Effectiveness of screening and brief alcohol intervention in primary care (SIPS trial): pragmatic...
14
Effectiveness of screening and brief alcohol intervention in primary care (SIPS trial): pragmatic cluster randomised controlled trial OPEN ACCESS Eileen Kaner professor of public health research 1 , Martin Bland professor of health statistics 2 , Paul Cassidy general practitioner 3 , Simon Coulton professor of health services research 4 , Veronica Dale trial statistician 2 , Paolo Deluca trial manager 5 , Eilish Gilvarry consultant psychiatrist and honorary professor of addiction psychiatry 6 , Christine Godfrey emeritus professor of health economics 2 , Nick Heather emeritus professor of drug and alcohol studies 7 , Judy Myles consultant psychiatrist 8 , Dorothy Newbury-Birch lecturer in public health 1 , Adenekan Oyefeso honorary reader and consultant clinical psychologist 8 , Steve Parrott health economics 2 , Katherine Perryman PhD student 9 , Tom Phillips clinical doctoral research fellow 10 , Jonathan Shepherd professor of oral and maxillofacial surgery 11 , Colin Drummond professor of addiction psychiatry 5 1 Institute of Health and Society, Newcastle University, Newcastle NE2 4AX, UK; 2 Department of Health Sciences, University of York, UK; 3 Teams Family Practice, Gateshead, UK; 4 Centre for Health Service Studies, University of Kent, Canterbury, UK; 5 National Addiction Centre, Institute of Psychiatry, King’s College London, UK; 6 Northumberland, Tyne and Wear NHS Foundation Trust, Newcastle, UK; 7 Department of Psychology, Faculty of Health and Life Sciences, Northumbria University, UK; 8 Division of Public Health Science and Education, St George’s University of London, UK; 9 Greater Manchester CLAHRC Practitioner theme, University of Manchester, UK; 10 Humber Mental Health and Teaching NHS Trust, Willerby, UK; 11 Violence Research Group, Cardiff University, UK Abstract Objective To evaluate the effectiveness of different brief intervention strategies at reducing hazardous or harmful drinking in primary care. The hypothesis was that more intensive intervention would result in a greater reduction in hazardous or harmful drinking. Design Pragmatic cluster randomised controlled trial. Setting Primary care practices in the north east and south east of England and in London. Participants 3562 patients aged 18 or more routinely presenting in primary care, of whom 2991 (84.0%) were eligible to enter the trial: 900 (30.1%) screened positive for hazardous or harmful drinking and 756 (84.0%) received a brief intervention. The sample was predominantly male (62%) and white (92%), and 34% were current smokers. Interventions Practices were randomised to three interventions, each of which built on the previous one: a patient information leaflet control group, five minutes of structured brief advice, and 20 minutes of brief lifestyle counselling. Delivery of the patient leaflet and brief advice occurred directly after screening and brief lifestyle counselling in a subsequent consultation. Main outcome measures The primary outcome was patients’ self reported hazardous or harmful drinking status as measured by the alcohol use disorders identification test (AUDIT) at six months. A negative AUDIT result (score <8) indicated non-hazardous or non-harmful drinking. Secondary outcomes were a negative AUDIT result at 12 months, experience of alcohol related problems (alcohol problems questionnaire), health utility (EQ-5D), service utilisation, and patients’ motivation to change drinking behaviour (readiness to change) as measured by a modified readiness ruler. Results Patient follow-up rates were 83% at six months (n=644) and 79% at 12 months (n=617). At both time points an intention to treat analysis found no significant differences in AUDIT negative status between the three interventions. Compared with the patient information Correspondence to: E Kaner [email protected] Extra material supplied by the author (see http://www.bmj.com/content/346/bmj.e8501?tab=related#webextra) PaT plot of procedures Results of interaction tests Mean alcohol problems questionnaire (APQ) score by intervention group No commercial reuse: See rights and reprints http://www.bmj.com/permissions Subscribe: http://www.bmj.com/subscribe BMJ 2013;346:e8501 doi: 10.1136/bmj.e8501 (Published 9 January 2013) Page 1 of 14 Research RESEARCH
Transcript of Effectiveness of screening and brief alcohol intervention in primary care (SIPS trial): pragmatic...

Effectiveness of screening and brief alcoholintervention in primary care (SIPS trial): pragmaticcluster randomised controlled trial
OPEN ACCESS
Eileen Kaner professor of public health research 1, Martin Bland professor of health statistics 2, PaulCassidy general practitioner 3, Simon Coulton professor of health services research 4, Veronica Daletrial statistician 2, Paolo Deluca trial manager 5, Eilish Gilvarry consultant psychiatrist and honoraryprofessor of addiction psychiatry 6, Christine Godfrey emeritus professor of health economics 2, NickHeather emeritus professor of drug and alcohol studies 7, Judy Myles consultant psychiatrist 8,Dorothy Newbury-Birch lecturer in public health1, Adenekan Oyefeso honorary reader and consultantclinical psychologist 8, Steve Parrott health economics 2, Katherine Perryman PhD student 9, TomPhillips clinical doctoral research fellow 10, Jonathan Shepherd professor of oral and maxillofacialsurgery 11, Colin Drummond professor of addiction psychiatry 5
1Institute of Health and Society, Newcastle University, Newcastle NE2 4AX, UK; 2Department of Health Sciences, University of York, UK; 3TeamsFamily Practice, Gateshead, UK; 4Centre for Health Service Studies, University of Kent, Canterbury, UK; 5National Addiction Centre, Institute ofPsychiatry, King’s College London, UK; 6Northumberland, Tyne and Wear NHS Foundation Trust, Newcastle, UK; 7Department of Psychology,Faculty of Health and Life Sciences, Northumbria University, UK; 8Division of Public Health Science and Education, St George’s University of London,UK; 9Greater Manchester CLAHRC Practitioner theme, University of Manchester, UK; 10Humber Mental Health and Teaching NHS Trust, Willerby,UK; 11Violence Research Group, Cardiff University, UK
AbstractObjective To evaluate the effectiveness of different brief interventionstrategies at reducing hazardous or harmful drinking in primary care.The hypothesis was that more intensive intervention would result in agreater reduction in hazardous or harmful drinking.
Design Pragmatic cluster randomised controlled trial.
Setting Primary care practices in the north east and south east ofEngland and in London.
Participants 3562 patients aged 18 or more routinely presenting inprimary care, of whom 2991 (84.0%) were eligible to enter the trial: 900(30.1%) screened positive for hazardous or harmful drinking and 756(84.0%) received a brief intervention. The sample was predominantlymale (62%) and white (92%), and 34% were current smokers.
Interventions Practices were randomised to three interventions, eachof which built on the previous one: a patient information leaflet controlgroup, five minutes of structured brief advice, and 20 minutes of brief
lifestyle counselling. Delivery of the patient leaflet and brief adviceoccurred directly after screening and brief lifestyle counselling in asubsequent consultation.
Main outcome measures The primary outcome was patients’ selfreported hazardous or harmful drinking status asmeasured by the alcoholuse disorders identification test (AUDIT) at six months. A negative AUDITresult (score <8) indicated non-hazardous or non-harmful drinking.Secondary outcomes were a negative AUDIT result at 12 months,experience of alcohol related problems (alcohol problems questionnaire),health utility (EQ-5D), service utilisation, and patients’ motivation tochange drinking behaviour (readiness to change) as measured by amodified readiness ruler.
Results Patient follow-up rates were 83% at six months (n=644) and79% at 12 months (n=617). At both time points an intention to treatanalysis found no significant differences in AUDIT negative statusbetween the three interventions. Compared with the patient information
Correspondence to: E Kaner [email protected]
Extra material supplied by the author (see http://www.bmj.com/content/346/bmj.e8501?tab=related#webextra)
PaT plot of proceduresResults of interaction testsMean alcohol problems questionnaire (APQ) score by intervention group
No commercial reuse: See rights and reprints http://www.bmj.com/permissions Subscribe: http://www.bmj.com/subscribe
BMJ 2013;346:e8501 doi: 10.1136/bmj.e8501 (Published 9 January 2013) Page 1 of 14
Research
RESEARCH

leaflet group, the odds ratio of having a negative AUDIT result for briefadvice was 0.85 (95% confidence interval 0.52 to 1.39) and for brieflifestyle counselling was 0.78 (0.48 to 1.25). A per protocol analysisconfirmed these findings.
Conclusions All patients received simple feedback on their screeningoutcome. Beyond this input, however, evidence that brief advice or brieflifestyle counselling provided important additional benefit in reducinghazardous or harmful drinking compared with the patient informationleaflet was lacking.
Trial registration Current Controlled Trials ISRCTN06145674.
IntroductionInternational studies have shown that 20-30% of patients whoroutinely present in primary care are hazardous or harmfuldrinkers.1 Hazardous drinking is a repeated pattern of drinkingthat increases the risk of physical or psychological problems,2whereas harmful drinking is defined by the presence of theseproblems.3 Several meta-analyses have shown that screeningusing short questionnaires followed by brief intervention(comprising simple advice or psychological counselling)significantly reduces alcohol consumption in primary carepopulations.4-8 A Cochrane Collaboration systematic review of29 primary care trials reported that brief intervention in patientswas associated with a statistically significant reduced alcoholconsumption of 38 g a week (95% confidence interval 23 g to54 g) at one year compared with controls typically receivingassessment only, treatment as usual, or written information.8Given that a standard drink unit in the United Kingdom contains8 g of ethanol,9 this is equivalent to a reduction of 4 or 5 unitsa week. Nevertheless, brief alcohol intervention is rarelydelivered in practice10 and this gap in implementation has beenascribed to several limitations in the current evidence.Brief intervention trials have been criticised for being efficacystudies (optimising internal validity) rather than pragmatictrials.11 Most trials have also focused on middle aged maledrinkers, with other groups under-represented.8 12Moreover, theoptimal intensity of brief intervention is currently unclear. Onestudy8 reported no significant additional benefit of longerinterventions compared with brief ones. However, althoughthree systematic reviews found a benefit of motivationalinterviewing compared with no input (controls) in reducingalcohol consumption, their conclusions on its impact comparedwith other active interventions, including giving advice,differed.13-15 Thus the present trial occurred in a context wherebrief intervention was widely regarded as being effective atreducing hazardous and harmful drinking. Nevertheless, thenecessary length or modality input of brief intervention has yetto be determined. We carried out a pragmatic trial of theeffectiveness of three different brief intervention strategies atreducing hazardous and harmful drinking in primary care. Thisstudy was one of three trials in the Screening and InterventionProgramme for Sensible drinking (SIPS) study. The two linkedtrials were based in emergency departments16 and probationoffices.17
MethodsDetails of this trial protocol have been published.18 The trialincorporated cluster randomisation of practices to avoid the riskof contamination between the trial arms. The overall trial hada 2×2×2×3 nested factorial design encompassing geographicalarea (north east and south east of England and London),screening approach (universal screening of all patients versustargeted screening focused on presentations where alcohol wasmost likely to be relevant), screening tool (either the fast alcohol
screening test19 or a modified single alcohol screeningquestionnaire),20 and three interventions (patient informationleaflet, five minutes of brief advice, and 20 minutes of brieflifestyle counselling). Targeted screening focused onpresentations linked to mental health, gastrointestinal problems,hypertension, minor injuries, and new patient registrations. Thescreening results are reported in detail elsewhere.21 This paperfocuses on patient level outcomes after brief alcohol interventionrather than trial process measures.
SettingsWe initially recruited 24 practices across London and the southeast and north east of England, plus five standby sites in caseof dropouts. All practices delivered the full range of generalmedical services and covered a range of urban and rural areas,socially deprived and affluent communities, and culturallydiverse populations. Recruitment spanned 15months fromMay2008 to July 2009. Fifteen practices completed their targetrecruitment of 31 patients but nine practices (six in London andthree in the north east) only partially recruited this target (threepatient information leaflet, one brief advice, and five brieflifestyle counselling). Thus we subsequently utilised the fivestandby practices. In addition, five practices that had completedthe full recruitment agreed to be reallocated to a more intensiveintervention than their original allocation. Thus we included 34practice clusters in the final analysis.
Inclusion and exclusion criteriaWe included patients who screened positive for an alcohol usedisorder and who were alert and oriented, aged 18 or more,resident within 20 miles of the practice, and able to understandEnglish sufficiently to complete study questionnaires. Weexcluded patients already involved in an alcohol research studyor who were specifically seeking help for alcohol problems andthose who were severely injured or unwell, had a serious mentalhealth problem, were grossly intoxicated, or had no fixed abode.
RandomisationA secure remote randomisation service carried outrandomisation. Twenty four allocations were initially generatedfor each of the possible factorial combinations of screeningapproach, screening tool, and intervention. Randomisation wasstratified by geographical area (north versus south). The standbyand reallocated practices were subsequently randomly allocatedin a similar manner.
ConsentPrimary care staff initially established verbal consent withpatients to check eligibility for the trial. At this stage theycollected basic personal information and screened the patientusing the fast alcohol screening test19 or modified single alcoholscreening questionnaire.20 Patients who screened positive werethen invited to provide written consent for the trial. Allconsenting patients entered the intervention part of the trial.
InterventionsImmediately after the screening process (in the sameconsultation), trial participants received a short assessment oftheir drinking behaviour, and brief intervention was deliveredaccording to the intervention to which the practice had beenrandomised. All intervention materials are available from thestudy website (www.sips.iop.kcl.ac.uk/pil.php).
No commercial reuse: See rights and reprints http://www.bmj.com/permissions Subscribe: http://www.bmj.com/subscribe
BMJ 2013;346:e8501 doi: 10.1136/bmj.e8501 (Published 9 January 2013) Page 2 of 14
RESEARCH

Patient information leaflet—Patients received simple feedbackon their screening outcome and a patient information leaflet thathad been developed by the Department of Health in EnglandcalledHowmuch is too much? (www.sips.iop.kcl.ac.uk/pil.php).This 16 page leaflet describes the effects of alcohol on healthand wellbeing and shows the number of units contained inpopular alcoholic drinks to help the reader understand howmuchthey are drinking. The back page lists two internet help sitesplus details of a national Drinkline number. The onlymodification to this leaflet was the addition of an adhesive labelon the back page with contact details of local alcohol treatmentagencies relevant to the practice setting.Brief advice—Patients received feedback on screening and thepatient information leaflet plus five minutes of structured briefadvice from practice staff based on theHow much is too much?brief intervention programme.22 In addition to providing specificdetails about the health and social consequences of hazardousand harmful drinking, patients were shown a sex specific graph,which indicated that their drinking exceeded that of most of thepopulation, and a list of benefits that would result from reduceddrinking. Thereafter patients were taken through a menu oftechniques to help reduce drinking and asked to consider apersonal target for an achievable reduction in drinking.Brief lifestyle counselling—Patients received feedback onscreening plus the patient information leaflet and structuredbrief advice in the initial consultation. They were then asked tomake an appointment for a follow-up consultation within twoweeks for a 20 minute session of brief lifestyle counselling.22The counselling was based on a condensed form of motivationalinterviewing called health behaviour change.23 The patients firstdescribed their typical drinking day and then rated theimportance of changing their drinking and their confidenceabout changing their drinking on a 10 point scale (where a highernumber indicated greater importance or confidence and viceversa). The practitioner then worked with these ratings toestablish why they were at the current level and how they mightbe increased to a higher point, before eliciting both pros andcons of drinking and finally working through a six step plan tohelp reduce drinking levels.
Training and supportImplementation of the protocol in this pragmatic trial variedacross practices according to their size, level of interest, andavailable resources. Practice based training was delivered to195 people (including all participating clinicians) in designatedteam meetings. The training included general information onalcohol epidemiology and UK standard drinks, an introductionto the trial protocol, demonstration of the relevant screeningand brief intervention approaches, and role play to practisedelivery. Research associates delivered training in the patientinformation leaflet and brief advice group. An alcohol healthworker who was experienced in alcohol counselling deliveredthe training in brief lifestyle counselling. In this group brieflifestyle counselling was practised with trained actors and taperecorded. The competency of counselling was checked usingthe behaviour change counselling index.24 Only practitionerswho reached a required standard (agreed by inter-rater consensusbetween three independent clinical assessors) were approvedto deliver brief lifestyle counselling in the trial.
ImplementationA mixture of general practitioners and practice care nursesdelivered 95% of screening and brief intervention activity inthis trial. A graphical summary of the trial procedures has been
provided to clarify the sequence and timing of screening,assessment, brief intervention, and follow-up activity (seesupplementary diagram 1, PaT plot). Seventy per cent of targetpatient recruitment occurred within six months, with theremaining 30% over nine months. Owing to this slowrecruitment, research staff who had delivered training in studyprocedures supported screening and brief intervention deliveryin 10 practices and recruited 152 patients, which was 5% of thetotal number of trial participants.
MeasuresBaselineThe primary outcome was drinking status at six months asmeasured by the alcohol use disorders identification test(AUDIT, score range 0-40),25 which has been validated for useas an outcome measure in primary care.26 A score of ≥8 on thistest indicates hazardous or harmful drinking or the likelihoodof dependent drinking, with a sensitivity of 92% and specificityof 94%.25 Since brief interventions aim to reduce hazardous orharmful drinking, the primary outcome measure was negativestatus on the test (proportion of participants scoring <8) at sixmonths.Participants also completed the EuroQol to measure quality oflife,27 a short service use questionnaire,28 and a modifiedreadiness ruler with one question (and four response categories)to measure patients’ motivation or “readiness to change” theirdrinking behaviour.29 The use of such readiness to changemeasures has been recommended in clinical practice to helptailor brief interventions and also predict subsequent drinkingoutcomes.30
Follow-upAt six and 12months after randomisation researchers who wereblinded to the allocated intervention contacted the participantsby telephone or post. Researchers administered the sameinstruments as at baseline plus the alcohol problemsquestionnaire.31A short patient satisfaction questionnaire32wasalso administered at 12 months.
Financial incentivesEach practice received £3000 to cover staff time and disruption.Payments were staged and occurred after training, on completionof participant recruitment, and at the end of data collection.Modelled on smoking cessation payments in the Quality andOutcomes Framework,33 screening and brief intervention wasincentivised as £1 per patient screened (€1.26 or $1.85, allconversions at 2008 exchange rates), £8 per brief advice, and£32 per brief lifestyle counselling. Each patient participantreceived a £10 voucher shortly after completing the baselineassessment and at each follow-up interview.
Sample size calculationAcomprehensivemeta-analysis4 suggested a clinically importantdifference in negative status on AUDIT between briefintervention and controls of 13% (5% reduction in controls and18% in brief intervention recipients). Detecting this differenceat the 5% significance level with 80% power (with a two sidedtest), required 109 patients per group (total 327). Assuming aloss to follow-up of 25%, the sample size was inflated to 145per group (total 435). To account for potential cluster effectswe used an intraclass correlation coefficient of 0.04 based onour experience of primary care trials.34 Assuming a cluster sizeof 31 patients per practice, this inflated the calculation by a
No commercial reuse: See rights and reprints http://www.bmj.com/permissions Subscribe: http://www.bmj.com/subscribe
BMJ 2013;346:e8501 doi: 10.1136/bmj.e8501 (Published 9 January 2013) Page 3 of 14
RESEARCH

factor of 1.7. Hence we required 248 patients per group (total744), with an expectation that at least 558 would be followedup at six months.
Statistical analysisAnalysis was by intention to treat, with patients analysed in thegroup to which they had been randomised. We used logisticregression to analyse the primary outcome, negative status onAUDIT at six months. Included in the model were screeningapproach, screening tool, and intervention, and the model wasadjusted for age, sex, and baseline AUDIT score. To takeaccount of the cluster study design we used theHuber-White-sandwich estimator, robust standard errorsmethod.As a factorial study, interaction effects were considered. To themodel we individually added three two-way interactions,screening approach*tool, screening approach*intervention, andscreening tool*intervention and compared the result with amodel without interactions. If the interaction was found to besignificant we included it in the final model.Data were presented as odds ratios and corresponding 95%confidence intervals. We carried out secondary analyses usingappropriate methods for the outcomes (linear, logistic, or ordinalregression) controlling for the same covariates as the primaryoutcome and adjusting for the clustered nature of the study.Intervention efficacy was also explored in a per protocolanalysis.To assess the impact of missing data on the primary outcome,we carried out multiple imputation using the ICE procedure inSTATA. We tested several models for the prediction; the finalmodel used AUDIT negative status at six months as thedependent variable, baseline AUDIT score, screening approach,screening tool, intervention, sex, and age. A series of 10imputations was done.We combined these using theMIcombinecommand in STATA. The imputation confirmed the initialanalysis where only those actually followed up were included.
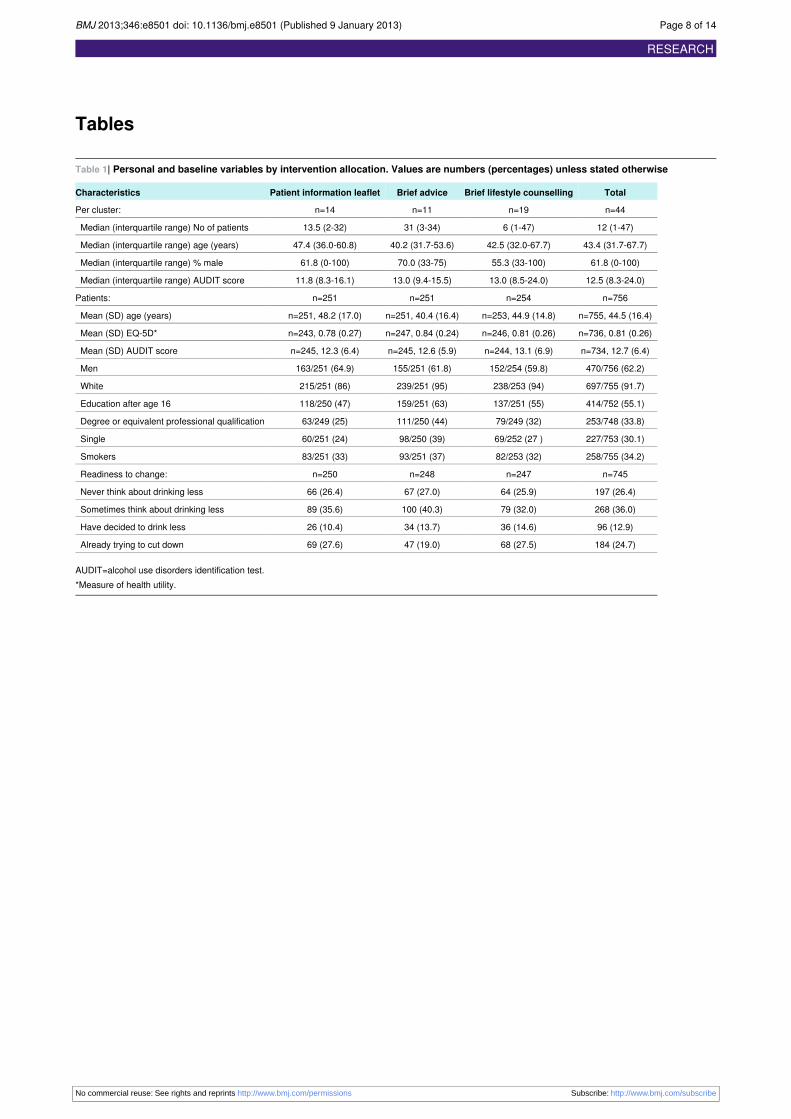
ResultsOf 3562 presenting patients, 2991 (84.0%) were eligible forscreening; 900 (30.1%) of these patients were identified ashazardous or harmful drinkers. Overall, 756 (84.0%) consentedto participate in the trial; consent rates were similar betweenthe three interventions (fig 1⇓). All participants received apatient information leaflet, whereas 99% (n=250) of thoseallocated to the other two interventions received brief advice.However, just 57% (n=143) of relevant patients returned andreceived the brief lifestyle counselling intervention.At six months the follow-up rates were 85% (patient informationleaflet 85% (n=212), brief advice 86% (n=215), and brieflifestyle counselling 85% (n=217)) and at 12 months 82%(patient information leaflet 79% (n=197), brief advice 83%(n=209), brief lifestyle counselling 83% (n=211)). Follow-uprates between the interventions did not differ significantly.However, those followed up at six months had lower meanbaseline AUDIT scores than those not followed up: 12.4 (SE0.25) v 14.3 (SE 0.66).The average age of participants was 45 years, 62% (n=756) ofparticipants were men, 92% (n=755) were white, 34% (n=253)had attained higher degree level, and 34% (n=258) were smokers(table 1⇓). At baseline 82% (n=611) of participants wereidentified as hazardous or harmful drinkers by the AUDIT, withan average score of 12.7 (SD 6.4). Reported readiness to changevaried across the three interventions, although 62% (n=465) of
patients reported never or only sometimes thinking aboutdrinking less.
Primary outcomeThe proportions of patients with a negative AUDIT statusincreased at six months in all three interventions (fig 2⇓). Thedifferences between the interventions were not, however,significant (table 2⇓). None of the interactions tested weresignificant (see supplementary table S1) so the model withoutinteractions was used to estimate the differences betweeninterventions. The odds ratios of having a negative AUDITstatus for brief advice compared with the patient informationleaflet was 0.85 (95% confidence interval 0.52 to 1.39) and forbrief lifestyle counselling compared with the patient informationleaflet was 0.78 (0.48 to 1.25). The primary outcome was notaffected by missing data (table 3⇓).
Secondary analysesAt 12 months there were no statistically significant differencesbetween the three interventions in the proportions of patientswith a negative AUDIT result (table 2). Compared with thepatient information leaflet intervention, at 12 months the oddsratio of having a negative AUDIT result was 0.91 (0.53 to 1.56)for brief advice and 0.99 (0.60 to 1.62) for brief lifestylecounselling. A per protocol analysis, including just those whoreceived their allocated treatment, and an analysis combiningthe more intensive interventions (brief advice plus brief lifestylecounselling versus patient information leaflet) also indicatedno significant differences between the interventions at six or 12months.In addition, there were no statistically significant differences inmean AUDIT score by intervention or over time (table 4⇓). Atsix months, the mean difference between brief advice and thepatient information leaflet was 0.06 (−0.70 to 0.83) and betweenbrief lifestyle counselling and the patient information leafletwas −0.38 (−1.51 to 0.75). At 12months these mean differenceswere larger but not statistically significant. Compared with thepatient information leaflet, the mean difference for brief advicewas −0.20 (−0.83 to 0.43) and for brief lifestyle counsellingwas −0.25 (−1.19 to 0.68). The estimates were derived frommodels without interactions.At six months there were differences in reported readiness tochange (table 5⇓), with 32% (n=65) of patients in the patientinformation leaflet group reporting “trying to cut down”compared with 34% (n=69) receiving brief advice and 45%(n=93) receiving brief lifestyle counselling. The expectedordered odds for brief lifestyle counselling compared with thepatient information leaflet increased by 1.74 (95% confidenceinterval 1.27 to 2.39, P=0.001) with a shift to the next highercategory—that is, a greater readiness to change. For brief advicecompared with the patient information leaflet, the expectedordered odds increased by 1.37 (0.95 to 1.98, P=0.095). Asimilar finding occurred at 12months, with 32% (n=61) of thosein the patient information leaflet group trying to cut downcompared with 37% (n=74) receiving brief advice and 48%(n=95) receiving brief lifestyle counselling. For brief lifestylecounselling compared with the patient information leaflet, theexpected ordered odds increased by 1.86 (1.31 to 2.65, P=0.001).For brief advice compared with the patient information leaflet,the expected ordered odds increased by 1.24 (0.83 to 1.87,P=0.293).Participants who received brief lifestyle counselling alsoreported greater satisfaction than those who received the patientinformation leaflet (table 6⇓) based on general communication
No commercial reuse: See rights and reprints http://www.bmj.com/permissions Subscribe: http://www.bmj.com/subscribe
BMJ 2013;346:e8501 doi: 10.1136/bmj.e8501 (Published 9 January 2013) Page 4 of 14
RESEARCH

(mean difference 0.13, 95% confidence interval 0.01 to 0.26)and the interpersonal manner of the clinician delivering theintervention (mean difference 0.10, 0.002 to 0.19). Thesedifferences were not observed between brief advice and thepatient information leaflet interventions.
Interaction with earlier screening activityAt six months there was a significant interaction between briefintervention and earlier screening approach, therefore the resultsare presented as six separate groups (see supplementary table2). Each groupwas compared with the reference group of patientinformation leaflet/universal screening. At the initial follow-uppoint, patients in the brief lifestyle counselling/universalscreening group (mean difference −0.78, 95% confidenceinterval −1.53 to −0.03) and the patient informationleaflet/targeted screening group (mean difference −0.77, −1.42to −0.12) had significantly lower scores on the alcohol problemsquestionnaire. But the other four combinations of briefintervention and screening approach did not differ significantly.Furthermore, outcomes measured by the alcohol problemsquestionnaire at 12 months did not differ significantly (seesupplementary table S2).
DiscussionAll patients in this trial received feedback on their hazardousor harmful drinking status immediately after the screeningprocess. At two follow-up points, however, brief advice andbrief lifestyle counselling did not provide a statisticallysignificant additional benefit in reducing hazardous or harmfuldrinking compared with the provision of a patient informationleaflet. Brief lifestyle counselling significantly increasedpatients’ motivation to reduce their drinking through a positiveshift in readiness to change compared with those receiving thepatient information leaflet. Moreover, these patients alsoreported greater satisfaction with the brief intervention processthan those in the patient information leaflet group. However,no significant differences between the brief interventions werefound for alcohol related problems or health related quality oflife. This study therefore does not support the additional deliveryof five minutes of brief advice or 20 minutes of brief lifestylecounselling over and above the delivery of feedback onscreening plus a patient information leaflet.
Strengths and weaknesses of the studyThis trial was a large pragmatic multicentre evaluation ofscreening and brief intervention in typical primary careconditions. Cluster randomisation avoided the potential problemsof contamination between the trial arms and thus subversion ofthe study protocol. Five practices delivered more than one briefintervention but only after they had successfully completedrecruitment for the intervention to which they had beenoriginally allocated. These reallocated practices subsequentlydelivered a more intensive brief intervention approach aftertraining in the new procedure.Other methodological strengths of the study were the use ofremote randomisation procedures and validated outcomemeasures of clinical relevance. Rates of eligibility and patientconsent to the trial (84%) were higher than in most previoussimilar studies,35 which adds weight to the generalisability ofthe research. Furthermore, the study achieved its expectedsample size, and patient follow-up rates were higher thananticipated (>80%) with no differential loss to follow-upbetween the three interventions.
In terms of potential weaknesses, since direct monitoring of theconsultations would have undermined the pragmatic nature ofthe study, it was difficult to ascertain the extent to which theinterventions were delivered as intended. Moreover, trial staffdelivered screening and brief intervention to a small proportionof patients (5%) owing to flagging recruitment. It is possiblethat the lack of intervention differences may have been due tounsuccessful implementation of the brief intervention protocolsby the primary care clinicians. These clinicians often give adviceand lifestyle counselling in other areas of practice and theremay have been unconscious use of these skills with patientswho were not intended to receive them in this trial. The issueof intervention fidelity will be explored in an indepth qualitative(interview based) process study with clinicians from this trial,which occurred after patient follow-up was completed.Only 57% of patients in the brief lifestyle counselling groupactually received the intervention, which could have reducedits potential impact. But, as this was a pragmatic study this levelof return to a subsequent counselling session probably reflectswhat would happen in usual practice. A further issue ofpragmatism was our attempt to make baseline assessment asshort as possible. We were aware that extensive questioningabout alcohol could have acted as an intervention in its ownright. Hence we used the 10 itemAUDIT (alcohol use disordersidentification test) questionnaire to provide our primary outcomemeasure.26Although this tool did not allow detailedmeasurementof actual consumption levels (in terms of standard drink unitsdaily or weekly), it captured wider aspects of alcohol relatedrisk and harm through items on drinking quantity, frequency,intensity, and negative behavioural consequences.
Relevance of the findings to the disciplineNumerous systematic reviews and meta-analyses have nowshown benefits of screening and brief alcohol intervention inprimary care compared with a range of control conditions(typically assessment only, treatment as usual, or writteninformation). However, a consistent finding in this disciplineis significantly reduced alcohol consumption in both interventionand controls groups.36-38 One explanation for reduced drinkingin both intervention and control groups is regression to themean,in which extreme measures of behaviour tend to shift to lessextreme positions from one time point to another.39 We cannotfully discount this explanation for our findings. However, wethink it unlikely since levels of drinking in this trial, as shownby mean AUDIT scores, were not particularly extreme. Indeed,some patients were close to the threshold for hazardous drinking.In addition, the changes over time in our control condition weresimilar to mean effect sizes reported for brief intervention.8 37
An alternative explanation is that our control condition,consisting of simple feedback and written information aboutalcohol, may have contained active factors of behaviourchange.40 Indeed two controlled trials have reported significantclinical effects of screening41 and assessment alone42 on drinkingbehaviour. Consequently, it is likely that the cumulative impactof screening, assessment, simple feedback, and the delivery ofwritten information may have overwhelmed the additional inputof five minutes of structured brief advice both in terms ofelapsed time and the number of distinct behaviour changetechniques used.43
To conclusively demonstrate that providing feedback plus apatient information leaflet led to reduced rates of hazardous andharmful drinking, our trial would ideally have had an additionalno intervention arm. However, in view of the extensive evidencesupporting brief intervention effectiveness at the time of the
No commercial reuse: See rights and reprints http://www.bmj.com/permissions Subscribe: http://www.bmj.com/subscribe
BMJ 2013;346:e8501 doi: 10.1136/bmj.e8501 (Published 9 January 2013) Page 5 of 14
RESEARCH

trial, our control condition was considered to be the minimalethically acceptable input after screening activity.
Implications for clinicians, servicecommissioners, and policymakersThe high levels of consent to this trial and the high rates ofscreening and immediate delivery of brief intervention indicatethat routinely presenting patients in primary care are willing toreceive feedback, written information, and advice about theirdrinking behaviour. In addition, the high levels of patientsatisfaction after brief intervention in all three conditions supportthe acceptability of this type of input. However, the significantpatient attrition in the brief lifestyle counselling group suggeststhat there may be a benefit of delivering brief interventiondirectly after screening rather than delaying until a subsequentoccasion. In emergency care, it has been recommended that thetime between screening and brief intervention is minimised andideally occurs on the same day.44 Indeed it is likely that theprocess of identifying and quantifying alcohol related risk orharm may be a “teachable moment” where patients have aheightened receptivity to the idea of reducing their drinking.44
Nevertheless, in patients who returned to a subsequentconsultation for brief lifestyle counselling, there were significantpositive changes in motivation to reduce drinking and in patientsatisfaction levels. Consequently, it is possible that whereasmost hazardous and harmful drinkers in primary care requireminimal input after screening, there may be a group of patientswho would value and benefit from additional support. Hence astepped care approach might be helpful in this area. Here theleast intensive (less costly) intervention is used with mostpatients who present with alcohol related risk or harm, andfurther intervention is reserved for patients who do not respondor who ask for more support to help reduce their drinkingbehaviour. A previous study found that a stepped care alcoholintervention wasmore cost effective than aminimal interventionin primary care.34This approachwas also recommended in recentNational Institute for Health and Clinical Excellence guidelineson the prevention of alcohol problems in adults and youngpeople.45
Finally, given the extensive published evidence on theeffectiveness of screening and brief intervention in reducinghazardous and harmful drinking, the case for its widerimplementation in primary care is strong. Regarding thenecessary level of input, our findings confirm the conclusionof a Cochrane Collaboration systematic review that longer (moreintensive) brief interventions add no significant additionalbenefit over shorter input in primary care.8However, this reviewcontained just one trial, based in Finland, which directlycompared three differing intensities of brief intervention.Equivalent outcomes were reported for women46 and men47whoreceived simple feedback compared with three or seven briefintervention sessions. However, this finding was attributed toa failure to successfully implement the more intensive briefinterventions in routine practice rather than the merit of simplefeedback in itself. The current study strongly suggests thatscreening followed by simple feedback and written informationmay be the most appropriate strategy to reduce hazardous andharmful drinking in primary care.
This paper is published on behalf of the SIPS programme researchgroup. A full list of the research group members is available at http://sips.iop.kcl.ac.uk/contactus.php. We thank Ruth McGovern and RobertPatton for refining the study interventions and supporting theimplementation of this trial.
Contributors: All of the authors contributed to the design anddevelopment of this trial protocol. CD was the chief investigator of SIPSand EK was deputy chief investigator and lead for the primary care trial.Expertise on clinical aspects of the research was provided for primarycare by PC and JM, for nursing practice by TP and for psychiatry CDand EG. Statistical input was provided by SC, VD and MB. Healtheconomics input was provided by CG and SP. Trial conduct and deliveryexpertise was provided by PD, DNB and KP. Alcohol and policy expertisewas provided by AO and DS. Brief intervention expertise was providedby CD, EK, NH and JS. EK wrote the first draft of the paper and allauthors contributed to successive drafts. All authors read and approvedthe final manuscript.Funding: EK was part funded by Fuse the Centre for TranslationalResearch in Public Health. Fuse is a UKCRC Public Health ResearchCentre of Excellence, and funding comes from the British HeartFoundation, Cancer Research UK, Economic and Social ResearchCouncil, Medical Research Council, and the National Institute for HealthResearch. This study was funded by the Department of Health. Theviews expressed herein do not necessarily reflect those of theDepartment of Health or the National Health Service in England andWales.Competing interests: All authors have completed the ICMJE uniformdisclosure form at www.icmje.org/coi_disclosure.pdf (available onrequest from the corresponding author) and declare: all authors hadfinancial support from the Department of Health in England (AlcoholPolicy Unit) for the submitted work; no financial relationships with anyorganisations that might have an interest in the submitted work in theprevious three years; no other relationships or activities that could appearto have influenced the submitted work.Ethical approval: This study received multicentre ethical approval(06/MRE02/90) plus local agreement from all relevant local researchethics committees. Research governance approval was granted by allrelevant primary care trusts. The research was done in accordance withthe Helsinki declaration.Data sharing: No additional data available.
1 Funk M, Wutzke S, Kaner E, Anderson P, Pas L, McCormick R, et al. A multicountrycontrolled trial of strategies to promote dissemination and implementation of brief alcoholintervention in primary health care: findings of a World Health Organization collaborativestudy. J Stud Alcohol 2005;66:379-88.
2 Saunders JB, Lee NK. Hazardous alcohol use: its delineation as a subthreshold disorder,and approaches to its diagnosis and management. Compr Psychiatry 2000;41:95-103.
3 World Health Organization. International classification of diseases . 10th revision. WHO,1992.
4 Moyer A, Finney JW, Swearingen CE, Vergun P. Brief interventions for alcohol problems:a meta-analytic review of controlled investigations in treatment-seeking andnon-treatment-seeking populations. Addiction 2002;97:279-92.
5 Ballesteros JA, Duffy JC, Querejeta I, Arino J, Gonzalez-Pinto A. Efficacy of briefinterventions for hazardous drinkers in primary care: systematic review and meta-analysis.Alcohol, Clin Exp Res 2004;28:608-18.
6 Bertholet N, Daeppen J-B, Wietlisbach V, Fleming M, Burnand B. Brief alcohol interventionin primary care: systematic review and meta-analysis. Arch Intern Med 2005;165:986-95.
7 Whitlock EP, Polen MR, Green CA, Orleans T, Klein J. Behavioral counseling interventionsin primary care to reduce risky/harmful alcohol use by adults: a summary of the evidencefor the US Preventive Services Task Force. Ann Intern Med 2004;140:557-68.
8 Kaner E, Beyer F, Dickinson H, Pienaar E, Campbell F, Schlesinger C, et al. Effectivenessof brief alcohol interventions in primary care populations. Cochrane Database Syst Rev2007;(2):CD004148.
9 Miller W, Heather N, Hall W. Calculating standard drink units: international comparisons.Br J Addict 1991;86:43-7.
10 Kaner E. Brief alcohol intervention: time for translational research. Addiction2010;105:960-1.
11 Babor TF, Higgins-Biddle JC, Dauser D, Burleson JA, Zarkin GA, Bray J. Brief interventionsfor at-risk drinking: patient outcomes and cost-effectiveness in managed care organizations.Alcohol Alcohol 2006;41:624-31.
12 Edwards AGK, Rollnick S. Outcome studies of brief alcohol intervention in general practice:the problem of lost subjects. Addiction 1997;92:1699-704.
13 Burke BL, Arkowitz H, Menchola M. The efficacy of motivational interviewing: ameta-analysis of controlled clinical trials. J Consult Clin Psychol 2003;71:843-61.
14 Lundahl B, Kunz C, Brownell C, Tollefson D, Burke B. A meta-analysis of motivationalinterviewing: twenty five years of empirical studies. Res Soc Work Pract 2010;20:137-60.
15 Vasilaki E, Hosier S, CoxW. The efficacy of motivational interviewing as a brief interventionfor excessive drinking: a meta-analytic review. Alcohol Alcohol 2006;41:328-35.
16 Coulton S, Bland M, Cassidy P, Deluca P, Drummond C, Gilvarry E, et al. Screening andbrief intervention for hazardous and harmful alcohol use in accident and emergencydepartments: a randomised controlled trial protocol. BMC Health Serv Res 2009;9(14).
No commercial reuse: See rights and reprints http://www.bmj.com/permissions Subscribe: http://www.bmj.com/subscribe
BMJ 2013;346:e8501 doi: 10.1136/bmj.e8501 (Published 9 January 2013) Page 6 of 14
RESEARCH

What is already known on this topic
Around 20-30% of patients who routinely present in primary care are hazardous or harmful drinkersBrief alcohol intervention in primary care can significantly reduce hazardous and harmful drinkingHowever, the optimal intensity of brief intervention input is currently not clear
What this study adds
Brief advice and brief lifestyle counselling did not provide a statistically significant benefit in reducing hazardous or harmful drinkingcompared with a patient information leafletScreening followed by simple feedback and written information may be the most appropriate strategy to reduce hazardous and harmfuldrinking in primary care
17 Newbury-Birch D, BlandM, Cassidy P, Coulton S, Deluca P, Drummond C, et al. Screeningand brief interventions for hazardous and harmful alcohol use in probation services: acluster randomised controlled trial protocol. BMC Public Health 2009;9:418.
18 Kaner E, Bland M, Cassidy P, Coulton S, Deluca P, Drummond C, et al. Screening andbrief interventions for hazardous and harmful alcohol use in primary care: a clusterrandomised controlled trial protocol BMC Public Health 2009;9:287.
19 Hodgson R, Alwyn T, John B, Thom B, Smith A. The FAST alcohol screening test. AlcoholAlcohol 2002;37:61-6.
20 Canagasaby A, Vinson DC. Screening for hazardous or harmful drinking using one ortwo quantity-frequency questions. Alcohol Alcohol 2005;40:208-13.
21 Coulton S, Drummond C, Deluca P, Kaner E, Newbury-Birch D, Perryman K, et al. Theutility of different screeningmethods to detect hazardous drinking and alcohol use disordersin the screening and intervention programme for Sensible drinking (SIPS) programme.Addict Sci Clin Pract 2012;7(Suppl 1):A83.
22 Heather N, Girvan M, Kaner E, Cassidy P. Implementing screening and brief alcoholintervention in pilot general practices in the Tyne and Wear Health Action Zone (finalreport). A final report on research funded by the Tyne and Wear Health Action Zone.Northumbria University, 2008.
23 Rollnick S, Mason P, Butler C. Health behaviour change: a guide for practitioners. ChurchillLivingstone, 1999.
24 Lane C. The Behaviour Change Counselling Index (BECCI) Scale. University of Wales,2002.
25 Saunders JB, Aasland OG, Babor TF, De La Fuente JR, Grant M. Development of theAlcohol Use Disorders Identification Test (AUDIT): WHO Collaborative Project on EarlyDetection of Persons with Harmful Alcohol Consumption. Addiction 1993;88:791-804.
26 Bradley KA, McDonell MB, Bush K, Kivlahan DR, Diehr P, Fihn SD. The AUDIT alcoholconsumption questions: reliability, validity, and responsiveness to change in older maleprimary care patients. Alcohol Clin Exp Res 1998;22:1842-9.
27 Rabin R, Charro F. EQ-5D: a measure of health status from the euroqol group. Ann Med2001;33:337-43.
28 UKATT Research Team. Cost effectiveness of treatment for alcohol problems: findingsof the randomised UK alcohol treatment trial (UKATT). BMJ 2005;331:544.
29 Heather N, Smailes D, Cassidy P. Development of a Readiness Ruler for use with alcoholbrief interventions. Drug Alcohol Depend 2008;98:235-40.
30 Williams E, Horton N, Samet J, Saitz R. Do brief measures of readiness to change predictalcohol consumption and consequences in primary care patients with unhealthy alcoholuse? Alcohol Clin Exp Res 2007;31:428-35.
31 Drummond C. The relationship between alcohol dependence and alcohol-related problemsin a clinical population. Br J Addict 1990;85:357-66.
32 Ware J, Snyder M, Wright W, eds. Development and validation of scales to measurepatient satisfaction with medical care services. National Technical Information Service,1976.
33 NHS Employers. Clinical Directed Enhanced Service (DES) Guidance for GMS contract2008/9. NHS Employers and BMA, 2008.
34 Drummond C, Coulton S, James D, Godfrey C, Parrott S, Baxter J, et al. Effectivenessand cost-effectiveness of a stepped care intervention for alcohol use disorders in primarycare: pilot study. Br J Psychiatry 2009;195:448-56.
35 Beich A, Thorsen T, Rollnick S. Screening in brief intervention trials targeting excessivedrinkers in general practice: systematic review and meta-analysis. BMJ 2003;327:536-40.
36 Bernstein J, Bernstein E, Heeren T. Mechanisms of change in control group drinking inclinical trials of brief alcohol intervention: implications for bias towards the null. DrugAlcohol Rev 2010;29:498-507.
37 Jenkins RJ, McAlaney J, McCambridge J. Change over time in alcohol consumption incontrol groups in brief intervention studies: systematic review and meta-regression study.Drug Alcohol Depend 2009;100:107-14.
38 McCambridge J, Kypri K. Can simply answering research questions change behaviour?systematic review and meta analyses of brief alcohol intervention trials. PLOS One2011;6:e23748. doi:10.1371/journal.pone.0023748.
39 Bland J, Altman D. Regression towards the mean. BMJ 1994;308:1499.40 Michie S, Prestwich A, deBruin M. Importance of the nature of comparison conditions for
testing theory-based interventions: reply. Health Psychol 2010;29:468-70.41 McCambridge J, Day M. Randomized controlled trial of the effects of completing the
Alcohol Use Disorders Identification Test questionnaire on self-reported hazardous drinking.Addiction 2007;103:241-8.
42 Kypri K, Langley JD, Saunders JB, Cashell-SmithML. Assessment may conceal therapeuticbenefit: findings from a randomised controlled trial for hazardous drinking. Addiction2007;102:62-70.
43 Abraham C, Michie S. A taxonomy of behavour change techniques used in interventions.Health Psychol 2008;27:379-87.
44 Williams S, Brown A, Patton B, Crawford M, Touquet R. The half-life of the ‘teachablemoment’ for alcohol misusing patients in the emergency department.Drug Alcohol Depend2005;77:205-8.
45 National Institute for Health and Clinical Excellence. Alcohol-use disorders—preventingthe development of hazardous and harmful drinking. 2010. http://guidance.nice.org.uk/PH24.
46 Aalto M, Saksanen R, Laine P, Forsstrom R, Raikaa M, Kiviluto M, et al. Brief interventionfor female heavy drinkers in routine general practice: a 3-year randomized controlledstudy. Alcohol Clin Exp Res 2000;24:1680-6.
47 Aalto M, Seppa K, Mattila P, Mustonen H, Ruuth K, Hyvarinen H, et al. Brief interventionfor male heavy drinkers in routine general practice: a three year randomized controlledstudy. Alcohol Alcohol 2001;36:224-30.
Accepted: 7 November 2012
Cite this as: BMJ 2013;346:e8501This is an open-access article distributed under the terms of the Creative CommonsAttribution Non-commercial License, which permits use, distribution, and reproduction inany medium, provided the original work is properly cited, the use is non commercial andis otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/2.0/ and http://creativecommons.org/licenses/by-nc/2.0/legalcode.
No commercial reuse: See rights and reprints http://www.bmj.com/permissions Subscribe: http://www.bmj.com/subscribe
BMJ 2013;346:e8501 doi: 10.1136/bmj.e8501 (Published 9 January 2013) Page 7 of 14
RESEARCH
Tables
Table 1| Personal and baseline variables by intervention allocation. Values are numbers (percentages) unless stated otherwise
TotalBrief lifestyle counsellingBrief advicePatient information leafletCharacteristics
n=44n=19n=11n=14Per cluster:
12 (1-47)6 (1-47)31 (3-34)13.5 (2-32)Median (interquartile range) No of patients
43.4 (31.7-67.7)42.5 (32.0-67.7)40.2 (31.7-53.6)47.4 (36.0-60.8)Median (interquartile range) age (years)
61.8 (0-100)55.3 (33-100)70.0 (33-75)61.8 (0-100)Median (interquartile range) % male
12.5 (8.3-24.0)13.0 (8.5-24.0)13.0 (9.4-15.5)11.8 (8.3-16.1)Median (interquartile range) AUDIT score
n=756n=254n=251n=251Patients:
n=755, 44.5 (16.4)n=253, 44.9 (14.8)n=251, 40.4 (16.4)n=251, 48.2 (17.0)Mean (SD) age (years)
n=736, 0.81 (0.26)n=246, 0.81 (0.26)n=247, 0.84 (0.24)n=243, 0.78 (0.27)Mean (SD) EQ-5D*
n=734, 12.7 (6.4)n=244, 13.1 (6.9)n=245, 12.6 (5.9)n=245, 12.3 (6.4)Mean (SD) AUDIT score
470/756 (62.2)152/254 (59.8)155/251 (61.8)163/251 (64.9)Men
697/755 (91.7)238/253 (94)239/251 (95)215/251 (86)White
414/752 (55.1)137/251 (55)159/251 (63)118/250 (47)Education after age 16
253/748 (33.8)79/249 (32)111/250 (44)63/249 (25)Degree or equivalent professional qualification
227/753 (30.1)69/252 (27 )98/250 (39)60/251 (24)Single
258/755 (34.2)82/253 (32)93/251 (37)83/251 (33)Smokers
n=745n=247n=248n=250Readiness to change:
197 (26.4)64 (25.9)67 (27.0)66 (26.4)Never think about drinking less
268 (36.0)79 (32.0)100 (40.3)89 (35.6)Sometimes think about drinking less
96 (12.9)36 (14.6)34 (13.7)26 (10.4)Have decided to drink less
184 (24.7)68 (27.5)47 (19.0)69 (27.6)Already trying to cut down
AUDIT=alcohol use disorders identification test.*Measure of health utility.
No commercial reuse: See rights and reprints http://www.bmj.com/permissions Subscribe: http://www.bmj.com/subscribe
BMJ 2013;346:e8501 doi: 10.1136/bmj.e8501 (Published 9 January 2013) Page 8 of 14
RESEARCH

Table 2| Proportions of participants with negative alcohol use disorders identification test result at baseline and six and 12month follow-up.Values are numbers (percentages) unless stated otherwise
ICC (SE)
Odds ratio* (95% CI), P value
Brief lifestylecounsellingBrief advice
Patientinformation leafletTime point
Brief lifestylecounselling/patientinformation leaflet
Brief advice/patientinformation leaflet
0.02 (0.02)——37/249 (15)51/249 (20)50/247 (20)Baseline
0.03 (0.02)0.78 (0.48 to 1.25), 0.300.85 (0.52 to 1.39), 0.5159/205 (29)61/208 (29)72/202 (36)6 months
0.04 (0.02)0.99 (0.60 to 1.62), 0.960.91 (0.53 to 1.56), 0.7372/203 (36)72/205 (35)74/190 (39)12 months
ICC=intraclass correlation coefficient.*Odds ratio from logistic regression models adjusting for screening approach, screening tool, age, sex, and baseline alcohol use disorders identification test score.
No commercial reuse: See rights and reprints http://www.bmj.com/permissions Subscribe: http://www.bmj.com/subscribe
BMJ 2013;346:e8501 doi: 10.1136/bmj.e8501 (Published 9 January 2013) Page 9 of 14
RESEARCH
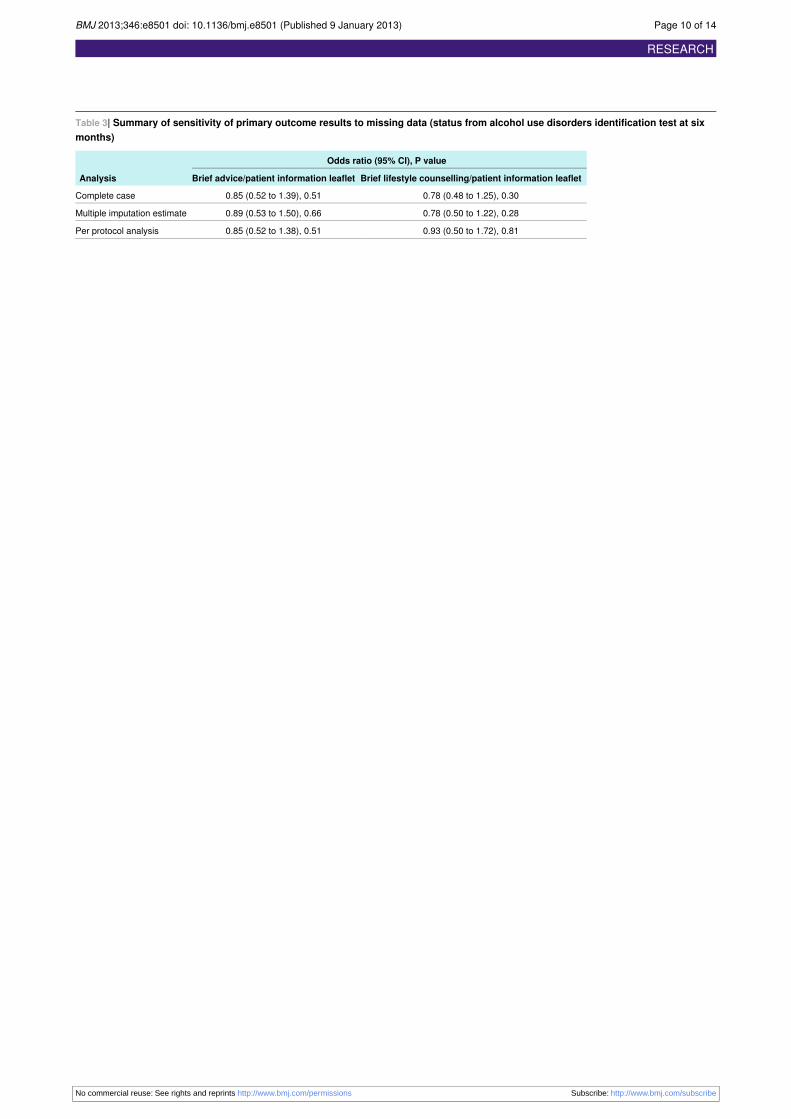
Table 3| Summary of sensitivity of primary outcome results to missing data (status from alcohol use disorders identification test at sixmonths)
Odds ratio (95% CI), P value
Analysis Brief lifestyle counselling/patient information leafletBrief advice/patient information leaflet
0.78 (0.48 to 1.25), 0.300.85 (0.52 to 1.39), 0.51Complete case
0.78 (0.50 to 1.22), 0.280.89 (0.53 to 1.50), 0.66Multiple imputation estimate
0.93 (0.50 to 1.72), 0.810.85 (0.52 to 1.38), 0.51Per protocol analysis
No commercial reuse: See rights and reprints http://www.bmj.com/permissions Subscribe: http://www.bmj.com/subscribe
BMJ 2013;346:e8501 doi: 10.1136/bmj.e8501 (Published 9 January 2013) Page 10 of 14
RESEARCH

Table 4| Alcohol use disorders identification test (AUDIT) scores by condition and over time
Mean difference (95% CI), P valueMean (SE) AUDIT score
Follow-up
Brief lifestylecounselling/patientinformation leaflet
Brief advice/patientinformation leaflet
Brief lifestylecounsellingBrief advice
Patient informationleaflet
−0.38 (−1.51 to 0.75), 0.500.06 (−0.70 to 0.83), 0.87n=205, 10.98 (0.49)n=208, 11.43 (0.23)n=202, 11.36 (0.31)6 months
−0.25 (−1.19 to 0.68), 0.59−0.20 (−0.83 to 0.43), 0.53n=203, 10.49 (0.40)n=205, 10.49 (0.17)n=195, 10.69 (0.24)12 months
*Estimates from linear regression models adjusting for screening approach, screening tool, age, sex, and baseline AUDIT score.
No commercial reuse: See rights and reprints http://www.bmj.com/permissions Subscribe: http://www.bmj.com/subscribe
BMJ 2013;346:e8501 doi: 10.1136/bmj.e8501 (Published 9 January 2013) Page 11 of 14
RESEARCH
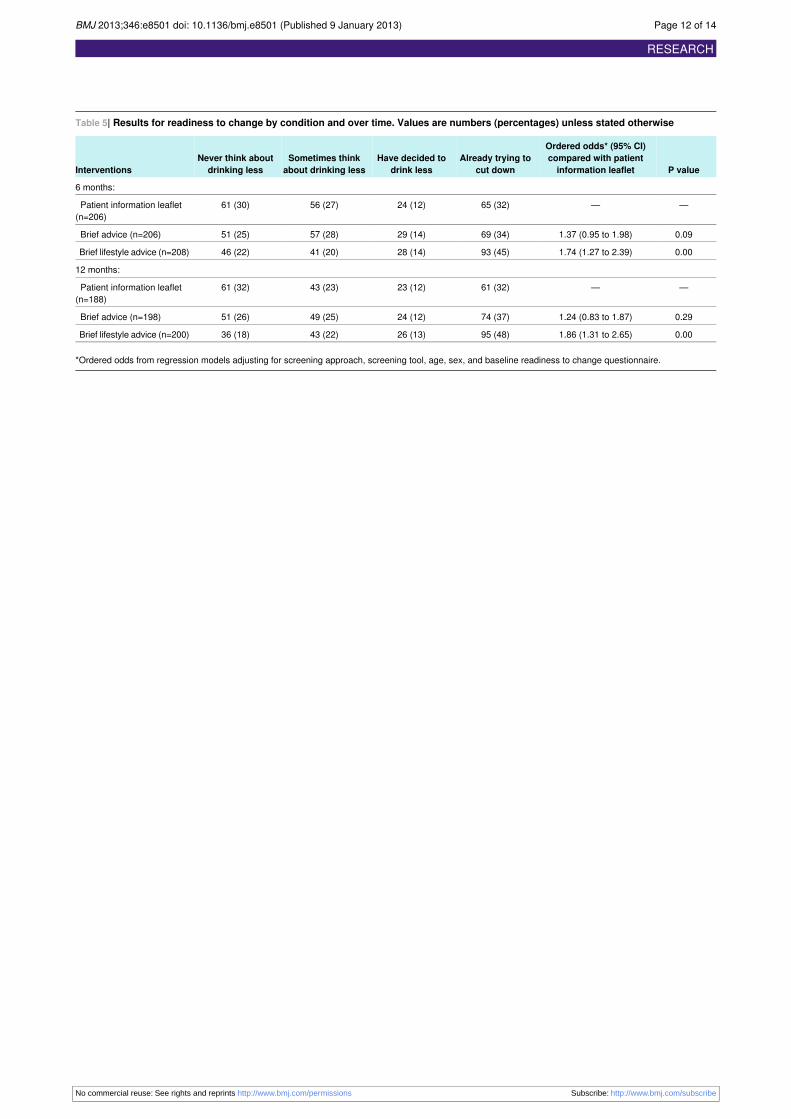
Table 5| Results for readiness to change by condition and over time. Values are numbers (percentages) unless stated otherwise
P value
Ordered odds* (95% CI)compared with patientinformation leaflet
Already trying tocut down
Have decided todrink less
Sometimes thinkabout drinking less
Never think aboutdrinking lessInterventions
6 months:
——65 (32)24 (12)56 (27)61 (30)Patient information leaflet(n=206)
0.091.37 (0.95 to 1.98)69 (34)29 (14)57 (28)51 (25)Brief advice (n=206)
0.001.74 (1.27 to 2.39)93 (45)28 (14)41 (20)46 (22)Brief lifestyle advice (n=208)
12 months:
——61 (32)23 (12)43 (23)61 (32)Patient information leaflet(n=188)
0.291.24 (0.83 to 1.87)74 (37)24 (12)49 (25)51 (26)Brief advice (n=198)
0.001.86 (1.31 to 2.65)95 (48)26 (13)43 (22)36 (18)Brief lifestyle advice (n=200)
*Ordered odds from regression models adjusting for screening approach, screening tool, age, sex, and baseline readiness to change questionnaire.
No commercial reuse: See rights and reprints http://www.bmj.com/permissions Subscribe: http://www.bmj.com/subscribe
BMJ 2013;346:e8501 doi: 10.1136/bmj.e8501 (Published 9 January 2013) Page 12 of 14
RESEARCH
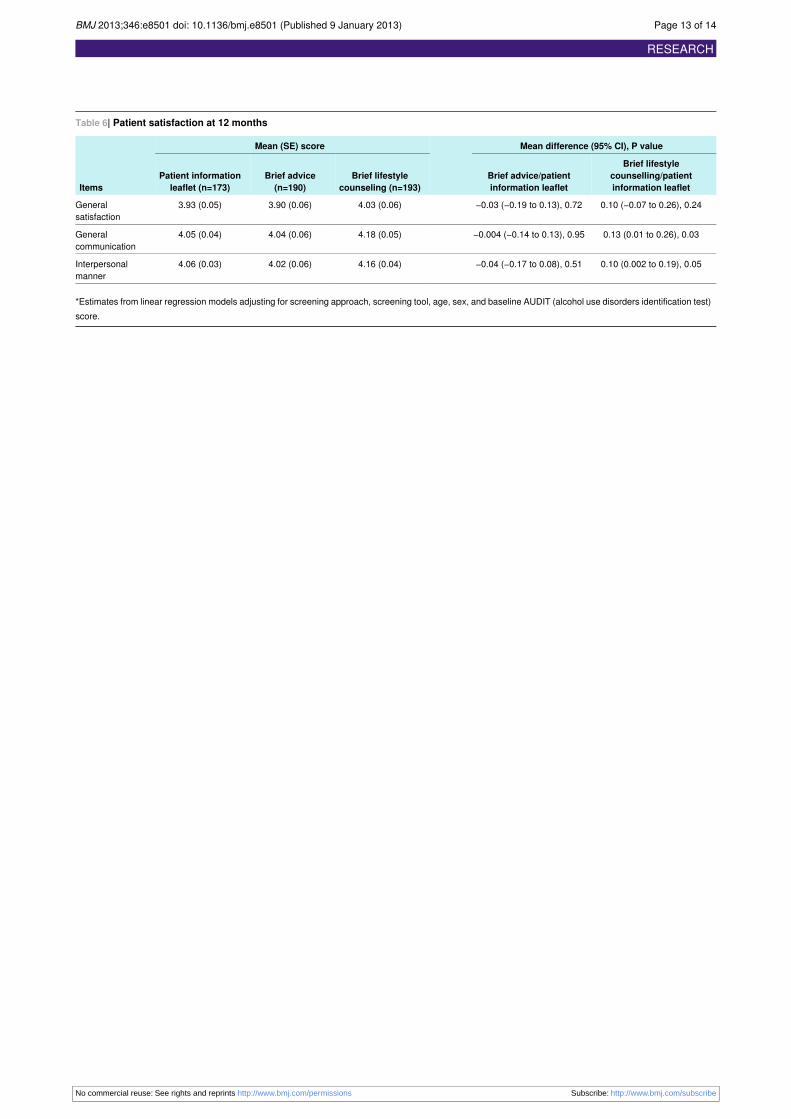
Table 6| Patient satisfaction at 12 months
Mean difference (95% CI), P valueMean (SE) score
Items
Brief lifestylecounselling/patientinformation leaflet
Brief advice/patientinformation leaflet
Brief lifestylecounseling (n=193)
Brief advice(n=190)
Patient informationleaflet (n=173)
0.10 (−0.07 to 0.26), 0.24−0.03 (−0.19 to 0.13), 0.724.03 (0.06)3.90 (0.06)3.93 (0.05)Generalsatisfaction
0.13 (0.01 to 0.26), 0.03−0.004 (−0.14 to 0.13), 0.954.18 (0.05)4.04 (0.06)4.05 (0.04)Generalcommunication
0.10 (0.002 to 0.19), 0.05−0.04 (−0.17 to 0.08), 0.514.16 (0.04)4.02 (0.06)4.06 (0.03)Interpersonalmanner
*Estimates from linear regression models adjusting for screening approach, screening tool, age, sex, and baseline AUDIT (alcohol use disorders identification test)score.
No commercial reuse: See rights and reprints http://www.bmj.com/permissions Subscribe: http://www.bmj.com/subscribe
BMJ 2013;346:e8501 doi: 10.1136/bmj.e8501 (Published 9 January 2013) Page 13 of 14
RESEARCH

Figures
Fig 1 Flow of participants through trial
Fig 2 Proportion of patients scoring <8 (negative status) on alcohol use disorders identification test, representingnon-hazardous or non-harmful drinking
No commercial reuse: See rights and reprints http://www.bmj.com/permissions Subscribe: http://www.bmj.com/subscribe
BMJ 2013;346:e8501 doi: 10.1136/bmj.e8501 (Published 9 January 2013) Page 14 of 14
RESEARCH