Clinical Outcomes for Patients Classified by Fear-Avoidance Beliefs and Centralization Phenomenon
10
ORIGINAL ARTICLE Clinical Outcomes for Patients Classified by Fear-Avoidance Beliefs and Centralization Phenomenon Mark W. Werneke, PT, MS, Dennis L. Hart, PT, PhD, Steven Z. George, PT, PhD, Paul W. Stratford, PT, MS, James W. Matheson, PT, DPT, Adrian Reyes, PT ABSTRACT. Werneke MW, Hart DL, George SZ, Stratford PW, Matheson JW, Reyes A. Clinical outcomes for patients classified by fear-avoidance beliefs and centralization phenom- enon. Arch Phys Med Rehabil 2009;90:768-77. Objectives: To (1) determine the prevalence of pain pattern classification subgroups (centralization, noncentralization, and not classified) observed during the initial evaluation of patients experiencing high versus low Fear-Avoidance Be- liefs Questionnaire for physical activity (FABQ-PA) scores, (2) examine the association between discharge pain intensity and functional status (FS) outcomes based on FABQ-PA and pain pattern subgroups, and (3) compare minimal clinically important improvement for FS and pain intensity for FABQ-PA and pain pattern classification subgroups. Design: Observational cohort design. Setting: Suburban hospital-based outpatient rehabilitation clinic. Participants: Consecutive patients with low back syn- dromes (N238, mean SD, 59.117.0y; minimum20, maximum91). Interventions: Interventions were designed to match patient classification by fear-avoidance level and pain pattern. Main Outcome Measures: Two outcome measures were assessed: patient self-reported FS and pain intensity. FS was assessed by using computerized adaptive testing methods. Maximal pain intensity was assessed by using an 11-point numeric pain scale: 0 (no pain) to 10 (worst imaginable pain). Results: There were no differences ( 2 2 3.7, P.16) in proportion of patients classified by pain pattern experiencing high or low fear-avoidance beliefs. After controlling for the effect of available risk-adjustment variables, only dual-level classification subgroups, symptom acuity, payer type, and in- take FS or pain intensity were associated with discharge FS or pain outcomes. The highest proportion of patients achieving minimal clinically important improvement in pain and FS were reported by the following patient subgroup: centralization and low fear. Conclusions: Pain pattern and FABQ-PA characteristics impacted rehabilitation outcomes. We recommend that both factors be considered when managing patients with low back pain in an effort to optimize rehabilitation outcomes. Key Words: Low back pain; Outcome assessment (health care); Rehabilitation. © 2009 by the American Congress of Rehabilitation Medicine T HE USE OF A BIOPSYCHOSOCIAL model 1,2 and mul- tilevel patient classification methods 3 that concurrently consider psychologic, social, and physical domains to evaluate and manage patients with nonspecific acute or chronic LBP syndromes has gained widespread acceptance. For example, such an approach is now recommended by clinical practice guidelines and by the World Health Organization’s Interna- tional Classification of Functioning, Disability and Health. 4,5 Consistent with these recommendations, there is evidence of the effectiveness for clinical assessment and management by physical therapists for pain-related fear 6,7 and the centralization of symptoms 8,9 experienced by patients with LBP. Pain-related fear is part of the Fear-Avoidance Model. 10 The Fear-Avoidance Model has been used to explain, in part, poor treatment outcomes, the transition between acute and chronic stages of pain, and the sustainability of chronic disability. 10-12 Patients with LBP syndromes and elevated fear-avoidance traits typically avoid spinal movements and activities of daily living in an effort to avoid pain or perceived harm. Over time, the avoidance of movement may sustain and/or contribute to chronic pain and disability troubles. 11 Recent studies have shown that the effectiveness of treatments in reducing disabil- ity for patients with lumbar impairment was associated with decreases in fear-avoidance beliefs. For example, exercise pro- grams to improve fitness and strength, 6,13-15 educational pro- grams to stay active and avoid unnecessary medical procedures and treatments, 16-18 and cognitive behavioral techniques to alter the patient’s exaggerated threat value of pain and to improve physical activity tolerance 19-23 were all successful in reducing fear-avoidance beliefs. Taken collectively, these stud- ies suggest that clinicians should emphasize and use treatment strategies specifically designed to reduce elevated pain-related fears to optimize patient outcomes. The centralization phenomenon is a common physical ex- amination sign to guide specific exercise prescription. 24,25 The centralization phenomenon is characterized by spinal-referred symptoms that are progressively abolished in a distal-to-prox- From the Spine Rehabilitation at CentraState Medical Center, Freehold, NJ (Werneke, Reyes); Focus On Therapeutic Outcomes Inc, White Stone, VA (Hart); Brooks Center for Rehabilitation Studies, University of Florida, Gainsville, FL (George); School of Rehabilitation Science and Department of Clinical Epidemiology and Biostatistics, McMaster University, Hamilton, ON, Canada (Stratford); and Therapy Partners Inc, Burnsville, MN (Matheson). A commercial party having a direct financial interest in the results of the research supporting this article has conferred or will confer a financial benefit on the author or one or more of the authors. Dr Hart is an investor in and employee of Focus On Therapeutic Outcomes Inc. Analyses of data and reporting of results of those analyses such as those reported in this manuscript are part of his routine, daily activities. Reprint requests to Mark W. Werneke, PT, MS, Dip. MDT at CentraState Medical Center, 901 West Main St, Freehold, NJ 07728, e-mail: [email protected]. 0003-9993/09/9005-00673$36.00/0 doi:10.1016/j.apmr.2008.11.008 List of Abbreviations CI confidence interval FS functional status FABQ Fear Avoidance Belief Questionnaire FABQ-PA Fear Avoidance Belief Questionnaire for Physical Activity LBP low back pain 768 Arch Phys Med Rehabil Vol 90, May 2009
Transcript of Clinical Outcomes for Patients Classified by Fear-Avoidance Beliefs and Centralization Phenomenon
O
CBMJ
Pce
capl(apiF
c
dm
c
aaMn
phectpmrl
i
(B(aT
soTs
C
768
A
RIGINAL ARTICLE
linical Outcomes for Patients Classified by Fear-Avoidanceeliefs and Centralization Phenomenon
ark W. Werneke, PT, MS, Dennis L. Hart, PT, PhD, Steven Z. George, PT, PhD, Paul W. Stratford, PT, MS,
ames W. Matheson, PT, DPT, Adrian Reyes, PTfp
c
M
TcassgtCtpo
FtsPtltcsidggaairisf
acs
ABSTRACT. Werneke MW, Hart DL, George SZ, StratfordW, Matheson JW, Reyes A. Clinical outcomes for patientslassified by fear-avoidance beliefs and centralization phenom-non. Arch Phys Med Rehabil 2009;90:768-77.
Objectives: To (1) determine the prevalence of pain patternlassification subgroups (centralization, noncentralization,nd not classified) observed during the initial evaluation ofatients experiencing high versus low Fear-Avoidance Be-iefs Questionnaire for physical activity (FABQ-PA) scores,2) examine the association between discharge pain intensitynd functional status (FS) outcomes based on FABQ-PA andain pattern subgroups, and (3) compare minimal clinicallymportant improvement for FS and pain intensity forABQ-PA and pain pattern classification subgroups.Design: Observational cohort design.Setting: Suburban hospital-based outpatient rehabilitation
linic.Participants: Consecutive patients with low back syn-
romes (N�238, mean � SD, 59.1�17.0y; minimum�20,aximum�91).Interventions: Interventions were designed to match patient
lassification by fear-avoidance level and pain pattern.Main Outcome Measures: Two outcome measures were
ssessed: patient self-reported FS and pain intensity. FS wasssessed by using computerized adaptive testing methods.aximal pain intensity was assessed by using an 11-point
umeric pain scale: 0 (no pain) to 10 (worst imaginable pain).Results: There were no differences (�2
2�3.7, P�.16) inroportion of patients classified by pain pattern experiencingigh or low fear-avoidance beliefs. After controlling for theffect of available risk-adjustment variables, only dual-levellassification subgroups, symptom acuity, payer type, and in-ake FS or pain intensity were associated with discharge FS orain outcomes. The highest proportion of patients achievinginimal clinically important improvement in pain and FS were
eported by the following patient subgroup: centralization andow fear.
Conclusions: Pain pattern and FABQ-PA characteristicsmpacted rehabilitation outcomes. We recommend that both
From the Spine Rehabilitation at CentraState Medical Center, Freehold, NJWerneke, Reyes); Focus On Therapeutic Outcomes Inc, White Stone, VA (Hart);rooks Center for Rehabilitation Studies, University of Florida, Gainsville, FL
George); School of Rehabilitation Science and Department of Clinical Epidemiologynd Biostatistics, McMaster University, Hamilton, ON, Canada (Stratford); andherapy Partners Inc, Burnsville, MN (Matheson).A commercial party having a direct financial interest in the results of the research
upporting this article has conferred or will confer a financial benefit on the author orne or more of the authors. Dr Hart is an investor in and employee of Focus Onherapeutic Outcomes Inc. Analyses of data and reporting of results of those analysesuch as those reported in this manuscript are part of his routine, daily activities.
Reprint requests to Mark W. Werneke, PT, MS, Dip. MDT at CentraState Medicalenter, 901 West Main St, Freehold, NJ 07728, e-mail: [email protected].
0003-9993/09/9005-00673$36.00/0doi:10.1016/j.apmr.2008.11.008
rch Phys Med Rehabil Vol 90, May 2009
actors be considered when managing patients with low backain in an effort to optimize rehabilitation outcomes.Key Words: Low back pain; Outcome assessment (health
are); Rehabilitation.© 2009 by the American Congress of Rehabilitationedicine
HE USE OF A BIOPSYCHOSOCIAL model1,2 and mul-tilevel patient classification methods3 that concurrently
onsider psychologic, social, and physical domains to evaluatend manage patients with nonspecific acute or chronic LBPyndromes has gained widespread acceptance. For example,uch an approach is now recommended by clinical practiceuidelines and by the World Health Organization’s Interna-ional Classification of Functioning, Disability and Health.4,5
onsistent with these recommendations, there is evidence ofhe effectiveness for clinical assessment and management byhysical therapists for pain-related fear6,7 and the centralizationf symptoms8,9 experienced by patients with LBP.
Pain-related fear is part of the Fear-Avoidance Model.10 Theear-Avoidance Model has been used to explain, in part, poor
reatment outcomes, the transition between acute and chronictages of pain, and the sustainability of chronic disability.10-12
atients with LBP syndromes and elevated fear-avoidanceraits typically avoid spinal movements and activities of dailyiving in an effort to avoid pain or perceived harm. Over time,he avoidance of movement may sustain and/or contribute tohronic pain and disability troubles.11 Recent studies havehown that the effectiveness of treatments in reducing disabil-ty for patients with lumbar impairment was associated withecreases in fear-avoidance beliefs. For example, exercise pro-rams to improve fitness and strength,6,13-15 educational pro-rams to stay active and avoid unnecessary medical proceduresnd treatments,16-18 and cognitive behavioral techniques tolter the patient’s exaggerated threat value of pain and tomprove physical activity tolerance19-23 were all successful ineducing fear-avoidance beliefs. Taken collectively, these stud-es suggest that clinicians should emphasize and use treatmenttrategies specifically designed to reduce elevated pain-relatedears to optimize patient outcomes.
The centralization phenomenon is a common physical ex-mination sign to guide specific exercise prescription.24,25 Theentralization phenomenon is characterized by spinal-referredymptoms that are progressively abolished in a distal-to-prox-
List of Abbreviations
CI confidence intervalFS functional statusFABQ Fear Avoidance Belief QuestionnaireFABQ-PA Fear Avoidance Belief Questionnaire for
Physical Activity
LBP low back pain
imsmticscmrd
(tfHirhttcwaorbiptTicvhtivpF
ttpoastbmbaatabgcpWiihwa
wba
S
wdp5wtwmOt
P
pdcdfswam
scllpf
wwwausFoslpoa0
cpbksUtccus
769FEAR-AVOIDANCE BELIEFS AND CENTRALIZATION PHENOMENON, Werneke
mal direction in response to a standard clinical assessmentethod in which the clinician documents the patient’s pain and
ymptom response(s) during repeated and end-range lumbarovement tests.25 The classification and management of pa-
ients with lumbar impairments based on centralization appearmportant because classification results have been used to suc-essfully direct treatment, and the presence of centralizingymptoms consistently predicts good short- and long-term out-omes.8,9,26-30 A standardized pain pattern assessment andeasurement technique to identify centralization have been
ecommended28 and supported by strong reliability and validityata.26,27,31,32
It seems theoretically feasible that combining both factorsie, fear avoidance and pain pattern) in a dual-level classifica-ion method and tailoring management techniques to eachactor might benefit patients with lumbar spine syndromes.owever, to date, research27,30 investigating the combined
nfluence of pain pattern and elevated fear-avoidance beliefs onehabilitation outcomes using multivariate regression modelsas been scant. George et al30 reported that both intake cen-ralization and elevated fear-avoidance beliefs of work activi-ies were important for explaining long-term disability out-omes from LBP. In contrast, Werneke and Hart27 reported thathen intake pain pattern classification and elevated fear avoid-
nce were in a multivariate model, only the noncentralizationf symptoms predicted disability at 1 year after discharge fromehabilitation. The ability to generalize these data are limitedy small sample sizes,30 selected patient characteristics includ-ng only young patients with acute onset of LBP27,30 or onlyatients whose symptoms centralized,30 and clinical interven-ions not matched to the level of fear avoidance at intake.27,30
herefore, further direction is needed for therapists interestedn managing patients based on the level of fear avoidance andentralization. For example, if a patient is experiencing ele-ated fear-avoidance beliefs of physical activity at intake ande/she is managed based solely on the Fear-Avoidance Model,he patient may be missing the beneficial effects of also mod-fying management based on pain pattern response. The con-erse may be true as well, with patients managed solely by painattern response missing the benefits of management by theear-Avoidance Model.We believe that the relative contribution or interaction be-
ween these factors during treatment is complex, and observa-ional data are lacking from the literature. Therefore, we im-lemented an exploratory study to improve our understandingf patient outcomes when patients are classified at intake usingdual-level classification scheme when both pain pattern clas-
ification and fear-avoidance belief levels are considered byreating clinicians. Clinicians assessed and classified patientsy pain pattern and FABQ-PA and administered specific treat-ents that have supporting evidence individually but have not
een studied well when performed concurrently. The specificims were to (1) determine the percentage of patients classifiedt intake by the centralization and noncentralization of symp-oms who experience either high or low levels of fear-avoid-nce beliefs of physical activity, (2) examine the associationetween discharge pain intensity and FS and patients sub-rouped by pain pattern and levels of fear at intake, and (3)ompare minimal clinically important improvement for FS andain intensity for patients subgrouped by pain pattern and fear.e hypothesized that the percentage of patients classified at
ntake by centralization would be the same for patients report-ng either low or high fear-avoidance beliefs. In addition, weypothesized that symptom centralization would be associatedith better outcomes regardless of the level of fear avoidance
nd noncentralization and high fear would be associated with c
orse outcomes. Study results may allow physical therapists toetter weigh the relative importance of 2 common initial ex-mination findings for patients with LBP.
METHODS
ubjectsThis study involved a secondary analysis of 238 patients
ith nonspecific lumbar spine syndromes from a previouslyescribed sample of patients.32 The original study32 was arospective observational cohort design collecting data from17 consecutive patients with mechanical neck or LBP whoere treated at 1 suburban hospital-based outpatient rehabili-
ation clinic between June 2003 and December 2004. The clinicas participating with Focus On Therapeutic Outcomes Inc, aedical rehabilitation data-management company.33,34 Focusn Therapeutic Outcomes Inc’s Institutional Review Board for
he Protection of Human Subjects approved the project.
roceduresPatient classification at intake. Procedures for patients’
hysical examination and data collection have been previouslyescribed.32 Briefly, all patients before physical examinationompleted a battery of questionnaires gathering functional andemographic information, pain, and psychosocial factors (ie,ear-avoidance belief questionnaire,35 depression, somatizationubscales36,37) by using Patient Inquiry software.a Patientsere evaluated by 1 of 2 physical therapists who were trained
nd credentialed at examining and classifying patients usingechanical diagnosis and therapy methods.25
For this study, patients were classified using a dual-level clas-ification method combining both pain pattern and FABQ-PAlassification subgroups as follows: centralization and fearow, centralization and fear high, noncentralization and fearow, noncentralization and fear high, not classified by painattern and fear low, and nonclassified by pain pattern andear high.
Patients were also classified at intake using the FABQ,hich has been recommended as a screening tool for patientsith lumbar spine syndromes who are fearful of physical orork activities.35 The FABQ-PA has been reported to exhibit
n acceptable level of test-retest reliability35,38 and has beensed to assess fear-avoidance beliefs in patients with lumbarpine syndromes.15,39,40 For this study, we included only theABQ-PA survey because many patients in our sample werelder than 65 years and retired, making the FABQ work sub-cale not applicable. We classified patients according to theirevel of fear of physical activities based on a median splitreviously recommended in the literature18 (ie, high fear wasperationally defined as FABQ-PA scores of 15 points or more,nd low fear was operationally defined as FABQ-PA scores ofto 14).In addition to FABQ-PA classification, patients were also
lassified at intake using pain pattern criteria for categorizingatients by centralization, noncentralization, and not classifiedy pain pattern.32 Although centralization is a commonlynown clinical phenomenon, operational definitions and as-essment methods to identify centralization vary widely.28,31
sing nonstandardized assessment methods and subjectiveechniques to identify centralization may explain variations inentralization’s prevalence rates and validity.41 We specificallyhose a standardized assessment and measurement techniquesing pain pattern criteria to identify centralization because oftrong reliability and validity data supporting this pain pattern
lassification method.26,27,31,32Arch Phys Med Rehabil Vol 90, May 2009

dplplbviiupprtmtwcw
I
ndtwwetFsletlsgupprtnstzrcd
O
aacg(hsvgest
npsc
D
aphpwdu
ccftt
rctvdpiftlve
camF
ilitsigpbasorapcMiss9
S
770 FEAR-AVOIDANCE BELIEFS AND CENTRALIZATION PHENOMENON, Werneke
A
Pain pattern classification methods have been described inetail elsewhere.32 Pain pattern is a method of classifyingatients with back pain according to a change in anatomicocation of pain reported in response to clinician-directed re-eated and end-range lumbar movements. All changes in painocation were measured using body diagrams and a numericody diagram overlay template tool, the reliability of which isery good.28 Because pain responses were numerically defined,f the patient’s pain location score immediately before mechan-cal diagnosis and therapy assessment was 0, the patient wasnable to be classified using this method.32 For example, ifatients, especially those patients 65 years of age or older withersistent yet intermittent pains during the subjective history,eport no pain immediately before repeated lumbar movementesting, they were classified as “not classified” using thisethod. Patients who could not be classified were retained in
he analyses to serve as a comparison group for those patientsho could be classified using pain pattern methods; the impli-
ations and limitations of not classified pain pattern subgroupill be discussed.
nterventionPatients were evaluated using a standard mechanical diag-
osis and therapy assessment method at intake and reassesseduring subsequent visits.25 Subsequent visits were scheduled athe therapist’s discretion. Both therapists were experiencedith intervention techniques described by McKenzie25 andith a specific cognitive-behavioral intervention “graded
xposure in vivo” described by Vlaeyen et al.20,42 Overallreatment strategies were guided by pain pattern and levels andABQ-PA observed during intake and over the treatment epi-ode. For instance, the patient subgroups centralization and fearow and centralization and fear high were prescribed specificxercises.25 For patients classified with elevated fear at intake,herapy treatment was augmented by integrating carefully se-ected educational information with an active managementtrategy based on “graded exposure in vivo” methods.21,42 Theraded exposure in vivo program was specifically designed bysing cognitive-behavioral techniques to change the patient’serception concerning hurt versus harm, to reduce the patient’sain-related fears, and to regain the patient’s confidence ineturning to physical activities, which were commonly part ofhe prescribed specific exercises. Treatments for patients withoncentralizing symptoms or patients who could not be clas-ified by pain pattern criteria consisted of reassurance, educa-ion to stay active, functional activities and exercises, mobili-ation/manipulation, and avoidance of passive modalities asecommended by recent clinical practice guidelines.5,43 Be-ause of this project’s observational cohort research design, weid not standardize care beyond these guidelines.
utcomesTwo primary outcome measures, patient self-reported FS
nd pain intensity, have been described in a prior study32 anddetailed technical report.44 Briefly, FS was assessed by using
omputerized adaptive testing methods.44-46 The FS measuresenerated from the computerized adaptive testing range from 0low) to 100 (high functioning) on a linear metric. The itemsave adequate internal consistency reliability (r�.86) and per-on separation (2.49).46,47 FS measures have good discriminantalidity for condition severity, symptom acuity, age, and sur-ical history, and FS measures estimated by using the comput-rized adaptive testing are sensitive to change (lumbar effectize�1.05).44 The maximal pain intensity experienced during
he preceding 24 hours was assessed by using an 11-point erch Phys Med Rehabil Vol 90, May 2009
umeric pain scale, 0 (no pain) to 10 (worst imaginableain).48,49 The reliability and validity for this 11-point paincale have been reported to be good and recommended forlinical assessment of subjective pain intensity.48,49
ata AnalysisTo better understand possible patient selection bias, we
ssessed differences between patients who had missing painattern and fear classification data compared with those whoad classification data, and we assessed differences betweenatients who dropped out of treatment compared with thoseho completed treatment by using chi-square tests of indepen-ence (dichotomous and categoric) or 2-sample t tests (contin-ous data) using available independent variables.For purpose 1, we calculated the percentage of patients
lassified for each pain pattern subgroup (centralization, non-entralization, not classified by pain pattern) and level ofear-avoidance beliefs (high, low fear) and tested differences inhe percentage of patients per subgroup by using chi-squareests for independence with standardized deviates.
For purpose 2, we used ordinary least squares multipleegressions to examine associations between intake patientlassification and characteristics and discharge functional sta-us and pain, which allowed us to control for risk-adjustmentariables. One regression was run for each dependent variable,ischarge FS and pain. The primary factor of interest wasatient dual-level classification (table 1). To control for thenfluence of important risk-adjustment factors, we included theollowing independent variables in the regression models: in-ake FS or pain, acuity, age, sex, surgical history, payer, painocation, and therapist. The importance of each level of eachariable was tested using a t statistic. The value for a type 1rror was set to .05 for all analyses.
For purpose 3, we compared the proportions of patientslassified by both pain pattern and levels of fear who achievedt least a minimal clinically important improvement as deter-ined by using receiver operating characteristics for change inS and pain intensity.The data analyses to calculate minimal clinically important
mprovement50-60 for FS and pain change were described atength in our original article.32 Minimal clinically importantmprovement represents the smallest observed change in pa-ients estimated to have important change.50 The external mea-ure or criterion standard to assess minimal clinically importantmprovement for FS and pain intensity change was a 15-pointlobal rating of change scale.55,58 For minimal clinically im-ortant improvement assessment, patients were dichotomizedy their global rating of change on a 15 point scale (�7 to 7)s patients who did not improve (ie, global rating of changecores �3) versus patients who improved (ie, global ratingf change scores �3).57 In addition, we used nonparametriceceiver operating characteristic analyses to quantify theccuracy52 of the change measures to discriminate betweenatients whose FS and pain had improved in an important wayompared with patients whose FS and pain had not improved.61
inimal clinically important improvement cut points weredentified by selecting the cut point with the largest averagepecificity/sensitivity. Receiver operator curve results were de-cribed using area under the receiver operator curves, SEs, and5% confidence intervals.
RESULTS
ubjectsOver the data-collection time, 517 consecutive patients with
ither lumbar spine or cervical syndromes were solicited to par-
tcescswd(wpbpc
P
Fephmpsm
cmcPswmwsptr
PP
itaito(
N(AW*
771FEAR-AVOIDANCE BELIEFS AND CENTRALIZATION PHENOMENON, Werneke
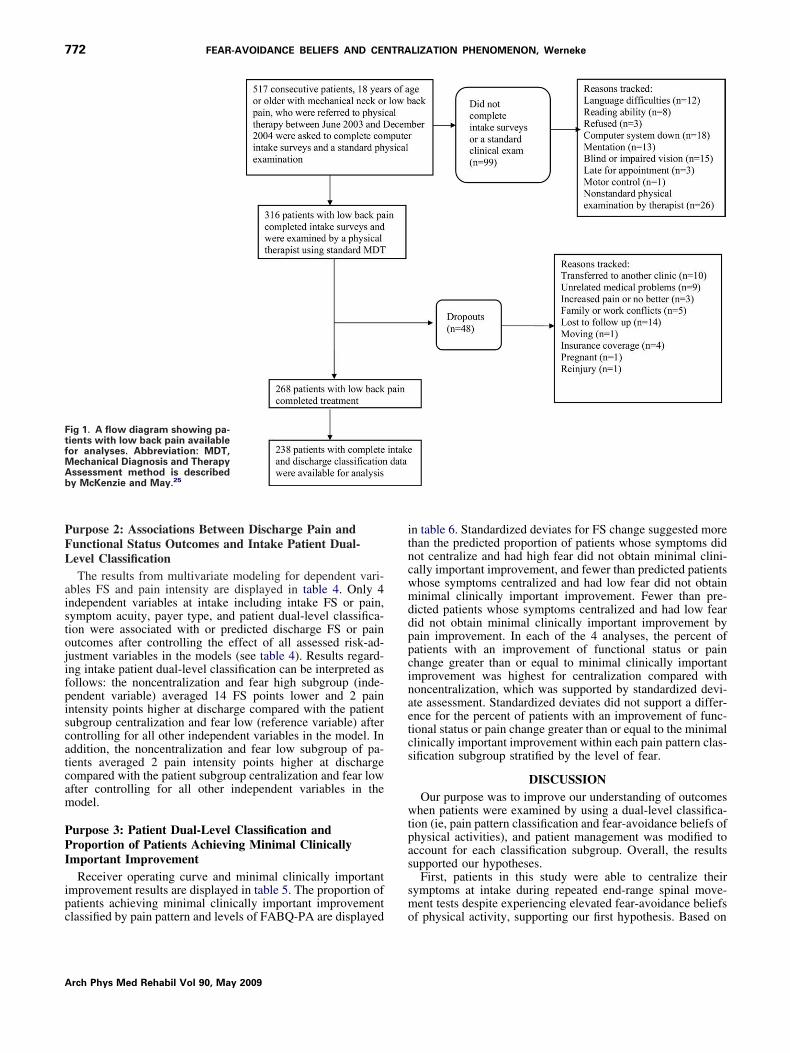
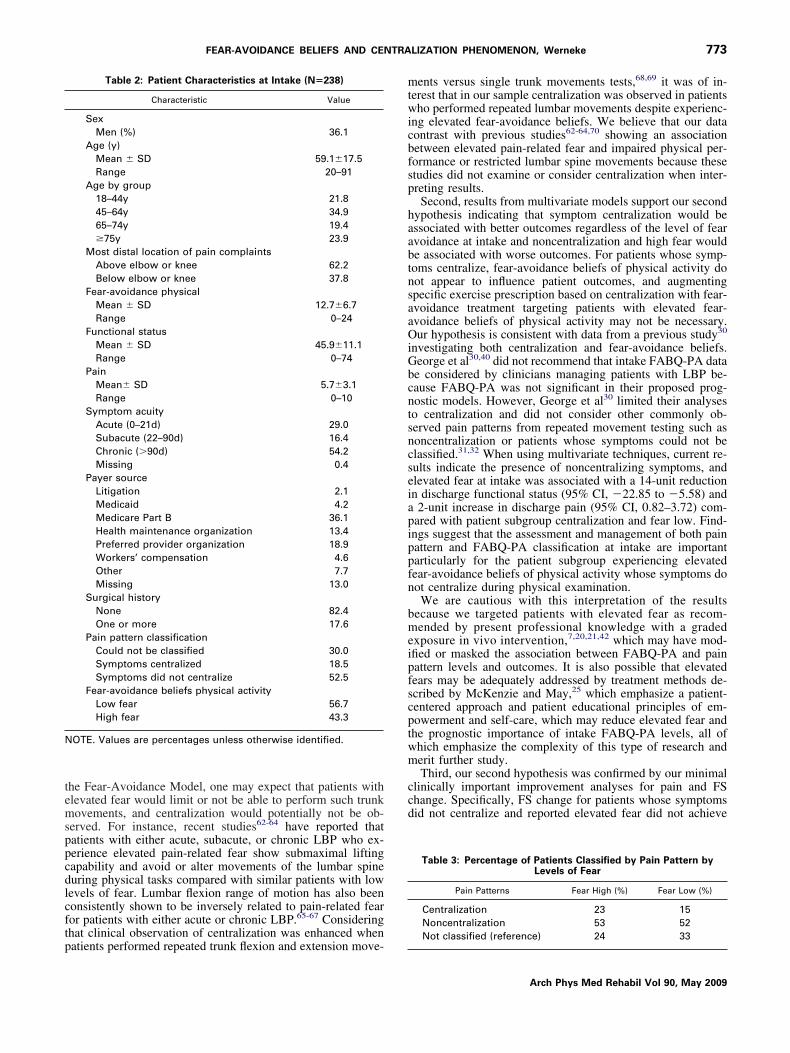
icipate in the original study (fig 1). Of these patients, 99 could notomplete intake surveys or did not receive a standard physicalxamination. Of the remaining 418 patients, 316 had lumbaryndromes, and, of these, 48 dropped out before treatment dis-harge. Patients who dropped out had lower intake functionaltatus measures (P�.005), higher pain at intake (P�.001), andere younger (P�.001), and proportionately fewer patients whoropped out could not be classified by pain pattern classificationP�.002). Of the remaining 268 patients with lumbar syndromesho started and completed treatment, 238 had complete painattern and FABQ-PA data (table 2). There were no differencesetween patients who were not classified at intake by both painattern and FABQ-PA (n�30) compared with patients who werelassified (n�238) for age, intake FS, fear, or pain (P�.05).
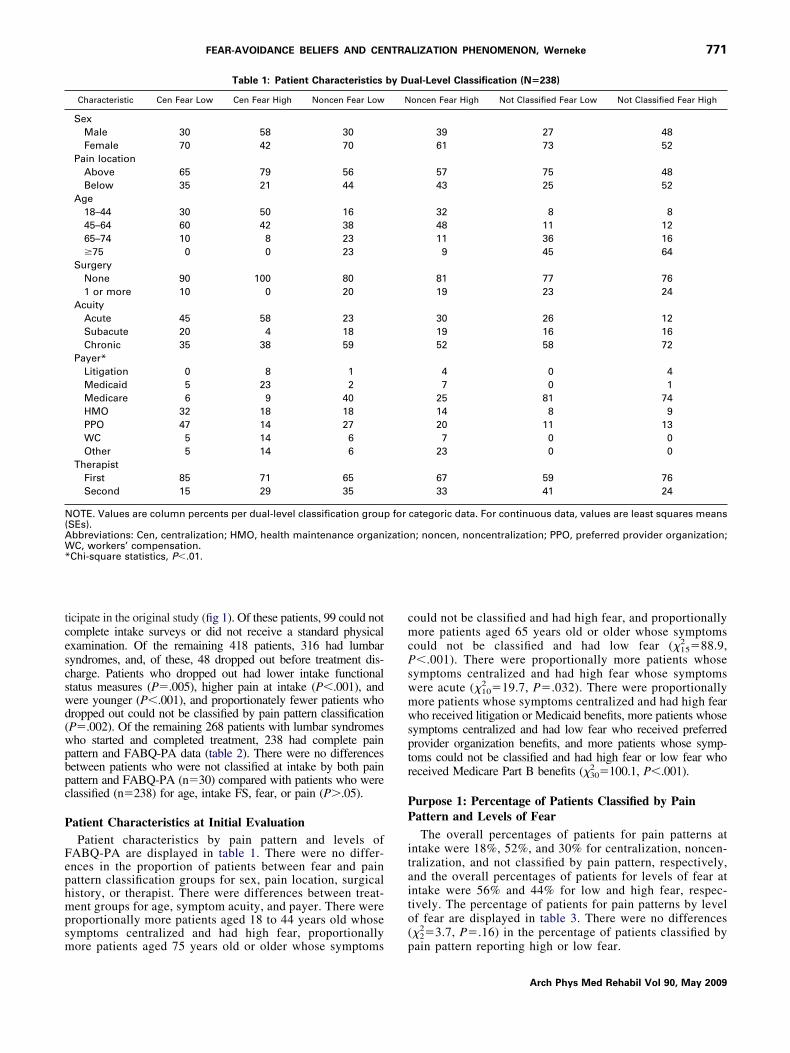
atient Characteristics at Initial EvaluationPatient characteristics by pain pattern and levels of
ABQ-PA are displayed in table 1. There were no differ-nces in the proportion of patients between fear and painattern classification groups for sex, pain location, surgicalistory, or therapist. There were differences between treat-ent groups for age, symptom acuity, and payer. There were
roportionally more patients aged 18 to 44 years old whoseymptoms centralized and had high fear, proportionally
Table 1: Patient Characteristics
Characteristic Cen Fear Low Cen Fear High Noncen Fear Low
SexMale 30 58 30Female 70 42 70
Pain locationAbove 65 79 56Below 35 21 44
Age18–44 30 50 1645–64 60 42 3865–74 10 8 23�75 0 0 23
SurgeryNone 90 100 801 or more 10 0 20
AcuityAcute 45 58 23Subacute 20 4 18Chronic 35 38 59
Payer*Litigation 0 8 1Medicaid 5 23 2Medicare 6 9 40HMO 32 18 18PPO 47 14 27WC 5 14 6Other 5 14 6
TherapistFirst 85 71 65Second 15 29 35
OTE. Values are column percents per dual-level classification groupSEs).bbreviations: Cen, centralization; HMO, health maintenance organC, workers’ compensation.
Chi-square statistics, P�.01.
ore patients aged 75 years old or older whose symptoms p
ould not be classified and had high fear, and proportionallyore patients aged 65 years old or older whose symptoms
ould not be classified and had low fear (�152 �88.9,
�.001). There were proportionally more patients whoseymptoms centralized and had high fear whose symptomsere acute (�10
2 �19.7, P�.032). There were proportionallyore patients whose symptoms centralized and had high fearho received litigation or Medicaid benefits, more patients whose
ymptoms centralized and had low fear who received preferredrovider organization benefits, and more patients whose symp-oms could not be classified and had high fear or low fear whoeceived Medicare Part B benefits (�30
2 �100.1, P�.001).
urpose 1: Percentage of Patients Classified by Painattern and Levels of FearThe overall percentages of patients for pain patterns at
ntake were 18%, 52%, and 30% for centralization, noncen-ralization, and not classified by pain pattern, respectively,nd the overall percentages of patients for levels of fear atntake were 56% and 44% for low and high fear, respec-ively. The percentage of patients for pain patterns by levelf fear are displayed in table 3. There were no differences�2�3.7, P�.16) in the percentage of patients classified by
al-Level Classification (N�238)
oncen Fear High Not Classified Fear Low Not Classified Fear High
39 27 4861 73 52
57 75 4843 25 52
32 8 848 11 1211 36 169 45 64
81 77 7619 23 24
30 26 1219 16 1652 58 72
4 0 47 0 1
25 81 7414 8 920 11 137 0 0
23 0 0
67 59 7633 41 24
categoric data. For continuous data, values are least squares means
n; noncen, noncentralization; PPO, preferred provider organization;
by Du
N
for
izatio
2
ain pattern reporting high or low fear.
Arch Phys Med Rehabil Vol 90, May 2009
PFL
aistojifpiscatcam
PPI
ipc
itncwmddppcinaetcs
wtpas
sm
FtfMAb
772 FEAR-AVOIDANCE BELIEFS AND CENTRALIZATION PHENOMENON, Werneke
A
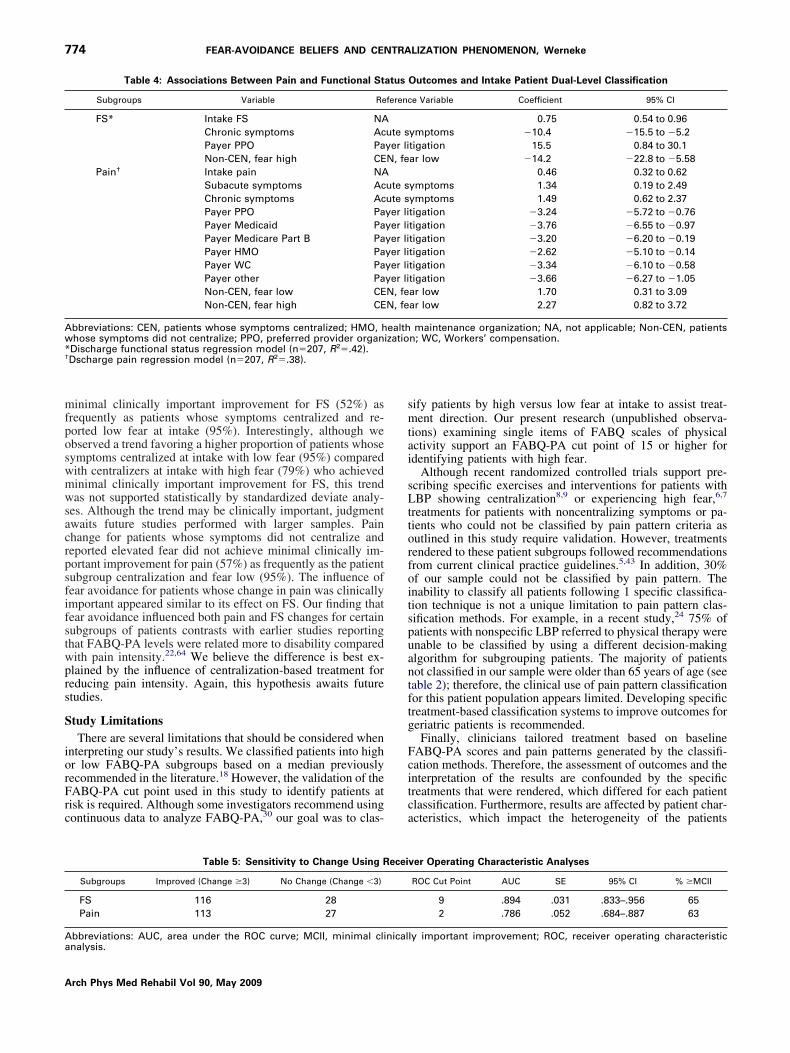
urpose 2: Associations Between Discharge Pain andunctional Status Outcomes and Intake Patient Dual-evel ClassificationThe results from multivariate modeling for dependent vari-
bles FS and pain intensity are displayed in table 4. Only 4ndependent variables at intake including intake FS or pain,ymptom acuity, payer type, and patient dual-level classifica-ion were associated with or predicted discharge FS or painutcomes after controlling the effect of all assessed risk-ad-ustment variables in the models (see table 4). Results regard-ng intake patient dual-level classification can be interpreted asollows: the noncentralization and fear high subgroup (inde-endent variable) averaged 14 FS points lower and 2 painntensity points higher at discharge compared with the patientubgroup centralization and fear low (reference variable) afterontrolling for all other independent variables in the model. Inddition, the noncentralization and fear low subgroup of pa-ients averaged 2 pain intensity points higher at dischargeompared with the patient subgroup centralization and fear lowfter controlling for all other independent variables in theodel.
urpose 3: Patient Dual-Level Classification androportion of Patients Achieving Minimal Clinicallymportant Improvement
Receiver operating curve and minimal clinically importantmprovement results are displayed in table 5. The proportion ofatients achieving minimal clinically important improvement
ig 1. A flow diagram showing pa-ients with low back pain availableor analyses. Abbreviation: MDT,
echanical Diagnosis and Therapyssessment method is describedy McKenzie and May.25
lassified by pain pattern and levels of FABQ-PA are displayed o
rch Phys Med Rehabil Vol 90, May 2009
n table 6. Standardized deviates for FS change suggested morehan the predicted proportion of patients whose symptoms didot centralize and had high fear did not obtain minimal clini-ally important improvement, and fewer than predicted patientshose symptoms centralized and had low fear did not obtaininimal clinically important improvement. Fewer than pre-
icted patients whose symptoms centralized and had low fearid not obtain minimal clinically important improvement byain improvement. In each of the 4 analyses, the percent ofatients with an improvement of functional status or painhange greater than or equal to minimal clinically importantmprovement was highest for centralization compared withoncentralization, which was supported by standardized devi-te assessment. Standardized deviates did not support a differ-nce for the percent of patients with an improvement of func-ional status or pain change greater than or equal to the minimallinically important improvement within each pain pattern clas-ification subgroup stratified by the level of fear.
DISCUSSIONOur purpose was to improve our understanding of outcomes
hen patients were examined by using a dual-level classifica-ion (ie, pain pattern classification and fear-avoidance beliefs ofhysical activities), and patient management was modified toccount for each classification subgroup. Overall, the resultsupported our hypotheses.
First, patients in this study were able to centralize theirymptoms at intake during repeated end-range spinal move-ent tests despite experiencing elevated fear-avoidance beliefs
f physical activity, supporting our first hypothesis. Based on
temsppcdlcftp
mtwicbfsp
haabtnsaaOiGbcntsncseiapippfn
bmeipfscptwm
ccd
N
773FEAR-AVOIDANCE BELIEFS AND CENTRALIZATION PHENOMENON, Werneke
he Fear-Avoidance Model, one may expect that patients withlevated fear would limit or not be able to perform such trunkovements, and centralization would potentially not be ob-
erved. For instance, recent studies62-64 have reported thatatients with either acute, subacute, or chronic LBP who ex-erience elevated pain-related fear show submaximal liftingapability and avoid or alter movements of the lumbar spineuring physical tasks compared with similar patients with lowevels of fear. Lumbar flexion range of motion has also beenonsistently shown to be inversely related to pain-related fearor patients with either acute or chronic LBP.65-67 Consideringhat clinical observation of centralization was enhanced when
Table 2: Patient Characteristics at Intake (N�238)
Characteristic Value
SexMen (%) 36.1
Age (y)Mean � SD 59.1�17.5Range 20–91
Age by group18–44y 21.845–64y 34.965–74y 19.4�75y 23.9
Most distal location of pain complaintsAbove elbow or knee 62.2Below elbow or knee 37.8
Fear-avoidance physicalMean � SD 12.7�6.7Range 0–24
Functional statusMean � SD 45.9�11.1Range 0–74
PainMean� SD 5.7�3.1Range 0–10
Symptom acuityAcute (0–21d) 29.0Subacute (22–90d) 16.4Chronic (�90d) 54.2Missing 0.4
Payer sourceLitigation 2.1Medicaid 4.2Medicare Part B 36.1Health maintenance organization 13.4Preferred provider organization 18.9Workers’ compensation 4.6Other 7.7Missing 13.0
Surgical historyNone 82.4One or more 17.6
Pain pattern classificationCould not be classified 30.0Symptoms centralized 18.5Symptoms did not centralize 52.5
Fear-avoidance beliefs physical activityLow fear 56.7High fear 43.3
OTE. Values are percentages unless otherwise identified.
atients performed repeated trunk flexion and extension move-
ents versus single trunk movements tests,68,69 it was of in-erest that in our sample centralization was observed in patientsho performed repeated lumbar movements despite experienc-
ng elevated fear-avoidance beliefs. We believe that our dataontrast with previous studies62-64,70 showing an associationetween elevated pain-related fear and impaired physical per-ormance or restricted lumbar spine movements because thesetudies did not examine or consider centralization when inter-reting results.Second, results from multivariate models support our second
ypothesis indicating that symptom centralization would bessociated with better outcomes regardless of the level of fearvoidance at intake and noncentralization and high fear woulde associated with worse outcomes. For patients whose symp-oms centralize, fear-avoidance beliefs of physical activity doot appear to influence patient outcomes, and augmentingpecific exercise prescription based on centralization with fear-voidance treatment targeting patients with elevated fear-voidance beliefs of physical activity may not be necessary.ur hypothesis is consistent with data from a previous study30
nvestigating both centralization and fear-avoidance beliefs.eorge et al30,40 did not recommend that intake FABQ-PA datae considered by clinicians managing patients with LBP be-ause FABQ-PA was not significant in their proposed prog-ostic models. However, George et al30 limited their analyseso centralization and did not consider other commonly ob-erved pain patterns from repeated movement testing such asoncentralization or patients whose symptoms could not belassified.31,32 When using multivariate techniques, current re-ults indicate the presence of noncentralizing symptoms, andlevated fear at intake was associated with a 14-unit reductionn discharge functional status (95% CI, �22.85 to �5.58) and
2-unit increase in discharge pain (95% CI, 0.82–3.72) com-ared with patient subgroup centralization and fear low. Find-ngs suggest that the assessment and management of both painattern and FABQ-PA classification at intake are importantarticularly for the patient subgroup experiencing elevatedear-avoidance beliefs of physical activity whose symptoms doot centralize during physical examination.We are cautious with this interpretation of the results
ecause we targeted patients with elevated fear as recom-ended by present professional knowledge with a graded
xposure in vivo intervention,7,20,21,42 which may have mod-fied or masked the association between FABQ-PA and painattern levels and outcomes. It is also possible that elevatedears may be adequately addressed by treatment methods de-cribed by McKenzie and May,25 which emphasize a patient-entered approach and patient educational principles of em-owerment and self-care, which may reduce elevated fear andhe prognostic importance of intake FABQ-PA levels, all ofhich emphasize the complexity of this type of research anderit further study.Third, our second hypothesis was confirmed by our minimal
linically important improvement analyses for pain and FShange. Specifically, FS change for patients whose symptomsid not centralize and reported elevated fear did not achieve
Table 3: Percentage of Patients Classified by Pain Pattern byLevels of Fear
Pain Patterns Fear High (%) Fear Low (%)
Centralization 23 15Noncentralization 53 52
Not classified (reference) 24 33Arch Phys Med Rehabil Vol 90, May 2009
mfposwmwsacrpsfifstwprs
S
iorFrc
smtai
sLttorfoitspuantftg
Fcitca
Aw*†
Aa
774 FEAR-AVOIDANCE BELIEFS AND CENTRALIZATION PHENOMENON, Werneke
A
inimal clinically important improvement for FS (52%) asrequently as patients whose symptoms centralized and re-orted low fear at intake (95%). Interestingly, although webserved a trend favoring a higher proportion of patients whoseymptoms centralized at intake with low fear (95%) comparedith centralizers at intake with high fear (79%) who achievedinimal clinically important improvement for FS, this trendas not supported statistically by standardized deviate analy-
es. Although the trend may be clinically important, judgmentwaits future studies performed with larger samples. Painhange for patients whose symptoms did not centralize andeported elevated fear did not achieve minimal clinically im-ortant improvement for pain (57%) as frequently as the patientubgroup centralization and fear low (95%). The influence ofear avoidance for patients whose change in pain was clinicallymportant appeared similar to its effect on FS. Our finding thatear avoidance influenced both pain and FS changes for certainubgroups of patients contrasts with earlier studies reportinghat FABQ-PA levels were related more to disability comparedith pain intensity.22,64 We believe the difference is best ex-lained by the influence of centralization-based treatment foreducing pain intensity. Again, this hypothesis awaits futuretudies.
tudy LimitationsThere are several limitations that should be considered when
nterpreting our study’s results. We classified patients into highr low FABQ-PA subgroups based on a median previouslyecommended in the literature.18 However, the validation of theABQ-PA cut point used in this study to identify patients atisk is required. Although some investigators recommend usingontinuous data to analyze FABQ-PA,30 our goal was to clas-
Table 4: Associations Between Pain and Functional St
Subgroups Variable Re
FS* Intake FS NAChronic symptoms AcPayer PPO PaNon-CEN, fear high CE
Pain† Intake pain NASubacute symptoms AcChronic symptoms AcPayer PPO PaPayer Medicaid PaPayer Medicare Part B PaPayer HMO PaPayer WC PaPayer other PaNon-CEN, fear low CENon-CEN, fear high CE
bbreviations: CEN, patients whose symptoms centralized; HMO, hhose symptoms did not centralize; PPO, preferred provider organDischarge functional status regression model (n�207, R2�.42).Dscharge pain regression model (n�207, R2�.38).
Table 5: Sensitivity to Change Using R
Subgroups Improved (Change �3) No Change (Change �3)
FS 116 28Pain 113 27
bbreviations: AUC, area under the ROC curve; MCII, minimal clinicalnalysis.
rch Phys Med Rehabil Vol 90, May 2009
ify patients by high versus low fear at intake to assist treat-ent direction. Our present research (unpublished observa-
ions) examining single items of FABQ scales of physicalctivity support an FABQ-PA cut point of 15 or higher fordentifying patients with high fear.
Although recent randomized controlled trials support pre-cribing specific exercises and interventions for patients withBP showing centralization8,9 or experiencing high fear,6,7
reatments for patients with noncentralizing symptoms or pa-ients who could not be classified by pain pattern criteria asutlined in this study require validation. However, treatmentsendered to these patient subgroups followed recommendationsrom current clinical practice guidelines.5,43 In addition, 30%f our sample could not be classified by pain pattern. Thenability to classify all patients following 1 specific classifica-ion technique is not a unique limitation to pain pattern clas-ification methods. For example, in a recent study,24 75% ofatients with nonspecific LBP referred to physical therapy werenable to be classified by using a different decision-makinglgorithm for subgrouping patients. The majority of patientsot classified in our sample were older than 65 years of age (seeable 2); therefore, the clinical use of pain pattern classificationor this patient population appears limited. Developing specificreatment-based classification systems to improve outcomes foreriatric patients is recommended.Finally, clinicians tailored treatment based on baseline
ABQ-PA scores and pain patterns generated by the classifi-ation methods. Therefore, the assessment of outcomes and thenterpretation of the results are confounded by the specificreatments that were rendered, which differed for each patientlassification. Furthermore, results are affected by patient char-cteristics, which impact the heterogeneity of the patients
Outcomes and Intake Patient Dual-Level Classification
e Variable Coefficient 95% CI
0.75 0.54 to 0.96ymptoms �10.4 �15.5 to �5.2tigation 15.5 0.84 to 30.1ar low �14.2 �22.8 to �5.58
0.46 0.32 to 0.62ymptoms 1.34 0.19 to 2.49ymptoms 1.49 0.62 to 2.37tigation �3.24 �5.72 to �0.76tigation �3.76 �6.55 to �0.97tigation �3.20 �6.20 to �0.19tigation �2.62 �5.10 to �0.14tigation �3.34 �6.10 to �0.58tigation �3.66 �6.27 to �1.05ar low 1.70 0.31 to 3.09ar low 2.27 0.82 to 3.72
maintenance organization; NA, not applicable; Non-CEN, patientsn; WC, Workers’ compensation.
ver Operating Characteristic Analyses
ROC Cut Point AUC SE 95% CI % �MCII
9 .894 .031 .833–.956 652 .786 .052 .684–.887 63
atus
ferenc
ute syer liN, fe
ute sute syer liyer liyer liyer liyer liyer liN, feN, fe
ealthizatio
ecei
ly important improvement; ROC, receiver operating characteristic

weatcn
cbsbcdttdbdcttrtrcdt
tptfmswfts
aafbs
mnhnaco
1
1
1
1
1
1
1
1
1
A
NwiA*o
775FEAR-AVOIDANCE BELIEFS AND CENTRALIZATION PHENOMENON, Werneke
ithin each treatment group. We attempted to control for theffect of patient differences by including several important andvailable independent variables in our regression models. Thus,he results of this study cannot be generalized to differentohorts with different independent variables and those who didot receive this type of classification and treatment.Despite these limitations, clinically logical trends and asso-
iations seem to be present in the current data, which mayenefit physical therapists interested in patient dual-level clas-ification and treatment by centralization and fear-avoidanceeliefs. Clinicians during routine clinical practice evaluate,lassify, and treat a heterogeneous group of patients withiverse presentations of LBP, many of which are different thanhose studied in randomized controlled trials.71,72 Therefore,here is a need to understand both the importance of using andifficulty investigating complex biopsychosocial treatment-ased classification systems3 in actual practice settings usingata from observational designs.73 Multilevel or dual-levellassification processes as examined in this study that are usedo direct the management of diverse patients add complexity tohe assessment of treatment outcomes. Further research is war-anted for not only examining the relationship between cen-ralization and fear-avoidance beliefs when collected concur-ently for patients with LBP syndromes in other treatmentohorts but also to concurrently investigate other importantemographic, biomedical, psychologic, and social constructshat could affect patient outcomes.73
Future randomized controlled trials are necessary to advancehe understanding of the effect of a dual-level classificationrocess when it seems clinically logical, and our data suggesthat patients could be classified 2 ways and treated accordinglyor better outcomes. Our findings suggest that pain pattern isore important than FABQ classifications for patients whose
ymptoms centralize, yet both appear important for patientshose symptoms do not centralize and in whom fear is high. If
uture analyses support the trends and associations observed inhese data, the management of patients with lumbar spineyndromes could benefit.
CONCLUSIONSThis study investigated clinical outcomes of patients man-
ged with treatments tailored to address both a psychosocialnd a physical domain commonly evaluated by clinicians (ie,ear-avoidance beliefs of physical activity and pain patternased on symptom change after physical examination). Results
Table 6: Proportion of Patients by Dual-Level Classificationchieving Minimal Clinically Important Improvement in Functional
Status or Pain
FS Change Pain ChangePatient Subgroups N�235* N�235*
Cen and fear low 95.0 95.0Cen and fear high 79.2 87.0Noncen and fear low 74.3 66.2Noncen and fear high 51.9 57.4Not classified and fear low 64.3 52.4Not classified and fear high 60.0 48.0
OTE. Values are percentages of patients whose changes scoresere equal to or greater than minimal clinically important
mprovement.bbreviations: Cen, centralization; Noncen, noncentralization.P�.01 for chi-square tests. Three patients did not have global ratingf change data.
uggest that when centralization is observed, augmenting treat-
ent for patients with LBP with a fear-avoidance program mayot be necessary. However, targeting patients experiencingigh fear and noncentralization of symptoms for formal cog-itive behavioral techniques appears important. Future studiesre recommended to understand interactions between multiplelassification and management strategies and their effect onutcomes.
References1. Waddell G. The back pain revolution. Edinburgh: Churchill Liv-
ingstone; 1998.2. Weiner BK. Spine update: the biopsychosocial model and spine
care. Spine 2008;33:219-23.3. McCarthy C, Arnall F, Strimpakos N, Freemont A, Oldham J. The
biopsychosocial classification of non-specific low back pain: asystematic review. Phys Ther Rev 2004;9:17-30.
4. World Health Organization. International Classification of Func-tioning, Disability and Health. Geneva: World Health Organiza-tion; 2001.
5. Rossignol M, Arsenault B, Dionne C, et al. Clinic on low-backpain in interdisciplinary practice (CLIP) guidelines. Montreal:Agence de la sante et des services sociaux de Montreal; 2006.
6. George SZ, Fritz JM, Bialosky JE, Donald DA. The effect of afear-avoidance-based physical therapy intervention for patientswith acute low back pain: results of a randomized clinical trial.Spine 2003;28:2551-60.
7. Leeuw M, Goossens ME, van Breukelen GJ, et al. Exposure invivo versus operant graded activity in chronic low back painpatients: results of a randomized controlled trial. Pain 2008;138:192-207.
8. Long A, Donelson R, Fung T. Does it matter which exercise? Arandomized control trial of exercise for low back pain. Spine2004;29:2593-602.
9. Browder DA, Childs JD, Cleland JA, Fritz JM. Effectiveness of anextension-oriented treatment approach in a subgroup of subjectswith low back pain: a randomized clinical trial. Phys Ther 2007;87:1608-18.
0. Lethem J, Slade PD, Troup JD, Bentley G. Outline of a Fear-Avoidance Model of exaggerated pain perception–I. Behav ResTher 1983;21:401-8.
1. Leeuw M, Goossens ME, Linton SJ, Crombez G, Boersma K,Vlaeyen JW. The fear-avoidance model of musculoskeletal pain:current state of scientific evidence. J Behav Med 2007;30:77-94.
2. Vlaeyen JW, Linton SJ. Fear-avoidance and its consequences inchronic musculoskeletal pain: a state of the art. Pain 2000;85:317-32.
3. Klaber Moffett JA, Carr J, Howarth E. High fear-avoiders ofphysical activity benefit from an exercise program for patientswith back pain. Spine 2004;29:1167-72.
4. Mannion AF, Junge A, Taimela S, Muntener M, Lorenzo K,Dvorak J. Active therapy for chronic low back pain: part 3.Factors influencing self-rated disability and its change followingtherapy. Spine 2001;26:920-9.
5. Marshall P, Murphy B. Self-report measures best explain changesin disability compared with physical measures after exercise re-habilitation for chronic low back pain. Spine 2008;33:326-38.
6. Buchbinder R, Jolley D. Effects of a media campaign on backbeliefs is sustained 3 years after its cessation. Spine 2005;30:1323-30.
7. Buchbinder R, Jolley D, Wyatt M. 2001 Volvo Award Winner inClinical Studies: effects of a media campaign on back pain beliefsand its potential influence on management of low back pain ingeneral practice. Spine 2001;26:2535-42.
8. Burton AK, Waddell G, Tillotson KM, Summerton N. Information
and advice to patients with back pain can have a positive effect. AArch Phys Med Rehabil Vol 90, May 2009
1
2
2
2
2
2
2
2
2
2
2
3
3
3
3
3
3
3
3
3
3
4
4
4
4
4
4
44
4
4
5
5
5
5
5
5
5
776 FEAR-AVOIDANCE BELIEFS AND CENTRALIZATION PHENOMENON, Werneke
A
randomized controlled trial of a novel educational booklet inprimary care. Spine 1999;24:2484-91.
9. Brox JI, Sorensen R, Friis A, et al. Randomized clinical trial oflumbar instrumented fusion and cognitive intervention and exer-cises in patients with chronic low back pain and disc degeneration.Spine 2003;28:1913-21.
0. Vlaeyen JW, de Jong J, Geilen M, Heuts PH, van Breukelen G.Graded exposure in vivo in the treatment of pain-related fear: areplicated single-case experimental design in four patients withchronic low back pain. Behav Res Ther 2001;39:151-66.
1. Vlaeyen JW, de Jong J, Geilen M, Heuts PH, van Breukelen G.The treatment of fear of movement/(re)injury in chronic low backpain: further evidence on the effectiveness of exposure in vivo.Clin J Pain 2002;18:251-61.
2. Woby SR, Watson PJ, Roach NK, Urmston M. Are changes infear-avoidance beliefs, catastrophizing, and appraisals of control,predictive of changes in chronic low back pain and disability? EurJ Pain 2004;8:201-10.
3. Woby SR, Watson PJ, Roach NK, Urmston M. Adjustment tochronic low back pain–the relative influence of fear-avoidancebeliefs, catastrophizing, and appraisals of control. Behav Res Ther2004;42:761-74.
4. Brennan GP, Fritz JM, Hunter SJ, Thackeray A, Delitto A, ErhardRE. Identifying subgroups of patients with acute/subacute “non-specific” low back pain: results of a randomized clinical trial.Spine 2006;31:623-31.
5. McKenzie R, May S. The lumbar spine: mechanical diagnosis andtherapy. 2nd ed. Waikanae: Spinal Publication; 2003.
6. Werneke M, Hart DL. Centralization phenomenon as a prognosticfactor for chronic low back pain and disability. Spine 2001;26:758-64.
7. Werneke MW, Hart DL. Categorizing patients with occupationallow back pain by use of the Quebec Task Force Classificationsystem versus pain pattern classification procedures: discriminantand predictive validity. Phys Ther 2004;84:243-54.
8. Aina A, May S, Clare H. The centralization phenomenon of spinalsymptoms–a systematic review [erratum appears in J OrthopSports Phys Ther 2007;37:769]. Man Ther 2004;9:134-43.
9. Fritz JM, Cleland JA, Childs JD. Subgrouping patients with lowback pain: evolution of a classification approach to physical ther-apy. J Orthop Sports Phys Ther 2007;37:290-302.
0. George SZ, Bialosky JE, Donald DA. The centralization phenom-enon and fear-avoidance beliefs as prognostic factors for acutelow back pain: a preliminary investigation involving patientsclassified for specific exercise. J Orthop Sports Phys Ther 2005;35:580-8.
1. Werneke M, Hart DL, Cook D. A descriptive study of the cen-tralization phenomenon. A prospective analysis. Spine 1999;24:676-83.
2. Werneke MW, Hart DL, Resnik L, Stratford PW, Reyes A.Centralization: prevalence and effect on treatment outcomes usinga standardized operational definition and measurement method.J Orthop Sports Phys Ther 2008;38:116-25.
3. Swinkels IC, van den Ende CH, de Bakker D, et al. Clinicaldatabases in physical therapy. Physiother Theory Pract 2007;23:153-67.
4. Deutscher D, Hart DL, Dickstein R, Horn SD, Gutvirtz M. Im-plementing an integrated electronic outcomes and electronichealth record process to create a foundation for clinical practiceimprovement. Phys Ther 2008;88:270-85.
5. Waddell G, Newton M, Henderson I, Somerville D, Main CJ. AFear-Avoidance Beliefs Questionnaire (FABQ) and the role offear-avoidance beliefs in chronic low back pain and disability.
Pain 1993;52:157-68.rch Phys Med Rehabil Vol 90, May 2009
6. Dionne CE. Psychological distress confirmed as predictor of long-term back-related functional limitations in primary care settings.J Clin Epidemiol 2005;58:714-8.
7. Dionne CE, Koepsell TD, Von Korff M, Deyo RA, Barlow WE,Checkoway H. Predicting long-term functional limitations amongback pain patients in primary care settings. J Clin Epidemiol1997;50:31-43.
8. Williamson E. Fear Avoidance Beliefs Questionnaire (FABQ).Aust J Physiother 2006;52:149.
9. George SZ. Fear: a factor to consider in musculoskeletal rehabil-itation. J Orthop Sports Phys Ther 2006;36:264-6.
0. George SZ, Fritz JM, Childs JD. Investigation of elevated fear-avoidance beliefs for patients with low back pain: a secondaryanalysis involving patients enrolled in physical therapy clinicaltrials. J Orthop Sports Phys Ther 2008;38:50-8.
1. Schmidt I, Rechter L, Hansen VK, Andreasen J, Overvad K.Prognosis of subacute low back pain patients according to painresponse. Eur Spine J 2008;17:57-63.
2. de Jong JR, Vlaeyen JW, Onghena P, Goossens ME, Geilen M,Mulder H. Fear of movement/(re)injury in chronic low back pain:education or exposure in vivo as mediator to fear reduction? ClinJ Pain 2005;21:9-17.
3. Chou R, Huffman LH. Nonpharmacologic therapies for acute andchronic low back pain: a review of the evidence for an AmericanPain Society/American College of Physicians clinical practiceguideline [erratum appears in Ann Intern Med 2008;148:247-8].Ann Intern Med 2007;147:492-504.
4. Hart D, Connolly J. Pay-for-performance for physical therapy andoccupational therapy: Medicare Part B Services. Grant #:18-P-93066/9-01: Health & Human Services/Centers for Medicare &Medicaid Services; 2006.
5. Wainer H, editor. Computerized adaptive testing. A primer. 2nded. Mahway: Lawrence Erlbaum Associates; 2000.
6. Wright B. Rating scale analysis. Chicago: Mesa Pr; 1982.7. Mallinson T, Stelmack J, Velozo C. A comparison of the separa-
tion ratio and coefficient alpha in the creation of minimum itemsets. Med Care 2004;42(1 Suppl):I17-24.
8. Childs JD, Piva SR, Fritz JM. Responsiveness of the numeric painrating scale in patients with low back pain. Spine 2005;30:1331-4.
9. Jensen MP, Turner JA, Romano JM, Fisher LD. Comparativereliability and validity of chronic pain intensity measures. Pain1999;83:157-62.
0. Beaton DE, Bombardier C, Katz JN, Wright JG. A taxonomy forresponsiveness. J Clin Epidemiol 2001;54:1204-17.
1. Crosby RD, Kolotkin RL, Williams GR. Defining clinically mean-ingful change in health-related quality of life. J Clin Epidemiol2003;56:395-407.
2. Deyo RA, Centor RM. Assessing the responsiveness of functionalscales to clinical change: an analogy to diagnostic test perfor-mance. J Chronic Dis 1986;39:897-906.
3. Hart DL, Wang YC, Stratford PW, Mioduski JE. Computerizedadaptive test for patients with knee impairments produced validand responsive measures of function. J Clin Epidemiol 2008;61:1113-24.
4. Hsieh YW, Wang CH, Wu SC, Chen PC, Sheu CF, Hsieh CL.Establishing the minimal clinically important difference of theBarthel Index in stroke patients. Neurorehabil Neural Repair2007;21:233-8.
5. Jaeschke R, Singer J, Guyatt GH. Measurement of health status.Ascertaining the minimal clinically important difference. ControlClin Trials 1989;10:407-15.
6. Lingard EA, Riddle DL. Impact of psychological distress on painand function following knee arthroplasty. J Bone Joint Surg Am
2007;89:1161-9.
5
5
5
6
6
6
6
6
6
6
6
6
6
7
7
7
7
a
777FEAR-AVOIDANCE BELIEFS AND CENTRALIZATION PHENOMENON, Werneke
7. Stratford PW, Binkley FM, Riddle DL. Health status measures:strategies and analytic methods for assessing change scores. PhysTher 1996;76:1109-23.
8. Stratford PW, Binkley J, Solomon P, Gill C, Finch E. Assessingchange over time in patients with low back pain. Phys Ther1994;74:528-33.
9. Tubach F, Ravaud P, Baron G, et al. Evaluation of clinicallyrelevant changes in patient reported outcomes in knee and hiposteoarthritis: the minimal clinically important improvement. AnnRheum Dis 2005;64:29-33.
0. Tubach F, Ravaud P, Beaton D, et al. Minimal clinically importantimprovement and patient acceptable symptom state for subjectiveoutcome measures in rheumatic disorders. J Rheumatol 2007;34:1188-93.
1. Hanley JA, McNeil BJ. The meaning and use of the area under areceiver operating characteristic (ROC) curve. Radiology 1982;143:29-36.
2. Thomas JS, France CR. Pain-related fear is associated with avoid-ance of spinal motion during recovery from low back pain. Spine2007;32:E460-6.
3. Swinkels-Meewisse IE, Roelofs J, Oostendorp RA, Verbeek AL,Vlaeyen JW. Acute low back pain: pain-related fear and paincatastrophizing influence physical performance and perceived dis-ability. Pain 2006;120:36-43.
4. Crombez G, Vlaeyen JW, Heuts PH, Lysens R. Pain-related fearis more disabling than pain itself: evidence on the role of pain-related fear in chronic back pain disability. Pain 1999;80:329-39.
5. Geisser ME, Haig AJ, Wallbom AS, Wiggert EA. Pain-relatedfear, lumbar flexion, and dynamic EMG among persons with
chronic musculoskeletal low back pain. Clin J Pain 2004;20:61-9.6. George SZ, Fritz JM, McNeil DW. Fear-avoidance beliefs asmeasured by the fear-avoidance beliefs questionnaire: change infear-avoidance beliefs questionnaire is predictive of change inself-report of disability and pain intensity for patients with acutelow back pain. Clin J Pain 2006;22:197-203.
7. Thomas JS, France CR. The relationship between pain-related fearand lumbar flexion during natural recovery from low back pain.Eur Spine J 2008;17:97-103.
8. Donelson R, Grant W, Kamps C, Medcalf R. Pain response tosagittal end-range spinal motion. A prospective, randomized, mul-ticentered trial. Spine 1991;16(6 Suppl):S206-12.
9. Wetzel FT, Donelson R. The role of repeated end-range/painresponse assessment in the management of symptomatic lumbardiscs. Spine J 2003;3:146-54.
0. Vlaeyen JW, Kole-Snijders AM, Boeren RG, van Eek H. Fear ofmovement/(re)injury in chronic low back pain and its relation tobehavioral performance. Pain 1995;62:363-72.
1. Horn SD. Performance measures and clinical outcomes. JAMA2006;296:2731-2.
2. Horn SD, DeJong G, Ryser DK, Veazie PJ, Teraoka J. Anotherlook at observational studies in rehabilitation research: goingbeyond the holy grail of the randomized controlled trial. ArchPhys Med Rehabil 2005;86(12 Suppl 2):S8-15.
3. Resnik L, Liu D, Hart DL, Mor V. Benchmarking physical therapyclinic performances: statistical methods to enhance internal valid-ity when using observational data. Phys Ther 2008;88:1078-87.
Supplier. Focus On Therapeutic Outcomes Inc, 6832 S Northshore Dr, Knox-
ville, TN 37919.
Arch Phys Med Rehabil Vol 90, May 2009