ENVISIONING THE FUTURE - CiteSeerX
351
R E M E M B E R I N G T H E P A S T WVMA CONVENTION 20 23 OCTOBER ENVISIONING THE FUTURE MADISON, WISCONSIN MONONA TERRACE 2011 PROCEEDINGS www.wvma.org
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of ENVISIONING THE FUTURE - CiteSeerX

REMEMBERING THE PAST
WVMA CONVENTION
2023OCTOBER
ENVISIONING THE FUTUREENVISIONING THE FUTURE
MADISON, WISCONSINMONONA TERRACE
2011PROCEEDINGS
www.wvma.org

Table of Contents 2011 Professional Education Committee .................................................................................................... 1 2011 WVMA Executive Board & Staff .......................................................................................................... 2
Small Animal Sessions Fred Born, DVM
The Early History of the Horse Doctor ............................................................................................. 3 Katie Diehl, DVM, DACVO
Catracts .......................................................................................................................................... 12
The Red Eye .................................................................................................................................... 21 Katie Diehl DVM, DACVO and Amy Pauli, DVM, DACVO
Ophthalmology Top 10 .................................................................................................................. 30 Meghan Herron, DVM, DACVB
Bite Prevention and Low Stress Handling in Clinical Practice ........................................................ 34
Don’t Leave Me Home Alone!: Diagnosis and Management of Canine Separation Anxiety ......... 42
Starting Off on the Right Paw: The Basics of Puppy Behavior and Problem Prevention ............... 48
Starting Off on the Right Paw: The Basics of Kitten Behavior and Problem Prevention ............... 57
Feline Aggression: An Overview of Common Problems ................................................................ 64
Feline Inappropriate Elimination ................................................................................................... 71 Kathy Linn, DVM
Orthopedic Examination for Forelimb Disorders ........................................................................... 79
Orthopedic Examination for Hind Limb Disorders ......................................................................... 81
Update on Cruciate Repair ............................................................................................................. 84
Those #*%$# Shoulder Problems .................................................................................................. 88 Fred Metzger, DVM, DABVP
Interpreting the Senior Hemogram – What Every Practitioner Should Know ............................... 92
Senior Liver Disease Case Challenge: Catching it BEFORE Your Patients Turn Yellow! ................. 95
The 2011 Video Practitioner's Case Challenge – Difficult Feline Cases ....................................... 102
The 2011 Video Practitioner's Case Challenge – The Emergency Patient ................................... 105
The 2011 Video Practitioner's Case Challenge – The “ADR” Patient ........................................... 110
The 2011 Video Practitioner's Case Challenge – The Senior Patient ........................................... 113 Amy Pauli, DVM, DACVO
Non‐healing Corneal Ulcers in Dogs ............................................................................................ 117
Non‐healing Corneal Ulcers in Cats ............................................................................................. 122 Sandy Sawchuck, DVM, MS
What is All This Interest in Raw Diets About? .............................................................................. 125 Margie Scherk, DVM, DABVP
Analgesia for Feline Arthritis ........................................................................................................ 130
Untangling the Complexities of the FLUTD Complex ................................................................... 139
Those Frustrating, Recurrent Diarrheas ....................................................................................... 148
Cholangitis‐cholangiohepatitis Complex in the Cat ..................................................................... 156
Snotting and Snuffling: The Cat With Chronic Upper Respiratory Disease ................................. 164 Rebecca Stepien, DVM, MS, DACVIM
Tips and Pitfalls in the Diagnosis of Canine Heart Failure ........................................................... 172
Treating Canine Heart Failure: As Easy As ABCD ......................................................................... 176
i

Challenging Canine Cases ............................................................................................................. 181
Confident Diagnosis and Treatment of Feline Heart Disease ...................................................... 184
Top 10 Misconceptions About Clinical Care of Cardiovascular Patients ..................................... 190
Large Animal Sessions Nigel Cook, BSc, BVSc, MRCVS, DECBHM
The Dairyland Initiative: Designing Welfare Friendly Facilities for Dairy Cattle .......................... 194 Todd Duffield, DVM, DVSc
Pain Considerations in Dehorning Dairy Calves ........................................................................... 202
Pain Management Factors at Parturition in Dairy Cows .............................................................. 209
Post‐Surgical and Disease‐Associated Pain Management Considerations in Dairy Practice ....... 213 Howard Ketover, DVM
Technical Large Animal Emergency Rescue: How Veterinarians Should Prepare ....................... 215
Managing the Equine Patient: Current Techniques and Pharmaceuticals Utilized in Common Equine Appointments and Emergencies ...................................................................... 218
Darlene Konkle, DVM, MS, DACVIM
Foreign Animal Disease Update Around the World ..................................................................... 225 Bill Manhanna, DVM, PhD, DACAN and Bill Seglar, DVM
Troubleshooting Silages – Field to Feedbunk Part I‐III ................................................................ 230 Matt Miesner, DVM, MS, DACVIM
Small Ruminant and Camelid Field Restraint ............................................................................... 252
Small Ruminant and Camelid Procedures .................................................................................... 261
Multimodal Bovine Restraint for More Enjoyable Challenges..................................................... 271
Rumen Troubles? Evaluation, Faunation, and Surgery ................................................................ 276
Addressing Problems of the Bovine Teat ..................................................................................... 283
Surgical Lameness of the Distal Limb ........................................................................................... 290
Case Discussions from the Teaching Hospital .............................................................................. 296 Lisa Nesson, DVM
Immunization and Parasite Control in Horses: A Practitioner’s Point of View ............................ 298 Mary Smith, DVM, DACT
Internal Parasite Control in Small Herds of Sheep or Goats ........................................................ 305
Urolithiasis and Copper Poisoning: Prevention of Two Deadly Nutritional Diseases in Small Ruminants .......................................................................................................................... 312
Neonatal Care of Small Ruminants and Monitoring Losses through Field Necropsies ............... 318 Richard Wallace, DVM, MS
2012 and Beyond: Where Are We Headed With Dairy Herd SCC? .............................................. 325
Improving the Value of Cull Cows ................................................................................................ 331
Join the Cause: Help Prevent and Reduce Antibiotic and Drug Residues in Meat and Milk ....... 336
Keynote Dennis Snow
Leading a Culture of Service Excellence ....................................................................................... 338
ii

Wisconsin Veterinary Medical Association 96th Annual Convention | October 20 - 23, 2011
Monona Terrace Convention Center | Madison, Wisconsin
Professional Education Committee
Our sincere appreciation is extended to the following committee members; the 96th Annual WVMA Convention is a result of their efforts.
Chairperson
Thomas Bach, DVM
Members Cheryl Kraft, DVM
Bruce R. Jens, DVM Amy B. Robinson, DVM
Chris J. Snyder, DVM Garrett R. Oetzel, DVM, MS
Thomas L. Strause, DVM Edward W. Loebach, DVM
Theresa Baker, SVM student representative Josh Heise, SVM student representative
Kasen Riemersma, SVM student representative Bill W. Nussdorfer, DVM, ex-officio
Dale Kressin, DVM, ex-officio Ryan Frazier, WVTA representative, ex-officio Lyn Schuh, WVMPA representative, ex-officio
The mission of the WVMA is to advocate and promote veterinary medicine, while enriching animal and human health.
1

Wisconsin Veterinary Medical Association 2011 Executive Board
President
Steven L. Erickson, DVM
President-Elect Robert J. Klostermann, DVM
Past President
Phillip C. Johnson, DVM
District 1 Peter J. Gaveras, DVM
District 3
Dale J. Kressin, DVM, FAVD, DAVDC
District 5 K.C. Brooks, DVM, DABVP
District 7
Bill W. Nussdorfer, DVM
District 9 Robert J. Zukowski, DVM
AVMA Delegate
Randy J. Schuett, DVM
State Veterinarian Robert G. Ehlenfeldt, DVM
Student Representative
Gina L. Laur
District 2
Zachary J. Janssen, DVM
District 4 Jessica M. Daul, DVM
District 6
John T. Been, DVM
District 8 Thomas H. Whitten, DVM
Treasurer
Thomas H. Howard, DVM
Dean, UW SVM Daryl D. Buss, DVM
WVDL Director
Thomas S. McKenna, DVM
Student Representative Marsh L. Bush
WVMA Staff
Executive Director Kim Brown Pokorny
Marketing & Communications Specialist
Sarah Young
Executive Assistant Torrie Kennedy
Marketing & Member Services Assistant
Amanda Veum
2

THE EARLY HISTORY OF THE HORSE DOCTOR
Fred J. Born, DVM This year, marks the world’s 250th anniversary of veterinary education that formally established the veterinary profession with founding of the world’s first veterinary school in Lyon, France, in 1761. This monumental work was followed shortly afterward by founding of the Alfort veterinary school, near Paris, in 1765. The establishment of both of these institutions was accomplished through the extraordinary vision and the initiative of French veterinarian Claude Bourgelat. As a result of his fruitful collaboration with human surgeons in Lyon, Bourgelat was also the first scientist who courageously suggested that studying animal biology and pathology would help to improve our understanding of human biology and pathology. With the cooperation of the Vet 2011 Executive Council (www.vet2011.org), and specifically Prof. Jean-Francois Chary, this illustrated lecture has been made available for presentation to interested groups in celebration of this most significant historical anniversary. The latest figures show Vet2011 has 1,377 corresponding members in 126 countries, where there are 52 national committees. Currently, 365 proposed events - 229 of which are accredited by Vet2011 - will take place or have already done so in 73 countries. Introduction Historians believe that the world’s greatest ancient discovery occurred about 8000 B.C., with the conversion of human beings from hunter-gatherers into farmers and keepers of livestock. We begin with Hippocrates 460 – 377 BC Father of Medicine, and even today the code of ethics written by this Greek physician and philosopher is the creed of every physician of human medicine. Hippocrates, whose name means “chief of horses,” and whose brother Sosander (“savior of men”) was reported to be one of the Greek hippiatroi (literally, horse doctors). The name hippopotamus is derived from the ancient Greek word for “river horse.” The hippology is the science of the horse. Medicine existed for centuries before him, and Hippocrates himself wrote a treatise entitled On Ancient Medicine. The medical knowledge of the ancients comes almost exclusively through the works of Hippocrates. All of what went before and much of what came immediately thereafter is lost in the dark of history. It can truly be said that Hippocrates invented modern medicine. Words such as malignant, benign, epidemic, and chronic fell from his pen as they are used today, just as are his treatments for dislocations of the hip, shoulder and jaw.
3

Hippocrates 460 – 377 B, Aristotle 384 - 322 BC Greek medicine had a greater impact upon veterinary medicine later in history, but both of these men were especially helpful in the development of the veterinary art. However, it was through the Hippocratic influence on Greek veterinary practitioners and writers of the Byzantine Period that veterinary medicine and human medicine grew. They were not colleagues, as Aristotle was only 7 years old when Hippocrates died. Aristotle was the student of Plato, Plato was the student of Socrates, much of philosophy and Western thought is a response to these three. Aristotle studied plants and animals and recorded his observations based on discovered facts. He classified animals according to their similarities of structure. He dissected more than 50 different animals and recorded the likenesses and differences in their structure. His works marks him as the father of biology. Claudius Galen 131- 201 AD A Greek physician and writer, who went to Rome and revived the ideas of Hippocrates and other Greek doctors. He was a gifted intellect who studied at the famous medical school in Alexandria in Egypt. At the age of 28, Galen became the surgeon to a school of gladiators. He was a genius, a born physiologist, a brilliant exponent of experimental methods, and a first-class anatomist. Rome gave us much of our current terminology relating to the veterinary profession, including veterinarius and equarius medicus. The oldest complete veterinary work known today is the Hippiatrika, which is a compilation of many texts by a number of Greek veterinarian authors who accompanied the Roman armies into Asia Minor during the Byzantine period (3rd-4th century AD). With the invention of the nailed-on iron horseshoe during the Roman period, horseshoeing became an adjunct to the craft of the ferrarious (ironworker, thus the farrier). Most physicians accepted astrology and some advised different treatments according to the position of the planets The Dark Ages The European Early Middle Ages (476-1000) Progress made by the Romans in the medical and veterinary science on the European Continent was destined to be short lived. The disuse of human and veterinary medical sciences during the Middle Ages brought obvious results. Human and animal plagues swept through all parts of Europe, taking a tremendous annual toll of life. Carts were piled high with human victims of smallpox and so-called plague, and then wheeled to the edge of the city so the bodies could be burned. Fields and farm lands frequently were littered with dead and dying domesticated animals. Superstition prevailed over reason and everything that happened was supposed to be the result of divine will. Hippocrates’ quest of natural causes was forgotten. Treatments for disease were usually absurd.
4

The Black Death Over the years, vast records of the Black Death document the greatest spread of terror in all of Western human history and because it involved a complex process that was not understood at that time, long before infectious diseases had been defined by Pasteur or even characterized clearly as contagious. As one of the most powerful historic examples of a great plague is that of the Black Death between 1333 and 1369. In 1347, this plague swept over Europe, ravaged cities causing wide-spread hysteria and death. One third of the population of Europe died. "The impact upon the future of England was greater than upon any other European country." (Cartwright, 1991) The primary culprits in transmitting this disease (bubonic plague) were oriental rat fleas carried on the back of black rats. While the plague was still active and spreading from town to town, men in Germany, Flanders, Hainault and Lorraine rose up and began a new sect on their own authority. Stripped to the waist, they gathered in large groups and bands and marched in procession throughout the crossroads and squares of cities and towns. They were men who did public penance and scourged themselves with whips of hard knotted leather with little iron spikes. The object of this penance was to put a stop to the mortality of that time. The Flagellants “This painting depicts the madness of penitent groups of flagellants, self-scourgers, who roamed through Europe in the thirteenth (also fourteenth) centuries and again in the sixteenth century.” Six Centuries of Islamic Influence 660-1258 All was not dark during the so-called Dark Ages, however; the flames of the Grecian cultural heritage never died in the Eastern or Byzantine part of the Roman Empire, around Constantinople. Then, too, beginning around 660 A.D., the Muslims (Mohammed 570-632) swept through Arabia, Syria and Persia and then across all of North Africa. The Arab Conquest 660-750 AD: The Omeyyade, the first Muslim dynasty By 715, the Islamic empire extended from Spain to the Indus River in India. After establishing their empire, the Muslims eagerly pursued all phases of learning. The works of the great philosophers, scientists and physicians, that were dormant for centuries, were revived by Arabian scholars and translated into Arabic. 750-1258 AD: The Abbasid Empire In 814, the Arabs adopted the concept of Indian numbers, including zero, to multiply by ten. In 975, the present mathematical notation was brought into Europe by the Arabs. Books dealing with the natural science were enriched by the observations of Arab scientists. Saracen or Arabian physicians added their own findings to the works of Hippocrates and Galen. The veterinary art, especially as it applied to the horse, was highly developed by Arab horsemen.
5

Improved knowledge in agriculture and veterinary medicine grew, improved and was disseminated in Arabic. The development of the sciences by the Islamic Empire influenced the people of Europe through Spain, Sicily and Asia Minor. During the twelfth (1100’s) century Arabic translations from the Greek were translated into Latin. These translations were written in monasteries throughout Europe, one such monastery reached its maximum splendor between the 11th and 12th centuries until its final decay in the 17th century. The legacy of ancient Greece was restored. Medieval depiction of a monk at work in a monastic (ma nas’ tik) scriptorium, in the 15th century.
This Catholic Benedictine monastery was built in 1120AD, in the small village of Engleberg, Switzerland and was one of many used by monks to do the translating of the Arabic texts into Latin. Latin scholars learned more of Aristotle by translating Arabic manuscripts based on Greek thought. The Gutenberg Printing Press Johannes Gutenberg (1398-1468) of Mainz, Germany was an inventor who drew upon known technology and adapted it for new uses. Movable type and the printing press had a revolutionary impact on Western Civilization. The first book he printed was the Bible that came to be known as the Gutenberg Bible, printed over a course of several years between 1445 and 1455. Gutenberg was also a German goldsmith, printer and publisher who introduced modern book printing. His invention of mechanical movable type printing started the Printing Revolution and is widely regarded as the most important event of the modern period. It played a key role in the development of the Renaissance, Reformation and the Scientific Revolution and laid the material basis for the modern knowledge-based economy and the spread of learning to the masses. With this one outstanding invention, books could be now printed with replaceable/moveable wooden or metal letters. In a time when books were printed by carving a complete page on a block of wood and printing it only for that particular book. By the 1500’s many types of books, including textbooks, were widely published. The wealthy developed private libraries of their own throughout Europe. Zodiac Horse Galenicals were originally “lunar medicines” prepared according to formulas of Claudius Galen. Galenicals owed their potency to the phase of the moon or the signs of the Zodiac. Leonardo da Vinci (1452-1519 AD) Leonardo da Vinci, as a youth, was an excellent horseman, had great physical strength and an intense curiosity of life. He dissected many animal and human bodies. He is known as the real Father of Modern Anatomy. With his anatomical work, he was the first
6
to draw accurate pictures, including the human skeleton. da Vinci was very interested in the anatomy of animals. Here is his drawing study of the uterus of a pregnant cow. The title page of the Hippiatria This veterinary text was printed in Paris, 1532. This work has many illustrations of stirrups and includes a lot of information about riding as well as healing. Libro De Albeyteria (1547) This is the only known printed copy of the first edition, by Francisco de la Reyna. In his book, Reyna postulated the circulation of the blood eighty years prior to Harvey’s famous discovery. The cover of this book is of plain vellum, with no illustrations. Veterinary medicine, for example, before the development of the veterinary sciences during the eighteenth century, was called veterinary art. An art is the development of skill along certain lines by means of experience, study or observation. This all changed with the Age of the Enlightenment (1650 -1789). (approx.140 years) Science, on the other, hand is knowledge based upon discovered facts and systematically arranged. Education in all phases of life grew. Veterinary medicine remained in the hands of farriers until the latter half of the eighteenth century, when great animal plagues in Europe made reforms in the system of veterinary education necessary. It was realized then that the system of apprenticeship training for farriers could not meet the demand for well-trained veterinary professionals. Remember that many of these farriers were still practicing by the principles of Galen (131 – 201 AD), over 1,500 years ago, using these Galenical medications as “lunar medicines” prepared according to formulas that owed their potency to the phase of the moon or the signs of the Zodiac. In 1753, Aristotle’s Compleat Master Piece, the Twenty-fifth Edition (including The Zodiac Man) was printed, just eight years before the first veterinary school was founded. Claude Bourgelat (1712- 1779) Claude Bourgelat was the son of a distinguished citizen of Lyon. In his youth, he was known to be a very intelligent young man and was an internationally-famous horseman. Bourgelat graduated from the University of Toulouse with a law degree, practiced law for a short time, joined a cavalry regiment and became an officer. In 1740, when he was 28 years old, he received his warrant as Grand Equerry of France and was made Director of the Lyon Academy of Horsemanship. The Academy at that time was a school ‘where young noblemen learned the equestrian arts and swordsmanship, together with mathematics, music and elegant manners’. At the age of 32, he published his first book (A New Treatise on Horsemanship). This original, instructive publication which developed a new approach to horsemanship
7
quickly brought him renowned recognition. Some preferred to call him the 'First Equerry of Europe.’ Bourgelat gained fame when he published “Elements of Hippiatry and New Knowledge of Equine Medicine” in three volumes, from 1750 to 1753 in which he encouraged the founding of a veterinary educational system. It also contained a series of papers on anatomy, morphology and medical treatment of Horses. In 1757, the New Practical Dictionary of Veterinary Medicine, Surgery and Hygiene,” (also in three volumes) by Bouley and Reynal, was published in Paris.T he combination of these six books, became the first veterinary classics. When Henri-Léonard Bertin was the Administrator of the region of Lyon from 1754 to 1757, he and Bourgelat became close friends. During the time Bertin spent in Lyon, Bourgelat convinced him that a veterinary school should be developed in Lyon. Bourgelat took an active part in the scientific affairs of France during the second half of the 18th century. The publication of (the 'Elements of Horsemanship') propelled him to the forefront of the writers of the time. His depth of understanding of the scientific methodology made him an outstanding leader in the field of medicine. He had acquired this through his association with human surgeons in Lyon, learning to perform dissections and surgical techniques from them. He developed a keen eye for detail of the anatomy of the horse. Because of this work, he was called to be a corresponding member of the Academy of Science in Paris. Diderot and d'Alembert then asked Bourgelat to work in collaboration on the Encyclopaedia, for which he was to write all the 'articles on horsemanship and farriery, and their related crafts'. After rectifying the contributions of preceding writers, he signed the first of some 250 articles in 1755. Because of these works, Bourgelat extended his acquaintances beyond the circle he knew in Lyon. Denis Diderot (1713-1784) Diderot was a French philosopher, art critic, and writer. He was a prominent figure during the Enlightenment and is best- known for serving as chief editor of and contributor to the creation of the Encyclopédie. The first volume was published in 1751. The Encyclopédie was an innovative encyclopedia in several respects. Among other things, it was the first encyclopedia to include contributions from many named contributors, and it was the first general encyclopedia to lavish attention on the mechanical arts. Still, the Encyclopédie is famous above all for representing the thought of the Enlightenment. According to Diderot, the Encyclopédie's aim was " to change the way people think". It was Bertin who pleaded his case with King Louis XV. In 1761, the government of King Louis XV chose to promote the prevention of cattle disease, develop soil conservation programs and the training of farmers. Bertin became the agent of this agricultural reform initiated by the King. He proposed that a veterinary school should be founded in Lyon, and that the director should be Bourgelat. He was well known as an international horseman, was very highly skilled with the whip and with his practical
8

experience in equine economics, was set apart as the man of choice to establish a new and strange departure in the educational system in France. It was obvious that there was no other figure in the animal industry of France that could meet this challenge. On August 4th, 1761, an order of the King's Council authorized Bourgelat to 'open a school in which the principles and methods whereby livestock diseases may be cured will be taught in public.’ The Veterinary School of Lyon Thus, the first veterinary school in the world had devoted most of its attention and resources to the diseases of the horse. The success of the Lyon school was immediate and became well-known throughout the world. This was a period of rapid expansion for the city of Lyon. It was at this time that the Hôtel-Dieu, like a temple to Medicine, was built as we still see it today. In 1762, Bourgelat signed a 6-year lease with the Rectors of the Hôtel-Dieu for a former inn in the Guillotiere district. The premises had two buildings which overlooked a large courtyard. The south side of the courtyard was closed by a porch which opened to the street; the north side faced a large meadow. The dissecting room and a large stable for 28 horses bounded the courtyard to the west. Two small stables to the east made possible the isolation of sick animals. On the upper floor, there was a large demonstration room, next to the Demonstrator's room and the office of the Director. The students were housed in dormitories above the stables. Never having taught or practiced, Bourgelat spent most of his energies in the administration of the veterinary schools, down to the smallest detail. He developed many sets of regulations. The good conduct of the students was one of his priorities. He aspired to make honest, educated men of them, and repeatedly underlined the good that the country could expect from them. August 5, 1761, was the official date of the founding of the first veterinary school opened the doors to students on January 2, 1762. The first class of 38 students attended classes studying the exterior anatomy of the horse, horsemanship, pharmacy, surgery and the principles of sterile procedures. Classes were scheduled, starting in the first year with a winter session, then a summer session. The only textbooks that were used in these classes were the ones that Bourgelat himself had written on the subjects. All of the students were required to know verbatim, the complete text from these books from beginning to end. Weekly oral tests were conducted by upperclassmen. Then, at the end of each course, the final oral test was given by the teaching professor. Students who had a good memory and were able to learn anatomy in two winters, could complete their course work in two and one half years, while many require four years.
9

One of many veterinary text books written by Bourgelat Students were required to practice horseshoeing and the use of the forge. The Instruction of making of horse shoes and farriery work was conducted by a “chief,” who is an upperclassman. A beautiful statue of Claude Bourgelat on the campus of the National Veterinary School of Lyon The second school built in 1765 at Alfort, France, became known as the National Veterinary School of Alfort. The School of Alfort displayed three different curricula: the classic one for the future veterinarians, similar to Lyon, the curriculum for the inspectors of stud farms and finally a specific teaching program intended for the military veterinarians. In 1765, Bertin ordered Bourgelat to create a school in Alfort, near Paris. The new veterinary school opened its doors in October 1766 and Honoré Fragonard became its first director; thus, Bourgelat was then assigned as the General Inspector of both French veterinary schools. The Alfort Veterinary School is still the oldest school in the world remaining on its original site, on the outskirts of Paris. It also houses the Fragonard Museum, which dates from 1766 and contains an impressive collection of anatomical items. The Paris Veterinary School would be Bourgelat’s final creation. This new school was established on the estate of the Alfort castle, its outbuildings would be on an approximately 25 acre park. The city map of Paris (currently 2010), showing Alfort-Maisons. Alfort is in a southeastern suburb of Paris, approx. 5 miles from the center of the city. During the later part of the eighteenth century, the population of Paris was est. at 600,000, compared to the present day population of approx. 12 million people in the metropolitan area (2007). All the founders of the European veterinary schools were trained in Lyon and Alfort near the end of the 18th century; they were either French and went on to live abroad, or foreigners that were eager to learn the fundamental talents of this new art of veterinary medicine. Later, more distant descendants of Bourgelat would establish the first schools in other continents. The reputation of the Lyon and Alfort schools attracted students from all over Europe, who in turn became the first leaders of veterinary schools in their countries. Thus, other European countries soon recognized the value of university-level education for veterinarians and also began to establish schools. Fifteen veterinary schools were developed over the next thirty-seven years. Then came the formation of the Royal Veterinary College in London (1791) and establishment of the Naples Veterinary School in Italy (1798). As you can see from this map, the spread of
10

veterinary schools crossed over the ocean to North America. The first North American veterinary college was the UNAM (Mexico City) in 1853, then Ontario Veterinary College in 1862, Montreal Veterinary College in 1866, then Cornell Veterinary College in 1868, then the New York City College of Veterinary Medicine in 1875 and then Iowa State College in 1879. The school at Toulouse was the 30th veterinary school to be developed in 12 countries over the next sixty years. The National Veterinary School of Toulouse was founded in 1828 at The University of Toulouse (the second-oldest university in France). All three of these French veterinary schools are still in existence. Bourgelat broke the bonds of quackery and superstition to a degree and gave science space and opportunity to develop. He extended his studies beyond the horse, seeing the necessity of studying the anatomy, physiology and pathology of all the domestic animals.
AS WE REFLECT ON THE HISTORY OF VETERINARY, MEDICINE FROM OUR CONTEMPORARY PERSPECTIVE, WE CAN VIEW IT IN THREE DEVELOPMENTAL PHASES:
The first phase of the development was the study of veterinary art, ranging over some 2,200 years of progress with Greek and Roman civilizations and characterized as 'one medicine' in so far as both humans and animals were concerned. The second phase of the development began 250 years ago with the founding of the veterinary profession and veterinary science, and the establishment of the first veterinary school in 1761 at Lyon, France and one medicine reaching a pinnacle about 1870-1920 The third phase is an increased emphasis today on specialization in veterinary medicine, public health, zoonotic diseases, and genomics, resulting in an increased focus on one health and one medicine. At the AVMA Convention, Sunday was devoted to Vet2011 and the Celebration of the 250th Anniversary. Our first speaker was Prof. Jean-Francois Chary, in his talk he quoted a speaker from a previous Vet2011 meeting this year, in Europe. The quote was as follows:
Physicians care for humans. Veterinarians care for humanity
11

Cataracts
Kathryn Diehl, DVM, MS, DACVO This lecture will briefly review clinically relevant lens anatomy and examination techniques to help identify and localize cataracts. It will then cover in depth different classification schemes of cataracts including causes. Finally, treatment of cataracts will be explained with concentration on a soon to be available promising medical treatment for diabetics, as well as surgery and indications for such. With respect to clinically applicable lens anatomy, it is often useful to think of and explain the lens like a peanut m & m shaped like a regular m & m. It is comprised of the (continuous anterior, equatorial and posterior) lens capsule and anteriorly, the associated epithelium as the “candy shell”, the cortex as the chocolate, and the dense central nucleus as the peanut. The actual lens cells or fibers are elongate, arising from the metabolically active equatorial region or lens bow and spanning from the front to the back of the lens, meeting at / forming the lens sutures. After being produced at the equator lens cells are sequentially compressed in to the lens center by new growth/cells. A cataract, by definition, is any opacity within the lens. Such opacities occur due to disruption of the normally perfect/orderly lamellar arrangement of the lens fibers and thus light’s passage through/interaction with (refraction (bending of light) and reflection) the structure. This disruption in varying degrees, may then affect the ability of the lens to “do its job” of focusing light (through refraction) and images onto the retina, with light scatter and ultimately blurred vision. Despite this potential visual impairment (with loss of menace response and/or object tracking), even with a complete cataract, the afferent (retina, optic nerve) and efferent (parasympathetic fibers of cranial nerve III, iris sphincter / pupil constrictor muscle) arms of the pupillary light reflex should be intact/functioning, and the pupil should react normally to light. To evaluate for cataracts, especially to pick up more subtle and/or posterior lesions, first perform an ophthalmic examination from arm’s distance away using a light source (pen light, transilluminator or otoscope head, direct ophthalmoscope (set at 0 diopters if looking through the ocular) in a darkened area. Collect a tapetal reflex to “back-light” the lens. Lens opacities will block the tapetal reflex and be highlighted as a darker or shadowed area within the pupil. Then perform a closer evaluation, ideally with a slit beam or other focused and bright light source (creating an optic cross section view or image) +/- magnification to localize a cataract within the lens and pharmacologic mydriasis (pupil dilation) with short-acting/diagnostic tropicamide (a topical anti-cholinergic / parasympatholytic agent). An optic cross section view provides Purkinje images where the first beam highlights the cornea, the black space the anterior chamber, the second beam the anterior lens capsule, the Tyndall effect of light scatter through the lens (protein) thickness including the anterior cortex, the nucleus and the posterior cortex, and finally the third beam the posterior lens capsule. Cataracts may be classified and named/diagnosed within several different categories, including their reason for development, size, location within the lens and age of onset.
12

Cataract cause classification scheme / reasons for cataract development: Inherited/genetic – This is the most common cause of cataracts in dogs. In this species cataracts should thus be presumed inherited until proven otherwise (known diabetes, trauma, etc.). Canine inherited cataracts occur in many breeds and in some there is a classic appearance. One common example is dominantly inherited triangular incipient posterior polar cataracts of Golden and Labrador Retrievers as well as some other large breed dogs. Fortunately these only rarely progress to cause clinical significance for the individual patient, but obviously affected animals should not be bred to avoid worse issues in the offspring. Metabolic Diabetes mellitus – A common cause of canine cataracts, the incidence of cataract formation in diabetic dogs is 80% within 16 months of diagnosis (Beam, S; Correa, MT: Davidson, MG. Vet. Ophthalmol. 1999; 2(3) 169-172), while it is rare in diabetic cats. Diabetic cataracts are usually bilateral, complete, develop rapidly and cause vision loss. Due to their tendency to occur and progress rapidly, they also commonly have Y suture clefting. Cataracts occur with diabetes due to altered lens metabolism of glucose. In a normoglycemic state, lens metabolism of glucose occurs first via breakdown of glucose by the enzyme hexokinase to glucose-6-phosphate. In a hyperglycemic state, hexokinase is overwhelmed and glucose metabolism is shifted to the enzyme aldose reductase and a pathway that produces sorbitol, which accumulates in the lens cells. Sorbitol is a large, osmotically-active molecule, and its accumulation ultimately leads to lens cell swelling and rupture. The disruption of lens fibers then leads to cataract formation. Hypocalcemia – An uncommon cause of cataracts with a typically bilateral, multi-focal punctate appearance similar to a “snow-globe” opacity appearance within the lens. This should not to be confused with that appearance within the vitreous, which indicates asteroid hyalosis, a degenerative or post-inflammatory change not uncommonly seen. The ophthalmic examination with an “optic cross section” is used to differentiate these locations/depth within the eye. Post-inflammatory – Inflammation is the most common cause of cataract formation in cats and horses. Particularly in those species then, but in dogs as well, it is important to look for hallmarks of (current/active with anterior chamber flare +/- relative miosis, red eye and low intraocular pressure and) prior inflammation (uveitis), including posterior synechiae (adhesions of the iris to the lens) and iris hyperpigmentation. Patients/eyes with cataracts in this category are generally poor candidates for cataract surgery due to significantly increased risk of post-operative complications of retinal detachment and secondary glaucoma. Traumatic – Cataracts may be caused by blunt or sharp/penetrating trauma to the eye. Blunt traumatic cataracts are managed as any other along with any other traumatic injury and likely uveitis present. Sharp traumatic cataracts are similarly managed but lens capsule integrity must also be considered as lens capsule tears pose an additional problem. Capsular tears greater than 1.5mm in length generally will not self-seal and this can lead to severe lens-induced uveitis that is refractory to treatment (phacoclastic uveitis) – an exception to this rule is found in puppies, which can often (though not always) overcome severe phacoclastic uveitis. Generally though in cases of phacoclastic uveitis, treatment is thus more urgent cataract surgery not only to address
13

the lens opacity as with typical cataract surgery, but also and almost more importantly to remove the inflammatory-inciting leaking lens material from the eye before secondary complications (retinal detachment, glaucoma) occur. In cats lens capsule damage is associated with the risk of post-traumatic sarcoma development, thus especially with sharp traumatic cataracts, long term close monitoring and ultimately possibly enucleation over cataract surgery is warranted. Electrocution may cause cataracts and is most often encountered in young animals chewing on electric cords or with lightning strikes. Obviously there may be other issues/injuries to attend to that “trump” the lens opacities. Nutritional cataracts can occur in orphaned or nutritionally supplemented/supported puppies (and some other species) fed milk replacer due to arginine and other amino acid deficiency. Some ophthalmologists advocate adding beef or liver baby food to the milk replacer to reduce this risk. Milk replacer-related cataracts typically occur bilaterally at the nuclear – cortical junction and fortunately, usually don’t progress and in fact become relatively smaller with age as the lens grows around them and compresses them centrally. Age-related or senile / degenerative with oxidative stress – These cataracts are incredibly common in older dogs with cumulative damage to the lens cells (by UV light, free radicals, etc.) but fortunately rarely affect vision and thus are often rightfully benignly neglected. They are often located at the equatorial cortex and wedge-shaped, as well as punctate cortical lesions. Radiation induced cataracts have been reported to occur in 10-28% of dogs with the eye in the field of ionizing radiation, even when appropriately/adequately protected or shielded. They generally occur 6-12 months following radiation therapy. The often start in the lens equator, as well as anterior and posterior subcapsular regions. They may or may not progress but are rarely treated surgically because of ocular surface / corneal disease (dry eye, keratitis) that is even more common in eyes in fields of RT +/- radiation retinopathy change preempting good candidacy and prognosis. Additionally there is often the “big-picture” disease and systemic status to consider in these cases (i.e., why the patient was receiving RT in the first place). Toxic cataracts may occur after exposure to certain drugs, most notably though still infrequent and not well described, ketoconazole. Toxic cataracts may also occur secondary to exposure to “natural” toxins such as those released into the vitreous and ultimately permeating the posterior lens capsule and lens tissue, from dying retinal cells (dialdehydes). This is common in dogs with progressive retinal atrophy (PRA) and is important to recognize as these patients are not good surgical candidates. This cause of / association with cataracts is one major reason for performing electroretinograms to assess retinal function before cataract surgery is performed, as if it is abnormally low, surgery may not be indicated to remove the opaque lens because the visual impairment is also and regardless (without treatment options available), retinally based. Prior to going down the road of pursuing pre-operative testing for cataract surgery though, signalment (PRA and secondary cataracts common in Labs and Poodles) and history can help suggest this underlying disease in patients being evaluated for cataracts as owners (especially when probed) often report dim light visual deficits and even blindness before, THEN the ocular cloudiness/opacity (of the cataracts).
14

Cataract size classification scheme Punctate - With the advantage of slit lamp biomicroscope evaluations, this is first category, which is as it sounds, a pin-head sized opacity. Incipient – These cataracts involve less than 10% of the lens volume and typically don’t affect vision. They can easily be missed on exam, especially when posterior, if diffuse retroillumination to back-light them with the tapetal reflex is not employed. Additionally, due to their small size and varying with location, they may be best visualized after pharmacologic mydriasis or dilation of the pupil (with tropicamide). Incomplete (immature) – These opacities involve greater than 10% of the lens volume but not the entire lens. As this is obviously a broad category, it is sometimes further subdivided into early and late incomplete cataracts. These lesions variably affect vision, depending on their size and location within the lens. Complete (mature) – These cataracts, as their name implies, involve the entire lens and are almost always associated with visual impairment (though slightly variable due to variable density of the opacity and “coping” function/ability of the patient. Resorbing (hypermature) – These cataracts are starting to liquefy; sort of the bodies way of doing its own cataract surgery. Cataract resorption often occurs with chronicity but also in very rapid-onset and progressive cataracts, for example in inherited, juvenile cataracts of Cocker Spaniels and several other breeds. Hallmarks of resorbing cataracts include a sparkly appearance, wrinkling of the anterior lens capsule, a deep anterior chamber and sometimes discernable (on exam itself and definitely with ocular ultrasound) decreased lens thickness. As lens resorption and leakage of lens proteins out of / through the lens capsule and into the eye often causes phacolytic lens-induced uveitis, other signs to look for are those associated with intraocular inflammation, including anterior chamber flare +/- relative miosis, red eye, low intraocular pressure, posterior synechiae and a velvety smooth and/or hyperpigmented iris. An uncommon specific type of resorbing cataract is a Morgagnian cataract, which occurs when the lens cortex is so markedly resorbed away that the residual nucleus sinks inferiorly within the lens capsule. Intumescent – In these cataracts, the lens fibers and thus the lens itself becomes markedly swollen and stretching the lens capsule. This results in shallowing of the anterior chamber and sometimes secondary pressure elevation or even overt glaucoma. It can also result in rupture (bursting) of the lens capsule (usually posteriorly where it is thinnest or near the equator) and then phacoclastic uveitis. This type of cataract is most commonly associated with diabetes. Cataract location classification scheme Recall the lens anatomy. An incomplete or smaller cataract can occupy a specific/focal region(s) within the lens and can thus be classified based on this location as below. During clinical examination, the location of lens opacities is most readily and best determined using a slit beam to create an optic cross section or slice through the eye and lens, highlighting the anterior and posterior lens capsule with bright, convex and concave respectively, lines of light, and then assessing relative depth and position of lesions.
15

Capsular – Capsular cataracts may affect the anterior or posterior lens capsule or shell. They rarely progress. Typical causes include uveitis, congenital / developmental abnormalities (especially incomplete regression of the embryologic vascular supply to the lens) and genetic. Subcapsular – anterior or posterior Cortical – Cortical cataracts may affect the anterior or posterior cortex. Anterior cortical cataracts are more likely to progress than posterior cortical ones. Equatorial (cortex) – This specific type of cortical cataract involves the equator or periphery of the lens and is often missed or difficult to see without retroillumination and ideally, for more thorough evaluation / assessment, pharmacologic mydriasis or pupil dilation. Cataracts in this location often progress (unless senile) because this is the most metabolically active region of the lens. Nuclear – Nuclear cataracts form in utero and are thus congenital. They may be inherited or associated with developmental accidents or “hiccups”. Fortunately they rarely progress and in fact, relatively-speaking, often become smaller with age as the nucleus is compressed centrally within the lens. Cataract age of onset classification Congenital – By definition, this type of cataract is present at birth. They may or may not be inherited. Juvenile – This type of cataract develops after birth and varying with breed, up to about six years of age. They are very commonly inherited in cause. Senile – As the name implies, this type of cataract occurs after about 6-10 years of age. Age-related cataracts are very common and one study documented some degree of cataract formation in all dogs greater than 13.5 years of age (Williams, DL; Heath, MF; Wallis, C. Vet. Ophthalmol. 2004; 7(1): 29-35). Fortunately these usually do not significantly affect vision nor progress. *Nuclear sclerosis is a normal age-related opacification of the lens nucleus associated with increased density due to lens fiber growth around it throughout life (without increase in lens size/volume) and resultant compression centrally. In dogs and cats it begins around age 6 years – though not really generally visibly so until 8-10 years. In humans it begins about age 40 years and results in decreased accommodative ability and presbyopia. Nuclear sclerosis should be differentiated from a true cataract opacity and can be as the former generally does not affect vision (whereas a complete or near complete cataract in the same central location likely would); and with nuclear sclerosis the tapetal reflex is still present and the fundus/retina can be visualized (not be the case with a complete or near complete cataract). Finally, differentiating nuclear sclerosis from cataract is often easier with pupil dilation allowing visualization of the clear(-er) cortical halo around the dense central nucleus. Once cataracts are identified and ideally classified, treatment options come into play. In terms of medical management, there have been some highly publicized/advertised/marketed topical
16

therapies that are touted to “melt away” cataracts. The old adage that says if it sounds too good to be true it probably is applies here. These eye drops are generally anti-oxidants, specifically N-acetyl carnosine and other ocular health vitamin supplement agents marketed under several names. They may in fact reduce oxidative damage to the lens and in a controversial study (as lens changes were very subtle and difficult to measure objectively with photographs as lighting and angle of exposure alter the results significantly and are nearly impossible to keep totally consistent, and the principle investigator refutes the findings stating his words have been manipulated by the pharmaceutical companies) did decrease lens opacity in cases of nuclear sclerosis and incomplete cataracts (Williams, DL; Munday, P. Vet. Ophthalmol. 2006; 9(5) 311-316. However, they do not eliminate or slow further progression of significant cataracts that we see in dogs that actually warrant treatment due to their visual impact (late incomplete and complete), probably due to the relatively large size of the canine lens and the high density of cataract opacities in this species. The bottom line is that these may be “useful” for cases where treatment is not really indicated as there is no visual impairment or other complication, but not for those already visually impaired. Furthermore, these medications are generally expensive, and can provide a false sense of security to clients as they think they’re managing things with the drops and thus seek veterinary evaluation and attention later in the disease course when secondary changes like lens induced uveitis, resorption, lens luxation, retinal detachment and/or secondary glaucoma, etc. may have already occurred with chronicity, and now preempt successful intervention. Ocu-GLO RxTM is a maybe more worthwhile oral nutraceutical containing a combination of 12 safe (and effective in generally supporting and protecting ocular health and normal function, boosting overall immune health, and scavenging destructive free radicals) antioxidant ingredients and formulated specifically for dogs. Considered a vision supplement, it is probably most useful in potentially delaying progression of retinal disease (progressive retinal atrophy (PRA) and other degenerative diseases, maybe sudden acquired retinal degeneration syndrome (SARDS) and immune-mediated retinopathies, etc) and cataracts that are secondary to such retinal disease (toxic cataracts) or prior to formation/early diabetic cataracts. It will not reduce existing opacities but depending on cause, might delay progression of such, and has possible utility in decreasing post-cataract surgery capsular scarring/fibrosis opacification. Finally, Ocu-GLO RxTM may also benefit (and it is certainly unlikely to harm though it is expensive) other ocular disease conditions such as uveitis, glaucoma, and Golden Retriever uveitis. A more promising potential medical therapy for diabetic cataracts is the use of aldose reductase inhibitors. This has been shown to be effective in delaying the onset and severity of cataracts in galactosemic (essentially an experimentally induced diabetic state) (Sato, S; Mori, K; Wyman, M; et. al.. Exp Eye Research 1998; 66(2) 217-222) and more recently diabetic dogs, and may ultimately also even be effective in treating these cataracts once they occur. Unfortunately these drugs (topical and systemic) are not commercially available for use at this time. Considering these issues with medical treatment options, at this time, surgery is the only proven and reliable, effective way to restore vision lost due to cataracts. Surgery employs phacoemulsification or ultrasound energy to break up the opaque lens and it is irrigated and aspirated out of the capsule. The success rate in good/ideal candidate canine patients is 90-95%.
17

The ideal candidate for cataract surgery is: -systemically healthy or at least managed/regulated/stable, -a manageable patient - intensive post-operative medical therapy and follow-up are vital to success and the patient, client/owner and veterinary ophthalmologist must be able to tolerate and handle this! -has vision affected by cataract/is impaired or functionally blind at least in the affected eye(s), making the potential benefit/gain of surgery worth the cost/risks, -has no or at least controlled lens induced uveitis - previous or refractory intraocular inflammation poses an increased risk of post-operative complication(s), especially retinal detachment and glaucoma) -does not have lens resorption – if present, this significantly increases the risk of pre-existing or post-operative retinal detachment -has normal pre-operative electroretinogram (ERG) and ocular ultrasound (normal lens shape and no capsule disruption, non-degenerate vitreous (as when present slightly increases the risk of retinal detachment), no pre-existing retinal detachment, no residual embryologic vascular supply) Risk factors for cataract surgery sort of naturally follow from the above list of qualities/factors of an ideal candidate. Specifically though, risk factors include lens induced uveitis (LIU) and lens resorption as above; breed predisposition to retinal detachment (in Bichon Frises and some other breeds as well as patients with significant vitreal degeneration); breed predisposition to glaucoma (Cocker Spaniels and many other breeds predisposed to primary glaucoma (and thus also secondary) with/by goniodysgenesis (an abnormal (narrowed) drainage angle)); and being a Boston Terrier – multiple studies have shown that the single biggest risk factor for serious (potentially devastating with ultimate blindness and loss of the eye/need for removal due to pain) post-operative complications (corneal ulceration, inflammation, retinal detachment, GLAUCOMA) is being a Boston Terrier! Several of the potential complications of surgery are eluded to above but most importantly, as they are vision threatening and in the latter case, painful, include retinal detachment and glaucoma. At surgery, inability to place an intraocular lens implant may occur, though even in this case, vision should still be improved, though far-sighted or hyperopic, like our vision underwater. Other possible issues include infection (potentially devastating endophthalmitis as the eye does not tolerate/handle infection and the associated secondary inflammation well); corneal ulceration, chronic and refractory inflammation/uveitis, posterior synechiae which may be cosmetic, increase the risk of secondary glaucoma or rarely be visually significant; and especially in young dogs, lens fiber regrowth often inciting lens induced uveitis and possibly though rarely affecting vision again – sometimes warranting surgery to alleviate the stimulus of inflammation and any visually significant opacity (remove regrowth). Also as mentioned above when discussing the ideal candidate for cataract surgery, indicated/appropriate pre-operative testing includes electroretinogram (measuring/assessing hopefully normal/adequate retinal function) and ocular ultrasound (hopefully ruling out pre-existing retinal detachment, etc. as above). These tests are warranted as for good surgical candidates likely complete or nearly so cataracts preclude retinal examination and these tests allow the best possible evaluation and assessment to determine that the retina “checks out” okay. If it does not, it probably doesn’t make sense to remove the cataract through somewhat invasive,
18
expensive surgery – this is sort of like the situation if there is no film/data card in the camera, there’s no point in removing the lens cover. Other cataract pre-operative testing indicated includes screening lab work to assess for underlying systemic disease that may have caused the cataracts in the first place but more importantly for safe candidacy for general anesthesia and aggressive peri- and post-operative anti-inflammatory medical therapy needed with this procedure. In diabetic patients for the same reasons, glucose regulation should be good and stable (clinical signs controlled, blood glucose curves with nadirs not lower than 80mg/dl and peaks less than 350mg/dl; fructosamine < 450-500). It is expected that they will suffer some dysregulation with the stress of anesthesia and surgery, and frequently with necessary aggressive peri-operative anti-inflammatory therapy, etc., so it is ideal if everyone is comfortable and on-board with where they were and stay the course without reactionary insulin dose changes in the “rough” period shortly afterwards. Additionally in diabetic patients a urine culture, even if not indicated by the sediment findings of the urinalysis, should be performed pre-operatively as these dogs are prone to silent urinary tract infections and any bacteria in the body can seed the eye particularly when peri-operative uveitis breaks down the blood aqueous barrier. Bacterial infection within the eye can result in devastating endophthalmitis, frequently with vision and ultimately eye loss (enucleation). For this same reason, skin should be assessed, especially in allergic or otherwise predisposed patients, for signs of pyoderma. In the case of UTI or pyoderma, appropriate antibiotic therapy should be initiated and continued through a negative culture and possibly the post-operative period to reduce risk of infection especially with intraocular lens implant (nidus potential). Finally, another pre-operative requirement or at least strong recommendation is good/reasonable periodontal health, again due to the risk of bacteremia with periodontal disease readily seeding the eye at surgery. Thus if/as indicated by oral/dental disease, a dental cleaning should be performed at least two weeks prior to cataract surgery, with peri-procedural antibiotics as indicated and also just time for expected bacteremia to clear. Though this all may seem excessive, remember that cataract surgery is an elective procedure with significant risk. Having all of the “ducks in a row” in an ideal candidate can maximize success. Surgery is performed with phacoemulsification under an operating microscope. An incision is made superiorly in the cornea paralleling the limbus. A capsulorrhexis (hole in the anterior lens capsule) is then made to access the lens contents. The phaco. needle delivers ultrasound energy to fragment the hard nucleus of the lens while continuous irrigation and aspiration flushes and vacuums it out. The remaining lens cortex is then aspirated out of the hopefully still intact (it is very thin and easy to rupture or tear during the procedure) lens capsular bag. An intraocular lens is then inserted into the capsular bag. These are generally foldable acrylic lenses of varying diameter sizes as indicated for the patient, and in dogs usually with dioptric power of 41 to restore normal/emmetropic vision (through bending of light rays through/by the lens into focus on the retina) in the majority of patients. They are injected with special cartridges and instruments. Previously and sometimes still currently on occasion, a rigid polymethylmethacrylate lens is used – this requires a larger corneal incision and generally longer surgical time. Regardless, the corneal incision is then closed and the road to recovery begins. The postoperative therapy is as important as what happens in the operating room / at surgery – it is absolutely vital to the success of the procedure and entails initially somewhat intense topical and systemic anti-inflammatory medications (ultimately slowly tapered as indicated) and
19

close/frequent monitoring with serial rechecks at increasing intervals. Because the inflammatory response incited by dogs to exposure to their own lens proteins (with any pre-operative lens induced uveitis and then at and after surgery itself) and the ultrasound energy requirement (high and long) to break up the relatively large and dense canine lens (about 8 times the size of a human lens and usually operated relatively later in the game when the lens is harder…) result in significant inflammation, afterwards weeks to months and even years are spent combating / hopefully controlling it and many canine post-cataract surgery patients remain on some level of topical therapy and monitoring long term to forever. What if cataract surgery is not an option? It may not be elected or the patient may not be a candidate, etc.. In these cases, it is still indicated to monitor and treat any lens induced uveitis (with topical anti-inflammatory medication) to avoid or at least decrease the risk of discomfort and secondary glaucoma or other complications. Occasionally, if lens resorption occurs and is advanced, without in the process inciting significant inflammation and causing retinal detachment or secondary glaucoma, it may result in enough clearing of the lens and visual axis that some vision (albeit far sighted/de-focused) may be restored/gained. In terms of visual impairment, if only one eye is affected, most veterinary patients function essentially normally, though longer-nosed and highly visually reliant working dogs may demonstrate some/more deficits on the affected side and astute owners may notice this. If patients are bilaterally affected and visually impaired to even completely functionally blind, fortunately the vast majority of dogs adapt amazingly well and have good quality of life, especially when their vision loss is gradual (with slow onset or progressing cataracts) or given time to adjust even when it is rapid. They will frequently memorize their environments and some owners don’t even recognize how impaired they are. However, with things out of place or novel environments, not surprisingly they may have more trouble, so ideally their environments should be kept as stable as possible to help them adjust and cope. This and other useful tips are available through many great resources for owners of visually impaired pets, in book and online forms.
20

The Red Eye
Kathryn Diehl, DVM, MS, DACVO
The red eye is a common presenting complaint in veterinary medicine. Unfortunately many ophthalmic diseases manifest with this clinical sign. This session’s objective is ultimately to help veterinarians consider, recognize and manage appropriate differential diagnoses through discussion of common causes from eyelids to globe. When presented with the client complaint of a red eye in a veterinary patient either over the phone or in person, knowing the differential diagnoses will help guide urgency, diagnostic work up and empiric +/- definitive treatment. Initially then, just quickly/briefly go through the differentials as follows: Blepharitis – usually obvious and involving the specialized skin (and associated glands) of the eyelids; not urgent Conjunctivitis – a diagnosis of exclusion with generally normal globe; not urgent; note though that the conjunctiva is often affected (hyperemic, swollen, etc.) as an extension of or reaction to other ocular disease but in those cases, not the primary problem (i.e., not conjunctivitis) Episcleritis – also a diagnosis of exclusion with generally normal globe; not urgent; note though, that like the conjunctiva, the episcleral tissues are also often affected (injected, etc.) as an extension of or reaction to other ocular disease but in those cases, not the primary problem (i.e., not episcleritis) Keratitis – corneal disease/inflammation with many potential underlying causes and types (ulcerative and non-); may be urgent due to potential risk of rupture with deep ulcers/thinned corneal tissue and this needs to be recognized! Diagnosis of true/primary keratitis may also be confounded by involvement by extension of intraocular diseases (e.g., corneal edema with uveitis, lens luxation and/or glaucoma, corneal vascularization with any chronic intraocular disease, etc., where the cornea is indeed abnormal but the diagnosis is not keratitis) Uveitis – intraocular inflammation that may be primary (or secondary, e.g. reflex uveitis with corneal disease) ophthalmic or associated with systemic disease and warranting screening diagnostic evaluation Hyphema (or subconjunctival, iris or retinal hemorrhage) – intraocular bleeding or ophthalmic petechiae/ecchymoses that may be primary ocular (from trauma or associated with systemic disease and warranting screening diagnostic evaluation Glaucoma – elevated intraocular pressure induced damage to the optic nerve +/- retina; may be primary (due to drainage angle abnormality) or secondary (to other ocular disease); urgent when acute in eye with visual potential due to risk of blindness and pain, thus needs to be recognized!
21

Keeping this cursory review of the differential diagnoses in mind, consider also the signalment and history. Many ophthalmic diseases have breed-inherited or breed-conformational bases that may help refine the differential diagnosis list. In terms of history, ophthalmic and any systemic signs noted at home, their chronicity, progression and response to any treatment may help define urgency as well as also refine the differential diagnoses list and guide work up and/or empiric (+/- definitive) treatment. The red eye diagnostic evaluation should be comprised of the ophthalmic examination and often a general physical examination. With regard to the ophthalmic exam, supportive tests including the Schirmer tear test (STT) (for quantitative tear film deficiency or keratoconjunctivitis sicca (KCS or dry eye), fluorescein staining (for corneal epithelial defects or ulcers) and tonometry or the measurement of intraocular pressure (IOP) (for glaucoma) may quickly provide most of or even all of the story of the case of the red eye! Note especially for the STT and tonometry, both eyes should always be checked, as there is variation of normal and the results in the other eye (which should be comparable) may help allow differentiation of such variation from pathologic results. Obviously, ultimately the complete ophthalmic examination allows identification of the cause of the red eye from amongst the differentials and they are each discussed in a little more detail below. Additionally, as many ophthalmic diseases are manifestations of systemic issues and systemic health status may impact the diagnostic work up and/or treatment of the ophthalmic disease, a thorough general physical examination is often indicated. The red eye differential diagnoses revisited: Blepharitis is inflammation of the specialized skin of the eyelids and associated meibomian glands resulting in variable swelling, erythema, ocular discharge, sensitivity, pruritis and alopecia. Blepharitis may occur focally as a hordeolum (stye), which is an acute abscess of meibomian glands, or as a chalazion, which is a chronic lipid granuloma that occurs secondary to a blocked meibomian gland duct. Blepharitis may also occur diffusely (affecting broader/larger regions or all of the eyelids) and in those cases may be a component of generalized dermatitis. Potential causes of blepharitis include: -infection bacterial (especially Staph.) fungal (including dermatophytosis, Malassezia and Candida which may be primary or secondary with immune-suppression and/or chronic topical cyclosporine use, and rarely deep fungal infection) parasitic -inflammatory immune-mediated including Staph. hypersensitivity meibomitis, granulomatous, uveodermatologic syndrome (an immune-mediated disease targeting pigmented cells at mucocutaneous junctions of the eyelids, nares, gums, vulva/prepuce and within the eye causing uveitis, chorioretinitis, retinal detachments and often secondary glaucoma; usually seen in Alaskan Malamutes, Akitas, Dachshunds, Samoyeds, Siberian Huskies) allergic – contact or atopic often with secondary traumatic component from pruritis and rubbing, insect hypersensitivity, drug reaction
22

-foreign body -neoplastic lymphosarcoma (including mycoses fungoides) mast cell tumor squamous cell carcinoma or solar-induced (especially in lightly pigmented eyelids) precursors to such (actinic inflammation, carcinoma in situ), etc. Blepharitis diagnostic evaluation includes close examination (ideally with magnification) of the eyelids/inflammation, general physical examination, often response to empiric therapy (antibiotic and/or anti-inflammatory), skin scrape cytology, culture, and/or biopsy. Treatment is obviously ideally based on definitive diagnosis though maintenance cleaning of discharge, warm compresses especially when meibomian glands are affected, and trial empiric therapy with topical steroid anti-inflammatory (assuming negative fluorescein stain indicates no concurrent corneal ulceration) and oral antibiotic (cephalexin, Clavamox or cefpodoxime (Simplicef)) and non-steroidal medications are often reasonable first steps. Note that for eyelid (essentially skin) disease, systemic administration of medications is generally more effective than topical. Also, when treating blepharitis empirically, even when immune-mediated disease is suspected, use systemic/oral steroid anti-inflammatory therapy with caution/awareness as it may worsen infectious disease and/or impair later ability to diagnose neoplastic conditions as well as their response to chemotherapy if pursued. Conjunctivitis is inflammation of the conjunctiva (palpebral, bulbar, nictitating membrane) with variable erythema, chemosis (edema of the conjunctiva), ocular discharge (serous, mucoid, mucopurulent, or with a characteristic thick, ropey nature with keratoconjunctivitis sicca) and follicular response (especially on the bulbar aspect of the third eyelid and with allergies or any other chronic cause of conjunctivitis). Causes of conjunctivitis include: -infection bacterial (uncommon in dogs unless puppies (ophthalmic neonatorum) or young with exposure; Chlamydophila, Mycoplasmal, Bartonellosis in cats) viral (especially feline herpes virus (EXTREMELY common) and Calicivirus in cats) parasitic (Thelazia, Onchocerca and Habronema – latter two mainly in horses) -immune-mediated allergic very common in dogs (atopic, food) eosinophilic in cats contact allergy/drug reaction especially with neomycin, antivirals, pilocarpine, acetylcysteine and others -decreased tear production (keratoconjunctivitis sicca or other tear film deficiencies) with characteristic ocular discharge -foreign body or other cause of physical/mechanical irritation (as sometimes with eyelid masses, notch defects, exposure, etc.) -neoplastic Conjunctivitis diagnostic evaluation includes assessment of the Schirmer tear test and close examination (ideally with magnification) of the tissue, possibly with application of topical
23

anesthetic and manual retraction of the third eyelid to allow assessment of its bulbar aspect. Additionally, again general physical examination may be useful in narrowing or identifying the specific underlying cause, and often response to empiric therapy (topical antibiotic and/or anti-inflammatory), conjunctival scrape cytology, culture, and/or biopsy are helpful/diagnostic. Treatment is obviously ideally based on definitive diagnosis but may involve removal of any irritant (drug or mechanical), saline eye wash rinsing, topical and/or oral antimicrobials (antibiotic, antiviral for cats though usually only if severe and/or concurrent corneal involvement), topical steroidal or other anti-inflammatories (contraindicated with even possible feline herpes viral infection), and tear stimulants (cyclosporine, tacrolimus). Episcleritis is inflammation of the episcleral tissues and it may be focal/nodular (nodular granulomatous episcleritis) or diffuse and usually bilateral (though not always symmetric). Besides inflammation with erythema and focal or diffuse swelling or thickening, often the limbal cornea is edematous and sometimes vascularized; crystalline corneal lipid/cholesterol deposits of inflammation/degeneration may also occur adjacent to areas of episcleral inflammation. Patients are often not bothered by these signs/lesions except in more severe cases. The cause of episcleritis is almost always immune-mediated, however, neoplasia is possible and especially with more aggressive diffuse (anterior and posterior) necrotizing episcleritis, underlying systemic disease (infectious, neoplastic, etc.) may be at play. Work up may thus include *ruling out other causes of red eye (this is a diagnosis of exclusion)*, assessment to response to initial empiric therapy (again with caution and informed consent with oral steroid use in this manner), lesion scrape or ideally aspirate cytology and/or better yet, biopsy. Depending on severity and with slow taper long term to the lowest amount that keeps things in check, treatment generally involves some combination of topical (even injected sub-bulbar conjunctivally) steroid and other anti-inflammatories, as well as oral anti-inflammatories and immune-modulative drugs (NSAIDs OR prednisone, tetracycline/doxycycline and niacinamide, cyclosporine, azathioprine) with appropriate work up first and still some caution. Finally, surgical debulking and adjunctive cryotherapy may benefit refractory lesions. Inflammation is rarely severe enough to significantly damage the eye, though in severe cases may be very aggressive ultimately resulting in enucleation if refractory and blinding by extension to other ocular tissues. Keratitis is corneal disease or inflammation that has numerous potential underlying causes and types. Clinical signs include variable squinting, discharge and ocular redness due to conjunctival hyperemia and episcleral injection. Additionally, variable corneal opacities including edema, infiltrate and vascularization, as well as malacia (melting due to corneal “digestion” by collagenases/proteinases) and stromal loss (corneal thinning from superficial to deep, even down to Descemet’s membrane, with significantly increased risk of rupture) may be present. Positive fluorescein staining or uptake of fluorescein dye is the hallmark of “active” corneal ulceration (surface epithelial defect), though lesions down to Descemet’s membrane will not retain stain in their beds, and lesions that epithelialize prior to remodeling/rebuilding stromal loss may be fluorescein negative but still thinned (facet). Finally, variable reflex uveitis (intraocular inflammation) may also be present, especially with infected corneal ulcers and in horses, even with uncomplicated surface issues.
24

Ulcerative keratitis is usually initially traumatic in origin +/- secondary bacterial infection in all species, with underlying herpes virus also incredibly common in cats, but exposure (in brachycephalic patients and others with altered blink reflex), lid abnormalities, tear film deficiencies (KCS so check STT!) and neurologic conditions can predispose and even cause ulceration in some cases and thus should be considered in the work up and management of corneal ulcers. Superficial / uncomplicated ulcers should be treated with a prophylactic topical antibiotic to prevent secondary infection until healing (generally within a few days to a week depending on size) and negative fluorescein stain are achieved. Topical atropine to dilate the pupil and alleviate pain associated with ciliary spasm of reflex uveitis (though not in patients with dry eye or a predisposition to / risk for glaucoma) is occasionally warranted, as are sometimes short courses of an oral non-steroidal anti-inflammatory drug (as long as not otherwise contraindicated) and/or tramadol. An e-collar may be indicated to prevent self-traumatic exacerbation of disease through rubbing. Spontaneous chronic corneal epithelial defects (SCCED) or primary non-healing or “Boxer” or “indolent” ulcers are frequently persistent/difficult to get healed though remain superficial and have a characteristic loose epithelial edge. Therapy is similar to that for uncomplicated ulcers above, but also usually requires at least epithelial debridement, +/- stromal alterations (grid keratotomy, anterior stromal puncture), bandage contact lens placement or third eyelid flap, gluing, thermokeratoplasty or even keratectomy. Complicated or deep (best determined by seeing a divot or ideally assessing with a focused slit beam to determine corneal depth/loss of thickness), melting and/or infected corneal ulcers warrant urgent and aggressive attention/intervention due to their potential risk of rapid progression to rupture with threat to vision and the globe itself. Infected ulcers tend to have corneal infiltrate (warranting at least cytology +/- culture as part of the diagnostic work up) and often more significant uveitis. Medical management consists of combination, broad spectrum, “big gun” and frequently administered (initially up to hourly) topical antibiotics (generally ophthalmic cefazolin and a fluoroquinolone) in solution form (ointments should not be used in eyes with current or possible impending perforation). Collagenase/proteinase inhibitors such as serum, EDTA or N-acetyl-L-cysteine can help reduce further malacia/melting. As with superficial ulcers, mydriatic-cycloplegic atropine may also be indicated in these cases also to achieve and maintain pupil dilation, reducing the risk of visually significant synechiae, and stabilizing the blood aqueous barrier / decreasing vascular permeability reducing further uveitis. Again though, it should not be used in patients with dry eye or (a risk of) glaucoma. Additionally, systemic anti-inflammatory therapy for common associated reflex uveitis and pain is often indicated, though this may somewhat delay vascularization and thus healing and administration decisions should balance comfort and healing “enhancement”. Topical anti-inflammatory medications, especially steroids should NOT be used as they readily delay healing and potentiate infection and malacia through potentiating collagenases. Finally, other considerations for management include additional or alternate pain control with opioid tramadol or others, activity restriction (possibly with sedation as necessary for the patient) due to risk of rupture, and e-collar placement.
25

Surgical stabilization may also be indicated if the lesion depth is greater than 50%, the ulcer is rapidly progressive or melting, there is a lack of or limited vascularization (which is how these more serious corneal ulcers will ultimately combat infection and heal (remodel and epithelialize)), or the defect is actively leaking, and there is a potential for vision or owner desire to save a blind eye. Immune-mediated (generally non-ulcerative) keratitis is not uncommon in dogs, especially Shih tzus, Shelties (associated with deposits of dystrophy), Dachshunds, German Shepherds and their relatives (as chronic superficial keratitis or “pannus”) and some other breeds, and also can occur in cats as eosinophilic keratitis (EK) and/or a stromal variant of herpes virus among other causes. Clinical signs generally include corneal vascularization and variable fibrosis and infiltrate (especially in the case of EK in cats). Corneal scrape cytology (of infiltrate) may be of diagnostic benefit. In these cases of immune-mediated keratitis though, with caution, treatment is generally with topical steroid and/or other anti-inflammatory to achieve control / remission, then long term tapered to the lowest amount that keeps things in check, while also balancing side effects and risk of use. Uveitis or inflammation of the uveal tract is essentially the medical term for intraocular inflammation. Clinical signs of uveitis include variable blepharospasm or squinting / photophobia, red eye due to conjunctival, episcleral and possibly even intraocular hyperemia/injection or even bleeding, corneal edema, aqueous humor flare (the hallmark of the clinical condition and diagnosis) +/- anterior chamber hypopyon (settled out white blood cells), relative miosis (pupil constriction) with resistance to pharmacologic mydriasis, low intraocular pressure, posterior synechiae (adhesions of the iris to the lens), iris hyperpigmentation and a velvety smooth texture change of the iris tissue. These latter three signs may be present during active inflammation or seen as remnants of disease after things are quiet. Uveitis may be caused by primary ophthalmic diseases such as blunt or sharp trauma, corneal disease (reflex uveitis), immune-mediated disease specific to the eye(s), lens-induced as with cataracts, developmental abnormalities, etc.. However it may also be caused by potentially serious underlying systemic disease, including broadly, infection (deep fungal, tick borne, etc.), immune-mediated disorders and neoplasia, thus warranting screening diagnostic evaluation. Due to the enormous differential diagnosis list for uveitis, unless a primary ophthalmic cause is known/obvious or for some reason suspected (e.g., there was trauma and only one eye is affected; inflammation is occurring in an eye with chronic cataract or a residual embryologic vascular structure, etc.), and certainly if there are any other signs of illness, and/or the cause is unknown (especially if both eyes are affected) and initial empiric therapy fails to improve things, an initially broad systemic work up with thorough general physical examination, lab work (complete blood count, chemistry profile, urinalysis, +/- titers for some of the more common infectious disease causes of uveitis based on exposure/risk and other signs if present) and imaging (chest radiographs, abdominal ultrasound, +/- ocular ultrasound if the posterior segment cannot be visualized and evaluated) ultimately narrowed based on any results, should be at least considered. In cases where the eye(s) is irreversibly blind from inflammatory damage or common secondary glaucoma, and often at least intermittently painful especially if refractory to
26

therapy, diagnostic (through biopsy) and therapeutic (alleviating pain and the need to treat) enucleation may actually be of highest/most direct yield and benefit. Regardless in the meantime of pending work up, empiric, symptomatic aggressive (based on severity of inflammation) anti-inflammatory therapy for the eye(s) with topical* steroid +/- non-steroid (contraindicated with elevated intraocular pressure - beware even a normal intraocular pressure in a uveitic eye as it should be low, and normal to elevated pressure indicates secondary glaucoma), and oral non-steroidal** (potentially later steroidal depending on the case and cause, etc.) should be initiated. Cycloplegic treatment with atropine or shorter acting tropicamide (a little safer/less risky in case secondary glaucoma arises though neither should be used if there is already pressure elevation and both should be stopped if such arises during treatment) alleviates pain from ciliary spasm, decreases the risk of visually significant synechiae formation and helps stabilize the blood aqueous barrier, reducing further inflammation. Any pressure elevation should also be addressed with topical carbonic anhydrase inhibitor and/or beta blocker therapy. Monitoring should assess for inflammation to subside and remain controlled, as well as pressure to stay appropriate, again with further work up and/or treatment based on response to therapy. Ultimate prognosis depends on the underlying cause (and ideally detection and management of that) as well as severity of inflammation and secondary changes, but this can certainly be a vision and comfort threatening condition. (*Assuming there is no contraindicating concurrent corneal ulceration. **Assuming there is no systemic contraindication.) Hyphema is hemorrhage within the anterior chamber and it along with subconjunctival, iris, vitreal or retinal hemorrhage are forms of ophthalmic bleeding or petechiae/ecchymoses that like uveitis may be due to primary ocular disease (from trauma, chronic inflammation, intraocular tumors, congenital anomalies such as Collie eye anomaly, merle ocular dysgenesis, vitreoretinal dysplasia and/or residual embryologic vascular structure (e.g., persistent hyaloids artery), retinal detachment, etc.) or associated with underlying systemic diseases that result in bleeding tendencies, thus warranting screening diagnostic evaluation. Very much like uveitis, with slightly different (again, more focused on bleeding tendency and including things like rodenticide toxicity or other causes of coagulopathy, immune-mediated or other thrombocytopenia, anemia, very commonly lymphoma but also other neoplasias, vasculitis – infectious or otherwise, systemic hypertension (esp. in cats), hyperviscosity syndrome with multiple myeloma, Ehrlichiosis, etc., etc.) but still overlapping differential diagnosis list, unless a primary ophthalmic cause is known/obvious or suspected, and certainly if there are any other signs of illness, and/or the cause is unknown (especially if both eyes are affected) and initial empiric therapy and a little time fails to improve things, a broad systemic work up is likewise indicated. In addition to those tests recommended for uveitis, coagulation profile testing and blood pressure measurement may also be specifically warranted depending on the situation. Again, enucleation for irreversibly blind (and painful) eyes may ultimately be indicated and can be of both diagnostic and therapeutic value. Again, regardless and in the meantime, while an underlying cause is hopefully sought, detected and treated / addressed specifically, the affected eye(s) should be treated with topical +/- systemic (though especially with an NSAID, with some increased risk in further increasing
27

bleeding tendency) anti-inflammatory and topical cycloplegic (assuming pressure is appropriately low) therapy. Specific intraocular pressure lowering / anti-glaucoma management should be employed when there is concern for or overt secondary glaucoma and regardless, monitoring for such should be done. Glaucoma is a term that encompasses a diverse group of diseases united by the common theme of an intraocular pressure that is too high for the optic nerve (and retina) to function normally, frequently rapidly resulting in the loss of some or all vision and pain. This pressure elevation essentially always occurs due to obstruction of outflow of continually produced/flowing aqueous humor from the eye. This obstruction and thus glaucoma may be primary (due to a congenital or inherited drainage angle abnormality/narrowing) or secondary (to other ocular disease such as uveitis (with inflammatory debris in and scarring of the drainage angle), lens luxation (with mechanical obstruction to fluid flow by the displaced lens), etc.) and these are treated differently and thus should be differentiated. Clinical signs of glaucoma include variable pain (from overt/dramatic with head shying, etc. to more subtle with decreased attitude, activity and/or appetite), squinting and third eyelid elevation, ocular redness due to conjunctival and episcleral vascular congestion as well as injection due to frequently associated mild inflammation (secondary uveitis), corneal edema from endothelial cell dysfunction with pressure elevation, mydriasis or pupil dilation due to iris sphincter muscle impairment at pressures over 40mmHg and/or as an afferent pupillary deficit from damage to the optic nerve, vision change (often hard for clients to detect when only one eye is affected), optic nerve head inflammation, peripapillary hyperreflectivity (conus) and eventually cupping due to both mechanical pressure bowing and eventually tissue atrophy, and, finally, the hallmark of diagnosis, elevated intraocular pressure. In terms of diagnostic evaluation, besides the ophthalmic examination (especially with respect to visual (potential) assessment with pupillary light and dazzle reflexes and the presence of any antecedent ocular disease (indicating secondary glaucoma)) and tonometry, fluorescein staining is indicated as secondary corneal ulcers are common and may alter prognosis and treatment (no topical steroid until healed and may be difficult to get healed depending on overall ocular health/disease severity). Also, general physical examination may be indicated in secondary cases, particularly due to uveitis, hypema or neoplasia (in case metastatic from the eye – more common in cats; or secondary from elsewhere in the body to the eye). Treatment considerations include differentiation of primary from secondary glaucoma and though this can be difficult, breed predisposition (Cocker Spaniel, Bassett Hound, Siberian Husky and other arctic circle breeds, etc. with an unfortunately growing list) and lack of other ocular abnormalities support a diagnosis of primary glaucoma. The referral procedure gonioscopy, evaluating the drainage angle for abnormalities, of the affected but more importantly other/”good” eye can also strongly support a diagnosis of primary glaucoma if it is abnormal (goniodysgenesis). Probably even more important with regard to treatment though is determining the visual potential and thus urgency of disease. If the eye is still visual, has a fairly healthy optic nerve and most importantly has a consensual pupillary light reflex (PLR) to the other eye, there is the potential for maintenance / return of vision and urgent and aggressive, even heroic with glaucoma filtering and laser surgery, may be indicated if elected. If the
28

condition is chronic, especially with buphthalmos (globe enlargement), optic nerve head cupping and/or loss of consensual PLR to the other eye, then urgency is alleviated and the goals of treatment shift to comfort and ideally maintenance of a blind, but pain-free eye, with salvage surgery to remove it if this cannot be achieved with reasonably tolerated (by both client and patient) medical therapy. With the potential for vision / goal of therapy, and differentiation of primary and secondary glaucoma in mind, treatment recommendations/options are as follows: For primary glaucoma in dogs – prompt referral if elected and condition is acute, especially with potential for vision and possible interest in surgery; otherwise/regardless, prostaglandin analogue (latanoprost) BID-TID, topical steroid anti-inflammatory (unless contraindicated by concurrent corneal ulceration), +/- topical and/or oral carbonic anhydrase inhibitor and/or beta blocker; osmotic diuretic (mannitol) administration intravenously may be used for urgent pressure reduction if prostaglandin analogue fails to reduce it within an hour or so with repeated doses (which is also a poor prognostic indicator) and there is potential for vision; pain management with oral anti-inflammatory and/or tramadol *”prophylactic” topical beta blocker (timolol) BID in other / “good” eye to delay onset and severity of disease, though usually eventually occurs For secondary glaucoma – ideally identify and manage the underlying issue (uveitis, lens luxation, etc.) and in the meantime, try to control pressure with topical and/or oral carbonic anhydrase inhibitor +/- beta blocker therapy. Note that prostaglandin analogues are contraindicated with secondary glaucoma as they exacerbate uveitis. They also are not effective at lowering intraocular pressure in cats. Topical steroid and oral non-steroidal (unless otherwise contraindicated), as well as tramadol or other pain management therapy, are almost always also indicated for secondary glaucoma. Enucleation of irreversibly blind and painful eyes with primary and this (secondary) condition is not uncommon as they are often refractory to treatment – sadly enough, it can thus be quite effective and rewarding.
29

Ophthalmology Top 10
Amy Pauli, DVM, DACVO Kathryn Diehl, DVM, MS, DACVO
In this lecture we will discuss what we consider to be the top 10 most important tips for the general practitioner regarding ocular examination techniques, ophthalmic diseases, and ophthalmic medications. 1. Pupillary light reflex (PLR) – The PLR assesses the integrity of the retina, optic nerve, parasympathetic fibers of cranial nerve III, and iris sphincter muscle. Localize a lesion along the PLR pathway using the swinging flashlight test, in which a bright light is alternately shined in one eye and then the other every 2-3 seconds. The direct PLR is constriction of the illuminated pupil. The consensual PLR is constriction of the contralateral pupil. An afferent pupillary defect, characterized by an absent direct and consensual (to the other eye) PLR, is indicative of retinal or optic nerve disease. An efferent pupillary defect, characterized by an absent direct PLR but positive consensual (to other eye) PLR, is indicative of cranial nerve III or iris disease. The PLR is useful in the initial evaluation for the cause of acute blindness. As a general rule of thumb, if a patient with acute blindness has a normal PLR the vision loss is likely associated with a central lesion, whereas if the patient has dilated pupils that are non-responsive to light the vision loss is likely associated with an ophthalmic lesion (retinal and/or optic nerve disease). One exception to this rule is Sudden Acquired Retinal Degeneration Syndrome (SARDS), in which the PLR is often relatively normal, at least initially. In addition, ophthalmic examination of patients with SARDS is unremarkable early in the course of the disease. Therefore, these patients may be suspected of having a central lesion. Diagnosis of SARDS is made with a retinal function test called an electroretinogram (ERG). A patient with SARDS will have a flat line response, indicating absent retinal function, while a patient with central blindness would be expected to have a normal ERG waveform. Another important use of the PLR is assessing the potential for return of vision in patients with a ruptured corneal ulcer, glaucoma, proptosis, etc. An absent consensual PLR from the effected eye to the contralateral eye indicates a low potential for restoration of vision. Therefore, aggressive measures to save the eye may not be recommended. 2. Tonometry tips – Tonometry, or assessement of the intraocular pressure (IOP), is an important part of the ophthalmic examination. Assess the IOP of both eyes whenever possible, as there is a wide range of normal variation and the pressure of the other eye can help provide a “normal” for that patient. The pressure of both eyes should be within a few mmHg of each other. Tonometry should be avoided in an eye with a deep or perforated corneal ulcer. There are several options for tonometers. The Schiotz tonometer is an indentation tonometer, which works by indenting the cornea with weight. Topical anesthesia is necessary, and this instrument should not be used on eyes that have deep or perforated corneal ulcers. Zero the Schiotz prior to each use using the stainless steel “eye” provided with the instrument. The
30

Schiotz tonometer must be positioned vertically; therefore, the patient should be in a sitting position with its nose pointed upward, or on its back. A high scale reading indicates a low IOP, and a low scale reading indicates a high IOP. When converting the instrument reading to an IOP, use the human (not canine) conversion chart provided with the instrument. The TonoPen is an applanation tonometer, which assesses the amount of force required to flatten a portion of the cornea. This instrument may be used with or without topical anesthesia. It should be used on the central cornea, and use the gentlest touch necessary to obtain readings. Align yourself perpendicular to the length of the instrument to see contact of the TonoPen tip on the corneal surface. The TonoPen is generally accurate even with corneal disease (scarring, etc.). The TonoVet is a rebound tonometer, which assesses the IOP using the deceleration characteristics of a magnetized probe after it bounces off the corneal surface. Topical anesthesia should not be used with this instrument. The TonoVet must be held horizontally or vertically. Its accuracy in the face of corneal disease has not been fully assessed, although it has been shown to be less accurate than the TonoPen when corneal edema is present. Many factors can affect IOP. Uveitis and increasing age are associated with a lower IOP. Factors associated with an increased IOP include glaucoma and stress/excitement. In addition, neck pressure during restraint of the patient, excessive traction on the eyelids or pressure on the globe when performing tonometry can all increase the IOP. 3. Buphthalmos versus exophthalmos – Buphthalmos refers to an enlarged globe secondary to chronic IOP elevation. Usually a buphthalmic eye will have a significantly elevated IOP at the time of examination. An eye that is buphthalmic is almost always blind with an afferent PLR defect (exceptions include puppies and some breeds, including the Shar Pei, which have an increased amount of elastin in the sclera). The corneal diameter can be compared to that of the other eye to confirm globe enlargement. Exophthalmia refers to a prominent eye due to anterior displacement of the globe, as with orbital disease. The easiest way to assess for anterior globe displacement is to point the patient’s face downward and view from above. Assess for resistance to retropulsion of the globe (compare to other eye), which is expected with orbital disease. An exophthalmic eye may be sighted or blind depending on whether the optic nerve is affected. The intraocular pressure of an exophthalmic eye may be normal to mildly elevated. Oral examination and imaging of the orbit with ultrasound, CT, or MRI can be helpful for evaluation of the cause of exophthalmia. 4. Complicated/malacic/infected/deep corneal ulcers – Infected corneal ulcers are common in veterinary medicine, particularly in brachycephalic dogs. Ophthalmic exam findings suggestive of corneal infection include corneal infiltrates (inflammatory cells), malacia (corneal “melting”), a corneal divot (consistent with loss of corneal thickness), clearing within the center of the ulcer (suggestive of corneal thinning), or excessive reflex uveitis. Aggressive medical management of infected corneal ulcers may prevent progression (especially further deepening of the ulcer) and need for surgery. Frequent (up to hourly) treatment with broad spectrum antibiotics (a fluoroquinolone such as ofloxacin or ciprofloxacin, in combination with cefazolin), as well serum, which has anti-collagenase and anti-proteinase activity to help reduce corneal melting, is
31

recommended. Treatment with atropine can also be helpful to help improve comfort and reduce formation of visually-impairing synechia, although this medication should be avoided in patients with KCS or glaucoma. Oral anti-inflammatory and/or pain management medications as well as e-collar placement are also often components of management. Patients with a complicated corneal ulcer should be monitored closely (recheck every 1-2 days initially) to make sure the ulcer is not becoming deeper and the signs of infection (corneal infiltrates, malacia, reflex uveitis) are improving. Surgical management for a corneal ulcer should be considered when there is less than 50% corneal thickness remaining. Surgical options include various grafting techniques (conjunctival graft, corneal graft, corneoconjunctival transposition), or corneal gluing. Some treatments should be avoided when there is a deep or infected corneal ulcer. A third eyelid flap is not recommended because it can apply pressure to the globe, increasing the risk of globe rupture. In addition, the presence of the third eyelid flap obscures the view of the cornea, making it impossible to closely monitor response to therapy. Ointments should also be avoided when a deep or perforated corneal ulcer is present, as severe intraocular inflammation can occur if the ointment gets into the eye. Never perform a grid keratotomy for a deep or infected corneal ulcer, as this procedure may lead to rupture of the eye or spread of infection deeper into the corneal stroma. Corneal debridement should also generally be avoided for deep corneal ulcers, as this procedure involves application of some pressure to the eye, which increases the risk of globe rupture. 5. Eosinophilic keratitis (EK) – EK is an immune-mediated inflammatory disease affecting the cornea and conjunctiva of cats. Ophthalmic exam findings include pinkish-white plaques of the cornea and conjunctiva, with associated corneal vascularization. Affected eyes are variably painful. This condition may be associated with feline herpes virus. To diagnose this condition, perform cytology of the plaques. The presence of a single eosinophil is diagnostic. Treatment of EK involves local immune-suppressive / anti-inflammatory therapy, typically with a topical steroid (prednisolone acetate). Topical cyclosporine therapy can also be used. Oral treatment with Ovaban can be effective as well, but is generally reserved for cases refractory to topical therapy because of the risk of diabetes mellitus. Regardless of which immune-modulating drug is used, concurrent anti-viral therapy should be considered to help address any herpes viral component to the disease and reduce the risk of a flare-up of herpes viral disease in the face of immune suppression. The immune-suppressive therapy should be slowly tapered over weeks to months as the disease is controlled. Recurrences of EK are common, and for some cats life-long treatment at some level is necessary to maintain control of the disease and reduce recurrences. Treatment for EK sometimes involves a careful balancing act between managing EK and addressing flare-ups of feline herpes viral corneal ulceration. 6. Ophthalmic manifestations of systemic disease – Many ophthalmic diseases are actually manifestations of systemic disease, and it is important to recognize when an ocular change may warrant a systemic work-up. Uveitis, hyphema or other ophthalmic hemorrhages, retinal detachment and optic neuritis can be secondary to underlying internal disease. In dogs, common causes for uveitis (+/- retinal detachment) include infectious diseases (tick-borne or deep fungal infections), an immune-mediated process, or neoplasia. Hypertension is a common cause of retinal detachment in cats, and occasionally in dogs. Conditions to assess for when hyphema is
32

noted include hypertension, a coagulopathy, neoplasia (primary intraocular mass, lymphoma, or metastatic spread of tumors to the eye), or infectious disease (especially tick-borne infections). Finally, a dog with rapidly developing cataracts should be assessed for diabetes mellitus. 7. Golden Retriever Uveitis (GRU) – Also called pigmentary uveitis of the Golden Retriever. This is a poorly understood (immune-mediated?) inflammatory condition, although it is likely at least in part genetic. Outward signs of this condition early in the course of the disease may be limited to ocular redness and mild discharge. As the disease progresses, ocular pain, cloudiness, and/or loss of vision may also be noted. Ophthalmic examination findings typically include ocular redness, aqueous flare, pigmented cells in the anterior chamber, iris hyperpigmentation, pigment on the anterior lens capsule, and uveal cysts. Post-inflammatory cataracts and glaucoma are common complications of this condition. Early recognition and treatment of GRU may slow progression of this condition, maintaining ocular comfort and vision for as long as possible. Treatment is symptomatic, including anti-inflammatory therapy (topical steroids and/or NSAIDS) and occasionally cautious treatment with tropicamide to reduce synechia formation by keeping the pupil mobile. As the disease progresses, anti-glaucoma therapy may also be necessary. Frequent monitoring is recommended to assess response to therapy and monitor the IOP. 8. Neomycin use in cats – Neomycin (as in Neomycin-Polymyxin-Bacitracin, NeoPolyGramicidin, and NeoPolyDexamethasone, etc.) should be avoided in cats for ophthalmic use as it is often irritating to cats and has the potential to cause sudden death in this species. In addition, triple antibiotic ointment/solution is ineffective against the common causes of conjunctivitis in cats (Chlamydophila and Mycoplasma). Topical antibiotics that are effective against these infections include Terramycin, erythromycin, and the fluoroquinolones. If topical steroid therapy is indicated for cats, straight dexamethasone or prednisolone acetate are recommended. 9. Topical hydrocortisone – Hydrocortisone is not recommended for ophthalmic use because it is generally not potent enough to address even ocular surface inflammatory diseases that warrant intervention and it does not penetrate the cornea well. Therefore, it is useless for treatment of intraocular or deep corneal inflammation. Topical prednisolone acetate or dexamethasone are better choices. Topical steroid therapy should be used with particular caution in cats, as it can be associated with flare-ups of feline herpes viral disease. 10. Xalatan (latanoprost) – Latanoprost, a prostaglandin analog, is a potent anti-glaucoma medication for treatment of dogs with primary glaucoma. Its use is generally contra-indicated in cases of secondary glaucoma, as it tends to incite intraocular inflammation and causes extreme miosis. This extreme miosis is useful, though, in “trapping” a posteriorly luxated lens behind the iris, where it is less likely to cause issues than an anteriorly luxated lens. Note that latanoprost should never be used in a patient with an anterior lens luxation, as it tends to cause an increase in IOP due to increased blockage of aqueous flow at the level of the pupil. Latanoprost does not lower the IOP in cats, although it does cause miosis in this species. This medication has recently become available as a generic.
33

Bite Prevention and Low Stress Handling in Clinical Practice
Meghan E. Herron, DVM, DACVB The Ohio State University Veterinary Medical Center www.vet.osu.edu/behavior
Goals:
1. Foster a better understanding of canine and feline body language 2. Demonstrate how human body language affects the behavior of animals 3. Learn techniques to ease animal stress and fear associated with the shelter setting, thereby
reducing arousal and aggression 4. Promote safety for clinicians and staff 5. Increase your confidence in handling dogs and cats 6. Provide tools for safe and effective restraint of fractious animals
Canine body language: Signs of a RELAXED dog Posture: relaxed, weight carried evenly, may see play bow or body “wiggle” Tail: relaxed & neutral position, may be wagging Ears: Relaxed, neutral position Mouth: appears “soft”, may be open, tongue hanging out, mouth may be closed with lips relaxed over teeth Eyes: “soft”, relaxed, eyebrows neutral, normal pupil size, steady, relaxed gaze Signs of a defensively threatening dog Body Posture: muscles tense, weight shifted back, low to ground, may roll to expose belly, holding one paw up Tail: stiff, usually tucked or low to ground, may be wagging (slowly or rapidly) Piloerection: may or not be present, may be “blowing coat” Ears: pulled back against head Mouth: lips pulled back +/- growling/snarling, often see excessive panting, lip licking, chewing, yawning Eyes: Vigilant with pupils dilated, eyebrows furrowed, scanning/darting eyes, “whale eye” The defensively threatening dog: Is feeling threatened and is saying “I don’t like that, stop what you are doing!” This dog is trying to avoid a fight, and would rather run away… …But is likely to become OFFENSIVELY THREATENING if provoked further. DO NOT
ANTAGONIZE THIS DOG! Stop and make a behavior management plan Signs of an offensively threatening dog Body posture: “hard & stiff”:muscles tensed, weight forward, may be very still Tail: carried high, often wagging slowly & methodically
34

Piloerection: usually present Ears: erect and forward, little movement Mouth: top lip pulled up (baring front teeth only), growling, snapping, barking Eyes: Hard stare, wide open or squinted/hooded, eyebrows tensed, pupils dilated The offensively threatening dog: This dog means business, is ready and willing to aggress, is not going to avoid it any longer
if a perceived threat continues. NOTE: It is VITAL to understand that while we may think this dog is acting “aggressively”
or “offensively”, the underlying motivation for this behavior is FEAR! Human vs. canine body language Our approach: we are taught to meet & greet people with a direct approach while making
direct eye contact, we often move rather quickly and lean forward to shake hands or offer a hug, etc
Dogs greet each other more indirectly – lateral approach, polite sniffing, averted gaze, play bow
Dogs who approach other dogs with forward, direct behavior are perceived as threatening and may elicit fear +/- aggression
Inherent miscommunication when an unfamiliar human approaches a dog; As humans, when we communicate directly, many dogs find it threatening
We must learn to use the appropriate body language to help dogs understand that we intend no harm. This is very important for fearful/aggressive dogs
Getting the fearful dog out of a cage
1. Turn your body sideways and crouch down outside the kennel 2. Offer a greeting with a soft, friendly voice, toss treats into the kennel 3. If the dog approaches, keep the treats coming… 4. Stay to the side of the kennel and slowly open kennel door, continue giving treats, slowly
place slip leash around neck, keeping your body facing sideways, avoiding eye contact 5. If the dog does not approach: leave treats on the floor of the cage and go away and try
again in a few minutes. The dog will likely come forward for the treats once you are out of sight…
6. Patience is key: you may need to repeat this exercise several times, eventually the dog learns that you are not a threat, but that good things (treats) happen when you approach.
7. Avoid placing fearful dogs on top cages Feline Body Language Mood scoring Head & Body Postures 1: Relaxed 2: Alert 3: Tense 4: Anxious 5: Fearful 6: Terrified
35

Relaxed Head: resting on surface or over body Eyes: closed to heavy, pupils slit to normal size Ears: turned slightly forward Sounds: none/purr Tail: extended or loosely wrapped; up or loosely down when standing Other: May see bunting Alert Head: over the body, some movement Eyes: open normally, pupils normal Ears: normal or erected to front or back Sounds: none or meow Tail: relaxed, some twitching Tense Head: over the body or pressed to body, little or no movement Eyes: wide open, pupils normal to partially dilated Ears: erected to front or back Tail: close to body; tense downwards or curled forward, may be twitching Other: ventral recumbency or “slinking” Sounds: none, meow, or plaintive meow Anxious Head: on the plane with body, little or no movement Eyes: wide open, pupils dilated Ears: partially flattened Tail: close to the body; may be curled forward close to body when standing Sounds: none, plaintive meow, growling, yowling Other: increased RR Fearful Head: tucked, still Eyes: wide open, pupils fully dilated Ears: fully flattened Tail: close to the body; curled under body when standing Sounds: none, plaintive meow, growling, yowling Other: freezing, fidgeting, escaping, aggression Terrified Head: lowered Eyes: pupils fully dilated Ears: fully flattened, back on head Tail: close to body Sounds: spitting, growling, yowling, hissing, shrieking Other: “Halloween Cat” – full piloerection, freezing, fidgeting, escaping, aggression
36

Aggression in a veterinary setting Defensive, variable degrees of aggression Fear or pain related aggression Confident aggression not seen in this setting Warning signs of an imminent cat bite
• Sudden dilation of pupils • Piloerection • Fast, jerky swishing of tail • Swatting with forearms • Vocalization – yowling, shrieking, spitting • Direct stare with open mouth vocalizations
Low stress handling and restraint
Environmental management Use of counter-conditioning in handling Safe restraint Canine and feline handling tools
Environmental management Starts when patient enters the lobby - for cats may start when enter carrier at home
• Is the lobby calm and inviting, or intimidating? • How do you manage the unruly or reactive pet in the lobby? • Do you have quiet areas for stressed patients? • Are you looking at the environment literally from the perspective of the animals
that enter? Everything that impacts their comfort and well-being happens at their level (visual field, odor, drafts….) Lobby Management: Cats
• ALL cats in carriers • Instruct owners on proper carrier training • Provide stable, high points to put carriers on to give cats a feeling of security • Segregate the lobby between dogs and cats • Feliway diffusers • Prevent clinic “mascot” cats from approaching carriers
**Lobby stress often a major contributing factor to fractious behavior during examination Lobby Management: Dogs
Separate “comfort” rooms for reactive dogs The more reactive they are in the lobby, the greater the chance for aggression during
exam No need for them to increase stress of other pets Ask owners of fractious pets to wait in car Call cell phone when ready Escort in through a side door
37

Best to make plan for owner ahead of time Fractious patients at slow time of day? DAP diffusers
Counter-conditioning (CC) Many animals have been inadvertently conditioned to fear the veterinary setting This fear often leads to dangerous and undesirable behavior towards the humans in this
setting Remember fear is not voluntary Use CC to change an animal’s negative (involuntary) emotional response to a positive one Instead of “here comes that scary person in scrubs,” it changes into, “here comes that great
person that brings me cheese/peanut butter/meat etc”. How do we accomplish this? FOOD! Food elicits an automatic (unconditioned) positive emotional response If paired with potentially aversive stimuli (injections, rectal temperature, nail trims, etc.) the
emotional response will transfer to the procedure “But if I feed a dog/cat that is being “bad”, aren’t I rewarding that dog/cat for “bad” behavior?” The answer is NO Not rewarding something that is under their voluntary control (like a sit) Changing their “emotional” state about strangers in a stressful environment Once the food reduces the fear, motivation for aggression is reduced Should we reserve food only for difficult patients? Nope. “An ounce of Prevention is Worth a Pound of Cure!” Most patients are at least mildly stressed Want to maintain positive experience to set them up for success with each visit Mitigate the environment to reduce stress Especially important for NPO patients or those who refuse palatable food Visual- turn down lights, block visual access to other people/animals; let cats hide head Auditory- speak softly and sparingly; select a quiet area; relaxing music -“Through a Dog’s Ear” Olfactory- avoid the pheromones of other stressed animals; use DAP and Feliway. Tactile- Touch animals as little as possible, or when needed touch them firmly & globally. Avoid cold, hot, or slippery surfaces. Use least restraint as necessary, depending on the individual animal and procedure No need to scruff or pin automatically Standing saphenous vs. lateral position
38

Safe restraint o When greater restraint needed, support the animal well o Provide firm, balanced restraint, preventing flailing, keeping control of head at all times o Should be able to move to lateral recumbency slowly and steadily o Utilize handling tools early, before animal becomes agitated o Do not put your face directly over or in front of any animal o Avoid reaching or petting head of fearful pets o Wait until the pet is relaxed and eating (if non-NPO) before procedures If pet struggles >3 seconds, stop the restraint and reposition to try again If after 2-3 restarts the pet is not relaxing after 3 seconds, or if arousal is escalating to panic or aggression, STOP If procedure is essential, use chemical restraint If nonessential, send patient home and create a behavior management plan for next visit Chemical restraint DO NOT WAIT for the animal to become fractious and highly agitated Use judgment to determine appropriate dosages and protocol selection based on age, temperament, and degree of health/disease. Canine handling tools Muzzles Nylon
o The stiffer the better o Only for short periods o Able to lick from front
Basket muzzles o Jafco o Wire cage o Center strap for short-nosed breeds
Use EARLY Use with food Proper muzzle placement o Stand to side of dog o Place from behind o Prevent backing up o Need to be quick and deliberate o Have owner place? o Gauze muzzle first if safe? Gauze muzzle o Start with a half throw with the knot on the top of the nose o Once slipped under chin, pull it tight quickly o Loop around mouth and tie o Can then place muzzle on top o Requires skill - practice on friendly dogs!
39

Towel restraint o For small dogs, control head, similar to cats o Can roll thick towel to create a buffer Calming Cap • Soft, sheer fabric • Limits visual stimuli • Prevents stress of procedure anticipation • Helpful for moving dogs with dog aggression problems • Can be used with muzzle D.A.P.™ - Dog Appeasing Pheromone o Analog of pheromone released from lactating bitch o Calming effect in nervous puppies and dogs o Spray (bandana or towel), collar, diffuser Squeeze cage o Reserved for dogs who cannot be safely muzzled o Use to administer chemical restraint Feline handling tools Muzzles
• Need to cover mouth and eyes • Use stiff leather or plastic for especially fractious cats • Soft muzzles help reduce stress by blocking visual access • Place from behind swiftly, supporting back end
Scruffing o Should not be automatic o Apply even, firm pressure o Support dorsum with forearm o Direct head away from clinician o Control back legs with secure, even pressure o Do not dangle! Towel restraint “Kitty burrito” Control head Provide lateral support Use multiple towels if unable to wrap Can also wear gloves for added protection (but less dexterity) Towel restraint of fractious cat
40

“Clipnosis” Pinch-induced behavioral inhibition Best used when patient is calm and quiet Not a tool for fractious cats! Utilize the carrier
• Allows cat to hide • Familiar place and scent • Keeps cat corralled • Can close lid quickly if needed
Feliway™ o Synthetic F3 fraction of facial pheromone o Available in diffuser and spray o Signal of contentment o Spray on towel on table, carrier, or cage o Diffuser in exam rooms, cat ward Cat Nabber o For feral or fractious cats o Capture for chemical restraint injection o Safe capture of fleeing cats
41

Don’t Leave Me Home Alone! : Diagnosis and Management of Canine Separation Anxiety
Meghan E. Herron, DVM, DACVB The Ohio State University Veterinary Medical Center www.vet.osu.edu/behavior
Separation anxiety disorder
Excessive and recurrent distress associated with separation from home or major attachment figure ◦ Children ◦ Adolescents ◦ Adults
Dogs and Cats
◦ Emotional distress Left alone in any environment Absence of favorite person Absence of pet companion
Separation anxiety in dogs
Social species Dogs show attachment to human companions Normal for puppies to show distress when separated from mother Normal for some level of distress when adults separated from companions Why do some dogs develop SAS? Genetic factors Early experience Degree of human attachment Traumatic separation Sociality of individual
Signs of separation anxiety
Signs occur when home alone only Vocalization
◦ Howling, barking, whining Elimination
◦ Urination and/or bowel movements Destructive behavior
◦ Chewing, scratching, digging Owner belongings?
Departure anxiety ◦ Clingy, following behaviors as owner prepares to leave ◦ May even see aggression ◦ Senses departure cues
42

Excessive greeting behaviors ◦ Difficulty settling down when owner returns home
Escape behaviors ◦ Escaping crate, windows, doors, etc.
Hypersalivation ◦ Excessive drooling when home alone ◦ Puddles of saliva in or around crate
Self-injury ◦ Tooth fracture, gum laceration, toenail injury ◦ Typically a result of panicked escape attempts ◦ Excessive grooming
Anorexia ◦ Unwilling to eat in owner’s absence ◦ Animals will not eat when they feel threatened, anxious or unsafe
Ruling out differential diagnoses
Housetraining problems Noise or thunderstorm fears Boredom/lack of appropriate outlets Territorial aggression Confinement anxiety Medical problem Differential diagnoses
Housetraining problems Does the animal also eliminate when owners are home?
Noise or thunderstorm fears
Do the owners notice nervous behaviors during storms/fireworks/loud noise when they are home?
Did the problem start on a storm day? Is the problem sporadic?
Boredom/lack of appropriate outlets
◦ Young, active dogs ◦ Destruction also occurs in presence of owners
Territorial aggression
◦ Behavior when owners are home? ◦ Focused on front windows?
Confinement anxiety
◦ How does the dog do when home alone and not crated? Medical problem
◦ Epilepsy, incontinence, dementia ◦ Acute onset in geriatric patient?
43
How to rule in SAS Thorough behavioral history Medical work up
◦ Minimum database, especially if elimination problems reported, acute onset, or geriatric patient
VIDEO RECORDING! ◦ When home alone ◦ In crate and out of crate
Predisposing factors
Traumatic separation ◦ Strays, shelter and rescue animals ◦ Abnormal bonding?
Sudden change in routine ◦ Owner returns to work ◦ Child moves away to college
Major household changes ◦ Death or departure of family member
Greyhounds? Rescued greyhounds
Inexperience with being left alone in a home environment Dramatic change in routine/environment Highly social breed
◦ Strong owner attachment Inadequate environmental socialization
◦ Stairs? ◦ Flooring?
Treatment
Encourage independence Create a safe environment Downplay departures and arrivals Decrease overall anxiety
Encourage independence
Relaxation exercises ◦ “Settle mat” ◦ Down-stay exercises ◦ Food toys - tethered ◦ Do not encourage clingy behavior ◦ “Social Skills”
44

Create a safe environment To crate or not to crate?
◦ Can be cause of severe injury ◦ Confinement exacerbates separation distress ◦ Some dogs panic if crate removed…. ◦ Typically avoid confinement if safe ◦ Block off areas that may be dangerous ◦ Remove valuable items
Enrichment ◦ Feed via puzzle toys
Kongs, Twist & Treat, Kibble Nibble, Dog Pyramid Canned food FROZEN, peanut butter, kibble, treats When alone AND when owner home Enrichment
Appropriate items to destroy ◦ Phone books, newspaper, pizza boxes, stuffed toys
Free-choice water – freeze it if needed Background noise
◦ White noise, classical music Remember to offer enrichment toys, play music/white noise, items to destroy at times
when owner IS HOME, as well as when owner is away Do not want enrichment to become a departure cue! NO PUNISHMENT for undesirable behaviors when home alone
◦ Will not associate punishment with act ◦ Will increase anxiety ◦ Creates fear of owner ◦ May exacerbate problem ◦ Coprophagia?
Downplay departures and arrivals
Neutral interactions 30 minutes prior Keep occupied during departure routine Prepare as much as possible ahead of time Avoid exposure to major triggers
◦ Keys ◦ Shoes ◦ Coat ◦ Downplay departures and arrivals
Set up enrichment toys, tethered “Sneak out” Different door Block sounds of departure
◦ White noise, classical music ◦ Neutral interactions upon arrival
45

Decrease overall anxiety Exercise
◦ Preferably BEFORE departures ◦ Long-brisk walks ◦ Energy outlet ◦ Typically not enough by itself ◦ Pheromones ◦ D.A.P. products
Diffuser, spray, collar Drug therapy
Standing drug ◦ Typically SSRI, or TCA ◦ Increase serotonin levels in CNS ◦ Daily anti-anxiety, takes 4-6 weeks to see full effect ◦ Continue until reach goal, then maintain an additional 3-6 months ◦ Gradual wean, 25% per 2 weeks
Be aware of drug interactions ◦ Tramadol, Promeris, Amitraz, Preventic collar…
Clomicalm ®
Clomipramine hydrochloride Tricyclic anti-depressant 1-3mg/kg BID target dose
◦ Side effects ◦ Anticholinergic effects possible
◦ Vomiting, constipation, urine retention, dry mouth ◦ Anti-histamine effects
◦ Mild sedation ◦ May offer greater “calming” of behavior
◦ Contraindications ◦ Seizures ◦ Male breeding dogs ◦ Renal or hepatic disease
46

Reconcile ® ◦ Fluoxetine hydrochloride ◦ Selective serotonin reuptake inhibitor ◦ 0.5-2.0mg/kg SID ◦ Side effects
Decreased appetite Lethargy Gastrointestinal upset (vomiting, diarrhea)
◦ Contraindications Seizures Existing poor appetite Renal/hepatic disease
Benzodiazepines ◦ Short-term sedative/anxiolytics
Valium, Xanax, Tranxene, Klonipin Anxiolysis, sedation, muscle relaxation, increase appetite within 30
minutes Given on departure days only
◦ Goal is to wean off of short-term drugs within 6-8 weeks
Trazodone ◦ Serotonin antagonist and reuptake inhibitor (SARI) ◦ Works synergistically with SSRIs and TCAs ◦ 1-5mg/kg BID, or PRN, not exceeding 300mg per dose, or 600mg daily ◦ Trazodone ◦ Side effects
Anti-histamine effects Sedation Priapism? (Humans)
◦ Contraindications Same as any serotonin-enhancing drug Can be used in place of or in addition to benzodiazepines if needed
Prevention
Teach independence early Set up an environment for success Keep a consistent routine Encourage time alone on days when home Avoid excitement around arrivals and departures
Discuss for every newly adopted shelter or rescue dog!
47

Starting Off on the Right Paw: Puppy Behavior Basics
Meghan E. Herron, DVM, DACVB The Ohio State University Veterinary Medical Center www.vet.osu.edu/behavior
Development Period Age Prenatal Conception to birth Neonatal 0-14 days Transitional 14-21 days Socialization 3-12 (14) weeks Juvenile 3-6 (7) months Sexual maturity reached 6-7 months Social maturity reached 18 months – 4 years Prenatal Period
Fetal development o Effects of stress o ↑ Cortisol o Changes ‘set point’ HPA axis o High emotionality as adults o Puppy mills?
Neonatal Period (0-13 days)
Born deaf and blind, poor smell
Eating and sleeping most of time
Anogenital stimulation required from bitch for elimination
Very limited learning capabilities, although they can learn to avoid bitter taste under 3 days
Transitional Period (14-20 days)
Eyes open
Tooth eruption
Able to stand
Anogenital stimulation not longer required for elimination
48

Transitional Period (14-20 days)
Learn to avoid pain o No emotional learning yet
No change in heart rate Don’t learn from bad experience
Startle response ENDS transitional period o Hearing begins
Socialization Period (3-12 weeks)
Gradual wean starts at 4 weeks
Leave nest to eliminate
Offer play behaviors
Social relationships develop o 6-8 week peak for human socialization
Avoidance response
Fearful postures develop
Learn from bad experiences
Early Illness predisposes to o Aggression problems o Fear of strangers and children o Separation-related problems
Isolation during this period leads to learning deficits and fear response o “kennel dog syndrome” o Dogs o Humans (children?) o Environmental changes o Sounds
Fear Period (8-10 weeks) Very sensitive to traumatic experience Single scary event can have life-long effects Can retain fear of person, dog, object HANDLE WITH CARE!
What is fearful behavior? Trembling Ears back Tail tucked Freezing Hiding Avoidance
49

Dilated pupils Growling Showing teeth Snapping/biting “Whale eye” Barking while backing away Excessive fidgeting Juvenile Period (3-6 months) Rapid growth Increasing independence Sexual interest begins Teething occurs
o Destructive chewing peaks Adolescence Time between sexual and social maturity Second fear period
o 3 weeks duration, between 4-11 months o Same rules apply – handle with care! o Maintain social experience and skills throughout adolescence
“Use it or lose it!” Social maturity As early as 18 months As late as 4 years More proactive defense Fearful puppies tend to become biters at this point
Puppy Prep School Set puppies up for success by covering the basics early:
o Socialization o Early low stress handling o Independence training o Housetraining o Crate training o Discouraging mouthing o Basic Manners o Avoidance of harsh punishment
50

Socialization People
o Age, race, sex Dogs
o Socially appropriate adult Leash, collar, head halter? Bikes, skateboards, wheelchairs Hats, winter clothing Crate, car Puppy Kindergarten “Taking a puppy to puppy class is the single best thing an owner can do to their dog in its entire life” -Andrew Luescher, DVM, PhD, DACVB
Study: Puppies that attended socialization class were more likely to be retained in their homes (Duxbury et al 2003)
Goal: Puppy socialization and owner education If your practice does not offer such classes, find one
Observe class yourself Puppies 4 months of age an younger Appropriate supervision
Train your staff to teach class Bonds clients to your practice
o DOGS! course o Offered for veterinarians and veterinary technicians at Purdue
University Vaccine Conundrum
Should we isolate puppies until they are fully vaccinated? o Absolutely not o More likely to lose pet over a behavior problem than from infectious disease
Make wise choices for socialization o Avoid dog parks, pet stores, etc. o Make play dates with healthy, socially mature, dogs with a history of appropriate
social behavior with dogs Early low-stress handling Remember that puppies are typically in their first fear period at the time of their first
vaccine appointment Potential frightening stimuli include:
o Cold exam table o Rectal temperature assessment o Vaccine injection o Nail trims o Physical manipulation by a stranger
51

How do we prevent long lasting fear of the veterinary clinic? ASSOCIATE FOOD WITH EVERYTHING!
o Squeeze cheese o Kong paste o Peanut butter o Canned food o “Behavior vaccine”
At home mock vet exam o Feet, ears, tail, mouth, exam table o Owner can use healthy treats to create a positive association
Independence Practice spending time alone Crate training Frozen food toys - tethered “Place” training D.A.P.® (Dog Appeasing Pheromone – synthetic version of pheromone released from
mammary area on lactating bitch) o Has been shown to reduce nighttime separation distress in puppies o Has been shown to decrease fear and improve socialization during puppy
kindergarten Always make the crate a positive experience! Housetraining
SUPERVISION o Must be able to SEE puppy at all times when loose in house
Frequent opportunities for success o Set a timer for every hour for first 2 weeks, o Also after play, sleeping, eating, etc.
Meal feeding o What goes in on schedule, should come out on schedule
Food and verbal rewards
Accompany pup outside
Give food reward and verbal praise immediately following urination and defecation o Do not wait until puppy comes back inside
Crate/Confinement o Can utilize when unable to supervise o Potty pads outside of crate if left alone for long periods
Interruption of indoor elimination rather than punishment o Clap hands, squeaker o Idea is to stop behavior without scaring the puppy o Do not want pup to be afraid of urinating in front of the owner o May just learn to go into another room o Punishment after the fact is ineffective at decreasing indoor elimination
52

Umbilical method o Owner attaches leash to belt loop o For difficult cases (small breeds)
Crate Training
Why crate train? o Housetraining o Safety o Independence o A place to escape
Pick a crate o Big enough to sit, stand, lie on side, and turn around o Can block off larger crates
Happy place! o Where family spends time o Meals, treats, Kongs o Access to water
• Ice cubes or frozen bowl if needed
Gradually increase time spent in crate • Start with door open
Bedtime • Move crate or place 2nd crate in bedroom • Don’t forget bedtime snack!
The mouthy pup
Normal behavior in young puppies o Taste and facial sensation are the 1st senses to develop o Information gathering and food seeking o Mother typically discourages rough or harsh biting
Persistent mouthing over 12 weeks of age may be a sign of o Premature maternal separation o Displacement behavior in anxious pups o Early signs of aggression if seen in the context of resource guarding and handling o Learned attention seeking behavior o Discouraging mouthy behavior
Avoid play with hands and feet
Avoid rough play or handling that increases arousal
Always have a toy available o Set puppy up for success o Mouth on toy, not on hand
53

Discouraging mouthy behavior
Provide appropriate chewing outlets o “Environment of plenty” o Nyla-bones o Kong toys o Busy Buddy toys o Durable stuffed toys o Meals via puzzle toys o Discouraging mouthy behavior
Remove all attention in response to mouthing o Pull hands away o Avoid eye contact o No talking
High pitched “ouch” works in some cases o Caution this does not provoke fear in puppy o Caution this does not increase arousal and inadvertently reward mouthing o Always redirect to a toy when once pup calms down
Basic Manners
Don’t encourage behaviors now that will not be desirable from an adult dog o Jumping o Pawing o Mouthing o Sitting on lap (owner preference)
“Sit” as default behavior o Every normal 8 week old puppy is capable of “sit” o Hold treat to nose, lure head back and up o Rear-end automatically goes down o No need to push on rump
“Sit” for attention “Sit” for food “Sit” for toys “Sit” for leash walks
Avoid punishment Does not teach appropriate behavior Inhibits learning and offering of new behaviors May have devastating effects during fear periods Can create fear of owner May exacerbate existing fear or aggression Attempts to punish aggression do not address underlying motivation and are
dangerous
54

Red flag alerts Avoidance of people, animals, objects
o Indication of fear – may progress to aggression during adolescence and social maturity
o Create a positive emotional response NOW Alarm barking, lunging, hackles up
o Not normal in a puppy – seek help NOW Excessive mouthing over handling
o May progress to aggression later – toenail trims? Vet exam? Ear cleaning? o Pain?
Reluctance to “sit” or “down” o PAIN! Hip and elbow dysplasia may manifest early in certain breeds o Anxiety
Anxious dogs have difficulty focusing and may not be comfortable with focused interactions
Often referred to as “stubborn” or “hyper” Excessive vocalization in crate or home alone Inability to settle in crate Pup will not eat food without owner present
o May all be indications of early separation or confinement anxiety Repeated elimination in appropriately-sized crate – NOT normal
o Learned helplessness o Crate anxiety o Congenital abnormality
Summary Be knowledgeable about developmental periods to maximize training success and
avoid detrimental effects during training. Advocate interruption rather than punishment. Be on the look out for early indications of anxiety and aggression and intervene or
refer immediately. The earlier the intervention the better the chance for change. How can we get all of this information to puppy owners? Make a checklist
o Include information on health, behavior, and nutrition Schedule extra time for puppy visits
o Divide topics among the vaccine appointments Ultimate Puppy ToolkitTM Puppy kindergarten Veterinary behaviorist
o Study: Puppies under 4 months of age whose owners met with a veterinary behaviorist for one hour showed fewer behavior problems as adults (Gazzano et al 2008)
o “Head Start” problem prevention appointments
55

Further Reading Before and After You Get Your Puppy – Ian Dunbar The Biology of Animal Stress – Gary Moberg and Joy Mench Domestic Animal Behavior – Katherine Houpt The Domestic Dog – James Serpell Genetics and the Social Behavior of the Dog – John Scott and John Fuller Handbook of Behavior Problems of the Dog and Cat – Gary Landsberg, Wayne
Hunthausen, Lowell Ackerman Low stress handling, restraint and behavior modification of dogs & cats : techniques
for developing patients who love their visits – Sophia Yin
56

Starting Off on the Right Paw: Kitten Behavior Basics
Meghan E. Herron, DVM, DACVB The Ohio State University Veterinary Medical Center www.vet.osu.edu/behavior
Development Neonatal Period (0-9days) Born blind and deaf “Teat order” formed by day 2 Guided by tactile, thermal and olfactory stimuli Hearing starts around day 5 Anogenital stimulation required for elimination Transitional Period (9-14days) Eyes open around day 7-10 Grooming emerges Start orienting to sound Begin standing and walking Socialization Period (2-7 weeks) Social relationships with people and animals formed Object and social play begins Spontaneous elimination Weaning starts around 4 weeks Learn to escape painful stimuli Fear response begins and persists Can learn from bad experiences Juvenile Period (7weeks - 5months) Weaning complete May suckle intermittently beyond 1 year Social play peaks and declines Independence increases Important for social interactions and handling to continue Sexual maturity reached between 5-9 months
57

Social Development Attachment to humans develops 2-7 weeks
– Early handling for 10 minutes twice daily increases friendliness – Strong paternal effect on friendliness – increased handing in kittens before 8 weeks of age increases boldness for the 1st year,
but genetics have a more substantial influence beyond 1 year of age Relationships with other animals
– Need exposure to other cats/kittens in a positive fashion before 12 weeks of age – If raised with puppies, they do not show fear of them as adults – If not exposed to dogs before 12 weeks of age, they show fearful, defensive behaviors – If raised with rats, will not hunt then as adults
Development of Play Social play with mother and siblings
– Begins around 3 weeks – Pawing, wrestling, rolling – 4 bouts of play per day – 1 hr per day spent on play at 9 weeks – Starts to decline around 12 weeks – Play takes on more of a predatory form as the socialization period progresses
•Stalking, staring, pouncing, biting, chasing •Normal part of play between kittens Object play high at 8 weeks
– Males and females with male littermates show more object contact – Early weaned cats show earlier object play – Kittens of undernourished mothers show more object play
Development of Predatory Behavior Queen brings prey to kittens around 4 weeks
– Begins with mother attacking and eating prey in front of kittens – Allows kittens to catch and eat over time – Kittens cannot kill prey on own until 8 weeks – Maternal preference for prey has strong influence on kitten choice later in life
Setting Up for Success
– Litter box training and hygiene – Socialization – Carrier training – Environment of plenty – Appropriate play outlets
58

The Litter Box Most cats have an innate preference to eliminate in fine, sandy substrates
– Litter box – Potted plants? – Sand box?
May need to confine kitten initially for first few days until reliably using box Dynamics of box Large
– Enter, turn around, dig, turn around, eliminate, turn around, cover, exit, shake off paws Uncovered
– Most cats prefer uncovered in a quiet area Clumping litter
– Preferred texture and keeps odor down Unscented litter
– Heavy perfumes can be aversive
Scoop daily – Consider this the “daily flush” – Some cats will not use an unscooped box
Change out monthly or as odor requires – Clean with warm, soapy water – Avoid bleach and ammonia-based cleaners
No liners – Claws can get caught when digging/covering and may lead to litter box aversion
Multiple boxes – “N + 1” rule: one litter box per number of cats plus one Multiple locations
– Easily accessible – Every floor of household – Especially important in multiple cat household
Socialization People
– Adults, children, visitors – Need to have a positive experience – FOOD and PLAY
Animals – Other cats, dogs – Must be kitten-appropriate and friendly
Handling – Nail trims, brushing, dental care – Associate with FOOD and PLAY
59

Veterinary clinic experience – Cold table – Thermometer – Injection – Nail trim
o ALL should be associated with FOOD o Squeeze cheese, canned food, fish heads, baby food
– “Clipnosis” – pinch-induced behavioral inhibition o Can induce relaxed state in most cats o Should also be associated with FOOD
Carrier Training Free Access Crate Training (FACT) - M. Milani
– Establishes a safe retreat for the cat – Need to create a positive association with the carrier over time – Start with just the bottom of the carrier, soft bedding, food and water – May add a small litter box if anticipate long periods of travel later in life – Place in a quiet area, preferably up off of the floor – Add top of carrier once using regularly – Add door and close periodically while cat is relaxed and has a food item
o Offering a highly palatable food item daily will help retain positive association –Squeeze cheese on inside walls, baby food, tuna or chicken bits, fish heads
Feliway spray may make carrier more appealing Take for short trips in the car once comfortable Work up to longer trips with time More positive travel experience at a young age will set them up for success with travel as
adults Environment of Plenty Resting areas Scratching options Entertainment “Safe haven” Chewing options Resting areas Kittens should have access to high resting places Provide multiple hiding options Soft bedding will make resting areas more appealing Appropriate scratching options Scratching is a NORMAL behavior
– Nail maintenance – Visual and olfactory marking
60

Vertical and horizontal options Rough and textured material is most appealing, such as corrugated cardboard or sisal Place posts close to resting areas
– Often scratch upon waking Cover or “booby trap” furniture that owner does not want damaged
– Double-sided tape panels – “Sticky Paws” – Cans on strings of yarn – caution if history of string ingestion – Ssscat motion-sensing spray deterrent
Kitty Entertainment Toys
– Interactive with owner preferred – Hidden hunting options – Rotate weekly
TV entertainment – “Video Catnip” DVD
Window perch – Bird feeder?
Safe Haven Quiet refuge Each cat should have his or her own area Access to own food, water, scratching post and litter box Electronic cat door access Chewing Options Remove toxic plants from household Provide safe, appealing options
– Kitty grass – Fresh catnip – Jerky
Make houseplants aversive if needed – Cayenne pepper – Hot sauce – Perfume
Appropriate Play Outlets Kittens typically have four play bouts per day One hour per day total play time is normal Morning and evening are times of highest activity
– Owners should anticipate these times – Kittens will find ways to meet these needs if owner does not provide them
61

Interactive play – Owner involvement
o Begin play session before kitten pesters for it o Interactive toys o Laser pointer o Always end laser games with a treat or toy to prevent frustration o Crinkly balls, balls with bells or food inside o AVOID rough play and play with owner hands and feet
– Self-entertaining play o Panic mouse – battery operated o Ping-pong balls in a bathtub o SlimCat food puzzle toy
– Another kitten o Can meet each other’s play needs o Familiarity increases time adults cat spend together
Training – Provides mental stimulation – Strengthens bond between owner and cat – Clicker training
o “Sit” o “Stay” o “Touch” o “High five”
Punishment in Kittens Avoid the use of direct punishment for inappropriate play, chewing, scratching, eliminating!
– Remember play, scratching, & chewing are NORMAL behaviors – Redirect to appropriate chew, scratch, play or elimination outlets – Confine to safe haven to give owner a break and allow kitten to utilize interactive food or
play toys if needed – Cats DO NOT learn by force – Punishment may create fear of owner and lead to aggression – Cats will likely learn to show undesirable behaviors when owner is not present – Remote, non-painful punishment as last resort
o “Booby traps”, Ssscat, foul tastes, etc.
62

How do we get all of this information to kitten owners? Allot more time for vaccine appointments
– Technician can provide most owner education before veterinary exam Check lists
– Divide behavior and health topics among the vaccine appointment series Handouts and reading lists Kitten kindergarten
o Set up your own! o Appropriate health screening
Veterinary Behaviorist – “Head Start” problem prevention appointments
63
Feline Aggression: An Overview of Common Problems
Meghan E. Herron, DVM, DACVB The Ohio State University Veterinary Medical Center www.vet.osu.edu/behavior
What is aggression, really? Function Communication – a distance increasing signal Threat to harm, often due to the cat’s perception of being threatened Predation? Is this really aggression?
o Does a yowling, hissing, growling cat catch many mice? Cat aggression Second most commonly reported cat behavior problem
o Feline inappropriate elimination is the only problem reported more frequently Damages the human/animal bond, putting the cat at risk of relinquishment or euthanasia
Cats are different “Overt” aggression – most owners can recognize this type of aggression “Covert” aggression – often owners are unaware of the problem until one cat starts
showing inappropriate elimination Intimidation The “stare down” Blocking another cat’s (or person’s?) access to resources Litter box, food, water, preferred resting places, rooms
Body language Offensive Staring Stiff, limbs extended Tail curving up then down or straight out, tip rotated outward May see piloerection on the tail Head held just below the line of the spine Ears erect or rotated Pupils typically narrow
64

Body Language Defensive “Halloween cat” Ears flattened or pointed back Crouching, may roll onto side or back with claws in ready position
o NOT a submissive roll as is sometimes seen in dogs Piloerection
o The further down the back the hair stands up, the greater the arousal Swatting Salivating, spitting, hissing Howling, yowling, growling, shrieking Dilated pupils May see a mix of both offensive and defensive signs if conflicted
Impact of Disease Metabolic disease Neurologic problems Dermatologic Musculoskeletal Urinary tract discomfort Any disease that causes discomfort or pain Primary central (brain) disease vs aggression due to irritability
How to Approach? Thorough behavioral and medical history Household changes, interactions between pets, outdoor cats, elimination problems,
recent traumatic event, what happened immediately prior to aggressive incident? Any history of urinary or gastrointestinal discomfort or disease? Lameness? Nausea? Changes in appetite or thirst? Current medications?
Medical workup Minimum database: Physical exam, including oral exam, CBC, chemistry, total T4,
urinalysis Behavior problem list Behavior differential diagnoses Video recording when necessary Map layout of house and locations of aggressive and/or elimination incidents Treatment plan Safety first – keep the owner and other animals safe Environmental management – reduce social and environmental stressors Behavior modification exercises – change underlying motivation for behavior Medication – as an adjunct to above changes Pheromones – as an adjunct to above changes
65

Behavior History Signalment? Who? Things are not always as they seem Perpetrator? Victim? When? Where? What? Claws? Teeth? Body language? Progression? Duration? Medical Workup Medical history Change in activity, appetite, thirst, hiding places, attention-seeking/other interactions Thorough physical examination by a veterinarian Minimum database plus additional diagnostics if indicated Differential diagnoses Inappropriate play behavior Aggression related to touch Fear related aggression Status related aggression Territorial aggression Pain related aggression Any type of aggression can be redirected Inappropriate play behavior/aggression Also referred to as play-related aggression Normal vs inappropriate play behavior History Orphaned kittens Inappropriate play by owners
Rarely vocalize Single cat household Victim can be a person or another animal May diminish as the cat matures Management
Avoid situations that provoke aggression Avoid play with hands & feet Provide appropriate scheduled play
66
“Environment of plenty” Anticipate and redirect (interrupt) Timed feeders Kitty haven
Management - other Belled collar Owner diary Another cat?
Video: http://www.youtube.com/watch?v=BvRg-F_1Q1Y Appropriate kitty entertainment – keeps distance between cat and owner
Laser pointers – always end with a treat or toy to prevent frustration Panic MouseTM Pavlov’s Cat Wand and feather toys
Aggression related to touch Descriptive diagnosis When petted, picked up or touched Tail thumping, excessive panniculus, rotation of ears, dilated pupils, +/- hissing, growling Management Change owner’s petting duration or style No petting - at least temporarily Brief petting Pet on the head and neck only Stop petting when cat displays signs of arousal
Interruption vs Punishment vs SIT STILL! Clicker training - Scheduled training sessions “Touch” Remember, not all cats like to be touched! Fear-related aggression “Affective” or emotional aggression Can be directed at a person or another animal Defensive body language Causes: Negative experience Pain Improper socialization Genetics Cat is trapped Learned component
67

Fear related aggression Directed toward people Familiar people Negative experience (+/-redirected) In specific contexts (tnt, putting in carrier, etc) Certain household members (antagonizing cat)
Unfamiliar people Strangers entering home Attempting to pet or pick up
Video: http://www.youtube.com/watch?v=u0Ys0J4rvFQ Directed towards other cats
Watch body language to ID fearful cat o Hissing, growling, running away, dilated pupils
Fear of outdoor cats or stimuli can be redirected to other household cats
Status related aggression Confident cat Directed toward a familiar individual within social group Most frequently directed toward other household cats Can be directed to owners, familiar people Related to resting places, interactions, and “personal space” Status related aggression Status related aggression directed towards other cats Confident body language Staring, ears forward, pupils narrow Blocks access to resources, litter box, food, resting places Can be covert Not a linear hierarchy - dyadic May not involve all cats in household “pariah cat” - tends to elicit aggression Video: http://www.youtube.com/watch?v=4NJQvswrSPg Status related aggression directed towards people Not frequently diagnosed Confident body language
Staring, ears forward, pupils narrow or dilated Can occur if cat disturbed when resting, location, interactions Arousal May also see aggression when touched
68

Territorial aggression Directed towards unfamiliar individuals – typically outdoor cats Often combined with fear Video: http://www.youtube.com/watch?v=Z1TEESDpk7A Pain-related aggression Veterinarians Underlying medical cause? Aggression associated with petting, picking up, other manipulations Body language consistent with avoidance and fear-related aggression Quickly becomes learned fear-related aggression Redirected aggression Not a diagnosis: find primary motivation Aggression directed toward a victim other than the inciting stimulus Triggers Outdoor cats** New odor Loud noise Any fear-producing stimulus
Does not have to be a temporal relationship between trigger and aggression Learning may result in development of fear-related aggression to victim Management of Aggression Aggression between household cats Properly identify perpetrator/victim Separate from victim with slow reintroduction Desensitization and counter-conditioning (DS &CC) cats to each other
o Often done by feeding each cat on opposite sides of a closed door o Gradually move bowls closer together and allow more exposure by opening the
door Interrupt (interruptor sound) and redirect tension or staring - before aggression escalates Provide core areas for each cat Increase the number of hiding/observation options for the fearful cat Belled collar on the offensive cat to alert victim cat Collar-controlled cat doors so that fearful cat has an escape route and safe haven Increase confidence of victim cat through training and medication Anti-anxiety medication to reduce fear of victim cat Exchange of odors Never separate fighting cats with hands or feet!!!
o Use blankets, pillows, water, large broom, etc.
69

Aggression to owners Avoid fear-eliciting stimuli Avoidance of petting (never touch an aroused cat!) Structure and predictability in daily routine Interrupt early signs of fear or tension with conditioned sound & redirect DS & CC to victim – clicker training Environmental enrichment Scheduled, structured play time Interactive toys, food toys High resting places, core area
Territorial aggression Keep cat indoors Block visual access outside
o “Frosty glass” window film Neuter
Pain related aggression Find and address cause Avoid situations that elicit pain Address any resulting fear-related aggression
Drug therapy Used to decrease reactivity/anxiety driving the aggression Minimum database (CBC, chemistry, total T4, urinalysis) Owner consent for extra-label use SSRIs Fluoxetine (Reconcile®, Prozac®) Paroxetine (Paxil®) Sertraline (Zoloft®)
TCAs Clomipramine (Clomicalm®) Amitriptyline (Elavil®)
Buspirone (BuSpar®) - contraindicated? General treatment guidelines Safety! – You may be liable for the recommendations you make.
Punishment vs. interruption Avoid interactions that provoke the cat No interactions for at least 1 hour after an aggressive incident Behavior modification Environmental modification Anxiety reduction through medication under the guidance of a veterinarian Referral when necessary
70

Feline Inappropriate Elimination
Meghan E. Herron, DVM, DACVB The Ohio State University Veterinary Medical Center www.vet.osu.edu.behavior
Would you use a toilet that had not been flushed in days? I didn’t think so – let’s not expect our cats to use one, either! The basics of the litter box: What do cats like? Clean Uncovered Clumping / sandy texture litter Large box:cat ratio
o Enter, turn around, dig, turn around, eliminate, turn around, cover Core area Easily accessible 1 litter box per cat +1 Multiple locations No liners Deep litter Other considerations Multiple litter box options in one location Location free from obstructions or agonistic encounters Adequate distance from food and water bowls What is feline inappropriate elimination (FIE)? Elimination outside of a designated area Is this truly inappropriate, or just undesirable? Most common cat behavior problem reported to veterinarians Leads to cat relinquishment to shelters Common cause for euthanasia Frequently can be resolved with appropriate treatment Consider the owner’s vs. the cat’s perspective
What’s a litter box? Laundry basket full of clean clothes bares a close resemblance….
71

Working it up… Behavior history Medical workup Behavior problem list List stressors and the inadequacies of the current environmental management …and making a treatment plan Medical rule-outs Treat all medical conditions Behavior differential diagnoses list Remedy environmental mismanagement Behavior modification Reduce anxiety as needed Behavioral history Be objective and ask open-ended questions about the environment and other household pets
o Signalment? o Where? o What? o When? o How? o Who?
Consider every cat in the household a suspect!
Progression and duration Acute onset? Household changes? New pets Addition or departure of family member Renovations Previous treatment and response? Litter box changes, medications, pheromones, punishment, clean up Behavioral history Beware of owner interpretations of their cat’s behavior
o “jealous” o “mad at me” o “spiteful”
When in doubt, consider normal cat behavior o 10% neutered males spray o 5% spayed females spray o Is this abnormal?
Remember – it’s an animal, not an adversary
72

Medical Workup Medical history
Change in weight, appetite, thirst, grooming History of lameness, abnormal stools, urinary disease Complete PE, CBC, chemistry, total T4, and U/A, fecal
Other useful tests: Urine culture and sensitivity Abdominal radiographs Abdominal ultrasound
Treat all medical conditions, including those not affecting GI or GU systems Differential diagnoses - medical
Bacterial cystitis Interstitial cystitis Cystic calculi Bladder neoplasia Renal neoplasia Diabetes mellitus Renal failure Pyelonephritis Hyperthyroidism Gastrointestinal disease Constipation Dietary etiology Liver insufficiency Neurologic disease Osteoarthritis Any causes of polyuria, polydypsia, pain and / or lethargy
Differential diagnoses - behavioral Urine marking/middening Inappropriate toileting Substrate preference Substrate aversion Location preference Location aversion Litter box aversion Anxiety-related elimination Contributing behavioral diagnoses Separation anxiety, territorial aggression
73

Differential diagnoses Remember that medical and behavior diagnoses are not mutually exclusive Often medical disease ecsacerbates behavioral pathology and visa versa Urine Marking - Characteristics Standing posture, tail up, tail shake Vertical surfaces
Baseboards, furniture, doors Small amounts of urine Absence of digging/covering before and after urination Socially relevant locations Items of certain household members Favored place of other pets Window/door frames New household items Urine Marking - Diagnoses Anxiety related
Generalized anxiety disorder Underlying stressors – changes in household, schedule, addition of new animals,
agonistic interactions Poor litter box management can be anxiety-provoking
Territorial Directed towards unfamiliar cats Outdoor cats (windows)
Sexual Estrus females – up to 1x/hour Intact males – up to 12x/hour
Medical Inappropriate Toileting
Squatting posture Horizontal surfaces Large amount Likely show digging before and covering behaviors after elimination
Causes of inappropriate toileting Anxiety/social stressors
Social group changes (animal, human) Environmental changes Schedule changes Cats outside the home Agonistic interactions Stress lowers threshold for tolerance of litter box management
74
Location Size of the box Substrate (type, amount, liners) Type of box Cat:box size ratio Cleanliness Number of boxes and cats Miscellaneous stimuli near box location
Litter box aversion
Something is wrong with the box Previous painful experience? Not cleaned/scooped properly Covers Plastic liners Motorized self-cleaning May eliminate right next to box Variable substrates and locations
Substrate aversion
Don’t like what’s in the box! Large, hard particles Strongly scented litter
Perch on the edge of the litter box Dig/cover outside of box rather than manipulate the litter
Substrate preference
Typically soft, clean substrates – carpet, bedding, laundry May develop as a result of substrate aversion
Location aversion
Agonistic interactions – ambush! Aversive stimuli in environment
o Washer/dryer, furnace, dogs o Not easily accessible
Location preference Preference for one or several locations in the house Variable substrates
Anxiety-related elimination
Urination or defection, or both Social and environmental factors Separation anxiety
75

Treatment Similar principles for marking and toileting
Improve litter box and social environment Behavior modification Medication when environment cannot meet cat’s needs
Litter box environment Make the litter box more attractive BIGGER – Large box:cat ratio CLEANER – scoop 1-2 times DAILY Change the box type entirely if needed More, more, more (n + 1) Location – 1 on every floor Litter box cafeteria Make the soiled areas less attractive Cleaners: enzymatic, fully soak Aversive stimuli Foil, upside-down carpet runner Decrease access Confinement to core area unless supervised may be indicated Improving litter box hygiene can decrease marking up to 50% Provide the desired environment for elimination Make the litter box the safest, most comfortable place to eliminate Acceptable area to mark? Improving the social environment Environment of plenty
Interactive toys, work for portion of food, “hunting” opportunities, scratching substrates, vertical resting options, hiding places
Separate core areas for each cat Feeding and water stations, litter boxes, resting places
Reduce agonistic interactions, such as punishment Decrease access to outside cats
Keep indoors only “frosty glass” window film ScareCrow® motion sensor sprinkler
76

Behavior modification Avoid positive punishment
Interruptor sound
Positive reinforcement of appropriate elimination
Teach new skills to improve confidence and safety in presence of owner
“touch”
“high five”
“sit” Medication Selective serotonin reuptake Inhibitors (SSRIs) Fluoxetine (Reconcile®, Prozac®)
0.25-1.0mg/kg SID 90% success rate for urine marking Decreased appetite and mild sedation most common side effects
Paroxetine (Paxil®) 0.25-1.0mg/kg SID Better choice for finicky eaters Anticholinergic side effects possible – constipation, urine retention, dry mouth,
arrhythmias Sertraline (Zoloft®)
0.25-0.5mg/kg SID No published reports in cats Fecal excretion
Contraindications: o Seizures, cardiovascular disease, hepatic dysfunction, renal disease (FLU, PAR),
constipation (PAR), obesity (FLU) Tricyclic antidepressants (TCAs) Clomipramine (Clomicalm®)
0.25-1.0mg/kg SID Approved for treatment of urine spraying in Canada Anticholinergic effects possible; sedating
Amitriptyline (Elavil®) 0.5-1.0mg/kg SID Higher side effect profile – anticholinergic; most sedating Extremely bitter
Contraindications: o Seizures, cardiovascular disease, hepatic dysfunction, renal disease, constipation,
owners opposed to sedative effects on their cat
77

Buspirone (Buspar®) 2.5-7.5mg per cat BID 55% success rate in urine marking Minimal side effects Contraindicated in aggression Benzodiazepines Diazepam (Valium®)
Up to 75% improvement Hepatotoxicity reported for PO administration in cats
Oxazepam (Serax®) 0.2-1.0mg/kg SID-BID Less potential for hepatotoxicity No active metabolites
Progestins
Megestrol acetate (Ovaban) and Medroxyprogesterone (DepoProvera) o Some efficacy in MC (50%), little in FS (10%) o Dangerous side effect profile
Pheromones Several studies showing efficacy To be used in combination with environmental changes Feliway® (Comfort Zone ®)
Synthetic F3 fraction of facial pheromone Available in diffuser and spray Signal of contentment (false signaling?) Antagonist of urine marking
Felifriend ® Synthetic F4 fraction of facial pheromone Allorubbing Antagonist of aggression or territorial activity Not available in the US
78

Orthopedic Examination for Forelimb Disorders
Kathleen Linn DVM, MS, Diplomate ACVS Western College of Veterinary Medicine
University of Saskatchewan
Gait Abnormalities to Look For: If the animal carries (or has a history of carrying) a limb, the problem is at or distal to the level of the elbow or stifle. Alternatively, you’re seeing evidence of nerve root compression. Dogs with sore shoulders or sore hips almost never hold the limb up—flexing those joints to carry the limb hurts more than using them.' Is the dog walking with his neck held low and stiff? Does she look over tops of her eyeglasses at you rather than moving her head? These are strong hints that the lameness may be due to a cervical nerve root compression.
Dogs with sore shoulders tend to walk with a rolling gait and a pronounced head nod. Dogs with sore elbows tend to take shorter, stiffer strides in the affected limb, and they rotate their elbows internally or externally. Carpal hyperextension is much easier to pick up while a dog is standing or walking than during palpation/manipulation of the carpus. Look for asymmetry in the amount of carpal “sinking” between forelimbs while the dog is fully weightbearing on each limb…keeping in mind that the condition can be bilateral.
Does the dog have a paddling gait in a forelimb, with that limb rotating externally when you pick up his front end? That’s classic for infraspinatus contracture.
Abnormalities to Look For on Palpation:
Digits: check for footpad abnormalities, torn or infected nails, swelling that may be indicative of fracture, infection or tumor, and interdigital masses or ulcers. Flex and extend each metacarpophalangeal junction, and stress it side to side: you’re looking for evidence of osteoarthritis and collateral ligament damage. Also feel for swelling and press over each set of sesamoid bones (located on the palmar side just proximal to the big metacarpal pad). Fractures, fragmentation and osteochondrosis of these bones can cause a lameness that is very hard to diagnose unless you think to look for it. Metacarpal bones: Palpate for pain and swelling that may indicate the presence of a fracture, remembering that there may not be crepitus evident if more than one bone remains intact. Generalized thickening of this area may be noted if hypertrophic osteopathy is present: this is the most common place for HO to manifest itself.
79

Carpus: Start by palpating the carpus—it should feel just like skin over bone, with no meatiness to it at all. Any thickening is abnormal and indicates swelling, such as you’ll get with polyarthritis or injury. Next, check for range of motion. You should be able to flex the carpus so that the toes touch the back of the antebrachium. You should not be able to extend the carpus more than 10 degrees off of vertical. Palpate the accessory carpal bone for swelling and pain, and feel for swelling of the palmar carpal ligament area.
Radius/ulna: Remember that the distal radius is the most common site for osteosarcoma to develop. Give it a squeeze to check for pain and swelling. Also squeeze the portions of ulna and radius not covered by muscle to check for the bone pain that goes with panosteitis in young dogs.
Elbow: This is a difficult joint to feel effusion in; if it’s severe you’ll feel some puffiness just axial to the humeral epicondylar ridges. Flex and extend the elbow to check for range of motion and crepitus (keeping in mind that a sensation of “popping” tendons is normal). You should be able to flex a normal elbow well beyond 90 degrees and to the point that the carpus almost but doesn’t quite touch the point of the shoulder (see what you can do with your own arm as a frame of reference…assuming, of course, that you’re normal!). If the elbow does not flex to that point, there is osteoarthritis—and probably elbow dysplasia-- present. Next, with the carpus and elbow flexed to 90 degrees, internally and externally rotate the carpus (this is called the Campbell test). You should be able to externally rotate a normal limb 45 and internally rotate it 70. If there is a collateral ligament rupture in the elbow, range of rotational motion doubles for the affected ligament (externally for the medial collateral and internally for the lateral collateral ligament). More commonly, however, you’ll find evidence of pain on external rotation of the carpus despite normal limits to the range of motion. This suggests the presence of a fragmented medial coronoid process, since this bit of bone underlies the medial collateral ligament being stressed. Humerus: This is one of the bones most commonly affected by panosteitis, so naturally it is also one of the most difficult to palpate without squeezing a lot of overlying muscle. Go for it medially in the middle portion of the bone and cranially in the proximal portion. Also keep in mind that the second most common site for osteosarcoma to appear is in the proximal humerus. Shoulder: Remember that the scapula is mobile, so trap it in place with your fingers over its cranial border when manipulating the shoulder joint. Dogs with osteochondritis dissecans are typically painful on full shoulder extension. Dogs with biceps tenosynovitis are most painful when the shoulder is flexed while the elbow is being extended. Do a shoulder abduction test by trapping the scapula in place with your fingers on the acromion process and then abducting the humerus at the shoulder joint. Normally you’ll be able to get just a tad over 30 degrees of abduction. If you can abduct the shoulder 50 degrees or more, that suggests a medial glenohumeral ligament or subscapularis tendon tear.
80

Orthopedic Examination for Hind Limb Disorders
Kathleen Linn DVM, MS, Diplomate ACVS Western College of Veterinary Medicine
University of Saskatchewan
Gait Abnormalities to Look For: The big thing to remember here is that if a dog holds up (or has a history of holding up) the limb, the problem is either at or distal to the stifle, or there’s a nerve root compression problem going on. Big dogs with bad hips almost never carry the affected limb (little dogs may, though). Hip soreness causes a base-narrow (“walking a tightrope”) gait and a sexy butt wiggle.
Stifle soreness produces a crouched, bow-legged gait with external rotation of the affected stifle(s). Remember: cranial cruciate rupture will be bilateral in half the affected dogs you see.
Cauda equina compression (lumbosacral disease) is a common problem that can produce a gait just like the one that comes with cruciate disease. Always check for lower back pain!
Does the dog sink (hyperflex the stifle) whenever he enters the stance phase of the gait? Look for either patellar tendon rupture or dysfunction of the femoral nerve/L4-6 spinal segments. The latter condition is associated with a normal-feeling patellar tendon and an absence of the patellar reflex.
Does the tarsus sink about 1/3 of the way to the floor lower than it should, and the toes seem to be hyperflexed (curling under) when weightbearing? There’s a disruption in the gastrocnemius musculotendinous unit—most commonly an avulsion of the gastrocnemius tendon from its mooring on the calcaneus.
Does the calcaneus rotate externally at the end of a stride, followed by a quick stomp of the foot to the ground? If so, you’re looking at classic contracture myopathy of the semimembranosis/gracilis muscles. This is mostly a German shepherd disease and can be associated with lumbosacral compressive disease.
Abnormalities to Look For on Palpation: Pes: the examination of the hindfoot up to the tarsus is identical to that for the manus. Tarsus: As with the carpus, any meatiness beyond the skin-over-bone feeling is evidence of joint effusion. If your patient is a young medium-to-large breed dog, suspect osteochondritis dissecans; if it’s an older dog, think about polyarthritis, or osteoarthritis secondary to OCD. Flex and extend the tarsus: this should only be possible at the level of the tarsocrural joint. If it bends anywhere else, there’s either a fracture/luxation or a hyperflexion injury present.
81

Calcaneus/common calcanean tendon: Palpate the Achilles tendon throughout its length to make sure it’s continuous with no swellings within its substance. Pay special attention to the area just proximal to the calcaneus: swelling here is most commonly indicative of a gastrocnemius tendon insertion rupture. Collies and shelties are prone to tears of the lateral retinaculum holding the superficial digital flexor in place as it courses over the tip of the calcaneus. If there is a rupture here there will be a “capped hock” appearance, and you will be able to move the tendon medially and laterally over the calcaneus (a sensation similar to what you feel with patellar luxation).
Tibia: sometimes gets panosteitis; osteosarcoma can occur at either the proximal or the distal end of this bone.
Stifle: Once again, check for evidence of swelling (rounded feeling to the stifle and loss of the dimples on either side of the patellar tendon). If effusion is present, be very, very suspicious of a cranial cruciate ligament tear, even if you can elicit no cranial drawer sign. Palpate for patellar luxation: first, just place your fingers lightly over the patella, flex and extend the stifle, and see if it pops out of the trochlear groove (or reduces back into it) spontaneously. Second, physically try to shove it medially and laterally out of the groove with the stifle in extension: if you can do this, patellar luxation is indeed present. Stress the joint medially and laterally to check for collateral ligament injury.
Check for cranial drawer sign, remembering to be very specific about landmarks. The thumb of your “proximal” hand should be on the lateral fabella (a vague bump in the back of the femoral condyle), and the index finger of this hand should be on the patella. This hand is the fixed point: you just use it to hold the femur in place. The thumb of your “distal” hand should rest on the prominent fibular head, and the index finger of this hand should be on the tibial tuberosity. Hold the femur steady and attempt to move the tibia forward (don’t flex or extend the stifle) by pushing on the fibular head from behind. A normal stifle feels rock solid. When cranial drawer sign is present you’ll feel slight movement, as if the stifle is held together with very heavy rubber bands. It’s usually more subtle that you’d expect.
Cranial tibial thrust is tested for by wrapping your “proximal" hand around the medial side of the stifle and placing your index finger on the tibial tuberosity. With your “distal” hand, flex the tarsus. If thrust is present, you’ll feel the tibial tuberosity move forward relative to the patella. Both cranial drawer sign and cranial tibial thrust are, of course, indicative of a cranial cruciate ligament rupture. Femur: this is another really difficult bone to palpate for pain. It is most exposed down by the condyle and up by the greater trochanter. Osteosarcoma can occur at either end. Palpate the muscle mass overlying it for evidence of swelling or pain…especially if your patient is a greyhound. Hip: For dogs over 18 months of age about all you need to do is check for evidence of pain on hip extension…if it’s there, think osteoarthritis secondary to dysplasia, but remember that dogs with lumbosacral disease are also often painful on hip extension, since this stretches the nerves that are being pinched. Check for evidence of hip luxation by feeling for thumb sign: find the dent between the greater trochanter and the ischial tuberosity and put a thumb in it. With your other hand, externally rotate the stifle. If the hip’s in joint, you’ll feel the greater trochanter rotate back to occupy the dent your thumb is in. If the hip is luxated, this dent will remain abnormally large.
82

Triangulation can also be used to see if the hip is in joint. Normally, the palpable bumps of the iliac crest, greater trochanter, and ischial tuberosity should form a right triangle. If a craniodorsal luxation is present, these points will be almost in a straight line. If a ventral luxation is present, you’ll have a really hard time finding the greater trochanter!
In dogs less than 18 months of age, check for the presence of hip laxity by testing for the presence of Ortolani sign. This test is performed with the dog in lateral recumbency and with both the hip and the stifle in 90 degrees of flexion. Place the palm of your “proximal” hand on top of the dog’s butt, and very lightly rest the thumb of this hand over the greater trochanter. It is essential to avoid placing any pressure over the greater trochanter, since this would prevent the subluxation you’re trying to elicit. Cup your other hand over the flexed stifle so that the thumb is lateral. This will place your fingers on the medial aspect of the femur. Using your thumb as the fulcrum, lever up on the femur with your fingers so that its proximal end will tend to be forced laterally. At the same time, push the femur proximally through the stifle. Abduct the hip. If you feel a click through the greater trochanter when you do this, you’ve elicited positive Ortolani sign. If performed in a dog older than 4 months of age, this is evidence of excessive hip laxity.
And now for a word about cats. Male (and rarely female) cats who have been neutered before skeletal maturity have a delay in the closure of their growth plates can develop capital femoral physeal fractures when they are 1-2 years of age. This problem is often bilateral. Suspect this problem if your patient has hip pain/ crepitus and is of a certain age.
Another word about cats: it is very rare for a cat to let you do an entire orthopedic exam in one go without sinking his canine teeth into your tendon sheaths. With cats plan to check out one limb at a time, with dashing-for-the-corner (the cat, not you) holidays in between. Usually the best form of restraint for the cat while you’re actively examining him is a single assistant's hand on his scruff.
83

Update on Cruciate Repair
Kathleen Linn DVM, MS, Diplomate ACVS Western College of Veterinary Medicine
University of Saskatchewan, Canada
Causes of Cranial Cruciate Ligament Rupture In human males, anterior cruciate ligament rupture usually results directly from trauma (there appear to be as-yet-unknown predisposing factors at work in human females). Cats follow the human male model of the disease and usually experience cranial cruciate ligament (CCL) ruptures due to bad landings or automobile accidents. In dogs, however, CCL ruptures are usually the result of degenerative disease. 50% of dogs with CCL ruptures have a history of slowly progressive lameness, and partial tears are common. Radiographic evidence of osteoarthritis frequently precedes palpable stifle instability, and 22-80% (it depends on whose study you are reading) of dogs with CCL rupture develop it bilaterally. The cause or causes of this degeneration are as yet unknown; here are the possibilities currently under investigation:
Age: all dogs over five years of age have microscopic evidence of cranial cruciate ligament degeneration
Collagen or related protein defects: Dogs with CCL rupture have a higher tendency than normal dogs of having other orthopedic problems
Immune disease: Dogs with CCL rupture have anti-collagen Type 2 antibodies in serum and synovial fluid and increased levels of IgG and IgM in synovial membranes. Immune changes are often also seen in the as-yet clinically unaffected contralateral stifles
Infection: bacterial DNA is present in a high proportion if stifles with CCL rupture but not in stifles that are osteoarthritic secondary to osteochondritis dissecans
Excessive tibial plateau slope, which often follows proximal tibial physeal fractures in puppies and which may also follow delayed closure of the tibial tuberosity apophysis, can place abnormal strain on the cranial cruciate ligament, leading to its ultimate rupture. However, most dogs who rupture their CCLs have normal tibial plateau slopes, so this can't be the whole story.
Concurrent Problems
Osteoarthritis is an expected sequela of CCL rupture--even if clinically successful surgical stabilization of the stifle has been accomplished.
Meniscal tears are present in 30-70% of canine stifles with CCL rupture. These cause exacerbated lameness and accelerated osteoarthritis. The caudal horn of the medial meniscus is by far the most common site of injury, but radial and complex tears of the lateral meniscus are also often present if you look for them.
Is surgery really better than medical management of CCL rupture? Conservative (medical) management of CCL rupture includes weight management, physical rehabilitation, anti-inflammatory and analgesic medication and disease-modifying ("chondroprotective") medication for osteoarthritis. A study done by Vasseur and team in 1984 showed that medical management of CCL rupture had a success rate of 50-83% in dogs weighing less than 15 kilograms and a 13-20% success rate for dogs weighing more than 15 kg.
84

By contrast, regardless of patient body weight, reported surgical success rates (no matter what technique is used) are generally in the 85-90% range. However, the definition of what constitutes a successful result varies from study to study. Numerous studies have shown that the degree of stability conferred by various surgical techniques does not correlate well with postoperative function. To further muddy the waters, when the 1984 study on conservative management was done, physical rehabilitation and disease-modifying drugs for osteoarthritis were not in common use. So where does the science stand on this question right now? It turns out there's not very much of it.
Chauvet et al., 1996: This study included 61 large breed dogs with CCL rupture; 22 stifles had fibular head transposition, 39 had lateral suture stabilization, and 11 were treated with aspirin and rest (selections as to treatment were nonrandom). Owners' impressions as to their dogs' function favored lateral suture stabilization. Veterinary analysis (including force plate testing and radiography) at six weeks after treatment showed no difference in results among methods. However, six weeks after surgery is awfully early for drawing conclusions about ultimate function.
Tivers et al., 2009: In this study, out of 31 large breed dogs with CCL rupture and concurrent medial meniscal tears, 22 were treated with caudal pole meniscectomy (of the medial meniscus), and 9 were treated with caudal pole meniscectomy alone--without any attempts made to stabilize the stifle. Evaluations--done by owner questionnaire a median of 25 months after treatment--showed no difference in outcome.
The bottom line here is that there is need for good controlled studies, with similar drug and rehabilitation treatments for both groups, to compare outcomes for surgical and nonsurgical treatment of CCL rupture, especially in large breed dogs. How well do stifle braces work? Over the past five years various braces purporting to control cranial tibial thrust have become commercially available. To date there have been no studies testing efficacy of any brace in limiting cranial tibial thrust and no studies objectively measuring clinical effectiveness of braces in dogs. Lateral Suture Stabilization Advances Lateral suture stabilization (LSS; always done in combination with arthrotomy or arthroscopy so that meniscal debridement can be performed if necessary) has been the method with the most durability: it is always to some form of this technique that veterinary surgeons have reverted when the popular stabilization method of a given decade has fallen out of favor. Recent tweaks to LSS have included:
The quest for isometric points: A number of studies have been aimed at identifying points for suture fixation that will result in the stabilization suture being equally taut throughout the full range of motion of the stifle. The thought here is that isometrically placed sutures will better stabilize the joint and be less prone to slipping, stretching or breaking. However, as the cranial cruciate ligament itself is not equally taut throughout the stifle's range of motion, this quest may be somewhat futile. So far it has been found
85

that the best spot to anchor a suture is just cranial to the distal pole of the lateral fabella. The best tibial anchor point for a single suture is just caudal to the groove of the long digital extensor and just distal to the joint line; the best tibial anchor spot for a suture loop may be in the more traditional location just caudal to the distal pole of the tibial tuberosity. No studies have been done comparing clinical efficacy of the various anchor points, however.
Bone anchors for suture fixation: a variety of bone anchors and suture materials have become available. Potential advantages to using them include the ability to place sutures minimally invasively, with no worry about having them slip out of place. Recovery to full weightbearing may be faster when bone anchors are used, since passage of tight sutures around the lateral fabella seems to be a source of postoperative pain for at least some dogs. However, suture anchors can fail by either pulling out of the bone (it is critical that femoral anchors be placed at the femoral isometric point) or by breaking the suture as it passes the edges of the eyelets (thus eyelet positioning is an important detail to attend to). No studies have been done to compare clinical results between bone anchor-fixed and more traditional fabellotibial sutures.
Suture loop configuration: The standard two single loops of suture turns out to be a relatively weak configuration. The strongest tested so far is one doubled, interlocking loop.
Suture materials: Materials in current use for LSS include monofilament nylon leader line (strong, cheap, minimal harboring of bacteria but quite large and stiff), nylon and polypropylene suture materials (weaker than leader line) and new braided polymer materials (OrthoFiber, Fiberwire, Fibertape), which are strong and relatively stiff but provide places for bacteria to hide. I know you're tired of hearing this, but they have not yet been compared for efficacy/complications in a clinical setting.
TightRope technique: This method uses medially-placed toggle buttons to anchor a very strong, braided suture that then passes through bone tunnels drilled through the femur and tibia over to the lateral side. This method offers very positive suture fixation along with an ability for the suture to adjust its tension to suit various stifle positions. It can be performed in a minimally invasive manner. However, there are not yet a lot of data comparing clinical effects of TightRope with those of LSS.
Which is better--lateral suture or tibial plateau leveling osteotomy? Potential benefits of LSS over TPLO include:
LSS controls internal rotation of the tibia; TPLO does not Failure of LSS is seldom catastrophic LSS can be done minimally invasively LSS has a lower infection rate than TPLO
Potential benefits of TPLO over LSS include:
More rapid return to good weightbearing Once the osteotomy has healed, stability should be permanent with TPLO, while with
LSS suture failure may result in return of instability Postoperative meniscal tear rate seems to be lower with TPLO than with LSS Partial cruciate ligament ruptures do not always progress when TPLO is performed
86

Still--where does the science stand on clinical effectiveness of TPLO versus LSS? Conzemius et al., 2005: Evaluation methods included force plate testing. There were no
significant differences in outcome between LSS and TPLO at 2 and 6 months after surgery
Cook et al., 2010: In a runoff between TPLO and TightRope method, there were no significant differences in outcome at 6 months after surgery
Lazar et al., 2005: Here no difference in degree of radiographic degenerative change was found in long-term comparisons between TPLO and LSS-treated stifles.
Millis et al., 2008: No long-term differences between TPLO and LSS on kinetic and kinematic studies
Au, Gordon-Evans et al., 2010: 65 dogs who received either LSS or TPLO were followed for 2 years using (among other evaluation methods) force plate testing and radiographs. Dogs received identical physical rehabilitation postoperatively. However, LSS patients tended to be a bit smaller than TPLO dogs. No difference in outcome was found.
Gordon-Evans et al., 2010: Here 40 large-breed dogs received LSS and 40 received TPLO; owners and evaluators were blinded as to treatment. Identical postoperative rehabilitation was done, and outcome was evaluated using radiographs, force plate testing, thigh circumference and subjective scales. This study will continue for 2 years, but so far the 6-month data are available. Here dogs weighing over 36 kg did better on force plate testing at the trot if they had been treated with TPLO (this was the only difference noted).
So at this point in time, TPLO gets a slight nod over LSS for dogs exceeding 36 kg in body weight. Both methods are effective treatments for CCL rupture in dogs of all sizes. How does TPLO compare with tibial tuberosity advancement (TTA) techniques? Not a lot of direct comparisons have been made between the two techniques, and they are generally viewed as being basically equivalent. Here's a summary of the TPLO-vs.-TTA studies that have been done:
Vezzoni, 2010: 85 stifles received TPLO, 85 received TTA, and dogs were followed up for 6 months after surgery clinically and radiographically (no force plate testing). Success rates were not reported, but the author's subjective impression was that outcomes were equivalent.
Kim, Pozzi et al: This was a biomechanical cadaver-limb study. Contact mechanics and tibial alignment were unchanged from normal when TTA was the treatment. TPLO led to a slight tibial varus with resultant overloading of the cartilage on the medial side of the joint.
That's it. The bottom line is that the two techniques are close to equivalent in outcome. TTA, correctly performed, gets awarded the win on a biomechanical basis, although TPLO may be applicable in more situations (like excessive tibial plateau slope) than is TTA.
87

Those #%*$# Shoulder Problems
Kathleen Linn DVM, MS, Diplomate ACVS Western College of Veterinary Medicine
University of Saskatchewan
Shoulder Joint Anatomy The scapula is attached to the body only by musculature: the serratis ventralis, rhomboideus, trapezius, and omotransversarius muscles. The pectoral and latissimus dorsi muscles also help connect the forelimb with the rest of the body, but they attach to the proximal aspect of the humerus. The shoulder is a ball and socket joint with a wide range of motion, primarily in flexion and extension. The glenoid lip is extended by a cartilage labrum in people, but this seems to be only occasionally the case in dogs. Even so, the actual area of contact between glenoid and humerus is smaller than you’d think. The greater tubercle of the humerus is not part of the joint itself, but it is the attachment point for the supraspinatus tendon. The supraglenoid tubercle of the scapula forms part of the articular surface of the joint and is also the origin of the biceps tendon. The biceps, by the way, spans two joints, the shoulder and the elbow, before finally inserting on the proximal part of both the radius and the ulna. The medial and lateral glenohumeral ligaments are the collateral ligaments of the joint. Tendons that cross the joint also aid in stability, especially the subscapularis tendon, with help from the biceps, supraspinatus, teres minor and infraspinatus (these last four form the rotator cuff in people). Clinical Signs of Shoulder Lameness
Head nod or a rolling gait Moderately prominent scapular spine on affected side due to muscle atrophy Pain on shoulder extension, flexion and/or simultaneous flexion of the shoulder and extension of the
elbow
Osteochondritis Dissecans (OCD) of the Humeral Head This one's easy to diagnose, so we'll just summarize the high points.
Occurs in medium to giant breed dogs Onset of lameness usually 6-12 , occasionally up to 18 months of age Weightbearing lameness that often gets worse after exercise Moderate amount of scapular muscle atrophy; pain on shoulder
extension and flexion Defect is bilateral 50% of the time, although usually asymmetric in
degree (so radiograph both shoulders!) Radiographic findings: divot in subchondral bone of the caudal aspect
of the humeral head (or the head just looks flattened here). Occasionally the defect leans over onto the medial side of the humeral
88

head, making it hard to pick up on a lateral view, so if you have suspicions of OCD and you're not finding it, add in a lateral shot while you're externally rotating the shoulder. Treatment of Humeral Head OCD Treatment with conservative therapy can be considered: 50% of affected dogs go sound within 6 months if you wait things out. We think this happens when the cartilage flap breaks free, attaches to the joint capsule, and (if you’re lucky) gets resorbed. Some people advocate rest during this waiting period, while others advocate heavy exercise to help break the flap free: in reality it doesn’t seem to matter which way you go. With surgical treatment 90% of dogs go sound within 6 weeks. Surgery involves removing the cartilage flap and curetting the subchondral bed, either via arthrotomy or via arthroscopy. Although some osteoarthritic change will happen on postoperative radiographs, long-term prognosis with surgical treatment is excellent.
Joint Capsule/Collateral Ligament Injuries These are THE most common causes of shoulder lameness. These injuries include glenohumeral ligament (most often the medial one) tears, subscapularis tendon tears, labral tears (when a labrum is present), and simple joint capsule tears. Diagnosis of Joint Capsule/ Collateral Tears
Occur mostly in young adult to middle-aged, medium to large breed dogs Cause a chronic, sometimes intermittent, mild to moderate lameness Pain on shoulder flexion/extension Can abduct humerus of extended shoulder >50 degrees, or at least considerably more than the
opposite humerus (normal degree of abduction is about 30 degrees) Radiography: usually normal or showing vague degenerative change Ultrasonography—can be done but takes an experienced ultrasonographer to pick up problems MRI: useful for diagnosis, given a good machine and an experienced interpreter Arthroscopy: the most sensitive and specific test for this condition
Treatment of Joint Capsule/Collateral Tears
Rest (six weeks of short leash walks only) and NSAIDs, followed by physical rehabilitation: this will work in a significant, but unknown, proportion of dogs.
Intra-articular injection of corticosteroids (triamcinolone or methylprednisolone acetate), combined with 6 weeks rest may help, simply because we know that most dogs diagnosed with “bicipital tenosynovitis” in the past actually had this condition instead…and there was an 80% success rate reported for this treatment.
Arthroscopic radiofrequency shrinkage of affected tissue can yield successful results, but prolonged immobilization (over 6 weeks) of shoulder joints after surgery is necessary as tensile strength of treated tissue decreases during the first couple of months.
Prosthetic ligament reconstruction is probably the most successful route to take with chronic, significant tears of the glenohumeral ligaments. This can be done arthroscopically in people (and the same repair has been reported in dogs), but it is usually done via an open surgical approach in dogs (arthroscopic implants are pricey and difficult to place in small joints).
89

Supraspinatus Calcifying Tendinopathy (SCT) and Supraspinatus Tendinopathy
This is thought to occur secondary to injury (either acute or due to repetitive strain) of the supraspinatus tendon. If you're lucky, portions of the core of the tendon fill with calcified goo, making radiographic diagnosis easy. However, about a third of affected dogs do not develop calcification. Just to confuse things, the tendon mineralization is often an incidental finding in asymptomatic shoulders--so diagnosis of this condition requires that you rule out concomitant conditions as the cause of lameness (this requires shoulder arthroscopy or monitoring response to treatment of presumptive SCT). This is usually a big dog (especially Labrador and rottweiler) problem. It can cause a chronic, often intermittent lameness. It usually produces a unilateral lameness despite being frequently bilateral on radiographs. Affected dogs may be painful on pressure over the greater tubercle (which is where the supraspinatus tendon inserts). Radiographs will show a mineral density just cranial to the supraglenoid tubercle; if you take a skyline view of the shoulder, this density will be over the greater tubercle or just medial to its ridge, rather than deep within the intertubercular groove (this latter position would indicate a problem with the biceps tendon instead). Ultrasonography and MRI are the way to make the diagnosis when mineralization is not present: they show enlargement of the tendon, often to the point where it is impinging on the adjacent biceps tendon. Treatment of Supraspinatus Tendinopathy
Rest-n-NSAID therapy is seldom successful. Extracorporeal shockwave therapy often works nicely to resolve clinical signs Surgical treatment: When mineralization is present, longitudinal incisions are made
in the tendon insertion to allow removal of the calcified goo (which is generally very much like toothpaste). When mineralization is not present, longitudinal incisions, often combined with resection of the most diseased portion of the tendon, is done. Success rate is about 75%.
Stem cell therapy: currently, information is anecdotal and unpublished. Injection of mesenchymal or adipose-derived stem cells into the abnormal portion of the tendon, combined with physical rehabilitation, may be helpful in resolving the lameness.
Biceps Tenosynovitis/Partial Avulsion
The biceps brachii tendon crosses both the shoulder and the elbow joint, so it is maximally stressed when the shoulder is flexed while the elbow is extended. The tendon originates on the supraglenoid tubercle, passes through the shoulder joint and then down in a groove between the greater and lesser tubercles (the intertubercular groove). While it is in the groove it is surrounded by an outpouching of the shoulder joint capsule. The biceps tendon can be injured either acutely or as a result of repetitive stress. Diagnosis of problems can be difficult (tendons don’t show up on radiographs), but testing may include:
90

Physical findings: pain on simultaneous flexion of shoulder/extension of elbow. The cross-chest test for pain on insertion of the biceps tendon on radius and ulna may be positive.
Radiography: sometimes mild nonspecific degenerative changes of the shoulder and intertubercular groove will be seen. If you’re lucky, you’ll see avulsion fragments just distal to the supraglenoid tubercle or a line of osteophytes along the intertubercular groove. A skyline view of the intertubercular groove may show an osteophyte or calcifications within the groove.
Arthrography: contrast arthrography may show filling defects in the outpouching of the joint capsule that accompanies the biceps tendon in the intertubercular groove. Not used so much these days, now that there's...
Ultrasonography: may show tendon abnormalities (if you have bribed the radiologist appropriately)
Magnetic resonance imaging (MRI): With the right eyes, you can see useful stuff. *Arthroscopy*: this is the gold standard for diagnosis—you can see the tendon and what it’s up
to…and do something about it while you’re there!
Treatment of Biceps Tendon Problems Rest +/- intraarticular corticosteroid injection: 60-80% success rate Biceps tenodesis: This involves cutting the tendon free of its origin on the supraglenoid tubercle
and sticking it down to the humerus somewhere. This means it doesn’t get stressed by crossing the shoulder. Biceps tenodesis has an 80% success rate, but lameness may persist for several months after surgery.
Biceps release: This means simply cutting the biceps tendon off of the supraglenoid tubercle and letting it go goodness knows where. This can be done either through a small approach to the intertubercular groove or via shoulder arthroscopy. The brachialis muscle replicates the function of the biceps, so no worries there. The success rate of this technique is unreported but it seems to be similar to tenodesis with less postoperative down time: surgery itself causes transient or no lameness. ☼Biceps tenosynovitis used to be the catchall diagnosis for soft tissue shoulder lameness. Now that we have better diagnostic tools, we know that this is an uncommon disease.
Infraspinatus Contracture Hunting dogs are most commonly affected with this condition. It occurs about three weeks after a tear of the infraspinatus tendon has occurred: a fibrous scar forms and is accompanied by muscle contracture. This produces external rotation of the humerus and a resultant mechanical lameness. Affected dogs have external rotation of the forelimb, which produces a paddling gait. The external rotation is particularly evident when you hold the dog’s front end up off of the ground. Ultrasonography may show scarring (hyperechogenicity) of the affected infraspinatus muscle. Radiographs are usually normal. Treatment of Infraspinatus Contracture Remove a segment from the affected tendon—who really needs an infraspinatus anyway? Success rate for return to normal function is high.
91

Interpreting the Senior Hemogram: What Every Practitioner Should Know!
Fred Metzger DVM, DABVP Metzger Animal Hospital
State College, Pennsylvania The complete blood count provides a broad overview of the general health status of the patient. For this reason, hematology becomes a critical component of laboratory evaluation of patients. The peripheral blood serves as the transport medium between the bone marrow and the tissues; consequently, the complete blood count provides a snap shot of the hematopoetic system at a specific point in time. Complete blood counts should be included in evaluations of every sick patient, every patient with vague signs of disease, every pre-anesthetic evaluation, every wellness and geriatric profile and as a recheck test for patients previously diagnosed with erythrocyte, leukocyte or thrombocyte abnormalities. Evaluating the white blood cells Leukogram data include total and differential white blood cell counts and a description of white blood cell morphology from the peripheral blood film. Differential cell counts should always be expressed and interpreted in absolute numbers, not percentages. All leukocyte compartments - neutrophils and their precursors, eosinophils, basophils, monocytes and lymphocytes must be counted. White blood cell data are used to answer the following questions: 1) is there evidence of inflammation? 2) Is there evidence of a glucocorticoid (stress) or epinephrine (excitement) response? 3) Is there a demand for phagocytosis or evidence of tissue necrosis? 4) If inflammation is present, can it be further classified as acute, chronic, or overwhelming? And 5) Is there evidence of systemic toxemia? Is there evidence of inflammation? Neutrophilic left shifts, persistent eosinophilia, and monocytosis are the best indicators of inflammation. Left shifts (increased numbers of immature [band] neutrophils in circulation) indicate increased turnover and tissue use of neutrophils. Persistent peripheral eosinophilia indicates a systemic allergic or hypersensitivity reaction. Monocytosis is seen in peripheral blood when there is a demand for phagocytosis. It is possible to have inflammatory leukograms without any of the above changes, but they are harder to recognize. For example, a mild leukocytosis with mature neutrophilia may indicate inflammation, but it may also represent a physiologic response to an epinephrine surge (excitement leukocytosis) or a response to endogenous or exogenous glucocorticoids. When the results of a leukogram are ambiguous, they can sometimes be clarified by repeating the CBC over several hours or days. Left shifts may develop with time.
92

Is there evidence of a glucocorticoid (stress) or epinephrine (excitement) response? High levels of circulating glucocorticoids cause a mild mature neutrophilia, lymphopenia and eosinopenia, and mild monocytosis. Of these changes, lymphopenia is the most consistent and reliable indicator of stress. In dogs and cats, we regard lymphocyte counts of 1,000 to 1,500/µl as marginal lymphopenia, whereas lymphocyte counts below 1,000/µl are absolute lymphopenias. When lymphocyte counts drop below 600/µl, other causes of lymphopenia such as chylous effusions, lymphangiectasia, and malignant lymphoma should also be considered. Is there a demand for phagocytosis or evidence of tissue necrosis? Monocytosis indicates a demand for phagocytosis or tissue necrosis. Monocytosis is almost always seen in chronic inflammatory conditions, but can also occur with acute inflammation. Whenever a severe monocytosis is observed (>4,000/µl), a buffy coat smear should be prepared in attempt to identify any particles or causative agents that have been phagocytosed by circulating monocytes (e.g. opsonized red blood cells in immune hemolytic anemia, Ehrlichia canis, Histoplasma capsulatum). Is there evidence of systemic toxemia? Circulating toxins (i.e. systemic toxemia) can arrest development of neutrophil precursors in the bone marrow. Either cytoplasmic or nuclear development can be affected. The abnormal neutrophils produced in this way are recognized on the peripheral blood film as toxic neutrophils. Cytoplasmic features of toxicity include foamy basophilia and the presence of small basophilic precipitates known as Döhle bodies. Döhle bodies are a sign of mild toxicity in cats (often seen in low numbers in normal cats), but indicate serious toxicity in dogs. Nuclear changes of toxicity include bizarre nuclear shapes and cellular giantism. Systemic toxemia is usually associated with bacterial endotoxins. Infectious diseases commonly accompanied by severe toxicity include feline pyothorax, pyometra, and severe canine prostatitis. Toxemia can also be associated with noninfectious causes such as tissue necrosis, heavy metal toxicosis, or cytotoxic drug therapy. Evaluating the red blood cells Red blood cell data include the hematocrit (hct), absolute reticulocyte count (if available), red blood cell count, hemoglobin (hgb) concentration, and indices like mean cell volume (mcv), mean cell hemoglobin concentration (mchc) and RDW (red cell distribution width). As stated earlier, we include total protein concentration as a part of the red blood cell evaluation. The red blood cell data are used to address the following central issue: Is the red blood cell mass normal, reduced, or increased? Classifying anemias If red blood cell mass is reduced, then the animal is anemic. The degree of anemia should be further considered in conjunction with plasma protein concentrations. If protein concentrations are elevated, then the animal may be dehydrated, and the anemia may be more severe than red blood cell mass measures indicate. Once anemia is recognized, the next issue of concern is bone marrow responsiveness: Is the anemia regenerative or nonregenerative? If the red blood cell marrow responds with an increase in production of appropriate magnitude, the anemia is regenerative (responsive). On the other
93

hand, the anemia is nonregenerative (nonresponsive) when there is not an effective increase in the production of red blood cells. The absolute reticulocyte count is the most objective measure of current bone marrow responsiveness. Classifying polycythemia If red blood cell mass is increased, then the animal is polycythemic. This then raises the question: Is the polycythemia relative or absolute? Relative polycythemia, the most common polycythemia recognized in veterinary medicine, is the result of hemoconcentration. It is generally established based on the clinical history and signs consistent with dehydration, as well as an elevated total protein concentration. Polycythemia in the absence of these findings is absolute. Absolute polycythemia can be either primary or secondary. Evaluating the platelets An assessment of platelet numbers is an important part of every cbc. As with red blood cells, the principal issue is whether platelet numbers are normal, increased (thrombocytosis), or reduced (thrombocytopenia).
94

Senior Liver Disease Case Challenge: Catching it BEFORE your Patients Turn Yellow
Fred Metzger DVM, DABVP
Metzger Animal Hospital State College, Pennsylvania
THE LIVER PROFILE Alanine Aminotransferase (ALT) – ALT is a cytosolic enzyme relatively specific for hepatocytes that serves as an excellent parameter in the dog and cat to detect hepatocellular injury. Increases in ALT are immediate following significant injury to the cell and if the injury is not ongoing, ALT values return to their baseline relatively rapidly. The circulating half-life of ALT is reportedly wide in the veterinary literature, but clinically, a 2-3 day half-life time period proves effective in interpreting serial ALT values. A decrease of 50% of a serum ALT value within 2-3 days indicates that either the hepatocellular injury is subsiding and the process is resolving or there are no additional hepatocytes remaining to injure. The latter process should be relatively easy to distinguish clinically from the former in that the clinical condition should be extremely severe. The vast majority of increases in ALT in the dog and cat are specific indicators of hepatocellular injury. Profile Parameters Associated with Cholestasis: Cholestasis can be seen with a variety of hepatic as well as post hepatic pathologic processes. Interferences with bilirubin metabolism and excretion can be seen at the hepatocellular level where intra-hepatocellular accumulations of bilirubin occurs (intra-cellular cholestasis). Blockage of bilirubin and bile salt passage through the early bile canalicular system between hepatocytes with mild to moderate hepatocellular swelling associated with both reversible and irreversibly injury is possible also. In addition, more significant blockage of the biliary system can be seen with accumulations of bilirubin and bile salts within bile ducts within the hepatic parenchyma due to pathologic changes in the periportal regions due to infiltrative inflammatory and neoplastic processes or changes such as fibrosis. Post hepatic obstruction associated with pathologic changes near the common bile duct result in similar parameter changes associated with this cholestatic process also. These various cholestatic processes result in similar profile changes with slight variations in timing of changes of the different parameters or different degrees of parameter change. Alkaline Phosphatase (ALP) – ALP is an extremely sensitive indicator of cholestasis in the dog (most cases of cholestasis will have increases in ALP); however, specificity varies between the dog and cat. Because of non-hepatic sources of ALP (tissue specific isozymes) and the presence of these isozymes in the serum of dogs, mild increases in ALP are extremely nonspecific. Bone ALP isozyme is commonly seen in young growing animals and sources such as intestinal epithelium, renal epithelium, and placenta are found in the serum of dogs in both health and disease. In addition, specific to the dog, there is a glucocorticoid-induced form of ALP that is commonly seen increased with a wide variety of disorders, not just hepatic disorders. Therefore, mild increases in ALP in
95

the dog are extremely nonspecific. If ALP values reach to levels greater than 3-4 fold above the high end of the reference range, some specificity is allowed. These degrees of changes are associated with either cholestasis or glucocorticoid-induced ALP origin. Use of other profile parameters and clinical information is required to make a proper interpretation of these types of ALP increases in the dog. In the cat, ALP is highly specific but not very sensitive for identifying a cholestatic disorder. With the exception of the glucocorticoid-induced isozyme, other tissue isozymes are also experienced in the cat. The reason that these isozymes are not interfering with the interpretation is because they have extremely short half-life and they do not accumulate in the plasma. The hepatic (cholestasis-associated) isozyme of ALP has a very short half-life also, which relates to its low sensitivity, but even this short half-life is longer than most of the other isozyme forms. Interpretation of ALP related to hepatic disease is different from the indicators of hepatocellular injury. ALP is primarily a membrane-associated enzyme that increases in plasma concentration due primarily due to increased (induced) production and concentration within membranes rather than “leakage” from the cytosol or mitochondria. Because of this difference, increases in ALP are not seen immediately, there is a lag time between cholestatic process and ALP increases. Similarly, discussions about half-life is of little value, because there is a lag time for the decreasing of this enzyme that is variable depending upon the primary stimulus for increased production to begin with. In general, following serial ALP values is of very little value shorter than a period 3-4 days. Location within the liver is primarily on hepatocyte membranes along bile canaliculi and increases from the liver typically have general hepatic involvement. Gamma Glutamyltransferase (GGT) – GGT is also a membrane-associated enzyme that increases and decreases in what clinically appears as a “lag time” relative to clinical disease. GGT is present in many tissues, primarily secretory tissues, with high concentrations per gram tissue weight in the pancreas, kidney, mammary gland and even the lung in addition to the liver. Within the liver, it is present in highest concentrations on membranes of bile ductular epithelial cells with much less associated with hepatocytes; therefore, increases are generally indicative of pathologic changes associated with periportal regions of the liver. When increases are seen in the plasma, it is typically of hepatic (cholestatic) origin because with the other tissue sources, the enzyme is lost within the secretory component of the tissues since it is associated with the apical membranes of the various tissues. As with ALP, interpretation of half-life is difficult with GGT and serial value determinations should are of very little value shorter than a period of 3-4 days. Bilirubin – Bilirubin is a hemoglobin breakdown product and may be present in circulation in a variety of forms. The simple profile provided by most reference laboratories includes total bilirubin, unconjugated bilirubin (form being delivered to the hepatocyte most immediately related to hemoglobin breakdown), and conjugated bilirubin (form processed by the liver making the breakdown product water soluble and freely passable in the biliary tree). Increases in unconjugated bilirubin (also identified as
96

Indirect Bilirubin) can be seen with decreased concentration of hepatocytes (decreased hepatic mass) associated with hepatic insufficiency but may also be seen with intravascular and extravascular hemolytic disease as well as selected internal hemorrhage situations where there is an increased turn-over of erythrocytes and excess hemoglobin breakdown compared to normal. The increase in unconjugated bilirubin associated with hemolytic disease is most likely seen when there is a concomitant insult to the liver and its functionality, which is commonly seen with the more severe hemolytic or hemorrhagic processes due to hypoxic injury. Increases in conjugated bilirubin are seen with post-hepatocellular events. Disruption of bile flow from partial or complete blockage of the biliary system anywhere from the bile canaliculus to the common bile duct entering the duodenum can result in increases in conjugated bilirubin. Bile Acids – Bile acids are produced in the liver, stored and secreted from the gall bladder, and mostly (95%) re-absorbed from the intestinal tract and re-circulated for re-use. Normally there is a small amount of bile acids in circulation and increases can prove extremely sensitive to hepatic disorders including hepatic insufficiency; however, bile acids are relatively nonspecific related to the type of hepatobiliary disease present. It can increase related to disturbances in circulation to the liver (entero-hepatic circulation / shunts) since the bile acids do not get delivered to the hepatocytes for uptake and re-utilization. It can increase related to hepatocellular injury, necrosis or decreased numbers since the hepatocytes are not available for uptake and the bile acids circulate longer than normal. It can also increase related to biliary stasis / obstruction where there is regurgitation of bile acids into circulation. Where bile acids are of particular value are related to cases of suspect circulatory shunts or if there is strong clinical suspect of underlying hepatic disease even though the primary and secondary hepatic panels have no significant changes. If there is already evidence of hepatocellular injury, cholestasis or hepatic insufficiency, bile acid profiling may prove not to be useful. Ammonia Tolerance Testing – Resting blood ammonia and more effectively, ammonia tolerance testing can be highly supportive of underlying hepatic insufficiency. Only rarely seen cases or urinary bacterial infections with urea splitting bacteria and circulating high circulating ammonia levels can be confused with true ammonia increases related to inability of the liver to metabolize ammonia to urea (hepatic insufficiency THE KIDNEY PROFILE PRIMARY RENAL PROFILE BUN – Urea produced from ammonia is produced in the body at a relatively constant rate and it is primarily removed from the body through excretion through the kidney, therefore, it becomes a commonly evaluated parameter in the chemistry profile. When the total nephron unit is affected and there are decreased numbers of intact nephrons, increases in BUN because of decreased excretion will be seen in most cases. However, one must also consider other causes for increased BUN that are not primarily renal in cause as well as reasons why BUN is not increased significantly in the case of true renal disease.
97

Specifically related to renal function one must remember the sensitivity of BUN in detecting decreased renal function. In most species, we need approximately 25% residual renal function before it is detected with an increased BUN. Therefore, rather significant renal disease will be present before any abnormality is identified. When present, increases in BUN typically represent decreased glomerular filtration rate (GFR), which in many cases truly represents renal disease. Not all increases in BUN though are directly related to renal disease. The primary cause for decreased GFR not related to renal disease is dehydration. Decreased perfusion of the kidney not associated with renal disease results in a decreased GFR and mild increases in BUN. In addition, if there is an increase in BUN in the circulation not related to renal disease, it is natural to understand that increased BUN concentrations will be seen even if the kidney is functioning normally because the plasma concentration of BUN is just at a higher level than normal. To properly interpret increases in BUN, one must have a urine specific gravity also. In cases of increases of BUN related to decreased vascular perfusion such as with dehydration (Pre-renal azotemia), urine specific gravity should be increased since the body is attempting to retain water and the kidney is still functioning properly. In cases of increases of BUN related to increased protein intake and increased production of urea, urine specific gravity values will relate to the current hydration status of the animal. If the animal is slightly in negative water balance, the specific gravity will be increased since the renal function is not altered with this cause of increased BUN. In cases of increases of BUN related to true renal disease (Renal azotemia), urine specific gravity should be within the isosthenuric range. Loss of tubular concentrating ability typically is lost before increased in BUN are detected with true renal disease. Post-renal azotemia associated with urethral or ureteral obstruction or potential rupture of the urinary bladder, urethra or ureter. In this latter case of non-renal origin azotemia, the urine specific gravity could be of any value. Other diagnostic modalities are required to identify these processes accurately and obviously, diagnostic imaging becomes an extremely valuable tool. Decreases in BUN are not typically associated with renal disease. In most cases, it is related to either decreased urea production (hepatic insufficiency) or increased glomerular filtration rate and increased renal excretion. This latter situation is seen in cases of overhydration or other causes of polyuria and diuresis. Creatinine – Creatinine is also a commonly measured analyte for purposes of screening for renal function abnormalities. Creatinine originates from the muscle metabolite creatine, which is non-enzymatically transformed to creatinine and then cleared with renal excretion, primarily to passive filtration. Since the metabolite from muscle, creatine, is freely filtered in the kidney, cases of muscle cell injury typically do not result in an increase in creatinine. When observed, increases in creatinine are associated with decreased GFR.
98

Increased GFR can be associated with either renal origin and decreased function or associated with conditions such as decreased vascular perfusion as might be seen with significant dehydration. Increased protein intake and metabolism will not affect creatinine values as it will with BUN. Urine specific gravity measurement is essential to proper interpretation of serum creatinine values. Similar to BUN, decreases in creatinine are possible with increased GFR associated with cases of overhydration or other causes of polyuria and diuresis. In some cases of marked muscle atrophy, decreases in creatine that will eventually be transformed to creatinine may be seen and a resulting decreased serum creatinine may be identified. Urine Specific Gravity – As was mentioned above, urine specific gravity is an essential component to the primary renal profile. It is required to properly interpret both BUN and Creatinine. It is easily and accurately determined with a refractometer; however, it is important to periodically check the refractometer to assure accurate results are obtained. Purchase of a refractometer that can be calibrated and checking calibration with distilled water, which should have a specific gravity of 1.000, is recommended. Use of urine test strip pads for specific gravity measurement in animals is not recommended since inaccurate results are common. Urine specific gravity will vary in normal animals because of the varying hydration status throughout the day. Urine specific gravity values between 1.008 and 1.012 are considered isosthenuric, which indicate that there has been no kidney alteration of the glomerular filtrate. In the dog, values greater than 1.030 suggest adequate concentration and values between 1.013 and 1.029 are considered concentrated but not concentrated enough to accurately document decreased renal tubular dysfunction and decreased ability to concentrate. In the cat, values greater than 1.035 indicate adequate renal function and values between 1.013 and 1.034 are considered concentrated but not concentrated enough to accurately document decreased renal tubular dysfunction. Interpretation of urine specific gravity relative to renal function requires either accurate assessment of hydration status of the animal in question or serial evaluations in conjunction with other testing. If a value of urine specific gravity is between 1.007 and 1.030 in a dog that is clinically dehydrated, this can be used strongly to support renal insufficiency but if the hydration status cannot be accurately assessed, changes in urine specific gravity during a water deprivation test or following serial measurements over a wider time period will be needed. Complete Urinalysis – Potential valuable additional information can be obtained with a complete urinalysis. A complete urinalysis includes not only the gross inspection of the urine, but also a complete chemical (Dipstick) and microscopic (urine sediment) evaluation. Urinalysis to many is merely a urine specific gravity and a Dipstick evaluation, but it is much more. Information beyond the kidney is obtained with the complete urinalysis; therefore, it is commonly used in most general health screen profiles to help identify potential underlying disease in the kidney, liver, and other organ systems
99

Microscopic evaluation of urine sediment – Characterization of the cellular response (inflammation, neoplasia, bacteria, etc.) can provide relative specific information associated with different types of renal disease. In addition, the identification of various crystals can provide information about the composition of the urine that may be associated with renal disease as well as non-renal systemic disease. SECONDARY RENAL PROFILE Phosphorus – Phosphorus metabolism is relatively complex with involvement with the gastrointestinal tract (absorption), skeletal system (storage), endocrine system (regulation) and kidney where primary excretion takes place. If there is decreased GFR, increases in serum Phosphorus is commonly seen. However, there are many other causes of hyperphosphatemia beyond primary renal disease and renal failure. Young growing animals will have high phosphorus values because of normal bone growth but hyperphosphatemia will also be seen in conditions such as pre-renal and post-renal azotemia, primary hyperparathyroidism, nutritional secondary hyperparathyroidism, hypervitaminosis D, osteolytic diseases, marked cell necrosis (rhabdomyolysis and tumor necrosis following therapy), and others. Calcium – Like phosphorus, calcium metabolism is relatively complex and renal excretion plays a role in the complexity. Cases of decreased GFR both from renal and non-renal origin can result with both acute and chronic renal failure but since there are so many other influencing factors, hypercalcemia is not a reliable parameter to follow to predict the presence or absence of renal disease. Electrolytes and acid-base status – The kidney plays an essential role for “filtering” excess electrolyte concentrations in the plasma through both passive and active processes along the intact nephron. In addition, normal glomerular filtration is essential in removing a variety of organic acids (sulphates, phosphates, etc.). When there is a decrease in this functional filtering activity of these acids, metabolic acidosis is possible; therefore, complete electrolyte profiling including measurement of Sodium, Potassium, Chloride, and Bicarbonate is needed to calculate Anion Gaps and characterize the acid-base status of the animal. This does not really assist in the identification of renal disease, but is essential in evaluating the whole animal and the secondary affects of renal disease. THE PANCREAS PROFILE Amylase – Amylase, although in high concentrations within exocrine pancreatic glandular epithelial cells is not solely specific for this tissue. Significant amylase activity is found in small intestinal mucosal epithelial cells also. Increased serum or plasma amylase activity can be seen in several primary conditions including exocrine pancreatic glandular epithelial cell injury. Simple blockage of the pancreatic duct from a variety of conditions can theoretically result in decreased release of this enzyme into the intestinal tract and possible regurgitation into the plasma. Gastrointestinal and hepatic disease may be associated with mild increases in amylase primarily through release from injured mucosal epithelial cells. .
100

Lipase – As with amylase, although there is a significant amount of lipase located in the exocrine pancreatic glandular epithelial cell, it is not restricted to this epithelium. Different forms of lipase are found in the pancreas, adipose tissue, gastric mucosal epithelial cells, and duodenal mucosal epithelial cells. Based on this knowledge, one can immediately recognize a potential problem with mild increases in lipase activity just as it is difficult, if not impossible, to interpret mild increases in amylase. Renal disease / dysfunction commonly a result in mild increases in lipase just as it does with amylase; however, the specific underlying mechanism is not clear. Hepatic disease is commonly implicated with mild increases in lipase also. It is unlikely that this is a result of release from injured hepatocytes but the potential of decreased deactivation of pancreatic lipase by fixed macrophages of the liver must be considered just as it is for increases in serum amylase during active hepatic disease. Gastrointestinal disease has been reported to be associated with 2-5 fold increases in serum lipase activity above the high end of the reference range. Source of these increases is presumed in most cases to be from injured gastric and duodenal mucosal epithelial cells but the potential of secondary pancreatitis or simple partial obstruction of the pancreatic duct during primary active gastroenteritis should be considered also. Interpretation of increased serum lipase activity, as with amylase increases, can be difficult because of the various sources of amylase and the various affects by other organ systems within the abdominal cavity. The table below provides a quick guide to the interpretation of increased amylase activity relative to the presence or absence of active pancreatitis. Hypocalcemia – Hypocalcemia is commonly seen transiently during an active pancreatitis episode. Hyperglycemia – Mild to moderate hyperglycemia may be seen in patients with active pancreatitis due to a variety and combination of factors. Transient diabetes can occur with pancreatitis and true diabetes can occur with more chronic pancreatitis where there is significant loss of functional islet cell tissue. Canine Pancreatic Specific Lipase (spec CPL) –In 2006 the investigators in the Gastrointestinal Laboratory and IDEXX worked together to develop a more stable assay for canine pancreas specific lipase (SPEC-cPL) that is now available daily from the various IDEXX laboratories throughout the United States as well as world-wide through various IDEXX reference laboratories. This has made testing to support the veterinarian’s clinical suspect of active pancreatitis much more readily available and it has become a valuable adjunct diagnostic test as well as a test to allow accurate monitoring of the progression or regression of pancreatic acinar tissue injury. Preliminary data demonstrates high correlation with true cases (histologically confirmed) of active pancreatitis. In 2007 a patient-side SNAP® cPL™ assay was released to the veterinary market by IDEXX Laboratories. This test is a highly valuable adjunct to the clinical patient when pancreatitis is suspected; confirmation is possible within minutes following collection of a blood sample.
101

The 2011 Video Practitioner’s Case Challenge: Difficult Feline Cases
Fred Metzger DVM, Diplomate ABVP Metzger Animal Hospital
State College, PA Feline Hyperthyroidism Excessive secretion of the thyroid hormones, T4 and T3, results in signs that reflect an increased metabolic rate and produces clinical hyperthyroidism. It is most common in middle-aged to old cats but also develops rarely in dogs. Functional thyroid adenoma (adenomatous hyperplasia) is the most common cause of feline hyperthyroidism; in ~70% of cases, both thyroid lobes are enlarged. Thyroid carcinoma, the primary cause of hyperthyroidism in dogs, is rare in cats (1-2% of hyperthyroidism cases). The most common signs include weight loss, increased appetite, hyper excitability, polydipsia, polyuria, and palpable enlargement of the thyroid gland. GI signs are also common and may include vomiting, diarrhea, and increased fecal volume. Cardiovascular signs include tachycardia, systolic murmurs, dyspnea, cardiomegaly, and congestive heart failure. Rarely, hyperthyroid cats will exhibit apathetic signs (eg, anorexia, lethargy, and depression); weight loss remains a common sign in these cats. High basal serum total thyroid hormone concentration is the hallmark of hyperthyroidism and confirms the diagnosis. Although serum total T4 concentrations are high in most cats with hyperthyroidism, ~5-10% of cats have normal T4 values. Most cats with normal serum T4 values have either mild or early hyperthyroidism or hyperthyroidism with concurrent nonthyroidal illness, which has caused suppression of a high total T4 concentration to within reference range limits. In these cats, a high free T4 concentration along with consistent history and physical examination findings is diagnostic of hyperthyroidism. Cats with hyperthyroidism can be treated by radioiodine therapy, thyroidectomy, or chronic administration of an antithyroid drug. Radioactive iodine provides a simple, effective, and safe treatment and is considered the treatment of choice. The radioiodine is concentrated within the thyroid tumor, where it selectively irradiates and destroys hyper functioning thyroid tissue. Feline Pancreatitis Pancreatitis, an inflammatory condition of the exocrine pancreas, is a multifactorial disease in cats with a variable clinical course and outcome. Feline pancreatitis is more common than many practitioners realize and diagnosis of this elusive disease can be extremely challenging. Recognizing these challenges, Dr. Jörg Steiner and Dr. David Williams developed and validated the feline pancreatic lipase immunoreactivity (fPLI) assay for the diagnosis of pancreatitis at the Gastrointestinal Laboratory at Texas A&M University. The fPLI test has been shown to be both sensitive for detecting significant pancreatitis and specific for helping to rule out pancreatitis.
102

Previously, IDEXX had collaborated with Drs. Steiner and Williams to develop the Spec cPL® or canine pancreas-specific lipase test to assist in the diagnosis of pancreatitis in dogs. The acceptance of this test has been overwhelmingly positive. The most frequent question asked of IDEXX has been “when is the cat test going to be available?” In response to these inquiries, IDEXX has continued to work with Drs. Steiner and Williams to develop the Spec fPL™ (feline pancreas-specific lipase) assay. The Spec fPL assay utilizes monoclonal antibody and recombinant antigen technology and is available through IDEXX Reference Laboratories.
Prevalence of Pancreatitis in Cats
A 2007 study published in The Journal of Veterinary Pathology found 67% of cats presented for necropsy, irrespective of the cause of death, had histologic evidence of pancreatitis, including 45% in apparently healthy cats. Chronic pancreatitis was more common than acute pancreatitis (60% versus 15.7%).1 Although the prevalence of clinically significant pancreatitis is likely not this high, these findings suggest that pancreatic inflammation likely occurs with a wide variety of clinical conditions and potentially explains why mild pancreatic lesions are common even in clinically healthy animals.1 Cats with other common aliments, including diabetes mellitus, inflammatory bowel disease, cholangiohepatitis and hepatic lipidosis, often have concurrent pancreatitis that is usually overlooked.2–5
Clinical Signs
Cats with pancreatitis typically present with nonspecific signs of illness including lethargy, decreased appetite, dehydration and weight loss.6 Vomiting and abdominal pain are hallmarks of this disease in dogs, but in cats vomiting may be absent or intermittent and abdominal pain is rarely recognized. Diarrhea can be associated with pancreatitis or secondary to concurrent gastrointestinal disease. Icterus, fever and a palpable abdominal mass may be found on physical examination.
Laboratory Findings
Routine laboratory findings in cats with pancreatitis may be normal, nonspecific or attributed to concurrent conditions which are common in this species. CBC changes most commonly seen in cats with pancreatitis are nonregenerative anemia, leukocytosis and leukopenia.6 Increased liver enzymes, hyperbilirubinemia, hyperglycemia, azotemia, electrolyte imbalances and hypocalcemia can be seen on a complete biochemical profile.6 Serum activities of amylase and lipase are not helpful in diagnosing pancreatitis in cats.7 Serum trypsin-like immunoreactivity (TLI) concentration is specific for exocrine pancreatic function and is the test of choice for diagnosing exocrine pancreatic insufficiency in cats. However, in cats with clinical signs of pancreatitis, serum fTLI concentration has been shown to be poorly associated with histopathologic diagnosis and overall sensitivity of 28% and specificity of 75% for the diagnosis of pancreatitis.
103

Feline Hepatic Lipidosis Feline idiopathic hepatic lipidosis is the most common cause of feline hepatopathy. The etiology is undetermined but is associated with a period of anorexia (few days to several weeks), especially in obese cats. Factors that may trigger anorexia include a change of diet to initiate weight loss or other stressful events (eg, moving, boarding, death of other pets or owners). Secondary hepatic lipidosis is associated with either a primary metabolic (eg, diabetes mellitus) or GI disease (eg, inflammatory bowel disease, gastric foreign bodies, pancreatitis, or cholangiohepatitis) that can cause anorexia. Regardless of the inciting cause, the end result is excessive accumulation of triglycerides (fat) within the liver, which leads to severe intrahepatic cholestasis and hepatic failure. Clinical signs are variable but can include dramatic weight loss (30-40% of body weight, experimentally) due to anorexia, vomiting, lethargy, and diarrhea. Signs of hepatic encephalopathy are unusual, as are bleeding tendencies, but can be noted in advanced disease. Icterus or pale mucous membranes, ptyalism, hepatomegaly, and decreased body condition with retention of abdominal fat are commonly seen. Laboratory abnormalities include a nonregenerative anemia with poikilocytosis, stress leukogram, hyperbilirubinemia and bilirubinuria, mild to moderate increases in AST and ALT and marked increase in AP; GGT values are usually normal or mildly elevated. Hypoalbuminemia, prolonged coagulation profile, and hyperammonemia have been reported in advanced disease. If the cat is not icteric, bile acids can be evaluated. Postprandial values may be difficult to obtain if the cat cannot be force-fed. However, in most cases, fasting bile acids will be abnormal, precluding the need for the postprandial sample. Peritoneal effusion may be seen on radiographs. On ultrasonographic evaluation, the liver often appears diffusely hyperechoic when compared with the falciform ligament. If pancreatitis is also present, abdominal effusion and pancreatic changes can be identified with ultrasonography. Histopathology or cytology reveals vacuolated hepatocytes and cholestasis; lipid is identified within the vacuoles using Sudan black or oil Red O stain.
104

The 2011 Video Practitioner’s Case Challenge: The Emergency Patient
Fred Metzger DVM, DABVP Metzger Animal Hospital
State College, PA Hematology The hemogram is an important component in the workup of any emergency patient because erythrocyte, leukocyte and thrombocyte abnormalities are common in patients presenting to emergency practices. The three-minute peripheral blood film evaluation is an especially important tool to the emergency veterinarian and technician. ERYTHROCYTE QUESTIONS Is there evidence of erythrocyte regeneration? (Is there significant polychromasia/ reticulocytosis?) Polychromatophils are immature red blood cells that stain bluish because they contain RNA. Polychromatophils on blood smears prepared with Wright’s or modified Wright’s stain roughly correspond to reticulocytes on smears prepared with new methylene blue stain. Are nucleated RBC’s present? An inappropriate nucleated red blood cell response occurs when greater than 5 nucleated red blood cells per 100 white blood cells are present in the absence of polychromasia. Is auto agglutination present? Agglutination is unorganized three dimensional clumping of erythrocytes which must be differentiated from Rouleaux formation. When confirmed, agglutination suggests the presence of an immune mediated process with the likelihood of antibodies on the surfaces of the erythrocytes resulting in cross-linking of cells and the resulting agglutination. Are significant numbers of poikilocytes (abnormally shaped RBC’s) present? Abnormally shaped erythrocytes are termed poikilocytes and include artifactual changes (crenation) as well as true abnormalities (spherocytes, acanthocytes, schistocytes and leptocytes among others).
105

Are red blood cell inclusions present? Accurate characterization of various inclusions is an important aspect of blood film evaluation. Inclusions may include Heinz bodies, basophilic stippling, Howell Jolly bodies and certain infectious agents. PLATELET QUESTIONS Are platelet numbers normal, decreased or increased? On a well-prepared peripheral blood film where there is no significant platelet clumping at the feathered edge, the average number of platelets observed per 100x oil immersion monolayer field multiplied by 20,000 provides a good estimate of the number of platelets per micro liter. As a general rule, one should see a minimum of 8-10 platelets and a maximum of 35-40 platelets per 100 x oil immersion monolayer field of view. LEUKOCYTE QUESTIONS Is the total WBC count elevated, normal or decreased? Experience is required to make accurate cell count estimations directly from blood films. Subjective analysis of total leukocyte numbers may be performed by counting several 20X objective fields with 10-20 WBC’s/20X field considered as normal in dogs and cats. Another method utilizes counting several 100X oil immersion monolayer fields then multiplying the average number of leukocytes/100X oil immersion field by 2,000 to obtain a final estimated total WBC. Is a left shift present? Left shifts are characterized by increased numbers of immature neutrophils (band cells, metamyelocytes, etc.) in circulation. On blood films, band cells are distinguished from mature neutrophils in that the nucleus of the band neutrophil typically has parallel sides whereas that of the mature neutrophil is distinctly segmented. A left shift is a hallmark of inflammation; therefore, the accurate identification of band cells is extremely valuable to the veterinarian. A left shift may be the only indicator of active inflammation in veterinary patients because total white cell and neutrophil counts are frequently within the normal reference range.
106

Is toxicity present? Toxic neutrophils are a result of an accelerated rate of neutrophil production in response to inflammatory signals received by the bone marrow. Systemic toxemia is often associated with bacterial endotoxins but non-infectious causes also occur. Infectious diseases commonly accompanied by severe toxicity include feline pyothorax, pyometra, and severe canine prostatitis. Noninfectious causes associated with toxemia include immune-mediated hemolytic anemia, acute pancreatitis, tissue necrosis, zinc and lead toxicosis and cytotoxic drug therapy among others. Blood gases Metabolic acidosis is the most common acid base disturbance in veterinary practice however other disorders can occur with findings summarized: Primary Changes & Compensatory Response for Simple Acid-Base Disorders Primary Disturbance
pH Change Primary Change
Compensatory Response
Metabolic Acidosis ↓ pH ↓ HCO3 / BE ↓ PCO2
Metabolic Alkalosis ↑ pH ↑ HCO3 / BE ↑ PCO2
Respiratory Acidosis
↑ pH ↑ PCO2 ↑ HCO3
Respiratory Alkalosis
↓ pH ↓ PCO2 ↓ HCO3
Anion Gap
AG (mEq/L) = [(Na+ + K+) – (Cl- + HCO3-)] The AG is a major tool used to evaluate acid-base disorders Normal Values: 15-25 (dogs) High Values: Lactic acidosis, diabetic ketoacidosis, dehydration, ethylene glycol toxicity, hypocalcemia Low Values: protein wasting disorders, hypercalcemia Note that two relatively common presentations to emergency practice include ethylene glycol toxicosis and diabetic ketoacidosis which typically result in a normochloremic high anion gap metabolic acidosis.
107

Lactate Reference range: < 2.5 mmol/L 3- 5 mmol/L indicates mild systemic tissue hypoperfusion 5-7 mmol/L moderate tissue hypoperfusion >7 mmol/L severe tissue hypoperfusion Conditions associated with increased lactate: Physiologic: restraint, exercise, seizures Pathologic: (tissue hypoperfusion)
Bloat (GDV)- Cardiovascular disease -Pulmonary disease Sepsis-Hemorrhage Feline- saddle thrombus Heartworm disease (caval syndrome)
If blood lactate can not be sufficiently decreased after 1 hour of aggressive therapy then alternative treatment should be considered. In one study of GDV patients survival was 99% if the lactate was < 6 prior to surgery; decreased to 58% if > 6 prior to surgery. The positive predicted value of lactate to predict gastric necrosis was 75%. Coagulation The bleeding patient is a relatively common presentation to the emergency practitioner. Evaluation of primary and secondary hemostasis plus the fibrinolytic systems are important diagnostically in bleeding patients. Evaluation of platelet numbers and function Platelet defects can be quantitative defects (thrombocytopenia / thrombocytosis) or qualitative defects (abnormal function/thrombopathy). Domestic animals have a tremendous platelet reserve, so animals that have platelet defects may not have clinical evidence of bleeding. Normal platelet numbers for domestic animals are between 200,000 and 500,000 platelets / ul. The platelet count must drop below 50,000 platelets / ul before an animal has increased bleeding secondary to trauma. Spontaneous hemorrhage due to thrombocytopenia alone generally will not occur until the platelet count drops below 25,000 platelets / ul, if the platelet function is normal. -Adequate: For platelet numbers to be assessed as adequate, at least 8 platelets /oil power field, on average, should be present. Remember that only moderate and marked thrombocytopenias are readily recognized by blood smear evaluation. Bleeding time is an in-house test used to assess platelet numbers, platelet function, von Willebrand's factor, and vessel wall integrity. It measures the duration of bleeding from a small stab incision, usually made on the inside of the lip, called a buccal mucosal bleeding time. This test is helpful if a patient has nonspecific hemorrhage and adequate platelet numbers. It is best if this test can be performed while the patient still has clinical evidence of spontaneous hemorrhage.
108

LABORATORY EVALUATION OF COAGULATION/HEMOSTASIS The initial evaluation of bleeding disorders should include a platelet count, followed by a bleeding time test if thrombocytopenia is not present. The APTT tests for abnormalities in both the intrinsic and common pathways. This test measures the time required for fibrin clot formation in citrated plasma after the addition of reagents, which include calcium, a platelet substitute phospholipid, and a contact activator of the intrinsic pathway. This test is not affected by platelet numbers. Prolonged PTT occurs with factor deficiency in the intrinsic and/or common pathways. The OSPT tests for abnormalities in both the extrinsic and common pathways. This test measures the time required for fibrin clot formation in citrated plasma after the addition of calcium and tissue thromboplastin. This test is not affected by platelet numbers. Prolonged PT occurs with factor deficiency in the extrinsic and/or common pathways. Fibrinogen concentration may be measured directly with a fibrometer, or indirectly by a heat precipitation method. The heat precipitation method is too insensitive to detect hypofibrinogenemia, but is useful for evaluation of hyperfibrinogenemia. Fibrinogen concentration increases with many inflammatory disorders, and decreases with DIC, primary fibrinolysis, and defects (inherited or acquired) of fibrinogen production. A test for fibrin degradation products (FDPs) may be performed to test for excessive plasmin activity. Elevated FDPs indicate excess plasmin activity. This most commonly occurs with disseminated intravascular coagulation (DIC), although severe internal hemorrhage (from any cause), and primary fibrinolysis (a very rare condition) may also result in elevated FDPs.
109

The 2011 Video Practitioner’s Case Challange: The “ADR” Patient
Fred Metzger DVM, DABVP Metzger Animal Hospital
State College, PA 16801
Canine Hyperadrenocorticism (Cushing’s Disease) Hyperadrenocorticism can be pituitary-dependent (PDH), secondary to an adrenal tumor, or iatrogenic. The diagnostic approach to a dog with suspected hyperadrenocorticism involves the confirmation of hyperadrenocorticism followed by differentiation between PDH and an adrenal tumor. The most important diagnostic tests for hyperadrenocorticism are a careful and complete history, including recent corticosteroid administration (including eye, ear, and topical preparations), and a thorough physical examination. Also important is a minimal data base (CBC, chemistry and urinalysis). It is important to determine if signs of hyperadrenocorticism are present and to exclude nonadrenal illness. LABORATORY FINDINGS The hemogram may reveal a stress leukogram and mild erythrocytosis. Up to 80% of dogs with hyperadrenocorticism have high serum alkaline phosphatase level. Increased serum ALT and AST levels are common. Elevated serum cholesterol and mild hyperglycemia are common. Overt diabetes mellitus (glucose >250 mg/dl) occurs in up to 5% of dogs with untreated hyperadrenocorticism. Urinalysis often reveals a low specific gravity <1.020). Proteinuria is occasionally seen and can result from glomerular disease or urinary tract infection. All pituitary-adrenal function tests used to diagnose hyperadrenocorticism may show false-positive results in dogs with nonadrenal disease. Whenever possible pituitary-adrenal function testing should be postponed until the nonadrenal disease has been resolved. It is important for the clinician to be aware of the limitations and potential pitfall of pituitary-adrenal function tests. Also, a working understanding of the epidemiologic parameters sensitivity, specificity, prevalence and positive predictive value is helpful. Tests for diagnosing hyperadrenocorticism include the ACTH stimulation test, the low dose dexamethasone suppression test and the urine cortisol: creatinine ratio. Imaging studies and plasma ACTH levels and sometimes the high-dose dexamethasone suppression test or CT and MRI are used to differentiate PDH from adrenal tumors. DIAGNOSIS The ACTH stimulation test has a higher number of false negative results than the low-dose dexamethasone suppression test in dogs with naturally occurring HAC. The ACTH stimulation test is the best test to differentiate spontaneous from iatrogenic hyperadrenocorticism. Dogs with iatrogenic hyperadrenocorticism have a “blunted” or no response to ACTH administration. The ACTH stimulation test is performed by obtaining a serum sample for cortisol determination before and 1 hour after IV injection of 5 ug/kg of the synthetic ACTH (Cortrosyn). Once
110

reconstituted, the solution appears to be stable for at least 4 weeks if refrigerated. Alternatively, the remaining solution can be aliquoted and frozen. Alternatively, ACTH gel can be used. Acthar Gel (80 U/ml, Rhone Poulenc) is available but is very expensive. ACTH gel (usually 40 U/ml) is available from various compounding pharmacies. A recent study evaluated a few of these products and demonstrated adequate stimulation of the adrenal glands but varying peak response times. The reproducibility of these various formulations has not been stringently evaluated. Therefore, it may be prudent to assess the activity of each new vial by performing an ACTH stimulation test on a normal dog. The low-dose dexamethasone suppression test is useful in confirming the diagnosis of hyperadrenocorticism with an overall sensitivity of 90–95%. The low dose dexamethasone suppression test is performed by obtaining serum samples for cortisol determination before and 4 and 8 hrs after IV or IM administration of 0.01 or 0.015 mg/kg dexamethasone. In normal dogs, serum cortisol concentrations are suppressed below 1 ug/dl by 4 hrs after administration of dexamethasone and remain suppressed at 8 hrs. In contrast, cortisol concentrations in most dogs with hyperadrenocorticism remain above 1 ug/dl. Some laboratories use a 1.5 ug/dl cutoff for the diagnosis of hyperadrenocorticism and consider the 1.0 to 1.5 ug/dl range a “grey zone”. About 25% of dogs show a pattern of “escape” from suppression, a pattern diagnostic for PDH. The urine cortisol: creatinine ratio is a convenient screening test for hyperadrenocorticism. A morning sample should be collected at home by the owner. A normal value virtually excludes a diagnosis of hyperadrenocorticism. A positive (elevated) result must be confirmed with an ACTH stimulation test or a low-dose dexamethasone suppression test, due to high number of false positive test results. Endogenous plasma ACTH determination reliably distinguishes PDH from adrenal tumors in most cases. Contact the appropriate laboratory for collection and shipping instructions. Dogs with PDH have a normal to high ACTH levels, whereas dogs with adrenal tumors have low or undetectable plasma levels of ACTH. The high-dose dexamethasone suppression test can be used to differentiate dogs PDH from AT. The test is easily performed in practice. Dogs with adrenal tumors do not have suppression of cortisol after administration of a high dose of dexamethasone, with serum cortisol concentrations remaining >1.5 ug/dl during the testing period. Suppression of serum cortisol concentration to <1.5 ug/dl excludes an adrenal tumor. About 20% of dogs with PDH fail to demonstrate adequate cortisol suppression Additional testing is necessary to distinguish these dogs from those with an adrenal tumor. Many dogs with nonsuppressible PDH have large pituitary tumors. The use of percentage of suppression to differentiate between PDH and AT can be misleading in some cases. Canine Hypoadrenocorticism (Addison’s disease) Hypoadrenocorticism is an uncommon endocrinopathy, typically seen in young to middle-aged female dogs. No set of clinical signs is pathognomonic for hypoadrenocorticism and the severity and duration varies greatly between dogs. Moreover, the typical signs are seen in a wide variety of common diseases.
111

LABORATORY FINDINGS The classic laboratory abnormalities are hyperkalemia, hyponatremia, azotemia, mild to moderate acidosis and the absence of a stress leukogram. Hypercalcemia is seen in up to 30% of cases. The electrolyte abnormalities cannot be used to diagnose hypoadrenocorticism as they can occur in a variety of other diseases. Azotemia is typically prerenal in origin and resolves with appropriate fluid therapy. Urinalysis often reveals a decreased specific gravity, especially in the context of azotemia. Over 50% of dogs have an impaired ability to concentrate urine (USG < 1.030) in the presence of azotemia, which can cause confusion with primary renal failure. In some dogs the specific gravity is in the isosthenuric range. Electrocardiographic abnormalities are not uncommon in dogs with hypoadrenocorticism and radiographic abnormalities are occasionally seen. DIAGNOSIS Definitive diagnosis of hypoadrenocorticism requires the demonstration of inadequate adrenal reserve with an ACTH stimulation test. Serum cortisol levels are measured before and 1 hour after the intravenous administration of 5 micrograms/kg of synthetic ACTH. We prefer synthetic ACTH to compounded gel formulations. Cortisol levels can be measured in house or sent to the diagnostic laboratory. The ACTH stimulation test can be done immediately or after initial stabilization. In dogs with hypovolemia or significant dehydration, waiting until after initial fluid replacement may be advisable. Dexamethasone SP does not cross react with the cortisol assay and should be used in the initial treatment of acute adrenocortical insufficiency. In dogs that have received prednisone, prednisolone or hydrocortisone, glucocorticoid therapy is changed to dexamethasone for at least 24 hours before an ACTH stimulation test is done. Electrolyte abnormalities (hyperkalemia and hyponatremia) coupled with a subnormal response to ACTH indicate primary hypoadrenocorticism. Remember that some dogs with secondary hypoadrenocorticism may have hyponatremia. A plasma ACTH level is used to differentiate atypical primary hypoadrenocorticism from secondary hypoadrenocorticism and must be drawn before therapy is initiated. Plasma concentration of ACTH is high (often �500 pg/ml) in dogs with primary hypoadrenocorticism and very low or undetectable with secondary hypoadrenocorticism. This assay is available at several diagnostic laboratories. Contact the appropriate laboratory for collection, shipping and handling instructions. The authors would like to thank Peter Kintzer DVM, DACVIM for his assistance with this manuscript.
112

The 2011 Video Practitioner’s Case Challenge: The Senior Patient
Fred Metzger DVM, DABVP Metzger Animal Hospital
State College, Pennsylvania Chronic Renal Failure Chronic renal failure (CRF) is the most frequently encountered urinary system disease in geriatric dogs and especially cats. Laboratory profile abnormalities commonly associated with chronic renal failure include: anemia, azotemia, hyperphosphatemia, hyperkalemia/hypokalemia, metabolic acidosis and isosthenuria. Hemogram Anemia is a frequent finding with CRF patients. Underlying mechanisms include decreased renal erythropoietin production, decreased erythrocyte survival and possible uremic induced gastrointestinal ulceration with blood loss. The anemia associated with chronic renal failure is typically mild to moderate and generally non-regenerative. If bleeding associated with anemia is a prominent finding, some evidence of regeneration may be observed. Biochemical Profile Blood Urea Nitrogen (BUN) and Creatinine (Cr) Azotemia is defined as increased circulating levels of nitrogenous wastes and is characterized by elevated BUN and creatinine levels. Elevated BUN and creatinine are typical in CRF. BUN and creatinine are indicators of glomerular filtration rate but do not elevate in renal disease until greater than 3/4 of the nephrons are non-functional. BUN and creatinine must be interpreted in light of urine specific gravity. If BUN and creatinine are elevated and urine specific gravity >1.035 in dogs and 1.040 in cats, then the azotemia is most likely prerenal (resulting from hemoconcentration). If urine specific gravity is isosthenuric (between 1.008 and 1.017, essentially the specific gravity of plasma), then primary renal disease is suspected. It is important to note that the occasional feline patient may concentrate urine to 1.035 and still have renal failure-a paradoxical finding that is unique in feline patients. Phosphorus Phosphorus is also cleared via glomerular filtration and hyperphosphatemia occurs late in renal disease. In general, phosphorous levels correlate with BUN elevations. Phosphorus levels should be closely monitored during treatment for CRF because chronic hyperphosphatemia may result in renal secondary hyperparathyroidism and soft tissue mineralization.
113

Potassium Potassium is predominantly an intracellular ion so serum potassium levels do not necessarily reflect total body potassium. Both hyperkalemia (increased serum potassium) and hypokalemia (decreased serum potassium) can be seen in CRF. Hyperkalemia is seen in renal failure in association with metabolic acidosis caused by circulating uremic acids (sulfates and phosphates). In acidosis, hydrogen ions move into tissue cells in exchange for potassium ions which migrate from within cells into blood. Hypokalemia occurs when total body stores of potassium are depleted due to decreased renal tubular absorption and increased renal excretion. Under these circumstances, serum potassium levels may be low even in the face of acidosis. This can be a life-threatening event. Hypokalemia can occur in CRF, particularly in cats. Total T4 Decreased total T4 levels may be seen as a result of non-thyroidal illness in CRF patients. Total T4 should always be evaluated in any feline CRF patient because hyperthyroidism may occur concurrently with CRF or CRF may result from the decreased glomerular filtration associated with the treatment of hyperthyroidism. Urinalysis Urinalysis is critical to making the diagnosis of CRF but findings may be somewhat variable depending on the underlying etiologic mechanism causing the CRF. The most consistent finding is isothenuria (urine specific gravity between 1.008 and 1.017, the specific gravity of plasma). Casts may or may not be present. In true end stage renal disease, casts are rare to occasional and consist principally of granular or waxy casts. If the underlying cause is pyelonephritis, white cell casts may be seen. In this circumstance white cells and red cells may also be present in the urine. Protein is variable, again, dependent upon underlying cause of the chronic renal disease. Canine Hyperadrenocorticism (HAC) occurs when the adrenal gland produces excess adrenal hormones. The clinical signs and laboratory abnormalities are largely the result of excessive circulating levels of cortisol. The majority of cases are usually a result of a pituitary tumor (85-90%) causing adrenal hyperplasia or a primary adrenal tumor (10-15%). Most HAC patients are older dogs and clinical signs can be quite variable and include polyuria/polydipsia, bilateral alopecia, muscular weakness, and pendulous abdomen. Hemogram The most common hemogram change is the stress leukogram (leukocytosis characterized by lymphopenia, mature neutrophilia, eosinopenia, and variable monocytosis). Steroid hormones stimulate red cell production so high normal to mildly polycythemic red cell counts are not uncommon. Mild inappropriate nucleated red cell responses (5 to 10 nRBC/100WBC in the absence of polychromasia) are also sometimes present.
114

Biochemical Profile Hepatic Enzymes Elevated circulating corticosteroids induce production of a steroid specific hepatic isoenzyme of ALP. As a consequence, it is estimated that approximately 80% of all canine Cushing’s patients have elevated levels of ALP. High levels of circulating glucocorticoids also cause hepatocellular swelling with vacuolar degeneration (steroid hepatopathy). Steroid hepatopathy is associated with mild to moderate elevations in ALT as well as elevations in GGT. GGT elevations are probably secondary to intrahepatic cholestasis. Glucose Glucocorticoids are gluconeogenic, and Cushing’s syndrome is commonly associated with mild to moderate elevations in blood glucose. Values generally fall between the upper end of the reference interval (approximately 120 mg/dl) and the renal threshold (180 mg/dl). Roughly 10% of all dogs with Cushing’s also suffer from overt diabetes mellitus with fasting glucose levels of 250 mg/dl or higher. Total T4 Cushing’s patients may have decreased total T4 concentrations from non-thyroidal illness. Confirmatory thyroid testing (free T4, TSH assay) is recommended to differentiate thyroidal from non-thyroidal causes. Urinalysis Glucocorticoids block ADH receptors in the kidney, thereby inducing polydipsia and polyuria. As a result, urine specific gravity is often 1.020 or less. If diabetes mellitus is present, glucosuria with or without ketonuria (ketoacidosis) may Feline Hyperthyroidism Feline hyperthyroidism is a multisystemic metabolic disease and is the most common endocrinopathy in older cats. Hyperfuntioning adenomatous hyperplasia of the thyroid gland results in a variety of clinical signs and laboratory abnormalities. Thyroid evaluation (Total T4) should always be performed when evaluating the laboratory profiles of geriatric felines. Hemogram Slight polycythemia is found in more than 50% of hyperthyroid cats and macrocytosis may cause an elevation in the mean cell volume. Biochemical profile Elevations in ALT and ALP occur singly or in combination in 50 to 75% of hyperthyroid cats.
115

Closely monitor renal function because hyperthyroidism may mask decreased reduced glomerular filtration rates as a result of increased cardiac output associated with elevated thyroid levels. Total T4 The majority of hyperthyroid patients have elevated total T4 concentrations which confirm the diagnosis in cats with compatible clinical signs. Total T4 may be within the normal reference interval in patients with concurrent hyperthyroidism and non-thyroidal illness illnesses (chronic renal failure, diabetes, etc.). Confirmatory thyroid testing (free T4, T3 suppression test, thyroid radio nucleotide imaging) is recommended in cats with signs compatible with hyperthyroidism but normal total T4 levels. Urinalysis Urinalysis is usually unremarkable but watch for decompensating renal function when treatment for hyperthyroidism is initiated.
116
Non-healing Corneal Ulcers in Dogs
Amy Pauli, DVM, DACVO
There are many potential causes of delayed corneal healing in dogs. In this lecture we will first focus on contributing factors to delayed corneal healing. Then, we will discuss a specific form of chronic corneal ulceration called an indolent ulcer or SCCED (Spontaneous Chronic Corneal Epithelial Defect). 1. Ectopic cilia – These are hairs that protrude through the palpebral conjunctiva, typically several millimeters posterior to the eyelid margin. Ectopic cilia are usually present in young (less than one year of age) dogs, most commonly in Golden Retrievers, Shih Tzus, and Boxers. Dogs with ectopic cilia may have a history of a chronic corneal ulcer, recurrent corneal ulcer in the same location, or chronic ocular discomfort (especially with a “jerky blink”) without corneal ulceration. Detection of ectopic cilia can be very tough (especially in Golden Retrievers, as the cilia tend to be blond), and use of magnification is often necessary. Evert the eyelid to evaluate the palpebral conjunctiva several millimeters posterior to the eyelid margin, and focus your search in the area of the lid that lines up with the corneal ulceration. The most common location for ectopic cilia is in the central portion of the superior eyelid. Treatment for ectopic cilia is surgical excision of the hair and associated follicle, +/- adjunctive cryotherapy. This procedure is performed under an operating microscope. 2. Distichiasis – These are eyelashes that protrude from the eyelid margin. Distichia are common in dogs and often are an insignificant finding. However, when numerous or stout, they can cause ocular irritation. In addition, if distichia line up with an area of corneal ulceration, they may contribute to delayed corneal healing. Treatment (when indicated) consists of plucking the hair(s) (temporary fix) or cryotherapy. 3. Foreign body – Foreign material may be located in the conjunctiva, cornea, or behind the third eyelid. Foreign bodies are particularly common in hunting dogs. Magnification may be necessary in order to find the foreign body. The presence of a “jerky blink” in a patient should increase your index of suspicion for the presence of a foreign body. 4. Eyelid defects – Common eyelid defects that can contribute to corneal ulcer development and to delayed healing of corneal ulcers include eyelid margin masses, notch defects, and entropion. Treatment to aid healing of a corneal ulcer associated with one of these conditions can include contact lens placement or surgical correction of the eyelid defect. In cases of corneal ulceration associated with entropion, it is important to determine whether the entropion is primary (anatomic) or secondary (spastic). Patient signalment and history can help to make this determination. Placement of a contact lens or temporary tacking sutures to evert the eyelid are useful to temporarily alleviate the trichiasis to allow the corneal ulcer to heal. Once the ulcer has healed, re-evaluate whether the entropion is primary or secondary and thus whether or not permanent corrective surgery is indicated for the entropion.
117

5. Tear deficiency – There are two types of tear film abnormalities, including a quantitative tear film disorder (keratoconjunctivitis sicca) and qualitative tear film disorder (associated with a deficiency of lipid or mucin). Typical ophthalmic examination findings include thick, ropey ocular discharge that often clings to the ocular surface, corneal vascularization (especially located superiorly) and edema, a lackluster appearance to the cornea, and ocular discomfort (variable). In cases of corneal ulceration associated with a tear film deficiency, it can sometimes be difficult to know whether or not to continue (or initiate) tear stimulant therapy. If the corneal ulcer is superficial and not infected, tear stimulant therapy may aid corneal healing by improving the tear film. However, if the ulcer is not progressing toward healing within a week or two, consider discontinuing the tear stimulant as it may contribute to delayed corneal wound healing. Tear stimulant therapy may be contraindicated in treatment of deep or infected corneal ulcers as this therapy slows corneal vascularization (and thus corneal remodeling) and may potentiate infection. In addition, ointment formulations of tear stimulants (or any other medication) should be avoided in cases of deep or perforated corneal ulcers. 6. Corneal infection – In dogs, corneal infection is almost always associated with bacteria, and rarely with fungal organisms. Ophthalmic examination findings suggesting corneal infection include corneal infiltrate, corneal malacia (“melting”), loss of corneal thickness (possibly with a visible “divot”), reflex uveitis, and excessive ocular pain. The presence of corneal infection can be confirmed through cytology and culture, although caution should be used in collecting a sample for these tests if the ulcer is deep. Aggressive medical management or referral for surgical stabilization (conjunctival graft, etc.) should be performed, as indicated and elected by the client. Procedures like debridement and grid keratotomy are contraindicated in cases of deep or infected corneal ulcers as they increase the risk of corneal perforation. In addition, a grid keratotomy can spread infection deeper into the corneal stroma. 7. Self trauma – Self trauma is a common contributing factor in delayed healing of corneal ulcers. Therefore, an E-collar is often recommended for dogs with non-healing corneal ulcers. 8. Deficiency of corneal innervation – The cornea is innervated by the ophthalmic branch of the trigeminal nerve. Normal corneal innervation and sensitivity are essential for normal corneal wound healing. Potential causes of reduced corneal sensitivity include diabetes mellitus, chronic glaucoma, prior proptosis, as well as cavernous sinus and orbital fissure syndromes (which can affect cranial nerves III, IV, V, and VI). In addition, brachycephalics tend to have reduced corneal sensitivity. Delayed corneal wound healing should be expected in patients with a deficiency of corneal innervation. 9. Lagophthalmia – Lagophthalmia is defined as the inability to blink completely. This can be associated with exophthalmos [either pathologic (associated with a retrobulbar mass) or physiologic (common in brachycephalics with shallow orbits)], buphthalmos, or facial nerve paralysis. Frequent application of topical lubricants can aid healing of corneal ulcers associated with lagophthalmia. Placement of a partial temporary tarsorraphy suture to close down the palpebral fissure and reduce corneal exposure can also be helpful.
118

10. Corneal endothelial disease – The main function of the corneal endothelium is to keep the cornea dehydrated. The corneal endothelium is composed of a single layer of hexagonal cells that have little to no regenerative capability in adults. The number of endothelial cells decreases with age and secondary to some ophthalmic diseases. Cells can spread out to some degree to maintain their barrier and pump functions, but eventually decompensation occurs leading to corneal edema. Corneal edema due to corneal endothelial degeneration can contribute to delayed healing of corneal ulcers. Corneal endothelial degeneration can also be associated with a condition called bullous keratopathy. In this condition, corneal bullae (“blisters”) form when the corneal edema becomes severe enough. These bullae can rupture, resulting in formation of corneal ulcers. Treatment for corneal ulcers associated with corneal endothelial degeneration is primarily symptomatic, including hypertonic saline solution or ointment and topical antibiotic therapy. Surgical treatment is sometimes necessary. Options include thermokeratoplasty (in which a hand held thermal cautery unit is used to make superficial burns in the corneal surface to create scarring to reduce the formation of corneal bullae), corneal gluing, conjunctival flap placement, or corneal transplant. 11. Spontaneous Chronic Corneal Epithelial Defect (SCCED) – AKA Boxer ulcer, indolent ulcer, non-healing ulcer, rodent ulcer, etc. This type of chronic (>2 weeks duration) ulcer can occur in any breed of dog, and usually affected dogs are middle-aged to older. SCCEDs can occur spontaneously or in association with trauma. Ophthalmic examination findings include a superficial corneal ulcer with loose epithelial margins (look for fluorescein undermining, in which there is a halo of faint fluorescein staining around the margin of the ulcer associated with leakage of the dye under this loosely adherent rim of epithelial cells). These ulcers are variably painful (with chronicity, these ulcers are often better tolerated). There is a variable degree of corneal vascularization and edema associated with the SCCED (to some extent, this is also associated with the degree of chronicity), and this vascularization, if severe, can contribute to delayed corneal healing. The pathophysiology of this ulcer is not completely understood, but histologically the basement membrane of the corneal epithelium in the region of the erosion is completely absent or present in discontinuous segments. In addition, a superficial stromal hyaline acellular zone was found in 92% of SCCEDs in one study.1 It is thought that anterior stromal changes may prevent formation of adhesion complexes between the corneal epithelial cells and anterior stroma. Most treatment options for SCCED work by altering the physical or chemical environment of the anterior corneal stroma. The most commonly used treatments for SCCEDs include corneal debridement and grid keratotomy. Debridement involves use of cotton tipped applicators (or sometimes other instruments, such as an Excimer laser spatula or corneal burr) to remove the loose epithelial margins of the ulcer under topical anesthesia. The success rate for healing of SCCEDs with this treatment alone (using CTAs) is about 50%. A grid keratotomy is performed following debridement. In this procedure, a superficial grid is created across the ulcerated corneal surface and extending 1-2mm into the surrounding cornea using a small gauge needle (either a 25g needle in which a sterile hemostat has been used to bend the tip of the needle to limit the depth of penetration, or commercially available stromal puncture needle that already has a hooked end). An anterior stromal puncture (ASP) is performed similarly, but superficial dot micropunctures are created in the ulcerated corneal surface instead of a grid pattern. These
119

procedures can usually be performed with good restraint and topical anesthesia alone, but sedation may be needed for wiggly patients. The success rate for debridement with grid keratotomy (or ASP) is about 80%. These procedures can be performed every couple weeks as needed until the ulcer heals. Never perform a grid keratotomy or ASP in an infected or deep corneal ulcer, and NEVER perform these procedures in cats (grid keratotomy has been linked with corneal sequestrum formation in cats). Placement of a bandage soft contact lens can also be helpful, often in conjunction with debridement and grid keratotomy / ASP, to improve comfort and aid healing. Contact lenses can also be useful as a “shield” in cases of distichia (in which there are too many to pluck), entropion, or other eyelid abnormalities. Other treatment options include corneal gluing, thermokeratoplasty (described above), and superficial keratectomy (in which the superficial stroma in the region of corneal ulceration is excised with the aid of an operating microscope; requires general anesthesia). Corneal gluing involves application of a thin layer of tissue glue to the thoroughly dried ulcerated corneal surface following debridement. This procedure often requires sedation, as the eyelids must be held open for several minutes to allow the glue to polymerize. A contact lens may be placed following corneal gluing to aid glue retention and improve comfort. The glue sloughs on its own as the corneal ulcer epithelializes. Topical antibiotic treatment is indicated to help prevent secondary bacterial infection of the corneal ulcer. A recent study demonstrated that Terramycin actually aids healing of SCCEDs by increasing TGF-β, which helps the corneal epithelium slide across and adhere to the underlying corneal stroma.2 Gentamicin should usually be avoided for treatment of SCCEDs because it delays corneal wound healing. Topical and/or oral analgesic therapy should also be considered. Topical options include an opioid (morphine or nalbuphine) or NSAID (such as flurbiprofen). Caution should be used when treating with a topical NSAID in the face of corneal ulceration, though, as topical NSAIDs have been associated with sterile corneal melting. A topical cycloplegic (atropine) can also be considered, although atropine is contraindicated in patients with KCS or glaucoma. Oral treatment with tramadol and/or an NSAID may also be considered. Serum is also sometimes used for treatment of SCCEDs. Serum has anti-collagenolytic properties and thus aids healing of deep, “melting” corneal ulcers. At least one study demonstrated that serum had no effect on healing time of SCCEDs. Patients with SCCED should be rechecked every one to two weeks, and treatments (debridement, grid keratotomy, etc.) can be repeated as needed. Referral of these cases to an ophthalmologist may be considered at any point, but particularly if you are not seeing improvement (smaller ulcer with tighter epithelial margins) after one or two attempts at debridement (+/- grid keratotomy). Unfortunately, once a dog has developed this type of corneal ulcer once, he or she is predisposed to recurrence of SCCED in either eye.
120

References: 1. Bentley E, Abrams GA, Covitz D, et al. Morphology and immunohistochemistry of spontaneous chronic corneal epithelial defects (SCCED) in dogs. Invest Ophthalmol Vis Sci 2001 Sep;42(10):2262-2269. 2. Chandler HL, Gemensky-Metzler AJ, Bras ID, et al. In vivo effects of adjunctive tetracycline treatment on refractory corneal ulcers in dogs; J Am Vet Med Assoc 2010 Aug 15;237(4):378-386.
121

Non-healing Corneal Ulcers in Cats
Amy Pauli, DVM, DACVO
In this lecture we will discuss common causes for delayed healing of corneal ulcers in cats. An emphasis will be placed on feline herpes virus and its ocular manifestations. 1. Feline herpes virus 1 (FHV-1) – This virus is a member of the family Herpes-viridae and subfamily Alphaherpesviridae. The hallmark of this family of herpes viruses is latency that develops after the primary infection. FHV is readily transmissible between cats, and almost all cats have been exposed to this infection. Ophthalmic manifestations of FHV include conjunctivitis, symblepharon (areas of adhesion of conjunctival tissue, often involving the third eyelid), blepharitis, corneal ulceration, eosinophilic keratitis (EK), non-ulcerative stromal keratitis, corneal sequestrum, and keratoconjunctivitis sicca (KCS). There are many diagnostic tests available for FHV, including conjunctival cytology for evaluation of intranuclear inclusion bodies, conjunctival swabs and scrapings for PCR, virus isolation, and IFA, and serology. However, these tests are not commonly performed, as there are many false positives and false negatives. As a rule of thumb, a positive value is of limited value in the diagnosis of FHV-1 associated disease in cats, but a negative result via multiple testing methods may be helpful in ruling out FHV-1. Corneal ulceration associated with FHV tends to be either dendritic or geographic. Dendritic corneal ulcers are linear, branching ulcers. Often, there are multiple dendritic ulcers present. These ulcers are nearly pathognomonic for FHV. Geographic corneal ulcers are larger areas of corneal ulceration that are typically superficial and variably vascularized. Treatment of presumed FHV corneal ulceration consists of administration of topical and/or oral anti-viral and topical antibiotic medications. Options for topical anti-virals include 0.5% cidofovir, which has the advantage of being effective at twice daily administration, or idoxuridine or Trifluridine, which both should be administered at least 4-6 times daily. Famciclovir is an oral anti-viral medication that is generally safe for cats (use with caution in cats with renal or hepatic disease) and usually well tolerated. There is a wide range of published doses for this medication for cats. Lysine is an amino acid with anti-viral properties that is probably most useful between active flare-ups of FHV-related ophthalmic disease to reduce the frequency and severity of flare-ups. Topical antibiotics to consider include Terramycin, erythromycin, or a fluoroquinolone (ofloxacin or ciprofloxacin). Topical medications containing neomycin, including NeoPolyBacitracin, are not recommended for cats, as neomycin tends to be irritating, is not effective against the common causes of conjunctivitis in cats (Chlamydophila and Mycoplasma), and can potentially cause sudden death in cats. Corneal debridement and contact lens placement are sometimes used to aid healing of corneal ulcers in cats. NEVER perform a grid keratotomy in cats, as this procedure has been linked to corneal sequestrum formation in this species.
122

Follow up for patients with presumed FHV corneal ulceration includes rechecks every 1-2 weeks to evaluate for progress toward healing, and to assess for signs of possible secondary bacterial infection (corneal “melting”, infiltrates, or loss of corneal thickness). Although these ulcers can have a relatively chronic course even without complicating factors, cats with diabetes and those with a compromised immune system (older cats, those receiving systemic steroid therapy, and those with chronic systemic disease) should be expected to have even further delayed corneal healing. 2. Corneal sequestrum – A condition unique to cats in which there is an area of dead or devitalized corneal stroma. Potential causes of corneal sequestrum include FHV-1 and chronic ocular irritation (entropion, lagophthalmia, chronic corneal ulceration, etc.). The latter is a common cause in brachycephalic cats. Corneal sequestra are variable in appearance, from a poorly defined area of amber discoloration of the cornea (“tea staining”), to a well-demarcated, dark corneal lesion. Sequestra may be superficial or extend deeply into the corneal stroma, and they are variably vascularized. They are often associated with overlying and/or surrounding corneal ulceration. The clinical course of sequestra is variable. Some slough on their own as corneal vascularization extends deep to the sequestrum. However, the time frame for this to occur is variable, taking months or even longer in some cats. In some cases, a deep corneal defect results when the sequestrum sloughs, and this may warrant urgent surgical intervention. Treatment options for corneal sequestra include medical management (while waiting for the sequestrum to slough) with a topical antibiotic if there is an associated corneal ulcer, as well as a topical lubricating agent (ophthalmic gel or ointment) to help improve comfort. Surgical management includes a keratectomy (+/- conjunctival or corneal graft). Unfortunately, there is a risk of recurrence of the sequestrum, especially if there is some corneal staining remaining following surgery or sloughing of the sequestrum. 3. Entropion – In-rolling of the eyelid can be anatomic (primary) or spastic (secondary) in cats, as in dogs. Cats with chronic spastic entropion are more likely than dogs to require surgical correction because of more extensive hypertrophy of the orbicularis oculi muscle in cats. Temporary measures including contact lens placement or temporary tacking sutures should be used for entropion suspected to be (at least in part) spastic until the underlying issue (corneal ulceration, etc.) resolves. 4. Lagophthalmia – An incomplete blink can be associated with exophthalmos [either pathologic (associated with a retrobulbar mass) or physiologic (common in brachycephalics with shallow orbits)], buphthalmos, facial nerve paralysis, or eyelid agenesis (in which a portion of the eyelid does not form, allowing the facial hair to contact the cornea and also causing exposure, often with corneal ulceration). Frequent application of topical lubricants can aid healing of corneal ulcers associated with lagophthalmia. Placement of a partial temporary tarsorrhaphy suture to close down the palpebral fissure and reduce corneal exposure can also be helpful in some cases. Lagophthalmia associated with eyelid agenesis often requires surgery to recreate a more functional eyelid margin (sliding and rotational skin flaps, etc.). Cryotherapy can also be helpful in these cases to address the trichiasis.
123

5. Keratoconjunctivitis sicca (KCS) – In cats, KCS is most often associated with chronic FHV-1 related disease. When performing a Schirmer tear test (STT) in cats, keep in mind that stressed cats can often “turn down” their tear production. Therefore, do not make a diagnosis of KCS in a cat unless there is a low STT along with corneal changes (corneal vascularization, especially superiorly, a lackluster appearance to the cornea, etc.) and clinical signs (thick, ropey ocular discharge, blepharospasm, etc.) of dry eye. Treatment of KCS in cats consists of cautious use of a tear stimulant such as topical cyclosporine. This therapy may promote flare-ups of FHV ocular disease. Therapy for corneal ulceration associated with KCS in cats consists of use of a topical antibiotic to help prevent secondary bacterial infection, +/- a topical lubricating agent, +/- topical or oral anti-viral medication(s), +/- tear stimulant therapy. 6. Bacterial infection – Signs of possible bacterial infection of a corneal ulcer include corneal malacia (“melting”), corneal infiltrates, loss of corneal thickness, reflex anterior uveitis, and increased ocular pain. Corneal swab samples may be collected for cytology and culture to help direct therapy. However, samples should probably not be collected from the surface of a deep corneal ulcer as this risks rupture of the eye. Aggressive medical management consists of frequent application of potent, broad-spectrum topical antibiotics (such as combination therapy with ofloxacin and cefazolin solutions) and serum (canine serum is safe and effective for use in cats). Oral antibiotic therapy is not necessary unless the corneal ulcer has perforated. Mydriatic/cycloplegic therapy (atropine) can also be used to help improve comfort, although cats tend to be very sensitive to the bitter taste of atropine (with associated salivation and sometimes vomiting).
124

Should I Feed My Pet a Raw Diet?
Sandi Sawchuk DVM MSClinical InstructorUW Madison School of Veterinary Medicine
www.rawfeddogs.net
Raw feeding recipes Cow’s foot Goat Goat head Goat leg Lamb head Rat Water buffalo ribs Etc., etc. etc………
Sheep Head Recipe
1 sheep head Take the sheep head
and hand it to the dog. This can be fed as a stand-alone meal or with a side of organ meat. This meal may require several sittings for your dog to consume.
Categories of Raw Diets
Commercial available “complete” diets
Combination diets – grain /supplement mix to be added to raw meat
Home-prepared complete raw food (B.A.R.F.)
Why Raw (or homemade)?
Provides owner with a sense of involvement
Allows selection for specific ingredients
Avoid ingredients that owner perceives to be unhealthy (grains, by-products)
Diet can be customized for the pet’s preferences
Unsubstantiated Reasons
Improved longevity Superior oral care Disease resolution especially GI
issues Provides natural enzymes Commercial foods are filled with
toxic chemicals that will weaken the pet’s immune system and even kill them (melamine recall)
125

Dogs are not prone to clinical bacterial infections such as Salmonella and E. coli
No doggy odor – end ear infections once and for all
Decreased to non-existent vet bills Develops jaw, neck and shoulder muscles Less arthritis Dogs choke on kibble more than bones
The Opposition on Raw
Nutritional adequacy questionable Foreign body ingestion
GI obstruction Broken teeth Gut perforations
Infectious diseases
Nutritional Inadequacies
85 published recipes for dog and cat home-prepared diets Evaluated by AAFCO standards
86% inadequate in at least one nutrient 55% deficient in protein 77% deficient in taurine
Lauten S, et al. Computer Analysis of Nutrient Sufficiency of Published Home-Cooked Diets for Dogs and Cats Proc ACVIM Forum Baltimore, MD, 2005
Generic Pet Food Recipes
Vague ingredients Ground beef – how much fat? Cooked chicken – cut and cooking
method? Multivitamin – pet or human?
Problematic ingredients Bone meal, onions, garlic
Recipes may be outdated
Dog Sliders
Yunhee Kim By: Rachael Ray From: Lunch
Mini-burgers for the whole family—furry friends included. Always check with your vet about which foods are appropriate for you to share with your pet.
Ingredients: 1/2 pound ground lamb or chicken 1/2 cup cooked white or brown rice 1/4 cup plain yogurt 1/2 teaspoon ground cumin (eyeball it) Pinch of allspice ½ teaspoon salt Extra-virgin olive oil (EVOO), for drizzling 4 small round dinner rolls, split
Directions: Combine the meat, rice, yogurt, cumin, allspice and salt in a medium bowl. Form 4 patties and drizzle
each on 1 side with EVOO. Heat a nonstick skillet over medium-high heat and cook the patties, olive oil side down, for 3 to 4 minutes per side for well done but still juicy. Place the burgers on the rolls, chop into pieces and serve.
Infectious Diseases
Salmonella spp. Campylobacter Clostridium difficile, C.
perfringens,C. botulinum E. coli Yersinia enterocolitica Listeria monocytogenes Entertoxic Staphylococcus aureus
126

Even commercial frozen diets can be contaminated.
Salmonella spp. from 22% of commercial frozen diets
Spore forming bacteria from 100% C. difficile from 8% Chicken diets 4X more likely to
contain Salmonella Finley R. MSc Thesis, University of
Guelph, 2005
Fecal Shedding of Pathogens
7/16 dogs fed a single meal of contaminated raw meat shed Salmonella (0/12 fed a non-contaminated diet) Shed for up to 11 days
Finley R, et al. The risk of salmonellae shedding by dogs fed Salmonella-contaminated commercial raw food diets. Can Vet J. 2007;8:69-75
So what is the problem with this?
Your pet may get sick Reports on Salmonella gastroenteritis in Greyhounds and
cats The environment is being contaminated
Food bowls (metal and plastic) inoculated with Salmonellaand then cultured after cleaning 100% in controls (no cleaning) 96% with warm water rinse 96% in the rinse and scrub group 79% in the scrub with soap group 71% in the 10% bleach soak 67% in the 85°C dishwasher group 42% in the scrub plus bleach soak group No difference between metal and plastic
Survival of Salmonella Copenhagen in food bowl following contamination with experimentally inoculated raw meat: Effects of time, cleaning and disinfection. Weese JS, Rouseau J. Can Vet J 47:887-889, 2006
And…you could get sick.
Update: Recall of Dry Dog and Cat Food Products Associated with Human Salmonella Schwarzengrund Infections ---United States, 2008 (cdc.gov) Multi-state outbreak of infection with
Salmonella enterica If it can happen with dry it can happen
with raw Young, elderly and immunocompromized
people are especially at risk
CDC Pet Food Handling Guidelines
Washing hands is the most important step to prevent illness. Wash your hands for 20 seconds with water and soap right after handling pet food and treats, and especially before preparing, serving or eating food, drinks or preparing baby bottles
Preferably, people should feed their pet in areas other than the kitchen.
Wash pet food bowls, dishes and scooping utensils with soap and hot water regularly. Avoid washing these items in the kitchen sink or bathtubs to prevent cross-contamination. In households where there is no alternative, the sink area should be adequately sanitized after these items have been cleaned and removed.
Infants should not be bathed in kitchen sinks because of the risk of cross-contamination.
Do not use the pet’s feeding bowl as a scooping utensil – use a clean, dedicated scoop, spoon, or cup.
But Doc, I’m using “Human Grade Meat”…and I freeze it before feeding.
“Human Grade” ≠ absence of contamination “Human Grade” has no regulatory
definition Pet food manufactured under FDA
authority – not subject to USDA inspection
Freezing prevents bacterial growth – does not kill contaminants
127
Other Bugs….
Helminths and protozoans Toxoplasmosis Trichinella Tapeworms Taenia, Echinococcus Roundworms Sarcocystis
Viruses and Prions Pseudorabies (not in US-raised pigs) Avian influenza Spongiform encephalopathies (BSE, CWD)
Other Issues
Costs more Time consuming to prepare Lack specificity about the exact amount to
feed a particular pet “diet drift” – substitution or elimination of
ingredients over time Using pork chop instead of pork loin causes
increase in fat content and lower protein Are the nutrients digestible and
bioavailable? Many raw diets rely on bones as calcium
source – bioavailability can vary
Some clinics refuse to hospitalize a pet being feed a raw diet Risk of contaminating other pets and
staff Most boarded veterinary
nutritionists will not balance a raw diet if consulted
Delta Society’s Raw Protein Diet Policy
July 9, 2010 “After careful consideration of known scientific
facts, and on the unanimous advice of the Delta society Advisory Group, who reviewed and took under advisement recommendations made by experts in animal-assisted interventions, infection control, public health and veterinary medicine from Canada and the United States, the Board of Directors voted to preclude animals eating raw protein foods from participating in Delta Society’s Pet Partners Program.”
What About Grain-free Diets?
Grains ≠ carbohydrates Carbohydrates are essential fibers, sugars
and starches Root vegetables (potatoes, yams), yucca
(tapioca), taro root Grains (barley, wheat, corn, oats)
contain: Digestible and indigestible carbohydrates Fatty acids Proteins, vitamins and minerals
Do grains cause allergies?
Most common allergens (in descending order)
Dogs: beef, dairy, wheat, egg, chicken, lamb, soy, pork, rabbit, fish
Cats: beef, dairy, fish, lamb, poultry, barley/wheat, egg/rabbit
128

If it is kibble, it contains carbohydrates.
“sweet potatoes, peas, potatoes… potato protein”
Not carbohydrate-less
Homemade Diets
Do the five food groups appear in the recipe? A carbohydrate source from a cooked cereal
grain A protein source, preferably of animal origin A fat source A source of minerals, particularly calcium A multivitamin and trace mineral source
What is the type and quantity of the primary protein source? Animal-source higher quality than vegetable-source All animal sources are generally equivalent Final food should have 25 to 30% cooked meat for
dogs, and 35 to 50% cooked meat for cats
Is the carbohydrate source a cooked cereal? Is CHO present in a higher or equal quantity than
the meat source? 1:1 to 2:1 CHO to protein for cats 2:1 to 3:1 CHO to protein for dogs
129

ANALGESIA FOR FELINE ARTHRITIS
Margie Scherk, DVM, Dip ABVP (feline practice) Vancouver, B.C., Canada
Over the last two decades, the realization that we need to provide analgesia to cats has gradually gained ground. Most people accept that cats experience pain in the same way that we do. We know that the effects of pain are detrimental to well being in the short term, and that over longer periods, pain interferes with healing and causes disease. More recently, it has become clear that cats develop and suffer from degenerative joint disease (DJD). Our therapeutic options have expanded in pharmacological agents available as well as adjunctive approaches and we have a better idea how to use the drugs available to us to optimize efficacy and minimize adverse effects. UNDERSTANDING PAIN1,2
Pain evolved as a protective mechanism. Certain types of pain, such as physiologic pain, are beneficial for survival. For example, if you touch a hot stove, you withdraw your hand. Conditions resulting in damage to tissues or nerves, however, are pathological and include visceral and neuropathic forms of maladaptive pain. The nociceptive response begins with the free nerve endings signaling potential or actual tissue injury. (Figure 1) This results from a combination of mechanical (crush), chemical (mediators) or thermal input being translated (transduced) into electric impulses. These impulses are transmitted via the primary afferent (1st order) neuron to the spinal cord where they are modulated in the dorsal horn. The impulse is further transmitted via 2nd order neurons in the spinal tract to the thalamus where the message is received by a 3rd order neuron to be projected to the somatosensory cortex. It is at this
point that the impulse is experienced as pain and an appropriate response, such as moving away from the source of the damage, may be generated.
Figure 1: Pain pathway (Descartes)
The clinical implications of understanding this pathway are important. Rather than addressing the alleviation of pain at only one level, we have multiple points to target. Using a combination of agents in a multimodal/balanced approach is often more effective as well as safer than using a single modality to treat and prevent pain. (Figure 2) A
130

second concept, namely pre-emptive analgesia, is important especially in care of the patient who will undergo an elective procedure. By preventing the initial transduction and transmission of input before the insult occurs, it is much easier to keep patients comfortable than by trying to eliminate a process in progress. The term “pre-emptive analgesia” has now been expanded to include treatment for the appropriate duration of time, as premature withdrawal of treatment may reactive a pain process negating the previous use of analgesics. Figure 2: Sites of analgesic action
(Note: An alpha-2 agonist would not be a suitable choice in most older patient.) Obviously we must be cognizant of potential or known adverse effects of analgesic agents; these depend on both the type of drug and the underlying status of the patient. These include the integrity of renal and hepatic function, state of hydration and intestinal health. However, pain itself is dangerous: the cascade of catabolic and detrimental effects that occur as a result of uncontrolled pain may be a greater risk for the patient than the drugs are. The cycle of chronic pain impacts on quality of life dramatically. The patient who is unable to lie comfortably and does not sleep properly, becomes inappetent, resents being handled, and may appear to give up with the result that the client and veterinary team conclude that euthanasia is warranted.
131

Persistent pain results in negative physiologic and hormonal responses that are detrimental, prevent healing and may cause progression of underlying disease. Initially, the stress response increases survival (short-term) by increasing sympathetic tone. Through vasoconstriction, the benefits of an increased heart rate and cardiac output are realized. Resultant redistribution of blood flow favours muscles and respiratory drive simultaneously decreasing gastrointestinal tone. By enabling fight or flight, this may save the individual’s life. If this process doesn’t stop however, it results in muscle fatigue and low end-tissue oxygen levels. Occurring simultaneously, but with a less immediate effect, are the endocrine responses to pain. These include changes in many hormone levels. These changes, if persistent, are detrimental to the individual. Some of the hormones that are released include corticotropin, cortisol, more catecholamines, growth hormone, and glucagon to provide energy in the form of cAMP. This results in protein catabolism with concurrent decreased ability to heal and lipolysis. All three components of the renin, angiotensin and aldosterone system are increased which, along with anti-diuretic hormone, result in retention of water and sodium, increased potassium excretion and decreased glomerular filtration rate (GFR). Decreased insulin and testosterone are released, the former resulting in hyperglycemia and an impaired nutrient delivery to cells. Along with sleep deprivation from discomfort and fear, the patient may succumb to chronic physiologic and emotional exhaustion. RECOGNIZING PAIN
The signs of pain are generally more subtle in cats than in dogs. Some objective clinical signs indicative of pain include: 1-3
Inability to rest/sleep Inappropriate activity level Sitting in the back of the kennel Mental attitude/demeanour (stupor or anxiety) Changes in attitude/personality Poor hair coat Lack of comfort when palpated Facial expression, staring, fixed gaze, dilated pupils, “squinting” Lack of appetite and thirst (Self-mutilation) Vocalizations Posture Tachycardia Tachypnea Body temperature and blood pressure may be increased or decreased.
132

If a procedure is to be performed in an arthritic patient, given the similarities in pain perception between humans and cats, we may assume that the cat’s experience is similar to that of a human and risk erring on the side of humaneness. Pain affects psychological and emotional well-being negatively. Adults and older individuals are generally more stoic making it even harder to detect pain than in kittens. Seriously ill or obtunded patients are especially difficult to assess for pain as they are less likely to display behavioural signs of distress when compared to an otherwise healthy cat who has been injured.4 By taking the time to assess a cat’s body posture, facial expression, and response to handling, including gentle palpation of the painful site will provide a lot of information. The experience of pain is individual, and the patient’s response should be re-evaluated at each visit and several times a day when hospitalized. The truest assessment of the presence of pain is response to analgesics resulting in return to normal behaviours.3 However, the current adage is to treat predictable pain and one can safely predict that arthritis is painful. We can’t always know that it does hurt but we can know that it doesn’t. CHRONIC OSTEOARTHRITIC PAIN Recognition of chronic pain and arthritic pain is a relatively recent event. The incidence of osteoarthritis or degenerative joint disease appears to be much more common that previously thought and is probably a major cause of discomfort in ageing cats. Secondary osteoarthritis may be caused by joint trauma (i.e., fractures or ligamentous injuries), infectious or immune-mediated inflammation, compensation for congenital and developmental, as well as neoplastic, endocrine (diabetic) or metabolic conditions. Osteoarthritis involves cascade of mechanical and biochemical events resulting in articular cartilage deterioration, synovial membrane inflammation, soft tissue changes and osteophyte formation, with bone remodelling. In one study of the prevalence of degenerative joint disease (DJD) in cats5, Hardie et al reviewed 100 radiographs (taken as part of a diagnostic workup for multiple reasons) of cats over 12 years of age finding that 90% of these cats showed evidence of DJD. Interestingly, in only 4 of these patients’ medical records was a concern noted for DJD. Does this mean that, as in dogs, the clinical signs of OA do not correlate well with radiographic findings or does this mean that we are very poor at recognizing the signs? Godfrey6 performed another retrospective radiographic study looking at cats of all ages. This study showed radiographic changes suggestive of OA in 22% of cats; in 33% of these cats’ medical records, clinical signs were noted. In a third study 7, the prevalence of radiographic signs of DJD or OA in 218 cats was 33.9%, of clinical signs was 16.5% and most of these were in cats over 10 years of age. The most recent study8 prospectively evaluated cats of all ages to determine the prevalence of radiographic signs of DJD in cats of all ages. Most (92%) cats had radiographic evidence of DJD; 91% had at least 1 site of appendicular DJD and 55% had > 1 site of axial column DJD. Affected joints in descending order of frequency were hip, stifle, tarsus, and elbow. The thoracic segment of the spine was more frequently affected than the lumbosacral segment. Using a scale (0–4) to grade the severity of each of the radiographic changes identified, they found that for each 1-year increase in cat age, the expected total DJD score increased by an estimated 13.6%. They concluded that radiographically visible DJD is very common in domesticated cats, even in young animals and is strongly associated with age.
133

Lameness is uncommonly a clinical sign of this problem. Rather, the signs are insidious or attributed to ageing. Problems with movement include constipation, defecating outside of the litter box, falling when jumping onto or off of the bed, inability to climb stairs, inability to crouch to eat resulting in weight loss. Decreased grooming, objecting to being combed, reluctance to jump up or down, sleeping more, moving less, withdrawing from human interaction, and possibly even hiding are other signs of joint pain. When activity monitors have been attached to cats’ collars9, activity counts increased with NSAID (meloxicam) treatment suggesting alleviation of musculoskeletal discomfort. Regular nail trimming helps by maintaining proper joint relationships. Ramps and steps to favourite sleeping spots are helpful. Warm, soft, padded sleeping places for stiff, painful, possibly bony joints should be considered. Adding a litter box to reduce the distance between boxes may reduce accidents as well as encourage regular voiding and defecation. The rim of the box mustn’t be too high, nor the opening into the box too small. It should be scooped several times a day to encourage use. THERAPEUTIC OPTIONS The cat with joint pain is often an older patient who may have concurrent problems (e.g., renal disease) including some that may affect drug metabolism.10 Like painful patients of any age, they may be in a physiologic state that affects drug disposition, the most common ones being dehydration, inadequate tissue oxygenation, electrolyte or acid-base imbalances and malnutrition. The most common concern regarding NSAID side effects is the possible consequence of using this class of drug in a dehydrated patient resulting in effects on gastric mucosal health or on renal function. 11 Dehydration may be subclinical and difficult to assess in the very young and in the older cat due to the unreliability of skin elasticity in these age groups. Stool character (i.e., pellets rather than formed logs) can be helpful in evaluating hydration. Opioids are safe for pain relief in any age group and are excellent when used at the same time as other agents, especially NSAIDs. They are not, however, a first drug of choice for cats with arthritic pain as they are not very effective for DJD. This is not to suggest that they shouldn’t be used for “break-through” pain or for comfort during diagnostic testing. If they produce adverse side effects (euphoria, constipation and inappetence) in an individual patient they may be reserved for palliative hospice care. Pharmacokinetic data is lacking for safe, long-term use of many NSAIDs in cats. Carprofen half-life varies from nine to over 40 hours in cats12,13. As most NSAIDs have long half-lives in cats when compared to other species, one precaution to avoid toxicity is to reduce the frequency of administration. Metacam 0.5 mg/ml oral suspension has been granted a licence in the EU for the alleviation of inflammation and pain in chronic musculoskeletal disorders in cats. Pharmacokinetic studies as well as safety and efficacy studies have been performed to the satisfaction of the regulatory bodies. The registered dose is 0.1 mg/kg on the first day followed by 0.05 mg/kg orally once daily. This is the first NSAID licensed for long-term use in cats. In one study14, cats were treated for one month with meloxicam, clients felt that their cats were more willing to jump and the height of jumping increased during the study. Evaluation of the
134

cats by the veterinarian at the end of the month showed a significant reduction of gait stiffness. Two studies have evaluated long-term safety of this agent in older cats; one concluded that this agent is safe, efficacious and palatable for OA pain at 0.01-0.03 mg/kg PO q24h for a mean treatment duration of 5.8 months; no deleterious effect on renal function was detected in cats studied. Gastrointestinal upset in 4% of cats was the only adverse effect noted.15 The second, reviewed the medical records of cats over seven years of age treated for a minimum of 6 months with a daily maintenance dose of 0.02 mg/kg meloxicam and concluded that this dose does not hasten progression of renal disease in aged cats or aged cats with pre-existent stable IRIS stage 1-3 renal disease.16
A recently published study has shown that after oral administration, the major route of excretion of meloxicam in the cat is fecal and that the main pathway of biotransformation of meloxicam in the cat is oxidation. This is of importance because in cats, glucuronidation is limited as a metabolic pathway, whereas oxidation is not. Additionally, 21% of the recovered drug was eliminated in urine (2% as unchanged meloxicam, 19% as metabolites) and 79% in the feces (49% as unchanged meloxicam, 30% as metabolites). This is significant because it means that the product was already metabolized and inactivated by the time it reached the kidneys.17 After reviewing 108 papers on NSAIDs including all of the studies to date on their use in cats the International Society for Feline Medicine (ISFM) and the American Association of Feline Practitioners (AAFP) made the following summary point statement in their recently released document providing guidelines on the long-term use of NSAIDs in cats18: “to date, published studies of the medium-to long-term use of the COX-1 sparing drug meloxicam in older cats and cats with chronic kidney disease provides encouraging data that these drugs can be used safely and should be used to relieve pain when needed” This document can be found at: www.catvets.com/professionals/guidelines/publications as well as at: www.isfm.net/toolbox/info_sheets/NSAIDs_guidelines.pdf with a client brochure to educate regarding the safe use of NSAIDs in cats at: www.isfm.net/toolbox/info_sheets/NSAIDs_client%20leaflet.pdf. A suitable protocol for a cat with pain from DJD might be baseline NSAID (such as meloxicam) with intermittent use of an opioid (such as burprenorphine) when break-through pain is evidenced by a decrease in appetite or mobility or social withdrawal. The key to safe chronic NSAID administration in cats is the use of the lowest effective dose and avoiding use, or using lower initial doses (based on lean body weight), in cats with renal disease. Ensure the patient is hydrated and give the NSAID with food. Individual patients respond differently to the same agent and dose. In most cases, NSAIDs are most effective when used in conjunction with other treatment modalities. Disease Modifying Osteoarthritis Agents19 One approach that has received a lot of attention and research in the past ~15 years, has been looking for ways to slow the progression of cartilage degradation as well as to promote rebuilding of healthy matrix. Products have been developed that, in research on humans and dogs, have been shown to be beneficial in enhancing hyaluronic acid production, inhibiting
135

catabolic enzymes in osteoarthritic joints, and encouraging normalization of the synovial fluid and joint cartilage matrix. Studies using radio-labelled compounds have shown that 87% of orally administered glucosamine is absorbed and is incorporated into the cartilage matrix. Glucosamine provides raw materials for synthesis of glycosaminoglycans. Since chondrocytes obtain preformed glucosamine from the circulation (or synthesize it from glucose and amino acids), adequate glucosamine levels in the body are essential for synthesis of glycosaminoglycans in cartilage. Glucosamine is required for the production of hyaluronic acid by synoviocytes. In vitro studies indicate that administration of glucosamine may normalize cartilage metabolism and stimulates the synthesis of proteoglycans. In one study, glucosamine stimulated synthesis of glycosaminolgycans, prostaglandin and collagen by chondrocytes and fibroblasts, suggesting it may actually up-regulate their synthesis. Chondroitin Sulfate (CS) is a long chain polymer of repeating disaccharide units. It is the predominant glycosaminolycan found in articular cartilage and can be purified from bovine, whale, and shark cartilage sources. Bioavailibilty studies in rats, dogs and humans have shown that 70% of orally administered CS is absorbed, some of it instact. Studies in rats and humans using radiolabeled CS have shown that CS does reach synovial fluid and articular cartilage. Hyaluronate concentrations and viscosity were shown to be increased, and collagenolytic activity was decreased, in the synovial fluid of human osteoarthritis patients treated with CS for 10 days. Both oral preparations (CosequinR) and parenterally injected preparations (AdequanR) have been shown to have therapeutic benefit in in vivo studies. One factor of note is that a polysulfated glycosaminoglycan, such as AdequanR, is a heparin analog, resulting in a transient prolonged partial thromboplastin time. Avoid using it in cats with bleeding disorders or pre-operatively and do not use it concurrently with NSAIDs that have potent anti-thromboxane activity. Cartrofen VetR is a pentosan polysulfate that is approved in Canada and Europe. In osteoarthritic dogs clinical improvement was noted with its use. Like AdequanR, it should not be used concurrently with NSAIDs with anti-thromboxane activity. Diet Weight loss should be encouraged in the obese, arthritic cat to reduce the pressure on joints10. The addition of omega 3 fatty acids may be beneficial by blocking the production of prostaglandins from arachadonic acid in the inflammatory cascade. A therapeutic prescription diet for joint health (Hill’s j/d, 505.7 kcal/cup) is available in both a canned and a dry formulation; to date the author is not aware of peer-reviewed papers on this diet. Royal Canin has developed Mobility Support (391 kcal/cup) for cats. A recently published study20 comparing this diet to the identical diet without the added high levels of eicosapentaenoic acid (EPA), and docosahexaenoic acid (DHA) and supplemented with green-lipped mussel (GLM) extract and glucosamine/chondroitin sulfate. Forty cats with not detectable systemic disease but with radiographic evidence of at least one affected joint and who showed an aversive response to manipulation of that joint were fed one of the two diets (control or test diet) for nine weeks. Interestingly, clients reported an improvement in quality of life regardless of diet fed, but when objective measures were evaluated including accelerometry to assess mobility, cats on the test
136

diet had significantly greater improvements. These included an increased ability to jump, increased time spent eating, less time sleeping, increased playing and interacting with other pets. In an earlier study21 that looked at efficacy and tolerance of an extract of GLM in dogs with DJD, a similar subjective improvement was noted by clients whether the dogs were receiving placebo extract or GLM extract. Over time, by 56 days, a difference was noted and the dogs on the test extract showed significant improvement. Thus, dietary modulation might be one modality to include in the therapy of cats with DJD-associated pain. Therapeutic exercise Moderate exercise has benefits in maintaining range of motion in the face of joint capsule fibrosis, to maintain/build muscle mass and maintain/build healthy articular cartilage. In acute flare-ups, restricting activity may be warranted. Additional therapeutic considerations Pain pre-exists in a visiting or hospitalized cat with arthritis and may be part of the condition for which the patient is presented to us. Nursing care can go a long way to improving the patient’s experience. Thoughtful and gentle handling goes a long way to reduce the stress, distress and discomfort of the hospital visit. Be cognisant of positioning and pay attention to padding surfaces. If a patient is uncomfortable when an elbow is extended for blood collection or catheter placement, consider using the medial saphenous vein instead. Soft, warm places to lie and hide are desirable. Quiet, calm surroundings decrease the stress. Clean litter trays should be as spacious as possible and have low edges for ease of access. These considerations translate into the home environment as well: ramps and steps may help the cat access favourite resting places and the distance to any litter box should be minimal. Acupuncture may be considered and can safely be combined with pharmacologic approaches. While efficacy has been shown for acupuncture in a few conditions in humans, there is no solid scientific evidence at the time of writing that clearly supports its efficacy in cats.22
References 1. Lamont LA, Tranquilli WJ, Grimm KA. Physiology of Pain. Vet Clin North Am Small Anim
Pract 1997; 27(4): 703-728. 2. Mathews KA. Relieving Pain: Assessment and Management of Post-Operative Pain in Dogs
and Cats. CD: www.jonkar.ca 3. Mathews KA. Pain Assessment and General Approach to Management. Vet Clin North Am
Small Anim Pract 1997; 27(4): 729-755. 4. Hansen B. Acute Pain Management. Vet Clin North Am Small Anim Pract 2000; 30 (4): 899-
916. 5. Hardie EM, Roe SC, Martin FR. Radiographic evidence of degenerative joint disease in
geriatric cats: 100 cases (1994-1997). J Am Vet Med Assoc 2002: 220(5): 628-32. 6. Godfrey DR Osteoarthritis in cats: a retrospective radiological study. J Small Anim Pract
2005: 46, 425-429. 7. Clarke SP, Mellor D, Clements DN, et al. Prevalence of radiographic signs of degenerative
joint disease in a hospital population of cats. Vet Rec 2005:157, 793-799.
137

8. Lascelles NDX, Henry JB, Brown J, et al: Cross-Sectional Study of the Prevalence of Radiographic Degenerative Joint Disease in Domesticated Cats. Vet Surg 39 (2010) 535–544.
9. Lascelles BD, Hansen BD, Roe S, et al. Evaluation of client specific outcome measures and activity monitoring to measure pain relief in cats with osteoarthritis. J Vet Intern Med 2007; 21:410–416.
10. Beale BS. Orthopedic problems in geriatric dogs and cats. Vet Clin North Am Small Anim Pract 2005; 35 (3): 655-74.
11. Clark TP. The clinical pharmacology of cyclooxygenase-2-selective and dual inhibitors. Vet Clin North Am Small Anim Pract 2006; 36 (5): 1061-85.
12. Taylor PM, Delatour P, Landoni FM, et al. Pharmacodynamics and enantioselective pharmacokinetics of carprofen in the cat. Res Vet Sci 1996:60, 144-151.
13. Parton K, Balmer TV, Boyle J, et al. The pharmacokinetics and effects of intravenously administered carprofen and salicylate on gastrointestinal mucosa and selected biochemical measurements in healthy cats. J Vet Pharmacol Ther 2000:23, 73-79.
14. Clarke SP, Bennett D. Feline osteoarthritis: a prospective study 28 cases. J Small Anim Pract 2006: 47, 439-445.
15. Gunew MN, Menrath VH, Marshall RD. Long-term safety, efficacy and palatability of oral meloxicam at 0.01-0.03 mg/kg for treatment of osteoarthritic pain in cats. J Feline Med Surg 2008;10(3):235-41.
16. Gowan R, Lingard A, Johnston L, et al. Retrospective case control study of the effects of long-term dosing with meloxicam on renal function in aged cats with degenerative joint disease. J Feline Med Surg 2011 (accepted, in press).
17. Grude´ P, Guittard J, Garcia C, et al. Excretion mass balance evaluation, metabolite profile analysis and metabolite identification in plasma and excreta after oral administration of [14C]-meloxicam to the male cat: preliminary study. J. Vet. Pharmacol. Therap. 2010; 33, 396–407.
18. Sparkes AH, Helene R, Lascelles BCX, et al. ISFM and AAFP consensus guidelines: Long-term use of NSAIDs in cats. J Fel Med Surg 2010: 12 (7): 521-538.
19. McLaughlin R. Management of Chronic Osteoarthritic Pain. Vet Clin North Am Small Anim Pract 2000; 30(4): 933-49.
20. Lascelles BDX, Depuy V, Thomson A, et al. Evaluation of a therapeutic diet for feline degenerative joint disease. J Vet Intern Med 2010 May-Jun;24(3):487-95.
21. Pollard B, Guilford WG, Ankenbauer-Perkins KL, et al. Clinical efficacy and tolerance of an extract of green-lipped mussel (Perna canaliculus) in dogs presumptively diagnosed with degenerative joint disease. New Zealand Veterinary Journal 54 (3); 2006, 114-118
22. The National Institutes of Health (NIH) Consensus Development Program: Acupuncture (website) http://consensus.nih.gov/1997/1997Acupuncture107html.htm Accessed January 8, 2010.
138

UNTANGLING THE COMPLEXITIES OF THE FLUTD COMPLEX
Margie Scherk, DVM, Dip ABVP (feline practice)
Vancouver, B.C., Canada
The characteristic signs of feline lower urinary tract disease (FLUTD), regardless of etiology, are hematuria, stranguria and pollakiuria. There are numerous causes for these signs, and they merely localize the problem to the bladder or urethra. Thus, In addition to the aforementioned clinical signs, a cat may urinate in inappropriate and/or unacceptable places (periuria), may vocalize or be agitated from discomfort, and, in the case of urethral obstruction, may present with dysuria (difficulty urinating). Clients may mistake the staining for difficulties defecating or may notice excessive grooming of the ventral abdominal or perineal region. The purpose of this presentation is to look at the FLUTD from a pathomechanical perspective as a means to identify causes, to interpret sometimes confusing urinalyses and to guide in deciding when to pursue further diagnostics. The goal of investigative testing is to determine whether a cat has a specific disorder rather than an idiopathic one and, in the former case, what the appropriate therapy is. Inflammation, regardless of cause (crystals, stones, infection, idiopathic) results in pain upon distention of the bladder or urethra. This pain causes the patient to empty their bladder more often, resulting in smaller volumes of urine being voided. Blood may be present as the fragile epithelial lining is stretched or from trauma caused by crystals or stones. The bladder will be small or even empty upon examination of the patient. These clinical signs localize the problem to the lower urinary tract. But they do not reveal the cause. Should there be sufficient protein and or debris to cause intraluminal urethral obstruction, the patient will strain ineffectually producing minimal or no urine but present with a large, full bladder. If the urethral wall itself is thickened (e.g., urethral tumour) or the outflow tract is compressed by a structure external to it (e.g., prostate, caudal abdominal mass), the presenting signs (voiding frequency, volume, bladder size) will be as noted. Regardless of cause, life-threatening systemic effects (depression, acute renal failure, hyperkalemic bradyarrythmia, etc) will occur if the obstruction is not resolved. Table 1: Etiologic categories to consider when evaluating a cat with LUTD Metabolic (e.g., struvite crystalluria, calcium oxalate uroliths) Infectious (e.g., bacterial cystitis: hematogenous or ascending) Trauma (e.g., sacrocaudal fracture, urethral catherization trauma) Neurogenic (e.g., sacrocaudal disease, dysautonomia) Iatrogenic (e.g., trauma to urethra from catheterization; irritation from reverse flushing solutions) Anatomic abnormalities (e.g., congenital urethrorectal fistula, urachal diverticulum) Neoplastic (transitional cell carcinoma of bladder, prostatic adenocarcinoma) Idiopathic (e.g., interstitial/sterile/idiopathic cystitis) In young cats, the largest proportion of cases of LUTD are idiopathic in origin with uroliths and urethral plugs as the other two major etiologies. Over the past 20 years, the composition of urinary crystals and stones has shifted away from struvite as the main type, to calcium oxalate. Plugs remain composed of inflammatory protein matrix (Tamm Horsfall mucoproteins) and trapped sediment components. In cats over ten years of age however, bacterial cystitis and ureteronephroliths are the most common causes of lower urinary tract disease, with a small proportion of cats in this age group having neoplasia.
139

The frequency of feline lower urinary tract neoplasia is rare; over a ten year period, the Veterinary Medical Data Base recorded only 69 urinary bladder tumours. Transitional cell carcinoma is the most common urinary bladder tumour in the cat. The history and examination of the patient will help to identify predisposing factors for lower urinary tract disease. These include being overweight (body condition score); Persian cats are over-represented in cats afflicted with Feline Idiopathic Cystitis (FIC); Persians, Himalayan and Burmese are over-represented in cats with CaOx susceptibility; male cats are more likely to become obstructed; older cats are more likely to have bacterial infections or neoplastic conditions of the lower urinary tract. Younger cats with the aforementioned clinical signs are more likely to have urolithiasis as the cause. Living strictly indoors, in a multicat environment, being fed dry food and having a nervous temperament have been associated with greater incidence for FIC. A key concept in pathophysiology that applies to diseases of the lower urinary tract as well is that of a susceptible individual in a provocative environment (internal or external). For example, not every Persian or cat in a multicat household experiencing similar degrees of social stress or eating a diet that results in a specific urinary pH will succumb to FIC or urolithiasis; the individual has to be predisposed and a threshold is exceeded. History Questions to ask include those regarding the initial episode, frequency of recurrence and duration of clinical signs. If there is a seasonal pattern or if signs follow a disruption, FIC may be more likely. If the cat lives alone, there may be sources of stress (emotional/psychological or nutritional). If the affected cat lives with other cats it is important to try to ascertain how well the individuals co-exist. Are the resources (food, water, resting perches, clean litter) plentiful and in multiple locations? If inappropriate urination is occurring, are the locations selected random or is there a clear preference for location or substrate? If there appears to be, a behavioural component may be considered more likely. (It is a fine line between purely physical and behavioural causes as the former may result in distress as well as negative associations with the litter box.) Examination With regards to the lower urinary tract, determining the size of the bladder directs preliminary therapies and diagnostics. Cats often resent palpation of the caudal abdomen when they have LUTD. A large bladder raises concern for urethral obstruction; should the patient be depressed or obtunded, therapeutic intervention to stabilize cardiovascular function, restore electrolyte balance and relieve the obstruction become the priorities with evaluation of urinalysis to determine cause taking a lesser urgency. If the cat is alert, relief of obstruction, analgesia and diagnostics are appropriate goals. If the bladder is small and the patient is alert, relief of pain and diagnostics are warranted. If the cat has a small bladder and is depressed, consideration should be given to the possibility of a ruptured bladder subsequent to trauma or obstruction; this is cause for urgent evaluation of electrolyte status and surgery may be required. When urethral obstruction exists, cardiac irregularity and bradycardia may indicate significant hyperkalaemia. In male cats, bruising of the penis and prepuce +/- swelling may be present when obstruction (partial or complete) play a role.
140

Diagnostics If a cat is extremely depressed or unconscious upon presentation or is anaesthetized for the relief of obstruction or radiographic contrast studies, a rectal examination should be performed as stones may be located and manipulated allowing easier, less traumatic passage of a urethral catheter. The urethra and prostate should be assessed digitally for evidence of thickening (fibrosis, neoplasia, abscessation) as well. Serum biochemistries and hematology are part of a minimum database. In the case of unobstructed disease in a cat without concurrent systemic disease (e.g., chronic renal insufficiency or diabetes in an older cat), the results of these tests should fall within reference intervals. The obstructed cat may have dramatic hyperkalemia +/- hypocalcemia with academia, hyperglycemia and marked azotemia with variable elevations of creatine phosphokinase. Subsequent to relief of obstruction, diuresis and a reduction in azotemia may be anticipated; resolution of acute renal failure is facilitated through appropriate fluid support and will take several days-weeks. Urinalysis: Key to this discussion is the urinalysis. In the cat who is not obstructed and who ahs a small bladder, therapy prior to urinalysis should be restricted to analgesia (and fluid therapy if needed). Assumptions should be avoided as to etiology of the LUTD as treatments may be of no value, interfere with future diagnostics or be harmful. In the case of FIC, diagnostics may appear to be helpful but, as it shows a waxing-waning course and clinical signs pass in approximately ten days, resolution of signs may be misinterpreted as therapeutic success. The method of collection of the urine sample must be considered in interpreting results. Wherever possible, shaking/agitating the bladder to resuspend gravitationally dependent sediment components before collecting the sample will improve the yield of the urinalysis. The optimal sample is collected via cystocentesis. Advantages to this technique include greatest reliability for culture and sensitivity (C&S) results. The presence of small amounts of blood can be misleading; examining a small amount of voided urine for blood and hemoglobin helps to determine whether blood was technique induced. This technique evaluates renal, ureteral and bladder health but fails to assess urethra and prostate. Voided samples may be collected ideally mid-stream, however this occurs infrequently and even when caught in a collection device may be contaminated by running over perineal fur. Thus, >10,000 colony forming units (cfu)/ml of a single organism should be grown on C&S to consider the urinary tract as being the source of the bacteria. Samples so collected do, however, offer the advantage of reflecting the entirety of the urogenital tract as well as being reliable as regards the presence of lesion-sourced blood or hemoglobin. More often, voided samples are collected from the treatment table, cage floor or carrier. They can be collected from a disinfected litter tray filled with (washed and dried) aquarium gravel. Because the bladder is not agitated prior to collection, they fail to reflect sediment proportionately as sediment remains in the bladder as it contracts, thus samples collected in this manner may underestimate the degree of inflammation, crystalluria, etc. Samples collected during catheterization for relief of obstruction may be useful for initial evaluation, however, C&S results may be affected by the difficulties in maintaining sterile procedure during catheterization resulting in the introduction of bacteria.
141

A urinalysis consists of macroscopic evaluation (appearance, concentration, semiquantitative urine biochemical dip strip tests for pH and urine constituents: protein, glucose, blood, etc.), urine specific gravity assessment and microscopic evaluation of spun urine sediment (cells, crystals, bacteria, etc.). Urinalysis is a procedure that is susceptible to many variables (e.g., age of sample, temperature, etc.), making consistency in protocol and technique very important. The length of these proceedings notes prevents a complete discussion; selected points are included. Samples evaluated within 30 minutes of collection at body temperature will provide the most reliable results. If it cannot be examined in this time frame the following suggestions will help to preserve the integrity of the specimen. 1. Refrigerate at 5C for two-three hours or possibly overnight. The sample should be warmed to
room temperature before analysis for accuracy of urine specific gravity and for glucose assessment. Do not freeze the sample.
2. Protect the sample from light. Bilirubin becomes undetectable within one hour of exposure to sunlight.
3. Casts and cellular material deteriorate in alkaline urine. Over time, more crystals will develop depending on the pH of the sample therefore the pH should be determined promptly.
4. Regarding materials used: urine strips should be kept dark and cool (but not refrigerated) and the refractometer should be kept at room temperature.
Colour, turbidity and odour should all be noted on the room or body-temperature sample. The concentration of the sample is very important in interpreting the significance of various findings. Urine specific gravity (usg) is valid when measured using a refractometer as the pad for usg incorporated on some urine strips is developed for human urine, detecting a maxiumum usg of 1.030, which is inadequate for feline urine. Veterinary refractometers measure the widest range of specific gravity and are, therefore best suited for cat urine, which may have a usg in excess of 1.080. Urine biochemical evaluation relies on the dip strip dry chemistry reactions. In addition to the usg, nitrate and leukocyte pads are inaccurate in non human animals. Interpretation of all of these colourometric tests relies on subjective evaluation by different individuals of variably coloured urine in often poorly lit areas thus require careful interpretation. Colour comparisons are subjective, are affected by coloured urine constituents. They should be done by a trained individual, in a consistently, well lit area with fresh urine. The most over-interpreted parameter is pH. The pH of urine in the healthy “normal” cat generally ranges between 6.0-7.5. The pH of urine least likely to result in crystal formation is 6.2-6.4 however, in dilute enough urine, crystals are unlikely to form, regardless of pH. Measured pH values are accurate only to within 0.5 units, meaning that the colour subjectively translated into a pH value is x +/- 0.5, resulting in one whole unit variability: pH meters are inexpensive and are most accurate. However, many patient factors affect urine pH. The pH of the urine at the time of sampling is a reflection of many factors summated over the past hours during which the urine was being produced. Factors such as fear and stress tend to raise the urine pH; this may be misleading. During the postprandial period the total body pH rises because of HCl acid secretion into the stomach, resulting in a temporarily higher urine pH.
142

While we associate Ca oxalate crystals with an acidic pH, in fact they can occur at any urine pH. Monohydrate crystals at a low specific gravity reflect toxicosis such as from ethylene glycol; monohydrate crystals at a normal or high urine specific gravity (usg) reflect dietary cause or normal physiologic mechanisms. A few Ca oxalate crystals may be completely normal and may have just precipitated out over time. As obligate carnivores, cats have evolved to have alkaline urine and a few struvite crystals in alkaline urine may be absolutely normal and not the cause for hematuria. These occur in neutral to alkaline pH. Sediment evaluation is part of a urinalysis. It is akin to exfoliative cytology of the urinary tract and is critically important in the interpretation of colour, specific gravity, turbidity, protein, pH, occult blood, etc. Without this procedure, it is not possible to differentiate, for example, proteinuria originating from glomerular disease from that of inflammatory response to bacterial insult in the urinary tract (at any level) or genital tract. Similarly, the sediment cannot be interpreted without knowledge of the physical and biochemical characteristics of the sample. Crystals occur commonly in normal cat urine and can precipitate rapidly as it cools. The presence of crystals without appropriate concurrent inflammatory cells should be questioned. Fat droplets of various sizes are commonly seen in cat urine: they may be mistaken them for crystals, cells or bacteria. Examining unstained sediment using a subdued light intensity (by lowering the condenser or closing the iris diaphragm of the microscope) helps reduce some mistaken identification of “bacteria” and other components. Stain artifact may include bacteria growing in the stain and foreign material. Stain should be filtered weekly or monthly (depending on number of samples being looked at) and should be kept in the refrigerator. Cats are able to produce highly concentrated acidic urine with a high urea concentration. In addition, they possess the characteristics of other species for bacterial resistance, namely complete and frequent unidirectional voiding, mucosal defense barriers and acquired resistance factors from previous encounters with microbes. Bacterial urinary tract infections are most common in cats with low usg (e.g. renal insufficiency) or glucosuria (e.g. diabetes mellitus). As concentrated urine is inhospitable to bacteria and wbcs, culturing urine with a usg > 1.050 is unlikely to be rewarding and contracted epithelial cells may look like wbcs. Below 1.040, culture is indicated if wbcs are seen. White blood cells reflect inflammation or infection, therefore culture and treat according to the sensitivity results for 3-5 weeks, reculturing after one week into therapy to determine that therapy is effective. Remember that a low usg may mask a bacteruria. The feline urinary tract generally resists infection better than those of other species because of numerous features. Below 1.025 low numbers of wbcs (or even none) may be significant and culture may in fact be indicated in the symptomatic cat. Reculture one week after cessation of therapy to confirm that there is no recurrence. It is also important to interpret the results of a urine culture and sensitivity in light of the other urinalysis parameters and the method of collection. Inflammatory cells indicating a response to infection should be present. (Acute pyelonephritis is an underdiagnosed condition in the cat and should be included in the differentials for the cat with vague signs of "ain't doing right" without obvious signs of perirenal pain.) Recurrence of infection warrants further diagnostics to assess the possibility of urolith, anatomic anomaly or neoplasia.
143

Possible causes for lack of growth on culture when bacteria were identified in sediment. 1. Bacteria nonviable in the urine at collection (e.g., antimicrobial therapy, immunological defences) 2. Urine sample improperly handled/preserved causing death of bacteria. 3. Organisms fastidious and did not survive time between collection and culture outside of the body. 4. Improper culture technique (e.g., anaerobic organism processed as an aerobe). 5. Bacteria misidentified in sediment (look-alikes). Diagnostic Imaging: Survey and contrast radiography as well as ultrasound are routinely indicated in untangling the cat with LUTD. Plain radiographs are valuable for the identification of radiodense stones in the kidneys, ureters, bladder or urethra; the lateral view will be more helpful than the VD. They may also identify masses external to but compressing the urinary tract. Double contrast cysto-urethrography helps to identify detect radiolucent bladder stones, bladder diverticula, urethral strictures, anatomical defects, neoplasia, or polyps. This technique is also helpful to assess bladder wall thickness. Compressing the bladder gently with a wooden spoon during radiography is helpful to move the dye into the distal ureters. (IV pyelogram/IV urogram is indicated when evaluation of the renal pelvis and ureters is desired.) Ultrasound, while non-invasive, fails to evaluate the urethra. It images hyperechoic material within the bladder including crystal sludge (“sand”) blood clots, mural irregularities including diverticulae, and thickening of the bladder wall. In addition, one can determine whether a lucent mass is an air bubble, whether a mass is sediment rather than tumour by rolling the cat during the procedure. Cystoscopy, where available, may reveal evidence of increased mucosal vascularity, urothelial ulceration, or focal areas of submucosal haemorrhage (“glomerulations”) suggestive of, but not pathognomonic for FIC. Figure 1: Algorithm for cats with LUTD Urethral ObstructionYes No Stabilize, anaesthetize, rectal exam, unblock, then proceed as No Collect urine for urinalysis If usg < 1.025, look for renal insufficiency, diabetes If usg > 1.025 perform urine C&S g if growth, 1st episode, treat 3-5 weeks, reculture after off antibiotics 1 week
for 2nd and subsequent episodes, treat 5-8 weeks and look for underlying cause with diagnostic imaging (start with survey radiographs)
if no growth, survey radiographs looking for bladder stones if yes, treat for bladder stones (hydropropulsion or cystotomy) if no, proceed with cysto-urethrography +/- abdominal ultrasound to look for
radiolucent bladder stones, bladder diverticula, urethral strictures, anatomical defects, neoplasia, or polyps
if physical defect found, treat accordingly if none seen, cystoscopy or presumptive dx of FIC
144

References and Further Reading Achar E, Achar RAN, Paiva TB, Campos AH, Schor N. Amitriptyline eliminates calculi
through urinary tract smooth muscle relaxation. Kidney International, 2003, 64: 1356-1364 Achar E, Maciel TT, Collares CF, Teixeira VPC, Schor N. Amitriptyline attenuates
interstitial inflammation and ameliorates the progression of renal fibrosis. Kidney International, 2009, 75: 596-604
Bass M, Howard J, Gerber B, Messmer M. Retrospective study of indications for and outcome of perineal urethrostomy in cats. JSAP, 2005, 46: 227-231
Buffington CAT, Chew DJ, DiBartola SP. Lower urinary tract disease in cats: Is diet still a cause? JAVMA, 205 (11): 1524-1527, 1994
Buffington CAT, Chew DJ, DiBartola SP. Interstitial cystitis in cats. Vet Clin , 26 (2): 317-326, 1996
Buffington CAT, Chew DJ, Woodworth BE. Feline interstitial cystitis. JAVMA, 215 (5): 682-687, 1999
Buffington CAT, Westropp JL, Chew DJ, Bolus RR. Risk factors associated with clinical signs of lower urinary tract disease in indoor-housed cats. JAVMA 228(5): 722-725, 2006
Buffington CAT, Westropp JL, Chew DJ, Bolus RR. Clinical evaluation of multimodal environmental modification (MEMO) in the management of cats with idiopathic cystitis. JFMS 8: 241-268, 2006
Cameron E, Casey RA, Bradshaw JWS, Waran NK, Gunn-Moore DA. A study of the environmental and behavioural factors that may be associated with feline idiopathic cystitis. JSAP, 45, 144-147, 2004
Davies M Urinary System. In: Manual of Small Animal Clinical Pathology. Eds Davidson M, Else R, Lumsden J. BSAVA, Cheltenham, 1998, p 287-336
Gerber B, Eichenberger S, Reusch CE. Guarded log-term prognosis in male cats with urethral obstruction. JFMS 10: 16-23, 2008
Gunn-Moore DA. Feline Lower Urinary Tract Disease. In Practice, 22(9), 534-542, 2000 Gunn-Moore DA. Pathophysiology of feline lower urinary tract disease (FLUTD). UK Vet,
6(5), 20-26, 2001; Treatment of feline lower urinary tract disease (FLUTD). UK Vet, 6(5), 27-32, 2001; Investigation of feline lower urinary tract disease (FLUTD). UK Vet, 7(1), 49-58, 2002
Gunn-Moore DA. Feline Lower Urinary Tract Disease. Proceedings of the ESFM Feline Congress, Stockholm 2002. JFMS, 5(2):134-138, 2003
Gunn-Moore DA, Cameron ME. A pilot study using synthetic feline facial pheromone for the management of feline idiopathic cystitis. JFMS, 6: 133-138, 2004
Gunn-Moore DA, Shenoy CM. Oral glucosamine and the management of feline idiopathic cystitis. JFMS, 6, 219-225, 2004
Hostutler RA, Chew DJ, DiBartola SP. Recent concepts in feline lower urinary tract disease. VetClinSmallAnim 35: 147-170, 2005
Houston D, Moore A, Favrin M et al: Feline urethral plugs and bladder uroliths: a review of 5484 submissions 1998-2003, Can Vet J 44:974, 2003.
Houston DM, Moore AEP: Canine and feline urolithiasis: examination of over 50,000 urolith submissions to the Canadian Veterinary Urolith Centre from 1998 to 2008, Can Vet J 50:1263, 2009.
145
Houston DM, Rinkardt NE, Hilton J: Evaluation of the efficacy of a commercial diet in the dissolution of feline struvite bladder uroliths, Vet Ther 5:187, 2004.
Kalkstein TS, Kruger JM, Osborne CA. Feline Idiopathic Lower Urinary Tract Disease. Part I. Clinical Manifestations. CompContEdPractVet, 21 (1): 15-26, 1999; Part II. Potential Causes. CompContEdPractVet, 21 (2): 148-154, 1999; Part III. Diagnosis. CompContEdPractVet, 21 (5): 387-448, 1999; Part IV. Therapeutic Options. CompContEdPractVet, 21 (6): 497-509, 1999
Kraijer M, Fink-Gremmels J,Nickel RF. The short-term clinical efficiency of amitriptyline in the management of idiopathic feline lower urinary tract disease: a controlled clinical study. JFSM, 5:191-196, 2003
Kruger JM, Osborne CA, Goyal SM, Wickstrom SL, Johnston GR, Fletcher TF, Brown PA. Clinical evaluation of cats with lower urinary tract disease. JAVMA, 199: 211-216, 1991
Kruger JM, Conway TS, Kaneene JB, Perry RL, Hagenlocker E, Golombek A, Stuhler J. Randomized controlled trial of the efficacy of short-term amitriptyline administration for treatment of acute, nonobstructive, idiopathic lower urinary tract disease in cats. JAVMA, 222(6):749-58, 2003
Lee JA, Drobatz KJ. Characterization of the clinical characteristics, electrolytes, acid-base, and renal parameters in male cats with urethral obstruction. J Vet Emerg Critical Care, 13(4): 227-233, 2003
Lekcharoensuk C, Osborne CA, Lulich JP. Epidemiological study of risk factors for lower urinary tract diseases in cats. Journal of the American Veterinary Medicine Association, 218 (9): 1429-35, 2001
Lulich JP, Osborne CA. Management of urocystoliths by voiding urohydropropulsion. VetClinNorthAm, 26 (3): 629-638, 1996
Markwell PJ, Buffington CAT, Chew DJ, Kendell MS, Harte JG, DiBartola SP. Clinical evaluation of commercially available urinary acidification diets in the management of idiopathic cystitis in cats. JAVMA, 214 (3): 361-365, 1999
Mayer-Ronne B, Goldstein RE, Erb HN. Urinary tract infections in cats with hyperthyroidism, diabetes mellitus and chronic kidney disease. JFMS, 9(2): 124-32, 2006
Osborne CA, Kruger JP, Lulich JP, Bartges JW, Polzin DJ, Molitor T, Beauclair KD, Onffroy J. Feline matrix-crystalline urethral plugs: A unifying hypothesis of causes. JSAP, 33: 172-177, 1992
Straeter-Knowlen IM, Marks SL, Speth RC, Wirth W, Knowlen GG. Effect of succinylcholine, diazepam, and dantrolene on the urethral pressure profile of anesthetized, healthy, sexually intact male cats. AmJVetRes, 55(12): 1739-1744, 1994
Straeter-Knowlen IM, Marks SL, Rishniw M, Speth RC, Wirth W and Knowlen GG. Urethral pressure response to smooth and skeletal muscle relaxants in anesthetized, adult male cats with naturally acquired urethral obstruction. AmJVetRes, 56(7): 919-923, 1995
Sturgess CP, Hesford A, Owen H, Privett R. An investigation into the effects of storage on the diagnosis of crystalluria in cats. JFMS, 3(2):81-85, 2001
Thumchai R, Lulich J, Osborne CA, King VL, Lund EM, Marsh WE, Ulrich LK, Koehler LA, Bird KA. Epizootiologic evaluation of urolithiasis in cats: 3498 cases (1982-1992). JAVMA, 208: 547-551, 1996
146

Westropp JL, Buffington CA. Feline idiopathic cystitis: current understanding of pathophysiology and management. Vet ClinNorthAm, Small Anim Pract, 34: 1043-1055, 2004
Westropp JL, Kass PH, Buffington CA. Evaluation of stress in cats with idiopathic cystitis. AJVR 67(4): 731-736, 2006.
Westropp JL, Kass PH, Buffington CA. In vivo evaluation of a2-adrenoceptors in cats with idiopathic cystitis. AJVR 68 (2): 203-207, 2007
Wallius BM, Tidholm AE. Use of pentosan polysulphate in cats with idiopathic non-obstructive lower urinary tract disease: a double-blind randomised placebo-controlled trial. JFMS, 11:409-412, 2009
Xu H, Laflamme DPL, Long GJ. Effects of dietary sodium chloride on health parameters in mature cats. JFMS 11: 435-441, 2009
147

RECURRENT FELINE DIARRHEA: A FRUSTRATING DILEMMA
Margie Scherk, DVM, Dip ABVP (feline practice) Vancouver, B.C., Canada
Diarrhea is a common problem in feline practice. Recurrent diarrhea frustrating to the client and can affect the trust they have in the competence of the clinician. Localizing the anatomic source of the diarrhea helps determine what specific tests to choose and then direct therapy. Etiology and Pathophysiology While most often a sign of intestinal disease, diarrhea can also be a result of extra-intestinal problems, notably cholangiohepatitis, pancreatitis, hyperthyroidism, systemic infections, and less often, exocrine pancreatic insufficiency (EPI). Diarrhea is defined as the abnormal frequency and liquidity of fecal discharges. It is the most common sign associated with intestinal disease. Other signs of intestinal disease include anorexia, weight loss, abdominal discomfort and vomiting. In considering the cause and possible therapy for diarrhea in a patient, it is first necessary to determine whether the problem is acute or chronic in nature as well as its duration. It is equally vital to clarify whether the problem is localized predominantly to the small or large bowel. Remembering that the colon acts like a reservoir and that inflammation is the process resulting in diarrhea in colitis is helpful in recalling the distinctions. Occasionally, chronic disease may affect both regions making localization by history difficult. Small bowel diarrhea Large bowel diarrhea Frequency of bowel movement
Normal or increased Often increased
Volume Usually increased Normal or decreased Blood Uncommon (melena) Common (frank blood) Mucus Absent Common Presence of undigested food
May occur Absent
Abnormal colour May occur Absent Steatorrhea Uncommon Absent Weight loss May occur Rare Polyphagia May occur Rare Urgency Absent May occur Straining Uncommon May occur Vomiting May occur May occur A thorough history (including that of travel) will also help to clarify possible causes of the diarrhea. Ascertaining the age, retrovirus status, and environmental conditions (indoors/outdoors, multiple cat household and health of those cats, other animals) of the cat is helpful. One should know whether the cat has experienced previous illness as well as whether he/she is currently on any medications or supplements. Similarly, a detailed query regarding the
148
current diet (types, quantities and duration of feeding) should be made as well as finding out what the cat has been fed in the past. Physical examination should pay particular attention to mucous membrane colour (intestinal blood loss), coat quality and skin turgor (protein loss, dehydration), the presence of effusion or edema (hypoalbuminemia), palpation of the thyroid as well as the intestinal loops and abdomen in general. Assessment of abdominal discomfort should be made. Causes of recurrent or chronic diarrhea in cats: Infectious: Tritrichomonas foetus, Giardia sp., Cryptosporidium sp., ascarids, tapeworms,
whipworms, hookworms, Strongyloides sp.; FeLV, FIV; Salmonella sp., Campylobacter jejuni, Clostridium sp.; Histoplasma capsulatum
Inflammatory: lymphoplasmacytic, eosinophilic, neutrophilic etc enterocolitis (inflammatory bowel diseases)
Neoplasia: alimentary lymphoma, adenocarcinoma, intestinal mast cell disease Metabolic/systemic: hyperthyroidism, cholangiohepatitis, pancreatitis, EPI, portosystemic
shunt, cobalamin deficiency, folate deficiency Toxic/drug-induced: house plants, insecticides, NSAIDs, anthelmentics, antibacterials,
lactulose Diet-associated: intolerance (milk, spicy foods), indiscretions (garbage, hair, bones, plants,
string, etc), specific protein hypersensitivities Tritrichomonas foetus has recently been recognized as a common cause for recurrent large bowel diarrhea in North America. In a study of 117 cats at a cat show, the prevalence of T. foetus was 31%, of Giardia lambia, 31% and of coinfections with both protozoal parasites, 12%. The conclusion was that T. foetus infected catteries are common. There is no evidence to show transmission of T. foetus by water, food or contact with other species. In contrast, Giardia sp. infection is significantly associated with source of water and direct contact with other indoor-outdoor species. Most cats experience spontaneous resolution of diarrhea within 2 years (with a median of six months) after the diagnosis, despite persistence of infection on the basis of fecal PCR. Changes in diet, administration of medication or other stressors result in recurrences of diarrhea in approximately 50% of the cats. By 2-5 years after diagnosis, infection was no longer detectable in 50% of the cats by PCR so the conclusion was made that the long-term prognosis for resolution and cure is good for cats infected with T. foetus. Since 2006, reports on the prevalence of T. foetus infection in cats with diarrhea have come out of the United Kingdom, Switzerland, Australia and Greece showing that this problem is worldwide. Recently, work studying IBD has attempted to identify the pattern of cytokine up-regulation, immune cell infiltration and morphologic changes in cats with spontaneous inflammatory bowel disease. Results have revealed that inflammatory bowel disease in cats is characterized by the concurrent activation of pro-inflammatory (IFNγ, IL-1,-6,-8 and-12) and immunomodulatory cytokines (IL-10, but not IL-4). Cytokine up regulation correlated more strongly with villus atrophy and fusion, and epithelial changes, than with the overall density of the cellular reaction. (Goldstein)
149

More work done by Kenny Simpson’s group at Cornell has discovered that there are increased numbers of mucosa-associated Enterobacteraceae, based on fluorescent in situ hybridization (FISH technique) with probes for 16s rDNA. Total numbers of mucosal bacteria strongly correlate with changes in mucosal architecture (namely villous atrophy and fusion), density of cellular infiltrates (esp. macrophages). In addition to Enterobacteraceae, invasive Clostridium spp and E. coli were found. (Simpson 2006) Diagnostics A minimum database for chronic diarrhea of undisclosed cause includes a complete blood count and biochemistry profile, retroviral serology, fecal flotation for ova as well as a fecal saline wet mount for protozoa. A serum tetraiodothyronine test should be run in older cats. Detection of Giardia is best accomplished using serial zinc sulfate flotation tests and may require up to three tests run on samples collected 48 hours apart. Alternately, the ProSpecT® Giardia Microplate ELISA Assay has equivalent sensitivity and specificity. Cryptosporidium parvum is a tiny coccidia (approximately 5 microns) that commonly infects people and may cause severe gastrointestinal disease. Cryptosporidial oocysts are directly infectious when passed with feces. The presence of oocysts or antigen has been documented in the feces of many cats with or without diarrhea. The prevalence of infection with this organism is equal to or greater than with Giardia spp. in two recent studies in New York state and Colorado. While infection with this organism in people is usually from contaminated water, zoonotic spread from infected cats is possible. Fortunately, the organism is shed in small numbers and only intermittently in the feces. Unfortunately, this makes it difficult to diagnose. Diagnosis may be pursued using modified Ziehl-Neelsen or Kinyoun acid-fast staining techniques, immunofluorescence detection (more sensitive and specific) or the Alexon ProSpecT® Cryptosporidium Microplate enzyme immunoassay. The “Rapid” version of this (and the Giardia test) is not as sensitive. Tritrichomonas foetus may be identified with light microscopy as a motile flagellated organism, which looks similar to Giardia. A commercially available test, (InPouch Feline TF®) has been validated as an excellent way to specifically identify this organism and is sensitive and specific for detection of T. foetus in feline feces. Inoculate a pouch with 0.025-0.05g of fresh feces (peppercorn or grain of rice size), then incubate it standing upright, at room temperature (optimally 25C), in the dark and examine the pouch for trophozoites at 20X every other day for 12 days. Approximately 50% of infected samples tested will be positive in three days. Light microscopy (on either a wet mount or rectal cytology), InPouch culture (or modified Diamond culture in commercial laboratory) may result in false negative results. A third type of test, PCR for Tritrichomonas may be submitted to the appropriate facility. It is more sensitive and exquisitely specific and is the gold standard; it may also occasionally fail to detect the organism in an affected cat. Fecal culture may be considered when specific pathogens need to be investigated. Routine culturing is not recommended because results will be difficult to interpret. Growth of Salmonella, Campylobacter sp., or Clostridium sp. may be attempted on specific culture media
150

when these agents are suspected, such as in an acute (or recurrent) outbreak of diarrhea after showing or in multiple cats in a household. For large bowel diarrhea, cytology from rectal scrapings and gram stain of prepared slides may be very helpful in achieving a definitive diagnosis in many cases of large bowel diarrhea. This test harvests cells and organisms from the lumen-colon wall interface. Insert a moistened sterile culture swab 2-3 cm into the rectum of the cat and rotate it gently. Roll this swab gently and thoroughly on two microscope slides and store the swab in the culturette medium. Submit the slides for cytology plus gram stain and follow with the swab as indicated by the cytology results. Rectal cytology may diagnose bacterial or non-septic suppurative colitis, Cryptosporidium, Giardia, Tritrichomonas, Campylobacter infections as well as fungal hyphae. The presence of clostridial spores must be interpreted carefully and a fecal enterotoxin assay should be performed to determine if disease-causing clostridial enterotoxin is present or not. For recurrent or non-resolving small or large bowel diarrhea, imaging may be the next step. Abdominal radiographs are low yield other than for foreign body or intussusceptions. With ultrasound it is possible to appreciate changes in intestinal wall architecture suggestive of inflammatory or infiltrative disease as well as alterations in hepatic, pancreatic and lymph node structure. Biopsies or aspiration may be performed using ultrasound guidance. Serum folate and cobalamin assays are available to detect deficiencies, which may be implicated in non-resolving chronic diarrhea. Exocrine pancreatic insufficiency may be definitively diagnosed by measurement of subnormal feline trypsin-like immunoreactivity (fTLI) levels. Surgically or endoscopically obtained biopsies are required to confirm suspicion of an inflammatory bowel disease and to differentiate IBD from neoplastic disease. Full thickness biopsies may be needed to diagnose the latter group of conditions because superficial histologic changes may be indistinguishable from IBD. Therapeutics In recurrent and chronic diarrhea more than supportive fluid and electrolyte care is required. Cats must be fed because enterocytes and colonocytes meet their metabolic needs from direct contact with ingesta. In general, a diet that is highly digestible with moderate protein, low to moderate fat and carbohydrate levels is suitable. A low residue diet is preferable as an initial choice. The presence of some fiber is essential for mucosal health. Soluble (highly fermentable) fibers (oat bran, pectin, beet pulp, vegetable gums, psylium) are readily digested by bacteria and provide large quantities of short chain fatty acids, which are beneficial for colonic health. Because sodium and water are coupled with the uptake of butyrate, soluble fibers may help ameliorate large bowel diarrhea. (These should not be used where there is suspicion of luminal enterotoxins.) Soluble fibers create gels. In nature, most fibers are not strictly insoluble or soluble, but can be considered to have a greater or lesser percentage of soluble fiber. Psyllium (Metamucil) has 79% soluble fiber (with 21% insoluble), oat bran has 50%, wheat bran has 11 % and cooked white rice has 0% soluble fiber.
151

Fiber in Common Foods and Pet Foods Soluble Fiber Metamucil 79% Corn gluten meal 51% Oat bran 50% Beet pulp 50% Bran flake cereal 33% Barley 29% Whole wheat bread 20% All-Bran cereal 14% Brewer’s grains 11% Wheat bran 11% Wheat middling 11% 100% bran cereal 11% Corn 0% Cooked white rice 0%
Adapted from: Buffington CAT, et al. Manual of Veterinary Dietetics, Saunders, 2004: Table 5-16. Insoluble fibers (cellulose, lignin, wheat bran) are less able to absorb water. They are able to bind toxins, bile acids and may help normalize transit time. Judicious addition of this class of fiber may be helpful in some patients with small bowel diarrhea, however, in many individuals, their action is laxative. Antibiotics should be avoided unless specific bacterial pathogens have been identified. An exception may be the use of metronidazole (10 mg/kg PO q12h) for its immunoregulatory actions; if the patient has concurrent hepatic disease, the dose should be reduced to 7.5 mg/kg PO q12h. Metronidazole benzoate is flavourless and has been shown to have the same pharmacokinetic profile as the traditionally used metronidazole salt (Flagyl). For giardiasis, metronidazole should be administered at the dose of 25 mg/kg PO q12h X 5-10 days; for giardia that is resistant to this therapy, consider furazolidone (4 mg/kg PO q12h X 5 days) or fenbendazole 50 mg/kg PO q24h for 3 days and repeated after three weeks. For cryptosporidium, the treatment of choice is azithromycin (7.5-10 mg/kg PO q12-72h) or tylosin administered at 15 mg/kg PO q12h for 10 days. Paromomycin has a very narrow safety margin and is not recommended in cats. Tylosin is also a useful drug in the treatment of Clostridia and Campylobacter infections. Amoxicillin or metronidazole may be considered in the treatment of Clostridia. Ronidazole and tinidazole have been evaluated for efficacy both clinically as well as for their ability to eliminate infection based on PCR. Using tinidazole at 30 mg/kg PO BID X 14 days. At the end of this therapeutic course, amoxicillin was administered to induce diarrhea successfully resulting in recrudescence of T foetus in some of the cats. The conclusion at this time is that ronidazole remains more efficacious for the treatment and elimination of T foetus in cats at 30
152

mg/kg PO SID. Higher doses are not more effective and at higher doses, there is a risk of neurotoxicity. Anthelmentics should be used when specific parasites have been identified. The presence of globule leukocytes on a histology report from intestinal biopsy indicates parasitic involvement and treatment with ivermectin (200 m/kg SC every 2 weeks for 3 treatments) is suggested. Immunosuppressive therapy for chronic diarrhea is indicated when a diagnosis of IBD has been achieved through biopsy. Prednisolone may be started at 1-2 mg/kg PO q12h and should not be tapered before the patient has been in remission from diarrhea for at least two weeks; therapy should be continued for a minimum of three months. Should the condition not be responsive to corticosteroid therapy or the patient intolerant of it, chlorambucil may be considered (2 mg PO twice a week). In severe cases, or in small cell lymphoma, the two agents may be used concurrently. Sulfazalazine (10-15 mg/kg PO q12h X 7-10 days) may be more effective in inflammatory colitis than prednisolone. Azathioprine should be reserved for extremely difficult cases: dose cautiously (0.06 mg/kg PO q48h). Non-specific therapies may be helpful: Oral protectants act locally and adsorb bacteria, toxins and protect the mucosa. Bismuth subsalicylate (Pepto-Bismol =17.5 mg/ml bismuth + 8.7 mg/m salicylate: 0.5-1
ml/kg PO q12h for 3 days). Bismuth has antibacterial, antienterotoxic, antisecretory and antiinflammatory properties.
Kaopectate (1-2 ml/kg PO q2-6h) may also be used but is not as effective as bismuth. Motility modifiers should be avoided if the pathophysiology of the diarrhea includes invasive microorganisms. Loperimide (0.1-0.2 mg/kg PO q8h) is effective in slowing motility. What about antioxidants? Clinical usefulness of Vitamins E and C in treating diarrhea is as yet unproven. The ideal ratio and composition of n3 fatty acids for the reduction of inflammation in cats remains to be determined. While prebiotic and probiotic therapy have been investigated in human gastroenterology, controlled studies to support their use in cats are lacking. Cobalamin supplementation may be warranted in cats with chronic small intestinal diarrhea where the disease process either through inflammation or chronic fibrosis has resulted in a reduction of small intestinal absorption of this vitamin (250 mcg SC once weekly X 4 weeks). (Ruaux 2005) Additional Detail List of infectious causes of gastrointestinal diseases in cats from Dr. Mike Lappin: There are many infectious agents associated with vomiting or diarrhea in cats. Primary
clinical signs associated with infectious causes of gastrointestinal tract diseases are abbreviated as follows: S = small bowel; M = mixed bowel; L = large bowel; V = vomiting. Any of the agents that induce diarrhea potentially can induce vomiting as well.
The primary bacteria associated with gastrointestinal tract disease in cats include Salmonella spp. (S,M, L), Campylobacter jejuni (M,L), Clostridium perfringens (L,rare), Helicobacter spp.(V), bacterial overgrowth syndrome (S), bacterial peritonitis (S), and bacterial cholangiohepatitis (S).
153

The primary viral agents include feline coronaviruses (S), feline leukemia virus (FeLV; V,S,M,L), feline immunodeficiency virus (FIV; V,S,M,L), and feline panleukopenia virus (V infrequently, S).
The primary helminths are Ancylostoma/Uncinaria (S,M), Strongyloides cati (S,M, rare), Dirofilaria immitis (V), Toxocara cati (V), Toxascaris leonina (V), Ollulanus tricuspis (V), and Physaloptera spp. (V).
Enteric protozoans include Giardia spp. (S,M), Cystoisospora spp. (Isospora; M,L), Cryptosporidium spp. (S,M), Entamoeba histolytica (L, rare), and Tritrichomonas foetus (L).
The cestodes Taenia, Dipylidium, and Echinococcus generally cause subclinical infection. Summary With a structured approach, the frustration of recurrent diarrhea can be solved. Chronic and recurrent diarrhea must be approached with diligence and patience. The first step is to determine the source of the diarrhea. Is it extra vs. Intra-intestinal? If gastrointestinal, localize to large or small bowel. Once localized, specific diagnostics can be selected and used logically. In situations in which treatment does not exist or cure is not possible (neoplasia) knowledge of the cause enables the practitioner to counsel and empower the client. References/Suggested Reading 1. Foster DM, Gookin JL, Poore MF et al. Outcome of Cats with Diarrhea and Tritrichomonas
Foetus. ACVIM Forum 2003 2. Gookin JL, Riviere JE, Gilger BC et al. Acute renal failure in four cats treated with
paromomycin. J Am Vet Med Assoc 1999; 215 (12): 1806, 1821-3 3. Gookin JL, Foster DM, Poore MF et al. Use of a Commercially Available Culture System for
Diagnosis of Tritrichomonas foetus Infection in Cats. J Am Vet Med Assoc 222[10]: 1376-9 2003.
4. Gookin JL, Stebbins ME, Adams E. Prevalence and Risk of T. foetus Infection in Cattery Cats. ACVIM Forum 2003
5. Gunn-Moore DA, McCann TM, Reed N, et al. Prevalence of Tritrichomonas foetus infection in cats with diarrhoea in the UK. J Feline Med Surg;9(3):214-8 2007
6. Gookin JL, Copple CN, Papich MG, et al. Efficacy of ronidazole for treatment of feline Tritrichomonas foetus infection. J Vet Int Med 20 (3): 536-43 2006
7. Gookin JL, Stauffer SH, Coccaro MR et al. Efficacy of tinidazole for treatment of cats experimentally infected with Tritrichomonas foetus. Am J Vet Res. 68(10):1085-8 2007
8. Gookin JL, Stauffe SH, Coccar .R et al. Efficacy of tinidazole for treatment of cats experimentally infected with Tritrichomonas foetus. Am J Vet Res. 68(10): 1085-8 2007
9. Goldstein RE, Greiter-Wilke A, McDonough SP et al. Quantitative Evaluation of Inflammatory and Immune Responses in Cats with Inflammatory Bowel Disease. ACVIM Forum 2003.
10. Hall JA. Clinical approach to chronic diarrhea. In August J (ed) Consultations in feline Internal medicine, Volume 4, Saunders, 127-35, 2001.
11. Hill S, Lappin MR, Cheney J, et al: Prevalence of enteric zoonotic agents in cats. J Am Vet Med Assoc 216: 687-92, 2000.
12. Latimer KS. Cytologic evaluation of rectal mucosal scrapings. Proc 11th Annual ACVIM Forum, 1993.
154

13. Ruaux CG, Steiner JM, Williams DA. Early biochemical and clinical responses to cobalamin supplementation in cats with signs of gastrointestinal disease and severe hypocobalaminemia. J Vet Int Med 19 (2): 155-60 2005.
14. Simpson KW. Do mucosa-associated bacteria have a role in IBD? ACVIM Forum 2006. 15. Spain CV, Scarlett JM, Wade SE et al: Prevalence of enteric zoonotic agents in cats less than
1 year old in central New York State. J Vet Int Med 15: 33-8, 2001. 16. Zoran DL. Diet and Drugs: The Keys to Managing Feline Colonic Disease Compend Contin
Educ Pract Vet 21[8]: 731-48 1999 17. Xenoulis PG, Saridomichelakis MN, Read SA, et al. Detection of Tritrichomonas foetus in
cats in Greece. J Feline Med Surg 12: 832-833, 2010
155

CHOLANGITIS-CHOLANGIOHEPATITIS COMPLEX IN THE CAT
Margie Scherk, DVM, Dip ABVP (feline practice) Vancouver, B.C., Canada
Feline cholangitis/cholangiohepatitis complex (CCH) is a group of disorders, which affect either the biliary tree alone or the biliary tree and the liver. A major difference between dogs and cats is that inflammatory disease originating in the liver is rare. Instead, the primary source of inflammation is most commonly in the biliary tree (cholangitis, C) with possible extension to the liver (cholangiohepatitis, CH) with lesions oriented around the portal triad. CCH may be suppurative or, more commonly, non-suppurative in nature. The non-suppurative variant may further be described as cholangiohepatitis (acute and chronic forms), lymphocytic portal hepatitis and slowly progressive lymphoproliferative disease (which is a low grade lymphoma). Determining what form of cholangitis or cholangiohepatitis as well as concurrent problems (pancreas, duodenum, etc.) is critical to developing a rational therapeutic plan. Etiology and Pathophysiology An appreciation of the microanatomy of the liver is helpful to understanding the pathophysiology affecting the liver.
Image from Crawford JM: The Gastrointestinal Tract, in Cotran RS, Kumar V, Robbins SL (eds): Robbins Pathologic Basis of Disease. Philadelphia, WB Saunders Co, 1994, p 755-829. The liver receives 75% of its blood directly from splanchnic (visceral) venous drainage via the portal circulation. The hepatic artery provides the remainder of the blood. Blood from the intestinal tract travels laden with nutrients and toxins to the liver via the portal vein (PV); the mesenteric lymph nodes responding to immunologic threats. The liver is a potential target for hematogenously transmitted bacteria. In a
156

gut with a healthy and intact mucosal barrier, this doesn’t pose a problem as few noxious elements pass into portal circulation. This blood then is filtered through the liver, draining into the terminal hepatic venules (THV), converging into the caudal vena cava. Nutrition for the liver comes to this organ by way of the hepatic artery (HA), originating at the aorta. The bile ducts and ductules (BD), are in close proximity to the “portal triad” each consisting of a portal venule, hepatic arteriole and bile ductule. The importance of this anatomic relationship is to help understand the implications of histologic findings as they suggest the etiologic source of the irritant. Histopathology provides the architecture which is extremely helpful/essential in determining etiology. Histology looks at the proximity to the THV in acinar “zones” or metabolic regions. If the portal blood absorbing from the gut or hepatic arterial blood contain bacteria or is consistently being challenged by antigen, damage will be most severe in the parenchymal structures closest to the portal triad, (periportal zone 1). Should there be hypoxia or toxins however, damage will be evident farther from the triad in the centrilobular region/zone 3. Acute cholangitis is generally suppurative and likely from ascending bacteria from the gut in the biliary tree. This results in an infiltration of neutrophils in the lumen or epithelial lining of the biliary ducts. With greater severity of disease (local necrosis), neutrophils will be located in the hepatic parenchyma in the periportal region (CH). Over time (1-3 weeks), the inflammatory infiltrate may include smaller numbers of lymphocytes and portal fibrosis with bile duct proliferation may occur. The suppurative process may also arise from hematogenous spread from the hepatic artery or portal vein. Chronic CCH is the more common form and is believed to be immune-mediated in origin. It may be lymphoplasmacytic, lymphocytic or sclerosing. Cats with CCH often have hyperbilirubinemia and bilirubinuria. These do not differentiate the conditions from other hepatic, pre-hepatic or post-hepatic causes of icterus. In patients with bilirubinuria, Increases in activities of serum alkaline phosphatase (ALP), alanine transferase (ALT) and gamma glutamyl transferase (GGT) may be present to varying degrees but do not distinguish between suppurative and non-suppurative CCH. Cats with hepatic lipidosis usually have markedly increased ALP activity compared to ALT activity and have normal GGT activity. In contrast, cats with CCH usually have ALP and ALT increases of equal magnitude or the increase in ALT is greater than ALP; GGT activity is usually increased as well. Bilirubinuria is significant in the cat because of the high renal threshold for bilirubin in the feline kidney. It is important to realize that some patients may have chronic CCH resulting in decreased functional liver mass and therefore no increases in ALT, ALP or bilirubin may occur. There may be variable changes in albumin, glucose, BUN, cholesterol. If you believe that liver disease is possible, a liver function test (pre- and postprandial serum bile acid) is indicated. Clinical Presentation and Diagnosis: Suppurative Clinical signs in the cat with suppurative CCH differ from those in the cat with non-suppurative disease. Because the former disease is associated with ascending bacterial infection, cats are sicker. The signalment includes more males and younger cats than the signalment for the patient with non-suppurative disease. Cats are presented for acute onset vomiting, lethargy, fever, dehydration, jaundice +/-
157

diarrhea. Abdominal pain may be noted. Concurrent conditions compromising bile duct health such as IBD, pancreatitis or extrahepatic bile duct obstruction (EHBDO) may be present. The complete blood count (CBC) reflects dehydration and stress. A left shift with toxic neutrophils may be present. Serum biochemical changes are rapid with moderate increases in ALT +/- gamma GT, mild in alkaline phosphatase (SAP) unless there is concurrent EHBDO. Other biochemical and electrolyte changes depend on the degree of dehydration and vomiting. Radiographs are generally unrewarding. On ultrasound, inflammation and thickening of extrahepatic biliary tree as well as inflammation within the intrahepatic bile ducts may be seen. Histologically, this translates as dilation of bile ducts, periportal edema and an accumulation of exudates within the biliary tree. Over time, uncontrolled, this will progress to periductal fibrosis, bile duct proliferation and biliary hyperplasia. Ultrasound is valuable to assess concurrent problems as well as enabling guided transhepatic aspiration of bile for cytology and culture. The information gleaned from ultrasound, assists in determining whether or not surgical exploration is warranted. Disorders associated with suppurative CCH in the cat:Primary bacterial infection Septicemia Chronic bacterial infections: Sinusitis/dental
Splenic abscess Pyelonephritis
Cholecystitis Cholelithiasis Pancreatitis Inflammatory bowel disease Extrahepatic bile duct obstruction Acute trematode infection Toxoplasmosis
Organisms that have been associated with suppurative cholangitis/cholangiohepatitis are (listed in descending order of frequency) E. coli, alpha hemolytic Streptococcus, Actinomyces, Enterobacter, Enterococcus, Staphylococcus, Bacillus, Bacteroides and Clostridia. Note that toxoplasmosis can be an underlying infection. The presence of Bacteroides suggests a polymicrobial infection. Inability to culture organisms may be a result of the type of bacteria (e.g., anaerobe) or because of previous antimicrobial therapy. Infection with Helicobacter spp. is linked with hepatobiliary inflammation and neoplasia in people and in a variety of animals. A study was performed to determine whether infection with this family of bacteria plays a role in feline cholangiohepatitis. The DNA sequences of hepatic Helicobacter species were distinct from those found in the stomach and are broadly consistent with those identified in cat intestine and bile, and hepatobiliary disease in people and rodents. Hepatic biopsy is preferred over FNA or Tru-cut biopsy. With FNA, not only are you restricted in what you harvest, but also the condition of that sample is mutilated by the aspiration action and slide preparation. Some types of cells do not exfoliate readily (mesenchymal neoplasias such as fibrosarcoma for example) resulting in a cytological diagnosis of whatever cells are sampled easily and may not get a real picture of the
158

underlying disease process. Additionally, orientation of the cellular reaction within tissue is critical in defining different disease processes affecting therapeutic recommendations. One can improve the diagnostic yield by using a passive stabbing technique rather than the traditional aspiration technique. Nevertheless, as seen in a pivotal study which compared the results of needle biopsy (18G) samples to those collected via wedge biopsy, discrepancy between results may be dishearteningly misleading. Morphologic diagnoses assigned to needle biopsy specimens concurred with the definitive histopathologic diagnosis (wedge biopsy) for 59 of 124 (48%) animals. This suggests that needle biopsy cytology should be interpreted with caution. A better correlation is found with greater number of needle biopsies taken to ensure a minimum of 15 portal triads are harvested to demonstrate the distribution and cellular character of a lesion. Cytologic samples are required for identification of bacteria as the preparation of samples for histopathology removes bacteria. Therefore, making a touch-impression of a surgically or laparoscpically obtained sample prior to placement in formalin is extremely helpful diagnostically. Additionally, samples for culture and gram stain should be taken at this time. Therapy: Suppurative Therapy for acute suppurative CCH, centers around antimicrobial therapy with concurrent fluid and nutritional support. Antimicrobials should be chosen based on sensitivity patterns that will be concentrated in the liver and bile, that are non-toxic to cats, can be given continuously for three to six months. Should sensitivities not be available, then gram stained organisms may be helpful. As first tier antibiotics, consider ampicillin, cephalexin or amoxicillin- clavulanic acid. Metronidazole is useful as adjunctive therapy for its anaerobic bactericidal, anti-inflammatory and anti-endotoxic effects; it penetrates liver and bile well. Avoid the following antibiotics in liver disease because they are biotransformed, activated or eliminated by the liver or because they promote lipid accumulation or may produce hepatic injury: chloramphenicol, clindamycin, erythromycin, lincomycin, hetacillin, streptomycin, sulfonamides, trimethoprim sulfas and oxy- or chlortetracycline. When fibrosis is present, D-penacillamine or methotrexate may be beneficial in slowing its progression. Colchicine may be used at a dosage of 0.03 mg/kg SID in attempt to reduce fibrosis although controlled studies have yet to be reported. (Jergens A, ACVIM, 2011 Proceedings) Cats with mechanical or functional extrahepatic bile duct obstruction (e.g., fibrosed or severely edematous bile duct) need prompt surgical intervention. If biliary tree decompression cannot be achieved conservatively, then biliary diversion is vital to prevent septicemia. Cholecystoduoden-ostomy is preferable to cholecystojejunostomy if the duodenal area isn’t compromised by pancreatic inflammation.
159

Drugs, Dosages and Indications: Suppurative Drug Dose Range Frequency Route Indications Ampicillin* 22 mg/kg TID PO, SC, IV First tier: gram
positive, many anaerobes
Cephalexin* 15 mg/kg TID PO, SC, IV First tier: gram positive, many anaerobes
Ticarcillin* 55 mg/kg TID IV Enterobacteraceae Piperacillin* 30 mg/kg TID- QID IV Enterobacteraceae Enrofloxacin* 5 mg/kg SID PO, IV Second tier: Gram
positive, many gram negative, anaerobes, Bacteroides fragilis
Metronidazole* 7.5 mg/kg BID PO, IV, rectal
Anaerobes
Vancomycin** 20 mg/kg BID Slow IV infusion
Resistant Enterococcus
* for 3-6 months; ** for 7-10 days only, then switch antibiotics Clinical Presentation and Diagnosis: Non- suppurative Most cats are middle aged or older and have had a long course (several weeks or more) of vague illness. The clinical presentation includes a vague history of inappetance/anorexia OR polyphagia, lethargy, as well as possibly nausea, vomiting, diarrhea and weight loss. The signs may have a chronic intermittent occurrence. On physical examination, signs of dehydration, weight loss, muscle wasting, icterus, salivation, palpable liver margins, cranial abdominal tenderness or firmness may be present. A key differential is hyperthyroidism. Non-suppurative is the most common form of CCH in cats. The course of the disease is chronic, vague and episodic; by the time a cat is presented and a diagnosis is achieved, the condition may have been going on for several months. It is often lymphocytic-plasmacytic in character and believed to involve immune mediated mechanisms. Cats with non-suppurative CCH often have co-existent IBD and low-grade pancreatitis. Disorders associated with non- suppurative CCHC in the cat: Inflammatory bowel disease Primary cholangitis Pancreatitis Extrahepatic bile duct obstruction Cholelithiasis Cholecystitis Neoplasia: Gallbladder
adenocarcinoma Bile duct cystadenoma Malformation: choledochal cyst Chronic trematode infestation Chronic bacterial infection
160

Cats with non-suppurative, inflammatory CCHC have variable increases in ALT, SAP, gamma GT, but, in general, those with lymphoplasmacytic inflammation have greater increases than those with lymphocytic inflammation do. They are hyperbilirubinemic and most have increased globulins. Diagnosis cannot be made by liver cytology; histopathology is required. Lymphocytic or lymphocytic-plasmacytic infiltrates surround and invade portal triads. There is bile duct hypertrophy and hyperplasia initially. If the disease progresses, bile ducts may “drop out” and bridging portal fibrosis develops to fill in the gaps. Rarely, this may progress to end-stage biliary cirrhosis; usually cats die before they reach this stage. Therapy: Non-suppurative The cornerstones for treating the non-suppurative forms of CCH in cats are those agents that aid in suppression of the dysfunctional immune system. Corticosteroids, metronidazole and a limited antigen diet along with the other general supportive treatments for all types of CCH are recommended. Drugs, Dosages and Indications: Non-suppurative
Drug Dose Range Frequency Route Indications Prednisolone 1-2 mg/kg* BID PO Immunosuppression Metronidazole 7.5 mg/kg BID PO, IV,
rectal Immunomodulation
*Taper after 2 weeks free from clinical illness; taper by 25-50% to lowest effective maintenance dose reducing dose every 10-14 days
Therapy common to suppurative and non-suppurative forms As with other diseases, general treatment includes ensuring the adequate provision of a balanced diet, rehydration and maintenance of hydration (for circulating volume and blood pressure), supplemental B vitamins, Additionally, Vitamin K1 should be given to any cat with liver disease, particularly if they are clinically jaundiced as the hepatic Vitamin K epoxidase recycling system is impaired in liver disease and because an inappetant patient is not ingesting adequate amounts of this micronutrient. If there is significant concurrent small intestinal disease, its absorption will be impaired and finally, should the patient have been on antimicrobials, the bacteria needed to manufacture Vitamin K may be lacking. Oral administration is not advised as gut disease or impaired enterohepatic circulation may result in poor absorption. Ursodeoxycholic acid has immunomodulatory, antifibrotic and choleretic effects. 1) It suppresses aberrant expression of major histocompatibility foci on hepatocytes and biliary
epithelium, thereby making them less evident to inflammatory mechanisms; 2) It affects lymphocyte activity; 3) It minimizes the immunosuppressive effects of cholestasis by 4) Promoting hydrocholeresis, and 5) Supports membrane integrity and flexibility by modulating the noxious bile acid population.
161

Antioxidant therapy is indicated in therapy to help protect against inflammation-induced free radicals. The liver has endogenous antioxidants to deal with toxic and noxious effects of products it is exposed to from gastrointestinal venous blood. These include zinc, glutathione, S-Adenosyl-L-Methionine (SAMe), Vitamin E, Vitamin C, beta-carotene, coenzyme Q10, and super oxide dismutase. Drugs, Dosages and Indications: Both Forms
Drug Dose Range Frequency
Route Indications
Balanced calories*
40-60 kcal/kg ideal weight/day
PO, via tube
Vitamin K1 0.5-1.5 mg/kg Q12h** SC, IM Jaundice Ursodeoxycholic acid
10 mg/kg SID PO Cholestasis
SAMe 200 mg SID PO Glutathione donor Lactulose 0.25-0.5 ml/kg
taper to effect of several soft stools/day
BID PO Hepatic encephalopathy
* convalescent or maintenance diet for suppurative form; limited antigen diet for non-suppurative form; ** for three doses Monitoring and Prognosis Frequent monitoring of serum biochemistries will help to ascertain whether the infection is resolving or the inflammation is controlled. It is extremely important to realize that should fibrosis/sclerosis be occurring, that the liver enzyme markers may decrease as there is less tissue to manufacture them. This may be seen in a patient whose values are improving yet the patient themselves is not. Regardless of whether a cat suffers from acute suppurative CCH or chronic non-suppurative CCH, survival time is good. Accurate definition of the type of disease requires histopathologic examination of liver biopsy. Cats with the lymphocytic portal hepatitis have an even better prognosis with very slowly progressive disease. Summary Appropriate and successful treatment of CCH in cats requires an accurate, histopathologic description. This enables both the appropriate therapeutics and duration of treatment to be recommended. Frequent monitoring of the patient and serum biochemistries is helpful in evaluating progress. With suitable therapy, a good prognosis may be expected. References/Suggested Reading Center SA: Diseases of the gall bladder and biliary tree. In Guilford WG (ed).
Strombeck’s Small Animal Gastroenterology, Philadelphia, WB Saunders Co, 1996, pp 860-888.
Cole TL, Center SA, Flood SN, et al: Diagnostic comparison of needle and wedge biopsy specimens of the liver in dogs and cats. J Am Vet Med Assoc. May 2002; 220 (10): 1483-90.
162

Gagne JM, Armstrong PJ, Weiss DJ, et al: Clinical features of inflammatory liver disease in cats: 41 cases (1983-1993). J Am Vet Med Assoc. February 1999; 214 (4): 513-6.
Greiter-Wilke A, Scanziani E, Soldati S, et al: Association of Helicobacter with cholangiohepatitis in cats. J Vet Intern Med. 2006 Jul-Aug; 20 (4): 822-7.
Liptak JM: Hepatobiliary tumors: Cancer of the gastrointestinal tract. In Withrow S, Vail D (eds). Withrow and MacEwen’s Small Animal Clinical Oncology, ed 4, Philadelphia, 2006, Saunders, 455-510.
Richter K. Use of SAMe (s-adenosylmethionine) in Liver Disease at Western Veterinary Conference 2004
Greiter-Wilke A, Scanziani E, Soldati S, et al: Association of Helicobacter with Cholangiohepatitis in Cats. J Vet Intern Med. 2006;20:822–827
163

SNOTS & SNUFFLES: THE CAT WITH CHRONIC UPPER RESPIRATORY DISEASE
Margie Scherk DVM, Dip ABVP (feline practice)
Vancouver, BC, Canada
INTRODUCTION The chronic feline snuffler is a frustrating patient to treat. The longer the course, the more severe the consequences to affected tissues are and the more debilitating it is to the patient. A logical diagnostic plan to differentiate probable etiologies and to rule-out non-viral causes results in appropriate therapeutic choices. Even with a viral etiology, therapies to reduce the pathological consequences of the infection may modulate and help control the clinical signs. Novel choices and drug combinations are discussed.
HISTORY & PRESENTATION Chronic, recurrent rhinosinusitis can occur in cats of any age. Cats are presented because of sneezing, nasal discharge, and noisy breathing with or without inappetence. Sneezing occurs because of stimulation of irritant receptors in the nasal and sinus subepithelium. Knowing the timing, onset, duration and frequency of sneezing can be helpful. With chronicity, inflammatory changes this response may be abolished resulting in accumulation of discharge. Nasal discharge may be serous, mucoid, purulent, or sanguinous. It is helpful to know whether the discharge has changed, whether it changes throughout the day or season, and especially whether it is unilateral or bilateral. Respiratory patterns and sounds may be abnormal. Clients may comment on the cat sounding hoarse or even silent when meowing or that his/her purr is different. In general, sounds heard on inspiration are associated with larger airways whereas expiratory sounds are associated with smaller, lower airways. Snorting occurs with accumulation of discharges in the nasal passages or with secretions coughed into the oropharynx (e.g., from pneumonia). A snoring, stertorous sound is associated with proximal upper respiratory occlusion, such as with a polyp or foreign body obstruction or functional inflammatory obstruction. Stridor is an inspiratory wheeze that reflects changes in the larynx. An expiratory wheeze, crackles and rales reflect small airway involvement. A complete lack of bronchovesicular sounds occurs when there is pulmonary consolidation or inflammation. If the breathing is “worse at night” this could reflect bronchitis or merely the time that the client is at home to observe the cat. Sounds that are worse after exercise or at rest may reflect the severity of the respiratory interference or the movement of secretions. Some cats have seasonal flare-ups suggesting an allergic or contact irritant component. Assess facial symmetry both face on and from above the head. Palpate the face to further look for swelling, invagination or discomfort. Thoroughly evaluate teeth and alveolar bone for evidence of periodontal disease, abscessation or inflammation. Look at and palpate the hard and soft palate, where feasible, looking for oronasal fistula or mass
164

lesions or ulceration. If a cat retches or yawns, the tonsils may be visualized. By opening the mouth we can evaluate neurologic competency: jaw tone (motor V), position, movements and symmetry of the tongue (XII), and gag reflex (IX, X). Evaluate nasal passage patency using a small mirror (compact or dental) or a glass slide that has been kept in the freezer. Wisps of cotton are also helpful. Palpate the trachea to see if this elicts a cough. It is helpful to auscult the trachea as well as three locations (dorsal cranial and caudal and craniaoventral) bilaterally to define the primary location of the lesion. Occasionally auscultation of the frontal sinuses may be revealing. For this, a small pediatric bell is used. For pulmonary auscultation, use two heads, the standard bell and a plexiglass scope (e.g., UltrascopeTM) as they provide different sensitivities and frequencies. A thorough physical examination should be performed. Fundic examination should be performed to look for Cryptococcus and other signs of systemic disease. Enlargement of regional lymph nodes or generalized node enlargement should be assessed. ETIOLOGIES AND PATHOGENESIS Chronic rhinitis may be a sequel to acute rhinitis but it may be a separate condition, all together. It may represent an ineffective immune response to persistent viral infection (1). Feline herpesvirus 1 (FHV-1) may be the common denominator initiating turbinate resorption, with subsequent secondary bacterial infections and unchecked inflammation exacerbating the problem. This is especially bad in anatomically predisposed individuals (conformation, anomalies). Irreversible destruction of the turbinates may result in viral or inflammatory mediator-induced cytolysis. Reactivation of herpesvirus from infected trigeminal ganglion may result in recurrent destruction. All of these are possible pathogenic strategies; it is not possible to determine the course/cause in a given individual. Caliciviruses infection results in a carrier state with continuous shedding for variable periods of time. FHV-1, like other herpesviruses, results in a state of latency and approximately 80% of infected cats are permanent carriers. Latency accounts for recurrence of clinical signs during periods of physiological or psychological stress. Primary bacterial agents include Bordetella bronchiseptica, commonly found as a commensal without causing morbidity. Mycoplasma spp. may be cultured from some individuals, but their true incidence remains unknown due to the difficulty of isolating these fastidious organisms. Chlamydophyliosis is not common, and infection is limited to varying degrees conjunctivitis. L-forms may also be involves but require specific targeted culture techniques for verification. In one study (2) aerobic bacteria were cultured from biopsy samples from twice as many clinically affected cats (4/10) than controls (2/7) while anaerobic infection occurred in only the affected cats (2/10). Flush samples were collected from the same cats with aerobes in 5/7 controls, and 9/10 affected cats; anaerobes in 3/10 and Mycoplasma spp. in 2/10 affected cats. Interestingly, FHV-1 was not cultured from any of the cats, but viral
165

DNA was detected in 4/7 control and 3/10 affected cats by PCR implying that the virus was not viable. Less frequently isolated bacteria worthy of journal publication have included Actinomyces sp., Haemophilus sp. (3), and Capnocytophaga sp. (4). Bartonella henselae is commonly detected by serology (antibody titres), yet its true role in the chronically infected cat is not as relevant as its serologic exposure. One study (5) showed that “Serological screening for Bartonella antibodies may not be useful for the identification of bacteremic cats (positive predictive value = 46.4%), but the lack of antibodies to B. henselae was highly predictive of the absence of bacteremia (negative predictive value = 89.7%).” The fact that cats on antibiotics often improve clinically, would support the role of bacteria; the fact that signs recur, despite therapy, implies that bacteria are only part of the cause of the illness. When antimicrobial therapy of 7-10 day duration fails to result in resolution of disease, then a thorough diagnostic work-up should be recommended. The main fungal organisms causing chronic upper respiratory disease, are Cryptococcus neoformans var. neoformans and gattii. These classically cause severe inflammation resulting in facial deformity and skin ulceration along with unilateral (> bilateral) nasal discharge. Aspergillosis sp. and Penicillium spp. have also been isolated (6). Trauma, congenital and conformational aspects, polyps, periodontal disease and foreign bodies all predispose to chronic infection (7). Any factors contributing to alterations in the structure or function of the upper airways, be they primary inflammation (lymphoplasmacytic rhinitis) or that secondary to the noxious effects of infection, will compromise normal function and predispose to chronic damage if the cat is unable to resolve the underlying factors. Chondritis and osteomyelitis are often sequellae to infection/inflammation. There is some suggestion that chronic rhinitis/sinusitis may predispose to nasal lymphoma in cats. Neoplasia further alters function and form, allowing secondary changes, which may be more worrisome to the client than the underlying cancer. If there are concurrent stressors (sub-optimal nutrition, social distress, environmental factors) or outright immunocompromise/suppression (e.g., retroviruses), the likelihood of infectious agent involvement and the inability to clear these is increased. Most feline nasal tumours are malignant. They tend to be locally invasive (frontal and paranasal sinuses) without metastasizing distantly. Similar to other types of cancer in cats, the older cat is over-represented. Clinical signs will vary depending on the location of the tumour. Nasal tumours result in sneezing and unilateral nasal discharge; nasopharyngeal masses present with stertorous respiration. Further signs include variable facial deformity, epistaxis and epiphora.
DIAGNOSTICS When rhinitis or rhinosinusitis is a recurrent or chronic problem, a logical and thorough diagnostic plan should be followed. Start with a minimum database of a CBC, serum
166

biochemistry, retroviral serology, urinalysis and blood pressure determination, if not already done in the earlier examination. If rhinoscopy is considered or if epistaxis has been part of the process, a coagulation panel should be performed. Any medications affecting hemostasis (e.g., aspirin, alpha antagonists) should be temporarily discontinued. If regionally appropriate, perform Aspergillus and Cryptococcus serologic titres. If lymph nodes are enlarged, cytologic specimens should be collected to use for staging in case neoplasia is diagnosed by histopathology. Skull radiography or CT/MRI to image dentition, nasal passages and sinuses as well as bone health will require general anaesthesia. Conventional radiography underestimates the extent of disease. Probe all periodontal pockets, retract the soft palate to look for polyps and palpate the soft palate. Three standard radiographic views should be exposed using high detail films and screens. 1) Open mouth ventrodorsal view assesses the nasal cavity and bullae. Symmetry is essential for evaluation of changes. 2) A lateral view allows evaluation of the frontal sinuses; if a change is suspected, it may be followed by an oblique lateral view to focus on the sinus in question. 3) A skyline view of the frontal sinuses is valuable and is performed with the cat in dorsal recumbency, pulling the mandible out of the way. Following imaging, samples should be harvested. Michiels et al (8) evaluated the records of 40 cats who had undergone rhinoscopy for chronic nasal disease to compare relative diagnostic yield. Specimens in 17 cases were collected by brush cytology (higher yield than flush cytology). Concurrent biopsies were collected for histopathologic evaluation. Only 25% of the cases showed agreement. The conclusion was that cytology (even brush cytology) does not appear to be a reliable means for the detection of chronic inflammation and evaluation of chronic rhinitis in cats. The small size of cats makes scoping challenging: a flexible endoscope may be retroflexed around the soft palate if retraction of the soft palate using a dental mirror was unrevealing. To evaluate the more rostral portions of the nasal passage, a rigid 1.9 mm arthroscope with a 30 degree viewing angle may be used if a small flexible scope is unavailable. Irrigation with sterile saline is essential for optimal visualization. Mucus exudation, a polyp or mass, foreign body or “webbing” (nasopharyngeal stenosis) may be seen. If unilateral disease is present, evaluation of the unaffected side first is recommended. Normal turbinate mucosa should be pale pink and smooth. Hyperemia, irregular turbinate surfaces and moderate amounts of discharge suggest pathology. Fungal plaques may be seen and biopsied. While adenocarcinoma or sarcoma appear as a discrete mass, lymphoma may present as a mass or as a diffuse infiltrate. Even if the mucosa looks normal, biopsies should be taken in a cat with chronic disease, as gross appearance may be misleading. The entire cavity (rostral and caudal) should be examined before biopsying to avoid bleeding which interferes with visualization. Sedation may be desirable upon recovery and overnight hospitalization prevents excessive movement allowing hemostasis to occur.
167

Concurrently, samples should be collected for culture. Aerobic and anaerobic cultures may be set up but results must be interpreted with caution because there are large numbers of normal flora in the nasal cavity. One can improve diagnostic yield by obtaining cultures from deep within the nasal cavity avoiding superficial contamination. Calicivirus identification requires virus isolation (VI). VI may also be attempted for FHV-1, however exposure to FHV-1, Chlamydophyla and Mycoplasma may be determined using PCR. A recent study (9) assessed the relative sensitivity of PCR assays for the detection of FHV-1 DNA in clinical samples and commercial vaccines. It concluded that none of the assays was able to distinguish between wild-type virus and vaccine virus. Additionally, test sensitivity (detection limits and rates) varies greatly between the tests used. Before recovering the patient from anaesthesia, flush gently and thoroughly to remove and aspirate the discharge to help the patient during and after recovery. The endotracheal tube must be well cuffed and the oropharynx should be packed with a known number of swabs to prevent fluid aspiration.
THERAPEUTICS: SPECIFIC Practitioners frequently choose antibiotics to treat the cat with upper respiratory disease. But do we know what organism is involved? If multiple organisms are grown on culture, the significance of the growth is questionable. Should a single bacterial species grow on culture that is NOT a normal commensal, sensitivity results may be used. Therapy should be continued for 6-8 weeks without changing the antibiotic if there is an initial positive response to the antibiotic, so the antibiotic should be safe for long-term use. Antibiotics should be chosen that reach the site of infection at effective therapeutic concentrations. Antibiotics that penetrate cartilage and bone are of value making amoxicillin- clavulanic acid, clindamycin and chloramphenicol reasonable choices. Clindamycin, doxycyline and chloramphenicol are effective against Mycoplasma spp.; metronidazole and doxycycline modulate the immune response thereby reducing inflammation somewhat. Doxycycline is effective against Chlamydophyla and L-forms. Azithromycin (5-10 mg/kg PO q24h for 5 days, then q72h long term) is popular because of its long duration of action. Pulse or intermittent therapy (e.g., one week/month) predisposes to the development of antibiotic resistance and cannot be recommended. Administration of antibiotic ophthalmic drops may be included because they can be used as direct topical therapy to the nasal passage. Should Cryptococcus sp. or Aspergillus sp. be cultured, specific antifungal protocols should be followed (discussed elsewhere). If an allergic component is suspected because of seasonal recurrence, antihistamines may be considered. Chlorpheniramine maleate 1-2 mg/cat PO q12h may be used. Less sedative antihistamines (e.g., AllegraTM, ClaritinTM), selectively inhibit peripheral H1 receptors. For FHV-1 infection, administration of the intranasal herpes and calicivirus vaccine two to three times a year may be beneficial in stimulating local immunity. L-lysine helps to reduce the frequency of herpesviral recrudescence by competing with arginine needed for viral replication. The dose is 250 (kittens) – 500 (adults) mg PO q12h long term.
168

Interferon alpha at 30 units PO q24h may also help modulate FHV-1 infection. Similarly, ophthalmic administration of alpha interferon in saline has been recommended for cats with herpes virus keratitis or conjunctivitis. Acyclovir is an anti-herpes drug used in humans. Because of potential toxicity in cats, it should only be used in cats with confirmed herpes infection and started at a low dose (10-25 mg/kg PO q12h) monitoring the CBC every 2-3 weeks. Polyps and foreign bodies should be removed. A novel approach to the removal of a polyp originating in a frontal sinus was recently reported (10). Because of the small size of the patient, an endoscope was passed orad through the cardia of the stomach, into the esophagus and orophaynx allowing retrieval of several polypoid masses. Nasophyaryngeal stenosis/”webbing” requires surgical resection via a transpalatine approach. Like polyps, webs may reoccur. Dental disease should be treated, repairing fistulae if present. Surgical drainage and flushing may be warranted for some patients with chronic sinusitis. After openings are drilled into the frontal sinus, histopathologic samples and bacterial samples may be collected. Trypsin-containing solutions may help break up heavy mucus. Sinus ablation has also been described in which the frontal sinus is opened by bone flap, the mucoperiosteal lining is removed, necrotic nasal turbinates are removed, the opening between the sinus and nasal passages is obliterated with a piece of temporal muscle fascia and the frontal sinus is packed with a piece of ventral abdominal fat. This technique has shown success and fat is preferable to the use of polymethylmethacralate.
THERAPEUTICS: NON-SPECIFIC Maintaining hydration is essential for tissue perfusion, but also to make secretions less viscous and to improve cell function (e.g., their ability to clear mucus via the muco-ciliary apparatus). Thus, humidifying the air around patients with chronic airway narrowing is beneficial be it by steaming the bathroom or instilling saline into the nostrils to stimulate sneezing and clearance of the nasal passages. Oral decongestants include diphenhydramine HCl 2-4mg/kg PO q8h, or dimenhydrinate 4mg/cat PO q8h, or pseudoephedrine 1 mg/kg PO q8h. Nasal decongestant drops are challenging to administer, but can be very helpful (pediatric OtrivinTM = 0.05% xylometazoline 1 drop into each nostril SID for three days only to avoid rebound congestion). Anti-inflammatories play a role. By reducing airway swelling, breathing improves and less secretion is produced making the patient more comfortable. Glucocorticoids may help by retarding leukocyte function and migration, block phospholipase A, decreased release of lytic enzymes, suppress delayed hypersensitivity reactions. This makes them candidates for use in lymphoplasmacytic rhinitis, the most common form of chronic rhinitis. Because the condition itself is not life-threatening, glucocorticoids should be used intermittently rather than continuously long-term. The author uses prednisolone daily for a week, and reduces to q48h over the next week. The concern with the use of glucocorticoids is the possibility that they might result in recrudescence of the virus or virus shedding. Non-steroidal anti-inflammatories are alternate options; they should be given with food and dosed based on lean body weight. Piroxicam (0.3 mg/kg PO q48h)
169

or meloxicam (0.05 mg/kg SID) may help. Leukotriene blockers may also be considered to reduce inflammatory cell infiltration. SingulairTM: 0.25mg-0.5mg/kg q24h (= 1/8th of a 10 mg tab); AccolateTM: 0.5mg-1mg/kg q12-24h It is critical to pay attention to nutrition in quality, balance and quantity. In addition to the frequently used antihistamine, anti-serotonin drug cyproheptadine (1 mg PO q12h), mirtazapine at 3-4 mg/cat PO q72h is a newly recognized appetite stimulant for cats.
PROGNOSIS It is important that clients understand that a cat with chronic rhinitis/rhinosinusitis will never be cured. With on-going management, the patient’s quality of life can be improved with a reduction in sneezing and nasal discharge. References 1. Veir JK, et al. J Fel Med Surg 2006;8(6):400-411. 2. Johnson LR, et al. J Am Vet Med Assoc 2005; 227[4]:579, 3. Milner RJ, et al. J S Afr Vet Assoc 2004; 75[2]:103, 4. Frey E, et al. J Clin Microbiol 2003; 41[11]:5321, 5. Chomel BB, et al. J Clin Microbiol 1995; 33 [9]:2445, 6. Tomsa K, et al. J Am Vet Med Assoc 2003; 222[10]:1380, 7. Henderson SM, et al. J Feline Med Surg 2004; 6[4]:245, 8. Michiels L, et al. J Feline Med Surg 2003; 5[5]:279, 9. Maggs DJ, et al. Am J Vet Res 2005; 66 [9]:1550, 10. Esterline ML, et al. J Feline Med Surg 2005; 7 [2]:121
Appendix: Feline Upper Respiratory Therapy: drugs and doses Antihistamines Amitriptyline (Elavil): 5-10 mg/cat q 12-24 hours Chlorpheniramine (Chlor-Trimeton): 1-2 mg/cat q 12-24 hours Clemastine (Tavist): 0.68 mg/cat or 0.05 mg/kg q 12 hours Cyproheptadine (Periactin): 1 mg/cat q 12 hours Diphenhydramine (Benadryl): 2-4 mg/cat q 8-12 hours Hydroxyzine (Atarax): 5-10 mg/cat or 2.2 mg/kg q 8-12 hours Trimeprazine (Temaril): 0.5-1 mg/kg q 8-12 hours Cetirizine (Zyrtec): 5 mg/cat q 12 hours Fexofenadine (Allegra): 10 mg/cat q 12 hours Claritin: 0.5 mg/kg/day Decongestants: Diphenhydramine HCl 2-4mg/kg PO q8h Dimenhydrinate 4mg/cat PO q8h Pseudoephedrine 1 mg/kg PO q8h
170
Nasal decongestant drops: Pediatric otrivin=0.05% xylometazoline (1 drop into each nostril SID for three days only to avoid rebound congestion). "Little Noses" Saline Spray/Drops non medicated "Little Noses" Decongestant Nose Drops with phenylephrine hydrochloride Afrin (oxymetazoline) Note, with any topical, medicated decongestant, you may get rebound effect due to secondary Beta adrenergic stimulation after three days. Not dangerous, just more congested. Treatments for feline herpesvirus Famcyclovir 15mg/kg PO BID (62.5 mg) X 2 weeks, assess response and decide whether or not to continue. Generic is fine. 10,000 U/kg a 2 b interferon SC SID during hospitalization Herpetic keratitis: Cidofovir eye drops: 0.5% solution in 1% methylcellulose, 1 drop BID in affected eye(s) duration dependent on response. Does not burn or cause inflammatory conjunctival reaction. Gary Newton: Rx Center 2.5 ml approx $ USD 56.40 US: 1-800-682-4662, Canada: 910-485-2167
171

Tips And Pitfalls In The Diagnosis of Canine Heart Failure
Rebecca L. Stepien DVM, MS, DACVIM (Cardiology)
I. Prevalence and types of canine heart disease
A. Valvular disease affects 70% of canine patients presented for cardiac evaluation
B. Myocardial disease (DCM) is dramatic, but affects only about 8% of canine heart patients
C. Large dogs may have anything, but miniature breeds seldom have DCM
II. Heart disease vs. heart failure
A. The purpose of the cardiovascular system is to maintain adequate blood pressure (BP) to supply organ perfusion.
1. Heart disease: physical or functional abnormality of component(s) of the CV system
2. Heart failure: CO is inadequate to support BP despite normal hydration
a. Low cardiac output = signs of low BP (hypotension)
b. Sodium/water retention = congestion/edema/fluid accumulation
3. Compensatory mechanisms: renin-angiotensin-aldosterone, sympathetic nervous system, antidiuretic hormone
B. Why bother?
1. HEART DISEASE----(usually)------- MONITOR
2. HEART FAILURE-----(almost always)--- TREAT
III. Identifying heart failure based on history
A. Heart disease (HD):
1. someone (maybe you) informed owners of abnormal physical findings consistent with heart disease OR the animal was screened based on breed
2. the owner detects no abnormalities in the dog (appetite, activity etc.)
3. abnormal physical findings: typically murmur, gallop or arrhythmia
B. Heart failure (HF):
1. physical findings consistent with heart disease are present
2. owner reports outward clinical signs of CV dysfunction
a. signs of low output: inability to maintain an exercising state, FATIGUE, (decreased activity in general)
b. signs of water retention: shortness of breath (pulmonary edema or pleural effusion), abdominal fluid accumulation
172

C. Common historical reports to listen for (or directly ask about)
1. unexplained weight loss
2. difficulty sleeping (dog “can’t get comfortable at night”)
3. cough: usually a sign of cardiac enlargement, may be worse in some positions
IV. Identifying heart failure based on physical examination
A. General appearance
1. HD: no outward abnormalities related to CV system
2. HF: weakness, fatigue, abdominal fluid, dyspnea at rest, cyanosis
a. left sided: dyspnea, cyanosis, cold extremities
b. right-sided: ascites, inability to lie sternally or laterally
B. Heart rate
1. HD: usually normal (70-80120-140 bpm) - not breed related
2. HF: often elevated at rest (>120 bpm)
C. Rhythm (extra heart sounds [gallop] may be present in HD or HF)
1. HD: usually regular or SINUS ARRHYTHMIA at normal heart rate
2. HF: regular or arrhythmia (irregular rhythm with pulse deficits)
D. Heart murmurs: intensity
1. cannot differentiate HD vs. HF
2. louder murmurs are worse in animals with valvular disease
3. softer murmurs are worse in myocardial disease
E. Heart murmur: point of maximal intensity and timing (systolic/diastolic etc.)
1. cannot differentiate HD vs. HF
2. useful to diagnose exact disease
3. descriptive modifiers are not helpful and should be avoided (“holosystolic”)
F. Pulse strength: reflects cardiac function but not HD vs. HF
G. Jugular examination:
1. HD: may be jugular pulsation if severe tricuspid insufficiency or arrhythmia
2. HF: jugular distension indicates elevated RA pressure HF (± pulsation)
173

H. Pulmonary auscultation:
1. HD: breath sounds audible all fields, may be accentuated if animal is breathing heavily, cough may be present if LA impinges on bronchus or airway collapse is present
2. HF: crackles and wheezes may be present if pulmonary edema, especially caudal dorsal lung fields on deep inspiration. Muffled sounds ventrallypleural effusion
I. Biochemical findings:
1. HD: biochemical findings reflect concurrent disease states
2. HF: azotemia, decreased PaO2 responsive to oxygen, mild ALT elevations
V. Thoracic radiographs: best documentation of fluid retention
A. HD: changes in cardiac size and shape, no changes in vessels size, no infiltrates
B. HF: HD findings PLUS infiltrates and vascular congestion OR pleural effusion
1. infiltrates consistent with HF: vascular, interstitial and alveolar patterns
2. NOT consistent: bronchial (unless pre-existing), nodular, mass lesions
3. Things to watch for:
a. pulmonary edema is usually bilateral
b. predictable pattern: LA enlargementpulmonary vascular congestioninterstitial leading to alveolar infiltrates (dorsal caudal, then ventral caudal, then ventral cranial)
c. hepatomegaly with enlarged caudal vena cava (± ascites) = right heart failure
VI. Staging heart failure: a guide
A. Once HF is present – how severe is it?
B. Clinical guide for treatment
1. New York Heart Association (NYHA): based on FUNCTION (difficult in dogs)
2. ACC/AHA: based on radiographs and clinical signs (most useful)
174

American College of Cardiology/American Heart Assoc (ACC/AHA) Classification System
At risk for heart failure
STAGE A No structural disease, but high risk for developing heart disease
STAGE B1 Asymptomatic disease, minimal remodeling
STAGE B2 Asymptomatic disease, significant remodeling
Heart failure
STAGE C Past or current signs/symptoms of CHF
STAGE D End stage CHF, signs refractory to Rx
1) Staging system as a guide for therapy:
(a) most therapy begins at Stage C, when clinical signs are present
(b) exception: some therapies for DCM begin in Stage B1 or B2 if systolic dysfunction is detected
(c) once in Stage C, continue medical therapy is required (cannot go back to B2)
(d) system does NOT take arrhythmias into account: may be present and need to be treated at Stages B1-D
175

Treating Canine Heart Failure: As Easy as ABCD
Rebecca L. Stepien DVM, MS, DACVIM (Cardiology)
I. Goals of heart failure therapy
A. Acute stabilization of critical patients
B. Maintain quality of life chronically
1. Maintain breathing comfort
2. Maintain ability to exercise
3. Avoid complications
C. Extend the length of good quality life
II. Factors to consider when deciding on specific therapies
A. Do the life-threatening clinical signs indicate congestive or low output (hypotensive) problems?
1. Congestive Signs: require furosemide, mechanical drainage, oxygen
a. Pulmonary edema
b. Ascites
c. Pleural effusion (less common in dogs)
2. Low output signs: require fluid and inotropic support
a. Hypotension
b. Cold extremities
c. Pallor, weak pulses, slow CRT
B. Are the clinical signs typical of right-sided, left-sided or biventricular heart failure?
1. Right-sided HF: jugular distension, hepatomegaly, ascites and/or pleural effusion - often require mechanical drainage acutely
2. Left-sided HF: cough, coughing up foam, dyspnea, pulmonary crackles and cyanosis - requires oxygen and immediate diuretic therapy
C. Presence of arrhythmia
1. May require direct therapy
2. May be the immediate cause of CHF
3. Resolution may be required in order to resolve CHF
176

III. Which medications should I keep on hand?
A. Acute: oxygen, injectable furosemide, pimobendan
B. Chronic: oral furosemide, pimobendan, angiotensin-converting enzyme inhibitors (ACEI), spironolactone (other vasodilators for late stage patients: amlodipine, hydralazine)
C. Anti-arrhythmic medications: IV lidocaine, oral digoxin, diltiazem, sotalol and mexiletine
D. Anti-anxiety: injectable butorphanol or buprenorphine, midazolam
IV. Acute therapy of heart failure
A. Recognize general signs of acute heart failure
1. History: auscultably abnormal heart, dyspnea, abdominal swelling, cyanosis, exercise intolerance due to dyspnea or cough, pet may not have slept for several days
2. PE: weakness, depression, anxiety/panic and tachycardia (arrhythmias may be detected)
B. Recognize signs typical of left sided failure
1. Gallop rhythm, coughing up foam, dyspnea, harsh lung sounds or pulmonary crackles, left-sided heart murmurs
2. Problems to attack
a. Dyspnea due to pulmonary edema:
i. Oxygen: oxygen cage, mask, nasal cannula
Blood gas not needed
When in doubt, oxygenate
ii. IV furosemide (2-4 mg/kg IV, repeat in ½ hour if no overt improvement)
Still the “go to” diuretic
Given IV, produces clinical effects within ~15-30 minutes
Provide urination opportunities
b. Decreased cardiac performance: pimobendan for vasodilating and inotropic effects
i. Pimobendan: combined inotrope and vasodilator (0.3 mg/kg PO)
Indicated when left-sided CHF is present
Oral medication, but effective within 1-2 hours after administration
177

ii. Dobutamine: positive inotrope, given as continuous rate infusion
c. Stress related to discomfort and anxiety: sedation with (usually) opioids
C. Recognize signs typical of right sided failure
1. Jugular distension, dull heart and breath sounds, hepatomegaly, dyspnea/open mouthed breathing if pleural effusion, positional discomfort if ascites and a right-sided heart murmur
2. Problems to attack
a. Must acutely rule out pericardial effusion (by radiograph or echo)
b. Relieve dyspnea/discomfort/anxiety related to severe fluid accumulations via centesis
i. Pericardiocentesis: if needed, remove as much as possible, analyze
ii. Thoracocentesis: remove as much fluid as possible, analyze (furosemide is not a substitute for centesis, but can be a helpful follow-up)
iii. Abdominocentesis: remove approximately 2/3 of amount in abdomen
D. Additional Testing Recommended
1. 6 second (or more) lead II (or equivalent) ECG strip
2. thoracic radiographs: if feasible:
a. Should not be pushed in dyspneic animals unless diagnosis is in doubt and waiting may kill the patient
b. Even single and crooked views can help!
V. Therapy of Chronic Congestive Heart Failure
A. Medications to treat chronic left-sided heart failure due to CVD or DCM
1. Diuretics: decrease the inflated circulating blood volume
a. Furosemide: still the mainstay diuretic
b. (Spironolactone: more of a neurohormonal modulator than diuretic)
2. Neurohormonal blockade
a. Angiotensin-converting enzyme inhibitors: block conversion of angiotensin I to angiotensin II, which blocks the ATII-induced vasoconstriction (relative vasodilation) and reduces ATII-induced production of aldosterone, decreasing sodium retention.
178

b. Spironolactone: competitive blockade of aldosterone receptors, reduces effect of any aldosterone made through non-ATII mechanisms
c. Digoxin: modulates the reactivity of the sympathetic nervous system in heart failure and decreases “cross-excitation” of renin-angiotensin-aldosterone and vasopressin systems
3. Positive inotropes: increasing the contractile force of the heart
a. Pimobendan: a newer positive inotrope that increases actin-myosin interaction by sensitizing the contractile proteins to the existing amount of intracellular calcium, rather than increasing intracellular calcium
b. Digoxin: a weak positive inotrope that increases cross-bridging of actin and myosin fibrils in myocytes by increasing intracellular calcium
4. Vasodilators: decreasing afterload (arterial) and preload (venous)
a. Angiotensin-converting enzyme inhibitors: decrease the amount of vasoconstriction rather that causing primary vasodilation. Effective but less powerful than direct-acting vasodilators.
b. Amlodipine: direct arterial dilator, effective and long-acting. Less useful in acute heart failure due to prolonged onset of effects.
c. Hydralazine: potent and direct-acting, leads to rapid and significant decreases in arterial pressure
d. Pimobendan: often thought of as more of a positive inotrope, pimobendan has significant vasodilating properties due to the inhibition of phosphodiesterase III (PDE III and V) activity
B. Approach: choose medications based on underlying disease and clinical signs (=stage of heart failure)
1. Underlying disease
a. Adult onset left-sided diseases (chronic valvular disease or DCM) are treated the same EXCEPT for pre-clinical phases)
b. Adult onset right-sided diseases are treated based on individual disease (e.g. heartworm disease vs. pericardial effusion vs. chronic tricuspid insufficiency)
2. Stage of Disease (ACC/AHA classification) for left heart failure
a. Stage A: at risk for heart disease but no evidence of disease: no treatment
b. Stage B1: heart disease is present but heart is not enlarged: no treatment
179

c. Stage B2: heart disease is present with cardiac enlargement
i. No treatment vs.
ii. ACEI for chronic valvular disease vs.
iii. ACEI + beta blocker (carvedilol) for DCM
d. Stage C: heart disease and heart failure are present: first offenders: TRIPLE THERAPY (furosemide, ACEI, pimobendan), + spironolactone
e. Stage D: repeat CHF, refractory CHF: adding inotropes short term, additional vasodilators, consider therapy for pulmonary hypertension if present
C. Recurrence of CHF after previously stable period: consider
1. Disruption of normal lifestyle (stress, boarding, change in exercise or weather)
2. Change in medication compliance or misunderstanding of medication
3. Occurrence of new arrhythmia
4. Development of complication: pulmonary hypertension, azotemia, diarrhea
5. If all previous ruled out…consider advancement of disease process and add appropriate medications
180

Challenging Canine Cases
Rebecca L. Stepien DVM, DAVIM (Cardiology)
Accurate diagnosis and staging of the cardiovascular patient are the necessary first steps toward choosing a successful treatment strategy. Diagnosis and staging are based on patient history, physical examination findings and thoracic radiographic findings. American College of Cardiology/American Heart Assoc (ACC/AHA) Classification System At risk for heart failure STAGE A No structural disease, but high risk for developing heart disease STAGE B1 Asymptomatic disease, minimal remodeling STAGE B2 Asymptomatic disease, significant remodeling Heart failure STAGE C Past or current signs/symptoms of CHF STAGE D End stage CHF, signs refractory to Rx
1) Staging system as a guide for therapy:
(a) most therapy begins at Stage C, when clinical signs are present (b) exception: some therapies for DCM begin in Stage B1 or B2 if systolic
dysfunction is detected (c) once in Stage C, continue medical therapy is required (cannot go back to B2) (d) system does NOT take arrhythmias into account: may be present and need to be
treated at Stages B1-D Once therapy has been instituted, unexpected developments may occur in a previously stable cardiovascular patient due to worsening of the cardiac disease, development of complications of that disease, or development of a concurrent, unrelated illness that is interacting with the cardiac disease. The assessment of patients with any of these causes of unexpected developments is similar, beginning with reassessment of cardiovascular status, assessment for new cardiovascular complications, and a larger look at the whole patient for other concurrent diseases. Heart failure that doesn’t respond to typical aggressive therapy is often referred to as “refractory” heart failure. This term may also be used to describe sequential recurrence of heart failure signs that increase in severity over time as the heart disease progresses, necessitating step-wise increases in medical therapy. Altering or adding further medications is tempting but hazardous because heart failure patients are often hemodynamically and metabolically fragile. The goals of therapy in refractory patients are the same as in “naïve” HF patients: improving quality of life and extending life.
181

The most common reasons for recurrent or refractory congestive heart failure include: Diagnosis of CHF was not correct, or not quite correct Development of new systemic abnormalities Progression of underlying abnormalities not previously recognized Medication-related problems (cardiac or other medications) Complication of current cardiac disease Progression of cardiac disease without “new” complications
General Clinical Approach to the Patient History: Any recent changes in the patient’s life should be investigated.
Have there been changes in routine? Kenneling? Medications? Weight? Geriatric patients are at increased risk for stress during holidays that include new
visitors, changes in daily routines and access to new or unusual food. Check the owner’s report of medication doses and schedule – it is often NOT what it
says in the record. Physical examination: Physical examination of the patient may reveal evidence of concurrent systemic illness.
Are the signs of heart failure the same as previously or are they new signs? Is an arrhythmia present or has the patient’s arrhythmia changed?
Recommended diagnostic approach for the chronic heart failure patient with new illness: The diagnostic testing choices for newly decompensated chronic heart failure patients or those with concurrent illness are based on what type of problem the animal is exhibiting.
Blood testing can be very helpful in cases where a new disease is suspected, and usually includes hematology, chemistry and urinalysis to detect new diseases or new complications.
Thoracic radiographs are used to assess heart failure status and in some cases, can be helpful to identify dehydration.
An ECG is warranted if a new or different arrhythmia is present. Additional testing that can be performed on patients in which it is indicated are serum
digoxin concentration and baseline or post-pill thyroxine concentration. An echocardiogram should be considered in cases where the manifestation of heart
failure is unexpected (e.g. a dog with chronic left-sided heart failure now has ascites and pulmonary hypertension is suspected), if a cause for new signs may be found (e.g. intracardiac thrombus in a cat with signs of peripheral embolism, or a ruptured chordae tendineae in a dog with acute, fulminant pulmonary edema). In general, if findings may change therapy, echocardiography is justified.
182

Once initial testing has been performed, a prioritized problem list should be developed. Is the new problem a magnified version of the historical disease, or is it completely
different? Which conditions are life-threatening and require immediate assistance? What effects might a suspected new disease have on the heart (e.g. development of
systemic hypertension may make left-sided heart failure more difficult to resolve)? Development of a new therapeutic plan: A new therapeutic plan must take into account the systemic illnesses or abnormalities that may be present as well as the underlying chronic heart disease itself. Rebalancing the decompensated patient may involve short term lifestyle change, short or long term changes in medications or a change in the way a patient’s medications are administered. Systemic illness: Temporary adjustments of cardiac medications may be necessary during the acute pre-treated stages of systemic illness (e.g. brief discontinuation of diuretics in severely hypotensive dehydrated animals). As the problem is resolved, medications will likely be restarted and gradually need to be increased to previous dose levels. If systemic illness occurs BECAUSE of cardiac medications, there may be permanent changes in dose (e.g. electrolyte imbalances, azotemia, inappetence). New cardiac signs: New cardiac signs may develop if new complications of old diseases are present, such as ruptured chordae tendineae or left atrium, new arrhythmias or pulmonary hypertension from left-sided failure leading to right-sided failure. In addition, new signs may develop due to distant complications or new cardiovascular disease, such as thromboembolism (systemic or pulmonary), dirofilariasis or cardiac tumors. These new complications are often uncovered with standard diagnostic tests, including radiographs, echocardiography and directed laboratory testing.
183

Confident Diagnosis and Treatment of Feline Heart Disease
Rebecca L. Stepien DVM, MS, DACVIM (Cardiology) HEART DISEASE VS. HEART FAILURE: CATS vs. DOGS In dogs, the difference between heart disease and heart failure is usually the difference between treatment and no treatment. In cats, the situation is not as straightforward, primarily based on the prevalence of functional murmurs in cats and the controversies surrounding dynamic left ventricular outflow tract obstruction that may cause these murmurs. When a diagnosis of heart disease or congestive heart failure is considered, the patient typically undergoes some amount of diagnostic testing, often receives therapeutic recommendations, and leaves the clinic. Many resources address medication recommendations and dosages, but the clinician may left wondering what to do when medications don’t work as anticipated, or how to monitor the chronic heart disease patient compared to the heart failure patient. Heart Disease vs. Heart Failure The first step in successful management of feline cardiac patients is to decide whether the patient has heart disease (anatomic or functional abnormality of the heart) or heart failure (heart disease plus clinical signs of congestion or low cardiac output). In general, congestive signs in cats usually are detected as tachypnea or dyspnea due to pulmonary edema, pleural effusion or both. Mild signs of low cardiac output (e.g. fatigue) may be difficult to discern in cats, but severely decreased cardiac output results in hypotension, with clinical signs of weak pulses, decreased core temperature and bradycardia. This differentiation guides immediate and long term therapy, as heart disease without heart failure is treated medically only in specific circumstances, and heart failure is always treated, with the severity of the failure dictating the aggressiveness of the therapy. DIAGNOSIS OF HEART FAILURE WHEN HEART DISEASE IS PRESENT Heart disease may be initially identified in cats with no clinical signs based on physical examination findings. In cats, identification of a heart murmur, a gallop rhythm, an irregular heart rhythm or any combination of these findings may indicate the presence of heart disease. Of these, gallop or irregular heart rhythms are highly suggestive of cardiac abnormality, while heart murmurs may be heard in some cats without identifiable cardiac abnormality or cardiac changes secondary to systemic problems (e.g. anemia). Recent studies suggest that 15-30% of random healthy cats have discernable heart murmurs and that approximately 1/3 of cats with murmurs will have detectable heart disease on investigation. Taken together, this makes identification of Stage B1 heart disease (cardiac abnormality without remodeling or clinical signs) more problematic in cats than it is in dogs. In young to middle-aged cats without clinical signs, assessment of NT-proBNP concentration may add information and in some cases, answer the question of whether diagnostic cardiac evaluation (e.g. echocardiogram) is needed. NT-proBNP is released from “stressed” ventricles, and is typically elevated in cats with structural heart disease even when heart failure is not present. The test is quite reliable in cats, and may be used clinically to assess the importance of a
184

murmur in a clinically normal animal. If NT-proBNP is elevated in this type of patient, further diagnostics are indicated but if the NT-proBNP is within the normal range, there is a greater likelihood that the patient’s heart is not significantly abnormal. A diagnosis of heart failure is based on compatible findings in the patient’s history (decreased activity, decreased appetite, dyspnea or tachypnea), physical examination findings (heart murmur/gallop rhythm/ arrhythmia, pulmonary crackles, jugular distension, dull heart sounds or percussion) and thoracic radiographs (to identify cardiomegaly, pulmonary vascular congestion, pulmonary edema and/or pleural effusion). In some cases, thoracocentesis may be performed based on physical examination findings and pleural effusion diagnosed without radiographic imaging. In these cases, post-centesis radiographs and fluid analysis are suggested to confirm the diagnosis of heart failure. GENERAL APPROACH TO THE PATIENT Whether a patient has heart disease or heart failure, the same areas of concern can be covered as treatment is considered:
Initial staging (diagnosis of problem, identification of concurrent problems) Decision regarding use of medical therapy Client education Treatment and monitoring schedule
Heart Disease Initial Staging: When auscultable cardiac abnormalities are detected in a cat with no clinical signs, further investigation is recommended, especially in older cats, cats in which anesthesia is anticipated, or cats with vague clinical abnormalities that may or may not reflect heart disease. Typical diagnostic testing includes thoracic radiographs, echocardiography, an electrocardiogram if an irregular heart rhythm is detected, blood pressure assessment and thyroid evaluation (if age appropriate). Identification of systemic abnormalities present at the time of heart disease detection may require additional biochemical testing, urinalysis and other imaging, as appropriate for the individual patient. In many cases, establishing “baseline” biochemical and urinalysis findings while the patient is without clinical signs is helpful as a comparison for future testing. Echocardiographic examination establishes the exact cardiac diagnosis (e.g. HCM), may provide clues reflecting systemic illness (e.g. left ventricular hypertrophy in systemic hypertension), reveals complications (e.g. the presence of intracardiac thrombi) and may allow “fine-tuning” of the diagnosis in ways that may affect therapy (e.g. dynamic left ventricular outflow tract obstruction due to systolic anterior motion of the mitral valve [SAM]). Importantly, echocardiographic findings may identify no cause for an ausculted heart murmur or identify a benign cause for an ausculted abnormality (e.g. dynamic right ventricular outflow tract obstruction). In these cases, the echocardiographic evaluation can rule OUT heart disease, and decrease the concerns of the clinician and the owner. Thoracic radiographs are an important part of the diagnostic evaluation even in cats without clinical signs, primarily to detect other thoracic abnormalities, subclinical heart failure, or cardiomegaly alone. The degree of cardiomegaly in the cat with heart disease but no clinical
185

signs allows planning of future re-evaluation, with cats with marked cardiomegaly scheduled for cardiac recheck more frequently than cats with normal cardiac size. Medical Therapy Recommendations: Specific cardiac therapy is generally not recommended in cats with identified heart disease but no evidence of heart failure, with the exception of some animals with dynamic left ventricular outflow tract obstruction. Diltiazem, previously commonly recommended for cats with HCM with the aim of promoting diastolic dysfunction, has fallen out of favor due to lack of evidence of efficacy. Diltiazem is still used as an antiarrhythmic medication in cats, especially those with atrial fibrillation. Cats with evidence of dynamic left ventricular outflow tract obstruction due to systolic anterior motion of the mitral valve and left ventricular hypertrophy may benefit from chronic beta blocker therapy; this treatment decreases HR and the extent of LV outflow tract obstruction, but long term benefit has yet to be proven. Now (when the patient is outwardly normal) is the time to optimize the patient's diet and weight. Client Education: In cats with proven heart disease but no clinical signs, the emphasis of information given to clients should center around supplying basic, current information about the disease, preparing the clients for potential modifications or problems that may be anticipated with regard to elective procedures/anesthesthetic events and discussing which clinical signs they should watch for and what to do if problems occur. This is a good time to introduce the concept of home monitoring of respiratory rate so that the client can identify a "typical" baseline respiratory rate for the patient. This serves two purposes: to give the client a numerical scale to monitor the patient at home (with instructions on what to do if resting respiratory rate increases) and to provide the owner with a "sanity check" for use in case they think that they may be imagining increased breathing rate in their pet. Monitoring Schedule: Systemic hypertension and/or hyperthyroidism should be treated primarily in affected patients. Once blood pressure has been normalized in hypertensive patients, routine blood pressure and physical rechecks (including retinal exams) should occur approximately every 3 months in most patients. For primary cardiac disease without heart failure, recheck appointments can be scheduled at 6 month to one year intervals with instructions to the owner to "call sooner if any questions or problems occur". Heart Failure Initial Staging: When congestive is diagnosed, treatment should begin immediately if the patient is exhibiting overt dyspnea or markedly increased respiratory effort. If physical examination findings are consistent with pulmonary edema (increased respiratory sounds, pulmonary crackles), parenteral furosemide should be administered. If pleural effusion is limiting respiration, thoracocentesis (with concurrent oxygen support) can be life-saving and should be performed prior to any other diagnostic or therapeutic manipulation. Medical Therapy Recommendations: As is the case in dogs, medical therapy of congestive heart failure in cats once acute signs have been stabilized relies on a combination of diuretics, vasodilators, inotropes and neurohormonal blockade.
Furosemide: Parenteral or oral furosemide (1-4 mg/kg q 8-12 hours) is still the mainstay diuretic used to treat heart failure in cats. Cats are prone to hypokalemia when receiving
186

furosemide, particularly if they are inappetent. Serum potassium concentrations should be monitored acutely and over time, and potassium supplements are recommended to maintain serum potassium concentrations of at least 4 mmol/L.
Angiotensin-converting enzyme inhibitors (ACEI): Medications like enalapril or benazepril (0.5 mg/kg q 12-24 hrs) should always be administered to patients that are receiving chronic furosemide therapy to limit neurohormonal activation and provide vasodilation. Contraindications for initiating include dehydration or hypernatremia, but ACEI may be started once these problems are resolved by appropriate therapy.
Pimobendan: Pimobendan is not approved for use in cats at this time, but has shown promise in the therapy of heart failure associated with cardiomyopathies in cats. Although classically categorized as a positive inotrope and vasodilator, pimobendan also has had pro-diastolic effects (positive lusitropy) documented in dogs. It is likely that the combination of these mechanisms proves beneficial in cats with congestive heart failure regardless of the type of dysfunction (systolic, diastolic or combined) present. The anecdotal dose is similar to that in dogs (approximately 0.25 mg/kg PO q 12 hrs or 1.25 mg per cats q 12 hrs). Although few side effects have been seen in feline patients thus far, some cats and clients may object to the size of the tablets.
Spironolactone: Spironolactone may be introduced to the stable patient’s treatment regimen as a long-term “care-taking” medication that limits neurohormonal activation. This medication may be especially useful in patients with pleural effusion to limit sodium and water retention leading to body cavity fluid accumulation, but is also used chronically in patients without effusions to (theoretically) decrease development of myocardial fibrosis and limit chronic neurohormonal activation.
187

The sequence of use of these medications typically begins with oxygen, furosemide and thoracocentesis if needed in the emergency patient, and proceeds to oral furosemide/pimobendan/ACEI in the first week of home therapy and addition of spironolactone, if desired, at the first recheck (approximately one week). Client Education: When acute congestive heart failure has occurred, it is often a highly stressful situation for the client as well as the patient. Once acute stabilization has been achieved, a discussion with the client regarding the logic, sequence and details of therapy is an important part of increasing client compliance and improving quality and length of life in the patient. Specific points that can be addressed are drug administration details (which medications must be given on a fairly strict schedule e.g. diltiazem, and which drugs may be given as needed in an emergency, e.g. furosemide), the importance of maintaining food intake and the importance of monitoring respiratory rate. Owners can be easily taught to monitor their heart failure patient’s respiratory rate in order to monitor for recurrence of pulmonary edema or pleural effusion. When initial heart failure has been treated and the patient is released, the owner can take the cat’s minute respiratory rate for several evenings in a row to identify the cat’s basal rate when not in heart failure. Over time, the clients can either take the respiratory rate on a schedule (e.g. several times per week) or at least have a baseline for comparison for some future moment when the cat appears to be “breathing funny”. Respiratory rates over about 30 per minute, especially if the rate has increased suddenly, may be used as an indication to contact the veterinarian or, if dyspnea is present, administer an extra dose of furosemide and then call the veterinarian for more advice. Monitoring Schedule: Discharge from the hospital after first occurrence of heart failure may occur after a day evaluation or several days of intensive management. Ideally, if the patient has been treated with high doses of diuretics for several days, serum creatinine and potassium status should be determined before discharge so that appropriate medication adjustments, including potassium supplementation, can be made. The first recheck evaluation usually occurs within one week, with some cats rechecked in 3-5 days if the patient is not doing well. For patients on shaky ground at discharge, a 24 hour phone check can be extremely helpful to ascertain the patient’s status and answer new questions that may have arisen since the patient arrived home. At the one week check-up, previous problems should be re-evaluated specifically in addition to an overall status check. For example, radiographs should be obtained if the patient had pulmonary edema or pleural effusion at original presentation, or an ECG should be recorded if arrhythmias are being treated. It is usually useful to check renal and electrolyte status at the one week recheck, but full chemistries and blood counts are usually not required. As soon as the patient is stable on medications (at one week check or subsequently), we usually recommend recheck appointments every 3-6 months, with specific instructions for owners to contact us in the interim if any problems come up.
188

Special Victims Unit: The Hypotensive Patient: The typical presentation for this type of “low output” heart failure patient is that of a patient already being treated for heart failure with diuretics and vasodilators who then stops eating for any reason. Dehydration results in decreased cardiac output, with clinical signs of low heart rate (often in the 120-140 bpm range), low rectal temperature, cool extremities and depression/lethargy. Temporarily discontinuing the dehydrating medications while provide cautious fluid support can bring these patients back to baseline with the goal of returning to a normal appetite. These patients require intensive management but usually only for a short time, until electrolyte disturbances and prerenal azotemia can be addressed. Acute monitoring of rehydration of the hypotensive patient: Careful observation of the patient’s urinary output will help judge the adequacy of rehydration efforts. This need not (and usually should not) involve invasive monitoring. If the patient is allowed the opportunity to urinate and does so after fluid administration, some efficacy can be assumed. Alternatively, bladder filling can be assessed by simple palpation or even “quick” ultrasound checks. Respiratory rate is a valuable indication of “overhydration” – when a patient’s resting respiratory rate (non-panting) climbs to > 30-~30 breaths per minute during fluid therapy, fluid therapy rate should be reassessed. Return to normal temperature, heart rate and appetite are indications of successful therapy but the patient may require 2-3 days of careful support before recovery is evident. An important component of care at this stage is frank discussion with the owner regarding the delicacy of the treatment protocol and the importance of not rushing the therapy in these fragile patients.
189

Top 10 Misconceptions in Clinical Care of Cardiovascular Patients
Rebecca L. Stepien DVM, MS, DACVIM (Cardiology)
The dictionary describes a “misconception” as a “mistaken idea”. In clinical medicine, most cases are complicated enough that many pieces of information must be integrated and coordinated, and when large numbers of diagnoses, medications and concurrent problems are involved, it is almost impossible to proceed without some questions or misunderstandings. In cardiovascular medicine, some misconceptions are well-entrenched, perhaps because the misunderstanding of the topic is widespread, the situation in cats/dogs differs from conventional wisdom for similar human patients, or because the facts are counter-intuitive. The following misconceptions are common, widespread, and can negatively affect patient care and the clinical success of therapy. Please note that the following ideas are FALSE: 1. Angiotensin-converting enzyme inhibitors cause renal failure, but benazepril is less “toxic”.
Due to the mechanism of action of these medications, most changes in renal values and electrolytes associated with their use are due to poor renal perfusion and can be avoided by only using ACEI in hydrated patients.
Acute CHF can be treated without ACEI in the short term, and these long-term medications can be started safely when the patient is hydrated and eating.
Enalapril and benazepril do not differ in their mechanism of action, only in their metabolic disposition. Enalapril is eliminated primarily via the kidneys, and benazepril via the liver. Therefore, benazepril is recommended in patients with known renal disease to avoid decreased elimination.
2. Dental disease is a frequent cause of canine valve disease.
Dental disease is a risk factor for many co-morbidities, but valvular heart disease is not one of them. There has been a single well-documented case of endocarditis following a dental procedure, and no good data in dogs regarding any relationship between dental disease and degenerative valve disease, the most common type of heart disease in dogs.
Bacteremia during dental procedures has been well-documented and poses a risk to many vital organs, especially the kidneys. This fact provides a rational argument for peri-procedural antibiotic administration.
Supportive fluid administration and limiting the length of the procedure can protect the patient from renal complications post-anesthesia.
190

3. Patients with heart disease cannot be vaccinated or anesthetized safely. Patients with active congestive heart failure have limited ability to respond to
physical or medical challenges and most routine elective procedures (e.g. vaccinations, dips and extensive grooming, dental procedures) should be postponed until the patient is clinically stable.
Patients without CHF or those who are being treated chronically and are stable may receive all routine care as usual.
Stable cardiovascular patients can be anesthetized safely, using cardiac-friendly medications and good monitoring. Xylazine, medetomidine and dexmedetomidine are not appropriate for patients with stable or unstable cardiac conditions, and ketamine should be avoided if possible.
4. Chronic cardiac medications should not be given on the morning of anesthesia.
The day of anesthesia, with its associated cardiorespiratory challenges, is not a good day to suddenly stop chronic cardiac medications.
Cardiac medications should be given as usual but without food on the morning of anesthesia. The patient should have access to water until induction.
Fluid therapy during anesthesia is an important contributor to renal-safe anesthesia in cardiac patients and the usual standards for fluid administration to anesthetized patients should be followed.
Close attention to blood pressure during anesthesia allows early detection of hypotension.
5. Elderly patients are like everyone else, only older.
Geriatric patients are often surprisingly resilient to heart disease and therapy for heart disease, so much so that the clinician often forgets how elderly patients differ from younger patients. Older patients are more likely to have concurrent disease that limits drug
metabolism or appetite. Older patients are often thin and may be debilitated, and have difficulty
tolerating “usual” doses of medication. Older patients may receive multiple non-cardiac medications, which may
provide opportunities for adverse drug interactions to occur. NSAIDs have multiple side effects that may be exacerbated by use of cardiac medications and should be used with great care, if at all, in these fragile patients.
The advantage of working with geriatric patients is that they are usually highly valued as part of the family and often have very dedicated owners.
191

6. ECG machines and monitoring devices are more accurate than people.
Reading ECGs is challenging for human beings. It’s hard to expect that machines can do better at counting heart rate during arrhythmias, and at diagnosing arrhythmias, and monitors will sometimes arrive at interesting diagnoses such as “signal detection failure”.
Heart rate identification is the easiest part of assessing rhythm abnormalities, and should be performed by a human being to avoid machine error.
7. Patients with abdominal fluid need an exploratory for liver disease.
Abdominal distention due to fluid accumulation without the presence of a heart murmur is often misdiagnosed as non-cardiac in origin.
Pericardial effusion is a very common cause of accumulation of abdominal fluid, and should be ruled out prior to further diagnostics for liver disease.
Pericardial effusion can cause sudden death if unrecognized; a survey lateral thoracic radiograph is indicated for any patient with abdominal fluid accumulation.
8. Patients usually only have one disease at a time, therefore, clinical abnormalities in a patient with heart disease are due to that disease.
It’s tempting to assume that once a patient has serious disease of any major organ, most new clinical signs will be referable to that disease.
In cardiac patients, the extended survival that is becoming the norm for CHF patients allows time for other diseases to develop. Some of these problems may have a clinical presentation that looks like cardiac disease.
9. Assessing for systemic hypertension can be difficult; luckily it’s rare and causes few problems – BP measurement is more trouble than it’s worth.
Systemic hypertension can be a clinically silent disease and requires a high index of suspicion for diagnosis.
Unrecognized systemic hypertension can result in permanent blindness, progressive renal deterioration and unexpected congestive heart failure after fluid administration.
The presence of retinal detachment, retinal hemorrhage or intraocular hemorrhage (hyphema) should be considered a strong indication for measurement of blood pressure in cats and dogs.
Renal disease, especially proteinuric renal disease, is a significant risk factor for development of systemic hypertension.
Systemic hypertension in cats tends to be stable once successfully treated, but in dogs, hypertension tends to be progressive over time and may require additional medication after an initial period of stable response to antihypertensive medications.
192

10. Congestive heart failure patients have a poor prognosis, and since they’re often old, it’s better to “not put them through” therapy for the disease.
Newer treatments for CHF that are applicable in both dogs and cats have significantly prolonged survival for veterinary patients with congestive heart failure, and most of these medications have very tolerable side effect profiles.
Because these medications improve quality of life, patients can enjoy longer periods of clinical stability and therefore, prolonged survival.
Many problems that arise with first therapy of CHF can be fixed with medication adjustment or substitution.
Prolonged high quality of life survival in these patients enhances their lives with their owners and provides ample opportunity for veterinarians to both educate and learn from their clients.
193

The Dairyland Initiative: Building Welfare Friendly Facilities For Dairy Cattle
Nigel B. Cook ABSTRACT Major consumer concerns exist over current dairy practices that relate to herd housing, herd size and ‘factory farming’, lack of grazing in our production systems, and the ‘hyper-production’ of our dairy cows. If we are to believe animal activists and main-stream media, large scale confinement dairy herds are places where cows are forced to milk around the clock, where individuals are pushed to breaking point with the use of hormones and feed additives, resulting in metabolic disease, poor well-being and premature death. In our Wisconsin dairy industry, while we can find examples of poor management and housing in both small and large herds, we generally find excellent standards of care and well-being in our dairy herds and we work with the industry to continue improvement in this area. Our experiences have culminated in ‘The Dairyland Initiative’ – a web-based program designed to facilitate the construction of welfare friendly housing for dairy cattle, which we believe is essential to the prosperity of our dairy industry. KEY WORDS: Welfare friendly housing, dairy cattle INTRODUCTION For years, the US dairy industry has forged ahead, becoming increasingly industrialized, adopting scientific enhancements to feed and productivity, with the primary goal of producing a plentiful supply of cheap, safe food at least cost. In recent years we have seen the emergence of large confinement housed facilities for dairy cattle with several thousand cattle housed in one site and this has been associated with increasing concerns for animal welfare. There are a number of reasons for the growing concern over the welfare of our food-producing animals. One can look at the increasing urban-rural disconnect. Fewer families have relatives that are involved in farming, and many are completely unaware of how meat and milk are produced. The growth in disposable income also carries with it a desire and ability to purchase better quality food and allows the consumer to exercise greater choice – concern over the care of the animals producing that food is central to many when they make that choice. Concerns over food safety are real, and the recent meat recalls for E.coli 0157 and Salmonella issues have raised awareness and the belief that our food is no longer as safe as we once thought it was. With the industrialization of the dairy industry, many people find themselves living near a large dairy herd (In the US referred to as a Concentrated Animal Feeding Operation or ‘CAFO’) and one has only to read the newspaper or watch TV to ‘know’ that these animal factories are mistreating animals and polluting the environment. With such a backdrop, it is not surprising for authors such as Michael Pollan, for mainstream films such as Food Inc. and for animal activism, led by organizations such as
194

PETA and HSUS, to increasingly shed doubt on modern farming practices and spread the word that we should all ‘shop local’ and vegetarianism is the healthier way to live if we are to stop needless animal cruelty and global warming. Within this argument, it appears that animal housing has become ‘bad’ and something ‘unnatural’. So, are they right? Have we got it wrong? Have we developed a monster in our back yards that we need to distance ourselves from as veterinarians? Specifically, are we putting our cows in large animal factories, pushing them to metabolic breaking point with no regard for animal well-being? Or is the truth rather different? In this article I will focus on concerns over housing systems and what we can do to improve them. Our approach in Wisconsin is to bring the producers together with construction professionals, consultants and agricultural lenders and promote the concept of welfare friendly housing. This has culminated in the launch of ‘The Dairyland Initiative’ last year – a web-based program to facilitate the flow of ideas and information related to housing dairy cattle. GRAZING AND ORGANIC The general public’s idealized vision of the dairy industry – one that marketers have used and misused in recent times in an attempt to enhance milk sales, consists of a well managed grazing dairy herd, where cows have access to pasture almost year round with good health and fertility producing ~25 l of milk per cow per day predominantly from forage, organically labeled without the use of ‘dangerous’ antibiotics, hormones and pesticides. Proponents of grazing point to the fact that the dairy cattle are managed in their natural state, eating a feed that they have been designed to harvest and magically convert into a nutritious food for humans. Freedom to exhibit natural behavior is of major importance to those that wish to ensure good welfare, and grazing certainly fits that requirement well. There is some evidence that grazing herds have a lower prevalence of lameness, and the lower production may help reduce the risk for metabolic disease. Recent evidence would also suggest that allowing lame cows access to pasture might help to improve locomotion (Hernandez-Mendo et al., 2007). Recent choice experiments where cows are allowed to decide whether to access pasture or housing have yielded some surprising results. In one study, when given the choice of housing or pasture, cows selectively preferred housing during the day and pasture during the night (Legrand et al., 2009). In another study, cows chose to remain housed twice as often as moving to pasture when they were allowed the same choice after each milking, with high production level and rainfall influencing that choice toward housing (Charlton et al., 2011). These data suggest that while cows may prefer to graze pasture at least some of the time, and it may be ‘good’ for them, the choice may not be as important to them as we may wish to make it from our preconceived notions. Grazing isn’t without its problems. Environmental regulations would not allow all herds to graze because of the risk of manure run off contaminating waterways. The lower production from grazing, if taken to a national scale, would take us back to the 1940s and
195

the market for milk would be such that we would need many more cattle to sustain the production required to meet the demand. Many of the same people that feel good about grazing cattle are also the same people that are trying to reduce their carbon footprint and help prevent global warming. Finding that the US current carbon footprint for the dairy industry is 37 % less than it was in the 1940s may surprise some and perhaps paint a different picture (Capper et al., 2009). Given that the FAO warns that we will need 100% more feed to provide to the 9 million people that will inhabit the planet in 2050, it is hard to believe that this increased production is going to come from an industry that returns to grazing. Finally, anyone involved in managing dairy herds at grass knows that they are not without their problems. Grass staggers in the spring, parasitism, ketosis in early lactation and lameness – especially when young-stock transition from pasture to the milking herd at the time of first calving, and where track maintenance is poor causing injuries as cows walk great distances to and from the milking center, can all be serious welfare issues. Dealing with inclement weather during the winter can present a major challenge for udder health and the provision of adequate feed year round can in some situations be problematic – leading to what can only be described as controlled starvation. Heat stress in the summer can also be a major concern in some climates where there is inadequate shade. For these reasons it is common for grazing herds to construct winter housing to confine the animals in the winter – creating a facility that they use only part of the year, with many of the limitations that we complain about in herds that house year-round. Because organic marketing is so tightly associated with grazing, it is sometimes hard to separate the two. However, organic is a management choice, not a housing choice - in fact, Langford et al. (2008) have shown that there is no difference in the quality of housing between organic and non-organic herds. Some organic dairy herds have excellent standards of management and care, however some do not. Like some conventional herds, they are poorly managed and badly housed. In fact there is little scientific evidence for organic herds having improved health and welfare (Huzley et al., 2004), although one study recently showed a lower prevalence of lameness (Rutherford et al., 2009). The organic movement’s desire to promote their product as antibiotic and hormone free is also damaging to the industry as a whole as it implies that conventional milk is somehow contaminated. If we follow the science, it clearly shows that there is no significant difference in the hormonal content of milk from organic dairies and conventional dairy herds that either use or do not use BST. Some organic milk actually contains significantly more estrogen and progesterone than conventional milk (Vicini et al., 2008). In short, organic does not mean better or healthier, in my view, it just means the management used to produce the milk was different and followed a different philosophy, which consumers should be allowed to support, provided they are aware of the truth. The vast majority of grazing herds also utilize winter housing for half of the year, so this management approach does not preclude the need to improve the quality of housing and reduce any potential negative impact on welfare.
196

CONFINEMENT FACTORY FARMING By definition in the US, any dairy herd with more than 700 cows is a CAFO (a Concentrated Animal Feeding Operation) typically with all-year-round total confinement of animals in large freestall barns with a milking parlor operating around the clock. This would fit many people’s definition of a ‘factory farm’, even though the majority are owned by a single or group of families and hence, by definition, are family farms. The term CAFO is actually used to place more stringent controls on manure and waste handling and clean water management for large livestock units. Depending on the day, if we visit such a farm we may find the problems that our confinement housed dairy industry commonly faces – too many dead cows, too many lame cows, and fresh cows suffering from retained placenta, metritis, and displaced abomasum. A 3% death rate looks very different on a 50 cow dairy compare to a 5,000 cow dairy on any given day. These production-related diseases maybe associated by some with confinement and the ‘hyperproduction’ induced by genetic manipulation, production enhancers and genetically modified feeds, and used as an example of why we should move away from this style of production system. We can certainly find associative evidence in the scientific literature that cows with high milk production are more susceptible to sub-acute ruminal acidosis, lameness, infertility and metabolic disease to ‘prove’ this point. Without a doubt, there is significant concern expressed by the general public regarding the size of these production units. In trying to determine an answer to the question ‘How big is too big?’ I made an assessment of the factors that impact a cows’ daily time budget that are influenced by herd size (Cook, 2008). These include:
1. Milking time and time away from the pen, reducing the time available for rest 2. Walking distance to and from the parlor resulting in excessive hoof wear, thin
soles and lameness 3. Our ability to detect a sick fresh cow in a pen of other fresh cows leading to
unrecognized health problems that are left untreated The impact of the first two factors can be lessened by milking with a larger parlor, and compressing the floor-plan of the barn using mechanical ventilation systems. However, it is difficult to overcome the limitations of trying to find a sick cow in a pen of fresh cows that gets larger and larger as herd size increases. Such a limitation puts a limit on herd size of ~ 2,000 cows by my estimations, if we are to preserve 12 h per day for rest and maintain excellent standards of fresh cow health. This number is a lot larger than the answer most people who ask me the question have in their own mind, and it is not to say that there aren’t many well-run dairy herds larger than this. It does however make people stop and think and perhaps consider that bigger isn’t always better, and that there are limiting factors associated with herd size, but perhaps these factors come into play at herd sizes much larger than we have traditionally been comfortable with. In 2010, from our Wisconsin DHIA records system, there are 697 herds larger than 150 cows on test. The largest herd on test has 6,508 lactating cows. For the most part, we
197

assume that these herds are predominantly freestall housed and of these herds, 99 achieve a rolling herd average milk production greater than 13,000 liters. They are the elite of the industry and we have had the pleasure of working with 42 of these herds in recent years. 88% of these herds utilize sand for bedding their freestalls and they achieve excellent levels of performance (Table 1). While performance does not always equate to good welfare, the very fact that these herds exist would suggest that the perception that large dairy herds are by definition bad for cows is erroneous.
Table 1. Performance of elite herds with more than 150 milking cows (assumed to be freestall housed) with rolling herd average milk production greater than 13,000 liters.
Herd
Size Transition Cow Index
Weighted Annual Mean SCC
Age at 1st Calving
Days Dry Turnover Rate
Mean 691 848 205 24 57 36 Range 158-6508 -944-2590 80-407 21-28 36-79 20-58 Some would look at the production of these herds and suggest that these cows are genetic monsters bred to be production units – frail animals pushed to their limits, living on a knife-edge and on the brink of metabolic exhaustion. That is what the animal activist groups would like to have us think, but we do not believe that this is the case. It is true to say that in the mid-90s our genetic indices favored selection for production over conformation and health/fitness traits, but that is no longer true. Figure 1 shows the current (2009) weighting of genetic indices around the world for Holstein cattle. The US ranks 3rd and 5th in the world for indices that use the most conformation and health/fitness traits, bested only by Scandinavia and the Netherlands. The UK is 7th on the list.
198

Figure 1. Relative contribution of production, conformation and health/fitness traits to genetic selection indices around the world in 2009.
If we take the time to visit these elite US herds, we generally find that behind these numbers are animals that are well-cared for, with excellent standards of health and welfare. Almost uniformly, these herds have lameness under control and excellent cow comfort and owners that are passionate about the health of their stock. THE WISCONSIN BLUEPRINT Our research on these high producing dairy herds would suggest that there are environmental and management changes that can be made that will reduce the risk for the common production related diseases. We believe that they are not an inevitable consequence of milking the kind of cow that we have bred, but a failure to provide her with the things she needs to be successful. Improvements in stall design lead to increased milk production and a reduction in lameness. Provision of enough bunk space for all of the pre-fresh and fresh cows to eat at the same time has reduced the incidence of ketosis, displaced abomasum and other peri-parturient diseases. Use of positive pressure ventilation systems reduces the incidence of respiratory disease in youngstock. Our research on the risk factors associated with mastitis, lameness, calf morbidity and fresh cow health has culminated in the creation of a set of guidelines for housing and management – The Wisconsin Blueprint. Rather than try to come up with a set of ‘ideal’ plans that farmers can attempt to duplicate, we have tried to sell a set of ideas and principles that farmers and construction professionals can use to build into there own ideas and create a facility that works best for their cattle and for them.
199

The aims of the Wisconsin Blueprint are to:
1. Accommodate cows and calves in groups which are socially stable over time, and manage groups to minimize movements between them
2. Wherever possible provide exposure to natural light and ventilation, but to utilize mechanical assistance where needed
3. Provide a comfortable place to rest for a target period of 12 h/d for both lame and non-lame cows which is designed to meet the space requirement of the animal, and not inhibit rising or lying movements
4. Provide enough feed and water space for each animal to optimize metabolic health 5. Design barn layouts that do not result in undue time out of the pen and minimize
trauma to the cows’ feet 6. Minimize morbidity and mortality rates
To achieve these goals, we have incorporated as many science based recommendations as we can find to create ‘biological’ standards to use along-side engineering standards and practices in the construction of superior dairy cattle facilities that are both economically viable and welfare friendly. We now have many examples of well-managed confinement housed freestall dairy herds where production and welfare are harmonious – to the benefit of the producer and the cow. In October 2010, we launched a web-site ‘http://thedairylandinitiative.vetmed.wisc.edu/’ that incorporates the Wisconsin Blueprint along with virtual tours of facilities we have assisted in the design and creation of. From the farm office, producers and their consultants can tour different facilities and use the blueprint to answer questions that they have related to the design of dairy cattle housing. We have also used the program to create dialogue between agricultural lenders and construction professionals in the State to learn from mistakes that have been made and fine-tune the advice being given. Because it is a web-site, the updates can be rapid and we use Facebook and Twitter to notify those interested of changes that are made. In order to make it self-sustaining, the site is restricted access and there is a fee of $100 for a 2-year subscription. However, we have also obtained sponsorship to make access free to farmers, extension and veterinarians in Wisconsin. The web-site is available to subscribers world-wide. CONCLUSION My belief is that dairy cows benefit from improvements to housing to enhance welfare in a variety of different management systems, and The Dairyland Initiative is being used to make these enhancements. In the future we must continue to question what we are doing and provide farmers solutions to promote economic survival and at the same time ensure that our cattle are well cared for. Consumers have diverse tastes and viewpoints and we will not please all of the people all of the time. Farmers should be able to graze their cattle if they choose, and people should be able to buy organic milk if they wish to do so. At the same time, the dairy industry has to be accountable and create improvements where it is needed. We must question how big a herd is ‘too big’, what kind of lying surface is best for our cows, what pen design is optimal for transition cows and how best to ventilate our calf barns. The Dairyland Initiative is providing a forum for that discussion by soliciting input from farmers, consultants, builders and lenders.
200

ACKNOWLEDGEMENTS The Dairyland Initiative is funded by the Ira and Ineva Baldwin Wisconsin Idea Endowment and sponsored by commercial companies listed at http://thedairylandinitiative.vetmed.wisc.edu/prv_supporters.htm REFERENCES
1. Capper J.L., Cady R.A., Bauman D.E. (2009) Environmental impact of dairy production: 1944 compared with 2007. J Anim. Sci. 87: 2160-2167
2. Charlton G.L., Rutter S.M., East M., Sinclair L.A. (2011) Preference of dairy cows: Indoor cubicle housing with access to a total mixed ration vs. access to pasture. Appl. Anim. Behav. Sci. 130: 1-9
3. Cook N.B. (2008) Designing welfare friendly housing for dairy cows. Proc. Am. Assoc. Bov. Pract. Conf. 41: 78-84
4. Hernandez-Mendo O., von Keyserlingk M.A.G., Veira D.M., Weary D.M. (2007) Effect of pasture versus freestall housing on lameness in dairy cows. J. Dairy Sci. 90: 1209-1214
5. Huxley J.N., Burke J., Roderick S., Main D.C.J., Whay H.R. (2004) Animal welfare assessent benchmarking as a tool for health and welfare planning in organic herds. Vet. Rec. 155: 237-239
6. Langford F.M., Rutherford K.M.D., Jack M.C., Sherwood L., Lawrence A.B., Haskell M.J. (2009) A comparison of management practices, farmer perceived disease incidence and winter housing on organic and non-organic dairy farms in the UK. J. Dairy Res. 76: 6-14
7. Legrand A.L., von Keyserlingk M.A.G., Weary D.M. (2009) Preference and usage of pasture versus free-stall housing by lactating dairy cattle. J. Dairy Sci. 92: 3651-3658
8. Rutherford K.M.D., Langford F.M., Jack M.J., Sherwood L., Lawrence A.B., Haskell M.J. (2009) Lameness prevalence and risk factors in organic and non-organic dairy herds in the United Kingdom. The Vet. J. 180: 95-105
9. Vicini J., Etherton T., Kris-Etherton P., Ballam J., Denham S., Staub R., Goldstein D., Cady R., McGrath M., Lucy M. (2008) Survey of retail milk composition as affected by label claims regarding farm-management practices. J. Am. Diet. Assoc. 108: 1198-1203
201

Pain Considerations in Dehorning Dairy Calves
Todd F. Duffield, DVM, DVSc, Professor, Department of Population Medicine, OVC,
University of Guelph
Modified from a proceedings published in the AABP Proceedings, September 2008, Charlotte, North Carolina Abstract Dehorning calves is a necessary practice that should be conducted as early as possible and with appropriate anesthetic/analgesia. With the possible exception of caustic paste, calves perceive and react to acute pain during dehorning, regardless of method, when no local anesthetic is used. Extensive research has shown that dehorning stimulates both an acute pain response and a delayed inflammatory reaction. These effects have been measured through physiological, behavioural, and pain sensitivity responses. The best method to fully address pain management for dehorning should include both a local cornual nerve block and systemic analgesia, particularly when calves are dehorned at or beyond 4 weeks of age. Current adoption rates of farm operator’s use of local anesthetics and/or systemic analgesia for dehorning are extremely low. Veterinarians are influential in designing dehorning protocols for on-farm use. A routine dehorning service conducted by trained technicians through a veterinary practice is one means of controlling dehorning protocols on –farm. Introduction Dehorning is a necessary task on dairy farms aimed at reducing the risk of injury to handlers and other cattle. Choosing whether or not to dehorn calves, therefore, is not a debate. However, how we dehorn calves is open for criticism and discussion. Genetic control of dehorning through breeding polled cattle is possible but is not a practical solution, at least in the short term. Agricultural practices are coming under increasing scrutiny from the public. Common management practices such as dehorning may be negatively perceived and lower the reputation of the industry. Considering this it is important for all of us within the industry – advisors and farm personnel to carefully choose a dehorning protocol that is aimed at minimizing pain. Several surveys in North America have recently been conducted that are informative with respect to current dehorning practices on dairy farms. In the U.S. it was reported that of 113 dairy farms in the Midwest and New York, 12% used anesthetic and 2% analgesia for dehorning.3 The most common method used for dehorning was electric or gas hot iron (67% of calves), followed by caustic paste (10%), and gouging (9%).3 The majority of calves were dehorned prior to 12 weeks of age. Similar calf dehorning demographic findings were reported in a Canadian survey conducted in the dairy industry in the province of Ontario.14 That survey indicated that the most common age in Ontario for dehorning dairy calves was 4 to 8 weeks of age, and the most common method was using a hot-iron electric (Rhinehart) dehorner. Producers in that province dehorn 78% of dairy calves, with the remainder performed by veterinarians.14 Survey respondents reported that 23% of producers who dehorned their own calves used lidocaine nerve blocks for reducing acute pain at dehorning. Of the veterinarians surveyed, 92% used local
202

anesthetics for dehorning. Putting these two figures together indicates that only 35 to 40% of dairy calves in Ontario receive the benefit of a local anesthetic at the time of dehorning. A cross Canada survey of veterinarians indicates that fewer veterinarians provide analgesia for dehorning beef calves compared to dairy calves.7 However, the decision by veterinarians to use analgesia for dehorning is more complicated than whether the animal is a beef or a dairy calf. Veterinarians are more likely to use analgesia for dehorning if they perceive dehorning as painful of if they are concerned with personal safety; while they are less likely to consider analgesia or to consider dehorning painful if they perceive that owners are unwilling to pay for it.8 The Ontario survey respondents were asked why they used or didn’t use local anesthetic. Common reasons for not using it included: cost, time, unaware of it, considered it unnecessary.14 Producers who administered local anesthetic used lidocaine primarily for pain management, but considered it cheap and enhanced the safety of the procedure for both the handler and the animal.14 Methods of Pain Control Age It is generally accepted that the younger the animal is the less painful the dehorning procedure is. This is most likely a function of dehorning a smaller horn bud and causing less trauma rather than being a function of a physiologic age response. There have been many dehorning experiments conducted on dairy calves of various ages. However, it is extremely difficult to compare age responses because of both the inherent confounding of the calves themselves as well as methodological differences between studies. In experiments conducted at the University of Guelph (data unpublished) using similar methods, younger calves (<4 weeks old) dehorned with a butane dehorner had substantially fewer head shakes, head rubs, and ear flicks (behaviours associated with dehorning pain) in the hours following the procedure, compared with older calves (6-10 weeks old) dehorned with an electric dehorner (Rhinehart). The electric hot iron device leaves a much greater burn diameter than the smaller butane dehorner. Method of Dehorning The older the calf and the larger the horn, the more painful the procedure becomes. Thus instead of waiting to use gougers, keystones, or wire on larger horns, it is best to do the calves at a younger age. In older calves (5-6 months) a comparison of gougers, keystones or wire revealed no differences in the cortisol responses between these methods (Sylvester et al, 1998a). 19 Some studies have suggested that cautery in addition to gouging may help reduce the pain response (ie lower cortisol concentrations).15, 20 However, use of a hot iron on its own still elicits measurable cortisol and behavioural responses for several hours post-dehorning. 2, 5 Even within the options for burning horns, the smaller devices – Buddex, Portasol, etc are probably a better choice and likely inflict less post-surgical pain than the Rhinehart or similar device. Another option for dehorning is caustic paste. Some research on caustic paste indicates that a local anesthetic block is unnecessary and the pain response following dehorning is minimal when animals are sedated with xylazine.21 However, other research has demonstrated that a lidocaine block controls pain associated with caustic paste disbudding for about an hour, after which pain returns (Stillwell et al, 2008). The main reported problems with caustic paste are either applying too much which can lead to eye ablation in severe cases, or applying too little which results in regrowth of the horn. However, in a study conducted at a custom heifer rearing facility, we observed no
203

regrowth or eye problems in over 200 calves dehorned with caustic paste (data unpublished). Careful attention was given to a controlled application of the caustic paste in that study. Pain of Dehorning Virtually all of the dehorning research on pain of dehorning and its control has been conducted on dairy heifer or bull calves, with limited or no data on beef calves. Pain elicited from dehorning can be divided into 2 categories: 1. acute (at the time of dehorning) and 2. inflammatory (pain derived from the dehorning insult on tissues). The acute phase of pain for dehorning is marked by a rapid rise in cortisol concentrations that peak within several minutes and then decline to a plateau above the starting baseline and remain at that level for several hours. 9, 20 There is typically a ‘rebound’ in cortisol in 2-4 hours coincident with the local anesthetic block wearing off.9 In calves that are not blocked at dehorning, heart rate remains elevated for nearly 4 hours.5 A recent study measured significant responses with an electroencephalograph and increased heart rate in calves dehorned under a light general anesthetic (halothane) but no block when compared to the same anesthesia but with a cornual nerve block.4 Many people object to using a block, particularly with smaller calves because they say they can’t tell if the block worked. A study was conducted in 27 calves, where 9 received lidocaine, and the others received saline.4 The technician administering the blocks was blinded to the treatments and yet was able to correctly identify all 9 calves that were blocked. Further, the behaviour of these calves at the time of dehorning was recorded. The most common behaviour in the non-blocked calves was foot stamping. Calves not receiving a block stamped their feet on average 22 times during butane dehorning compared to an average of 4 foot stamps in the blocked calf group. Other behaviours associated with pain (not being blocked) were vocalization, rearing, kicking, and falling. Not all non-blocked calves vocalized (less than half), but vocalization only occurred in this group. Other studies have also demonstrated kicking and struggling at dehorning as evidence of a reduced effective block.1, 16 Important behavioural indicators of pain following dehorning include – head shakes, head rubs, ear flicks and tail flicks. Various studies involving the use of non-steroidal anti-inflammatory drugs (NSAID’s) have indicated benefits in the reduction of these behaviours for anywhere from 6 to as long as 24 hours after dehorning depending on the therapeutic regimen.2, 10 Administering of Cornual Nerve blocks Routinely administering a lidocaine cornual nerve block is not that difficult and becomes part of the dehorning routine once the decision is made to do it. Although some have used ring blocks for blocking horns 2, 21 in addition to the cornual nerve block, we find this unnecessary provided the block is performed correctly with adequate volume. Volume of local anesthetic per nerve block has ranged from as little as 3 mL of 2% lignocaine 15 to as much as 6 ml per side of either 2% lignocaine or 0.25% bupivicaine.16 We use 5 mL of 2% lidocaine on each side injected with an 18 gauge 1 ½ inch needle. We find that the best injection site is usually 1/3 of the distance from the edge of the eye to the horn, but injected at the approximate level of the eye, below the frontal crest bone (ridge of bone running to toward the horn). It is helpful to fan the lidocaine out by slightly angling the injection in different directions. Depositing approximately 1 mL as you withdraw the needle appears to improve success.
204

Use of Non-Steroidal Anti-inflammatory drugs (NSAID’s) These drugs include flunixin meglumine, ketoprofen, acetylsalicylic acid, meloxicam and phenylbutazone. However, many of these drugs are not approved for food animal use in all or any North American countries. Several studies have shown that with most dehorning procedures, the cornual nerve block only manages the acute pain. Inflammatory pain is experienced at the time the local anesthetic wears off, regardless of whether the block is extended up to 8 hours post dehorning.9 Thus, there is an important role for NSAID’s and there is a need to encourage regulatory agencies and pharmaceutical companies to consider pain management as a label claim for some of these efficacious products. The purpose of administering these products in calves is to help manage pain following the dehorning procedure. There have been several studies now that have found benefits to the additional use of NSAID’s when administered with lidocaine at the time of the cornual nerve block. In calves aged 3-4 months dehorned by gouging, a local anesthetic (6 ml per site) and administration of ketoprofen (1.4 mg/lb BW or 3mg/ kg BW) 20 minutes prior to dehorning reduced ear flicking and tail flicking and improved rumination.11 Calves of the same age dehorned with the same methods also had improved cortisol responses.10,
18 Faulkner and Weary (2000) showed that there were reductions in ear flicks, head shakes and head rubs for calves receiving ketoprofen (3mg/kg BW) and local anesthetic compared with just a local block in 4 to 8 week old calves dehorned with an electric hot iron device.2 However, in that study calves were treated with ketoprofen orally at 2 hours pre-dehorning, and again at 2 and 7 hours post-dehorning. We have found benefits in terms of reduced ear flicks and improved calf starter intake when ketoprofen (1.4 mg/lb (3 mg/kg) intramuscular injection) is administered at the time of the cornual nerve block, approximately 10 minutes prior to dehorning in calves 6-10 weeks old dehorned with the Rhinehart electric dehorner. The best way to avoid a reason to use these NSAID’s may be to simply dehorn the calves when they are young. Despite subtle reductions in serum cortisol, there was no additional behavioural benefit (in addition to lidocaine) of using ketoprofen in young calves (< 4 weeks old) dehorned with a butane dehorner.12 To our knowledge the use of flunixin meglumine has not been investigated for alleviation of pain response from dehorning. Phenylbutazone was found ineffective at altering cortisol patterns in one study.18 Recently, we have evaluated meloxicam at the time of dehorning (currently unapproved for food animals in the U.S. or Canada). Use of meloxicam (0.22 mg/lb (0.5 mg/kg) intramuscular injection) at the time of lidocaine nerve block (approximately 10 minutes prior to dehorning) for dehorning calves 10 to 12 weeks of age with an electric hot iron device (rhinehart) caused reductions in ear flicks, head shakes, head rubs, tail flicks, pain sensitivity (measured at 4 hours post-dehorning with an algometer), and serum cortisol concentrations.6 Behavioural benefits of meloxicam in this study have been observed for up to 44 hours post-dehorning indicating that calves feel pain from dehorning for at least this duration. This study and a similar unpublished study with ketoprofen have both shown tendencies for NSAID treated calves to eat more on the day following dehorning. Faulkner and Weary (2000) reported a tendency for ketoprofen-treated calves to gain more weight during the 24 hours following dehorning.2 Sedation Many people like to use sedation (usually xylazine (Rompun)) for dehorning calves. A recent survey indicated that 44% of veterinarians in Ontario use xylazine for dehorning.14 Primarily veterinarians indicated that safety, restraint, and pain control were reasons for use. It should be
205

noted that there is little pain control benefit to xylazine. Calves given xylazine and butorphonol without a local anesthetic nerve block and dehorned with electric cautery, had similar cortisol patterns to untreated dehorned calves and elevated heart rates for 4 hours post-dehorning.17 If calves aren’t blocked, they won’t always respond to the dehorning procedure (because of the sedation) but they will still feel it. Thus xylazine without lidocaine is not an acceptable method of pain management for dehorning. Role of the Technician in Dehorning There is a tremendous opportunity for technician dehorning combined with improving pain management of dehorning within the dairy industry. Offering a technician service to clients allows a dehorning protocol to be implemented, ensures regular dehorning at the appropriate age and even provides opportunity for some heifer health monitoring. At the Ontario Veterinary College we have had a technician organize and conduct dehorning visits on most of our dairies for many years. Recently, we conducted a dehorning trial on a large local dairy that previously was fitting dehorning into their schedule when they could find time. At the end of the study, they wanted us to provide the dehorning service because of the advantages listed above. I know a very large dairy practice in New Zealand that has recently started a similar service for the same reasons. Interestingly, analysis of the Ontario dehorning survey data indicated that the use of lidocaine in 100% of the calves for dehorning was over 20 times more likely if the veterinary practice utilized a technician for dehorning dairy calves.14 Recommendations for Dehorning 1. Devise calf dehorning protocols with your clients and teach the technical skills such as
administering a local nerve block. 2. Dehorn calves at a young age (< 4 weeks old) 3. If possible choose either:
A. Small dehorner (Portasol or Buddex) + Nerve Block B. Caustic Paste – (no nerve block required?) 4. Administer approved NSAID’s for calves dehorned > 4 weeks of age. REFERENCES 1. Doherty, T.J., HG Kattesh, R J Adcock,MG Welborn, AM Saxton,JL Morrow, and JW Dailey. Effects of a Concentrated Lidocaine Solution on the Acute Phase Stress Response to Dehorning in Dairy Calves. J. Dairy Sci. 90:4232–4239, 2007 2. Faulkner PM, Weary DM. Reducing pain after dehorning in dairy calves. J Dairy Sci 2000;83:2037-2041. 3. Fulwider,WK, T. Grandin, BE Rollin,TE Engle, NL Dalsted, and WD Lamm. Survey of Dairy Management Practices on One Hundred Thirteen North Central and Northeastern United States Dairies. J. Dairy Sci. 91:1686–1692, 2008.
206

4. Gibson, T.J., C.B. Johnson, K.J. Stafford, S.L. Mitchinson, and D.J. Mellor. Validation of the acute electroencephalographic response of calves to noxious stimulus with scoop dehorning. NZ Vet. J. 55:152-157, 2007. 5. Grøndahl-Nielsen C, Simonsen HB, Damkjer Lund J, Hesselholt H. Behavioural, endocrine and cardiac responses in young calves undergoing dehorning without and with the use of sedation and analgesia. Vet J 1999;158:14-20. 6. Heinrich, A. An Investigation of meloxicam for the relief of pain associated with dehorning of dairy calves. MSc Thesis Dissertation. University of Guelph, Guelph, ON, Canada, 2007. 7. Hewson, C J, IR Dohoo, KA Lemke, HW Barkema. Canadian veterinarians’ use of analgesics in cattle, pigs, and horses in 2004 and 2005. Can Vet J 48:155–164, 2007a. 8. Hewson, C J, IR Dohoo, KA Lemke, HW Barkema. Factors affecting Canadian veterinarians’ use of analgesics when dehorning beef and dairy calves, Can Vet J 48:1129–1136, 2007b. 9. McMeekan, CM, DJ Mellor, , KJ Stafford, RA Bruce, RN Ward, and NG Gregory. Effects of local anaesthesia of 4 to 8 hours’ duration on the acute cortisol response to scoop dehorning in calves. Aust Vet J 76:281-285, 1998a. 10. McMeekan, CM, KJ Stafford, DJ Mellor, RA Bruce, RN Ward, and NG Gregory. Effects of regional analgesia and/or a non-steroidal anti-inflammatory analgesic on the acute cortisol response to dehorning in calves. Res. Vet. Sci. 64:147-150, 1998b. 11. McMeekan, C.M., K. J. Stafford, D. J. Mellor, R. A. Bruce, R. N. Ward, and N. G. Gregory. Effects of local anesthetic and a non-steroidal anti-inflammatory analgesic on the behavioural responses of calves to dehorning. NZ Vet. J. 47:92-96, 1999. 12. Milligan, B.N., Duffield, T. , Lissemore, K. The utility of ketoprofen for alleviating pain following dehorning in young dairy calves. Can. Vet. J., 45: 140-143, 2004. 13. Millman, S., Duffield, T., Lissemore, K., James, S., Misch, L. Does ketoprofen alleviate acute pain during dehorning? American Dairy Science Association Annual Meeting, Cincinnati, Ohio. J. Dairy Sci: 88: (Suppl1) p374, 2005 14. Misch, L, K. Lissemore, S. Millman, T. F. Duffield. A survey of dehorning practices in Ontario dairy calves. Canadian Veterinary Journal. Can. Vet. J. 48: 1259-1254, 2007. 15. Petrie, N.J., D.J. Mellor, K.J. Stafford, R.A. Bruce, and R.N. Ward. Cortisol responses of calves to two methods of disbudding used with or without local anaesthetic. NZ Vet. J. 44:9-14, 1996. 16. Schwartzkopf-Genswein, KS, ME. Booth-McLean, TA McAllister, and GJ. Mears Physiological and behavioural changes in Holstein calves during and after dehorning or castration. Can. J. Anim. Sci. 85:131-138, 2005.
207

17. Stafford, KJ, DJ Mellor, SE Todd, RN Wardand CM McMeekan. The effect of different combinations of lignocaine, ketoprofen, xylazine and tolazoline on the acute cortisol response to dehorning in calves. N. Z. Vet. J. 51: 219-226, 2003. 18. Stilwell G., Campos de Carvalho R., Lima M.S., Broom D.M. Effect of caustic paste disbudding, using local anesthesia with and without analgesia, on behavior and cortisol in calves. 2008. Appl. Anim. Behav. Sci. doi:10.1016/j.applanim.2008.06.008 18. Sutherland, MA., DJ Mellor, KJ Stafford, NG Gregory, RA Bruce, and RN Ward. Cortisol responses to dehorning of calves given a 5-h local anaesthetic regimen plus phenylbutazone, ketoprofen or adrenocorticotropic hormone prior to dehorning. Res. Vet. Sci. 73:115-123, 2002. 19. Sylvester, SP, KJ Stafford, DJ Mellor, RA Bruce and RN Ward Acute cortisol responses of calves to four methods of dehorning by amputation. Aust Vet J 76:123-126,1998a. 20. Sylvester, SP, DJ Mellor, KJ Stafford, RA Bruce and RN Ward. Acute cortisol responses of calves to scoop dehorning using local anaesthesia and/or cautery of the wound. Aust Vet J 76:118-122, 1998b. 21. Vickers, K.J., L. Niel, L. M. Kiehlbauch, and D. M. Weary Calf response to caustic paste and hot-iron dehorning using sedation with and without local anesthetic J Dairy Sci 2005 88: 1454-1459.
208

Pain Management Factors at Parturition in Dairy Cows
Todd F. Duffield, DVM, DVSc, Professor, Department of Population Medicine, OVC,
University of Guelph
Introduction The identification of sick animals is a key component of any dairy herd health program. Early identification or prediction of disease can curb economic losses that result from reduced milk yield, compromised reproductive performance and cow welfare. Despite decades of nutritional and epidemiological work, the incidence of disease around the calving period in lactating dairy cattle remains high, underscoring the need for a more comprehensive understanding of the biological mechanisms associated with illness combined with the need to explore alternative management schemes that minimize the incidence of illness. During the transition period cows face a number of stressors, including several diet changes and social regroupings, as well as hormonal and physiological changes associated with calving and the onset of lactation. One of the main challenges for transition dairy cows is a sudden increase in nutrient requirements to support the onset of lactation, at a time when dry matter intake (DMI), and thus nutrient supply, lags far behind (Drackley, 1999). The constraints imposed by the decline in DMI, coupled with the other stressors associated with the transition period, no doubt contribute to the high incidences metabolic and infectious diseases during this time (Drackley, 1999). It has been documented that approximately 50% of cows have one or more adverse health events during this time (Ferguson, 2001). Clearly, any practices that can help reduce disease at the time of calving will result in improved welfare and profitability, and are thus of broad relevance to both the dairy industry and society. Research is needed to identify the factors that contribute to successful coping strategies as a step in designing management practices that reduce illness during the time immediately following parturition when dairy cattle are most vulnerable to disease. A huge stress that all cows go through is calving. Calving is an inflammatory event and it seems reasonable that pain following calving may interfere with social behaviour and the ability to compete at the feed bunk or the motivation to consume feed. Alleviation of this pain at or shortly following calving may have huge benefits in improving eating behaviour, dry matter intake and subsequently reducing disease risk. Impact of Dystocia on Dry matter Intake (DMI) and Milk Production Changes in dry matter intake in the periparturient cow have been used as a tool to identify cows at risk of postpartum complications (Drackley, 1999; Grummer et al., 2004). Proudfoot et al. (2009) have shown that the dry matter intake for cows that experienced dystocia was lower 24-48 hours prior to calf delivery and 48 hours after calf delivery compared to cows that were not assisted. Since feed intake and milk production are closely related, a decrease in feed intake will correspond to a decrease in milk production. There has been little research to examine the effects of dystocia levels on feed intake and milk production in dairy cattle.
209
Dystocia and Haptoglobin Calving is an inflammatory event, and studies have shown an increase in acute phase inflammatory proteins, such as haptoglobin, following parturition (Koets et al., 1998; Humblet et al. 2006). Schonfelder et al. (2005) observed higher levels of haptoglobin concentration in animals with dystocia after uterine torsion compared to animals with natural parturition after 5 days postpartum. No studies in cattle have examined haptoglobin concentrations following different dystocia categories. Behavioral Changes Associated with Dystocia The activity of the cow increases quite dramatically prior to calving. It has been suggested that this increased restlessness may be due to discomfort (von Keyserlingk and Weary, 2007). Houwing et al. (1990) reported a significant increase in the number of standing bouts within the three hours immediately prepartum. Huzzey et al. (2005) found that during the three days prior to calving, the number of standing bouts increased by 80% in dairy cows housed indoors. Lying time was shorter and lying bouts more frequent in cows requiring calving assistance (Misch et al, 2006). Cows that were treated with disinfectants to induce vaginal irritation (as might be created by tears or lacerations following birth) showed specific behavioural changes – tail lifting and pressing and occasionally groaning (Grussel and Busch, 1998). Thermal nociception testing has also been used successfully in cows to assess pain response (Machado et al, 1997). Dystocia and Analgesia Society expects agriculture to consider animal welfare a priority in animal production. Parturition is necessary for production and this event happens nearly every day on dairy farms across Ontario. Dystocia rates are much higher in NA (>10%) compared with other parts of the world (<5%) and regardless of country are much higher in primiparous animals (Mee, 2008). In some animals, this event is likely painful and may remain painful for several days. Yet, we know little about the effect of this pain on production or health. In addition there is a paucity of data on control of this pain with appropriate medication. Of the small body of work that does exist on this topic, consumption of the amniotic fluid by the cow was shown to provide some analgesic effect (Machado et al, 1997). This effect of amniotic fluid has also been documented in rats (Kristal et al, 1990). Because of our management recommendations, many dairy cattle may not get the benefit of ingestion of amniotic fluid. It is much better for calf health if the calves are removed from their dams immediately after birth. Also, most dystocias result in rupture and dispelling of most of the amniotic fluid prior to the delivery of the calf. In addition, up to 10% of dairy calves may be stillborn and, the amniotic fluid from these dystocia’s may not provide the same degree of analgesia as a normal calving. From the literature, clear hormonal changes that are related to the severity of labour have been documented to occur during parturition in both heifers and goats (Hydbring et al, 1999). Both vasopressin and oxytocin were greater in heifers that needed assistance. Cows that were treated with disinfectants to induce vaginal irritation (as might be created by tears or lacerations following birth) showed specific behavioural changes – tail lifting and pressing and occasionally groaning (Grussel and Busch, 1998). Thermal nociception testing has also been used successfully in cows to assess pain response (Machado et al, 1997). Rates of metabolic disease in dairy cows are expected to increase with age. Yet, on many of our dairies, rates of displaced
210

abomasums are as high or higher in first pairy animals compared with third lactation and greater animals. It is possible that some of this increased risk is related to management factors and social interactions amongst younger and older animals. However, primiparous heifers have the highest rate of dystocia on most dairy farms. It is possible that the untreated pain resulting from these difficult births is a contributing cause of suboptimal milk production and impaired cow health issues. Treatment of dairy cows at calving with flunixin meglumine has been shown to have negative effects, including decreased DMI (Shwartz et al, 2009) and increased risk of retained placenta (Duffield et al, 2009). However, treatment with ketoprofen on the day of, and day following, calving tended to reduce the incidence of retained placenta (Richards et al, 2009). Impact of meloxicam on alleviation of pain around calving in dairy cattle is currently unknown.
REFERENCES
Bareille, N. Beaudeau, F., Billon, S., Robert, A., Faverdin, P. 2003. Effects of health disorders on feed intake and milk production in dairy cows. Livestock Prod. Sci. 83:53-62
Chan, J.P.-W., Chu, C.C., Fung, H.P., Chuang, S.T., Lin, Y.C., Chu, R.M., Lee, S.L. 2004. Serum haptoglobin concentration in cattle. J. Vet. Med. Sci. 66:43-46
Drackley, J.K. Biology of Dairy Cows During the Transition Period: the Final Frontier J Dairy Sci 1999 82: 2259-2273.
Duffield, T. F., Putnam-Dingwell, H., Weary, D., Skidmore, A., Neuder, L., Raphael, W., Millman, S., Newby, N., Leslie, K. E. Effect of flunixin meglumine treatment following parturition on cow health and milk production. American Dairy Science Association Annual Meeting, Montreal, Canada. J. Dairy Sci. Vol. 92, (E-Suppl.1) p 118, 2009.
Grüssel, T and W. Busch. 1998. Behavioral response of cows after intrauterine application of disinfectants for treatment of endometritis. Tierarztl Prax Ausg G Grosstiere Nutztiere. Apr. 26(2):67-72.
Houwing, H., J. F. Hurnik and N. J. Lewis. 1990. Behaviour of periparturient dairy cows and their calves. Can. J. Anim. Sci. 70:355-362.
Huzzey, J. M., M. A. von Keyserlingk and D. M. Weary. 2005. Changes in feeding, drinking, and standing behavior of dairy cows during the transition period. J. Dairy Sci. 88:2454-2461.
Humblet, M.-F., Guyot, H., Boudry, B., Mbayahi, F., Hanzen, C., Rollin, F., Godeau, J.-M. 2006. Relationship between haptoglobin, serum amyloid A, and clinical status in a survey of dairy herds during a 6-month period. Vet. Clin. Path. 35:188-193
Koets, A.P., De Schwartz, N., Tooten, P. 1998. Release of proinflammatory cytokines related to luteolysis and the periparturient acute phase response in prostaglandin-induced parturition in cows. Theriogenology. 49:797-812
211

Machado F, L. C. P., J. F. Hurnik and G. J. King. 1997. Timing of the attraction towards the placenta and amniotic fluid by the parturient cow. Applied Animal Behaviour Science. 53:183-192.
Misch, L., H. Putnam, T. Duffield, S. Millman, K. Lissemore, K. Leslie. 1996. A retrospective video analysis of behavior of periparturient dairy cattle. Proceedings of the American Association of Bovine Practitioners. St. Paul, Minnesota, p. 124-125.
Mee, J. F. 2004. Managin the dairy cow at calving time. Vet. Clin. Food Anim. 20:521-546
Mee, J.F. 2008. Prevalence and risk factors for dystocia in dairy cattle. Vet. J. 176:93-101
Proudfoot, K.L., Huzzey, J.M., von Keyserlingk, M.A.G. 2009. The effect of dystocia on the dry matter intake and behaviour of Holstein cows. J. Dairy Sci. 92:4937-4944
Rajala, P.J., Grohn, Y.T. 1998. Effects of dystocia, retained placenta, and metritis on milk yield in dairy cows. J. Dairy Sci. 81:3172-3181
Richards, B. D., D. H. Black, R. M. Christley, M. D. Royal, R. F. Smith, H. Dobson. 2009. Effects of the administration of ketoprofen at parturition on the milk yield and fertility of Holstein-Friesian cattle. Vet. Rec. 165: 102-106.
Schonfelder, A., Schrodl, W., Kruger, M., Ricjter, A., Sobiraj, A. 2005. The change in acute phase protein haptoglobin in cattle during spontaneous labor and Caesarean section with or without torsio uteri intrapartum. Berl Munch Tierarztl Wochenschr. 118:240-246
Shwartz, G., K. L. Hill, M. J. VanBaale, and L. H. Baumgard. 2009. Effects of flunixin meglumine on pyrexia and bioenergetic variables in postparturient dairy cows. J. Dairy Sci. 92:1963-1970.
van Werven, T., Schukken, Y.H., Lloyd, J., Brand, A., Heeringa, H.Tj., Shea, M. 1992. The effects of duration of retained placenta on reproduction, milk production, postpartum disease and culling rate. Theriogenology. 37:1191-1203
von Keyserlingk, M. A. and D. M. Weary. 2007. Maternal behavior in cattle. Horm. Behav. 52:106-113.
Wathes, D.C., Cheng, Z., Bourne, N., Taylor, V.J., Coffey, M.P., Brotherstone, S. 2007. Differences between primiparous and multiparous dairy cows in the inter-relationships between metabolic traits, milk yield and body condition score in the periparturient period. Domest. Anim. Endocrinol. 33:203-225
212

Post-Surgical and Disease-Associated Pain Management Considerations in Dairy Practice
Todd F. Duffield, DVM, DVSc, Professor, Department of Population Medicine, OVC,
University of Guelph Introduction Although pain management is a routine consideration in small animal practice, both research and adoption of pain management considerations in food animal practice has been lacking. Beyond discussions of pain management of dehorning, castration, and other routine procedures, pain management following surgical procedures in cows such as for left displaced abomasums is worth evaluating and considering. Additionally, there may be a number of diseases that have associated pain, such as mastitis and diarrhea where pain management could potentially benefit the animal and enhance recovery. LDA Surgery The incidence of displaced abomasum has been in the range of 3 to 6% in several recent studies conducted in Ontario and the North Eastern United States. The majority of these animals are subjected to surgical correction in an attempt to return the cow to normal production. Traditional ancillary treatments include postsurgical antibiotics, intravenous dextrose, and propylene glycol drench. While some veterinary practitioners may consider and use non steroidal anti-inflammatory drugs (NSAID) there is limited research data on its benefits post surgery in the bovine. Non-steroidal anti-inflammatory drugs have been administered in rodents after surgery for pain relief and to reduce inflammation and prostaglandin synthesis (Pairet and Ruckebusch, 1989; DeWinter et al, 1998). NSAID therapy has been used to alleviate signs of visceral pain in cattle, and as a preoperative treatment to make an animal less likely to lie down during a standing laparotomy. It was found that the treated cow may still lie down at the time of painful viscera manipulation (Constable et al, 1997; Van Metre et al, 2005). However, it is not common practice to administer NSAID therapy after LDA surgery. Ketoprofen has been used as method of managing postsurgical pain following dehorning. In a Canadian study, one intramuscular injection of ketoprofen at the time of a cornual nerve block resulted in reduced serum cortisol in young calves dehorned with a butane dehorner (Milligan et al, 2004). A follow-up study of the same design but in older calves dehorned with an electric cautery device resulted in significant reductions in pain related bevaviour (ear flicks) and improved feed intake (Duffield et al, 2010). There is currently no research on postsurgical pain management following LDA surgery. However, if cows were less painful after receiving ketoprofen or other NSAID’s, dry matter intake might be improved which could reduce the level on ketone bodies, specfically beta-hydroxybutyrate, and subsequently could lead to improved milk production. Diarrhea Research on 62 calves with a high exposure risk for Cryptosporidum parvum diarrhea investigated the role of meloxicam as an adjunctive therapy, in addition to routine fluid administration. Researchers concluded that meloxicam is an effective supportive therapy for neonatal calf diarrhea complex, as evidenced by the stronger appetite for milk during sickness,
213

improved starter ration consumption, earlier time to weaning and a reduction in pain related behaviour (Todd et al, 2010). This research led to an approval in Canada for meloxicam use as an adjunctive treatment for diarrhea. Mastitis NSAID use as an adjunctive therapy for mastitis has been utilized in practice for many years. Some NSAID’s have specific label claims in certain countries for use in mastitis (ie meloxicam). However, research on pain mitigation with NSAID’s in mastitis. Several research projects are underway investigate pain mitigation with different NSAID’s in LPS induction models. REFERENCES 1. Pairet M, Ruckebusch Y. 1989. On the relevance of non-steroidal anti-inflammatory
drugs in the prevention of paralytic ileus in rodents. Journal of Pharmacy and Pharmacology 41:757–761.
2. De Winter B.Y., Boeckxstaens, G.E., de Man J.G, Moreels, T.G., Herman, A.G., Pelckmans, P.A. 1998. Differential effect of indomethacin and ketorolac on postoperative ileus in rats. European Journal of Pharmacology 344:71–76.
3. Constable, P.D., St Jean G, Hull BL, Rings, D.M., Morin, D.E., Nelson, D.R. 1997. Intussusception in cattle: 336 cases (1964–1993). Journal of the American Veterinary Medical Association 210(4):531–6.
4. Van Metre , D.C, Callan, R.J., Holt, T,N., Garry, F.B. 2005. Abdominal Emergencies in Cattle. Veterinary Clinics of North America: Food Animal Practice 21:655–696
5. Milligan, B.N., Duffield, T. , Lissemore, K. The utility of ketoprofen for alleviating pain following dehorning in young dairy calves. Can. Vet. J., 45: 140-143, 2004
6. Duffield, T.F., Heinrich, A., Millman, S.T.,DeHaan, A., James, S., Lissemore, K. Reduction in pain response by combined use of local lidocaine anesthesia and systemic ketoprofen in dairy calves dehorned by heat cauterization. Can. Vet. J. 51: 283-288, 2010.
7. Todd, C. G., Millman, S. T., McKnight ,D. R., Duffield, T. F. , Leslie, K. E. Nonsteroidal anti-inflammatory drug therapy for neonatal calf diarrhea complex: effects on calf performance. J. Anim. Sci. 88: 2019-2028, 2010.
214

Technical Large Animal Emergency Rescue: How Veterinarians Should Prepare
Howard Ketover, DVM
Large animals can be unpredictable, especially when they are in a desperate life or death situation. Horses and cattle, when stressed and trapped, have the capacity to hurt themselves further and cause significant damage to property. When animals are involved in an incident, handlers and rescuers are inclined to place themselves in perilous positions, risking life and limb without even knowing it. Whether it be involved in a trailer accident, submerged in mud, fallen into a ravine while on a ride or in the pasture, cast in a stall, or simply an animal that has fallen on barnyard ice and can’t get up, we as animal professionals want to help them. However these are dangerous circumstances that can cause further injury to animal or human if the rescue is not performed in an organized, efficient and safe manner. Technical rescue training and the use of proper equipment can help to procure the best possible outcome and avoid unnecessary secondary injuries to the animal or to the responders trying to help. Knowledge of correct techniques such as how to configure straps, ropes, and other rescue equipment, as well as scene management and secondary animal confinement can offer animal owners, veterinarians, and the first responders’ direction and purpose in their rescue efforts. Veterinarians play a crucial role in any animal rescue or extraction. With the education, training, and life experiences the veterinarian has gained, he or she serves as a resource for the individual client, first responders and community. In an emergency, the veterinarian serves as the authority on animal health and is best qualified to assess the animals condition, direct and perform health and life preserving procedures such as sedation, intravenous fluids and if necessary euthanasia services. Veterinarians serve as an advocate for the animals and lend credibility to any rescue effort that comes under public scrutiny. While education and daily practice generates many tools for the veterinarian to choose from in a rescue scenario, some of the common practices taken for granted could potentially lead to more harm to the patient. Common areas where “normal veterinary practices” could be considered contraindicated are the following. Utilizing sedation or general anesthesia when the animal cannot protect itself from further injury or using sedation if the rescuers are planning to allow the animal to help extract its’ self to facilitate the rescue. Placing straps on the distal limbs or head/neck to pull or move an animal across a surface that offers significant friction versus the same strap placement for a vertical lift performed during surgical procedures can cause trauma that the animal cannot recover from. In some instances, the body of the animal may be recovered but the life is lost even if the animal walks away from the initial incident; death may follow in hours or days. It is the veterinarian’s role to limit any iatrogenic injuries during the rescue procedure that would limit future health. Additional continuing education is recommended and is offered to first responders, animal control officers, veterinarians, and animal professionals in large animal rescue techniques. This training not only improves the veterinarian’s response in critical emergency situations, but also
215

offers tools that veterinarians can utilize in daily practice to improve the outcome in some critical medical situations that are handled quietly on the farm or in the clinic. An important finding in training courses is that first responders and veterinarians begin to have a common language and understand each other’s strengths and limitations in regards to various rescue scenarios. Many of the classes take place over two to three days and offer hands on scenarios utilizing full size mannequins or live animals. If additional training in large animal rescue is planned, consider sponsoring and taking classes with a first responder from the community. This will create a much stronger approach for cohesive organized response when the emergency arises. If additional training is not currently practical or possible, simply meeting with the local first responders may gain significant ground in creating a balanced, trusting team approach to handling large animal emergencies in the community. Should the first time you meet your local first responders be at an incident, communication, trust, and a positive outcome will be challenging but not impossible. Researching, reading, and planning for emergencies in personal, professional and community scenarios will aid in private practice, as well as in high stress emergency situations. Meeting with, organizing and getting commitments from local equipment retailers, livestock haulers, and livestock removal providers will save time and increase the likelihood of a successful outcome should you be faced with an emergency/disaster scenario. The internet provides nearly unlimited resources for education, equipment, and templates to model your emergency response planning. The resources listed below provide a strong starting point for any level of interest and preparedness, from training opportunities to complete equipment purchases. Equipment can be very specialized and expensive or as simple as tow straps or used fire hose that can be obtained, often free of cost, from many fire departments. Often times utilizing the simplest, lowest tech approach to a rescue will lead to the fastest, safest, most effective outcome. Training classes/instructors/websites: www.largeanimalrescue.com www.tlaer.org www.code3associates.org http://www.avma.org/disaster/default.asp http://training.fema.gov/EMIWeb/IS/IS100b.asp Introduction to Incident Command System http://training.fema.gov/EMIWeb/IS/IS11a.asp Animals in Disasters: Community Planning http://edis.ifas.ufl.edu/vm117 Emergency Considerations for Beef Cattle
216

Textbooks and printed resources: Technical Large Animal Rescue
Rebecca Gimenez, PhD, Major; Thomas Gimenez, DVM; and Kimberly A May, DVM, MS, ACVS Wiley-Blackwell, 2008
How to Effectively Perform Emergency Rescue of Equines Tomas Gimenez, DVM; Rebecca M. Gimenez, PhD, CPT; Janice L. Baker, DVM; and Douglas T. Johannessen, BS Vol. 48, AAEP PROCEEDINGS, 2002
Save Your Horse Michelle Staples Red Jeans Ink, 2007
217

Managing the Equine Patient: Current Techniques and Pharmaceuticals Utilized in Common Equine Appointments and Emergencies
Howard Ketover, DVM
Due to the nature of the current equine health care market and the potential for significant financial gain, many products and medical techniques are available that may have limited or no practical application. In addition, certain aspects of equine health care have been driven based primarily on historical perspective or anecdotal evidence. While all aspects of medicine are prone to these forces, it is not uncommon for equine clients to base the treatment of their horses upon recommendations from fellow horse owners, great grandfathers and the internet. In today’s equine veterinary market, we have products that have been proven to provide safe, effective, and predicable outcomes for our patients. Today’s equine client is driven to achieve the best possible outcome for their animals and is willing to seek out and provide the level of care needed. Typically this requires education, demonstrations, and time to overcome the clients’ preexisting misconceptions. Utilizing and incorporating the products and techniques listed below may improve the patients’ outcome and decrease the time required to return them to production, be it performance, reproduction or pleasure riding. Non-Steroidal Anti-Inflammatory Drugs (NSAIDs) Surpass® (1% diclofenac sodium) Surpass is a topical anti-inflammatory cream that is indicated for the control of pain and inflammation associated with osteoarthritis (OA) in horses. Surpass topical cream contains 1% diclofenac sodium with the carrier Wisdom® as a liposomal agent. Diclofenac is a non-steroidal anti-inflammatory drug (NSAID) of the phenylacetic acid class that is believed to function by the inhibition of cyclooxygenase activity. As a class, NSAIDs may be associated with gastrointestinal and renal toxicity, but the targeted use of a topical NSAID allows for localized therapy with decreased concerns for systemic adverse effects to the gastrointestinal tract and renal tissues. Care should be taken during administration by wearing rubber gloves to prevent absorption into the hands. Recommended dosage is to apply a five-inch (5") ribbon twice daily over the affected joint for up to ten days. Surpass is manufactured for Boehringer Ingelheim Vetmedica, Inc. EQUIOXX® (firocoxib) – Oral and Intravenous Equioxx is the first coxb class non-steroidal anti-inflammatory drug (NSAID) approved for horses in the US and is formulated especially to alleviate the pain and inflammation associated with osteoarthritis (OA). Equioxx targets COX-2 (cyclooxygenase-2), while sparing COX-1 (cycloxygenase-1). Equioxx Oral Paste can be administered solely for the treatment of OA or in conjunction with Equioxx Injection. The recommended dosage of Equioxx Injection for intravenous administration in horses is 0.04 mg/lb (0.09 mg/kg) of body weight once daily for up to 5 days. If further treatment is needed, Equioxx Oral Paste for horses can be used at a dosage of 0.045 mg/lb (0.1 mg/kg) body weight for up to an additional 9 days of treatment. The overall duration of treatment with Equioxx Injection and Equioxx Oral Paste will be dependent on the response observed, but should not exceed 14 days. While IV or oral dosing reach similar plasma concentrations after 2 hours the IV dose reached peak concentration after 1 minute where as oral
218

delivery required the full two hours. Equioxx Oral Paste is administered by once daily dosing giving 24 hours of pain relief. Equioxx is manufactured for Boehringer Ingelheim Vetmedica, Inc. Clarification regarding substitution of Previcox® for Equioxx® “May 11, 2010 The AVMA was recently made aware that there were questions surrounding the legality of treating a horse with Previcox® (firocoxib), a non-steroidal anti-inflammatory drug (NSAID) product labeled for dogs. Since there is a firocoxib product, Equioxx®, labeled for use in horses, then the canine product cannot be used in an extra-label fashion. Selecting the canine product over the equine product for any reason, including economic, is not acceptable. It is only if or when the approved equine drug were judged clinically ineffective for that labeled use that a veterinarian could use another animal approved drug, in an extra-label manner. Some may have heard that economic reasons are valid reasons to use a drug in an extra-label manner – this is true only in that a veterinarian can select an approved human drug to relieve pain and suffering in a non-food animal even when an identical approved animal drug is available. The spirit of AMDUCA is to allow veterinarians flexibility in administering therapies that will help relieve animal pain and suffering. The over arching premise for AMDUCA is that extra-label use is for filling a medical need when an animal's health is threatened.” – AVMA Sedatives and Analgesics Sedivet® (romifidine hydrochloride) Sedivet 1.0% Injection is a α2-adrenoceptor agonist with sedative and analgesic properties. It is utilized to facilitate handling, as a standing sedative and analgesic for clinical examinations and procedures, minor surgical procedures in adult horses, and as a general anesthesia premedication. To achieve sedation and analgesia: Administer Sedivet slowly as a single IV injection using a dosage range of 40-120 µg/kg (0.4 1.2 mL/100 kg body weight) depending on the depth and duration of sedation that is required. As a preanesthesia agent, use a single IV injection dosed at 100 µg/kg (1.0 mL/100 kg body weight ). Anesthesia should be induced after maximum sedation is achieved typically within 2-4 minutes. When utilizing Ketamine and Diazepam for field anesthesia, recovery typically begins with sternal recumbency occurring within 12-83 minutes, followed by standing in 17-84 minutes. While recovery occurs over a longer duration it tends to be more even and controlled. Sedivet is manufactured for Boehringer Ingelheim Vetmedica, Inc. Dormosedan Gel® (detomidine hydrochloride) Dormosedan Gel is a α2-adrenoreceptor agonist oromucosal gel which produces sedation and restraint in horses. It is dose dependent in its depth and duration and is an effective and safe option for needle-shy horses. It selectively binds to the α2-adrenoceptors, causing the nerve to stop releasing norepinephrine and blocking the nerve impulse. Unlike injectable detomidine hydrochloride, the gel does not provide analgesia and should not use for painful procedures. Onset of sedation is approximately 40 minutes with a duration of 90 to 180 minutes. Dormosedan Gel produces sedation when administered sublingually at 0.018 mg/lb (0.040
219

mg/kg). The tube is designed for single use and should be safely discarded with the remaining contents. Precautions, such as impermeable gloves, should be taken when utilizing Dormosedan Gel because it can be absorbed following direct exposure to skin, eyes, or mouth. Accidental human exposure could cause adverse reactions, including sedation, hypotension and bradycardia. Seek medical attention immediately but do not drive because sedation or changes in blood pressure may occur. Dormosedan Gel is distributed by Pfizer Animal Health. Buscopan™ Injectable Solution (N-butylscopolammonium bromide, 20 mg/mL) Buscopan is a antispasmodic and anticholinergic drug for intravenous use which suppresses spasms of the digestive system. Buscopan’s spasmolytic action is based on anticholinergic effects resulting from competitive inhibition of parasympathetic activation (via muscarinic receptors) of smooth muscle cells. It is indicated for the control of abdominal pain associated with spasmodic colic, flatulent colic, and simple impactions in horses. Intravenous dosage is a single injection of 0.3 mg/kg body weight (0.14 mg/lb), 1.5 mL of Buscopan injectable solution per 100 kg (220 pounds) body weight. Intravenous administration of Buscopan results in heart rate elevation which invalidates heart rate as an indicator of pain for 30 minutes following IV injection. A recent study performed in 2010, demonstrated that N-Butylscopolammonium bromide can be administered safely and effectively to horses intramuscularly. Duration of gastrointestinal effect was prolonged with IM administration and tachycardia was not as dramatic. Buscopan has been recommended to aid in the relief of distal esophageal obstruction by inducing relaxation of the esophageal muscles. Recent clinical trials have supported anecdotal information that administration of Buscopan also induces rectal relaxation and may reduce the potential risk of rectal tears during medical or reproductive examination, a total dose of 20–40 mg in a 500-kg mare was utilized to facilitate rectal examinations and reproductive procedures. Buscopan is manufactured for Boehringer Ingelheim Vetmedica, Inc. EXCEDE(Ceftiofur Crystalline Free Acid) Excede is a broad spectrum cephalosporin antibiotic active against Gram-positive and Gram-negative bacteria including ß-lactamase-producing strains. Like other cephalosporins, ceftiofur is bactericidal, in vitro, resulting from inhibition of cell wall synthesis. Each mL of this ready-to-use sterile suspension contains ceftiofur crystalline free acid equivalent to 200 mg ceftiofur, in a caprylic/capric triglyceride. Excede is indicated for the treatment of lower respiratory tract infections in horses caused by susceptible strains of Streptococcus equi ssp. zooepidemicus. Excede is labeled for intramuscular injection in the horse. Administer two intramuscular injections to horses, 4 days apart, at a dose of 3.0 mg/lb (6.6 mg/kg). A maximum of 20 mL per injection site may be administered with no more than 10 mL placed prior to redirecting the needle. Therapeutic drug concentrations are maintained for 6 days after the second injection. Excede is distributed by Pfizer Animal Health. GastroGard & UlcerGard (Omeprazole) Omeprazole is a gastric acid pump inhibitor that regulates the final step in hydrogen ion production and blocks gastric acid secretion. It is indicated for the treatment and prevention of recurrent gastric ulcers in horses and foals 4 weeks of age and older. Equine stomach ulcers, also called Equine Gastric Ulcer Syndrome or EGUS, create a painful condition that can reduce
220

performance, generate symptoms of colic, and give a general appearance of ill thrift. Omeprazole at 4 mg/kg daily for 28 days, effectively healed or reduced the severity of gastric ulcers. Omeprazole at 0.9 mg/lb (2 mg/kg) prevented recurrence and formation of new gastric ulcers. GastroGard and UlcerGard are manufactured for Merial LLC. Wound management Many hallmarks of wound management are conserved between species, but due to the nature of the equine distal limb and the propensity for exuberant granulation tissue production, many of the therapies and ointments that have been utilized historically may have in fact delayed and prevented healing. Initial therapies by the owner should be directed towards gross decontamination of the wound and bandaging with no use of topical medication until evaluation by the veterinarian. Initial and prolonged cleaning of equine wounds especially in the distal limb should be targeted to optimize healing and limit cellular damage. Products such as Hydrogen Peroxide (3%) are not recommended for wound cleansing due to the narrow antibacterial spectrum and fact that it is damaging to tissue and causes thrombosis of microvasculature. Povodine - Iodine (10%) diluted to 0.1-0.2% (10-20ml/L) is recommended for general wound cleaning as it has a wide antibacterial and antifungal activities. Chlorhexidine (2%) diluted to a 0.05% concentration (25ml to 975 saline solution) is also recommended due to its prolonged residual antibacterial activity and broad spectrum antibacterial effect. High concentrations of Cholrohexadine greater than 0.05 % will delay wound healing and should be avoided in treating equine wounds. General rule: “The solution to pollution is dilution.” Common topical ointments utilized in the equine with great effectiveness are triple antibiotic cream, and Silver sulfadiazine (SSD). A very common ointment found in most equine barns that should be used with caution in the distal limb is Nitofurazone ointment. This ointment will delay wound healing and increase the production of exuberant granulation tissue. Additional topical medications are available from natural/ herbal preparations to sprays and ointments. While many products lack evidence based medicine to prove efficacy in the equine, particularly in the limb, the anecdotal reports have been promising, however, additional research should be completed prior to wide spread utilization. The use of regional limb perfusions should be considered and utilized due to the ability to get very high concentrations of antibiotics locally, typically many times the MIC. This effect allows for the use of costly antibiotics that could be otherwise economically prohibitive and/or contraindicated in the patient. Regional limb perfusion Management of infection or sepsis in the equine limb following trauma or iatrogenic synovial sepsis can be challenging and unrewarding for clients and veterinarians alike. The use of regional limb perfusions can be a first round treatment option that is highly effective and relatively easy to offer in the standing horse. Multiple studies have demonstrated the efficacy of intravenous digital perfusions with aminoglycacides (amikacin or gentamicin) that result in high concentrations of antibiotics within synovial fluid in the treated region. One study demonstrated a minimum inhibitory concentration 25 to 50 times the requirement to kill pathogenic bacteria.
221

To perform a regional perfusion, systemic sedation and regional anesthesia should be utilized. Placement of an Esmarch bandages proximally and if applicable, distal to the affected region will need to be applied. A 25 gauge butterfly catheter can be placed in the regional vein and utilized to inject 1 gram of amikacin diluted in 20-40 mL of normal saline depending on location and region being treated. Some veterinarians have utilized lidocaine in the injection to provide regional anesthesia versus performing distal limb blocks prior to placement of the Esmarch bandage. Regional limb perfusion of equine limbs results in locally high concentrations of antibiotics that are effective in treating local sepsis when used in conjunction with systemic antibiotic therapies and proper wound management. The procedure requires no specialized equipment and can be performed in a standing equine. Impaction colic While the underlying etiology of impaction colic is unknown, it is the most common cause of obstruction colic in the horse. Definitive diagnosis of an impaction is commonly achieved by direct rectal palpation. Historically, mineral oil has been utilized to manage impaction colic. Recent evidence exists demonstrating the use of oral or intravenous fluids to be a much more effective treatment choice. Anecdotal evidence was thought to demonstrate that a state of “over hydration” could be achieved with the use of intravenous fluids allowing fluids to leak into the gastrointestinal lumen, directly hydrating the ingesta. This theory has been proven to be incorrect, but utilization of intravenous fluids does facilitate systemic hydration allowing for normalization of fluid content in the digesta, possibly due to normal saliva production and decreased absorption of oral fluids administered via nasogastric tubing and normal access to clean warm water. Balanced electrolyte solutions via nasogastric tube have been shown to rehydrate the impaction and improve systemic hydration while using many types of hypertonic or hypotonic fluids, such as tap water, have demonstrated limited effects on the ingesta and adverse effects on systemic electrolyte levels, so their use should be limited. Oral balanced electrolyte fluids at a rate of 5-10 liters per an hour have been shown to be highly effective in treating large colon impactions. Upward fixation of the patella Upward fixation of the patella is a condition that affects horses most commonly when they are returned to work after an extended period of rest that resulted in loss of quadriceps muscle strength. Often the condition will resolve with exercise (hill work, trotting over poles, and backing), anti-inflammatories and time. Historically, internal blisters have been utilized over the medial and middle patellar ligaments, with medial patellar desmotomy being the final salvage procedure for the condition, but recently medial patellar ligament splitting has been demonstrated to be highly effective in resolving upward fixation of the patella. This procedure can be performed on the farm in the standing horse utilizing a 14 or 18 gauge needle. This procedure requires little down time, allowing the horse to return to work more quickly, typically within three days and carries less risk than internal blisters.
222

Additional reading and resources Pharmacokinetics, Pharmacodynamics, and Safety of N-Butylscopolammonium Bromide Administered Intramuscularly Versus Intravenously Joseph J. Bertone, DVM, MS; Holly M. Greene, MS; Margaret Sislak, DVM; Heidi Agnic, DVM; Melodee Heidmiller; Scott Stanley, PhD; and Steven J. Wickler, DVM, PhD AAEP PROCEEDINGS Vol. 56 2010 279 Clinical Cases in Equine Reproduction Patrick M. McCue, DVM, PhD, Diplomate ACT AAEP PROCEEDINGS Vol. 52 2006 594 What’s New and Innovative in Wound Management: Problems and Solutions Christine L. Theoret, DMV, PhD AAEP PROCEEDINGS Vol. 52 2006 265 EQUINE WOUND MANAGEMENT 2nd Edition Editors: Ted S. Stashak and Christine L. Theoret Wiley Blackwellne Vet Rev 1998; 3(4):27-29. How to Perform Regional Limb Perfusion in the Standing Horse Scott E. Palmer, VMD; and Patricia M. Hogan, VMD AAEP PROCEEDINGS Vol. 45 1999 127 Local antibiotic perfusion of the distal limb of horses Murphey ED, Santschi EM, Papich MG. AAEP PROCEEDINGS Vol. 40 1994 141–142. Evaluation of Regional Limb Perfusion With Amikacin Using the Saphenous, Cephalic, and Palmar Digital Veins Gal Kelmer, DVM, MS, Diplomate ACVS; Gillian C. Bell, BS; Tomas Martin-Jimenez, DVM, PhD, Diplomate ACVCP, Diplomate ECVPT; Arnold M. Saxton, PhD; Christina Catasus, BS; Sarah B. Elliott, BS; and Bernd Meibohm, PhD, FCP AAEP PROCEEDINGS Vol. 55 2009 251 Critical Decisions in Colic Anthony Blikslager, DVM, PhD, Diplomate ACVS AAEP PROCEEDINGS _ Vol. 55 _ 2009 201-207 Advances in Management of Large Intestinal Colic Alison J. Morton, DVM, MSpVM, Diplomate ACVS AAEP PROCEEDINGS Vol. 55 2009 212-218
223

Treatments for Colic Nathaniel A. White II, DVM, MS, Diplomate ACVS AAEP PROCEEDINGS Vol. 52 2006 153-169 Prospective study of equine colic incidence and mortality Tinker MK, White NA, Lessard P, et al. Equine Vet J 1997; 29:448–453 Treatment of impaction colics White NA II, Dabareiner RM. Vet Clin North Am Equine Pract 1997;13:243–259 How to Perform a Standing Medial Patellar Ligament Splitting Scott R. Reiners, DVM, Diplomate ACVS; Kim May, DVM, Diplomate ACVS; Wynne DiGrassie, DVM, MS, Diplomate ACT; and Tabitha Moore, DVM, MS AAEP PROCEEDINGS Vol. 51 2005 483
224

Foreign Animal Disease Update Around the World
Darlene Konkle, DVM, MS Wisconsin Department of Agriculture, Trade and Consumer Protection
What is at stake: Foreign and emerging diseases threaten the livestock and poultry industries of the United States. In Wisconsin alone, agriculture is a $59 billion industry. Our nearly 13,000 dairy farms produce over 25 billion pounds of milk annually. The economic and societal impact of a foreign animal disease introduction would be devastating for Wisconsin and the nation. Introduction of a foreign animal disease into the United States would greatly reduce our ability to trade animals and animal products internationally, and would also affect interstate movement. The discovery of Bovine Spongiform Encephalopathy in a Washington cow in 2003 still has an impact on the international trade of beef today. The H1N1 outbreak in 2009, labeled ‘swine flu’ by international media, has cost the U.S. swine industry hundreds of millions of dollars in lost revenue. The United States Department of Agriculture and the Department of Homeland Security recognize 17 diseases as significant threats to US agriculture: Foot and Mouth Disease, Rift Valley Fever, Highly Pathogenic Avian Influenza, Exotic Newcastle Disease, Nipah and Hendra Virus, Classical Swine Fever, African Swine Fever, Bovine Spongiform Encephaopathy, Rinderpest, Japanese Encephalitis, African Horse Sickness, Venezuelan Equine Encephalitis, Eastern Equine Encephalitis, Contagious Bovine Pleuropneumonia, Ehrlichia ruminatium (Heartwater), Coxiella burnetii, and Akabane virus. This presentation will describe recent outbreaks of some of these diseases worldwide, and the implications of their introduction into the United States. Overview of recent outbreaks: Foot and Mouth Disease (FMD) is one of the diseases considered most potentially devastating to the U.S. livestock industry. FMD is highly contagious, and affects cloven-hoofed species. Although not a public health threat, FMD causes painful vesicular lesions in affected animals, leading to lameness, salivation, as well as decreased weight gain and milk production. The 2001 outbreak in Great Britain is an example of the economic and social impacts of an FMD outbreak in a previously free country. FMD remains endemic in 2/3 of the world today, including Africa, Asia, and South America. Two major outbreaks have occurred recently in Japan and in South Korea. The Japan FMD outbreak began in April 2010 in the Miyazaki province and spread throughout that province into the month of July. In total, 292 farms were affected. Over 200,000 animals were affected, including 37,000 cattle and 174,000 hogs. The Japanese government employed vaccination for FMD, and vaccinated over 100,000 animals. Both infected and vaccinated animals were destroyed. The source of the infection was thought to be infected rice straw imported from China. The outbreak is estimated to have cost $200 billion US dollars. Over 7500 veterinarians were employed in this FMD response.
225

The FMD outbreak in South Korea began in November 2010, and was a recurrence of a previous outbreak of FMD Serotype O. The response in South Korea involved mass culling of 3 million cattle and hogs. The government employed FMD vaccination as a control measure in December, 2010. The South Korea outbreak made international headlines when it was reported that animals were buried alive due to shortages of euthanasia drugs, and the need to depopulate quickly. South Korea utilized mass burial for carcass disposal, and was faced with water quality issues post-outbreak. As with the Japan 2010 outbreak, in South Korea the virus spread rapidly through the area, affecting hundreds of farms. Highly pathogenic avian influenza H5N1 continues to circulate in Indonesia, Egypt and eastern Asia. South Korea and Japan both reported highly pathogenic H5N1 in 2010. The H5N1 virus circulates in wild birds, and has been reported in domestic poultry in these countries. Since 2003, approximately 400 people have died from highly pathogenic H5N1 influenza. These people have had very close contact with infected poultry. In very few cases (1-2 worldwide) there has been evidence of human to human transmission of the virus. In these cases, infected people had very close contact with ill family members. Although H5N1 did not evolve into the human pandemic some had feared, its continued circulation and transmission to domestic poultry and humans offers potential for re-assortment of the virus. Hendra virus has re-emerged in horses in Australia. Hendra is a zoonotic disease of horses and humans spread by bats in Australia. Since 1994, there have been 40 cases affecting horses. Hendra virus causes rapidly progressing respiratory and neurologic signs. Reported case fatality rates are over 70% in horses. Additionally, humans in close contact with infected horses have been infected with the Hendra virus. Of 7 humans known to have been infected with the disease, 4 have died. In July 2011, there have been outbreaks of Hendra virus in horses in Queensland and New South Wales. Thirteen horses have died, and the people in close contact with these horses have been tested. One of the farm dogs was also confirmed positive for Hendra virus via antibody detection methods. The dog was euthanized. Risks: An astounding number of people, animals and animal products move across United States borders. United States Customs and Border Protection officials process over 1 million people, 70,000 containers, and 330,000 vehicles entering the United States from abroad each day. What is inspected represents a small fraction of goods and containers entering the U.S. In addition to the legal movement of people, animals and animal products, the U.S. is also at risk from smuggling of plant and animal products, and intentional adulteration of our food supply. United States Customs and Border Protection officials intercept over 4,000 prohibited meat, plant and animal products at ports of entry each day.
226
Roles for veterinarians and producers: The clinical signs of foreign animal diseases often closely resemble those of domestic diseases of livestock and poultry. This makes early detection and response a challenge, but a rapid response is critical to eliminating the disease. Private practitioners and producers are the first lines of defense against foreign animal diseases. Practitioners and producers will likely recognize the first warning signs of a potential foreign disease, and timely reporting to the appropriate state and federal authorities is needed. Practitioners and producers also control what comes on and off the farm. Good bio-security plans, record keeping and documentation of visitors are all important. Practitioners and producers can be also part of a trained volunteer cadre to respond to a foreign animal disease through membership in the Wisconsin Animal Response Corps. For veterinarians and veterinary technicians willing to respond to a disease event outside of Wisconsin, the National Animal Health Emergency Response Corps is also recruiting members.
Wisconsin Foreign Animal Disease Response Plan Executive Summary
Purpose: This plan defines the framework needed to detect, control, and eradicate a highly contagious foreign animal disease (FAD) in order to return Wisconsin agriculture to normal production, and the United States to disease free status, as efficiently as possible. Situation: Wisconsin has extensive and varied dairy, livestock and poultry industries, with cash receipts totaling over $3 billion annually. These industries are highly vulnerable to an outbreak of a foreign animal disease. During the past several years, foreign animal disease outbreaks have occurred in other states and countries resulting in devastating economic consequences. Control and eradication of these diseases consumes enormous amounts of resources and results in trade and national income loss. Response Coordination: In contrast to the initial emergency response to a fire, flood, or tornado, a foreign animal disease (FAD) response will require a rapid initial response from state agencies with special expertise. Statutory authority to conduct an FAD response is held by the Wisconsin Department of Agriculture, Trade and Consumer Protection (DATCP) under Wis. Stat. 93.07(10). Further, veterinarians and laboratories are required to report suspicion of a foreign animal disease to DATCP. The technical veterinary expertise required to implement measures to control the disease will be provided by DATCP and the US Department of Agriculture, Animal and Plant Health Inspection Service - Veterinary Services (USDA-VS). The USDA Veterinary Services has responsibility, expertise and authority to address animal diseases that threaten U.S. agriculture. The USDA provides the bulk of the funding at the local, state and national level for response to disease outbreaks because they all have a national impact. This funding may be delivered directly from USDA to supporting agencies
227

such as DATCP. Consequently, DATCP and USDA maintain a unique relationship of cooperation in safeguarding Wisconsin’s livestock resources. Upon discovery of a FAD in Wisconsin, DATCP and USDA/VS will work with local officials to coordinate the response for the incident. To most efficiently coordinate the response, the state and federal animal health agencies will operate in Unified Command under the Incident Command System. DATCP and USDA-VS will also contact local officials and offer to provide an Advance Team of 2-4 individuals to the affected county. The Advance Team will coordinate with local officials to gather and share information, assess the need for resources, and identify the roles of the county and local entities in managing the FAD response. In a large incident, the Unified Command may request that the State Emergency Operations Center be activated to provide support and coordinate resources as needed. Initial Reporting and Investigation (1st Response): Any member of the agriculture or animal health community might first detect the abnormal situation indicating a possible FAD. Ideally, this detection will occur soon after the disease is introduced and will be reported to DATCP or Wisconsin’s APHIS/VS Area Office. Together, the State Veterinarian and the USDA/VS Area Veterinarian-in-Charge (AVIC) for Wisconsin will send a Foreign Animal Disease Diagnostician (FADD) to follow up on a report of a possible FAD. A Foreign Animal Disease Diagnostician in Wisconsin is designated by the State Veterinarian and the AVIC, is a state or federally employed veterinarian, and is trained to recognize signs of a foreign animal disease, collect appropriate diagnostic samples, and take initial actions. The FADD will make a field diagnosis and in consultation with the State Veterinarian and the AVIC and will determine the likelihood of an FAD. Samples will be collected from affected animals and submitted for testing to a federal laboratory. Response Activities: When laboratory results, combined with compatible clinical signs and epidemiologic information, indicate a foreign animal disease is strongly suspected, the USDA-APHIS/VS and DATCP will initiate the response coordination. Response activities are intended to prevent the spread of the disease and determine the likely route of introduction while also eliminating the disease-causing agent using the following principles:
1) detect the disease quickly; 2) prevent contact between susceptible animals and the disease causing agent; 3) stop production of the disease-causing agent by infected animals; and 4) increase the disease resistance of susceptible animals.
228

The following activities are used to accomplish control and eradication: Stop animal movement (quarantine) to and from the affected premises Implement bio-security measures on the premises to ensure the disease organism
will not be a) moved off the farm through movement of vehicles or people or b) spread to other susceptible groups of animals on the farm.
Initiate an epidemiological investigation to: o Identify contacts (animals, people, vehicles) who have recently moved on
or off the premises and quarantine additional premises associated by contact
o Identify all properties in the appropriate area with susceptible animals and monitor these animals for signs of the disease
o Determine the possible contact between wildlife and infected animals and implement a plan to detect and control the disease in wildlife.
Establish a control zone and surveillance zone around infected premises which defines the activities to be conducted to detect and control the disease
o Define permitted movement of products and non susceptible animals o Define affected “compartments” within the industry and which other
compartments can continue to operate with additional control measures and assessment
Consider all options for depopulation of the affected animals after determining the value of the herd or flock
o Controlled slaughter o Humane euthanasia and disposal without spreading the disease
Clean and disinfect affected premises Initiate the information management plan Prepare to receive vaccine and develop vaccination plan if vaccination becomes a
viable control measure.
229

Troubleshooting Silage Yeast, Mold, VFA and Feeding Problems
Bill Mahanna and Bill SeglarPioneer Nutritional Sciences Pioneer, A DuPont Business
http://www.pioneer.com/home/site/us/livestock-feed-nutrition/
Bunker Safety Message
Think Safety---------- Forwarded message ----------From: Luciana Jonkman <[email protected]>Date: Tue, Sep 1, 2009 at 12:06 AMSubject: Doug crushed by silage last Thursday!
Last Thursday my friend and partner Doug DeGroff was crushed by a silage pile. He is thankfully laying in a hospital bed as I write this able to move all his limbs.
The situation was as follows:
Doug was sampling silage from the “ramp” portion of 2009 silage. This was the second sample he had taken of this pile and at this point the pile was about 12-14 feet high. Doug was going to take a picture of the pile because it had such a well maintained and flat face. The dairy uses a facer to remove silage from the pile. He was standing in front of the pile taking a sample when all of a sudden the silage hit him from the side. Doug was unable to move and was buried by the silage with just an arm sticking out. He dug his face clear of silage and when the feeder return to the pile he pulled him from avalanched area that buried him. Doug drove himself to the emergency room without shoes! The weight of the silage broke his back in two spots just above his waist line. He has many torn ligaments, 4 injured discs and bruises. I write because I feel I must remind everyone, including myself, of the risk we put ourselves in when we take silage samples. Pray for a full and speedy recovery for Doug.
Luciana LC Jonkman, MS
Progressive Dairy Solutions, Inc.
Lets start with my favorite little critters…YEAST
Different types of beers (e.g. ales, stouts, etc) are distinguished primarily by their yeast,
• van Leeuwenhoek (Father of Microbiology, 1632-
1723) was the first to observe yeast cells
• The yeast species Saccharomycescerevisiae has been used in baking and fermenting alcoholic beverages for thousands of years
• Other genus of yeast, such as Candida are opportunistic pathogens and can cause infection in humans
•Yeasts have recently been used to generate electricity in microbial fuel cells and produce ethanol for the biofuel industry.
I would like to recognize the contributions to this presentation by Pioneer microbiologist, Dr. Scott Dennis
( Ph.D. under Erle Bartley, K-State, Bloat Guard ® , Starea ® , Bovatec ®) Yeast • Yeasts are eukaryotic micro-organisms classified in the
kingdom Fungi, with about 1,500 species currently described.
• Yeasts do not form an exact taxonomic or phylogeneticgrouping. At present it is estimated that only 1% of all yeast species have been described.
• The term "yeast" is often taken as a synonym for S. cerevisiae, but the phylogenetic diversity of yeasts is shown by their placement in both divisions Ascomycotaand Basidiomycota. The budding yeasts ("true yeasts") are classified in the order Saccharomycetales]
• Most reproduce asexually by budding although a few do so by binary fission.
• Yeasts are unicellular, although some species with yeast forms may become multicellular through the formation of a string of connected budding cells known as pseudohyphae or false hyphae as seen in most mold
• Yeast are relatively large by microbe standard and size can vary greatly depending on the species, typically measuring 3–4 µm in diameter, although some yeasts can reach over 40 µm.
230
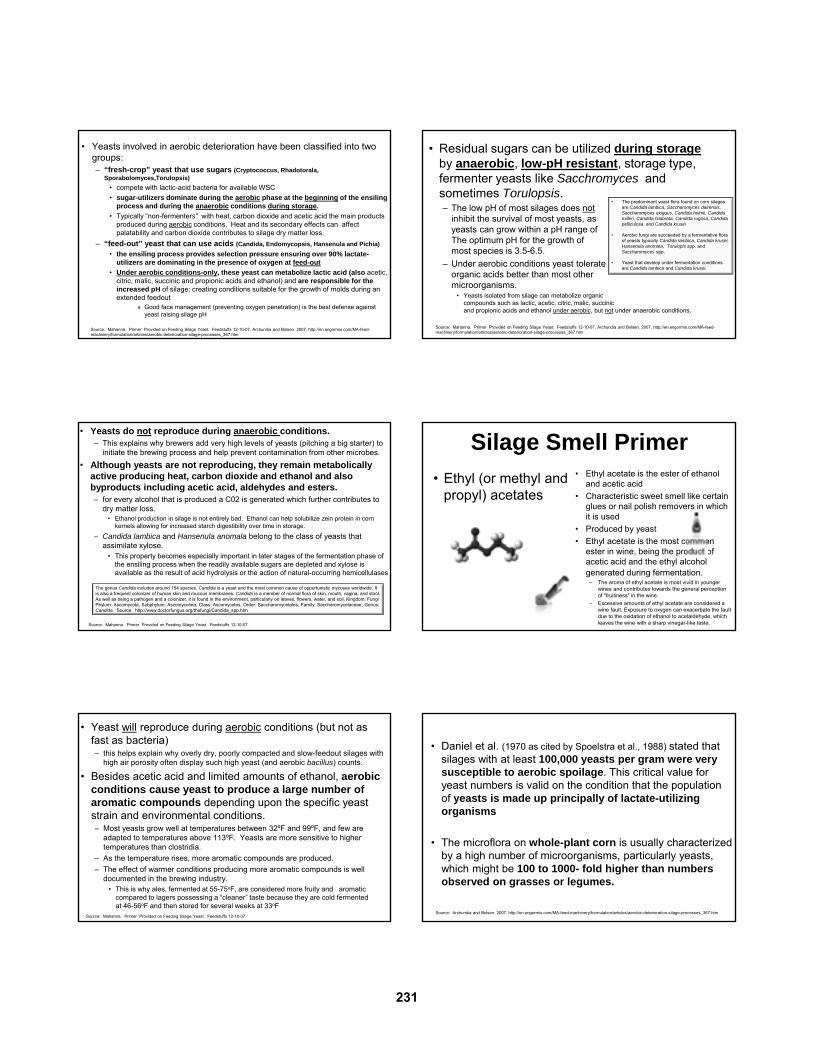
• Yeasts involved in aerobic deterioration have been classified into two groups: – “fresh-crop” yeast that use sugars (Cryptococcus, Rhadotorala,
Sporabolomyces,Torulopsis)
• compete with lactic-acid bacteria for available WSC
• sugar-utilizers dominate during the aerobic phase at the beginning of the ensiling process and during the anaerobic conditions during storage.
• Typically “non-fermenters” with heat, carbon dioxide and acetic acid the main products produced during aerobic conditions. Heat and its secondary effects can affect palatability and carbon dioxide contributes to silage dry matter loss.
– “feed-out” yeast that can use acids (Candida, Endomycopsis, Hansenula and Pichia)
• the ensiling process provides selection pressure ensuring over 90% lactate-utilizers are dominating in the presence of oxygen at feed-out
• Under aerobic conditions-only, these yeast can metabolize lactic acid (also acetic, citric, malic, succinic and propionic acids and ethanol) and are responsible for the increased pH of silage; creating conditions suitable for the growth of molds during an extended feedout
» Good face management (preventing oxygen penetration) is the best defense against yeast raising silage pH
Source: Mahanna. Primer Provided on Feeding Silage Yeast. Feedstuffs 12-10-07. Archundia and Bolsen. 2007. http://en.engormix.com/MA-feed-machinery/formulation/articles/aerobic-deterioration-silage-processes_367.htm
• Residual sugars can be utilized during storageby anaerobic, low-pH resistant, storage type, fermenter yeasts like Sacchromyces and sometimes Torulopsis.– The low pH of most silages does not
inhibit the survival of most yeasts, as yeasts can grow within a pH range of 3-8. The optimum pH for the growth of most species is 3.5-6.5.
– Under aerobic conditions yeast tolerate organic acids better than most other microorganisms.
• Yeasts isolated from silage can metabolize organic compounds such as lactic, acetic, citric, malic, succinicand propionic acids and ethanol under aerobic, but not under anaerobic conditions.
Source: Mahanna. Primer Provided on Feeding Silage Yeast. Feedstuffs 12-10-07. Archundia and Bolsen. 2007. http://en.engormix.com/MA-feed-machinery/formulation/articles/aerobic-deterioration-silage-processes_367.htm
• The predominant yeast flora found on corn silages are Candida lambica, Saccharomyces dairensis, Saccharomyces exiguus, Candida holmii, Candida milleri, Candida Glabrata, Candida rugosa, Candida pelliculosa and Candida krusei
• Aerobic fungi are succeeded by a fermentative flora of yeasts typically Candida lambica, Candida krusei, Hansenula anomala, Torulopis spp. and Saccharomyces spp.
• Yeast that develop under fermentation conditions are Candida lambica and Candida krusei.
• Yeasts do not reproduce during anaerobic conditions. – This explains why brewers add very high levels of yeasts (pitching a big starter) to
initiate the brewing process and help prevent contamination from other microbes.
• Although yeasts are not reproducing, they remain metabolically active producing heat, carbon dioxide and ethanol and also byproducts including acetic acid, aldehydes and esters. – for every alcohol that is produced a C02 is generated which further contributes to
dry matter loss. • Ethanol production in silage is not entirely bad. Ethanol can help solubilize zein protein in corn
kernels allowing for increased starch digestibility over time in storage.
– Candida lambica and Hansenula anomala belong to the class of yeasts that assimilate xylose.
• This property becomes especially important in later stages of the fermentation phase of the ensiling process when the readily available sugars are depleted and xylose is available as the result of acid hydrolysis or the action of natural-occurring hemicellulases
Source: Mahanna. Primer Provided on Feeding Silage Yeast. Feedstuffs 12-10-07.
The genus Candida includes around 154 species. Candida is a yeast and the most common cause of opportunistic mycoses worldwide. It is also a frequent colonizer of human skin and mucous membranes. Candida is a member of normal flora of skin, mouth, vagina, and stool. As well as being a pathogen and a colonizer, it is found in the environment, particularly on leaves, flowers, water, and soil. Kingdom: FungiPhylum: Ascomycota, Subphylum: Ascomycotina, Class: Ascomycetes, Order: Saccharomycetales, Family: Saccharomycetaceae, Genus: Candida. Source: http://www.doctorfungus.org/thefungi/Candida_spp.htm
Silage Smell Primer
• Ethyl (or methyl and propyl) acetates
• Ethyl acetate is the ester of ethanol and acetic acid
• Characteristic sweet smell like certain glues or nail polish removers in which it is used
• Produced by yeast
• Ethyl acetate is the most common ester in wine, being the product of acetic acid and the ethyl alcohol generated during fermentation.
– The aroma of ethyl acetate is most vivid in younger wines and contributes towards the general perception of "fruitiness" in the wine.
– Excessive amounts of ethyl acetate are considered a wine fault. Exposure to oxygen can exacerbate the fault due to the oxidation of ethanol to acetaldehyde, which leaves the wine with a sharp vinegar-like taste.
• Yeast will reproduce during aerobic conditions (but not as fast as bacteria) – this helps explain why overly dry, poorly compacted and slow-feedout silages with
high air porosity often display such high yeast (and aerobic bacillus) counts.
• Besides acetic acid and limited amounts of ethanol, aerobic conditions cause yeast to produce a large number of aromatic compounds depending upon the specific yeast strain and environmental conditions. – Most yeasts grow well at temperatures between 32ºF and 99ºF, and few are
adapted to temperatures above 113ºF. Yeasts are more sensitive to higher temperatures than clostridia.
– As the temperature rises, more aromatic compounds are produced.
– The effect of warmer conditions producing more aromatic compounds is well documented in the brewing industry.
• This is why ales, fermented at 55-75oF, are considered more fruity and aromatic compared to lagers possessing a “cleaner” taste because they are cold fermented at 46-56oF and then stored for several weeks at 33oF
Source: Mahanna. Primer Provided on Feeding Silage Yeast. Feedstuffs 12-10-07.
• Daniel et al. (1970 as cited by Spoelstra et al., 1988) stated that silages with at least 100,000 yeasts per gram were very susceptible to aerobic spoilage. This critical value for yeast numbers is valid on the condition that the population of yeasts is made up principally of lactate-utilizing organisms
• The microflora on whole-plant corn is usually characterized by a high number of microorganisms, particularly yeasts, which might be 100 to 1000- fold higher than numbers observed on grasses or legumes.
Source: Archundia and Bolsen. 2007. http://en.engormix.com/MA-feed-machinery/formulation/articles/aerobic-deterioration-silage-processes_367.htm
231

http://blog.foragelab.com/2010/01/mold-yeast-dount-distributions-cvas-fall-2009/
Real World Data Corn Silage harvested Fall 2006 on a West-Central Minnesota dairy
competitor
0 C
1st peak typically yeast and aerobic bacterial induced 2nd peak typically mold
and fungal induced
0 point = baseline = temp of room held at 22C (72F)
9F
Honig Aerobic Stability Method
23 F
When silage heats over this line, it is aerobically UNSTABLE
Fermentation Pathway of Lactobacillus buchneri
2 Lactic Acid 2 Acetic Acid
1 Acetic Acid + 1 1,2 Propanediol
Propanol + Propionic Acid
or
or
Degrading the preformed lacticacid is why it takes 3-4 weeksfor maximum aerobic stabilitybenefits to be achieved with
products containing L. buchneri
Other silage microflora make this conversion, it is not absolutely clear that L. buchneri initiate this last step.
Source: Driehuis, F, S.J.W.H Oude Elferink and S.F. Spoelstra. 1999. Anaerobic lactic acid degradation during ensilage of whole crop maize inoculated with Lactobacillus buchneri inhibits yeast growth and improves aerobic stability. Journal of Applied Microbiology 87:583-94.
The combination of lactic acid+ acetic acid + these other compounds inhibits yeast
growth which initiates silage heating
The combination of lactic acid+ acetic acid + these other compounds inhibits yeast
growth which initiates silage heating
Volatile Fatty Acid patterns differ depending on the strains found in the Inoculant
VFA profile typical of products containing both homo-fermentative
and L. buchneri strains
VFA profile typical of products containing only Homofermentative strains
It Makes a Difference Which Organism
Produces the Acetic Acid
• Silages treated with bacterial products containing L. buchneri typically exhibit lower lactic:acetic acid ratios (e.g. as low as 1:1) due to increased production of acetic and propionic acids. Research studies by Kung, Taylor, Combs and Driehuis indicate that silages treated with additives resulting in these altered VFA profiles generally have improved bunklife and exert no negative impact on dry matter intake; as opposed to elevated acetic acid levels caused by detrimental organisms commonly found on the crop such as: 1) yeast, 2) gram-negative acetic acid producers (e.g. enterobacter sp.) or 3) heterofermentative lactic-acid bacteria (e.g. leuconostocsp.) which may contribute to poor bunklife or feeding issues.
232

Impact of Corn Silage Feeding on MFD
• Corn silage is rapidly becoming the major forage in many dairy rations and may cause herds to be more susceptible to MFD unless careful consideration is directed at a corn silage-based TMR potential to alter rumen pH.
• Corn silage is unique in that it contributes high levels of digestible fiber from the stover with highly digestible starch and approximately 55% unsaturated linoleic acid in the grain. – The problem is production of trans-10, cis-12 conjugated linoleic acid (CLA),
which escape the rumen and signal a decrease in lipoganic enzymes reducing mammary tissue fat synthesis
• This makes it difficult to separate the effect of starch on rumen pH versus the contribution of additional linoleic acid when diagnosing the causes of MFD in high corn silage rations(Van Amburgh et al., 2008).
Source: Mahanna, B. 2009. Milk fat depression involves many factors. Feedstuffs Vol. 81, No 42 October 12, 2009
Nutritionists should probably start MFD troubleshooting by first investigating…
• Reviewing the current ration and feed delivery status of the herd for issues which have the greatest potential to altered rumen pH. These include: 1) ration starch content, 2) changes in starch digestibility due to:
a. particle size in concentrates, b. moving to wetter high-moisture corn, c. changes in the degree of kernel damage in corn silage and d. adjusting for length of time silage or high-moisture corn was in fermented
storage, 33) physically effective NDF of the ration, 4) feed mixing issues contributing to further particle size reductions, 5) recent changes in dry matter intake causing higher rumen turnover rates, 6) cud-chewing and saliva flow, 7) abrupt changes to new-crop or a different bunker,8) moving into aerobically unstable silages, 9) ration sorting 10)excess particles in the bottom pan of the Penn State Particle Separator.
Source: Mahanna, B. 2009. Milk fat depression involves many factors. Feedstuffs Vol. 81, No 42 October 12, 2009
What Else to Monitor• Rumen load of unsaturated fatty acids, particularly
linoleic (18:2) acid, delivered in the total ration.– Linoleic acid is the primary unsaturated fatty acid in
cottonseed, soybeans, corn and corn byproducts such as distiller grains.
• Concerns for MFD may exist when:– Total unsaturated fatty acids in the entire ration
exceed 500-600 g/day. – When CPM or CNCPS predicts intakes of C18:1C
exceeding 150 g/day• The biohydrogenation of 18:1 (oleic) to 18:0
(stearic) is rate limiting and can cause a buildup of problematic C18:1T
– in CPM, C18:1T includes all the trans forms, not just the ones implicated to MFD. This is why the thumb-rule of C18:1T exceeding 100 g/day to the duodenum may not be very predictive of MFD (Overton, 2009)
– Researchers in this area are more reluctant to assign a specific threshold levels of total rumen unsaturated fatty acids because it is such a variable, moving target highly dependent on dietary components and interactions.
• Attention should also be focused on the unsaturated fatty acid loads coming from various “ruminally inert” commercial fat sources in addition to the variability in fat content (5-15% of DM) commonly observed with distillers’ grains.
Source: Mahanna, B. 2009. Milk fat depression involves many factors. Feedstuffs Vol. 81, No 42 October 12, 2009 and Overtom, T, Novus CPM Training, World Dairy Expo 093009
• Research has shown that the combination of elevated levels of high-starch corn silage, with supplemental oil-based energy sources (such as cottonseed or distillers’ grains) and the inclusion of an additive such as monensin, can initiate a negative stepwise effect on MFD, demonstrating the need to focus on the additive effect of various ration ingredients (Van Amburgh et al., 2008).
Impact of Corn Silage Feeding on MFD
Source: Mahanna, B. 2009. Milk fat depression involves many factors. Feedstuffs Vol. 81, No 42 October 12, 2009
High Acetic Acid or Yeasty Silages• Researchers have questioned if abnormally fermented (e.g. high
acetic acid) might exhibit an altered fatty acid profile contributing to MFD. – Florida researchers (Amaral, et al., 2009) have reported changes in fatty acid
profiles with abnormal silages but further research is needed to determine if undesirable trans-intermediates are actually being produced during silage fermentation.
• Field experiences have also led some nutritionists to correlate high yeast silages with MFD. – While these may be contributing factors, more research is required to
determine specific cause and effect, such as specific genus/species/strain at fault, given the recent molecular research showing the complexity of microbial populations involved in the silage ecosystem (Ahmad et al., 2009, 2009a).
• It may be premature to get overly focused on this one dietary/management aspect given the limited capabilities for silage microbial/fungi identification and enumeration currently available to consulting nutritionists; especially if aerobically-challenged silages become the MFD scapegoat and other factors are not seriously investigated
Source: Mahanna, B. 2009. Milk fat depression involves many factors. Feedstuffs Vol. 81, No 42 October 12, 2009
Potential Impact of Spoilage Yeast in Silage on Rumen FermentationSantos Et Al, Proc. 2011 ASAS/ADSA, #146, p.91.
• Candida valida detected at 106 and 105 CFU/g in 35% of high moisture corn and 31% of corn silage samples from U.S. dairy farms.
• Tested in vitro effects on NDFD with 104, 106, 108 CFU/ml C. valida
– At 12 h, NDFD depressed only at 108 cfu/ml yeast level.– At 24 h, NDFD depressed linearly from 59 to 52% only at 108
cfu/ml yeast level
• Higher acetate/propionate at 108 log
• No change in biohydrogenation products
– Significance: first known study that indicates spoilage yeast do not impact milk fat depression
233

Molds and Mycotoxins in Grains and Forages
Field-Produced MoldsAnd Mycotoxins
Storage-Produced MoldsAnd Mycotoxins
• Typically less frequent in silage than with grain because • harvest is earlier • fungi have less time to grow
• Typically levels do not increase once silage is fermented unless poor fermentation and feed-out management
• Difficult to detect – not evenly distributed in silages
• Several types may be present at once
What Are They Are, What Do They Do??? Thousands of molds exist
– field and storage molds
– each has it’s own unique environment
• “Common link between different mycotoxins and their mode of action they are all produced by fungi!” Ronald Riley, USDA/ARS
Greater than 300 mycotoxins identified
– secondary metabolites
– most considered harmless
Several metabolites have toxic effect on livestock
Field Fungi• Mold spores are virtually everywhere and easily survive
over winter in soil and plant residues.
• The most common method of fungi entry in corn is:– own silk channels during pollination
– plant wounds from environmental or insect injury
– through the roots during the seedling stage
• Common field-fungi are capable of producing toxins such as aflatoxin, vomitoxin (DON), fumonisin, zearalenone and T-2.
• Almost all field produced mycotoxins are already on the plant prior to harvest and ensiling
• Presence of visible ear molds does not correlate well with mycotoxin contamination.
Pioneer’s Ear mold nurseries - USA
Napolean,OH
Ithaca, NY
GibberellaDiplodia
Fusarium
Strip Testing at Pioneer Ear Mold Nurseries
Mapping Disease Resistance:Major efforts underway to identify resistance and incorporate into new genetics. True for DIPERS, GIBERS and FUSERS.
234

Corn Field Molds With Toxin-Producing Potential
Penicillium Spp.
Fusarium graminearum Spp.(also called Gibberella zeae or Gibb)
Aspergillus Spp.
Fusarium (moniliforme) stalk rotFusarium (moniliforme) stalk rot
Fusarium verticillioides (F. moniliforme)
ear rot
Gibb stalk rot
Gibb ear rot
Aspergillus FusariumGibberella
(F. graminearum)
Temperature Optimum 90º + F Optimum 80-85º Optimum ~75º F
Moisture Grain-fill drought stress Early drought, humidity Wet during flowering
Insects Important Very important Less important
Metabolite Production
Purpose• Free up nutrient from host for self
preservation
• Invade and attack other parasitic micro-organisms that compete for similar nutrients
• Fungus uses metabolite production for domination
More aggressive under plant stress
• “Life is good” for mold growth = fewer metabolites
• “Life is challenging” for fungal growth = more metabolites
Why Mycotoxin Can Be Present in Absence of Visible Mold
Mycotoxins and Dairy Health/Productivity
• Associated symptoms– Depressed feed intakes
– Unthriftiness
– Rough hair coat
– Poor body condition
– Suppressed immunity
– Reproductive issues
– Fresh cow metabolic disorders
• Problem: – Limited research exists to identify mode of action (in vitro vs. in vivo)
– Lack of mycotoxin research studies on high production dairy cattle
– Monogastric studies referenced to explain mode of action on ruminants
Ruminal Digestionby Microbes
Intestinal Digestionby Animal Enzymes
Starch
Kp
KdId
rumen by-pass (is usually degraded)
rumen by-pass fiber can be lost (up to 70%)
Starch
Fiber
Kp = rate of passageKd = rate of digestion
Hindgut Digestionby Microbes
Starch
FiberHigh Production Dairy Cows Likely are Less Likely to Degrade Mycotoxins Compared to Beef Cows
Mycotoxins Undergo Ruminal Bioconversion
High Quality Forage For Mycotoxin Rumen DegradationpH and Rumen Flora
Source: Kaufman et al (1980)
High concentrate feeding will lower rumen pH, create acidosis,and lessen the likelihood of mycotoxin degradation
Rumen Fermentation Dynamics and Presence of Deoxynivalenol DON• 2009 Japanese study indicates bioconversion of
DON more effective in high forage compared to high concentration ration
• In vitro study using corn starch and cellulose carbon sources– 40 mg/kg DON
– Results• Cellulose source resulted in 14% more DON degradation
at P<0,01
• Starch resulted in Ammonia-N, Acetate, and Propionate reduction at P<0.01
235
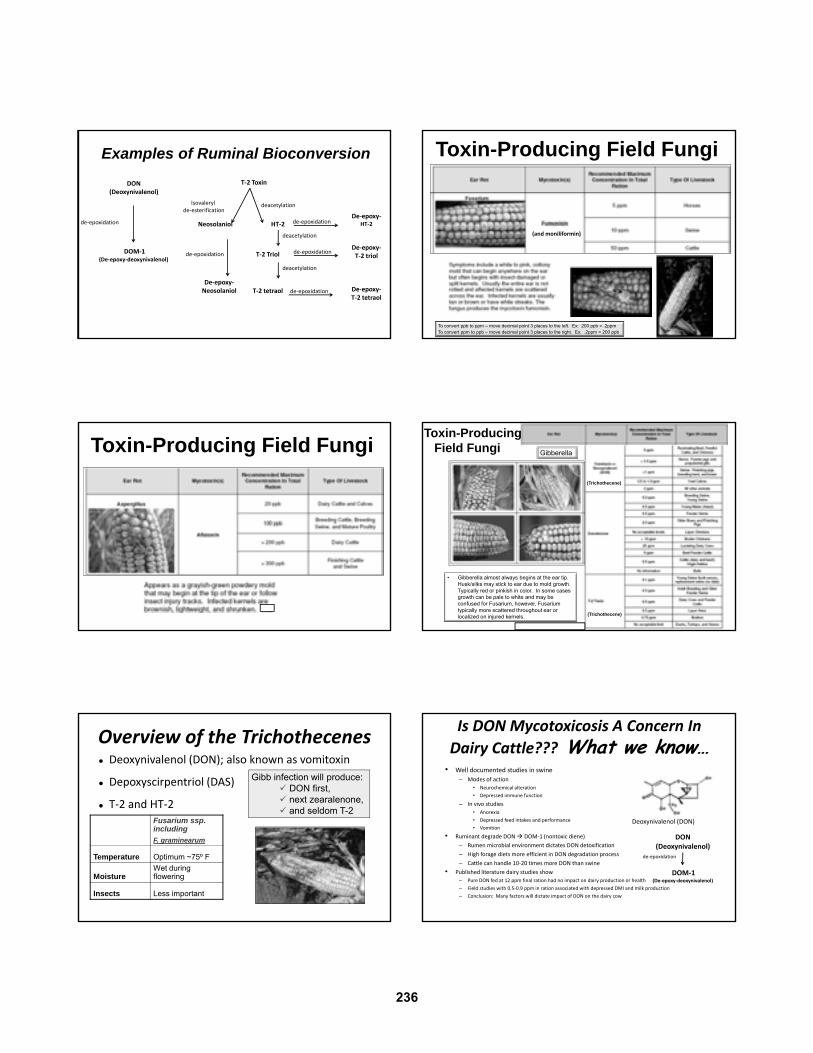
Examples of Ruminal Bioconversion
de‐epoxidation
DON(Deoxynivalenol)
DOM‐1(De‐epoxy‐deoxynivalenol)
T‐2 Toxin
Isovalerylde‐esterification
deacetylation
Neosolaniol
De‐epoxy‐Neosolaniol
de‐epoxidation
HT‐2De‐epoxy‐
HT‐2de‐epoxidation
de‐epoxidation
de‐epoxidation
T‐2 TriolDe‐epoxy‐T‐2 triol
deacetylation
T‐2 tetraol
deacetylation
De‐epoxy‐T‐2 tetraol
Toxin-Producing Field Fungi
To convert ppb to ppm – move decimal point 3 places to the left. Ex: 200 ppb = .2ppmTo convert ppm to ppb – move decimal point 3 places to the right. Ex: .2ppm = 200 ppb
(and moniliformin)
Toxin-Producing Field Fungi
(Trichothecene)
(Trichothecene)
• Gibberella almost always begins at the ear tip. Husk/silks may stick to ear due to mold growth. Typically red or pinkish in color. In some cases growth can be pale to white and may be confused for Fusarium, however, Fusarium typically more scattered throughout ear or localized on injured kernels.
Gibberella
Toxin-Producing Field Fungi
Overview of the Trichothecenes Deoxynivalenol (DON); also known as vomitoxin
Depoxyscirpentriol (DAS)
T‐2 and HT‐2
Gibb infection will produce: DON first, next zearalenone, and seldom T-2
Fusarium ssp. including
F. graminearum
Temperature Optimum ~75º F
MoistureWet during flowering
Insects Less important
Is DON Mycotoxicosis A Concern In
Dairy Cattle??? What we know…• Well documented studies in swine
– Modes of action
• Neurochemical alteration
• Depressed immune function
– In vivo studies
• Anorexia
• Depressed feed intakes and performance
• Vomition
• Ruminant degrade DON DOM‐1 (nontoxic diene)
– Rumen microbial environment dictates DON detoxification
– High forage diets more efficient in DON degradation process
– Cattle can handle 10‐20 times more DON than swine
• Published literature dairy studies show
– Pure DON fed at 12 ppm final ration had no impact on dairy production or health
– Field studies with 0.5‐0.9 ppm in ration associated with depressed DMI and milk production
– Conclusion: Many factors will dictate impact of DON on the dairy cow
Deoxynivalenol (DON)
de‐epoxidation
DON(Deoxynivalenol)
DOM‐1(De‐epoxy‐deoxynivalenol)
236
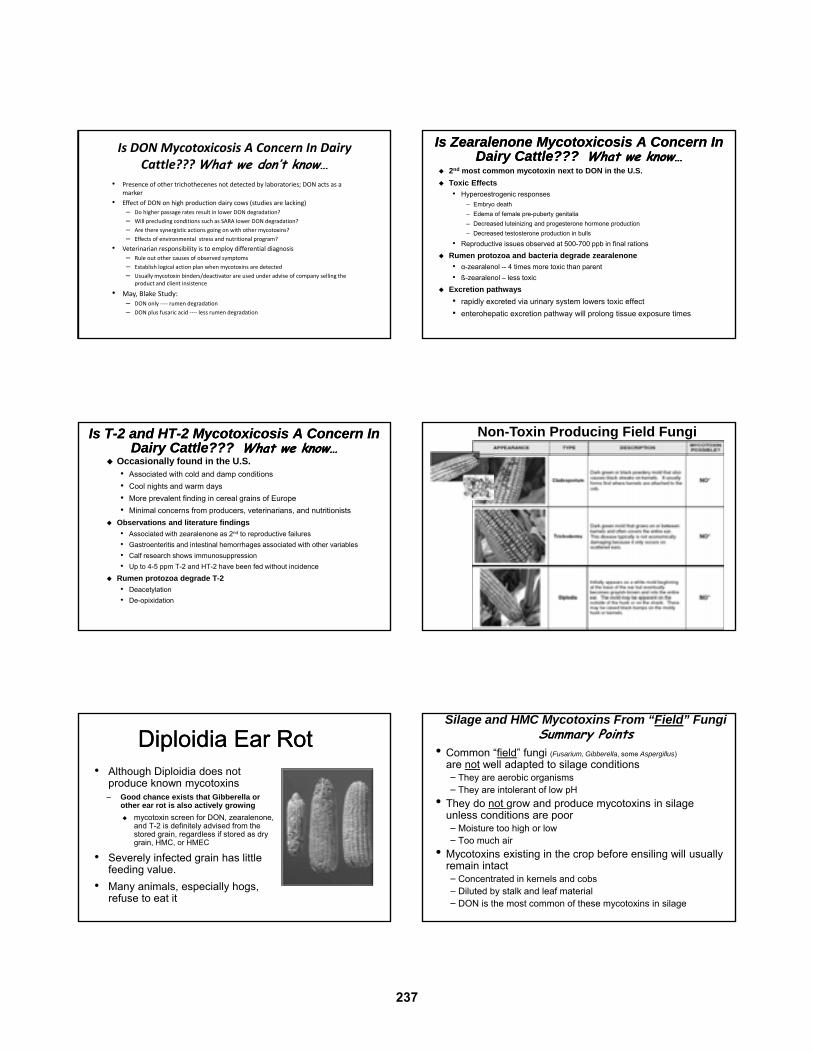
• Presence of other trichothecenes not detected by laboratories; DON acts as a marker
• Effect of DON on high production dairy cows (studies are lacking)
– Do higher passage rates result in lower DON degradation?
– Will precluding conditions such as SARA lower DON degradation?
– Are there synergistic actions going on with other mycotoxins?
– Effects of environmental stress and nutritional program?
• Veterinarian responsibility is to employ differential diagnosis
– Rule out other causes of observed symptoms
– Establish logical action plan when mycotoxins are detected
– Usually mycotoxin binders/deactivator are used under advise of company selling the product and client insistence
• May, Blake Study: – DON only ‐‐‐‐ rumen degradation
– DON plus fusaric acid ‐‐‐‐ less rumen degradation
Is DON Mycotoxicosis A Concern In Dairy Cattle??? What we don’t know…
Is Zearalenone Mycotoxicosis A Concern In Dairy Cattle??? What we know…
Is Zearalenone Mycotoxicosis A Concern In Dairy Cattle??? What we know…
2nd most common mycotoxin next to DON in the U.S.
Toxic Effects
• Hyperoestrogenic responses
– Embryo death
– Edema of female pre-puberty genitalia
– Decreased luteinizing and progesterone hormone production
– Decreased testosterone production in bulls
• Reproductive issues observed at 500-700 ppb in final rations
Rumen protozoa and bacteria degrade zearalenone
• α-zearalenol -- 4 times more toxic than parent
• ß-zearalenol – less toxic
Excretion pathways
• rapidly excreted via urinary system lowers toxic effect
• enterohepatic excretion pathway will prolong tissue exposure times
Is T-2 and HT-2 Mycotoxicosis A Concern In Dairy Cattle??? What we know…
Is T-2 and HT-2 Mycotoxicosis A Concern In Dairy Cattle??? What we know…
Occasionally found in the U.S.• Associated with cold and damp conditions
• Cool nights and warm days
• More prevalent finding in cereal grains of Europe
• Minimal concerns from producers, veterinarians, and nutritionists
Observations and literature findings
• Associated with zearalenone as 2nd to reproductive failures
• Gastroenteritis and intestinal hemorrhages associated with other variables
• Calf research shows immunosuppression
• Up to 4-5 ppm T-2 and HT-2 have been fed without incidence
Rumen protozoa degrade T-2
• Deacetylation
• De-opixidation
Non-Toxin Producing Field Fungi
Diploidia Ear RotDiploidia Ear Rot• Although Diploidia does not
produce known mycotoxins– Good chance exists that Gibberella or
other ear rot is also actively growing
mycotoxin screen for DON, zearalenone, and T-2 is definitely advised from the stored grain, regardless if stored as dry grain, HMC, or HMEC
• Severely infected grain has little feeding value.
• Many animals, especially hogs, refuse to eat it
Silage and HMC Mycotoxins From “Field” Fungi Summary Points
• Common “field” fungi (Fusarium, Gibberella, some Aspergillus)
are not well adapted to silage conditions− They are aerobic organisms− They are intolerant of low pH
• They do not grow and produce mycotoxins in silage unless conditions are poor−Moisture too high or low− Too much air
• Mycotoxins existing in the crop before ensiling will usually remain intact−Concentrated in kernels and cobs−Diluted by stalk and leaf material−DON is the most common of these mycotoxins in silage
237

Practical approaches to minimizing field‐produced molds and toxins
1. Reduce fungi populations and access sites by planting hybrids with insect, stalk rot and ear mold resistance,
2. Harvest in a timely manner with particular attention to proper moisture levels,
3. Isolate silages from crops exposed to severe drought or hail damage,
4. Consider traditional tillage methods to reduce fungal spore loads in crop residues
Note: No silage acid or inoculant product is capable of degrading preformed, field-produced toxins
Source: Hoard’s Dairyman August 10, 2002
Percent of Corn Acres Under No-Till U.S., 1989-2004
Logic Would Indicate Increase in Conservation Tillage Means More Residue, Which Serves as the Source of Disease!
Are Prevalence of Mycotoxin Levels Increasing with
Modern Crop Production?
References:2004 and 2008 data: North Dakota State University Veterinary
Diagnostic Laboratory (sample submissions)1990-1999 data: Casper H.H., Tacke, B.K., Iverson D.M.. 2000.
Experiences in Mycotoxin Testing. Proc 21st Western Nutrition Conference, Winnipeg, Manitoba. P 75-80.
Comparison of DON Levels Over Time• 2004 was a stress year in that many samples were hail damaged
• 2008 was considered a normal year, both 2004 and 2008 had similar weather growing patterns
0.00
5.00
10.00
15.00
20.00
25.00
30.00
35.00
40.00
45.00
0.5 – 0.9 1.0 – 1.9 2.0 – 2.9 3.0 – 3.9 4.0 – 4.9 5.0 – 9.9 >10.0
Percent of Samples
PPM Ranges
DON2004
DON2008
DON1990‐1999
Comparison of Zearalenone Levels Over Time• 2004 was a stress year in that many samples were hail damaged
• 2008 was considered a normal year, both 2004 and 2008 had similar weather growing patterns
0.00
10.00
20.00
30.00
40.00
50.00
60.00
70.00
0.5 – 0.9 1.0 – 1.9 2.0 – 2.9 3.0 – 3.9 4.0 – 4.9 5.0 – 9.9 >10.0
Percent of Samples
PPM Ranges
ZEN2004
ZEN2008
ZEN1990‐1999
238

Are Prevalence of Mycotoxin Levels Increasing with Modern
Crop Production?………………………..
Results Show: 1. No Difference For Past Two Decades
2. It Appears Transitioning From Moldboard to Minimal Tillage Practices Has Not Impacted Mycotoxin Incidence
References:2004 and 2008 data: North Dakota State University Veterinary
Diagnostic Laboratory (sample submissions)1990-1999 data: Casper H.H., Tacke, B.K., Iverson D.M.. 2000.
Experiences in Mycotoxin Testing. Proc 21st Western Nutrition Conference, Winnipeg, Manitoba. P 75-80.
Environmental Growing Conditions Drives Likelihood of Mycotoxin Prevalence
Environmental Growing Conditions Drives Likelihood of Mycotoxin Prevalence
2010 Map2009 Map
Produced when heat moisture, and oxygen are present stable silages are less prone to become moldy.
• Mold growth is facilitated by an elevated pH due to aerobic lactic acid consuming yeast that become active when oxygen penetrates into the silo.
– Candida and Hansula yeast are lactate consumers that usually precede mold activity
Storage Fungi Environmental Differences Between Field and Silage Produced Molds
Environmental Differences Between Field and Silage Produced Molds
Oxygen rich
Neutral pH
High humidity Micro-aerophilic
Acidic pH
High humidity
Mucor (white/gray fluffy) 45%
Penicillium (green/blue) 45%
Aspergillus (yellow/green) 7%
Monilia (white/yellow) 3% (not pictured)
Source: Bill Seglar, Pioneer Technical Service Sample Summary
MucorMucor AspergillusAspergillusPenicilliumPenicillium
Common Molds Found in US Silages and HM Grains
Incidence of Molds in Silage from International Studies
Penicillium roqueforti - most prevalent
Aspergillus fumigatus - 2nd most prevalent
Monascus ruber - 3rd most prevalentSource: J. Fink-Gremmels, Netherlands The Mycotoxin Blue Book Mycotoxins in Forages Ch 11, p 258-259
239
Penicillium Are Adapted to Low pH Environments(isolated from corn silage by Dr. Al Gotlieb, University of Vermont)• All Penicillium alter silage quality
‐ Reduced palatability‐ Depressed feed intakes‐Result in production loss and health problems
• Metabolic end‐products produced and classified as mycotoxins
• Primary onesPR toxinmycophenolic acidroquefortinepatulinpenicillic acid
• Many others…….
Source: J. Fink-Gremmels, Netherlands The Mycotoxin Blue Book Mycotoxins in Forages Ch 11, p 258-259
Characteristics of PenicilliumCharacteristics of Penicillium References on the Impact of Penicillium roqueforti Mycotoxins on Cattle
References on the Impact of Penicillium roqueforti Mycotoxins on Cattle
Modified ruminal fermentation• Antimicrobial effect on rumen microbes• Research
– P. roqueforti: Source: Holterschinken et al 2005. Europe – Patulin: Source: Tapia, et al. 2005. UMN
Altered central nervous system• Neurotoxins (at high doses)
– Patulin– Roquefortine C
• Source: Kellerman et al 1984
Localized inflammatory responses • Rumenitis in cattle
– Penicillic acid– Mycophenolic acid
• Source: Kopp-Holtwiesche and Rehm. 1990. Italy
Characteristics of Aspergillus fumigatusCharacteristics of Aspergillus fumigatus
Common soil contaminant Altered silage quality
• Reduced palatability• Depressed feed intakes• Result in production loss and health
problems
Mycotic infections• Sporadic abortions (Sarfati et al.1996)
• From consumption, orifice entry, and mold dust inhalation
Metabolic end-products produced and classified as mycotoxins • Primary ones
– verrucolegen– fumitremorgens– Penitrem A– gliotoxin
Source: J. Fink-Gremmels, Netherlands The Mycotoxin Blue Book Mycotoxins in Forages Ch 11, p 258-259
References on the Impact of Aspergillus fumigatus Mycotoxins on Cattle
References on the Impact of Aspergillus fumigatus Mycotoxins on Cattle
Hemorrhagic jejunal syndrome• Immune Suppression• Gliotoxin + effects of T-2• Source: Forsburg et al. Oregon
Therapy resistant mastitis• Fungus crosses intestinal barrier
– produces glioitoxin in various tissues• Source: Bauer et al. 1989
Powerful immunosuppressive agent – Mycotoxins
gliotoxin verrucolegen fumitremorgens fumagillin helvolic acid
• Source: Watanabe et al. 2003
Some Molds Can Produce Brilliant ColorsMonascus ruber Monascus ruber
Common soil contaminant More common in grass silages
• Presence reduces prevalence of P. rouquefortii
Altered silage quality• Reduced palatability• Depressed feed intakes• Result in production loss and health problems
Mycotic infections• From consumption, orifice entry, and mold dust
inhalation
Metabolic end-products produced and classified as mycotoxins • Citrinin
– Hepatotoxic– Nephrotoxic – Antimicrobial effect…therefore likely impacts
rumen function
Source: J. Fink-Gremmels, Netherlands The Mycotoxin Blue Book Mycotoxins in Forages Ch 11, p 258-259
Mycotoxin Diagnostic ConsiderationsMycotoxin Diagnostic Considerations Sampling protocol makes huge differences in results
Description of values
• Parts per million = ppm (mg/kg)
• Parts per billion = ppb (µg/kg)
Reported values
• As fed basis
• Dry matter basis
Wide variety of tests available with different sensitivities.
Make sure you are comparing apples to apples (different labs, different tests used).
Know the laboratory: testing provided by Universities, Government Agencies, Private Laboratories.
240

Mycotoxin Analysis ELISA (enzyme-linked-immunosorbent assay)
─ fast, in house test─ inexpensive─ general screen designed for grains only─ false positives in forages
− Forage debris causes problems− Most ELISA kits don’t have clean up procedure
Chromatography─ slower lab test─ more expensive ─ types
HPLC (high pressure liquid chromatography) GC (gas chromatography) TLC (thin layer chromatography)
As an industry, we may be severely underestimating the
contribution of toxins to production problems because
they can often exist in conjugated forms (primarily with sugars) which escape laboratory
detection (Whitlow, 2007). These undetected toxins can
then exert their toxic and immunosuppressive effects when disassociated in the
digestive tract (Kendra, 2005).
Example of HPLC Lab Report That Screens for Parent and Derivative Toxins
Example of HPLC Lab Report That Screens for Parent and Derivative Toxins
Introduction of Conjugated MycotoxinsIntroduction of Conjugated Mycotoxins “Masked” forms incorporated into or
attached to macromolecules of• Living plants
• Fungi
• Mammals
Bound form of toxin is expressed after animal consumes feedstuff
Not detected by current mycotoxin tests
Current area of mycotoxin detection research
Mycotoxins Not Routinely Diagnosed
• PR from Penicillium rouquefortii• Citrinin from Penicillium, Aspergillums, Monascus• Patulin from Penicillium• Myenophenolic Acid from Penicillium• Ochratoxin from Penicillium and Aspergillus
Laboratory decision to test is based upon research that associates animal health with metabolites.
Idea for potential presence of silage mold mycotoxins: Use a mycology laboratory to have silage fungi isolated and
identified. If the isolated fungi are from toxigenic species, then toxins become a plausible, whether or not random feed sampling
detected the actual presence of a mycotoxin
Use Discretion With Choice of Laboratory for Yeast and Molds
• Quick tests only approximatecfu counts
– Speed should not be priority over quality
– Designed for users not experienced with advanced mycological techniques
• Isolation techniques should include speciation of different yeasts and molds in addition to cfu counts
• Must grow cultures at 25o
and 37o C.– E.G.: A. fumigatus won’t grow at 25o C
– Accurate population counts occur at 37o C
Penicillium roquefortii
Monascus ruberAspergillus flavus
Watch for mycotoxins in straw, not just silage!(especially if feeding straw to transition cows)
Source: Kurt Cotanch. Miner Farm Report March, 2010
241

Remediation Steps• Dilution is the best solution
– Avoid feeding to young stock and transition cows
• Feed additives:– Binders (clay, yeast cell walls)
• Primarily effective on toxins with suitably located polar groups
– aflatoxin and to a lesser degree fumonisins
– Deactivators• Enzymatically alter molecular structure
– More effective on trichothecenes (DON, T‐2) and zearalenones which lack suitably located polar groups
Source: Mike Watkins. Biomin GmbH. Manage mycotoxins in rations. Feedstuffs. 11/9/09
Some nutritionists use a mycology laboratory to have silage fungi
isolated and identified. If the isolated fungi are from toxigenic species, then toxins become a plausible, whether or not random feed sampling detected the actual presence of a mycotoxin
Classes of Mycotoxin Remediation in Livestock
Classes of Mycotoxin Remediation in Livestock
Dilution is the solution!!!
High forage rations
Balanced diets for carbohydrates, protein, and mineral/vitamin needs
Antioxidant products• Immune stimulation
• Reactive Oxygen Species (ROS)
• E.g.: Vitamin E, Selenium products
Adsorbents and deactivators• Adsorbent: Binds mycotoxin
• Deactivator: enzymatically alters mycotoxin
Nutrients That Enhance the Immune System That Will Lessen Stress and Lessen Mycotoxin Risk
Nutrients That Enhance the Immune System That Will Lessen Stress and Lessen Mycotoxin Risk
Carotenoids
Vitamin E / Selenium
Omega-3 and -6 fatty acids
Chromium
Copper
Zinc
Cell wall fractions
Direct Fed Microbials
Mycotoxin AdsorbentsMycotoxin Adsorbents Most common class: aluminosilicates of clay
origin• Bentonite
• Montmorellonite,
• Zeolites
• Hydrated sodium calcium aluminosilicates (HSCAS)
Efficacy of product must be known• Needs a suitable polar group location
• Must have a level of solubility
• Size and shape must be in relation to that of the mycotoxin
Why most adsorbents won’t bind trichothecenes, but will bind aflatoxin• Aflatoxin = 0.2-0.8 nm
• Trichothecenes = 1.5 – 4.0 nm
Mycotoxin DeactivatorsMycotoxin Deactivators Enzymatically alter the
molecular structure of trichothecene and zearalenone mycotoxins
Breaks apart the molecular ring structure that makes mycotoxins toxic
Current class of feed additives that show promise for mycotoxin remediation
Deoxynivalenol (DON)
Zearalenone
Concluding Remarks Regarding Mycotoxicosis in Dairy Cattle
Concluding Remarks Regarding Mycotoxicosis in Dairy Cattle
Complex set of variable will determine severity of mycotoxins in dairy cattle
Veterinarians should objectively complete differential diagnosis of herd problem
Detected mycotoxin on lab report is not a diagnosis
Awareness must be given to mycotoxin methodology (e.g.: ELISA to chromatography)
Dairy producers need to practice best management skills with feeding, herd health, and cow comfort
Dairy management skill set implementation should precede investment of antioxidants, deactivators and adsorbants
242

Interest exploded with Oct 1999 article in Dairy Herd Managementand the increased availability of VFA analysis from commercial
laboratories
One hybrid (34A89)from Several Small Fields (60 acres)
Harvested within 2-Days(No inoculant used)
8ft(2.4 m)
32ft (9.7 m)
Source: Dann Bolinger, Pioneer Dairy Specialist, Michigan
One hybrid, Similar Growing Environments Equals Improved Consistency but it Still Needs Managing
Lack of inoculation resultedin a very poor lactic:acetic ratio
(either limited lactic production or excess acetic from yeast growth)
Source: Dann Bolinger, Pioneer Dairy Specialist, Michigan
What About Numerous Hybrids from Many Fields (~1,000 acres)(inoculated with a non-Pioneer homo-fermentative inoculant) 26ft
(8m)
90ft (27.5m)
Source: Dann Bolinger, Pioneer Dairy Specialist, Michigan
1B was in a wet zone
Z is what mostnutritionists
would analyze
4C was from a fill line
Lots of variation just like in the Cornell (Bill Stone) study
Source: Dann Bolinger, Pioneer Dairy Specialist, Michigan
Blend your Feed…. before you Mix It
Source: Dann Bolinger, Pioneer Dairy Specialist, Michigan
243

Where VFA analysis has merit C. butyricum
C. paraputrificum
C. tyrobutyricum
C. bifermentens C. sporogenes
C. perfringens C. sphenoides
Lactate Fermenters Amino Acid Fermenters Others
Source: McDonald’s Biochemistry Of Silage, 1991
Environmental Conditions That Contribute To Clostridial Activity
Source: Jonsson, 1991
• Low dry matter silages
• Low water soluble carbohydrate content
• High silage temperatures
• High buffering capacity of the crop
• Elevated ash content (>5% in CS, >8-10% in alfalfa/grass silage)
Source: Dan Undersander, UW Extension
Ash Content of Forage Samples
UW Marshfield Lab
Type Statistic % Ash
Haylage Avg 12.3
Max 18.0
Min 5.7
Hay Average 10.3
Max 17.6
Min 8.8
Plant content of ash is 6% for grass and 8% for alfalfa…the rest of ash is from soilcontamination contamination
Measurable Indicators of Clostridial Fermentation
– high moisture content (>65%)
– elevated pH (>4.5)
– elevated butyric acid (>0.1%)
– elevated ammonia nitrogen (>5-10%)
Working with Clostridial silages Keep them away from transition
(and high production) cows
“Aerating” these feeds can volatize some noxious components heating is not an issue
Source: B. Stone, Cornell Nutrition Conference, 2004
Likely reduction in DMI
No water soluble carbohydrates
Loss of amino acids
Increase in blood ketones
244

“Venting Off” Undesirable Silage VFA’sby “mismanaging” the silage face
• Case Study Example: – 16 lbs of clostridial haylage DM/cow/day in TMR
• 3.2% butyric acid on haylage taken from face of the bunker = 323 g/c/d intake
• After loosening face and left in pile for 24 hours haylage now 2.1% butyric acid = 152 g/c/c intake
• After mixing in TMR for one hour haylage now 1.8% butyric = 130g/c/d intake
– Watch this method if relying heavily on haylage for peNDF
– Only way to get to 50 gm/c/d intakes or less is to reduce inclusion rate of haylage in TMR
Source: Ruppel, Kurt. 2004. Move forage storage to a higher level. Northeast Dairy Business Pro-Dairy. ¼. Pg 30-32.
(e.g. knocking down and aerate – remember, butyric silages will not heat)
% Butyric Acid in
silage (DM basis)
mg/lb 50g/c/d 150g/c/d 250g/c/d
0.25 1.1 44.1 132.2 220.3
0.50 2.3 22.0 66.1 110.1
0.75 3.4 14.7 44.1 73.4
1.00 4.5 11.0 33.0 55.1
1.25 5.7 8.8 26.4 44.1
1.50 6.8 7.3 22.0 36.7
1.75 7.9 6.3 18.9 31.5
2.00 9.1 5.5 16.5 27.5
2.25 10.2 4.9 14.7 24.5
2.50 11.4 4.4 13.2 22.0
2.75 12.5 4.0 12.0 20.0
3.00 13.6 3.7 11.0 18.4
3.25 14.8 3.4 10.2 16.9
3.50 15.9 3.1 9.4 15.7
3.75 17.0 2.9 8.8 14.7
4.00 18.2 2.8 8.3 13.8
4.50 20.4 2.4 7.3 12.2
5.00 22.7 2.2 6.6 11.0
5.50 25.0 2.0 6.0 10.0
6.00 27.2 1.8 5.5 9.2
6.50 29.5 1.7 5.1 8.5
7.00 31.8 1.6 4.7 7.9
8.00 36.3 1.4 4.1 6.9
9.00 40.9 1.2 3.7 6.1
Butyric acid concentrationsand pounds of silage DM intake to reach butyric acid doses of:• 50g – reduced DM intake and
risk of ketosis to early lactation cows
• 150g – high risk of ketosis inearly lactation cows
• 250g – high risk of ketosis inall lactating cows
Source: Dairyland Laboratories, Inc. 12/2000 andGary Oetzel, DVM – University of Wisconsin
Butyric Acid Dose Calculator
Table values indicates how many lbs of silage DM you can feed to stay below these threshold levels
• Dairy cattle can produce as many as 160 moles of fermentation acids per day. Source: Dr. Jim Russell, page 9 of his 2002 text ”Rumen Microbiology and Its Role in Ruminant Nutrition”
• If a cow is eating 20 lbs of CS dry matter per day….how many moles of fermentation acids is that contributing? Assumptions: example based on typical VFA profiles for CS ensiled at about 35% DM. There are a number of other VFA’s that are ignored since they contribute so little compared to the major VFA’s.
• Typical CS VFA profile: – Lactate (molar mass=90.1): assume 7% lactate on a DM basis = 70 (g/kg)/(2.2 lb/kg) = 31.8 g/lb
– Acetate (molar mass= 60): assume 3% acetate on a DM basis = 30 (g/kg)/(2.2 lb/kg) = 13.6 g/lb
– Propionic (molar mass=74.1): assume 1% propionic acid on a DM basis = 10 (g/kg)/(2.2 lb/kg) = 4.5 g/lb
• Amount of acid and divide by the molar mass to get the number of moles of acid present:
– Lactate (MM 90.1) 31.8 (g/lb)/90.1 g/mole = 0.35 moles lactate
– Acetate (MM 60) 13.6 (g/lb)/60 = 0.23 moles acetate
– Propionic (MM 74.1) 4.5 (g/lb)/74.1 = 0.06 moles prop
• Multiply the number of moles by 20 lb DM to get the total consumption of VFA/day
– Lactate (MM 90.1) 31.8 (g/lb)/90.1 g/mole = 0.35 moles lactate * 20 = 7 moles lactate/day
– Acetate (MM 60) 13.6 (g/lb)/60 = 0.23 moles acetate * 20 = 4.6 moles/day
– Propionic (MM 74.1) 4.5 (g/lb)/74.1 = 0.06 moles prop * 20 = 1.2 moles/day
• Total all these up and the total consumption of VFA from silage is 12.8 moles VFA/day or about 8% of the total VFA in the rumen come from the corn silage in this example.
Do Silage Acids Cause Acidosis?
Source: Bill Rutherford, Ph.D. Pioneer Senior Research Scientist
Pioneer has had a long-established research focus on silage bio-security and improvement of feeding quality….
Silage Management is Still a Top Priority!
Heating: Look for a heat layer 1–2 meters behind the face (it quickly dissipates from the face surface)
Insufficient Compactation,High Porosity
Superior Compactation,Low Porosity
Pioneer was the very first company toIntroduce bunker density probes to N. America
KontrolleControl
Thermal Imaging Helps Demonstratethe Cost of Silage Face Heating
Caused by Yeast, Bacillus and MoldsPioneer was the very first company to
Introduce bunker thermal imaging to N. America
245

Real World Data....Corn Silage harvested Fall 2006 on a 20,000 cow dairy, located in Central Minnesota
competitor
0 C
1st peak typically yeast and aerobic bacterial induced 2nd peak typically mold
and fungal induced
Base = 72F, 22C9F
Honig Aerobic Stability Method
23 F
Not all silage bacteria are the same….despite product labels showing the same genus and species
Source: Pioneer Microbial Research
pH activity in alfalfa and whole plant corn broths at 28oC. These are strains that lower pH better than target levels in both alfalfa and corn
silage
This strain works well in alfalfa but not in
corn silage
Worse than target pH in alfalfa
This strain works well in corn silage but not in alfalfa
Homofermentative rods
Heterofermentative rods
Heterofermentative cocci
Homofermentative cocci
Non-gas producers
Gas producers
Heterofermentative gas producers that do not do well at rapidly lowering pH like
homofermenters although L. buchneri can be used in combination with homofermentative strains to achieve both low pH and improve
bunklife.
Wo
rse
than
targ
et p
H in
cor
n si
lage
Population of enterococci that
work well to initiate fermentation but can
not induce low terminal pH’s.
Plot of >7000 Pioneer LAB strains used for visualize strain differences, relationships, and patterns to help determine future prototype product candidates
Pioneer is the only seed company with a dedicated livestock forage research center
- and we openly share our understanding of fiber digestion methodologies -
Animal trials measuring digestibility or production remain the “gold standard” Among the possible assay methods, in situ methods appear
to be the most “animal relevant” procedure to predict differences in NDF digestibility observed with animals.
60,000 in situ bags hung annually
(16 reps of each sample)
Dr. Fred Owens, Pioneer Research ScientistLesa Nuzback – Pioneer Senior Research AssociatePresenting poster on in situ methodology at International Silage Conference, Madison, WI, July 2009
Pioneer ® Brand Fiber Technology Products
Grass and cereal silage specific
Corn silage specific
Since 2007
Corn silage specific
Introduced Spring 2011
1. Reduces “front-end” fermentation losses from the homfermentative strains
2. Reduces heating at feed-out from the L. buchneri strain
3. Increased fiber digestibility (NDFD) by an average of 4 % units From the Pioneer L. buchneri strain in
FT inoculants, not all L. buchneri strains have this enzyme-producing capability
FT “Triple” Activity 1. Reduces “front-end” fermentation losses
from the homfermentative strains
2. Reduces heating at feed-out from the L. buchneri strain
3. Increased fiber digestibility (NDFD) by an average of 4% units From the Pioneer L. buchneri strain in FT
inoculants, not all L. buchneri strains have this enzyme-producing capability
FT “Triple” Activity
For the Cow - Increase rate of fiber digestibility
For the Dairyman - Ability to feed more forage and reduce concentrates
246

Lignin “binds up” cell wall constituents thus limiting the rate at which bacteria can
access and digest the cell walls
CFT breaks this ester bond with an enzyme produced in the bunker by our L. buchneri strain, allowing rumen bacteria to digest the cell wall much faster because it is separated from the lignin.
Before FT
After FT
Another way to visualize FT
45
50
55
60
65
70
75
80
Trial 1 Trial 2 Trial 3 Trial 4 Trial 5 Trial 6
% N
DF
Dig
esti
bilit
y
11CFT Lamb NDF Digestion Studies (Pioneer Livestock Nutrition Center)
Control
CFT
Hyb
rid A
with
C
FT
in y
ear
1
Hyb
rid A
with
out
CF
T in
yea
r 2
Will CFT work the same every year?
1. Improved dry matter intake 2. Improved NDF digestibility 3. Improved gain/tonne of silage fed 4. Improved feed efficiency 5. Reduced heating at feeding 6. Reduced dry matter loss at feeding
Pioneer has received official Canadian government approval to make the following claims for 11CFT:
Registration received on January 5, 2007
11GFT (Grass Fiber Technology) launched in Canada & US in 2010Launched in Europe in 2009
247

1. Assume slightly higher intakes (hence more starch intake)
Not as high as experienced with BMR corn silage
2. Be sure ration has adequate effective fiber (peNDF, scratch)
3. Increase the energy density of CFT-silage by assuming a 4-percentage point increase in NDFD
These are still valid, but #3 did not provide adequate direction for consulting nutritionists
If nutritionists use Net Energy (NE-L), changing NDFD 4-points results in very minor changes in NE-L estimates that will NOT be sensitive
enough to the digestion rate changes caused by CFT.
4 points of NDFD only increased NE-L .01 Mcals
FastKd’s
SlowKd’s
CNCPS V6.1
CPM
NDFD can be used to adjust NDF (B3) digestion rates (Kd’s) with this Cornell spreadsheet
Dr. Mike VanAmburgh’s NDFD Kd calculator available from Cornell University or Pioneer
In this corn silage example, a 4-point increase in NDFD translates to a 15% higher Kd
Using FermentricsTM and CNCPS to Quantify Value of Fiber Technology Products
248

Dairyland Laboratories introduced Jay Johnston’s gas method (Fermentricstm) to a wider audience at 2010 World Dairy Expo
Fermentricstm allows for estimating pool sizes and rates of digestion in TMR’s or individual feedstuffs
http://www.ritchiefeed.com/Lab_%20Research/Lab_Research.htmlJay Johnston, CEO RFS
Batch culture system400 mg samples
Rumen fluid from lactating cows
http://www.dairylandlabs.com/• Producers or consultants can
submit samples to Dairyland Laboratories (analyzed, dried, ground
(6mm), over-nighted to Canada for incubation)
• Requires 2 qt representative sample of TMR or feedstuff
• Conservative 7-day turnaround (more likely 4-5 days)
Farm Name:Farm Name:
Total gas produced(black curve)
Gas produced from fast pool (orange curve). Do not like to see this much higher than 40 ml of gas indicating too much acetate (which produces gas) and not as much propionate (no gas,
more ATP) coming from the fast pool nutrients
Gas produced from slow pool (green curve)
A Partitioning Factor: larger number (>4) means more efficient fermentation with less gas
(acetate) and propionate driving more energy (ATP) and microbial biomass yield.
PF is calculated as:(VFA + microbial protein)/gas production
More gas = less efficient with less ATP
Estimated Kd’s for B1, B2 and B3 pools. Fast pool rates should be greater than B1 rates as the fast pool also contains soluble fibers, pectins etc.
Prefer the B1 rate ~18-20%/hr and B3 rate ~ 5-6%/hr
Amount of gas from the fast pool vs. slow pool. Over 40ml gas from fast pool indicates
considerable acetate production and less propionate production as propionate produces
minimal gas.
More than a 10-hour difference in “Time to Max” between fast vs. slow pools can lead to asynchrony of
digestion causing production problems.
SP (microbial) value per Broderick incubation approach The value is considered low in this example. Goal is high
30’s. It is commonly believed that current methods (Buffer-Borate System) tend to overestimate SP levels. If
low and you supplement more SP, it should reduce energy-spilling by rumen bacteria allowing them to
increase their populations to improve MBP
Four Quadrants for “Benchmarking” TMR’s Control
CFT
CFT sample demonstrates:– Faster rate of the (pink) B3 (slow pool)
5.4 vs. 4.21%/hr– Faster rate of (blue) B1 (fast pool)
13.9 vs. 9.06%/hr
1st Page from both sample reports
249

Fiber Technology-Silage Feeding GuidelinesFeeding FT-silage typically allows for reduction in both “fast pool” nutrients (e.g. starch) and protein (from increased microbial protein production). In practice, this means reducing grain and protein in the TMR to offset increased availability of fiber components and the shifting of “slow pool” nutrients (B3) to the “fast pools” (B1 and B2). Using CFT-corn silage as an example, in typical dairy rations containing 50 lbs of corn silage/cow/day (as fed), field experience has shown that about 2 lbs of corn meal and 0.75 lbs of 44% crude protein soybean meal can be removed from the diet without any change in cow production or body condition (corn silage intake was increased to offset the removal of grain and protein). This provides the economic advantage to FT-silages to compliment value associated with faster silage fermentation, reduced silage face heating/spoilage and improved ration bunklife.
Intakes may also be elevated in FT-silages, further increasing total daily starch loads. This is magnified if corn or cereal silage inclusion rates are significantly increased when feeding FT-silage. Adjustments will also be necessary for increased starch digestibility over time in storage for corn or cereal silage (and high-moisture corn).
Field experience with herds who experienced milkfat depression problems when starting to feed FT-silage, were typically borderline for effective fiber and/or acidosis issues and quickly resolved the problem (and lowered feed costs) by reducing grain (especially high-moisture corn), increasing silage inclusion rates (and effective fiber) and/or adding co-products such as soyhulls (additional source of soluble fiber).
Gas-production laboratory comparisons and field experience suggest that carbohydrate pool digestion rates be increased as follows (if specific carbohydrate digestion rates are not measured) to reflect the enzymatic activity of FT products and their impact on altering rates and/or shifting nutrient pools (example: FT-corn silage book value B3 rate of 3.4%/ hour should be increased by 35% to 4.6%/hour).
CFT/GFT AFT
B1 50% 60%
B2 30% 60%
B3 35% 20%
When feeding high levels of highly digestible forages (corn silage, grass or legumes), it is helpful to frequently monitor cud-chewing, TMR particle size consistency and sorting issues due to changes in TMR mixing/delivery, along with ensuring adequate levels of ration NDF and peNDF (>23%). The peNDF or fragility of fiber in CFT-silage appears similar to that of conventional corn silages. As with any ration, observing animal performance, intakes, effective fiber levels, and manure consistency will help nutritionists further refine FT-silage-based rations.
Corn Silage profiles from CNCPS V6.1.32 CS directly from
CNCPS feed libraryCFT-treated CS with B1, B2, B3 Kd’s changed per gas analysis
CHO-B3 Kd
Corn Silage profiles from CNCPS V6.1.32 CS directly from
CNCPS feed libraryCFT-treated CS with B1, B2, B3 Kd’s changed per gas analysis
CHO-B1 KdCHO-B2 Kd
Balanced withFeed LibraryCorn Silage
Balanced withCFT-Corn Silage
(B1, B2, B3 Kd’s per gas prod)
ME Milk (lb) 89.94 92.04 (+2.1)
MP Milk (lb) 93.81 99.07 (+5.26)
Microbial Protein (g) 1326 1422 (+96)
Example ration that came pre-loaded in CNCPS V6.1.3290 lbs milk, 62 lbs as fed CS
Balanced withFeed LibraryCorn Silage
Balanced withCFT-Corn Silage
(B1, B2, B3 Kd’s per gas prod)
ME Milk (lb) 89.94 92.04 (+2.1)
MP Milk (lb) 93.81 99.07 (+5.26)
Microbial Protein (g) 1326 1422 (+96)
The true value of CFT…reducing feed cost, NOT promising more milk!
How much could corn grain and SBM be reduced to bring ME, MP and MP yield back to
original levels while maintaining equal DM intakes
True value of CFT: how much could corn grain and SBM be reduced to bring
ME and MP predicted milk back to original levels while maintaining equal DM intakes
Reducing corn grain by 1.6 lb and SBM by 1.0 lb saved
~ 35 cents/c/d
Treating with the original 62 lbs of CS with CFT cost ~ 9 cents/c/d
Increasing CFT-corn silage by 6 lbs (as fed) to keep DMI the same
cost ~ 11 cents/c/d(includes cost of CFT)
NET GAIN: 15 cents/cow/day
-and better rumen health-(this does not include the added
value of reduced silage shrink and improved palatability with CFT)
Now only 4 lbs corn grain,1.3 lbs soybean meal
and CFT-corn silage increased to 68 lbs
250
NEWSpring 2011
Introducing……. CFT and AFT Feed Cost Savings Are Additive
Original Ration Inclusion Rates
Rebalanced Ration Inclusion
Rates(ME and MP milk same as
original ration)
Savings/Cowfrom reduced soybean
meal and grain supplementation*
700‐Cow Herd Savings
11AFT Alfalfa Silage 20 lbs /day 21.5 lbs/day 4.25¢/day $29.75
11CFT Corn Silage 63 lbs /day 68 lbs/day 15.0¢/day $105.00
Savings/Cow/Day(includes cost of inoculation and increased forage intake)
19.25¢/day $134.75
Savings per 300‐day Lactation(assuming one‐group TMR for the entire lactation to help replace body reserves lost during early lactation)
$57.75/ Lactation
$40,425/year
* Soybean meal was valued at $350/ton and corn grain at $6.00/bu
Ration formulated with CNCPS V6.136 balanced for 90 lbs milk/3.6%BF with cows fed 62.3 lbs corn silage and 20 lbs alfalfa silage (as fed)
Plus Value of Reduced Shrink: at 70 lbs CS/day x 300 days = 21,000 lbs /cow/year = 10.5 tons/cow x 700 cows = 7350 tons x value of conservatively reducing shrink from 15% to 12.5% of %1.89/ton when the DM loss is replaced with corn valued at $6/bu = $13,891 shrink savings on the corn silage /700 cow dairy. The same logic on 3.3 tons of alfalfa silage/cow/year = $4,365/700 cows. Grand total = $18,256
$58,681 including savings from reduced
shrink losses
Thank You……
Bill Mahanna, Ph.D., Dipl ACANNutritional Sciences ManagerPioneer, A DuPont [email protected]
515.229.3409
Bill Seglar, DVM, PASNutritional Sciences Veterinarian
Pioneer, A DuPont [email protected]
515.360.9690
251

Small Ruminant and Camelid Field Restraint
Matt D. Miesner, DVM, MS, DACVIM (LAIM)
Introduction A regularly encountered subject during consultation with practicing veterinarians in the field, involves recommendations for chemical restraint and analgesia to accomplish various procedures in camelids and small ruminants. Relative unfamiliarity with the species and potentially the drugs used, present an uneasy feeling when preparing for the task at hand. Single drugs or combinations of α2 agonists, opioids, ketamine with or without local anesthetics are excellent and safe methods for sedating, anesthetizing and providing analgesia. With camelids, physical restraint alone when performing painful procedures, may pose greater risks to the welfare of the patient than anesthesia or sedation. Key points: Describe approaches to field restraint, sedation and analgesia in South American
Camelids and small ruminants. Provide the practitioner with methods that have proven beneficial with the author
and colleagues. Present information regarding techniques in pain management that may be
utilized in practice situations. Utilizing anesthetics and analgesics in combination when needed, enhance the
quality of the procedure and makes the job more enjoyable for the client, patient and veterinarian.
For optimal pain management, three actions should occur: 1) Restoration of normal physiologic protective pain mechanisms; 2) preemption of the pain cascade; 3) attack of the pain at various places along the cascade, called multimodal or balanced analgesia.
PROCEDURAL PAIN It is well documented that analgesics are more effective when given before the initiation of the pain cascade. We do not have control of this in naturally-occurring disease. We do, however, have absolute control over this when we will be performing what we know to be painful procedures. In order to provide the most effective analgesia, our analgesic agents must be given before beginning the procedure.
252

Castration All castration methods cause acute pain. In camelids, frequently we choose to perform castration in recumbency. The cocktail we use at KSU for castrations or any other procedure where recumbency is desired utilizes an IM combination of butorphanol + xylazine + ketamine: These drugs are combined into one syringe and given intramuscularly which avoids the inherent difficulties of intravenous injection in camelids.[Table 1] Note, alpacas appear to be slightly more resistant to sedation than llamas.
Table 1. Summary of INTRAMUSCULAR Butorphanol-Xylazine-Ketamine combined anesthesia for multiple procedures requiring recumbent anesthesia for up to 30 minutes. Administering 50% of the original dose (ketmine and xylazine) can be used during anesthesia to prolong the effect up to 15 minutes.
Alpacas 0.021 mg/lb butorphanol (0.046 mg/kg)
0.21 mg/lb xylazine (0.46 mg/kg)
2.1 mg/kg ketamine (4.6 mg/kg)
Llamas 0.017 mg/lb butorphanol (0.037 mg/kg)
0.17 mg/lb xylazine (0.37mg/kg)
1.7 mg/lb ketamine (3.7 mg/kg)
If I am performing “mass castration” on 3 or more animals, I will make up a bottle of the cocktail. To a 1 gram (10ml) bottle of ketamine, add; 10mg (1ml) butorphanol and 100mg (1ml) of xylazine. This mixture is then dosed at 1mL/40# (18kg) for alpacas, or 1ml/50# (22kg) for llamas. In my experience, very few of these animals, if handled quietly and plenty of time is given before starting the incisions, will need additional local anesthetic of the scrotum or spermatic cords. Expect 20 minutes of surgical time and the patient should stand 45 min to 1 hour after injection. I also have performed castrations standing by giving 0.4 mg/kg xylazine IM in alpacas and then infiltrating 1-1.5mL of 2% lidocaine into the median raphe of the scrotum and 2-3mL lidocaine into each spermatic cord. Many animals will lay down with this protocol when placed in a chute, likely behavioral and not related to over-sedation. Nevertheless, control over position and procedure is decreased. Another method for standing castration utilizes intramuscular butorphanol (0.15 mg/kg IM) in combination with local lidocaine anesthesia as described above. Butorphanol alone will not cause the degree of sedation as xylazine, and the patient will appear alert. The butorphanol should be administered 10 minutes before local anesthesia and castration to allow time for it to take effect.[1]
253

Additionally, caudal epidural may be used for routine castrations. A clinical study reported on three different methods in alpacas. Method 1; 1.5 mL of 2% lidocaine epidural, which provided perineal analgesia in 2 minutes, but did not alleviate discomfort associated with exteriorization of emasculation of the testicles. Method 2; used 20mg of 20mg/mL xylazine IM and 1 mL lidocaine as an epidural, both 10 min before surgery. This also did not fully alleviate discomfort associated with emasculation. Method 3; used 20mg/mL xylazine added 1:1 with lidocaine, with 0.75mL of the total solution given epidurally. This also did not fully anesthetize the spermatic cord. It is believed that such low-volume caudal epidurals do not move cranially enough to block the lumbosacral plexus, which feeds the structures of the spermatic cord. So, caudal epidurals should be increased in volume, or lidocaine should be infiltrated into the spermatic cords prior to emasculation or ligation.[2] The procedure used for castration also has some effect on pain responses. A publication reported that prescrotal castration, with primary closure, resulted in less incisional pain than did bilateral scrotal castration left open. Prescrotal castration does take longer, controlled patient positioning, and requires more attention to sterility, but may be most appropriate for some owners and during fly season.[3] Wound / Fracture/ Treatment of Limbs Regional IV anesthesia of the foot may be attained by placement of a tourniquet proximal to the fetlock with injection of 5-10 mL 2% lidocaine into any superficial vein. I more commonly utilize the common interdigital vessels between the pastern bones just proximal to the interdigital cleft of the foot. This is a blind stick, but the vessels are there. A 20ga butterfly catheter is sufficient, but for repeated infusions, an IV catheter may be placed. Alternatively, for more proximal lesions, the tourniquet may be placed proximal to the carpus or hock and 10-15mL of lidocaine infused into a vein. An interdigital block for foot analgesia may be performed by using an 18ga, 1-1.5” needle inserted into the dorsal interdigital space of the foot where the interdigital skin forms a “v” and directed toward the heel, parallel to the coronary band. The needle should be long enough to nearly exit the interdigital skin at the heel. Withdraw the needle, while injecting 5-10mL of lidocaine to anesthetize the axial nerves. Aspirate occasionally to avoid intravenous lidocaine injection. Abaxial nerves may be palpated on the medial and lateral aspects of the fetlock. 2-3mL of lidocaine injected over each of these nerves, in addition to the interdigital block, provides complete foot anesthesia. Dystocia Dystocia is mentioned here as there are some important things to keep in mind when selecting analgesics and sedatives. Low volume lidocaine caudal epidurals (1 mL/200#)
254

are most commonly used, but do not block the cranial vagina and cervix, and therefore may not provide analgesia sufficient to reduce straining and adverse behaviors. Higher volumes (2-3mL/adult female alpaca) provide a greater area of analgesia, but may result in some temporary loss of motor function to the hindlimbs. Butorphanol 0.05mg/kg, IV
is an excellent analgesic and sedative in addition to a lidocaine caudal epidural. α2
agonists should be used cautiously systemically or as part of an epidural when attempting to deliver live crias, as, in cattle studies, they have been shown to sedate the calf and reduce uterine blood flow and oxygen delivery. In the situation where dam sedation is required, acepromazine (0.02mg/kg, IV) is a better choice, although it does not provide analgesia. I prefer to use a combination of ace and butorphanol. The author does use xylazine for management of uterine torsion and cesarean section (see field surgical techniques proceedings by author at this conference) despite the potential risks to the fetus. However, by utilizing a combination of butorphanol for these procedures, the volume of xylazine can be reduced. Recognize the potential adverse affects on the fetus and be prepared for management. Frequently for Small ruminant Cesarean sections, tube cystostomy, perineal urethrostomy, prolapsed amputation, etc, I use lumbosacral lidocaine epidurals in addition to some mild sedation. (See below). DISEASE PAIN A variety of disease processes cause discomfort and pain of varying degrees to our camelid patients. For some diseases, such as septic arthritis, an obvious lameness alerts us to pain. For visceral diseases, pain responses tend to be more cryptic in prey species. In camelids, colic, fractures and trauma are all commonly encountered painful conditions. Pain signs include guarding affected area, reactivity to touch, vocalization, grunting, depression, recumbency, anorexia, isolation, elbow abduction, and bruxism. Rolling and kicking are not frequently seen in ruminants with visceral pain, and, when present, indicate severe pain. When these signs are present, we know that an analgesic should be included in our treatment plan, however, individual pain tolerance may alter the clinical presentation significantly.
Generalized Pain Management Techniques All of the classes of analgesics listed above can function in “whole body” pain managment. NSAIDs and α2 agonists are the classes most commonly used for this purpose, as they are relatively inexpensive and we tend to be comfortable with them. For all of the classes of drugs listed below, what we know primarily from cattle will be the information presented, as no drugs are labeled for and little is known about their activity in camelids.
255

NSAIDs are some of the most widely used analgesics and include flunixin, aspirin, ketoprofen, meloxicam, carprofen, phenylbutazone and many others. They have varying degrees of antipyretic, analgesic and anti-inflammatory effects by inhibiting the cyclooxygenase, lipoxygenase and thromboxane enzymes, all involved in the arachidonic acid pathway of inflammation. COX-2 is known to play a role in central sensitization from pain. As many painful conditions in camelids are inflammatory in origin, NSAIDs are an excellent choice, as they are the only drug class that directly addresses both the pain and the cause. Unfortunately, the NSAIDs vary in their analgesic and anti-inflammatory potency and are often inadequate for very painful conditions. Flunixin meglumine, ketoprofen and phenylbutazone are nonspecific COX inhibitors, used with the most success in ruminants. Etodolac, meloxicam and carprofen are more specific COX-2 inhibitors, making them theoretically safer, but these drugs have yielded disappointing analgesic results in ruminants. It is important to ensure adequate hydration in patients, particularly neonates, receiving any NSAIDs. Flunixin is labeled in the US and Canada for the control of pyrexia associated with bovine respiratory disease, endotoxemia and acute bovine mastitis and inflammation associated with endotoxemia, with a dose rate of 1.1-1.2mg/kg IV q 12h. The duration of analgesia ranges from 6-12 hours. There is little information regarding its analgesic qualities, but clinical experience is that it provides better visceral analgesia than musculoskeletal analgesia. Phenylbutazone is clinically believed to be superior for musculoskeletal injuries over flunixin. It is extensively protein bound and has a very long half-life, increasing its dosing interval. It is usually used orally in ruminants at 10mg/kg once, then 5mg/kg every other day thereafter. I have never used phenylbutazone in camelids due to toxicity concerns. Α2 agonists, including xylazine, detomidine and medetomidine, inhibit release for norepinephrine presynaptically in the dorsal horn of the spinal cord, managing peripheral sensitization. In addition to analgesia, these agents provide sedation and muscle relaxation. Side effects include cardiac arrhythmias, bloat, aspiration and increased myometrial activity. These drugs also sensitize the heart to catecholamine-induced arrhythmias and therefore should not be used as the sole analgesic for very painful procedures. It is also important to remember that these drugs greatly increase urine output, and should, therefore, not be used in animals suspected to have urinary tract obstruction.
256

Xylazine is our most commonly used drug of this class, used at dosages of 0.1-0.3 mg/kg IV, IM or SC. The analgesic properties of this drug last less time than its sedation does and animals are prone to laying down. This is particularly true for camelids, who are prone to “pout”. It provides similar visceral analgesia to opioids and flunixin, but its duration is much shorter than flunixin. The preferred reversal agent for xylazine is tolazoline (1-2 mg/kg), given IM or SQ. IV administration (especially the labeled dose) of tolazoline should be avoided as adverse reactions have occurred.[4] Local Anesthetics include lidocaine, mepivicaine, bupivicaine and procaine. These block nerve conduction of motor, pain and proprioceptive nerve fibers. They can be used as both local and systemic analgesics, with abilities to stimulate gastrointestinal motility and counter inflammation. Given IV, they act to limit central sensitization in the pain pathway. Local anesthetic side effects depend on the location used, but can include cardiac arrhythmias and ataxia. Toxic doses for small ruminants are much lower than those for large ruminants. Lidocaine used as a systemic analgesic is often overlooked. The drug itself is inexpensive, but it can be labor and equipment intensive to administer for this purpose. It must be given IV as a constant rate infusion (CRI), usually requiring a fluid pump. An initial lidocaine bolus of 1.3 mg/kg is given slowly IV followed by a CRI of 0.05 mg/kg/min. This is particularly useful postoperatively after intestinal surgery to potentially stimulate GI motility and provide visceral analgesia. Opioids include morphine, butorphanol, buprenorphine, meperidine and fentanyl. They inhibit the release of some neurotransmitters, hyperpolarize neurons and inhibit spinal pain transmission. Side effects seen in other species with opioids, such as hyperexcitability, are not as commonly seen in ruminants. It is important to remember that opioids exhibit a ceiling effect, such that once all receptors are bound, no additional drug will be effective. Butorphanol is the drug with which we have the most success in all ruminant-types. The dose is 0.1 mg/kg IV, IM, or SC, given q 4-6 hours. In a study of llamas, the elimination half-life for this dose IV was 15.9 +/- 9.1 minutes, while for IM dosing it was 66.8 +/- 13.5 minutes. Therefore, if analgesia is needed for a longer duration than a quick procedure, it should be given IM or SC. We perceive that it provides excellent visceral analgesia in 8/10 animals and is probably the best drug we have for established pain. Morphine is much less expensive than is butorphanol, but we perceive it to provide good analgesia in only about 1/3 of patients. Butorphanol has about 5 times the potency as morphine, so adjust systemic doses accordingly. Unlike butorphanol, morphine may be used epidurally as well. One paper of llamas suggests a dose of 0.25 mg/kg IV q 4 hours, which provided the most tolerance to electrical stimuli.[5]
257

Fentanyl may be used parenterally, but most frequently used transdermally. Both methods have produced varied responses in small ruminants and swine. I have used the transdermal patches in small ruminants primarily, using a 50ug/h patch for a 30-50kg animal. In mature llamas weighing 150 +/- 18 kg, four 75 ug/hr patches placed on the clipped antebrachial area provided serum levels of ~0.3 ng/mL within 12h and lasted for 72 hours. Other analgesics must be provided until the patch kicks in, and a new patch should be placed about 48 hours after the first, as each patch works for about 3 days. It can get costly, but it provides cost savings over butorphanol, if the animal requires analgesia over a period of time. Ketamine is a dissociative anesthetic that blocks NMDA and other receptors pre and post synaptically, which play a key role in the pain process of central sensitization. Additionally, it may have potent anti-inflammatory effects, suppressing cytokines and neutrophil chemotaxis. Ketamine is good for established pain, provides analgesia at microdoses, and can be safely used long-term. It does not last long and therefore, needs to be given constantly at 0.4-1.2 mg/kg/hr as a CRI. This is a dosage for cattle and I know of no studies using it in camelids. Synergistic Groupings of Drugs. As stated before, it is a good idea to use drugs in combination in order to stop the pain cascade at multiple points, and to overcome the inevitable shortfalls of each drug as an individual. Some synergistic groupings include: 1) Xylazine + Opioids, 2) NSAIDs + Opioids, 3) Local anesthetics + Opioids, 4) Ketamine + Xylazine + Opioid + Local anesthetics Epidural Techniques Many of the painful conditions we see in small ruminants involve the pelvis, hindlimbs or caudal abdomen. The use of caudal and lumbosacral epidurals can provide regional analgesia, often avoiding systemic side-effects and reducing drug costs. Caudal epidurals, administered between the first two caudal vertebrae, provide analgesia to the perineum. 2% lidocaine at1mL/200# is the most commonly used drug for this purpose, providing perineal analgesia and motor loss for about 90 minutes. Higher volume caudal epidural with lidocaine 2% at 2-3 mL/adult alpaca or increased in volume by addition of saline, provides pelvic and caudal abdominal analgesia, in addition to ataxia or motor loss to hindlimbs. To provide longer duration, bupivicaine may be used, providing analgesia for ~4 hours. Α2 agonists may also be used in epidurals, either alone or in addition to local anesthetics. Xylazine 20 mg + 1mL of 2% lidocaine, given to an adult alpaca, provides prolonged analgesia, with minimal motor interference. Ketamine may also be used for caudal epidurals, providing analgesia without sedation. For a solution of 5% ketamine: 5mL as a caudal epidural to an adult cow provides analgesic
258

onset at 6.5 min, duration 17 min; 10mL to adult cow; onset at 5 min, lasts 34 min +/- hindlimb ataxia; 20mL to adult cow; onset at 5 min, lasts 62 min + hindlimb ataxia. These doses are for cattle and may be scaled back for camelid use. Lumbosacral epidurals are a little trickier than caudal epidurals and require aseptic technique, but provide analgesia to the hindlimbs, caudal abdomen and pelvis. These can be done with 2% lidocaine, and remember, hindlimb motor loss will occur. In small ruminants and camelids, 3 mg/kg of 2% lidocaine induces analgesia and motor loss that is good for C-sections, umbilical surgery and relief of urinary obstruction.[6] As an alternative, morphine epidurals work well in ruminants, providing good analgesia to the hindquarters, perineum and caudal abdomen without causing motor loss. A dose of 0.1 mg/kg (you may see dose ranges of 0.5-1 mg/kg) may be given epidurally q 12 hours with a spinal needle. This could also be combined with xylazine. Indwelling epidural catheters are a great consideration for cases that require longer-term analgesic administration. I have used these to reduce straining in many species with prolapses, straining in general, and to give repeated analgesic epidurals to animals with hindlimb fractures or claw amputations. There are several brands available and they typically come in 18 or 19 ga sizes. They may be placed at the LS junction or as for a caudal epidural; at either site, the area should be clipped and surgically prepped. A slightly curved needle (provided with the kit) is inserted into the epidural space, the catheter introduced through the needle several centimeters, the needle removed and the catheter sutured to the skin. An injection port is placed on the catheter and I usually make an adhesive patch (Elastikon) over the catheter-skin interface to keep the area clean. If placed aseptically and bandaged, these can be maintained for up to 1-2 weeks. Summary For most procedures, combinations of drugs are administered for full benefit of anesthetic and analgesic properties. The author utilizes xylazine alone frequently for short, relatively benign procedures. Combinations of xylazine, butorphanol, and ketamine are used for field procedures which may be painful and require recumbency of up to 30 minutes. Additional local anesthetics/analgesics greatly enhance patient comfort and smoothness of anesthesia. Endotracheal intubation greatly reduces the subconscious hypoxia stress enhancing patient cooperation. The summary of analgesic methods are presented as options (not practical in all practices) for managing prolonged or severe pain and discomfort in patients.
259

References: 1. Barrington GM, Meyer TF, Parish SM. Standing castration of the llama using
butorphanol tartrate and local anesthesia. Equine Pract. 1993;15:35-39. 2. Padula AM. Clinical evaluation of caudal epidural anaesthesia for neutering of
alpacas. Vet Rec 2005;156:616-17. 3. Baird AN, Pugh DG, Wenzel JG, et al. Comparison of two techniques for castration
of llamas. JAVMA 1996;208(2):261-2 4. Read MR, Duke T, Toews AR. Suspected tolazoline toxicosis in a llama. JAVMA
2000; 216(2):227-29. 5. Uhrig SR, Papich MG, Kukanich B, et al. Pharmacokinetics and pharmacodynamics
of morphine in llamas. AJVR 2007;68(1):25-34. 6. Scott PR. Extradural Analgesia for Field Surgery in Sheep. Compendium, Food
Animal Supplement, March 2000 22(3);S68-S75.
260

Small Ruminant and Camelid Procedures
Matt D. Miesner, DVM, MS, DACVIM(LAIM)
Introduction Camelid and small ruminant owners continue to play a significant part in the life of the mixed animal practitioner. The hobby farmer, 4Hers, and spontaneous salebarn purchasers make up a significant portion of the clientele in many practices these days. Therefore they are less likely than the experienced lifelong herdspeople of tradition. In addition, the standard of care expectation may be a little more involved as well. Owners are eager to find a veterinarian in the area to establish a working relationship and primary care for their animals and are willing to accept financial duty of professional care. I have found that the large majority of these clients dearly respect the veterinarian’s contributions to their animals, understand limitations and provide for a financially sound branch of a practice willing to work with them. As primary care veterinarians we are regularly called upon for elective procedures and intervention during emergency situations that are best addressed on the farm. The primary goal of this seminar is to familiarize the practicing veterinarian with some of these regularly encountered procedures and how the author chooses to handle them. Presentation Goals. Familiarize practitioners with field surgical techniques and procedures regularly
encountered in camelids and small ruminants Describe restraint methods and surgical techniques that can be performed in the
field. IV Catheterization in Camelids: Venous access during procedures is occasionally nice to have but sometimes intimidating. Jugular vein catheterization: supplies: 14ga to 16 ga 3 ½ inch (juvenile to adult) and 18ga to 20 ga 1 ½ to 2 inch catheters (crias), Vet-wrap or elastic tape, short extension and catheter cap. Soft, long term type catheters can be used but are sometimes difficult to feed through the skin.
261

The jugular veins in camelids are protected by the transverse processes of the cervical vertebrae and tough skin. The thick, tough skin in males is more pronounced than in females. The veins lie just medial and ventral to the transverse processes and in close proximity to the carotid artery which lies deep to the vein.
Best performed in the upper middle 1/3 of the neck.
Difficult to visualize jugular fill in camelids.
Palpate the transverse processes and clip and prepare the area medial to the processes toward midline. Locate atleast two transverse processes to estimate the orientation of the vein.
14 gauge needle (juveniles and adults) can be used to pierce the skin before the catheter is inserted, alternatively, a scalpel stab incision
Suturing the catheter in place is not required and can be sufficiently held in place with vet-wrap or elastic tape.
Other venous access sites for catheterization in include the medial saphenous, cephalic and ear. These sites are similarly catheterized as in other species. The cephalic vein is less visible as that in small animals, but in the same location. Castration Anesthesia: For additional options, see author’s section on field anesthesia in these proceedings. For nearly all castrations, the combination of butorphanol, xylazine, and ketamine (BXK)is used. [table 1] Note the ratios of the drug doses in the cocktail, the author and colleagues have adjusted most commonly reported doses to help make them easier to remember. If standing castration is to be performed, a minimum of systemic sedation with an α-2 / butorphanol and local anesthetic are recommended.1
Table 1. Summary of INTRAMUSCULAR Butorphanol-Xylazine-Ketamine combined anesthesia for multiple procedures requiring recumbent anesthesia for up to 30 minutes. Administering 50% of the original dose (ketmine and xylazine) can be used during anesthesia to prolong the effect up to 15 minutes.
Alpacas 0.021 mg/lb butorphanol (0.046 mg/kg)
0.21 mg/lb xylazine (0.46 mg/kg)
2.1 mg/kg ketamine (4.6 mg/kg)
Llamas 0.017 mg/lb butorphanol (0.037 mg/kg)
0.17 mg/lb xylazine (0.37mg/kg)
1.7 mg/lb ketamine (3.7 mg/kg)
262

Procedure: Precautions should be taken prior due castration during positioning and during anesthesia to ensure safety for the patient: 1) Support the head and neck at all times. Cervical-vertebral subluxation risk increases as the animal looses stability during sedation. 2) Camelids (ruminants for that matter) produce a significant amount of saliva. Therefore position the head so that saliva will drain away from the oral cavity. A rolled towel under the atlanto-occipital region of the neck, caudal to the ramus of the mandible, while in lateral recumbency works well. 3) Have the client withhold feed (not water) 12 hours prior to castration. 4) Due to hormonal influence on skeletal growth, camelids should not be castrated until 18-24 months of age.2
The castration can be performed with either pre-scrotal or scrotal approaches. The pre-scrotal method utilizing two incisions over each testicle and second-intention postoperative healing is preferred by this author, since nearly all are done in recumbency. I don’t feel confident enough that sufficient asepsis is maintained during the procedure in the field, to safely warrant primary closure. Some clinicians prefer pre-scrotal castration (one or two incisions) with primary closure and may provide for less post-operative discomfort and be more aesthetically pleasing to the client.3 Standing castration will be limited to a scrotal approach. The testicular cord should either be ligated with absorbable suture or emasculated. I prefer ligatures as the cord is small and doesn’t crush well will emasculators. Assure the patient is current on clostridial vaccinations. Cesarean Section/Uterine torsion correction Luckily dystocia is relatively uncommon in camelids. The most common causes of dystocia are fetal mal-positioning, uterine torsion, and limited cervical dilation or vaginal relaxation (possibly scarring due to previous dystocia). Critically assess the systemic stability of the dam for clinical signs of dehydration, hypotension, and shock and place IV catheter for triage with fluids and anti-inflammatories. Avoid dexamethazone as it may intiate metabolic derangements in the dam and/or fetus. Assess the cause for dystocia. Take precautions with vaginal delivery as the uterine and vaginal walls, and cervix in camelids are not as resilient to trauma as cattle. If the cervix is closed, try to obtain viability of the fetus by ultrasonography if possible. A fetal heart rate of between 80 to 120 is normal, bradycardia indicates fetal stress. Uterine fluid should normally appear clear. Rectal palpation, to detect uterine torsion, is possible in most llamas and multiparous alpaca females for clinicians comfortably wearying a 7 ½ surgery glove. In dystocia, if the uterus or fetus is not accessible or the cervix is closed, immediate c-section is indicated.
263

In cases of uterine torsion, external (rolling) should be attempted initially. The author and colleagues generally give the patient a “two strikes and you’re out” chance. If the torsion is not corrected in two rolling attempts, laparotomy is performed. Cesarean section may or may not be performed. Anesthesia: An IV catheter is in place at the time of surgery and the left flank is surgically prepared. The dam is given 0.05 to 0.1 mg/kg xylazine IV and 0.2mg/kg butorphanol IM. A caudal epidural, 2 to 3ml 2% Lidocaine is administered to reduce straining. A local line block of 2% lidocaine is administered in the left flank where the incision will be made. I prefer to limit my total lidocaine administration to 10mg/kg including the epidural. Dilute the lidocaine for the line block as needed with saline. The length of the incision will be approximately 20 cm. The dam is placed and maintained in right lateral recumbency with ropes tied over the back in a cushed position. Procedure: Approach to the abdomen can be through the flank or by midline celiotomy. The author prefers the left flank approach. Precautions should be taken to assure tissues will be accurately re-apposed during closure. An oblique incision following the orientation of the muscle fibers of the internal abdominal oblique (caudo-dorsal to cranio-ventral) allows accurate re-apposition in a three layer closure. The uterus should be isolated and in cases of uterine torsion, visually assess uterine wall health. Fetal viability can be assessed by placing an ultrasound probe in a sterile rectal sleeve. Re-assess after detorsion of the uterus. If cesarean section is to be performed, exteriorize the uterine horn and remove the fetus. Suture the uterus with size No. 0 absorbable suture material in an inverting pattern. Due to the diffuse epitheliochorial placentation, I prefer a two layer closure with the first layer only slightly inverting (nearly appositional), with a second inverting pattern (cushing). Suture the body wall in three layers (transversus and peritoneum + internal abdominal oblique + external abdominal oblique). Post-operative care should include antibiotics (7 to 10 days) and NSAIDS (3 days). Prolong therapy as needed depending on initial presentation and surgical complications. If the placenta is retained after the first 24 hours after surgery (ie failure of cervical dilation), 250µg of cloprostenol IM (2 doses q 24 hours) can be given. Do NOT give Lutalyse® as toxicity and death has been reported.4
264

Trimming Teeth (incisors, fighting teeth) and removing retained deciduous incisors A common procedure performed in camelids involves trimming the sharp canines and possibly the sharp upper incisor in camelids to prevent injury among herdmates and handlers. Occasionally retained deciduous incisors need removed and also excessive overgrowth of permanent incisors. Incisor and canine dental formulas and eruption times are summarized in table 2.
Table 2: Incisor and canine dental formula in camelids. Adapted from Fowler ME, 1998.4
Incisors (per side)
Canines (per side)
-Note: camelids’ one upper incisor (caudally positioned) functions as “canine”. - Lower incisors erupt: I-1(2-2.5yr), I-2(3yr), I-3(3-6yr) -Canines (upper and lower) erupt: (2-7yrs) *present in small percentage of males at birth.
Deciduous 1/ 3 at birth *1/1 Permanent 1/3 **1/1
** The lower canine is positioned just caudal to the last lower incisor (I-3). Mature male camelids may appear to have two upper "canines" (one is actually an incisor), and one lower canine. Females and castrated males may or may not have canine teeth.
Anesthesia: Xylazine alone or xylazine + butorphanol may be sufficient. Alternatively, the BXK combination cocktail may be used. Procedures: Trimming fighting teeth is quite simple. A wire saw is often used to trim the teeth. I have found that a Dremel™ tool fitted with a diamond cutting blade (found at nearly all hardware stores for ~$15) does the job quicker, cleaner and safer. Cut the canines and sharp incisors to within 1-2 mm of the gingiva. You can then round the edges of the cut tooth with a sanding burr that also fits the Dremel™ tool. The lower incisors can be trimmed when the jet out in front of the nasal filtrum. Overgrown incisors don’t necessarily impede grazing, but may put the animal at risk for trauma and are unsightly to look at. Trimming incisors may be performed with the same instruments used in cutting fighting teeth. Attempt to trim the incisors level of the dental pad when the molars are apposed. Occasionally deciduous incisors are retained during permanent incisor eruption. This poses a potential problem with malocclusion as well as accumulation of feed material between the two rows of teeth causing premature decay and tooth root infection/degeneration. Invariably the front row of incisors are the retained teeth. A periosteal elevator, gingiva elevator, equine wolf tooth extractor or pliers can be used. Try not to fracture the tooth at the root.
265

Managing Nasolacrimal Ducts Causes: Nasolacrimal duct obstruction may either be congenital or acquired. Congenital nasolacrimal duct atresia is suspected when clear to cloudy ocular discharge is noted at or soon after birth. Obstruction is suspected if discharge develops a few weeks to months after birth and is occasionally seen in adults. There are two medial canthus puncta (dorsal and ventral) that merge and drain to a single nasal opening near the nares. The nasal opening is a faint depression seen on the abaxial ridge near the opening at the nares. Anesthesia: Xylazine is usually sufficient for routine flushing of a duct. Topical lidocaine anesthetics in the nares and ocular proparacaine provide additional local anesthesia . Techniques: Obstruction of normal ducts: A polypropylene tomcat catheter may be sufficient for catheterizing and flushing small ducts or locating the puncta. A longer polypropylene catheter with a wider lumen will be needed if we want to leave a temporary “stent” with monofilament suture material in place. The easiest way to flush a duct is to enter from the nasal opening and advance the catheter until it stops. Attach a syringe with saline and apply pressure over the catheter to prevent backflush. Apply pressure to the syringe in a “pulsing” motion and observe the medial canthus for fluid. Alternatively, attempt to pass the catheter from the puncta of the medial canthus. Naso lacrimal duct atresia: Various degrees of segmental aplasia occur. If either a opening exists, follow instructions above. While pulsing the saline, look for a “bulge” in the soft tissues. Lance the distended area with a 14 ga needle and advance the catheter. Monofilament suture material can be passed through the lumen of the catheter which is then removed. The suture is tied back to itself to provide a stent to keep the duct patent during the post-op phase of healing. Leave the suture in place for a week to 10 days. Have the client treat the eye topically. Complete atresia may necessitate a nasolacrimal rhinostomy. Tube Cystostomy Urinary obstruction is a commonly encountered problem in small ruminants. There are many methods for relieving the obstruction, which is almost always due to obstructive calculi. Relieving the obstruction by retrograde urinary catheterization is highly unlikely to be achieved, in ruminants and pigs, due to the urethral diverticulum present at the ischial arch of the penis. In addition, dynamic and physiologic healing characteristics of the ruminant urethra result in a strong likelihood for lumenal stricture formation as a result of trauma from calculi, attempted catheterization or surgically induced (ie
266

urethrostomy). Tube cystostomy is a viable option for curative (long term) relief of urethral obstruction as well as maintaining functional breeding males. Anesthesia General anesthesia is Not essential for successfully performing a tube cystostomy, however this luxury allows the surgeon more time to flush the bladder and attempt normograde catheterization for hydropulsion of stones from the urethra. Induction with “double drip” (Guafenesin and Ketamine), tracheal intubation with maintainence on a small animal anesthesia machine is easily performed in small ruminants. An alternative to general anesthesia would be lidocaine epidural and local anesthesia with xylazine/ketamine sedation. Care should be taken when using lidocaine in goats (toxic dose 5-10mg/kg). Xylazine should also be used with caution due to its hypotensive and diuretic effects. The metabolic and electrolyte imbalances should be considered (hyponatremia, hypochloremia, and possibly hyperkalemia) and either measured or empirically treated. A method for percutaneous tube cystostomy and vesicular irrigation has been described.1 Risks with this procedure include, bowel perforation and increased risk of peritonitis. Ultrasound guidance is highly recommended. Anesthetic, Fluid and Electrolyte considerations Surgical success when dealing with urinary obstruction largely depends on duration of disease, and correction of fluid and electrolyte derangements prior or during surgery. Not using hypotensive drugs and quickly replacing fluid volume is probably of primary importance. The severity of these electrolyte changes vary with duration and if the bladder is ruptured. Potassium levels can be variable in ruminants, even with ruptured bladder. When dealing with a ruminant, we have to keep in mind that they have a second set of kidneys (salivary glands). Azotemia, hyperkalemia and hyperphosphatemia can generally be tolerated by large ruminants to a greater degree due to recirculation through the salivary glands. Small ruminants (especially sheep), however, seem to be affected more often with the hyperkalemic acidosis syndrome that we see in small animals and foals. Whether performing a tube cystostomy in the field or in the hospital, try to avoid longer acting hypotensives such as xylazine. Most ruminants are very sensitive to xylazine and it also has quite significant diuretic affects. Hyperkalemic animals can have significant adverse cardiovascular effects with xylazine and it also sensitizes the heart to catecholamine induced tachyarrhythmias. 5% Guafenesin mixed with 1mg/ml of ketamine is adequate for intubation and could also be used to maintain a surgical plane of
267

anesthesia. For surgical induction or intubation, the dose of the “Double drip” mixture is about 0.75 to 1 ml per pound of body weight. Be sure to dose to effect as the onset of anesthesia is slow. If you are going to intubate the patient, I would recommend using a stylet (polypropylene dog catheter) to guide the endotracheal tube through the larynx. The replacement fluid of choice is 0.9% NaCl. If you suspect the animal has been obstructed for longer than 36 to 48hr or has a ruptured bladder, anticipate the potassium to be elevated. If the potassium levels are high, consider adding dextrose to make a 2.5 to 5% solution to your sodium chloride and possibly using insulin. This will induce endogenous insulin release to drive dextrose into the cells and take the potassium with it. Potassium also exerts an inhibitory effect on cardiac muscle resulting in bradycardia. Adding 20ml of Calcium borogluconate per liter of fluids will aid muscle contractility of the heart. Atropine can be used as well to combat bradycardia usually at a dose of 1ml per 40 to 80 pounds of bodyweight. If you have the ability to perform an electrolyte and acid-base panel prior to surgery, you may want to consider some more technical ways of supporting the critical patient during surgery. Use the potassium level as a marker for determining the degree of intervention. Sodium bicarbonate can be used to correct acidosis and decrease hyperkalemia. These general rules of thumb can be used in conjunction with fluid therapy. Example 1. Mild acidosis and Potassium level 5 to 6, normal heart rate.
0.1 IU/kg of regular insulin and 0.4 Gm/kg Dextrose IV
Less effect and shorter duration
Can be used even when estimating clinical derangements Example 2. Moderate acidosis and Potassium level >7, bradycardia
0.5 IU/kg of regular insulin and 1Gm/kg of Dextrose IV
More dramatic effect and longer duration
Monitor for severe hypoglycemia, will likely need to maintain on CRI of 5% dextrose for 24 hr.
Procedure Approach The procedure is easiest to perform in dorsal recumbency. The approach is paramedian, so as to avoid the penis. The penis can also be reflected and the abdominal incision made through the linea alba. The incision should be approximately six inches long with the posterior extent of the incision ending just anterior to the teat. Cystotomy Once in the abdomen, locate the bladder and place two stay sutures in the bladder wall to maintain the bladder at the incision once decompressed. Decompress the bladder with a sharp stab incision with a #10 scalpel blade between the stay sutures. Extend the incision enough to insert a finger or two to palpate the trigone of the bladder for stones. Lavage
268

the bladder with saline to remove all stones and debris that may have accumulated. Attempt normograde passage of a polypropylene urinary catheter to flush stones from the urethra. I have found it to be difficult to pass the catheter in most cases, but unsuccessful attemp does not preclude failure of the procedure. Prolonged attempts at normograde catheterization should be avoided to prevent excessive trauma to the urethral mucosa. Don’t force it, all is not lost. Tube Cystostomy The next step is to place the Foley catheter through the abdominal wall first and then into the bladder through a separate stab incision adjacent to the celiotomy and cystotomy. The size of the tube should be large enough to flow freely and allow passage of small blood clots without becoming obstructed. I rarely use less than an 18Fr. A stab incision is made about two inches lateral to the laparotomy incision towards the posterior 1/3 of its extent. The tip of the catheter is then passed through the abdominal wall. It is easiest to pass a hemostat from interior (peritoneum) to exterior (skin) and pull the catheter through. Another stab incision is made about an inch lateral to the cystotomy incision where the foley will be inserted and the bulb filled with approximately 10ml of saline. Be sure to have checked the volume limit of the bulb as well as if it is free from leaks. Some surgeons will then place a purse-string suture around the insersion of the catheter into the bladder. Close the cystotomy incision with a one or two layer, inverting pattern. Finally, close the laparotomy incision. The portion of the Foley catheter exiting the abdomen should be anchored to the skin. We prefer to use a “fingertrap” suture to anchor the tube where it exits the body wall, followed by a few additional interrupted sutures placed around the tube in a few places to prevent the tube from dragging the ground or being stepped on. Consider an Elisabethan-type collar for some goats (especially Pigmies). Post-Op Care Don’t worry if you were unable to achieve a patent urethra during surgery. In many cases where we were certain that there were stones still obstructing the urethra after surgery, it took an average of 14 days before the animal was able to urinate successfully. Also, we have left tubes in for over a month before the animal urinated normally. Our success rate for long term cure (greater than one year) is about 70%.2 Allow at least 7 days to pass after surgery before attempting to clamp off the catheter to assess urethral patency. Sometimes the animal is already urinating normally with the catheter still in place before being clamped. Clamp the catheter and leave in place for a couple of hours or until the animal shows discomfort. The clamp is then removed and not attempted until the next day. This process is repeated daily for several days or every
269

other day. Once the patient is able to urinate will for 24hours, the Foley is removed. Urine leakage from the insertion site may be noted, but will soon be closed. Potential complications from urethral obstruction are hydronephrosis,, cystitis, pyelonephritis, atonic bladder from overdistention, urethral stricture due to trauma from the calculi, failure to pass the obstruction, and erectile dysfunction in breeding males due to circulatory damage. The potential complications should be discussed with the client prior to treatment.
References:
1. Streeter RN, Washburn KE, McCauley CT. Percutaneous tube cystostomy and vesicular irrigation for treatment of obstructive urolithiasis in a goat. JAVMA (2002) August 15;221(4):546-49.
2. Ewoldt J, Anderson DE, Miesner MD, Saville W. Long Term Survival with tube cystostomy as treatment for urolithiasis in goats. Vet Surg. 2006 Jul;35(5):417-22.
References:
1. Barrington GM, Meyer TF, Parish SM. Standing castration of the llama using butorphanol tartrate and local anesthesia. Equine Prac 1993;15(5):35-39.
2. Smith BB, Timm KI, Reed PJ. Morphometric evaluation of growth in llamas (lama glama) from birth to maturity. JAVMA 1992;200(8):1095-1100.
3. Baird AN, Pugh DG, Wenzel JG, et al. Comparison of two techniques for castration of llamas. JAVMA 1996:208(2):261-2.
4. Fowler ME, Bravo PW. Reproduction. In: Fowler, ME (Ed), Medicine and Surgery in South American Camelids, second ed. Iowa State University Press, Ames, USA, pp. 381-429.
270

Multimodal Bovine Restraint
Matt D. Miesner, DVM, MS, DACVIM (LAIM)
Introduction Bovine practice has many physical and mental challenges, among them is safely and effectively restraining cattle for procedures. We accept the challenge as part of the job, but relish the thought of not having to hit a moving target with the suture needle, dodge the flying hoof like an inside fastball, or be forced to practice our box waltz steps. But mostly we want to provide the most safe, secure, and pleasant care we can while we’re doing what we need to do. We have tried and true, very effective methods for physical restraint which can keep our patients “still”, including chutes and tables when available and rope restraint methods. Lidocaine and local anesthesthesia prevent the “ouch” at the focal location, but many of us have been smashed or kicked working on that totally numb flank. Sedatives, dissociatives and systemic analgesics provide the mental distraction needed to reduce reflex reactions and over-ride learned behavior, but ideally want to be used at the minimally effective doses to avoid adverse side effects. To achieve this goal, consider “multimodal” anesthetic and analgesic protocols. Restraint through low stress handling, secure physical restraint, local/regional anesthesia, and “chemical reasoning” share the role of addressing pain and stress management, reducing risk and increasing safety in both patients and handlers. We can look at this as “multimodal” restraint. Environment, situation, breed, etc., necessitate adjustments. This discussion will provide situations encountered by the author requiring restraint and how they are addressed. By no means is this proceedings meant to act as a formulary replacement for published drug recommendations. Physical Restraint Learn how to make a halter. Dr. Dee Griffin has a nice description in text and picture.2 Knowing how to fashion your own head restraint allows you to tailor the length of lead you may need in the field or incorporate the lead in various rope casting methods. Even in squeeze chutes with various head catches, the head has enough movement to cause harm to handlers and the patient, not to mention making it really challenging to accurately incise skin during cosmetic dehorn for example. The halter should be easy to remove and not constrict the airway. Rope casting methods are a very helpful safety net even in field anesthetized patients. The two most commonly performed are; 1) the Double half hitch, also referred to as the “reefing” method, and 2) the “running W” a.k.a “criss-cross” a.k.a “over and under”. Both methods have their pros and cons, but both are safe and effective for inducing and restraining cattle in recumbency. The author prefers the “running W” for midline cesarean sections, as it allows access to the surgical field, and provides hindlimb stabilization all in one. The running W is not ideal for a recumbent flank approach. Invest in chutes and tables that allow safe access to the ventrum and feet. Portable units are very helpful and endless possibilities exist with modifications made to adapt pulley systems and support straps for various situations.
271

Local/Regional/Epidural Anesthesia Block regions when possible, versus locations. Local and regional anesthetics are commonly used in bovine practice for various procedures for both diagnostic and treatment regimes. Local infiltration of lidocaine into infected tissue or inflamed tissue can be ineffective, not to mention potentially scattering the infection with multiple injections. Therefore, when possible utilize local anesthetics at distal locations to the point of interest. Paravertebral blocks for the flank, intravenous regional limb blocks, ring blocks, and point blocks for distal limbs and feet, and epidural blocks for perineal surgery are all well described and effective. The distal limb can be anesthetized for localizing lameness and surgery by way of intravenous administration of lidocaine after applying a tourniquet proximal to the region allowing for diffusion of anesthetic throughout the distal limb. I have performed this procedure on standing cattle multiple times to addresses problems distal to the carpus/tarsus. After applying the tourniquet, allow several minutes to pass before attempting to insert the needle in the desired vein, usually blindly into the dorsal common digital vein. Delay after tourniquet application allows for the distal limb to desensitize to the insertion of the needle. A short extension line from the needle to the syringe is helpful to prevent perivascular injection during inevitable movement by the patient. Alternatively, a “four point” block of the abaxial pastern and interdigital region can be performed for coffin joint lesions or sole abscesses. Epidural anesthesia with lidocaine at high volumes (~20 to 50 ml (adult cow) in the tail head epidural space) will cause recumbency due to paralysis of the hind quarters. It is recommended that the animal be hobbled for recovery due to the extended time for the anesthetic effects to wear off. Combined with casting rope restraint, a pinch of opioid and a sprinkle of ketamine parenterally make midline cesarean sections a lot more palatable. Field Anesthesia and Sedation Chemical restraint can make procedures more pleasant for practitioners and patients, whether it be light or heavy sedation, or general anesthesia. The enhanced level of cooperation of the patient often improves efficiency to help counterbalance the cost of the drugs used. Of course, individual considerations with drug class use have to be made as to regulatory cost:benefits. Finally, food animals require food safety guidelines and drug residue avoidance decisions to be considered with use of sedatives as well as antibiotics. Little is published in this area, and frequently changes. Call FARAD and consider the T1/2 of the drug used. I am comfortable using short acting drugs where elimination is nearly always less than healing times or antibiotic withdrawals for meat. Sedation for examination only, requires an educated estimate. Milk withdrawals “should be” even shorter, but test when possible. A few things should be taken into consideration when sedating or anesthetizing ruminants to aid in prevention of undue complications. First, ruminants produce a significant amount of saliva while under sedation or anesthesia. Thus, it is important that the patient’s head be positioned so that the saliva runs out of the mouth, which is particularly important when the animal is in lateral or dorsal recumbency. As important as salivary pooling in the larynx, is rumen contents from a drug induced rumen atony and positional disruption of the rumen contents. This can be achieved simply by placing a pad under the neck just behind the ramus of the mandible or mid cervical region. The protocols that I will present should allow for some degree of “protective” laryngeal
272

reflexes to remain intact to help prevent aspiration of saliva or rumen contents. Atropine does not necessarily reduce the amount of saliva produced in ruminants, but does make it more viscus which may be detrimental in itself. Atropine also causes reduced intestinal motility and risk of rumen atony. Try to perform as many procedures with the animal standing or in at least semi-sternal recumbency to help prevent or more readily recognize rumen tympani and decrease the adverse cardio-respiratory effects. Also, consider other concurrent affects of the the drug used, such as xylazine’s increase in uterine tone, in addition to sedation of the fetus. Is there a dose dependent effect of the drug used? For the most part there is, therefore using low dose combinations of different drugs may provide desirable restraint without overwhelming individual mechanisms and saturating receptors.
Xylazine: A suggested dose: Standing sedation (0.01 to 0.015 mg/lb ( .02 to .03 mg/kg) IV), Recumbency 0.05 mg/lb ( 0.1 mg/kg) IV)1 This is the most common drug used in chemical restraint of ruminants, either by itself or in combination with other pharmaceuticals. I rarely use the intramuscular route of administration as I am unsure of the ultimate effects that will be achieved and under what time frame they will occur. Intravenous administration provides me with a more predictable and faster onset of anesthesia and analgesia, and I can give multiple smaller doses to titrate the effect to the desired level of anesthesia or sedation. All levels of sedation from standing to recumbency can be achieved with xylazine alone. The initial demeanor of the patient does mediate the effect obtained to some extent. There are some dose dependent side effects of decreased GI motility and cardio-respiratory function and increases in uterine tone in late gestation. Use cautiously in compromised patients and/or reverse upon completion of the procedure. I will commonly reverse the effects of xylazine with tolazoline after the procedure, particularly if large amounts of xylazine were given to produce recumbency. Yohimbine has not proven to be as affective of a reversal agent as tolazoline in my hands with ruminants. I use tolazoline at a dose a lot less than the label and have had good success and smooth reversals. The dose I use for tolazoline is about 3X to 5X the milligrams of xylazine given, intramuscularly, dependent on the duration of the procedure and the time the last dose of xylazine was given. The recommended emergency reversal dose of tolazoline is 1.8mg/lb (4mg/kg) IV but that is a whopping dose to reverse routine sedation in the author’s opinion and mortal complications have been reported. Combination anesthetic protocols are handy for standing and recumbent procedures and can provide the multimodal goal of anesthetic enhanced restraint. The author feels comfortable using an opiate, alpha-2, and dissociative combination for most procedures.
Intramuscular Butorphanol + Xylazine + Ketamine (BXK): Butorphanol (0.005 – 0.013 mg/lb (0.01 - 0.025 mg/kg)) + Xylazine (0.01-0.025 mg/lb (0.02 – 0.05 mg/kg)) + Ketamine (0.02-0.05mb/lb (0.04 – 0.1 mg/kg)).1 From this combination we get the benefit of a fairly potent ruminant sedative from xylazine but at low dose. Butorphanol, a mild sedative modulates some of xylazines potency as well as providing analgesia and euphoria. Ketamine provides our dissociative limb of the combination with its affects of amnesia and catalepsy as well as analgesia. At first glance of this dosage recommendation, it seems a little busy. But if you calculate this dose out for a 1000lb (450 kg) animal you come up with a dose of about:
5mg Butorphanol, 10mg Xylazine, 20 mg Ketamine at the low range, and 10mg Butorphanol, 20mg Xylazine, 40mg Ketamine at the high range.
273

Notice that we are administering about 2X the amount of xylazine as butorphanol, and 2X the amount of Ketamine as Xylazine. The “5-10-20” is good starting point for tame cattle and Brahman cattle. From this starting point we estimate changes in doses administered. We don’t give more than 10 mg of butorphanol, or 20 mg of Xylazine in the initial dose. I personally have given up to 80mg of Ketamine and still maintained a standing patient. If we are going to re-dose during a procedure (try to give 30-40 minutes for the initial dose to fully take effect), then you can re-dose with ½ of your initial Ketamine dose and ¼ of the initial xylazine dose. In general we have noted up to an hour of cooperation from patients using this protocol. As with anything however, the attitude of the patient prevents blanket success, and we have had some go down, but restraint was maintained. Other drug combinations for achieving recumbency or subduing wild patients may need to be used in certain situations. The following combinations are some suggestions that the author has used and feels comfortable with.1
Intramuscular Xylazine – Ketamine: Xylazine (0.05mg/lb (0.11mg/kg)) – Ketamine (2mg/lb (4.4mg/kg)) administered together in one syringe.
Extremely unruly patients may not go down in a timely fashion with this combination without some assistance. The level of anesthesia and analgesia seems to vary remarkably from patient to patient. Additional IV ketamine or “triple drip” (see below) can be administered to enhance the level of anesthesia and analgesia, if needed. Note that when using ketamine in combination with xylazine, it is important to allow sufficient time for the ketamine anesthesia to resolve (30-45 minutes post IM and 15-20 minutes post IV) before reversing the xylazine. Intravenous drips can be used to produce and/or sustain anesthesia. Sometimes severely cold ambient temperatures may necessitate the use of a warm water bath to run the IV line through if used.
Triple Drip – Ruminant (GKX-Ru):
Triple Drip is 5% guaifenesin to which ketamine (1mg/ml) and xylazine (0.1 mg/ml) have been added. The resulting mixture is administered as a slow IV infusion of 0.5-0.75 ml per pound (1.1 – 1.5 ml/ kg) for induction of anesthesia and can be continued at an infusion rate of ~ 1.2 ml/lb/hr (2.6ml/kg/hr). Recovery time will be prolonged with prolonged duration of infusion during the procedure.
Double Drip: Double drip is 5% guaifenesin to which only ketamine (1mg/ml) has been added. Dose at 0.75-1 ml/lb (1.5-2.2 ml/kg) of BW. The benefit is less risk of cardiovascular compromise, but a downfall is a decreased level of analgesia. We commonly use this method for induction prior to starting the patient on inhalant anesthetics. If it were to be used in the field for a compromised patient, an analgesic such as Morphine (0.025 – 0.1 mg/lb (0.05 - .2 mg/kg) IM) or butorphanol (0.025 – 0.1 mg/lb (0.05 -.2mg/kg) IM) could be administered.
274

Telazol-Ketamine-Xylazine cocktail: Instead of reconstiting the telazol with 5ml of sterile water, reconstitute it with 250 mg (2.5 ml) of ketamine and 250 mg (2.5ml) of xylazine. Dose 1ml per 275 lb (120kg) IM. This combination has been beneficial for various proceedures with rodeo bulls. The cocktail can be given IM and recumbency generally occurs within 10 minutes and provides 45 to 50 minutes of proceedure time. The volume of xylazine in this cocktail can become uncomfortably high especially for Brahman influence variation in sensitivity. The author frequently reduces the reconstituted dose of xylazine to 200 mg and increases the dose fo ketamine to 300 mg. Another option is to reduce the initial dose rate by 25% and redose as needed. Conclusion Multimodal overall restraint is enhanced through multimodal chemical restraint techniques. References
1. Abrahamsen, EJ. Chemical Restraint in Ruminants. In; VCNA-food animal practice, Field surgery of cattle part 1. July 2008;24(2):227-243.
2. Griffin, D. Easy halter or foot-restraint rope. Bovine Veterinarian supplement Jan 2009; p19.
Recommended Reading
Fowler ME. Restraint and handlinig of wild and domestic animals, 2nd Edition. Wiley-Blackwell, 1995.
275

Rumen Trouble? Evaluation, Faunation and Surgery
Matt D. Miesner, DVM, MS, DACVIM(LAIM)
Rumen Evaluation for Disease Normal rumen contractions are smooth and consistent with about one to two contractions every three minutes. Succussion of fluid and percussion of “pings” are indicative of rumen indigestion. When the resonating “ping” is due to rumen gas or rumen “collapse” the sound is more like a low pitched “pong” than the typical high pitched resonating ping of a left displaced abomasum. Rumen pongs also tend to remain the same pitch over several moments of evaluation, versus a left displaced abomasum which will commonly change pitch with changes in wall tension as the rumen contracts deep to it. Rumen Fluid Analysis Rumen fluid can be collected through a common stomach tube, double bore tube, or a Derksen® rumen fluid collector. As long as enough fluid (~200ml) is collected to decrease the effects of saliva contamination to offset the actual rumen pH, any method is sufficient. If the rumen fluid pH is around 7.5 to 8.5, saliva contamination has likely occurred or the patient has ingested a high protein source (urea, placenta, etc). Normal rumen pH is between 6 and 7, depending on diet. Rumenocentesis can also be performed through aspiration of rumen fluid in the lower left flank with a 14 – 16 ga needle and syringe. Ruminocentesis is frequently reserved for collection of fluid when many samples are required during herd investigations of disease possibly arising from dietary causes. A smaller volume of fluid for analysis is required as salivary contamination is not a factor in analysis, therefore 10-15 ml is sufficient. A methylene blue reduction test (10ml rumen fluid: 0.5ml newmethylene blue (.04%)) in a capped red top tube is an indication of bacterial flora health in the rumen. The bacteria should reduce the blue color within 8-10 minutes, possibly <5min. Failure to do so within 15 to 20 minutes indicates a dead bacterial population. When rumen pH is less than 5.5 the test becomes much less predictable and valid. A very active diverse group of protozoa should be evident with a fresh drop of rumen fluid evaluated under a microscope. Different sizes of both ciliated and flagellated protozoa should be seen. An indication of carbohydrate overload is observed when there are more flagellated protozoa than ciliates, and a more alkaline rumen environment tends to favor ciliates. High rumen chloride levels can be indicative of a pyloric outflow obstruction or vagal indigestion at the level of the abomasum, allowing backflow of chloride from the abomasum to the rumen. Normal rumen chloride should be less than 30-40mEq/L. Clinical Indications for Rumen Evaluation/Surgery We recognize clinical signs associated with rumen disruption or overt rumen disease and thus indications to target rumen evaluation and associated therapy. Rumen bloat, atony/hypomotility, and indigestion are definitely important and should be readily recognized. However, at this point I feel it is important to recognize that absence of clinical signs (systemic or specific), such as
276

seen in the “failure to thrive” patient or herd, should stimulate the clinician’s interest in focusing on rumen evaluation as a source of the problem. Occasionally, rumen transfaunation is a diagnosed cure for an individual animal with vague clinical signs of lethargy after evaluating rumen contents. Ruminal Tympany (Bloat) Excessive accumulation of rumen fermentation gasses in the form of free gas or a frothy foam that occurs when fermentation rate exceeds eructation rate or ability. A complete inability to eructate occurs with esophageal occlusion (choke, mediastinal masses). Bloat can result from dietary imbalances of carbohydrate and protein as with grain overload or risky forages such as clovers and perennial grasses. Bloat may be primarily neurogenic (vagal indigestion), physical disruption of normal motility (adhesions, abscess, left abomasal displacement), a result of pain induced atony (reticular foreign body), toxicoinfectious (tetanus), drug induced (xylazine, atropine), metabolic (milk fever) and causic irritation. Pre-ruminating calves may be affected with rumen bloat during rumen putrefaction where milk accumulates in the rumen instead of the abomasum. Whatever the inciting cause excessive rumen distention occurs and can become life threatening. Once the smooth muscle of the rumen is stretched too far, motility is further inhibited and therefore relieving the distention will allow rumen motility to return in some cases. Passing a oral-rumen tube to attempt decompression is the frequently the first therapeutic step when the clinician is presented with a case of bloat. Free-gas bloat in the absence of esophageal obstruction is easily relieved in this manner, whereas frothy bloat is not. Evaluation of the contents of the tube after being withdrawn from the rumen should be performed to attempt classification of potential inciting causes for disease. Animals that are severely bloated and recumbent often require rumen trocarization to relieve the bloat, and escaping fluid from the trocar should be analyzed as well. Rumen Impaction During physical examination, palpation of the left paralumbar fossa or rectal palpation of the rumen reveals a firm or “doughy” rumen. Frequently, during right paralumbar exploratory surgery for other diseases (ex LDA), a firm or “impacted” rumen is detected. Usually the cause for decreased fluid and apparent increased solids within the rumen is dehydration, where simply rehydrating the rumen by oral fluid administration is sufficient for therapy. If one suspects a specific dietary indiscretion, investigate further through signalment and history given by the owner. Rumen foreign body (ex baling twine or plastic bag) should be included in the differential list. Rumen fluid evaluation is difficult as collection is hindered by the lack of fluid within the rumen. Succussion of Fluid in the rumen This is a frequently overlooked physical examination technique. Placing the bell of the stethoscope over the left mid-flank and vigorously compressing the abdominal wall during auscultation may reveal the sounds of fluid sloshing within the rumen. This physical finding indicates a disturbance in the normal rumen environment, with loss of the fiber mat layer. Loss of the fiber mat within the rumen allows fluid to slosh back and forth and radiate fluid sounds during auscultation. This finding may indicate a simple indigestion which frequently accompanies a lack of systemic clinical signs of disease. Succussion of fluid with systemic
277

disease indicates indigestion due to a separate primary problem such as traumatic reticulitis, LDA, acidosis, ketosis, etc. Rumen fluid is easily collected for evaluation. Abnormal transabdominal ultrasound findings A valuable diagnostic tool for evaluating rumen pathology/reticulitis/peritonitis is the use of ultrasound. Scanning the ventral thoracic/abdominal region left and right of the sternum dorsally to the level of the elbows is performed. Using a 7.5 MHz linear probe, which is commonly used for reproductive ultrasound, will allow visualization of the proximity of the reticular rumen wall and motility, but limits depth of penetration. If a 3.5 MHz probe is available, depth and clarity is much improved and visualization of the ruminoreticular groove (left of midline) and the omasum, abomasum and the liver can be visualized from midline to right paramedian respectively. Stationary viewing of the reticular-rumen motility reveals potential adhesions, fibrin formation and potentially abscessation between the peritoneum and forestomach viscera. For a more complete review:
1. Braun U, Iselin U, Lischer C, et al. Ultrasonographic findings in five cows before and after treatment of reticular abscesses. Vet Rec, Feb 21, 1998;142:pp184-189.
2. Braun U. Ultrasound as a Decision-Making Tool in Abdominal Surgery in Cows. VCNA;Food Animal Practice. 2005 (March); 21(1), pp33-53.
Reduced production parameters or increased incidence of disease at the Herd level. An overall decrease in average milk production, increased lameness, increased incidence of metritis/mastitis in dairy cattle may stem from dietary intake. Increased bloat incidence, diarrhea, lameness, etc in intensively fed cattle populations such as feedlots may stem from dietary intake. Feed analysis should be performed and further classification of disease can be performed through evaluation of rumen contents. Therapy for Rumen Disorders Transfaunation Transfaunation is the removal of ruminal fluid and microbes from one animal, and the transfer of that material to a different animal. Attempts to diagnose the primary cause of abnormal ruminal flora in the patient should be made and possibly corrected prior to transfaunation. The rumen environment must be receptive and conducive to microbial life prior to introduction of new microbes. Rumen Trocarization Relief of bloat when life threatening emergency arises can be performed by trocarizing the rumen with designated rumen trocars. Blindly puncturing the rumen percutaneous will relieve the accumulated gases (unless frothy in nature). However as the free gas escapes, the rumen wall retracts form the peritoneum and away from the trocar allowing rumen fluids to contaminate the abdomen causing peritonitis. If a trocar is used, it is recommended that a type that engages the rumen wall to “fix” it to the peritoneum is used. An alternative method is described below to be used when time allows or in cases of recurrent chronic bloat.
278

Oral Anti-foaming agents and fluids. Frothy bloat occasionally requires emergency rumenotomy (see below). When time allows, or in cases of recurrent bloat, rumenostomy may be a better choice. Initial medical therapy by ororumen drenching of emulsifying (anti-foaming) agents should be attempted. Anti-foaming agents to break up air bubbles in the foam include poloxalene, dioctyl sodium sulfosuccinate, and oils (mineral or vegetable). Use caution when using oils in bloated animals as aspiration pneumonia during regurgitation can result. Surgery of the Rumen. Rumenotomy and Rumenostomy are frequently performed. Rumenotomy refers to opening the rumen for temporary exploration of its contents. It is performed when removing rumino-reticular foreign bodies (“Hardware”) or abnormal rumen contents (froth, excessive carbohydrates, toxins), and/or lancing peri-reticular abscesses into the lumen of the reticulum. Rumenostomy refers to surgery to achieve prolonged (technically permanent) communication between the rumen lumen and outside world. Rumenostomy is performed when installing a rumen cannula, cases of recurrent bloat, and also a portal for enteric nutritional support. Rumenostomy for relief of recurrent bloat or temporary nutritional support, will often be allowed to close by second intention. Rumenotomy. A left flank laparotmy is performed intially to provide exploration of the abdomen and reticulo-rumen as well as approach for rumenotomy. Little visualization of the abdominal contents can be achieved, however palpation of the right and caudal abdomen should be performed. In addition, palpation of the reticular surface should be done to detect areas of inflammation or adhesions. The laparotomy incision is approximately a hands width (8-10cm) caudal to the last rib and about 15 cm below the transverse processes of the lumbar vertebrae. The length of the laparotomy incision is approximately 15-20cm, or such that the surgeon can comfortably insert their arm for exploratoring the abdomen. Attempt to palpate the medial side of the reticulum between the omasum for a peri-reticular abscess as this is a common location of abscess formation and would need to be drained into the reticular lumen after the rumenotomy is performed. The rumenotomy can be performed by first securing the dorsal sac of the rumen to the skin. A continuous inverting suture pattern is efficient and secure. The author prefers to use #2 or #3 braunamid suture to secure the rumen with hemi-circumferential runs in a continuous inverting pattern. The outer skin will contact the rumen serosa when finished. It is important to protect the muscle layers and abdomen from contamination of the rumen contents. Another method described is by using a rumen board to temporarily attach the rumen serosa, however this technique limits the extent one can reach cranially toward the reticulum in larger cattle. After the rumen is secured to the skin, incise the rumen wall sufficiently to allow the surgeon’s arm to enter the opening. Exploring the rumen may begin with removal of sufficient contents to facilitate exploration and explore the fiber contents for trapped foreign material. Next, locate the reticulum by following the dorsal wall of the rumen into the reticular lumen which has a unique “honeycomb” mucosa. Grasp the reticular mucosa and “roll” it between your fingers. Often reticular foreign bodies
279

become embedded within the mucosa and deep palpation is required to locate them. Attempt to palpate the esophageal reticular orifice and the reticular-omasal orifice. Palpate the medial wall of the reticulum for swelling ventral to the reticular-omasal orifice and areas where the omasal mucosa is “smooth”. As mentioned before, peri-reticular abscesses commonly form in this area and drainage of the abscess into the reticular lumen is to be performed. Close the rumenotomy site using a one to two layer inverting suture pattern with absorbable suture. Often, we close the first layer initially followed by a second layer staged during release of the skin sutures which allows a more thorough closure. Close the abdominal wall and skin in normal fashion. Rumenostomy By definition, a rumenostomy would imply surgical formation of a permanent rumen fistula. This is best described during insertion of a rumen cannula for easy access to rumen contents for research purposes or occasional transfaunation procedures in other patients. Rumenostomy for Cannula placement Placing a rumen cannula is often performed in practice to allow access to rumen contents for transfaunating patients that can benefit from renewed rumen nutrients. The implant is inserted into a rumenostomy site per manufacturer’s instructions. The centerpiece of the implant can be removed and replaced after rumen contents are collected. (See attached reference below). Rumenostomy for bloat therapy Rumenostomy can also be performed as a therapeutic option for bloat, particularly recurrent bloat. The procedure is safer than blind rumen trocarization as there is less risk of abdominal contamination and peritonitis. Many clinicians that perform this procedure have described different preferred techniques. The goal is to pexy the rumen to the body wall to prevent contamination of the abdomen but that is large enough to allow excess gas to escape yet small enough to potentially close by second intention over an extended period of time. The author will describe his technique in this text. An approximately 2-3cm elliptical skin incision is made and the skin is removed. A small elliptical section of the external abdominal oblique muscle is also excised. The internal abdominal oblique and transversus abdominus muscles and peritoneum are incised in a grid fashion. The rumen wall is then pexied to the external abdominal oblique muscle using absorbable suture material in an interrupted pattern to sufficiently prevent abdominal contamination of draining rumen contents. The rumen wall is then incised and sutured at four points to the skin. What should happen is when the rumen gas accumulates in excess, the fistula opens to allow gas to escape and closes when the rumen collapses. Often the fistula closes over a period of weeks to months as the animal’s recurrent bloat resolves. Rumenostomy for nutritional support Providing nutritional support is possible through rumenostomy. This can be done in animals with conditions preventing normal feed consumption, such as mandibular fractures and
280

esophageal trauma. The procedure is similar to rumenostomy for bloat therapy described above, however, a larger fistula is formed to accompany tube placement of sufficient diameter to pass processed feedstuffs. To limit trauma or disruption of the intial surgery site, a 12cc or 20cc syringe case can be cut and fixed into the rumenostomy site to allow frequent passage of the feeding tube. Rumen Canulation. * For full length article on rumen cannulation, and step by step photographs, refer to the following reference. * Laflin SL, Gnad DP. Rumen Cannulation: Procedure and Use of a Cannulated Bovine. VCNA, Food Animal Practice. 2008 (July); 24(2);335-340.
Rumen cannula Variable models and sizes of rumen cannulas are commercially available for use. The use of a flexible rumen cannula will be described within this discussion. The flexible cannula allows for slight growth in the individual, wear easier, and are easier to place and replace in my opinion. Cannulas are available in different sizes and should be matched to the potential donor. Guidelines are often available from the manufacturer. Submerge the cannula in hot water to make it more pliable for manipulation. Although actual insertion may vary, surgical approach and preparation will not vary for different brands of flexible cannulas. Within the context of this discussion, preparation and usage of the Bar Diamond (Bar Diamond Company, Parma, ID) cannula is considered. Complete instructions are supplied with the cannula.
Pre-surgical preparation of the donor Hold donor off feed (24hrs) and water (12hrs) prior to surgery, to facilitate cannula insertion and lessen contamination Standing surgery of the left paralumbar fossa is clipped and surgically scrubbed. A local paravertebral or inverted L block with 2% lidocaine is applied. Light sedation may be helpful in some cases but not necessary. Pre-surgical, broad-spectrum antibiotics and non-steriodal antiinflammatories are recommended. Post-operative antibiotics are also preferred for 5-7 days.
Surgical technique The appropriate area for the fistula is in the upper middle part of the left paralumbar fossa, approximately 4-5 inches ventral to the transverse processes. Appropriate positioning will allow for the outer ring of the cannula to be confined within the paralumbar fossa (transverse processes, rib and the tuber coxae). A circular area of the skin approximately 0.5 inches smaller in diameter than the inside diameter of the cannula is excised. It is helpful to use a template and mark the area prior to beginning the excision to prevent improper fit of the cannula and potentially terminal consequences for the potential donor. Finish the abdominal approach by “gridding” of the abdominal oblique and transversus abdominus musculature parallel to the respective muscle fibers. This approach allows for a more
281

form fitting mold of the abdominal wall after placement of the cannula. Carefully incise the peritoneum avoiding the rumen, enlarge the peritoneum manually to the size of the muscular opening. Grasp the rumen with sterile 4 X 4 gauze pads or suitable tissue forceps and exteriorize the rumen wall through the laparotomy site. Sometimes with a taught rumen wall, a stay suture or two will help exteriorize the rumen. Horizontal mattress stay sutures are placed at the 12, 3, 6 and 9 o’clock margins of the incision to secure the rumen to the body wall. These stay sutures are placed partial thickness through the rumen wall and full thickness body wall to prevent possible contamination of the surgery site. The sutures should be far enough from the periphery of the cut edge of the skin and rumen to allow room for unhindered rumen mucosa to skin apposition. I prefer to leave these sutures in place and remove them one week after surgery. The rumen wall is then exteriorized to encompass an area approximately equal to the inner circumference of the cannula and allow for complete circumferential suture placement without putting tension on the rumen wall. Begin suturing the exposed rumen mucosa to the skin margin in an everting fashion (mucosa to skin). Incise a small portion of rumen and suture sequentially to avoid excess exposure and contamination. Continue until the entire circumference in completed.
Once the rumen has been sutured to the skin, the cannula is placed into the surgery site after removing it from the hot water bath. Evert ½ of the inner flange to form a conical shape to place through the rumenostomy. After placement, reach into the center of the cannula and replace the flange to its original shape within the rumen. Finally, insert the stopper into the cannula.
Post-operative care
The surgical site and the surface of the cannula’s outer rim next to the skin should be cleaned daily for five to seven days with a dilute antiseptic solution. Don’t remove the cannula daily to do this. Approximately 10 days post-surgery, remove the cannula by reaching through the center of the cannula and pulling the inner flange into the center. A necrotic ring of rumen tissue and any remaining suture material should be removed from the edge of the fistula. Once the wound is cleaned, the cannula is replaced. Clean the area every couple of weeks for a couple of months after that. The wound should be protected from flies, and a broad spectrum antibiotic should be administered for seven days following surgery.
Application
One quart (~1L) of rumen fluid is adequate to transfaunate ruminating calves, and a minimum of three quarts (~3L) should be administered to adult cattle.1 Rumen fluid for transfaunation purposes can be obtained from an abattoir or from a cannulated animal. Transfaunate is best when used immediately following collection, but contains viable organisms for up to nine hours at room temperature, and for 24 hours if refrigerated. Be sure to keep in containers which allow excess fermented gas to excape to avoid rupture of the container.
1. Garry F: Diagnosing and treating indigestion caused by fermentative disorders. Vet Med 1990; June 660-670.
282

Problems and Solutions of the Teat and Udder
Matt D. Miesner, DVM, MS, DACVIM(LAIM)
ANATOMY See slides 1 and 2 at the end of text The Teat : (Teat wall, Teat Cistern, “Rosette of Furstenberg, Streak canal, and Teat Sphincter) 5 tissue layers compose the teat wall, and are: (beginning with most superficial layer)
Stratified squamous epithelium Muscular layer (circular and longitudinal) Connective tissue (highly vascular) Submucosa Mucosa
The Teat Cistern is surrounded by the wall and is a continuation of the gland cistern. It begins proximally at the annular ring or vascular ring which is a large vein surrounding the teat at the base, and ends distally at the streak canal. The Rosette of Furstenberg is created where the teat cistern mucosa meets the stratified squamous epithelium of the streak canal. The Teat sphincter lies deep to the rosette. The streak canal, also known as the papillary duct, is less than a centimeter long and ends at the teat orifice. The Udder: Blood Supply and Support Vascular supply and drainage. Cranial and caudal quarters of each side share blood supply from their respective pudendal arteries, and drain from their respective veins. Blood supply to the teat is oriented in a vertical manner.
External pudendal artery which branches into the cranial and caudal mammary arteries.
Perineal artery (minimal supply) Venous drainage is from the Subcutaneous abdominal veins
(milk veins), external pudendal veins and the perineal veins. Support structures are the medial and lateral suspensory ligaments of each half of the udder. TEAT AND UDDER ABNORMALITIES Always evaluate the gland cistern in conjunction with teat abnormalities. It doesn’t matter what you do to the teat, if there is severe glandular fibrosis there will be no milk to get out of the teat. Supernumerary teats. This is the most common congenital anomaly. The teat is not functional, but a mere blemish and is not attached to the mucosa of the primary teat of that quarter. The supernumerary teat is frequently removed, not only for cosmetics, but to maintain a proper fit of the milking claw and prevent mastitis. Preferably, removal is
283

done when the animal is 4-6 months of age and removed with scissors. If the patient is older, but not springing, use an emasculatome prior to sharp removal to control hemorrhage. Springer heifers and mature cows should be left alone until dry off, or surgically removed and sutured. Care should be taken to avoid damage to the underlying gland cistern. The elliptical incision around the teat with the long axis of the ellipse oriented cranial-caudal should be made. Suture subcutaneous tissue and skin separately. Conjoined (“Web”) teat. This is a supernumerary teat that is conjoined with the primary teat mucosa. A web teat may or may not have a teat orifice and its own glandular tissue. The entire web teat needs to be removed to the primary teat cistern and/or any separate glandular tissue. The surgical incision should be an elliptical incision oriented with the long axis of the primary teat. The resulting surgical wound into the primary teat cistern must be closed in three layers. Distal Teat obstruction. This usually just refers to atresia (imperforate skin) at the distal end of the teat when seen in heifers. When attempting to express milk, a bulge of tissue is noted at the teat orifice. Correction is simple by cutting the tissue with a 14 gauge needle or a #11 scalpel blade. Express the teat well. Have the milker roll the teat end with fingers for a few days at milking time. Teat Cistern Obstruction. Refers to fibrosis or scaring within the teat cistern possibly due to previous trauma or congenital atresia. Be sure to check the quarter for congenital atresia as well “Blind Quarter”. This also occurs in heifers due to heifer/calfhood mastitis or pre-milking trauma. Evaluate the extent of scarring with ultrasound. A small scar may be relieved through the teat orifice. More often a thelotomy is performed to remove the defect more thoroughly. Close the mucosa where the defect was removed and follow with a three layer closure of the thelotomy site. A large amount of scar tissue may require a teat implant to maintain patency of the teat cistern. A teat implant is made by sterilizing a section of plastic tubing (ie nasogastric tube). The tube is then sutured into the teat cistern prior to closure. Basically it becomes a stent for the teat cistern. Annular Ring Obstruction. This can be a thin membrane separating the gland cistern from the teat cistern that can be corrected through the teat orifice by making an “X” incision in the membrane. Do NOT cut too deep which may result in lacerating the vascular ring. More often the obstruction is a thick band of tissue requiring a thelotomy and teat implant. Tight Teat Sphincter (“Hard Milker”) SEE slide 3 below. “Hard Milker” is a term generally refers to difficulty expressing milk from the teat as a result of teat-end trauma. Trauma may have been self inflicted or a result of malfunction or maladjusted milking machines. Teat dilation devides are available for attempting to stretch the streak canal and distal teat cistern. Surgical enlargement of the teat orifice yields better results when done properly. Remember that you want to preserve the keratin lining of the streak canal. Perform surgery prior to morning milking if possible. Insert a teat knife (Ex. Lichty Teat knife) through the orifice to the rosette of Furstenberg, angle 45 degrees and cut outward while withdrawing the knife. Assess progress by forcefully milking teat to determine
284

flow. May need to make a second incision at 180 degrees to the first cut, repeat at 90 degrees for third and fourth cut. Before making each cut, evaluate flow of milk. You do not want to overly enlarge the teat orifice. A rule of thumb for knowing when to stop is when the teat end drips a small stream of milk for a minute or two after forcefully milking the teat. Strip the teat every 15 to 30 minutes for the next three hours and then once every hour until the next milking. Enlarged Teat Orifice. Usually a result of overzealous cutting when treating a “hard milker” (see above). Difficult to treat successfully. Attempts can be made to cause swelling in the submucosa of the teat by injecting iodine solution, however success is difficult to achieve without detrimental side-effects. Teat Fistula. Fistulas involving the teat can occur for several reasons: Congenital, inadequate healing after trauma (ie laceration) or incomplete closure after thelotomy. When attempting repair of the fistula, first resolve any infection/mastitis that may be present. Surgically excise the fistula similar to web teat removal. Dissect the fistula to the mucosa of the primary teat. Close the defect with a three layer closure. Teat “Spider”. (Mass of Scar tissue in teat cistern preventing flow of milk) The scar tissue is a localized mural mass that may or may not be pedunculated. The mass protrudes from the mucosa and impairs flow of milk in the teat cistern. Occasionally the scar tissue is a freely floating mass of tissue within the cistern. The scar tissue results from trauma, either acute or chronic (improper milking). Removal through the teat orifice is difficult and often unrewarding. The aid of theloscopy can facilitate removal of pedunculated masses or free floating tissue. Broadly attached mural masses are best removed through thelotomy. TEAT LACERATIONS Pre-Treatment Evaluation Ask yourself three simple questions to assess feasibility and prognosis: Duration? Thickness? Orientation?
1. Duration? For primary closure to be a feasible option, it must be attempted within the first 2-3 hours. There is little room for debridement, therefore the cut edges must be fresh.
2. Thickness? If the laceration enter the teat cistern at any point, the mucosa must be closed to prevent a fistula from forming.
3. Orientation? Horizontal or circumferential lacerations will greatly affect blood supply to the laceration during healing.
Treatment Technique Anesthesia and restraint can usually be done with local lidocaine infusion (ring block at base of teat) and light sedation. Rarely is one case identical to the next. Repair should therefore follow principles rather than rules. Asepsis, tension relief and accurate apposition of teat wall layers (i.e. mucosa, sub-mucosa and skin must appose accurately). Therefore a three layer closure is recommended. Continuous patterns of absorbable suture for the mucosa and sub-mucosa, followed by a tension relieving interrupted pattern
285

with soft non-absorbable suture in the skin. Often three separate layers cannot be identified due to the nature of the trauma that occurred. A one or two layer appositional suture to re-appose the cut edges initially with the intent on a second repair implied is quite all right. Post-operative care It is generally recommended that the teat receive little manipulation after the repair. Mastitis resulting from the contaminants that inoculated the teat during trauma is possible, therefore one would want to continue to milk the cow or cannulate the teat frequently to drain the contaminated udder. However, it is best to balance drainage of the udder with allowing the inflammation and edema at trauma site to subside to promote healing. Therefore, a “3 X 3 X 3” protocol is often followed post-operatively as follows: Step 1: Repair the laceration and drain the quarter with a teat cannula. Step 2: Infuse the quarter with approved intra-mammary antimicrobial. Step 3: Insert teat canal implant and bandage teat. Don’t remove bandage for 3 days unless outward appearance of mastitis Step 4: At Day 3 remove bandage and GENTLY drain quarter with teat cannula, infuse quarter with intramammary antimicrobial. Reapply bandage and implant. Step 5: Repeat Step 4 on Day 6 and Day 9. Finally: Milk cow as usual. Remove skin sutures on day 14. TEAT AMPUTATION See slide 4 below Occasionally the trauma to the teat is irreparable or continuous drainage of an affected quarter is the only option for treatment. Therefore, amputating the teat provides continuous ventral drainage and the quarter will eventually dry off. This procedure can be done by first using a crushing instrument (such as an emasculatome) then suturing the remaining teat open for continuous drainage and hemostasis. Some veterinarians don’t suture, but fatal hemorrhage has resulted. UDDER AMPUTATION Merely a large mass removal An elliptical incision is begun on the lateral side of the udder, through skin, subcutaneous tissue and lateral suspensory ligaments until the external pudendal artery and vein can be isolated. First, ligate the external pudendal artery it exits the inguinal ring, then ligate the external pudendal vein. The external pudendal arteries and veins can be ligated together but the chance of forming an arterio-venous fistula is a potential concern. Repeat the pudendal ligation on the opposite side. Continue the incision around the udder cranially and ligate the subcutaneous abdominal veins and their branches. Continue posterior and ligate the perineal arteries and veins. Remove the remainder of the udder from the body wall by cutting the median suspensory apparatus. Leave about 1-2 cm of median suspensory ligament attached to the body wall.
286

Close the defect with one layer of tension relieving sutures. The author prefers intermittent #6 braunamid using a vertical mattress pattern, followed by a forward interlocking pattern with the same suture material. If you have left 1-2 cm or so of median suspensory ligament attached to body wall you can anchor the central part of the defect to it to decrease dead space and tension. Place a drain between the skin and abdominal wall prior to closure. One layer skin closure is all that is needed, utilizing a tension relieving pattern. PHYSIOLOGIC MASTECTOMY Refer to reference below By ligating the blood supply to the udder, the effect will be controlled avascular necrosis and tissue will slough. This is a salvage procedure to remove the severely infected udder and prevent the infection from causing life-threatening illness in the cow. There are a few described techniques for performing this procedure. I will discuss a standing technique developed by Professors at Washington State University College of Veterinary Medicine (Parish SP, et al) for use in cattle. The procedure is performed through a flank incision and the external pudendal arteries and veins are ligated as they enter the inguinal ring. This is a blind suture technique done by palpation.
287
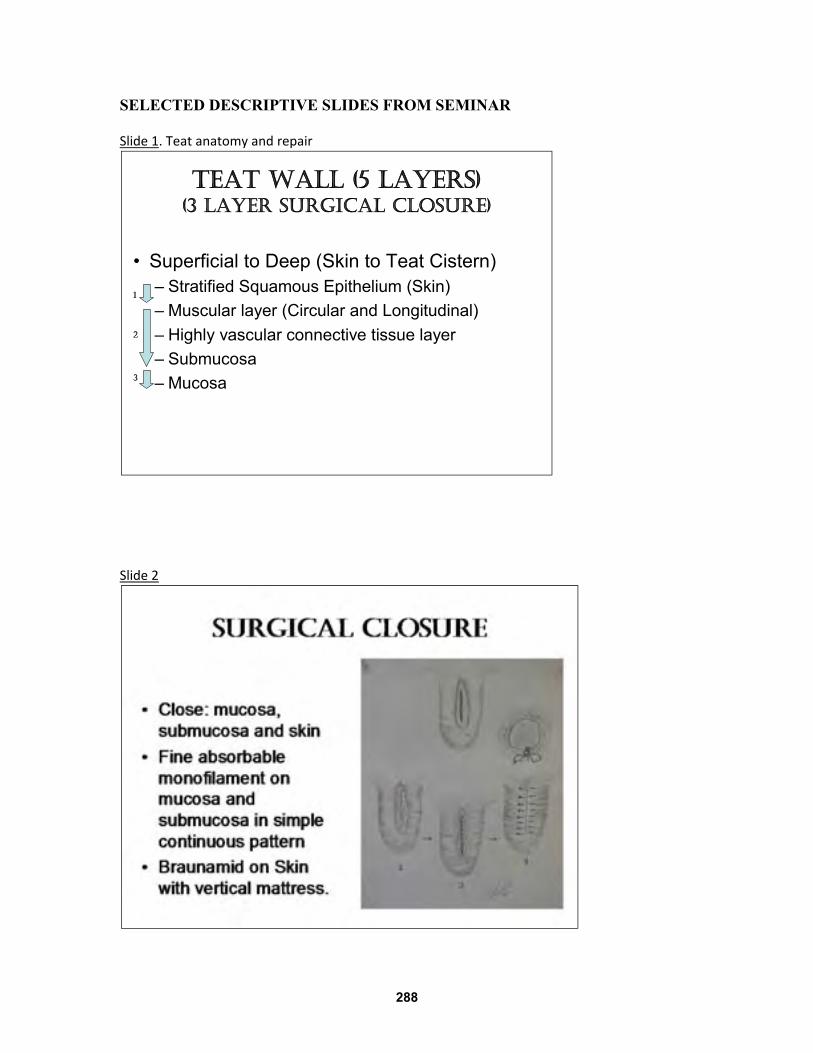
SELECTED DESCRIPTIVE SLIDES FROM SEMINAR Slide 1. Teat anatomy and repair
Slide 2
TEAT WALL (5 LAYERS)(3 LAYER SURGICAL CLOSURE)
• Superficial to Deep (Skin to Teat Cistern)– Stratified Squamous Epithelium (Skin)
– Muscular layer (Circular and Longitudinal)
– Highly vascular connective tissue layer
– Submucosa
– Mucosa
1
2
3
288
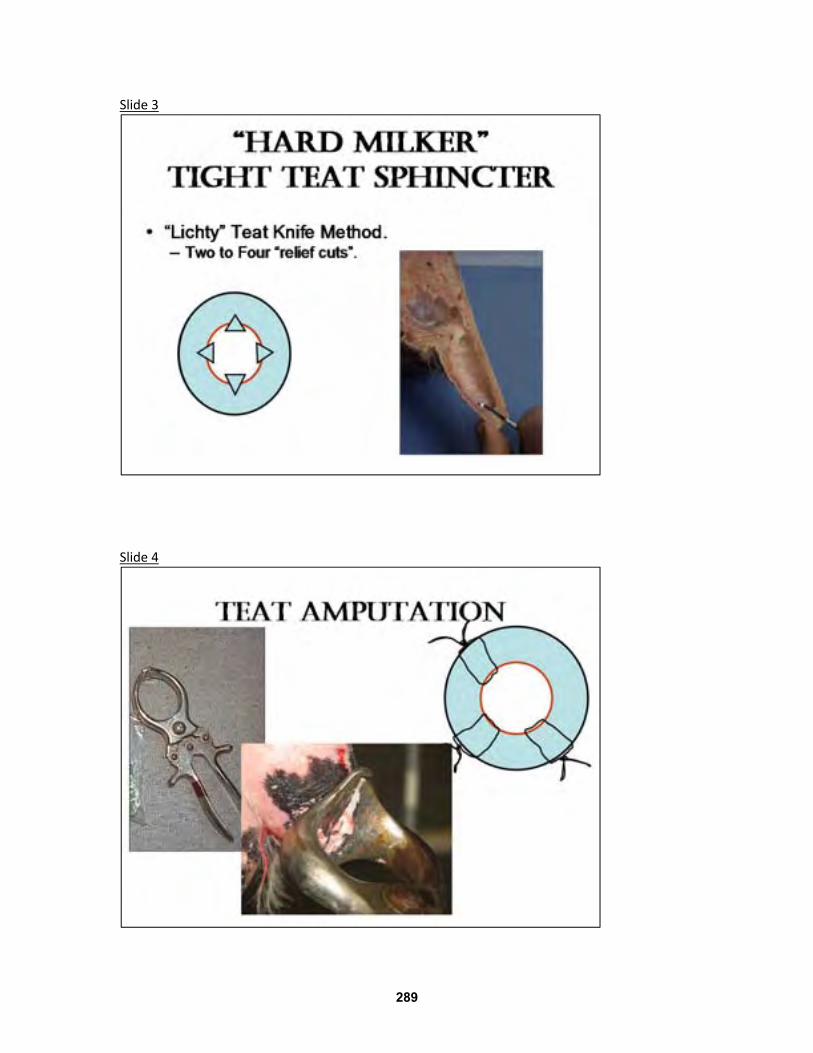
Slide 3
Slide 4
289

Surgical Lameness of the Bovine Distal Limb
Matt D. Miesner, DVM, MS, DACVIM (LAIM)
Bovine Distal Limb Lameness A vast amount of information regarding clinical conditions of the hoof, from which roughly 90% of lameness arises, exists in the literature. Sole ulcers, sole abscesses, papillomatous digital dermatitis and interdigital phlegmon (foot rot) are the most prevalent. The 2002 NAHMS survey reported that digital papillomatous dermatitis (PDD or hairy heel warts) was the caused 50% of the lamenesses diagnosed in the United States. Interdigital phlegmon and PDD are considered to be conditions resulting from primary infectious causes and poor environmental hygiene rather than mechanical causes. Claw disorders such as sole hemorrhages, ulcers, abscesses, and cracks appear to be affected primarily by mechanical forces such as interactive ground pressures and abrasive surfaces. Though cause and effect has yet to be proven, an association exists between type of flooring and claw health and hoof horn lesions. The effects of flooring on claw health have to be evaluated in light of management, genetics, nutrition and physiologic states that also influence claw health. Afterall, we still see these lesions in beef cattle on pasture and drylots. Claw horn health, growth, and wear characteristics can differ based on the hydration state of horn tissue, biotin level in the diet, footing type, and hardness of the hoof horn.4 Phenotypic or genotypic expression of pigmented hoof horn has been debated as a factor of hoof horn disease resistance. Many consider that pigmented horn is more resistant to disease than non-pigmented horn. A case-control study on lameness, comprising 62 dairy herds in New Zealand, found the prevalence of lameness and the percentage of cattle with non-pigmented hoof horn to be positively correlated. A correlation also existed between lameness and herds with the fewest number of Jersey cows, a breed with pigmented hoof horn.5 Pigmented horn has been shown to be negatively correlated to sole bruising.6
However, sole contusions would also be more difficult to detect in dark horn than lighter colored horn. Hardness of the hoof may be more dependent on hydration status, mineral composition, and other environmental factors rather than pigment based on previous observations.4
Studies of the gait and weight distribution over the claws of cattle have been performed for decades, though early instrumentation was technically limited. Literature regarding the pressure distribution differences between claws is limited and none exist comparing potential differences between breeds. It is widely accepted that cattle bear the majority of the weight on the medial claw of the front feet and the lateral claw of the hind feet. More recent evaluations of pressure distributions, reinforced the substantiation of pressure difference between the medial and lateral claws in both standing and walking cattle.7,8 Location of lesions within the claw may also represent overloading of specific regions of solear or hoof wall areas.
290

Relevant claw anatomy and physiology Structure and Function Hoof horn is produced from a germinal layer (epidermis) which is supported by its corresponding dermal layer (corium). The horn making up the hoof capsule is not consistent with respect to hardness, consistency and appearance. This is due to the fact that there are four different regions of corium within the hoof capsule and each region makes a functionally and structurally different type of horn.
The claws house the distal phalange and the distal interphalangeal joint of the third and fourth digits. The three layers of the claw are the horn wall, corium, and the coronary/digital cushion, which correspond to the epidermis, dermis and subcutis respectively. Only two regions of the claw have a subcutis layer, the region beneath the perioplic (coronary) corium and the region below the sole and heel corium, also known as the digital cushion. The digital cushion, which is comprised of three fat cylinders, aids in shock absorption during locomotion, as well as movement of the distal phalange.
The corium does not produce horn, but provides support and vascular nutrition to the stratum basale and stratum germinativum. The blood supply is a vast and intricate network of paired arterioles and venules, each connected to an extensive capillary bed, arranged to interdigitate with its respective epidermis. This interdigitation is also referred to as a vascular peg. The vascular pegs are arranged perpendicular to the solear surface in each region. Keratinocytes of the basement membrane in each anatomic epidermal region of the hoof are responsible for horn production. The cells are adhered together tightly by a cell membrane coating substance, giving them enhanced stability and moisture resistance. Arrangement of the cells is either tubular (from the apex of the vascular peg) or intertubular (between tubular horn) in all regions other than the laminar epithelium which is thus termed laminar horn. The tubular horn is the strongest, followed by the intertubular horn and the laminar horn is the weakest. The horn of the sole and the heel have approximately one-fourth the tubular density as the wall.
291

The healthy claw is quite resistant to damage or disease. Alterations in weight bearing surfaces of the claws, flooring types, metabolic diseases, and dietary nutrients can disrupt the anatomical structures or the processes of horn growth discussed above. Rates of keratinization and horn production can differ between regions of the claw and faster rates can be associated with vascular damage, particularly in the white line. Bearing an excessive amount of weight on individual claws, the “overburdening of the pododerm” theory, may increase the rate of horn growth, predisposing to keratinization disruption and/or mechanical alteration leading to further trauma. Metabolic and traumatic causes of poor hoof horn quality and disease likely are linked. For example, changes in the suspensory apparatus resulting in instability and sinking of the distal phalange to the inner hoof wall occurs in recently fresh cattle without clinical signs of laminitis. Sole (Rusterholz) ulcers, or “typical” ulcers occur in the posterior sole region of the hind lateral claw. Occurrence is believed to be from damaged corium leading to solear hemorrhages and eventual ulceration. Controversy exists as to whether there is a primary laminitis event, from any metabolic alteration, leading to sinking and rotation of P3 or if the cause is due to degeneration of the digital cushion.9,10 Investigators admit that continued research is needed to determine cause and effect.
Corium Region Location Type of Horn Notes Perioplic Skin-horn junction
(cornonet) and extending to the hell bulbs
Soft, pliable horn Susceptible to environmental challenges resulting in heel erosion
Coronary Just distal to the perioplic corium at the coronet.
Hardest horn in the hoof capsule.
Grows at approximately ¼ in. per month.
Solar Sole Medium hardness ~ 1/8 in. per month Lamellar Horn of the white
line, derived from sensitive laminae.
Soft and flexible. “Suspensory apparatus” for coffin bone. High turnover rate.
Relevant distal limb anatomy and pathology Knowledge of the anatomic location of muscle-tendon units, osseous/joint structures, and neurovascular anatomy of the distal limb is imperative for successful evaluation and treatment of lamenesses arising within the claw (ex coffin joint) and above the coronary band (ex septic tenosynovitis). Intravenous regional anesthesia (Baer Block) is frequently performed to anesthetize the distal limb for therapeutic intervention, but can also be a useful tool for localizing lameness when obvious lesions are undetected during exam. The procedure is performed by placing a tourniquet below the carpus/tarsus and injecting local anesthetic intravenously distal to the tourniquet. Any vessel distal to the tourniquet can be utilized, the goal is to inject enough anesthetic into the vessel that it will diffuse from the occluded area to surrounding local structures. The author prefers to use the dorsal axial common digital vein which is located between the claws distal to the fetlock and proximal to the
292

interdigital cleft. This is a “blind” stick as you cannot visualize this vessel. However, often severe swelling/ cellulitis prevents visualization of any of the vessels of the distal limb. Septic Coffin (P-3) joint. Infection within the joint may arise from direct trauma, penetrating wounds, hematogenous, or extensive local infection (ex interdigital disease or untreated sole abscess). Lameness is very pronounced. Surgical drainage of the joint and debridement of the affected bone and cartilage which facilitates the goal of Ankylosis of the joint is indicated. Elevating the unaffected claw with a hoof block will alleviate pressure on the affected claw. Claw amputation may be performed in animals not intended to be retained in the herd for longevity. Facilitated Ankylosis preserves stability within the distal limb once the joint is fused but requires longer duration of treatment. Coffin bone (P-3) fractures. Often occur in conjunction with infection, however can occur spontaneously. Fluoride toxicosis (fluorosis) may be a cause for apparent outbreaks of P-3 fractures in cattle. Treatment of P-3 fractures in cattle is often as basic as elevating the unaffected claw with a block. Occasionally, casting or wiring the claws together is needed to decrease motion and pain until the fracture heals sufficiently (3-4 weeks). Navicular bursitis involves inflammation within the navicular bursa. The lameness is very pronounced and may occur concurrently with a septic coffin joint. Again surgical drainage and debridement (sometimes the entire navicular bone) is indicated. However the deep digital flexor tendon is often damaged severely, resulting in abnormal weight bearing and hoof growth in the affected claw. Septic flexor tenosynovitis. Can be an extension of hoof sepsis. Diagnosis is facilitated by use of ultrasound. Therapy is aimed at tenovaginotomy (opening the tendon sheath) for drainage and lavage of the flexor tendon sheath. Often the infection is unilateral. Making two incisions dorsal and distal to the dewclaw will facilitate lavage. Septic physes. On multiple occasions I have encountered septic or inflamed growth plates of the distal metacarpal or metatarsals. This can occur in young growing cattle that are pushed hard on feed for growth recognized by flaring/widening of the physes on radiographs. Limited concentrate feed management can be curative in many of those cases. Hematogenous seeding and trauma to the distal limb may lead to sequestration or sepsis within the physis. The condition presents a confusing picture with significant lameness and often little swelling. Swelling may be diffuse around the fetlock joint. Radiographs are needed, focused over the physis. In cases of sepsis or trauma with sequestra, the area needs to be debrided and lavaged. Casting may be required and elevated hoof block applied to non affected side with unilateral disease. Distal limb Fractures. Growth plate fractures often occur in calves and the distal metacarpal/metatarsal physis. Simple re-alignment and casting for 3-4 weeks is often curative due to the characteristics of the growth plate. Mid diaphyseal metatarsal fractures can often be successfully casted due to the angles and shared forces of the
293

hindlimb. Metacarpal fractures are more difficult to successfully cast due to the straight column of bone and compression and rotation exerted directly onto the fracture site. Metacarpal fractures often require a “pin-cast”, where intramedullary pins are inserted proximal to the fracture site then incorporated into a cast. It is important to note that when casting, the cast should extend completely to the ground and incorporate the hoof. Hoof Growth Defects. Review the following references for hoof trimming techniques. The topic is too vast to cover within the allotted time of this seminar.
1. Toussaint Raven E: Cattle Foot Care and Claw Trimming, Ipswich, UK, Farming Press. 1989.
2. Shearer JK, van Amstel SR. Functional and Corrective Claw Trimming. Vet Clin N Am; Food animal Practice: Lameness. 2001, March; 17(1), 53-72.
References: 1. USDA. 2002 Part III. Reference of dairy cattle health and health management practices in the U.S. USDA-APHIS, N.A.H.M.S survey. 2002; p 35-37. 2. Melendez P, Bartolome J, Archbald LF, Donovan A. The association between lameness, ovarian cysts and fertility in lactating dairy cows. Theriogenology 2003;59:927-37. 3. Fatehi J, Stella A, Shannon JJ, Boettcher PJ. Genetic parameters for feet and leg traits evaluated in different environments. J. Dairy Sci. 2003;86:661-666. 4. Vermunt JJ, Greenough PR. Structural characteristics of the bovine claw: Horn growth and wear, horn hardness and claw conformation. Br. Vet. J. 1995;151:157-180. 5. Chesterton RN, Pfeiffer DU, Morris RS, Tanner CM. Environmental and behavioural factors affecting the prevalence of foot lameness in New Zealand dairy herds - a case- control study. New Zealand Vet. J. 1989;37:135-42. 6. Petersen PH, Nielsen AS, Buchwald E, et al. Genetic studies on hoof characters in dairy cows. Zeit. Fur Tierz. Zuchtungs. 1982;99:286-91. 7. van der Tol PPJ, Metz JHM, Noordhuizen-Stassen EN, et al. The pressure distribution under the bovine claw during square standing on a flat substrate. J. Dairy Sci. 2002;85:1476-1481. 8. van der Tol PPj, Metz EN, Noordhuizen-Stassen EN, et al. The vertical ground reaction force and the pressure distribution on the claws of dairy cows while walking on a flat substrate. J. Dairy Sci. 2003;86:2875-2883. 9. Logue DN, Offer JE, McGovern RD. The bovine digital cushion – how crucial is it to contusions on the bearing surface of the claw of the cow. The Vet Journ 2004;167:220-221. 10. Raber M, Lischer ChJ, Geyer H, Osent P. The bovine digital cushion – a descriptive anatomical study. The Vet Journ. 2004;167:258-264.
294

Recommended Reading 1. van Amstel SR, Shearer JK. Abnormalities of hoof growth and development.
VCNA, FA practice. 17 (1), March 2001, p 73. 2. Sprecher, DL, et al. A lameness Scoring system that uses posture and gait to
predict dairy cattle reproductive performance. Theriogenology, 1997, 47:1179. 3. Anderson DE (guest editor). The Veterinary Clinics of North America; food
animal practice. Lameness. March 2001, 17(1). Topics Presented during lecture:
1. Complicated Sole ulcers, abscesses 2. Septic Arthritis, navicular bursitis, flexor tenosynovitis 3. Coffin bone (P3) fractures 4. Foreign bodies/ bone sequestra and septic physitis
295

Cases Discussions from the Teaching Hospital
Matt D. Miesner, DVM, MS, DACVIM (LAIM)
Case 1: Bilateral Epistaxis and Fecal Occult Blood in a 2 year old Devon Bull.
Case 2: Exercise Intolerance in a 4 Year Old Longhorn
296

Case 3: Lame 4 month old Calf
Case 4: Bloated 5 year old Angus Bull
297

IMMUNIZATION AND PARASITE CONTROL IN HORSES: A PRACTITIONER’S POINT OF VIEW
Lisa M. Nesson, DVM
Since the mid to late 1990’s, several events have occurred in the fields of equine infectious disease and immunology that influence how veterinarians immunize horses. First, West Nile Virus Encephalitis was introduced to the United States in 1999 and several vaccines were developed to address the new disease situation. Second, the AAEP published its Vaccination Guidelines on-line outlining core vaccinations that include West Nile and rabies in addition to recommendations on changes to vaccination protocols for foals and unvaccinated horses utilizing a primary series of three doses for several vaccines. Third, modified live intranasal vaccines became available for two highly contagious respiratory diseases, equine influenza and strangles West Nile appeared in the United States in August 1999, starting with a human case in Queens, New York, followed by a number of equine cases in the same region and spreading westward over the next 5 years. West Nile virus causes encephalitis with a wide range of neurologic signs including: ataxia, weakness, muzzle twitching, obtundation, recumbency, lip droop, hyper-responsiveness/hyperesthesia, teeth- grinding, dog-sitting, thoracic limb collapse, compulsive walking, muscle atrophy, seizure, blindness, circling and head pressing. One fourth of affected horses also have mild to moderate fever at the time of presentation. A one to two week incubation period is typical in outbreaks. The virus, an arbovirus, is spread from bird reservoirs by mosquito vectors to humans, horses and other susceptible mammals. Horses and humans are considered dead end hosts for this virus so horse to horse or horse to human transmission does not occur. It is currently the leading cause of arboviral encephalitis in horses and humans in the US. Approximately 97% of non-human mammalian cases are seen in horses. The case fatality rate for infected horses is 33% with 40% of those that survive infection having residual neurologic abnormalities 6 months post infection. A conditional use killed vaccine, West Nile-Innovator, was introduced by Fort Dodge in August 2001. Since that time, Fort Dodge’s vaccine has received full approval and two others have been introduced, PreveNile West Nile Virus Vaccine from Intervet and Recombitek Equine West Nile Virus for Merial. PreveNile is a chimera virus vaccine based on an attenuated yellow fever virus backbone and requires only a single dose for primary vaccination. Merial’s Recombitek West Nile vaccine is a recombinant modified-live vaccine in a pigeon pox virus vector. Vaccination for this disease has become standard in most parts of the country, annually or semi-annually, based on the mosquito population and West Nile prevalence for each region. Cases are typically seen in unvaccinated or incompletely vaccinated horses during the vector season, with most cases in late summer. The vaccination series should be completed one month prior to the onset of the mosquito season in a given area. In 2008, the AAEP published new guidelines covering the immunization of horses. These guidelines are intended to be viewed as dynamic instructions that change with current research and have stepped up equine practitioner’s standard of care requirements. They are available on the organization’s website for practitioners as well as the public at www.aaep.org. Outlined in these guidelines are core versus risk based vaccinations for horses. Core vaccinations, as defined
298
by the AVMA, are those “that protect from diseases that are endemic to a region, those with potential public health significance, required by law, virulent/highly infectious, and/or those posing a risk of severe disease. Core vaccines have clearly demonstrated efficacy and safety, and thus exhibit a high enough level of patient benefit and low enough level of risk to justify their use in the majority of patients.” The core vaccines for horses, as outlined in the guidelines include: tetanus, Eastern and Western Equine Encephalomyelitis, West Nile Virus Encephalitis and rabies. The addition of West Nile and rabies to this category has revised the standard of care for equine practitioners. These core vaccines should be discussed with all clients when designing the immunization protocol for their individual horses. Rabies vaccination has become more wide spread since the release of these guidelines, in part, due to increased client awareness from veterinarians having these discussions and also due to owner’s finding this information on the Internet and initiating the conversation with their veterinarians. Risk based vaccinations are those that are included in a vaccination program after considering the likelihood that a given horse will be exposed to a given disease. This group will vary based on geography, population of horses and between individuals within a population. Examples of vaccines in this category include but are not limited to influenza, equine herpes virus 1 & 4, Potomac Horse Fever, strangles, botulism and Equine Viral Arteritis.
The AAEP guidelines also incorporate new recommendations based on current research for the initial vaccination of foals from vaccinated and unvaccinated dams and the initial vaccination of unvaccinated adults. These animals are to receive an initial series of three doses for all killed vaccines in an effort to achieve optimal effective, long lasting immunity. Two-dose protocols have been shown to be ineffective when using killed antigens. The age to start vaccinating foals depends on whether the foal’s dam was vaccinated four to six weeks prior to foaling and the foal received adequate colostrum from that mare. Maternal antibodies interfere with the early vaccination of foals, so foals from vaccinated mares should not be vaccinated prior to four to six months for most vaccines (six months for rabies and nine months for influenza). Foals from unvaccinated mares or mares of unknown history should be vaccinated starting at two to four months, depending on the vaccine given. All foals should receive a three dose series for killed vaccines, with the first and second doses separated by three to four weeks and the third dose given at 10-12 months of age, prior to the onset of the next vector season.
Intranasal vaccines for influenza and strangles became available for horses in the mid to late 1990’s. These vaccines have been proven effective and are fairly widely accepted by clients, perhaps less so by patients. This advent has significantly improved our defense against Streptococcus equi in that the modified live intranasal vaccine (Pinnacle IN, Pfizer) has been shown to be more effective in the prevention of clinical strangles and with fewer side effects to the vaccination than the older intramuscular Streptococcus equi vaccines were. The vaccine is given in a two dose initial series with the doses three weeks apart and protective immunity develops two weeks after the booster vaccination. Side effects are rare but include nasal discharge for one to three days, abscess formation if given intramuscularly either accidentally or through contaminated injection procedures and possibly purpura if the animal’s pre-vaccination antibody titer is elevated due to prior exposure through disease or vaccination. It is recommended to either give no other injections on the same day as the intranasal strangles vaccine or give all other injections prior to giving the intranasal strangles vaccine to minimize
299

the risk of inadvertently creating an abscess. FluAvert (Pfizer) is a modified live intranasal influenza vaccine that conveys 12 months of immunity after a single initial dose, though the label claim is for six months. Research has also shown that it produces an antibody response within seven days of vaccination so it could be a useful aide in the face of an outbreak. It can be used to booster other intramuscular influenza vaccinations. Foals can be vaccinated with FluAvert at six months of age with a second booster being given at 11 months of age. Vaccination reactions are rare. In summary on the topic of vaccinations, the conversation with horse owners regarding appropriate vaccines for their horse should include the core vaccines (Eastern/Western Encephalitis, West Nile Encephalitis, tetanus and rabies) and any risk based vaccines that are deemed appropriate based on the horse’s risk of exposure. The risk of exposure should be assessed by the veterinarian and horse owner after discussing the horse’s age, health status, living situation and intended use or travel plans of the horse. For the past decade, more and more has been published documenting the growing issue of anthelmintic resistance to common equine internal parasites, especially cyathasomins and Parascaris equorum. This issue has been created in part by the minor role many veterinarians play in the development of equine deworming protocols for their clients because anthelmintics are now available over the counter. Also, many owners are continuing to deworm based on the calendar or eight week intervals rather than based on the actual needs of the horse. These practices, in addition to faulty dosing, have resulted in increased selective pressure on parasite populations and the development of drug resistance. Equine practitioners have been cautioned to use the remaining effective anthelmintics selectively, much like antibiotics – right drug at the right time, to slow further development of resistance. Drug manufacturers predict that it will be at least another ten years before any new anthelmintics will become available, further emphasizing the need to make our existing drugs effective for as long as possible. Therefore, more and more practices are implementing strategic or targeted deworming protocols for their clients and patients. These programs can provide better care for the horses, prevent or control resistance issues and provide a much needed profit center in these tough economic times by involving the veterinarian in an important area of equine preventative health care. Strategic or targeted deworming programs are designed to control clinical parasitism due primarily to small strongyles and tapeworms, to control environmental contamination, to determine if anthelmintic resistance exists on a given farm and to slow the development of parasite resistance to anthelmintics in use currently. The program is based on the fecal egg count or eggs per gram (epg) of feces that the horse is producing. The modified McMaster technique is the method used by our clinic to quantify eggs per gram. Once this is known, the horses are categorized as either low (<200epg), moderate (200-500epg) or high shedders (>500epg) and dewormed appropriately for each shedder class. Once a horse reaches maturity, they tend to shed a consistent number of eggs and therefore stay in their respective shedder categories. Changes in a given horse’s immune status may cause them to demonstrate less immunity to parasites and therefore they may start shedding more eggs and change shedder category. The parasite burden of a given horse is influenced primarily by its’ innate immunity or susceptibility of the individual animal to the parasites it is exposed to as well as any resistance patterns that exist on a given farm. In any given population, 20% of the horses are producing 80% of the eggs
300

in the environment so it is essential to identify that 20%. These horses will be treated more frequently than the low shedders to control the number of eggs they are putting into the environment. Selling this program to clients may at first seem daunting but it can and should be done. In addition to educating the clients and barn managers/owners, veterinarians must educate themselves, their technicians and lay staff in the details of the proposed program so the entire staff is in agreement on how to proceed and present a clear, uniform message to clients. How to market and introduce the program to clients and farm owners, how to collect the samples, where and how they will be run in an efficient, effective, economical way, who will manage the required client communication that is generated by the data and how the program will be sustained going forward are all areas that must be considered when designing and implementing this approach to parasite control. Our practice started working on this program in 2008 and introduced it to our clients in 2009 through client education seminars and barn meetings as well as on our website and Facebook page. It required and continues to require ongoing education from all levels of our staff but has gained more and more acceptance from clients as they come to understand what the goal of the program is – to take better care of their horses and prevent resistance from becoming more prevalent. All horses in the herd should be tested. Ideally, samples are collected by the veterinarian or their staff directly from the horse’s rectum. Lacking this direct approach, a sample (one fecal ball is sufficient) taken from the middle of a manure pile that is less than two hours old will suffice as long as it is free of dirt and bedding. The sample should be placed in a sealed zipper plastic bag with all the air removed and refrigerated until it is run (up to 10 days for an anaerobic, refrigerated sample). The samples must not be frozen. Bags should be labeled with owner’s name, date collected, horse’s name, age, date of last deworming and product used. Providing owners with preprinted labels/bags will ensure that all needed information is collected. Training owners and barn managers to collect samples is possible, but it is best if they are collected by the veterinarian or their staff in an effort to get reliable results. In order to get fecal egg counts that can be used to categorize the horses into low, moderate or high shedder groups, an appropriate period of time must have elapsed since the last anthelmintic treatment. This time period is dependent on which anthelmintic was used last: wait 12 weeks after ivermectin treatment, 16 weeks after moxidectin treatment and 10 weeks after benzimidazole or pyrantel treatment. Our practice elected to utilize our technical staff (CVT) to run the fecal egg counts in an effort to get reliable results in an economical way for our clients. Sending samples to an outside lab will result in a higher cost to the client. In order to market the program, FEC testing is moderately priced so owners are more willing to consent to testing as needed throughout the year. Fecal egg count reduction testing (FECRT) is recommended for all high shedders if there is concern that there may be a resistance issue on a particular farm. To perform a FECRT, a FEC is done, the horse is treated with the anthelmintic to be tested based on the horse’s weight and a second FEC it performed within 10 to 14 days following treatment. There should be a 90-95% decrease in the FEC following treatment if the anthelmintic was effective (90% for the benimidazoles and pyrimidines, 95% for ivermectin/moxidectin). Ideally, all the anthelmintics to be used on the
301

farm will be tested for efficacy so that only effective dewormers are being used in a given program. The results are conveyed to the attending veterinarian, the owner and possibly the barn manager/owner if the entire farm is on the program. A spreadsheet is developed for each farm to convey the results for each horse, outline the horses in each category and detail the treatment schedule to be followed for each category. The flow chart included at the end of these Proceedings is an example of a targeted program designed for adult equine in Northern climates like Wisconsin. Treating the individual horse is not the only component to the program. Environmental control is also important. Management practices that should be considered and utilized, when possible, include the following: pick-up and disposal of manure in pastures and stalls regularly. Fresh manure should not be spread on pastures as this leads to more contamination and exposure of grazing animals to infective larvae. Mowing or harrowing pastures to break up manure piles and expose parasite eggs and larvae to the weather should be done during hot (temperature is >85 F), dry periods leaving the pastures empty for four weeks afterward. Rotating pastures with other livestock, such as ruminants, to break up life cycles of parasites and avoiding over-stocking pastures and over-grazing which forces horses to graze closer to manure piles within a pasture. While targeted or strategic parasite control is not without its challenges, it has been well received by most clients once they understand the goals of the program and is worth the effort involved in development, implementation and marketing.
302

March / April Fecal Egg Count
Eggs per gram (epg)
<200 epg 200-500 epg >500 epg
Do Nothing
FEC in Oct/Nov
Ivermectin
with Praziquantel in November
Moxidectin in Mar/April
FEC in Oct/Nov
Ivermectin
with Praziquantel in November
Moxidectin in Mar/April
Deworm in
June/July with Pyrantel or
Benzimadazole
FEC in Oct/Nov
Ivermectin with Praziquantel in
November
Moxidectin in Mar/April
Deworm in
June/July with Pyrantel
Deworm in
July/Aug with Ivermectin
FEC in Nov
Ivermectin with Praziquantel in
November
Repeat process in March/April
303

Suggested Readings/Sources/Acknowledgements: MacKay RJ: West Nile Encephalitis. Current Therapy in Equine Medicine 6, 2009. American Association of Equine Practitioners Vaccination Guidelines: www.aaep.org. True CK, et al. How to implement an internal parasite control program based on fecal egg counts, in Proceedings. 56th Annual American Association of Equine Practitioners Convention 2010;258-260. Kaplan RM. Anthelmintic resistance of nematodes in horses. Vet Res 2002;33:491-507. Reinemeyer RM. Controlling strongyle parasites of the horse: mandate for change, in Proceedings. 55th Annual American Association of Equine Practitioners Convention 2009;352-360. Nielsen MK, et al. Practical aspects of equine parasite control: A review based upon a workshop discussion consensus. Equine Veterinary Journal (2010) 42 (5) 460-468. Tigert R, CVT: Assistance with deworming flow chart
304

Internal Parasite Control in Small Herds of Sheep or Goats
Mary C. Smith DVM Ambulatory and Production Medicine Cornell University, Ithaca NY 14853
• An excellent factsheet “Sustainable Control of Internal Parasites in Small Ruminant Production” is available for free at the SARE site: http://www.sare.org/Learning-Center/Fact-Sheets/View-all-fact-sheets • Additional information is available at the website of the Southern Consortium for Small Ruminant Parasite Control, http://www.scsrpc.com/ • Small Ruminant Pastures, Parasites, and Profits was the topic of a series of producer seminars in Ohio in 2011. Recordings are available online at http://vet.osu.edu/extension/sare/parasite_control • Also see Luginbuhl JM. Gastrointestinal parasite management of meat goats. Available on line at http://www.cals.ncsu.edu/an_sci/extension/animal/meatgoat/MGWormer.htm Briefly, the concepts recommended include: Smart Drenching
• Identify which dewormers will work on the farm by performing a fecal egg count reduction test or a DrenchRite ® larval development assay (Ray Kaplan, University of Georgia). • Deliver the proper dose of dewormer for the weight and species of animal. Goats typically require 1.5 to 2 times the sheep dose of a drug for the same effect. • If safe to do so, withhold feed 12 to 24 hours before drenching with a benzimidazole or avermectin. Benzimidazole efficacy may be enhanced by repeating the drench 12 hours after the first dose. • Deliver the dewormer over the tongue in the back of the throat with a drench tip or drench gun.
• Drench only the animals that need treatment according to anemia score, body condition score, or presence of diarrhea. Untreated animals harbor worms (refugia) that will stay more vulnerable to dewormers.
Pasture Management • Maintain forage height of at least 4 inches. Most parasite larvae migrate in water droplets on grass, but usually to heights no greater than 3 inches. When grazing cool-season forages, such as fescue or orchardgrass, move animals to a new paddock or section when the forage stubble height reaches 3 to 4 inches. This promotes faster regrowth while maintaining forage above the infected zone. • If feasible, remove small ruminants from pastures for 3 to 6 months to allow worm larvae on pasture to die off. Winter kills many parasites in the Northeast. • Hay heavily contaminated pastures to reduce the parasite population in the pasture. • Plant winter and summer annual forages in a tilled or disked seedbed to break the worm cycle and drastically reduce the worm population on the pasture. • Alternate or co-graze pastures with horses or adult cattle, as these are not affected by sheep and goat parasites. They can serve as dead-end hosts for the parasites, lowering the
305

parasite population on the pasture. • Maintain appropriate stocking rates for the pasture. High stocking rates will increase parasite loads on the pasture. • Avoid over-grazing, which forces animals to feed close to the soil, where worm larvae live. • Allow goats to browse upright plants rather than grasses, as goats are especially vulnerable to re-infection through close-to-the-ground grazing.
FAMACHA© FAMACHA© uses a color chart that shows five consecutive grades of goat or sheep eyelid pallor, ranging from 1 (red color; not anemic) to 5 (very pale; anemic). Five is fatal. Owners can only get a color card after they have been trained in its proper use. When Haemonchus is the problem, only animals in the palest categories are dewormed. Other strongyles can cause severe weight loss and diarrhea without anemia, so pallor is not the only indication for deworming. Records of treatments are kept and animals that require frequent deworming should be culled. The most infection-resistant animals are kept for breeding, parasite levels on pasture are reduced by culling heavily infected animals, the development of resistance to dewormers is slowed, and drug expenditures are reduced. It is especially important to select breeding males that are resistant or resilient to parasites.
Copper Oxide Wire Particles COWP (given by bolus or mixed with highly palatable feed) are helpful for controlling Haemonchus but not intestinal worms. Do NOT use if the animals already have a high copper load. A 2 gram dose is given to adults, and 0.5 to 1 g to lambs and kids.
Sericea lespedeza This is a perennial summer legume with a relatively high condensed-tannin content. Grazing the plant will decrease the fecal egg count, but other techniques will also be needed for full parasite control.
Chicory has been investigated for similar use in Ohio. Use Resistant Breeds
Sheep breeds that have demonstrated some level of resistance to internal parasite infection include St. Croix, Barbados Blackbelly, Gulf Coast or Florida Native, and Katahdin. Preliminary research indicates Spanish, Kiko and Myotonic goat breeds may offer some genetic resistance to parasite infections.
Other Techniques Garlic and diatomaceous earth are not effective. Zero grazing and supplementing protein when the diet is otherwise deficienct in protein are helpful.
How to Apply These Concepts to the Farms You Serve
Parasite control programs must be tailored to fit the herd, its size, its environment, and its management. The parasite burdens in sheep and goat herds should be monitored by physical examination and semiquantitative fecal exams that technicians or owners can do. Emphasis should be placed on keeping the animals in balance with their worms and coccidia and following smart drenching principles to maintain refugia and delay anthelmintic resistance. As was outlined above, delay the development of resistance by decreasing the frequency of exposure to
306

dewormers. Decrease the pasture contamination by tilling, harvesting hay, grazing with other species such as cattle or horses, and allowing the pastures to go ungrazed for 6 months to a year or more. Moving the group to clean pasture after deworming will delay reinfestation. Unfortunately, this also selects for resistant worms. In the Northeast, long winters insure that the pastures are relatively worm free in the spring. If the sheep and goats are dewormed before being turned out to pasture, they will vacuum up the larvae that did survive the winter. A repeat deworming 3 weeks later is analogous to emptying the vacuum cleaner bag, but may not be necessary in small flocks with ample pasture. If parturition occurs on pasture, it is also helpful to deworm at that time, as the phenomenon of periparturient rise greatly increases the shedding of eggs. In the MidAtlantic states and the Southeast, many producers in the past treated their herds monthly around the year. Resistance has developed to the anthelmintics used in these programs. No new classes of drugs are apt to reach us soon, and in some areas the parasites are now resistant to the benzimidazoles, the avermectins, and the cholinergic agonists such as levamisole and morantel. Also very alarming is the frequent recommendation from owners and over the counter drug catalogs that moxidectin (Cydectin®) be used routinely in small ruminants. Parasitologists have considered this drug to be the reserve treatment when all others have failed - and with continued overuse resistance to moxidectin will become the norm; there will be no reserve drug. Dewormers should be rotated, probably on an annual basis. More frequent rotation merely speeds the development of resistance to multiple drugs. When treating a group, dose for the highest, not the average weight. Because of differences in drug metabolism, goats require 150 to 200% of the sheep drug dose per pound. Goats also have less inherent resistance than sheep, probably because they evolved as browsers, not grazers. The drugs should be given orally for fast kill of parasites and equally fast removal of the anthelmintic from the body. Avermectins should not be given by injection, as the slow decline in drug concentration will select for establishment of resistant populations. Obviously, this last bit of advice goes counter to P. tenuis control programs for camelids, and continued high frequency use of avermectins in camelids has produced resistance in gastrointestinal nematodes and fatal haemonchosis. It is easy to import resistant parasites onto a farm with the purchase of carrier animals. All incoming small ruminants and camelids (such as guard llamas) should be dewormed before mixing with the group or being turned out on pasture. Ideally, a double dose of two different anthelmintics, from two different classes should be used. Levamisole is too toxic to permit doubling the dose. Fasting the animal overnight before giving a benzimidazole drug increases efficacy, as does treating two or three days in a row. Check the results of treatment with a fecal exam before lifting the quarantine. On each routine (or emergency) farm visit, as many animals as possible should be assessed for body condition (1 is emaciated and 5 is fat), rate of growth or production, anemia (by examining the conjunctival mucosa of the lower eyelid, the FAMACHA© score), and presence of diarrhea. Animals that are in good body condition and pink with formed fecal pellets are unlikely to need a dewormer at that time. During warm, wet weather worm populations can increase very quickly,
307

so owners should be advised to continue monitoring their apparently healthy animals at least every two weeks. Also verify that the diet seems appropriate for the species, age, and purpose in terms of energy, protein, and vitamin and mineral content. If an individual is very heavily parasitized (severe anemia or severe diarrhea and weight loss) you cannot afford to guess wrong on which drugs are effective on the farm. Consider using a benzimidazole and oral moxidectin simultaneously for these animals. Do a fecal egg count reduction test, in case resistance to both classes of anthelmintics is already present. Also draw an EDTA sample for PCV and total protein. Anemic goats can be supplemented with a product such as RedCell, 10 cc to an adult the first day followed by 5 cc per day. Supply a palatable, high protein forage also. Young lambs and kids with severe diarrhea should be treated for coccidiosis while fecal analysis is pending. If you choose to not deworm a group of animals, because they look good, a few semiquantitative fecals (see below) will confirm the appropriateness of the decision. If deworming is selected, take fecal samples on the same animals before and 10 days after deworming, to verify the efficacy of the dewormer that was used. If an individual animal is heavily infested with parasites while the remainder of the flock appears to be healthy, test for paratuberculosis with the Johne’s small ruminant AGID (available from the Animal Health Diagnostic Center at Cornell), fecal culture of goats, and histology of the ileocecal junction and associated lymph node. Also investigate the possibility that selenium or copper deficiency, especially in goats, has impaired immune function. Haemonchus The blood sucking Haemonchus contortus severely limits small ruminant production in regions that have a warm, wet season of the year. A heavy load can remove one fifth of the animal’s blood volume per day. Haemonchus has a short generation time and is a heavy egg producer. Animals can die of haemonchosis even with monthly deworming. Thus pasture management is critical. Studies have shown that 85% of the worms are in 15% of the sheep in a flock, so culling the persistently anemic animals improves both genetics and pasture contamination. Other Intestinal Nematodes Other species of importance to small ruminants include Teladorsagia (was Ostertagia), Trichostrongylus, Nematodirus, and Trichuris. They lead to weight loss or poor production, diarrhea, and hypoproteinemia which appears clinically as bottle jaw. Ostertagia, Trichostrongylus, and Haemonchus all have identical appearing eggs. It is impossible to know which of these worm species are causing a clinical problem unless larval culture or postmortem examination of the gastrointestinal tract is performed or a peanut lectin assay for Haemonchus eggs is requested (University of Georgia and Oregon State). Nematodirus (large egg) and Trichuris (whipworm, doubly operculated egg) have distinctive eggs but are not well controlled by ivermectin. Fenbendazole has been suggested for treating these parasites in camelids, at 15 mg/kg for 1 to 3 days.
308

Coccidiosis Lambs and kids over 3 weeks of age with diarrhea "have coccidiosis until proven otherwise." "Mucky butt" is a common presentation in lambs. There is diarrhea and illthrift; only rarely and with massive exposure is the diarrhea bloody. At necropsy there may be raised white foci in the wall of the intestine, but don’t count on this. Weaning, crowding, poor nutrition (including vitamin E/selenium deficiencies), wet environment, feet and feces in feeders all predispose to coccidiosis. Eimeria species that cause coccidiosis are host species-specific. The chickens will not give coccidia to the goats, neither will the sheep. Fecals may be negative for oocysts early in the disease, while animals in balance with less pathogenic species may have 100,000 oocysts/gram. No treatments are legally available to kill the coccidia. Drugs just slow multiplication to allow the animal to develop immunity and decrease environmental contamination to protect others. A rebound of fecal oocyst counts occurs after treatment. It is typical to see higher counts 10 days after than before treatment. Once clinical signs appear, treatments have little effect on weight gain but do limit shedding. Treat all animals in the group, prophylactically. Group by age (no more than 2 weeks difference) to avoid deaths in late-born lambs and kids. Drugs for coccidiosis control in small ruminants, given orally (note that none is allowed on
organic farms): Sulfonamides (Albon®) for 5 days - typical oral dose is 50 mg/kg/day (100 mg/kg loading dose first day) Amprolium (Corid®) - 25 to 50 mg/kg/day orally once daily for 5 days (1cc of solution per 8 pounds body weight per day) Monensin (Rumensin®) - approved for goats at 20 g/ton feed Lasalocid (Bovatec®) - approved for sheep at 20-30 g/ton feed Decoquinate (Deccox®) - approved for sheep and goats at 0.5 mg/kg body wt. No LD50.
Routinely medicate starter and creep rations. Shedding from adults can be limited by mixing one of the last 3 drugs with salt, but only do this to protect neonates. The safest example is 2 pounds of Deccox® premix added to 50 pounds of salt. These drugs are not permitted in dairy animals. Be sure selenium status is adequate for immunity. Fecal Examination Monitor the parasite load and development of anthelmintic resistance with quantitative fecal exams. A plastic McMasters slide is available from Chalex Corporation (http://www.vetslides.com/), P.O. Box 187, Wallowa, OR. 97885, fax 541-886-3300. Counting chambers with etched grids are about $15; those with higher contrast green grids are about $20 each. If you are having trouble seeing the lines, close the condenser and focus on the bubbles. To clean the chamber, rinse under a stream of cold water. Procedure for Quantitative Fecal Examination 1. Place beaker on balance and tare it. 2. Using tongue depressor, weigh out 4 gm of feces into beaker. 3. Add approximately 20 ml flotation solution.
309

4. Mix well with tongue depressor to break up lumps. 5. Bring up to 60 ml with flotation solution. 6. Add stir bar, and stir at medium speed for 5 min. 7. While mixture is still stirring, draw about 0.6 to1 ml fecal suspension into a 1 ml syringe. 8. Load one side of counting chamber carefully to avoid producing bubbles. 9. Repeat sampling and loading procedure for second side of chamber. 10. Let preparation stand 5(zinc flotation solution) or 10 (sugar) min but examine it at least by 20
minutes. 11. Place chamber on microscope and examine with 10X objective. 12. Count eggs in both sides of chamber, counting those eggs located under the grid. 13. Calculate eggs per gram: for 60 ml final volume, epg = (side 1 + side 2) x 50 Do fecal egg counts on animals before deworming and repeat on the same animals 10 days later. If the counts do not decrease by at least 90%, resistance is present. Owners will see a clinical response to treatment of parasitized animals with as little as 30% efficacy, so do not trust “response to therapy.” A possible threshold for treatment is 500 to 1000 eggs per gram in sheep and goats. The lower threshold would be appropriate early in the grazing season, when it is important to limit pasture contamination, and for young growing animals with little immunity or reserves. Procedures for Qualitative Fecal Examination A proper quantitative fecal examination is seen as requiring a lot of effort (or expense), and therefore is not done as frequently as it should be. A semi-quantitative examination is certainly better than none at all and often is adequate for monitoring purposes. In the centrifugation method (preferred), the sample is first dispersed in tap water, then strained through cheese cloth or an opened gauze sponge, then centrifuged to wash it. After the wash solution has been poured off the flotation solution is added and the sample is centrifuged again. The parasite eggs and cysts are harvested from the film at the top of the centrifuged sample. Procedure with centrifugation: 1. Measure out approximately 1 gm (1 cc) of feces into a paper cup, using 2 applicator sticks or a
tongue depressor to move feces. 2. Add about 15 ml tap water and disperse the feces in the water vigorously with the applicator
sticks 3. While swirling, sieve the fecal matter by pouring the contents of the cup through a layer of
cheese cloth into a second cup. 4. Pour the sieved fecal mater into a 13 x 100 mm test tube. 5. Balance with a similar tube and centrifuge at 600-800 x g; 1 min. 6. Decant. 7. Add flotation medium to fill the tube approximately 2/3 full and resuspend the pellet
vigorously with two applicator sticks. 8. Fill the tube with the same flotation solution to slightly overfill the tube so there is a slight
bulging of the surface film above the rim of the tube, and add a coverslip before centrifuging. 9.Centrifuge for three minutes if using ZnS04 or MgS04. If sugar solution is used, centrifuge for
8-10 minutes.
310

10. Remove the coverslip by lifting straight up so that a drop adheres to it; place the coverslip on a slide, and examine with a compound microscope at 10X. Count all the parasite eggs or oocysts seen.
If no centrifuge is available, the tube needs to sit for 20 minutes or more if saturated sugar solution is used, and not as many eggs will be recovered. It is customary in the student parasitology labs at Cornell to count all of the parasites seen on the slide prepared in this method, and report according to the following chart. This will give a rough approximation of the results of a quantitative fecal examination.
Parasites counted on slide Interpretation
0 NPS
1-5 few
6-15 several
16-50 low
50-100 moderate
low hundreds many
high hundreds many!
thousands many!!
wall to wall many!!!
Flotation solutions: Zinc sulfate solution, specific gravity 1.18 (about 33 grams of crystals in 100 ml distilled water). Using a hydrometer check the specific gravity, adjust accordingly to read 1.18 spg. Saturated sugar solution, specific gravity at least 1.31 at room temperature. Add granulated table sugar to boiling water, stirring continuously until no more will dissolve. Cool. Add 3 g phenol crystals or 10 ml formalin per liter to discourage mold growth, otherwise refrigerate. A website describes how owners can do fecals with simple equipment: http://microscope-microscope.org/applications/animals/fecal_analysis.htm
311

Urolithiasis and Copper Poisoning: Prevention of Two Deadly Nutritional Diseases
Mary C. Smith DVM Ambulatory and Production Medicine Cornell University, Ithaca NY 14853
Urolithiasis and copper poisoning are easy to diagnose but hard to treat. Prevention will require evaluating the nutrition and management during each and every farm visit and spotting potential dangers stemming from lack of owner education or presence of multiple species and their feeds on the farm.
Urolithiasis
Any male or castrated sheep or goat that is "sick" or off feed should be presumed to have urolithiasis unless seen to urinate freely! Pygmy goats are at high risk because the castrated males are retained as pets and the diet is rarely appropriate. Males of fiber producing breeds (Angoras and Cashmeres) are also kept. Whenever males and wethers are found on a farm, a discussion of the risks of urolithiasis is appropriate. And if the owner is thinking about getting additional animals, a reminder that females rarely get this problem may be your best preventive strategy.
The portion of the urinary outflow tract with the smallest diameter is the urethral process, which extends beyond the end of the glans penis. At birth the urethral process and the glans penis are adhered to the lining of the prepuce. These adhesions break down under the influence of testosterone near puberty. This may be as early as 3 months of age in a well-fed buck kid, later in most breeds of sheep. The penis has a sigmoid flexure, and calculi may also lodge in this narrow portion of the urethra. The other anatomic feature of note is the urethral recess (also referred to as a diverticulum) dorsal to the urethra near the ischiatic arch. When a catheter is passed up the urethra it usually enters this recess and does not reach the bladder. Obstruction of urinary outflow is a problem for males; the female has a wider urethra and can pass sand and calculi. Excess minerals and inadequate water consumption to keep the minerals in solution lead to calculi formation. Texel sheep are especially prone to calculi because they absorb and excrete more phosphorus into the urine. Infections, mucoproteins, or sloughed epithelial cells may contribute to nidus formation. Calculi generally form in the renal medulla. Primary urethral obstruction rather than ureteral blockage is usually observed. Urethral rupture occurs where the calculus is lodged or where the urethra is damaged by attempts to catheterize. Bladder rupture may occur instead of urethral rupture.
312

The composition of the calculi is variable but possibilities include: magnesium ammonium phosphate silica oxalate (rhubarb blades, Halogeton, Rumex, moldy feeds) calcium carbonate - look like gold BB's The Minnesota Urolith lab will analyze small ruminant calculi for free: find on the web or call 612-625-4221 Magnesium and calcium phosphates will precipitate in urine at a pH of more than 6.8 and the urine of sheep and goats is usually alkaline. Calcium carbonate is also more apt to precipitate at high urine pH. Note that siliceous calculi form in urine of low pH and calcium oxalate is insoluble at any urine pH. Much lip service is given to the importance of delaying castration to permit the diameter of the urethra to increase. Published statistics for the difference in diameter are weak, but the preputial adhesions in early castrated wethers are indisputable. Many intact males also obstruct if improperly fed. Delaying castration more than one or two months to reduce the risk of urolithiasis increases the risks from surgery and the chance that bucks will breed females on the farm or begin to stink. Suggest a female pet instead. Do not castrate lambs and kids that will be slaughtered young. Clinical signs often begin with depression and anorexia, though the animals may eat briefly after transport even though still obstructed. Signs more specific to the urinary tract include stranguria, anuria, dribbling urine, or bloody urine. The animal stretches out to urinate, the urethra pulsates, and a goat may vocalize. The owner often diagnoses bloat or constipation. Straining may stop when the bladder ruptures. Bruxism is a nonpsecific sign of pain. Gritty material may accumuluate on the prepuce. Fluid accumulation subcutaneously near the prepuce ("water belly") is a sign that the urethra has ruptured. If instead the bladder ruptures, the abdomen will be distended with a fluid wave, but remember that Pygmy goats normally appear to have a distended abdomen. Diagnosis often is made by finding a calculus or amorphous sediment obstructing the urethral process. A sheep is easiest to examine while sitting on its rump, body slightly forward of vertical. One hand pushes prepuce down while the other pushes up on the shaft of the penis. This is easy in intact males, may be impossible in fat wethers castrated early. Goats do not sit quietly in this position. If xylazine is given for tranquilization, remember that it is cleared through the urine - the animal will remain "depressed" until urination resumes. Also, xylazine increases urine production. Sedation with diazepam (0.1 mg/kg slowly IV) may be preferable. If no obstruction is visualized or the penis cannot be extruded, place the animal on a dry cement floor or wrap the body with paper toweling to observe for urination. Often, the stress of trying to examine the penis is enough to make an unobstructed goat urinate as soon as it is released! If you still are not sure of the diagnosis, draw blood for serum urea nitrogen and creatinine. Note that SUN can be normal in a recently obstructed animal that still has a functional rumen to degrade recycled urea. If possible, ultrasound for size (or presence) of a bladder. If no bladder is seen but peritoneal fluid is increased and smells like urine when warmed, suspect rupture and check urea nitrogen, creatinine, and potassium relative to serum levels.
313

Once the diagnosis of urolithiasis is made, assuming the bladder has not yet ruptured, the next step is usually amputation of the urethral process with scissors and averted gaze. Usually multiple calculi are present in the bladder and the animal re-obstructs within hours or days. Expect approximately 70% to re-obstruct. Carefully flush the distal urethra if necessary. Start a large sheep or goat (150 to 200 pounds) on 12 grams (1 tablespoon) ammonium chloride twice a day to acidify urine, but decrease the dose after 3 days. Too much ammonium chloride can be fatal, and we don't know how much is too much. Or substitute your favorite acidifier, such as dl-methionine (Methio-Form, efficacy unproven in ruminants). Vitamin C is probably not appropriate, as it is metabolized to oxalates by ruminants. Also try flunixin (IV best, oral possible) to control pain and reduce swelling. Surgical management is far beyond the scope of this talk and what we are trying to prevent ever having to deal with. Perineal urethrostomy is done under general or epidural anesthesia. This is a salvage technique, not appropriate for breeding animals or pets, and too expensive for commercial wethers raised for meat. Start near the castration scar, in case you have to repeat the surgery higher up. Urethrostomy and urethrotomy have been associated with stricture formation and recurrence of urethral obstruction. Urine scald is troublesome in managing the pet animal. Currently a preferred means of correcting an obstruction is a tube cystostomy. Surgeons have experimented with a percutaneous bladder drainage catheter to decrease the cost of treatment but peritonitis has been a problem with this technique and it is definitely out of favor except for temporary relief of obstruction. Laparoscopic placement is now being tried. Bladder marsupialization requires much shorter hospitalization and less postoperative care, but leaves the animal incontinent. Thus this technique is not suitable for house pets. Mild urine scald occurs but ascending infection is uncommon. It is possible that breeding soundness could be retained. Secondary closure of the stoma could be attempted to resolve the incontinence if the urethral obstruction is relieved without permanent damage, or to correct bladder prolapse through the stoma. Infusion of Walpole’s solution (sodium acetate and glacial acetic acid, pH 4.5) by ultrasound-guided cystocentesis can also relieve obstruction; see JAVMA 234:249-252, 2009. Now we get to the purpose of this seminar: prevention through nutritional management. The following discussion points should be considered. 1. Provide fresh clean water at all times, including during the winter, although this may require a heated or insulated waterer. Flavoring with orange juice or molasses or sugar free drink mixes may increase consumption. Place water buckets high enough that they do not get contaminated by feces. If one fecal pellet is found in the water, immediately empty and clean the bucket before refilling. Goats are discriminating creatures! 2. Provide salt free choice at all times (but avoid red salt in sheep, as it may lead to copper poisoning). Up to 4% salt can be added to the ration on a dry matter basis to encourage water consumption. Spray a saturated salt solution directly onto the hay.
314

3. Keep pets on mostly high quality grass hay. Feed some alfalfa hay to animals on mostly concentrate diet, but not to pets. The alfalfa is high in calcium and helps to get the high grain diet back near the recommended calcium : phosphorus ratio in the diet of 2:1. Keep the total quantities of calcium, phosphorus, and magnesium in the normal range so that the animal does not have to excrete excess minerals in the urine. 4. Magnesium excess is involved frequently, but concentration of this mineral is not indicated on the feed tag. Does feeding alfalfa help because high potassium interferes with magnesium absorption or because increasing dietary calcium decreases urinary magnesium? Keep the dietary magnesium below 0.2%. 5. Avoid high concentrate and high protein diets that favor production of urinary mucoproteins, which have a cementing effect. Limit adult Pygmy goats to 1/2 cup grain per day. 6. Market lambs and meat goats are usually fed a lot of concentrate, and for them a commercial lamb finisher pellet (such as Blue Seal) or a meat goat pellet with ammonium chloride premixed as a urinary acidifier is recommended. In home-mixed feeds, include ammonium chloride at 2% of the ration. For mature pets who don't need any grain anyway, ammonium chloride can be given, perhaps a teaspoon three times a week, but this is unlikely to change the urine pH for long. They usually don’t like it, so make into jello jigglers. Biochlor (anionic salts for transition dairy cows, 1/8 pound per day) has been used in pack goats and seems to be more palatable than ammonium chloride. 7. Provide adequate vitamin A. The current recommendation is 105 IU per kg body weight per day for maintenance and 333 IU/kg/day for growing animals. Browse and green leafy hays are good sources. An on-line Paper on urolithiasis by Dave Van Metre at CSU is posted at www.aasrp.org under “News and Topics of Interest”
Copper Poisoning
Copper accumulates in the liver (and kidney) over a period of weeks to months with no clinical signs. After a stress (shearing, transport, predator attack, starvation) acute illness occurs characterized by hemolytic crisis when copper is released from the liver into the blood stream. Copper accumulation: Sheep need at least 4-6 ppm (DM) copper in the diet to avoid copper deficiency. A normal copper level for sheep would be 8-11 ppm. Even this level can be toxic if other factors favor accumulation of copper. Molybdenum in the diet is a copper antagonist: it reduces absorption and increases excretion from the liver. Sulfates in the diet also decrease copper accumulation, as insoluble copper thio-molybdate forms in the rumen. Dietary Cu:Mo should be 6:1 to 10:1.
315

Sources of excess copper: Look for these on every farm visit! a. Trace mineralized salts formulated for cattle or horses. In the Northeast, sheep salts should have no copper added. b. Concentrates: If < 15 ppm copper, often OK; if > 20 ppm definite hazard. Swine feeds may be up to 250 ppm copper for growth promotant effect, horse sweet feeds up to 80 ppm. Modern dairy cow rations have added copper for improved fertility, and concentrates may be up to 100 ppm copper. Check feed tags, have owner date and save. c. Soybean meal and corn distillers grain are naturally high in copper. d. Copper rich swine or poultry manure spread on grass, poultry litter eaten by sheep. e. Footbaths using copper sulfate, drinking water treated with copper to control algae or snails. f. Mistaken feeding of excess copper for parasite control (need copper oxide wire particles instead) Other predisposing factors: a. Increased availability of copper if diet is low in calcium, molybdenum, zinc, sulfate. Molybdenum uptake by forage is reduced on acid (pH < 6.5) soils. b. Liver damage due to consumption of plants containing pyrrolizidine alkaloids (Heliotropium, Echium, Senecio) increases copper storage. Called enzootic jaundice or enzootic icterus in Australia. In the US, sheep are used for biologic control of Senecio, and both liver disease and copper poisoning are rarely reported in sheep eating this weed. c. Breed susceptibility: Suffolk and Texel (and their crosses) more susceptible because absorb copper more efficiently. East Friesian dairy sheep are at risk, but this may be partly because fed more concentrates to support milk production. Pathogenesis: Copper crisis may occur several months after excessive intake of copper stops. Prehemolytic necrosis in liver - sheep is clinically normal but LDH and AST increase 6-8 weeks before hemolytic crisis. Plasma copper increases 24-48 hours before clinical signs appear. Copper increases in red blood cells and glutathione decreases. Methemoglobin is produced and Heinz bodies are formed. Splenic sequestration or intravascular hemolysis occurs. At death, PCV often 6-10%, hemoglobin 5-6 g/dl. Clinical signs of copper poisoning: Anorexia, lethargy, increased respiratory rate. Methemoglobinemia, icterus (muddy yellow mucous membranes and sclera). Discolored urine due to hemoglobinuria ("constant"). Arched back from renal pain. Course 1-4 days. [Petechial hemorrhages and photosensitization without icterus reported in Sweden.] [Bloody urine, tubular necrosis and high liver copper without icterus reported from western US.]
316

Leptospirosis is an important differential to copper poisoning. Signs include fever, hemolytic anemia, hemoglobinuria, icterus, and abortion. Several serotypes may be involved. Most cases are mild. Diagnosis is based on abortion work-up and fluorescent antibody testing or silver staining of liver and kidney of animals that die. Treat with oxytetracycline. Sheep and goats are usually not vaccinated. If it’s a sheep, think copper first! And second! And third! Necropsy findings of copper poisoning: Yellow (-brown) mucous membranes and body fat. Dark (gun metal gray) kidneys due to hemoglobinuric nephrosis. Coffee colored urine. Spongy degeneration in midbrain, pons, cerebellum Single cell necrosis is seen in liver, especially if > 300 ppm copper wet weight. Copper is stored in lysosomes. Pyrrolizidine alkaloids are antimitotic, so that liver cells can't be replaced after apoptosis. Confirm with copper analyses, but each text gives different reference ranges and beware wet weight versus dry weight values. Ex. Liver copper > 150 ppm wet weight (> 800 ppm dry weight basis). Kidney copper > 15 ppm wet weight. Treatment: Intravenous fluids to flush kidneys, blood transfusions if very anemic. Penicillamine mentioned, used in referral hospitals, but expensive. Oral ammonium molybdate (50 to 500 mg) plus sodium sulfate (0.3 to 1 g) daily for 3 weeks. Recent report of mixing livestock salt: gypsum (76% calcium sulfate) 2:1 free choice. If off feed, gave 2 ounces of mixture orally in gelatin capsules, daily for 10 days and saved 10 lambs weighing 120#. (Bovine Practitioner 35:70-72, 2001) Treat other at risk sheep to remove copper from liver before hemolysis occurs. Goats are much more resistant than sheep but toxicity is possible (kids on milk replacer high in copper, pet goats eating rabbit or swine feeds, high copper show goat rations). Goats usually have no problems with red salt blocks. In a recent report (J. Cornish et al.: Copper toxicosis in a dairy goat herd. JAVMA 231:586-589, 2007) goats died after being fed a beef cattle loose mineral mix that was 3,050 ppm copper for 9 months. These goats were NOT icteric but did have extensive hepatic necrosis and hemorrhage histologically. Because the feed company was to blame, the animals were treated with penicillamine 50 mg/kg orally daily for 7 days, and milk could not be sold until 21 days after the last treatment. The cost of the penicilliamine was approximately $165 for each 50 kg goat.
317

Neonatal Care of Small Ruminants and Monitoring Losses through Field Necropsies
Mary C. Smith DVM Ambulatory and Production Medicine Cornell University, Ithaca NY 14853
Early care of dam-reared and artificially-reared lambs and kids is crucial for their well being. Hypothermic and hypoglycemic neonates need to be identified and treated quickly. Quick field necropsies will identify the cause of death in most instances. Necropsy findings and review of management protocols will help to prevent further losses.
Normal Parturition Despite the frequency of multiple births, most ewes and does complete parturition without assistance. Softening and total disappearance of the ligaments around the base of the tail is a good indication that parturition will occur in the next 12 hours. The mother often waits until the barn is quiet and may isolate herself from the flock or others may back away or be driven away (goats) to give her room. First stage labor, when uterine contractions force placenta, fetus, and fluids against the cervix to dilate it, lasts up to 12 hours in primiparous animals. Multiparous females typically proceed faster. Second stage labor, which is accompanied by straining, typically lasts two hours or less and is completed by expulsion of the last fetus. The third stage involves expulsion of the placenta, which normally occurs within 4 hours. Lochia, which should not have a foul odor, is normally discharged for 2 to 3 weeks. Owners may choose to clip or wash the tail of a goat to prevent unsightly accumulations of lochia. Correction of Dystocia As a guide for when to interfere, use the 30-30-30 rule. If a ewe or doe goes into labor or part of the fetus or placenta shows, allow 30 minutes for delivery to be completed before examining the dam. Of course, this rule does not apply if the animal is found to be in labor after a long period without observation. Another exception would be if the lamb or kid is yellow with meconium, indicating that it is already hypoxic and needs to be delivered rapidly. If everything appears to be in normal position and posture, allow a further 30 minutes before delivering the lamb or kid. If the mother has had one or more fetuses unassisted but an additional fetus is believed to be present (part visible, further straining, fetus ballottable through the abdominal wall) allow a further 30 minutes to elapse before delivering the next fetus. It is imperative to wash the vulva (use a mild dish detergent or betadine), wear a sterile glove (for protection of the ewe or doe as well as for protection of the examiner from zoonotic diseases), and use plenty of lubricant when examining the birth canal or manipulating a fetus. A head snare (available from many supply catalogs including Nasco as a “lamb puller”) is very useful for correcting a head back position. If the uterus is tight around the fetus(es), try epinephrine (1 ml IM) to relax the uterine wall and provide room to work. Most lambs and kids
318

can be delivered in either anterior or posterior presentation with one limb retained. Swing the newborn, clear its nose, and place it in front of the dam. Check for an additional fetus, and follow up with antibiotics if any major manipulation was required. If you pull one, pull the rest. Do not hesitate to cut off a swollen head with a scalpel blade if the fetus is dead and room is needed to retrieve a retained front limb. Subcutaneous fetotomy techniques quickly remove limbs of tangled dead twins and triplets. Cut through the skin encircling the leg just above the carpus and it will be easy to pull off the front limb of a rotten fetus. Reposition the dam (roll over or elevate the hindquarters) to aid manipulation or repulsion of the fetus. Flunixin (Banamine®,1 ml per 100 pounds IV or orally) is used for pain relief. A lidocaine - xylazine epidural early in a dystocia will provide analgesia, limit straining, and simplify a C-section if surgery is ultimately required. The dose is 0.07 mg/kg xylazine added to 2% lidocaine to give 2 ml of solution and the injection is given at the sacro-caudal space. Antibiotics by injection are indicated after a difficult dystocia or delivery of emphysematous fetuses. Caesarian sections on small ruminants are relatively easy to perform. Common indications include failure of cervical dilation (“ringwomb”), uterine torsion, and fetal oversize. Left flank, ventral midline (directly in front of the udder), and ventral paramedian approaches have all been used. Surgery can be done standing or down. Some veterinarians like to do standing surgery with the patient in a bathtub, for containment and easy cleanup. The anesthesia can be supplied with a line block, inverted L block, paravertebral block (1-2 ml lidocaine above and below the tips of the transverse processes of L1, L2, and L4), caudal epidural injection of lidocaine with xylazine, or gas anesthesia. Avoid xylazine tranquilization of the dam if possible, as pulmonary alveolar hemorrhage and depression of both dam and fetuses are likely adverse sequelae. A blindfold is very helpful for restraining small ruminants. Diazepam (0.2 to 0.4 mg/kg IV) can also be used for tranquilization. Normally all fetuses are removed through one incision. One or two layers of inverting absorbable suture are used to close the uterus. Penicillin is an appropriate antibiotic in most instances. If fetuses are fresh and the uterus intact at the time of surgery, the prognosis for rebreeding is good. Neonatal Care Human involvement during indoor lambing or kidding begins with “Clip, Dip, Strip, Sip”. Shorten the umbilical stump with scissors if it is long and dip the umbilicus into 2 to 7% tincture of iodine. A film canister or small paper cup holds the right amount of iodine and avoids contamination of a larger stock bottle. Strip the plugs out of each teat so that the lamb or kid doesn't have to suck very hard to get its first drink, then leave mother and young together but watch closely that the neonate actually sucks. A lamb or kid that has eaten will have a bulging belly when it is held up by the front legs. If the forage locally is selenium deficient and the dams have not been adequately supplemented throughout pregnancy, a subcutaneous injection of vitamin E/selenium (BoSe® - 0.25 to 1.0 ml) may improve the strength and immune function of the newborn. The ewe needs time and protection from interference (lamb stealing) while she licks her lambs dry and learns to recognize and count them. The lambs have to find the udder and learn to recognize their mother. Counting is difficult for sheep, so the ewes are typically kept in a
319

claiming pen for one day for every lamb being raised. Thus a ewe with a single is released to the mixing pen after one day, a ewe with twins stays two days, and the ewe raising triplets is given three days to figure everything out. A normal, dry neonate that is nursing well can withstand very cold temperatures. Shearing the ewe prelambing encourages her to seek a sheltered spot to lie down and permits heat transfer from mother to the offspring lying beside her. The weak lamb or kid may benefit from a knitted sweater, old sock with the toe cut out, or a sweatshirt sleeve as a coat. Cut holes for the front legs and provide a slit ventrally for urination by the male. One piece body suits for human babies have also been placed on lambs and kids. The warmth goes with the youngster wherever it goes and there is no danger of a barn fire. In rainy climates, plastic raincoats have been used successfully to keep young lambs alive in wet cold spring weather. The coat may only stay on a few days or weeks but certainly saves lives if the weather is bad. Lambs are occasionally grafted onto a different mother. A slime graft is performed by rubbing birth fluids or placenta onto an orphan lamb and putting that lamb in front of the ewe that delivered a dead lamb or a single and has enough milk for another lamb. Acceptance may be improved by placing a gloved fist into the dam’s vagina for several minutes, then popping the hand out to simulate passage of another fetus. A skin graft is performed by cutting the skin off the ewe's own dead lamb and putting the skin onto an orphan as a coat. The coat is removed a few days later after the ewe's milk has passed through the lamb. An older and vigorous orphan can have its limbs tied together to make it flop around more like a neonate. Tying or stanchioning the ewe so it can't evade or head butt the lamb may also lead to adoption after a few days to a week or more. If is very helpful to identify neonatal lambs by ear tag or paint branding/spray marker before releasing them from the claiming pen. In larger flocks, spray painting the same number on the side of both the ewe and her lambs allows a lost lamb to be rapidly reunited with the ewe. Also, the lambs can be easily located for special attention if the ewe becomes sick. Different colors or marking conventions can be used to identify singles, twins, and triplets. Colostrum Management If kids and lambs are dam reared, nutrition of the doe must be good if enough colostrum is to be produced. A little colostrum should be stripped from each teat by hand to ensure that dry plugs in the teats do not prevent suckling and that mastitis is not present. Obviously, if the lambs or kids are nursing their dams normally you have no way to know how much they are drinking - just that they are active, not hunched, and look full. If lambs die of starvation at 24 hours but the mother’s udder is full of colostrum at that point, check for protein deficiency in the diet, leading to delayed colostrum production. If the udder is over full or unbalanced, enough colostrum should be stripped out to make suckling easier for the neonates. This colostrum can be tube fed to weak or slow to nurse lambs or kids or can be frozen in 240 ml (1 cup) quantities for later use in other lambs or kids.
320
When artificially reared, the lamb or kid should consume 1 ounce of colostrum per pound body weight three times during the first 24 hours. Thus an 8 pound lamb would receive 8 ounces (about 240 ml) every 8 hours for 3 feedings if hand fed. Owners with lots of time can divide this into more, smaller feedings. The first feeding should be given as soon as possible (tube fed if necessary), and certainly within 6 hours after birth. When triplets or quadruplets are born, the smaller size of the neonate predisposes it to chilling while it may be weaker or even premature when compared with a single or twin. Additionally, the dam may not have enough colostrum during the first few hours after delivery to adequately feed a large litter. When disease control programs (such as CAE eradication) require hand rearing and heat treatment of colostrum, under feeding is common, which leads to increased susceptibility to enteric infections and septicemia. Hypothermia and Hypoglycemia The lamb or kid that is not licked dry by its mother quickly becomes chilled and looks hunched. The neonate with hypothermia needs to be dried off and warmed up. The brown fat around the heart and kidneys that supplies nonshivering heat production is often exhausted by 5 hours if no colostrum is consumed. Then hypoglycemia develops in addition to the initial hypothermia. The lamb that is older and dry also becomes hunched and has a tucked up abdomen if it does not nurse successfully. It cries plaintively and is suffering from starvation. If a lamb has a temperature of 99 to 102F (mild hypothermia), it should be dried off and fed by stomach tube. The ewe and lamb should be provided with shelter. If the lamb’s temperature is below 99 F and it is less than 5 hours old, it should be toweled dry and rewarmed and then tube fed before being returned to its dam. Rewarming can be done in a box or dog crate with warm air forced through it, monitoring the temperature with a thermometer to avoid overheating. This is preferable to a simple heat lamp, which may overheat one side of the neonate or start a barn fire if knocked down. Another method of rewarming used by some producers is to place the lamb in a water-tight plastic bag, tied around the neck, and submerge all but the head into warm water. It is also possible to heat several large bath towels in the clothes drier, turn the drier off, and install the chilled lamb into the warm nest of towels. If one lamb in a litter needs to be revived, remove the entire litter so that the mother is more apt to accept the treated one when it is returned along with its siblings. If the cold lamb is older than 5 hours but able to hold its head up, it should be dried and tube fed, then rewarmed until the temperature rises above 99 F and tube fed again, then returned to the ewe. If the hypothermic lamb is over 5 hours old and unable to hold its head up it needs an injection of intraperitoneal dextrose before it is rewarmed. After warming it should be tube fed and returned to its mother or transferred to a weak lamb unit. To stomach tube a neonate, an 18 French red rubber feeding tube is inserted through the mouth to the level of the last rib. No mouth gag is needed in the neonate and the stomach tube can be palpated between the trachea and the cervical vertebrae when positioned properly. A 60 cc dosing syringe fits on the stomach tube. Colostrum or milk can be delivered by gravity, using the barrel of the syringe as a funnel, or can be injected slowly.
321

The intraperitoneal glucose is given with a 1 inch 20 gauge needle, one inch lateral and one inch caudal to the umbilicus. The lamb is suspended by its front limbs during injection. Using a 20% solution of dextrose warmed to body temperature, administer 25 ml to a small lamb, 35 ml to a medium lamb, and 50 ml to a large lamb. Follow with a subcutaneous injection of long acting antibiotic. Now rewarm the lamb and feed it. Do not use this technique on an older lamb with enteritis and diarrhea, as peritonitis is likely to develop. Post-colostral Feeding of the Neonatal Dairy Kid Goat kids can thrive on goat milk (dam fed or bottle/pan fed), whole cow milk, or high quality goat, lamb, or calf milk replacers. In general, the milk replacer should be 16 to 24% fat and 20 to 28% protein, with milk based protein more digestible than plant protein sources. The milk replacer may be fed warm or cold, but quantities need to be increased in the face of cold ambient temperatures or suboptimal housing conditions. By 1 week of age, the dairy kid can do well on 2 or 3 feedings of warm milk per day totaling 1 liter, with a maximum of 1.5 to 2 liter offered by 2 weeks of age. Concentrate (20% protein) is fed to permit continued good growth while the milk intake remains constant until weaning when a body weight of approximately 22 pounds (10 kg) has been achieved. Delaying weaning until the kid is significantly larger is advantageous if the owner is willing to continue milk feeding. Necropsy Examination Whenever possible, veterinarians and producers should necropsy neonates that are found dead or die within the first few days. Dead lambs or kids often pile up on a commercial farm when many prolific animals give birth each day. Keeping these losses below 10% is a real challenge. Spending a few minutes a piece to necropsy many neonates and tallying the results by category will give more useful information to direct management changes than will spending a long time doing an exhaustive examination of one or two animals. Charge by the hour. Ask the owner to identify each dead lamb or kid by writing the dam, date, and circumstances of death on a piece of waterproof tape wrapped around a leg or attached to a plastic grocery bag. The necropsy examination should be done in a warm and well lit area, on a surface that can be easily sterilized. Allow for safe disposal of the bodies afterwards, by burning, burial, composting, or pickup with other farm refuse. Start by assembling gloves, a sharp knife, and containers and supplies for samples for various tests including formalin for fixation of tissues for histological exam. If a regular necropsy or hunter’s knife is not available, the job can be done with a number 22 scalpel blade to cut soft tissues and footrot shears to cut the ribs. Note any tattoos or tags. Record the weight of the lamb or kid (you can weigh with a fish scale) and whether it is a single, twin, or higher multiple. Briefly inspect the body for wounds, abnormal swellings, skin lesions, discharges or fecal staining from diarrhea. Place the body with left side down and the feet pointing towards you. The initial incision is made by inserting the point of the knife into the axilla and cutting the skin from the inside out (to avoid dulling the knife on hair). Next cut through the muscles supporting the scapula and reflect the front limb away from you. For access to tongue, pharynx, trachea, and esophagus extend the skin incision up the neck along the jugular furrow to (and in young animal through) the mandibular
322

symphysis. Now cut into the hip joint. Cut skin and muscles as needed to reflect the hind limb away from you. Next, still cutting from inside the skin, cut the skin in a line from axilla to hip, then reflect skin dorsally and ventrally. Carefully cut through the muscles of the abdominal wall just behind the costochondral arch with the belly of the knife blade and reflect a large triangle of body wall to expose the abdominal contents. Now puncture the diaphragm near its attachment to the ribs and cut it free from the ribs. Cut from inside out (avoid going so deep that the heart is penetrated) along the cartilage of the costochondral junctions with knife or rib cutters. The entire rib cage can be reflected dorsally by breaking the ribs near their attachment to the spine in young animals or cutting the ribs with branch loppers in adult sheep and goats. Sheep and goats normally have abundant internal fat, and that fat is very white, except where stained by apposition to the gall bladder. The skin turns blue-green soon after death in warm weather and even in the winter, unless the animal was a preruminant or had been off feed so long that there was little or no bacterial fermentation in the rumen to keep the carcass warm after death. A rapid but systematic examination of internal organs exposed by this time in the necropsy will often yield a probable cause of death. The remainder of this presentation will emphasize what to look for in neonates. Abortions and Stillbirths If more than 2% of a large sheep flock aborts, an infectious abortion disease is probably present. If due dates are not available, a diagnosis of abortion will be based on small fetal size or delivery in advance of the earliest possible due date, determined from date of introduction of the males. Gestation length averages 150 days for most goats and 146 days for many breeds of sheep. Triplets and quadruplets are apt to be delivered a few days early but are also most apt to cause pregnancy toxemia in the dam or to become tangled, resulting in dystocia and stillbirth. As the season progresses, the distinction between abortion and stillbirth is not very meaningful, as many abortion diseases also cause stillbirths or weak liveborns. To determine if the fetus was dead when delivered, check the lungs for inflation which would be proof that it breathed. The lungs of a stillborn animal will not float in water. Milk in the abomasum, manure on the bottom of the feet, and iodine on the umbilical stump all indicate a live birth. If the lamb or kid was stillborn but large or yellow from meconium staining, a simple dystocia rather than an abortion disease will be suspected. A swollen, edematous head is a good indicator of death due to dystocia. If all evidence points towards an abortion problem, samples need to be submitted to a diagnostic laboratory to obtain an etiologic diagnosis. The placenta is especially important, and without it many diseases cannot be diagnosed. Chlamydiosis and Q fever cause a generalized placentitis whereas toxoplasmosis is suspected when small white necrotic foci are found in the cotyledons. An acid fast stain of impression smears of placenta or abomasal fluid will demonstrate Chlamydophila abortus and Coxiella burnetii. It is also common to have a live and an autolyzed or mummified fetus delivered together when the naive sheep or goat has been exposed to toxoplasmosis during pregnancy. Placenta, abomasal contents, lung and liver are all useful for culture of bacterial agents. Occasionally lambs aborted with campylobacteriosis have grossly visible necrotic liver lesions or
323

pleuritis. Thoracic fluid can be used to demonstrate antibodies, as to toxoplasmosis. Remove the skull cap with heavy scissors and observe for malformations of the brain (bluetongue, Cache Valley virus). Histology of the brain is another useful test for toxoplasmosis. Goiters occur with iodine deficiency or feeding of brassicas during pregnancy. Hypothermia and Starvation If the lamb or kid was alive at delivery, note if it has nursed (milk in abomasum) and if it has a normal, copious supply of brown fat covering the kidneys and pericardium. Neonates delivered in inclement weather and not licked dry can die very quickly of hypothermia, before they use up their brown fat for nonshivering thermogenesis. They will have no or very little milk in the abomasum, unless fed terminally. The animal that lives beyond 5 hours without adequate colostral intake will become hypoglycemic as it exhausts its reserves. Scant red connective tissue replaces the brown fat. Failure to pen ewe and lamb together for bonding, mismothering by an inexperienced or sick mother, and colostrum deficiency because of inadequate maternal nutrition in late pregnancy are possible, correctable causes of hypothermia and starvation. Neonatal Infections If the animal has eaten, an infectious disease such as pneumonia or septicemia is more likely to be present. If umbilical infections and liver abscesses or swollen, infected joints are identified, check for iodine staining around the umbilicus. Prompt dipping of the navel in 7% tincture of iodine should be advised in flocks experiencing umbilical infections and associated septicemia. Sanitation of the birthing area, including liberal use of dry clean bedding, and tube feeding colostrum to weak neonates are other appropriate recommendations. If instead of abscesses originating from the umbilicus the liver contains numerous microabscesses, suspect septicemic listeriosis and submit liver for culture. Other neonates in the flock may be aborted or stillborn because of listeriosis but lack gross lesions. Feeding of poor quality silage or manger sweepings is frequently the cause of these problems. Mannheimia (Pasteurella) haemolytica is a frequent cause of septicemia or pneumonia in young lambs. The right apical lung lobe is involved first and most severely, as it has a separate bronchus. The affected lung lobes are firm but friable, and usually redder than the normal, unaffected dorsal areas. Selenium and/or vitamin E deficiency (leading to inhalation pneumonia), inadequate colostrum, dirty wet bedding, and poor ventilation all increase the risk of pneumonia. Some flocks have serious lamb pneumonia problems even when management appears adequate.
324

2012 and Beyond: Where Are We Headed with Dairy Herd SCC?
Richard L. Wallace, DVM, MS Take Home Messages • Begin monitoring milk quality practices by recording bulk tank data, DHIA
somatic cell count (SCC) information, and clinical mastitis treatments. • High bulk tank bacteria counts usually indicate improper milking machine
sanitation or poor teat hygiene prior to milking unit attachment. • Elevated bulk tank SCC indicates herd level infection status with mastitis
pathogens. • Keep track of clinical mastitis episodes. About 88% of the losses associated with
each case of clinical mastitis are due to discarded milk and decreased milk production.
Introduction Many dairy producers have implemented the NMC ten step approach to mastitis control. The NMC program includes the three basic principles of mastitis control: elimination of existing infections, prevention of new intramammary infections (IMI) and monitoring infection status. Several steps deal with elimination of existing infections. These steps involve effective dry cow management (Step 3), appropriate treatment of clinical mastitis during lactation (Step 4), and culling chronically infected cows (Step 5). Prevention practices are found elsewhere. Steps 1 and 2 (proper maintenance and use of milking equipment, and employment of proper milking procedure) deal with preventing new IMI during the milking process. Step 7 (maintenance of a clean environment) deals with controlling new infections between milking times. Segregating infected cows, screening herd replacements and improving cow resistance factors are other preventive measures mentioned within the first seven steps. Monitoring procedures are found in Steps 6, 8, 9, and 10. Good record keeping, regular evaluations of udder health status, periodic review of the mastitis control program and goal setting for udder health status are the essential ingredients of these steps. The monitoring process is commonly the weakest link in most mastitis control programs. Yet, the success of any control program rests on the ability and desire to monitor progress. Monitoring Milk Quality Monitoring milk quality is essential for production of a safe food product that meets consumer acceptance standards. Specific traits such as milk composition, flavors and odors, bacterial content, somatic cell count (SCC), and drug residues are important to
325

maintain consumer demand for dairy products. Most milk processors pay additional premiums for “high quality” milk. Break points are different between processors, but in this case, lower are better. Federal milk order pricing also includes a small bonus for low somatic cell count milk. Goals for quality milk are presented in Table 1. Monitoring Bacterial Content Monitoring bacteria in milk is routinely performed by regulatory agencies through dairy cooperatives and milk processing plants. Although these procedures are quantitative in nature, some attempt is made to differentiate between psychrotrophic and thermoduric bacteria. Psychrotrophic bacteria are cold-enduring organisms. They secrete enzymes that are proteolytic and lipolytic. These organisms cause spoilage in refrigerated milk and reduce shelf life. Pseudomonas is the most common of the non-pathogenic bacteria found, with Enterobacter, Acinetobacter, and Flavobacterium also isolated. Pathogenic psychrotrophic bacteria include Yersinia enterocolytica and Listeria monocytogenes. These organisms have been implicated in food-borne disease outbreaks. Most psychrotrophic bacteria are readily destroyed by pasteurization but their proteolytic and lipolytic enzymes can remain active. The most common sources of these organisms are water, soil, contaminated teat ends and milking equipment, and post-pasteurization contamination. Control measures include proper teat preparation, cleaning and sanitizing milk contact surfaces on farm and at the processing plant, appropriate temperature controls, and prevention of contamination from environmental sources from the farm to the store shelves. Thermoduric bacteria are proteolytic organisms from the genera Bacillus and Clostridium. These bacteria are capable of surviving pasteurization temperatures but their enzymes are destroyed in the process. These organisms are found when poor sanitary practices are employed. Mastitis pathogens can also be found in milk, but unlike psychrotrophic bacteria, they only grow at near body temperatures. In general, when bulk tank milk shipped from dairy farms contains environmental mastitis pathogens the source is not from the milk but rather from improper sanitation. Milk processors can use several quantitative methods to evaluate raw milk. The particular objectives of these procedures are to indicate the total number of organisms per milliliter of raw milk in order to reflect the level of sanitation, storage, and handling practices performed at the farm level. The Standard Plate Count (SPC) is the accepted regulatory test. With the dilution factor considered, the SPC is reported as bacteria/ml of raw milk. The Grade A regulations requires that on-farm milk contain less than 100,000 bacteria/ml. Most producers should be able to maintain levels below 5,000 to 10,000 bacteria/ml. Preliminary Incubation (PI) count is designed to encourage growth of psychrotrophic bacteria. After the raw milk has been incubated for 18 hours at 55F, another SPC is performed. The PI count cannot be interpreted accurately without a concurrent SPC. The ratio of bacteria detected before and after incubation is closely associated with milking system sanitation. The Laboratory Pasteurization Count (LPC) helps detect the level of thermoduric bacteria in raw farm milk. Initially the milk sample is pasteurized at 145F for 30 minutes, then the SPC is performed and again the ratio of before and after is determined. Since these organisms are routinely found in the cows'
326

environment, the LPC is considered a good indicator of farm sanitation. These regulatory tests make no attempt at qualitative evaluation of the organisms found in raw farm milk. A bullk tank culture would provide that information. Monitoring Somatic Cells Monitoring somatic cells can demonstrate the dairy producer's ability manage clean cows and produce quality milk. Somatic cells in milk above 50,000 per ml are an indication of injury or inflammation. Milk with elevated SCC has higher proteolytic and lipolytic activity. Plasmin, a proteolytic enzyme from serum can reduce casein levels in secreted milk. Casein is the primary protein utilized in dairy products. Lipases from white blood cells can react with milk triglycerides causing release of free fatty acids, which leads to off flavors. Several different measures of somatic cells are available both at the farm level and at the level of the milk processing laboratory. The California Mastitis Test (CMT) utilizes a reagent that causes somatic cells to rupture then forms a gel with the cellular DNA. The thickness of the gel indicates the amount of somatic cells present. A score of "zero" (no gel formation) signifies a SCC range from 0 to 100,000/ml. A score of "trace" (slight gel formation) indicates a SCC range from 200,000 to 400,000/ml. Scores of 1, 2, or 3 (distinct gel formation) are all representations of high SCC. Too much emphasis is placed on distinguishing the difference between these positive scores. It is well established that cows with SCC greater than 400,000/ml have either subclinical or clinical mastitis. For this reason, CMT scores are best interpreted as; negative, trace or positive. Most milk processing laboratories and DHIA centers use automated, electronic cell counters (ECC). The use of computerized records and ECC has greatly enhanced the ability to monitor SCC and milk quality. Monitoring Udder Health / Subclinical Mastitis Although subclinical mastitis cannot be seen by the producer, it represents the largest single loss (65-70%) of the total mastitis cost. Evaluation of SCC and microbiologic culturing of milk are the primary monitoring methods to evaluate udder health. The availability of accurate records will determine the depth and breadth of the monitoring program. Many dairy producers are not enrolled in DHIA and the SCC program. Monitoring subclinical mastitis in these herds will be more difficult, but is not impossible. Some dairy cooperatives offer individual cow SCC data and milk culturing on an as needed basis. If the herd veterinarian is not performing in-house culturing, there are laboratories available to accomplish this task. The use of a CMT paddle can offer much information if used at milking time.
327

Measures at the Bulk Tank The most basic level of measurement of subclinical mastitis and udder health is the bulk tank somatic cell count (BTSCC). This value is reported to the dairy producer several times each month. Often milk processors can make BTSCC available from each milk pick up. This data is essential for initial evaluation of herd udder health. The legal limit for BTSCC in milk sold for Grade A purposes is 750,000/ml. Herds with BTSCC above 600,000 have approximately 80% of their cows infected and are losing between 12 and 15 % in milk production. These herds have increased incidence of clinical cases and are discarding milk due to antibiotic residues. Even at low BTSCC levels (200,000 to 299,000/ml), one third of the herd is most likely infected. Graphing these values is simple and herd level trends can be evaluated. Monthly bulk tank culturing has proven useful in monitoring udder health, particularly with regard to contagious pathogens (Staphylococcus aureus, Streptococcus agalactia and Mycoplasma bovis). As stated previously, sanitation problems should be suspected if bulk tank milk contains multiple environmental pathogens (Coliforms and fecal Streptococci). The sensitivity of a single bulk tank culture for contagious organisms is fairly low, especially when the herd prevalence of contagious mastitis is low as well. In other words, often one bulk tank sample will be culture negative for S. aureus or S. agalactia even though a herd may have cows infected with one or both of these organisms. The specificity of bulk tank cultures for contagious organisms is high (94%). So it is rare that a bulk tank culture will be positive when in reality no cows in the herd have contagious mastitis. Multiple sampling will improve the sensitivity of bulk tank culturing, particularly with intermittently shedding organisms like S. aureus. Most dairy herds have every-other-day milk pick up. Serial testing can be performed by having the producer aseptically collect an agitated bulk tank sample in a sterile container. This procedure can be repeated every other day when the bulk tank contains four milkings. The samples can be frozen immediately after they are obtained and delivered to the testing facility once each month. Screening for contagious pathogens can be performed on the samples and management practices can be modified as needed. Herd Level Evaluation Individual cow data has more significance when grouped and evaluated on a herd basis. Initially the proportion of cows harboring mastitis pathogens needs to be determined (defined as prevalence). Once control measures are implemented, the monitoring process determines the number of new infections occurring (defined as incidence) and old infections resolving or eliminated. Vital to this analysis is regular milk culturing and monthly SCC data. Somatic cell count data from DHIA is conveniently grouped by parity and stage of lactation. Somatic cell score (SCS) is the logarithmic transformation of the SCC. Each doubling of the SCC increases the SCS by one score. The relationship between lost milk production and SCS becomes linear and easier to evaluate. Beginning at an SCS of 3.0
328

(mid-point SCC of 100,000/ml) mature cows will lose 1.5 lb of milk production per day. As the SCS increases by one log score, the loss increases by 1.5 lb/day, so that an SCS of 6.0 would be associated with a milk loss of 6.0 lb/day. Values for lost milk production in first calf heifers is half that of mature cows. At least 90% of first calf heifers should have SCS of 4.0 or less. Eighty percent of mature cows should be in the low SCS range (4.0 or less). A herd goal is 85% with low SCS. This value can be graphed over time just like the BTSCC discussed previously. Whole herd, quarter milk samples may be necessary for research purposes but are impractical for field monitoring of subclinical mastitis. Using individual cow SCS to determine which cows to culture helps streamline the process. Keep in mind that one high score may not be indicative of a chronic infection. Cows with multiple scores above 4.0 are most likely to be infected. The monthly DHIA somatic cell data is generated from a composite sample. Average SCC when one quarter is infected is 500,000/ml. When 2 or 3 quarters are infected the average SCC can reach 700,000 or 1,500,000/ml, respectively. Once cows to sample are selected, the CMT can be used to determine which quarter(s) to culture. If SCC data is unavailable then the CMT paddle can be used on the entire herd. Individual quarter samples are preferred to composite milk samples. Even under the best conditions many composite samples become contaminated. Contaminated milk samples are impossible to interpret and a waste of resources. A small (3-5 ml), sterile quarter sample is preferable to a voluminous contaminated one. Cultures should be immediately chilled and if microbiologic procedures are to be delayed, the samples should be frozen. Culturing all cows and heifers at 2 to 3 weeks postpartum may be helpful. This will assess the efficacy of the dry cow program and offer assurance that reservoirs of contagious organisms are not introduced to the herd. Monitoring Clinical Mastitis Of all the costs associated with clinical mastitis, 88% of the losses are due to milk withheld because of drug residues and decreased milk production. Other costs include increased labor, veterinary services, treatment expenses, culling and death loss. Typically, cows with more genetic merit are higher milk producers, are under more stress during early lactation, and are more susceptible to clinical mastitis. Cows that develop clinical mastitis are two to three times more likely to be culled. Premature culling can be costly in terms of genetic progress as well as cash flow. Availability of accurate, up-to-date farm records is essential to an effective clinical mastitis monitoring program. These records are also vital to the Milk and Dairy Beef Quality Assurance Program. Changes in the incidence of clinical mastitis can be evaluated. The total number of days that milk was discarded and an estimation of lost milk production can be extremely revealing. DHIA records can offer some useful information. The percent of cows with clinical mastitis that died or were culled will indicate the extent of any existing problems. An obvious goal for death loss due to clinical mastitis is zero. Cull rates should be below 5%. On a monthly basis, no more than 3% of the herd should be affected by mastitis. Clinical cases should be cultured to determine the causative agent of the infection. Once
329

the cause(s) is determined, management changes can be recommended versus treatment options. Treatments used for clinical mastitis are the most common causes of antibiotic residues in raw milk. Cows with repeat or recurring cases of clinical mastitis have been shown to be responsible for the majority of the discarded milk. Therapeutic efficacy of antibiotics for most mastitis pathogens has been questioned. Ultimately, the success of mastitis therapy should not be measured by the elimination of bacteria, the reduction of SCC, or reducing the cow's rectal temperature, but by the ability to increase the amount of quality milk shipped from the farm. Table 1. Interpretation of bulk tank analysis for bacteria and SCC in raw milk.
Test Procedure
Excellent Good
Concern
SPC 1,000 10,000 20,000
PI 10,000 20,000 50,000
LPC 100 300
500
SCC
100,000 200,000
400,000
Contagious pathogens
None None
Present
Source: Shearer, J. et. al. 1992
330

Improving the Value of Cull Cows
Richard L. Wallace, DVM, MS Take Home Messages
Culling and transporting decisions are an important part of dairy farming. Occasionally, an animal that is ambulatory on the farm may not be suitable for
transport to a packing or processing facility. Consider the “Top 10 Considerations for Culling and Transporting Dairy Animals
to a Packing or Processing Facility” to make appropriate decisions on the suitability of an animal to be shipped.
All production animals eventually become market animals. Within the food production system, dairy producers wear several “hats.” The largest and most obvious “hat” is the production of raw milk shipped from the dairy operation. The quality of the raw milk produced will not improve once it has been harvested from the cows. Every effort should be made to present the highest quality, most wholesome product to the milk processor. A less obvious “hat” that dairy producers wear is the generation of calves and cows for the beef market. Cull cows and bull calves can represent between 10-15 percent of the gross farm income. With proper management and timely marketing, the value of market cows and bull calves can be increased. This paper will focus on the considerations dairy producers must make when culling and transporting cattle from their operations. The National Milk Producers Federation has published a document outlining the “Top 10 Considerations for Culling and Transporting Dairy Animals to a Packing or Processing Facility.” Leaders in the dairy industry have been working on a dairy beef quality assurance program for years. The Humane Society of the United States release of the Heartland Packing Plant video showing inhumane treatment of dairy cattle propagated the release of this document.
1. Do not move non-ambulatory animals to market under any circumstances. (Only allow ambulatory animals to be shipped to market).
2. Make the decision to treat, to cull, or to euthanize animals promptly. Sick and injured animals should be segregated from the herd.
3. Delay transport of an animal that appears to be exhausted or dehydrated until the animal is rested and re-hydrated.
4. Milk all cows that are still lactating just prior to transporting to a packing or processing facility.
5. Use a transportation company that is knowledgeable about your animal care expectations and provides for the safety and comfort of the animals during transport.
331

6. Do not transport animals to a packing or processing facility until all proper treatment withdrawal times have been followed.
7. Do not transport animals with a poor body condition, generally a Body Condition Score of less than 2 (1-5 scale).
8. Do not transport animals that require mechanical assistance to rise and are reluctant or unable to walk, except for veterinary treatment. When using any handling device, abuse must not be tolerated.
9. Do not transport animals with bone fractures of the limbs or injuries to the spine. Animals with a recent fracture unrelated to mobility should be culled and transported directly to a packing or processing facility.
10. Do not transport animals with conditions that will not pass pre-slaughter inspection at a packing or processing facility. If unsure, consult with your veterinarian before transporting an animal to a packing or processing facility.
The dairy industry needs to shift our thought processes regarding the classification of surplus animals. There are actually two classes of animals on dairy farms, production animals and market animals. Production animals would include lactating cows, dry cows, replacement heifers and potentially bulls for breeding. Market animals would include cull cows and bull calves. All production animals eventually become market animals! To that end, the dairy industry should discontinue using terms like cull, spent, salvage, junk and surplus, and begin using the term market when referring to animals that are no longer economically productive. Market cattle, non-fed beef and dairy animals supply 20 percent of the total beef produced in the United States. In 1998, 2.5 billion pounds of market cow beef was produced in the U.S. with nearly half of that amount from dairy cows. Almost three quarters of the market cow beef is destined for processed beef products. Most dairy producers assume that the major product from market cows is ground beef sold as hamburgers through fast-food restaurants. In reality, ground beef is a very important product from market cattle, but it is only one of many products. Depending upon the operation, market cow packers utilize tenderloins, ribeyes and strip loins, particularly from younger cows as well as the hide and many other inedible products. The decision to market a cow is a complex one. When making a marketing decision, dairy producers may consider many cow factors, such as age, stage of lactation, milk production, health status, disposition, and reproductive performance. Other economic factors such as current milk price, market cow price, as well as cost and availability of replacement heifers may have a role in determining whether or not to market a cow. Dairy cow marketing decisions have an important influence on the financial success of the dairy. Marketing decisions can function as a component of genetic improvement programs designed for long-term gain and improved production efficiency (voluntary marketing). At the same time, marketing may also represent failure or limited success of health programs resulting in cows leaving the herd prematurely due to death, disease or health-related problems (involuntary marketing).
332

Annual market rates for DHIA Holstein herd herds in Illinois and the Midwest as of September 2008 are shown below. The data is averaged for the bottom, middle and top third of herds based on rolling herd average milk production. Location/RHA < 18,000 18,001-22,000 > 22,001 Illinois 33.4 (126) 36.4 (172) 36.1 (107) Midwest 34.3 (1583) 35.2 (2508) 36.3 (2271)
Marketing decisions are important from several different perspectives. Costs for replacement heifers may represent up to 20 percent of the dairy operating budget (Fetrow 1988, AABP). Negative cash flows occur when a cow is sold for beef and a heifer is added to the lactating herd as a replacement. Cows retained in the herd represent capital investments, which are subject to various forms of risk that may alter the earnings from those investments. Cows have different risks of being marketed depending on their age. Although there is a tendency for increased marketing rates with advancing age, management constraints and biases can modify this relationship. The typical cow remains in the milking herd less than 4 years even though peak milk production related to maturity ordinarily does not decline until 8 or 9 years of age. The reluctance of some producers to market first calf heifers and choosing instead to give them a second chance is an example of management bias affecting marketing policy. A recent study (Bascom and Young, JDS 1998) summarized the reasons dairies market cows and determined whether cows were marketed for multiple reasons. Dairy producers identified a secondary reason for marketing 35 percent of the time, and a tertiary reason for marketing 11 percent of the time. Unfortunately, DHIA data only provides the producer with one choice when categorizing marketing decisions. The most prevalent reason for marketing was reproduction. Producers may be unaware of the cost associated with reproductive marketing. In herds with less than optimal reproductive performance, dairy operators must find a balance between income loss caused by excessive days open and income loss caused by high marketing rates. The second most prevalent reason for marketing was mastitis. High somatic cell count (SCC) was rarely used as the reason for marketing, however, clinical mastitis was the primary reason for 15 percent of the cows marketed in this study. How producers interpret the difference between mastitis and high SCC is unknown, and marketing for mastitis may include both categories. Cows may be marketed for mastitis because they never recover from chronic infections or because of reduced milk production due to elevated SCC. In 1994, the National Cattlemen’s Association performed an audit of market beef cows, market dairy cows, and market bulls. This study was conducted to determine areas for improvement in the manner by which these classes of animals were marketed. In 1999, the study was repeated to see if the concerns found five years previously had changed. Slightly over 6 million head of market cows and bulls were assessed in the 1999 audit. In general, producers did a good job of managing and marketing surplus animals. However,
333

quality defects in only 1% of market cows and bulls indicate that thousands of cattle are below acceptable standards. On average, 3 percent of all market dairy cows are condemned at USDA packing plants. Considering only emaciated and disabled cattle, over 40 percent of these market cows are condemned. Lameness and disabled cattle represent a problem to the industry from a public perception standpoint. Many lame cattle, however, are the result of failure to market animals before feet and leg problems progress. The packer is required to remove all tissue associated with an arthritic joint. More than 7 percent of cattle had at least one arthritic joint, and nearly 4 percent had two bad joints. With an average trim loss of 40 pounds, more than 37 million pounds of product would have been lost in 1999 due to joint problems alone. Packers listed arthritis as one of their top concerns. Since lean muscle is the principal end product of market cattle, it is important that market animals do have adequate muscling and do not have excessive amounts of fat. However, the 1999 audit suggested that over 70 percent of dairy cows were inadequately muscled. Certainly, dairy cows are not genetically designed for extreme muscling, but of greater concern is that the poor meat yield due to emaciation. Extremely thin cows amounted to 4.5 percent of dairy cows harvested in the 1999 audit. In many cases, the most valuable part of a thin cow is her hide. Emaciated cows are much more prone to bruising because they have no fat to serve as padding and they are more likely to be disabled upon arrival at the packing plant. The primary concern of packers in the 1999 audit was the high incidence of bruising. Only 11.8 percent of cow carcasses did not have a bruise (down from the 1994 audit). Minor, medium, major and extreme bruises results in 0.69, 1.42, 4.78 and 15 pounds of trim loss, respectively. Using these estimates, more than 14 million pounds of product were lost due to bruising. Unfortunately, the bruises do not just occur on the lower-valued portion of the carcass. The 1999 audit revealed that trim loss was observed in the top sirloin, loin, rib, round and chuck. When a bruise is created on an animal, it takes time for the body to heal. Handling practices at the farm are very important in minimizing bruises. It is estimated that one-third of bruises occur on the farm and the other two-thirds occur in transport and marketing. Close scrutiny of handling facilities to eliminate sharp, protruding corners can help reduce bruising. Producers should also merchandise market cattle before they become emaciated and are more susceptible to bruises. Another major concern of packers was the incidence of injection-site lesions and the potential for antibiotic residues. A recent study at Colorado State University revealed that approximately 29 percent of the rounds of market cows contain an injection-site lesion. Most of these lesions were detected in the upper portions of the hip. These lesions do not represent a food safety concern, but they are a beef quality problem. Scar tissue from intramuscular (IM) injections of antibiotics or vaccines causes the muscle tissue to be tougher, producing a product that may be unacceptable to the consumer. Producers should carefully avoid marketing cattle that have been treated with antibiotics until the specified withdrawal time has ended. The USDA currently monitors the
334

incidence of antibiotic residues in market cattle, and a trace-back system is already in place through the use of back tags at the auction barn. In the 1994 audit, dairy cows and veal calves were the two classes with the highest level of violative antibiotic residues, 1.5 and 1.8 percent, respectively. By 1999, the violation level in dairy cows had dropped to 1.1 percent (415 positives from 37,308 cattle tested). Inspectors at packing plants identify animals to be tested both ante mortem and post mortem. Nearly 85 percent of the residue violations were from post mortem-identified high risk cattle. The leading causes of antibiotic contamination included gentamycin (39%), penicillin (25%), sulfadimethoxine (12%), streptomycin (9%), tetracyclines (6%) and several others. Gentamycin may not be as commonly used as some of these other antibiotics, but the prolonged tissue retention may explain the reason this drug is at the top of the list. When you look at the overall picture, the 1999 audit suggests that nearly $70 is lost in value for every market cow or bull that is merchandised. Most of this loss comes from merchandising thin, emaciated animals that are more susceptible to bruises and trim loss and have poor yields. Dairy Beef Quality Assurance (DBQA) addresses the day-to-day management practices that influence safety, quality, and wholesomeness of beef and beef products. Reducing the problem starts on the dairy and suggested changes involve seven steps.
1. Use the neck or shoulder as preferred injection site, when possible. 2. Read and understand injection product labels. 3. Avoid intramuscular (IM) injections when other labeled administration routes are
available. 4. Products approved for subcutaneous injection should be done with the tenting
technique by lifting animal hide between fingers and inject into the "tent." 5. Avoid mixing products as this causes more tissue damage, reduces product
efficacy, and extends withdrawal times. 6. Ask your veterinarian about comparable tissue damage from different products. 7. Encourage promotion of tissue reaction information from pharmaceutical
companies that produce injectable products. The first step may be the biggest obstacle. Typically, large groups of dairy cows are not run through squeeze chutes like beef cattle. Injections in cows tossing their heads while in the stanchion can be dangerous. Is there an economic incentive from the buyer to justify the extra effort by the dairy personnel to reduce hindquarter injections? Tracing antibiotic residues is currently being pursued in dairy market cow carcasses. Tracing carcass quality (injection site lesions) back to the dairy would be needed to promote this type of quality assurance. Quality assurance is not an all or none situation and partial improvements could be beneficial.
335

Dai
ry B
eef R
egul
ator
y A
utho
rity
Sys
tem
Farm
Vete
rinar
y/C
lient
/Pat
ient
R
elat
ions
hip
(VC
PR)
Slau
ghte
rPl
ant
Truc
kers
, Dea
lers
&
Mar
kets
FSIS
Aut
horit
y
FDA
A
utho
rity
FDA
A
utho
rity
USD
A A
utho
rity
336

Regulatory Process, Definitions and Findings for Drug Tissue Residue
90% of violations originate from dairy
70% cull cows, 20% bob veal (under 150 pounds)
Top Tissue Violator Drugs
Cull cows (in order) Bob Veal (in order)
1. Penicillin 1. Neomycin
2. Flunixin 2. Sulfas
3. Sulfas 3. Gentamicin
4. Desfuroylceftiofur 4. Flunixin
5. Gentamicin
Top three reasons for violations during on-farm investigations:
1. Failure to maintain records, no farm treatment records
2. Overdose without adjusting withdrawal times
3. Failure to identify treated animals, lack of animal ID
(In most places there is no veterinary-client- patient- relationship (VCPR) in place.)
Number one concern was the amount of prescription drugs utilized without a VCPR.
Food & Drug Administration (FDA )– has jurisdiction over animals from farm to the slaughterhouse door. FDA takes enforcement
action against FSIS reported residue violators.
United States Department of Agriculture (USDA)/Food Safety Inspection Service (FSIS) – has jurisdiction at the slaughter plant.
Conducts ante and post mortem inspection and collection of tissue samples from animals slaughtered in the U.S. Reports violations
to the FDA for possible enforcement action.
Sampling process: two types sampling: 1) scheduled (random) sampling and, 2) inspector generated samples.* If a positive sample
is found, a certified letter is sent to the producer and then the information is entered into an automated system accessible by the
FDA. FDA determines which farms to investigate. Only 35% of drug residue violations are investigated.
*Inspector generated sampling is driven by visual evaluation of the animal and suspicion of recent drug use. Include but not
limited to: mastitis, metritis, recent surgeries, injection lesions and pneumonia.
WI Dept. of Agriculture & Consumer Protection (DATCP) – state inspected plants slaughter about 2,000 head dairy/year and follow
the USDA directive and Federal Meat Inspection Act.
VCPR Overview:
A relationship exists between the veterinarian, the client and the patient which the following apply:
a) Veterinarian has responsibility for medical oversight of patient
b) Client agrees to accept the veterinarian oversight and related instructions
c) To make diagnosis the veterinarian must have sufficient medical knowledge of the patient and have timely visits to the
premise
d) Veterinarian must be readily available for follow-up treatment, in case of adverse reactions
For the legal definition of the VCPR, see: WI Chapter 453.02(8) and FDA Title 21, Part 530.3 of CFR
Same Source Suppliers, Repeat Violators
http://www.fsis.usda.gov/science/Chemistry/index.asp
FDA Warning Letters:
http://www.fda.gov/ICECI/EnforcementActions/WarningLetters/default.htm
337

Leading a Culture of Service Excellence
Presented at the
2011 WVMA Convention
by Dennis Snow
Snow & Associates, Inc. Phone: 407.294.1855
Email: [email protected] Website: www.snowassociates.com
338

2011 WVMA Convention
©2011 Snow & Associates, Inc. Phone: 407.294.1855 E-mail: [email protected]
1
The Customer Experience
“Simplicity is the ultimate sophistication”
Leonardo da Vinci
Many (most) organizations overcomplicate any initiative they undertake. Because of this over complication, these organizations tend to freeze and never finish what they start. Employees and management become frustrated by the never-ending flow of new initiatives that come and go. This is where the “flavor of the month” reputation begins to haunt any new initiative. The key is to keep it simple! The following service model is simple and straightforward. It is easily communicated to everyone in the organization and can provide a foundation or anchor for the improvement effort.
Customer Service Delivery
Service Environment
Processes
Processes
339

2011 WVMA Convention
©2011 Snow & Associates, Inc. Phone: 407.294.1855 E-mail: [email protected]
2
Service Map
Process Analyzed: _____________________
The customer… The customer… The customer…
The customer… The customer… The customer…
The customer… The customer… The customer…
8 9 7
6 5 4
3 21
Step 1: List process steps in each block Step 2: Which blocks present immediate areas of opportunity? (List in Step 3)
340

2011 WVMA Convention
©2011 Snow & Associates, Inc. Phone: 407.294.1855 E-mail: [email protected]
3
Step 3: For each block identified in step 2, describe what would be considered mediocre service and what would be considered excellent service.
Block Number
Mediocre Service
Excellent Service
Step 4: Choose one or two processes to work towards improving customer service and determine improvement strategies.
341

2011 WVMA Convention
©2011 Snow & Associates, Inc. Phone: 407.294.1855 E-mail: [email protected]
4
Everything Speaks
Every detail of the service experience is saying something about your organization. Everything the customer sees, hears, smells, tastes, or touches impacts the experience. Anything that is out of alignment causes a disconnect in the mind of the customer. Everything Speaks! They may not consciously notice every detail, but subconsciously clues to your culture are being communicated. What is your service environment saying about your organization?
Be sure to include physical and “attitudinal” elements.
Everything Speaks
Distracter Everything Speaks
Commitment
342

2011 WVMA Convention
©2011 Snow & Associates, Inc. Phone: 407.294.1855 E-mail: [email protected]
5
Customer Expectations
Advice
Partnership
Availability
Adapted from Gallup Research
Service Behaviors
Accuracy
Availability
Partnership
Advice
Accuracy
343

2011 WVMA Convention
©2011 Snow & Associates, Inc. Phone: 407.294.1855 E-mail: [email protected]
6
Service Improvement Meeting
1. Put employees at ease by holding the meeting in a distraction-free environment. Silence phones, etc.
2. State the purpose of the discussion: To identify obstacles that are in the
way of creating an exceptional customer experience.
3. Re-emphasize that continuous improvement is not directed at blaming people, but at improving processes.
4. Establish a cooperative environment at the meeting, following the rules for
successful brainstorming.
5. Decide on a customer process on which to focus. • Ask, “What operational barriers impede our ability to provide an
exceptional experience every time with this process?” • Set allotted time for brainstorming. • Record all obstacles on flipchart or worksheet. • Encourage all participation, not permitting critical comments.
6. After discussion, select one or two obstacles that are a major source of
customer complaints or frustration.
7. Generate as many potential solutions to the obstacle as possible. Often, the solution will be generated on the spot. The key is to keep an open mind and build on ideas. While not every solution presented will be feasible, it’s important to respect the contribution.
8. For those solutions that will require time and study to implement, discuss
and agree on who will be responsible to work on a solution and others who need to be involved. The more involvement from the team, the greater the resulting buy-in.
9. Set a date to report back on status of obstacle and solution.
344

2011 WVMA Convention
©2011 Snow & Associates, Inc. Phone: 407.294.1855 E-mail: [email protected]
7
Unleashing Excellence The Complete Guide to Ultimate Customer Service
2nd Edition By Dennis Snow and Teri Yanovitch
Originally published in 2003, this quintessential how-to guide has now been expanded and extensively updated to include the latest tools, best practices, and invaluable lessons learned from companies that have actually applied the authors’ comprehensive system for building a first-rate customer service culture from the ground up! Filled with vital information, this second edition of Unleashing Excellence literally walks you through every aspect of the nine leadership actions required to compete in a global marketplace where products and services are becoming increasingly commoditized and the Internet provides dissatisfied customers with a powerful forum. Nothing is left out of Unleashing Excellence: The Complete Guide to Ultimate Customer Service. If you’ve been searching for a blueprint for building a customer service program, you’ll find it here. The book’s chapters include: • The “DNA” of Service Excellence • Creating a Service Improvement Team • Developing Your Service “Non-negotiables” • Communicating the Service Strategy to
Your Team • Service Training and Education
• Interviewing For Service Excellence • Developing Effective Service
Measurements • Recognition and Reward Systems • Implementing a Service Obstacle System • Building a Culture of Accountability
Praise for Unleashing Excellence: ‘‘Customer service is key to the success of any company. I recommend Unleashing Excellence to any company needing a ‘how to’ and ‘can do’ manual to implement service excellence in their organization.’’ —Richard A. Nunis, Retired Chairman, Walt Disney Parks & Resorts ‘‘If your organization is not fully committed to service excellence, don’t read this book. If you are fully committed, then you MUST read this book. It provides all the nuts and bolts of how to create and sustain a service culture.’’ —Pamela Paulk, Vice President, Human Resources Johns Hopkins Health System ‘‘In the restaurant business, achieving and maintaining excellent customer service is of paramount importance. Unleashing Excellence is a must read that would benefit any industry. It gives step by step guidelines that can be implemented with ease and invaluable insights that will help encourage your customers to keep coming back for more instead of leaving before the first bite.’’ —Fred DeLuca, President and Co-Founder Subway Restaurants Available now in bookstores or at Amazon.com, BarnesandNoble.com
345

2011 WVMA Convention
©2011 Snow & Associates, Inc. Phone: 407.294.1855 E-mail: [email protected]
8
Available at online bookstores or www.snowassociates.com
Lessons From the Mouse A Guide for Applying Disney World’s Secrets of Success
to Your Organization, Your Career, and Your Life What can a mouse teach you? When that mouse has been delighting and entertaining hundreds of millions of people for decades, it turns out there is plenty to learn! Dennis Snow’s book, Lessons From the Mouse provides ten no-nonsense, practical principles that anyone, anywhere can apply. He entertains while he educates with chapters like “’What Time is the 3:00 Parade?’ Is Not a Stupid Question.”
The mouse is very candid here – no Disney pixie dust blinds the reader. Backstage snafus, onstage errors, and occasional chaos emerge in all their drama, humor, or irony. At its heart, though, Lessons From the Mouse presents ten lessons that guide readers in applying excellence in their own organizations, careers, and lives. The ten lessons include: • Never Let Backstage Come Onstage • What Time is the 3:00 Parade? Is Not a
Stupid Question • Little Wows Add Up • Have Fun With the Job – No Matter How
Miserable You Feel • Don’t Be a Customer Service Robot
• Pay Attention to the Details – Everything Speaks
• Never, Ever Say, “That’s Not My Job” – Don’t Even Think It!
• Everyone Has a Customer • Figure Out What Ticks Off Your Customers
– And Do Something About It • Take Responsibility for Your Own Career
Available at www.snowassociates.com Creating a Culture of Service Excellence (DVD) Dennis’s customer service presentation is now available on DVD. This informative 45-minute DVD covers topics like:
• Looking at your organization through the “lens of the customer.”
• Paying attention to the details because “everything speaks.” • Delighting your customers by creating “little wows.”
Featuring a keynote speech presented before a live audience, the DVD includes the service principles and stories that bring the principles to life. The content is designed to be entertaining, informative and practical. Use this DVD to:
• Provide content for in-house training programs. • Introduce new employees to the service standards they are expected to demonstrate. • Revitalize a company’s focus on customer service. • Re-familiarize employees with the key drivers of a service-driven organization
346

Author Index
Born, Fred .......................................................................................................................... 3
Cook, Nigel ..................................................................................................................... 194
Diehl, Katie .......................................................................................................... 12, 21, 30
Duffield, Todd ................................................................................................ 202, 209, 213
Herron, Meghan ................................................................................. 34, 42, 48, 57, 64, 71
Ketover, Howard .................................................................................................... 215, 218
Konkle, Darlene ............................................................................................................. 225
Linn, Kathy ...................................................................................................... 79, 81, 84, 88
Manhanna, Bill ............................................................................................................... 230
Metzger, Fred ............................................................................. 92, 95, 102, 105, 110, 113
Miesner, Matt ................................................................. 252, 261, 271, 276, 283, 290, 296
Nesson, Lisa ................................................................................................................... 298
Pauli, Amy .............................................................................................................. 117, 122
Pauli, Amy ........................................................................................................................ 30
Sawchuck, Sandy ........................................................................................................... 125
Scherk, Margie ................................................................................ 130, 139, 148, 156, 164
Seglar, Bill ...................................................................................................................... 230
Smith, Mary ................................................................................................... 305, 312, 318
Snow, Dennis ................................................................................................................. 338
Stepien, Rebecca ............................................................................ 172, 176, 181, 184, 190
Wallace, Richard ............................................................................................ 325, 331, 336
347

www.wvma.org
2801 Crossroads Drive, Suite 1200 | Madison, WI 53718608-257-3665 | Fax 608-257-8989