Self-evaluation.pdf - Faculty of Medicine and Health Sciences

HELSINGIN YLIOPISTO
ARVIOINTEJA
11 | 2003
EVALUATION PROJECTS
OF THE UNIVERSITY OF HELSINKI
Kaarlo Simojoki (Ed.)
Final Report on the Evaluationof the Faculty of Medicine
Evaluation of the Quality of Education and the Degree Programmesof the University of Helsinki

Evaluation of the Quality of Education and the Degree Programmes of the
University of Helsinki
Final Report on the Evaluationof the Faculty of Medicine
The following persons took part in the writing of the final report:
Satu Alaluusua Eeva PyöräläPirkko Heasman Hilpi RautelinHeikki Hervonen Juha Ruotoistenmäki
Timo Kuusi Antti SajantilaKirsti Lonka Mikko Salaspuro
Pekka Louhiala Martti SiimesTuomas Lähdeoja Kaarlo Simojoki
Tom Pettersson Ismo Virtanen
U N I V E R S I T Y O F H E L S I N K I

2
Cover design by Reija Jokinen
Layout: Sirpa Eskolin
Contact person of the publisher:Rebekka Niskanen, Academic Affairs,P.O.Box 3, 00014 University of Helsinki, Finland
ISBN 952-10-0968-3
Helsinki University Printing House 2003

3
Preface
This report is part of the evaluation of the quality of education and the degree pro-grammes of the University of Helsinki. For the medical faculty the evaluation processstarted at a point where educational reforms had been rolled out for several years andit was time to look for a new direction. Many details of the reforms had not been easyand had demanded the participation of many faculty staff members. However, theevaluation gave the possibility to slow down for a while and to reflect on the changesand work done.
The evaluation process itself included a lot of work, but it also provided the possibilityfor open discussion. Happily enough this option was actively used by the faculty staffmembers. As a result, a firmer joint vision for the future direction of curriculumdevelopment was achieved. The panelists’ report also had an important impact on thefaculty opinion climate by giving positive feedback and recognizing the extensive workdone.
This is an appropriate opportunity to thank all the teachers, faculty staff and studentswho have been a crucial part of the development process during the last years at ourfaculty. Without their dedicated involvement this faculty could not have been twicenominated a unit of excellence in the field of education.
But we should not forget that curriculum development is a never-ending processcreating again and again new challenges. Together we will move on to meet them.
Professor Matti J. Tikkanen Professor Mikko SalaspuroDean, Faculty of Medicine Dean of Education, Faculty
of Medicine

4

5
Contents
Preface .................................................................................................................. 3
1 Introduction ...................................................................................................... 7
2 Description of the field of education ................................................................ 8
3 Present state and development prospects of medical education ........................ 113.1 Undergraduate training at the University of Helsinki ............................. 113.2 Recent trends in undergraduate training at the University of Helsinki ... 113.3 The administrative organization of undergraduate studies ...................... 123.4 The aims of the undergraduate curriculum reform ................................. 133.5 The Helsinki 2000 curriculum ................................................................ 143.6 ”Growing to be a physician” ................................................................... 143.7 Objective structured clinical examination (OSCE) ................................. 153.8 The Learning Centre concept .................................................................. 153.9 Educational technology ........................................................................... 153.10 The Development and Research Unit ...................................................... 153.11 Staff development and teacher training ................................................... 163.12 The evaluation procedures ....................................................................... 16
4 The Self-evaluation process .............................................................................. 174.1 The Co-operation Group ........................................................................... 174.2 The panel visit ........................................................................................... 17
5 Panel report – Development by Rotation ......................................................... 195.1 Introduction ............................................................................................. 195.2 General observations ............................................................................... 215.3 Educational philosophy ........................................................................... 225.4 Curriculum design ................................................................................... 225.5 Organization of the curriculum ............................................................... 245.6 Learning environment ............................................................................. 265.7 Assessment ............................................................................................... 285.8 Learning results/student’s comments ....................................................... 295.9 Relationship between teaching and research ........................................... 305.10 Quality assurance ..................................................................................... 305.11 International activities/bilingualism. ....................................................... 315.12 PhD/MD-PhD/Specialist training/Dentistry ............................................ 325.13 Strengths and weaknesses, a summary .................................................... 33
6 Students and the second phase of the evaluation .............................................. 34
7 Conclusions and measures taken ....................................................................... 367.1 General observations ................................................................................. 367.2 The Development & Research Unit for Medical Education ..................... 367.3 The shared vision ...................................................................................... 367.4 Key issues .................................................................................................. 37
References ............................................................................................................. 42

6

7
1 Introduction
As part of its strategy for the years 2001–2003, the University of Helsinki decided tocarry out a comprehensive evaluation of its education. As specified in the decision ofthe University Senate, the aim of the evaluation project was:• to develop teaching and learning on the basis of the evaluation• to offer departments and faculties the opportunity to receive international feed-
back on their teaching• to improve the quality of degrees• to investigate how well the aims set for education and degrees are achieved• to develop evaluation systems and an evaluation culture at the departments and
faculties.
The evaluation will lead to the following concrete measures:• the feedback received will be made use of in the drawing up of future plans
for the development of teaching and studies at the departments, faculties, andthe University as a whole
• the most successful fields of education will be rewarded either by a non-recurring performance-based grant or fixed-term performance-based fund-ing in 2003 and/or during the planning period 2004–2006
• projects designed to meet development needs and amend deficiencies will begranted funding for the planning period 2004–2006.
The ultimate aim of the evaluation is to improve teaching and degrees, develop qualityassurance for degrees and compare the quality of degrees with European standards.The University did not wish to connect the evaluation of education with the allocationof basic funding, so the evaluation exercise yields no numerical results that could havean impact on the distribution of resources. As the aim of the evaluation project is toencourage the academic community to develop its work further, it was estimated thata direct connection to the allocation of basic resources might discourage an honestand self-critical evaluation. Project funding and other resources will be reserved formeeting development challenges and amending detected deficiencies. In addition, fieldsof education of a high quality may be rewarded by performance-based grants. Asuccessful evaluation is a learning situation which may result in reforms that are notdirectly dependent on available resources.
The starting points and criteria of the evaluation, as well as the university-wide resultswill be presented in a final report (Tuomi & Pakkanen: Towards Excellence in Teach-ing. Publications of the Finnish Higher Education Evaluation Council 18:2002). Theevaluation project has covered all fields of education of the University of Helsinki. Forthe purpose of the evaluation, these fields were divided into fifteen groups. The presentfield-specific report is one of a series of thirteen equivalent reports.

8
The evaluation of each field of education took place in five stages as illustrated by thefigure below:
1. SELF-EVALUATION, part 1
2. PANEL EVALUATION
3. SELF-EVALUATION, part 2
4. FINAL REPORTS
5. PROJECT PROPOSALS AND OTHER MEASURES
2 Description of the field of education
Faculty of Medicine
In the Faculty of Medicine the basic degree is the Licentiate (medicine 250 credits,dentistry 200 credits). In the study of both medicine and dentistry the two first yearsare spent learning about the structure and functioning of a normal human being. Thelater stages are arranged separately and spent in learning the skills, knowledge andattitudes needed in clinical practice.
The Licentiate degrees provide the qualification for working as a physician or dentistand prepare students for postgraduate studies. The degrees also provide the qualifica-tion for teaching and research work and for administrative duties which require ex-pertise in these fields.
The Faculty of Medicine of the University of Helsinki has the only Swedish languageprogramme of medical studies in Finland.

9
Structure of the Licentiate Degree
Structure of the Licentiate Degree Programme in Medicine, 250 credits Licentiate ofMedicine (Lic.Med.) The Medical studies are divided into three phases (203 credits):
• Phase 1 (pre-clinical studies)• Phase 2 (clinical theoretical studies)• Phase 3 (clinical studies)
Advanced Studies: 10 creditsPractical Training: 24 creditsLanguage and Communication Skills: 3 creditsElective Studies: 10 credits
Phases 1 and 2 take 2.5 years and comprise mainly biomedical and other subjectstudies.Phase 3 takes 3.5 years and comprises most of the clinical subject studies, advancedstudies and practical training.
Structure of the Licentiate Degree Programme in Dentistry, 200 creditsLicentiate of Dentistry (Lic.Dent.)
The Dentistry studies are divided into two stages (141.5 credits):
Pre-Clinical Stage, 2 yearsClinical Stage, 3 yearsAdvanced Studies: 8 creditsPractical Training: 36 creditsLanguage and Communication Skills: 4.5 creditsElective Studies: 10 credits
MD/Ph.D. Programme
The special MD/Ph.D. programme at the Faculty of Medicine admits ten medical anddental students each year during their first year in Medical School. The goal of theprogramme is to provide research training with the aim of helping students mastermodern techniques in cell and molecular biology, molecular medicine and medicalgenetics. Its goal is also to assure that, at the time of their graduation from this pro-gramme, the students will be capable of performing high-quality research in variousfields of the medical sciences.
Structure of the Postgraduate DegreesDoctor of Medical Science (D.Med.Sc.)Doctor of Dental Science (D.Dent.Sc.)Doctor of Philosophy (Ph.D.)The Specialist Degrees in Medicine and Dentistry are professional postgraduate de-grees.

10
Doctoral Degrees in Medicine and Dentistry
Nearly 20% of all medical graduates continue their studies and complete a doctorate.In order to obtain the degree, a doctoral candidate must conduct research, write andpublish a doctoral dissertation and defend it in a public debate. In addition, the candi-date must participate in theoretical research training, the extent of which is 20 credits.The training includes prescribed courses concerning general postgraduate training (5credits) and specialised training (15 credits) in the chosen topic. The preparation ofthe doctorate corresponds to 3–4 years of full-time work.
A Master’s degree holder can obtain a Doctor of Philosophy (Ph.D.) degree. Theextent of the theoretical research training for the Ph.D. is 40 credits. Otherwise, therequirements are similar to those of the degree of Doctor of Medical/Dental Science.The language of instruction in some of these postgraduate courses is English.
Specialist Degree in Medicine
Specialist degree in medicine can be taken by medical graduates licensed by the Na-tional Board of Medicolegal Affairs. A licensed physician should first apply for entryto a university training programme. There are 49 specialisation programmes at theUniversity of Helsinki. Completion of a Specialist degree takes 5 or 6 years. It con-sists of:
• 6 month service in primary health care and 4.5 or 5.5 years of special trainingin a university hospital or other hospitals which are approved as teachinghospitals.
• at least 80 hours of theoretical courses: 60 hours in the relevant specialisationand 20 hours in health administration and management
• a written national specialist examination • participation in the evaluation and development of the specialist programme.
Specialist Degree in Dentistry
This degree takes three years to complete, oral and maxillofacial surgery degree takessix years. The specialist degree in dentistry consists of general training, special train-ing and a written examination. Specialist studies can be begun after two years experi-ence as a dentist and having obtained a specialisation post.

11
3 Present state and developmentprospects of medical education
3.1 Undergraduate training at the University ofHelsinki
Finnish research on medical education suggests that traditional ways of teaching med-icine may not always lead to optimal learning results (e.g., 1, 2, 3, 4). While a varietyof often highly conservative teaching methods have managed to produce competentphysicians over the past century, it is our view that instructional procedures shouldalways find support from latest research.
In the course of their studies, medical students tend to develop a professional orienta-tion in which priority is given to simple and directly applicable information (1). How-ever, the medical profession in its current form also calls for scientific thinking skillsand a capacity for life-long learning.
Learning problems within a traditional curriculum have been explained by means ofthe so-called two-world hypothesis (5), which may be summarized as a gap betweenbasic scientific concepts and their translation into practical applications. A combina-tion of practical experience with real patients, tutorial groups and self-study may leadto an improved integration between acquired knowledge and the relevant clinical con-cepts, i.e. efficient knowledge encapsulation (6). Previous research suggests that withinproblem-based (PBL) curricula, students are more likely to study for meaning and lesslikely to study for reproduction of information (7). This may be one of the reasonswhy PBL has spread to an increasing number of medical faculties throughout theworld, including older and traditionally oriented universities (8).
Students have claimed that medical training and clinical practice are two separateworlds. An integrated curriculum based on PBL is one solution to this problem. Thisis the line that our Faculty has chosen to follow.
3.2 Recent trends in undergraduate training at theUniversity of Helsinki
At the University of Helsinki, the main objective of the Programme for the Develop-ment of Teaching and Studies for the years 1998–2000 is “to shift the emphasis ofteaching from a teacher-centred approach to a student-centred one with an emphasison supporting the students’ learning processes.” (9, p.10). The Faculty of Medicineat the University of Helsinki began to evaluate and reform the curriculum in 1994. Theprocess encompassed not only the content, but also instructional procedures and theplanning organization.

12
In fulfilling the general objective described above, the role of the Faculty of Medicinehas been imperative: “The largest individual development project to be carried out inrecent years has been the reform of medical studies. The most essential points of thereform were the launching of the parallel track with problem-based learning as thestarting point and a study programme designed for all medical students, focusing onprofessional interactive skills. The reform of the study system has drawn attention tolearning environments and learning centres (three centres have already been estab-lished). Throughout the reform process, significant information has been gained aboutthe role of the teacher as a supervisor of the studies and support person of learning.What has also become clear is that when radical reforms of the study systems arecarried out, teachers need staff development training.” (9, p. 23.)
3.3 The administrative organization ofundergraduate studies
The Medical Faculty consists of six departments, with the Dean as head of the Facul-ty. The Faculty council and the Dean make the decisions for the Faculty. The FacultyCouncil consists of 27 members: 13 professors, 7 medical teachers and other staff,and 7 students. The Departmental Boards and the Chairs are responsible for the ad-ministration of the individual departments. It is worth noting that student representa-tives have a significant role in all planning and decision-making in the Faculty.
Integration of the different medical sub-domains is emphasized in the reformed Hel-sinki 2000 undergraduate curriculum. The departments form the planning networkresponsible for planning the programme and developing the integrated blocks. Thedepartments are also responsible for learning results. The planning organization forundergraduate medical education is under constant development. The criteria for dis-tributing economic resources are also under constant scrutiny and development.
The Planning Committee for Undergraduate Medical Education is in charge of theplanning, development and co-ordination of undergraduate education and preparesand develops the curriculum and required regulations. The Committee consists of theChair, 7 other Faculty members, 8 students, and visiting experts (e.g. from the D & RUnit for Medical Education).
In addition to the Planning Committee, the Faculty has the following preparatory com-mittees:
1) Growing to be a physician2) Undergraduate clinical studies3) Clinical Assessment4) Preclinical Assessment5) Term coordinators6) Swedish-language education7) Dental undergraduate education8) Specialist training9) Specialist dental training

13
10) Scientific training11) Research-oriented undergraduate training12) Entrance exams13) Docents14) Administration15) Information Technology and Computers.
All matters concerning studies are presented to the Faculty Council by the PlanningCommittee or by the preparatory committees.
In the Study Office, there are two full-time and three part-time study advisors. Inaddition, there is a dental studies advisor at the Ruskeasuo Campus. Advanced stu-dents systematically tutor freshmen groups according to the general tutoring systemof the University. Each course also has an unofficial “host” or “hostess”, who acts asa contact person for students and interacts with the Faculty and Study Office.
3.4 The aims of the undergraduate curriculumreform
The task of the Faculty of Medicine is to train competent medical doctors and den-tists. Furthermore, it must guarantee the availability of professional and scientificpostgraduate studies. The Faculty carries out multidisciplinary research both in Fin-land and internationally. The quality of research and instruction have a strong impacton the health services of Finland and therefore on the health and well-being of thepopula-tion.
In the initial stages, the Educational Development Group analysed the needs for edu-cational reform. The main objectives were listed as follows: Those who complete theprogramme will have a better capability of fulfilling the needs of individuals and thesociety as a physician or dentist. The study orientation should move away from teach-er-centred teaching towards student-centred learning. This means that the quality ofmedical knowledge, clinical competence, and attitudes will be enhanced particularlyvis-a à-vis doctor-patient relationships and communication skills. In order to ensurethat these objectives are met, competence-based assessment will be introduced. Mo-tivation, enthusiasm and creativity will be encouraged. The students’ natural readinessfor life-long learning will be supported. Scientific thinking skills will be promoted.
The main task of our Faculty is to produce physicians and dentists with the appropri-ate knowledge and skills as well as a capability for independent, critical and scientificthinking. They should be able to analyze problem situations and to acquire and use thenecessary knowledge for solving problems at hand. In addition, young doctors shouldbe able to communicate and co-operate with patients and other professionals in theteam.
The students first learn the fundamentals of the biomedical sciences, then those of theclinical-theoretical sciences, and, finally, of the clinical sciences. In the pre-clinical

14
phase, the approach is based on the normal structure, functioning and behaviour ofhumans. In the following clinical-theoretical phase, patophysiological pathophysiolog-ical processes are introduced, and in the final clinical phase, clinical diagnosis andtreatment are emphasized. Each phase expands on the previous one in terms of knowl-edge, skills and understanding. However, the basic idea of an integrated and mainlyproblem-based curriculum is to motivate students by presenting them with clinicalproblems during the first years of study. The Growing to bBe a Physician programmeis developed in step with student progress through all phases of study, and its themesare integrated into and applied to each phase. The structure and contents of the pro-gramme may be viewed at http://www.ltdk.helsinki.fi/english/education/ or http://www.ltdk.helsinki.fi/opiskelu/.
3.5 The Helsinki 2000 curriculumThe Helsinki 2000, a unified problem-based curriculum, was introduced in 1998. Thenew curriculum was a hybrid of the Main Curriculum and the Parallel Track, empha-sizing problem-based learning. The curriculum of the first two years was commonfor both medical and dental students.
The problem was that students from the main curriculum had to move directly into aPBL curriculum in their clinical phase of studying without previous experience of thisinstructional method. Instead of merely transmitting knowledge, the tutors assist thelearning process and help students in knowledge construction (i.e., finding relevantinformation). As it is imperative that the tutors are specialists in content and that theyalso understand the learning process, they are systematically trained in these areas.During the first two years, studies proceed according to the Seven Steps method (10)developed at the University of Maastricht. In the third year – called the clinical-theoretical phase – autopsies and laboratory work are introduced. This phase of studyis not yet along the lines of a typical PBL curriculum, but many shapeup improve-ments in teaching have been made. The last three clinical years, consisting of clinicalblocks and bedside teaching, are mainly organised around so-called mentor sessions.In mentor sessions, the tutor acts as a clinical mentor whose role is more active thanthe role of the tutor during the pre-clinical years.
3.6 “Growing to be a Physician”The objective of the Growing to be a Physician programme is integrated competence(13, 14) based on the teaching of content knowledge together with physician-patientinteraction, teamwork and leadership, ethics, and scientific thinking (Evidence-BasedMedicine). Communication in health-care has been the most extensively covered areain the programme. Teaching methods vary from patient simulations to visits to health-care centres where students follow the work of experienced general practitioners.Strong emphasis is also placed on rehearsals simulated training in talking to patientsabout their state of health and especially in breaking bad news to them.
The programme has been thoroughly evaluated throughout its existence. In general,the feedback has been positive, even though there is a small minority of students who

15
give negative feedback. Over the past few years, some of the courses (Learning inter-view format through role plays and patient simulations and Learning the delivery oftest results, diagnosis and information on treatment with simulated patients) havereceived highly positive feedback and, according to student evaluation, are today amongthe most popular courses in the Faculty of Medicine.
3.7 Objective structured clinical examination (OSCE)The OSCE was introduced in the spring term 2000. It has been arranged once peryear in the sixth study year and consists of 10 different assignments on major medicalissues – not only clinical skills but also interaction with simulated patients played bytrained actors.
3.8 The Learning Centre conceptProblem-based and self-regulated learning call for flexible facilities, which may bemodified according to instructional innovations. The Learning Centre of the Facultyof Medicine aims at designing environments that support the use of technology as anaid for learning. The Learning Centre currently functions in four different locations:preclinical studies are located at the Biomedicum, clinical studies at the HaartmanInstitute and the Library for the Health Sciences, and dental studies, forensic medi-cine, and public health in Ruskeasuo. Previously these facilities were located in onseparate campuses, but they are now in on or near the Meilahti Campus, close to theUniversity Central Hospital.
3.9 Educational technologyThe aim of the national “IT culture in medical education” project in Finland (TheUniversities of Helsinki, Turku and Kuopio) was to enhance the opportunities provid-ed for medical education by information technology. The project was funded by theMinistry of Education and focused on attitudes towards IT and on its current useamong teachers and students. The conclusions were that medical teachers and stu-dents had a highly positive attitude toward advances in modern technology (15). Com-puter-related technology was also widely applied. Teachers, however, used informa-tion technology more in their research work than in teaching. This finding is a chal-lenge for medical education and emphasises the importance of pedagogical compe-tence in combination with technical skills.
3.10 The Development and Research UnitThe Development and Research Unit was founded in 1996. It is a part of the LearningCentre concept and directly controlled by the Dean. The main responsibilities of theUnit are related to the training of medical teachers and the development of evaluationprocedures, such as the course feedback system. The Unit also provides expert con-sultation in, for instance, designing exams and instructional procedures. Its speciali-

16
ties are cross-disciplinary co-operation and research on the learning process by usingpsychological theories and methods. The Unit’s latest innovation is a counselling serv-ice for medical students who need help in study strategies, motivation or other study-related problems. Prior to the evaluation the Unit had a small task force of two exter-nally funded researchers and two part-time research assistants in addition to the Direc-tor, Ph.D. (Psychology) Kirsti Lonka.
3.11 Staff development and teacher trainingOriginally, only few of our teachers had pedagogical training, and their understandingof the psychology of learning was rather modest. It was therefore necessary to trainthem in the application of new instructional procedures. Knowledge about problem-based learning was not enough by itself. The teachers had to learn a whole newapproach to teaching and learning. A good lecturer was not necessarily a good smallgroup tutor. Problem-based learning requires medical teachers to re-examine the rela-tionship between what they do and what students learn (15); they have to internalise anew, more active view of learning in which students are active constructors as op-posed to passive recipients of knowledge (4). The Growing to bBe a Physician Pro-gramme as well as the Objective Structured Clinical Examination (OSCE) also call fornew forms of training. To date, the R&D Unit has trained more than 200 teachers ofthe Faculty. One problem is the constant turnover and heavy workload of the academ-ic staff. The fact that many of the trained teachers have been on temporary contractshas not helped in creating an atmosphere of continuity.
3.12 The evaluation proceduresThe curriculum is subject to systematic evaluation the aims of which are twofold:First, good and innovative teachers should be given credit for their contribution. Sec-ond, information is needed about the advantages and disadvantages of instruction.Which procedures receive the best feedback while being, at the same time, successfulin terms of the learning results. The teachers have been evaluated and rewarded on thebasis of three main criteria:A) The Teacher of the Year Award: The Medical Students’ Union chooses the Memberof the Teaching stuff Staff of the Year, the Lecturer of the Year and the Small-GroupTutor of the Year.B) The Course Feedback System: Since 1994, a feedback form approved by the Fac-ulty has been systematically collected from the students on each course. Courses getextra funding depending on their ranking. The ranking procedure is based on struc-tured items (Likert-type questions).C)The Term Feedback Form: In 2000, a new instrument was developed in order tocollect more comprehensive feedback. Each student was sent a questionnaire afterthe Autumn Term 2000 and Spring Term 2001. In these questionnaires, the studentswere asked to evaluate each course separately and also to give feedback for the termas a whole in order to spot any overlaps or gaps between individual courses. Theywere also asked to name the best lecturer, the best tutor, and the best clinical teacherof the term.

17
4 The self-evaluation process
4.1 The Co-operation Group
Self-evaluation on the basis of course feedback, discussions, and reform groups goeson constantly. The official self-evaluation process started in 2000, when the Universi-ty of Helsinki decided to evaluate all programs and studies. The Faculty decided toform a Co-operation Group in January 2001. The group consisted of the representa-tives of all Departments and programs:
Pirkko Heasman (Professional Growth, Clinical)Heikki Hervonen (Biomedical studies)Timo Kuusi (Clinical studies)Päivi Kärnä (International studies)Kirsti Lonka (Director, D & R Unit for Medical Education)Pekka Louhiala (Public Health)Niina Paganus (Secretary, D & R Unit for Medical Education)Tom Pettersson (Medical education in Swedish)Kaisu Pitkälä (Professional Growth, EBM, Clinical)Eeva Pyörälä (Professional Growth, Preclinical)Hilpi Rautelin (Clinical-theoretical studies)Juha Ruotoistenmäki (Dentist Program)Antti Sajantila (Forensic medicine)Mikko Salaspuro (Chair of the Planning Committee of Undergraduate Studies)Martti Siimes (Professional postgraduate training)Ismo Virtanen (Scientific training)Satu Alaluusua (Chair of the Planning Committee of UndergraduateDental Studies)Student representatives:Camilla Krogerus, Tuomas Lähdeoja, Jan Selenius, and Suoma Toivanen.
Each member of the co-operation group was responsible for the discussion and eval-uation of their own Department or programme. The D & R Unit provided informationconcerning course feedback. The task of each representative was to come up with abrief self-evaluation report.
4.2 The panel visitThe members of our external evaluation panel were Professor Robert Schaub, Assist-ant Professor Gege Blok and Professor Amos Pasternack.
All our panellists work in faculties that have extensive experience of problem-basedlearning. Professor Schaub, the chairman of the panel, is the Dean of dental studies atDental and Oral Hygiene school at the University of Groningen and professor inpublic oral health since 1996. He has a long experience in developing medical educa-

18
tion curricula. Gege Blok is has an M.A. in clinical psychology and anthropology andis a consultant in psychotherapy. She is currently an assistant professor at the Depart-ment of Educational Development & Research, Faculty of Health Sciences, at theUniversity of Maastricht. She has carried out research on and contributed to commu-nication skills training. Professor Pasternack, is a panel member from the Universityof Tampere, Finland, where he has been Professor of Internal mMedicine, vice deanand also dean of the medical faculty until 2001.
The panellists worked intensively within a tight timetable during their four-day visit.Quite a lot of time with students was included in order to give the panel an opportunityto find out how students perceive their learning environment. The panel interviewedboth medical and dental undergraduates from each study year. Postgraduate studentsand students in training for a specialist degree in a variety of medical sub-domainswere also interviewed. The learning facilities were shown to the panel by students.The panel met our curriculum planners and other key personnel in curriculum devel-opment. The panel also had meetings with the representatives of all of our six depart-ments – i.e., the Haartman Institute, the Institute of Biomedicine, the Institute ofClinical Medicine, the Department of Dentistry, the Department of the Forensic Med-icine and the Department of Public Health – as well as with representatives of special-ist training and of the Swedish curriculum, and with staff developing assessmentmethods. The panel also observed teaching situations, visiting two study groups (oneof 2nd year and one of 4th year students).
At the end of each day, the panellists held their own conclusion session, discussedtheir observations and outlined their evaluation report. On the final day, an open feed-back session was arranged: the panellists gave a brief presentation of their observa-tions and suggested key development areas. This session was highly useful, and ourfaculty staff felt that the feedback came at a critical juncture in our reform process.
The next step was to extract the main criticisms and recommendations from thereport. These were presented on several occasions to the members of the faculty tostimulate discussion on common goals to be decided. These presentations were led bythe Dean who then appointed a second co-operation group consisting of representa-tives of the different departments and students to work out the final report (see be-low). It was also discussed in the departmental boards before being finalized and sentto the central administration of the University of Helsinki.
Heikki Hervonen (Biomedical studies)Timo Kuusi (Clinical studies)Päivi Kärnä (International studies)Kirsti Lonka (D & R Unit for Medical Education)Pekka Louhiala (Public Health)Niina Paganus (D & R Unit for Medical Education)Tom Pettersson (Medical education in Swedish)Leila Niemi-Murola (Professional Growth, EBM, Clinical)Eeva Pyörälä (Professional Growth, Preclinical)Kirsi Rauhala (Professional postgraduate training)Hilpi Rautelin (Clinical-theoretical studies)Juha Ruotoistenmäki (Dentist program)

19
Antti Sajantila (Forensic medicine)Mikko Salaspuro (Chair of the Planning Committee of Undergraduate Studies)Martti Siimes (Professional postgraduate training)Kaarlo Simojoki (Director, D & R Unit for Medical Education)Ismo Virtanen (Scientific training)Satu Alaluusua (Chair of the Planning Committee of UndergraduateDental Studies)Student representatives:Anne Riihimäki, Tuomas Lähdeoja
5 Panel report – Development by Rotation
Evaluation panel
Prof. R.M.H. Schaub, University of Groningen, the Netherlands, chairmanProf. G.A. Blok, University of Maastricht, the NetherlandsProf. A. Pasternack, Tampere, Finland
5.1 IntroductionIn line with the ‘Programme for Development of Teaching and Studies at the Univer-sity of Helsinki, 2001–2003’, the University of Helsinki is currently executing a com-prehensive evaluation of the teaching and degrees in all faculties. Within this policy anevaluative site visit was carried out of educational programs of the Medical Faculty inNovember 2001 by an international panel. The educational programs are concernedwith medicine, dentistry, MD/PhD stream, postgraduate training, specialist training.
The panel appointed by the Rector of the University of Helsinki had the followingmembers:
– Prof. A. Pasternack, MD, PhD. Professor Pasternack is a medical specialistin the area of internal medicine. For many years he was dean of the MedicalFaculty of the University of Tampere.
– Prof. G. A. Blok. Mrs. Blok is a psychologist, specialised in education, withan emphasis on assessment. She holds a position of assistant professor in theDepartment of Educational Development and Research at the University ofMaastricht, the Netherlands.
– Prof. R.M.H. Schaub, BDS, PhD. Professor Schaub is a dentist. His chair isin Oral Health Care. He is curriculum coordinator of dental studies in theMedical Faculty of the University of Groningen, the Netherlands.
The panel had the task of evaluating and reporting to the Rector their findings on:– teaching and studies of the Medical Faculty– the meeting of objectives set for education and degrees.

20
Based on guidelines set by the University the panel reports their findings in the fol-lowing chapters.
There are two matters to consider in reading this evaluation. Firstly, the internationalpanel consists of three panellists who, though familiar with several educational phi-losophies, are presently mostly involved in the systems of Problem Based Learning(PBL). Secondly, the Faculty of Medicine has only recently introduced a new educa-tional approach (1998), and is in the middle of a transitional process.
The University of Helsinki gave the panel the following policies as a basis for evalua-tion: ‘The results should be valuable for the Medical Faculty to improve teaching. The
process of evaluation should enhance an evaluation culture’. ‘The core of a degree obtained from the University of Helsinki consists of pro-
found competence and expertise in one’s field. Other important components of ahigh-quality degree include general academic skills, such as co-operation and com-munication skills, cultural knowledge, and openness to international interaction.The emphasis in teaching and learning is clearly shifting from a teacher-orientedapproach to a student-oriented one. More important than teaching is learning1’.
Education in the medical faculty in Helsinki used to be discipline-based and ratherteacher-oriented. The Faculty decided several years ago upon introducing a curricu-lum reform, the objectives of which are:– To educate doctors who will better meet the needs of society and individuals– To improve the weaknesses in the old curriculum with an emphasis on:
• A learning-centered approach• Developing skills and attitudes• Motivation, enthusiasm and creativity• Evaluation by competence• Life-long learning skills to facilitate maintenance of competence• Scientific thinking
The implementation of new educational approaches has already gone through severalstages. The first stage began in 1994 and included the introduction of an integratedpre-clinical curriculum and early patient contacts with special emphasis on the doc-tor-patient-relationship.
The second stage began in August 1995, when a PBL program started with 14 volun-tary students (‘parallel track’). Starting from 1998–1999 the ‘parallel track’ and the‘main track’ have been integrated as a PBL program. All of the students now studyaccording to the new Helsinki-2000 study programme characterised by an increase inthe amount of self-directed learning, small group work and personal guidance, and adecrease in the number of lectures’2.
1 Letter of the Vice-Rector, appointing the panel.2 Ulla Anttila, Juha Ruotoisenmäki (Eds.). (2000) Faculty of Medicine ECTS Information package2000–2001.

21
5.2 General observationsThe Medical Faculty of the University of Helsinki, together with the university hospi-tal, are well known institutions concerning medical and dental, both basic and clinical,research and patient care. A large number of experts, often with a PhD degree, consti-tute the faculty. The institute has a strong organization. Output is high, both under-graduate and graduate. Remarkable is the large number of PhD’s in medicine. Togeth-er with the MD/PhD programme this shows the strong research orientation of theMedical Faculty. Without hesitation it can be said that graduating dentists and doctorsmeet the requirements laid down in the EU-guidelines for the qualifications of theseprofessionals.
Programs of teaching and training are well thought of. None of the programs gov-erned by the Medical Faculty seems to be in competition with other programs. Re-garding the Dental Programs, this close relationship with the Medical Program is astrength. Quite innovative is the organization of oral health care by the Helsinki Pub-lic Health service, serving at the same time the clinical training of dental and dentalhygiene students, a development sought by many dental schools in the world.
Concerning education, large efforts have successfully been made to meet the require-ments of the present and the future. It is well recognised that the overwhelmingamount of knowledge available, together with the high speed of developments in med-icine and dentistry, require specific methods for teaching and learning. Self directedlearning, problem solving and lifelong learning are the keyissues. The Medical Facultytherefore has adopted the philosophy of student-oriented learning. In order to achievethis, the Medical Faculty has gone as far as to reduce the number of departments andto combine disciplines (Institute of Biomedicine, Haartman institute, Institute of Clin-ical Medicine) to facilitate the integration of disciplines. Co-ordinating tasks within theprograms have been allocated (Swedish program, vertical integration). Teachers arebeing trained to improve educational skills. A Development and Research Unit to sup-port the development of education has been established. Altogether the Medical Facul-ty has undertaken, and still is undertaking, tremendous efforts to develop educationalprograms based on defined educational principles to be able to continue the training ofdoctors and dentists in the future.
General recommendation:
The Faculty should broadly in all areas maintain and strengthen the high quality ofresearch and expertise. It is however apparent that the Medical Faculty needs to takefurther steps in the development of their educational system. Strengthening of policiesand organization are key issues in this respect. Undoubtedly such steps would haveoccurred without this evaluation, as they are natural steps in the process that theMedical Faculty is undertaking. May this report strengthen the developments.

22
5.3 Educational philosophyThe Medical Faculty has adopted the philosophy of student oriented learning by imple-menting the methods of Problem Based Learning (PBL). Integration of disciplines andsmall groupwork has been implemented. At this point in time most emphasis has beenput on ‘horizontal integration’, where disciplines within one phase (in time) of thecurriculum are being presented to students in an integrated way around problems andtasks.
It has been observed, however, that the educational philosophy is not well establishedwithin the body of the faculty. A large variety of theories about education and interpre-tations of educational methods are to be found. The result is a hybrid educationalapproach where a variety of approaches concerning student oriented learning arecombined with more traditional educational approaches. The hybridity varies substan-tially between the various parts of the curriculum. In the first part of the curriculumstudent-oriented learning based on PBL is quite strongly present. During this phase,but much more in the later phases, also a large variety of (innovative) approaches tostudent oriented learning can be found, such as IC-supported learning and a portfoliolearning. Often such innovations are applied in isolation. It appears that a central phi-losophy and guidance are absent. Departments are left much freedom to create theirown programme and teaching methods. Both teachers and students therefore arequite confused, both in teaching and learning, resulting in programs becoming lessefficient and possibly less effective.
Recommendations:
The Medical Faculty should further develop a clear philosophy regarding its educa-tional methods, which can be carried by the majority of faculty. This philosophyshould at least include:
– the reasons for implementing the principles of student oriented learning– a clear choice of educational method(s), which should be consistently ap-
plied; PBL is only one of several approaches to student oriented learning.– a clear explanation as to the nature of the method (e.g. PBL does not exclude
the use of lectures, whereas portfolio learning also allows for written tests).– clear guidelines for a core curriculum.
The Medical Faculty also should develop strategies to achieve the objectives laid downin the philosophy and to building on the strategic steps already taken (reduction ofdepartments, horizontal integration, D&R unit, application of PBL-principles). Somesuggestions for a further strategy are made in the following chapters.
5.4 Curriculum designThe medical program is made up of three phases: a two-year preclinical phase, a oneterm clinical-theoretical phase and a three year clinical phase. The dental programconsists of two years of preclinical theory, studied jointly with medical students and athree-year clinical phase. In all of the phases in principle horizontal integration be-tween disciplines is applied, however not in every part of the program (hybrid educa-

23
tional system). For instance some of the clinical disciplines are not integrated. Alsowithin the preclinical and clinical-theoretical phases integration is not always accom-plished. Between the different phases co-ordination seems poor, however. This con-cerns both medical and dental undergraduate training.
Special attention is to be paid to the ‘Growing to be a physician/dentist’ programs.These programs are aimed at integrated competence based on the teaching of contentknowledge in harmony with physician/dentist-patient interaction; teamwork and lead-ership; ethic and scientific thinking. Students are sensitised to ethical issues and madeaware of relevant interpersonal factors and skills in the communication with patientsand the other professions. Stimulation to develop a critical attitude towards accom-plishments in science and medical practice is addressed in the course on evidencebased medicine. The concept is innovative and well received; students value some ofthe communication skills training for instance very high. The actual implementation ofthe programs, however, on the whole is not optimal, as the programs are not integrat-ed with other parts of the curriculum. A long-term perspective which links the differ-ent segments of the programme therefore is not clear to the students. The program iscarried out in a fragmented way, for instance concerning training communicationskills. There are also logistic problems, which have a negative influence on the stu-dent’s evaluations.
The evidence based medicine course seems to be an isolated part even within theseprogrammes.
This design of the curriculum reflects the current stage of development of the educa-tional philosophy of the Medical Faculty, described before. Elements originating fromdifferent educational philosophies are combined. Those educational methods thatwere successful in the traditional curriculum were combined with successful ele-ments in problem-based learning from the former ‘parallel-track’.
For the dental curriculum the current design results in a disengagement of the preclin-ical phase from the clinical phase. In itself the principle of combined learning of dentaland medical students during the preclinical phase is a worthwhile achievement to bestrengthened. The achievement of clinical training based on comprehensive patientcare is unfortunately not in line with disciplinebased theoretical education.
Recommendations:
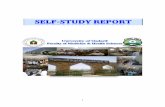
A central strategy to further develop education within the Medical Faculty could be torotate the program by 90 degrees. The main objective would be to enhance verticalintegration from basic sciences to clinical disciplines, which is necessary to createoptimal circumstances for student oriented learning and specifically PBL. It wouldalso prevent horizontal integration to become an objective in itself. ‘Rotation’ canenhance the process of vertical integration wanted by many and for which recently aco-ordinator is appointed.
At the moment the programs are based on three (dentistry) to four (medicine) sepa-rate parts (phases): preclinical phase, clinical-theoretical phase (medicine only), clini-cal phase, and the programs ‘Growing to be a physician/dentist’. These parts are

24
separately developed and executed: they are self contained, like locomotives of atrain, that can be connected for a common task but also can function on their own.‘Rotation of the curriculum’ would make the different parts dependent on each other.The structure then is like a tower, where the different components are interrelatedotherwise the tower would collapse. Eventually a true tower should develop where thedifferent parts are difficult to identify. This is desirable in student oriented learning:sometimes basic sciences can more effectively been studied late in the program; on theother hand students should be exposed to clinical problems early on. If the currentphases have each a separate colour nowadays; the rotation of the curriculum shouldresult eventually in a variety of colours without too much distinction like in a rain-bow.
It is strongly recommended to maintain the ‘Growing to be..’ programs though inte-grate them strongly with other parts of the curriculum. The vertical integration there-fore provides excellent opportunities. There can be clear links with the subject matterstudied, theory can be put into practice and can be related to ethical and societaldiscussions. It is to be advised to train communication skills in a systematic way,throughout the curriculum. These skills can be tested in an OSCE.
In general more consistency of the learning process is to be recommended. Forinstance the learning goals have to be clearly defined at all levels. The tutorial sessionsshould end up with a comparison of the goals set up by the planning group (those whowrote the problem) with those defined by the students (see also assessment).Freshmen students have to be introduced to the philosophy of PBL. This is accom-plished by an introductory course of three weeks. More emphasis should be paid onthis very important phase of the studies, e.g. create more training sessions, so that thestudents know exactly what is expected of them and acquire the appropriate skills.
5.5 Organization of the curriculumThe curricula for the different programs are developed and executed within the Med-ical Faculty. The Faculty of Medicine is made up out of The Institute of Biomedicine,The Haartman Institute, The Institute of Clinical Medicine, The Department of Den-tistry, The Department of Forensic Medicine, and The Department of Public Health.
The faculty is chaired by the Dean who has the final responsibility, controlled by theFaculty Council. Mechanisms to enforce educational policies or for incenting groupsor individuals because of educational efforts are only available on a limited scale.
Current design Rotated design Fully integrated design
▲ ▲

25
The Planning Committee for Undergraduate Medical Education plays a central role inplanning, developing, and co-ordination of education. A number of (sub) committeesis responsible for the development and co-ordination of education in certain areas, forinstance the Committee for the Development of Preclinical Education.The unit for Development and Research, a direct responsibility of the Dean, supportsthe development of education, for instance by regular evaluation.
From the discussions it appears that there is ample discussion among teachers regard-ing the development and execution of programs. It is of great value that on all levelsstudents are participating. Nevertheless in some cases it was felt that programs andteaching methods were more or less imposed. This in turn resulted in behaviour ‘re-sisting’ new teaching methods. On the other hand it was mentioned that little guidancewas given in producing and executing education. Although this ‘freedom’ was appre-ciated it was equally felt disappointing that no integration with others could be estab-lished. Consequently some experienced insecurity in considering integration their sub-jects with others, because of the concern to loose control over content and quality. Asa result there is a risk for lack of continuity in contents and lack of collaborationwhich does not further vertical integration. Lack of collaboration leads to repetition ofcontents.An example of efforts to solve these problems can be found in the Swedishprogramme, where a co-ordinator is appointed, and objectives are defined.
The responsibility for the MD/PhD and postgraduate programs belongs to the Dean.The actual training and support of students is left to professors. A common approachin education seems only partly present. The specialist training ends up with a special-ist university degree since 1986. New regulations became effective in 1999, whichreduced the number of specialities from 92 to 49 and called for better learning andevaluation. The training and specialist education is a co-operation between the facul-ties and the university hospitals. Also other hospitals and institutes participate. Thefaculty has a Specialist Training Committee for co-ordination and has nominatedabout 50 professors to be responsible for the training and education in all differentspecialities. The process of change from teaching to improved learning is in its devel-oping phase. Efforts have been made to structure the studies (logbooks for the resi-dents, training course for teachers and trainers, net-based registration and monitoringof residents etc.)
In conclusion it can be said, that in the organization of the curricula to some extentlacks guidance but also a lack of participation of departments, teachers and others isto be found.
Recommendations:
It should be considered to give either the dean budgetary responsibility on teaching, orappoint a vice-dean with this task.
The organizational structure should be changed in such a way that the departmentsand the representatives of the disciplines are encouraged to participate more activelyin the planning process. Participation should be awarded. It is to be considered toestablish an educational institute to be headed by the (vice-) dean for education, whichhas the full organizational responsibility for education. The main task of this institute

26
is the implementation and maintenance of the curricula. Guiding should concern theobjectives and strategies mentioned before, such as vertical integration. The instituteshould have its own budget in order to have the curricula carried out by departmentsbased on the teaching philosophies adopted by the Medical Faculty. The D & R unitshould be part of the institute, with certain independence in evaluation. The unit hasthe responsibility to support teachers and departments by training and otherwise.
Existing committees should be strengthened or new ones installed for materialisationof central strategic issues such as the curriculum design, the core curriculum, and thevertical integration. Other committees should be aimed at for instance controlling theconsistency in assessment methods (e.g. in accordance with the educational philoso-phy).
An important measure can be the defining of specific educational units within thecurriculum for which co-ordinators are appointed with the responsibility to co-ordi-nate this part (e.g. a specific period such as a semester or a specific line of education,such as ‘Growing to be…’). A defined format for organising education would be veryhelpful. A co-ordinator would be advised to install a planning committee. In all com-mittees, representatives of all institutes and disciplines, and also students should par-ticipate. The instalment of educational ‘roles’, each role representing a specified numberof hours, would allow departments and institutes control over contents as well as overthe amount of time spent on education. The teaching institute will have a clear over-view of the investments of the institutes and departments in the educational process.Roles could be e.g. co-ordinator of an educational unit, member of a planning com-mittee, co-ordinator of a training, tutor, or trainer.
It would strengthen the MD/PhD and PhD programme if a co-ordinator were ap-pointed with the task to ensure formal scientific training. This could take the format ofa graduate school. This would probably also help to solve problems of funding thePhD-students, where nowadays undesirable inequalities can be observed.
5.6 Learning environmentDuring the last few years the Medical Faculty has made considerable investments inimproving the learning facilities. A new central library with a learning centre has beenbuilt and it provides the students with excellent access to a variety of learning material.Computers, IT-material, and journals are available. The facilities for selfconductedstudies are good. The services provided by the library staff are of a high quality. Thestudents thought that there should be more of the distinguished IT-software that isavailable. A problem is the fact that textbooks (needed throughout the curriculum andfor exams) are too few. The principle is to have one textbook per ten students, whichseems not entirely sufficient.
Another remarkable investment has been the establishment of the Biomedicum Helsin-ki, a huge complex, which brings together all departments within the Institute ofBiomedicine, clinical research laboratories, dental science laboratories and a greatnumber of other related medical scientific activities. Thereby a fruitful atmospherehas been established for further development of research and academic education in

27
the field of health sciences. From the educational point of view this environmentcreates the milieu where vertical integration of the medical studies has its possibilitiesto be fostered.
The reduction of the great number of departmental and discipline based institutes toonly five medical institutes should also be seen as an effort towards better cowork andintegration between the disciplines with teaching duties. This is already used effec-tively in the way of horizontal integration of the studies but may be also helpful inimplementing vertical integration in the future.
The location of the activities of the Institute of Dentistry far away from the medicalinstitutes is a drawback, as is the fact that the dental clinical activities are in threelocations far from each other.
The medical students are also obliged to move to many faraway places for their clin-ical studies. This is due to the fact that a lot of clinical teaching has to be effected invarious hospitals and health centres. The visits to health care centres create goodpossibilities for students to get acquainted with clinical practice. As it is, this part ofthe programme is not consistent satisfactory. A main reason seems to be, that stu-dents encounter a quite strong variety in health care staff, concerning motivation tocreate learning opportunities.
A serious problem, common to many medical schools , is the availability of clinicalteachers. The fact is that hospital administrators often engage clinical teachers inheavy clinical duties, which limits the time available for teaching. It is to be appreciat-ed that the Medical Faculty opened a number of clinical teacher’s posts. To someextent this seems to apply to the dental school as well, now that patient care is in thehands of the Helsinki Public Health Service.
The availability of teachers appointed by the faculty is also sometimes a problem. Thishas to do with the fact that a great proportion of posts are held by temporary peopledue to frequent absences (scientific work, studies abroad etc.) of the permanent staff.
The decision to apply student oriented and problem based learning has resulted in ademand of pedagogic activities. The faculty has in co-operation with its Unit of Devel-opment and Research established a program for tutor education through which thecompetency has distributed to a great number of potential tutors.The faculty has to be aware of the fact that heavy engagement in educational dutiesmay be a hinder for further career development. A system has to be accepted whereeducational merits are taken into account in deciding upon appointments.
Recommendations:
It is to be advised to increase (even more) access to books and other informationcarriers which are essential in student oriented learning.
The much needed integration of dental with medical studies will eventually requirehousing on the hospital grounds, as is already the case with research.

28
Dislocations in the clinical stage are inevitable, however should be avoided or beingaccounted when the timetables are constructed.
Negotiations between the university and the university hospital should be started orstrengthened to get an increase of teaching efforts from clinicians. A likewise recom-mendation is to make to the dental school concerning the Helsinki Public HealthService.
All potential teachers, in fact all of the faculty and also clinicians, should engage inpedagogic training to acquire essential knowledge and skills regarding (under)graduatetraining. Good teachers should be awarded and they should feel that they are safe inthe university hierarchy.
The organization and contents of the visits of the health care centres need improve-ment to overcome the variety in quality. It is advised to evaluate the problems in depth,not only students’ evaluations but also those of the staff in the health care centres.Inclusion of the health care centres’ staff in the design of the programme and discus-sion about the aims might help to solve some of the existing problems.
5.7 AssessmentThe policy and practice of assessment of the students vary between the three differ-ent study periods: preclinical, clinical-theoretical, and clinical. In the preclinical stud-ies there are 12 courses (‘blocks’) that end with an exam. The topics of learning aredealt with partly in a horizontally integrated way. Each discipline produces its ownquestions for the exam and no integration takes place. Some of the teachers in laterphases of the curriculum have complained that the students lack essential knowledgein anatomy and physiology. Whether that is due to defects in teaching or ill definedlearning goals and thereby goals of assessment, is not known. In order to avoid thatthe students select the disciplines they try to learn, a 0-rule has been applied.
In line with the principles of PBL a progress test is taken twice a year during thepreclinical studies. This is a positive way of following acquired knowledge both forthe faculty and the students. The clinical-theoretical disciplines exert their own examsat the end of the courses. Bacteriology and virology are assessed in a common examhaving only two essay questions of each discipline.
The assessment during the clinical studies consists of block-tests after each block.Recently the method of OSCE at the end of year 5 has been introduced, which can betaken as an important step towards student oriented learning. The OSCE is an impor-tant instrument in assessing the clinical skills acquired. The final clinical exam con-sists of 160 true false statements and 18 essays mostly based on short case reports.The true false statements are randomly selected from a bank consisting currently ofabout 3000 questions to represent in a proportional way the volumes of the clinicaldisciplines of the curriculum. The students at the Institute of Dentistry pointed to thefact that there are a great number of course-exams that cover very short courses (0.3– 1.0 credits).

29
Recommendations:
In general exams should be aimed more adequately at the learning goals, to be morecongruent with the integration during the learning process; an advice is to form exam-groups for each block, who can be responsible for integrated questions.
Exams should have a greater number of questions to cover the fields.
The preclinical phase ends with a final exam that covers the whole curriculum hither-to. Considering the above-mentioned complaint of the clinical teachers increasingemphasis should be put on the quality of this exam. The participation of the teachersfrom various clinics in writing the tests should be improved. The 0-rule might not bethe adequate response.
In order to get an impression of how skills have accumulated during the studies theOSCE should be repeated at least once a year during the clinical studies. Skills taughtin the ‘Growing to be…’programme should also be included. It is important that thetest is tailored so that the students are familiar with what they are exposed to at thestations.
In principle a progress test, in order to serve its purposes, should be applied all overthe curriculum, not only during the two first years. In order to get more informationof accumulated factual knowledge it would be rational to use the question-bank toestablish a progress test, based on the true-false concept, to which the students areexposed to several times during their clinical studies. A progress test would probablyalso bring the disciplines closer to each other and thereby be a way to enhance verticalintegration.
In order not to be a disturbing element in the progress of studies, small exams shouldbe avoided or integrated into larger entities.
5.8 Learning results/student’s commentsIn general the results of the Medical Faculty are good. 80 % of the students enrollingwill receive a degree in medicine or dentistry. Per year 10 students enrol the MD/PhDprogram. Usually they get their degree in medicine and their doctoral degree in 6.5 to7 years. A relatively high number of students enrol the PhD program. Remarkable isthe large number of PhD degrees, in 2000 even exceeding the number of medicaldegrees. This does unfortunately not apply to the dental school. About 200 specialistdegrees are granted annually.
Students generally are satisfied with their education. Medical students praise the facil-ities, such as the Biomedicum, and the learning centres as in the library. They appre-ciate clinical teaching. More critical are students concerning the sizes of groups andthe large variety in tutors. The students in general sense the lack of a strong educationphilosophy; they experience large differences between teachers. The programs “Grow-ing to be…’ are not always valued, for instance as sometimes one comes to closewithin each others personal space. The medical students vary in their appreciation ofvisits to health care centres in the region due to logistic problems and less motivated

30
health care staff. The dental students are more positive about the visits.Dental students have difficulty to integrate the knowledge from the first two years.They experience a repetition in the third year. Also it is not easy to identify withdentistry in this period.
MD/PhD and PhD students appreciate their opportunities greatly. It is however notalways easy to acquire funding, frustrating the opportunities given. Specialist students(residents) usually have difficulties in finding time for their theoretical studies and alsopossibilities to take part in courses.
Recommendation:
See other paragraphs.
5.9 Relationship between teaching and researchThe faculty has a very high record in scientific activities. In many fields the researchis at a very high international level. As almost all teachers are involved in research;contents of the teaching is in a way based on research. Evidence based medicine-wayof thinking is stressed along the curriculum.
Students have on obligatory 10-credit part of the studies, which is tailored to givethem an introduction to scientific work. The module ends with a written scientificessay based on research that they have conducted or a scientific review on a giventopic. The curriculum also contains other scientific elements: epidemiology, biomet-rics, ethics, evidence-based medicine.
The Medical Faculty has a fairly large programme for MD/PhD and PhD students. Onan individual level students expressed satisfaction with these programs. At the sametime there seems a lack of organised formal scientific training, despite a requirementof 20 credits in this area.
Recommendations:
To strengthen and broaden the scientific educational element in the studies it could beworth while to nominate a co-ordinator with the responsibility to take care of theprocedures and quality control. This also accounts for the MD/PhD and PhD pro-grammes.
5.10 Quality assuranceThe Development and Research Unit is responsible for the quality control in the facul-ty. Quality control means faculty development regarding educational philosophy andmethods and evaluation of education and assessment. In recent years the Unit hastrained 200 teachers in problem-based learning, i.e. the role of the tutor. Other tasks of

31
the D&R are expert consultation in designing exams and instructional procedures,cross-disciplinary co-operation and research on the learning process by using psycho-logical theories and methods and a counselling service for students regarding studystrategies, motivation or other problems related to learning. D&R is also performingevaluations of courses, e.g. all first and second year tutorials are evaluated. In theacademic year 2001-2002 the term-evaluation was introduced. Results of which werenot available yet. Systematic observation of tutorial groups has started in the spring of2001. This is not obligatory. In the spring of 2001 all teachers were sent question-naires about their workload and teaching ideas. Results of this were not available.
The Unit is also responsible for the contents of the training of the PBL academic skillsof the students: the training in the first three weeks is run by the Department of PublicHealth.
Recommendations:
The D&R unit could be more involved in the direct development of the curricula. Tothis end it would be desirable to include the D&R unit to a teaching institute to beestablished within the Medical Faculty.
One of the main recommendations for the D&R Unit is to develop instruments toevaluate the whole curriculum and that innovations are guided by close evaluation ofprocess and results. Improvement of the current student and teacher training is nec-essary. Precautions should be taken to restrict evaluation to students only.
Faculty development regarding designing exams and instructional procedures needsimprovement; this should be a part of the transition to vertical integration.
D&R should support innovations within the curriculum on the basis of research(“evidence based education’). It is very important that the results of evaluations aredisseminated throughout the faculty The D&R unit has a vital role in the implementa-tion of the vertical integration, mainly through proper evaluation of all stages andfaculty development programmes which are consisted with the educational innova-tions made. Its role should be to advise both the educational institute and the individualdepartments and institutes.
5.11 International activities/bilingualismThe Medical Faculty has a number of student and staff exchanges every year. It is tobe appreciated, that the language is an important factor in the limited opportunities toincrease the volume of this exchange program. Possibly a program in English willenhance this enlargement.
Clear policies are defined and measures are taken (appointment of a co-ordinator)policies to achieve an improved Swedish program. Within the Medical Faculty feelingsand experiences regarding Swedish spoken education were mixed.

32
Recommendations:
It is to be considered to increase education in Swedish and English to give the MedicalFaculty a better position in the international market of higher education. Such pro-grams based on the application of consistent educational philosophies couldfurther strengthen this position.
5.12 PhD/MD-PhD/Specialist training/DentistryA substantial program for doctoral degrees, starting after or even during undergradu-ate training is to be highly valued. Most of the students feel this way, although fundingis not always easy. Formal scientific training sometimes is sometimes difficult tofollow because of requirements made by the research group.
Specialist training has not received extra resources since the responsibility of theuniversities was established. There is therefore potential competition between resourcesand interest for specialist training and education and time and efforts dedicated forundergraduate education.
Generally the specialists in training thought they had sufficient background. Whenattention was paid to increase the quality in training (e.g. paediatrics) satisfaction hasrisen. There is a general complaint that there is too much work to be done in patientcare both in medical and dental specialties, which makes it hard to study for thetheoretical courses, which are usually in lecture-format. Another complication is thatthey have to register for courses; there is no room for all. Often they are given veryshort notice when e.g. seminars have to be prepared.
In surgery there seemed to be no right balance between policlinical and clinical work;it was felt that there was not enough opportunity to do operations.
The training of dentists has a slightly isolated position, whereas at the same time therelation with medical training is intense. In the first two years the undergraduate pro-grams are alike. Also physically the dental school is somewhat isolated. With its posi-tion within the Medical Faculty the training of dentists has great opportunities to antic-ipate on future developments, such as an increased demand for medical knowledgeand skills of dentists.
Giving patient care in the hands of the Helsinki Public Health Service, although onpragmatic reasons, is an innovation, as it requires comprehensive clinical training.Unfortunately theoretical education seems mostly disciplinebased. It is noticed thatresearch related education (PhD) is low because of lack of funds.
Recommendations:
It is to be considered to increase co-ordination of the MD/PhD and PhD programs.
A clear balance is necessary between learning and patient care within specialist train-ing. Also guarding is necessary to avoid competition between undergraduate and spe-

33
cialist training. The allocation of educational ‘roles’ could help to clarify responsibil-ities and to quantify the amount of time spent on each programme.
Most importantly the Medical Faculty should really integrate dentistry as an area ofmedical education. Dental training should become part of all of the educational or-ganizations, ranging from the responsible (vice-) dean to co-ordinators for parts ofthe curriculum and members of committees. Most of the recommendations made inthis report also apply to the dental school. Possibly more financial means could beallocated to the doctoral programs.
5.13 Strengths and weaknesses, a summary
Strengths:
The broadness and high quality of research. This applies to both basic and clinicalresearch. This in theory fosters a fruitful background for scientific and also practicalmedical education.A strong desire is present to apply educational methods aimed at current and futureneeds, combined with the establishment of pilot programs (former ‘parallel track’),horizontal integration of disciplines, and training of teachers.
The establishment of institutes combining several disciplines, fostering horizontal in-tegration between disciplines being taught within the same phase of the curriculum.This has the potential of being helpful in constructing a further, vertically integratedcurriculum.
The Meilahti campus with its new library and the Biomedicum Helsinki offer extreme-ly good facilities for the development of the educational programmes. This also can besaid of the dental school. The students have excellent possibilities to visit learningcentres and have access to various IT-based learning procedures and material.
The co-operation of the dental school with the Helsinki Public Health Service in oralhealth care combined with clinical teaching.
Weaknesses:
A clear philosophy about learning and teaching is missing, as are strategies to achievesuch goals. This has resulted in a hybrid model, of which the structure is clear, but theinternal consistency is missing. It seems that lack of being explicit about the reasonsfor transformation into a student-oriented curriculum has led to a situation in whichdepartments and individuals that are not in favor of the reform could maintain theirpractices.
The lack of rewards for spending time in educational development and the currentinfrastructure are such that not all have a lot enthusiasm and stamina to keep theinnovations up to date. The lack of vertical integration has lead to a situation in whichthere are actually three different sub-curricula within the curriculum.

34
The structure of the studies, where the principle is that of basics first, and where thedisciplines have their right of maintaining their traditional teaching does not fit to theprinciples of problem based learning. Student orientation as well as problem- basedlearning principles cannot be accomplished in a milieu where lectures and other teach-er-dominated approaches are in majority of learning methods.
The infrastructure to develop and execute consistently curricula within the MedicalFaculty is inadequate.Students are confronted with mutually contrasting ways of learning. As the assess-ment has not really changed compared to the situation before the reform: students willstill be oriented to reproduction of information. A clear philosophy about assessmentis missing. It is not consistent with a student-oriented approach to have a graduation-test aiming at reproduction of knowledge at the end of undergraduate training.
Lack of consistent integration of the dental school in the Medical Faculty.
6 Students and the second phase of theevaluation
In general, the students’ evaluations were in line with the international panel. Theirobservations on the curriculum captured addressed the most prominent problems,and their suggestions for improvements were useful. The interpretation of the reportpresented by the Dean of the Faculty reflected these sentiments and was well receivedby the students.
Perhaps predictably, lack of resources was perceived as the first and greatest obstacleto a better learning environment. All other points presented below require more timeand effort from the teachers – if they cannot allocate time for teaching, or for theplanning of teaching, and if they are not competitively rewarded, nothing can be ex-pected to change. Currently the teachers are slowly burning out under their teachingload, and the need for more resources cannot be overemphasized. Monetary rewardfor good teaching should be seriously considered.
The “examination game” is a powerful indicator of learning and studying strategies.Changes in the learning philosophy must begin from the examinations. A change fromquestions on minute detail towards questions requiring actual understanding and theinterplay of details is essential in this process. Continuous learning could be supportedby non-obligatory mid-course examinations. There are many possible ways of imple-menting this: (1) the mid-course exams could give extra points for the final exam ofthe course, (2) the whole course can be passed by passing all the mid-course examsand (3) the total points gathered from the mid-course exams can be used to pass thecourse. The mid-course exams could be written, oral, individual or group exams.

35
Learning can could also be supported by smaller hearings exams during group tuitionsessions. Every exam should also be a learning experience, not just a technical meas-urement of the student’s knowledge. The mid-course exams can could be one-timetries; itis would not be necessary to arrange retries retakes of exams in the fashion offinal course exams. The students also support the idea of a faculty-wide progress testas a good motivator for the studies.
The panel suggested an annual OSCE for the clinical phase. This, however, is a moreexpensive method of either testing or learning than traditional exams. The resourcescan probably be used in a more cost-effective way. The block exams or mid-courseexams could, for example, adopt pieces parts of the OSCE philosophy by includingpractical questions either with real patients or actors or, for example, by suturing apig leg.
The greatest concern of the students is the vagueness of the learning goals. Thefaculty needs a solid, well defined Collection of Learning Goals. This is a detailedthree-tiered list, presented course by course and listing first first the things which astudent should master actively after passing the course (the so-called Core Curricu-lum). The second tier is composed of things of which the student should know theessentials, and information about where to quickly review his knowledge should heneed it. The third tier is the whole field of medical science related to the course, a “funto know”-level, of which the student should be able to find information after thecourse if need be. It should be noted that the terminology varies from place to place;the Karolinska Institutet at Stockholm, for example, uses the term Core Curriculumfor the whole Collection of Learning Goals. Therefore simple measures such as stand-ard term definitions are also important here. The Collection of Learning Goals shouldbe a publication handed to the student at the beginning of the studies. As for thelearning goals, each course should have a course booklet which includes all the rele-vant information, the learning goals, times, places etc. The content of the education(i.e. also the content of the individual sessions) must be consistent and include thesame items regardless of the location of the session. Currently the content of thesessions varies from one hospital to another.
The Faculty should adopt and define an explicit educational philosophy, and all mem-bers should be committed to it. Of course, the methods can, and must, depend on thepersonality of the teacher and the subject matter at hand, but the philosophy and spiritshould be the same: activity-encouraging and student-oriented.
In order to integrate the education vertically, the Faculty needs a common denomina-tor. The Collection of Learning Goals is an important part of this. Before the construc-tion of a comprehensive view of what to teach, when, why, in which context and towhom, it is impossible to achieve true vertical integration. Co-operation between thedifferent departments and divisions and their personnel is extremely important - it’stime to move from defending territory to contributing to a common cause.
The pre-clinical phase is comparatively lightweight and could accommodate moresubject matter; the clinical-theoretical phase is balanced, while the clinical phase isoverloaded. The vertical integration could be better used to balance the studies, but thetotal study time should stay the same.

36
The increase in starting places admissions inevitably increases the number of studentsin the Swedish-language track. This must be followed by a proportional increase inthe Swedish-language teaching positions, or, at the very least, a sufficient number ofteachers must be fluent in Swedish.
Finally, the students would like to see teaching and scientific work merited moreequally than today. Perhaps devoting positions to teaching would be fruitful: the teach-ers would not have to prioritize one sphere of work over the other. This would beespecially useful during the preclinical phase, where the subject matter of the tuitionteaching and the narrow research field of the teacher often fail to meet - somebodyproficient in a wider field might be better suited and more interested in teaching.
7 Conclusions and measures taken
7.1 General observationsThe evaluation of the Medical Faculty took place when the stabilisation phase of thenew curriculum was reached. The conclusions and recommendations of the panelseem highly useful. As a result of a number of open discussions based on the panelreport, a common position for future actions in the faculty, including shared visionsand subject specific actions, has begun to crystallize. These concern issues of struc-ture and substance and also organizational reforms. An important change was theestablishment of the position of an educational dean with a specific responsibility forthe education provided by the faculty. He has a separate budget for various develop-ment projects as well as extra funding granted to courses on the basis of their rankingin the course feedback system. There are many new projects which are beyond thescope of this report but which will feature in future plans and development processes.
7.2 The Development & Research Unit for MedicalEducationSoon after the panellist visit, the Development & Research Unit for Medical Educationwas established with the education dean as director. The persons involved in edu-cation development and coordination were posted into in the new unit to achieveorganizational and substantial synergies at faculty level. Each program and specialunit has now has an appointed coordinator working in the unit.
7.3 The shared visionOne of the main themes of the panel report was athe lack of a shared vision of educa-tion in the Faculty. Different groups have different views on educational philosophyand, in particular, on how it should be expressed in teaching. This means that there are

37
too many approaches to teaching within the Faculty. This is confusing especially forthe students, but also for members of the teaching staff. In order to strengthen thereforms of recent years and to get the most out of them in the future, the facultyshould define a common educational philosophy. This process should involve all groupsof the faculty in an open debate.
The main question is: what do we mean by the Helsinki 2000 curriculum? A mutualunderstanding should be reached on teaching methods and how they reflect the sharededucation philosophy. This does not mean just listing permitted teaching methods; itrequires an agreement on the different teaching methods employed in the Faculty. Outof these, each department should define the most suitable methods for their particularsubjects. Also, if there are existing structures which that are found useful, theseshould be retained and integrated into a hybrid curriculum. Vertical integration shouldbe achieved also in these cases.
As recommended by the panel, more emphasis will also be placed on introducing thePBL philosophy to first-year students to make sure that they know exactly what isexpected of them and are able to acquire the appropriate skills.
The development of the assessment methods is a crucial part of the Helsinki 2000curriculum, and more effort will be put into creating a constructive alignment, whichmeans that curriculum design, instructional procedures, and assessment methods forma coherent whole.
7.4 Key issuesIn faculty discussions on the panel report, some issues have been highlighted.
Defining the core curriculum
The volume of medical knowledge has grown rapidly in recent years. This, togetherwith changes in teaching methods, has forced medical faculties to evaluate their cur-riculum content. In order to meet the demands of modern health care, it is crucial thatwe define the skills and knowledge each graduated physician has to master upongraduation – i.e., their core competence. Without such a foundation, it will be difficultto maintain a high quality medical care in the future. Well-defined outcomes will alsoserve as a starting point for building the integrated curriculum starting from day oneand ending at graduation. If we do not know the “what“, it is hard to work out the“how”.
This process was initiated in the Faculty last year and is now given top priority. We arein the middle of the process of evaluating and restructuring our core curriculum atthree different levels: (1) Kknowledge and skills (i.e., competences) that everybodymust possess at maximum level, (2) basic principles and mechanisms that must beknown at least at a theoretical level, and (3) awareness and understanding of rareproblems that one may face in clinical work, and the capacity to learn more aboutthem. Not all problems can be solved on the basis of undergraduate education, andtherefore a capacity for life-long learning must be encouraged. A working group is

38
Current design Rotated design Fully integrated design
▲ ▲
currently defining a structured process description to help the departments with corecurricula qualifying. Co-operation with other Nordic countries will also be initiated.
Vertical integration
The Faculty has also has to deal with the issue, so far undiscussed, issue of verticalintegration between undergraduate education and specialist training. The latter hasbeen reformed dramatically since 1999 based on new guidelines for assessment, self-evaluation and curriculum design. The opportunity for mutually beneficial co-opera-tion should be launched in the near future. With a good working integration, bothprogrammes could become more effective and reach higher quality standards.
This topic was strongly highlighted by the panel, who and gave the report the title“Development by 90 degree rotation”. It was also prioritised during the Faculty dis-cussions in which it emerged as one of the most controversial issues. The problem isthat there seems to be no clear idea of what vertical integration means in practice.There are also fears that the different subjects will lose their identity.
The faculty has now hired a planning officer to co-ordinate the process of verticalintegration, which is linked closely to the definition of core curriculum.
An important challenge of vertical integration is more intense co-operation betweenundergraduate education and specialist training. Emphasis should be placed on creat-ing an ongoing common educational framework, especially in content definitions andthe possibility to start of starting a “Growing to be a specialist” programme.
Assessment
Although teaching methods have been revamped, assessment has not kept up with thechanges, and continues more or less as before. This has created major problems andfrustration especially among students, as exams have oriented them towards inappro-priate types of knowledge. Besides medical content, this conflict also affects otherareas of core competence such as communication skills, teamwork and leadership,ethics and scientific thinking. More co-operation in assessment is also needed in un-dergraduate education and specialist training.

39
Exams: The faculty has started to re-activate existing working groups in evaluatingand planning the different exam types used in the departments. It has also been decid-ed that teachers from the different phases will participate in the planning of exams.
For example, at the Institute of Biomedicine special effort has been put in developingassessment in accordance with the change in the teaching/learning philosophy. Eachexam has its own planning group, and the preclinical final exam has a planning groupof its own, with special effort directed to creating well-planned integrated questions.The panel suggests that also the representatives of various clinics should participate inthe planning of the exams. This is an excellent idea, and a broad-based planning groupis now in the pipeline.
Progress test: The Institute of Biomedicine has arranged progress-tests for some years.In the spring of 2002, the faculty decided to establish a progress test for all phases ofthe studies. It will be arranged twice a year and participation is voluntary. If a studentfails to participate, the counselling psychologists of the D & R Unit will contact him orher to offer guidance in study processes. Similarly, if the exam result is below averageseveral times, the student will be offered help to improve his/her performance.
WWW based evaluation tool: The field of medical education is constantly under pres-sure to maintain a high standard and to develop. Ongoing evaluation is crucial if wewish to uphold and enhance the quality of learning of future doctors. Student feed-back is an essential tool for controlling the quality of instruction. Furthermore, suchfeedback provides useful information for the development of medical education. InHelsinki, a pilot project to shift the evaluation process into WWW environment wasstarted in 2001. By giving feedback, students evaluate both the quality of instructionand their own learning processes. As suggested by the panellist report, new areas ofthe studies such as clinical internment will be integrated into the system. The facultyhas also reached a decision that giving feedback will be a crucial part of the studiesand no longer a voluntary sideline. The effects of this decision on the feedback will beevaluated before making a final decision on the issue.
The OSCE
In line with the panel’s recommendation, an OSCE coordinator has been appointed.The position is located in the D & R Unit. Besides co-ordinating the OSCE, she is alsoresponsible for the “Growing to be a physician” programme in the clinical phase. Thecontent of the OSCE is under continuous development, and the examination is also asubject of academic research.
The “Growing to be a physician” programme
The panellists pointed out that students rate parts of the communication skills trainingvery high. They suggested, however, that the actual implementation of the programmeon the whole is not optimal. The students do not have a holistic picture of the pro-gramme but see it in a fragmented way. They strongly recommend integrating the“Growing to be a physician” both horizontally and vertically with other parts of thecurriculum and training the students’ communication skills in a systematic way through-out their studies.

40
In addition to special courses on communication skills during the clinical stage, thetraining of communication skills could be integrated into the learning of clinical skillsby embedding feedback on the students’ communication skills into group discussionsafter contacts with real patients. The students are able and willing to give feedback oncommunication: at the preclinical stage they have had several courses on communica-tion skills using role plays, simulated patients and video-recorded patient interviewsin which feedback sessions are always included. The implementation of this view-point into clinical teaching would require training for the clinical teachers, some extratime in each teaching session and relatively small student groups.
A course of evidence-based medicine is a part of the “Growing to be a physician”programme. At present, it is a theoretical course, without any integration into theprogramme as a whole. However, the method helps the students to critically evaluatethe scientific articles they search and read for their PBL sessions. EBM could beimplemented toin clinical teaching by using the method in every clinical PBL session.
These panellists’ observations are in line with our own feedback and reflections on thestate of the programme. The reform began eight years ago at a time when there washardly any communication skills training in medical studies. The learning methodsused in the “Growing to be a physician” programme, such as patient simulations, roleplays and portfolios, were new in the Faculty of Medicine. In the course of the pasteight years, the programme has become an established part of the curriculum. Fur-thermore, the rest of the curriculum has undergone a radical reform, and new educa-tion approaches have been adopted almost throughout the curriculum. It is now timeto reconsider the ideology of the “Growing to be a physician” programme in order tointegrate it both horizontally and vertically into undergraduate medical studies.
Involvement to in constantly improvement
One major problem in Helsinki – as seems to be the case practically everywhere – isthe fact that teaching is not perceived as an opportunity to achieve academic merit.Research merit still tends to be more emphasised when filling posts in the faculty.There has been improvement in some departments, but all too often pedagogic merit isnot given sufficient emphasis even when filling teaching positions.
The inflexibility of the payroll system makes it difficult to provide financial rewardsfor teachers getting good feedback from students. The University has effected somepolicy changes earlier this year, and the Faculty has started to make use of these newpossibilities.
As the financial situation of Finnish universities has weakened over the last few years,a major part of the funding of Departments is based on strict calculations,. This hascreated limitations for projects to improve teaching. The faculty has allocated fundsfrom its budget to support development processes.
All potential teachers – in fact all of the Faculty and also clinicians – should engage inpedagogic training to acquire essential knowledge and skills in undergraduate andpostgraduate training. One major task of the new D & R Unit is to provide morepedagogic training and consultation on teaching issues. The departments and hospitals

41
have to improve the possibilities for their teaching staff to attend academic trainingduring working hours.
Educational technology
For some years, the University of Helsinki has funded senior lecturer positions, whichcan be applied for by faculties for a five year term. This year, it was possible to applyfor a senior lecturer position specializing in educational technology. The medical fac-ulty applied for and was granted one such post. The senior lecturer has now beenappointed and will start work in the D & R unit for medical education in September2002.
Bilingualism
The panel recommends that the Medical Faculty considers an increaseing in the edu-cation in Swedish and English in order to give the Faculty a better position in theinternational market. In recent years, bilingualism and medical education in Swedishhave been strengthened by an official programme for bilingualism and by the appoint-ment of a co-ordinator for the Swedish training programme. This programme formsan integral part of the education throughout the curriculum. Structurally, qualitativelyand pedagogically there should be no differences between the Swedish and the Finn-ish training programmes.
The current situation and the aims of the Swedish training programme are clearlystated in the programme of bilingualism, which in turn relies on the general pro-gramme of bilingualism approved of by the University Council. A further aim of theprogramme is that every physician graduating from the Medical Faculty should beable to speak with his/her patient in the patient’s mother tongue, either Finnish orSwedish. In practice, education in Swedish takes place when the students meet thePprofessors or junior teachers whose positions are dedicated to the Swedish lan-guage.
As the intake of medical students and, consequently, also those attending the Swedishtraining programme will be increased, guaranteeing the number of teachering posi-tions dedicated to the Swedish programme will be a major challenge for the Faculty.

42
References
(1) Hyppölä, H., Kumpusalo, E., Neittaanmäki, L., Mattila, K., Virjo, I., Kujala, S., Luhtala, R., Halila, H.,& Isokoski, M. (1996) Where should special attention be paid in undergraduate medical education? Twosurveys among Finnish doctors. Medical Education, 30, 31–37.
(2) Hyppölä, H. (2001). Development and evaluation of undergraduate medical education in Finland.Doctoral dissertation. Department of Public Health and General Practice, University of Kuopio.
(3) Lindblom-Ylänne, S. (1999). Studying in traditional medical curriculum. Study success, orientations tostudying, and problems that arise. Doctoral dissertation. Faculty of Medicine, University of Helsinki.
(4) Lonka, K. (1997). Explorations of constructive processes in student learning. Doctoral dissertation.Department of Psychology, University of Helsinki.
(5) Patel, V.L., Evans, D.A., & Groen, G.J. (1989). Biomedical knowledge and clinical reasoning. In D.A.Evans & V.L. Patel (Eds.), Cognitive science in medicine: Biomedical modeling. (pp. 53–112) Cambridge,MA: The MIT Press.
(6) van de Wiel, M. W. J. (1997). Knowledge encapsulation. Studies on the development of medicalexpertise. Doctoral dissertation. University of Maastricht.
(7) Albanese, M.A., & Mitchell, S. (1993). Problem-based learning: A review of literature on its outcomesand implementation issues. Academic Medicine, 68, 52–81.
(8) Lowry, S. (1993). Making change happen. British Medical Journal, 306, 320–322.
(9) Frimodig, M., Pakkanen, P., & Venna, M. (1997, Eds.) University of Helsinki. Programme for thedevelopment of teaching and studies 1998–2000. Student and Academic Affairs Department, Develop-ment of Studies Unit. University of Helsinki.
(10) Schmidt, H. G. (1983) Problem-based learning: Rationale and description. Medical Education, 17,11–16.
(11) Weston, W.W. & Lipkin, M. (1990.) Doctors learning communication skills: developmental issues.In: Stewart, M. & Roter, D. (Eds.), Communicating with medical patients. Newbury Park: Sage Publica-tions. (pp. 43–57.)
(12) Mäntyranta, T., Lonka, K., Järvinen, A., & Pitkälä, K. (1996). Raportti ja esitys juonteen jatkamisentarpeesta kliiniseen vaiheeseen. Helsingin yliopisto. Lääketieteellisen tiedekunta. (A report on teachingcommunication skills in the clinical phase of studying. Faculty of Medicine, University of Helsinki.)
(13) Lonka, K., Mäntyranta, T., Kekki-Karppinen, P., Paavonen, J., Palo, J., Pitkälä, K., & Tenhunen,A. (1997, August) Becoming a Physician - an integrated study program. A short communication present-ed at AMEE Conference, Vienna, Austria, August 31-September 2, 1997.
(14) Hager, P., & Gonczi, A. (1996). What is competence? Medical Teacher, 18, 15–18.
(15) Wilkerson, L. (1994). Faculty development. In Tosteson, D.C., Adelsten, S.J., & Carver, S. T. Newpathways to medical education. (pp. 79–99.) Cambridge, MA: Harvard University Press.

43
Appendix 1 : Panel program
Evaluation of the Quality of Education and the Degree Programmes ofthe University of Helsinki
PROGRAMME/Medicine: 12th November – 15th November, 2001Institute of Biomedicum (in Meilahti) Institute of Dentistry (in Ruskeasuo)Haartmaninkatu 8 Mannerheimintie 17200014 University of Helsinki 00014 University of HelsinkiCoordinator: Ms Niina Paganus
Monday 12th November: Meilahti /Biomedicum8.30 Departure from the University Guest Rooms/Hotel9.00 Organisation of the panels (University Main Building, 2nd floor, room nr 2056)
10.00 Departure to Meilahti (Biomedicum)10.30 Welcome to Biomedicum (Faculty Club)11.00 Interview: 1. General policies of the Faculty, 2. Communication skill training
(Meeting room 8–9)12.30 LUNCH (Meeting room 4)13.30 Interview: Representatives from the Haartman Institute (Meeting room 3)14.15 Break14.30 Interview: Graduate Students (Meeting room 3)16.00 Return to the city centre16.30 Conclusion (University Main Building, 2nd floor, room nr 2056)
Tuesday 13th November: Meilahti/Biomedicum8.30 Departure from the University Guest Rooms/Hotel9.00 Interview: Representatives from the Institute of Biomedicine
(Meeting room 3)10.30 Interview: Representatives from the Institute of Clinical Medicine (Meeting
room 3)11.30 Interview: Staff of the Faculty office (Meeting room 3)12.00 LUNCH (Faculty Club)13.00 Observing of teaching14.00 Interview: Postgraduate students (Room 8-9)15.00 Premises and facilities by the students16.00 Return to the city centre16.30 Conclusion (University Main Building, 2nd floor, room nr 2056)
– – – –
19.00 Dinner offered by the Rector, Prof. Kari Raivio(Restaurant Svenska Klubben, Maurinkatu 6)
Wednesday 14th November: Ruskeasuo8.30 Departure from the University Guest Rooms/Hotel9.00 Welcome to Ruskeasuo9.30 Presentation of premises and facilities (Phantom lab)

44
10.00– Interview: Representatives from the Department of Dentistry: Department10.45 leadership and staff responsible for teaching (seminar room Apex, 4th floor)11.00 Interview: Representatives from the Department of Dentistry: Senior lectur-
ers and clinical instructors12.00 LUNCH (In the company with the Vice-Rector, Prof. Raija Sollamo, and Co-
ordinator Bettina Lindfors)13.00 Interview: Representatives from the Department of Forensic Medicine13.45 Interview: Representatives from the Department of Public Health14.45 Interview: Dental graduate students (seminar room Apex, 4th floor)16.00 Return to the city centre16.30 Conclusion (University Main Building, 2nd floor, room nr 2056)
Thursday 15th November: Meilahti/Biomedicum8.30 Departure from the University Guest Rooms/Hotel9.00– Interview: Representatives from the Specialist degree education9.45 (Meeting room 1)
10.00 Interview: Dean Matti J. Tikkanen and Ms Petra Wickholm (Meeting room 1)10.45 Interview: Specialist degree students (Meeting room 1)11.30 Return to the city centre12.00 LUNCH13.00– Final report (University Main Building, 2nd floor, room nr 2056)17.00
Refreshments are included in the mornings and in the afternoons

45
Appendix II: Participation list
MondayMeilahti/Biomedicum
10.30–11.00:Welcome to BiomedicumProf. Matti Tikkanen (Dean)Prof. Mikko Salaspuro (Department of Medicine)Scientific director Kirsti Lonka (Development and Research Unit)Prof. Martti Siimes (Hospital of Children and Adolescents)Ms Anne Riihimäki (Student representative)Ms Niina Paganus (Coordinator)
11.00–12.30:a) 11.00–12.00Scientific director Kirsti Lonka (Development and Research Unit)Prof. Mikko SalaspuroPlanning officer Kaarlo SimojokiClinical lecturer Tom Pettersson (Coordinator of the medical education in Swedish)Clinical lecturer Timo KuusiProf. Satu Alaluusua
b) 12.00–12.30Senior lecturer Eeva PyöräläClinical lecturer Leila Niemi-MurolaD.D.S. Juha Ruotoistenmäki
14.00–14.45:Haartman InstituteProf. Antti Vaheri (Head of the Department)Senior lecturer Timo HyypiäSenior lecturer Kristiina AittomäkiSenior lecturer Hilpi RautelinSenior lecturer Tuomo TimonenSenior lecturer Ilmo Leivo
14.30–16.00:Graduate StudentsMs Anne Riihimäki (Coordinator)

46
TuesdayMeilahti/Biomedicum
9.00–10.30Institute of BiomedicineProf. Ismo Virtanen (Head of the Department)Prof. Heikki Hervonen (Coordinator)Senior lecturer Nils Bäck
Pharmacology:Senior lecturer Pekka RauhalaAssistant Riikka Nevala
Bio-Chemistry:Prof. Tuomas HaltiaAssistant Otso Lindy
Physiology:Prof. Dag StenbergSenior lecturer Erkki Jyväsjärvi
10.30–11.30:Institute of Clinical MedicineProf. Reijo Tilvis (Head of the Department)Clinical lecturer Timo Kuusi (Coordinator)Prof. Eero KivilaaksoProf. Leila LaatikainenProf. Jorma PaavonenClinical lecturer Tom Pettersson (Coordinator of the medical education in Swedish)Prof. Annamari RankiProf. Carl-Gustaf Standerskjöld-NordenstamProf. Olavi Ylikorkala
11.30–12.00Staff of the Faculty officeMs Päivi Kärnä (International Affairs Coordinator)Clinical lecturer Raili Kauppinen (Coordinator for International Educationin Medicine)Ms Paula Paqvalin (Planning officer, doctoral studies)
13.00–14.00Observing of teachingPlease notice that various alternatives will be offered
14.00–15.00Post-graduate studentsMs Heini Lassus (Coordinator)

47
15.00–16.00Presentation of premises and facilities by studentsMs Anne Riihimäki (Coordinator)Mr Kalle Romanov (Teacher of medical informatics)
19.00Dinner offered by the Rector of the University of Helsinki, Prof. Kari Raivio:Prof. Matti J. Tikkanen (Dean)Prof. Tomi Mäkelä (Director, Biomedical Graduate School)Prof. Heikki HervonenProf. Sinikka Pirinen (Department of Dentistry)Ms Anne Riihimäki (Student representative)Prof. Mikko SalaspuroProf. Martti SiimesDr Ossi Tuomi
WednesdayRuskeasuo/Institute of Dentistry
9.00–9.30:Welcome to Ruskeasuo:Prof. Jukka H. Meurman (Head of the Department)Dr Kimmo SuomalainenD.D.S. Juha Ruotoistenmäki (Coordinator)Prof. Mauno KönönenProf. Heikki MurtomaaMs Anu Kiukkonen (Student)
9.30–10.00Please see above
10.00–10.45Please see above
11.00–12.00Anja Nieminen, Riitta Suuronen, Kimmo Suomalainen, Kirsti Liede(Senior lecturers)Hanna Pajukoski, Terhi Karaharju-Suvanto (Clinical instructors)
12.00–13.00LunchVice-Rector Raija SollamoMs Bettina Lindfors

48
13.00–13.45Department of Forensic MedicineSenior lecturer Antti Sajantila (Coordinator)Prof. Antti PenttiläProf. Erkki VuoriAssistant Päivi Mäkelä-Bengs
13.45–14.45Department of Public HealthProf. Risto Tuominen (Coordinator)Prof. Matti KlockarsProf. Eero Lahelma
14.45–16.00Graduate Students in DentistryMr Tuomas Pakkala (Coordinator)
ThursdayMeilahti/Biomedicum
9.00–9.45Prof. Martti SiimesKirsi Rauhala (Student secretary)Prof. Christian LindqvistProf. Reijo Tilvis
10.00–10.45Prof. Matti J. Tikkanen (Dean)Petra Wickholm (Head of Student Affairs)
10.45–11.30Specialist degree studentsOuti Nylander-Koski (Coordinator)

49
PUBLICATIONS IN THE SERIES ‘EVALUATIONPROJECTS OF THE UNIVERSITY OF HELSINKI’
1. Universitas renovata. Helsingin yliopiston arviointiryhmän raportti ja ehdotukset.Helsingin yliopisto 1993.
2. Universitas renovata continuata. Helsingin yliopiston arviointiryhmän raportti.Helsingin yliopisto 1994.
3. Hyvärinen, Kaarina & Hämäläinen, Kauko & Pakkanen, Päivi: Institutional Re-sponses to Quality Assessment. Quality Management, Quality Assessment andDecision-Making Processes in the University of Helsinki. University of Helsinki1996.
4. Hyvärinen, Kaarina & Hämäläinen, Kauko & Pakkanen, Päivi: ArviointihankkeetHelsingin yliopistossa 1990-luvulla ja niiden vaikutukset toimintaan. Helsinginyliopisto 1996.
5. An Internationalisation Quality Review Process: University of Helsinki. Univer-sity of Helsinki 1996 (1997).
6. Hämäläinen, Esa (ed.): Research Assessment Exercise 1999. University of Helsinki2000.
7. Geleijnse, Hans & Gellerstam, Göran & Mowat, Ian R.M. & Ruokonen, Kyllikki:Helsinki University Libraries. – Report of an Assessment Panel. University ofHelsinki 2000.
8. Mäkinen, Riitta & Virtanen, Aimo: Helsingin yliopiston kirjastot – hakua vaivientiä? Helsingin yliopisto 2000.
9. Tuomi, Ossi & Pakkanen, Päivi: Koulutuksen ja tutkintojen laatu Helsinginyliopistossa – Kansainvälisen arvioinnin loppuraportti. Helsingin yliopisto 2003.
10. Kaitajärvi, Riitta & Ryhänen, Sanna (Eds.): Final Report on the Evaluation ofthe Faculty of Veterinary Medicine. Evaluation of the Quality of Education andthe Degree Programmes of the University of Helsinki. University of Helsinki 2003.

U N I V E R S I T A S H E L S I N G I E N S I S
ISBN 952-10-0968-3ISSN 1239-8667Helsinki 2003Yliopistopaino
Copyright © 2022 FDOKUMEN