Empagli ozin induced diabetes ketoacidosis - Research Square
26
Page 1/26 Empagliozin induced diabetes ketoacidosis: a review of literature Lida Shojaei Kermanshah University of Medical Sciences Kolsoom Majidzadeh Kermanshah University of Medical Sciences foroud shahbazi ( [email protected] ) Kermanshah University of Medical Sciences https://orcid.org/0000-0002-0640-356X Research Article Keywords: Diabetic ketoacidosis, Sodium-Glucose Transporter 2 Inhibitors, Risk factors, Presentations, Management Posted Date: April 14th, 2022 DOI: https://doi.org/10.21203/rs.3.rs-1505037/v1 License: This work is licensed under a Creative Commons Attribution 4.0 International License. Read Full License
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Empagli ozin induced diabetes ketoacidosis - Research Square

Page 1/26
Empagli�ozin induced diabetes ketoacidosis: a review of literatureLida Shojaei
Kermanshah University of Medical SciencesKolsoom Majidzadeh
Kermanshah University of Medical Sciencesforoud shahbazi ( [email protected] )
Kermanshah University of Medical Sciences https://orcid.org/0000-0002-0640-356X
Research Article
Keywords: Diabetic ketoacidosis, Sodium-Glucose Transporter 2 Inhibitors, Risk factors, Presentations, Management
Posted Date: April 14th, 2022
DOI: https://doi.org/10.21203/rs.3.rs-1505037/v1
License: This work is licensed under a Creative Commons Attribution 4.0 International License. Read Full License

Page 2/26
Abstract
BackgroundSodium-Glucose Co-Transporter 2 inhibitors have been proven to have positive effects on blood glucose control and decrease major atherosclerosiscardiac and renal outcomes. Diabetic ketoacidosis and genitourinary infections are two major side effects of this class. Hyper-, normo- orhypoglycemic diabetic ketoacidosis has been reported with SGLT2is. In this study, we report two cases of empagli�ozin-associated diabeticketoacidosis (DKA).
Aimin this narrative review we summarized cases of Sodium-Glucose Co-Transporter 2 inhibitors associated diabetes ketoacidosis. First, we describedtwo cases of empagli�ozin induced diabetes ketoacidosis.
MethodDatabases including PubMed, Scopus, Cochrane library, and Google scholar were searched for eligible reports during February 2022.
ResultsA review on etiology, signs, symptoms, laboratory data, and treatments for diabetic ketoacidosis associated sodium glucose transporter 2 inhibitorsare provided here.
ConclusionEarly recognition, good past medical history taking, discontinuation before/during invasive procurers and acute illness, appropriate �uid and insulinreplacement therapy are cornerstones of treatment.
Impacts On PracticeThe SGLT2is are responsible for 6.6% of all cases of the DKA
The SGLT2is associated DKA may be severe and life-threatening
The SGLT2is should be discontinued 24-72 hours before planed surgeries and in acute illness
IntroductionSodium glucose cotransporter 2 inhibitors (SGLT2is) are a group of medications that inhibit glucose reuptake in the S1 segment of proximal tubuleand pancreatic alpha cells [1]. In the normal conditions, only 500 mg from 180 g daily �ltered glucose is excreted in urine [2]. Sodium glucosecotransporter is responsible for 90% of glucose reabsorption in the kidney [2]. However, following the use of SGLT2is up to 50% (90g) of �lteredglucose (180g) was excreted in urine per day [3]. SGLT2is lowers blood glucose, HgbA1c, blood pressure, sympathetic activities, in�ammation, bodyweight, and plasma volume [4, 5]. Cardiovascular bene�ts of the SGLT2is were medicated through the preload reduction, natriuresis,sodium/hydrogen exchange inhibition, reducing cardiac necrosis or �brosis, and lower in�ammatory cytokines [6, 7]. These agents reduced the riskof cardiovascular, renal events, cerebrovascular events, heart failure exacerbation, and death [8]. They also reduced all causes of mortality,cardiovascular mortality, hospitalization, myocardial infarction, and renal events in patients with diabetes [9]. The recent ESC guidelines recommendSGLT2is along with angiotensin blockers, beta-blockers, and aldosterone antagonists for patients with heart failure with a decreased ejectionfraction [10]. In addition, a recent meta-analysis suggested that empagli�ozin can be the best option for patients with cardiovascular diseases inorder to decrease renal and cardiac outcomes [11]. However, this group can increase the risk of diabetes ketoacidosis (DKA) genital infections [10].The most recent UK guidelines for diagnosis and management of diabetes ketoacidosis de�ned the DKA as having diabetes mellitus or blood sugar(BS) > 11 mmol/l (198mg/dl), positive serum (> 3.0 mmol/L) or urine ketone (2 + or higher), and acidosis (either pH < 7.3 or bicarbonate < 15 mmol/l)[12].
CasesCase 1

Page 3/26
A 72-year-old diabetic patient who had been diagnosed with diabetes 20 years ago was brought to the emergency department with severe malaiseand a decreased level of consciousness. Her blood sugar was partially controlled by glyburide (5 mg twice daily), metformin (500 mg twice daily),and empagli�ozin (10 mg/day) combination regimen (fasting blood sugar < 110-180 mg/dl, HgA1c = 7.5%). The later was introduced 2 monthsbefore hospitalization by the patient without prescription (self-prescription). Three days before hospitalization, the patient experienced malaise,nausea, two episodes of vomiting, and one episode of diarrhea. She reported having a poor intake for three days. The malaise was deteriorated herdisease and she was brought to the emergency department with decreased consciousness and severe malaise. During the initial examination, thepatient was found paled. However, no polyuria, kussmaul sign, abdominal tenderness, fever, shivering, and hypotension was observed in the earlyexamination in the emergency department. All the oral antihyperglycemic agents were discontinued and the patient was transferred to the IntensiveCare Unit (ICU). Although, the initial vital signs were BP=110/70 mmHg, PR:100/min, RR:23 beats/min, O2 saturation: 98%, T:37.3 C., the patientdeveloped hypotension and tachycardia (80/50 mmHg, HR 120 /min). So, she was transferred to the ICU. The initial signi�cant lab data were asfollows: blood sugar (BS) = 250 mg/dl, pH = 6.94, PCO2: 18.5 mmHg, PO2: 49 mmHg, O2 saturation: 60.9%, serum HCO3- 3.4 mmol/L, and baseexcess -18 mmol/lit. The other lab data are presented in Table 1. The urine ketone body was positive (3+).
With diagnosis of the DKA, 1000 ml saline 0.9% and 50-ml sodium bicarbonate were initially infused over an hour in the emergency department andthe patient was transferred to the ICU. Continuous insulin infusion (2-6 units/h), �uid (dextrose 5% and saline 0.9%), and sodium bicarbonate50meq/lit at dose of 100-150 ml/hour were continued in the ICU. 20 hours of the vasopressor therapy with norepinephrine (4-10 mcg/min) wasrequired. Intravenous bicarbonate was continued for 24 hours. The acidosis responded to the treatment slowly. Continuous infusion of �uid (saline0.9% and dextrose 5%) and insulin after about 4 days was stopped after the patients reached pH = 7.4 and HCO3- = 18, and base excess = -12meq/l.However, after 12 hours, the pH and bicarbonate levels decreased to 7.3 and 12.5 mmol/l, respectively. Therefore, intravenous sodium chloride(0.9%) or half-saline with dextrose (5%) (to maintain blood glucose at 150-200 mg/dl) at a rate of 70-150 ml/hour (depending on the patient's bloodsugar and �uid status) along with insulin at a dose of 2-5 unit/hour was continued for a total of 144 hours in order to correct the negative baseexcess and ketonuria. Acidosis slowly responded to the treatment (Fig 1 and 2). Finally, the patient was discharged with insulin (NPH 12 unit 6-AM,and 8 unit 6-PM) on the 7th day of hospitalization with pH = 7.40, HCO3- = 19 mmol/l, negative urine and serum ketone, and normal base excess.
Case 2
A 65 years old female patient with a 10-year history of T2DM was brought to the emergency department with a decreased level of consciousness,tachycardia (125/min), and tachypnea (30/min). Her blood sugar was controlled by empagli�ozin/linagliptin (25/5) and gliclazide. She had ahistory of laparoscopic cholecystectomy 5 days before the current presentation. Empagli�ozin was discontinued 24 hours before the surgery andreintroduced again the day after surgery. The initial lab values included pH 7.11, bicarbonate 6.4 mmol/lit, ketone 3 +, base excess -26, PCO2 20mmHg, and PaO2 40 mmHg. Continuous �uid infusion of 300 ml/hr (dextrose 5%/saline0.9%), and 1-4 unites insulin were initiated, which werecontinued for 52 hours, and piperacillin-tazobactam was initiated for her. The pH and base excess were normalized (pH 7.39, bicarbonate 15.6mmol/lit, base excess -8, negative ketone). Blood culture results showed pseudomonas aeruginosa and susceptibility to piperacillin-tazobactam andmeropenem. Piperacillin-tazobactam was continued for 10 days. The patient was discharged with insulin NPH 6 unites thrice daily and metformin.Empagli�ozin was discontinued permanently.
Ethics
Informed consent was obtained from the patients for publishing data.
MethodWe searched PubMed, Cochrane Library, Scopus databases, and google scholar on January 2022. The key words used were “empagli�ozin” or“dapagli�ozin” or “canagli�ozin” or “Sodium glucose cotransporter 2 inhibitors” AND “diabetes ketoacidosis SGLT2 inhibitors”, “DKA AND SGLT2inhibitors”. Two authors searched on these databases independently. Article references were also assessed for related studies. All eligible casereports (73 case reports and two case series) included in the present review. Data including signs, symptoms, tigers, lab data, and treatmentmodalities are summarized here.
Results And DiscussionCanagli�ozin was the �rst Sodium-glucose cotransporter 2 inhibitor that has been approved by the FDA in march 2013 for glycemic control alongwith diet. Followed by empagli�ozin in August 2014. Empagli�ozin also lowers cardiovascular mortality, hospitalization, and renal outcomes inpatients with heart failures [13, 14]. Subsequently, empagli�ozin was approved for cardiovascular risk reduction in patients with Type 2 diabetesmellites (T2DM), treatment of patients with decreased ejection fraction, cardiovascular death, and hospitalization in patients with heart failure andlow ejection fraction. These agents lower blood sugar through increasing urinary glucose elimination. The SGLT2is prescriptions have increased overrecent years [15]. Although all available studies do not show an association between the SGLT2is and DKA versus other agents [16, 17]. However, theSGLT2is are responsible for 6.6% of all cases of the DKA [18]. The rate of the DKA in the SGLT2is is twice as dipeptidyl peptidase inhibitors in 180days after initiation [19]. The overall incidence of the DKA associated with the SGLT2is was estimated as 0.1–0.43% by the studies [20, 21]. The

Page 4/26
incidence of the SGLT2is -induced DKA is 0.6 to 4.9 events per 1000 patient-years in recent studies [22–24]. In a meta-analysis on 59,747 patients,an odds ratio of 2.86 (1.39–5.86) versus placebo for the DKA was obtained [9]. A recent systematic review and meta-analysis found a hazard ratioof (HR 0.96–2.14) for the DKA with uncertainty [25]. In other words, these medications increase the risk of DKA by 2–3 times [23, 26, 27]. Similar�ndings were also obtained by another meta-analysis [27]. The FDA warned about the association between the diabetes ketoacidosis (DKA) and theSGLT2is [22]. The incidence of hyperglycemic, euglycemic (de�ned as BS < 250 mg/dl, arterial pH < 7.3, HCO3- < 18 meq/L, and anion gap > 10), andhypoglycemic DKA associated with SGLT2is were 0.34%, 0.26%, and 0.08%, respectively, in a recent cohort [21].
A recent multicenter study on 500 patients with DKA showed hazard ratios of 1.86, 2.52, and 3.58 for dapagli�ozin, empagli�ozin, and canagli�ozin,respectively [26]. Euglycemic DKA may be more prevalent with canagli�ozin, followed by empagli�ozin and dapagli�ozin [21]. Lower selectivity ofcanagli�ozin for SGLT2/SGLT1 versus dapagli�ozin and empagli�ozin can be responsible for these differences [28]. DKA associated with the higherdoses of sotagli�ozin (400 mg vs. 200 mg) is greater and occurs in a shorter time [29]. Different mechanisms including lowering serum insulinlevels, along with increased glucagon, counter regulators hormones, lipolysis, and ketone bodies serum concentration have been proposed for theSGLT2is induced DKA [30–32]. An increase in the circulatory concentration of ketone bodies through an increased tubular reabsorption occurs after14 days of the SGLT2is [33, 34].
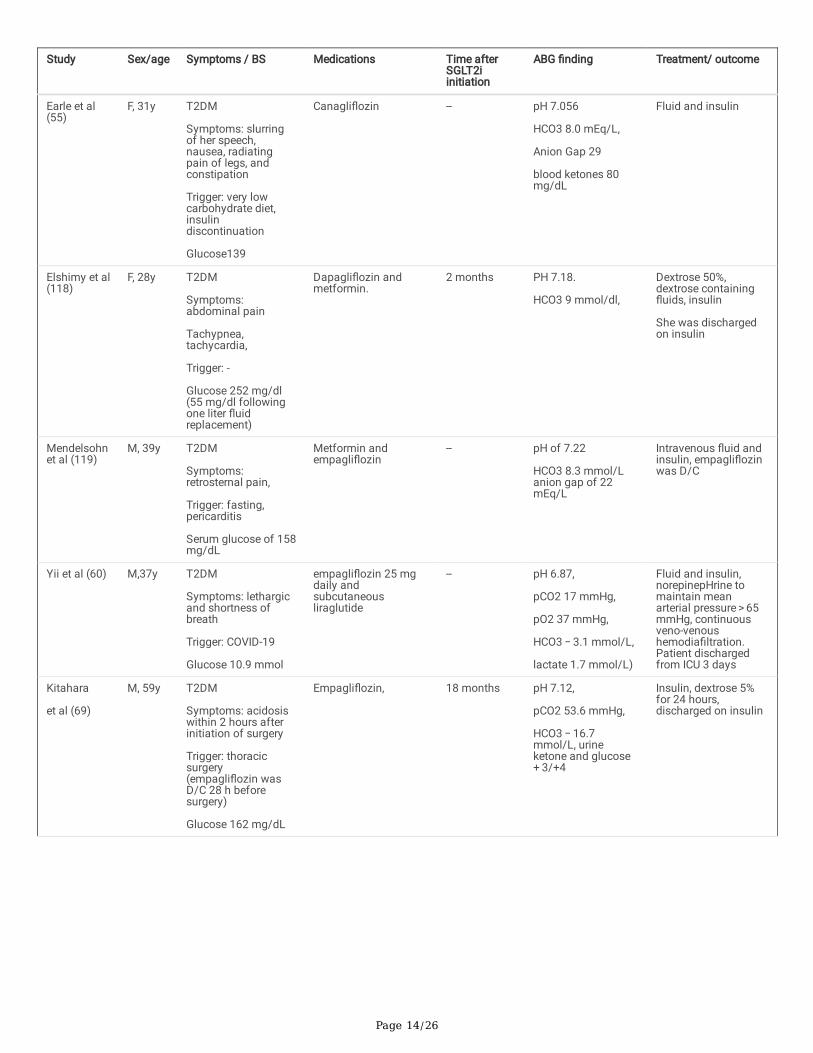
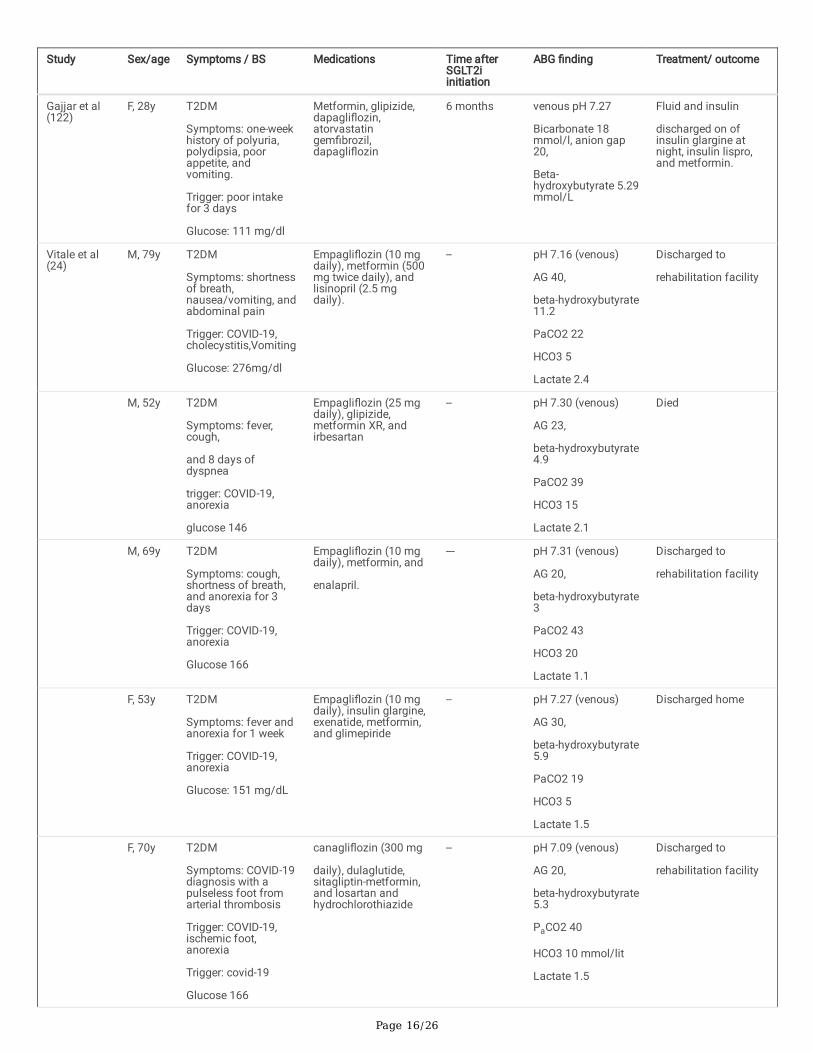
Vomiting, nausea, abdominal pain, tachycardia, malaise, tachypnea, tachypnea, altered mental status, dizziness, syncope, and diarrhea were amongthe most frequently reported signs in patients with the SGLT2is -induced DKA (Table 2). Severe acidosis and hypotension, shock, acute kidney injury,volume depletion are other life-threatening symptoms. In one of the largest case series, Meyer et al. found that 6 out of the 13 patient who developedDKA following SGLT2is used had reductions of missed insulin doses [35]. In 20 patients with DKA or diabetes ketosis, acute illness (70%), insulindose reduction, alcoholism, low medication adherence, fasting, and low body weight were reported as the major risk factors for DKA following theseagents [36]. The risk factors include the Latent Autoimmune Diabetes in Adults (LADA), discontinuing or lowering the dose of insulin, surgery,trauma, pregnancy, increased physical activity, decreased preoperative alcohol intake, starvation or low-calorie diets, fasting, acute coronarysyndromes, heart failure, previous DKA, acute pancreatitis, and acute infections have been proposed as causes for the DKA associated with SGLT2is[37–48]. Nausea, vomiting, dehydration, severe exercise, omit insulin doses, viral and bacterial infections, COVID-19 infection, and acute illness canprecipitate the DKA in SGLT2is s users [24, 35, 49–51]. Low carbohydrate (< 30-50g carbohydrate/day) and ketogenic diets can precipitate the DKAin patients based on the SGLT2is [45, 52–55]. Cardiothoracic surgery is considered as a risk factor for the SGLT2is associated DKA [56–60]. PriorDKA background, higher HA1c (> 10%), baseline bicarbonate levels of < 18 meq/l, use of dementia medications, and digoxin use are other risk factorsproposed in a recent cohort study [24].
Page 5/26
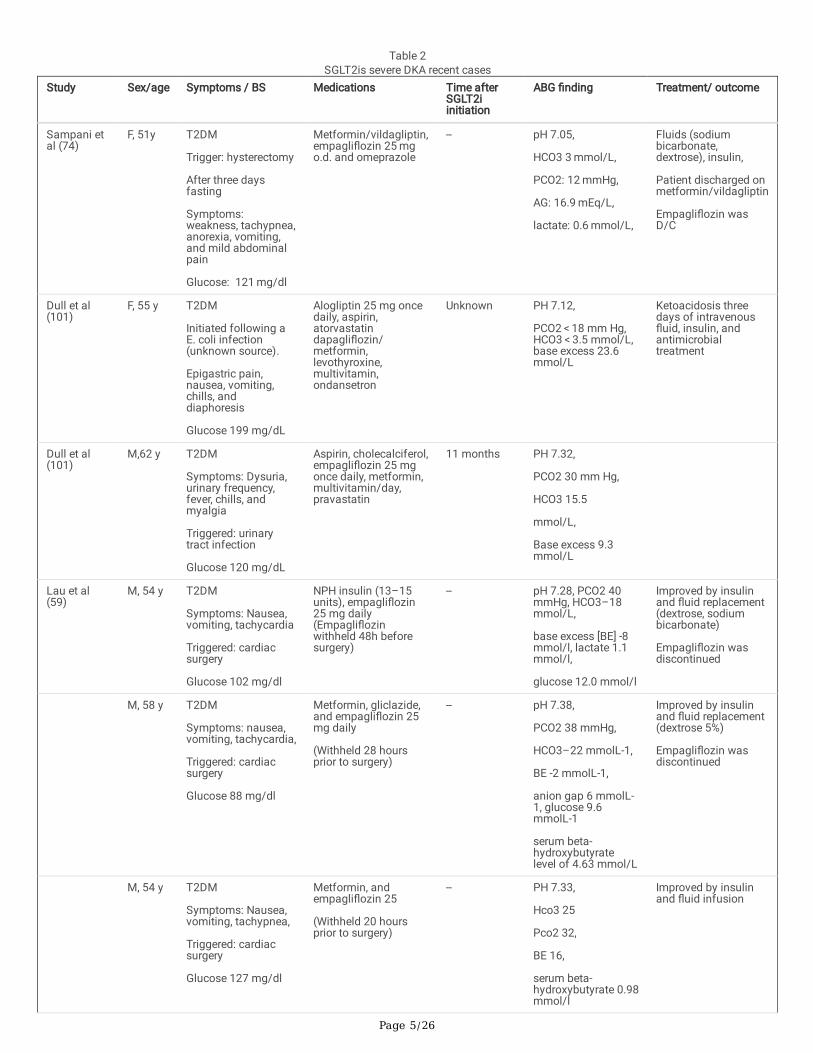
Table 2SGLT2is severe DKA recent cases
Study Sex/age Symptoms / BS Medications Time afterSGLT2iinitiation
ABG �nding Treatment/ outcome
Sampani etal (74)
F, 51y T2DM
Trigger: hysterectomy
After three daysfasting
Symptoms:weakness, tachypnea,anorexia, vomiting,and mild abdominalpain
Glucose: 121 mg/dl
Metformin/vildagliptin,empagli�ozin 25 mgo.d. and omeprazole
-- pH 7.05,
HCO3 3 mmol/L,
PCO2: 12 mmHg,
AG: 16.9 mEq/L,
lactate: 0.6 mmol/L,
Fluids (sodiumbicarbonate,dextrose), insulin,
Patient discharged onmetformin/vildagliptin
Empagli�ozin wasD/C
Dull et al(101)
F, 55 y T2DM
Initiated following aE. coli infection(unknown source).
Epigastric pain,nausea, vomiting,chills, anddiaphoresis
Glucose 199 mg/dL
Alogliptin 25 mg oncedaily, aspirin,atorvastatindapagli�ozin/metformin,levothyroxine,multivitamin,ondansetron
Unknown PH 7.12,
PCO2 < 18 mm Hg,HCO3 < 3.5 mmol/L,base excess 23.6mmol/L
Ketoacidosis threedays of intravenous�uid, insulin, andantimicrobialtreatment
Dull et al(101)
M,62 y T2DM
Symptoms: Dysuria,urinary frequency,fever, chills, andmyalgia
Triggered: urinarytract infection
Glucose 120 mg/dL
Aspirin, cholecalciferol,empagli�ozin 25 mgonce daily, metformin,multivitamin/day,pravastatin
11 months PH 7.32,
PCO2 30 mm Hg,
HCO3 15.5
mmol/L,
Base excess 9.3mmol/L
Lau et al(59)
M, 54 y T2DM
Symptoms: Nausea,vomiting, tachycardia
Triggered: cardiacsurgery
Glucose 102 mg/dl
NPH insulin (13–15units), empagli�ozin25 mg daily(Empagli�ozinwithheld 48h beforesurgery)
-- pH 7.28, PCO2 40mmHg, HCO3–18mmol/L,
base excess [BE] -8mmol/l, lactate 1.1mmol/l,
glucose 12.0 mmol/l
Improved by insulinand �uid replacement(dextrose, sodiumbicarbonate)
Empagli�ozin wasdiscontinued
M, 58 y T2DM
Symptoms: nausea,vomiting, tachycardia,
Triggered: cardiacsurgery
Glucose 88 mg/dl
Metformin, gliclazide,and empagli�ozin 25mg daily
(Withheld 28 hoursprior to surgery)
-- pH 7.38,
PCO2 38 mmHg,
HCO3–22 mmolL-1,
BE -2 mmolL-1,
anion gap 6 mmolL-1, glucose 9.6mmolL-1
serum beta-hydroxybutyratelevel of 4.63 mmol/L
Improved by insulinand �uid replacement(dextrose 5%)
Empagli�ozin wasdiscontinued
M, 54 y T2DM
Symptoms: Nausea,vomiting, tachypnea,
Triggered: cardiacsurgery
Glucose 127 mg/dl
Metformin, andempagli�ozin 25
(Withheld 20 hoursprior to surgery)
-- PH 7.33,
Hco3 25
Pco2 32,
BE 16,
serum beta-hydroxybutyrate 0.98mmol/l
Improved by insulinand �uid infusion

Page 6/26
Study Sex/age Symptoms / BS Medications Time afterSGLT2iinitiation
ABG �nding Treatment/ outcome
Latif et al(75)
F, 43 y T2DM
Symptoms: vomiting,cough, shortness ofbreath andgeneralized weakness
Trigger: Ketogenicdiet
Glucose: 169 mg/dl
Empagli�ozin 25mg/d,metformin 1000mg/bd
2 months pH of 7.01,
PO2 119mm Hg,
CO2 5mm Hg,
HCO3: 5 mmol/L
Fluid and insulininfusion
Puls et al(77)
(Mediandata)
5patients(3 wereM)
57 y(43, 53,57, 63,73)
T2DM
Symptoms: Nausea(60%), vomiting (60%)and fatigue (40%),one patient (20%)loss ofconsciousness
Glucose 191 mg/dl
(176, 190, 191, 192,215)
Not speci�ed (at leastthree oral agents)
20 months(17, 20, 21)
PH 7.01
(6.95, 7.01, 7.01,7.10, 7.30)
HCO3 = 8
(6, 7, 8, 9, 13)
AG 27
(26, 27, 27, 28, 31),
serum beta-hydroxybutyrate
9.9 mmol/L
(9.2, 9.4, 9.9, 11.4,12.3)
urine ketones 150mg/dL (150–150).
Fluid and Insulintreatment for median23.82 hours
Meyer et al(35)
12patients(9female)
with euglycemic DKA
8/13 T2DM, 5 T1DM
Trigger (somepatients may havemultiple risk factors):
Surgery orpreoperative (13/13),
Acute coronarysyndrome (2/13),
Infections (4/13),
Reduced oral intake(1/13)
CABG (1/13)
Missed insulin (5/13),
Chemotherapy (1/13),cardiomyopathy,cardiogenic shock(1/13)
Renal or kidneyimpairment (2/13)
No risk (1/13)
Blood glucose
<250 mg/dl
13 patients with DKA(9/13) dapagli�ozin(10 mg/d) and 4/13empagli�ozin (10-25mg/d)
Metformin 13/13,
Sitagliptin orlinagliptin 3/13,
gliclazide 1/13,acarbose 1/13
< 1month(3/13),
1–3 months(2/13)
> 3 months(6/13)
Unknown(2/13)
PH
6.9(2/13)
7 (1/13)
7.1(2/13)
7.2(1/13)
7.3(2/13)
unknow(5/13)
HCO3
2–4(3/13)
5–9(6/13)
10–14(4/13)
Time to resolution24–48 hours,
Death (1/13)

Page 7/26
Study Sex/age Symptoms / BS Medications Time afterSGLT2iinitiation
ABG �nding Treatment/ outcome
Sethi et al(102)
F, A 55y T2DM
Symptoms: Low-grade fever, vomiting,and lethargy
Triggered: lowerrespiratory infection
Glucose 125-175mg/dL
Dapagli�ozin 10 mg/d
glimepiride 2 mg, andinsulin glargine 18units at bedtime
Notmentioned
pH 7.18,
pCO2 14.3 mmHg,
pO2 107 mmHg,
HCO3 5.2 mmol/L
Insulin and hydration
Chou et al(76)
F, 61 y T2DM
Symptoms:weakness, nausea,vomiting, abdominalpain, Kussmaulbreathing, sunkeneyes, dry oralmucosa, reduced skinturgor
Trigger: Reducedintake due totoothache,
Glucose 180 mg/dl
Dapagli�ozin 10mg/day, metforminand glibenclamide
2 weeks pH 6.986,
CO2 20.9 mm Hg,HCO3− 7.0 mEq/L,anion gap 20 mEq/L
Dapagli�ozin d/c
Discharged after twodays of insulin �uidreplacement
Iqbal et al(103)
F,74y T2DM
Symptoms:Confusion and lossof consciousness,hypotension,bradycardia
Trigger: in�uenza
Glucose 187 mg/dL
Metformin,pioglitazone,amlodipine,atorvastatin, andezetimibe,dapagli�ozin
2 weeks pH: 7.009,
pCO2: 18.2 mmHg,HCO3: 5.1 mmol/L.
Serum osmolarity312 mOsm/kg,
osmolar anion gapof 12 mOsm/kg.
Dapagli�ozin d/c
Fluid and insulin for15 hours
Hussaini etal (63)
M, 49y T2DM
Craniotomy (right-sided middle
cerebral artery stroke)
Glucose 163 mg/dl
Sitagliptin/metformin,gliclazide,dapagli�ozin 10 mgdaily
5 years (DKAwas occurred72 hours afterdapagli�ozinD/C
Arterial pH 7.168,
HCO3 12 mmol/l,
Pco2 37,
anion gap 20.7,
Intravenous �uids,dextrose, and insulin
Osafehinti etal (57)
M, 60y T2DM,
Asymptomatic
Trigger: CABG
Glucose 138mg/dl
Glimepiride,metformin,subcutaneoussemaglutide,empagli�ozin (10 mgorally daily)
1 year pH 7.275,
HCO3 15 mmol/L,
anion gap of 25mmol/L,
Insulin and infusion of5% dextrose for 3days
norepinepHrine (for 24hours)
Alabdaljabaret al (58)
M, 52y T2DM
Triger: CABG
Asymptomatic
Glucose 166 mg/dl
vildagliptin-metformin,empagli�ozin (10 mg),pioglitazone,irbesartan-hydrochlorothiazide,atorvastatin (20 mg),aspirin
(Empagli�ozin wasD/C 24 hours beforesurgery)
-- pH of 7.225,
HCO3 − 14.60 mmol/L
anion gap of 17.40
sodium 152 mg/dl
urine ketone 3+
urine glucose 4+
IV �uids and insulininfusion (12 hours)

Page 8/26
Study Sex/age Symptoms / BS Medications Time afterSGLT2iinitiation
ABG �nding Treatment/ outcome
Steinmetz-Wood et al(54)
M, 47y T2DM
Symptoms:weakness,intermittent chestdiscomfort, andshortness ofbreath (�rst episode)
Symptoms:tachypneic andtachycardic and hadmild abdominaltenderness
(Second episodes)
Trigger: ketogenicdiet/ low intake, andurinary tract infection
Glucose 269 mg/dl
glucose 269 mg/dl
Metformin andempagli�ozin
-- pH 7.22
HCO3 13 mmol/L
anion gap of 21,
second episode:
pH 6.94,
HCO3 5 mmol/L,
3 + urinary ketones,
beta-hydroxybutyratelevel of 8.9 mmol/L,
Fluid and insulin,
In the �rst episodeketogenic diet wasconsideredresponsible for DKA
Empagli�ozin D/C atthe secondpresentationinde�nitely
Wang et al(30)
40y, F T2DM
Symptoms(associated):
slurred speech, MRIshowed acute leftanterior cerebralinfarct
Trigger: cerebralrevascularizationpostoperatively,
Atorvastatin,levothyroxine,metformin,pioglitazone, andempagli�ozin.
-- pH of 7.01,
PCO2 11 mm Hg,
anion gap 27,
HCO3 not mentioned
Patients treated forone day (iv �uid andinsulin),pHenylepHrine, and�udrocortisone.
Patient died due toacute stroke
Yasuma etal (104)
F, 43y T2DM
Trigger: insulin D/C
Symptoms: fatigueand vomiting
Glucose 184 mg/dl
Switched from insulinto metformin 500mg/d, empagli�ozin10 mg/d, andvildagliptin 100 mg/d.
4 days pH, 7.18;
pCO2, 18 mmHg;
HCO3, 6.6 mEq/L;
base excess, -19.3mmol/L;
A-gap, 27.6 mmol/L
Fluid and insulin fortwo days,
Lindsay et al(44)
M, 51y T2DM,
Trigger: gangreneFournier
glucose level of 212mg/dL
Empagli�ozin 25 mgdaily, metformin 1000mg twice daily,lisinopril 10 mg daily,atorvastatin 20 mgdaily and aspirin 81mg daily
-- pH 7.12,
anion gap 31),
low bicarbonate level(6 mmol/L),
elevated creatinine(1.64 mg/dL)
All oral medicationsd/c 24 h beforepresentation, DKAresolved after �uid,insulin and few hoursvasopressor therapy
Kasbawalaet al (46)
F, 37y T2DM
Symptoms: Dysuria,pain
Trigger: gangreneFournier
Glucose 402 mg/dL
Canagli�ozin,Cetirizine, Citalopram,Levothyroxine,levothyroxine,pantoprazole,pravastatin, Sitagliptin-metformin, trazodone,valacyclovir
1 month b-hydroxybutyrate of2.49 mmol/L.
pH of 7.23
PCO2 34 mmHg.
Insulin infusion withaggressive �uidresuscitation
canagli�ozin was D/C
Page 9/26
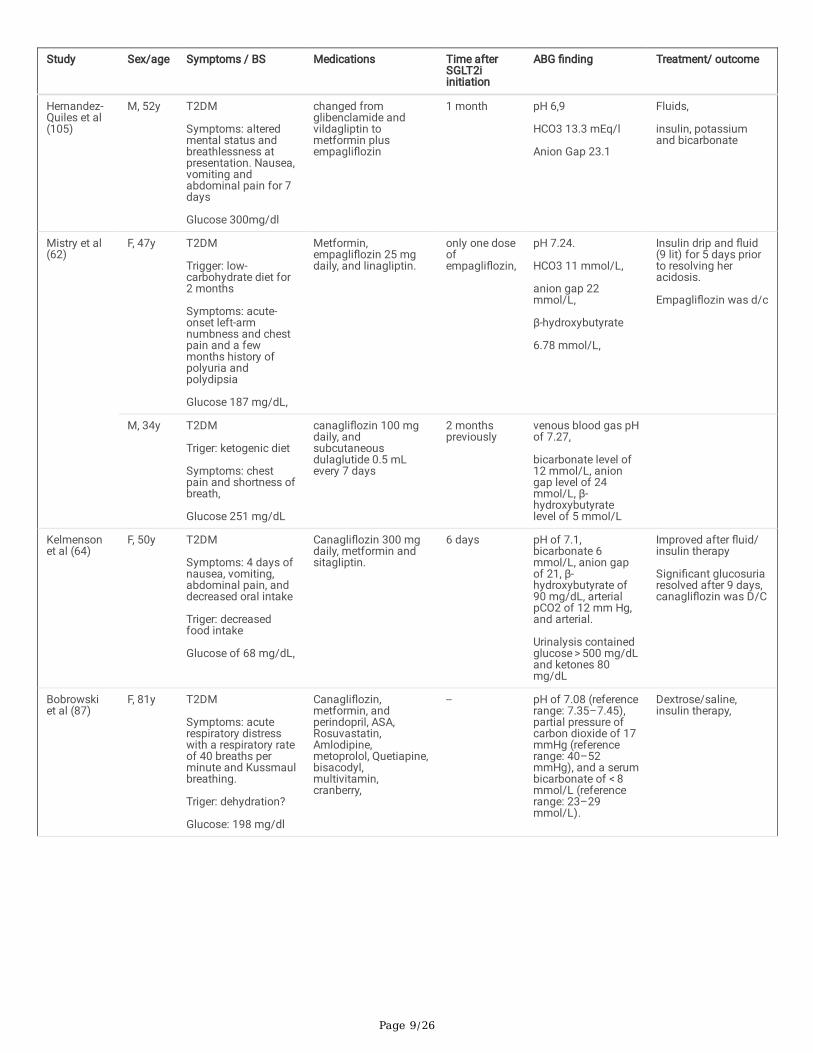
Study Sex/age Symptoms / BS Medications Time afterSGLT2iinitiation
ABG �nding Treatment/ outcome
Hernandez-Quiles et al(105)
M, 52y T2DM
Symptoms: alteredmental status andbreathlessness atpresentation. Nausea,vomiting andabdominal pain for 7days
Glucose 300mg/dl
changed fromglibenclamide andvildagliptin tometformin plusempagli�ozin
1 month pH 6,9
HCO3 13.3 mEq/l
Anion Gap 23.1
Fluids,
insulin, potassiumand bicarbonate
Mistry et al(62)
F, 47y T2DM
Trigger: low-carbohydrate diet for2 months
Symptoms: acute-onset left-armnumbness and chestpain and a fewmonths history ofpolyuria andpolydipsia
Glucose 187 mg/dL,
Metformin,empagli�ozin 25 mgdaily, and linagliptin.
only one doseofempagli�ozin,
pH 7.24.
HCO3 11 mmol/L,
anion gap 22mmol/L,
β-hydroxybutyrate
6.78 mmol/L,
Insulin drip and �uid(9 lit) for 5 days priorto resolving heracidosis.
Empagli�ozin was d/c
M, 34y T2DM
Triger: ketogenic diet
Symptoms: chestpain and shortness ofbreath,
Glucose 251 mg/dL
canagli�ozin 100 mgdaily, andsubcutaneousdulaglutide 0.5 mLevery 7 days
2 monthspreviously
venous blood gas pHof 7.27,
bicarbonate level of12 mmol/L, aniongap level of 24mmol/L, β-hydroxybutyratelevel of 5 mmol/L
Kelmensonet al (64)
F, 50y T2DM
Symptoms: 4 days ofnausea, vomiting,abdominal pain, anddecreased oral intake
Triger: decreasedfood intake
Glucose of 68 mg/dL,
Canagli�ozin 300 mgdaily, metformin andsitagliptin.
6 days pH of 7.1,bicarbonate 6mmol/L, anion gapof 21, β-hydroxybutyrate of90 mg/dL, arterialpCO2 of 12 mm Hg,and arterial.
Urinalysis containedglucose > 500 mg/dLand ketones 80mg/dL
Improved after �uid/insulin therapy
Signi�cant glucosuriaresolved after 9 days,canagli�ozin was D/C
Bobrowskiet al (87)
F, 81y T2DM
Symptoms: acuterespiratory distresswith a respiratory rateof 40 breaths perminute and Kussmaulbreathing.
Triger: dehydration?
Glucose: 198 mg/dl
Canagli�ozin,metformin, andperindopril, ASA,Rosuvastatin,Amlodipine,metoprolol, Quetiapine,bisacodyl,multivitamin,cranberry,
-- pH of 7.08 (referencerange: 7.35–7.45),partial pressure ofcarbon dioxide of 17mmHg (referencerange: 40–52mmHg), and a serumbicarbonate of < 8mmol/L (referencerange: 23–29mmol/L).
Dextrose/saline,insulin therapy,

Page 10/26
Study Sex/age Symptoms / BS Medications Time afterSGLT2iinitiation
ABG �nding Treatment/ outcome
Yehya et al(89)
F, 57y T2DM
Triger: breast abscess(right breasttenderness andfever),
Glucose 469 mg/dl at�rst course oftherapy, < 150 mg/dlat the second course(de�nite diagnosis ofempagli�ozin relatedDKA)
Metformin,pioglitazone,
empagli�ozin 25 mg
3 weeks Bicarbonate 5mEq/L, elevatedanion
gap of 29 mEq/L,glucosuria 3+,
7 hours aftertreatment d/c: 7hours later 7 mEq/L,anion gap increasedto 22 mEq/L, andBHOB
increased to 6.45mmol/L
Early �uid and insulintherapy improvedABG, however,
28 hours �uid(saline/dextrose) andinsulin therapy
Adachi et al(106)
F, 27y T2DM
Symptoms: dizziness,and then upperabdominal pain, thirstand malaise, andpolyuria (> 5l/day)
Triger: lowcarbohydrate diet
Glucose: 240 mg/dL
Gliclazide, metformin,sitagliptin, andcanagli�ozin (300mg/day)
3 months pH 6.906, pCO216.6mmHg, pO2128.2(mmHg),Bicarbonate(mmol/L) 6.6, Baseexcess(mmol/L)-28.5
Improved after 4 daysof �uid therapy,
Aggarwal etal (107)
M, 53y T2DM
Trigger: laparoscopicappendectomy?
Symptoms:generalizedabdominal pain, non-exertional shortnessof breath, and fever.Fever, tachycardia,tachypnea, lowoxygen saturation.
Glucose 126 mg/dL
Metformin andcanagli�ozin,
-- pH 7.21, Bicarbonate17 mEq/L, bloodurea nitrogen (BUN)11 mg/dL, andcreatinine 0.9mg/dL, anion gap of20.8 mEq/L,glucosuria (urineglucose > 1500mg/dL) andketonuria
Canagli�ozin was d/c,insulin drip with 10%dextrose for two days,
Fieger etal(108)
F, 42y T2DM,
Symptoms: nauseaand vomiting,tachypnea,tachycardia,
Trigger: very lowcarbohydrateketogenic diet, insulind/c
Blood glucose was152 mg/dL
Insulin and glyburide,sitagliptin-metformin.
Insulin and glyburided/c and canagli�ozinwas started two weeksbefore presentations.
Two weeks pH of 7.11 and apCO2 of 16 mm Hg,Urinalysis ketones of80 mg/dL,glucosuria at > 500mg/dL
PCO2 7 mmol/L,anion gap of 19mmol/L
four days of �uid andinsulin treatment.discharged on 30units of glargineinsulin daily,sitagliptin-metformin50 mg/1,000 mg twicea da
Kapila et al(109)
F, 51y T2DM
Symptoms:generalizedabdominal pain,shortness of breath,and fever.
Trigger: ketogenic dietfor two weeks andsleeve surgery
Blood glucose 150 to180 mg/dL
insulin aspart, insulinglargine, metformin,and canagli�ozin
-- pH of 7.21,bicarbonate 8mEq/L, Pco2 60mmHg, anion gap of37 mEq/L.
Three days of �uid(dextrose 5%) andinsulin therapy,canagli�ozin D/c
Page 11/26
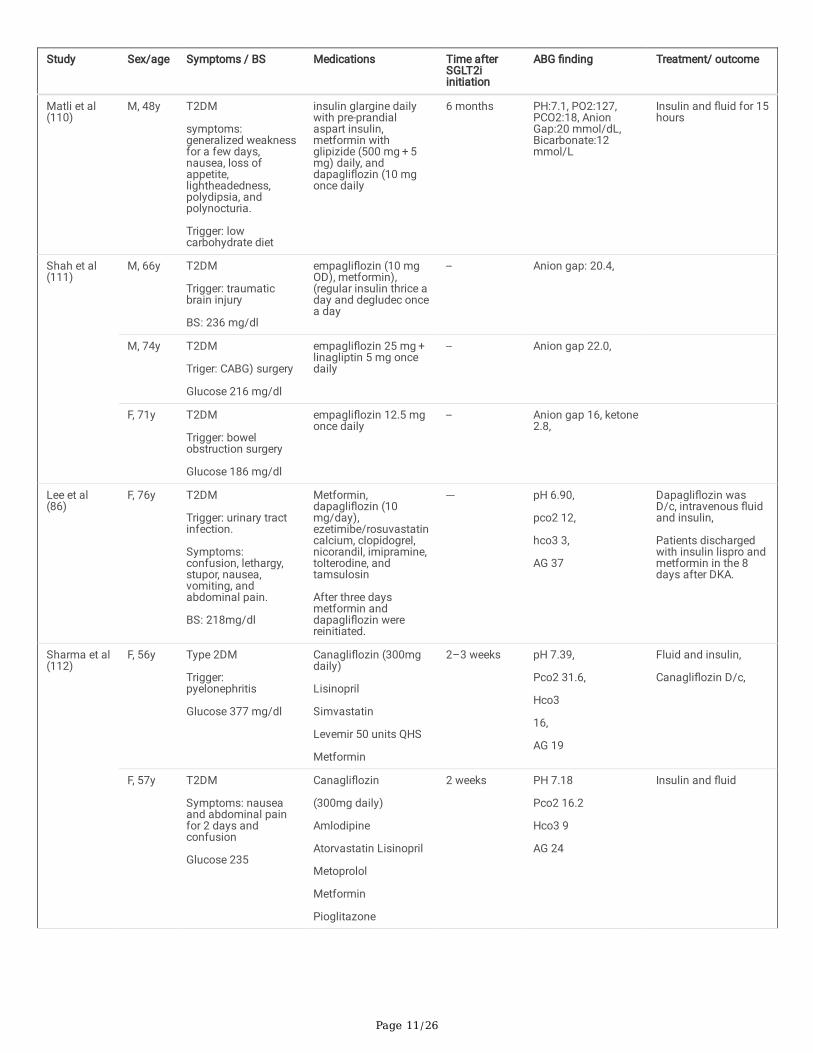
Study Sex/age Symptoms / BS Medications Time afterSGLT2iinitiation
ABG �nding Treatment/ outcome
Matli et al(110)
M, 48y T2DM
symptoms:generalized weaknessfor a few days,nausea, loss ofappetite,lightheadedness,polydipsia, andpolynocturia.
Trigger: lowcarbohydrate diet
insulin glargine dailywith pre-prandialaspart insulin,metformin withglipizide (500 mg + 5mg) daily, anddapagli�ozin (10 mgonce daily
6 months PH:7.1, PO2:127,PCO2:18, AnionGap:20 mmol/dL,Bicarbonate:12mmol/L
Insulin and �uid for 15hours
Shah et al(111)
M, 66y T2DM
Trigger: traumaticbrain injury
BS: 236 mg/dl
empagli�ozin (10 mgOD), metformin),(regular insulin thrice aday and degludec oncea day
-- Anion gap: 20.4,
M, 74y T2DM
Triger: CABG) surgery
Glucose 216 mg/dl
empagli�ozin 25 mg + linagliptin 5 mg oncedaily
-- Anion gap 22.0,
F, 71y T2DM
Trigger: bowelobstruction surgery
Glucose 186 mg/dl
empagli�ozin 12.5 mgonce daily
-- Anion gap 16, ketone2.8,
Lee et al(86)
F, 76y T2DM
Trigger: urinary tractinfection.
Symptoms:confusion, lethargy,stupor, nausea,vomiting, andabdominal pain.
BS: 218mg/dl
Metformin,dapagli�ozin (10mg/day),ezetimibe/rosuvastatincalcium, clopidogrel,nicorandil, imipramine,tolterodine, andtamsulosin
After three daysmetformin anddapagli�ozin werereinitiated.
--- pH 6.90,
pco2 12,
hco3 3,
AG 37
Dapagli�ozin wasD/c, intravenous �uidand insulin,
Patients dischargedwith insulin lispro andmetformin in the 8days after DKA.
Sharma et al(112)
F, 56y Type 2DM
Trigger:pyelonephritis
Glucose 377 mg/dl
Canagli�ozin (300mgdaily)
Lisinopril
Simvastatin
Levemir 50 units QHS
Metformin
2–3 weeks pH 7.39,
Pco2 31.6,
Hco3
16,
AG 19
Fluid and insulin,
Canagli�ozin D/c,
F, 57y T2DM
Symptoms: nauseaand abdominal painfor 2 days andconfusion
Glucose 235
Canagli�ozin
(300mg daily)
Amlodipine
Atorvastatin Lisinopril
Metoprolol
Metformin
Pioglitazone
2 weeks PH 7.18
Pco2 16.2
Hco3 9
AG 24
Insulin and �uid

Page 12/26
Study Sex/age Symptoms / BS Medications Time afterSGLT2iinitiation
ABG �nding Treatment/ outcome
F, 46y T2DM
Symptoms:
Trigger: nausea anddiarrhea for two days
Glucose 203
Canagli�ozin
(300 mg daily)
Pioglitazone
Metformin
Atorvastatin
5 days PH 7.04
Pco2 20
Hco3 8
AG 23
Fluid and insulin
Canagli�ozin D/C,insulin detemir wasadd to medications
F, 63y T2DM
Symptoms:generalizedweakness, abdominalpain, nausea,vomiting and diarrheafor four days
Trigger: poorcompliance tomedications (insulinand metformin),bacteremia
Glucose 400 mg/dl
Dulaglutide
Metformin
Empagli�ozin
(10mg daily)
Unknown PH 7.24
Pco2 20
Hco3 9
AG 22
Insulin and �uid
Badwal et al(113)
M, 25y T2DM
Trigger: acutepancreatitis,
Symptoms:tachypnea andtachycardia
BS: 120mg/dl and200mg/dl
Type II diabetes onmetformin, sitagliptin,and dapagli�ozin
All were continueduntil diagnosis of DKA
--- PH 7.14
Pco2 20
Hco3 5
AG 32
Fluid and insulin
Dapagli�ozin,pioglitazone andsitagliptin was D/C,
Morrison etal (50)
M, 40y T2DM
Symptoms: non-bloody, non-biliousvomiting, and poororal intake,diaphoretic
Trigger: COVID-19,poor intake,
glucose 177 mg/dL
empagli�ozin 25mg/daily, semaglutide,metformin,atorvastatin, moda�nil
--- pH of 7.06,
PCo2 37 mm Hg,
PaO2 31 mm Hg,bicarbonate 10.0mEq/L, lactate 2.3mmol/L.
Fluid and insulin for 3days, discharged after4 days on glargine
Brown et al(114)
M, 53y T2DM
symptoms: nausea,vomiting, anorexia,and generalized
abdominal pain.
trigger: poor intake
glucose 162 mg/dL
Metformin,dapagli�ozin,omeprazole,perindopril,atorvastatin, andamitriptyline
-- PH 7.24,
Anion gap of 30, andlactate of 4.5mmol/L
Insulin and �uid
Allison et al(115)
M, 47y T2DM
Symptoms:generalized weakness
Trigger:
Glucose 216 mg/dL
teri�unomide for thetreatment of MS,subcutaneous regularinsulin taken withmeals, metformin, andempagli�ozin
--- bicarbonate 10mmol/L, anion gapwas 24. Urineketones 4 + and 3 + glucose.
Fluid and insulin

Page 13/26
Study Sex/age Symptoms / BS Medications Time afterSGLT2iinitiation
ABG �nding Treatment/ outcome
Goto et al(73)
Female,52y
T2DM
symptoms:tachypnea, vomiting,and decreased bloodpressure
Trigger: low intakedue to dental pain
glucose: 178 mg/dL
empagli�ozin 10 mgsitagliptin), ezetimibe10 rosuvastatin,clopidogrel 75
-- pH, 6.84; HCO3–level, 2.1 mEq/L;base excess, − 20.0mmol/L; anion gap,31.9 mmol/L; andlactate level, 2.4mmol/L
Empagli�ozin D/C,�uid, bicarbonate,insulin, vasopressor
F, 76-y Type 2 diabetesmellitus
Trigger: gastrojejunalbypass surgery
Symptoms: cardiacarrest due toacidemia,
Glucose: 140 mg/dL
canagli�ozin 100 mgdaily and metformin,cilnidipine, feno�brate
--- pH, 7.25; HCO3–level, − 17.3 mEq/L;base excess, − 9.1;anion gap, 16.2mmol/L; and lactatelevel, 0.8 mmol/L
Fluid and insulintreatment,
Fukuda et al(72)
F, 71y T2DM
Symptoms: malaise,nausea andabdominal pain
Trigger: reduced oralintake for two weeks
Glucose: 259 mg/dL.
canagli�ozin,metformin, andsaxagliptin
1 month pH, 6.860; CO2, 8mmHg, HCO3, − 1.0mEq/L; base excess:− 31.3 mmol/L
Chai et al(116)
F, 55y T2DM
Symptoms: nausea,vomiting, abdominalpain, and polyuriaover 24 hours,
Glucose 366 mg/dl
Canagli�ozin 300 mg -- PH 7.09
Hco3 8.8
Pco2 29
Anion gap:32
Canagli�ozin wasD/C, insulin and �uidwas initiated. Patientdischarged onmetformin andglipizide
M, 54 y T1DM
Symptoms:abdominal pain,nausea, vomiting, andabdominal pain
Glucose327 mg/dL
insulin (humalog25/35 AM/PM),albiglutide 50 mg, andcanagli�ozin 300 mgPO daily
--- PH 7.15
Hco3 10
Pco2 29
Anion gap:27
Fluid and insulin
Lucero et al(117)
F, 50y T2DM
Symptoms: diarrheaand vomiting
Glucose 165 mg/dl
Dapagli�ozin 10mg/day, and NPHinsulin at 40 and 60 IU.
-- PH 7.13
Hco3 2
BE -23.7
AG 32
Fluid and insulin
Sloan et al(88)
M, 63y T2DM
Symptoms: vomiting,diarrhea, anorexiaand right upperquadrant abdominalpain
glucose: 239 mmol/L
Metformin, aspirin,simvastatin and twicedaily pre-mixed
insulin. canagli�ozin
7 months blood glucose was
13.3mmol/L and 3-hydroxybutyrate5.2mmol/L.
Venous bloodglucose wasdetermined; pH: 7.15and
bicarbonate:8mmol/L
All medications wereD/C, Fluid and insulinafter improvement inglucose, pH,bicarbonate and 3-hydroxybutyratesubcutaneous insulinwas initiated on day 3.However, ketonemiaaggravated andadditional two days(total 5 days) wasrequired tobiochemicalimprovement.
Page 14/26
Study Sex/age Symptoms / BS Medications Time afterSGLT2iinitiation
ABG �nding Treatment/ outcome
Earle et al(55)
F, 31y T2DM
Symptoms: slurringof her speech,nausea, radiatingpain of legs, andconstipation
Trigger: very lowcarbohydrate diet,insulindiscontinuation
Glucose139
Canagli�ozin -- pH 7.056
HCO3 8.0 mEq/L,
Anion Gap 29
blood ketones 80mg/dL
Fluid and insulin
Elshimy et al(118)
F, 28y T2DM
Symptoms:abdominal pain
Tachypnea,tachycardia,
Trigger: -
Glucose 252 mg/dl(55 mg/dl followingone liter �uidreplacement)
Dapagli�ozin andmetformin.
2 months PH 7.18.
HCO3 9 mmol/dl,
Dextrose 50%,dextrose containing�uids, insulin
She was dischargedon insulin
Mendelsohnet al (119)
M, 39y T2DM
Symptoms:retrosternal pain,
Trigger: fasting,pericarditis
Serum glucose of 158mg/dL
Metformin andempagli�ozin
-- pH of 7.22
HCO3 8.3 mmol/Lanion gap of 22mEq/L
Intravenous �uid andinsulin, empagli�ozinwas D/C
Yii et al (60) M,37y T2DM
Symptoms: lethargicand shortness ofbreath
Trigger: COVID-19
Glucose 10.9 mmol
empagli�ozin 25 mgdaily andsubcutaneousliraglutide
-- pH 6.87,
pCO2 17 mmHg,
pO2 37 mmHg,
HCO3 − 3.1 mmol/L,
lactate 1.7 mmol/L)
Fluid and insulin,norepinepHrine tomaintain meanarterial pressure > 65mmHg, continuousveno-venoushemodia�ltration.Patient dischargedfrom ICU 3 days
Kitahara
et al (69)
M, 59y T2DM
Symptoms: acidosiswithin 2 hours afterinitiation of surgery
Trigger: thoracicsurgery(empagli�ozin wasD/C 28 h beforesurgery)
Glucose 162 mg/dL
Empagli�ozin, 18 months pH 7.12,
pCO2 53.6 mmHg,
HCO3 − 16.7mmol/L, urineketone and glucose + 3/+4
Insulin, dextrose 5%for 24 hours,discharged on insulin

Page 15/26
Study Sex/age Symptoms / BS Medications Time afterSGLT2iinitiation
ABG �nding Treatment/ outcome
Nappi
et al (68)
F, 67 F T2DM
Symptoms:abdominal pain andimpaired levelconscious,tachypnea,tachycardia,hypotension, acutekidney injury,dehydration.
Trigger: low caloryregimen, infection
Glucose 299mg/dl
Empagli�ozin 25mg/day, metformin,NSAIDS,
1 month PH 6.91
Hco3 1.8
AG 31
Lactate 1.3
Pco2 9
Pao2 138
Insulin, �uid,bicarbonate, renalreplacement therapy,
Patient discharged oninsulin
Dorcely et al(120)
M, 61y T2DM
Symptoms: nauseaand right-sided chestpain
Trigger: ketogenic diet
glucose 84 mg/dl
Empagli�ozin 10 mgdaily, metforminliraglutide,rosuvastatin,ezetimibe, omeprazole
3 years PH ---
anion gap 17
bicarbonate 17
beta hydroxybutyricacid 4.1
Fluid (3 lit) andinsulin, empagli�ozinwas d/c
Improved after 24hours
Polina et al(121)
F, 45y T1DM
Symptoms:weakness, nausea,and emesis, chills,fatigue, and polyuriathe day prior topresentation, non-bloody emesis
Trigger:
Glucose: 224 mg/dl
Canagli�ozin, andinsulin pump
-- pH of 7.199
AG 32,
beta-hydroxybutyrate5.89.
PaCO2 20
Fluid and insulin
Yeo et al
(47)
F, 23y T2DM
Symptoms: severeabdominal pain
Trigger: pancreatic,clostridium infection
Glucose 148mg/dl
Metformin anddapagli�ozin (10 mg,once a day) as oralhypoglycemic
2 years H, 7.029;
HCO3- 1.8 mmol/L;serum ketone, 2+;
Urine ketone, 2+
continuous renalreplacement therapy,dapagli�ozin was D/C
discharged onmetformin and insulin
Bitar et al(81)
F, 64y T2DM
Symptoms:headaches andbreathlessness,tachycardia,tachypnea,hypotension
Trigger:
Glucose: 90 mg/dl
GlucopHage/da-pagli�ozin, aspirin, andatorvastatin
4 weeks PH 6.6
HCO3, mmol/L5
Lactate, mmol/L1.2
Anion gap38
β-hydroxybutyrate,mmol9
Intravenous �uid,insulin (up to 10units/hour), anddextrose, andbicarbonate
Insulin was continuedfor 48 hours
Discharged onglargine basal insulin,insulin aspart, beforemeals, andGlucopHage
M, 56y T1DM
Symptoms: dizziness,tachycardia,
Insulin aspart beforeeach meal, insulindegludec (ultralong-acting basal insulin),and liraglutide
semaglutide
2 months PH 6.9
HCO3, mmol/L8.8
Lactate, mmol/L1.4
β-hydroxybutyrate,mmol6.9
urine ketones +++++
intravenous dextrose�uid with normalsaline and insulininfusion in twodifferent intravenouslines, with a bolus ofNa2HCO3 to keep thepH above 7
Page 16/26
Study Sex/age Symptoms / BS Medications Time afterSGLT2iinitiation
ABG �nding Treatment/ outcome
Gajjar et al(122)
F, 28y T2DM
Symptoms: one-weekhistory of polyuria,polydipsia, poorappetite, andvomiting.
Trigger: poor intakefor 3 days
Glucose: 111 mg/dl
Metformin, glipizide,dapagli�ozin,atorvastatingem�brozil,dapagli�ozin
6 months venous pH 7.27
Bicarbonate 18mmol/l, anion gap20,
Beta-hydroxybutyrate 5.29mmol/L
Fluid and insulin
discharged on ofinsulin glargine atnight, insulin lispro,and metformin.
Vitale et al(24)
M, 79y T2DM
Symptoms: shortnessof breath,nausea/vomiting, andabdominal pain
Trigger: COVID-19,cholecystitis,Vomiting
Glucose: 276mg/dl
Empagli�ozin (10 mgdaily), metformin (500mg twice daily), andlisinopril (2.5 mgdaily).
-- pH 7.16 (venous)
AG 40,
beta-hydroxybutyrate11.2
PaCO2 22
HCO3 5
Lactate 2.4
Discharged to
rehabilitation facility
M, 52y T2DM
Symptoms: fever,cough,
and 8 days ofdyspnea
trigger: COVID-19,anorexia
glucose 146
Empagli�ozin (25 mgdaily), glipizide,metformin XR, andirbesartan
-- pH 7.30 (venous)
AG 23,
beta-hydroxybutyrate4.9
PaCO2 39
HCO3 15
Lactate 2.1
Died
M, 69y T2DM
Symptoms: cough,shortness of breath,and anorexia for 3days
Trigger: COVID-19,anorexia
Glucose 166
Empagli�ozin (10 mgdaily), metformin, and
enalapril.
--- pH 7.31 (venous)
AG 20,
beta-hydroxybutyrate3
PaCO2 43
HCO3 20
Lactate 1.1
Discharged to
rehabilitation facility
F, 53y T2DM
Symptoms: fever andanorexia for 1 week
Trigger: COVID-19,anorexia
Glucose: 151 mg/dL
Empagli�ozin (10 mgdaily), insulin glargine,exenatide, metformin,and glimepiride
-- pH 7.27 (venous)
AG 30,
beta-hydroxybutyrate5.9
PaCO2 19
HCO3 5
Lactate 1.5
Discharged home
F, 70y T2DM
Symptoms: COVID-19diagnosis with apulseless foot fromarterial thrombosis
Trigger: COVID-19,ischemic foot,anorexia
Trigger: covid-19
Glucose 166
canagli�ozin (300 mg
daily), dulaglutide,sitagliptin-metformin,and losartan andhydrochlorothiazide
-- pH 7.09 (venous)
AG 20,
beta-hydroxybutyrate5.3
PaCO2 40
HCO3 10 mmol/lit
Lactate 1.5
Discharged to
rehabilitation facility

Page 17/26
Study Sex/age Symptoms / BS Medications Time afterSGLT2iinitiation
ABG �nding Treatment/ outcome
Calçada etal (61)
M, 70y T2DM
Symptoms: epigastricpain and vomiting for3 days, tachycardia(116/min), fever(38C)
Trigger: pancreatitis
Glucose: 188 mg/dL
Dipeptidyl peptidase-4inhibitor, biguanideand sulfonylurea,empagli�ozin
1 days pH 7.28;
pCO2 22 mmHg;HCO3 − 10.3 mEq/L;lactate 2.0 mmol/L;
AG 26 mmol/L
Ketone 6.6 mmol/L
Saline0.9%, dextrose5%, insulin
Yeoh et al(123)
M, 61y T2DM
Symptoms: -
Trigger: vertebralfracture
Glucose: 149 mg/dl
Metformin,Empagli�ozin 10 mgat night
Aspirin, Bisoprolol,Atorvastatin, Fish oilcapsules, Calciumsupplement
3 months pH 7.12,
HCO3 8.3 meq/l
anion gap 18.7mmol/L,
base excess − 19.4mmol/L
urine ketones (2+),serum ketones 6mmol/l
sodium bicarbonate8.4% 200 mL of over 1hour, saline 0.9% 2L/day and Hartmann’ssolution 1 L/day
patient ABG wasnormalized after44hours
Dyatlova etal (92)
F, 23 y T2DM
Symptoms: shortnessof breath, dry cough,chills, malaise,diaphoresis,tachycardia andtachypnea
Trigger: COVID-19
Blood glucose: 181mg/dl
Not mentioned.
Oral hypoglycemicagents includingEmpagli�ozin (poorlycontrolled T2DM)
-- pH of 7.02, PCO216.7, PO2 67, andHCO3 4.
Urinalysis waspositive for glucose,protein, and ketones
Oral hypoglycemicagents werediscontinued, slidingscale insulin didn’timprove HCO3.
Sodium bicarbonate,saline, insulininfusion.
Ozer et al(124)
F, 42 y T2DM
Symptoms: nausea,vomiting anddyspnea, tachypnea,tachycardia
Trigger: COVID-19
Glucose: 196 mg/dl,
Metformin, andempagli�ozin (10mg/day)
-- pH7.08,
Hco3 8.9 mmol/L,anion gap 20 mEq/L,and urine ketones 2+
Isotonic �uids,dextrose 5%, andinsulin infusion
Oral agents were D/C,
Acidosis resolvedafter 12 hours
Smyth et al(90)
M, 54 T2DM
Symptoms:
Metformin anddapagli�ozin
Dapagli�ozin was hold24 before CABG
2 months pH 7.2
Hco3 6.7mmol/lit
Base excess − 7.7mmol/l)
Serum ketone 4.9mmol/l
Urine ketone 3+
Dextrose/ insulininfusion for 90 hours
Mackintoshet al (125)
F, 68Y T2DM
Symptoms: lethargicwith confusion andworsening expressiveaphasia,
Trigger: craniotomy
Glucose 140–160mg/dl
empagli�ozin 10 mgonce daily
-- pH of 7.2.
Hco3 9 mmol/L,
AG 21,
Blood serum b-hydroxybutyrate,positive urineketones,
urine glucose > 1000mg/dL
Fluid and insulin for 2days
Neurologic symptomswere improved

Page 18/26
Study Sex/age Symptoms / BS Medications Time afterSGLT2iinitiation
ABG �nding Treatment/ outcome
Chaudhry etal (48)
M,41y T2DM
Symptoms: right-sided chestdiscomfort, nausea,and two episodes ofnonbilious and non-bloody vomiting
Trigger: acutepancreatitis
metformin,empagli�ozin 12.5 mgPO BID, andsemaglutide 1 mg
-- pH of 7.21,
pCO2 16 mmHg,
pO2 107 mmHg,
HCO3 6.4 mmol/L
Second ABG
pH of 7.17,
AG 26
pCO2 17 mmHg,
pO2 68 mmHg,
HCO3 6.2 mol/lit
Fluid, bicarbonate,and insulin infusion
Discharged onmetformin 500 mgtwice daily andglimepiride 5mg/day
Smith et al(126)
F, 51 y T2DM
Symptoms: lethargyand tachycardia,
Trigger: sleevesurgery
glucose 160 mg/dL
canagli�ozin-metformin insulin,metoprolol
-- pH of 7.21
HCO3- of 3 mmol/L
AG 37 mmol/L
Ringer lactate,bicarbonate, insulininfusion
Patient wasdischarged on insulin
In the present case, self-prescribing empagli�ozin as well as decreased intake due to nausea and vomiting were major risk factors of the DKA [38].Although they are likely to occur at any time, even after a single dose [18, 61], most cases occur within the �rst six months after SGLT2is initiation[35, 36, 62–64]. However, a recent systematic review and meta-analysis showed that the mean age > 60-year-old and longer duration of therapy (> 52weeks) are the major risk factors for the SGLT2is-induced DKA in patients with type 2 diabetes [65]. A systematic review on 47 patients (42 ofwhom were euglycemic) with perioperative SGLT2is-associated DKA found that most cases occur within the �rst few hours to 6 weeks after surgery[66]. Bariatric, abdominal, gynecologic, and cardiac surgery were the major operations associated with DKA [66].
some research claimed that female gender is more susceptible to the euglycemic DKA [36]. However, it was not shown in all studies [26]. It seemsthat male or female susceptibility to the SGLT2is induced DKA is related to other precipitating risk factors rather than gender. However, furtherstudies are needed to con�rm that.
The normal or moderate hyperglycemia (< 300 mg/dl) should not preclude ketone and blood gas assessment body measurement. The urine ketonebody can be negative due to its tubular reabsorption or positivity [67, 68]. Therefore, blood ketone is more sensitive for detection of the DKA. Earlyclinical and biochemical (e.g., serum or capillary ketone bodies venous blood gas) monitoring for susceptible patients can be helpful [69].
About 70% of DKA episodes that are associated with SGLT2is are euglycemic (BS < 250mg/dl) [18, 31]. However, mild hyperglycemia andhypoglycemic DKA are possible [44, 64]. Therefore, the absence of hyperglycemia does not rule out the DKA [64, 70]. Euglycemia and hypoglycemiacan be due to increased urinary glucose elimination. Cases of the SGLT2is-induced DKA can be severe in nature.
One of the largest case series on euglycemic DKA was reported by Meyer’s et al. study conducted on 13 (including 9 female) patients, 8 of whomhad type 2 diabetes and the remaining 5 patients had LADA [35]. Dapagli�ozin (9/13) and empagli�ozin (4/13) with mean duration of 11.6 weekswere used along with the SGLT2is [35].
Several cases of DKA with life-threatening acidosis have been reported [71–73]. Soni et al. reported 8 patients with euglycemic DKA followingempagli�ozin initiation. 5 patients had bicarbonate levels of < 10 mmol/l and 3 had PH < 7.1 [71]. In addition, Goto et al. reported one patient withsevere life-threatening DKA who received empagli�ozin before elective coronary artery bypass grafting surgery [73]. Tachypnea, vomiting,hypotension, and severe acidosis (pH = 6.84; HCO3-level = 2.1 mEq/L; base excess = -20 mmol/L; anion gap = 31.9 mmol/L; and lactate level = 2.4mmol/L) were the main clinical and metabolic factors in the patient. Metabolic acidosis was improved after two days of insulin and glucose/salineinfusion [73]. Sampani et al. reported one patient with the DKA who developed severe metabolic acidosis (pH = 7.05; HCO3- = 3 mmol/l) followinghysterectomy surgery [74]. Latif et al. reported one case of empagli�ozin-associated DKA with malaise, nausea, vomiting, cough, shortness andsevere acidosis (pH = 7.01, HCO3- = 5 meq/l) [75]. Chou et al. reported one patient with tachycardia, tachypnea, kaussmal signs, dry mucus, sunkeneyes, and metabolic acidosis (pH = 6.986; CO2 = 20.9mm Hg; HCO3- = 7.0 mEq/L; and anion gap = 20mEq/L) [76]. In addition, Puls et al. described 5cases (60% male) of severe euglycemic DKA with mean pH = 7.01, HCO3- 8 = meq/l, anion gap = 27 mEq/L, after averagely 20 months of the

Page 19/26
SGLT2is therapy [77]. Euglycemic DKA with respiratory alkalosis were likely to occur [78]. Death have been reported in the SGLT2is -associated DKA[30, 35].
No universal guideline is available for the treatment of the SGLT2is s-associated DKA in T2DM. Discontinuation of the SGLT2is, �uid replacement,and insulin therapy are the mainstays of treatment (Table 2) and (Fig. 3). Continuation of the SGLT2is s after the �rst episode of DKA can be a riskfactor for subsequent attacks [54]. Therefore, reintroduction of SGLT2is is not recommended after the �rst occurrence of DKA. Unfortunately, ourpatients did not eat well for 2–3 days before admission, which could in�uence acidosis. Similar to our cases, Karakaya et al. reported one patientwith severe DKA associated with canagli�ozin (pH = 6.9; CO2 = 16.6 mmHg; HCO3- = 9.2 mmol/L; anion gap = 20.7 mEq/L; and blood ketones level = 8.0mmol/L), who was successfully treated following rehydration, insulin, bicarbonate, and potassium replacement [79]. Recently, Yeo et al. reporteda case of dapagli�ozin-associated DKA with PH = 7.04 and HCO3- = 1.8 meq/l in a patient with pseudo-membrane colitis, which becamecomplicated by septic shock and acute kidney injury [47]. The patient was effectively treated with continuous renal replacement therapy [47].Although the infusion of sodium bicarbonate for patients with PH < 7 and/or renal replacement was successful [47, 80, 81]. However, it was noteffective in all the patients with euglycemic DKA [42]. Intravenous infusion of sodium bicarbonate can paradoxically exacerbate acidosis and reduceserum potassium levels; therefore, it is only recommended for patients with pH < 6.9 [82]. In addition, empagli�ozin use can either increase ordecrease serum potassium level [83]. Prophylactic hydration and insulin infusion can prevent euglycemic diabetic ketoacidosis associated withsodium-glucose cotransporter 2 inhibitors in high-risk patients [84, 85]. Lee and Ahn reported DKA in a patient with loss of consciousness,pyelonephritis and acute kidney injury receiving metformin, dapagli�ozin, clopidogrel, nicorandil, imipramine, tolterodine, and tamsulosin. The initiallab data included pH = 6.904, Pco2 = 12.0 mmHg, HCO3- = 3.1 mmol/L, BS = 150–200 mg/dl, sodium = 162 meg/l, and potassium = 2.5 meq/l [86].The patient improved in the 7th day after discontinuation of dapagli�ozin and hydration [86]. Similar cases with prolonged acidosis or glucosuriawere also reported by other studies [52, 64, 76, 87]. Bobrowski et al. studied cases with prolonged metabolic recovery and showed that some casescan recover 10 (4–12) days after initial presentations [87]. Furthermore, it seems that the time for recovery from the DKA based on the SGLT2is,insulin infusion, the amount required �uid, and duration of hospitalization is longer than the time for recovery from the DKA based on other causes[64, 68, 80, 88]. Early discontinuation of �uid and insulin treatment can be associated with return of the symptoms [88–90]. Consequently, precisemedications history and monitoring of patients for at least �ve half-lives and longer after SGLT2is discontinuation are recommended [87]. The renalclearance of empagli�ozin is signi�cantly higher than that of dapagli�ozin and canagli�ozin [91]. Therefore, a decreased renal function results in anincrease in empagli�ozin concentration [91]. Patients’ blood pressure monitoring due to osmotic diuresis and electrolyte abnormalities (e.g.,hypokalemia and hypernatremia) is necessary [68]. Short-term vasopressor therapy may be required for some patients, in particular for those withhigh anion-gap metabolic acidosis [44, 57]. Treatment with intravenous insulin, �uids (e.g., saline 0.9% or half-saline, with or without dextrose 5%),vasopressors, bicarbonate, and renal replacement therapy should be individualized. The most recent UK guidelines on management of DKArecommend stopping of the SGLT2is and replacement of �uid with dextrose 10% along with insulin (0.05–0.1 unit/kg) for euglycemic DKA [12].Sliding scale insulin treatment can lead to an increase in the severity of acidosis [92]. Goldenberg et al. proposed the STOP DKA protocol for patientswith type 1 diabetes mellites [93]. The Stop SGLT2is when patient is symptomatic for the DKA, Test for ketone body and blood sugar every 2–4hours, Oral intake (250–500 cc �uid every 2 hours and up to 60 g carbohydrate ever 2–4 hours), and Protocol instruction (insulin and carbohydrateuse) are recommended [93]. An international panel of experts recommends St (STOP SGLT2is), Insulin, Carbohydrate intake, and Hydration withsuitable �uids for lower risk of DKA in type 1 diabetic patients [94].
Although most of the presented case reports followed such approach. However, this protocol has not been validated in patients with type 2 diabetes.
ConclusionIn the present literature review, we summarized available cases of the SGLT2is-induced DKA. Case reports can be of value about presentation,complications, risk factors, and management plans of the SGLT2is-induced DKA. However, the self-medication practice is relatively high in diabeticpatients [95]. In the meta-analysis of the EMPEROR-Reduced and DAPA-HF trials, no case of the the DKA was seen in the patients with non-diabeticheart failure [96]. The SGLT2is should be discontinued in the case of acute illnesses at least 24 (24–72) hours before elective surgery, and forpatients with the DKA [44, 97]. In terms of the SGLT2is users, during acute illness episodes, patients should check blood ketone, and patients withpositive ketone should be instructed to receive bolus insulin injection, adequate �uid intake, carbohydrate ingestion (at least 30 gram/day), andcheck serum ketone concentration every four hours [82, 98]. Patients should seek emergency department if ketosis not resolved of the DKAsymptoms appears [98]. Although, no case of the DKA was observed in the patients with acute heart failure in the EMPULSE trial [99]. As prescribingof the SGLT2is increases [100], clinicians should be aware of the DKA in patients with diabetes with polyuria, abdominal pain, nausea/vomiting, andconfusion.
DeclarationsEthical statement:
This study approved by ethics committee of Kermanshah University of Medical Sciences, Kermanshah, Iran.
This material is the authors' own original work, which has not been previously published elsewhere.

Page 20/26
The patient gave their informed consent prior to their inclusion in the study
The paper is not currently being considered for publication elsewhere.
All sources used are properly disclosed (correct citation). Literally copying of text must be indicated as such by using quotation marks and givingproper reference.
All authors have been personally and actively involved in substantial work leading to the paper, and will take public responsibility for its content.
Con�ict of interest statement:
The authors declare that they have no con�ict of interests.
References1. Heerspink HJ, Perkins BA, Fitchett DH, Husain M, Cherney DZ. Sodium Glucose Cotransporter 2 Inhibitors in the Treatment of Diabetes Mellitus:
Cardiovascular and Kidney Effects, Potential Mechanisms, and Clinical Applications. Circulation. 2016;134(10):752–72.
2. Bakris GL, Fonseca VA, Sharma K, Wright EM. Renal sodium-glucose transport: role in diabetes mellitus and potential clinical implications.Kidney Int. 2009;75(12):1272–7.
3. Neumiller JJ. Empagli�ozin: a new sodium-glucose co-transporter 2 (SGLT2) inhibitor for the treatment of type 2 diabetes. Drugs Context.2014;3:212262-.
4. Frampton JE. Empagli�ozin. A Review in Type 2 Diabetes. Drugs. 2018;78(10):1037–48.
5. Zelniker TA, Braunwald E. Mechanisms of Cardiorenal Effects of Sodium-Glucose Cotransporter 2 Inhibitors: JACC State-of-the-Art Review. J AmColl Cardiol. 2020;75(4):422–34.
�. Verma S, McMurray JJV. SGLT2 inhibitors and mechanisms of cardiovascular bene�t: a state-of-the-art review. Diabetologia.2018;61(10):2108–17.
7. Lopaschuk GD, Verma S. Mechanisms of Cardiovascular Bene�ts of Sodium Glucose Co-Transporter 2 (SGLT2) Inhibitors: A State-of-the-ArtReview. JACC Basic Transl Sci. 2020;5(6):632–44.
�. Zelniker TA, Wiviott SD, Raz I, Im K, Goodrich EL, Bonaca MP, et al. SGLT2 inhibitors for primary and secondary prevention of cardiovascular andrenal outcomes in type 2 diabetes: a systematic review and meta-analysis of cardiovascular outcome trials. Lancet. 2019;393(10166):31–9.
9. Salah HM, Al'Aref SJ, Khan MS, Al-Hawwas M, Vallurupalli S, Mehta JL, et al. Effect of sodium-glucose cotransporter 2 inhibitors oncardiovascular and kidney outcomes-Systematic review and meta-analysis of randomized placebo-controlled trials. Am Heart J. 2021;232:10–22.
10. McDonagh TA, Metra M, Adamo M, Gardner RS, Baumbach A, Böhm M, et al. 2021 ESC Guidelines for the diagnosis and treatment of acute andchronic heart failure. Eur Heart J. 2021;42(36):3599–726.
11. Martínez-Vizcaíno V, Díez-Fernández A, Álvarez-Bueno C, Martínez-Alfonso J, Cavero-Redondo I. Safety and E�cacy of SGLT2 Inhibitors: AMultiple-Treatment Meta-Analysis of Clinical Decision Indicators. J Clin Med. 2021;10(12).
12. Dhatariya KK. The management of diabetic ketoacidosis in adults-An updated guideline from the Joint British Diabetes Society for InpatientCare. Diabet Med. 2022:e14788.
13. Anker SD, Butler J, Filippatos G, Ferreira JP, Bocchi E, Böhm M, et al. Empagli�ozin in Heart Failure with a Preserved Ejection Fraction. N Engl JMed. 2021;385(16):1451–61.
14. Packer M, Anker SD, Butler J, Filippatos G, Pocock SJ, Carson P, et al. Cardiovascular and Renal Outcomes with Empagli�ozin in Heart Failure. NEngl J Med. 2020;383(15):1413–24.
15. Bramlage P, Tittel SR, Wagner C, König K, Raddatz D, Weber-Lauffer R, et al. The DIVE/DPV registries: evolution of empagli�ozin use in clinicalpractice in Germany. BMJ Open Diabetes Research & Care. 2020;8(1):e001486.
1�. Kim YG, Jeon JY, Han SJ, Kim DJ, Lee KW, Kim HJ. Sodium-glucose co-transporter-2 inhibitors and the risk of ketoacidosis in patients with type2 diabetes mellitus: A nationwide population-based cohort study. Diabetes Obes Metab. 2018;20(8):1852–8.
17. Han SJ, Ha KH, Lee N, Kim DJ. Effectiveness and safety of sodium-glucose co-transporter-2 inhibitors compared with dipeptidyl peptidase-4inhibitors in older adults with type 2 diabetes: A nationwide population-based study. Diabetes Obes Metab. 2021;23(3):682–91.
1�. Clark A, Mohammed AS, Raut A, Moore S, Houlden R, Awad S. Prevalence and Clinical Characteristics of Adults Presenting With Sodium-GlucoseCotransporter-2 Inhibitor-Associated Diabetic Ketoacidosis at a Canadian Academic Tertiary Care Hospital. Can J Diabetes. 2021;45(3):214–9.
19. Fralick M, Schneeweiss S, Patorno E. Risk of Diabetic Ketoacidosis after Initiation of an SGLT2 Inhibitor. N Engl J Med. 2017;376(23):2300–2.
20. Erondu N, Desai M, Ways K, Meininger G. Diabetic Ketoacidosis and Related Events in the Canagli�ozin Type 2 Diabetes Clinical Program.Diabetes Care. 2015;38(9):1680–6.
Page 21/26
21. Ata F, Yousaf Z, Khan AA, Razok A, Akram J, Ali EAH, et al. SGLT-2 inhibitors associated euglycemic and hyperglycemic DKA in a multicentriccohort. Sci Rep. 2021;11(1):10293.
22. Blau JE, Tella SH, Taylor SI, Rother KI. Ketoacidosis associated with SGLT2 inhibitor treatment: Analysis of FAERS data. Diabetes Metab ResRev. 2017;33(8).
23. Colacci M, Fralick J, Odutayo A, Fralick M. Sodium-Glucose Cotransporter-2 Inhibitors and Risk of Diabetic Ketoacidosis Among Adults WithType 2 Diabetes: A Systematic Review and Meta-Analysis. Can J Diabetes. 2022;46(1):10 – 5.e2.
24. Fralick M, Redelmeier DA, Patorno E, Franklin JM, Razak F, Gomes T, et al. Identifying Risk Factors for Diabetic Ketoacidosis Associated withSGLT2 Inhibitors: a Nationwide Cohort Study in the USA. J Gen Intern Med. 2021;36(9):2601–7.
25. Caparrotta TM, Greenhalgh AM, Osinski K, Gifford RM, Moser S, Wild SH, et al. Sodium-Glucose Co-Transporter 2 Inhibitors (SGLT2i) Exposureand Outcomes in Type 2 Diabetes: A Systematic Review of Population-Based Observational Studies. Diabetes Ther. 2021;12(4):991–1028.
2�. Douros A, Lix LM, Fralick M, Dell'Aniello S, Shah BR, Ronksley PE, et al. Sodium-Glucose Cotransporter-2 Inhibitors and the Risk for DiabeticKetoacidosis: A Multicenter Cohort Study. Ann Intern Med. 2020;173(6):417–25.
27. Lin DS, Lee JK, Chen WJ. Clinical Adverse Events Associated with Sodium-Glucose Cotransporter 2 Inhibitors: A Meta-Analysis Involving 10Randomized Clinical Trials and 71 553 Individuals. J Clin Endocrinol Metab. 2021;106(7):2133–45.
2�. Faillie JL. Pharmacological aspects of the safety of gli�ozins. Pharmacol Res. 2017;118:71–81.
29. Deeks ED. Sotagli�ozin. A Review in Type 1 Diabetes. Drugs. 2019;79(18):1977–87.
30. Wang KM, Isom RT. SGLT2 Inhibitor-Induced Euglycemic Diabetic Ketoacidosis: A Case Report. Kidney Med. 2020;2(2):218–21.
31. Goldenberg RM, Berard LD, Cheng AYY, Gilbert JD, Verma S, Woo VC, et al. SGLT2 Inhibitor-associated Diabetic Ketoacidosis: Clinical Review andRecommendations for Prevention and Diagnosis. Clin Ther. 2016;38(12):2654-64.e1.
32. Singh AK. Sodium-glucose co-transporter-2 inhibitors and euglycemic ketoacidosis: Wisdom of hindsight. Indian J Endocrinol Metab.2015;19(6):722–30.
33. Ferrannini E, Baldi S, Frascerra S, Astiarraga B, Barsotti E, Clerico A, et al. Renal Handling of Ketones in Response to Sodium-GlucoseCotransporter 2 Inhibition in Patients With Type 2 Diabetes. Diabetes Care. 2017;40(6):771–6.
34. Gri�n M, Rao VS, Ivey-Miranda J, Fleming J, Mahoney D, Maulion C, et al. Empagli�ozin in Heart Failure: Diuretic and Cardiorenal EffectsCirculation. 2020;142(11):1028–39.
35. Meyer EJ, Gabb G, Jesudason D. SGLT2 Inhibitor-Associated Euglycemic Diabetic Ketoacidosis: A South Australian Clinical Case Series andAustralian Spontaneous Adverse Event Noti�cations. Diabetes Care. 2018;41(4):e47-e9.
3�. Limenta M, Ho CSC, Poh JWW, Goh SY, Toh DSL. Adverse Drug Reaction Pro�le of SGLT2 Inhibitor-Associated Diabetic Ketosis/Ketoacidosis inSingapore and their Precipitating Factors. Clin Drug Investig. 2019;39(7):683–90.
37. Diaz-Ramos A, Eilbert W, Marquez D. Euglycemic diabetic ketoacidosis associated with sodium-glucose cotransporter-2 inhibitor use: a casereport and review of the literature. Int J Emerg Med. 2019;12(1):27.
3�. Bamgboye AO, Oni IO, Collier A. Predisposing factors for the development of diabetic ketoacidosis with lower than anticipated glucose levels intype 2 diabetes patients on SGLT2-inhibitors: a review. Eur J Clin Pharmacol. 2021;77(5):651–7.
39. Burke KR, Schumacher CA, Harpe SE. SGLT2 Inhibitors: A Systematic Review of Diabetic Ketoacidosis and Related Risk Factors in the PrimaryLiterature. Pharmacotherapy. 2017;37(2):187–94.
40. Nasa P, Chaudhary S, Shrivastava PK, Singh A. Euglycemic diabetic ketoacidosis: A missed diagnosis. World J Diabetes. 2021;12(5):514–23.
41. Popli R, Chao JH. Precipitation of Euglycemic DKA (euDKA) From the Initiation of SGLT2 Inhibitor (SGLT2i) and 0-Carb Diet Inpatient. J EndocrSoc. 2021;5(Supplement_1):A395-A.
42. Goto S, Ishikawa JY, Idei M, Iwabuchi M, Namekawa M, Nomura T. Life-Threatening Complications Related to Delayed Diagnosis of EuglycemicDiabetic Ketoacidosis Associated with Sodium-Glucose Cotransporter-2 Inhibitors: A Report of 2 Cases. Am J Case Rep. 2021;22:e929773.
43. Ehrmann D, Kulzer B, Roos T, Haak T, Al-Khatib M, Hermanns N. Risk factors and prevention strategies for diabetic ketoacidosis in people withestablished type 1 diabetes. Lancet Diabetes Endocrinol. 2020;8(5):436–46.
44. Lindsay PJ, Gibson LE, Bittner EA, Berg S, Chang MG. Sodium-glucose cotransporter-2 (SGLT2) inhibitor-induced euglycemic diabeticketoacidosis complicating the perioperative management of a patient with type 2 diabetes mellitus (T2DM) and Fournier's gangrene: A casereport. Int J Surg Case Rep. 2020;77:463–6.
45. Paul N, Jonklaas J. Low carbohydrate diet while taking dapagli�ozin: A case report and review of literature. Diabetes Metab Syndr.2021;15(1):361–3.
4�. Kasbawala K, Stamatiades GA, Majumdar SK. Fournier's Gangrene and Diabetic Ketoacidosis Associated with Sodium Glucose Co-Transporter 2(SGLT2) Inhibitors: Life-Threatening Complications. Am J Case Rep. 2020;21:e921536.
47. Yeo SM, Park H, Paek JH, Park WY, Han S, Park SB, et al. Ketoacidosis with euglycemia in a patient with type 2 diabetes mellitus takingdapagli�ozin: A case report. Med (Baltim). 2019;98(3):e14150.
Page 22/26
4�. Chaudhry A, Biggiani C, Afzal M, Chaudhry S, Vwich Y. Acute Pancreatitis-Induced Euglycemic Diabetic Ketoacidosis. Cureus.2021;13(6):e15949-e.
49. Musso G, Saba F, Cassader M, Gambino R. Diabetic ketoacidosis with SGLT2 inhibitors. BMJ. 2020;371:m4147.
50. Morrison N, Barnett K, Tantum J, Morrison HK, Whalen M. A Case of Euglycemic Diabetic Ketoacidosis in a Patient With Type 2 DiabetesMellitus and COVID-19. Cureus. 2020;12(12):e12029-e.
51. Batista DV, Vieira C, Costa TA, Lima EG. COVID-19-associated euglycemic diabetic ketoacidosis in a patient with type 2 diabetes on SGLT2inhibitor: a case report. Diabetol Int. 2021;12(3):313–6.
52. Lucero P, Chapela S. Euglycemic Diabetic Ketoacidosis in the ICU: 3 Case Reports and Review of Literature. Case Rep Crit Care.2018;2018:1747850-.
53. Kapila V, Topf J. Sodium-Glucose Co-transporter 2 Inhibitor-Associated Euglycemic Diabetic Ketoacidosis After Bariatric Surgery: A Case andLiterature Review. Cureus. 2021;13(8):e17093-e.
54. Steinmetz-Wood S, Gilbert M, Menson K. A Case of Diabetic Ketoacidosis in a Patient on an SGLT2 Inhibitor and a Ketogenic Diet: A Critical TrioNot to Be Missed. Case Rep Endocrinol. 2020;2020:8832833.
55. Earle M, Ault B, Bonney C. Euglycemic Diabetic Ketoacidosis in Concurrent Very Low-carbohydrate Diet and Sodium-glucose Transporter-2Inhibitor Use: A Case Report. Clin Pract Cases Emerg Med. 2020;4(2):185–8.
5�. Wohlrab P, Kainz M, Schiferer A, Zapletal B, Tschernko E. Euglycemic Diabetic Ketoacidosis After Cardiac Surgery in a Patient Treated WithEmpagli�ozin for Type 2 Diabetes Mellitus: A Case Report. J Cardiothorac Vasc Anesth. 2021.
57. Osafehinti DA, Okoli OJ, Karam JG. A Case of SGLT2 Inhibitor-Associated Euglycemic Diabetic Ketoacidosis Following Coronary Artery BypassSurgery. AACE Clin Case Rep. 2021;7(1):20–2.
5�. Alabdaljabar MS, Abdullah KM, Almasood A, Ali SS, Ashmeg A. Euglycemic Diabetic Ketoacidosis in a Sedated Patient after Coronary ArteryBypass Grafting: A Case Report and Literature Review. Case Rep Med. 2021;2021:2086520.
59. Lau A, Bruce S, Wang E, Ree R, Rondi K, Chau A. Perioperative implications of sodium-glucose cotransporter-2 inhibitors: a case series ofeuglycemic diabetic ketoacidosis in three patients after cardiac surgery. Can J Anaesth. 2018;65(2):188–93.
�0. Yii ESS, Azli AW, Sitaram PN. Sodium-glucose cotransporter 2 inhibitor-induced euglycemic diabetic ketoacidosis in a patient with coronavirusdisease 2019: a case report. J Med Case Rep. 2022;16(1):17.
�1. Calçada MB, Fernandes L, Soares Costa R, Montezinho S, Martins Duarte F, Frutuoso L, et al. Euglycemic Diabetic Ketoacidosis after a SingleDose of Empagli�ozin in a Patient with Pancreatitis. Clin Pract. 2021;11(2):216–8.
�2. Mistry S, Eschler DC. Euglycemic Diabetic Ketoacidosis Caused by SGLT2 Inhibitors and a Ketogenic Diet: A Case Series and Review ofLiterature. AACE Clin case Rep. 2020;7(1):17–9.
�3. Hussaini SA, Aziz A, Musa M, Alamin M, Danjuma M. Late-Onset Euglycemic Diabetic Ketoacidosis in a Patient With Massive Stroke RequiringDecompressive Craniectomy: A Case Report. Cureus. 2021;13(10):e18629.
�4. Kelmenson DA, Burr K, Azhar Y, Reynolds P, Baker CA, Rasouli N. Euglycemic Diabetic Ketoacidosis With Prolonged Glucosuria Associated Withthe Sodium-Glucose Cotransporter-2 Canagli�ozin. J Investig Med High Impact Case Rep. 2017;5(2):2324709617712736.
�5. Liu J, Li L, Li S, Wang Y, Qin X, Deng K, et al. Sodium-glucose co-transporter-2 inhibitors and the risk of diabetic ketoacidosis in patients withtype 2 diabetes: A systematic review and meta-analysis of randomized controlled trials. Diabetes Obes Metab. 2020;22(9):1619–27.
��. Thiruvenkatarajan V, Meyer EJ, Nanjappa N, Van Wijk RM, Jesudason D. Perioperative diabetic ketoacidosis associated with sodium-glucose co-transporter-2 inhibitors: a systematic review. Br J Anaesth. 2019;123(1):27–36.
�7. Fleming N, Hamblin PS, Story D, Ekinci EI. Evolving Evidence of Diabetic Ketoacidosis in Patients Taking Sodium-Glucose Cotransporter 2Inhibitors. J Clin Endocrinol Metab. 2020;105(8).
��. Nappi F, La Verde A, Carfora G, Garofalo C, Provenzano M, Sasso FC, et al. Nephrology Consultation for Severe SGLT2 Inhibitor-InducedKetoacidosis in Type 2 Diabetes: Case Report. Medicina (Kaunas). 2019;55(8).
�9. Kitahara C, Morita S, Kishimoto S, Matsuno S, Uraki S, Takeshima K, et al. Early detection of euglycemic ketoacidosis during thoracic surgeryassociated with empagli�ozin in a patient with type 2 diabetes: A case report. J Diabetes Investig. 2021;12(4):664–7.
70. Isaacs M, Tonks KT, Green�eld JR. Euglycaemic diabetic ketoacidosis in patients using sodium-glucose co-transporter 2 inhibitors. Intern Med J.2017;47(6):701–4.
71. Soni P, Kumar V, Saradna A, Kupfer Y. Empagli�ozin-Associated Euglycemic Diabtetic Ketoacidosis. Am J Ther. 2018;25(6):e740-e1.
72. Fukuda M, Nabeta M, Muta T, Fukami K, Takasu O. Euglycemic diabetic ketoacidosis caused by canagli�ozin: a case report. Int J Emerg Med.2020;13(1):2.
73. Goto S, Ishikawa J-Y, Idei M, Iwabuchi M, Namekawa M, Nomura T. Life-Threatening Complications Related to Delayed Diagnosis of EuglycemicDiabetic Ketoacidosis Associated with Sodium-Glucose Cotransporter-2 Inhibitors: A Report of 2 Cases. Am J Case Rep. 2021;22:e929773-e.
74. Sampani E, Sara�dis P, Dimitriadis C, Kasimatis E, Daikidou D, Bantis K, et al. Severe euglycemic diabetic ketoacidosis of multifactorial etiologyin a type 2 diabetic patient treated with empagli�ozin: case report and literature review. BMC Nephrol. 2020;21(1):276.
Page 23/26
75. Latif A, Gastelum AA, Sood A, Reddy JT. Euglycaemic diabetic ketoacidosis in a 43-year-old woman with type 2 diabetes mellitus on SGLT-2inhibitor (empagli�ozin). BMJ Case Rep. 2020;13(6).
7�. Chou YM, Seak CJ, Goh ZNL, Seak JC, Seak CK, Lin CC. Euglycemic diabetic ketoacidosis caused by dapagli�ozin: A case report. Med (Baltim).2018;97(25):e11056.
77. Puls HA, Haas NL, Franklin BJ, Theyyunni N, Harvey CE. Euglycemic diabetic ketoacidosis associated with SGLT2i use: Case series. Am J EmergMed. 2021;44:11–3.
7�. Farjo PD, Kidd KM, Reece JL. A Case of Euglycemic Diabetic Ketoacidosis Following Long-term Empagli�ozin Therapy. Diabetes Care.2016;39(10):e165-6.
79. Karakaya Z, Topal FE, Topal F, Payza U, Akyol PY. Euglisemic diabetic ketoacidotic coma caused by dapagli�ozin. Am J Emerg Med.2018;36(11):2136. .e1-.e2.
�0. Papanastasiou L, Glycofridi S, Gravvanis C, Skarakis N, Papadimitriou I, Kanti G, et al. Diabetic ketoacidosis in patients treated with SGLT2inhibitors: experience at a tertiary hospital. Horm (Athens). 2021;20(2):369–76.
�1. Bitar ZI, Maadarani OS, Alabdali F, Teama A, Elsawah W, Mohsen MJ, et al. Sodium-glucose cotransporter-2 inhibitors induced euglycemicdiabetic ketoacidosis: Two case reports and a review of the literature. Clin Case Rep. 2022;10(2):e05440.
�2. Karslioglu French E, Donihi AC, Korytkowski MT. Diabetic ketoacidosis and hyperosmolar hyperglycemic syndrome: review of acutedecompensated diabetes in adult patients. BMJ. 2019;365:l1114.
�3. Ferreira JP, Butler J, Zannad F, Filippatos G, Schueler E, Steubl D, et al. Mineralocorticoid Receptor Antagonists and Empagli�ozin in PatientsWith Heart Failure and Preserved Ejection Fraction. J Am Coll Cardiol. 2022;79(12):1129–37.
�4. Ito T, Sugasawa G, Suzuki F, Sunada M, Iwamuro K, Nakano T, et al. Insulin and glucose infusion could prevent euglycemic diabetic ketoacidosisassociated with sodium-glucose cotransporter 2 inhibitors. Indian J Thorac Cardiovasc Surg. 2022;38(1):87–91.
�5. Cianciolo G, De Pascalis A, Capelli I, Gasperoni L, Di Lullo L, Bellasi A, et al. Mineral and Electrolyte Disorders With SGLT2i Therapy. JBMR Plus.2019;3(11):e10242-e.
��. Lee IH, Ahn DJ. Dapagli�ozin-associated euglycemic diabetic ketoacidosis in a patient with type 2 diabetes mellitus: A case report. Medicine.2020;99(21):e20228-e.
�7. Bobrowski D, Kumar R, Wu PE, Lapointe-Shaw L. Prolonged ketosis and glycosuria secondary to SGLT2 inhibitor therapy. Clin Case Rep.2021;9(11):e05057.
��. Sloan G, Kakoudaki T, Ranjan N. Prolonged diabetic ketoacidosis associated with canagli�ozin. Endocrinol Diabetes Metab Case Rep.2018;2018.
�9. Yehya A, Sadhu A. Sodium-Glucose Cotransporter 2 Inhibitor-Associated Prolonged Euglycemic Diabetic Ketoacidosis in Type 2 Diabetes: ACase Report and Literature Review. Clin Diabetes. 2020;38(1):112–6.
90. Smyth CC, Collins M, McCarthy J, Galvin S. The catabolic triad: case report of fasting, major cardiac surgery and sodium-glucose co-transporter2 inhibitors leading to perioperative euglycaemic ketoacidosis. Interact Cardiovasc Thorac Surg. 2021;33(3):494–5.
91. Scheen AJ. Pharmacokinetic and pharmacodynamic pro�le of empagli�ozin, a sodium glucose co-transporter 2 inhibitor. Clin Pharmacokinet.2014;53(3):213–25.
92. Dyatlova N, Omotosho YB, Sherchan R, Shrestha J, Buddharaju V. A Case of Severe Metabolic Acidosis due to Jardiance-Induced EuglycemicDiabetic Ketoacidosis. Cureus. 2021;13(4):e14580.
93. Goldenberg RM, Gilbert JD, Hramiak IM, Woo VC, Zinman B. Sodium-glucose co-transporter inhibitors, their role in type 1 diabetes treatment anda risk mitigation strategy for preventing diabetic ketoacidosis: The STOP DKA Protocol. Diabetes Obes Metab. 2019;21(10):2192–202.
94. Danne T, Garg S, Peters AL, Buse JB, Mathieu C, Pettus JH, et al. International Consensus on Risk Management of Diabetic Ketoacidosis inPatients With Type 1 Diabetes Treated With Sodium-Glucose Cotransporter (SGLT) Inhibitors. Diabetes Care. 2019;42(6):1147–54.
95. Aziz MM, Masood I, Yousaf M, Saleem H, Ye D, Fang Y. Pattern of medication selling and self-medication practices: A study from Punjab,Pakistan. PLoS ONE. 2018;13(3):e0194240.
9�. Zannad F, Ferreira JP, Pocock SJ, Anker SD, Butler J, Filippatos G, et al. SGLT2 inhibitors in patients with heart failure with reduced ejectionfraction: a meta-analysis of the EMPEROR-Reduced and DAPA-HF trials. Lancet. 2020;396(10254):819–29.
97. Tamargo J. Sodium-glucose Cotransporter 2 Inhibitors in Heart Failure: Potential Mechanisms of Action, Adverse Effects and FutureDevelopments. Eur Cardiol. 2019;14(1):23–32.
9�. Garg SK, Peters AL, Buse JB, Danne T. Strategy for Mitigating DKA Risk in Patients with Type 1 Diabetes on Adjunctive Treatment with SGLTInhibitors: A STICH Protocol. Diabetes Technol Ther. 2018;20(9):571–5.
99. Voors AA, Angermann CE, Teerlink JR, Collins SP, Kosiborod M, Biegus J, et al. The SGLT2 inhibitor empagli�ozin in patients hospitalized foracute heart failure: a multinational randomized trial. Nat Med. 2022.
100. Honigberg MC, Vardeny O, Vaduganathan M. Practical Considerations for the Use of Sodium-Glucose Co-Transporter 2 Inhibitors in HeartFailure. Circ Heart Fail. 2020;13(2):e006623.

Page 24/26
101. Dull RB, Spangler ML, Knezevich EL, Lau BM. Euglycemic Diabetic Ketoacidosis Associated With Sodium-Glucose Cotransporter Type 2Inhibitors in Patients With Type 2 Diabetes Mellitus Receiving Oral Therapy. J Pharm Pract. 2019;32(2):240–3.
102. Sethi SM, Vohra M, Ali SA. EUGLYCEMIC DIABETIC KETOACIDOSIS (EDKA) IN A PATIENT RECEIVING DAPAGLIFLOZIN. Acta Endocrinol(Buchar). 2021;17(2):266–9.
103. Iqbal I, Hamid M, Khan MAA, Kainat A, Tariq S. Dapagli�ozin-induced Late-onset Euglycemic Diabetic Ketoacidosis. Cureus. 2019;11(11):e6089.
104. Yasuma T, Okano Y, Tanaka S, Nishihama K, Eguchi K, Inoue C, et al. Sodium-glucose co-transporter-2 inhibitor-associated euglycemic diabeticketoacidosis that prompted the diagnosis of fulminant type-1 diabetes: A case report. World J Clin Cases. 2021;9(13):3163–9.
105. Hernandez-Quiles C, Ramirez-Duque N, Acosta-Delgado D. Ketoacidosis Due to Empagli�ozin, a Paradigm Shift: Case Report and Review ofLiterature. Curr Diabetes Rev. 2019;15(4):259–62.
10�. Adachi J, Inaba Y, Maki C. Euglycemic Diabetic Ketoacidosis with Persistent Diuresis Treated with Canagli�ozin. Intern Med. 2017;56(2):187–90.
107. Aggarwal A, Jain A, Sachdeva S, Kulairi ZI. Prolonged Glucosuria With Sodium-Glucose Cotransporter-2 (SGLT2) Inhibitors: A Case Report andReview of Literature. Cureus. 2020;12(11):e11554.
10�. Fieger EI, Fadel KM, Modarres AH, Wickham EP 3rd, Wolver SE. Successful reimplementation of a very low carbohydrate ketogenic diet aftersglt2 inhibitor associated euglycemic diabetic ketoacidosis. AACE Clin Case Rep. 2020;6(6):e330-e3.
109. Kapila V, Topf J. Sodium-Glucose Co-transporter 2 Inhibitor-Associated Euglycemic Diabetic Ketoacidosis After Bariatric Surgery: A Case andLiterature Review. Cureus. 2021;13(8):e17093.
110. Matli VVK, Fariduddin MM, Asafo-Agyei KO, Bansal N. Normoglycemic diabetic ketoacidosis in a type 2 diabetes patient on dapagli�ozin: A casereport. Clin Case Rep. 2021;9(12):e05144.
111. Shah M, Pathrose E, Bhagwat NM, Chandy D. "The Bitter Truth of Sugar"-Euglycemic Diabetic Ketoacidosis due to Sodium-glucoseCotransporter-2 Inhibitors: A Case Series. Indian J Crit Care Med. 2022;26(1):123–6.
112. Sharma PV, Jobanputra YB, Lewin K, Bagatell S, Lichtstein DM. Diabetic Ketoacidosis in Patients with Type 2 Diabetes on Sodium-GlucoseCotransporter-2 Inhibitors - A Case Series. Rev Recent Clin Trials. 2018;13(2):156–60.
113. Thawabi M, Studyvin S. Euglycemic Diabetic Ketoacidosis, a Misleading Presentation of Diabetic Ketoacidosis. N Am J Med Sci.2015;7(6):291–4.
114. Brown F, McColl T. Euglycemic Diabetic Ketoacidosis Secondary to Dapagli�ozin Use: A Case Report. J Emerg Med. 2018;54(1):109–11.
115. Allison R, Goldstein D, Musso MW. Challenges in the Diagnosis of Euglycemic Diabetic Ketoacidosis in a Patient With Multiple Sclerosis Takinga Sodium-Glucose Cotransporter 2 Inhibitor. J Emerg Med. 2019;57(1):e1–3.
11�. Chai PR, Bonney C, Blohm E, Boyer EW, Babu KM. Canagli�ozin-associated diabetic ketoacidosis: a case report. Toxicol Commun. 2017;1(1):2–5.
117. Lucero P, Chapela S. Euglycemic Diabetic Ketoacidosis in the ICU: 3 Case Reports and Review of Literature. Case Rep Crit Care.2018;2018:1747850.
11�. Elshimy G, Correa R. Sudden-onset Hypoglycemia Following Fluid Replacement in a Patient with Dapagli�ozin-induced Diabetic KetoacidosisWithout Prior Insulin Use: Case Report. Cureus. 2019;11(8):e5448-e.
119. Mendelsohn RA, Taveras AN, Mazer BA, Clayton LM. Euglycemic Diabetic Ketoacidosis Precipitated by SGLT-2 Inhibitor Use, Pericarditis, andFasting: A Case Report. Clin Pract Cases Emerg Med. 2020;4(3):389–92.
120. Dorcely B, Nitis J, Schwartzbard A, Newman JD, Goldberg IJ, Sum M. A Case Report: Euglycemic Diabetic Ketoacidosis Presenting as Chest Painin a Patient on a Low Carbohydrate Diet. Curr Diabetes Rev. 2021;17(2):243–6.
121. Trachuk P, Shihadeh S, Choi E. Euglycemic diabetic ketoacidosis in a patient on canagli�ozin. Chest. 2015;148(4):257A.
122. Gajjar K, Luthra P. Euglycemic Diabetic Ketoacidosis in the Setting of SGLT2 Inhibitor Use and Hypertriglyceridemia: A Case Report and Reviewof Literature. Cureus. 2019;11(4):e4384.
123. Yeoh HL, Lee M, Pan WJ, Ong HY. Case of sodium-glucose cotransporter-2 inhibitor-associated euglycaemic diabetic ketoacidosis. BMJ CaseRep. 2021;14(8).
124. Ozer O, Yorulmaz G. Euglycemic Diabetic Ketoacidosis Associated with Empagli�ozin Use in the Course of the SARS-Cov-2 Pandemic. J CollPhysicians Surg Pak. 2020;30(10):110–1.
125. Mackintosh C, Tewari A, Siegel J, Wang RD, Freeman W. Postoperative Euglycemic Diabetic Ketoacidosis and Encephalopathy Related to SGLT-2Inhibitors: A Case Report and Discussion of Diabetes Treatment and "Sweet Pee Encephalopathy" in Perioperative Hospital Management.Neurohospitalist. 2020;10(1):51–4.
12�. Smith A, Holtrop J, Sadoun M. Post-Operative Euglycemic Diabetic Ketoacidosis in a Patient With SGLT-2 Inhibitor Use and Recent SleeveGastrectomy. Cureus. 2021;13(4):e14297-e.
Table

Page 25/26
Table 1 is not available with this version
Figures
Figure 1
Bicarbonate concentration during the hospitalization period
Figure 2
PH during the hospitalization period

Page 26/26
Figure 3
Legend not included with this version