
caledonian society for endocrinology - Edinburgh Diabetes
48
caledonian society for endocrinology and diabetes www.calsoc.org CalSoc 2017 Crieff Hydro November 24 th /25 th @CalSocEndo
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of caledonian society for endocrinology - Edinburgh Diabetes

caledoniansocietyforendocrinologyanddiabetes
www.calsoc.org
CalSoc2017
CrieffHydroNovember24th/25th
@CalSocEndo

@CalSocEndo
#CalSoc2017

Contents
1CalSoc2017
PageProgrammeofevents 2Welcome 4AHendeelist 5
InvitedspeakersProfRebeccaReynolds 6ProfSimonPearce 10DrPetrosPerros 14DrPaulNewey 18ProfRobertSemple 21
Abstractpresenta1onsDrDhruOBhaH 23DrLauraReid 26DrSharonMackin 29DrNyoNyoTun 32DrCatrionaFarrell 35DrMarcusLyall 37DrCatrionaKyle 40

ProgrammeofEvents
13.00–14.30 RegistraOon
Friday24thNovember
Session1
Chair:DrAnnaDoverConsultantPhysician/HonorarySeniorLecturerRoyalInfirmaryofEdinburgh/UniversityofEdinburgh
14.30–15.15 Obesity&DiabetesinPregnancy:Highlightsin2017ProfessorRebeccaReynoldsProfessorofMetabolicMedicineUniversityofEdinburgh
15.15–16.00 Addison’sDiseaseUpdateProfessorSimonPearceProfessorofEndocrinologyNewcastleUniversity
16.00–16.15 Coffee
16.15–17.00 HypothyroidismgoestotheScoKshParliamentDrPetrosPerrosConsultantEndocrinologist/HonorarySeniorLecturerRoyalVictoriaInfirmary,Newcastle/NewcastleUniversity
17.00–17.30 DevelopingaScoKshEndocrineITsystem
19.30 Dinner
2 CalSoc2017
13.15–14.00 MeettheExpert–Traineesession–ThyroidDrPetrosPerros/ProfSimonPearce

ProgrammeofEvents
08.45–09.00 CalSocAnnualGeneralMeeOng
Saturday25thNovember
Session2
DrMarieFreelConsultantEndocrinologist/HonoraryAssociateClinicalProfessorQueenElizabethUniversityHospital,Glasgow/UniversityofGlasgow
09.00–09.45 U1lityandChallengesofGene1cTes1nginEndocrinologyDrPaulNeweySeniorLecturerinEndocrinologySchoolofMedicine,UniversityofDundee
09.45–10.45 AbstractPresenta1onsDrDhruOBhaHDrLauraReidDrSharonMackinDrNyoNyoTun
10.45–11.00 Coffee
11.00–11.45 AbstractPresenta1onsDrCatrionaFarrellDrMarcusLyallDrCatrionaKyle
11.45–12.30 UpdateoninsulinresistanceProfessorRobertSempleProfessorofTranslaOonalMolecularMedicineUniversityofEdinburgh
Chair:
3CalSoc2017

WelcometoCalSoc2017WelcometoCrieffforthe37thwintermeeOngoftheCaledonianSocietyforEndocrinology.Thisyear’smeeOngpromisestocoverawiderangeofclinicallyrelevanttopicsacrossbothdiabetesandendocrinology,deliveredbyinternaOonallyrecognisedexpertsintheirfield.ArecurringquesOonatrecentmeeOngshasbeen‘HowcanweuseCalSoctoharnesstheenthusiasmandexperOseoftheScofshendocrinecommunitytodeliveranaOonalprogrammeofclinicalresearch?’Thishasinvolvedexploringthepossibilityofdevelopinganendocrineequivalentofourworld-leadingSCI-Diabetessystem.Partofthisyear’smeeOngwillbedevotedtoprovidinganupdateonprogressandcanvassingopinionaboutwhatsuchasystemwouldlooklikeandhowwemightachieveit.ManythankstoourgrowingnumberofsupportersfromthepharmaceuOcalindustry.ThisyearwewelcomeNAPPandPfizer,aswellaslong-termsponsorsNovoNordisk,Lilly,Sanofi,MSDandIpsen.ThemeeOngcouldnottakepartwithouttheircontribuOonandIwouldencourageyoutovisittheirstandsbetweensessions.DrFraserGibbOnbehalfoftheCalSocCommiHee
ProfessorGrahamLeeseConsultantPhysicianandHonoraryProfessorNinewellsHospital/UniversityofDundee
DrRussellDrummondConsultantPhysicianandHonoraryClinicalAssociateProfessorGlasgowRoyalInfirmary/UniversityofGlasgow
DrFraserGibb(Secretary-Treasurer)ConsultantPhysicianandHonorarySeniorClinicalLecturerRoyalInfirmaryofEdinburgh/UniversityofEdinburgh
DrSamPhilipConsultantPhysicianandHonoraryClinicalLecturerAberdeenRoyalInfirmary/UniversityofAberdeen
CalSocCommi\ee
'CaledonianSocietyforEndocrinology&DiabetesAnnualMeeOng'hasbeensubmiHedtotheFederaOonoftheRoyalCollegesofPhysiciansoftheUnitedKingdomfor6category1(external)CPDcredits.Approvalpending.
4 CalSoc2017
DrLouiseClarkConsultantPhysicianDumfriesandGallowayRoyalInfirmary

AHendees
5CalSoc2017
Firstname SecondName Grade Loca1on Role
Prakash Abraham Cons Aberdeen AHendee
Melisande Addison Trainee Edinburgh AHendee
Ganesh Arungirinathan Cons Edinburgh AHendee
MohammedAzharuddin Cons Greenock AHendee
DhruO BhaH Trainee Aberdeen Oral
Chad Bisambar Trainee Ayr AHendee
Luke Boyle Trainee Edinburgh AHendee
Geraldine Brennan Cons Monklands AHendee
Linda Buchanan Cons ForthValley AHendee
David Carty Cons Glasgow AHendee
Tom Chambers Trainee Edinburgh AHendee
Louise Clark Cons Dumfries AHendee
Catriona Clarke Biochemist Edinburgh AHendee
Alan Connacher Cons Perth AHendee
Jenna Cowan Cons Crosshouse AHendee
Marion Devers Cons Monklands AHendee
Anna Dover Cons Edinburgh AHendee
Jane DymoH Cons Aberdeen AHendee
Catriona Farrell Trainee Dundee Oral
Marie Freel Cons Glasgow AHendee
Priya George Trainee Dundee AHendee
Fraser Gibb Cons Edinburgh AHendee
Saket Gupta Cons Fife AHendee
Kate Hughes Cons Glasgow AHendee
Emma Johns Trainee Glasgow AHendee
Chris Jones Cons Greenock AHendee
Pauline Jones Cons Edinburgh AHendee
Brian Kennon Cons Glasgow AHendee
Chris Kueh Trainee Glasgow AHendee
Catriona Kyle Trainee Edinburgh Oral
Graham Leese Cons Dundee AHendee
Robert Lindsay Cons Glasgow AHendee
Rachel Livingstone Trainee Glasgow AHendee
Marcus Lyall Trainee Edinburgh Oral
Firstname SecondName Grade LocaOon Role
Alison MacEwen Cons Ayrshire AHendee
David Macfarlane Cons Inverness AHendee
ScoH Mackenzie Cons Edinburgh AHendee
Alasdair Mackie Cons Dundee AHendee
Sharon Mackin Trainee Glasgow Oral
Hannah Macpherson Trainee Edinburgh AHendee
Iqbal Malik Cons Dundee AHendee
Susan McGeoch Cons Aberdeen AHendee
Louise McKenna Trainee Glasgow AHendee
Frances McManus Cons Glasgow AHendee
Emily McMurray Cons Edinburgh AHendee
Kenneth Muir Cons Inverness AHendee
Paul Newey Cons Dundee Speaker
Rose Norton Student Edinburgh AHendee
Mo Oroko Trainee Glasgow AHendee
Simon Pearce Cons Newcastle Speaker
Petros Perros Cons Newcastle Speaker
Colin Perry Cons Glasgow AHendee
Sam Philip Cons Aberdeen AHendee
Laura Reid Trainee Edinburgh Oral
Rebecca Reynolds Cons Edinburgh Speaker
Robert Semple Cons Edinburgh Speaker
Anne Sillars Trainee Glasgow AHendee
Lee Sit Trainee Edinburgh AHendee
Karen Smith Biochemist Glasgow AHendee
Alison Stewart Cons Glasgow AHendee
Roland SOmson Cons Edinburgh AHendee
Mark Strachan Cons Edinburgh AHendee
Sandeep Thekkepat Cons Monklands AHendee
Chris Thompson Cons Dublin AHendee
Joe Timmons Trainee Glasgow AHendee
NyoNyo Tun Trainee Edinburgh Oral
Liesbeth VanLook Cons Livingston AHendee
MinChong Zhuo Trainee Glasgow AHendee

ProfRebeccaReynoldsBiographyProfessorReynoldsisProfessorofMetabolicMedicine,UniversityofEdinburghandHonoraryConsultantPhysicianinDiabetes&Endocrinology,NHSLothianandDeputyHeadoftheCentreforCardiovascularSciences,UniversityofEdinburgh.HermainresearchinterestisintheearlylifeoriginsofhealthanddiseaseandshewasawardedtheNickHalesAwardin2011bytheInternaOonalSocietyfortheDevelopmentalOriginsofHealthandDiseaseandtheCurtRichterAwardin2012bytheInternaOonalSocietyofPsychoneuronendocrinologyinrecogniOonofthiswork.SheisChairoftheDiabetesUKClinicalStudiesGroup‘CausesofDiabetes’.Herresearchspans‘processtopopulaOon’egexperimentalmedicinestudiesinpregnantwomenandtheirchildren,detailedmechanisOcstudiesusingplacentalOssue,randomisedcontrolledtrialstesOngintervenOonsinpregnancytoimproveoutcomesandepidemiologicaldata-linkagestudiesusing‘bigdata’inScotland.Herclinicalworkincludesgeneralandantenataldiabetesandendocrinology,andreproducOveendocrinology.SheismoduleleadforUniversityofEdinburghMBChBEndocrinology&Diabetes.
AbstractObesityandDiabetesinPregnancy:Highlightsin2017ObesityanddiabetesrepresentthemostcommonpregnancycomplicaOonsindevelopedcountries.BothofthesecondiOonshaveshorttermrisksduringpregnancyforbothmotherandchild(1),withincreasingevidencedemonstraOngthattherearealsolongertermrisksoftheseexposuresinpregnancyimpacOngonhealthacrossthelifespan(2,3).ResearchersandcliniciansinScotlandhavecontributedtosomeofthelandmarkclinicaltrialspublishedin2017.Allthesetrialsaimedtoimprovetreatmentandclinicaloutcomesforwomenwithobesityand/ordiabetesinpregnancy.ThispresentaOonwilldiscusstheresultsofthesekeytrialsincludingtheCONCEPTTtrialtesOngtheuOlityofconOnuousglucosemonitoringinpregnantwomenwithtype1diabetes(4),theGRACEStrial,tesOngwhetherthecombinaOonoforalhypoglycaemicagentsmepormin+glibenclamidewouldbepreferabletostandardcareofmepormin+insulinforwomenwithgestaOonaldiabetes(5)andtrialsofintervenOonsinobesepregnancywithmepormin(EMPOWARandMOPS)(6,7),diet/lifestyleintervenOons(8),orbariatricsurgery(9).ParOcipaOoninthesestudieshasdemonstratedourabilitytoparOcipatein/and/orleadimportantclinicaltrialsinpregnancy,chimingwiththeChiefMedicalOfficerforEngland’svisiontoopOmisewomen’shealth.ReferencesKallialaIetalObesityandgynaecologicalandobstetriccondiOons:umbrellareviewoftheliterature.BMJ.2017Oct26;359:j4511.doi:10.1136/bmj.j4511.LeeKetalMaternalObesityDuringPregnancyAssociatesWithPrematureMortalityandMajorCardiovascularEventsinLaterLife.Hypertension.2015Nov;66(5):938-44.doi:10.1161/HYPERTENSIONAHA.115.05920ReynoldsRMetalMaternalobesityduringpregnancyandprematuremortalityfromcardiovasculareventinadultoffspring:follow-upof1323275personyears.BMJ.2013Aug13;347:f4539.doi:10.1136/bmj.f4539.FeigDSetalConOnuousglucosemonitoringinpregnantwomenwithtype1diabetes(CONCEPTT):amulOcentreinternaOonalrandomisedcontrolledtrial.Lancet.2017Sep15.pii:S0140-6736(17)32400-5.doi:10.1016/S0140-6736(17)32400-5ReynoldsRMetalGlibenclamideandmepoRminversusstAndardcareingEstaOonaldiabeteS(GRACES):afeasibilityopenlabelrandomisedtrial.BMCPregnancyChildbirth.2017Sep22;17(1):316.doi:10.1186/s12884-017-1505-3.ChiswickCetalEffectofmeporminonmaternalandfetaloutcomesinobesepregnantwomen(EMPOWaR):arandomised,double-blind,placebo-controlledtrial.LancetDiabetesEndocrinol.2015Oct;3(10):778-86.doi:10.1016/S2213-8587(15)00219-3.Epub2015Jul9.SyngelakiAetalMeporminversusPlaceboinObesePregnantWomenwithoutDiabetesMellitus.NEnglJMed.2016Feb4;374(5):434-43.doi:10.1056/NEJMoa1509819.RogozińskaEetalEffectsofantenataldietandphysicalacOvityonmaternalandfetaloutcomes:individualpaOentdatameta-analysisandhealtheconomicevaluaOon.HealthTechnolAssess.2017Aug;21(41):1-158.doi:10.3310/hta21410.JohanssonKetalOutcomesofpregnancyawerbariatricsurgery.NEnglJMed.2015Feb26;372(9):814-24.doi:10.1056/NEJMoa1405789.
6 CalSoc2017

ProfRebeccaReynolds
7CalSoc2017
Primary outcome
*
CGMControl
*mean difference -0.19%; 95% CI -0.34—0.03; p = 0.0207
• LGA 53% CGM vs 69% control; Odds ratio 0.51; 95%CI 0.28—0.90, p=0.0210
• Neonatal hypoglycaemia requiring iv treatment 15% vs 28%;Odds ratio 0.45; 95%CI 0.22—0.89, p=0.0250
• NICU admission>24hrs; 27% CGM vs 43% control;Odds ratio 0.48; 95% CI 0.26-0.86; p=0.0157
Summary of neonatal outcomes
NNT 6
NNT 8
NNT 6

ProfRebeccaReynolds
8 CalSoc2017
Obesity and obstetric conditions: umbrella review of 144 meta-analyses of cohort studies
Strong evidence for increased risk of :Maternal adverse outcomes• Pre-eclampsia • Gestational Diabetes• Antenatal depression• Total and emergency caesarean sectionFetal adverse outcomes• Fetal macrosomia• Low Apgar score at 1 minute• Stillbirth Kalliala et al BMJ 2017; 359; j4511
Conclusions• A randomised trial of glibenclamide v insulin in
women with GDM and who need a second line therapy in addition to metformin would be “feasible” but would require 30-60 centres recruiting for 3 years
• In this small sample, no woman had a symptomatic hypoglycaemic episode
• Preference for glibenclamide over insulin is not universal
• Preliminary data suggests that insulin gives superior control, with fewer excursions < 3.3 mmol/l
ProfRebeccaReynolds
9CalSoc2017
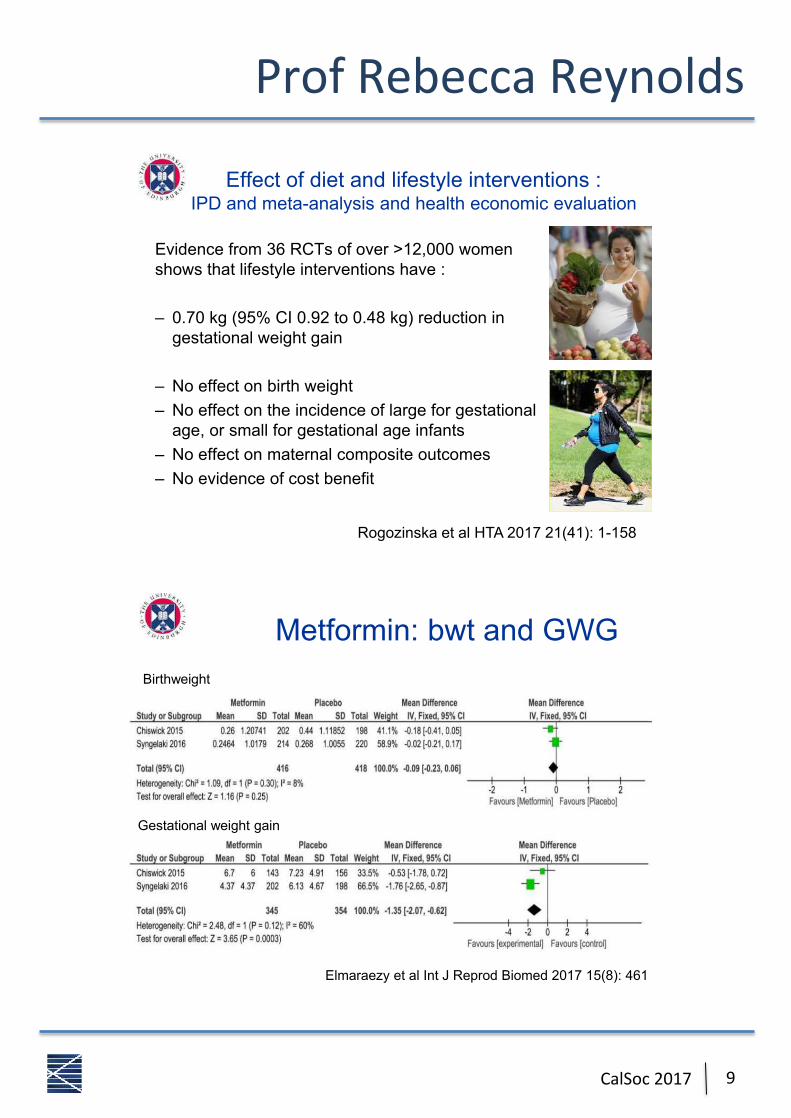
Effect of diet and lifestyle interventions : IPD and meta-analysis and health economic evaluation
Evidence from 36 RCTs of over >12,000 women shows that lifestyle interventions have :
– 0.70 kg (95% CI 0.92 to 0.48 kg) reduction in gestational weight gain
– No effect on birth weight– No effect on the incidence of large for gestational
age, or small for gestational age infants– No effect on maternal composite outcomes– No evidence of cost benefit
Rogozinska et al HTA 2017 21(41): 1-158
Metformin: bwt and GWG
Elmaraezy et al Int J Reprod Biomed 2017 15(8): 461
Birthweight
Gestational weight gain
ProfSimonPearceBiographySimonPearcequalifiedinMedicineMB,BS1stclasshonoursfromNewcastleUniversity.Followinginternalmedicinetraining,heundertookpostgraduateeducaOoninendocrinologyinRajThakker’slabatHammersmith,followedbyspellsatBrigham&Women’sHospital,Boston;andlaHerlybackinNewcastle,UK.HewasappointedasSeniorLecturerinEndocrinologyin2001atNewcastleUniversity,andpromotedtoProfessorin2007,affiliatedtotheInsOtuteofGeneOcMedicineandtheRoyalVictoriaInfirmary.Hehaspublishedmorethan170papersoverthelast25years,mainlyonparathyroidcalcium-sensing,thyroiddiseaseandAddison’sdisease.
Summaryoftalk•ThefirstpresentaOonofapaOentwithadrenalinsufficiencyisfrequentlyoverlookedbyhealthcareprofessionals.•FoodpoisoningandgastroenteriOsarethecommonestcauseofAddisoniancrisis.•SaltdepleOondueto(relaOve)mineralocorOcoiddeficiencyisresponsibleformuchofthepathophysiologyofadrenalcrisis.•ExcellentpaOentengagementandsteroideducaOoniskeytoallowingpeoplewithAddison’sdiseasetosafelymanagetheircondiOon,day-to-day.•SmallandowendosesofhydrocorOsonegivebeHersteroidexposureprofiles.•Fine-tuningofmineralocorOcoidreplacementandsaltintakeinAddison’spaOentsisimportantforadrenalcrisisprevenOonandopOmalwellbeing,andisowenneglectedbyphysicians.•Bothmodified-releasehydrocorOsonetabletsandconOnuoussubcutaneoushydrocorOsoneinfusionsoffercloserapproximaOonstohealthyplasmacorOsolrhythmsthanmulOdose,immediate-releaseoralhydrocorOsone.•Greaterclinicalexperiencewiththesenovelreplacementtherapiesneedstobegainedfortheirroleinthemanagementofadrenalinsufficiencytobeestablished.•ThereisdurableresidualadrenalfuncOoninaproporOonofpaOentswithAddison’sdisease,andthisisafuturetherapeuOctarget.References:PazderskaA,PearceSH.Adrenalinsufficiency-recogniOonandmanagement.ClinMed(Lond)2017;17:258-262.doi:10.7861/clinmedicine.17-3-258.GanEH,PearceSH.RegeneraOvetherapiesinautoimmuneAddison'sdisease.EurJEndocrinol2017;176:R123-R135.doi:10.1530/EJE-16-0581.HusebyeES,AllolioB,ArltW,BadenhoopK,BensingS,BeHerleC,FalorniA,GanEH,HulOngAL,Kasperlik-ZaluskaA,KämpeO,LøvåsK,MeyerG,PearceSH.Consensusstatementonthediagnosis,treatmentandfollow-upofpaOentswithprimaryadrenalinsufficiency.JInternMed2014;275:104-15.doi:10.1111/joim.12162.GanEH,MacArthurK,MitchellAL,HughesBA,PerrosP,BallSG,JamesRA,QuintonR,ChenS,FurmaniakJ,ArltW,PearceSH.ResidualadrenalfuncOoninautoimmuneAddison'sdisease:improvementawertetracosacOde(ACTH1-24)treatment.JClinEndocrinolMetab2014;99:111-8.doi:10.1210/jc.2013-2449
10 CalSoc2017

ProfSimonPearce
11CalSoc2017
• 67%$of$pa)ents$had$3$or$more$encounters$with$features$of$adrenal$failure$before$Δ$
• 50%$of$men,$70%$of$women$had$complained$of$symptoms$>$6$months$
• 68%$had$a$different$ini)al$diagnosis$– Mental$health$– Gastrointes)nal$
Bleicken$B$et$al.$Am$J$Med$Sci$2010$
Pa3ent,Educa3on,• Steroid$card$&$Medical$alert$jewellery$
• iPhone$medic$alert$home$screens$
• �Sick$day$rules�$– Fever,$diarrhoea$– Minor$procedures$(den)st,$gastroscopy)$
– Vomi)ng$
• How$&$when$to$inject$with$IM$hydrocor)sone$
• www.addisons.org.uk$

ProfSimonPearce
12 CalSoc2017
Pa3ent,Educa3on,• Steroid$card$&$Medical$alert$jewellery$
• iPhone$medic$alert$home$screens$
• �Sick$day$rules�$– Fever,$diarrhoea$– Minor$procedures$(den)st,$gastroscopy)$
– Vomi)ng$
• How$&$when$to$inject$with$IM$hydrocor)sone$
• www.addisons.org.uk$
Ask the patient 10 questions 1. Do you have low spots during the day? 2. Are you clock-watching for one particular dose? 3. Do you often miss a dose because you haven�t
noticed the time? 4. What time is bedtime? 5. Do you sleep okay? 6. How do you feel first thing in the morning? 7. How are your general energy levels/ get up & go? 8. Are you napping during the day? 9. Changes in pigmentation? 10. Changes in weight?

ProfSimonPearce
13CalSoc2017
Chronic,Management:,mineralocor3coid,
• Fludrocor)sone$50`500mcg$daily$
• Younger$people$need$more$
• Discuss$salt$cravings,$including$typical$foods$
• Consider$salt$tablets$(NaCl$1.8`3.6$g/d)$
• Titrate$according$to$Na+/K+,$BP,$renin$
Model of evolving Addison�s disease
• Insidious onset of disease • ACTH vs Immune destruction
ACTH
Immune system attack Failure to make steroids Adrenal becomes dormant
ACTH stimulation Adrenal cells proliferate
Regeneration

DrPetrosPerrosBiographyPetrosPerrosisaconsultantendocrinologistattheRoyalVictoriaInfirmary,Newcastleandhonoraryseniorlecturer,NewcastleUniversity.HequalifiedfromNewcastleUniversityandtrainedinNewcastle,GlasgowandEdinburgh.Hisclinicalandresearchinterestsincludethyroidcancer,thyroideyediseaseandneuroendocrinetumours.HeisapastpresidentoftheEuropeanGrouponGraves’OrbitopathyandiscurrentlyconvenoroftheSocietyforEndocrinologythyroidnetwork.
AbstractHypothyroidismgoestotheScofshParliamentSomaOcandcogniOvesymptomsarefoundabout10%ofthegeneralpopulaOonandinpaOentswithhypothyroidism.ClaimsthattreatmentwithT3-containingpreparaOonsincombinaOonwithT4aresuperiortoT4alonehavenotbeenconfirmedbyseveralrandomisedclinicaltrials.SomepaOentgroupsarecampaigningforwideuseofT3incombinaOonwithT4ordesiccatedanimalthyroidextract.TwoplausiblehypotheseshavebeenputforwardtoexplainpersistentsymptomsintreatedhypothyroidpaOents:funcOonalsomatoformdisorder,andinabilityofavailablethyroidhormonereplacementtherapiestorestorenormalphysiology.Concernsaboutlong-termsafetyofcombinaOontherapiespersist.
14 CalSoc2017
• T4 alone resulted in normal TSH but low serum and tissue T3 levels
• Serum T3, T4 and TSH and tissue T3 were only restored with continuous T4 + T3 administration
• Patterns of gene expression in tissues were only restored with continuous T4 + T3 administration
Biological basis Pathophysiology of OTAST
Moreales-Escobar et al, 1996, Werneck de Castro et al, 2015)
Thyroidectomised rats treated with: -T4 alone -T4 + boluses of T3 -T4 + continuous T3 infusion

DrPetrosPerros
15CalSoc2017
Biological basis MCT10 and D2 Gene Polymorphisms:
preference for T4+T3 treatment
Carle et al, 2017
Pathophysiology of OTAST
% Responsers
100 80 60 40 20 0
Neither n=19
One n=19
Both n=7
p<0.05
Taylor et al, 2014
TSH threshold for starting treatment
10% 51%
Trends in diagnosis and treatment of hypothyroidism
Pathophysiology of OTAST

DrPetrosPerros
16 CalSoc2017
Prescriptions 2001-2013 (PCA)
10
8
6
4
2
0
Fold increase
T4 T3 Animal thyroid extract
TFTs
Pathophysiology of OTAST
Mean FT3 Values
2.80
3.60
4.40
5.20
6.00
6.80
0.00 4.00 8.00 12.00 16.00 20.00 24.00
Hours Post-Dose
FT
3 -
No
rmal
Ran
ge
(pm
ol/L
)
P atientsC ontro ls
Potential harm of T3 + T4 treatments
Biochemical thyrotoxicosis almost inevitable in T3 treated patients

DrPetrosPerros
17CalSoc2017
Risk of future AF
Cappola et al 2006
HR =1.98 (1.29-3.03)
Potential harm of T3 + T4 treatments
Extrapolations from subclinical hyperthyroidism paradigm
Haemtkens et al 2008
Potential harm of T3 + T4 treatments
Mortality
Extrapolations from subclinical hyperthyroidism paradigm

DrPaulNewey
18 CalSoc2017
BiographyDrPaulNeweyisaSeniorLecturerinEndocrinologyandHonoraryConsultantPhysicianattheUniversityofDundee,Scotland.HeundertookhismedicalstudiesattheUniversityofEdinburghbeforemovingtoOxfordforhisSpecialtyTraining.DuringthisperiodhewasawardedaDPhilforhisstudiesonhereditaryendocrinedisordersincludingMulOpleEndocrineNeoplasiaType1(MEN1).HewassubsequentlyappointedaNIHRClinicalLecturerinOxfordundertakingpost-doctoralresearchinthefieldofendocrinetumourigenesis.In2014,DrNeweymovedtotheUniversityofDundeetoestablishhisownresearchgroupconOnuinghisinterestinendocrinetumourigenesis.In2015,hewasawardedaNRSScofshSeniorClinicalFellowship.DrNewey’smainareaofresearchisunderstandingthegeneOcbasisofendocrinediseasewithafocusonneuroendocrinetumoursanddisordersofcalciumhomeostasis.
AbstractUOlityandChallengesofGeneOcTesOnginEndocrinologyTheadventofhigh-throughputDNAsequencingtechnologyhasacceleratedtheidenOficaOonofgenesresponsibleforbothhereditaryandsporadicendocrinediseasesandisincreasinglyappliedintheclinicalsefngtoguidepaOentmanagement.However,thisaccessibilityandscopeofgeneOctesOngbringsmanychallenges,includinginherentdifficulOesindatainterpretaOon.Thesechallenges,whichincludeestablishingaccurateesOmatesofvariantpathogenicityandpenetrance,mayresultindiagnosOcconfusion.ThistalkwillprovideanoverviewofthecurrentapproachestoclinicalgeneOctesOnginendocrinologyandhighlightmanyofthecontemporarychallengesfaced.

DrPaulNewey
19CalSoc2017
TheGene'cTes'ngWorkflow–WhichTest?
TheGene'cTes'ngWorkflow–Pre-TestConsidera'ons

DrPaulNewey
20 CalSoc2017
TheGene'cTes'ngWorkflow–Communica'ngResults
TheGene'cTes'ngWorkflow–Intepreta'on

ProfRobertSempleBiographyRobertSempleisanerrantScotwho,unOlOctober,hadspenthisenOreprofessionalcareerinEngland.HereadNaturalSciencesandthenMedicineattheUniversityofCambridgebeforeinternalmedicalpostsinLondon.HereturnedtoCambridgeforspecialisttraininginDiabetesandEndocrinology,interruptedbydoctoralstudieswithProfSirStephenO'Rahilly,focusingontranscripOonalregulaOonofadiposeOssuemetabolism.Forthepast12yearshisresearchhasfocusedonrarehumandisordersofinsulinacOonand/orgrowth,withtheaimofidenOfyingnovelacquiredorgeneOcdefectsunderlyinginsulinresistanceandrelatedcondiOons,bothtoacceleratediagnosisandtreatmentofaffectedpaOents,andtogaininsightsintodiseasemechanism.InOctoberhetookupachairofTranslaOonalMolecularMedicineattheUniversityofEdinburgh,andaswellasre-establishingaresearchgroupfocusingoncausesandconsequencesofinsulinresistance,heaimstoprovideaclinicalrouteofreferralinScotlandforpaOentswithrelatedproblems.
AbstractAcquiredandgeneOcdisordersofadiposeOssuedevelopmentorfuncOonand/orsevereinsulinresistanceareaheterogenousgroupofcondiOonswhichareunderdiagnosedyetimposeahugeburdenofprematuremorbidityandmortalityonaffectedpaOents.Drawingonexperienceof15yearsofresearch,translaOonalandclinicalexperienceinCambridge,encompassingtheEnglishNHSSevereInsulinResistanceService,apracOcalaccountwillbegivenofthecondiOonsmostlikelytobeseeninendocrine/diabetespracOce,withafocusontherequirementsforspecificdiagnosisandmanagement.
21CalSoc2017

ProfRobertSemple
22 CalSoc2017

DrDhruOBhaH
23CalSoc2017
BiographyIgraduatedfromtheUniversityofSheffieldin2009andmovedtoNorthofScotlandforfoundaOonandcoremedicaltraining.IcommencedspecialisttraininginDiabetesandEndocrinologyin2014andamcurrentlyinmypenulOmateyearoftrainingatAberdeenRoyalInfirmary.
AbstractIs11C-methioninePETco-registeredwithMRIagamechangerforchallengingfunc1oningpituitarytumours–AberdeenexperienceinAcromegalyandCushing’sdisease.DhruOBhaH1,JackStraiton2,MahmoudKamel3,AlexGraveling1,SamPhilip1,PrakashAbraham1.DepartmentofEndocrinology1,DepartmentofClinicalRadiologyandNuclearMedicine2,DepartmentofNeurosurgery3,AberdeenRoyalInfirmary,Aberdeen,U.K.Aims:11C-methioninepositronemissiontomographyco-registeredwithMRI(met-PET/MRI)isanewimagingtechniqueusedforfuncOoningpituitaryadenomas.InpaOentswithpersistentacromegalyawerprimarytherapyandotherfuncOoningpituitaryadenomas,met-PET/MRIcanhelpidenOfythesite(s)ofresidualpituitaryadenomawhenMRIappearancesareinconclusiveanddirectfurthertargetedintervenOon(Trans-sphenoidalsurgery-TSSorradiotherapy).Methods:ProspecOvestudyofpaOentswithacromegalyunderacOvefollow-upinateachinghospital.Datawascollectedfrompaperandelectronicrecords(2009onwards).Anarbitraryagecut-offof75wasusedwhenconsideringsuitabilityforrepeatTSS.RemainingpaOentsweredividedintothreecategories.P1:poorlycontrolledonsomatostaOnanalogue(SSA)therapyand/orpegvisomant.P2:wellcontrolledonSSA.P3:poorlycontrolledondopamineagonist(DA)therapy.ForCushing’sdiseasetargetedpaOentswerereferredfromothercentres.Results:Acromegalycohort:Outofthefiwy-onepaOentsincluded,twenty-threepaOentsundertheageof75wereonacOvetreatment(P1:10,P2:8andP3:3).Annualcost(BNF2017)ofmedicalendocrinetherapyforP1categorypaOentswas£150,829andP2categorypaOentswas£73,466.NineP1categorypaOents,willingforfurtherintervenOon,haveagreedtomet-PET/MRIand2paOentshaveundergoneTSS.IllustraOvecase:AyoungfemalepaOentwithacromegalyonSSA+DA(P1)andDM(diabetesmellitus)on120unitsofinsulin/day,bothpoorlycontrolled,underwentredoTSSinfluencedbymet-PET/MRI(fusedimages).Shewasdischargedoffinsulinandwithintactsteroidaxis.Cushing’sdiseasecohort:Sofar3paOents(1eachfromAberdeen/Dundee/Inverness)withCushing’sdiseasehavehadposiOveoutcomesfollowingTSSinfluencedbymet-PET/MRI.IllustraOvecases1:A67yearoldwomanwithpreviousrightadrenalectomyandsubsequentACTHdependantCushing’ssyndromeviasuppressionandCRHtests.BIPSSandMRIx2negaOve,met-PET/MRIconfirmedanadenomaandunderwentsurgery;2A28yearoldmanwithrecurrentCushing’sdiseaseandType2DMunderwentTSSawerthemet-PET/MRIclarifiedthefuncOoningareafrompostsurgicalchange.Comment:Sofar,ourpaOentswhohaveundergonemet-PET/MRIhaveshownidenOfiableresidualfuncOoningpituitaryadenoma.IthasinfluencedourdecisiontoputthesepaOentsforwardforTSS.TherearepotenOalcostsavingsinvolvediftheyareabletocomeoffmedicaltherapiesorevendecreasefrequencyoftheseinjecOons.Acknowledgements–Cambridgeteamforassistancesefngupmet-PET/MRI.EurJEndocrinol.2016Nov;175(5):485-498.ProfGrahamLeese,DundeeandDrSaOnderBal,InvernessforreferralandinformaOonabouttheirpaOents.

DrDhruOBhaH
24 CalSoc2017
Outline
• MET-PET• Poten+alapplica+ons
– Cambridgeexperiencesince2011–200+– AberdeenstartupDec2016–9cases(6pipeline)
• Acromegaly–4(2illustra+vecasesdiscussed)• Cushings–3(1eachfromAberdeen/Dundee/Inverness–2illustra+vecasesdiscussed)
• TSHoma-1• EctopicACTH-1
• Poorlycontrolledonsomatosta0nanalogue(SSA)therapyand/orpegvisomant
• 10pa0ents• Meanannualcostoftherapy-£15,083
P1• WellcontrolledonSSA• 8pa0ents• Meanannualcostoftherapy-£9,183P2• Poorlycontrolledondopamineagonist(DA)therapy• 3pa0ents• Meanannualcostoftherapy-£455P3
• Poorlycontrolledonsomatosta0nanalogue(SSA)therapyand/orpegvisomant
• 10pa0ents• Meanannualcostoftherapy-£15,083
P1
• WellcontrolledonSSA• 8pa0ents• Meanannualcostoftherapy-£9,183
P2
• Poorlycontrolledondopamineagonist(DA)therapy
• 3pa0ents• Meanannualcostoftherapy-£455
P3
Figure1:Pa0entcategoryandtotalannualcost
Acromegaly–Illustra1vecase-1• 26,F,presentedin2011• IGF1-150(9-42nmol/l)atdiagnosis,OGTTlowestGH83mcg/l
andnewdiagnosisofDM• TSS-2011–Improvedvision,butremnant• Radiotherapy–2013;Pegvisamontallergy,OnLanreoSde
120mg4weeklyandCabergoline• Singleparent,Smoker,Poorcompliance• 2016:IGF145-60(15-40nmol/L);HBA1c:127-151mmol/molonHumalogMix25–60unitsbd

DrDhruOBhaHBiographyXX
25CalSoc2017
Case1:-
Radiology–PreandPost-op
CoronalMRI-Pre-op CoronalT1wMRI+Gd–Pre-op/met-PETMRI
CoronalMRI-Post-op
Biochemicalprofile Pre-op(Feb’17)
Post-op(Jul’17)
IGF-1(15-40nmol/L) 63.2 16.9GHug/L 1.55 1.31Cor<sol,nmol/L - 894HbA1c(20-42mmol/mol) 120 88
Prolac<n(59-619mu/l) <40 <40
FT4(10-25pmol/L) 17 22
Case1:resultscon=nued

DrLauraReid
26 CalSoc2017
BiographyLaurastudiedmedicineatClareCollege,Cambridge,graduaOngin2010.ShecompletedherfoundaOonandcoremedicaltraininginNorthernIreland,beforespendingayearworkinginMelbourne,Australia.ShemovedtoEdinburghin2015tocommencetrainingindiabetesandendocrinology.ShehasrecentlystartedworkonanMD,focusingonglycaemicvariabilityanddiabeOcreOnopathyprogressioninpeoplewithtype1diabetespreandpostcommencementofinsulinpumptherapyortreatmentwithisletcelltransplantaOon.
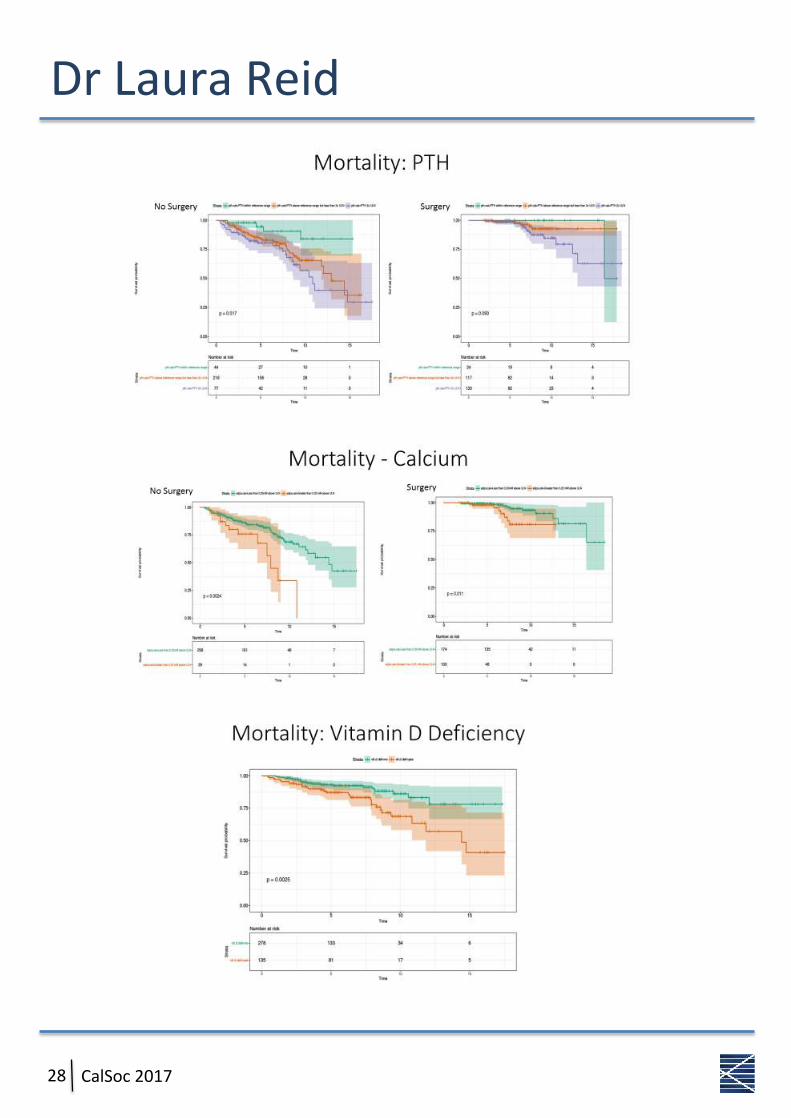
AbstractPredictorsofnephrolithiasis,osteoporosisandmortalityinprimaryhyperparathyroidismLauraJReid,BalaMuthukrishnan,FraserWGibbIntroduc1on:Primaryhyperparathyroidism(PHPT)isoneofthecommonestendocrinedisorderswithaprevalenceofatleast1in1000.Nephrolithiasisandosteoporosisaremorecommoninpeoplewithprimaryhyperparathyroidism,althoughtheclinicalfactorsassociatedwiththisriskarenotwellcharacterised.RecentevidencehassuggestedparathyroidhormoneconcentraOon,butnotcalcium,isassociatedwithmortalityinPHPT.Objec1ves:ToreviewprevalenceofnephrolithiasisandosteoporosisinpaOentswithPHPTinEdinburgh,andassessfactorsassociatedwiththesecomplicaOons.ToassessfactorsassociatedwithmortalityinPHPT.Methods:AllpaOentsassessedattheEdinburghCentreforEndocrinology&Diabetes,between2006–2014,withadiagnosisofPHPTwereidenOfied(n=611).PresenOngclinicalfeatures,biochemistryresultsandimagingresultswereobtainedfromtheelectronicpaOentrecord.Results:Intotal,85/611(13.9%)ofpaOentshadadiagnosisofnephrolithiasis.Adjustedcalciumatdiagnosis(2.76[2.65–2.91]vs.2.72[2.65–2.82],p=0.08)andPTH(12.7[9.9–19.6]vs.12.0[9.3–16.7],p=0.07)werenotsignificantlydifferentinthosewithahistoryofrenalstonescomparedtothosewithnorenalstones.Onlyage(OR0.97,p<0.001)andmalegender(OR2.32,p=0.003)weresignificantlyassociatedwithnephrolithiasisinlogisOcregressionanalysis.BoneMineralDensity(BMD)datawasavailablein461paOentsofwhom223hadosteoporosis;184osteopeniaand54normalBMD.Age(p<0.001),BMI(p<0.001),Gender(p=0.044)andPTHatdiagnosis(p=0.047)weresignificantlyassociatedwithosteoporosis.Parathyroidsurgery(HR0.25,p=0.005),VitaminDdeficiency(HR1.23,p=0.007)adjustedcalciumatdiagnosis(HR1.15,p=0.03)wereindependentlyassociatedwithmortality;PTHwasnot(HR0.99,p=0.74).Conclusions:• NephrolithiasisismostcommoninyoungermenwithPHPT.• OsteoporosisiscommoninPHPTbutthisis,inpart,aconsequenceoftheageandgenderofthosepresenOng
withthiscondiOon.• PTH,ratherthancalcium,ismorestronglycorrelatedwithbonemineraldensity.• ParathyroidsurgeryisassociatedwithlowerratesofmortalitybutthisisalmostcertainlyareflecOonofselecOon
bias(i.e.lesssurgeryinfrailpaOents).• HigherPTHisassociatedwithhighermortality,butthisismostlikelyareflecOonoflowervitaminDlevels,which
aremorerobustlyassociatedwithmortality.• Contrarytoearlierreports,thesedatasuggestadjustedcalciumandnotPTHisthemostsignificantbiochemical
signalformortalityriskinPHPT.

DrLauraReid
27CalSoc2017
DrLauraReid
28 CalSoc2017

DrSharonMackin
29CalSoc2017
BiographyIgraduatedfromtheUniversityofDundeein2009andthereawermovedtoGlasgowformyclinicaltraining,progressingthroughthetradiOonalfoundaOonandcoretrainingroutes.ItookupmyspecialtypostinDiabetesandEndocrinologybackin2013andamnowST6.Morerecently,IhavebeenawardedapersonalfellowshipfromtheGlasgowChildren’sHospitalCharitytoresearchtheroleofglucose-loweringonmaternalandplacentalvascularfuncOoningestaOonaldiabetes.MyresearchisbeingconductedattheUniversityofGlasgow’sInsOtuteofCardiovascularandMedicalSciencesunderthesupervisionofDrRobertLindsayandProfessorChrisOanDelles,andIhavebeeninpostsinceAugust2017.
AbstractKenneyCaffeySyndrome2:AnextremelyrarecaseofhypoparathyroidismandrecurrenthypomagnesaemiaSharonTMackin,RhianMTouyz,ColinPerryWepresentadiagnosOcallychallengingcaseofa22-yearoldfemalewithshortstatureandcongenitalhypoparathyroidismwithrecurrentadmissionsforseverehypocalcaemia,hypokalaemiaandhypomagnesaemia.CaseOurpaOentwasbornat38weeksgestaOontounrelated,healthyparentsofaverageheight,followingapregnancycomplicatedbyintrauterinegrowthrestricOon.Shewasasmallinfantwithabirthweightof2.4kg(-1.7SD),alengththatwasalmost4SDbelowexpectedandasmallheadcircumferenceof31cm(-2.2SD).Shehadfacialdysmorphicfeaturesoffrontalbossing,microphthalmiaandmid-facialhypoplasia.GrowthfailurewasapersistentproblemduringchildhooddespitenormalsOmulatedGHandIGF-1levels.SkeletalsurveysrevealedgracileboneswithcorOcalthickening,hypoplasOcmandiblesandaj-shapedsella.Pituitaryimagingandbiochemistrywerenormal.GHtherapywastrialledseveralOmesbutcomplicatedpre-exisOnghypermetropiawithmacularoedema.Recurrentseverehypocalcaemia,hypomagnesaemiaandhypokalaemiahasresultedinfrequenthospitalisaOonsinceinfancy.BiochemicaltesOngconfirmspersistenthypoparathyroidism,highurinarymagnesiumandpotassiumexcreOonbutnormalcalcium:creaOnine,reninandaldosterone.Sheistreatedwithalfacalcidol1microgramdailyandvaryingdosesofcalciumcarbonate,magnesiumandpotassiumreplacement.DespiteextensiveinvesOgaOon,nounifyingdiagnosiswasachievedunOlattheageof21years,wholegenomicsequencingconfirmedade-novoheterozygousc.1706G>AtransiOonintheFAM111AgenediagnosOcofKenny-CaffeySyndrome2.Kenny-CaffeySyndrome2(KCS2)KCS2isextremelyrarewithlessthan60casesreportedintheEnglishliterature.Theclinicalfeaturesofshortstature,skeletalabnormaliOesandhypoparathyroidismwerefirstdescribedinamotherandsonin1966byKennyandLinarelli.1In2013,genomicsequencingoffiveunrelated,affectedindividualsidenOfiedamutaOonintheFAM111Agenelocatedonchromosome11.2FAM111Acodesfora611aminoacidproteinwhichbearshomologytotrypsinbutitsfuncOonisunclear.3ExisOngclinicalcaseseries’hypothesiseanimportantroleinparathyroidhormoneregulaOonandbonegrowth.TherecurrenthypomagnesaemiaandhypokalaemiaseeninourcasesuggestsapotenOalmechanisminvolvingmagnesiumregulaOon.WeareconducOngfurtherresearchintounderstandingtheroleofFAM111Ainmagnesiumhomeostasis.KennyFM,LinarelliL(1966).DwarfismandcorOcalthickeningoftubularbones:transienthypocalcemiainamotherandson.AmJDisChild111:201–207UngerS,GornaMW,LeBechecAetal(2013).FAM111AmutaOonsresultinhypoparathyroidismandimpairedskeletaldevelopment.AmJHumGenet92:990–995FineDA,RozenblaH-RozenO,PadiMetal(2012)IdenOficaOonofFAM111AasanSV40hostrangerestricOonandadenovirushelperfactor.PLoSPathog.8(10):e1002949

DrSharonMackin
30 CalSoc2017
DrSharonMackin
31CalSoc2017

DrNyoNyoTun
32 CalSoc2017
AbstractTestosteroneDeficiencyinT2DMisaCondi1onofRela1veEstrogenExcess,ElevatedAdiposeAromataseExpressionandHighLep1nDrNyoNyoTun,DrDawnLivingstone&DrFraserWGibbBackground:Androgendeficiency(AD)isobservedinupto50%ofmenwithT2DM.IthasbeenproposedthisisaconsequenceofelevatedaromataseacOvityfromanexpandedadiposecompartment,howeverthishasbeencalledintoquesOonaslowerestradiolconcentraOonshavebeenreportedinmenwithT2DMrelatedhypogonadism.Acomplementaryhypothesispositsthepro-inflammatorystateassociatedwithT2DMasapotenOalcontributor.WesoughttoinvesOgatepredicOvefactorsforADinalargecohortofmenwithT2DM.Methods:228menwithT2DMundertheageof65wererecruitedandunderwent:fasOngbloodsampling,anthropometricmeasurements,bioimpedancebodyfatesOmaOon,AMSandSF-36quesOonnairesandsubcutaneousadiposeneedlebiopsy(n=150).Sexsteroids(includingTandE2)weremeasuredbyLCMS/MS.15geneOcvariantsrelatedtosex-steroidswereanalysedandsubcutaneousadiposemRNAexpressionof23genesofinterestwasassessedbyRT-PCR.TandE2wereconvertedtoz-scoresandthedifferencebetweenz-scoresusedasameasureofdivergence.Results:AD(definedastotalT<10nM)waspresentin34.3%.IndividualfactorsassociatedwithADincludedBMI(33.2vs.30.5mg/kg2,P<0.001),HbA1c(58vs.51mmol/mol,P<0.001),HOMA-IR(6.2vs.4.6,P=0.008),differencebetweenTandE2z-score(-0.6,vs.0.40,P<0.001–lessthan0indicatesrelaOveE2excess),plasmalepOn(21350vs.14600pg/ml,P<0.001)andadiposearomataseexpression(2.45vs.1.87,P<0.05).Age,smoking,alcoholconsumpOon,IL-6,IL-8,MCP-1andTNF-αwerenotassociatedwithtestosteronedeficiency.ModestassociaOonswithADwereobservedin5ofthe15geneOcvariantsassessed.LogisOcregressionidenOfiedT–E2z-scoredifference(P<0.001),insulinresistance(P=0.03)andplasmalepOn(P0.05)asthestrongestindependentpredictorsofAD.Conclusions:PreviousdemonstraOonoflowerE2levelsinhypogonadalmenwithT2DMisconfoundedbyfailuretoadjustforlowersubstrateandrogenlevels.Ourfindingssupportthehypothesisthatadiposity(highlepOn),higheraromataseexpressionandrelaOveestrogenexcessarekeydeterminantsofhypogonadisminT2DM.IncontrastcirculaOngandadiposemeasuresofinflammaOonwerenotassociatedwithhypogonadism.
BiographyIgraduatedfromUniversityofEdinburghin2007.MyfoundaOonandcoremedicaltrainingyearswerespentinGlasgowandAberdeen.IreturnedtoEdinburghin2013toundertakespecialtytrainingandtookOmeoutofprogrammetoundertakeanMDlookingintopredicOvefactorsofandrogendeficiencyinmenwithtype2diabetesunderthesupervisionofDr.DawnLivingstoneandDr.FraserGibb.

DrNyoNyoTun
33CalSoc2017
Δ=-3
Lessthan0=rela0veestradiolexcess
EdinburghEndocrinology
Rela0veTandE2balanceDifferencebetweenz-scores
Rela%veTandE2balanceDifferencebetweenz-scores
EdinburghEndocrinology
Rela%veestrogenexcess
Rela%veandrogenexcess
Limitedton=196menwithnormalrangeLH

DrNyoNyoTun
34 CalSoc2017
HbA1cLowerTassociatedwithhigherHbA1c
EdinburghEndocrinology
Totaltestosterone
R-0.287,P<0.001
P<0.001
Freetestosterone
R–0.173,P=0.016
P=0.108
Estradiol
R0.085,P=0.239
Lep$nAssociatedwithlowerTandhigherE2
EdinburghEndocrinology
Totaltestosterone
R-0.351,P<0.001
P=0.002
Freetestosterone
R-0.331,P<0.001
P=0.002
Estradiol
R0.143,P0.046
CYP19expressionAssociatedwithlowerCFTandhigherE2
EdinburghEndocrinology
Totaltestosterone
R-0.100,P=0.308
P=0.090
Freetestosterone
R-0.205,P=0.035
P=0.266
Estradiol
R0.301,P=0.002
HOMA-IRInsulinresistanceassociatedwithlowT
EdinburghEndocrinology
Totaltestosterone
R-0.272,P<0.001
P=0.011
Freetestosterone
R-0.167,P=0.019
P=0.025
Estradiol
R0.086,P=0.232
AgeAssociatedwithE,CFTbutnottotalT
EdinburghEndocrinology
Totaltestosterone
R-0.023,P=0.744
P=0.820
Freetestosterone
R-0.218,P=0.002
P=0.019
Estradiol
R-0.157,P=0.028
BMIDivergentassocia1onwithTandE2
EdinburghEndocrinology
Totaltestosterone
R-0.291,P<0.001
P=0.002
Freetestosterone
R-0.332,P<0.001
P<0.001
Estradiol
R0.257,P<0.001

DrCatrionaFarrell
35CalSoc2017
BiographyCatrionaFarrellgraduatedinmedicinefromGlasgowUniversityin2010whereshewentontocompleteFoundaOonandCoreMedicalTraining.ShemovedtotheEastofScotlandin2015tocommencehigherspecialtytraininginDiabetesandEndocrinology.In2017CatrionawasawardedtheDiabetesUKSirGeorgeAlberOResearchFellowshiptoundertakeaPhD,shewillbelookingintotheuseofhighintensityexerciseasanoveltreatmentofimpairedawarenessofhypoglycaemiaintype1diabetesunderthesupervisionofProfRoryMcCrimmonattheUniversityofDundee.
AbstractPancrea1cNeuroendocrineTumourassociatedwithHypoglycaemia;Tumour,TreatmentorTransforma1on?CatrionaFarrell,AsaDahle-Smith,GrahamLeese,PaulNeweyPancreaOcneuroendocrinetumours(PanNETs)occurinfrequently,withanannualincidenceof~1/100,000andaretypicallyclassifiedintofuncOoningandnon-funcOoningsubgroupsdependingonthesecretoryprofileofthetumour.ForindividualspresenOngwithadvancedfuncOonaltumours(e.g.insulinoma,gastrinoma,glucagonoma)treatmentstrategiesneednotonlyaddresscontrollingdiseaseprogressionbutmustalsocontrolsymptomsassociatedwithhormoneexcess.FailuretorecogniseoradequatelytreatsuchhormonesecreOonmayresultinsignificantmorbidityand/ormortality.Here,weillustratesomeofthesechallengesinapaOentdiagnosedwithanadvancedPanNET,whosubsequentlydevelopedmarkedhypoglycaemia.The57-yearoldmalepaOentiniOallypresentedwithweightlossandjaundice.Imagingrevealedthepresenceofahead-of-pancreasmassassociatedwithmulOplelivermetastases.SubsequentpancreaOcbiopsyindicatedalow-gradepancreaOcneuroendocrinetumour,whilstfurtherevaluaOonindicatedmarkedelevaOonofserumchromograninA,modestelevaOonofglucagon(X2ULN),andaviduptakeonoctreoOdescanning.Inviewofdiseaseburden,medicalmanagementwasrecommendedandhecommencedlong-acOngsomatostaOnanalogue(SSA)therapy.ThreemonthsawercommencingSSAtherapy,thepaOentdevelopedsymptomssuggesOveofhypoglycaemiaculminaOnginaroadtrafficaccidentassociatedwithlossofconsciousness.SubsequentreferraltoendocrinologyconfirmedendogenoushyperinsulinaemichypoglycaemiaanddiazoxidewasstartedwithparOalamelioraOonofsymptoms.Inviewofminordiseaseprogressiononimaging,SSAtherapywasdisconOnuedandeverolimuscommenced,withexcellentcontrolofhypoglycaemia.Diseaseburdenhasremainedstableoncurrenttherapy.InthispresentaOonwewillreviewtheuseofeverolimusasaninsulinomatreatmentandconsiderthethreepossibiliOesforthepresentaOonofhypoglycaemiainthiscase:(1)misseddiagnosisofmetastaOcinsulinomaatpresentaOon;(2)precipitaOonofhypoglycaemiabySSAtherapy;or(3)tumourtransformaOontoasecretoryphenotype.

DrCatrionaFarrell
36 CalSoc2017
Background–Pancrea/cNeuroendocrineTumours(PanNETs)
1
• PanNETSareaheterogeneousgroupofneoplasmsarisingfromendocrinecellsofthepancrea9cislets
• Incidenceandprevalenceincreasingover
past20years• Func9oningvsnon-func9oning• Advanceddiseaseisfrequentlyevidentat
the9meofdiagnosis• Currenttherapiesaimtocontroldisease
progressionandsymptomsrelatedtoexcesshormonesecre9on
Age-adjustedincidenceofPancrea3cNETS(DatafromSEERRegistry)
• Surgical–shouldbeofferedtoallpa0entsifnonresectablemetasta0cdiseaseisnotpresent– Laparoscopic– Abla0on(percutaneous,endoscopic)
• Medical–priortosurgery,ormalignantorrecurrentcases
– Frequentsmallmeals– Diazoxide– Somatosta0nanalogues– mTORinhibitor(Everolimus)– Pep0deReceptorRadionuclideTherapy(PRRT)– Chemoembolisa0on
Management–Insulinoma
0123456789
01/03/13
01/04/13
01/05/13
01/06/13
01/07/13
01/08/13
01/09/13
Glucosemmol/l
0500
10001500200025003000
01/03/13
01/04/13
01/05/13
01/06/13
01/07/13
01/08/13
01/09/13
Proinsulinpmol/l
00.51
1.52
2.53
3.54
4.5
01/03/13
01/04/13
01/05/13
01/06/13
01/07/13
01/08/13
01/09/13
CPep1de(nmol/l)
0
50
100
150
200
250
01/03/13
01/04/13
01/05/13
01/06/13
01/07/13
01/08/13
01/09/13
InsulinmU/l
ResponsetoEverolimus
DrMarcusLyallBiographyMarcusLyallisaClinicalLecturerattheBHFCentreforCardiovascularScienceattheUniversityofEdinburgh.HavinggraduatedinbiochemistryandthensubsequentlymedicinefromtheUniversityofDundee,hetookupaspecialtytrainingpostindiabetesandendocrinologyinLothianin2011beforeobtainingapositonontheEdinburghClinicalAcademicTraining(ECAT)Schemein2012.HisPhDresearchunderthesupervisionofDrMandyDrakeandProfessorRichardMeehan,focusedontheinteracOonbetweenglucosemetabolismandtheepigenomeinmetabolicliverdisease.OtherresearchinterestsincludeinvitrostemcellmodellingofNAFLDandsteroidinducedhyperglycaemiaincancertherapy.
AbstractIsReninaUsefulMarkerofMineralocorOcoidReplacementinAddison’sDisease?MarcusJLyall1,TarekMohamedElsayedSalem2,FraserWGibb31University/BHFCentreforCardiovascularScience,EndocrinologyUnit,UniversityofEdinburgh.2Alexandriauniversity,Egypt.3EdinburghCentreforEndocrinologyandDiabetes,RoyalInfirmaryofEdinburgh.IntroducOonTheuOlityofreninmeasurementinguidingmineralocorOcoidreplacementisunclear.Toaddressthis,weretrospecOvelyexaminedtheparametersandtreatmentof97paOentswithAddison’sdiseaseoverafiveyearperiod.MethodsAdrenalreplacement,bloodpressure(BP),orthostaOcbloodpressureresponse,urea,sodium,potassiumandreninlevelsof97paOentsaHendingourclinicwerecollectedovertheperiod2012-2016.DatawereanalysedandgraphicaloutputsgeneratedinRversion3.3.2.Results97paOentsaHendingfor397appointmentswerereviewed.Reninlevelwasmeasuredon227(57%)ofaHendancesatanesOmatedcostof£5500.68%ofreninmeasurementswereelevated(>45mU/L)with48%above90mu/Landamedianlevelof82mU/L.AweakbutsignificantnegaOveassociaOonwithplasmasodium(P<0.001,R20.072)wasnotedhowevernoassociaOonwaspresentbetweenreninlevelandpotassiumlevel,systolicordiastolicbloodpressureororthostaOcresponse.Areninlevel>90mu/Lwas63%sensiOveand57%specificfordetecOnganotherfeatureofmineralocorOcoiddeficiency(Na<135mmol/l,K>5.0mmol/l,orthostaOchypotension).Areninlevel>45ml/lwas76%sensiOvebutonly36%sensiOve.ReceiveroperaOngcharacterisOccurvedemonstratedthatelevatedreninwasavalidbutsubopOmaltestforidenOfyingotherfeaturesofmineralocorOcoiddeficiency(AUC0.649,pvalue<0.01).InpaOentswithnormalbiochemistryandorthostaOcbloodpressureresponse,derangedreninlevelalonesignificantlyinfluencedtheincidenceoffludrocorOsonedoseOtraOon(renin<5or>90mU/l,P<0.001chi-squaredtest).Conclusion.OurstudysuggeststhatserumreninminimallycorrelateswithclinicalandbiochemicalfeaturesofmineralocorOcoidstateandthathighreninlevelshaveonlymodestsensiOvityandlowspecificityfordetecOngfeaturesofmineralocorOcoiddeficiency.Despitethis,reninconOnuestobemeasuredrouOnelyatsignificantcostandtreatmentdecisionsconOnuetobemadebasedonlyonreninleveltheclinicaloutcomeofwhichremainsunclear.
37CalSoc2017

DrMarcusLyall
38 CalSoc2017
• Renin level was measured on 227/397 (57%) of attendances
• The majority of patients with PAI remain hyper-reninaemic despite fludrocortisone replacement (Median 82mu/l).
• 68% of measurements were above the reference range (45mU/L) with 48% greater than 90mU/l.
Renindistribu,onofpa,entsonmineralocor,coidreplacement.
SerumreninmU/l
45 82
EdinburghEndocrinology
Statistic >45mU/l >90mU/l
Sensitivity 76.47% 62.75%
Specificity 34.09 % 56.82 %
Positive Predictive Value 25.16% 29.63%
Negative Predictive Value 83.33 % 84.03 %
Disease prevalence 22.47% 22.47%
• Reninreninisavalidbutsubop1maltestforiden1fyingotherfeaturesofmineralocor1coid
• serumNa<135mmol/l,• serumK+>5.0mmol/lor• posturaldropof
≥10mmHgdiastolicor≥20mmHgsystolic
AUC = 0.649
P Value = 0.0012
Doeselevatedserumreninpredictotherfeaturesofmineralocor4coiddeficiency?
EdinburghEndocrinology

DrMarcusLyall
39CalSoc2017
not measured
**
*
**
ns
Changeinfludrocor/sonedoseinresponsetoreninlevelinpa/entswithnormalelectrolytes,bloodpressureandorthosta/cresponse,stra/fiedbyreninlevel.*P<0.01**P<0.001Chi squared test compared to ‘notmeasured’.
Arewemakingclinicaldecisionsbasedonreninlevelalone?
• Inpa/entswithnormalbiochemistryandorthosta/cbloodpressureresponse,derangedreninlevelalonesignificantlyinfluencedtheincidenceoffludrocor/sonedose/tra/on.
EdinburghEndocrinology
Conclusions • This study suggests that serum renin minimally correlates with
clinical and biochemical features of mineralocorticoid state.
• Despite this, renin continues to be measured routinely, at significant cost, and treatment decisions continue to be made based on renin level alone
• How this impacts on clinical outcomes is unclear.
• Further work is required to investigate how renin level relates to incidence of hospital admission, antihypertensive treatment and cardiovascular outcome.
EdinburghEndocrinology

DrCatrionaKyleBiographyIgraduatedfromAberdeenUniversityin2008andcompletedmyfoundaOonandcoremedicaltraininginGlasgow.In2012,ImovedtoEdinburghtoundertakespecialisttraininginDiabetesandEndocrinology.Awer2years,ItookOmeoutofprogrammetoundertakeaPhDwithProfessorBrianWalkerandDrRolandSOmsoninvesOgaOngthecontribuOonsofcorOsolandcorOcosteronetometabolicregulaOoninhumans.IreturnedtoclinicaltraininginAugust2017andamcurrentlyworkingintheRoyalInfirmaryofEdinburgh.
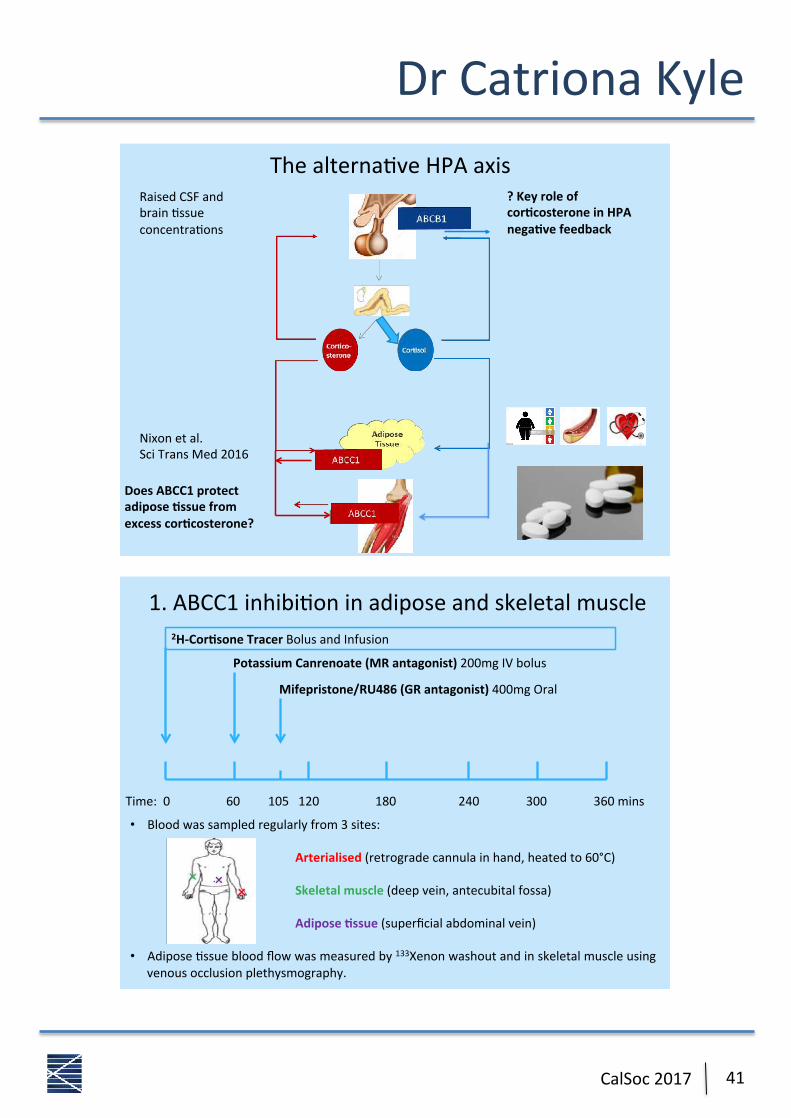
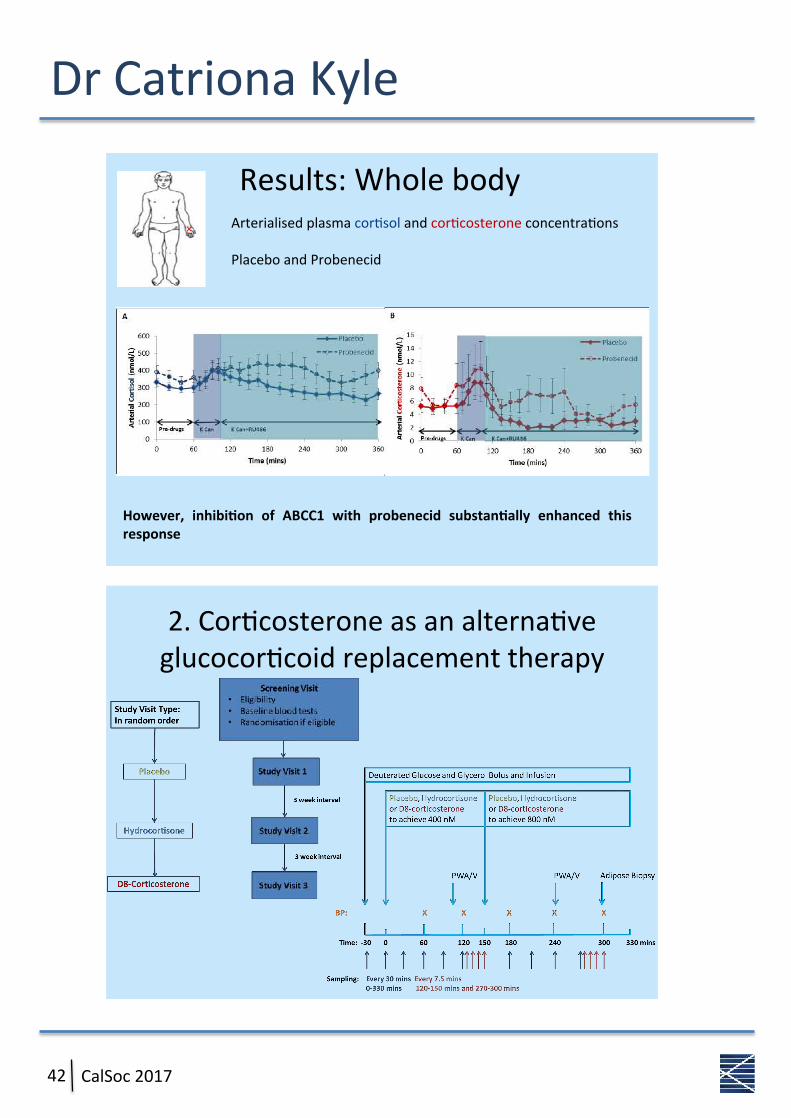
AbstractContribu1onsofcor1solandcor1costeronetometabolicregula1oninhumansCatrionaJKyle1,MarkNixon1,AliceOstojic1,LukeBoyle1,NatalieZHomer1,RuthAndrew1,RolandHSOmson1,BrianRWalker1.1BHFCentreforCardiovascularScience,Queen’sMedicalResearchInsOtute,UniversityofEdinburgh,UKBackgroundBothcorOsolandcorOcosteronecirculateinhumanplasmahowevercorOcosteronehasbeenrelaOvelyneglectedinhumanresearchtodate.ThereisevidenceofdisOnctregulaOonwithindifferentOssues:thetransmembraneATP-bindingcasseHe(ABC)transporterABCB1,highlyexpressedinthebrain,exportscorOsolbutnotcorOcosterone,likelyaccounOngfortherelaOveaccumulaOonofcorOcosteroneinthecentralnervoussystem(CNS).Incontrast,ABCC1,highlyexpressedinadiposeOssueandskeletalmuscle,exportscorOcosteronebutnotcorOsol,suggesOngcorOsolhasadisproporOonatelygreatereffectintheseOssues.WehypothesizedthatcorOcosteroneplaysanimportantroleincentralhypothalamic-pituitary-adrenalaxisfeedbackandthatcorOcosteronemightbeabeHerglucocorOcoidforreplacementincongenitaladrenalhyperplasia(CAH)duetoanimprovedmetabolicsideeffectprofile.MethodsTodeterminewhethertheABCC1transporterisresponsiblefordifferenOalbindingofcorOsolandcorOcosteronetoGR/MRinadiposeOssueandskeletalmuscle,weexaminedcorOcosteroidreceptoroccupancyofglucocorOcoidscentrallyandperipherallywithandwithoutABCC1inhibiOonin14healthyindividualsinarandomisedcrossoverdesign.ToexploretheefficacyofcorOcosteroneasanoveltreatmentforCAHinhumans,wecomparedtheefficacyofcorOcosteronecomparedwithhydrocorOsoneandplaceboinsuppressingtheHPAaxisinpaOentswithCAH.ResultsABCC1inhibiOonincreasedHPAaxisacOvitybutdidnotincreaseadiposeOssueorskeletalmuscleglucocorOcoidreceptoroccupancyfollowingcombinedglucocorOcoidandmineralocorOcoidreceptorantagonism,highlighOngapreviouslyundiscoveredcentralroleforABCC1.CorOcosteroneinfusionsuppressedACTHandadrenalandrogenstoasimilarextentashydrocorOsoneinCAHpaOents,providingproof-of-conceptofitsefficacy.ConclusionsThesedatashowthatthereareimportantdifferencesbetweencorOcosteroneandcorOsolphysiologyinhumans.ThisisinpartduetotheeffectsofABCC1whichplaysanimportantroleinregulaOonoftheHPAaxisinaddiOontoregulaOngperipheralglucocorOcoidacOon.CorOcosteroneacutelysuppressestheHPAaxisinCAH,highlighOngitspotenOalasanalternaOvetohydrocorOsoneforglucocorOcoidreplacementtherapy.
40 CalSoc2017
DrCatrionaKyle
41CalSoc2017
Thealterna*veHPAaxis?Keyroleofcor+costeroneinHPAnega+vefeedback
DoesABCC1protectadipose+ssuefromexcesscor+costerone?
RaisedCSFandbrain*ssueconcentra*ons
Nixonetal.SciTransMed2016
• Bloodwassampledregularlyfrom3sites:
Arterialised(retrogradecannulainhand,heatedto60°C)
Skeletalmuscle(deepvein,antecubitalfossa)
Adipose2ssue(superficialabdominalvein)
• AdiposeCssuebloodflowwasmeasuredby133Xenonwashoutandinskeletalmuscleusing
venousocclusionplethysmography.
1.ABCC1inhibiConinadiposeandskeletalmuscle
2H-Cor2soneTracerBolusandInfusion
Time:060105120180240300360mins
PotassiumCanrenoate(MRantagonist)200mgIVbolus
Mifepristone/RU486(GRantagonist)400mgOral
DrCatrionaKyle
42 CalSoc2017
However, inhibi-on of ABCC1 with probenecid substan-ally enhanced thisresponse
Results:WholebodyArterialisedplasmacor6solandcor6costeroneconcentra6onsPlaceboandProbenecid
2.Cor'costeroneasanalterna'veglucocor'coidreplacementtherapy

DrCatrionaKyle
43CalSoc2017
Results:PlasmaACTHACTHsuppressionapparentwithbothglucocor:coids
%ACTHsuppressionagainstGCconcentra:on
PlaceboCor+solD8-cor+costerone
Cor:sol333.1±31.0nmol/LD8-cor:costerone:535.2±53.6nmol/L

Notes
44 CalSoc2017

Notes
45CalSoc2017

CalSoc2017registraOon,mealsandaccommodaOonwerecoveredbyoursponsors:




















