prescribing by Oxford University Hospitals (OUH)
only, in accordance with NICE TA 319.
3. Prescribing by consultant oncologists (Melanoma) at
OUH only. To be used In combination with nivolumab for
treating advanced melanoma in accordance with NICE
TA 400, Jul 16 and NHSE Letter ref 1640 from end Oct
2016.
8.1
.5 (
Ipili
mu
ma
b)
Sep-1
6
Se
p 1
6.4
Add Trametinib 0.5mg,
2mg film-coated
tablets
in combination with
dabrafenib for treating
unresectable or metastatic
melanoma in accordance
with NICE TA 396, June 16
and NHSE Letter 1639
funded by NHSE from 20th
Sept 2016
Consultant
Oncologists
(Melanoma) at OUH
only
Re
d
Y
NICE TA 396, June 16 and NHSE letter 1639 published FOR ALL PRESCRIBING - a completed and approved
HIGH COST DRUG compliance form, via BLUETEQ, is
required.
Restricted - prescribing by Consultant Oncologists
(Melanoma) at OUH only
Use in combination with dabrafenib for treating
unresectable or metastatic melanoma in accordance with
NICE TA 396, June 16 and NHSE Letter 1639
8.1
.5 (
pro
tein
kin
ase
inh
ibito
rs)
Sep-1
6
Se
p 1
6.3

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Se
p 1
6.5
Amend
indication
Ezetimibe 10mg
tablets
Monotherapy or co-
administration with a statin
in accordance with NICA
TA 385 and CG 71
Initiation and
continuation in
secondary or primary
care
Gre
en
Y
• The Bucks Lipid modification guideline 104FM.2 recommends
ezetimibe monotherapy in secondary prevention of CVD as an
option when all statins are unsuitable due to intolerance or
contraindications, in line with NICE TA 132.
• NICE TA 132 has been replaced by NICE TA 385 Ezetimibe
for treating primary heterozygous-familial and non-familial
hypercholesterolaemia; NICE CG 71 Familial
hypercholesterolaemia has been updated to reflect TA 385.
Approved for treatment of primary heterozygous-familial (FH)
and non-familial (NF) hypercholesterolaemia in accordance
with NICE TA 385 and in the updated 104FM.3 Bucks Lipid
modification for secondary and primary prevention of CVD in
adult patients guideline. The amendments re. ezetimibe in the
guideline were approved. The revised place of ezetimibe is as
follows:
plus a maximum potency tolerated statin (usually atorvastatin
80mg) is fourth line. Ezetimibe monotherapy would be fifth line.
or ezetimibe plus a maximum potency tolerate statin are also
used for primary prevention of CVD
familial and familial hypercholesterolaemia : prescribing
initiation and continuation in secondary or primary care (Green
on TLL)
Restricted for treatment of primary heterozygous-familial
(FH) and non-familial (NF) hypercholesterolaemia in
accordance with NICE TA 385 and in the updated
104FM.3 Bucks Lipid modification for secondary and
primary prevention of CVD in adult patients guideline
(guideline awaited). See link above for Bucks lipid
modification for secondary and primary prevention of
CVD in adult patients guideline (BHTCG 104FM).
2.1
2
Sep-1
6
Add drug Alirocumab 75mg/ml,
150mg/ml injection
(pre-filled pen or
syringe)
Treatment of primary
hypercholesterolaemia
(heterozygous familial and
non-familial) and mixed
dyslipidaemia in
accordance with NICE TA
393 (alirocumab) and NICE
TA 394 (evolocumab) and
Bucks guideline 104FM.3
Lipid Modification for
secondary and primary
prevention of
cardiovascular disease
(CVD) in adult patients
Prescribing initiation
and continuation by
Consultant Chemical
Pathologists
(Lipidologists) only
Re
d
Y
New NICE TA 393 and NICE TA 394 published.
Approved for treatment of primary hypercholesterolaemia
(heterozygous familial and non-familial) and mixed
dyslipidaemia in accordance with NICE TA 393 (alirocumab)
and NICE TA 394 (evolocumab) and Bucks guideline 104FM.3
Lipid Modification for secondary and primary prevention of
cardiovascular disease (CVD) in adult patients
FOR ALL PRESCRIBING - a completed and approved
HIGH COST DRUG compliance form is required.
Prescribing initiation and continuation by Consultant
Chemical Pathologists (Lipidologists) only.
For treatment of primary hypercholesterolaemia
(heterozygous familial and non-familial) and mixed
dyslipidaemia in accordance with NICE TA 393
(alirocumab) and Bucks guideline 104FM.3 Lipid
Modification for secondary and primary prevention of
cardiovascular disease (CVD) in adult patients (guideline
awaited)
2.1
2
Sep-1
6
Se
p 1
6.6

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Add drug Evolocumab 140mg/ml
injection (pre-filled
pen or syringe)
Treatment of primary
hypercholesterolaemia
(heterozygous familial and
non-familial) and mixed
dyslipidaemia in
accordance with NICE TA
393 (alirocumab) and NICE
TA 394 (evolocumab) and
Bucks guideline 104FM.3
Lipid Modification for
secondary and primary
prevention of
cardiovascular disease
(CVD) in adult patients
Prescribing initiation
and continuation by
Consultant Chemical
Pathologists
(Lipidologists) only
Re
d
Y
New NICE TA 393 and NICE TA 394 published.
Approved for treatment of primary hypercholesterolaemia
(heterozygous familial and non-familial) and mixed
dyslipidaemia in accordance with NICE TA 393 (alirocumab)
and NICE TA 394 (evolocumab) and Bucks guideline 104FM.3
Lipid Modification for secondary and primary prevention of
cardiovascular disease (CVD) in adult patients
FOR ALL PRESCRIBING - a completed and approved
HIGH COST DRUG compliance form is required.
Prescribing initiation and continuation by Consultant
Chemical Pathologists (Lipidologists) only.
For treatment of primary hypercholesterolaemia
(heterozygous familial and non-familial) and mixed
dyslipidaemia in accordance with NICE TA 394
(evolocumab) and Bucks guideline 104FM.3 Lipid
Modification for secondary and primary prevention of
cardiovascular disease (CVD) in adult patients (guideline
awaited)
2.1
2
Sep-1
6
Se
p 1
6.8
Add
indication
Adalimumab 40mg
(Humira®)
(injection, prefilled
pen or syringe)
Treatment of moderate to
severe hidradenitis
suppurativa in accordance
with NICE TA 392 and
NHSE circular 1643
September 2016
Prescribing initiation
by Specialist Centre
Consultant
Dermatologists e.g;
OUH and continued
by BHT Consultant
Dermatologists
Re
d
Y
• Approved for treatment of moderate to severe hidradenitis
suppurativa in accordance with NICE TA 392 and NHSE
circular 1643 September 2016
• Prescribing initiation by Specialist Centre Consultant
Dermatologists e.g; OUH and continued by BHT Consultant
Dermatologists after NICE compliance and funding approval
has been confirmed
FOR ALL PRESCRIBING - a completed and approved
HIGH COST DRUG compliance form is required.
1. Restricted - to prescribing by Dermatology consultants
only, in accordance with Biologics for Psoriasis guideline
(BHTCG 738FM) and NICE TA 146.
2. Restricted - to prescribing by Rheumatology or
Dermatology consultants only, in accordance with
Biologics for Psoriatic arthritis guideline (BHTCG 740FM)
and NICE TA 199.
3. Restricted - prescribing initiation by Specialist Centre
Consultant Dermatologists e.g; OUH and continued by
BHT Consultant Dermatologists in accordance with
NICE TA 392 and NHSE circular 1643 September 2016
13
.5.3
Sep-1
6
Se
p 1
6.6

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Se
p 1
6.9
Add Flucloxacillin 12g, 18g
24 hour infusers
• Patients with the following
infections who are unable
to receive suitable oral
antibiotic(s) and who are
suitable to receive out-
patient antimicrobial
therapy (OPAT)
penicillinase producing
staphylococci and other
gram-positive organisms
susceptible to this anti-
infective including MSSA
bacteriaemias associated
with cellulitis, osteomyelitis,
endocarditis and of
unknown source.
OPAT team on the
advice of
Microbiologists and
in conjunction with
the team responsible
for the patient
Re
d
N
• Flucloxacillin is first line for treating cellulitis and has the best
efficacy and safety profile. It is administered in hospital as
intermittent doses but on discharge is switched to IV ceftriaxone
or teicoplanin to facilitate administration in the outpatient
setting.
• Flucloxacillin administered via a 24 hour infuser has
demonstrated equivalent efficacy to flucloxacillin administered
intermittently.
Flucloxacillin 12g and 18g 24 hour controlled infusion devices
were approved for formulary inclusion as follows
• Patients with the following infections who are unable to
receive suitable oral antibiotic(s) and who are suitable to
receive out-patient antimicrobial therapy (OPAT)
other gram-positive organisms susceptible to this anti-infective
including MSSA bacteriaemias associated with cellulitis,
osteomyelitis, endocarditis and of unknown source.
• Prescribing by the OPAT team on the advice of
Microbiologists and in conjunction with the team responsible
for the patient
Restricted - to prescribing by OPAT team on the advice
of microbiologists and in conjunction with the team
responsible for the patient.
For patients with the following infections who are unable
to receive suitable oral antibiotic(s) and who are suitable
to receive out-patient antimicrobial therapy (OPAT):
- infections due to penicillinase producing staphylococci
and other gram-positive organisms susceptible to this
anti-infective including MSSA bacteriaemias associated
with cellulitis, osteomyelitis, endocarditis and of unknown
source
5.1
.1.2
Sep-1
6
Se
p 1
6.1
0
Add Piperacillin /
tazobactam 13.5g, 18g
controlled infusion
devices
Patients with the following
infections who are unable
to receive suitable oral
antibiotic(s) and who are
suitable to receive out-
patient antimicrobial
therapy (OPAT)
including hospital-acquired
pneumonia
infections (including
pyelonephritis)
infections
soft tissue infections
(including diabetic foot
infections)
in association with, or is
suspected to be associated
with, any of the infections
listed above.
OPAT team on the
advice of
Microbiologists and
in conjunction with
the team responsible
for the patient
Re
d
N
• Two systematic reviews with meta-analyses have
demonstrated a lower mortality rate with continuous extended
infusions of Pip/Taz compared to intermittent dosing,.
The incidence of adverse effects was found to be similar
between the two regimens
• In hospital, current practice for bronchiectasis patients
infected with Ps.aeruginosa is to administer Pip/Taz three times
daily for two weeks. Transfer to OPAT will reduce duration of
admission for medically stable patients.
Approved for:
• Patients with the following infections who are unable to
receive suitable oral antibiotic(s) and who are suitable to
receive out-patient antimicrobial therapy (OPAT)
foot infections)
to be associated with, any of the infections listed above.
• Prescribing by the OPAT team on the advice of
Microbiologists in conjunction with the team responsible for the
patient
Restricted - to prescribing by OPAT team on the advice
of microbiologists and in conjunction with the team
responsible for the patient.
Patients with the following infections who are unable to
receive suitable oral antibiotic(s) and who are suitable to
receive out-patient antimicrobial therapy (OPAT)
pneumonia
pyelonephritis)
diabetic foot infections)
suspected to be associated with, any of the infections
listed above.
5.1
.1.4

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Se
p 1
6.1
1
Add
indication
Metformin 500mg,
850mg (tablet)
For treatment of women
with polycystic ovary
syndrome (PCOS) as
second line to hormonal
contraceptive
Any prescriber in
hospital or primary
care
Gre
en
N
• PCOS is an unlicensed indication for use of metformin. This
use has been standard treatment for many years but is not
currently on the Bucks formulary
Approved for:
• Treatment of women with polycystic ovary syndrome (PCOS)
as second line to hormonal contraceptives. Hormonal
See separate entry and restrictions when using to control
weight gain in Oxfordshire Health paediatric patients
receiving antipsychotic therapy.
1. For use in accordance with Type 2 Diabetes; blood-
glucose-lowering therapy - Primary/Secondary Care
6.1
.2.2
Sep-1
6
Add Canagliflozin 100mg,
300mg
(tablet)
As monotherapy for
treating type 2 diabetes in
adults in accordance with
NICE TA 390 May 16
No restrictions
Gre
en
Y
NICE TA 390 published in May 2016
Approved for:
• As monotherapy for treating type 2 diabetes in adults in
accordance with NICE TA 390, i.e. when metformin is
unsuitable due to contraindications or intolerance when diet and
exercise alone do not provide adequate glycaemic control,
when a DPP-4 inhibitor would otherwise be prescribed and a
sulfonylurea or pioglitazone are inappropriate
• Prescribing by primary and secondary care
3rd Choice SGLT2 Inhibitor after Dapagliflozin and
Empagliflozin
Restricted - for use in accordance with The Management
of Type 2 Diabetes: Blood-Glucose Lowering therapy -
Primary/Secondary Care guideline (BHTCG 667FM)
(updated guideline awaited- see link above) :
1.For the treatment of adults with Type 2 diabetes in
accordance with NICE TA315 in the following
circumstances, when dapagliflozin cannot be used:
- in dual therapy with metformin for patients over 75
years of age when sitagliptin is not suitable or,
- in triple therapy with metformin and a sulphonylurea
when sitagliptin is not suitable.
2. As monotherapy for treating type 2 diabetes in adults
in accordance with NICE TA 390, i.e. when metformin is
unsuitable due to contraindications or intolerance when
diet and exercise alone do not provide adequate
glycaemic control, when a DPP-4 inhibitor would
otherwise be prescribed and a sulfonylurea or
pioglitazone are inappropriate
6.1
.2.3
Sep-1
6
Add Dapagliflozin 5mg,
10mg
(tablet)
As monotherapy for
treating type 2 diabetes in
adults in accordance with
NICE TA 390 May 16
No restrictions
Gre
en
Y
NICE TA 390 published in May 2016
Approved for:
• As monotherapy for treating type 2 diabetes in adults in
accordance with NICE TA 390, i.e. when metformin is
unsuitable due to contraindications or intolerance when diet and
exercise alone do not provide adequate glycaemic control,
when a DPP-4 inhibitor would otherwise be prescribed and a
sulfonylurea or pioglitazone are inappropriate
• Prescribing by primary and secondary care
1st Choice SGLT2 Inhibitor
Restricted - for use in accordance with The Management
of Type 2 Diabetes: Blood-Glucose Lowering therapy -
Primary/Secondary Care guideline (BHTCG 667FM)
(updated guideline awaited- see link above) :
1. In combination with other blood-glucose-lowering
therapies
2. As monotherapy for treating type 2 diabetes in adults
in accordance with NICE TA 390, i.e. when metformin is
unsuitable due to contraindications or intolerance when
diet and exercise alone do not provide adequate
glycaemic control, when a DPP-4 inhibitor would
otherwise be prescribed and a sulfonylurea or
pioglitazone are inappropriate
6.1
.2.3
Sep-1
6
Se
p 1
6.1
3

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Add Empagliflozin 10mg,
25mg
(tablet)
As monotherapy for
treating type 2 diabetes in
adults in accordance with
NICE TA 390 May 16
No restrictions
Gre
en
Y
NICE TA 390 published in May 2016
Approved for:
• As monotherapy for treating type 2 diabetes in adults in
accordance with NICE TA 390, i.e. when metformin is
unsuitable due to contraindications or intolerance when diet and
exercise alone do not provide adequate glycaemic control,
when a DPP-4 inhibitor would otherwise be prescribed and a
sulfonylurea or pioglitazone are inappropriate
• Prescribing by primary and secondary care
2nd Choice SGLT2 Inhibitor after dapagliflozin
Restricted - for use in accordance with The Management
of Type 2 Diabetes: Blood-Glucose Lowering therapy -
Primary/Secondary Care guideline (BHTCG 667FM)
(updated guideline awaited- see link above) :
1. In combination with other blood-glucose-lowering
therapies in accordance with NICE TA 336.
2. As monotherapy for treating type 2 diabetes in adults
in accordance with NICE TA 390, i.e. when metformin is
unsuitable due to contraindications or intolerance when
diet and exercise alone do not provide adequate
glycaemic control, when a DPP-4 inhibitor would
otherwise be prescribed and a sulfonylurea or
pioglitazone are inappropriate
6.1
.2.3
Sep-1
6
Amend
traffic light
restriction
and
formulary
wording
Exenatide
5micrograms/dose,
10micrograms/dose
(Byetta®)
(injection)
Initiation by hospital
Diabetes consultants
or Hospital Diabetes
specialist nurses or
by GPs who have
received training
Gre
en
Y
Traffic light re-classification AI to green
Approved for:
Initiation by hospital Diabetes consultants or Hospital Diabetes
specialist nurses or by GPs who have received training
NOTE: 5microgram pre-filled pen only, to be used when
initiating treatment in secondary care. 10microgram pre-
filled pen to be used in primary care, and in secondary
care only for continuation of in-patient treatment.
Restricted -Initiation by hospital Diabetes consultants or
Hospital Diabetes specialist nurses or by GPs who have
received training in accordance with NICE CG 87 Type 2
Diabetes with the exception of the last criteria which is
changed to: BMI 30-35kg/m2 and insulin is unacceptable
because of occupational implication or weight loss would
benefit other co-morbidities in accordance with Glucagon-
like peptide-1 (GLP-1) Agonist Injectable Therapy -
Primary/ Secondary Care guideline (BHT CG109FM).
Also see Type 2 Diabetes: blood-glucose-lowering
therapy guideline (BHTCG 667FM)(see link above)
EXENATIDE and INSULIN
Exenatide in combination with insulin may only be
initiated by Consultant Diabetologists with continuation
by GPs, in accordance with the criteria defined in the
High Cost Drug compliance form - see link from
Formulary home page. The decision to continue or stop
therapy to be made by Consultant Diabetologist at 6
months.
6.1
.2.3
Sep-1
6
Se
p 1
6.1
3A
pr
16
.8

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Amend
traffic light
restriction
and
formulary
wording
Exenatide 2mg
(Bydureon®)
(MR injection, vial and
pre-filled pen)
Initiation by hospital
Diabetes consultants
or Hospital Diabetes
specialist nurses or
by GPs who have
received training
Gre
en
Y
Traffic light re-classification AI to green
Approved for:
Initiation by hospital Diabetes consultants or Hospital Diabetes
specialist nurses or by GPs who have received training
Restricted - initiation by hospital Diabetes consultants or
Hospital Diabetes specialist nurses or by primary care
health professionals who have received training in
accordance with Glucagon-like peptide-1 (GLP-1)
Agonist Injectable Therapy - Primary/ Secondary Care
guideline (BHT CG109FM) and NICE TA 248. Also see
Type 2 Diabetes blood glucose-lowering therapy
(BHTCG 667FM) (see link above)
EXENATIDE and INSULIN
Exenatide in combination with insulin may only be
initiated by Consultant Diabetologists with continuation
by GPs, in accordance with the criteria defined in the
High Cost Drug compliance form - see link from
Formulary home page. The decision to continue or stop
therapy to be made by Consultant Diabetologist at 6
months.
6.1
.2.3
Sep-1
6
Amend
traffic light
restriction
and
formulary
wording
Liraglutide 6mg/mL
(injection, 3mL
prefilled pen)
Initiation by hospital
Diabetes consultants
or Hospital Diabetes
specialist nurses or
by GPs who have
received training Gre
en
Y
Traffic light re-classification AI to green
Approved for:
Initiation by hospital Diabetes consultants or Hospital Diabetes
specialist nurses or by GPs who have received training
Restricted - to prescribing by hospital Diabetes
consultants or Hospital Diabetes specialist nurses or by
primary care health professionals who have received
training, in accordance with Glucagon-like peptide-1
(GLP-1) Agonist Injectable Therapy - Primary/
Secondary Care guideline (BHT CG109FM)and NICE TA
203, and in line with Type 2 Diabetes blood glucose-
lowering therapy guideline (BHTCG 667FM)(see above)
6.1
.2.3
Sep-1
6
Se
p 1
6.1
9
Amend
traffic light
restriction
Minoxidil (Regaine®)
Bla
ck
Y
Minoxidil, all topical forms are Nationally blacklisted Non-formulary black listed
13
.9
Sep-1
6
Se
p 1
6.1
9
formatting -
combine
entries
Octreotide
50micrograms/1mL,
100micrograms/1mL,
500micrograms/1mL,
1g/5mL Various
Y
Currently 3 entries with different TLL positions on the formulary.
To be combined into one entry. TLL positions to remain the
same
RED
1. Restricted - prescribing by Oncology team.
2. Restricted - prescribing by Paediatric consultants for
insulin resistance (Congenital Hyperinsulinism (CHI)) in
paediatric patients (as shared care with tertiary referral
centres)(Unlicensed Use)
8.3
.4.3
Sep-1
6
Se
p 1
6.1
9 Add link Formulary Chapter 25:
A2 - Borderline
substances
Add link to link to chapter A2 - 'Healthcare professional
guidance: Cows' milk protein allergy in infants' (CCG guideline)
http://www.bucksformulary.nhs.uk/docs/avc/CMPAguidance121
214.pdf
A2
Sep-1
6
Ap
r 1
6.8
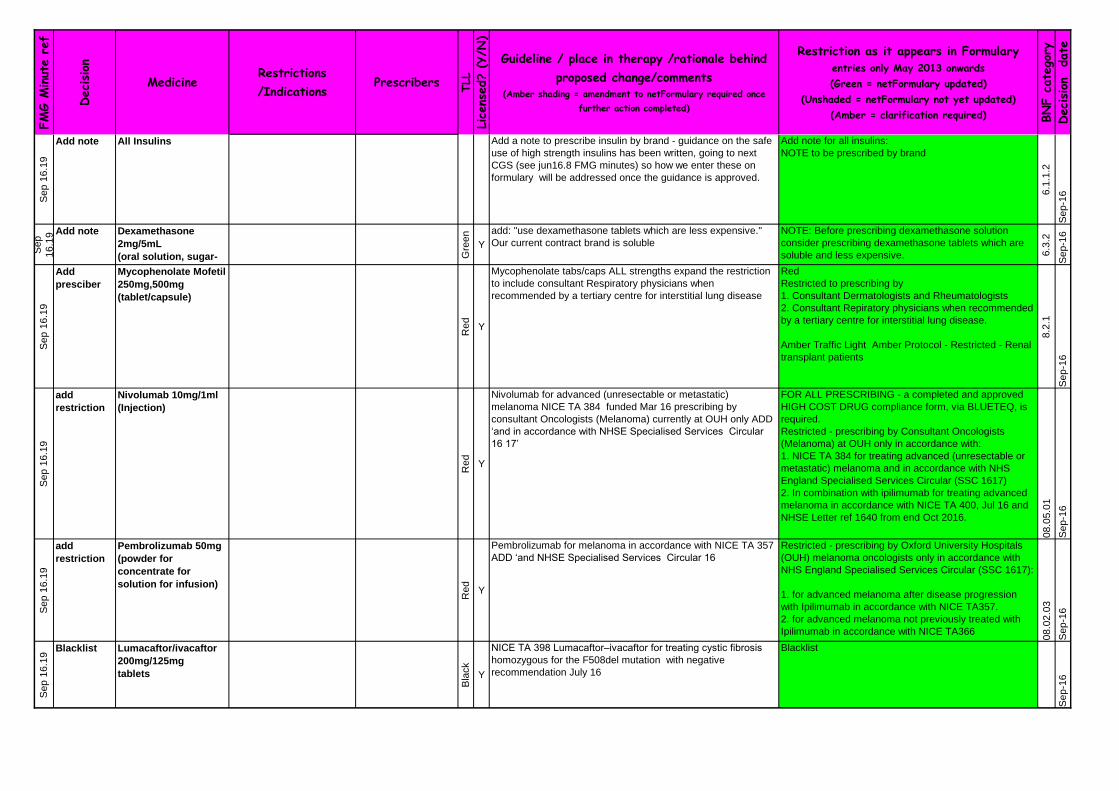
FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Se
p 1
6.1
9
Add note All Insulins Add a note to prescribe insulin by brand - guidance on the safe
use of high strength insulins has been written, going to next
CGS (see jun16.8 FMG minutes) so how we enter these on
formulary will be addressed once the guidance is approved.
Add note for all insulins:
NOTE to be prescribed by brand
6.1
.1.2
Sep-1
6
Sep
16
.19 Add note Dexamethasone
2mg/5mL
(oral solution, sugar-
free)
Gre
en
Y
add: "use dexamethasone tablets which are less expensive."
Our current contract brand is soluble
NOTE: Before prescribing dexamethasone solution
consider prescribing dexamethasone tablets which are
soluble and less expensive. 6.3
.2
Sep-1
6
Se
p 1
6.1
9
Add
presciber
Mycophenolate Mofetil
250mg,500mg
(tablet/capsule)
Re
d
Y
Mycophenolate tabs/caps ALL strengths expand the restriction
to include consultant Respiratory physicians when
recommended by a tertiary centre for interstitial lung disease
Red
Restricted to prescribing by
1. Consultant Dermatologists and Rheumatologists
2. Consultant Repiratory physicians when recommended
by a tertiary centre for interstitial lung disease.
Amber Traffic Light Amber Protocol - Restricted - Renal
transplant patients
8.2
.1
Sep-1
6
Se
p 1
6.1
9
add
restriction
Nivolumab 10mg/1ml
(Injection)
Re
dY
Nivolumab for advanced (unresectable or metastatic)
melanoma NICE TA 384 funded Mar 16 prescribing by
consultant Oncologists (Melanoma) currently at OUH only ADD
‘and in accordance with NHSE Specialised Services Circular
16 17’
FOR ALL PRESCRIBING - a completed and approved
HIGH COST DRUG compliance form, via BLUETEQ, is
required.
Restricted - prescribing by Consultant Oncologists
(Melanoma) at OUH only in accordance with:
1. NICE TA 384 for treating advanced (unresectable or
metastatic) melanoma and in accordance with NHS
England Specialised Services Circular (SSC 1617)
2. In combination with ipilimumab for treating advanced
melanoma in accordance with NICE TA 400, Jul 16 and
NHSE Letter ref 1640 from end Oct 2016.
08
.05
.01
Sep-1
6
Se
p 1
6.1
9
add
restriction
Pembrolizumab 50mg
(powder for
concentrate for
solution for infusion)
Re
d
Y
Pembrolizumab for melanoma in accordance with NICE TA 357
ADD ‘and NHSE Specialised Services Circular 16
Restricted - prescribing by Oxford University Hospitals
(OUH) melanoma oncologists only in accordance with
NHS England Specialised Services Circular (SSC 1617):
1. for advanced melanoma after disease progression
with Ipilimumab in accordance with NICE TA357.
2. for advanced melanoma not previously treated with
Ipilimumab in accordance with NICE TA366
08
.02
.03
Sep-1
6
Se
p 1
6.1
9
Blacklist Lumacaftor/ivacaftor
200mg/125mg
tablets
Bla
ck
Y
NICE TA 398 Lumacaftor–ivacaftor for treating cystic fibrosis
homozygous for the F508del mutation with negative
recommendation July 16
Blacklist
Sep-1
6

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Se
p 1
6.1
9
Blacklist Azacitidine 100mg
(injection)
Bla
ck
Y
NICE TA 399 Azacitidine for treating AML in more than 30%
bone marrow blasts has negative recommendation July 16
Blacklist
8.1
.3
Sep-1
6
Apr
16
.1
Add Zolmitriptan
5mg/0.1mL
(nasal spray)
in accordance with Bucks
Headache management for
adults guideline gre
en
yFor the acute treatment of migraine attacks with or without aura
for patients unsuitable for two oral triptans (sumatriptan and
almotriptan) due to prominent vomiting or treatment failure at
For the acute treatment of migraine attacks for patients
unsuitable for two oral triptans due to prominent vomiting
or treatment failure at maximum tolerated dose and in 04
.07
.
04
.01
Apr-
16
Apr
16
.4
Add Etanercept biosimilar
50mg injection
(Benepali®)
As Enbrel Consultant
Rheumatologists,
Dermatologists
Re
d
Y
As for Etanercept previously except Benepali® is not licensed
for use in Juvenile Idiopathic Arthritis or in paediatric plaque
psoriasis as it is only currently available as a 50mg dose
NOTE: ALL prescribing of etanercept must include
generic and brand name.
Benepali® is first choice etanercept preparation for the 10
.01
.
03
A
pr-
16
Ap
r 1
6.7 Amend Gluten-free and Sip
Feed formulary
chapter revision
The amendments to the Gluten-free and SIP feed formulary
chapter, as listed below under CCG FORMULARY CHANGE
TRACKING DOCUMENT - PROPOSED CHANGES FOR
APRIL 2016 FMG, were approved
A2
.06
.0
1A
pr-
16
Apr
16
.8
Add new section to Bucks
Formulary Policy
Bucks Formulary Policy: NEW section re. Process for NHSE
Clinical commissioning policies and circulars
the process was approved Apr-
16
Apr
16
.10 Add link to Rx guidelines
app
Inclusion of new link to Rx guidelines app (mainly hospital
antibiotic guidelines) on Formulary home page
Dapagliflozin 5mg,
10mg
MHRA Drug Saftey Update - April 2016 - SGLT2 inhibitors:
updated advice on the risk of diabetic ketoacidosisNatalizumab
300mg/15mL
(concentrate for
intravenous infusion)
MHRA Drug Saftey Update - April 2016 - Natalizumab
(Tysabri▼): progressive multifocal
leukoencephalopathy—updated advice to support early
detection
FMG DECISIONS APRIL 2016
Ap
r 1
6.1
0
Add links to
MHRA drug
safety
updates

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Dimethyl Fumarate
120mg, 240mg
(capsule)
MHRA Drug Saftey Update - April 2016 - Dimethyl fumarate
(Tecfidera): updated advice on risk of progressive multifocal
leukoencephalopathy
Fingolimod
500micrograms
(capsule)
MHRA Drug Saftey Update - April 2016 - Fingolimod
(Gilenya▼): risks of progressive multifocal
leukoencephalopathy, basal-cell carcinoma, and opportunistic
infections
Chapter 14:
Immunological
products and vaccines
MHRA drug safety update - April 2016 - Live attenuated
vaccines: avoid in those who are clinically immunosuppressed
Oct
15
.6
Add Perampanel 2mg,
4mg, 6mg, 8mg, 10mg,
12mg (Fycompa®)
(Tablet)
Consultant
Neurologists at BHT
and the national
centre of epilepsy
AI
y
For the adjunctive treatment of partial-onset seizures with or
without secondarily generalised seizures in people aged 12
years and older with epilepsy for whom first line and ‘standard
adjunct therapy are ineffective or unsuitable and for whom
lacosamide, phenobarbital, phenytoin, vigabatrin, zonisamide
and retigabine are ineffective or unsuitable
Restricted - prescribing initiation by consultant
neurologists at BHT and the National Society for
Epilepsy for the first 6 months with continuation by GPs
when patient is stabilised
04
.08
.01
r
Ap
r 1
6.1
0
Add links to
MHRA drug
safety
updates

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Ju
n 1
5.5
Add Capsaicin 0.075%
(Axsain®)
(cream)
in accordance with
Pharmacological treatment
of chronic pain following
spinal cord injury in adults
guideline(BHTCG 375FM)
Spinal consultants or
pain team
Re
d
n
Treatment of localized neuropathic pain for Spinal Cord Injury
(SCI) patients who cannot tolerate, or have failed to respond to,
or are contraindicated to maximum doses of oral treatment with
Tricyclic antidepressants (TCAs), Gabapentinoids, and
Duloxetine
Restricted - prescribing by spinal consultants or pain
team for the treatment of localized neuropathic pain for
spinal cord injury (SCI) patients who cannot tolerate, or
who have failed to respond to, or are contra-indicated to
maximum doses of oral treatment with tricyclic
antidepressants, gabapentinoids and duloxetine and in
accordance with Pharmacological treatment of chronic
pain following spinal cord injury in adults
guideline(BHTCG 375FM)
10
.03
.02
Ju
n 1
5.6
Add
IndicationLidocaine 5%
(700mg/medicated
plaster)
and in accordance with
Pharmacological treatment
of chronic pain following
spinal cord injury in adults
guideline(BHTCG 375FM)
Spinal consultants or
pain team
Re
d
xlvii. Treatment of localized neuropathic pain for Spinal Cord
Injury (SCI) patients who cannot tolerate, or have failed to
respond to, or are contraindicated to oral treatment with TCA’s,
Gabapentinoids, Duloxetine, and topical Capsaicin 0.075%
Cream
Restricted - prescribing by spinal consultants or pain
team for the treatment of localized neuropathic pain for
spinal cord injury (SCI) patients who cannot tolerate, or
who have failed to respond to, or are contra-indicated to
maximum doses of oral treatment with tricyclic
antidepressants, gabapentinoids, duloxetine and topical
capsaicin 0.075% cream and in accordance with
Pharmacological treatment of chronic pain following
spinal cord injury in adults guideline(BHTCG 375FM)
15
.02
De
c 1
5.3
Add Midodrine 2.5mg, 5mg
(tablet)
in accordance with amber
initiation guideline
Initiation by
consultant
neurologists and
spinal also
appropriate
consultant e.g.
cardiologists
continuation by GPs
AI
y
Midodrine has recently received a licence for use in orthostatic
hypotension due to autonomic dysfunction
Restricted - Initiation by hospital consultants with
continuation by GPs in accordance with amber initiation
guideline (awaiting upload) for use when all other
corrective factors have failed and other treatment is
ineffective or not tolerated
1. Initiation by consultant neurologists and spinal for the
treatment of orthostatic hypotension due to autonomic
dysfunction
2. Initiation by appropriate consultant e.g. cardiologists
for unprovoked vasovagal syncope (where no reversible
cause can be found)
02
.07
.02
Apr-
16
De
c 1
5.1
2
Add Brinzolamide/Brimoni
dine 10mg/2mg in 1mL
(ophthalmic
suspension, preserved
consultant
ophthalmologists
AI
y
second line to the individual components prescribed
concomitantly - For use in adults with open angle glaucoma /
intra-ocular hypertension for whom beta blockers and
prostaglandin analogues are unsuitable and the use of the two
components (brimonidine/brinzolamide) as separate entities is
inappropriate
Restricted - to initiation by Consultant Ophthalmologists
with continuation by GPs for use in adults with open
angle glaucoma/intra-ocular hypertension for whom beta
blockers and prostaglandin analogues are unsuitable
and the use of the two components
(brinzolamide/brimonidine) as separate entities in
inappropriate
11
.06
Apr-
16

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
De
c 1
5.1
3 Add Tafluprost/Timolol
15micrograms/5mg in
1mL
(eye drops, unit dose,
preservative-free
consultant
ophthalmologists
AI
y
As a third line preservative free Prostaglandin analogue
inhibitor/Beta Blocker combination eye drop for patients who
have not responded to or are unsuitable for other PF formulary
choices
Restricted - to initiation by Consultant Ophthalmologists
with continuaton by GPs as a third line preservative free
prostaglandin analogue (PGA)/beta blocker combination
eye drop in patients who are using both a PGA and beta
blocker in preservative free forms but a combination may
11
.06
Apr-
16
Fe
b 1
4.9
Add TLL
amend
restriction
Sevelamer
Hydrochloride 800mg
(Renagel®)
(tablet)
Renal team
Re
d
y
previous proposed AI traffic light position changed to red for all
patients (new and established)
Restricted - prescribing by the Renal team only.
Red traffic light position applies to new and established
patients
09
.05
.02
.02
Apr-
16
Ap
r 1
6.9 Add
restrictionTemozolomide 5mg,
20mg, 100mg, 250mg
(capsules)
in accordance with NICE
TA23, updated March 2016
consultant
oncologists - OUH
only Re
d
y
Restricted - prescribing by consultant oncologists at
OUH in accordance with NICE TA 23, updated March
2016 for the treatment of recurrent malignant glioma
(brain cancer) 08
.01
.05
Apr-
16
Ap
r 1
6.9
Add Nivolumab 10mg/1ml
(Injection)
in accordance with NICE
TA384
Consultant
Oncologists
(melanoma) at OUH
only
Re
d
y
Restricted - prescribing by Consultant Oncologists
(melanoma) at OUH only in accordance with NICE TA
384 for treating advanced (unresectable or metastatic)
melanoma Apr-
16
Ap
r 1
6.9 Add Elosulfase alfa
5mg/5ml
(concentrate for
solution for infusion)
in accordance with NICE
HST2 and the Managed
Access Scheme
consultant
paediatricians on
initiation by a Highly
Specialised Service
Re
d
Initiation by a Highly Specialised Centre Restricted - prescribing by consultant paediatricians in
accordance with NICE HST2 and the Managed Access
Scheme on initiation by a Highly Specialised Service for
treating mucopolysaccharidosis type IVa
16
.01
Apr-
16
Add Irinotecan, oxaliplatin
and raletrexed
PbR excluded, NHSE
NICE TA 93 published Aug
2005
NICE CG 131
Consultant
Oncologists only
red y
NICE TA 93 published Aug 2005 Colorectal cancer (advanced)
- irinotecan, oxaliplatin and raletrexed. It was noticed this is not
reflected in the formulary. Irinotecan, oxaliplatin are on
formulary for other indications, ralitrexed not on formulary at all
NICE TA93 has now been replaced with NICE CG131
Colorectal cancer: diagnosis and management
Restricted - prescribing by consultant oncologists only in
accordance with NICE clinical guideline 131
8.0
1
Apr-
16
Add Vortioxetine
5mg, 10mg, 20mg
Tablets
in accordance with NICE
TA 367
Prescribing by Oxford
Health Consultant
Psychiatrists only red y
for major depressive disorder in accordance with NICE TA 367.
Red on TLL; Prescribing by Oxford Health Consultant
Psychiatrists only
Restricted - prescribing by Oxford Health Consultant
Psychiatrists only in accordance with NICE TA367 -
Vortioxetine for treating major depressive episodes 04
.03
.04
01
-ma
r-1
6A
pr-
16
Add Darunavir 800mg
tablet
PbR excluded, NHSE
in accordance with BHIVA
2013 HIV
HIV and Specialist
Sexual Health
consultants (GUM
and Contraception)
teams red
y
150mg, 400mg and 600mg already on formulary. 800mg is
used via Homecare a lot. 800mg same price as 400mg tablets
tablets and offer improved compliance for patients requiring this
medicine.
Restricted – to be prescribed by HIV and Specialist
Sexual Health consultants (GUM and Contraception)
teams in accordance with BHIVA 2013 HIV treatment
guidelines.
05
.03
.01
Apr-
16
BHT FORMULARY CHANGE TRACKING DOCUMENT - PROPOSED FORMULARY CHANGES FOR NOTE APRIL 2016 FMG

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Add Meningococcal group
B Vaccine (injection)
in accordance with the
recommendations in the
immunisation schedule. gre
en
y
To be used in accordance with the recommendations in
the immunisation schedule.
14
.04
Apr-
16
remove
unlicensed Glycopyrronium
Bromide 1mg, 2mg these are now licensed
Re
d
y consultant Paediatricians only Restricted - prescribing by consultant Paediatricians
only. Supply on a named patient basis
15.
01.
Add note to
verify
funding has
been
approved
Pirfenidone 267mg
(hard capsule)
PbR excluded, NHSE
Initiation by consultant
Respiratory physicians in
named Specialist Services
only but prescribing may
be continued in BHT by
red
Re
d
It must be verified, via blueteq, that funding approval has been
obtained.
Restricted - prescribing in accordance with NICE TA 282
with initiation by consultant Respiratory physicians in
named Specialist Services only (Oxford University
Hospitals NHS Trust, Interstitial Lung Disease Service
(ILD Service), University Hospital Southampton NHS
03
.11
Azithromycin 250mg
capsules
gre
en
y
Ceftazidime 250mg,
500mg, 1g, 2g
injection red
y
Ceftriaxone 250mg,
1g, 2g injection
red y
Add
restrictionCabergoline
500micrograms, 1mg,
2mg Tablets
AI
y
included in O+G guidelines as a single dose for suppression of
lactation
Guideline 437 Induction of Labour (IOL) for fetal death from 20
weeks gestation
Guideline 662 Termination of pregnancy (TOP) for fetal
abnormality)
Restricted - initiation by consultant endocrinologists and
continuation by GPs.
In secondary care - also for use in lactation supression
as a SINGLE dose in accordance with Guideline 437
Induction of Labour (IOL) for fetal death from 20 weeks
gestation or Guideline 662 Termination of pregnancy
(TOP) for fetal abnormality
06
.07
.01
Add
restriction
included in secondary care
guideline 133 Management
and antibiotic therapy for
respiratory tract conditions
in adults
In secondary care restricted - in accordance with
Guideline 133 - Management and antibiotic therapy for
respiratory tract conditions in adults 05
.01

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Uploaded The routine
immunisation
schedule from Spring
2016
to replace previous version
Add Desmopressin
120 microgram,
240 microgram
Oral lyophilisates,
green; 2nd line
Gre
en
Required as a 2nd line choice for children with primary
nocturnal enuresis who cannot swallow tablets. More
expensive than tablets but in use (CCG spend over £40K a
year on this and it is regularly recommended by BHT clinicians).
Mentioned in the existing NICE clinical guideline 111 -
nocturnal enuresis
Restricted - as a 2nd line choice for children with primary
nocturnal enuresis who cannot swallow tablets
06
.05
.02
Delete
Vitasavoury 200
(sip feed) Discontinued Jan 2016
A2
.02
Add Slo Milkshake In primary care initiation on
the recommendation of a
Dietitian only AR
In Primary Care - Initiation on the recommendation of a
dietitian only.
In Secondary Care, not stocked. Requires dietitian input
regarding appropriate alternative A2
.02
change
switch
recommend
ation
Barkat®
(500 G Multigrain
bread (sliced))
AR
In Primary Care - Less cost effective choice for people with
coeliac disease or dermatitis herpetiformis. Consider switching
to - currently Dietary Specials Loaf Sliced Multigrain to be
changed to Glutafin Select Sliced seeded loaf
In Primary Care - Less cost effective choice for people
with coeliac disease or dermatitis herpetiformis.
Consider switching to Glutafin Select Sliced seeded loaf A2
.06
.01
Apr-
16
change
switch
recommend
ation
Ener-G
(474g Brown or white
rice bread (sliced))
AR
In Primary Care - Less cost effective choice for people with
coeliac disease or dermatitis herpetiformis. Switch to -
currently EnerG Rice Loaf (sliced) Proceli Brown Rice Bread.
To delete Proceli Brown Rice Bread
In Primary Care - Less cost effective choice for people
with coeliac disease or dermatitis herpetiformis. Switch
to EnerG Rice Loaf (sliced) A2
.06
.01
Apr-
16
change
switch
recommend
ation
Proceli®
(8 x 34g White lunch
rolls)
AR
In Primary Care - Less cost effective choice for people with
coeliac disease or dermatitis herpetiformis. Consider switching
to - currently Livwell White rolls, to be changed to Lifestyle
Bread rolls (white)
In Primary Care - Less cost effective choice for people
with coeliac disease or dermatitis herpetiformis.
Consider switching to Lifestyle Bread rolls (white) A2
.06
.01
Apr-
16
change
switch
recommend
ation
Livwell® (4 x 50g
Toasting Bread Buns)
AR
In Primary Care - Less cost effective choice for people with
coeliac disease or dermatitis herpetiformis. Consider switching
to -currently Livwell White rolls, to be changed to Lifestyle
Bread rolls (white)
In Primary Care - Less cost effective choice for people
with coeliac disease or dermatitis herpetiformis.
Consider switching to Lifestyle Bread rolls (white) A2
.06
.01
Apr-
16
CCG FORMULARY CHANGE TRACKING DOCUMENT - PROPOSED CHANGES FOR APRIL 2016 FMG
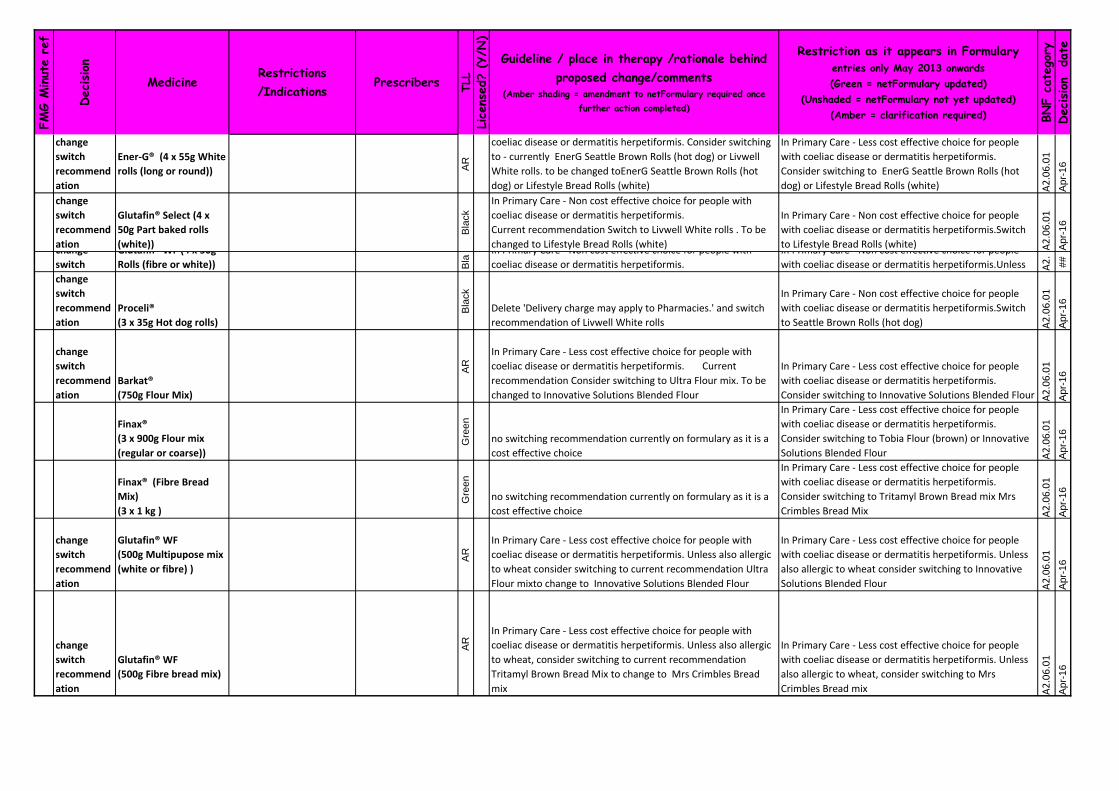
FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
change
switch
recommend
ation
Ener-G® (4 x 55g White
rolls (long or round)) AR
In Primary Care - Less cost effective choice for people with
coeliac disease or dermatitis herpetiformis. Consider switching
to - currently EnerG Seattle Brown Rolls (hot dog) or Livwell
White rolls. to be changed toEnerG Seattle Brown Rolls (hot
dog) or Lifestyle Bread Rolls (white)
In Primary Care - Less cost effective choice for people
with coeliac disease or dermatitis herpetiformis.
Consider switching to EnerG Seattle Brown Rolls (hot
dog) or Lifestyle Bread Rolls (white) A2
.06
.01
Apr-
16
change
switch
recommend
ation
Glutafin® Select (4 x
50g Part baked rolls
(white))
Bla
ck
In Primary Care - Non cost effective choice for people with
coeliac disease or dermatitis herpetiformis.
Current recommendation Switch to Livwell White rolls . To be
changed to Lifestyle Bread Rolls (white)
In Primary Care - Non cost effective choice for people
with coeliac disease or dermatitis herpetiformis.Switch
to Lifestyle Bread Rolls (white) A2
.06
.01
Apr-
16
change
switch
Glutafin® WF (4 x 50g
Rolls (fibre or white)) Bla
In Primary Care - Non cost effective choice for people with
coeliac disease or dermatitis herpetiformis.
In Primary Care - Non cost effective choice for people
with coeliac disease or dermatitis herpetiformis.Unless A2
.
##
change
switch
recommend
ation
Proceli®
(3 x 35g Hot dog rolls)
Bla
ck
Delete 'Delivery charge may apply to Pharmacies.' and switch
recommendation of Livwell White rolls
In Primary Care - Non cost effective choice for people
with coeliac disease or dermatitis herpetiformis.Switch
to Seattle Brown Rolls (hot dog) A2
.06
.01
Apr-
16
change
switch
recommend
ation
Barkat®
(750g Flour Mix)
AR
In Primary Care - Less cost effective choice for people with
coeliac disease or dermatitis herpetiformis. Current
recommendation Consider switching to Ultra Flour mix. To be
changed to Innovative Solutions Blended Flour
In Primary Care - Less cost effective choice for people
with coeliac disease or dermatitis herpetiformis.
Consider switching to Innovative Solutions Blended Flour A2
.06
.01
Apr-
16
Finax®
(3 x 900g Flour mix
(regular or coarse)) G
reen
no switching recommendation currently on formulary as it is a
cost effective choice
In Primary Care - Less cost effective choice for people
with coeliac disease or dermatitis herpetiformis.
Consider switching to Tobia Flour (brown) or Innovative
Solutions Blended Flour A2
.06
.01
Apr-
16
Finax® (Fibre Bread
Mix)
(3 x 1 kg )
Gre
en
no switching recommendation currently on formulary as it is a
cost effective choice
In Primary Care - Less cost effective choice for people
with coeliac disease or dermatitis herpetiformis.
Consider switching to Tritamyl Brown Bread mix Mrs
Crimbles Bread Mix A2
.06
.01
Apr-
16
change
switch
recommend
ation
Glutafin® WF
(500g Multipupose mix
(white or fibre) )
AR
In Primary Care - Less cost effective choice for people with
coeliac disease or dermatitis herpetiformis. Unless also allergic
to wheat consider switching to current recommendation Ultra
Flour mixto change to Innovative Solutions Blended Flour
In Primary Care - Less cost effective choice for people
with coeliac disease or dermatitis herpetiformis. Unless
also allergic to wheat consider switching to Innovative
Solutions Blended Flour A2
.06
.01
Apr-
16
change
switch
recommend
ation
Glutafin® WF
(500g Fibre bread mix)
AR
In Primary Care - Less cost effective choice for people with
coeliac disease or dermatitis herpetiformis. Unless also allergic
to wheat, consider switching to current recommendation
Tritamyl Brown Bread Mix to change to Mrs Crimbles Bread
mix
In Primary Care - Less cost effective choice for people
with coeliac disease or dermatitis herpetiformis. Unless
also allergic to wheat, consider switching to Mrs
Crimbles Bread mix A2
.06
.01
Apr-
16

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
change
switch
recommend
ation
Glutafin® Select
(500g Fibre Bread mix)
AR
In Primary Care - Less cost effective choice for people with
coeliac disease or dermatitis herpetiformis. Consider switching
to current recommentdation Tritamyl Brown Bread mix to
change to Mrs Crimbles Bread Mix
In Primary Care - Less cost effective choice for people
with coeliac disease or dermatitis herpetiformis.
Consider switching to Mrs Crimbles Bread Mix A2
.06
.01
Apr-
16
change
switch
recommend
ation
Glutafin® Select
(500g Multipupose mix
(white or fibre) )
AR
In Primary Care - Less cost effective choice for people with
coeliac disease or dermatitis herpetiformis. Consider switching
to current recommendation Ultra Flour mix To change to
Innovative Solutions Blended Flour or Tobia Flour (brown)
In Primary Care - Less cost effective choice for people
with coeliac disease or dermatitis herpetiformis.
Consider switching to Innovative Solutions Blended Flour
or Tobia Flour (brown) A2
.06
.01
Apr-
16
change
switch
recommend
ation
Heron Foods® (500g Hi
fibre bread mix)
Bla
ck
In Primary Care - Non cost effective choice for people with
coeliac disease or dermatitis herpetiformis. Switch to current
recommendation Tritamyl Brown Bread mix to change to Mrs
Crimbles Bread mix
In Primary Care - Non cost effective choice for people
with coeliac disease or dermatitis herpetiformis. Switch
to Mrs Crimbles Bread mix A2
.06
.01
Apr-
16
Add switch
recommend
ation
change TLL
Orgran® (250g Pasta
spirals (buckwheat
corn, rice & millet, rice,
rice & maize))
AR
current: green TLL
In primary care - a cost effective choice for patients with coeliac
disease or dermatitis herpetiformis. No longer cost effective so
add consider switch to Rizopia fusilli
In Primary Care - Less cost effective choice for people
with coeliac disease or dermatitis herpetiformis.
Consider switching to Rizopia fusilli A2
.06
.01
Apr-
16
change
switch
recommend
ation
Barkat® (500G pasta
(spaghetti, spirals,
tagliatelle, animal
shapes, macaroni))
AR
In Primary Care - Less cost effective choice for people with
coeliac disease or dermatitis herpetiformis.
Currently - Consider switching to Rizopia spaghetti, fusilli or
penne or Orgran Rice and Corn Macaroni or EnerG macaroni
(white rice) . nolonger recommend switch to EnerG macaroni
In Primary Care - Less cost effective choice for people
with coeliac disease or dermatitis herpetiformis.
Consider switching to Rizopia spaghetti, fusilli or penne
or Orgran Rice and Corn Macaroni(white rice) A2
.06
.01
Apr-
16
change
switch
recommend
ation
Proceli® (250g Pasta
macaroni, penne)
AR
In Primary Care - Less cost effective choice for people with
coeliac disease or dermatitis herpetiformis.
Consider switching to currently Rizopia penne or EnerG
macaroni (white rice)to be tanged to Rizopia penne or Orgran
Rice and Corn Macaroni
In Primary Care - Less cost effective choice for people
with coeliac disease or dermatitis herpetiformis.
Consider switching to Rizopia penne or Orgran Rice and
Corn Macaroni A2
.06
.01
Apr-
16

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
change
switch
recommend
ation
BiAlimenta® (6 x 500g
pasta (spiral, grains,
sagnette, penne,
mixed))
AR
In Primary Care - Less cost effective choice for people with
coeliac disease or dermatitis herpetiformis.Consider switching
to current - Rizopia spaghetti, fusilli or penne or EnerG
macaroni (white rice) or EnerG pasta (small shells) To remove
EnerG macaroni (white rice) or EnerG pasta (small shells)
In Primary Care - Less cost effective choice for people
with coeliac disease or dermatitis herpetiformis.
Consider switching to Rizopia spaghetti, fusilli or penne A2
.06
.01
Apr-
16
change
switch
recommend
ation
Juvela® GF (6 x 500g
Penne (fibre))
AR
In Primary Care - Less cost effective choice for people with
coeliac disease or dermatitis herpetiformis.Consider switching
to current recommendation Glutafin Fibre pasta Spirals. to
change to Glutafin Fibre pasta Fusilli
In Primary Care - Less cost effective choice for people
with coeliac disease or dermatitis herpetiformis.Consider
switching to Glutafin Fibre pasta Fusilli A2
.06
.01
Apr-
16
change
switch
recommend
ation
Juvela® GF (8 x 250g
Tagliatelle)
current formulary wording - In primary care - a LESS cost
effective choice for patients with coeliac disease or dermatitis
herpetiformis Consider switching to Rizopia spaghetti or Juvela
GF fibre linguine
In Primary Care - Less cost effective choice for people
with coeliac disease or dermatitis herpetiformis.Consider
switching to Rizopia spaghetti or Juvela GF fibre linguine.
Not Barkat Pasta Tagliatelle Apr-
16
Glutafin®
(250g Pasta (lasagne,
tagliatelle))
In primary care - a LESS cost effective choice for patients with
coeliac disease or dermatitis herpetiformis. Current
recommendatiion - Consider switching to Rizopia
lasagne/spaghetti
In Primary Care - Less cost effective choice for people
with coeliac disease or dermatitis herpetiformis.
Consider switching to Rizopia Lasagne or Juvela Fibre
linguine. Apr-
16
change
switch
recommend
ation
Juvela® GF (6 x 500g
Spaghetti, macaroni,
fusilli)
AR
In Primary Care - Less cost effective choice for people with
coeliac disease or dermatitis herpetiformis. Consider switching
to current recommendations Rizopia spaghetti, fusilli or penne
or Dietary specials pasta fusilli, spaghetti or EnerG macaroni
(white rice) . To change to to Rizopia spaghetti, fusilli or penne
or Orgran Rice and corn macaroni
In Primary Care - Less cost effective choice for people
with coeliac disease or dermatitis herpetiformis.
Consider switching to Rizopia spaghetti, fusilli or penne
or Orgran Rice and corn macaroni A2
.06
.01
Apr-
16
change
switch
recommend
ation
Orgran® (150g Lasagne
(rice & maize))
Bla
ck
In Primary Care - Non cost effective choice for people with
coeliac disease or dermatitis herpetiformis.
Switch to current recommendation is EnerG Lasagne (white
rice) to change to Rizopia Lasagne
In Primary Care - Non cost effective choice for people
with coeliac disease or dermatitis herpetiformis.
Switch to Rizopia Lasagne A2
.06
.01
Apr-
16
change
switch
recommend
ation
Ener-G (300G
Vermicelli)
Bla
ck
In Primary Care - Non cost effective choice for people with
coeliac disease or dermatitis herpetiformis.
Switch to current recommendation Rizopia Spaghetti or EnerG
pasta (small shells). To delete recommmendation for EnerG
pasta (small shells).
In Primary Care - Non cost effective choice for people
with coeliac disease or dermatitis herpetiformis.
Switch to Rizopia Spaghetti. A2
.06
.01
Apr-
16

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Proceli® (4 x 50G
Bread buns) Bla
ck
A2
.06
Proceli® (4 x 35G Part
Baked white dinner
rolls) Bla
ck
A2
.06
.0
Fe
b 1
6.4
Add
indication
Docetaxel
20mg/0.5ml/80mg/2ml
(infusion)
in accordance with NHS
England Clinical
Commissioning Policy
B15/PS/a
Prescribing by
consultant
Oncologists
(Prostate)
red
n
For the treatment of hormone naïve metastatic prostate cancer
In combination with androgen deprivation therapy in
accordance with NHS England Clinical Commissioning Policy
B15/PS/a
Restricted - prescribing by Consultant Oncologists
(Prostate) for the treatment of hormone naïve metastatic
prostate cancer in combination with androgen
deprivation therapy in accordance with NHS England
Clinical Commissioning Policy B15/PS/a
08
.01
.05
Fe
b-1
6
Fe
b 1
6.6
Add Radium-223 dichloride
1000 kBq/ml (Xofigo®)
(solution for injection)
PbR excl, NHS
England
in accordance with NICE
TA 376
Prescribing by
consultant
Oncologists at OUH
only
For the treatment of hormone-relapsed prostate cancer with
bone metastases in accordance with NICE TA 376, Prescribing
by consultant Oncologists at OUH only.
Restricted - prescribing by consultant oncologists at
OUH only for the treatment of hormone-relapsed
prostate cancer with bone metastases in accordance
with NICE TA 376
08
.03
.04
.02
Fe
b-1
6
Fe
b 1
6.7
Add Ciclosprin
1mg/ml (Ikervis®)
(eye drops, emulsion)
in accordance with NICE
TA 369and the Ocular
Lubricants guideline
371FM (to be updated)
Consultant
Ophthalmologists in
the Corneal Clinic
red
y
For the treatment of severe keratitis in adult patients with dry
eye disease that has not improved despite treatment with tear
substitutes in accordance with NICE TA 369 and the Ocular
Lubricants guideline 371FM (to be updated). In this cohort,
ciclosporin eye drops 0.1% would be used after all formulary
ocular lubricant choices had been found to be unsuitable due to
Restricted - prescribing by consultant ophthalmologists
in the corneal clinic
1. for the treatment of severe keratitis in adult patients
with dry eye disease that has not improved despite
treatment with tear substitutes in accordance with NICE
TA369 and the Ocular Lubricants Guideline (BHTCG
11
.04
.02
Fe
b-1
6
Fe
b 1
6.7
Delete Ciclosporin 0.2%
(Eye ointment)
(unlicensed) n
Replaced by licensed Ciclosprin 1mg/ml (Ikervis®) (eye drops,
emulsion). See above
11
.99
.99
Fe
b-1
6
the following no longer have delivery charges
FMG DECISIONS FEBRUARY 2016

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Fe
b 1
6.1
2
Add Tolvaptan 15mg,
30mg, 45mg, 60mg,
90mg (Jinarc®)
PbR excl, CCG
(Tablets)
in accordance with NICE
TA358 and the OUH
Tolvaptan guideline
Oxford renal
consultants
Re
d
Y
The NICE TA is being implemented by the OUH Renal Service
for treatment of autosomal dominant polycystic kidney disease
in accordance with NICE TA258. Prescribing by OUH Renal
consultants
Restricted - prescribing by Oxford renal consultants for
treatment of autosomal dominant polycystic kidney
disease in accordance with NICE TA258 and the Oxford
University Hospitals Tolvaptan guideline.
Fe
b-1
6
Add
prescribing
restriction
Add MHRA
warning
Change TLL
Intra-uterine
Progestogen Only
System (Mirena®)
(intrauterine system)
Jaydess® 13.5mg
(intrauterine delivery
system)
Fe
b 1
6.1
7
Add Nintedanib
100mg, 150mg (Ofev®)
(capsule)
PbR excl, NHS
England
restricted to prescribing by
a Tertiary Centre
NICE TA
Re
d
y
Restricted - to prescribing by a tertiary centre (e.g
Brompton) for idiopathic pulmonary fibrosis - NICE TA
379
03
.11
Fe
b-1
6
Fe
b 1
6.1
3
Sodium valproate
MR tablet, crushable
tablet, ec tablet, oral
solution
Prescribing initiation
by a consultant
Neurologist,
Psychiatrist,
Paediatrician or Pain
consultant only,
continuation by GPs
AI
y
MHRA Drug Safety Update - February 2016: Valproate and risk
of abnormal pregnancy outcomes
Sodium valproate oral preparations for use in all patients are to
receive the following amended formulary restriction: Prescribing
initiation by a consultant Neurologist, Psychiatrist, Paediatrician
or Pain consultant only, continuation by GPs
https://www.gov.uk/drug-safety-update/valproate-and-of-risk-of-
abnormal-pregnancy-outcomes-new-communication-materials
Prescribing generically or by brand is discretionary
Restricted - prescribing initiation by a consultant
Neurologist, Psychiatrist, Paediatrician or Pain
consultant only, continuation by GPs
07
.03
.02
.03
Fe
b-1
6
BHT FORMULARY CHANGE TRACKING DOCUMENT - PROPOSED FORMULARY CHANGES FOR NOTE FEBRUARY 2016 FMG
04
.08
.01
Fe
b-1
6
Fe
b 1
6.1
6
Add MHRA
warning
Gre
en
y
MHRA Drug Safety Alert - Levonorgestrel-releasing IUDs
should be prescribed by brand
Levonogestrol-releasing IUDs should be prescribed by
brand (see MHRA drug safety update, link below)

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Add
Esmolol 100mg/10ml
Injection
red
y
currently 2.5g in 10ml (injection concentrate) is on the
formulary, to remain on for time being. 02
.04
.0 0F
eb
-16
Add
indication
Tacrolimus
500micrograms, 1mg
Capsules
Consultant
Gastroenterologists
red
y
For autoimmune hepatitis
No policy / guideline to refer to
Two patients per year
Restricted - to prescribing by Consultant
Gastroenterologists for autoimmune hepatitis 13
.05
.0 3F
eb
-16
Add
Bupivacaine 0.125%
epidural inj 250ml bagpain team
red
y to align with epidural guideline 15
.02
#####
Add
Tacrolimus
500micrograms, 1mg,
5mg Capsules Adoport®
brand
red
y
Adoport is used by the Renal and Transplant Units at OUH so
standardise brand at BHT .
patients should be switched from PROGRAF brand where
possible. PROGRAF to remain on formulary until patients have
been switched.
08
.02
.02
13
.05
.03
Fe
b-1
6
Add MHRA
warning
Tacrolimus
500micrograms, 1mg,
5mg Capsules
red
y
MHRA Drug Saftey Update june 2012 says potential for
inadvertent switching between products, which has been
associated with reports of toxicity and graft rejection. Therefore,
to ensure maintenance of therapeutic response when a patient
is stabilised on a particular brand, oral tacrolimus products
should be prescribed and dispensed by brand name only.
Oral Tacrolimus products should be prescribed and
dispensed by brand name only (MHRA drug safety
update, June 2012)
08
.02
.02
13
.05
.03
Fe
b-1
6
Add MHRA
warning
Vemurafenib 240mg
Tablets
red
y
MHRA Drug Saftey Update - Vemurafenib : risk of potentiation
of radiation toxicity
Nov 2015 08
.01
.0 5F
eb
-16
Add
Clotrimazole 10%
vaginal cream gre
en
y
Included in Management of Infection Guidance for Primary
Care which was approvedat CGS Feb16
Use in accordance with Management of Infection
Guidance for Primary Care 07
.02
.0 2F
eb
-16
Add
Tisseel Ready To Use
Solutions for Sealant
(fibrin sealant)
Spinal surgeons
red
y restricted to hosp only, red, use for Spinal surgeons only Restricted - for use by spinal surgeons only 16
.01
.0 0F
eb
-16
Delete
Amitryptiline
hydrochloride 50mg in
5ml oral solution gre
en
y
rationalise to keep only 25mg in 5ml
04
.03
.0 1F
eb
-16
Delete
Furosemide 1mg in 1ml
red
n
keep only 40mg in 5ml
02
.02
.0 2F
eb
-16
Delete
Haloperidol 5mg in 5ml
red
Y
keep only 10mg in 5ml
04
.02
.0 1F
eb
-16
FMG DECISIONS DECEMBER 2015

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
de
c1
5.1
Add indications Lidocaine Hydrochloride
1%
(100mg/10mL,
200mg/20mL)
(injection) when used as
Lidocaine infusion
In accordance with
Administration of
Intravenous Lidocaine for
Neuropathic Paine
Guideline (BHTCG 673FM)
Prescribing by the
Pain Service on the
advice of a consultant
anaesthetist (Pain
specialist)
Re
d
n
• As a diagnostic tool for neuropathic pain. Where a positive
response will guide subsequent management e.g. the use of
membrane stabilizing drugs
• For the treatment of neuropathic pain where all other agents
are ineffective or not tolerated at maximum doses
• To put a ceiling on high levels of neuropathic pain in patients
taking very high doses of neuropathic pain agents
When used as an intravenous infusion (unlicensed use),
restricted to prescribing by the pain service on the
advice of a consultant anaesthetist (pain specialist) in
accordance with The Administration of Intravenous
Lidocaine for Neuropathic Pain Management (BHTCG
673FM) Guideline
1.As a diagnostic tool for neuropathic pain. Where a
positive response will guide subsequent management
e.g. the use of membrane stabilising drugs
2.For the treatment of neuropathic pain where all other
agents are ineffective or not tolerated at maximum
doses.
3.To put a ceiling on high levels of neuropathic pain in
patients taking very high doses of neuropathic pain
agents
15
.02
De
c-1
5
de
c 1
5.4
Add Naloxegol 12.5mg,
25mg Tablets
For treatment of opioid
induced constipation in
adults whose constipation
has not adequately
responded to laxatives in
accordance with NICE TA
345
on the
recommendation of a
hospital consultant,
continuation by GPs
AR y
Prescribing on the recommendation of a hospital consultant e.g.
Palliative care, Spinal, Pain, MfOP consultant), continuation by
GPs For treatment of opioid induced constipation in adults
whose constipation has not adequately responded to laxatives
in accordance with NICE TA 345.
Consider use when there has been an inadequate response to
at least two oral and one rectal laxative at maximum tolerated
doses for at least two weeks. E.gs are macrogol (Laxido®),
docusate, senna, bisacodyl
Patients to be reviewed for efficacy at one month. If this is
positive, it may be appropriate to stop the naloxegol and return
to earlier treatment options
Restricted - prescribing on the recommendation of a
hospital consultant with continuation by GPs for
treatment of opioid induced constipation in adults whose
constipation has not adequately responded to laxatives
in accordance with NICE TA345, when there has been
an inadequate response to at least two oral and one
rectal laxative at maximum tolerated doses for a least
two weeks.
Patients to be reviewed for efficacy at 1 month and if
positive it may be appropriate to stop
01
.06
De
c-1
5
de
c 1
5.5
Amend
restrictionViekirax 12.5 mg/75
mg/50 mg tablet
Ombitasvir/Paritaprevi
r/Ritonavir
PbR excl, NHSE, PAS
with or without dasabuvir
for treating adults with
chronic hepatitis C in
accordance with NICE
TA365 and NHSE
commissioning policy 1524
Consultant
Gastroenterologists/
Hepatologists and
Associate Specialist
Gastroenterology
Re
d
y
Already on formulary for use in cirrhotic hepatitis C patients in
accordance with NHSE Commissioning policy 1524 June 2015
NICE TA365 subsequently published in November 2015
FOR ALL PRESCRIBING - a completed and approved
HIGH COST DRUG compliance form, via BLUETEQ, is
required.
Restricted - prescribing by Consultant
Gastroenterologists/Hepatologists and Associate
Specialist (Gastroenterology), as part of Thames Valley
ODN in accordance with NICE TA 365 or NHSE
Commissioning Policy statement 1524, June 2015 -
Hepatitis C with cirrhosis. All patients will be discussed in
the ODN MDT. De
c-1
5
de
c 1
5.5
Amend
restrictionSofosbuvir/Ledipasvir
400mg/90mg tablets
PbR excl, NHSE, PAS
For treating chronic
hepatitis C in accordance
with NICE TA 363 and
NHSE commissioning
policy 1524
Consultant
Gastroenterologists/
Hepatologists and
Associate Specialist
Gastroenterology
Re
d
y
Already on formulary for use in cirrhotic hepatitis C patients in
accordance with NHSE Commissioning policy 1524 June 2015
NICE TA363 subsequently published in November 2015
FOR ALL PRESCRIBING - a completed and approved
HIGH COST DRUG compliance form, via BLUETEQ, is
required.
Restricted - prescribing by Consultant
Gastroenterologists/Hepatologists and Associate
Specialist (Gastroenterology), as part of Thames Valley
ODN in accordance with NICE TA 363 or NHSE
Commissioning Policy statement 1524, June 2015 -
Hepatitis C with cirrhosis. All patients will be discussed in
the ODN MDT. De
c-1
5

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
de
c 1
5.5
Amend
restrictionDaclatasvir 30mg,
60mg tablets
PbR excl, NHSE, PAS
for treating chronic
hepatitis C in accordance
with NICE TA 364 and
NHSE commissioning
policy 1524
Consultant
Gastroenterologists/
Hepatologists and
Associate Specialist
Gastroenterology
Re
d
y
Already on formulary for use in cirrhotic hepatitis C patients in
accordance with NHSE Commissioning policy 1524 June 2015
NICE TA364 subsequently published in November 2016
FOR ALL PRESCRIBING - a completed and approved
HIGH COST DRUG compliance form, via BLUETEQ, is
required.
Restricted - prescribing by Consultant
Gastroenterologists/Hepatologists and Associate
Specialist (Gastroenterology), as part of Thames Valley
ODN in accordance with NICE TA 364 or NHSE
Commissioning Policy statement 1524, June 2015 -
Hepatitis C with cirrhosis. All patients will be discussed in
the ODN MDT. De
c-1
5
de
c 1
5.6
Add Idelalisib 100mg,
125mg Tablets
PbR excl, NHSE, PAS
NICE TA359 Idelalisib for
treating chronic
lymphoblastic leukaemia
Consultant
Haematologists
red y
1. untreated chronic lymphocytic leukaemia in adults with a 17p
deletion or TP53 mutation or
2. chronic lymphocytic leukaemia in adults when the disease
has been treated but has relapsed within 24 months.
For patients in category 1, prior to NICE TA359, alemtuzumab
would have been used (if fit enough) or dexamethasone (if unfit
for alemtuzumab).
For patients in category 2, prior to and following NICE TA359,
Ibrutinib (Cancer Drugs Fund) is the first choice agent.
However, if patients relapse within 24 months of ibrutinib,
idelalisib will be used
FOR ALL PRESCRIBING - NICE compliance form
required - see link from Formulary homepage. NICE
compliance to be verified if form not yet available
Restricted - prescribing by Consultant Haematologists in
accordance with NICE TA359
08
.01
.05
De
c-1
5
de
c
15. Add Indications Rotigotine patch 1mg,
2mg,3mg, 4mg, 6mg,
Neurology team or
PD nurses red
y Indications added -
1b patients unable to swallow and discharged to palliative care
Restricted - to prescribing by Neurology team or PD
nurses for Parkinson's disease
##
de
c 1
5.8
Remove Co-
careldopa/Entacapone
7 strengths
Stalevo® brand
recommendation by
Clinical Nurse
Specialist
(Parkinson's) or
Neurology team
AR y
see entry ref Jun15.9
Sastravi® has been use in six Stalevo® naïve patients. No
clinical issues have arisen and the use of Sastravi® instead of
Stalevo® as a Bucks wide formulary decision was felt
appropriate
Restricted - recommendation by Clinical Nurse Specialist
(Parkinson's) or Neurology team
Where suitable the separate component parts may be
used at the discretion of the Parkinson's nurses
New patient suitable for the combined product will be
initiated on Sastravi®. Existing patients on Stalevo® will
be switched to Sastravi®.
Switching of existing patients from Stalevo® to Sastravi®
may be undertaken by the GP
04
.09
.01
De
c-1
5
de
c 1
5.1
Revise TLL Fosfomycin Trometamol
3g sachet
recommendation by
microbiology
AR y
Oral fosfomycin trometamol (Monuril®) is now newly available
as a licensed product in the UK. To improve accessibility and
timely administration the formulary status changed from Red to
Amber Recommended so that GPs may prescribe it based
upon sensitivity results released by Microbiology.
Restricted - to be prescribed on the recommendation of
microbiology sensitivity results.
When results are given in response to a secondary care
initiated sample, clear communication between the
secondary care clinician and GP should take place.
05
.01
.05
De
c-1
5
de
c 1
5.1
1
Add indication Chlorhexidine
Gluconate 2% in
Isopropyl Alcohol 70%
(ChloraPrep®)
(cutaneous solution,
3mL)
red y
Extend use of chlorhexidine 2% in 70% IPA (Chloraprep®) to
include use to prepare skin pre-operatively for breast surgery
Chlorhexidine products review
In secondary care restricted -
1. to areas where central venous catheters, mid and
PICC lines are inserted
2. to prepare skin pre-operatively for breast surgery
13
.11
.02
De
c-1
5

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
de
c 1
5.1
1
Amend
restrictionsChlorhexidine
Gluconate 2% (Clinell®)
(wash cloth (4 per
pack)) red
n
Indication for “pre-op cleansing regimen” removed in
accordance with MHRA /RCS statement on use of topical
chlorhexidine for skin preparation prior to surgery. This is
supported by correspondence from MHRA and does not
represent a change to practice as the wash cloths are not used
for pre-op cleansing.
Chlorhexidine products review
unlicensed - low risk
Restricted - for skin cleansing in patients receiving
inpatient care in ICU.
13
.11
.02
De
c-1
5
de
c 1
5.1
1 Add indication Chlorhexidine
Gluconate 2% in
Isopropyl Alcohol 70%
(200mL)
red
n
Add for disinfection prior to trauma surgery.previously only prior
to orthopaedic surgery
Chlorhexidine products review
unlicensed - low risk
In secondary care restricted - only for disinfection prior to
trauma and orthopaedic surgery 13
.11
.02
De
c-1
5
de
c 1
5.1
1 Delete Chlorhexidine/Cetrimide
0.015%/0.15%
(Tisept®)
sachets 25ml
To be replace by Chlorhexidine gluconate 0.05% (Unisept®)
pink single use 25mL, 100mL sachets
Chlorhexidine products review
13
.11
.02
De
c-1
5
de
c 1
5.1
1
Add Chlorhexidine
Gluconate 0.05%
(Unisept®)
(sterile solution, 100mL
sachet)
gre
en
y
see above (Tisept® entry)
new size added, 100ml 25ml size already on fromulary
13
.11
.02
De
c-1
5
de
c
15
.11
TLL change Chlorhexidine Acetate
0.05%
(sterile solution, 1L) red y
TLL changed from AR to red - Chlorhexidine products review
13
.11
.02
De
c-1
5
de
c 1
5.1
1
Additional
presentation
and restriction
Chlorhexidine
Gluconate 0.5% in
Denatured Ethanol 70%
(solution, 600mL, 500ml
spray bottle)
500ml spray bottle presentation added for use by podiatry only 500ml spray bottle restricted to podiatry for pre and post
intervention skin disinfection
13
.11
.02
De
c-1
5
de
c 1
5.6
Delete Ethinylestradiol
10 microgram,
50 microgram and 1mg
tablets
Due to the high cost of the branded generic decision made to
delete. Agreed with SDU Lead Obs/Gynaecology:
06
.04
.01
De
c-1
5
De
c 1
5.2
0
Add Pembrolizumab
50 mg powder for
concentrate for solution
for infusion
NICE TA357 and NICE
TA366
prescribing by OUH
Melanoma
Oncologists
Re
d
y
Restricted - prescribing by Oxford University Hospitals
(OUH) melanoma oncologists only
Restricted - prescribing by OUH Oncologists only
1. for advanced melanoma after disease progression
with Ipilimumab in accordance with NICE TA357.
2. for advanced melanoma not previously treated with
Ipilimumab in accordance with NICE TA366.

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Se
p 1
5.1
Add Indication Omalizumab 150mg
prefilled syringe
PBr excl CCG
NICE TA 339 Consultant
dermatologists
Re
d
y
Desicion at Dec15 FMG was
in accordance with formal shared care arrangements between
BHT and a Highly Specialised Service (in line with NHS
England commissioning guidance) as add-on therapy for the
treatment of chronic spontaneous urticaria in adult and
adolescent (12 years and above) patients with inadequate
response to H1 antihistamine treatment in accordance with
NICE TA 339
Post Dec FMG, A circular from NHSE to Acute Trusts has
confirmed that NHSE have re-classified omalizumab for
urticaria as a non- Highly Specialised Centre use. This is based
on NICE confirming the wording of their TA. It is now expected
FOR ALL PRESCRIBING - NICE compliance form
required - see link from Formulary homepage
Restricted - prescribing by Consultant Dermatologists in
accordance with NICE TA339 for previously treated
chronic spontaneous urticaria
change wording Cefotaxime inj (all
strengths)
gre
en y In primary care stat dose is green on Traffic lights list when
used for meningitis infections in penicillin allergic patients. ARG
agreed, this use has always been in primary care antibiotic
guidance
In primary care for use as a stat dose in suspected
meningitis when penicillin allergic
05
.01
.02
.01
05
.01
.02
.01
change wording metronidazole 0.75%
vaginal gel
gre
en y In primary care recommended when other choices not suitable.
ARG agreed, this use has always been in primary care
antibiotic guidance
In primary care only recommended when other choices
not suitable
07
.02
.02
07
.02
.02
BHT FORMULARY CHANGE TRACKING DOCUMENT - PROPOSED FORMULARY CHANGES FOR NOTE DECEMBER 2015 FMG

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
change wording Clindamycin 2% vaginal
cream
gre
en y In primary care recommended when other choices not suitable.
ARG agreed, this use has always been in primary care
antibiotic guidance
In primary care only recommended when other choices
not suitable
07
.02
.02
07
.02
.02
change wording Add wording to all
ketone monitoring sticks
on the formulary as per
published low priority
statement (Policy No.
TVPC 13 issued
Aug15)
AR y There is insufficient evidence to recommend routine
measurement of ketones in patients with type 1 or type 2
diabetes. The proposed policy recommends that the following
high risk patients should receive ketone testing strips to self-
monitor when required:
- Insulin pump users
- Patients with a history of admissions with ketoacidosis within
last 5 years
- HbA1c >11% (97 mmol/mol) or blood glucose often > 20
mmol/l
- Pregnant patients with type 1 diabetes
- Newly diagnosed type 1 diabetes
6.1
.6
6.1
.6
WC
F N
ov1
5
add for
evaluationKliniderm Foam Silicone
Border adhesive foam
dressing
7.5cm x 7.5cm
10cm x 10cm
12.5cm x 12.5cm
15cm x 15cm
17.5cm x17.5cm
Added to formulary for evaluation by Spinal, Paediatrics and
Burns/Plastics. Evaluation comparing Mepilex Border against
Kliniderm and Biatain Silicon will run from December 2015 to
end of February 2016.
During January 2016, as part of a controlled evaluation
only, available on formulary for use by Spinal (St
Patrick's Ward), Burns and Plastics and Paediatric
Ward. Evaluation forms to be completed for each use in
these areas. A5
,2,5
WOUNDCARE FORMULARY COMMITTEE DECISIONS NOVEMBER 2015

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
WC
F N
ov1
5
add for
evaluationBiatain Silicon adhesive
foam dressing
7.5cm x 7.5cm
10cm x 10cm
12.5cm x 12.5cm
15cm x 15cm
17.5cm x17.5cm
Added to formulary for evaluation by Spinal, Paediatrics and
Burns/Plastics. Evaluation comparing Mepilex Border against
Kliniderm and Biatain Silicon will run from December 2015 to
end of February 2016.
During February 2016, as part of a controlled evaluation
only, available on formulary for use by Spinal (St
Patrick's Ward), Burns and Plastics and Paediatric
Ward. Evaluation forms to be completed for each use in
these areas.
A5
,2,5
Delete Steripaste No longer available 7.5cm x 7.5cm
A5
.8.9
WC
F
No
v1 Delete Drymax super
absorbent dressing
Spend on super absorbers increased since introduction.
Change to Kerramax now cheaper. xxx
WC
F N
ov1
5
revise
restriction, add
size
Kerramax super
absorbent dressing
20 x 30cm
gre
en
No longer only restricted to nursing home use
xxx
WC
F
No
v1 Add Biatain Ag Silicone
7.5cm x7.5cm
10cm x 10cm
gre
en Savings with switcfh to Biatain Ag Silicone from existing Biatain
Ag adhesive and non-adhesive.
Three smallest sizes available in primary care as stock
through the On-line Non-Prescription Ordering System
(ONPOS), Largest two sizes available on prescription
A5
.3.
3
Delete Biatain Ag adhesive and
non-adhesive - all sizes
Replaced by Biatain Ag
Silicon
NOTE: to be replaced with Biatain Ag Silicone low
adherence dressing, see entry below
A5
.3.3

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
WC
F N
ov1
5
ADD Medi Derma-S barrier
cream
2g sachet, 28g, 90g
tube
Replacing Cavilon barrier
products
gre
en
2g sachet barrier cream
28g, 90g tube barrier cream
All above, except 90g tube, available in primary care as
stock through On-line Non-Prescription Ordering System
(ONPOS)
Apply sparingly For each buttock only a pea-sized
quantity required.
WC
F N
ov 1
5
WC
F N
ov1
5
ADD Medi Derma-S barrier
film
1mL, 3mL foam
applicator (sterile),
30mL non-sting pump
spray
Replacing Cavilon barrier
products
gre
en
1mL, 3mL foam applicator (sterile)
30mL non-sting pump spray
Available in primary care as stock through the On-line
Non-Prescription Ordering System (ONPOS)
In secondary care obtain from Supplies
WC
F N
ov 1
5
WC
F
No
v1
5
Delete Cavilon No Sting Barrier
film
1ml, 3mL applicator
Replaced by Medi Derma-
S barrier products
bla
ck
NOTE: will become non-formulary from 2016
WC
F N
ov
WC
F
No
v1
5
Delete Cavilon Durable barrier
cream 2g sachet, 28g,
98g tube.
Replaced by Medi Derma-
S barrier products
bla
ck
NOTE: will become non-formulary from 2016
WC
F N
ov
Oc
t 1
5.4 Add Edoxaban 15mg, 30mg,
60mg Tablets
In accordance with NICE
TA 354 and the Bucks
NOACs for use in DVT/PE
amber initiation guideline.
Consultant
Haematologists or
NOAC pharmacists.
In hospital, any
consultant physician
may refer DVT / PE
cases to the NOAC
service for decision
about choice of
treatment after
dalteparin has
already been initiated
red
un
til g
uid
elin
e a
pp
rove
d
y
Place in therapy has been shown in the Table of Considerations
in the NOACs for DVT/PE guideline (FMG 15.9)
An alternative to Rivaroxaban, Dabigatran and Apixaban
for the treatment of DVT and PE, and prevention of
recurrent DVT and PE in adult patients unsuitable for
warfarin for whom dalteparin would otherwise be
considered in accordance with NICE TA 354 and the
Bucks NOACs for use in DVT/PE guideline (not yet
uploaded)
The choice of NOAC will be based upon the table of
considerations for choosing a NOAC described in the
NOACs for DVT/PE guideline
Restricted to initiation by
1. Consultant haematologists or NOAC pharmacists with
continuation by GPs
2. In hospital any consultant physician may refer DVT/PE
cases to the NOAC service for decision about treatment
after dalteparin has already been initiated
Traffic light red until guideline approved
02
.08
.02
Oct-
15
FMG DECISIONS OCTOBER 2015

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Oc
t 1
5.5 Add Edoxaban 15mg, 30mg,
60mg Tablets
In accordance with NICE
TA 355 and the NOACs for
stroke prevention in AF
amber initiation guideline.
1. Consultant Stroke
physicians .
2. NOAC Pharmacy
service.
3. Consultant
Cardiologists for
urgent AF patients
Prescribing for
emergency cover
only
All patients initiated
by consultants to be
referred to the NOAC
service for next
working day follow-
up.
red
un
til g
uid
elin
e a
pp
rove
d
y
Place in therapy has been shown in the Table of Considerations
in the NOACs for AF guideline (FMG Sep 15.10)
This updated NOACs for AF guideline
- has revised the definition of an urgent patient 'without a
previous stroke or TIA but with a CHADSVASC2 of 5 or more
should be referred to the NOAC clinic for an urgent initial
appointment. ' (previously CHA2DS2VASc of 6 or more)
- includes a table of considerations for choosing a NOAC upon
which the choice of treatment should be made
- Includes emergency prescribing by consultant Cardiologists
when NOAC service not available at weekends
NOTE 1. Any urgent patient without a previous stroke or
TIA but with a CHA2DS2VASc of 5 or more should be
referred to the NOAC Service for an urgent initial
appointment.
Red Traffic Light For preventing stroke and systemic
embolism in adults with non-valvular atrial fibrillation in
accordance with the NICE TA355 and the NOACs for
stroke prevention in AF amber initiation guideline. The
choice of NOAC will be based upon the Table of
considerations for choosing a NOAC described in the
NOACs for stroke prevention AF guideline (not yet
uploaded)
Restricted to prescribing by
1. Consultant stroke physicians for urgent patients who
have had a previous stroke or TIA. All patients initiated
by consultants to be subsequently referred to the NOAC
service for follow-up.
2. NOAC Pharmacy service
3. Consultant cardiologists for urgent AF patients with a
CHA2DSVASc of 5 or more when the consultant has
confirmed with the NOAC service that the patient cannot
be seen the next working day due to the weekend.
Prescribing for emergency cover only (normally 3 days'
supply) All patients initiated by consultants to be referred
to the NOAC service for next working day follow up.
02
.08
.02
Oct-
15

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Se
p 1
5.1
0 Amend
restrictionApixaban 2.5mg, 5mg
tablet
1. Consultant Stroke
physicians .
2. NOAC Pharmacy
service.
3. Consultant
Cardiologists for
urgent AF patients
Prescribing for
emergency cover
only
All patients initiated
by consultants to be
referred to the NOAC
service for next
working day follow-
up.
Continuation by GPs AI
y
Updated NOACs for AF guideline
- has revised the definition of an urgent patient 'without a
previous stroke or TIA but with a CHADSVASC2 of 5 or more
should be referred to the NOAC clinic for an urgent initial
appointment.' (previously CHA2DS2VASc of 6 or more)
- includes a table of considerations for choosing a NOAC upon
which the choice of treatment should be made
- Includes emergency prescribing by consultant Cardiologists
when NOAC service not available at weekends
NOTE 1. Any urgent patient without a previous stroke or
TIA but with a CHA2DS2VASc of 5 or more should be
referred to the NOAC Service for an urgent initial
appointment.
NOTE 2. In secondary care tablets can be
dissolved/crushed and administered via
nasogastric/PEG tubes.
Amber Traffic Light for preventing stroke and systemic
embolism in adults with non-valvular atrial fibrillation in
accordance with NICE TA 275 and Dabigatran,
Rivaroxaban and Apixaban for Atrial Fibrillation - Amber
Initiation guideline (BHTCG 313FM) (to be replaced by
the NOACs for stroke prevention in AF amber initiation
guideline)
The choice of NOAC will be based upon the Table of
Considerations for choosing a NOAC described in the
NOACs for stroke prevention AF guideline (awaited)
Restricted to initiation by (with continuation by GPs)
1. Stroke physicians for urgent patients who have had a
previous stroke or TIA. All patients initiated by
consultants to be subsequently referred to the NOAC
service for follow-up.
2. NOAC pharmacy service
3. Consultant Cardiologists for urgent AF patients with a
CHA2DS2VASc of 5 or more when the consultant has
confirmed with the NOAC service that the patient cannot
be seen the next working day due to the weekend.
Prescribing for emergency cover only (normally 3 days'
supply) All patients initiated by consultants to be referred
to the NOAC service for next working day follow-up.
02
.08
.02
Oct-
15
Se
p 1
5.1
0 Amend
restrictionDabigatran etexilate
110mg, 150mg
capsules
In accordance with NICE
TA249 and the NOACs for
stroke prevention in AF
amber initiation guideline.
as for Edoxaban
tablets in AF above
with continuation by
GPs
AI
y
Updated NOACs for AF guideline
- has revised the definition of an urgent patient 'without a
previous stroke or TIA but with a CHADSVASC2 of 5 or more
should be referred to the NOAC clinic for an urgent initial
appointment.' (previously CHA2DS2VASc of 6 or more)
- includes a table of considerations for choosing a NOAC upon
which the choice of treatment should be made
- Includes emergency prescribing by consultant Cardiologists
when NOAC service not available at weekends
as for Edoxaban tablets in AF above
02
.08
.02
Oct-
15

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Se
p 1
5.1
0 Amend
restrictionRivaroxaban 15mg,
20mg Tablets
In accordance with NICE
TA256 and the NOACs for
stroke prevention in AF
amber initiation guideline.
as for Edoxaban
tablets in AF above
with continuation by
GPs
AI
y
Updated NOACs for AF guideline
- has revised the definition of an urgent patient 'without a
previous stroke or TIA but with a CHADSVASC2 of 5 or more
should be referred to the NOAC clinic for an urgent initial
appointment.' (previously CHA2DS2VASc of 6 or more)
- includes a table of considerations for choosing a NOAC upon
which the choice of treatment should be made
- Includes emergency prescribing by consultant Cardiologists
when NOAC service not available at weekends
as for Edoxaban tablets in AF above
02
.08
.02
Oct-
15
Fe
b 1
5.2
an
d S
ep
15
.9 Amend wording Dabigatran 110mg,
150mg capsules
in accordance with NICE
TA327 and the Bucks
NOACs for use in DVT/PE
amber initiation guideline.
(awaited)
as for Edoxaban
tablets in DVT/PE
above with
continuation by GPs
AI
Updated NOACs for DVT/PE guideline (FMG 15.9) includes a
table of considerations for choosing a NOAC upon which the
choice of NOAC should be made
as for Edoxaban tablets in DVT/PE above
02
.08
.02
Oct-
15
Se
p 1
5.8 Amend wording Apixaban 2.5mg, 5mg
Tablets
In accordance with NICE
TA341 and the Bucks
NOACs for use in DVT/PE
amber initiation guideline.
(awaited)
as for Edoxaban
tablets in DVT/PE
above with
continuation by GPs
red
un
til g
uid
elin
e
y
Updated NOACs for DVT/PE guideline (FMG 15.9) includes a
table of considerations for choosing a NOAC upon which the
choice of NOAC should be made
as for Edoxaban tablets in DVT/PE above
02
.08
.02
Oct-
15
Se
p 1
5.8 Amend wording Rivaroxaban 15mg,
20mg Tablets
In accordance with NICE
TA 261 and TA 287, and
the Bucks NOACs for use
in DVT/PE amber initiation
guideline. (awaited)
as for Edoxaban
tablets in DVT/PE
above with
continuation by GPs AI
Updated NOACs for DVT/PE guideline (FMG 15.9) includes a
table of considerations for choosing a NOAC upon which the
choice of NOAC should be made
as for Edoxaban tablets in DVT/PE above
02
.08
.02
Oct-
15
Oc
t 1
5.7 Add Glatiramer acetate
40mg/ml pre-filled
syringe
PbR excl - NHS
England
In accordance with NHS
England circular SSC1534
Consultant
Neurologists and
Clinical Nurse
Specialists (MS)
red
y
NHS England commissioning circular SSC1534 confirms
commissioning of two new products for RRMS both of which
have demonstrated similar efficacy and tolerability to their
current formulary alternatives and have price parity
FOR ALL PRESCRIBING - NICE compliance form
required - see link from Formulary home page. NICE
compliance to be verified if form not yet available
Restricted - prescribing by Consultant Neurologists and
clinical nurse specialists (MS) as a first line treatment
option for adults with relapsing-remitting multiple
sclerosis in accordance with: NHS England circular
SSC1534.
08
.02
.04
Oct-
15

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Oc
t 1
5.7 Add Peginterferon beta-1a
125 micrograms/0.5ml
pre-filled pen
63micrograms in 0.5ml
and 94micrograms in
0.5ml pre-filled pens
(treatment initiation
pack)
PbR excl - NHS
England
In accordance with NHS
England circular SSC1535
Consultant
Neurologists and
Clinical Nurse
Specialists (MS)
red y
NHS England commissioning circular SSC1534 confirms
commissioning of two new products for RRMS both of which
have demonstrated similar efficacy and tolerability to their
current formulary alternatives and have price parity
FOR ALL PRESCRIBING - Compliance form required -
see link from Formulary home page. Compliance to be
verified if form not yet available
Restricted - prescribing by Consultant Neurologists and
clinical nurse specialists (MS) as a first line treatment
option for adults with relapsing-remitting multiple
sclerosis in accordance with NHS England circular
SSC1534 08
.02
.04
Oct-
15
Oc
t 1
5.9 Add Dexamethasone
700microgram
intravitreal implant
PbR excluded CCG
For diabetic macular
oedema (DMO) in
accordance with NICE
TA349
Consultant
Ophthalmologists
red
y
Dexamethasone implant is a second line option in
pseudophakic lensed DMO patients for whom antiVEGF
treatment fails or is unsuitable due to intolerance or
contraindications
FOR ALL PRESCRIBING - NICE compliance form
required - see link form Formulary home page.
Restricted - prescribing by consultant ophthalmologists
as a 2nd line option in pseudophakic diabetic macular
oedema patients for whom anti VEGF treatment fails or
is unsuitable due to intolerance or contraindications in
accordance with NICE TA 349.
11
.04
.01
Oct-
15
Oc
t 1
5.1
0 Add Aflibercept 40mg/ml
solution for
intravitreal injection
PbR excluded CCG
For diabetic macular
oedema (DMO) in
accordance with NICE
TA346
Consultant
Ophthalmologists
red
y
Aflibercept would be an alternative first and second line
antiVEGF to first choice ranibizumab for treatment of DMO as
described in the draft Intravitreal injections algorithm and based
upon the principle that ’When all clinical considerations are
equal, priority will be given to the product with the greatest
experience and lowest short and long term treatment costs’
FOR ALL PRESCRIBING - NICE compliance form
required - see link from Formulary homepage.
Restricted - prescribing by consultant Ophthalmologists:
As an alternative 1st and 2nd line anti VEGF to 1st
choice ranibizumab for treating visual impairment caused
by diabetic macular oedema in accordance with NICE TA
346 and as described in the draft intravitreal injections
algorithm and based upon the principle that 'when all
clinical considerations are equal, priority will be given to
the product with greatest experience and lowest short
and long term treatment costs'
11
.08
.02
Oct-
15
Oc
t 1
5.1
1 Add Vedolizumab 300mg
intravenous infusion
PbR excluded CCG
PAS
in accordance with
Biologics Crohn's disease
guideline (in development)
and NICE TA 352
Consultant
Gastroenterologists
red
y
NICE TA 352. Biologics in Crohn's Disease algorithm being
developed
FOR ALL PRESCRIBING: NICE compliance form
required - see link from Formulary homepage. NICE
compliance to be confirmed if form not yet available.
Restricted - For treatment of moderate to severe active
Crohn’s disease in adult patients in accordance with
biologics Crohn's disease algorithm (in development)
and NICE TA 352 Vedolizumab for treating moderately to
severely active Crohn's disease after prior therapy
01
.05
.03
Oct-
15
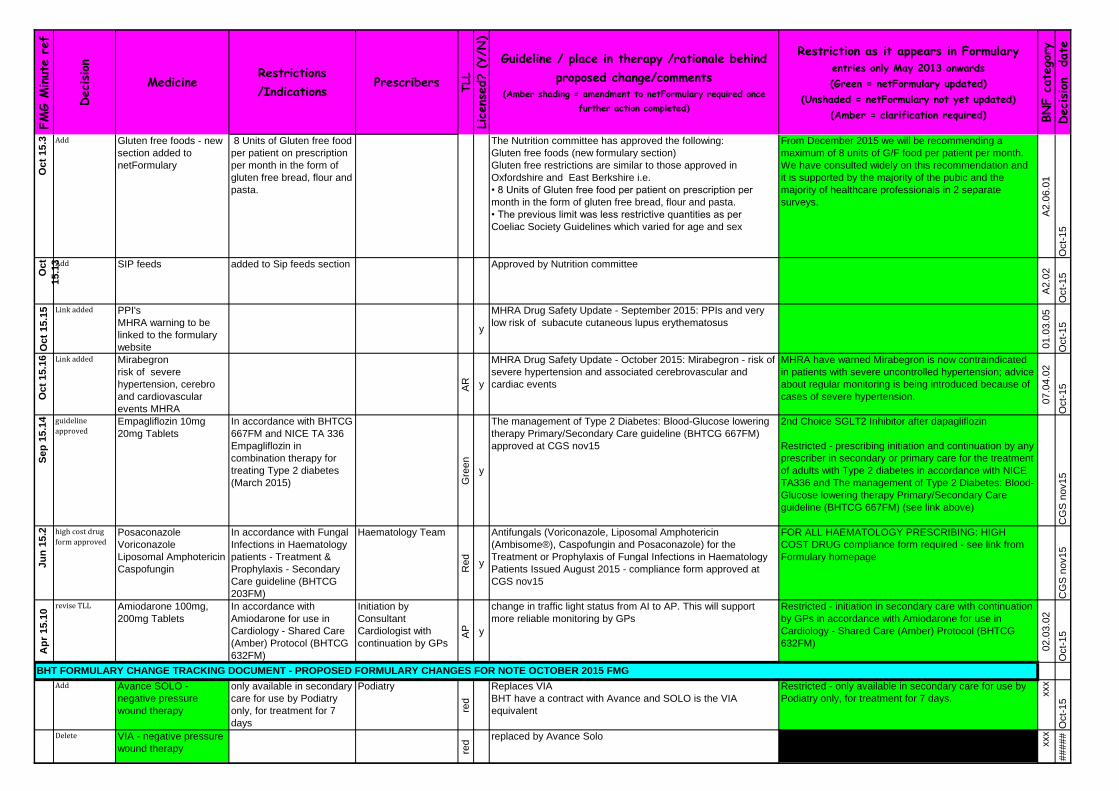
FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Oc
t 1
5.3 Add Gluten free foods - new
section added to
netFormulary
8 Units of Gluten free food
per patient on prescription
per month in the form of
gluten free bread, flour and
pasta.
The Nutrition committee has approved the following:
Gluten free foods (new formulary section)
Gluten free restrictions are similar to those approved in
Oxfordshire and East Berkshire i.e.
• 8 Units of Gluten free food per patient on prescription per
month in the form of gluten free bread, flour and pasta.
• The previous limit was less restrictive quantities as per
Coeliac Society Guidelines which varied for age and sex
From December 2015 we will be recommending a
maximum of 8 units of G/F food per patient per month.
We have consulted widely on this recommendation and
it is supported by the majority of the pubic and the
majority of healthcare professionals in 2 separate
surveys.
A2
.06
.01
Oct-
15
Oct
15
.13Add SIP feeds added to Sip feeds section Approved by Nutrition committee
A2
.02
Oct-
15
Oc
t 1
5.1
5 Link added PPI's
MHRA warning to be
linked to the formulary
website
y
MHRA Drug Safety Update - September 2015: PPIs and very
low risk of subacute cutaneous lupus erythematosus
01
.03
.05
Oct-
15
Oc
t 1
5.1
6 Link added Mirabegron
risk of severe
hypertension, cerebro
and cardiovascular
events MHRA
AR y
MHRA Drug Safety Update - October 2015: Mirabegron - risk of
severe hypertension and associated cerebrovascular and
cardiac events
MHRA have warned Mirabegron is now contraindicated
in patients with severe uncontrolled hypertension; advice
about regular monitoring is being introduced because of
cases of severe hypertension. 07
.04
.02
Oct-
15
Se
p 1
5.1
4 guideline
approvedEmpagliflozin 10mg
20mg Tablets
In accordance with BHTCG
667FM and NICE TA 336
Empagliflozin in
combination therapy for
treating Type 2 diabetes
(March 2015) Gre
en
y
The management of Type 2 Diabetes: Blood-Glucose lowering
therapy Primary/Secondary Care guideline (BHTCG 667FM)
approved at CGS nov15
2nd Choice SGLT2 Inhibitor after dapagliflozin
Restricted - prescribing initiation and continuation by any
prescriber in secondary or primary care for the treatment
of adults with Type 2 diabetes in accordance with NICE
TA336 and The management of Type 2 Diabetes: Blood-
Glucose lowering therapy Primary/Secondary Care
guideline (BHTCG 667FM) (see link above)
CG
S n
ov1
5
Ju
n 1
5.2 high cost drug
form approvedPosaconazole
Voriconazole
Liposomal Amphotericin
Caspofungin
In accordance with Fungal
Infections in Haematology
patients - Treatment &
Prophylaxis - Secondary
Care guideline (BHTCG
203FM)
Haematology Team
Re
d
y
Antifungals (Voriconazole, Liposomal Amphotericin
(Ambisome®), Caspofungin and Posaconazole) for the
Treatment or Prophylaxis of Fungal Infections in Haematology
Patients Issued August 2015 - compliance form approved at
CGS nov15
FOR ALL HAEMATOLOGY PRESCRIBING: HIGH
COST DRUG compliance form required - see link from
Formulary homepage
CG
S n
ov1
5
Ap
r 1
5.1
0
revise TLL Amiodarone 100mg,
200mg Tablets
In accordance with
Amiodarone for use in
Cardiology - Shared Care
(Amber) Protocol (BHTCG
632FM)
Initiation by
Consultant
Cardiologist with
continuation by GPs
AP y
change in traffic light status from AI to AP. This will support
more reliable monitoring by GPs
Restricted - initiation in secondary care with continuation
by GPs in accordance with Amiodarone for use in
Cardiology - Shared Care (Amber) Protocol (BHTCG
632FM) 02
.03
.02
Oct-
15
Add Avance SOLO -
negative pressure
wound therapy
only available in secondary
care for use by Podiatry
only, for treatment for 7
days
Podiatry
red
Replaces VIA
BHT have a contract with Avance and SOLO is the VIA
equivalent
Restricted - only available in secondary care for use by
Podiatry only, for treatment for 7 days.
xxx
Oct-
15
Delete VIA - negative pressure
wound therapy red
replaced by Avance Solo
xxx
#####
BHT FORMULARY CHANGE TRACKING DOCUMENT - PROPOSED FORMULARY CHANGES FOR NOTE OCTOBER 2015 FMG

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Note on
FormularyMelatonin 3mg tablets
(Bio-Melatonin brand)
Paediatrics team
red n
To encourage use of less expensive tablets rather than the
more costly liquid, add note to say tablets can be dissolved in a
small amount of water if broken and stirred, or can be crushed
to a fine powder and mixed with water, or given with cold soft
food such as a teaspoon of Yoghurt or jam.
Brand name added to formulary entry
6Jul15
NOTE: Tablets can be dissolved in a small amount of
water if broken and stirred, or can be crushed to a fine
powder and mixed with water, or given with cold soft food
such as a teaspoon of yoghurt or jam.
4.1
.1
Oct-
15
Add Amoxicillin 1g IV MHRA drug alert (July
2014)
red y
Currentlycontracted to Wockhardt but Due to MHRA drug alert
(July 2014) advising not to use any Wockhardt Amoxicillin
Sodium Powder for Solution for Injection (all batches) in
patients <1 year of age. BHT have switched to using Bowmed
(off contract) for all patients to avoid Wockhardt products being
used in this patient group inadvertantly. Currently issues
obtaining the 500mg vial amoxicillin and as a result, the Trust is
using a high volume of the 250mg vials.
The 1g injection is also useful to keep on the formulary for
patients on doses of 1g TDS (CAP) and 2g every 4 hours
(Listerial meningitis/ Native valve endocarditis)
05
.01
.01
.03
Oct-
15
revise restriction
for BHT useRifampicin
tablets, syrup, injection
red and green entries
red
an
d g
ree
n
y
approval from Microbiology no longer needed for legionnarires
disease
In secondary care restricted - for use in mycobacterial
infections, Legionnaire's disease and for meningococcal
contacts. Microbiology approval required for all other
uses.
05
.01
.09
Oct-
15
remove brand Hydrocortisone sodium
phosphate 100ml/1ml
injection
glass ampoules
gre
en
y
Used to be Efcortesol brand but no longer called this, therefore
remove brand name
06
.03
.02
Oct-
15
Combining
entriesEpoetin Alfa,
Darbepoetin, Epoetin
Beta, Aripiprazole tabs,
orodisp tabs, oral
solution,
Chlorpromazine tablet
and oral solution,
Promazine tablets and
oral solution,
Pivmecillinam
Drugs in this list were listed as separate entries each with a
different traffic light status. These have now been combined
into one entry and each entry contains two or more traffic light
sections.
Oct-
15
Add Haloperidol oral
solution 5mg/5mL
red y In wide use across the Trust but not on the formulary.
10mg/5mL sugar-free is on formulary, green on TLL. Both
strengths similar cost although one is half the strength.
To be added as TLL red for now. The trust may want to
consider removing 5mg in 5ml from the formulary
4.2
.1
Oct-
15
Add Clonidine tablets
25microgram
In secondary care
restricted - for use in
Spinal patients only
for spinal patients
only
gre
en y omitted to be added to formulary when merge took place. Is in
use by Spinal patients using 25-50mcg qds for BP control
In secondary care restricted - for use in Spinal patients
only. 2.5
.2
Oct-
15
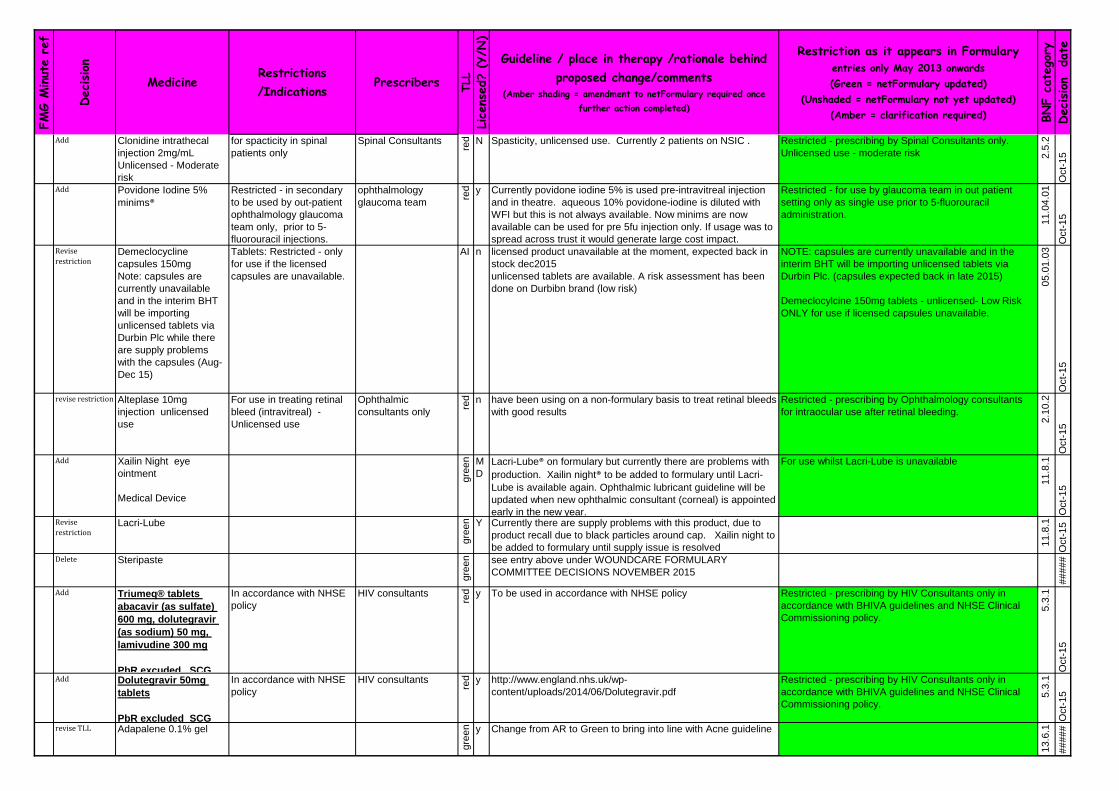
FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Add Clonidine intrathecal
injection 2mg/mL
Unlicensed - Moderate
risk
for spacticity in spinal
patients only
Spinal Consultants
red N Spasticity, unlicensed use. Currently 2 patients on NSIC . Restricted - prescribing by Spinal Consultants only.
Unlicensed use - moderate risk 2.5
.2
Oct-
15
Add Povidone Iodine 5%
minims®
Restricted - in secondary
to be used by out-patient
ophthalmology glaucoma
team only, prior to 5-
fluorouracil injections.
ophthalmology
glaucoma team
red y Currently povidone iodine 5% is used pre-intravitreal injection
and in theatre. aqueous 10% povidone-iodine is diluted with
WFI but this is not always available. Now minims are now
available can be used for pre 5fu injection only. If usage was to
spread across trust it would generate large cost impact.
Restricted - for use by glaucoma team in out patient
setting only as single use prior to 5-fluorouracil
administration.
11
.04
.01
Oct-
15
Revise
restrictionDemeclocycline
capsules 150mg
Note: capsules are
currently unavailable
and in the interim BHT
will be importing
unlicensed tablets via
Durbin Plc while there
are supply problems
with the capsules (Aug-
Dec 15)
Tablets: Restricted - only
for use if the licensed
capsules are unavailable.
AI n licensed product unavailable at the moment, expected back in
stock dec2015
unlicensed tablets are available. A risk assessment has been
done on Durbibn brand (low risk)
NOTE: capsules are currently unavailable and in the
interim BHT will be importing unlicensed tablets via
Durbin Plc. (capsules expected back in late 2015)
Demeclocylcine 150mg tablets - unlicensed- Low Risk
ONLY for use if licensed capsules unavailable.
05
.01
.03
Oct-
15
revise restriction Alteplase 10mg
injection unlicensed
use
For use in treating retinal
bleed (intravitreal) -
Unlicensed use
Ophthalmic
consultants only
red n have been using on a non-formulary basis to treat retinal bleeds
with good results
Restricted - prescribing by Ophthalmology consultants
for intraocular use after retinal bleeding.
2.1
0.2
Oct-
15
Add Xailin Night eye
ointment
Medical Device
gre
en M
D
Lacri-Lube® on formulary but currently there are problems with
production. Xailin night® to be added to formulary until Lacri-
Lube is available again. Ophthalmic lubricant guideline will be
updated when new ophthalmic consultant (corneal) is appointed
early in the new year.
For use whilst Lacri-Lube is unavailable
11
.8.1
Oct-
15
Revise
restrictionLacri-Lube
gre
en Y Currently there are supply problems with this product, due to
product recall due to black particles around cap. Xailin night to
be added to formulary until supply issue is resolved 11
.8.1
Oct-
15
Delete Steripaste
gre
en see entry above under WOUNDCARE FORMULARY
COMMITTEE DECISIONS NOVEMBER 2015
#####
Add Triumeq® tablets
abacavir (as sulfate)
600 mg, dolutegravir
(as sodium) 50 mg,
lamivudine 300 mg
PbR excuded SCG
In accordance with NHSE
policy
HIV consultants
red y To be used in accordance with NHSE policy Restricted - prescribing by HIV Consultants only in
accordance with BHIVA guidelines and NHSE Clinical
Commissioning policy.
5.3
.1
Oct-
15
Add Dolutegravir 50mg
tablets
PbR excluded SCG
In accordance with NHSE
policy
HIV consultants
red y http://www.england.nhs.uk/wp-
content/uploads/2014/06/Dolutegravir.pdf
Restricted - prescribing by HIV Consultants only in
accordance with BHIVA guidelines and NHSE Clinical
Commissioning policy.
5.3
.1
Oct-
15
revise TLL Adapalene 0.1% gel
gre
en y Change from AR to Green to bring into line with Acne guideline
13
.6.1
#####

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
revise TLL Tretinoin 0.025% lotion
gre
en y Change from AR to Green to bring into line with Acne guideline
13
.6.1
#####
revise restriction
until stock
depleted, then
delete
Diclofenac dispersible
tablets 50mg
gre
en y Advised by Pharmacy Procurement that now discontinued and
no replacement available. To be left on formulary with a note to
say discontinued for a period of time to allow stock to be used
up.
NOTE: diclofenac 50mg dispersible tablets now
discontinued
10
.1.1
Oct-
15
Revise
restrictionCaspofungin 50mg,
70mg IV infusion
In secondary care
restricted for Haematology
in accordance with Fungal
Infections in Haematology
Patients - Treatment and
Prophylaxis Secondary
Care guideline (BHTCG
203FM) or on Microbiology
approval
Consultant
Haematologists
red y Caspofungin to be used in accordance with the guideline
203FM where it is first line in some conditions and 3rd line in
others.
In secondary care Restricted - for Haematology in
accordance with Fungal Infections in Haematology
Patients - Treatment and Prophylaxis Secondary Care
guideline (BHTCG 203FM) or on Microbiology approval
5.2
.4
Oct-
15
Add Triomel Supplemented
N4-700E (FKCN
12001)
NOTE: the first 14 days
is in tariff and after 14
days, funded by NHS
England.
red N First of possibly several different TPN products used in BHT.
This section of the formulary has never been populated so
spoken with Aseptics to see what they use. Baxter Triomel N4-
700E 2.5L supplemented is the only standard formulary choice.
All other requirements are bespoke and outsourced to ITH
pharma.
SS
9.3
Oct-
15
revise restriction Oxybutynin tablets
2.5mg, 5mg
NOTE: tablets may be
crushed/dispersed in
10mL water and
administered orally or
via NG/PEG tubes.
gre
en y Change in restriction to oxybutynin liquid (see below) so add
note to Formulary as per info from MI regarding crushing of
tablets and mixing with water and administering. Suitable for
admin via nasogastric and PEG tubes. (info from Medicines
Information)
NOTE: immediate release (ordinary) tablets can be
dispersed/crushed in 10mL water and administered
orally or via NG/PEG tubes
7.4
.2
Oct-
15
Add Pilocarpine
hydrochloride tablets
5mg
Requests have come form
specialist centres in
London and Swindon.
Currently being approved
on NF basis in CCG. No
use in BHT
gre
en y Restricted - for use to increase secretions in sjogren's
syndrome
12
.3.5
Oct-
15
revise restriction Oxybutynin oral solution
2.5mg/5mL
to be prescribed for
paediatric patients only
red y Current liq is now discontinued, 2.5mgin 5ml unlicensed. A new
licensed liquid is now being made at greatly increaed cost. MI
have confirmed it is possible to crush tablets.
Restrict use to Paediatrics.
Restricted - to be prescribed for paediatric patients only.
NOTE: immediate release (ordinary) tablets can be
dispersed/crushed in 10mL water and administered
orally or via NG/PEG tub es. .
7.4
.2
Oct-
15
TLL change Fludroxycortide
0.0125% cream
(Haelan)
Was agreed Red at Dec 14
FMG subject to
Dermatology agreeing but
at Dermatology meeting
recently agreed to change
to green
gre
en y Agreed at dermatology SDU Meeting 6th Oct 2015 Potency: Moderate
13
.4
Oct-
15

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Add Diflucortolone valerate
0.1% oily cream
gre
en y Agreed at dermatology SDU Meeting 6th Oct 2015
Green on Traffic Light List, Post meeting proposal: 3rd choice
Potency: potent
13
.4
Oct-
15
Add Diflucortolone valerate
0.3% oily cream
Potency - Very Potent
gre
en y Agreed at dermatology SDU Meeting 6th Oct 2015
Add as an alternative to Dermovate when there are Dermovate
supply problems.
Green on Traffic Light List, 2nd choice
Potency: Very Potent
2nd line to Dermovate when there are Dermovate supply
problems.
In primary care try to avoid using very potent topical
steroids
In primary care try to avoid using very potent topical
steroids
13
.4
Oct-
15
Add Epimax
emollient cream
gre
en y Agreed at dermatology SDU Meeting 6th Oct 2015 In primary care - first choice basic emollient.
Note - patients may be prescribed an alternative if it is
not found suitable
13
.02
.01
Oct-
15
Add Clobetasol propionate
0.05% shampoo
(Etrivex®) (Levon®)
2nd line for use when
dermovate scalp
application not available
gre
en Agreed at dermatology SDU Meeting 6th Oct 2015 Potency: Very Potent
Second choice after Dermovate® scalp application when
this is not available
In primary care try to avoid using very potent topical
steroids
Choice Immunoglobulin
Privigen 1st Choice
consultants only
red y Privigen is stored at room temp and everything else being equal
to Octagam including use in Paeds
First choice Immunoglobulin is Privigen®
14
.05
.0 1O
ct-
15
Add Cheapest
brand Colecalciferol/Calcium
Carbonate
10micrograms
(400units)/1.5g
Accrete D3
greeny Accrete® is the cheapest Ca/vit D product on the market.
Currently Primary care recommend Calceos which will
gradually be phased out over 6 months.
Review Calceos in 6 months
In primary care Accrete D3® preferred brand
previous prefered brand Calceos® to be phased out over
6 months
9.6
.4
Oct-
15
new restriction Glibenclamide 2.5mg,
5mg tablet
gr
ee
n
y glibenclamide is no longer recommended because the long half
life means a greater risk of hypos
Restricted - New patients not to be started on
glibenclamide because long half life increases the risk of
hypoglycaemia 6.1
.2.1
Oct-
15
new restriction Tolbutamide 500mg tabletNot a 1st choice treatment
because of the interactions
in use.
greeny F Restricted - not to be used as a first choice treatment
because of the interactions in use
6.1
.2.1
Oct-
15
Swap Macrogol Oral Powder,
Compound.
gr
ee
n
y Cosmocol is a cheaper brand (compared to Movicol). In
Primary care savings can be achieved by actively switching.
Formulary states Macrogol Oral Powder Compound with no
brand names stated so no changes made.
CCG will actively switch to this brand and BHT will remain with
contract product.
1.6
.4
Oct-
15
CCG FORMULARY CHANGE TRACKING DOCUMENT - PROPOSED CHANGES FOR SEPTEMBER -NOVEMBER 2015 FMG

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Add Methylphenidate
Hydrochloride MR tablet
54mg (Concerta XL)
Restricted - initiation by
Consultant Paediatricians
specialising in childhood
behavioural disorders or
Child or Adult Mental
Health Specialist
initiation by
Consultant
Paediatricians
specialising in
childhood behavioural
disorders or Child or
Adult Mental Health
Specialist
A
P
y New strentgth MR tablet, in use in primary care Restricted - initiation by Consultant Paediatricians
specialising in childhood behavioural disorders or Child
or Adult Mental Health Specialist with continuation by
GPs for the treatment of ADHD in children over 6 years
and in accordance with ADHD amber protocol (BHTCG
796FM)
4.4
Oct-
15
Se
p 1
5.2
Add Secukinumab 150mg
pre-filled pen
PbR excl- CCG
funded. PAS
NICE TA350 Secukinumab
for treating moderate to
severe plaque psoriasis
(July 2015)
Consultant
Dermatologists
red y
Add although NICE form awaited. FOR ALL PRESCRIBING - NICE compliance form
required - see link from Formulary homepage. NICE
compliance to be confirmed if form not yet available.
Restricted - prescribing by Consulant Dermatologists for
moderate to severe plaque psoriasis in adults, in
accordance with Psoriasis Biologics treatment guidline
(BHTCG 738FM) and NICE TA 350.
13
.5.3
Sep-1
5
Sep
15
.3
Update Biologics in Psoriasis
algorithm (BHTCG
738FM)
Updated guideline approved (awaiting upload)
Sep-1
5
Sep
15
.4
Update Biologics in Psoriatic
arthritis algorithm
(BHTCG 740FM)
Updated guideline approved (awaiting upload)
Sep-1
5
Se
p 1
5.5
Revise
restrictionCertolizumab pegol
200mg pre-filled
syringe
Consultant
Rheumatologistsre
d
y
Add note regarding restricted use in BHT. FOR ALL PRESCRIBING - NICE compliance form
required - see link from Formulary homepage
1. Restricted - prescribing by Consultant
Rheumatologists only, in accordance Biologics for
Rheumatoid Arthritis guideline (BHTCG 749FM) and
NICE TA 186.
NOTE: use restricted in BHT to rheumatoid arthritis
patients with a low number of co-morbidities and low risk
of infection and is subject to further audit.
10
.1.3
Sep-1
5
Se
p 1
5.7
Add Ofatumumab 100mg,
1000mg concentrate
for infusion
PbR excl - SCG. PAS
NICE TA 344 Ofatumumab
in combination with
chlorambucil or
bendamustine for
untreated lymphocytic
leukaemia
Consultant
Haematologists
red
y
• To replace rituximab and chlorambucil as the standard of care
for less fit newly diagnosed CLL patients.
• The choice between ofatumumab and obinutuzumab will be
made by the lymphoma MDT
FOR ALL PRESCRIBING - NICE compliance form
required - see link from Formulary homepage. NICE
compliance to be confirmed if form not yet available.
Restricted - prescribing by Consultant Haematologists in
accordance with NICE TA 344. To replace rituximab and
chlorambucil as the standard of care for less fit newly
diagnosed CLL patients. The choice between
ofatumumab and obinutuzumab will be made by the
Lymphoma MDT.
8.2
.3
Sep-1
5
FMG DECISIONS SEPTEMBER 2015

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Se
p 1
5.7
Add Obinutuzumab
1000mg concentrate
for infusion
PbR excl - SCG. PAS
NICE TA 343
Obinutuzumab in
combination with
chlorambucil for untreated
lymphocytic leukaemia.
Consultant
Haematologists
red
y
• To replace rituximab and chlorambucil as the standard of care
for less fit newly diagnosed CLL patients.
• The choice between ofatumumab and obinutuzumab will be
made by the lymphoma MDT
FOR ALL PRESCRIBING - NICE compliance form
required - see link from Formulary homepage. NICE
compliance to be confirmed if form not yet available.
Restricted - prescribing by Consultant Haematologists in
accordance with NICE TA 343. To replace rituximab and
chlorambucil as the standard of care for less fit newly
diagnosed CLL patients. The choice between
ofatumumab and obinutuzumab will be made by the
Lymphoma MDT.
8.2
.3
Sep-1
5
Se
p 1
5.8
?
Add Apixaban 2.5mg, 5mg
tablet
NICE TA 341 Apixaban for
treatment and secondary
prevention of DVT and PE.
Initiation by
Consultant
Haematologists in the
DVT clinic, or NOAC
service, with
continuation by GPs.
In hospital, any
consultant physician
(POD) may refer DVT
cases to the
Haemostasis or
NOAC clinic for
decision about choice
of treatment after
dalteparin has been
initiated
AI
y
As an alternative to rivaroxaban and dabigatran for the
treatment of DVT and PE, and prevention of recurrent DVT and
PE in adult patients unsuitable for warfarin for whom dalteparin
would otherwise be considered in accordance with NICE TA
341 and the Bucks NOACs for use in DVT/PE amber initiation
guideline.
Red traffic light symbol in place initially becoming AI for the
entire entry after guideline approved (AI guideline awaited)
2. Restricted - to initiation by Consultant
Haematologists in the DVT clinic, or NOAC service, with
continuation by GPs. In hospital, any consultant
physician (POD) may refer DVT cases to the
Haemostasis or NOAC clinic for decision about choice of
treatment after dalteparin has been initiated.
To be used as an alternative to rivaroxaban and
dabigatran for the treatment of DVT and PE, and
prevention of recurrent DVT and PE in adult patients
unsuitable for warfarin, for whom dalteparin would
otherwise be considered, in accordance with NICE TA
341 and the Bucks NOACs for use in DVT/PE Amber
Initiation guideline. (guideline awaited and traffic light
status is RED until guideline uploaded and available)
2.8
.2
Sep-1
5
Se
p1
5.1
3
Add Daclatasvir tablet
30mg, 60mg (Daklinza)
PbR excl - NHSE PAS
NHSE Commissioning
policy 1524 June 2015 -
Hepatitis C with cirrhosis.
Consultant
Gastroenterologists/H
epatologists and
Associate Specialist
Gastroenterology red
y
Link to NHSE Commissioning policy statement June 2015 FOR ALL PRESCRIBING - a completed and approved
HIGH COST DRUG compliance form via BLUETEQ is
required
Restricted - prescribing by Consultant
Gastroenterologists/Hepatologists and Assoicate
Specialist (Gastroenterology), as part of ODN in
accordance with NHSE Commissioning Policy statement
June 2015 - Hepatitis C with Cirrhosis
5.3
.3.2
Sep-1
5
Add Viekirax 12.5 mg/75
mg/50 mg tablet
Ombitasvir/Paritaprevi
r/Ritonavir
NHSE Commissioning
policy 1524 June 2015 -
Hepatitis C with cirrhosis.
Consultant
Gastroenterologists/H
epatologists and
Associate Specialist
Gastroenterology red
y
FOR ALL PRESCRIBING - a completed and approved
HIGH COST DRUG compliance form via BLUETEQ is
required
Restricted - prescribing by Consultant
Gastroenterologists/Hepatologists and Assoicate
Specialist (Gastroenterology), as part of ODN in
accordance with NHSE Commissioning Policy statement
June 2015 - Hepatitis C with Cirrhosis
5.3
.3.2
Sep-1
5

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Add Dasabuvir 250mg
tablet
PbR excl - NHSE PAS
NHSE Commissioning
policy 1524 June 2015 -
Hepatitis C with cirrhosis.
Consultant
Gastroenterologists/H
epatologists and
Associate Specialist
Gastroenterology red
y
FOR ALL PRESCRIBING - a completed and approved
HIGH COST DRUG compliance form via BLUETEQ is
required
Restricted - prescribing by Consultant
Gastroenterologists/Hepatologists and Assoicate
Specialist (Gastroenterology), as part of ODN in
accordance with NHSE Commissioning Policy statement
June 2015 - Hepatitis C with Cirrhosis
5.3
.3.2
Sep-1
5
Add Sofosbuvir/Ledipasvir
400mg/90mg tablet
(Harvoni)
PbR excl - NHSE PAS
NHSE Commissioning
policy 1524 June 2015 -
Hepatitis C with cirrhosis.
Consultant
Gastroenterologists/H
epatologists and
Associate Specialist
Gastroenterology red
y
FOR ALL PRESCRIBING - a completed and approved
HIGH COST DRUG compliance form via BLUETEQ is
required
Restricted - prescribing by Consultant
Gastroenterologists/Hepatologists and Assoicate
Specialist (Gastroenterology), as part of ODN in
accordance with NHSE Commissioning Policy statement
June 2015 - Hepatitis C with Cirrhosis
5.3
.3.2
Sep-1
5
Add Sofosbuvir 400mg
tablet
PbR excl - NHSE PAS
NHSE Commissioning
policy 1524 June 2015 -
Hepatitis C with cirrhosis.
Consultant
Gastroenterologists/H
epatologists and
Associate Specialist
Gastroenterology red
y
FOR ALL PRESCRIBING - a completed and approved
HIGH COST DRUG compliance form via BLUETEQ is
required
2...Restricted - prescribing by Consultant
Gastroenterologists/Hepatologists and Assoicate
Specialist (Gastroenterology), as part of ODN in
accordance with NHSE Commissioning Policy statement
June 2015 - Hepatitis C with Cirrhosis
5.3
.3.2
Sep-1
5
Se
p1
5.1
4
Add Empagliflozin 10mg,
25mg tablet
NICE TA 336 Empagliflozin
in combination therapy for
treating Type 2 diabetes
(March 2015) gre
en
y
Guideline (update awaited) 2nd Choice SGLT2 Inhibitor afater Dapagliflozin
Restricted - for the treatment of adults with Type 2
diabetes in accordance with NICE TA336 and Type 2
Diabetes guideline (BHTCG 667FM) (guideline being
updated)(see link above)
6.1
.2.3
Sep-1
5
Oct1
4.2
Add Rifaximin 550mg tablet
(Targaxan)
NICE TA 337 Rifaximin for
preventing epiosdes of
overt hepatic
encephalopathy
Consultants
Gastroenterologists
and Hepatologists
red
Y
Confirm funding SCG/CCG? FOR ALL PRESCRIBING - NICE compliance form
required - see link from Formulary homepage. NICE
compliance to be confirmed if form not yet available.
Prescribing by Consultant Gastroenterologists and
Hepatologists for reduction in recurrence of episodes of
overt hepatic encephalopathy in patients over 18 years
of age in accordance with NICE TA 337. When following
up at 1 and 6 months NICE form to be completed each
time.
5.1
.7
Sep-1
5
Se
p 1
5.1
1
Add Vedolizumab 300mg
powder for
concentrate for
solution for infusion
PbR Excl CCG PAS
NICE TA 342 Vedolizumab
for treating moderately to
severely active ulcerative
colitis
Consultant
Gastroenterologists
red
y
FOR ALL PRESCRIBING - NICE compliance form
required - see link from Formulary homepage. NICE
compliance to be confirmed if form not yet available.
Prescribing by Consultant Gastroenterologists in
accordance with NICE TA 342 and Biologics in
Ulcerative Colitis guideline (awaited)
1.5
.3
Sep-1
5
BHT FORMULARY CHANGE TRACKING DOCUMENT - PROPOSED FORMULARY CHANGES FOR NOTE APRIL 2015 FMG

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Se
p 1
5. Revise
restriction Rifampicin 150mg,
300mg capsules and
syrup 100mg/5mL
Respiratory physicians
able to prescribe for
Legionnaire's disease
without Micro approval
gre
en
y
In secondary care restricted - for use in mycobacterial
infections, Legionnaire's disease and for meningococcal
contacts. Microbiology approval required for all other
uses
5.1
.9
FM
G
Add Adalimumab 40mg
prefilled pen or
syringe
Infliximab 100mg
infusion
Golimumab 50mg
prefilled pen or
syringe
PbR excl CCG funded
in accordance with NICE
TA329 Infliximab,
adalimumab and
golimumab for treating
moderately to severely
active ulcerative colitis
after the failure of
conventional therapy
(including review of TA140
and TA262)
Prescribing by
Consultant
Gastroenterologists
red y
NOTE (added in full to adalimumab and infliximab entry and in
part to golimumab entry)
In NICE TA 329, adalimumab is the first choice biologic for
adult use and infliximab for paediatric use; in NICE TA 163
infliximab is approved for acute exacerbations. If a patient on
infliximab for NICE TA 163 continues treatment long term in
accordance with NICE TA 329, infliximab should be the drug of
choice and switching to adalimumab should not take place
It should be noted that NICE TA 329 recommends titrating up to
weekly dosing for adalimumab. This is in contrast to current
Thames Valley Priorities Committee recommendations and
supersedes them.
FOR ALL PRESCRIBING - NICE compliance form
required - see link from Formulary homepage. NICE
compliance to be confirmed if form not yet available.
Restricted - to prescribing by Consultant
Gastroenterologists in accordance with NICE TA329
Infliximab, adalimumab and golimumab for treating
moderately to severely active ulcerative colitis after the
failure of conventional therapy and in accordance with
BHT Ulcerative Colitis treatment algorithm (in
development)
NOTE (see adjacent column) added to adalimumaband
infliximab and in part to golimumab
1.5
.3
Ju
ne
15
FM
G
Add Eculizumab 300mg
concentrate for
solution for infusion
PbR excl NHSE
NICE Highly Specialised
Technology guidance 1:
Eculizumab for treating
atypical haemolytic
uraemic syndrome
Restricted - to
prescribing by
consultant
paediatricians in
shared care with
tertiary centres
red
y
FOR ALL PRESCRIBING - NICE compliance form
required - see link from Formulary homepage. NICE
compliance to be confirmed if form not yet available.
Restricted - prescribing by Consultant Paediatricians in
shared care with tertiary centres only.
un
kn
ow
n
Ju
ne
15
FM
G
Add Axitinib 1mg, 3mg,
5mg, 7mg tablet
PbR excl NHSE
Treatment of advanced
renal cell cancer after
failure of prior systemic
treatments in accordance
with NICE TA 333
Prescribing initiation
by consultant
oncologist (renal) or
consultant oncologist
SDU Lead,
continuation by
consultant
oncologists (all)
red y
Cost impact to be circulated electronically and NICE form
upload awaited. Coming to CGS Aug15
FOR ALL PRESCRIBING - NICE compliance form
required - see link from Formulary homepage. NICE
compliance to be confirmed if form not yet available.
Restricted - prescribing to be initiated by Consultant
Oncologist (renal) or their SDU Lead, with continuation
by all Consultant Oncologists in accordance with NICE
TA 333 Axitinib for the treatment of advanced renal cell
carcinoma after failure of prior systemic treatment.
8.1
.5
Ju
ne
15
FM
G
Add Use of Exenatide with
Insulin
Use of exenatide and
insulin in combination in
accordance with criteria
defined in HCD compliance
form
Diabetes consultant
only
AI
HCD form completed and awaiting upload. Wording added to
exenatide entries.
EXENATIDE and INSULIN
Exenatide in combination with insulin may only be
initiated by Consultant Diabetologists with continuation
by GPs, in accordance with the criteria defined in the
High Cost Drug compliance form - see link from
Formulary home page. The decision to continue or stop
therapy to be made by Consultant Diabetologist at 6
months.
6.1
.2.3
Ju
ne
15
FM
G
FMG DECISIONS JUNE 2015

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Updated Lipid Modification for
secondary and primary
prevention of
cardiovascular disease
(CVD) in adult patients
guideline
Updated, approved and uploaded to website.
Ju
ne
15
FM
G
Ju
ne
15
.1
Add Infliximab biosimilars
Inflectra® and
Remsima® 100mg
intravenous infusion
PbR excluded - CCG
funded
Consultant
Gastroenterologists,
Rheumatologists,
Dermatologists
Re
d
y
As for infliximab previously. HCD updates still awaited. FOR ALL PRESCRIBING - NICE compliance form
required - see link from Formulary homepage. NICE
compliance to be verified if form not yet available.
NOTE:
ALL prescribing of infliximab must include generic and
brand name.
Inflectra® is first choice infliximab biosimilar for all new
patients, with Remsima® second choice only when first
choice is more expensive or not available.
Infliximab biosimilars may be prescribed for patients
currently receiving Remicade® brand when considered
clinically appropriate by the relevant consultant and with
consent of the patient.
1.5
.3,
10
.1.3
, 1
3.5
.3
Ju
ne
15
FM
G
Ju
ne
15
.2
Add Ustekinemab 45mg
pre-filled syringe
PbR excl - CCG
funded
NICE TA 340 Ustekinumab
for treating active psoriatic
arthritis (rapid review of TA
313) June 2015
Consultant
Rheumatologists and
Dermatologists
Re
d
y
Added to formulary with note informing: not funded until end of
August 2015. Updated Biologics guideline for Psoriatic arthritis
in process.
Wording removed as now funded.
FOR ALL PRESCRIBING: NICE compliance form
required - see link from Formulary homepage
Restricted to:
1. Prescribing by Consultant Dermatologists only, in
accordance with Biologics for Psoriasis guideline
(BHTCG 738FM) and NICE TA 180.
2. From September 2015 - Prescribing by Consultant
Dermatologists and Rheumatologists, in accordance with
Biologics for Psoriatic Arthritis guideline (BHTCG
740FM)(updating in process) and NICE TA 340. (NOTE:
not funded for NICE TA 340 until after August 2015)
10
.1.3
, 1
3.5
.3
Ju
ne
15
FM
G
Add Rituximab 1400mg sub-
cutaneous injection
PbR excl - NHS
England
NICE TA 226 Rituximab for
first line maintenance
therapy of folllicular non-
Hodgkin's lymphoma (June
2011)
Consultant
Haematologists only
Re
d
y
Link active to England Specialised services circular (PDF
uploaded to website)
HCD form needs updating - awaited
FOR ALL PRESCRIBING - NICE compliance form
required - see link from Formulary homepage. NICE
compliance to be verified if form not yet available.
1. Restricted - prescribing by Haematologists only, in
accordance with NICE TA 226 and in accordance with
NHS England Specialised Services Circular (see link
below).
1. Restricted - prescribing by Haematologists only, in
accordance with NICE TA 226.
8.2
.3
Ju
ne
15
FM
G

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Ju
n 1
5.7
Add Rivaroxaban 2.5mg NICE TA 335 Riva for
preventing adverse
outcomes after acute
management of acute
coronary syndromes
Consultant
Cardiologists and
continuation by GPs
AI
y
add but AI guideline in development. Restricted - prescribing by Consultant Cardiologists with
continuation by GPs, in accordance with NICE TA 335.
To be stopped by the GP at 12 months, at the same time
as clopidogrel unless consultant clearly specifies at
discharge that treatmetn is lifelong (for a small cohort of
patients each year)
02
.8.2
Ju
ne
15
FM
G
Ju
n 1
5.8
Add Aromatherapy in Labour FMG acknowledged and accepted the use of aromatherapy for
patients' wellbeing in the Midwife led Unit in BHT.
16sep15 add in accordance with guideline BHT CG500 to be
added to formulary
The aromatherapy oils do not need to be prescribed nor be
included on the formulary.
For use in accordance with Aromatherapy in Labour
guidleline (BHTCG 500) (awaited)(BHT users only)
Ju
ne
15
FM
G
Ju
n 1
5.9
Add Co-
careldopa/Entacapone
7 strengths
Sastravi® (generic
Stalevo® equivalent)
Advice Clinical Nurse
Specialist
(Parkinson's) or
Neurology team with
continuation by GPS AR y
Sastravi® is product of choice.
The choice between prescribing separate component parts or
the combined product is made on the recommendation of the
PArkinson's Nurse/Neurology team, with continuation by GPs.
Restricted - the choice between prescribing the separate
component parts or the combined product is made on
the recommendation of the Clinical Nurse Specialist
(Parkinson's)/Neurology team with continuation by GPs.
If the combined product is recommended then Sastravi®
is first choice for Stalevo® naive patients.
Ju
ne
15
FM
G
Ju
n 1
5.1
0
revise
restrictionMultiple sclerosis
therapy - beta-
interferon, glatiramer,
natalizumab and
fingolimod
PbR excl - NHS
England
NHSE Clinical
Commissioning Policy -
Disease Modifying
Therapies for Patients with
Multiple Sclerosis
as for individual drug
red
y
Link to NHSE Clinical Commissioning Policy - Disease
Modifying Therapies for Patients with MS added to website,
section 8.2.4 and reference to policy added to the named
drugs.
Copy link to formulary.
Restricted - prescribing by Neurologists only in
accordance with NHSE Clinical Commissioning Policy -
Disease Modifying Therapies for Patients with MS (see
link above)
8.2
.4
Ju
ne
15
FM
G
Ap
ril 1
5.1
4
Add Sofosbuvir 400mg
tablet
PbR excl - NHS
England
NICE TA 330 Sofosbuvir
for treating chronic
hepatitis C
Consultant
Gastroenterologists
and Associate
Specialist (Gastro)
Re
d
y
Prescribing in accordance with NICE TA 331 and with
Operational Delivery network as defined by NHS England. Not
funded until August 2015 - noted on formulary entry on website.
16sep remove funding note need to add using blueteq
FOR ALL PRESCRIBING - NICE compliance form
required - see link from Formulary homepage. NICE
compliance to be confirmed if form not yet available.
NOTE: Only funded from August 2015 onwards as per
NICE and NHS England and as defined in NICE TA 331
Restricted - prescribing by Consultant
Gastroenterologists and Associate Specialist
Gastroenterology in accordance with NICE TA330 and
within the framework of an Operational Delivery Network
in accordance with NHSE Specialized Commissioning.
1.5
.3.
Ju
ne
15
FM
G

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Fe
b 1
5.4
Add Brimonidine (Mirvaso)
3mg/g (0.33%) gel
(brimonidine tartrate
5mg/g
Treatment of moderate to
severe persistent facial
erythema assoicated with
rosacea
Consultant
Dermatologists only
Re
d
y
Restricted - prescribing by Consultant Dermatologists
only for the treatment of moderate to severe persistent
facial erythema associated with rosacea. Patient to be
reviewed by consultant one month after commencing
treatment.
Efficacy and safety to be audited with review of results
after 6 months (March 2016)
13
.6.3
Ju
ne
15
FM
G
Add Botulinum toxin type
A (Dysport) 300units
red
y PROPOSAL: add Dysport 300 Units to the formulary for all
restrictions / indications/ specialties currently applied to Dysport
500 units.
Not to be used for the treatment of hyperhidrosis.
NOTE: When writing prescriptions for botulinum toxin
Type A or B, both the GENERIC and BRAND name
MUST be included.
1. Restricted - prescribing by Opthalmology, consultant
Neurologists and Spinal Unit Specialist Clinic.
2. Restricted - prescribing by colorectal surgeons. For
use (unlicensed)when glyceryl trinitrate and diltiazem
ointments have failed, in line with the poisiton statement
on the management of anal fissures produced by the
Association of Coloproctology in 2008.
3. Restricted - prescribing by Paediatric consultant (Jo
Hicks) only, for cerebral palsy spasticity.
11
.99
4.9
.3Ju
ne
15
FM
G
Revise
restrictionAll botulinum injections
add this note:
red
y and add a note for all botulinum injections: “All prescribing of
botulinum toxin type A or B to be written by generic AND brand
name”
NOTE: When writing prescriptions for botulinum toxin
Type A or B, both the GENERIC and BRAND name
MUST be included.
11
.99
4.9
.3Ju
ne
15
Classification Biologic Drugs
red
Not classified as cytotoxics. Agreed at DTC. Also reflected in
National Injectables Guide and also verified in BS
Rhematology. Therefore biologics not listed as cytotoxic.
8.2
.3
Ju
ne
15
Add link Stribild tablets HIV Consultants only
red
Clinical Commissioning policy updated. Linked to formulary
now
Contains: cobicistat 150mg/elvitegravir
150mg/emtricitabine 200mg/tenofovir disoproxil 245mg
Restricted - prescribing by HIV Consultants only in
accordance with BHIVA guidelines and NHSE Clinical
Commissioning policy.
5.3
.1
Ju
ne
15
FM
G
Revise
restrictionOxybutynin MR 5mg,
10mg tablets
gre
en
y Clarify prescribing in primary care with addition of primary care
statement.
In secondary care restricted - for use on the Spinal Unit
or for prescribing by consultants only, when the ordinary
tablets are not suitable or there are problems with
compliance
In primary care may be used where ordinary tablets have
caused side effects or where concordance is an issue.
7.4
.2
Ju
ne
15
FM
G
BHT FORMULARY CHANGE TRACKING DOCUMENT - PROPOSED FORMULARY CHANGES FOR NOTE JUNE 2015 FMG

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Revise
restrictionTetanus
Immunoglobulin
250units red
Addition of link to guidance and reworded restriction. Restricted - to be prescribed in accordance with Public
Health England - HPA expert working group interim
guidance on the use of tetanus immunoglobulin for the
treatment of Tetanus.
14
.5
Ju
ne
15
Add Co-trimoxazole tablets
960mg
red
y The shortage of IV CTX is resolving slowly. 960mg tablets to
be added to the formulary and restricted to use in patients
suffering from pneumocystis pneumonia (PCP) to aid
compliance given the large tablet load.
Restricted - only to be prescribed for patients with
pneumocystis pneumonia (PCP) to aid compliance. 5.1
.8
Ju
ne
15
Revise
restrictionNitrofurantoin 100mg
MR tablet
gre
en
y Green (current status)- Removed restriction to patients unable
to tolerate capsules/ suspension and can now be used as joint
first line formulation (with non-MR)
For use in uncomplicated urinary tract infections as 1st line
therapy for lower UTI with eGFR >45mL/min. Female patients 3-
5 day course and male patients 7-10day course.
Evidence - Public Health England: Management of Infection
Guidance for primary care for consultation and local adaptation.
October 2014. Guidance written in accordance with PHE Urine,
SIGN, CKS women, CKS men, RCGP UTI clinical module and
SAPG UTI. Modified-release preparations can be used to
reduce dosing frequency. Reduced dosing frequency (e.g. from
four times a day to twice a day) improves compliance.
In primary care = a first choice for UTI
5.1
.13
Ju
ne
15
FM
G
Add Nifedipine oral drops
20mg/mL 30mL
Autonomic dysflexia Initiation by
Consultant
Paediatricians and
Spinal ConsultantsA
I
N Used for autonomic dysreflexia and patients require urgently. Unlicensed - Medium Risk
Restricted - initiation by Consultant Paediatricians and
Spinal Consultants for treatment of autonomic
dysreflexia in paediatric patients only.
2.6
.2
Ju
ne
15
Nifedipine oral drops
20mg/mL 30mL
(£85.11 excl VAT)
Alcura red
n Used on the advice of a tertiary referral centre only (GOS or
Oxford) and not expected that patient would be discharged into
community requiring this.
Unlicensed - Medium Risk
Restricted - to paediatric patient prescribing in secondary
care only.
NOTE: for treatment of autonomic dysreflexia see
separate amber initiationa entry
2.6
.2
Ju
ne
15
FM
G

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
TLL from
Autumn 2015
and revise
restriction
Pivmecillinam
hydrochloride 200mg
tablet
AR
y Following specialist advice from PHE based on National data of
culture and sensitivity results. Is it possible to make this clear
on the formulary so that the Microbiology department are not
inundated with unnecessarily calls?
The advantages of pivmecillinam are that it is a narrower
spectrum drug which will provide excellent cover for gram
negative organisms (including some resistant ones) and it is not
as broad-spectrum as co-amoxiclav and so is less likely to
cause C.difficile infections.
The urinary tract infection is an important section in the Adult
Flashcard which we need to review ready for the new doctors in
August so if possible, could we ask that this is reviewed
urgently?
NOTE: from Autumn 2015 Microbiology will provide urine
sensitivity results for mecillinam (pivmecillinam is the pro-
drug). When treating UTIs, until such sensitivities are
provided, follow the GREEN entry for pivmecillinam (see
below)
Restricted - to be recommended by Microbiology with
continuation by GPs except when prescribing for urinary
tract infections where pivmecillinam is the 3rd line
choice. If Microbiology release mecillinam on urine
reports this constitutes 'recommendation by
Microbiology' and GPs to prescribe pivmecillinam
accordingly. Microbiology may also recommend in the
absence of results.
In secondary care nitrofurantoin MR is 1st line and
trimethoprim is 2nd line, in accordance with urinary tract
infection guidance and in primary care nitrofurantoin and
trimethoprim are 1st line.
5.1
.1.5
Ju
ne
15
FM
G
TLL change &
revise restrictionPivmecillinam
hydrochloride 200mg
tablet
gre
en
Y Add additional note to formulary until Autumn 2015. Green until
Micro begin providing sensitivities, then go back to AR
Restricted - to be recommended by Microbiology with
continuation by GPs except when prescribing for urinary
tract infections where, until pivmecillinam sensitivities
are provided by Microbiology (expected Autumn 2015),
pivmecillinam to be prescribed 3rd line for urinary tract
infections. In secondary care nitrofurantoin MR is 1st line
and trimethoprim is 2nd line, in accordance with urinary
tract infection guidance. In primary care nitrofurantoin
and trimethoprim are 1st line.
5.1
.1.5
Ju
ne
15
FM
G
Revise
restrictionTrimethoprim tablets
100mg, 200mg and
Trimethoprim
suspension 50mg/5mL
gre
en
y Updated BHT UTI guideline, recommend as 2nd line treatment
after nitrofurantoin.
Add note to formulary stating 2nd line for UTI
In secondary care - 2nd line treatment for urinary tract
infections after nitrofurantoin. 5.1
.8
Ju
ne
15
Add NeoNatal TPN
NeoStart and NeoMain
aqueous parenteral
nutrition bags.
SMOFlipid
PbR excl - CCG
NeoStart and NeoMain
aqueous standard 500 ml
PN bags, SMOF 120 lipid
standard PN 120ml bag as
per Oxford tertiary centre.
Manufacturered by Baxter. red
N Only recently approved TPN products are currently listed on the
formulary.
Restricted - for use as per Oxforde Tertiary centre
9.3
Ju
ne
15
FM
G
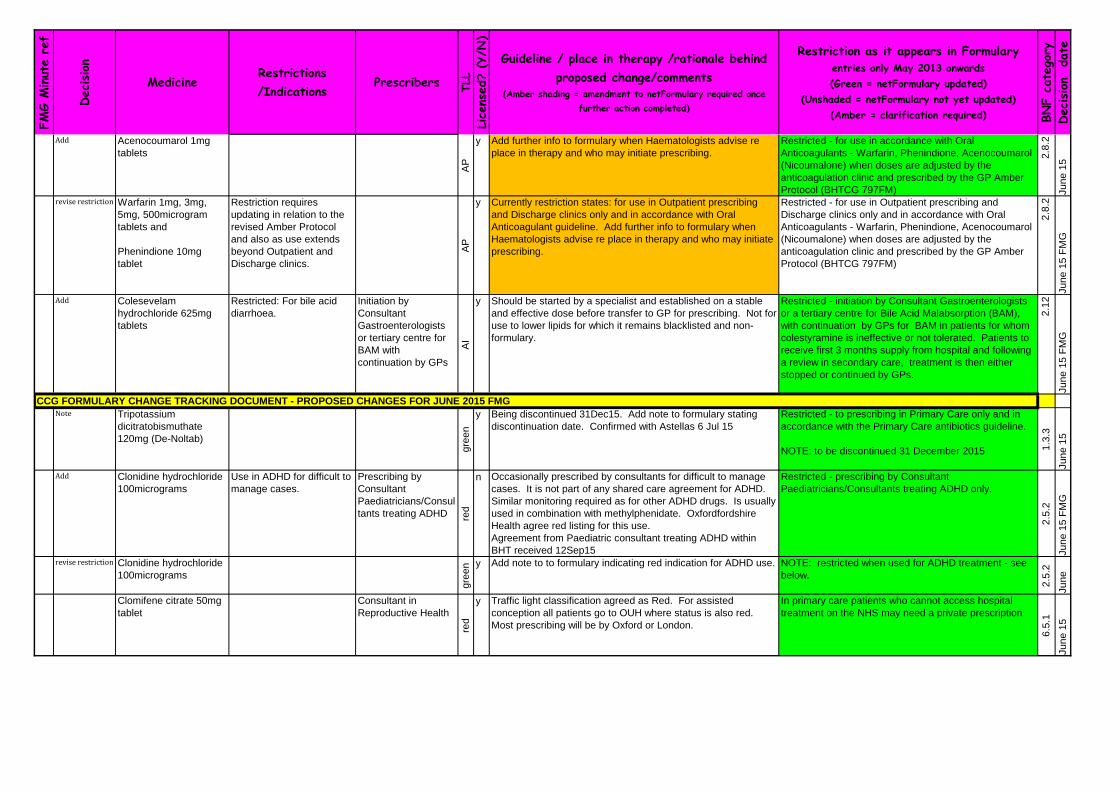
FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Add Acenocoumarol 1mg
tablets
AP
y Add further info to formulary when Haematologists advise re
place in therapy and who may initiate prescribing.
Restricted - for use in accordance with Oral
Anticoagulants - Warfarin, Phenindione, Acenocoumarol
(Nicoumalone) when doses are adjusted by the
anticoagulation clinic and prescribed by the GP Amber
Protocol (BHTCG 797FM)
2.8
.2
Ju
ne
15
revise restriction Warfarin 1mg, 3mg,
5mg, 500microgram
tablets and
Phenindione 10mg
tablet
Restriction requires
updating in relation to the
revised Amber Protocol
and also as use extends
beyond Outpatient and
Discharge clinics.
AP
y Currently restriction states: for use in Outpatient prescribing
and Discharge clinics only and in accordance with Oral
Anticoagulant guideline. Add further info to formulary when
Haematologists advise re place in therapy and who may initiate
prescribing.
Restricted - for use in Outpatient prescribing and
Discharge clinics only and in accordance with Oral
Anticoagulants - Warfarin, Phenindione, Acenocoumarol
(Nicoumalone) when doses are adjusted by the
anticoagulation clinic and prescribed by the GP Amber
Protocol (BHTCG 797FM)
2.8
.2
Ju
ne
15
FM
G
Add Colesevelam
hydrochloride 625mg
tablets
Restricted: For bile acid
diarrhoea.
Initiation by
Consultant
Gastroenterologists
or tertiary centre for
BAM with
continuation by GPs
AI
y Should be started by a specialist and established on a stable
and effective dose before transfer to GP for prescribing. Not for
use to lower lipids for which it remains blacklisted and non-
formulary.
Restricted - initiation by Consultant Gastroenterologists
or a tertiary centre for Bile Acid Malabsorption (BAM),
with continuation by GPs for BAM in patients for whom
colestyramine is ineffective or not tolerated. Patients to
receive first 3 months supply from hospital and following
a review in secondary care, treatment is then either
stopped or continued by GPs.
2.1
2
Ju
ne
15
FM
G
CCG FORMULARY CHANGE TRACKING DOCUMENT - PROPOSED CHANGES FOR JUNE 2015 FMGNote Tripotassium
dicitratobismuthate
120mg (De-Noltab)
gre
en
y Being discontinued 31Dec15. Add note to formulary stating
discontinuation date. Confirmed with Astellas 6 Jul 15
Restricted - to prescribing in Primary Care only and in
accordance with the Primary Care antibiotics guideline.
NOTE: to be discontinued 31 December 2015 1.3
.3
Ju
ne
15
Add Clonidine hydrochloride
100micrograms
Use in ADHD for difficult to
manage cases.
Prescribing by
Consultant
Paediatricians/Consul
tants treating ADHD red
n Occasionally prescribed by consultants for difficult to manage
cases. It is not part of any shared care agreement for ADHD.
Similar monitoring required as for other ADHD drugs. Is usually
used in combination with methylphenidate. Oxfordfordshire
Health agree red listing for this use.
Agreement from Paediatric consultant treating ADHD within
BHT received 12Sep15
Restricted - prescribing by Consultant
Paediatricians/Consultants treating ADHD only.
2.5
.2
Ju
ne
15
FM
G
revise restriction Clonidine hydrochloride
100micrograms
gre
en y Add note to to formulary indicating red indication for ADHD use. NOTE: restricted when used for ADHD treatment - see
below.
2.5
.2
Ju
ne
Clomifene citrate 50mg
tablet
Consultant in
Reproductive Health
red
y Traffic light classification agreed as Red. For assisted
conception all patients go to OUH where status is also red.
Most prescribing will be by Oxford or London.
In primary care patients who cannot access hospital
treatment on the NHS may need a private prescription
6.5
.1
Ju
ne
15

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Add Prednisolone solution
1mg/mL, 10x5mL
gre
en
Y New, licensed and less costly alternative to prednisolone
soluble tablets. Soluble tablets will remain on formulary for a
transition period. Review January 2016
From SPC: Single-dose polyethylene containers containing 5 ml
of oral solution, grouped in strips of five containers. All opened
units should be discarded once the required dose is removed.
Each unit carton contains two over-pouches (ten single-doses),
a patient leaflet and a measuring spoon (dosing 3.75 ml, 2.5 ml
and 1.25 ml, corresponding to partial doses).
In secondary care restricted - only for use in paediatric
patients, who cannot manage the crushed and dispersed
tablets or where the dose required is less than 5mg.
NOTE: it is most cost effective to use ordinary 5mg
tablets which can be crushed, dispersed in water and
administered orally or via PEG/NG tubes
NOTE: All opened units should be discarded once the
required dose is removed
6.3
.2
Ju
ne
15
FM
G
revise restriction Prednisolone soluble
tablets 5mg x 30
Could replace solution
completely. Until this
happens revise restriction
slightly to encourage use
of the oral solution over the
soluble tablets. Also
strengthen the note
regarding cost
effectiveness.
Review for possible
deletion Dec 2015
gre
en
y To remain on formulary for a period of time to allow transition to
1mg/mL licensed solution. Review usage in January
In secondary care restricted - only for use in paediatric
patients and only when prednisolone oral solution
1mg/mL is not available or suitable and patients cannot
manage the crushed and dispersed tablets.
NOTE: it is most cost effective to use ordinary 5mg
tablets which can be crushed, dispersed in water and
administered orally or via PEG/NG tubes.
6.3
.2
Ju
ne
15
FM
G
Ap
r 1
5.1
a
Revise
restrictionSugammadex
200mg/2mL,
500mg/5mL injection
Reversal of neuromuscular
blockade caused by
vecuronium bromide or
recuronium bromide.
Anaesthetics Team
red
y
Removed requirement for replacement of stock only on receipt
of completed audit form for a previous patient.
Revised audit form and guideline approved CGS June 15.
Restricted - prescribing by Anaesthetics team for
reversal of neuromuscular blockade caused by
vecuronium bromide or rocuronium bromide in
accordance with Sugammadex for reversal of
Neuromuscular blockade in Theatres (BHTCG 151) 15
.1.6
FM
G A
pr1
5
FMG DECISIONS APRIL 2015

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Ap
r 1
5.2
Add Posaconazole 100mg
tablet, 200mg/5mL
suspension and
300mg concentrate for
solution for infusion
PbR excl - NHS
England funded
Fungal infection -
treatment and prophylaxis
in accordance with BHT
guideline 203 The
treatment and prophylaxis
of fungal infections in
Haematology patients
Haematology team
and Microbiology
consultants .
red
y
(E
U)
Indications as per FMG April 2015 Decision
Added from application: where possible use tablets instead of
oral suspension as tablets have higher bioavailability. The
suspension is NOT interchangeable with the tablets on a mg-for-
mg basis.
Restricted - to prescribing by Haematology Team and
Microbiology consultants in accordance with the
treatment and prophylaxis of fungal infections in
Haematology patients (BHTCG 203) for:
Treatment of invasive fungal infections (IFI)
- Fourth line antifungal for the empirical treatment of
presumed invasive fungal infection or confirmed invasive
aspergillosis. Alternative oral agent if voriconazole
toxicity or intolerance occurs and triazole antifungal
required. (1st line voriconazole; 2nd line liposomal
amphotericin; 3rd line caspofungin)
- Second line antifungal for the treatment of other
moulds or proven sinus infections or deep seated
mycoses (1st line liposomal amphotericin).
Prophylaxis of IFI
- Empirical prophylaxis for patients receiving remission-
induction chemotherapy for AML or myelodysplastic
syndromes (MDS) expected to result in prolonged
neutropenia who are at high risk of developing invasive
fungal infections.
High Cost Drug form awaited
5.2
1.
FM
G A
pr1
5
Ap
r 1
5.4
Add Imatinib 100mg,
400mg tablet
PbR excl - funded NHS
England
For adjuvant treatment of
gastrointestinal stromal
tumours (GIST) in
accordance with NICE TA
326
Consultant
Oncologist (Gastro)re
d y
GIST in accordance with NICE TA 326
NICE TA 326 replaces NICE TA 196.
NICE TA 86 moved to NICE static list
FOR ALL PRESCRIBING - NICE compliance form
required - see link from Formulary homepage. NICE
compliance to be confirmed if form not yet available.
Restricted - to prescribing by Consultant Oncologist
(Gastro) for adjuvant treatment of gastrointestinal
stromal tumours (GIST) in accordance with NICE TA
326 (review NICE TA 196).
8.1
.5
Add NexoBrid 2g, 5g powder Consultant Burns and
Plastic
red
y (
EU
)
• Prescribing by consultant Burns and Plastics
• For adults with deep partial and full thickness thermal burns
up to a maximum of 15% TBSA who would normally be
considered for surgical debridement
Audit form awaited
Set up on netFormulary but not live yet
Restricted - to prescribing by Consultant Burns and
Plastic for adults with deep partial and full thickness
thermal burns up to a maximum of 15% total body
surface area (TBSA) who would normally be considered
for surgical debridement. 99

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Fe
b 1
5.9
Simeprevir 150mg
capsules
PbR excl - funded NHS
England
Chronic Hepatitis C in
accordance with NICE TA
331
Consultant
Gastroenterologists
and Associate
Specialist (Gastro)
red y
see sofosbuvir FOR ALL PRESCRIBING - NICE compliance form
required - see link from Formulary homepage. NICE
compliance to be confirmed if form not yet available.
Restricted - to prescribing by Consultant
Gastroenterologists and Associate Specialist (Gastro) in
accordance with NICE TA 331 Simeprevir in combination
with peginterferon alfa and ribavirin for treating
genotypes 1 and 4 chronic hepatitis C and within the
framework of an Operational Delivery Network in
accordance with NHSE Specialized Commissioning.
Add Bimatoprost
100micrograms/mL
eyedrops
Consultant
Ophthalmologists with
continuation by GPs
AI
y To replace the discontinued 0.03%. If a generic 0.01%
becomes available to be reconsidered
2nd Choice of prostaglandin analogue eyedrops if
300microgram/mL product no longer available.
Restricted - to initiation by Consultant Ophthalmologist
with continuation by GPs
Branded Lumigan®, bimatoprost 300micrograms/mL
eyedrops are being discontinued by the manufacturer. A
generic equivalent is planned but not yet available. If
the 300micrograms/mL (0.03%) strength cannot be
obtained the GP may transfer prescribing to the
100microgram/mL (0.01%) strength, which has a similar
effect. This has been agreed with BHT
Ophthalmologists. A small number of patients may need
300microgram/mL preservative-free unit dose eyedrops.
Such patients will be identified by BHT Ophthalmologists
and a request for a repeat prescription will be made in
the discharge letter to the GP.
11
.6
FM
G A
pr1
5
revise restriction Bimatoprost
300micrograms/mL
eyedrops
Consultant
Ophthalmologists with
continuation by GPs
AI
y To be discontinued from 1 May 2015. Bring in the 0.01% for
use once stock of 0.03% runs out.
Generic product may be available from Sandoz in the near
future.
2nd Choice of prostaglandin analogue eyedrops if
300microgram/mL product no longer available.
Restricted - to initiation by Consultant Ophthalmologist
with continuation by GPs
Branded Lumigan®, bimatoprost 300micrograms/mL
eyedrops are being discontinued by the manufacturer. A
generic equivalent is planned but not yet available. If
the 300micrograms/mL (0.03%) strength cannot be
obtained the GP may transfer prescribing to the
100microgram/mL (0.01%) strength, which has a similar
effect. This has been agreed with BHT
Ophthalmologists. A small number of patients may need
300microgram/mL preservative-free unit dose eyedrops.
Such patients will be identified by BHT Ophthalmologists
and a request for a repeat prescription will be made in
the discharge letter to the GP.
11
.6
FM
G A
pr1
5
Add Calcium chloride
10mmol in 10mL
ampoules
Only for use with CRRT
red y Required for use with CRRT solutions (Prismacitrate, Prismocal
and Phoxilium) now available on ITU. Calcium chloride
ampoules required rather than pre-filled syringes.
Restricted - only for use within clinical areas using CRRT
(Continuous Renal Replacement Therapy)
9.5
.1.1
FM
G
BHT FORMULARY CHANGE TRACKING DOCUMENT - PROPOSED FORMULARY CHANGES FOR NOTE APRIL 2015 FMG
Fo
rmu
lary
Ch
an
ge
s f
or
No
tin
g A
pril 2
01
5

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
revise restriction Rifampicin injection
600mg IV infusion
red y Restriction currently states, "in secondary care restricted - for
use in mycobacterial infections and for meningococcal
contacts. Microbiology approval required for all others uses".
Add , "and for the treatment of endocarditis in accordance with
Investigation and Antimicrobial treatment of Infective
Endocarditis in Adults (BHTCG 236)"
In secondary care restricted - for use in mycobacterial
infections, for meningococcal contacts and for the
treatment of endocarditis in accordance with
Investigation and Antimicrobial treatment of Infective
Endocarditis in Adults (BHTCG 236). Microbiology
approval required for all other uses.
5.1
.9
FM
G A
pr1
5
Add Lenograstim
13.4million units
(105mg), 33.6million
units (263mg) vial
injection
PbR excl NHS
England funded
Consultant Paediatric
Oncologists
red y For use in paediatrics in accordance with Oxford protocol
(shared care from tertiary referral centre). We are treating the
patients here under a shared care agreement with Oxford and
so should stay on the treatment they are started on by Oxford -
Lenograstim. Oxford would not want the patient to be changed
onto a different GSCF. Patients who are on protocols are
usually supplied their lenograstim from Oxford which is
administered by the community nurses but very occasionally we
may need to supply doses if they don’t have enough, this is
very rare. GSCF is not used routinely for neutropenia unless
the counts do not improve, in which case Lenograstim is
recommended by Oxford.
Restricted - to prescribing by Consultant Paediatric
Oncologists in accordance with Oxford protocol (Shared
care from tertiary referral centre)
9.1
.6
FM
G A
pr1
5
Add Sodium nitroprusside
50mg/5mL infusion
red no Now unlicensed and imported from Spain via UL Medicines.
Risk Assessed as Moderate
Agreed
Note: Powder for dilution and use as an infusion
Unlicensed - Medium Risk
2.5
.1
FM
G
Add link Chapter 14 Vaccines Add link to The Green Book - Immunisation Against Infection
Disease. Public Health England
https://www.gov.uk/government/collections/immunisation-
against-infectious-disease-the-green-book
FM
G
Add Naloxone injection
400micrograms/1mL
PFS
red y Injection listed on formulary but pre-filled syringes also need to
be listed.
Restricted for use in Emergency Treatment of opiate
Overdosage.
15
.1.7
FM
G
Add Vitamins A
5000unit/Vitamin D
400unit capsule
gre
en no The product which is available and is being supplied to
community pharmacies and hospital pharmacies is the
5000unit/400unit capsules made by Alissa Healthcare.
Restricted - for use in accordance with Vitamin
Supplementation for Paediatric Cystic Fibrosis (CF)
Patients - Primary/Secondary Care guideline (BHTCG
378FM)
NOTE: Product containing Vitamin A 4000units and
Vitamin D 400units no longer available.
09
.06
.01
FM
G A
pr1
5
revised
restriction Mupirocin 2% in WSP
Nasal cream (Bactroban
Nasal)
gre
en y Mupirocin is 1st Choice for MRSA decolonisation but
Dermatology may use Naseptin first line for other staphy aureus
infections. Request that we provide link to guidelines 14 B and
C
1st Choice - when used for MRSA decolonisation in
accordance with, Suppression of MRSA Colonisation -
patients only (BHTCG 14B) and Eradication of MRSA
Colonisation - patients only (BHTCG 14C)
12
.2.3
FM
G A
pr1
5
revised
restrictionChlorhexidine
Hydrochloride 0.1% with
Neomycin Sulphate
0.5% Nasal cream
(Naseptin)
gre
en y Naseptin is 2nd Choice for MRSA decolonisation. Request also
that we provide link to guidelines 14 B and C
2nd Choice - when used for MRSA decolonisation in
accordance with, Suppression of MRSA Colonisation -
patients only (BHTCG 14B) and Eradication of MRSA
Colonisation - patients only (BHTCG 14C)
12
.2.3
FM
G A
pr1
5
Fo
rmu
lary
Ch
an
ge
s f
or
No
tin
g A
pril 2
01
5

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
revise restriction Prontoderm Nasal Gel
Light
gre
en y Revised wording: Restricted - for use only as 3rd line for MRSA
decolonisation when 1st and 2nd line agents cannot be used
i.e. MRSA is resistant to mupirocin, MRSA is resistant to
neomycin (Naspetin®), product unavailability, patient allergic to
the ingredients/excipients contained in mupirocin or Naseptin®
The guidelines for which Prontoderm may be used do not
include use in neonates. A separate guideline exists for
neonatal MRSA decolonisation.
Restricted - for use only as 3rd line for MRSA
decolonisation when 1st and 2nd line agents cannot be
used ie. MRSA is resistant to mupirocin, MRSA is
resistant to chlorhexidine hydrochloride 0.1%/neomycin
sulphate 0.5% (Naseptin®), product unavailability,
patient allergic to the ingredients/excipients contained in
mupirocin or Naseptin®. To be used in accordance with,
Suppression of MRSA Colonisation - patients only
(BHTCG 14B) and Eradication of MRSA Colonisation -
patients only (BHTCG 14C)
12
.2.3
FM
G A
pr1
5
Now licensed Magnaspartate
(magnesium aspartate
oral granules) 243mg
(10mmol magnesium)
powder for oral solution
(sachet)
red y Now available as a licensed product was previously Unlicensed
- Low Risk.
Restricted - for treatment of post chemotherapy induced
Mg loss in children. Named Patient. An alternative to
Magnesium glycerophosphate tablets in young children
who cannot swallow large tablets.
Contains Mg2+
10mmol per sachet
9.5
.1.3
FM
G A
pr1
5
revise restriction Ferric Carboxymaltose
(Ferinject) 100mg/2mL,
500mg/10mL and
1g/20mL injection
Haematology team
and Oxford Renal
Service
red y in accordance with Oxford renal formulary. BHT reimbursed for
all renal drugs
Restricted - prescribing by Haematology team in
accordance with Parenteral Iron for Iron Deficiency
Anaemia (BHTCG 58) and for renal patients in
accordance with Oxford Renal formulary
9.1
.1.2
FM
G
Revise TLL Montelukast Granules
4mg x 28 gre
e y Part of Step 2 in asthma guidelines (BTS) Restricted - only for use in children who cannot manage
chewable tablets 3.3
.2
FM
G
CCG FORMULARY CHANGE TRACKING DOCUMENT - PROPOSED CHANGES FOR APRIL 2015 FMGadd note Pipothiazine depot
injection
bl
ac
k
has been discontinued, please add a note which says
discontinued April 15 patients on this depot will need a
specialist review to determine the most appropriate choice of
therapy. Mental Health Trust advocating change to
paliperidone which is a redlisted choice.
No longer available.
Patients on this depot will need a specialist review to
determine the most appropriate choice of therapy.
4.2
.2
FM
G A
pr1
5
Add Paliperidone pre-filled
syringe 50mg, 75mg,
100mg, 150mg
re
d
Mental Health Trust only and recommended by Mental Health
Trust for patients discontinued from pipothiazine
Restricted - prescribing by Mental Health Trust only and
recommended for patinets discontinued from
pipothiazine depot injection.
4.2
.2
FM
G
Revise
restrictionSildenafil 25mg, 50mg,
100mg tablet
gr
ee
n
y
South Central Priorities Committee, April 2015 states: Funding
for the treatment of generic sildenafil in the minimum effective
dose is recommended for any man with erectile dysfunction,
with a frequency of dosing of two times per month.
Discussed with Spinal Pharmacist. Restriction is correct for
secondary care but remove reference to DoH as prescribing
restrictions removed for Sildenafil.
In secondary care restricted - to Spinal patients only.
Doses are provided for the initial dose calibration and
then for Spinal in-patients on weekend leave (2 doses
per weekend)
In primary care for erectile dysfunction restricted to
2/month
7.4
.5
FM
G A
pr1
5
change TLL
status
Nitrazepam tablets and
liquid
AI
Change from green to amber initiation to reduce initiation Restricted - initiation in secondary care with continuation
by GPs
4.1
.1
FM
G
change TLL
status
Zolpidem tartrate 5mg,
10mg tabletsre
d
Changed from black to red with prescribing by Mental Health
Trust team only
Restricted - prescribing by Mental Health Trust team only
4.1
.1
FM
G
Fo
rmu
lary
Ch
an
ge
s f
or
No
tin
g A
pril 2
01
5

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
change TLL
status
Cloral betaine 707mg
tablet and 143.3mg/5mL
elixirbl
ac
k
Large increase in cost, no use across Trust. Agreed to black
list
4.1
.1
FM
G
change TLL
status
Clomethiazole 192mg
capsule bl
ac
k
Green to Black-listed. No longer recommended in BNF for
indication used for.
4.1
.1
FM
G
change TLL
status
Oxazepam 10mg tablet
AI
Restriction was Mental Health Trust initiation only, now
requested change to black. Small use by BHT therefore agreed
to restrict and not recommended for initiation.
Restricted - to continuation only and not recommended
for initiation.
4.1
.2
FM
G
change TLL
status
Benperidol
250microgram tablet bl
ac
k
Mental Health Trust requesting change from AI & Mental Health
Trust only to black
4.1
.2
FM
G
change TLL
status
Chlorpromazine
hydrochloride tablets
25mg, 50mg, 100mg
and oral solution
25mg/5mL, 100mg/5mL
AI
for all traditional antipsychotic use Restricted - to initiation in secondary care with
continuation by GPs, when used for traditional
antipsychotic treatment.
4.2
.1
FM
G A
pr1
5
revise restriction
Chlorpromazine
hydrochloride tablets
25mg, 50mg, 100mg
and oral solution
25mg/5mL, 100mg/5mL
gr
ee
n
for treatment of nausea or for prescribing in Palliative Care Restricted - for treatment of nausea or for prescribing in
Palliatve Care (for traditional antipsychotic use see
separate amber initiation entry)
4.2
.1
FM
G A
pr1
5
change TLL
status
Pericyazine 10mg tablet
bl
ac
k
Mental Health Trust requested red to black
4.2
.1
FM
G
change TLL
status
Flupentixol
500micrograms, 1mg,
3mg tablets AI
Licensed for schizophrenia and other psychoses Restricted - to initiation in secondary care with
continuation by GPs.
4.2
.1
FM
G
change TLL
status
Pimozide 4mg tablet
bl
ac
k
7 scripts in last 3 months in primary care. No use across Trust
since 2008.
4.2
.1
FM
G
change TLL
status
Promazine 25mg,
50mg tabs and
25mg/5mL, 50mg/5mL
oral solution AI
for all traditional antipsychotic use . Licensed as adjunct to
short-term treatment of moderate to severe psychomotor
agitation and agitation and restlessness in the elderly
Restricted - to initiation in secondary care with
continuation by GPs, when used for traditional
antipsychotic treatment.
4.2
.1
FM
G
change TLL
status
Promazine 25mg,
50mg tabs and
25mg/5mL, 50mg/5mL
oral solution
gr
ee
n
for treatment of nausea or for prescribing in Palliative Care Restricted - for treatment of nausea or for prescribing in
Palliatve Care (for traditional antipsychotic use see
separate amber initiation entry)
4.2
.1
FM
G

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
change TLL
status
Sulpiride 200mg, 400mg
tablets and oral solution
200mg/5mL
AI
Licensed for acute and chronic schizophrenia Restricted - to initiation in secondary care with
continuation by GPs.
4.2
.1
FM
G
change TLL
status
Zuclopenthixol
Decanoate 200mg/1mL,
500mg/1mL depot
injection A
P
Amber protocol in development Protocol in development
4.2
.2
FM
G A
pr1
5
change TLL
status
Zuclopenthixol tabs
2mg, 10mg, 25mgAI
Licensed for psychoses and schizophrenia Restricted - to initiation in secondary care with
continuation by GPs.
4.2
.1
FM
G
typo
Amisulpiride 100mg/mL
solution and 50mg,
200mg tablets
AI
typo change neurologist to psychiatrists; 2 entries Restricted - initiation by Consultant Psychiatrists with
continuation by GPs
4.2
.1
FM
G
change TLL
status
Aripiprazole solution,
tablets & orodispersible
tablets AI
Licensed for schizophrenia in adults and in adolescents aged
15years and older, for moderate to severe manic episodes. Ar
to AI
Restricted - initiation by Psychiatric (Mental Health Trust)
team.
4.2
.1
FM
G
change TLL
status
Olanzapine tablets and
orodispersible tablets,
all strengths.
AI
green to AI Restricted - initiation by Consultant Psychiatrist (Mental
Health Trust) only, with continuation by GPs.
4.2
.1
FM
G
change TLL
status
Sertindole
bl
ac
k
Mental Health trust agreed to red list but not available or listed
in Mims, BNF etc, therefore remove
4.2
.1
FM
G
change TLL
status
Risperidone all oral
formulationsAI
Green to Amber Initiation Restricted - to initiation in secondary care and
continuation by GPs
4.2
.1
FM
G
change TLL
status
Olanzapine embonate
injection 210mg,
300mg, 405mg
Prescribing only by
Mental Health Trustre
d
Restricted - prescribing by Mental Health Trust only
4.2
.2
FM
G
change TLL
status
Asenapine tablet 5mg,
10mgPrescribing only by
Mental Health Trust
re
d
Restricted - prescribing by Mental Health Trust only
4.2
3.
FM
G
change TLL
status
Amitriptyline
hydrochloride/Perphena
zine 25mg/2mg tabletbl
ac
k
Not in use in primary or secondary care
4.3
.1
FM
G
change TLL
status
Clomipramine
Hydrochloride 10mg,
25mg, 50mg tabletgr
ee
n
green on TLL
4.3
.1
FM
G
change TLL
status
Mianserin 10mg 30mg
tablets
AI
Agreed to leave on formulary with recommendation that it not
be initiated. (MHTrust requested black but some use in BHT)
Restricted - recommended not to be initiated
4.3
.1
FM
G
change TLL
status
Phenelzine 15mg tablet
AI
1st choice traditional MAOI with tranylcypromine and
isocarboxid 2nd line.
Restricted - initiation by Consultant Psychiatrist (Mental
Health Trust) only.
4.3
.2
FM
G

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
change TLL
status
Isocarboxazid tablet
10mg Initiation by Mental
Health Trust only
AI
Non-formulary to Amber initiation. Restricted - to initiation by Mental Health Trust only
4.3
.2
FM
G
Fe
b1
5.7
Revised
wordingNalmefene 18mg tablet For reducing alcohol
consumption in people with
alcohol dependence in
accordance with NICE TA
325
Prescribing on advice
of Drug and Alcohol
Advisory Team
(DAAT) red y
• For reducing alcohol consumption in people with alcohol
dependence in accordance with NICE TA 325
• Prescribing on the advice of the Drug and Alcohol Advisory
Team (DAAT)
Restricted - prescribing on the advice of the Drug and
Alchohol Advisory Team (DAAT) in accordance with
NICE TA 325 Nalmefene for reducing alcohol
consumption in people with alcohol dependence
4.1
0.1
Fe
b-1
5
De
c 1
4.6
Revise TLL Naproxen suspension
125mg/5mL
Secondary care
Re
d
n
Since naproxen suspension has not been used in the past 5
years and it is an unlicensed product which is particularly
expensive to primary care, it should be red on the traffic light
list for the time being
Restricted - prescribing in secondary care only.
In primary care this is a pharmaceutical special
Use in accordance with NSAIDs in Adults -
Primary/Secondary Care guideline (BHTCG 299FM) Fe
b-1
5
De
c 1
4.4
Add Colecalciferol capsules
20,000units
gre
en
yThere are two licensed brands available: Aviticol and Fultium
D3. Neither contain peanut oil or lactose, but do contain
gelatine.
Restricted - 1st Choice product for the treatment of
Vitamin D deficiency in accordance with Vitamin D
Testing and Treatment in Adults (BHTCG 785FM) - see
above
9.6
.4
Fe
b-1
5
Fe
b
15
.8
Add link Hydroxyzine - all dose
forms
Awareness of EMA PRAC
advice
lenol
gre
en
y
Ensure prescribers are made aware of report and its
recommendations so that they can be considered.
Medicines Information to send email alert to all BHT doctors to
make them aware of risk.
Dermatology have reviewed at SDU Governance meeting (Feb
2015)
Link to EMA PRAC - Hydroxyzine review
3.4
.1
Fe
b-1
5
Fe
b
15
.6
Review Gliptins review Sitagliptin will remain the only DPP-4 inhibitor on the Bucks
formulary. Although alogliptin is currently 20% cheaper than all
other DPP-4 inhibitors, a review of its evidence led the FMG to
decide to avoid its formulary inclusion at this time.
6.1
.2.3
Fe
b-1
5
Fe
b
15
.6
Black list Alopgliptin
Saxagliptin
Vildagliptin
Sitagliptin - only gliptin to
be on formulary
bla
ck
y
6.1
.2.3
Fe
b-1
5
Fe
b 1
5.3
Add Epoetin (Eprex®)
PbR excluded Funded
NHS England)
For use in accordance with
NICE TA 323
Oncology and
Haematology teams
red
y
Formulary not yet updated - awaiting NICE compliance form
approval/upload
FOR ALL PRESCRIBING - NICE compliance form
required - see link from Formulary homepage
1st Choice
Restricted - prescribing by Oncology and Haematology
teams for use in accordance with NICE TA 323
Erythropoiesis stimulating agents (Epoetin and
Darbepoetin) for treating anaemia in people with cancer
having chemotherapy (supersedes NICE TA142)
9.1
.3
Fe
b-1
5
NOTE - drugs above shaded peach (Flupentixol, Sulpiride, Aripiprazole and Zuclopentixol) were to be split into 2 entries: AI for traditional anti-psychotic use and Green for use in
palliative care and treatment of nausea. Palliative Care Team do not use these drugs for palliative care treatment and they are not licensed for nausea treatment. Therefore CCG
and BHT have agreed to leave as one entry for antipsychotic use as amber initiation. 12June15
FMG DECISIONS FEBRUARY 2015

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Fe
b 1
5.3
Add Darbepoetin alfa
PbR excluded Funded
NHS England
For use in accordance with
NICE TA 323
Oncology and
Haematology teams
red
y
Formulary not yet updated - awaiting NICE compliance form
approval/upload
FOR ALL PRESCRIBING - NICE compliance form
required - see link from Formulary homepage
2nd Choice , if patients cannot have Epoetin alfa
(Eprex®)
Restricted - prescribing by Oncology and Haematology
teams for use in accordance with NICE TA 323
Erythropoiesis stimulating agents (Epoetin and
Darbepoetin) for treating anaemia in people with cancer
having chemotherapy (supersedes NICE TA142)
9.1
.3
Fe
b-1
5
Fe
b 1
5.2
Add Dabigatran for DVT/PE as an alternative to
rivaroxaban for treatment
DVT/PE and prevention
recurrent DVT/PE in
accordance NICE TA 327
Initiation by
Consultant
Haematologists in the
DVT clinic, or NOAC
Pharmacy service
with continuation by
GPs.
AI
y
Formulary not yet updated - await Rivaroxaban for DVT/PE
Amber Initiation guideline(BHTCG 295FM) approval/upload
FOR ALL PRESCRIBING - NICE compliance form
required - see link from Formulary homepage
Restricted - to initiation by Consultant Haematologists in
the DVT clinic, or NOAC Pharmacy service with
continuation by GPs, as an alternative to rivaroxaban for
the treatment of DVT and PE and prevention of recurrent
DVT and PE in accordance with NICE TA 327 and Bucks
criteria for use of NOACs in DVT/PE (described in
Rivaroxaban for DVT/PE Amber Initiation
guideline(BHTCG 295FM)). Rivaroxaban is 1st choice
NOAC for DVT and PE. Dabigatran to be reserved for
patients on medicines which interact with rivaroxaban,
intolerance to rivaroxaban or other clinical situations
deemed appropriate. In hospital, any consultant
physician (POD) may refer DVT cases to the
Haemostasis or NOAC clinic for a decision regarding
choice of treatment after dalteparin has been initiated.
2.8
.2
Fe
b-1
5
Fe
b1
5.1
a
Audit 2014 Audit Data for
Rivaroxaban DVT/PE
Showed more than 95% patients were prescribed in accordance
with BHTCG 295FM. It was felt that formulary approved criteria
for use are reasonable and do not require changing
2015 data to be reviewed February 2016
Fe
b-1
5
Oct
14
.6
Add Prismocitrate 18/0
solution
For critically ill patients who
require continuous renal
replacement therapy
(CRRT) and are not
contraindicated for RCA.
These include but are not
restricted to, metabolic
disturbance, renal
impairment, poisoning
cases cleared by dialysis
and septic multi-organ
failure
Consultant
Anaesthetists
Re
d
y
guideline approved at CGS Feb 2015 and storage
arrangements confirmed to be in place.
Add reference to guideline once uploaded
Restricted - to prescribing by Consultant Anaesthetists
only, for critically ill patients who require continuous
renal replacement therapy (CRRT) and are not
contraindicated for RCA, in accordance with Continuous
Renal Replacement Therapy (CRRT) using Citrate
(BHTCG 404FM)
no
t in
BN
F-
99
Fe
b-1
5

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Oct
14
.6
Add Prism0cal B22
Bicarbonate-buffered
dialysis solution
For critically ill patients who
require continuous renal
replacement therapy
(CRRT) and are not
contraindicated for RCA.
These include but are not
restricted to, metabolic
disturbance, renal
impairment, poisoning
cases cleared by dialysis
and septic multi-organ
failure
Consultant
Anaesthetists
Re
d
y
guideline approved at CGS Feb 2015 and storage
arrangements confirmed to be in place.
Add reference to guideline once uploaded
Restricted - to prescribing by Consultant Anaesthetists
only, for critically ill patients who require continuous
renal replacement therapy (CRRT) and are not
contraindicated for RCA, in accordance with Continuous
Renal Replacement Therapy (CRRT) using Citrate
(BHTCG 404FM)
no
t in
BN
F-
99
Fe
b-1
5
Oct
14
.6
Add Phoxilium 1.2mmol/L
phosphate solution
For critically ill patients who
require continuous renal
replacement therapy
(CRRT) and are not
contraindicated for RCA.
These include but are not
restricted to, metabolic
disturbance, renal
impairment, poisoning
cases cleared by dialysis
and septic multi-organ
failure
Consultant
Anaesthetists
Re
d
y
guideline approved at CGS Feb 2015 and storage
arrangements confirmed to be in place.
Add reference to guideline once uploaded
Restricted - to prescribing by Consultant Anaesthetists
only, for critically ill patients who require continuous
renal replacement therapy (CRRT) and are not
contraindicated for RCA, in accordance with Continuous
Renal Replacement Therapy (CRRT) using Citrate
(BHTCG 404FM)
no
t in
BN
F-
99
Fe
b-1
5
Ma
y1
3.3
Add AquADEKs liquid, 60mL Approved for CF patients
who cannot swallow tablets
and who require Vitamin K
supplementation
Initiation by
Consultant
Paediatricians and
continuation by GPs AI
n
Aquadeks® liquid was approved for formulary inclusion for CF
patients who cannot swallow tablets and has been on the
formulary but now there is a guideline available..
Restricted - initiation by Consultant Paediatricians with
continuation by GPs for cystic fibrosis patients who cannot
swallow tablets.
Restricted - initiation by Consultant Paediatricians with
continuation by GPs for cystic fibrosis patients requiring
Vitamin K supplementation, who cannot swallow tablets
and to be used in accordance with Vitamin
Supplementation for Paediatric Cystic Fibrosis Patients -
Primary/Secondary care guideline (BHTCG 378FM)
Ma
y-1
3
Se
p1
4.8
Add Hepatitis A and B
Vaccine - Primary Care
Travel Guidance
Guideline approved at CGS
Link to be added to Chapter 14 when guideline uploaded to
netFormulary 14
Fe
b-1
5
CCG FORMULARY CHANGE TRACKING DOCUMENT - PROPOSED CHANGES FOR FEB 2015 FMGadd ibuprofen 5% gel, 30g,
50g, 100g
NICE CG on osteoarthritis
suggests topical NSAID
with paracetamol is 1st
choice
gre
en y In primary care consider patient purchasing - often
cheaper than paying a prescription charge.
10
.3.
2
Fe
b-1
5
add ibuprofen 10% gel, 30g,
50g, 100g
NICE CG on osteoarthritis
suggests topical NSAID
with paracetamol is 1st
choice
gre
en y In primary care consider patient purchasing - often
cheaper than paying a prescription charge.
10
.3.
2
Fe
b-1
5
add diclofenac gel 1.16% NICE CG on osteoarthritis
suggests topical NSAID
with paracetamol is 1st
choice
gre
en y In primary care consider patient purchasing - often
cheaper than paying a prescription charge.
10
.3.
2
Fe
b-1
5
In primary care consider patient purchasing -often cheaper than
a prescription charge.
Consultant Rheumatologist, Malgosia Magliano commonly
recommends diclofenac and ibuprofen gel in patients with hand
OA
MI Response April 15: NICE do not specify which topical NSAID
to use for osteoarthritis of the knee in their guidelines. A
Cochrane review in 2010 found insufficient data to reliably
compare individual topical NSAIDs with each other. Another
Cochrane review in 2012 which looked at the use of topical
NSAIDs for chronic musculoskeletal pain in adults found that
the best data were for topical diclofenac in osteoarthritis where
the NNT for at least 50% pain relief over 8 to 12 weeks

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
new wording Helicobacter Test
INFAI®
un
sp
eciif
ied ? In primary care the CCGs commission a service from
GPs to test for helicobacter status. Within this service
the kit to test for helicobacter can be ordered (free) from
Stoke Mandevilla Hospital Pharmacy using the specific
form.
2
Fe
b-1
5
Choice of
therapy 1st 2nd
3rd line
Mupiricin 2% in WSP
Nasal cream (Bactroban
Nasal)
1st Choice - recommended
by ARG and in MRSA
guideline
gre
en y NOTE: if unavailable, Chlorhexidine hydrochloride 0.1%
with Neomycin sulphate 0.5% (Naspetin) nasal cream
recommended as there is no direct equivalent.
y
Fe
b-1
5
Choice of
therapy 1st 2nd
3rd line
Chlorhexidine
Hydrochloride 0.1% with
Neomycin Sulphate
0.5% Nasal cream
(Naseptin)
nd Choice - recommended
by ARG and in MRSA
guideline
gre
en y y
Fe
b-1
5
Choice of
therapy 1st 2nd
3rd line
Prontoderm Nasal Gel
Light 3rd
Choice
3rd Choice - recommended
by ARG
gre
en BHT agree 3rd choice. (not for neonates due to a lack of
experience) Neonate comment not confirmed by BHT and
Prontoderm not included in MRSA guideline but was only
approved at December 14 FMG
Restricted - for use only as 3rd line for MRSA
decolonisation if mupirocin is unavailable and Naseptin
nasal cream is unsuitable due to resistance or if patients
are allergic to the ingredients/excipients contained in
mupirocin or Naseptin..
y
Fe
b-1
5
Add Montelukast Granules
4mg x 28
Prophylaxis of asthma in
children who cannot
manage the chewable
tablets.
Initiation by
Consultant
Paediatricians and
continuation by GPs
AI y Montelukast sits in Step 2 of BTS guidelines for paediatric
patients. Amber initiation agreed but will apply for green
status at April FMG
Restricted - initiation by Consultant Paediatricians with
continuation by GPs for use in children who cannot
manage chewable tablets.
3.3
.2
Fe
b-1
5
Revise
restrictionMontelukast 4mg, 5mg
tablet
Existing restriction
states: In secondary
care - restricted to
prescribing by
respiratory, ENT and
Dermatology teams only
Consider removing all
restrictions so it can
prescribed throughout the
hospital. emove restrictions
in secondary care
Gre
en y
3.3
.2
Fe
b-1
5
Revise
restrictionMontelukast 10mg
tablet
Existing restriction
states: In secondary
care - restricted to
prescribing by
respiratory, ENT and
Dermatology teams only
Consider removing all
restrictions so it can
prescribed throughout the
hospital.
Gre
en y
3.3
.2
Fe
b-1
5
BHT FORMULARY CHANGE TRACKING DOCUMENT - PROPOSED FORMULARY CHANGES FOR NOTE FEBRUARY 2015 FMG

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Add Carbex for radiology Each 2.8g sachet contains
sodium bicarbonate and
simethicone. Each 10mL
bottle of Carbex contains
citric acid.. Gas producing
agend for double contract
radiography of the
gastrointestinal tract.
Carbex is given orally.
Radiology use only
red PGD written for this product. Restricted - prescribing by Radiology team only
Mis
ce
llan
ou
e
Fe
b-1
5
Add Barium sulphate 100%
(Baritop 100)
X-ray contract medium for
use in the radiological
examination fo GI tract.
Radiology use only
red Restricted - prescribing by Radiology team only
Mis
ce
llan
ou e
Fe
b-1
5
Add E-Z-HD 98% barium
sulphate
Barium sulphate 98.45%
powder for oral suspension
for use as a radiopaque
agent during X-ray
visualisation of the upper
gastrointestinal tract.
Radiology use only
red PGD written for this product. Radiology order directly from
Bracco UK .
Restricted - prescribing by Radiology team only
Mis
ce
llan
ou
e
Fe
b-1
5
Revise
restrictionFondaparinux
2.5mg/0.5mL
Acute Medical Team
or Consultant
Haematologists
Re
d y Haematologists have requested add to formulary for prescribing
by Consultant Haematologists for patients intolerant of
dalteparin eg. due to heparin-induced thrombocytopenia (HITT),
skin rash.
Restricted to:
1. Prescribing by acute medical team for suspected
ACS. Refer to ICP for ACS
2. Prescribing by Consultant Haematologists for patients
intolerant of dalteparin (eg. Due to heparin-induced
thrombocytopenia (HITT), skin rash)
2.8
.1
Fe
b-1
5
Revise TLL Pivmecillinam
hydrochloride 200mg
tablet
Pivmecillinam is part of the
penicillins group, however,
it is in a class of its own
(5.1.1.5 mecillinams) as it
has additional activity
against gram negative
organisms that are
ESBL/AMPC producers. It
should never be used if
amoxicillin can be, from a
cost and preservation
perspective, but offers a
valuable oral agent for the
treatment of resistant
organisms that otherwise
require IV antibiotics.
Microbiology to
recommend.
AR y Change from Red to AR. Restrict to recommendation by
Microbiology with GPs to prescribe.
Restricted - in secondary care, to be recommended by
Microbiology and,
- in primary care, Microbiology to recommend and GPs
prescribe.
5.1
.1.5
Fe
b-1
5
Revise
restrictionPrednisolone tablets
5mg soluble
gre
en y Add a restriction in secondary care to restrict use to paediatrics
only. Also add note: Normal tablets are suitable to be crushed
and administered down PEG/NG tubes.
5mgx28 tabs £1.33 compared to £47 for soluble tablets.
In secondary care restricted - for use in paediatric
patients only.
NOTE: ordinary 5mg tablets are able to be crushed,
dispersed in water and administered orally or via
PEG/NG tube.
6.3
.2
Fe
b-1
5

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
revise restriction Haloperidol injection
5mg/mL
red No longer licensed for IV use. Some IV use may occur but
restricted to Critical Care areas. Also sub-cutaneous use
ongoing. Formulary worded to say IV use now unlicensed and
restricted to Critical Care areas only
NOTE: Intravenous use is now an unlicensed use. All IV
use restricted to Critical Care areas only. 4.2
.1
Fe
b-1
5
revise restriction Rifampicin injection
300mg
red Restriction currently states, "in secondary care restricted - for
use in mycobacterial infections and for meningococcal
contacts. Microbiology approval required for all others uses".
Add , "and for the treatment of endocarditis in accordance with
Investigation and Antimicrobial treatment of Infective
Endocarditis in Adults (BHTCG 236)"
In secondary care restricted - for use in mycobacterial
infection, for meningococcal contacts and for the
treatment of endocarditis in accordance with
Investigation and Antimicrobial treatment of Infective
Endocarditis in Adults (BHTCG 236). Microbiology
approval required for all other uses.
5.1
.9
Fe
b-1
5
Unlic Clonazepam injection
1mg/mL
Used in epilepsy but not
first line.
Some use in ITU to control
dystonic reactions. Often
other alternatives have
been tried (eg midazolam,
lorazepam)
red no No longer manufactured in the UK. Unlicensed - Medium Risk
Cloazepam 1mg/mL in solvent, for dilution with 1mL
water for injections immediately before injection.
4.8
.2
Fe
b-1
5
DELETE Diprobath additive
(contained isopropyl
myristate and liquid
paraffin)
gre
en y No longer available therefore removed from formulary.
Dermatology agree remaining emollient bath and shower
preparations are sufficient for formulary purposes. 13
.2.1
.1
Fe
b-1
5
Add Urea 10% cream
(Hydromol Intensive)
30g, 100g
gre
en y Dermatology and CCG agree cheapest as 1st Choice ie
Hydromol Intensive. Dermatology also requested both products
remain on formulary. 13
.2.1
Fe
b-1
5
Add Betamethasone
dipropionate
0.05%/salicylic acid 2%
in alcoholic basis.
(Diprosalic Scalp
Application) 100mL
(Potent)
Diprosalic ointment is on
the formulary and the scalp
application has been
requested by Dermatology.
gre
en y Potency: Potent
13
.4
Fe
b-1
5
Add Dermol Cream 100g,
500g pump
Dermol 500 lotion is on
formulary and cream also
requested by Dermatology
gre
en y
13
.2.1
Fe
b-1
5
Add Stribild (cobicistat
150mg/elvitegravir
150mg/emtricitabine
200mg/tenofovir
disoproxil 245mg)
tablets
£1034.72 (excl
VAT)/30tabs
Restricted - to prescribing
by HIV Consultants only in
accordance with BHIVA
guidelines.
red y Contains: cobicistat 150mg/ elvitegravir 150mg/
emtricitabine 200mg/ tenofovir disoproxil 245mg
Restricted - prescribing by HIV Consultants only in
accordance with BHIVA guidelines.
5.3
.1
Fe
b-1
5

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Change
(Remove and
Add)
REMOVE
Calcium Sandoz liquid
108mg or 2.7mmol
Ca/5mL licensed but
no longer manufactured
ADD
Calcium syrup
102mg/5mL
(2.55mmol/5mL) to be
added to formulary
(unlicensed)(food
supplement)
for use in paediatric
patients only
gre
en n Calcium-Sandoz liquid no longer manufactured by Alliance due
to inability to source one of ingredients. Therefore remove from
formulary. Small amount of use at BHT .
Alliance now making Alliance Calcium syrup 102mg calcium in
5mL (2.55mmol/5mL) £8.71/250mL for children over 4 yrs.
Calcium-Sandoz was £3.74/300mL (£4.49 incl VAT)
Calcium Sandoz tablets 1000 (25mmol) disperse in 200mL
water and this equates to 20mL QDS for a one year old
compared to 5mL of the liquid. Also need to consider the
sodium content of some of the effervescent products especially
if renal patient.
16Mar15 Emailed Alexa to query frequency of monitoring in
secondary care, if patient requires long-term treatment. May
put note on formulary.
Restricted - for use in paediatric patients only. Adults
requiring a soluble form of calcium should use
soluble/dispersible calcium tablets 9.5
.1.1
Fe
b-1
5
Add Vitamins A and D
(Vitamin A 4000 units,
Vitamin D 400 units) 84
capsules pack
required as in guideline for
children with CF
gre
en BNF states may be difficult to obtain. Product available and
sold via wholesalers contains 5000units Vitamin A. 4000 unit
product not available. Formulary amended to include 5000unit
product
Restricted - for use in accordance with Vitamin
Supplementation for Paediatric Cystic Fibrosis (CF)
Patients (BHTCG 378FM)
9.6
.4
Fe
b-1
5
Delete De Kristol 20,000
tablets (unlicensed)
remove as licensed
capsules now available
gre
en no Now non-formulary as licensed capsules are now
available.
CAUTION: this product is NOT peanut-free, NOT
suitable for patients with peanut allergy
Unlicensed - Medium risk (IDIS)
9.6
.4
Fe
b-1
5
Choice change InVita D3 ampoule Licensed capsules now
available as 1 st Choice
product for Vitamin D
replacement with InVita D3
now 2nd Choice for
patients who cannot
manage the capsules
gre
en y NOTE: dose NOT contain peanut, gelatine or lactose
Restricted - 2nd Choice product for use in patients who
cannot manage capsules, in accordance with Vitamin D
Testing and Treatment in Adults guideline (BHTCG
785FM)
9.6
.4
Fe
b-1
5
revise restriction Nicotine Invisi Patch
10mg.
gre
en y All patches listed in formulary are available in primary care.
Only the 25mg Invisi patch was recommended for hospital use
however Smoking Cessation team agree a lower strength patch
would be useful for stepping down in secondary care.
NRT guideline updated by Smoking Cessation Team and
awaiting approval.
releasing approx. 10mg, 15mg or 25mg over 16 hours
Restricted - in secondary care use in accordance with
Guidelines for Nicotine Replacement Therapy (NRT) for
Inpatients (BHTCG 369). The '25mg' patch should be
used initially, with the '10mg' patch only for use for
"stepping down" from the '25mg' patch if required, or for
very light smokers (0-5 cigarettes/day)
4.1
0.2
Fe
b-1
5
revise
restriction for
BHT use
Apixaban 2.5mg, 5mg
tablet
as listed in formulary Consultant Stroke
Physicians/NOAC
service to initiate,
continuation by GPs
AI
y Manufacturer has advised it is possible to crush/dissolve
tablets and administer via nasogastric/PEG tube - add note to
formulary to reflect this for use in secondary care.
Added :
NOTE 2. In secondary care tablets can be
dissolved/crushed and administered via nasgastric/PEG
tubes.
2.8
.2
Fe
b-1
5

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
new dose form Exenatide 2mg PFS pen
(Bydureon Pen) - new
presentation to replace
the Bydureon vial.
Initiation by Diabetes
Team with
continuation by GPS
AI
y Patent expiry on Bydureon confirm with Astra Zeneca 2023. No
price difference. New product launched Jan 15, withdrawal of
vial in 2015, date as yet unknown
Listed on the formulary as modified release injection (vial and
pre-filled pen)
Restricted - initiation by Diabetes team in accordance
with NICE TA 248 Exenatide pro-longed release
suspension for injection in combination with oral
antidiabetic therapy for the treatment of type 2 diabetes,
and Exenatide (Twice Daily or Once Weekly) for use in
Type 2 Diabetes amber initiation guideline (BHTCG
83FM). Also see Type 2 Diabetes blood-glucose
lowering therapy (BHTCG 667FM) (see link above)
6.1
.2.3
Fe
b-1
5
Revise
restrictionEpoprostenol
500microgram infusion
Prescribing in
secondary care only
red y Previous restriction referred to use for ischaemic limbs. MI has
requested this be removed as it is not used for ischaemic limbs.
Restricted - for use on NICU, ITU and SCBU only
2.8
.1
Fe
b-1
5
De
c 1
4.1 Add Abatacept
subcutaneous 125mg
pre-filled syringe
PbR excluded CCg
funded
For Rheumatoid Arthritis as
an alternative to abatacept
IV and in accordance with
NICE TA 280 and TA 195
Consultant
Rheumatologists Re
d y Abatacept should remain on formulary
Preferred choice for treatment of Rheumatoid Arthritis when
abatacept IV is recommended NICE TA280 and TA195 and in
accordance with Biologics for Rheumatoid Arthritis (BHTCG
749)
FOR ALL PRESCRIBING - NICE compliance form
required - see link from Formulary homepage. (NICE
compliance to be verified if NICE compliance form not
yet available)
Restricted - to prescribing by Consultant
Rheumatologists only for the treatment of rheumatoid
arthritis, as the preferred choice when abatacept IV is
recommended in NICE TA280 and in accordance with
Biologics for Rheumatoid Arthritis (BHTCG 749)
NOTE If patients fail to respond to one route they may
not try the alternative route.
10
.1.3
FM
G D
ec1
4
De
c 1
4.1 Revise
restrictionAbatacept 250mg
intravenous infusion
PbR excluded, CCG
funded
For Rheumatoid Arthritis in
accordance with NICE TA
280 and TA 195
Consultant
Rheumatologists
red y To remain on formulary for use when Abatacept SC is
inappropriate eg. Inability to self-administer, intolerance etc.
Restricted - ro Rheumatology consultant prescribing
only, in accordance with NICE TA195, NICE TA280 and
Biologics for Rheumatoid Arthritis (BHTCG 749)
NOTE 1: to remain on formulary for use when abatacept
sub-cutaneous is inappropriate eg. Inability to self-
administer, intolerance etc.
NOTE 2: If patients fail to respond to one route they may
not use the alternative route.
10
.1.3
FM
G D
ec1
4
De
c 1
4.4 revise
restrictionCholecalciferol oral
solution (InVita D3)
25,000 IU in 1mL
gre
en Jan CGS
Note - does not contain peanut, gelatine or lactose.
NOTE: does NOT contain peanut, gelatine or lactose
Restricted - for use in accordance with Vitamin D Testing
and Treatment in Adults guidleline (BHTCG 785FM)
9.6
.4
FM
G
De
c 1
4.4 revise
restrictionCholecalciferol
(Dekristol) 20,000 IU
gre
en JanCGS - remove reference in guideline CAUTION: this product is NOT peanut-free. Not suitable
for use in patients with peanut allergy.
Unlicensed - Medium risk (imported from IDIS)
Restricted - to be used as second choice product for the
treatment of Vitamin D deficiency in adults only if InVita
D3 is unavailable and in accordance with Vitamin D
Testing and Treatment in Adults (BHTCG 785FM) - see
link below
9.6
.4
FM
G D
ec1
4
FMG DECISIONS DECEMBER 2014

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Oct
14
.1 Add Tocilizumab 162mg
pre-filled syringe,
subcutaneous
injection
PBR excluded
CCG funded
For Rheumatoid Arthritis as
an alternative to
tocilizumab IV and in
accordance with NICE TA
247
Consultant
Rheumatologists Re
d y FOR ALL PRESCRIBING - NICE compliance form
required - see link from Formulary homepage. (NICE
compliance to be verified if NICE compliance form not
yet available)
Restricted - to prescribing by Consultant
Rheumatologists only for the treatment of rheumatoid
arthritis, as an alternative to tocilizumab IV
recommendations in NICE TA247 and in accordance
with Biologics for Rheumatoid Arthritis (BHTCG 749)
Patients should use either IV or SC tocilizumab. If they
fail on either of the routes, they may not use the
alternative route.
10
.1.3
FM
G D
ec1
4
Oct
14
.5 revised TLL
positionOctreotide/Lanreotide For use in palliative care Palliative Care Team
AR y Restricted - recommendation by Palliative Care Team
8.3
.4.3
FM
G
Se
p 1
4.1
1 Add Canagliflozin 100mg,
300mg tablet
gre
en y add as per decision and say Await update of Diabetes guideline Restricted - for the treatment of adults with Type 2
diabetes in accordance with NICE TA315 and Type 2
Diabetes guidelin (BHTCG 667FM) (guideline being
updated) in the following circumstances, when
dapagliflozin cannot be used:
- in dual therapy with metformin for patients over 75
years of age when sitagliptin is not suitable or,
- in triple therapy with metformin and a sulphonylurea
when sitagliptin is not suitable.
6.1
.2.3
FM
G D
ec1
4
Se
p1
4.5 Revised
guidelineContraceptive Guideline links all active
xxx
FM
G
Se
p 1
4.2 Revised
guidelinePsoriasis Bioligcs
guideline
Links to guideline in place from drugs included in guideline eg
adalimumab, etanercept, infliximab and ustekinumab
xxx
FM
G

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
revise restriction Avance Negative
Pressure Wound
Therapy
NPWT is approved for
formulary inclusion for the
healing of a wound which
has excessive exudate
levels and is not
progressing towards
healing.
to included Tissue
Viability nurses
red
me
dic
al d
evic
e Formulary restriction is widened to include initiation in primary
care by Tissue Viability ONLY with supply via ONPOS for
patients who have been or need to be discharged on NPWT
from an out-of-area acute Trust and require continued NPWT or
patients who need NPWT to help prevent admission or re-
admission to hospital.
NOt to be prescribed on FP10s
Restricted -
1. In secondary care to be initiated by Tissue Viability,
Spinal, Burns & Plastics, Orthopaedics and General
Surgery.
2. In primary care, intiation by Tissue Viability ONLY
with supply via ONPOS for patient who:
- have been, or need to be, discharged on NPWT from
an out-of-area acute Trust and require continued NPWT
or,
- need NPWT to help prevent admission or readmission
to hospital
NOTE: NOT to be prescribed on FP10
After initiation of treatment, patients should be reviewed
weekly under the direction/supervision of the Tissue
Viability Team. If no significant improvement is seen in 2
weeks therapy will be stopped. If improvement is
confirmed then the usual length of treatment is 4 weeks
although occasionally patients may require longer
treatment (generally a maximum of 8 weeks)
[Audit results to FMG after 20 patients have received
treatment initiated in primary care using either Avance or
PICO NPWT]
xxx
FM
G D
ec1
4
De
c 1
4.9 Add PICO Negative
Pressure Wound care
dressing 15cm x 15cm,
10cm x 20cm
small, highly exuding
wounds for a maximum of
4 weeks.
recommendation by
Tissue Viability only
in Primary Care.
red
me
dic
al d
evic
e Use on 20 patients per year approved. Audit results, once the
first 20 patients have been treated, to come to FMG.
NOT TO BE USED IN SECONDARY CARE - ONLY FOR
USE IN PRIMARY CARE
In primary care restricted to recommendation by TV only
for short term use (not exceeding 4 weeks), on small,
highly exuding wounds.
- Patients require regular TV specialist review. In
community must be supplied through TV nurse who will
organise supplies to go to the patient's nurse.
- Not to be prescribed on FP10.
- In primary care restricted to TV recommendation
ONLY.
xxx
FM
G D
ec1
4
De
c 1
4.8 Add Lenalidomide 5mg,
10mg, 15mg, 25mg
capsule
PbR excluded, NHSE
funded
For myelodysplastic
syndromes associated with
an isolated deletion 5q
cytogenetic abnormality
NICE TA322
Cons Haematologists
red y Check whether need to add note as per BNF: NOTE: patient,
prescriber and supplying pharmacy must comply with a
pregnancy prevention programme. Every prescription must be
accompanied by a completed Prescription Authorisation Form
FOR ALL PRESCRIBING - NICE compliance form
required - see link from Formulary homepage. (NICE
compliance to be verified if NICE compliance form not
yet available)
Restricted - to prescribing by Consultant Haematologists
for myelodysplastic syndromes in accordance with NICE
TA 322 Lenalidomide for treating myelodysplastic
syndromes associated with an isolated deletion 5q
cytogenetic abnormality.
8.2
.4
FM
G D
ec1
4

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
De
c 1
4.6 revise restriction Celecoxib 100mg,
200mg capsule
When used in
secondary care,
restricted to
prescribing by
Consultant
Rheumatologists
gre
en y in accordance with NSAIDs guideline In secondary care - restricted to prescribing by
Consultant Rheumatologists only.
Use in accordance with NSAIDs in Adult -
Primary/Secondary Care guideline (BHTCG 299FM) -
see link above.
10
.1.1
FM
G D
ec1
4
CCG FORMULARY CHANGE TRACKING DOCUMENT - PROPOSED CHANGES FOR DECEMBER 2014 FMGRevise
restrictionsLiothyronine
5micrograms and 20
micrograms
AI
y In secondary care liothyronine has the advantage of a shorter
halflife and faster onset of action. Apart from this acute use,
which is usually short term, liothyronine should not be used as a
1st line treatment choice when prescribed on the NHS. Use in
primary care should only be in patients who have had a
therapeutic trial of levothyroxine and failed to derive adequate
benefits from this treatment.
2nd line to levothyroxine
Problem in primary care of privately initiated treatments being
requested for ongoing prescribing on NHS. Restriction should
help restrict use on NHS after private initiation.
Restricted - initiation in secondary care with continuation
by GPs. 2nd line to levothyroxine.
6.2
FM
G D
ec1
4
BHT FORMULARY CHANGE TRACKING DOCUMENT - PROPOSED FORMULARY CHANGES FOR NOTE DECEMBER 2014 FMGRevise
restrictionsOseltamivir 30mg,
45mg, 75mg (Tamiflu)
caps
Influenza post-exposure
prophylaxis and treatment
gre
en
y
Restrictions revised to reflect latest PHE guidance. Restricted - for seasonal influenza post-exposure
prophylaxis and treatment (see Public Health England
(PHE) advice/local guidance above), or when there is a
high level of seasonal influenza circulating as
determined by PHE.
NICE guidance should be considered by all clinicians
(primary and secondary).
In secondary care - clinicians should use their clinical
judgement to prescribe antivirals, particularly for patients
with proven or suspected influenza whose overal clinical
condition required admission.
In primary care - prescribe when directed by PHE and
GPs may, at their discretion, prescribe antiviral
medicines for people who may not be in the specified at-
risk groups but who they believe would suffer serious
complications if not treated with an antiviral medicine eg
those whoare clinically very unwell or at risk of hospital
admission.
5.3
.4
FM
G D
ec1
4
Revise
restrictionsOseltamivir 6mg/ml
(30mg/5mL) Tamiflu
oral suspension
Restricted - only for use
in children less than 1
year of age
Restricted - as above
for oseltamivir tablets
Influenza post-exposure
prophylaxis and treatment
gre
en
y
and restriction also includes "only for use in children less than
1 year of age."
5.3
.4
FM
G D
ec1
4

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Revise
restrictionsZanamivir 5mg blister
for inhalation (Relenza)
dry powder for
inhalation disks
Restriction - as for
oseltamivir tablets
above
Influenza post-exposure
prophylaxis and treatment
gre
en
y
Restrictions revised to reflect latest PHE guidance.
5.3
.4
FM
G D
ec1
4
Revise
restrictionsZanamivir 200mg/20mL
(Relenza) aqueous
solution
Influenza post-exposure
prophylaxis and treatment
red
N
Restriction revised to include manufacturer and phone number Unlicensed - Medium risk
Available on a named patient basis from
GlaxoSmithKline (0800 036 1060) for patients who fit the
Public Health England criteria (BHTCG 302)
5.3
.4
FM
G
Supply
problemsAlprostadil
10micrograms,
20micrograms
(Caverject Dual
Chamber)
Ai a
nd
Re
d y Availability problems. Add comment to both Red and AI entries
on formulary
If problems with supply, please use Viridal® Duo
7.4
.5
Add Alprostadil
10micrograms,
20micrograms (Viridal
Duo)
Re
d a
nd
AI
-
y Add to formulary whilst supply problems For use while supply problems exist with Caverject® Dual
Chamber 7.4
.5
Add Raltegravir 400mg
tablet Re
d y NHSE have produced new post exposure prophylaxis guidance.
1st line PEP (post exposure prophylaxis for occupational and
non-occupational use)
For PEP (post-exposure prophylaxis), to be used in
combination with tenofovir disoproxil/emtricitabine
(Truvada) and in accordance with November 2014
guidance from EAGA (Expert Advisory Group on AIDS)
5.3
.1
Revise
restrictionZidovudine/Lamivudine
300mg/150mg tablet
(Combivir)
Re
d y Restricted - prescribing for the prevention of maternal to foetal
HIV transmission. See protocol by Obs & Gynae Depts
Restricted - prescribing for patients treated for PEP (post
exposure prophylaxis), in combination with lopinavir/ritonavir.
Initial 5 day treatment followed by a further 25 days if
appropriate.
The latter restriction should be removed.
1. Restricted - prescribing for the prevention of maternal
to foetal HIV transmission. See protocol by Obs &
Gynae Depts.
2. Restricted - prescribing for patients treated for PEP
(post-exposure prophylaxis), in combination with
lopinavir/ritonavir. Initial 5 day treatment followed by a
further 25 days if appropriate.
NOTE: New guidance from EAGA (Expert advisory
Group on AIDS) states PEP prophylaxis to change to
Raltegravir and Truvada from November 2014 (see
entries for Raltegravir and Truvada)
5.3
.1
Revise
restrictionTenofovir
Disoproxil/Emtricitabine
245mg/200mg
(Truvada) tablet
Re
d y For PEP (post exposure prophylaxis)
5.3
.1
Delete Fluenz nasal spray
influenza vaccine Re
d y Discontinued 14
Add Fluenz Tetra nasal
spray influenza vaccine Re
d y replaced Fluenz 14
replacement Urokinase 10,000units
red We removed 5000U as no longer available but didn’t add in the
10,000units which is what the nurses have been using for ages
to give the dose of 5000units now. Done already as I didn't
want to cause issues with something that has been this way for
a long time.
Available on a named patient basis for central line
blockages - see hospital protocol
2.1
0.2

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Revise
restrictionCalcium folinate 15mg
tablet
red Presently on formulary for Methotrexate rescue only. It is
included in the Uveitis guideline and therefore propose adding
as separate entry, as Red on TLL, for use in accordance with
Uveitis Guideline for the treatment of toxoplasmosis.
Restricted - for use in accordance with Uveitis guideline
(BHTCG 374FM)
8.1
Remove Pyrimethamine/sulfadox
ine tablet 25mg/500mg
bla
ck? No longer in Uveitis guideline. Remove as long as no other use
across Trust.
Available on a named patient basis for central line
blockages - see hospital protocol 5.4
.1
Add Nicotine inhalator
15mg/cartridge x 4 pack
gre
en y For use in accordance with NRT guideline
Additional pack size. More cost effective for use in hospital
rather than the 36 cartridge pack presently in use.
Community are discussing their needs regarding this size.
Clare Hodsdon and Nicky Blyth
Restricted - in secondary care use in accordance with
NRT guideline
4.1
0.2
revise
restriction Omeprazole injection
40mg
Omeprazole infusion to be used across Trust (and not
omeprazole IV) To avoid potential for error and confusion.
Don't want to delete from formulary as if in future there were to
be supply issues the IV product may be required. Therefore
tightly restrict and word formulary accordingly. Agreed with
Tracy Percival
NOTE: Omeprazole intravenous infusion to be used.
Omeprazole injection is not to be used unless the
infusion is unavailable due to supply problems. (If using
the injection, restrictions apply as for the infusion above)
Revise
restrictionMirabegron 25mg,
50mg
AR y Add Consultant neurologists as prescribers for recommendation Restricted - recommendation by Consultant
Urogynaeacologists, Consultant Urologists, Neurologists
and Spinal Consultants with continuation by GPs, as an
option when patients fail on, or are intolerant of,
solifenacin or for whom anticholinergics are
contraindicated. To be used in accordance with, Over-
Active Bladder - Medical Management -
Primary/Secondary Care guideline (BHTCG 110FM) (see
link above) and NICE TA 290 Overactive bladder -
Mirabegron.
7.4
.2
ADD Ametop cream
gre
e y requested by CCG during Chapter 15 netformulary review Restricted - for use in primary care.
REVISE Captopril suspension
5mg/5mL
AI
y Now a licensed preparation therefore remove unlicensed
wording from formulary.
Restricted - to initiation by Paediatric consultants with
continuation by GPs.
2.5
.5.1
Add Formoterol
12micrograms/metered
inhalation, dry powder
for inhalation
(Easyhaler)
gre
en y Listed in COPD guideline but missed Restricted - may be used as an alternative to salmeterol
for treatment of COPD. See COPD Inhaled Treatment
algorithm (BHTCG 726FM) 3.1
.1.1
Add Formoterol
12micrograms/metered
inhalation, aerosol
inhalation (Atimos
Modulite)
gre
en y Listed in COPD guideline but missed Restricted - may be used as an alternative to salmeterol
for treatment of COPD. See COPD Inhaled Treatment
algorithm (BHTCG 726FM) 3.1
.1.1

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Add Prontoderm Nasal Gel
Light 30mL
gre
en y as 3rd line agent for MRSA decolonisation as there continues to
be supply issues with Mupirocin Nasal and an alternative is
required in case of Naseptin resistance or if patients are allergic
to the ingredients/excipients (chlorhexidine, arachis oil)
30mL £4.45 (Mupirocin £4.25 and Naseptin £1.67)
Estimated use - one patient per month.
Sodium fusidate is an alternative but resistance is an issue.
Polyfax eye ointment (£3.26 excl VAT) was also a possibility.
Restricted - for use only as 3rd line for MRSA
decolonisation if mupirocin is unavailable and Naseptin
nasal cream is unsuitable due to resistance or if patients
are allergic to the ingredients/excipients contained in
mupirocin or Naseptin..
no
t in
BN
F
Add Dabrafenib 50mg, 75mg
capsule
red y NICE TA 321 Dabrafenib for treating unresectable or metastatic
BRAF V600 mutation positive melanoma.
No use at BHT
This Specialty is entirely based at OUH and all patients with this
condition needing dabrafenib are treated there.
Restricted - prescribing byt Oxfdord University Hospitals
(OUH) only, in accordance with NICE TA 321 Dabrafenib
for treating unresectable or metastatic BRAF V600
mutation positive melanoma.
8.1
.5
Add Omeprazole MUPS
20mg
gre
en y In secondary care restricted - for use in patients who cannot
swallow because they are in ITU or have a NG/PEG tube and
paediatric patients
In primary care only for use in patients unable to swallow the
capsules
NOTE: Before prescribing omeprazole MUPS consider
lansoprazole Fastab as they are the most cost effective
dispersible tablet
In secondary care restricted - for use in patients who
cannot swallow because they are in ITU or have a
NG/PEG tube and paediatric patients
In primary care only for use in patients unable to swallow
the capsules
NOTE: Before prescribing omeprazole MUPS consider
lansoprazole Fastab as they are the most cost effective
dispersible tablet
1.3
.5
Revise
restrictionOmeprazole MUPS
10mg, 20mg dispersible
tablet
gre
en y Added paed patients and Note regarding use of Lansoprazole
FasTabs
In secondary care restricted - for use in patients who
cannot swallow because they are in ITU or have a
NG/PEG tube and paediatric patients
In primary care only for use in patients unable to swallow
the capsules
NOTE: Before prescribing omeprazole MUPS consider
lansoprazole Fastab as they are the most cost effective
dispersible tablet
1.3
.5
Revise
restrictionLansoprazole 15mg,
30mg (FasTab
(orodispersible))
gre
en y Added use for paediatrics and cost effective NOTE In secondary care restricted - for use in patients who
cannot swallow because they are in ITU or have a
NG/PEG tube and paediatric patients
In primary care only for use in patients unable to swallow
the capsules
NOTE: Lansoprazole Fastab are the most cost effective
dispersible tablet
1.3
.5
FMG DECISIONS OCTOBER 2014

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Oct
14
.3 Add Lubiprostone
24micrograms capsule
Chronic idiopathic
constipation in accordance
with NICE TA 318
Consultant
Gastroenterologists
and Spinal
Consultants with
continuation by GP
AI
y For adults in whom treatment with at least two laxatives from
different classes at the highest tolerated recommended doses
for at least 6 months has failed to provide adequate relief and
for whom invasive treatment for constipation is being
considered.
The first course will be initiated by the consultants and reviewed
at the end of the course (two weeks) to consider the benefit of
treatment; second and subsequent courses will be initiated by
GPs on the advice of the consultant.
At first initiation consultants to provide GPs with clear guidance
regarding expected duration of ongoing treatment.
Restricted - initiation by Gastroenterologists and Spinal
Consultants, with continuation by GPs in accordance
with NICE TA318, for adults in whom treatment with at
least two laxatives from different classes at the highest
tolerated recommended doses for at least 6 months has
failed to provide adequate relief and for whom invasive
treatment for constipation is being considered.
When first course initiated, consultant to:
- provide GPs with clear guidance regarding the
expected duration of ongoing treatment and,
- review patient at the end of the initial 2 week course to
consider the benefit of treatment.
Second and subsequent courses to be initiated by GPs
on the advice of the consultant.
1.6
.7
FM
G O
ct1
4
Oct
14
.3 Revise
restrictionPrucalopride 1mg, 2mg
tablet
Spinal Consultant
may also prescribe
AI
y see formulary restriction Restricted - initiation by Gastroenterologists and Spinal
Consultants, with continuation by GPs after first hospital
review at 4 weeks, in accordance with NICE TA 211
Prucalopride for the treatment of chronic constipation in
women. A supply of 2 weeks to be provided by the
hospital after the first review at four weeks ie. total of 6
weeks supply from hospital
1.6
.7
FM
G O
ct1
4
OC
t14
.5 revised TLL
positionOctreotide/Lanreotide For use in cancer Oncology team
red y Restricted - prescribing by Oncology team
8.3
.4.3
FM
G
Oct
14
.5 revised TLL
positionOctreotide/Lanreotide For use in insulin
resistance (CHI -
Congenital
Hyperinsulinism) in
paediatric patients. (As
shared care with tertiary
referral centres)
Paediatriciansre
d y Unlicensed Use
Restricted - prescribing by Consultant Paediatricians for
use in insulin resistance (Congenital Hyperinsulinism
(CHI)) in paediatric patients (as shared care with tertiary
referral centres)
8.3
.4.3
FM
G O
ct1
4
Oct
14
.5 revised TLL
positionOctreotide/Lanreotide Acromegaly Consultant
Paediatricians and
Endocrinologists
AP y Restricted - prescribing by Consultant Paediatricians and
Endocrinologists for the treatment of acromegaly.
(shared care protocol awaited) 8.3
.4.3
FM
G
Oct
14
.7 Add Trastuzumab s.c
injection 600mg
PBr excluded funded
NHS England
same as entry on formulary
but not for GIST. In
accordance with NICE TA
34 and NICE TA107 for
adjuvant for HER2 positive
breast cancer
Breast oncologists
red y FOR ALL PRESCRIBING - NICE compliance form
required - see link from Formulary homepage. (NICE
compliance to be verified if NICE compliance form not
yet available)
Restricted - prescribing by Breast Oncologists for:
1. use in accordance with NICE TA34 for advanced
breast cancer
2. use in accordance with NICE TA107 for the adjuvant
treatment of early-stage HER2-positive breast cancer
8.1
.5
FM
G O
ct1
4

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Se
pt
14
.4 Add Levonorgestrel IUD
(Jaydess)
use in Women's health in
primary and secondary
care in accordance with the
Contraceptives guideline
BHTCG updated NOv2014
gre
en M
D
Not on formulary until mid-November (after APC and CGS) To be used in accordance with Contraception (Summary
of Key Messages) (BHTCG 783FM)
In secondary care restricted - to Family Planning and
Obs & Gynae Consultants/SPRs only
In primary care GP must have undergone training on
insertion
7.3
.2.3
FM
G O
ct1
4
Se
p 1
4.5 Add Alemtuzumab 12mg
concentrate for
solution for infusion
PBr excl. Funded NHS
England
treatment of adults with
relapsing remitting multiple
sclerosis with active
disease in accordance with
NICE TA 312
Consultant
Neurologists and
Clinical Nurse
Specialist for
Neurology
red y HCD Form approved Dec 2014 - NICE wording to be removed FOR ALL PRESCRIBING - NICE compliance form
required - see link from Formulary homepage. (NICE
compliance to be verified if form not yet available)
Restricted - prescribing by Consultant Neurologists and
Clinical Nurse Specialist for Neurology for the treatment
of adults with relapsing remitting multiple sclerosis with
active disease in accordance with NICE TA312.
8.2
.3
FM
G O
ct1
4
Se
p 1
4.6 Add Dimethyl fumarate
120mg, 240mg
capsules
PBR excl Funded NHS
England
treatment of adults with
relapsing remitting multiple
sclerosis with active
disease in accordance with
NICE TA 320
Consultant
Neurologists and
Clinical Nurse
Specialist for
Neurology
red y HCD Form approved Dec 2014 - NICE wording to be removed FOR ALL PRESCRIBING - NICE compliance form
required - see link from Formulary homepage. (NICE
compliance to be verified if form not yet available)
Restricted - prescribing by Consultant Neurologists and
Clinical Nurse Specialist for Neurology for the treatment
of adults with relapsing remitting multiple sclerosis with
active disease in accordance with NICE TA320.
8.2
.4
FM
G O
ct1
4
Se
p 1
4.7 Add Enzalutamide 40mg
capsules
PBR excl Funded NHS
England
for treatment of metastatic
hromone-relapse prostate
cancer in adults whose
disease has progressed
during or after docetaxel-
containing chemotherapy
in accordance with NICE
TA 316
Consultant
Oncologists
(Prostate)
red y HCD Form approved Dec 2014 - NICE wording to be removed FOR ALL PRESCRIBING - NICE compliance form
required - see link from Formulary homepage. (NICE
compliance to be verified if form not yet available)
Restricted - prescribing by Consultant Oncologists
(Prostate) for the treatment of metastatic hormone-
relapsed prostate cancer in adults whose disease has
progressed during or after docetaxel-containing
chemotherapy in accordance with NICE TA316
8.3
.4.2
FM
G O
ct1
4
Fe
b1
4.6 Add Ranolazine MR 375mg,
500mg, 750mg tablets
treatment of stable angina
only in patients who
symptoms are not
adequately controlled or
there is intolerance or
contraindications to four
anti-anginal medicines
(beta-blockers, calcium
channel blockers, long-
acting nitrates and
nicorandil) and where
revascularisation is not
appropriate.
Initiation by
Consultant
Cardiologist with
continuation by GPs
AI
y Not added to formulary until mid-November. (CGS and APC
Nov 6th and 12th)
Restricted - initiation by Consultant Cardiologists with
continuation by GPs, in accordance with Ranolazine
Amber Initiation guideline (BHTCG ), for the
treatment of stable angina only in patients whose
symptoms are not adequately controlled or there is
intolerance or contraindications to four anti-anginal
medicines (beta-blockers, calcium channel blockers,
long-acting nitrates and nicorandil) and where
revascularisation is not appropriate.
2.6
.3
FM
G O
ct1
4
CCG FORMULARY CHANGE TRACKING DOCUMENT - PROPOSED CHANGES FOR OCTOBER 2014 FMGChange TLL
positionHydrocortisone (as
sodium phosphate)
100mg/1mL (Efcortesol)
injection Gre
en
y
Reclassified from red to green so available as ready made
preparation for Doctors bag in primary care
Glass ampoules in case of latex allergy.
Comes as a ready diluted form, so may be more suitable
for GP emergency bags than Solu-Cortef
6.3
.2
FM
G O
CT

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Blacklist/NF Lactase 50,000units/g
(Colief)
Bla
ck
y
DROP list recomends listing as NF. In primary care may be
purchased OTC, should be listed as NF
If required may be purchase OTC
A2
.5.1
FM
G O
CT
Blacklist/NF Fentanyl lozenge
(Buccal) all strengths
(Actiq) Bla
ck
y
Black list and NF as per DROP list
4.7
.2
FM
G
Blacklist/NF Fentanyl tablets
(buccal), all strengths
(Effentora)
Bla
ck
y
Black list and NF as per DROP list
4.7
.2
FM
G O
CT
Blacklist/NF Fentanyl tablets
(sublingual) all strengths
(Abstral) Bla
ck
y
Black list and NF as per DROP list
4.7
.2
FM
G
Blacklist/NF Fentanyl nasal spray, all
strengths (Instanyl)
Bla
ck
y
Black list and NF as per DROP list
4.7
.2
FM
G
Blacklist/NF Fentanyl nasal spray, all
strengths (PecFent)
Bla
ck
y
Black list and NF as per DROP list
4.7
.2
FM
G O
CT
Choice added Resource Thicken-Up
Clear
AR
List as 1st choice thickener Initiation on recommendation of SALT only
A2
.5.2
FM
G O
CT
Choice added Thick and Easy
AR
List as 2nd choice thickener Initiation on recommendation of SALT only
A2
.5.2
FM
G O
CT
Add Lurasidone
Hydrochloride tablet
18.5mg, 37mg, 74mg
Restriction - only for
patients with schizophrenia
who cannot tolerate or who
have contraindications to
usual 1st or 2nd choices or
aripiprazole
Consultant
Psychiatrist
Re
d y
E
U
Queried with SC whether any further detail re 1st and 2nd
Choices required?
Restricted - prescribing by Consultant Psychiatrist only
for patients with schizophrenia who cannot tolerate, or
have contraindications to, commonly presribed
antipsychotics or aripirazole.
4.7
.2
FM
G O
CT
14

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Remove Multivitamins BPC
y
Traffic light position not yet agreed.
Do not contain RDA of vitamins. If a multivitamin is needed use
alternative such as Forceval or Multivitamins with minerals.
Agreed to add note to say not recommended for initiation as
does not contain RDA of vitamins and note to say in primary
care it is recommended that all patients are stopped or
switched to a suitable alternative and should be purchased over
the counter.
Not recommended for initiation as does not contain RDA
of vitamins. In primary care it is recommended that all
patients are stopped or switched to a suitable alternative
and should be purchased over the counter.
9.6
.7
FM
G O
CT
14
Add Cholecalciferol oral
solution (InVita D3)
25,000 IU in 1mL
Licensed Vitamin D in a
liquid form. This could
replace unlicensed high
dose (DeKristol). Restrict
use in accordance with
Adult Vitamin D guideline
In last year 56 issues
Colecalciferol 20,000U
(DeKristol) caps £11.52
(excl VAT) £650
3 ampoules per pack £3.89
(excl VAT). SPC states for
Vit D deficiency
50,000U/week for 6-8
weeks. Ie 2amps weekly
for 6 weeks = 300,000U 4x
£3.89 = £15.56 (£18.67 incl
VAT) (similar to Vit D
guideline DeKristol
2x20,000 caps for 7 days,
14caps=£3.22)
Gre
en
y
Agree to add, pending confirmation from Vit D subgroup and
subsequent amending of Vit D guidelines. Green list and place
note restricting use in patients for whom DeKristol is not
suitable, for eg peanut allergy.
Also added warning regarding peanut allergy to DeKristol entry
Restricted - only for use in patients recommneded by
Heatherwood and Wexham Park Trust or in patients for
whom colecalciferol 20,000unit capsules (DeKristol) is
not suitable, for eg. in peanut allergy
(Restriction to be revised following discussion/approval
by Bucks Vitamin D subgroup and amendment of
Vitamin D guideline)
9.6
.4
FM
G O
CT
14
Add Oxybutynin patches
3.9mg/24hours
Dose: 1 patch twice
weekly
gre
en y Cost effective alternative to the more costly unlicensed
solutions. Restrict use on formulary for patients unable to
swallow the tablets and for whom the solution might otherwise
be considered
£23.80 (£28.56 incl VAT) / 8 patches
Licensed 2.5mg/5mL (£7.22 incl VAT /150mL) 5mg tds for 1
month = £43.32 (6 bottles)[Approx £700 last yr approx 104
issues]
Unlicensed 5mg/5mL (£52.20 incl VAT/125mL) 5mg tds for 1
month = £187.92 [87 issues £4541.40]
Restricted - for use only in patients unable to swallow
tablets and for whom the oral liquid, which is more
costly, might otherwise be considered.
7.4
.2
FM
G O
CT
14
Reinstate Metolazone tablet 5mg
Re
d no Licensed product was discontinued and metolazone was
removed from formulary.On reflection this was hasty as stocks
have been used up in Pharmacy and problems have occurred
due to its absence from the formulary. It is available as a
special now and has been requested several times recently for
heart failure.
MSt/SS agreed to restore metolazone to the formulary (Red
TLL) until cardiology are able to reach a decision given latest
information from MI
Unlicensed
Restricted - prescribing by secondary care only. 2.2
.1
FM
G O
CT
14
BHT FORMULARY CHANGE TRACKING DOCUMENT - PROPOSED FORMULARY CHANGES FOR NOTE OCTOBER 2014 FMG

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Missed during
Netformulary
population
Diclofenac 12.5mg,
25mg, 50mg, 100mg
suppositories
gre
en y Diclofenac suppositories were inadvertently missed during
establishment of netFormulary
10
.1.1
FM
G
Add Fluarix Tetra
vaccination Re
d y For use in Influenza Vaccination in Special Schools where
Fluenz is not appropriate.
Restricted - only for use in Influenza Vaccination in
Special Schools where Fluenz is not appropriate.
14
.04
FM
G O
CT
Delete Urokinase 5000units
Re
d no Not available therefore remove, but added 10,000u as nurses
use this to give 5000u dose.
Available on a named patient basis for central line
blockages - see hospital protocol
2.1
0.2
FM
G O
CT
Change Fentanyl & Bupivacaine
Re
d
y Licensed preparation is now available - so remove "unlicensed "
wording from formulary 15
.2
FM
G O
CT
Delete Dexamethasone
4mg/mL injection
Gre
en y There were supply problems with this product which has now
been remarketed as 3.8mg/mL. To avoid confusion remove
from formulary leaving only the 3.3mg/mL product.
MHRA Alert Oct 14
Added to formulary a note stating:
(Dexamethasone injection 4mg/mL is no longer available
and is non-formulary)
6.3
.2
FM
G O
CT
Se
p1
4.1 Add Prilocaine Hydrochloride
20mg/Ml (2%), glucose
60mg/mL, 5ml Ampoule
Adults for spinal
anaesthesia in short term
surgical procedures.
Consultant
Anaestthetistsre
d y
Restricted - prescribing by Consultant Anaesthetists for
Day Case procedures where surgical anaesthesia is
required for approximately 60-90 minutes.
15
.2
Sep-1
4
Se
p1
4.3 Add Cefuroxime 50mg
powder for solution for
intracameral injection
As a replacement for sub-
conjunctival cefuroxime to
be used routinely for all
cataract procedures
performed at SMH and
WYC.
Ophthalmology team
red y
Uptake should be aimed to be achieved by all consultants
within three months . Confirmation of this (or explanation of
cause of delay) via SDU Governance meeting minutes is
requested.
Audit of rate of endophthalmitis for cataract surgery patients to
be reported to FMG twelve months after uptake (December
2015)
Restricted - prescribing by Ophthalmology team as a stat
dose immediately after cataract surgery.
11
.08
.02
Sep-1
4
CCG FORMULARY CHANGE TRACKING DOCUMENT - PROPOSED CHANGES FOR SEPTEMBER 2014 FMG
Add Glucose Rx Nexus
meter
gre
en
yJoint 1st Choice in primary care for all type 2 diabetics
6.1
.6
#####
Add Glucose Rx Nexus
blood glucose strips
gre
en
yJoint 1st Choice in primary care for all type 2 diabetics
6.1
.6
#####
Add Supecheck 2 meter
gre
en
yJoint 1st Choice in primary care for all type 2 diabetics
6.1
.6
#####
Add Supercheck 2 strips
gre
en
yJoint 1st Choice in primary care for all type 2 diabetics
6.1
.6
#####
FMG DECISIONS SEPT 2014
FORMULARY TRACKING DOCUMENT- CHANGES FOR NOTE (including Woundcare Formulary)- AGREED SEPTEMBER 2014 FMG
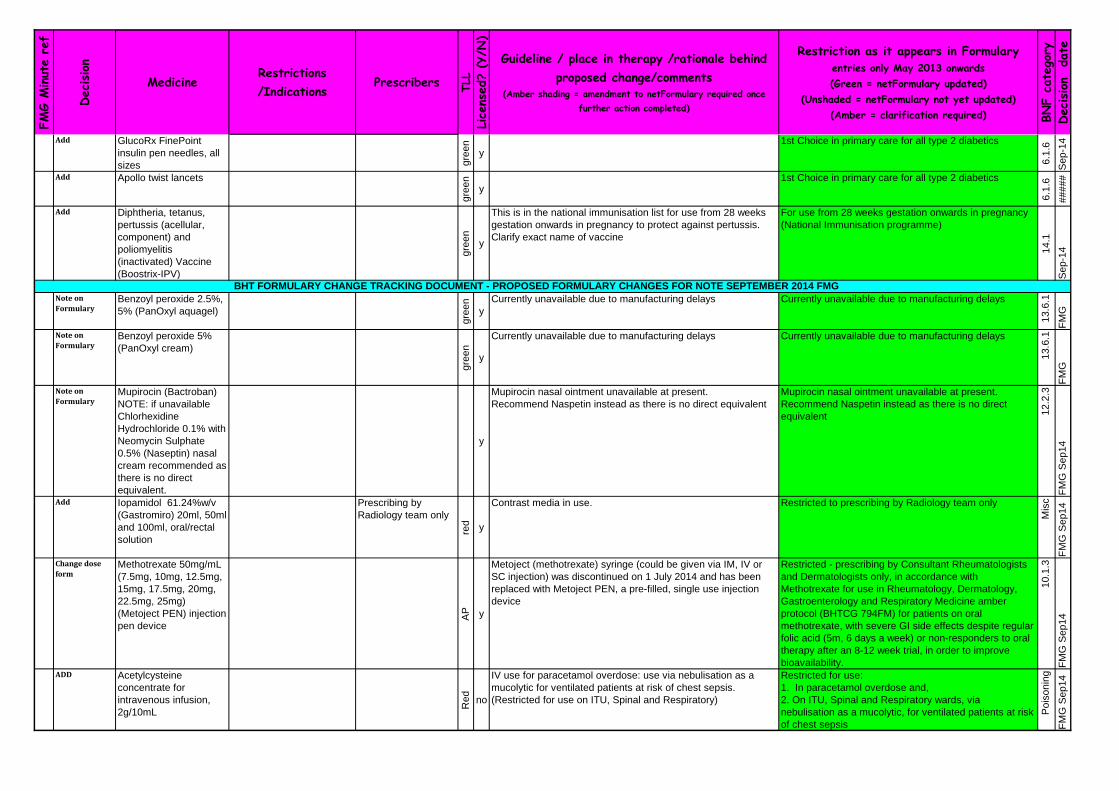
FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Add GlucoRx FinePoint
insulin pen needles, all
sizes gre
en
y
1st Choice in primary care for all type 2 diabetics
6.1
.6
Sep-1
4
Add Apollo twist lancets
gre
en
y1st Choice in primary care for all type 2 diabetics
6.1
.6
#####
Add Diphtheria, tetanus,
pertussis (acellular,
component) and
poliomyelitis
(inactivated) Vaccine
(Boostrix-IPV)
gre
en
y
This is in the national immunisation list for use from 28 weeks
gestation onwards in pregnancy to protect against pertussis.
Clarify exact name of vaccine
For use from 28 weeks gestation onwards in pregnancy
(National Immunisation programme)
14
.1
Sep-1
4
Note on
FormularyBenzoyl peroxide 2.5%,
5% (PanOxyl aquagel)
gre
en
y
Currently unavailable due to manufacturing delays Currently unavailable due to manufacturing delays
13
.6.1
FM
G
Note on
FormularyBenzoyl peroxide 5%
(PanOxyl cream)
gre
en
y
Currently unavailable due to manufacturing delays Currently unavailable due to manufacturing delays
13
.6.1
FM
G
Note on
FormularyMupirocin (Bactroban)
NOTE: if unavailable
Chlorhexidine
Hydrochloride 0.1% with
Neomycin Sulphate
0.5% (Naseptin) nasal
cream recommended as
there is no direct
equivalent.
y
Mupirocin nasal ointment unavailable at present.
Recommend Naspetin instead as there is no direct equivalent
Mupirocin nasal ointment unavailable at present.
Recommend Naspetin instead as there is no direct
equivalent 12
.2.3
FM
G S
ep
14
Add Iopamidol 61.24%w/v
(Gastromiro) 20ml, 50ml
and 100ml, oral/rectal
solution
Prescribing by
Radiology team only
red y
Contrast media in use. Restricted to prescribing by Radiology team only
Mis
c
FM
G S
ep
14
Change dose
formMethotrexate 50mg/mL
(7.5mg, 10mg, 12.5mg,
15mg, 17.5mg, 20mg,
22.5mg, 25mg)
(Metoject PEN) injection
pen device
AP y
Metoject (methotrexate) syringe (could be given via IM, IV or
SC injection) was discontinued on 1 July 2014 and has been
replaced with Metoject PEN, a pre-filled, single use injection
device
Restricted - prescribing by Consultant Rheumatologists
and Dermatologists only, in accordance with
Methotrexate for use in Rheumatology, Dermatology,
Gastroenterology and Respiratory Medicine amber
protocol (BHTCG 794FM) for patients on oral
methotrexate, with severe GI side effects despite regular
folic acid (5m, 6 days a week) or non-responders to oral
therapy after an 8-12 week trial, in order to improve
bioavailability.
10
.1.3
FM
G S
ep
14
ADD Acetylcysteine
concentrate for
intravenous infusion,
2g/10mL
Re
d
no
IV use for paracetamol overdose: use via nebulisation as a
mucolytic for ventilated patients at risk of chest sepsis.
(Restricted for use on ITU, Spinal and Respiratory)
Restricted for use:
1. In paracetamol overdose and,
2. On ITU, Spinal and Respiratory wards, via
nebulisation as a mucolytic, for ventilated patients at risk
of chest sepsis
Po
iso
nin
g
FM
G S
ep
14
BHT FORMULARY CHANGE TRACKING DOCUMENT - PROPOSED FORMULARY CHANGES FOR NOTE SEPTEMBER 2014 FMG

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Add
temporarilyKetamine 50mg/5mL
(injection) - unlicensed
red no
Ketamine is already on the formulary and always has been.
The licensed product is not available at present and we are
buying in an Unlicensed injection from Germany. Risk
assessment to be noted on formulary - Low Risk
Unlicensed - Low Risk
NOTE: The licensed product is currently unavailable
Restricted - treated as a CD inthis Trust. Order, store
and record all issues as per a controlled drug.
15
.1.1
FM
G
ADD Sodium Tetradecyl
Sulphate 3% (Fibro-
Vein) 3% STD
Local sclerosant Prescribing by
vascular team only red
In accordance with NICE CG Varicose veins in the legs CG168.
To be prescribed by vascular team
Restricted - prescribing by vascular team only in
accordance with NICE CG168 Varicose veins in the legs. 2.1
3
FM
G
ADD Ferric carboxymaltose
injection (Ferinject) 1g
vial
Iron Deficiency anaemai Haematology team
only
red y
Additional size now available. More cost effective Resticted - prescribing by Haematology team only in
accordance with Parenteral Iron for Iron Deficiency
Anaemia (BHTCG 58) 9.1
.1.2
FM
G
Add Chlorhexidine gluconate
2% in isopropyl alcohol
70% (ChloraPrep with
tint cutaneous solution,
3mL)
red y
Already on formulary without tint. Price difference minimal.
Current restriction to remain (in secondary care restricted to
areas where central venous catheters, mid and PIC lines are
inserted)
In secondary care restricted - to areas where central
venous catheters, mid and PIC lines are inserted
13
.11
.2
FM
G S
ep
14
Add Biotin 5mg tablet Consultant
Paediatricians on
recommendation of
tertiary Paediatric
specialist.
red no
Mitochondrial metabolic disorder in paeds patient on
recommendation of tertiary Paediatrics Specialist. To be
prescribed by consultant Paediatricians; one patient per year
(COST PRESSURE from Nicky T/F)
Unlicensed - Medium Risk
Restricted - to prescribing by Consultant Paediatricians
on the recommendation of tertiary Paediatric specialists
only
9.8
.1
FM
G S
ep
14
Add Ipilimumab
50mg/10mL,
200mg/40mL
(concentrate for
intravenous infusion)
PbR excl - SCG funded
ORH Oncology
consultants only
red
y
NICE TA 319 Previously untreated advanced (unresectable or
metastatic) melanoma.
No use at BHT
This Specialty is entirely based at OUH and all patients with this
condition needing ipilimumab are treated there. 2 patients per
year estimate.
Restricted:
2. Prescribing by Oxford University Hospitals (OUH)
only, in accordance with NICE TA 319 Ipilimumab for
previously UNtreated advanced (unresctable or metstatic
) melanoma.
8.1
.5
FM
G S
ep
14
Add Hydroxycarbamide
100mg tablets
Chemotherapy funded
by SCG
red y
500mg capsules already on formulary. Additional strengths
required.
Restriction wording? Discussed with Maire and decided to leave
without restriction.
8.1
.5
FM
G S
ep
14
Add new dose
formRanibizumab 1.65mg
in 0.165mL PFS
PbR excl - CCG
red y
reduced risk of infection. Vials to remain on formulary. If price
of vials is less than the PFS then the use of the PFS/formulary
inclusion to be re-considered
Restriction as it appears in Formulary for Ranibizumab
2.3mg in 0.23mL intravitreal injection
11
.8.2
FM
G
Add Methylprednisolone
acetate 40mg with
lidocaine hydrochloride
10mg in 1mL
red
y
Has been in use across Trust by physiotherapists for a long
time. Breda discovered not on formulary whilst checking a
PGD. 10
.1.2
FM
G
Added use Midazolam
2.5mg/0.5mL
oromucosal solution,
prefilled syringe.
red Y
Already on formulary for several other clinical situations.
Included in guidelines for use in MRI sedation
Restricted - prescribing only in accordance with
Guidelines for the sedation of children undergoing MRI
or CT scan (BHTCG 343) 15
.1.4
.1
FM
G

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Added use Midazolam 5mg/mL
injection
red y
On formulary but use restricted to anaesthesia and intensive
care sedation and in clinical areas where its use has been
formally risk assessed.
Restricted - use of all 5mg/mL and 2mg/mL strengths is
restricted to anaesthesia and intensive care sedation
and in clinical areas where its use has been formally risk
assessed.
15
.1.4
.1
FM
G
Added use Alimemazine 30mg/5ml
Re
d
y
Included in a guideline for sedation in children.
Paediatrics usage is usually the 30mg/5mL therefore some
concerns re both strengths being used in the Paed
environment. May need further investigation into which is the
best strength to use in this group of patients.
Restricted - prescribing only in accordance with
Guidelines for the sedation of children undergoing MRI
or CT scan (BHTCG 343)
3.4
.1
FM
G S
ep
14
Revise
restrictionCo-trimoxazole oral
suspension
240mg/5mL,
480mg/5mL and tablet
480mg
AR y
Included in Rheumatology guidelines for PCP prophylaxis for
patients who have oral/iv cyclophosphamide.
No chewable/soluble tablets available.
In secondary care restricted - for use in Rheumatology
for PCP prophylaxis for patients receiving oral/iv
cyclophosphamide or for use in Genitourinary Medicine.
Microbiology approval required for all other uses. May
be recommended by secondary care for prescribing by
GPs.
5.1
.8
FM
G S
ep
14
place in
therapyCarvedilol tablets
3.125mg, 6.25mg.
12.5mg, 25mg
gre
en
y
Carvedilol green on formulary but strength of tablets not
included. Also make 2nd line after bisprolol
2nd Choice after bisoprolol
2.4
FM
G
revise License
statusProflavine cream BPC
Re
d
no
Add unlicensed product status
CCG do not want unlicensed version to be used in community.
Is there an alternative?
Unlicensed - Low Risk
Licensed product is presently unavailable. Unlicensed
product not to be prescribed in secondary care. 13
.10
.5
FM
G
Amend entry Proflavine cream BPCgre
en
y
Put note on formulary re manufacturing problems Currently unavailable due to manufacturing delays
13
.10
. 5F
MG
Add Sitagliptin tablets 25mg,
50mg
gre
en
yAdditional strengths to be added to formulary for use in renal
impairment
Restriction - as per formulary entry - no change with the
addition of alternate strength tablets
6.1
.2.3
FM
G
ADD New Poisoning section added to netFormulary. All drugs
mentioned based on College of Emergency Medicine guidelines
which state which drugs should be immediately available in
areas where treatment of poisoning might occur and other
drugs which should be available within an hour (in the hospital
setting) and some rare drugs which are seldom required.
Po
iso
nin
g S
ectio
n
FM
G S
ep
14
Oct
12
.7 Add Erlotinib 25mg,
100mg, 150mg tablet
PBr - SCG
NICE TA 258 Erlotinib first
line treatment of locally
advanced or metastatic
EGFR-TK mutation positive
non-SCLC
Consultant
Oncologists (Lung)
red y
NICE Form approved FOR ALL PRESCRIBING: NICE compliance form
required - see link from Formulary homepage. .....
2. Restricted - prescribing by Consultant Oncologist
(Lung) as 1st line treatment of locally advanced or
metastatic EGFR-TK mutation positive non-SCLC, in
accordance with NICE TA258
8.1
.5
Ju
n-1
4
Poisoning Section - was originally part of the formulary prior to population of
netformulary. The following drugs to be included: acetylcysteine 2g,
activated charcoal suspension 50g/250mL, atropine injection, calcium
folinate injection, calcium chloride injection, calcium gluconate gel 2.5%,
dantrolene injection, desferrioxamine injection, diazepam injection, dicobalt
edetate injection, absolute alcohol injection, flumazenil injection, glucagon
injection, haloperidol injection, isoprenaline injection, lorazepam injection,
FMG DECISIONS JUNE 2014

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
De
c 1
3.8 Add Ciclesonide
80micrograms,
160micrograms per
metered inhalation, 60
and 120 dose units
For treatment of astma for
patients who required an
inhaled steroid, with
unacceptable side effects
(dyphonia, oropharyngeal
candidiasis, cough, throat
irritation and reflex
bronchospasm) caused by
standard and high dose
inhaled corticosteroids
despite thorough post-dose
mouth rinsing, use of
spacer and treatment of
candidiasis.
Initiated by consultant
respiratory physicians
with continuation by
GPs
AI
y
Approved at CGS Restricted - to initiation by Consultant Respiratory
Physicians with continuation by GPs, for patients who
require an inhaled corticosteroid who have unacceptable
side effects (dysphonia, oropharyngeal candidiasis,
cough, throat irritation and reflex bronchospasm) caused
by standard and high dose corticosteroid inhalers
(budesonide, fluticasone or beclometasone) despite
thorough post-dose mouth rinsing, use of a spacer and
treatment of candidiasis, and in accordance with
Ciclesonide Amber Initiation guideline (BHTCG 744FM)
3.2
Ju
n-1
4
Ju
n1
4..
4 revise
restrictionDomperidone
gre
en
y
Add link to MHRA Drug Safety Update May 2014 Restricted - MHRA have advised should only to be
used for nausea and vomiting. It's use is contraindicated
in patients with underlying cardiovascular conditions and
risk factors. Dose and duration have been revised to a
maximum of 10mg three times daily for one week in
adults. For more details see MHRA link below
4.6
Ju
n-1
4
Fe
b 1
4.1
0 Updated TLL
and place in
therapy
Strontium ranelate 6th Choice for secondary
prevention of osteoporosis.
Initiation by
Endocrinologists,
Rheumatologists
AR y
IN accordance with Strontium for Secondary Fracture
Prevention in Osteoporosis (BHTCG 802FM) and Osteoporosis
Secondary Fracture Prevention over 50years (BHTCG 403FM)
6th Choice for Osteoporosis: Secondary fracture
prevention (not recommended for primary prevention)
Restricted - to be prescribed by GPs on the
recommendation of Pheumatology or Endocrinology
teams, in accordance with Osteoporosis: Secondary
fracture prevention over 50 yrs (BHTCG 403FM)(see link
above) and with Strontium for Secondary Fracture
Prevention in OSteoporosis (BHTCG 802FM)
6.6
.2
Ju
n-1
4
Ju
ne
14
.5 Add Sodium benzoate
100mg/mL
50mg, 250mg, 400mg,
500mg capsules,
500mg tablets,
2g/10mL injection
PbR excl - SCG
Treatment of metabolic
disorders after initiation by
tertiary centres in
accordance with NHS
England commissioning of
highly specialised
metabolic disorders
services
Continuaton by
Consultant Paeds
red
N
All unlicensed Unlicensed
Restricted - to initiation by Consultant Paediatricians for
the treatment of metabolic disorders, on the advice of
the teritiary care centre in accordance with NHS
England commissioning of highly specialised metabolic
disorder services.
9.8
.1
Ju
n-1
4
Ju
ne
14
.5 Add Sodium
phenylbutyrate 500mg
tablet, syrup
250mg/mL, Injection
2g/10mL
PbR excl - SCG
Treatment of metabolic
disorders after initiation by
tertiary centres in
accordance with NHS
England commissioning of
highly specialised
metabolic disorders
services
Continuaton by
Consultant Paeds
red
N
&
Y
Tablets are licensed, the rest unlicensed and formulary
annotated accordingly
Unlicensed
Restricted - to initiation by Consultant Paediatricians for
the treatment of metabolic disorders, on the advice of
the teritiary care centre in accordance with NHS
England commissioning of highly specialised metabolic
disorder services.
9.8
.1
Ju
n-1
4

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Ju
ne
14
.5 Add L-arginine 100mg/mL
syrup, 5g/10mL
injection, 500mg tabs
PbR - SCG
Treatment of metabolic
disorders after initiation by
tertiary centres in
accordance with NHS
England commissioning of
highly specialised
metabolic disorders
services
Continuaton by
Consultant Paeds
red N
All unlicensed Unlicensed
Restricted - to initiation by Consultant Paediatricians for
the treatment of metabolic disorders, on the advice of
the teritiary care centre in accordance with NHS
England commissioning of highly specialised metabolic
disorder services.
9.8
.1
Ju
n-1
4
Ju
ne
14
.12 Revise
restriction Colistimethate Sodium
injection 1million units
(Colomycin and generic
brands)
Initiation in secondary
care with continuation
by GPs
AI
Y
For treatment of conditions other than cycstic bibrosis (eg
bronchiectasis). This is an interim decision until the exact place
in therapy is fully established
For uses, other than cystic fibrosis (see separate entry
above), to be initiated in secondary care, with approval
from Microbiology, and continuation by GPs. (Guideline
under development)
5.1
.7
Ju
n-1
4
Ju
ne
14
.2 Add Bortezomib injection
3.5mg
PbR Excl - SCG
In combination with
dexamethasone or
dexamethasone and
thalidomide for induction
treatment of patients with
previously untreated
multiple myeloma in line
with NICE TA 311
Consulant
Haematologists
red y
NICE prescribing statement and compliance form approved FOR ALL PRESCRIBING - NICE compliance form
required - see link from Formulary homepage.
Restricted - prescribing by Consultant Haematologists in
combination with dexamethasone or dexamethasone
and thalidomide for induction treatment of patients with
previously untreated multiple myeloma in accordance
with NICE TA311.
8.1
.5
Ju
l-1
4
Ap
ril 1
4.2 Add Probenecid 500mg
tablet
Treatment chronic gout in
patients with normal renal
function who are intolerant
or have contraindications
to, allopurinol , febuxostat
and benzbromarone. To
be prescribed in in
accordance with Bucks
Management of Gout
guideline
Initiation by
Consultant
Rheumatologists with
continuation by GPs
AI
n
Unlicensed - needs risk assessment Restricted - to initiation by Consultant Rheumatologists
with continuation by GPs for treatment of gout ibn
patients with normal renal function who are intolerant of,
or have contraindications to, allopurinol, febuxostat and
benzbromarone. To be prescribed in accordance with
Management of Gout guideline (upload awaited)
10
.1.4
Ju
l-1
4
Ap
ril 1
4.2 Add Sulphinpyrazone
100mg, 200mg
Treatment chronic gout in
patients with normal renal
function who are intolerant
or have contraindications
to, allopurinol , febuxostat
and benbromarone. To be
prescribed in in
accordance with Bucks
Management of Gout
guideline
Initiation by
Consultant
Rheumatologists with
continuation by GPs
AI
y
Restricted - to initiation by Consultant Rheumatologists
with continuation by GPs for treatment of gout ibn
patients with normal renal function who are intolerant of,
or have contraindications to, allopurinol, febuxostat and
benzbromarone. To be prescribed in accordance with
Management of Gout guideline (upload awaited)
10
.1.4
Ju
l-1
4

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Ap
ril 1
4.1 Add Benzbromarone 50mg,
100mg tablets
Treatment chronic gout in
patients with mild to
moderate renal impairment
who are intolerant or have
contraindications to,
allopurinol and febuxostat.
To be prescribed in in
accordance with Bucks
Management of Gout
guideline.
Consultant
Rheumatologists
red n
Unlicensed Risk Assessment - HIGH risk Unlicensed - High Risk
Restricted - prescribing by Consultant Rheumatologists
for treatment of chronic gout in patients with mild to
moderate renal impairment who are intolerant or have
contraindications to, allopurinol and febuxostat. To be
prescribed in accordance with Management of Gout
guideline (upload awaited)
10
.1.4
Ju
l-1
4
Ju
ne
14
.9 Add Rituximab
100mg/10mL
concentrate for
intravenous infusion
PbR excl - SCG
Treatment of ANCA-
associated vasculitis in
accordance with NICE TA
308
Consultant physicians
with an interest in
vasculitis
red y
Need another NICE link on formulary
FOR ALL PRESCRIBING - NICE compliance form
required - see link from Formulary homepage.
Restricted - prescribing by Consultant Physicians with an
interest in vasculitis for the treatment of ANCA-
associated vasculitis in accordance with NICE TA 308
8.2
.3
Ju
l-1
4
Ju
ne
14
.8 Add Beclometasone
dipropionate/Formoterol
100micrograms/6microg
rams aerosol inhalation
(Fostair)
For the treatment of
COPD. 1st Choice ICS
LABA when an MDI is
appropriate, in accordance
with COPD guideline
gre
en
y
in COPD guideline for sizes Restricted - for the treatment of COPD. 1st Choice
LABA when an MDI is appropriate, in accordance with
COPD Inhaled Treatment algorithm (BHTCG 726FM)
3.2
Ju
l-1
4
Ju
n e
14
.7 Rejected Fluticasone
furoate/Vilatnerol
(Relvar)
For the treatment of
COPD.
bla
ck
y
Rejected for inclusion on formulary due to concerns about the
potential for patient perception of the product as a "reliever"
rather than a "preventer" which could lead to ICS overdose.
Also there is a lack of wider experience with use of both active
ingredients of the product. Increasing concern about links
between fluticasone compared to less potent ICS with
pneumonia. Ju
n-1
4
Ju
ne
14
.3 Add Pixantrone injection
29mg
PbR exclu - SCG
Treatment with multiple
relapsed or refractory
aggressive non-Hodgkins
lymphoma in accordance
with NICE TA 306
Consultant
Haematologists
red y
NICE prescribing statement and compliance form approved FOR ALL PRESCRIBING - NICE compliance form
required - see link from Formulary homepage. 8.1
.2
Ju
l-1
4
Ju
n1
4.1 Add Afatinib 20mg, 30mg,
40mg, 50mg tablet
PbR excluded - SCG
Treatment of adults with
locally advanced or
metastatic non- SCLC if
tests positive for EGFR-TK
mutation. Patient has not
previously had a EGFR-TK
inhibitor in line with NICE
TA 310
Consultant
oncologists (Lung)
red y
NICE prescribing statement and compliance form approved FOR ALL PRESCRIBING - NICE compliance form
required - see link from Formulary homepage.
Restricted - prescribing by Consultant Oncologists
(Lung) only for treatment of adults with locally advanced
or metastatic non-SCLC if tests positive for EGFR-TK
mutation. PAtient has not previously had a EGRF-TK
inhibitor, in line iwth NICE TA310
8.1
.5
Ju
l-1
4
Fe
b
14
.11Add Dapagliflozin tablet
5mg, 10mg
Diabetes treatment in
accordance with Diabetes
Type 2 guideline gre
en
y
For use in accordance with The Management of Type 2
Diabetes: Blood Glucose -lowering therapy -
Primary/Secondary Care guideline (BHTCG 667FM)
6.1
.2
Fe
b-1
4
CCG FORMULARY CHANGE TRACKING DOCUMENT - PROPOSED CHANGES FOR JUNE 2014 FMG
FORMULARY CHANGES FOR NOTE - AGREED June 2014 FMG

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
add Peptac suspension Cheaper alternative to
Gaviscon Advance. GPs
use widely and we have a
switch on their software to
encourage this. It is a 1st
line antacid
gre
en
y
Restricted - only for use in Primary Care - it is a 1st
Choice antacid, for use as a cheaper alternative to
Gaviscon Advance. Patients coming from secondary
care who may have been prescribed Gaviscon Advance
to be switched to Peptac suspension.
1.1
.2
Ju
n-1
4
Add Colistimethate
nebuliser powder
(Promixin®) 1million-
unit vial
Consultant
Paediatricians
red y
Expected patient numbers = 5
Note: Promixin 1MU is therapeuticlaly equivalent to 2MU
standard vials - to be clearly stated on formulary
Cost pressure if 5 patients use Promixin instead of 2megaunits
of Colomycin twice daily: £17,388 - 12,247 = £5141 (( £4.83-
£3.40 ) x2 x30 x12 x5 )
Benefits - improved compliance. Shared device (I-neb) can
also be used for tobramycin.
In use by local specialist centres and paid for by NHS England,
who name it as a funded line in their CF commissioning
statement 2013 (SC)
Restricted - prescribing by Consultant Paediatricians for
the treatment of cystic fibrosis in children in accordance
with "Clinical Commissioning Policy Statement: Inhaled
Therapy for Adults and Children with Cystic Fibrosis April
2013 (see link below)
NOTE: Promixin 1million units is therapeutically
equivalent to 2million units standard colistimethate
sodium (eg Colomycin) ONLY if Promixin is nebulised
via the I-Neb device.
5.1
Ju
n-1
4
Revise
restrictionCiprofloxacin - tablet
(250mg, 500mg),
suspension
(250mg/5mL), iv
infusion 400mg in
glucose 5%,
100mg/50mL,
200mg/100mL,
400mg/200mLg
ree
n (
tab
s&
su
sp
), r
ed
(IV
)
5.
1.
12
Secondary care Gastroenteritis guideline (2011) recommends
using ciprofloxacin first line without consulting micro. The
formulary needs to be altered to reflect this. It was picked up
during recent review of the gastroenteritis guideline (new
guideline yet to be uploaded BHTCG 204) and has been agreed
with David Waghorn, Consultant Microbiologist.
Need to ensure formulary makes clear that use for enteric fever
is within secondary care only.
In secondary care restricted to:-
1. TTO and Outpatient prescriptions,
2. Inpatient urology and respiratory patients where no
other suitable alternative,
3. Use by Ophthalomology and Obstetrics and
Gynaecology,
4. Treatment of enteric fever as described in the hospital
guideline for Antimicrobial Therapy for Infectious
Gastroenteritis (BHTCG 204)
5.1
.12
Ju
n-1
4
Replacement Trichloracetic acid 90% Prescribing by
Specialist Sexual
Health consultants
(GUM and
Contraception)
red N
80% no longer available. GUM staff prefer 90%
Risk assessment to be completed by Rachel
Restricted - use by Specialist Sexual Health consultants
(GUM and Contraception) for the treatment of anogenital
warts only.
13
.7
Ju
n-1
4
Add Taurolidine/Citrate 4%
with Heparin
500units/mL
(Taurolock® Hep 500)
Renal Physicians
Only
red xx
x
FR CAUTION - always double check you have selected the
correct Taurolock® product.
Restricted - prescribing by Renal Physicians Only for
locking haemodialysis and haemofiltration lines
Ju
n-1
4
Add Taurolidine/Citrate 4%
with Urokinase
25,000units/mL
(Taurolock®Urokinase
25,000)
Renal Physicians
Only
red xx
x
FR CAUTION - always double check you have selected the
correct Taurolock® product.
Restricted - prescribing by Renal Physicians Only for
locking haemodialysis and haemofiltration lines
Ju
n-1
4
BHT FORMULARY CHANGE TRACKING DOCUMENT - PROPOSED FORMULARY CHANGES FOR NOTE JUNE 2014 FMG

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Add Creon Micro Gastro
resistant granules 20g
Consultant
Paediatricians
AR
1.
9.
4
For pancreatic enzyme deficiency in infants with cystic fibrosis.
When infants are diagnosed this product needs to be
immediately available. Time is lost following the non-formulary
process for these babies.
Expected numbers = 2
£27.56 (£33.07 incl VAT) every months, x12 = £396.84 per yr
per patients, x2 = £794 for 2 patients per year.
Restricted - to be recommended by Consultant
Paediatricians for the treatment of cystic fibrosis in
infants.
1.9
.4
Ju
n-1
4
Delete Metformin 500mg
sachets
discontinued
bla
ck
6.
1.
2.
2
Discontinued product
Agre
ed
Ju
n-1
4
Delete Metformin 1000mg
sachets
to be discontinued. To
remain on formulary until
no longer available. Added
syrup as replacement
6.
1.
2.
2
To be discontinued but to remain on formulary until no
longer available
Agre
ed
Ju
n-1
4
Add Metformin Oral solution
500mg/5mL, sugar free
sachets discontinued
gre
en
y
Restricted - to patients who cannot swallow metformin
hydrochloride tablets.
Agre
ed
Ju
n-1
4
Delete Chlorhexidine
acetate1% dusting
powder Bla
ck
long term supply problems. Dr Waghorn has advised
colleagues to stop requesting on prescription and is not
concerned about sourcing an alternative. They will stick with
standard MRSA suppression kits.
Non-formulary - due to ongoing supply problems
13
.11
.2
Ju
n-1
4

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Add Fomepizole injection
red
y
The College of Emergency Medicine and Toxbase recommend
this over absolute alcohol (updated recommendation Dec 13).
Four patients treated for this type of poisoning in last FY with
absolute alcohol. Absolute alcohol unavailable indefinitely.
Predict four patients to be treated with fomepizole in 14-15 at a
cost of £5013 per patient. This is PbR excluded funded by
CCGs. Included in horizon scanning / budget setting for 14-15
with Bucks CCGs.
HCD compliance form will be needed
For emergency treatment of ethylene glycol and
methanol poisoning in accordance with National
Poisoning Information Centre (Toxbase)
recommendations.
FOR ALL PRESCRIBING - completion of Compliance
form required. If Compliance form not yet available
confimation that National Poisoning Information Centre
recommendations are met, is required.
Ag
ree
d t
o a
dd
to
fo
rmu
lary
su
bje
ct
to t
he
de
ve
lop
me
nt
an
d a
pp
rova
l o
f a
Co
mp
lian
ce
Fo
rm o
r so
me
oth
er
ag
ree
d m
ea
ns o
f ca
ptu
rin
g a
nd
en
su
rin
g c
om
plia
nce
with
Na
tio
na
l
Ju
n-1
4
Clarify
guidance for
use
Digoxin specific
antibody fragments
40mg
red
y
CCG now responsible for payments, urgently need a NICE
compliance form, or some agreed way of ensuring appropriate
usage.
If used in accordance with National Poisoning
Information Centre (Toxbase) recommendations. FOR
ALL PRESCRIBING - completion of Compliance form
required. If Compliance form not yet available
confimation that National Poisoning Information Centre
recommendations are met, is required.
2.1
.1
Ju
n-1
4
Revise
restrictionMiragbegron and
Solifenacin for OAB
Spinal Consultants
may initiate for OAB
AI
y
Spinal consultants also initiate treatment of OAB and need to
be included in the restriction for initiation of miragbegron and
solifenacin. Use of solifenacin and mirabegron by Spinal
consultants currently being agreed via NF approval process in
BHT
Both presently have restriction which says: "Restricted -
initiation by Consultant Urogynaecologists and Consultant
Urologists…."
The new restriction would also include Spinal Consultants.
LInk to new guideline
Restricted - to initiation by Urologists, Uro-
gynaecologists and Spinal Consultants only, with
continuation by GPs…….
7.4
.2
Ju
n-1
4

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Add Gelatin - Gelaspan change brand from
Gelofusin to Gelaspan red y 9.3
#####
Delete Dexamethasone 4mg/ml
injection
Supply problems ongoing
bla
ck
y
Not available at present due to ongoing supply problems.
See Dexamethasone injection 3.3mg/mL entry above
and note important dosing information
6.3
.2
Ju
n-1
4
Add Dexamethasone
3.3mg/ml injection
ON contract. Savings to be
made and 4mg/ml very
difficult to assure
regularsupply
£3.75/10 (excl VAT)
£9.90/5 (excl VAT) PASA
contract
gre
en
y
There are several preparations of intravenous
dexamethasone available in different concentrations.
Check carefully that the preparation administered
provides the prescribed dose.
Dexamethasone injection 4mg/mL is currently
unavailable.
Dexamethasone injection 3.3mg/mL is available
Most prescriptions for dexamthasone injection will be
4mg (or a multiple of). So please follow one of the
options below:
1. The patient can be converted to 3.3mg (of multiples
of, as appropriate) - doctors will need to rewrite the
prescription so that this dose can be given OR
2. Use 1.2mL of dexamethasone injection 3.3mg/mL
(approximately equal to 4mg dexamethasone injection)
6.3
.2
Ju
n-1
4
Delete Domperidone suppositories 30mgNo longer available
bla
ck y no longer available
4.6
#####
Ap
r 1
4.4 Add Aflibercept 4mg/0.1mL
solution for
intravitreal injection
PBT excl CCG
For Central Retinal Vein
Occlusion NICE TA 305
Consultant
Ophthalmologists
Re
d
Y
2nd line option to Ranibizumab
HCD drug form approved
FOR ALL PRESCRIBING - NICE compliance form
required - see link from Formulary homepage.
Restricted - to prescribing by Consultant
Ophthalmologists, as a 2nd line option after ranibizumab,
for Central Retinal Vein Occlusion in accordance with
NICE TA 305.
11
.8.2
Ju
n-1
4
Ap
r 1
4.9 Additional
adviceJext and Epipen, adult
and junior strengths
gre
en
y
Additional advice: ensure that training is given to all patients,
for all prescriptions for Jext and Epipen, irrespective of whether
patients have received or used the product previously - added
to all 4 entries on formulary
NOTE: Ensure that training is given to all patients, for all
prescriptions, irrespective of whether patients have
received or used the product previously.
3.4
.3
Apr-
14
Ap
r 1
4.7 Add Aclidinium inhaler
400micrograms/metered
inhalation
Treatment of COPD in
adults
In secondary care to
be initiated by
Respiratory team only
gre
en
y
2nd line to tiotropium in patients for whom tiotropium is
unsuitable due to intolerance or contraindications
1st line LAMA in renal impairment.
IN secondary care to be initiated by Respiratory team in
accordance with COPD Inhaled Treatment algorithmin BHTCG
726FM - updated version approved CGS May14 awaiting APC
July 16th
Restricted - to be prescribed in accordance with COPD
Inhaled Treatment algorithm (BHTCG 726FM)(see link
above) as:
1. To be prescribed 2nd line to tiotropium in patients for
whom tiotropium is unsuitable due to intolerance or
contraindications or,
2. 1st line LAMA in renal impairment.
In secondary care to be initiated by the Respiratory team
only.
3.1
2.
Apr-
14
FMG DECISIONS APRIL 2014

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Fe
b 1
4.2 TLL Revision
and Restriction
revisions
Rivaroxaban Treatment of DVT and PE Initiation by
Consultant
Haematologistsand
NOAC (not cardiology
or stroke team)
AI
Y
NICE HCD approved
Await upload. Approved at CGS (JUNE 14) but waiting for APC
(July 16th)
FOR ALL PRESCRIBING - NICE compliance form
required - see link from Formulary homepage.
1. Restricted - initiation by Consultant Haematologists or
NOAC Pharmacy service for patients unsuitable for
warfarin for whom dalteparin would otherwise be
considered and only in accordance with;
NICE TA 261 Rivaroxaban for the treatment of deep vein
thrombosis and prevention of recurrent DVT and PE and
NICE TA 287 Pulmonary embolism and recurrent venous
thromboembolism - rivaroxaban,
and in accordance with Rivaroxaban for DVT and PE -
Amber initiation guideline (BHTCG 295FM)
2.8
.2
Ju
l-1
4
Fe
b 1
4.3 Revised TLL Apixaban Prevention stroke in AF same as dabi and
riva
AI
Y
NICE HCD approved - same wording as for dabi and riva
guideline for dabi and riva, sep guidelines for AF need to be
replace with combined guideline which lists 3 drugs and this
was approved at CGS
Dabi for AF and Riva for AF guidelines to be removed and
replaced by Riva, Dabi and Apixa for AF once approved at
APC. CGS approved.
NOTE: Any urgent patient without a previous stroke or
TIA but with a CHA2DS2VASc of 6 or more should be
referred to the NOAC Service for an urgent initial
appointment.
Restricted - to initiation by:
1. Consultant Stroke physicians for urgent patients who
have had a previous stroke or TIA. All patients initiated
by consultants to be subsequently referred to NOAC
clinic for follow-up
2. NOAC Service
for the prevention of stroke and systemic embolism in
patients with AF when a NOAC is indicated, in
accordance with Dabigatran, Rivaroxaban and Apixaban
for Atrial Fibrillation - Amber Initiation guideline (BHTCG
313FM) and the patient has had a GI disturbance or
bleeding with dabigatran and rivaroxaban OR the patient
is unable to take either dabigatran or rivaroxaban due to
a history of GI bleeding or ulceration and in accordance
with NICE TA275 Apixaban for preventing stroke and
systemic embolism in people with nonvalvular atrial
fibrillation.
2.8
.2
Ju
l-1
4
Rejected Domperidone For increased milk supply Breastfeeding
Service only
AI
In light of the MHRA Drug Safety Update, the use of
domperidone should be restricted to one week due to potential
adverse effects and therefore Obs & Gynae have requested it
be removed from the formulary for enhanced breast milk
production. Ju
n-1
4
Fe
b 1
4.8 Add Chapter 25 Borderline
substances (Sip Feeds
and Fluid Thickeners)
• Chapter 25 Borderline substances (sip feeds and fluid
thickeners) as described in the draft Bucks formulary (date of
access April 9th 2014) was approved.
,
Ch
ap
ter
25
FM
G A
pril

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Fe
b 1
4.8 Add Ames Shake • Ames Shake® was approved for inclusion on the formulary
for use in primary care. It replaces Complan Shake as first
choice prescribed sip feed when evidence of malnutrition has
been established and the ‘food first’ approach alone has proven
to be inadequate
CCG to manage formulary entries in Chapter 25
Ch
ap
ter
25
FM
G A
pril 1
4
De
c 1
3.3 Add Ranibizumab
2.3mg/0.23mL
intravitreal injection
PbR - CCG
For treatment of visual
impairment due to
choroidal
neovascularisation (CNV)
secondary to pathologic
myopia, NICE TA 298
Consultant
Ophthalmologists
red
y
NICE HCD approved FOR ALL PRESCRIBING: NICE compliance form
required - see link from Formulary homepage.
Restricted - prescribing by Consultant Ophthalmologists
only for the treatment of visual impairment due to
choroidal neovascularisation (CNV) secondary to
pathologic myopia in accordance with NICE TA298.
11
.8.2
Ma
y-1
4
Add Teriflunomide 40mg
tablet
PBR excl SCG
NICE TA 303
Teriflunomide for treating
Relapsing-remitting
Multiple Sclerosis.
Consultant
Neurologist and
Clinical Nurse
Specialist
Re
d
Y
NICE HCD form approved at CGS May14 FOR ALL PRESCRIBING - NICE compliance form
required - see link from Formulary homepage.
Restricted - prescribing by Consultant Neurologists and
Clinical Nurse Specialists for Relapsing-remitting
Multiple Sclerosis in accordance with NICE TA 303
Teriflunomide for treating Relapsing-remitting Multiple
Sclerosis in accordance with NICE TA 303 Teriflunomide
for treating Relapsing-remitting Multiple Sclerosis
8.2
.4
CG
S M
Ay1
4
Ap
r 1
4.8 Revise Choice Sodium cromoglicate
2% eye drops
gre
en
y
Agreed 1st Choice 1st Choice
In primary care consider if more suitable for patients to
purchase over the counter. 11
.4.2
FM
G A
pril
Ap
r 1
4.8 Revise Choice Olopatadine 1mg/mL
eye drops
gre
en
y
Historic "choice" related only to use within secondary care and
did not accurately reflect across joint formulary
11
.4.2
FM
G A
pril
Ap
r 1
4.8 Revise Choice Lodoxamide 0.1% eye
drops
gre
en
y
Historic "choice" related only to use within secondary care and
did not accurately reflect across joint formulary
11
.4.2
FM
G A
pril
Ap
r 1
4.8 Revise Choice Emedastine 0.05% eye
drops
gre
en
y
Historic "choice" related only to use within secondary care and
did not accurately reflect across joint formulary
11
.4.2
FM
G A
pril
Apr
14
.8Add Fenofibrate 200mg
capsule
gre
en
y
Addition of cheaper product in this class of medicines.
Agreed as 1st Choice with Bezafibrate now 2nd Choice.
Lipid guideline to be reviewed and updated Oct 14 approx.
1st Choice
2.1
2
FM
G
Ap
r 1
4.8 Add Resource Thicken-Up
Clear
Restricted Use. Only for patients who have diagnosed
dysphagia and have been advised by SALT to thicken fluids (to
reduce risk of aspiration). More cost effective that Thick and
Easy. Already in use and recommended by SALT and hospital
and community dieticians.
CCG to manage formulary entries in Chapter 26 25
FM
G A
pril
FORMULARY TRACKING DOCUMENT- CHANGES FOR NOTE (including Woundcare Formulary)- AGREED APRIL 2014 FMG

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Ap
r 1
4.8 Add Alendronic acid oral
solution 70mg/100mL,
sugar-free
gre
en
y
Restricted - only for use in patients who cannot swallow
alendronic acid tablets. 6.6
.2
FM
G A
pril
Ap
r 1
4.8 revise
restrictionAlimemazine
suspension 30mg/5mL
Recommendation by
Paediatric or
Haematology teams
and continuation by
GPs
AR y
Restricted - recommendation by Paediatric or
Haematology teams with continuation by GPs 3.4
.1
FM
G A
pril
Apr
14
.8revise
restrictionAlimemazine
suspension 7.5mg/5mL
Recommendation by
Spinal team and
continuation by GPs
AR y
Restricted - recommendation by Spinal team with
continuation by GPs 3.4
.1
FM
G
Ap
r 1
4.8 revise
restrictionPeg-asparaginase
3750units injection
PbR excl - SCG
Haematology
Consultants
red
N
The UKALL 2003 trial is still ongoing, for one patient in the
Trust. The trial is for children and young adults. It is closed to
new patients and expected to conclude June 2014.
Although patients have their chemotherapy treatment in
Oxford, some of the follow-up treatment, such as peg-
asparaginase, may be given at BHT. The UKALL 2011 trial (2
year trial)is ongoing and were patients to receive treatment at
BHT it would be under the supervision of Consultant
Haematologists.
Unlicensed - High Risk
Restricted - use by Haematology Consultants for
Treatment of Childhood ALL in MRC UK ALL 2003 and
2001 trials (inpatients only). Named patient basis.
8.1
.5
FM
G A
pril 1
4
Ap
r 1
4.8 Add Botulinum toxin type
A (Dysport) 500units
vial
PbR excl - CCG
10 patients per year
PBr excluded, CCG funded
Paediatric consultant
red Y
Previously patients were seen at Oxford but are now seen at
SMH every 3 months. It is used for relieving spasticity in
cerebral palsy patients.
3. Restricted - prescribing by Paediatric consultant (Jo
Hicks) only. For cerebral palsy spacticity. 4.9
.3
FM
G A
pril
Ap
r 1
4.8 Rename GUM Ulipristal Acetate 30mg
tablet (EllaOne)
Prevention of pregnancy
after unprotected
intercourse when patients
present at more than 72
hours and less than 120
hours and an IUD is not a
suitable option.
A&E, Specialist
Sexual Health
consultants (GUM
and Contraception),
GPs gre
en
y
GUM consultans and Family Planning Clinics to be replaced by
Specialist Sexual Health consultants (GUM and Contraception)
Restricted - prescribing in secondary care by A&E and
Specialist Sexual Health consultants (GUM and
Contraception) and by GPs and Family Planning Clinics,
for the prevention of pregnancy after unprotected
intercourse when patients present at more than 72 hours
and less than 120 hours and an IUD is not a suitable
option.
7.3
.5
FM
G A
pril 1
4
Ap
r 1
4.8 Add Calcium carbonate 1.5g
and colecalciferol
10micrograms (Adcal-
D3 Dissolve)
effervescent tablet
For use in hospital in
patients who required
calcium and vitamin D
administration via a PEG. red Y
Additional NOTE: For patients discharged from secondary care
on Adcal-D3 effervescent tablets, a switch to Calfovit powder is
recommended.
Restricted - only for use in secondary care for patients
who require calcium and colecalciferol administration via
a PEG
NOTE: For patients discharged from secondary care on
Adcal-D3 Dissolve effervescent tablets a switch to
Calfovit powder is recommended.
9.6
.4
FM
G A
pril 1
4
Ap
r 1
4.8 Add Calcium phosphate
3.1g and colecalciferol
20micrograms (Calfovit
D3) Powder gre
en
Y
Calfovit is in use in primary care Restricted - for use in primary care only.
NOTE: if patients are discharged from secondary care
on Adcal-D3 Dissolve effervescent tablets a switch to
Calfovit D3 powder is recommended
9.6
.4
FM
G A
pril

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Ap
r 1
4.8 Revise
restrictionFludroxycortide 4
micrograms/cm2
(Haelan tape)
Restriction revised and
agreed by Woundcare
Formulary subgroup
gre
en
Y
NOT TO BE USED FOR COSMETIC ONLY USE
Restricted - only for use in the following:
1. Wound care - only to be used for over granulation
tissued on wounds/ulcers for 5 days and then review.
2. Eczema - for skin cracks/fissures in areas difficult to
treat with conventional methods eg. hands and feet
3. Painful keloid scars
13
.4
FM
G A
pril 1
4
Ap
r 1
4.8 Delete Olanzepine injection
10mg/2mL
red Y
No longer available no longer available
FM
G A
pril
Ap
r 1
4.8 Add Sodium amidotrizoate /
Meglumine
amidotrizoate
100mg/660mg in 1mL
(Gastrografin),
gastroenteral solution
Radiology use only
red Y
In use in radiology. Restricted - to use by Radiology team only
16
.01
FM
G A
pril 1
4
Apr
14
.8Add Pyrimethamine 25mg
tablet
Treatment of
toxoplasmosis in uveitis
guideline BHTCG 374
Consultant
Ophthalmologists
red Y
Restricted - prescribing by Consultant Ophthalmologists
for the treatment of tocoplasmosis in accordance with
Uveitis guidelines (BHTCG 374)
5.4
.7
Ap
r 1
4.8 New Entry Colistimethate injection
1,000,000units
Consultant
Paediatricians,
Respiratory
Physicians and
Consultant
MicrobiologistsR
ed
y
Colistimethate is available on the formulary. The existing
restriction is under revision. For cystic fibrosis patients only
agree the inclusion of Colomycin brand injection, licensed for
nebulisation.
Antimicrobial pharmacists recommend Colomycin brand be
stocked and named on formulary as it is licensed for
nebulisation. The generic injection is not licensed for this use.
Promixin injection is not licensed for nebulisation because
Promixin powder for nebulisation is available
Restricted - prescribing by Respiratory Physicians,
Consultant Paediatricians and Consultant Microbiologists
for use in cystic fibrosis only.
NOTE: Colomycin® injection is licensed for nebulisation
and may be given by inhalation as a nebulised solution
as an adjunct to standard antibacterial therapy in cystic
fibrosis patients with severe pseudomonal chest
infections.
5.1
.7
Ap
r 1
4.8 Add Actifast bandage
10.75cm, 7.5cm and
5cm - all 10metre
lengths
red
In use across Trust. All 10m lengths restricted and only
available in secondary care.
10.75cm, 7.5cm and 5cm x 10m lengths only available in
secondary care.
In primary care 1m and 5m lengths available as stock
through the On-line Non-Prescription Orderin System
(ONPOS)
A5
.8.3
Apr
14
.8Delete Chlorhexidine aqueous
solution 0.5% (blue)
No longer available therefore removed from formulary
13
.11
.2
Ap
r 1
4.8 Revise
Restriction Sudocrem Restrict for use on intact
skin only.
Not for use on incontinent
patients - consider Cavilon
Durable Barrier cream and
Honey as an alternative
gre
en
y
Woundcare formulary committee have considered and revised
restriction
Restricted for use on intact skin only
NOTE: Not for use on incontinent patients - consider
Cavilon Durable Barrier cream + Honey as an alternative
for incontinent patients.
13
.2.2
FMG DECISIONS FEBRUARY 2014

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Fe
b 1
4.1 Add Eltrombopag tablet
25mg, 50mg
PbR excl - CCG
Chronic IPT in accordance
with NICE TA 293
Consultant
Haematologists only
red Y
NICE compliance form is complete FOR ALL PRESCRIBING - NICE compliance form
required - see link from Formulary homepage.
Restricted - to prescribing by Consultant Haematologists
only for Chronic Idiopathic Thrombocytopenic purpura
(ITP) in accordance with NICE TA 293
Thrombocytopenic purpura - Eltrombopag.
9.1
.4
FM
G F
eb
14
Fe
b 1
4.5 Delete Omacor Post MI no longer
recommended by NICE CG
172 MI Secondary
prevention published 2013 bla
ck
To be removed from Formulary as no longer recommended by
NICE.
This was restricted to adjuvant treatment in secondary
prevention after myocardial infarction in addition to other
standard therapy in accordance with NICE clinical guideline NO.
48
2.1
2
FM
G F
eb
14
Fe
b 1
4.7 Add Oxycodone
Hydrochloride MR tablet
5mg, 10mg, 20mg
Oxycodone
Hydrochloride Oral
Solution 5mg/5mL
For pain management in
enhanced recovery for hip
and knee arthroplasty and
colorectal surgical patients
Initiation by
Anesthetics team and
continuation by Pain
team and Ward
Surgical and
Orthopaedia doctors
red Y
Unless patients are admitted on oxycodone, the TTOS should
not include it unless countersigned by a Consultant
Anaethetist.
Oxycodone liquid and tabs use as second line when morphine
is unsuitable (green)
Red as first line analgesia in enhanced recovery for stated
conditions.
Restricted - to initiation by Anaesthetics team and
continuation by the Pain team and ward surgical and
othopaedic doctors for pain management in enhanced
recovery for hip and knee arthroplasty and colorectal
surgical patients.
NOTE: unless patients are admitted on oxycodone, the
TTOs should not include it unless countersigned by a
Consultant Anaesthetist.
4.7
.2
FM
G F
eb
14
De
c1
3.1 Add Fluocinolone
Acetonide intravitreal
implant
190micrograms
PbR excl - CCG
chronic diabetic macular
oedema
Consultant
Ophthalmologists
red Y
in accordance with NICE TA 301
Plus NICE statement for approved form
http://guidance.nice.org.uk/TA301
FOR ALL PRESCRIBING - NICE compliance form
required - see link from Formulary homepage.
Restricted - prescribing by Consultant Ophthalmologists
in accordance with NICE TA 301 Fluocinolone acetonide
intravitreal implant for treating chronic diabetic macular
oedema after an inadequate response to prior therapy.
11
.4.1
FM
G F
eb
14
De
c 1
3.2 Add Ocriplasmin intravitreal
injection 0.5mg in
0.2mL
treatment of vitromacular
traction (VMT)
Consultant
Ophthalmologists
red Y
in accordance with NICE TA 297
plus NICE statement for approved form
http://guidance.nice.org.uk/TA297
FOR ALL PRESCRIBING - NICE compliance form
required - see link from Formulary homepage.
Restricted - prescribing by Consultant Ophthalmologists
in accordance with NICE TA 297 Vitreomacular traction -
ocriplasmin
11
.99
FM
G F
eb
14
De
c 1
3.6 Add Fluticasone
Propionate/Formoterol
Fumarate (Flutiform)
50micrograms/5microgr
ams,
125micrograms/5microg
rams,
250micrograms/10micro
grams
for treatment of asthma.
gre
en
Y
For patients who required ICS /LABA combination MDI in
accordance with Joint Asthma in Adults guideline awaited
upload
To be used in accordance with Joint Asthma in Adults
guideline (upload awaited) for patients who require
ICS/LABA combination MDI.
3.2
FM
G F
eb
14
De
c
13
.6reject Fostair for treatment of asthma.
bla
ck
Y
The lack of three strengths does not allow clear monitoring that
doses have been stepped down.
FM
G

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
De
c 1
3.7
Add Asthma guideline Note to "see link above: Asthma - Inhaled Treatment Algorithm -
Adults (BHTCG 803FM)" added to all drugs mentioned in
guideline
FM
G
De
c 1
3.1
1 Add Glaucoma prescribing
guideline
Glaucoma prescribing guideline added to netformulary by
CCGs
FM
G
Dec
13.
12
Add Insulin Degludec 100units/mL
Tresiba, 3ml cartridge, 3mL
FlexTouch prefilled
disposable injection device.
Type I Diabetes when nocturnal
hypoglycaemia is a problem in
spite of treatment with isophane
insulin
Consultant Diabetologists
and continuation by GPs
AI
Y
Restricted - initiation by Consultant Diabetologists with continuation by
GPs for the treatment of Type I diabetes in patients with problematic
nocturnal hypoglycaemia who are unable to achieve adequate blood
glucose control. This is inspite of treatment with basal insulin
analogue therapy, with insulin glargine, which has been optimised in
terms of insulin delivery, dosage and timing.
FM
G F
eb
14
Oct
13
.3
revised
guidelineDrug Treatment for
Urinary Incontinence
Revised guideline uploaded
FM
G
Ma
y 1
3.4
Add Aprepitant capsule
80mg, 125mg
PbR excl - SCG
Chemotherapy induced
nausea and vomiting for
patients on highly
emetogenic regimens (FEC
100 or Cisplatin
>70mg/m2) only in
accordance with the TVCN
CINV guidelines
Consultant
Oncologists
red Y
Restricted - prescribing by Consultant Oncologists for
chemotherapy induced nausea and vomiting to patients
on highly emetogenic regimens (FEC 100 or Cisplatin
>70mg/m2) only, in accordance with TVCN CINV guidelines
4.6
FM
G F
eb
14
Ma
r 1
1.2 Revise
restrictionMelatonin 3mg
immediate release
tablet
Paediatric team
red
N
Unlicensed - Low Risk
1. Restricted - prescribing by Paediatrics team only for
Pre-EEG sedation.
2. Restricted - prescribing by Consultant Paediatricians
only, for induction of normal sleep pattern in ADHD and
neuro-developmental paediatric patients.
4.1
.1
FM
G F
eb
14
Au
g 1
0.2 Add Lidocaine plaster 5%
(700mg/medicated
plaster)
Neuropathic pain in the
palliative care setting only
Initiation by Palliative
Care Team only and
continuation by GPS AI
Y
in accordance with Neuropathic Pain in Palliative Care guideline
BHTCG
Restricted - to initiation by Palliative Care team only with
continuation by GPs, in accordance with the Neuropathic
Pain in Palliative Care in Adults (BHTCG 275FM)
15
.2
FM
G
Fe
b-1
4 Delete Otosporin ear drops
Y
product discontinued -remove
Alternatives include Betnesol N, Otomize and Otocomb Otic
(unlicensed). MI have contacted Mr Bottrill and he is happy
with the alternatives. So MI have not investigated the
availability of any unlicensed versions of Otosporin.
Add comment to formulary in the non-formulary part
giving alternatives: Betnesol N and Otomize or Otocomb
Otic 12
.1.2
FM
G F
eb
14
##### Delete Clinitest
Yproduct discontinued -remove
6.1
.6
FM
G
FORMULARY CHANGES FOR NOTE - AGREED FEBRUARY 2014 FMG
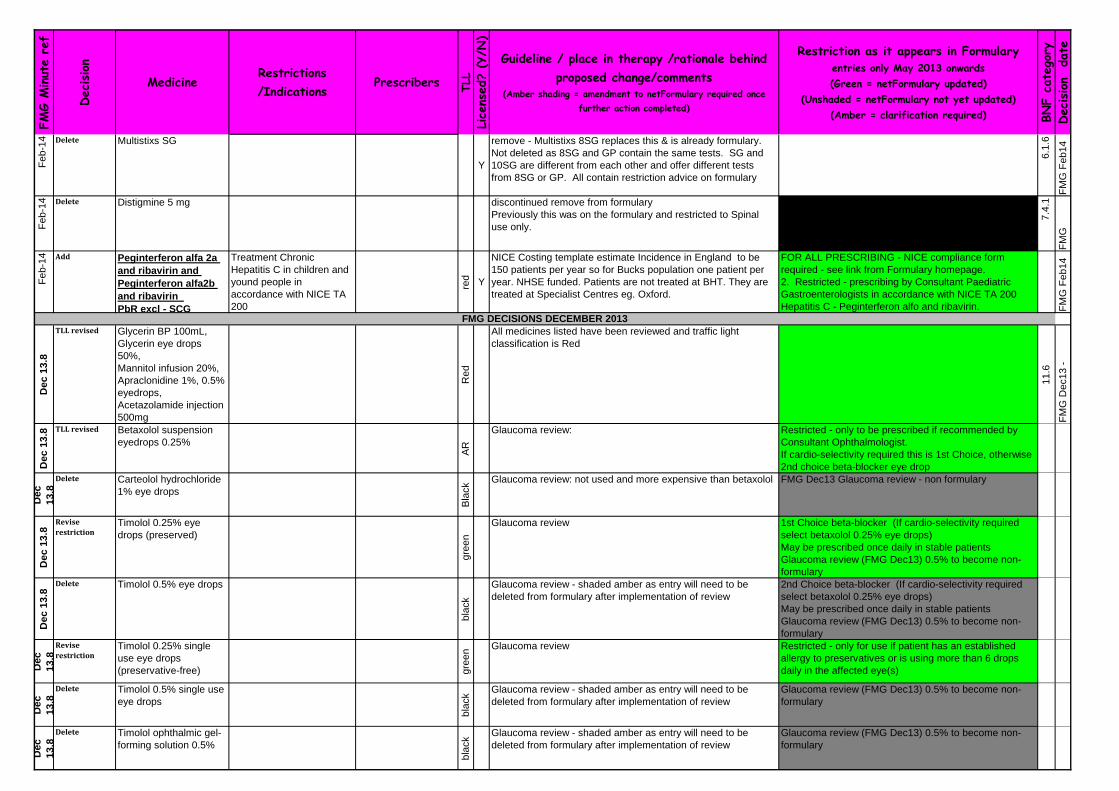
FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Fe
b-1
4 Delete Multistixs SG
Y
remove - Multistixs 8SG replaces this & is already formulary.
Not deleted as 8SG and GP contain the same tests. SG and
10SG are different from each other and offer different tests
from 8SG or GP. All contain restriction advice on formulary
6.1
.6
FM
G F
eb
14
Fe
b-1
4 Delete Distigmine 5 mg discontinued remove from formulary
Previously this was on the formulary and restricted to Spinal
use only.
7.4
.1
FM
G
Fe
b-1
4 Add Peginterferon alfa 2a
and ribavirin and
Peginterferon alfa2b
and ribavirin
PbR excl - SCG
Treatment Chronic
Hepatitis C in children and
yound people in
accordance with NICE TA
200
red Y
NICE Costing template estimate Incidence in England to be
150 patients per year so for Bucks population one patient per
year. NHSE funded. Patients are not treated at BHT. They are
treated at Specialist Centres eg. Oxford.
FOR ALL PRESCRIBING - NICE compliance form
required - see link from Formulary homepage.
2. Restricted - prescribing by Consultant Paediatric
Gastroenterologists in accordance with NICE TA 200
Hepatitis C - Peginterferon alfo and ribavirin. FM
G F
eb
14
De
c 1
3.8
TLL revised Glycerin BP 100mL,
Glycerin eye drops
50%,
Mannitol infusion 20%,
Apraclonidine 1%, 0.5%
eyedrops,
Acetazolamide injection
500mg
Re
d
All medicines listed have been reviewed and traffic light
classification is Red
11
.6
FM
G D
ec1
3 -
De
c 1
3.8 TLL revised Betaxolol suspension
eyedrops 0.25%
AR
Glaucoma review: Restricted - only to be prescribed if recommended by
Consultant Ophthalmologist.
If cardio-selectivity required this is 1st Choice, otherwise
2nd choice beta-blocker eye drop
De
c
13
.8
Delete Carteolol hydrochloride
1% eye drops
Bla
ck
Glaucoma review: not used and more expensive than betaxolol FMG Dec13 Glaucoma review - non formulary
De
c 1
3.8
Revise
restrictionTimolol 0.25% eye
drops (preserved)
gre
en
Glaucoma review 1st Choice beta-blocker (If cardio-selectivity required
select betaxolol 0.25% eye drops)
May be prescribed once daily in stable patients
Glaucoma review (FMG Dec13) 0.5% to become non-
formulary
De
c 1
3.8
Delete Timolol 0.5% eye drops
bla
ck
Glaucoma review - shaded amber as entry will need to be
deleted from formulary after implementation of review
2nd Choice beta-blocker (If cardio-selectivity required
select betaxolol 0.25% eye drops)
May be prescribed once daily in stable patients
Glaucoma review (FMG Dec13) 0.5% to become non-
formulary
De
c
13
.8
Revise
restrictionTimolol 0.25% single
use eye drops
(preservative-free) gre
en
Glaucoma review Restricted - only for use if patient has an established
allergy to preservatives or is using more than 6 drops
daily in the affected eye(s)
De
c
13
.8
Delete Timolol 0.5% single use
eye drops
bla
ck
Glaucoma review - shaded amber as entry will need to be
deleted from formulary after implementation of review
Glaucoma review (FMG Dec13) 0.5% to become non-
formulary
De
c
13
.8
Delete Timolol ophthalmic gel-
forming solution 0.5%
bla
ck
Glaucoma review - shaded amber as entry will need to be
deleted from formulary after implementation of review
Glaucoma review (FMG Dec13) 0.5% to become non-
formulary
FMG DECISIONS DECEMBER 2013
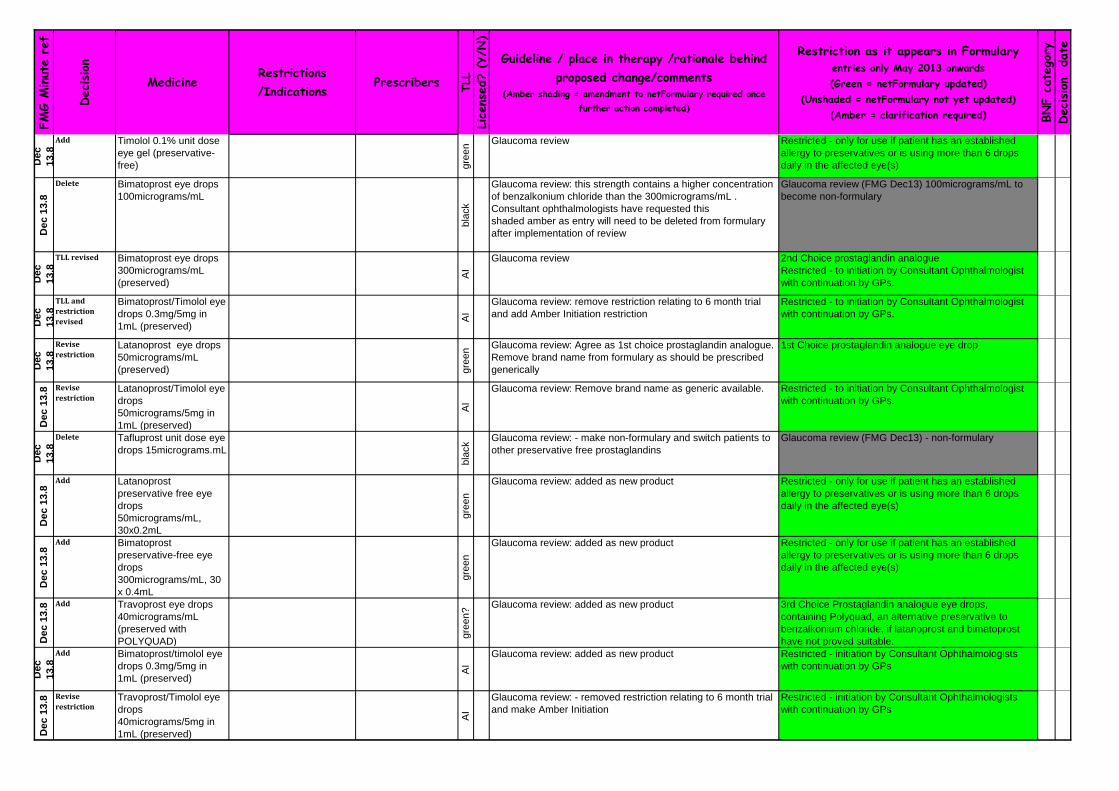
FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
De
c
13
.8
Add Timolol 0.1% unit dose
eye gel (preservative-
free) gre
en
Glaucoma review Restricted - only for use if patient has an established
allergy to preservatives or is using more than 6 drops
daily in the affected eye(s)
De
c 1
3.8
Delete Bimatoprost eye drops
100micrograms/mL
bla
ck
Glaucoma review: this strength contains a higher concentration
of benzalkonium chloride than the 300micrograms/mL .
Consultant ophthalmologists have requested this
shaded amber as entry will need to be deleted from formulary
after implementation of review
Glaucoma review (FMG Dec13) 100micrograms/mL to
become non-formulary
De
c
13
.8
TLL revised Bimatoprost eye drops
300micrograms/mL
(preserved)
AI
Glaucoma review 2nd Choice prostaglandin analogue
Restricted - to initiation by Consultant Ophthalmologist
with continuation by GPs.
De
c
13
.8
TLL and
restriction
revised
Bimatoprost/Timolol eye
drops 0.3mg/5mg in
1mL (preserved)
AI
Glaucoma review: remove restriction relating to 6 month trial
and add Amber Initiation restriction
Restricted - to initiation by Consultant Ophthalmologist
with continuation by GPs.
De
c
13
.8
Revise
restrictionLatanoprost eye drops
50micrograms/mL
(preserved) gre
en
Glaucoma review: Agree as 1st choice prostaglandin analogue.
Remove brand name from formulary as should be prescribed
generically
1st Choice prostaglandin analogue eye drop
De
c 1
3.8 Revise
restrictionLatanoprost/Timolol eye
drops
50micrograms/5mg in
1mL (preserved)
AI
Glaucoma review: Remove brand name as generic available. Restricted - to initiation by Consultant Ophthalmologist
with continuation by GPs.
De
c
13
.8
Delete Tafluprost unit dose eye
drops 15micrograms.mL
bla
ck
Glaucoma review: - make non-formulary and switch patients to
other preservative free prostaglandins
Glaucoma review (FMG Dec13) - non-formulary
De
c 1
3.8
Add Latanoprost
preservative free eye
drops
50micrograms/mL,
30x0.2mL
gre
en
Glaucoma review: added as new product Restricted - only for use if patient has an established
allergy to preservatives or is using more than 6 drops
daily in the affected eye(s)
De
c 1
3.8
Add Bimatoprost
preservative-free eye
drops
300micrograms/mL, 30
x 0.4mL
gre
en
Glaucoma review: added as new product Restricted - only for use if patient has an established
allergy to preservatives or is using more than 6 drops
daily in the affected eye(s)
De
c 1
3.8 Add Travoprost eye drops
40micrograms/mL
(preserved with
POLYQUAD)
gre
en?
Glaucoma review: added as new product 3rd Choice Prostaglandin analogue eye drops,
containing Polyquad, an alternative preservative to
benzalkonium chloride, if latanoprost and bimatoprost
have not proved suitable.
De
c
13
.8
Add Bimatoprost/timolol eye
drops 0.3mg/5mg in
1mL (preserved)
AI
Glaucoma review: added as new product Restricted - initiation by Consultant Ophthalmologists
with continuation by GPs
De
c 1
3.8 Revise
restrictionTravoprost/Timolol eye
drops
40micrograms/5mg in
1mL (preserved)
AI
Glaucoma review: - removed restriction relating to 6 month trial
and make Amber Initiation
Restricted - initiation by Consultant Ophthalmologists
with continuation by GPs

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
De
c
13
.8
Revise TLL Brimonidine tartrate eye
drops 0.2% (preserved)
AI
Glaucoma review: - add TLL classification Alphagan®
Restricted - initiation by Consultant Ophthalmologists
with continuation by GPs
De
c
13
.8
Revise
restrictionBrimonidine
tartrate/Timolol eye
drops 0.2%/0,5%
AI
Glaucoma review: - removed restriction relating tocompliance
issues and make Amber Initiation
Combigan®
Restricted - initiation by Consultant Ophthalmologists
with continuation by GPs
De
c
13
.8
Delete Dipivefrin hydrochloride
eye drops 0.1%
bla
ck
Glaucoma review: - discontinued. If unlicensed product is
being used TLL is Red.
De
c
13
.8
TLL revised Acetazolamide 250mg
tablet, 250mg MR
capsule
AI
Glaucoma review - add TLL classification Restricted - initiation by Consultant Ophthalmologists
with continuation by GPs
De
c 1
3.8 TLL revised Dorzolamide eye drops
2% (preserved)
AI
Glaucoma review - add TLL classification Trusopt®
1st Choice topical carbonic anhydrase inhibitors
Restricted - initiation by Consultant Ophthalmologists
with continuation by GPs
De
c 1
3.8 TLL revised Brinzolamide eye drops
10mg/1mL (preserved)
AI
Glaucoma review - add TLL classification Azopt®
2nd Choice topical carbonic anhydrase inhibitors
Restricted - initiation by Consultant Ophthalmologists
with continuation by GPs
De
c
13
.8
TLL revised Dorzolamide/Timolol
eye drops 2%/0.5%,
0.2mL (preserved)
AI
Glaucoma review - add TLL classification
15Jan14 Added as inadvertently omitted from initial list
Restricted - initiation by Consultant Ophthalmologists
with continuation by GPs
De
c 1
3.8 TLL revised Dorzolamide/Timolol
preservative-free unit
dose eye drops
2%/0.5%, 0.2mL
AI
Glaucoma review - add TLL classification Restricted - initiation by Consultant Ophthalmologists
with continuation by GPs for patients who have an
established allergy to preservatives or who are using
more than 6 drops daily in the affected eye(s)
De
c 1
3.8 TLL revised Brinzolamide / Timolol
ophthalmic suspension
10mg/5mg per mL
(preserved)
AI
Glaucoma review - add TLL classification Azarga®
Restricted - initiation by Consultant Ophthalmologists
with continuation by GPs
De
c 1
3.8 TLL revised Pilocarpine
hydrochloride eye drops
1%, 2% (preserved) AI
Glaucoma review - add TLL classification Restricted - initiation by Consultant Ophthalmologists
with continuation by GPs
De
c 1
3.8
TLL revised Pilocarpine
hydrochloride eye drops
2% single use eye
drops (preservative-
free)
AI
Glaucoma review - add TLL classification Restricted - initiation by Consultant Ophthalmologists
with continuation by GPs for patients who have an
established allergy to preservatives or who are using
more than 6 drops daily in the affected eye(s)
De
c 1
3.8
Delete Pilocarpine
hydrochloride eye drops
4%, single use 4% and
ophthalmic gel 4% bla
ck
Glaucoma review - delete from formulary Glaucoma review (FMG Dec13) - non-formulary
FORMULARY CHANGES FOR NOTE - AGREED DECEMBER 2013 FMG

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
add Nalmefene 18mg tablet
red y
Oxfordshire Health decision Restricted - to be prescribed only by Oxford Health
NOTE: Not to be prescribed or dispensed by
Buckinghamshire Hospitals NHS Trust 4.1
0.1
DE
CE
MB
E
revise
restrictionPhenytoin
Carbamazepine
Phenobarbital
Primidone
NO
Label to prescribe by brand and state brand used in hospital as
"in secondary care the usual brand used is….."
Prescribe by brand to ensure patient is maintained on
specific manufacturer's product. In secondary care the
usual brand stocked is……..
4.8
.1
revise
restrictionSodium valproate
Lamotrigine
Retigabine
Clobazam
Clonazepam
Oxcarbazepine
Zonisamide
Topiramate
add usual brand stocked by hospital, prescribing generically or
by brand is discretionary and this decision should be taken in
consultation with the patient
Prescribing generically or by brand is discretionary
4.8
.1
Add wording to
NF entryPermanel
Rufinamide
Eslicarbazepine
Tiagabine
Pregabalin (epilepsy NF
entry only)
add usual brand stocked by hospital, prescribing generically or
by brand is discretionary and this decision should be taken in
consultation with the patient
List medicines as non-formulary and refer to MHRA warning
See link to MHRA warning above
4.8
.1
Revise
restrictionLevetiracetam
Lacosamide
Gabapentin
Ethosuximide
Vigabatrin
Prescibe generically May be prescribed generically
4.8
.1
add drug as a
2nd line
treatment
choice
varenicline
green
(this drug has been available in the community for years but is
not listed in the formulary currently).
Usually started on the advice of the smoking cessation team,
along with psychological support. In secondary care not to be
started for in patients - but available for continuation in
established patients.
Restricted - to be used in accordance with NICE TA123
Varenicline for smoking cessation and Public Health
guidance Volumne 10, 200, as second line therapy when
NRT has failed.
4.1
0.3
Revise
restrictionFluticasone
Propionate/Salmeterol
250micrograms/50micro
grams per blister
(Seretide 250
accuhaler) dry powder
for inhalation
gre
en
y
Using the Seretide 500 accuhaler is more cost effective than
the Seretide 250
Add note to state that for COPD the Seretide 500 accuhaler
should be used (see COPD guideline)
Using the Seretide 500 Accuhaler for COPD treatment
is more cost effective than the Seretide 250 Accuhaler.
(See link to Bucks COPD guideline above)
3.2
FM
GD
EC
13
Add Thiopental 500mg in
2mL prefilled syringes
red N
Maternity theatres requesting
Less work for aseptic unit who are presently making.
Several risk assessments have been done for various
manufacturers the most recent being Medium Risk from UDG.
All risk assessments have come out as medium and all were
completed Dec12, Feb13 and Mar13.
Unlicensed - Medium Risk
Restricted - for use in Maternity Theatres only
15
.1.1
FM
GD
EC
13
All epilepsy medication listed below - revised restriction as a result of CHM warning regarding brand dispensing

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Revise
restrictionCeftriaxone 250mg, 1g,
2g injection
red ye
s
Antibiotic guideline for gastroenteritis states ceftriaxone can be
used for enteric fever. Need to add this as a restriction. (Added
to formulary by SS
In secondary care restricted - Paediatrics, suspected
meningitis or meningococcal septicasemia, serious
Orthopaedic infections; cellulitis; pelvic inflammatory
disease; enteric fever and sexually transmitted
infections. Also for use in accordance with Guidelines
for antibiotic treatment of infections within Obstetrics and
Gynaecology (BHTCG 207) May also be used in
accordance with OPAT guideline 103 (Empirical short
course home antibiotic regimens)
Microbiology approval required for all other uses.
In primary care not listed in local antibiotic guide.
5.1
.2.1
FM
GD
EC
13
Add Bupropion hydrochloride
150mg MR tablet
gre
en ye
s
The position of bupropion needs clarification with respect to the
NRT guideline and factsheet.
Bupropion is on the formulary for the community LES services
and it is in the Service Spec that it is offered through GP
prescription. In community varenicline is low priority drug and
should be prescribed 2nd line after therapy has failed, with
bupropion available as 3rd line. (confirmed with Val Mills
11Dec13)
In primary care - only to be prescribed as a 3rd line
treatment if 1st line treatment with nicotine replacement
therapy (NRT) has not been successful and second line
treatment with varenicline is not appropriate. To be used
in accordance with NRT guideline
In secondary care - only to be supplied to inpatients for
continuation of existing treatment in accordance with
NRT guideline.
4.1
0.2
FM
GD
EC
13
Add Miconazole ovule 1.2g
available to replace
100mg pessary gre
en ye
s
Miconazole pessary 100mg was 2nd choice after clotrimazole.
The ovule is now second choice 7.2
.2
FM
GD
E
Delete Miconazole pessary
100mggre
en
no longer available.
7.2
.2
FM
GD
EC
1
Add Adrenaline /
Epinephrine
150micrograms (child)
(Epipen Jr Auto-injector
0.15mg
gre
en ye
s
Jext® have recently recalled many batches due to a potential
problem with the delivery of adrenaline, which has led to
insufficient stocks in primary care. The availability of Epipen®
on formulary as a back up for such situations is proposed
Restricted - 2nd Choice adrenaline auto-injector pen only
to be used when there are supply issues with the Jext
brand
03
.04
.03
FM
GD
EC
13
Add Adrenaline /
Epinephrine
300micrograms (adult)
(Epipen Auto-injector
0.3mg
gre
en ye
s
Restricted - 2nd Choice adrenaline auto-injector pen only
to be used when there are supply issues with the Jext
brand
03
.04
.03
FM
GD
EC
13
Add Nystatin 100,000 units
vaginal cream
For vaginal candidiasis
resistant to clotrimazole
GUM team only
red no
The licensed product is no longer manufactured.
If to be prescribed more widely will be discussed at subsequent
meeting and traffic light position to be reviewed.
Unlicensed - Medium Rsk
Restricted - prescribing by GUM team only for vaginal
candidiasis resistant to clotrimazole.
13
.10
.02
FM
GD
EC
1
Add Iobitridol (Xenetix)
300mg iodine/mL and
350mg iodine/mL
Consultant
Radiologists only
red
In regular use in radiology Restricted - prescribing by Consultant Radiologists only
no
t in
BN
F
FM
GD
EC
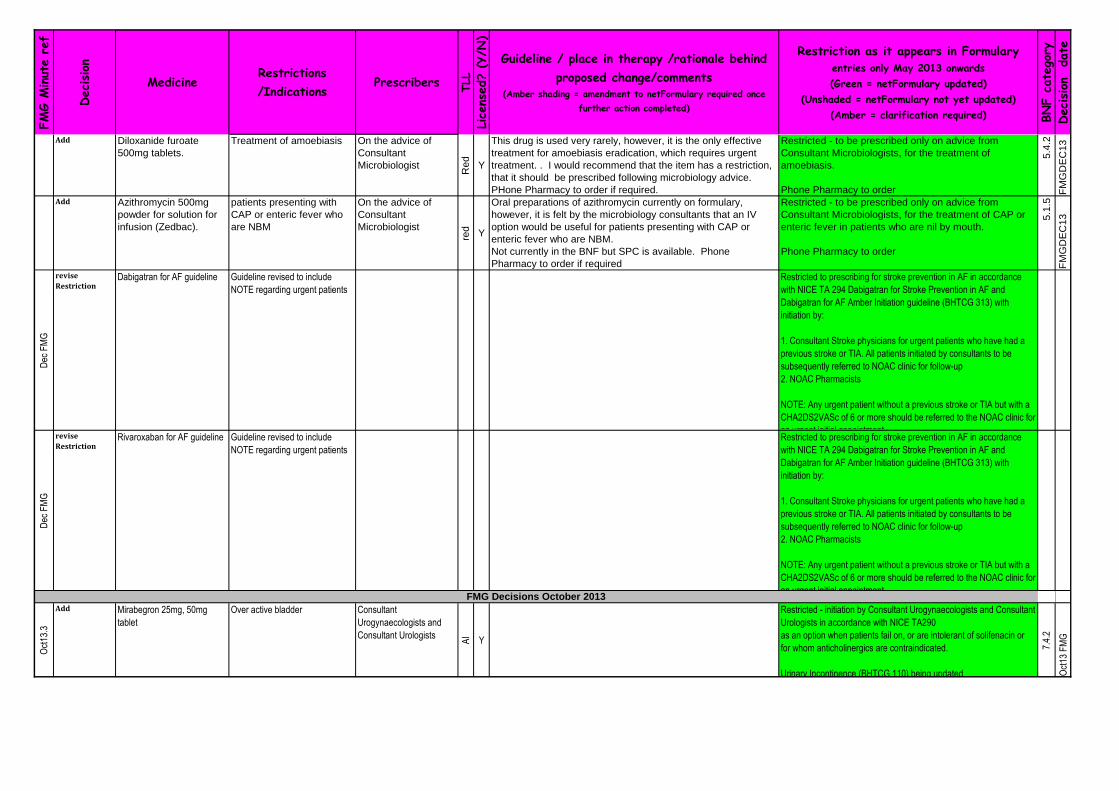
FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Add Diloxanide furoate
500mg tablets.
Treatment of amoebiasis On the advice of
Consultant
Microbiologist
Re
d
Y
This drug is used very rarely, however, it is the only effective
treatment for amoebiasis eradication, which requires urgent
treatment. . I would recommend that the item has a restriction,
that it should be prescribed following microbiology advice.
PHone Pharmacy to order if required.
Restricted - to be prescribed only on advice from
Consultant Microbiologists, for the treatment of
amoebiasis.
Phone Pharmacy to order
5.4
.2
FM
GD
EC
13
Add Azithromycin 500mg
powder for solution for
infusion (Zedbac).
patients presenting with
CAP or enteric fever who
are NBM
On the advice of
Consultant
Microbiologist
red Y
Oral preparations of azithromycin currently on formulary,
however, it is felt by the microbiology consultants that an IV
option would be useful for patients presenting with CAP or
enteric fever who are NBM.
Not currently in the BNF but SPC is available. Phone
Pharmacy to order if required
Restricted - to be prescribed only on advice from
Consultant Microbiologists, for the treatment of CAP or
enteric fever in patients who are nil by mouth.
Phone Pharmacy to order
5.1
.5
FM
GD
EC
13
Dec
FM
G
revise
RestrictionDabigatran for AF guideline Guideline revised to include
NOTE regarding urgent patients
Restricted to prescribing for stroke prevention in AF in accordance
with NICE TA 294 Dabigatran for Stroke Prevention in AF and
Dabigatran for AF Amber Initiation guideline (BHTCG 313) with
initiation by:
1. Consultant Stroke physicians for urgent patients who have had a
previous stroke or TIA. All patients initiated by consultants to be
subsequently referred to NOAC clinic for follow-up
2. NOAC Pharmacists
NOTE: Any urgent patient without a previous stroke or TIA but with a
CHA2DS2VASc of 6 or more should be referred to the NOAC clinic for
an urgent initial appointment.
Dec
FM
G
revise
RestrictionRivaroxaban for AF guideline Guideline revised to include
NOTE regarding urgent patients
Restricted to prescribing for stroke prevention in AF in accordance
with NICE TA 294 Dabigatran for Stroke Prevention in AF and
Dabigatran for AF Amber Initiation guideline (BHTCG 313) with
initiation by:
1. Consultant Stroke physicians for urgent patients who have had a
previous stroke or TIA. All patients initiated by consultants to be
subsequently referred to NOAC clinic for follow-up
2. NOAC Pharmacists
NOTE: Any urgent patient without a previous stroke or TIA but with a
CHA2DS2VASc of 6 or more should be referred to the NOAC clinic for
an urgent initial appointment.
Oct
13.3
Add Mirabegron 25mg, 50mg
tablet
Over active bladder Consultant
Urogynaecologists and
Consultant Urologists
AI
Y
Restricted - initiation by Consultant Urogynaecologists and Consultant
Urologists in accordance with NICE TA290
as an option when patients fail on, or are intolerant of solifenacin or
for whom anticholinergics are contraindicated.
Urinary Incontinence (BHTCG 110) being updated
7.4.
2
Oct
13 F
MG
FMG Decisions October 2013

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Oct
13.
5
Add Rivaroxaban 15mg, 20mg Treatment PE and prevention PE
and DVT
Consultant Haematologists
Red Y
NICE compliance form required.
In accordance with NICE TA 297 and in accordance with awaited guideline.
FOR ALL PRESCRIBING - NICE compliance form required - see link
from Formulary homepage. Named patient approval only as
NICE/HCD compliance form awaited.
2. Restricted - prescribing by Consultant Haematologists for patients
unsuitable for warfarin in accordance with NICE TA287 Pulmonary
embolism and recurrent venous thromboembolism - rivaroxaban and
in accordance with BHT guideline (awaited).
Audit results to be brought to FMG February 2014
2.8.
2
Oct
13 F
MG
Oct
13.7
Reject Linaclotide Symptomatic treatment of
patients with moderate to severe
constipation predominant irritable
bowel syndrome which hasn't
responded to laxatives and anti-
spasmodics
Bla
ck
Y
Rejected because evidence of efficacy could not confirm that linaclotide would
provide at least equivalent levels of efficacy to standard treatment
1.6.
7
Oct
13 F
MG
Oct
Reject Esomeprazole All licensed indications
Bla
ck
Y
Rejected because no evidence to support its superior efficacy or safety
compared to other PPIs at equivalent acid suppression doses.
1.3.
5
Oct
13
May
13.5
Add Ibandronic acid 50mg tablets Prevention of skeletal events in
patients with breast cancer and
bone metastases. For patients
not receiving IV therapy for their
breast cancer
Initiation by Consultant
Breast Oncologists and
continuation by GPs AI
Y
Restricted - initiation by Consultant Breast Oncologists with
continuation by GPs.for metastatic bone disease in cancer patients
not receiving iv therapy, in accordance with Ibandronic Acid for
treatment of metastatic bone disease in breast cancer (BHTCG
307FM)
06.0
6.02
Oct
13
FM
G
Revise
restrictionSeretide evohaler,
Symbicort and Flixotide
inhalers - all strengths
Initiation by
respiratory teamgre
en
Y
Seretide 50 Evohaler already restricted for treatment of asthma
in accordance with British Guideline on the Management of
Asthma revised 2009
Seretide 125 Evohaler - restricted. May ony be used for
continuation of therapy. Not to be initiated as not cost effective
compared to other strengths.
In secondary care - restricted to initiation by respiratory
team only
3.2
FM
G O
ct1
3
Add FreeStyle Optium
glucose test strips
gre
en
YRecently agreed for Trust. Not aligned with primary care Restricted - only for use by patients using FreeStyle
Optium beta-ketone test strips.
6.1
.6
FM
G
Add FreeStyle Optium beta-
ketone test strips
gre
en
Y
Recently agreed for Trust. Not aligned with primary care Restricted for Type 1 Diabetics and patients on insulin
6.1
.6
FM
G
Delete Ascensia glucose and
ketone blood testing
products
?? Y
Still in use in the community along with ketone test strips.
Added ketone test strips to formulary
6.1
.6
FM
G
Revise TLL
classificationLanreotide 60mg
(Somatuline Autogel®)
(injection, prefilled
syringe)
PbR excluded SCG
funded
Paediatric
consultants
Re
d
U
nli
c
U
se
SCP with GOS; Bucks GPs do not wish to 'share care' with
GOS for this drug because it is a very rare condition,
Unlicensed indication, not a routinely used medication for a GP
(even in adults), commissioned by specialist commissioning
according to their manual.
GOS guideline states Somatuline Autogel 60mg syringes (Nicky
Greenberg 8Nov13)
Unlicensed use.
Restricted - prescribing by Paediatric consultants for
Congenital Hyperinsulinism (CHI) in accordance with
Great Ormond Street hospital guidelines
8.3
.4.3
.
FM
G O
ct1
3
Formulary Changes for Note FMG October 2013

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Revise TLL
classificationOctreotide
50micrograms/1mL,
100micrograms/1mL,
500micrograms/1mL,
1g/5mL
(injection)
PbR excluded SCG
funded
Re
d
U
nli
c
U
se
SCP with GOS; Bucks GPs do not wish to 'share care' with
GOS for this drug because it is a very rare condition,
Unlicensed indication, not a routinely used medication for a GP
(even in adults), commissioned by specialist commissioning
according to their manual.
Clarify strengths required according to GOS guideline
Unlicensed use.
Restricted - prescribing by Paediatric consultants for
Congenital Hyperinsulinism (CHI) in accordance with
Great Ormond Street hospital guidelines
8.3
.4.3
.
FM
G O
ct1
4
Add Colistimethate sodium
1,662,500IU inhalation
powder, hard capsules
for use with
Turbospin® powder
inhaler Colobreathe®
DPI (dry powder
inhaler)
PbR excluded SCG
funded
Consultants Paed
specialising in Cystic
Fibrosis management
red
Y
NICE TA 276 (March 2013) Colistimethate sodium dry powder
inhaler is recommended for use in patients unsuitable or unable
to use colistimethate sodium nebulisers. Colistimethate sodium
nebuliser remains the first line agent for the management of
chronic pulmonary infections due to Pseudomonas aeruginosa
in patients with Cystic Fibrosis,. Colistin inhaler is similar in
price to Tobramycin POD haler. Both have the same place in
therapy and NICE TA. Colistin inhaler was not included in the
Tobi Podhaler application in May 13 as it was not marketed at
the time. Approx 2 patients per year
Restricted - prescribing by consultant Paediatricians
specialising in Cystic Fibrosis for the management of
chronic pulmonary infection due to Pseudomonas
aeruginosa in patients with cystic fibrosis aged 6 years
and older if nebulised colistin is not tolerated or if clinical
progress is unsatisfactory. To be used in accordance
with NICE TA276 Colistimethat sodium and tobramycin
dry powders for inhalation for treating pseudomonas lung
infection in cystic fibrosis.
5.1
.4
FM
G O
ct1
3
Revise Cetraben emollient
cream 50g, 500g, 150g,
1.05kg pump packs
gre
en
Y
Clarification of sizes on formulary. Secondary care require 50g
and 500g. 50g, 150g, 500g and 1.05kg requested for use in
primary care. Cetraben already on formulary. Address sizes
required as result of Woundcare Formulary merge action and in
line with moisturizing and cleansing advice from Dermatology.
In Primary care all sizes available.
In Secondary care 50g and 500g available
13
.02
.01
.01
FM
G O
ct1
3
Add Diprobase cream 50g
tube
gre
en
Y
Diprobase already on formulary. This convenient 50g size to be
added as a result of Woundcare Formulary merge action and in
line with moisturizine and cleansing advice from Dermatology.
13
.02
.01
.0
1F
MG
Revise
restrictionDenosumab 60mg/1mL
(Prolia)
Osteoporosis Consultant
Endocrinologists and
Consultant
Rheumatologists with
continuation by GPs
AP Y
NOTE: Denosumab 120mg (Xgeva®) is administered monthly.
Denosumab 60mg (Prolia®) is administered every six months.
Apply notes to both entries on Formulary to alert users to the
potential for confusion between the two drugs and highlight
need for care when prescribing and administering
Add: "WARNING: There are TWO brands of denosumab, each
a different strength - take extra care and attention when
prescribing and administering.
Combined entry from CCG adding in 4th Choice
4th Choice for secondary prevention of osteoporosis (not
recommended for primary prevention)
WARNING: - There are TWO brands of denosumab,
each a different strength - take extra care when
prescibing and administering.
NOTE: Prolia® is administered every six months
Restricted - to prescribing by Rheumatologists and
Endocrinologists only, with continuation by GPs, in
accordance with: Denosumab for primary and secondary
fracture prevention in men and women over 50 years
(BHTCG 401) and BHTCG 402 and 403 (see above link
to osteoporosis guidelines) for patients with confirmed
intolerance or contraindications to oral bishosphonates
and strontium ranelate and in accordance with NICE TA
204 Osteoporotic fractures - Denosumab.
6.6
.2
FM
G O
ct1
3

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Revise
restrictionDenosumab vial
120mg/1.7mL (XGEVA)
Bone Metastases in Solid
Tumours
Consultant Breast
Oncologists
Re
d
Y
NOTE: Denosumab 120mg (Xgeva®) is administered monthly.
Denosumab 60mg (Prolia®) is administered every six months.
Apply notes to both entries on Formulary to alert users to the
potential for confusion between the two drugs and highlight
need for care when prescribing and administering
Add: "WARNING: There are TWO brands of denosumab, each
a different strength - take extra care and attention when
prescribing and administering.
WARNING: - There are TWO brands of denosumab,
each a different strength - take extra care when
prescibing and administering.
NOTE: XGEVA® is administered monthly
FOR ALL PRESCRIBING - NICE compliance form
required - see link from Formulary homepage.
Restricted - prescribing by Consultant Breast
Oncologists in accordance with Denosumab for Bone
Metastases in Solid Tumours (BHTCG 305FM) and in
accordance with NICE TA265
6.6
.2
FM
G O
ct1
3
Revise
restrictionBendroflumethiazide
2.5mg, 5mg
gre
en
Y
NOTE: in accordance with Clinical Management of
Hypertension in Adults BHTCG 227 bendroflumethiazide is
ONLY for continuation in stable patients and is NOT to be
initiated for treatment of hypertension
Restricted - when used for hypertension to be prescribed
in accordance with Clinical Management of Hypertension
in Adults (BHTCG 227) and only for continuation in
stable patients and NOT to be initiated for the treatment
of hypertension.
02
.02
.01
FM
G O
ct1
3
Revise
restrictionBendroflumethiazide
5mg
gre
en
Y
Split into 2 entries with 5mg only for use with loop diuretics for
treating oedema.
Restricted - only for use with loop diuretics for controlling
oedema.
NOTE: Use 2.5mg only when treating hypertension (see
entry below) 02
.02
.01
FM
G O
ct1
3
Revise
restrictionTenofovir Disoproxil
245mg/Emtricitabine
200mg tablet (Truvada)
HIV/GUM team
red Y
Advice to Phone Pharmacy was added originally to ensure that
the prescriber knew where to obtain stocks from IF the patient
could not have a standard PEP pack but Truvada is also used
for treatment as well as PEP so to avoid confusion restriction is
removed... Normal restriction to HIV and GUM consultant
prescribing still stands across the whole group.
05
.03
.01
FM
G O
ct1
3
Add Darunavir 150mg,
400mg, 600mg tablet
PbR excluded SCG
funded
HIV/GUM team
Re
d
Y
treatment of HIV in accordance with BHIVA 2012 HIV
treatment guidelines
Restricted - to be prescribed by HIV and GUM teams in
accordance with BHIVA 2012 HIV treatment guidelines
05
.03
.01
FM
G O
ct1
3
Add Rilpivirine 25mg tablet
PbR excluded SCG
funded
HIV/GUM team
Re
d
Y
Treatment of HIV in accordance with BHIVA 2012 HIV
treatment guidelines. For patients who are unable to take first
line anti-retrovirals due to resistance or as a alternative to
- efavirenz where tolerability is/has potential (e.g. due to
working patterns)to be a problem due to adverse effects
- nevirapine - due to adverse effects or high CD4 levels
- protease inhibitors - to spare these and in view of possible
long term metabolic side effects. Max 10 patients per year.
Funded by SCG as included in BHIVA guidelines
Restricted - prescribing by HIV and GUM teams in
accordance with BHIVA 2012 HIV treatment guidelines
and restricted to patients who are unable to take first line
anti-retrovirals due to resistance or as an alternative to:
- efavirenz - where tolerability is/has potential (eg. due to
working patterns) to be a problem due to adverse effects
- nevirapine - due to adverse effects or high CD4 levels,
or
- protease inhibitors - to spare these and in view of
possible long term metabolic side effects.
05
.03
.01
FM
G O
ct1
3

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Add Emtricitabine 200mg,
rilpivirine 25mg and
tenofovir disoproxil
245mg tablet
(Eviplera®)
PbR excluded, SCG
funded
HIV/GUM team
Re
d
Y
treatment of HIV in accordance with BHIVA 2012 HIV
treatment guidelines. To be used in patients who experience
side effects from efavirenz. Max 10 patients per year. Funded
by SCG as included in BHIVA guidelines
Restricted - to be prescribed by HIV and GUM teams in
accordance with BHIVA 2012 HIV treatment guidelines
forpatients who experience side effects from efavirenz.
05
.03
.01
FM
G O
ct1
3
Add Nevirapine 400mg MR
tablet
PbR excluded, SCG
funded
HIV/GUM team
Re
d
Y
treatment of HIV in accordance with BHIVA 2012 HIV treatment
guidelines
Treatment of HIV in accordance with BHIVA 2012 HIV
treatment guidelines
05
.03
.01
FM
G O
ct1
3
expand
restrictionRibavirin oral solution
200mg/5mL
PBr excl SCG
Unexplained acute
encephalopathy
Paediatric team
red
Y
Short course of treatment (3 days)
Prescribing by Paed team.in accordance with BHTCG 771
which recommends use for children with measles who have not
been vaccinated against it.
Restricted - to prescribing by Paediatric team in
accordance with Investigation of unexplained acute
encephalopathy in paediatrics (BHTCG 771)
05
.03
.05
FM
G
expand
restrictionRibavirin 200mg tablet
PBr excl SCG
Unexplained acute
encephalopathy
Paediatric team
red
Y
Short course of treatment (3 days)
Prescribing by Paed team.in accordance with BHTCG 771
which recommends use for children with measles who have not
been vaccinated against it.
Restricted - to prescribing by Paediatric team in
accordance with Investigation of unexplained acute
encephalopathy in paediatrics (BHTCG 771)
05
.03
.05
FM
G
Delete Metaraminol 10mg in
1ml injection
red
N
Unlicensed - Medium Risk. To be deleted and replaced by a
lower strength for reasons of safety.
NOTE: This strength will be deleted from the formulary once
there is an assured supply of the lower strength.
Unlicensed - Medium risk
WARNING: Take extra care when prescribing and
administering as there are TWO different strengths of
this drug.
NOTE: This strength will be deleted from the formulary
once there is an assured supply of the lower strength
02
.07
.02
FM
G O
ct1
3
Add Metaraminol 2.5mg in
5ml injection (all sizes)
red N
Unlicensed LOW risk. Unlicensed - Low risk
WARNING: Take extra care when prescribing and
administering as there are TWO different strengths of
this drug.
02
.07
.02
FM
G O
ct1
3
Add Paracetamol
suppositories 60mg,
125mg, 250mg, 500mg,
1g
gre
en
Y
All available as licensed products 60mg suppository: Unlicensed - Low Risk
In primary care the licensed 60mg, 125mg, 250mg,
500mg, 1g preferred
In secondary care the unlicensed 60mg, 120mg and
240mg to be deleted and the licensed 60mg, 125mg,
250mg, 500mg and 1g suppositories to be introduced.
04
.07
.01
FM
G O
ct1
3
delete Paracetamol
suppositories 60mg
(unlicensed), 120mg,
240mg and 500mg
gre
en
N
These strengths are on formulary. Licensed strengths now
available to replace 60mg and the other two strengths no
licensed product available.
To be deleted once new licensed strengths are introduced and
implemented
60mg suppository: Unlicensed - Low Risk
In primary care the licensed 60mg, 125mg, 250mg,
500mg, 1g preferred
In secondary care the unlicensed 60mg, 120mg and
240mg to be deleted and the licensed 60mg, 125mg,
250mg, 500mg and 1g suppositories to be introduced.
04
.07
.01
FM
G O
ct1
3

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
revise
restrictionBevacizumab
2.5mg/0.1mL
red
N
Update restriction which was out of date and include direction to
complete NICE form (MSt, 18Sep13)
Unlicensed - High Risk
FOR ALL PRESCRIBING - NICE compliance form
required - see link from Formulary homepage.
Restricted - prescribing by consultant Ophthalmologists
for treatment of non-AMD choroidal neovascular
membranes, rubeotic glaucoma and as an adjunct to
vitrectomy for proliferative diabetic retinopathy
11
.08
.02
FM
G O
ct1
3
add Sildenafil
800micrograms in
1mL injection, 20mL
vial
PBr excluded drug
SCG
Primary pulmonary arterial
hypertension
red
Y
primary pulmonary arterial hypertension in patients who cannot
swallow tablets
For treatment of pulmonary arterial hypertension.
FIRST DOSE MUST BE GIVEN IN HOSPITAL - risk of
first-dose hypotension.
Restricted - only for patients who are unable to swallow
the tablets with initiation by Respiratory consultants in
secondary or tertiary care. See European Society of
Cardiology guideline on diagnosis and treatment of
pulmonary arterial hypertension, European Heart Journal
2004.
02
.05
.01
FM
G O
ct1
3
Add Peginterferon alfa 2b
pens
Hepatitis C,Christine
Helmer
red
Y
prefilled syringes are already on formulary and the cost is the
same.
Left entry unaltered as only changing from prefilled pen to a
click device prefilled pen
FOR ALL PRESCRIBING: NICE compliance form
required - see link from Formulary homepage.
Restricted - prescribing by Gastroenterologists and
Associate Specialist Gastroenterology in accordance
with NICE TA 75 Interferon alfa and ribavirin for the
treatment of chronic hepatitis, NICE TA 106
Peginterferon alfa and ribavirin for the treatment of mild
hepatitis C and NICE TA 200 Hepatitis C - peginterferon
alfa and ribavirin.
FM
G O
ct1
3
Add Palivizumab 50mg,
100mg vial
PbR excluded funded
by SCG
Prevention of RSV
(Respiratory Syncytial
Virus) infection
Consultant
Paediatricians
Re
d
Y
Used to be approved via IFR at PCT. This is now funded by
SCG and they do not want to use IFRs for this product unless
the JCVI criteria are not met. BHT internal approval process
with NICE / HCD compliance form will be used instead
FOR ALL PRESCRIBING - NICE compliance form
required - see link from Formulary homepage. NICE
compliance to be confirmed if form not available.
Restricted - prescribing by Consultant Paediatricians
only in accordance with JCVI criteria. Approval required
prior to initiation.
05
.03
.05
FM
G O
ct1
3
Add choice Indapamide 2.5 mg
gre
en
Y
1st choice thiazide for hypertension 1st Choice thiazide for treatment of hypertension
For use in accordance with Clinical management of
hypertension in adults (BHTCG 227)(see link above)
2.2
.1
FM
G
Add choice Alendronic acid 70mg
gre
en
Y1st choice for osteoporosis 1st Choice for osteoporosis
6.6
.2
FM
G
Add choice Risedronate 35 mg
gre
en
Y
2nd choice for osteoporosis 2nd line treatment when intolerant to Alendronate
6.6
.2
FM
G

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Add choice Strontium
gre
en
Y
3rd choice for osteoporosis treatment (but not recommended
for primary prevention)
3rd Choice for Osteoporosis treatment (but not
recommended for primary prevention)
Restricted to Consultant Rheumatologists and Care of
the Elderly for treatment of post menopausal
osteoporosis to reduce the risk of vertebral and hip
fractures.
6.6
.2
FM
G O
ct1
3
Add choice Denosumab s/c 60mg
AP Y
4th choice for secondary prevention of osteoporosis (not
recommended for primary prevention)
see entry above
6.6
.2
FM
G
Add Varicella-Zoster vaccine
(Zostavax®)
gre
en
YAdd as part of 1ary care national immunisation programme for
adults aged 70 and 79 14
.4
FM
G
Add Pneumococcal vaccine
(Prevenar 13®)
gre
en
YAdd as part of 1ary care national immunisation programme
14
.4
FM
G
Add Rotavirus vaccine
(Rotarix®) oral
suspension 1.5mL
prefilled oral syringe
gre
en
Y
Add as part of 1ary care national immunisation programme
14
.4
FM
G
Add Influenza vaccine
(Fluenz®) nasal spray,
0.2mL nasal applicator
gre
en
Y
Add as part of 1ary care national immunisation programme for
childrens aged 2 and 3
14
.4
FM
G
Add new
indicationAripipazole - all
strengths and dose
forms
Moderate to severe manic
episodes in adolescents
aged 13-18 with bipolar
disorder within its
marketing authorisation (ie
up to 12 weeks of
treatment for moderate to
severe manic episodes in
bipolar disorder)
Oxford Health
initiation onlyre
d
Y
TA292 Aripiprazole is recommended as an option for treating
moderate to severe manic episodes in adolescents aged 13-18
with bipolar I disorder, within its marketing authorisation (that is,
up to 12 weeks of treatment for moderate to severe manic
episodes in bipolar disorder)
Restricted - prescribing by Psychiatric (Mental Health
Trust) team only.
NICE TA292 - Aripiprazole is recommended as an option
for treating moderate to severe manic episodes in
adolescents aged 13-18 years, with bipolar 1 disorder,
within its marketing authorisation (ie. up to 12 weeks of
treatment for moderate to severe manic episodes in
bipolar disorder)(see link above)
4.2
.1
FM
G O
ct1
3
Add Eurax HC®
gre
en
Y
As recommended in Dermatolog referral guidelines; it does not
pose a cost pressure
This is still manufactured even though not mentioned in BNF 13
.3
FM
G
Add Emulsiderm liquid
emulsion
gre
en
Y
As recommended in Dermatolog referral guidelines; it does not
pose a cost pressure
13
.2.1
.
1F
MG
Add Alphosyl 2 in 1®
shampoo
gre
en
Y
As recommended in Dermatolog referral guidelines; it does not
pose a cost pressure
13
.9
FM
G
Add Lisdexamphetamine
Mesilate capsule 30mg,
50mg, 70mg
Oxfordshire Health
red Y
3rd line for ASHD instaed of dexampheatamine - reviewed by
Oxford Health DTC
not listed in BNF
Restricted - to be prescribed only by Oxford Health
NOTE: Not to be prescribed or dispensed by
Buckinghamshire Hospitals NHS Trust FM
G

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
revise
restrictionMetformin 500mg,
850mg tablet
gre
en
Y
See separate entry and restrictions when using to
control weight gain in Oxfordshire Health
paediatric patients receiving antipsychotic
therapy.
6.1
.2.2
FM
G
Add new
indicationMetformin 850mg tab Oxfordshire Health
red N
OH protocol approved by their DTC to control weight gain in
Oxfordshire Health paediatric patients
Unlicensed Use
Restricted - prescribing and management by Oxfordshire
Health only when used to control weight gain in
paediatrics caused by antipsychotic therapy.
6.1
.2.2
FM
G O
ct1
3
Au
g 1
3.1 Add Ranibizumab
2.3mg/0.23mL
(Lucentis) intravitreal
injection
PBR excl CCG
Macular Oedema caused
by retinal vein occlusion
(NICE TA 283)
Consultant
Ophthalmologosts
red y
Dexamethasone implant is the first line treatment for macular
oedema caused by CRVO or BRVO. Ranibizumab may be used
as a second line treatment instead of dexamethasone implant
when dexamethasone is deemed unsuitable in the following
circumstances:
Audit results for one year, for the relative use of ranibizumab
and dexamethasone to come back to FMG Sept 14
FOR ALL PRESCRIBING - NICE compliance form
required - see link from Formulary homepage.
1. Restricted - Prescribing by Ophthalmologists only for
the treatment of Age Related Macular Degeneration.
Intravitreal use only.
See Guideline: Ranibizumab for the treatment of age-
related macular degeneration (based upon NICE TA
155).
2. Restricted - Prescribing by Ophthalmologists only in
accordance with NICE TA 274 Ranibizumab for the
treatment of Diabetic Macular Oedema (DMO).
3. Restricted - Prescribing by Ophthalmologists only as
second line treatment, instead of dexamethasone
implant, when dexamethasone is deemed unsuitable in
the following circumstances: raised intraocular pressure
or a strong family history of raised intraocular pressure
and in accordance with NICE TA 283 Macular oedema
(retinal vein occlusion) ranibizumab.
Audit results confirming the relative use of ranibizumab
and dexamethasone in one year to be brought back to
FMG September 2014
11
.08
.02
Sep-1
3
Au
g1
3.2 Add Aflibercept 4mg in
0.1mL solution for
intravitreal injection
PBR excl CCG
Wet Age Related Macular
degeneration
Consultant
Ophthalmologists
red
y
NOT AVAILABLE UNTIL LATE OCTOBER WHEN FUNDING
AGREED - NOT ENTERED ON NET FORMULARY
Approved as alternative to ranibizumab as a first line treatment
for wet AMD in accordance with NICE TA 294
Audit results for one year, for the relative use of ranibizumab
and dexamethasone to come back to FMG Sept 14
NICE Compliance form approved CGS Sept 13
FOR ALL PRESCRIBING - NICE compliance form
required - see link from Formulary homepage.
1. Restricted - Prescribing by Ophthalmologists as an
alternative to ranibizumab as a first line treatment for wet
Age Related Macular Degeneration (AMD) in accordance
with NICE TA 294 Macular degeneration (wet age-
related) aflibercept (1st line)
Audit results confirming the relative use of ranibizumab
and aflibercept in one year to be brought back to FMG
September 2014
11
.08
.02
Sep-1
3
FMG Decisions August 2013
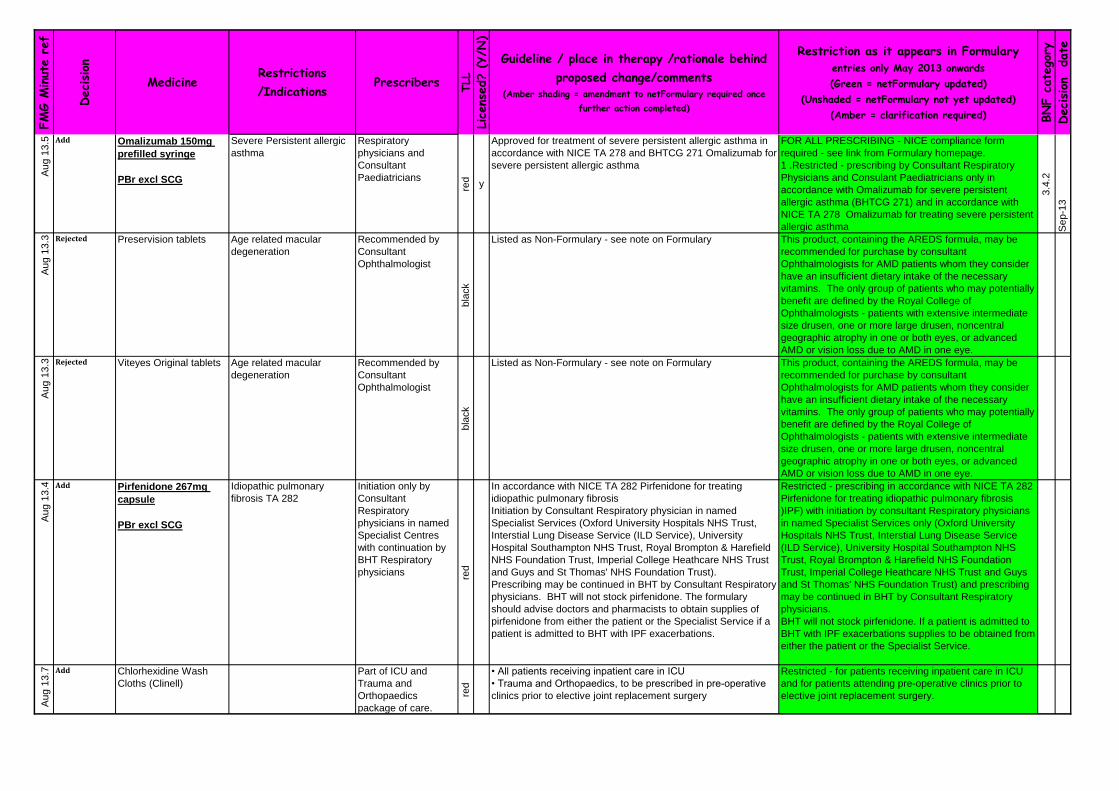
FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Au
g 1
3.5 Add Omalizumab 150mg
prefilled syringe
PBr excl SCG
Severe Persistent allergic
asthma
Respiratory
physicians and
Consultant
Paediatricians
red y
Approved for treatment of severe persistent allergic asthma in
accordance with NICE TA 278 and BHTCG 271 Omalizumab for
severe persistent allergic asthma
FOR ALL PRESCRIBING - NICE compliance form
required - see link from Formulary homepage.
1 .Restricted - prescribing by Consultant Respiratory
Physicians and Consulant Paediatricians only in
accordance with Omalizumab for severe persistent
allergic asthma (BHTCG 271) and in accordance with
NICE TA 278 Omalizumab for treating severe persistent
allergic asthma
3.4
.2
Sep-1
3
Au
g 1
3.3 Rejected Preservision tablets Age related macular
degeneration
Recommended by
Consultant
Ophthalmologist
bla
ck
Listed as Non-Formulary - see note on Formulary This product, containing the AREDS formula, may be
recommended for purchase by consultant
Ophthalmologists for AMD patients whom they consider
have an insufficient dietary intake of the necessary
vitamins. The only group of patients who may potentially
benefit are defined by the Royal College of
Ophthalmologists - patients with extensive intermediate
size drusen, one or more large drusen, noncentral
geographic atrophy in one or both eyes, or advanced
AMD or vision loss due to AMD in one eye.
Au
g 1
3.3 Rejected Viteyes Original tablets Age related macular
degeneration
Recommended by
Consultant
Ophthalmologist
bla
ck
Listed as Non-Formulary - see note on Formulary This product, containing the AREDS formula, may be
recommended for purchase by consultant
Ophthalmologists for AMD patients whom they consider
have an insufficient dietary intake of the necessary
vitamins. The only group of patients who may potentially
benefit are defined by the Royal College of
Ophthalmologists - patients with extensive intermediate
size drusen, one or more large drusen, noncentral
geographic atrophy in one or both eyes, or advanced
AMD or vision loss due to AMD in one eye.
Au
g 1
3.4 Add Pirfenidone 267mg
capsule
PBr excl SCG
Idiopathic pulmonary
fibrosis TA 282
Initiation only by
Consultant
Respiratory
physicians in named
Specialist Centres
with continuation by
BHT Respiratory
physicians red
In accordance with NICE TA 282 Pirfenidone for treating
idiopathic pulmonary fibrosis
Initiation by Consultant Respiratory physician in named
Specialist Services (Oxford University Hospitals NHS Trust,
Interstial Lung Disease Service (ILD Service), University
Hospital Southampton NHS Trust, Royal Brompton & Harefield
NHS Foundation Trust, Imperial College Heathcare NHS Trust
and Guys and St Thomas' NHS Foundation Trust).
Prescribing may be continued in BHT by Consultant Respiratory
physicians. BHT will not stock pirfenidone. The formulary
should advise doctors and pharmacists to obtain supplies of
pirfenidone from either the patient or the Specialist Service if a
patient is admitted to BHT with IPF exacerbations.
Restricted - prescribing in accordance with NICE TA 282
Pirfenidone for treating idiopathic pulmonary fibrosis
)IPF) with initiation by consultant Respiratory physicians
in named Specialist Services only (Oxford University
Hospitals NHS Trust, Interstial Lung Disease Service
(ILD Service), University Hospital Southampton NHS
Trust, Royal Brompton & Harefield NHS Foundation
Trust, Imperial College Heathcare NHS Trust and Guys
and St Thomas' NHS Foundation Trust) and prescribing
may be continued in BHT by Consultant Respiratory
physicians.
BHT will not stock pirfenidone. If a patient is admitted to
BHT with IPF exacerbations supplies to be obtained from
either the patient or the Specialist Service.
Au
g 1
3.7 Add Chlorhexidine Wash
Cloths (Clinell)
Part of ICU and
Trauma and
Orthopaedics
package of care.
red
• All patients receiving inpatient care in ICU
• Trauma and Orthopaedics, to be prescribed in pre-operative
clinics prior to elective joint replacement surgery
Restricted - for patients receiving inpatient care in ICU
and for patients attending pre-operative clinics prior to
elective joint replacement surgery.

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Au
g 1
3.6 Rejected Glycopyrronium
inhalation powder
50micrograms
Treatment of COPD
bla
ck
• Aclidinium inhaler and glycopyrronium inhaler were not
approved for formulary inclusion as an alternative to Tiotropium
in moderate to severe COPD. The duration of trial evidence
was short in the treatment of COPD which is a chronic
condition. Aclidinium was studied for 12 and 24 weeks.
Glycopyrronium was only studied for 26 and 52 weeks.
Au
g 1
3.6 Rejected Aclidinium inhaler
400micrograms/metered
inhalation
Treatment of COPD
bla
ck
• Aclidinium inhaler and glycopyrronium inhaler were not
approved for formulary inclusion as an alternative to Tiotropium
in moderate to severe COPD. The duration of trial evidence
was short in the treatment of COPD which is a chronic
condition. Aclidinium was studied for 12 and 24 weeks.
Glycopyrronium was only studied for 26 and 52 weeks.
Au
g 1
3.8 Add Sucrose 24% oral
solution
Re
d
Y
• Sucrose 24% is approved as a first line agent in addition to
the use of current non-pharmacological strategies for the
treatment of procedural pain in neonates, to be used in
accordance with the draft guideline
Restricted - prescribing by paediatrics team for
procedural pain in neonates, in accordance with Sucrose
Solution for Pain Relief Guidelines (BHTCG 326).
Au
g 1
3.1
0 Add Caffeine citrate solution
for infusion and oral
solution 20mg/mL
(Peyona)
Treatment of primary
apnoea of premature
newborns
Paediatrics team in
NICU only
red y
Each ml contains 20mg caffeine citrate (equivalent to
10mg caffeine).
Restricted - prescribing by paediatrics team in NICU only
in accordance with Neonatal Dosage Guidelines
(BHTCG 69).
Aug
13
.13 New All traffic light related
guidelines agreed
review date of 3 years.
Ma
y1
3.9 Add
Audit: April 14Dexmedetomidine
200micrograms/2mL,
400micrograms/4mL,
1mg/10mL
For sedation in ICU Consultant
Anaesthetists on ITU
red y
In accordance with Dexmedetomidine (Dexdor) Use in ICU
(BHTCG 50)
Guideline approved CGS June 13, Audit protocol approved
FMG Aug 13. Addition of protocol to guideline due for approval
CGS Sept 13 Therefore formulary inclusion after CGS Sept 13
Restricted - to prescribing by Consultant Anaesthetists
on ICU in accordance with Dexmedetomidine (Dexdor)
Use in ICU (BHTCG 50)
Audit results to be reviewed at FMG April 2014
Ma
r13
.4 NF process
notedTolvaptan 15mg, 30mg
tablets
PBr excl SCG
Hyponatraemia Endocrinologists
red
y
Tolvaptan for hyponatraemia secondary to SIADH and
hyponatraemia guideline
Ja
n 1
3.3 Guideline
AddedRetigabine for use as
adjunctive treatment for
partial seizures clinical
guideline
AI
BHT CG 801
Ja
n 1
3.3 Add Retigabine tablet, 50mg,
100mg, 200mg, 300mg,
400mg
Adjunct treatment epilepsy Initiation Consultant
Neurologist and
continuation by GPs AI
y
Restricted - initiation by Consultant Neurologists with
continuation by GPs, in accordance with NICE TA 232
Retigabine for the adjunctive treatment of partial onset
seizures in epilepsy and Retigabine for use as adjunctive
treatment for partial seizures (BHTCG 801)
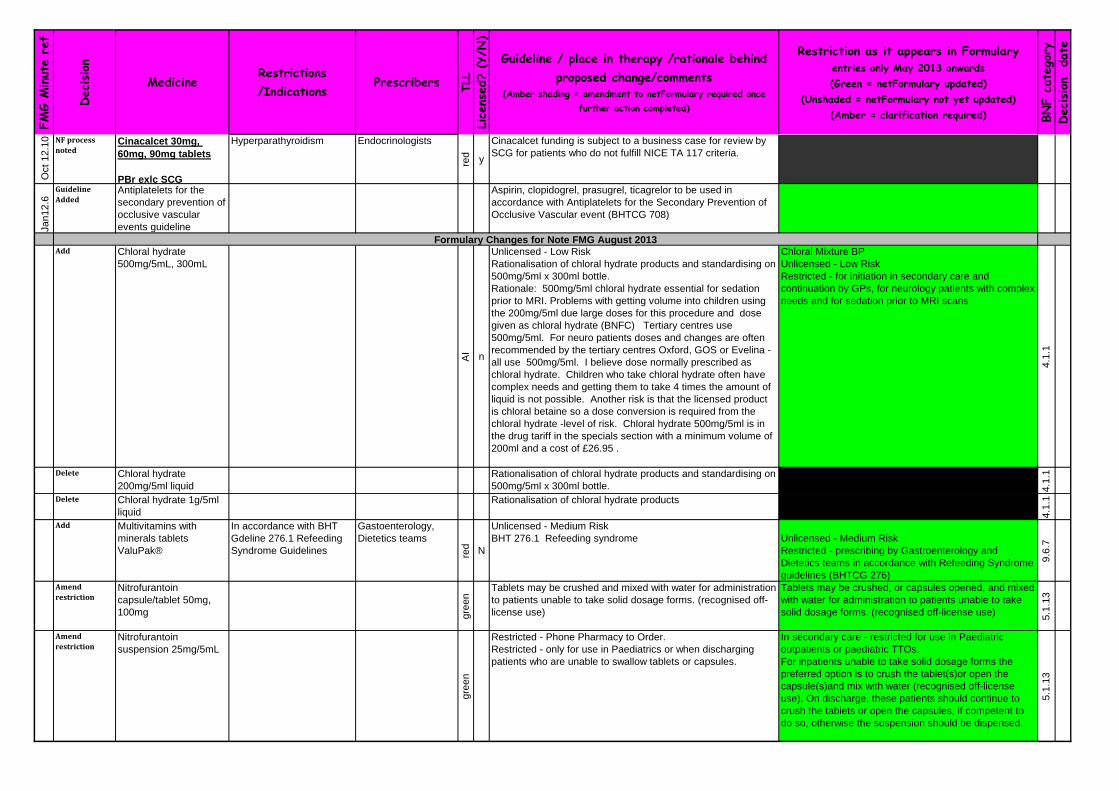
FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Oct
12
.10 NF process
notedCinacalcet 30mg,
60mg, 90mg tablets
PBr exlc SCG
Hyperparathyroidism Endocrinologists
red
y
Cinacalcet funding is subject to a business case for review by
SCG for patients who do not fulfill NICE TA 117 criteria.
Ja
n1
2.6
Guideline
AddedAntiplatelets for the
secondary prevention of
occlusive vascular
events guideline
Aspirin, clopidogrel, prasugrel, ticagrelor to be used in
accordance with Antiplatelets for the Secondary Prevention of
Occlusive Vascular event (BHTCG 708)
Add Chloral hydrate
500mg/5mL, 300mL
AI
n
Unlicensed - Low Risk
Rationalisation of chloral hydrate products and standardising on
500mg/5ml x 300ml bottle.
Rationale: 500mg/5ml chloral hydrate essential for sedation
prior to MRI. Problems with getting volume into children using
the 200mg/5ml due large doses for this procedure and dose
given as chloral hydrate (BNFC) Tertiary centres use
500mg/5ml. For neuro patients doses and changes are often
recommended by the tertiary centres Oxford, GOS or Evelina -
all use 500mg/5ml. I believe dose normally prescribed as
chloral hydrate. Children who take chloral hydrate often have
complex needs and getting them to take 4 times the amount of
liquid is not possible. Another risk is that the licensed product
is chloral betaine so a dose conversion is required from the
chloral hydrate -level of risk. Chloral hydrate 500mg/5ml is in
the drug tariff in the specials section with a minimum volume of
200ml and a cost of £26.95 .
Chloral Mixture BP
Unlicensed - Low Risk
Restricted - for initiation in secondary care and
continuation by GPs, for neurology patients with complex
needs and for sedation prior to MRI scans
4.1
.1
Delete Chloral hydrate
200mg/5ml liquid
Rationalisation of chloral hydrate products and standardising on
500mg/5ml x 300ml bottle. 4.1
.1
Delete Chloral hydrate 1g/5ml
liquid
Rationalisation of chloral hydrate products
4.1
.1
Add Multivitamins with
minerals tablets
ValuPak®
In accordance with BHT
Gdeline 276.1 Refeeding
Syndrome Guidelines
Gastoenterology,
Dietetics teams
red N
Unlicensed - Medium Risk
BHT 276.1 Refeeding syndrome Unlicensed - Medium Risk
Restricted - prescribing by Gastroenterology and
Dietetics teams in accordance with Refeeding Syndrome
guidelines (BHTCG 276)
9.6
.7
Amend
restrictionNitrofurantoin
capsule/tablet 50mg,
100mg gre
en
Tablets may be crushed and mixed with water for administration
to patients unable to take solid dosage forms. (recognised off-
license use)
Tablets may be crushed, or capsules opened, and mixed
with water for administration to patients unable to take
solid dosage forms. (recognised off-license use)
5.1
.13
Amend
restrictionNitrofurantoin
suspension 25mg/5mL
gre
en
Restricted - Phone Pharmacy to Order.
Restricted - only for use in Paediatrics or when discharging
patients who are unable to swallow tablets or capsules.
In secondary care - restricted for use in Paediatric
outpatients or paediatric TTOs.
For inpatients unable to take solid dosage forms the
preferred option is to crush the tablet(s)or open the
capsule(s)and mix with water (recognised off-license
use). On discharge, these patients should continue to
crush the tablets or open the capsules, if competent to
do so, otherwise the suspension should be dispensed.
5.1
.13
Formulary Changes for Note FMG August 2013
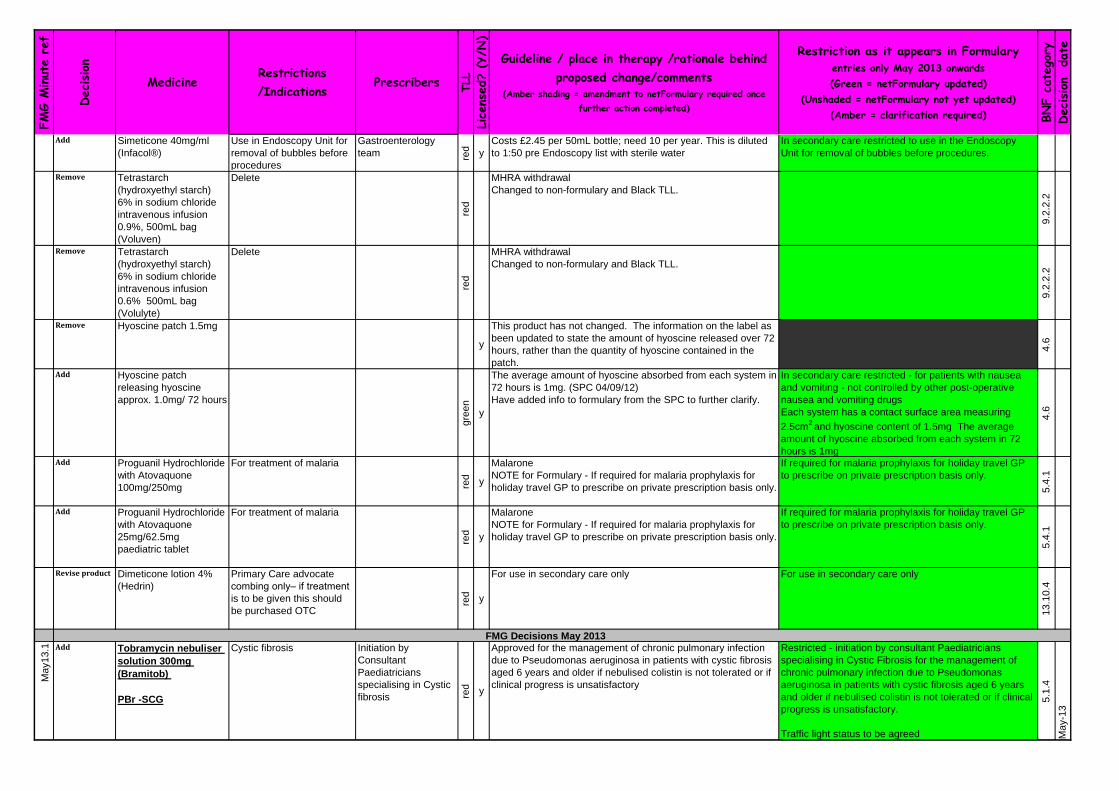
FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Add Simeticone 40mg/ml
(Infacol®)
Use in Endoscopy Unit for
removal of bubbles before
procedures
Gastroenterology
team red y
Costs £2.45 per 50mL bottle; need 10 per year. This is diluted
to 1:50 pre Endoscopy list with sterile water
In secondary care restricted to use in the Endoscopy
Unit for removal of bubbles before procedures.
Remove Tetrastarch
(hydroxyethyl starch)
6% in sodium chloride
intravenous infusion
0.9%, 500mL bag
(Voluven)
Delete
red
MHRA withdrawal
Changed to non-formulary and Black TLL.
9.2
.2.2
Remove Tetrastarch
(hydroxyethyl starch)
6% in sodium chloride
intravenous infusion
0.6% 500mL bag
(Volulyte)
Delete
red
MHRA withdrawal
Changed to non-formulary and Black TLL.
9.2
.2.2
Remove Hyoscine patch 1.5mg
y
This product has not changed. The information on the label as
been updated to state the amount of hyoscine released over 72
hours, rather than the quantity of hyoscine contained in the
patch.
4.6
Add Hyoscine patch
releasing hyoscine
approx. 1.0mg/ 72 hours
gre
en
y
The average amount of hyoscine absorbed from each system in
72 hours is 1mg. (SPC 04/09/12)
Have added info to formulary from the SPC to further clarify.
In secondary care restricted - for patients with nausea
and vomiting - not controlled by other post-operative
nausea and vomiting drugs
Each system has a contact surface area measuring
2.5cm2 and hyoscine content of 1.5mg The average
amount of hyoscine absorbed from each system in 72
hours is 1mg
4.6
Add Proguanil Hydrochloride
with Atovaquone
100mg/250mg
For treatment of malariare
d
y
Malarone
NOTE for Formulary - If required for malaria prophylaxis for
holiday travel GP to prescribe on private prescription basis only.
If required for malaria prophylaxis for holiday travel GP
to prescribe on private prescription basis only.
5.4
.1
Add Proguanil Hydrochloride
with Atovaquone
25mg/62.5mg
paediatric tablet
For treatment of malaria
red y
Malarone
NOTE for Formulary - If required for malaria prophylaxis for
holiday travel GP to prescribe on private prescription basis only.
If required for malaria prophylaxis for holiday travel GP
to prescribe on private prescription basis only.
5.4
.1
Revise product Dimeticone lotion 4%
(Hedrin)
Primary Care advocate
combing only– if treatment
is to be given this should
be purchased OTC
red
y
For use in secondary care only For use in secondary care only
13
.10
.4
Ma
y1
3.1 Add Tobramycin nebuliser
solution 300mg
(Bramitob)
PBr -SCG
Cystic fibrosis Initiation by
Consultant
Paediatricians
specialising in Cystic
fibrosis red y
Approved for the management of chronic pulmonary infection
due to Pseudomonas aeruginosa in patients with cystic fibrosis
aged 6 years and older if nebulised colistin is not tolerated or if
clinical progress is unsatisfactory
Restricted - initiation by consultant Paediatricians
specialising in Cystic Fibrosis for the management of
chronic pulmonary infection due to Pseudomonas
aeruginosa in patients with cystic fibrosis aged 6 years
and older if nebulised colistin is not tolerated or if clinical
progress is unsatisfactory.
Traffic light status to be agreed
5.1
.4
Ma
y-1
3
FMG Decisions May 2013

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Ma
y 1
3.1 Add Tobramycin dry
powder for inhalation
Tobi Podhaler
28mg/capsule
Cystic fibrosis Initiation by
Consultant
Paediatricians
specialising in Cystic
fibrosis
red
y
Approved for the management of chronic pulmonary infection
due to Pseudomonas aeruginosa in patients with cystic fibrosis
aged 6 years and older in accordance with NICE TA 276. To be
used as a second line to tobramycin nebuliser solution
Bramitob)
30Oct13 removed comment re TLL to be agreed. Agreed red
Restricted - initiation by consultant Paediatricians
specialising in Cystic Fibrosis for the management of
chronic pulmonary infection due to Pseudomonas
aeruginosa in patients with cystic fibrosis aged 6 years
and older in accordance with NICE TA 276
To be used second line to tobramycin nebuliser solution
(Bramitob®)
5.1
.4
Ma
y-1
3
Ma
y 1
3.3 Add AquADEKs liquid Initiation by
Consultant
Paediatricians and
continuation by GPs
AI
n
Aquadeks® liquid is approved for formulary inclusion for CF
patients who cannot swallow tablets.
Restricted - initiation by Consultant Paediatricians with
continuation by GPs for cystic fibrosis patients who
cannot swallow tablets.
Ma
y-1
3
Ma
y1
3.3 Rejected Aquadeks soft gel
capsules and chewable
tablets bla
ck
n
Children over 6 who are able to swallow tablets/capsules to be
prescribed the 3 separate products of vitamin A and D
capsules, vitamin E capsules and menadiol tablets, the latter if
required. Ma
y-1
3
MA
y1
3.8 Add Apixaban tablet 2.5mg,
5mg
Prevention of stroke and
systemic embolism in
patients with AF when a
NOAC is indicated
according to the Bucks
local criteria and the
patient has had GI
disturbance or bleeding
with dabigatran and
rivaroxaban OR the
patient is unable to take
either dabigatran or
rivaroxaban due to a
history of GI bleeding or
ulceration
Initiated and
continued by NOAC
clinic only
Re
d
y
review TLL position once protocol available. Traffic light
position to change to AI once protocol approved
Restricted - initiation and continuation by NOAC clinic
only for the prevention of stroke and systemic embolism
in patients with AF when a NOAC is indicated according
to the Bucks local criteria and the patient has had a GI
disturbance or bleeding with dabigatran and rivaroxaban
OR the patient is unable to take either dabigatran or
rivaroxaban due to a history of GI bleeding or ulceration.
2.8
.2
Ma
y-1
3
Ma
r 1
3.3 Add Ranibizumab solution
for intravitreal injection,
2.3mg/0.23mL
Diabetic Macular Oedema Consultant
Ophthalmologists
red y
NICE compliance in accordance with NICE TA 274 FOR ALL PRESCRIBING - NICE compliance form
required - see link from Formulary homepage.
1. Restricted - Prescribing by Ophthalmologists only for
the treatment of Age Related Macular Degeneration
(AMD). Intravitreal use only. Traffic light list: Red
See Guideline: Ranibizumab for the treatment of age-
related macular degeneration (based upon NICE TA
155).
2. Restricted - Prescribing by Ophthalmologists only in
accordance with NICE TA 274 Ranibizumab for the
treatment of Diabetic Macular Oedema (DMO).
Intravitreal use only. Traffic light list: Red
11
.8.2
Ju
n-1
3
Revise
restricionMinocycline 50mg,
100mg capsules and
Minocycline MR 100mg
For treatment of
dermatological conditions
other than acne AI
y
In accordance with Dermatology Referral guidelines Restricted - for treatment of dermatological conditions
OTHER than acne in accordance with Dermatology
Referral guidelines.
For all other uses - Microbiology approval required 5.1
.3

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Revise
restricionMinocycline 50mg,
100mg capsules and
Minocycline MR 100mg
for treatment of acne
gre
en
y
In accordance with Dermatology Referral guidelines - only
100mg m/r strength used in acne
for the treatment of acne.
5.1
.3
Change Betamethasone
0.05%/calcipotriol
50micrograms/g
ointment, 60g
(Dovobet)
Prescribing by
Dermatology team
red y
Dovobet® may be therapeutically substituted with
betamethasone dipropionate ointment 0.05% (Diprosone®) and
calcipotriol ointment 50micrograms/g in accordance with
primary care current practice
Dovobet®
In secondary care restricted - to prescribing by
Dermatology team.
Dovobet® ointment may be therapeutically substituted
with betamethasone dipropionate ointment 0.05%
(Diprosone®) and calcipotriol ointment 50micrograms/g,
in accordance with primary care current practice
13
.5.1
Add Betamethasone
dipropionate 0.05%
ointment (Diprosone) gre
en
y
Added as per above statement regarding substitution of
Dovobet.
Diprosone
13
.4
Add or amend Nicotine"10mg",
"15mg","25mg" patch
NRT for primary care use,
except for 25mg patch
gre
en
y
Nicorette Invisi patches releasing approx. 10mg, 15mg
or 25mg over 16 hours.
Restricted - use in accordance with NRT guideline. All
strengths available for use in Primary Care. In
Secondary Care only the "25mg" patch may be used.
4.1
0.2
Add Nicotine "7mg", "14mg",
"21mg" patch
NRT for primary care use
gre
en
y
NiQuitin patch
Releasing approx. 7mg, 14mg or 21mg over 24 hours
Restricted - for use in Primary Care only 4.1
0.2
De
c
12
.3 Revise Nicotine lozenge, sugar-
free 1.5mg, 4mg
gre
en
y
NiQuitin Mini lozenge
4.1
0.2
De
c
12
.3 Add Nicotine inhalator
15mg/cartridge, 36
cartridges gre
en
y
Nicorette
Restricted - use in accordance with NRT guideline
4.1
0.2
Add Nicotine 1mg, 2mg,
4mg lozenge, sugar-free
NRT for primary care use
gre
en
y
Restricted - for use in Primary Care only.
NiQuitin® Minis lozenge 1.5mg and 4mg available for
use in Secondary Care (see entry above) 4.1
0.2
Add Nicotine 2mg sublingual
tablet
NRT for primary care use
gre
en
yNicorette Microtab
Restricted - for use in Primary Care only
4.1
0.2
Add Nicotine chewing gum,
2mg, 4mg
NRT for primary care use
gre
en
yRestricted - for use in Primary Care only
4.1
0.2
Add Nicotine
500micrograms/metered
spray
NRT for primary care use
gre
en
y
Restricted - for use in Primary Care only
4.1
0.2
Add Sodium hypochlorite
320mg tablet (Milton®)
Disinfection of diagnostic
contact lenses
Ophthalmology team
red
yRCog guidelines; ‘Managing CJD/vCJD risk in opthalmology’ Restricted - for use by Ophthalmology team only for
disinfection of diagnostic contact lenses xx
#####
Reinstate Carmustine 100mg
injection red
?
Was deleted as thought no longer available but is required
occasionally and now obtainable through IDIS. (ask MTS)
8.1
.1
#####
Formulary Changes for Note FMG May 2013

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Add isosorbide mononitrate
M/R 40mg and 60mg
tablet
gre
en
y
For use when there is a shortage of isosorbide mononitrate
immediate release 10mg, 20mg and 40mg tablets, change to
the modified release tablets on a mg - mg basis. For example,
isosorbide mononitrate 20mg twice daily should be changed to
isosorbide mononitrate MR 40mg once daily.
Restricted - only for use if there is a shortage of
immediate release 10mg, 20mg and 40mg tablets.
Change to SR tablets on a mg to mg basis. Eg.
Isosorbide 20mg twice daily should be changed to
isosorbide SR 40mg daily.
2.6
.1
Ma
y-1
3
Revise
restrictionBotulinum toxin type B
Neurobloc® brand
Consultant
Neurologists
red y
Cervical dystonia (Spasmodic torticollis) in accordance with the
SPC and MHRA advice Feb 2013
Restricted - prescribing by Consultant Neurologists
1. When resistance to Botulinum toxin type A has been
confirmed
2. For cervical dystonia (spasmodic torticollis) in
accordance with the SPC and MHRA advice Feb 2013
4.9
.3
Ma
y-1
3
Specify brand Carmellose 0.5%
Celluvisc® eye drops
Hospital diagnostic contact
lenses. For all other
indications the generic
product may be used
Hospital
Ophthalmology team
red y
Celluvisc® brand restricted - for use by hospital
ophthalmology team only for contact lens diagnostics.
For all other indications generic product to be used.
Traffic light list: Red 11
.8.1
Ma
y-1
3
Add C1 esterase inhibitor
injection 500units
Treatment of acute attacks
of potentially life
threatening hereditary
angioedema in accordance
with MOBBB Policy
statement 87 dated
September 2012
On the advice of A&E
consultants only
red
To be used in accordance with criteria defined in I MOBBB
Policy statement for acute life threatening attacks of HO only
when symptoms described in the policy statement are
confirmed to be present,
Restricted - prescribed only on advice of A&E
consultants in accordance with criteria defined in
MOBBB Policy statement 27 for acute life threatening
attacks of hereditary angioedema only when symptoms
described in policy statement are confirmed to be
present Traffic light list: Red
3.4
.3
Ma
y-1
3
Revise
restricitonRemifentanil injection all
strengths
PCA in labour where
epidural or pethidine is not
an option
consultant
anaesthetists
red
n
23. Guideline for remifentanil PCA in labour Restricted to prescribing by Consultant Anaesthetists
only.
1. Use in accordance with Guidelines for the use of
Intravenous (IV) infusion of remifentanil for sedation in
the general ICU (BHTCG 735) Use to be recorded and
reviewed on the Remifentanil Sedation in Adult Patients
on ITU - Compliance Form
2. Use in accordance with Guideline for Remifentanil
PCA in Labour (BHTCG 23)
15
.1.4
.3
Ma
y-1
3
Add Bivalirudin 250mg
injection
STENI ACS in accordance
with NICE TA 230
Consultant
Cardiologists
red y
For patients intolerant to first line treatment options Restricted - prescribing by Cardiologists only for patients
intolerant to first line treatment options for ACS STEMI
and in accordance with NICE TA 230 Bivalirudin for the
treatment of ST-segment-elevation myocardial infarction.
Traffic light list: Red
2.8
.1
Ma
y-1
3
Add Precision Xceed Pro
blood test strips
For use within secondary
care for blood glucose and
ketone testing red
Ongoing discussion between trust and CCGs for product
choice.
From Abbott Diabetes Care. Entered on netFormulary
23Feb15. Unsure of outcome of discussion between CCG and
BHT but these products are in regular use in BHT.
For use within secondary care for blood glucose and
ketone testing
6.1
.6
Ma
y-1
3
Add Precision Xceed Pro
ketone test strips red
For use within secondary care for blood glucose and
ketone testing
6.1
.6
#####
Add Medisense Control
solution (High/low) red
For use within secondary care for blood glucose and
ketone testing
6.1
.6
#####

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Add Medisense QC solution
(high/low)
For use within primary care
for blood glucose and
ketone testing gre
en 23 Feb15 Check if actually in use in primary care before
entering on netFormulary.
For use within primary care for blood glucose and ketone
testing
6.1
.6
#####
Delete Halothane No longer available
15
.1.2
#####
Revise
restrictionBone Cement with
gentamicin and
vancomycin
(Copal G+V)
red
Microbiology do not need to give approval for use therefore
remove restriction
Medical Device
xx
Ma
y-1
3
De
c1
2.2 Revise
restrictionBotulinum type A for migraine
red
NICE compliance form not yet available. Going to CGS June13 1. Restricted - prescribing by Ian Currie, Consultant
Urogynaecologist and Mr Greenland, Consultant
Urologist, for treatment of detrusor overactivity. Named
patient. Unlicensed use.
2. Restricted - prescribing by Matthew Koshy,
Consultant Neuro-rehabilitation medicine for Spasticity.
3. Restricted - prescribing by Consultant Neurologists
and Chronic Pain consultants only in accordance with
NICE TA 260 Botulinum toxin type A for the prevention
of headaches in adults with chronic migraine. ALL
PRESCRIBING in accordance with NICE TAs - NICE
compliance form required - see link from Formulary
homepage.
4.9
.3
Add Crotamiton cream
gre
en
#####
not added Eurax HC No longer available
#####
Add Methylphenidate MR
(Concerta XL) 27mg
for treatment of ADHD in
children over 6 years
Initiation by Cons
Paediatricians who
specialise in
behavioural disorders
and continued by
GPs
AP y
Added as included in updated SCP for ADHD Restricted - initiation by Consultant Paediatricians
specialising in childhood behavioural disorders or Child
or Adult Mental Health Specialist with continuation by
GPs for the treatment of ADHD in children over 6 years
and in accordance with ADHD amber protocol (BHTCG
796)
4.4
Ma
y-1
3
Add Methylphenidate MR
(Equasym XL) 20mg
for treatment of ADHD in
children over 6 years
Initiation by Cons
Paediatricians who
specialise in
behavioural disorders
and continued by
GPs
AP y
Added as included in updated SCP for ADHD Restricted - initiation by Consultant Paediatricians
specialising in childhood behavioural disorders or Child
or Adult Mental Health Specialist with continuation by
GPs for the treatment of ADHD in children over 6 years
and in accordance with ADHD amber protocol (BHTCG
796)
4.4
Ma
y-1
3
Add Atomoxetine capsules
80mg
for treatment of ADHD in
children over 6 years
Initiation by Cons
Paediatricians who
specialise in
behavioural disorders
and continued by
GPs
AP y
Added as included in updated SCP for ADHD Restricted - initiation by Consultant Paediatricians
specialising in childhood behavioural disorders or Child
or Adult Mental Health Specialists with continuation by
GPs for the treatment of ADHD in children over 6 years
and in accordance with ADHD amber protocol (BHTCG
796)
4.4
Ma
y-1
3

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Add Nevirapine 400mg
prolonged release cap
HIV Treatment GUM consultants
red
y
Alternative to the standard 200mg immediate release
formulation. It reduces the pill burden once patients are
established & tolerate the treatment Used in Oxford where
patients are treated under shared arrangements
All HIV drugs are on the formulary as being restricted to
prescribing by GUM consultants only and TLL is Red
5.3
.1
Ma
y-1
3
Revis UMP risk
ratingVinblastine injection Haematology indications Haematology and
Oncology teams
red
N
Unlicensed medicine - Medium Risk - risk increased because
licensed manufacturer supply difficulties. Expected to be
resolved by September 2013
Should risk be high as CYTO?
Unlicensed - High Risk
8.1
.4
Ma
y-1
3
Reinstate Gadofosveset
(Ablavar®)
Contrast agent Consultant
Radiologists
red
N
Unlicensed - Low Risk
Identical to the UK licensed Vasovist® brand which was on
formulary but discontinued. Ablavar® is a US licensed
equivalent product
Unlicensed - Low Risk
Restricted - prescribing by Consultant Radiologists only
Mis
c
Ma
y-1
3
Add Healthy Start Children's
vitamin drops
Paediatrics team,
Health visitors,
Womens and
Childrens team
red
n
Daily dose of 5 drops contains: 233micrograms Vitamin A,
20mg Vitamins C and 7.5micrograms Vitamin D3
In accordance with DOH guidance and the Bucks Vitamin D
guidelines
Service commissioned via BHT via District Nurses
Daily dose of 5 drops contains approx. 233micrograms
Vitamin A 700units (233micrograms), Vitamin C 20mg
and Vitamin D 300units (7.5microgams)
Restricted to prescribing by Paediatric team, Health
Visitors, Women's and Children's team in accordance
with DOH guidance and the Bucks Vitamin D guidelines.
Service commissioned via BHT via District Nurses.
9.6
.1
Ma
y-1
3
Add Healthy Start vitamins
for women
Paediatrics team,
Health visitors,
Womens and
Childrens team
red
n
One tablet daily contains: 70mg Vitamin C, 10micrograms
Vitamin D and 400micrograms Folic Acid
in accordance with DOH guidance and the Bucks Vitamin D
guidelines
Service commissioned via BHT via District Nurses
Each tablet contains approx. Vitamin C 70mg, Vitamin D
10micrograms and Folic Acid 400micrograms.
Restricted to prescribing by Paediatric team, Health
Visitors, Women's and Children's team in accordance
with DOH guidance and the Bucks Vitamin D guidelines.
Service commissioned via BHT via District Nurses.
9.6
.1
Ma
y-1
3
Ma
y 1
3.2 Add Mannitol 40mg powder
for inhalation
Cystic fibrosis in adults Respiratory
consultants
red
In accordance with NICE TA 266 Mannitol dry powder for
inhalation recommended as an option for treating cystic fibrosis
in adults: who cannot use rhDNase because of neligibility,
intolerance or inadequate response to rhDNase and whose
lung function is rapidly declining (forced expiratory volume in 1
second [FEV1] decline greater than % annually) and for whom
other osmotic agents are not considered appropriate. Not used
in BHT as all adult CF patients are treated at Oxford or in
London.
FOR ALL PRESCRIBING - NICE compliance to be
verified.
Restricted - to prescribing by Respiratory consultants in
accordance with NICE TA 266 Mannitol as an option for
treating cystic fibrosis in adults.
NOTE: Unlikely to be used in BHT as all adult CF
patients are treated in Oxford or London.
3.7
Ma
y-1
3
Ma
r 1
3.2 Add Methylphenidate MR
(Medikinet XL) 5mg,
10mg, 20mg, 30mg,
40mg
for treatment of ADHD in
children over 6 years
Initiation by Cons
Paediatricians and
Child/Adult Mental
Health specialists and
continued by GPs
AP y
In accordance with shared care protocol
4.4
Ma
r-1
3
Ja
n1
3. 2 Revise
restrictionTicagrelor tablet 90mg see BHT CG Antiplatelet
guideline
Cardiology team only
with continuation by
GPs
AI
y
In accordance with BHT CG Antiplatelet guideline
2.9
Ma
r-1
3
FMG Decision March 2013

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Ja
n
13
.5 Revise TLL
classificationVoriconazole
red y
Restricted – Haematology and Oncology consultants, GUM and
solid organ transplant patients. Microbiology approval required
for all other uses. Traffic light list: Red.
Ma
r-1
3
Oct
12
.1 Revise
restrictionMinocycline
y
Uses see guideline
Ma
r-1
3
Oct1
2.1 2 Guideline
approved CGSSomatropin Paediatric
red y
Ma
r-1
3
De
c
12
.3 Add Nicotine inhalator
15mg/cartridge
Additional NRT product for
hospital to use
gre
en
y
Nicorette SEE BELOW
4.1
0.2
Ma
r-1
3
Ma
y1
1.4 Add Colecalcifierol capsules
20,000units
Vitamin D deficiency
gre
en
n
Unlicensed Medium risk
Dekristol® Imported via IDIS
Restricted - for use in accordance with BHT CG 785.1 Vitamin
D Testing and Treatment in Adults. Ma
r-1
3
Add Ergocalciferol i.m.
injection 7.5mg
(300,000units/mL)
Vitamin D deficiency
gre
en
y
Restricted - for use in accordance with BHT CG 785.1 Vitamin
D Testing and Treatment in Adults.
9.6
.4
Ma
r-1
3
Ja
n1
3.1 Add Ivabradine tablet 5mg,
7.5mg
For Chronic Heart Failure
in accordance with NICE
TA 267
Initiated by
Consultant
Cardiologists on
name patient
approval until NICE
compliance form
approved and GP
continuation
AI
y
Named patient approval only until AI guideline in place
2.6
.3
Ja
n-1
3
Ja
n1
3.3 Add Retigabine tablet, 50mg,
100mg, 200mg, 300mg,
400mg
For adjuvant treatment of
epilepsy in accordance
with NICE TA 232
Initiated by
Consultant
Neurologists with GP
continuation
AI
y
Named patient approval only until AI guideline in place
4.8
.1
Ja
n-1
3
De
c1
2.2 Add Botulinum toxin type A
(Botox brand)
For prevention of
headache in patients with
migraine in accordance
NICE TA260
Prescibing by
Consultant
Neurologist and
Consultant Chronic
Pain only
Re
d
y
4.9
.3
Ja
n-1
3
Oct
12
.9 Guideline
approved CGSTriptorelin for use in
Obs & Gynae AR
guideline
AR
Ja
n-1
3
Ma
y1
2.5 Guideline
approved CGSBHT CG315 Protease
Inhibitors Telaprevir and
Boceprevir for the
treatment of Genotype 1
Chronic Hepatitus C
in accordance with NICE
TA 252 and TA253
Ja
n-1
3
Ma
r12
. 4 Guideline
approved CGSActinic keratoses
guideline
Ja
n-1
3
FMG Decisions January 2013

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
OC
t11
. 1 Guideline
approved CGSIntranasal Steroid
Guideline
Ja
n-1
3
Add Bone Cement with
gentamicin and
vancomycin
(Copal G+V)
Revision total hip
replacemen t surgery
Orthopaedics
consultants only, on
the advice of
Microbiology and
named patient
advanced formulary
approval
red y
Palacos R is being used at present and this does not contain
vancomycin. Vancomycin is currently being added to Palacos R
by mixing it manually in theatres. Microbiology recommend the
use of Copal G+V for specific patients undergoing orthopaedic
surgery where risk of non-union due to infection is high .
Named patient approval by Microbiologist required.
£270 per 40g powder. Palacos R 2x40g £54
xx
Ja
n-1
3
Add Ipilimumab
concentrate for IV
infusion vial
50mg/10mL,
200mg/40mL
previously treated
advanced (unresectable or
metastatic) melanoma in
accordance with NICE TA
268
ORH Oncology
consultants
red Y
Horizon scanning identified zero patients for treatment at BHT.
Any patients will be referred to ORH and use with be in
accordance with TVCN Protocol. NICE TA costing template
estimates very little cost pressure 8.1
.5
Ja
n-1
3
Add Vemurafenib tablet
240mg
treating locally advanced
or metastatic BRAF V600
mutation-positive
malignant melanoma
ORH Oncology
consultants
red y
Horizon scanning identified zero patients for treatment at BHT.
Any patients will be referred to ORH and use with be in
accordance with TVCN Protocol. NICE TA costing template
estimates 4 patients for Bucks population with a cost pressure
of 205,372.
8.1
.5
Ja
n-1
3
Add Vitamin A and D
capsules
4000units/400units
(10micrograms)
Prophylaxis of vitamin A
and D deficiency in
paediatric cystic fibrosis
patients
Paediatrics team
initiation, continuation
by GPs gre
en
y
BNF price is 3.44 per pack. 20 CF patients under BHT
Paediatrics team care each year. Mainly prescribed by GPs for
these patients 9.6
.1
Ja
n-1
3
Ja
n
13
.4 Add Calcitriol (Silkis®)
ointment
3micrograms/g, 100g gre
en
13
.5.2
Ja
n-1
3
Ja
n 1
3.4 Add Hydrocortisone ointment
0.5%, 15g, 30g
gre
en
Potency: Mild
13
.4
Ja
n-1
3
Ja
n
13
.4 Add Hydrocortisone/Urea
cream 1%/10%, 30g,
100g (Alphaderm®) gre
en Potency: Moderate
13
.4
Ja
n-1
3
Ja
n
13
.4 Add Azelaic acid cream
20%, 30g
Skinoren® gre
en
13
.6.1
Ja
n-1
3
Ja
n
13
.4 Add Azelaic acid gel 15%,
30g
Finacea® gre
en
13
.6.1
Ja
n-1
3
Ja
n 1
3.4 Add Benzoyl
peroxide/potassium
hydroxyquinoline sulfate
cream 5%/0.5%, 50g
and 10%/0.5%, 25g,
50g (Quinoderm®)
gre
en
13
.6.1
Ja
n-1
3

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Ja
n
13
.4 Add Benzoyl peroxide cream
4%, 40g (Brevoxyl®)
gre
en
13
.6.1
Ja
n-1
3
Ja
n
13
.4 Add Coal tar extract
shampoo 2%, 125mL,
250mL (T/Ggel®) gre
en
13
.9
Ja
n-1
3
Ja
n 1
3.4 Add Isopropyl myristate/
Liquid paraffin gel
15%/15%, 100g, 500g
(Doublebase®)
gre
en
13
.2.1
Ja
n-1
3
Ma
r
12
.4 Guideline
approved CGSActinic Keratoses
guideline
Ja
n-1
3
Ma
r
12
.3 Add Fluorouracil/salicyclic
acid 0.5%/10% solution,
25mL
For actinic keratoses
gre
en
y
Actikerall®
To be used in accordance with CG365 Treatment of Actinic
Keratoses 13
.8.1
De
c-1
2
Ma
r 1
2.3 Add Diclofenac sodium 3%
in a sodium hyaluronate
gel basis, 50g
For actinic keratoses
gre
en
y
Solaraze
In accordance with AK guideline
13
.8.1
De
c-1
2
Oct
12
.9 Add Triptorelin MR i.m.
injection 3mg
Recommendation of
Obs and Gynae team
with continuation by
GPsA
R y
On recommendation of Obs and Gynae team for treatment of
endometriosis and reducing the size of uterine fibroids
6.7
.2
De
c-1
2
Oct1
2.9 Add Triptorelin MR i.m.
injection 11.25mg
AR y
Decapeptyl SR® (11.25mg i.m. injection every 3 months)
Restricted to prescribing in Primary care only (not to be
prescribed in Secondary care)
May be used for treatment of endometriosis and reducing the
size of uterine fibroids on the recomendation of Obs & Gynae
team with continuation by GPs. Traffic light list: Amber
recommendation
6.7
.2
De
c-1
2
Oct
12
.8 Add
NICE
compliance
form awaited
Abiraterone NICE TA 259 Abiraterone
acetate for castration-
resistant metastatic
prostate cancer previously
treated with a docetaxel-
containing regime
Consultant
Oncologists for
patients with prostate
cancer red y
8.3
.4
De
c-1
2
Oct
12
.6 Add
NICE
compliance
form awaited
Imatinib (standard
dose)
PBR excl funded NHS
England
For CML in accordance
NICE TA 251 Dasatanib,
standard dose imatinib and
nilotinib for CML (dasatanib
not recommended)
Consultant
Haematologists
red y
De
c-1
2
Oct
12
.6 Add
NICE
compliance
form awaited
Nilotinib
PBR Excl funded NHS
England
For CML in accordance
NICE TA 251 Dasatanib,
standard dose imatinib and
nilotinib for CML (dasatanib
not recommended)
Consultant
Haematologists
red y
De
c-1
2
FMG Decision December 2012

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Oct
12
.4 Add
NICE
compliance
form awaited
Nilotinib
PBR Excl funded NHS
England
For CML in accordance
NICE TA 241 Dasatanib,
high dose imatinib and
nilotinib for CML (dasatanib
and high dose imatinib not
recommended)
Consultant
Haematologists
red
y
De
c-1
2
Oct
12
.3 Add
NICE/HCD form
awaited
Hospital
guideline
awaited
Rivaroxaban Treatment of DVT and
prevention of recurrent
DVT and PE.
NICE TA 261
Consultant
Haematologists
red y
Named patient approval only as NICE/HCD compliance form
awaited.
De
c-1
2
Aug
12
.6 Guideline
approved CGSHypertension gudieline Hypertension NICE CG
127
De
c-1
2
Oct1
2.5 Add
HCD form
awaited
Rituximab Follicular lymphoma NICE
TA 243
Haematologists
red
y
In accordance with NICE TA 243
NICE compliance form required
De
c-1
2
Aug
12
.5 Add Indapamide 2.5mg Hypertension NICE CG
127
gre
en
y
In accordance with NICE CG 127 Hypertension and BHT CG
227 Clinical Management of Hypertension is Adults
2.5
.5.1
De
c-1
2
Aug
12
.6 Guideline
approved CGSHypertension guideline Hypertension NICE CG
127
De
c-1
2
Aug
12
.9 HCD form
approvedGolimumab psoriatic arthritis NICE TA
220
consultant
rheumatologistsre
d y
Psoriatic arthritis in accordance with NICE TA 220. NICE
compliance form required
In accordance with BHT CG Biologics in Psoriatic Arthritis. 10
.1.3
De
c-1
2
Add Nicotine (NiQuitin)
lozenge 1.5mg, 4mg
additional NRT product for
immediate use, the
NiQuitin lozenge (NiQuitin
Minis) 1.5mg and 4mg
were approved as an
interim measure.
gre
en
y
4.1
0.2
De
c-1
2
Remove Oseltamivir 15mg/ml
liquid unlicensed
Treatment of influenza in
infants less than one year
of age; Prophylaxis of
influenza in children aged
one year or more
n
Not required as licensed 6mg/ml product available
5.3
.4
De
c-1
2
Delete Carmustine injection
100mg
No longer available
8.1
.1
#####

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Change Mesalazine MR 400mg
tablets
1st Choice - Mesren MR®.
(bioequivalent to Asacol
MR®)
Mesren MR® to be
prescribed 1st line instead
of Asacol MR®. Patients
stabilised on Asacol MR®
should not to be switched
unless prescribed
generically.
gre
en
y
1st Choice - Octasa MR®. (bioequivalent to Asacol MR®)
Octasa MR® to be prescribed 1st line instead of Asacol MR®.
Patients stabilised on Asacol MR® should not to be switched
unless prescribed generically.
1.5
.1
De
c-1
2
Add Adenosine infusion
130mg in 130mL red N
MPSA Safety Alert 20 recommend using ready prepared
solutions where available.
2.3
.2
#####
Add Atropine injection
1mg/mL red
New strength due to lack of availability of other strength.
15
.1.3
#####
Update
restrictionAlteplase infusion 50mg Ischaemic stroke Stroke team and A&E
senior physicians
red
y
In accordance with NICE TA 264. NOTE: BHT Clinical
Guideline 146.4 Management of Acute Stroke and 12.1 Stroke
Thombolysis Protocol will need to be amended in line with NICE
TA 264. De
c-1
2
Add Seretide® 50 inhaler Paediatric respiratory
disorders
gre
en
y
For treatment of asthma in accordance with British Thoracic
Society BTS Guideline on the Management of Asthma revised
2009
3.2
De
c-1
2
Add Triptorelin 22.5mg vial For locally advanced non-
metastatic prostate cancer
Consultant Urologists
or Oncologists, and
continuation by GPs AP y
Restricted - for use in Primary Care only for patients who are
receiving triptorelin 3 monthly as Shared Care and are deemed
suitable for the 6 monthly injections.
No cost difference 3/12 £207 and 6/12 £414
8.3
.4
De
c-1
2
Oct
12
.3 Add Rivaroxaban Treatment of DVT and
prevention of recurrent
DVT and PE.
Consultant
Haematologists
Re
d
y
Use NICE compliance form
NICE TA 261 Rivaroxaban for the treatment of deep vein
thrombosis and
prevention of recurrent DVT and PE. To be used for patients
unsuitable for warfarin for whom dalteparin would otherwise be
considered,
2.8
.2
Oct-
12
Au
g 1
2.8 Add Tocilizumab Rheumatoid Arthritis Consultant
Rheumatologists
Re
d
y
Use NICE compliance form
NICE TA 247 Tocilizumab in Rheumatoid Arthritis and in
accordance with BHT CG 749 Biologics Rheumatoid Arthritis
guideline
10
.1.3
Oct-
12
Ma
y 1
2.5 Add Telaprevir Hepatitis C Consultant
Gastroenterologist
and Associate
Specialist
Gastroenterology Re
d
y
Use NICE compliance form
NICE TA 252 Telaprevir for the treatment of genotype 1 chronic
hepatitis C and TA253 Boceprevir for the treatment of genotype
1 chronic hepatitis C and in accordance with BHT CG Protease
Inhibitors Telaprevir and Boceprevir for the treatment of
Genotype 1
Chronic Hepatitis C
5.3
.3.2
Oct-
12
FMG Decision October 2012

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Ma
y 1
2.5 Add Boceprevir Hepatitis C Consultant
Gastroenterologist
and Associate
Specialist
Gastroenterology Re
d
y
Use NICE compliance form
NICE TA 252 Telaprevir for the treatment of genotype 1 chronic
hepatitis C and TA253 Boceprevir for the treatment of genotype
1 chronic hepatitis C and in accordance with BHT CG Protease
Inhibitors Telaprevir and Boceprevir for the treatment of
Genotype 1
Chronic Hepatitis C
5.3
.3.2
Oct-
12
De
c 1
1.4 Add Adrenaline (Jext) auto-
injector 150micrograms
and 300micrograms
Emergency treatment of
acute anaphylaxis
In secondary care
restricted to
prescribing by middle
grade doctors and
above.
Gre
en
y
All prescribing to ensure patient has 2 devices. Prescriptions
may be written for up to 2 devices per patient at one time for
adults and children.
3.4
.3
Oct-
12
De
c1
1.4 Delete Adrenaline (Epipen)
auto-injector
150micrograms and
300micrograms
Emergency treatment of
acute anaphylaxis
Gre
en
y
3.4
.3
Oct-
12
Fo
r n
otin
g Revised
restrictionClindamycin capsules,
injection and
suspension
Microbiology
y/
n
Restricted - Microbiology approval required for use in patients
over 85 years of age, but caution in prescribing for any patient
over 65 years due to increased risk of Clostridium difficile
associated diarrhoea
5.1
.6
Oct-
12
Fo
r
no
tin
g Revised
formulary
entry
MS treatment algorithm All DMTs to be used in
accordance with BHT CG
MS treatment algorithm
Oct-
12
Au
g 1
2.1 Revise TLL
classificationSomatropin Growth deficiency Consultant
Paediatricians and
Consultant
Endocrinologists
(adults)
AI/
Re
dAI for adults. Hospital only for new paediatrics. Existing
paediatrics to become Hospital Only from April 2013.
Guidelines awaited
6.5
.1
Oct-
12
Aug
12
.3 Add Fingolimod Multiple Sclerosis Consultant
Neurologists
Re
d
y
NICE compliance form required
To be used in accordance with NICE TA 254 MS (Relapsing-
remitting) and BHT CG MS Algorithm 8.2
.4
Oct-
12
Aug
12
.4 Revised TLL
classificationRiluzole Motor Neurone disease Consultant
Neurologists
Re
d
y
To be used in accordance with Hospital Only Riluzole guideline
4.9
.3
Oct-
12
Ma
y 1
2.1 Add Dabigatran Stoke prevention in AF in
accordance with NICE TA
249
INITIATION
Consultant
Cardiologists, Stroke
and Haematologists
(urgent cases only,
NOAC Pharmacist
(all other patients)
CONTINUATION
GPs
AI
y
All patients initiated by consultants to be referred to NOAC
clinic for followup in accordance with Dabigatran for Stroke and
AF AI guideline.
2.8
.2
Oct-
12

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Oct
10
.1 Add Almotriptan Treatment of migraine
gre
en
y
In accordance with BHT CG First and Second line treatments
for migraine
4.7
.4.1
Oct-
12
Add Rotigotine patch 1mg,
2mg,3mg, 4mg, 6mg,
8mg per 24 hours.
Parkinson's disease PD nurse or
Neurology team only
red y
Restricted - to prescribing by Neurology team or PD Nurses for
Parkinson's Disease when there is no other route of
administration possible. Patients are NOT to be discharged on
this product. Strengths other than 2mg and 4mg, are Phone
Pharmacy to Order.
4.9
.1
Oct-
12
Add Estradiol vaginal tablet
10micrograms
Vaginal atrophy
gre
en
y25microgram tablet already on formulary and 10microgram
required for initial use.
7.2
.1
#####
Ma
r12
.1 revised
restrictionDalteparin
subcutaneous injection
all strengths
For treatment and
prevention DVT and PE
AI
y
Treatment doses (exceeding 5000 units daily) and all
indications for use within obstetrics and gynaecology are
hospital only and Red on the TLL
For amber initiation indications see Amber Initiation guideline.
Note:for amber initiation the first 6 weeks supply to be provided
by hospital.
2.8
.1
Aug-1
2
Oct
11
.23 NICE form
approvedBortezomib and
thalidomide
1st line treatment of
multiple myeloma
Consultant
Haematologists
Re
d
Y
Use NICE compliance form
NICE 228 for multiple myeloma
8.1
.5
8.1
.3A
ug-1
2
Aug
11
.2 NICE form
approvedRituximab Follicular non-Hodgkin's
lymphoma
Haematologists
red
Use NICE compliance form
NICE TA 226 for first-line maintenance of follicular non-
Hodgkins' lymphoma 8.2
.3
Aug-1
2
Ma
y 1
1.3 NICE form
approvedPeginterferon alfa 2a
or 2b and ribavirin for
Hepatitis C
Hepatitis C Consultant and
Assoc. Spec in
Gastroenterology Re
d
y
Use NICE compliance form
In accordance with NICE TA 200
8.2
.4,5
.3.
5A
ug-1
2
ADD additional
strengthRibavirin 400mg tablet hepatitis C Consultant
Gastroenterologist,
Associate Specialist
Gastroenteroly and
Consultant
Paediatrician
red
y
Use in accordance with NICE TA 75 Interferon alfa and ribavirin
for the treatment of chronic hepatitis, NICE TA 106
Peginterferon alfa and ribavirin for the treatment of mild
hepatitis C and NICE TA 200 Hepatitis C - peginterferon alfa
and ribavirin. FOR ALL PRESCRIBING: NICE compliance form
required - see link from Formulary homepage. NICE
compliance to be verified if form not yet available.
5.3
.5
Aug-1
2
REVISE
restriction to
align with TLL
Rosuvastatin tablets (all
strengths)
Hyperlipidaemia Lipid clinic initiation;
continuation by GP AI
Ytreatment of hyperlipidaemia in patients who are intolerant of all
high intensity statins.
2.1
2
#####
FMG Decision August 2012
Formulary changes noted at FMG August 2012

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
REVISE
restrictionPatent blue injection sentinel node biopsy Plastic surgeons
red
n
m
ed
ris
k
sentinel node biopsy in malignant melanoma patients (already
on formulary for use in breast surgery)
Aug-1
2
ADD Klean-Prep® paediatric patients with
bowel obstruction
Paeds team
red y
1.6
.5
#####
REVISE
restrictionBevacizumab PFS
1.25mg in 0.5ml
Sight threatening
disorders: pre vitrectomy
for proliferative diabetic
retinopathy, rubeotic
glaucoma, non AMD
choroidal neo-vascular
membranes,
Consultant
ophthalmologists
red
n
REMOVE retinal venous occlusions (MOBBB 57), diabetic
macular oedema (MOBBB 56)
Aug-1
2
ADD Pentamidine isetionate
Injection 300mg
Prophylaxis of
Pneumocystis jirovecii
(Pneumocystis carinii)
pneumonia, by inhalation
of nebulised solution (using
suitable
equipment—consult
product literature
on recommendation
of Microbiology team
red y
Caution in handling Pentamidine isetionate is toxic and
personnel should be adequately protected during handling and
administration—consult product literature
5.4
.8
Aug-1
2
Revise
restrictionDapsone 50mg tablets Prophylaxis of
Pneumocystis jirovecii
(Pneumocystis carinii)
pneumonia,
on recommendation
of Microbiology teamre
dy
5.1
.10
Aug-1
2
ADD Indocyanine green dye
25mg in 5ml
Ophthalmology diagnostic
use
ophthalmology team
red
n
hi
gh
ris
k
Aug-1
2
ADD Insuman brands of
insulin 6.1
#####
REVISE
RESTRICTIONAdalimumab sc inj severe Crohn's disease in
adults (18YRS AND
OLDER)
consultant
Gastroenterologists
red y
in accordance with MOBBB Policy recommendation 61 'Dose
escalation therapy with infliximab and adalimumab in patients
with severe Crohn's disease Dec 2011 NOTE Dose Escalation
for severe Crohn's in 6-17 years age group (MOBBB
recommendation 62). and for active fistulising Crohn's (MOBBB
policy 600 are Nonformulary
1.5
.3
Aug-1
2
REVISE
RESTRICTIONInfliximab inj severe Crohn's disease in
adults (18YRS AND
OLDER)
consultant
Gastroenterologists
red y
in accordance with MOBBB Policy recommendation 61 'Dose
escalation therapy with infliximab and adalimumab in patients
with severe Crohn's disease Dec 2011 NOTE Dose Escalation
for severe Crohn's in 6-17 years age group (MOBBB
recommendation 62). and for active fistulising Crohn's (MOBBB
policy 600 are Nonformulary
1.5
.3
Aug-1
2

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
ADD Buprenorphine 400mcg
S/L tab
adjunct in the treatment of
opioid dependence
initiation by the
CAMS team
gre
en
Y
In accordance with NICE TA 114 - Methadone and
Buprenorphine for management of opioid dependence (Jan07)
4.1
0.3
Aug-1
2
Ma
y 1
2.3 Revised TLL
classificationMercaptopurine - use in
Gastroenterology –
traffic light review and
draft Shared Care
Protocol
AP
1.5
.3
Ju
n-1
2
Ja
n 1
2.2 ADD Febuxostat for gout (NICE TA 164) Restricted - to
prescribing by GPs
on the
recommendation of
the rheumatology
team.
AR
In accordance with amber recommendation guidance
10
.1.4
Apr-
12
De
c 1
1.5 APROVED Traffic light system
process version 2.1 (for
incorporation into the
Policy for Managed
Entry of New Medicines
Ma
y-1
2
Ma
r12
.6 Guideline
approvedMidazolam oromucosal
solution 5mg/mL
0.5mL (2.5mg),
1mL (5mg),
1.5mL (7.5mg),
2mL (10mg) prefilled
syringe
Epilepsy Adults: restricted to
initiation by
consultant
neurologists only.
Children: Restricted
to initiation by
Consultant
Paediatricians and
Neurologists, teams
from National Society
for Epilepsy Centre
and Ridgeway
Partnership (for
learning disabiltiy)
AI
for
ad
ults a
nd
pa
ed
s
Y
Buccolam®
in accordance with Status epilepticus algorithm and CG384.1
Buccal midazolam treatment algorithm. Traffic light list: Amber
Initiation.
4.8
.2
Ma
y-1
2
Ja
n1
2.8 Add Exenatide modified
release injection 2mg
vial, once weekly
Type 2 Diabetes Diabetes team
AI
Y
Restricted - initiation by Diabetes team in accordance with
NICE TA 248 Exenatide prolonged-release suspension for
injection in combination with oral antidiabetic therapy for the
treatment of type 2 diabetes and BHT CG83.1 Exenatide (Twice
Daily or Once Weekly) for use in Type 2 Diabetes amber
initiation guideline. Traffic light list: Amber initiation
6.1
.2.3
Ju
n-1
2
De
c1
1.1 add for primary
preventionDenosumab injection
pre-filled syringe
60mg/mL
Osteoporosis Cons Rheumatologist
and Endocrinologists
Re
d
y
To be prescribed in accordance with BHT CG 402 Osteoporosis
– Primary fracture prevention guidelines in men and women
over the age of 50 with risk factors and BHT CG 403
Osteoporosis – Secondary fracture prevention guidelines in
men and women over the age of 50 who sustain fragility
fracture and NICE TA 204 Osteoporotic fractures - Denosumab
6.6
.2
Ju
n-1
2
FMG May 12 decisions

FM
G M
inut
e r
ef
Decision
MedicineRestrictions
/IndicationsPrescribers
TLL
Licens
ed? (Y/N
)
Guideline / place in therapy /rationale behind
proposed change/comments(Amber shading = amendment to netFormulary required once
further action completed)
Restriction as it appears in Formulary
entries only May 2013 onwards
(Green = netFormulary updated)
(Unshaded = netFormulary not yet updated)
(Amber = clarification required) BNF c
ate
gory
Decision
date
Oct1
1.7 APPROVED Osteoporosis guidelines
for primary and
secondary fracture
prevention Ju
n-1
2
Oct1
1.2 2 Add Golimumab Ankylosing spondylitis Consultant
Rheumatologist
Re
d
y
In accordance with NICE TA 233 Golimumab for Ank Spond
10
.1.3
Ju
l-1
2
Au
g 1
1.3 Add Golimumab for Rheu Arthritis after
failure of previous disease
modifying anti-rheumatic
drugs
Consultant
Rheumatologist
Re
d
y
In accordance with NICE TA 225 Golimumab for Rheu Arthritis
after failure of previous disease modifying anti-rheumatic drugs
10
.1.3
Ju
l-1
2
Ma
y1
1.5 Add Ferric carboxymaltose Iron Deficiency anaemia Restricted -
prescribing by
Haematology team
only in accordance
with BHT CG
Re
d
Y
In accordance with BHT CG 58 Parenteral Iron for Iron
Deficiency Anaemia.
9.1
.1
Ma
y-1
2
Au
g 1
0.1 ADD Sugammadex for reversal of
neuromuscular block
produced by vecuronium or
rocuronium
restricted to
prescribing by
Anaesthetics team. red
In accordance with BHT CG151 Sugammadex for Reversal of
Neuromuscular blockade in Theatres.
15
.1.6
Ja
n-1
2
Ma
r
12
.2 Revised TLL
classificationFluorouracil cream
(Efudix®)
for use in Dermatology:
traffic light classification
review
Initiation by
Dermatology team AI
to be used in accordance with AK algorithm
13
.8.1
Ma
r-1
2
Ma
r
12
.5 REJECTED Linagliptin for Type 2 Diabetes
6.1
.2.3
Ma
r-1
2
Ja
n
12
.1 Revised TLL
classificationMycophenolate mofetil
(MMF)
in rheumatology traffic light
classification review
Consultant
Rheumatologists and
Dermatologists
red
8.2
.1
Apr-
12
Ja
n
12
.5 Add new
indicationClopidogrel for secondary prevention of
TIA
GR
EE
N
y 2.9
Ma
r-1
2
Ja
n
12
.7
Rationalised Contraceptives –
formulary review
In accordance with guideline BHT CG 783
7.3
Apr-
12
Ja
n
12
.9 ADD Ticagrelor for ACS – NICE TA 236
October 2011
Restricted to
prescribing by
Cardiology team
red
for in-patients with ACS (unstable angina, nSTEMI) who have
had an angiogram, are not suitable for PCI and are awaiting a
CABG
2.9
Ja
n-1
2
FMG March 12 decisions
FMG January 12 decisions




















