
Provisional appointment as Library Assistant District Cadre ...
Upload
khangminh22Category
view
3download
0
Centralized Appointment Scheduling:
Industry Leading Access to Primary Care Services
American College of Medical Practice Executives Professional Paper
- FOCUS PAPER -
Paper being submitted in partial fulfillment of the requirements for election
to Fellow

1
Focus Paper Title – Centralized Appointment Scheduling: Industry Leading Access to Primary Care Services
Introduction
The purpose of this paper is to discuss the need for healthcare organizations or systems
to adopt or refine centralized appointment scheduling for primary care services to assist
in providing greater access for patients. Independent healthcare providers are
integrating their operations into health systems unlike any time in the past and it’s easy
for this integration activity to distract from key operational issues. Ensuring efficient
operations is paramount in today’s healthcare environment, considering continual
reimbursement pressures on operating margins as well as patients’ expectations of
service being provided without delay. The front door to any health system is through
primary care services and, whether one is new to the community or a long-time health
system user in the community, the first point of contact that patients have with primary
care is often over the phone. More than ever before, it is critical to offer new primary
care patients and returning patients an experience over the phone, which is
dependable, timely, and patient-centric. This experience can be achieved through
appointment scheduling by phone that is offered in a centralized fashion and
transparent to patients. Additionally, this work must be surrounded by a health system
that embraces a standardized approach in how services are offered so that patients
receive a consistent positive experience that meets and exceeds expectations regardless
of location.
2
Overall objective of this paper
a. Focus
The author of this paper has researched best practices in the management of
primary care patient appointment scheduling within health systems
interested in providing greater patient access. A few decades of direct
industry knowledge and first-hand experience will be offered in this paper.
b. Purpose
The ideas presented in this paper will provide suggested approaches to
address patients’ appointment needs and to monitor related outcomes, in a
timely and cost-efficient manner. It will be suggested that by using an
approach of organizing centralized primary care appointment scheduling
systems, there would be an improvement in efficiency and a minimizing of
expenses. According to Moody’s Investors Service, the median annual
expense growth rate in 2016 was 7.1% compared to the median annual
revenue growth rate of 6.1%, a difference of 1.0%. The negative margin
between expenses and revenues increased even more in 2017 with expenses
growing at 5.7% compared to revenue at 4.6%, a difference of 1.1%
(Sanborn, 2018). Similar projections were expected throughout 2019 with
expenses anticipated to end in the range of 4 to 5% and revenues anticipated
in the range of 3 to 4% (Kacik, 2018) concluding, that health systems which
fail to standardize and consolidate operations will be left behind in a
healthcare environment in which expense growth outpaces revenue growth.

3
c. Situation being analyzed
The traditional medical practice environment has team members who check-
in and check-out patients to and from their medical appointments while
simultaneously answering incoming phone calls and making outbound phone
calls. Alternatively, they might have individuals who are separated from this
front-office activity to answer phone calls to schedule patient appointments
and to address other patient issues over the phone. In many cases, this
phone activity may only have one or two individuals assigned to it. Phones,
check-in lines, check-out lines, and team members can easily get backed up
and patients quickly become irritated and frustrated with apparently
inefficient service. Add to these challenges a team member who calls off sick
and suddenly one-third or half of the front office team is unavailable, and the
concerns have escalated. While this represents the challenges of one
medical practice location, increasing the number of locations only adds to
the potential for ineffective operations as well as patient confusion due to
multiple phone numbers and departments.
What will be covered in this paper?
First, an analysis and discussion will be presented about current health
system approaches to scheduling primary care patient appointments. With
this information in hand and having the goal of maximizing patient
satisfaction and minimizing cost, alternative approaches for organizing
primary care appointment scheduling centers will be presented along with
4
possible outcomes that health systems could expect. Appointment
scheduling centers are not to be confused with call centers which handle
every type of incoming call, regardless of reason. This paper will conclude
with a discussion about the approaches to primary care appointment
scheduling and the significance of the findings.
How will the key topic be addressed?
The primary issue at hand is identifying how health industry leaders can best
meet the ever-increasing needs and expectations of patients, who want to
minimize the time they wait for services, and still achieve financial and
operational goals. The key topic being addressed in this paper is meeting
these needs and expectations through cost-efficient and effective scheduling
of primary care medical appointments. This will be addressed by analyzing
current approaches and outcomes and comparing these to other methods of
organizing team members to achieve positive results with patients, while
minimizing health system costs.
Explanation of the research methodology used
a. Literature search
Many health systems have attempted to address the issue of scheduling
timely primary care medical appointments in a patient-centric manner. As
such, numerous articles and perspectives were taken into consideration
while comparing approaches, to discover best practice models. While there
is much discussion in the industry on this topic, it was somewhat surprising

5
to discover that there is not much in the way of standardized or
benchmarkable metrics. There are many individual health systems and
studies that present data in their own non-standardized way however, there
is not an industry-wide common view for this information.
b. Interviews
Individual interviews and discussions, as well as group discussions and
analysis, were conducted on a limited basis to inform the methods presented
in this paper. Individual practice managers, practice directors, physicians,
medical directors and patients were queried for their perspectives on the
advantages and disadvantages of patient scheduling environments, and the
benefits and shortfalls of each.
c. Experience
The author of this paper contributes over 30 years of health industry
experience which has included the implementation and use of various
methods of patient appointment scheduling. In evaluating these methods,
consideration was given to the needs, desires and input of patients who seek
responsive services, providers who want to maximize quality and
productivity, and team members who listen to patients and know first-hand
about their challenges and concerns. Because of the author’s career
involvement with patient scheduling within a few health systems, more
emphasis was placed on the research methodology of experience, as
compared to interviews.
6
Background/Context
Importance of patient access to care
Difficulties with access and long wait times are associated with negative
patient outcomes. Patients who have experienced long wait times, even for
non-urgent needs, have been shown to have higher rates of noncompliance
and appointment no-shows. According the Vitals Index, 84% of patients
believe that wait time is either somewhat important or very important to the
overall experience at a doctor’s office. In fact, 30% of patients have walked
out before being seen due to long wait times and 1 in 5 patients report that
they have changed doctors because of long wait times. (Business Wire,
2018). This represents not only an increase in costs to patients’ care but also
a lost service opportunity for the providers of care. Additionally, it is
apparent that inefficiencies in healthcare processes result in lower levels of
patient satisfaction and contribute to provider dissatisfaction and burnout, a
growing concern in healthcare that is partly the result of these inefficiencies.
The role of patient appointment scheduling in providing patient access to care
One of the most critical aspects about patient appointment scheduling is that
it must be surrounded by standard provider templates and scheduling
guidelines. Recognizing this allows for consistency of experience for patients,
for improved scheduling accuracy, for reduced call wait times, and for a
simplified process for patients who are selecting new providers. Each of
these factors allows patients to feel that getting access to a new provider or
7
their existing provider is simple and convenient. Having a larger pool of
scheduling staff for multiple practices allows for better absorption of the
ebbs and flows in call volume that individual practices may experience, and
this results in improved speed to answer calls, reduction in call abandonment
rates due to shorter call answer times, and better overall service levels.
It is reported that 80% of medical groups are working to improve patient
access in some way. However, the data suggests that groups are still failing
to meet some critical patient demands for access. Specifically, two
accessibility-related demands are not being consistently met: (1) extended
office hours and (2) centralized scheduling services. (Advisory Board, 2018).
Models used to schedule patient appointments
The traditional independent medical practice, as well as many health systems
with expanding medical practices and sites of care, employ medical
receptionists that are responsible for both the check-in and check-out of
patients and the answering of phones which includes scheduling of patient
appointments. Alternatively, grouping medical practice sites of care, in order
to offer centralized appointment scheduling, is an ongoing trend that allows
for much greater operational efficiency, better patient access to their
providers, and flexibility in operations. Variations are also possible in the
way that practice types are grouped together (e.g. primary care, surgical,
specialty, therapies, etc.) or the way in which geographical locations are
grouped together. Having one physical location is not necessarily the best
8
answer since other issues need to be considered. These issues include
redundancy that is needed for system outages or site emergencies, backup
support for times of excess volume, the pool of candidates who qualify for
these positions of employment in a specific geographical area, and even
office space constraints. With these issues in mind, two or more “scheduling
hubs” have proven to be very beneficial for health systems.
While the focus in this paper is on phone appointment scheduling, other
options include on-line appointment scheduling and in-person appointment
scheduling. Additionally, open scheduling for new patients, in which these
individuals can obtain access to appointments either through the health
system’s on-line scheduling or through independent vendors, can provide
similar on-line access to appointments.
Standard work that impacts the patient scheduling process
If patients find it difficult to locate the phone number of a primary care
medical practice, they will often move on to the next provider in the area,
due to lack of convenience. Having one phone number for all health system
primary care locations allows patients to quickly identify with the health
system. From there, the appointment schedulers can assist in finding the
best provider for the patient throughout the various sites of care. Another
area of standardization which impacts patients would be the steps the
patient goes through on each call, allowing them consistency with their
provider of care. With standardized scripting and workflows in patient
9
scheduling, the patients begin to learn the order of questions, regardless of
the individual scheduler who is helping them, and they become better
prepared with the answers and information. The accuracy of scheduling
should improve with the same team members having responsibility for the
scheduling function. Versus the inefficient decentralized environment in
which team members may have to be temporarily pulled from other
responsibilities when a scheduler is gone, or heavy call volume requires the
additional help. In these cases, the lack of knowledge and experience
negatively impacts accuracy. Additionally, minimizing the choice amongst
visit types in the electronic health record (EHR) allows for ease of selection
by the scheduler and reduction of errors by providers and team members
due to the multitude of visit types being properly identified and scheduled.
This author is aware of health systems that only allow for two visit types in
the EHR – a short visit and a long visit - while others have literally hundreds
of visit types available for team members to choose. Lastly, having one
supervisor or manager responsible for all appointment scheduling activities,
regardless of number of “scheduling hubs”, will help drive the desired
consistency and standardization for the health system.
Review of key stakeholders
There are many stakeholders that have a part in maximizing the appointment
scheduling experience for patients. Besides the patient being the chief
stakeholder, other stakeholders include physicians, advanced practice

10
providers (APPs), practice managers, medical receptionists, medical
assistants, registered nurses, triage staff, senior administrators and more.
In any health system review, most often it is the patient that gets forgotten
when it comes to pulling together key stakeholders. It is assumed that we
are all patients and have the best perspective of our patients in mind.
However, health care workers tend to forget that they approach problems
and solutions with their employee “hat” on which will inevitably bias their
perspective on what is best for the patient.
The other stakeholders that are often left on the sidelines are the physicians
and APPs. They are often viewed as being too busy and that caution should
be taken to include them because of patient care responsibilities and
concerns with lost productivity and revenue. It is extremely imperative that
they are well represented at the table, especially considering the need to
establish consistent and standardized scheduling guidelines and provider
templates.
Another important stakeholder(s) is health system senior administration. At
a bare minimum, there should be one senior administration champion who
stands behind the initiative and who can routinely provide updates to others
in administration. Without this support, the importance and urgency of the
work will not be recognized.
Practice managers and directors will likely handle the greatest share of work
to be done in leading information gathering, provider preferences for

11
scheduling, provider template rebuilding, staff education, patient
communication, and more. These individuals are the conduit of
communication and are pivotal in guiding the initiative forward and are
absolutely pivotal to its success or failure.
Lastly, and certainly not least, is the input and involvement of clinical support
staff team members. The breadth of this representation will be beneficial by
incorporating individuals such as nurse assistants, medical assistants, medical
receptionists, nurses, social workers and others.
In the end, having a representative cross-section of individuals, that is of a
reasonable and manageable size to serve on a steering committee, will help
lead the initiative forward. The number of stakeholders that can provide
input can be unlimited however, the committee should consist of no more
than 7 to 10 individuals. Keeping to this size allows for a finite number of
opinions and perspectives which are well respected by others in the health
system.
Body of the Focus Paper
Key considerations
There are many factors to consider when transitioning to a centralized
appointment scheduling system. First and foremost, one must engage with a
cross-section of the key stakeholders who are most willing to think about
things differently, who are open to change, and who want to do what is best
for the health system and its patients. It will also be valuable to include

12
some who may resist change, in order to consider all perspectives and to gain
insight from the “devil’s advocate”. Second, key appointment scheduling
team members will have the greatest level of knowledge when it comes to
what patients like or do not like. Third, it will be beneficial to understand
how others in the industry operate and what we can learn from them. While
it is difficult to find a consistent set of industry benchmarks for centralized
appointment centers, there is enough data available that can give a sense on
whether one is moving in the right direction. In the end, the best way to
measure is against your own health system trends and to incrementally
improve upon these results, in areas where there is a sense of opportunity.
There are so many variables that each health system must navigate, and no
two health systems are alike. So, knowing your own trends over the course
of time and how your current performance compares to the past will give the
best indication of how well one is doing. Some common things to measure,
in no specific order, include average number of seconds to answer, service
level percentage, percentage of calls converted to appointments, call
abandonment rate, percentage of calls handled, call duration/handle time in
minutes and seconds, scheduler quality score, and patient satisfaction.
Effective approaches to patient appointment scheduling
As discussed earlier, grouping medical practices and offering centralized
appointment scheduling is an efficient and effective approach that offers
greater access within a more cost sensitive model. There can be variations in
13
how this centralized approach is handled, considering the nuances of each
health system. Thinking about the geography of medical practices, health
systems may find it beneficial to group practices by type (e.g. primary care,
surgical, specialty, therapies, etc.) or by geography, to take advantage of
common knowledge or of local labor pools, especially if the population base
is largely rural. Health systems must always consider other aspects, such as
system redundancy. What happens if a natural disaster hits the area or if a
section of the electrical power grid in the area is disabled for hours or even a
couple of days? How then are these calls being answered when the primary
care medical practice doors are still open for business? Therefore,
consideration should be given to having more than one physical location with
the capability to have calls immediately migrate to the other location if there
is an outage. As a health system is considering the possible transition to
centralized appointment scheduling, one extremely important aspect to
consider is the roll out of the implementation. The author of this paper and
others feel strongly about staggering the implementation to the central
location with one clinic location at a time. Allowing at least three or four
weeks in between each clinic location implementation is not unusual and
allows for several benefits including immediate feedback specific to the
nuances of each clinic, an opportunity to adjust or change workflow based on
lessons learned, a chance to pause the implementation for other clinics if a
14
significant challenge needs to be addressed, and time for team members at
each clinic to adapt to the centralized workflow.
Alternative approaches and methods
In our age of technology, there is clearly a move towards increased use of on-
line appointment scheduling. This author is aware of actual data that the top
10% performers in 2017, who were using the industry leading EHR, were
seeing on-line appointment use at a rate of 2.4%. Data available in 2019
indicated that this top 10% performing group was seeing on-line
appointments at 4.8%. While this is not a significant shift, it is relatively clear
that this trend will continue in the direction of increased use, and ongoing
efforts to allow patients this type of access is certainly increasing. While this
may appear at the surface to relieve health systems from the intensity of
appointment scheduling, it must recognize that these appointments have to
be carefully monitored and managed, often with every appointment being
validated for accuracy. The resulting corrections may require additional
phone calls to patients to clarify needs or to schedule a different
appointment time, depending on the type of error that occurred.
Another approach allowing greater patient access is called open scheduling.
This approach takes the scheduling challenges one step further allowing not
only established patients to schedule appointments but also new patients
who have never seen a primary care provider within the health system.
Again, the types of appointments that patients can choose must be carefully

15
monitored and managed, in order to reduce scheduling errors. A health
system may have the best design that controls and guides patients into the
most appropriate scheduling slots however, errors will still occur.
This author is also aware of a health system which uses an approach called
wave scheduling. With this approach, all patients are scheduled at the top of
the hour so that partway through the hour you know if you will have no-
shows. If there is an open patient slot available, a provider then knows they
can see a walk-in or urgent patient need. The hope with this approach is to
help the provider, who might have patients with a lot of same day needs, to
better manage their patient panel. There is a variation to this wave
scheduling approach which is called modified wave scheduling. The concept
with this approach is generally the same and the main difference is that only
two or three patients are scheduled at the top of the hour and additional
patients are scattered throughout the hour, again with the understanding
that there is likelihood for a higher than normal no-show rate, typically found
in a lower-income population.
Review of process
Maximizing efficiency in key areas can make a significant impact on the
performance of any health system. Take, for example, a health system that
historically had a call duration of 4 minutes and 30 seconds. It handles
15,000 calls each month, resulting in 67,500 minutes of phone time per
month or 1125 hours. Through process improvement, standardization, and
16
centralization, this same health system finds itself managing each call in an
average of 3 minutes and 30 seconds. Upon further review, this health
system recognizes that it has shaved 250 hours of talk time per month,
representing about 1.5 full time equivalents (FTEs)! Double the number of
calls in this example for a larger health system and the staff savings could
represent 3 FTEs.
If an organization is considering implementation of a centralized group, the
team must provide high quality services with knowledge and expertise right
from the start. In the absence of this type of implementation, the confidence
of the patients and physicians will quickly deteriorate, and they will want
their prior scheduling system restored. Additionally, clinics which are yet to
be integrated with the health system will strongly resist joining the new
appointment system structure, making it extremely difficult to have a
successful path forward.
Expected outcomes
There are specific outcomes that each health system needs to measure in
order to understand the impact of its work and the impact of incremental
changes that it chooses to make, whether through lean or kaizen
approaches, to improve the workflow. While industry benchmarks can be
found, they are not broadly accepted and adopted, although they do provide
a sense for whether a health system is moving in the right direction. Without
a doubt, the best measure of success is through an evaluation of internal

17
trend data while understanding the impact of individual changes. Having
said this, some of the most important elements to measure include:
a. Average time to answer: The ways to measure this in the industry
vary including an overall average or a percentage answered within
so many seconds; typical benchmarks noted with this research
include average time to answer of 50 seconds or less, with best
performers answering 90% of their calls within 20 seconds.
b. Call abandonment rate: For clarification, the abandonment rate is
the percentage of inbound phone calls made to an appointment
center that are abandoned by the patient before speaking to a
team member and it is calculated as abandoned calls divided by
total inbound calls. Abandon rates have a direct relation to
waiting times. Typical goals for this category are less than 4% and
best performers are less than 2%, although some of the data
suggests that less than 4% is a best performer.
c. Call duration / handle time: Often less than 3 minutes and 30
seconds with best performers closer to 3 minutes.
d. Patient satisfaction: While the type of question will help
determine the percentage, achieving satisfaction rates of 95% or
higher are clearly industry best, while the average performer
hopes to exceed 80%.
18
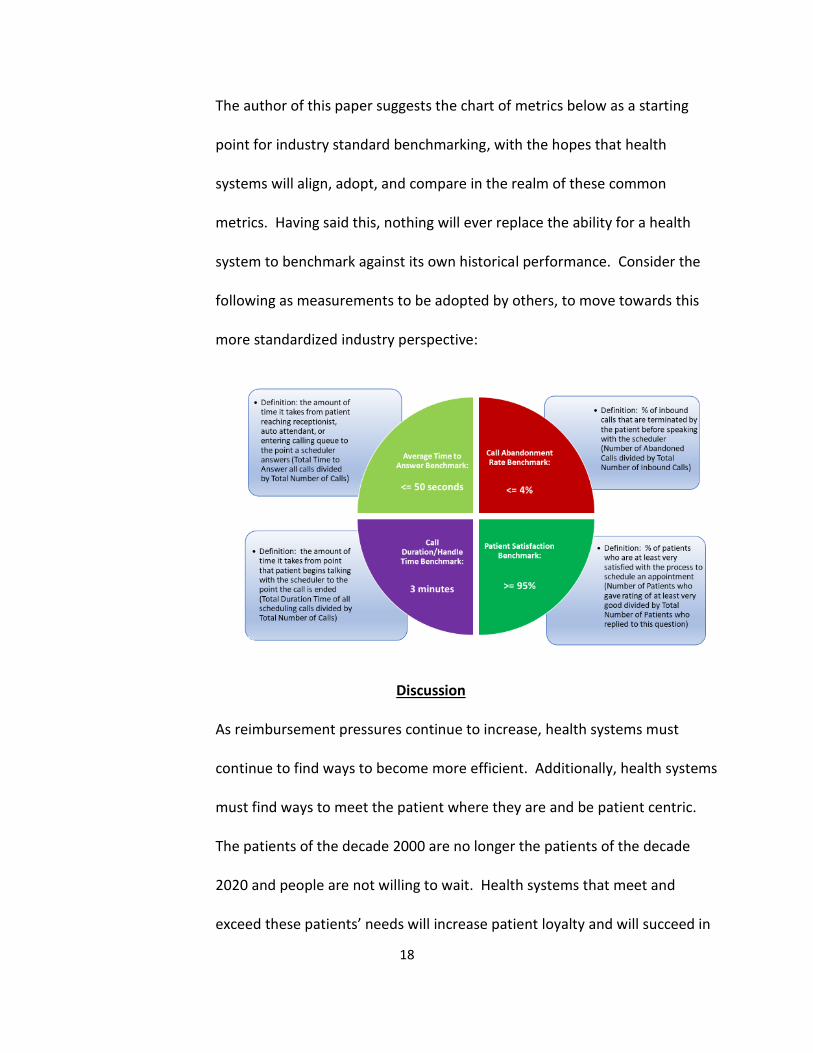
The author of this paper suggests the chart of metrics below as a starting
point for industry standard benchmarking, with the hopes that health
systems will align, adopt, and compare in the realm of these common
metrics. Having said this, nothing will ever replace the ability for a health
system to benchmark against its own historical performance. Consider the
following as measurements to be adopted by others, to move towards this
more standardized industry perspective:
Discussion
As reimbursement pressures continue to increase, health systems must
continue to find ways to become more efficient. Additionally, health systems
must find ways to meet the patient where they are and be patient centric.
The patients of the decade 2000 are no longer the patients of the decade
2020 and people are not willing to wait. Health systems that meet and
exceed these patients’ needs will increase patient loyalty and will succeed in
19
the competitive healthcare environment. Technology will continue to
advance and alternative ways to monitor one’s health and to communicate
with healthcare providers will evolve. Keeping abreast of these technological
advancements will be important however, the author of this paper expects
most patients to rely on the long-standing approach of scheduling medical
appointments by using the telephone and talking directly to their health
system of choice. The basis for this prediction is that on-line appointment
scheduling has been available to patients for several years, yet the adoption
rate has experienced relatively slow growth.
Significance of the findings
a. So, what does this mean?
It means that health systems must answer their phones more promptly, it
means that key details about the patient must be understood in a timely
fashion and known into the future, it means that the time patients spend on
the phone must be kept to a minimum, and all of this means that patients
will ultimately be more pleased with the care they receive.
b. What if nothing was done?
Solutions in healthcare are not “one size fits all” and the author of this paper
is not advocating that centralizing appointment scheduling in primary care is
the best and only solution for every health system. Maintaining
decentralized, independent appointment scheduling locations can be
successful, when the patient is kept at the center of the approach. Having a
20
couple of star-employees can have a very positive impact on the perception
and satisfaction that patients have about their experience and it can be
difficult to duplicate a personalized level of service within a centralized
environment, especially as the number of team members grows. Having said
this, it is likely difficult to gain the desired level of system standardization and
efficiencies within a decentralized approach, and the cost savings
opportunities that are missed must be made up in other ways. As discussed
earlier, health systems with expense growth outpacing revenue growth must
find every way that they can to maximize the efficiency of its work.
Additionally, if a health system maintains a decentralized approach,
consideration should be given for how peak volume of phone calls will be
handled when there are limited team members who can flex with the
demands. Perhaps other team members should be cross trained to provide
back-up support for this work or maybe other sites of care can serve as
support for call volume overflow.
c. Summary of what others may learn.
Technology seems to have no boundary, and this leaves the door open for
other advances in service to patients for years to come. Emerging models of
care means that healthcare will continue to evolve and be delivered in ways
never imagined and we must remain flexible in our approaches. As the
author of this paper was “penning” the finishing touches, COVID-19 was
ramping up in the United States. Who would have thought that our globe

21
would have experienced such a crisis! So, what is the point about this? Well,
how does this change our world and how do events of the future change our
world, in ways that we never thought? How much will the COVID-19 crisis
change the way we care for patients and distance ourselves socially from
others? What then can be expected when it comes to expanding virtual
patient visits including video, telephonic and electronic health record
messaging? And as patients become more comfortable with technology in
healthcare, how will this change the ways in which patients communicate
with their healthcare provider, including scheduling of appointments? Will
more health systems shift towards a portion of the labor pool working from
home? We have seen home-based positions in the areas of billing and
coding however, it has not seemed to shift much to other disciplines.
Significant events certainly have and will place a new and different
perspective on the entire healthcare landscape. Throughout it all, and never
ending, will be the fact that the patient remains at the center, with ever
increasing demands and expectations.
d. Areas for further research.
The focus of this paper has been on primary care appointment scheduling.
Areas for continued growth and learning include specialty care, surgical care,
radiology, lab, and rehab appointment scheduling. And while primary care
appointment scheduling has been at the center of this paper, additional
research needs to be conducted on best practices relative to the possible
22
centralization of referral coordination, of prior authorizations, of medication
refills, of triage services and more. Also, as referenced earlier in this paper,
on-line appointment scheduling has not gained adequate following to allow
the industry enough experience with this modality. Further understanding
and research will be beneficial for development of this approach.
Final Comments
There are many “front doors” to a health system and each one can have a significant
impact on its success. Meeting and exceeding the needs and expectations of patients is
critical in the competitive healthcare environment in which we live and must be done
with efficient operations in a time when operating margins are narrowing or
disappearing. Since one of the front doors is through primary care services, and a front
door to primary care is through its answering of phones and having simple and available
appointment solutions, the structure of these operations is extremely important to the
patients’ experience. Providing these patients with a consistent, standardized, and
positive interaction with team members will go a long way in securing their confidence
and loyalty. There are many aspects to consider when organizing primary care
centralized appointment scheduling in a health system, and there are many benefits and
advantages to establishing this centralized structure. While there are complexities to
this model, a well planned and collaborative approach will lend to the success of these
services and the success of the health system.
23
Bibliography
Advisory Board. (2016). 10 Steps to Centralized Scheduling. Washington D.C.: Advisory Board.
Advisory Board. (2018). Five Must-Have Characteristics of the Consumer-Focused Physician.
Washington D.C.: Advisory Board.
AHC Media. (2013). Switch to centralized scheduling. Atlanta: AHC Media.
Association, A. M. (2014). One Destination, Two Journeys: Call Center Centralization at Henry
Ford Medical Group and The Jackson Clinic. Alexandria: American Medical Group Association.
Brandenburg, G. S. (2015). Innovation and Best Practices in Health Care Scheduling. Washington
D.C.: Institute of Medicine of the National Academes.
Business Wire. (2018). 9th Annual Vitals Wait Time Report Released. New York: Business Wire.
Chan, T. (2014). How Aurora Medical Group reinvented the scheduling wheel. Washington D.C.:
Advisory Board.
Creech, M. D. (2017). Save money and reduce stress with centralized scheduling in healthcare.
Chicago: Becker's Hospital Review.
Heath, S. (2017). Centralized Appointment Scheduling Aids Patient Experience. Danvers: Patient
EngagementHIT.
Institute for Healthcare Improvement. (n.d.). Reduce Scheduling Complexity. Boston: Institute
for Healthcare Improvement.
Kacik, A. (2018). Not-for-profit hospital expenses will continue to outpace revenue in 2019.
Chicago: Modern Healthcare.
Krim, T. (2012). Leading Trends in Patient Access. Beverly Hills: American Health Connection.
Kumar, S. S. (2014). Healthcare Systems and Services Practice - The access imperative. New York
City: McKinsey & Company.
Relate Care. (2016). The Centralization of Primary Care Scheduling. Cleveland: Relate Care.
Sanborn, B. J. (2018). Moody's data shows expenses continue to outpace revenue for nonprofit
hospitals. Healthcare Finance.
Wilkins, A. (2018). A Review of Centralized Scheduling Implementation in Pediatric Ambulatory
Care.
Williams, M. (2015). Online Appointment Scheduling Expected to Increase in Healthcare.
Horsham: VAR insights.
Copyright © 2022 FDOKUMEN




















